User login
5 Must-Do’s for Hospitalists in 2010
For the ambitious hospitalist, 2010 will be an eventful year. The next 12 months will be filled with new and exciting opportunities to establish credentials in the specialty and to find venues for continuing education.
But the time to start is now.
The new Recognition of Focused Practice (RFP) in Hospital Medicine application process begins this month and, if last year is any indicator, SHM’s annual conference in April will sell out well in advance.
Begin the RFP Application Process
Don’t wait for HM10 to begin applying for the RFP in HM designation. American Board of Internal Medicine (ABIM)-certified diplomates don’t have to wait for their maintenance of certification (MOC) to expire in order to apply. Instead, typical hospitalists can begin the process if they:
- Have completed training in internal medicine;
- Are certified in internal medicine; and
- Have engaged for at least three years in a practice that focuses primarily on HM.
Award-winning HOSPITAL CEO is Featured SPEAKER at HM10

For Paul Levy, addressing hospitalists as a featured presenter at HM10 in Washington, D.C., makes perfect sense. As president and CEO of Beth Israel Deaconess Medical Center in Boston, he sees firsthand the value hospitalists bring to patients and the 621-bed academic hospital.
“We place a heavy emphasis on eliminating harm, and hospitalists are key in that effort,” Levy says. “They have constant contact with the systems and patients on the floor, and they’re people we count on to come up with solutions.”
Though the conference is months away, Levy already knows the general focus of his presentation: eliminating preventable harm. He plans to talk about the medical center’s progress in reducing preventable harm, ideas for the future, the role of transparency, and different approaches to process improvement.
Given that Beth Israel Deaconess Medical Center was one of three AHA-McKesson Quest for Quality Prize honorees in 2009, he will be speaking from a position of authority. “It’s really nice to be recognized for what we’re doing, but we’re only taking baby steps in elimination of harm and process improvement,” he says. “We take those awards as encouragement to do even better.”
For 2010, Levy predicts an increased role for hospitalists in new programs at Beth Israel Deaconess. In particular, Project GRACE, a “geriatric bundle” of care for elderly patients that pairs the medical center’s gerontologists with hospitalists, was in pilot stage in 2009 and will be rolled out in full this year.
Paul Levy’s blog, Running a Hospital, is available at http://runningahospital.blogspot.com.
Hospitalists who satisfy those requirements can begin the process this month by developing and submitting attestations that demonstrate their focus on HM and their commitment to the specialty. The certification process requires that the hospitalist and a senior executive at his or her hospital each submit an attestation.
Once the attestations are submitted and accepted, ABIM will provide more information on the exam, which is scheduled for October. Registration for the exam will begin in May. Detailed information about the application process will be presented at the ABIM pre-course at HM10. For more information, visit www.abim.org.
Register for HM10
With an agenda packed with networking events, eight pre-courses and more than 90 educational sessions, Hospital Medicine 2010 in Washington, D.C., promises to be the event for hospitalists of all stripes. The conference begins with pre-courses on Thursday, April 8, and runs through Sunday, April 11.
This year’s pre-courses will cover a range of topics, from critical care to practice management and quality improvement (QI). New hospitalists can receive an introduction to the specialty at “Early Career Hospitalist: Skills for Success,” while physicians certified by ABIM can participate in the interactive MOC learning sessions. The ABIM session will include information about the inaugural MOC through the RFP in HM.
SHM’s annual meeting kicks off on Friday, April 9, with featured speaker Paul Levy, president and CEO of Beth Israel Deaconess Medical Center in Boston. His presentation will focus on the role hospitalists will play in the hospital of the future.
On Sunday, HM thought-leader Robert Wachter, MD, FHM, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World, will share his thoughts about how healthcare reform will change HM, and vice versa.
Sandwiched in between will be sessions on every area of hospital medicine, including:
- Quality improvement;
- Hospitalist practice management;
- New research in HM;
- Clinical practice; and
- Pediatric HM.
For more information, visit the HM10 section of www.hospitalmedicine.org.
Apply for FHM, SFHM
The deadline for SHM Fellow applications is Jan. 15. This year, in addition to new fellows, the first class of senior fellows (SFHM) will be inducted at HM10.
More than 500 hospitalists were a part of the inaugural class of fellows introduced at HM09. Since then, the letters have begun to pop up everywhere. Hospitalists across the country are attaching “FHM” to their name and credentials for additional prestige and credibility among their peers.
Based on SHM’s Core Competencies in Hospital Medicine, the FHM and SFHM designations represent a hospitalist’s commitment to excellence, systems change, and QI. In addition to demonstrated experience in teamwork, leadership, and QI (scored on a point-based system), all qualified candidates must have:
- Five years completed as a practicing hospitalist;
- No disciplinary action that resulted in the suspension or revocation of credentials or license within five years; and
- Two SHM member endorsements.
Requirements for the SFHM designation are similar to that of FHM but require additional experience in leadership. In addition to using the SFHM designation, all fellows receive a personalized certificate from SHM, a listing on the SHM Web site, and a discount on SHM events and materials.
For more information, visit www. hospitalmedicine.org/fellows.
Get Involved in Advocacy
The future of healthcare delivery is being formed now. And it will change how every provider works.
Hospitalists will play a major role in healthcare reform, but it doesn’t end there. The extent of their impact will depend on their knowledge of the issues and their ability to reach out to members of Congress and others in government.
SHM’s Advocacy section at www.hospitalmedicine.org provides members all the information and resources to make a real difference, including:
- Resources from SHM, including position papers and public letters to government officials;
- Resources from other influential healthcare organizations;
- Monthly updates on legislation and other government activities that affect hospital medicine; and
- SHM’s Legislative Action Center.
For hospitalists new to public advocacy, SHM’s Legislative Action Center is a one-stop shop for learning more about the most pressing policy issues affecting HM. In less than 10 minutes, visitors can get up to speed on the issues and contact their members of Congress with a customizable e-mail or personal note. To get involved, visit www.hosp italmedicine.org/advocacy.
SHM Junior Faculty Development Award
For junior hospitalist faculty at academic hospital centers, making ends meet as you apply for such research grants as the U.S. Department of Health and Human Services K Awards or the Veterans Administration’s Career Development Awards can be daunting or even prohibitive.
SHM is launching a program to assist two junior academic hospitalists: the SHM Junior Faculty Development Award. Two successful applicants will be awarded $25,000 a year for two years, and will receive mentoring from senior SHM faculty and the recipients’ host institutions.
To qualify, applicants must have an MD or a DO degree, have completed or be in the final year of a two- to three-year HM fellowship (or an equivalent post-residency program), and submit a research project proposal on a topic related to HM (e.g., QI, patient safety, or critical care). Full eligibility criteria are included in the request for application (RFA).
The program has two main goals: The new award aims to not only promote promising young academic hospitalists in a critical juncture of their careers, but it also aims to generate peer-reviewed research that will help all hospitalists to better practice in the specialty.
The deadline for submissions is Feb. 15. Winners will be notified April 5.
For details about the SHM Junior Faculty Development Award, including the RFA, contact Claudia Stahl at [email protected]. TH
Brendon Shank is a freelance writer based in Philadelphia.
For the ambitious hospitalist, 2010 will be an eventful year. The next 12 months will be filled with new and exciting opportunities to establish credentials in the specialty and to find venues for continuing education.
But the time to start is now.
The new Recognition of Focused Practice (RFP) in Hospital Medicine application process begins this month and, if last year is any indicator, SHM’s annual conference in April will sell out well in advance.
Begin the RFP Application Process
Don’t wait for HM10 to begin applying for the RFP in HM designation. American Board of Internal Medicine (ABIM)-certified diplomates don’t have to wait for their maintenance of certification (MOC) to expire in order to apply. Instead, typical hospitalists can begin the process if they:
- Have completed training in internal medicine;
- Are certified in internal medicine; and
- Have engaged for at least three years in a practice that focuses primarily on HM.
Award-winning HOSPITAL CEO is Featured SPEAKER at HM10
For Paul Levy, addressing hospitalists as a featured presenter at HM10 in Washington, D.C., makes perfect sense. As president and CEO of Beth Israel Deaconess Medical Center in Boston, he sees firsthand the value hospitalists bring to patients and the 621-bed academic hospital.
“We place a heavy emphasis on eliminating harm, and hospitalists are key in that effort,” Levy says. “They have constant contact with the systems and patients on the floor, and they’re people we count on to come up with solutions.”
Though the conference is months away, Levy already knows the general focus of his presentation: eliminating preventable harm. He plans to talk about the medical center’s progress in reducing preventable harm, ideas for the future, the role of transparency, and different approaches to process improvement.
Given that Beth Israel Deaconess Medical Center was one of three AHA-McKesson Quest for Quality Prize honorees in 2009, he will be speaking from a position of authority. “It’s really nice to be recognized for what we’re doing, but we’re only taking baby steps in elimination of harm and process improvement,” he says. “We take those awards as encouragement to do even better.”
For 2010, Levy predicts an increased role for hospitalists in new programs at Beth Israel Deaconess. In particular, Project GRACE, a “geriatric bundle” of care for elderly patients that pairs the medical center’s gerontologists with hospitalists, was in pilot stage in 2009 and will be rolled out in full this year.
Paul Levy’s blog, Running a Hospital, is available at http://runningahospital.blogspot.com.
Hospitalists who satisfy those requirements can begin the process this month by developing and submitting attestations that demonstrate their focus on HM and their commitment to the specialty. The certification process requires that the hospitalist and a senior executive at his or her hospital each submit an attestation.
Once the attestations are submitted and accepted, ABIM will provide more information on the exam, which is scheduled for October. Registration for the exam will begin in May. Detailed information about the application process will be presented at the ABIM pre-course at HM10. For more information, visit www.abim.org.
Register for HM10
With an agenda packed with networking events, eight pre-courses and more than 90 educational sessions, Hospital Medicine 2010 in Washington, D.C., promises to be the event for hospitalists of all stripes. The conference begins with pre-courses on Thursday, April 8, and runs through Sunday, April 11.
This year’s pre-courses will cover a range of topics, from critical care to practice management and quality improvement (QI). New hospitalists can receive an introduction to the specialty at “Early Career Hospitalist: Skills for Success,” while physicians certified by ABIM can participate in the interactive MOC learning sessions. The ABIM session will include information about the inaugural MOC through the RFP in HM.
SHM’s annual meeting kicks off on Friday, April 9, with featured speaker Paul Levy, president and CEO of Beth Israel Deaconess Medical Center in Boston. His presentation will focus on the role hospitalists will play in the hospital of the future.
On Sunday, HM thought-leader Robert Wachter, MD, FHM, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World, will share his thoughts about how healthcare reform will change HM, and vice versa.
Sandwiched in between will be sessions on every area of hospital medicine, including:
- Quality improvement;
- Hospitalist practice management;
- New research in HM;
- Clinical practice; and
- Pediatric HM.
For more information, visit the HM10 section of www.hospitalmedicine.org.
Apply for FHM, SFHM
The deadline for SHM Fellow applications is Jan. 15. This year, in addition to new fellows, the first class of senior fellows (SFHM) will be inducted at HM10.
More than 500 hospitalists were a part of the inaugural class of fellows introduced at HM09. Since then, the letters have begun to pop up everywhere. Hospitalists across the country are attaching “FHM” to their name and credentials for additional prestige and credibility among their peers.
Based on SHM’s Core Competencies in Hospital Medicine, the FHM and SFHM designations represent a hospitalist’s commitment to excellence, systems change, and QI. In addition to demonstrated experience in teamwork, leadership, and QI (scored on a point-based system), all qualified candidates must have:
- Five years completed as a practicing hospitalist;
- No disciplinary action that resulted in the suspension or revocation of credentials or license within five years; and
- Two SHM member endorsements.
Requirements for the SFHM designation are similar to that of FHM but require additional experience in leadership. In addition to using the SFHM designation, all fellows receive a personalized certificate from SHM, a listing on the SHM Web site, and a discount on SHM events and materials.
For more information, visit www. hospitalmedicine.org/fellows.
Get Involved in Advocacy
The future of healthcare delivery is being formed now. And it will change how every provider works.
Hospitalists will play a major role in healthcare reform, but it doesn’t end there. The extent of their impact will depend on their knowledge of the issues and their ability to reach out to members of Congress and others in government.
SHM’s Advocacy section at www.hospitalmedicine.org provides members all the information and resources to make a real difference, including:
- Resources from SHM, including position papers and public letters to government officials;
- Resources from other influential healthcare organizations;
- Monthly updates on legislation and other government activities that affect hospital medicine; and
- SHM’s Legislative Action Center.
For hospitalists new to public advocacy, SHM’s Legislative Action Center is a one-stop shop for learning more about the most pressing policy issues affecting HM. In less than 10 minutes, visitors can get up to speed on the issues and contact their members of Congress with a customizable e-mail or personal note. To get involved, visit www.hosp italmedicine.org/advocacy.
SHM Junior Faculty Development Award
For junior hospitalist faculty at academic hospital centers, making ends meet as you apply for such research grants as the U.S. Department of Health and Human Services K Awards or the Veterans Administration’s Career Development Awards can be daunting or even prohibitive.
SHM is launching a program to assist two junior academic hospitalists: the SHM Junior Faculty Development Award. Two successful applicants will be awarded $25,000 a year for two years, and will receive mentoring from senior SHM faculty and the recipients’ host institutions.
To qualify, applicants must have an MD or a DO degree, have completed or be in the final year of a two- to three-year HM fellowship (or an equivalent post-residency program), and submit a research project proposal on a topic related to HM (e.g., QI, patient safety, or critical care). Full eligibility criteria are included in the request for application (RFA).
The program has two main goals: The new award aims to not only promote promising young academic hospitalists in a critical juncture of their careers, but it also aims to generate peer-reviewed research that will help all hospitalists to better practice in the specialty.
The deadline for submissions is Feb. 15. Winners will be notified April 5.
For details about the SHM Junior Faculty Development Award, including the RFA, contact Claudia Stahl at [email protected]. TH
Brendon Shank is a freelance writer based in Philadelphia.
For the ambitious hospitalist, 2010 will be an eventful year. The next 12 months will be filled with new and exciting opportunities to establish credentials in the specialty and to find venues for continuing education.
But the time to start is now.
The new Recognition of Focused Practice (RFP) in Hospital Medicine application process begins this month and, if last year is any indicator, SHM’s annual conference in April will sell out well in advance.
Begin the RFP Application Process
Don’t wait for HM10 to begin applying for the RFP in HM designation. American Board of Internal Medicine (ABIM)-certified diplomates don’t have to wait for their maintenance of certification (MOC) to expire in order to apply. Instead, typical hospitalists can begin the process if they:
- Have completed training in internal medicine;
- Are certified in internal medicine; and
- Have engaged for at least three years in a practice that focuses primarily on HM.
Award-winning HOSPITAL CEO is Featured SPEAKER at HM10
For Paul Levy, addressing hospitalists as a featured presenter at HM10 in Washington, D.C., makes perfect sense. As president and CEO of Beth Israel Deaconess Medical Center in Boston, he sees firsthand the value hospitalists bring to patients and the 621-bed academic hospital.
“We place a heavy emphasis on eliminating harm, and hospitalists are key in that effort,” Levy says. “They have constant contact with the systems and patients on the floor, and they’re people we count on to come up with solutions.”
Though the conference is months away, Levy already knows the general focus of his presentation: eliminating preventable harm. He plans to talk about the medical center’s progress in reducing preventable harm, ideas for the future, the role of transparency, and different approaches to process improvement.
Given that Beth Israel Deaconess Medical Center was one of three AHA-McKesson Quest for Quality Prize honorees in 2009, he will be speaking from a position of authority. “It’s really nice to be recognized for what we’re doing, but we’re only taking baby steps in elimination of harm and process improvement,” he says. “We take those awards as encouragement to do even better.”
For 2010, Levy predicts an increased role for hospitalists in new programs at Beth Israel Deaconess. In particular, Project GRACE, a “geriatric bundle” of care for elderly patients that pairs the medical center’s gerontologists with hospitalists, was in pilot stage in 2009 and will be rolled out in full this year.
Paul Levy’s blog, Running a Hospital, is available at http://runningahospital.blogspot.com.
Hospitalists who satisfy those requirements can begin the process this month by developing and submitting attestations that demonstrate their focus on HM and their commitment to the specialty. The certification process requires that the hospitalist and a senior executive at his or her hospital each submit an attestation.
Once the attestations are submitted and accepted, ABIM will provide more information on the exam, which is scheduled for October. Registration for the exam will begin in May. Detailed information about the application process will be presented at the ABIM pre-course at HM10. For more information, visit www.abim.org.
Register for HM10
With an agenda packed with networking events, eight pre-courses and more than 90 educational sessions, Hospital Medicine 2010 in Washington, D.C., promises to be the event for hospitalists of all stripes. The conference begins with pre-courses on Thursday, April 8, and runs through Sunday, April 11.
This year’s pre-courses will cover a range of topics, from critical care to practice management and quality improvement (QI). New hospitalists can receive an introduction to the specialty at “Early Career Hospitalist: Skills for Success,” while physicians certified by ABIM can participate in the interactive MOC learning sessions. The ABIM session will include information about the inaugural MOC through the RFP in HM.
SHM’s annual meeting kicks off on Friday, April 9, with featured speaker Paul Levy, president and CEO of Beth Israel Deaconess Medical Center in Boston. His presentation will focus on the role hospitalists will play in the hospital of the future.
On Sunday, HM thought-leader Robert Wachter, MD, FHM, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World, will share his thoughts about how healthcare reform will change HM, and vice versa.
Sandwiched in between will be sessions on every area of hospital medicine, including:
- Quality improvement;
- Hospitalist practice management;
- New research in HM;
- Clinical practice; and
- Pediatric HM.
For more information, visit the HM10 section of www.hospitalmedicine.org.
Apply for FHM, SFHM
The deadline for SHM Fellow applications is Jan. 15. This year, in addition to new fellows, the first class of senior fellows (SFHM) will be inducted at HM10.
More than 500 hospitalists were a part of the inaugural class of fellows introduced at HM09. Since then, the letters have begun to pop up everywhere. Hospitalists across the country are attaching “FHM” to their name and credentials for additional prestige and credibility among their peers.
Based on SHM’s Core Competencies in Hospital Medicine, the FHM and SFHM designations represent a hospitalist’s commitment to excellence, systems change, and QI. In addition to demonstrated experience in teamwork, leadership, and QI (scored on a point-based system), all qualified candidates must have:
- Five years completed as a practicing hospitalist;
- No disciplinary action that resulted in the suspension or revocation of credentials or license within five years; and
- Two SHM member endorsements.
