User login
Surgery in an aging population
Men and women older than 65 years make up the fastest-growing portion of the U.S. population. By 2020, more than 16% of the American population is projected to be older than 65 years of age, according to projections by the U.S. Census.
As the population ages, an increasing proportion of our patients will be considered elderly (greater than 65 years), and up to 50% of surgeries will be performed in these patients. Perioperative mortality has decreased over the past 50 years in all patients, but elderly patients continue to have higher perioperative morbidity and mortality than their younger counterparts (Mt. Sinai J. Med. 2012;79:95-106). This increased morbidity is particularly relevant to gynecologists as 60% of the population older than 65 years is female. It is also important to note that 30-day mortality is higher in patients older than 80 years.

Significant risk factors in any surgical population include underlying cardiac and pulmonary disease, smoking, obesity, prior or current abdominal/thoracic surgery, and type of anesthesia (Prim. Care 1989;16:361-76).
Studies conflict on whether age alone is an independent risk factor for perioperative morbidity and mortality. Older patients tend to have more underlying diseases, thus placing them at increased risk for perioperative morbidity. Unfortunately, the presence of coexisting comorbidities does not alone account for poor outcomes. In one large population-based study, even healthy elderly patients continued to have higher morbidity and mortality. This is likely because elderly patients respond differently to perioperative physiologic stressors and pharmacologic interventions (Anesthesiology 2009;110:1176-81).
Organ function declines with age, but there is wide inter- and intraindividual variability in the rate of decline (Anesthesiology 2009;110:1176-81). Because of the potential for interpatient aging differences, gynecologists must assess each patient; chronologic age and biologic age can differ significantly (Semin. Perioper. Nurs. 1997;6:14-20). There are changes in pharmacokinetics and pharmacodynamics related to age and organ function changes. Alterations in kidney and liver function result in slower rates of drug metabolism, potentially increasing concentrations of medications in older patients. In addition to considering alterations in dosing, physicians must consider the possibility of increased or decreased sensitivities to medications resulting from alterations in pharmacodynamics.

Patients over 80 years old have increased perioperative morbidity and mortality. Respiratory and urinary tract complications are the most common, but cardiac complications are more severe in these patients (Mt. Sinai J. Med. 2012;79:95-106). Respiratory complications account for 40% of surgical complications and up to 20% of all surgery-related deaths. Respiratory morbidity is increased in patients who are under anesthesia for more than 3 hours or have abdominal and/or thoracic incisions (Can. Oper. Room Nurs. J. 2007;25:34-5, 37-41). Although less prevalent, cardiovascular complications can be devastating short term, accounting for 50% of postoperative mortality in the elderly. Complications increase with age, and 20% of patients older than 80 years experience at least one complication, which is particularly concerning given that the presence of one complication increases mortality sixfold.
In addition to being at greater risk for physical complications, elderly patients are at increased risk of experiencing psychological and neurologic complications in the postoperative period. Up to 15% of elderly patients can develop postoperative delirium, which is associated with longer hospital stays and other long-term consequences (Prim. Care 1989;16:361-76). Postoperative cognitive decline is a research finding of deterioration in neurocognitive testing that is also seen in elderly patients. Practically, this decline is manifested by a decreased ability to perform activities of daily living and instrumental activities of daily living. This decline may resolve over the first year postoperatively, and the incidence ranges from 5% to 15%. Patients older than 70 years are more likely to experience postoperative delirium and cognitive decline (Curr. Opin. Anaesthesiol. 2010;23:201-8).
As the population ages, gynecologists are going to face an increase in the number of women requiring surgical intervention for both benign and malignant indications. A thorough knowledge of the risks associated with this population is of the utmost importance so that we can appropriately counsel our patients and their families and take steps to minimize complications.
Dr. Hacker is a rising fourth-year resident in the department obstetrics and gynecology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. Dr. Hacker and Dr. Gehrig said they had no relevant financial disclosures.
Men and women older than 65 years make up the fastest-growing portion of the U.S. population. By 2020, more than 16% of the American population is projected to be older than 65 years of age, according to projections by the U.S. Census.
As the population ages, an increasing proportion of our patients will be considered elderly (greater than 65 years), and up to 50% of surgeries will be performed in these patients. Perioperative mortality has decreased over the past 50 years in all patients, but elderly patients continue to have higher perioperative morbidity and mortality than their younger counterparts (Mt. Sinai J. Med. 2012;79:95-106). This increased morbidity is particularly relevant to gynecologists as 60% of the population older than 65 years is female. It is also important to note that 30-day mortality is higher in patients older than 80 years.
Significant risk factors in any surgical population include underlying cardiac and pulmonary disease, smoking, obesity, prior or current abdominal/thoracic surgery, and type of anesthesia (Prim. Care 1989;16:361-76).
Studies conflict on whether age alone is an independent risk factor for perioperative morbidity and mortality. Older patients tend to have more underlying diseases, thus placing them at increased risk for perioperative morbidity. Unfortunately, the presence of coexisting comorbidities does not alone account for poor outcomes. In one large population-based study, even healthy elderly patients continued to have higher morbidity and mortality. This is likely because elderly patients respond differently to perioperative physiologic stressors and pharmacologic interventions (Anesthesiology 2009;110:1176-81).
Organ function declines with age, but there is wide inter- and intraindividual variability in the rate of decline (Anesthesiology 2009;110:1176-81). Because of the potential for interpatient aging differences, gynecologists must assess each patient; chronologic age and biologic age can differ significantly (Semin. Perioper. Nurs. 1997;6:14-20). There are changes in pharmacokinetics and pharmacodynamics related to age and organ function changes. Alterations in kidney and liver function result in slower rates of drug metabolism, potentially increasing concentrations of medications in older patients. In addition to considering alterations in dosing, physicians must consider the possibility of increased or decreased sensitivities to medications resulting from alterations in pharmacodynamics.
Patients over 80 years old have increased perioperative morbidity and mortality. Respiratory and urinary tract complications are the most common, but cardiac complications are more severe in these patients (Mt. Sinai J. Med. 2012;79:95-106). Respiratory complications account for 40% of surgical complications and up to 20% of all surgery-related deaths. Respiratory morbidity is increased in patients who are under anesthesia for more than 3 hours or have abdominal and/or thoracic incisions (Can. Oper. Room Nurs. J. 2007;25:34-5, 37-41). Although less prevalent, cardiovascular complications can be devastating short term, accounting for 50% of postoperative mortality in the elderly. Complications increase with age, and 20% of patients older than 80 years experience at least one complication, which is particularly concerning given that the presence of one complication increases mortality sixfold.
In addition to being at greater risk for physical complications, elderly patients are at increased risk of experiencing psychological and neurologic complications in the postoperative period. Up to 15% of elderly patients can develop postoperative delirium, which is associated with longer hospital stays and other long-term consequences (Prim. Care 1989;16:361-76). Postoperative cognitive decline is a research finding of deterioration in neurocognitive testing that is also seen in elderly patients. Practically, this decline is manifested by a decreased ability to perform activities of daily living and instrumental activities of daily living. This decline may resolve over the first year postoperatively, and the incidence ranges from 5% to 15%. Patients older than 70 years are more likely to experience postoperative delirium and cognitive decline (Curr. Opin. Anaesthesiol. 2010;23:201-8).
As the population ages, gynecologists are going to face an increase in the number of women requiring surgical intervention for both benign and malignant indications. A thorough knowledge of the risks associated with this population is of the utmost importance so that we can appropriately counsel our patients and their families and take steps to minimize complications.
Dr. Hacker is a rising fourth-year resident in the department obstetrics and gynecology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. Dr. Hacker and Dr. Gehrig said they had no relevant financial disclosures.
Men and women older than 65 years make up the fastest-growing portion of the U.S. population. By 2020, more than 16% of the American population is projected to be older than 65 years of age, according to projections by the U.S. Census.
As the population ages, an increasing proportion of our patients will be considered elderly (greater than 65 years), and up to 50% of surgeries will be performed in these patients. Perioperative mortality has decreased over the past 50 years in all patients, but elderly patients continue to have higher perioperative morbidity and mortality than their younger counterparts (Mt. Sinai J. Med. 2012;79:95-106). This increased morbidity is particularly relevant to gynecologists as 60% of the population older than 65 years is female. It is also important to note that 30-day mortality is higher in patients older than 80 years.
Significant risk factors in any surgical population include underlying cardiac and pulmonary disease, smoking, obesity, prior or current abdominal/thoracic surgery, and type of anesthesia (Prim. Care 1989;16:361-76).
Studies conflict on whether age alone is an independent risk factor for perioperative morbidity and mortality. Older patients tend to have more underlying diseases, thus placing them at increased risk for perioperative morbidity. Unfortunately, the presence of coexisting comorbidities does not alone account for poor outcomes. In one large population-based study, even healthy elderly patients continued to have higher morbidity and mortality. This is likely because elderly patients respond differently to perioperative physiologic stressors and pharmacologic interventions (Anesthesiology 2009;110:1176-81).
Organ function declines with age, but there is wide inter- and intraindividual variability in the rate of decline (Anesthesiology 2009;110:1176-81). Because of the potential for interpatient aging differences, gynecologists must assess each patient; chronologic age and biologic age can differ significantly (Semin. Perioper. Nurs. 1997;6:14-20). There are changes in pharmacokinetics and pharmacodynamics related to age and organ function changes. Alterations in kidney and liver function result in slower rates of drug metabolism, potentially increasing concentrations of medications in older patients. In addition to considering alterations in dosing, physicians must consider the possibility of increased or decreased sensitivities to medications resulting from alterations in pharmacodynamics.
Patients over 80 years old have increased perioperative morbidity and mortality. Respiratory and urinary tract complications are the most common, but cardiac complications are more severe in these patients (Mt. Sinai J. Med. 2012;79:95-106). Respiratory complications account for 40% of surgical complications and up to 20% of all surgery-related deaths. Respiratory morbidity is increased in patients who are under anesthesia for more than 3 hours or have abdominal and/or thoracic incisions (Can. Oper. Room Nurs. J. 2007;25:34-5, 37-41). Although less prevalent, cardiovascular complications can be devastating short term, accounting for 50% of postoperative mortality in the elderly. Complications increase with age, and 20% of patients older than 80 years experience at least one complication, which is particularly concerning given that the presence of one complication increases mortality sixfold.
In addition to being at greater risk for physical complications, elderly patients are at increased risk of experiencing psychological and neurologic complications in the postoperative period. Up to 15% of elderly patients can develop postoperative delirium, which is associated with longer hospital stays and other long-term consequences (Prim. Care 1989;16:361-76). Postoperative cognitive decline is a research finding of deterioration in neurocognitive testing that is also seen in elderly patients. Practically, this decline is manifested by a decreased ability to perform activities of daily living and instrumental activities of daily living. This decline may resolve over the first year postoperatively, and the incidence ranges from 5% to 15%. Patients older than 70 years are more likely to experience postoperative delirium and cognitive decline (Curr. Opin. Anaesthesiol. 2010;23:201-8).
As the population ages, gynecologists are going to face an increase in the number of women requiring surgical intervention for both benign and malignant indications. A thorough knowledge of the risks associated with this population is of the utmost importance so that we can appropriately counsel our patients and their families and take steps to minimize complications.
Dr. Hacker is a rising fourth-year resident in the department obstetrics and gynecology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. Dr. Hacker and Dr. Gehrig said they had no relevant financial disclosures.

The authentic life of Henry Grunebaum
Henry Grunebaum wrote: "Dying need not be merely a matter of letting go, of disengaging from those most dear to us, but of giving meaning, hope and a vital part of oneself to those whose lives we have touched and have touched us" ("A Final Round of Therapy, Fulfilling the Needs of 2," New York Times, Oct. 5, 2009). The reciprocity of this remark is now apt for Henry: that in his dying, he gives us a vital part of his life.
Henry Grunebaum died at age 87 on Friday, April 11, 2014. He was a member of the Group for the Advancement of Psychiatry (GAP) Family Committee, which was meeting on that Friday. We missed him from his usual seat by the window. He had been a member of GAP for many decades.
Henry was one of the earliest family psychiatrists: Since the 1950s, he thought, wrote, and taught us about our responsibility in caring for families. This essay is a reflection on Henry’s place in the history of family psychiatry. By following Henry’s interests, we take a tour of many family concerns that remain unattended by psychiatrists today.
His earliest work and writings concerned the care of children when a parent has a mental illness (Am. J. Psychiatry 1963;119:927-33). He was an inspiration to many during family psychiatry’s formative years.
As part of an Association of Family Psychiatrists discussion group, family psychiatrist Lee Combrinck-Graham of Stamford, Conn., wrote in remembrance of Henry: "I was a first-year resident and we had a young woman with a very young baby who thought she was an apple. This apparently had something to do with the Garden of Eden and Original Sin, but it definitely distracted her from caring for her baby. So, we wrote to Henry and read his paper, and we invited her husband to bring in the baby, and they all stayed there, on 10 Gates at the Hospital of the University of Pennsylvania. She was certainly able to stay more involved with her baby in the setting where she was getting a lot of coaching and input and support from the nurses. It was difficult, because there were no provisions for babies in psychiatric units – and what Henry had done was to inspire us to do something that was right to do, and make it work, and we did."
Fast-forward to 2011, when the University of North Carolina at Chapel Hill inaugurated the first perinatal psychiatry inpatient unit in the United States. The most frequent admitting diagnosis is perinatal unipolar mood disorder (60.4%). The unit’s success is measured by the significant improvements in symptoms of depression, anxiety, and active suicidal ideation between admission and discharge (P less than 0.0001) (Arch. Womens Ment. Health 2014;17:107-13).
Henry reminded psychiatrists of his early family research when, in 2011, he wrote a letter to the editor of the American Journal of Psychiatry: "It may interest readers of the article by Wickramaratne et al. on the children of depressed mothers that a study of a similar population with similar goals was conducted four decades ago" (Am. J. Psychiatry 2011;168:1222-3).
We still have a long way to go in providing care for children who have parents with mental illness. A few individuals such as Dr. Michelle D. Sherman of Oklahoma City (http://www.ouhsc.edu/safeprogram/) and Dr. William Beardslee of Harvard University (http://fampod.org) have developed programs for these children that are accessible to all practitioners, but we still lag far behind places such as the United Kingdom and Australia, which provide state programs for children who have parents with mental illness.
Henry next became concerned about the therapeutic neglect of fathers (J. Child. Psychol. Psychiatry 1964;5:241-9). He enrolled fathers in group therapy and wrote empathically about their difficulties (Br. J. Med. Psychol. 1962,35:147-54). Psychiatry still lacks a focus on fathers, especially those with mental illness.
Next, Henry turned his attention to the topic of love. Psychiatrists rarely speak of love, except with caution and a lack of comprehension. What do we say to our patients who ask us about love? There is no psychiatric theory of love. Martin S. Bergmann, Ph.D., explained: "Freud approached the topic of love reluctantly, fearing to encroach on a territory of poets or philosophers like Plato and Schopenhauer endowed with poetic gifts. Not without irony he claimed that when psychoanalysis touches the subject of love, its touch must be clumsy by comparison with that of the poets" (J. Am. Psychoanal. Assoc.1988;36:653-72).
Psychiatrists have written for the public, explaining love through brain chemistry. "A General Theory of Love" (New York: Random House, 2000), written by psychiatrists Thomas Lewis, Fari Amini, and Richard Lannon, is immensely popular and has been translated into many languages. In "Can Love Last? The Fate of Romance Over Time" (New York: W.W. Norton & Co., 2003), Stephen A. Mitchell informed readers that "romance depends on mystery, but long-term relationships depend on understanding. Romance gets its fizz from sexuality, but partnership demands tenderness and caring, not lust. Romance is based on idealization of the other, and idealizing anyone is asking for trouble." Freud described his yearning patients neatly: "Where they love, they have no desire; where they desire, they cannot love." What hormones are important in love?
Oxytocin is a significant hormone involved in the neuroanatomy of intimacy. It has a role in many biological processes, such as the promotion of wound healing (Curr. Opinion Psychiatry;2012;25:135-40), and in human bonding. Researchers recently reported on the role of partners’ hormones at the initiation of romantic love (Soc. Neurosci. 2014;9:337-51). Test subjects were 40 singles and 120 new lovers (60 couples). Couples were assessed for empathy and hostility. Oxytocin showed direct partner effects: Individuals whose partners had higher oxytocin showed greater empathy. Low empathy, on the other hand, was associated with high cortisol, but only in the context of high partner’s cortisol. High cortisol in both partners is associated with relationship breakup. The mutual influences between hormones and behavior highlight the systemic nature of relationships.
Empathy also is important in the recovery from schizophrenia. Investigators have identified the importance of warmth in reducing relapse rates (J. Abnorm. Psychol. 2004;113:428-39). On the flip side, the role of criticism is a well-known key family factor linked to relapse in many illnesses, both psychiatric and medical. Putting those ideas into clinical practice, however, has proven to be difficult, and the gap between research and practice is still quite large.
Henry considered romantic problems from the perspective of a practicing clinician. He stated: "There are no easy solutions available to the clinician whose clients are experiencing problems with romantic/erotic love. There are no easy solutions, because love itself, in all of its manifestations and disguises, is complicated and perplexing. But why should we expect it to be less so than life? We desire to have another to love, for without one we will be lonely and there will be no one who truly knows us. We desire to become one with the other, to be selfless, and to lose ourselves in sexual intimacy. But we are also afraid of losing ourselves, for we know that the person we love is other, independent, and that we can never truly know him or her. This is the predicament of love" (J. Marital Fam. Ther. 1997;23:295-307).
A fairly recent study validated Henry’s focus on love. When couples are asked to describe the main themes that determine the quality and stability of their relationships, they answer decisively "love" (Fam. Process 2003;42:253-67).
Throughout his life, Henry continued to share his own experiences of therapy in an authentic way. When he wrote about his visits with a dying patient in the New York Times in 2009, Henry revealed his own personal reflections on illness and death. In that piece, he taught us to be always considering our responses to our patients. He also taught us that we are always learning.
His last published work is a reflection on the relationship between a patient and therapist when that relationship spans decades (Am. J. Psychiatry 2012;169:434). He asked whether this is therapy or companionship – and if this matters. Henry resisted biological reductionism in psychiatry with a gentle wisdom that pointed to the role of narrative and family throughout history and in our work. He still reminds us that love and compassion are needed to do our work well.
Henry’s legacy for family psychiatry is deep, and he had several lessons for those of us who attend to patients:
• Work to maintain the mother-child bond when maternal illness is present.
• Attend to fathers.
• Remember that romantic/erotic love is a topic of great importance to psychiatry and health.
• Keep in mind that relationships with patients hold truths that we may not yet fully understand.
• Believe that love and compassion make work into a life’s joy.
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. She is editor of the recently published book, "Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals" (New York: Routledge, 2013).
Henry Grunebaum wrote: "Dying need not be merely a matter of letting go, of disengaging from those most dear to us, but of giving meaning, hope and a vital part of oneself to those whose lives we have touched and have touched us" ("A Final Round of Therapy, Fulfilling the Needs of 2," New York Times, Oct. 5, 2009). The reciprocity of this remark is now apt for Henry: that in his dying, he gives us a vital part of his life.
Henry Grunebaum died at age 87 on Friday, April 11, 2014. He was a member of the Group for the Advancement of Psychiatry (GAP) Family Committee, which was meeting on that Friday. We missed him from his usual seat by the window. He had been a member of GAP for many decades.
Henry was one of the earliest family psychiatrists: Since the 1950s, he thought, wrote, and taught us about our responsibility in caring for families. This essay is a reflection on Henry’s place in the history of family psychiatry. By following Henry’s interests, we take a tour of many family concerns that remain unattended by psychiatrists today.
His earliest work and writings concerned the care of children when a parent has a mental illness (Am. J. Psychiatry 1963;119:927-33). He was an inspiration to many during family psychiatry’s formative years.
