User login
Happy Birthday, HM

Ah, 15 years. My, how time flies. August 1996 seems like yesterday. I had just moved to Denver. It was a hot summer. I still had hair, a normal BMI, and a social life. The world was gearing up for the Olympics in Atlanta; my adrenal glands were gearing up for the hypertrophying journey called internship. The films of ’96 seemed to portend ominously about my year ahead: Twister (a whirlwind ride?), Jerry Maguire (you complete me, internship?), Independence Day (apocalypse?), The Nutty Professor (research attendings on the wards?), Mission: Impossible (hmmm).
The Spice Girls were spreading girl power, this thing called the Internet was sort of catching on with 10 million (yes, that’s an “m,” not a “b”) users worldwide, and the dotcom era introduced us to eBay, which offered to sell your junk “online.”
In Scotland, Dolly the sheep was cloned and the world grappled with the ethical implications. In England, Diana and Charles divorced and cows became mad (coincidence?). Back home, Seinfeld, ER, and Friends teamed for “must-see” Thursday nights, the average car cost $16,000, and Federal Reserve Chairman Alan Greenspan wondered if the Dow Jones was overvalued at 6,400.
Oh, and on Aug. 15, the term “hospitalist” appeared in print for the first time, helping launch the fastest-growing medical specialty of all time.1
Labor & Delivery
I remember as an intern seeing the article by Drs. Wachter and Goldman. I guess I didn’t get it, really. Was it that easy to create a new specialty? Just take something and add “ist” to the end? As interns, we excitedly begin to create new fields to describe our work: “dump-ologists,” “failure-to-thrive-ists,” “rectalists.” Much like Jamiroquai, however, our specialties never really caught on.
But HM did, and this month we celebrate 15 years. Now, I’ll recognize that its impossible to pin an exact date on the creation of a specialty, and in fact, hospitalists clearly existed prior to the term. But in terms of identifying a start date, Aug. 15, 1996, is as good as any.
The Early Days: Doing It
I don’t remember the day I became a hospitalist. It all sort of just flowed together. I finished residency, did a chief year where I taught, attended on the wards, and didn’t do any clinic, and then I took a job at the Denver VA, where I taught, attended on the wards, and didn’t do any clinic. It felt kind of all the same.
But from the outside, this was a significant transition point. Until this time, subspecialists or general internists, family medicine doctors, and pediatricians provided nearly all inpatient ward attending (and indeed, community inpatient care). I recall vividly the reaction of others; it was a mixture of amazement (you do what all year?), concern (you’ll burn out), apprehension (I won’t be able to care for my patients in the hospital), and enmity (you’ll destroy the fabric of internal medicine!).
And this was the point of the first few years: survival. These were the formative years. It was all about showing HM was a sustainable model that could enhance, not detract, from the system of care. And it had its very vocal critics, who saw it as a flash in the pan. They assumed it would go the way of the Tickle Me Elmo doll (a fad, for the record, that needed to die).
And this was the importance of the creation of the National Association of Inpatient Physicians (now SHM), HM textbooks, the development of hospitalist researchers, a national meeting, the creation of sustainable community hospitalist jobs, the growth of academic HM groups, and studies showing the model could indeed be implemented and wouldn’t negatively impact patient outcomes or outpatient provider satisfaction. These things legitimized the field, gave it legs, propelled it to the next phase.
The Next Phase: Doing it Cheaper
To be fair, HM is not all about the money. Even in the early days, it was recognized that at its pinnacle HM was about improving the patient experience—higher quality, safety, and satisfaction. That said, it was Medicare’s diagnosis-related group (DRG) that drove the model forward. To be clear, there were other factors that helped propel the HM movement: staffing issues, the rise in complexity of care, many PCPs and specialists willingly leaving the hospital. But in the end, the bottom line drove many hospital administrations to adopt the HM model.
Most hospital care is reimbursed via prospective payment, which means hospital reimbursement is, in a sense, determined upon admission. Every dollar of that DRG payment that isn’t spent is pocketed by the hospital as profit. As expected, specialists in hospital care were able to significantly reduce the length of hospital stay, costs of care, and, ultimately, save hospitals many dollars for each dollar of investment.
And to be clear, there was nothing unsavory about this. It wasn’t done through rationing care or reducing access, but rather through systematically reducing some of the estimated 30% waste in healthcare. This was shown in numerous studies, with a 2002 report estimating average savings at about 13% per patient cared for in the HM model.2
The Current Phase: Doing it Better
Pretty impressive, but mostly unsatisfying. Yes, as a group director that has negotiated for nearly a decade with hospital administrators, I’m well aware of the power of cost savings. Yet, I didn’t go into medicine to save money. I did so to help patients, enhance their experience, and improve outcomes. And indeed, there are data that hospitalists do this. Two 2002 papers showed that hospitalist groups could reduce readmission rates as well as inpatient and 30-day mortality.3,4 A paper in 2004 showed that pairing hospitalists with orthopedic surgeons could reduce perioperative complications.5
Couple these studies with anecdotal experience and perusal of any issue of the Journal of Hospital Medicine, and its clear that hospitalists are fulfilling their promise of doing it better. But we have a long way to go. We must continue to innovative and create better, safer systems of care until we can be confident that not a single one of our patients is avoidably harmed by healthcare. That is the kind of care you’d want for your family member, for yourself.
Our Legacy, TBD
And here we are now, looking forward to the next 15 years. For many hospitalists, this will represent the twilight years of their careers. For others, it’ll be the formative years. What mark will we leave?
Clearly, the premium on patient safety and quality is increasing, morphing from word to deed as we speak. And hospitalists will find themselves in the middle of the fray. The healthcare reform alphabet soup calls for equal parts VBP and ACO, with a pinch of EHR, and a dash of PFP—boiled in a cost reduction. But more than ingredients, it requires a chef—someone to orchestrate the great change that is necessary in American healthcare.
Whether it’s leading inpatient safety, improving the quality of hospital care, bridging post-discharge transitions, or reducing readmissions, someone is required to tend these fires.
And I believe HM’s legacy will be forged in these flames of change. There is no single group as well positioned to impact the outcomes that matter most to healthcare reform now than hospitalists. In most hospitals, we will touch the majority of patients, control the spending of the majority of dollars, and be directly responsible for the majority of outcomes. This is an unfathomable position to be in for a specialty that is yet old enough to drive. Yet this is where we find ourselves.
Our legacy is being written. You are its author.
Dr. Glasheen is The Hospitalist’s physician editor.
References
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335:514-517.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287:487-494.
- Auerbach AD, Wachter RM, Katz P, Showstack J, Baron RB, Goldman L. Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137:859-865.
- Meltzer D, Manning WG, Morrison J, Shah MN, Jin L, Guth T, Levinson W. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137:866-874.
- Huddleston JM, Long KH, Naessens JM, et. al. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004;141:28-38.
Ah, 15 years. My, how time flies. August 1996 seems like yesterday. I had just moved to Denver. It was a hot summer. I still had hair, a normal BMI, and a social life. The world was gearing up for the Olympics in Atlanta; my adrenal glands were gearing up for the hypertrophying journey called internship. The films of ’96 seemed to portend ominously about my year ahead: Twister (a whirlwind ride?), Jerry Maguire (you complete me, internship?), Independence Day (apocalypse?), The Nutty Professor (research attendings on the wards?), Mission: Impossible (hmmm).
The Spice Girls were spreading girl power, this thing called the Internet was sort of catching on with 10 million (yes, that’s an “m,” not a “b”) users worldwide, and the dotcom era introduced us to eBay, which offered to sell your junk “online.”
In Scotland, Dolly the sheep was cloned and the world grappled with the ethical implications. In England, Diana and Charles divorced and cows became mad (coincidence?). Back home, Seinfeld, ER, and Friends teamed for “must-see” Thursday nights, the average car cost $16,000, and Federal Reserve Chairman Alan Greenspan wondered if the Dow Jones was overvalued at 6,400.
Oh, and on Aug. 15, the term “hospitalist” appeared in print for the first time, helping launch the fastest-growing medical specialty of all time.1
Labor & Delivery
I remember as an intern seeing the article by Drs. Wachter and Goldman. I guess I didn’t get it, really. Was it that easy to create a new specialty? Just take something and add “ist” to the end? As interns, we excitedly begin to create new fields to describe our work: “dump-ologists,” “failure-to-thrive-ists,” “rectalists.” Much like Jamiroquai, however, our specialties never really caught on.
But HM did, and this month we celebrate 15 years. Now, I’ll recognize that its impossible to pin an exact date on the creation of a specialty, and in fact, hospitalists clearly existed prior to the term. But in terms of identifying a start date, Aug. 15, 1996, is as good as any.
The Early Days: Doing It
I don’t remember the day I became a hospitalist. It all sort of just flowed together. I finished residency, did a chief year where I taught, attended on the wards, and didn’t do any clinic, and then I took a job at the Denver VA, where I taught, attended on the wards, and didn’t do any clinic. It felt kind of all the same.
But from the outside, this was a significant transition point. Until this time, subspecialists or general internists, family medicine doctors, and pediatricians provided nearly all inpatient ward attending (and indeed, community inpatient care). I recall vividly the reaction of others; it was a mixture of amazement (you do what all year?), concern (you’ll burn out), apprehension (I won’t be able to care for my patients in the hospital), and enmity (you’ll destroy the fabric of internal medicine!).
And this was the point of the first few years: survival. These were the formative years. It was all about showing HM was a sustainable model that could enhance, not detract, from the system of care. And it had its very vocal critics, who saw it as a flash in the pan. They assumed it would go the way of the Tickle Me Elmo doll (a fad, for the record, that needed to die).
And this was the importance of the creation of the National Association of Inpatient Physicians (now SHM), HM textbooks, the development of hospitalist researchers, a national meeting, the creation of sustainable community hospitalist jobs, the growth of academic HM groups, and studies showing the model could indeed be implemented and wouldn’t negatively impact patient outcomes or outpatient provider satisfaction. These things legitimized the field, gave it legs, propelled it to the next phase.
The Next Phase: Doing it Cheaper
To be fair, HM is not all about the money. Even in the early days, it was recognized that at its pinnacle HM was about improving the patient experience—higher quality, safety, and satisfaction. That said, it was Medicare’s diagnosis-related group (DRG) that drove the model forward. To be clear, there were other factors that helped propel the HM movement: staffing issues, the rise in complexity of care, many PCPs and specialists willingly leaving the hospital. But in the end, the bottom line drove many hospital administrations to adopt the HM model.
Most hospital care is reimbursed via prospective payment, which means hospital reimbursement is, in a sense, determined upon admission. Every dollar of that DRG payment that isn’t spent is pocketed by the hospital as profit. As expected, specialists in hospital care were able to significantly reduce the length of hospital stay, costs of care, and, ultimately, save hospitals many dollars for each dollar of investment.
And to be clear, there was nothing unsavory about this. It wasn’t done through rationing care or reducing access, but rather through systematically reducing some of the estimated 30% waste in healthcare. This was shown in numerous studies, with a 2002 report estimating average savings at about 13% per patient cared for in the HM model.2
The Current Phase: Doing it Better
Pretty impressive, but mostly unsatisfying. Yes, as a group director that has negotiated for nearly a decade with hospital administrators, I’m well aware of the power of cost savings. Yet, I didn’t go into medicine to save money. I did so to help patients, enhance their experience, and improve outcomes. And indeed, there are data that hospitalists do this. Two 2002 papers showed that hospitalist groups could reduce readmission rates as well as inpatient and 30-day mortality.3,4 A paper in 2004 showed that pairing hospitalists with orthopedic surgeons could reduce perioperative complications.5
Couple these studies with anecdotal experience and perusal of any issue of the Journal of Hospital Medicine, and its clear that hospitalists are fulfilling their promise of doing it better. But we have a long way to go. We must continue to innovative and create better, safer systems of care until we can be confident that not a single one of our patients is avoidably harmed by healthcare. That is the kind of care you’d want for your family member, for yourself.
Our Legacy, TBD
And here we are now, looking forward to the next 15 years. For many hospitalists, this will represent the twilight years of their careers. For others, it’ll be the formative years. What mark will we leave?
Clearly, the premium on patient safety and quality is increasing, morphing from word to deed as we speak. And hospitalists will find themselves in the middle of the fray. The healthcare reform alphabet soup calls for equal parts VBP and ACO, with a pinch of EHR, and a dash of PFP—boiled in a cost reduction. But more than ingredients, it requires a chef—someone to orchestrate the great change that is necessary in American healthcare.
Whether it’s leading inpatient safety, improving the quality of hospital care, bridging post-discharge transitions, or reducing readmissions, someone is required to tend these fires.
And I believe HM’s legacy will be forged in these flames of change. There is no single group as well positioned to impact the outcomes that matter most to healthcare reform now than hospitalists. In most hospitals, we will touch the majority of patients, control the spending of the majority of dollars, and be directly responsible for the majority of outcomes. This is an unfathomable position to be in for a specialty that is yet old enough to drive. Yet this is where we find ourselves.
Our legacy is being written. You are its author.
Dr. Glasheen is The Hospitalist’s physician editor.
References
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335:514-517.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287:487-494.
- Auerbach AD, Wachter RM, Katz P, Showstack J, Baron RB, Goldman L. Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137:859-865.
- Meltzer D, Manning WG, Morrison J, Shah MN, Jin L, Guth T, Levinson W. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137:866-874.
- Huddleston JM, Long KH, Naessens JM, et. al. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004;141:28-38.
Ah, 15 years. My, how time flies. August 1996 seems like yesterday. I had just moved to Denver. It was a hot summer. I still had hair, a normal BMI, and a social life. The world was gearing up for the Olympics in Atlanta; my adrenal glands were gearing up for the hypertrophying journey called internship. The films of ’96 seemed to portend ominously about my year ahead: Twister (a whirlwind ride?), Jerry Maguire (you complete me, internship?), Independence Day (apocalypse?), The Nutty Professor (research attendings on the wards?), Mission: Impossible (hmmm).
The Spice Girls were spreading girl power, this thing called the Internet was sort of catching on with 10 million (yes, that’s an “m,” not a “b”) users worldwide, and the dotcom era introduced us to eBay, which offered to sell your junk “online.”
In Scotland, Dolly the sheep was cloned and the world grappled with the ethical implications. In England, Diana and Charles divorced and cows became mad (coincidence?). Back home, Seinfeld, ER, and Friends teamed for “must-see” Thursday nights, the average car cost $16,000, and Federal Reserve Chairman Alan Greenspan wondered if the Dow Jones was overvalued at 6,400.
Oh, and on Aug. 15, the term “hospitalist” appeared in print for the first time, helping launch the fastest-growing medical specialty of all time.1
Labor & Delivery
I remember as an intern seeing the article by Drs. Wachter and Goldman. I guess I didn’t get it, really. Was it that easy to create a new specialty? Just take something and add “ist” to the end? As interns, we excitedly begin to create new fields to describe our work: “dump-ologists,” “failure-to-thrive-ists,” “rectalists.” Much like Jamiroquai, however, our specialties never really caught on.
But HM did, and this month we celebrate 15 years. Now, I’ll recognize that its impossible to pin an exact date on the creation of a specialty, and in fact, hospitalists clearly existed prior to the term. But in terms of identifying a start date, Aug. 15, 1996, is as good as any.
The Early Days: Doing It
I don’t remember the day I became a hospitalist. It all sort of just flowed together. I finished residency, did a chief year where I taught, attended on the wards, and didn’t do any clinic, and then I took a job at the Denver VA, where I taught, attended on the wards, and didn’t do any clinic. It felt kind of all the same.
But from the outside, this was a significant transition point. Until this time, subspecialists or general internists, family medicine doctors, and pediatricians provided nearly all inpatient ward attending (and indeed, community inpatient care). I recall vividly the reaction of others; it was a mixture of amazement (you do what all year?), concern (you’ll burn out), apprehension (I won’t be able to care for my patients in the hospital), and enmity (you’ll destroy the fabric of internal medicine!).
And this was the point of the first few years: survival. These were the formative years. It was all about showing HM was a sustainable model that could enhance, not detract, from the system of care. And it had its very vocal critics, who saw it as a flash in the pan. They assumed it would go the way of the Tickle Me Elmo doll (a fad, for the record, that needed to die).
And this was the importance of the creation of the National Association of Inpatient Physicians (now SHM), HM textbooks, the development of hospitalist researchers, a national meeting, the creation of sustainable community hospitalist jobs, the growth of academic HM groups, and studies showing the model could indeed be implemented and wouldn’t negatively impact patient outcomes or outpatient provider satisfaction. These things legitimized the field, gave it legs, propelled it to the next phase.
The Next Phase: Doing it Cheaper
To be fair, HM is not all about the money. Even in the early days, it was recognized that at its pinnacle HM was about improving the patient experience—higher quality, safety, and satisfaction. That said, it was Medicare’s diagnosis-related group (DRG) that drove the model forward. To be clear, there were other factors that helped propel the HM movement: staffing issues, the rise in complexity of care, many PCPs and specialists willingly leaving the hospital. But in the end, the bottom line drove many hospital administrations to adopt the HM model.
Most hospital care is reimbursed via prospective payment, which means hospital reimbursement is, in a sense, determined upon admission. Every dollar of that DRG payment that isn’t spent is pocketed by the hospital as profit. As expected, specialists in hospital care were able to significantly reduce the length of hospital stay, costs of care, and, ultimately, save hospitals many dollars for each dollar of investment.
And to be clear, there was nothing unsavory about this. It wasn’t done through rationing care or reducing access, but rather through systematically reducing some of the estimated 30% waste in healthcare. This was shown in numerous studies, with a 2002 report estimating average savings at about 13% per patient cared for in the HM model.2
The Current Phase: Doing it Better
Pretty impressive, but mostly unsatisfying. Yes, as a group director that has negotiated for nearly a decade with hospital administrators, I’m well aware of the power of cost savings. Yet, I didn’t go into medicine to save money. I did so to help patients, enhance their experience, and improve outcomes. And indeed, there are data that hospitalists do this. Two 2002 papers showed that hospitalist groups could reduce readmission rates as well as inpatient and 30-day mortality.3,4 A paper in 2004 showed that pairing hospitalists with orthopedic surgeons could reduce perioperative complications.5
Couple these studies with anecdotal experience and perusal of any issue of the Journal of Hospital Medicine, and its clear that hospitalists are fulfilling their promise of doing it better. But we have a long way to go. We must continue to innovative and create better, safer systems of care until we can be confident that not a single one of our patients is avoidably harmed by healthcare. That is the kind of care you’d want for your family member, for yourself.
Our Legacy, TBD
And here we are now, looking forward to the next 15 years. For many hospitalists, this will represent the twilight years of their careers. For others, it’ll be the formative years. What mark will we leave?
Clearly, the premium on patient safety and quality is increasing, morphing from word to deed as we speak. And hospitalists will find themselves in the middle of the fray. The healthcare reform alphabet soup calls for equal parts VBP and ACO, with a pinch of EHR, and a dash of PFP—boiled in a cost reduction. But more than ingredients, it requires a chef—someone to orchestrate the great change that is necessary in American healthcare.
Whether it’s leading inpatient safety, improving the quality of hospital care, bridging post-discharge transitions, or reducing readmissions, someone is required to tend these fires.
And I believe HM’s legacy will be forged in these flames of change. There is no single group as well positioned to impact the outcomes that matter most to healthcare reform now than hospitalists. In most hospitals, we will touch the majority of patients, control the spending of the majority of dollars, and be directly responsible for the majority of outcomes. This is an unfathomable position to be in for a specialty that is yet old enough to drive. Yet this is where we find ourselves.
Our legacy is being written. You are its author.
Dr. Glasheen is The Hospitalist’s physician editor.
References
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335:514-517.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287:487-494.
- Auerbach AD, Wachter RM, Katz P, Showstack J, Baron RB, Goldman L. Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137:859-865.
- Meltzer D, Manning WG, Morrison J, Shah MN, Jin L, Guth T, Levinson W. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137:866-874.
- Huddleston JM, Long KH, Naessens JM, et. al. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004;141:28-38.
A Critical First Step

For those of you who were kind enough to catch my column in last month’s issue of The Hospitalist (see “What Is Your Value,” p. 56), you spent a few minutes reading my thoughts on the value of hospitalists. I mentioned the fact that the U.S. is moving rapidly toward a value-based system of purchasing healthcare, and that all healthcare providers, including hospitalists, increasingly will be judged on the value of care they deliver to their patients and the healthcare system. (Remember, value=quality/cost.)
Hospitalists, like all other healthcare providers, can increase their “value” by improving the quality of care they provide and decreasing the cost of healthcare delivery. Seems simple enough, right? Take better care of patients and do so while minimizing unnecessary costs. (If you have figured out how to do this, I want to learn from you!)
As a doctor and as the leader of the hospitalist group at Beth Israel Deaconess Medical Center in Boston, I have given this topic considerable thought. How do I become a “high value” provider? How do I help my hospitalist colleagues become “high value” hospitalists? Another persistent thought that has crossed my mind is: “How do I know that I am not already a high-value hospitalist?”
Maybe all of my hospitalist colleagues at Beth Israel Deaconess Medical Center are high-value providers. Seems fair enough, right? Maybe each of us is providing “high quality” care and doing so while minimizing unnecessary costs.
I mean, who really wants to think of themselves as low-quality doctors spending a considerable amount of unnecessary resources?
Like many of you, it became evident to me that the first step to improving quality and/or decreasing cost is to define “quality” and “cost.”
The First Step
Although it might seem difficult for the individual hospitalist to know the cost of a patient’s hospitalization, such information is available, and your hospital administrator might be willing to share such information with you and your group. But when it comes to quality of care, I think most patients would expect that doctors should understand the definition of “high-quality care.”
So, what is the definition of “high-quality care?” Try asking this question of patients and doctors, and you are likely to get very different answers. Not surprised? Try asking this question just to doctors, and you are likely to get some different answers. (For fun, you could try this exercise with your hospitalist colleagues; I have.)
Honestly, none of us should be alarmed if a group of doctors cannot easily define “high-quality care.” Not being able to do so does not mean these are “bad” doctors. While it may not be easy to define high-quality care, I suspect most of us recognize it when we see it.