Requirements for the SFHM designation are similar to that of FHM but require additional experience in leadership. In addition to using the SFHM designation, all fellows receive a personalized certificate from SHM, a listing on the SHM Web site, and a discount on SHM events and materials.
For more information, visit www. hospitalmedicine.org/fellows.
Get Involved in Advocacy
The future of healthcare delivery is being formed now. And it will change how every provider works.
Hospitalists will play a major role in healthcare reform, but it doesn’t end there. The extent of their impact will depend on their knowledge of the issues and their ability to reach out to members of Congress and others in government.
SHM’s Advocacy section at www.hospitalmedicine.org provides members all the information and resources to make a real difference, including:
- Resources from SHM, including position papers and public letters to government officials;
- Resources from other influential healthcare organizations;
- Monthly updates on legislation and other government activities that affect hospital medicine; and
- SHM’s Legislative Action Center.
For hospitalists new to public advocacy, SHM’s Legislative Action Center is a one-stop shop for learning more about the most pressing policy issues affecting HM. In less than 10 minutes, visitors can get up to speed on the issues and contact their members of Congress with a customizable e-mail or personal note. To get involved, visit www.hosp italmedicine.org/advocacy.
SHM Junior Faculty Development Award
For junior hospitalist faculty at academic hospital centers, making ends meet as you apply for such research grants as the U.S. Department of Health and Human Services K Awards or the Veterans Administration’s Career Development Awards can be daunting or even prohibitive.
SHM is launching a program to assist two junior academic hospitalists: the SHM Junior Faculty Development Award. Two successful applicants will be awarded $25,000 a year for two years, and will receive mentoring from senior SHM faculty and the recipients’ host institutions.
To qualify, applicants must have an MD or a DO degree, have completed or be in the final year of a two- to three-year HM fellowship (or an equivalent post-residency program), and submit a research project proposal on a topic related to HM (e.g., QI, patient safety, or critical care). Full eligibility criteria are included in the request for application (RFA).
The program has two main goals: The new award aims to not only promote promising young academic hospitalists in a critical juncture of their careers, but it also aims to generate peer-reviewed research that will help all hospitalists to better practice in the specialty.
The deadline for submissions is Feb. 15. Winners will be notified April 5.
For details about the SHM Junior Faculty Development Award, including the RFA, contact Claudia Stahl at [email protected]. TH
Brendon Shank is a freelance writer based in Philadelphia.
Article on Anniversary of Medical Errors Report Missed Key Points
Donald Berwick, MD, MPP, FRCP, is honest, forthright, and accurate, as always. Christine Cassel, MD, is correct: We need to change the culture in medical school. However, diagnostic errors aren’t “emerging” as a medical error—they’ve been with us all along.
I would point to Maureen Thiel as one example. She was the victim of repeated diagnostic errors in the late 1990s. Her widower, Bill Thiel, has been a patient-safety advocate ever since (www.maureensmission.org).
“Failure to rescue” is an emerging medical error. Lori Nerbonne of New Hampshire Patient Voices has a story of a failure to rescue that ultimately took her mother’s life.
Lewis Blackman, a healthy 15-year-old boy, died in 2000. He slowly bled to death over the course of several days after being admitted to the hospital for an elective procedure. I’m sure his mother, Helen Haskell, can share his story. She is the director of the Empowered Patient Coalition. You can find her and other advocates listed at www.empoweredpatientcoalition.org/patient-advocate-directory.
What’s missing from your November cover story, “Medical Mistakes, 10 Years Post-Op,” and the accompanying timeline is what really sparked the patient-safety movement. It was the 100,000 Lives Campaign in tandem with medical-error victims and their families. Unfortunately, those numbers have grown exponentially in recent years.
With the exception of Dr. Berwick and Johns Hopkins, our nation’s political and healthcare “leaders” have not taken the initiative with patient safety. And make no mistake: They have been pushed.
Dr. Berwick is leading. We are pushing.
“To Err is Human—To Delay is Deadly” is the message patient-safety advocates took to Washington on Nov. 17, 2009. We think the IOM report should be acted on before it’s commemorated. It should not be a surprise that patient-safety advocates were excluded from this article. We have been dismissed and ignored by the medical profession for years. Why is that? History should not overlook the substantial contribution made by the grassroots advocates.
Lisa Lindell,
Webster, Texas
Author, PULSE of America
Coalition state coordinator
Donald Berwick, MD, MPP, FRCP, is honest, forthright, and accurate, as always. Christine Cassel, MD, is correct: We need to change the culture in medical school. However, diagnostic errors aren’t “emerging” as a medical error—they’ve been with us all along.
I would point to Maureen Thiel as one example. She was the victim of repeated diagnostic errors in the late 1990s. Her widower, Bill Thiel, has been a patient-safety advocate ever since (www.maureensmission.org).
“Failure to rescue” is an emerging medical error. Lori Nerbonne of New Hampshire Patient Voices has a story of a failure to rescue that ultimately took her mother’s life.
Lewis Blackman, a healthy 15-year-old boy, died in 2000. He slowly bled to death over the course of several days after being admitted to the hospital for an elective procedure. I’m sure his mother, Helen Haskell, can share his story. She is the director of the Empowered Patient Coalition. You can find her and other advocates listed at www.empoweredpatientcoalition.org/patient-advocate-directory.
What’s missing from your November cover story, “Medical Mistakes, 10 Years Post-Op,” and the accompanying timeline is what really sparked the patient-safety movement. It was the 100,000 Lives Campaign in tandem with medical-error victims and their families. Unfortunately, those numbers have grown exponentially in recent years.
With the exception of Dr. Berwick and Johns Hopkins, our nation’s political and healthcare “leaders” have not taken the initiative with patient safety. And make no mistake: They have been pushed.
Dr. Berwick is leading. We are pushing.
“To Err is Human—To Delay is Deadly” is the message patient-safety advocates took to Washington on Nov. 17, 2009. We think the IOM report should be acted on before it’s commemorated. It should not be a surprise that patient-safety advocates were excluded from this article. We have been dismissed and ignored by the medical profession for years. Why is that? History should not overlook the substantial contribution made by the grassroots advocates.
Lisa Lindell,
Webster, Texas
Author, PULSE of America
Coalition state coordinator
Donald Berwick, MD, MPP, FRCP, is honest, forthright, and accurate, as always. Christine Cassel, MD, is correct: We need to change the culture in medical school. However, diagnostic errors aren’t “emerging” as a medical error—they’ve been with us all along.
I would point to Maureen Thiel as one example. She was the victim of repeated diagnostic errors in the late 1990s. Her widower, Bill Thiel, has been a patient-safety advocate ever since (www.maureensmission.org).
“Failure to rescue” is an emerging medical error. Lori Nerbonne of New Hampshire Patient Voices has a story of a failure to rescue that ultimately took her mother’s life.
Lewis Blackman, a healthy 15-year-old boy, died in 2000. He slowly bled to death over the course of several days after being admitted to the hospital for an elective procedure. I’m sure his mother, Helen Haskell, can share his story. She is the director of the Empowered Patient Coalition. You can find her and other advocates listed at www.empoweredpatientcoalition.org/patient-advocate-directory.
What’s missing from your November cover story, “Medical Mistakes, 10 Years Post-Op,” and the accompanying timeline is what really sparked the patient-safety movement. It was the 100,000 Lives Campaign in tandem with medical-error victims and their families. Unfortunately, those numbers have grown exponentially in recent years.
With the exception of Dr. Berwick and Johns Hopkins, our nation’s political and healthcare “leaders” have not taken the initiative with patient safety. And make no mistake: They have been pushed.
Dr. Berwick is leading. We are pushing.
“To Err is Human—To Delay is Deadly” is the message patient-safety advocates took to Washington on Nov. 17, 2009. We think the IOM report should be acted on before it’s commemorated. It should not be a surprise that patient-safety advocates were excluded from this article. We have been dismissed and ignored by the medical profession for years. Why is that? History should not overlook the substantial contribution made by the grassroots advocates.
Lisa Lindell,
Webster, Texas
Author, PULSE of America
Coalition state coordinator
Growth Spurt
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.1,2
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture—it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
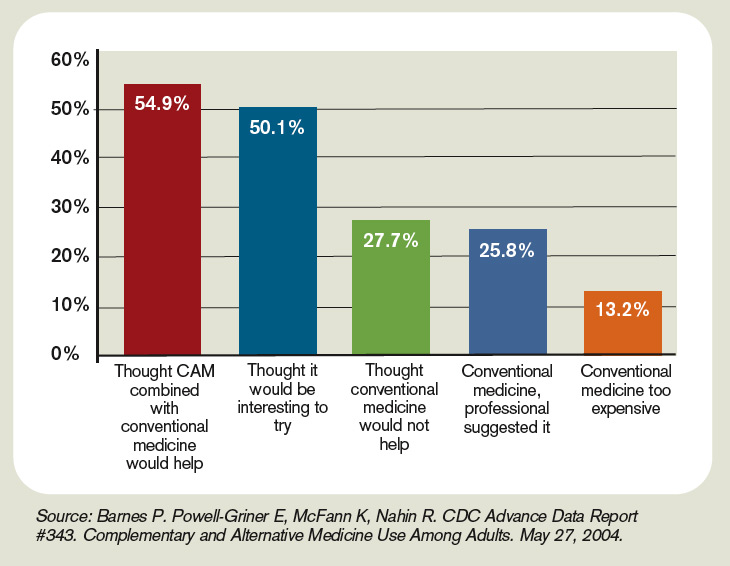
Even if your hospital does not offer complementary and alternative medicine (CAM), your patients are using CAM at ever-increasing rates. In 1993, 34% of Americans reported using some type of CAM (e.g., supplements, massage therapy, prayer, and so on). That number has almost doubled to 62%.3 Americans spend $47 billion a year—of their own money—for CAM therapies, chiropractors, acupuncturists, and massage therapists. And older patients with chronic conditions—the kind of patient hospitalists are most familiar with—tend to try CAM more than younger patients.4
These trends can directly affect hospitalists’ treatment decisions, but they also play a part in how you establish communication and trust with your patients, and how you keep your patients safe from adverse drug interactions. According to the National Academy of Sciences, in order to effectively counsel patients and ensure high-quality comprehensive care, conventional professionals need more CAM-related education.5


—Suzanne Bertisch, MD, MPH, fellow, Harvard Medical School’s Osher Research Center
Complementary Medicine: Online Resources

- National Center for Complementary and Alternative Medicine: http://nccam.nih.gov
- Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center’s About Herbs: www.mskcc.org/mskcc/html/11570.cfm
- Natural Standard: www.naturalstandard.com
- The M.D. Anderson Cancer Center’s Complementary/Integrative Medicine Education Resources: www.mdanderson.org/departments/CIMER
What Trends Show
In 2007, according to the American Hospital Association, 20.8% of community hospitals offered some type of care or treatment not based on traditional Western allopathic medicine. That’s up from 8.6% of reporting hospitals that offered those services in 1998.
The 1990s saw rapid growth of integrative medicine centers at major research institutions, and the majority of U.S. cancer centers now offer some form of complementary therapy, says Barrie R. Cassileth, MS, PhD, the Laurance S. Rockefeller Chair in Integrative Medicine and chief of the Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center in New York City.
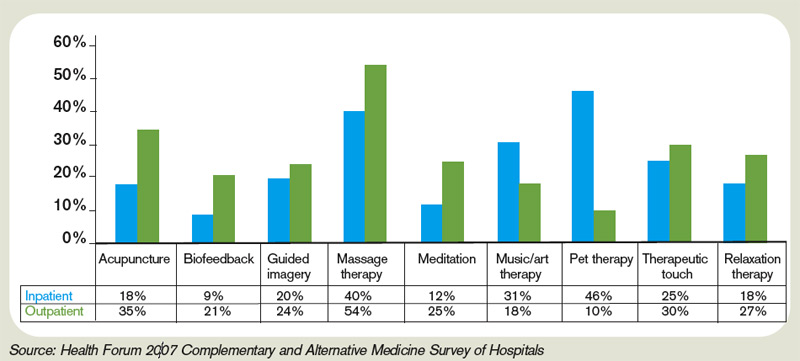
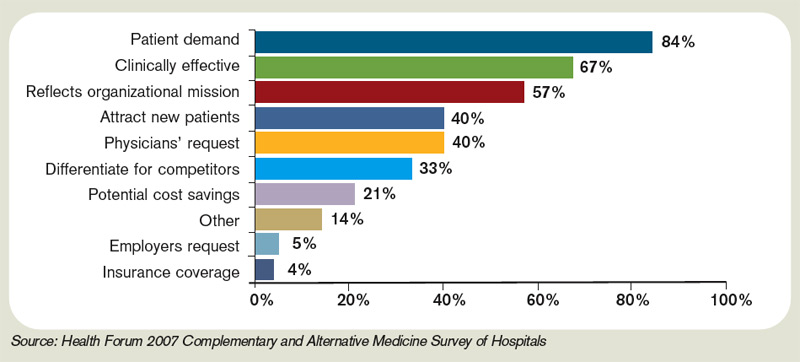
The 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals reported that complementary programs are more common in urban rather than rural hospitals; services vary by hospital size (see Figure 2, above); and the top six modalities offered on an inpatient basis are pet therapy, massage therapy, music/art therapy, guided imagery, acupuncture, and reiki (see “Glossary of Complementary Terms,” above). Eighty-four percent of hospitals offer complementary services due to patient demand, the survey showed.
Joseph Ming-Wah Li, MD, FHM, SHM board member and assistant professor of medicine at Harvard Medical School and director of the hospital medicine program and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston, doesn’t see a problem with modalities that can make his patients feel better. Patients at his hospital have access to pet therapy, massage, and acupuncture. “I don’t think these modalities hurt our patients, and there is very little downside, except for potential cost,” says Dr. Li, an SHM board member. “What’s not clear is whether these therapies work or not.”
What’s in a Name?
Numerous therapies and modalities crowd under the CAM umbrella, but most experts classify “complementary” modalities as those used in conjunction with conventional medicine to mitigate symptoms of disease or treatment, whereas “alternative” connotes therapies claiming to treat or cure the underlying disease. Some harmful, dangerous, and dishonest practices fall into the “alternative” category, such as Hulda Clark’s “Zapper” device, which was promoted as a cure for liver flukes, something she says cause everything from diabetes to heart disease. (For more on questionable practices, visit www.quackwatch.com or the National Council Against Health Fraud’s Web site at www.ncahf.org.)
The National Institutes of Health’s National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of “diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” Dr. Cassileth says the conflation of “complementary and alternative” into one neat acronym—CAM—causes confusion among patients and medical professionals. NCCAM will be changing its name soon, she says, to the National Center for Integrative Medicine, emphasizing the use of adjunctive modalities along with conventional medical treatments.
Hospitalist Suzanne Bertisch, MD, MPH, recently completed a research fellowship at Harvard Medical School’s Osher Research Center. She explains that integrative medicine uses a macro model of health, claiming a middle ground between the traditional, allopathic model of treating disease.
All Kinds of Evidence
Twenty years of complementary medicine research has yielded some information about safety—namely, what works and what doesn’t. For example, saw palmetto has not panned out as an effective treatment for benign prostatic hyperplasia; St. John’s wort, useful for mild depression, interferes with many medications, including cyclosporine and warfarin, and should be avoided at least five days prior to surgery.7,8
Since NCCAM’s inception in October 1998, its research portfolio has stirred debate in the scientific community. Part of the disagreement stems from the difficulty of fitting multidimensional interventions, some of which are provider-dependent (e.g., massage or acupuncture), into the gold standard of the randomized, double-blind, placebo-controlled trial, explains Darshan Mehta, MD, MPH, associate director of medical education at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. The manner in which the effectiveness of integrative techniques is assessed requires a higher sophistication of systems research, Dr. Mehta says.
“The way we construe evidence needs to change,” she adds.
Likely to Expand
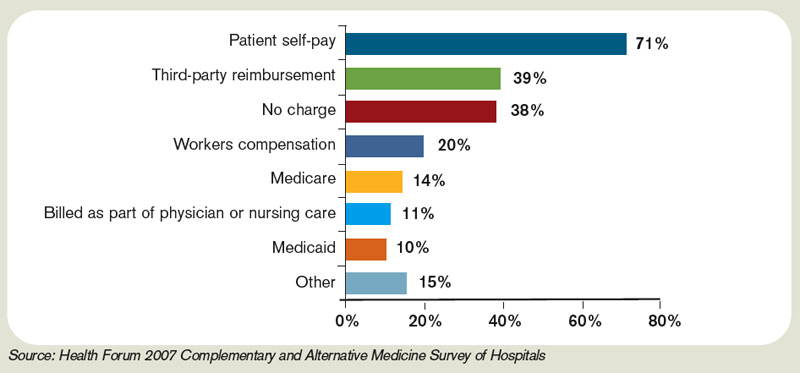
Most private health plans do not cover complementary services, although Medicare and numerous insurance plans will reimburse treatment in conjunction with physical therapy (e.g., massage) in the outpatient setting. Twenty-three states cover chiropractic care under Medicaid, and Medicare has begun to assess the cost-effectiveness of including acupuncture—especially for postoperative and chemotherapy-associated nausea and vomiting—in its benefits package.9 Other modalities, ranging from aromatherapy to guided imagery training, are paid for largely out-of-pocket.10
Dr. Rakel notes that the delivery of integrative medicine services at UW entails conversations with patients about out-of-pocket payments. “It can pose a barrier to the clinician-patient relationship if you give them acupuncture to help with their chemotherapy-induced nausea and then ask for their credit card,” he says.
Hospitalist Preparation
Most complementary therapies are currently offered on an outpatient basis. Because of this trend, and because they deal with acute conditions, hospitalists are less likely to be involved with complementary or integrative medicine services, says Beth Israel Deaconess Medical Center hospitalist Andrew C. Ahn, MD, MPH. But that’s not to say complementary medicine is something hospitalists should ignore; patients arrive at the hospital with CAM regimens in tow. It’s the No. 1 reason, Dr. Ahn says, hospitalists should be knowledgeable and exposed to CAM therapies.
Physicians must understand patient patterns and preferences regarding allopathic and complementary medicine, says Sita Ananth, MHA, director of knowledge services and optimal healing environments at the Samueli Institute in Alexandria, Va., and author of the 2007 AHA report. She points to a 2006 survey conducted by AARP and NCCAM that found almost 70% of respondents did not tell their physicians about their complementary medicine approaches. These patients are within the age range most likely to be cared for by hospitalists, and failure to communicate about complementary treatment, such as supplemental vitamin use, could lead to safety issues. Moreover, without complete disclosure, the patient-physician relationship might not be as open as possible, Dr. Ananth says.