As part of an Association of Family Psychiatrists discussion group, family psychiatrist Lee Combrinck-Graham of Stamford, Conn., wrote in remembrance of Henry: "I was a first-year resident and we had a young woman with a very young baby who thought she was an apple. This apparently had something to do with the Garden of Eden and Original Sin, but it definitely distracted her from caring for her baby. So, we wrote to Henry and read his paper, and we invited her husband to bring in the baby, and they all stayed there, on 10 Gates at the Hospital of the University of Pennsylvania. She was certainly able to stay more involved with her baby in the setting where she was getting a lot of coaching and input and support from the nurses. It was difficult, because there were no provisions for babies in psychiatric units – and what Henry had done was to inspire us to do something that was right to do, and make it work, and we did."
Fast-forward to 2011, when the University of North Carolina at Chapel Hill inaugurated the first perinatal psychiatry inpatient unit in the United States. The most frequent admitting diagnosis is perinatal unipolar mood disorder (60.4%). The unit’s success is measured by the significant improvements in symptoms of depression, anxiety, and active suicidal ideation between admission and discharge (P less than 0.0001) (Arch. Womens Ment. Health 2014;17:107-13).
Henry reminded psychiatrists of his early family research when, in 2011, he wrote a letter to the editor of the American Journal of Psychiatry: "It may interest readers of the article by Wickramaratne et al. on the children of depressed mothers that a study of a similar population with similar goals was conducted four decades ago" (Am. J. Psychiatry 2011;168:1222-3).
We still have a long way to go in providing care for children who have parents with mental illness. A few individuals such as Dr. Michelle D. Sherman of Oklahoma City (http://www.ouhsc.edu/safeprogram/) and Dr. William Beardslee of Harvard University (http://fampod.org) have developed programs for these children that are accessible to all practitioners, but we still lag far behind places such as the United Kingdom and Australia, which provide state programs for children who have parents with mental illness.
Henry next became concerned about the therapeutic neglect of fathers (J. Child. Psychol. Psychiatry 1964;5:241-9). He enrolled fathers in group therapy and wrote empathically about their difficulties (Br. J. Med. Psychol. 1962,35:147-54). Psychiatry still lacks a focus on fathers, especially those with mental illness.
Next, Henry turned his attention to the topic of love. Psychiatrists rarely speak of love, except with caution and a lack of comprehension. What do we say to our patients who ask us about love? There is no psychiatric theory of love. Martin S. Bergmann, Ph.D., explained: "Freud approached the topic of love reluctantly, fearing to encroach on a territory of poets or philosophers like Plato and Schopenhauer endowed with poetic gifts. Not without irony he claimed that when psychoanalysis touches the subject of love, its touch must be clumsy by comparison with that of the poets" (J. Am. Psychoanal. Assoc.1988;36:653-72).
Psychiatrists have written for the public, explaining love through brain chemistry. "A General Theory of Love" (New York: Random House, 2000), written by psychiatrists Thomas Lewis, Fari Amini, and Richard Lannon, is immensely popular and has been translated into many languages. In "Can Love Last? The Fate of Romance Over Time" (New York: W.W. Norton & Co., 2003), Stephen A. Mitchell informed readers that "romance depends on mystery, but long-term relationships depend on understanding. Romance gets its fizz from sexuality, but partnership demands tenderness and caring, not lust. Romance is based on idealization of the other, and idealizing anyone is asking for trouble." Freud described his yearning patients neatly: "Where they love, they have no desire; where they desire, they cannot love." What hormones are important in love?
Oxytocin is a significant hormone involved in the neuroanatomy of intimacy. It has a role in many biological processes, such as the promotion of wound healing (Curr. Opinion Psychiatry;2012;25:135-40), and in human bonding. Researchers recently reported on the role of partners’ hormones at the initiation of romantic love (Soc. Neurosci. 2014;9:337-51). Test subjects were 40 singles and 120 new lovers (60 couples). Couples were assessed for empathy and hostility. Oxytocin showed direct partner effects: Individuals whose partners had higher oxytocin showed greater empathy. Low empathy, on the other hand, was associated with high cortisol, but only in the context of high partner’s cortisol. High cortisol in both partners is associated with relationship breakup. The mutual influences between hormones and behavior highlight the systemic nature of relationships.
Empathy also is important in the recovery from schizophrenia. Investigators have identified the importance of warmth in reducing relapse rates (J. Abnorm. Psychol. 2004;113:428-39). On the flip side, the role of criticism is a well-known key family factor linked to relapse in many illnesses, both psychiatric and medical. Putting those ideas into clinical practice, however, has proven to be difficult, and the gap between research and practice is still quite large.
Henry considered romantic problems from the perspective of a practicing clinician. He stated: "There are no easy solutions available to the clinician whose clients are experiencing problems with romantic/erotic love. There are no easy solutions, because love itself, in all of its manifestations and disguises, is complicated and perplexing. But why should we expect it to be less so than life? We desire to have another to love, for without one we will be lonely and there will be no one who truly knows us. We desire to become one with the other, to be selfless, and to lose ourselves in sexual intimacy. But we are also afraid of losing ourselves, for we know that the person we love is other, independent, and that we can never truly know him or her. This is the predicament of love" (J. Marital Fam. Ther. 1997;23:295-307).
A fairly recent study validated Henry’s focus on love. When couples are asked to describe the main themes that determine the quality and stability of their relationships, they answer decisively "love" (Fam. Process 2003;42:253-67).
Throughout his life, Henry continued to share his own experiences of therapy in an authentic way. When he wrote about his visits with a dying patient in the New York Times in 2009, Henry revealed his own personal reflections on illness and death. In that piece, he taught us to be always considering our responses to our patients. He also taught us that we are always learning.
His last published work is a reflection on the relationship between a patient and therapist when that relationship spans decades (Am. J. Psychiatry 2012;169:434). He asked whether this is therapy or companionship – and if this matters. Henry resisted biological reductionism in psychiatry with a gentle wisdom that pointed to the role of narrative and family throughout history and in our work. He still reminds us that love and compassion are needed to do our work well.
Henry’s legacy for family psychiatry is deep, and he had several lessons for those of us who attend to patients:
• Work to maintain the mother-child bond when maternal illness is present.
• Attend to fathers.
• Remember that romantic/erotic love is a topic of great importance to psychiatry and health.
• Keep in mind that relationships with patients hold truths that we may not yet fully understand.
• Believe that love and compassion make work into a life’s joy.
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. She is editor of the recently published book, "Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals" (New York: Routledge, 2013).
Henry Grunebaum wrote: "Dying need not be merely a matter of letting go, of disengaging from those most dear to us, but of giving meaning, hope and a vital part of oneself to those whose lives we have touched and have touched us" ("A Final Round of Therapy, Fulfilling the Needs of 2," New York Times, Oct. 5, 2009). The reciprocity of this remark is now apt for Henry: that in his dying, he gives us a vital part of his life.
Henry Grunebaum died at age 87 on Friday, April 11, 2014. He was a member of the Group for the Advancement of Psychiatry (GAP) Family Committee, which was meeting on that Friday. We missed him from his usual seat by the window. He had been a member of GAP for many decades.
Henry was one of the earliest family psychiatrists: Since the 1950s, he thought, wrote, and taught us about our responsibility in caring for families. This essay is a reflection on Henry’s place in the history of family psychiatry. By following Henry’s interests, we take a tour of many family concerns that remain unattended by psychiatrists today.
His earliest work and writings concerned the care of children when a parent has a mental illness (Am. J. Psychiatry 1963;119:927-33). He was an inspiration to many during family psychiatry’s formative years.
As part of an Association of Family Psychiatrists discussion group, family psychiatrist Lee Combrinck-Graham of Stamford, Conn., wrote in remembrance of Henry: "I was a first-year resident and we had a young woman with a very young baby who thought she was an apple. This apparently had something to do with the Garden of Eden and Original Sin, but it definitely distracted her from caring for her baby. So, we wrote to Henry and read his paper, and we invited her husband to bring in the baby, and they all stayed there, on 10 Gates at the Hospital of the University of Pennsylvania. She was certainly able to stay more involved with her baby in the setting where she was getting a lot of coaching and input and support from the nurses. It was difficult, because there were no provisions for babies in psychiatric units – and what Henry had done was to inspire us to do something that was right to do, and make it work, and we did."
Fast-forward to 2011, when the University of North Carolina at Chapel Hill inaugurated the first perinatal psychiatry inpatient unit in the United States. The most frequent admitting diagnosis is perinatal unipolar mood disorder (60.4%). The unit’s success is measured by the significant improvements in symptoms of depression, anxiety, and active suicidal ideation between admission and discharge (P less than 0.0001) (Arch. Womens Ment. Health 2014;17:107-13).
Henry reminded psychiatrists of his early family research when, in 2011, he wrote a letter to the editor of the American Journal of Psychiatry: "It may interest readers of the article by Wickramaratne et al. on the children of depressed mothers that a study of a similar population with similar goals was conducted four decades ago" (Am. J. Psychiatry 2011;168:1222-3).
We still have a long way to go in providing care for children who have parents with mental illness. A few individuals such as Dr. Michelle D. Sherman of Oklahoma City (http://www.ouhsc.edu/safeprogram/) and Dr. William Beardslee of Harvard University (http://fampod.org) have developed programs for these children that are accessible to all practitioners, but we still lag far behind places such as the United Kingdom and Australia, which provide state programs for children who have parents with mental illness.
Henry next became concerned about the therapeutic neglect of fathers (J. Child. Psychol. Psychiatry 1964;5:241-9). He enrolled fathers in group therapy and wrote empathically about their difficulties (Br. J. Med. Psychol. 1962,35:147-54). Psychiatry still lacks a focus on fathers, especially those with mental illness.
Next, Henry turned his attention to the topic of love. Psychiatrists rarely speak of love, except with caution and a lack of comprehension. What do we say to our patients who ask us about love? There is no psychiatric theory of love. Martin S. Bergmann, Ph.D., explained: "Freud approached the topic of love reluctantly, fearing to encroach on a territory of poets or philosophers like Plato and Schopenhauer endowed with poetic gifts. Not without irony he claimed that when psychoanalysis touches the subject of love, its touch must be clumsy by comparison with that of the poets" (J. Am. Psychoanal. Assoc.1988;36:653-72).
Psychiatrists have written for the public, explaining love through brain chemistry. "A General Theory of Love" (New York: Random House, 2000), written by psychiatrists Thomas Lewis, Fari Amini, and Richard Lannon, is immensely popular and has been translated into many languages. In "Can Love Last? The Fate of Romance Over Time" (New York: W.W. Norton & Co., 2003), Stephen A. Mitchell informed readers that "romance depends on mystery, but long-term relationships depend on understanding. Romance gets its fizz from sexuality, but partnership demands tenderness and caring, not lust. Romance is based on idealization of the other, and idealizing anyone is asking for trouble." Freud described his yearning patients neatly: "Where they love, they have no desire; where they desire, they cannot love." What hormones are important in love?
Oxytocin is a significant hormone involved in the neuroanatomy of intimacy. It has a role in many biological processes, such as the promotion of wound healing (Curr. Opinion Psychiatry;2012;25:135-40), and in human bonding. Researchers recently reported on the role of partners’ hormones at the initiation of romantic love (Soc. Neurosci. 2014;9:337-51). Test subjects were 40 singles and 120 new lovers (60 couples). Couples were assessed for empathy and hostility. Oxytocin showed direct partner effects: Individuals whose partners had higher oxytocin showed greater empathy. Low empathy, on the other hand, was associated with high cortisol, but only in the context of high partner’s cortisol. High cortisol in both partners is associated with relationship breakup. The mutual influences between hormones and behavior highlight the systemic nature of relationships.
Empathy also is important in the recovery from schizophrenia. Investigators have identified the importance of warmth in reducing relapse rates (J. Abnorm. Psychol. 2004;113:428-39). On the flip side, the role of criticism is a well-known key family factor linked to relapse in many illnesses, both psychiatric and medical. Putting those ideas into clinical practice, however, has proven to be difficult, and the gap between research and practice is still quite large.
Henry considered romantic problems from the perspective of a practicing clinician. He stated: "There are no easy solutions available to the clinician whose clients are experiencing problems with romantic/erotic love. There are no easy solutions, because love itself, in all of its manifestations and disguises, is complicated and perplexing. But why should we expect it to be less so than life? We desire to have another to love, for without one we will be lonely and there will be no one who truly knows us. We desire to become one with the other, to be selfless, and to lose ourselves in sexual intimacy. But we are also afraid of losing ourselves, for we know that the person we love is other, independent, and that we can never truly know him or her. This is the predicament of love" (J. Marital Fam. Ther. 1997;23:295-307).
A fairly recent study validated Henry’s focus on love. When couples are asked to describe the main themes that determine the quality and stability of their relationships, they answer decisively "love" (Fam. Process 2003;42:253-67).
Throughout his life, Henry continued to share his own experiences of therapy in an authentic way. When he wrote about his visits with a dying patient in the New York Times in 2009, Henry revealed his own personal reflections on illness and death. In that piece, he taught us to be always considering our responses to our patients. He also taught us that we are always learning.
His last published work is a reflection on the relationship between a patient and therapist when that relationship spans decades (Am. J. Psychiatry 2012;169:434). He asked whether this is therapy or companionship – and if this matters. Henry resisted biological reductionism in psychiatry with a gentle wisdom that pointed to the role of narrative and family throughout history and in our work. He still reminds us that love and compassion are needed to do our work well.
Henry’s legacy for family psychiatry is deep, and he had several lessons for those of us who attend to patients:
• Work to maintain the mother-child bond when maternal illness is present.
• Attend to fathers.
• Remember that romantic/erotic love is a topic of great importance to psychiatry and health.
• Keep in mind that relationships with patients hold truths that we may not yet fully understand.
• Believe that love and compassion make work into a life’s joy.
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. She is editor of the recently published book, "Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals" (New York: Routledge, 2013).

ASCO at 50 … we’ve come a long way, we know a lot, but we’ve only just begun
I recently had both the pleasure and the challenge of attending ASCO 2014, the annual meeting of the American Society of Clinical Oncology. It was my first official ASCO meeting, and as an almost-third-year fellow in oncology, no amount of reading, research, scheduling, ASCO 2014 iPad app organizing, or even attending the day 1 early morning How to Navigate the Annual Meeting seminar could have prepared me for the experience…
Click on the PDF icon at the top of this introduction to read the full article.
I recently had both the pleasure and the challenge of attending ASCO 2014, the annual meeting of the American Society of Clinical Oncology. It was my first official ASCO meeting, and as an almost-third-year fellow in oncology, no amount of reading, research, scheduling, ASCO 2014 iPad app organizing, or even attending the day 1 early morning How to Navigate the Annual Meeting seminar could have prepared me for the experience…
Click on the PDF icon at the top of this introduction to read the full article.
I recently had both the pleasure and the challenge of attending ASCO 2014, the annual meeting of the American Society of Clinical Oncology. It was my first official ASCO meeting, and as an almost-third-year fellow in oncology, no amount of reading, research, scheduling, ASCO 2014 iPad app organizing, or even attending the day 1 early morning How to Navigate the Annual Meeting seminar could have prepared me for the experience…
Click on the PDF icon at the top of this introduction to read the full article.
Encouraging data at ASCO 2014 for survival and fertility in some cancers
The American Society of Clinical Oncology marked its 50th anniversary at this year’s annual conference in Chicago, where it showcased the latest scientific advances in oncology and explored the translation of research findings into practice under its umbrella theme, Science and Society.
Drug combo extends survival by more than 1 year in metastatic prostate cancer patients
Key clinical finding Adding docetaxel to hormonal therapy at the time of diagnosis of metastatic prostate cancer extends survival. Major finding Patients receiving docetaxel and androgen deprivation therapy at the time of diagnoses had median overall survival that was 13.6 months longer than men who received androgen deprivation therapy alone. Data source Randomized trial in 790 men with newly diagnosed metastatic hormone-sensitive prostate cancer...
Click on the PDF icon at the top of this introduction to read the full article.
The American Society of Clinical Oncology marked its 50th anniversary at this year’s annual conference in Chicago, where it showcased the latest scientific advances in oncology and explored the translation of research findings into practice under its umbrella theme, Science and Society.
Drug combo extends survival by more than 1 year in metastatic prostate cancer patients
Key clinical finding Adding docetaxel to hormonal therapy at the time of diagnosis of metastatic prostate cancer extends survival. Major finding Patients receiving docetaxel and androgen deprivation therapy at the time of diagnoses had median overall survival that was 13.6 months longer than men who received androgen deprivation therapy alone. Data source Randomized trial in 790 men with newly diagnosed metastatic hormone-sensitive prostate cancer...
Click on the PDF icon at the top of this introduction to read the full article.
The American Society of Clinical Oncology marked its 50th anniversary at this year’s annual conference in Chicago, where it showcased the latest scientific advances in oncology and explored the translation of research findings into practice under its umbrella theme, Science and Society.
Drug combo extends survival by more than 1 year in metastatic prostate cancer patients
Key clinical finding Adding docetaxel to hormonal therapy at the time of diagnosis of metastatic prostate cancer extends survival. Major finding Patients receiving docetaxel and androgen deprivation therapy at the time of diagnoses had median overall survival that was 13.6 months longer than men who received androgen deprivation therapy alone. Data source Randomized trial in 790 men with newly diagnosed metastatic hormone-sensitive prostate cancer...
Click on the PDF icon at the top of this introduction to read the full article.
Should lithium and ECT be used concurrently in geriatric patients?
Delirium has been described as a potential complication of concurrent lithium and electroconvulsive therapy (ECT) for depression, in association with a range of serum lithium levels. Although debate persists about the safety of continuing previously established lithium therapy during a course of ECT for mood symptoms, withholding lithium for 24 hours before administering ECT and measuring the serum lithium level before ECT were found to decrease the risk of post-ECT neurocognitive effects.1
We have found that the conventional practice of holding lithium for 24 hours before ECT might need to be re-evaluated in geriatric patients, as the following case demonstrates. Only 24 hours of holding lithium therapy might result in a lithium level sufficient to contribute to delirium after ECT.
CASE REPORT
An older woman with recurrent unipolar psychotic depression
Mrs. A, age 81, was admitted to the hospital with a 1-week history of depressed mood, anhedonia, insomnia, anergia, anorexia, and nihilistic somatic delusions that her organs were “rotting and shutting down.” Treatment included nortriptyline, 40 mg/d; lithium, 150 mg/d; and haloperidol, 0.5 mg/d. Her serum lithium level was 0.3 mEq/L (reference range, 0.6 to 1.2 mEq/L); the serum nortriptyline level was 68 ng/mL (reference range, 50 to 150 ng/mL). CT of the head and an electrocardiogram were unremarkable.
A twice-weekly course of ECT was initiated.
The day before Treatment 1 of ECT, the serum lithium level (drawn 12 hours after the last dose) was 0.4 mEq/L. Lithium was withheld 24 hours before ECT; nortriptyline and haloperidol were continued at prescribed dosages.
Right unilateral stimulation was used at 50%/mC energy (Thymatron DG, with methohexital anesthesia, and succinylcholine for muscle relaxation). Seizure duration, measured by EEG, was 57 seconds.
Mrs. A developed postictal delirium after the first 2 ECT sessions. The serum lithium level was unchanged. Subsequently, lithium treatment was discontinued and ECT was continued; once lithium was stopped, delirium resolved. ECT sessions 3 and 4 were uneventful, with no post-treatment delirium. Seizure duration for Treatment 4 was 58 seconds. She started breathing easily after all ECT sessions.
After Treatment 4, Mrs. A experienced full remission of depressive and psychotic symptoms. Repeat CT of head, after Treatment 4, was unchanged from baseline.
What is the role of lithium?
Mrs. A did not exhibit typical signs of lithium intoxication (diarrhea, vomiting, tremor). Notably, lithium has an intrinsic anticholinergic activity2; concurrent nortriptyline, a secondary amine tricyclic antidepressant with fewer anticholinergic side effects than other tricyclics,2 could precipitate delirium in a vulnerable patient secondary to excessive cumulative anticholinergic exposure.
No prolonged time-to-respiration or time-to-awakening occurred during treatments in which concurrent lithium and ECT were used; seizure duration with and without concurrent lithium was relatively similar.
There are potential complications of concurrent use of lithium and ECT:
• prolongation of the duration of muscle paralysis and apnea induced by commonly used neuromuscular-blocking agents (eg, succinylcholine)
• post-ECT cognitive disturbance.1,3,4
There is debate about the safety of continuing lithium during, or in close proximity to, ECT. In a case series of 12 patients who underwent combined lithium therapy and ECT, the authors concluded that this combination can be safe, regardless of age, as long as appropriate clinical monitoring is provided.4 In Mrs. A’s case, once post-ECT delirium was noted, lithium was discontinued for subsequent ECT sessions.
