User login
Consider developmental issues when treating teen sports injuries
BUENA VISTA, FLA – The cups and ribbons that young athletes bring home sometimes come with a price – injuries that can sideline them for a few games or haunt them for the rest of their lives.
Teenagers are more likely than adults to sustain sports injuries, Dr. Ilene Claudius said at a meeting sponsored by the American College of Emergency Physicians and the American Academy of Pediatrics. Immature bones, strong tendons, and a general tendency to brush off aches and pains all conspire to increase the risk.
Open epiphyseal plates are always points of weakness on a growing bone, said Dr. Claudius of the University of Southern California, Los Angeles. "During periods of rapid growth, the epiphyses are incredibly weak, so boys in their early teens get a lot of sports injuries. They also have strong tendons that insert there and set those kids up for inflammation."

Most of these stress injuries occur in runners, jumpers, and dancers, she said – but they can be seen in those who play other sports. The risk is highest in two periods during a young athlete’s career – just as they delve enthusiastically into their sport and when they reach an elite level, during which time physical efforts grow even more demanding.
"Think about what that person has been doing that might predispose him to an injury: the couch potato who has been doing nothing for 12 years and then starts running every day, the elite athlete who excels in a sport and never deviates from that sport, or the athlete who has played a single sport for years and then takes up a new one, which uses an entirely different set of muscles and bones."
Muscles and bones grow rapidly to accommodate new activities, Dr. Claudius said. Muscles increase in mass and pull on bones, increasing bone mass. It takes a full 14 months for skeletal remodeling. But, in the meantime, when bone absorption outstrips bone repair, stress fractures can occur.
With some ice, rest, and NSAIDs, most of these injuries will heal within 8 weeks. Occasionally, stress fractures appear in more concerning places, like the navicular bone, femur, or femoral neck "These have a higher risk of complete fracture, so they need more aggressive treatment."
Gymnastics, football, and wrestling predispose athletes to hyperextension injuries. Symptoms include lower back pain that radiates to the buttocks and gets worse with exercise. Affected teens can present with paresthesia. These patients usually respond to a few months of activity modification and some physical therapy.
Repetitive hyperextension injuries can leave a lasting effect in the form of traction apophysitis, impingement of the spinous processes, or pseudoarthrosis of the transitional vertebrae.
Concussion is probably the most-feared sports injury. Every time an athlete sustains a concussion, the chances of getting another are increased and the time it takes to recover is extended.
Repeated head trauma can lead to a chronic traumatic encephalopathy. The latency period is 6-10 years, after which the athlete may begin to express emotional disorders, paranoia, memory problems, and even suicidal ideation. "Pathologically, it looks a lot like Alzheimer’s," Dr. Claudius said.
Concussion isn’t always easy to identify on the field or in the emergency department. Preseason neurocognitive testing can make diagnosis easier. "This gives you a baseline; if a concussion is present, the score typically decreases by 10% or more."
While adults typically return to normal in 4 or 5 days, research shows that young people have a much longer recovery time. For a teenager, up to 3 weeks or recovery is not unusual. Any kind of return to full play is absolutely contraindicated during recovery, and resting the brain is just as important as resting other parts of the body.
Cognitive rest can be a difficult concept for the teen to grasp. Dr. Claudius said. "We always need to tailor our message to the audience, and in this case, our audience is an adolescent. A week of cognitive rest means more than just a few days off school. It means not staying up late; it means no texting or video games. It means no sex."
When symptoms recede to mild – for example, sustained attention for 30 minutes without the return of somatic symptoms- the teen can take on a limited amount of school work. It’s important to get up out of bed and start returning to regular activities, with the exception of sports.
"They should avoid aerobic activity until they’re completely asymptomatic," Dr. Claudius said. "Then there can be a careful program that includes light aerobic exercise."
This should be followed by sport-specific training, then noncontact training, followed by full contact practice and, finally, returning to the game.
"Athletes should stay at each level until are completely asymptomatic for 24 hours. If they become symptomatic, they need to drop back to the prior level and stay there until they are."
Dr. Claudius had no financial disclosures.
BUENA VISTA, FLA – The cups and ribbons that young athletes bring home sometimes come with a price – injuries that can sideline them for a few games or haunt them for the rest of their lives.
Teenagers are more likely than adults to sustain sports injuries, Dr. Ilene Claudius said at a meeting sponsored by the American College of Emergency Physicians and the American Academy of Pediatrics. Immature bones, strong tendons, and a general tendency to brush off aches and pains all conspire to increase the risk.
Open epiphyseal plates are always points of weakness on a growing bone, said Dr. Claudius of the University of Southern California, Los Angeles. "During periods of rapid growth, the epiphyses are incredibly weak, so boys in their early teens get a lot of sports injuries. They also have strong tendons that insert there and set those kids up for inflammation."
Most of these stress injuries occur in runners, jumpers, and dancers, she said – but they can be seen in those who play other sports. The risk is highest in two periods during a young athlete’s career – just as they delve enthusiastically into their sport and when they reach an elite level, during which time physical efforts grow even more demanding.
"Think about what that person has been doing that might predispose him to an injury: the couch potato who has been doing nothing for 12 years and then starts running every day, the elite athlete who excels in a sport and never deviates from that sport, or the athlete who has played a single sport for years and then takes up a new one, which uses an entirely different set of muscles and bones."
Muscles and bones grow rapidly to accommodate new activities, Dr. Claudius said. Muscles increase in mass and pull on bones, increasing bone mass. It takes a full 14 months for skeletal remodeling. But, in the meantime, when bone absorption outstrips bone repair, stress fractures can occur.
With some ice, rest, and NSAIDs, most of these injuries will heal within 8 weeks. Occasionally, stress fractures appear in more concerning places, like the navicular bone, femur, or femoral neck "These have a higher risk of complete fracture, so they need more aggressive treatment."
Gymnastics, football, and wrestling predispose athletes to hyperextension injuries. Symptoms include lower back pain that radiates to the buttocks and gets worse with exercise. Affected teens can present with paresthesia. These patients usually respond to a few months of activity modification and some physical therapy.
Repetitive hyperextension injuries can leave a lasting effect in the form of traction apophysitis, impingement of the spinous processes, or pseudoarthrosis of the transitional vertebrae.
Concussion is probably the most-feared sports injury. Every time an athlete sustains a concussion, the chances of getting another are increased and the time it takes to recover is extended.
Repeated head trauma can lead to a chronic traumatic encephalopathy. The latency period is 6-10 years, after which the athlete may begin to express emotional disorders, paranoia, memory problems, and even suicidal ideation. "Pathologically, it looks a lot like Alzheimer’s," Dr. Claudius said.
Concussion isn’t always easy to identify on the field or in the emergency department. Preseason neurocognitive testing can make diagnosis easier. "This gives you a baseline; if a concussion is present, the score typically decreases by 10% or more."
While adults typically return to normal in 4 or 5 days, research shows that young people have a much longer recovery time. For a teenager, up to 3 weeks or recovery is not unusual. Any kind of return to full play is absolutely contraindicated during recovery, and resting the brain is just as important as resting other parts of the body.
Cognitive rest can be a difficult concept for the teen to grasp. Dr. Claudius said. "We always need to tailor our message to the audience, and in this case, our audience is an adolescent. A week of cognitive rest means more than just a few days off school. It means not staying up late; it means no texting or video games. It means no sex."
When symptoms recede to mild – for example, sustained attention for 30 minutes without the return of somatic symptoms- the teen can take on a limited amount of school work. It’s important to get up out of bed and start returning to regular activities, with the exception of sports.
"They should avoid aerobic activity until they’re completely asymptomatic," Dr. Claudius said. "Then there can be a careful program that includes light aerobic exercise."
This should be followed by sport-specific training, then noncontact training, followed by full contact practice and, finally, returning to the game.
"Athletes should stay at each level until are completely asymptomatic for 24 hours. If they become symptomatic, they need to drop back to the prior level and stay there until they are."
Dr. Claudius had no financial disclosures.
BUENA VISTA, FLA – The cups and ribbons that young athletes bring home sometimes come with a price – injuries that can sideline them for a few games or haunt them for the rest of their lives.
Teenagers are more likely than adults to sustain sports injuries, Dr. Ilene Claudius said at a meeting sponsored by the American College of Emergency Physicians and the American Academy of Pediatrics. Immature bones, strong tendons, and a general tendency to brush off aches and pains all conspire to increase the risk.