Many acute-care hospitalists do not have formal dietary supplement policies, and less than half of U.S. children’s hospitals require documentation of a check for drug or dietary supplement interaction.11,12 As a safety issue, it is always incumbent on hospitalists, says Dr. Li, to ask about any supplements or therapies patients are trying on their own as part of the history and physical examination. The policy at Memorial Sloan-Kettering Cancer Center, Dr. Cassileth says, is that patients on chemotherapy or who are undergoing radiation or facing surgery must avoid herbal dietary supplements.
Beyond Safety
Dr. Bertisch advises hospitalists to pose questions about complementary therapies in an open manner, avoiding antagonistic discussions. “Even when I disagree, I try to guide them to issues about safety and nonsafety, and coax in my concerns,” she says. “The most challenging part about complementary medicine is that patients’ beliefs in these therapies may be so strong that even if the doctor says it won’t work, that will not necessarily change that belief.” A 2001 study in the Archives of Internal Medicine revealed that 70% of respondents would continue to take supplements even if a major study or their physician told them they didn’t work.13
The attraction to complementary medicine often reflects patients’ preferences for a holistic approach to health, says Dr. Ahn, or it may emanate from traditions carried with them from their country of origin. “Once you do understand their reasons for using CAM, then the patient-physician relationship can be significantly strengthened,” he says. With nearly two-thirds of Americans using some form of CAM, hospitalists need to engage in this dialogue.
Dr. Rakel agrees understanding patient culture is vital to uncovering useful information. “Most clinicians would agree that if we can match a therapy to the patient culture and belief system, we are more likely to get buy-in from the patient,” he says.
Dr. Mehta also is a clinical instructor of medicine at Harvard Medical School. He teaches his residents to educate themselves about credentialing, certification, and licensure of complementary providers. He also asks them to maintain an open mind. He says the most important preparation for hospitalists right now is to help educate their patients to be more proactive in their own healthcare. “An engaged patient,” he says, “is better than a disengaged patient.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Deng G, Cassileth BR, Yeung KS. Complementary therapies for cancer-related symptoms. J Support Oncol. 2004;2(5):419-426.
- Kahn ST, Johnstone PA. Management of xerostomia related to radiotherapy for head and neck cancer. Oncology. 2005;19(14):1827-1832.
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;27(343):1-19.
- Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280(18):1569-1575.
- Committee on the Use of Complementary and Alternative Medicine by the American Public. Complementary and Alternative Medicine in the United States. Washington, D.C: National Academies Press; 2005.
- Ananth S. 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals. Health Forum LLC. 2008.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-566.
- Bauer BA. The herbal hospitalist. The Hospitalist. 2006;10(2);16-17.
- Ananth S. Applying integrative healthcare. Explore. 2009;5(2):119-120.
- Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med. 1993;328:246-52
- Bassie KL, Witmer DR, Pinto B, Bush C, Clark J, Deffenbaugh J Jr. National survey of dietary supplement policies in acute care facilities. Am J Health Syst Pharm. 2006;63(1):65-70.
- Gardiner P, Phillips RS, Kemper KJ, Legedza A, Henlon S, Woolf AD. Dietary supplements: inpatient policies in US children’s hospitals. Pediatrics. 2008;121(4):e775-781.
- Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE. Americans’ views on the use and regulation of dietary supplements. Arch Intern Med. 2001;161(6):805-810.
Top Image Source: TETRA IMAGES
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.1,2
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture—it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
Even if your hospital does not offer complementary and alternative medicine (CAM), your patients are using CAM at ever-increasing rates. In 1993, 34% of Americans reported using some type of CAM (e.g., supplements, massage therapy, prayer, and so on). That number has almost doubled to 62%.3 Americans spend $47 billion a year—of their own money—for CAM therapies, chiropractors, acupuncturists, and massage therapists. And older patients with chronic conditions—the kind of patient hospitalists are most familiar with—tend to try CAM more than younger patients.4
These trends can directly affect hospitalists’ treatment decisions, but they also play a part in how you establish communication and trust with your patients, and how you keep your patients safe from adverse drug interactions. According to the National Academy of Sciences, in order to effectively counsel patients and ensure high-quality comprehensive care, conventional professionals need more CAM-related education.5
—Suzanne Bertisch, MD, MPH, fellow, Harvard Medical School’s Osher Research Center
Complementary Medicine: Online Resources
- National Center for Complementary and Alternative Medicine: http://nccam.nih.gov
- Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center’s About Herbs: www.mskcc.org/mskcc/html/11570.cfm
- Natural Standard: www.naturalstandard.com
- The M.D. Anderson Cancer Center’s Complementary/Integrative Medicine Education Resources: www.mdanderson.org/departments/CIMER
What Trends Show
In 2007, according to the American Hospital Association, 20.8% of community hospitals offered some type of care or treatment not based on traditional Western allopathic medicine. That’s up from 8.6% of reporting hospitals that offered those services in 1998.
The 1990s saw rapid growth of integrative medicine centers at major research institutions, and the majority of U.S. cancer centers now offer some form of complementary therapy, says Barrie R. Cassileth, MS, PhD, the Laurance S. Rockefeller Chair in Integrative Medicine and chief of the Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center in New York City.
The 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals reported that complementary programs are more common in urban rather than rural hospitals; services vary by hospital size (see Figure 2, above); and the top six modalities offered on an inpatient basis are pet therapy, massage therapy, music/art therapy, guided imagery, acupuncture, and reiki (see “Glossary of Complementary Terms,” above). Eighty-four percent of hospitals offer complementary services due to patient demand, the survey showed.
Joseph Ming-Wah Li, MD, FHM, SHM board member and assistant professor of medicine at Harvard Medical School and director of the hospital medicine program and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston, doesn’t see a problem with modalities that can make his patients feel better. Patients at his hospital have access to pet therapy, massage, and acupuncture. “I don’t think these modalities hurt our patients, and there is very little downside, except for potential cost,” says Dr. Li, an SHM board member. “What’s not clear is whether these therapies work or not.”
What’s in a Name?
Numerous therapies and modalities crowd under the CAM umbrella, but most experts classify “complementary” modalities as those used in conjunction with conventional medicine to mitigate symptoms of disease or treatment, whereas “alternative” connotes therapies claiming to treat or cure the underlying disease. Some harmful, dangerous, and dishonest practices fall into the “alternative” category, such as Hulda Clark’s “Zapper” device, which was promoted as a cure for liver flukes, something she says cause everything from diabetes to heart disease. (For more on questionable practices, visit www.quackwatch.com or the National Council Against Health Fraud’s Web site at www.ncahf.org.)
The National Institutes of Health’s National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of “diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” Dr. Cassileth says the conflation of “complementary and alternative” into one neat acronym—CAM—causes confusion among patients and medical professionals. NCCAM will be changing its name soon, she says, to the National Center for Integrative Medicine, emphasizing the use of adjunctive modalities along with conventional medical treatments.
Hospitalist Suzanne Bertisch, MD, MPH, recently completed a research fellowship at Harvard Medical School’s Osher Research Center. She explains that integrative medicine uses a macro model of health, claiming a middle ground between the traditional, allopathic model of treating disease.
All Kinds of Evidence
Twenty years of complementary medicine research has yielded some information about safety—namely, what works and what doesn’t. For example, saw palmetto has not panned out as an effective treatment for benign prostatic hyperplasia; St. John’s wort, useful for mild depression, interferes with many medications, including cyclosporine and warfarin, and should be avoided at least five days prior to surgery.7,8
Since NCCAM’s inception in October 1998, its research portfolio has stirred debate in the scientific community. Part of the disagreement stems from the difficulty of fitting multidimensional interventions, some of which are provider-dependent (e.g., massage or acupuncture), into the gold standard of the randomized, double-blind, placebo-controlled trial, explains Darshan Mehta, MD, MPH, associate director of medical education at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. The manner in which the effectiveness of integrative techniques is assessed requires a higher sophistication of systems research, Dr. Mehta says.
“The way we construe evidence needs to change,” she adds.
Likely to Expand
Most private health plans do not cover complementary services, although Medicare and numerous insurance plans will reimburse treatment in conjunction with physical therapy (e.g., massage) in the outpatient setting. Twenty-three states cover chiropractic care under Medicaid, and Medicare has begun to assess the cost-effectiveness of including acupuncture—especially for postoperative and chemotherapy-associated nausea and vomiting—in its benefits package.9 Other modalities, ranging from aromatherapy to guided imagery training, are paid for largely out-of-pocket.10
Dr. Rakel notes that the delivery of integrative medicine services at UW entails conversations with patients about out-of-pocket payments. “It can pose a barrier to the clinician-patient relationship if you give them acupuncture to help with their chemotherapy-induced nausea and then ask for their credit card,” he says.
Hospitalist Preparation
Most complementary therapies are currently offered on an outpatient basis. Because of this trend, and because they deal with acute conditions, hospitalists are less likely to be involved with complementary or integrative medicine services, says Beth Israel Deaconess Medical Center hospitalist Andrew C. Ahn, MD, MPH. But that’s not to say complementary medicine is something hospitalists should ignore; patients arrive at the hospital with CAM regimens in tow. It’s the No. 1 reason, Dr. Ahn says, hospitalists should be knowledgeable and exposed to CAM therapies.
Physicians must understand patient patterns and preferences regarding allopathic and complementary medicine, says Sita Ananth, MHA, director of knowledge services and optimal healing environments at the Samueli Institute in Alexandria, Va., and author of the 2007 AHA report. She points to a 2006 survey conducted by AARP and NCCAM that found almost 70% of respondents did not tell their physicians about their complementary medicine approaches. These patients are within the age range most likely to be cared for by hospitalists, and failure to communicate about complementary treatment, such as supplemental vitamin use, could lead to safety issues. Moreover, without complete disclosure, the patient-physician relationship might not be as open as possible, Dr. Ananth says.
Many acute-care hospitalists do not have formal dietary supplement policies, and less than half of U.S. children’s hospitals require documentation of a check for drug or dietary supplement interaction.11,12 As a safety issue, it is always incumbent on hospitalists, says Dr. Li, to ask about any supplements or therapies patients are trying on their own as part of the history and physical examination. The policy at Memorial Sloan-Kettering Cancer Center, Dr. Cassileth says, is that patients on chemotherapy or who are undergoing radiation or facing surgery must avoid herbal dietary supplements.
Beyond Safety
Dr. Bertisch advises hospitalists to pose questions about complementary therapies in an open manner, avoiding antagonistic discussions. “Even when I disagree, I try to guide them to issues about safety and nonsafety, and coax in my concerns,” she says. “The most challenging part about complementary medicine is that patients’ beliefs in these therapies may be so strong that even if the doctor says it won’t work, that will not necessarily change that belief.” A 2001 study in the Archives of Internal Medicine revealed that 70% of respondents would continue to take supplements even if a major study or their physician told them they didn’t work.13
The attraction to complementary medicine often reflects patients’ preferences for a holistic approach to health, says Dr. Ahn, or it may emanate from traditions carried with them from their country of origin. “Once you do understand their reasons for using CAM, then the patient-physician relationship can be significantly strengthened,” he says. With nearly two-thirds of Americans using some form of CAM, hospitalists need to engage in this dialogue.
Dr. Rakel agrees understanding patient culture is vital to uncovering useful information. “Most clinicians would agree that if we can match a therapy to the patient culture and belief system, we are more likely to get buy-in from the patient,” he says.
Dr. Mehta also is a clinical instructor of medicine at Harvard Medical School. He teaches his residents to educate themselves about credentialing, certification, and licensure of complementary providers. He also asks them to maintain an open mind. He says the most important preparation for hospitalists right now is to help educate their patients to be more proactive in their own healthcare. “An engaged patient,” he says, “is better than a disengaged patient.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Deng G, Cassileth BR, Yeung KS. Complementary therapies for cancer-related symptoms. J Support Oncol. 2004;2(5):419-426.
- Kahn ST, Johnstone PA. Management of xerostomia related to radiotherapy for head and neck cancer. Oncology. 2005;19(14):1827-1832.
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;27(343):1-19.
- Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280(18):1569-1575.
- Committee on the Use of Complementary and Alternative Medicine by the American Public. Complementary and Alternative Medicine in the United States. Washington, D.C: National Academies Press; 2005.
- Ananth S. 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals. Health Forum LLC. 2008.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-566.
- Bauer BA. The herbal hospitalist. The Hospitalist. 2006;10(2);16-17.
- Ananth S. Applying integrative healthcare. Explore. 2009;5(2):119-120.
- Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med. 1993;328:246-52
- Bassie KL, Witmer DR, Pinto B, Bush C, Clark J, Deffenbaugh J Jr. National survey of dietary supplement policies in acute care facilities. Am J Health Syst Pharm. 2006;63(1):65-70.
- Gardiner P, Phillips RS, Kemper KJ, Legedza A, Henlon S, Woolf AD. Dietary supplements: inpatient policies in US children’s hospitals. Pediatrics. 2008;121(4):e775-781.
- Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE. Americans’ views on the use and regulation of dietary supplements. Arch Intern Med. 2001;161(6):805-810.
Top Image Source: TETRA IMAGES
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.1,2
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture—it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
Even if your hospital does not offer complementary and alternative medicine (CAM), your patients are using CAM at ever-increasing rates. In 1993, 34% of Americans reported using some type of CAM (e.g., supplements, massage therapy, prayer, and so on). That number has almost doubled to 62%.3 Americans spend $47 billion a year—of their own money—for CAM therapies, chiropractors, acupuncturists, and massage therapists. And older patients with chronic conditions—the kind of patient hospitalists are most familiar with—tend to try CAM more than younger patients.4
These trends can directly affect hospitalists’ treatment decisions, but they also play a part in how you establish communication and trust with your patients, and how you keep your patients safe from adverse drug interactions. According to the National Academy of Sciences, in order to effectively counsel patients and ensure high-quality comprehensive care, conventional professionals need more CAM-related education.5
—Suzanne Bertisch, MD, MPH, fellow, Harvard Medical School’s Osher Research Center
Complementary Medicine: Online Resources
- National Center for Complementary and Alternative Medicine: http://nccam.nih.gov
- Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center’s About Herbs: www.mskcc.org/mskcc/html/11570.cfm
- Natural Standard: www.naturalstandard.com
- The M.D. Anderson Cancer Center’s Complementary/Integrative Medicine Education Resources: www.mdanderson.org/departments/CIMER
What Trends Show
In 2007, according to the American Hospital Association, 20.8% of community hospitals offered some type of care or treatment not based on traditional Western allopathic medicine. That’s up from 8.6% of reporting hospitals that offered those services in 1998.
The 1990s saw rapid growth of integrative medicine centers at major research institutions, and the majority of U.S. cancer centers now offer some form of complementary therapy, says Barrie R. Cassileth, MS, PhD, the Laurance S. Rockefeller Chair in Integrative Medicine and chief of the Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center in New York City.
The 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals reported that complementary programs are more common in urban rather than rural hospitals; services vary by hospital size (see Figure 2, above); and the top six modalities offered on an inpatient basis are pet therapy, massage therapy, music/art therapy, guided imagery, acupuncture, and reiki (see “Glossary of Complementary Terms,” above). Eighty-four percent of hospitals offer complementary services due to patient demand, the survey showed.
Joseph Ming-Wah Li, MD, FHM, SHM board member and assistant professor of medicine at Harvard Medical School and director of the hospital medicine program and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston, doesn’t see a problem with modalities that can make his patients feel better. Patients at his hospital have access to pet therapy, massage, and acupuncture. “I don’t think these modalities hurt our patients, and there is very little downside, except for potential cost,” says Dr. Li, an SHM board member. “What’s not clear is whether these therapies work or not.”
What’s in a Name?
Numerous therapies and modalities crowd under the CAM umbrella, but most experts classify “complementary” modalities as those used in conjunction with conventional medicine to mitigate symptoms of disease or treatment, whereas “alternative” connotes therapies claiming to treat or cure the underlying disease. Some harmful, dangerous, and dishonest practices fall into the “alternative” category, such as Hulda Clark’s “Zapper” device, which was promoted as a cure for liver flukes, something she says cause everything from diabetes to heart disease. (For more on questionable practices, visit www.quackwatch.com or the National Council Against Health Fraud’s Web site at www.ncahf.org.)
The National Institutes of Health’s National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of “diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” Dr. Cassileth says the conflation of “complementary and alternative” into one neat acronym—CAM—causes confusion among patients and medical professionals. NCCAM will be changing its name soon, she says, to the National Center for Integrative Medicine, emphasizing the use of adjunctive modalities along with conventional medical treatments.
Hospitalist Suzanne Bertisch, MD, MPH, recently completed a research fellowship at Harvard Medical School’s Osher Research Center. She explains that integrative medicine uses a macro model of health, claiming a middle ground between the traditional, allopathic model of treating disease.
All Kinds of Evidence
Twenty years of complementary medicine research has yielded some information about safety—namely, what works and what doesn’t. For example, saw palmetto has not panned out as an effective treatment for benign prostatic hyperplasia; St. John’s wort, useful for mild depression, interferes with many medications, including cyclosporine and warfarin, and should be avoided at least five days prior to surgery.7,8
Since NCCAM’s inception in October 1998, its research portfolio has stirred debate in the scientific community. Part of the disagreement stems from the difficulty of fitting multidimensional interventions, some of which are provider-dependent (e.g., massage or acupuncture), into the gold standard of the randomized, double-blind, placebo-controlled trial, explains Darshan Mehta, MD, MPH, associate director of medical education at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. The manner in which the effectiveness of integrative techniques is assessed requires a higher sophistication of systems research, Dr. Mehta says.
“The way we construe evidence needs to change,” she adds.
Likely to Expand
Most private health plans do not cover complementary services, although Medicare and numerous insurance plans will reimburse treatment in conjunction with physical therapy (e.g., massage) in the outpatient setting. Twenty-three states cover chiropractic care under Medicaid, and Medicare has begun to assess the cost-effectiveness of including acupuncture—especially for postoperative and chemotherapy-associated nausea and vomiting—in its benefits package.9 Other modalities, ranging from aromatherapy to guided imagery training, are paid for largely out-of-pocket.10
Dr. Rakel notes that the delivery of integrative medicine services at UW entails conversations with patients about out-of-pocket payments. “It can pose a barrier to the clinician-patient relationship if you give them acupuncture to help with their chemotherapy-induced nausea and then ask for their credit card,” he says.