Because further ECT was uneventful without lithium, and no other clear acute cause of delirium could be identified, we concluded that lithium likely played a role in Mrs. A’s delirium. Notably, nortriptyline had been continued, suggesting that the degree of anticholinergic blockade provided by nortriptyline was insufficient to provoke delirium post-ECT in the absence of potentiation of this effect, as it had been when lithium also was used initially.
Guidelines for dosing and serum lithium concentrations in geriatric patients are not well-established; the current traditional range of 0.6 to 1.2 mEq/L, is too high for geriatric patients and can result in episodes of lithium toxicity, including delirium.5 Although our patient’s lithium level was below the reference range for all patients, a level of 0.3 mEq/L can be considered at the low end of the reference range for geriatric patients.5 Inasmuch as the lithium-assisted post-ECT delirium could represent a clinical sign of lithium toxicity, perhaps even a subtherapeutic level in a certain patient could be paradoxically “toxic.”
Although the serum lithium level in our patient remained below the toxic level for the general population (>1.5 mEq/L), delirium in a geriatric patient could result from:
• age-related changes in the pharmacokinetics of lithium, a water-soluble drug; these changes reduce renal clearance of the drug and extend plasma elimination half-life of a single dose to 36 hours, with the result that lithium remains in the body longer and necessitating a lower dosage (ie, a dosage that yields a serum level of approximately 0.5 mEq/L)
• the CNS tissue concentration of lithium, which can be high even though the serum level is not toxic
• an age-related increase in blood-brain barrier permeability, making the barrier more porous for drugs
• changes in blood-brain barrier permeability by post-ECT biochemical induction, with subsequent increased drug availability in the CNS.5,6
What we recommend
Possible interactions between lithium and ECT that lead to ECT-associated delirium need further elucidation, but discontinuing lithium during the course of ECT in a geriatric patient warrants your consideration. Following a safe interval after the last ECT session, lithium likely can be safely re-introduced 1) if there is clinical need and 2) as long as clinical surveillance for cognitive side effects is provided— especially if ECT will need to be reconsidered in the future.
Two additional considerations:
• Actively reassess lithium dosing in all geriatric psychiatric patients, especially those with renal insufficiency and other systemic metabolic considerations.
• Actively examine the use of all other anticholinergic agents in the course of evaluating a patient’s candidacy for ECT.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. A task force report of the American Psychiatric Association. 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
3. Hill GE, Wong KC, Hodges MR. Potentiation of succinylcholine neuromuscular blockade by lithium carbonate. Anesthesiology. 1976;44(5):439-442.
4. Dolenc TJ, Rasmussen KG. The safety of electroconvulsive therapy and lithium in combination: a case series and review of the literature. J ECT. 2005;21(3):165-170.
5. Shulman KI. Lithium for older adults with bipolar disorder: should it still be considered a first line agent? Drugs Aging. 2010;27(8):607-615.
6. Grandjean EM, Aubry JM. Lithium: updated human knowledge using an evidence-based approach. Part II: clinical pharmacology and therapeutic monitoring. CNS Drugs. 2009;23(4):331-349.
Delirium has been described as a potential complication of concurrent lithium and electroconvulsive therapy (ECT) for depression, in association with a range of serum lithium levels. Although debate persists about the safety of continuing previously established lithium therapy during a course of ECT for mood symptoms, withholding lithium for 24 hours before administering ECT and measuring the serum lithium level before ECT were found to decrease the risk of post-ECT neurocognitive effects.1
We have found that the conventional practice of holding lithium for 24 hours before ECT might need to be re-evaluated in geriatric patients, as the following case demonstrates. Only 24 hours of holding lithium therapy might result in a lithium level sufficient to contribute to delirium after ECT.
CASE REPORT
An older woman with recurrent unipolar psychotic depression
Mrs. A, age 81, was admitted to the hospital with a 1-week history of depressed mood, anhedonia, insomnia, anergia, anorexia, and nihilistic somatic delusions that her organs were “rotting and shutting down.” Treatment included nortriptyline, 40 mg/d; lithium, 150 mg/d; and haloperidol, 0.5 mg/d. Her serum lithium level was 0.3 mEq/L (reference range, 0.6 to 1.2 mEq/L); the serum nortriptyline level was 68 ng/mL (reference range, 50 to 150 ng/mL). CT of the head and an electrocardiogram were unremarkable.
A twice-weekly course of ECT was initiated.
The day before Treatment 1 of ECT, the serum lithium level (drawn 12 hours after the last dose) was 0.4 mEq/L. Lithium was withheld 24 hours before ECT; nortriptyline and haloperidol were continued at prescribed dosages.
Right unilateral stimulation was used at 50%/mC energy (Thymatron DG, with methohexital anesthesia, and succinylcholine for muscle relaxation). Seizure duration, measured by EEG, was 57 seconds.
Mrs. A developed postictal delirium after the first 2 ECT sessions. The serum lithium level was unchanged. Subsequently, lithium treatment was discontinued and ECT was continued; once lithium was stopped, delirium resolved. ECT sessions 3 and 4 were uneventful, with no post-treatment delirium. Seizure duration for Treatment 4 was 58 seconds. She started breathing easily after all ECT sessions.
After Treatment 4, Mrs. A experienced full remission of depressive and psychotic symptoms. Repeat CT of head, after Treatment 4, was unchanged from baseline.
What is the role of lithium?
Mrs. A did not exhibit typical signs of lithium intoxication (diarrhea, vomiting, tremor). Notably, lithium has an intrinsic anticholinergic activity2; concurrent nortriptyline, a secondary amine tricyclic antidepressant with fewer anticholinergic side effects than other tricyclics,2 could precipitate delirium in a vulnerable patient secondary to excessive cumulative anticholinergic exposure.
No prolonged time-to-respiration or time-to-awakening occurred during treatments in which concurrent lithium and ECT were used; seizure duration with and without concurrent lithium was relatively similar.
There are potential complications of concurrent use of lithium and ECT:
• prolongation of the duration of muscle paralysis and apnea induced by commonly used neuromuscular-blocking agents (eg, succinylcholine)
• post-ECT cognitive disturbance.1,3,4
There is debate about the safety of continuing lithium during, or in close proximity to, ECT. In a case series of 12 patients who underwent combined lithium therapy and ECT, the authors concluded that this combination can be safe, regardless of age, as long as appropriate clinical monitoring is provided.4 In Mrs. A’s case, once post-ECT delirium was noted, lithium was discontinued for subsequent ECT sessions.
Because further ECT was uneventful without lithium, and no other clear acute cause of delirium could be identified, we concluded that lithium likely played a role in Mrs. A’s delirium. Notably, nortriptyline had been continued, suggesting that the degree of anticholinergic blockade provided by nortriptyline was insufficient to provoke delirium post-ECT in the absence of potentiation of this effect, as it had been when lithium also was used initially.
Guidelines for dosing and serum lithium concentrations in geriatric patients are not well-established; the current traditional range of 0.6 to 1.2 mEq/L, is too high for geriatric patients and can result in episodes of lithium toxicity, including delirium.5 Although our patient’s lithium level was below the reference range for all patients, a level of 0.3 mEq/L can be considered at the low end of the reference range for geriatric patients.5 Inasmuch as the lithium-assisted post-ECT delirium could represent a clinical sign of lithium toxicity, perhaps even a subtherapeutic level in a certain patient could be paradoxically “toxic.”
Although the serum lithium level in our patient remained below the toxic level for the general population (>1.5 mEq/L), delirium in a geriatric patient could result from:
• age-related changes in the pharmacokinetics of lithium, a water-soluble drug; these changes reduce renal clearance of the drug and extend plasma elimination half-life of a single dose to 36 hours, with the result that lithium remains in the body longer and necessitating a lower dosage (ie, a dosage that yields a serum level of approximately 0.5 mEq/L)
• the CNS tissue concentration of lithium, which can be high even though the serum level is not toxic
• an age-related increase in blood-brain barrier permeability, making the barrier more porous for drugs
• changes in blood-brain barrier permeability by post-ECT biochemical induction, with subsequent increased drug availability in the CNS.5,6
What we recommend
Possible interactions between lithium and ECT that lead to ECT-associated delirium need further elucidation, but discontinuing lithium during the course of ECT in a geriatric patient warrants your consideration. Following a safe interval after the last ECT session, lithium likely can be safely re-introduced 1) if there is clinical need and 2) as long as clinical surveillance for cognitive side effects is provided— especially if ECT will need to be reconsidered in the future.
Two additional considerations:
• Actively reassess lithium dosing in all geriatric psychiatric patients, especially those with renal insufficiency and other systemic metabolic considerations.
• Actively examine the use of all other anticholinergic agents in the course of evaluating a patient’s candidacy for ECT.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Delirium has been described as a potential complication of concurrent lithium and electroconvulsive therapy (ECT) for depression, in association with a range of serum lithium levels. Although debate persists about the safety of continuing previously established lithium therapy during a course of ECT for mood symptoms, withholding lithium for 24 hours before administering ECT and measuring the serum lithium level before ECT were found to decrease the risk of post-ECT neurocognitive effects.1
We have found that the conventional practice of holding lithium for 24 hours before ECT might need to be re-evaluated in geriatric patients, as the following case demonstrates. Only 24 hours of holding lithium therapy might result in a lithium level sufficient to contribute to delirium after ECT.
CASE REPORT
An older woman with recurrent unipolar psychotic depression
Mrs. A, age 81, was admitted to the hospital with a 1-week history of depressed mood, anhedonia, insomnia, anergia, anorexia, and nihilistic somatic delusions that her organs were “rotting and shutting down.” Treatment included nortriptyline, 40 mg/d; lithium, 150 mg/d; and haloperidol, 0.5 mg/d. Her serum lithium level was 0.3 mEq/L (reference range, 0.6 to 1.2 mEq/L); the serum nortriptyline level was 68 ng/mL (reference range, 50 to 150 ng/mL). CT of the head and an electrocardiogram were unremarkable.
A twice-weekly course of ECT was initiated.
The day before Treatment 1 of ECT, the serum lithium level (drawn 12 hours after the last dose) was 0.4 mEq/L. Lithium was withheld 24 hours before ECT; nortriptyline and haloperidol were continued at prescribed dosages.
Right unilateral stimulation was used at 50%/mC energy (Thymatron DG, with methohexital anesthesia, and succinylcholine for muscle relaxation). Seizure duration, measured by EEG, was 57 seconds.
Mrs. A developed postictal delirium after the first 2 ECT sessions. The serum lithium level was unchanged. Subsequently, lithium treatment was discontinued and ECT was continued; once lithium was stopped, delirium resolved. ECT sessions 3 and 4 were uneventful, with no post-treatment delirium. Seizure duration for Treatment 4 was 58 seconds. She started breathing easily after all ECT sessions.
After Treatment 4, Mrs. A experienced full remission of depressive and psychotic symptoms. Repeat CT of head, after Treatment 4, was unchanged from baseline.
What is the role of lithium?
Mrs. A did not exhibit typical signs of lithium intoxication (diarrhea, vomiting, tremor). Notably, lithium has an intrinsic anticholinergic activity2; concurrent nortriptyline, a secondary amine tricyclic antidepressant with fewer anticholinergic side effects than other tricyclics,2 could precipitate delirium in a vulnerable patient secondary to excessive cumulative anticholinergic exposure.
No prolonged time-to-respiration or time-to-awakening occurred during treatments in which concurrent lithium and ECT were used; seizure duration with and without concurrent lithium was relatively similar.
There are potential complications of concurrent use of lithium and ECT:
• prolongation of the duration of muscle paralysis and apnea induced by commonly used neuromuscular-blocking agents (eg, succinylcholine)
• post-ECT cognitive disturbance.1,3,4
There is debate about the safety of continuing lithium during, or in close proximity to, ECT. In a case series of 12 patients who underwent combined lithium therapy and ECT, the authors concluded that this combination can be safe, regardless of age, as long as appropriate clinical monitoring is provided.4 In Mrs. A’s case, once post-ECT delirium was noted, lithium was discontinued for subsequent ECT sessions.
Because further ECT was uneventful without lithium, and no other clear acute cause of delirium could be identified, we concluded that lithium likely played a role in Mrs. A’s delirium. Notably, nortriptyline had been continued, suggesting that the degree of anticholinergic blockade provided by nortriptyline was insufficient to provoke delirium post-ECT in the absence of potentiation of this effect, as it had been when lithium also was used initially.
Guidelines for dosing and serum lithium concentrations in geriatric patients are not well-established; the current traditional range of 0.6 to 1.2 mEq/L, is too high for geriatric patients and can result in episodes of lithium toxicity, including delirium.5 Although our patient’s lithium level was below the reference range for all patients, a level of 0.3 mEq/L can be considered at the low end of the reference range for geriatric patients.5 Inasmuch as the lithium-assisted post-ECT delirium could represent a clinical sign of lithium toxicity, perhaps even a subtherapeutic level in a certain patient could be paradoxically “toxic.”
Although the serum lithium level in our patient remained below the toxic level for the general population (>1.5 mEq/L), delirium in a geriatric patient could result from:
• age-related changes in the pharmacokinetics of lithium, a water-soluble drug; these changes reduce renal clearance of the drug and extend plasma elimination half-life of a single dose to 36 hours, with the result that lithium remains in the body longer and necessitating a lower dosage (ie, a dosage that yields a serum level of approximately 0.5 mEq/L)
• the CNS tissue concentration of lithium, which can be high even though the serum level is not toxic
• an age-related increase in blood-brain barrier permeability, making the barrier more porous for drugs
• changes in blood-brain barrier permeability by post-ECT biochemical induction, with subsequent increased drug availability in the CNS.5,6
What we recommend
Possible interactions between lithium and ECT that lead to ECT-associated delirium need further elucidation, but discontinuing lithium during the course of ECT in a geriatric patient warrants your consideration. Following a safe interval after the last ECT session, lithium likely can be safely re-introduced 1) if there is clinical need and 2) as long as clinical surveillance for cognitive side effects is provided— especially if ECT will need to be reconsidered in the future.
Two additional considerations:
• Actively reassess lithium dosing in all geriatric psychiatric patients, especially those with renal insufficiency and other systemic metabolic considerations.
• Actively examine the use of all other anticholinergic agents in the course of evaluating a patient’s candidacy for ECT.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. A task force report of the American Psychiatric Association. 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
3. Hill GE, Wong KC, Hodges MR. Potentiation of succinylcholine neuromuscular blockade by lithium carbonate. Anesthesiology. 1976;44(5):439-442.
4. Dolenc TJ, Rasmussen KG. The safety of electroconvulsive therapy and lithium in combination: a case series and review of the literature. J ECT. 2005;21(3):165-170.
5. Shulman KI. Lithium for older adults with bipolar disorder: should it still be considered a first line agent? Drugs Aging. 2010;27(8):607-615.
6. Grandjean EM, Aubry JM. Lithium: updated human knowledge using an evidence-based approach. Part II: clinical pharmacology and therapeutic monitoring. CNS Drugs. 2009;23(4):331-349.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. A task force report of the American Psychiatric Association. 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
3. Hill GE, Wong KC, Hodges MR. Potentiation of succinylcholine neuromuscular blockade by lithium carbonate. Anesthesiology. 1976;44(5):439-442.
4. Dolenc TJ, Rasmussen KG. The safety of electroconvulsive therapy and lithium in combination: a case series and review of the literature. J ECT. 2005;21(3):165-170.
5. Shulman KI. Lithium for older adults with bipolar disorder: should it still be considered a first line agent? Drugs Aging. 2010;27(8):607-615.
6. Grandjean EM, Aubry JM. Lithium: updated human knowledge using an evidence-based approach. Part II: clinical pharmacology and therapeutic monitoring. CNS Drugs. 2009;23(4):331-349.
Combo appears safe and active in CLL, NHL

Credit: Linda Bartlett
KOHALA COAST, HAWAII—Early results of a small, phase 1 study suggest a novel combination treatment is active and generally well-tolerated in relapsed or refractory patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) or non-Hodgkin lymphomas (NHLs).
The treatment consists of ublituximab (TG-1101), a monoclonal antibody that targets a unique epitope on the CD20 antigen, and TGR-1202, a next-generation PI3K delta inhibitor.
The combination appeared to be well tolerated overall, although infusion-related reactions were common, and nearly a quarter of patients experienced grade 3/4 neutropenia.
Four of 5 CLL/SLL patients experienced a partial response (PR), and the remaining patient had stable disease (SD). Among the 10 NHL patients, 1 had progressive disease, 7 had SD, and 2 achieved a PR.
Matthew Lunning, DO, of the University of Nebraska Medical Center in Omaha, and his colleagues presented these results in a poster at the 2014 Pan Pacific Lymphoma Conference.
The study is sponsored by TG Therapeutics, the company developing both drugs.
The researchers presented results from 8 patients with CLL/SLL, 7 patients with diffuse large B-cell lymphoma (DLBCL), 5 with follicular lymphoma (FL), and 1 patient with Richter’s syndrome (RS).
Patients had a median age of 64 years (range, 35-82), and they had received a median of 3 prior therapies (range, 1-9). Fifty-seven percent of patients had received 3 or more prior therapies, and 38% were refractory to their prior therapy.
The patients received escalating doses of TGR-1202, with a fixed dose of ublituximab—900 mg for patients with NHL and 600 mg for patients with CLL.
As of the data cutoff, all 21 patients were evaluable for safety, but only 15 were evaluable for efficacy.
Adverse events
The most common adverse event was infusion-related reactions, which occurred in 48% of patients. All of these events were manageable without dose reductions, and all but 1 event was grade 1 or 2 in severity.
Neutropenia was also common, occurring in 38% of patients. Grade 3/4 neutropenia occurred in 24% of patients. One CLL patient required a dose delay for neutropenia in cycle 1, which met the criteria for a dose-limiting toxicity.
No additional dose-limiting toxicities have been observed to date. Likewise, none of the patients has required dose reductions for either drug, and there were no drug-related AST/ALT elevations.
On the other hand, 1 patient did come off the study due to grade 1 itching that was possibly related to TGR-1202.
Other common adverse events associated with treatment included diarrhea (29%), nausea (29%), hoarseness (10%), muscle aches (10%), and fatigue (10%).
Activity in CLL/SLL
Of the 8 CLL/SLL patients enrolled to date, 5 were evaluable for efficacy. Four patients achieved a PR at the first efficacy assessment. The remaining patient, a CLL patient with both 17p and 11q del, achieved SD with a 44% nodal reduction at the first assessment.
All 5 patients achieved a greater-than-50% reduction in ALC by the first efficacy assessment. One patient achieved complete normalization of ALC (less than 4000/uL), and the other 4 patients achieved at least an 80% reduction by the first efficacy assessment.
The lymphocytosis generally observed in CLL patients treated with TGR-1202, similar to other PI3K delta and BTK inhibitors, appears to be mitigated by the addition of ublituximab.
Activity in NHL
Of the 13 patients in this group, 10 were evaluable for efficacy, including 5 with DLBCL, 4 with FL, and 1 with RS. Results were not as favorable in this group as they were among CLL/SLL patients, but, as the researchers pointed out, these patients were heavily pretreated.
Among the DLBCL patients, 2 achieved PRs with TGR-1202 and ublituximab. Both of these responses occurred at the higher dose of TGR-1202.
Two DLBCL patients had SD, and 1 patient progressed. DLBCL patients had a median of 3 prior treatment lines, and 3 patients had GCB DLBCL, with 1 patient classified as triple-hit lymphoma (overexpression of BCL2, BCL6, and MYC rearrangements).
In the FL group, all 4 patients had SD after treatment and exhibited a reduction in tumor mass at the first assessment. These patients had advanced disease and a median of 6 prior lines of therapy.
The RS patient also had SD following TGR-1202 and ublituximab.
“We have been very impressed with the safety profile and the level of activity observed to date in all patient groups with TGR-1202 in combination with ublituximab, particularly given the advanced stage of disease . . . ,” said Susan O’Brien, MD, a professor at MD Anderson Cancer Center in Houston and study chair for the CLL patient group.
