User login
Activities of Daily Living
Tears well up in my eyes. Not from pain, but frustration.
I pleaded with my 3‐year‐olds to come to me, so I could help them wash and dress for the day. Ordinarily, I would have come into their room, leaned over their beds, and whispered good morning into their ears.
Four days after surgery, I wasn't able to do that. Not without the crutches. Even with the crutches, I was moving slowly. I scooted up, put a few pillows behind my back, and carefully lifted up my leg. Putting on the knee immobilizer would take too long; I would only be crossing the hall.
Weighing less than 800 g, the immobilizer is an adjustable aluminum frame attached to foam rubber and 4 wide Velcro straps. It is a device of torment. I can never seem to find the proper fit. If it is too tight, my leg hurts and starts turning blue. When it is too loose, it pulls on my incision, multiplying the pain. You put it on while sitting, but you only discover whether it is too tight or too loose when you stand up.
With one foot on the floor at the edge of the bed, I took one crutch in hand, shifted to the left, and grabbed for the other crutch. I squeezed the handgrips of the crutches tightly and pulled myself up.
Put your weight on your hands, NOT your armpits, the instructions said. Easier said than done, because my armpits were now sore too.
Keep your crutches even with each other. I tried to remember to make an equilateral triangle with my good foot and 2 crutches, but the instructions only seemed to account for movement in a straight line.
Keep your elbows slightly bent and close to your sides to help keep the crutches under your arm. I am trying that too.
Lock your elbows. This instruction contradicts the previous one. Which should I follow?
Place your crutches 2 to 3 inches outside of each foot. How do I do this and keep my elbows close to my sides?
Swing your injured leg through first. But not too much, or I'll pole vault across the room.
After 3 steps, my leg started to throb, and my quadriceps went into a spasm. I needed to sit down, immediately.
Non‐weight‐bearing for next 4 weeks, was written on the doctor's note. Four weeks feels like an eternity. If my heel or toe even touched the ground, I felt an immediate throb of pain in my knee.
How do my orthopedic patients do it: those with broken hips and bad or broken knees, with hip replacements, or knee replacements? I was sensitive to their pain and could optimize control. Postoperatively, I could support gastrointestinal and other organ systems. I made sure that the basic weight‐bearing order was correct. I carefully followed the physical and/or occupational therapy recommendation for home, rehabilitation, or a nursing home. I spoke with families. Yet I did not dwell on activities of daily living nor how my patients felt to be dependent on others for simple things they needed. Some patients were non‐weight‐bearing for weeks, some for months, others never walked again. How can one deeply understand it if one has never experienced it?
According to Centers for Disease Control and Prevention (CDC) statistics,1 unintentional injuries are the leading cause of death between the ages of 1 and 44 years. Accidents are again the leading cause of death after age 75 years. More startling is the fact that these numbers have not been significantly reduced since these data were first collected. Nor do these numbers reveal the number of those debilitated, but still living. In my case, I was not playing basketball, water skiing, or rock climbing: I slipped and fell while stepping into a wading pool with my children, severing ligaments, tearing meniscus, and creating a hairline fracture of my tibia.
Expect to move slowly with the crutches. Yes, I am moving very slowly, only 1 to 2 feet with each stride. If I take a longer stride, I lose my balance.
Learn to sit down with the crutches. Learn to stand up. Learn to get into a car.
Learn to go up the stairs. Learn to go down the stairs.
Avoid wet surfaces. Otherwise you'll start skating and reinjure that knee.
It was effortless to think of patients and colleagues of mine. Mr. S., how do you do it? At age 30 years, he was quadriplegic from falling from a tree as a teenager. Mr. D, how about you, in a wheelchair, after being hit by a car and multiple postoperative leg infections and amputations: living in hotels, with estranged family and no social support. How did you do it, while we nagged you about controlling your glucose. Dr. J? The sadness fills my heart. At only 60 years old, my wonderful professor now made rounds in an electric wheelchair, the victim of amyotrophic lateral sclerosis (ALS). My fate, in comparison, is fortunate; my immobility only temporary. I can still think. And talk. And use a phone. And eat, as well as write this essay. And, best of all, read stories to my children. Be careful about this leg, I remind them. Don't come too close!
Maybe what life is trying to tell you is, slow down. In fact, it's forcing you to do that, a colleague and friend said. I had prided myself in thorough and compassionate doctoring. Now, having been a patient on crutches, I have a greater understanding of how limits to mobility can impact daily living on my patients after I discharge them. And the mundane subject of accident prevention has gained a new urgency.
- ,,,.Deaths: final data for 2005.Natl Vital Stat Rep.2008;56(10):1–120.
Tears well up in my eyes. Not from pain, but frustration.
I pleaded with my 3‐year‐olds to come to me, so I could help them wash and dress for the day. Ordinarily, I would have come into their room, leaned over their beds, and whispered good morning into their ears.
Four days after surgery, I wasn't able to do that. Not without the crutches. Even with the crutches, I was moving slowly. I scooted up, put a few pillows behind my back, and carefully lifted up my leg. Putting on the knee immobilizer would take too long; I would only be crossing the hall.
Weighing less than 800 g, the immobilizer is an adjustable aluminum frame attached to foam rubber and 4 wide Velcro straps. It is a device of torment. I can never seem to find the proper fit. If it is too tight, my leg hurts and starts turning blue. When it is too loose, it pulls on my incision, multiplying the pain. You put it on while sitting, but you only discover whether it is too tight or too loose when you stand up.
With one foot on the floor at the edge of the bed, I took one crutch in hand, shifted to the left, and grabbed for the other crutch. I squeezed the handgrips of the crutches tightly and pulled myself up.
Put your weight on your hands, NOT your armpits, the instructions said. Easier said than done, because my armpits were now sore too.
Keep your crutches even with each other. I tried to remember to make an equilateral triangle with my good foot and 2 crutches, but the instructions only seemed to account for movement in a straight line.
Keep your elbows slightly bent and close to your sides to help keep the crutches under your arm. I am trying that too.
Lock your elbows. This instruction contradicts the previous one. Which should I follow?
Place your crutches 2 to 3 inches outside of each foot. How do I do this and keep my elbows close to my sides?
Swing your injured leg through first. But not too much, or I'll pole vault across the room.
After 3 steps, my leg started to throb, and my quadriceps went into a spasm. I needed to sit down, immediately.
Non‐weight‐bearing for next 4 weeks, was written on the doctor's note. Four weeks feels like an eternity. If my heel or toe even touched the ground, I felt an immediate throb of pain in my knee.
How do my orthopedic patients do it: those with broken hips and bad or broken knees, with hip replacements, or knee replacements? I was sensitive to their pain and could optimize control. Postoperatively, I could support gastrointestinal and other organ systems. I made sure that the basic weight‐bearing order was correct. I carefully followed the physical and/or occupational therapy recommendation for home, rehabilitation, or a nursing home. I spoke with families. Yet I did not dwell on activities of daily living nor how my patients felt to be dependent on others for simple things they needed. Some patients were non‐weight‐bearing for weeks, some for months, others never walked again. How can one deeply understand it if one has never experienced it?
According to Centers for Disease Control and Prevention (CDC) statistics,1 unintentional injuries are the leading cause of death between the ages of 1 and 44 years. Accidents are again the leading cause of death after age 75 years. More startling is the fact that these numbers have not been significantly reduced since these data were first collected. Nor do these numbers reveal the number of those debilitated, but still living. In my case, I was not playing basketball, water skiing, or rock climbing: I slipped and fell while stepping into a wading pool with my children, severing ligaments, tearing meniscus, and creating a hairline fracture of my tibia.
Expect to move slowly with the crutches. Yes, I am moving very slowly, only 1 to 2 feet with each stride. If I take a longer stride, I lose my balance.
Learn to sit down with the crutches. Learn to stand up. Learn to get into a car.
Learn to go up the stairs. Learn to go down the stairs.
Avoid wet surfaces. Otherwise you'll start skating and reinjure that knee.
It was effortless to think of patients and colleagues of mine. Mr. S., how do you do it? At age 30 years, he was quadriplegic from falling from a tree as a teenager. Mr. D, how about you, in a wheelchair, after being hit by a car and multiple postoperative leg infections and amputations: living in hotels, with estranged family and no social support. How did you do it, while we nagged you about controlling your glucose. Dr. J? The sadness fills my heart. At only 60 years old, my wonderful professor now made rounds in an electric wheelchair, the victim of amyotrophic lateral sclerosis (ALS). My fate, in comparison, is fortunate; my immobility only temporary. I can still think. And talk. And use a phone. And eat, as well as write this essay. And, best of all, read stories to my children. Be careful about this leg, I remind them. Don't come too close!
Maybe what life is trying to tell you is, slow down. In fact, it's forcing you to do that, a colleague and friend said. I had prided myself in thorough and compassionate doctoring. Now, having been a patient on crutches, I have a greater understanding of how limits to mobility can impact daily living on my patients after I discharge them. And the mundane subject of accident prevention has gained a new urgency.
Tears well up in my eyes. Not from pain, but frustration.
I pleaded with my 3‐year‐olds to come to me, so I could help them wash and dress for the day. Ordinarily, I would have come into their room, leaned over their beds, and whispered good morning into their ears.
Four days after surgery, I wasn't able to do that. Not without the crutches. Even with the crutches, I was moving slowly. I scooted up, put a few pillows behind my back, and carefully lifted up my leg. Putting on the knee immobilizer would take too long; I would only be crossing the hall.
Weighing less than 800 g, the immobilizer is an adjustable aluminum frame attached to foam rubber and 4 wide Velcro straps. It is a device of torment. I can never seem to find the proper fit. If it is too tight, my leg hurts and starts turning blue. When it is too loose, it pulls on my incision, multiplying the pain. You put it on while sitting, but you only discover whether it is too tight or too loose when you stand up.
With one foot on the floor at the edge of the bed, I took one crutch in hand, shifted to the left, and grabbed for the other crutch. I squeezed the handgrips of the crutches tightly and pulled myself up.
Put your weight on your hands, NOT your armpits, the instructions said. Easier said than done, because my armpits were now sore too.
Keep your crutches even with each other. I tried to remember to make an equilateral triangle with my good foot and 2 crutches, but the instructions only seemed to account for movement in a straight line.
Keep your elbows slightly bent and close to your sides to help keep the crutches under your arm. I am trying that too.
Lock your elbows. This instruction contradicts the previous one. Which should I follow?
Place your crutches 2 to 3 inches outside of each foot. How do I do this and keep my elbows close to my sides?
Swing your injured leg through first. But not too much, or I'll pole vault across the room.
After 3 steps, my leg started to throb, and my quadriceps went into a spasm. I needed to sit down, immediately.
Non‐weight‐bearing for next 4 weeks, was written on the doctor's note. Four weeks feels like an eternity. If my heel or toe even touched the ground, I felt an immediate throb of pain in my knee.
How do my orthopedic patients do it: those with broken hips and bad or broken knees, with hip replacements, or knee replacements? I was sensitive to their pain and could optimize control. Postoperatively, I could support gastrointestinal and other organ systems. I made sure that the basic weight‐bearing order was correct. I carefully followed the physical and/or occupational therapy recommendation for home, rehabilitation, or a nursing home. I spoke with families. Yet I did not dwell on activities of daily living nor how my patients felt to be dependent on others for simple things they needed. Some patients were non‐weight‐bearing for weeks, some for months, others never walked again. How can one deeply understand it if one has never experienced it?
According to Centers for Disease Control and Prevention (CDC) statistics,1 unintentional injuries are the leading cause of death between the ages of 1 and 44 years. Accidents are again the leading cause of death after age 75 years. More startling is the fact that these numbers have not been significantly reduced since these data were first collected. Nor do these numbers reveal the number of those debilitated, but still living. In my case, I was not playing basketball, water skiing, or rock climbing: I slipped and fell while stepping into a wading pool with my children, severing ligaments, tearing meniscus, and creating a hairline fracture of my tibia.
Expect to move slowly with the crutches. Yes, I am moving very slowly, only 1 to 2 feet with each stride. If I take a longer stride, I lose my balance.
Learn to sit down with the crutches. Learn to stand up. Learn to get into a car.
Learn to go up the stairs. Learn to go down the stairs.
Avoid wet surfaces. Otherwise you'll start skating and reinjure that knee.
It was effortless to think of patients and colleagues of mine. Mr. S., how do you do it? At age 30 years, he was quadriplegic from falling from a tree as a teenager. Mr. D, how about you, in a wheelchair, after being hit by a car and multiple postoperative leg infections and amputations: living in hotels, with estranged family and no social support. How did you do it, while we nagged you about controlling your glucose. Dr. J? The sadness fills my heart. At only 60 years old, my wonderful professor now made rounds in an electric wheelchair, the victim of amyotrophic lateral sclerosis (ALS). My fate, in comparison, is fortunate; my immobility only temporary. I can still think. And talk. And use a phone. And eat, as well as write this essay. And, best of all, read stories to my children. Be careful about this leg, I remind them. Don't come too close!
Maybe what life is trying to tell you is, slow down. In fact, it's forcing you to do that, a colleague and friend said. I had prided myself in thorough and compassionate doctoring. Now, having been a patient on crutches, I have a greater understanding of how limits to mobility can impact daily living on my patients after I discharge them. And the mundane subject of accident prevention has gained a new urgency.
- ,,,.Deaths: final data for 2005.Natl Vital Stat Rep.2008;56(10):1–120.
- ,,,.Deaths: final data for 2005.Natl Vital Stat Rep.2008;56(10):1–120.
IVIG for Severe Colitis
Clostridium difficile colitis (CDC) is the most common cause of hospital‐acquired diarrhea.1 The incidence of CDC has sharply increased over the past decade despite increasing awareness among health care professionals.24 C. difficile pathogenic strains induce diarrhea through the elaboration and secretion of 2 exotoxins: toxin A and toxin B. Toxin A is an inflammatory toxin, leading to fluid secretion, increased mucosal permeability, and marked enteritis and colitis.5 Toxin B is cytotoxic, leading to cell injury and apoptosis.5 Combined, toxin A and toxin B can cause a wide spectrum of clinical presentations, ranging from mild diarrhea that resolves with the discontinuation of antibiotics to a fulminant colitis requiring surgical intervention.
The severity of clinical manifestations has been shown to be inversely proportional to the host anti‐toxin A antibody level in response to toxin exposure. Kyne et al.6 demonstrated that asymptomatic C. difficile carriers produced significantly higher anti‐toxin A immunoglobulin G (IgG) levels compared to symptomatic patients. Among the latter group, patients with mild disease had a higher antibody level compared to those with severe colitis.6, 7 Additional risk factors predisposing to severe colitis are advanced age, severe underlying illness,8 and immunocompromised state.9
Recently, a new C. difficile strain (BI/NAP1) with a mutated toxin A and toxin B promoter silencer, a binary toxin gene, and fluoroquinolone resistance has been described in Canada and the United States.3, 10 This strain has been associated with an increased incidence of CDC among hospitalized patients, especially the incidence of severe disease requiring colectomy. At the same time, several reports describing metronidazole treatment failure have been published.1114 These recent findings emphasize the importance of finding alternative treatments for CDC.
Intravenous immunoglobulin (IVIG) was used to treat CDC for the first time in 1991.15 Since then, 12 case reports and small case series, along with 1 case‐control study have been published documenting IVIG treatment outcomes.1527 However, only 5 reports to date examined patients with severe CDC.2125 In the present study, we report the largest series of patients with severe CDC treated with IVIG in the literature to our knowledge.
Patients and Methods
Case Series
We used CareScience software (CareScience, Inc., Philadelphia, PA) to retrospectively identify all patients admitted to our institution with a primary or secondary diagnosis of CDC (code 00845) between July 1, 2002 and May 1, 2006. CareScience is commercially available software that tracks all admissions to our institution and allows the performance of patient searches with a wide spectrum of user‐defined search criteria. Using the same software, we further identified those patients who received IVIG during their hospital stay. We then obtained the hospital chart for each patient, from the medical records department and established the study database.
A case was defined as a patient with diarrhea (at least 3 loose stools daily) for at least 2 days who had C. difficile cytotoxin‐positive feces and at least 1 of the following criteria: clinical symptoms (abdominal pain and/or distension and fever); leukemoid reaction (defined as white blood cell count of 20,000 cells/mm3 or above. This cutoff value was chosen as it has been used previously as a prognostic factor)4; radiographic evidence of colitis by computed tomography (CT) of the abdomen; and/or the presence of pseudomembranes on flexible sigmoidoscopy or colonoscopy. We excluded all patients who received IVIG for an indication other than CDC treatment (n = 3). There were no other exclusion criteria.
We used a standardized data collection tool and recorded demographics (age, gender, principal diagnosis), past medical and surgical history, other risk factors for C. difficile infection (previous CDC, antibiotics received during hospital stay, immunosuppressive medications or organ transplantation within the previous 6 weeks, history of malignancy or diabetes mellitus); clinical presentation (abdominal distention, abdominal pain, diarrhea, fever, leukemoid reaction, and hypotension defined as systolic blood pressure <85 mm Hg despite at least 1 L of intravenous normal saline administration and the need for vasopressor use); colonoscopy findings; CT scan and x‐ray findings; laboratory values; date and dose of IVIG infused and other C. difficile pharmacological treatments; and Acute Physiological Assessment and Chronic Health Evaluation (APACHE II) score28 at the first day of IVIG infusion. The primary outcomes were survival at the end of the hospital stay and clinical disease resolution, defined as 2 formed bowel movements or less per day without abdominal pain or distention.
The decision to initiate IVIG therapy and the dose to be used was made by the individual attending physician.
Statistical Analysis
Single (univariate) and multiple (multivariate) logistic regression analysis were applied to identify variables among the ones collected that are independent predictors of CDC mortality. All statistical analyses were completed with the STATA 10 software package (StatCorp LP, College Station, TX).
Review of the Literature
We used PubMed, Web of Science, Scopus, and Excerpta Medica databases to search for any publication in a peer‐reviewed journal on the use of IVIG for the treatment of severe CDC. We used the search words: IVIG or intravenous immunoglobulin and clostridium difficile. Only publications published in English were selected. The date range used was January 1, 1950 to January 7, 2009. We were able to find 5 publications using this search criteria.
Results
Study Population
Of the 1230 patients diagnosed with CDC over the 4‐year study period, 21 patients were treated with IVIG. Table 1 summarizes the patients' characteristics. There were 13 women and 8 men. The mean age was 68 years, with a standard deviation (SD) of 13 years. Sepsis was the primary diagnosis in all patients. Sixteen patients had predisposing risk factors for CDC, including immunosuppression (immunosuppressive medication [n = 2], human immunodeficiency virus [HIV] infection [n = 2]); cancer (n = 3); recent surgery (n = 3); and diabetes mellitus (n = 11). Nine patients had documented previous CDC episodes. The indications for IVIG administration were evidence of pancolitis on abdominal CT scan (n = 12) or severe ileus with cessation of diarrhea, abdominal distention, and requirement for total parenteral nutrition (n = 5), or severe hypotension (n = 4) (defined as systolic blood pressure <85 mm Hg despite at least 1 L of intravenous normal saline administration and the subsequent need for vasopressor use).
| Patient | Age (gender) | Diagnosis | Medical and Surgical History | CDC History | Colonoscopy Findings | Radiographic Findings |
|---|---|---|---|---|---|---|
| ||||||
| A | 40 (female) | CDC with sec. sepsis | Gastric stapling | Yes | * | Diffuse colitis |
| B | 86 (female) | Fulminant CDC | Metastatic ovarian carcinoma | PC | No colonic thickening | |
| C | 72 (male) | Sepsis | Acute pancreatitis with sec. pseudocyst, DM | Yes | PC | Diffuse colitis |
| D | 78 (male) | Discitis | Delayed: normal mucosa | Dilation of small and large bowel | ||
| E | 98 (female) | Urosepsis | Yes | * | No bowel distention | |
| F | 90 (female) | Right lower extremity cellulitis | DM | * | Concentric thickening of rectal wall | |
| G | 64 (male) | Ischemic colitis | DM, recent Hartman pouch closure | Marked inflammation | Diffuse colitis | |
| H | 78 (female) | Toe osteomyelitis and CDC with sec. sepsis | DM | * | Diffuse colitis | |
| I | 35 (female) | Sepsis | Yes | * | Diffuse nonspecific colitis, minimal ascites | |
| J | 47 (female) | Pneumonia and sec. sepsis | * | Diffuse colitis | ||
| K | 56 (female) | Urosepsis | HIV | Yes | * | Colitis involving the right colon |
| L | 76 (male) | CDC with sec. sepsis | Sigmoid bladder fistula repair, DM | * | Diffuse colitis | |
| M | 71 (female) | Pneumonia with sec. sepsis | * | Diffuse colitis | ||
| N | 63 (male) | Urosepsis | DM, lymphoma resection from small intestine | PC | Marked small and large bowel distention | |
| O | 86 (male) | Enterococcus‐induced sepsis | Rheumatoid arthritis on methotrexate | * | Fat stranding suggesting peritonitis | |
| P | 60 (female) | Gastrointestinal bleed and CDC | DM with neuropathy and retinopathies | Yes | * | Thickening of wall of colon in most of the colon |
| Q | 57 (female) | Sepsis | DM | Yes | * | Normal |
| R | 67 (female) | CDC with sec. sepsis | Candidal esophagitis | Yes | * | Large amount of peritoneal fluid, mild small bowel thickening |
| S | 60 (female) | Sepsis sec. to S. aureus and P. aerogenosa | DM, renal transplant (myco, prednisone) | * | Ileus with air fluid level in the small intestine | |
| T | 80 (female) | Sepsis | DM | Yes | * | Thickening of descending colon consistent with colitis |
| U | 72 (male) | CDC, widespread metastatic cancer | DM, metastatic cancer (unknown primary site) | * | Severe colitis up to the splenic flexure | |
Table 2 describes disease severity in these patients. Since CDC starts locally in the colon then secondarily involves multiple organs as part of the systemic inflammatory response syndrome (SIRS), 2 scales were used to characterize the disease in each patient: (1) extent of local colonic inflammation, and (2) severity of systemic involvement. Extensive colonic involvement was evidenced in all patients by pancolitis on abdominal imaging modalities (12 patients), severe ileus requiring total parenteral nutrition (13 patients), or referral for surgical consultation for possible colectomy (12 patients).
| Patient | Complications During the Hospital Stay | APACHE II Score | Monitored Unit | WBC* | K | Alb | Lactate | Cr | Hospital Stay (days) | Surgical Consult/Surgery | TPN for Colitis |
|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||
| A | Sepsis, DIC, ARDS, intubation | 15 | Yes | 48 | 4 | 1.1 | 2.9 | 1.3 | 26 | No/No | Yes |
| B | Dehydration, weakness | 12 | No | 19 | 3.4 | 3.1 | 1.1 | 16 | No/No | Yes | |
| C | HTP, GI bleed, ischemic colitis, F | 22 | Yes | 21 | 2.7 | 2.5 | 1.3 | ESRD | 34 | Yes/No | Yes |
| D | AD, megacolon, HT, intubation, ARF | 18 | Yes | 25 | 3.4 | 1.4 | 1.1 | 2.6 | 52 | Yes/No | Yes |
| E | Exacerbation of CHF with respiratory distress, Bipap support, confusion | 21 | No | 10 | 2.6 | 2.3 | 1 | 11 | No/No | No | |
| F | Confusion, gout acute attack | 21 | No | 33 | 3.1 | 2.6 | ESRD | 15 | No/No | No | |
| G | Intubation, cardiac arrest, AF with RVR, PNA, ARF, DVT, dysphagia, PEG | 6 | Yes | 15 | 3.1 | 1.7 | 1.9 | 2.2 | 32 | Yes/No | Yes |
| H | Sepsis, intubation, ARF, PEG, toe amputation, PNA, pulmonary edema, TPN, vitamin D deficiency | 34 | Yes | 59 | 2.8 | 1.5 | 4 | 3.8 | 17 | No/No | Yes |
| I | CHF, transient third cranial nerve palsy, DIC | 20 | Yes | 52 | 3.2 | 3.3 | 0.7 | ESRD | 11 | No/No | No |
| J | Aspiration PNA, sepsis, DIC, intubation, MI, F, HT | 32 | Yes | 17 | 2.7 | 1.8 | 14 | ESRD | 21 | Yes/no | No |
| K | Intubation, cardiac arrest, ARF, DIC, AP, F | 30 | Yes | 25 | 2.1 | 2.1 | 13 | 3.6 | 10 | Yes/no | No |
| L | Intubation, ARF, HTP, MI, AD, F | 23 | Yes | 69 | 3.2 | 1.8 | 1.4 | 3.6 | 23 | Yes/no | No |
| M | Intubation, DIC, ARF, GI bleeding, hypothermia, AD | 23 | Yes | 47 | 2.8 | 1.4 | 1.4 | 4.3 | 23 | Yes/no | Yes |
| N | Intubation, HTP, AD, F, ARF with HD, AF, osteomyelitis | 23 | Yes | 46 | 2.9 | 1.5 | 1.5 | 2.7 | 27 | Yes/no | Yes |
| O | Intubation, ARF, 2 cardiac arrests, GI bleed, UTI, rhabdomyolysis, liver shock, AF | 31 | Yes | 49 | 2.5 | 1.1 | 2.3 | 2.9 | 25 | Yes/no | Yes |
| P | Bowel ischemia with bowel resection, ARF, MI, ischemic bowel, fluid overload, respiratory failure | 23 | Yes | 26 | 2.6 | 0.8 | 2.9 | 3.1 | 9 | Yes/Yes | Yes |
| Q | Pulmonary embolism | 39 | Yes | 23 | 2.8 | 1.1 | 8.1 | ESRD | 9 | No/No | Yes |
| R | Fungal peritonitis, aspiration pneumonia, cardiac arrest | 26 | Yes | 30 | 4.1 | 1.1 | 0.9 | ESRD | 36 | No/No | Yes |
| S | Intubation, pneumothorax, CRT, pressor‐dependent shock, ARF | 36 | Yes | 46 | 3.1 | 1.8 | 2.1 | 5.4 | 64 | Yes/Yes | No |
| T | Pressor‐dependent sepsis, pulmonary edema, ARF with HD | 36 | Yes | 35 | 3.3 | 1.3 | 1.8 | 5.5 | 11 | Yes/No | Yes |
| U | Sepsis | 34 | Yes | 58 | 3.1 | 2.2 | 3.3 | 1.6 | 9 | No/No | No |
Of the 21 patients treated with IVIG, 9 did not receive a surgical consultation either because they responded to medical treatment promptly (6 patients), were too unstable for surgery (2 patients), or because the patient/family refused surgery (1 patient). Of the 12 patients who received surgical consultation, 2 underwent surgery. The remainder did not proceed to surgery for the following reasons: they were deemed medically unstable for surgery (6 patients), declined surgery (2 patients), were diagnosed with cancer on colonoscopy (1 patient), or improved with medical treatment (1 patient).
The severity of systemic involvement was measured using the APACHE II score on day 1 of IVIG infusion. The mean APACHE II score was 25. Eighteen patients were in a monitored unit when IVIG was administered. The study group had laboratory results in keeping with those previously used to define severe colitis:4, 9, 19 leukocytosis (defined as white blood cell count higher than 12,000 cells/mL [mean = 36,000 cells/mL]), hypoalbuminemia (mean = 1.78 g/dL, SD = 0.68 g/dL), hypokalemia (mean = 3.02 mg/dL, SD = 0.47 g/dL), and acute renal failure (defined as serum creatinine level >1.5 mg/dL [mean = 2.98 mg/dL, SD = 1.42 g/dL]).
IVIG Use
Table 3 describes the treatment patients received for CDC as well as the total number of antibiotics used throughout the hospital stay. IVIG was used as adjuvant treatment (defined as IVIG administration within 4 days or less after CDC diagnosis) in 8 patients and as second‐line treatment (defined as IVIG administration more than 4 days after CDC diagnosis) in 13 patients. Metronidazole, vancomycin, cholestyramine, and probiotic treatment alone or in different combinations were used for an average of 8 days (SD = 8 days; range, 025 days) before IVIG infusion. The total IVIG dose administered varied depending on the prescribing attending, with a range of 200 mg/kg to 1250 mg/kg and a mode of 250 mg/kg for 1 to 3 days. An average of 5 (SD = 2) different antibiotics that were not active against C. difficile were used per patient without being discontinued after a CDC diagnosis was made. The 3 most common were: cephalosporins (cefazolin, ceftriaxone, cefepime), fluoroquinolones (levofloxacin), and combination antibiotics (piperacillin and tazobactam or ampicillin and sulbactam).
| Patient | Number of Antibiotics | Duration of Treatment Before IVIG (days) | Treatment Before IVIG (days) | Total CDC Treatment (days) | IgG Level | IVIG Dose |
|---|---|---|---|---|---|---|
| ||||||
| A | 5 | 7 | Metro (7), Vanc (7), Choles (2) | Oral and rectal Vanc (26,19), IV Metro (19), Choles (2), Lacto (6) | Low | 300 mg/kg for 1 day |
| B | 1 | 13 | Metro (13), Vanc (13) | Oral Vanc (17) and IV Metro (12) | 300 mg/kg for 1 day | |
| C | 3 | 7 | Metro (7), Vanc (3) | IV Metro (28),Vanc oral and enema (18,3), Lacto (10) | Low | 125 mg/kg for 5 days |
| D | 5 | 25 | Metro (25), Vanc (15) | Oral then IV Metro (10,15), oral Vanc (25), Choles (7) and Lacto (13) | Low | 200 mg/kg for 1 day |
| E | 1 | 4 | Metro (1), Vanc (4), Choles(4) | IV Metro (8), oral Vanc (10) and Choles (4) | 75 mg/kg for 5 days | |
| F | 4 | 2 | Metro (2), Vanc (1) | IV Metro (8) and oral Vanc (9) | 250 mg/kg for 5 days | |
| G | 3 | 17 | Metro (17), Vanc (14) | IV Metro (49) and oral Vanc (61) | 250 mg/kg for 2 days | |
| H | 5 | 1 | Metro (1), Vanc (1) | Oral Metro (18), oral Vanc (22 ), IV Metro (3) | 250 mg/kg for 3 days | |
| I | 6 | 1 | Metro (1) | Oral and IV Metro (7,9), Vanc oral and enema (8,3) | 250 mg/kg for 2 days | |
| J | 8 | 16 | Metro (14), Vanc (2), Lacto (6) | Oral then IV Metro (10,5), oral and rectal Vanc (3,1), Lacto (6) | 300 mg/ kg for 1 day | |
| K | 6 | 7 | Metro (7), Vanc (3) | Oral then IV Metro (10) and oral Vanc (9) | Normal | 400 mg/kg for 2 days |
| L | 4 | 0 | None | IV then oral Metro (7,10), oral Vanc (23), Choles (7), and Lacto (5) | 150 mg/kg for 5 days | |
| M | 6 | 1 | Metro (1) | IV Metro (23) and oral Vanc (9) | 250 mg/kg for 2 days | |
| N | 7 | 1 | Metro (1), Vanc (1) | IV Metro (16), oral Vanc (14), oral Metro (7) | 250 mg /kg for 2 days | |
| O | 6 | 7 | Metro (6), Vanc (4) | IV Metro (6) and oral Vanc (22) | Low | 250 mg/kg for 2 days |
| P | 3 | 6 | Metro (6), Vanc (6) | IV Metro (25) and oral Vanc (17) | 150 mg/kg fro 3 days | |
| Q | 3 | 4 | Metro (4), Vanc (3) | Oral Metro (8),Vanc oral and enema (6,3) | 250 mg/kg for 3 days | |
| R | 5 | 9 | Vanc (9) | Vanc oral and enema (5,4), IV Metro (2) | 250 mg/kg for 1 day | |
| S | 8 | 23 | Metro (23), Vanc (23) | Oral then IV Metro (12,22), oral Vanc (39) | 250 mg/kg for 3 days | |
| T | 4 | 6 | Metro (6), Vanc (1) | Oral Vanc and IV Metro (11) | 250 mg/kg for 1 day | |
| U | 4 | 2 | Metro (2), Vanc (2) | Oral Vanc and IV Metro (6) | 250 mg/kg for 3 days | |
Survival with IVIG Use
Nine patients (43%) survived their illness and were discharged from the hospital. They experienced complete clinical resolution after an average of 10 days from IVIG administration (range, 220 days) (Table 4). The other 12 patients (57%) died during the index hospitalization. The average length of stay was 23 (range, 964) days.0
| Patient | Disposition | Clearance of Clostridium difficile Colitis? | Days to Resolution |
|---|---|---|---|
| |||
| A | Alive | Loose BM persisted but diarrhea resolved 9 days after IVIG. | 9 |
| B | Alive | BM became formed and diarrhea resolved 48 hours after IVIG. | 2 |
| C | Alive | Diarrhea resolved 20 days post‐IVIG infusion. CAT scan: colonic thickening improved. | 20 |
| D | Alive | Diarrhea resolved on discharge. Response to IVIG started next day after administration. | 18 |
| E | Alive | Diarrhea improved next day after IVIG administration and resolved on discharge. | 5 |
| F | Alive | Diarrhea resolved 5 days after IVIG administration. | 5 |
| G | Alive | Diarrhea resolved. C. difficile test became negative. | 13 |
| H | Alive | Diarrhea resolved 2 days before discharge. | 15 |
| I | Alive | Diarrhea slowly improved and resolved 4 days before discharge. | 7 |
| J | Deceased | ||
| K | Deceased | ||
| L | Deceased | ||
| M | Deceased | ||
| N | Deceased | ||
| O | Deceased | ||
| P | Deceased | ||
| Q | Deceased | ||
| R | Deceased | ||
| S | Deceased | ||
| T | Deceased | ||
| U | Deceased | ||
| Study | Number of Patients | Age (SD) (years) | Male | Female | Severity Definition | IVIG Dose | Days to Resolution | Days IVIG Infused | Alive? (%) | Recurrence |
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
| Salcedo et al.22 | 2 | 63, 64 | 1 | 1 | Pancolitis or thumbprinting on CAT scan | 200300 mg/kg once | 12 | 59 | 100 | 1 out of 2 |
| McPherson et al.21 | 8 | 72 (12) | ? | ? | Pancolitis | 200400 mg/kg twice | 226 | 1165 | 75 | 2 out of 6 |
| Juang et al.25 | 18 | 67 (17.4) | 5 | 13 | Modified Rubin et al.9 criteria | 200300 mg/kg once | ? | ? | 83 | ? |
| Hassoun et al.24 | 1 | 72 | 1 | 0 | Pancolitis | 400 mg/kg once | 6 | 15 | 100 | None |
| Chandrasekar et al.23 | 1 | 67 | 0 | 1 | Shock requiring inotropic support and pseudomembranes on colonoscopy | 400 mg/kg for 5 doses | 16 | 35 | 100 | ? |
| This paper | 21 | 68 (16) | 7 | 14 | Pancolitis and APACHE II score | 300 mg/kg once; 250 mg/kg for 5 doses | 220 | 025 | 43 | ? |
To further assess the impact of IVIG on colitis resolution, we investigated all variables in the data set that may have been associated with mortality using univariate Cox regression analysis. Those variables were as follows: APACHE II score on the first day of IVIG infusion, age, sex, previous history of CDC, number of days before IVIG use, peak white blood cell count, serum potassium level and creatinine level, lactate level on first day of IVIG infusion, and number of antibiotics administered that are not active against CDC. Only the APACHE II score (P = 0.006) and lactate level on the day of IVIG infusion (P = 0.004) were (positively) associated with CDC mortality. The positive association between CDC mortality and APACHE II score remained significant (P = 0.04) after adjusting for sex, previous history of CDC, number of days before IVIG use, lactate level on first day of IVIG infusion, and number of antibiotics administered that are not active against CDC using a multivariate Cox regression analysis model. No adjustments were made for age, white blood cell count, potassium level, or creatinine level as those are included within the APACHE II score. The positive association between lactate level on the first day of IVIG infusion and CDC mortality was not statistically significant after adjusting for the factors listed above in the same model (P = 0.13).
Discussion
To our knowledge, the present study is the largest series published in the literature to date on the use of IVIG for severe CDC. It is also the first study to report a high mortality rate compared to the 5 previous smaller studies on this topic. In the first report on IVIG use for CDC, Leung et al.15 used IVIG to treat 5 pediatric patients suffering from chronic relapsing CDC. It was not until 7 years later, in 1997, that the first IVIG use for severe CDC was reported.22 Since then, a total of 13 works have been published on IVIG for CDC treatment, and only in 5 of these was IVIG administered for severe CDC treatment:2125 3 case reports, 1 case series, and 1 case‐control study. Although the 4 uncontrolled reports concluded that IVIG is beneficial for severe CDC, the only controlled study reported no significant difference between cases and controls for all‐cause mortality, length of stay, and colectomy rate.25
The definition of severe CDC varied between reports, making comparison difficult. McPherson et al.21 and Hassoun and Ibrahim24 defined severe disease as one causing pancolitis on CT scan either with or without megacolon. In the study by Juang et al.,25 disease severity was assessed using the modified criteria of Rubin et al.9 Salcedo et al.22 defined severe CDC as one causing pancolitis in one patient and thumbprinting on CT scan in another, whereas Chandrasekar et al.23 defined it as one causing shock requiring inotropic support and presence of pseudomembranes on colonoscopy.
The present report is unique in that it provided 2 scales to characterize disease in each patient. The first scale measured colonic involvement anatomically and physiologically using a combination of computerized axial tomography (CAT) scan findings, presence or absence of ileus or referral for possible colectomy. This is not a prognostic scale, however, since CAT scan findings have been previously shown to be poor predictors of treatment outcome.29 The second scale measured the severity of systemic involvement using a well‐validated and standardized scale, the APACHE II score. We have shown in this report that it is associated with prognosis in the context of IVIG use.
Our study reports a higher mortality rate than previously described, and suggests that risk stratification and patient selection are important before IVIG administration, since not all patients seem to benefit from this treatment as previously suggested by smaller case series. Previously, several physical findings and laboratory values were found to be associated with worse outcome in CDC. These were increasing age, immunosuppression, shock requiring vasopressors, peak white blood cell count, peak serum lactate level, hypoalbuminemia, a fall in serum albumin level of >1.1 g/dL at the onset of CDC symptoms, use of 3 or more antibiotics, comorbid disease, previous history of CDC, acute renal failure and hypotension, underlying altered or depressed mental status, abdominal pain or distention, white blood cell count over 20,000/mm3 or <1500/mm3 and/or a >10% band forms on the white blood cell differential count, and ascites or pneumatosis coli by abdominal imaging.9, 3033 Using the APACHE II scale for the same purpose has the advantage of utilizing a well‐validated and objective scale that is expected to measure the degree of systemic involvement more reliably compared to the clinical and laboratory values above.
Timing of IVIG infusion remains controversial. Due to the lack of randomized controlled trials, the current practice is guided by expert opinion, leading to wide variations between reports. Since the APACHE II score was positively associated with mortality in the setting of IVIG treatment, the same scale could be used to guide decisions regarding timing of IVIG infusion. Our results suggest that IVIG should be preferentially used while the APACHE II score is still relatively low. This association and the specific APACHE II score at which to initiate or hold treatment need to be validated in the setting of a randomized controlled study before being used in clinical practice.
Although the current study was not designed to test this theory, IVIG could be associated conceptually with treatment success for patients with severe disease that is still restricted to the colon (without other organ dysfunction or at least at an early stage of extracolonic organ failure and thus associated with a low APACHE II score) but not for severe colonic disease with secondary multiple organ failure (high APACHE II score). This may be because colonic disease is toxin‐mediated whereas secondary systemic involvement is mediated through toxin‐induced inflammatory mediators (interleukin‐8, macrophage‐inflammatory protein‐2, substance P, tumor necrosis factor‐alpha) released locally in the colon,3436 triggering a SIRS and hematogenous translocation of colonic bacteria,37 both of which are poorly responsive to immunoglobulin infusion. Along the same lines, waiting for failure of conventional therapy before IVIG use might result in IVIG treatment failure because of disease progression and secondary sepsis, at which point no treatment may be effective. No study thus far has addressed this issue specifically.
Overall, the combined cohort of patients with severe CDC treated with IVIG in the literature includes 51 patients (Table 4). The current report contributes 41% of these patients. The patients' average age was 68 years, with a 2 to 1 female‐male ratio. The dose of IVIG used varied largely also, with 400 mg/kg being the mode (range, 75400 mg/kg from 1 to 5 doses). This dose is significantly below the doses used in the treatment of other diseases, like Guillain‐Barr syndrome, myasthenia gravis, Kawasaki disease, autoimmune hemolytic anemia, agammaglobulinemia, and hypogammaglobulinemia, where the usual dose is 400 mg/kg for 5 days. The resolution of diarrhea in these cases occurred after an average of 9 (range, 142) days. The index hospitalization survival rate varied from 43% to 100%. Patients received standard treatment for an average of 13 (range, 065) days before IVIG infusion. Thirty‐two of 51 patients survived their illness (63%). Neither total IgG nor anti‐toxin A IgG levels were measured in any of the reports. Of the 32 patients who had clinical resolution, 3 (10%) experienced symptoms recurrence in a follow‐up period of 1 to 13 months. This number is most probably an underestimation of the true recurrence rate resulting from an incomplete reporting because there was no uniform or active recurrence ascertainment mechanism in any of the studies. The recurrences were at 10, 14, and 30 days posttreatment. Since standard treatment was not discontinued in any of the reports once IVIG was given, the relative contribution and the ideal timing for IVIG infusion are still unclear.
The mechanism of action of IVIG is passive immunization (with anti‐toxin A and anti‐toxin B antibodies present in the pooled immunoglobulin) of a host who is usually unable to mount an adequate protective immune response.15, 22 IVIG is formed from pooling immunoglobulin from several random donors. It has been shown that many such donors express high anti‐toxin A and anti‐toxin B antibody serum titers.38, 39 In addition, high levels of anti‐toxin A and anti‐toxin B antibodies were present in the IVIG preparations and the recipients after infusion.1517, 22 Although constituting only a small fraction of the total IVIG administered, these antitoxin antibodies are believed to neutralize toxin A and B and help the host recover from the disease. In fact, Babcock et al.40 used an experimental hamster model of CDC to demonstrate a mortality reduction from 100% to 55% postinfusion of combined anti‐toxin A and anti‐toxin B antibodies. While some early reports indicated that anti‐toxin B antibodies were the major determinants of protection against colitis,41 later reports correlated disease severity pathologically42 and clinically43, 44 with anti‐toxin A levels. Anti‐toxin B antibodies were later shown to play an adjunctive role in conferring immunity against CDC40, 45, 46 when added to anti‐toxin A antibodies, but not to have any significant role on their own.
However, IVIG has been shown to contain IgG, but not IgA, anti‐toxin A and anti‐toxin B antibodies while it is only the IgA class of anti‐toxin A antibodies, and not the IgG class, that could neutralize toxin A in vitro and in vivo.47, 48 Babcock et al.40 solved this apparent dilemma by showing that a combination of 3 different monoclonal IgG anti‐toxin A antibodies could neutralize toxin A activity in vitro and prevent disease in the hamster model in vivo. Each of the 3 antibodies recognized a different toxin A domain: the first neutralized toxin A enzymatic activity, while the second prevented toxin A binding to its receptor on enterocytes, and the third prevented toxin internalization after binding to the receptor.
Thus, the mechanism of action of IVIG is most likely through the transfer of IgG anti‐toxin A antibodies that gain access to the intestinal lumen presumably secondary to inflammation‐induced mucosal damage and neutralize toxin A. Transfer of yet undetected IgA anti‐toxin A antibodies that prevent toxin A from binding to its receptor is much less likely, although possible.
The present study has limitations. As in all retrospective studies, selection bias was unavoidable. In addition, the decision to initiate IVIG administration was dependent on the attending physician, who also decided the dose, leading to heterogeneity in the total dose of IVIG infused. Such heterogeneity, however, is primarily the result of a lack of a standard dose for IVIG infusion for CDC in the published literature, as reported above. In addition, since IVIG is not yet approved by the U.S. Food and Drug Administration (FDA) for the treatment of severe CDC, standard treatment was not discontinued in any of the reports to date, including ours.
Choosing appropriate controls for patients suffering from severe CDC is challenging. This patient population is usually frail, with severe and multiple underlying diseases. The deteriorating clinical condition (and subsequently the need for multiple antibiotics) may be either the result of or the cause of CDC. Furthermore, IVIG has been in short supply for several years and therefore it has been expensive, making its administration to the number of patients needed to design adequately‐powered controlled studies difficult. These are mainly the reasons no randomized, multicenter, placebo‐controlled trial on IVIG use in severe CDC has been conducted to date.
Conclusions
In the present study, we report the results of IVIG use for the treatment of 21 patients with severe CDC. This is the largest cohort to our knowledge in the literature. Unlike previous studies on the subject, the present report provided 2 scales for disease assessment: the first based on the extent of colonic involvement and the second measuring the severity of systemic involvement using the APACHE II score. The latter was positively associated with mortality in this context. Of the 21 study patients treated with IVIG, only 9 patients (43%) survived their illness. This is the highest reported mortality rate among all studies on this subject so far. Further studies on the ideal timing of IVIG infusion, dose, and patient selection are needed before accepting IVIG as a standard of care for severe CDC treatment. The role of APACHE II score in the decision to use IVIG is promising and should be validated in randomized controlled trials.
Acknowledgements
The authors thank Indrani Mukherjee, MD, for her help and expertise in proofreading the manuscript.
- ,,.Secular trends in hospital‐acquired Clostridium difficile disease in the United States, 1987–2001.J Infect Dis.2004;189:1585–1589.
- ,,, et al.Fulminant Clostridium difficile: an underappreciated and increasing cause of death and complications.Ann Surg.2002;235:363–372.
- ,,, et al.An epidemic, toxin gene‐variant strain of Clostridium difficile.N Engl J Med.2005;353:2433–2441.
- ,,, et al.Clostridium difficile‐associated diarrhea in a region of Quebec from 1991 to 2003: a changing pattern of disease severity.CMAJ.2004;171:466–472.
- ,,.Comparison of two toxins produced by Clostridium difficile.Infect Immun.1981;34:1036–1043.
- ,,,.Asymptomatic carriage of Clostridium difficile and serum levels of IgG antibody against toxin A.N Engl J Med.2000;342:390–397.
- ,,,.Human antibody response to Clostridium difficile toxin A in relation to clinical course of infection.Infect Immun.1994;62:384–389.
- ,,.Risk factors for Clostridium difficile carriage and C. difficile‐associated diarrhea in a cohort of hospitalized patients.J Infect Dis.1990;162:678–684.
- ,,.Severe Clostridium difficile colitis.Dis Colon Rectum.1995;38:350–354.
- ,, et al.A predominantly clonal multi‐institutional outbreak of Clostridium difficile‐associated diarrhea with high morbidity and mortality.N Engl J Med.2005;353:2442–2449.
- ,,.Factors associated with failure of metronidazole in Clostridium difficile‐associated disease.J Clin Gastroenterol.2004;38:414–418.
- ,,.Treatment of Clostridium difficile‐associated disease: old therapies and new strategies.Lancet Infect Dis.2005;5:549–557.
- ,,, et al.Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole.Clin Infect Dis.2005;40:1586–1590.
- ,,, et al.Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada.Clin Infect Dis.2005;40:1591–1597.
- ,,,,,.Treatment with intravenously administered gamma globulin of chronic relapsing colitis induced by Clostridium difficile toxin.J Pediatr.1991;118:633–637.
- ,,,.Gamma globulin administration in relapsing Clostridium difficile‐induced pseudomembranous colitis with a defective antibody response to toxin A.Acta Clin Belg.1995;50:36–39.
- ,,,.Recurrent Clostridium difficile infection in a patient with selective IgG1 deficiency treated with intravenous immune globulin and Saccharomyces boulardii.Clin Infect Dis.1995;20(suppl 2):S266–S268.
- .Intravenous immunoglobulin for recurrent Clostridium difficile diarrhoea.Gut.2002;51:456.
- .Descriptive study of intravenous immunoglobulin for the treatment of recurrent Clostridium difficile diarrhoea.J Antimicrob Chemother.2004;53:882–884.
- ,,.Intravenous immunoglobulin for resistant Clostridium difficile infection.Age Ageing.2006;35:85–86.
- ,,,,.Intravenous immunoglobulin for the treatment of severe, refractory, and recurrent Clostridium difficile diarrhea.Dis Colon Rectum.2006;49:640–645.
- ,,, et al.Intravenous immunoglobulin therapy for severe Clostridium difficile colitis.Gut.1997;41:366–370.
- ,,, et. al.Intravenous immunoglobulin therapy for refractory Clostridium difficile toxin colitis in chronic kidney disease: case reports and literature review.NDT Plus.2008;1:20–22.
- ,.Use of intravenous immunoglobulin for the treatment of severe Clostridium difficile colitis.Am J Geriatr Pharmacother.2007;5:48–51.
- ,,, et al.Clinical outcomes of intravenous immune globulin in severe clostridium difficile‐associated diarrhea.Am J Infect Control.2007;35:131–137.
- ,,,.Successful treatment of Clostridium difficile colitis with intravenous immunoglobulin.J Gastrointestin Liver Dis.2008;17:353–359.
- ,,, et al.A durable response to relapsing Clostridium difficile colitis may require combined therapy with high‐dose oral Vancomycin and intravenous immune globulin.Infect Dis Clin Pract.2006;14:217–220.
- ,,,.APACHE II: a severity of disease classification system.Crit Care Med.1985;13:818–829.
- ,,,,,.Colonic abnormalities on CT in adult hospitalized patients with Clostridium difficile colitis: prevalence and significance of findings.AJR Am J Roentgenol.2006;186:1393–1400.
- ,,,.Clostridium difficile‐associated diarrhea: predictors of severity in patients presenting to the emergency department.Can J Gastroenterol.2003;17:369–373.
- ,,, et al.Impact of emergency colectomy on survival of patients with fulminant Clostridium difficile colitis during an epidemic caused by a hypervirulent strain.Ann Surg.2007;245:267–272.
- ,, et al.Risk factors for severity and relapse of pseudomembranous colitis in an elderly population.Colorectal Dis.2007;9:173–177.
- ,,,,.Prognostic criteria in Clostridium difficile colitis.Am J Gastroenterol.1996;91:460–464.
- ,,, et al.Clostridium difficile toxin a stimulates macrophage‐inflammatory protein‐2 production in rat intestinal epithelial cells.J Immunol.1998;160:6039–6045.
- ,,, et al.Increased substance P responses in dorsal root ganglia, intestinal macrophages during Clostridium difficile toxin a enteritis in rats.Proc Natl Acad Sci U S A.1997;94:4788–4793.
- ,,,,,.Cytokine response by human monocytes to Clostridium difficile toxin a and toxin B.Infect Immun.1991;59:3659–3666.
- ,,,.Bacterial translocation, intestinal microflora and morphological changes of intestinal mucosa in experimental models of Clostridium difficile infection.J Med Microbiol.1998;47:591–598.
- ,.Immunoglobulin G directed against toxins A and B of Clostridium difficile in the general population and patients with antibiotic‐associated diarrhea.Diagn Microbiol Infect Dis.1994;18:205–209.
- ,,, et al.Serum antibody response to toxins A and B of Clostridium difficile.J Infect Dis.1983;148:93–100.
- ,,, et al.Human monoclonal antibodies directed against toxins A and B prevent Clostridium difficile‐induced mortality in hamsters.Infect Immun.2006;74:6339–6347.
- ,,,.Serum antibody response to Clostridium difficile toxins in patients with Clostridium difficile diarrhoea.Infection.1985;13:97–101.
- ,,,.Relationship between levels of Clostridium difficile toxin A and toxin B and cecal lesions in gnotobiotic mice.Infect Immun.1989;57:2123–2127.
- ,,,,.Protection against experimental pseudomembranous colitis in gnotobiotic mice by use of monoclonal antibodies against Clostridium difficile toxin A.Infect Immun.1991;59:1192–1195.
- ,,.Systemic and mucosal antibody responses to toxin A in patients infected with Clostridium difficile.J Infect Dis.1992;166:1287–1294.
- ,,, et al.Transcutaneous immunization with Clostridium difficile toxoid A induces systemic and mucosal immune responses and toxin A‐neutralizing antibodies in mice.Infect Immun.2007;75:2826–2832.
- ,,, et al.Serum antitoxin antibodies mediate systemic and mucosal protection from Clostridium difficile disease in hamsters.Infect Immun.1999;67:527–538.
- ,,,.Human colonic aspirates containing immunoglobulin A antibody to Clostridium difficile toxin A inhibit toxin A‐receptor binding.Gastroenterology.1992;102:35–40.
- ,,,,.Selective neutralization of a bacterial enterotoxin by serum immunoglobulin A in response to mucosal disease.Infect Immun.1995;63:3166–3173.
Clostridium difficile colitis (CDC) is the most common cause of hospital‐acquired diarrhea.1 The incidence of CDC has sharply increased over the past decade despite increasing awareness among health care professionals.24 C. difficile pathogenic strains induce diarrhea through the elaboration and secretion of 2 exotoxins: toxin A and toxin B. Toxin A is an inflammatory toxin, leading to fluid secretion, increased mucosal permeability, and marked enteritis and colitis.5 Toxin B is cytotoxic, leading to cell injury and apoptosis.5 Combined, toxin A and toxin B can cause a wide spectrum of clinical presentations, ranging from mild diarrhea that resolves with the discontinuation of antibiotics to a fulminant colitis requiring surgical intervention.
The severity of clinical manifestations has been shown to be inversely proportional to the host anti‐toxin A antibody level in response to toxin exposure. Kyne et al.6 demonstrated that asymptomatic C. difficile carriers produced significantly higher anti‐toxin A immunoglobulin G (IgG) levels compared to symptomatic patients. Among the latter group, patients with mild disease had a higher antibody level compared to those with severe colitis.6, 7 Additional risk factors predisposing to severe colitis are advanced age, severe underlying illness,8 and immunocompromised state.9
Recently, a new C. difficile strain (BI/NAP1) with a mutated toxin A and toxin B promoter silencer, a binary toxin gene, and fluoroquinolone resistance has been described in Canada and the United States.3, 10 This strain has been associated with an increased incidence of CDC among hospitalized patients, especially the incidence of severe disease requiring colectomy. At the same time, several reports describing metronidazole treatment failure have been published.1114 These recent findings emphasize the importance of finding alternative treatments for CDC.
Intravenous immunoglobulin (IVIG) was used to treat CDC for the first time in 1991.15 Since then, 12 case reports and small case series, along with 1 case‐control study have been published documenting IVIG treatment outcomes.1527 However, only 5 reports to date examined patients with severe CDC.2125 In the present study, we report the largest series of patients with severe CDC treated with IVIG in the literature to our knowledge.
Patients and Methods
Case Series
We used CareScience software (CareScience, Inc., Philadelphia, PA) to retrospectively identify all patients admitted to our institution with a primary or secondary diagnosis of CDC (code 00845) between July 1, 2002 and May 1, 2006. CareScience is commercially available software that tracks all admissions to our institution and allows the performance of patient searches with a wide spectrum of user‐defined search criteria. Using the same software, we further identified those patients who received IVIG during their hospital stay. We then obtained the hospital chart for each patient, from the medical records department and established the study database.
A case was defined as a patient with diarrhea (at least 3 loose stools daily) for at least 2 days who had C. difficile cytotoxin‐positive feces and at least 1 of the following criteria: clinical symptoms (abdominal pain and/or distension and fever); leukemoid reaction (defined as white blood cell count of 20,000 cells/mm3 or above. This cutoff value was chosen as it has been used previously as a prognostic factor)4; radiographic evidence of colitis by computed tomography (CT) of the abdomen; and/or the presence of pseudomembranes on flexible sigmoidoscopy or colonoscopy. We excluded all patients who received IVIG for an indication other than CDC treatment (n = 3). There were no other exclusion criteria.
We used a standardized data collection tool and recorded demographics (age, gender, principal diagnosis), past medical and surgical history, other risk factors for C. difficile infection (previous CDC, antibiotics received during hospital stay, immunosuppressive medications or organ transplantation within the previous 6 weeks, history of malignancy or diabetes mellitus); clinical presentation (abdominal distention, abdominal pain, diarrhea, fever, leukemoid reaction, and hypotension defined as systolic blood pressure <85 mm Hg despite at least 1 L of intravenous normal saline administration and the need for vasopressor use); colonoscopy findings; CT scan and x‐ray findings; laboratory values; date and dose of IVIG infused and other C. difficile pharmacological treatments; and Acute Physiological Assessment and Chronic Health Evaluation (APACHE II) score28 at the first day of IVIG infusion. The primary outcomes were survival at the end of the hospital stay and clinical disease resolution, defined as 2 formed bowel movements or less per day without abdominal pain or distention.
The decision to initiate IVIG therapy and the dose to be used was made by the individual attending physician.
Statistical Analysis
Single (univariate) and multiple (multivariate) logistic regression analysis were applied to identify variables among the ones collected that are independent predictors of CDC mortality. All statistical analyses were completed with the STATA 10 software package (StatCorp LP, College Station, TX).
Review of the Literature
We used PubMed, Web of Science, Scopus, and Excerpta Medica databases to search for any publication in a peer‐reviewed journal on the use of IVIG for the treatment of severe CDC. We used the search words: IVIG or intravenous immunoglobulin and clostridium difficile. Only publications published in English were selected. The date range used was January 1, 1950 to January 7, 2009. We were able to find 5 publications using this search criteria.
Results
Study Population
Of the 1230 patients diagnosed with CDC over the 4‐year study period, 21 patients were treated with IVIG. Table 1 summarizes the patients' characteristics. There were 13 women and 8 men. The mean age was 68 years, with a standard deviation (SD) of 13 years. Sepsis was the primary diagnosis in all patients. Sixteen patients had predisposing risk factors for CDC, including immunosuppression (immunosuppressive medication [n = 2], human immunodeficiency virus [HIV] infection [n = 2]); cancer (n = 3); recent surgery (n = 3); and diabetes mellitus (n = 11). Nine patients had documented previous CDC episodes. The indications for IVIG administration were evidence of pancolitis on abdominal CT scan (n = 12) or severe ileus with cessation of diarrhea, abdominal distention, and requirement for total parenteral nutrition (n = 5), or severe hypotension (n = 4) (defined as systolic blood pressure <85 mm Hg despite at least 1 L of intravenous normal saline administration and the subsequent need for vasopressor use).
| Patient | Age (gender) | Diagnosis | Medical and Surgical History | CDC History | Colonoscopy Findings | Radiographic Findings |
|---|---|---|---|---|---|---|
| ||||||
| A | 40 (female) | CDC with sec. sepsis | Gastric stapling | Yes | * | Diffuse colitis |
| B | 86 (female) | Fulminant CDC | Metastatic ovarian carcinoma | PC | No colonic thickening | |
| C | 72 (male) | Sepsis | Acute pancreatitis with sec. pseudocyst, DM | Yes | PC | Diffuse colitis |
| D | 78 (male) | Discitis | Delayed: normal mucosa | Dilation of small and large bowel | ||
| E | 98 (female) | Urosepsis | Yes | * | No bowel distention | |
| F | 90 (female) | Right lower extremity cellulitis | DM | * | Concentric thickening of rectal wall | |
| G | 64 (male) | Ischemic colitis | DM, recent Hartman pouch closure | Marked inflammation | Diffuse colitis | |
| H | 78 (female) | Toe osteomyelitis and CDC with sec. sepsis | DM | * | Diffuse colitis | |
| I | 35 (female) | Sepsis | Yes | * | Diffuse nonspecific colitis, minimal ascites | |
| J | 47 (female) | Pneumonia and sec. sepsis | * | Diffuse colitis | ||
| K | 56 (female) | Urosepsis | HIV | Yes | * | Colitis involving the right colon |
| L | 76 (male) | CDC with sec. sepsis | Sigmoid bladder fistula repair, DM | * | Diffuse colitis | |
| M | 71 (female) | Pneumonia with sec. sepsis | * | Diffuse colitis | ||
| N | 63 (male) | Urosepsis | DM, lymphoma resection from small intestine | PC | Marked small and large bowel distention | |
| O | 86 (male) | Enterococcus‐induced sepsis | Rheumatoid arthritis on methotrexate | * | Fat stranding suggesting peritonitis | |
| P | 60 (female) | Gastrointestinal bleed and CDC | DM with neuropathy and retinopathies | Yes | * | Thickening of wall of colon in most of the colon |
| Q | 57 (female) | Sepsis | DM | Yes | * | Normal |
| R | 67 (female) | CDC with sec. sepsis | Candidal esophagitis | Yes | * | Large amount of peritoneal fluid, mild small bowel thickening |
| S | 60 (female) | Sepsis sec. to S. aureus and P. aerogenosa | DM, renal transplant (myco, prednisone) | * | Ileus with air fluid level in the small intestine | |
| T | 80 (female) | Sepsis | DM | Yes | * | Thickening of descending colon consistent with colitis |
| U | 72 (male) | CDC, widespread metastatic cancer | DM, metastatic cancer (unknown primary site) | * | Severe colitis up to the splenic flexure | |
Table 2 describes disease severity in these patients. Since CDC starts locally in the colon then secondarily involves multiple organs as part of the systemic inflammatory response syndrome (SIRS), 2 scales were used to characterize the disease in each patient: (1) extent of local colonic inflammation, and (2) severity of systemic involvement. Extensive colonic involvement was evidenced in all patients by pancolitis on abdominal imaging modalities (12 patients), severe ileus requiring total parenteral nutrition (13 patients), or referral for surgical consultation for possible colectomy (12 patients).
| Patient | Complications During the Hospital Stay | APACHE II Score | Monitored Unit | WBC* | K | Alb | Lactate | Cr | Hospital Stay (days) | Surgical Consult/Surgery | TPN for Colitis |
|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||
| A | Sepsis, DIC, ARDS, intubation | 15 | Yes | 48 | 4 | 1.1 | 2.9 | 1.3 | 26 | No/No | Yes |
| B | Dehydration, weakness | 12 | No | 19 | 3.4 | 3.1 | 1.1 | 16 | No/No | Yes | |
| C | HTP, GI bleed, ischemic colitis, F | 22 | Yes | 21 | 2.7 | 2.5 | 1.3 | ESRD | 34 | Yes/No | Yes |
| D | AD, megacolon, HT, intubation, ARF | 18 | Yes | 25 | 3.4 | 1.4 | 1.1 | 2.6 | 52 | Yes/No | Yes |
| E | Exacerbation of CHF with respiratory distress, Bipap support, confusion | 21 | No | 10 | 2.6 | 2.3 | 1 | 11 | No/No | No | |
| F | Confusion, gout acute attack | 21 | No | 33 | 3.1 | 2.6 | ESRD | 15 | No/No | No | |
| G | Intubation, cardiac arrest, AF with RVR, PNA, ARF, DVT, dysphagia, PEG | 6 | Yes | 15 | 3.1 | 1.7 | 1.9 | 2.2 | 32 | Yes/No | Yes |
| H | Sepsis, intubation, ARF, PEG, toe amputation, PNA, pulmonary edema, TPN, vitamin D deficiency | 34 | Yes | 59 | 2.8 | 1.5 | 4 | 3.8 | 17 | No/No | Yes |
| I | CHF, transient third cranial nerve palsy, DIC | 20 | Yes | 52 | 3.2 | 3.3 | 0.7 | ESRD | 11 | No/No | No |
| J | Aspiration PNA, sepsis, DIC, intubation, MI, F, HT | 32 | Yes | 17 | 2.7 | 1.8 | 14 | ESRD | 21 | Yes/no | No |
| K | Intubation, cardiac arrest, ARF, DIC, AP, F | 30 | Yes | 25 | 2.1 | 2.1 | 13 | 3.6 | 10 | Yes/no | No |
| L | Intubation, ARF, HTP, MI, AD, F | 23 | Yes | 69 | 3.2 | 1.8 | 1.4 | 3.6 | 23 | Yes/no | No |
| M | Intubation, DIC, ARF, GI bleeding, hypothermia, AD | 23 | Yes | 47 | 2.8 | 1.4 | 1.4 | 4.3 | 23 | Yes/no | Yes |
| N | Intubation, HTP, AD, F, ARF with HD, AF, osteomyelitis | 23 | Yes | 46 | 2.9 | 1.5 | 1.5 | 2.7 | 27 | Yes/no | Yes |
| O | Intubation, ARF, 2 cardiac arrests, GI bleed, UTI, rhabdomyolysis, liver shock, AF | 31 | Yes | 49 | 2.5 | 1.1 | 2.3 | 2.9 | 25 | Yes/no | Yes |
| P | Bowel ischemia with bowel resection, ARF, MI, ischemic bowel, fluid overload, respiratory failure | 23 | Yes | 26 | 2.6 | 0.8 | 2.9 | 3.1 | 9 | Yes/Yes | Yes |
| Q | Pulmonary embolism | 39 | Yes | 23 | 2.8 | 1.1 | 8.1 | ESRD | 9 | No/No | Yes |
| R | Fungal peritonitis, aspiration pneumonia, cardiac arrest | 26 | Yes | 30 | 4.1 | 1.1 | 0.9 | ESRD | 36 | No/No | Yes |
| S | Intubation, pneumothorax, CRT, pressor‐dependent shock, ARF | 36 | Yes | 46 | 3.1 | 1.8 | 2.1 | 5.4 | 64 | Yes/Yes | No |
| T | Pressor‐dependent sepsis, pulmonary edema, ARF with HD | 36 | Yes | 35 | 3.3 | 1.3 | 1.8 | 5.5 | 11 | Yes/No | Yes |
| U | Sepsis | 34 | Yes | 58 | 3.1 | 2.2 | 3.3 | 1.6 | 9 | No/No | No |
Of the 21 patients treated with IVIG, 9 did not receive a surgical consultation either because they responded to medical treatment promptly (6 patients), were too unstable for surgery (2 patients), or because the patient/family refused surgery (1 patient). Of the 12 patients who received surgical consultation, 2 underwent surgery. The remainder did not proceed to surgery for the following reasons: they were deemed medically unstable for surgery (6 patients), declined surgery (2 patients), were diagnosed with cancer on colonoscopy (1 patient), or improved with medical treatment (1 patient).
The severity of systemic involvement was measured using the APACHE II score on day 1 of IVIG infusion. The mean APACHE II score was 25. Eighteen patients were in a monitored unit when IVIG was administered. The study group had laboratory results in keeping with those previously used to define severe colitis:4, 9, 19 leukocytosis (defined as white blood cell count higher than 12,000 cells/mL [mean = 36,000 cells/mL]), hypoalbuminemia (mean = 1.78 g/dL, SD = 0.68 g/dL), hypokalemia (mean = 3.02 mg/dL, SD = 0.47 g/dL), and acute renal failure (defined as serum creatinine level >1.5 mg/dL [mean = 2.98 mg/dL, SD = 1.42 g/dL]).
IVIG Use
Table 3 describes the treatment patients received for CDC as well as the total number of antibiotics used throughout the hospital stay. IVIG was used as adjuvant treatment (defined as IVIG administration within 4 days or less after CDC diagnosis) in 8 patients and as second‐line treatment (defined as IVIG administration more than 4 days after CDC diagnosis) in 13 patients. Metronidazole, vancomycin, cholestyramine, and probiotic treatment alone or in different combinations were used for an average of 8 days (SD = 8 days; range, 025 days) before IVIG infusion. The total IVIG dose administered varied depending on the prescribing attending, with a range of 200 mg/kg to 1250 mg/kg and a mode of 250 mg/kg for 1 to 3 days. An average of 5 (SD = 2) different antibiotics that were not active against C. difficile were used per patient without being discontinued after a CDC diagnosis was made. The 3 most common were: cephalosporins (cefazolin, ceftriaxone, cefepime), fluoroquinolones (levofloxacin), and combination antibiotics (piperacillin and tazobactam or ampicillin and sulbactam).
| Patient | Number of Antibiotics | Duration of Treatment Before IVIG (days) | Treatment Before IVIG (days) | Total CDC Treatment (days) | IgG Level | IVIG Dose |
|---|---|---|---|---|---|---|
| ||||||
| A | 5 | 7 | Metro (7), Vanc (7), Choles (2) | Oral and rectal Vanc (26,19), IV Metro (19), Choles (2), Lacto (6) | Low | 300 mg/kg for 1 day |
| B | 1 | 13 | Metro (13), Vanc (13) | Oral Vanc (17) and IV Metro (12) | 300 mg/kg for 1 day | |
| C | 3 | 7 | Metro (7), Vanc (3) | IV Metro (28),Vanc oral and enema (18,3), Lacto (10) | Low | 125 mg/kg for 5 days |
| D | 5 | 25 | Metro (25), Vanc (15) | Oral then IV Metro (10,15), oral Vanc (25), Choles (7) and Lacto (13) | Low | 200 mg/kg for 1 day |
| E | 1 | 4 | Metro (1), Vanc (4), Choles(4) | IV Metro (8), oral Vanc (10) and Choles (4) | 75 mg/kg for 5 days | |
| F | 4 | 2 | Metro (2), Vanc (1) | IV Metro (8) and oral Vanc (9) | 250 mg/kg for 5 days | |
| G | 3 | 17 | Metro (17), Vanc (14) | IV Metro (49) and oral Vanc (61) | 250 mg/kg for 2 days | |
| H | 5 | 1 | Metro (1), Vanc (1) | Oral Metro (18), oral Vanc (22 ), IV Metro (3) | 250 mg/kg for 3 days | |
| I | 6 | 1 | Metro (1) | Oral and IV Metro (7,9), Vanc oral and enema (8,3) | 250 mg/kg for 2 days | |
| J | 8 | 16 | Metro (14), Vanc (2), Lacto (6) | Oral then IV Metro (10,5), oral and rectal Vanc (3,1), Lacto (6) | 300 mg/ kg for 1 day | |
| K | 6 | 7 | Metro (7), Vanc (3) | Oral then IV Metro (10) and oral Vanc (9) | Normal | 400 mg/kg for 2 days |
| L | 4 | 0 | None | IV then oral Metro (7,10), oral Vanc (23), Choles (7), and Lacto (5) | 150 mg/kg for 5 days | |
| M | 6 | 1 | Metro (1) | IV Metro (23) and oral Vanc (9) | 250 mg/kg for 2 days | |
| N | 7 | 1 | Metro (1), Vanc (1) | IV Metro (16), oral Vanc (14), oral Metro (7) | 250 mg /kg for 2 days | |
| O | 6 | 7 | Metro (6), Vanc (4) | IV Metro (6) and oral Vanc (22) | Low | 250 mg/kg for 2 days |
| P | 3 | 6 | Metro (6), Vanc (6) | IV Metro (25) and oral Vanc (17) | 150 mg/kg fro 3 days | |
| Q | 3 | 4 | Metro (4), Vanc (3) | Oral Metro (8),Vanc oral and enema (6,3) | 250 mg/kg for 3 days | |
| R | 5 | 9 | Vanc (9) | Vanc oral and enema (5,4), IV Metro (2) | 250 mg/kg for 1 day | |
| S | 8 | 23 | Metro (23), Vanc (23) | Oral then IV Metro (12,22), oral Vanc (39) | 250 mg/kg for 3 days | |
| T | 4 | 6 | Metro (6), Vanc (1) | Oral Vanc and IV Metro (11) | 250 mg/kg for 1 day | |
| U | 4 | 2 | Metro (2), Vanc (2) | Oral Vanc and IV Metro (6) | 250 mg/kg for 3 days | |
Survival with IVIG Use
Nine patients (43%) survived their illness and were discharged from the hospital. They experienced complete clinical resolution after an average of 10 days from IVIG administration (range, 220 days) (Table 4). The other 12 patients (57%) died during the index hospitalization. The average length of stay was 23 (range, 964) days.0
| Patient | Disposition | Clearance of Clostridium difficile Colitis? | Days to Resolution |
|---|---|---|---|
| |||
| A | Alive | Loose BM persisted but diarrhea resolved 9 days after IVIG. | 9 |
| B | Alive | BM became formed and diarrhea resolved 48 hours after IVIG. | 2 |
| C | Alive | Diarrhea resolved 20 days post‐IVIG infusion. CAT scan: colonic thickening improved. | 20 |
| D | Alive | Diarrhea resolved on discharge. Response to IVIG started next day after administration. | 18 |
| E | Alive | Diarrhea improved next day after IVIG administration and resolved on discharge. | 5 |
| F | Alive | Diarrhea resolved 5 days after IVIG administration. | 5 |
| G | Alive | Diarrhea resolved. C. difficile test became negative. | 13 |
| H | Alive | Diarrhea resolved 2 days before discharge. | 15 |
| I | Alive | Diarrhea slowly improved and resolved 4 days before discharge. | 7 |
| J | Deceased | ||
| K | Deceased | ||
| L | Deceased | ||
| M | Deceased | ||
| N | Deceased | ||
| O | Deceased | ||
| P | Deceased | ||
| Q | Deceased | ||
| R | Deceased | ||
| S | Deceased | ||
| T | Deceased | ||
| U | Deceased | ||
| Study | Number of Patients | Age (SD) (years) | Male | Female | Severity Definition | IVIG Dose | Days to Resolution | Days IVIG Infused | Alive? (%) | Recurrence |
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
| Salcedo et al.22 | 2 | 63, 64 | 1 | 1 | Pancolitis or thumbprinting on CAT scan | 200300 mg/kg once | 12 | 59 | 100 | 1 out of 2 |
| McPherson et al.21 | 8 | 72 (12) | ? | ? | Pancolitis | 200400 mg/kg twice | 226 | 1165 | 75 | 2 out of 6 |
| Juang et al.25 | 18 | 67 (17.4) | 5 | 13 | Modified Rubin et al.9 criteria | 200300 mg/kg once | ? | ? | 83 | ? |
| Hassoun et al.24 | 1 | 72 | 1 | 0 | Pancolitis | 400 mg/kg once | 6 | 15 | 100 | None |
| Chandrasekar et al.23 | 1 | 67 | 0 | 1 | Shock requiring inotropic support and pseudomembranes on colonoscopy | 400 mg/kg for 5 doses | 16 | 35 | 100 | ? |
| This paper | 21 | 68 (16) | 7 | 14 | Pancolitis and APACHE II score | 300 mg/kg once; 250 mg/kg for 5 doses | 220 | 025 | 43 | ? |
To further assess the impact of IVIG on colitis resolution, we investigated all variables in the data set that may have been associated with mortality using univariate Cox regression analysis. Those variables were as follows: APACHE II score on the first day of IVIG infusion, age, sex, previous history of CDC, number of days before IVIG use, peak white blood cell count, serum potassium level and creatinine level, lactate level on first day of IVIG infusion, and number of antibiotics administered that are not active against CDC. Only the APACHE II score (P = 0.006) and lactate level on the day of IVIG infusion (P = 0.004) were (positively) associated with CDC mortality. The positive association between CDC mortality and APACHE II score remained significant (P = 0.04) after adjusting for sex, previous history of CDC, number of days before IVIG use, lactate level on first day of IVIG infusion, and number of antibiotics administered that are not active against CDC using a multivariate Cox regression analysis model. No adjustments were made for age, white blood cell count, potassium level, or creatinine level as those are included within the APACHE II score. The positive association between lactate level on the first day of IVIG infusion and CDC mortality was not statistically significant after adjusting for the factors listed above in the same model (P = 0.13).
Discussion
To our knowledge, the present study is the largest series published in the literature to date on the use of IVIG for severe CDC. It is also the first study to report a high mortality rate compared to the 5 previous smaller studies on this topic. In the first report on IVIG use for CDC, Leung et al.15 used IVIG to treat 5 pediatric patients suffering from chronic relapsing CDC. It was not until 7 years later, in 1997, that the first IVIG use for severe CDC was reported.22 Since then, a total of 13 works have been published on IVIG for CDC treatment, and only in 5 of these was IVIG administered for severe CDC treatment:2125 3 case reports, 1 case series, and 1 case‐control study. Although the 4 uncontrolled reports concluded that IVIG is beneficial for severe CDC, the only controlled study reported no significant difference between cases and controls for all‐cause mortality, length of stay, and colectomy rate.25
The definition of severe CDC varied between reports, making comparison difficult. McPherson et al.21 and Hassoun and Ibrahim24 defined severe disease as one causing pancolitis on CT scan either with or without megacolon. In the study by Juang et al.,25 disease severity was assessed using the modified criteria of Rubin et al.9 Salcedo et al.22 defined severe CDC as one causing pancolitis in one patient and thumbprinting on CT scan in another, whereas Chandrasekar et al.23 defined it as one causing shock requiring inotropic support and presence of pseudomembranes on colonoscopy.
The present report is unique in that it provided 2 scales to characterize disease in each patient. The first scale measured colonic involvement anatomically and physiologically using a combination of computerized axial tomography (CAT) scan findings, presence or absence of ileus or referral for possible colectomy. This is not a prognostic scale, however, since CAT scan findings have been previously shown to be poor predictors of treatment outcome.29 The second scale measured the severity of systemic involvement using a well‐validated and standardized scale, the APACHE II score. We have shown in this report that it is associated with prognosis in the context of IVIG use.
Our study reports a higher mortality rate than previously described, and suggests that risk stratification and patient selection are important before IVIG administration, since not all patients seem to benefit from this treatment as previously suggested by smaller case series. Previously, several physical findings and laboratory values were found to be associated with worse outcome in CDC. These were increasing age, immunosuppression, shock requiring vasopressors, peak white blood cell count, peak serum lactate level, hypoalbuminemia, a fall in serum albumin level of >1.1 g/dL at the onset of CDC symptoms, use of 3 or more antibiotics, comorbid disease, previous history of CDC, acute renal failure and hypotension, underlying altered or depressed mental status, abdominal pain or distention, white blood cell count over 20,000/mm3 or <1500/mm3 and/or a >10% band forms on the white blood cell differential count, and ascites or pneumatosis coli by abdominal imaging.9, 3033 Using the APACHE II scale for the same purpose has the advantage of utilizing a well‐validated and objective scale that is expected to measure the degree of systemic involvement more reliably compared to the clinical and laboratory values above.
Timing of IVIG infusion remains controversial. Due to the lack of randomized controlled trials, the current practice is guided by expert opinion, leading to wide variations between reports. Since the APACHE II score was positively associated with mortality in the setting of IVIG treatment, the same scale could be used to guide decisions regarding timing of IVIG infusion. Our results suggest that IVIG should be preferentially used while the APACHE II score is still relatively low. This association and the specific APACHE II score at which to initiate or hold treatment need to be validated in the setting of a randomized controlled study before being used in clinical practice.
Although the current study was not designed to test this theory, IVIG could be associated conceptually with treatment success for patients with severe disease that is still restricted to the colon (without other organ dysfunction or at least at an early stage of extracolonic organ failure and thus associated with a low APACHE II score) but not for severe colonic disease with secondary multiple organ failure (high APACHE II score). This may be because colonic disease is toxin‐mediated whereas secondary systemic involvement is mediated through toxin‐induced inflammatory mediators (interleukin‐8, macrophage‐inflammatory protein‐2, substance P, tumor necrosis factor‐alpha) released locally in the colon,3436 triggering a SIRS and hematogenous translocation of colonic bacteria,37 both of which are poorly responsive to immunoglobulin infusion. Along the same lines, waiting for failure of conventional therapy before IVIG use might result in IVIG treatment failure because of disease progression and secondary sepsis, at which point no treatment may be effective. No study thus far has addressed this issue specifically.
Overall, the combined cohort of patients with severe CDC treated with IVIG in the literature includes 51 patients (Table 4). The current report contributes 41% of these patients. The patients' average age was 68 years, with a 2 to 1 female‐male ratio. The dose of IVIG used varied largely also, with 400 mg/kg being the mode (range, 75400 mg/kg from 1 to 5 doses). This dose is significantly below the doses used in the treatment of other diseases, like Guillain‐Barr syndrome, myasthenia gravis, Kawasaki disease, autoimmune hemolytic anemia, agammaglobulinemia, and hypogammaglobulinemia, where the usual dose is 400 mg/kg for 5 days. The resolution of diarrhea in these cases occurred after an average of 9 (range, 142) days. The index hospitalization survival rate varied from 43% to 100%. Patients received standard treatment for an average of 13 (range, 065) days before IVIG infusion. Thirty‐two of 51 patients survived their illness (63%). Neither total IgG nor anti‐toxin A IgG levels were measured in any of the reports. Of the 32 patients who had clinical resolution, 3 (10%) experienced symptoms recurrence in a follow‐up period of 1 to 13 months. This number is most probably an underestimation of the true recurrence rate resulting from an incomplete reporting because there was no uniform or active recurrence ascertainment mechanism in any of the studies. The recurrences were at 10, 14, and 30 days posttreatment. Since standard treatment was not discontinued in any of the reports once IVIG was given, the relative contribution and the ideal timing for IVIG infusion are still unclear.
The mechanism of action of IVIG is passive immunization (with anti‐toxin A and anti‐toxin B antibodies present in the pooled immunoglobulin) of a host who is usually unable to mount an adequate protective immune response.15, 22 IVIG is formed from pooling immunoglobulin from several random donors. It has been shown that many such donors express high anti‐toxin A and anti‐toxin B antibody serum titers.38, 39 In addition, high levels of anti‐toxin A and anti‐toxin B antibodies were present in the IVIG preparations and the recipients after infusion.1517, 22 Although constituting only a small fraction of the total IVIG administered, these antitoxin antibodies are believed to neutralize toxin A and B and help the host recover from the disease. In fact, Babcock et al.40 used an experimental hamster model of CDC to demonstrate a mortality reduction from 100% to 55% postinfusion of combined anti‐toxin A and anti‐toxin B antibodies. While some early reports indicated that anti‐toxin B antibodies were the major determinants of protection against colitis,41 later reports correlated disease severity pathologically42 and clinically43, 44 with anti‐toxin A levels. Anti‐toxin B antibodies were later shown to play an adjunctive role in conferring immunity against CDC40, 45, 46 when added to anti‐toxin A antibodies, but not to have any significant role on their own.
However, IVIG has been shown to contain IgG, but not IgA, anti‐toxin A and anti‐toxin B antibodies while it is only the IgA class of anti‐toxin A antibodies, and not the IgG class, that could neutralize toxin A in vitro and in vivo.47, 48 Babcock et al.40 solved this apparent dilemma by showing that a combination of 3 different monoclonal IgG anti‐toxin A antibodies could neutralize toxin A activity in vitro and prevent disease in the hamster model in vivo. Each of the 3 antibodies recognized a different toxin A domain: the first neutralized toxin A enzymatic activity, while the second prevented toxin A binding to its receptor on enterocytes, and the third prevented toxin internalization after binding to the receptor.
Thus, the mechanism of action of IVIG is most likely through the transfer of IgG anti‐toxin A antibodies that gain access to the intestinal lumen presumably secondary to inflammation‐induced mucosal damage and neutralize toxin A. Transfer of yet undetected IgA anti‐toxin A antibodies that prevent toxin A from binding to its receptor is much less likely, although possible.
The present study has limitations. As in all retrospective studies, selection bias was unavoidable. In addition, the decision to initiate IVIG administration was dependent on the attending physician, who also decided the dose, leading to heterogeneity in the total dose of IVIG infused. Such heterogeneity, however, is primarily the result of a lack of a standard dose for IVIG infusion for CDC in the published literature, as reported above. In addition, since IVIG is not yet approved by the U.S. Food and Drug Administration (FDA) for the treatment of severe CDC, standard treatment was not discontinued in any of the reports to date, including ours.
Choosing appropriate controls for patients suffering from severe CDC is challenging. This patient population is usually frail, with severe and multiple underlying diseases. The deteriorating clinical condition (and subsequently the need for multiple antibiotics) may be either the result of or the cause of CDC. Furthermore, IVIG has been in short supply for several years and therefore it has been expensive, making its administration to the number of patients needed to design adequately‐powered controlled studies difficult. These are mainly the reasons no randomized, multicenter, placebo‐controlled trial on IVIG use in severe CDC has been conducted to date.
Conclusions
In the present study, we report the results of IVIG use for the treatment of 21 patients with severe CDC. This is the largest cohort to our knowledge in the literature. Unlike previous studies on the subject, the present report provided 2 scales for disease assessment: the first based on the extent of colonic involvement and the second measuring the severity of systemic involvement using the APACHE II score. The latter was positively associated with mortality in this context. Of the 21 study patients treated with IVIG, only 9 patients (43%) survived their illness. This is the highest reported mortality rate among all studies on this subject so far. Further studies on the ideal timing of IVIG infusion, dose, and patient selection are needed before accepting IVIG as a standard of care for severe CDC treatment. The role of APACHE II score in the decision to use IVIG is promising and should be validated in randomized controlled trials.
Acknowledgements
The authors thank Indrani Mukherjee, MD, for her help and expertise in proofreading the manuscript.