Hospitalist Preparation
Most complementary therapies are currently offered on an outpatient basis. Because of this trend, and because they deal with acute conditions, hospitalists are less likely to be involved with complementary or integrative medicine services, says Beth Israel Deaconess Medical Center hospitalist Andrew C. Ahn, MD, MPH. But that’s not to say complementary medicine is something hospitalists should ignore; patients arrive at the hospital with CAM regimens in tow. It’s the No. 1 reason, Dr. Ahn says, hospitalists should be knowledgeable and exposed to CAM therapies.
Physicians must understand patient patterns and preferences regarding allopathic and complementary medicine, says Sita Ananth, MHA, director of knowledge services and optimal healing environments at the Samueli Institute in Alexandria, Va., and author of the 2007 AHA report. She points to a 2006 survey conducted by AARP and NCCAM that found almost 70% of respondents did not tell their physicians about their complementary medicine approaches. These patients are within the age range most likely to be cared for by hospitalists, and failure to communicate about complementary treatment, such as supplemental vitamin use, could lead to safety issues. Moreover, without complete disclosure, the patient-physician relationship might not be as open as possible, Dr. Ananth says.
Many acute-care hospitalists do not have formal dietary supplement policies, and less than half of U.S. children’s hospitals require documentation of a check for drug or dietary supplement interaction.11,12 As a safety issue, it is always incumbent on hospitalists, says Dr. Li, to ask about any supplements or therapies patients are trying on their own as part of the history and physical examination. The policy at Memorial Sloan-Kettering Cancer Center, Dr. Cassileth says, is that patients on chemotherapy or who are undergoing radiation or facing surgery must avoid herbal dietary supplements.
Beyond Safety
Dr. Bertisch advises hospitalists to pose questions about complementary therapies in an open manner, avoiding antagonistic discussions. “Even when I disagree, I try to guide them to issues about safety and nonsafety, and coax in my concerns,” she says. “The most challenging part about complementary medicine is that patients’ beliefs in these therapies may be so strong that even if the doctor says it won’t work, that will not necessarily change that belief.” A 2001 study in the Archives of Internal Medicine revealed that 70% of respondents would continue to take supplements even if a major study or their physician told them they didn’t work.13
The attraction to complementary medicine often reflects patients’ preferences for a holistic approach to health, says Dr. Ahn, or it may emanate from traditions carried with them from their country of origin. “Once you do understand their reasons for using CAM, then the patient-physician relationship can be significantly strengthened,” he says. With nearly two-thirds of Americans using some form of CAM, hospitalists need to engage in this dialogue.
Dr. Rakel agrees understanding patient culture is vital to uncovering useful information. “Most clinicians would agree that if we can match a therapy to the patient culture and belief system, we are more likely to get buy-in from the patient,” he says.
Dr. Mehta also is a clinical instructor of medicine at Harvard Medical School. He teaches his residents to educate themselves about credentialing, certification, and licensure of complementary providers. He also asks them to maintain an open mind. He says the most important preparation for hospitalists right now is to help educate their patients to be more proactive in their own healthcare. “An engaged patient,” he says, “is better than a disengaged patient.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Deng G, Cassileth BR, Yeung KS. Complementary therapies for cancer-related symptoms. J Support Oncol. 2004;2(5):419-426.
- Kahn ST, Johnstone PA. Management of xerostomia related to radiotherapy for head and neck cancer. Oncology. 2005;19(14):1827-1832.
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;27(343):1-19.
- Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280(18):1569-1575.
- Committee on the Use of Complementary and Alternative Medicine by the American Public. Complementary and Alternative Medicine in the United States. Washington, D.C: National Academies Press; 2005.
- Ananth S. 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals. Health Forum LLC. 2008.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-566.
- Bauer BA. The herbal hospitalist. The Hospitalist. 2006;10(2);16-17.
- Ananth S. Applying integrative healthcare. Explore. 2009;5(2):119-120.
- Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med. 1993;328:246-52
- Bassie KL, Witmer DR, Pinto B, Bush C, Clark J, Deffenbaugh J Jr. National survey of dietary supplement policies in acute care facilities. Am J Health Syst Pharm. 2006;63(1):65-70.
- Gardiner P, Phillips RS, Kemper KJ, Legedza A, Henlon S, Woolf AD. Dietary supplements: inpatient policies in US children’s hospitals. Pediatrics. 2008;121(4):e775-781.
- Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE. Americans’ views on the use and regulation of dietary supplements. Arch Intern Med. 2001;161(6):805-810.
Top Image Source: TETRA IMAGES
Step-by-Step Medicine
Evidence-based practice guidelines are key tools to help hospitalists practice high-quality medicine and demonstrate the value of their inpatient care model. Guidelines are designed to produce superior care outcomes and resource utilization efficiencies by encouraging proven medical practices and discouraging ineffective or unproven ones. Yet inefficiencies, variation, and quality gaps persist in medical care—much to the chagrin of policymakers.
Is the answer more guidelines, and better implementation of existing ones?
Research experts and many HM leaders say yes.
In fact, HM is leading the way in an important new area for which there is little uniform guidance: optimal care transitions during patient handoffs. Care transitions are a pivotal time in the patient care process and are replete with avoidable service duplication, poor communication among providers, gaps in care reconciliation, and patient-safety issues.
SHM has joined five other organizations in issuing a Transitions of Care Consensus Policy Statement, which promises more systematic, safe, and efficient patient handoffs.1 SHM also is targeting care-transition improvement in a variety of other venues, all of which can help hospitalists demonstrate more persuasively the value they bring to healthcare delivery.
Guidelines Work
Practice guidelines work, in the sense that they help providers practice in ways consistent with what the best aggregate knowledge and expert opinion says is most effective. The evidence allows physicians to avoid expending scarce resources on ineffective clinical services. Their importance is magnified by the current urgency given to value-based purchasing in healthcare reform. “The right care, for the right patient, at the right time” is the new mantra of payors and policymakers, many of whom are demanding the best and most efficient healthcare delivery at the lowest cost.

“When providers are not providing the right care at the right time to patients, we find that the patient often gets more services … that they didn’t need. That oftentimes exposes them to potential harm and (services) that are wasteful of resources,” says Janet M. Corrigan, PhD, MBA, president and CEO of the National Quality Forum (NQF), a standard-setting organization that convenes national experts to apply “gold standard” endorsement of guidelines developed by professional medical societies and other entities. “Guidelines are a way of synthesizing evidence and translating it into action steps that providers can follow so that they get the best results that we know how to get for their patients.”
Clinicians and healthcare organizations have several sources for guidelines. The Agency for Healthcare Research and Quality (AHRQ) systematically reviews and vets guidelines submitted for inclusion in its National Guideline Clearinghouse (www.guideline.gov), and makes them available for evidence-based clinical decision-making, says Jean Slutsky, director of AHRQ’s Center for Outcomes and Evidence. AHRQ also offers public access to the National Quality Measure Clearinghouse and the Health Care Innovations Exchange, repositories of searchable quality measures and tools relevant to an array of diseases and conditions.
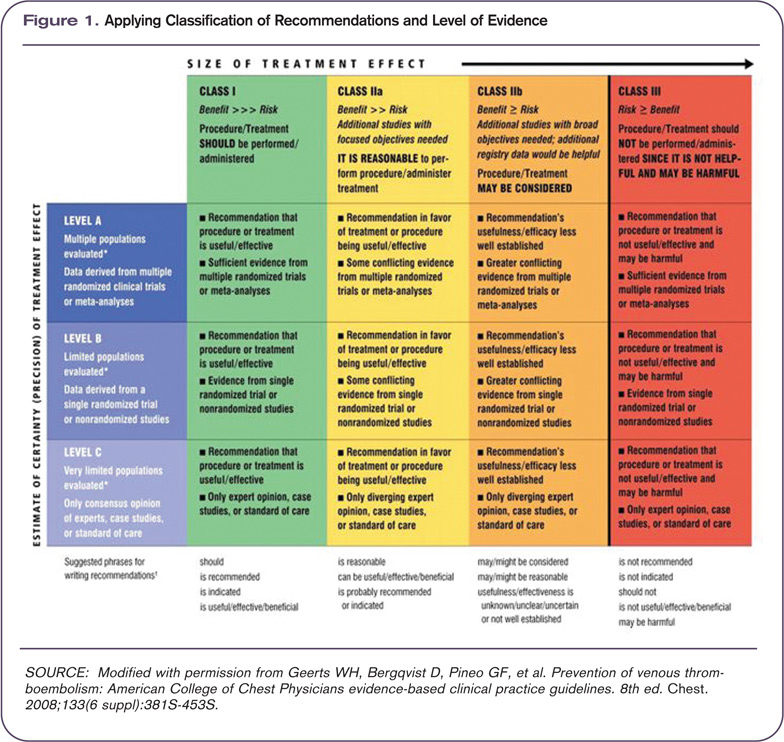
The Institute for Healthcare Improvement (IHI), an independent nonprofit organization, helps frontline physicians implement guidelines, and also helps provider teams decide which guidelines are most appropriate to achieve their desired outcomes, according to Amy E. Boutwell, MD, MPP, IHI’s director of health policy strategy.
Hospitalists use an array of disease-specific practice guidelines from different specialty societies for diagnoses they frequently encounter, such as chest pain, stroke, pneumonia, myocardial infarction, gastrointestinal bleeding, asthma, and chronic obstructive pulmonary disease (COPD). “Most hospitalists want to keep up with the best available evidence,” says Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., and chair of SHM’s Performance and Standards Committee. “The recently updated American College of Cardiology (ACC) and American Heart Association (AHA) guidelines on heart failure are exceptional. The American College of Chest Physicians has an extremely comprehensive set of guidelines on thrombosis, which is the bible for handling anticoagulation.”
Studies are published every month demonstrating that physicians who implement national guidelines at the local level improve such patient outcomes as mortality, length of stay, and time to clinical stability. Dr. Corrigan notes that there are abundant examples of guideline adherence boosting quality outcomes, and cites as a prime example the AHA’s Get With the Guidelines program (www.american heart.org/presenter.jhtml?identifier=1165), which has documented quality gains in coronary artery disease, stroke, and heart failure patients.

—William T. Ford, MD, FHM, section chief of hospital medicine, Temple University Hospital, Philadelphia
Barriers to Acceptance and Adherence
But there are obstacles to guideline adherence, and widespread practice pattern variation remains a huge national problem. Providers in some regions of the country can use twice the resources as their counterparts in other regions and bring no additional benefit to patients (see “Medicare Fee Inspection,” p. 30). The Dartmouth Atlas of Health Care says unwarranted practice variation is responsible for as much as 30% of wasted healthcare spending in the U.S.—a cost that reformers are anxious to eliminate.
The traditional culture of autonomy in the medical profession is perhaps the most difficult and enduring barrier to reducing unjustified practice variation: clinicians don’t automatically follow guidelines, many treat them more as options than as true standards, and organizations do not sufficiently enforce or reward adherence to guidelines, wrote researchers in a special 2005 issue of Health Affairs focusing on guidelines.2
“In an age of mandated cost control and resource limitation under managed care,” the researchers wrote, some physicians still regard practice guidelines as “cookbook medicine” that threatens the use of clinical judgment and encourages treating patients as essentially interchangeable. In the face of that perceived threat, the researchers added, many physicians continue to uphold a traditional view of medicine as an art “in which individual expertise and technique are allowed to shine through and ultimately result in a higher standard of patient care.”
Dr. Corrigan acknowledges the significant obstacles to successful practice guideline implementation:
- Guidelines are developed by various sources, particularly specialty societies, who do not always coordinate their activities. Physicians are left with overlapping and sometimes contradictory guidelines for managing the same disease or condition.
- Guidelines must be maintained and kept current, or physicians will lose confidence and not follow them.
- Guidelines are of varying quality. Some provide clear clinical direction; others are not written in a way that physicians can clearly translate into clinical practice.
- There are significant gaps in the evidence basis for guideline development. Much more comparative effectiveness research needs to be conducted to develop more valid and meaningful guidelines.
- Guidelines must be communicated effectively to physicians, making them available and convenient at the point of clinical care. Electronic health records with user-friendly decision support functions show great promise in “making the right thing the easy thing to do.”
- The fee-for-service payment system encourages greater volume of services, irrespective of guideline recommendations.
Physicians also recognize inherent limitations of guidelines. “Guidelines typically apply across populations. Adding levels of clinical complexity gets further away from a guideline’s applicability. Many physicians will tell you that the patient in front of them is a special case requiring a modification of the protocol,” Dr. Boutwell explains. For example, diabetic management guidelines are based on what is best for a population of diabetics, versus what is best for said hospitalist’s patient who has eight co-morbidities, one of which is diabetes, Boutwell notes. “Guidelines come disease-specific. Patients don’t,” she adds.
Nevertheless, Dr. Boutwell notes, there are robust guidelines and the IHI tries to help front-line physicians and care teams to implement them reliably and effectively.
An obstacle that inhibits hospitalists from implementing guidelines in an optimal fashion “is that we’re not one specialty—we deal with it all—and that complexity can be overwhelming. There is no central repository where all of the guidelines can be found in one place,” according to William T. Ford, MD, FHM, program medical director for Cogent Healthcare and section chief of hospital medicine for Temple University Hospital in Philadelphia.
Make Guidelines Work
Researchers say guidelines are most successful when they are well-supported and uncomplicated, backed by strong leadership and sufficient resources, and are used as “rallying points” to stimulate interdependent and collaborative care among physicians, nurses, pharmacists, equipment suppliers, administrators, and patients.
“Guidelines are really the foundation for determining best practices,” Dr. Torcson says. “There is no shortage of excellent guidelines, or proof that specific interventions do improve outcomes. The key is achieving more uniform implementation. We need tools like pre-printed orders in electronic health records (EHR) to effectively integrate these guidelines into hospitalists’ practice.”
More widespread EHR adoption with user-friendly medical decision-support systems will play a huge role in boosting guideline adoption and effectiveness, says Mary Nix, MS, MT(ASCP)SBB, health science administrator at AHRQ and project officer for the agency’s Center for Outcomes and Evidence.
Dr. Ford says HM groups must evaluate the top 10 to 15 diagnosis-related groups (DRGs) that they see each day (e.g., congestive heart failure, acute kidney failure, pneumonia, cellulitis, or acute coronary syndrome) and come to consensus on which guidelines best address them.
HM groups must then secure buy-in to those guidelines from everyone in the group; from the subspecialists they work with; and from their hospital’s chief medical, financial, and utilization officers.
Care-Transition Guidelines: Opportunity for Hospitalists
A particularly important HM opportunity is improving care transitions. Deficits in communication and information transfer between hospital-based and primary-care physicians (PCPs) are “substantial and ubiquitous,” while delays and omissions are consistently large, and traditional methods of completing and delivering discharge summaries are “suboptimal for communicating timely, accurate, and medically important data to the physicians who will be responsible for follow-up care,” according to a hospitalist-authored Feb. 28, 2007, article in the Journal of the American Medical Association.3 PCPs routinely are not notified about patient admissions or complications during the hospital stay, and some PCPs fail to provide sufficient information to hospitalists at admission, fail to visit or call hospitalized patients, or fail to participate in discharge planning, the study’s researchers noted. For patients with chronic illnesses and frequent hospitalization, those deficits are multiplied, making completeness of information handoffs particularly important.
Because patient handoffs have notoriously been fraught with miscommunication and poor information exchange between providers, adopting a professional consensus on what constitutes the best, safest, and most effective activities during these handoffs is sorely needed.
“Care-transition guidelines can have tremendous power because they affect every hospital patient—each of whom experiences care transitions,” says Rusty Holman, MD, FHM, chief operating officer of Brentwood, Tenn.-based Cogent Healthcare and past president of SHM. “It is an area undergoing rapid development, evolution, and discovery, and hospitalists have positioned themselves as leaders and owners of this particular scenario.”

As care-transition guidelines emerge and mature, Holman thinks they eventually will be tied to value-based healthcare purchasing programs that affect hospitalists’ reimbursement equations and further boost incentives to follow those guidelines. A prime example: Medicare calculated it could save $12 billion annually by reducing preventable 30-day hospital readmissions and will soon stop paying for them. Perhaps 3% to 5% of a hospital’s DRG reimbursement will be at risk under Medicare’s proposal, Dr. Torcson notes.
“Hospitals are going to be much more motivated to build systems and engage physicians, especially hospitalists, to lower readmission rates. Hospitalists will be focusing more and more on how care-transition process improvements can lower those rates,” Dr. Holman says. “That’s a huge opportunity for hospitalists to make a business case for the value they bring to their institutions, and will further justify the financial support they already receive.”
Dr. Ford is more cautious in his appraisal of the financial rewards of better guideline implementation. “We do not capture that much revenue per patient, and even a length-of-stay reduction is difficult for a hospital’s CFO to extrapolate how much money hospitalists save,” he says. “I don’t think hospitalists will be paid more, even if they save the hospital money. You’re just doing your job, but you’re going to keep your job, and you’ll have an enormous bargaining chip when renegotiating contracts with hospitals.”
Still, a prevented readmission might mean a bed for a revenue-generating elective surgery, something that adds to the reward equation.

—Patrick Torcson, MD, MMM, FACP, director of hospital medicine, St. Tammany Parish Hospital, Covington, La., SHM Performance and Standards Committee chair
Transition Evolution
SHM and other sources offer physicians and hospitals expert assistance in implementing care-transition guidelines (see “Care-Transition Guidance,” p. 7). The transitions-of-care policy statement jointly issued by the SHM and five other specialty societies further demonstrates that hospitalists play a key leadership role on this front.1
The policy statement emerged from a multi-stakeholder consensus conference convened by SHM, the American College of Physicians (ACP), and the Society of General Internal Medicine, which was attended by more than 30 medical specialty societies, governmental agencies, and performance measure developers. Participants focused on what standard pieces of information should be exchanged among providers during inpatient to outpatient transitions, and they issued a set of standards for improving those transitions (see “Managing Transitions in Care Between the Inpatient and Outpatient Settings,” p. 7).
“This consensus statement has enormous significance,” Dr. Ford says. “We’re finally shedding light on how to tackle patient handoff and hospital readmission issues, and we as a specialty have to take on care-transition improvement as our mantra. If we were to solve just that one piece, we can more easily start implementing other clinical guidelines. Care-transition guidelines are a fundamental tool to build consensus within your own group and with other clinicians in a team approach.”
Dr. Corrigan applauds the physician groups for publishing the transitions-of-care statement and encourages the societies to work together to “take it to the next step, which is to develop the measures and get them endorsed through the NQF process.”
SHM members are participating in workgroups convened by the NQF to identify standardized performance measures and to develop action plans over the next few months for several national priority areas—one of which is care coordination. “We have a ways to go to achieve better patient handoffs and information exchange between hospitals and other settings in the community. Hospitalists can drive the development of those guidelines and protocols,” Dr. Corrigan says. TH
Christopher Guadagnino, PhD, is a freelance medical writer based in Pennsylvania.