“Of particular interest is the absence of observed elevations in AST/ALT with TGR-1202, which is a known adverse event associated with other PI3K delta inhibitors. We look forward to continuing enrollment at all trial centers of this exciting combination and presenting data on more patients at upcoming medical meetings.” ![]()
Credit: Linda Bartlett
KOHALA COAST, HAWAII—Early results of a small, phase 1 study suggest a novel combination treatment is active and generally well-tolerated in relapsed or refractory patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) or non-Hodgkin lymphomas (NHLs).
The treatment consists of ublituximab (TG-1101), a monoclonal antibody that targets a unique epitope on the CD20 antigen, and TGR-1202, a next-generation PI3K delta inhibitor.
The combination appeared to be well tolerated overall, although infusion-related reactions were common, and nearly a quarter of patients experienced grade 3/4 neutropenia.
Four of 5 CLL/SLL patients experienced a partial response (PR), and the remaining patient had stable disease (SD). Among the 10 NHL patients, 1 had progressive disease, 7 had SD, and 2 achieved a PR.
Matthew Lunning, DO, of the University of Nebraska Medical Center in Omaha, and his colleagues presented these results in a poster at the 2014 Pan Pacific Lymphoma Conference.
The study is sponsored by TG Therapeutics, the company developing both drugs.
The researchers presented results from 8 patients with CLL/SLL, 7 patients with diffuse large B-cell lymphoma (DLBCL), 5 with follicular lymphoma (FL), and 1 patient with Richter’s syndrome (RS).
Patients had a median age of 64 years (range, 35-82), and they had received a median of 3 prior therapies (range, 1-9). Fifty-seven percent of patients had received 3 or more prior therapies, and 38% were refractory to their prior therapy.
The patients received escalating doses of TGR-1202, with a fixed dose of ublituximab—900 mg for patients with NHL and 600 mg for patients with CLL.
As of the data cutoff, all 21 patients were evaluable for safety, but only 15 were evaluable for efficacy.
Adverse events
The most common adverse event was infusion-related reactions, which occurred in 48% of patients. All of these events were manageable without dose reductions, and all but 1 event was grade 1 or 2 in severity.
Neutropenia was also common, occurring in 38% of patients. Grade 3/4 neutropenia occurred in 24% of patients. One CLL patient required a dose delay for neutropenia in cycle 1, which met the criteria for a dose-limiting toxicity.
No additional dose-limiting toxicities have been observed to date. Likewise, none of the patients has required dose reductions for either drug, and there were no drug-related AST/ALT elevations.
On the other hand, 1 patient did come off the study due to grade 1 itching that was possibly related to TGR-1202.
Other common adverse events associated with treatment included diarrhea (29%), nausea (29%), hoarseness (10%), muscle aches (10%), and fatigue (10%).
Activity in CLL/SLL
Of the 8 CLL/SLL patients enrolled to date, 5 were evaluable for efficacy. Four patients achieved a PR at the first efficacy assessment. The remaining patient, a CLL patient with both 17p and 11q del, achieved SD with a 44% nodal reduction at the first assessment.
All 5 patients achieved a greater-than-50% reduction in ALC by the first efficacy assessment. One patient achieved complete normalization of ALC (less than 4000/uL), and the other 4 patients achieved at least an 80% reduction by the first efficacy assessment.
The lymphocytosis generally observed in CLL patients treated with TGR-1202, similar to other PI3K delta and BTK inhibitors, appears to be mitigated by the addition of ublituximab.
Activity in NHL
Of the 13 patients in this group, 10 were evaluable for efficacy, including 5 with DLBCL, 4 with FL, and 1 with RS. Results were not as favorable in this group as they were among CLL/SLL patients, but, as the researchers pointed out, these patients were heavily pretreated.
Among the DLBCL patients, 2 achieved PRs with TGR-1202 and ublituximab. Both of these responses occurred at the higher dose of TGR-1202.
Two DLBCL patients had SD, and 1 patient progressed. DLBCL patients had a median of 3 prior treatment lines, and 3 patients had GCB DLBCL, with 1 patient classified as triple-hit lymphoma (overexpression of BCL2, BCL6, and MYC rearrangements).
In the FL group, all 4 patients had SD after treatment and exhibited a reduction in tumor mass at the first assessment. These patients had advanced disease and a median of 6 prior lines of therapy.
The RS patient also had SD following TGR-1202 and ublituximab.
“We have been very impressed with the safety profile and the level of activity observed to date in all patient groups with TGR-1202 in combination with ublituximab, particularly given the advanced stage of disease . . . ,” said Susan O’Brien, MD, a professor at MD Anderson Cancer Center in Houston and study chair for the CLL patient group.
“Of particular interest is the absence of observed elevations in AST/ALT with TGR-1202, which is a known adverse event associated with other PI3K delta inhibitors. We look forward to continuing enrollment at all trial centers of this exciting combination and presenting data on more patients at upcoming medical meetings.” ![]()
Credit: Linda Bartlett
KOHALA COAST, HAWAII—Early results of a small, phase 1 study suggest a novel combination treatment is active and generally well-tolerated in relapsed or refractory patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) or non-Hodgkin lymphomas (NHLs).
The treatment consists of ublituximab (TG-1101), a monoclonal antibody that targets a unique epitope on the CD20 antigen, and TGR-1202, a next-generation PI3K delta inhibitor.
The combination appeared to be well tolerated overall, although infusion-related reactions were common, and nearly a quarter of patients experienced grade 3/4 neutropenia.
Four of 5 CLL/SLL patients experienced a partial response (PR), and the remaining patient had stable disease (SD). Among the 10 NHL patients, 1 had progressive disease, 7 had SD, and 2 achieved a PR.
Matthew Lunning, DO, of the University of Nebraska Medical Center in Omaha, and his colleagues presented these results in a poster at the 2014 Pan Pacific Lymphoma Conference.
The study is sponsored by TG Therapeutics, the company developing both drugs.
The researchers presented results from 8 patients with CLL/SLL, 7 patients with diffuse large B-cell lymphoma (DLBCL), 5 with follicular lymphoma (FL), and 1 patient with Richter’s syndrome (RS).
Patients had a median age of 64 years (range, 35-82), and they had received a median of 3 prior therapies (range, 1-9). Fifty-seven percent of patients had received 3 or more prior therapies, and 38% were refractory to their prior therapy.
The patients received escalating doses of TGR-1202, with a fixed dose of ublituximab—900 mg for patients with NHL and 600 mg for patients with CLL.
As of the data cutoff, all 21 patients were evaluable for safety, but only 15 were evaluable for efficacy.
Adverse events
The most common adverse event was infusion-related reactions, which occurred in 48% of patients. All of these events were manageable without dose reductions, and all but 1 event was grade 1 or 2 in severity.
Neutropenia was also common, occurring in 38% of patients. Grade 3/4 neutropenia occurred in 24% of patients. One CLL patient required a dose delay for neutropenia in cycle 1, which met the criteria for a dose-limiting toxicity.
No additional dose-limiting toxicities have been observed to date. Likewise, none of the patients has required dose reductions for either drug, and there were no drug-related AST/ALT elevations.
On the other hand, 1 patient did come off the study due to grade 1 itching that was possibly related to TGR-1202.
Other common adverse events associated with treatment included diarrhea (29%), nausea (29%), hoarseness (10%), muscle aches (10%), and fatigue (10%).
Activity in CLL/SLL
Of the 8 CLL/SLL patients enrolled to date, 5 were evaluable for efficacy. Four patients achieved a PR at the first efficacy assessment. The remaining patient, a CLL patient with both 17p and 11q del, achieved SD with a 44% nodal reduction at the first assessment.
All 5 patients achieved a greater-than-50% reduction in ALC by the first efficacy assessment. One patient achieved complete normalization of ALC (less than 4000/uL), and the other 4 patients achieved at least an 80% reduction by the first efficacy assessment.
The lymphocytosis generally observed in CLL patients treated with TGR-1202, similar to other PI3K delta and BTK inhibitors, appears to be mitigated by the addition of ublituximab.
Activity in NHL
Of the 13 patients in this group, 10 were evaluable for efficacy, including 5 with DLBCL, 4 with FL, and 1 with RS. Results were not as favorable in this group as they were among CLL/SLL patients, but, as the researchers pointed out, these patients were heavily pretreated.
Among the DLBCL patients, 2 achieved PRs with TGR-1202 and ublituximab. Both of these responses occurred at the higher dose of TGR-1202.
Two DLBCL patients had SD, and 1 patient progressed. DLBCL patients had a median of 3 prior treatment lines, and 3 patients had GCB DLBCL, with 1 patient classified as triple-hit lymphoma (overexpression of BCL2, BCL6, and MYC rearrangements).
In the FL group, all 4 patients had SD after treatment and exhibited a reduction in tumor mass at the first assessment. These patients had advanced disease and a median of 6 prior lines of therapy.
The RS patient also had SD following TGR-1202 and ublituximab.
“We have been very impressed with the safety profile and the level of activity observed to date in all patient groups with TGR-1202 in combination with ublituximab, particularly given the advanced stage of disease . . . ,” said Susan O’Brien, MD, a professor at MD Anderson Cancer Center in Houston and study chair for the CLL patient group.
“Of particular interest is the absence of observed elevations in AST/ALT with TGR-1202, which is a known adverse event associated with other PI3K delta inhibitors. We look forward to continuing enrollment at all trial centers of this exciting combination and presenting data on more patients at upcoming medical meetings.” ![]()
Fasting can have beneficial effects in cancer setting

in the bone marrow
New research indicates that cycles of prolonged fasting may prevent chemotherapy-induced immunosuppressive toxicity and induce regeneration of the hematopoietic system.
Long periods of fasting reduced damage in bone marrow stem and progenitor cells and protected both mice and humans from chemotoxicity.
In mice, the fasting cycles “flipped a regenerative switch,” changing the signaling pathways for hematopoietic stem cells (HSCs).
Researchers reported these results in Cell Stem Cell.
“We could not predict that prolonged fasting would have such a remarkable effect in promoting stem cell-based regeneration of the hematopoietic system,” said study author Valter Longo, PhD, of the University of Southern California in Los Angeles.
“When you starve, the system tries to save energy, and one of the things it can do to save energy is to recycle a lot of the immune cells that are not needed, especially those that may be damaged. What we started noticing in both our human work and animal work is that the white blood cell count goes down with prolonged fasting. Then, when you re-feed, the blood cells come back. So we started thinking, well, where does it come from?”
The researchers found that prolonged fasting reduced the enzyme PKA, which regulates HSC self-renewal and pluripotency.
“PKA is the key gene that needs to shut down in order for these stem cells to switch into regenerative mode,” Dr Longo said. “It gives the ‘okay’ for stem cells to go ahead and begin proliferating and rebuild the entire system.”
Prolonged fasting also lowered levels of IGF-1, a growth-factor hormone that has been linked to aging, tumor progression, and cancer risk.
In addition to downregulating the IGF-1/PKA pathway in HSCs, prolonged fasting protected hematopoietic cells from chemotoxicity and promoted HSC self-renewal to reverse immunosuppression.
Experiments revealed that inhibiting IGF-1 or PKA signaling mimicked the effects of prolonged fasting.
The researchers also analyzed a small group of patients from a pilot study evaluating the effects of fasting before chemotherapy. Fasting for 72 hours, but not 24 hours, ensured that patients had normal lymphocyte counts and maintained a normal lineage balance in white blood cells after chemotherapy.
Dr Longo’s lab is now conducting further research on controlled dietary interventions and stem cell regeneration in both animal and clinical studies. ![]()
in the bone marrow
New research indicates that cycles of prolonged fasting may prevent chemotherapy-induced immunosuppressive toxicity and induce regeneration of the hematopoietic system.
Long periods of fasting reduced damage in bone marrow stem and progenitor cells and protected both mice and humans from chemotoxicity.
In mice, the fasting cycles “flipped a regenerative switch,” changing the signaling pathways for hematopoietic stem cells (HSCs).
Researchers reported these results in Cell Stem Cell.
“We could not predict that prolonged fasting would have such a remarkable effect in promoting stem cell-based regeneration of the hematopoietic system,” said study author Valter Longo, PhD, of the University of Southern California in Los Angeles.
“When you starve, the system tries to save energy, and one of the things it can do to save energy is to recycle a lot of the immune cells that are not needed, especially those that may be damaged. What we started noticing in both our human work and animal work is that the white blood cell count goes down with prolonged fasting. Then, when you re-feed, the blood cells come back. So we started thinking, well, where does it come from?”
The researchers found that prolonged fasting reduced the enzyme PKA, which regulates HSC self-renewal and pluripotency.
“PKA is the key gene that needs to shut down in order for these stem cells to switch into regenerative mode,” Dr Longo said. “It gives the ‘okay’ for stem cells to go ahead and begin proliferating and rebuild the entire system.”
Prolonged fasting also lowered levels of IGF-1, a growth-factor hormone that has been linked to aging, tumor progression, and cancer risk.
In addition to downregulating the IGF-1/PKA pathway in HSCs, prolonged fasting protected hematopoietic cells from chemotoxicity and promoted HSC self-renewal to reverse immunosuppression.
Experiments revealed that inhibiting IGF-1 or PKA signaling mimicked the effects of prolonged fasting.
The researchers also analyzed a small group of patients from a pilot study evaluating the effects of fasting before chemotherapy. Fasting for 72 hours, but not 24 hours, ensured that patients had normal lymphocyte counts and maintained a normal lineage balance in white blood cells after chemotherapy.
Dr Longo’s lab is now conducting further research on controlled dietary interventions and stem cell regeneration in both animal and clinical studies. ![]()
in the bone marrow
New research indicates that cycles of prolonged fasting may prevent chemotherapy-induced immunosuppressive toxicity and induce regeneration of the hematopoietic system.
Long periods of fasting reduced damage in bone marrow stem and progenitor cells and protected both mice and humans from chemotoxicity.
In mice, the fasting cycles “flipped a regenerative switch,” changing the signaling pathways for hematopoietic stem cells (HSCs).
Researchers reported these results in Cell Stem Cell.
“We could not predict that prolonged fasting would have such a remarkable effect in promoting stem cell-based regeneration of the hematopoietic system,” said study author Valter Longo, PhD, of the University of Southern California in Los Angeles.
“When you starve, the system tries to save energy, and one of the things it can do to save energy is to recycle a lot of the immune cells that are not needed, especially those that may be damaged. What we started noticing in both our human work and animal work is that the white blood cell count goes down with prolonged fasting. Then, when you re-feed, the blood cells come back. So we started thinking, well, where does it come from?”
The researchers found that prolonged fasting reduced the enzyme PKA, which regulates HSC self-renewal and pluripotency.
“PKA is the key gene that needs to shut down in order for these stem cells to switch into regenerative mode,” Dr Longo said. “It gives the ‘okay’ for stem cells to go ahead and begin proliferating and rebuild the entire system.”
Prolonged fasting also lowered levels of IGF-1, a growth-factor hormone that has been linked to aging, tumor progression, and cancer risk.
In addition to downregulating the IGF-1/PKA pathway in HSCs, prolonged fasting protected hematopoietic cells from chemotoxicity and promoted HSC self-renewal to reverse immunosuppression.
Experiments revealed that inhibiting IGF-1 or PKA signaling mimicked the effects of prolonged fasting.
The researchers also analyzed a small group of patients from a pilot study evaluating the effects of fasting before chemotherapy. Fasting for 72 hours, but not 24 hours, ensured that patients had normal lymphocyte counts and maintained a normal lineage balance in white blood cells after chemotherapy.
Dr Longo’s lab is now conducting further research on controlled dietary interventions and stem cell regeneration in both animal and clinical studies. ![]()
Drug approved to treat NHL in Israel

The Israeli Ministry of Health has granted approval for the antineoplastic agent pixantrone (Pixuvri).
The drug is now approved as monotherapy for adults with relapsed or refractory aggressive B-cell non-Hodgkin lymphoma (NHL) who have received fewer than 4 previous courses of treatment.
The benefit of pixantrone has not been established when used as fifth-line or greater treatment in patients who were refractory to their last therapy.
Pixantrone will be distributed in Israel by the Neopharm Group.
“The approval of Pixuvri in Israel provides patients with aggressive B-cell NHL who have failed second- or third-line therapy a new approved option, where none existed before, that can effectively treat their disease with manageable side effects,” said Abraham Avigdor, MD, of Tel Aviv University.
“Patients who have relapsed after second-line therapy have a poor survival outcome. It is vital to have additional treatment options available, like Pixuvri, so we can provide these patients the best care possible and help them battle their disease.”
The main study of pixantrone, the phase 3 EXTEND PIX301 trial, compared the drug to other chemotherapeutic agents in patients with relapsed or refractory NHL. The response rate was 20% in the pixantrone arm and 6% in the comparator arm.
In addition, patients receiving pixantrone had longer progression-free survival than patients in the comparator group, with a median of 10.2 months and 7.6 months, respectively.
However, grade 3/4 adverse events—including neutropenia, leukopenia, and thrombocytopenia—were more common in the pixantrone arm.
Pixantrone is already marketed in the European Union. In 2012, the European Commission granted conditional marketing authorization for the drug as monotherapy for adults with relapsed or refractory aggressive B-cell NHL.
Under the provisions of the conditional marketing authorization, Cell Therapeutics, Inc., the company developing pixantrone, will be required to complete a post-marketing study aimed at confirming the drug’s clinical benefit.
The European Medicines Agency’s Committee for Medicinal Products for Human Use has accepted PIX306, a randomized, phase 3 trial comparing pixantrone plus rituximab to gemcitabine plus rituximab in patients who have relapsed after 1 to 3 prior regimens for aggressive B-cell NHL and who are not eligible for autologous stem cell transplant.
As a condition of approval, Cell Therapeutics has agreed to have the trial data available by June 2015.
Pixantrone is not approved for use in the US. ![]()
The Israeli Ministry of Health has granted approval for the antineoplastic agent pixantrone (Pixuvri).
The drug is now approved as monotherapy for adults with relapsed or refractory aggressive B-cell non-Hodgkin lymphoma (NHL) who have received fewer than 4 previous courses of treatment.
The benefit of pixantrone has not been established when used as fifth-line or greater treatment in patients who were refractory to their last therapy.
Pixantrone will be distributed in Israel by the Neopharm Group.
“The approval of Pixuvri in Israel provides patients with aggressive B-cell NHL who have failed second- or third-line therapy a new approved option, where none existed before, that can effectively treat their disease with manageable side effects,” said Abraham Avigdor, MD, of Tel Aviv University.
“Patients who have relapsed after second-line therapy have a poor survival outcome. It is vital to have additional treatment options available, like Pixuvri, so we can provide these patients the best care possible and help them battle their disease.”
The main study of pixantrone, the phase 3 EXTEND PIX301 trial, compared the drug to other chemotherapeutic agents in patients with relapsed or refractory NHL. The response rate was 20% in the pixantrone arm and 6% in the comparator arm.
In addition, patients receiving pixantrone had longer progression-free survival than patients in the comparator group, with a median of 10.2 months and 7.6 months, respectively.
However, grade 3/4 adverse events—including neutropenia, leukopenia, and thrombocytopenia—were more common in the pixantrone arm.
Pixantrone is already marketed in the European Union. In 2012, the European Commission granted conditional marketing authorization for the drug as monotherapy for adults with relapsed or refractory aggressive B-cell NHL.
Under the provisions of the conditional marketing authorization, Cell Therapeutics, Inc., the company developing pixantrone, will be required to complete a post-marketing study aimed at confirming the drug’s clinical benefit.
The European Medicines Agency’s Committee for Medicinal Products for Human Use has accepted PIX306, a randomized, phase 3 trial comparing pixantrone plus rituximab to gemcitabine plus rituximab in patients who have relapsed after 1 to 3 prior regimens for aggressive B-cell NHL and who are not eligible for autologous stem cell transplant.
As a condition of approval, Cell Therapeutics has agreed to have the trial data available by June 2015.
Pixantrone is not approved for use in the US. ![]()
The Israeli Ministry of Health has granted approval for the antineoplastic agent pixantrone (Pixuvri).