Open epiphyseal plates are always points of weakness on a growing bone, said Dr. Claudius of the University of Southern California, Los Angeles. "During periods of rapid growth, the epiphyses are incredibly weak, so boys in their early teens get a lot of sports injuries. They also have strong tendons that insert there and set those kids up for inflammation."
Most of these stress injuries occur in runners, jumpers, and dancers, she said – but they can be seen in those who play other sports. The risk is highest in two periods during a young athlete’s career – just as they delve enthusiastically into their sport and when they reach an elite level, during which time physical efforts grow even more demanding.
"Think about what that person has been doing that might predispose him to an injury: the couch potato who has been doing nothing for 12 years and then starts running every day, the elite athlete who excels in a sport and never deviates from that sport, or the athlete who has played a single sport for years and then takes up a new one, which uses an entirely different set of muscles and bones."
Muscles and bones grow rapidly to accommodate new activities, Dr. Claudius said. Muscles increase in mass and pull on bones, increasing bone mass. It takes a full 14 months for skeletal remodeling. But, in the meantime, when bone absorption outstrips bone repair, stress fractures can occur.
With some ice, rest, and NSAIDs, most of these injuries will heal within 8 weeks. Occasionally, stress fractures appear in more concerning places, like the navicular bone, femur, or femoral neck "These have a higher risk of complete fracture, so they need more aggressive treatment."
Gymnastics, football, and wrestling predispose athletes to hyperextension injuries. Symptoms include lower back pain that radiates to the buttocks and gets worse with exercise. Affected teens can present with paresthesia. These patients usually respond to a few months of activity modification and some physical therapy.
Repetitive hyperextension injuries can leave a lasting effect in the form of traction apophysitis, impingement of the spinous processes, or pseudoarthrosis of the transitional vertebrae.
Concussion is probably the most-feared sports injury. Every time an athlete sustains a concussion, the chances of getting another are increased and the time it takes to recover is extended.
Repeated head trauma can lead to a chronic traumatic encephalopathy. The latency period is 6-10 years, after which the athlete may begin to express emotional disorders, paranoia, memory problems, and even suicidal ideation. "Pathologically, it looks a lot like Alzheimer’s," Dr. Claudius said.
Concussion isn’t always easy to identify on the field or in the emergency department. Preseason neurocognitive testing can make diagnosis easier. "This gives you a baseline; if a concussion is present, the score typically decreases by 10% or more."
While adults typically return to normal in 4 or 5 days, research shows that young people have a much longer recovery time. For a teenager, up to 3 weeks or recovery is not unusual. Any kind of return to full play is absolutely contraindicated during recovery, and resting the brain is just as important as resting other parts of the body.
Cognitive rest can be a difficult concept for the teen to grasp. Dr. Claudius said. "We always need to tailor our message to the audience, and in this case, our audience is an adolescent. A week of cognitive rest means more than just a few days off school. It means not staying up late; it means no texting or video games. It means no sex."
When symptoms recede to mild – for example, sustained attention for 30 minutes without the return of somatic symptoms- the teen can take on a limited amount of school work. It’s important to get up out of bed and start returning to regular activities, with the exception of sports.
"They should avoid aerobic activity until they’re completely asymptomatic," Dr. Claudius said. "Then there can be a careful program that includes light aerobic exercise."
This should be followed by sport-specific training, then noncontact training, followed by full contact practice and, finally, returning to the game.
"Athletes should stay at each level until are completely asymptomatic for 24 hours. If they become symptomatic, they need to drop back to the prior level and stay there until they are."
Dr. Claudius had no financial disclosures.
EXPERT ANALYSIS AT THE ADVANCED PEDIATRIC EMERGENCY MEDICINE ASSEMBLY

ONLINE EXCLUSIVE:
Enter text here
Enter text here
Enter text here
SHM Names Masters of Hospital Medicine, Board of Directors for 2013

SHM has named its 2013-2014 board of directors and three new Masters in Hospital Medicine, the highest designation in the HM specialty.
The Master in Hospital Medicine (MHM) designation is reserved for hospitalists who have distinguished themselves in the specialty through the excellence and significance of their contributions to hospital medicine and health care as a whole. Nominations were reviewed by SHM’s Masters Selection Committee and the board of directors. The MHM designation was introduced in 2010; this year’s designees bring the total number of MHMs to 13.
The 2013 Masters in Hospital Medicine are:

Scott A. Flanders, MD, MHM, professor in the division of general internal medicine at the University of Michigan in Ann Arbor, where he serves as associate division chief of general medicine for inpatient programs and associate director of inpatient programs for the department of internal medicine. He is also the director of the University of Michigan’s hospitalist program.

David O. Meltzer, MD, PhD, MHM, chief of the section of hospital medicine, director of the Center for Health and the Social Sciences, associate professor in the medicine and economics departments and the Harris School of Public Policy Studies, at the University of Chicago.

Jeffrey G. Wiese, MD, MHM, professor of medicine and associate dean for graduate medical education at the Tulane University Health Sciences Center, as well as associate chair of medicine and the chief of the charity medical service. He is also the director of Tulane’s internal-medicine residency program.
The new MHMs will take the stage to officially be inducted, along with more than 200 Fellows and Senior Fellows, on May 18 at HM13, SHM’s annual meeting (www.hospitalmedicine2013.org) at the Gaylord National Resort and Conference Center in National Harbor, Md.
“SHM’s Masters in Hospital Medicine are truly the hall of fame of the hospital medicine specialty,” says SHM President Shaun Frost, MD, SFHM. “It is an honor to recognize their contributions to hospitalists and patients alike.”
Nominations for all three levels of SHM’s Fellows program are accepted throughout the year. For details, visit www.hospitalmedicine.org/fellows.
SHM also announced the election of three new board members; each will serve a three-year term beginning this month. The new board members are:

Howard Epstein, MD, FHM, chief health systems officer at the Institute for Clinical Systems Improvement in Bloomington, Minn.

Bradley Sharpe, MD, FACP, SFHM, professor of medicine at the University of California at San Francisco’s department of medicine, associate program director for UCSF’s internal medicine residency program and associate division chief in the division of hospital medicine.

Patrick J. Torcson, MD, MMM, SFHM, vice president and chief integration officer, and director of hospital medicine for St. Tammany Parish Hospital, Covington, La.
“We welcome these new faces to the SHM board of directors and appreciate the commitment of their time and expertise to the goals of SHM, hospitalists, and hospitalized patients everywhere,” Dr. Frost says.
For more information about SHM’s leadership and nomination process, visit www.hospitalmedicine.org.
Brendon Shank is SHM’s associate vice president of communications.
SHM has named its 2013-2014 board of directors and three new Masters in Hospital Medicine, the highest designation in the HM specialty.
The Master in Hospital Medicine (MHM) designation is reserved for hospitalists who have distinguished themselves in the specialty through the excellence and significance of their contributions to hospital medicine and health care as a whole. Nominations were reviewed by SHM’s Masters Selection Committee and the board of directors. The MHM designation was introduced in 2010; this year’s designees bring the total number of MHMs to 13.
The 2013 Masters in Hospital Medicine are:
Scott A. Flanders, MD, MHM, professor in the division of general internal medicine at the University of Michigan in Ann Arbor, where he serves as associate division chief of general medicine for inpatient programs and associate director of inpatient programs for the department of internal medicine. He is also the director of the University of Michigan’s hospitalist program.
David O. Meltzer, MD, PhD, MHM, chief of the section of hospital medicine, director of the Center for Health and the Social Sciences, associate professor in the medicine and economics departments and the Harris School of Public Policy Studies, at the University of Chicago.
Jeffrey G. Wiese, MD, MHM, professor of medicine and associate dean for graduate medical education at the Tulane University Health Sciences Center, as well as associate chair of medicine and the chief of the charity medical service. He is also the director of Tulane’s internal-medicine residency program.
The new MHMs will take the stage to officially be inducted, along with more than 200 Fellows and Senior Fellows, on May 18 at HM13, SHM’s annual meeting (www.hospitalmedicine2013.org) at the Gaylord National Resort and Conference Center in National Harbor, Md.
“SHM’s Masters in Hospital Medicine are truly the hall of fame of the hospital medicine specialty,” says SHM President Shaun Frost, MD, SFHM. “It is an honor to recognize their contributions to hospitalists and patients alike.”