References
- Kripalani S, LeFevre F, Phillips CO, Williams MV; Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831-841.
- Timmermans S, Mauck A. The promises and pitfalls of evidence-based medicine. Health Affairs. 2005; 24(1):18-28.
- Snow V, Beck D, Budnitz T, et al. Transitions of care consensus policy statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, Society of Academic Emergency Medicine. J Hosp Med. 2009: 4(6)364-370.
Top Image Source: GOLDEN PIXELS LLC/ALAMY
Managing Transitions of Care Between the Inpatient and Outpatient Settings

The following are joint recommendations from SHM, ACP, SGIM, AGS, ACEP, and SAEM, based upon a multi-stakeholder consensus conference in July 2007 and published in the July/August Journal of Hospital Medicine (http://onlinelibrary.wiley.com/doi/10.1002/jhm.510/full):
- Communication and information exchange between the sending and receiving provider should be timely, as dictated by clinical presentation and urgency of follow-up care required.
- The transition record should always include at least these data elements: principal diagnosis, medication list, contact information of the transferring physician, patient’s cognitive status, test results or pending results. An ideal transition record would add six more elements.
- All communications need to be secure, private, HIPAA-compliant, and accessible to patients and their providers.
- Communities need to develop standard data transfer forms, with the ability to modify information as a patient’s condition changes.
- The sending provider maintains responsibility for the care of the patient until the receiving provider confirms that the transfer is complete. The sending provider should be available to clarify issues of care, and the patient should be able to identify the responsible provider.
- Information transfer should be timely, as determined by transition setting, patient circumstances, level of acuity, and clear transition responsibility.
- Medical institutions must adopt national standards and establish processes to promote effective transitions of care.
- Standardized and evidence-based metrics related to these standards should be used for monitoring and improving transitions.
Evidence-based practice guidelines are key tools to help hospitalists practice high-quality medicine and demonstrate the value of their inpatient care model. Guidelines are designed to produce superior care outcomes and resource utilization efficiencies by encouraging proven medical practices and discouraging ineffective or unproven ones. Yet inefficiencies, variation, and quality gaps persist in medical care—much to the chagrin of policymakers.
Is the answer more guidelines, and better implementation of existing ones?
Research experts and many HM leaders say yes.
In fact, HM is leading the way in an important new area for which there is little uniform guidance: optimal care transitions during patient handoffs. Care transitions are a pivotal time in the patient care process and are replete with avoidable service duplication, poor communication among providers, gaps in care reconciliation, and patient-safety issues.
SHM has joined five other organizations in issuing a Transitions of Care Consensus Policy Statement, which promises more systematic, safe, and efficient patient handoffs.1 SHM also is targeting care-transition improvement in a variety of other venues, all of which can help hospitalists demonstrate more persuasively the value they bring to healthcare delivery.
Guidelines Work
Practice guidelines work, in the sense that they help providers practice in ways consistent with what the best aggregate knowledge and expert opinion says is most effective. The evidence allows physicians to avoid expending scarce resources on ineffective clinical services. Their importance is magnified by the current urgency given to value-based purchasing in healthcare reform. “The right care, for the right patient, at the right time” is the new mantra of payors and policymakers, many of whom are demanding the best and most efficient healthcare delivery at the lowest cost.
“When providers are not providing the right care at the right time to patients, we find that the patient often gets more services … that they didn’t need. That oftentimes exposes them to potential harm and (services) that are wasteful of resources,” says Janet M. Corrigan, PhD, MBA, president and CEO of the National Quality Forum (NQF), a standard-setting organization that convenes national experts to apply “gold standard” endorsement of guidelines developed by professional medical societies and other entities. “Guidelines are a way of synthesizing evidence and translating it into action steps that providers can follow so that they get the best results that we know how to get for their patients.”
Clinicians and healthcare organizations have several sources for guidelines. The Agency for Healthcare Research and Quality (AHRQ) systematically reviews and vets guidelines submitted for inclusion in its National Guideline Clearinghouse (www.guideline.gov), and makes them available for evidence-based clinical decision-making, says Jean Slutsky, director of AHRQ’s Center for Outcomes and Evidence. AHRQ also offers public access to the National Quality Measure Clearinghouse and the Health Care Innovations Exchange, repositories of searchable quality measures and tools relevant to an array of diseases and conditions.
The Institute for Healthcare Improvement (IHI), an independent nonprofit organization, helps frontline physicians implement guidelines, and also helps provider teams decide which guidelines are most appropriate to achieve their desired outcomes, according to Amy E. Boutwell, MD, MPP, IHI’s director of health policy strategy.
Hospitalists use an array of disease-specific practice guidelines from different specialty societies for diagnoses they frequently encounter, such as chest pain, stroke, pneumonia, myocardial infarction, gastrointestinal bleeding, asthma, and chronic obstructive pulmonary disease (COPD). “Most hospitalists want to keep up with the best available evidence,” says Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., and chair of SHM’s Performance and Standards Committee. “The recently updated American College of Cardiology (ACC) and American Heart Association (AHA) guidelines on heart failure are exceptional. The American College of Chest Physicians has an extremely comprehensive set of guidelines on thrombosis, which is the bible for handling anticoagulation.”
Studies are published every month demonstrating that physicians who implement national guidelines at the local level improve such patient outcomes as mortality, length of stay, and time to clinical stability. Dr. Corrigan notes that there are abundant examples of guideline adherence boosting quality outcomes, and cites as a prime example the AHA’s Get With the Guidelines program (www.american heart.org/presenter.jhtml?identifier=1165), which has documented quality gains in coronary artery disease, stroke, and heart failure patients.
—William T. Ford, MD, FHM, section chief of hospital medicine, Temple University Hospital, Philadelphia
Barriers to Acceptance and Adherence
But there are obstacles to guideline adherence, and widespread practice pattern variation remains a huge national problem. Providers in some regions of the country can use twice the resources as their counterparts in other regions and bring no additional benefit to patients (see “Medicare Fee Inspection,” p. 30). The Dartmouth Atlas of Health Care says unwarranted practice variation is responsible for as much as 30% of wasted healthcare spending in the U.S.—a cost that reformers are anxious to eliminate.
The traditional culture of autonomy in the medical profession is perhaps the most difficult and enduring barrier to reducing unjustified practice variation: clinicians don’t automatically follow guidelines, many treat them more as options than as true standards, and organizations do not sufficiently enforce or reward adherence to guidelines, wrote researchers in a special 2005 issue of Health Affairs focusing on guidelines.2
“In an age of mandated cost control and resource limitation under managed care,” the researchers wrote, some physicians still regard practice guidelines as “cookbook medicine” that threatens the use of clinical judgment and encourages treating patients as essentially interchangeable. In the face of that perceived threat, the researchers added, many physicians continue to uphold a traditional view of medicine as an art “in which individual expertise and technique are allowed to shine through and ultimately result in a higher standard of patient care.”
Dr. Corrigan acknowledges the significant obstacles to successful practice guideline implementation:
- Guidelines are developed by various sources, particularly specialty societies, who do not always coordinate their activities. Physicians are left with overlapping and sometimes contradictory guidelines for managing the same disease or condition.
- Guidelines must be maintained and kept current, or physicians will lose confidence and not follow them.
- Guidelines are of varying quality. Some provide clear clinical direction; others are not written in a way that physicians can clearly translate into clinical practice.
- There are significant gaps in the evidence basis for guideline development. Much more comparative effectiveness research needs to be conducted to develop more valid and meaningful guidelines.
- Guidelines must be communicated effectively to physicians, making them available and convenient at the point of clinical care. Electronic health records with user-friendly decision support functions show great promise in “making the right thing the easy thing to do.”
- The fee-for-service payment system encourages greater volume of services, irrespective of guideline recommendations.
Physicians also recognize inherent limitations of guidelines. “Guidelines typically apply across populations. Adding levels of clinical complexity gets further away from a guideline’s applicability. Many physicians will tell you that the patient in front of them is a special case requiring a modification of the protocol,” Dr. Boutwell explains. For example, diabetic management guidelines are based on what is best for a population of diabetics, versus what is best for said hospitalist’s patient who has eight co-morbidities, one of which is diabetes, Boutwell notes. “Guidelines come disease-specific. Patients don’t,” she adds.
Nevertheless, Dr. Boutwell notes, there are robust guidelines and the IHI tries to help front-line physicians and care teams to implement them reliably and effectively.
An obstacle that inhibits hospitalists from implementing guidelines in an optimal fashion “is that we’re not one specialty—we deal with it all—and that complexity can be overwhelming. There is no central repository where all of the guidelines can be found in one place,” according to William T. Ford, MD, FHM, program medical director for Cogent Healthcare and section chief of hospital medicine for Temple University Hospital in Philadelphia.
Make Guidelines Work
Researchers say guidelines are most successful when they are well-supported and uncomplicated, backed by strong leadership and sufficient resources, and are used as “rallying points” to stimulate interdependent and collaborative care among physicians, nurses, pharmacists, equipment suppliers, administrators, and patients.
“Guidelines are really the foundation for determining best practices,” Dr. Torcson says. “There is no shortage of excellent guidelines, or proof that specific interventions do improve outcomes. The key is achieving more uniform implementation. We need tools like pre-printed orders in electronic health records (EHR) to effectively integrate these guidelines into hospitalists’ practice.”
More widespread EHR adoption with user-friendly medical decision-support systems will play a huge role in boosting guideline adoption and effectiveness, says Mary Nix, MS, MT(ASCP)SBB, health science administrator at AHRQ and project officer for the agency’s Center for Outcomes and Evidence.
Dr. Ford says HM groups must evaluate the top 10 to 15 diagnosis-related groups (DRGs) that they see each day (e.g., congestive heart failure, acute kidney failure, pneumonia, cellulitis, or acute coronary syndrome) and come to consensus on which guidelines best address them.
HM groups must then secure buy-in to those guidelines from everyone in the group; from the subspecialists they work with; and from their hospital’s chief medical, financial, and utilization officers.
Care-Transition Guidelines: Opportunity for Hospitalists
A particularly important HM opportunity is improving care transitions. Deficits in communication and information transfer between hospital-based and primary-care physicians (PCPs) are “substantial and ubiquitous,” while delays and omissions are consistently large, and traditional methods of completing and delivering discharge summaries are “suboptimal for communicating timely, accurate, and medically important data to the physicians who will be responsible for follow-up care,” according to a hospitalist-authored Feb. 28, 2007, article in the Journal of the American Medical Association.3 PCPs routinely are not notified about patient admissions or complications during the hospital stay, and some PCPs fail to provide sufficient information to hospitalists at admission, fail to visit or call hospitalized patients, or fail to participate in discharge planning, the study’s researchers noted. For patients with chronic illnesses and frequent hospitalization, those deficits are multiplied, making completeness of information handoffs particularly important.
Because patient handoffs have notoriously been fraught with miscommunication and poor information exchange between providers, adopting a professional consensus on what constitutes the best, safest, and most effective activities during these handoffs is sorely needed.
“Care-transition guidelines can have tremendous power because they affect every hospital patient—each of whom experiences care transitions,” says Rusty Holman, MD, FHM, chief operating officer of Brentwood, Tenn.-based Cogent Healthcare and past president of SHM. “It is an area undergoing rapid development, evolution, and discovery, and hospitalists have positioned themselves as leaders and owners of this particular scenario.”
As care-transition guidelines emerge and mature, Holman thinks they eventually will be tied to value-based healthcare purchasing programs that affect hospitalists’ reimbursement equations and further boost incentives to follow those guidelines. A prime example: Medicare calculated it could save $12 billion annually by reducing preventable 30-day hospital readmissions and will soon stop paying for them. Perhaps 3% to 5% of a hospital’s DRG reimbursement will be at risk under Medicare’s proposal, Dr. Torcson notes.
“Hospitals are going to be much more motivated to build systems and engage physicians, especially hospitalists, to lower readmission rates. Hospitalists will be focusing more and more on how care-transition process improvements can lower those rates,” Dr. Holman says. “That’s a huge opportunity for hospitalists to make a business case for the value they bring to their institutions, and will further justify the financial support they already receive.”
Dr. Ford is more cautious in his appraisal of the financial rewards of better guideline implementation. “We do not capture that much revenue per patient, and even a length-of-stay reduction is difficult for a hospital’s CFO to extrapolate how much money hospitalists save,” he says. “I don’t think hospitalists will be paid more, even if they save the hospital money. You’re just doing your job, but you’re going to keep your job, and you’ll have an enormous bargaining chip when renegotiating contracts with hospitals.”
Still, a prevented readmission might mean a bed for a revenue-generating elective surgery, something that adds to the reward equation.
—Patrick Torcson, MD, MMM, FACP, director of hospital medicine, St. Tammany Parish Hospital, Covington, La., SHM Performance and Standards Committee chair
Transition Evolution
SHM and other sources offer physicians and hospitals expert assistance in implementing care-transition guidelines (see “Care-Transition Guidance,” p. 7). The transitions-of-care policy statement jointly issued by the SHM and five other specialty societies further demonstrates that hospitalists play a key leadership role on this front.1
The policy statement emerged from a multi-stakeholder consensus conference convened by SHM, the American College of Physicians (ACP), and the Society of General Internal Medicine, which was attended by more than 30 medical specialty societies, governmental agencies, and performance measure developers. Participants focused on what standard pieces of information should be exchanged among providers during inpatient to outpatient transitions, and they issued a set of standards for improving those transitions (see “Managing Transitions in Care Between the Inpatient and Outpatient Settings,” p. 7).
“This consensus statement has enormous significance,” Dr. Ford says. “We’re finally shedding light on how to tackle patient handoff and hospital readmission issues, and we as a specialty have to take on care-transition improvement as our mantra. If we were to solve just that one piece, we can more easily start implementing other clinical guidelines. Care-transition guidelines are a fundamental tool to build consensus within your own group and with other clinicians in a team approach.”
Dr. Corrigan applauds the physician groups for publishing the transitions-of-care statement and encourages the societies to work together to “take it to the next step, which is to develop the measures and get them endorsed through the NQF process.”
SHM members are participating in workgroups convened by the NQF to identify standardized performance measures and to develop action plans over the next few months for several national priority areas—one of which is care coordination. “We have a ways to go to achieve better patient handoffs and information exchange between hospitals and other settings in the community. Hospitalists can drive the development of those guidelines and protocols,” Dr. Corrigan says. TH
Christopher Guadagnino, PhD, is a freelance medical writer based in Pennsylvania.
References
- Kripalani S, LeFevre F, Phillips CO, Williams MV; Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831-841.
- Timmermans S, Mauck A. The promises and pitfalls of evidence-based medicine. Health Affairs. 2005; 24(1):18-28.
- Snow V, Beck D, Budnitz T, et al. Transitions of care consensus policy statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, Society of Academic Emergency Medicine. J Hosp Med. 2009: 4(6)364-370.
Top Image Source: GOLDEN PIXELS LLC/ALAMY
Managing Transitions of Care Between the Inpatient and Outpatient Settings
The following are joint recommendations from SHM, ACP, SGIM, AGS, ACEP, and SAEM, based upon a multi-stakeholder consensus conference in July 2007 and published in the July/August Journal of Hospital Medicine (http://onlinelibrary.wiley.com/doi/10.1002/jhm.510/full):
- Communication and information exchange between the sending and receiving provider should be timely, as dictated by clinical presentation and urgency of follow-up care required.
- The transition record should always include at least these data elements: principal diagnosis, medication list, contact information of the transferring physician, patient’s cognitive status, test results or pending results. An ideal transition record would add six more elements.
- All communications need to be secure, private, HIPAA-compliant, and accessible to patients and their providers.
- Communities need to develop standard data transfer forms, with the ability to modify information as a patient’s condition changes.
- The sending provider maintains responsibility for the care of the patient until the receiving provider confirms that the transfer is complete. The sending provider should be available to clarify issues of care, and the patient should be able to identify the responsible provider.
- Information transfer should be timely, as determined by transition setting, patient circumstances, level of acuity, and clear transition responsibility.
- Medical institutions must adopt national standards and establish processes to promote effective transitions of care.
- Standardized and evidence-based metrics related to these standards should be used for monitoring and improving transitions.
Evidence-based practice guidelines are key tools to help hospitalists practice high-quality medicine and demonstrate the value of their inpatient care model. Guidelines are designed to produce superior care outcomes and resource utilization efficiencies by encouraging proven medical practices and discouraging ineffective or unproven ones. Yet inefficiencies, variation, and quality gaps persist in medical care—much to the chagrin of policymakers.
Is the answer more guidelines, and better implementation of existing ones?
Research experts and many HM leaders say yes.
In fact, HM is leading the way in an important new area for which there is little uniform guidance: optimal care transitions during patient handoffs. Care transitions are a pivotal time in the patient care process and are replete with avoidable service duplication, poor communication among providers, gaps in care reconciliation, and patient-safety issues.
SHM has joined five other organizations in issuing a Transitions of Care Consensus Policy Statement, which promises more systematic, safe, and efficient patient handoffs.1 SHM also is targeting care-transition improvement in a variety of other venues, all of which can help hospitalists demonstrate more persuasively the value they bring to healthcare delivery.
Guidelines Work
Practice guidelines work, in the sense that they help providers practice in ways consistent with what the best aggregate knowledge and expert opinion says is most effective. The evidence allows physicians to avoid expending scarce resources on ineffective clinical services. Their importance is magnified by the current urgency given to value-based purchasing in healthcare reform. “The right care, for the right patient, at the right time” is the new mantra of payors and policymakers, many of whom are demanding the best and most efficient healthcare delivery at the lowest cost.
“When providers are not providing the right care at the right time to patients, we find that the patient often gets more services … that they didn’t need. That oftentimes exposes them to potential harm and (services) that are wasteful of resources,” says Janet M. Corrigan, PhD, MBA, president and CEO of the National Quality Forum (NQF), a standard-setting organization that convenes national experts to apply “gold standard” endorsement of guidelines developed by professional medical societies and other entities. “Guidelines are a way of synthesizing evidence and translating it into action steps that providers can follow so that they get the best results that we know how to get for their patients.”
Clinicians and healthcare organizations have several sources for guidelines. The Agency for Healthcare Research and Quality (AHRQ) systematically reviews and vets guidelines submitted for inclusion in its National Guideline Clearinghouse (www.guideline.gov), and makes them available for evidence-based clinical decision-making, says Jean Slutsky, director of AHRQ’s Center for Outcomes and Evidence. AHRQ also offers public access to the National Quality Measure Clearinghouse and the Health Care Innovations Exchange, repositories of searchable quality measures and tools relevant to an array of diseases and conditions.