The process of defining the quality of care involves capturing the essence of what we see. For example, can we agree that prescribing aspirin for patients with acute coronary syndrome is optimal care? If so, it stands to reason that a patient with acute coronary syndrome who did not receive aspirin received suboptimal care.
This is how a group of hospitalists can go about creating a quality standard. If you are a hospitalist or HM group leader who is interested in improving the quality of care you and your colleagues are providing to your patients, defining a quality standard is the critical first step to process improvement. Do not limit yourself to clinical processes. Although clinical processes are important, so are communication and documentation processes.
For example, most of us, as hospitalists, believe that communication with outpatient providers is important to the provision of high-quality inpatient care. How often do your hospitalists communicate with patients’ primary-care providers? Is this a quality standard for your hospitalist group? What about the documentation of a patient’s code status at the time of admission or documentation of a patient’s functional status in the discharge summary?
If you believe these are important, your group should include these as quality standards. You should be measuring them and reporting the results to individual providers.
Start with Definition
At this point, some of us might be tempted to get ahead of ourselves and worry about what standards we can or cannot measure, but I urge you to complete this first step of defining “high-quality care” before worrying about anything else. (In other words, don’t start running before you can walk.)
Another suggestion: Please don’t try to do too much all at once. Nobody is going to argue that patients with acute coronary syndrome should not receive aspirin. Reaching consensus on other quality standards might not be as easy. But do not get bogged down trying to create too many quality standards all at once. Start with a few and get yourself and your colleagues accustomed to the process.
Remember, when it comes to doctors, we have centuries of history of not knowing exactly what we are doing. I hope it won’t take centuries to fix this problem, but I also know we are not going to fix this in a few days or weeks. Small victories along the way are important if we hope to succeed.
Once you and your hospitalist colleagues arrive at a mutually agreed upon quality standard, the next step is performance measurement. I honestly believe performance measurement is easy when we spend the time understanding and agreeing to the most appropriate quality standards for our hospitalist groups.
I am interested in learning about your efforts to define the quality standards for your hospitalist group. Feel free to email me at [email protected].
Dr. Li is president of SHM.
For those of you who were kind enough to catch my column in last month’s issue of The Hospitalist (see “What Is Your Value,” p. 56), you spent a few minutes reading my thoughts on the value of hospitalists. I mentioned the fact that the U.S. is moving rapidly toward a value-based system of purchasing healthcare, and that all healthcare providers, including hospitalists, increasingly will be judged on the value of care they deliver to their patients and the healthcare system. (Remember, value=quality/cost.)
Hospitalists, like all other healthcare providers, can increase their “value” by improving the quality of care they provide and decreasing the cost of healthcare delivery. Seems simple enough, right? Take better care of patients and do so while minimizing unnecessary costs. (If you have figured out how to do this, I want to learn from you!)
As a doctor and as the leader of the hospitalist group at Beth Israel Deaconess Medical Center in Boston, I have given this topic considerable thought. How do I become a “high value” provider? How do I help my hospitalist colleagues become “high value” hospitalists? Another persistent thought that has crossed my mind is: “How do I know that I am not already a high-value hospitalist?”
Maybe all of my hospitalist colleagues at Beth Israel Deaconess Medical Center are high-value providers. Seems fair enough, right? Maybe each of us is providing “high quality” care and doing so while minimizing unnecessary costs.
I mean, who really wants to think of themselves as low-quality doctors spending a considerable amount of unnecessary resources?
Like many of you, it became evident to me that the first step to improving quality and/or decreasing cost is to define “quality” and “cost.”
The First Step
Although it might seem difficult for the individual hospitalist to know the cost of a patient’s hospitalization, such information is available, and your hospital administrator might be willing to share such information with you and your group. But when it comes to quality of care, I think most patients would expect that doctors should understand the definition of “high-quality care.”
So, what is the definition of “high-quality care?” Try asking this question of patients and doctors, and you are likely to get very different answers. Not surprised? Try asking this question just to doctors, and you are likely to get some different answers. (For fun, you could try this exercise with your hospitalist colleagues; I have.)
Honestly, none of us should be alarmed if a group of doctors cannot easily define “high-quality care.” Not being able to do so does not mean these are “bad” doctors. While it may not be easy to define high-quality care, I suspect most of us recognize it when we see it.
The process of defining the quality of care involves capturing the essence of what we see. For example, can we agree that prescribing aspirin for patients with acute coronary syndrome is optimal care? If so, it stands to reason that a patient with acute coronary syndrome who did not receive aspirin received suboptimal care.
This is how a group of hospitalists can go about creating a quality standard. If you are a hospitalist or HM group leader who is interested in improving the quality of care you and your colleagues are providing to your patients, defining a quality standard is the critical first step to process improvement. Do not limit yourself to clinical processes. Although clinical processes are important, so are communication and documentation processes.
For example, most of us, as hospitalists, believe that communication with outpatient providers is important to the provision of high-quality inpatient care. How often do your hospitalists communicate with patients’ primary-care providers? Is this a quality standard for your hospitalist group? What about the documentation of a patient’s code status at the time of admission or documentation of a patient’s functional status in the discharge summary?
If you believe these are important, your group should include these as quality standards. You should be measuring them and reporting the results to individual providers.
Start with Definition
At this point, some of us might be tempted to get ahead of ourselves and worry about what standards we can or cannot measure, but I urge you to complete this first step of defining “high-quality care” before worrying about anything else. (In other words, don’t start running before you can walk.)
Another suggestion: Please don’t try to do too much all at once. Nobody is going to argue that patients with acute coronary syndrome should not receive aspirin. Reaching consensus on other quality standards might not be as easy. But do not get bogged down trying to create too many quality standards all at once. Start with a few and get yourself and your colleagues accustomed to the process.
Remember, when it comes to doctors, we have centuries of history of not knowing exactly what we are doing. I hope it won’t take centuries to fix this problem, but I also know we are not going to fix this in a few days or weeks. Small victories along the way are important if we hope to succeed.
Once you and your hospitalist colleagues arrive at a mutually agreed upon quality standard, the next step is performance measurement. I honestly believe performance measurement is easy when we spend the time understanding and agreeing to the most appropriate quality standards for our hospitalist groups.
I am interested in learning about your efforts to define the quality standards for your hospitalist group. Feel free to email me at [email protected].
Dr. Li is president of SHM.
For those of you who were kind enough to catch my column in last month’s issue of The Hospitalist (see “What Is Your Value,” p. 56), you spent a few minutes reading my thoughts on the value of hospitalists. I mentioned the fact that the U.S. is moving rapidly toward a value-based system of purchasing healthcare, and that all healthcare providers, including hospitalists, increasingly will be judged on the value of care they deliver to their patients and the healthcare system. (Remember, value=quality/cost.)
Hospitalists, like all other healthcare providers, can increase their “value” by improving the quality of care they provide and decreasing the cost of healthcare delivery. Seems simple enough, right? Take better care of patients and do so while minimizing unnecessary costs. (If you have figured out how to do this, I want to learn from you!)
As a doctor and as the leader of the hospitalist group at Beth Israel Deaconess Medical Center in Boston, I have given this topic considerable thought. How do I become a “high value” provider? How do I help my hospitalist colleagues become “high value” hospitalists? Another persistent thought that has crossed my mind is: “How do I know that I am not already a high-value hospitalist?”
Maybe all of my hospitalist colleagues at Beth Israel Deaconess Medical Center are high-value providers. Seems fair enough, right? Maybe each of us is providing “high quality” care and doing so while minimizing unnecessary costs.
I mean, who really wants to think of themselves as low-quality doctors spending a considerable amount of unnecessary resources?
Like many of you, it became evident to me that the first step to improving quality and/or decreasing cost is to define “quality” and “cost.”
The First Step
Although it might seem difficult for the individual hospitalist to know the cost of a patient’s hospitalization, such information is available, and your hospital administrator might be willing to share such information with you and your group. But when it comes to quality of care, I think most patients would expect that doctors should understand the definition of “high-quality care.”
So, what is the definition of “high-quality care?” Try asking this question of patients and doctors, and you are likely to get very different answers. Not surprised? Try asking this question just to doctors, and you are likely to get some different answers. (For fun, you could try this exercise with your hospitalist colleagues; I have.)
Honestly, none of us should be alarmed if a group of doctors cannot easily define “high-quality care.” Not being able to do so does not mean these are “bad” doctors. While it may not be easy to define high-quality care, I suspect most of us recognize it when we see it.
The process of defining the quality of care involves capturing the essence of what we see. For example, can we agree that prescribing aspirin for patients with acute coronary syndrome is optimal care? If so, it stands to reason that a patient with acute coronary syndrome who did not receive aspirin received suboptimal care.
This is how a group of hospitalists can go about creating a quality standard. If you are a hospitalist or HM group leader who is interested in improving the quality of care you and your colleagues are providing to your patients, defining a quality standard is the critical first step to process improvement. Do not limit yourself to clinical processes. Although clinical processes are important, so are communication and documentation processes.
For example, most of us, as hospitalists, believe that communication with outpatient providers is important to the provision of high-quality inpatient care. How often do your hospitalists communicate with patients’ primary-care providers? Is this a quality standard for your hospitalist group? What about the documentation of a patient’s code status at the time of admission or documentation of a patient’s functional status in the discharge summary?
If you believe these are important, your group should include these as quality standards. You should be measuring them and reporting the results to individual providers.
Start with Definition
At this point, some of us might be tempted to get ahead of ourselves and worry about what standards we can or cannot measure, but I urge you to complete this first step of defining “high-quality care” before worrying about anything else. (In other words, don’t start running before you can walk.)
Another suggestion: Please don’t try to do too much all at once. Nobody is going to argue that patients with acute coronary syndrome should not receive aspirin. Reaching consensus on other quality standards might not be as easy. But do not get bogged down trying to create too many quality standards all at once. Start with a few and get yourself and your colleagues accustomed to the process.
Remember, when it comes to doctors, we have centuries of history of not knowing exactly what we are doing. I hope it won’t take centuries to fix this problem, but I also know we are not going to fix this in a few days or weeks. Small victories along the way are important if we hope to succeed.
Once you and your hospitalist colleagues arrive at a mutually agreed upon quality standard, the next step is performance measurement. I honestly believe performance measurement is easy when we spend the time understanding and agreeing to the most appropriate quality standards for our hospitalist groups.
I am interested in learning about your efforts to define the quality standards for your hospitalist group. Feel free to email me at [email protected].
Dr. Li is president of SHM.
The Tablet Revolution
In his June 3 blog post at CIO.com, Tom Kaneshige asks: “Can the iPad cure what ails us?” He goes on to describe new applications for iPads in Texas hospitals, including the remote monitoring of patients’ EKGs by nurses roaming the hospital.
“The big revolution in tablet computing for hospitalists, which has been right around the corner for the past decade, hasn’t quite arrived yet,” says Russ Cucina, MD, MS, hospitalist and medical director of information technology at the University of California San Francisco Medical Center. “But I think we’re getting close, even though I’m not convinced that the iPad will be the vehicle.”
One of the hallmarks of such a technological revolution will be to free up hospitalists and other workers from computer work stations, where they are increasingly removed from face-to-face interactions. “Something gets lost in the name of efficiency,” Dr. Cucina says.
Hurdles to the tablet revolution include:
- Short battery life and the lack of rechargeable batteries. “Doctors need to be on the floor longer than eight hours,” Dr. Cucina says.
- Interacting with a tablet using thumbs and a touchscreen is fundamentally different from using a laptop, and applications should recognize the differences.
- Wireless access to secure electronic health records (EHR) throughout the hospital. “This is more of a cost issue than a technical problem,” Dr. Cucina explains. “It’s also incumbent upon us as physicians to develop good security practices with our tablets.”
- The skills to use the screen in the presence of others—in other words, What is the proper etiquette in front of care team members, patients, their families, etc.?
Hospitalists Look to Partner with New Quality Institute
Don’t be surprised if HM eventually gets a piece of the new Armstrong Institute for Patient Safety and Quality at Johns Hopkins University School of Medicine in Baltimore.
The center, funded through a $10 million gift from Johns Hopkins Medicine board of trustees chairman C. Michael Armstrong, will become the umbrella arm in charge of reducing preventable harm and improving healthcare quality.
Eric Howell, MD, SFHM, associate professor of medicine at Johns Hopkins University and director of Johns Hopkins Bayview Medical Center’s HM division, already sees that as hospitalist turf and could easily see HM partnering with the new institute. Dr. Howell, who already has reached out to the institute’s head, checklist guru Peter Pronovost, MD, PhD, wrote in an email to The Hospitalist: “Hospitalists at Hopkins have a long tradition of exactly this type of work.”
Dr. Howell points to recent HM-driven research and initiatives to reduce “red alerts,” the term for ambulance diversions in the ICU, and streamlining the admission process to allow outpatient doctors to bypass the ED for patients for whom hospitalist admission is needed. At Howard County General Hospital, a suburb about 15 miles southwest of Baltimore, the HM group is running all rapid response team (RRT) events.
“In short,” Dr. Howell writes, “the Armstrong Institute will find hospitalists to be a willing partner.”
Hospitalists Must Prepare for Primary-Care Shortfalls
The Milwaukee-based American Society for Quality (ASQ) recently surveyed healthcare quality professionals about anticipated shortages of primary-care physicians (PCPs) and other medical staff, particularly as more Americans gain health insurance under the Accountable Care Act and Medicare). The trend is real, says Joseph Fortuna, MD, chair of ASQ’s Health Care Division, and hospitalists will face challenges in discharging patients who lack a defined PCP.
Survey respondents highlighted some strategies for dealing with the primary-care shortage, including the EHR for improving efficiency, teamwork, and checklists. Dr. Fortuna suggests HM groups:
- Work with PCPs and federally qualified health centers to enhance integrated relationships and improve handoffs. Local public health departments will be important collaborators.
- Define quality not just clinically, but also in terms of financial, operational, and cultural domains, using techniques of change management, root cause analysis, and other quality tools.
- Be involved in patient-centered medical homes as “catalysts, coordinators, and facilitators.”
HM Group Redesigns Workflow to Comply with ACGME Rules and Improve Continuity
As academic HM groups react to the new Accreditation Council for Graduation Medical Education (ACGME) guidelines on how long residents can work, they might want to keep the Toyota Production System (TPS) in mind.
Diana Mancini, MD, a hospitalist at Denver Health Medical Center and associate program director of the University of Colorado Internal Medicine Residency, presented data in the Research, Innovations, and Clinical Vignettes competition at HM11 that showed how the use of continuous workflow and standardized tasks—hallmarks of TPS—helped redesign the medicine ward system to both comply with the ACGME rules and improve continuity of care.
The project replaced the traditional call system, and its corresponding floats and moonlighters, with a shift system comprised of two teams of six interns and three residents. At night, one intern worked a “continuity shift.” Using administrative data, Dr. Mancini and colleagues projected that 89% of patients admitted on a continuity shift would be discharged by the end of that intern’s five consecutive shifts. And, by dividing admissions among two teams, the “bolus” effect was halved, she says.
“The continuity shift is crucial for both the patient safety/continuity and educational content/value for the housestaff,” Dr. Mancini wrote in an email. “With the new work hours coming ... the hours would have to be adjusted … but the continuity could most certainly be maintained.”
Feds Delay Deadline for Stage 2 “Meaningful Use” Application Process
If your HM group is among the first cohort that reaches Stage 1 attestation this year for meaningful use of electronic health records (EHR), you may get more time to reach Stage 2. The federal Health Information Technology (HIT) policy committee has voted for a 12-month delay in implementing the criteria for that second stage, agreeing with those who say the current deadline of October 2013 “poses a nearly insurmountable timing challenge.”
The HIT is pushing to delay the deadline until 2014, which would mean providers have three years to verify that they have met Stage 1 meaningful use requirements, according to Government HealthIT. A cadre of medical trade groups, led by the AMA, is now pushing the Department of Health and Human Services to adopt the new timeline.
The ultimate decision rests with the Centers for Medicaid & Medicare Services (CMS).
By the numbers
Number of months without a central-line-associated bloodstream infection (BSI) on the eight-bed ICU at Beaufort Memorial Hospital, a 197-bed community hospital in Beaufort, S.C.
The hospital, which had a higher rate of BSIs than the national average in 2005, created a team to reduce its BSIs, led by infection-prevention specialist Beverly Yoder, RN, and involving hospitalists. Beaufort joined the Institute for Healthcare Improvement’s 100K Lives Campaign and the South Carolina Hospital Association’s Stop BSI Project.
The team implemented a central-line “bundle” of quality practices, then simplified the bundle and incorporated it into its EHR. The unit celebrated its 30-month achievement with a luncheon in June.
For information, contact critical-care director Diane Razo, RN, MSN, PCCN, at [email protected]. (For more information about central-line infection prevention, visit SHM's Resource Room (www.hospitalmedicine.org/resource)
In his June 3 blog post at CIO.com, Tom Kaneshige asks: “Can the iPad cure what ails us?” He goes on to describe new applications for iPads in Texas hospitals, including the remote monitoring of patients’ EKGs by nurses roaming the hospital.
“The big revolution in tablet computing for hospitalists, which has been right around the corner for the past decade, hasn’t quite arrived yet,” says Russ Cucina, MD, MS, hospitalist and medical director of information technology at the University of California San Francisco Medical Center. “But I think we’re getting close, even though I’m not convinced that the iPad will be the vehicle.”
One of the hallmarks of such a technological revolution will be to free up hospitalists and other workers from computer work stations, where they are increasingly removed from face-to-face interactions. “Something gets lost in the name of efficiency,” Dr. Cucina says.
Hurdles to the tablet revolution include:
- Short battery life and the lack of rechargeable batteries. “Doctors need to be on the floor longer than eight hours,” Dr. Cucina says.
- Interacting with a tablet using thumbs and a touchscreen is fundamentally different from using a laptop, and applications should recognize the differences.
- Wireless access to secure electronic health records (EHR) throughout the hospital. “This is more of a cost issue than a technical problem,” Dr. Cucina explains. “It’s also incumbent upon us as physicians to develop good security practices with our tablets.”
- The skills to use the screen in the presence of others—in other words, What is the proper etiquette in front of care team members, patients, their families, etc.?
Hospitalists Look to Partner with New Quality Institute
Don’t be surprised if HM eventually gets a piece of the new Armstrong Institute for Patient Safety and Quality at Johns Hopkins University School of Medicine in Baltimore.
The center, funded through a $10 million gift from Johns Hopkins Medicine board of trustees chairman C. Michael Armstrong, will become the umbrella arm in charge of reducing preventable harm and improving healthcare quality.
Eric Howell, MD, SFHM, associate professor of medicine at Johns Hopkins University and director of Johns Hopkins Bayview Medical Center’s HM division, already sees that as hospitalist turf and could easily see HM partnering with the new institute. Dr. Howell, who already has reached out to the institute’s head, checklist guru Peter Pronovost, MD, PhD, wrote in an email to The Hospitalist: “Hospitalists at Hopkins have a long tradition of exactly this type of work.”
Dr. Howell points to recent HM-driven research and initiatives to reduce “red alerts,” the term for ambulance diversions in the ICU, and streamlining the admission process to allow outpatient doctors to bypass the ED for patients for whom hospitalist admission is needed. At Howard County General Hospital, a suburb about 15 miles southwest of Baltimore, the HM group is running all rapid response team (RRT) events.
“In short,” Dr. Howell writes, “the Armstrong Institute will find hospitalists to be a willing partner.”
Hospitalists Must Prepare for Primary-Care Shortfalls
The Milwaukee-based American Society for Quality (ASQ) recently surveyed healthcare quality professionals about anticipated shortages of primary-care physicians (PCPs) and other medical staff, particularly as more Americans gain health insurance under the Accountable Care Act and Medicare). The trend is real, says Joseph Fortuna, MD, chair of ASQ’s Health Care Division, and hospitalists will face challenges in discharging patients who lack a defined PCP.
Survey respondents highlighted some strategies for dealing with the primary-care shortage, including the EHR for improving efficiency, teamwork, and checklists. Dr. Fortuna suggests HM groups:
- Work with PCPs and federally qualified health centers to enhance integrated relationships and improve handoffs. Local public health departments will be important collaborators.
- Define quality not just clinically, but also in terms of financial, operational, and cultural domains, using techniques of change management, root cause analysis, and other quality tools.
- Be involved in patient-centered medical homes as “catalysts, coordinators, and facilitators.”
HM Group Redesigns Workflow to Comply with ACGME Rules and Improve Continuity
As academic HM groups react to the new Accreditation Council for Graduation Medical Education (ACGME) guidelines on how long residents can work, they might want to keep the Toyota Production System (TPS) in mind.
Diana Mancini, MD, a hospitalist at Denver Health Medical Center and associate program director of the University of Colorado Internal Medicine Residency, presented data in the Research, Innovations, and Clinical Vignettes competition at HM11 that showed how the use of continuous workflow and standardized tasks—hallmarks of TPS—helped redesign the medicine ward system to both comply with the ACGME rules and improve continuity of care.
The project replaced the traditional call system, and its corresponding floats and moonlighters, with a shift system comprised of two teams of six interns and three residents. At night, one intern worked a “continuity shift.” Using administrative data, Dr. Mancini and colleagues projected that 89% of patients admitted on a continuity shift would be discharged by the end of that intern’s five consecutive shifts. And, by dividing admissions among two teams, the “bolus” effect was halved, she says.
“The continuity shift is crucial for both the patient safety/continuity and educational content/value for the housestaff,” Dr. Mancini wrote in an email. “With the new work hours coming ... the hours would have to be adjusted … but the continuity could most certainly be maintained.”
Feds Delay Deadline for Stage 2 “Meaningful Use” Application Process
If your HM group is among the first cohort that reaches Stage 1 attestation this year for meaningful use of electronic health records (EHR), you may get more time to reach Stage 2. The federal Health Information Technology (HIT) policy committee has voted for a 12-month delay in implementing the criteria for that second stage, agreeing with those who say the current deadline of October 2013 “poses a nearly insurmountable timing challenge.”