The drug is now approved as monotherapy for adults with relapsed or refractory aggressive B-cell non-Hodgkin lymphoma (NHL) who have received fewer than 4 previous courses of treatment.
The benefit of pixantrone has not been established when used as fifth-line or greater treatment in patients who were refractory to their last therapy.
Pixantrone will be distributed in Israel by the Neopharm Group.
“The approval of Pixuvri in Israel provides patients with aggressive B-cell NHL who have failed second- or third-line therapy a new approved option, where none existed before, that can effectively treat their disease with manageable side effects,” said Abraham Avigdor, MD, of Tel Aviv University.
“Patients who have relapsed after second-line therapy have a poor survival outcome. It is vital to have additional treatment options available, like Pixuvri, so we can provide these patients the best care possible and help them battle their disease.”
The main study of pixantrone, the phase 3 EXTEND PIX301 trial, compared the drug to other chemotherapeutic agents in patients with relapsed or refractory NHL. The response rate was 20% in the pixantrone arm and 6% in the comparator arm.
In addition, patients receiving pixantrone had longer progression-free survival than patients in the comparator group, with a median of 10.2 months and 7.6 months, respectively.
However, grade 3/4 adverse events—including neutropenia, leukopenia, and thrombocytopenia—were more common in the pixantrone arm.
Pixantrone is already marketed in the European Union. In 2012, the European Commission granted conditional marketing authorization for the drug as monotherapy for adults with relapsed or refractory aggressive B-cell NHL.
Under the provisions of the conditional marketing authorization, Cell Therapeutics, Inc., the company developing pixantrone, will be required to complete a post-marketing study aimed at confirming the drug’s clinical benefit.
The European Medicines Agency’s Committee for Medicinal Products for Human Use has accepted PIX306, a randomized, phase 3 trial comparing pixantrone plus rituximab to gemcitabine plus rituximab in patients who have relapsed after 1 to 3 prior regimens for aggressive B-cell NHL and who are not eligible for autologous stem cell transplant.
As a condition of approval, Cell Therapeutics has agreed to have the trial data available by June 2015.
Pixantrone is not approved for use in the US. ![]()
Military technology has application for malaria

Credit: Peter H. Seeberger
Researchers have used military technology to develop a test for detecting malaria parasites in the blood.
The team used a detector known as a focal plane array (FPA), which was originally developed for heat-seeking missiles.
The FPA gives highly detailed information on a sample area in minutes. The heat-seeking detector, which is coupled to an infrared imaging microscope, could detect the malaria parasite in a single red blood cell.
The infrared signature from the fatty acids of the parasites allowed the researchers to detect the parasite at its earliest stages and determine the number of parasites in a blood smear.
The team described the technology in Analyst.
“Our test detects malaria at its very early stages, so that doctors can stop the disease in its tracks before it takes hold and kills,” said study author Bayden Wood, PhD, of Monash University in Victoria, Australia. “We believe this sets the gold standard for malaria testing.”
“There are some excellent tests that diagnose malaria. However, the sensitivity is limited, and the best methods require hours of input from skilled microscopists, and that’s a problem in developing countries where malaria is most prevalent.”
The new test, on the other hand, gives an automatic diagnosis within 4 minutes and doesn’t require a specialist technician.
Study author Leann Tilley, PhD, of the University of Melbourne in Australia, said the test could make an impact in large-scale screening of malaria parasite carriers who do not present with the classic fever-type symptoms associated with the disease.
“In many countries, only people who display signs of malaria are treated,” Dr Tilley said. “But the problem with this approach is that some people don’t have typical flu-like symptoms associated with malaria, and this means a reservoir of parasites persists that can reemerge and spread very quickly within a community.”
“Our test works because it can detect the malaria parasite at the very early stages and can reliably detect it in an automated manner in a single red blood cell. No other test can do that.”
FPA detectors were originally developed for Javelin Portable anti-tank missiles in the 1990s. The heat-seeking detector is used on shoulder-fired missiles but can also be installed on tracked, wheeled, or amphibious vehicles, providing spatial and spectral information in a matter of seconds.
The FPA detector used in this project was coupled to a synchrotron source located at the InfraRed Environmental Imaging facility at the Synchrotron Radiation Center in Wisconsin.
For the next phase of this research, Dr Wood’s team is collaborating with Patcharee Jearanaikoon, PhD, of Kohn Kaen University in Thailand, to test the technology in clinics. ![]()
Credit: Peter H. Seeberger
Researchers have used military technology to develop a test for detecting malaria parasites in the blood.
The team used a detector known as a focal plane array (FPA), which was originally developed for heat-seeking missiles.
The FPA gives highly detailed information on a sample area in minutes. The heat-seeking detector, which is coupled to an infrared imaging microscope, could detect the malaria parasite in a single red blood cell.
The infrared signature from the fatty acids of the parasites allowed the researchers to detect the parasite at its earliest stages and determine the number of parasites in a blood smear.
The team described the technology in Analyst.
“Our test detects malaria at its very early stages, so that doctors can stop the disease in its tracks before it takes hold and kills,” said study author Bayden Wood, PhD, of Monash University in Victoria, Australia. “We believe this sets the gold standard for malaria testing.”
“There are some excellent tests that diagnose malaria. However, the sensitivity is limited, and the best methods require hours of input from skilled microscopists, and that’s a problem in developing countries where malaria is most prevalent.”
The new test, on the other hand, gives an automatic diagnosis within 4 minutes and doesn’t require a specialist technician.
Study author Leann Tilley, PhD, of the University of Melbourne in Australia, said the test could make an impact in large-scale screening of malaria parasite carriers who do not present with the classic fever-type symptoms associated with the disease.
“In many countries, only people who display signs of malaria are treated,” Dr Tilley said. “But the problem with this approach is that some people don’t have typical flu-like symptoms associated with malaria, and this means a reservoir of parasites persists that can reemerge and spread very quickly within a community.”
“Our test works because it can detect the malaria parasite at the very early stages and can reliably detect it in an automated manner in a single red blood cell. No other test can do that.”
FPA detectors were originally developed for Javelin Portable anti-tank missiles in the 1990s. The heat-seeking detector is used on shoulder-fired missiles but can also be installed on tracked, wheeled, or amphibious vehicles, providing spatial and spectral information in a matter of seconds.
The FPA detector used in this project was coupled to a synchrotron source located at the InfraRed Environmental Imaging facility at the Synchrotron Radiation Center in Wisconsin.
For the next phase of this research, Dr Wood’s team is collaborating with Patcharee Jearanaikoon, PhD, of Kohn Kaen University in Thailand, to test the technology in clinics. ![]()
Credit: Peter H. Seeberger
Researchers have used military technology to develop a test for detecting malaria parasites in the blood.
The team used a detector known as a focal plane array (FPA), which was originally developed for heat-seeking missiles.
The FPA gives highly detailed information on a sample area in minutes. The heat-seeking detector, which is coupled to an infrared imaging microscope, could detect the malaria parasite in a single red blood cell.
The infrared signature from the fatty acids of the parasites allowed the researchers to detect the parasite at its earliest stages and determine the number of parasites in a blood smear.
The team described the technology in Analyst.
“Our test detects malaria at its very early stages, so that doctors can stop the disease in its tracks before it takes hold and kills,” said study author Bayden Wood, PhD, of Monash University in Victoria, Australia. “We believe this sets the gold standard for malaria testing.”
“There are some excellent tests that diagnose malaria. However, the sensitivity is limited, and the best methods require hours of input from skilled microscopists, and that’s a problem in developing countries where malaria is most prevalent.”
The new test, on the other hand, gives an automatic diagnosis within 4 minutes and doesn’t require a specialist technician.
Study author Leann Tilley, PhD, of the University of Melbourne in Australia, said the test could make an impact in large-scale screening of malaria parasite carriers who do not present with the classic fever-type symptoms associated with the disease.
“In many countries, only people who display signs of malaria are treated,” Dr Tilley said. “But the problem with this approach is that some people don’t have typical flu-like symptoms associated with malaria, and this means a reservoir of parasites persists that can reemerge and spread very quickly within a community.”
“Our test works because it can detect the malaria parasite at the very early stages and can reliably detect it in an automated manner in a single red blood cell. No other test can do that.”
FPA detectors were originally developed for Javelin Portable anti-tank missiles in the 1990s. The heat-seeking detector is used on shoulder-fired missiles but can also be installed on tracked, wheeled, or amphibious vehicles, providing spatial and spectral information in a matter of seconds.
The FPA detector used in this project was coupled to a synchrotron source located at the InfraRed Environmental Imaging facility at the Synchrotron Radiation Center in Wisconsin.
For the next phase of this research, Dr Wood’s team is collaborating with Patcharee Jearanaikoon, PhD, of Kohn Kaen University in Thailand, to test the technology in clinics. ![]()
EHR Impact on Patient Experience
Delivering patient‐centered care is at the core of ensuring patient engagement and active participation that will lead to positive outcomes. Physician‐patient interaction has become an area of increasing focus in an effort to optimize the patient experience. Positive patient‐provider communication has been shown to increase satisfaction,[1, 2, 3, 4] decrease the likelihood of medical malpractice lawsuits,[5, 6, 7, 8] and improve clinical outcomes.[9, 10, 11, 12, 13] Specifically, a decrease in psychological symptoms such as anxiety and stress, as well as perception of physical symptoms have been correlated with improved communication.[9, 12] Furthermore, objective health outcomes, such as improvement in hypertension and glycosylated hemoglobin, have also been correlated with improved physician‐patient communication.[10, 11, 13] The multifaceted effects of improved communication are impactful to both the patient and the physician; therefore, it is essential that we understand how to optimize this interaction.
Patient‐centered care is a critical objective for many high‐quality healthcare systems.[14] In recent years, the use of electronic health records (EHRs) has been increasingly adopted by healthcare systems nationally in an effort to improve the quality of care delivered. The positive benefits of EHRs on the facilitation of healthcare, including consolidation of information, reduction of medical errors, easily transferable medical records,[15, 16, 17] as well as their impact on healthcare spending,[18] are well‐documented and have been emphasized as reasons for adoption of EHRs by the Patient Protection and Affordable Care Act. However, EHR implementation has encountered some resistance regarding its impact on the patient experience.
As EHR implementation is exponentially increasing in the United States, there is limited literature on the consequences of this technology.[19] Barriers reported during EHR implementation include the limitations of standardization, attitudinal and organizational constraints, behavior of individuals, and resistance to change.[20] Additionally, poor EHR system design and improper use can cause errors that jeopardize the integrity of the information inputted, leading to inaccuracies that endanger patient safety or decrease the quality of care.[21]
One of the limitations of EHRs has been the reported negative impact on patient‐centered care by decreasing communication during the hospital visit.[22] Although the EHR has enhanced internal provider communication,[23] the literature suggests a lack of focus on the patient sitting in front of the provider. Due to perceived physician distraction during the visit, patients report decreased satisfaction when physicians spend a considerable period of time during the visit at the computer.[22] Furthermore, the average hospital length of stay has been increased due to the use of EHRs.[22]
Although some physicians report that EHR use impedes patient workflow and decreases time spent with patients,[23] previous literature suggests that EHRs decrease the time to develop a synopsis and improve communication efficiency.[19] Some studies have also noted an increase in the ability for medical history retrieval and analysis, which will ultimately increase the quality of care provided to the patient.[24] Physicians who use the EHR adopted a more active role in clarifying information, encouraging questions, and ensuring completeness at the end of a visit.[25] Finally, studies show that the EHR has a positive return on investment from savings in drug expenditures, radiology tests, and billing errors.[26] Given the significant financial and time commitment that health systems and physicians must invest to implement EHRs, it is vital that we understand the multifaceted effects of EHRs on the field of medicine.
METHODS
The purpose of this study was to assess the physician‐patient communication patterns associated with the implementation and use of an EHR in a hospital setting.
ARC Medical Program
In 2006, the Office of Patient Experience at University of California, Los Angeles (UCLA) Health, in conjunction with the David Geffen School of Medicine at UCLA, launched the Assessing Residents' CI‐CARE (ARC) Medical Program. CI‐CARE is a protocol that emphasizes for medical staff and providers to Connect with their patients, Introduce themselves, Communicate their purpose, Ask or anticipate patients' needs, Respond to questions with immediacy, and to Exit courteously. CI‐CARE represents the standards for staff and providers in any encounter with patients or their families. The goals of the ARC Medical Program are to monitor housestaff performance and patient satisfaction while improving trainee education through timely and patient‐centered feedback. The ARC Medical Program's survey has served as an important tool to assess and improve physician professionalism and interpersonal skills and communication, 2 of the Accreditation Council for Graduate Medical Education core competencies.[27]
The ARC program is a unique and innovative volunteer program that provides timely and patient‐centered feedback from trainees' daily encounters with hospitalized patients. The ARC Medical Program has an established infrastructure to conduct evaluations on a system‐wide scale, including 9 departments within UCLA Health. ARC volunteers interview patients using a CI‐CARE Questionnaire (ARC survey) to assess their resident physician's communication patterns. The ARC Survey targets specific areas of the residents' care as outlined by the CI‐CARE Program of UCLA Health.
As part of UCLA Health's mission to ensure the highest level of patient‐centered care, the CI‐CARE standards were introduced in 2006, followed by implementation of the EHR system. Given the lack of previous research and conflicting results on the impact of EHRs on the patient experience, this article uses ARC data to assess whether or not there was a significant difference following implementation of the EHR on March 2, 2013.
The materials and methods of this study are largely based on those of a previous study, also published by the ARC Medical Program.[27]
CI‐CARE QuestionnaireARC Survey
The CI‐CARE Questionnaire is a standardized audit tool consisting of a total of 20 questions used by the facilitators who work with ARC. There are a total of 20 items on the ARC survey, including 18 multiple‐choice, polar, and Likert‐scale questions, and 2 free‐response questions that assess the patients' overall perception of their resident physician and their hospital experience. Questions 1 and 2 pertain to the recognition of attending physicians and resident physicians, respectively. Questions 3, 4, 6, 7, and 8 are Likert‐scalebased questions assessing the residents' professionalism. Questions 9 through 14 are Likert‐scalebased items included to evaluate the quality of communication between patient and provider. We categorized questions 5 and 15 as relating to diagnostics.[27] In 2012, ARC implemented 3 additional questions that assessed residents' communication skills (question 16), level of medical expertise (question 17), and quality of medical care (question 18). We chose to examine the CI‐CARE Questionnaire instead of a standard survey such as the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), because it examines the physician‐patient interaction in more detail. The survey can be reviewed in Figure 1.
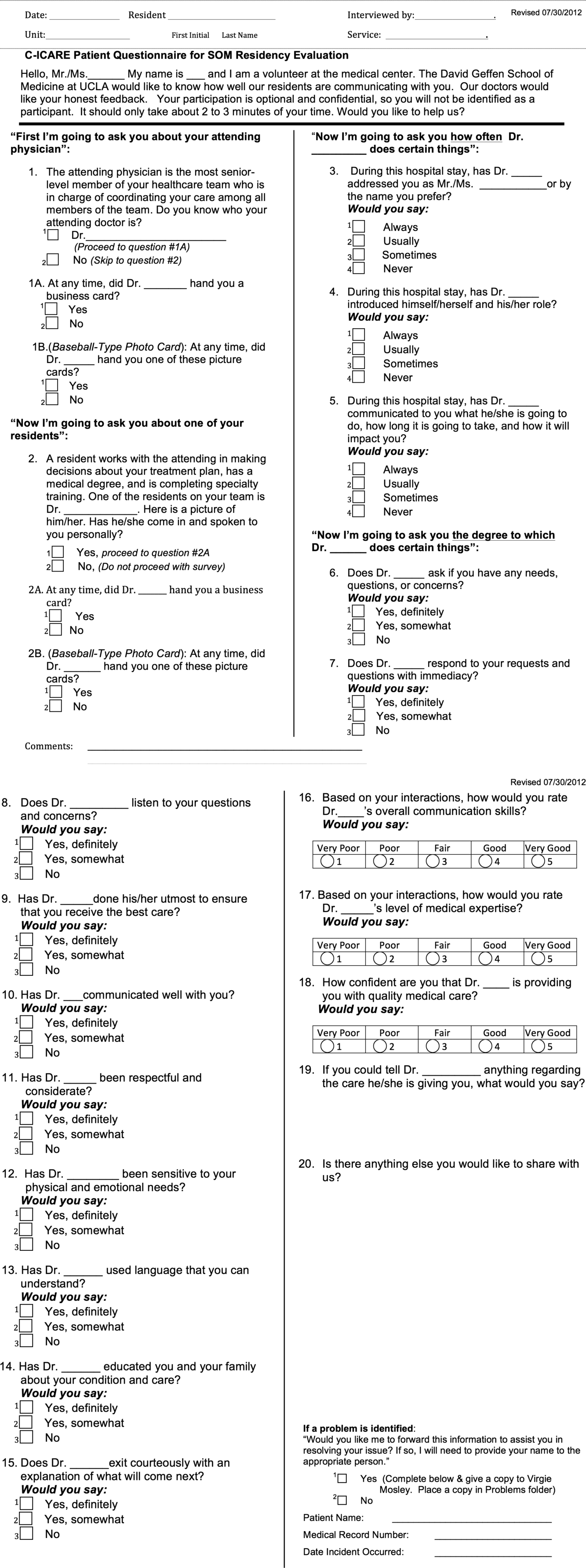
Interview Procedure
The ARC Medical Program is comprised of 47 premedical UCLA students who conducted the surveys. New surveyors were trained by the senior surveyors for a minimum of 12 hours before conducting a survey independently. All surveyors were evaluated biyearly by their peers and the program director for quality assurance and to ensure uniform procedures. The volunteers' surveying experience on December 1, 2012 was as follows: (=10 months [237 months], =10 months).
Prior to the interview, the surveyor introduces himself or herself, the purpose and length of the interview, and that the patient's anonymous participation is optional and confidential. Upon receiving verbal consent from the patient, the surveyor presents a picture card to the patient and asks him or her to identify a resident who was on rotation who treated them. If the patient is able to identify the resident who treated them, the surveyor asks each question and records each response verbatim. The surveyors are trained not to probe for responses, and to ensure that the patients answer in accordance with the possible responses. Although it has not been formally studied, the inter‐rater reliability of the survey is likely to be very high due to the verbatim requirements.
Population Interviewed
A total of 3414 surveys were collected from patients seen in the departments of internal medicine, family medicine, pediatrics, general surgery, head and neck surgery, orthopedic surgery, neurosurgery, neurology, and obstetrics and gynecology in this retrospective cohort study. Exclusion criteria included patients who were not awake, were not conscious, could not confidently identify a resident, or stated that they were not able to confidently complete the survey.
Data Analysis
The researchers reviewed and evaluated all data gathered using standard protocols. Statistical comparisons were made using [2] tests. All quantitative analyses were performed in Excel 2010 (Microsoft Corp., Redmond, WA) and SPSS version 21 (IBM Corp., Armonk, NY).
Institutional Review Board
This project received an exemption by the UCLA institutional review board.