Clostridium difficile colitis (CDC) is the most common cause of hospital‐acquired diarrhea.1 The incidence of CDC has sharply increased over the past decade despite increasing awareness among health care professionals.24 C. difficile pathogenic strains induce diarrhea through the elaboration and secretion of 2 exotoxins: toxin A and toxin B. Toxin A is an inflammatory toxin, leading to fluid secretion, increased mucosal permeability, and marked enteritis and colitis.5 Toxin B is cytotoxic, leading to cell injury and apoptosis.5 Combined, toxin A and toxin B can cause a wide spectrum of clinical presentations, ranging from mild diarrhea that resolves with the discontinuation of antibiotics to a fulminant colitis requiring surgical intervention.
The severity of clinical manifestations has been shown to be inversely proportional to the host anti‐toxin A antibody level in response to toxin exposure. Kyne et al.6 demonstrated that asymptomatic C. difficile carriers produced significantly higher anti‐toxin A immunoglobulin G (IgG) levels compared to symptomatic patients. Among the latter group, patients with mild disease had a higher antibody level compared to those with severe colitis.6, 7 Additional risk factors predisposing to severe colitis are advanced age, severe underlying illness,8 and immunocompromised state.9
Recently, a new C. difficile strain (BI/NAP1) with a mutated toxin A and toxin B promoter silencer, a binary toxin gene, and fluoroquinolone resistance has been described in Canada and the United States.3, 10 This strain has been associated with an increased incidence of CDC among hospitalized patients, especially the incidence of severe disease requiring colectomy. At the same time, several reports describing metronidazole treatment failure have been published.1114 These recent findings emphasize the importance of finding alternative treatments for CDC.
Intravenous immunoglobulin (IVIG) was used to treat CDC for the first time in 1991.15 Since then, 12 case reports and small case series, along with 1 case‐control study have been published documenting IVIG treatment outcomes.1527 However, only 5 reports to date examined patients with severe CDC.2125 In the present study, we report the largest series of patients with severe CDC treated with IVIG in the literature to our knowledge.
Patients and Methods
Case Series
We used CareScience software (CareScience, Inc., Philadelphia, PA) to retrospectively identify all patients admitted to our institution with a primary or secondary diagnosis of CDC (code 00845) between July 1, 2002 and May 1, 2006. CareScience is commercially available software that tracks all admissions to our institution and allows the performance of patient searches with a wide spectrum of user‐defined search criteria. Using the same software, we further identified those patients who received IVIG during their hospital stay. We then obtained the hospital chart for each patient, from the medical records department and established the study database.
A case was defined as a patient with diarrhea (at least 3 loose stools daily) for at least 2 days who had C. difficile cytotoxin‐positive feces and at least 1 of the following criteria: clinical symptoms (abdominal pain and/or distension and fever); leukemoid reaction (defined as white blood cell count of 20,000 cells/mm3 or above. This cutoff value was chosen as it has been used previously as a prognostic factor)4; radiographic evidence of colitis by computed tomography (CT) of the abdomen; and/or the presence of pseudomembranes on flexible sigmoidoscopy or colonoscopy. We excluded all patients who received IVIG for an indication other than CDC treatment (n = 3). There were no other exclusion criteria.
We used a standardized data collection tool and recorded demographics (age, gender, principal diagnosis), past medical and surgical history, other risk factors for C. difficile infection (previous CDC, antibiotics received during hospital stay, immunosuppressive medications or organ transplantation within the previous 6 weeks, history of malignancy or diabetes mellitus); clinical presentation (abdominal distention, abdominal pain, diarrhea, fever, leukemoid reaction, and hypotension defined as systolic blood pressure <85 mm Hg despite at least 1 L of intravenous normal saline administration and the need for vasopressor use); colonoscopy findings; CT scan and x‐ray findings; laboratory values; date and dose of IVIG infused and other C. difficile pharmacological treatments; and Acute Physiological Assessment and Chronic Health Evaluation (APACHE II) score28 at the first day of IVIG infusion. The primary outcomes were survival at the end of the hospital stay and clinical disease resolution, defined as 2 formed bowel movements or less per day without abdominal pain or distention.
The decision to initiate IVIG therapy and the dose to be used was made by the individual attending physician.
Statistical Analysis
Single (univariate) and multiple (multivariate) logistic regression analysis were applied to identify variables among the ones collected that are independent predictors of CDC mortality. All statistical analyses were completed with the STATA 10 software package (StatCorp LP, College Station, TX).
Review of the Literature
We used PubMed, Web of Science, Scopus, and Excerpta Medica databases to search for any publication in a peer‐reviewed journal on the use of IVIG for the treatment of severe CDC. We used the search words: IVIG or intravenous immunoglobulin and clostridium difficile. Only publications published in English were selected. The date range used was January 1, 1950 to January 7, 2009. We were able to find 5 publications using this search criteria.
Results
Study Population
Of the 1230 patients diagnosed with CDC over the 4‐year study period, 21 patients were treated with IVIG. Table 1 summarizes the patients' characteristics. There were 13 women and 8 men. The mean age was 68 years, with a standard deviation (SD) of 13 years. Sepsis was the primary diagnosis in all patients. Sixteen patients had predisposing risk factors for CDC, including immunosuppression (immunosuppressive medication [n = 2], human immunodeficiency virus [HIV] infection [n = 2]); cancer (n = 3); recent surgery (n = 3); and diabetes mellitus (n = 11). Nine patients had documented previous CDC episodes. The indications for IVIG administration were evidence of pancolitis on abdominal CT scan (n = 12) or severe ileus with cessation of diarrhea, abdominal distention, and requirement for total parenteral nutrition (n = 5), or severe hypotension (n = 4) (defined as systolic blood pressure <85 mm Hg despite at least 1 L of intravenous normal saline administration and the subsequent need for vasopressor use).
| Patient | Age (gender) | Diagnosis | Medical and Surgical History | CDC History | Colonoscopy Findings | Radiographic Findings |
|---|---|---|---|---|---|---|
| ||||||
| A | 40 (female) | CDC with sec. sepsis | Gastric stapling | Yes | * | Diffuse colitis |
| B | 86 (female) | Fulminant CDC | Metastatic ovarian carcinoma | PC | No colonic thickening | |
| C | 72 (male) | Sepsis | Acute pancreatitis with sec. pseudocyst, DM | Yes | PC | Diffuse colitis |
| D | 78 (male) | Discitis | Delayed: normal mucosa | Dilation of small and large bowel | ||
| E | 98 (female) | Urosepsis | Yes | * | No bowel distention | |
| F | 90 (female) | Right lower extremity cellulitis | DM | * | Concentric thickening of rectal wall | |
| G | 64 (male) | Ischemic colitis | DM, recent Hartman pouch closure | Marked inflammation | Diffuse colitis | |
| H | 78 (female) | Toe osteomyelitis and CDC with sec. sepsis | DM | * | Diffuse colitis | |
| I | 35 (female) | Sepsis | Yes | * | Diffuse nonspecific colitis, minimal ascites | |
| J | 47 (female) | Pneumonia and sec. sepsis | * | Diffuse colitis | ||
| K | 56 (female) | Urosepsis | HIV | Yes | * | Colitis involving the right colon |
| L | 76 (male) | CDC with sec. sepsis | Sigmoid bladder fistula repair, DM | * | Diffuse colitis | |
| M | 71 (female) | Pneumonia with sec. sepsis | * | Diffuse colitis | ||
| N | 63 (male) | Urosepsis | DM, lymphoma resection from small intestine | PC | Marked small and large bowel distention | |
| O | 86 (male) | Enterococcus‐induced sepsis | Rheumatoid arthritis on methotrexate | * | Fat stranding suggesting peritonitis | |
| P | 60 (female) | Gastrointestinal bleed and CDC | DM with neuropathy and retinopathies | Yes | * | Thickening of wall of colon in most of the colon |
| Q | 57 (female) | Sepsis | DM | Yes | * | Normal |
| R | 67 (female) | CDC with sec. sepsis | Candidal esophagitis | Yes | * | Large amount of peritoneal fluid, mild small bowel thickening |
| S | 60 (female) | Sepsis sec. to S. aureus and P. aerogenosa | DM, renal transplant (myco, prednisone) | * | Ileus with air fluid level in the small intestine | |
| T | 80 (female) | Sepsis | DM | Yes | * | Thickening of descending colon consistent with colitis |
| U | 72 (male) | CDC, widespread metastatic cancer | DM, metastatic cancer (unknown primary site) | * | Severe colitis up to the splenic flexure | |
Table 2 describes disease severity in these patients. Since CDC starts locally in the colon then secondarily involves multiple organs as part of the systemic inflammatory response syndrome (SIRS), 2 scales were used to characterize the disease in each patient: (1) extent of local colonic inflammation, and (2) severity of systemic involvement. Extensive colonic involvement was evidenced in all patients by pancolitis on abdominal imaging modalities (12 patients), severe ileus requiring total parenteral nutrition (13 patients), or referral for surgical consultation for possible colectomy (12 patients).
| Patient | Complications During the Hospital Stay | APACHE II Score | Monitored Unit | WBC* | K | Alb | Lactate | Cr | Hospital Stay (days) | Surgical Consult/Surgery | TPN for Colitis |
|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||
| A | Sepsis, DIC, ARDS, intubation | 15 | Yes | 48 | 4 | 1.1 | 2.9 | 1.3 | 26 | No/No | Yes |
| B | Dehydration, weakness | 12 | No | 19 | 3.4 | 3.1 | 1.1 | 16 | No/No | Yes | |
| C | HTP, GI bleed, ischemic colitis, F | 22 | Yes | 21 | 2.7 | 2.5 | 1.3 | ESRD | 34 | Yes/No | Yes |
| D | AD, megacolon, HT, intubation, ARF | 18 | Yes | 25 | 3.4 | 1.4 | 1.1 | 2.6 | 52 | Yes/No | Yes |
| E | Exacerbation of CHF with respiratory distress, Bipap support, confusion | 21 | No | 10 | 2.6 | 2.3 | 1 | 11 | No/No | No | |
| F | Confusion, gout acute attack | 21 | No | 33 | 3.1 | 2.6 | ESRD | 15 | No/No | No | |
| G | Intubation, cardiac arrest, AF with RVR, PNA, ARF, DVT, dysphagia, PEG | 6 | Yes | 15 | 3.1 | 1.7 | 1.9 | 2.2 | 32 | Yes/No | Yes |
| H | Sepsis, intubation, ARF, PEG, toe amputation, PNA, pulmonary edema, TPN, vitamin D deficiency | 34 | Yes | 59 | 2.8 | 1.5 | 4 | 3.8 | 17 | No/No | Yes |
| I | CHF, transient third cranial nerve palsy, DIC | 20 | Yes | 52 | 3.2 | 3.3 | 0.7 | ESRD | 11 | No/No | No |
| J | Aspiration PNA, sepsis, DIC, intubation, MI, F, HT | 32 | Yes | 17 | 2.7 | 1.8 | 14 | ESRD | 21 | Yes/no | No |
| K | Intubation, cardiac arrest, ARF, DIC, AP, F | 30 | Yes | 25 | 2.1 | 2.1 | 13 | 3.6 | 10 | Yes/no | No |
| L | Intubation, ARF, HTP, MI, AD, F | 23 | Yes | 69 | 3.2 | 1.8 | 1.4 | 3.6 | 23 | Yes/no | No |
| M | Intubation, DIC, ARF, GI bleeding, hypothermia, AD | 23 | Yes | 47 | 2.8 | 1.4 | 1.4 | 4.3 | 23 | Yes/no | Yes |
| N | Intubation, HTP, AD, F, ARF with HD, AF, osteomyelitis | 23 | Yes | 46 | 2.9 | 1.5 | 1.5 | 2.7 | 27 | Yes/no | Yes |
| O | Intubation, ARF, 2 cardiac arrests, GI bleed, UTI, rhabdomyolysis, liver shock, AF | 31 | Yes | 49 | 2.5 | 1.1 | 2.3 | 2.9 | 25 | Yes/no | Yes |
| P | Bowel ischemia with bowel resection, ARF, MI, ischemic bowel, fluid overload, respiratory failure | 23 | Yes | 26 | 2.6 | 0.8 | 2.9 | 3.1 | 9 | Yes/Yes | Yes |
| Q | Pulmonary embolism | 39 | Yes | 23 | 2.8 | 1.1 | 8.1 | ESRD | 9 | No/No | Yes |
| R | Fungal peritonitis, aspiration pneumonia, cardiac arrest | 26 | Yes | 30 | 4.1 | 1.1 | 0.9 | ESRD | 36 | No/No | Yes |
| S | Intubation, pneumothorax, CRT, pressor‐dependent shock, ARF | 36 | Yes | 46 | 3.1 | 1.8 | 2.1 | 5.4 | 64 | Yes/Yes | No |
| T | Pressor‐dependent sepsis, pulmonary edema, ARF with HD | 36 | Yes | 35 | 3.3 | 1.3 | 1.8 | 5.5 | 11 | Yes/No | Yes |
| U | Sepsis | 34 | Yes | 58 | 3.1 | 2.2 | 3.3 | 1.6 | 9 | No/No | No |
Of the 21 patients treated with IVIG, 9 did not receive a surgical consultation either because they responded to medical treatment promptly (6 patients), were too unstable for surgery (2 patients), or because the patient/family refused surgery (1 patient). Of the 12 patients who received surgical consultation, 2 underwent surgery. The remainder did not proceed to surgery for the following reasons: they were deemed medically unstable for surgery (6 patients), declined surgery (2 patients), were diagnosed with cancer on colonoscopy (1 patient), or improved with medical treatment (1 patient).
The severity of systemic involvement was measured using the APACHE II score on day 1 of IVIG infusion. The mean APACHE II score was 25. Eighteen patients were in a monitored unit when IVIG was administered. The study group had laboratory results in keeping with those previously used to define severe colitis:4, 9, 19 leukocytosis (defined as white blood cell count higher than 12,000 cells/mL [mean = 36,000 cells/mL]), hypoalbuminemia (mean = 1.78 g/dL, SD = 0.68 g/dL), hypokalemia (mean = 3.02 mg/dL, SD = 0.47 g/dL), and acute renal failure (defined as serum creatinine level >1.5 mg/dL [mean = 2.98 mg/dL, SD = 1.42 g/dL]).
IVIG Use
Table 3 describes the treatment patients received for CDC as well as the total number of antibiotics used throughout the hospital stay. IVIG was used as adjuvant treatment (defined as IVIG administration within 4 days or less after CDC diagnosis) in 8 patients and as second‐line treatment (defined as IVIG administration more than 4 days after CDC diagnosis) in 13 patients. Metronidazole, vancomycin, cholestyramine, and probiotic treatment alone or in different combinations were used for an average of 8 days (SD = 8 days; range, 025 days) before IVIG infusion. The total IVIG dose administered varied depending on the prescribing attending, with a range of 200 mg/kg to 1250 mg/kg and a mode of 250 mg/kg for 1 to 3 days. An average of 5 (SD = 2) different antibiotics that were not active against C. difficile were used per patient without being discontinued after a CDC diagnosis was made. The 3 most common were: cephalosporins (cefazolin, ceftriaxone, cefepime), fluoroquinolones (levofloxacin), and combination antibiotics (piperacillin and tazobactam or ampicillin and sulbactam).
| Patient | Number of Antibiotics | Duration of Treatment Before IVIG (days) | Treatment Before IVIG (days) | Total CDC Treatment (days) | IgG Level | IVIG Dose |
|---|---|---|---|---|---|---|
| ||||||
| A | 5 | 7 | Metro (7), Vanc (7), Choles (2) | Oral and rectal Vanc (26,19), IV Metro (19), Choles (2), Lacto (6) | Low | 300 mg/kg for 1 day |
| B | 1 | 13 | Metro (13), Vanc (13) | Oral Vanc (17) and IV Metro (12) | 300 mg/kg for 1 day | |
| C | 3 | 7 | Metro (7), Vanc (3) | IV Metro (28),Vanc oral and enema (18,3), Lacto (10) | Low | 125 mg/kg for 5 days |
| D | 5 | 25 | Metro (25), Vanc (15) | Oral then IV Metro (10,15), oral Vanc (25), Choles (7) and Lacto (13) | Low | 200 mg/kg for 1 day |
| E | 1 | 4 | Metro (1), Vanc (4), Choles(4) | IV Metro (8), oral Vanc (10) and Choles (4) | 75 mg/kg for 5 days | |
| F | 4 | 2 | Metro (2), Vanc (1) | IV Metro (8) and oral Vanc (9) | 250 mg/kg for 5 days | |
| G | 3 | 17 | Metro (17), Vanc (14) | IV Metro (49) and oral Vanc (61) | 250 mg/kg for 2 days | |
| H | 5 | 1 | Metro (1), Vanc (1) | Oral Metro (18), oral Vanc (22 ), IV Metro (3) | 250 mg/kg for 3 days | |
| I | 6 | 1 | Metro (1) | Oral and IV Metro (7,9), Vanc oral and enema (8,3) | 250 mg/kg for 2 days | |
| J | 8 | 16 | Metro (14), Vanc (2), Lacto (6) | Oral then IV Metro (10,5), oral and rectal Vanc (3,1), Lacto (6) | 300 mg/ kg for 1 day | |
| K | 6 | 7 | Metro (7), Vanc (3) | Oral then IV Metro (10) and oral Vanc (9) | Normal | 400 mg/kg for 2 days |
| L | 4 | 0 | None | IV then oral Metro (7,10), oral Vanc (23), Choles (7), and Lacto (5) | 150 mg/kg for 5 days | |
| M | 6 | 1 | Metro (1) | IV Metro (23) and oral Vanc (9) | 250 mg/kg for 2 days | |
| N | 7 | 1 | Metro (1), Vanc (1) | IV Metro (16), oral Vanc (14), oral Metro (7) | 250 mg /kg for 2 days | |
| O | 6 | 7 | Metro (6), Vanc (4) | IV Metro (6) and oral Vanc (22) | Low | 250 mg/kg for 2 days |
| P | 3 | 6 | Metro (6), Vanc (6) | IV Metro (25) and oral Vanc (17) | 150 mg/kg fro 3 days | |
| Q | 3 | 4 | Metro (4), Vanc (3) | Oral Metro (8),Vanc oral and enema (6,3) | 250 mg/kg for 3 days | |
| R | 5 | 9 | Vanc (9) | Vanc oral and enema (5,4), IV Metro (2) | 250 mg/kg for 1 day | |
| S | 8 | 23 | Metro (23), Vanc (23) | Oral then IV Metro (12,22), oral Vanc (39) | 250 mg/kg for 3 days | |
| T | 4 | 6 | Metro (6), Vanc (1) | Oral Vanc and IV Metro (11) | 250 mg/kg for 1 day | |
| U | 4 | 2 | Metro (2), Vanc (2) | Oral Vanc and IV Metro (6) | 250 mg/kg for 3 days | |
Survival with IVIG Use
Nine patients (43%) survived their illness and were discharged from the hospital. They experienced complete clinical resolution after an average of 10 days from IVIG administration (range, 220 days) (Table 4). The other 12 patients (57%) died during the index hospitalization. The average length of stay was 23 (range, 964) days.0
| Patient | Disposition | Clearance of Clostridium difficile Colitis? | Days to Resolution |
|---|---|---|---|
| |||
| A | Alive | Loose BM persisted but diarrhea resolved 9 days after IVIG. | 9 |
| B | Alive | BM became formed and diarrhea resolved 48 hours after IVIG. | 2 |
| C | Alive | Diarrhea resolved 20 days post‐IVIG infusion. CAT scan: colonic thickening improved. | 20 |
| D | Alive | Diarrhea resolved on discharge. Response to IVIG started next day after administration. | 18 |
| E | Alive | Diarrhea improved next day after IVIG administration and resolved on discharge. | 5 |
| F | Alive | Diarrhea resolved 5 days after IVIG administration. | 5 |
| G | Alive | Diarrhea resolved. C. difficile test became negative. | 13 |
| H | Alive | Diarrhea resolved 2 days before discharge. | 15 |
| I | Alive | Diarrhea slowly improved and resolved 4 days before discharge. | 7 |
| J | Deceased | ||
| K | Deceased | ||
| L | Deceased | ||
| M | Deceased | ||
| N | Deceased | ||
| O | Deceased | ||
| P | Deceased | ||
| Q | Deceased | ||
| R | Deceased | ||
| S | Deceased | ||
| T | Deceased | ||
| U | Deceased | ||
| Study | Number of Patients | Age (SD) (years) | Male | Female | Severity Definition | IVIG Dose | Days to Resolution | Days IVIG Infused | Alive? (%) | Recurrence |
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
| Salcedo et al.22 | 2 | 63, 64 | 1 | 1 | Pancolitis or thumbprinting on CAT scan | 200300 mg/kg once | 12 | 59 | 100 | 1 out of 2 |
| McPherson et al.21 | 8 | 72 (12) | ? | ? | Pancolitis | 200400 mg/kg twice | 226 | 1165 | 75 | 2 out of 6 |
| Juang et al.25 | 18 | 67 (17.4) | 5 | 13 | Modified Rubin et al.9 criteria | 200300 mg/kg once | ? | ? | 83 | ? |
| Hassoun et al.24 | 1 | 72 | 1 | 0 | Pancolitis | 400 mg/kg once | 6 | 15 | 100 | None |
| Chandrasekar et al.23 | 1 | 67 | 0 | 1 | Shock requiring inotropic support and pseudomembranes on colonoscopy | 400 mg/kg for 5 doses | 16 | 35 | 100 | ? |
| This paper | 21 | 68 (16) | 7 | 14 | Pancolitis and APACHE II score | 300 mg/kg once; 250 mg/kg for 5 doses | 220 | 025 | 43 | ? |
To further assess the impact of IVIG on colitis resolution, we investigated all variables in the data set that may have been associated with mortality using univariate Cox regression analysis. Those variables were as follows: APACHE II score on the first day of IVIG infusion, age, sex, previous history of CDC, number of days before IVIG use, peak white blood cell count, serum potassium level and creatinine level, lactate level on first day of IVIG infusion, and number of antibiotics administered that are not active against CDC. Only the APACHE II score (P = 0.006) and lactate level on the day of IVIG infusion (P = 0.004) were (positively) associated with CDC mortality. The positive association between CDC mortality and APACHE II score remained significant (P = 0.04) after adjusting for sex, previous history of CDC, number of days before IVIG use, lactate level on first day of IVIG infusion, and number of antibiotics administered that are not active against CDC using a multivariate Cox regression analysis model. No adjustments were made for age, white blood cell count, potassium level, or creatinine level as those are included within the APACHE II score. The positive association between lactate level on the first day of IVIG infusion and CDC mortality was not statistically significant after adjusting for the factors listed above in the same model (P = 0.13).
Discussion
To our knowledge, the present study is the largest series published in the literature to date on the use of IVIG for severe CDC. It is also the first study to report a high mortality rate compared to the 5 previous smaller studies on this topic. In the first report on IVIG use for CDC, Leung et al.15 used IVIG to treat 5 pediatric patients suffering from chronic relapsing CDC. It was not until 7 years later, in 1997, that the first IVIG use for severe CDC was reported.22 Since then, a total of 13 works have been published on IVIG for CDC treatment, and only in 5 of these was IVIG administered for severe CDC treatment:2125 3 case reports, 1 case series, and 1 case‐control study. Although the 4 uncontrolled reports concluded that IVIG is beneficial for severe CDC, the only controlled study reported no significant difference between cases and controls for all‐cause mortality, length of stay, and colectomy rate.25
The definition of severe CDC varied between reports, making comparison difficult. McPherson et al.21 and Hassoun and Ibrahim24 defined severe disease as one causing pancolitis on CT scan either with or without megacolon. In the study by Juang et al.,25 disease severity was assessed using the modified criteria of Rubin et al.9 Salcedo et al.22 defined severe CDC as one causing pancolitis in one patient and thumbprinting on CT scan in another, whereas Chandrasekar et al.23 defined it as one causing shock requiring inotropic support and presence of pseudomembranes on colonoscopy.
The present report is unique in that it provided 2 scales to characterize disease in each patient. The first scale measured colonic involvement anatomically and physiologically using a combination of computerized axial tomography (CAT) scan findings, presence or absence of ileus or referral for possible colectomy. This is not a prognostic scale, however, since CAT scan findings have been previously shown to be poor predictors of treatment outcome.29 The second scale measured the severity of systemic involvement using a well‐validated and standardized scale, the APACHE II score. We have shown in this report that it is associated with prognosis in the context of IVIG use.
Our study reports a higher mortality rate than previously described, and suggests that risk stratification and patient selection are important before IVIG administration, since not all patients seem to benefit from this treatment as previously suggested by smaller case series. Previously, several physical findings and laboratory values were found to be associated with worse outcome in CDC. These were increasing age, immunosuppression, shock requiring vasopressors, peak white blood cell count, peak serum lactate level, hypoalbuminemia, a fall in serum albumin level of >1.1 g/dL at the onset of CDC symptoms, use of 3 or more antibiotics, comorbid disease, previous history of CDC, acute renal failure and hypotension, underlying altered or depressed mental status, abdominal pain or distention, white blood cell count over 20,000/mm3 or <1500/mm3 and/or a >10% band forms on the white blood cell differential count, and ascites or pneumatosis coli by abdominal imaging.9, 3033 Using the APACHE II scale for the same purpose has the advantage of utilizing a well‐validated and objective scale that is expected to measure the degree of systemic involvement more reliably compared to the clinical and laboratory values above.
Timing of IVIG infusion remains controversial. Due to the lack of randomized controlled trials, the current practice is guided by expert opinion, leading to wide variations between reports. Since the APACHE II score was positively associated with mortality in the setting of IVIG treatment, the same scale could be used to guide decisions regarding timing of IVIG infusion. Our results suggest that IVIG should be preferentially used while the APACHE II score is still relatively low. This association and the specific APACHE II score at which to initiate or hold treatment need to be validated in the setting of a randomized controlled study before being used in clinical practice.
Although the current study was not designed to test this theory, IVIG could be associated conceptually with treatment success for patients with severe disease that is still restricted to the colon (without other organ dysfunction or at least at an early stage of extracolonic organ failure and thus associated with a low APACHE II score) but not for severe colonic disease with secondary multiple organ failure (high APACHE II score). This may be because colonic disease is toxin‐mediated whereas secondary systemic involvement is mediated through toxin‐induced inflammatory mediators (interleukin‐8, macrophage‐inflammatory protein‐2, substance P, tumor necrosis factor‐alpha) released locally in the colon,3436 triggering a SIRS and hematogenous translocation of colonic bacteria,37 both of which are poorly responsive to immunoglobulin infusion. Along the same lines, waiting for failure of conventional therapy before IVIG use might result in IVIG treatment failure because of disease progression and secondary sepsis, at which point no treatment may be effective. No study thus far has addressed this issue specifically.
Overall, the combined cohort of patients with severe CDC treated with IVIG in the literature includes 51 patients (Table 4). The current report contributes 41% of these patients. The patients' average age was 68 years, with a 2 to 1 female‐male ratio. The dose of IVIG used varied largely also, with 400 mg/kg being the mode (range, 75400 mg/kg from 1 to 5 doses). This dose is significantly below the doses used in the treatment of other diseases, like Guillain‐Barr syndrome, myasthenia gravis, Kawasaki disease, autoimmune hemolytic anemia, agammaglobulinemia, and hypogammaglobulinemia, where the usual dose is 400 mg/kg for 5 days. The resolution of diarrhea in these cases occurred after an average of 9 (range, 142) days. The index hospitalization survival rate varied from 43% to 100%. Patients received standard treatment for an average of 13 (range, 065) days before IVIG infusion. Thirty‐two of 51 patients survived their illness (63%). Neither total IgG nor anti‐toxin A IgG levels were measured in any of the reports. Of the 32 patients who had clinical resolution, 3 (10%) experienced symptoms recurrence in a follow‐up period of 1 to 13 months. This number is most probably an underestimation of the true recurrence rate resulting from an incomplete reporting because there was no uniform or active recurrence ascertainment mechanism in any of the studies. The recurrences were at 10, 14, and 30 days posttreatment. Since standard treatment was not discontinued in any of the reports once IVIG was given, the relative contribution and the ideal timing for IVIG infusion are still unclear.
The mechanism of action of IVIG is passive immunization (with anti‐toxin A and anti‐toxin B antibodies present in the pooled immunoglobulin) of a host who is usually unable to mount an adequate protective immune response.15, 22 IVIG is formed from pooling immunoglobulin from several random donors. It has been shown that many such donors express high anti‐toxin A and anti‐toxin B antibody serum titers.38, 39 In addition, high levels of anti‐toxin A and anti‐toxin B antibodies were present in the IVIG preparations and the recipients after infusion.1517, 22 Although constituting only a small fraction of the total IVIG administered, these antitoxin antibodies are believed to neutralize toxin A and B and help the host recover from the disease. In fact, Babcock et al.40 used an experimental hamster model of CDC to demonstrate a mortality reduction from 100% to 55% postinfusion of combined anti‐toxin A and anti‐toxin B antibodies. While some early reports indicated that anti‐toxin B antibodies were the major determinants of protection against colitis,41 later reports correlated disease severity pathologically42 and clinically43, 44 with anti‐toxin A levels. Anti‐toxin B antibodies were later shown to play an adjunctive role in conferring immunity against CDC40, 45, 46 when added to anti‐toxin A antibodies, but not to have any significant role on their own.
However, IVIG has been shown to contain IgG, but not IgA, anti‐toxin A and anti‐toxin B antibodies while it is only the IgA class of anti‐toxin A antibodies, and not the IgG class, that could neutralize toxin A in vitro and in vivo.47, 48 Babcock et al.40 solved this apparent dilemma by showing that a combination of 3 different monoclonal IgG anti‐toxin A antibodies could neutralize toxin A activity in vitro and prevent disease in the hamster model in vivo. Each of the 3 antibodies recognized a different toxin A domain: the first neutralized toxin A enzymatic activity, while the second prevented toxin A binding to its receptor on enterocytes, and the third prevented toxin internalization after binding to the receptor.
Thus, the mechanism of action of IVIG is most likely through the transfer of IgG anti‐toxin A antibodies that gain access to the intestinal lumen presumably secondary to inflammation‐induced mucosal damage and neutralize toxin A. Transfer of yet undetected IgA anti‐toxin A antibodies that prevent toxin A from binding to its receptor is much less likely, although possible.
The present study has limitations. As in all retrospective studies, selection bias was unavoidable. In addition, the decision to initiate IVIG administration was dependent on the attending physician, who also decided the dose, leading to heterogeneity in the total dose of IVIG infused. Such heterogeneity, however, is primarily the result of a lack of a standard dose for IVIG infusion for CDC in the published literature, as reported above. In addition, since IVIG is not yet approved by the U.S. Food and Drug Administration (FDA) for the treatment of severe CDC, standard treatment was not discontinued in any of the reports to date, including ours.
Choosing appropriate controls for patients suffering from severe CDC is challenging. This patient population is usually frail, with severe and multiple underlying diseases. The deteriorating clinical condition (and subsequently the need for multiple antibiotics) may be either the result of or the cause of CDC. Furthermore, IVIG has been in short supply for several years and therefore it has been expensive, making its administration to the number of patients needed to design adequately‐powered controlled studies difficult. These are mainly the reasons no randomized, multicenter, placebo‐controlled trial on IVIG use in severe CDC has been conducted to date.
Conclusions
In the present study, we report the results of IVIG use for the treatment of 21 patients with severe CDC. This is the largest cohort to our knowledge in the literature. Unlike previous studies on the subject, the present report provided 2 scales for disease assessment: the first based on the extent of colonic involvement and the second measuring the severity of systemic involvement using the APACHE II score. The latter was positively associated with mortality in this context. Of the 21 study patients treated with IVIG, only 9 patients (43%) survived their illness. This is the highest reported mortality rate among all studies on this subject so far. Further studies on the ideal timing of IVIG infusion, dose, and patient selection are needed before accepting IVIG as a standard of care for severe CDC treatment. The role of APACHE II score in the decision to use IVIG is promising and should be validated in randomized controlled trials.
Acknowledgements
The authors thank Indrani Mukherjee, MD, for her help and expertise in proofreading the manuscript.
- ,,.Secular trends in hospital‐acquired Clostridium difficile disease in the United States, 1987–2001.J Infect Dis.2004;189:1585–1589.
- ,,, et al.Fulminant Clostridium difficile: an underappreciated and increasing cause of death and complications.Ann Surg.2002;235:363–372.
- ,,, et al.An epidemic, toxin gene‐variant strain of Clostridium difficile.N Engl J Med.2005;353:2433–2441.
- ,,, et al.Clostridium difficile‐associated diarrhea in a region of Quebec from 1991 to 2003: a changing pattern of disease severity.CMAJ.2004;171:466–472.
- ,,.Comparison of two toxins produced by Clostridium difficile.Infect Immun.1981;34:1036–1043.
- ,,,.Asymptomatic carriage of Clostridium difficile and serum levels of IgG antibody against toxin A.N Engl J Med.2000;342:390–397.
- ,,,.Human antibody response to Clostridium difficile toxin A in relation to clinical course of infection.Infect Immun.1994;62:384–389.
- ,,.Risk factors for Clostridium difficile carriage and C. difficile‐associated diarrhea in a cohort of hospitalized patients.J Infect Dis.1990;162:678–684.
- ,,.Severe Clostridium difficile colitis.Dis Colon Rectum.1995;38:350–354.
- ,, et al.A predominantly clonal multi‐institutional outbreak of Clostridium difficile‐associated diarrhea with high morbidity and mortality.N Engl J Med.2005;353:2442–2449.
- ,,.Factors associated with failure of metronidazole in Clostridium difficile‐associated disease.J Clin Gastroenterol.2004;38:414–418.
- ,,.Treatment of Clostridium difficile‐associated disease: old therapies and new strategies.Lancet Infect Dis.2005;5:549–557.
- ,,, et al.Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole.Clin Infect Dis.2005;40:1586–1590.
- ,,, et al.Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada.Clin Infect Dis.2005;40:1591–1597.
- ,,,,,.Treatment with intravenously administered gamma globulin of chronic relapsing colitis induced by Clostridium difficile toxin.J Pediatr.1991;118:633–637.
- ,,,.Gamma globulin administration in relapsing Clostridium difficile‐induced pseudomembranous colitis with a defective antibody response to toxin A.Acta Clin Belg.1995;50:36–39.
- ,,,.Recurrent Clostridium difficile infection in a patient with selective IgG1 deficiency treated with intravenous immune globulin and Saccharomyces boulardii.Clin Infect Dis.1995;20(suppl 2):S266–S268.
- .Intravenous immunoglobulin for recurrent Clostridium difficile diarrhoea.Gut.2002;51:456.
- .Descriptive study of intravenous immunoglobulin for the treatment of recurrent Clostridium difficile diarrhoea.J Antimicrob Chemother.2004;53:882–884.
- ,,.Intravenous immunoglobulin for resistant Clostridium difficile infection.Age Ageing.2006;35:85–86.
- ,,,,.Intravenous immunoglobulin for the treatment of severe, refractory, and recurrent Clostridium difficile diarrhea.Dis Colon Rectum.2006;49:640–645.
- ,,, et al.Intravenous immunoglobulin therapy for severe Clostridium difficile colitis.Gut.1997;41:366–370.
- ,,, et. al.Intravenous immunoglobulin therapy for refractory Clostridium difficile toxin colitis in chronic kidney disease: case reports and literature review.NDT Plus.2008;1:20–22.
- ,.Use of intravenous immunoglobulin for the treatment of severe Clostridium difficile colitis.Am J Geriatr Pharmacother.2007;5:48–51.
- ,,, et al.Clinical outcomes of intravenous immune globulin in severe clostridium difficile‐associated diarrhea.Am J Infect Control.2007;35:131–137.
- ,,,.Successful treatment of Clostridium difficile colitis with intravenous immunoglobulin.J Gastrointestin Liver Dis.2008;17:353–359.
- ,,, et al.A durable response to relapsing Clostridium difficile colitis may require combined therapy with high‐dose oral Vancomycin and intravenous immune globulin.Infect Dis Clin Pract.2006;14:217–220.
- ,,,.APACHE II: a severity of disease classification system.Crit Care Med.1985;13:818–829.
- ,,,,,.Colonic abnormalities on CT in adult hospitalized patients with Clostridium difficile colitis: prevalence and significance of findings.AJR Am J Roentgenol.2006;186:1393–1400.
- ,,,.Clostridium difficile‐associated diarrhea: predictors of severity in patients presenting to the emergency department.Can J Gastroenterol.2003;17:369–373.
- ,,, et al.Impact of emergency colectomy on survival of patients with fulminant Clostridium difficile colitis during an epidemic caused by a hypervirulent strain.Ann Surg.2007;245:267–272.
- ,, et al.Risk factors for severity and relapse of pseudomembranous colitis in an elderly population.Colorectal Dis.2007;9:173–177.
- ,,,,.Prognostic criteria in Clostridium difficile colitis.Am J Gastroenterol.1996;91:460–464.
- ,,, et al.Clostridium difficile toxin a stimulates macrophage‐inflammatory protein‐2 production in rat intestinal epithelial cells.J Immunol.1998;160:6039–6045.
- ,,, et al.Increased substance P responses in dorsal root ganglia, intestinal macrophages during Clostridium difficile toxin a enteritis in rats.Proc Natl Acad Sci U S A.1997;94:4788–4793.
- ,,,,,.Cytokine response by human monocytes to Clostridium difficile toxin a and toxin B.Infect Immun.1991;59:3659–3666.
- ,,,.Bacterial translocation, intestinal microflora and morphological changes of intestinal mucosa in experimental models of Clostridium difficile infection.J Med Microbiol.1998;47:591–598.
- ,.Immunoglobulin G directed against toxins A and B of Clostridium difficile in the general population and patients with antibiotic‐associated diarrhea.Diagn Microbiol Infect Dis.1994;18:205–209.
- ,,, et al.Serum antibody response to toxins A and B of Clostridium difficile.J Infect Dis.1983;148:93–100.
- ,,, et al.Human monoclonal antibodies directed against toxins A and B prevent Clostridium difficile‐induced mortality in hamsters.Infect Immun.2006;74:6339–6347.
- ,,,.Serum antibody response to Clostridium difficile toxins in patients with Clostridium difficile diarrhoea.Infection.1985;13:97–101.
- ,,,.Relationship between levels of Clostridium difficile toxin A and toxin B and cecal lesions in gnotobiotic mice.Infect Immun.1989;57:2123–2127.
- ,,,,.Protection against experimental pseudomembranous colitis in gnotobiotic mice by use of monoclonal antibodies against Clostridium difficile toxin A.Infect Immun.1991;59:1192–1195.
- ,,.Systemic and mucosal antibody responses to toxin A in patients infected with Clostridium difficile.J Infect Dis.1992;166:1287–1294.
- ,,, et al.Transcutaneous immunization with Clostridium difficile toxoid A induces systemic and mucosal immune responses and toxin A‐neutralizing antibodies in mice.Infect Immun.2007;75:2826–2832.
- ,,, et al.Serum antitoxin antibodies mediate systemic and mucosal protection from Clostridium difficile disease in hamsters.Infect Immun.1999;67:527–538.
- ,,,.Human colonic aspirates containing immunoglobulin A antibody to Clostridium difficile toxin A inhibit toxin A‐receptor binding.Gastroenterology.1992;102:35–40.
- ,,,,.Selective neutralization of a bacterial enterotoxin by serum immunoglobulin A in response to mucosal disease.Infect Immun.1995;63:3166–3173.
- ,,.Secular trends in hospital‐acquired Clostridium difficile disease in the United States, 1987–2001.J Infect Dis.2004;189:1585–1589.
- ,,, et al.Fulminant Clostridium difficile: an underappreciated and increasing cause of death and complications.Ann Surg.2002;235:363–372.
- ,,, et al.An epidemic, toxin gene‐variant strain of Clostridium difficile.N Engl J Med.2005;353:2433–2441.
- ,,, et al.Clostridium difficile‐associated diarrhea in a region of Quebec from 1991 to 2003: a changing pattern of disease severity.CMAJ.2004;171:466–472.
- ,,.Comparison of two toxins produced by Clostridium difficile.Infect Immun.1981;34:1036–1043.
- ,,,.Asymptomatic carriage of Clostridium difficile and serum levels of IgG antibody against toxin A.N Engl J Med.2000;342:390–397.
- ,,,.Human antibody response to Clostridium difficile toxin A in relation to clinical course of infection.Infect Immun.1994;62:384–389.
- ,,.Risk factors for Clostridium difficile carriage and C. difficile‐associated diarrhea in a cohort of hospitalized patients.J Infect Dis.1990;162:678–684.
- ,,.Severe Clostridium difficile colitis.Dis Colon Rectum.1995;38:350–354.
- ,, et al.A predominantly clonal multi‐institutional outbreak of Clostridium difficile‐associated diarrhea with high morbidity and mortality.N Engl J Med.2005;353:2442–2449.
- ,,.Factors associated with failure of metronidazole in Clostridium difficile‐associated disease.J Clin Gastroenterol.2004;38:414–418.
- ,,.Treatment of Clostridium difficile‐associated disease: old therapies and new strategies.Lancet Infect Dis.2005;5:549–557.
- ,,, et al.Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole.Clin Infect Dis.2005;40:1586–1590.
- ,,, et al.Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada.Clin Infect Dis.2005;40:1591–1597.
- ,,,,,.Treatment with intravenously administered gamma globulin of chronic relapsing colitis induced by Clostridium difficile toxin.J Pediatr.1991;118:633–637.
- ,,,.Gamma globulin administration in relapsing Clostridium difficile‐induced pseudomembranous colitis with a defective antibody response to toxin A.Acta Clin Belg.1995;50:36–39.
- ,,,.Recurrent Clostridium difficile infection in a patient with selective IgG1 deficiency treated with intravenous immune globulin and Saccharomyces boulardii.Clin Infect Dis.1995;20(suppl 2):S266–S268.
- .Intravenous immunoglobulin for recurrent Clostridium difficile diarrhoea.Gut.2002;51:456.
- .Descriptive study of intravenous immunoglobulin for the treatment of recurrent Clostridium difficile diarrhoea.J Antimicrob Chemother.2004;53:882–884.
- ,,.Intravenous immunoglobulin for resistant Clostridium difficile infection.Age Ageing.2006;35:85–86.
- ,,,,.Intravenous immunoglobulin for the treatment of severe, refractory, and recurrent Clostridium difficile diarrhea.Dis Colon Rectum.2006;49:640–645.
- ,,, et al.Intravenous immunoglobulin therapy for severe Clostridium difficile colitis.Gut.1997;41:366–370.
- ,,, et. al.Intravenous immunoglobulin therapy for refractory Clostridium difficile toxin colitis in chronic kidney disease: case reports and literature review.NDT Plus.2008;1:20–22.
- ,.Use of intravenous immunoglobulin for the treatment of severe Clostridium difficile colitis.Am J Geriatr Pharmacother.2007;5:48–51.
- ,,, et al.Clinical outcomes of intravenous immune globulin in severe clostridium difficile‐associated diarrhea.Am J Infect Control.2007;35:131–137.
- ,,,.Successful treatment of Clostridium difficile colitis with intravenous immunoglobulin.J Gastrointestin Liver Dis.2008;17:353–359.
- ,,, et al.A durable response to relapsing Clostridium difficile colitis may require combined therapy with high‐dose oral Vancomycin and intravenous immune globulin.Infect Dis Clin Pract.2006;14:217–220.
- ,,,.APACHE II: a severity of disease classification system.Crit Care Med.1985;13:818–829.
- ,,,,,.Colonic abnormalities on CT in adult hospitalized patients with Clostridium difficile colitis: prevalence and significance of findings.AJR Am J Roentgenol.2006;186:1393–1400.
- ,,,.Clostridium difficile‐associated diarrhea: predictors of severity in patients presenting to the emergency department.Can J Gastroenterol.2003;17:369–373.
- ,,, et al.Impact of emergency colectomy on survival of patients with fulminant Clostridium difficile colitis during an epidemic caused by a hypervirulent strain.Ann Surg.2007;245:267–272.
- ,, et al.Risk factors for severity and relapse of pseudomembranous colitis in an elderly population.Colorectal Dis.2007;9:173–177.
- ,,,,.Prognostic criteria in Clostridium difficile colitis.Am J Gastroenterol.1996;91:460–464.
- ,,, et al.Clostridium difficile toxin a stimulates macrophage‐inflammatory protein‐2 production in rat intestinal epithelial cells.J Immunol.1998;160:6039–6045.
- ,,, et al.Increased substance P responses in dorsal root ganglia, intestinal macrophages during Clostridium difficile toxin a enteritis in rats.Proc Natl Acad Sci U S A.1997;94:4788–4793.
- ,,,,,.Cytokine response by human monocytes to Clostridium difficile toxin a and toxin B.Infect Immun.1991;59:3659–3666.
- ,,,.Bacterial translocation, intestinal microflora and morphological changes of intestinal mucosa in experimental models of Clostridium difficile infection.J Med Microbiol.1998;47:591–598.
- ,.Immunoglobulin G directed against toxins A and B of Clostridium difficile in the general population and patients with antibiotic‐associated diarrhea.Diagn Microbiol Infect Dis.1994;18:205–209.
- ,,, et al.Serum antibody response to toxins A and B of Clostridium difficile.J Infect Dis.1983;148:93–100.
- ,,, et al.Human monoclonal antibodies directed against toxins A and B prevent Clostridium difficile‐induced mortality in hamsters.Infect Immun.2006;74:6339–6347.
- ,,,.Serum antibody response to Clostridium difficile toxins in patients with Clostridium difficile diarrhoea.Infection.1985;13:97–101.
- ,,,.Relationship between levels of Clostridium difficile toxin A and toxin B and cecal lesions in gnotobiotic mice.Infect Immun.1989;57:2123–2127.
- ,,,,.Protection against experimental pseudomembranous colitis in gnotobiotic mice by use of monoclonal antibodies against Clostridium difficile toxin A.Infect Immun.1991;59:1192–1195.
- ,,.Systemic and mucosal antibody responses to toxin A in patients infected with Clostridium difficile.J Infect Dis.1992;166:1287–1294.
- ,,, et al.Transcutaneous immunization with Clostridium difficile toxoid A induces systemic and mucosal immune responses and toxin A‐neutralizing antibodies in mice.Infect Immun.2007;75:2826–2832.
- ,,, et al.Serum antitoxin antibodies mediate systemic and mucosal protection from Clostridium difficile disease in hamsters.Infect Immun.1999;67:527–538.
- ,,,.Human colonic aspirates containing immunoglobulin A antibody to Clostridium difficile toxin A inhibit toxin A‐receptor binding.Gastroenterology.1992;102:35–40.
- ,,,,.Selective neutralization of a bacterial enterotoxin by serum immunoglobulin A in response to mucosal disease.Infect Immun.1995;63:3166–3173.
Copyright © 2010 Society of Hospital Medicine
Evidence‐Based Strategies for VTE
Pretest probability assessment is an important first step in the diagnosis of venous thromboembolism (VTE) and models incorporating Wells criteria1 can be used accurately in emergency department (ED) and inpatient settings.2 Gestalt has the disadvantage of poor interobserver reliability,3 and use of clinical prediction rules has been advocated instead.4 In academic institutions, trainees frequently first evaluate patients with suspected VTE, and although gestalt improves with degree of experience, the performance of gestalt in 1 study5 was better for attendings than interns or residents (for whom it was equivalent), suggesting that structured pretest probability assessment may be more important for trainees.
From an imaging perspective, multidetector computed tomography (CT),6 is more accurate than ventilation perfusion (VP) scanning7, 8 in diagnosing VTE in any setting, including the critically ill.9, 10 Lower extremity CT venography (LECTV) has comparable sensitivity to contrast venography and sonography,11 and in combination with computed tomographic pulmonary angiography (CTPA) is important when imaging results are discordant with pretest probability.12 Guidelines for diagnostic pathways in VTE based on published literature incorporating D‐dimer testing have been updated recently,13 the degree of adoption and use of diagnostic algorithms among trainees has been understudied.
Clinical trials14, 15 have confirmed the safety and efficacy of low molecular weight heparin (LMWH) in the treatment of pulmonary embolism (PE) in inpatients, but the degree of adoption of this therapy is unclear. The primary objective of our survey of was to assess the knowledge, attitudes, practices, and preferences of trainees and attendings who order and evaluate the results of diagnostic studies in the management of VTE. A secondary objective was to assess willingness to use LMWH to treat VTE in the inpatient setting among non‐ED respondents.
Methods
Survey Design and Administration
The study was cross‐sectional and was approved by the institutional review board. The survey was paper‐based and anonymous, and the requirement for written informed consent was waived. The survey instrument was reviewed for clarity, lack of bias, and accuracy by a panel of hospitalists at the State University of New York (SUNY) Downstate Medical Center. Closed‐ended questions were used, including a 5‐point Likert scale (1 = strongly agree, 5 = strongly disagree) and multiple‐choice queries. Between October 2006 and March 2008, paper‐based survey questionnaires were distributed to internal medicine (IM) attendings, residents, and students from institutions in the New York, New Jersey, and Connecticut tri‐state area taking medicine review courses in New York City and attending grand rounds at SUNY Downstate. Of 319 non‐ED respondents, 116 (30%) were from the SUNY Downstate system. All third‐year medical students (58/116) were from the SUNY Downstate training program. representing 5 different training institutions for medical students and 4 institutions for residents. ED physicians (n = 46) were selected randomly and telephoned at work and questioned about their practices with an abbreviated version of the survey. Response rates were 80% for the paper‐based surveys and 20% for the ED physicians. Data was recorded into an electronic database (Microsoft Access; Microsoft Corp., Redmond, WA). Simple clinical vignettes were used to assess diagnostic and therapeutic strategies in the setting of VTE for non‐ED respondents only.
Data Analysis
Descriptive statistics were used to report respondents' demographic information and work environments. Data are expressed as proportions, means SD, or medians with interquartile range. Differences in response levels between groups were compared by Fisher's exact test, chi square test, or the Kruskal‐Wallis test, where appropriate. Two‐sided P values of less than 0.05 were considered significant. Since no difference in the ability of residents and interns to predict PE has been noted,5 both groups were analyzed together, as were third‐year and fourth‐year medical students. JMP version 7.0 software (SAS Institute, Cary, NC) was used to perform all analyses.
Results
Table 1 lists the characteristics of respondents. Medical attendings reported practicing in up to 5 different institutions, and residents reported rotating through up to 10 different institutions during their residency. Students reported rotating through up to 11 different institutions.
| n (%) | Institutions Rotated Through [median (IQR)] | |
|---|---|---|
| ||
| Emergency department attendings | 46 | |
| Medicine attendings | 46 | 1 (12) |
| Residents | 139 | 3 (23) |
| PGY1 | 39 (28) | |
| PGY2 | 27 (19) | |
| PGY3 | 34 (24) | |
| PGY4 | 3 (2) | |
| PGY5 | 19 (14) | |
| Year not checked | 17 (13) | |
| Medical students | 134 | 3 (15) |
| Third year | 58 (43) | |
| Fourth year | 76 (57) | |
Pretest Probability Assessment
Table 2 depicts differences between ED and IM attending responses. More than 60% of all attendings used no structured pretest probability assessment; the rest reported using the Wells criteria. An equivalent proportion of ED and IM attendings thought prediction rules were too complex to use (P = 0.2). Years of attending experience did not predict responses regarding perceptions of the complexity of prediction rules (P = 0.5). More IM attendings than residents or students felt that prediction rules were too complex for routine use (P = 0.02). Among trainees, significantly more residents than students reported using the Wells model (P < 0.001); 40% of residents did not use any model. Advanced years in training among residents did not predict an increased likelihood of using prediction rules.
| ED Attendings (n = 46) | IM Attendings (n = 43) | P Value | |
|---|---|---|---|
| |||
| Years of experience [median (interquartile range)] | 12.5 (7.521) | 6 (214) | <0.001 |
| Academic practice [n (%)] | 23 (50) | 27 (63) | 0.7 |
| Do not use prediction rules [n (%)] | 28 (61) | 28 (65) | 0.8 |
| Prediction rules too complex to use [n (% agree)] | 22 (48) | 13 (30) | 0.5 |
| Aware of a written algorithm for diagnosis of VTE [n (%)] | 2 (4) | 21 (50) | <0.001 |
D‐Dimer Testing
Among trainees, 25% of residents and students and 20% of IM attendings were unaware of the sensitivity or specificity of D‐dimer assays in use in their institution (P = 0.8), and 70% of ED attendings were unaware. Almost all residents, students, and IM attendings were unable to identify the name of the D‐dimer test used in their institutions (>95% in each category); while 54% of ED attendings were also unable to do so (P < 0.0001).
Imaging Strategies
Table 3 depicts responses regarding knowledge about various VTE imaging strategies. The majority of students responded that they would use VP scanning as the initial modality and a substantial number of attendings and residents would too. All ED attendings reported using CTPA as the initial modality of choice. A substantial number of students, residents, and IM attendings did not know whether LECTV had to be ordered separately or was done by default and a large proportion incorrectly surmised that the sensitivity of LECTV was not equivalent to lower extremity Doppler.
| ED Attending (n = 46) | IM Attending (n = 43) | Residents (n = 139) | Medical Students (n = 134) | P value | |
|---|---|---|---|---|---|
| |||||
| VP scanning test of choice in suspected PE [n (%)] | 0 (0) | 9 (22) | 24 (17) | 78 (58) | <0.001 |
| CTV ordered separate from or with CTPA by default [n (% unaware)] | 12 (27) | 53 (38) | 96 (72) | <0.001 | |
| Sensitivity of CTV = LE US [n (% agree)] | 22 (51) | 69 (50) | 42 (31) | 0.01 | |
Clinical Vignettes
Table 4 depicts responses by non‐ED respondents to various clinical scenarios presented. Faced with a dyspneic patient 2 days after a hip fracture and a negative CTPA alone, almost 25% of all respondents would incorrectly withhold anticoagulation. In outpatients with low probability Wells score for DVT and a negative D‐dimer, substantial proportions of all respondents would incorrectly order further imaging. For treatment of inpatients with DVT and non‐massive PE, 17% of students disagreed that LMWH was appropriate, and similar proportions of residents (12%) and IM attendings (13%) disagreed.
| IM Attending (n = 46) | Residents (n = 139) | Medical Students (n = 134) | P Value | |
|---|---|---|---|---|
| ||||
| Anticoagulate high risk patient with negative CTPA alone [n (% agree)] | 35 (76) | 104 (75) | 99 (74) | 0.9 |
| Order further imaging in outpatient with negative D‐dimer and low probability for DVT [n (% agree)] | 25 (54) | 68 (49) | 59 (44) | 0.6 |
| LMWH appropriate for DVT and non‐massive PE among inpatients [n (% agree)] | 40 (88) | 119 (86) | 88 (66) | 0.02 |
Discussion
Pretest Probability Assessment
Our findings that only a minority of trainees and practicing physicians calculate pretest probability using a prediction score translate into potentially inferior (and more costly) care for patients with suspected VTE. This is especially true for academic institutions, where trainees are ordinarily first responders. Among practitioners in the United States,16 72.5% prefer an unstructured approach to pretest assessment, whereas 22.9% use published prediction rules. In this survey, more residents than students or attendings used the Wells criteria for pretest probability testing. The majority of ED attendings surveyed (61%) used no structured pretest probability assessment, consistent with a retrospective study published recently17; however, this may have been because of the relatively experienced group sampled (median number of years in practice was 12.5 compared to 6 years among IM attendings). Students may not be receiving training to use prediction rules because attendings may feel they are too complex to use and/or may not use these rules themselves. A substantial proportion of residents (40% in our study) do not use them. Awareness of written algorithms was reported by a minority of all respondents, but did not translate into greater use of prediction rules.
D‐Dimer Testing
Only a few highly sensitive quantitative assays (VIDAS, Tinaquant, Liatest, and Simplired)1821 have been validated in large clinical trials incorporating structured pretest probability assessment and CTPA. Guidelines for diagnosis of VTE recommend that physicians be informed about the type of D‐dimer being used in their practice setting given the substantial variation in D‐dimer sensitivity.22 The sensitivities of quantitative enzyme‐linked immunosorbent assays (ELISAs) are clinically and statistically superior to other types of D‐dimer tests among patients with VTE.23 Over 20% of all non‐ED respondents did not know the sensitivity and specificity of the D‐dimer assay in use in their respective institutions and most (>70% in each category) could not name the assay, resulting in potentially inappropriate decision making if nonquantitative ELISA D‐dimers were used alone or gestalt were used, especially by trainees.
Imaging Strategies
Weiss et al.24 surveyed U.S. clinicians and found a clear preference for CTPA as the initial imaging modality in patients with suspected PE but did not include the trainee perspective. As level of training progressed, we found a decrease in the percentage of respondents that preferred VP scanning over CTPA as the first test of choice; however, 25% of residents and 17% of attendings still designated VP scanning as their first choice. The perception of the majority of students in our survey is that VP scanning is the preferred initial test. We conjecture that students do not receive the pertinent training from supervising clinicians in this regard. All ED attendings surveyed used CTPA as their first choice of imaging. Knowledge about whether LECTV was ordered separately from CTPA or done by default was lacking in over 25% of all non‐ED respondents. The lower the level of experience, the more incorrect answers were given. Apropos of the PIOPED II study,12 lack of awareness about lower extremity imaging in association with CTPA may therefore contribute to inappropriate decision making, especially in patients with high pretest probability of PE and a negative CTPA alone.
Clinical Vignettes
Two studies25, 26 analyzed outcomes in patients with low to intermediate pretest probability PE and negative CTPA alone who did not receive anticoagulation. Both suggest that withholding anticoagulation in these patients is safe. The 25% of non‐ED respondents who would consider withholding anticoagulation in high‐risk settings translates into a large number of potentially inappropriate decisions, especially if gestalt is used in pretest probability assessment. This is in line with recommendations from the PIOPED II study that lower extremity imaging and, if necessary, serial lower extremity ultrasonography be performed in high‐risk groups.11, 12 A negative validated D‐dimer study and a low pretest probability exclude the need for further testing in outpatients with suspected DVT27; however, 50% of all respondents would order further testing. Thus, regardless of experience, a disparity exists between practice and published literature among both trainees and attendings, especially since further imaging in this setting is not cost effective.28
Use of LMWH
In a cohort of 946 inpatients in one study,29 only 56.1% of inpatients with DVT or PE were treated with LMWH. In our survey a substantial minority of IM attendings, residents, and students (12%, 13%, and 17%, respectively) would not consider LMWH one of the prefered therapies for VTE in the right clinical setting.
Limitations
The cross‐sectional nature of the survey and localization of non‐ED respondents to the New York, New Jersey, and Connecticut tri‐state region, limits generalizability to other geographic regions of the country. Responses of ED attendings were sampled nationally. The attendings (ED and IM) sampled were a relatively experienced group (6‐12 years of practice) and this may explain the relatively low adoption of prediction rules reflecting the use of gestalt in this group. Additionally, over time, knowledge (and use) of validated D‐dimer assays may have increased in the practices evaluated. Among non‐ED respondents, 30% (116/319) were from a single training program (SUNY Downstate) and the responses of these respondents may reflect practice in the institutions sampled, limiting nationwide generalization with the potential for selection bias. The low rate of response from ED physicians (20%) was presumably a result of being called at work. We believe the responses are still a valuable insight into the real‐time practices of the clinicians surveyed and do not preclude a meaningful comparison to the rest of the respondents especially given the significant differences between ED and IM attending knowledge and awareness (Tables 3 and 4).
Conclusions
Our survey identifies the use of evidence‐based strategies in the management of VTE among trainees, a perspective that has been lacking in other studies of physicians in practice.16, 24, 27 Substantial variability in attending practice identified in this survey may impede the adoption of a structured approach to the diagnosis of VTE among trainees, and this survey raises major concerns about mechanisms of diagnosis of VTE. Caprini et al.29 believe that physician knowledge, attitudes, and beliefs are partially responsible for the gap between actual practice and international guidelines.27 The results of our survey extend this suggestion to trainees and imply that supervisor attitudes may negatively influence trainee practices. Development of written protocols or standardized pathway order sets based on published evidence‐based guidelines13 in the management of VTE could improve the use of structured pretest probability determination and use of evidence‐based strategies among trainees. Finally, comparisons of outcomes using algorithms and usual practice could provide valuable, clinically important data that could inform clinical practice.
- ,,, et al.Assessment of pretest probability of pulmonary embolism in the emergency department by physicians in training using the Wells model.Thromb Res.2007;120(2):173–179.
- ,,,.A prospective reassessment of the utility of the Wells score in identifying pulmonary embolism.Med J Aust.2007;187(6):333–336.
- ,,,,.The interobserver reliability of pretest probability assessment in patients with suspected pulmonary embolism.Thromb Res.2005;116(2):101–107.
- ,,, et al.Does this patient have pulmonary embolism?JAMA.2003;290(21):2849–2858.
- ,,,,.Does a physician's ability to accurately assess the likelihood of pulmonary embolism increase with training?Acad Med.2000;75(12):1199–1205.
- ,,, et al.Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and D‐dimer.Ann Intern Med.2001;135(2):98–107.
- ,,, et al.Pulmonary embolism revealed on helical CT angiography: comparison with ventilation perfusion radionuclide lung scanning.AJR Am J Roentgenol.2000;174:1041–1047.
- ,,, et al.Clinical validity of a negative computed tomography scan in patients with suspected pulmonary embolism: a systematic review.JAMA.2005;293(16):2012–2017.
- ,,,,.Multidetector CT: a new gold standard in the diagnosis of pulmonary embolism? State of the art and diagnostic algorithms.Radiol Med.2005;109(1–2):49–61.
- ,,,,.Multidetector row CT pulmonary angiography and indirect venography for the diagnosis of venous thromboembolic disease in intensive care unit patients.Acad Radiol.2006;13(4):486–495.
- ,,.The role of multidetector computed tomography angiography for the diagnosis of pulmonary embolism.Semin Nucl Med.2008;38:418–431.
- ,,, et al.Multidetector computed tomography for acute pulmonary embolism.N Engl J Med.2006;354:2317–2327.
- Institute for Clinical Systems Improvement. Venous Thromboembolism Diagnosis and Treatment. Available at: http://www.icsi.org. Accessed October2009.
- The Columbus Investigators.Low‐molecular‐weight heparin in the treatment of patients with venous thromboembolism.N Engl J Med.1997;337:657–662.
- ,,, et al.A comparison of low‐molecular‐weight heparin with unfractionated heparin for acute pulmonary embolism. The THESEE Study Group.N Engl J Med.1997;337(10):663–669.
- ,,,,,.Pretest risk assessment in suspected acute pulmonary embolism.Acad Radiol.2008;15(1):3–14.
- ,,,.Is pretest probability assessment on emergency department patients with suspected venous thromboembolism documented before SimpliRED D‐dimer testing?CJEM.2008;10(6):519–523.
- ,,,,,.Exclusion of DVT with D‐dimer testing: comparison of 13 D‐dimer methods in 99 outpatients suspected of DVT using venography as a standard.Thromb Haemost.2000;83:191–198.
- ,,, et al.Multidetector‐row computed tomography in suspected pulmonary embolism.N Engl J Med.2005;352(17):1760–1768.
- ,,, et al.Simple and safe exclusion of pulmonary embolism in outpatients using quantitative D‐dimer and Wells' simplified decision rule.Thromb Haemost.2007;97(1):146–150.
- ,,,,;ANTELOPE Study Group. The performance of two rapid quantitative D‐dimer assays in 287 patients with clinically suspected pulmonary embolism.Thromb Res.2002;107(6):283–286.
- ,,, et al.Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians.Ann Fam Med.2007;5:57–62.
- ,,, et al.D‐dimer for the exclusion of acute venous thrombosis and pulmonary embolism. A systematic review.Ann Intern Med.2004;140:589–602.
- ,,, et al.CT pulmonary angiography is the first‐line imaging test for acute pulmonary embolism: a survey of US clinicians.Acad Radiol.2006;13:434–446.
- ,,, et al.Outcomes after withholding anticoagulation from patients with suspected pulmonary embolism and negative computed tomographic findings: a cohort study.Mayo Clin Proc.2002;77:130–138.
- ,,,.Meta‐analysis: outcomes in patients with suspected pulmonary embolism managed with computed tomographic pulmonary angiography.Ann Intern Med.2004;141:866–874.
- ,,, et al.Does this patient have deep vein thrombosis?JAMA.2006;295(2):199–207.
- ,,, et al.Measurement of the clinical and cost‐effectiveness of non‐invasive diagnostic testing strategies for deep vein thrombosis.Health Technol Assess.2006;10(15):1–168.
- ,,, et al.NABOR Steering Committee. Treatment of venous thromboembolism: adherence to guidelines and impact of physician knowledge, attitudes, and beliefs.J Vasc Surg.2005;42(4):726–733.
Pretest probability assessment is an important first step in the diagnosis of venous thromboembolism (VTE) and models incorporating Wells criteria1 can be used accurately in emergency department (ED) and inpatient settings.2 Gestalt has the disadvantage of poor interobserver reliability,3 and use of clinical prediction rules has been advocated instead.4 In academic institutions, trainees frequently first evaluate patients with suspected VTE, and although gestalt improves with degree of experience, the performance of gestalt in 1 study5 was better for attendings than interns or residents (for whom it was equivalent), suggesting that structured pretest probability assessment may be more important for trainees.
From an imaging perspective, multidetector computed tomography (CT),6 is more accurate than ventilation perfusion (VP) scanning7, 8 in diagnosing VTE in any setting, including the critically ill.9, 10 Lower extremity CT venography (LECTV) has comparable sensitivity to contrast venography and sonography,11 and in combination with computed tomographic pulmonary angiography (CTPA) is important when imaging results are discordant with pretest probability.12 Guidelines for diagnostic pathways in VTE based on published literature incorporating D‐dimer testing have been updated recently,13 the degree of adoption and use of diagnostic algorithms among trainees has been understudied.
Clinical trials14, 15 have confirmed the safety and efficacy of low molecular weight heparin (LMWH) in the treatment of pulmonary embolism (PE) in inpatients, but the degree of adoption of this therapy is unclear. The primary objective of our survey of was to assess the knowledge, attitudes, practices, and preferences of trainees and attendings who order and evaluate the results of diagnostic studies in the management of VTE. A secondary objective was to assess willingness to use LMWH to treat VTE in the inpatient setting among non‐ED respondents.
Methods
Survey Design and Administration
The study was cross‐sectional and was approved by the institutional review board. The survey was paper‐based and anonymous, and the requirement for written informed consent was waived. The survey instrument was reviewed for clarity, lack of bias, and accuracy by a panel of hospitalists at the State University of New York (SUNY) Downstate Medical Center. Closed‐ended questions were used, including a 5‐point Likert scale (1 = strongly agree, 5 = strongly disagree) and multiple‐choice queries. Between October 2006 and March 2008, paper‐based survey questionnaires were distributed to internal medicine (IM) attendings, residents, and students from institutions in the New York, New Jersey, and Connecticut tri‐state area taking medicine review courses in New York City and attending grand rounds at SUNY Downstate. Of 319 non‐ED respondents, 116 (30%) were from the SUNY Downstate system. All third‐year medical students (58/116) were from the SUNY Downstate training program. representing 5 different training institutions for medical students and 4 institutions for residents. ED physicians (n = 46) were selected randomly and telephoned at work and questioned about their practices with an abbreviated version of the survey. Response rates were 80% for the paper‐based surveys and 20% for the ED physicians. Data was recorded into an electronic database (Microsoft Access; Microsoft Corp., Redmond, WA). Simple clinical vignettes were used to assess diagnostic and therapeutic strategies in the setting of VTE for non‐ED respondents only.
Data Analysis
Descriptive statistics were used to report respondents' demographic information and work environments. Data are expressed as proportions, means SD, or medians with interquartile range. Differences in response levels between groups were compared by Fisher's exact test, chi square test, or the Kruskal‐Wallis test, where appropriate. Two‐sided P values of less than 0.05 were considered significant. Since no difference in the ability of residents and interns to predict PE has been noted,5 both groups were analyzed together, as were third‐year and fourth‐year medical students. JMP version 7.0 software (SAS Institute, Cary, NC) was used to perform all analyses.
Results
Table 1 lists the characteristics of respondents. Medical attendings reported practicing in up to 5 different institutions, and residents reported rotating through up to 10 different institutions during their residency. Students reported rotating through up to 11 different institutions.
| n (%) | Institutions Rotated Through [median (IQR)] | |
|---|---|---|
| ||
| Emergency department attendings | 46 | |
| Medicine attendings | 46 | 1 (12) |
| Residents | 139 | 3 (23) |
| PGY1 | 39 (28) | |
| PGY2 | 27 (19) | |
| PGY3 | 34 (24) | |
| PGY4 | 3 (2) | |
| PGY5 | 19 (14) | |
| Year not checked | 17 (13) | |
| Medical students | 134 | 3 (15) |
| Third year | 58 (43) | |
| Fourth year | 76 (57) | |
Pretest Probability Assessment
Table 2 depicts differences between ED and IM attending responses. More than 60% of all attendings used no structured pretest probability assessment; the rest reported using the Wells criteria. An equivalent proportion of ED and IM attendings thought prediction rules were too complex to use (P = 0.2). Years of attending experience did not predict responses regarding perceptions of the complexity of prediction rules (P = 0.5). More IM attendings than residents or students felt that prediction rules were too complex for routine use (P = 0.02). Among trainees, significantly more residents than students reported using the Wells model (P < 0.001); 40% of residents did not use any model. Advanced years in training among residents did not predict an increased likelihood of using prediction rules.
| ED Attendings (n = 46) | IM Attendings (n = 43) | P Value | |
|---|---|---|---|
| |||
| Years of experience [median (interquartile range)] | 12.5 (7.521) | 6 (214) | <0.001 |
| Academic practice [n (%)] | 23 (50) | 27 (63) | 0.7 |
| Do not use prediction rules [n (%)] | 28 (61) | 28 (65) | 0.8 |
| Prediction rules too complex to use [n (% agree)] | 22 (48) | 13 (30) | 0.5 |
| Aware of a written algorithm for diagnosis of VTE [n (%)] | 2 (4) | 21 (50) | <0.001 |
D‐Dimer Testing
Among trainees, 25% of residents and students and 20% of IM attendings were unaware of the sensitivity or specificity of D‐dimer assays in use in their institution (P = 0.8), and 70% of ED attendings were unaware. Almost all residents, students, and IM attendings were unable to identify the name of the D‐dimer test used in their institutions (>95% in each category); while 54% of ED attendings were also unable to do so (P < 0.0001).
Imaging Strategies
Table 3 depicts responses regarding knowledge about various VTE imaging strategies. The majority of students responded that they would use VP scanning as the initial modality and a substantial number of attendings and residents would too. All ED attendings reported using CTPA as the initial modality of choice. A substantial number of students, residents, and IM attendings did not know whether LECTV had to be ordered separately or was done by default and a large proportion incorrectly surmised that the sensitivity of LECTV was not equivalent to lower extremity Doppler.
| ED Attending (n = 46) | IM Attending (n = 43) | Residents (n = 139) | Medical Students (n = 134) | P value | |
|---|---|---|---|---|---|
| |||||
| VP scanning test of choice in suspected PE [n (%)] | 0 (0) | 9 (22) | 24 (17) | 78 (58) | <0.001 |
| CTV ordered separate from or with CTPA by default [n (% unaware)] | 12 (27) | 53 (38) | 96 (72) | <0.001 | |
| Sensitivity of CTV = LE US [n (% agree)] | 22 (51) | 69 (50) | 42 (31) | 0.01 | |
Clinical Vignettes
Table 4 depicts responses by non‐ED respondents to various clinical scenarios presented. Faced with a dyspneic patient 2 days after a hip fracture and a negative CTPA alone, almost 25% of all respondents would incorrectly withhold anticoagulation. In outpatients with low probability Wells score for DVT and a negative D‐dimer, substantial proportions of all respondents would incorrectly order further imaging. For treatment of inpatients with DVT and non‐massive PE, 17% of students disagreed that LMWH was appropriate, and similar proportions of residents (12%) and IM attendings (13%) disagreed.
| IM Attending (n = 46) | Residents (n = 139) | Medical Students (n = 134) | P Value | |
|---|---|---|---|---|
| ||||
| Anticoagulate high risk patient with negative CTPA alone [n (% agree)] | 35 (76) | 104 (75) | 99 (74) | 0.9 |
| Order further imaging in outpatient with negative D‐dimer and low probability for DVT [n (% agree)] | 25 (54) | 68 (49) | 59 (44) | 0.6 |
| LMWH appropriate for DVT and non‐massive PE among inpatients [n (% agree)] | 40 (88) | 119 (86) | 88 (66) | 0.02 |
Discussion
Pretest Probability Assessment
Our findings that only a minority of trainees and practicing physicians calculate pretest probability using a prediction score translate into potentially inferior (and more costly) care for patients with suspected VTE. This is especially true for academic institutions, where trainees are ordinarily first responders. Among practitioners in the United States,16 72.5% prefer an unstructured approach to pretest assessment, whereas 22.9% use published prediction rules. In this survey, more residents than students or attendings used the Wells criteria for pretest probability testing. The majority of ED attendings surveyed (61%) used no structured pretest probability assessment, consistent with a retrospective study published recently17; however, this may have been because of the relatively experienced group sampled (median number of years in practice was 12.5 compared to 6 years among IM attendings). Students may not be receiving training to use prediction rules because attendings may feel they are too complex to use and/or may not use these rules themselves. A substantial proportion of residents (40% in our study) do not use them. Awareness of written algorithms was reported by a minority of all respondents, but did not translate into greater use of prediction rules.
D‐Dimer Testing
Only a few highly sensitive quantitative assays (VIDAS, Tinaquant, Liatest, and Simplired)1821 have been validated in large clinical trials incorporating structured pretest probability assessment and CTPA. Guidelines for diagnosis of VTE recommend that physicians be informed about the type of D‐dimer being used in their practice setting given the substantial variation in D‐dimer sensitivity.22 The sensitivities of quantitative enzyme‐linked immunosorbent assays (ELISAs) are clinically and statistically superior to other types of D‐dimer tests among patients with VTE.23 Over 20% of all non‐ED respondents did not know the sensitivity and specificity of the D‐dimer assay in use in their respective institutions and most (>70% in each category) could not name the assay, resulting in potentially inappropriate decision making if nonquantitative ELISA D‐dimers were used alone or gestalt were used, especially by trainees.
Imaging Strategies
Weiss et al.24 surveyed U.S. clinicians and found a clear preference for CTPA as the initial imaging modality in patients with suspected PE but did not include the trainee perspective. As level of training progressed, we found a decrease in the percentage of respondents that preferred VP scanning over CTPA as the first test of choice; however, 25% of residents and 17% of attendings still designated VP scanning as their first choice. The perception of the majority of students in our survey is that VP scanning is the preferred initial test. We conjecture that students do not receive the pertinent training from supervising clinicians in this regard. All ED attendings surveyed used CTPA as their first choice of imaging. Knowledge about whether LECTV was ordered separately from CTPA or done by default was lacking in over 25% of all non‐ED respondents. The lower the level of experience, the more incorrect answers were given. Apropos of the PIOPED II study,12 lack of awareness about lower extremity imaging in association with CTPA may therefore contribute to inappropriate decision making, especially in patients with high pretest probability of PE and a negative CTPA alone.
Clinical Vignettes
Two studies25, 26 analyzed outcomes in patients with low to intermediate pretest probability PE and negative CTPA alone who did not receive anticoagulation. Both suggest that withholding anticoagulation in these patients is safe. The 25% of non‐ED respondents who would consider withholding anticoagulation in high‐risk settings translates into a large number of potentially inappropriate decisions, especially if gestalt is used in pretest probability assessment. This is in line with recommendations from the PIOPED II study that lower extremity imaging and, if necessary, serial lower extremity ultrasonography be performed in high‐risk groups.11, 12 A negative validated D‐dimer study and a low pretest probability exclude the need for further testing in outpatients with suspected DVT27; however, 50% of all respondents would order further testing. Thus, regardless of experience, a disparity exists between practice and published literature among both trainees and attendings, especially since further imaging in this setting is not cost effective.28
Use of LMWH
In a cohort of 946 inpatients in one study,29 only 56.1% of inpatients with DVT or PE were treated with LMWH. In our survey a substantial minority of IM attendings, residents, and students (12%, 13%, and 17%, respectively) would not consider LMWH one of the prefered therapies for VTE in the right clinical setting.
Limitations
The cross‐sectional nature of the survey and localization of non‐ED respondents to the New York, New Jersey, and Connecticut tri‐state region, limits generalizability to other geographic regions of the country. Responses of ED attendings were sampled nationally. The attendings (ED and IM) sampled were a relatively experienced group (6‐12 years of practice) and this may explain the relatively low adoption of prediction rules reflecting the use of gestalt in this group. Additionally, over time, knowledge (and use) of validated D‐dimer assays may have increased in the practices evaluated. Among non‐ED respondents, 30% (116/319) were from a single training program (SUNY Downstate) and the responses of these respondents may reflect practice in the institutions sampled, limiting nationwide generalization with the potential for selection bias. The low rate of response from ED physicians (20%) was presumably a result of being called at work. We believe the responses are still a valuable insight into the real‐time practices of the clinicians surveyed and do not preclude a meaningful comparison to the rest of the respondents especially given the significant differences between ED and IM attending knowledge and awareness (Tables 3 and 4).
Conclusions
Our survey identifies the use of evidence‐based strategies in the management of VTE among trainees, a perspective that has been lacking in other studies of physicians in practice.16, 24, 27 Substantial variability in attending practice identified in this survey may impede the adoption of a structured approach to the diagnosis of VTE among trainees, and this survey raises major concerns about mechanisms of diagnosis of VTE. Caprini et al.29 believe that physician knowledge, attitudes, and beliefs are partially responsible for the gap between actual practice and international guidelines.27 The results of our survey extend this suggestion to trainees and imply that supervisor attitudes may negatively influence trainee practices. Development of written protocols or standardized pathway order sets based on published evidence‐based guidelines13 in the management of VTE could improve the use of structured pretest probability determination and use of evidence‐based strategies among trainees. Finally, comparisons of outcomes using algorithms and usual practice could provide valuable, clinically important data that could inform clinical practice.
Pretest probability assessment is an important first step in the diagnosis of venous thromboembolism (VTE) and models incorporating Wells criteria1 can be used accurately in emergency department (ED) and inpatient settings.2 Gestalt has the disadvantage of poor interobserver reliability,3 and use of clinical prediction rules has been advocated instead.4 In academic institutions, trainees frequently first evaluate patients with suspected VTE, and although gestalt improves with degree of experience, the performance of gestalt in 1 study5 was better for attendings than interns or residents (for whom it was equivalent), suggesting that structured pretest probability assessment may be more important for trainees.
From an imaging perspective, multidetector computed tomography (CT),6 is more accurate than ventilation perfusion (VP) scanning7, 8 in diagnosing VTE in any setting, including the critically ill.9, 10 Lower extremity CT venography (LECTV) has comparable sensitivity to contrast venography and sonography,11 and in combination with computed tomographic pulmonary angiography (CTPA) is important when imaging results are discordant with pretest probability.12 Guidelines for diagnostic pathways in VTE based on published literature incorporating D‐dimer testing have been updated recently,13 the degree of adoption and use of diagnostic algorithms among trainees has been understudied.
Clinical trials14, 15 have confirmed the safety and efficacy of low molecular weight heparin (LMWH) in the treatment of pulmonary embolism (PE) in inpatients, but the degree of adoption of this therapy is unclear. The primary objective of our survey of was to assess the knowledge, attitudes, practices, and preferences of trainees and attendings who order and evaluate the results of diagnostic studies in the management of VTE. A secondary objective was to assess willingness to use LMWH to treat VTE in the inpatient setting among non‐ED respondents.
Methods
Survey Design and Administration
The study was cross‐sectional and was approved by the institutional review board. The survey was paper‐based and anonymous, and the requirement for written informed consent was waived. The survey instrument was reviewed for clarity, lack of bias, and accuracy by a panel of hospitalists at the State University of New York (SUNY) Downstate Medical Center. Closed‐ended questions were used, including a 5‐point Likert scale (1 = strongly agree, 5 = strongly disagree) and multiple‐choice queries. Between October 2006 and March 2008, paper‐based survey questionnaires were distributed to internal medicine (IM) attendings, residents, and students from institutions in the New York, New Jersey, and Connecticut tri‐state area taking medicine review courses in New York City and attending grand rounds at SUNY Downstate. Of 319 non‐ED respondents, 116 (30%) were from the SUNY Downstate system. All third‐year medical students (58/116) were from the SUNY Downstate training program. representing 5 different training institutions for medical students and 4 institutions for residents. ED physicians (n = 46) were selected randomly and telephoned at work and questioned about their practices with an abbreviated version of the survey. Response rates were 80% for the paper‐based surveys and 20% for the ED physicians. Data was recorded into an electronic database (Microsoft Access; Microsoft Corp., Redmond, WA). Simple clinical vignettes were used to assess diagnostic and therapeutic strategies in the setting of VTE for non‐ED respondents only.
Data Analysis
Descriptive statistics were used to report respondents' demographic information and work environments. Data are expressed as proportions, means SD, or medians with interquartile range. Differences in response levels between groups were compared by Fisher's exact test, chi square test, or the Kruskal‐Wallis test, where appropriate. Two‐sided P values of less than 0.05 were considered significant. Since no difference in the ability of residents and interns to predict PE has been noted,5 both groups were analyzed together, as were third‐year and fourth‐year medical students. JMP version 7.0 software (SAS Institute, Cary, NC) was used to perform all analyses.
Results
Table 1 lists the characteristics of respondents. Medical attendings reported practicing in up to 5 different institutions, and residents reported rotating through up to 10 different institutions during their residency. Students reported rotating through up to 11 different institutions.
| n (%) | Institutions Rotated Through [median (IQR)] | |
|---|---|---|
| ||
| Emergency department attendings | 46 | |
| Medicine attendings | 46 | 1 (12) |
| Residents | 139 | 3 (23) |
| PGY1 | 39 (28) | |
| PGY2 | 27 (19) | |
| PGY3 | 34 (24) | |
| PGY4 | 3 (2) | |
| PGY5 | 19 (14) | |
| Year not checked | 17 (13) | |
| Medical students | 134 | 3 (15) |
| Third year | 58 (43) | |
| Fourth year | 76 (57) | |
Pretest Probability Assessment
Table 2 depicts differences between ED and IM attending responses. More than 60% of all attendings used no structured pretest probability assessment; the rest reported using the Wells criteria. An equivalent proportion of ED and IM attendings thought prediction rules were too complex to use (P = 0.2). Years of attending experience did not predict responses regarding perceptions of the complexity of prediction rules (P = 0.5). More IM attendings than residents or students felt that prediction rules were too complex for routine use (P = 0.02). Among trainees, significantly more residents than students reported using the Wells model (P < 0.001); 40% of residents did not use any model. Advanced years in training among residents did not predict an increased likelihood of using prediction rules.
| ED Attendings (n = 46) | IM Attendings (n = 43) | P Value | |
|---|---|---|---|
| |||
| Years of experience [median (interquartile range)] | 12.5 (7.521) | 6 (214) | <0.001 |
| Academic practice [n (%)] | 23 (50) | 27 (63) | 0.7 |
| Do not use prediction rules [n (%)] | 28 (61) | 28 (65) | 0.8 |
| Prediction rules too complex to use [n (% agree)] | 22 (48) | 13 (30) | 0.5 |
| Aware of a written algorithm for diagnosis of VTE [n (%)] | 2 (4) | 21 (50) | <0.001 |
D‐Dimer Testing
Among trainees, 25% of residents and students and 20% of IM attendings were unaware of the sensitivity or specificity of D‐dimer assays in use in their institution (P = 0.8), and 70% of ED attendings were unaware. Almost all residents, students, and IM attendings were unable to identify the name of the D‐dimer test used in their institutions (>95% in each category); while 54% of ED attendings were also unable to do so (P < 0.0001).