The HIT is pushing to delay the deadline until 2014, which would mean providers have three years to verify that they have met Stage 1 meaningful use requirements, according to Government HealthIT. A cadre of medical trade groups, led by the AMA, is now pushing the Department of Health and Human Services to adopt the new timeline.
The ultimate decision rests with the Centers for Medicaid & Medicare Services (CMS).
By the numbers
Number of months without a central-line-associated bloodstream infection (BSI) on the eight-bed ICU at Beaufort Memorial Hospital, a 197-bed community hospital in Beaufort, S.C.
The hospital, which had a higher rate of BSIs than the national average in 2005, created a team to reduce its BSIs, led by infection-prevention specialist Beverly Yoder, RN, and involving hospitalists. Beaufort joined the Institute for Healthcare Improvement’s 100K Lives Campaign and the South Carolina Hospital Association’s Stop BSI Project.
The team implemented a central-line “bundle” of quality practices, then simplified the bundle and incorporated it into its EHR. The unit celebrated its 30-month achievement with a luncheon in June.
For information, contact critical-care director Diane Razo, RN, MSN, PCCN, at [email protected]. (For more information about central-line infection prevention, visit SHM's Resource Room (www.hospitalmedicine.org/resource)
In his June 3 blog post at CIO.com, Tom Kaneshige asks: “Can the iPad cure what ails us?” He goes on to describe new applications for iPads in Texas hospitals, including the remote monitoring of patients’ EKGs by nurses roaming the hospital.
“The big revolution in tablet computing for hospitalists, which has been right around the corner for the past decade, hasn’t quite arrived yet,” says Russ Cucina, MD, MS, hospitalist and medical director of information technology at the University of California San Francisco Medical Center. “But I think we’re getting close, even though I’m not convinced that the iPad will be the vehicle.”
One of the hallmarks of such a technological revolution will be to free up hospitalists and other workers from computer work stations, where they are increasingly removed from face-to-face interactions. “Something gets lost in the name of efficiency,” Dr. Cucina says.
Hurdles to the tablet revolution include:
- Short battery life and the lack of rechargeable batteries. “Doctors need to be on the floor longer than eight hours,” Dr. Cucina says.
- Interacting with a tablet using thumbs and a touchscreen is fundamentally different from using a laptop, and applications should recognize the differences.
- Wireless access to secure electronic health records (EHR) throughout the hospital. “This is more of a cost issue than a technical problem,” Dr. Cucina explains. “It’s also incumbent upon us as physicians to develop good security practices with our tablets.”
- The skills to use the screen in the presence of others—in other words, What is the proper etiquette in front of care team members, patients, their families, etc.?
Hospitalists Look to Partner with New Quality Institute
Don’t be surprised if HM eventually gets a piece of the new Armstrong Institute for Patient Safety and Quality at Johns Hopkins University School of Medicine in Baltimore.
The center, funded through a $10 million gift from Johns Hopkins Medicine board of trustees chairman C. Michael Armstrong, will become the umbrella arm in charge of reducing preventable harm and improving healthcare quality.
Eric Howell, MD, SFHM, associate professor of medicine at Johns Hopkins University and director of Johns Hopkins Bayview Medical Center’s HM division, already sees that as hospitalist turf and could easily see HM partnering with the new institute. Dr. Howell, who already has reached out to the institute’s head, checklist guru Peter Pronovost, MD, PhD, wrote in an email to The Hospitalist: “Hospitalists at Hopkins have a long tradition of exactly this type of work.”
Dr. Howell points to recent HM-driven research and initiatives to reduce “red alerts,” the term for ambulance diversions in the ICU, and streamlining the admission process to allow outpatient doctors to bypass the ED for patients for whom hospitalist admission is needed. At Howard County General Hospital, a suburb about 15 miles southwest of Baltimore, the HM group is running all rapid response team (RRT) events.
“In short,” Dr. Howell writes, “the Armstrong Institute will find hospitalists to be a willing partner.”
Hospitalists Must Prepare for Primary-Care Shortfalls
The Milwaukee-based American Society for Quality (ASQ) recently surveyed healthcare quality professionals about anticipated shortages of primary-care physicians (PCPs) and other medical staff, particularly as more Americans gain health insurance under the Accountable Care Act and Medicare). The trend is real, says Joseph Fortuna, MD, chair of ASQ’s Health Care Division, and hospitalists will face challenges in discharging patients who lack a defined PCP.
Survey respondents highlighted some strategies for dealing with the primary-care shortage, including the EHR for improving efficiency, teamwork, and checklists. Dr. Fortuna suggests HM groups:
- Work with PCPs and federally qualified health centers to enhance integrated relationships and improve handoffs. Local public health departments will be important collaborators.
- Define quality not just clinically, but also in terms of financial, operational, and cultural domains, using techniques of change management, root cause analysis, and other quality tools.
- Be involved in patient-centered medical homes as “catalysts, coordinators, and facilitators.”
HM Group Redesigns Workflow to Comply with ACGME Rules and Improve Continuity
As academic HM groups react to the new Accreditation Council for Graduation Medical Education (ACGME) guidelines on how long residents can work, they might want to keep the Toyota Production System (TPS) in mind.
Diana Mancini, MD, a hospitalist at Denver Health Medical Center and associate program director of the University of Colorado Internal Medicine Residency, presented data in the Research, Innovations, and Clinical Vignettes competition at HM11 that showed how the use of continuous workflow and standardized tasks—hallmarks of TPS—helped redesign the medicine ward system to both comply with the ACGME rules and improve continuity of care.
The project replaced the traditional call system, and its corresponding floats and moonlighters, with a shift system comprised of two teams of six interns and three residents. At night, one intern worked a “continuity shift.” Using administrative data, Dr. Mancini and colleagues projected that 89% of patients admitted on a continuity shift would be discharged by the end of that intern’s five consecutive shifts. And, by dividing admissions among two teams, the “bolus” effect was halved, she says.
“The continuity shift is crucial for both the patient safety/continuity and educational content/value for the housestaff,” Dr. Mancini wrote in an email. “With the new work hours coming ... the hours would have to be adjusted … but the continuity could most certainly be maintained.”
Feds Delay Deadline for Stage 2 “Meaningful Use” Application Process
If your HM group is among the first cohort that reaches Stage 1 attestation this year for meaningful use of electronic health records (EHR), you may get more time to reach Stage 2. The federal Health Information Technology (HIT) policy committee has voted for a 12-month delay in implementing the criteria for that second stage, agreeing with those who say the current deadline of October 2013 “poses a nearly insurmountable timing challenge.”
The HIT is pushing to delay the deadline until 2014, which would mean providers have three years to verify that they have met Stage 1 meaningful use requirements, according to Government HealthIT. A cadre of medical trade groups, led by the AMA, is now pushing the Department of Health and Human Services to adopt the new timeline.
The ultimate decision rests with the Centers for Medicaid & Medicare Services (CMS).
By the numbers
Number of months without a central-line-associated bloodstream infection (BSI) on the eight-bed ICU at Beaufort Memorial Hospital, a 197-bed community hospital in Beaufort, S.C.
The hospital, which had a higher rate of BSIs than the national average in 2005, created a team to reduce its BSIs, led by infection-prevention specialist Beverly Yoder, RN, and involving hospitalists. Beaufort joined the Institute for Healthcare Improvement’s 100K Lives Campaign and the South Carolina Hospital Association’s Stop BSI Project.
The team implemented a central-line “bundle” of quality practices, then simplified the bundle and incorporated it into its EHR. The unit celebrated its 30-month achievement with a luncheon in June.
For information, contact critical-care director Diane Razo, RN, MSN, PCCN, at [email protected]. (For more information about central-line infection prevention, visit SHM's Resource Room (www.hospitalmedicine.org/resource)
How Do I Determine if My Patient has Decision-Making Capacity?
Case
A 79-year-old male with coronary artery disease, hypertension, non-insulin-dependent mellitus, moderate dementia, and chronic renal insufficiency is admitted after a fall evaluation. He is widowed and lives in an assisted living facility. He’s accompanied by his niece, is alert, and oriented to person. He thinks he is in a clinic and is unable to state the year, but the remainder of the examination is unremarkable. His labs are notable for potassium of 6.3 mmol/L, BUN of 78 mg/dL, and Cr of 3.7 mg/dL. The niece reports that the patient is not fond of medical care, thus the most recent labs are from two years ago (and indicate a BUN of 39 and Cr of 2.8, with an upward trend over the past decade). You discuss possible long-term need for dialysis with the patient and niece, and the patient clearly states "no." However, he also states that it is 1988. How do you determine if he has the capacity to make decisions?
Overview
Hospitalists are familiar with the doctrine of informed consent—describing a disease, treatment options, associated risks and benefits, potential for complications, and alternatives, including no treatment. Not only must the patient be informed, and the decision free from any coercion, but the patient also must have capacity to make the decision.
Hospitalists often care for patients in whom decision-making capacity comes into question. This includes populations with depression, psychosis, dementia, stroke, severe personality disorders, developmental delay, comatose patients, as well as those with impaired attentional capacity (e.g. acute pain) or general debility (e.g. metastatic cancer).1,2
ave for the comatose patient, whether the patient has capacity might not be obvious. However, addressing the components of capacity (communication, understanding, appreciation, and rationalization) by using a validated clinical tool, such as the MacCAT-T, or more simply by systematically applying those four components to the clinical scenario under consideration, hospitalists can make this determination.
Review of the Literature
It is important to differentiate capacity from competency. Competency is a global assessment and a legal determination made by a judge in court. Capacity, on the other hand, is a functional assessment regarding a particular decision. Capacity is not static, and it can be performed by any clinician familiar with the patient. A hospitalist often is well positioned to make a capacity determination given established rapport with the patient and familiarity with the details of the case.
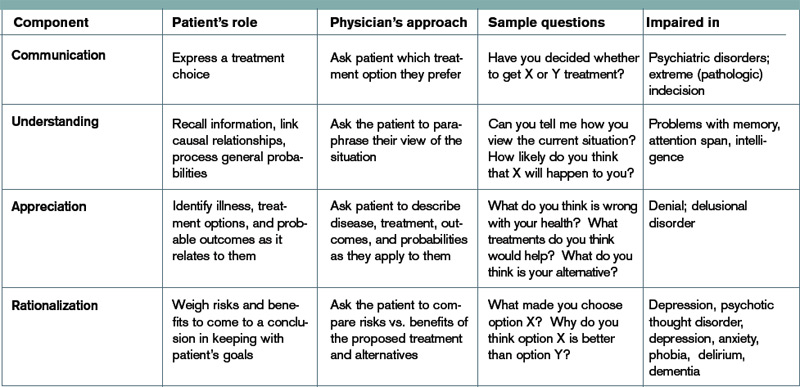
To make this determination, a hospitalist needs to know how to assess capacity. Although capacity usually is defined by state law and varies by jurisdiction, clinicians generally can assume it includes one or more of the four key components:
- Communication. The patient needs to be able to express a treatment choice, and this decision needs to be stable enough for the treatment to be implemented. Changing one’s decision in itself would not bring a patient’s capacity into question, so long as the patient was able to explain the rationale behind the switch. Frequent changes back and forth in the decision-making, however, could be indicative of an underlying psychiatric disorder or extreme indecision, which could bring capacity into question.
- Understanding. The patient needs to recall conversations about treatment, to make the link between causal relationships, and to process probabilities for outcomes. Problems with memory, attention span, and intelligence can affect one’s understanding.
- Appreciation. The patient should be able to identify the illness, treatment options, and likely outcomes as things that will affect him or her directly. A lack of appreciation usually stems from a denial based on intelligence (lack of a capability to understand) or emotion, or a delusion that the patient is not affected by this situation the same way and will have a different outcome.
- Rationalization or reasoning. The patient needs to be able to weigh the risks and benefits of the treatment options presented to come to a conclusion in keeping with their goals and best interests, as defined by their personal set of values. This often is affected in psychosis, depression, anxiety, phobias, delirium, and dementia.3
Several clinical capacity tools have been developed to assess these components:
Clinical tools.
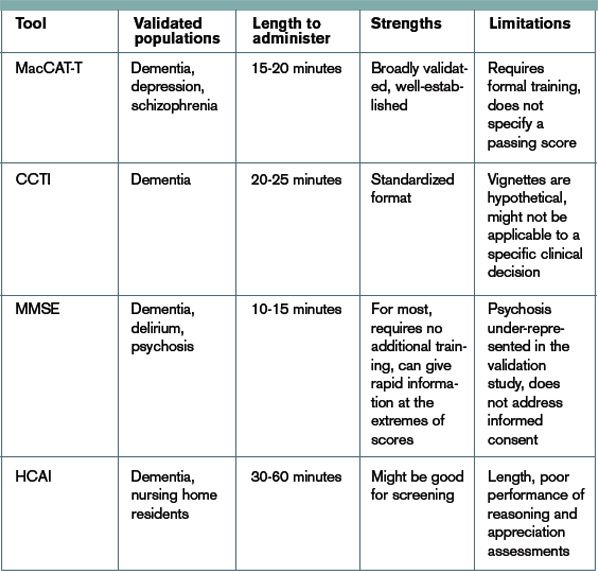
The Mini-Mental Status Examination (MMSE) is a bedside test of a patient’s cognitive function, with scores ranging from 0 to 30.4 Although it wasn’t developed for assessing decision-making capacity, it has been compared with expert evaluation for assessment of capacity; the test performs reasonably well, particularly with high and low scores. Specifically, a MMSE >24 has a negative likelihood ratio (LR) of 0.05 for lack of capacity, while a MMSE <16 has a positive LR of 15.5 Scores from 17 to 23 do not correlate well with capacity, and further testing would be necessary. It is easy to administer, requires no formal training, and is familiar to most hospitalists. However, it does not address any specific aspects of informed consent, such as understanding or choice, and has not been validated in patients with mental illness.
The MacArthur Competence Assessment Tools for Treatment (MacCAT-T) is regarded as the gold standard for capacity assessment aids. It utilizes hospital chart review followed by a semi-structured interview to address clinical issues relevant to the patient being assessed; it takes 15 to 20 minutes to complete.6 The test provides scores in each of the four domains (choice, understanding, appreciation, and reasoning) of capacity. It has been validated in patients with dementia, schizophrenia, and depression. Limiting its clinical applicability is the fact that the MacCAT-T requires training to administer and interpret the results, though this is a relatively brief process.
The Capacity to Consent to Treatment Instrument (CCTI) uses hypothetical clinical vignettes in a structured interview to assess capacity across all four domains. The tool was developed and validated in patients with dementia and Parkinson’s disease, and takes 20 to 25 minutes to complete.7 A potential limitation is the CCTI’s use of vignettes as opposed to a patient-specific discussion, which could lead to different patient answers and a false assessment of the patient’s capacity.
The Hopemont Capacity Assessment Interview (HCAI) utilizes hypothetical vignettes in a semi-structured interview format to assess understanding, appreciation, choice, and likely reasoning.8,9 Similar to CCTI, HCAI is not modified for individual patients. Rather, it uses clinical vignettes to gauge a patient’s ability to make decisions. The test takes 30 to 60 minutes to administer and performs less well in assessing appreciation and reasoning than the MacCAT-T and CCTI.10
It is not necessary to perform a formal assessment of capacity on every inpatient. For most, there is no reasonable concern for impaired capacity, obviating the need for formal testing. Likewise, in patients who clearly lack capacity, such as those with end-stage dementia or established guardians, formal reassessment usually is not required. Formal testing is most useful in situations in which capacity is unclear, disagreement amongst surrogate decision-makers exists, or judicial involvement is anticipated.
The MacCAT-T has been validated in the broadest population and is probably the most clinically useful tool currently available. The MMSE is an attractive alternative because of its widespread use and familiarity; however, it is imprecise with scores from 17 to 23, limiting its applicability.
At a minimum, familiarity with the core legal standards of capacity (communication of choice, understanding, appreciation, and reasoning) will improve a hospitalist’s ability to identify patients who lack capacity. Understanding and applying the defined markers most often provides a sufficient capacity evaluation in itself. As capacity is not static, the decision usually requires more than one assessment.
Equally, deciding that a patient lacks capacity is not an end in itself, and the underlying cause should be addressed. Certain factors, such as infection, medication, time of day, and relationship with the clinician doing the assessment, can affect a patient’s capacity. These should be addressed through treatment, education, and social support whenever possible in order to optimize a patient’s performance during the capacity evaluation. If the decision can be delayed until a time when the patient can regain capacity, this should be done in order to maximize the patient’s autonomy.11
Risk-related standards of capacity.
Although some question the notion, given our desire to facilitate management beneficial to the patient, the general consensus is that we have a lower threshold for capacity for consent to treatments that are low-risk and high-benefit.12,13 We would then have a somewhat higher threshold for capacity to refuse that same treatment. Stemming from a desire to protect patients from harm, we have a relatively higher threshold for capacity to make decisions regarding high-risk, low-benefit treatments. For the remainder of cases (low risk/low benefit; high risk/high benefit), as well as treatments that significantly impact a patient’s lifestyle (e.g. dialysis, amputation), we have a low capacity to let patients decide for themselves.11,14
Other considerations.
Clinicians should be thorough in documenting details in coming to a capacity determination, both as a means to formalize the thought process running through the four determinants of capacity, and in order to document for future reference. Cases in which it could be reasonable to call a consultant for those familiar with the assessment basics include:
- Cases in which a determination of lack of capacity could adversely affect the hospitalist’s relationship with the patient;
- Cases in which the hospitalist lacks the time to properly perform the evaluation;
- Particularly difficult or high-stakes cases (e.g. cases that might involve legal proceedings); and
- Cases in which significant mental illness affects a patient’s capacity.11
Early involvement of potential surrogate decision-makers is wise for patients in whom capacity is questioned, both for obtaining collateral history as well as initiating dialogue as to the patient’s wishes. When a patient is found to lack capacity, resources to utilize to help make a treatment decision include existing advance directives and substitute decision-makers, such as durable power of attorneys (DPOAs) and family members. In those rare cases in which clinicians are unable to reach a consensus about a patient’s capacity, an ethics consult should be considered.
Back to the Case.
Following the patient’s declaration that dialysis is not something he is interested in, his niece reports that he is a minimalist when it comes to interventions, and that he had similarly refused a cardiac catheterization in the 1990s. You review with the patient and niece that dialysis would be a procedure to replace his failing kidney function, and that failure to pursue this would ultimately be life-threatening and likely result in death, especially in regard to electrolyte abnormalities and his lack of any other terminal illness.
The consulting nephrologist reviews their recommendations with the patient and niece as well, and the patient consistently refuses. Having clearly communicated his choice, you ask the patient if he understands the situation. He says, "My kidneys are failing. That’s how I got the high potassium." You ask him what that means. "They aren’t going to function on their own much longer," he says. "I could die from it."
You confirm his ideas, and ask him why he doesn’t want dialysis. "I don’t want dialysis because I don’t want to spend my life hooked up to machines three times a week," the patient explains. "I just want to let things run their natural course." The niece says her uncle wouldn’t have wanted dialysis even if it were 10 years ago, so she’s not surprised he is refusing now.
Following this discussion, you feel comfortable that the patient has capacity to make this decision. Having documented this discussion, you discharge him to a subacute rehabilitation facility.
Bottom Line.
In cases in which capacity is in question, a hospitalist’s case-by-case review of the four components of capacity—communicating a choice, understanding, appreciation, and rationalization and reasoning—is warranted to help determine whether a patient has capacity. In cases in which a second opinion is warranted, psychiatry, geriatrics, or ethics consults could be utilized.
Drs. Dastidar and Odden are hospitalists at the University of Michigan in Ann Arbor.
References
- Buchanan A, Brock DW. Deciding for others. Milbank Q. 1986;64(Suppl. 2):17-94.
- Guidelines for assessing the decision-making capacities of potential research subjects with cognitive impairment. American Psychiatric Association. Am J Psychiatry. 1998;155(11):1649-50.
- Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988;319(25):1635-1638.
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-198.
- Etchells E, Darzins P, Silberfeld M, et al. Assessment of patient capacity to consent to treatment. J Gen Intern Med. 1999;14:27-34.
- Grisso T, Appelbaum PS, Hill-Fotouhi C. The MacCAT-T: a clinical tool to assess patients’ capacities to make treatment decisions. Psychiatr Serv. 1997;48:1415- 1419.
- Marson DC, Ingram KK, Cody HA, Harrell LE. Assessing the competency of patients with Alzheimer’s disease under different legal standards. A prototype instrument. Arch Neurol. 1995;52:949-954.
- Edelstein B. Hopemont Capacity Assessment Interview Manual and Scoring Guide. 1999: Morgantown, W.V.: West Virginia University.
- Pruchno RA, Smyer MA, Rose MS, Hartman-Stein PE, Henderson-Laribee DL. Competence of long-term care residents to participate in decisions about their medical care: a brief, objective assessment. Gerontologist. 1995;35:622-629.
- Moye J, Karel M, Azar AR, Gurrera R. Capacity to consent to treatment: empirical comparison of three instruments in older adults with and without dementia. Gerontologist. 2004;44:166-175.
- Grisso T, Appelbaum PS. Assessing competence to consent to treatment: a guide for physicians and other health professionals. 1998; New York: Oxford University Press, 211.
- Cale GS. Risk-related standards of competence: continuing the debate over risk-related standards of competence. Bioethics. 1999;13(2):131-148.
- Checkland D. On risk and decisional capacity. J Med Philos. 2001;26(1):35-59.
- Wilks I. The debate over risk-related standards of competence. Bioethics. 1997;11(5):413-426.
- Ganzini L, Volicer L, Nelson WA, Fox E, Derse AR. Ten myths about decision-making capacity. J Am Med Dir Assoc. 2004;5(4):263-267.