RESULTS
There were a total of 3414 interviews conducted and completed from December 1, 2012 to May 30, 2013. Altogether, 1567 surveys were collected 3 months prior to EHR implementation (DecemberFebruary), and 1847 surveys were collected 3 months following implementation (MarchMay). The survey breakdown is summarized in Table 1.
| Department | Pre (N) | Post (N) | Total (N) |
|---|---|---|---|
| |||
| Family medicine | 65 | 128 | 193 |
| General surgery | 226 | 246 | 472 |
| Head and neck surgery | 43 | 65 | 108 |
| Internal medicine | 439 | 369 | 808 |
| Neurology | 81 | 98 | 179 |
| Neurosurgery | 99 | 54 | 153 |
| OB/GYN | 173 | 199 | 372 |
| Orthopedic surgery | 117 | 128 | 245 |
| Pediatrics | 324 | 563 | 887 |
| Totals | 1,567 | 1,850 | 3,417 |
2 analysis revealed that the residents received significantly better feedback in the 3 months following EHR implementation, compared to the 3 months prior to implementation on questions 3, addressing the patient by their preferred name; 4, introducing themselves and their role; 5, communicating what they will do, how long it will take, and how it will impact the patient; 7, responding to the patient's requests and questions with immediacy; 8, listening to the patient's questions and concerns; 9, doing their utmost to ensure the patient receives the best care; 10, communicating well with the patient; 11, being respectful and considerate; and 12, being sensitive to the patient's physical and emotional needs (P<0.05) (Table 2).
| Question | Pre‐EHR % Responses (n=1,567) | Post‐EHR % Responses (n=1,850) | 2 Significance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |||
| ||||||||||||
| 3 | Address you by preferred name? | 90.1 | 3.8 | 2.7 | 3.4 | 91.5 | 3.6 | 1.3 | 3.6 | 0.032* | ||
| 4 | Introduce himself/herself? | 88.3 | 6.4 | 3.2 | 2.1 | 93.1 | 3.6 | 1.8 | 1.5 | 0.000* | ||
| 5 | Communicate what he/she will do? | 83.1 | 9.3 | 4.5 | 3.2 | 86.9 | 6.4 | 3.5 | 3.3 | 0.006* | ||
| 6 | Ask if you have any questions? | 90.9 | 6.2 | 2.9 | 92.4 | 4.9 | 2.7 | 0.230 | ||||
| 7 | Respond with immediacy? | 92.5 | 5.4 | 2.2 | 94.6 | 3.4 | 2.1 | 0.015* | ||||
| 8 | Listens to your questions and concerns? | 94.8 | 4.0 | 1.1 | 96.6 | 2.4 | 1.0 | 0.022* | ||||
| 9 | Ensure you received the best care? | 92.4 | 6.3 | 1.3 | 95.2 | 3.9 | 1.0 | 0.003* | ||||
| 10 | Communicates well with you? | 92.3 | 6.3 | 1.5 | 94.8 | 4.2 | 0.9 | 0.009* | ||||
| 11 | Is respectful and considerate? | 96.5 | 2.7 | 0.8 | 98.0 | 1.6 | 0.4 | 0.025* | ||||
| 12 | Sensitive to your physical and emotional needs? | 90.4 | 6.9 | 2.7 | 94.5 | 3.9 | 1.6 | 0.000* | ||||
| 13 | Uses language that you can understand? | 96.5 | 2.8 | 0.7 | 96.9 | 2.8 | 0.4 | 0.431 | ||||
| 14 | Educated you/family about condition/care? | 84.0 | 8.6 | 7.4 | 86.6 | 7.4 | 6.0 | 0.111 | ||||
| 15 | Exit courteously? | 89.7 | 6.6 | 3.6 | 91.7 | 5.2 | 3.1 | 0.130 | ||||
| 16 | Communication skills? | 75.6 | 19.5 | 3.6 | 0.7 | 0.7 | 78.6 | 16.9 | 3.9 | 0.4 | 0.3 | 0.077 |
| 17 | Medical expertise? | 79.5 | 15.9 | 3.5 | 0.7 | 0.4 | 80.0 | 16.5 | 2.7 | 0.5 | 0.2 | 0.398 |
| 18 | Quality medical care? | 82.5 | 13.0 | 2.8 | 0.8 | 0.9 | 82.6 | 13.6 | 2.7 | 0.7 | 0.5 | 0.754 |
ARC surveyed for 10 weeks prior to our reported sample (OctoberDecember) and 22 weeks prior to EHR implementation total (OctoberMarch). To rule out resident improvement due to the confounding effects of time and experience, we compared the data from the first 11 weeks (OctoberDecember) to the second 11 weeks (DecemberMarch) prior to EHR implementation. [2] analysis revealed that only 6 of the 16 questions showed improvement in this period, and just 1 of these improvements (question 3) was significant. Furthermore, 10 of the 16 questions actually received worse responses in this period, and 2 of these declines (questions 9 and 12) were significant (Table 3).
| Question | First 11 Weeks' Responses (n=897) | Second 11 Weeks' Responses (n=1,338) | 2 Significance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |||
| ||||||||||||
| 3 | Address you by preferred name? | 87.1 | 6.4 | 4.6 | 2.0 | 90.7 | 3.7 | 2.3 | 3.4 | 0.000* | ||
| 4 | Introduce himself/herself? | 87.7 | 6.9 | 4.1 | 1.2 | 88.3 | 6.1 | 3.3 | 2.3 | 0.174 | ||
| 5 | Communicate what he/she will do? | 82.9 | 8.2 | 5.1 | 3.7 | 83.2 | 9.1 | 4.3 | 3.4 | 0.698 | ||
| 6 | Ask if you have any questions? | 92.0 | 5.9 | 2.1 | 90.7 | 6.1 | 3.1 | 0.336 | ||||
| 7 | Respond with immediacy? | 91.2 | 6.6 | 2.2 | 92.8 | 5.2 | 2.1 | 0.353 | ||||
| 8 | Listens to your questions and concerns? | 94.6 | 3.9 | 1.4 | 95.0 | 3.8 | 1.2 | 0.868 | ||||
| 9 | Ensure you received the best care? | 94.4 | 5.0 | 0.6 | 92.1 | 6.5 | 1.4 | 0.049* | ||||
| 10 | Communicates well with you? | 93.3 | 5.9 | 0.8 | 92.4 | 5.9 | 1.7 | 0.167 | ||||
| 11 | Is respectful and considerate? | 97.3 | 2.1 | 0.6 | 96.4 | 2.7 | 0.9 | 0.455 | ||||
| 12 | Sensitive to your physical and emotional needs? | 93.2 | 5.5 | 1.3 | 90.3 | 6.9 | 2.8 | 0.022* | ||||
| 13 | Uses language that you can understand? | 96.2 | 3.5 | 0.3 | 96.4 | 2.8 | 0.7 | 0.327 | ||||
| 14 | Educated you/family about condition/care? | 85.7 | 8.9 | 5.4 | 83.8 | 8.7 | 7.5 | 0.141 | ||||
| 15 | Exit courteously? | 89.7 | 7.8 | 2.5 | 89.6 | 6.6 | 3.8 | 0.124 | ||||
| 16 | Communication skills? | 78.7 | 17.1 | 2.9 | 0.7 | 0.7 | 75.9 | 19 | 3.6 | 0.7 | 0.8 | 0.633 |
| 17 | Medical expertise? | 82.3 | 13.3 | 3.9 | 0.1 | 0.4 | 78.9 | 16.1 | 3.6 | 0.8 | 0.5 | 0.062 |
| 18 | Quality medical care? | 82.7 | 13.5 | 2.6 | 0.8 | 0.4 | 82.1 | 13.0 | 3.0 | 0.9 | 1.0 | 0.456 |
DISCUSSION
The adoption of EHRs has been fueled by their suggested improvement on healthcare quality and spending.[15, 16, 17, 18] Few studies have investigated the patient experience and its relation to EHR implementation. Furthermore, these studies have not yielded consistent results,[19, 20, 21, 22, 23, 25] raising uncertainty about the effects of EHRs on the patient experience. Possible barriers that may contribute to the scarcity of literature include the relatively recent large‐scale implementation of EHRs and a lack of programs in place to collect extensive data on the physician‐patient relationship.
In a field with increasing demands on patient‐centered care, we need to find ways to preserve and foster the patient‐physician relationship. Given that improvements in the delivery of compassionate care can positively impact clinical outcomes, the likelihood of medical malpractice lawsuits, and patient satisfaction,[1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13] the need to improve the patient‐provider relationship is tremendously important. Following EHR implementation, residents were perceived to provide more frequent diagnostics information including the nature, impact, and treatment of conditions. Furthermore, they were perceived to provide significantly better communication quality following implementation, through care monitoring, respectful and sensitive communication, and enhanced patient and family education. Residents were also perceived as being more professional following implementation, as indicated by positive assessments of several interpersonal communication questions. These results suggest that implementing an EHR may be an effective way to meet these increasing demands on patient‐centered care.
Limitations to this study should be considered. The ARC Medical Program is primarily used as an education tool for resident physicians, so all of our data are specific to resident physicians. It would be interesting and important to observe if EHRs affect nurse or attending‐patient interactions. Furthermore, we did not have access to any patient demographic or clinical data. However, we did not anticipate a significant change in the patient population that would alter the survey responses during this 6‐month period. Patients were required to recognize their resident on a photo card presented to them by the surveyor, which likely favored patients with strong feelings toward their residents. Due to this, our population sampled may not be indicative of the entire patient population. All findings were simply correlational. Due to the nature of our data collection, we were unable to control for many confounding variables, thus causal conclusions are difficult to draw from these results.
There are a few important trends to note. No question on the ARC survey received lower scores following implementation of the EHR. Furthermore, 9 of the 16 questions under investigation received significantly higher scores following implementation. The residents largely received positive responses both before and after EHR implementation, so despite the statistically significant improvements, the absolute differences are relatively small. These significant differences were likely not due to the residents improving through time and experience. We observed relatively insignificant and nonuniform changes in responses between the two 11‐week periods prior to implementation.
One possible reason for the observed significant improvements is that EHRs may increase patient involvement in the healthcare setting,[28] and this collaboration might improve resident‐patient communication.[29] Providing patients with an interactive tablet that details their care has been suggested to increase patient satisfaction and comfort in an inpatient setting.[30] In this light, the EHR can be used as a tool to increase these interactions by inviting patients to view the computer screen and electronic charts during data entry, which allows them to have a participatory role in their care and decision‐making process.[31] Although the reasons for our observed improvements are unclear, they are noteworthy and warrant further study. The notion that implementing an EHR might enhance provider‐patient communication is a powerful concept.
This study not only suggests the improvement of resident‐patient communication due to the implementation of an EHR, but it also reveals the value of the ARC Medical Program for studying the patient experience. The controlled, prolonged, and efficient nature of the ARC Medical Program's data collection was ideal for comparing a change in resident‐patient communication before and after EHR implementation at UCLA Health. ARC and UCLA Health's EHR can serve as a model for residency programs nationwide. Future studies can assess the changes of the patient‐provider interaction for any significant event, as demonstrated by this study and its investigation of the implementation of UCLA Health's EHR.
Acknowledgements
The authors acknowledge the UCLA Health Office of the Patient Experience and UCLA Health for allowing for this unique partnership with the David Geffen School of Medicine to improve physician‐patient communication. Furthermore, the authors thank the student volunteers and interns of the ARC Medical program for their commitment and effort to optimize the patient experience. Additionally, the authors thank the program directors of the David Geffen School of Medicine residency physician training programs for their outstanding support of the ARC Medical Program.
Disclosures: C.W.M. and A.A.N. contributed equally to this manuscript. C.W.M. and A.A.N. collected data, performed statistical analyses, and drafted and revised the manuscript. A.A.N. and V.N.M. oversaw the program. N.A. provided faculty support and revised the manuscript. The authors report no conflicts of interest.
- , , . Doctor‐patient communication and patient satisfaction: a review. Fam Pract. 1998;15(5):480–492.
- . Patient satisfaction in primary health care: a literature review and analysis. Eval Program Plann. 1983;6:185–210.
- , . The significance of patients' perceptions of physician conduct. J Community Health. 1980;6(1):18–34.
- , , , . Predicting patient satisfaction from physicians' nonverbal communication skills. Med Care. 1980;18(4):376–387.
- , , . Why do people sue doctors? A study of patients and relatives. Lancet. 1994;343:1609–1613.
- , , . Reducing legal risk by practicing patient‐centered medicine. Arch Intern Med. 2002;162(11):1217–1219.
- , . Listening and talking. West J Med. 1993;158:268–272.
- , , . Medical malpractice: the effect of doctor‐patient relations on medical patient perceptions and malpractice intentions. West J Med. 2000;173(4):244–250.
- . Effective physician‐patient communication and health outcomes: a review. CMAJ. 1995;152(9):1423–1433.
- , , , , . Patients' participation in medical care: effects on blood sugar control and quality of life in diabetes. J Intern Med. 1988;3:448–457.
- , , . Assessing the effects of physician‐patient interactions on the outcomes of chronic disease. Med Care. 1989;27(3 suppl):S110–S127.
- , , . Expanding patient involvement in care. Ann Intern Med. 1985;102:520–528.
- , , , , . Patient exposition and provider explanation in routine interviews and hypertensive patients' blood control. Health Psychol. 1987;6(1):29–42.
- , , . A framework for making patient‐centered care front and center. Perm J. 2012;16(3):49–53.
- . Interoperability: the key to the future health care system. Health Aff. 2005;5(21):19–21.
- , . Physicians' use of electronic medical records: barriers and solutions. Health Aff. 2004;23(2):116–126.
- , . Do hospitals with electronic medical records (EMRs) provide higher quality care?: an examination of three clinical conditions. Med Care Res Rev. 2008;65(4):496–513.
- , , , et al. Can electronic medical record systems transform health care? Potential health benefits, savings, and costs. Health Aff. 2005;24(5):1103–1117.
- , , , . An electronic medical record in primary care: impact on satisfaction, work efficiency and clinic processes. AMIA Annu Symp.2006:394–398.
- , . Barriers to implement electronic health records (EHRs). Mater Sociomed. 2013;25(3):213–215.
- . Impact of electronic health record systems on information integrity: quality and safety implications. Perspect Health Inf Manag. 2013;10:1c.eCollection 2013.
- , , , , . Electronic medical record use and physician–patient communication: an observational study of Israeli primary care encounters. Patient Educ Couns. 2006;61:134–141.
- , , , et al. EHR implementation in a new clinic: a case study of clinician perceptions. J Med Syst. 2013;37(9955):1–6.
- , , . Accuracy and speed of electronic health record versus paper‐based ophthalmic documentation strategies. Am J Ophthalmol. 2013;156(1):165–172.
- , , . The use of electronic medical records communication patterns in outpatient encounters. J Am Informatics Assoc. 2001:610–616.
- , , . Cost‐benefit analysis of electronic medical record system at a tertiary care hospital. Healthc Inform Res. 2013;19(3):205–214.
- , , , . Promoting patient‐centred care through trainee feedback: assessing residents' C‐I‐CARE (ARC) program. BMJ Qual Saf. 2012;21(3):225–233.
- . Electronic health records?: can we maximize their benefits and minimize their risks? Acad Med. 2012;87(11):1456–1457.
- , . Let the left hand know what the right is doing: a vision for care coordination and electronic health records. J Am Med Inform Assoc. 2014;21(1):13–16.
- , , , et al. A tablet computer application for patients to participate in their hospital care. AMIA Annu Symp Proc. 2011;2011:1428–1435.
- , . Enhancing patient‐centered communication and collaboration by using the electronic health record in the examination room. J Am Med Assoc. 2013;309(22):2327–2328.
Delivering patient‐centered care is at the core of ensuring patient engagement and active participation that will lead to positive outcomes. Physician‐patient interaction has become an area of increasing focus in an effort to optimize the patient experience. Positive patient‐provider communication has been shown to increase satisfaction,[1, 2, 3, 4] decrease the likelihood of medical malpractice lawsuits,[5, 6, 7, 8] and improve clinical outcomes.[9, 10, 11, 12, 13] Specifically, a decrease in psychological symptoms such as anxiety and stress, as well as perception of physical symptoms have been correlated with improved communication.[9, 12] Furthermore, objective health outcomes, such as improvement in hypertension and glycosylated hemoglobin, have also been correlated with improved physician‐patient communication.[10, 11, 13] The multifaceted effects of improved communication are impactful to both the patient and the physician; therefore, it is essential that we understand how to optimize this interaction.
Patient‐centered care is a critical objective for many high‐quality healthcare systems.[14] In recent years, the use of electronic health records (EHRs) has been increasingly adopted by healthcare systems nationally in an effort to improve the quality of care delivered. The positive benefits of EHRs on the facilitation of healthcare, including consolidation of information, reduction of medical errors, easily transferable medical records,[15, 16, 17] as well as their impact on healthcare spending,[18] are well‐documented and have been emphasized as reasons for adoption of EHRs by the Patient Protection and Affordable Care Act. However, EHR implementation has encountered some resistance regarding its impact on the patient experience.
As EHR implementation is exponentially increasing in the United States, there is limited literature on the consequences of this technology.[19] Barriers reported during EHR implementation include the limitations of standardization, attitudinal and organizational constraints, behavior of individuals, and resistance to change.[20] Additionally, poor EHR system design and improper use can cause errors that jeopardize the integrity of the information inputted, leading to inaccuracies that endanger patient safety or decrease the quality of care.[21]
One of the limitations of EHRs has been the reported negative impact on patient‐centered care by decreasing communication during the hospital visit.[22] Although the EHR has enhanced internal provider communication,[23] the literature suggests a lack of focus on the patient sitting in front of the provider. Due to perceived physician distraction during the visit, patients report decreased satisfaction when physicians spend a considerable period of time during the visit at the computer.[22] Furthermore, the average hospital length of stay has been increased due to the use of EHRs.[22]
Although some physicians report that EHR use impedes patient workflow and decreases time spent with patients,[23] previous literature suggests that EHRs decrease the time to develop a synopsis and improve communication efficiency.[19] Some studies have also noted an increase in the ability for medical history retrieval and analysis, which will ultimately increase the quality of care provided to the patient.[24] Physicians who use the EHR adopted a more active role in clarifying information, encouraging questions, and ensuring completeness at the end of a visit.[25] Finally, studies show that the EHR has a positive return on investment from savings in drug expenditures, radiology tests, and billing errors.[26] Given the significant financial and time commitment that health systems and physicians must invest to implement EHRs, it is vital that we understand the multifaceted effects of EHRs on the field of medicine.
METHODS
The purpose of this study was to assess the physician‐patient communication patterns associated with the implementation and use of an EHR in a hospital setting.
ARC Medical Program
In 2006, the Office of Patient Experience at University of California, Los Angeles (UCLA) Health, in conjunction with the David Geffen School of Medicine at UCLA, launched the Assessing Residents' CI‐CARE (ARC) Medical Program. CI‐CARE is a protocol that emphasizes for medical staff and providers to Connect with their patients, Introduce themselves, Communicate their purpose, Ask or anticipate patients' needs, Respond to questions with immediacy, and to Exit courteously. CI‐CARE represents the standards for staff and providers in any encounter with patients or their families. The goals of the ARC Medical Program are to monitor housestaff performance and patient satisfaction while improving trainee education through timely and patient‐centered feedback. The ARC Medical Program's survey has served as an important tool to assess and improve physician professionalism and interpersonal skills and communication, 2 of the Accreditation Council for Graduate Medical Education core competencies.[27]
The ARC program is a unique and innovative volunteer program that provides timely and patient‐centered feedback from trainees' daily encounters with hospitalized patients. The ARC Medical Program has an established infrastructure to conduct evaluations on a system‐wide scale, including 9 departments within UCLA Health. ARC volunteers interview patients using a CI‐CARE Questionnaire (ARC survey) to assess their resident physician's communication patterns. The ARC Survey targets specific areas of the residents' care as outlined by the CI‐CARE Program of UCLA Health.
As part of UCLA Health's mission to ensure the highest level of patient‐centered care, the CI‐CARE standards were introduced in 2006, followed by implementation of the EHR system. Given the lack of previous research and conflicting results on the impact of EHRs on the patient experience, this article uses ARC data to assess whether or not there was a significant difference following implementation of the EHR on March 2, 2013.
The materials and methods of this study are largely based on those of a previous study, also published by the ARC Medical Program.[27]
CI‐CARE QuestionnaireARC Survey
The CI‐CARE Questionnaire is a standardized audit tool consisting of a total of 20 questions used by the facilitators who work with ARC. There are a total of 20 items on the ARC survey, including 18 multiple‐choice, polar, and Likert‐scale questions, and 2 free‐response questions that assess the patients' overall perception of their resident physician and their hospital experience. Questions 1 and 2 pertain to the recognition of attending physicians and resident physicians, respectively. Questions 3, 4, 6, 7, and 8 are Likert‐scalebased questions assessing the residents' professionalism. Questions 9 through 14 are Likert‐scalebased items included to evaluate the quality of communication between patient and provider. We categorized questions 5 and 15 as relating to diagnostics.[27] In 2012, ARC implemented 3 additional questions that assessed residents' communication skills (question 16), level of medical expertise (question 17), and quality of medical care (question 18). We chose to examine the CI‐CARE Questionnaire instead of a standard survey such as the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), because it examines the physician‐patient interaction in more detail. The survey can be reviewed in Figure 1.