Imaging Strategies
Table 3 depicts responses regarding knowledge about various VTE imaging strategies. The majority of students responded that they would use VP scanning as the initial modality and a substantial number of attendings and residents would too. All ED attendings reported using CTPA as the initial modality of choice. A substantial number of students, residents, and IM attendings did not know whether LECTV had to be ordered separately or was done by default and a large proportion incorrectly surmised that the sensitivity of LECTV was not equivalent to lower extremity Doppler.
| ED Attending (n = 46) | IM Attending (n = 43) | Residents (n = 139) | Medical Students (n = 134) | P value | |
|---|---|---|---|---|---|
| |||||
| VP scanning test of choice in suspected PE [n (%)] | 0 (0) | 9 (22) | 24 (17) | 78 (58) | <0.001 |
| CTV ordered separate from or with CTPA by default [n (% unaware)] | 12 (27) | 53 (38) | 96 (72) | <0.001 | |
| Sensitivity of CTV = LE US [n (% agree)] | 22 (51) | 69 (50) | 42 (31) | 0.01 | |
Clinical Vignettes
Table 4 depicts responses by non‐ED respondents to various clinical scenarios presented. Faced with a dyspneic patient 2 days after a hip fracture and a negative CTPA alone, almost 25% of all respondents would incorrectly withhold anticoagulation. In outpatients with low probability Wells score for DVT and a negative D‐dimer, substantial proportions of all respondents would incorrectly order further imaging. For treatment of inpatients with DVT and non‐massive PE, 17% of students disagreed that LMWH was appropriate, and similar proportions of residents (12%) and IM attendings (13%) disagreed.
| IM Attending (n = 46) | Residents (n = 139) | Medical Students (n = 134) | P Value | |
|---|---|---|---|---|
| ||||
| Anticoagulate high risk patient with negative CTPA alone [n (% agree)] | 35 (76) | 104 (75) | 99 (74) | 0.9 |
| Order further imaging in outpatient with negative D‐dimer and low probability for DVT [n (% agree)] | 25 (54) | 68 (49) | 59 (44) | 0.6 |
| LMWH appropriate for DVT and non‐massive PE among inpatients [n (% agree)] | 40 (88) | 119 (86) | 88 (66) | 0.02 |
Discussion
Pretest Probability Assessment
Our findings that only a minority of trainees and practicing physicians calculate pretest probability using a prediction score translate into potentially inferior (and more costly) care for patients with suspected VTE. This is especially true for academic institutions, where trainees are ordinarily first responders. Among practitioners in the United States,16 72.5% prefer an unstructured approach to pretest assessment, whereas 22.9% use published prediction rules. In this survey, more residents than students or attendings used the Wells criteria for pretest probability testing. The majority of ED attendings surveyed (61%) used no structured pretest probability assessment, consistent with a retrospective study published recently17; however, this may have been because of the relatively experienced group sampled (median number of years in practice was 12.5 compared to 6 years among IM attendings). Students may not be receiving training to use prediction rules because attendings may feel they are too complex to use and/or may not use these rules themselves. A substantial proportion of residents (40% in our study) do not use them. Awareness of written algorithms was reported by a minority of all respondents, but did not translate into greater use of prediction rules.
D‐Dimer Testing
Only a few highly sensitive quantitative assays (VIDAS, Tinaquant, Liatest, and Simplired)1821 have been validated in large clinical trials incorporating structured pretest probability assessment and CTPA. Guidelines for diagnosis of VTE recommend that physicians be informed about the type of D‐dimer being used in their practice setting given the substantial variation in D‐dimer sensitivity.22 The sensitivities of quantitative enzyme‐linked immunosorbent assays (ELISAs) are clinically and statistically superior to other types of D‐dimer tests among patients with VTE.23 Over 20% of all non‐ED respondents did not know the sensitivity and specificity of the D‐dimer assay in use in their respective institutions and most (>70% in each category) could not name the assay, resulting in potentially inappropriate decision making if nonquantitative ELISA D‐dimers were used alone or gestalt were used, especially by trainees.
Imaging Strategies
Weiss et al.24 surveyed U.S. clinicians and found a clear preference for CTPA as the initial imaging modality in patients with suspected PE but did not include the trainee perspective. As level of training progressed, we found a decrease in the percentage of respondents that preferred VP scanning over CTPA as the first test of choice; however, 25% of residents and 17% of attendings still designated VP scanning as their first choice. The perception of the majority of students in our survey is that VP scanning is the preferred initial test. We conjecture that students do not receive the pertinent training from supervising clinicians in this regard. All ED attendings surveyed used CTPA as their first choice of imaging. Knowledge about whether LECTV was ordered separately from CTPA or done by default was lacking in over 25% of all non‐ED respondents. The lower the level of experience, the more incorrect answers were given. Apropos of the PIOPED II study,12 lack of awareness about lower extremity imaging in association with CTPA may therefore contribute to inappropriate decision making, especially in patients with high pretest probability of PE and a negative CTPA alone.
Clinical Vignettes
Two studies25, 26 analyzed outcomes in patients with low to intermediate pretest probability PE and negative CTPA alone who did not receive anticoagulation. Both suggest that withholding anticoagulation in these patients is safe. The 25% of non‐ED respondents who would consider withholding anticoagulation in high‐risk settings translates into a large number of potentially inappropriate decisions, especially if gestalt is used in pretest probability assessment. This is in line with recommendations from the PIOPED II study that lower extremity imaging and, if necessary, serial lower extremity ultrasonography be performed in high‐risk groups.11, 12 A negative validated D‐dimer study and a low pretest probability exclude the need for further testing in outpatients with suspected DVT27; however, 50% of all respondents would order further testing. Thus, regardless of experience, a disparity exists between practice and published literature among both trainees and attendings, especially since further imaging in this setting is not cost effective.28
Use of LMWH
In a cohort of 946 inpatients in one study,29 only 56.1% of inpatients with DVT or PE were treated with LMWH. In our survey a substantial minority of IM attendings, residents, and students (12%, 13%, and 17%, respectively) would not consider LMWH one of the prefered therapies for VTE in the right clinical setting.
Limitations
The cross‐sectional nature of the survey and localization of non‐ED respondents to the New York, New Jersey, and Connecticut tri‐state region, limits generalizability to other geographic regions of the country. Responses of ED attendings were sampled nationally. The attendings (ED and IM) sampled were a relatively experienced group (6‐12 years of practice) and this may explain the relatively low adoption of prediction rules reflecting the use of gestalt in this group. Additionally, over time, knowledge (and use) of validated D‐dimer assays may have increased in the practices evaluated. Among non‐ED respondents, 30% (116/319) were from a single training program (SUNY Downstate) and the responses of these respondents may reflect practice in the institutions sampled, limiting nationwide generalization with the potential for selection bias. The low rate of response from ED physicians (20%) was presumably a result of being called at work. We believe the responses are still a valuable insight into the real‐time practices of the clinicians surveyed and do not preclude a meaningful comparison to the rest of the respondents especially given the significant differences between ED and IM attending knowledge and awareness (Tables 3 and 4).
Conclusions
Our survey identifies the use of evidence‐based strategies in the management of VTE among trainees, a perspective that has been lacking in other studies of physicians in practice.16, 24, 27 Substantial variability in attending practice identified in this survey may impede the adoption of a structured approach to the diagnosis of VTE among trainees, and this survey raises major concerns about mechanisms of diagnosis of VTE. Caprini et al.29 believe that physician knowledge, attitudes, and beliefs are partially responsible for the gap between actual practice and international guidelines.27 The results of our survey extend this suggestion to trainees and imply that supervisor attitudes may negatively influence trainee practices. Development of written protocols or standardized pathway order sets based on published evidence‐based guidelines13 in the management of VTE could improve the use of structured pretest probability determination and use of evidence‐based strategies among trainees. Finally, comparisons of outcomes using algorithms and usual practice could provide valuable, clinically important data that could inform clinical practice.
- ,,, et al.Assessment of pretest probability of pulmonary embolism in the emergency department by physicians in training using the Wells model.Thromb Res.2007;120(2):173–179.
- ,,,.A prospective reassessment of the utility of the Wells score in identifying pulmonary embolism.Med J Aust.2007;187(6):333–336.
- ,,,,.The interobserver reliability of pretest probability assessment in patients with suspected pulmonary embolism.Thromb Res.2005;116(2):101–107.
- ,,, et al.Does this patient have pulmonary embolism?JAMA.2003;290(21):2849–2858.
- ,,,,.Does a physician's ability to accurately assess the likelihood of pulmonary embolism increase with training?Acad Med.2000;75(12):1199–1205.
- ,,, et al.Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and D‐dimer.Ann Intern Med.2001;135(2):98–107.
- ,,, et al.Pulmonary embolism revealed on helical CT angiography: comparison with ventilation perfusion radionuclide lung scanning.AJR Am J Roentgenol.2000;174:1041–1047.
- ,,, et al.Clinical validity of a negative computed tomography scan in patients with suspected pulmonary embolism: a systematic review.JAMA.2005;293(16):2012–2017.
- ,,,,.Multidetector CT: a new gold standard in the diagnosis of pulmonary embolism? State of the art and diagnostic algorithms.Radiol Med.2005;109(1–2):49–61.
- ,,,,.Multidetector row CT pulmonary angiography and indirect venography for the diagnosis of venous thromboembolic disease in intensive care unit patients.Acad Radiol.2006;13(4):486–495.
- ,,.The role of multidetector computed tomography angiography for the diagnosis of pulmonary embolism.Semin Nucl Med.2008;38:418–431.
- ,,, et al.Multidetector computed tomography for acute pulmonary embolism.N Engl J Med.2006;354:2317–2327.
- Institute for Clinical Systems Improvement. Venous Thromboembolism Diagnosis and Treatment. Available at: http://www.icsi.org. Accessed October2009.
- The Columbus Investigators.Low‐molecular‐weight heparin in the treatment of patients with venous thromboembolism.N Engl J Med.1997;337:657–662.
- ,,, et al.A comparison of low‐molecular‐weight heparin with unfractionated heparin for acute pulmonary embolism. The THESEE Study Group.N Engl J Med.1997;337(10):663–669.
- ,,,,,.Pretest risk assessment in suspected acute pulmonary embolism.Acad Radiol.2008;15(1):3–14.
- ,,,.Is pretest probability assessment on emergency department patients with suspected venous thromboembolism documented before SimpliRED D‐dimer testing?CJEM.2008;10(6):519–523.
- ,,,,,.Exclusion of DVT with D‐dimer testing: comparison of 13 D‐dimer methods in 99 outpatients suspected of DVT using venography as a standard.Thromb Haemost.2000;83:191–198.
- ,,, et al.Multidetector‐row computed tomography in suspected pulmonary embolism.N Engl J Med.2005;352(17):1760–1768.
- ,,, et al.Simple and safe exclusion of pulmonary embolism in outpatients using quantitative D‐dimer and Wells' simplified decision rule.Thromb Haemost.2007;97(1):146–150.
- ,,,,;ANTELOPE Study Group. The performance of two rapid quantitative D‐dimer assays in 287 patients with clinically suspected pulmonary embolism.Thromb Res.2002;107(6):283–286.
- ,,, et al.Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians.Ann Fam Med.2007;5:57–62.
- ,,, et al.D‐dimer for the exclusion of acute venous thrombosis and pulmonary embolism. A systematic review.Ann Intern Med.2004;140:589–602.
- ,,, et al.CT pulmonary angiography is the first‐line imaging test for acute pulmonary embolism: a survey of US clinicians.Acad Radiol.2006;13:434–446.
- ,,, et al.Outcomes after withholding anticoagulation from patients with suspected pulmonary embolism and negative computed tomographic findings: a cohort study.Mayo Clin Proc.2002;77:130–138.
- ,,,.Meta‐analysis: outcomes in patients with suspected pulmonary embolism managed with computed tomographic pulmonary angiography.Ann Intern Med.2004;141:866–874.
- ,,, et al.Does this patient have deep vein thrombosis?JAMA.2006;295(2):199–207.
- ,,, et al.Measurement of the clinical and cost‐effectiveness of non‐invasive diagnostic testing strategies for deep vein thrombosis.Health Technol Assess.2006;10(15):1–168.
- ,,, et al.NABOR Steering Committee. Treatment of venous thromboembolism: adherence to guidelines and impact of physician knowledge, attitudes, and beliefs.J Vasc Surg.2005;42(4):726–733.
- ,,, et al.Assessment of pretest probability of pulmonary embolism in the emergency department by physicians in training using the Wells model.Thromb Res.2007;120(2):173–179.
- ,,,.A prospective reassessment of the utility of the Wells score in identifying pulmonary embolism.Med J Aust.2007;187(6):333–336.
- ,,,,.The interobserver reliability of pretest probability assessment in patients with suspected pulmonary embolism.Thromb Res.2005;116(2):101–107.
- ,,, et al.Does this patient have pulmonary embolism?JAMA.2003;290(21):2849–2858.
- ,,,,.Does a physician's ability to accurately assess the likelihood of pulmonary embolism increase with training?Acad Med.2000;75(12):1199–1205.
- ,,, et al.Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and D‐dimer.Ann Intern Med.2001;135(2):98–107.
- ,,, et al.Pulmonary embolism revealed on helical CT angiography: comparison with ventilation perfusion radionuclide lung scanning.AJR Am J Roentgenol.2000;174:1041–1047.
- ,,, et al.Clinical validity of a negative computed tomography scan in patients with suspected pulmonary embolism: a systematic review.JAMA.2005;293(16):2012–2017.
- ,,,,.Multidetector CT: a new gold standard in the diagnosis of pulmonary embolism? State of the art and diagnostic algorithms.Radiol Med.2005;109(1–2):49–61.
- ,,,,.Multidetector row CT pulmonary angiography and indirect venography for the diagnosis of venous thromboembolic disease in intensive care unit patients.Acad Radiol.2006;13(4):486–495.
- ,,.The role of multidetector computed tomography angiography for the diagnosis of pulmonary embolism.Semin Nucl Med.2008;38:418–431.
- ,,, et al.Multidetector computed tomography for acute pulmonary embolism.N Engl J Med.2006;354:2317–2327.
- Institute for Clinical Systems Improvement. Venous Thromboembolism Diagnosis and Treatment. Available at: http://www.icsi.org. Accessed October2009.
- The Columbus Investigators.Low‐molecular‐weight heparin in the treatment of patients with venous thromboembolism.N Engl J Med.1997;337:657–662.
- ,,, et al.A comparison of low‐molecular‐weight heparin with unfractionated heparin for acute pulmonary embolism. The THESEE Study Group.N Engl J Med.1997;337(10):663–669.
- ,,,,,.Pretest risk assessment in suspected acute pulmonary embolism.Acad Radiol.2008;15(1):3–14.
- ,,,.Is pretest probability assessment on emergency department patients with suspected venous thromboembolism documented before SimpliRED D‐dimer testing?CJEM.2008;10(6):519–523.
- ,,,,,.Exclusion of DVT with D‐dimer testing: comparison of 13 D‐dimer methods in 99 outpatients suspected of DVT using venography as a standard.Thromb Haemost.2000;83:191–198.
- ,,, et al.Multidetector‐row computed tomography in suspected pulmonary embolism.N Engl J Med.2005;352(17):1760–1768.
- ,,, et al.Simple and safe exclusion of pulmonary embolism in outpatients using quantitative D‐dimer and Wells' simplified decision rule.Thromb Haemost.2007;97(1):146–150.
- ,,,,;ANTELOPE Study Group. The performance of two rapid quantitative D‐dimer assays in 287 patients with clinically suspected pulmonary embolism.Thromb Res.2002;107(6):283–286.
- ,,, et al.Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians.Ann Fam Med.2007;5:57–62.
- ,,, et al.D‐dimer for the exclusion of acute venous thrombosis and pulmonary embolism. A systematic review.Ann Intern Med.2004;140:589–602.
- ,,, et al.CT pulmonary angiography is the first‐line imaging test for acute pulmonary embolism: a survey of US clinicians.Acad Radiol.2006;13:434–446.
- ,,, et al.Outcomes after withholding anticoagulation from patients with suspected pulmonary embolism and negative computed tomographic findings: a cohort study.Mayo Clin Proc.2002;77:130–138.
- ,,,.Meta‐analysis: outcomes in patients with suspected pulmonary embolism managed with computed tomographic pulmonary angiography.Ann Intern Med.2004;141:866–874.
- ,,, et al.Does this patient have deep vein thrombosis?JAMA.2006;295(2):199–207.
- ,,, et al.Measurement of the clinical and cost‐effectiveness of non‐invasive diagnostic testing strategies for deep vein thrombosis.Health Technol Assess.2006;10(15):1–168.
- ,,, et al.NABOR Steering Committee. Treatment of venous thromboembolism: adherence to guidelines and impact of physician knowledge, attitudes, and beliefs.J Vasc Surg.2005;42(4):726–733.
Copyright © 2010 Society of Hospital Medicine
Management of Ischemic Stroke: Part 1
The term stroke is defined by the World Health Organization as rapidly developed clinical signs of focal (or global) disturbance of cerebral function lasting more than 24 hours (unless interrupted by surgery or death), with no apparent cause other than a vascular origin; it includes patients presenting clinical signs and symptoms suggestive of subarachnoid hemorrhage (SAH), intracerebral hemorrhage, or cerebral ischemic necrosis.1 Stroke is 1 of the leading causes of death and the number 1 cause of long‐term disability in the United States, with over 700,000 strokes and over 150,000 stroke deaths each year.2
Given the projections of 30,000 hospitalists nationally by 2010 (
Case Presentation
A 76‐year‐old right‐handed male with a history of hyperlipidemia and myocardial infarction was found at 7 AM with right‐sided paralysis and poor responsiveness on the morning of admission. He seemed to prefer looking to the left and to understand what was being said to him, but had great difficulty speaking. When he went to bed at 9 PM, he was at his neurological baseline. Upon finding him that morning, his wife called 911.
With increased knowledge regarding the pathophysiology of stroke, it has become clear that timeliness is of utmost importance (time is brain) and that acute stroke should be regarded as an acute medical/neurological emergency.
This article reviews the approach in evaluating an acute stroke patient, management strategies, and treatment options. Where not otherwise referenced, data to support our comments come from the recently updated and exhaustive American Heart Association (AHA)/American Stroke Association (ASA) Guidelines for the Early Management of Adults With Ischemic Stroke and will be referred to herein as the Guidelines.4 Harborview Medical Center in Seattle is a Joint Commissioncertified Primary Stroke Center and the home hospital of 2 of the authors (C.L.E., D.L.T.); it is referred to herein as Harborview.
Emergency Room Care (see Acute Stroke Algorithm, Figure 1)
The First 15 Minutes
After assuring stable airway, breathing, and circulation, immediate (STAT) blood draws should be performed, including full complete blood count (CBC) with platelets, international normalized ratio/prothrombin time/partial thromboplastin time (INR/PT/PTT), full electrolytes, and glucose (finger‐stick blood glucose also recommended). Glasgow Coma Scale (GCS) score and NIH Stroke Scale (NIHSS) score should be established via a focused history and physical exam. The GCS is most appropriate for patients with a significantly depressed level of consciousness, while the NIHSS can be scored for any stroke patient (1‐page version of NIHSS used at Harborview is shown in Figure 2). By quantifying stroke severity, the NIHSS score helps both to facilitate communication about neurologic deficit as well as serve as a documented baseline in case of subsequent clinical change. Emergency department (ED) physicians, hospitalists, neurologists, and nursing staff regularly caring for acute stroke patients would be well‐served by obtaining certification in the NIHSS (available free online at
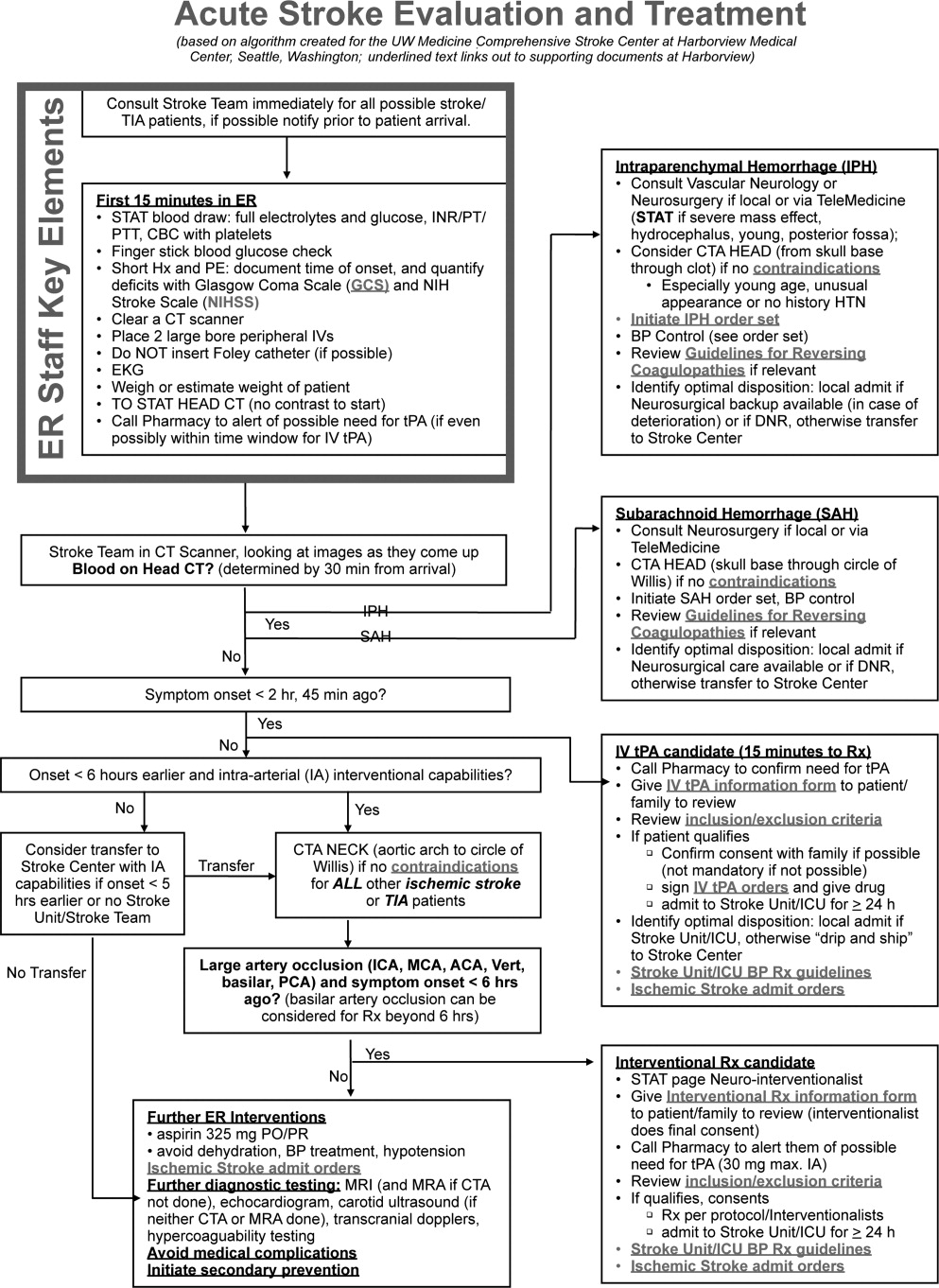
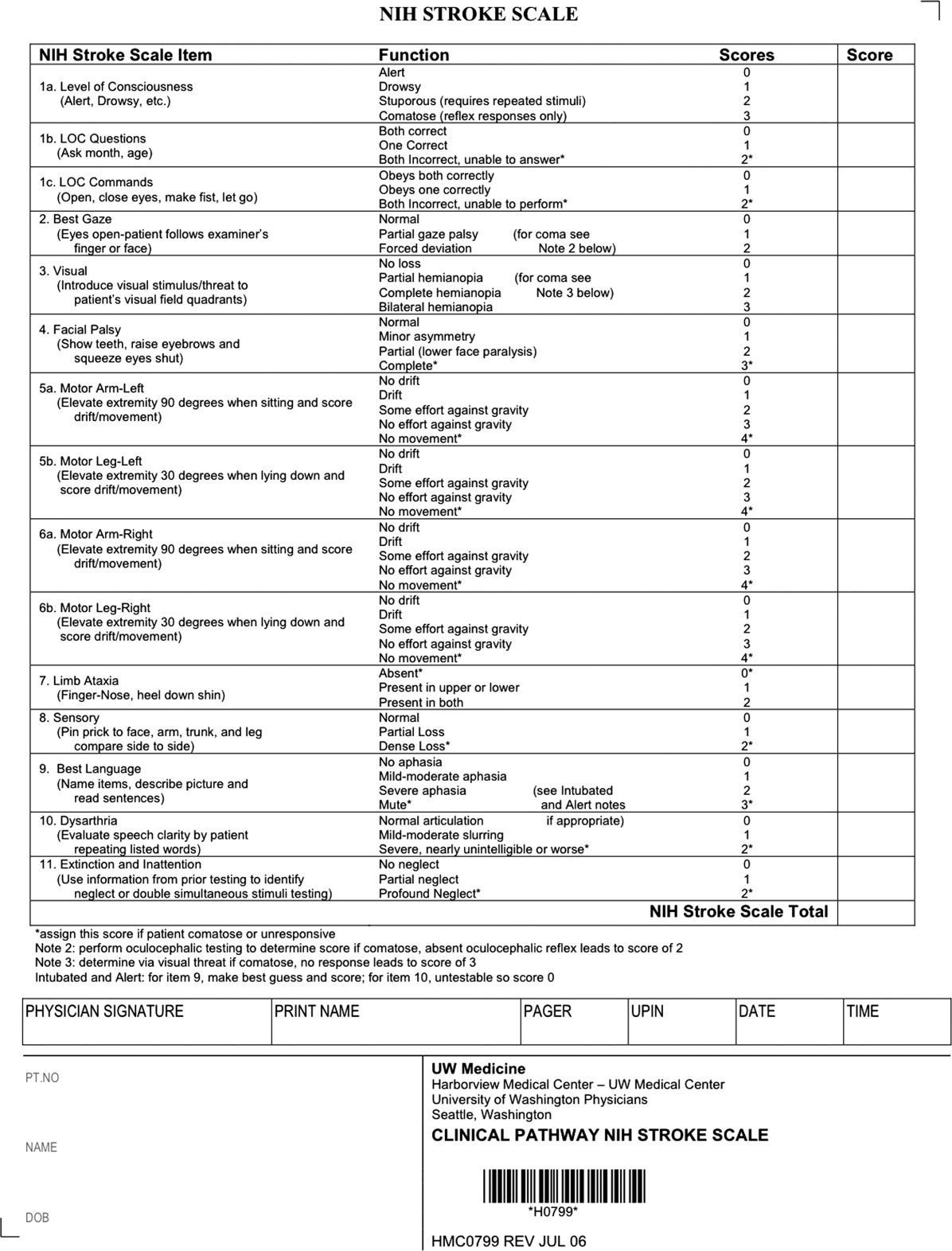
Our case patient's initial NIHSS score was 15, with points given for drowsiness, inability to answer questions, partial facial palsy, no movement in right arm or leg, mild‐moderate aphasia, and mild‐moderate dysarthria (Figure 2).
Differential Diagnosis
Many acute conditions can mimic stroke, and 1 of the goals of the initial emergency room (ER) evaluation is to rule out such stroke mimics. A report of 411 initial ER stroke diagnoses identified 19% as stroke mimics; the most common mimic diagnoses were seizure, systemic infection, brain tumor, and toxic‐metabolic.5 The same study identified decreased level of alertness as associated with a final mimic diagnosis and history of angina as associated with a final diagnosis of stroke. Another study looked at 350 presentations with an initial stroke diagnosis and found 31% stroke mimics; similarly, the main alternative diagnoses were seizure, sepsis, toxic‐metabolic, space‐occupying lesion, and syncope/presyncope.6 Findings associated with a mimic diagnosis included no cognitive impairment and abnormal findings in any other system, while findings associated with a stroke diagnosis were a definite history of focal neurological symptoms, NIHSS score, stroke type classification possible, an exact onset that could be determined, and abnormal vascular findings on imaging.6
Initial Imaging
The patient should receive a STAT noncontrast head CT to evaluate for the presence or absence of blood. At this time, magnetic resonance imaging (MRI) is not essential to confirm the diagnosis of ischemic stroke, as diagnosis is based on clinical suspicion. MRI is more sensitive at imaging acute ischemia (on diffusion‐weighted sequences) and recently has been shown to be equally sensitive in identifying acute blood (previously thought to be a relative advantage of CT).7, 8 Practical and pervasive barriers to emergent MRI include study duration, significant patient cooperation, and that few hospitals are currently set up to perform such rapid MRIS. The Guidelines specifically state that In most instances, CT will provide the information to make decisions about emergency management (p. 1668),4 that vascular imaging should not delay treatment of patients whose symptoms started 3 hours ago and who have acute ischemic stroke, and that emergency treatment of stroke should not be delayed in order to obtain multimodal imaging studies (p. 1669).4
Our case patient's initial imaging, a noncontrast head CT (Supporting Figures 1 and 2), showed subtle clues consistent with the diagnosis of acute ischemic stroke. These include a hyperdense middle cerebral artery (MCA) sign (presumably representing thrombus), possible obscuration of the basal ganglia, and, importantly, no acute intraparenchymal (IPH), SAH, or subdural hemorrhage.
Acute Treatments
After the patient's head CT is completed, the next steps are dependent upon what was seen on the scan and the time from symptom onset.
Blood on the CT Scan
If the initial brain imaging reveals IPH or SAH, further diagnostic testing and early treatments are quite different than for ischemic stroke. New guidelines are available for IPH management,9 and there have been recent review articles of care for SAH.1012 At the authors' institutions, early care of such patients always involves aggressive reversal of any antithrombotic medications the patient was taking prior to presentation. Our approach to warfarin reversal includes vitamin K and fresh frozen plasma (FFP) to achieve an INR 1.4; others have used prothrombin complex concentrate (PCC).13 Blood pressure (BP) treatment goals are generally more aggressive than for ischemic stroke, while supportive care to avoid aspiration, hyperglycemia, fever, and venous thrombosis (here initially with sequential compression devices alone) are similar. Early estimation of prognosis for these patients with IPH and SAH and discussions with families about continued aggressive care are of utmost importance, and should involve providers with sufficient expertise. Care should be taken to avoid overly pessimistic early prognostication, as early do not resuscitate (DNR) decisions in intercranial hemorrhage (ICH) can become a self‐fulfilling prophecy.1416 If the decision is to continue aggressive and supportive care, or if an appropriately expert consultation is not available at the presentation hospital, IPH and SAH patients should be considered for transfer to a hospital with the appropriate resources (including emergency access to neurosurgeons) or be evaluated by such an expert by telemedicine if available.
No Blood on the CT Scan, Results Back in 3 Hours From Symptom Onset
If such a patient is not rapidly resolving their symptoms, and the diagnosis continues to remain clear, inclusion/exclusion criteria for IV tPA should be reviewed (Table 1). Consent should be obtained much like any other procedure with significant risk. As many consider tPA to be standard of care, it is reasonable to proceed in cases of unobtainable consent as one would with any other emergent therapy. This situation is a topic of ongoing debate.17, 18 The Guidelines state that although written consent is not necessary before administration of recombinant tPA (rtPA) for treatment of stroke, a full discussion of the potential risks and benefits of treatment with rtPA with the family and the patient if possible is recommended (p. 1676).4 After tPA is given in the ER, the patient should be admitted to an intensive care unit (ICU) setting for 24 hours for careful monitoring of BP, avoidance of invasive procedures, and no use of antithrombotic medications during that period of time.
| Comments (from the authors) | |
|---|---|
| |
| Inclusion criteria | |
| Diagnosis of ischemic stroke causing measurable neurological deficit | Usually NIHSS > 4 |
| Neurological signs should not be clearing spontaneously | Such a patient may do well without tPA, but there is debate82 |
| Neurological signs should not be minor and isolated. | |
| Onset of symptoms >3 hours before beginning treatment | |
| Patient or family members understand the potential risks and benefits from treatment | Debated, as tPA considered standard of care by many |
| Cautionary criteria | |
| Caution should be exercised in treating a patient with major deficits | Higher risk of hemorrhage, but still may benefit from treatment |
| Exclusion criteria | |
| Symptoms of stroke should not be suggestive of subarachnoid hemorrhage | |
| No head trauma or prior stroke in previous 3 months | |
| No myocardial infarction in the previous 3 months | |
| No gastrointestinal or urinary tract hemorrhage in previous 21 days | |
| No major surgery in the previous 14 days | |
| No arterial puncture at a noncompressible site in the previous 7 days | |
| No history of previous intracranial hemorrhage | |
| Blood pressure not elevated (systolic >185 mm Hg or diastolic 110 mm Hg) | Okay to bring down with labetolol, nitropaste, or nicardipine* |
| No evidence of active bleeding or acute trauma (fracture) on examination | |
| Not taking an oral anticoagulant or, if anticoagulant being taken, INR 1.7 | |
| If receiving heparin in previous 48 hours, aPTT must be in normal range | |
| Platelet count 100,000 mm3 | |
| Blood glucose concentration 50 mg/dL (2.7 mmol/L) | |
| Seizure with postictal residual neurological impairments | Not absolute if treating physician feels stroke also present, or if confirmed by imaging |
| CT does not show a multilobar infarction (hypodensity >1/3 cerebral hemisphere) | Not strictly evidence based, in NINDS trial this finding did not preclude benefit of tPA |
Based mainly on the results of the National Institute of Neurological Disorders and Stroke (NINDS) tPA trial,19 and recently supported by a large Phase IV observational study from the European Union,20 IV tPA for acute ischemic stroke is approved for use in many countries and is endorsed for the treatment of carefully selected ischemic stroke patients in a number of practice guidelines.4 Despite this, the emergency medicine community has been less enthusiastic about the use of IV tPA.21, 22 Although the risk of hemorrhagic complications is greater in certain subgroups of patients (ie, the most severe strokes, significant early CT changes, older age), there is no definitive evidence to suggest that these groups do not still benefit from the treatment.23 It is also clear that if patients are not carefully selected, meeting strict inclusion and exclusion criteria, the rate of complications is increased.24 Thus, as summarized in a practice statement of the American College of Emergency Physicians, There is insufficient evidence at this time to endorse the use of intravenous tPA in clinical practice when systems are not in place to ensure that the inclusion/exclusion criteria established by the NINDS guidelines for tPA use in acute stroke are followed.21 When counseling patients and their families about the benefits and risks of IV tPA, one should keep in mind that the NINDS trial demonstrated increased odds of excellent outcomes despite a significant 10‐fold increase in the risk of symptomatic intracranial hemorrhage (6.4% vs. 0.6%), and did not alter 30‐day mortality. The largest Phase IV cohort study of IV tPA treatment, Safe Implementation of Thrombolysis in Stroke Monitoring Study (SITS‐MOST) was mandated by the European Union upon approval of the medication for use in acute ischemic stroke.20 The results in 6483 patients showed that tPA, when used in strict accordance with published inclusion and exclusion criteria, could perform as well as it did in randomized trials.
The recently published European Cooperative Acute Stroke Study3 (ECASS‐3) trial demonstrated that IV tPA has efficacy with adequate safety up to 4.5 hours after the onset of symptoms. A total of 821 patients were enrolled and 375 received tPA. Exclusion criteria included diabetes being treated with medication with a history of prior stroke, an NIHSS score >25, or treatment with warfarin. The rates of hemorrhage (27.0% vs. 17.6%, P = 0.001) were in line with those of the SITS‐MOST study patients who were treated within the 3‐hour time window. There was no significant difference in mortality (7.7% tPA vs. 8.4% placebo). This study is relatively new; therefore, the data have not been reviewed by guideline committees.25
No Blood on the CT Scan, Results Back in >3 Hours, but 8 Hours, From Symptom Onset
Unfortunately as with our patient, most people do not present to an ER in a timely fashion. Nonetheless, there may be other treatments and interventions possible. If the patient arrives 8 hours from onset of symptoms, intraarterial (IA) interventions are a possibility. In such a case, a CT angiogram (CTA) of the neck from the arch of the aorta to the circle of Willis is recommended (barring any contraindications such as renal failure or iodine allergy). The rationale behind this study is that other treatment options, such as IA tPA or mechanical thrombectomy may be considered if a large arterial occlusion is identified. CTA is preferred over magnetic resonance angiography (MRA) due to the same time and patient cooperation issues mentioned above, though some expert centers may be set up to perform MRI and MRA rapidly in the acute setting. CTA or MRA is of great value early on in the emergent assessment of ischemic stroke patients, as it allows detailed evaluation of the cerebral vasculature; this knowledge helps define the pathophysiology of the ongoing stroke (eg, is there a larger artery occlusion?) and can help inform the approach to subsequent therapies.
The Guidelines (p. 1678)4 recommend IA thrombolysis as a treatment option if it can be started within 6 hours, based on results from the Prolyse in Acute Cerebral Thromboembolism (PROACT) II trial. This study involved angiography with identification of the occluded vessel (the proximal MCA‐M1 in this study) and administration of recombinant pro‐urokinase to the clot with functional outcome as the primary endpoint.26 At 3 months, patients who received the IA thrombolytic had a 40% chance of slight disability; unable to carry out all previous activities, but able to look after own affairs without assistance or better (ie, a modified Rankin Scale score of 2) vs. 25% of those not receiving the IA thrombolytic. Pro‐urokinase is not available in the United States; therefore, many institutions substitute IA tPA. The Guidelines further state that IA thrombolysis can be considered for use in some patients with contraindications to IV tPA (eg, recent surgery), but should not be used instead of IV tPA in patients otherwise eligible (p. 1678).4
There are now two U.S. Food and Drug Administration (FDA)‐approved devices for mechanical cerebral vasculature thrombectomy for use up to 8 hours from symptom onset. The mechanical embolus removal in cerebral ischemia (MERCI) clot retrieval device was originally approved by the FDA in August 2004 for restoring blood flow in the neurovasculature by removing thrombus in patients experiencing ischemic stroke. Modified devices have been approved as recently as January 2007.27 The Penumbra System was FDA‐approved in December 2007 for revascularization of patients with acute ischemic stroke secondary to intracranial large vessel occlusive disease.28 In both cases, the FDA approval was based on demonstration of safety in case series of patients treated with the devices.2931 No randomized trials have shown the use of these devices improves outcomes for stroke patients. The Guidelines state that Although the MERCI device is a reasonable intervention for extraction of IA thrombi in carefully selected patients, the panel also recognizes that the utility of the device in improving outcomes after stroke is unclear (p. 1684);4 this statement applies similarly to the Penumbra device.
More complex imaging techniques, including multimodal CT (CT, CTA, and CT perfusion) and MR (MRI with diffusion, MRA, and MR perfusion) are being used in some stroke centers to make decisions about acute ischemic stroke treatments.32, 33 The theory is that by using these techniques, one can determine the presence or absence of a mismatch, whereby the perfusion imaging suggests more tissue at risk of infarction than is seen as already abnormal on MR diffusion‐weighted images or compared to a clinical assessment. These mismatch patients are then seen as appropriate candidates for the more aggressive interventions (ie, late IV tPA or IA interventions).34 Unfortunately, the 2 largest randomized trials to look at this issue with respect to >3‐hour IV tPA both failed to show a benefit for patients selected in this manner.35, 36 Standardized definitions of mismatch are still needed, and larger randomized trials are needed before this approach can be suggested for routine care.3739
More complex interventions, available only at tertiary or comprehensive stroke centers, include a bridging approach in which IV tPA (at 2/3 standard dose) is followed by IA tPA, IV tPA with transcranial Doppler (TCD)‐enhanced thrombolysis or IA rescue thrombectomy when vascular imaging after IV tPA shows a persistent large artery occlusion. The Guidelines suggests that these more complex combinations of interventions to restore perfusion cannot be recommended outside the setting of clinical trials (p. 1685).4
No Blood on the CT Scan, Results Back in >8 Hours From Symptom Onset (or if Contraindications to Above Interventions)
This time frame takes the more aggressive interventions off the table. Per the Guidelines, 325 mg of aspirin is the default antiplatelet agent for use, and has been shown in 2 very large randomized trials to reduce early death and longer‐term disability vs. placebo after acute ischemic stroke.40, 41 Importantly, all patients who do not qualify for thrombolysis in the 0‐hour to 8‐hour time window should receive aspirin.
Although a number of small or pilot studies suggest a benefit of the addition of clopidogrel to aspirin for a period (13 months) immediately after ischemic stroke,4244 this more aggressive antiplatelet intervention is not an endorsed standard of care. As described below, the long‐term use of this antiplatelet combination has been consistently associated with a higher risk of hemorrhagic complications. There are no published data regarding the use of aspirin plus dipyridamole in the acute stroke setting. A number of randomized trials have now been performed that have consistently failed to show a benefit of heparin, or heparin‐like medications, for the routine treatment of acute ischemic stroke. Despite this, a number of exceptions exist, based more on tradition and theory than on evidence. These exceptions, for which an IV heparin drip will at times still be considered, include acute ischemic stroke due to dissection of the carotid or vertebral arteries, cardioembolic stroke with fresh clot seen on echocardiogram (ECHO), and a clinically progressive syndrome suggestive of basilar artery occlusion (see below).45, 46 Good evidence exists to specifically recommend the use of full‐dose heparin in the setting of cerebral venous sinus thrombosis.47
Basilar Artery Occlusion Syndromes
Basilar artery occlusion syndromes warrant special mention. These may involve patients who present with quadriparesis, altered mental status, vertigo, diplopia, and other brainstem signs. Conventional treatment of basilar artery occlusion has been associated with 40% mortality with 65% of survivors having severe disability.48 If suspected, an urgent CTA can usually confirm the diagnosis, and urge the clinician to expeditiously consider aggressive intervention. Only case series have been reported regarding basilar artery thrombosis and acute treatments. Based on these studies, it is generally agreed upon that patients who appear comatose or quadriplegic for more than 3 hours will likely have a very poor functional outcome regardless of treatment, and interventional treatment is withheld. If a basilar occlusion patient presents within the 3‐hour time window for IV tPA, they are thus treated, with follow‐up vascular imaging, and possible rescue IA mechanical thrombectomy if recanalization from the IV tPA does not occur. However, if the patient still has preserved neurologic function, or is waxing and waning, there is no clear time limit for IA interventions and they may be useful a day or more after presentation. For basilar occlusion patients with severe stenoses not responsive to lysis, or continuing to be symptomatic, angioplasty and stenting has also been used.46 Despite a lack of evidence, many stroke clinicians will use an IV heparin drip for treatment of acute basilar occlusive disease.
Malignant Middle Cerebral Artery (MCA) Infarction
Malignant MCA infarction is another specific clinical syndrome worthy of special consideration. It is most generally defined as a large infarction (1/2 or 2/3) of the MCA territory, somewhat depressed level of consciousness, and high stroke scale scores (ie, severe deficits) that goes on to severe cerebral edema, mass effect, and often herniation with death.49, 50 Associated patient characteristics include younger age, abnormal (incomplete) ipsilateral collateral circulation, and internal carotid artery occlusion.51 Maximal edema occurs 2 to 5 days from stroke onset and, despite best intensive therapy, has been associated with mortality rates of 70% to 80%.49, 50 A recent pooling of 3 small randomized trials of early decompressive hemicraniectomy and durotomy showed a 50% absolute risk reduction for mortality and a 23% absolute benefit in long‐term independence (modified Rankin scale 3).49 This treatment option should be strongly considered in carefully selected patients., Transfer to an appropriately equipped facility should be offered if not available at your hospital.
Returning to our case patient, upon arrival to the ED with symptoms of partial aphasia, right hemiplegia, and left gaze preference, there was a high suspicion for a left MCA stroke. Unfortunately, he was excluded from receiving IV tPA or any other interventions, as the last time he was known to be neurologically intact was the prior evening, which is taken to be the time of onset. Antiplatelet therapy was continued, and the patient was admitted for further workup.
The initial care of the patient with a cerebrovascular event is often quite complicated. Assimilation of a great deal of data must occur and decisions around therapy must be made in a timely fashion. In prior years there was little to offer in the way of therapy, which also meant there was little initial potential for iatrogenic complication. Both diagnostic and therapeutic options are evolving rapidly. We now have much to offer these patients both emergently and in areas of secondary prevention. In part 2 of this article, the patient's inpatient course and therapy will be reviewed.
- Organization WH. MONICA Manual, Part IV: Event Registration. Available at: http://www.ktl.fi/publications/monica/manual/part4/iv‐2.htm#s2. Accessed May2009.
- ,,, et al.Heart disease and stroke statistics 2008 update. A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee.Circulation.200829;117(4):e25–e146.
- .Neurology in the next two decades: report of the Workforce Task Force of the American Academy of Neurology.Neurology.2000;54(4):787–789.
- ,,, et al.Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists.Stroke.2007;38(5):1655–1711.
- ,,,.Conditions that mimic stroke in the emergency department. Implications for acute stroke trials.Arch Neurol.1995;52(11):1119–1122.
- ,,,,.Distinguishing between stroke and mimic at the bedside: the brain attack study.Stroke.2006;37(3):769–775.
- ,,, et al.Stroke magnetic resonance imaging is accurate in hyperacute intracerebral hemorrhage: a multicenter study on the validity of stroke imaging.Stroke.2004;35(2):502–506.
- ,,, et al.Comparison of MRI and CT for detection of acute intracerebral hemorrhage.JAMA.2004;292(15):1823–1830.
- ,,, et al.Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group.Stroke.2007;38(6):2001–2023.
- ,,.Aneurysmal subarachnoid hemorrhage.N Engl J Med.2006;354(4):387–396.
- ,,,.Subarachnoid haemorrhage.BMJ.2006;333(7561):235–240.
- ,,.Subarachnoid haemorrhage.Lancet.2007;369(9558):306–318.
- ,,.Intracerebral hemorrhage associated with oral anticoagulant therapy: current practices and unresolved questions.Stroke.2006;37(1):256–262.
- ,,, et al.Withdrawal of support in intracerebral hemorrhage may lead to self‐fulfilling prophecies.Neurology.2001;56(6):766–772.
- ,,,.Hospital usage of early do‐not‐resuscitate orders and outcome after intracerebral hemorrhage.Stroke.2004;35(5):1130–1134.
- ,,, et al.Early care limitations independently predict mortality after intracerebral hemorrhage.Neurology.2007;68(20):1651–1657.
- ,,,.Consent for intravenous thrombolysis in acute stroke: review and future directions.Arch Neurol.2007;64(6):785–792.
- .Thrombolysis (tissue plasminogen activator) in stroke: a medicolegal quagmire.Stroke.2006;37(7):1917–1922.
- Tissue plasminogen activator for acute ischemic stroke.The National Institute of Neurological Disorders and Stroke rt‐PA Stroke Study Group.N Engl J Med.1995;333(24):1581–1587.
- ,,, et al.Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke‐Monitoring Study (SITS‐MOST): an observational study.Lancet.2007;369(9558):275–282.
- American College of Emergency Physicians (ACEP). Use of Intravenous tPA for the Management of Acute Stroke in the Emergency Department. ACEP Policy Statement. February 2002. Available at: http://www.acep.org/practres.aspx?id=29834. Accessed May2009.
- American Academy of Emergency Medicine (AAEM). Position statement on the use of intravenous thrombolytic therapy in the treatment of stroke. January 2002. Available at: http://aaem.org/positionstatements/thrombolytictherapy.php. Accessed May2009.
- ,,, et al.Lack of clinical significance of early ischemic changes on computed tomography in acute stroke.JAMA.2001;286(22):2830–2838.
- ,,,,.Thrombolysis for acute stroke in routine clinical practice.Arch Intern Med.2002;162(17):1994–2001.
- ,,, et al.Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke.N Engl J Med.2008;359:1317–1329,1393–1395.
- ,,, et al.Intra‐arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism.JAMA.1999;282(21):2003–2011.
- Modified MERCI Retriever FDA marketing approval letter. Available at: www.fda.gov/cdrh/pdf6/K062046.pdf. Accessed May2009.
- Penumbra System FDA marketing approval letter. Available at: www.fda.gov/cdrh/pdf7/K072718.pdf. Accessed May2009.
- .Safety of mechanical thrombectomy and intravenous tissue plasminogen activator in acute ischemic stroke. Results of the multi mechanical embolus removal in cerebral ischemia (MERCI) trial, part I.AJNR Am J Neuroradiol.2006;27(6):1177–1182.
- ,,, et al.Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial.Stroke.2005;36(7):1432–1438.
- ,,, et al.The Penumbra System: a mechanical device for the treatment of acute stroke due to thromboembolism.AJNR Am J Neuroradiol.2008;29(7):1409–1413.
- ,,, et al.Comparison of CT perfusion and angiography and MRI in selecting stroke patients for acute treatment.Neurology.2007;68(9):694–697.
- ,,, et al.Combined intravenous and intraarterial revascularization therapy using MRI perfusion/diffusion mismatch selection for acute ischemic stroke at 3–6 h after symptom onset.Neurocrit Care.2008;8(3):353–359.
- ,,, et al.Refining the perfusion‐diffusion mismatch hypothesis.Stroke.2005;36(6):1153–1159.
- . DIAS‐2: no benefit of desmoteplase in acute ischemic stroke. Available at: www.medscape.com/viewarticle/557663. Accessed May2009.
- ,,, et al.Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo‐controlled randomised trial.Lancet Neurol.2008;7(4):299–309.
- ,,.Magnetic resonance perfusion diffusion mismatch and thrombolysis in acute ischaemic stroke: a systematic review of the evidence to date.J Neurol Neurosurg Psychiatry.2007;78(5):485–491.
- ,,, et al.Optimal definition for PWI/DWI mismatch in acute ischemic stroke patients.J Cereb Blood Flow Metab.2008;28(5):887–891.
- ,,, et al.Rapid assessment of perfusion‐diffusion mismatch.Stroke.2008;39(1):75–81.
- CAST: randomised placebo‐controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke.CAST (Chinese Acute Stroke Trial) Collaborative Group.Lancet.1997;349(9066):1641–1649.
- The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke.International Stroke Trial Collaborative Group.Lancet.1997;349(9065):1569–1581.
- ,,, et al.Dual antiplatelet therapy with clopidogrel and aspirin in symptomatic carotid stenosis evaluated using doppler embolic signal detection: the clopidogrel and aspirin for reduction of emboli in symptomatic carotid stenosis (CARESS) trial.Circulation.2005;111(17):2233–2240.
- ,,, et al.Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population‐based sequential comparison.Lancet.2007;370(9596):1432–1442.
- ,,,,,.Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): a randomised controlled pilot trial.Lancet Neurol.2007;6(11):961–969.
- ,,, et al.Antiplatelets versus anticoagulation in cervical artery dissection.Stroke.2007;38(9):2605–2611.
- ,,.Basilar artery occlusion.Neurocrit Care.2004;1(3):319–329.
- ,.Cerebral venous thrombosis: an update.Lancet Neurol.2007;6(2):162–170.
- ,,,,.Outcome in patients with basilar artery occlusion treated conventionally.J Neurol Neurosurg Psychiatry.2005;76(9):1238–1241.
- ,,, et al.Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomised controlled trials.Lancet Neurol.2007;6(3):215–222.
- ,,,,,.‘Malignant’ middle cerebral artery territory infarction: clinical course and prognostic signs.Arch Neurol.1996;53(4):309–315.
- ,,,,.Predictors for malignant middle cerebral artery infarctions: a postmortem analysis.Neurology. 282006;66(6):815–820.
- ,,,,,.Poor outcomes in patients who do not receive intravenous tissue plasminogen activator because of mild or improving ischemic stroke.Stroke.2005;36(11):2497–2499.
The term stroke is defined by the World Health Organization as rapidly developed clinical signs of focal (or global) disturbance of cerebral function lasting more than 24 hours (unless interrupted by surgery or death), with no apparent cause other than a vascular origin; it includes patients presenting clinical signs and symptoms suggestive of subarachnoid hemorrhage (SAH), intracerebral hemorrhage, or cerebral ischemic necrosis.1 Stroke is 1 of the leading causes of death and the number 1 cause of long‐term disability in the United States, with over 700,000 strokes and over 150,000 stroke deaths each year.2
Given the projections of 30,000 hospitalists nationally by 2010 (
Case Presentation
A 76‐year‐old right‐handed male with a history of hyperlipidemia and myocardial infarction was found at 7 AM with right‐sided paralysis and poor responsiveness on the morning of admission. He seemed to prefer looking to the left and to understand what was being said to him, but had great difficulty speaking. When he went to bed at 9 PM, he was at his neurological baseline. Upon finding him that morning, his wife called 911.
With increased knowledge regarding the pathophysiology of stroke, it has become clear that timeliness is of utmost importance (time is brain) and that acute stroke should be regarded as an acute medical/neurological emergency.
This article reviews the approach in evaluating an acute stroke patient, management strategies, and treatment options. Where not otherwise referenced, data to support our comments come from the recently updated and exhaustive American Heart Association (AHA)/American Stroke Association (ASA) Guidelines for the Early Management of Adults With Ischemic Stroke and will be referred to herein as the Guidelines.4 Harborview Medical Center in Seattle is a Joint Commissioncertified Primary Stroke Center and the home hospital of 2 of the authors (C.L.E., D.L.T.); it is referred to herein as Harborview.
Emergency Room Care (see Acute Stroke Algorithm, Figure 1)
The First 15 Minutes
After assuring stable airway, breathing, and circulation, immediate (STAT) blood draws should be performed, including full complete blood count (CBC) with platelets, international normalized ratio/prothrombin time/partial thromboplastin time (INR/PT/PTT), full electrolytes, and glucose (finger‐stick blood glucose also recommended). Glasgow Coma Scale (GCS) score and NIH Stroke Scale (NIHSS) score should be established via a focused history and physical exam. The GCS is most appropriate for patients with a significantly depressed level of consciousness, while the NIHSS can be scored for any stroke patient (1‐page version of NIHSS used at Harborview is shown in Figure 2). By quantifying stroke severity, the NIHSS score helps both to facilitate communication about neurologic deficit as well as serve as a documented baseline in case of subsequent clinical change. Emergency department (ED) physicians, hospitalists, neurologists, and nursing staff regularly caring for acute stroke patients would be well‐served by obtaining certification in the NIHSS (available free online at
Our case patient's initial NIHSS score was 15, with points given for drowsiness, inability to answer questions, partial facial palsy, no movement in right arm or leg, mild‐moderate aphasia, and mild‐moderate dysarthria (Figure 2).
Differential Diagnosis
Many acute conditions can mimic stroke, and 1 of the goals of the initial emergency room (ER) evaluation is to rule out such stroke mimics. A report of 411 initial ER stroke diagnoses identified 19% as stroke mimics; the most common mimic diagnoses were seizure, systemic infection, brain tumor, and toxic‐metabolic.5 The same study identified decreased level of alertness as associated with a final mimic diagnosis and history of angina as associated with a final diagnosis of stroke. Another study looked at 350 presentations with an initial stroke diagnosis and found 31% stroke mimics; similarly, the main alternative diagnoses were seizure, sepsis, toxic‐metabolic, space‐occupying lesion, and syncope/presyncope.6 Findings associated with a mimic diagnosis included no cognitive impairment and abnormal findings in any other system, while findings associated with a stroke diagnosis were a definite history of focal neurological symptoms, NIHSS score, stroke type classification possible, an exact onset that could be determined, and abnormal vascular findings on imaging.6
Initial Imaging
The patient should receive a STAT noncontrast head CT to evaluate for the presence or absence of blood. At this time, magnetic resonance imaging (MRI) is not essential to confirm the diagnosis of ischemic stroke, as diagnosis is based on clinical suspicion. MRI is more sensitive at imaging acute ischemia (on diffusion‐weighted sequences) and recently has been shown to be equally sensitive in identifying acute blood (previously thought to be a relative advantage of CT).7, 8 Practical and pervasive barriers to emergent MRI include study duration, significant patient cooperation, and that few hospitals are currently set up to perform such rapid MRIS. The Guidelines specifically state that In most instances, CT will provide the information to make decisions about emergency management (p. 1668),4 that vascular imaging should not delay treatment of patients whose symptoms started 3 hours ago and who have acute ischemic stroke, and that emergency treatment of stroke should not be delayed in order to obtain multimodal imaging studies (p. 1669).4
Our case patient's initial imaging, a noncontrast head CT (Supporting Figures 1 and 2), showed subtle clues consistent with the diagnosis of acute ischemic stroke. These include a hyperdense middle cerebral artery (MCA) sign (presumably representing thrombus), possible obscuration of the basal ganglia, and, importantly, no acute intraparenchymal (IPH), SAH, or subdural hemorrhage.
Acute Treatments
After the patient's head CT is completed, the next steps are dependent upon what was seen on the scan and the time from symptom onset.
Blood on the CT Scan
If the initial brain imaging reveals IPH or SAH, further diagnostic testing and early treatments are quite different than for ischemic stroke. New guidelines are available for IPH management,9 and there have been recent review articles of care for SAH.1012 At the authors' institutions, early care of such patients always involves aggressive reversal of any antithrombotic medications the patient was taking prior to presentation. Our approach to warfarin reversal includes vitamin K and fresh frozen plasma (FFP) to achieve an INR 1.4; others have used prothrombin complex concentrate (PCC).13 Blood pressure (BP) treatment goals are generally more aggressive than for ischemic stroke, while supportive care to avoid aspiration, hyperglycemia, fever, and venous thrombosis (here initially with sequential compression devices alone) are similar. Early estimation of prognosis for these patients with IPH and SAH and discussions with families about continued aggressive care are of utmost importance, and should involve providers with sufficient expertise. Care should be taken to avoid overly pessimistic early prognostication, as early do not resuscitate (DNR) decisions in intercranial hemorrhage (ICH) can become a self‐fulfilling prophecy.1416 If the decision is to continue aggressive and supportive care, or if an appropriately expert consultation is not available at the presentation hospital, IPH and SAH patients should be considered for transfer to a hospital with the appropriate resources (including emergency access to neurosurgeons) or be evaluated by such an expert by telemedicine if available.
No Blood on the CT Scan, Results Back in 3 Hours From Symptom Onset
If such a patient is not rapidly resolving their symptoms, and the diagnosis continues to remain clear, inclusion/exclusion criteria for IV tPA should be reviewed (Table 1). Consent should be obtained much like any other procedure with significant risk. As many consider tPA to be standard of care, it is reasonable to proceed in cases of unobtainable consent as one would with any other emergent therapy. This situation is a topic of ongoing debate.17, 18 The Guidelines state that although written consent is not necessary before administration of recombinant tPA (rtPA) for treatment of stroke, a full discussion of the potential risks and benefits of treatment with rtPA with the family and the patient if possible is recommended (p. 1676).4 After tPA is given in the ER, the patient should be admitted to an intensive care unit (ICU) setting for 24 hours for careful monitoring of BP, avoidance of invasive procedures, and no use of antithrombotic medications during that period of time.
| Comments (from the authors) | |
|---|---|
| |
| Inclusion criteria | |
| Diagnosis of ischemic stroke causing measurable neurological deficit | Usually NIHSS > 4 |
| Neurological signs should not be clearing spontaneously | Such a patient may do well without tPA, but there is debate82 |
| Neurological signs should not be minor and isolated. | |
| Onset of symptoms >3 hours before beginning treatment | |
| Patient or family members understand the potential risks and benefits from treatment | Debated, as tPA considered standard of care by many |
| Cautionary criteria | |
| Caution should be exercised in treating a patient with major deficits | Higher risk of hemorrhage, but still may benefit from treatment |
| Exclusion criteria | |
| Symptoms of stroke should not be suggestive of subarachnoid hemorrhage | |
| No head trauma or prior stroke in previous 3 months | |
| No myocardial infarction in the previous 3 months | |
| No gastrointestinal or urinary tract hemorrhage in previous 21 days | |
| No major surgery in the previous 14 days | |
| No arterial puncture at a noncompressible site in the previous 7 days | |
| No history of previous intracranial hemorrhage | |
| Blood pressure not elevated (systolic >185 mm Hg or diastolic 110 mm Hg) | Okay to bring down with labetolol, nitropaste, or nicardipine* |
| No evidence of active bleeding or acute trauma (fracture) on examination | |
| Not taking an oral anticoagulant or, if anticoagulant being taken, INR 1.7 | |
| If receiving heparin in previous 48 hours, aPTT must be in normal range | |
| Platelet count 100,000 mm3 | |
| Blood glucose concentration 50 mg/dL (2.7 mmol/L) | |
| Seizure with postictal residual neurological impairments | Not absolute if treating physician feels stroke also present, or if confirmed by imaging |
| CT does not show a multilobar infarction (hypodensity >1/3 cerebral hemisphere) | Not strictly evidence based, in NINDS trial this finding did not preclude benefit of tPA |
Based mainly on the results of the National Institute of Neurological Disorders and Stroke (NINDS) tPA trial,19 and recently supported by a large Phase IV observational study from the European Union,20 IV tPA for acute ischemic stroke is approved for use in many countries and is endorsed for the treatment of carefully selected ischemic stroke patients in a number of practice guidelines.4 Despite this, the emergency medicine community has been less enthusiastic about the use of IV tPA.21, 22 Although the risk of hemorrhagic complications is greater in certain subgroups of patients (ie, the most severe strokes, significant early CT changes, older age), there is no definitive evidence to suggest that these groups do not still benefit from the treatment.23 It is also clear that if patients are not carefully selected, meeting strict inclusion and exclusion criteria, the rate of complications is increased.24 Thus, as summarized in a practice statement of the American College of Emergency Physicians, There is insufficient evidence at this time to endorse the use of intravenous tPA in clinical practice when systems are not in place to ensure that the inclusion/exclusion criteria established by the NINDS guidelines for tPA use in acute stroke are followed.21 When counseling patients and their families about the benefits and risks of IV tPA, one should keep in mind that the NINDS trial demonstrated increased odds of excellent outcomes despite a significant 10‐fold increase in the risk of symptomatic intracranial hemorrhage (6.4% vs. 0.6%), and did not alter 30‐day mortality. The largest Phase IV cohort study of IV tPA treatment, Safe Implementation of Thrombolysis in Stroke Monitoring Study (SITS‐MOST) was mandated by the European Union upon approval of the medication for use in acute ischemic stroke.20 The results in 6483 patients showed that tPA, when used in strict accordance with published inclusion and exclusion criteria, could perform as well as it did in randomized trials.
The recently published European Cooperative Acute Stroke Study3 (ECASS‐3) trial demonstrated that IV tPA has efficacy with adequate safety up to 4.5 hours after the onset of symptoms. A total of 821 patients were enrolled and 375 received tPA. Exclusion criteria included diabetes being treated with medication with a history of prior stroke, an NIHSS score >25, or treatment with warfarin. The rates of hemorrhage (27.0% vs. 17.6%, P = 0.001) were in line with those of the SITS‐MOST study patients who were treated within the 3‐hour time window. There was no significant difference in mortality (7.7% tPA vs. 8.4% placebo). This study is relatively new; therefore, the data have not been reviewed by guideline committees.25
No Blood on the CT Scan, Results Back in >3 Hours, but 8 Hours, From Symptom Onset
Unfortunately as with our patient, most people do not present to an ER in a timely fashion. Nonetheless, there may be other treatments and interventions possible. If the patient arrives 8 hours from onset of symptoms, intraarterial (IA) interventions are a possibility. In such a case, a CT angiogram (CTA) of the neck from the arch of the aorta to the circle of Willis is recommended (barring any contraindications such as renal failure or iodine allergy). The rationale behind this study is that other treatment options, such as IA tPA or mechanical thrombectomy may be considered if a large arterial occlusion is identified. CTA is preferred over magnetic resonance angiography (MRA) due to the same time and patient cooperation issues mentioned above, though some expert centers may be set up to perform MRI and MRA rapidly in the acute setting. CTA or MRA is of great value early on in the emergent assessment of ischemic stroke patients, as it allows detailed evaluation of the cerebral vasculature; this knowledge helps define the pathophysiology of the ongoing stroke (eg, is there a larger artery occlusion?) and can help inform the approach to subsequent therapies.
The Guidelines (p. 1678)4 recommend IA thrombolysis as a treatment option if it can be started within 6 hours, based on results from the Prolyse in Acute Cerebral Thromboembolism (PROACT) II trial. This study involved angiography with identification of the occluded vessel (the proximal MCA‐M1 in this study) and administration of recombinant pro‐urokinase to the clot with functional outcome as the primary endpoint.26 At 3 months, patients who received the IA thrombolytic had a 40% chance of slight disability; unable to carry out all previous activities, but able to look after own affairs without assistance or better (ie, a modified Rankin Scale score of 2) vs. 25% of those not receiving the IA thrombolytic. Pro‐urokinase is not available in the United States; therefore, many institutions substitute IA tPA. The Guidelines further state that IA thrombolysis can be considered for use in some patients with contraindications to IV tPA (eg, recent surgery), but should not be used instead of IV tPA in patients otherwise eligible (p. 1678).4
There are now two U.S. Food and Drug Administration (FDA)‐approved devices for mechanical cerebral vasculature thrombectomy for use up to 8 hours from symptom onset. The mechanical embolus removal in cerebral ischemia (MERCI) clot retrieval device was originally approved by the FDA in August 2004 for restoring blood flow in the neurovasculature by removing thrombus in patients experiencing ischemic stroke. Modified devices have been approved as recently as January 2007.27 The Penumbra System was FDA‐approved in December 2007 for revascularization of patients with acute ischemic stroke secondary to intracranial large vessel occlusive disease.28 In both cases, the FDA approval was based on demonstration of safety in case series of patients treated with the devices.2931 No randomized trials have shown the use of these devices improves outcomes for stroke patients. The Guidelines state that Although the MERCI device is a reasonable intervention for extraction of IA thrombi in carefully selected patients, the panel also recognizes that the utility of the device in improving outcomes after stroke is unclear (p. 1684);4 this statement applies similarly to the Penumbra device.
More complex imaging techniques, including multimodal CT (CT, CTA, and CT perfusion) and MR (MRI with diffusion, MRA, and MR perfusion) are being used in some stroke centers to make decisions about acute ischemic stroke treatments.32, 33 The theory is that by using these techniques, one can determine the presence or absence of a mismatch, whereby the perfusion imaging suggests more tissue at risk of infarction than is seen as already abnormal on MR diffusion‐weighted images or compared to a clinical assessment. These mismatch patients are then seen as appropriate candidates for the more aggressive interventions (ie, late IV tPA or IA interventions).34 Unfortunately, the 2 largest randomized trials to look at this issue with respect to >3‐hour IV tPA both failed to show a benefit for patients selected in this manner.35, 36 Standardized definitions of mismatch are still needed, and larger randomized trials are needed before this approach can be suggested for routine care.3739
More complex interventions, available only at tertiary or comprehensive stroke centers, include a bridging approach in which IV tPA (at 2/3 standard dose) is followed by IA tPA, IV tPA with transcranial Doppler (TCD)‐enhanced thrombolysis or IA rescue thrombectomy when vascular imaging after IV tPA shows a persistent large artery occlusion. The Guidelines suggests that these more complex combinations of interventions to restore perfusion cannot be recommended outside the setting of clinical trials (p. 1685).4
No Blood on the CT Scan, Results Back in >8 Hours From Symptom Onset (or if Contraindications to Above Interventions)
This time frame takes the more aggressive interventions off the table. Per the Guidelines, 325 mg of aspirin is the default antiplatelet agent for use, and has been shown in 2 very large randomized trials to reduce early death and longer‐term disability vs. placebo after acute ischemic stroke.40, 41 Importantly, all patients who do not qualify for thrombolysis in the 0‐hour to 8‐hour time window should receive aspirin.
Although a number of small or pilot studies suggest a benefit of the addition of clopidogrel to aspirin for a period (13 months) immediately after ischemic stroke,4244 this more aggressive antiplatelet intervention is not an endorsed standard of care. As described below, the long‐term use of this antiplatelet combination has been consistently associated with a higher risk of hemorrhagic complications. There are no published data regarding the use of aspirin plus dipyridamole in the acute stroke setting. A number of randomized trials have now been performed that have consistently failed to show a benefit of heparin, or heparin‐like medications, for the routine treatment of acute ischemic stroke. Despite this, a number of exceptions exist, based more on tradition and theory than on evidence. These exceptions, for which an IV heparin drip will at times still be considered, include acute ischemic stroke due to dissection of the carotid or vertebral arteries, cardioembolic stroke with fresh clot seen on echocardiogram (ECHO), and a clinically progressive syndrome suggestive of basilar artery occlusion (see below).45, 46 Good evidence exists to specifically recommend the use of full‐dose heparin in the setting of cerebral venous sinus thrombosis.47
Basilar Artery Occlusion Syndromes
Basilar artery occlusion syndromes warrant special mention. These may involve patients who present with quadriparesis, altered mental status, vertigo, diplopia, and other brainstem signs. Conventional treatment of basilar artery occlusion has been associated with 40% mortality with 65% of survivors having severe disability.48 If suspected, an urgent CTA can usually confirm the diagnosis, and urge the clinician to expeditiously consider aggressive intervention. Only case series have been reported regarding basilar artery thrombosis and acute treatments. Based on these studies, it is generally agreed upon that patients who appear comatose or quadriplegic for more than 3 hours will likely have a very poor functional outcome regardless of treatment, and interventional treatment is withheld. If a basilar occlusion patient presents within the 3‐hour time window for IV tPA, they are thus treated, with follow‐up vascular imaging, and possible rescue IA mechanical thrombectomy if recanalization from the IV tPA does not occur. However, if the patient still has preserved neurologic function, or is waxing and waning, there is no clear time limit for IA interventions and they may be useful a day or more after presentation. For basilar occlusion patients with severe stenoses not responsive to lysis, or continuing to be symptomatic, angioplasty and stenting has also been used.46 Despite a lack of evidence, many stroke clinicians will use an IV heparin drip for treatment of acute basilar occlusive disease.
Malignant Middle Cerebral Artery (MCA) Infarction
Malignant MCA infarction is another specific clinical syndrome worthy of special consideration. It is most generally defined as a large infarction (1/2 or 2/3) of the MCA territory, somewhat depressed level of consciousness, and high stroke scale scores (ie, severe deficits) that goes on to severe cerebral edema, mass effect, and often herniation with death.49, 50 Associated patient characteristics include younger age, abnormal (incomplete) ipsilateral collateral circulation, and internal carotid artery occlusion.51 Maximal edema occurs 2 to 5 days from stroke onset and, despite best intensive therapy, has been associated with mortality rates of 70% to 80%.49, 50 A recent pooling of 3 small randomized trials of early decompressive hemicraniectomy and durotomy showed a 50% absolute risk reduction for mortality and a 23% absolute benefit in long‐term independence (modified Rankin scale 3).49 This treatment option should be strongly considered in carefully selected patients., Transfer to an appropriately equipped facility should be offered if not available at your hospital.
Returning to our case patient, upon arrival to the ED with symptoms of partial aphasia, right hemiplegia, and left gaze preference, there was a high suspicion for a left MCA stroke. Unfortunately, he was excluded from receiving IV tPA or any other interventions, as the last time he was known to be neurologically intact was the prior evening, which is taken to be the time of onset. Antiplatelet therapy was continued, and the patient was admitted for further workup.
The initial care of the patient with a cerebrovascular event is often quite complicated. Assimilation of a great deal of data must occur and decisions around therapy must be made in a timely fashion. In prior years there was little to offer in the way of therapy, which also meant there was little initial potential for iatrogenic complication. Both diagnostic and therapeutic options are evolving rapidly. We now have much to offer these patients both emergently and in areas of secondary prevention. In part 2 of this article, the patient's inpatient course and therapy will be reviewed.
The term stroke is defined by the World Health Organization as rapidly developed clinical signs of focal (or global) disturbance of cerebral function lasting more than 24 hours (unless interrupted by surgery or death), with no apparent cause other than a vascular origin; it includes patients presenting clinical signs and symptoms suggestive of subarachnoid hemorrhage (SAH), intracerebral hemorrhage, or cerebral ischemic necrosis.1 Stroke is 1 of the leading causes of death and the number 1 cause of long‐term disability in the United States, with over 700,000 strokes and over 150,000 stroke deaths each year.2
Given the projections of 30,000 hospitalists nationally by 2010 (
Case Presentation
A 76‐year‐old right‐handed male with a history of hyperlipidemia and myocardial infarction was found at 7 AM with right‐sided paralysis and poor responsiveness on the morning of admission. He seemed to prefer looking to the left and to understand what was being said to him, but had great difficulty speaking. When he went to bed at 9 PM, he was at his neurological baseline. Upon finding him that morning, his wife called 911.
With increased knowledge regarding the pathophysiology of stroke, it has become clear that timeliness is of utmost importance (time is brain) and that acute stroke should be regarded as an acute medical/neurological emergency.
This article reviews the approach in evaluating an acute stroke patient, management strategies, and treatment options. Where not otherwise referenced, data to support our comments come from the recently updated and exhaustive American Heart Association (AHA)/American Stroke Association (ASA) Guidelines for the Early Management of Adults With Ischemic Stroke and will be referred to herein as the Guidelines.4 Harborview Medical Center in Seattle is a Joint Commissioncertified Primary Stroke Center and the home hospital of 2 of the authors (C.L.E., D.L.T.); it is referred to herein as Harborview.
Emergency Room Care (see Acute Stroke Algorithm, Figure 1)
The First 15 Minutes
After assuring stable airway, breathing, and circulation, immediate (STAT) blood draws should be performed, including full complete blood count (CBC) with platelets, international normalized ratio/prothrombin time/partial thromboplastin time (INR/PT/PTT), full electrolytes, and glucose (finger‐stick blood glucose also recommended). Glasgow Coma Scale (GCS) score and NIH Stroke Scale (NIHSS) score should be established via a focused history and physical exam. The GCS is most appropriate for patients with a significantly depressed level of consciousness, while the NIHSS can be scored for any stroke patient (1‐page version of NIHSS used at Harborview is shown in Figure 2). By quantifying stroke severity, the NIHSS score helps both to facilitate communication about neurologic deficit as well as serve as a documented baseline in case of subsequent clinical change. Emergency department (ED) physicians, hospitalists, neurologists, and nursing staff regularly caring for acute stroke patients would be well‐served by obtaining certification in the NIHSS (available free online at
Our case patient's initial NIHSS score was 15, with points given for drowsiness, inability to answer questions, partial facial palsy, no movement in right arm or leg, mild‐moderate aphasia, and mild‐moderate dysarthria (Figure 2).
Differential Diagnosis
Many acute conditions can mimic stroke, and 1 of the goals of the initial emergency room (ER) evaluation is to rule out such stroke mimics. A report of 411 initial ER stroke diagnoses identified 19% as stroke mimics; the most common mimic diagnoses were seizure, systemic infection, brain tumor, and toxic‐metabolic.5 The same study identified decreased level of alertness as associated with a final mimic diagnosis and history of angina as associated with a final diagnosis of stroke. Another study looked at 350 presentations with an initial stroke diagnosis and found 31% stroke mimics; similarly, the main alternative diagnoses were seizure, sepsis, toxic‐metabolic, space‐occupying lesion, and syncope/presyncope.6 Findings associated with a mimic diagnosis included no cognitive impairment and abnormal findings in any other system, while findings associated with a stroke diagnosis were a definite history of focal neurological symptoms, NIHSS score, stroke type classification possible, an exact onset that could be determined, and abnormal vascular findings on imaging.6
Initial Imaging
The patient should receive a STAT noncontrast head CT to evaluate for the presence or absence of blood. At this time, magnetic resonance imaging (MRI) is not essential to confirm the diagnosis of ischemic stroke, as diagnosis is based on clinical suspicion. MRI is more sensitive at imaging acute ischemia (on diffusion‐weighted sequences) and recently has been shown to be equally sensitive in identifying acute blood (previously thought to be a relative advantage of CT).7, 8 Practical and pervasive barriers to emergent MRI include study duration, significant patient cooperation, and that few hospitals are currently set up to perform such rapid MRIS. The Guidelines specifically state that In most instances, CT will provide the information to make decisions about emergency management (p. 1668),4 that vascular imaging should not delay treatment of patients whose symptoms started 3 hours ago and who have acute ischemic stroke, and that emergency treatment of stroke should not be delayed in order to obtain multimodal imaging studies (p. 1669).4
Our case patient's initial imaging, a noncontrast head CT (Supporting Figures 1 and 2), showed subtle clues consistent with the diagnosis of acute ischemic stroke. These include a hyperdense middle cerebral artery (MCA) sign (presumably representing thrombus), possible obscuration of the basal ganglia, and, importantly, no acute intraparenchymal (IPH), SAH, or subdural hemorrhage.
Acute Treatments
After the patient's head CT is completed, the next steps are dependent upon what was seen on the scan and the time from symptom onset.
Blood on the CT Scan
If the initial brain imaging reveals IPH or SAH, further diagnostic testing and early treatments are quite different than for ischemic stroke. New guidelines are available for IPH management,9 and there have been recent review articles of care for SAH.1012 At the authors' institutions, early care of such patients always involves aggressive reversal of any antithrombotic medications the patient was taking prior to presentation. Our approach to warfarin reversal includes vitamin K and fresh frozen plasma (FFP) to achieve an INR 1.4; others have used prothrombin complex concentrate (PCC).13 Blood pressure (BP) treatment goals are generally more aggressive than for ischemic stroke, while supportive care to avoid aspiration, hyperglycemia, fever, and venous thrombosis (here initially with sequential compression devices alone) are similar. Early estimation of prognosis for these patients with IPH and SAH and discussions with families about continued aggressive care are of utmost importance, and should involve providers with sufficient expertise. Care should be taken to avoid overly pessimistic early prognostication, as early do not resuscitate (DNR) decisions in intercranial hemorrhage (ICH) can become a self‐fulfilling prophecy.1416 If the decision is to continue aggressive and supportive care, or if an appropriately expert consultation is not available at the presentation hospital, IPH and SAH patients should be considered for transfer to a hospital with the appropriate resources (including emergency access to neurosurgeons) or be evaluated by such an expert by telemedicine if available.
No Blood on the CT Scan, Results Back in 3 Hours From Symptom Onset
If such a patient is not rapidly resolving their symptoms, and the diagnosis continues to remain clear, inclusion/exclusion criteria for IV tPA should be reviewed (Table 1). Consent should be obtained much like any other procedure with significant risk. As many consider tPA to be standard of care, it is reasonable to proceed in cases of unobtainable consent as one would with any other emergent therapy. This situation is a topic of ongoing debate.17, 18 The Guidelines state that although written consent is not necessary before administration of recombinant tPA (rtPA) for treatment of stroke, a full discussion of the potential risks and benefits of treatment with rtPA with the family and the patient if possible is recommended (p. 1676).4 After tPA is given in the ER, the patient should be admitted to an intensive care unit (ICU) setting for 24 hours for careful monitoring of BP, avoidance of invasive procedures, and no use of antithrombotic medications during that period of time.
| Comments (from the authors) | |
|---|---|
| |
| Inclusion criteria | |
| Diagnosis of ischemic stroke causing measurable neurological deficit | Usually NIHSS > 4 |
| Neurological signs should not be clearing spontaneously | Such a patient may do well without tPA, but there is debate82 |
| Neurological signs should not be minor and isolated. | |
| Onset of symptoms >3 hours before beginning treatment | |
| Patient or family members understand the potential risks and benefits from treatment | Debated, as tPA considered standard of care by many |
| Cautionary criteria | |
| Caution should be exercised in treating a patient with major deficits | Higher risk of hemorrhage, but still may benefit from treatment |
| Exclusion criteria | |
| Symptoms of stroke should not be suggestive of subarachnoid hemorrhage | |
| No head trauma or prior stroke in previous 3 months | |
| No myocardial infarction in the previous 3 months | |
| No gastrointestinal or urinary tract hemorrhage in previous 21 days | |
| No major surgery in the previous 14 days | |
| No arterial puncture at a noncompressible site in the previous 7 days | |
| No history of previous intracranial hemorrhage | |
| Blood pressure not elevated (systolic >185 mm Hg or diastolic 110 mm Hg) | Okay to bring down with labetolol, nitropaste, or nicardipine* |
| No evidence of active bleeding or acute trauma (fracture) on examination | |
| Not taking an oral anticoagulant or, if anticoagulant being taken, INR 1.7 | |
| If receiving heparin in previous 48 hours, aPTT must be in normal range | |
| Platelet count 100,000 mm3 | |
| Blood glucose concentration 50 mg/dL (2.7 mmol/L) | |
| Seizure with postictal residual neurological impairments | Not absolute if treating physician feels stroke also present, or if confirmed by imaging |
| CT does not show a multilobar infarction (hypodensity >1/3 cerebral hemisphere) | Not strictly evidence based, in NINDS trial this finding did not preclude benefit of tPA |
Based mainly on the results of the National Institute of Neurological Disorders and Stroke (NINDS) tPA trial,19 and recently supported by a large Phase IV observational study from the European Union,20 IV tPA for acute ischemic stroke is approved for use in many countries and is endorsed for the treatment of carefully selected ischemic stroke patients in a number of practice guidelines.4 Despite this, the emergency medicine community has been less enthusiastic about the use of IV tPA.21, 22 Although the risk of hemorrhagic complications is greater in certain subgroups of patients (ie, the most severe strokes, significant early CT changes, older age), there is no definitive evidence to suggest that these groups do not still benefit from the treatment.23 It is also clear that if patients are not carefully selected, meeting strict inclusion and exclusion criteria, the rate of complications is increased.24 Thus, as summarized in a practice statement of the American College of Emergency Physicians, There is insufficient evidence at this time to endorse the use of intravenous tPA in clinical practice when systems are not in place to ensure that the inclusion/exclusion criteria established by the NINDS guidelines for tPA use in acute stroke are followed.21 When counseling patients and their families about the benefits and risks of IV tPA, one should keep in mind that the NINDS trial demonstrated increased odds of excellent outcomes despite a significant 10‐fold increase in the risk of symptomatic intracranial hemorrhage (6.4% vs. 0.6%), and did not alter 30‐day mortality. The largest Phase IV cohort study of IV tPA treatment, Safe Implementation of Thrombolysis in Stroke Monitoring Study (SITS‐MOST) was mandated by the European Union upon approval of the medication for use in acute ischemic stroke.20 The results in 6483 patients showed that tPA, when used in strict accordance with published inclusion and exclusion criteria, could perform as well as it did in randomized trials.
The recently published European Cooperative Acute Stroke Study3 (ECASS‐3) trial demonstrated that IV tPA has efficacy with adequate safety up to 4.5 hours after the onset of symptoms. A total of 821 patients were enrolled and 375 received tPA. Exclusion criteria included diabetes being treated with medication with a history of prior stroke, an NIHSS score >25, or treatment with warfarin. The rates of hemorrhage (27.0% vs. 17.6%, P = 0.001) were in line with those of the SITS‐MOST study patients who were treated within the 3‐hour time window. There was no significant difference in mortality (7.7% tPA vs. 8.4% placebo). This study is relatively new; therefore, the data have not been reviewed by guideline committees.25
No Blood on the CT Scan, Results Back in >3 Hours, but 8 Hours, From Symptom Onset
Unfortunately as with our patient, most people do not present to an ER in a timely fashion. Nonetheless, there may be other treatments and interventions possible. If the patient arrives 8 hours from onset of symptoms, intraarterial (IA) interventions are a possibility. In such a case, a CT angiogram (CTA) of the neck from the arch of the aorta to the circle of Willis is recommended (barring any contraindications such as renal failure or iodine allergy). The rationale behind this study is that other treatment options, such as IA tPA or mechanical thrombectomy may be considered if a large arterial occlusion is identified. CTA is preferred over magnetic resonance angiography (MRA) due to the same time and patient cooperation issues mentioned above, though some expert centers may be set up to perform MRI and MRA rapidly in the acute setting. CTA or MRA is of great value early on in the emergent assessment of ischemic stroke patients, as it allows detailed evaluation of the cerebral vasculature; this knowledge helps define the pathophysiology of the ongoing stroke (eg, is there a larger artery occlusion?) and can help inform the approach to subsequent therapies.
The Guidelines (p. 1678)4 recommend IA thrombolysis as a treatment option if it can be started within 6 hours, based on results from the Prolyse in Acute Cerebral Thromboembolism (PROACT) II trial. This study involved angiography with identification of the occluded vessel (the proximal MCA‐M1 in this study) and administration of recombinant pro‐urokinase to the clot with functional outcome as the primary endpoint.26 At 3 months, patients who received the IA thrombolytic had a 40% chance of slight disability; unable to carry out all previous activities, but able to look after own affairs without assistance or better (ie, a modified Rankin Scale score of 2) vs. 25% of those not receiving the IA thrombolytic. Pro‐urokinase is not available in the United States; therefore, many institutions substitute IA tPA. The Guidelines further state that IA thrombolysis can be considered for use in some patients with contraindications to IV tPA (eg, recent surgery), but should not be used instead of IV tPA in patients otherwise eligible (p. 1678).4
There are now two U.S. Food and Drug Administration (FDA)‐approved devices for mechanical cerebral vasculature thrombectomy for use up to 8 hours from symptom onset. The mechanical embolus removal in cerebral ischemia (MERCI) clot retrieval device was originally approved by the FDA in August 2004 for restoring blood flow in the neurovasculature by removing thrombus in patients experiencing ischemic stroke. Modified devices have been approved as recently as January 2007.27 The Penumbra System was FDA‐approved in December 2007 for revascularization of patients with acute ischemic stroke secondary to intracranial large vessel occlusive disease.28 In both cases, the FDA approval was based on demonstration of safety in case series of patients treated with the devices.2931 No randomized trials have shown the use of these devices improves outcomes for stroke patients. The Guidelines state that Although the MERCI device is a reasonable intervention for extraction of IA thrombi in carefully selected patients, the panel also recognizes that the utility of the device in improving outcomes after stroke is unclear (p. 1684);4 this statement applies similarly to the Penumbra device.