Acknowledgements:The authors would like to thank Dr. Jeff Rohde for reviewing a copy of the manuscript, and Dr. Amy Rosinski for providing direction from the psychiatry standpoint
Case
A 79-year-old male with coronary artery disease, hypertension, non-insulin-dependent mellitus, moderate dementia, and chronic renal insufficiency is admitted after a fall evaluation. He is widowed and lives in an assisted living facility. He’s accompanied by his niece, is alert, and oriented to person. He thinks he is in a clinic and is unable to state the year, but the remainder of the examination is unremarkable. His labs are notable for potassium of 6.3 mmol/L, BUN of 78 mg/dL, and Cr of 3.7 mg/dL. The niece reports that the patient is not fond of medical care, thus the most recent labs are from two years ago (and indicate a BUN of 39 and Cr of 2.8, with an upward trend over the past decade). You discuss possible long-term need for dialysis with the patient and niece, and the patient clearly states "no." However, he also states that it is 1988. How do you determine if he has the capacity to make decisions?
Overview
Hospitalists are familiar with the doctrine of informed consent—describing a disease, treatment options, associated risks and benefits, potential for complications, and alternatives, including no treatment. Not only must the patient be informed, and the decision free from any coercion, but the patient also must have capacity to make the decision.
Hospitalists often care for patients in whom decision-making capacity comes into question. This includes populations with depression, psychosis, dementia, stroke, severe personality disorders, developmental delay, comatose patients, as well as those with impaired attentional capacity (e.g. acute pain) or general debility (e.g. metastatic cancer).1,2
ave for the comatose patient, whether the patient has capacity might not be obvious. However, addressing the components of capacity (communication, understanding, appreciation, and rationalization) by using a validated clinical tool, such as the MacCAT-T, or more simply by systematically applying those four components to the clinical scenario under consideration, hospitalists can make this determination.
Review of the Literature
It is important to differentiate capacity from competency. Competency is a global assessment and a legal determination made by a judge in court. Capacity, on the other hand, is a functional assessment regarding a particular decision. Capacity is not static, and it can be performed by any clinician familiar with the patient. A hospitalist often is well positioned to make a capacity determination given established rapport with the patient and familiarity with the details of the case.
To make this determination, a hospitalist needs to know how to assess capacity. Although capacity usually is defined by state law and varies by jurisdiction, clinicians generally can assume it includes one or more of the four key components:
- Communication. The patient needs to be able to express a treatment choice, and this decision needs to be stable enough for the treatment to be implemented. Changing one’s decision in itself would not bring a patient’s capacity into question, so long as the patient was able to explain the rationale behind the switch. Frequent changes back and forth in the decision-making, however, could be indicative of an underlying psychiatric disorder or extreme indecision, which could bring capacity into question.
- Understanding. The patient needs to recall conversations about treatment, to make the link between causal relationships, and to process probabilities for outcomes. Problems with memory, attention span, and intelligence can affect one’s understanding.
- Appreciation. The patient should be able to identify the illness, treatment options, and likely outcomes as things that will affect him or her directly. A lack of appreciation usually stems from a denial based on intelligence (lack of a capability to understand) or emotion, or a delusion that the patient is not affected by this situation the same way and will have a different outcome.
- Rationalization or reasoning. The patient needs to be able to weigh the risks and benefits of the treatment options presented to come to a conclusion in keeping with their goals and best interests, as defined by their personal set of values. This often is affected in psychosis, depression, anxiety, phobias, delirium, and dementia.3
Several clinical capacity tools have been developed to assess these components:
Clinical tools.
The Mini-Mental Status Examination (MMSE) is a bedside test of a patient’s cognitive function, with scores ranging from 0 to 30.4 Although it wasn’t developed for assessing decision-making capacity, it has been compared with expert evaluation for assessment of capacity; the test performs reasonably well, particularly with high and low scores. Specifically, a MMSE >24 has a negative likelihood ratio (LR) of 0.05 for lack of capacity, while a MMSE <16 has a positive LR of 15.5 Scores from 17 to 23 do not correlate well with capacity, and further testing would be necessary. It is easy to administer, requires no formal training, and is familiar to most hospitalists. However, it does not address any specific aspects of informed consent, such as understanding or choice, and has not been validated in patients with mental illness.
The MacArthur Competence Assessment Tools for Treatment (MacCAT-T) is regarded as the gold standard for capacity assessment aids. It utilizes hospital chart review followed by a semi-structured interview to address clinical issues relevant to the patient being assessed; it takes 15 to 20 minutes to complete.6 The test provides scores in each of the four domains (choice, understanding, appreciation, and reasoning) of capacity. It has been validated in patients with dementia, schizophrenia, and depression. Limiting its clinical applicability is the fact that the MacCAT-T requires training to administer and interpret the results, though this is a relatively brief process.
The Capacity to Consent to Treatment Instrument (CCTI) uses hypothetical clinical vignettes in a structured interview to assess capacity across all four domains. The tool was developed and validated in patients with dementia and Parkinson’s disease, and takes 20 to 25 minutes to complete.7 A potential limitation is the CCTI’s use of vignettes as opposed to a patient-specific discussion, which could lead to different patient answers and a false assessment of the patient’s capacity.
The Hopemont Capacity Assessment Interview (HCAI) utilizes hypothetical vignettes in a semi-structured interview format to assess understanding, appreciation, choice, and likely reasoning.8,9 Similar to CCTI, HCAI is not modified for individual patients. Rather, it uses clinical vignettes to gauge a patient’s ability to make decisions. The test takes 30 to 60 minutes to administer and performs less well in assessing appreciation and reasoning than the MacCAT-T and CCTI.10
It is not necessary to perform a formal assessment of capacity on every inpatient. For most, there is no reasonable concern for impaired capacity, obviating the need for formal testing. Likewise, in patients who clearly lack capacity, such as those with end-stage dementia or established guardians, formal reassessment usually is not required. Formal testing is most useful in situations in which capacity is unclear, disagreement amongst surrogate decision-makers exists, or judicial involvement is anticipated.
The MacCAT-T has been validated in the broadest population and is probably the most clinically useful tool currently available. The MMSE is an attractive alternative because of its widespread use and familiarity; however, it is imprecise with scores from 17 to 23, limiting its applicability.
At a minimum, familiarity with the core legal standards of capacity (communication of choice, understanding, appreciation, and reasoning) will improve a hospitalist’s ability to identify patients who lack capacity. Understanding and applying the defined markers most often provides a sufficient capacity evaluation in itself. As capacity is not static, the decision usually requires more than one assessment.
Equally, deciding that a patient lacks capacity is not an end in itself, and the underlying cause should be addressed. Certain factors, such as infection, medication, time of day, and relationship with the clinician doing the assessment, can affect a patient’s capacity. These should be addressed through treatment, education, and social support whenever possible in order to optimize a patient’s performance during the capacity evaluation. If the decision can be delayed until a time when the patient can regain capacity, this should be done in order to maximize the patient’s autonomy.11
Risk-related standards of capacity.
Although some question the notion, given our desire to facilitate management beneficial to the patient, the general consensus is that we have a lower threshold for capacity for consent to treatments that are low-risk and high-benefit.12,13 We would then have a somewhat higher threshold for capacity to refuse that same treatment. Stemming from a desire to protect patients from harm, we have a relatively higher threshold for capacity to make decisions regarding high-risk, low-benefit treatments. For the remainder of cases (low risk/low benefit; high risk/high benefit), as well as treatments that significantly impact a patient’s lifestyle (e.g. dialysis, amputation), we have a low capacity to let patients decide for themselves.11,14
Other considerations.
Clinicians should be thorough in documenting details in coming to a capacity determination, both as a means to formalize the thought process running through the four determinants of capacity, and in order to document for future reference. Cases in which it could be reasonable to call a consultant for those familiar with the assessment basics include:
- Cases in which a determination of lack of capacity could adversely affect the hospitalist’s relationship with the patient;
- Cases in which the hospitalist lacks the time to properly perform the evaluation;
- Particularly difficult or high-stakes cases (e.g. cases that might involve legal proceedings); and
- Cases in which significant mental illness affects a patient’s capacity.11
Early involvement of potential surrogate decision-makers is wise for patients in whom capacity is questioned, both for obtaining collateral history as well as initiating dialogue as to the patient’s wishes. When a patient is found to lack capacity, resources to utilize to help make a treatment decision include existing advance directives and substitute decision-makers, such as durable power of attorneys (DPOAs) and family members. In those rare cases in which clinicians are unable to reach a consensus about a patient’s capacity, an ethics consult should be considered.
Back to the Case.
Following the patient’s declaration that dialysis is not something he is interested in, his niece reports that he is a minimalist when it comes to interventions, and that he had similarly refused a cardiac catheterization in the 1990s. You review with the patient and niece that dialysis would be a procedure to replace his failing kidney function, and that failure to pursue this would ultimately be life-threatening and likely result in death, especially in regard to electrolyte abnormalities and his lack of any other terminal illness.
The consulting nephrologist reviews their recommendations with the patient and niece as well, and the patient consistently refuses. Having clearly communicated his choice, you ask the patient if he understands the situation. He says, "My kidneys are failing. That’s how I got the high potassium." You ask him what that means. "They aren’t going to function on their own much longer," he says. "I could die from it."
You confirm his ideas, and ask him why he doesn’t want dialysis. "I don’t want dialysis because I don’t want to spend my life hooked up to machines three times a week," the patient explains. "I just want to let things run their natural course." The niece says her uncle wouldn’t have wanted dialysis even if it were 10 years ago, so she’s not surprised he is refusing now.
Following this discussion, you feel comfortable that the patient has capacity to make this decision. Having documented this discussion, you discharge him to a subacute rehabilitation facility.
Bottom Line.
In cases in which capacity is in question, a hospitalist’s case-by-case review of the four components of capacity—communicating a choice, understanding, appreciation, and rationalization and reasoning—is warranted to help determine whether a patient has capacity. In cases in which a second opinion is warranted, psychiatry, geriatrics, or ethics consults could be utilized.
Drs. Dastidar and Odden are hospitalists at the University of Michigan in Ann Arbor.
References
- Buchanan A, Brock DW. Deciding for others. Milbank Q. 1986;64(Suppl. 2):17-94.
- Guidelines for assessing the decision-making capacities of potential research subjects with cognitive impairment. American Psychiatric Association. Am J Psychiatry. 1998;155(11):1649-50.
- Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988;319(25):1635-1638.
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-198.
- Etchells E, Darzins P, Silberfeld M, et al. Assessment of patient capacity to consent to treatment. J Gen Intern Med. 1999;14:27-34.
- Grisso T, Appelbaum PS, Hill-Fotouhi C. The MacCAT-T: a clinical tool to assess patients’ capacities to make treatment decisions. Psychiatr Serv. 1997;48:1415- 1419.
- Marson DC, Ingram KK, Cody HA, Harrell LE. Assessing the competency of patients with Alzheimer’s disease under different legal standards. A prototype instrument. Arch Neurol. 1995;52:949-954.
- Edelstein B. Hopemont Capacity Assessment Interview Manual and Scoring Guide. 1999: Morgantown, W.V.: West Virginia University.
- Pruchno RA, Smyer MA, Rose MS, Hartman-Stein PE, Henderson-Laribee DL. Competence of long-term care residents to participate in decisions about their medical care: a brief, objective assessment. Gerontologist. 1995;35:622-629.
- Moye J, Karel M, Azar AR, Gurrera R. Capacity to consent to treatment: empirical comparison of three instruments in older adults with and without dementia. Gerontologist. 2004;44:166-175.
- Grisso T, Appelbaum PS. Assessing competence to consent to treatment: a guide for physicians and other health professionals. 1998; New York: Oxford University Press, 211.
- Cale GS. Risk-related standards of competence: continuing the debate over risk-related standards of competence. Bioethics. 1999;13(2):131-148.
- Checkland D. On risk and decisional capacity. J Med Philos. 2001;26(1):35-59.
- Wilks I. The debate over risk-related standards of competence. Bioethics. 1997;11(5):413-426.
- Ganzini L, Volicer L, Nelson WA, Fox E, Derse AR. Ten myths about decision-making capacity. J Am Med Dir Assoc. 2004;5(4):263-267.
Acknowledgements:The authors would like to thank Dr. Jeff Rohde for reviewing a copy of the manuscript, and Dr. Amy Rosinski for providing direction from the psychiatry standpoint
Case
A 79-year-old male with coronary artery disease, hypertension, non-insulin-dependent mellitus, moderate dementia, and chronic renal insufficiency is admitted after a fall evaluation. He is widowed and lives in an assisted living facility. He’s accompanied by his niece, is alert, and oriented to person. He thinks he is in a clinic and is unable to state the year, but the remainder of the examination is unremarkable. His labs are notable for potassium of 6.3 mmol/L, BUN of 78 mg/dL, and Cr of 3.7 mg/dL. The niece reports that the patient is not fond of medical care, thus the most recent labs are from two years ago (and indicate a BUN of 39 and Cr of 2.8, with an upward trend over the past decade). You discuss possible long-term need for dialysis with the patient and niece, and the patient clearly states "no." However, he also states that it is 1988. How do you determine if he has the capacity to make decisions?
Overview
Hospitalists are familiar with the doctrine of informed consent—describing a disease, treatment options, associated risks and benefits, potential for complications, and alternatives, including no treatment. Not only must the patient be informed, and the decision free from any coercion, but the patient also must have capacity to make the decision.
Hospitalists often care for patients in whom decision-making capacity comes into question. This includes populations with depression, psychosis, dementia, stroke, severe personality disorders, developmental delay, comatose patients, as well as those with impaired attentional capacity (e.g. acute pain) or general debility (e.g. metastatic cancer).1,2
ave for the comatose patient, whether the patient has capacity might not be obvious. However, addressing the components of capacity (communication, understanding, appreciation, and rationalization) by using a validated clinical tool, such as the MacCAT-T, or more simply by systematically applying those four components to the clinical scenario under consideration, hospitalists can make this determination.
Review of the Literature
It is important to differentiate capacity from competency. Competency is a global assessment and a legal determination made by a judge in court. Capacity, on the other hand, is a functional assessment regarding a particular decision. Capacity is not static, and it can be performed by any clinician familiar with the patient. A hospitalist often is well positioned to make a capacity determination given established rapport with the patient and familiarity with the details of the case.
To make this determination, a hospitalist needs to know how to assess capacity. Although capacity usually is defined by state law and varies by jurisdiction, clinicians generally can assume it includes one or more of the four key components:
- Communication. The patient needs to be able to express a treatment choice, and this decision needs to be stable enough for the treatment to be implemented. Changing one’s decision in itself would not bring a patient’s capacity into question, so long as the patient was able to explain the rationale behind the switch. Frequent changes back and forth in the decision-making, however, could be indicative of an underlying psychiatric disorder or extreme indecision, which could bring capacity into question.
- Understanding. The patient needs to recall conversations about treatment, to make the link between causal relationships, and to process probabilities for outcomes. Problems with memory, attention span, and intelligence can affect one’s understanding.
- Appreciation. The patient should be able to identify the illness, treatment options, and likely outcomes as things that will affect him or her directly. A lack of appreciation usually stems from a denial based on intelligence (lack of a capability to understand) or emotion, or a delusion that the patient is not affected by this situation the same way and will have a different outcome.
- Rationalization or reasoning. The patient needs to be able to weigh the risks and benefits of the treatment options presented to come to a conclusion in keeping with their goals and best interests, as defined by their personal set of values. This often is affected in psychosis, depression, anxiety, phobias, delirium, and dementia.3
Several clinical capacity tools have been developed to assess these components:
Clinical tools.
The Mini-Mental Status Examination (MMSE) is a bedside test of a patient’s cognitive function, with scores ranging from 0 to 30.4 Although it wasn’t developed for assessing decision-making capacity, it has been compared with expert evaluation for assessment of capacity; the test performs reasonably well, particularly with high and low scores. Specifically, a MMSE >24 has a negative likelihood ratio (LR) of 0.05 for lack of capacity, while a MMSE <16 has a positive LR of 15.5 Scores from 17 to 23 do not correlate well with capacity, and further testing would be necessary. It is easy to administer, requires no formal training, and is familiar to most hospitalists. However, it does not address any specific aspects of informed consent, such as understanding or choice, and has not been validated in patients with mental illness.
The MacArthur Competence Assessment Tools for Treatment (MacCAT-T) is regarded as the gold standard for capacity assessment aids. It utilizes hospital chart review followed by a semi-structured interview to address clinical issues relevant to the patient being assessed; it takes 15 to 20 minutes to complete.6 The test provides scores in each of the four domains (choice, understanding, appreciation, and reasoning) of capacity. It has been validated in patients with dementia, schizophrenia, and depression. Limiting its clinical applicability is the fact that the MacCAT-T requires training to administer and interpret the results, though this is a relatively brief process.
The Capacity to Consent to Treatment Instrument (CCTI) uses hypothetical clinical vignettes in a structured interview to assess capacity across all four domains. The tool was developed and validated in patients with dementia and Parkinson’s disease, and takes 20 to 25 minutes to complete.7 A potential limitation is the CCTI’s use of vignettes as opposed to a patient-specific discussion, which could lead to different patient answers and a false assessment of the patient’s capacity.
The Hopemont Capacity Assessment Interview (HCAI) utilizes hypothetical vignettes in a semi-structured interview format to assess understanding, appreciation, choice, and likely reasoning.8,9 Similar to CCTI, HCAI is not modified for individual patients. Rather, it uses clinical vignettes to gauge a patient’s ability to make decisions. The test takes 30 to 60 minutes to administer and performs less well in assessing appreciation and reasoning than the MacCAT-T and CCTI.10
It is not necessary to perform a formal assessment of capacity on every inpatient. For most, there is no reasonable concern for impaired capacity, obviating the need for formal testing. Likewise, in patients who clearly lack capacity, such as those with end-stage dementia or established guardians, formal reassessment usually is not required. Formal testing is most useful in situations in which capacity is unclear, disagreement amongst surrogate decision-makers exists, or judicial involvement is anticipated.
The MacCAT-T has been validated in the broadest population and is probably the most clinically useful tool currently available. The MMSE is an attractive alternative because of its widespread use and familiarity; however, it is imprecise with scores from 17 to 23, limiting its applicability.
At a minimum, familiarity with the core legal standards of capacity (communication of choice, understanding, appreciation, and reasoning) will improve a hospitalist’s ability to identify patients who lack capacity. Understanding and applying the defined markers most often provides a sufficient capacity evaluation in itself. As capacity is not static, the decision usually requires more than one assessment.
Equally, deciding that a patient lacks capacity is not an end in itself, and the underlying cause should be addressed. Certain factors, such as infection, medication, time of day, and relationship with the clinician doing the assessment, can affect a patient’s capacity. These should be addressed through treatment, education, and social support whenever possible in order to optimize a patient’s performance during the capacity evaluation. If the decision can be delayed until a time when the patient can regain capacity, this should be done in order to maximize the patient’s autonomy.11
Risk-related standards of capacity.
Although some question the notion, given our desire to facilitate management beneficial to the patient, the general consensus is that we have a lower threshold for capacity for consent to treatments that are low-risk and high-benefit.12,13 We would then have a somewhat higher threshold for capacity to refuse that same treatment. Stemming from a desire to protect patients from harm, we have a relatively higher threshold for capacity to make decisions regarding high-risk, low-benefit treatments. For the remainder of cases (low risk/low benefit; high risk/high benefit), as well as treatments that significantly impact a patient’s lifestyle (e.g. dialysis, amputation), we have a low capacity to let patients decide for themselves.11,14
Other considerations.
Clinicians should be thorough in documenting details in coming to a capacity determination, both as a means to formalize the thought process running through the four determinants of capacity, and in order to document for future reference. Cases in which it could be reasonable to call a consultant for those familiar with the assessment basics include:
- Cases in which a determination of lack of capacity could adversely affect the hospitalist’s relationship with the patient;
- Cases in which the hospitalist lacks the time to properly perform the evaluation;
- Particularly difficult or high-stakes cases (e.g. cases that might involve legal proceedings); and
- Cases in which significant mental illness affects a patient’s capacity.11
Early involvement of potential surrogate decision-makers is wise for patients in whom capacity is questioned, both for obtaining collateral history as well as initiating dialogue as to the patient’s wishes. When a patient is found to lack capacity, resources to utilize to help make a treatment decision include existing advance directives and substitute decision-makers, such as durable power of attorneys (DPOAs) and family members. In those rare cases in which clinicians are unable to reach a consensus about a patient’s capacity, an ethics consult should be considered.
Back to the Case.
Following the patient’s declaration that dialysis is not something he is interested in, his niece reports that he is a minimalist when it comes to interventions, and that he had similarly refused a cardiac catheterization in the 1990s. You review with the patient and niece that dialysis would be a procedure to replace his failing kidney function, and that failure to pursue this would ultimately be life-threatening and likely result in death, especially in regard to electrolyte abnormalities and his lack of any other terminal illness.
The consulting nephrologist reviews their recommendations with the patient and niece as well, and the patient consistently refuses. Having clearly communicated his choice, you ask the patient if he understands the situation. He says, "My kidneys are failing. That’s how I got the high potassium." You ask him what that means. "They aren’t going to function on their own much longer," he says. "I could die from it."
You confirm his ideas, and ask him why he doesn’t want dialysis. "I don’t want dialysis because I don’t want to spend my life hooked up to machines three times a week," the patient explains. "I just want to let things run their natural course." The niece says her uncle wouldn’t have wanted dialysis even if it were 10 years ago, so she’s not surprised he is refusing now.
Following this discussion, you feel comfortable that the patient has capacity to make this decision. Having documented this discussion, you discharge him to a subacute rehabilitation facility.
Bottom Line.
In cases in which capacity is in question, a hospitalist’s case-by-case review of the four components of capacity—communicating a choice, understanding, appreciation, and rationalization and reasoning—is warranted to help determine whether a patient has capacity. In cases in which a second opinion is warranted, psychiatry, geriatrics, or ethics consults could be utilized.
Drs. Dastidar and Odden are hospitalists at the University of Michigan in Ann Arbor.
References
- Buchanan A, Brock DW. Deciding for others. Milbank Q. 1986;64(Suppl. 2):17-94.
- Guidelines for assessing the decision-making capacities of potential research subjects with cognitive impairment. American Psychiatric Association. Am J Psychiatry. 1998;155(11):1649-50.
- Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988;319(25):1635-1638.
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-198.
- Etchells E, Darzins P, Silberfeld M, et al. Assessment of patient capacity to consent to treatment. J Gen Intern Med. 1999;14:27-34.