The Institute for Healthcare Improvement (IHI), an independent nonprofit organization, helps frontline physicians implement guidelines, and also helps provider teams decide which guidelines are most appropriate to achieve their desired outcomes, according to Amy E. Boutwell, MD, MPP, IHI’s director of health policy strategy.
Hospitalists use an array of disease-specific practice guidelines from different specialty societies for diagnoses they frequently encounter, such as chest pain, stroke, pneumonia, myocardial infarction, gastrointestinal bleeding, asthma, and chronic obstructive pulmonary disease (COPD). “Most hospitalists want to keep up with the best available evidence,” says Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., and chair of SHM’s Performance and Standards Committee. “The recently updated American College of Cardiology (ACC) and American Heart Association (AHA) guidelines on heart failure are exceptional. The American College of Chest Physicians has an extremely comprehensive set of guidelines on thrombosis, which is the bible for handling anticoagulation.”
Studies are published every month demonstrating that physicians who implement national guidelines at the local level improve such patient outcomes as mortality, length of stay, and time to clinical stability. Dr. Corrigan notes that there are abundant examples of guideline adherence boosting quality outcomes, and cites as a prime example the AHA’s Get With the Guidelines program (www.american heart.org/presenter.jhtml?identifier=1165), which has documented quality gains in coronary artery disease, stroke, and heart failure patients.
—William T. Ford, MD, FHM, section chief of hospital medicine, Temple University Hospital, Philadelphia
Barriers to Acceptance and Adherence
But there are obstacles to guideline adherence, and widespread practice pattern variation remains a huge national problem. Providers in some regions of the country can use twice the resources as their counterparts in other regions and bring no additional benefit to patients (see “Medicare Fee Inspection,” p. 30). The Dartmouth Atlas of Health Care says unwarranted practice variation is responsible for as much as 30% of wasted healthcare spending in the U.S.—a cost that reformers are anxious to eliminate.
The traditional culture of autonomy in the medical profession is perhaps the most difficult and enduring barrier to reducing unjustified practice variation: clinicians don’t automatically follow guidelines, many treat them more as options than as true standards, and organizations do not sufficiently enforce or reward adherence to guidelines, wrote researchers in a special 2005 issue of Health Affairs focusing on guidelines.2
“In an age of mandated cost control and resource limitation under managed care,” the researchers wrote, some physicians still regard practice guidelines as “cookbook medicine” that threatens the use of clinical judgment and encourages treating patients as essentially interchangeable. In the face of that perceived threat, the researchers added, many physicians continue to uphold a traditional view of medicine as an art “in which individual expertise and technique are allowed to shine through and ultimately result in a higher standard of patient care.”
Dr. Corrigan acknowledges the significant obstacles to successful practice guideline implementation:
- Guidelines are developed by various sources, particularly specialty societies, who do not always coordinate their activities. Physicians are left with overlapping and sometimes contradictory guidelines for managing the same disease or condition.
- Guidelines must be maintained and kept current, or physicians will lose confidence and not follow them.
- Guidelines are of varying quality. Some provide clear clinical direction; others are not written in a way that physicians can clearly translate into clinical practice.
- There are significant gaps in the evidence basis for guideline development. Much more comparative effectiveness research needs to be conducted to develop more valid and meaningful guidelines.
- Guidelines must be communicated effectively to physicians, making them available and convenient at the point of clinical care. Electronic health records with user-friendly decision support functions show great promise in “making the right thing the easy thing to do.”
- The fee-for-service payment system encourages greater volume of services, irrespective of guideline recommendations.
Physicians also recognize inherent limitations of guidelines. “Guidelines typically apply across populations. Adding levels of clinical complexity gets further away from a guideline’s applicability. Many physicians will tell you that the patient in front of them is a special case requiring a modification of the protocol,” Dr. Boutwell explains. For example, diabetic management guidelines are based on what is best for a population of diabetics, versus what is best for said hospitalist’s patient who has eight co-morbidities, one of which is diabetes, Boutwell notes. “Guidelines come disease-specific. Patients don’t,” she adds.
Nevertheless, Dr. Boutwell notes, there are robust guidelines and the IHI tries to help front-line physicians and care teams to implement them reliably and effectively.
An obstacle that inhibits hospitalists from implementing guidelines in an optimal fashion “is that we’re not one specialty—we deal with it all—and that complexity can be overwhelming. There is no central repository where all of the guidelines can be found in one place,” according to William T. Ford, MD, FHM, program medical director for Cogent Healthcare and section chief of hospital medicine for Temple University Hospital in Philadelphia.
Make Guidelines Work
Researchers say guidelines are most successful when they are well-supported and uncomplicated, backed by strong leadership and sufficient resources, and are used as “rallying points” to stimulate interdependent and collaborative care among physicians, nurses, pharmacists, equipment suppliers, administrators, and patients.
“Guidelines are really the foundation for determining best practices,” Dr. Torcson says. “There is no shortage of excellent guidelines, or proof that specific interventions do improve outcomes. The key is achieving more uniform implementation. We need tools like pre-printed orders in electronic health records (EHR) to effectively integrate these guidelines into hospitalists’ practice.”
More widespread EHR adoption with user-friendly medical decision-support systems will play a huge role in boosting guideline adoption and effectiveness, says Mary Nix, MS, MT(ASCP)SBB, health science administrator at AHRQ and project officer for the agency’s Center for Outcomes and Evidence.
Dr. Ford says HM groups must evaluate the top 10 to 15 diagnosis-related groups (DRGs) that they see each day (e.g., congestive heart failure, acute kidney failure, pneumonia, cellulitis, or acute coronary syndrome) and come to consensus on which guidelines best address them.
HM groups must then secure buy-in to those guidelines from everyone in the group; from the subspecialists they work with; and from their hospital’s chief medical, financial, and utilization officers.
Care-Transition Guidelines: Opportunity for Hospitalists
A particularly important HM opportunity is improving care transitions. Deficits in communication and information transfer between hospital-based and primary-care physicians (PCPs) are “substantial and ubiquitous,” while delays and omissions are consistently large, and traditional methods of completing and delivering discharge summaries are “suboptimal for communicating timely, accurate, and medically important data to the physicians who will be responsible for follow-up care,” according to a hospitalist-authored Feb. 28, 2007, article in the Journal of the American Medical Association.3 PCPs routinely are not notified about patient admissions or complications during the hospital stay, and some PCPs fail to provide sufficient information to hospitalists at admission, fail to visit or call hospitalized patients, or fail to participate in discharge planning, the study’s researchers noted. For patients with chronic illnesses and frequent hospitalization, those deficits are multiplied, making completeness of information handoffs particularly important.
Because patient handoffs have notoriously been fraught with miscommunication and poor information exchange between providers, adopting a professional consensus on what constitutes the best, safest, and most effective activities during these handoffs is sorely needed.
“Care-transition guidelines can have tremendous power because they affect every hospital patient—each of whom experiences care transitions,” says Rusty Holman, MD, FHM, chief operating officer of Brentwood, Tenn.-based Cogent Healthcare and past president of SHM. “It is an area undergoing rapid development, evolution, and discovery, and hospitalists have positioned themselves as leaders and owners of this particular scenario.”
As care-transition guidelines emerge and mature, Holman thinks they eventually will be tied to value-based healthcare purchasing programs that affect hospitalists’ reimbursement equations and further boost incentives to follow those guidelines. A prime example: Medicare calculated it could save $12 billion annually by reducing preventable 30-day hospital readmissions and will soon stop paying for them. Perhaps 3% to 5% of a hospital’s DRG reimbursement will be at risk under Medicare’s proposal, Dr. Torcson notes.
“Hospitals are going to be much more motivated to build systems and engage physicians, especially hospitalists, to lower readmission rates. Hospitalists will be focusing more and more on how care-transition process improvements can lower those rates,” Dr. Holman says. “That’s a huge opportunity for hospitalists to make a business case for the value they bring to their institutions, and will further justify the financial support they already receive.”
Dr. Ford is more cautious in his appraisal of the financial rewards of better guideline implementation. “We do not capture that much revenue per patient, and even a length-of-stay reduction is difficult for a hospital’s CFO to extrapolate how much money hospitalists save,” he says. “I don’t think hospitalists will be paid more, even if they save the hospital money. You’re just doing your job, but you’re going to keep your job, and you’ll have an enormous bargaining chip when renegotiating contracts with hospitals.”
Still, a prevented readmission might mean a bed for a revenue-generating elective surgery, something that adds to the reward equation.
—Patrick Torcson, MD, MMM, FACP, director of hospital medicine, St. Tammany Parish Hospital, Covington, La., SHM Performance and Standards Committee chair
Transition Evolution
SHM and other sources offer physicians and hospitals expert assistance in implementing care-transition guidelines (see “Care-Transition Guidance,” p. 7). The transitions-of-care policy statement jointly issued by the SHM and five other specialty societies further demonstrates that hospitalists play a key leadership role on this front.1
The policy statement emerged from a multi-stakeholder consensus conference convened by SHM, the American College of Physicians (ACP), and the Society of General Internal Medicine, which was attended by more than 30 medical specialty societies, governmental agencies, and performance measure developers. Participants focused on what standard pieces of information should be exchanged among providers during inpatient to outpatient transitions, and they issued a set of standards for improving those transitions (see “Managing Transitions in Care Between the Inpatient and Outpatient Settings,” p. 7).
“This consensus statement has enormous significance,” Dr. Ford says. “We’re finally shedding light on how to tackle patient handoff and hospital readmission issues, and we as a specialty have to take on care-transition improvement as our mantra. If we were to solve just that one piece, we can more easily start implementing other clinical guidelines. Care-transition guidelines are a fundamental tool to build consensus within your own group and with other clinicians in a team approach.”
Dr. Corrigan applauds the physician groups for publishing the transitions-of-care statement and encourages the societies to work together to “take it to the next step, which is to develop the measures and get them endorsed through the NQF process.”
SHM members are participating in workgroups convened by the NQF to identify standardized performance measures and to develop action plans over the next few months for several national priority areas—one of which is care coordination. “We have a ways to go to achieve better patient handoffs and information exchange between hospitals and other settings in the community. Hospitalists can drive the development of those guidelines and protocols,” Dr. Corrigan says. TH
Christopher Guadagnino, PhD, is a freelance medical writer based in Pennsylvania.
References
- Kripalani S, LeFevre F, Phillips CO, Williams MV; Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831-841.
- Timmermans S, Mauck A. The promises and pitfalls of evidence-based medicine. Health Affairs. 2005; 24(1):18-28.
- Snow V, Beck D, Budnitz T, et al. Transitions of care consensus policy statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, Society of Academic Emergency Medicine. J Hosp Med. 2009: 4(6)364-370.
Top Image Source: GOLDEN PIXELS LLC/ALAMY
Managing Transitions of Care Between the Inpatient and Outpatient Settings
The following are joint recommendations from SHM, ACP, SGIM, AGS, ACEP, and SAEM, based upon a multi-stakeholder consensus conference in July 2007 and published in the July/August Journal of Hospital Medicine (http://onlinelibrary.wiley.com/doi/10.1002/jhm.510/full):
- Communication and information exchange between the sending and receiving provider should be timely, as dictated by clinical presentation and urgency of follow-up care required.
- The transition record should always include at least these data elements: principal diagnosis, medication list, contact information of the transferring physician, patient’s cognitive status, test results or pending results. An ideal transition record would add six more elements.
- All communications need to be secure, private, HIPAA-compliant, and accessible to patients and their providers.
- Communities need to develop standard data transfer forms, with the ability to modify information as a patient’s condition changes.
- The sending provider maintains responsibility for the care of the patient until the receiving provider confirms that the transfer is complete. The sending provider should be available to clarify issues of care, and the patient should be able to identify the responsible provider.
- Information transfer should be timely, as determined by transition setting, patient circumstances, level of acuity, and clear transition responsibility.
- Medical institutions must adopt national standards and establish processes to promote effective transitions of care.
- Standardized and evidence-based metrics related to these standards should be used for monitoring and improving transitions.
Borderline or bipolar? Don't skimp on the life story
Shift-work disorder
The burden of shift-work disorder (SWD) is multifactorial—affecting relationships, health, and work performance. Lack of support, research, and treatment for SWD has economic and safety consequences for society in general. In this supplement, sleep experts suggest practical steps to relieve the adverse effects of SWD.
The burden of shift-work disorder (SWD) is multifactorial—affecting relationships, health, and work performance. Lack of support, research, and treatment for SWD has economic and safety consequences for society in general. In this supplement, sleep experts suggest practical steps to relieve the adverse effects of SWD.
The burden of shift-work disorder (SWD) is multifactorial—affecting relationships, health, and work performance. Lack of support, research, and treatment for SWD has economic and safety consequences for society in general. In this supplement, sleep experts suggest practical steps to relieve the adverse effects of SWD.
Support
Support for the publication of this supplement was provided by Cephalon, Inc. Editorial assistance was provided by Anthemis Consulting Ltd and supported by Cephalon, Inc.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily represent those of Cephalon, Inc., or the publishers. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested by the authors should not be used by clinicians without evaluation of their patients’ conditions and possible contraindications or dangers in use, review of any applicable manufacturer’s product information, and comparisons with the recommendations of other authorities. Content may include product information that is inconsistent with or outside the approved labeling for these products in the United States. Before prescribing any medication, you must familiarize yourself with the manufacturer’s product information.
This material was submitted by Anthemis Consulting Ltd on behalf of the authors. It has been edited and peer reviewed by The Journal of Family Practice.
Should we routinely screen for hypercapnia in sleep apnea patients before elective noncardiac surgery?
Yes. Obesity hypoventilation syndrome (OHS) is often undiagnosed and greatly increases perioperative risk. Therefore, we recommend trying to detect OHS in a timely manner. Treatment should begin without delay to avoid adverse perioperative outcomes, which can include acute-on-chronic respiratory failure requiring intensive-care monitoring and invasive mechanical ventilation, or death.
ALSO CALLED PICKWICKIAN SYNDROME
OHS is also known as Pickwickian syndrome, named for a character—a “fat boy” who is constantly falling asleep—in The Posthumous Papers of the Pickwick Club by Charles Dickens.
Salient features of OHS are:
- Obesity (body mass index ≥ 30 kg/m2)
- Sleep-disordered breathing (most patients with OHS are morbidly obese and have severe obstructive sleep apnea1)
- Chronic daytime alveolar hypoventilation: ie, Paco2 ≥ 45 mm Hg (normal range 35–45 mm Hg) and Pao2 < 70 mm Hg1 (normal range 85–95 mm Hg)
- No other identifiable cause of hypoventilation such as pulmonary disease (severe obstructive or restrictive), chest wall deformities, severe hypothyroidism, or neuromuscular disease.
WHY SCREEN FOR OHS?
Both obstructive sleep apnea and OHS worsen quality of life and increase the risk of serious disease and death.2–3 Patients with severe sleep apnea, particularly those with hypercapnia (ie, OHS) are at higher risk of cardiopulmonary complications in the perioperative period.
Compared with eucapnic patients with obstructive sleep apnea, patients with OHS have higher health care expenses, are at higher risk of developing serious cardiovascular diseases such as pulmonary hypertension and congestive heart failure, and are more likely to die sooner.4,5
Nowbar et al5 prospectively followed a group of severely obese patients after hospital discharge. At 18 months, 23% of those with OHS had died, compared with 9% of those without OHS. The groups were well matched for body mass index, age, and a number of comorbid conditions. Most of the deaths occurred in the first 3 months after hospital discharge. During the hospital stay, more patients with OHS were admitted to the intensive care unit and needed endotracheal intubation and mechanical ventilation, and more were discharged to a long-term facility.
A high level of suspicion can lead to early recognition and treatment, which may reduce the rate of adverse outcomes associated with undiagnosed and untreated OHS. Routine screening for hypercapnia in patients with sleep apnea might help to identify patients with OHS and allow for modifications in surgical approach, anesthetic technique, and postoperative monitoring, increasing patient safety.
HOW PREVALENT IS OHS?
Obstructive sleep apnea affects up to 20% of US adults and is undiagnosed and untreated in up to 90% of cases.6 Simple screening questionnaires have been shown to reliably identify patients at risk.7,8
To date, no population-based prevalence studies of OHS have been done.
The overall prevalence of OHS in patients with obstructive sleep apnea is better studied: multiple prospective and retrospective studies across various geographic regions with a variety of racial or ethnic populations have shown it to be between 10% and 20%.1,9 This range is very consistent among studies performed in Europe, the United States, and Japan, whether retrospective or prospective, and whether large or small.
The prevalence of OHS in the general adult population in the United States can, however, be estimated. If approximately 5% of the general US population has severe obesity (body mass index ≤ 40 kg/m2), if half of patients with severe obesity have obstructive sleep apnea,10 and if 15% of severely obese patients with sleep apnea have OHS, then a conservative estimated prevalence of OHS in the general adult US population is 0.37% (1 in 270 adults).
WHAT CAN BE DONE BEFORE ELECTIVE SURGERY?
Patients with OHS have an elevated serum bicarbonate level due to metabolic compensation for chronic respiratory acidosis. Moreover, they may have mild hypoxemia during wakefulness as measured by finger pulse oximetry.
The serum venous bicarbonate level is an easy and reasonable test to screen for hypercapnia in obese patients with obstructive sleep apnea because it is readily available, physiologically sensible, and less invasive than arterial puncture to measure blood gases.9
Arterial blood gas measurements, however, should be obtained to confirm the presence and severity of daytime hypercapnia in obese patients with hypoxemia during wakefulness or an elevated serum bicarbonate level.
Pulmonary function testing and chest imaging can exclude other causes of hypercapnia if hypercapnia is confirmed.
An overnight, attended polysomnographic study in a sleep laboratory is ultimately needed to establish the diagnosis and severity of obstructive sleep apnea and to titrate continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BPAP) therapy. Since most patients with OHS have severe obstructive sleep apnea, in-laboratory attended polysomnography allows the clinician to both diagnose and intervene with PAP therapy (a “split-night” study). Home titration with an auto-CPAP device is not recommended because it does not have the ability to titrate PAP pressures in response to hypoxemia or hypoventilation. Patients with OHS require attended, laboratory-based PAP titration with or without supplemental oxygen.
CPAP or BPAP therapy should be started during the few days or weeks before surgery, and adherence should be emphasized. Anesthesiologists might reconsider the choice of anesthetic technique in favor of regional anesthesia and modify postoperative pain management to reduce opioid requirements. Reinstituting CPAP or BPAP therapy upon extubation or arrival in the postoperative recovery unit can further reduce the risk of respiratory complications. Additional monitoring such as continuous pulse oximetry when the patient is on the general ward should be considered.