More complex imaging techniques, including multimodal CT (CT, CTA, and CT perfusion) and MR (MRI with diffusion, MRA, and MR perfusion) are being used in some stroke centers to make decisions about acute ischemic stroke treatments.32, 33 The theory is that by using these techniques, one can determine the presence or absence of a mismatch, whereby the perfusion imaging suggests more tissue at risk of infarction than is seen as already abnormal on MR diffusion‐weighted images or compared to a clinical assessment. These mismatch patients are then seen as appropriate candidates for the more aggressive interventions (ie, late IV tPA or IA interventions).34 Unfortunately, the 2 largest randomized trials to look at this issue with respect to >3‐hour IV tPA both failed to show a benefit for patients selected in this manner.35, 36 Standardized definitions of mismatch are still needed, and larger randomized trials are needed before this approach can be suggested for routine care.3739
More complex interventions, available only at tertiary or comprehensive stroke centers, include a bridging approach in which IV tPA (at 2/3 standard dose) is followed by IA tPA, IV tPA with transcranial Doppler (TCD)‐enhanced thrombolysis or IA rescue thrombectomy when vascular imaging after IV tPA shows a persistent large artery occlusion. The Guidelines suggests that these more complex combinations of interventions to restore perfusion cannot be recommended outside the setting of clinical trials (p. 1685).4
No Blood on the CT Scan, Results Back in >8 Hours From Symptom Onset (or if Contraindications to Above Interventions)
This time frame takes the more aggressive interventions off the table. Per the Guidelines, 325 mg of aspirin is the default antiplatelet agent for use, and has been shown in 2 very large randomized trials to reduce early death and longer‐term disability vs. placebo after acute ischemic stroke.40, 41 Importantly, all patients who do not qualify for thrombolysis in the 0‐hour to 8‐hour time window should receive aspirin.
Although a number of small or pilot studies suggest a benefit of the addition of clopidogrel to aspirin for a period (13 months) immediately after ischemic stroke,4244 this more aggressive antiplatelet intervention is not an endorsed standard of care. As described below, the long‐term use of this antiplatelet combination has been consistently associated with a higher risk of hemorrhagic complications. There are no published data regarding the use of aspirin plus dipyridamole in the acute stroke setting. A number of randomized trials have now been performed that have consistently failed to show a benefit of heparin, or heparin‐like medications, for the routine treatment of acute ischemic stroke. Despite this, a number of exceptions exist, based more on tradition and theory than on evidence. These exceptions, for which an IV heparin drip will at times still be considered, include acute ischemic stroke due to dissection of the carotid or vertebral arteries, cardioembolic stroke with fresh clot seen on echocardiogram (ECHO), and a clinically progressive syndrome suggestive of basilar artery occlusion (see below).45, 46 Good evidence exists to specifically recommend the use of full‐dose heparin in the setting of cerebral venous sinus thrombosis.47
Basilar Artery Occlusion Syndromes
Basilar artery occlusion syndromes warrant special mention. These may involve patients who present with quadriparesis, altered mental status, vertigo, diplopia, and other brainstem signs. Conventional treatment of basilar artery occlusion has been associated with 40% mortality with 65% of survivors having severe disability.48 If suspected, an urgent CTA can usually confirm the diagnosis, and urge the clinician to expeditiously consider aggressive intervention. Only case series have been reported regarding basilar artery thrombosis and acute treatments. Based on these studies, it is generally agreed upon that patients who appear comatose or quadriplegic for more than 3 hours will likely have a very poor functional outcome regardless of treatment, and interventional treatment is withheld. If a basilar occlusion patient presents within the 3‐hour time window for IV tPA, they are thus treated, with follow‐up vascular imaging, and possible rescue IA mechanical thrombectomy if recanalization from the IV tPA does not occur. However, if the patient still has preserved neurologic function, or is waxing and waning, there is no clear time limit for IA interventions and they may be useful a day or more after presentation. For basilar occlusion patients with severe stenoses not responsive to lysis, or continuing to be symptomatic, angioplasty and stenting has also been used.46 Despite a lack of evidence, many stroke clinicians will use an IV heparin drip for treatment of acute basilar occlusive disease.
Malignant Middle Cerebral Artery (MCA) Infarction
Malignant MCA infarction is another specific clinical syndrome worthy of special consideration. It is most generally defined as a large infarction (1/2 or 2/3) of the MCA territory, somewhat depressed level of consciousness, and high stroke scale scores (ie, severe deficits) that goes on to severe cerebral edema, mass effect, and often herniation with death.49, 50 Associated patient characteristics include younger age, abnormal (incomplete) ipsilateral collateral circulation, and internal carotid artery occlusion.51 Maximal edema occurs 2 to 5 days from stroke onset and, despite best intensive therapy, has been associated with mortality rates of 70% to 80%.49, 50 A recent pooling of 3 small randomized trials of early decompressive hemicraniectomy and durotomy showed a 50% absolute risk reduction for mortality and a 23% absolute benefit in long‐term independence (modified Rankin scale 3).49 This treatment option should be strongly considered in carefully selected patients., Transfer to an appropriately equipped facility should be offered if not available at your hospital.
Returning to our case patient, upon arrival to the ED with symptoms of partial aphasia, right hemiplegia, and left gaze preference, there was a high suspicion for a left MCA stroke. Unfortunately, he was excluded from receiving IV tPA or any other interventions, as the last time he was known to be neurologically intact was the prior evening, which is taken to be the time of onset. Antiplatelet therapy was continued, and the patient was admitted for further workup.
The initial care of the patient with a cerebrovascular event is often quite complicated. Assimilation of a great deal of data must occur and decisions around therapy must be made in a timely fashion. In prior years there was little to offer in the way of therapy, which also meant there was little initial potential for iatrogenic complication. Both diagnostic and therapeutic options are evolving rapidly. We now have much to offer these patients both emergently and in areas of secondary prevention. In part 2 of this article, the patient's inpatient course and therapy will be reviewed.
- Organization WH. MONICA Manual, Part IV: Event Registration. Available at: http://www.ktl.fi/publications/monica/manual/part4/iv‐2.htm#s2. Accessed May2009.
- ,,, et al.Heart disease and stroke statistics 2008 update. A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee.Circulation.200829;117(4):e25–e146.
- .Neurology in the next two decades: report of the Workforce Task Force of the American Academy of Neurology.Neurology.2000;54(4):787–789.
- ,,, et al.Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists.Stroke.2007;38(5):1655–1711.
- ,,,.Conditions that mimic stroke in the emergency department. Implications for acute stroke trials.Arch Neurol.1995;52(11):1119–1122.
- ,,,,.Distinguishing between stroke and mimic at the bedside: the brain attack study.Stroke.2006;37(3):769–775.
- ,,, et al.Stroke magnetic resonance imaging is accurate in hyperacute intracerebral hemorrhage: a multicenter study on the validity of stroke imaging.Stroke.2004;35(2):502–506.
- ,,, et al.Comparison of MRI and CT for detection of acute intracerebral hemorrhage.JAMA.2004;292(15):1823–1830.
- ,,, et al.Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group.Stroke.2007;38(6):2001–2023.
- ,,.Aneurysmal subarachnoid hemorrhage.N Engl J Med.2006;354(4):387–396.
- ,,,.Subarachnoid haemorrhage.BMJ.2006;333(7561):235–240.
- ,,.Subarachnoid haemorrhage.Lancet.2007;369(9558):306–318.
- ,,.Intracerebral hemorrhage associated with oral anticoagulant therapy: current practices and unresolved questions.Stroke.2006;37(1):256–262.
- ,,, et al.Withdrawal of support in intracerebral hemorrhage may lead to self‐fulfilling prophecies.Neurology.2001;56(6):766–772.
- ,,,.Hospital usage of early do‐not‐resuscitate orders and outcome after intracerebral hemorrhage.Stroke.2004;35(5):1130–1134.
- ,,, et al.Early care limitations independently predict mortality after intracerebral hemorrhage.Neurology.2007;68(20):1651–1657.
- ,,,.Consent for intravenous thrombolysis in acute stroke: review and future directions.Arch Neurol.2007;64(6):785–792.
- .Thrombolysis (tissue plasminogen activator) in stroke: a medicolegal quagmire.Stroke.2006;37(7):1917–1922.
- Tissue plasminogen activator for acute ischemic stroke.The National Institute of Neurological Disorders and Stroke rt‐PA Stroke Study Group.N Engl J Med.1995;333(24):1581–1587.
- ,,, et al.Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke‐Monitoring Study (SITS‐MOST): an observational study.Lancet.2007;369(9558):275–282.
- American College of Emergency Physicians (ACEP). Use of Intravenous tPA for the Management of Acute Stroke in the Emergency Department. ACEP Policy Statement. February 2002. Available at: http://www.acep.org/practres.aspx?id=29834. Accessed May2009.
- American Academy of Emergency Medicine (AAEM). Position statement on the use of intravenous thrombolytic therapy in the treatment of stroke. January 2002. Available at: http://aaem.org/positionstatements/thrombolytictherapy.php. Accessed May2009.
- ,,, et al.Lack of clinical significance of early ischemic changes on computed tomography in acute stroke.JAMA.2001;286(22):2830–2838.
- ,,,,.Thrombolysis for acute stroke in routine clinical practice.Arch Intern Med.2002;162(17):1994–2001.
- ,,, et al.Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke.N Engl J Med.2008;359:1317–1329,1393–1395.
- ,,, et al.Intra‐arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism.JAMA.1999;282(21):2003–2011.
- Modified MERCI Retriever FDA marketing approval letter. Available at: www.fda.gov/cdrh/pdf6/K062046.pdf. Accessed May2009.
- Penumbra System FDA marketing approval letter. Available at: www.fda.gov/cdrh/pdf7/K072718.pdf. Accessed May2009.
- .Safety of mechanical thrombectomy and intravenous tissue plasminogen activator in acute ischemic stroke. Results of the multi mechanical embolus removal in cerebral ischemia (MERCI) trial, part I.AJNR Am J Neuroradiol.2006;27(6):1177–1182.
- ,,, et al.Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial.Stroke.2005;36(7):1432–1438.
- ,,, et al.The Penumbra System: a mechanical device for the treatment of acute stroke due to thromboembolism.AJNR Am J Neuroradiol.2008;29(7):1409–1413.
- ,,, et al.Comparison of CT perfusion and angiography and MRI in selecting stroke patients for acute treatment.Neurology.2007;68(9):694–697.
- ,,, et al.Combined intravenous and intraarterial revascularization therapy using MRI perfusion/diffusion mismatch selection for acute ischemic stroke at 3–6 h after symptom onset.Neurocrit Care.2008;8(3):353–359.
- ,,, et al.Refining the perfusion‐diffusion mismatch hypothesis.Stroke.2005;36(6):1153–1159.
- . DIAS‐2: no benefit of desmoteplase in acute ischemic stroke. Available at: www.medscape.com/viewarticle/557663. Accessed May2009.
- ,,, et al.Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo‐controlled randomised trial.Lancet Neurol.2008;7(4):299–309.
- ,,.Magnetic resonance perfusion diffusion mismatch and thrombolysis in acute ischaemic stroke: a systematic review of the evidence to date.J Neurol Neurosurg Psychiatry.2007;78(5):485–491.
- ,,, et al.Optimal definition for PWI/DWI mismatch in acute ischemic stroke patients.J Cereb Blood Flow Metab.2008;28(5):887–891.
- ,,, et al.Rapid assessment of perfusion‐diffusion mismatch.Stroke.2008;39(1):75–81.
- CAST: randomised placebo‐controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke.CAST (Chinese Acute Stroke Trial) Collaborative Group.Lancet.1997;349(9066):1641–1649.
- The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke.International Stroke Trial Collaborative Group.Lancet.1997;349(9065):1569–1581.
- ,,, et al.Dual antiplatelet therapy with clopidogrel and aspirin in symptomatic carotid stenosis evaluated using doppler embolic signal detection: the clopidogrel and aspirin for reduction of emboli in symptomatic carotid stenosis (CARESS) trial.Circulation.2005;111(17):2233–2240.
- ,,, et al.Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population‐based sequential comparison.Lancet.2007;370(9596):1432–1442.
- ,,,,,.Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): a randomised controlled pilot trial.Lancet Neurol.2007;6(11):961–969.
- ,,, et al.Antiplatelets versus anticoagulation in cervical artery dissection.Stroke.2007;38(9):2605–2611.
- ,,.Basilar artery occlusion.Neurocrit Care.2004;1(3):319–329.
- ,.Cerebral venous thrombosis: an update.Lancet Neurol.2007;6(2):162–170.
- ,,,,.Outcome in patients with basilar artery occlusion treated conventionally.J Neurol Neurosurg Psychiatry.2005;76(9):1238–1241.
- ,,, et al.Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomised controlled trials.Lancet Neurol.2007;6(3):215–222.
- ,,,,,.‘Malignant’ middle cerebral artery territory infarction: clinical course and prognostic signs.Arch Neurol.1996;53(4):309–315.
- ,,,,.Predictors for malignant middle cerebral artery infarctions: a postmortem analysis.Neurology. 282006;66(6):815–820.
- ,,,,,.Poor outcomes in patients who do not receive intravenous tissue plasminogen activator because of mild or improving ischemic stroke.Stroke.2005;36(11):2497–2499.
- Organization WH. MONICA Manual, Part IV: Event Registration. Available at: http://www.ktl.fi/publications/monica/manual/part4/iv‐2.htm#s2. Accessed May2009.
- ,,, et al.Heart disease and stroke statistics 2008 update. A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee.Circulation.200829;117(4):e25–e146.
- .Neurology in the next two decades: report of the Workforce Task Force of the American Academy of Neurology.Neurology.2000;54(4):787–789.
- ,,, et al.Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists.Stroke.2007;38(5):1655–1711.
- ,,,.Conditions that mimic stroke in the emergency department. Implications for acute stroke trials.Arch Neurol.1995;52(11):1119–1122.
- ,,,,.Distinguishing between stroke and mimic at the bedside: the brain attack study.Stroke.2006;37(3):769–775.
- ,,, et al.Stroke magnetic resonance imaging is accurate in hyperacute intracerebral hemorrhage: a multicenter study on the validity of stroke imaging.Stroke.2004;35(2):502–506.
- ,,, et al.Comparison of MRI and CT for detection of acute intracerebral hemorrhage.JAMA.2004;292(15):1823–1830.
- ,,, et al.Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group.Stroke.2007;38(6):2001–2023.
- ,,.Aneurysmal subarachnoid hemorrhage.N Engl J Med.2006;354(4):387–396.
- ,,,.Subarachnoid haemorrhage.BMJ.2006;333(7561):235–240.
- ,,.Subarachnoid haemorrhage.Lancet.2007;369(9558):306–318.
- ,,.Intracerebral hemorrhage associated with oral anticoagulant therapy: current practices and unresolved questions.Stroke.2006;37(1):256–262.
- ,,, et al.Withdrawal of support in intracerebral hemorrhage may lead to self‐fulfilling prophecies.Neurology.2001;56(6):766–772.
- ,,,.Hospital usage of early do‐not‐resuscitate orders and outcome after intracerebral hemorrhage.Stroke.2004;35(5):1130–1134.
- ,,, et al.Early care limitations independently predict mortality after intracerebral hemorrhage.Neurology.2007;68(20):1651–1657.
- ,,,.Consent for intravenous thrombolysis in acute stroke: review and future directions.Arch Neurol.2007;64(6):785–792.
- .Thrombolysis (tissue plasminogen activator) in stroke: a medicolegal quagmire.Stroke.2006;37(7):1917–1922.
- Tissue plasminogen activator for acute ischemic stroke.The National Institute of Neurological Disorders and Stroke rt‐PA Stroke Study Group.N Engl J Med.1995;333(24):1581–1587.
- ,,, et al.Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke‐Monitoring Study (SITS‐MOST): an observational study.Lancet.2007;369(9558):275–282.
- American College of Emergency Physicians (ACEP). Use of Intravenous tPA for the Management of Acute Stroke in the Emergency Department. ACEP Policy Statement. February 2002. Available at: http://www.acep.org/practres.aspx?id=29834. Accessed May2009.
- American Academy of Emergency Medicine (AAEM). Position statement on the use of intravenous thrombolytic therapy in the treatment of stroke. January 2002. Available at: http://aaem.org/positionstatements/thrombolytictherapy.php. Accessed May2009.
- ,,, et al.Lack of clinical significance of early ischemic changes on computed tomography in acute stroke.JAMA.2001;286(22):2830–2838.
- ,,,,.Thrombolysis for acute stroke in routine clinical practice.Arch Intern Med.2002;162(17):1994–2001.
- ,,, et al.Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke.N Engl J Med.2008;359:1317–1329,1393–1395.
- ,,, et al.Intra‐arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism.JAMA.1999;282(21):2003–2011.
- Modified MERCI Retriever FDA marketing approval letter. Available at: www.fda.gov/cdrh/pdf6/K062046.pdf. Accessed May2009.
- Penumbra System FDA marketing approval letter. Available at: www.fda.gov/cdrh/pdf7/K072718.pdf. Accessed May2009.
- .Safety of mechanical thrombectomy and intravenous tissue plasminogen activator in acute ischemic stroke. Results of the multi mechanical embolus removal in cerebral ischemia (MERCI) trial, part I.AJNR Am J Neuroradiol.2006;27(6):1177–1182.
- ,,, et al.Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial.Stroke.2005;36(7):1432–1438.
- ,,, et al.The Penumbra System: a mechanical device for the treatment of acute stroke due to thromboembolism.AJNR Am J Neuroradiol.2008;29(7):1409–1413.
- ,,, et al.Comparison of CT perfusion and angiography and MRI in selecting stroke patients for acute treatment.Neurology.2007;68(9):694–697.
- ,,, et al.Combined intravenous and intraarterial revascularization therapy using MRI perfusion/diffusion mismatch selection for acute ischemic stroke at 3–6 h after symptom onset.Neurocrit Care.2008;8(3):353–359.
- ,,, et al.Refining the perfusion‐diffusion mismatch hypothesis.Stroke.2005;36(6):1153–1159.
- . DIAS‐2: no benefit of desmoteplase in acute ischemic stroke. Available at: www.medscape.com/viewarticle/557663. Accessed May2009.
- ,,, et al.Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo‐controlled randomised trial.Lancet Neurol.2008;7(4):299–309.
- ,,.Magnetic resonance perfusion diffusion mismatch and thrombolysis in acute ischaemic stroke: a systematic review of the evidence to date.J Neurol Neurosurg Psychiatry.2007;78(5):485–491.
- ,,, et al.Optimal definition for PWI/DWI mismatch in acute ischemic stroke patients.J Cereb Blood Flow Metab.2008;28(5):887–891.
- ,,, et al.Rapid assessment of perfusion‐diffusion mismatch.Stroke.2008;39(1):75–81.
- CAST: randomised placebo‐controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke.CAST (Chinese Acute Stroke Trial) Collaborative Group.Lancet.1997;349(9066):1641–1649.
- The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke.International Stroke Trial Collaborative Group.Lancet.1997;349(9065):1569–1581.
- ,,, et al.Dual antiplatelet therapy with clopidogrel and aspirin in symptomatic carotid stenosis evaluated using doppler embolic signal detection: the clopidogrel and aspirin for reduction of emboli in symptomatic carotid stenosis (CARESS) trial.Circulation.2005;111(17):2233–2240.
- ,,, et al.Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population‐based sequential comparison.Lancet.2007;370(9596):1432–1442.
- ,,,,,.Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): a randomised controlled pilot trial.Lancet Neurol.2007;6(11):961–969.
- ,,, et al.Antiplatelets versus anticoagulation in cervical artery dissection.Stroke.2007;38(9):2605–2611.
- ,,.Basilar artery occlusion.Neurocrit Care.2004;1(3):319–329.
- ,.Cerebral venous thrombosis: an update.Lancet Neurol.2007;6(2):162–170.
- ,,,,.Outcome in patients with basilar artery occlusion treated conventionally.J Neurol Neurosurg Psychiatry.2005;76(9):1238–1241.
- ,,, et al.Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomised controlled trials.Lancet Neurol.2007;6(3):215–222.
- ,,,,,.‘Malignant’ middle cerebral artery territory infarction: clinical course and prognostic signs.Arch Neurol.1996;53(4):309–315.
- ,,,,.Predictors for malignant middle cerebral artery infarctions: a postmortem analysis.Neurology. 282006;66(6):815–820.
- ,,,,,.Poor outcomes in patients who do not receive intravenous tissue plasminogen activator because of mild or improving ischemic stroke.Stroke.2005;36(11):2497–2499.
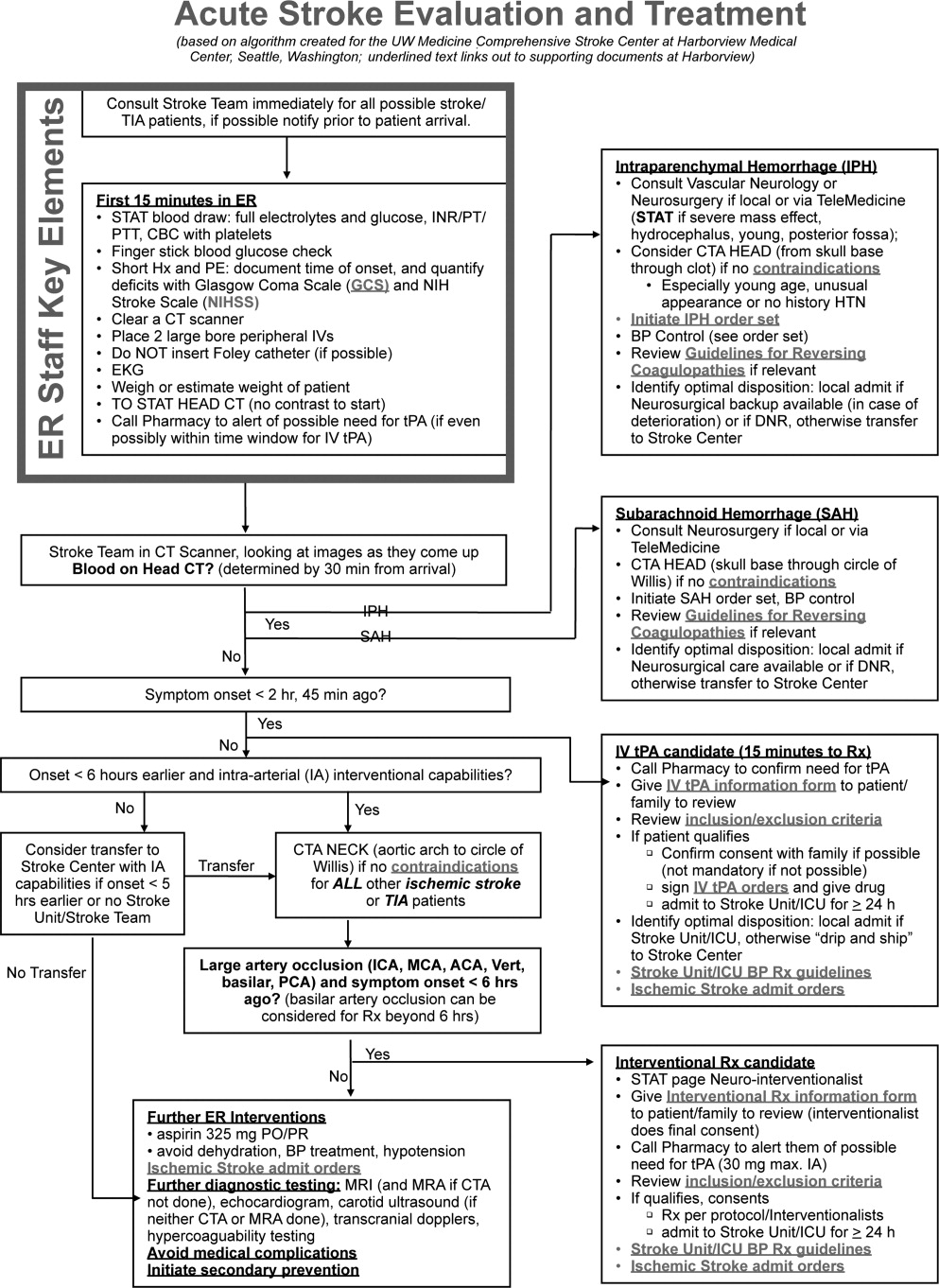
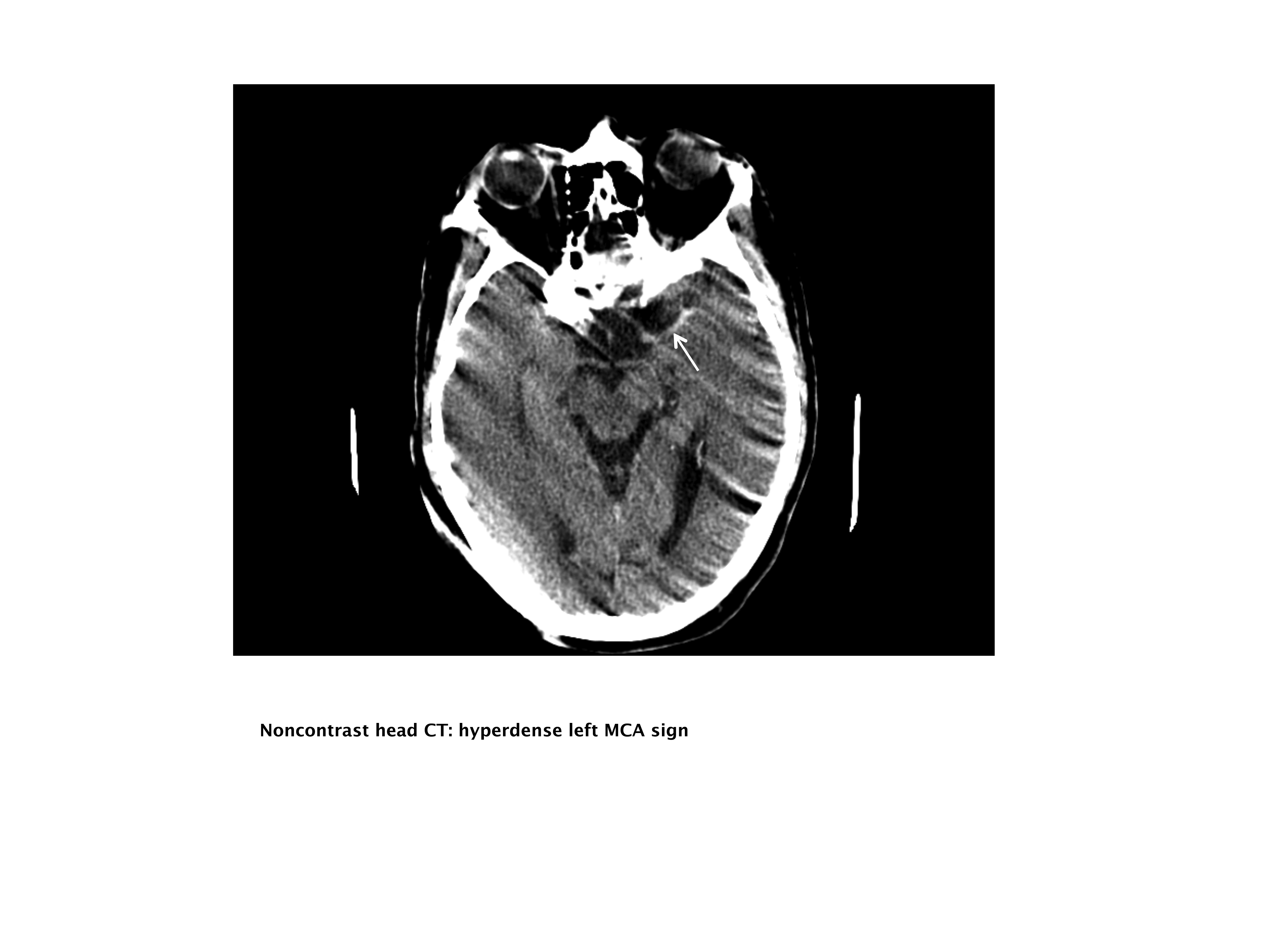
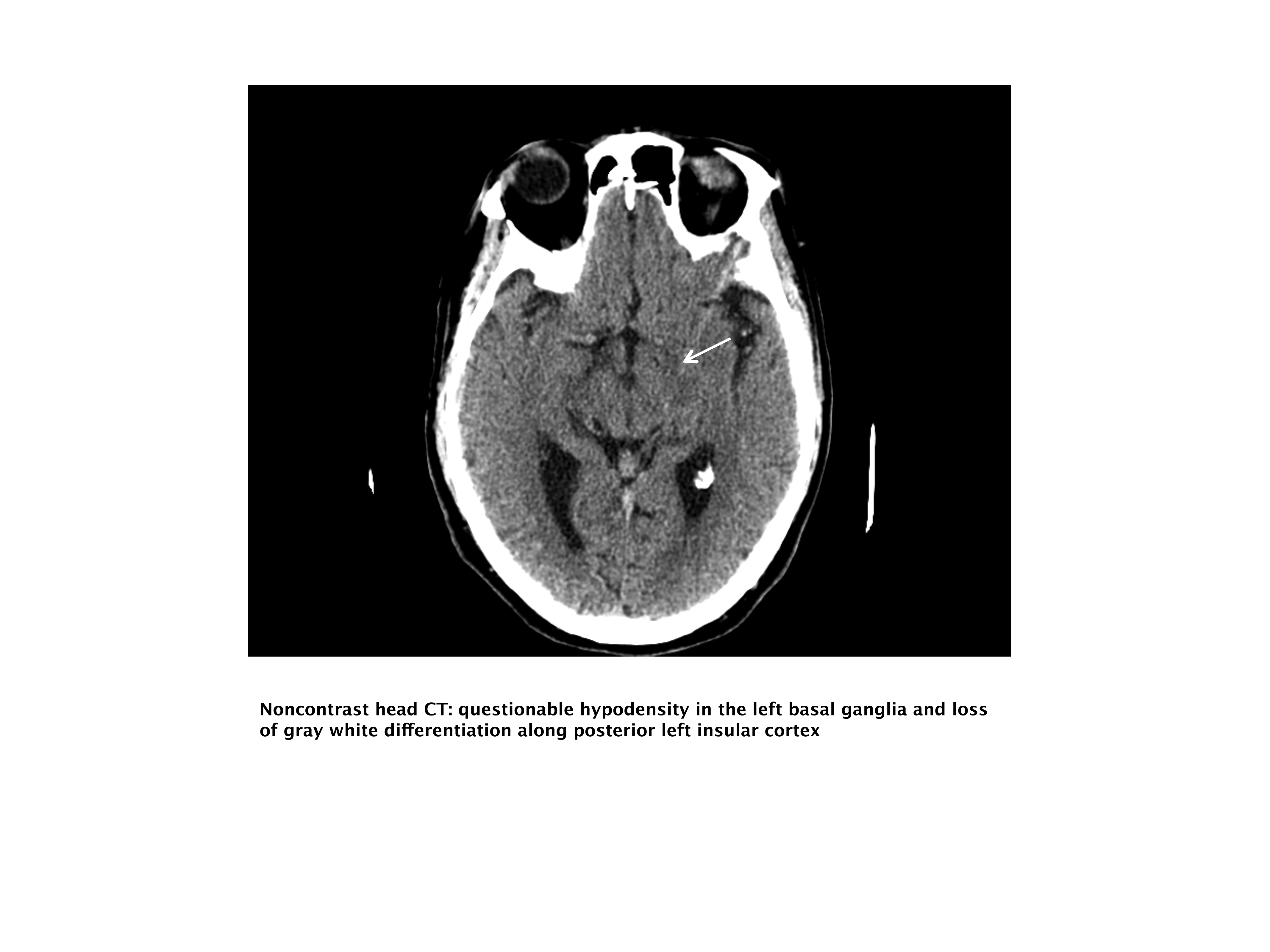
The Hospitalist and NSF
What Is Nephrogenic Systemic Fibrosis?
Nephrogenic systemic fibrosis (NSF) is a systemic fibrosing disease that occurs after exposure to gadolinium‐based contrast (GBC) in the presence of severe renal failure of acute or chronic nature.1, 27 As suggested by its former name, nephrogenic fibrosing dermopathy, the cardinal feature of this disorder is skin involvement. Symptoms begin anywhere from 2 to 75 days after exposure to GBC, though usually within 2 months.27 Initial signs and symptoms may include sharp and sometimes excruciating pain, tightening and burning of the skin associated with redness and swelling, symmetrical involvement, distribution with predilection for the extremities more than the trunk, and sparing of the face. The dependent lower extremities are more severely involved than the upper extremities. Dermal induration may occur in the form of plaques, nodules, and papules resulting in a woody texture on palpation. These findings usually progress over weeks to months with extensive dermal fibrosis involving entire limbs. Ultimately the patient may develop severe joint contractures and marked limitations in mobility.8 A fulminant presentation is seen in approximately 5% of patients who develop a rapidly progressive course over as short a time period as 2 weeks.
Systemic organ involvement including fibrosis of the heart, lung, diaphragm, skeletal muscles, and other organs has been described and has been associated with fatal outcomes.79
Though more frequent in those with end‐stage renal disease (ESRD), NSF has been seen in those with stage 4 and 5 chronic kidney disease (CKD) and acute kidney injury (AKI). Incidence rates have been difficult to calculate due to lack of exposure data in most studies, though 1 small case‐control study found 4.3 cases per 1000 patient years among hemodialysis patients with an absolute risk of 3.4% in the exposed patient.4 Interestingly, incident NSF rates published in a Centers for Disease Control case‐control study of 19 NSF sufferers were much higher for peritoneal dialysis (4.6 cases/100 patients) than for hemodialysis (0.61/100 patients).2 This is likely related to the different GBC clearance achieved with these modalities.
NSF has no predilection for gender, race, nationality or age group. Those with liver disease and lower body weight or lower muscle mass appear to be at greater risk, which may be related to overestimation of glomerular filtration rate (GFR) with falsely low creatinines seen in such patients. Risk is likely increased as well by multiple exposures to GBC in close proximity. Related host cofactors have not been identified, though elevated serum calcium and phosphate concentrations, exposure to high dose erythropoietin, and iron overload have been considered.10, 11
The diagnosis of NSF requires compatible clinical findings along with consistent histopathology. Suspicious clinical findings in a patient with underlying kidney disease (AKI, CKD stages 4 and 5) who has been exposed to a GBC agent, should prompt skin biopsy. An incisional or deep punch biopsy to allow examination of dermis, epidermis and subcutaneous fat is required. The primary feature is the presence of collagen bundles with increased dermal spindle cells that stain for CD34 and procollagen I. Importantly, an inflammatory infiltrate is absent.12, 13
The major differential diagnosis includes scleroderma, eosinophilic fasciitis, morphea, scleromyxedema, and calcific uremic arteriolopathy. Scleroderma is distinguished by clinical findings such as facial involvement, Raynaud's phenomenon, and sclerodactyly with histology demonstrating normal or decreased numbers of fibroblasts on skin biopsy. Scleromyxedema is marked clinically by facial involvement, paraproteinemia on laboratory testing, and presence of inflammation sometimes seen on biopsy. Calcific uremic arteriolopathy (called calciphylaxis by some), which also occurs in those with kidney failure, is distinguished clinically by usually focal skin changes with cutaneous necrosis and ulceration and livedo reticularis; skin biopsy often reveals medial calcification of the vasculature with intimal fibrosis and luminal thrombosis.
What Is the Role of GBC in NSF?
The cause of NSF remained elusive for several years. Initially described in 2006 with several case series confirming the association, the role GBC agents in the pathogenesis of NSF gained widespread acceptance.1, 27 It should be noted that there are 5 cases of NSF described in kidney transplant patients where no exposure to Gadolinium was found.14, 15 Therefore, the possibility of other triggers remains.
The currently proposed pathogenesis needs to be understood in the context of gadolinium's pharmacologic properties. Gadolinium in its free ionic form (Gd3+) is highly toxic and therefore is sequestered by a non‐toxic organic molecule called a chelate.16, 17 Dissociation of the Gd3+ from a chelate may occur through a process called transmetallation when the chelate binds with another endogenous metal such as zinc or copper, allowing the release of free Gd3+. It is this free gadolinium that appears to be culpable in development of NSF.18 GBC chelates can be categorized based on their biochemical structure (linear vs. macrocyclic) and their charge (ionic vs. non‐ionic). Macrocyclic chelates bind Gd3+ more tightly than linear chelates and possess lower dissociation rates,19 which may have implications for possible toxicity.
The prolonged half‐life of GBC in the context of renal failure appears to predispose GBC to transmetallation and dissociation of Gd3+ from its chelate. Following intravenous injection, GBC is excreted unchanged by the kidneys via glomerular filtration. As a result, elimination half‐life, which is approximately 1.6 hours in normal individuals, is increased approximately 4‐ to 33‐fold in renal failure, depending on the level of GFR.16, 17, 20, 21 This increases the potential for Gd3+ dissociation through prolonged circulation times.
It has been postulated that once dissociated, deposition of the Gd3+ ion into skin and other organs sets off a cascade of poorly understood events that result in edema and fibrosis.18 Recent findings of gadolinium deposition in the skin of patients with NSF as well as an animal model of NSF following GBC exposure support this hypothesis.2225 It appears that vascular trauma, endothelial dysfunction or transudation (edema) allows the Gd3+ metal to enter the tissues. This may explain the preponderance of initial symptoms in dependent areas of the limbs.
What Can Be Done to Prevent NSF?
Avoid GBC Exposure in at Risk Patients
GBC agents are contraindicated in those with ESRD, CKD with estimated GFR 30 mL/minute/1.73 m2 (stages 4 and 5) and AKI. It has become common practice to use the 4‐variable Modification of Diet in Renal Disease (MDRD) formula in estimating GFR.26 Importantly, no estimating formula can be used in the context of a rising serum creatinine concentration as occurs with AKI. If a patient has AKI, one must assume a GFR 15 mL/minute until proven otherwise.
In those with low muscle mass the MDRD estimated GFR may overestimate the true GFR.27 Therefore, the Cockcroft‐Gault estimated creatinine clearance or a 24 hour urine‐based creatinine clearance may be useful in identifying at risk patients with underlying CKD.
Choose the Lowest Risk GBC Agent
When GBC use is deemed necessary in the high risk individual, an agent with a macrocyclic chelate (gadoteridol in the United States) is recommended.28 No published cases of NSF have been described with singular use of such agents. In addition, a retrospective study demonstrated no cases of NSF in ESRD patients on hemodialysis exposed to gadoteridol over a 7‐year period.29 This is not unexpected given the pharmacologic properties of this GBC agent.
Gadodiamide, a linear, non‐ionic agent, appears to produce the greatest risk of NSF as the largest number of NSF cases has been reported with this agent. By October 2007, 283 of 447 cases reported to the Food and Drug Administration (FDA) were exposed to gadodiamide.28 The significant preponderance with this agent is unlikely related to market share, reporting bias or publication bias. Gadopentetate, a linear, ionic agent, which had the greatest market share during this time, was responsible for approximately a quarter of cases reported to the FDA.28 Based on these data, gadodiamide and gadopentetate (and probably all linear agents) should be avoided in high risk patients.
Use Lower Doses of GBC
The FDA approved dose of all GBC agents, except the macrocyclic agent gadoteridol, is 0.1 mmol/kg.30 It appears that higher off‐label doses of GBC agents (0.3‐0.4 mmol/kg) which have been utilized for vascular studies (magnetic resonance angiography [MRA]), may have contributed to the emergence of NSF several years after these agents became available.
Develop a Protocol With Radiology and Nephrology Departments
Assessment of Renal Function Prior to Contrast Administration Is Required
Radiology departments should identify those with ESRD, CKD with estimated GFR 30 mL/minute/1.73 m2 (stages 4 and 5) and AKI. Using the 4‐variable MDRD formula in estimating GFR with the caveats previously noted, radiology departments will identify most at‐risk patients. Since the MDRD formula will be inaccurate in the setting of ESRD and AKI, these diagnoses should be determined through other means (for example, the patient's medical history) as part of the consent process.
Alternative Radiologic Imaging Modalities to GBC Enhanced Magnetic Resonance Imaging Should Be Utilized When Suitable in Those at High Risk
Newer techniques should be investigated as alternatives to GBC exposure. These include Magnetic Resonance Imaging (MRI) without GBC‐enhancement, where options such as 3D time‐of‐flight MRA, phase‐contrast angiography, and arterial spin labeling‐MR provide excellent information about blood vessels and blood flow.31 MRI with ultra‐small paramagnetic iron oxide particles may offer a future alternative in those that need a contrast‐based scan for diagnosis.32
However, since contrast enhanced MRI/MRA studies remain extremely important imaging modalities, their use may be required in some high risk individuals. In this circumstance, a macrocyclic chelate employed at the lowest dose possible, is recommended. The radiologist and nephrologist should be consulted in these instances.
Hemodialysis
Although hemodialysis efficiently clears GBC, its removal is not complete. Furthermore, it is not clear whether the damage has already occurred by the time a hemodialysis treatment can be instituted.33 It should be recognized that GBC removal after one treatment averages 65% to 73.8%; 3 to 4 sessions are required to remove 99% of the contrast agent.21, 34 Peritoneal dialysis on the other hand is an ineffective method of GBC removal (T1/2 of 52.7 hours).21 Because not all of the circulating Gd3+ is removed with a single hemodialysis treatment, prolonged tissue exposure occurs in these patients. This is reflected by the development of NSF in patients despite undergoing consecutive hemodialysis treatments following GBC exposure.3 Therefore, based on incomplete GBC removal with hemodialysis and the lack of evidence supporting prevention of NSF with this modality, we and others33, 35 strongly recommend avoidance of GBC in all patients with advanced kidney disease (GFR 30), regardless of the availability of hemodialysis. As such, the ability to perform hemodialysis after GBC in and of itself does not justify such exposure. However, if GBC use is deemed essential, then immediate hemodialysis should be strongly considered after exposure with further treatment on consecutive days.
Once NSF Develops, What Treatments Options are Available?
Unfortunately there is lack of a universally effective therapy for NSF. Several interventions have been described mainly in anecdotal case reports and very small case series. They have been recently reviewed (Table 2).360
| GBC Formulation | Year of Approval | Charge | Molecular Structure | Probable Risk of NSF* |
|---|---|---|---|---|
| Gadopentetate (Magnevist) | 1988 | Ionic | Linear | Medium |
| Gadoteridol (Prohance) | 1992 | Non‐ionic | Cyclic | Very low |
| Gadodiamide (Omniscan) | 1993 | Non‐ionic | Linear | High |
| Gadoversetamide (OptiMARK) | 1999 | Non‐ionic | Linear | Medium |
| Gadobenate (MultiHance) | 2004 | Ionic | Linear | Low |
|
| Therapies most likely to benefit |
| Kidney transplant (in ESRD) |
| Physical therapy |
| Pain control |
| Therapies with anecdotal success |
| Extracorporeal photopharesis |
| Sodium thiosulfate |
| Therapies with limited success |
| Drugs: Glucocorticoids, Pentoxifylline, Cyclophosphamide, Thalidomide |
| Immunomodulatory: Plasmapharesis, Intravenous immunoglobulin |
| Local: Intralesional IFN‐alpha, topical calcipotriene, other phototherapy |
Physical therapy is the mainstay of treatment for NSF. Physical therapy (and occupational therapy if needed) is essential to help prevent or slow the progression of joint contractures. Adequate pain relief, often with narcotics, is essential for patient comfort and to allow tolerance of physical therapy. Therapies with anecdotal benefit include extracorporeal photopheresis and infusions of sodium thiosulfate, a substance with chelating properties. Other interventions, such as immunosuppressive agents, topical agents and other phototherapies have shown limited success.
AKI resolution has been observed to result in regression of lesions.1, 3740 Presumably, resolution of the AKI allows for clearance of gadolinium and other profibrotic mediators, though definitive evidence of this is not available. Based on the observed response to AKI recovery, it is not surprising that improvement after kidney transplantation has also been described.1, 41 However, responses have not been consistent.39, 42
Consensus Guidelines and Recommendations
Nephrology societies have not yet developed consensus guidelines. Only the European Society of Urogenital Radiology has issued guidelines to date.43 These guidelines are consistent with expert opinions published elsewhere and are reflected in our approach regarding prevention of NSF (Table 3).
|
| 1. GBC agents are contraindicated in patients on dialysis regardless of availability of rapid treatment after exposure |
| 2. Avoid MRI with GBC in those with GFR 30 ml/min (estimated by MDRD formula) |
| MDRD formula may overestimate GFR in those of low weightconsider Cockcroft‐Gault calculation or 24 hour urine collection for creatinine clearance |
| MDRD is invalid in patient with a rising serum creatinine concentration. Assume GFR 30 in those with acutely rising serum creatinine concentration |
| 3. Consider alternative imaging studies or MRI studies without Gadolinium consult radiologist |
| 4. If GBC study is a necessity, then as low a dose as possible of a macrocyclic chelate would be recommended |
| 5. If an exposure to gadolinium occurs in ESRD, hemodialysis should be performed as soon as possible and repeated on consecutive days |
| 6. If an exposure to gadolinium occurs in CKD 4 or 5 or AKI patient (not on dialysis), an individualized approach should be undertaken when considering temporary catheter placement and initiation of hemodialysis |
The FDA has sent out several alerts since June 2006, the most recent in May 2007.30, 4446 In its Information for Healthcare Professionals alert, the FDA outlines recommendations. These are included in our final recommendations shown in Table 3.30 Those with a recent liver transplant, or those with chronic liver disease, who have associated kidney insufficiency of any severity, have also been identified by the FDA as an at risk group. This is based on reports of NSF occurring more commonly in patients with AKI who have these underlying conditions.47
Conclusions
With the high and increasing rates of AKI, CKD and ESRD seen among hospitalized patients,48 the need for vigilance when obtaining imaging with GBC agents becomes particularly important in the inpatient setting. As a preventable disease, it is incumbent upon us to fully understand the risk factors and potential pitfalls that may result in a patient exposed to these agents. The hospitalist has the unique role of acting as a firewall between the patient and the imaging study that may put him or her at risk for this devastating disorder.
Identification of GBC as a major culprit in the development of NSF and hence avoidance of this agent in those at the highest risk is expected to reduce the incidence of NSF. It is likely that the future will bring further understanding of the underlying mechanisms of gadolinium‐induced NSF and with this understanding, even safer strategies for GBC usage. However, until safer contrast agents become available, avoidance of GBC exposure in those with advanced acute or CKD remains our most important defense.
- .Gadolinium–a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis?Nephrol Dial Transplant.2006;21(4):1104–1108.
- Nephrogenic fibrosing dermopathy associated with exposure to gadolinium‐containing contrast agents–St. Louis, Missouri, 2002–2006.MMWR Morb Mortal Wkly Rep.2007;56(7):137–141.
- ,,,,,.Gadodiamide‐associated nephrogenic systemic fibrosis: why radiologists should be concerned.AJR Am J Roentgenol.2007;188(2):586–592.
- ,,.Nephrogenic systemic fibrosis: a population study examining the relationship of disease development to gadolinium exposure.Clin J Am Soc Nephrol.2007;2(2):264–267.
- ,,,,.Nephrogenic systemic fibrosis: a review of 6 cases temporally related to gadodiamide injection (omniscan).Invest Radiol.2007;42(2):139–145.
- ,,, et al.Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast‐enhanced magnetic resonance imaging.J Am Soc Nephrol.2006;17(9):2359–2362.
- ,,, et al.Nephrogenic systemic fibrosis: risk factors and incidence estimation.Radiology.2007;243(1):148–157.
- ,,.Nephrogenic systemic fibrosis (nephrogenic fibrosing dermopathy).Curr Opin Rheumatol.2006;18(6):614–617.
- . Nephrogenic Fibrosing Dermopathy [NFD/NSF Website]. 2001–2007. Available at http://www.icnfdr.org. Accessed December 2009.
- ,,,,.Case‐control study of gadodiamide‐related nephrogenic systemic fibrosis.Nephrol Dial Transplant.2007;22(11):3174–3178.
- ,,, et al.Nephrogenic fibrosing dermopathy and high‐dose erythropoietin therapy.Ann Intern Med.2006;145(3):234–235.
- ,.Nephrogenic systemic fibrosis: an update.Curr Rheumatol Rep.2006;8(2):151–157.
- ,.Nephrogenic systemic fibrosis: early recognition and treatment.Semin Dial.2008;21(2):123–128.
- ,,.Gadolinium is not the only trigger for nephrogenic systemic fibrosis: insights from two cases and review of the recent literature.Am J Transplant.2007;7(10):2425–2432.
- .Nephrogenic systemic fibrosis associated with gadolinium based contrast agents: a summary of the medical literature reporting.Eur J Radiol.2008;66(2):230–234.
- .MR contrast agents, the old and the new.Eur J Radiol.2006;60(3):314–323.
- ,,,,,.Magnetic resonance contrast agents: from the bench to the patient.Curr Pharm Des.2005;11(31):4079–4098.
- .Tissue deposition of gadolinium and development of NSF: a convergence of factors.Semin Dial.232008.
- .Safety of magnetic resonance contrast media.Top Magn Reson Imaging.2001;12(4):309–314.
- ,,, et al.Safety and pharmacokinetic profile of gadobenate dimeglumine in subjects with renal impairment.Invest Radiol.1999;34(7):443–448.
- ,,.Pharmacokinetics of gadodiamide injection in patients with severe renal insufficiency and patients undergoing hemodialysis or continuous ambulatory peritoneal dialysis.Acad Radiol.1998;5(7):491–502.
- ,,.Gadolinium deposition in nephrogenic fibrosing dermopathy.J Am Acad Dermatol.2007;56(1):27–30.
- ,,,,.Gadolinium is detectable within the tissue of patients with nephrogenic systemic fibrosis.J Am Acad Dermatol.2007;56(1):21–26.
- ,,.Gadolinium is quantifiable within the tissue of patients with nephrogenic systemic fibrosis.J Am Acad Dermatol.2007;56(4):710–712.
- ,,,,,.A preclinical study to investigate the development of nephrogenic systemic fibrosis: a possible role for gadolinium‐based contrast media.Invest Radiol.2008;43(1):65–75.
- ,,,.A simplified equation to predict GFR from S‐creatinine [abstract].J Am Soc Nephrol.2000;11:155A.
- ,,,.Assessing kidney function–measured and estimated glomerular filtration rate.N Engl J Med.2006;354(23):2473–2483.
- ,.Nephrogenic systemic fibrosis risk: is there a difference between gadolinium‐based contrast agents?Semin Dial.2008;21(2):129–134.
- .Risk for nephrogenic systemic fibrosis with gadoteridol (ProHance) in patients who are on long‐term hemodialysis.Clin J Am Soc Nephrol.2008;3(3):747–751.
- US Food and Drug Administration: Information for Healthcare Professionals: Gadolinium‐Containing Contrast Agents for Magnetic Resonance Imaging (MRI) ProHance, and MultiHance). Available at: http://www.fda.gov/cder/drug/InfoSheets/HCP/gcca_200705HCP.pdf. Accessed December 2009.
- ,.Nephrogenic systemic fibrosis: non‐gadolinium options for the imaging of CKD/ESRD patients.Semin Dial.2008;21(2):160–165.
- ,,, et al.Ultrasmall superparamagnetic iron oxides (USPIOs): a future alternative magnetic resonance (MR) contrast agent for patients at risk for nephrogenic systemic fibrosis (NSF)?Kidney Int.2008;75(5):465–474.
- .Dialytic therapies to prevent NSF following gadolinium exposure in high‐risk patients.Semin Dial.2008;21(2):145–149.
- ,,,,.Dialyzability of gadodiamide in hemodialysis patients.Radiat Med.2006;24(6):445–451.
- ,,,,,.Nephrogenic systemic fibrosis and its association with gadolinium exposure during MRI.Cleve Clin J Med.2008;75(2):95–97, 103–104, 106 passim.
- ,,.Treatment of nephrogenic systemic fibrosis: limited options but hope for the future.Semin Dial.2008;21(2):155–159.
- ,,,,.Nephrogenic fibrosing dermopathy.Am J Dermatopathol.2001;23(5):383–393.
- ,,,,.Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure.Am J Med.2003;114(7):563–572.
- ,,,.Nephrogenic systemic fibrosis: relationship to gadolinium and response to photopheresis.Arch Dermatol.2007;143(8):1025–1030.
- ,,,.A case of nephrogenic fibrosing dermopathy.Ann Acad Med Singapore.2004;33(4):527–529.
- ,,,,,.Nephrogenic fibrosing dermopathy: two pediatric cases.J Pediatr.2003;143(5):678–681.
- ,,.Nephrogenic fibrosing dermopathy in children.Pediatr Nephrol.2006;21(9):1307–1311.
- .ESUR guideline: gadolinium‐based contrast media and nephrogenic systemic fibrosis.Eur Radiol.2007;17(10):2692–2696.
- US Food and Drug Administration: FDA News: FDA Requests Boxed Warning for Contrast Agents Used to Improve MRI Images. Available at: http://www.fda.gov/bbs/topics/NEWS/2007/NEW01638.html. Accessed December 2009.
- US Food and Drug Administration: Public Health Advisory: Gadolinium‐containing Contrast Agents for Magnetic Resonance Imaging (MRI): Omniscan, OptiMARK, Magnevist, ProHance, and MultiHance. Available at: http://www.fda.gov/cder/drug/advisory/gadolinium_agents.htm. Accessed December 2009.
- US Food and Drug Administration: Public Health Advisory: Update on Magnetic Resonance Imaging (MRI) Contrast Agents Containing Gadolinium and Nephrogenic Fibrosing Dermopathy. Available at: http://www.fda.gov/cder/drug/advisory/gadolinium_agents_20061222.htm. Accessed December 2009.
- ,,, et al.Nephrogenic systemic fibrosis among liver transplant recipients: a single institution experience and topic update.Am J Transplant.2006;6(9):2212–2217.
- Hospitalization discharge diagnoses for kidney disease–United States, 1980–2005.MMWR Morb Mortal Wkly Rep. 282008;57(12):309–312.
- ,,,.Response to the FDA's May 23, 2007, nephrogenic systemic fibrosis update.Radiology.2008;246(1):11–14.
- .How should nephrologists approach gadolinium‐based contrast imaging in patients with kidney disease?Clin J Am Soc Nephrol.2008;3(3):649–651.
What Is Nephrogenic Systemic Fibrosis?
Nephrogenic systemic fibrosis (NSF) is a systemic fibrosing disease that occurs after exposure to gadolinium‐based contrast (GBC) in the presence of severe renal failure of acute or chronic nature.1, 27 As suggested by its former name, nephrogenic fibrosing dermopathy, the cardinal feature of this disorder is skin involvement. Symptoms begin anywhere from 2 to 75 days after exposure to GBC, though usually within 2 months.27 Initial signs and symptoms may include sharp and sometimes excruciating pain, tightening and burning of the skin associated with redness and swelling, symmetrical involvement, distribution with predilection for the extremities more than the trunk, and sparing of the face. The dependent lower extremities are more severely involved than the upper extremities. Dermal induration may occur in the form of plaques, nodules, and papules resulting in a woody texture on palpation. These findings usually progress over weeks to months with extensive dermal fibrosis involving entire limbs. Ultimately the patient may develop severe joint contractures and marked limitations in mobility.8 A fulminant presentation is seen in approximately 5% of patients who develop a rapidly progressive course over as short a time period as 2 weeks.
Systemic organ involvement including fibrosis of the heart, lung, diaphragm, skeletal muscles, and other organs has been described and has been associated with fatal outcomes.79
Though more frequent in those with end‐stage renal disease (ESRD), NSF has been seen in those with stage 4 and 5 chronic kidney disease (CKD) and acute kidney injury (AKI). Incidence rates have been difficult to calculate due to lack of exposure data in most studies, though 1 small case‐control study found 4.3 cases per 1000 patient years among hemodialysis patients with an absolute risk of 3.4% in the exposed patient.4 Interestingly, incident NSF rates published in a Centers for Disease Control case‐control study of 19 NSF sufferers were much higher for peritoneal dialysis (4.6 cases/100 patients) than for hemodialysis (0.61/100 patients).2 This is likely related to the different GBC clearance achieved with these modalities.
NSF has no predilection for gender, race, nationality or age group. Those with liver disease and lower body weight or lower muscle mass appear to be at greater risk, which may be related to overestimation of glomerular filtration rate (GFR) with falsely low creatinines seen in such patients. Risk is likely increased as well by multiple exposures to GBC in close proximity. Related host cofactors have not been identified, though elevated serum calcium and phosphate concentrations, exposure to high dose erythropoietin, and iron overload have been considered.10, 11
The diagnosis of NSF requires compatible clinical findings along with consistent histopathology. Suspicious clinical findings in a patient with underlying kidney disease (AKI, CKD stages 4 and 5) who has been exposed to a GBC agent, should prompt skin biopsy. An incisional or deep punch biopsy to allow examination of dermis, epidermis and subcutaneous fat is required. The primary feature is the presence of collagen bundles with increased dermal spindle cells that stain for CD34 and procollagen I. Importantly, an inflammatory infiltrate is absent.12, 13
The major differential diagnosis includes scleroderma, eosinophilic fasciitis, morphea, scleromyxedema, and calcific uremic arteriolopathy. Scleroderma is distinguished by clinical findings such as facial involvement, Raynaud's phenomenon, and sclerodactyly with histology demonstrating normal or decreased numbers of fibroblasts on skin biopsy. Scleromyxedema is marked clinically by facial involvement, paraproteinemia on laboratory testing, and presence of inflammation sometimes seen on biopsy. Calcific uremic arteriolopathy (called calciphylaxis by some), which also occurs in those with kidney failure, is distinguished clinically by usually focal skin changes with cutaneous necrosis and ulceration and livedo reticularis; skin biopsy often reveals medial calcification of the vasculature with intimal fibrosis and luminal thrombosis.
What Is the Role of GBC in NSF?
The cause of NSF remained elusive for several years. Initially described in 2006 with several case series confirming the association, the role GBC agents in the pathogenesis of NSF gained widespread acceptance.1, 27 It should be noted that there are 5 cases of NSF described in kidney transplant patients where no exposure to Gadolinium was found.14, 15 Therefore, the possibility of other triggers remains.
The currently proposed pathogenesis needs to be understood in the context of gadolinium's pharmacologic properties. Gadolinium in its free ionic form (Gd3+) is highly toxic and therefore is sequestered by a non‐toxic organic molecule called a chelate.16, 17 Dissociation of the Gd3+ from a chelate may occur through a process called transmetallation when the chelate binds with another endogenous metal such as zinc or copper, allowing the release of free Gd3+. It is this free gadolinium that appears to be culpable in development of NSF.18 GBC chelates can be categorized based on their biochemical structure (linear vs. macrocyclic) and their charge (ionic vs. non‐ionic). Macrocyclic chelates bind Gd3+ more tightly than linear chelates and possess lower dissociation rates,19 which may have implications for possible toxicity.
The prolonged half‐life of GBC in the context of renal failure appears to predispose GBC to transmetallation and dissociation of Gd3+ from its chelate. Following intravenous injection, GBC is excreted unchanged by the kidneys via glomerular filtration. As a result, elimination half‐life, which is approximately 1.6 hours in normal individuals, is increased approximately 4‐ to 33‐fold in renal failure, depending on the level of GFR.16, 17, 20, 21 This increases the potential for Gd3+ dissociation through prolonged circulation times.
It has been postulated that once dissociated, deposition of the Gd3+ ion into skin and other organs sets off a cascade of poorly understood events that result in edema and fibrosis.18 Recent findings of gadolinium deposition in the skin of patients with NSF as well as an animal model of NSF following GBC exposure support this hypothesis.2225 It appears that vascular trauma, endothelial dysfunction or transudation (edema) allows the Gd3+ metal to enter the tissues. This may explain the preponderance of initial symptoms in dependent areas of the limbs.
What Can Be Done to Prevent NSF?
Avoid GBC Exposure in at Risk Patients
GBC agents are contraindicated in those with ESRD, CKD with estimated GFR 30 mL/minute/1.73 m2 (stages 4 and 5) and AKI. It has become common practice to use the 4‐variable Modification of Diet in Renal Disease (MDRD) formula in estimating GFR.26 Importantly, no estimating formula can be used in the context of a rising serum creatinine concentration as occurs with AKI. If a patient has AKI, one must assume a GFR 15 mL/minute until proven otherwise.
In those with low muscle mass the MDRD estimated GFR may overestimate the true GFR.27 Therefore, the Cockcroft‐Gault estimated creatinine clearance or a 24 hour urine‐based creatinine clearance may be useful in identifying at risk patients with underlying CKD.
Choose the Lowest Risk GBC Agent
When GBC use is deemed necessary in the high risk individual, an agent with a macrocyclic chelate (gadoteridol in the United States) is recommended.28 No published cases of NSF have been described with singular use of such agents. In addition, a retrospective study demonstrated no cases of NSF in ESRD patients on hemodialysis exposed to gadoteridol over a 7‐year period.29 This is not unexpected given the pharmacologic properties of this GBC agent.
Gadodiamide, a linear, non‐ionic agent, appears to produce the greatest risk of NSF as the largest number of NSF cases has been reported with this agent. By October 2007, 283 of 447 cases reported to the Food and Drug Administration (FDA) were exposed to gadodiamide.28 The significant preponderance with this agent is unlikely related to market share, reporting bias or publication bias. Gadopentetate, a linear, ionic agent, which had the greatest market share during this time, was responsible for approximately a quarter of cases reported to the FDA.28 Based on these data, gadodiamide and gadopentetate (and probably all linear agents) should be avoided in high risk patients.
Use Lower Doses of GBC
The FDA approved dose of all GBC agents, except the macrocyclic agent gadoteridol, is 0.1 mmol/kg.30 It appears that higher off‐label doses of GBC agents (0.3‐0.4 mmol/kg) which have been utilized for vascular studies (magnetic resonance angiography [MRA]), may have contributed to the emergence of NSF several years after these agents became available.
Develop a Protocol With Radiology and Nephrology Departments
Assessment of Renal Function Prior to Contrast Administration Is Required
Radiology departments should identify those with ESRD, CKD with estimated GFR 30 mL/minute/1.73 m2 (stages 4 and 5) and AKI. Using the 4‐variable MDRD formula in estimating GFR with the caveats previously noted, radiology departments will identify most at‐risk patients. Since the MDRD formula will be inaccurate in the setting of ESRD and AKI, these diagnoses should be determined through other means (for example, the patient's medical history) as part of the consent process.
Alternative Radiologic Imaging Modalities to GBC Enhanced Magnetic Resonance Imaging Should Be Utilized When Suitable in Those at High Risk
Newer techniques should be investigated as alternatives to GBC exposure. These include Magnetic Resonance Imaging (MRI) without GBC‐enhancement, where options such as 3D time‐of‐flight MRA, phase‐contrast angiography, and arterial spin labeling‐MR provide excellent information about blood vessels and blood flow.31 MRI with ultra‐small paramagnetic iron oxide particles may offer a future alternative in those that need a contrast‐based scan for diagnosis.32
However, since contrast enhanced MRI/MRA studies remain extremely important imaging modalities, their use may be required in some high risk individuals. In this circumstance, a macrocyclic chelate employed at the lowest dose possible, is recommended. The radiologist and nephrologist should be consulted in these instances.
Hemodialysis
Although hemodialysis efficiently clears GBC, its removal is not complete. Furthermore, it is not clear whether the damage has already occurred by the time a hemodialysis treatment can be instituted.33 It should be recognized that GBC removal after one treatment averages 65% to 73.8%; 3 to 4 sessions are required to remove 99% of the contrast agent.21, 34 Peritoneal dialysis on the other hand is an ineffective method of GBC removal (T1/2 of 52.7 hours).21 Because not all of the circulating Gd3+ is removed with a single hemodialysis treatment, prolonged tissue exposure occurs in these patients. This is reflected by the development of NSF in patients despite undergoing consecutive hemodialysis treatments following GBC exposure.3 Therefore, based on incomplete GBC removal with hemodialysis and the lack of evidence supporting prevention of NSF with this modality, we and others33, 35 strongly recommend avoidance of GBC in all patients with advanced kidney disease (GFR 30), regardless of the availability of hemodialysis. As such, the ability to perform hemodialysis after GBC in and of itself does not justify such exposure. However, if GBC use is deemed essential, then immediate hemodialysis should be strongly considered after exposure with further treatment on consecutive days.
Once NSF Develops, What Treatments Options are Available?
Unfortunately there is lack of a universally effective therapy for NSF. Several interventions have been described mainly in anecdotal case reports and very small case series. They have been recently reviewed (Table 2).360
| GBC Formulation | Year of Approval | Charge | Molecular Structure | Probable Risk of NSF* |
|---|---|---|---|---|
| Gadopentetate (Magnevist) | 1988 | Ionic | Linear | Medium |
| Gadoteridol (Prohance) | 1992 | Non‐ionic | Cyclic | Very low |
| Gadodiamide (Omniscan) | 1993 | Non‐ionic | Linear | High |
| Gadoversetamide (OptiMARK) | 1999 | Non‐ionic | Linear | Medium |
| Gadobenate (MultiHance) | 2004 | Ionic | Linear | Low |
|
| Therapies most likely to benefit |
| Kidney transplant (in ESRD) |
| Physical therapy |
| Pain control |
| Therapies with anecdotal success |
| Extracorporeal photopharesis |
| Sodium thiosulfate |
| Therapies with limited success |
| Drugs: Glucocorticoids, Pentoxifylline, Cyclophosphamide, Thalidomide |
| Immunomodulatory: Plasmapharesis, Intravenous immunoglobulin |
| Local: Intralesional IFN‐alpha, topical calcipotriene, other phototherapy |
Physical therapy is the mainstay of treatment for NSF. Physical therapy (and occupational therapy if needed) is essential to help prevent or slow the progression of joint contractures. Adequate pain relief, often with narcotics, is essential for patient comfort and to allow tolerance of physical therapy. Therapies with anecdotal benefit include extracorporeal photopheresis and infusions of sodium thiosulfate, a substance with chelating properties. Other interventions, such as immunosuppressive agents, topical agents and other phototherapies have shown limited success.
AKI resolution has been observed to result in regression of lesions.1, 3740 Presumably, resolution of the AKI allows for clearance of gadolinium and other profibrotic mediators, though definitive evidence of this is not available. Based on the observed response to AKI recovery, it is not surprising that improvement after kidney transplantation has also been described.1, 41 However, responses have not been consistent.39, 42
Consensus Guidelines and Recommendations
Nephrology societies have not yet developed consensus guidelines. Only the European Society of Urogenital Radiology has issued guidelines to date.43 These guidelines are consistent with expert opinions published elsewhere and are reflected in our approach regarding prevention of NSF (Table 3).
|
| 1. GBC agents are contraindicated in patients on dialysis regardless of availability of rapid treatment after exposure |
| 2. Avoid MRI with GBC in those with GFR 30 ml/min (estimated by MDRD formula) |
| MDRD formula may overestimate GFR in those of low weightconsider Cockcroft‐Gault calculation or 24 hour urine collection for creatinine clearance |
| MDRD is invalid in patient with a rising serum creatinine concentration. Assume GFR 30 in those with acutely rising serum creatinine concentration |
| 3. Consider alternative imaging studies or MRI studies without Gadolinium consult radiologist |
| 4. If GBC study is a necessity, then as low a dose as possible of a macrocyclic chelate would be recommended |
| 5. If an exposure to gadolinium occurs in ESRD, hemodialysis should be performed as soon as possible and repeated on consecutive days |
| 6. If an exposure to gadolinium occurs in CKD 4 or 5 or AKI patient (not on dialysis), an individualized approach should be undertaken when considering temporary catheter placement and initiation of hemodialysis |
The FDA has sent out several alerts since June 2006, the most recent in May 2007.30, 4446 In its Information for Healthcare Professionals alert, the FDA outlines recommendations. These are included in our final recommendations shown in Table 3.30 Those with a recent liver transplant, or those with chronic liver disease, who have associated kidney insufficiency of any severity, have also been identified by the FDA as an at risk group. This is based on reports of NSF occurring more commonly in patients with AKI who have these underlying conditions.47
Conclusions
With the high and increasing rates of AKI, CKD and ESRD seen among hospitalized patients,48 the need for vigilance when obtaining imaging with GBC agents becomes particularly important in the inpatient setting. As a preventable disease, it is incumbent upon us to fully understand the risk factors and potential pitfalls that may result in a patient exposed to these agents. The hospitalist has the unique role of acting as a firewall between the patient and the imaging study that may put him or her at risk for this devastating disorder.
Identification of GBC as a major culprit in the development of NSF and hence avoidance of this agent in those at the highest risk is expected to reduce the incidence of NSF. It is likely that the future will bring further understanding of the underlying mechanisms of gadolinium‐induced NSF and with this understanding, even safer strategies for GBC usage. However, until safer contrast agents become available, avoidance of GBC exposure in those with advanced acute or CKD remains our most important defense.
What Is Nephrogenic Systemic Fibrosis?
Nephrogenic systemic fibrosis (NSF) is a systemic fibrosing disease that occurs after exposure to gadolinium‐based contrast (GBC) in the presence of severe renal failure of acute or chronic nature.1, 27 As suggested by its former name, nephrogenic fibrosing dermopathy, the cardinal feature of this disorder is skin involvement. Symptoms begin anywhere from 2 to 75 days after exposure to GBC, though usually within 2 months.27 Initial signs and symptoms may include sharp and sometimes excruciating pain, tightening and burning of the skin associated with redness and swelling, symmetrical involvement, distribution with predilection for the extremities more than the trunk, and sparing of the face. The dependent lower extremities are more severely involved than the upper extremities. Dermal induration may occur in the form of plaques, nodules, and papules resulting in a woody texture on palpation. These findings usually progress over weeks to months with extensive dermal fibrosis involving entire limbs. Ultimately the patient may develop severe joint contractures and marked limitations in mobility.8 A fulminant presentation is seen in approximately 5% of patients who develop a rapidly progressive course over as short a time period as 2 weeks.
Systemic organ involvement including fibrosis of the heart, lung, diaphragm, skeletal muscles, and other organs has been described and has been associated with fatal outcomes.79
Though more frequent in those with end‐stage renal disease (ESRD), NSF has been seen in those with stage 4 and 5 chronic kidney disease (CKD) and acute kidney injury (AKI). Incidence rates have been difficult to calculate due to lack of exposure data in most studies, though 1 small case‐control study found 4.3 cases per 1000 patient years among hemodialysis patients with an absolute risk of 3.4% in the exposed patient.4 Interestingly, incident NSF rates published in a Centers for Disease Control case‐control study of 19 NSF sufferers were much higher for peritoneal dialysis (4.6 cases/100 patients) than for hemodialysis (0.61/100 patients).2 This is likely related to the different GBC clearance achieved with these modalities.
NSF has no predilection for gender, race, nationality or age group. Those with liver disease and lower body weight or lower muscle mass appear to be at greater risk, which may be related to overestimation of glomerular filtration rate (GFR) with falsely low creatinines seen in such patients. Risk is likely increased as well by multiple exposures to GBC in close proximity. Related host cofactors have not been identified, though elevated serum calcium and phosphate concentrations, exposure to high dose erythropoietin, and iron overload have been considered.10, 11
The diagnosis of NSF requires compatible clinical findings along with consistent histopathology. Suspicious clinical findings in a patient with underlying kidney disease (AKI, CKD stages 4 and 5) who has been exposed to a GBC agent, should prompt skin biopsy. An incisional or deep punch biopsy to allow examination of dermis, epidermis and subcutaneous fat is required. The primary feature is the presence of collagen bundles with increased dermal spindle cells that stain for CD34 and procollagen I. Importantly, an inflammatory infiltrate is absent.12, 13
The major differential diagnosis includes scleroderma, eosinophilic fasciitis, morphea, scleromyxedema, and calcific uremic arteriolopathy. Scleroderma is distinguished by clinical findings such as facial involvement, Raynaud's phenomenon, and sclerodactyly with histology demonstrating normal or decreased numbers of fibroblasts on skin biopsy. Scleromyxedema is marked clinically by facial involvement, paraproteinemia on laboratory testing, and presence of inflammation sometimes seen on biopsy. Calcific uremic arteriolopathy (called calciphylaxis by some), which also occurs in those with kidney failure, is distinguished clinically by usually focal skin changes with cutaneous necrosis and ulceration and livedo reticularis; skin biopsy often reveals medial calcification of the vasculature with intimal fibrosis and luminal thrombosis.
What Is the Role of GBC in NSF?
The cause of NSF remained elusive for several years. Initially described in 2006 with several case series confirming the association, the role GBC agents in the pathogenesis of NSF gained widespread acceptance.1, 27 It should be noted that there are 5 cases of NSF described in kidney transplant patients where no exposure to Gadolinium was found.14, 15 Therefore, the possibility of other triggers remains.
The currently proposed pathogenesis needs to be understood in the context of gadolinium's pharmacologic properties. Gadolinium in its free ionic form (Gd3+) is highly toxic and therefore is sequestered by a non‐toxic organic molecule called a chelate.16, 17 Dissociation of the Gd3+ from a chelate may occur through a process called transmetallation when the chelate binds with another endogenous metal such as zinc or copper, allowing the release of free Gd3+. It is this free gadolinium that appears to be culpable in development of NSF.18 GBC chelates can be categorized based on their biochemical structure (linear vs. macrocyclic) and their charge (ionic vs. non‐ionic). Macrocyclic chelates bind Gd3+ more tightly than linear chelates and possess lower dissociation rates,19 which may have implications for possible toxicity.
The prolonged half‐life of GBC in the context of renal failure appears to predispose GBC to transmetallation and dissociation of Gd3+ from its chelate. Following intravenous injection, GBC is excreted unchanged by the kidneys via glomerular filtration. As a result, elimination half‐life, which is approximately 1.6 hours in normal individuals, is increased approximately 4‐ to 33‐fold in renal failure, depending on the level of GFR.16, 17, 20, 21 This increases the potential for Gd3+ dissociation through prolonged circulation times.
It has been postulated that once dissociated, deposition of the Gd3+ ion into skin and other organs sets off a cascade of poorly understood events that result in edema and fibrosis.18 Recent findings of gadolinium deposition in the skin of patients with NSF as well as an animal model of NSF following GBC exposure support this hypothesis.2225 It appears that vascular trauma, endothelial dysfunction or transudation (edema) allows the Gd3+ metal to enter the tissues. This may explain the preponderance of initial symptoms in dependent areas of the limbs.
What Can Be Done to Prevent NSF?
Avoid GBC Exposure in at Risk Patients
GBC agents are contraindicated in those with ESRD, CKD with estimated GFR 30 mL/minute/1.73 m2 (stages 4 and 5) and AKI. It has become common practice to use the 4‐variable Modification of Diet in Renal Disease (MDRD) formula in estimating GFR.26 Importantly, no estimating formula can be used in the context of a rising serum creatinine concentration as occurs with AKI. If a patient has AKI, one must assume a GFR 15 mL/minute until proven otherwise.
In those with low muscle mass the MDRD estimated GFR may overestimate the true GFR.27 Therefore, the Cockcroft‐Gault estimated creatinine clearance or a 24 hour urine‐based creatinine clearance may be useful in identifying at risk patients with underlying CKD.
Choose the Lowest Risk GBC Agent
When GBC use is deemed necessary in the high risk individual, an agent with a macrocyclic chelate (gadoteridol in the United States) is recommended.28 No published cases of NSF have been described with singular use of such agents. In addition, a retrospective study demonstrated no cases of NSF in ESRD patients on hemodialysis exposed to gadoteridol over a 7‐year period.29 This is not unexpected given the pharmacologic properties of this GBC agent.
Gadodiamide, a linear, non‐ionic agent, appears to produce the greatest risk of NSF as the largest number of NSF cases has been reported with this agent. By October 2007, 283 of 447 cases reported to the Food and Drug Administration (FDA) were exposed to gadodiamide.28 The significant preponderance with this agent is unlikely related to market share, reporting bias or publication bias. Gadopentetate, a linear, ionic agent, which had the greatest market share during this time, was responsible for approximately a quarter of cases reported to the FDA.28 Based on these data, gadodiamide and gadopentetate (and probably all linear agents) should be avoided in high risk patients.
Use Lower Doses of GBC
The FDA approved dose of all GBC agents, except the macrocyclic agent gadoteridol, is 0.1 mmol/kg.30 It appears that higher off‐label doses of GBC agents (0.3‐0.4 mmol/kg) which have been utilized for vascular studies (magnetic resonance angiography [MRA]), may have contributed to the emergence of NSF several years after these agents became available.
Develop a Protocol With Radiology and Nephrology Departments
Assessment of Renal Function Prior to Contrast Administration Is Required
Radiology departments should identify those with ESRD, CKD with estimated GFR 30 mL/minute/1.73 m2 (stages 4 and 5) and AKI. Using the 4‐variable MDRD formula in estimating GFR with the caveats previously noted, radiology departments will identify most at‐risk patients. Since the MDRD formula will be inaccurate in the setting of ESRD and AKI, these diagnoses should be determined through other means (for example, the patient's medical history) as part of the consent process.
Alternative Radiologic Imaging Modalities to GBC Enhanced Magnetic Resonance Imaging Should Be Utilized When Suitable in Those at High Risk
Newer techniques should be investigated as alternatives to GBC exposure. These include Magnetic Resonance Imaging (MRI) without GBC‐enhancement, where options such as 3D time‐of‐flight MRA, phase‐contrast angiography, and arterial spin labeling‐MR provide excellent information about blood vessels and blood flow.31 MRI with ultra‐small paramagnetic iron oxide particles may offer a future alternative in those that need a contrast‐based scan for diagnosis.32
However, since contrast enhanced MRI/MRA studies remain extremely important imaging modalities, their use may be required in some high risk individuals. In this circumstance, a macrocyclic chelate employed at the lowest dose possible, is recommended. The radiologist and nephrologist should be consulted in these instances.
Hemodialysis
Although hemodialysis efficiently clears GBC, its removal is not complete. Furthermore, it is not clear whether the damage has already occurred by the time a hemodialysis treatment can be instituted.33 It should be recognized that GBC removal after one treatment averages 65% to 73.8%; 3 to 4 sessions are required to remove 99% of the contrast agent.21, 34 Peritoneal dialysis on the other hand is an ineffective method of GBC removal (T1/2 of 52.7 hours).21 Because not all of the circulating Gd3+ is removed with a single hemodialysis treatment, prolonged tissue exposure occurs in these patients. This is reflected by the development of NSF in patients despite undergoing consecutive hemodialysis treatments following GBC exposure.3 Therefore, based on incomplete GBC removal with hemodialysis and the lack of evidence supporting prevention of NSF with this modality, we and others33, 35 strongly recommend avoidance of GBC in all patients with advanced kidney disease (GFR 30), regardless of the availability of hemodialysis. As such, the ability to perform hemodialysis after GBC in and of itself does not justify such exposure. However, if GBC use is deemed essential, then immediate hemodialysis should be strongly considered after exposure with further treatment on consecutive days.
Once NSF Develops, What Treatments Options are Available?
Unfortunately there is lack of a universally effective therapy for NSF. Several interventions have been described mainly in anecdotal case reports and very small case series. They have been recently reviewed (Table 2).360
| GBC Formulation | Year of Approval | Charge | Molecular Structure | Probable Risk of NSF* |
|---|---|---|---|---|
| Gadopentetate (Magnevist) | 1988 | Ionic | Linear | Medium |
| Gadoteridol (Prohance) | 1992 | Non‐ionic | Cyclic | Very low |
| Gadodiamide (Omniscan) | 1993 | Non‐ionic | Linear | High |
| Gadoversetamide (OptiMARK) | 1999 | Non‐ionic | Linear | Medium |
| Gadobenate (MultiHance) | 2004 | Ionic | Linear | Low |
|
| Therapies most likely to benefit |
| Kidney transplant (in ESRD) |
| Physical therapy |
| Pain control |
| Therapies with anecdotal success |
| Extracorporeal photopharesis |
| Sodium thiosulfate |
| Therapies with limited success |
| Drugs: Glucocorticoids, Pentoxifylline, Cyclophosphamide, Thalidomide |
| Immunomodulatory: Plasmapharesis, Intravenous immunoglobulin |
| Local: Intralesional IFN‐alpha, topical calcipotriene, other phototherapy |
Physical therapy is the mainstay of treatment for NSF. Physical therapy (and occupational therapy if needed) is essential to help prevent or slow the progression of joint contractures. Adequate pain relief, often with narcotics, is essential for patient comfort and to allow tolerance of physical therapy. Therapies with anecdotal benefit include extracorporeal photopheresis and infusions of sodium thiosulfate, a substance with chelating properties. Other interventions, such as immunosuppressive agents, topical agents and other phototherapies have shown limited success.
AKI resolution has been observed to result in regression of lesions.1, 3740 Presumably, resolution of the AKI allows for clearance of gadolinium and other profibrotic mediators, though definitive evidence of this is not available. Based on the observed response to AKI recovery, it is not surprising that improvement after kidney transplantation has also been described.1, 41 However, responses have not been consistent.39, 42
Consensus Guidelines and Recommendations
Nephrology societies have not yet developed consensus guidelines. Only the European Society of Urogenital Radiology has issued guidelines to date.43 These guidelines are consistent with expert opinions published elsewhere and are reflected in our approach regarding prevention of NSF (Table 3).
|
| 1. GBC agents are contraindicated in patients on dialysis regardless of availability of rapid treatment after exposure |
| 2. Avoid MRI with GBC in those with GFR 30 ml/min (estimated by MDRD formula) |
| MDRD formula may overestimate GFR in those of low weightconsider Cockcroft‐Gault calculation or 24 hour urine collection for creatinine clearance |
| MDRD is invalid in patient with a rising serum creatinine concentration. Assume GFR 30 in those with acutely rising serum creatinine concentration |
| 3. Consider alternative imaging studies or MRI studies without Gadolinium consult radiologist |
| 4. If GBC study is a necessity, then as low a dose as possible of a macrocyclic chelate would be recommended |
| 5. If an exposure to gadolinium occurs in ESRD, hemodialysis should be performed as soon as possible and repeated on consecutive days |
| 6. If an exposure to gadolinium occurs in CKD 4 or 5 or AKI patient (not on dialysis), an individualized approach should be undertaken when considering temporary catheter placement and initiation of hemodialysis |
The FDA has sent out several alerts since June 2006, the most recent in May 2007.30, 4446 In its Information for Healthcare Professionals alert, the FDA outlines recommendations. These are included in our final recommendations shown in Table 3.30 Those with a recent liver transplant, or those with chronic liver disease, who have associated kidney insufficiency of any severity, have also been identified by the FDA as an at risk group. This is based on reports of NSF occurring more commonly in patients with AKI who have these underlying conditions.47
Conclusions
With the high and increasing rates of AKI, CKD and ESRD seen among hospitalized patients,48 the need for vigilance when obtaining imaging with GBC agents becomes particularly important in the inpatient setting. As a preventable disease, it is incumbent upon us to fully understand the risk factors and potential pitfalls that may result in a patient exposed to these agents. The hospitalist has the unique role of acting as a firewall between the patient and the imaging study that may put him or her at risk for this devastating disorder.
Identification of GBC as a major culprit in the development of NSF and hence avoidance of this agent in those at the highest risk is expected to reduce the incidence of NSF. It is likely that the future will bring further understanding of the underlying mechanisms of gadolinium‐induced NSF and with this understanding, even safer strategies for GBC usage. However, until safer contrast agents become available, avoidance of GBC exposure in those with advanced acute or CKD remains our most important defense.
- .Gadolinium–a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis?Nephrol Dial Transplant.2006;21(4):1104–1108.
- Nephrogenic fibrosing dermopathy associated with exposure to gadolinium‐containing contrast agents–St. Louis, Missouri, 2002–2006.MMWR Morb Mortal Wkly Rep.2007;56(7):137–141.
- ,,,,,.Gadodiamide‐associated nephrogenic systemic fibrosis: why radiologists should be concerned.AJR Am J Roentgenol.2007;188(2):586–592.
- ,,.Nephrogenic systemic fibrosis: a population study examining the relationship of disease development to gadolinium exposure.Clin J Am Soc Nephrol.2007;2(2):264–267.
- ,,,,.Nephrogenic systemic fibrosis: a review of 6 cases temporally related to gadodiamide injection (omniscan).Invest Radiol.2007;42(2):139–145.
- ,,, et al.Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast‐enhanced magnetic resonance imaging.J Am Soc Nephrol.2006;17(9):2359–2362.
- ,,, et al.Nephrogenic systemic fibrosis: risk factors and incidence estimation.Radiology.2007;243(1):148–157.
- ,,.Nephrogenic systemic fibrosis (nephrogenic fibrosing dermopathy).Curr Opin Rheumatol.2006;18(6):614–617.