- Grisso T, Appelbaum PS, Hill-Fotouhi C. The MacCAT-T: a clinical tool to assess patients’ capacities to make treatment decisions. Psychiatr Serv. 1997;48:1415- 1419.
- Marson DC, Ingram KK, Cody HA, Harrell LE. Assessing the competency of patients with Alzheimer’s disease under different legal standards. A prototype instrument. Arch Neurol. 1995;52:949-954.
- Edelstein B. Hopemont Capacity Assessment Interview Manual and Scoring Guide. 1999: Morgantown, W.V.: West Virginia University.
- Pruchno RA, Smyer MA, Rose MS, Hartman-Stein PE, Henderson-Laribee DL. Competence of long-term care residents to participate in decisions about their medical care: a brief, objective assessment. Gerontologist. 1995;35:622-629.
- Moye J, Karel M, Azar AR, Gurrera R. Capacity to consent to treatment: empirical comparison of three instruments in older adults with and without dementia. Gerontologist. 2004;44:166-175.
- Grisso T, Appelbaum PS. Assessing competence to consent to treatment: a guide for physicians and other health professionals. 1998; New York: Oxford University Press, 211.
- Cale GS. Risk-related standards of competence: continuing the debate over risk-related standards of competence. Bioethics. 1999;13(2):131-148.
- Checkland D. On risk and decisional capacity. J Med Philos. 2001;26(1):35-59.
- Wilks I. The debate over risk-related standards of competence. Bioethics. 1997;11(5):413-426.
- Ganzini L, Volicer L, Nelson WA, Fox E, Derse AR. Ten myths about decision-making capacity. J Am Med Dir Assoc. 2004;5(4):263-267.
Acknowledgements:The authors would like to thank Dr. Jeff Rohde for reviewing a copy of the manuscript, and Dr. Amy Rosinski for providing direction from the psychiatry standpoint
A Chilly Reception
The reviews are in, and most healthcare provider groups are finding little to their liking in the proposed rules for the Centers for Medicare & Medicaid Services’ (CMS) voluntary Accountable Care Organization (ACO) program. Organizations like SHM have publically supported the concept of an ACO, but details in the 128 pages of proposed rules released March 31 apparently were not what they had in mind. The problem, as many provider groups detailed in a flurry of letters sent before the June 6 deadline for comments, is too much stick and not enough carrot.
The Patient Protection and Affordable Care Act of 2010, which authorized the program, stipulates that any Medicare savings deriving from ACOs must be divided between CMS and participating organizations. Organizations can choose between two financial models: One track allows participants to retain 60% of overall savings but also requires them to assume financial risk from the start; a second track delays any risk until the third year and offers 50% savings. In exchange, ACOs must achieve an average savings of 2% per patient, as well as meet or beat thresholds for 65 measures of quality.
Organizational Uproar
Critics contend that the recommended rules are so onerous and bureaucratic that the program is likely to attract few takers. In its comment letter, SHM expressed an opinion shared by many: "Although the ACO concept holds much promise, the proposed rule as written presents many barriers to successful ACO development and operations. Establishing an ACO will require an enormous upfront investment from participating providers, but the proposed rule does not allow for enough flexibility to ensure a reasonable return on investment." (Read SHM’s response letter at www.hospital medicine.org/advocacy.)
The American College of Physicians similarly warned that the proposed rules set the bar too high for many would-be participants. "The required administrative, infrastructure, service delivery, and financial resources and the need to accept risk will effectively limit participation to those few large entities already organized under an ACO-like structure; that already have ready access to capital, substantial infrastructure development, and experience operating under an integrative service/payment model (e.g. Medicare Advantage)," the ACP wrote in its response letter (www.acponline.org/run ning_practice/aco/acp_comments.pdf).
The tone was markedly different in letters from consumer and advocacy groups, including one by the Campaign for Better Care, signed by more than 40 organizations (www.nationalpartnership.org). "Overall we believe you are moving in the right direction with the proposed rule, and we applaud your commitment to ensuring ACOs deliver truly patient-centered care," the letter stated. Acknowledging the negative feedback, the letter continued, "While some are concerned about asking too much of ACOs, we cannot expect genuine transformation to be easy, and we know that these new models must be held to standards that ensure they deliver on the promise of better care, better health, and lower cost."
—Michael W. Painter, JD, MD, senior program officer, Robert Wood Johnson Foundation, Princeton, N.J.
Accountability Gap
Michael W. Painter, JD, MD, senior program officer at the Robert Wood Johnson Foundation in Princeton, N.J., helped research and write the foundation’s own comment letter, which he says tried to bridge the divide between provider and patient groups.
"We did get behind the notion of ratcheting up the accountability for quality and cost, including the risk, as soon as it makes sense to do it," he says. "Not dragging our feet, recognizing that we have to do it rapidly, but it has to be balanced by being reasonable to help move from where we are."
Given the mandate for change, Dr. Painter says, the negative tone of many letters from provider organizations shouldn’t be surprising. "What we’re asking the hospital, the health professionals, to do is to change fairly radically and embrace this accountability. So as you just walk through the door of this conversation, it’s not surprising that they would balk," he says. "Nobody wants to take on all of this new responsibility. It’s no fault of theirs; they’ve just been following the rules of the road of the current system and the payment schemes to try to be successful in that environment."
Success, of course, depends on financial stability, and Dr. Painter says the worry that participating ACOs could open themselves up to financial risk too soon is "absolutely a legitimate concern." CMS, he says, should give providers clear guidance and assistance, as well as assurance that the regulations won’t change on them once they’ve enrolled.
So far, at least, CMS has not swayed some of the very institutions that government officials have lauded as examples of how ACOs should be run. In June, the Mayo Clinic in Rochester, Minn., announced that it would not participate. As reported by the Minneapolis Star Tribune, clinic officials said the proposed regulations clashed with Mayo’s existing Medicare operations. One of the clinic’s chief complaints is the proposed requirement that patients be added to oversight boards charged with assessing performance, something that Mayo argues is unnecessary to deliver patient-centered care. Antitrust rules represent another major concern for Mayo and others that argue their dominant position as healthcare providers in rural communities could run afoul of the regulations.
Cleveland Clinic likewise blasted the proposed ACO rules in a letter. "Rather than providing a broad framework that focuses on results as the key criteria of success, the Proposed Rule is replete with (1) prescriptive requirements that have little to do with outcomes, and (2) many detailed governance and reporting requirements that create significant administrative burdens," stated Delos Cosgrove, MD, the clinic’s CEO and president.
Furthermore, Cosgrove’s letter concluded that the shared-savings component "is structured in such a way that creates real uncertainty about whether applicants will be able to achieve success."
The American Medical Group Association went so far as to include in its letter the results of a member survey, which showed 93% would not enroll under the current ACO rules.
No Turning Back
Dr. Painter says the pushback is to be expected. Although the country has no choice but to move toward more accountability, he says, it’s impossible for the first attempt at a proposed rule to be the "magic bullet" that gets it exactly right. "One, this is a radical departure, and two, when you get into the nitty-gritty of the proposed rule and people crunch the numbers, if it’s not going to work for them or it’s simply not enticing enough for them, they [CMS] need to go back to the table and make it that way," he says.
Organizations like the American Medical Association have been particularly vocal about asking CMS to delay issuing its final rule, slated for January. So far, Dr. Painter says, CMS officials have indicated that the timeline will proceed according to schedule, though he notes that providers have raised plenty of valid concerns that should be addressed.
"Would I be surprised if there’s a delay? No. This is a big deal," he says.
Along with some expected rule changes, he says the newly formed Center for Medicare and Medicaid Innovation could play a key role in offering assistance and developing alternative ACO models and pilot programs.
Regardless of whether the voluntary CMS program ultimately pleases both providers and patients, though, one thing seems certain: The accountable-care concept is here to stay.
Bryn Nelson is a freelance medical writer based in Seattle
The reviews are in, and most healthcare provider groups are finding little to their liking in the proposed rules for the Centers for Medicare & Medicaid Services’ (CMS) voluntary Accountable Care Organization (ACO) program. Organizations like SHM have publically supported the concept of an ACO, but details in the 128 pages of proposed rules released March 31 apparently were not what they had in mind. The problem, as many provider groups detailed in a flurry of letters sent before the June 6 deadline for comments, is too much stick and not enough carrot.
The Patient Protection and Affordable Care Act of 2010, which authorized the program, stipulates that any Medicare savings deriving from ACOs must be divided between CMS and participating organizations. Organizations can choose between two financial models: One track allows participants to retain 60% of overall savings but also requires them to assume financial risk from the start; a second track delays any risk until the third year and offers 50% savings. In exchange, ACOs must achieve an average savings of 2% per patient, as well as meet or beat thresholds for 65 measures of quality.
Organizational Uproar
Critics contend that the recommended rules are so onerous and bureaucratic that the program is likely to attract few takers. In its comment letter, SHM expressed an opinion shared by many: "Although the ACO concept holds much promise, the proposed rule as written presents many barriers to successful ACO development and operations. Establishing an ACO will require an enormous upfront investment from participating providers, but the proposed rule does not allow for enough flexibility to ensure a reasonable return on investment." (Read SHM’s response letter at www.hospital medicine.org/advocacy.)
The American College of Physicians similarly warned that the proposed rules set the bar too high for many would-be participants. "The required administrative, infrastructure, service delivery, and financial resources and the need to accept risk will effectively limit participation to those few large entities already organized under an ACO-like structure; that already have ready access to capital, substantial infrastructure development, and experience operating under an integrative service/payment model (e.g. Medicare Advantage)," the ACP wrote in its response letter (www.acponline.org/run ning_practice/aco/acp_comments.pdf).
The tone was markedly different in letters from consumer and advocacy groups, including one by the Campaign for Better Care, signed by more than 40 organizations (www.nationalpartnership.org). "Overall we believe you are moving in the right direction with the proposed rule, and we applaud your commitment to ensuring ACOs deliver truly patient-centered care," the letter stated. Acknowledging the negative feedback, the letter continued, "While some are concerned about asking too much of ACOs, we cannot expect genuine transformation to be easy, and we know that these new models must be held to standards that ensure they deliver on the promise of better care, better health, and lower cost."
—Michael W. Painter, JD, MD, senior program officer, Robert Wood Johnson Foundation, Princeton, N.J.
Accountability Gap
Michael W. Painter, JD, MD, senior program officer at the Robert Wood Johnson Foundation in Princeton, N.J., helped research and write the foundation’s own comment letter, which he says tried to bridge the divide between provider and patient groups.
"We did get behind the notion of ratcheting up the accountability for quality and cost, including the risk, as soon as it makes sense to do it," he says. "Not dragging our feet, recognizing that we have to do it rapidly, but it has to be balanced by being reasonable to help move from where we are."
Given the mandate for change, Dr. Painter says, the negative tone of many letters from provider organizations shouldn’t be surprising. "What we’re asking the hospital, the health professionals, to do is to change fairly radically and embrace this accountability. So as you just walk through the door of this conversation, it’s not surprising that they would balk," he says. "Nobody wants to take on all of this new responsibility. It’s no fault of theirs; they’ve just been following the rules of the road of the current system and the payment schemes to try to be successful in that environment."
Success, of course, depends on financial stability, and Dr. Painter says the worry that participating ACOs could open themselves up to financial risk too soon is "absolutely a legitimate concern." CMS, he says, should give providers clear guidance and assistance, as well as assurance that the regulations won’t change on them once they’ve enrolled.
So far, at least, CMS has not swayed some of the very institutions that government officials have lauded as examples of how ACOs should be run. In June, the Mayo Clinic in Rochester, Minn., announced that it would not participate. As reported by the Minneapolis Star Tribune, clinic officials said the proposed regulations clashed with Mayo’s existing Medicare operations. One of the clinic’s chief complaints is the proposed requirement that patients be added to oversight boards charged with assessing performance, something that Mayo argues is unnecessary to deliver patient-centered care. Antitrust rules represent another major concern for Mayo and others that argue their dominant position as healthcare providers in rural communities could run afoul of the regulations.
Cleveland Clinic likewise blasted the proposed ACO rules in a letter. "Rather than providing a broad framework that focuses on results as the key criteria of success, the Proposed Rule is replete with (1) prescriptive requirements that have little to do with outcomes, and (2) many detailed governance and reporting requirements that create significant administrative burdens," stated Delos Cosgrove, MD, the clinic’s CEO and president.
Furthermore, Cosgrove’s letter concluded that the shared-savings component "is structured in such a way that creates real uncertainty about whether applicants will be able to achieve success."
The American Medical Group Association went so far as to include in its letter the results of a member survey, which showed 93% would not enroll under the current ACO rules.
No Turning Back
Dr. Painter says the pushback is to be expected. Although the country has no choice but to move toward more accountability, he says, it’s impossible for the first attempt at a proposed rule to be the "magic bullet" that gets it exactly right. "One, this is a radical departure, and two, when you get into the nitty-gritty of the proposed rule and people crunch the numbers, if it’s not going to work for them or it’s simply not enticing enough for them, they [CMS] need to go back to the table and make it that way," he says.
Organizations like the American Medical Association have been particularly vocal about asking CMS to delay issuing its final rule, slated for January. So far, Dr. Painter says, CMS officials have indicated that the timeline will proceed according to schedule, though he notes that providers have raised plenty of valid concerns that should be addressed.
"Would I be surprised if there’s a delay? No. This is a big deal," he says.
Along with some expected rule changes, he says the newly formed Center for Medicare and Medicaid Innovation could play a key role in offering assistance and developing alternative ACO models and pilot programs.
Regardless of whether the voluntary CMS program ultimately pleases both providers and patients, though, one thing seems certain: The accountable-care concept is here to stay.
Bryn Nelson is a freelance medical writer based in Seattle
The reviews are in, and most healthcare provider groups are finding little to their liking in the proposed rules for the Centers for Medicare & Medicaid Services’ (CMS) voluntary Accountable Care Organization (ACO) program. Organizations like SHM have publically supported the concept of an ACO, but details in the 128 pages of proposed rules released March 31 apparently were not what they had in mind. The problem, as many provider groups detailed in a flurry of letters sent before the June 6 deadline for comments, is too much stick and not enough carrot.
The Patient Protection and Affordable Care Act of 2010, which authorized the program, stipulates that any Medicare savings deriving from ACOs must be divided between CMS and participating organizations. Organizations can choose between two financial models: One track allows participants to retain 60% of overall savings but also requires them to assume financial risk from the start; a second track delays any risk until the third year and offers 50% savings. In exchange, ACOs must achieve an average savings of 2% per patient, as well as meet or beat thresholds for 65 measures of quality.
Organizational Uproar
Critics contend that the recommended rules are so onerous and bureaucratic that the program is likely to attract few takers. In its comment letter, SHM expressed an opinion shared by many: "Although the ACO concept holds much promise, the proposed rule as written presents many barriers to successful ACO development and operations. Establishing an ACO will require an enormous upfront investment from participating providers, but the proposed rule does not allow for enough flexibility to ensure a reasonable return on investment." (Read SHM’s response letter at www.hospital medicine.org/advocacy.)
The American College of Physicians similarly warned that the proposed rules set the bar too high for many would-be participants. "The required administrative, infrastructure, service delivery, and financial resources and the need to accept risk will effectively limit participation to those few large entities already organized under an ACO-like structure; that already have ready access to capital, substantial infrastructure development, and experience operating under an integrative service/payment model (e.g. Medicare Advantage)," the ACP wrote in its response letter (www.acponline.org/run ning_practice/aco/acp_comments.pdf).
The tone was markedly different in letters from consumer and advocacy groups, including one by the Campaign for Better Care, signed by more than 40 organizations (www.nationalpartnership.org). "Overall we believe you are moving in the right direction with the proposed rule, and we applaud your commitment to ensuring ACOs deliver truly patient-centered care," the letter stated. Acknowledging the negative feedback, the letter continued, "While some are concerned about asking too much of ACOs, we cannot expect genuine transformation to be easy, and we know that these new models must be held to standards that ensure they deliver on the promise of better care, better health, and lower cost."
—Michael W. Painter, JD, MD, senior program officer, Robert Wood Johnson Foundation, Princeton, N.J.
Accountability Gap
Michael W. Painter, JD, MD, senior program officer at the Robert Wood Johnson Foundation in Princeton, N.J., helped research and write the foundation’s own comment letter, which he says tried to bridge the divide between provider and patient groups.
"We did get behind the notion of ratcheting up the accountability for quality and cost, including the risk, as soon as it makes sense to do it," he says. "Not dragging our feet, recognizing that we have to do it rapidly, but it has to be balanced by being reasonable to help move from where we are."
Given the mandate for change, Dr. Painter says, the negative tone of many letters from provider organizations shouldn’t be surprising. "What we’re asking the hospital, the health professionals, to do is to change fairly radically and embrace this accountability. So as you just walk through the door of this conversation, it’s not surprising that they would balk," he says. "Nobody wants to take on all of this new responsibility. It’s no fault of theirs; they’ve just been following the rules of the road of the current system and the payment schemes to try to be successful in that environment."
Success, of course, depends on financial stability, and Dr. Painter says the worry that participating ACOs could open themselves up to financial risk too soon is "absolutely a legitimate concern." CMS, he says, should give providers clear guidance and assistance, as well as assurance that the regulations won’t change on them once they’ve enrolled.
So far, at least, CMS has not swayed some of the very institutions that government officials have lauded as examples of how ACOs should be run. In June, the Mayo Clinic in Rochester, Minn., announced that it would not participate. As reported by the Minneapolis Star Tribune, clinic officials said the proposed regulations clashed with Mayo’s existing Medicare operations. One of the clinic’s chief complaints is the proposed requirement that patients be added to oversight boards charged with assessing performance, something that Mayo argues is unnecessary to deliver patient-centered care. Antitrust rules represent another major concern for Mayo and others that argue their dominant position as healthcare providers in rural communities could run afoul of the regulations.
Cleveland Clinic likewise blasted the proposed ACO rules in a letter. "Rather than providing a broad framework that focuses on results as the key criteria of success, the Proposed Rule is replete with (1) prescriptive requirements that have little to do with outcomes, and (2) many detailed governance and reporting requirements that create significant administrative burdens," stated Delos Cosgrove, MD, the clinic’s CEO and president.
Furthermore, Cosgrove’s letter concluded that the shared-savings component "is structured in such a way that creates real uncertainty about whether applicants will be able to achieve success."
The American Medical Group Association went so far as to include in its letter the results of a member survey, which showed 93% would not enroll under the current ACO rules.
No Turning Back
Dr. Painter says the pushback is to be expected. Although the country has no choice but to move toward more accountability, he says, it’s impossible for the first attempt at a proposed rule to be the "magic bullet" that gets it exactly right. "One, this is a radical departure, and two, when you get into the nitty-gritty of the proposed rule and people crunch the numbers, if it’s not going to work for them or it’s simply not enticing enough for them, they [CMS] need to go back to the table and make it that way," he says.
Organizations like the American Medical Association have been particularly vocal about asking CMS to delay issuing its final rule, slated for January. So far, Dr. Painter says, CMS officials have indicated that the timeline will proceed according to schedule, though he notes that providers have raised plenty of valid concerns that should be addressed.
"Would I be surprised if there’s a delay? No. This is a big deal," he says.
Along with some expected rule changes, he says the newly formed Center for Medicare and Medicaid Innovation could play a key role in offering assistance and developing alternative ACO models and pilot programs.
Regardless of whether the voluntary CMS program ultimately pleases both providers and patients, though, one thing seems certain: The accountable-care concept is here to stay.
Bryn Nelson is a freelance medical writer based in Seattle
In the Literature: Research You Need to Know
In This Edition
Literature At A Glance
A guide to this month’s studies
- Screening for AAA
- Adverse events in atrial fibrillation
- Biological treatment of inflammatory bowel diseases
- Steroid treatment of inflammatory bowel diseases
- Levofloxacin for H. pylori
- Natural history of tako-tsubo cardiomyopathy
- Predicting postoperative pulmonary complications
- Code status and goals of care in the ICU
New Screening Strategy To Identify Large Abdominal Aortic Aneurysms
Clinical question: Can an effective scoring system be developed to better identify patients at risk for large abdominal aortic aneurysms (AAA)?
Background: Screening reduces AAA-related mortality by about half in men aged >65. The United States Preventive Services Task Force (USPSTF) has recommended screening for AAA in men aged 65 to 75 with a history of smoking. However, more than 50% of AAA ruptures occur in individuals outside this patient cohort, and only some AAAs detected are large enough to warrant surgery.
Study design: Retrospective, observational cohort study.
Setting: More than 20,000 screening sites across the U.S.
Synopsis: Researchers collected demographics and risk factors from 3.1 million people undergoing ultrasound screening for AAA by Life Line Screening Inc. At the screening visit, subjects completed a questionnaire about their health status and medical history. Screening data also included diameter of the infrarenal abdominal aorta. To construct and test a risk model, the screened individuals were randomly allocated into two equal groups: a data set used for model development and one for validation.
Most of the AAAs greater than 5 cm in diameter discovered were in males (84.4%) and among subjects with a smoking history (83%). Other risk factors for large AAAs included advanced age, peripheral arterial disease, and obesity. The authors estimate that there are about 121,000 people with >5.0 cm aneurysms in the general population. Current guidelines would detect only 33.7% of the existing large AAAs. Study limitations include possible selection bias, as a majority of patients were self-referred. Also, the database did not include all comorbidities that could affect the risk of AAA. The self-reported nature of health data might cause misclassification of a patient’s true health status.
Bottom line: A screening strategy based on a newly developed scoring system is an effective way to identify patients at risk of large abdominal aortic aneurysms.
Citation: Greco G, Egorova NN, Gelijns AC, et al. Development of a novel scoring tool for the identification of large >5 cm abdominal aortic aneurysms. Ann Surg. 2010;252(4):675-682.
Risk Factors for Adverse Events in Patients with Symptomatic Atrial Fibrillation
Clinical question: What are the predictors of 30-day adverse events in ED patients evaluated for symptomatic atrial fibrillation?
Background: Atrial fibrillation (AF) affects more than 2 million people in the U.S. and accounts for nearly 1% of ED visits. Physicians have little information to guide risk stratification, and they admit more than 65% of patients. A strategy to better define the ED management of patients presenting with atrial fibrillation is required.