Nominations for all three levels of SHM’s Fellows program are accepted throughout the year. For details, visit www.hospitalmedicine.org/fellows.
SHM also announced the election of three new board members; each will serve a three-year term beginning this month. The new board members are:
Howard Epstein, MD, FHM, chief health systems officer at the Institute for Clinical Systems Improvement in Bloomington, Minn.
Bradley Sharpe, MD, FACP, SFHM, professor of medicine at the University of California at San Francisco’s department of medicine, associate program director for UCSF’s internal medicine residency program and associate division chief in the division of hospital medicine.
Patrick J. Torcson, MD, MMM, SFHM, vice president and chief integration officer, and director of hospital medicine for St. Tammany Parish Hospital, Covington, La.
“We welcome these new faces to the SHM board of directors and appreciate the commitment of their time and expertise to the goals of SHM, hospitalists, and hospitalized patients everywhere,” Dr. Frost says.
For more information about SHM’s leadership and nomination process, visit www.hospitalmedicine.org.
Brendon Shank is SHM’s associate vice president of communications.
SHM has named its 2013-2014 board of directors and three new Masters in Hospital Medicine, the highest designation in the HM specialty.
The Master in Hospital Medicine (MHM) designation is reserved for hospitalists who have distinguished themselves in the specialty through the excellence and significance of their contributions to hospital medicine and health care as a whole. Nominations were reviewed by SHM’s Masters Selection Committee and the board of directors. The MHM designation was introduced in 2010; this year’s designees bring the total number of MHMs to 13.
The 2013 Masters in Hospital Medicine are:
Scott A. Flanders, MD, MHM, professor in the division of general internal medicine at the University of Michigan in Ann Arbor, where he serves as associate division chief of general medicine for inpatient programs and associate director of inpatient programs for the department of internal medicine. He is also the director of the University of Michigan’s hospitalist program.
David O. Meltzer, MD, PhD, MHM, chief of the section of hospital medicine, director of the Center for Health and the Social Sciences, associate professor in the medicine and economics departments and the Harris School of Public Policy Studies, at the University of Chicago.
Jeffrey G. Wiese, MD, MHM, professor of medicine and associate dean for graduate medical education at the Tulane University Health Sciences Center, as well as associate chair of medicine and the chief of the charity medical service. He is also the director of Tulane’s internal-medicine residency program.
The new MHMs will take the stage to officially be inducted, along with more than 200 Fellows and Senior Fellows, on May 18 at HM13, SHM’s annual meeting (www.hospitalmedicine2013.org) at the Gaylord National Resort and Conference Center in National Harbor, Md.
“SHM’s Masters in Hospital Medicine are truly the hall of fame of the hospital medicine specialty,” says SHM President Shaun Frost, MD, SFHM. “It is an honor to recognize their contributions to hospitalists and patients alike.”
Nominations for all three levels of SHM’s Fellows program are accepted throughout the year. For details, visit www.hospitalmedicine.org/fellows.
SHM also announced the election of three new board members; each will serve a three-year term beginning this month. The new board members are:
Howard Epstein, MD, FHM, chief health systems officer at the Institute for Clinical Systems Improvement in Bloomington, Minn.
Bradley Sharpe, MD, FACP, SFHM, professor of medicine at the University of California at San Francisco’s department of medicine, associate program director for UCSF’s internal medicine residency program and associate division chief in the division of hospital medicine.
Patrick J. Torcson, MD, MMM, SFHM, vice president and chief integration officer, and director of hospital medicine for St. Tammany Parish Hospital, Covington, La.
“We welcome these new faces to the SHM board of directors and appreciate the commitment of their time and expertise to the goals of SHM, hospitalists, and hospitalized patients everywhere,” Dr. Frost says.
For more information about SHM’s leadership and nomination process, visit www.hospitalmedicine.org.
Brendon Shank is SHM’s associate vice president of communications.
Work-Hour Restrictions Impact Staffing, Education for Academic Hospital Medicine
Source: 2012 State of Hospital Medicine report


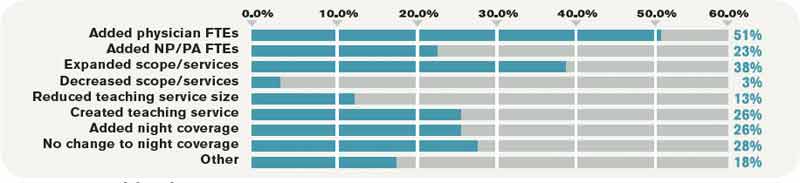
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
Source: 2012 State of Hospital Medicine report
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
Source: 2012 State of Hospital Medicine report
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
SHM Supports Clarification to Observational Status Loophole for Medicare Patients
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
We Welcome the Newest SHM Members
- D. Hinton, RN, Alabama
- M. Irfan, MD, Alabama
- V. Patel, MD, Alabama
- Z. Zhou, MD, Alabama
- J. Song, MD, Arizona
- M. Ahmad, MD, Arizona
- W. Chun, MD, Arizona
- L. Fox, FAAP, Arizona
- N. Iqbal, MD, FACP, Arizona
- M. Brewer, PA, Arkansas
- V. Chinta, MD, Arkansas
- M. Measel, MD, Arkansas
- J. Smith Jr., Arkansas
- T. Daltoe, Brazil
- G. Frandoloso, MD, Brazil
- R. Rodrigues, Brazil
- D. Ampie, MPAS, PA-C, California
- B. Carl, MBA, RN, California
- A. Carlile, MD, California
- F. Chan, Med, California
- Y. Ding, California
- E. Kaldor, California
- B. Kwan, MD, California
- J. Levay, DO, California
- Z. Shaikh, MD, California
- A. Smith, MHA, California
- K. Tumber, DO, California
- P. Wallace, ANP, California
- R. White, MD, California
- C. Wilkinson, MD, California
- L. Orellana, Chile
- G. Hartsuiker, PA, Colorado
- E. Marcum, MD, Colorado
- H. Mazzola, ACNP, FNP, Colorado
- N. Amoah, Connecticut
- E. Massey, APRN, Connecticut
- M. Longo, MD, Delaware
- M. Haider, MD, District of Columbia
- A. Elochukwu, Florida
- S. Gupta, MD, Florida
- N. Hector, MD, Florida
- F. Rodriguez, MD, Florida
- M. Weiner, MD, Florida
- M. Zelfman, DO, Florida
- I. Davis, DO, Georgia
- M. Dhawan, MHA, Georgia
- L. Doerr, MD, Georgia
- B. Majewski, MD, Georgia
- P. Carullo, Illinois
- A. Encinas, MD, Illinois
- J. Fischer, Illinois