Interview Procedure
The ARC Medical Program is comprised of 47 premedical UCLA students who conducted the surveys. New surveyors were trained by the senior surveyors for a minimum of 12 hours before conducting a survey independently. All surveyors were evaluated biyearly by their peers and the program director for quality assurance and to ensure uniform procedures. The volunteers' surveying experience on December 1, 2012 was as follows: (=10 months [237 months], =10 months).
Prior to the interview, the surveyor introduces himself or herself, the purpose and length of the interview, and that the patient's anonymous participation is optional and confidential. Upon receiving verbal consent from the patient, the surveyor presents a picture card to the patient and asks him or her to identify a resident who was on rotation who treated them. If the patient is able to identify the resident who treated them, the surveyor asks each question and records each response verbatim. The surveyors are trained not to probe for responses, and to ensure that the patients answer in accordance with the possible responses. Although it has not been formally studied, the inter‐rater reliability of the survey is likely to be very high due to the verbatim requirements.
Population Interviewed
A total of 3414 surveys were collected from patients seen in the departments of internal medicine, family medicine, pediatrics, general surgery, head and neck surgery, orthopedic surgery, neurosurgery, neurology, and obstetrics and gynecology in this retrospective cohort study. Exclusion criteria included patients who were not awake, were not conscious, could not confidently identify a resident, or stated that they were not able to confidently complete the survey.
Data Analysis
The researchers reviewed and evaluated all data gathered using standard protocols. Statistical comparisons were made using [2] tests. All quantitative analyses were performed in Excel 2010 (Microsoft Corp., Redmond, WA) and SPSS version 21 (IBM Corp., Armonk, NY).
Institutional Review Board
This project received an exemption by the UCLA institutional review board.
RESULTS
There were a total of 3414 interviews conducted and completed from December 1, 2012 to May 30, 2013. Altogether, 1567 surveys were collected 3 months prior to EHR implementation (DecemberFebruary), and 1847 surveys were collected 3 months following implementation (MarchMay). The survey breakdown is summarized in Table 1.
| Department | Pre (N) | Post (N) | Total (N) |
|---|---|---|---|
| |||
| Family medicine | 65 | 128 | 193 |
| General surgery | 226 | 246 | 472 |
| Head and neck surgery | 43 | 65 | 108 |
| Internal medicine | 439 | 369 | 808 |
| Neurology | 81 | 98 | 179 |
| Neurosurgery | 99 | 54 | 153 |
| OB/GYN | 173 | 199 | 372 |
| Orthopedic surgery | 117 | 128 | 245 |
| Pediatrics | 324 | 563 | 887 |
| Totals | 1,567 | 1,850 | 3,417 |
2 analysis revealed that the residents received significantly better feedback in the 3 months following EHR implementation, compared to the 3 months prior to implementation on questions 3, addressing the patient by their preferred name; 4, introducing themselves and their role; 5, communicating what they will do, how long it will take, and how it will impact the patient; 7, responding to the patient's requests and questions with immediacy; 8, listening to the patient's questions and concerns; 9, doing their utmost to ensure the patient receives the best care; 10, communicating well with the patient; 11, being respectful and considerate; and 12, being sensitive to the patient's physical and emotional needs (P<0.05) (Table 2).
| Question | Pre‐EHR % Responses (n=1,567) | Post‐EHR % Responses (n=1,850) | 2 Significance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |||
| ||||||||||||
| 3 | Address you by preferred name? | 90.1 | 3.8 | 2.7 | 3.4 | 91.5 | 3.6 | 1.3 | 3.6 | 0.032* | ||
| 4 | Introduce himself/herself? | 88.3 | 6.4 | 3.2 | 2.1 | 93.1 | 3.6 | 1.8 | 1.5 | 0.000* | ||
| 5 | Communicate what he/she will do? | 83.1 | 9.3 | 4.5 | 3.2 | 86.9 | 6.4 | 3.5 | 3.3 | 0.006* | ||
| 6 | Ask if you have any questions? | 90.9 | 6.2 | 2.9 | 92.4 | 4.9 | 2.7 | 0.230 | ||||
| 7 | Respond with immediacy? | 92.5 | 5.4 | 2.2 | 94.6 | 3.4 | 2.1 | 0.015* | ||||
| 8 | Listens to your questions and concerns? | 94.8 | 4.0 | 1.1 | 96.6 | 2.4 | 1.0 | 0.022* | ||||
| 9 | Ensure you received the best care? | 92.4 | 6.3 | 1.3 | 95.2 | 3.9 | 1.0 | 0.003* | ||||
| 10 | Communicates well with you? | 92.3 | 6.3 | 1.5 | 94.8 | 4.2 | 0.9 | 0.009* | ||||
| 11 | Is respectful and considerate? | 96.5 | 2.7 | 0.8 | 98.0 | 1.6 | 0.4 | 0.025* | ||||
| 12 | Sensitive to your physical and emotional needs? | 90.4 | 6.9 | 2.7 | 94.5 | 3.9 | 1.6 | 0.000* | ||||
| 13 | Uses language that you can understand? | 96.5 | 2.8 | 0.7 | 96.9 | 2.8 | 0.4 | 0.431 | ||||
| 14 | Educated you/family about condition/care? | 84.0 | 8.6 | 7.4 | 86.6 | 7.4 | 6.0 | 0.111 | ||||
| 15 | Exit courteously? | 89.7 | 6.6 | 3.6 | 91.7 | 5.2 | 3.1 | 0.130 | ||||
| 16 | Communication skills? | 75.6 | 19.5 | 3.6 | 0.7 | 0.7 | 78.6 | 16.9 | 3.9 | 0.4 | 0.3 | 0.077 |
| 17 | Medical expertise? | 79.5 | 15.9 | 3.5 | 0.7 | 0.4 | 80.0 | 16.5 | 2.7 | 0.5 | 0.2 | 0.398 |
| 18 | Quality medical care? | 82.5 | 13.0 | 2.8 | 0.8 | 0.9 | 82.6 | 13.6 | 2.7 | 0.7 | 0.5 | 0.754 |
ARC surveyed for 10 weeks prior to our reported sample (OctoberDecember) and 22 weeks prior to EHR implementation total (OctoberMarch). To rule out resident improvement due to the confounding effects of time and experience, we compared the data from the first 11 weeks (OctoberDecember) to the second 11 weeks (DecemberMarch) prior to EHR implementation. [2] analysis revealed that only 6 of the 16 questions showed improvement in this period, and just 1 of these improvements (question 3) was significant. Furthermore, 10 of the 16 questions actually received worse responses in this period, and 2 of these declines (questions 9 and 12) were significant (Table 3).
| Question | First 11 Weeks' Responses (n=897) | Second 11 Weeks' Responses (n=1,338) | 2 Significance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |||
| ||||||||||||
| 3 | Address you by preferred name? | 87.1 | 6.4 | 4.6 | 2.0 | 90.7 | 3.7 | 2.3 | 3.4 | 0.000* | ||
| 4 | Introduce himself/herself? | 87.7 | 6.9 | 4.1 | 1.2 | 88.3 | 6.1 | 3.3 | 2.3 | 0.174 | ||
| 5 | Communicate what he/she will do? | 82.9 | 8.2 | 5.1 | 3.7 | 83.2 | 9.1 | 4.3 | 3.4 | 0.698 | ||
| 6 | Ask if you have any questions? | 92.0 | 5.9 | 2.1 | 90.7 | 6.1 | 3.1 | 0.336 | ||||
| 7 | Respond with immediacy? | 91.2 | 6.6 | 2.2 | 92.8 | 5.2 | 2.1 | 0.353 | ||||
| 8 | Listens to your questions and concerns? | 94.6 | 3.9 | 1.4 | 95.0 | 3.8 | 1.2 | 0.868 | ||||
| 9 | Ensure you received the best care? | 94.4 | 5.0 | 0.6 | 92.1 | 6.5 | 1.4 | 0.049* | ||||
| 10 | Communicates well with you? | 93.3 | 5.9 | 0.8 | 92.4 | 5.9 | 1.7 | 0.167 | ||||
| 11 | Is respectful and considerate? | 97.3 | 2.1 | 0.6 | 96.4 | 2.7 | 0.9 | 0.455 | ||||
| 12 | Sensitive to your physical and emotional needs? | 93.2 | 5.5 | 1.3 | 90.3 | 6.9 | 2.8 | 0.022* | ||||
| 13 | Uses language that you can understand? | 96.2 | 3.5 | 0.3 | 96.4 | 2.8 | 0.7 | 0.327 | ||||
| 14 | Educated you/family about condition/care? | 85.7 | 8.9 | 5.4 | 83.8 | 8.7 | 7.5 | 0.141 | ||||
| 15 | Exit courteously? | 89.7 | 7.8 | 2.5 | 89.6 | 6.6 | 3.8 | 0.124 | ||||
| 16 | Communication skills? | 78.7 | 17.1 | 2.9 | 0.7 | 0.7 | 75.9 | 19 | 3.6 | 0.7 | 0.8 | 0.633 |
| 17 | Medical expertise? | 82.3 | 13.3 | 3.9 | 0.1 | 0.4 | 78.9 | 16.1 | 3.6 | 0.8 | 0.5 | 0.062 |
| 18 | Quality medical care? | 82.7 | 13.5 | 2.6 | 0.8 | 0.4 | 82.1 | 13.0 | 3.0 | 0.9 | 1.0 | 0.456 |
DISCUSSION
The adoption of EHRs has been fueled by their suggested improvement on healthcare quality and spending.[15, 16, 17, 18] Few studies have investigated the patient experience and its relation to EHR implementation. Furthermore, these studies have not yielded consistent results,[19, 20, 21, 22, 23, 25] raising uncertainty about the effects of EHRs on the patient experience. Possible barriers that may contribute to the scarcity of literature include the relatively recent large‐scale implementation of EHRs and a lack of programs in place to collect extensive data on the physician‐patient relationship.
In a field with increasing demands on patient‐centered care, we need to find ways to preserve and foster the patient‐physician relationship. Given that improvements in the delivery of compassionate care can positively impact clinical outcomes, the likelihood of medical malpractice lawsuits, and patient satisfaction,[1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13] the need to improve the patient‐provider relationship is tremendously important. Following EHR implementation, residents were perceived to provide more frequent diagnostics information including the nature, impact, and treatment of conditions. Furthermore, they were perceived to provide significantly better communication quality following implementation, through care monitoring, respectful and sensitive communication, and enhanced patient and family education. Residents were also perceived as being more professional following implementation, as indicated by positive assessments of several interpersonal communication questions. These results suggest that implementing an EHR may be an effective way to meet these increasing demands on patient‐centered care.
Limitations to this study should be considered. The ARC Medical Program is primarily used as an education tool for resident physicians, so all of our data are specific to resident physicians. It would be interesting and important to observe if EHRs affect nurse or attending‐patient interactions. Furthermore, we did not have access to any patient demographic or clinical data. However, we did not anticipate a significant change in the patient population that would alter the survey responses during this 6‐month period. Patients were required to recognize their resident on a photo card presented to them by the surveyor, which likely favored patients with strong feelings toward their residents. Due to this, our population sampled may not be indicative of the entire patient population. All findings were simply correlational. Due to the nature of our data collection, we were unable to control for many confounding variables, thus causal conclusions are difficult to draw from these results.
There are a few important trends to note. No question on the ARC survey received lower scores following implementation of the EHR. Furthermore, 9 of the 16 questions under investigation received significantly higher scores following implementation. The residents largely received positive responses both before and after EHR implementation, so despite the statistically significant improvements, the absolute differences are relatively small. These significant differences were likely not due to the residents improving through time and experience. We observed relatively insignificant and nonuniform changes in responses between the two 11‐week periods prior to implementation.
One possible reason for the observed significant improvements is that EHRs may increase patient involvement in the healthcare setting,[28] and this collaboration might improve resident‐patient communication.[29] Providing patients with an interactive tablet that details their care has been suggested to increase patient satisfaction and comfort in an inpatient setting.[30] In this light, the EHR can be used as a tool to increase these interactions by inviting patients to view the computer screen and electronic charts during data entry, which allows them to have a participatory role in their care and decision‐making process.[31] Although the reasons for our observed improvements are unclear, they are noteworthy and warrant further study. The notion that implementing an EHR might enhance provider‐patient communication is a powerful concept.
This study not only suggests the improvement of resident‐patient communication due to the implementation of an EHR, but it also reveals the value of the ARC Medical Program for studying the patient experience. The controlled, prolonged, and efficient nature of the ARC Medical Program's data collection was ideal for comparing a change in resident‐patient communication before and after EHR implementation at UCLA Health. ARC and UCLA Health's EHR can serve as a model for residency programs nationwide. Future studies can assess the changes of the patient‐provider interaction for any significant event, as demonstrated by this study and its investigation of the implementation of UCLA Health's EHR.
Acknowledgements
The authors acknowledge the UCLA Health Office of the Patient Experience and UCLA Health for allowing for this unique partnership with the David Geffen School of Medicine to improve physician‐patient communication. Furthermore, the authors thank the student volunteers and interns of the ARC Medical program for their commitment and effort to optimize the patient experience. Additionally, the authors thank the program directors of the David Geffen School of Medicine residency physician training programs for their outstanding support of the ARC Medical Program.
Disclosures: C.W.M. and A.A.N. contributed equally to this manuscript. C.W.M. and A.A.N. collected data, performed statistical analyses, and drafted and revised the manuscript. A.A.N. and V.N.M. oversaw the program. N.A. provided faculty support and revised the manuscript. The authors report no conflicts of interest.
Delivering patient‐centered care is at the core of ensuring patient engagement and active participation that will lead to positive outcomes. Physician‐patient interaction has become an area of increasing focus in an effort to optimize the patient experience. Positive patient‐provider communication has been shown to increase satisfaction,[1, 2, 3, 4] decrease the likelihood of medical malpractice lawsuits,[5, 6, 7, 8] and improve clinical outcomes.[9, 10, 11, 12, 13] Specifically, a decrease in psychological symptoms such as anxiety and stress, as well as perception of physical symptoms have been correlated with improved communication.[9, 12] Furthermore, objective health outcomes, such as improvement in hypertension and glycosylated hemoglobin, have also been correlated with improved physician‐patient communication.[10, 11, 13] The multifaceted effects of improved communication are impactful to both the patient and the physician; therefore, it is essential that we understand how to optimize this interaction.
Patient‐centered care is a critical objective for many high‐quality healthcare systems.[14] In recent years, the use of electronic health records (EHRs) has been increasingly adopted by healthcare systems nationally in an effort to improve the quality of care delivered. The positive benefits of EHRs on the facilitation of healthcare, including consolidation of information, reduction of medical errors, easily transferable medical records,[15, 16, 17] as well as their impact on healthcare spending,[18] are well‐documented and have been emphasized as reasons for adoption of EHRs by the Patient Protection and Affordable Care Act. However, EHR implementation has encountered some resistance regarding its impact on the patient experience.
As EHR implementation is exponentially increasing in the United States, there is limited literature on the consequences of this technology.[19] Barriers reported during EHR implementation include the limitations of standardization, attitudinal and organizational constraints, behavior of individuals, and resistance to change.[20] Additionally, poor EHR system design and improper use can cause errors that jeopardize the integrity of the information inputted, leading to inaccuracies that endanger patient safety or decrease the quality of care.[21]
One of the limitations of EHRs has been the reported negative impact on patient‐centered care by decreasing communication during the hospital visit.[22] Although the EHR has enhanced internal provider communication,[23] the literature suggests a lack of focus on the patient sitting in front of the provider. Due to perceived physician distraction during the visit, patients report decreased satisfaction when physicians spend a considerable period of time during the visit at the computer.[22] Furthermore, the average hospital length of stay has been increased due to the use of EHRs.[22]
Although some physicians report that EHR use impedes patient workflow and decreases time spent with patients,[23] previous literature suggests that EHRs decrease the time to develop a synopsis and improve communication efficiency.[19] Some studies have also noted an increase in the ability for medical history retrieval and analysis, which will ultimately increase the quality of care provided to the patient.[24] Physicians who use the EHR adopted a more active role in clarifying information, encouraging questions, and ensuring completeness at the end of a visit.[25] Finally, studies show that the EHR has a positive return on investment from savings in drug expenditures, radiology tests, and billing errors.[26] Given the significant financial and time commitment that health systems and physicians must invest to implement EHRs, it is vital that we understand the multifaceted effects of EHRs on the field of medicine.
METHODS
The purpose of this study was to assess the physician‐patient communication patterns associated with the implementation and use of an EHR in a hospital setting.
ARC Medical Program
In 2006, the Office of Patient Experience at University of California, Los Angeles (UCLA) Health, in conjunction with the David Geffen School of Medicine at UCLA, launched the Assessing Residents' CI‐CARE (ARC) Medical Program. CI‐CARE is a protocol that emphasizes for medical staff and providers to Connect with their patients, Introduce themselves, Communicate their purpose, Ask or anticipate patients' needs, Respond to questions with immediacy, and to Exit courteously. CI‐CARE represents the standards for staff and providers in any encounter with patients or their families. The goals of the ARC Medical Program are to monitor housestaff performance and patient satisfaction while improving trainee education through timely and patient‐centered feedback. The ARC Medical Program's survey has served as an important tool to assess and improve physician professionalism and interpersonal skills and communication, 2 of the Accreditation Council for Graduate Medical Education core competencies.[27]
The ARC program is a unique and innovative volunteer program that provides timely and patient‐centered feedback from trainees' daily encounters with hospitalized patients. The ARC Medical Program has an established infrastructure to conduct evaluations on a system‐wide scale, including 9 departments within UCLA Health. ARC volunteers interview patients using a CI‐CARE Questionnaire (ARC survey) to assess their resident physician's communication patterns. The ARC Survey targets specific areas of the residents' care as outlined by the CI‐CARE Program of UCLA Health.
As part of UCLA Health's mission to ensure the highest level of patient‐centered care, the CI‐CARE standards were introduced in 2006, followed by implementation of the EHR system. Given the lack of previous research and conflicting results on the impact of EHRs on the patient experience, this article uses ARC data to assess whether or not there was a significant difference following implementation of the EHR on March 2, 2013.
The materials and methods of this study are largely based on those of a previous study, also published by the ARC Medical Program.[27]
CI‐CARE QuestionnaireARC Survey
The CI‐CARE Questionnaire is a standardized audit tool consisting of a total of 20 questions used by the facilitators who work with ARC. There are a total of 20 items on the ARC survey, including 18 multiple‐choice, polar, and Likert‐scale questions, and 2 free‐response questions that assess the patients' overall perception of their resident physician and their hospital experience. Questions 1 and 2 pertain to the recognition of attending physicians and resident physicians, respectively. Questions 3, 4, 6, 7, and 8 are Likert‐scalebased questions assessing the residents' professionalism. Questions 9 through 14 are Likert‐scalebased items included to evaluate the quality of communication between patient and provider. We categorized questions 5 and 15 as relating to diagnostics.[27] In 2012, ARC implemented 3 additional questions that assessed residents' communication skills (question 16), level of medical expertise (question 17), and quality of medical care (question 18). We chose to examine the CI‐CARE Questionnaire instead of a standard survey such as the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), because it examines the physician‐patient interaction in more detail. The survey can be reviewed in Figure 1.
Interview Procedure
The ARC Medical Program is comprised of 47 premedical UCLA students who conducted the surveys. New surveyors were trained by the senior surveyors for a minimum of 12 hours before conducting a survey independently. All surveyors were evaluated biyearly by their peers and the program director for quality assurance and to ensure uniform procedures. The volunteers' surveying experience on December 1, 2012 was as follows: (=10 months [237 months], =10 months).
Prior to the interview, the surveyor introduces himself or herself, the purpose and length of the interview, and that the patient's anonymous participation is optional and confidential. Upon receiving verbal consent from the patient, the surveyor presents a picture card to the patient and asks him or her to identify a resident who was on rotation who treated them. If the patient is able to identify the resident who treated them, the surveyor asks each question and records each response verbatim. The surveyors are trained not to probe for responses, and to ensure that the patients answer in accordance with the possible responses. Although it has not been formally studied, the inter‐rater reliability of the survey is likely to be very high due to the verbatim requirements.