- Mokhlesi B, Kryger MH, Grunstein RR. Assessment and management of patients with obesity hypoventilation syndrome. Proc Am Thorac Soc 2008; 5:218–225.
- Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. JAMA 2005; 293:1861–1867.
- Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008; 31:1071–1078.
- Berg G, Delaive K, Manfreda J, Walld R, Kryger MH. The use of health-care resources in obesity-hypoventilation syndrome. Chest 2001; 120:377–383.
- Nowbar S, Burkart KM, Gonzales R, et al. Obesity-associated hypoventilation in hospitalized patients: prevalence, effects, and outcome. Am J Med 2004; 116:1–7.
- Kapur V, Strohl KP, Redline S, Iber C, O'Connor G, Nieto J. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep Breath 2002; 6:49–54.
- Finkel KJ, Searleman AC, Tymkew H, et al. Prevalence of undiagnosed obstructive sleep apnea among adult surgical patients in an academic medical center. Sleep Med 2009; 10:753–758.
- Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008; 108:812–821.
- Mokhlesi B, Tulaimat A, Faibussowitsch I, Wang Y, Evans AT. Obesity hypoventilation syndrome: prevalence and predictors in patients with obstructive sleep apnea. Sleep Breath 2007; 11:117–124.
- Lee W, Nagubadi S, Kryger MH, Mokhlesi B. Epidemiology of obstructive sleep apnea: a population-based perspective. Expert Rev Respir Med 2008; 2:349–364.
Yes. Obesity hypoventilation syndrome (OHS) is often undiagnosed and greatly increases perioperative risk. Therefore, we recommend trying to detect OHS in a timely manner. Treatment should begin without delay to avoid adverse perioperative outcomes, which can include acute-on-chronic respiratory failure requiring intensive-care monitoring and invasive mechanical ventilation, or death.
ALSO CALLED PICKWICKIAN SYNDROME
OHS is also known as Pickwickian syndrome, named for a character—a “fat boy” who is constantly falling asleep—in The Posthumous Papers of the Pickwick Club by Charles Dickens.
Salient features of OHS are:
- Obesity (body mass index ≥ 30 kg/m2)
- Sleep-disordered breathing (most patients with OHS are morbidly obese and have severe obstructive sleep apnea1)
- Chronic daytime alveolar hypoventilation: ie, Paco2 ≥ 45 mm Hg (normal range 35–45 mm Hg) and Pao2 < 70 mm Hg1 (normal range 85–95 mm Hg)
- No other identifiable cause of hypoventilation such as pulmonary disease (severe obstructive or restrictive), chest wall deformities, severe hypothyroidism, or neuromuscular disease.
WHY SCREEN FOR OHS?
Both obstructive sleep apnea and OHS worsen quality of life and increase the risk of serious disease and death.2–3 Patients with severe sleep apnea, particularly those with hypercapnia (ie, OHS) are at higher risk of cardiopulmonary complications in the perioperative period.
Compared with eucapnic patients with obstructive sleep apnea, patients with OHS have higher health care expenses, are at higher risk of developing serious cardiovascular diseases such as pulmonary hypertension and congestive heart failure, and are more likely to die sooner.4,5
Nowbar et al5 prospectively followed a group of severely obese patients after hospital discharge. At 18 months, 23% of those with OHS had died, compared with 9% of those without OHS. The groups were well matched for body mass index, age, and a number of comorbid conditions. Most of the deaths occurred in the first 3 months after hospital discharge. During the hospital stay, more patients with OHS were admitted to the intensive care unit and needed endotracheal intubation and mechanical ventilation, and more were discharged to a long-term facility.
A high level of suspicion can lead to early recognition and treatment, which may reduce the rate of adverse outcomes associated with undiagnosed and untreated OHS. Routine screening for hypercapnia in patients with sleep apnea might help to identify patients with OHS and allow for modifications in surgical approach, anesthetic technique, and postoperative monitoring, increasing patient safety.
HOW PREVALENT IS OHS?
Obstructive sleep apnea affects up to 20% of US adults and is undiagnosed and untreated in up to 90% of cases.6 Simple screening questionnaires have been shown to reliably identify patients at risk.7,8
To date, no population-based prevalence studies of OHS have been done.
The overall prevalence of OHS in patients with obstructive sleep apnea is better studied: multiple prospective and retrospective studies across various geographic regions with a variety of racial or ethnic populations have shown it to be between 10% and 20%.1,9 This range is very consistent among studies performed in Europe, the United States, and Japan, whether retrospective or prospective, and whether large or small.
The prevalence of OHS in the general adult population in the United States can, however, be estimated. If approximately 5% of the general US population has severe obesity (body mass index ≤ 40 kg/m2), if half of patients with severe obesity have obstructive sleep apnea,10 and if 15% of severely obese patients with sleep apnea have OHS, then a conservative estimated prevalence of OHS in the general adult US population is 0.37% (1 in 270 adults).
WHAT CAN BE DONE BEFORE ELECTIVE SURGERY?
Patients with OHS have an elevated serum bicarbonate level due to metabolic compensation for chronic respiratory acidosis. Moreover, they may have mild hypoxemia during wakefulness as measured by finger pulse oximetry.
The serum venous bicarbonate level is an easy and reasonable test to screen for hypercapnia in obese patients with obstructive sleep apnea because it is readily available, physiologically sensible, and less invasive than arterial puncture to measure blood gases.9
Arterial blood gas measurements, however, should be obtained to confirm the presence and severity of daytime hypercapnia in obese patients with hypoxemia during wakefulness or an elevated serum bicarbonate level.
Pulmonary function testing and chest imaging can exclude other causes of hypercapnia if hypercapnia is confirmed.
An overnight, attended polysomnographic study in a sleep laboratory is ultimately needed to establish the diagnosis and severity of obstructive sleep apnea and to titrate continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BPAP) therapy. Since most patients with OHS have severe obstructive sleep apnea, in-laboratory attended polysomnography allows the clinician to both diagnose and intervene with PAP therapy (a “split-night” study). Home titration with an auto-CPAP device is not recommended because it does not have the ability to titrate PAP pressures in response to hypoxemia or hypoventilation. Patients with OHS require attended, laboratory-based PAP titration with or without supplemental oxygen.
CPAP or BPAP therapy should be started during the few days or weeks before surgery, and adherence should be emphasized. Anesthesiologists might reconsider the choice of anesthetic technique in favor of regional anesthesia and modify postoperative pain management to reduce opioid requirements. Reinstituting CPAP or BPAP therapy upon extubation or arrival in the postoperative recovery unit can further reduce the risk of respiratory complications. Additional monitoring such as continuous pulse oximetry when the patient is on the general ward should be considered.
Yes. Obesity hypoventilation syndrome (OHS) is often undiagnosed and greatly increases perioperative risk. Therefore, we recommend trying to detect OHS in a timely manner. Treatment should begin without delay to avoid adverse perioperative outcomes, which can include acute-on-chronic respiratory failure requiring intensive-care monitoring and invasive mechanical ventilation, or death.
ALSO CALLED PICKWICKIAN SYNDROME
OHS is also known as Pickwickian syndrome, named for a character—a “fat boy” who is constantly falling asleep—in The Posthumous Papers of the Pickwick Club by Charles Dickens.
Salient features of OHS are:
- Obesity (body mass index ≥ 30 kg/m2)
- Sleep-disordered breathing (most patients with OHS are morbidly obese and have severe obstructive sleep apnea1)
- Chronic daytime alveolar hypoventilation: ie, Paco2 ≥ 45 mm Hg (normal range 35–45 mm Hg) and Pao2 < 70 mm Hg1 (normal range 85–95 mm Hg)
- No other identifiable cause of hypoventilation such as pulmonary disease (severe obstructive or restrictive), chest wall deformities, severe hypothyroidism, or neuromuscular disease.
WHY SCREEN FOR OHS?
Both obstructive sleep apnea and OHS worsen quality of life and increase the risk of serious disease and death.2–3 Patients with severe sleep apnea, particularly those with hypercapnia (ie, OHS) are at higher risk of cardiopulmonary complications in the perioperative period.
Compared with eucapnic patients with obstructive sleep apnea, patients with OHS have higher health care expenses, are at higher risk of developing serious cardiovascular diseases such as pulmonary hypertension and congestive heart failure, and are more likely to die sooner.4,5
Nowbar et al5 prospectively followed a group of severely obese patients after hospital discharge. At 18 months, 23% of those with OHS had died, compared with 9% of those without OHS. The groups were well matched for body mass index, age, and a number of comorbid conditions. Most of the deaths occurred in the first 3 months after hospital discharge. During the hospital stay, more patients with OHS were admitted to the intensive care unit and needed endotracheal intubation and mechanical ventilation, and more were discharged to a long-term facility.
A high level of suspicion can lead to early recognition and treatment, which may reduce the rate of adverse outcomes associated with undiagnosed and untreated OHS. Routine screening for hypercapnia in patients with sleep apnea might help to identify patients with OHS and allow for modifications in surgical approach, anesthetic technique, and postoperative monitoring, increasing patient safety.
HOW PREVALENT IS OHS?
Obstructive sleep apnea affects up to 20% of US adults and is undiagnosed and untreated in up to 90% of cases.6 Simple screening questionnaires have been shown to reliably identify patients at risk.7,8
To date, no population-based prevalence studies of OHS have been done.
The overall prevalence of OHS in patients with obstructive sleep apnea is better studied: multiple prospective and retrospective studies across various geographic regions with a variety of racial or ethnic populations have shown it to be between 10% and 20%.1,9 This range is very consistent among studies performed in Europe, the United States, and Japan, whether retrospective or prospective, and whether large or small.
The prevalence of OHS in the general adult population in the United States can, however, be estimated. If approximately 5% of the general US population has severe obesity (body mass index ≤ 40 kg/m2), if half of patients with severe obesity have obstructive sleep apnea,10 and if 15% of severely obese patients with sleep apnea have OHS, then a conservative estimated prevalence of OHS in the general adult US population is 0.37% (1 in 270 adults).
WHAT CAN BE DONE BEFORE ELECTIVE SURGERY?
Patients with OHS have an elevated serum bicarbonate level due to metabolic compensation for chronic respiratory acidosis. Moreover, they may have mild hypoxemia during wakefulness as measured by finger pulse oximetry.
The serum venous bicarbonate level is an easy and reasonable test to screen for hypercapnia in obese patients with obstructive sleep apnea because it is readily available, physiologically sensible, and less invasive than arterial puncture to measure blood gases.9
Arterial blood gas measurements, however, should be obtained to confirm the presence and severity of daytime hypercapnia in obese patients with hypoxemia during wakefulness or an elevated serum bicarbonate level.
Pulmonary function testing and chest imaging can exclude other causes of hypercapnia if hypercapnia is confirmed.
An overnight, attended polysomnographic study in a sleep laboratory is ultimately needed to establish the diagnosis and severity of obstructive sleep apnea and to titrate continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BPAP) therapy. Since most patients with OHS have severe obstructive sleep apnea, in-laboratory attended polysomnography allows the clinician to both diagnose and intervene with PAP therapy (a “split-night” study). Home titration with an auto-CPAP device is not recommended because it does not have the ability to titrate PAP pressures in response to hypoxemia or hypoventilation. Patients with OHS require attended, laboratory-based PAP titration with or without supplemental oxygen.
CPAP or BPAP therapy should be started during the few days or weeks before surgery, and adherence should be emphasized. Anesthesiologists might reconsider the choice of anesthetic technique in favor of regional anesthesia and modify postoperative pain management to reduce opioid requirements. Reinstituting CPAP or BPAP therapy upon extubation or arrival in the postoperative recovery unit can further reduce the risk of respiratory complications. Additional monitoring such as continuous pulse oximetry when the patient is on the general ward should be considered.
- Mokhlesi B, Kryger MH, Grunstein RR. Assessment and management of patients with obesity hypoventilation syndrome. Proc Am Thorac Soc 2008; 5:218–225.
- Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. JAMA 2005; 293:1861–1867.
- Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008; 31:1071–1078.
- Berg G, Delaive K, Manfreda J, Walld R, Kryger MH. The use of health-care resources in obesity-hypoventilation syndrome. Chest 2001; 120:377–383.
- Nowbar S, Burkart KM, Gonzales R, et al. Obesity-associated hypoventilation in hospitalized patients: prevalence, effects, and outcome. Am J Med 2004; 116:1–7.
- Kapur V, Strohl KP, Redline S, Iber C, O'Connor G, Nieto J. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep Breath 2002; 6:49–54.
- Finkel KJ, Searleman AC, Tymkew H, et al. Prevalence of undiagnosed obstructive sleep apnea among adult surgical patients in an academic medical center. Sleep Med 2009; 10:753–758.
- Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008; 108:812–821.
- Mokhlesi B, Tulaimat A, Faibussowitsch I, Wang Y, Evans AT. Obesity hypoventilation syndrome: prevalence and predictors in patients with obstructive sleep apnea. Sleep Breath 2007; 11:117–124.
- Lee W, Nagubadi S, Kryger MH, Mokhlesi B. Epidemiology of obstructive sleep apnea: a population-based perspective. Expert Rev Respir Med 2008; 2:349–364.
- Mokhlesi B, Kryger MH, Grunstein RR. Assessment and management of patients with obesity hypoventilation syndrome. Proc Am Thorac Soc 2008; 5:218–225.
- Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. JAMA 2005; 293:1861–1867.
- Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008; 31:1071–1078.
- Berg G, Delaive K, Manfreda J, Walld R, Kryger MH. The use of health-care resources in obesity-hypoventilation syndrome. Chest 2001; 120:377–383.
- Nowbar S, Burkart KM, Gonzales R, et al. Obesity-associated hypoventilation in hospitalized patients: prevalence, effects, and outcome. Am J Med 2004; 116:1–7.
- Kapur V, Strohl KP, Redline S, Iber C, O'Connor G, Nieto J. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep Breath 2002; 6:49–54.
- Finkel KJ, Searleman AC, Tymkew H, et al. Prevalence of undiagnosed obstructive sleep apnea among adult surgical patients in an academic medical center. Sleep Med 2009; 10:753–758.
- Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008; 108:812–821.
- Mokhlesi B, Tulaimat A, Faibussowitsch I, Wang Y, Evans AT. Obesity hypoventilation syndrome: prevalence and predictors in patients with obstructive sleep apnea. Sleep Breath 2007; 11:117–124.
- Lee W, Nagubadi S, Kryger MH, Mokhlesi B. Epidemiology of obstructive sleep apnea: a population-based perspective. Expert Rev Respir Med 2008; 2:349–364.
Food allergy and eosinophilic esophagitis: Learning what to avoid
More children and even adults seem to be allergic to various foods these days than in the past. Also apparently on the rise is a linked condition, eosinophilic esophagitis.
The reason for these increases is not clear. This article confines itself to what we know about the mechanisms of food allergies and eosinophilic esophagitis, how to diagnose them, and how to treat them.
FOOD ALLERGIES ARE COMMON, AND MORE PREVALENT THAN EVER
Food allergies—abnormal immune responses to food proteins1—affect an estimated 6% to 8% of young children and 3% to 4% of adults in the United States,2,3 and their prevalence appears to be rising in developed countries. Studies in US and British children indicate that peanut allergy has doubled in the past decade. 4
Any food can provoke a reaction, but only a few foods account for most of the significant allergic reactions: cow’s milk, soy, wheat, eggs, peanuts, tree nuts, fish, and shellfish.
Approximately 80% of allergies to milk, egg, wheat, and soy resolve by the time the patient reaches early adolescence.6 Fewer cases resolve in children with tree nut allergies (approximately 9%) or peanut allergy (20%),7,8 and allergies to fish and shellfish often develop or persist in adulthood.
A family history of an atopic disease such as asthma, allergic rhinitis, eczema, or food allergy is a risk factor for developing a food allergy. 3 Considering that the rate of peanut allergy has doubled in children over the past 10 years, environmental factors may also play a role.3
How we tolerate foods or become allergic to them
The gut, the largest mucosal organ in the body, is exposed to large quantities of foreign proteins daily. Most protein is broken down by stomach acid and digestive enzymes into lessantigenic peptides or is bound by secretory immunoglobulin A (IgA), which prevents it from being absorbed. Further, the epithelial cells lining the gut do not allow large molecules to pass easily, having tight intracellular junctions and being covered with mucus.
For these reasons, less than 2% of the protein in food is absorbed in an allergenic form.9 The reason food allergies are more prevalent in children is most likely that children have an immature gut barrier, lower IgA levels, a higher gastric pH, and lower proteolytic enzyme levels.
When dietary proteins do cross the gut barrier, the immune system normally suppresses the allergic response. Regulatory T cells, dendritic cells, and local immune responses play critical roles in the development of tolerance. Several types of regulatory T cells, such as Tr1 cells (which secrete interleukin 10), TH3 cells (which secrete transforming growth factor beta), CD4+CD25+ regulatory T cells, gamma-delta T cells, and CD8+ suppressor cells can all contribute to suppressing allergic responses.10 Dendritic cells also help induce tolerance by stimulating CD4+ T cells to secrete transforming growth factor beta, which leads to the production of interleukin 10 and additional transforming growth factor beta.11
Factors that contribute to food allergy
Many factors may contribute to whether a person becomes tolerant to or sensitized to a specific food protein.
The dose of antigen. Tolerance can develop after either high or low doses of antigens, but by different mechanisms.
The antigen structure. Soluble antigens are less sensitizing than particulate antigens.12,13
Processing of foods. Dry-roasted peanuts are more allergenic than raw or boiled peanuts, partly because they are less soluble.13
The route of initial exposure. Sensitization to food proteins can occur directly through the gut or the skin. Alternatively, it can occur indirectly via the respiratory tract. Skin exposure may be especially sensitizing in children with atopic dermatitis.14,15
The gut flora. When mice are raised in a germ-free environment, they fail to develop normal tolerance.16 They are also more likely to become sensitized if they are treated with antibiotics or if they lack toll-like receptors that recognize bacterial lipopolysaccharides.17 Furthermore, human studies suggest that probiotics promote tolerance, especially in preventing atopic dermatitis, although the studies have had conflicting results.18–21
The gastric pH. Murine and human studies reveal that antacid medications increase the risk of food allergy.22,23
Genetic susceptibility. A child with a sibling who is allergic to peanuts is approximately 10 times more likely to be allergic to peanuts than predicted by the rate in the general population. Although no risk-conferring gene has been identified, a study of twins showed concordance for peanut allergy in 64.3% of identical twins vs 6.8% of fraternal twins.24
Three types of immune responses to food
Immunologic reactions to foods can be divided into three categories: mediated by immunoglobulin E (IgE), non-IgE-mediated, and mixed. Therefore, these disorders can present as an acute, potentially life-threatening reaction or as a chronic disease such as eosinophilic gastoenteropathy.