- K. Kakac, Illinois
- W. Le, MD, Illinois
- R. Mayhew, MD, Illinois
- P. McLoone, MD, Illinois
- J. Wener, MD, Illinois
- S. Khatib, MD, Indiana
- M. Knutson, DO, Indiana
- W. Turton, Indiana
- M. Alam, MD, Iowa
- T. Farley, PharmD, Iowa
- M. Otto, MD, Iowa
- T. Smith, NP, Iowa
- A. Humpert, MD, Kansas
- M. Lewis, MD, Kentucky
- M. Russell, Kentucky
- B. Thompson, MD, Kentucky
- J. Tovar, MD, Kentucky
- L. Bazzano, MD, Louisiana
- M. Zickerman, MD, Louisiana
- M. Lefebvre, NP, Maine
- T. Merza, MD, Maine
- M. Moffatt, DO, Maine
- V. Munusamy, MD, Maine
- Z. Ahmed, MD, Maryland
- A. Desai, DO, Maryland
- E. Gillespie, Maryland
- P. Martin, PA-C, Maryland
- B. McMullen, PA-C, Maryland
- F. Randhawa, MBBS, PA-C, Maryland
- A. Rivera Jr., MD, Maryland
- F. Sarabchi, MD, Maryland
- W. Furness, MS, Massachusetts
- J. Goldman, MD, Massachusetts
- M. Goodwin, PharmD, Massachusetts
- J. Moyer, Massachusetts
- S. Quadri, Massachusetts
- J. Walter, Massachusetts
- I. Arboleda, MD, Michigan
- R. Barnett, DO, Michigan
- K. Crosby, PA-C, Michigan
- D. Engers, MD, Michigan
- J. Hwang, DO, Michigan
- R. Ishaq, MBchB, Michigan
- M. Kyriacou, MD, Michigan
- J. Lee, PA-C, Michigan
- M. Moses, PA, Michigan
- P. Mussman, PA-C, Michigan
- L. Page, Michigan
- A. Podczervinski, PA-C, Michigan
- A. Pohl, DO, Michigan
- N. Rousse, NP-C, Michigan
- R. Shyamraj, MD, MHSA, Michigan
- V. Worthington, MSN, FNP, Michigan
- M. Abdissa, MD, Minnesota
- W. Evavold, MD, Minnesota
- M. Fredrickson, MD, Minnesota
- J. Selickman, USN, Minnesota
- D. Skinner, PAC, Minnesota
- S. Freer, BSN, RN, CMSRN, Missouri
- T. Hofmeister, Missouri
- E. Kinports, MD, Missouri
- P. Klaus, MBA, Missouri
- N. Levy, MD, Missouri
- A. Houlihan, NP, Nebraska
- R. Runge, MD, Nebraska
- C. Shore-Anderson, ACNP, Nebraska
- R. Pua, MD, Nevada
- B. Horrigan, PA, New Hampshire
- A. Angelow, NP, New Jersey
- R. Arerangaiah, MD, New Jersey
- J. Burgos-Dago-oc, MD, New Jersey
- K. Doktor, MD, New Jersey
- D. Fabius, DO, New Jersey
- C. Keresztury, NP, New Jersey
- O. Kocia, MD, New Jersey
- J. Lim, MD, New Jersey
- M. Mangold, DO, New Jersey
- E. Pierre, MD, New Jersey
- R. Rondanina, MD, New Jersey
- S. Siddiqui, MD, New Jersey
- C. Sipaco-Ong, NP, New Jersey
- N. Siu, NP, New Jersey
- R. Verma, MD, New Jersey
- W. Zaeeter, MD, New Jersey
- S. Modi, New Mexico
- D. Rao, MD, New Mexico
- S. Behuria, MD, New York
- N. Hung, New York
- H. Cho, MD, New York
- R. Duszak, New York
- S. Hoag, MD, New York
- F. Masrur, MBBS, New York
- C. Mensah, New York
- M. Nagasaka, MD, New York
- A. Nagpaul, New York
- A. Narayan, New York
- V. Punnam, New York
- D. Scime, ANP, BC, New York
- T. Shirani, New York
- S. Stewart, New York
- S. Brown, MD, North Carolina
- I. Mitropoulos, PharmD, North Carolina
- K. Reschly, MD, North Carolina
- K. Rutterer, MD, North Carolina
- J. Singh, MD, North Carolina
- J. Anwar, MD, Ohio
- P. Betkerur, USA, Ohio
- C. Demian, MD, Ohio
- S. Demian, MD, MBBch, Ohio
- K. Geckle, ANP, Ohio
- J. Moore, MD, Ohio
- K. Pestak, DO, Ohio
- V. Porter, Ohio
- S. Shenoy, MD, Ohio
- J. Zang, MD, Ohio
- T. Jones, Oklahoma
- K. Shah, MD, Oklahoma
- M. Nag, MSc, Ontario, Canada
- J. Meghashyam, MD, Oregon
- G. Regalbuto, MD, Oregon
- X. Song, MD, Oregon
- E. Weeks, MD, Oregon
- D. Ebhaleme, MD, Pennsylvania
- Y. Li, Pennsylvania
- R. Lynn, MD, Pennsylvania
- K. Repine, Pennsylvania
- P. Scoble, PharmD, Pennsylvania
- M. Sharma, DO, Pennsylvania
- N. Sinha, MD, Pennsylvania
- A. Somasundaram, Pennsylvania
- P. Timon, Pennsylvania
- A. Weber, DO, Pennsylvania
- D. Zielinski, MD, Pennsylvania
- K. O’Neil, MD, Prince Edward Island, Canada
- J. Patel, MD, MBBS, South Carolina
- M. Acha, Spain
- A. de Arcaya, Spain
- F. Garrido, MD, Spain
- A. Gonzalez, Spain
- V. Clark, MD, Tennessee
- G. Dutta, MD, Tennessee
- J. Gonce, MD, Tennessee
- R. Kunder, Tennessee
- C. Davenport, FAAP, Texas
- C. Gordon, Texas
- F. Hernandez, MD, Texas
- C. Jones, Texas
- S. Prihoda, CPCS, Texas
- A. Stock, AHIP, Texas
- J. Wilson, MD, Texas
- J. Zepeda, MD, Texas
- C. Stratis, MD, United Arab Emirates
- E. Guenzel, MD, Utah
- K. Chewning, MD, Virginia
- R. Gadesam, MD, MBBS, Virginia
- T. Jones, MD, Virginia
- B. Montgomery, MD, Virginia
- M. Shah, MD, Virginia
- A. Torralba, MD, Virginia
- A. Ulrich, Virginia
- R. Cupp, PA-C, Washington
- J. Remington, MD, Washington
- A. Harsanyne, FNP, West Virginia
- M. Lilly, PA, West Virginia
- K. Patra, MBBS, West Virginia
- S. Aman, MD, Wisconsin
- S. Dean, Wisconsin
- J. Friday, APRNBC, MSN, Wisconsin
- J. Kurman, MD, MBA, Wisconsin
- D. Miller, Wisconsin
- D. Hinton, RN, Alabama
- M. Irfan, MD, Alabama
- V. Patel, MD, Alabama
- Z. Zhou, MD, Alabama
- J. Song, MD, Arizona
- M. Ahmad, MD, Arizona
- W. Chun, MD, Arizona
- L. Fox, FAAP, Arizona
- N. Iqbal, MD, FACP, Arizona
- M. Brewer, PA, Arkansas
- V. Chinta, MD, Arkansas
- M. Measel, MD, Arkansas
- J. Smith Jr., Arkansas
- T. Daltoe, Brazil
- G. Frandoloso, MD, Brazil
- R. Rodrigues, Brazil
- D. Ampie, MPAS, PA-C, California
- B. Carl, MBA, RN, California
- A. Carlile, MD, California
- F. Chan, Med, California
- Y. Ding, California
- E. Kaldor, California
- B. Kwan, MD, California
- J. Levay, DO, California
- Z. Shaikh, MD, California
- A. Smith, MHA, California
- K. Tumber, DO, California
- P. Wallace, ANP, California
- R. White, MD, California
- C. Wilkinson, MD, California
- L. Orellana, Chile
- G. Hartsuiker, PA, Colorado
- E. Marcum, MD, Colorado
- H. Mazzola, ACNP, FNP, Colorado
- N. Amoah, Connecticut
- E. Massey, APRN, Connecticut
- M. Longo, MD, Delaware
- M. Haider, MD, District of Columbia
- A. Elochukwu, Florida
- S. Gupta, MD, Florida
- N. Hector, MD, Florida
- F. Rodriguez, MD, Florida
- M. Weiner, MD, Florida
- M. Zelfman, DO, Florida
- I. Davis, DO, Georgia
- M. Dhawan, MHA, Georgia
- L. Doerr, MD, Georgia
- B. Majewski, MD, Georgia
- P. Carullo, Illinois
- A. Encinas, MD, Illinois
- J. Fischer, Illinois
- K. Kakac, Illinois
- W. Le, MD, Illinois
- R. Mayhew, MD, Illinois
- P. McLoone, MD, Illinois
- J. Wener, MD, Illinois
- S. Khatib, MD, Indiana
- M. Knutson, DO, Indiana
- W. Turton, Indiana
- M. Alam, MD, Iowa
- T. Farley, PharmD, Iowa
- M. Otto, MD, Iowa
- T. Smith, NP, Iowa
- A. Humpert, MD, Kansas
- M. Lewis, MD, Kentucky
- M. Russell, Kentucky
- B. Thompson, MD, Kentucky
- J. Tovar, MD, Kentucky
- L. Bazzano, MD, Louisiana
- M. Zickerman, MD, Louisiana
- M. Lefebvre, NP, Maine
- T. Merza, MD, Maine