- . Nephrogenic Fibrosing Dermopathy [NFD/NSF Website]. 2001–2007. Available at http://www.icnfdr.org. Accessed December 2009.
- ,,,,.Case‐control study of gadodiamide‐related nephrogenic systemic fibrosis.Nephrol Dial Transplant.2007;22(11):3174–3178.
- ,,, et al.Nephrogenic fibrosing dermopathy and high‐dose erythropoietin therapy.Ann Intern Med.2006;145(3):234–235.
- ,.Nephrogenic systemic fibrosis: an update.Curr Rheumatol Rep.2006;8(2):151–157.
- ,.Nephrogenic systemic fibrosis: early recognition and treatment.Semin Dial.2008;21(2):123–128.
- ,,.Gadolinium is not the only trigger for nephrogenic systemic fibrosis: insights from two cases and review of the recent literature.Am J Transplant.2007;7(10):2425–2432.
- .Nephrogenic systemic fibrosis associated with gadolinium based contrast agents: a summary of the medical literature reporting.Eur J Radiol.2008;66(2):230–234.
- .MR contrast agents, the old and the new.Eur J Radiol.2006;60(3):314–323.
- ,,,,,.Magnetic resonance contrast agents: from the bench to the patient.Curr Pharm Des.2005;11(31):4079–4098.
- .Tissue deposition of gadolinium and development of NSF: a convergence of factors.Semin Dial.232008.
- .Safety of magnetic resonance contrast media.Top Magn Reson Imaging.2001;12(4):309–314.
- ,,, et al.Safety and pharmacokinetic profile of gadobenate dimeglumine in subjects with renal impairment.Invest Radiol.1999;34(7):443–448.
- ,,.Pharmacokinetics of gadodiamide injection in patients with severe renal insufficiency and patients undergoing hemodialysis or continuous ambulatory peritoneal dialysis.Acad Radiol.1998;5(7):491–502.
- ,,.Gadolinium deposition in nephrogenic fibrosing dermopathy.J Am Acad Dermatol.2007;56(1):27–30.
- ,,,,.Gadolinium is detectable within the tissue of patients with nephrogenic systemic fibrosis.J Am Acad Dermatol.2007;56(1):21–26.
- ,,.Gadolinium is quantifiable within the tissue of patients with nephrogenic systemic fibrosis.J Am Acad Dermatol.2007;56(4):710–712.
- ,,,,,.A preclinical study to investigate the development of nephrogenic systemic fibrosis: a possible role for gadolinium‐based contrast media.Invest Radiol.2008;43(1):65–75.
- ,,,.A simplified equation to predict GFR from S‐creatinine [abstract].J Am Soc Nephrol.2000;11:155A.
- ,,,.Assessing kidney function–measured and estimated glomerular filtration rate.N Engl J Med.2006;354(23):2473–2483.
- ,.Nephrogenic systemic fibrosis risk: is there a difference between gadolinium‐based contrast agents?Semin Dial.2008;21(2):129–134.
- .Risk for nephrogenic systemic fibrosis with gadoteridol (ProHance) in patients who are on long‐term hemodialysis.Clin J Am Soc Nephrol.2008;3(3):747–751.
- US Food and Drug Administration: Information for Healthcare Professionals: Gadolinium‐Containing Contrast Agents for Magnetic Resonance Imaging (MRI) ProHance, and MultiHance). Available at: http://www.fda.gov/cder/drug/InfoSheets/HCP/gcca_200705HCP.pdf. Accessed December 2009.
- ,.Nephrogenic systemic fibrosis: non‐gadolinium options for the imaging of CKD/ESRD patients.Semin Dial.2008;21(2):160–165.
- ,,, et al.Ultrasmall superparamagnetic iron oxides (USPIOs): a future alternative magnetic resonance (MR) contrast agent for patients at risk for nephrogenic systemic fibrosis (NSF)?Kidney Int.2008;75(5):465–474.
- .Dialytic therapies to prevent NSF following gadolinium exposure in high‐risk patients.Semin Dial.2008;21(2):145–149.
- ,,,,.Dialyzability of gadodiamide in hemodialysis patients.Radiat Med.2006;24(6):445–451.
- ,,,,,.Nephrogenic systemic fibrosis and its association with gadolinium exposure during MRI.Cleve Clin J Med.2008;75(2):95–97, 103–104, 106 passim.
- ,,.Treatment of nephrogenic systemic fibrosis: limited options but hope for the future.Semin Dial.2008;21(2):155–159.
- ,,,,.Nephrogenic fibrosing dermopathy.Am J Dermatopathol.2001;23(5):383–393.
- ,,,,.Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure.Am J Med.2003;114(7):563–572.
- ,,,.Nephrogenic systemic fibrosis: relationship to gadolinium and response to photopheresis.Arch Dermatol.2007;143(8):1025–1030.
- ,,,.A case of nephrogenic fibrosing dermopathy.Ann Acad Med Singapore.2004;33(4):527–529.
- ,,,,,.Nephrogenic fibrosing dermopathy: two pediatric cases.J Pediatr.2003;143(5):678–681.
- ,,.Nephrogenic fibrosing dermopathy in children.Pediatr Nephrol.2006;21(9):1307–1311.
- .ESUR guideline: gadolinium‐based contrast media and nephrogenic systemic fibrosis.Eur Radiol.2007;17(10):2692–2696.
- US Food and Drug Administration: FDA News: FDA Requests Boxed Warning for Contrast Agents Used to Improve MRI Images. Available at: http://www.fda.gov/bbs/topics/NEWS/2007/NEW01638.html. Accessed December 2009.
- US Food and Drug Administration: Public Health Advisory: Gadolinium‐containing Contrast Agents for Magnetic Resonance Imaging (MRI): Omniscan, OptiMARK, Magnevist, ProHance, and MultiHance. Available at: http://www.fda.gov/cder/drug/advisory/gadolinium_agents.htm. Accessed December 2009.
- US Food and Drug Administration: Public Health Advisory: Update on Magnetic Resonance Imaging (MRI) Contrast Agents Containing Gadolinium and Nephrogenic Fibrosing Dermopathy. Available at: http://www.fda.gov/cder/drug/advisory/gadolinium_agents_20061222.htm. Accessed December 2009.
- ,,, et al.Nephrogenic systemic fibrosis among liver transplant recipients: a single institution experience and topic update.Am J Transplant.2006;6(9):2212–2217.
- Hospitalization discharge diagnoses for kidney disease–United States, 1980–2005.MMWR Morb Mortal Wkly Rep. 282008;57(12):309–312.
- ,,,.Response to the FDA's May 23, 2007, nephrogenic systemic fibrosis update.Radiology.2008;246(1):11–14.
- .How should nephrologists approach gadolinium‐based contrast imaging in patients with kidney disease?Clin J Am Soc Nephrol.2008;3(3):649–651.
- .Gadolinium–a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis?Nephrol Dial Transplant.2006;21(4):1104–1108.
- Nephrogenic fibrosing dermopathy associated with exposure to gadolinium‐containing contrast agents–St. Louis, Missouri, 2002–2006.MMWR Morb Mortal Wkly Rep.2007;56(7):137–141.
- ,,,,,.Gadodiamide‐associated nephrogenic systemic fibrosis: why radiologists should be concerned.AJR Am J Roentgenol.2007;188(2):586–592.
- ,,.Nephrogenic systemic fibrosis: a population study examining the relationship of disease development to gadolinium exposure.Clin J Am Soc Nephrol.2007;2(2):264–267.
- ,,,,.Nephrogenic systemic fibrosis: a review of 6 cases temporally related to gadodiamide injection (omniscan).Invest Radiol.2007;42(2):139–145.
- ,,, et al.Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast‐enhanced magnetic resonance imaging.J Am Soc Nephrol.2006;17(9):2359–2362.
- ,,, et al.Nephrogenic systemic fibrosis: risk factors and incidence estimation.Radiology.2007;243(1):148–157.
- ,,.Nephrogenic systemic fibrosis (nephrogenic fibrosing dermopathy).Curr Opin Rheumatol.2006;18(6):614–617.
- . Nephrogenic Fibrosing Dermopathy [NFD/NSF Website]. 2001–2007. Available at http://www.icnfdr.org. Accessed December 2009.
- ,,,,.Case‐control study of gadodiamide‐related nephrogenic systemic fibrosis.Nephrol Dial Transplant.2007;22(11):3174–3178.
- ,,, et al.Nephrogenic fibrosing dermopathy and high‐dose erythropoietin therapy.Ann Intern Med.2006;145(3):234–235.
- ,.Nephrogenic systemic fibrosis: an update.Curr Rheumatol Rep.2006;8(2):151–157.
- ,.Nephrogenic systemic fibrosis: early recognition and treatment.Semin Dial.2008;21(2):123–128.
- ,,.Gadolinium is not the only trigger for nephrogenic systemic fibrosis: insights from two cases and review of the recent literature.Am J Transplant.2007;7(10):2425–2432.
- .Nephrogenic systemic fibrosis associated with gadolinium based contrast agents: a summary of the medical literature reporting.Eur J Radiol.2008;66(2):230–234.
- .MR contrast agents, the old and the new.Eur J Radiol.2006;60(3):314–323.
- ,,,,,.Magnetic resonance contrast agents: from the bench to the patient.Curr Pharm Des.2005;11(31):4079–4098.
- .Tissue deposition of gadolinium and development of NSF: a convergence of factors.Semin Dial.232008.
- .Safety of magnetic resonance contrast media.Top Magn Reson Imaging.2001;12(4):309–314.
- ,,, et al.Safety and pharmacokinetic profile of gadobenate dimeglumine in subjects with renal impairment.Invest Radiol.1999;34(7):443–448.
- ,,.Pharmacokinetics of gadodiamide injection in patients with severe renal insufficiency and patients undergoing hemodialysis or continuous ambulatory peritoneal dialysis.Acad Radiol.1998;5(7):491–502.
- ,,.Gadolinium deposition in nephrogenic fibrosing dermopathy.J Am Acad Dermatol.2007;56(1):27–30.
- ,,,,.Gadolinium is detectable within the tissue of patients with nephrogenic systemic fibrosis.J Am Acad Dermatol.2007;56(1):21–26.
- ,,.Gadolinium is quantifiable within the tissue of patients with nephrogenic systemic fibrosis.J Am Acad Dermatol.2007;56(4):710–712.
- ,,,,,.A preclinical study to investigate the development of nephrogenic systemic fibrosis: a possible role for gadolinium‐based contrast media.Invest Radiol.2008;43(1):65–75.
- ,,,.A simplified equation to predict GFR from S‐creatinine [abstract].J Am Soc Nephrol.2000;11:155A.
- ,,,.Assessing kidney function–measured and estimated glomerular filtration rate.N Engl J Med.2006;354(23):2473–2483.
- ,.Nephrogenic systemic fibrosis risk: is there a difference between gadolinium‐based contrast agents?Semin Dial.2008;21(2):129–134.
- .Risk for nephrogenic systemic fibrosis with gadoteridol (ProHance) in patients who are on long‐term hemodialysis.Clin J Am Soc Nephrol.2008;3(3):747–751.
- US Food and Drug Administration: Information for Healthcare Professionals: Gadolinium‐Containing Contrast Agents for Magnetic Resonance Imaging (MRI) ProHance, and MultiHance). Available at: http://www.fda.gov/cder/drug/InfoSheets/HCP/gcca_200705HCP.pdf. Accessed December 2009.
- ,.Nephrogenic systemic fibrosis: non‐gadolinium options for the imaging of CKD/ESRD patients.Semin Dial.2008;21(2):160–165.
- ,,, et al.Ultrasmall superparamagnetic iron oxides (USPIOs): a future alternative magnetic resonance (MR) contrast agent for patients at risk for nephrogenic systemic fibrosis (NSF)?Kidney Int.2008;75(5):465–474.
- .Dialytic therapies to prevent NSF following gadolinium exposure in high‐risk patients.Semin Dial.2008;21(2):145–149.
- ,,,,.Dialyzability of gadodiamide in hemodialysis patients.Radiat Med.2006;24(6):445–451.
- ,,,,,.Nephrogenic systemic fibrosis and its association with gadolinium exposure during MRI.Cleve Clin J Med.2008;75(2):95–97, 103–104, 106 passim.
- ,,.Treatment of nephrogenic systemic fibrosis: limited options but hope for the future.Semin Dial.2008;21(2):155–159.
- ,,,,.Nephrogenic fibrosing dermopathy.Am J Dermatopathol.2001;23(5):383–393.
- ,,,,.Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure.Am J Med.2003;114(7):563–572.
- ,,,.Nephrogenic systemic fibrosis: relationship to gadolinium and response to photopheresis.Arch Dermatol.2007;143(8):1025–1030.
- ,,,.A case of nephrogenic fibrosing dermopathy.Ann Acad Med Singapore.2004;33(4):527–529.
- ,,,,,.Nephrogenic fibrosing dermopathy: two pediatric cases.J Pediatr.2003;143(5):678–681.
- ,,.Nephrogenic fibrosing dermopathy in children.Pediatr Nephrol.2006;21(9):1307–1311.
- .ESUR guideline: gadolinium‐based contrast media and nephrogenic systemic fibrosis.Eur Radiol.2007;17(10):2692–2696.
- US Food and Drug Administration: FDA News: FDA Requests Boxed Warning for Contrast Agents Used to Improve MRI Images. Available at: http://www.fda.gov/bbs/topics/NEWS/2007/NEW01638.html. Accessed December 2009.
- US Food and Drug Administration: Public Health Advisory: Gadolinium‐containing Contrast Agents for Magnetic Resonance Imaging (MRI): Omniscan, OptiMARK, Magnevist, ProHance, and MultiHance. Available at: http://www.fda.gov/cder/drug/advisory/gadolinium_agents.htm. Accessed December 2009.
- US Food and Drug Administration: Public Health Advisory: Update on Magnetic Resonance Imaging (MRI) Contrast Agents Containing Gadolinium and Nephrogenic Fibrosing Dermopathy. Available at: http://www.fda.gov/cder/drug/advisory/gadolinium_agents_20061222.htm. Accessed December 2009.
- ,,, et al.Nephrogenic systemic fibrosis among liver transplant recipients: a single institution experience and topic update.Am J Transplant.2006;6(9):2212–2217.
- Hospitalization discharge diagnoses for kidney disease–United States, 1980–2005.MMWR Morb Mortal Wkly Rep. 282008;57(12):309–312.
- ,,,.Response to the FDA's May 23, 2007, nephrogenic systemic fibrosis update.Radiology.2008;246(1):11–14.
- .How should nephrologists approach gadolinium‐based contrast imaging in patients with kidney disease?Clin J Am Soc Nephrol.2008;3(3):649–651.
Advice and Preparedness to Quit Smoking
Hospitalization may offer a natural opportunity to screen and advise patients on the advantages of quitting smoking due to a variety of reasons, such as the smoke‐free environment, availability of medical personnel, suitability of tailoring information, and the potential to catch a teachable moment.1, 2 Additionally, a recent meta‐analysis suggested that hospital‐based cessation programs and referrals to cardiac rehabilitation result in significantly higher rates of cessation among discharged smokers.3 In 2008, the U.S. Public Health Service Task Force on Clinical Practice Guidelines for Treating Tobacco Use and Dependence in hospitalized smokers recommended listing smoking status on problem lists, evaluating a smoker's preparedness to quit, providing counseling and medications to treat in‐hospital withdrawal symptoms, and arranging discharge follow‐up to help smokers remain abstinent.4 To promote these practices, the Center for Medicaid and Medicare Services (CMS) has made smoking cessation counseling a quality of care indicator for patients hospitalized with congestive heart failure (CHF), acute myocardial infarction (AMI), or pneumonia. This indicator is a critical step in recognizing the importance of smoking cessation counseling in improving mortality and morbidity for these patients.
Despite the importance of promoting smoking cessation among hospitalized patients, few studies have looked at whether or not hospitalized patients are prepared to quit smoking. Ascertaining patients' preparedness to quit smoking is an important first step in understanding a patient's readiness to change their health behaviors because smoking cessation is the culmination of a lengthy process of behavior change.5 Studies of healthy factory workers suggest that smokers who were more prepared to quit smoking had a higher number of previous quit attempts and perceived coworker encouragement.6
Understanding patient preparedness to quit smoking is especially important among African American smokers, who face a disproportionate health burden due to smoking‐related illness. Studies show that African Americans are less likely than other racial groups to engage in formal tobacco cessation interventions and have lower long‐term quit rates, despite a higher desire to quit smoking.5, 79 Understanding preparedness to quit among this particular group of hospitalized patients may be an important first step in identifying those most likely to quit and benefit from tailored, intensive interventions, such as using medications to assist in combination with postdischarge tobacco cessation counseling.
The aim of this study was to characterize the preparedness to quit smoking and to assess quit attempts made, methods used for quitting, and the success of such quit attempts at 1‐month follow‐up in a group comprised of a high proportion of underserved African American hospitalized smokers. In addition, the relationship of hospitalized patients' preparedness to quit and the effect of inpatient advice on the likelihood of subsequent tobacco cessation were examined.
Patients and Methods
The data used for this study were collected for the Cardiology Quality of Care Study, an ongoing prospective study of patients hospitalized on the inpatient cardiology service at the University of Chicago Medical Center. Newly admitted patients were approached by research assistants and consented to the study using a previously described protocol for enrolling hospitalized patients.10 Patients that lacked decisional capacity (score of <17 on the telephone version of the Mini‐Mental Status Exam)11 were excluded. Patients did not receive any scripted intervention during this admission to assist with cessation. The study left cessation counseling and advice to quit up to the discretion of the individual physician caring for the patient in the hospital. The Institutional Review Board at the University of Chicago approved this study.
Inpatient Interview
The inpatient interview is a 60‐item questionnaire taking approximately 15 minutes to administer by trained research assistants. The questionnaire is designed to assess demographic characteristics (race, socioeconomic status, education, sex, and age), smoking habits, and preparedness to quit. Demographics were collected on all consented patients. Seven items focused on cigarette smoking, consistent with questions in the National Health Information Survey.12 Patients were classified as lifetime smokers if they smoked at least 100 cigarettes in their lifetime. To identify current smokers on admission, patients were asked if they now smoke cigarettes some days or everyday. Additionally, smokers were asked if they had made any quit attempts in the past 12 months.
Patients rated their level of preparedness using a modified version of the Biener Abrams Contemplation Ladder. The Contemplation Ladder is an easily‐administered tool represented by a ladder image of rungs with anchor statements developed as an alternative method to the Prochaska and DiClemente Stages of Change.13 The 10‐point scale ranges from 1 (I enjoy smoking and have decided not to quit smoking for my lifetime; I have no interest in quitting) to 10 (I have quit smoking and will never smoke again.) Tobacco users may rank their current level of motivation to quit. A level of 6 (I definitely plan to quit smoking in the next 6 months) or higher is consistent with preparedness to quit. The Contemplation Ladder was validated by Biener and Abrams6 in a work site study which demonstrated that subjects with higher Ladder scores (score 6) were more likely than those with lower Ladder scores (scores < 6) to participate in awareness activities (eg, educational session) and make a quit attempt in 6 months. This instrument is easier to administer than the more well known Transtheoretical Model of Change, given that it is an ordinal scale with clear steps that may be more user‐friendly for both clinicians and patients.6 In a prior study of emergency room patients, an individual's Ladder score was shown to be significantly associated with a patient's reported intention to quit, number of previous quit attempts, perceived coworker encouragement, and socioeconomic status.14
Admission Diagnoses
Chart audit was performed by trained research assistants at the time of the inpatient interview (within 24 hours of admission) to assess whether patients were admitted with the potential diagnoses of AMI, CHF, neither, or both. All were based on the chart documentation of the patients' clinical presentation. This information was used to assess which CMS Quality Indicators applied to cardiology patients, given that smoking cessation is now a quality indicator for patients with AMI or CHF.
Thirty‐day Follow‐up Telephone Survey
Trained research assistants interviewed patients by telephone at approximately 1 month postdischarge. The follow‐up telephone survey included routine questions concerning follow‐up appointments, readmissions, emergency room visits, and patient satisfaction.15, 10 An additional 5 questions related to smoking cessation were added for this study. Questions were developed using the CMS quality indicators16 or were taken from the National Health Information Survey.12 Patients were asked to self‐report quit attempts made postdischarge, whether or not these quit attempts were associated with success (self‐reported abstinence at the time of follow‐up), and what methods were used to quit (ie, nicotine replacement therapy [NRT], other pharmacotherapy, quit line, pamphlet, counseling group, or cold turkey.) Patients were also asked if they recalled receiving advice to quit during their hospitalization from either a nurse or physician.
Data Analysis
Descriptive statistics were used to summarize Contemplation Ladder scores and types of quit methods used. Chi square tests were used to assess the effect of preparedness (Ladder score 6) on quit behaviors. The main quit behavior was any self‐reported quit attempt made within 1 month after discharge. Additionally, the relationship between preparedness and making a successful quit attempt (defined as a self‐report of not smoking as a result of this quit attempt in the last month) was examined. Multivariate logistic regression, controlling for demographic characteristics, was performed to test the effect of preparedness on quit behaviors (any quit attempt after discharge, or successful quit attempt). While not a primary aim of this study, the association between recall of in‐hospital advice and quit behaviors after discharge was also examined using chi square tests and multivariate logistic regression models, controlling for the demographic characteristics as above. Models also tested the effect of preparedness and recall of in‐hospital advice as independent predictors on quit behaviors and whether or not an interaction between preparedness and advice existed. A linear test of trend was also performed on preparedness and advice. All statistical tests were performed using Intercooled Stata 9.0 (Stata Corporation, College Station, TX), with statistical significance defined as P < 0.05.
Results
From February 2006 through July 2007, 86% (2906/3364) of all cardiology inpatients approached were interviewed. Fifteen percent (436/2906) of patients enrolled in the study indicated that they were current smokers. Contemplation Ladder scores were obtained on 95% (415/436) of the current smokers, and 1‐month postdischarge follow‐up telephone surveys were completed in 67% (276/415) of the current smokers. Three attempts were made to contact patients who were lost to follow‐up (Figure 1). The major reasons for inability to contact patients included wrong telephone numbers, disconnected phone lines, or no method to leave a message for the patient (ie, no answering machine). Given that we were only able to complete follow‐up interviews on 276 patients, we conducted our analyses on only this group of patients.
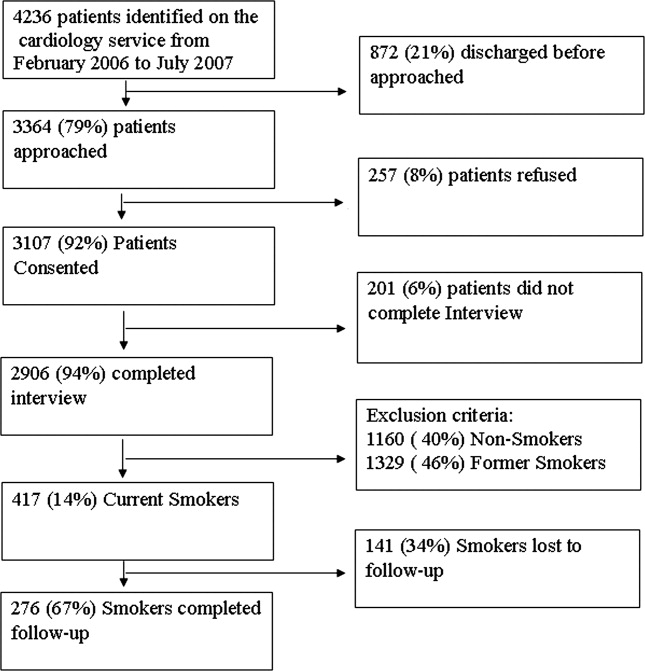
The average age of current smokers in the sample was 55 years (95% confidence interval [CI], 54‐58). Most current smokers were of the African American race (83%; 224/276). More than 65% of smokers had completed high school or higher, and nearly one‐half (46%) had an average household income of $25,000 or less before taxes. The most common admitting diagnoses per chart audit among current inpatient smokers were AMI (31%) and CHF (27%). The vast majority (95%) of hospitalized smokers in this sample were first‐time admissions to the University of Chicago. Table 1 shows the demographic data for current smokers compared to former smokers (those who have quit smoking prior to admission). Current smokers were more likely to be African American, had lower income levels, and were less likely to have completed high school. Additionally, current smokers were more likely to carry a potential diagnosis of AMI or CHF and to be a first‐time admission (Table 1).
| Demographic Variables | Current Smokers (n = 276)* | Nonsmoker (n = 1329)* | P Value |
|---|---|---|---|
| |||
| Male sex | 156 (57) | 705 (53) | 0.22 |
| African American race | 224 (83) | 886 (67) | <0.001 |
| Age (years) | 55.3 | 64.0 | <0.001 |
| Highest completed level of education | 0.02 | ||
| Junior high school or less | 15 (6) | 98 (7) | |
| Some high school | 67 (25) | 230 (17) | |
| High school graduate | 81 (30) | 403 (31) | |
| Some college education | 68 (25) | 313 (24) | |
| College graduate | 19 (7) | 135 (10) | |
| Graduate level education | 11 (4) | 96 (7) | |
| Household income before taxes | 0.001 | ||
| <$2500 | 33 (12) | 79 (6) | |
| $2501‐$15,000 | 66 (24) | 334 (26) | |
| $15,001‐$50,000 | 51 (19) | 311 (24) | |
| 50,001‐$100,000 | 22 (8) | 126 (9) | |
| >$100,001 | 11 (4) | 50 (4) | |
| Did not answer | 88 (33) | 422 (32) | |
| Diagnosis on admission | 0.02 | ||
| AMI | 66 (31) | 269 (24) | |
| CHF | 58 (27) | 287 (25) | |
| Both | 49 (23) | 273 (24) | |
| Neither | 42 (19) | 305 (27) | |
| Admission status | |||
| New admission | 258 (95) | 1,154 (87) | 0.051 |
| Readmission | 14 (5) | 175 (13) | |
Approximately three‐quarters (76%; 210/276) of current smokers were identified as prepared to quit, with a Ladder score 6. There was a wide distribution of Ladder scores, with one‐third (31%; 86/276) of smokers reporting a Ladder score of 8, indicating that they still smoke, but are ready to set a quit date and another 34% (95/276 patients) with Ladder scores of either 6 or 7 also indicating they were planning to quit smoking (Figure 2). A significant portion of smokers (71%; 195/276) reported making a quit attempt after discharge, and 38% of smokers (106/276) self‐reported that their quit attempt was successful (ie, no longer smoking at 1 month post discharge). Note that the quit rate is reduced to 26% (106/415) at 1 month if one conservatively assumes that those who did not take part in follow‐up were relapsers. Among those who did participate in follow‐up, as shown in Figure 3, the most frequently reported (53%; 145/276) method used to quit smoking was cold turkey. Thirteen percent (37/276) of patients reported making a quit attempt using pharmacological therapy (ie, NRT or bupropion) and only 4% (12/276) of patients reported making a quit attempt using the help of a smoking cessation program (Figure 3).
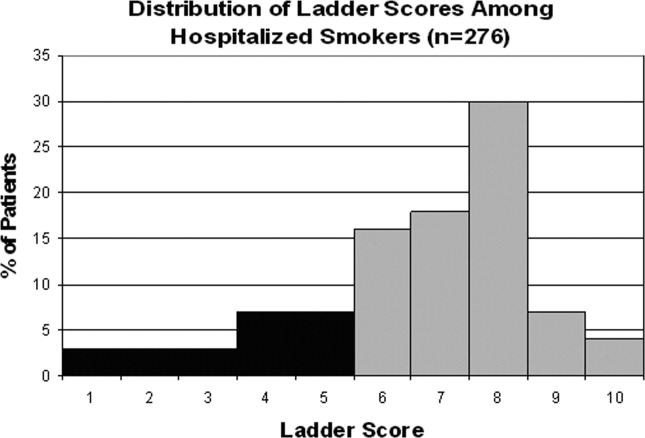

Preparedness was an important predictor of making a quit attempt. Prepared patients (ie, Ladder score 6) were significantly more likely than patients who were less prepared to report making a quit attempt after discharge (163/212 [77%] vs. 32/64 [50%], respectively; P < 0.001). This result remained significant after adjusting for sociodemographic characteristics with a similar effect size (adjusted estimates 76% [95% CI, 75.7‐76.7] prepared vs. 49% [95% CI, 48.5‐49.8]; P < 0.001). These results also remained significant with a similar effect size in analyses using multivariate logistic regression (Table 2). Of those patients who made quit attempts, prepared patients were slightly more likely to report a successful quit attempt (90/163; 55%) than were less‐prepared patients (16/32; 50%), though this was not significant (P = 0.205).
| Statistical test | Quit Behavior | Prepared % (95% CI) | Unprepared % (95% CI) | P Value |
|---|---|---|---|---|
| ||||
| Chi square tests | Any quit attempt made after discharge | 76.9 (71.2‐82.6) | 50.0 (37.8‐62.2) | <0.001 |
| Successful quit attempt at time of follow‐up | 55.0 (45.9‐60.2) | 50.0 (25.4‐58.2) | 0.20 | |
| Multivariate logistic regression* | Any quit attempt made after discharge | 76.2 (75.7‐76.7) | 49.2 (48.5‐49.9) | <0.001 |
In the follow‐up sample, 17% could not remember if they received advice to quit smoking. Among those who were able to recall receiving advice, the majority (78%; 180/230) reported that they received advice from a nurse or physician during hospitalization, compared to 22% who did not recall ever being advised to quit by any healthcare provider during the admission. Patients who reported receiving advice to quit were more likely to report making a quit attempt postdischarge as compared to those that did not recall receiving advice (70% vs. 46%, respectively; P = 0.002). In a multivariate logistic regression, controlling for demographic factors and admitting diagnosis, both preparedness and receipt of in‐hospital advice were independent predictors of making a future quit attempt (odds ratio [OR] = 4.05; 95% CI, 1.91‐8.60; P < 0.001 for preparedness; OR = 3.96; 95% CI, 1.84‐8.54; P < 0.001 for advice). Additionally, there was no significant interaction or synergistic effect between being prepared to quit smoking and receiving in‐hospital advice to quit (OR = 1.24; 95% CI, 0.17‐9.21; P = 0.836) (Figure 4). When analyzing the effects of preparedness and advice on quit attempts, only preparedness to quit remained a significant predictor of a successful quit attempt (OR = 2.93; 95% CI, 1.13‐7.60; P = 0.027 for preparedness; OR = 2.16; 95% CI, 0.85‐5.49; P = 0.10 for advice to quit). As demonstrated in Table 2, a higher percentage of prepared patients made a quit attempt after discharge (76.9% vs. 50%) and had a successful quit attempt and short‐term abstinence (55% prepared patients vs. 50% less prepared patients).
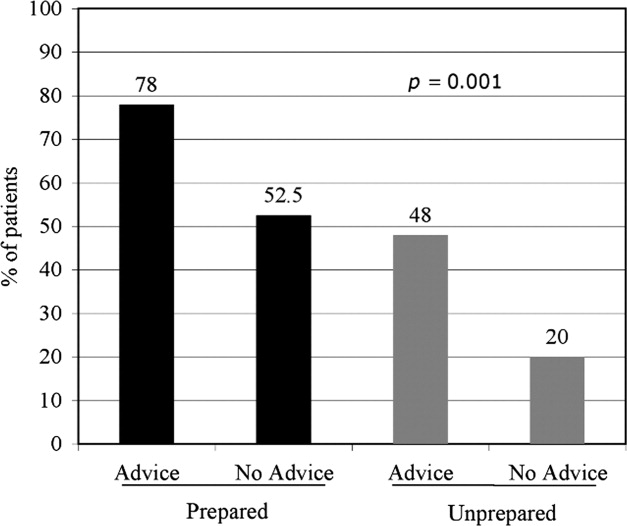
Discussion
This study demonstrated that in a group of hospitalized underserved, and predominantly African American smokers, the majority of patients reported being prepared to quit smoking at the time of hospitalization. Prepared patients were more likely to report making a quit attempt after discharge and more likely to report being successful in their quit attempt than patients who reported being less prepared to quit during their hospitalization. Nevertheless, approximately one‐half of unprepared patients did make a quit attempt 1 month after discharge, demonstrating a desire to quit smoking after hospitalization among this population. However, short‐term success rates in this group were lower than in patients prepared to quit. In addition, preparedness to quit and receipt of in‐hospital advice to quit smoking were both found to be independent predictors of making a quit attempt, with nearly identical ORs; however, only preparedness remained significant after controlling for advice to quit. Last, although the majority of hospitalized cardiac patients were making quit attempts after discharge, most patients reported using the least effective quit methods (ie, cold turkey) rather than more effective and intensive interventions such as counseling in combination with pharmacotherapy.
These findings have important implications for current quality initiatives targeted at promoting smoking cessation among cardiac patients. First, these results highlight the need for evidence‐based methods to be made available to hospitalized smokers who are prepared to quit. Our results are consistent with other studies reporting rare use (5.2%) of NRT in the hospital setting, despite the proven benefit in treating nicotine withdrawal symptoms.17 This is also consistent with data reporting that among nonhospitalized smokers, quitting cold turkey was the most commonly used and least effective cessation method.18 Second, the rate of recall of in‐hospital advice among patients (78%) was generally consistent with those reported to CMS (most recent quarter 95% for AMI and 88% for CHF).19
In addition to receiving advice, preparedness to quit was associated with higher quit attempts, therefore highlighting the importance of assessing level of preparedness in addition to giving advice. The fact that most quit attempts were made using cold turkey and resulted in low short‐term success rates underscores the need to reevaluate the current CMS quality indicator of advice alone for hospitalized smokers. Furthermore, the recently updated 2008 U.S. Public Health guidelines recently recommend, in addition to advice, that all hospitalized smokers be assessed for readiness to change, be assisted in quitting with pharmacotherapy, and be arranged follow‐up for tobacco cessation postdischarge, highlighting the inadequacy of advice alone.4 While it is important to continue to advise all hospitalized smokers to quit, the study findings demonstrate that assessing preparedness may result in targeting more prepared patients with more intensive interventions. Further policy implications include that less prepared patients may need motivational techniques to increase their level of preparedness to quit during hospitalization.
Several limitations are worth mentioning. First, the study included a relatively small sample size drawn from a single urban medical center. The prevalence of current smokers in our sample was 15%, which is lower than many studies looking at cardiology inpatient smokers.3, 20 This limitation of our study may be attributed to the advanced age of the majority of our patients, as compared with other studies, as well as the possibility of socially desirable response bias that many low‐income African American smokers may experience, leaving them less likely to admit to smoking at the time of hospitalization. Second, there was a low follow‐up rate, with 66% of patients undergoing follow‐up postdischarge. While this may raise the concerns of differences between ladder scores in those patients that participated in follow‐up and those that did not, analyses show no significant difference between level of preparedness in these 2 groups (68% prepared in patients who received follow‐up vs. 63% prepared patients in those who did not participate in follow‐up; P = 0.36). Third, follow‐up of quit attempts and receipt of advice were all assessed using self‐report, and, therefore, were limited by lack of verification and lack of assessment for potential recall bias. Fourth, in this pilot study, the follow‐up period was relatively short at 1 month postdischarge. It is likely that rates of successful quit attempts would be lower with longer‐term follow‐up periods, given previous literature demonstrating the difficulty with long‐term abstinence.21 Last, the study was not able to account for potential effects that hospitalization itself may have on preparedness, as patients may be more likely to report being prepared to quit when in the face of a health shock,22 as well as the fact that some patients may demonstrate a socially desirable response bias influenced by hospitalization.
In conclusion, the majority of underserved smokers with cardiac disease reported being prepared to quit smoking and were more likely to self‐report making a quit attempt after discharge. However, the majority of these quit attempts were made via cold turkey, without the support of available evidence‐based methods to quit. It is possible that by directly providing education, access to pharmacotherapy, and counseling options, the utilization rates for more efficacious treatments would increase in cardiac patients who are prepared to quit. While recall of in‐hospital advice was associated with future quit attempts, prepared patients who recalled receiving advice were more likely to make a quit attempt than prepared patients who did not recall receiving advice, as well as unprepared patients. Together, these findings highlight the need to consider a patient's level of preparedness to quit in understanding the success of in‐hospital advice and the importance of making evidence‐based cessation methods available to hospitalized smokers who are prepared to quit. Additionally, identifying patients not prepared to quit may help in providing them with appropriate motivational therapy, to move them along the stages of change, as well as educational information on how to quit once they have decided to do so.
- ,,.Helping hospitalized smokers quit: new directions for treatment and research.J Consult Clin Psychol.1993;61:778–789.
- ,.Smokers who are hospitalized: a window of opportunity for cessation interventions.Prev Med.1992;21:262–269.
- ,,, et al.Predictors of smoking cessation after a myocardial infarction: the role of institutional smoking cessation programs in improving success.Arch Intern Med.2008;168(18):1961–1967.
- Guideline Panel.Clinical Practice Guidelines: Treating Tobacco Use and Dependence.Washington, DC:Public Health Service, U.S. Department of Health and Human Services;2008.
- ,.Stages and processes of self‐change in smoking: toward an integrative model of change.J Consult Clin Psychol.1983;51:390–395.
- ,.The Contemplation Ladder: validation of a measure of readiness to consider smoking cessation.Health Psychol.1991;10(5):360–365.
- ,,,,.Smoking cessation factors among African Americans and Whites.Am J Public Health.1993;83(2):220–226.
- U.S. Department of Health and Human Services.The Health Benefits of Smoking Cessation.Rockville, MD:Office on Smoking and Health, Centers for Chronic Disease Prevention and Health Promotion, Public Health Service,U.S. Department of Health and Human Services,Washington, DC;2000.
- ,,,,.Trends in cigarette smoking in the United States. the changing influence of gender and race.JAMA.1989;261(1):49–55.
- ,,, et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137(11):866–874.
- ,,,.Validation of a telephone version of the Mini‐Mental State Examination.J Am Geriatr Soc.1992;40(7):697–702.
- National Health Information Survey Questionnaire, Sample Adult,Adult Health Behaviors;2004.
- ,,, et al.The Marijuana Ladder: measuring motivation to change marijuana use in incarcerated adolescents.Drug Alcohol Depend.2006;83:42–48.
- ,,,,.Motivation for stopping tobacco use among emergency department patients.Acad Emerg Med.2005;12:568–571.
- Picker‐Commonwealth Survey of Patient‐Centered Care.Health Aff.1991.
- Hospital Quality Initiatives. Centers for Medicare and Medicaid Services (CMS). Available at: http://www.cms.hhs.gov/HospitalQualtiyInits. Accessed April2009.
- ,,, et al.The use of nicotine replacement therapy by hospitalized smokers.Am J Prev Med.1999;17(4):255–259.
- ,,,,.Methods used to quit smoking in the United States: do cessation programs help?JAMA.1990;263(20):2795–2796.
- U.S. Department of Health and Human Services.Hospital Compare.2006 Data Graphs. Available at: http://www.hospitalcompare.hhs.gov. Accessed April2009.
- ,,, et al.Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Cigarette smoking among adults—United States, 2006.MMWR Morb Mortal Wkly Rep.2007;56:1157–1161.
- ,,.Smoking cessation interventions for hospitalized smokers.Arch Intern Med.2008;168(18):1950–1960.
- ,.Health beliefs and smoking patterns in heart patients and their wives: a longitudinal study.Am J Public Health.1977;67:921–930.
Hospitalization may offer a natural opportunity to screen and advise patients on the advantages of quitting smoking due to a variety of reasons, such as the smoke‐free environment, availability of medical personnel, suitability of tailoring information, and the potential to catch a teachable moment.1, 2 Additionally, a recent meta‐analysis suggested that hospital‐based cessation programs and referrals to cardiac rehabilitation result in significantly higher rates of cessation among discharged smokers.3 In 2008, the U.S. Public Health Service Task Force on Clinical Practice Guidelines for Treating Tobacco Use and Dependence in hospitalized smokers recommended listing smoking status on problem lists, evaluating a smoker's preparedness to quit, providing counseling and medications to treat in‐hospital withdrawal symptoms, and arranging discharge follow‐up to help smokers remain abstinent.4 To promote these practices, the Center for Medicaid and Medicare Services (CMS) has made smoking cessation counseling a quality of care indicator for patients hospitalized with congestive heart failure (CHF), acute myocardial infarction (AMI), or pneumonia. This indicator is a critical step in recognizing the importance of smoking cessation counseling in improving mortality and morbidity for these patients.
Despite the importance of promoting smoking cessation among hospitalized patients, few studies have looked at whether or not hospitalized patients are prepared to quit smoking. Ascertaining patients' preparedness to quit smoking is an important first step in understanding a patient's readiness to change their health behaviors because smoking cessation is the culmination of a lengthy process of behavior change.5 Studies of healthy factory workers suggest that smokers who were more prepared to quit smoking had a higher number of previous quit attempts and perceived coworker encouragement.6
Understanding patient preparedness to quit smoking is especially important among African American smokers, who face a disproportionate health burden due to smoking‐related illness. Studies show that African Americans are less likely than other racial groups to engage in formal tobacco cessation interventions and have lower long‐term quit rates, despite a higher desire to quit smoking.5, 79 Understanding preparedness to quit among this particular group of hospitalized patients may be an important first step in identifying those most likely to quit and benefit from tailored, intensive interventions, such as using medications to assist in combination with postdischarge tobacco cessation counseling.
The aim of this study was to characterize the preparedness to quit smoking and to assess quit attempts made, methods used for quitting, and the success of such quit attempts at 1‐month follow‐up in a group comprised of a high proportion of underserved African American hospitalized smokers. In addition, the relationship of hospitalized patients' preparedness to quit and the effect of inpatient advice on the likelihood of subsequent tobacco cessation were examined.
Patients and Methods
The data used for this study were collected for the Cardiology Quality of Care Study, an ongoing prospective study of patients hospitalized on the inpatient cardiology service at the University of Chicago Medical Center. Newly admitted patients were approached by research assistants and consented to the study using a previously described protocol for enrolling hospitalized patients.10 Patients that lacked decisional capacity (score of <17 on the telephone version of the Mini‐Mental Status Exam)11 were excluded. Patients did not receive any scripted intervention during this admission to assist with cessation. The study left cessation counseling and advice to quit up to the discretion of the individual physician caring for the patient in the hospital. The Institutional Review Board at the University of Chicago approved this study.
Inpatient Interview
The inpatient interview is a 60‐item questionnaire taking approximately 15 minutes to administer by trained research assistants. The questionnaire is designed to assess demographic characteristics (race, socioeconomic status, education, sex, and age), smoking habits, and preparedness to quit. Demographics were collected on all consented patients. Seven items focused on cigarette smoking, consistent with questions in the National Health Information Survey.12 Patients were classified as lifetime smokers if they smoked at least 100 cigarettes in their lifetime. To identify current smokers on admission, patients were asked if they now smoke cigarettes some days or everyday. Additionally, smokers were asked if they had made any quit attempts in the past 12 months.
Patients rated their level of preparedness using a modified version of the Biener Abrams Contemplation Ladder. The Contemplation Ladder is an easily‐administered tool represented by a ladder image of rungs with anchor statements developed as an alternative method to the Prochaska and DiClemente Stages of Change.13 The 10‐point scale ranges from 1 (I enjoy smoking and have decided not to quit smoking for my lifetime; I have no interest in quitting) to 10 (I have quit smoking and will never smoke again.) Tobacco users may rank their current level of motivation to quit. A level of 6 (I definitely plan to quit smoking in the next 6 months) or higher is consistent with preparedness to quit. The Contemplation Ladder was validated by Biener and Abrams6 in a work site study which demonstrated that subjects with higher Ladder scores (score 6) were more likely than those with lower Ladder scores (scores < 6) to participate in awareness activities (eg, educational session) and make a quit attempt in 6 months. This instrument is easier to administer than the more well known Transtheoretical Model of Change, given that it is an ordinal scale with clear steps that may be more user‐friendly for both clinicians and patients.6 In a prior study of emergency room patients, an individual's Ladder score was shown to be significantly associated with a patient's reported intention to quit, number of previous quit attempts, perceived coworker encouragement, and socioeconomic status.14
Admission Diagnoses
Chart audit was performed by trained research assistants at the time of the inpatient interview (within 24 hours of admission) to assess whether patients were admitted with the potential diagnoses of AMI, CHF, neither, or both. All were based on the chart documentation of the patients' clinical presentation. This information was used to assess which CMS Quality Indicators applied to cardiology patients, given that smoking cessation is now a quality indicator for patients with AMI or CHF.
Thirty‐day Follow‐up Telephone Survey
Trained research assistants interviewed patients by telephone at approximately 1 month postdischarge. The follow‐up telephone survey included routine questions concerning follow‐up appointments, readmissions, emergency room visits, and patient satisfaction.15, 10 An additional 5 questions related to smoking cessation were added for this study. Questions were developed using the CMS quality indicators16 or were taken from the National Health Information Survey.12 Patients were asked to self‐report quit attempts made postdischarge, whether or not these quit attempts were associated with success (self‐reported abstinence at the time of follow‐up), and what methods were used to quit (ie, nicotine replacement therapy [NRT], other pharmacotherapy, quit line, pamphlet, counseling group, or cold turkey.) Patients were also asked if they recalled receiving advice to quit during their hospitalization from either a nurse or physician.
Data Analysis
Descriptive statistics were used to summarize Contemplation Ladder scores and types of quit methods used. Chi square tests were used to assess the effect of preparedness (Ladder score 6) on quit behaviors. The main quit behavior was any self‐reported quit attempt made within 1 month after discharge. Additionally, the relationship between preparedness and making a successful quit attempt (defined as a self‐report of not smoking as a result of this quit attempt in the last month) was examined. Multivariate logistic regression, controlling for demographic characteristics, was performed to test the effect of preparedness on quit behaviors (any quit attempt after discharge, or successful quit attempt). While not a primary aim of this study, the association between recall of in‐hospital advice and quit behaviors after discharge was also examined using chi square tests and multivariate logistic regression models, controlling for the demographic characteristics as above. Models also tested the effect of preparedness and recall of in‐hospital advice as independent predictors on quit behaviors and whether or not an interaction between preparedness and advice existed. A linear test of trend was also performed on preparedness and advice. All statistical tests were performed using Intercooled Stata 9.0 (Stata Corporation, College Station, TX), with statistical significance defined as P < 0.05.
Results
From February 2006 through July 2007, 86% (2906/3364) of all cardiology inpatients approached were interviewed. Fifteen percent (436/2906) of patients enrolled in the study indicated that they were current smokers. Contemplation Ladder scores were obtained on 95% (415/436) of the current smokers, and 1‐month postdischarge follow‐up telephone surveys were completed in 67% (276/415) of the current smokers. Three attempts were made to contact patients who were lost to follow‐up (Figure 1). The major reasons for inability to contact patients included wrong telephone numbers, disconnected phone lines, or no method to leave a message for the patient (ie, no answering machine). Given that we were only able to complete follow‐up interviews on 276 patients, we conducted our analyses on only this group of patients.
The average age of current smokers in the sample was 55 years (95% confidence interval [CI], 54‐58). Most current smokers were of the African American race (83%; 224/276). More than 65% of smokers had completed high school or higher, and nearly one‐half (46%) had an average household income of $25,000 or less before taxes. The most common admitting diagnoses per chart audit among current inpatient smokers were AMI (31%) and CHF (27%). The vast majority (95%) of hospitalized smokers in this sample were first‐time admissions to the University of Chicago. Table 1 shows the demographic data for current smokers compared to former smokers (those who have quit smoking prior to admission). Current smokers were more likely to be African American, had lower income levels, and were less likely to have completed high school. Additionally, current smokers were more likely to carry a potential diagnosis of AMI or CHF and to be a first‐time admission (Table 1).
| Demographic Variables | Current Smokers (n = 276)* | Nonsmoker (n = 1329)* | P Value |
|---|---|---|---|
| |||
| Male sex | 156 (57) | 705 (53) | 0.22 |
| African American race | 224 (83) | 886 (67) | <0.001 |
| Age (years) | 55.3 | 64.0 | <0.001 |
| Highest completed level of education | 0.02 | ||
| Junior high school or less | 15 (6) | 98 (7) | |
| Some high school | 67 (25) | 230 (17) | |
| High school graduate | 81 (30) | 403 (31) | |
| Some college education | 68 (25) | 313 (24) | |
| College graduate | 19 (7) | 135 (10) | |
| Graduate level education | 11 (4) | 96 (7) | |
| Household income before taxes | 0.001 | ||
| <$2500 | 33 (12) | 79 (6) | |
| $2501‐$15,000 | 66 (24) | 334 (26) | |
| $15,001‐$50,000 | 51 (19) | 311 (24) | |
| 50,001‐$100,000 | 22 (8) | 126 (9) | |
| >$100,001 | 11 (4) | 50 (4) | |
| Did not answer | 88 (33) | 422 (32) | |
| Diagnosis on admission | 0.02 | ||
| AMI | 66 (31) | 269 (24) | |
| CHF | 58 (27) | 287 (25) | |
| Both | 49 (23) | 273 (24) | |
| Neither | 42 (19) | 305 (27) | |
| Admission status | |||
| New admission | 258 (95) | 1,154 (87) | 0.051 |
| Readmission | 14 (5) | 175 (13) | |
Approximately three‐quarters (76%; 210/276) of current smokers were identified as prepared to quit, with a Ladder score 6. There was a wide distribution of Ladder scores, with one‐third (31%; 86/276) of smokers reporting a Ladder score of 8, indicating that they still smoke, but are ready to set a quit date and another 34% (95/276 patients) with Ladder scores of either 6 or 7 also indicating they were planning to quit smoking (Figure 2). A significant portion of smokers (71%; 195/276) reported making a quit attempt after discharge, and 38% of smokers (106/276) self‐reported that their quit attempt was successful (ie, no longer smoking at 1 month post discharge). Note that the quit rate is reduced to 26% (106/415) at 1 month if one conservatively assumes that those who did not take part in follow‐up were relapsers. Among those who did participate in follow‐up, as shown in Figure 3, the most frequently reported (53%; 145/276) method used to quit smoking was cold turkey. Thirteen percent (37/276) of patients reported making a quit attempt using pharmacological therapy (ie, NRT or bupropion) and only 4% (12/276) of patients reported making a quit attempt using the help of a smoking cessation program (Figure 3).
Preparedness was an important predictor of making a quit attempt. Prepared patients (ie, Ladder score 6) were significantly more likely than patients who were less prepared to report making a quit attempt after discharge (163/212 [77%] vs. 32/64 [50%], respectively; P < 0.001). This result remained significant after adjusting for sociodemographic characteristics with a similar effect size (adjusted estimates 76% [95% CI, 75.7‐76.7] prepared vs. 49% [95% CI, 48.5‐49.8]; P < 0.001). These results also remained significant with a similar effect size in analyses using multivariate logistic regression (Table 2). Of those patients who made quit attempts, prepared patients were slightly more likely to report a successful quit attempt (90/163; 55%) than were less‐prepared patients (16/32; 50%), though this was not significant (P = 0.205).
| Statistical test | Quit Behavior | Prepared % (95% CI) | Unprepared % (95% CI) | P Value |
|---|---|---|---|---|
| ||||
| Chi square tests | Any quit attempt made after discharge | 76.9 (71.2‐82.6) | 50.0 (37.8‐62.2) | <0.001 |
| Successful quit attempt at time of follow‐up | 55.0 (45.9‐60.2) | 50.0 (25.4‐58.2) | 0.20 | |
| Multivariate logistic regression* | Any quit attempt made after discharge | 76.2 (75.7‐76.7) | 49.2 (48.5‐49.9) | <0.001 |
In the follow‐up sample, 17% could not remember if they received advice to quit smoking. Among those who were able to recall receiving advice, the majority (78%; 180/230) reported that they received advice from a nurse or physician during hospitalization, compared to 22% who did not recall ever being advised to quit by any healthcare provider during the admission. Patients who reported receiving advice to quit were more likely to report making a quit attempt postdischarge as compared to those that did not recall receiving advice (70% vs. 46%, respectively; P = 0.002). In a multivariate logistic regression, controlling for demographic factors and admitting diagnosis, both preparedness and receipt of in‐hospital advice were independent predictors of making a future quit attempt (odds ratio [OR] = 4.05; 95% CI, 1.91‐8.60; P < 0.001 for preparedness; OR = 3.96; 95% CI, 1.84‐8.54; P < 0.001 for advice). Additionally, there was no significant interaction or synergistic effect between being prepared to quit smoking and receiving in‐hospital advice to quit (OR = 1.24; 95% CI, 0.17‐9.21; P = 0.836) (Figure 4). When analyzing the effects of preparedness and advice on quit attempts, only preparedness to quit remained a significant predictor of a successful quit attempt (OR = 2.93; 95% CI, 1.13‐7.60; P = 0.027 for preparedness; OR = 2.16; 95% CI, 0.85‐5.49; P = 0.10 for advice to quit). As demonstrated in Table 2, a higher percentage of prepared patients made a quit attempt after discharge (76.9% vs. 50%) and had a successful quit attempt and short‐term abstinence (55% prepared patients vs. 50% less prepared patients).
Discussion
This study demonstrated that in a group of hospitalized underserved, and predominantly African American smokers, the majority of patients reported being prepared to quit smoking at the time of hospitalization. Prepared patients were more likely to report making a quit attempt after discharge and more likely to report being successful in their quit attempt than patients who reported being less prepared to quit during their hospitalization. Nevertheless, approximately one‐half of unprepared patients did make a quit attempt 1 month after discharge, demonstrating a desire to quit smoking after hospitalization among this population. However, short‐term success rates in this group were lower than in patients prepared to quit. In addition, preparedness to quit and receipt of in‐hospital advice to quit smoking were both found to be independent predictors of making a quit attempt, with nearly identical ORs; however, only preparedness remained significant after controlling for advice to quit. Last, although the majority of hospitalized cardiac patients were making quit attempts after discharge, most patients reported using the least effective quit methods (ie, cold turkey) rather than more effective and intensive interventions such as counseling in combination with pharmacotherapy.
These findings have important implications for current quality initiatives targeted at promoting smoking cessation among cardiac patients. First, these results highlight the need for evidence‐based methods to be made available to hospitalized smokers who are prepared to quit. Our results are consistent with other studies reporting rare use (5.2%) of NRT in the hospital setting, despite the proven benefit in treating nicotine withdrawal symptoms.17 This is also consistent with data reporting that among nonhospitalized smokers, quitting cold turkey was the most commonly used and least effective cessation method.18 Second, the rate of recall of in‐hospital advice among patients (78%) was generally consistent with those reported to CMS (most recent quarter 95% for AMI and 88% for CHF).19
In addition to receiving advice, preparedness to quit was associated with higher quit attempts, therefore highlighting the importance of assessing level of preparedness in addition to giving advice. The fact that most quit attempts were made using cold turkey and resulted in low short‐term success rates underscores the need to reevaluate the current CMS quality indicator of advice alone for hospitalized smokers. Furthermore, the recently updated 2008 U.S. Public Health guidelines recently recommend, in addition to advice, that all hospitalized smokers be assessed for readiness to change, be assisted in quitting with pharmacotherapy, and be arranged follow‐up for tobacco cessation postdischarge, highlighting the inadequacy of advice alone.4 While it is important to continue to advise all hospitalized smokers to quit, the study findings demonstrate that assessing preparedness may result in targeting more prepared patients with more intensive interventions. Further policy implications include that less prepared patients may need motivational techniques to increase their level of preparedness to quit during hospitalization.
Several limitations are worth mentioning. First, the study included a relatively small sample size drawn from a single urban medical center. The prevalence of current smokers in our sample was 15%, which is lower than many studies looking at cardiology inpatient smokers.3, 20 This limitation of our study may be attributed to the advanced age of the majority of our patients, as compared with other studies, as well as the possibility of socially desirable response bias that many low‐income African American smokers may experience, leaving them less likely to admit to smoking at the time of hospitalization. Second, there was a low follow‐up rate, with 66% of patients undergoing follow‐up postdischarge. While this may raise the concerns of differences between ladder scores in those patients that participated in follow‐up and those that did not, analyses show no significant difference between level of preparedness in these 2 groups (68% prepared in patients who received follow‐up vs. 63% prepared patients in those who did not participate in follow‐up; P = 0.36). Third, follow‐up of quit attempts and receipt of advice were all assessed using self‐report, and, therefore, were limited by lack of verification and lack of assessment for potential recall bias. Fourth, in this pilot study, the follow‐up period was relatively short at 1 month postdischarge. It is likely that rates of successful quit attempts would be lower with longer‐term follow‐up periods, given previous literature demonstrating the difficulty with long‐term abstinence.21 Last, the study was not able to account for potential effects that hospitalization itself may have on preparedness, as patients may be more likely to report being prepared to quit when in the face of a health shock,22 as well as the fact that some patients may demonstrate a socially desirable response bias influenced by hospitalization.
In conclusion, the majority of underserved smokers with cardiac disease reported being prepared to quit smoking and were more likely to self‐report making a quit attempt after discharge. However, the majority of these quit attempts were made via cold turkey, without the support of available evidence‐based methods to quit. It is possible that by directly providing education, access to pharmacotherapy, and counseling options, the utilization rates for more efficacious treatments would increase in cardiac patients who are prepared to quit. While recall of in‐hospital advice was associated with future quit attempts, prepared patients who recalled receiving advice were more likely to make a quit attempt than prepared patients who did not recall receiving advice, as well as unprepared patients. Together, these findings highlight the need to consider a patient's level of preparedness to quit in understanding the success of in‐hospital advice and the importance of making evidence‐based cessation methods available to hospitalized smokers who are prepared to quit. Additionally, identifying patients not prepared to quit may help in providing them with appropriate motivational therapy, to move them along the stages of change, as well as educational information on how to quit once they have decided to do so.
Hospitalization may offer a natural opportunity to screen and advise patients on the advantages of quitting smoking due to a variety of reasons, such as the smoke‐free environment, availability of medical personnel, suitability of tailoring information, and the potential to catch a teachable moment.1, 2 Additionally, a recent meta‐analysis suggested that hospital‐based cessation programs and referrals to cardiac rehabilitation result in significantly higher rates of cessation among discharged smokers.3 In 2008, the U.S. Public Health Service Task Force on Clinical Practice Guidelines for Treating Tobacco Use and Dependence in hospitalized smokers recommended listing smoking status on problem lists, evaluating a smoker's preparedness to quit, providing counseling and medications to treat in‐hospital withdrawal symptoms, and arranging discharge follow‐up to help smokers remain abstinent.4 To promote these practices, the Center for Medicaid and Medicare Services (CMS) has made smoking cessation counseling a quality of care indicator for patients hospitalized with congestive heart failure (CHF), acute myocardial infarction (AMI), or pneumonia. This indicator is a critical step in recognizing the importance of smoking cessation counseling in improving mortality and morbidity for these patients.
Despite the importance of promoting smoking cessation among hospitalized patients, few studies have looked at whether or not hospitalized patients are prepared to quit smoking. Ascertaining patients' preparedness to quit smoking is an important first step in understanding a patient's readiness to change their health behaviors because smoking cessation is the culmination of a lengthy process of behavior change.5 Studies of healthy factory workers suggest that smokers who were more prepared to quit smoking had a higher number of previous quit attempts and perceived coworker encouragement.6
Understanding patient preparedness to quit smoking is especially important among African American smokers, who face a disproportionate health burden due to smoking‐related illness. Studies show that African Americans are less likely than other racial groups to engage in formal tobacco cessation interventions and have lower long‐term quit rates, despite a higher desire to quit smoking.5, 79 Understanding preparedness to quit among this particular group of hospitalized patients may be an important first step in identifying those most likely to quit and benefit from tailored, intensive interventions, such as using medications to assist in combination with postdischarge tobacco cessation counseling.
The aim of this study was to characterize the preparedness to quit smoking and to assess quit attempts made, methods used for quitting, and the success of such quit attempts at 1‐month follow‐up in a group comprised of a high proportion of underserved African American hospitalized smokers. In addition, the relationship of hospitalized patients' preparedness to quit and the effect of inpatient advice on the likelihood of subsequent tobacco cessation were examined.
Patients and Methods
The data used for this study were collected for the Cardiology Quality of Care Study, an ongoing prospective study of patients hospitalized on the inpatient cardiology service at the University of Chicago Medical Center. Newly admitted patients were approached by research assistants and consented to the study using a previously described protocol for enrolling hospitalized patients.10 Patients that lacked decisional capacity (score of <17 on the telephone version of the Mini‐Mental Status Exam)11 were excluded. Patients did not receive any scripted intervention during this admission to assist with cessation. The study left cessation counseling and advice to quit up to the discretion of the individual physician caring for the patient in the hospital. The Institutional Review Board at the University of Chicago approved this study.
Inpatient Interview
The inpatient interview is a 60‐item questionnaire taking approximately 15 minutes to administer by trained research assistants. The questionnaire is designed to assess demographic characteristics (race, socioeconomic status, education, sex, and age), smoking habits, and preparedness to quit. Demographics were collected on all consented patients. Seven items focused on cigarette smoking, consistent with questions in the National Health Information Survey.12 Patients were classified as lifetime smokers if they smoked at least 100 cigarettes in their lifetime. To identify current smokers on admission, patients were asked if they now smoke cigarettes some days or everyday. Additionally, smokers were asked if they had made any quit attempts in the past 12 months.
Patients rated their level of preparedness using a modified version of the Biener Abrams Contemplation Ladder. The Contemplation Ladder is an easily‐administered tool represented by a ladder image of rungs with anchor statements developed as an alternative method to the Prochaska and DiClemente Stages of Change.13 The 10‐point scale ranges from 1 (I enjoy smoking and have decided not to quit smoking for my lifetime; I have no interest in quitting) to 10 (I have quit smoking and will never smoke again.) Tobacco users may rank their current level of motivation to quit. A level of 6 (I definitely plan to quit smoking in the next 6 months) or higher is consistent with preparedness to quit. The Contemplation Ladder was validated by Biener and Abrams6 in a work site study which demonstrated that subjects with higher Ladder scores (score 6) were more likely than those with lower Ladder scores (scores < 6) to participate in awareness activities (eg, educational session) and make a quit attempt in 6 months. This instrument is easier to administer than the more well known Transtheoretical Model of Change, given that it is an ordinal scale with clear steps that may be more user‐friendly for both clinicians and patients.6 In a prior study of emergency room patients, an individual's Ladder score was shown to be significantly associated with a patient's reported intention to quit, number of previous quit attempts, perceived coworker encouragement, and socioeconomic status.14
Admission Diagnoses
Chart audit was performed by trained research assistants at the time of the inpatient interview (within 24 hours of admission) to assess whether patients were admitted with the potential diagnoses of AMI, CHF, neither, or both. All were based on the chart documentation of the patients' clinical presentation. This information was used to assess which CMS Quality Indicators applied to cardiology patients, given that smoking cessation is now a quality indicator for patients with AMI or CHF.
Thirty‐day Follow‐up Telephone Survey
Trained research assistants interviewed patients by telephone at approximately 1 month postdischarge. The follow‐up telephone survey included routine questions concerning follow‐up appointments, readmissions, emergency room visits, and patient satisfaction.15, 10 An additional 5 questions related to smoking cessation were added for this study. Questions were developed using the CMS quality indicators16 or were taken from the National Health Information Survey.12 Patients were asked to self‐report quit attempts made postdischarge, whether or not these quit attempts were associated with success (self‐reported abstinence at the time of follow‐up), and what methods were used to quit (ie, nicotine replacement therapy [NRT], other pharmacotherapy, quit line, pamphlet, counseling group, or cold turkey.) Patients were also asked if they recalled receiving advice to quit during their hospitalization from either a nurse or physician.
Data Analysis
Descriptive statistics were used to summarize Contemplation Ladder scores and types of quit methods used. Chi square tests were used to assess the effect of preparedness (Ladder score 6) on quit behaviors. The main quit behavior was any self‐reported quit attempt made within 1 month after discharge. Additionally, the relationship between preparedness and making a successful quit attempt (defined as a self‐report of not smoking as a result of this quit attempt in the last month) was examined. Multivariate logistic regression, controlling for demographic characteristics, was performed to test the effect of preparedness on quit behaviors (any quit attempt after discharge, or successful quit attempt). While not a primary aim of this study, the association between recall of in‐hospital advice and quit behaviors after discharge was also examined using chi square tests and multivariate logistic regression models, controlling for the demographic characteristics as above. Models also tested the effect of preparedness and recall of in‐hospital advice as independent predictors on quit behaviors and whether or not an interaction between preparedness and advice existed. A linear test of trend was also performed on preparedness and advice. All statistical tests were performed using Intercooled Stata 9.0 (Stata Corporation, College Station, TX), with statistical significance defined as P < 0.05.
Results
From February 2006 through July 2007, 86% (2906/3364) of all cardiology inpatients approached were interviewed. Fifteen percent (436/2906) of patients enrolled in the study indicated that they were current smokers. Contemplation Ladder scores were obtained on 95% (415/436) of the current smokers, and 1‐month postdischarge follow‐up telephone surveys were completed in 67% (276/415) of the current smokers. Three attempts were made to contact patients who were lost to follow‐up (Figure 1). The major reasons for inability to contact patients included wrong telephone numbers, disconnected phone lines, or no method to leave a message for the patient (ie, no answering machine). Given that we were only able to complete follow‐up interviews on 276 patients, we conducted our analyses on only this group of patients.
The average age of current smokers in the sample was 55 years (95% confidence interval [CI], 54‐58). Most current smokers were of the African American race (83%; 224/276). More than 65% of smokers had completed high school or higher, and nearly one‐half (46%) had an average household income of $25,000 or less before taxes. The most common admitting diagnoses per chart audit among current inpatient smokers were AMI (31%) and CHF (27%). The vast majority (95%) of hospitalized smokers in this sample were first‐time admissions to the University of Chicago. Table 1 shows the demographic data for current smokers compared to former smokers (those who have quit smoking prior to admission). Current smokers were more likely to be African American, had lower income levels, and were less likely to have completed high school. Additionally, current smokers were more likely to carry a potential diagnosis of AMI or CHF and to be a first‐time admission (Table 1).
| Demographic Variables | Current Smokers (n = 276)* | Nonsmoker (n = 1329)* | P Value |
|---|---|---|---|
| |||
| Male sex | 156 (57) | 705 (53) | 0.22 |
| African American race | 224 (83) | 886 (67) | <0.001 |
| Age (years) | 55.3 | 64.0 | <0.001 |
| Highest completed level of education | 0.02 | ||
| Junior high school or less | 15 (6) | 98 (7) | |
| Some high school | 67 (25) | 230 (17) | |
| High school graduate | 81 (30) | 403 (31) | |
| Some college education | 68 (25) | 313 (24) | |
| College graduate | 19 (7) | 135 (10) | |
| Graduate level education | 11 (4) | 96 (7) | |
| Household income before taxes | 0.001 | ||
| <$2500 | 33 (12) | 79 (6) | |
| $2501‐$15,000 | 66 (24) | 334 (26) | |
| $15,001‐$50,000 | 51 (19) | 311 (24) | |
| 50,001‐$100,000 | 22 (8) | 126 (9) | |
| >$100,001 | 11 (4) | 50 (4) | |
| Did not answer | 88 (33) | 422 (32) | |
| Diagnosis on admission | 0.02 | ||
| AMI | 66 (31) | 269 (24) | |
| CHF | 58 (27) | 287 (25) | |
| Both | 49 (23) | 273 (24) | |
| Neither | 42 (19) | 305 (27) | |
| Admission status | |||
| New admission | 258 (95) | 1,154 (87) | 0.051 |
| Readmission | 14 (5) | 175 (13) | |
Approximately three‐quarters (76%; 210/276) of current smokers were identified as prepared to quit, with a Ladder score 6. There was a wide distribution of Ladder scores, with one‐third (31%; 86/276) of smokers reporting a Ladder score of 8, indicating that they still smoke, but are ready to set a quit date and another 34% (95/276 patients) with Ladder scores of either 6 or 7 also indicating they were planning to quit smoking (Figure 2). A significant portion of smokers (71%; 195/276) reported making a quit attempt after discharge, and 38% of smokers (106/276) self‐reported that their quit attempt was successful (ie, no longer smoking at 1 month post discharge). Note that the quit rate is reduced to 26% (106/415) at 1 month if one conservatively assumes that those who did not take part in follow‐up were relapsers. Among those who did participate in follow‐up, as shown in Figure 3, the most frequently reported (53%; 145/276) method used to quit smoking was cold turkey. Thirteen percent (37/276) of patients reported making a quit attempt using pharmacological therapy (ie, NRT or bupropion) and only 4% (12/276) of patients reported making a quit attempt using the help of a smoking cessation program (Figure 3).
Preparedness was an important predictor of making a quit attempt. Prepared patients (ie, Ladder score 6) were significantly more likely than patients who were less prepared to report making a quit attempt after discharge (163/212 [77%] vs. 32/64 [50%], respectively; P < 0.001). This result remained significant after adjusting for sociodemographic characteristics with a similar effect size (adjusted estimates 76% [95% CI, 75.7‐76.7] prepared vs. 49% [95% CI, 48.5‐49.8]; P < 0.001). These results also remained significant with a similar effect size in analyses using multivariate logistic regression (Table 2). Of those patients who made quit attempts, prepared patients were slightly more likely to report a successful quit attempt (90/163; 55%) than were less‐prepared patients (16/32; 50%), though this was not significant (P = 0.205).
| Statistical test | Quit Behavior | Prepared % (95% CI) | Unprepared % (95% CI) | P Value |
|---|---|---|---|---|
| ||||
| Chi square tests | Any quit attempt made after discharge | 76.9 (71.2‐82.6) | 50.0 (37.8‐62.2) | <0.001 |
| Successful quit attempt at time of follow‐up | 55.0 (45.9‐60.2) | 50.0 (25.4‐58.2) | 0.20 | |
| Multivariate logistic regression* | Any quit attempt made after discharge | 76.2 (75.7‐76.7) | 49.2 (48.5‐49.9) | <0.001 |
In the follow‐up sample, 17% could not remember if they received advice to quit smoking. Among those who were able to recall receiving advice, the majority (78%; 180/230) reported that they received advice from a nurse or physician during hospitalization, compared to 22% who did not recall ever being advised to quit by any healthcare provider during the admission. Patients who reported receiving advice to quit were more likely to report making a quit attempt postdischarge as compared to those that did not recall receiving advice (70% vs. 46%, respectively; P = 0.002). In a multivariate logistic regression, controlling for demographic factors and admitting diagnosis, both preparedness and receipt of in‐hospital advice were independent predictors of making a future quit attempt (odds ratio [OR] = 4.05; 95% CI, 1.91‐8.60; P < 0.001 for preparedness; OR = 3.96; 95% CI, 1.84‐8.54; P < 0.001 for advice). Additionally, there was no significant interaction or synergistic effect between being prepared to quit smoking and receiving in‐hospital advice to quit (OR = 1.24; 95% CI, 0.17‐9.21; P = 0.836) (Figure 4). When analyzing the effects of preparedness and advice on quit attempts, only preparedness to quit remained a significant predictor of a successful quit attempt (OR = 2.93; 95% CI, 1.13‐7.60; P = 0.027 for preparedness; OR = 2.16; 95% CI, 0.85‐5.49; P = 0.10 for advice to quit). As demonstrated in Table 2, a higher percentage of prepared patients made a quit attempt after discharge (76.9% vs. 50%) and had a successful quit attempt and short‐term abstinence (55% prepared patients vs. 50% less prepared patients).
Discussion
This study demonstrated that in a group of hospitalized underserved, and predominantly African American smokers, the majority of patients reported being prepared to quit smoking at the time of hospitalization. Prepared patients were more likely to report making a quit attempt after discharge and more likely to report being successful in their quit attempt than patients who reported being less prepared to quit during their hospitalization. Nevertheless, approximately one‐half of unprepared patients did make a quit attempt 1 month after discharge, demonstrating a desire to quit smoking after hospitalization among this population. However, short‐term success rates in this group were lower than in patients prepared to quit. In addition, preparedness to quit and receipt of in‐hospital advice to quit smoking were both found to be independent predictors of making a quit attempt, with nearly identical ORs; however, only preparedness remained significant after controlling for advice to quit. Last, although the majority of hospitalized cardiac patients were making quit attempts after discharge, most patients reported using the least effective quit methods (ie, cold turkey) rather than more effective and intensive interventions such as counseling in combination with pharmacotherapy.
These findings have important implications for current quality initiatives targeted at promoting smoking cessation among cardiac patients. First, these results highlight the need for evidence‐based methods to be made available to hospitalized smokers who are prepared to quit. Our results are consistent with other studies reporting rare use (5.2%) of NRT in the hospital setting, despite the proven benefit in treating nicotine withdrawal symptoms.17 This is also consistent with data reporting that among nonhospitalized smokers, quitting cold turkey was the most commonly used and least effective cessation method.18 Second, the rate of recall of in‐hospital advice among patients (78%) was generally consistent with those reported to CMS (most recent quarter 95% for AMI and 88% for CHF).19
In addition to receiving advice, preparedness to quit was associated with higher quit attempts, therefore highlighting the importance of assessing level of preparedness in addition to giving advice. The fact that most quit attempts were made using cold turkey and resulted in low short‐term success rates underscores the need to reevaluate the current CMS quality indicator of advice alone for hospitalized smokers. Furthermore, the recently updated 2008 U.S. Public Health guidelines recently recommend, in addition to advice, that all hospitalized smokers be assessed for readiness to change, be assisted in quitting with pharmacotherapy, and be arranged follow‐up for tobacco cessation postdischarge, highlighting the inadequacy of advice alone.4 While it is important to continue to advise all hospitalized smokers to quit, the study findings demonstrate that assessing preparedness may result in targeting more prepared patients with more intensive interventions. Further policy implications include that less prepared patients may need motivational techniques to increase their level of preparedness to quit during hospitalization.
Several limitations are worth mentioning. First, the study included a relatively small sample size drawn from a single urban medical center. The prevalence of current smokers in our sample was 15%, which is lower than many studies looking at cardiology inpatient smokers.3, 20 This limitation of our study may be attributed to the advanced age of the majority of our patients, as compared with other studies, as well as the possibility of socially desirable response bias that many low‐income African American smokers may experience, leaving them less likely to admit to smoking at the time of hospitalization. Second, there was a low follow‐up rate, with 66% of patients undergoing follow‐up postdischarge. While this may raise the concerns of differences between ladder scores in those patients that participated in follow‐up and those that did not, analyses show no significant difference between level of preparedness in these 2 groups (68% prepared in patients who received follow‐up vs. 63% prepared patients in those who did not participate in follow‐up; P = 0.36). Third, follow‐up of quit attempts and receipt of advice were all assessed using self‐report, and, therefore, were limited by lack of verification and lack of assessment for potential recall bias. Fourth, in this pilot study, the follow‐up period was relatively short at 1 month postdischarge. It is likely that rates of successful quit attempts would be lower with longer‐term follow‐up periods, given previous literature demonstrating the difficulty with long‐term abstinence.21 Last, the study was not able to account for potential effects that hospitalization itself may have on preparedness, as patients may be more likely to report being prepared to quit when in the face of a health shock,22 as well as the fact that some patients may demonstrate a socially desirable response bias influenced by hospitalization.
In conclusion, the majority of underserved smokers with cardiac disease reported being prepared to quit smoking and were more likely to self‐report making a quit attempt after discharge. However, the majority of these quit attempts were made via cold turkey, without the support of available evidence‐based methods to quit. It is possible that by directly providing education, access to pharmacotherapy, and counseling options, the utilization rates for more efficacious treatments would increase in cardiac patients who are prepared to quit. While recall of in‐hospital advice was associated with future quit attempts, prepared patients who recalled receiving advice were more likely to make a quit attempt than prepared patients who did not recall receiving advice, as well as unprepared patients. Together, these findings highlight the need to consider a patient's level of preparedness to quit in understanding the success of in‐hospital advice and the importance of making evidence‐based cessation methods available to hospitalized smokers who are prepared to quit. Additionally, identifying patients not prepared to quit may help in providing them with appropriate motivational therapy, to move them along the stages of change, as well as educational information on how to quit once they have decided to do so.
- ,,.Helping hospitalized smokers quit: new directions for treatment and research.J Consult Clin Psychol.1993;61:778–789.
- ,.Smokers who are hospitalized: a window of opportunity for cessation interventions.Prev Med.1992;21:262–269.
- ,,, et al.Predictors of smoking cessation after a myocardial infarction: the role of institutional smoking cessation programs in improving success.Arch Intern Med.2008;168(18):1961–1967.
- Guideline Panel.Clinical Practice Guidelines: Treating Tobacco Use and Dependence.Washington, DC:Public Health Service, U.S. Department of Health and Human Services;2008.
- ,.Stages and processes of self‐change in smoking: toward an integrative model of change.J Consult Clin Psychol.1983;51:390–395.
- ,.The Contemplation Ladder: validation of a measure of readiness to consider smoking cessation.Health Psychol.1991;10(5):360–365.
- ,,,,.Smoking cessation factors among African Americans and Whites.Am J Public Health.1993;83(2):220–226.
- U.S. Department of Health and Human Services.The Health Benefits of Smoking Cessation.Rockville, MD:Office on Smoking and Health, Centers for Chronic Disease Prevention and Health Promotion, Public Health Service,U.S. Department of Health and Human Services,Washington, DC;2000.
- ,,,,.Trends in cigarette smoking in the United States. the changing influence of gender and race.JAMA.1989;261(1):49–55.
- ,,, et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137(11):866–874.
- ,,,.Validation of a telephone version of the Mini‐Mental State Examination.J Am Geriatr Soc.1992;40(7):697–702.
- National Health Information Survey Questionnaire, Sample Adult,Adult Health Behaviors;2004.
- ,,, et al.The Marijuana Ladder: measuring motivation to change marijuana use in incarcerated adolescents.Drug Alcohol Depend.2006;83:42–48.
- ,,,,.Motivation for stopping tobacco use among emergency department patients.Acad Emerg Med.2005;12:568–571.
- Picker‐Commonwealth Survey of Patient‐Centered Care.Health Aff.1991.
- Hospital Quality Initiatives. Centers for Medicare and Medicaid Services (CMS). Available at: http://www.cms.hhs.gov/HospitalQualtiyInits. Accessed April2009.
- ,,, et al.The use of nicotine replacement therapy by hospitalized smokers.Am J Prev Med.1999;17(4):255–259.
- ,,,,.Methods used to quit smoking in the United States: do cessation programs help?JAMA.1990;263(20):2795–2796.
- U.S. Department of Health and Human Services.Hospital Compare.2006 Data Graphs. Available at: http://www.hospitalcompare.hhs.gov. Accessed April2009.
- ,,, et al.Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Cigarette smoking among adults—United States, 2006.MMWR Morb Mortal Wkly Rep.2007;56:1157–1161.
- ,,.Smoking cessation interventions for hospitalized smokers.Arch Intern Med.2008;168(18):1950–1960.
- ,.Health beliefs and smoking patterns in heart patients and their wives: a longitudinal study.Am J Public Health.1977;67:921–930.
- ,,.Helping hospitalized smokers quit: new directions for treatment and research.J Consult Clin Psychol.1993;61:778–789.
- ,.Smokers who are hospitalized: a window of opportunity for cessation interventions.Prev Med.1992;21:262–269.
- ,,, et al.Predictors of smoking cessation after a myocardial infarction: the role of institutional smoking cessation programs in improving success.Arch Intern Med.2008;168(18):1961–1967.
- Guideline Panel.Clinical Practice Guidelines: Treating Tobacco Use and Dependence.Washington, DC:Public Health Service, U.S. Department of Health and Human Services;2008.
- ,.Stages and processes of self‐change in smoking: toward an integrative model of change.J Consult Clin Psychol.1983;51:390–395.
- ,.The Contemplation Ladder: validation of a measure of readiness to consider smoking cessation.Health Psychol.1991;10(5):360–365.
- ,,,,.Smoking cessation factors among African Americans and Whites.Am J Public Health.1993;83(2):220–226.
- U.S. Department of Health and Human Services.The Health Benefits of Smoking Cessation.Rockville, MD:Office on Smoking and Health, Centers for Chronic Disease Prevention and Health Promotion, Public Health Service,U.S. Department of Health and Human Services,Washington, DC;2000.
- ,,,,.Trends in cigarette smoking in the United States. the changing influence of gender and race.JAMA.1989;261(1):49–55.
- ,,, et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137(11):866–874.
- ,,,.Validation of a telephone version of the Mini‐Mental State Examination.J Am Geriatr Soc.1992;40(7):697–702.
- National Health Information Survey Questionnaire, Sample Adult,Adult Health Behaviors;2004.
- ,,, et al.The Marijuana Ladder: measuring motivation to change marijuana use in incarcerated adolescents.Drug Alcohol Depend.2006;83:42–48.
- ,,,,.Motivation for stopping tobacco use among emergency department patients.Acad Emerg Med.2005;12:568–571.
- Picker‐Commonwealth Survey of Patient‐Centered Care.Health Aff.1991.
- Hospital Quality Initiatives. Centers for Medicare and Medicaid Services (CMS). Available at: http://www.cms.hhs.gov/HospitalQualtiyInits. Accessed April2009.
- ,,, et al.The use of nicotine replacement therapy by hospitalized smokers.Am J Prev Med.1999;17(4):255–259.
- ,,,,.Methods used to quit smoking in the United States: do cessation programs help?JAMA.1990;263(20):2795–2796.
- U.S. Department of Health and Human Services.Hospital Compare.2006 Data Graphs. Available at: http://www.hospitalcompare.hhs.gov. Accessed April2009.
- ,,, et al.Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Cigarette smoking among adults—United States, 2006.MMWR Morb Mortal Wkly Rep.2007;56:1157–1161.
- ,,.Smoking cessation interventions for hospitalized smokers.Arch Intern Med.2008;168(18):1950–1960.
- ,.Health beliefs and smoking patterns in heart patients and their wives: a longitudinal study.Am J Public Health.1977;67:921–930.
Copyright © 2010 Society of Hospital Medicine
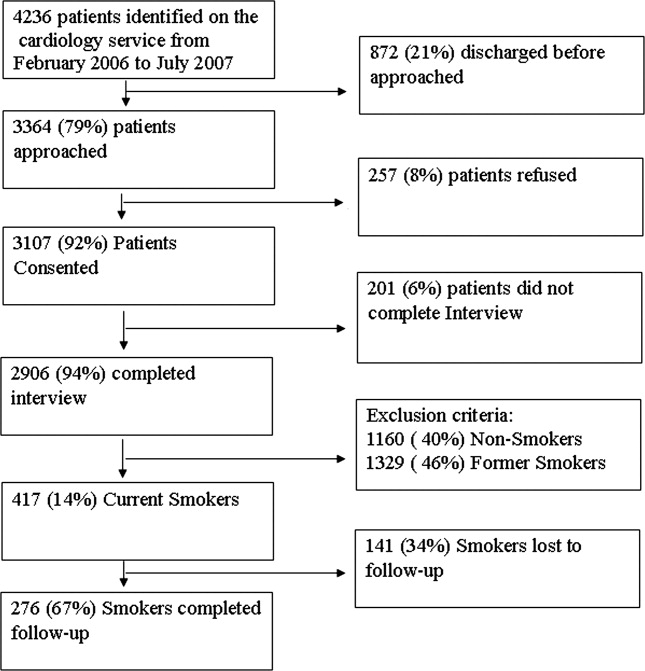
Performance of MEWS Max
Matching the severity of illness to the appropriate intensity of care is important for the effective delivery of medical care. Overtriage to critical care units results in unnecessary resource consumption. Undertriage to the wards may result in worsening of physiologic parameters1, 2 that often go unnoticed or unaddressed for more than 24 hours.3 Therefore, it is important for emergency department (ED) admission decisions to be accurate with respect to the level of care. Because of the importance of this decision, objective criteria to aid in this decision process, if accurate, would improve medical care delivery.
Physiologic measurements and procedural interventions appear to predict the need for a higher level of care among inpatients.2, 4, 5 This knowledge has led to the development of tools meant to identify inpatients on general wards who are at risk for deterioration. Such tools for identification of inpatients at risk generally use single threshold models triggered by a single abnormal physiologic value, or models that combine multiple parameters into a summative score.6, 7 The performance of previously described risk stratification tools has generally been to exhibit high sensitivity at the sacrifice of low specificity and discriminatory value.8
The value of these models as they apply in the emergency department is less well characterized. Because derangements in physiologic parameters are common among ED patients, one might expect that single‐threshold systems would exhibit high sensitivity at the expense of specificity when applied to this population. In contrast, a summative risk score may be better suited for the complexities of illness in undifferentiated ED patients and offer better discriminatory value in this population. Summative scoring systems have been shown to retain a higher specificity as the score increases compared to single‐threshold systems.8
The Modified Early Warning Score (MEWS)9 is a predictive tool for higher level of care that has been tested in the ED setting. This tool produces a summative score using temperature, respiratory rate, heart rate, level of consciousness, and systolic blood pressure. In a single‐site study from the United Kingdom, MEWS, when calculated at the time of ED presentation, did not improve decision making over a commonly used triage system, exhibiting inadequate sensitivity in identifying patients who would be admitted to the intensive care unit (ICU).10 However, as a result of the care delivered in the ED, patients' conditions can change significantly throughout their stay. Therefore we postulate that the MEWS calculated at a single time in the ED (eg, at the time of admission) is not the most accurate predictor of care intensity requirements.