Study design: Retrospective, observational cohort study.
Setting: Urban academic tertiary-care referral center with an adult ED.
Synopsis: A systematic review of the electronic medical records of all ED patients presenting with symptomatic atrial fibrillation over a three-year period was performed. Predefined adverse outcomes included 30-day ED return visits, unscheduled hospitalizations, cardiovascular complications, or death.
Of 832 eligible patients, 216 (25.9%) experienced at least one of the 30-day adverse events. Adverse events occurred in 181 of the 638 (28.4%) admitted patients and 35 of the 192 (18.2%) patients discharged from the ED. Increasing age, complaint of dyspnea, smoking history, inadequate ventricular rate control, and patients receiving beta-blockers were factors independently associated with higher risk for adverse events.
Study results were limited by a number of factors. This was a single-center, retrospective, observational study, with all of its inherent limitations. The predictor model did not include laboratory data, such as BNP or troponin. Patients might have experienced additional events within the 30 days that were treated at other hospitals and not recorded in the database. Patient disposition might have affected the results, as patients initially admitted from the ED had a higher rate of 30-day adverse events than patients who were discharged from the ED.
Bottom line: Patients with increased age, smoking history, complaints of dyspnea, inadequate ventricular rate control in the ED, and home beta-blocker therapy are more likely to experience an atrial-fibrillation-related adverse event within 30 days.
Citation: Barrett TW, Martin AR, Storrow AB, et al. A clinical prediction model to estimate risk for 30-day adverse events in emergency department patients with symptomatic atrial fibrillation. Ann Emerg Med. 2011;57 (1):1-12.
Biological Therapies Are Effective in Inducing Remission in Inflammatory Bowel Disease
Clinical question: Are biological therapies useful in the treatment of ulcerative colitis (UC) and Crohn’s disease (CD)?
Background: Patients with CD and UC often experience flares of disease activity, despite maintenance therapy with 5-aminosalicylic acid compounds. These flares are usually treated with corticosteroids, which carry numerous adverse side effects. The role of biological therapies in inducing remission is uncertain.
Study design: Systematic review and meta-analysis.
Setting: Twenty-seven randomized controlled trials involving 7,416 patients.
Synopsis: Anti-TNF α antibodies and natalizumab were both superior to placebo in inducing remission of luminal CD (RR of no remission 0.87 and 0.88, respectively). Anti-TNF antibodies also were superior to placebo in preventing relapse of luminal CD (RR of relapse=0.71). Infliximab was superior to placebo in inducing remission of moderate to severely active UC (RR=0.72; 95% CI, 0.57-0.91). There were no significantly increased adverse drug effects with anti-TNF α antibodies or with infliximab compared with placebo. Natalizumab caused significantly higher rates of headache.
Limitations include risk of publication bias inherent in meta-analyses. There also was evidence of moderate heterogeneity in the studies analyzed. Finally, not every study was consistent in reporting adverse drug effects.
Bottom line: Biological therapies are superior to placebo in inducing remission of active UC and CD, as well as preventing relapse of quiescent CD.
Citation: Ford AC, Sandborn WJ, Khan KJ, Hanauer SB, Talley NJ, Moayyedi P. Efficacy of biological therapies in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2011; 106(4):644-659.
Glucocorticosteroids Probably Effective in Treatment of Inflammatory Bowel Disease, Primarily in Active Ulcerative Colitis
Clinical question: Is glucocorticosteroid therapy effective in the treatment of active IBD and in preventing relapses?
Background: Crohn’s disease (CD) and ulcerative colitis (UC) are chronic inflammatory bowel diseases of unclear etiology. Use of standard glucocorticosteroids and budesonide is widespread in inflammatory bowel disease (IBD) treatment. To date, there has been no large-scale meta-analysis to examine the effectiveness of both treatments in CD and UC.
Study design: Systematic review and meta-analysis.
Setting: Twenty randomized controlled trials totaling 2,398 patients.
Synopsis: Standard glucocorticosteroids were superior to placebo for UC remission (RR of no remission=0.65; 95% CI, 0.45-0.93). Both trials of standard glucocorticosteroids in CD remission reported a statistically significant effect, but the overall effect was not significant due to heterogeneity of the studies. Budesonide was superior to placebo for CD remission (RR=0.73; 95% CI, 0.63-0.84) but not in preventing CD relapse (RR=0.93; 95% CI, 0.83-1.04). Standard glucocorticosteroids were superior to budesonide for CD remission (RR=0.82; 95% CI, 0.68-0.98) but with more adverse effects (RR=1.64; 95% CI, 1.34-2.00).
The limitations of the study include the poor overall quality of the studies included in the meta-analysis, with only one study judged as low risk of bias. There was intermediate to high heterogeneity between study results.
Bottom line: Standard glucocorticosteroids are likely effective in inducing remission in UC and, possibly, in CD. Budesonide probably is effective at inducing remission in active CD. Neither therapy was recommended in preventing relapse of UC and CD.
Citation: Ford AC, Bernstein CN, Khan KJ, et al. Glucocorticosteroid therapy in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2011;106(4):590-599.
Levofloxacin Effective in Treatment of H. Pylori in Settings of High Clarithromycin Resistance
Clinical question: In areas with high H. pylori clarithromycin resistance rates, is levofloxacin more effective in eradicating H. pylori than standard clarithromycin, based treatment regimens?
Background: The rise in antimicrobial drug resistance is a major cause for the decreasing rate of H. pylori eradication. In areas with higher than 15% H. pyloriclarithromycin-resistant strains, quadruple therapy has been suggested as first-line therapy. The efficacy of a levofloxacin-based sequential therapy in eradicating H. pylori is undetermined.
Study design: Prospective, randomized, controlled multicenter study with a parallel-group design.
Setting: Five gastroenterology clinics in Italy.
Synopsis: Researchers randomly assigned 375 patients who were infected with H. pylori and naive to treatment to one of three groups. All three treatment groups received an initial five days of omeprazole 20 mg BID and amoxicillin 1 gm BID, then five days of omeprazole 20 mg BID and tinidazole 500 mg BID. The groups also received either clarithromycin 500 mg BID, levofloxacin 250 mg BID, or levofloxacin 500 mg BID, respectively, during the second five days of treatment.
Eradication rates were 80.8% (95% CI, 72.8% to 87.3%) with clarithromycin sequential therapy, 96.0% (95% CI, 90.9% to 98.7%) with levofloxacin-250 sequential therapy, and 96.8% (95% CI, 92.0% to 99.1%) with levofloxacin-500 sequential therapy.
The clarithromycin-group eradication rate was significantly lower than both levofloxacin groups. No significant difference was observed between the levofloxacin-250 and levofloxacin-500 groups. No differences in prevalence of antimicrobial resistance or incidence of adverse events were observed between the groups. Levofloxacin-250 therapy does offer cost savings when compared with clarithromycin sequential therapy.
A potential limitation to the study is referral bias, as each of the patients first were sent by their primary physicians to a specialized GI clinic.
Bottom line: In areas with a high prevalence of clarithromycin-resistant strains of H. pylori levofloxacin-containing sequential therapy should be considered for a first-line eradication regimen.
Citation: Romano M, Cuomo A, Gravina AG, et al. Empirical levofloxacin-containing versus clarithromycin-containing sequential therapy for Helicobacter pylori eradication: a randomised trial. Gut. 2010;59(11):1465-1470.
Tako-Tsubo Cardiomyopathy Is Associated with Higher Hospital Readmission Rates and Long-Term Mortality
Clinical question: What is the natural history of patients who develop tako-tsubo cardiomyopathy?
Background: Stress-induced or tako-tsubo cardiomyopathy (TTC) is a rare acute cardiac syndrome, characterized by chest pain or dyspnea, ischemic electrocardiographic changes, transient left ventricular (LV) dysfunction, and limited release of cardiac injury markers, in the absence of epicardial coronary artery disease (CAD). The long-term outcome of this condition is unknown.
Study design: Prospective, case-control study.
Setting: Five urban-based hospitals in Italy.
Synopsis: One hundred-sixteen patients with TTC were included in the five-year study period. Patients were followed up at one and six months, then annually thereafter. Primary endpoints were death, TTC recurrence, and rehospitalization for any cause.
Mean initial LV ejection fraction (LVEF) was 36%. Two patients died of refractory heart failure during hospitalization. Of the patients who were discharged alive, all except one showed complete LV functional recovery.
At follow-up (mean two years), only 64 (55%) patients were asymptomatic. Rehospitalization rate was high (25%), with chest pain and dyspnea the most common causes. Only two patients had a recurrence of TTC. Eleven patients died (seven from cardiovascular causes). There was no significant difference in mortality or in other clinical events between patients with and without severe LV dysfunction at presentation. The standardized mortality ratio was 3.40 (95% CI, 1.83-6.34) in the TTC population, compared with the age- and sex-specific mortality of the general population.
The study is limited by a lack of patients with subclinical TTC disease and those who might have suffered from sudden cardiac death prior to enrollment, leading to a possible sampling bias, as well as the nonrandomized use of beta-blockers.
Bottom line: Tako-tsubo disease is associated with rare recurrence of the disease, common recurrence of chest pain and dyspnea, and three times the mortality rate of the general population.
Citation: Parodi G, Bellandi B, Del Pace S, et al. Natural history of tako-tsubo cardiomyopathy. Chest. 2011;139(4):887-892.
Seven Independent Risk Factors Predict Postoperative Pulmonary Complications
Clinical question: What are the clinical risk factors that predict higher rates of postoperative pulmonary complications?
Background: Postoperative pulmonary complications (PPCs) are a major cause of postoperative morbidity, mortality, and prolonged hospital stays. Previous studies looking at risk factors for PPCs were limited by sampling bias and small sample sizes.
Study design: Prospective, randomized-sample cohort study.
Setting: Fifty-nine participating Spanish hospitals (community, intermediate referral, or major tertiary-care facilities).
Synopsis: Patients undergoing surgical procedures with general, neuraxial, or regional anesthesia were selected randomly. The main outcome was the development of at least one of the following: respiratory infection, respiratory failure, bronchospasm, atelectasis, pleural effusion, pneumothorax, or aspiration pneumonitis. Of 2,464 patients enrolled, 252 events were observed in 123 patients (5%). The 30-day mortality rate was significantly higher in patients suffering a PPC than those who did not (19.5% vs. 0.5%). Additionally, regression modeling identified seven independent risk factors: low preoperative arterial oxygen saturation, acute respiratory infection within one month of surgery, advanced age, preoperative anemia, upper abdominal or intrathoracic surgery, surgical duration more than two hours, and emergency surgery.
The study was underpowered to assess the significance of all potential risk factors for PPCs. Also, given the number of centers involved in the study, variation in assessing development of PPCs is likely.
Bottom line: Postoperative pulmonary complications are a major cause of morbidity and mortality. Seven independent risk factors were identified for the development of PPCs, which could be useful in preoperative risk stratification.
Citation: Canet J, Gallart L, Gomar C, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338-1350.
Code Status Orders and Goals of Medical ICU Care
Clinical question: How familiar are patients in the medical ICU (MICU) or their surrogates regarding code-status orders and goals of care, what are their preferences, and to what extent do they and their physicians differ?
Background: Discussions about code-status orders and goals of care carry great import in the MICU. However, little data exist on patients’ code-status preferences and goals of care. More knowledge of these issues can help physicians deliver more patient-centered care.
Study design: Prospective interviews.
Setting: Twenty-six-bed MICU at a large Midwestern academic medical center.
Synopsis: Data were collected from December 2008 to December 2009 on a random sample of patients—or their surrogates—admitted to the MICU. Of 135 eligible patients/surrogates, 100 completed interviews. Patients primarily were white (95%) and from the ages of 41 to 80 (79%).
Only 28% of participants recalled having a discussion about CPR and one goal of care, while 27% recalled no discussion at all; 83% preferred full code status but had limited knowledge of CPR and its outcomes in the hospital setting. Only 4% were able to identify all components of CPR, and they estimated the mean probability of survival following in-hospital arrest with CPR to be 71.8%, although data suggest survival is closer to 18%. There was a correlation between a higher estimation of survival following CPR and preference for it. After learning about the evidence-based likelihood of a good neurologic outcome following CPR, 8% of the participants became less interested.
Discrepancies between patients’ stated code status and that in the medical record was identified 16% of the time. Additionally, 67.7% of participants differed with their physicians regarding the most important goal of care.
Bottom line: Discussions about code status and goals of care in the MICU occur less frequently than recommended, leading to widespread discrepancies between patients/surrogates and their physicians regarding the most important goal of care. This is compounded by the fact that patients and their surrogates have limited knowledge about in-hospital CPR and its likelihood of success.
Citation: Gehlbach TG, Shinkunas LA, Forman-Hoffman VL, Thomas KW, Schmidt GA, Kaldjian LC. Code status orders and goals of care in the medical ICU. Chest. 2011;139:802-809. TH
In This Edition
Literature At A Glance
A guide to this month’s studies
- Screening for AAA
- Adverse events in atrial fibrillation
- Biological treatment of inflammatory bowel diseases
- Steroid treatment of inflammatory bowel diseases
- Levofloxacin for H. pylori
- Natural history of tako-tsubo cardiomyopathy
- Predicting postoperative pulmonary complications
- Code status and goals of care in the ICU
New Screening Strategy To Identify Large Abdominal Aortic Aneurysms
Clinical question: Can an effective scoring system be developed to better identify patients at risk for large abdominal aortic aneurysms (AAA)?
Background: Screening reduces AAA-related mortality by about half in men aged >65. The United States Preventive Services Task Force (USPSTF) has recommended screening for AAA in men aged 65 to 75 with a history of smoking. However, more than 50% of AAA ruptures occur in individuals outside this patient cohort, and only some AAAs detected are large enough to warrant surgery.
Study design: Retrospective, observational cohort study.
Setting: More than 20,000 screening sites across the U.S.
Synopsis: Researchers collected demographics and risk factors from 3.1 million people undergoing ultrasound screening for AAA by Life Line Screening Inc. At the screening visit, subjects completed a questionnaire about their health status and medical history. Screening data also included diameter of the infrarenal abdominal aorta. To construct and test a risk model, the screened individuals were randomly allocated into two equal groups: a data set used for model development and one for validation.
Most of the AAAs greater than 5 cm in diameter discovered were in males (84.4%) and among subjects with a smoking history (83%). Other risk factors for large AAAs included advanced age, peripheral arterial disease, and obesity. The authors estimate that there are about 121,000 people with >5.0 cm aneurysms in the general population. Current guidelines would detect only 33.7% of the existing large AAAs. Study limitations include possible selection bias, as a majority of patients were self-referred. Also, the database did not include all comorbidities that could affect the risk of AAA. The self-reported nature of health data might cause misclassification of a patient’s true health status.
Bottom line: A screening strategy based on a newly developed scoring system is an effective way to identify patients at risk of large abdominal aortic aneurysms.
Citation: Greco G, Egorova NN, Gelijns AC, et al. Development of a novel scoring tool for the identification of large >5 cm abdominal aortic aneurysms. Ann Surg. 2010;252(4):675-682.
Risk Factors for Adverse Events in Patients with Symptomatic Atrial Fibrillation
Clinical question: What are the predictors of 30-day adverse events in ED patients evaluated for symptomatic atrial fibrillation?
Background: Atrial fibrillation (AF) affects more than 2 million people in the U.S. and accounts for nearly 1% of ED visits. Physicians have little information to guide risk stratification, and they admit more than 65% of patients. A strategy to better define the ED management of patients presenting with atrial fibrillation is required.
Study design: Retrospective, observational cohort study.
Setting: Urban academic tertiary-care referral center with an adult ED.
Synopsis: A systematic review of the electronic medical records of all ED patients presenting with symptomatic atrial fibrillation over a three-year period was performed. Predefined adverse outcomes included 30-day ED return visits, unscheduled hospitalizations, cardiovascular complications, or death.
Of 832 eligible patients, 216 (25.9%) experienced at least one of the 30-day adverse events. Adverse events occurred in 181 of the 638 (28.4%) admitted patients and 35 of the 192 (18.2%) patients discharged from the ED. Increasing age, complaint of dyspnea, smoking history, inadequate ventricular rate control, and patients receiving beta-blockers were factors independently associated with higher risk for adverse events.
Study results were limited by a number of factors. This was a single-center, retrospective, observational study, with all of its inherent limitations. The predictor model did not include laboratory data, such as BNP or troponin. Patients might have experienced additional events within the 30 days that were treated at other hospitals and not recorded in the database. Patient disposition might have affected the results, as patients initially admitted from the ED had a higher rate of 30-day adverse events than patients who were discharged from the ED.
Bottom line: Patients with increased age, smoking history, complaints of dyspnea, inadequate ventricular rate control in the ED, and home beta-blocker therapy are more likely to experience an atrial-fibrillation-related adverse event within 30 days.
Citation: Barrett TW, Martin AR, Storrow AB, et al. A clinical prediction model to estimate risk for 30-day adverse events in emergency department patients with symptomatic atrial fibrillation. Ann Emerg Med. 2011;57 (1):1-12.
Biological Therapies Are Effective in Inducing Remission in Inflammatory Bowel Disease
Clinical question: Are biological therapies useful in the treatment of ulcerative colitis (UC) and Crohn’s disease (CD)?
Background: Patients with CD and UC often experience flares of disease activity, despite maintenance therapy with 5-aminosalicylic acid compounds. These flares are usually treated with corticosteroids, which carry numerous adverse side effects. The role of biological therapies in inducing remission is uncertain.
Study design: Systematic review and meta-analysis.
Setting: Twenty-seven randomized controlled trials involving 7,416 patients.
Synopsis: Anti-TNF α antibodies and natalizumab were both superior to placebo in inducing remission of luminal CD (RR of no remission 0.87 and 0.88, respectively). Anti-TNF antibodies also were superior to placebo in preventing relapse of luminal CD (RR of relapse=0.71). Infliximab was superior to placebo in inducing remission of moderate to severely active UC (RR=0.72; 95% CI, 0.57-0.91). There were no significantly increased adverse drug effects with anti-TNF α antibodies or with infliximab compared with placebo. Natalizumab caused significantly higher rates of headache.
Limitations include risk of publication bias inherent in meta-analyses. There also was evidence of moderate heterogeneity in the studies analyzed. Finally, not every study was consistent in reporting adverse drug effects.
Bottom line: Biological therapies are superior to placebo in inducing remission of active UC and CD, as well as preventing relapse of quiescent CD.
Citation: Ford AC, Sandborn WJ, Khan KJ, Hanauer SB, Talley NJ, Moayyedi P. Efficacy of biological therapies in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2011; 106(4):644-659.
Glucocorticosteroids Probably Effective in Treatment of Inflammatory Bowel Disease, Primarily in Active Ulcerative Colitis
Clinical question: Is glucocorticosteroid therapy effective in the treatment of active IBD and in preventing relapses?
Background: Crohn’s disease (CD) and ulcerative colitis (UC) are chronic inflammatory bowel diseases of unclear etiology. Use of standard glucocorticosteroids and budesonide is widespread in inflammatory bowel disease (IBD) treatment. To date, there has been no large-scale meta-analysis to examine the effectiveness of both treatments in CD and UC.
Study design: Systematic review and meta-analysis.
Setting: Twenty randomized controlled trials totaling 2,398 patients.
Synopsis: Standard glucocorticosteroids were superior to placebo for UC remission (RR of no remission=0.65; 95% CI, 0.45-0.93). Both trials of standard glucocorticosteroids in CD remission reported a statistically significant effect, but the overall effect was not significant due to heterogeneity of the studies. Budesonide was superior to placebo for CD remission (RR=0.73; 95% CI, 0.63-0.84) but not in preventing CD relapse (RR=0.93; 95% CI, 0.83-1.04). Standard glucocorticosteroids were superior to budesonide for CD remission (RR=0.82; 95% CI, 0.68-0.98) but with more adverse effects (RR=1.64; 95% CI, 1.34-2.00).
The limitations of the study include the poor overall quality of the studies included in the meta-analysis, with only one study judged as low risk of bias. There was intermediate to high heterogeneity between study results.
Bottom line: Standard glucocorticosteroids are likely effective in inducing remission in UC and, possibly, in CD. Budesonide probably is effective at inducing remission in active CD. Neither therapy was recommended in preventing relapse of UC and CD.
Citation: Ford AC, Bernstein CN, Khan KJ, et al. Glucocorticosteroid therapy in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2011;106(4):590-599.
Levofloxacin Effective in Treatment of H. Pylori in Settings of High Clarithromycin Resistance
Clinical question: In areas with high H. pylori clarithromycin resistance rates, is levofloxacin more effective in eradicating H. pylori than standard clarithromycin, based treatment regimens?
Background: The rise in antimicrobial drug resistance is a major cause for the decreasing rate of H. pylori eradication. In areas with higher than 15% H. pyloriclarithromycin-resistant strains, quadruple therapy has been suggested as first-line therapy. The efficacy of a levofloxacin-based sequential therapy in eradicating H. pylori is undetermined.
Study design: Prospective, randomized, controlled multicenter study with a parallel-group design.
Setting: Five gastroenterology clinics in Italy.
Synopsis: Researchers randomly assigned 375 patients who were infected with H. pylori and naive to treatment to one of three groups. All three treatment groups received an initial five days of omeprazole 20 mg BID and amoxicillin 1 gm BID, then five days of omeprazole 20 mg BID and tinidazole 500 mg BID. The groups also received either clarithromycin 500 mg BID, levofloxacin 250 mg BID, or levofloxacin 500 mg BID, respectively, during the second five days of treatment.
Eradication rates were 80.8% (95% CI, 72.8% to 87.3%) with clarithromycin sequential therapy, 96.0% (95% CI, 90.9% to 98.7%) with levofloxacin-250 sequential therapy, and 96.8% (95% CI, 92.0% to 99.1%) with levofloxacin-500 sequential therapy.
The clarithromycin-group eradication rate was significantly lower than both levofloxacin groups. No significant difference was observed between the levofloxacin-250 and levofloxacin-500 groups. No differences in prevalence of antimicrobial resistance or incidence of adverse events were observed between the groups. Levofloxacin-250 therapy does offer cost savings when compared with clarithromycin sequential therapy.