- M. Moffatt, DO, Maine
- V. Munusamy, MD, Maine
- Z. Ahmed, MD, Maryland
- A. Desai, DO, Maryland
- E. Gillespie, Maryland
- P. Martin, PA-C, Maryland
- B. McMullen, PA-C, Maryland
- F. Randhawa, MBBS, PA-C, Maryland
- A. Rivera Jr., MD, Maryland
- F. Sarabchi, MD, Maryland
- W. Furness, MS, Massachusetts
- J. Goldman, MD, Massachusetts
- M. Goodwin, PharmD, Massachusetts
- J. Moyer, Massachusetts
- S. Quadri, Massachusetts
- J. Walter, Massachusetts
- I. Arboleda, MD, Michigan
- R. Barnett, DO, Michigan
- K. Crosby, PA-C, Michigan
- D. Engers, MD, Michigan
- J. Hwang, DO, Michigan
- R. Ishaq, MBchB, Michigan
- M. Kyriacou, MD, Michigan
- J. Lee, PA-C, Michigan
- M. Moses, PA, Michigan
- P. Mussman, PA-C, Michigan
- L. Page, Michigan
- A. Podczervinski, PA-C, Michigan
- A. Pohl, DO, Michigan
- N. Rousse, NP-C, Michigan
- R. Shyamraj, MD, MHSA, Michigan
- V. Worthington, MSN, FNP, Michigan
- M. Abdissa, MD, Minnesota
- W. Evavold, MD, Minnesota
- M. Fredrickson, MD, Minnesota
- J. Selickman, USN, Minnesota
- D. Skinner, PAC, Minnesota
- S. Freer, BSN, RN, CMSRN, Missouri
- T. Hofmeister, Missouri
- E. Kinports, MD, Missouri
- P. Klaus, MBA, Missouri
- N. Levy, MD, Missouri
- A. Houlihan, NP, Nebraska
- R. Runge, MD, Nebraska
- C. Shore-Anderson, ACNP, Nebraska
- R. Pua, MD, Nevada
- B. Horrigan, PA, New Hampshire
- A. Angelow, NP, New Jersey
- R. Arerangaiah, MD, New Jersey
- J. Burgos-Dago-oc, MD, New Jersey
- K. Doktor, MD, New Jersey
- D. Fabius, DO, New Jersey
- C. Keresztury, NP, New Jersey
- O. Kocia, MD, New Jersey
- J. Lim, MD, New Jersey
- M. Mangold, DO, New Jersey
- E. Pierre, MD, New Jersey
- R. Rondanina, MD, New Jersey
- S. Siddiqui, MD, New Jersey
- C. Sipaco-Ong, NP, New Jersey
- N. Siu, NP, New Jersey
- R. Verma, MD, New Jersey
- W. Zaeeter, MD, New Jersey
- S. Modi, New Mexico
- D. Rao, MD, New Mexico
- S. Behuria, MD, New York
- N. Hung, New York
- H. Cho, MD, New York
- R. Duszak, New York
- S. Hoag, MD, New York
- F. Masrur, MBBS, New York
- C. Mensah, New York
- M. Nagasaka, MD, New York
- A. Nagpaul, New York
- A. Narayan, New York
- V. Punnam, New York
- D. Scime, ANP, BC, New York
- T. Shirani, New York
- S. Stewart, New York
- S. Brown, MD, North Carolina
- I. Mitropoulos, PharmD, North Carolina
- K. Reschly, MD, North Carolina
- K. Rutterer, MD, North Carolina
- J. Singh, MD, North Carolina
- J. Anwar, MD, Ohio
- P. Betkerur, USA, Ohio
- C. Demian, MD, Ohio
- S. Demian, MD, MBBch, Ohio
- K. Geckle, ANP, Ohio
- J. Moore, MD, Ohio
- K. Pestak, DO, Ohio
- V. Porter, Ohio
- S. Shenoy, MD, Ohio
- J. Zang, MD, Ohio
- T. Jones, Oklahoma
- K. Shah, MD, Oklahoma
- M. Nag, MSc, Ontario, Canada
- J. Meghashyam, MD, Oregon
- G. Regalbuto, MD, Oregon
- X. Song, MD, Oregon
- E. Weeks, MD, Oregon
- D. Ebhaleme, MD, Pennsylvania
- Y. Li, Pennsylvania
- R. Lynn, MD, Pennsylvania
- K. Repine, Pennsylvania
- P. Scoble, PharmD, Pennsylvania
- M. Sharma, DO, Pennsylvania
- N. Sinha, MD, Pennsylvania
- A. Somasundaram, Pennsylvania
- P. Timon, Pennsylvania
- A. Weber, DO, Pennsylvania
- D. Zielinski, MD, Pennsylvania
- K. O’Neil, MD, Prince Edward Island, Canada
- J. Patel, MD, MBBS, South Carolina
- M. Acha, Spain
- A. de Arcaya, Spain
- F. Garrido, MD, Spain
- A. Gonzalez, Spain
- V. Clark, MD, Tennessee
- G. Dutta, MD, Tennessee
- J. Gonce, MD, Tennessee
- R. Kunder, Tennessee
- C. Davenport, FAAP, Texas
- C. Gordon, Texas
- F. Hernandez, MD, Texas
- C. Jones, Texas
- S. Prihoda, CPCS, Texas
- A. Stock, AHIP, Texas
- J. Wilson, MD, Texas
- J. Zepeda, MD, Texas
- C. Stratis, MD, United Arab Emirates
- E. Guenzel, MD, Utah
- K. Chewning, MD, Virginia
- R. Gadesam, MD, MBBS, Virginia
- T. Jones, MD, Virginia
- B. Montgomery, MD, Virginia
- M. Shah, MD, Virginia
- A. Torralba, MD, Virginia
- A. Ulrich, Virginia
- R. Cupp, PA-C, Washington
- J. Remington, MD, Washington
- A. Harsanyne, FNP, West Virginia
- M. Lilly, PA, West Virginia
- K. Patra, MBBS, West Virginia
- S. Aman, MD, Wisconsin
- S. Dean, Wisconsin
- J. Friday, APRNBC, MSN, Wisconsin
- J. Kurman, MD, MBA, Wisconsin
- D. Miller, Wisconsin
- D. Hinton, RN, Alabama
- M. Irfan, MD, Alabama
- V. Patel, MD, Alabama
- Z. Zhou, MD, Alabama
- J. Song, MD, Arizona
- M. Ahmad, MD, Arizona
- W. Chun, MD, Arizona
- L. Fox, FAAP, Arizona
- N. Iqbal, MD, FACP, Arizona
- M. Brewer, PA, Arkansas
- V. Chinta, MD, Arkansas
- M. Measel, MD, Arkansas
- J. Smith Jr., Arkansas
- T. Daltoe, Brazil
- G. Frandoloso, MD, Brazil
- R. Rodrigues, Brazil
- D. Ampie, MPAS, PA-C, California
- B. Carl, MBA, RN, California
- A. Carlile, MD, California
- F. Chan, Med, California
- Y. Ding, California
- E. Kaldor, California
- B. Kwan, MD, California
- J. Levay, DO, California
- Z. Shaikh, MD, California
- A. Smith, MHA, California
- K. Tumber, DO, California
- P. Wallace, ANP, California
- R. White, MD, California
- C. Wilkinson, MD, California
- L. Orellana, Chile
- G. Hartsuiker, PA, Colorado
- E. Marcum, MD, Colorado
- H. Mazzola, ACNP, FNP, Colorado
- N. Amoah, Connecticut
- E. Massey, APRN, Connecticut
- M. Longo, MD, Delaware
- M. Haider, MD, District of Columbia
- A. Elochukwu, Florida
- S. Gupta, MD, Florida
- N. Hector, MD, Florida
- F. Rodriguez, MD, Florida
- M. Weiner, MD, Florida
- M. Zelfman, DO, Florida
- I. Davis, DO, Georgia
- M. Dhawan, MHA, Georgia
- L. Doerr, MD, Georgia
- B. Majewski, MD, Georgia
- P. Carullo, Illinois
- A. Encinas, MD, Illinois
- J. Fischer, Illinois
- K. Kakac, Illinois
- W. Le, MD, Illinois
- R. Mayhew, MD, Illinois
- P. McLoone, MD, Illinois
- J. Wener, MD, Illinois
- S. Khatib, MD, Indiana
- M. Knutson, DO, Indiana
- W. Turton, Indiana
- M. Alam, MD, Iowa
- T. Farley, PharmD, Iowa
- M. Otto, MD, Iowa
- T. Smith, NP, Iowa
- A. Humpert, MD, Kansas
- M. Lewis, MD, Kentucky
- M. Russell, Kentucky
- B. Thompson, MD, Kentucky
- J. Tovar, MD, Kentucky
- L. Bazzano, MD, Louisiana
- M. Zickerman, MD, Louisiana
- M. Lefebvre, NP, Maine
- T. Merza, MD, Maine
- M. Moffatt, DO, Maine
- V. Munusamy, MD, Maine
- Z. Ahmed, MD, Maryland
- A. Desai, DO, Maryland
- E. Gillespie, Maryland
- P. Martin, PA-C, Maryland
- B. McMullen, PA-C, Maryland
- F. Randhawa, MBBS, PA-C, Maryland
- A. Rivera Jr., MD, Maryland
- F. Sarabchi, MD, Maryland
- W. Furness, MS, Massachusetts
- J. Goldman, MD, Massachusetts
- M. Goodwin, PharmD, Massachusetts
- J. Moyer, Massachusetts
- S. Quadri, Massachusetts
- J. Walter, Massachusetts
- I. Arboleda, MD, Michigan
- R. Barnett, DO, Michigan