The primary objective of this research was to add to the literature provided by Subbe et al.10 by describing the performance characteristics and discriminatory ability of the most abnormal MEWS (MEWS Max) score during the entire ED stay in predicting the need for higher levels of care among ED patients presenting to a tertiary care facility in North America.
Patients and Methods
Study Design
To determine the performance characteristics of the MEWS in ED patients, we used a structured explicit retrospective chart review on a random sample of ED patients being admitted to the hospital.
Study Setting
The study was conducted at 1 tertiary care academic medical center in the United States, consisting of 830 beds, approximately 125 of which provide a higher level of care, defined as intensive care, intermediate care, or acute care. The ED volume in 2005 was 75,000 with an admission rate of 20%. In the ED, patients are primarily seen by residents who are supervised by board‐certified or board‐eligible emergency medicine attendings.
Study Population
All patients presenting to the ED of Wake Forest University Baptist Medical Center in 2005 were considered for inclusion. From these patients, a listing was created of all hospital admissions through the ED in 2005. Because trauma and cardiology patients have disease‐specific risk stratification tools that are used to guide admission,11, 12 they were then removed from this list and excluded. Additionally, pediatric patients were excluded from this listing as the MEWS score relies on vital sign abnormalities, which have varying ranges of normal in children. From this list, 500 charts were randomly selected for further review. Additional criteria were applied at the time the charts were reviewed to exclude those: without an ED record matching the date of admission, without 1 complete set of ED vitals, receiving mechanical ventilation at the time of presentation, or patients currently receiving hospice or comfort care. Charts from the list of 500 were reviewed sequentially until the goal number of charts had been completed. The number of charts reviewed was selected to allow relatively precise 95% confidence intervals [CIs] around sensitivity (10%) based on the assumptions of 80% sensitivity and a 20% incidence of the primary outcome. Based on this, the intent was to abstract information from 300 patient charts.
Study Protocol
A standardized data abstraction template was created. Data abstractors included 2 physicians and 2 nurses. Group training for the abstractors was provided by the primary investigator and included performance review and feedback until competence was demonstrated. Data abstractors used the paper copy of the ED nursing notes (and physician notes if clarification required) to abstract data from the medical record. Abstractors were not aware of the patient's outcome at the time of data abstraction as this information was contained in a separate database. During the chart review, and blinded to the abstractors, 25 charts were selected for abstraction by all data abstractors to allow calculation of interobserver agreement.
Clinical outcomes were determined by referencing hospital databases and the medical record if clarification was needed. The admission bed location and changes in patient location throughout the hospital stay were used to track the need for a higher level of care. The outcome of death was determined by cross‐referencing study participants with hospital mortality data, and the medical record, if needed.
Predictor Score Calculation
Abstracted data were used to calculate the MEWS score according to the criteria specified in Table 1 at the initial ED presentation (MEWS Initial), the maximum during the ED stay (MEWS Max), and prior to admission (MEWS Admit). Parameters not repeated after arrival were carried forward from the most recent recording. An adaptation of the MEWS score was required by replacing the alert/verbal/painful/unresponsive (AVPU) scale to determine the level of consciousness with the Glascow Coma Scale (GCS), a conversion that has been previously described.13, 14
| 3 Points | 2 Points | 1 Point | 0 Points | 1 Point | 2 Points | 3 Points | |
|---|---|---|---|---|---|---|---|
| |||||||
| Systolic blood pressure | <70 | 71‐80 | 81‐100 | 101‐199 | 200 | ||
| Heart rate | <40 | 41‐50 | 51‐100 | 101‐110 | 111‐129 | 130 | |
| Respiratory rate | <9 | 9‐14 | 15‐20 | 21‐29 | 30 | ||
| Temperature | <95 | 95‐101.1 | 101.2 | ||||
| GCS | 15 | 11‐14 | 7‐10 | 6 | |||
Clinical Endpoint Definitions and Outcomes
Need for higher level of care was defined as initial admission from the ED or transfer within 24 hours to a nonfloor bed (acute care, intermediate care unit, or critical care unit). Acute care beds at the study hospital have a lower bed‐to‐nurse ratio and more intensive monitoring (beside vs. radiotelemetry, vitals signs every 2 hours compared to every 4 hours) than floor beds. Intermediate care beds fulfill a gap between these and critical care, with dedicated respiratory therapists, the ability for invasive monitoring, and ventilator management. In addition, the hospital's burn, bone marrow transplant (BMT), and cardiac care units (CCU) are intensive carelevel units, and were included when measuring the need for higher level of care. Mortality was defined as death during the index hospitalization. The primary outcome was the composite need for a higher level of care or mortality within 24 hours of ED presentation.
Data Analysis
Calculation of interobserver agreement for data obtained from the chart abstraction was performed using Kappa coefficients. Descriptive statistics were used to summarize the patient characteristics separately for those who did and did not need higher levels of care. Fisher exact tests and Wilcoxon rank‐sum tests were used to assess group differences in the categorical and continuous patient characteristics, respectively. A frequency table was used to display the cross‐tabulation of MEWS Max scores with the need for higher levels of care, and the sensitivity and specificity were calculated for each cutpoint of the predictor scores. These measurements were plotted against one another in receiver‐operating characteristic (ROC) curves and the optimal cutpoint chosen as the one that gave the greatest sum of sensitivity and specificity. The area under the ROC curves and approximate 95% CIs were calculated. The Cochran‐Armitage trend test1517 was used to assess the association between risk score and outcome. Logistic regression was used to model the log odds of needing higher levels of care as a function of the MEWS Max score. Calibration of the model was assessed by analyzing the performance of the MEWS Max score among patient subgroups and comparing observed and expected events. Performance was also assessed among sextiles of risk using the Hosmer and Lemshow18 goodness‐of‐fit test.
As a secondary objective, additional covariates were added to the logistic model including MEWS to see if model performance could be improved. First, a simple logistic regression was used to determine the most significant MEWS score measurements among the 3 that were measured (MEWS Initial, MEWS Max, and MEWS Admit). Only 1 MEWS measurement was considered for the final model to avoid colinearity. The selected MEWS measurement was then entered into a multivariable logistic model along with age 60 years, gender, race/ethnicity (white, black, Hispanic, other), method of arrival (ambulatory or by ambulance), ED length of stay (recorded to the nearest minute, then converted to hours at the second significant digit), intravenous (IV) antibiotics in the ED, and antibiotics prior to ED arrival. Candidate variables were chosen considering both the plausibility to be associated with the outcome and the reliability of the data elements considering our retrospective methods. Forward selection, stepwise selection, and backward elimination with a significance level of 0.20 to enter and/or stay in the model were used to obtain a predictive model.
In order to assess the risk stratification potential for the MEWS Max model and the exploratory model (MEWS Plus), the ability to classify subjects by their probability of experiencing the outcome was assessed. Because an established consensus does not exist in the literature for these cutoffs, it was hypothesized that 4 risk categories (0‐10%, >10‐40%, >40‐70%, and >70%) would be clinically useful to clinicians allowing categorization into low‐, intermediate‐, high‐, and very‐high‐risk‐groups for requiring a higher level of care.
Results
Complete chart abstraction was performed for 299 patient encounters. After abstraction, 19 charts were excluded from final analysis due to missing outcome data (n = 6) or implausible and/or missing crucial data values (n = 13). Pairwise kappa values for abstraction of the MEWS Max score demonstrated agreement ranging from good to very good (0.67‐0.88). Of the 280 analyzed encounters, 76 (27%) met the primary composite outcome of death (n = 1) or need for higher care (n = 76). Of these 76 patients, 69 were admitted from the ED to a high level of care, and 7 were initially admitted to a lower level of care and required transfer to a higher level of care within 24 hours. Thirty‐seven patients requiring a higher level of care were admitted to an ICU (ICU = 31; BMT, CCU, and burn unit with 2 patients each), 9 to intermediate care, and 30 to an acute care bed.
Demographics and presenting characteristics from the study participants can be seen in Table 2. The mean age of participants was 56 years and was similar for the 2 groups. Approximately one‐half of the study participants were female (49%) and there was no statistical association between experiencing the composite outcome and gender (P = 0.28). The majority (64%) of participants were Caucasian, followed by African American (33%) and Hispanic or other (2%). Similar distributions were seen when stratified by outcome. Vital signs of the participants in total and stratified by outcome fell within normal parameters. ED length of stay was similar among those meeting and not meeting the composite outcome (5.5 hours vs. 5.8 hours, P = 0.15). Patients who met the composite outcome were more likely to have arrived by ambulance (63% vs. 43%, P = 0.004).
| Patient Characteristics | Composite Endpoint Not Met (n = 204)* | Composite Endpoint Met (n = 76)* | P Value |
|---|---|---|---|
| |||
| Demographics | |||
| Age (years) | 56 (42, 73) | 55 (41, 71) | 0.66 |
| Female sex (%) | 51 | 43 | 0.28 |
| White race (%) | 65 | 63 | 0.91 |
| Arrival via ambulance (%) | 43 | 63 | 0.004 |
| Length of stay (hours) | 5.8 (4.6, 7.2) | 5.5 (4.3, 6.9) | 0.15 |
| Presenting characteristics | |||
| Systolic BP (mmHg) | 132 (117, 148) | 135 (118, 159) | 0.26 |
| Heart rate (beats/minute) | 87 (74, 100) | 96 (82, 111) | 0.003 |
| Respiratory rate (breaths/minute) | 20 (18, 22) | 20 (18, 24) | 0.26 |
| Temperature (degrees F) | 97.9 (97.1, 98.8) | 97.8 (96.8, 99.6) | 0.78 |
| Glasgow coma scale | 15 (15, 15) | 15 (14, 15) | <0.001 |
| Antibiotic therapy | |||
| On antibiotics at arrival (%) | 9 | 9 | 1.00 |
| IV antibiotics in the ED (%) | 31 | 34 | 0.67 |
The distribution of scores and the proportion of participants with each score that met the composite outcome are shown in Figure 1. The MEWS Max was significantly associated with the primary composite outcome (P < 0.001, Cochran‐Armitage trend test). The scoring system demonstrates an increase in the proportion of participants meeting the composite endpoint as the score increases, and all participants with a MEWS Max score 9 met the composite outcome.
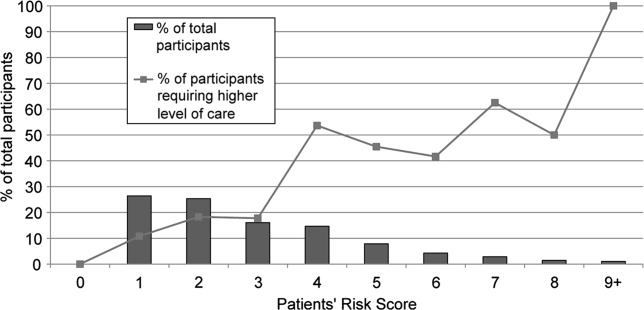
ROC are shown in Figure 2. The optimum threshold for MEWS Max based on the sum of sensitivity and specificity is 4, associated with a sensitivity of 62% and a specificity of 79% (Table 3) The predictive ability of the MEWS Max was moderate (C statistic MEWS Max 0.73; 95% CI, 0.66‐0.79), with each 1‐point increase in the MEWS Max score associated with a 60% increase in the odds of meeting the composite endpoint (odds ratio [OR], 1.6; 95% CI, 1.3‐1.8).

| MEWS Max Cutoff | Number at or Above the Cutoff Needing a Higher Level of Care | Sensitivity % (95% CI) | Specificity % (95% CI) | Positive Predictive Value (%) | Negative Predictive Value (%) |
|---|---|---|---|---|---|
| |||||
| 1 | 76 | 100 (95‐100) | 0 (0‐2) | 27 | NA |
| 2 | 68 | 89 (80‐95) | 32 (26‐39) | 33 | 89 |
| 3 | 55 | 72 (61‐82) | 61 (54‐68) | 41 | 86 |
| 4 | 47 | 62 (50‐73) | 79 (73‐84) | 52 | 85 |
| 5 | 25 | 33 (23‐45) | 88 (83‐92) | 51 | 78 |
| 6 | 15 | 20 (11‐30) | 94 (90‐97) | 56 | 76 |
| 7 | 10 | 13 (6‐23) | 98 (94‐99) | 67 | 75 |
| 8 | 5 | 7 (2‐15) | 99 (97‐100) | 71 | 74 |
| 9 | 3 | 4 (1‐11) | 100 (98‐100) | 100 | 74 |
Table 4 shows calibration of the model using different subgroups of the patient population. Grouping patients by age or gender did not reveal a higher event rate in any particular group. Using the Hosmer and Lemeshow18 goodness‐of‐fit test to stratify by risk category, no evidence for lack of fit was found (P = 0.06).
| Characteristic | Total Participants | Observed Events | Expected Events | Observed/ Expected |
|---|---|---|---|---|
| ||||
| Age | ||||
| >45 years | 87 | 24 | 23.8 | 1.01 |
| 45‐70 years | 118 | 33 | 32.8 | 1.01 |
| >70 years | 75 | 19 | 19.4 | 0.98 |
| Sex* | ||||
| Male | 142 | 43 | 37.4 | 1.15 |
| Female | 137 | 33 | 38.5 | 0.86 |
| Sextile of risk with MEWS Max | ||||
| First | 27 | 15 | 17.8 | 0.84 |
| Second | 22 | 10 | 10.1 | 0.99 |
| Third | 41 | 22 | 14.4 | 1.53 |
| Fourth | 45 | 8 | 11.6 | 0.69 |
| Fifth | 71 | 13 | 12.9 | 1.01 |
| Sixth | 74 | 8 | 9.2 | 0.87 |
In the exploratory analysis, 267 subjects had complete data for all candidate variables. Simple logistic regression revealed that the most predictive MEWS measurement was the MEWS Max (C statistic MEWS Max 0.725, MEWS Initial 0.668, MEWS Admit 0.653). Stepwise selection, forward selection, and backward elimination produced the same model containing method of arrival (P = 0.03), MEWS Max (P < 0.001), IV antibiotics in the ED (P = 0.17), length of stay (P = 0.05), and gender (P = 0.12). In the subset of subjects with these complete data elements (n = 268), the inclusion of the additional measures increased the C statistic to 0.76 (95% CI, 0.69‐0.82), a 0.04 increase over the model that only included MEWS Max in the same subset of subjects.
MEWS Max resulted in no patients being classified as low‐risk, with the majority (81.7%) classified as intermediate‐risk, 15.7% classified as high‐risk, and 2.6% classified as very high risk (Table 5). In all categories the actual event rate fell within the predicted event rate interval. The addition of variables included in MEWS Plus resulted in 14.6% of patients being classified as low‐risk, 64.0% as intermediate risk, 17.2% with high‐risk, and 4.1% as very‐high‐risk. In 58 cases (21.7%), using MEWS Plus would have placed patients in a more appropriate risk category than that assigned by MEWS Max; ie, a lower risk category for those who did not have events, and a higher risk category for those experiencing events. The majority of this correct reclassification was seen in the intermediate risk group by MEWS Max, where 17.6% were appropriately reclassified. Alternatively, 5.6% of cases would have resulted in inappropriate reclassification. Again, the actual event rate fell within the boundaries of predicted risk in all cases.
| MEWS Plus* | Events | ||||||
|---|---|---|---|---|---|---|---|
| MEWS Max | 0‐10 | >10‐40 | >40‐70 | >70 | Row Totals (%) | Correctly Reclassified (%) | Incorrectly Reclassified (%) |
| |||||||
| Total (%) | 39 (14.6) | 171 (64.0) | 46 (17.2) | 11 (4.1) | 267 | 58 (21.7) | 15 (5.6) |
| Events (% of total) | 2 (5.1) | 39 (22.8) | 24 (52.2) | 8 (72.7) | 73 (27.3) | ||
| Nonevents (% of total) | 37 (94.9) | 132 (77.2) | 22 (47.8) | 3 (27.3) | 194 (72.7) | ||
| 0‐10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Events | 0 | 0 | 0 | 0 | 0 | ||
| Nonevents | 0 | 0 | 0 | 0 | 0 | ||
| >10‐40 | 39 | 162 | 17 | 0 | 218 (81.7) | 47 (17.6) | 9 (3.4) |
| Events | 2 | 36 | 10 | 0 | 48 (22.0) | ||
| Nonevents | 37 | 126 | 7 | 0 | 170 (78.0) | ||
| >40‐70 | 0 | 9 | 27 | 6 | 42 (15.7) | 10 (3.7) | 5 (1.9) |
| Events | 0 | 3 | 13 | 4 | 20 (47.6) | ||
| Nonevents | 0 | 6 | 14 | 2 | 22 (52.4) | ||
| >70 | 0 | 0 | 2 | 5 | 7 (2.6) | 1 (0.4) | 1 (0.4) |
| Events | 0 | 0 | 1 | 4 | 5 (71.4) | ||
| Nonevents | 0 | 0 | 1 | 1 | 2 (28.6) | ||
Discussion
Matching the initial level of care to the patient's severity of illness can be expected to improve the efficiency of health care delivery. The MEWS is a simple prediction instrument that can be calculated at the bedside and would be ideal for this purpose. The MEWS has good predictive ability among patients on the wards or awaiting admission,9, 10 and in this investigation a variation of MEWS appears to have potential to discriminate among high‐risk and low‐risk ED patients.
Examination of the ROC curve for the MEWS Max score demonstrates a fair performance (C statistic = 0.73). In this analysis, we created low‐risk, intermediate‐risk, high‐risk, and very‐high‐risk groups. The strength of the MEWS Max rests in its ability to classify patients as high‐risk or very‐high‐risk. Approximately 16% of patients are classified by MEWS Max as high‐risk, and 3% as very‐high‐risk, making the practitioner more confident in the decision to admit to a high level of care. However, MEWS Max classifies no patients as low risk and approximately 80% of patients are classified as intermediate‐risk. The majority of patients being classified into this gray zone and the inability to classify patients as low‐risk significantly limits the utility of MEWS Max.
In exploratory analysis, these data propose a model using additional readily available parameters that when added to the MEWS Max can improve patient classification. Of particular interest is the ability of the MEWS Plus model to more accurately identify patients at low risk of requiring a higher level of care. When compared to MEWS Max, approximately 22% of patients were correctly reclassified by MEWS Plus, with only 5% incorrectly reclassified. Importantly, MEWS Plus is able to reduce the size of the intermediate‐risk group, predominantly by reclassifying patients as low risk. Forty‐seven (17.6%) of the patients previously categorized as intermediate risk with MEWS Max were reclassified, with 39 of them becoming low risk, 2 (5.1%) of whom had events. However, the major limitation of the MEWS Plus is that it is currently not able to be calculated at the bedside as many of the included variables are time dependent. More analysis is needed to validate precisely which variables are most important, determine how they add to the calculation, and understand when or how often during the ED visit risk should be calculated. Further exploration and validation of this model is necessary.
The results of this investigation add in important ways to a previous study of the MEWS in ED patient triage.10 Subbe et al.10 examined the ability of the MEWS to improve admission decisions beyond those recommended by the Manchester Triage System. Their investigation was conducted among 153 ED patients who belonged to 1 of 3 cohorts being admitted from the ED in the United Kingdom. They concluded that the MEWS was unable to significantly improve admission level of care decisions over the Manchester Triage System. Our investigation differs from that reported by Subbe et al.10 in several important ways. Methodologically, we chose to include a broad population of ED patients rather than selecting 3 cohorts for comparison, and excluded trauma and cardiology patients due to suspected differences in admission patterns in these patients. Further, we conducted our analysis using the maximum MEWS score obtained during a patient's encounter. We felt that using the maximum MEWS score takes full of advantage of all clinical data obtained during the patient's ED visit rather than relying on their severity of illness when the patient first arrives. Additionally, we selected an outcome measure that was determined at 24 hours because we feel events occurring within 24 hours of admission are more likely to reflect a progression of a disease process present at the time of the ED evaluation. Subbe et al.10 analyzed ICU admissions after any duration of hospitalization on the wards. However, ICU admission after several days of ward care may neither be avoidable, nor predictable, while the patient is in the ED.
Subbe et al.10 concluded that the MEWS score did not significantly add to triage decisions aided by the Manchester Triage System. However, in their results, a MEWS score >2 would have classified 7 additional patients as high risk out of 50 who required a transfer to a higher level of care when compared to the Manchester Triage System. Our findings explore the discriminatory value of the maximum MEWS score for a patient throughout the ED visit. This approach, combined with our methodologic differences, have led to more encouraging findings about the utility of the MEWS Max score, especially when combined with a few simple and reliably abstracted variables, to predict the required level of care within 24 hours.
Limitations to our results mainly relate to the study design. We chose a nonconcurrent cohort design using an explicit chart review. Chart reviews have inherent limitations that can include inaccuracy of abstracted data elements, missing data, systematic bias imposed by the abstraction process, and unmeasured confounding. To minimize avoidable biases and maintain accuracy while conducting this chart review, we followed well‐described methods.19 However, because we were relying on retrospective data, some data elements were incomplete. For instance, not all participants had multiple sets of vital signs recorded, which could have affected the predictive accuracy of the risk scores. Anticipating this difficulty, we had algorithms established to handle missing data, which we feel minimized this effect. However, despite this effort, 13 patients had to be excluded due to incomplete data. During review, it was noted that some patients admitted due to a traumatic mechanism were included in the final data analysis despite our intent to exclude them. We expect that this was a very small number, and should have had a minimal effect on risk score calculation. In addition, we modified the original MEWS model in that the GCS was used in substitution for the AVPU score. The conversion of the AVPU score to the GCS is well‐described and is unlikely to have affected the accuracy of the MEWS. We did not adjust for ED length of stay in our primary MEWS model. It is possible that more severely ill patients were in the ED longer and therefore had more opportunity to have abnormal vital signs recorded. ED length of stay was incorporated into the MEWS Plus model. Another limitation relates to our reference standard. We chose a composite of the need for a higher level of care or death within 24 hours. The need for higher care is a subjective endpoint. However, we felt this reflection of actual decision making is more informing than comparisons to other objective, unvalidated scoring systems. As more robust scoring systems are developed, researchers will need to consider developing a reference standard employing blinded adjudicators. Pediatric, cardiology, and trauma patients were excluded from this analysis and therefore our results cannot be extrapolated to these populations. MEWS model calibration was performed using the same data set as that on which the model was tested. This may have resulted in overfit of the model to the data, possibly leading to an overstatement of the model's predictive ability. Additionally, the MEWS Plus model requires validation in another study population. A final limitation is that in performing the study at 1 institution, the results may not be generalizable to other settings.
Building on previous work in defining and testing risk scores to predict poor outcomes, we have shown that the MEWS Max is a potentially useful tool to categorize patients as high‐risk or very‐high‐risk for requiring a higher level of care. MEWS Max suffers from the creation of a large intermediate risk group and the inability to classify patients as low‐risk. Adding further variables to MEWS Max creates a model with improved performance (MEWS Plus). This model may allow for 15% of admissions to be classified as low‐risk and shows promise as a tool to be used in ED triage of patients who are being admitted. Further work should attempt to further refine and validate the MEWS Plus model and examine the effect of implementation of these models on admission decision making and clinical outcomes.
Acknowledgements
Special gratitude is extended to Ronald H. Small, M.B.A., Vice President of the Division of Healthcare Research and Quality, for his assistance.
- ,,,.The longer patients are in hospital before intensive care admission the higher their mortality.Intensive Care Med.2004;30(10):1908–1913.
- ,,.Physiological values and procedures in the 24 h before ICU admission from the ward.Anaesthesia.1999;54(6):529–534.
- ,.Can some in‐hospital cardio‐respiratory arrests be prevented?A prospective survey. Resuscitation.1998;37(3):133–137.
- ,.Physiological abnormalities in early warning scores are related to mortality in adult inpatients.Br J Anaesth.2004;92(6):882–884.
- ,,,,,.Recognising clinical instability in hospital patients before cardiac arrest or unplanned admission to intensive care. A pilot study in a tertiary‐care hospital.Med J Aust.1999;171(1):22–25.
- ,,,,,.Improving the utilization of medical crisis teams (Condition C) at an urban tertiary care hospital.J Crit Care.2003;18(2):87–94.
- ,,,.The medical emergency team.Anaesth Intensive Care.1995;23(2):183–186.
- ,,, et al.Systematic review and evaluation of physiological track and trigger warning systems for identifying at‐risk patients on the ward.Intensive Care Med.2007;33(4):667–679.
- ,,,.Validation of a modified early warning score in medical admissions.QJM.2001;94(10):521–526.
- ,,,.Validation of physiological scoring systems in the accident and emergency department.Emerg Med J.2006;23(11):841–845.
- ,,, et al.The TIMI risk score for unstable angina/non‐ST elevation MI: a method for prognostication and therapeutic decision making.JAMA.2000;284(7):835–842.
- ,.Trauma scoring systems: a review.J Am Coll Surg.1999;189(5):491–503.
- ,,.Comparison of consciousness level assessment in the poisoned patient using the alert/verbal/painful/unresponsive scale and the Glasgow Coma Scale.Ann Emerg Med.2004;44(2):108–113.
- ,.Simple bedside assessment of level of consciousness: comparison of two simple assessment scales with the Glasgow Coma scale.Anaesthesia.2004;59(1):34–37.
- ,,.Exact inference for contingency tables with ordered categories.J Am Stat Assoc.1990(85):453–458.
- .Tests for trends in proportions. In: Klotz S, Johnson NH, eds. Encyclopedia of Statistical Sciences. Vol 9.New York:John Wiley and Sons, Inc.;1988:334–336.
- SAS Institute I. Cochran Armitage Test for Trend.SAS OnlineDoc 9.1.3.Cary, NC:SAS Institute, Inc.;2007.
- ,.Applied Logistic Regression.2nd ed.New York:John Wiley and Sons;2000.
- ,,,,.Chart reviews in emergency medicine research: Where are the methods?Ann Emerg Med.1996;27(3):305–308.
Matching the severity of illness to the appropriate intensity of care is important for the effective delivery of medical care. Overtriage to critical care units results in unnecessary resource consumption. Undertriage to the wards may result in worsening of physiologic parameters1, 2 that often go unnoticed or unaddressed for more than 24 hours.3 Therefore, it is important for emergency department (ED) admission decisions to be accurate with respect to the level of care. Because of the importance of this decision, objective criteria to aid in this decision process, if accurate, would improve medical care delivery.
Physiologic measurements and procedural interventions appear to predict the need for a higher level of care among inpatients.2, 4, 5 This knowledge has led to the development of tools meant to identify inpatients on general wards who are at risk for deterioration. Such tools for identification of inpatients at risk generally use single threshold models triggered by a single abnormal physiologic value, or models that combine multiple parameters into a summative score.6, 7 The performance of previously described risk stratification tools has generally been to exhibit high sensitivity at the sacrifice of low specificity and discriminatory value.8
The value of these models as they apply in the emergency department is less well characterized. Because derangements in physiologic parameters are common among ED patients, one might expect that single‐threshold systems would exhibit high sensitivity at the expense of specificity when applied to this population. In contrast, a summative risk score may be better suited for the complexities of illness in undifferentiated ED patients and offer better discriminatory value in this population. Summative scoring systems have been shown to retain a higher specificity as the score increases compared to single‐threshold systems.8
The Modified Early Warning Score (MEWS)9 is a predictive tool for higher level of care that has been tested in the ED setting. This tool produces a summative score using temperature, respiratory rate, heart rate, level of consciousness, and systolic blood pressure. In a single‐site study from the United Kingdom, MEWS, when calculated at the time of ED presentation, did not improve decision making over a commonly used triage system, exhibiting inadequate sensitivity in identifying patients who would be admitted to the intensive care unit (ICU).10 However, as a result of the care delivered in the ED, patients' conditions can change significantly throughout their stay. Therefore we postulate that the MEWS calculated at a single time in the ED (eg, at the time of admission) is not the most accurate predictor of care intensity requirements.
The primary objective of this research was to add to the literature provided by Subbe et al.10 by describing the performance characteristics and discriminatory ability of the most abnormal MEWS (MEWS Max) score during the entire ED stay in predicting the need for higher levels of care among ED patients presenting to a tertiary care facility in North America.
Patients and Methods
Study Design
To determine the performance characteristics of the MEWS in ED patients, we used a structured explicit retrospective chart review on a random sample of ED patients being admitted to the hospital.
Study Setting
The study was conducted at 1 tertiary care academic medical center in the United States, consisting of 830 beds, approximately 125 of which provide a higher level of care, defined as intensive care, intermediate care, or acute care. The ED volume in 2005 was 75,000 with an admission rate of 20%. In the ED, patients are primarily seen by residents who are supervised by board‐certified or board‐eligible emergency medicine attendings.
Study Population
All patients presenting to the ED of Wake Forest University Baptist Medical Center in 2005 were considered for inclusion. From these patients, a listing was created of all hospital admissions through the ED in 2005. Because trauma and cardiology patients have disease‐specific risk stratification tools that are used to guide admission,11, 12 they were then removed from this list and excluded. Additionally, pediatric patients were excluded from this listing as the MEWS score relies on vital sign abnormalities, which have varying ranges of normal in children. From this list, 500 charts were randomly selected for further review. Additional criteria were applied at the time the charts were reviewed to exclude those: without an ED record matching the date of admission, without 1 complete set of ED vitals, receiving mechanical ventilation at the time of presentation, or patients currently receiving hospice or comfort care. Charts from the list of 500 were reviewed sequentially until the goal number of charts had been completed. The number of charts reviewed was selected to allow relatively precise 95% confidence intervals [CIs] around sensitivity (10%) based on the assumptions of 80% sensitivity and a 20% incidence of the primary outcome. Based on this, the intent was to abstract information from 300 patient charts.
Study Protocol
A standardized data abstraction template was created. Data abstractors included 2 physicians and 2 nurses. Group training for the abstractors was provided by the primary investigator and included performance review and feedback until competence was demonstrated. Data abstractors used the paper copy of the ED nursing notes (and physician notes if clarification required) to abstract data from the medical record. Abstractors were not aware of the patient's outcome at the time of data abstraction as this information was contained in a separate database. During the chart review, and blinded to the abstractors, 25 charts were selected for abstraction by all data abstractors to allow calculation of interobserver agreement.
Clinical outcomes were determined by referencing hospital databases and the medical record if clarification was needed. The admission bed location and changes in patient location throughout the hospital stay were used to track the need for a higher level of care. The outcome of death was determined by cross‐referencing study participants with hospital mortality data, and the medical record, if needed.
Predictor Score Calculation
Abstracted data were used to calculate the MEWS score according to the criteria specified in Table 1 at the initial ED presentation (MEWS Initial), the maximum during the ED stay (MEWS Max), and prior to admission (MEWS Admit). Parameters not repeated after arrival were carried forward from the most recent recording. An adaptation of the MEWS score was required by replacing the alert/verbal/painful/unresponsive (AVPU) scale to determine the level of consciousness with the Glascow Coma Scale (GCS), a conversion that has been previously described.13, 14
| 3 Points | 2 Points | 1 Point | 0 Points | 1 Point | 2 Points | 3 Points | |
|---|---|---|---|---|---|---|---|
| |||||||
| Systolic blood pressure | <70 | 71‐80 | 81‐100 | 101‐199 | 200 | ||
| Heart rate | <40 | 41‐50 | 51‐100 | 101‐110 | 111‐129 | 130 | |
| Respiratory rate | <9 | 9‐14 | 15‐20 | 21‐29 | 30 | ||
| Temperature | <95 | 95‐101.1 | 101.2 | ||||
| GCS | 15 | 11‐14 | 7‐10 | 6 | |||
Clinical Endpoint Definitions and Outcomes
Need for higher level of care was defined as initial admission from the ED or transfer within 24 hours to a nonfloor bed (acute care, intermediate care unit, or critical care unit). Acute care beds at the study hospital have a lower bed‐to‐nurse ratio and more intensive monitoring (beside vs. radiotelemetry, vitals signs every 2 hours compared to every 4 hours) than floor beds. Intermediate care beds fulfill a gap between these and critical care, with dedicated respiratory therapists, the ability for invasive monitoring, and ventilator management. In addition, the hospital's burn, bone marrow transplant (BMT), and cardiac care units (CCU) are intensive carelevel units, and were included when measuring the need for higher level of care. Mortality was defined as death during the index hospitalization. The primary outcome was the composite need for a higher level of care or mortality within 24 hours of ED presentation.
Data Analysis
Calculation of interobserver agreement for data obtained from the chart abstraction was performed using Kappa coefficients. Descriptive statistics were used to summarize the patient characteristics separately for those who did and did not need higher levels of care. Fisher exact tests and Wilcoxon rank‐sum tests were used to assess group differences in the categorical and continuous patient characteristics, respectively. A frequency table was used to display the cross‐tabulation of MEWS Max scores with the need for higher levels of care, and the sensitivity and specificity were calculated for each cutpoint of the predictor scores. These measurements were plotted against one another in receiver‐operating characteristic (ROC) curves and the optimal cutpoint chosen as the one that gave the greatest sum of sensitivity and specificity. The area under the ROC curves and approximate 95% CIs were calculated. The Cochran‐Armitage trend test1517 was used to assess the association between risk score and outcome. Logistic regression was used to model the log odds of needing higher levels of care as a function of the MEWS Max score. Calibration of the model was assessed by analyzing the performance of the MEWS Max score among patient subgroups and comparing observed and expected events. Performance was also assessed among sextiles of risk using the Hosmer and Lemshow18 goodness‐of‐fit test.
As a secondary objective, additional covariates were added to the logistic model including MEWS to see if model performance could be improved. First, a simple logistic regression was used to determine the most significant MEWS score measurements among the 3 that were measured (MEWS Initial, MEWS Max, and MEWS Admit). Only 1 MEWS measurement was considered for the final model to avoid colinearity. The selected MEWS measurement was then entered into a multivariable logistic model along with age 60 years, gender, race/ethnicity (white, black, Hispanic, other), method of arrival (ambulatory or by ambulance), ED length of stay (recorded to the nearest minute, then converted to hours at the second significant digit), intravenous (IV) antibiotics in the ED, and antibiotics prior to ED arrival. Candidate variables were chosen considering both the plausibility to be associated with the outcome and the reliability of the data elements considering our retrospective methods. Forward selection, stepwise selection, and backward elimination with a significance level of 0.20 to enter and/or stay in the model were used to obtain a predictive model.
In order to assess the risk stratification potential for the MEWS Max model and the exploratory model (MEWS Plus), the ability to classify subjects by their probability of experiencing the outcome was assessed. Because an established consensus does not exist in the literature for these cutoffs, it was hypothesized that 4 risk categories (0‐10%, >10‐40%, >40‐70%, and >70%) would be clinically useful to clinicians allowing categorization into low‐, intermediate‐, high‐, and very‐high‐risk‐groups for requiring a higher level of care.
Results
Complete chart abstraction was performed for 299 patient encounters. After abstraction, 19 charts were excluded from final analysis due to missing outcome data (n = 6) or implausible and/or missing crucial data values (n = 13). Pairwise kappa values for abstraction of the MEWS Max score demonstrated agreement ranging from good to very good (0.67‐0.88). Of the 280 analyzed encounters, 76 (27%) met the primary composite outcome of death (n = 1) or need for higher care (n = 76). Of these 76 patients, 69 were admitted from the ED to a high level of care, and 7 were initially admitted to a lower level of care and required transfer to a higher level of care within 24 hours. Thirty‐seven patients requiring a higher level of care were admitted to an ICU (ICU = 31; BMT, CCU, and burn unit with 2 patients each), 9 to intermediate care, and 30 to an acute care bed.
Demographics and presenting characteristics from the study participants can be seen in Table 2. The mean age of participants was 56 years and was similar for the 2 groups. Approximately one‐half of the study participants were female (49%) and there was no statistical association between experiencing the composite outcome and gender (P = 0.28). The majority (64%) of participants were Caucasian, followed by African American (33%) and Hispanic or other (2%). Similar distributions were seen when stratified by outcome. Vital signs of the participants in total and stratified by outcome fell within normal parameters. ED length of stay was similar among those meeting and not meeting the composite outcome (5.5 hours vs. 5.8 hours, P = 0.15). Patients who met the composite outcome were more likely to have arrived by ambulance (63% vs. 43%, P = 0.004).
| Patient Characteristics | Composite Endpoint Not Met (n = 204)* | Composite Endpoint Met (n = 76)* | P Value |
|---|---|---|---|
| |||
| Demographics | |||
| Age (years) | 56 (42, 73) | 55 (41, 71) | 0.66 |
| Female sex (%) | 51 | 43 | 0.28 |
| White race (%) | 65 | 63 | 0.91 |
| Arrival via ambulance (%) | 43 | 63 | 0.004 |
| Length of stay (hours) | 5.8 (4.6, 7.2) | 5.5 (4.3, 6.9) | 0.15 |
| Presenting characteristics | |||
| Systolic BP (mmHg) | 132 (117, 148) | 135 (118, 159) | 0.26 |
| Heart rate (beats/minute) | 87 (74, 100) | 96 (82, 111) | 0.003 |
| Respiratory rate (breaths/minute) | 20 (18, 22) | 20 (18, 24) | 0.26 |
| Temperature (degrees F) | 97.9 (97.1, 98.8) | 97.8 (96.8, 99.6) | 0.78 |
| Glasgow coma scale | 15 (15, 15) | 15 (14, 15) | <0.001 |
| Antibiotic therapy | |||
| On antibiotics at arrival (%) | 9 | 9 | 1.00 |
| IV antibiotics in the ED (%) | 31 | 34 | 0.67 |
The distribution of scores and the proportion of participants with each score that met the composite outcome are shown in Figure 1. The MEWS Max was significantly associated with the primary composite outcome (P < 0.001, Cochran‐Armitage trend test). The scoring system demonstrates an increase in the proportion of participants meeting the composite endpoint as the score increases, and all participants with a MEWS Max score 9 met the composite outcome.
ROC are shown in Figure 2. The optimum threshold for MEWS Max based on the sum of sensitivity and specificity is 4, associated with a sensitivity of 62% and a specificity of 79% (Table 3) The predictive ability of the MEWS Max was moderate (C statistic MEWS Max 0.73; 95% CI, 0.66‐0.79), with each 1‐point increase in the MEWS Max score associated with a 60% increase in the odds of meeting the composite endpoint (odds ratio [OR], 1.6; 95% CI, 1.3‐1.8).
| MEWS Max Cutoff | Number at or Above the Cutoff Needing a Higher Level of Care | Sensitivity % (95% CI) | Specificity % (95% CI) | Positive Predictive Value (%) | Negative Predictive Value (%) |
|---|---|---|---|---|---|
| |||||
| 1 | 76 | 100 (95‐100) | 0 (0‐2) | 27 | NA |
| 2 | 68 | 89 (80‐95) | 32 (26‐39) | 33 | 89 |
| 3 | 55 | 72 (61‐82) | 61 (54‐68) | 41 | 86 |
| 4 | 47 | 62 (50‐73) | 79 (73‐84) | 52 | 85 |
| 5 | 25 | 33 (23‐45) | 88 (83‐92) | 51 | 78 |
| 6 | 15 | 20 (11‐30) | 94 (90‐97) | 56 | 76 |
| 7 | 10 | 13 (6‐23) | 98 (94‐99) | 67 | 75 |
| 8 | 5 | 7 (2‐15) | 99 (97‐100) | 71 | 74 |
| 9 | 3 | 4 (1‐11) | 100 (98‐100) | 100 | 74 |
Table 4 shows calibration of the model using different subgroups of the patient population. Grouping patients by age or gender did not reveal a higher event rate in any particular group. Using the Hosmer and Lemeshow18 goodness‐of‐fit test to stratify by risk category, no evidence for lack of fit was found (P = 0.06).
| Characteristic | Total Participants | Observed Events | Expected Events | Observed/ Expected |
|---|---|---|---|---|
| ||||
| Age | ||||
| >45 years | 87 | 24 | 23.8 | 1.01 |
| 45‐70 years | 118 | 33 | 32.8 | 1.01 |
| >70 years | 75 | 19 | 19.4 | 0.98 |
| Sex* | ||||
| Male | 142 | 43 | 37.4 | 1.15 |
| Female | 137 | 33 | 38.5 | 0.86 |
| Sextile of risk with MEWS Max | ||||
| First | 27 | 15 | 17.8 | 0.84 |
| Second | 22 | 10 | 10.1 | 0.99 |
| Third | 41 | 22 | 14.4 | 1.53 |
| Fourth | 45 | 8 | 11.6 | 0.69 |
| Fifth | 71 | 13 | 12.9 | 1.01 |
| Sixth | 74 | 8 | 9.2 | 0.87 |
In the exploratory analysis, 267 subjects had complete data for all candidate variables. Simple logistic regression revealed that the most predictive MEWS measurement was the MEWS Max (C statistic MEWS Max 0.725, MEWS Initial 0.668, MEWS Admit 0.653). Stepwise selection, forward selection, and backward elimination produced the same model containing method of arrival (P = 0.03), MEWS Max (P < 0.001), IV antibiotics in the ED (P = 0.17), length of stay (P = 0.05), and gender (P = 0.12). In the subset of subjects with these complete data elements (n = 268), the inclusion of the additional measures increased the C statistic to 0.76 (95% CI, 0.69‐0.82), a 0.04 increase over the model that only included MEWS Max in the same subset of subjects.
MEWS Max resulted in no patients being classified as low‐risk, with the majority (81.7%) classified as intermediate‐risk, 15.7% classified as high‐risk, and 2.6% classified as very high risk (Table 5). In all categories the actual event rate fell within the predicted event rate interval. The addition of variables included in MEWS Plus resulted in 14.6% of patients being classified as low‐risk, 64.0% as intermediate risk, 17.2% with high‐risk, and 4.1% as very‐high‐risk. In 58 cases (21.7%), using MEWS Plus would have placed patients in a more appropriate risk category than that assigned by MEWS Max; ie, a lower risk category for those who did not have events, and a higher risk category for those experiencing events. The majority of this correct reclassification was seen in the intermediate risk group by MEWS Max, where 17.6% were appropriately reclassified. Alternatively, 5.6% of cases would have resulted in inappropriate reclassification. Again, the actual event rate fell within the boundaries of predicted risk in all cases.
| MEWS Plus* | Events | ||||||
|---|---|---|---|---|---|---|---|
| MEWS Max | 0‐10 | >10‐40 | >40‐70 | >70 | Row Totals (%) | Correctly Reclassified (%) | Incorrectly Reclassified (%) |
| |||||||
| Total (%) | 39 (14.6) | 171 (64.0) | 46 (17.2) | 11 (4.1) | 267 | 58 (21.7) | 15 (5.6) |
| Events (% of total) | 2 (5.1) | 39 (22.8) | 24 (52.2) | 8 (72.7) | 73 (27.3) | ||
| Nonevents (% of total) | 37 (94.9) | 132 (77.2) | 22 (47.8) | 3 (27.3) | 194 (72.7) | ||
| 0‐10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Events | 0 | 0 | 0 | 0 | 0 | ||
| Nonevents | 0 | 0 | 0 | 0 | 0 | ||
| >10‐40 | 39 | 162 | 17 | 0 | 218 (81.7) | 47 (17.6) | 9 (3.4) |
| Events | 2 | 36 | 10 | 0 | 48 (22.0) | ||
| Nonevents | 37 | 126 | 7 | 0 | 170 (78.0) | ||
| >40‐70 | 0 | 9 | 27 | 6 | 42 (15.7) | 10 (3.7) | 5 (1.9) |
| Events | 0 | 3 | 13 | 4 | 20 (47.6) | ||
| Nonevents | 0 | 6 | 14 | 2 | 22 (52.4) | ||
| >70 | 0 | 0 | 2 | 5 | 7 (2.6) | 1 (0.4) | 1 (0.4) |
| Events | 0 | 0 | 1 | 4 | 5 (71.4) | ||
| Nonevents | 0 | 0 | 1 | 1 | 2 (28.6) | ||
Discussion
Matching the initial level of care to the patient's severity of illness can be expected to improve the efficiency of health care delivery. The MEWS is a simple prediction instrument that can be calculated at the bedside and would be ideal for this purpose. The MEWS has good predictive ability among patients on the wards or awaiting admission,9, 10 and in this investigation a variation of MEWS appears to have potential to discriminate among high‐risk and low‐risk ED patients.
Examination of the ROC curve for the MEWS Max score demonstrates a fair performance (C statistic = 0.73). In this analysis, we created low‐risk, intermediate‐risk, high‐risk, and very‐high‐risk groups. The strength of the MEWS Max rests in its ability to classify patients as high‐risk or very‐high‐risk. Approximately 16% of patients are classified by MEWS Max as high‐risk, and 3% as very‐high‐risk, making the practitioner more confident in the decision to admit to a high level of care. However, MEWS Max classifies no patients as low risk and approximately 80% of patients are classified as intermediate‐risk. The majority of patients being classified into this gray zone and the inability to classify patients as low‐risk significantly limits the utility of MEWS Max.
In exploratory analysis, these data propose a model using additional readily available parameters that when added to the MEWS Max can improve patient classification. Of particular interest is the ability of the MEWS Plus model to more accurately identify patients at low risk of requiring a higher level of care. When compared to MEWS Max, approximately 22% of patients were correctly reclassified by MEWS Plus, with only 5% incorrectly reclassified. Importantly, MEWS Plus is able to reduce the size of the intermediate‐risk group, predominantly by reclassifying patients as low risk. Forty‐seven (17.6%) of the patients previously categorized as intermediate risk with MEWS Max were reclassified, with 39 of them becoming low risk, 2 (5.1%) of whom had events. However, the major limitation of the MEWS Plus is that it is currently not able to be calculated at the bedside as many of the included variables are time dependent. More analysis is needed to validate precisely which variables are most important, determine how they add to the calculation, and understand when or how often during the ED visit risk should be calculated. Further exploration and validation of this model is necessary.
The results of this investigation add in important ways to a previous study of the MEWS in ED patient triage.10 Subbe et al.10 examined the ability of the MEWS to improve admission decisions beyond those recommended by the Manchester Triage System. Their investigation was conducted among 153 ED patients who belonged to 1 of 3 cohorts being admitted from the ED in the United Kingdom. They concluded that the MEWS was unable to significantly improve admission level of care decisions over the Manchester Triage System. Our investigation differs from that reported by Subbe et al.10 in several important ways. Methodologically, we chose to include a broad population of ED patients rather than selecting 3 cohorts for comparison, and excluded trauma and cardiology patients due to suspected differences in admission patterns in these patients. Further, we conducted our analysis using the maximum MEWS score obtained during a patient's encounter. We felt that using the maximum MEWS score takes full of advantage of all clinical data obtained during the patient's ED visit rather than relying on their severity of illness when the patient first arrives. Additionally, we selected an outcome measure that was determined at 24 hours because we feel events occurring within 24 hours of admission are more likely to reflect a progression of a disease process present at the time of the ED evaluation. Subbe et al.10 analyzed ICU admissions after any duration of hospitalization on the wards. However, ICU admission after several days of ward care may neither be avoidable, nor predictable, while the patient is in the ED.
Subbe et al.10 concluded that the MEWS score did not significantly add to triage decisions aided by the Manchester Triage System. However, in their results, a MEWS score >2 would have classified 7 additional patients as high risk out of 50 who required a transfer to a higher level of care when compared to the Manchester Triage System. Our findings explore the discriminatory value of the maximum MEWS score for a patient throughout the ED visit. This approach, combined with our methodologic differences, have led to more encouraging findings about the utility of the MEWS Max score, especially when combined with a few simple and reliably abstracted variables, to predict the required level of care within 24 hours.
Limitations to our results mainly relate to the study design. We chose a nonconcurrent cohort design using an explicit chart review. Chart reviews have inherent limitations that can include inaccuracy of abstracted data elements, missing data, systematic bias imposed by the abstraction process, and unmeasured confounding. To minimize avoidable biases and maintain accuracy while conducting this chart review, we followed well‐described methods.19 However, because we were relying on retrospective data, some data elements were incomplete. For instance, not all participants had multiple sets of vital signs recorded, which could have affected the predictive accuracy of the risk scores. Anticipating this difficulty, we had algorithms established to handle missing data, which we feel minimized this effect. However, despite this effort, 13 patients had to be excluded due to incomplete data. During review, it was noted that some patients admitted due to a traumatic mechanism were included in the final data analysis despite our intent to exclude them. We expect that this was a very small number, and should have had a minimal effect on risk score calculation. In addition, we modified the original MEWS model in that the GCS was used in substitution for the AVPU score. The conversion of the AVPU score to the GCS is well‐described and is unlikely to have affected the accuracy of the MEWS. We did not adjust for ED length of stay in our primary MEWS model. It is possible that more severely ill patients were in the ED longer and therefore had more opportunity to have abnormal vital signs recorded. ED length of stay was incorporated into the MEWS Plus model. Another limitation relates to our reference standard. We chose a composite of the need for a higher level of care or death within 24 hours. The need for higher care is a subjective endpoint. However, we felt this reflection of actual decision making is more informing than comparisons to other objective, unvalidated scoring systems. As more robust scoring systems are developed, researchers will need to consider developing a reference standard employing blinded adjudicators. Pediatric, cardiology, and trauma patients were excluded from this analysis and therefore our results cannot be extrapolated to these populations. MEWS model calibration was performed using the same data set as that on which the model was tested. This may have resulted in overfit of the model to the data, possibly leading to an overstatement of the model's predictive ability. Additionally, the MEWS Plus model requires validation in another study population. A final limitation is that in performing the study at 1 institution, the results may not be generalizable to other settings.
Building on previous work in defining and testing risk scores to predict poor outcomes, we have shown that the MEWS Max is a potentially useful tool to categorize patients as high‐risk or very‐high‐risk for requiring a higher level of care. MEWS Max suffers from the creation of a large intermediate risk group and the inability to classify patients as low‐risk. Adding further variables to MEWS Max creates a model with improved performance (MEWS Plus). This model may allow for 15% of admissions to be classified as low‐risk and shows promise as a tool to be used in ED triage of patients who are being admitted. Further work should attempt to further refine and validate the MEWS Plus model and examine the effect of implementation of these models on admission decision making and clinical outcomes.
Acknowledgements
Special gratitude is extended to Ronald H. Small, M.B.A., Vice President of the Division of Healthcare Research and Quality, for his assistance.
Matching the severity of illness to the appropriate intensity of care is important for the effective delivery of medical care. Overtriage to critical care units results in unnecessary resource consumption. Undertriage to the wards may result in worsening of physiologic parameters1, 2 that often go unnoticed or unaddressed for more than 24 hours.3 Therefore, it is important for emergency department (ED) admission decisions to be accurate with respect to the level of care. Because of the importance of this decision, objective criteria to aid in this decision process, if accurate, would improve medical care delivery.
Physiologic measurements and procedural interventions appear to predict the need for a higher level of care among inpatients.2, 4, 5 This knowledge has led to the development of tools meant to identify inpatients on general wards who are at risk for deterioration. Such tools for identification of inpatients at risk generally use single threshold models triggered by a single abnormal physiologic value, or models that combine multiple parameters into a summative score.6, 7 The performance of previously described risk stratification tools has generally been to exhibit high sensitivity at the sacrifice of low specificity and discriminatory value.8
The value of these models as they apply in the emergency department is less well characterized. Because derangements in physiologic parameters are common among ED patients, one might expect that single‐threshold systems would exhibit high sensitivity at the expense of specificity when applied to this population. In contrast, a summative risk score may be better suited for the complexities of illness in undifferentiated ED patients and offer better discriminatory value in this population. Summative scoring systems have been shown to retain a higher specificity as the score increases compared to single‐threshold systems.8
The Modified Early Warning Score (MEWS)9 is a predictive tool for higher level of care that has been tested in the ED setting. This tool produces a summative score using temperature, respiratory rate, heart rate, level of consciousness, and systolic blood pressure. In a single‐site study from the United Kingdom, MEWS, when calculated at the time of ED presentation, did not improve decision making over a commonly used triage system, exhibiting inadequate sensitivity in identifying patients who would be admitted to the intensive care unit (ICU).10 However, as a result of the care delivered in the ED, patients' conditions can change significantly throughout their stay. Therefore we postulate that the MEWS calculated at a single time in the ED (eg, at the time of admission) is not the most accurate predictor of care intensity requirements.
The primary objective of this research was to add to the literature provided by Subbe et al.10 by describing the performance characteristics and discriminatory ability of the most abnormal MEWS (MEWS Max) score during the entire ED stay in predicting the need for higher levels of care among ED patients presenting to a tertiary care facility in North America.
Patients and Methods
Study Design
To determine the performance characteristics of the MEWS in ED patients, we used a structured explicit retrospective chart review on a random sample of ED patients being admitted to the hospital.
Study Setting
The study was conducted at 1 tertiary care academic medical center in the United States, consisting of 830 beds, approximately 125 of which provide a higher level of care, defined as intensive care, intermediate care, or acute care. The ED volume in 2005 was 75,000 with an admission rate of 20%. In the ED, patients are primarily seen by residents who are supervised by board‐certified or board‐eligible emergency medicine attendings.
Study Population
All patients presenting to the ED of Wake Forest University Baptist Medical Center in 2005 were considered for inclusion. From these patients, a listing was created of all hospital admissions through the ED in 2005. Because trauma and cardiology patients have disease‐specific risk stratification tools that are used to guide admission,11, 12 they were then removed from this list and excluded. Additionally, pediatric patients were excluded from this listing as the MEWS score relies on vital sign abnormalities, which have varying ranges of normal in children. From this list, 500 charts were randomly selected for further review. Additional criteria were applied at the time the charts were reviewed to exclude those: without an ED record matching the date of admission, without 1 complete set of ED vitals, receiving mechanical ventilation at the time of presentation, or patients currently receiving hospice or comfort care. Charts from the list of 500 were reviewed sequentially until the goal number of charts had been completed. The number of charts reviewed was selected to allow relatively precise 95% confidence intervals [CIs] around sensitivity (10%) based on the assumptions of 80% sensitivity and a 20% incidence of the primary outcome. Based on this, the intent was to abstract information from 300 patient charts.
Study Protocol
A standardized data abstraction template was created. Data abstractors included 2 physicians and 2 nurses. Group training for the abstractors was provided by the primary investigator and included performance review and feedback until competence was demonstrated. Data abstractors used the paper copy of the ED nursing notes (and physician notes if clarification required) to abstract data from the medical record. Abstractors were not aware of the patient's outcome at the time of data abstraction as this information was contained in a separate database. During the chart review, and blinded to the abstractors, 25 charts were selected for abstraction by all data abstractors to allow calculation of interobserver agreement.
Clinical outcomes were determined by referencing hospital databases and the medical record if clarification was needed. The admission bed location and changes in patient location throughout the hospital stay were used to track the need for a higher level of care. The outcome of death was determined by cross‐referencing study participants with hospital mortality data, and the medical record, if needed.
Predictor Score Calculation
Abstracted data were used to calculate the MEWS score according to the criteria specified in Table 1 at the initial ED presentation (MEWS Initial), the maximum during the ED stay (MEWS Max), and prior to admission (MEWS Admit). Parameters not repeated after arrival were carried forward from the most recent recording. An adaptation of the MEWS score was required by replacing the alert/verbal/painful/unresponsive (AVPU) scale to determine the level of consciousness with the Glascow Coma Scale (GCS), a conversion that has been previously described.13, 14
| 3 Points | 2 Points | 1 Point | 0 Points | 1 Point | 2 Points | 3 Points | |
|---|---|---|---|---|---|---|---|
| |||||||
| Systolic blood pressure | <70 | 71‐80 | 81‐100 | 101‐199 | 200 | ||
| Heart rate | <40 | 41‐50 | 51‐100 | 101‐110 | 111‐129 | 130 | |
| Respiratory rate | <9 | 9‐14 | 15‐20 | 21‐29 | 30 | ||
| Temperature | <95 | 95‐101.1 | 101.2 | ||||
| GCS | 15 | 11‐14 | 7‐10 | 6 | |||
Clinical Endpoint Definitions and Outcomes
Need for higher level of care was defined as initial admission from the ED or transfer within 24 hours to a nonfloor bed (acute care, intermediate care unit, or critical care unit). Acute care beds at the study hospital have a lower bed‐to‐nurse ratio and more intensive monitoring (beside vs. radiotelemetry, vitals signs every 2 hours compared to every 4 hours) than floor beds. Intermediate care beds fulfill a gap between these and critical care, with dedicated respiratory therapists, the ability for invasive monitoring, and ventilator management. In addition, the hospital's burn, bone marrow transplant (BMT), and cardiac care units (CCU) are intensive carelevel units, and were included when measuring the need for higher level of care. Mortality was defined as death during the index hospitalization. The primary outcome was the composite need for a higher level of care or mortality within 24 hours of ED presentation.
Data Analysis
Calculation of interobserver agreement for data obtained from the chart abstraction was performed using Kappa coefficients. Descriptive statistics were used to summarize the patient characteristics separately for those who did and did not need higher levels of care. Fisher exact tests and Wilcoxon rank‐sum tests were used to assess group differences in the categorical and continuous patient characteristics, respectively. A frequency table was used to display the cross‐tabulation of MEWS Max scores with the need for higher levels of care, and the sensitivity and specificity were calculated for each cutpoint of the predictor scores. These measurements were plotted against one another in receiver‐operating characteristic (ROC) curves and the optimal cutpoint chosen as the one that gave the greatest sum of sensitivity and specificity. The area under the ROC curves and approximate 95% CIs were calculated. The Cochran‐Armitage trend test1517 was used to assess the association between risk score and outcome. Logistic regression was used to model the log odds of needing higher levels of care as a function of the MEWS Max score. Calibration of the model was assessed by analyzing the performance of the MEWS Max score among patient subgroups and comparing observed and expected events. Performance was also assessed among sextiles of risk using the Hosmer and Lemshow18 goodness‐of‐fit test.
As a secondary objective, additional covariates were added to the logistic model including MEWS to see if model performance could be improved. First, a simple logistic regression was used to determine the most significant MEWS score measurements among the 3 that were measured (MEWS Initial, MEWS Max, and MEWS Admit). Only 1 MEWS measurement was considered for the final model to avoid colinearity. The selected MEWS measurement was then entered into a multivariable logistic model along with age 60 years, gender, race/ethnicity (white, black, Hispanic, other), method of arrival (ambulatory or by ambulance), ED length of stay (recorded to the nearest minute, then converted to hours at the second significant digit), intravenous (IV) antibiotics in the ED, and antibiotics prior to ED arrival. Candidate variables were chosen considering both the plausibility to be associated with the outcome and the reliability of the data elements considering our retrospective methods. Forward selection, stepwise selection, and backward elimination with a significance level of 0.20 to enter and/or stay in the model were used to obtain a predictive model.
In order to assess the risk stratification potential for the MEWS Max model and the exploratory model (MEWS Plus), the ability to classify subjects by their probability of experiencing the outcome was assessed. Because an established consensus does not exist in the literature for these cutoffs, it was hypothesized that 4 risk categories (0‐10%, >10‐40%, >40‐70%, and >70%) would be clinically useful to clinicians allowing categorization into low‐, intermediate‐, high‐, and very‐high‐risk‐groups for requiring a higher level of care.
Results
Complete chart abstraction was performed for 299 patient encounters. After abstraction, 19 charts were excluded from final analysis due to missing outcome data (n = 6) or implausible and/or missing crucial data values (n = 13). Pairwise kappa values for abstraction of the MEWS Max score demonstrated agreement ranging from good to very good (0.67‐0.88). Of the 280 analyzed encounters, 76 (27%) met the primary composite outcome of death (n = 1) or need for higher care (n = 76). Of these 76 patients, 69 were admitted from the ED to a high level of care, and 7 were initially admitted to a lower level of care and required transfer to a higher level of care within 24 hours. Thirty‐seven patients requiring a higher level of care were admitted to an ICU (ICU = 31; BMT, CCU, and burn unit with 2 patients each), 9 to intermediate care, and 30 to an acute care bed.
Demographics and presenting characteristics from the study participants can be seen in Table 2. The mean age of participants was 56 years and was similar for the 2 groups. Approximately one‐half of the study participants were female (49%) and there was no statistical association between experiencing the composite outcome and gender (P = 0.28). The majority (64%) of participants were Caucasian, followed by African American (33%) and Hispanic or other (2%). Similar distributions were seen when stratified by outcome. Vital signs of the participants in total and stratified by outcome fell within normal parameters. ED length of stay was similar among those meeting and not meeting the composite outcome (5.5 hours vs. 5.8 hours, P = 0.15). Patients who met the composite outcome were more likely to have arrived by ambulance (63% vs. 43%, P = 0.004).
| Patient Characteristics | Composite Endpoint Not Met (n = 204)* | Composite Endpoint Met (n = 76)* | P Value |
|---|---|---|---|
| |||
| Demographics | |||
| Age (years) | 56 (42, 73) | 55 (41, 71) | 0.66 |
| Female sex (%) | 51 | 43 | 0.28 |
| White race (%) | 65 | 63 | 0.91 |
| Arrival via ambulance (%) | 43 | 63 | 0.004 |
| Length of stay (hours) | 5.8 (4.6, 7.2) | 5.5 (4.3, 6.9) | 0.15 |
| Presenting characteristics | |||
| Systolic BP (mmHg) | 132 (117, 148) | 135 (118, 159) | 0.26 |
| Heart rate (beats/minute) | 87 (74, 100) | 96 (82, 111) | 0.003 |
| Respiratory rate (breaths/minute) | 20 (18, 22) | 20 (18, 24) | 0.26 |
| Temperature (degrees F) | 97.9 (97.1, 98.8) | 97.8 (96.8, 99.6) | 0.78 |
| Glasgow coma scale | 15 (15, 15) | 15 (14, 15) | <0.001 |
| Antibiotic therapy | |||
| On antibiotics at arrival (%) | 9 | 9 | 1.00 |
| IV antibiotics in the ED (%) | 31 | 34 | 0.67 |
The distribution of scores and the proportion of participants with each score that met the composite outcome are shown in Figure 1. The MEWS Max was significantly associated with the primary composite outcome (P < 0.001, Cochran‐Armitage trend test). The scoring system demonstrates an increase in the proportion of participants meeting the composite endpoint as the score increases, and all participants with a MEWS Max score 9 met the composite outcome.
ROC are shown in Figure 2. The optimum threshold for MEWS Max based on the sum of sensitivity and specificity is 4, associated with a sensitivity of 62% and a specificity of 79% (Table 3) The predictive ability of the MEWS Max was moderate (C statistic MEWS Max 0.73; 95% CI, 0.66‐0.79), with each 1‐point increase in the MEWS Max score associated with a 60% increase in the odds of meeting the composite endpoint (odds ratio [OR], 1.6; 95% CI, 1.3‐1.8).
| MEWS Max Cutoff | Number at or Above the Cutoff Needing a Higher Level of Care | Sensitivity % (95% CI) | Specificity % (95% CI) | Positive Predictive Value (%) | Negative Predictive Value (%) |
|---|---|---|---|---|---|
| |||||
| 1 | 76 | 100 (95‐100) | 0 (0‐2) | 27 | NA |
| 2 | 68 | 89 (80‐95) | 32 (26‐39) | 33 | 89 |
| 3 | 55 | 72 (61‐82) | 61 (54‐68) | 41 | 86 |
| 4 | 47 | 62 (50‐73) | 79 (73‐84) | 52 | 85 |
| 5 | 25 | 33 (23‐45) | 88 (83‐92) | 51 | 78 |
| 6 | 15 | 20 (11‐30) | 94 (90‐97) | 56 | 76 |
| 7 | 10 | 13 (6‐23) | 98 (94‐99) | 67 | 75 |
| 8 | 5 | 7 (2‐15) | 99 (97‐100) | 71 | 74 |
| 9 | 3 | 4 (1‐11) | 100 (98‐100) | 100 | 74 |
Table 4 shows calibration of the model using different subgroups of the patient population. Grouping patients by age or gender did not reveal a higher event rate in any particular group. Using the Hosmer and Lemeshow18 goodness‐of‐fit test to stratify by risk category, no evidence for lack of fit was found (P = 0.06).
| Characteristic | Total Participants | Observed Events | Expected Events | Observed/ Expected |
|---|---|---|---|---|
| ||||
| Age | ||||
| >45 years | 87 | 24 | 23.8 | 1.01 |
| 45‐70 years | 118 | 33 | 32.8 | 1.01 |
| >70 years | 75 | 19 | 19.4 | 0.98 |
| Sex* | ||||
| Male | 142 | 43 | 37.4 | 1.15 |
| Female | 137 | 33 | 38.5 | 0.86 |
| Sextile of risk with MEWS Max | ||||
| First | 27 | 15 | 17.8 | 0.84 |
| Second | 22 | 10 | 10.1 | 0.99 |
| Third | 41 | 22 | 14.4 | 1.53 |
| Fourth | 45 | 8 | 11.6 | 0.69 |
| Fifth | 71 | 13 | 12.9 | 1.01 |
| Sixth | 74 | 8 | 9.2 | 0.87 |
In the exploratory analysis, 267 subjects had complete data for all candidate variables. Simple logistic regression revealed that the most predictive MEWS measurement was the MEWS Max (C statistic MEWS Max 0.725, MEWS Initial 0.668, MEWS Admit 0.653). Stepwise selection, forward selection, and backward elimination produced the same model containing method of arrival (P = 0.03), MEWS Max (P < 0.001), IV antibiotics in the ED (P = 0.17), length of stay (P = 0.05), and gender (P = 0.12). In the subset of subjects with these complete data elements (n = 268), the inclusion of the additional measures increased the C statistic to 0.76 (95% CI, 0.69‐0.82), a 0.04 increase over the model that only included MEWS Max in the same subset of subjects.
MEWS Max resulted in no patients being classified as low‐risk, with the majority (81.7%) classified as intermediate‐risk, 15.7% classified as high‐risk, and 2.6% classified as very high risk (Table 5). In all categories the actual event rate fell within the predicted event rate interval. The addition of variables included in MEWS Plus resulted in 14.6% of patients being classified as low‐risk, 64.0% as intermediate risk, 17.2% with high‐risk, and 4.1% as very‐high‐risk. In 58 cases (21.7%), using MEWS Plus would have placed patients in a more appropriate risk category than that assigned by MEWS Max; ie, a lower risk category for those who did not have events, and a higher risk category for those experiencing events. The majority of this correct reclassification was seen in the intermediate risk group by MEWS Max, where 17.6% were appropriately reclassified. Alternatively, 5.6% of cases would have resulted in inappropriate reclassification. Again, the actual event rate fell within the boundaries of predicted risk in all cases.
| MEWS Plus* | Events | ||||||
|---|---|---|---|---|---|---|---|
| MEWS Max | 0‐10 | >10‐40 | >40‐70 | >70 | Row Totals (%) | Correctly Reclassified (%) | Incorrectly Reclassified (%) |
| |||||||
| Total (%) | 39 (14.6) | 171 (64.0) | 46 (17.2) | 11 (4.1) | 267 | 58 (21.7) | 15 (5.6) |
| Events (% of total) | 2 (5.1) | 39 (22.8) | 24 (52.2) | 8 (72.7) | 73 (27.3) | ||
| Nonevents (% of total) | 37 (94.9) | 132 (77.2) | 22 (47.8) | 3 (27.3) | 194 (72.7) | ||
| 0‐10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Events | 0 | 0 | 0 | 0 | 0 | ||
| Nonevents | 0 | 0 | 0 | 0 | 0 | ||
| >10‐40 | 39 | 162 | 17 | 0 | 218 (81.7) | 47 (17.6) | 9 (3.4) |
| Events | 2 | 36 | 10 | 0 | 48 (22.0) | ||
| Nonevents | 37 | 126 | 7 | 0 | 170 (78.0) | ||
| >40‐70 | 0 | 9 | 27 | 6 | 42 (15.7) | 10 (3.7) | 5 (1.9) |
| Events | 0 | 3 | 13 | 4 | 20 (47.6) | ||
| Nonevents | 0 | 6 | 14 | 2 | 22 (52.4) | ||
| >70 | 0 | 0 | 2 | 5 | 7 (2.6) | 1 (0.4) | 1 (0.4) |
| Events | 0 | 0 | 1 | 4 | 5 (71.4) | ||
| Nonevents | 0 | 0 | 1 | 1 | 2 (28.6) | ||
Discussion
Matching the initial level of care to the patient's severity of illness can be expected to improve the efficiency of health care delivery. The MEWS is a simple prediction instrument that can be calculated at the bedside and would be ideal for this purpose. The MEWS has good predictive ability among patients on the wards or awaiting admission,9, 10 and in this investigation a variation of MEWS appears to have potential to discriminate among high‐risk and low‐risk ED patients.
Examination of the ROC curve for the MEWS Max score demonstrates a fair performance (C statistic = 0.73). In this analysis, we created low‐risk, intermediate‐risk, high‐risk, and very‐high‐risk groups. The strength of the MEWS Max rests in its ability to classify patients as high‐risk or very‐high‐risk. Approximately 16% of patients are classified by MEWS Max as high‐risk, and 3% as very‐high‐risk, making the practitioner more confident in the decision to admit to a high level of care. However, MEWS Max classifies no patients as low risk and approximately 80% of patients are classified as intermediate‐risk. The majority of patients being classified into this gray zone and the inability to classify patients as low‐risk significantly limits the utility of MEWS Max.
In exploratory analysis, these data propose a model using additional readily available parameters that when added to the MEWS Max can improve patient classification. Of particular interest is the ability of the MEWS Plus model to more accurately identify patients at low risk of requiring a higher level of care. When compared to MEWS Max, approximately 22% of patients were correctly reclassified by MEWS Plus, with only 5% incorrectly reclassified. Importantly, MEWS Plus is able to reduce the size of the intermediate‐risk group, predominantly by reclassifying patients as low risk. Forty‐seven (17.6%) of the patients previously categorized as intermediate risk with MEWS Max were reclassified, with 39 of them becoming low risk, 2 (5.1%) of whom had events. However, the major limitation of the MEWS Plus is that it is currently not able to be calculated at the bedside as many of the included variables are time dependent. More analysis is needed to validate precisely which variables are most important, determine how they add to the calculation, and understand when or how often during the ED visit risk should be calculated. Further exploration and validation of this model is necessary.
The results of this investigation add in important ways to a previous study of the MEWS in ED patient triage.10 Subbe et al.10 examined the ability of the MEWS to improve admission decisions beyond those recommended by the Manchester Triage System. Their investigation was conducted among 153 ED patients who belonged to 1 of 3 cohorts being admitted from the ED in the United Kingdom. They concluded that the MEWS was unable to significantly improve admission level of care decisions over the Manchester Triage System. Our investigation differs from that reported by Subbe et al.10 in several important ways. Methodologically, we chose to include a broad population of ED patients rather than selecting 3 cohorts for comparison, and excluded trauma and cardiology patients due to suspected differences in admission patterns in these patients. Further, we conducted our analysis using the maximum MEWS score obtained during a patient's encounter. We felt that using the maximum MEWS score takes full of advantage of all clinical data obtained during the patient's ED visit rather than relying on their severity of illness when the patient first arrives. Additionally, we selected an outcome measure that was determined at 24 hours because we feel events occurring within 24 hours of admission are more likely to reflect a progression of a disease process present at the time of the ED evaluation. Subbe et al.10 analyzed ICU admissions after any duration of hospitalization on the wards. However, ICU admission after several days of ward care may neither be avoidable, nor predictable, while the patient is in the ED.
Subbe et al.10 concluded that the MEWS score did not significantly add to triage decisions aided by the Manchester Triage System. However, in their results, a MEWS score >2 would have classified 7 additional patients as high risk out of 50 who required a transfer to a higher level of care when compared to the Manchester Triage System. Our findings explore the discriminatory value of the maximum MEWS score for a patient throughout the ED visit. This approach, combined with our methodologic differences, have led to more encouraging findings about the utility of the MEWS Max score, especially when combined with a few simple and reliably abstracted variables, to predict the required level of care within 24 hours.
Limitations to our results mainly relate to the study design. We chose a nonconcurrent cohort design using an explicit chart review. Chart reviews have inherent limitations that can include inaccuracy of abstracted data elements, missing data, systematic bias imposed by the abstraction process, and unmeasured confounding. To minimize avoidable biases and maintain accuracy while conducting this chart review, we followed well‐described methods.19 However, because we were relying on retrospective data, some data elements were incomplete. For instance, not all participants had multiple sets of vital signs recorded, which could have affected the predictive accuracy of the risk scores. Anticipating this difficulty, we had algorithms established to handle missing data, which we feel minimized this effect. However, despite this effort, 13 patients had to be excluded due to incomplete data. During review, it was noted that some patients admitted due to a traumatic mechanism were included in the final data analysis despite our intent to exclude them. We expect that this was a very small number, and should have had a minimal effect on risk score calculation. In addition, we modified the original MEWS model in that the GCS was used in substitution for the AVPU score. The conversion of the AVPU score to the GCS is well‐described and is unlikely to have affected the accuracy of the MEWS. We did not adjust for ED length of stay in our primary MEWS model. It is possible that more severely ill patients were in the ED longer and therefore had more opportunity to have abnormal vital signs recorded. ED length of stay was incorporated into the MEWS Plus model. Another limitation relates to our reference standard. We chose a composite of the need for a higher level of care or death within 24 hours. The need for higher care is a subjective endpoint. However, we felt this reflection of actual decision making is more informing than comparisons to other objective, unvalidated scoring systems. As more robust scoring systems are developed, researchers will need to consider developing a reference standard employing blinded adjudicators. Pediatric, cardiology, and trauma patients were excluded from this analysis and therefore our results cannot be extrapolated to these populations. MEWS model calibration was performed using the same data set as that on which the model was tested. This may have resulted in overfit of the model to the data, possibly leading to an overstatement of the model's predictive ability. Additionally, the MEWS Plus model requires validation in another study population. A final limitation is that in performing the study at 1 institution, the results may not be generalizable to other settings.
Building on previous work in defining and testing risk scores to predict poor outcomes, we have shown that the MEWS Max is a potentially useful tool to categorize patients as high‐risk or very‐high‐risk for requiring a higher level of care. MEWS Max suffers from the creation of a large intermediate risk group and the inability to classify patients as low‐risk. Adding further variables to MEWS Max creates a model with improved performance (MEWS Plus). This model may allow for 15% of admissions to be classified as low‐risk and shows promise as a tool to be used in ED triage of patients who are being admitted. Further work should attempt to further refine and validate the MEWS Plus model and examine the effect of implementation of these models on admission decision making and clinical outcomes.
Acknowledgements
Special gratitude is extended to Ronald H. Small, M.B.A., Vice President of the Division of Healthcare Research and Quality, for his assistance.
- ,,,.The longer patients are in hospital before intensive care admission the higher their mortality.Intensive Care Med.2004;30(10):1908–1913.
- ,,.Physiological values and procedures in the 24 h before ICU admission from the ward.Anaesthesia.1999;54(6):529–534.
- ,.Can some in‐hospital cardio‐respiratory arrests be prevented?A prospective survey. Resuscitation.1998;37(3):133–137.
- ,.Physiological abnormalities in early warning scores are related to mortality in adult inpatients.Br J Anaesth.2004;92(6):882–884.
- ,,,,,.Recognising clinical instability in hospital patients before cardiac arrest or unplanned admission to intensive care. A pilot study in a tertiary‐care hospital.Med J Aust.1999;171(1):22–25.
- ,,,,,.Improving the utilization of medical crisis teams (Condition C) at an urban tertiary care hospital.J Crit Care.2003;18(2):87–94.
- ,,,.The medical emergency team.Anaesth Intensive Care.1995;23(2):183–186.
- ,,, et al.Systematic review and evaluation of physiological track and trigger warning systems for identifying at‐risk patients on the ward.Intensive Care Med.2007;33(4):667–679.
- ,,,.Validation of a modified early warning score in medical admissions.QJM.2001;94(10):521–526.
- ,,,.Validation of physiological scoring systems in the accident and emergency department.Emerg Med J.2006;23(11):841–845.
- ,,, et al.The TIMI risk score for unstable angina/non‐ST elevation MI: a method for prognostication and therapeutic decision making.JAMA.2000;284(7):835–842.
- ,.Trauma scoring systems: a review.J Am Coll Surg.1999;189(5):491–503.
- ,,.Comparison of consciousness level assessment in the poisoned patient using the alert/verbal/painful/unresponsive scale and the Glasgow Coma Scale.Ann Emerg Med.2004;44(2):108–113.
- ,.Simple bedside assessment of level of consciousness: comparison of two simple assessment scales with the Glasgow Coma scale.Anaesthesia.2004;59(1):34–37.
- ,,.Exact inference for contingency tables with ordered categories.J Am Stat Assoc.1990(85):453–458.
- .Tests for trends in proportions. In: Klotz S, Johnson NH, eds. Encyclopedia of Statistical Sciences. Vol 9.New York:John Wiley and Sons, Inc.;1988:334–336.
- SAS Institute I. Cochran Armitage Test for Trend.SAS OnlineDoc 9.1.3.Cary, NC:SAS Institute, Inc.;2007.
- ,.Applied Logistic Regression.2nd ed.New York:John Wiley and Sons;2000.
- ,,,,.Chart reviews in emergency medicine research: Where are the methods?Ann Emerg Med.1996;27(3):305–308.
- ,,,.The longer patients are in hospital before intensive care admission the higher their mortality.Intensive Care Med.2004;30(10):1908–1913.
- ,,.Physiological values and procedures in the 24 h before ICU admission from the ward.Anaesthesia.1999;54(6):529–534.
- ,.Can some in‐hospital cardio‐respiratory arrests be prevented?A prospective survey. Resuscitation.1998;37(3):133–137.
- ,.Physiological abnormalities in early warning scores are related to mortality in adult inpatients.Br J Anaesth.2004;92(6):882–884.
- ,,,,,.Recognising clinical instability in hospital patients before cardiac arrest or unplanned admission to intensive care. A pilot study in a tertiary‐care hospital.Med J Aust.1999;171(1):22–25.
- ,,,,,.Improving the utilization of medical crisis teams (Condition C) at an urban tertiary care hospital.J Crit Care.2003;18(2):87–94.
- ,,,.The medical emergency team.Anaesth Intensive Care.1995;23(2):183–186.
- ,,, et al.Systematic review and evaluation of physiological track and trigger warning systems for identifying at‐risk patients on the ward.Intensive Care Med.2007;33(4):667–679.
- ,,,.Validation of a modified early warning score in medical admissions.QJM.2001;94(10):521–526.
- ,,,.Validation of physiological scoring systems in the accident and emergency department.Emerg Med J.2006;23(11):841–845.
- ,,, et al.The TIMI risk score for unstable angina/non‐ST elevation MI: a method for prognostication and therapeutic decision making.JAMA.2000;284(7):835–842.
- ,.Trauma scoring systems: a review.J Am Coll Surg.1999;189(5):491–503.
- ,,.Comparison of consciousness level assessment in the poisoned patient using the alert/verbal/painful/unresponsive scale and the Glasgow Coma Scale.Ann Emerg Med.2004;44(2):108–113.
- ,.Simple bedside assessment of level of consciousness: comparison of two simple assessment scales with the Glasgow Coma scale.Anaesthesia.2004;59(1):34–37.
- ,,.Exact inference for contingency tables with ordered categories.J Am Stat Assoc.1990(85):453–458.
- .Tests for trends in proportions. In: Klotz S, Johnson NH, eds. Encyclopedia of Statistical Sciences. Vol 9.New York:John Wiley and Sons, Inc.;1988:334–336.
- SAS Institute I. Cochran Armitage Test for Trend.SAS OnlineDoc 9.1.3.Cary, NC:SAS Institute, Inc.;2007.
- ,.Applied Logistic Regression.2nd ed.New York:John Wiley and Sons;2000.
- ,,,,.Chart reviews in emergency medicine research: Where are the methods?Ann Emerg Med.1996;27(3):305–308.
Copyright © 2010 Society of Hospital Medicine
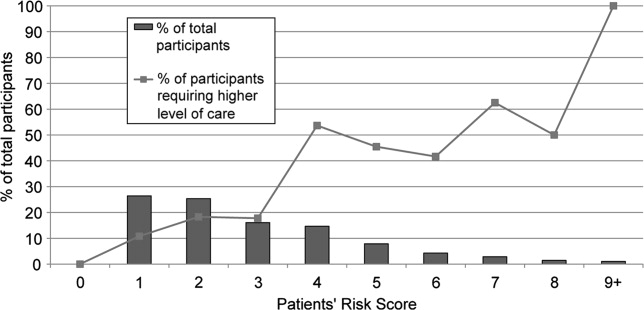
Implementing a Smoke‐Free Medical Campus
Even though imposition of smoke‐free policies and workplaces comprise one of the most effective antismoking strategies,1 hospital administrators hesitate to implement a smoke‐free medical campus policy.2 They fear losing patients who smoke because these patients will opt for other facilities that permit smoking.
Apart from studies evaluating Joint Commission on Accreditation of Healthcare Organizations (JCAHO)‐required indoor smoking bans in hospitals in 1992,3, 4 there are few published studies or formal evaluations of the impact of medical campuses going smoke‐free. One study of the implementation of a smoke‐free medical campus policy at a university hospital in Little Rock, AR, showed that the policy had no impact on employee retention, bed occupancy, or mean daily census; however, inpatient smoking status was not ascertained.5 Most (83%) employees were supportive of the policy. More importantly, employees at 2 university medical centers reported reduced cigarette consumption and increased attempts to quit after implementation of a smoke‐free medical campus policy.6, 7
Our hospital is 180‐bed, acute care inpatient teaching facility in upstate New York. Prior to the implementation of the smoke‐free medical campus policy, it was common to see employees, visitors, and patients lined up outdoors around the main hospital entrances and smoking just beyond the no smoking signage. Inpatients could look out their windows at the main entrance or into the courtyard and see hospital staff, other patients, and visitors smoking.
This study prospectively evaluates the impact of implementing the smoke‐free medical campus policy and starting an inpatient smoking cessation service. It addresses the following questions that have also been raised by the Task Force for Community Preventive Services.8 Does the institution of hospital smoking bans reduce the percentage of inpatients who smoke or increase the percentage who sign out against medical advice? What are the extended effects (beyond 1 year after implementation) of medical campus smoking bans on employee smoking rates?
Materials and Methods
Policy Implementation
As prior studies have shown that institution of a smoke‐free medical campus policy involves much more than just posting signage,9, 10 a detailed multidisciplinary work plan was implemented starting 1.5 years prior to the date our policy went into effect on July 1, 2006. The Implementing a Smoke‐Free Environment plan, produced by the University of Michigan,11 which includes a 15‐step checklist, was used to guide this policy change.12 As part of that plan, employees were offered on‐site smoking cessation services, including nicotine replacement therapy (NRT), and 150 employees participated in this program prior to July 1, 2006. Staff, community, and patient education was also completed. A new campus map delineating the smoke‐free border was disseminated. Signage was posted in areas used in the past for smoking. In addition to implementing this plan, an inpatient smoking cessation service was started 3 months prior to July 1, 2006. In addition to supporting the enforcement of the smoke‐free medical campus, our inpatient smoking cessation program was designed to help inpatients with nicotine withdrawal as well as smoking cessation, if they were ready to quit.
Data Collection and Analysis
The inpatient electronic medical record (EMR) was used to monitor the smoking status of patients admitted to hospital on a monthly basis. On admission to the hospital, the admitting nurse screened patients for current smoking status. This information was entered into the EMR starting in April 2006; therefore, pre‐ban screening data were limited to 2 months prior to the ban. Inpatients too sick to complete this screening process, women admitted for labor and delivery, and inpatients boarded in the emergency department were not screened. No identifiers were used in compiling these monthly data.
Nursing reports of inpatients signing out against medical advice (AMA) were compiled in order to compare incidence of AMA pre‐ban to post‐ban. AMA documentation in our hospital takes the form of a structured incident report that is reliably documented by nursing staff and signed by the attending physician of service.
Computerized inpatient doctors' orders to pharmacy for NRT, dispensed as gum or patch, were monitored 2 years preinitiation and postinitiation of the inpatient smoking cessation service on April 1, 2006. As varenicline was nonformulary and bupropion was used for other indications than smoking cessation, these medications were not included in this review. The Chow test was used to measure and test for significant breaks in a time series analysis of the NRT orders.