A potential limitation to the study is referral bias, as each of the patients first were sent by their primary physicians to a specialized GI clinic.
Bottom line: In areas with a high prevalence of clarithromycin-resistant strains of H. pylori levofloxacin-containing sequential therapy should be considered for a first-line eradication regimen.
Citation: Romano M, Cuomo A, Gravina AG, et al. Empirical levofloxacin-containing versus clarithromycin-containing sequential therapy for Helicobacter pylori eradication: a randomised trial. Gut. 2010;59(11):1465-1470.
Tako-Tsubo Cardiomyopathy Is Associated with Higher Hospital Readmission Rates and Long-Term Mortality
Clinical question: What is the natural history of patients who develop tako-tsubo cardiomyopathy?
Background: Stress-induced or tako-tsubo cardiomyopathy (TTC) is a rare acute cardiac syndrome, characterized by chest pain or dyspnea, ischemic electrocardiographic changes, transient left ventricular (LV) dysfunction, and limited release of cardiac injury markers, in the absence of epicardial coronary artery disease (CAD). The long-term outcome of this condition is unknown.
Study design: Prospective, case-control study.
Setting: Five urban-based hospitals in Italy.
Synopsis: One hundred-sixteen patients with TTC were included in the five-year study period. Patients were followed up at one and six months, then annually thereafter. Primary endpoints were death, TTC recurrence, and rehospitalization for any cause.
Mean initial LV ejection fraction (LVEF) was 36%. Two patients died of refractory heart failure during hospitalization. Of the patients who were discharged alive, all except one showed complete LV functional recovery.
At follow-up (mean two years), only 64 (55%) patients were asymptomatic. Rehospitalization rate was high (25%), with chest pain and dyspnea the most common causes. Only two patients had a recurrence of TTC. Eleven patients died (seven from cardiovascular causes). There was no significant difference in mortality or in other clinical events between patients with and without severe LV dysfunction at presentation. The standardized mortality ratio was 3.40 (95% CI, 1.83-6.34) in the TTC population, compared with the age- and sex-specific mortality of the general population.
The study is limited by a lack of patients with subclinical TTC disease and those who might have suffered from sudden cardiac death prior to enrollment, leading to a possible sampling bias, as well as the nonrandomized use of beta-blockers.
Bottom line: Tako-tsubo disease is associated with rare recurrence of the disease, common recurrence of chest pain and dyspnea, and three times the mortality rate of the general population.
Citation: Parodi G, Bellandi B, Del Pace S, et al. Natural history of tako-tsubo cardiomyopathy. Chest. 2011;139(4):887-892.
Seven Independent Risk Factors Predict Postoperative Pulmonary Complications
Clinical question: What are the clinical risk factors that predict higher rates of postoperative pulmonary complications?
Background: Postoperative pulmonary complications (PPCs) are a major cause of postoperative morbidity, mortality, and prolonged hospital stays. Previous studies looking at risk factors for PPCs were limited by sampling bias and small sample sizes.
Study design: Prospective, randomized-sample cohort study.
Setting: Fifty-nine participating Spanish hospitals (community, intermediate referral, or major tertiary-care facilities).
Synopsis: Patients undergoing surgical procedures with general, neuraxial, or regional anesthesia were selected randomly. The main outcome was the development of at least one of the following: respiratory infection, respiratory failure, bronchospasm, atelectasis, pleural effusion, pneumothorax, or aspiration pneumonitis. Of 2,464 patients enrolled, 252 events were observed in 123 patients (5%). The 30-day mortality rate was significantly higher in patients suffering a PPC than those who did not (19.5% vs. 0.5%). Additionally, regression modeling identified seven independent risk factors: low preoperative arterial oxygen saturation, acute respiratory infection within one month of surgery, advanced age, preoperative anemia, upper abdominal or intrathoracic surgery, surgical duration more than two hours, and emergency surgery.
The study was underpowered to assess the significance of all potential risk factors for PPCs. Also, given the number of centers involved in the study, variation in assessing development of PPCs is likely.
Bottom line: Postoperative pulmonary complications are a major cause of morbidity and mortality. Seven independent risk factors were identified for the development of PPCs, which could be useful in preoperative risk stratification.
Citation: Canet J, Gallart L, Gomar C, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338-1350.
Code Status Orders and Goals of Medical ICU Care
Clinical question: How familiar are patients in the medical ICU (MICU) or their surrogates regarding code-status orders and goals of care, what are their preferences, and to what extent do they and their physicians differ?
Background: Discussions about code-status orders and goals of care carry great import in the MICU. However, little data exist on patients’ code-status preferences and goals of care. More knowledge of these issues can help physicians deliver more patient-centered care.
Study design: Prospective interviews.
Setting: Twenty-six-bed MICU at a large Midwestern academic medical center.
Synopsis: Data were collected from December 2008 to December 2009 on a random sample of patients—or their surrogates—admitted to the MICU. Of 135 eligible patients/surrogates, 100 completed interviews. Patients primarily were white (95%) and from the ages of 41 to 80 (79%).
Only 28% of participants recalled having a discussion about CPR and one goal of care, while 27% recalled no discussion at all; 83% preferred full code status but had limited knowledge of CPR and its outcomes in the hospital setting. Only 4% were able to identify all components of CPR, and they estimated the mean probability of survival following in-hospital arrest with CPR to be 71.8%, although data suggest survival is closer to 18%. There was a correlation between a higher estimation of survival following CPR and preference for it. After learning about the evidence-based likelihood of a good neurologic outcome following CPR, 8% of the participants became less interested.
Discrepancies between patients’ stated code status and that in the medical record was identified 16% of the time. Additionally, 67.7% of participants differed with their physicians regarding the most important goal of care.
Bottom line: Discussions about code status and goals of care in the MICU occur less frequently than recommended, leading to widespread discrepancies between patients/surrogates and their physicians regarding the most important goal of care. This is compounded by the fact that patients and their surrogates have limited knowledge about in-hospital CPR and its likelihood of success.
Citation: Gehlbach TG, Shinkunas LA, Forman-Hoffman VL, Thomas KW, Schmidt GA, Kaldjian LC. Code status orders and goals of care in the medical ICU. Chest. 2011;139:802-809. TH
In This Edition
Literature At A Glance
A guide to this month’s studies
- Screening for AAA
- Adverse events in atrial fibrillation
- Biological treatment of inflammatory bowel diseases
- Steroid treatment of inflammatory bowel diseases
- Levofloxacin for H. pylori
- Natural history of tako-tsubo cardiomyopathy
- Predicting postoperative pulmonary complications
- Code status and goals of care in the ICU
New Screening Strategy To Identify Large Abdominal Aortic Aneurysms
Clinical question: Can an effective scoring system be developed to better identify patients at risk for large abdominal aortic aneurysms (AAA)?
Background: Screening reduces AAA-related mortality by about half in men aged >65. The United States Preventive Services Task Force (USPSTF) has recommended screening for AAA in men aged 65 to 75 with a history of smoking. However, more than 50% of AAA ruptures occur in individuals outside this patient cohort, and only some AAAs detected are large enough to warrant surgery.
Study design: Retrospective, observational cohort study.
Setting: More than 20,000 screening sites across the U.S.
Synopsis: Researchers collected demographics and risk factors from 3.1 million people undergoing ultrasound screening for AAA by Life Line Screening Inc. At the screening visit, subjects completed a questionnaire about their health status and medical history. Screening data also included diameter of the infrarenal abdominal aorta. To construct and test a risk model, the screened individuals were randomly allocated into two equal groups: a data set used for model development and one for validation.
Most of the AAAs greater than 5 cm in diameter discovered were in males (84.4%) and among subjects with a smoking history (83%). Other risk factors for large AAAs included advanced age, peripheral arterial disease, and obesity. The authors estimate that there are about 121,000 people with >5.0 cm aneurysms in the general population. Current guidelines would detect only 33.7% of the existing large AAAs. Study limitations include possible selection bias, as a majority of patients were self-referred. Also, the database did not include all comorbidities that could affect the risk of AAA. The self-reported nature of health data might cause misclassification of a patient’s true health status.
Bottom line: A screening strategy based on a newly developed scoring system is an effective way to identify patients at risk of large abdominal aortic aneurysms.
Citation: Greco G, Egorova NN, Gelijns AC, et al. Development of a novel scoring tool for the identification of large >5 cm abdominal aortic aneurysms. Ann Surg. 2010;252(4):675-682.
Risk Factors for Adverse Events in Patients with Symptomatic Atrial Fibrillation
Clinical question: What are the predictors of 30-day adverse events in ED patients evaluated for symptomatic atrial fibrillation?
Background: Atrial fibrillation (AF) affects more than 2 million people in the U.S. and accounts for nearly 1% of ED visits. Physicians have little information to guide risk stratification, and they admit more than 65% of patients. A strategy to better define the ED management of patients presenting with atrial fibrillation is required.
Study design: Retrospective, observational cohort study.
Setting: Urban academic tertiary-care referral center with an adult ED.
Synopsis: A systematic review of the electronic medical records of all ED patients presenting with symptomatic atrial fibrillation over a three-year period was performed. Predefined adverse outcomes included 30-day ED return visits, unscheduled hospitalizations, cardiovascular complications, or death.
Of 832 eligible patients, 216 (25.9%) experienced at least one of the 30-day adverse events. Adverse events occurred in 181 of the 638 (28.4%) admitted patients and 35 of the 192 (18.2%) patients discharged from the ED. Increasing age, complaint of dyspnea, smoking history, inadequate ventricular rate control, and patients receiving beta-blockers were factors independently associated with higher risk for adverse events.
Study results were limited by a number of factors. This was a single-center, retrospective, observational study, with all of its inherent limitations. The predictor model did not include laboratory data, such as BNP or troponin. Patients might have experienced additional events within the 30 days that were treated at other hospitals and not recorded in the database. Patient disposition might have affected the results, as patients initially admitted from the ED had a higher rate of 30-day adverse events than patients who were discharged from the ED.
Bottom line: Patients with increased age, smoking history, complaints of dyspnea, inadequate ventricular rate control in the ED, and home beta-blocker therapy are more likely to experience an atrial-fibrillation-related adverse event within 30 days.
Citation: Barrett TW, Martin AR, Storrow AB, et al. A clinical prediction model to estimate risk for 30-day adverse events in emergency department patients with symptomatic atrial fibrillation. Ann Emerg Med. 2011;57 (1):1-12.
Biological Therapies Are Effective in Inducing Remission in Inflammatory Bowel Disease
Clinical question: Are biological therapies useful in the treatment of ulcerative colitis (UC) and Crohn’s disease (CD)?
Background: Patients with CD and UC often experience flares of disease activity, despite maintenance therapy with 5-aminosalicylic acid compounds. These flares are usually treated with corticosteroids, which carry numerous adverse side effects. The role of biological therapies in inducing remission is uncertain.
Study design: Systematic review and meta-analysis.
Setting: Twenty-seven randomized controlled trials involving 7,416 patients.
Synopsis: Anti-TNF α antibodies and natalizumab were both superior to placebo in inducing remission of luminal CD (RR of no remission 0.87 and 0.88, respectively). Anti-TNF antibodies also were superior to placebo in preventing relapse of luminal CD (RR of relapse=0.71). Infliximab was superior to placebo in inducing remission of moderate to severely active UC (RR=0.72; 95% CI, 0.57-0.91). There were no significantly increased adverse drug effects with anti-TNF α antibodies or with infliximab compared with placebo. Natalizumab caused significantly higher rates of headache.
Limitations include risk of publication bias inherent in meta-analyses. There also was evidence of moderate heterogeneity in the studies analyzed. Finally, not every study was consistent in reporting adverse drug effects.
Bottom line: Biological therapies are superior to placebo in inducing remission of active UC and CD, as well as preventing relapse of quiescent CD.
Citation: Ford AC, Sandborn WJ, Khan KJ, Hanauer SB, Talley NJ, Moayyedi P. Efficacy of biological therapies in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2011; 106(4):644-659.
Glucocorticosteroids Probably Effective in Treatment of Inflammatory Bowel Disease, Primarily in Active Ulcerative Colitis
Clinical question: Is glucocorticosteroid therapy effective in the treatment of active IBD and in preventing relapses?
Background: Crohn’s disease (CD) and ulcerative colitis (UC) are chronic inflammatory bowel diseases of unclear etiology. Use of standard glucocorticosteroids and budesonide is widespread in inflammatory bowel disease (IBD) treatment. To date, there has been no large-scale meta-analysis to examine the effectiveness of both treatments in CD and UC.
Study design: Systematic review and meta-analysis.
Setting: Twenty randomized controlled trials totaling 2,398 patients.
Synopsis: Standard glucocorticosteroids were superior to placebo for UC remission (RR of no remission=0.65; 95% CI, 0.45-0.93). Both trials of standard glucocorticosteroids in CD remission reported a statistically significant effect, but the overall effect was not significant due to heterogeneity of the studies. Budesonide was superior to placebo for CD remission (RR=0.73; 95% CI, 0.63-0.84) but not in preventing CD relapse (RR=0.93; 95% CI, 0.83-1.04). Standard glucocorticosteroids were superior to budesonide for CD remission (RR=0.82; 95% CI, 0.68-0.98) but with more adverse effects (RR=1.64; 95% CI, 1.34-2.00).
The limitations of the study include the poor overall quality of the studies included in the meta-analysis, with only one study judged as low risk of bias. There was intermediate to high heterogeneity between study results.
Bottom line: Standard glucocorticosteroids are likely effective in inducing remission in UC and, possibly, in CD. Budesonide probably is effective at inducing remission in active CD. Neither therapy was recommended in preventing relapse of UC and CD.
Citation: Ford AC, Bernstein CN, Khan KJ, et al. Glucocorticosteroid therapy in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. 2011;106(4):590-599.
Levofloxacin Effective in Treatment of H. Pylori in Settings of High Clarithromycin Resistance
Clinical question: In areas with high H. pylori clarithromycin resistance rates, is levofloxacin more effective in eradicating H. pylori than standard clarithromycin, based treatment regimens?
Background: The rise in antimicrobial drug resistance is a major cause for the decreasing rate of H. pylori eradication. In areas with higher than 15% H. pyloriclarithromycin-resistant strains, quadruple therapy has been suggested as first-line therapy. The efficacy of a levofloxacin-based sequential therapy in eradicating H. pylori is undetermined.
Study design: Prospective, randomized, controlled multicenter study with a parallel-group design.
Setting: Five gastroenterology clinics in Italy.
Synopsis: Researchers randomly assigned 375 patients who were infected with H. pylori and naive to treatment to one of three groups. All three treatment groups received an initial five days of omeprazole 20 mg BID and amoxicillin 1 gm BID, then five days of omeprazole 20 mg BID and tinidazole 500 mg BID. The groups also received either clarithromycin 500 mg BID, levofloxacin 250 mg BID, or levofloxacin 500 mg BID, respectively, during the second five days of treatment.
Eradication rates were 80.8% (95% CI, 72.8% to 87.3%) with clarithromycin sequential therapy, 96.0% (95% CI, 90.9% to 98.7%) with levofloxacin-250 sequential therapy, and 96.8% (95% CI, 92.0% to 99.1%) with levofloxacin-500 sequential therapy.
The clarithromycin-group eradication rate was significantly lower than both levofloxacin groups. No significant difference was observed between the levofloxacin-250 and levofloxacin-500 groups. No differences in prevalence of antimicrobial resistance or incidence of adverse events were observed between the groups. Levofloxacin-250 therapy does offer cost savings when compared with clarithromycin sequential therapy.
A potential limitation to the study is referral bias, as each of the patients first were sent by their primary physicians to a specialized GI clinic.
Bottom line: In areas with a high prevalence of clarithromycin-resistant strains of H. pylori levofloxacin-containing sequential therapy should be considered for a first-line eradication regimen.
Citation: Romano M, Cuomo A, Gravina AG, et al. Empirical levofloxacin-containing versus clarithromycin-containing sequential therapy for Helicobacter pylori eradication: a randomised trial. Gut. 2010;59(11):1465-1470.
Tako-Tsubo Cardiomyopathy Is Associated with Higher Hospital Readmission Rates and Long-Term Mortality
Clinical question: What is the natural history of patients who develop tako-tsubo cardiomyopathy?
Background: Stress-induced or tako-tsubo cardiomyopathy (TTC) is a rare acute cardiac syndrome, characterized by chest pain or dyspnea, ischemic electrocardiographic changes, transient left ventricular (LV) dysfunction, and limited release of cardiac injury markers, in the absence of epicardial coronary artery disease (CAD). The long-term outcome of this condition is unknown.
Study design: Prospective, case-control study.
Setting: Five urban-based hospitals in Italy.
Synopsis: One hundred-sixteen patients with TTC were included in the five-year study period. Patients were followed up at one and six months, then annually thereafter. Primary endpoints were death, TTC recurrence, and rehospitalization for any cause.
Mean initial LV ejection fraction (LVEF) was 36%. Two patients died of refractory heart failure during hospitalization. Of the patients who were discharged alive, all except one showed complete LV functional recovery.
At follow-up (mean two years), only 64 (55%) patients were asymptomatic. Rehospitalization rate was high (25%), with chest pain and dyspnea the most common causes. Only two patients had a recurrence of TTC. Eleven patients died (seven from cardiovascular causes). There was no significant difference in mortality or in other clinical events between patients with and without severe LV dysfunction at presentation. The standardized mortality ratio was 3.40 (95% CI, 1.83-6.34) in the TTC population, compared with the age- and sex-specific mortality of the general population.
The study is limited by a lack of patients with subclinical TTC disease and those who might have suffered from sudden cardiac death prior to enrollment, leading to a possible sampling bias, as well as the nonrandomized use of beta-blockers.
Bottom line: Tako-tsubo disease is associated with rare recurrence of the disease, common recurrence of chest pain and dyspnea, and three times the mortality rate of the general population.
Citation: Parodi G, Bellandi B, Del Pace S, et al. Natural history of tako-tsubo cardiomyopathy. Chest. 2011;139(4):887-892.
Seven Independent Risk Factors Predict Postoperative Pulmonary Complications
Clinical question: What are the clinical risk factors that predict higher rates of postoperative pulmonary complications?
Background: Postoperative pulmonary complications (PPCs) are a major cause of postoperative morbidity, mortality, and prolonged hospital stays. Previous studies looking at risk factors for PPCs were limited by sampling bias and small sample sizes.
Study design: Prospective, randomized-sample cohort study.
Setting: Fifty-nine participating Spanish hospitals (community, intermediate referral, or major tertiary-care facilities).
Synopsis: Patients undergoing surgical procedures with general, neuraxial, or regional anesthesia were selected randomly. The main outcome was the development of at least one of the following: respiratory infection, respiratory failure, bronchospasm, atelectasis, pleural effusion, pneumothorax, or aspiration pneumonitis. Of 2,464 patients enrolled, 252 events were observed in 123 patients (5%). The 30-day mortality rate was significantly higher in patients suffering a PPC than those who did not (19.5% vs. 0.5%). Additionally, regression modeling identified seven independent risk factors: low preoperative arterial oxygen saturation, acute respiratory infection within one month of surgery, advanced age, preoperative anemia, upper abdominal or intrathoracic surgery, surgical duration more than two hours, and emergency surgery.
The study was underpowered to assess the significance of all potential risk factors for PPCs. Also, given the number of centers involved in the study, variation in assessing development of PPCs is likely.
Bottom line: Postoperative pulmonary complications are a major cause of morbidity and mortality. Seven independent risk factors were identified for the development of PPCs, which could be useful in preoperative risk stratification.
Citation: Canet J, Gallart L, Gomar C, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338-1350.
Code Status Orders and Goals of Medical ICU Care
Clinical question: How familiar are patients in the medical ICU (MICU) or their surrogates regarding code-status orders and goals of care, what are their preferences, and to what extent do they and their physicians differ?
Background: Discussions about code-status orders and goals of care carry great import in the MICU. However, little data exist on patients’ code-status preferences and goals of care. More knowledge of these issues can help physicians deliver more patient-centered care.
Study design: Prospective interviews.
Setting: Twenty-six-bed MICU at a large Midwestern academic medical center.
Synopsis: Data were collected from December 2008 to December 2009 on a random sample of patients—or their surrogates—admitted to the MICU. Of 135 eligible patients/surrogates, 100 completed interviews. Patients primarily were white (95%) and from the ages of 41 to 80 (79%).
Only 28% of participants recalled having a discussion about CPR and one goal of care, while 27% recalled no discussion at all; 83% preferred full code status but had limited knowledge of CPR and its outcomes in the hospital setting. Only 4% were able to identify all components of CPR, and they estimated the mean probability of survival following in-hospital arrest with CPR to be 71.8%, although data suggest survival is closer to 18%. There was a correlation between a higher estimation of survival following CPR and preference for it. After learning about the evidence-based likelihood of a good neurologic outcome following CPR, 8% of the participants became less interested.
Discrepancies between patients’ stated code status and that in the medical record was identified 16% of the time. Additionally, 67.7% of participants differed with their physicians regarding the most important goal of care.
Bottom line: Discussions about code status and goals of care in the MICU occur less frequently than recommended, leading to widespread discrepancies between patients/surrogates and their physicians regarding the most important goal of care. This is compounded by the fact that patients and their surrogates have limited knowledge about in-hospital CPR and its likelihood of success.
Citation: Gehlbach TG, Shinkunas LA, Forman-Hoffman VL, Thomas KW, Schmidt GA, Kaldjian LC. Code status orders and goals of care in the medical ICU. Chest. 2011;139:802-809. TH
SHM’S Leadership Academy Trains Next Generation of HM Leaders
As HM programs mature, seasoned leaders begin to evaluate the leadership potential of their staff, both clinical and administrative. Although the skills that brought each staff member to their current position often are well above average, the personal tools necessary to lead teams will ultimately come to the fore.
The need to develop and enhance leadership skills within hospitalist programs has attracted nearly 1,800 participants to SHM’s Leadership Academy courses.