- K. Crosby, PA-C, Michigan
- D. Engers, MD, Michigan
- J. Hwang, DO, Michigan
- R. Ishaq, MBchB, Michigan
- M. Kyriacou, MD, Michigan
- J. Lee, PA-C, Michigan
- M. Moses, PA, Michigan
- P. Mussman, PA-C, Michigan
- L. Page, Michigan
- A. Podczervinski, PA-C, Michigan
- A. Pohl, DO, Michigan
- N. Rousse, NP-C, Michigan
- R. Shyamraj, MD, MHSA, Michigan
- V. Worthington, MSN, FNP, Michigan
- M. Abdissa, MD, Minnesota
- W. Evavold, MD, Minnesota
- M. Fredrickson, MD, Minnesota
- J. Selickman, USN, Minnesota
- D. Skinner, PAC, Minnesota
- S. Freer, BSN, RN, CMSRN, Missouri
- T. Hofmeister, Missouri
- E. Kinports, MD, Missouri
- P. Klaus, MBA, Missouri
- N. Levy, MD, Missouri
- A. Houlihan, NP, Nebraska
- R. Runge, MD, Nebraska
- C. Shore-Anderson, ACNP, Nebraska
- R. Pua, MD, Nevada
- B. Horrigan, PA, New Hampshire
- A. Angelow, NP, New Jersey
- R. Arerangaiah, MD, New Jersey
- J. Burgos-Dago-oc, MD, New Jersey
- K. Doktor, MD, New Jersey
- D. Fabius, DO, New Jersey
- C. Keresztury, NP, New Jersey
- O. Kocia, MD, New Jersey
- J. Lim, MD, New Jersey
- M. Mangold, DO, New Jersey
- E. Pierre, MD, New Jersey
- R. Rondanina, MD, New Jersey
- S. Siddiqui, MD, New Jersey
- C. Sipaco-Ong, NP, New Jersey
- N. Siu, NP, New Jersey
- R. Verma, MD, New Jersey
- W. Zaeeter, MD, New Jersey
- S. Modi, New Mexico
- D. Rao, MD, New Mexico
- S. Behuria, MD, New York
- N. Hung, New York
- H. Cho, MD, New York
- R. Duszak, New York
- S. Hoag, MD, New York
- F. Masrur, MBBS, New York
- C. Mensah, New York
- M. Nagasaka, MD, New York
- A. Nagpaul, New York
- A. Narayan, New York
- V. Punnam, New York
- D. Scime, ANP, BC, New York
- T. Shirani, New York
- S. Stewart, New York
- S. Brown, MD, North Carolina
- I. Mitropoulos, PharmD, North Carolina
- K. Reschly, MD, North Carolina
- K. Rutterer, MD, North Carolina
- J. Singh, MD, North Carolina
- J. Anwar, MD, Ohio
- P. Betkerur, USA, Ohio
- C. Demian, MD, Ohio
- S. Demian, MD, MBBch, Ohio
- K. Geckle, ANP, Ohio
- J. Moore, MD, Ohio
- K. Pestak, DO, Ohio
- V. Porter, Ohio
- S. Shenoy, MD, Ohio
- J. Zang, MD, Ohio
- T. Jones, Oklahoma
- K. Shah, MD, Oklahoma
- M. Nag, MSc, Ontario, Canada
- J. Meghashyam, MD, Oregon
- G. Regalbuto, MD, Oregon
- X. Song, MD, Oregon
- E. Weeks, MD, Oregon
- D. Ebhaleme, MD, Pennsylvania
- Y. Li, Pennsylvania
- R. Lynn, MD, Pennsylvania
- K. Repine, Pennsylvania
- P. Scoble, PharmD, Pennsylvania
- M. Sharma, DO, Pennsylvania
- N. Sinha, MD, Pennsylvania
- A. Somasundaram, Pennsylvania
- P. Timon, Pennsylvania
- A. Weber, DO, Pennsylvania
- D. Zielinski, MD, Pennsylvania
- K. O’Neil, MD, Prince Edward Island, Canada
- J. Patel, MD, MBBS, South Carolina
- M. Acha, Spain
- A. de Arcaya, Spain
- F. Garrido, MD, Spain
- A. Gonzalez, Spain
- V. Clark, MD, Tennessee
- G. Dutta, MD, Tennessee
- J. Gonce, MD, Tennessee
- R. Kunder, Tennessee
- C. Davenport, FAAP, Texas
- C. Gordon, Texas
- F. Hernandez, MD, Texas
- C. Jones, Texas
- S. Prihoda, CPCS, Texas
- A. Stock, AHIP, Texas
- J. Wilson, MD, Texas
- J. Zepeda, MD, Texas
- C. Stratis, MD, United Arab Emirates
- E. Guenzel, MD, Utah
- K. Chewning, MD, Virginia
- R. Gadesam, MD, MBBS, Virginia
- T. Jones, MD, Virginia
- B. Montgomery, MD, Virginia
- M. Shah, MD, Virginia
- A. Torralba, MD, Virginia
- A. Ulrich, Virginia
- R. Cupp, PA-C, Washington
- J. Remington, MD, Washington
- A. Harsanyne, FNP, West Virginia
- M. Lilly, PA, West Virginia
- K. Patra, MBBS, West Virginia
- S. Aman, MD, Wisconsin
- S. Dean, Wisconsin
- J. Friday, APRNBC, MSN, Wisconsin
- J. Kurman, MD, MBA, Wisconsin
- D. Miller, Wisconsin
SHM To Award First Certificates of Leadership at HM13
This month, Thomas McIlraith, MD, SFHM, will be on stage at HM13 accepting one of the first SHM Certificates in Leadership. As chair of hospital medicine at Sacramento, Calif.-based Mercy Medical Group, Dr. McIlraith already is familiar with the need for leadership in our specialty and shares why SHM’s Leadership Academy and new certification have helped his hospital and his career.
Question: What made you apply for the Certificate in Leadership in the first place?
Answer: I have always felt that a young field like hospital medicine needs to have resources to develop leadership; I don’t think there is another place in the field of medicine that has more shared responsibility requiring coordinated response than hospital medicine.
I have always been impressed and grateful that SHM recognized this and put forth the considerable effort required to create and develop the Leadership Academies into the premiere institution that they have evolved into. That is why I not only got involved in the leadership academies personally, but also had my entire leadership team complete the curriculum.
Certification is the culmination of that experience for me; I am hoping it is not the end, however. I have had other leadership training course work, and while the SHM Leadership Academies and the certification process were the best experience, I have learned that you can never have too much leadership training.
There are always new challenges a leader will be called on to face, and leadership skills need to continually grow.
Q: What’s been the biggest impact on your career so far? How do you plan on using it in the future?
A: It is not enough to be successful; you have to be able to tell the story of your success. Most of us want to be humble and focus on serving our patients, but the tree that falls in the woods is applicable to successful hospital medicine programs: If nobody hears about it, are you really successful? Can you really drive change?
Lenny Marcus put it best in his SHM Leadership Academy session on meta-leadership: Learning how to communicate to your boss is leading up; communicating across the silos of your organization is meta-leadership. The academies teach you about the skills you need for leadership; certification allows you to put those skills into action.
I vividly remember the day that academy instructor Eric Rice called me up to give me feedback on the first draft of my project. I was already stressed out because in four days I knew I had to give a critical presentation to top hospital leadership and health plan medical directors about our group. We had two new hospital presidents and a new service area senior vice president that had already terminated their contract with the ED group that covered three of the four hospitals. I knew they were scrutinizing my group; the pressure was on.