New York State law requires an annual occupational health review to be completed by every hospital employee. At our hospital, this review included a question on tobacco use Do you smoke or chew tobacco? Although there has been a smoker/nonsmoker differential in the rates offered for supplemental life insurance since 1992, there were no wellness credits or other incentives for medical insurance offered in employee benefits that may predispose employees to underreport tobacco use. Using this question, employees were categorized as self‐reported current smokers or chew users. Employee smoking rates were estimated using different denominators to validate the direction of the trend. First, self‐reported smoking rates were compared pre‐ban and post‐ban among a stable cohort of hospital employees (n = 489), defined as hospital‐based employees with anniversary dates from March to June who reported in both 2005 and 2007. The McNemar test was used to test the statistical significance of the 2 smoking rates of paired replicates in this stable cohort of employees reporting pre‐ban and post‐ban. Second, all employees in the database reporting smoking status pre‐ban, March to June 2005, and then post‐ban, March to June 2006 and 2007, were compared in order to monitor trends in employee smoking overall. A t‐test was used to compare the statistical significance of the difference in the overall rates of smoking among all employees pre‐ban and post‐ban.
Internal review boards of our hospital and the New York State Department of Health reviewed and approved this study.
Results
Inpatient Outcomes
An average of 959 patients were admitted per month in the 18‐month period pre‐ban (January 2005 to June 2006) vs. 988 per month in the 23‐month period post‐ban (July 2006 to September 2008). A monthly average of 89% of inpatients were screened for tobacco use when admitted. The monthly average for the percentage of inpatients who currently smoke has been approximately 21.6% following the implementation of the smoke‐free hospital plan. There has been little variation (Figure 1) in the percentage of inpatients who smoke pre‐ban and post‐ban except for the startup period in 2006 and the onset of the 2007 respiratory illness season.
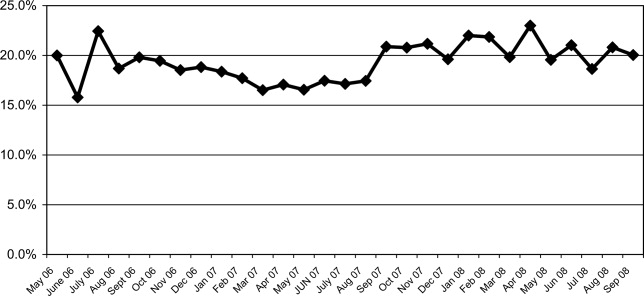
Among all inpatients who currently smoke, 69.8% received a brief nursing intervention at the time of admission and 25% received an inpatient visit from our part‐time smoking cessation specialist.
The percentage of inpatients who signed out against medical advice (AMA) with the reason of having to smoke was 13.8% (4/29) 6 months pre‐ban, and 13.6% (3/22) 6 months post‐ban. In 2007, there were no inpatients who signed out AMA stating that they needed to smoke. Because the reason for signing out AMA may be underreported, we also examined the rate of smoking among all inpatients who sign out AMA. Six months pre‐ban, this percentage was 48.3% (14/29), but increased 6 months post‐ban to 59% (13/22). In 2007, the percentage of smokers among inpatients who sign out AMA leveled off at 50.8% (29/57).
Review of computerized inpatient prescription orders shows that orders for NRT nearly tripled after the inpatient smoking cessation service started April 1, 2006 (3 months prior to the ban) (Figure 2). Inpatient orders for these medications increased from 832 in a 2‐year period before the ban (April 1, 2004 to March 31, 2006) to 2475 in the 2 years following the initiation of the inpatient smoking service (April 1, 2006 to March 31, 2008). The Chow test is highly significant for a break point in June 2006 (P = 0.008), 1 month prior to the ban.

Employee Smoking Rates
Among a cohort of 489 hospital‐based employees reporting in both 2005 and 2007, 12% reported smoking in 2005 and 7.5% in 2007 (McNemar was significant at P 0.001). Two employees reported using chewing tobacco in 2005 and only 1 in 2007.
Including all hospital employees reporting any 1 year during their anniversary dates, the self‐reported smoking rates were 14.3% (n = 624) in March to June 2005, 14.8% (n = 661) in March to June 2006, and 9.4% (n = 1,112) in March to June 2007 (P 0.0002). Because promotions change the anniversary date, and the database was expanded in 2007 to include new hires and managerial staff, these estimates represent the point prevalence among employees whose anniversary dates fall between March and June.
Discussion
Following implementation of a smoke‐free medical campus, no adverse effects were observed on inpatient volume at our hospital. The percentage of inpatients who smoke and the percentage of inpatients signing out AMA have remained stable after the smoke‐free policy went into effect. In addition, self‐reported employee smoking rates decreased significantly. Fears about losing inpatients (who smoke) following the implementation of a smoke‐free hospital plan were unfounded.
This study employs the electronic medical record to not only monitor trends in the proportion of inpatients who smoke pre‐ban and post‐ban, but also to notify our inpatient smoking cessation specialist, on the day of admission, to consult on patients who currently smoke. Unfortunately, our cessation specialist, who is part‐time, was unable to see all inpatients who smoke on account of the inpatient's acuity, pain, hospice status, weekend or night admission, or not being available due to testing, surgery, or other procedures. Nevertheless, use of NRT increased sharply following the initiation of this program. As shown in Figure 2, a linear rise in NRT orders was already underway starting April 2005, probably in anticipation of the ban and coinciding with the start of the inpatient smoking cessation program. However, the Chow test is highly significant for a breakpoint in June 2006 (P = 0.008), 1 month prior to the ban, meaning that the slope was climbing even more steeply after that point.
As hospitalized smokers may be more motivated to stop smoking, the updated 2008 clinical practice guidelines for Treating Tobacco Use and Dependence now recommend that all patients in the hospital be given medications, advised, counseled, and receive follow‐up after discharge.13 Although our inpatient cessation program was started before these clinical practice guidelines were available, we are currently evaluating the efficacy of our inpatient program by assessing self‐reported quit rates 6‐months posthospitalization (data collection in process). Provision of inpatient smoking cessation has been shown to be an effective smoking cessation intervention if combined with outpatient follow‐up.14 Our current program will be expanded to include outpatient follow‐up, if the inpatient's primary care provider is unable to provide it or if the inpatient refuses faxed referral to the New York State quit line program.
This study evaluates the impact of simultaneously introduced interventions such as medical campus smoking ban, inpatient smoking cessation program, hospital staff education, and other elements of the University of Michigan Smoke‐Free Hospital Implementation Plan. The role of individual components of the plan cannot be evaluated in this study as they were intentionally implemented simultaneously in order to achieve a synergistic effect.
Another limitation of this study is that smoking status is self‐reported and not validated biochemically. Although validated smoking status measures such as salivary cotinine testing would be more scientifically valid, it was not feasible to validate the smoking status of inpatients, nor that of employees. Thus smoking status, as ascertained in this study, is subject to underreporting. Social desirability bias has been recognized as potential limitation of self‐reported smoking status in other evaluations of smoke‐free policies.3, 4, 15
In the 1990s, the employee benefits of instituting indoor smoking bans in hospitals were theorized to include reduced employee sick time, break time, and tobacco use, as well as increased motivation for smoking cessation and reduced legitimacy of tobacco use.16, 17 Peer pressure, workplace socialization, and being forced to stay away from cigarettes for the length of entire workdays have been credited with helping hospital workers to quit.4, 7 In our study, extending the ban to the outdoor areas of our medical campus as well as provision of employee smoking cessation services may augment these mechanisms. This study extends findings of older studies that showed hospital smoking bans (primarily indoor) decreased hospital employee smoking rates. Currently, our reduced employee smoking rate approaches the Healthy People 2010 goal of 12%.18
In conclusion, implementing a smoke‐free medical campus does not adversely affect inpatient volume (even among smokers), does not increase inpatient signing out AMA and can significantly increase inpatient NRT use, which in turn can increase the success of a quit attempt.19 In addition, implementing an outdoor smoking ban further reduces hospital employee smoking rates.
Acknowledgements
The authors are grateful to the many Mary Imogene Bassett Hospital staff in administration, employee health, facilities management, human resources, inpatient pharmacy, medical education, patient care service, respiratory care, and security who provided policy support and/or data needed to evaluate policy implementation.
- Institute of Medicine.Ending the Tobacco Problem: A Blueprint for the Nation.Washington, DC:National Academies Press;2007.
- ,.Smoke‐Free Hospital Campus Policies.Washington, DC,Advisory Board Original Inquiry Brief. 2/1/2005. Available at: http://www.roswellpark.org/files/1_2_1/prevention/3%20‐%20‐Advisory% 20Board%20smoke%20free%20policies.pdf. Accessed March 2009.
- ,,,,.Effects of the implementation of a smoke‐free policy in a medical center.Chest.1992;102:1531–1536.
- ,,, et al.Hospital smoking bans and employee smoking behavior: results of a national survey.JAMA.1996;275(16):1252–1257.
- ,,, et al.Impact of a smoke‐free hospital campus policy on employee and consumer behavior.Public Health Rep.2007;122(6):744–752.
- ,,,.Employee attitudes and smoking behavior at the City of Hope National Medical Center smoke–free campus.J Natl Compr Canc Netw.2006;4(6):535–542.
- ,.Effect of a total work‐site ban on employee smoking and attitudes.J Occup Med.1991;33(8):884–890.
- ,,, et al.Reviews of evidence regarding interventions to reduce tobacco use and exposure to environmental tobacco smoke.Am J Prev Med.2001;20(2S):16–66.
- ,,.Smoking on hospital grounds and the impact of outdoor smoke‐free zones.Tob Control.1996;5:199–204.
- ,,,,.The making of a smoke free hospital may not be as easy as you think.Am J Prev Med.1991;7(4):214–218.
- University of Michigan Health System. Tobacco Consultation Service. Available at: http://www.med.umich.edu/mfit/tobacco/freeenvironment. htm. Accessed March2009.
- Michigan Health and Hospital Association. It's a matter of life and health: MHA campaign for smoke‐free hospitals. Available at: http://www. mhasmokefreecampus.org. Accessed March2009.
- Department of Health and Human Services (DHHS). Treating Tobacco Use and Dependence: 2008 Update. Chapter 7: Specific Populations and Other Topics. Available at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi? rid=hstat2.section.28504. Accessed March2009.
- ,,.Interventions for smoking cessation in hospitalized patients.Cochrane Database Syst Rev.2007;(3):CD001837.
- ,,, et al.Ending smoking at the Johns Hopkins Medical Institutions: an evaluation of smoking prevalence and indoor air pollution.JAMA.1990;264:1565–1569.
- .Toward smoke‐free medical facilities.Chest.1990;97:1027–1028.
- .The benefits of smoke‐free health care campuses.Am Fam Physician.1994;49(1):28–33.
- U.S. Department of Health and Human Services.Healthy People 2010. Vol 12nd ed.Washington, DC:U.S. Department of Health and Human Services;2000.
- ,,,.Effectiveness of smoking cessation therapies: a systematic review and meta‐analysis.BMC Public Health.2006;6:300.
Even though imposition of smoke‐free policies and workplaces comprise one of the most effective antismoking strategies,1 hospital administrators hesitate to implement a smoke‐free medical campus policy.2 They fear losing patients who smoke because these patients will opt for other facilities that permit smoking.
Apart from studies evaluating Joint Commission on Accreditation of Healthcare Organizations (JCAHO)‐required indoor smoking bans in hospitals in 1992,3, 4 there are few published studies or formal evaluations of the impact of medical campuses going smoke‐free. One study of the implementation of a smoke‐free medical campus policy at a university hospital in Little Rock, AR, showed that the policy had no impact on employee retention, bed occupancy, or mean daily census; however, inpatient smoking status was not ascertained.5 Most (83%) employees were supportive of the policy. More importantly, employees at 2 university medical centers reported reduced cigarette consumption and increased attempts to quit after implementation of a smoke‐free medical campus policy.6, 7
Our hospital is 180‐bed, acute care inpatient teaching facility in upstate New York. Prior to the implementation of the smoke‐free medical campus policy, it was common to see employees, visitors, and patients lined up outdoors around the main hospital entrances and smoking just beyond the no smoking signage. Inpatients could look out their windows at the main entrance or into the courtyard and see hospital staff, other patients, and visitors smoking.
This study prospectively evaluates the impact of implementing the smoke‐free medical campus policy and starting an inpatient smoking cessation service. It addresses the following questions that have also been raised by the Task Force for Community Preventive Services.8 Does the institution of hospital smoking bans reduce the percentage of inpatients who smoke or increase the percentage who sign out against medical advice? What are the extended effects (beyond 1 year after implementation) of medical campus smoking bans on employee smoking rates?
Materials and Methods
Policy Implementation
As prior studies have shown that institution of a smoke‐free medical campus policy involves much more than just posting signage,9, 10 a detailed multidisciplinary work plan was implemented starting 1.5 years prior to the date our policy went into effect on July 1, 2006. The Implementing a Smoke‐Free Environment plan, produced by the University of Michigan,11 which includes a 15‐step checklist, was used to guide this policy change.12 As part of that plan, employees were offered on‐site smoking cessation services, including nicotine replacement therapy (NRT), and 150 employees participated in this program prior to July 1, 2006. Staff, community, and patient education was also completed. A new campus map delineating the smoke‐free border was disseminated. Signage was posted in areas used in the past for smoking. In addition to implementing this plan, an inpatient smoking cessation service was started 3 months prior to July 1, 2006. In addition to supporting the enforcement of the smoke‐free medical campus, our inpatient smoking cessation program was designed to help inpatients with nicotine withdrawal as well as smoking cessation, if they were ready to quit.
Data Collection and Analysis
The inpatient electronic medical record (EMR) was used to monitor the smoking status of patients admitted to hospital on a monthly basis. On admission to the hospital, the admitting nurse screened patients for current smoking status. This information was entered into the EMR starting in April 2006; therefore, pre‐ban screening data were limited to 2 months prior to the ban. Inpatients too sick to complete this screening process, women admitted for labor and delivery, and inpatients boarded in the emergency department were not screened. No identifiers were used in compiling these monthly data.
Nursing reports of inpatients signing out against medical advice (AMA) were compiled in order to compare incidence of AMA pre‐ban to post‐ban. AMA documentation in our hospital takes the form of a structured incident report that is reliably documented by nursing staff and signed by the attending physician of service.
Computerized inpatient doctors' orders to pharmacy for NRT, dispensed as gum or patch, were monitored 2 years preinitiation and postinitiation of the inpatient smoking cessation service on April 1, 2006. As varenicline was nonformulary and bupropion was used for other indications than smoking cessation, these medications were not included in this review. The Chow test was used to measure and test for significant breaks in a time series analysis of the NRT orders.
New York State law requires an annual occupational health review to be completed by every hospital employee. At our hospital, this review included a question on tobacco use Do you smoke or chew tobacco? Although there has been a smoker/nonsmoker differential in the rates offered for supplemental life insurance since 1992, there were no wellness credits or other incentives for medical insurance offered in employee benefits that may predispose employees to underreport tobacco use. Using this question, employees were categorized as self‐reported current smokers or chew users. Employee smoking rates were estimated using different denominators to validate the direction of the trend. First, self‐reported smoking rates were compared pre‐ban and post‐ban among a stable cohort of hospital employees (n = 489), defined as hospital‐based employees with anniversary dates from March to June who reported in both 2005 and 2007. The McNemar test was used to test the statistical significance of the 2 smoking rates of paired replicates in this stable cohort of employees reporting pre‐ban and post‐ban. Second, all employees in the database reporting smoking status pre‐ban, March to June 2005, and then post‐ban, March to June 2006 and 2007, were compared in order to monitor trends in employee smoking overall. A t‐test was used to compare the statistical significance of the difference in the overall rates of smoking among all employees pre‐ban and post‐ban.
Internal review boards of our hospital and the New York State Department of Health reviewed and approved this study.
Results
Inpatient Outcomes
An average of 959 patients were admitted per month in the 18‐month period pre‐ban (January 2005 to June 2006) vs. 988 per month in the 23‐month period post‐ban (July 2006 to September 2008). A monthly average of 89% of inpatients were screened for tobacco use when admitted. The monthly average for the percentage of inpatients who currently smoke has been approximately 21.6% following the implementation of the smoke‐free hospital plan. There has been little variation (Figure 1) in the percentage of inpatients who smoke pre‐ban and post‐ban except for the startup period in 2006 and the onset of the 2007 respiratory illness season.
Among all inpatients who currently smoke, 69.8% received a brief nursing intervention at the time of admission and 25% received an inpatient visit from our part‐time smoking cessation specialist.
The percentage of inpatients who signed out against medical advice (AMA) with the reason of having to smoke was 13.8% (4/29) 6 months pre‐ban, and 13.6% (3/22) 6 months post‐ban. In 2007, there were no inpatients who signed out AMA stating that they needed to smoke. Because the reason for signing out AMA may be underreported, we also examined the rate of smoking among all inpatients who sign out AMA. Six months pre‐ban, this percentage was 48.3% (14/29), but increased 6 months post‐ban to 59% (13/22). In 2007, the percentage of smokers among inpatients who sign out AMA leveled off at 50.8% (29/57).
Review of computerized inpatient prescription orders shows that orders for NRT nearly tripled after the inpatient smoking cessation service started April 1, 2006 (3 months prior to the ban) (Figure 2). Inpatient orders for these medications increased from 832 in a 2‐year period before the ban (April 1, 2004 to March 31, 2006) to 2475 in the 2 years following the initiation of the inpatient smoking service (April 1, 2006 to March 31, 2008). The Chow test is highly significant for a break point in June 2006 (P = 0.008), 1 month prior to the ban.
Employee Smoking Rates
Among a cohort of 489 hospital‐based employees reporting in both 2005 and 2007, 12% reported smoking in 2005 and 7.5% in 2007 (McNemar was significant at P 0.001). Two employees reported using chewing tobacco in 2005 and only 1 in 2007.
Including all hospital employees reporting any 1 year during their anniversary dates, the self‐reported smoking rates were 14.3% (n = 624) in March to June 2005, 14.8% (n = 661) in March to June 2006, and 9.4% (n = 1,112) in March to June 2007 (P 0.0002). Because promotions change the anniversary date, and the database was expanded in 2007 to include new hires and managerial staff, these estimates represent the point prevalence among employees whose anniversary dates fall between March and June.
Discussion
Following implementation of a smoke‐free medical campus, no adverse effects were observed on inpatient volume at our hospital. The percentage of inpatients who smoke and the percentage of inpatients signing out AMA have remained stable after the smoke‐free policy went into effect. In addition, self‐reported employee smoking rates decreased significantly. Fears about losing inpatients (who smoke) following the implementation of a smoke‐free hospital plan were unfounded.
This study employs the electronic medical record to not only monitor trends in the proportion of inpatients who smoke pre‐ban and post‐ban, but also to notify our inpatient smoking cessation specialist, on the day of admission, to consult on patients who currently smoke. Unfortunately, our cessation specialist, who is part‐time, was unable to see all inpatients who smoke on account of the inpatient's acuity, pain, hospice status, weekend or night admission, or not being available due to testing, surgery, or other procedures. Nevertheless, use of NRT increased sharply following the initiation of this program. As shown in Figure 2, a linear rise in NRT orders was already underway starting April 2005, probably in anticipation of the ban and coinciding with the start of the inpatient smoking cessation program. However, the Chow test is highly significant for a breakpoint in June 2006 (P = 0.008), 1 month prior to the ban, meaning that the slope was climbing even more steeply after that point.
As hospitalized smokers may be more motivated to stop smoking, the updated 2008 clinical practice guidelines for Treating Tobacco Use and Dependence now recommend that all patients in the hospital be given medications, advised, counseled, and receive follow‐up after discharge.13 Although our inpatient cessation program was started before these clinical practice guidelines were available, we are currently evaluating the efficacy of our inpatient program by assessing self‐reported quit rates 6‐months posthospitalization (data collection in process). Provision of inpatient smoking cessation has been shown to be an effective smoking cessation intervention if combined with outpatient follow‐up.14 Our current program will be expanded to include outpatient follow‐up, if the inpatient's primary care provider is unable to provide it or if the inpatient refuses faxed referral to the New York State quit line program.
This study evaluates the impact of simultaneously introduced interventions such as medical campus smoking ban, inpatient smoking cessation program, hospital staff education, and other elements of the University of Michigan Smoke‐Free Hospital Implementation Plan. The role of individual components of the plan cannot be evaluated in this study as they were intentionally implemented simultaneously in order to achieve a synergistic effect.
Another limitation of this study is that smoking status is self‐reported and not validated biochemically. Although validated smoking status measures such as salivary cotinine testing would be more scientifically valid, it was not feasible to validate the smoking status of inpatients, nor that of employees. Thus smoking status, as ascertained in this study, is subject to underreporting. Social desirability bias has been recognized as potential limitation of self‐reported smoking status in other evaluations of smoke‐free policies.3, 4, 15
In the 1990s, the employee benefits of instituting indoor smoking bans in hospitals were theorized to include reduced employee sick time, break time, and tobacco use, as well as increased motivation for smoking cessation and reduced legitimacy of tobacco use.16, 17 Peer pressure, workplace socialization, and being forced to stay away from cigarettes for the length of entire workdays have been credited with helping hospital workers to quit.4, 7 In our study, extending the ban to the outdoor areas of our medical campus as well as provision of employee smoking cessation services may augment these mechanisms. This study extends findings of older studies that showed hospital smoking bans (primarily indoor) decreased hospital employee smoking rates. Currently, our reduced employee smoking rate approaches the Healthy People 2010 goal of 12%.18
In conclusion, implementing a smoke‐free medical campus does not adversely affect inpatient volume (even among smokers), does not increase inpatient signing out AMA and can significantly increase inpatient NRT use, which in turn can increase the success of a quit attempt.19 In addition, implementing an outdoor smoking ban further reduces hospital employee smoking rates.
Acknowledgements
The authors are grateful to the many Mary Imogene Bassett Hospital staff in administration, employee health, facilities management, human resources, inpatient pharmacy, medical education, patient care service, respiratory care, and security who provided policy support and/or data needed to evaluate policy implementation.
Even though imposition of smoke‐free policies and workplaces comprise one of the most effective antismoking strategies,1 hospital administrators hesitate to implement a smoke‐free medical campus policy.2 They fear losing patients who smoke because these patients will opt for other facilities that permit smoking.
Apart from studies evaluating Joint Commission on Accreditation of Healthcare Organizations (JCAHO)‐required indoor smoking bans in hospitals in 1992,3, 4 there are few published studies or formal evaluations of the impact of medical campuses going smoke‐free. One study of the implementation of a smoke‐free medical campus policy at a university hospital in Little Rock, AR, showed that the policy had no impact on employee retention, bed occupancy, or mean daily census; however, inpatient smoking status was not ascertained.5 Most (83%) employees were supportive of the policy. More importantly, employees at 2 university medical centers reported reduced cigarette consumption and increased attempts to quit after implementation of a smoke‐free medical campus policy.6, 7
Our hospital is 180‐bed, acute care inpatient teaching facility in upstate New York. Prior to the implementation of the smoke‐free medical campus policy, it was common to see employees, visitors, and patients lined up outdoors around the main hospital entrances and smoking just beyond the no smoking signage. Inpatients could look out their windows at the main entrance or into the courtyard and see hospital staff, other patients, and visitors smoking.
This study prospectively evaluates the impact of implementing the smoke‐free medical campus policy and starting an inpatient smoking cessation service. It addresses the following questions that have also been raised by the Task Force for Community Preventive Services.8 Does the institution of hospital smoking bans reduce the percentage of inpatients who smoke or increase the percentage who sign out against medical advice? What are the extended effects (beyond 1 year after implementation) of medical campus smoking bans on employee smoking rates?
Materials and Methods
Policy Implementation
As prior studies have shown that institution of a smoke‐free medical campus policy involves much more than just posting signage,9, 10 a detailed multidisciplinary work plan was implemented starting 1.5 years prior to the date our policy went into effect on July 1, 2006. The Implementing a Smoke‐Free Environment plan, produced by the University of Michigan,11 which includes a 15‐step checklist, was used to guide this policy change.12 As part of that plan, employees were offered on‐site smoking cessation services, including nicotine replacement therapy (NRT), and 150 employees participated in this program prior to July 1, 2006. Staff, community, and patient education was also completed. A new campus map delineating the smoke‐free border was disseminated. Signage was posted in areas used in the past for smoking. In addition to implementing this plan, an inpatient smoking cessation service was started 3 months prior to July 1, 2006. In addition to supporting the enforcement of the smoke‐free medical campus, our inpatient smoking cessation program was designed to help inpatients with nicotine withdrawal as well as smoking cessation, if they were ready to quit.
Data Collection and Analysis
The inpatient electronic medical record (EMR) was used to monitor the smoking status of patients admitted to hospital on a monthly basis. On admission to the hospital, the admitting nurse screened patients for current smoking status. This information was entered into the EMR starting in April 2006; therefore, pre‐ban screening data were limited to 2 months prior to the ban. Inpatients too sick to complete this screening process, women admitted for labor and delivery, and inpatients boarded in the emergency department were not screened. No identifiers were used in compiling these monthly data.
Nursing reports of inpatients signing out against medical advice (AMA) were compiled in order to compare incidence of AMA pre‐ban to post‐ban. AMA documentation in our hospital takes the form of a structured incident report that is reliably documented by nursing staff and signed by the attending physician of service.
Computerized inpatient doctors' orders to pharmacy for NRT, dispensed as gum or patch, were monitored 2 years preinitiation and postinitiation of the inpatient smoking cessation service on April 1, 2006. As varenicline was nonformulary and bupropion was used for other indications than smoking cessation, these medications were not included in this review. The Chow test was used to measure and test for significant breaks in a time series analysis of the NRT orders.
New York State law requires an annual occupational health review to be completed by every hospital employee. At our hospital, this review included a question on tobacco use Do you smoke or chew tobacco? Although there has been a smoker/nonsmoker differential in the rates offered for supplemental life insurance since 1992, there were no wellness credits or other incentives for medical insurance offered in employee benefits that may predispose employees to underreport tobacco use. Using this question, employees were categorized as self‐reported current smokers or chew users. Employee smoking rates were estimated using different denominators to validate the direction of the trend. First, self‐reported smoking rates were compared pre‐ban and post‐ban among a stable cohort of hospital employees (n = 489), defined as hospital‐based employees with anniversary dates from March to June who reported in both 2005 and 2007. The McNemar test was used to test the statistical significance of the 2 smoking rates of paired replicates in this stable cohort of employees reporting pre‐ban and post‐ban. Second, all employees in the database reporting smoking status pre‐ban, March to June 2005, and then post‐ban, March to June 2006 and 2007, were compared in order to monitor trends in employee smoking overall. A t‐test was used to compare the statistical significance of the difference in the overall rates of smoking among all employees pre‐ban and post‐ban.
Internal review boards of our hospital and the New York State Department of Health reviewed and approved this study.
Results
Inpatient Outcomes
An average of 959 patients were admitted per month in the 18‐month period pre‐ban (January 2005 to June 2006) vs. 988 per month in the 23‐month period post‐ban (July 2006 to September 2008). A monthly average of 89% of inpatients were screened for tobacco use when admitted. The monthly average for the percentage of inpatients who currently smoke has been approximately 21.6% following the implementation of the smoke‐free hospital plan. There has been little variation (Figure 1) in the percentage of inpatients who smoke pre‐ban and post‐ban except for the startup period in 2006 and the onset of the 2007 respiratory illness season.
Among all inpatients who currently smoke, 69.8% received a brief nursing intervention at the time of admission and 25% received an inpatient visit from our part‐time smoking cessation specialist.
The percentage of inpatients who signed out against medical advice (AMA) with the reason of having to smoke was 13.8% (4/29) 6 months pre‐ban, and 13.6% (3/22) 6 months post‐ban. In 2007, there were no inpatients who signed out AMA stating that they needed to smoke. Because the reason for signing out AMA may be underreported, we also examined the rate of smoking among all inpatients who sign out AMA. Six months pre‐ban, this percentage was 48.3% (14/29), but increased 6 months post‐ban to 59% (13/22). In 2007, the percentage of smokers among inpatients who sign out AMA leveled off at 50.8% (29/57).
Review of computerized inpatient prescription orders shows that orders for NRT nearly tripled after the inpatient smoking cessation service started April 1, 2006 (3 months prior to the ban) (Figure 2). Inpatient orders for these medications increased from 832 in a 2‐year period before the ban (April 1, 2004 to March 31, 2006) to 2475 in the 2 years following the initiation of the inpatient smoking service (April 1, 2006 to March 31, 2008). The Chow test is highly significant for a break point in June 2006 (P = 0.008), 1 month prior to the ban.
Employee Smoking Rates
Among a cohort of 489 hospital‐based employees reporting in both 2005 and 2007, 12% reported smoking in 2005 and 7.5% in 2007 (McNemar was significant at P 0.001). Two employees reported using chewing tobacco in 2005 and only 1 in 2007.
Including all hospital employees reporting any 1 year during their anniversary dates, the self‐reported smoking rates were 14.3% (n = 624) in March to June 2005, 14.8% (n = 661) in March to June 2006, and 9.4% (n = 1,112) in March to June 2007 (P 0.0002). Because promotions change the anniversary date, and the database was expanded in 2007 to include new hires and managerial staff, these estimates represent the point prevalence among employees whose anniversary dates fall between March and June.
Discussion
Following implementation of a smoke‐free medical campus, no adverse effects were observed on inpatient volume at our hospital. The percentage of inpatients who smoke and the percentage of inpatients signing out AMA have remained stable after the smoke‐free policy went into effect. In addition, self‐reported employee smoking rates decreased significantly. Fears about losing inpatients (who smoke) following the implementation of a smoke‐free hospital plan were unfounded.
This study employs the electronic medical record to not only monitor trends in the proportion of inpatients who smoke pre‐ban and post‐ban, but also to notify our inpatient smoking cessation specialist, on the day of admission, to consult on patients who currently smoke. Unfortunately, our cessation specialist, who is part‐time, was unable to see all inpatients who smoke on account of the inpatient's acuity, pain, hospice status, weekend or night admission, or not being available due to testing, surgery, or other procedures. Nevertheless, use of NRT increased sharply following the initiation of this program. As shown in Figure 2, a linear rise in NRT orders was already underway starting April 2005, probably in anticipation of the ban and coinciding with the start of the inpatient smoking cessation program. However, the Chow test is highly significant for a breakpoint in June 2006 (P = 0.008), 1 month prior to the ban, meaning that the slope was climbing even more steeply after that point.
As hospitalized smokers may be more motivated to stop smoking, the updated 2008 clinical practice guidelines for Treating Tobacco Use and Dependence now recommend that all patients in the hospital be given medications, advised, counseled, and receive follow‐up after discharge.13 Although our inpatient cessation program was started before these clinical practice guidelines were available, we are currently evaluating the efficacy of our inpatient program by assessing self‐reported quit rates 6‐months posthospitalization (data collection in process). Provision of inpatient smoking cessation has been shown to be an effective smoking cessation intervention if combined with outpatient follow‐up.14 Our current program will be expanded to include outpatient follow‐up, if the inpatient's primary care provider is unable to provide it or if the inpatient refuses faxed referral to the New York State quit line program.
This study evaluates the impact of simultaneously introduced interventions such as medical campus smoking ban, inpatient smoking cessation program, hospital staff education, and other elements of the University of Michigan Smoke‐Free Hospital Implementation Plan. The role of individual components of the plan cannot be evaluated in this study as they were intentionally implemented simultaneously in order to achieve a synergistic effect.
Another limitation of this study is that smoking status is self‐reported and not validated biochemically. Although validated smoking status measures such as salivary cotinine testing would be more scientifically valid, it was not feasible to validate the smoking status of inpatients, nor that of employees. Thus smoking status, as ascertained in this study, is subject to underreporting. Social desirability bias has been recognized as potential limitation of self‐reported smoking status in other evaluations of smoke‐free policies.3, 4, 15
In the 1990s, the employee benefits of instituting indoor smoking bans in hospitals were theorized to include reduced employee sick time, break time, and tobacco use, as well as increased motivation for smoking cessation and reduced legitimacy of tobacco use.16, 17 Peer pressure, workplace socialization, and being forced to stay away from cigarettes for the length of entire workdays have been credited with helping hospital workers to quit.4, 7 In our study, extending the ban to the outdoor areas of our medical campus as well as provision of employee smoking cessation services may augment these mechanisms. This study extends findings of older studies that showed hospital smoking bans (primarily indoor) decreased hospital employee smoking rates. Currently, our reduced employee smoking rate approaches the Healthy People 2010 goal of 12%.18
In conclusion, implementing a smoke‐free medical campus does not adversely affect inpatient volume (even among smokers), does not increase inpatient signing out AMA and can significantly increase inpatient NRT use, which in turn can increase the success of a quit attempt.19 In addition, implementing an outdoor smoking ban further reduces hospital employee smoking rates.
Acknowledgements
The authors are grateful to the many Mary Imogene Bassett Hospital staff in administration, employee health, facilities management, human resources, inpatient pharmacy, medical education, patient care service, respiratory care, and security who provided policy support and/or data needed to evaluate policy implementation.
- Institute of Medicine.Ending the Tobacco Problem: A Blueprint for the Nation.Washington, DC:National Academies Press;2007.
- ,.Smoke‐Free Hospital Campus Policies.Washington, DC,Advisory Board Original Inquiry Brief. 2/1/2005. Available at: http://www.roswellpark.org/files/1_2_1/prevention/3%20‐%20‐Advisory% 20Board%20smoke%20free%20policies.pdf. Accessed March 2009.
- ,,,,.Effects of the implementation of a smoke‐free policy in a medical center.Chest.1992;102:1531–1536.
- ,,, et al.Hospital smoking bans and employee smoking behavior: results of a national survey.JAMA.1996;275(16):1252–1257.
- ,,, et al.Impact of a smoke‐free hospital campus policy on employee and consumer behavior.Public Health Rep.2007;122(6):744–752.
- ,,,.Employee attitudes and smoking behavior at the City of Hope National Medical Center smoke–free campus.J Natl Compr Canc Netw.2006;4(6):535–542.
- ,.Effect of a total work‐site ban on employee smoking and attitudes.J Occup Med.1991;33(8):884–890.
- ,,, et al.Reviews of evidence regarding interventions to reduce tobacco use and exposure to environmental tobacco smoke.Am J Prev Med.2001;20(2S):16–66.
- ,,.Smoking on hospital grounds and the impact of outdoor smoke‐free zones.Tob Control.1996;5:199–204.
- ,,,,.The making of a smoke free hospital may not be as easy as you think.Am J Prev Med.1991;7(4):214–218.
- University of Michigan Health System. Tobacco Consultation Service. Available at: http://www.med.umich.edu/mfit/tobacco/freeenvironment. htm. Accessed March2009.
- Michigan Health and Hospital Association. It's a matter of life and health: MHA campaign for smoke‐free hospitals. Available at: http://www. mhasmokefreecampus.org. Accessed March2009.
- Department of Health and Human Services (DHHS). Treating Tobacco Use and Dependence: 2008 Update. Chapter 7: Specific Populations and Other Topics. Available at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi? rid=hstat2.section.28504. Accessed March2009.
- ,,.Interventions for smoking cessation in hospitalized patients.Cochrane Database Syst Rev.2007;(3):CD001837.
- ,,, et al.Ending smoking at the Johns Hopkins Medical Institutions: an evaluation of smoking prevalence and indoor air pollution.JAMA.1990;264:1565–1569.
- .Toward smoke‐free medical facilities.Chest.1990;97:1027–1028.
- .The benefits of smoke‐free health care campuses.Am Fam Physician.1994;49(1):28–33.
- U.S. Department of Health and Human Services.Healthy People 2010. Vol 12nd ed.Washington, DC:U.S. Department of Health and Human Services;2000.
- ,,,.Effectiveness of smoking cessation therapies: a systematic review and meta‐analysis.BMC Public Health.2006;6:300.
- Institute of Medicine.Ending the Tobacco Problem: A Blueprint for the Nation.Washington, DC:National Academies Press;2007.
- ,.Smoke‐Free Hospital Campus Policies.Washington, DC,Advisory Board Original Inquiry Brief. 2/1/2005. Available at: http://www.roswellpark.org/files/1_2_1/prevention/3%20‐%20‐Advisory% 20Board%20smoke%20free%20policies.pdf. Accessed March 2009.
- ,,,,.Effects of the implementation of a smoke‐free policy in a medical center.Chest.1992;102:1531–1536.
- ,,, et al.Hospital smoking bans and employee smoking behavior: results of a national survey.JAMA.1996;275(16):1252–1257.
- ,,, et al.Impact of a smoke‐free hospital campus policy on employee and consumer behavior.Public Health Rep.2007;122(6):744–752.
- ,,,.Employee attitudes and smoking behavior at the City of Hope National Medical Center smoke–free campus.J Natl Compr Canc Netw.2006;4(6):535–542.
- ,.Effect of a total work‐site ban on employee smoking and attitudes.J Occup Med.1991;33(8):884–890.
- ,,, et al.Reviews of evidence regarding interventions to reduce tobacco use and exposure to environmental tobacco smoke.Am J Prev Med.2001;20(2S):16–66.
- ,,.Smoking on hospital grounds and the impact of outdoor smoke‐free zones.Tob Control.1996;5:199–204.
- ,,,,.The making of a smoke free hospital may not be as easy as you think.Am J Prev Med.1991;7(4):214–218.
- University of Michigan Health System. Tobacco Consultation Service. Available at: http://www.med.umich.edu/mfit/tobacco/freeenvironment. htm. Accessed March2009.
- Michigan Health and Hospital Association. It's a matter of life and health: MHA campaign for smoke‐free hospitals. Available at: http://www. mhasmokefreecampus.org. Accessed March2009.
- Department of Health and Human Services (DHHS). Treating Tobacco Use and Dependence: 2008 Update. Chapter 7: Specific Populations and Other Topics. Available at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi? rid=hstat2.section.28504. Accessed March2009.
- ,,.Interventions for smoking cessation in hospitalized patients.Cochrane Database Syst Rev.2007;(3):CD001837.
- ,,, et al.Ending smoking at the Johns Hopkins Medical Institutions: an evaluation of smoking prevalence and indoor air pollution.JAMA.1990;264:1565–1569.
- .Toward smoke‐free medical facilities.Chest.1990;97:1027–1028.
- .The benefits of smoke‐free health care campuses.Am Fam Physician.1994;49(1):28–33.
- U.S. Department of Health and Human Services.Healthy People 2010. Vol 12nd ed.Washington, DC:U.S. Department of Health and Human Services;2000.
- ,,,.Effectiveness of smoking cessation therapies: a systematic review and meta‐analysis.BMC Public Health.2006;6:300.
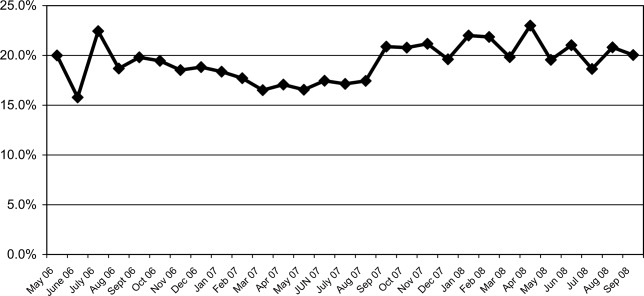
Consultative Pediatrics
In an ideal situation, a child could be cared for by 1 physician from childhood through adolescence. This physician could care for the child from the first days in the nursery, through multiple well‐child and sick visits, and during any hospitalizations. In 1992, the American Academy of Pediatrics (AAP) introduced the concept of the medical home to provide accessible, continuous, comprehensive, family‐centered, coordinated, and compassionate care for children.1 These ideals were reaffirmed in a 2002 AAP policy statement.2 The demands for outpatient care have become more intense and patient safety issues have become a public focus. Combined with the necessity for increased efficiency, the ideal medical home has become difficult to achieve simultaneously in both an outpatient and inpatient setting. This has led to the growth of the hospital specialist or hospitalist, a term first coined by Drs. Wachter and Goldman in August 1996.3 A hospitalist has been defined as a physician whose primary professional focus is the general medical care of hospitalized patients . . . teaching, research, and leadership related to hospital care.4 Despite early concerns voiced after the publication of this landmark article, there has been tremendous growth in the number of hospitalists nationwide.5 Initially, this growth was seen in adult medicine, but pediatric hospitalists have become increasingly more common. There are an estimated 10,000 to 20,000 hospitalists in the profession, with more than 30,000 expected by the end of the decade, with just over 10% being pediatric hospitalists.4 Several studies have shown the benefits of pediatric hospitalist programs with decreased length of stay, hospital charges, and utilization of unnecessary tests and therapies, and increased satisfaction among the physicians, students, and patients.611
History of the Diagnostic Referral Service
Despite the coining of the term hospitalist in 1996, specialization in inpatient care existed in various forms long before then.12 The Diagnostic Referral Service (DRS) at Children's Hospital of Pittsburgh (CHP) initially began under the guidance of Dr. Edmund R. McCluskey, chairman of the Department of Pediatrics at CHP, and Dr. Paul C. Gaffney, a beloved and revered clinician and educator. In 1951, Dr. Gaffney joined the full‐time CHP faculty after residency, chief residency, and a year of fellowship, providing his expertise in hematology and oncology. Over time, Dr. Gaffney's role expanded to that of a master physician, and pediatricians and family practitioners in the community began sending their most diagnostically challenging patients to be seen in his clinic. His activities further extended to providing inpatient care and consultations for complex patients.
With these growing responsibilities, Dr. Gaffney formed the DRS as a separate division within the Department of Pediatrics in the mid‐1970s and began developing the division. The group, then and now, is comprised of general pediatricians who provide multidisciplinary care for hospitalized children as well as for ambulatory consultations. The DRS was initially described in the literature 20 years ago; the roles of the 5 full‐time physicians at that time included a variety of clinical, teaching, and scholarly activities, as both inpatient and outpatient consultative physicians.13 Though much growth has occurred within the division since then, Dr. Gaffney's initial goals of providing excellent patient care and education in an academic setting still remain at the heart of each group member.
Growth of the Division
In March 2002, there were 4 full‐time physicians within the DRS. A remarkable increase in the group size has occurred since then, and currently there are 16 physicians. Each member of the division is assigned a specific activity, either outpatient or inpatient, for at least a 5‐day block. This allows the division to provide continuity in the care of complex patients in both settings and help maintain a medical home for these challenging patients. The primary care physician (PCP) remains responsible for primary care of the patient while the DRS can help manage the patient's complexities in the outpatient and inpatient setting. In essence, there is joint patient ownership between the DRS and the PCP, with relegation of different skill sets to provide a complete medical home for the patient.
The current activities of the group are summarized as follows.
Inpatient Activities
Inpatient Care
Corresponding to the growing pediatric hospitalist movement in the past decade, several area PCPs began requesting that their office patients be followed by the DRS when admitted to CHP. In 2003, the DRS physician referral list had 150 physicians, and it currently has over 325 physicians who refer the inpatient care of their patients to the DRS. These practices are located in a variety of locations in Western Pennsylvania, Ohio, and West Virginia. There are only 7 private practices that continue to maintain their admitting privileges to CHP, and these practices account for 0.5% of general pediatric admissions. The remaining admissions (those PCPs not on the DRS referral list or with admitting privileges) are covered by a rotating attending physician; 85% of the time this is a DRS physician. Therefore, while 0.5% of general pediatric admissions are cared for by private pediatricians, >95% of all general pediatric admissions are cared for by DRS, with the remaining patients cared for by a small number of pediatric subspecialists who occasionally serve as rotating attendings.
Associated with the increase in referrals has been a marked increase in inpatient activity (Figures 0, 0, 0, 13). Nearly 1 of every 4 CHP discharges and 1 of every 3 observation patients are cared for by the DRS.
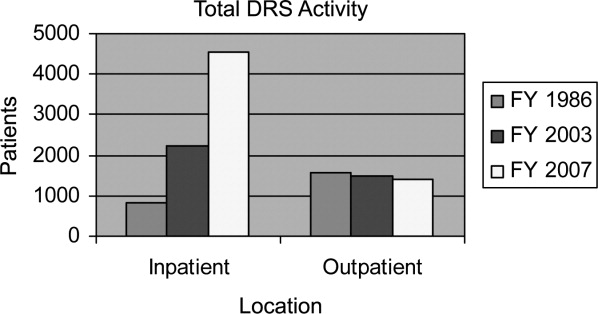
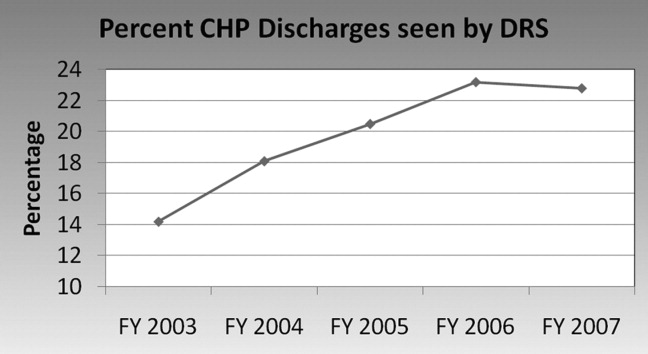
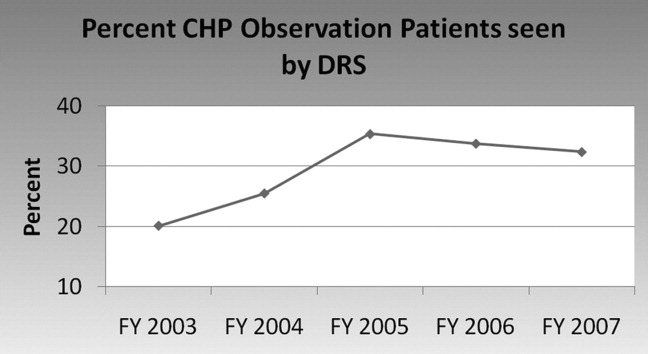
The DRS division has seen an increase in complex inpatient admissions as well as a much larger number of routine pediatric admissions from the community PCP referrals, as described above. Statistically, this has resulted in an overall stable to slightly increased inpatient complexity for the DRS group. During this same time period, there was a steep decrease in DRS inpatient length of stay followed by maintenance at the shorter length of stay thereafter. Inpatient complexity has increased throughout CHP, yet the same decreases in length of stay have not been seen universally in all the divisions (Figure 4). The advantage that a hospitalist group can bring in decreasing length of stay (and, thereby, hospital costs) has been seen in hospitalist programs around the country.6, 7
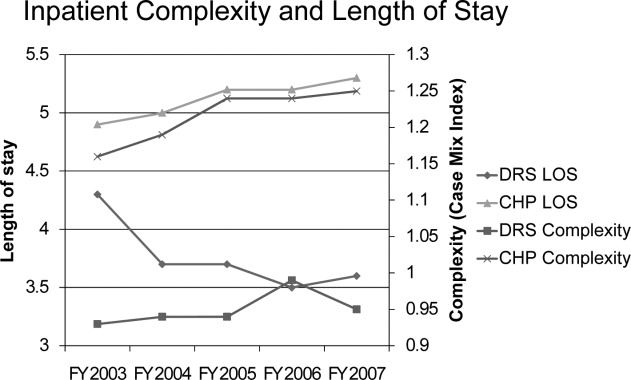
Each member of the group attends on the general pediatric ward for 9 to 10 months per year as compared to 2 months per year in 1986. In order to prevent job‐related fatigue, 6 to 8 members of the group typically attend on the ward at the same time so that individual patient volume is more manageable. On average, each individual physician is responsible for about 6 to 8 patients per day. This census allows for daily education of residents and medical students as well as faculty participation in a variety of administrative activities. Despite emphasis on careful documentation and billing for both inpatient and ambulatory activities, the division, like most other pediatric hospitalist divisions, depends upon financial support from CHP and the Department of Pediatrics.
There is a wide variety of diagnoses that are seen in the inpatient setting, with notable similarities and differences when compared to 2 decades ago (Table 1). For example, asthma, gastroenteritis, and bronchiolitis continue to be frequent diagnoses, with bronchiolitis admissions becoming more frequent, following national trends.14
| FY 1986 | FY 2007 | ||
|---|---|---|---|
| Rank | Diagnosis | Rank | Diagnosis |
| |||
| 1. | Asthma | 1. | Bronchiolitis |
| 2. | Gastroenteritis | 2. | Asthma |
| 3. | Failure to thrive | 3. | Pneumonia |
| 4. | Seizures | 4. | Dehydration |
| 5. | Bronchiolitis | 5. | Viral enteritis |
| 6. | Pneumonia | 6. | Viral infection, NOS |
| 7. | Suspected sepsis | 7. | Esophageal reflux |
| 8. | Apneic episodes | 8. | Fever |
| 9. | Meningitis | 9. | Cellulitis |
| 10. | Otitis media | 10. | Convulsions |
In general, a DRS faculty member becomes the primary resource for families with medically complex children. The same faculty member tends to follow the patient in the consultative ambulatory clinic, be available for phone calls, and, if possible, follow them as the attending physician when the patient is admitted. This provides a degree of continuity generally not seen in many other hospitalist programs and has the potential to increase patient and physician satisfaction as well as patient safety.
Limited Stay Unit
In addition to general inpatient care, the DRS developed and maintains the Limited Stay Unit (LSU). This unit was specifically created in 2001 to serve patients with uncomplicated diagnoses who are expected to be discharged within 48 hours. Up to 10 short‐stay/observation patients are admitted to this unit each day, with nurses and staff specially prepared to handle rapid patient turnover. A child's eligibility for the unit is determined by the Emergency Department physicians or by phone consultation between the referring physician and the attending LSU physician. The design of the LSU allows for efficient admission and discharges of patients admitted with uncomplicated diagnoses. Each morning, the LSU attending physician, nurse practitioner, and residents discuss each patient with the nursing team and assess discharge readiness. Prescriptions and other discharge paperwork are prepared before morning rounds in order to avoid delays when the child has met criteria for safe discharge. Initial internal data evaluating the efficiency of the LSU demonstrated shorter length of stay for similar diagnoses admitted to the general ward. This difference was not observed in a subsequent study, likely due to CHP initiatives to improve the efficiency of discharge processes throughout the hospital.
Inpatient Consultations
The DRS serves as the inpatient pediatric consultant for the medical and surgical subspecialties. In 2007, the division saw 292 inpatient consultations. Many of the consultations originate from the surgical subspecialties (eg, a consult from neurosurgery for vomiting in a child with a functioning ventriculoperitoneal shunt). Other consultations come from pediatric subspecialties (eg, a patient with a congenital heart defect managed by the pediatric cardiology service with recurrent aspiration pneumonia of unclear etiology). The consultation process begins with the primary service discussing the patient with a senior resident who performs the initial history and physical, formulates an assessment and recommendations, and discusses the case with the DRS physician. Any necessary changes to the recommendations are made and relayed to the primary service. In addition, the DRS consults on known chronically ill patients in the intensive care unit (ICU), providing support to the family, nuances of chronic care to the ICU team, and continuity of care when the patient is transferred to the general ward.
Evening Hospitalist Program
In September 2005, the DRS began to provide extended in‐house attending coverage until midnight on weekdays and 10 PM on weekends. The evening hospitalist (EH) not only sees the new DRS admissions during the evening but also is available for formal consultations from subspecialty services and informal consultations from house staff. The EH is responsible for resident and medical student education (including direct observation of history taking and physical exam skills), facilitation of early discharges for the following morning, and enhancement of patient safety. The EH is also a part of the Condition Help team,15 a novel patient safety initiative discussed below.
The EH program benefits patients and DRS members alike. Other members of the group are able to assume care of patients in the morning for whom the diagnostic evaluation has already been initiated by the EH. Therefore, definitive plans are in place earlier, and many laboratory tests, radiographs, and other tests have returned by the time the daytime attending sees the patient.
The EH program was structured to enhance patient care and resident supervision while avoiding scheduling that could adversely affect job sustainability and retention. As currently structured, the EH program offers numerous advantages over 24‐hour, 7‐days‐per‐week coverage. First, resident autonomy is crucial during their training.16 One significant early concern was that extending the hours of attending physician coverage could diminish this autonomy. To prevent this from occurring, the EH allows the senior residents to take ownership of patient care and provide the initial teaching and instructions to interns, students, and families before the EH becomes involved. This structure of the EH program enhances the development of resident autonomy, yet provides support for the residents either by the EH or on‐call attending through all hours of the night. Second, the senior residents meet with members of DRS each morning to discuss their decision‐making process for overnight admissions that arrive after the EH shift has ended. This allows analysis of house staff thought processes and discussion of considered alternatives. Third, with the recent resident work‐hour restrictions, several residency programs have moved to either daytime or nighttime shift‐based work for the residents. Therefore, having the same EH working each day for the week allows for more accurate assessment of the nighttime residents than scattered 24‐hour attending shifts. Fourth, evening coverage allows for simpler scheduling and a less disruptive sleep cycle for the EH than 24‐hour coverage could allow. Finally, the EH is able to transition to typical daytime hours following a week of evening shifts, which helps to enhance EH retention by providing opportunities for academic endeavors and peer interactions.
The Children's Home
Since August 2007, the DRS has provided inpatient care for children admitted to The Children's Home of Pittsburgh and Lemieux Family Center (TCH). This independent facility is administratively and geographically separate from CHP. The DRS manages a 6‐bed unit that specializes in transitional pediatric care and serves technology‐dependent infants and children in a family‐centered, home‐like environment. In general, patients who require these services are seen at CHP initially, medically stabilized, and then transferred to TCH to continue their care. There is 1 DRS physician assigned each week to providing care for these patients. Examples of patient problems cared for at this facility include feeding issues, long term intravenous (IV) antibiotic treatment (eg, neonates recovering from sepsis, meningitis, osteomyelitis), and family education for technology‐dependent children (eg, new tracheostomy or ostomy). The average length of stay is 10.2 days, which decreases CHP length of stay and promotes CHP savings during periods of high census.
Outpatient Activities
Outpatient Care
Many physicians in community clinics have large daily patient volumes, seeing upward of 30 to 40 patients per day. These added outpatient responsibilities can lead to decreased time available for a PCP to round on inpatients (hence, the nationwide growth of hospitalists).17 Additionally, this increased practice intensity may lead to less time to manage individual patients in the primary care setting.18
The pediatric patient has become significantly more complex, likely due to increased survival of patients with chronic medical problems.19 This is also evidenced at CHP by steadily increasing patient acuity scores (Figure 4). With this growing complexity, effective outpatient care in a standard 15‐minute to 20‐minute patient visit20 is difficult, especially given the AAP recommendations of providing an effective medical home for every patient.2 Since its inception, the DRS has provided ambulatory consultative services for the community. Sixty percent of the 1400 to 1900 patients seen each year are new patient referrals. The outpatient clinic activity has been essentially stable over the past several years (Figure 1), likely due to increased access to CHP subspecialty clinics and overall increased manpower in the Department of Pediatrics. A wide variety of diagnoses are made in the outpatient clinic (Table 2).
| Rank | Diagnosis |
|---|---|
| |
| 1. | Failure to thrive, poor weight gain, weight loss |
| 2. | Abdominal pain |
| 3. | Fever |
| 4. | Chronic fatigue |
| 5. | Syncope |
| 6. | Gastroesophageal reflux |
| 7. | Chest pain |
| 8. | Developmental delay |
| 9. | Headache |
| 10. | Coordination of care |
The DRS provides long‐term, multidisciplinary continuity of care for medically complex children. The child is seen by the same DRS physician during each clinic visit. If the patient is admitted to the hospital, every effort is made for the patient to be seen by the DRS physician who saw the patient in the clinic setting. This process allows for medically complex children to have the coordinated care that can be difficult to achieve if a different hospitalist physician is responsible for their care during each admission.
The DRS works closely with the PCP to augment continuity of care while the PCP continues to provide primary care services. This provides the PCP with assurance that the patient will remain in their practice while the patient's multiple medical needs are addressed by the DRS. In this manner, a complete medical home can be provided. Insurance companies have recognized members of the DRS to be specialists in general pediatric care and permit DRS faculty to bill as specialists.
Education
Teaching is a major role for the DRS, and the division is closely involved in leadership in medical education. Two members are directors of the pediatric physical exam course for first‐year and second‐year medical students, 2 members are the third‐year medical school Pediatric clerkship directors, 1 member is co‐director for the fourth‐year acting internship, 1 member is co‐director of the advanced pediatric interviewing program, 1 member is director of the pediatric medical education program, and 1 member is associate residency program director.
The entire group is involved with teaching at all of these levels. The majority of the group is involved with formal mentoring and advising of residents and medical students. The only general pediatric aspect of student and resident medical education in which the DRS is no longer involved is ambulatory pediatric medicine. The full‐time ambulatory faculty is responsible for the primary ambulatory care experience. However, many residents choose to complete an elective in DRS, including the outpatient clinic, to become exposed to the different diagnostic dilemmas and coordination of care visits that they may not see in their primary care continuity clinics.
The division always welcomes new teaching challenges and incorporates new methods of teaching as opportunities arise. For example, the recent family‐centered rounds initiative allowed for new teaching methods that were not previously possible. The team, comprised of a senior resident, 2 interns, 2 students, and an attending physician rounds at the bedside with permission from the parent. The patient's nurse, when available, and a pharmacist are often a part of the team. The case is presented by the student or intern (directed to the parent), and the case is discussed and clarified for the family. A plan for the day is presented and discussed with the family for approval. Through family‐centered rounds, the DRS attending provides patient specific teaching and role modeling during rounds that would not otherwise have been possible with classical didactic teaching. This method of daily rounding also allows for the patients, families, nurses, nursing students, medical students, and residents to be taught by the attending physician simultaneously. Additionally, it affords the nurses the opportunity to participate in medical decision‐making, and the house staff have perceived fewer pages by the nurses to clarify clinical issues.
The EH program also provided new teaching opportunities. Through the EH, the house staff and students are exposed to direct attending teaching in the evenings that otherwise would not occur, such as direct observation of student and resident histories and physical examinations. Based on resident evaluations and comments to the residency program directors, this teaching experience is deemed to be valuable and effective. In fact, since the EH program's inception 3 years ago, 2 EHs have been selected by the residents as Teacher of the Year.
Patient Safety
Patient safety and reduction of medical errors is a major focus of the entire group. One DRS member serves within the hospital administration as Medical Director for Clinical Excellence and Service to enhance patient safety hospital‐wide. One DRS member orchestrates a monthly house staff meeting entitled To Err is Human which provides a nonthreatening environment for residents to discuss medical errors or difficult situations that they have encountered. Two DRS members are part of the Physician Advisory Committee, which serves as a bridge between the information technology group and clinicians. This committee has aided in achieving a smooth transition to a completely electronic medical record (EMR) and works together to use the tools of an EMR to enhance patient safety. This successful EMR implementation was recognized by the Health Information Management Systems Society in October 2008. Additionally, stemming from several successful patient safety initiatives, CHP was 1 of only 7 children's hospitals recognized for patient safety in 2008 by Leapfrog, the nation's premier patient safety evaluation group.
Condition HELP
In February 2001, the death of 18‐month‐old Josie King at a leading children's hospital brought medical errors to the national forefront.21 In response to this tragedy, several hospitals in the University of Pittsburgh system began to implement a program called Condition HELP.22 Condition HELP gives parents the ability to have their child evaluated by a special medical team if they feel their child's immediate health is in danger or their concerns are not being addressed. In 2005, CHP was one of the first hospitals in the country to implement this type of system. The Condition HELP team consists of a physician, a nursing supervisor, and a patient advocate. During the evening hours, the DRS EH also participates in the calls. The team discusses the family's concern and, with the patient's attending physician, generates a plan of action to help remedy the issue. Usually within 5 days, each call is intensively reviewed for events leading up to the Condition HELP as part of the CHP's patient safety initiative. From September 2005 through August 2007, the CHP Condition HELP team responded to 42 calls from patients and parents, with the most issues found to be related to communication breakdown between caregivers and families. The involvement of this team helped to identify the root cause of the parent or patient's concern and implement measures to help to rectify the issue and increase patient safety.15
Scholarly Activity
Previously, the DRS was responsible for the general medical care of liver transplant recipients, and many prior publications from the division focused on these patients.13 The division no longer provides that service, and the current focus of scholarly activity is publication of case reports, book chapters, and review articles. There were 13 publications from the division members in the past 3 years. The group also serves as a major resource within the department by referring patients that fulfill the clinical criteria for ongoing clinical studies in other divisions.
One member of the group continues to serve as senior editor of the Atlas of Pediatric Physical Diagnosis, which is currently in its fifth edition. Several members of the group contribute chapters to this well‐known text. One member is an editor and another is a specialty reviewer for
At the University of Pittsburgh, both tenured and nontenured faculty promotions carry the same title without a prefix. Academic promotions for clinician‐educators center around clinical excellence and innovation in education. The 3 senior members of the group have been promoted to professor (1 tenured, 2 nontenured), and 2 other members are currently in consideration for promotion to associate professor. Two members of the group have been elected to the School of Medicine Academy of Master Educators, which recognizes and rewards excellence in education.
Future Goals
Future goals include expansion and refinement of the division's current inpatient and ambulatory activities. The group increased in size to 16 physicians in July 2008 due to the increased inpatient volume and growing demand for outpatient referrals. The family‐centered rounds initiative will continue to be refined to provide the best possible service to the patients and their families. The members of the group will have increased activity and involvement at the regional and national level with the growing pediatric hospitalist movement.
A pediatric hospitalist fellowship program certainly would be feasible in the current environment. At this writing, there are only 8 pediatric hospitalist fellowship programs nationwide. The outpatient/emnpatient environment that the DRS provides the community would certainly provide a unique training environment for a hospitalist fellowship. The diversity in hospitalist divisions nationwide and the standardization of fellowship training is an important task for the future.23
Discussion
Pediatrics has undergone major changes since the original description of the DRS 20 years ago.7 These changes have revolutionized the practice of pediatrics in both the ambulatory and inpatient settings. The DRS role has changed significantly along with the national trends in pediatric hospitalist growth over the past decade. Currently, 90% of the division's clinical activity is inpatient care. In essence, this is an extension of the original consultant role, but the model has been extended to provide inpatient multidisciplinary care for pediatric patients.
Despite the remarkable growth in inpatient activity, 1 unique advantage to the DRS model is maintenance of an active outpatient consultation clinic focused on providing a multidisciplinary medical home for chronically ill patients. DRS faculty are able to coordinate the care of these complex patients while not usurping the primary care responsibility of the community physician. The same faculty are able to extend the continuity of care to the inpatient setting should the patient require admission.
There have been several innovations that the DRS has implemented over the past decade. The LSU was designed to provide effective and efficient care. The EH program extends attending in‐house coverage without the disadvantages of 24‐hour, 7‐day‐per‐week coverage. Expanding services to include The Children's Home allows for easier transition to home for technology‐dependent patients and families. At the same time, DRS continues to strive for innovative clinical leadership as well as creative and effective student and resident education.
Conclusion
Despite the remarkable growth and increased clinical activity of the DRS since its inception, Dr. Gaffney's ideals continue to serve as the lifeline for the division. The DRS still maintains the consultative pediatric role that he originated, but the inpatient activity has grown with the pediatric hospitalist movement at the same time. The division also maintains an active outpatient clinic. This dual function allows the DRS to continue to serve the community in a unique manner.
- American Academy of Pediatrics.Ad hoc task force on definition of the medical home, the medical home.Pediatrics.1992;90:774.
- American Academy of Pediatrics.Medical Home Initiatives for Children with Special Needs Project Advisory Committee, The Medical Home.Pediatrics.2002;110:184–186.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- Society of Hospital Medicine. Home. Available at http://www.hospitalmedicine.org. Accessed June 2009.
- ,,, et al.The role of “hospitalists” in the health care system.N Engl J Med.1997;336:444–446.
- ,,,,,.Restructuring an academic pediatric inpatient service using concepts developed by hospitalists.Clin Pediatr.2001;40:653–660.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- ,,, et al.Impact of a hospitalist system on length of stay and cost for children with common conditions.Pediatrics.2007;120:267–274.
- ,,,.Pediatric hospitalists: a systematic review of the literature.Pediatrics.2006;117:1736–1744.
- ,.Evaluation of a pediatric hospitalist service: impact on length of stay and hospital charges.Pediatrics.2000;105:478–484.
- ,,,,,.Variations in management of common inpatient pediatric illnesses: hospitalists and community pediatricians.Pediatrics.2006;118:441–447.
- American Academy of Pediatrics.Section on Hospital Medicine. Guiding principles for pediatric hospitalist programs.Pediatrics.2005;115:1101–1102.
- ,,,,.Consultative pediatrics: a role for the generalist in an academic setting.J Pediatr.1988;112:1035–1038.
- ,,,,,.Bronchiolitis‐associated hospitalizations among U.S. children, 1980–1996.JAMA.1999:282:1440–1446.
- ,,,,,.Condition HELP: a pediatric rapid response team triggered by patients and parents.J Healthc Qual.2008;30:28–31.
- ,,,,,.Effect of a pediatric hospitalist system on housestaff education and experience.Arch Pediatr Adolesc Med.2002;156:877–883.
- .Clinical and behavioral adaptation to managed care: stepwise suggestions for survival.Pediatrics.1995;96:821–824.
- ,,,,,.Gatekeeping and referral of children and adolescents to specialty care.Pediatrics.1999;104:28–34.
- (Chair, AAP Council on Children with Disabilities). Written Statement on Behalf of the American Academy of Pediatrics: Presented to the Institute of Medicine Committee on Disability in America. January 9,2006. Available at: http://www.aap.org/advocacy/washing/Testimonies‐Statements‐Petitions/IOM_testimony.pdf. Accessed June 2009.
- ,,, et al.The duration of ambulatory visits to physicians.J Fam Pract.1999;48:264–271.
- .Systemic errors continue to plague many hospitals.Pittsburgh Post‐Gazette.2004 Dec 5: Sect. Living.
- Josie King Foundation: Creating a Culture of Patient Safety, Together. Available at http://www.josieking.org. Accessed June 2009.
- .Hospitalist fellowships: pro and con.Section on Hospital Medicine News.2006;1:7,9. Available at: https://www.aap.org/sections/hospcare/SOHMwinter06news.pdf. Accessed June 2009.
In an ideal situation, a child could be cared for by 1 physician from childhood through adolescence. This physician could care for the child from the first days in the nursery, through multiple well‐child and sick visits, and during any hospitalizations. In 1992, the American Academy of Pediatrics (AAP) introduced the concept of the medical home to provide accessible, continuous, comprehensive, family‐centered, coordinated, and compassionate care for children.1 These ideals were reaffirmed in a 2002 AAP policy statement.2 The demands for outpatient care have become more intense and patient safety issues have become a public focus. Combined with the necessity for increased efficiency, the ideal medical home has become difficult to achieve simultaneously in both an outpatient and inpatient setting. This has led to the growth of the hospital specialist or hospitalist, a term first coined by Drs. Wachter and Goldman in August 1996.3 A hospitalist has been defined as a physician whose primary professional focus is the general medical care of hospitalized patients . . . teaching, research, and leadership related to hospital care.4 Despite early concerns voiced after the publication of this landmark article, there has been tremendous growth in the number of hospitalists nationwide.5 Initially, this growth was seen in adult medicine, but pediatric hospitalists have become increasingly more common. There are an estimated 10,000 to 20,000 hospitalists in the profession, with more than 30,000 expected by the end of the decade, with just over 10% being pediatric hospitalists.4 Several studies have shown the benefits of pediatric hospitalist programs with decreased length of stay, hospital charges, and utilization of unnecessary tests and therapies, and increased satisfaction among the physicians, students, and patients.611
History of the Diagnostic Referral Service
Despite the coining of the term hospitalist in 1996, specialization in inpatient care existed in various forms long before then.12 The Diagnostic Referral Service (DRS) at Children's Hospital of Pittsburgh (CHP) initially began under the guidance of Dr. Edmund R. McCluskey, chairman of the Department of Pediatrics at CHP, and Dr. Paul C. Gaffney, a beloved and revered clinician and educator. In 1951, Dr. Gaffney joined the full‐time CHP faculty after residency, chief residency, and a year of fellowship, providing his expertise in hematology and oncology. Over time, Dr. Gaffney's role expanded to that of a master physician, and pediatricians and family practitioners in the community began sending their most diagnostically challenging patients to be seen in his clinic. His activities further extended to providing inpatient care and consultations for complex patients.
With these growing responsibilities, Dr. Gaffney formed the DRS as a separate division within the Department of Pediatrics in the mid‐1970s and began developing the division. The group, then and now, is comprised of general pediatricians who provide multidisciplinary care for hospitalized children as well as for ambulatory consultations. The DRS was initially described in the literature 20 years ago; the roles of the 5 full‐time physicians at that time included a variety of clinical, teaching, and scholarly activities, as both inpatient and outpatient consultative physicians.13 Though much growth has occurred within the division since then, Dr. Gaffney's initial goals of providing excellent patient care and education in an academic setting still remain at the heart of each group member.
Growth of the Division
In March 2002, there were 4 full‐time physicians within the DRS. A remarkable increase in the group size has occurred since then, and currently there are 16 physicians. Each member of the division is assigned a specific activity, either outpatient or inpatient, for at least a 5‐day block. This allows the division to provide continuity in the care of complex patients in both settings and help maintain a medical home for these challenging patients. The primary care physician (PCP) remains responsible for primary care of the patient while the DRS can help manage the patient's complexities in the outpatient and inpatient setting. In essence, there is joint patient ownership between the DRS and the PCP, with relegation of different skill sets to provide a complete medical home for the patient.
The current activities of the group are summarized as follows.
Inpatient Activities
Inpatient Care
Corresponding to the growing pediatric hospitalist movement in the past decade, several area PCPs began requesting that their office patients be followed by the DRS when admitted to CHP. In 2003, the DRS physician referral list had 150 physicians, and it currently has over 325 physicians who refer the inpatient care of their patients to the DRS. These practices are located in a variety of locations in Western Pennsylvania, Ohio, and West Virginia. There are only 7 private practices that continue to maintain their admitting privileges to CHP, and these practices account for 0.5% of general pediatric admissions. The remaining admissions (those PCPs not on the DRS referral list or with admitting privileges) are covered by a rotating attending physician; 85% of the time this is a DRS physician. Therefore, while 0.5% of general pediatric admissions are cared for by private pediatricians, >95% of all general pediatric admissions are cared for by DRS, with the remaining patients cared for by a small number of pediatric subspecialists who occasionally serve as rotating attendings.
Associated with the increase in referrals has been a marked increase in inpatient activity (Figures 0, 0, 0, 13). Nearly 1 of every 4 CHP discharges and 1 of every 3 observation patients are cared for by the DRS.
The DRS division has seen an increase in complex inpatient admissions as well as a much larger number of routine pediatric admissions from the community PCP referrals, as described above. Statistically, this has resulted in an overall stable to slightly increased inpatient complexity for the DRS group. During this same time period, there was a steep decrease in DRS inpatient length of stay followed by maintenance at the shorter length of stay thereafter. Inpatient complexity has increased throughout CHP, yet the same decreases in length of stay have not been seen universally in all the divisions (Figure 4). The advantage that a hospitalist group can bring in decreasing length of stay (and, thereby, hospital costs) has been seen in hospitalist programs around the country.6, 7
Each member of the group attends on the general pediatric ward for 9 to 10 months per year as compared to 2 months per year in 1986. In order to prevent job‐related fatigue, 6 to 8 members of the group typically attend on the ward at the same time so that individual patient volume is more manageable. On average, each individual physician is responsible for about 6 to 8 patients per day. This census allows for daily education of residents and medical students as well as faculty participation in a variety of administrative activities. Despite emphasis on careful documentation and billing for both inpatient and ambulatory activities, the division, like most other pediatric hospitalist divisions, depends upon financial support from CHP and the Department of Pediatrics.
There is a wide variety of diagnoses that are seen in the inpatient setting, with notable similarities and differences when compared to 2 decades ago (Table 1). For example, asthma, gastroenteritis, and bronchiolitis continue to be frequent diagnoses, with bronchiolitis admissions becoming more frequent, following national trends.14
| FY 1986 | FY 2007 | ||
|---|---|---|---|
| Rank | Diagnosis | Rank | Diagnosis |
| |||
| 1. | Asthma | 1. | Bronchiolitis |
| 2. | Gastroenteritis | 2. | Asthma |
| 3. | Failure to thrive | 3. | Pneumonia |
| 4. | Seizures | 4. | Dehydration |
| 5. | Bronchiolitis | 5. | Viral enteritis |
| 6. | Pneumonia | 6. | Viral infection, NOS |
| 7. | Suspected sepsis | 7. | Esophageal reflux |
| 8. | Apneic episodes | 8. | Fever |
| 9. | Meningitis | 9. | Cellulitis |
| 10. | Otitis media | 10. | Convulsions |
In general, a DRS faculty member becomes the primary resource for families with medically complex children. The same faculty member tends to follow the patient in the consultative ambulatory clinic, be available for phone calls, and, if possible, follow them as the attending physician when the patient is admitted. This provides a degree of continuity generally not seen in many other hospitalist programs and has the potential to increase patient and physician satisfaction as well as patient safety.
Limited Stay Unit
In addition to general inpatient care, the DRS developed and maintains the Limited Stay Unit (LSU). This unit was specifically created in 2001 to serve patients with uncomplicated diagnoses who are expected to be discharged within 48 hours. Up to 10 short‐stay/observation patients are admitted to this unit each day, with nurses and staff specially prepared to handle rapid patient turnover. A child's eligibility for the unit is determined by the Emergency Department physicians or by phone consultation between the referring physician and the attending LSU physician. The design of the LSU allows for efficient admission and discharges of patients admitted with uncomplicated diagnoses. Each morning, the LSU attending physician, nurse practitioner, and residents discuss each patient with the nursing team and assess discharge readiness. Prescriptions and other discharge paperwork are prepared before morning rounds in order to avoid delays when the child has met criteria for safe discharge. Initial internal data evaluating the efficiency of the LSU demonstrated shorter length of stay for similar diagnoses admitted to the general ward. This difference was not observed in a subsequent study, likely due to CHP initiatives to improve the efficiency of discharge processes throughout the hospital.
Inpatient Consultations
The DRS serves as the inpatient pediatric consultant for the medical and surgical subspecialties. In 2007, the division saw 292 inpatient consultations. Many of the consultations originate from the surgical subspecialties (eg, a consult from neurosurgery for vomiting in a child with a functioning ventriculoperitoneal shunt). Other consultations come from pediatric subspecialties (eg, a patient with a congenital heart defect managed by the pediatric cardiology service with recurrent aspiration pneumonia of unclear etiology). The consultation process begins with the primary service discussing the patient with a senior resident who performs the initial history and physical, formulates an assessment and recommendations, and discusses the case with the DRS physician. Any necessary changes to the recommendations are made and relayed to the primary service. In addition, the DRS consults on known chronically ill patients in the intensive care unit (ICU), providing support to the family, nuances of chronic care to the ICU team, and continuity of care when the patient is transferred to the general ward.
Evening Hospitalist Program
In September 2005, the DRS began to provide extended in‐house attending coverage until midnight on weekdays and 10 PM on weekends. The evening hospitalist (EH) not only sees the new DRS admissions during the evening but also is available for formal consultations from subspecialty services and informal consultations from house staff. The EH is responsible for resident and medical student education (including direct observation of history taking and physical exam skills), facilitation of early discharges for the following morning, and enhancement of patient safety. The EH is also a part of the Condition Help team,15 a novel patient safety initiative discussed below.
The EH program benefits patients and DRS members alike. Other members of the group are able to assume care of patients in the morning for whom the diagnostic evaluation has already been initiated by the EH. Therefore, definitive plans are in place earlier, and many laboratory tests, radiographs, and other tests have returned by the time the daytime attending sees the patient.
The EH program was structured to enhance patient care and resident supervision while avoiding scheduling that could adversely affect job sustainability and retention. As currently structured, the EH program offers numerous advantages over 24‐hour, 7‐days‐per‐week coverage. First, resident autonomy is crucial during their training.16 One significant early concern was that extending the hours of attending physician coverage could diminish this autonomy. To prevent this from occurring, the EH allows the senior residents to take ownership of patient care and provide the initial teaching and instructions to interns, students, and families before the EH becomes involved. This structure of the EH program enhances the development of resident autonomy, yet provides support for the residents either by the EH or on‐call attending through all hours of the night. Second, the senior residents meet with members of DRS each morning to discuss their decision‐making process for overnight admissions that arrive after the EH shift has ended. This allows analysis of house staff thought processes and discussion of considered alternatives. Third, with the recent resident work‐hour restrictions, several residency programs have moved to either daytime or nighttime shift‐based work for the residents. Therefore, having the same EH working each day for the week allows for more accurate assessment of the nighttime residents than scattered 24‐hour attending shifts. Fourth, evening coverage allows for simpler scheduling and a less disruptive sleep cycle for the EH than 24‐hour coverage could allow. Finally, the EH is able to transition to typical daytime hours following a week of evening shifts, which helps to enhance EH retention by providing opportunities for academic endeavors and peer interactions.
The Children's Home
Since August 2007, the DRS has provided inpatient care for children admitted to The Children's Home of Pittsburgh and Lemieux Family Center (TCH). This independent facility is administratively and geographically separate from CHP. The DRS manages a 6‐bed unit that specializes in transitional pediatric care and serves technology‐dependent infants and children in a family‐centered, home‐like environment. In general, patients who require these services are seen at CHP initially, medically stabilized, and then transferred to TCH to continue their care. There is 1 DRS physician assigned each week to providing care for these patients. Examples of patient problems cared for at this facility include feeding issues, long term intravenous (IV) antibiotic treatment (eg, neonates recovering from sepsis, meningitis, osteomyelitis), and family education for technology‐dependent children (eg, new tracheostomy or ostomy). The average length of stay is 10.2 days, which decreases CHP length of stay and promotes CHP savings during periods of high census.
Outpatient Activities
Outpatient Care
Many physicians in community clinics have large daily patient volumes, seeing upward of 30 to 40 patients per day. These added outpatient responsibilities can lead to decreased time available for a PCP to round on inpatients (hence, the nationwide growth of hospitalists).17 Additionally, this increased practice intensity may lead to less time to manage individual patients in the primary care setting.18
The pediatric patient has become significantly more complex, likely due to increased survival of patients with chronic medical problems.19 This is also evidenced at CHP by steadily increasing patient acuity scores (Figure 4). With this growing complexity, effective outpatient care in a standard 15‐minute to 20‐minute patient visit20 is difficult, especially given the AAP recommendations of providing an effective medical home for every patient.2 Since its inception, the DRS has provided ambulatory consultative services for the community. Sixty percent of the 1400 to 1900 patients seen each year are new patient referrals. The outpatient clinic activity has been essentially stable over the past several years (Figure 1), likely due to increased access to CHP subspecialty clinics and overall increased manpower in the Department of Pediatrics. A wide variety of diagnoses are made in the outpatient clinic (Table 2).
| Rank | Diagnosis |
|---|---|
| |
| 1. | Failure to thrive, poor weight gain, weight loss |
| 2. | Abdominal pain |
| 3. | Fever |
| 4. | Chronic fatigue |
| 5. | Syncope |
| 6. | Gastroesophageal reflux |
| 7. | Chest pain |
| 8. | Developmental delay |
| 9. | Headache |
| 10. | Coordination of care |
The DRS provides long‐term, multidisciplinary continuity of care for medically complex children. The child is seen by the same DRS physician during each clinic visit. If the patient is admitted to the hospital, every effort is made for the patient to be seen by the DRS physician who saw the patient in the clinic setting. This process allows for medically complex children to have the coordinated care that can be difficult to achieve if a different hospitalist physician is responsible for their care during each admission.
The DRS works closely with the PCP to augment continuity of care while the PCP continues to provide primary care services. This provides the PCP with assurance that the patient will remain in their practice while the patient's multiple medical needs are addressed by the DRS. In this manner, a complete medical home can be provided. Insurance companies have recognized members of the DRS to be specialists in general pediatric care and permit DRS faculty to bill as specialists.
Education
Teaching is a major role for the DRS, and the division is closely involved in leadership in medical education. Two members are directors of the pediatric physical exam course for first‐year and second‐year medical students, 2 members are the third‐year medical school Pediatric clerkship directors, 1 member is co‐director for the fourth‐year acting internship, 1 member is co‐director of the advanced pediatric interviewing program, 1 member is director of the pediatric medical education program, and 1 member is associate residency program director.
The entire group is involved with teaching at all of these levels. The majority of the group is involved with formal mentoring and advising of residents and medical students. The only general pediatric aspect of student and resident medical education in which the DRS is no longer involved is ambulatory pediatric medicine. The full‐time ambulatory faculty is responsible for the primary ambulatory care experience. However, many residents choose to complete an elective in DRS, including the outpatient clinic, to become exposed to the different diagnostic dilemmas and coordination of care visits that they may not see in their primary care continuity clinics.
The division always welcomes new teaching challenges and incorporates new methods of teaching as opportunities arise. For example, the recent family‐centered rounds initiative allowed for new teaching methods that were not previously possible. The team, comprised of a senior resident, 2 interns, 2 students, and an attending physician rounds at the bedside with permission from the parent. The patient's nurse, when available, and a pharmacist are often a part of the team. The case is presented by the student or intern (directed to the parent), and the case is discussed and clarified for the family. A plan for the day is presented and discussed with the family for approval. Through family‐centered rounds, the DRS attending provides patient specific teaching and role modeling during rounds that would not otherwise have been possible with classical didactic teaching. This method of daily rounding also allows for the patients, families, nurses, nursing students, medical students, and residents to be taught by the attending physician simultaneously. Additionally, it affords the nurses the opportunity to participate in medical decision‐making, and the house staff have perceived fewer pages by the nurses to clarify clinical issues.
The EH program also provided new teaching opportunities. Through the EH, the house staff and students are exposed to direct attending teaching in the evenings that otherwise would not occur, such as direct observation of student and resident histories and physical examinations. Based on resident evaluations and comments to the residency program directors, this teaching experience is deemed to be valuable and effective. In fact, since the EH program's inception 3 years ago, 2 EHs have been selected by the residents as Teacher of the Year.
Patient Safety
Patient safety and reduction of medical errors is a major focus of the entire group. One DRS member serves within the hospital administration as Medical Director for Clinical Excellence and Service to enhance patient safety hospital‐wide. One DRS member orchestrates a monthly house staff meeting entitled To Err is Human which provides a nonthreatening environment for residents to discuss medical errors or difficult situations that they have encountered. Two DRS members are part of the Physician Advisory Committee, which serves as a bridge between the information technology group and clinicians. This committee has aided in achieving a smooth transition to a completely electronic medical record (EMR) and works together to use the tools of an EMR to enhance patient safety. This successful EMR implementation was recognized by the Health Information Management Systems Society in October 2008. Additionally, stemming from several successful patient safety initiatives, CHP was 1 of only 7 children's hospitals recognized for patient safety in 2008 by Leapfrog, the nation's premier patient safety evaluation group.
Condition HELP
In February 2001, the death of 18‐month‐old Josie King at a leading children's hospital brought medical errors to the national forefront.21 In response to this tragedy, several hospitals in the University of Pittsburgh system began to implement a program called Condition HELP.22 Condition HELP gives parents the ability to have their child evaluated by a special medical team if they feel their child's immediate health is in danger or their concerns are not being addressed. In 2005, CHP was one of the first hospitals in the country to implement this type of system. The Condition HELP team consists of a physician, a nursing supervisor, and a patient advocate. During the evening hours, the DRS EH also participates in the calls. The team discusses the family's concern and, with the patient's attending physician, generates a plan of action to help remedy the issue. Usually within 5 days, each call is intensively reviewed for events leading up to the Condition HELP as part of the CHP's patient safety initiative. From September 2005 through August 2007, the CHP Condition HELP team responded to 42 calls from patients and parents, with the most issues found to be related to communication breakdown between caregivers and families. The involvement of this team helped to identify the root cause of the parent or patient's concern and implement measures to help to rectify the issue and increase patient safety.15
Scholarly Activity
Previously, the DRS was responsible for the general medical care of liver transplant recipients, and many prior publications from the division focused on these patients.13 The division no longer provides that service, and the current focus of scholarly activity is publication of case reports, book chapters, and review articles. There were 13 publications from the division members in the past 3 years. The group also serves as a major resource within the department by referring patients that fulfill the clinical criteria for ongoing clinical studies in other divisions.
One member of the group continues to serve as senior editor of the Atlas of Pediatric Physical Diagnosis, which is currently in its fifth edition. Several members of the group contribute chapters to this well‐known text. One member is an editor and another is a specialty reviewer for
At the University of Pittsburgh, both tenured and nontenured faculty promotions carry the same title without a prefix. Academic promotions for clinician‐educators center around clinical excellence and innovation in education. The 3 senior members of the group have been promoted to professor (1 tenured, 2 nontenured), and 2 other members are currently in consideration for promotion to associate professor. Two members of the group have been elected to the School of Medicine Academy of Master Educators, which recognizes and rewards excellence in education.