Population Interviewed
A total of 3414 surveys were collected from patients seen in the departments of internal medicine, family medicine, pediatrics, general surgery, head and neck surgery, orthopedic surgery, neurosurgery, neurology, and obstetrics and gynecology in this retrospective cohort study. Exclusion criteria included patients who were not awake, were not conscious, could not confidently identify a resident, or stated that they were not able to confidently complete the survey.
Data Analysis
The researchers reviewed and evaluated all data gathered using standard protocols. Statistical comparisons were made using [2] tests. All quantitative analyses were performed in Excel 2010 (Microsoft Corp., Redmond, WA) and SPSS version 21 (IBM Corp., Armonk, NY).
Institutional Review Board
This project received an exemption by the UCLA institutional review board.
RESULTS
There were a total of 3414 interviews conducted and completed from December 1, 2012 to May 30, 2013. Altogether, 1567 surveys were collected 3 months prior to EHR implementation (DecemberFebruary), and 1847 surveys were collected 3 months following implementation (MarchMay). The survey breakdown is summarized in Table 1.
| Department | Pre (N) | Post (N) | Total (N) |
|---|---|---|---|
| |||
| Family medicine | 65 | 128 | 193 |
| General surgery | 226 | 246 | 472 |
| Head and neck surgery | 43 | 65 | 108 |
| Internal medicine | 439 | 369 | 808 |
| Neurology | 81 | 98 | 179 |
| Neurosurgery | 99 | 54 | 153 |
| OB/GYN | 173 | 199 | 372 |
| Orthopedic surgery | 117 | 128 | 245 |
| Pediatrics | 324 | 563 | 887 |
| Totals | 1,567 | 1,850 | 3,417 |
2 analysis revealed that the residents received significantly better feedback in the 3 months following EHR implementation, compared to the 3 months prior to implementation on questions 3, addressing the patient by their preferred name; 4, introducing themselves and their role; 5, communicating what they will do, how long it will take, and how it will impact the patient; 7, responding to the patient's requests and questions with immediacy; 8, listening to the patient's questions and concerns; 9, doing their utmost to ensure the patient receives the best care; 10, communicating well with the patient; 11, being respectful and considerate; and 12, being sensitive to the patient's physical and emotional needs (P<0.05) (Table 2).
| Question | Pre‐EHR % Responses (n=1,567) | Post‐EHR % Responses (n=1,850) | 2 Significance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |||
| ||||||||||||
| 3 | Address you by preferred name? | 90.1 | 3.8 | 2.7 | 3.4 | 91.5 | 3.6 | 1.3 | 3.6 | 0.032* | ||
| 4 | Introduce himself/herself? | 88.3 | 6.4 | 3.2 | 2.1 | 93.1 | 3.6 | 1.8 | 1.5 | 0.000* | ||
| 5 | Communicate what he/she will do? | 83.1 | 9.3 | 4.5 | 3.2 | 86.9 | 6.4 | 3.5 | 3.3 | 0.006* | ||
| 6 | Ask if you have any questions? | 90.9 | 6.2 | 2.9 | 92.4 | 4.9 | 2.7 | 0.230 | ||||
| 7 | Respond with immediacy? | 92.5 | 5.4 | 2.2 | 94.6 | 3.4 | 2.1 | 0.015* | ||||
| 8 | Listens to your questions and concerns? | 94.8 | 4.0 | 1.1 | 96.6 | 2.4 | 1.0 | 0.022* | ||||
| 9 | Ensure you received the best care? | 92.4 | 6.3 | 1.3 | 95.2 | 3.9 | 1.0 | 0.003* | ||||
| 10 | Communicates well with you? | 92.3 | 6.3 | 1.5 | 94.8 | 4.2 | 0.9 | 0.009* | ||||
| 11 | Is respectful and considerate? | 96.5 | 2.7 | 0.8 | 98.0 | 1.6 | 0.4 | 0.025* | ||||
| 12 | Sensitive to your physical and emotional needs? | 90.4 | 6.9 | 2.7 | 94.5 | 3.9 | 1.6 | 0.000* | ||||
| 13 | Uses language that you can understand? | 96.5 | 2.8 | 0.7 | 96.9 | 2.8 | 0.4 | 0.431 | ||||
| 14 | Educated you/family about condition/care? | 84.0 | 8.6 | 7.4 | 86.6 | 7.4 | 6.0 | 0.111 | ||||
| 15 | Exit courteously? | 89.7 | 6.6 | 3.6 | 91.7 | 5.2 | 3.1 | 0.130 | ||||
| 16 | Communication skills? | 75.6 | 19.5 | 3.6 | 0.7 | 0.7 | 78.6 | 16.9 | 3.9 | 0.4 | 0.3 | 0.077 |
| 17 | Medical expertise? | 79.5 | 15.9 | 3.5 | 0.7 | 0.4 | 80.0 | 16.5 | 2.7 | 0.5 | 0.2 | 0.398 |
| 18 | Quality medical care? | 82.5 | 13.0 | 2.8 | 0.8 | 0.9 | 82.6 | 13.6 | 2.7 | 0.7 | 0.5 | 0.754 |
ARC surveyed for 10 weeks prior to our reported sample (OctoberDecember) and 22 weeks prior to EHR implementation total (OctoberMarch). To rule out resident improvement due to the confounding effects of time and experience, we compared the data from the first 11 weeks (OctoberDecember) to the second 11 weeks (DecemberMarch) prior to EHR implementation. [2] analysis revealed that only 6 of the 16 questions showed improvement in this period, and just 1 of these improvements (question 3) was significant. Furthermore, 10 of the 16 questions actually received worse responses in this period, and 2 of these declines (questions 9 and 12) were significant (Table 3).
| Question | First 11 Weeks' Responses (n=897) | Second 11 Weeks' Responses (n=1,338) | 2 Significance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |||
| ||||||||||||
| 3 | Address you by preferred name? | 87.1 | 6.4 | 4.6 | 2.0 | 90.7 | 3.7 | 2.3 | 3.4 | 0.000* | ||
| 4 | Introduce himself/herself? | 87.7 | 6.9 | 4.1 | 1.2 | 88.3 | 6.1 | 3.3 | 2.3 | 0.174 | ||
| 5 | Communicate what he/she will do? | 82.9 | 8.2 | 5.1 | 3.7 | 83.2 | 9.1 | 4.3 | 3.4 | 0.698 | ||
| 6 | Ask if you have any questions? | 92.0 | 5.9 | 2.1 | 90.7 | 6.1 | 3.1 | 0.336 | ||||
| 7 | Respond with immediacy? | 91.2 | 6.6 | 2.2 | 92.8 | 5.2 | 2.1 | 0.353 | ||||
| 8 | Listens to your questions and concerns? | 94.6 | 3.9 | 1.4 | 95.0 | 3.8 | 1.2 | 0.868 | ||||
| 9 | Ensure you received the best care? | 94.4 | 5.0 | 0.6 | 92.1 | 6.5 | 1.4 | 0.049* | ||||
| 10 | Communicates well with you? | 93.3 | 5.9 | 0.8 | 92.4 | 5.9 | 1.7 | 0.167 | ||||
| 11 | Is respectful and considerate? | 97.3 | 2.1 | 0.6 | 96.4 | 2.7 | 0.9 | 0.455 | ||||
| 12 | Sensitive to your physical and emotional needs? | 93.2 | 5.5 | 1.3 | 90.3 | 6.9 | 2.8 | 0.022* | ||||
| 13 | Uses language that you can understand? | 96.2 | 3.5 | 0.3 | 96.4 | 2.8 | 0.7 | 0.327 | ||||
| 14 | Educated you/family about condition/care? | 85.7 | 8.9 | 5.4 | 83.8 | 8.7 | 7.5 | 0.141 | ||||
| 15 | Exit courteously? | 89.7 | 7.8 | 2.5 | 89.6 | 6.6 | 3.8 | 0.124 | ||||
| 16 | Communication skills? | 78.7 | 17.1 | 2.9 | 0.7 | 0.7 | 75.9 | 19 | 3.6 | 0.7 | 0.8 | 0.633 |
| 17 | Medical expertise? | 82.3 | 13.3 | 3.9 | 0.1 | 0.4 | 78.9 | 16.1 | 3.6 | 0.8 | 0.5 | 0.062 |
| 18 | Quality medical care? | 82.7 | 13.5 | 2.6 | 0.8 | 0.4 | 82.1 | 13.0 | 3.0 | 0.9 | 1.0 | 0.456 |
DISCUSSION
The adoption of EHRs has been fueled by their suggested improvement on healthcare quality and spending.[15, 16, 17, 18] Few studies have investigated the patient experience and its relation to EHR implementation. Furthermore, these studies have not yielded consistent results,[19, 20, 21, 22, 23, 25] raising uncertainty about the effects of EHRs on the patient experience. Possible barriers that may contribute to the scarcity of literature include the relatively recent large‐scale implementation of EHRs and a lack of programs in place to collect extensive data on the physician‐patient relationship.
In a field with increasing demands on patient‐centered care, we need to find ways to preserve and foster the patient‐physician relationship. Given that improvements in the delivery of compassionate care can positively impact clinical outcomes, the likelihood of medical malpractice lawsuits, and patient satisfaction,[1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13] the need to improve the patient‐provider relationship is tremendously important. Following EHR implementation, residents were perceived to provide more frequent diagnostics information including the nature, impact, and treatment of conditions. Furthermore, they were perceived to provide significantly better communication quality following implementation, through care monitoring, respectful and sensitive communication, and enhanced patient and family education. Residents were also perceived as being more professional following implementation, as indicated by positive assessments of several interpersonal communication questions. These results suggest that implementing an EHR may be an effective way to meet these increasing demands on patient‐centered care.
Limitations to this study should be considered. The ARC Medical Program is primarily used as an education tool for resident physicians, so all of our data are specific to resident physicians. It would be interesting and important to observe if EHRs affect nurse or attending‐patient interactions. Furthermore, we did not have access to any patient demographic or clinical data. However, we did not anticipate a significant change in the patient population that would alter the survey responses during this 6‐month period. Patients were required to recognize their resident on a photo card presented to them by the surveyor, which likely favored patients with strong feelings toward their residents. Due to this, our population sampled may not be indicative of the entire patient population. All findings were simply correlational. Due to the nature of our data collection, we were unable to control for many confounding variables, thus causal conclusions are difficult to draw from these results.
There are a few important trends to note. No question on the ARC survey received lower scores following implementation of the EHR. Furthermore, 9 of the 16 questions under investigation received significantly higher scores following implementation. The residents largely received positive responses both before and after EHR implementation, so despite the statistically significant improvements, the absolute differences are relatively small. These significant differences were likely not due to the residents improving through time and experience. We observed relatively insignificant and nonuniform changes in responses between the two 11‐week periods prior to implementation.
One possible reason for the observed significant improvements is that EHRs may increase patient involvement in the healthcare setting,[28] and this collaboration might improve resident‐patient communication.[29] Providing patients with an interactive tablet that details their care has been suggested to increase patient satisfaction and comfort in an inpatient setting.[30] In this light, the EHR can be used as a tool to increase these interactions by inviting patients to view the computer screen and electronic charts during data entry, which allows them to have a participatory role in their care and decision‐making process.[31] Although the reasons for our observed improvements are unclear, they are noteworthy and warrant further study. The notion that implementing an EHR might enhance provider‐patient communication is a powerful concept.
This study not only suggests the improvement of resident‐patient communication due to the implementation of an EHR, but it also reveals the value of the ARC Medical Program for studying the patient experience. The controlled, prolonged, and efficient nature of the ARC Medical Program's data collection was ideal for comparing a change in resident‐patient communication before and after EHR implementation at UCLA Health. ARC and UCLA Health's EHR can serve as a model for residency programs nationwide. Future studies can assess the changes of the patient‐provider interaction for any significant event, as demonstrated by this study and its investigation of the implementation of UCLA Health's EHR.
Acknowledgements
The authors acknowledge the UCLA Health Office of the Patient Experience and UCLA Health for allowing for this unique partnership with the David Geffen School of Medicine to improve physician‐patient communication. Furthermore, the authors thank the student volunteers and interns of the ARC Medical program for their commitment and effort to optimize the patient experience. Additionally, the authors thank the program directors of the David Geffen School of Medicine residency physician training programs for their outstanding support of the ARC Medical Program.
Disclosures: C.W.M. and A.A.N. contributed equally to this manuscript. C.W.M. and A.A.N. collected data, performed statistical analyses, and drafted and revised the manuscript. A.A.N. and V.N.M. oversaw the program. N.A. provided faculty support and revised the manuscript. The authors report no conflicts of interest.
- , , . Doctor‐patient communication and patient satisfaction: a review. Fam Pract. 1998;15(5):480–492.
- . Patient satisfaction in primary health care: a literature review and analysis. Eval Program Plann. 1983;6:185–210.
- , . The significance of patients' perceptions of physician conduct. J Community Health. 1980;6(1):18–34.
- , , , . Predicting patient satisfaction from physicians' nonverbal communication skills. Med Care. 1980;18(4):376–387.
- , , . Why do people sue doctors? A study of patients and relatives. Lancet. 1994;343:1609–1613.
- , , . Reducing legal risk by practicing patient‐centered medicine. Arch Intern Med. 2002;162(11):1217–1219.
- , . Listening and talking. West J Med. 1993;158:268–272.
- , , . Medical malpractice: the effect of doctor‐patient relations on medical patient perceptions and malpractice intentions. West J Med. 2000;173(4):244–250.
- . Effective physician‐patient communication and health outcomes: a review. CMAJ. 1995;152(9):1423–1433.
- , , , , . Patients' participation in medical care: effects on blood sugar control and quality of life in diabetes. J Intern Med. 1988;3:448–457.
- , , . Assessing the effects of physician‐patient interactions on the outcomes of chronic disease. Med Care. 1989;27(3 suppl):S110–S127.
- , , . Expanding patient involvement in care. Ann Intern Med. 1985;102:520–528.
- , , , , . Patient exposition and provider explanation in routine interviews and hypertensive patients' blood control. Health Psychol. 1987;6(1):29–42.
- , , . A framework for making patient‐centered care front and center. Perm J. 2012;16(3):49–53.
- . Interoperability: the key to the future health care system. Health Aff. 2005;5(21):19–21.
- , . Physicians' use of electronic medical records: barriers and solutions. Health Aff. 2004;23(2):116–126.
- , . Do hospitals with electronic medical records (EMRs) provide higher quality care?: an examination of three clinical conditions. Med Care Res Rev. 2008;65(4):496–513.
- , , , et al. Can electronic medical record systems transform health care? Potential health benefits, savings, and costs. Health Aff. 2005;24(5):1103–1117.
- , , , . An electronic medical record in primary care: impact on satisfaction, work efficiency and clinic processes. AMIA Annu Symp.2006:394–398.
- , . Barriers to implement electronic health records (EHRs). Mater Sociomed. 2013;25(3):213–215.
- . Impact of electronic health record systems on information integrity: quality and safety implications. Perspect Health Inf Manag. 2013;10:1c.eCollection 2013.
- , , , , . Electronic medical record use and physician–patient communication: an observational study of Israeli primary care encounters. Patient Educ Couns. 2006;61:134–141.
- , , , et al. EHR implementation in a new clinic: a case study of clinician perceptions. J Med Syst. 2013;37(9955):1–6.
- , , . Accuracy and speed of electronic health record versus paper‐based ophthalmic documentation strategies. Am J Ophthalmol. 2013;156(1):165–172.
- , , . The use of electronic medical records communication patterns in outpatient encounters. J Am Informatics Assoc. 2001:610–616.
- , , . Cost‐benefit analysis of electronic medical record system at a tertiary care hospital. Healthc Inform Res. 2013;19(3):205–214.
- , , , . Promoting patient‐centred care through trainee feedback: assessing residents' C‐I‐CARE (ARC) program. BMJ Qual Saf. 2012;21(3):225–233.
- . Electronic health records?: can we maximize their benefits and minimize their risks? Acad Med. 2012;87(11):1456–1457.
- , . Let the left hand know what the right is doing: a vision for care coordination and electronic health records. J Am Med Inform Assoc. 2014;21(1):13–16.
- , , , et al. A tablet computer application for patients to participate in their hospital care. AMIA Annu Symp Proc. 2011;2011:1428–1435.
- , . Enhancing patient‐centered communication and collaboration by using the electronic health record in the examination room. J Am Med Assoc. 2013;309(22):2327–2328.
- , , . Doctor‐patient communication and patient satisfaction: a review. Fam Pract. 1998;15(5):480–492.
- . Patient satisfaction in primary health care: a literature review and analysis. Eval Program Plann. 1983;6:185–210.
- , . The significance of patients' perceptions of physician conduct. J Community Health. 1980;6(1):18–34.
- , , , . Predicting patient satisfaction from physicians' nonverbal communication skills. Med Care. 1980;18(4):376–387.
- , , . Why do people sue doctors? A study of patients and relatives. Lancet. 1994;343:1609–1613.
- , , . Reducing legal risk by practicing patient‐centered medicine. Arch Intern Med. 2002;162(11):1217–1219.
- , . Listening and talking. West J Med. 1993;158:268–272.
- , , . Medical malpractice: the effect of doctor‐patient relations on medical patient perceptions and malpractice intentions. West J Med. 2000;173(4):244–250.
- . Effective physician‐patient communication and health outcomes: a review. CMAJ. 1995;152(9):1423–1433.
- , , , , . Patients' participation in medical care: effects on blood sugar control and quality of life in diabetes. J Intern Med. 1988;3:448–457.
- , , . Assessing the effects of physician‐patient interactions on the outcomes of chronic disease. Med Care. 1989;27(3 suppl):S110–S127.
- , , . Expanding patient involvement in care. Ann Intern Med. 1985;102:520–528.
- , , , , . Patient exposition and provider explanation in routine interviews and hypertensive patients' blood control. Health Psychol. 1987;6(1):29–42.
- , , . A framework for making patient‐centered care front and center. Perm J. 2012;16(3):49–53.
- . Interoperability: the key to the future health care system. Health Aff. 2005;5(21):19–21.
- , . Physicians' use of electronic medical records: barriers and solutions. Health Aff. 2004;23(2):116–126.
- , . Do hospitals with electronic medical records (EMRs) provide higher quality care?: an examination of three clinical conditions. Med Care Res Rev. 2008;65(4):496–513.
- , , , et al. Can electronic medical record systems transform health care? Potential health benefits, savings, and costs. Health Aff. 2005;24(5):1103–1117.
- , , , . An electronic medical record in primary care: impact on satisfaction, work efficiency and clinic processes. AMIA Annu Symp.2006:394–398.
- , . Barriers to implement electronic health records (EHRs). Mater Sociomed. 2013;25(3):213–215.
- . Impact of electronic health record systems on information integrity: quality and safety implications. Perspect Health Inf Manag. 2013;10:1c.eCollection 2013.
- , , , , . Electronic medical record use and physician–patient communication: an observational study of Israeli primary care encounters. Patient Educ Couns. 2006;61:134–141.
- , , , et al. EHR implementation in a new clinic: a case study of clinician perceptions. J Med Syst. 2013;37(9955):1–6.
- , , . Accuracy and speed of electronic health record versus paper‐based ophthalmic documentation strategies. Am J Ophthalmol. 2013;156(1):165–172.
- , , . The use of electronic medical records communication patterns in outpatient encounters. J Am Informatics Assoc. 2001:610–616.
- , , . Cost‐benefit analysis of electronic medical record system at a tertiary care hospital. Healthc Inform Res. 2013;19(3):205–214.
- , , , . Promoting patient‐centred care through trainee feedback: assessing residents' C‐I‐CARE (ARC) program. BMJ Qual Saf. 2012;21(3):225–233.
- . Electronic health records?: can we maximize their benefits and minimize their risks? Acad Med. 2012;87(11):1456–1457.
- , . Let the left hand know what the right is doing: a vision for care coordination and electronic health records. J Am Med Inform Assoc. 2014;21(1):13–16.
- , , , et al. A tablet computer application for patients to participate in their hospital care. AMIA Annu Symp Proc. 2011;2011:1428–1435.
- , . Enhancing patient‐centered communication and collaboration by using the electronic health record in the examination room. J Am Med Assoc. 2013;309(22):2327–2328.
© 2014 Society of Hospital Medicine