Eric gave the feedback that I had been focusing on the clinical aspects of my project and said I needed to tell the economic story—to measure the economic impact of my intervention. Further, he advised me on how to get the data to tell that story. I knew that he had just given me the material I needed to blow away the upcoming presentation to the hospital presidents, but would I get the data in time? I called up the CFO of the hospital as Eric advised, told him that I needed the data for a presentation I was giving to his boss in four days.
I got the data in time and blew away the presentation. I got to inform one of the new presidents that we had improved the contribution margin in his ICU by half a million dollars and cut length of stay by 0.9 days, while dramatically improving sepsis mortality. I was then able to go on and tell the HM leaders of our entire hospital system about our intervention and encouraged them to take similar steps.
Someday I hope I get the chance to tell Lenny Marcus this story; I hope he will consider me a meta-leader.
After the dust settled from those successes, I went back to my computer to write up the final draft of my project and I was able to tell a much better story than I ever could have without that advice Eric Rice and the committee [gave me].
My new boss was at the presentation that I gave. We went to the American Medical Group Association conference recently, and he did not hesitate to walk around bragging about what we had done, often quoting the numbers I delivered in my presentation. In another coda to the story, the new service area senior vice president asked my wife and I to join him and his wife for dinner; we have struck up a very valuable friendship.
—Thomas McIlraith, MD, SFHM
Q: What would you say to others who are thinking about applying for the certificate?
A: What are you waiting for?
On a more serious note, we are all engaged with important projects to make our hospitals run better, to keep our patients safer, and give our patients better experience. In the certification process, you continue with that work while top leaders from the field of hospital medicine coach and advise you.
Not only do you come out with a better product in the short term, but also you have better skills for taking on projects in the future; you know what questions to ask and what stories to tell and to whom. That stays with you long after the certification project is over.
Q: How are the results of your project benefiting your institution?
A: My hospitalists are seeing increased productivity and my hospitals are seeing stronger contribution margin in tough economic times. Further, the successful completion of the project has elevated the reputation of my department.
This month, Thomas McIlraith, MD, SFHM, will be on stage at HM13 accepting one of the first SHM Certificates in Leadership. As chair of hospital medicine at Sacramento, Calif.-based Mercy Medical Group, Dr. McIlraith already is familiar with the need for leadership in our specialty and shares why SHM’s Leadership Academy and new certification have helped his hospital and his career.
Question: What made you apply for the Certificate in Leadership in the first place?
Answer: I have always felt that a young field like hospital medicine needs to have resources to develop leadership; I don’t think there is another place in the field of medicine that has more shared responsibility requiring coordinated response than hospital medicine.
I have always been impressed and grateful that SHM recognized this and put forth the considerable effort required to create and develop the Leadership Academies into the premiere institution that they have evolved into. That is why I not only got involved in the leadership academies personally, but also had my entire leadership team complete the curriculum.
Certification is the culmination of that experience for me; I am hoping it is not the end, however. I have had other leadership training course work, and while the SHM Leadership Academies and the certification process were the best experience, I have learned that you can never have too much leadership training.
There are always new challenges a leader will be called on to face, and leadership skills need to continually grow.
Q: What’s been the biggest impact on your career so far? How do you plan on using it in the future?
A: It is not enough to be successful; you have to be able to tell the story of your success. Most of us want to be humble and focus on serving our patients, but the tree that falls in the woods is applicable to successful hospital medicine programs: If nobody hears about it, are you really successful? Can you really drive change?
Lenny Marcus put it best in his SHM Leadership Academy session on meta-leadership: Learning how to communicate to your boss is leading up; communicating across the silos of your organization is meta-leadership. The academies teach you about the skills you need for leadership; certification allows you to put those skills into action.
I vividly remember the day that academy instructor Eric Rice called me up to give me feedback on the first draft of my project. I was already stressed out because in four days I knew I had to give a critical presentation to top hospital leadership and health plan medical directors about our group. We had two new hospital presidents and a new service area senior vice president that had already terminated their contract with the ED group that covered three of the four hospitals. I knew they were scrutinizing my group; the pressure was on.
Eric gave the feedback that I had been focusing on the clinical aspects of my project and said I needed to tell the economic story—to measure the economic impact of my intervention. Further, he advised me on how to get the data to tell that story. I knew that he had just given me the material I needed to blow away the upcoming presentation to the hospital presidents, but would I get the data in time? I called up the CFO of the hospital as Eric advised, told him that I needed the data for a presentation I was giving to his boss in four days.
I got the data in time and blew away the presentation. I got to inform one of the new presidents that we had improved the contribution margin in his ICU by half a million dollars and cut length of stay by 0.9 days, while dramatically improving sepsis mortality. I was then able to go on and tell the HM leaders of our entire hospital system about our intervention and encouraged them to take similar steps.
Someday I hope I get the chance to tell Lenny Marcus this story; I hope he will consider me a meta-leader.
After the dust settled from those successes, I went back to my computer to write up the final draft of my project and I was able to tell a much better story than I ever could have without that advice Eric Rice and the committee [gave me].
My new boss was at the presentation that I gave. We went to the American Medical Group Association conference recently, and he did not hesitate to walk around bragging about what we had done, often quoting the numbers I delivered in my presentation. In another coda to the story, the new service area senior vice president asked my wife and I to join him and his wife for dinner; we have struck up a very valuable friendship.
—Thomas McIlraith, MD, SFHM
Q: What would you say to others who are thinking about applying for the certificate?
A: What are you waiting for?
On a more serious note, we are all engaged with important projects to make our hospitals run better, to keep our patients safer, and give our patients better experience. In the certification process, you continue with that work while top leaders from the field of hospital medicine coach and advise you.
Not only do you come out with a better product in the short term, but also you have better skills for taking on projects in the future; you know what questions to ask and what stories to tell and to whom. That stays with you long after the certification project is over.
Q: How are the results of your project benefiting your institution?
A: My hospitalists are seeing increased productivity and my hospitals are seeing stronger contribution margin in tough economic times. Further, the successful completion of the project has elevated the reputation of my department.
This month, Thomas McIlraith, MD, SFHM, will be on stage at HM13 accepting one of the first SHM Certificates in Leadership. As chair of hospital medicine at Sacramento, Calif.-based Mercy Medical Group, Dr. McIlraith already is familiar with the need for leadership in our specialty and shares why SHM’s Leadership Academy and new certification have helped his hospital and his career.
Question: What made you apply for the Certificate in Leadership in the first place?
Answer: I have always felt that a young field like hospital medicine needs to have resources to develop leadership; I don’t think there is another place in the field of medicine that has more shared responsibility requiring coordinated response than hospital medicine.
I have always been impressed and grateful that SHM recognized this and put forth the considerable effort required to create and develop the Leadership Academies into the premiere institution that they have evolved into. That is why I not only got involved in the leadership academies personally, but also had my entire leadership team complete the curriculum.
Certification is the culmination of that experience for me; I am hoping it is not the end, however. I have had other leadership training course work, and while the SHM Leadership Academies and the certification process were the best experience, I have learned that you can never have too much leadership training.
There are always new challenges a leader will be called on to face, and leadership skills need to continually grow.
Q: What’s been the biggest impact on your career so far? How do you plan on using it in the future?
A: It is not enough to be successful; you have to be able to tell the story of your success. Most of us want to be humble and focus on serving our patients, but the tree that falls in the woods is applicable to successful hospital medicine programs: If nobody hears about it, are you really successful? Can you really drive change?
Lenny Marcus put it best in his SHM Leadership Academy session on meta-leadership: Learning how to communicate to your boss is leading up; communicating across the silos of your organization is meta-leadership. The academies teach you about the skills you need for leadership; certification allows you to put those skills into action.
I vividly remember the day that academy instructor Eric Rice called me up to give me feedback on the first draft of my project. I was already stressed out because in four days I knew I had to give a critical presentation to top hospital leadership and health plan medical directors about our group. We had two new hospital presidents and a new service area senior vice president that had already terminated their contract with the ED group that covered three of the four hospitals. I knew they were scrutinizing my group; the pressure was on.