Hundreds more are expected to attend the next academy, Sept. 12-15 at the historic Fontainebleau Miami Beach resort. Registration is available at www.hospitalmedicine.org/leadership.
To encourage HM programs to strengthen entire teams, SHM offers a $100 discount per person for groups of three or more hospitalists. Group leaders who bring their administrators receive a 10% discount.
First-time Leadership Academy participants will participate in the "Foundations for Effective Leadership" course. Those who already have completed "Foundations" will take their leadership skills to the next level with "Advanced Leadership: Personal Leadership Excellence."
Another advanced leadership course, "Strengthening Your Organization," will be presented in February 2012 in New Orleans.
"I send every hospitalist to Leadership Academy because I believe it makes them better team members," said Eric Howell, section chief of hospital medicine and deputy director of hospital operations for the Department of Medicine at Johns Hopkins Bayview Medical Center, in a video presented at HM11. Dr. Howell, an academy faculty member, says the training makes hospitalists "better problem-solvers. I believe it makes them better doctors." TH
As HM programs mature, seasoned leaders begin to evaluate the leadership potential of their staff, both clinical and administrative. Although the skills that brought each staff member to their current position often are well above average, the personal tools necessary to lead teams will ultimately come to the fore.
The need to develop and enhance leadership skills within hospitalist programs has attracted nearly 1,800 participants to SHM’s Leadership Academy courses.
Hundreds more are expected to attend the next academy, Sept. 12-15 at the historic Fontainebleau Miami Beach resort. Registration is available at www.hospitalmedicine.org/leadership.
To encourage HM programs to strengthen entire teams, SHM offers a $100 discount per person for groups of three or more hospitalists. Group leaders who bring their administrators receive a 10% discount.
First-time Leadership Academy participants will participate in the "Foundations for Effective Leadership" course. Those who already have completed "Foundations" will take their leadership skills to the next level with "Advanced Leadership: Personal Leadership Excellence."
Another advanced leadership course, "Strengthening Your Organization," will be presented in February 2012 in New Orleans.
"I send every hospitalist to Leadership Academy because I believe it makes them better team members," said Eric Howell, section chief of hospital medicine and deputy director of hospital operations for the Department of Medicine at Johns Hopkins Bayview Medical Center, in a video presented at HM11. Dr. Howell, an academy faculty member, says the training makes hospitalists "better problem-solvers. I believe it makes them better doctors." TH
As HM programs mature, seasoned leaders begin to evaluate the leadership potential of their staff, both clinical and administrative. Although the skills that brought each staff member to their current position often are well above average, the personal tools necessary to lead teams will ultimately come to the fore.
The need to develop and enhance leadership skills within hospitalist programs has attracted nearly 1,800 participants to SHM’s Leadership Academy courses.
Hundreds more are expected to attend the next academy, Sept. 12-15 at the historic Fontainebleau Miami Beach resort. Registration is available at www.hospitalmedicine.org/leadership.
To encourage HM programs to strengthen entire teams, SHM offers a $100 discount per person for groups of three or more hospitalists. Group leaders who bring their administrators receive a 10% discount.
First-time Leadership Academy participants will participate in the "Foundations for Effective Leadership" course. Those who already have completed "Foundations" will take their leadership skills to the next level with "Advanced Leadership: Personal Leadership Excellence."
Another advanced leadership course, "Strengthening Your Organization," will be presented in February 2012 in New Orleans.
"I send every hospitalist to Leadership Academy because I believe it makes them better team members," said Eric Howell, section chief of hospital medicine and deputy director of hospital operations for the Department of Medicine at Johns Hopkins Bayview Medical Center, in a video presented at HM11. Dr. Howell, an academy faculty member, says the training makes hospitalists "better problem-solvers. I believe it makes them better doctors." TH
Policy Corner: Obama Suggests Eliminating Wasteful Regulations
The federal government is taking a hard look at many of its regulations, and hospitalists might have the chance to help identify those that no longer make sense.
On Jan. 18, President Obama issued Executive Order 13563, which calls, in part, for a comprehensive retrospective review of existing government regulations. The stated goal of this review is to improve or remove those rules that are out of date, unnecessary, excessively burdensome, or in conflict with other rules.
The Office of Information and Regulatory Affairs (OIRA), the executive-level department charged with overseeing the execution of this order, asked federal agencies to submit preliminary plans for how they will conduct their internal reviews. The agencies responded, and on May 26, the White House released 30 agency preliminary plans to the public, including those prepared by the Department of Commerce, the Department of Energy, and the Department of Health and Human Services (HHS).
When reviewing some of these publicly available preliminary plans, the easy answer for some observers is to say that most rules should be eliminated. Rules requiring the use of such technologies as film X-rays instead of digital images are obvious culprits in the out-of date category; rules defining milk as "oil" (subjecting it to the same costly environmental safeguards as real oil) are just as absurd. Both of these regulations are being lifted as a result of the review.
In contrast, many rules actually do protect public health and safety and will not be subject to review. For example, as a result of federal rulemaking, highway deaths are at the lowest level in 60 years and the risk of contracting salmonella from eggs is relatively low.
As part of HHS, the Center for Medicare & Medicaid Services (CMS) specifically stated that "the goal of the retrospective review will be to identify opportunities to improve patient care and outcomes and reduce system costs by removing obsolete or burdensome requirements." A major CMS concern will be to prevent the elimination or revision of a regulation only to find that the problem it sought to solve resurfaces, or that its removal or revision results in unanticipated and more serious outcomes.
This review could significantly impact HM in areas of quality measurement and reporting requirements:
- What quality measurements might not accomplish their intent?
- What measures might result in more harm than good?
- What reporting or process requirements could be changed to make for less duplication?
- If requirements cannot be eliminated, how can they be improved?
Due to hospitalist expertise in quality-improvement (QI) efforts and cost containment, these stated goals and the concerns that come with them are areas where hospitalists are likely to have some good answers. Hospitalists should not hesitate to provide their input to SHM Government Relations staff so that your ideas can be shared with CMS.
A complete list of agency proposals is available at www.whitehouse.gov/21stcentury gov/actions/21st-century-regulatory-system.
The federal government is taking a hard look at many of its regulations, and hospitalists might have the chance to help identify those that no longer make sense.
On Jan. 18, President Obama issued Executive Order 13563, which calls, in part, for a comprehensive retrospective review of existing government regulations. The stated goal of this review is to improve or remove those rules that are out of date, unnecessary, excessively burdensome, or in conflict with other rules.
The Office of Information and Regulatory Affairs (OIRA), the executive-level department charged with overseeing the execution of this order, asked federal agencies to submit preliminary plans for how they will conduct their internal reviews. The agencies responded, and on May 26, the White House released 30 agency preliminary plans to the public, including those prepared by the Department of Commerce, the Department of Energy, and the Department of Health and Human Services (HHS).
When reviewing some of these publicly available preliminary plans, the easy answer for some observers is to say that most rules should be eliminated. Rules requiring the use of such technologies as film X-rays instead of digital images are obvious culprits in the out-of date category; rules defining milk as "oil" (subjecting it to the same costly environmental safeguards as real oil) are just as absurd. Both of these regulations are being lifted as a result of the review.
In contrast, many rules actually do protect public health and safety and will not be subject to review. For example, as a result of federal rulemaking, highway deaths are at the lowest level in 60 years and the risk of contracting salmonella from eggs is relatively low.
As part of HHS, the Center for Medicare & Medicaid Services (CMS) specifically stated that "the goal of the retrospective review will be to identify opportunities to improve patient care and outcomes and reduce system costs by removing obsolete or burdensome requirements." A major CMS concern will be to prevent the elimination or revision of a regulation only to find that the problem it sought to solve resurfaces, or that its removal or revision results in unanticipated and more serious outcomes.
This review could significantly impact HM in areas of quality measurement and reporting requirements:
- What quality measurements might not accomplish their intent?
- What measures might result in more harm than good?
- What reporting or process requirements could be changed to make for less duplication?
- If requirements cannot be eliminated, how can they be improved?
Due to hospitalist expertise in quality-improvement (QI) efforts and cost containment, these stated goals and the concerns that come with them are areas where hospitalists are likely to have some good answers. Hospitalists should not hesitate to provide their input to SHM Government Relations staff so that your ideas can be shared with CMS.
A complete list of agency proposals is available at www.whitehouse.gov/21stcentury gov/actions/21st-century-regulatory-system.
The federal government is taking a hard look at many of its regulations, and hospitalists might have the chance to help identify those that no longer make sense.
On Jan. 18, President Obama issued Executive Order 13563, which calls, in part, for a comprehensive retrospective review of existing government regulations. The stated goal of this review is to improve or remove those rules that are out of date, unnecessary, excessively burdensome, or in conflict with other rules.
The Office of Information and Regulatory Affairs (OIRA), the executive-level department charged with overseeing the execution of this order, asked federal agencies to submit preliminary plans for how they will conduct their internal reviews. The agencies responded, and on May 26, the White House released 30 agency preliminary plans to the public, including those prepared by the Department of Commerce, the Department of Energy, and the Department of Health and Human Services (HHS).
When reviewing some of these publicly available preliminary plans, the easy answer for some observers is to say that most rules should be eliminated. Rules requiring the use of such technologies as film X-rays instead of digital images are obvious culprits in the out-of date category; rules defining milk as "oil" (subjecting it to the same costly environmental safeguards as real oil) are just as absurd. Both of these regulations are being lifted as a result of the review.
In contrast, many rules actually do protect public health and safety and will not be subject to review. For example, as a result of federal rulemaking, highway deaths are at the lowest level in 60 years and the risk of contracting salmonella from eggs is relatively low.
As part of HHS, the Center for Medicare & Medicaid Services (CMS) specifically stated that "the goal of the retrospective review will be to identify opportunities to improve patient care and outcomes and reduce system costs by removing obsolete or burdensome requirements." A major CMS concern will be to prevent the elimination or revision of a regulation only to find that the problem it sought to solve resurfaces, or that its removal or revision results in unanticipated and more serious outcomes.
This review could significantly impact HM in areas of quality measurement and reporting requirements:
- What quality measurements might not accomplish their intent?
- What measures might result in more harm than good?
- What reporting or process requirements could be changed to make for less duplication?
- If requirements cannot be eliminated, how can they be improved?
Due to hospitalist expertise in quality-improvement (QI) efforts and cost containment, these stated goals and the concerns that come with them are areas where hospitalists are likely to have some good answers. Hospitalists should not hesitate to provide their input to SHM Government Relations staff so that your ideas can be shared with CMS.
A complete list of agency proposals is available at www.whitehouse.gov/21stcentury gov/actions/21st-century-regulatory-system.
Master in HM profile

Fifteen years ago, Bob Wachter, MD, MHM, and Lee Goldman, MD, introduced hospital medicine and the term "hospitalist" to modern medicine in an article in the New England Journal of Medicine. In it, they wrote, "we anticipate the rapid growth of a new breed of physicians we call ‘hospitalists’—specialists in inpatient medicine—who will be responsible for managing the care of hospitalized patients in the same way that primary care physicians are responsible for managing the care of outpatients."
Since that introduction in 1996, the term "hospitalist" has gone from concept to cutting edge, and now to a title that describes more than 30,000 caregivers in hospitals around the world.
The evolution and growth of the hospitalist specialty owes much to Dr. Wachter. In addition to coining the term, he wrote the specialty’s first textbook, led SHM as president in 2000, and in 2010 was one of three HM pioneers honored by SHM as the first group of Masters in Hospital Medicine.
For each of the past three years, Modern Healthcare has listed him as one of healthcare’s most influential physician-executives.
Dr. Wachter used his recent presentation at HM11 to reflect on the growth of hospital medicine, where he showed how the specialty’s early focus on quality and safety puts hospitalists in positions of authority among physicians and hospitals.
Today, he is professor and associate chairman of the Department of Medicine at the University of California at San Francisco and chief of the division of hospital medicine, and chief of the medical service at UCSF Medical Center.
In July, Dr. Wachter was named chair-elect of the American Board of Internal Medicine’s (ABIM) board of directors.
Fifteen years ago, Bob Wachter, MD, MHM, and Lee Goldman, MD, introduced hospital medicine and the term "hospitalist" to modern medicine in an article in the New England Journal of Medicine. In it, they wrote, "we anticipate the rapid growth of a new breed of physicians we call ‘hospitalists’—specialists in inpatient medicine—who will be responsible for managing the care of hospitalized patients in the same way that primary care physicians are responsible for managing the care of outpatients."
Since that introduction in 1996, the term "hospitalist" has gone from concept to cutting edge, and now to a title that describes more than 30,000 caregivers in hospitals around the world.
The evolution and growth of the hospitalist specialty owes much to Dr. Wachter. In addition to coining the term, he wrote the specialty’s first textbook, led SHM as president in 2000, and in 2010 was one of three HM pioneers honored by SHM as the first group of Masters in Hospital Medicine.
For each of the past three years, Modern Healthcare has listed him as one of healthcare’s most influential physician-executives.
Dr. Wachter used his recent presentation at HM11 to reflect on the growth of hospital medicine, where he showed how the specialty’s early focus on quality and safety puts hospitalists in positions of authority among physicians and hospitals.
Today, he is professor and associate chairman of the Department of Medicine at the University of California at San Francisco and chief of the division of hospital medicine, and chief of the medical service at UCSF Medical Center.
In July, Dr. Wachter was named chair-elect of the American Board of Internal Medicine’s (ABIM) board of directors.
Fifteen years ago, Bob Wachter, MD, MHM, and Lee Goldman, MD, introduced hospital medicine and the term "hospitalist" to modern medicine in an article in the New England Journal of Medicine. In it, they wrote, "we anticipate the rapid growth of a new breed of physicians we call ‘hospitalists’—specialists in inpatient medicine—who will be responsible for managing the care of hospitalized patients in the same way that primary care physicians are responsible for managing the care of outpatients."
Since that introduction in 1996, the term "hospitalist" has gone from concept to cutting edge, and now to a title that describes more than 30,000 caregivers in hospitals around the world.
The evolution and growth of the hospitalist specialty owes much to Dr. Wachter. In addition to coining the term, he wrote the specialty’s first textbook, led SHM as president in 2000, and in 2010 was one of three HM pioneers honored by SHM as the first group of Masters in Hospital Medicine.
For each of the past three years, Modern Healthcare has listed him as one of healthcare’s most influential physician-executives.
Dr. Wachter used his recent presentation at HM11 to reflect on the growth of hospital medicine, where he showed how the specialty’s early focus on quality and safety puts hospitalists in positions of authority among physicians and hospitals.
Today, he is professor and associate chairman of the Department of Medicine at the University of California at San Francisco and chief of the division of hospital medicine, and chief of the medical service at UCSF Medical Center.
In July, Dr. Wachter was named chair-elect of the American Board of Internal Medicine’s (ABIM) board of directors.
Hospitalists on the Move

Cogent HMG has announced its new executive team and outside directors following the merger of Cogent Healthcare and Hospitalists Management Group (HMG). Gene Fleming, formerly president and CEO of Cogent Healthcare, will serve as executive chairman, assisting CEO Stephen Houff, MD, founder and CEO of Hospitalists Management Group. Ron Greeno, MD, a founder of Cogent Healthcare, will serve as chief medical officer of Cogent HMG and will steer the consulting business and serve as an advisor to the board. Antoine Agassi will serve as president and oversee day-to-day business operations. Linda Ellis will serve as COO, directing all regional and site operations.

Other key executives: Rusty Holman, MD, chief clinical officer; Susan Brownie, chief financial officer; Doug Mefford, chief legal officer; Anna-Gene O’Neal, senior vice president of quality; and Cheryl Slack, senior vice president of human resources. In addition to Fleming and Houff, Cogent HMG board members include Gary Chartrand, executive chairman of Acosta Sales and Marketing; Mike Leavitt, founder and chairman of Leavitt Partners and former U.S. Secretary of Health and Human Services; and Mark Neaman, president and CEO of NorthShore University HealthSystem.

The St. Anthony’s Hospital Foundation in St. Petersburg, Fla., has announced five new members of its board of directors: Emery Ellinger, CEO of the brokerage firm Aberdeen Advisors; Vitalis Unaeze, MD; Brian McNulty of USI Insurance Services; Angela Rouson, a St. Petersburg resident with a history of community service; and Dan Masi of Bright House Networks, a telecommunications company. Karim Godamunne, MD, has been promoted from medical director to vice president of clinical systems integration at Eagle Hospital Physicians in Atlanta.

Dr. Godamunne won primary stroke center designation within eight months of adding a teleneurology program to an existing Eagle hospitalist program at South Fulton Medical Center in East Point, Ga. Caitlin B. Foxley, MD, has been elected hospital medicine service chief for the Nebraska Medical Center in Omaha. Dr. Foxley is a member of Team Hospitalist.
Cynthia Roldan, MD, director of Westminster, Md.-based Carroll Hospital Center’s pediatric hospitalist program, has been selected as the hospital’s June Physician of the Month. A physician affiliated with Carroll Hospital Center for four years, Roldan was nominated for exceptional patient care and education of new and expecting mothers.

Dixon, Ill.-based Katherine Shaw Bethea Hospital has announced that hospitalist Tim Appenheimer, MD, has been promoted to vice president and CMO. The move is meant to address the growing focus on improving quality and patient safety across the country.
Cogent HMG has announced its new executive team and outside directors following the merger of Cogent Healthcare and Hospitalists Management Group (HMG). Gene Fleming, formerly president and CEO of Cogent Healthcare, will serve as executive chairman, assisting CEO Stephen Houff, MD, founder and CEO of Hospitalists Management Group. Ron Greeno, MD, a founder of Cogent Healthcare, will serve as chief medical officer of Cogent HMG and will steer the consulting business and serve as an advisor to the board. Antoine Agassi will serve as president and oversee day-to-day business operations. Linda Ellis will serve as COO, directing all regional and site operations.
Other key executives: Rusty Holman, MD, chief clinical officer; Susan Brownie, chief financial officer; Doug Mefford, chief legal officer; Anna-Gene O’Neal, senior vice president of quality; and Cheryl Slack, senior vice president of human resources. In addition to Fleming and Houff, Cogent HMG board members include Gary Chartrand, executive chairman of Acosta Sales and Marketing; Mike Leavitt, founder and chairman of Leavitt Partners and former U.S. Secretary of Health and Human Services; and Mark Neaman, president and CEO of NorthShore University HealthSystem.
The St. Anthony’s Hospital Foundation in St. Petersburg, Fla., has announced five new members of its board of directors: Emery Ellinger, CEO of the brokerage firm Aberdeen Advisors; Vitalis Unaeze, MD; Brian McNulty of USI Insurance Services; Angela Rouson, a St. Petersburg resident with a history of community service; and Dan Masi of Bright House Networks, a telecommunications company. Karim Godamunne, MD, has been promoted from medical director to vice president of clinical systems integration at Eagle Hospital Physicians in Atlanta.
Dr. Godamunne won primary stroke center designation within eight months of adding a teleneurology program to an existing Eagle hospitalist program at South Fulton Medical Center in East Point, Ga. Caitlin B. Foxley, MD, has been elected hospital medicine service chief for the Nebraska Medical Center in Omaha. Dr. Foxley is a member of Team Hospitalist.
Cynthia Roldan, MD, director of Westminster, Md.-based Carroll Hospital Center’s pediatric hospitalist program, has been selected as the hospital’s June Physician of the Month. A physician affiliated with Carroll Hospital Center for four years, Roldan was nominated for exceptional patient care and education of new and expecting mothers.
Dixon, Ill.-based Katherine Shaw Bethea Hospital has announced that hospitalist Tim Appenheimer, MD, has been promoted to vice president and CMO. The move is meant to address the growing focus on improving quality and patient safety across the country.
Cogent HMG has announced its new executive team and outside directors following the merger of Cogent Healthcare and Hospitalists Management Group (HMG). Gene Fleming, formerly president and CEO of Cogent Healthcare, will serve as executive chairman, assisting CEO Stephen Houff, MD, founder and CEO of Hospitalists Management Group. Ron Greeno, MD, a founder of Cogent Healthcare, will serve as chief medical officer of Cogent HMG and will steer the consulting business and serve as an advisor to the board. Antoine Agassi will serve as president and oversee day-to-day business operations. Linda Ellis will serve as COO, directing all regional and site operations.
Other key executives: Rusty Holman, MD, chief clinical officer; Susan Brownie, chief financial officer; Doug Mefford, chief legal officer; Anna-Gene O’Neal, senior vice president of quality; and Cheryl Slack, senior vice president of human resources. In addition to Fleming and Houff, Cogent HMG board members include Gary Chartrand, executive chairman of Acosta Sales and Marketing; Mike Leavitt, founder and chairman of Leavitt Partners and former U.S. Secretary of Health and Human Services; and Mark Neaman, president and CEO of NorthShore University HealthSystem.
The St. Anthony’s Hospital Foundation in St. Petersburg, Fla., has announced five new members of its board of directors: Emery Ellinger, CEO of the brokerage firm Aberdeen Advisors; Vitalis Unaeze, MD; Brian McNulty of USI Insurance Services; Angela Rouson, a St. Petersburg resident with a history of community service; and Dan Masi of Bright House Networks, a telecommunications company. Karim Godamunne, MD, has been promoted from medical director to vice president of clinical systems integration at Eagle Hospital Physicians in Atlanta.
Dr. Godamunne won primary stroke center designation within eight months of adding a teleneurology program to an existing Eagle hospitalist program at South Fulton Medical Center in East Point, Ga. Caitlin B. Foxley, MD, has been elected hospital medicine service chief for the Nebraska Medical Center in Omaha. Dr. Foxley is a member of Team Hospitalist.
Cynthia Roldan, MD, director of Westminster, Md.-based Carroll Hospital Center’s pediatric hospitalist program, has been selected as the hospital’s June Physician of the Month. A physician affiliated with Carroll Hospital Center for four years, Roldan was nominated for exceptional patient care and education of new and expecting mothers.
Dixon, Ill.-based Katherine Shaw Bethea Hospital has announced that hospitalist Tim Appenheimer, MD, has been promoted to vice president and CMO. The move is meant to address the growing focus on improving quality and patient safety across the country.