Future Goals
Future goals include expansion and refinement of the division's current inpatient and ambulatory activities. The group increased in size to 16 physicians in July 2008 due to the increased inpatient volume and growing demand for outpatient referrals. The family‐centered rounds initiative will continue to be refined to provide the best possible service to the patients and their families. The members of the group will have increased activity and involvement at the regional and national level with the growing pediatric hospitalist movement.
A pediatric hospitalist fellowship program certainly would be feasible in the current environment. At this writing, there are only 8 pediatric hospitalist fellowship programs nationwide. The outpatient/emnpatient environment that the DRS provides the community would certainly provide a unique training environment for a hospitalist fellowship. The diversity in hospitalist divisions nationwide and the standardization of fellowship training is an important task for the future.23
Discussion
Pediatrics has undergone major changes since the original description of the DRS 20 years ago.7 These changes have revolutionized the practice of pediatrics in both the ambulatory and inpatient settings. The DRS role has changed significantly along with the national trends in pediatric hospitalist growth over the past decade. Currently, 90% of the division's clinical activity is inpatient care. In essence, this is an extension of the original consultant role, but the model has been extended to provide inpatient multidisciplinary care for pediatric patients.
Despite the remarkable growth in inpatient activity, 1 unique advantage to the DRS model is maintenance of an active outpatient consultation clinic focused on providing a multidisciplinary medical home for chronically ill patients. DRS faculty are able to coordinate the care of these complex patients while not usurping the primary care responsibility of the community physician. The same faculty are able to extend the continuity of care to the inpatient setting should the patient require admission.
There have been several innovations that the DRS has implemented over the past decade. The LSU was designed to provide effective and efficient care. The EH program extends attending in‐house coverage without the disadvantages of 24‐hour, 7‐day‐per‐week coverage. Expanding services to include The Children's Home allows for easier transition to home for technology‐dependent patients and families. At the same time, DRS continues to strive for innovative clinical leadership as well as creative and effective student and resident education.
Conclusion
Despite the remarkable growth and increased clinical activity of the DRS since its inception, Dr. Gaffney's ideals continue to serve as the lifeline for the division. The DRS still maintains the consultative pediatric role that he originated, but the inpatient activity has grown with the pediatric hospitalist movement at the same time. The division also maintains an active outpatient clinic. This dual function allows the DRS to continue to serve the community in a unique manner.
In an ideal situation, a child could be cared for by 1 physician from childhood through adolescence. This physician could care for the child from the first days in the nursery, through multiple well‐child and sick visits, and during any hospitalizations. In 1992, the American Academy of Pediatrics (AAP) introduced the concept of the medical home to provide accessible, continuous, comprehensive, family‐centered, coordinated, and compassionate care for children.1 These ideals were reaffirmed in a 2002 AAP policy statement.2 The demands for outpatient care have become more intense and patient safety issues have become a public focus. Combined with the necessity for increased efficiency, the ideal medical home has become difficult to achieve simultaneously in both an outpatient and inpatient setting. This has led to the growth of the hospital specialist or hospitalist, a term first coined by Drs. Wachter and Goldman in August 1996.3 A hospitalist has been defined as a physician whose primary professional focus is the general medical care of hospitalized patients . . . teaching, research, and leadership related to hospital care.4 Despite early concerns voiced after the publication of this landmark article, there has been tremendous growth in the number of hospitalists nationwide.5 Initially, this growth was seen in adult medicine, but pediatric hospitalists have become increasingly more common. There are an estimated 10,000 to 20,000 hospitalists in the profession, with more than 30,000 expected by the end of the decade, with just over 10% being pediatric hospitalists.4 Several studies have shown the benefits of pediatric hospitalist programs with decreased length of stay, hospital charges, and utilization of unnecessary tests and therapies, and increased satisfaction among the physicians, students, and patients.611
History of the Diagnostic Referral Service
Despite the coining of the term hospitalist in 1996, specialization in inpatient care existed in various forms long before then.12 The Diagnostic Referral Service (DRS) at Children's Hospital of Pittsburgh (CHP) initially began under the guidance of Dr. Edmund R. McCluskey, chairman of the Department of Pediatrics at CHP, and Dr. Paul C. Gaffney, a beloved and revered clinician and educator. In 1951, Dr. Gaffney joined the full‐time CHP faculty after residency, chief residency, and a year of fellowship, providing his expertise in hematology and oncology. Over time, Dr. Gaffney's role expanded to that of a master physician, and pediatricians and family practitioners in the community began sending their most diagnostically challenging patients to be seen in his clinic. His activities further extended to providing inpatient care and consultations for complex patients.
With these growing responsibilities, Dr. Gaffney formed the DRS as a separate division within the Department of Pediatrics in the mid‐1970s and began developing the division. The group, then and now, is comprised of general pediatricians who provide multidisciplinary care for hospitalized children as well as for ambulatory consultations. The DRS was initially described in the literature 20 years ago; the roles of the 5 full‐time physicians at that time included a variety of clinical, teaching, and scholarly activities, as both inpatient and outpatient consultative physicians.13 Though much growth has occurred within the division since then, Dr. Gaffney's initial goals of providing excellent patient care and education in an academic setting still remain at the heart of each group member.
Growth of the Division
In March 2002, there were 4 full‐time physicians within the DRS. A remarkable increase in the group size has occurred since then, and currently there are 16 physicians. Each member of the division is assigned a specific activity, either outpatient or inpatient, for at least a 5‐day block. This allows the division to provide continuity in the care of complex patients in both settings and help maintain a medical home for these challenging patients. The primary care physician (PCP) remains responsible for primary care of the patient while the DRS can help manage the patient's complexities in the outpatient and inpatient setting. In essence, there is joint patient ownership between the DRS and the PCP, with relegation of different skill sets to provide a complete medical home for the patient.
The current activities of the group are summarized as follows.
Inpatient Activities
Inpatient Care
Corresponding to the growing pediatric hospitalist movement in the past decade, several area PCPs began requesting that their office patients be followed by the DRS when admitted to CHP. In 2003, the DRS physician referral list had 150 physicians, and it currently has over 325 physicians who refer the inpatient care of their patients to the DRS. These practices are located in a variety of locations in Western Pennsylvania, Ohio, and West Virginia. There are only 7 private practices that continue to maintain their admitting privileges to CHP, and these practices account for 0.5% of general pediatric admissions. The remaining admissions (those PCPs not on the DRS referral list or with admitting privileges) are covered by a rotating attending physician; 85% of the time this is a DRS physician. Therefore, while 0.5% of general pediatric admissions are cared for by private pediatricians, >95% of all general pediatric admissions are cared for by DRS, with the remaining patients cared for by a small number of pediatric subspecialists who occasionally serve as rotating attendings.
Associated with the increase in referrals has been a marked increase in inpatient activity (Figures 0, 0, 0, 13). Nearly 1 of every 4 CHP discharges and 1 of every 3 observation patients are cared for by the DRS.
The DRS division has seen an increase in complex inpatient admissions as well as a much larger number of routine pediatric admissions from the community PCP referrals, as described above. Statistically, this has resulted in an overall stable to slightly increased inpatient complexity for the DRS group. During this same time period, there was a steep decrease in DRS inpatient length of stay followed by maintenance at the shorter length of stay thereafter. Inpatient complexity has increased throughout CHP, yet the same decreases in length of stay have not been seen universally in all the divisions (Figure 4). The advantage that a hospitalist group can bring in decreasing length of stay (and, thereby, hospital costs) has been seen in hospitalist programs around the country.6, 7
Each member of the group attends on the general pediatric ward for 9 to 10 months per year as compared to 2 months per year in 1986. In order to prevent job‐related fatigue, 6 to 8 members of the group typically attend on the ward at the same time so that individual patient volume is more manageable. On average, each individual physician is responsible for about 6 to 8 patients per day. This census allows for daily education of residents and medical students as well as faculty participation in a variety of administrative activities. Despite emphasis on careful documentation and billing for both inpatient and ambulatory activities, the division, like most other pediatric hospitalist divisions, depends upon financial support from CHP and the Department of Pediatrics.
There is a wide variety of diagnoses that are seen in the inpatient setting, with notable similarities and differences when compared to 2 decades ago (Table 1). For example, asthma, gastroenteritis, and bronchiolitis continue to be frequent diagnoses, with bronchiolitis admissions becoming more frequent, following national trends.14
| FY 1986 | FY 2007 | ||
|---|---|---|---|
| Rank | Diagnosis | Rank | Diagnosis |
| |||
| 1. | Asthma | 1. | Bronchiolitis |
| 2. | Gastroenteritis | 2. | Asthma |
| 3. | Failure to thrive | 3. | Pneumonia |
| 4. | Seizures | 4. | Dehydration |
| 5. | Bronchiolitis | 5. | Viral enteritis |
| 6. | Pneumonia | 6. | Viral infection, NOS |
| 7. | Suspected sepsis | 7. | Esophageal reflux |
| 8. | Apneic episodes | 8. | Fever |
| 9. | Meningitis | 9. | Cellulitis |
| 10. | Otitis media | 10. | Convulsions |
In general, a DRS faculty member becomes the primary resource for families with medically complex children. The same faculty member tends to follow the patient in the consultative ambulatory clinic, be available for phone calls, and, if possible, follow them as the attending physician when the patient is admitted. This provides a degree of continuity generally not seen in many other hospitalist programs and has the potential to increase patient and physician satisfaction as well as patient safety.
Limited Stay Unit
In addition to general inpatient care, the DRS developed and maintains the Limited Stay Unit (LSU). This unit was specifically created in 2001 to serve patients with uncomplicated diagnoses who are expected to be discharged within 48 hours. Up to 10 short‐stay/observation patients are admitted to this unit each day, with nurses and staff specially prepared to handle rapid patient turnover. A child's eligibility for the unit is determined by the Emergency Department physicians or by phone consultation between the referring physician and the attending LSU physician. The design of the LSU allows for efficient admission and discharges of patients admitted with uncomplicated diagnoses. Each morning, the LSU attending physician, nurse practitioner, and residents discuss each patient with the nursing team and assess discharge readiness. Prescriptions and other discharge paperwork are prepared before morning rounds in order to avoid delays when the child has met criteria for safe discharge. Initial internal data evaluating the efficiency of the LSU demonstrated shorter length of stay for similar diagnoses admitted to the general ward. This difference was not observed in a subsequent study, likely due to CHP initiatives to improve the efficiency of discharge processes throughout the hospital.
Inpatient Consultations
The DRS serves as the inpatient pediatric consultant for the medical and surgical subspecialties. In 2007, the division saw 292 inpatient consultations. Many of the consultations originate from the surgical subspecialties (eg, a consult from neurosurgery for vomiting in a child with a functioning ventriculoperitoneal shunt). Other consultations come from pediatric subspecialties (eg, a patient with a congenital heart defect managed by the pediatric cardiology service with recurrent aspiration pneumonia of unclear etiology). The consultation process begins with the primary service discussing the patient with a senior resident who performs the initial history and physical, formulates an assessment and recommendations, and discusses the case with the DRS physician. Any necessary changes to the recommendations are made and relayed to the primary service. In addition, the DRS consults on known chronically ill patients in the intensive care unit (ICU), providing support to the family, nuances of chronic care to the ICU team, and continuity of care when the patient is transferred to the general ward.
Evening Hospitalist Program
In September 2005, the DRS began to provide extended in‐house attending coverage until midnight on weekdays and 10 PM on weekends. The evening hospitalist (EH) not only sees the new DRS admissions during the evening but also is available for formal consultations from subspecialty services and informal consultations from house staff. The EH is responsible for resident and medical student education (including direct observation of history taking and physical exam skills), facilitation of early discharges for the following morning, and enhancement of patient safety. The EH is also a part of the Condition Help team,15 a novel patient safety initiative discussed below.
The EH program benefits patients and DRS members alike. Other members of the group are able to assume care of patients in the morning for whom the diagnostic evaluation has already been initiated by the EH. Therefore, definitive plans are in place earlier, and many laboratory tests, radiographs, and other tests have returned by the time the daytime attending sees the patient.
The EH program was structured to enhance patient care and resident supervision while avoiding scheduling that could adversely affect job sustainability and retention. As currently structured, the EH program offers numerous advantages over 24‐hour, 7‐days‐per‐week coverage. First, resident autonomy is crucial during their training.16 One significant early concern was that extending the hours of attending physician coverage could diminish this autonomy. To prevent this from occurring, the EH allows the senior residents to take ownership of patient care and provide the initial teaching and instructions to interns, students, and families before the EH becomes involved. This structure of the EH program enhances the development of resident autonomy, yet provides support for the residents either by the EH or on‐call attending through all hours of the night. Second, the senior residents meet with members of DRS each morning to discuss their decision‐making process for overnight admissions that arrive after the EH shift has ended. This allows analysis of house staff thought processes and discussion of considered alternatives. Third, with the recent resident work‐hour restrictions, several residency programs have moved to either daytime or nighttime shift‐based work for the residents. Therefore, having the same EH working each day for the week allows for more accurate assessment of the nighttime residents than scattered 24‐hour attending shifts. Fourth, evening coverage allows for simpler scheduling and a less disruptive sleep cycle for the EH than 24‐hour coverage could allow. Finally, the EH is able to transition to typical daytime hours following a week of evening shifts, which helps to enhance EH retention by providing opportunities for academic endeavors and peer interactions.
The Children's Home
Since August 2007, the DRS has provided inpatient care for children admitted to The Children's Home of Pittsburgh and Lemieux Family Center (TCH). This independent facility is administratively and geographically separate from CHP. The DRS manages a 6‐bed unit that specializes in transitional pediatric care and serves technology‐dependent infants and children in a family‐centered, home‐like environment. In general, patients who require these services are seen at CHP initially, medically stabilized, and then transferred to TCH to continue their care. There is 1 DRS physician assigned each week to providing care for these patients. Examples of patient problems cared for at this facility include feeding issues, long term intravenous (IV) antibiotic treatment (eg, neonates recovering from sepsis, meningitis, osteomyelitis), and family education for technology‐dependent children (eg, new tracheostomy or ostomy). The average length of stay is 10.2 days, which decreases CHP length of stay and promotes CHP savings during periods of high census.
Outpatient Activities
Outpatient Care
Many physicians in community clinics have large daily patient volumes, seeing upward of 30 to 40 patients per day. These added outpatient responsibilities can lead to decreased time available for a PCP to round on inpatients (hence, the nationwide growth of hospitalists).17 Additionally, this increased practice intensity may lead to less time to manage individual patients in the primary care setting.18
The pediatric patient has become significantly more complex, likely due to increased survival of patients with chronic medical problems.19 This is also evidenced at CHP by steadily increasing patient acuity scores (Figure 4). With this growing complexity, effective outpatient care in a standard 15‐minute to 20‐minute patient visit20 is difficult, especially given the AAP recommendations of providing an effective medical home for every patient.2 Since its inception, the DRS has provided ambulatory consultative services for the community. Sixty percent of the 1400 to 1900 patients seen each year are new patient referrals. The outpatient clinic activity has been essentially stable over the past several years (Figure 1), likely due to increased access to CHP subspecialty clinics and overall increased manpower in the Department of Pediatrics. A wide variety of diagnoses are made in the outpatient clinic (Table 2).
| Rank | Diagnosis |
|---|---|
| |
| 1. | Failure to thrive, poor weight gain, weight loss |
| 2. | Abdominal pain |
| 3. | Fever |
| 4. | Chronic fatigue |
| 5. | Syncope |
| 6. | Gastroesophageal reflux |
| 7. | Chest pain |
| 8. | Developmental delay |
| 9. | Headache |
| 10. | Coordination of care |
The DRS provides long‐term, multidisciplinary continuity of care for medically complex children. The child is seen by the same DRS physician during each clinic visit. If the patient is admitted to the hospital, every effort is made for the patient to be seen by the DRS physician who saw the patient in the clinic setting. This process allows for medically complex children to have the coordinated care that can be difficult to achieve if a different hospitalist physician is responsible for their care during each admission.
The DRS works closely with the PCP to augment continuity of care while the PCP continues to provide primary care services. This provides the PCP with assurance that the patient will remain in their practice while the patient's multiple medical needs are addressed by the DRS. In this manner, a complete medical home can be provided. Insurance companies have recognized members of the DRS to be specialists in general pediatric care and permit DRS faculty to bill as specialists.
Education
Teaching is a major role for the DRS, and the division is closely involved in leadership in medical education. Two members are directors of the pediatric physical exam course for first‐year and second‐year medical students, 2 members are the third‐year medical school Pediatric clerkship directors, 1 member is co‐director for the fourth‐year acting internship, 1 member is co‐director of the advanced pediatric interviewing program, 1 member is director of the pediatric medical education program, and 1 member is associate residency program director.
The entire group is involved with teaching at all of these levels. The majority of the group is involved with formal mentoring and advising of residents and medical students. The only general pediatric aspect of student and resident medical education in which the DRS is no longer involved is ambulatory pediatric medicine. The full‐time ambulatory faculty is responsible for the primary ambulatory care experience. However, many residents choose to complete an elective in DRS, including the outpatient clinic, to become exposed to the different diagnostic dilemmas and coordination of care visits that they may not see in their primary care continuity clinics.
The division always welcomes new teaching challenges and incorporates new methods of teaching as opportunities arise. For example, the recent family‐centered rounds initiative allowed for new teaching methods that were not previously possible. The team, comprised of a senior resident, 2 interns, 2 students, and an attending physician rounds at the bedside with permission from the parent. The patient's nurse, when available, and a pharmacist are often a part of the team. The case is presented by the student or intern (directed to the parent), and the case is discussed and clarified for the family. A plan for the day is presented and discussed with the family for approval. Through family‐centered rounds, the DRS attending provides patient specific teaching and role modeling during rounds that would not otherwise have been possible with classical didactic teaching. This method of daily rounding also allows for the patients, families, nurses, nursing students, medical students, and residents to be taught by the attending physician simultaneously. Additionally, it affords the nurses the opportunity to participate in medical decision‐making, and the house staff have perceived fewer pages by the nurses to clarify clinical issues.
The EH program also provided new teaching opportunities. Through the EH, the house staff and students are exposed to direct attending teaching in the evenings that otherwise would not occur, such as direct observation of student and resident histories and physical examinations. Based on resident evaluations and comments to the residency program directors, this teaching experience is deemed to be valuable and effective. In fact, since the EH program's inception 3 years ago, 2 EHs have been selected by the residents as Teacher of the Year.
Patient Safety
Patient safety and reduction of medical errors is a major focus of the entire group. One DRS member serves within the hospital administration as Medical Director for Clinical Excellence and Service to enhance patient safety hospital‐wide. One DRS member orchestrates a monthly house staff meeting entitled To Err is Human which provides a nonthreatening environment for residents to discuss medical errors or difficult situations that they have encountered. Two DRS members are part of the Physician Advisory Committee, which serves as a bridge between the information technology group and clinicians. This committee has aided in achieving a smooth transition to a completely electronic medical record (EMR) and works together to use the tools of an EMR to enhance patient safety. This successful EMR implementation was recognized by the Health Information Management Systems Society in October 2008. Additionally, stemming from several successful patient safety initiatives, CHP was 1 of only 7 children's hospitals recognized for patient safety in 2008 by Leapfrog, the nation's premier patient safety evaluation group.
Condition HELP
In February 2001, the death of 18‐month‐old Josie King at a leading children's hospital brought medical errors to the national forefront.21 In response to this tragedy, several hospitals in the University of Pittsburgh system began to implement a program called Condition HELP.22 Condition HELP gives parents the ability to have their child evaluated by a special medical team if they feel their child's immediate health is in danger or their concerns are not being addressed. In 2005, CHP was one of the first hospitals in the country to implement this type of system. The Condition HELP team consists of a physician, a nursing supervisor, and a patient advocate. During the evening hours, the DRS EH also participates in the calls. The team discusses the family's concern and, with the patient's attending physician, generates a plan of action to help remedy the issue. Usually within 5 days, each call is intensively reviewed for events leading up to the Condition HELP as part of the CHP's patient safety initiative. From September 2005 through August 2007, the CHP Condition HELP team responded to 42 calls from patients and parents, with the most issues found to be related to communication breakdown between caregivers and families. The involvement of this team helped to identify the root cause of the parent or patient's concern and implement measures to help to rectify the issue and increase patient safety.15
Scholarly Activity
Previously, the DRS was responsible for the general medical care of liver transplant recipients, and many prior publications from the division focused on these patients.13 The division no longer provides that service, and the current focus of scholarly activity is publication of case reports, book chapters, and review articles. There were 13 publications from the division members in the past 3 years. The group also serves as a major resource within the department by referring patients that fulfill the clinical criteria for ongoing clinical studies in other divisions.
One member of the group continues to serve as senior editor of the Atlas of Pediatric Physical Diagnosis, which is currently in its fifth edition. Several members of the group contribute chapters to this well‐known text. One member is an editor and another is a specialty reviewer for
At the University of Pittsburgh, both tenured and nontenured faculty promotions carry the same title without a prefix. Academic promotions for clinician‐educators center around clinical excellence and innovation in education. The 3 senior members of the group have been promoted to professor (1 tenured, 2 nontenured), and 2 other members are currently in consideration for promotion to associate professor. Two members of the group have been elected to the School of Medicine Academy of Master Educators, which recognizes and rewards excellence in education.
Future Goals
Future goals include expansion and refinement of the division's current inpatient and ambulatory activities. The group increased in size to 16 physicians in July 2008 due to the increased inpatient volume and growing demand for outpatient referrals. The family‐centered rounds initiative will continue to be refined to provide the best possible service to the patients and their families. The members of the group will have increased activity and involvement at the regional and national level with the growing pediatric hospitalist movement.
A pediatric hospitalist fellowship program certainly would be feasible in the current environment. At this writing, there are only 8 pediatric hospitalist fellowship programs nationwide. The outpatient/emnpatient environment that the DRS provides the community would certainly provide a unique training environment for a hospitalist fellowship. The diversity in hospitalist divisions nationwide and the standardization of fellowship training is an important task for the future.23
Discussion
Pediatrics has undergone major changes since the original description of the DRS 20 years ago.7 These changes have revolutionized the practice of pediatrics in both the ambulatory and inpatient settings. The DRS role has changed significantly along with the national trends in pediatric hospitalist growth over the past decade. Currently, 90% of the division's clinical activity is inpatient care. In essence, this is an extension of the original consultant role, but the model has been extended to provide inpatient multidisciplinary care for pediatric patients.
Despite the remarkable growth in inpatient activity, 1 unique advantage to the DRS model is maintenance of an active outpatient consultation clinic focused on providing a multidisciplinary medical home for chronically ill patients. DRS faculty are able to coordinate the care of these complex patients while not usurping the primary care responsibility of the community physician. The same faculty are able to extend the continuity of care to the inpatient setting should the patient require admission.
There have been several innovations that the DRS has implemented over the past decade. The LSU was designed to provide effective and efficient care. The EH program extends attending in‐house coverage without the disadvantages of 24‐hour, 7‐day‐per‐week coverage. Expanding services to include The Children's Home allows for easier transition to home for technology‐dependent patients and families. At the same time, DRS continues to strive for innovative clinical leadership as well as creative and effective student and resident education.
Conclusion
Despite the remarkable growth and increased clinical activity of the DRS since its inception, Dr. Gaffney's ideals continue to serve as the lifeline for the division. The DRS still maintains the consultative pediatric role that he originated, but the inpatient activity has grown with the pediatric hospitalist movement at the same time. The division also maintains an active outpatient clinic. This dual function allows the DRS to continue to serve the community in a unique manner.
- American Academy of Pediatrics.Ad hoc task force on definition of the medical home, the medical home.Pediatrics.1992;90:774.
- American Academy of Pediatrics.Medical Home Initiatives for Children with Special Needs Project Advisory Committee, The Medical Home.Pediatrics.2002;110:184–186.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- Society of Hospital Medicine. Home. Available at http://www.hospitalmedicine.org. Accessed June 2009.
- ,,, et al.The role of “hospitalists” in the health care system.N Engl J Med.1997;336:444–446.
- ,,,,,.Restructuring an academic pediatric inpatient service using concepts developed by hospitalists.Clin Pediatr.2001;40:653–660.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- ,,, et al.Impact of a hospitalist system on length of stay and cost for children with common conditions.Pediatrics.2007;120:267–274.
- ,,,.Pediatric hospitalists: a systematic review of the literature.Pediatrics.2006;117:1736–1744.
- ,.Evaluation of a pediatric hospitalist service: impact on length of stay and hospital charges.Pediatrics.2000;105:478–484.
- ,,,,,.Variations in management of common inpatient pediatric illnesses: hospitalists and community pediatricians.Pediatrics.2006;118:441–447.
- American Academy of Pediatrics.Section on Hospital Medicine. Guiding principles for pediatric hospitalist programs.Pediatrics.2005;115:1101–1102.
- ,,,,.Consultative pediatrics: a role for the generalist in an academic setting.J Pediatr.1988;112:1035–1038.
- ,,,,,.Bronchiolitis‐associated hospitalizations among U.S. children, 1980–1996.JAMA.1999:282:1440–1446.
- ,,,,,.Condition HELP: a pediatric rapid response team triggered by patients and parents.J Healthc Qual.2008;30:28–31.
- ,,,,,.Effect of a pediatric hospitalist system on housestaff education and experience.Arch Pediatr Adolesc Med.2002;156:877–883.
- .Clinical and behavioral adaptation to managed care: stepwise suggestions for survival.Pediatrics.1995;96:821–824.
- ,,,,,.Gatekeeping and referral of children and adolescents to specialty care.Pediatrics.1999;104:28–34.
- (Chair, AAP Council on Children with Disabilities). Written Statement on Behalf of the American Academy of Pediatrics: Presented to the Institute of Medicine Committee on Disability in America. January 9,2006. Available at: http://www.aap.org/advocacy/washing/Testimonies‐Statements‐Petitions/IOM_testimony.pdf. Accessed June 2009.
- ,,, et al.The duration of ambulatory visits to physicians.J Fam Pract.1999;48:264–271.
- .Systemic errors continue to plague many hospitals.Pittsburgh Post‐Gazette.2004 Dec 5: Sect. Living.
- Josie King Foundation: Creating a Culture of Patient Safety, Together. Available at http://www.josieking.org. Accessed June 2009.
- .Hospitalist fellowships: pro and con.Section on Hospital Medicine News.2006;1:7,9. Available at: https://www.aap.org/sections/hospcare/SOHMwinter06news.pdf. Accessed June 2009.
- American Academy of Pediatrics.Ad hoc task force on definition of the medical home, the medical home.Pediatrics.1992;90:774.
- American Academy of Pediatrics.Medical Home Initiatives for Children with Special Needs Project Advisory Committee, The Medical Home.Pediatrics.2002;110:184–186.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- Society of Hospital Medicine. Home. Available at http://www.hospitalmedicine.org. Accessed June 2009.
- ,,, et al.The role of “hospitalists” in the health care system.N Engl J Med.1997;336:444–446.
- ,,,,,.Restructuring an academic pediatric inpatient service using concepts developed by hospitalists.Clin Pediatr.2001;40:653–660.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- ,,, et al.Impact of a hospitalist system on length of stay and cost for children with common conditions.Pediatrics.2007;120:267–274.
- ,,,.Pediatric hospitalists: a systematic review of the literature.Pediatrics.2006;117:1736–1744.
- ,.Evaluation of a pediatric hospitalist service: impact on length of stay and hospital charges.Pediatrics.2000;105:478–484.
- ,,,,,.Variations in management of common inpatient pediatric illnesses: hospitalists and community pediatricians.Pediatrics.2006;118:441–447.
- American Academy of Pediatrics.Section on Hospital Medicine. Guiding principles for pediatric hospitalist programs.Pediatrics.2005;115:1101–1102.
- ,,,,.Consultative pediatrics: a role for the generalist in an academic setting.J Pediatr.1988;112:1035–1038.
- ,,,,,.Bronchiolitis‐associated hospitalizations among U.S. children, 1980–1996.JAMA.1999:282:1440–1446.
- ,,,,,.Condition HELP: a pediatric rapid response team triggered by patients and parents.J Healthc Qual.2008;30:28–31.
- ,,,,,.Effect of a pediatric hospitalist system on housestaff education and experience.Arch Pediatr Adolesc Med.2002;156:877–883.
- .Clinical and behavioral adaptation to managed care: stepwise suggestions for survival.Pediatrics.1995;96:821–824.
- ,,,,,.Gatekeeping and referral of children and adolescents to specialty care.Pediatrics.1999;104:28–34.
- (Chair, AAP Council on Children with Disabilities). Written Statement on Behalf of the American Academy of Pediatrics: Presented to the Institute of Medicine Committee on Disability in America. January 9,2006. Available at: http://www.aap.org/advocacy/washing/Testimonies‐Statements‐Petitions/IOM_testimony.pdf. Accessed June 2009.
- ,,, et al.The duration of ambulatory visits to physicians.J Fam Pract.1999;48:264–271.
- .Systemic errors continue to plague many hospitals.Pittsburgh Post‐Gazette.2004 Dec 5: Sect. Living.
- Josie King Foundation: Creating a Culture of Patient Safety, Together. Available at http://www.josieking.org. Accessed June 2009.
- .Hospitalist fellowships: pro and con.Section on Hospital Medicine News.2006;1:7,9. Available at: https://www.aap.org/sections/hospcare/SOHMwinter06news.pdf. Accessed June 2009.
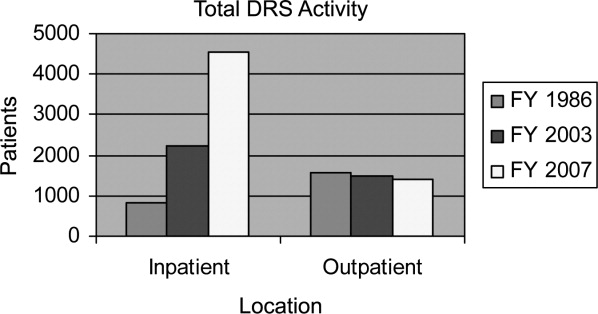
VTE Prevention in VA Hospitals
Pulmonary embolism (PE) is the most common preventable cause of death in hospitals,1 accounting for approximately 10% of hospital deaths. Most cases of PE result from dislodged lower extremity thrombi, so that deep vein thrombosis (DVT) and PE are manifestations of the same disorder, venous thromboembolism (VTE). Even though the majority of hospitalized patients are at increased risk for VTE and proven preventive measures have long been available, most patients do not receive appropriate care.2
Recent surgery is a well‐recognized risk factor for VTE, and surgeons have prescribed prophylactic therapies more consistently than other specialists.3 At the same time, prevention of VTE among hospitalized medical patients has been neglected.4 The American College of Chest Physicians recommends pharmacologic VTE prevention for most acutely ill medical patients, and advises prevention using mechanical devices when pharmacologic intervention is contraindicated.1
In Department of Veterans Affairs (VA) hospitals, compliance with preventive guidelines in surgical patients has been high. During October through December 2007, according to the Office of Quality and Performance, Veterans Health Administration, the national average for administration of VTE prophylaxis within 24 hours of surgery in VA hospitals was 92%. No comparable systemwide performance measure has been applied for medical patients, but an assessment involving intensive care unit patients has been completed and plans are underway for an evaluation of anticoagulant use among all inpatients considered to be at increased risk.
We sought to determine the extent to which hospitalized VA medical patients receive VTE preventive care in accordance with evidence‐based recommendations. Because quality of care may vary in hospitals based on teaching status,5 a secondary goal was to ascertain whether teaching and nonteaching facilities differ with respect to the delivery of care for VTE prevention.
Patient Populations Methods
We examined compliance with accepted VTE clinical practice guidelines in 2 patient populations. First, the care of patients at risk for developing VTE was evaluated for evidence of appropriate preventive measures. Second, the care of patients who developed PE while hospitalized was evaluated for evidence of preventive therapy prior to the event.
We identified patients discharged from VA acute care hospitals during the period April 1, 2006 to March 31, 2007, excluding patients hospitalized for less than 48 hours. We also excluded hospitalizations of VA patients at military and private hospitals because oversight of the quality of care provided at those facilities is beyond the purview of the Inspector General.
We then defined 2 distinct populations:
Medical patients at increased risk for VTE. These patients were identified by: (1) age 75 years at the time of admission; and (2) hospitalization with a principal discharge diagnosis of heart failure (International Classification of Diseases, 9th edition [ICD‐9] code 428). Elderly heart failure patients were chosen because advanced age and heart failure are recognized VTE risk factors, medical inpatients have been identified as being neglected in hospital VTE prevention efforts, and the VA was conducting no systemwide assessment of this aspect of care.
Patients with established PE. These patients had any discharge diagnosis pulmonary embolism and infarction (ICD‐9 codes 415.1 or 415.19), but those with the diagnostic code personal history of venous thrombosis and embolism (V12.51) were excluded.
Within each population, the discharge date defined an index hospitalization for evaluation. For patients discharged more than once with a qualifying diagnosis during the study period, we analyzed only the most recent hospitalization.
Characterization of Facilities
Hospitals were considered teaching hospitals if they were members of the Association of American Medical Colleges' Council of Teaching Hospitals and Health Systems (COTH).6 When COTH membership was through a Veterans Integrated Service Network, hospitals were judged to be teaching hospitals if they had 1 or more close university affiliations and/or management of medical inpatients by house staff.
Patient Selection and Medical Record Review
In order to ensure optimal representation of teaching and nonteaching hospitals, we stratified patients with increased VTE risk and those with diagnosed PE according to hospital teaching status, thereby creating 4 groups:
Patients at increased risk for VTEteaching hospitals;
Patients at increased risk for VTEnonteaching hospitals;
PE patientsteaching hospitals;
PE patientsnonteaching hospitals.
Within each group we assigned a random number to each patient, ordered the patients by random number, and selected patients sequentially until 50 patients were identified or no further eligible patients were available. For the heart failure patients, we assumed that all were at risk for VTE and required prophylaxis. For the group of patients with established PE, we excluded patients if the diagnosis was made prior to admission or in the first 2 hospital days, if there were no acute signs and symptoms and the diagnosis was chronic PE, or if there were no imaging studies or postmortem findings in support of the diagnosis.
In both groups, we assessed patients' records for VTE risk factors, evidence of preventive care, and contraindications.7 We considered pertinent VTE risk factors to be those included with published guidelines.1 In the care of patients with established PE, designation of adequate prophylactic therapy required at least 24 hours of treatment prior to diagnosis.
Appropriate VTE prophylaxis was defined as anticoagulant medications or, in the case of contraindications to anticoagulation, mechanical compression devices applied to the lower extremities with or without antiembolism stockings. Any administration of warfarin, lowmolecular‐weight heparin, or heparin by infusion, was considered adequate. Prophylaxis with subcutaneous unfractionated heparin was considered adequate only if at least 5000 units was administered 3 times daily.8 Aspirin and other antiplatelet agents were not considered to be anticoagulants.
We characterized hospitalizations of at‐risk individuals as missed opportunities for prevention if there were no contraindications to treatment and no evidence that adequate prophylactic therapy was provided.
Data Analysis
To determine sample size for each of the 2 study populations, we assumed the baseline rate of compliance with recommendations for VTE prophylaxis among medical inpatients to be 0.4 to 0.5.4 We further assumed that an observed compliance rate of 0.7 would be indicative of an important difference compared with published results (rate difference, 0.2‐0.3). With a Type 1 (alpha) error of 0.025 (1‐tailed), approximately 90 patients are required for a 0.9 probability of detecting a difference of at least 0.25.9
Comparisons between teaching and nonteaching hospitals were analyzed using chi‐square tests. Confidence intervals for estimates of overall compliance were calculated using a normal approximation to the binomial distribution.10
Results
Medical Patients at Increased Risk for VTE
We identified 4963 patients age 75 and older discharged after at least 2 days of acute hospitalization for heart failure: 3437 from 73 teaching hospitals and 1526 from 58 nonteaching hospitals. The 100 patients randomly selected for review ranged in age from 75 to 94 (median, 82) and had hospitalizations of 3 to 41 days (median, 6). Ninety‐eight were male. In this group of patients, we found 63 with evidence of adequate pharmacologic VTE prevention and 37 for which opportunities for prevention were not realized. At teaching hospitals, anticoagulation was effected with warfarin (13 cases), heparin (11), and enoxaparin (10). At nonteaching hospitals anticoagulants included warfarin (16), enoxaparin (11), and heparin (2). Twenty‐nine of the 63 patients who received anticoagulation (46%) were admitted while taking warfarin for chronic conditions. Teaching and nonteaching hospitals did not differ with respect to missed opportunities for prevention of VTE (37% in each group; Table 1).
| Hospital Type | |||
|---|---|---|---|
| Total | Teaching | Nonteaching | |
| |||
| Number of patients | 4963 | 3437 | 1526 |
| Randomly selected patients at risk | 100 | 54 | 46 |
| Received prophylactic anticoagulation | 63 | 34 | 29 |
| Missed opportunities for prevention | 37 | 20 | 17 |
| Percent (95% confidence interval) | 37 (27‐47) | 37 (23‐51) | 37 (22‐52) |
Patients With Established PE
We identified 1448 acute hospitalizations of at least 2 days duration for patients with PE, 1118 from 72 teaching hospitals and 330 from 51 nonteaching hospitals. We reviewed 779 medical records, 449 (40.2%) teaching cases and all 330 nonteaching cases. Chart review was completed after all nonteaching cases had been reviewed. In only 8.2% (64) of reviewed cases was the diagnosis of acute PE made after the first 2 hospital days and with accompanying objective evidence of VTE. Most cases (698; 89.6%) were excluded because there was only a remote history of PE or the diagnosis was made prior to admission. Additional cases (17; 2.2%) were excluded because the diagnosis was made during the first 2 hospital days; there were no acute signs and symptoms and the diagnosis was chronic PE; or there was no confirmation by computed tomography or ventilation‐perfusion scans, lower extremity ultrasonography in the setting of consistent clinical findings, or autopsy.
The 64 patients with confirmed in‐hospital PE ranged in age from 44 to 85 years (median, 65) and had hospitalizations of 4 to 53 days (median, 16). Sixty‐three were male. One of these patients had no definite risk factors for VTE and was ambulatory when acute symptoms occurred. Among the 63 patients who had unequivocal VTE risk factors, 34 (54%) received appropriate prophylactic treatment, and 29 (46%) received inadequate or no preventive therapy (Table 2). There was no significant difference between teaching and nonteaching hospitals with respect to missed opportunities for prevention (49% vs. 35%; P 0.3).
| Hospital Type | |||
|---|---|---|---|
| Total | Teaching | Nonteaching | |
| |||
| Number of patients | 1448 | 1118 | 330 |
| Randomly selected patients | 779 | 449 | 330 |
| Documented in‐hospital pulmonary embolism | 64 | 47 | 17 |
| No definite VTE risk factors | 1 | 0 | 1 |
| Received prophylactic anticoagulation | 30 | 20 | 10 |
| Anticoagulation contraindicated, received mechanical prophylaxis | 4 | 4 | 0 |
| Missed opportunities for prevention | 29 | 23 | 6 |
| Percent (95% confidence interval) | 45 (32‐58) | 49 (30‐68) | 35 (12‐58) |
Anticoagulants used at teaching hospitals included heparin (15 cases), enoxaparin (4), and warfarin (1), while at nonteaching hospitals enoxaparin (7) and heparin (3) were used.
Each of the 10 patients who received no anticoagulation had the VTE risk factor of recent immobility prior to PE. Nine of the 10 had active malignancies, and 4 of these had undergone recent surgery. None had evidence of hypercoagulable states (factor V Leiden, lupus anticoagulant, or anticardiolipin antibodies). Five of the 10 patients died in the year following pulmonary embolism, 3 prior to discharge or within 2 weeks of discharge.
Missed Opportunities for Prevention
Among the 66 patients whose hospitalizations were characterized as missed opportunities for prevention, 30 received no pharmacologic VTE prevention despite having no contraindications. Seven patients had contraindications to pharmacologic prophylaxis, but none of these patients had contraindications to mechanical prophylaxis. An additional 18 patients received mechanical prophylaxis only despite having no contraindications to anticoagulation. Eleven patients received inadequate heparin regimens with or without mechanical prophylaxis (Table 3).
| Hospital Type | |||
|---|---|---|---|
| Total | Teaching | Nonteaching | |
| Number of patients | 66 | 43 | 23 |
| No contraindications, no prophylaxis | 30 | 18 | 12 |
| Anticoagulation contraindicated, no mechanical prophylaxis | 7 | 3 | 4 |
| No contraindication to anticoagulation, mechanical prophylaxis only | 18 | 13 | 5 |
| Inadequate heparin regimen, no mechanical prophylaxis | 9 | 7 | 2 |
| Inadequate heparin regimen, mechanical prophylaxis | 2 | 2 | 0 |
Discussion
Based on a random sample of 4963 elderly heart failure patients admitted to VA hospitals during a 1‐year period, we estimated that 63% received recommended interventions aimed at preventing VTE. Although differences in methodology limit comparisons with published reports, this rate is similar to those observed at individual hospitals,1113 in large multicenter registries of patients with DVT or at risk for VTE,14, 15 and in a recent multinational cross‐sectional study.16 Notably, chronic outpatient anticoagulation that was continued during hospitalization accounted for nearly one‐half of patients receiving preventive care. Compliance did not differ between teaching and nonteaching hospitals.
In a complementary approach to examining the extent of preventive care, we identified 1448 patients discharged with a diagnosis of PE. Most of these patients were excluded because they did not have a new event while hospitalized. Eleven (17%) of the 64 patients with confirmed in‐hospital PE received no preventive care before the event. An additional 18 (28%) received suboptimal heparin regimens or mechanical prophylaxis in the absence of contraindications to anticoagulation. As with the patients at risk for VTE, patients with established PE at teaching and nonteaching hospitals received similar rates of preventive care. Contrary to our expectation, the observed difference in rates between types of hospitals favored nonteaching hospitals. However, the sample size for this comparison was small and the difference did not reach statistical significance.
This study's population‐based approach permits conclusions about the performance of the VA's entire system of acute care hospitals. The results indicate that proven preventive therapies are often neglected at VA hospitals, but overall performance is probably comparable to other settings. VA employs an extensively implemented electronic medical record (EMR) and superior performance might have been expected. However, these results suggest limitations in the EMR as it is currently deployed. Successful efforts probably require a multifaceted approach incorporating decision support and institutional standardization.17
Several additional findings warrant comment. Patients with malignancies accounted for 9 of 10 patients who had PE after receiving no prior anticoagulation. Recent surgery was also a contributing factor for 4 of these cancer patients. Although both cancer and surgery are well‐known risk VTE factors, clinicians may not appreciate the extremely high risk associated with the combination.18 Particular effort may be warranted to ensure prophylaxis in this group, and more intensive measures may be necessary.
These results reveal several barriers to the accurate retrospective measurement of preventable inpatient PE. First, the use of discharge diagnoses to monitor the occurrence of inpatient PE is fraught with hazard. In this study, even after excluding patients with a discharge diagnostic code indicating a past history of PE, very few identified patients in fact had an acute or recent event. In addition, many patients were clearly admitted after having the onset of symptoms as outpatients. Further, reliance on discharge diagnoses alone can lead to the inclusion of patients with a presumptive diagnosis made without the advantage of imaging studies or postmortem examination. Although we overcame these barriers through careful record review and strict diagnostic criteria, our results suggest that efficient performance improvement efforts may require ongoing concurrent review.
There are several limitations of this study. First, we excluded PE patients whose diagnoses were made before the third hospital day. Some of these patients may have had events attributable to recent prior hospitalizations and should have received VTE prophylaxis. Second, we considered preventive measures applied at least 24 hours prior to PE to be acceptable evidence of prevention, potentially neglecting prior periods without treatment that might confer increased risk. Bias due to either of these limitations could exaggerate the compliance rates we report. Finally, the retrospective design of this study did not allow for consistent assessments of whether patients had the risk factor of immobility. Nevertheless, immobility was obvious for the 10 patients with PE who had no prior anticoagulation, all of whom had 2 or more risk factors.
Despite an acknowledged need for improvements in clinical practice, past efforts have had mixed results. For instance, in 1 study at a hospital with a well‐established EMR, computer alerts led to substantial improvement in the use of preventive measures and in VTE outcomes, but overall compliance remained low.19 On the other hand, a multidisciplinary approach can achieve marked reductions in preventable VTE events.20 Key elements of such an approach are a simplified risk assessment tool and concurrent monitoring of patient treatments and outcomes. The Agency for Healthcare Research and Quality has recently published a guide that outlines strategies for achieving breakthrough levels of improvement in the prevention of VTE.21
In conclusion, this population‐based study of hospitalized veterans with PE or at risk for VTE found compliance comparable to rates in published reports. Missed opportunities for prevention included inappropriate and inadequate interventions. Using discharge diagnoses to monitor the occurrence of inpatient PE is of limited value, and efficient performance improvement efforts may require ongoing concurrent review.
Acknowledgements
The authors thank Greg Maynard, MD, MS for advice on study design, and Deborah Howard, RN, for assistance with medical record review.
- ,,.Prevention of venous thromboembolism. The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126:338S–400S.
- ,,,.Thromboprophylaxis rates in US medical centers: success or failure?J Thromb Haemost.2007;5:1610–1616.
- .Preventing venous thromboembolism in surgical patients.Cleve Clin J Med.2006;73:S88–S94.
- ,.Prevention of venous thromboembolism among hospitalized medical patients.Circulation.2005;111:e1–e3.
- ,,.Quality of care for the treatment of acute medical conditions in US hospitals.Arch Intern Med.2006;166:2511–2517.
- Association of American Medical Colleges (AAMC). Council of Teaching Hospitals and Health Systems (COTH). Available at: http://www.aamc. org/members/coth. Accessed August2009.
- Contraindications are those described in the Institute for Clinical Systems Improvement Health Care Guideline: Venous Thromboembolism Prophylaxis. 4th ed. June 2007, pp 13–14. Available at: http://www. icsi.org/guidelines_and_more/gl_os_prot/cardiovascular/venous_thromboem bolism_prophylaxis/venous_thromboembolism_prophylaxis_5.html. Accessed August2009.
- ,,, et al.Prevention and treatment of venous thromboembolism. International Consensus Statement.Int Angiol.2006;25:101–161.
- ,.Designing Clinical Research.Baltimore, MD:Williams 1988.
- ,,. Statistical Methods for Rates and Proportions.3rd ed.Hoboken, NJ:Wiley‐Interscience;2003;28,54.
- ,,.New onset of venous thromboembolism among hospitalized patients at Brigham and Women's Hospital is caused more often by prophylaxis failure than by withholding treatment.Chest.2000;118;1680–1684.
- ,,.Prophylaxis against venous thromboembolism in acutely ill medical patients: an observational study.Pharmacotherapy.2006;26:1086–1090.
- ,,.Hospital‐acquired venous thromboembolism and prophylaxis in an integrated hospital delivery system.J Clin Pharm Ther.2006;31:455–459.
- ,;DVT FREE Steering Committee.A prospective study of 5,451 patients with ultrasound‐confirmed deep vein thrombosis.Am J Cardiol.2004;15:259–262.
- ,,, et al.Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism.Chest.2007;132:936–945.
- ,,, et al.Venous thromboembolism risk and prophylaxis in the acute hospital care setting.Lancet.2008;371:387–394.
- .Medical admission order sets to improve deep vein thrombosis prevention: a model for others or a prescription for mediocrity?J Hosp Med.2009;4:77–80.
- ,,,,,.Prevention of venous thromboembolism in the cancer surgery patient.Cleve Clin J Med.2008;75(suppl 3):S17–S26.
- ,,, et al.Electronic alerts for hospitalized high‐VTE risk patients not receiving prophylaxis: a cohort study.J Thromb Thrombolysis.2008;25:146–150.
- ,,, et al. Prevention of hospital‐acquired venous thromboembolism: prospective validation of a VTE risk assessment model and protocol. Society of Hospital Medicine 2008 National Meeting. Electronic citation abstract #52, page 29. Available at: http://www.hospital medicine.org/Paperless2008/PDFs/Additional_Info/SHM08_Abstracts.pdf. Accessed August2009
- ,.Preventing Hospital‐Acquired Venous Thromboembolism: A Guide for Effective Quality Improvement. AHRQ Publication No. 08–0075.Rockville, MD:Agency for Healthcare Research and Quality;2008.
Pulmonary embolism (PE) is the most common preventable cause of death in hospitals,1 accounting for approximately 10% of hospital deaths. Most cases of PE result from dislodged lower extremity thrombi, so that deep vein thrombosis (DVT) and PE are manifestations of the same disorder, venous thromboembolism (VTE). Even though the majority of hospitalized patients are at increased risk for VTE and proven preventive measures have long been available, most patients do not receive appropriate care.2
Recent surgery is a well‐recognized risk factor for VTE, and surgeons have prescribed prophylactic therapies more consistently than other specialists.3 At the same time, prevention of VTE among hospitalized medical patients has been neglected.4 The American College of Chest Physicians recommends pharmacologic VTE prevention for most acutely ill medical patients, and advises prevention using mechanical devices when pharmacologic intervention is contraindicated.1
In Department of Veterans Affairs (VA) hospitals, compliance with preventive guidelines in surgical patients has been high. During October through December 2007, according to the Office of Quality and Performance, Veterans Health Administration, the national average for administration of VTE prophylaxis within 24 hours of surgery in VA hospitals was 92%. No comparable systemwide performance measure has been applied for medical patients, but an assessment involving intensive care unit patients has been completed and plans are underway for an evaluation of anticoagulant use among all inpatients considered to be at increased risk.
We sought to determine the extent to which hospitalized VA medical patients receive VTE preventive care in accordance with evidence‐based recommendations. Because quality of care may vary in hospitals based on teaching status,5 a secondary goal was to ascertain whether teaching and nonteaching facilities differ with respect to the delivery of care for VTE prevention.
Patient Populations Methods
We examined compliance with accepted VTE clinical practice guidelines in 2 patient populations. First, the care of patients at risk for developing VTE was evaluated for evidence of appropriate preventive measures. Second, the care of patients who developed PE while hospitalized was evaluated for evidence of preventive therapy prior to the event.
We identified patients discharged from VA acute care hospitals during the period April 1, 2006 to March 31, 2007, excluding patients hospitalized for less than 48 hours. We also excluded hospitalizations of VA patients at military and private hospitals because oversight of the quality of care provided at those facilities is beyond the purview of the Inspector General.
We then defined 2 distinct populations:
Medical patients at increased risk for VTE. These patients were identified by: (1) age 75 years at the time of admission; and (2) hospitalization with a principal discharge diagnosis of heart failure (International Classification of Diseases, 9th edition [ICD‐9] code 428). Elderly heart failure patients were chosen because advanced age and heart failure are recognized VTE risk factors, medical inpatients have been identified as being neglected in hospital VTE prevention efforts, and the VA was conducting no systemwide assessment of this aspect of care.
Patients with established PE. These patients had any discharge diagnosis pulmonary embolism and infarction (ICD‐9 codes 415.1 or 415.19), but those with the diagnostic code personal history of venous thrombosis and embolism (V12.51) were excluded.
Within each population, the discharge date defined an index hospitalization for evaluation. For patients discharged more than once with a qualifying diagnosis during the study period, we analyzed only the most recent hospitalization.
Characterization of Facilities
Hospitals were considered teaching hospitals if they were members of the Association of American Medical Colleges' Council of Teaching Hospitals and Health Systems (COTH).6 When COTH membership was through a Veterans Integrated Service Network, hospitals were judged to be teaching hospitals if they had 1 or more close university affiliations and/or management of medical inpatients by house staff.
Patient Selection and Medical Record Review
In order to ensure optimal representation of teaching and nonteaching hospitals, we stratified patients with increased VTE risk and those with diagnosed PE according to hospital teaching status, thereby creating 4 groups:
Patients at increased risk for VTEteaching hospitals;
Patients at increased risk for VTEnonteaching hospitals;
PE patientsteaching hospitals;
PE patientsnonteaching hospitals.
Within each group we assigned a random number to each patient, ordered the patients by random number, and selected patients sequentially until 50 patients were identified or no further eligible patients were available. For the heart failure patients, we assumed that all were at risk for VTE and required prophylaxis. For the group of patients with established PE, we excluded patients if the diagnosis was made prior to admission or in the first 2 hospital days, if there were no acute signs and symptoms and the diagnosis was chronic PE, or if there were no imaging studies or postmortem findings in support of the diagnosis.
In both groups, we assessed patients' records for VTE risk factors, evidence of preventive care, and contraindications.7 We considered pertinent VTE risk factors to be those included with published guidelines.1 In the care of patients with established PE, designation of adequate prophylactic therapy required at least 24 hours of treatment prior to diagnosis.
Appropriate VTE prophylaxis was defined as anticoagulant medications or, in the case of contraindications to anticoagulation, mechanical compression devices applied to the lower extremities with or without antiembolism stockings. Any administration of warfarin, lowmolecular‐weight heparin, or heparin by infusion, was considered adequate. Prophylaxis with subcutaneous unfractionated heparin was considered adequate only if at least 5000 units was administered 3 times daily.8 Aspirin and other antiplatelet agents were not considered to be anticoagulants.
We characterized hospitalizations of at‐risk individuals as missed opportunities for prevention if there were no contraindications to treatment and no evidence that adequate prophylactic therapy was provided.
Data Analysis
To determine sample size for each of the 2 study populations, we assumed the baseline rate of compliance with recommendations for VTE prophylaxis among medical inpatients to be 0.4 to 0.5.4 We further assumed that an observed compliance rate of 0.7 would be indicative of an important difference compared with published results (rate difference, 0.2‐0.3). With a Type 1 (alpha) error of 0.025 (1‐tailed), approximately 90 patients are required for a 0.9 probability of detecting a difference of at least 0.25.9
Comparisons between teaching and nonteaching hospitals were analyzed using chi‐square tests. Confidence intervals for estimates of overall compliance were calculated using a normal approximation to the binomial distribution.10
Results
Medical Patients at Increased Risk for VTE
We identified 4963 patients age 75 and older discharged after at least 2 days of acute hospitalization for heart failure: 3437 from 73 teaching hospitals and 1526 from 58 nonteaching hospitals. The 100 patients randomly selected for review ranged in age from 75 to 94 (median, 82) and had hospitalizations of 3 to 41 days (median, 6). Ninety‐eight were male. In this group of patients, we found 63 with evidence of adequate pharmacologic VTE prevention and 37 for which opportunities for prevention were not realized. At teaching hospitals, anticoagulation was effected with warfarin (13 cases), heparin (11), and enoxaparin (10). At nonteaching hospitals anticoagulants included warfarin (16), enoxaparin (11), and heparin (2). Twenty‐nine of the 63 patients who received anticoagulation (46%) were admitted while taking warfarin for chronic conditions. Teaching and nonteaching hospitals did not differ with respect to missed opportunities for prevention of VTE (37% in each group; Table 1).
| Hospital Type | |||
|---|---|---|---|
| Total | Teaching | Nonteaching | |
| |||
| Number of patients | 4963 | 3437 | 1526 |
| Randomly selected patients at risk | 100 | 54 | 46 |
| Received prophylactic anticoagulation | 63 | 34 | 29 |
| Missed opportunities for prevention | 37 | 20 | 17 |
| Percent (95% confidence interval) | 37 (27‐47) | 37 (23‐51) | 37 (22‐52) |
Patients With Established PE
We identified 1448 acute hospitalizations of at least 2 days duration for patients with PE, 1118 from 72 teaching hospitals and 330 from 51 nonteaching hospitals. We reviewed 779 medical records, 449 (40.2%) teaching cases and all 330 nonteaching cases. Chart review was completed after all nonteaching cases had been reviewed. In only 8.2% (64) of reviewed cases was the diagnosis of acute PE made after the first 2 hospital days and with accompanying objective evidence of VTE. Most cases (698; 89.6%) were excluded because there was only a remote history of PE or the diagnosis was made prior to admission. Additional cases (17; 2.2%) were excluded because the diagnosis was made during the first 2 hospital days; there were no acute signs and symptoms and the diagnosis was chronic PE; or there was no confirmation by computed tomography or ventilation‐perfusion scans, lower extremity ultrasonography in the setting of consistent clinical findings, or autopsy.
The 64 patients with confirmed in‐hospital PE ranged in age from 44 to 85 years (median, 65) and had hospitalizations of 4 to 53 days (median, 16). Sixty‐three were male. One of these patients had no definite risk factors for VTE and was ambulatory when acute symptoms occurred. Among the 63 patients who had unequivocal VTE risk factors, 34 (54%) received appropriate prophylactic treatment, and 29 (46%) received inadequate or no preventive therapy (Table 2). There was no significant difference between teaching and nonteaching hospitals with respect to missed opportunities for prevention (49% vs. 35%; P 0.3).
| Hospital Type | |||
|---|---|---|---|
| Total | Teaching | Nonteaching | |
| |||
| Number of patients | 1448 | 1118 | 330 |
| Randomly selected patients | 779 | 449 | 330 |
| Documented in‐hospital pulmonary embolism | 64 | 47 | 17 |
| No definite VTE risk factors | 1 | 0 | 1 |
| Received prophylactic anticoagulation | 30 | 20 | 10 |
| Anticoagulation contraindicated, received mechanical prophylaxis | 4 | 4 | 0 |
| Missed opportunities for prevention | 29 | 23 | 6 |
| Percent (95% confidence interval) | 45 (32‐58) | 49 (30‐68) | 35 (12‐58) |
Anticoagulants used at teaching hospitals included heparin (15 cases), enoxaparin (4), and warfarin (1), while at nonteaching hospitals enoxaparin (7) and heparin (3) were used.
Each of the 10 patients who received no anticoagulation had the VTE risk factor of recent immobility prior to PE. Nine of the 10 had active malignancies, and 4 of these had undergone recent surgery. None had evidence of hypercoagulable states (factor V Leiden, lupus anticoagulant, or anticardiolipin antibodies). Five of the 10 patients died in the year following pulmonary embolism, 3 prior to discharge or within 2 weeks of discharge.
Missed Opportunities for Prevention
Among the 66 patients whose hospitalizations were characterized as missed opportunities for prevention, 30 received no pharmacologic VTE prevention despite having no contraindications. Seven patients had contraindications to pharmacologic prophylaxis, but none of these patients had contraindications to mechanical prophylaxis. An additional 18 patients received mechanical prophylaxis only despite having no contraindications to anticoagulation. Eleven patients received inadequate heparin regimens with or without mechanical prophylaxis (Table 3).
| Hospital Type | |||
|---|---|---|---|
| Total | Teaching | Nonteaching | |
| Number of patients | 66 | 43 | 23 |
| No contraindications, no prophylaxis | 30 | 18 | 12 |
| Anticoagulation contraindicated, no mechanical prophylaxis | 7 | 3 | 4 |
| No contraindication to anticoagulation, mechanical prophylaxis only | 18 | 13 | 5 |
| Inadequate heparin regimen, no mechanical prophylaxis | 9 | 7 | 2 |
| Inadequate heparin regimen, mechanical prophylaxis | 2 | 2 | 0 |
Discussion
Based on a random sample of 4963 elderly heart failure patients admitted to VA hospitals during a 1‐year period, we estimated that 63% received recommended interventions aimed at preventing VTE. Although differences in methodology limit comparisons with published reports, this rate is similar to those observed at individual hospitals,1113 in large multicenter registries of patients with DVT or at risk for VTE,14, 15 and in a recent multinational cross‐sectional study.16 Notably, chronic outpatient anticoagulation that was continued during hospitalization accounted for nearly one‐half of patients receiving preventive care. Compliance did not differ between teaching and nonteaching hospitals.
In a complementary approach to examining the extent of preventive care, we identified 1448 patients discharged with a diagnosis of PE. Most of these patients were excluded because they did not have a new event while hospitalized. Eleven (17%) of the 64 patients with confirmed in‐hospital PE received no preventive care before the event. An additional 18 (28%) received suboptimal heparin regimens or mechanical prophylaxis in the absence of contraindications to anticoagulation. As with the patients at risk for VTE, patients with established PE at teaching and nonteaching hospitals received similar rates of preventive care. Contrary to our expectation, the observed difference in rates between types of hospitals favored nonteaching hospitals. However, the sample size for this comparison was small and the difference did not reach statistical significance.
This study's population‐based approach permits conclusions about the performance of the VA's entire system of acute care hospitals. The results indicate that proven preventive therapies are often neglected at VA hospitals, but overall performance is probably comparable to other settings. VA employs an extensively implemented electronic medical record (EMR) and superior performance might have been expected. However, these results suggest limitations in the EMR as it is currently deployed. Successful efforts probably require a multifaceted approach incorporating decision support and institutional standardization.17
Several additional findings warrant comment. Patients with malignancies accounted for 9 of 10 patients who had PE after receiving no prior anticoagulation. Recent surgery was also a contributing factor for 4 of these cancer patients. Although both cancer and surgery are well‐known risk VTE factors, clinicians may not appreciate the extremely high risk associated with the combination.18 Particular effort may be warranted to ensure prophylaxis in this group, and more intensive measures may be necessary.
These results reveal several barriers to the accurate retrospective measurement of preventable inpatient PE. First, the use of discharge diagnoses to monitor the occurrence of inpatient PE is fraught with hazard. In this study, even after excluding patients with a discharge diagnostic code indicating a past history of PE, very few identified patients in fact had an acute or recent event. In addition, many patients were clearly admitted after having the onset of symptoms as outpatients. Further, reliance on discharge diagnoses alone can lead to the inclusion of patients with a presumptive diagnosis made without the advantage of imaging studies or postmortem examination. Although we overcame these barriers through careful record review and strict diagnostic criteria, our results suggest that efficient performance improvement efforts may require ongoing concurrent review.
There are several limitations of this study. First, we excluded PE patients whose diagnoses were made before the third hospital day. Some of these patients may have had events attributable to recent prior hospitalizations and should have received VTE prophylaxis. Second, we considered preventive measures applied at least 24 hours prior to PE to be acceptable evidence of prevention, potentially neglecting prior periods without treatment that might confer increased risk. Bias due to either of these limitations could exaggerate the compliance rates we report. Finally, the retrospective design of this study did not allow for consistent assessments of whether patients had the risk factor of immobility. Nevertheless, immobility was obvious for the 10 patients with PE who had no prior anticoagulation, all of whom had 2 or more risk factors.
Despite an acknowledged need for improvements in clinical practice, past efforts have had mixed results. For instance, in 1 study at a hospital with a well‐established EMR, computer alerts led to substantial improvement in the use of preventive measures and in VTE outcomes, but overall compliance remained low.19 On the other hand, a multidisciplinary approach can achieve marked reductions in preventable VTE events.20 Key elements of such an approach are a simplified risk assessment tool and concurrent monitoring of patient treatments and outcomes. The Agency for Healthcare Research and Quality has recently published a guide that outlines strategies for achieving breakthrough levels of improvement in the prevention of VTE.21
In conclusion, this population‐based study of hospitalized veterans with PE or at risk for VTE found compliance comparable to rates in published reports. Missed opportunities for prevention included inappropriate and inadequate interventions. Using discharge diagnoses to monitor the occurrence of inpatient PE is of limited value, and efficient performance improvement efforts may require ongoing concurrent review.
Acknowledgements
The authors thank Greg Maynard, MD, MS for advice on study design, and Deborah Howard, RN, for assistance with medical record review.
Pulmonary embolism (PE) is the most common preventable cause of death in hospitals,1 accounting for approximately 10% of hospital deaths. Most cases of PE result from dislodged lower extremity thrombi, so that deep vein thrombosis (DVT) and PE are manifestations of the same disorder, venous thromboembolism (VTE). Even though the majority of hospitalized patients are at increased risk for VTE and proven preventive measures have long been available, most patients do not receive appropriate care.2
Recent surgery is a well‐recognized risk factor for VTE, and surgeons have prescribed prophylactic therapies more consistently than other specialists.3 At the same time, prevention of VTE among hospitalized medical patients has been neglected.4 The American College of Chest Physicians recommends pharmacologic VTE prevention for most acutely ill medical patients, and advises prevention using mechanical devices when pharmacologic intervention is contraindicated.1
In Department of Veterans Affairs (VA) hospitals, compliance with preventive guidelines in surgical patients has been high. During October through December 2007, according to the Office of Quality and Performance, Veterans Health Administration, the national average for administration of VTE prophylaxis within 24 hours of surgery in VA hospitals was 92%. No comparable systemwide performance measure has been applied for medical patients, but an assessment involving intensive care unit patients has been completed and plans are underway for an evaluation of anticoagulant use among all inpatients considered to be at increased risk.
We sought to determine the extent to which hospitalized VA medical patients receive VTE preventive care in accordance with evidence‐based recommendations. Because quality of care may vary in hospitals based on teaching status,5 a secondary goal was to ascertain whether teaching and nonteaching facilities differ with respect to the delivery of care for VTE prevention.
Patient Populations Methods
We examined compliance with accepted VTE clinical practice guidelines in 2 patient populations. First, the care of patients at risk for developing VTE was evaluated for evidence of appropriate preventive measures. Second, the care of patients who developed PE while hospitalized was evaluated for evidence of preventive therapy prior to the event.
We identified patients discharged from VA acute care hospitals during the period April 1, 2006 to March 31, 2007, excluding patients hospitalized for less than 48 hours. We also excluded hospitalizations of VA patients at military and private hospitals because oversight of the quality of care provided at those facilities is beyond the purview of the Inspector General.
We then defined 2 distinct populations:
Medical patients at increased risk for VTE. These patients were identified by: (1) age 75 years at the time of admission; and (2) hospitalization with a principal discharge diagnosis of heart failure (International Classification of Diseases, 9th edition [ICD‐9] code 428). Elderly heart failure patients were chosen because advanced age and heart failure are recognized VTE risk factors, medical inpatients have been identified as being neglected in hospital VTE prevention efforts, and the VA was conducting no systemwide assessment of this aspect of care.
Patients with established PE. These patients had any discharge diagnosis pulmonary embolism and infarction (ICD‐9 codes 415.1 or 415.19), but those with the diagnostic code personal history of venous thrombosis and embolism (V12.51) were excluded.
Within each population, the discharge date defined an index hospitalization for evaluation. For patients discharged more than once with a qualifying diagnosis during the study period, we analyzed only the most recent hospitalization.
Characterization of Facilities
Hospitals were considered teaching hospitals if they were members of the Association of American Medical Colleges' Council of Teaching Hospitals and Health Systems (COTH).6 When COTH membership was through a Veterans Integrated Service Network, hospitals were judged to be teaching hospitals if they had 1 or more close university affiliations and/or management of medical inpatients by house staff.
Patient Selection and Medical Record Review
In order to ensure optimal representation of teaching and nonteaching hospitals, we stratified patients with increased VTE risk and those with diagnosed PE according to hospital teaching status, thereby creating 4 groups:
Patients at increased risk for VTEteaching hospitals;
Patients at increased risk for VTEnonteaching hospitals;
PE patientsteaching hospitals;
PE patientsnonteaching hospitals.
Within each group we assigned a random number to each patient, ordered the patients by random number, and selected patients sequentially until 50 patients were identified or no further eligible patients were available. For the heart failure patients, we assumed that all were at risk for VTE and required prophylaxis. For the group of patients with established PE, we excluded patients if the diagnosis was made prior to admission or in the first 2 hospital days, if there were no acute signs and symptoms and the diagnosis was chronic PE, or if there were no imaging studies or postmortem findings in support of the diagnosis.
In both groups, we assessed patients' records for VTE risk factors, evidence of preventive care, and contraindications.7 We considered pertinent VTE risk factors to be those included with published guidelines.1 In the care of patients with established PE, designation of adequate prophylactic therapy required at least 24 hours of treatment prior to diagnosis.
Appropriate VTE prophylaxis was defined as anticoagulant medications or, in the case of contraindications to anticoagulation, mechanical compression devices applied to the lower extremities with or without antiembolism stockings. Any administration of warfarin, lowmolecular‐weight heparin, or heparin by infusion, was considered adequate. Prophylaxis with subcutaneous unfractionated heparin was considered adequate only if at least 5000 units was administered 3 times daily.8 Aspirin and other antiplatelet agents were not considered to be anticoagulants.
We characterized hospitalizations of at‐risk individuals as missed opportunities for prevention if there were no contraindications to treatment and no evidence that adequate prophylactic therapy was provided.
Data Analysis
To determine sample size for each of the 2 study populations, we assumed the baseline rate of compliance with recommendations for VTE prophylaxis among medical inpatients to be 0.4 to 0.5.4 We further assumed that an observed compliance rate of 0.7 would be indicative of an important difference compared with published results (rate difference, 0.2‐0.3). With a Type 1 (alpha) error of 0.025 (1‐tailed), approximately 90 patients are required for a 0.9 probability of detecting a difference of at least 0.25.9
Comparisons between teaching and nonteaching hospitals were analyzed using chi‐square tests. Confidence intervals for estimates of overall compliance were calculated using a normal approximation to the binomial distribution.10
Results
Medical Patients at Increased Risk for VTE
We identified 4963 patients age 75 and older discharged after at least 2 days of acute hospitalization for heart failure: 3437 from 73 teaching hospitals and 1526 from 58 nonteaching hospitals. The 100 patients randomly selected for review ranged in age from 75 to 94 (median, 82) and had hospitalizations of 3 to 41 days (median, 6). Ninety‐eight were male. In this group of patients, we found 63 with evidence of adequate pharmacologic VTE prevention and 37 for which opportunities for prevention were not realized. At teaching hospitals, anticoagulation was effected with warfarin (13 cases), heparin (11), and enoxaparin (10). At nonteaching hospitals anticoagulants included warfarin (16), enoxaparin (11), and heparin (2). Twenty‐nine of the 63 patients who received anticoagulation (46%) were admitted while taking warfarin for chronic conditions. Teaching and nonteaching hospitals did not differ with respect to missed opportunities for prevention of VTE (37% in each group; Table 1).
| Hospital Type | |||
|---|---|---|---|
| Total | Teaching | Nonteaching | |
| |||
| Number of patients | 4963 | 3437 | 1526 |
| Randomly selected patients at risk | 100 | 54 | 46 |
| Received prophylactic anticoagulation | 63 | 34 | 29 |
| Missed opportunities for prevention | 37 | 20 | 17 |
| Percent (95% confidence interval) | 37 (27‐47) | 37 (23‐51) | 37 (22‐52) |
Patients With Established PE
We identified 1448 acute hospitalizations of at least 2 days duration for patients with PE, 1118 from 72 teaching hospitals and 330 from 51 nonteaching hospitals. We reviewed 779 medical records, 449 (40.2%) teaching cases and all 330 nonteaching cases. Chart review was completed after all nonteaching cases had been reviewed. In only 8.2% (64) of reviewed cases was the diagnosis of acute PE made after the first 2 hospital days and with accompanying objective evidence of VTE. Most cases (698; 89.6%) were excluded because there was only a remote history of PE or the diagnosis was made prior to admission. Additional cases (17; 2.2%) were excluded because the diagnosis was made during the first 2 hospital days; there were no acute signs and symptoms and the diagnosis was chronic PE; or there was no confirmation by computed tomography or ventilation‐perfusion scans, lower extremity ultrasonography in the setting of consistent clinical findings, or autopsy.
The 64 patients with confirmed in‐hospital PE ranged in age from 44 to 85 years (median, 65) and had hospitalizations of 4 to 53 days (median, 16). Sixty‐three were male. One of these patients had no definite risk factors for VTE and was ambulatory when acute symptoms occurred. Among the 63 patients who had unequivocal VTE risk factors, 34 (54%) received appropriate prophylactic treatment, and 29 (46%) received inadequate or no preventive therapy (Table 2). There was no significant difference between teaching and nonteaching hospitals with respect to missed opportunities for prevention (49% vs. 35%; P 0.3).
| Hospital Type | |||
|---|---|---|---|
| Total | Teaching | Nonteaching | |
| |||
| Number of patients | 1448 | 1118 | 330 |
| Randomly selected patients | 779 | 449 | 330 |
| Documented in‐hospital pulmonary embolism | 64 | 47 | 17 |
| No definite VTE risk factors | 1 | 0 | 1 |
| Received prophylactic anticoagulation | 30 | 20 | 10 |
| Anticoagulation contraindicated, received mechanical prophylaxis | 4 | 4 | 0 |
| Missed opportunities for prevention | 29 | 23 | 6 |
| Percent (95% confidence interval) | 45 (32‐58) | 49 (30‐68) | 35 (12‐58) |
Anticoagulants used at teaching hospitals included heparin (15 cases), enoxaparin (4), and warfarin (1), while at nonteaching hospitals enoxaparin (7) and heparin (3) were used.
Each of the 10 patients who received no anticoagulation had the VTE risk factor of recent immobility prior to PE. Nine of the 10 had active malignancies, and 4 of these had undergone recent surgery. None had evidence of hypercoagulable states (factor V Leiden, lupus anticoagulant, or anticardiolipin antibodies). Five of the 10 patients died in the year following pulmonary embolism, 3 prior to discharge or within 2 weeks of discharge.
Missed Opportunities for Prevention
Among the 66 patients whose hospitalizations were characterized as missed opportunities for prevention, 30 received no pharmacologic VTE prevention despite having no contraindications. Seven patients had contraindications to pharmacologic prophylaxis, but none of these patients had contraindications to mechanical prophylaxis. An additional 18 patients received mechanical prophylaxis only despite having no contraindications to anticoagulation. Eleven patients received inadequate heparin regimens with or without mechanical prophylaxis (Table 3).
| Hospital Type | |||
|---|---|---|---|
| Total | Teaching | Nonteaching | |
| Number of patients | 66 | 43 | 23 |
| No contraindications, no prophylaxis | 30 | 18 | 12 |
| Anticoagulation contraindicated, no mechanical prophylaxis | 7 | 3 | 4 |
| No contraindication to anticoagulation, mechanical prophylaxis only | 18 | 13 | 5 |
| Inadequate heparin regimen, no mechanical prophylaxis | 9 | 7 | 2 |
| Inadequate heparin regimen, mechanical prophylaxis | 2 | 2 | 0 |
Discussion
Based on a random sample of 4963 elderly heart failure patients admitted to VA hospitals during a 1‐year period, we estimated that 63% received recommended interventions aimed at preventing VTE. Although differences in methodology limit comparisons with published reports, this rate is similar to those observed at individual hospitals,1113 in large multicenter registries of patients with DVT or at risk for VTE,14, 15 and in a recent multinational cross‐sectional study.16 Notably, chronic outpatient anticoagulation that was continued during hospitalization accounted for nearly one‐half of patients receiving preventive care. Compliance did not differ between teaching and nonteaching hospitals.
In a complementary approach to examining the extent of preventive care, we identified 1448 patients discharged with a diagnosis of PE. Most of these patients were excluded because they did not have a new event while hospitalized. Eleven (17%) of the 64 patients with confirmed in‐hospital PE received no preventive care before the event. An additional 18 (28%) received suboptimal heparin regimens or mechanical prophylaxis in the absence of contraindications to anticoagulation. As with the patients at risk for VTE, patients with established PE at teaching and nonteaching hospitals received similar rates of preventive care. Contrary to our expectation, the observed difference in rates between types of hospitals favored nonteaching hospitals. However, the sample size for this comparison was small and the difference did not reach statistical significance.
This study's population‐based approach permits conclusions about the performance of the VA's entire system of acute care hospitals. The results indicate that proven preventive therapies are often neglected at VA hospitals, but overall performance is probably comparable to other settings. VA employs an extensively implemented electronic medical record (EMR) and superior performance might have been expected. However, these results suggest limitations in the EMR as it is currently deployed. Successful efforts probably require a multifaceted approach incorporating decision support and institutional standardization.17
Several additional findings warrant comment. Patients with malignancies accounted for 9 of 10 patients who had PE after receiving no prior anticoagulation. Recent surgery was also a contributing factor for 4 of these cancer patients. Although both cancer and surgery are well‐known risk VTE factors, clinicians may not appreciate the extremely high risk associated with the combination.18 Particular effort may be warranted to ensure prophylaxis in this group, and more intensive measures may be necessary.
These results reveal several barriers to the accurate retrospective measurement of preventable inpatient PE. First, the use of discharge diagnoses to monitor the occurrence of inpatient PE is fraught with hazard. In this study, even after excluding patients with a discharge diagnostic code indicating a past history of PE, very few identified patients in fact had an acute or recent event. In addition, many patients were clearly admitted after having the onset of symptoms as outpatients. Further, reliance on discharge diagnoses alone can lead to the inclusion of patients with a presumptive diagnosis made without the advantage of imaging studies or postmortem examination. Although we overcame these barriers through careful record review and strict diagnostic criteria, our results suggest that efficient performance improvement efforts may require ongoing concurrent review.
There are several limitations of this study. First, we excluded PE patients whose diagnoses were made before the third hospital day. Some of these patients may have had events attributable to recent prior hospitalizations and should have received VTE prophylaxis. Second, we considered preventive measures applied at least 24 hours prior to PE to be acceptable evidence of prevention, potentially neglecting prior periods without treatment that might confer increased risk. Bias due to either of these limitations could exaggerate the compliance rates we report. Finally, the retrospective design of this study did not allow for consistent assessments of whether patients had the risk factor of immobility. Nevertheless, immobility was obvious for the 10 patients with PE who had no prior anticoagulation, all of whom had 2 or more risk factors.
Despite an acknowledged need for improvements in clinical practice, past efforts have had mixed results. For instance, in 1 study at a hospital with a well‐established EMR, computer alerts led to substantial improvement in the use of preventive measures and in VTE outcomes, but overall compliance remained low.19 On the other hand, a multidisciplinary approach can achieve marked reductions in preventable VTE events.20 Key elements of such an approach are a simplified risk assessment tool and concurrent monitoring of patient treatments and outcomes. The Agency for Healthcare Research and Quality has recently published a guide that outlines strategies for achieving breakthrough levels of improvement in the prevention of VTE.21
In conclusion, this population‐based study of hospitalized veterans with PE or at risk for VTE found compliance comparable to rates in published reports. Missed opportunities for prevention included inappropriate and inadequate interventions. Using discharge diagnoses to monitor the occurrence of inpatient PE is of limited value, and efficient performance improvement efforts may require ongoing concurrent review.
Acknowledgements
The authors thank Greg Maynard, MD, MS for advice on study design, and Deborah Howard, RN, for assistance with medical record review.
- ,,.Prevention of venous thromboembolism. The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126:338S–400S.
- ,,,.Thromboprophylaxis rates in US medical centers: success or failure?J Thromb Haemost.2007;5:1610–1616.
- .Preventing venous thromboembolism in surgical patients.Cleve Clin J Med.2006;73:S88–S94.
- ,.Prevention of venous thromboembolism among hospitalized medical patients.Circulation.2005;111:e1–e3.
- ,,.Quality of care for the treatment of acute medical conditions in US hospitals.Arch Intern Med.2006;166:2511–2517.
- Association of American Medical Colleges (AAMC). Council of Teaching Hospitals and Health Systems (COTH). Available at: http://www.aamc. org/members/coth. Accessed August2009.
- Contraindications are those described in the Institute for Clinical Systems Improvement Health Care Guideline: Venous Thromboembolism Prophylaxis. 4th ed. June 2007, pp 13–14. Available at: http://www. icsi.org/guidelines_and_more/gl_os_prot/cardiovascular/venous_thromboem bolism_prophylaxis/venous_thromboembolism_prophylaxis_5.html. Accessed August2009.
- ,,, et al.Prevention and treatment of venous thromboembolism. International Consensus Statement.Int Angiol.2006;25:101–161.
- ,.Designing Clinical Research.Baltimore, MD:Williams 1988.
- ,,. Statistical Methods for Rates and Proportions.3rd ed.Hoboken, NJ:Wiley‐Interscience;2003;28,54.
- ,,.New onset of venous thromboembolism among hospitalized patients at Brigham and Women's Hospital is caused more often by prophylaxis failure than by withholding treatment.Chest.2000;118;1680–1684.
- ,,.Prophylaxis against venous thromboembolism in acutely ill medical patients: an observational study.Pharmacotherapy.2006;26:1086–1090.
- ,,.Hospital‐acquired venous thromboembolism and prophylaxis in an integrated hospital delivery system.J Clin Pharm Ther.2006;31:455–459.
- ,;DVT FREE Steering Committee.A prospective study of 5,451 patients with ultrasound‐confirmed deep vein thrombosis.Am J Cardiol.2004;15:259–262.
- ,,, et al.Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism.Chest.2007;132:936–945.
- ,,, et al.Venous thromboembolism risk and prophylaxis in the acute hospital care setting.Lancet.2008;371:387–394.
- .Medical admission order sets to improve deep vein thrombosis prevention: a model for others or a prescription for mediocrity?J Hosp Med.2009;4:77–80.
- ,,,,,.Prevention of venous thromboembolism in the cancer surgery patient.Cleve Clin J Med.2008;75(suppl 3):S17–S26.
- ,,, et al.Electronic alerts for hospitalized high‐VTE risk patients not receiving prophylaxis: a cohort study.J Thromb Thrombolysis.2008;25:146–150.
- ,,, et al. Prevention of hospital‐acquired venous thromboembolism: prospective validation of a VTE risk assessment model and protocol. Society of Hospital Medicine 2008 National Meeting. Electronic citation abstract #52, page 29. Available at: http://www.hospital medicine.org/Paperless2008/PDFs/Additional_Info/SHM08_Abstracts.pdf. Accessed August2009
- ,.Preventing Hospital‐Acquired Venous Thromboembolism: A Guide for Effective Quality Improvement. AHRQ Publication No. 08–0075.Rockville, MD:Agency for Healthcare Research and Quality;2008.
- ,,.Prevention of venous thromboembolism. The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126:338S–400S.
- ,,,.Thromboprophylaxis rates in US medical centers: success or failure?J Thromb Haemost.2007;5:1610–1616.
- .Preventing venous thromboembolism in surgical patients.Cleve Clin J Med.2006;73:S88–S94.
- ,.Prevention of venous thromboembolism among hospitalized medical patients.Circulation.2005;111:e1–e3.
- ,,.Quality of care for the treatment of acute medical conditions in US hospitals.Arch Intern Med.2006;166:2511–2517.
- Association of American Medical Colleges (AAMC). Council of Teaching Hospitals and Health Systems (COTH). Available at: http://www.aamc. org/members/coth. Accessed August2009.
- Contraindications are those described in the Institute for Clinical Systems Improvement Health Care Guideline: Venous Thromboembolism Prophylaxis. 4th ed. June 2007, pp 13–14. Available at: http://www. icsi.org/guidelines_and_more/gl_os_prot/cardiovascular/venous_thromboem bolism_prophylaxis/venous_thromboembolism_prophylaxis_5.html. Accessed August2009.
- ,,, et al.Prevention and treatment of venous thromboembolism. International Consensus Statement.Int Angiol.2006;25:101–161.
- ,.Designing Clinical Research.Baltimore, MD:Williams 1988.
- ,,. Statistical Methods for Rates and Proportions.3rd ed.Hoboken, NJ:Wiley‐Interscience;2003;28,54.
- ,,.New onset of venous thromboembolism among hospitalized patients at Brigham and Women's Hospital is caused more often by prophylaxis failure than by withholding treatment.Chest.2000;118;1680–1684.
- ,,.Prophylaxis against venous thromboembolism in acutely ill medical patients: an observational study.Pharmacotherapy.2006;26:1086–1090.
- ,,.Hospital‐acquired venous thromboembolism and prophylaxis in an integrated hospital delivery system.J Clin Pharm Ther.2006;31:455–459.
- ,;DVT FREE Steering Committee.A prospective study of 5,451 patients with ultrasound‐confirmed deep vein thrombosis.Am J Cardiol.2004;15:259–262.
- ,,, et al.Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism.Chest.2007;132:936–945.
- ,,, et al.Venous thromboembolism risk and prophylaxis in the acute hospital care setting.Lancet.2008;371:387–394.
- .Medical admission order sets to improve deep vein thrombosis prevention: a model for others or a prescription for mediocrity?J Hosp Med.2009;4:77–80.
- ,,,,,.Prevention of venous thromboembolism in the cancer surgery patient.Cleve Clin J Med.2008;75(suppl 3):S17–S26.
- ,,, et al.Electronic alerts for hospitalized high‐VTE risk patients not receiving prophylaxis: a cohort study.J Thromb Thrombolysis.2008;25:146–150.
- ,,, et al. Prevention of hospital‐acquired venous thromboembolism: prospective validation of a VTE risk assessment model and protocol. Society of Hospital Medicine 2008 National Meeting. Electronic citation abstract #52, page 29. Available at: http://www.hospital medicine.org/Paperless2008/PDFs/Additional_Info/SHM08_Abstracts.pdf. Accessed August2009
- ,.Preventing Hospital‐Acquired Venous Thromboembolism: A Guide for Effective Quality Improvement. AHRQ Publication No. 08–0075.Rockville, MD:Agency for Healthcare Research and Quality;2008.
Copyright © 2010 Society of Hospital Medicine