Eric gave the feedback that I had been focusing on the clinical aspects of my project and said I needed to tell the economic story—to measure the economic impact of my intervention. Further, he advised me on how to get the data to tell that story. I knew that he had just given me the material I needed to blow away the upcoming presentation to the hospital presidents, but would I get the data in time? I called up the CFO of the hospital as Eric advised, told him that I needed the data for a presentation I was giving to his boss in four days.
I got the data in time and blew away the presentation. I got to inform one of the new presidents that we had improved the contribution margin in his ICU by half a million dollars and cut length of stay by 0.9 days, while dramatically improving sepsis mortality. I was then able to go on and tell the HM leaders of our entire hospital system about our intervention and encouraged them to take similar steps.
Someday I hope I get the chance to tell Lenny Marcus this story; I hope he will consider me a meta-leader.
After the dust settled from those successes, I went back to my computer to write up the final draft of my project and I was able to tell a much better story than I ever could have without that advice Eric Rice and the committee [gave me].
My new boss was at the presentation that I gave. We went to the American Medical Group Association conference recently, and he did not hesitate to walk around bragging about what we had done, often quoting the numbers I delivered in my presentation. In another coda to the story, the new service area senior vice president asked my wife and I to join him and his wife for dinner; we have struck up a very valuable friendship.
—Thomas McIlraith, MD, SFHM
Q: What would you say to others who are thinking about applying for the certificate?
A: What are you waiting for?
On a more serious note, we are all engaged with important projects to make our hospitals run better, to keep our patients safer, and give our patients better experience. In the certification process, you continue with that work while top leaders from the field of hospital medicine coach and advise you.
Not only do you come out with a better product in the short term, but also you have better skills for taking on projects in the future; you know what questions to ask and what stories to tell and to whom. That stays with you long after the certification project is over.
Q: How are the results of your project benefiting your institution?
A: My hospitalists are seeing increased productivity and my hospitals are seeing stronger contribution margin in tough economic times. Further, the successful completion of the project has elevated the reputation of my department.
Fellow in Hospital Medicine Spotlight: Mangla Gulati, MD, FACP, FHM

Dr. Gulati is a physician advisor, the medical director for clinical effectiveness, and an assistant professor in the division of general internal medicine at the University of Maryland School of Medicine. She is secretary of SHM’s Maryland chapter.
Undergraduate education: London.
Medical school: Dayanand Medical School, Ludhiana, Punjab, India.
Notable: An academic hospitalist, Dr. Gulati has been awarded the Physician-Colleague of the Year Award for her efforts to promote communication between doctors, nurses, and other nonphysician staff, as well as the Theodore Woodward Teaching Award for her exemplary teaching and patient care. One example of her unique teaching style is taking her residents and students to the patient placement center so that they understand the reality and importance of a timely discharge and how throughput affects an 800-bed facility. As a mentor for the first chief resident focused on patient safety and quality at the University of Maryland School of Medicine, she designed and developed a curriculum catered to the chief resident’s needs.
FYI: A fan of the outdoors, Dr. Gulati enjoys kayaking and loves to travel. She has camped in the Sahara and visited the Scandinavian peninsula. When not outdoors, she spends her time reading; her current favorite book is The Checklist Manifesto by Atul Gawande, MD.
Quotable: “I am honored to be a fellow in the Society of Hospital Medicine, as it gives credence to how I focus on patient care from beginning to end, and how it is essential to work with a multidisciplinary team to provide patient-centered, quality care across the continuum of care.”
Dr. Gulati is a physician advisor, the medical director for clinical effectiveness, and an assistant professor in the division of general internal medicine at the University of Maryland School of Medicine. She is secretary of SHM’s Maryland chapter.
Undergraduate education: London.
Medical school: Dayanand Medical School, Ludhiana, Punjab, India.
Notable: An academic hospitalist, Dr. Gulati has been awarded the Physician-Colleague of the Year Award for her efforts to promote communication between doctors, nurses, and other nonphysician staff, as well as the Theodore Woodward Teaching Award for her exemplary teaching and patient care. One example of her unique teaching style is taking her residents and students to the patient placement center so that they understand the reality and importance of a timely discharge and how throughput affects an 800-bed facility. As a mentor for the first chief resident focused on patient safety and quality at the University of Maryland School of Medicine, she designed and developed a curriculum catered to the chief resident’s needs.
FYI: A fan of the outdoors, Dr. Gulati enjoys kayaking and loves to travel. She has camped in the Sahara and visited the Scandinavian peninsula. When not outdoors, she spends her time reading; her current favorite book is The Checklist Manifesto by Atul Gawande, MD.
Quotable: “I am honored to be a fellow in the Society of Hospital Medicine, as it gives credence to how I focus on patient care from beginning to end, and how it is essential to work with a multidisciplinary team to provide patient-centered, quality care across the continuum of care.”
Dr. Gulati is a physician advisor, the medical director for clinical effectiveness, and an assistant professor in the division of general internal medicine at the University of Maryland School of Medicine. She is secretary of SHM’s Maryland chapter.
Undergraduate education: London.
Medical school: Dayanand Medical School, Ludhiana, Punjab, India.
Notable: An academic hospitalist, Dr. Gulati has been awarded the Physician-Colleague of the Year Award for her efforts to promote communication between doctors, nurses, and other nonphysician staff, as well as the Theodore Woodward Teaching Award for her exemplary teaching and patient care. One example of her unique teaching style is taking her residents and students to the patient placement center so that they understand the reality and importance of a timely discharge and how throughput affects an 800-bed facility. As a mentor for the first chief resident focused on patient safety and quality at the University of Maryland School of Medicine, she designed and developed a curriculum catered to the chief resident’s needs.
FYI: A fan of the outdoors, Dr. Gulati enjoys kayaking and loves to travel. She has camped in the Sahara and visited the Scandinavian peninsula. When not outdoors, she spends her time reading; her current favorite book is The Checklist Manifesto by Atul Gawande, MD.
Quotable: “I am honored to be a fellow in the Society of Hospital Medicine, as it gives credence to how I focus on patient care from beginning to end, and how it is essential to work with a multidisciplinary team to provide patient-centered, quality care across the continuum of care.”
SHM Welcomes Nonphysician Fellows to Hospital Medicine
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
HM13 At Hand App Puts Meeting Materials Within Easy Reach
As hospitalists pack their bags and head to Washington, D.C., this month for the annual meeting, it’s a sure bet most are packing a smartphone or a tablet—and many will be bringing both. If you’re one of them, you will find it easier than ever to pull up presentations, speaker bios, and many of the other materials you used to find on the annual meeting’s “paperless” website. This year, presentations, schedules, attendee contact information, and lots of other important HM13 information will be available at hospitalists’ fingertips via the HM13 At Hand app. Download the app today at www.eventmobi.com/hm13.
HM13 At Hand puts HM13 in your hands with meeting content and tools, such as:
- Presentations;
- Speaker information;
- HM13 schedule and agenda planner;
- “Scan to Win” contest;
- Real-time alerts and updates; and
- Links to other HM13 resources and social media.
As hospitalists pack their bags and head to Washington, D.C., this month for the annual meeting, it’s a sure bet most are packing a smartphone or a tablet—and many will be bringing both. If you’re one of them, you will find it easier than ever to pull up presentations, speaker bios, and many of the other materials you used to find on the annual meeting’s “paperless” website. This year, presentations, schedules, attendee contact information, and lots of other important HM13 information will be available at hospitalists’ fingertips via the HM13 At Hand app. Download the app today at www.eventmobi.com/hm13.
HM13 At Hand puts HM13 in your hands with meeting content and tools, such as:
- Presentations;
- Speaker information;
- HM13 schedule and agenda planner;
- “Scan to Win” contest;
- Real-time alerts and updates; and
- Links to other HM13 resources and social media.
As hospitalists pack their bags and head to Washington, D.C., this month for the annual meeting, it’s a sure bet most are packing a smartphone or a tablet—and many will be bringing both. If you’re one of them, you will find it easier than ever to pull up presentations, speaker bios, and many of the other materials you used to find on the annual meeting’s “paperless” website. This year, presentations, schedules, attendee contact information, and lots of other important HM13 information will be available at hospitalists’ fingertips via the HM13 At Hand app. Download the app today at www.eventmobi.com/hm13.
HM13 At Hand puts HM13 in your hands with meeting content and tools, such as:
- Presentations;
- Speaker information;
- HM13 schedule and agenda planner;
- “Scan to Win” contest;
- Real-time alerts and updates; and
- Links to other HM13 resources and social media.