IgE-mediated reactions are immediate hypersensitivity responses. In most patients, an IgE-mediated mechanism can be confirmed by a positive skin test or a test for food-specific IgE in the serum. In this article, the term “food allergy” refers to an IgE-mediated reaction to a food, unless otherwise indicated.
Non-IgE-mediated reactions have a delayed onset and chronic symptoms. Commonly, they are confined to the gastrointestinal tract; examples are food-protein-induced enterocolitis, proctitis, and proctocolitis and celiac disease.3,26,27 However, other diseases such as contact dermatitis, dermatitis herpetiformis, and food-induced pulmonary hemosiderosis (Heiner syndrome) are also considered non-IgE-mediated allergies.
Mixed-reaction disorders are chronic and include the eosinophilic gastroenteropathies, ie, eosinophilic proctocolitis, eosinophilic gastroenteritis, and eosinophilic esophagitis.28 The pathophysiology of these diseases is poorly understood. Many patients have evidence of allergic sensitivities to food or to environmental allergens, or both, but whether these sensitivities have a causal role in these disorders is not clear.
Atopic dermatitis, another complicated disease process, may be associated with mixedreaction food allergy, as approximately 35% of young children with moderate to severe atopic dermatitis have food allergies.29
Diagnosis of IgE-mediated food allergies
A thorough history and physical examination are key to diagnosing an IgE-mediated food allergy.
The history should include potential culprit foods, the quantity eaten, the timing of the onset of symptoms, and related factors such as exercise, alcohol intake, or medication use. Symptoms of an IgE-mediated reaction are generally rapid in onset but may be delayed up to a few hours, while non-IgE mediated symptoms may present several hours to days later.
Food challenge. A double-blind, placebocontrolled oral food challenge is the gold standard for the diagnosis of food allergies. (The food to be tested is hidden in other food or in capsules.) However, this test poses significant risks, and other diagnostic methods are more practical for screening.
Skin-prick tests with commercially available extracts are a rapid and sensitive method of screening for allergy to several foods.
Negative skin-prick tests have an estimated negative predictive value of more than 95% and can therefore exclude IgE-mediated food allergies.
A positive test indicates the presence of IgE against a specific food allergen and suggests a clinical food allergy, although the specificity of the test is only about 50%, making a positive result difficult to interpret. Although the size of the skin-test response does not necessarily correlate with the potential severity of a reaction, a response larger than 3 mm does indicate a greater likelihood of clinical reactivity. A positive test is most helpful in confirming the diagnosis of IgE-mediated food allergy when combined with a clear history of food-induced symptoms.
The proteins in commercially based extracts of most fruits and vegetables are often labile; therefore, skin testing with fresh fruits and vegetables may be indicated.30
Immunoassays. Radioallergosorbent tests (RASTs) and fluorescent enzyme immunoassays are used to identity food-specific IgE antibodies in the serum. The commercially available tests do not use radioactivity, but the term “RAST” is still commonly used.
Immunoassays are generally less sensitive and more costly than skin-prick tests, and their results are not immediately available, unlike those of skin-prick testing. However, these in vitro tests are not affected by antihistamine use and are useful in patients with severe dermatologic conditions or severe anaphylaxis, for whom skin-prick testing would not be appropriate.
However, unlike a negative skin-prick test, an undetectable serum food-specific IgE level has a low negative predictive value, and an undetectable level may be associated with symptoms of an allergic reaction for 10% to 25% of patients.29 Therefore, if one suspects an allergic reaction but no food-specific IgE can be detected in the serum, confirming the absence of a clinical allergy must be done with a skin-prick test or with a physician-supervised oral challenge, or both.
Managing food allergy by avoiding the allergen
Food allergies are managed by strictly avoiding food allergens and by taking medications such as self-injectable epinephrine for anaphylactic symptoms.
Patients and caregivers must be educated about reading food labels, avoiding high-risk situations such as eating at buffets and other restaurants with high risk of cross-contamination, wearing a medical-alert bracelet, recognizing and managing early symptoms of an allergic reaction, and calling for emergency services if they are having an allergic reaction. Since January 2006, the US Food and Drug Administration has required food manufacturers to list common food allergens on food labels (cow’s milk, soy, wheat, egg, peanut, tree nuts, fish, and shellfish), and the labeling must use simple, easily understood terms, such as “milk” instead of “whey.” However, it is still prudent to read all ingredients listed on the label.
Experimental treatments for food allergies
Humanized monoclonal anti-IgE antibodies such as talizumab (also known as TNX-901) and omalizumab (Xolair) have been developed, but their use in food allergy has been limited. In a study in patients with peanut allergy, injections of talizumab increased the threshold for sensitivity to peanuts in most patients, but 25% of the patients did not have any improvement.32 A study of omalizumab in patients with peanut allergy was stopped after adverse reactions developed during oral peanut challenges.33
Oral immunotherapy. Recent studies suggest it may be possible to induce oral tolerance in patients with IgE-mediated food allergy. Pilot studies have shown that frequent, increasing doses of food allergens (egg, milk, and peanut) may raise the threshold at which symptoms occur.34–36 Though these studies suggest that oral immunotherapy may protect some patients against a reaction if they accidentally ingest a food they are allergic to, some patients could not reach the goal doses because allergic symptoms were provoked.
At this early stage, these strategies must be considered investigational, and more randomized, placebo-controlled studies are needed. Further studies will also be needed to assess whether oral immunotherapy induces only short-term desensitization (in which case the allergen needs to be ingested daily to prevent reactions) or sustained tolerance (in which case the antigenic protein can be ingested without symptoms despite periods of abstinence).
THE ROLE OF FOOD ALLERGY IN EOSINOPHILIC ESOPHAGITIS
Eosinophilic esophagitis has been recognized with increasing frequency in both children and adults over the past several years. Symptoms can include difficulty feeding, failure to thrive, vomiting, epigastric or chest pain, dysphagia, and food impaction.
Diagnostic criteria for eosinophilic esophagitis are37:
- Clinical symptoms of esophageal dysfunction
- At least 15 eosinophils per high-power field in at least one esophageal biopsy specimen
- No response to a proton-pump inhibitor in high doses (up to 2 mg/kg/day) for 1 to 2 months, or normal results on pH probe monitoring of the esophagus (the reason for this criterion is that patients with gastroesophageal reflux disease can also have large numbers of eosinophils in the esophagus—more than 100 per highpower field38)
- Exclusion of other causes.
Though the cause of eosinophilic esophagitis is not completely understood, atopy has been strongly implicated as a factor. More than 50% of patients with eosinophilic esophagitis also have an atopic condition (eg, atopic dermatitis, allergic rhinitis, asthma), as well as positive results on skin-prick testing or measurement of antigen-specific IgE in the serum.39–41 Also, since most patients improve with either dietary restriction or elemental diets, food sensitization appears to play a considerable role.
As with atopic conditions such as asthma, atopic dermatitis, allergic rhinitis, and food allergy, eosinophilic esophagitis has been linked with immune responses involving helper T cell 2 (TH2). Adults and children with eosinophilic esophagitis have been found to have elevated eosinophil counts and total IgE levels in peripheral blood.37 In the esophagus, patients have elevated levels of the TH2 cytokines often seen in atopic patients (eg, interleukins 4, 5, and 13) and mast cells.42,43 In mice, eosinophilic esophagitis can be induced by allergen exposure and overexpression of TH2 cytokines.44,45 Expression of eotaxin-3, a potent eosinophil chemoattractant, was noted to be higher in children with eosinophilic esophagitis than in controls.46
Of interest, some patients with eosinophilic esophagitis say their symptoms vary with the seasons, correlating with seasonal changes in esophageal eosinophil levels.47,48
Studies linking eosinophilic esophagitis and food allergy in children
Kelly et al49 reported that 10 children with chronic symptomatic gastroesophageal reflux and eosinophilic esophagitis all had partial or complete resolution of symptoms on an elemental diet.
Markowitz et al50 found that symptoms of chronic reflux disease and eosinophilic esophagitis improved in 49 of 51 children on an elemental diet, and the number of eosinophils in the distal esophagus decreased significantly.
Liacouras et al39 reported similar findings in a 10-year experience. Of 132 children who had eosinophilic esophagitis, 75 improved with dietary restriction based on results of skin-prick and patch testing. The 57 patients who did not respond and 115 others were started on an elemental diet. Of the 164 patients who complied with the elemental diet, 160 had significant improvement of symptoms and a significant decrease in the number of eosinophils in the esophagus. Individual foods were reintroduced approximately every 5 days, and esophagogastroduodenoscopy with biopsies was performed 4 to 8 weeks after the last was reintroduced into the diet.
In a retrospective study, Kagalwalla et al51 reported that 60 children with eosinophilic esophagitis were treated with either an elemental diet or a six-food elimination diet (no milk, soy, wheat, egg, peanut, or seafood). The two groups showed similar clinical and histologic improvements.
Collectively, these studies in pediatric patients imply that food allergy is a significant factor in the pathogenesis of eosinophilic esophagitis.
Studies in adults
Fewer studies of the link between food allergy and eosinophilic esophagitis have been done in adults.
In a preliminary study, 18 adults followed the six-food elimination diet. Symptoms improved in 17 (94%), and histologic findings improved in 14 (78%).52
On the other hand, in six adult patients with eosinophilic esophagitis, Simon et al53 found that only one had improvement in symptoms after eliminating wheat and rye from the diet, and none had significant changes in the number of eosinophils in the esophagus.
In a 37-year-old man with eosinophilic esophagitis, symptoms improved after eliminating egg from his diet.54
Yamazaki et al55 measured expression of interleukin 5 and interleukin 13 in 15 adult patients with eosinophilic esophagitis. Food and aeroallergens that included milk, soy, dust mite, ragweed, and Aspergillus induced significantly more interleukin 5 production in these patients than in atopic controls, suggesting that both foods and aeroallergens may have a role in the pathogenesis of eosinophilic esophagitis in adults.
How to identify potential food triggers of eosinophilic esophagitis
Though elemental diets have been associated with a decrease in symptoms and esophageal eosinophilia, elemental formulas are expensive and unpalatable and pose a risk of nutritional deprivation. Identifying specific food allergens to eliminate from the diet in patients with eosinophilic esophagitis may be less expensive and more desirable than a very limited or elemental diet.
However, potential food triggers have been hard to identify in eosinophilic esophagitis. A recent consensus report did not recommend in vitro food allergy testing,37 owing to a lack of positive or negative predictive values for food-specific IgE level testing in eosinophilic esophagitis. Furthermore, the absence of IgE does not eliminate a food as a potential trigger, since non-IgE mechanisms may play a role.
Skin-prick testing is one of the currently validated diagnostic methods. Several studies have used skin-prick testing of foods in patients with eosinophilic esophagitis. In these studies, approximately two-thirds of patients had positive test reactions to at least one food, most often to common food allergens such as cow’s milk, egg, soy, wheat, and peanut, but also to rye, beef, and bean.37 In a recent article,56 81% of adult patients with eosinophilic esophagitis had one or more allergens identified by skin-prick testing, and 50% of the patients tested positive for one or more food allergens.
Atopy patch testing. The combination of skin-prick testing and atopy patch testing may be more effective than skin-prick testing alone in identifying potential food triggers. Atopy patch testing has been used in the diagnosis of non-IgE cell-mediated (delayed) immune responses, in which T cells may play a significant role.
Atopy patch testing is similar to patch testing for contact dermatitis. It involves placing a small quantity of food on the skin and evaluating for a local delayed reaction after a set time.
In two studies,50,57 146 children with biopsy-proven eosinophilic esophagitis had foods eliminated from the diet on the basis of positive skin-prick tests and atopy patch tests. Approximately 77% of the children had significant reduction of esophageal eosinophils in biopsy specimens (from 20 per high-power field to 1.1). The foods most commonly implicated by skin-prick testing were cow’s milk, egg, wheat, peanut, shellfish, peas, beef, fish, rye, and tomato; those identified by atopy patch testing were cow’s milk, egg, wheat, corn, beef, milk, soy, rye, chicken, oats, and potato. The combination of both types of testing had a negative predictive value of 88% to 100% for all foods except milk, while the positive predictive value was greater than 74% for the most common foods causing eosinophilic esophagitis.58
Though atopy patch testing shows some usefulness in identifying foods that may elicit non-IgE-mediated reactions, currently these tests are not validated and have been evaluated in only a small number of studies. Currently, no standardized testing materials, methods of application, or interpretation of results exist, and no studies have included a control population to validate atopy patch testing. More studies are needed to validate atopy patch testing as a reliable diagnostic tool before it can be recommended as a component of routine diagnostic evaluation in patients with eosinophilic esophagitis.
- Bruijnzeel-Koomen C, Ortolani C, Aas K, et al. Adverse reactions to food. European Academy of Allergology and Clinical Immunology Subcommittee. Allergy 1995; 50:623–635.
- Sampson HA. Update on food allergy. J Allergy Clin Immunol 2004; 113:805–819.
- Sicherer SH, Sampson HA. 9. Food allergy. J Allergy Clin Immunol 2006; 117 (suppl 2):S470–S475.
- Sicherer SH, Munoz-Furlong A, Sampson HA. Prevalence of peanut and tree nut allergy in the United States determined by means of a random digit dial telephone survey: a 5-year follow-up study. J Allergy Clin Immunol 2003; 112:1203–1207.
- American College of Allergy, Asthma, & Immunology. Food allergy: a practice parameter. Ann Allergy Asthma Immunol 2006; 96( suppl 2):S1–S68.
- Wood RA. The natural history of food allergy. Pediatrics 2003; 111:1631–1637.
- Hourihane JO, Roberts SA, Warner JO. Resolution of peanut allergy: case-control study. BMJ 1998; 316:1271–1275.
- Fleischer DM, Conover-Walker MK, Matsui EC, Wood RA. The natural history of tree nut allergy. J Allergy Clin Immunol 2005; 116:1087–1093.
- Husby S, Foged N, Host A, Svehag SE. Passage of dietary antigens into the blood of children with coeliac disease. Quantification and size distribution of absorbed antigens. Gut 1987; 28:1062–1072.
- Mowat AM. Anatomical basis of tolerance and immunity to intestinal antigens. Nat Rev Immunol 2003; 3:331–341.
- Frossard CP, Tropia L, Hauser C, Eigenmann PA. Lymphocytes in Peyer patches regulate clinical tolerance in a murine model of food allergy. J Allergy Clin Immunol 2004; 113:958–964.
- Jain SL, Barone KS, Flanagan MP, Michael JG. Activation patterns of murine B cells after oral administration of an encapsulated soluble antigen. Vaccine 1996; 14:1291–1297.
- Kopper RA, Odum NJ, Sen M, Helm RM, Stanley JS, Burks AW. Peanut protein allergens: the effect of roasting on solubility and allergenicity. Int Arch Allergy Immunol 2005; 136:16–22.
- Lack G. Epidemiologic risks for food allergy. J Allergy Clin Immunol 2008; 121:1331–1336.
- Lack G, Fox D, Northstone K, Golding J; Avon Longitudinal Study of Parents and Children Study Team. Factors associated with the development of peanut allergy in childhood. N Engl J Med 2003; 348:977–985.
- Sudo N, Sawamura S, Tanaka K, Aiba Y, Kubo C, Koga Y. The requirement of intestinal bacterial flora for the development of an IgE production system fully susceptible to oral tolerance induction. J Immunol 1997; 159:1739–1745.
- Bashir ME, Louie S, Shi HN, Nagler-Anderson C. Toll-like receptor 4 signaling by intestinal microbes influences susceptibility to food allergy. J Immunol 2004; 172:6978–6987.
- Kopp MV, Hennemuth I, Heinzmann A, Urbanek R. Randomized, double-blind, placebo-controlled trial of probiotics for primary prevention: no clinical effects of lactobacillus GG supplementation. Pediatrics 2008; 121:e850–e856.
- Kukkonen K, Savilahti E, Haahtela T, et al. Probiotics and prebiotic galacto-oligosaccharides in the prevention of allergic diseases: a randomized, double-blind, placebo-controlled trial. J Allergy Clin Immunol 2007; 119:192–198.
- Osborn DA, Sinn JK. Probiotics in infants for prevention of allergic disease and food hypersensitivity. Cochrane Database Syst Rev 2007;CD006475.
- Prescott SL, Bjorksten B. Probiotics for the prevention or treatment of allergic diseases. J Allergy Clin Immunol 2007; 120:255–262.
- Untersmayr E, Jensen-Jarolim E. The role of protein digestibility and antacids on food allergy outcomes. J Allergy Clin Immunol 2008; 121:1301–1308.
- Untersmayr E, Scholl I, Swoboda I, et al. Antacid medication inhibits digestion of dietary proteins and causes food allergy: a fish allergy model in BALB/c mice. J Allergy Clin Immunol 2003; 112:616–623.
- Sicherer SH, Furlong TJ, Maes HH, Desnick RJ, Sampson HA, Gelb BD. Genetics of peanut allergy: a twin study. J Allergy Clin Immunol 2000; 106:53–56.
- Sicherer SH, Sampson HA. Food allergy: recent advances in pathophysiology and treatment. Annu Rev Med 2009; 60:261–277.
- Sampson HA, Anderson JA. Summary and recommendations: classification of gastrointestinal manifestations due to immunologic reactions to foods in infants and young children. J Pediatr Gastroenterol Nutr 2000; 30( suppl 1):S87–S94.
- Sampson HA, Sicherer SH, Birnbaum AH. AGA technical review on the evaluation of food allergy in gastrointestinal disorders. American Gastroenterological Association. Gastroenterology 2001; 120:1026–1040.
- Spergel JM, Pawlowski NA. Food allergy. Mechanisms, diagnosis, and management in children. Pediatr Clin North Am 2002; 49:73–96.
- Sampson HA. Utility of food-specific IgE concentrations in predicting symptomatic food allergy. J Allergy Clin Immunol 2001; 107:891–896.
- Ortolani C, Ispano M, Pastorello EA, Ansaloni R, Magri GC. Comparison of results of skin prick tests (with fresh foods and commercial food extracts) and RAST in 100 patients with oral allergy syndrome. J Allergy Clin Immunol 1989; 83:683–690.
- Perry TT, Matsui EC, Kay Conover-Walker M, Wood RA. The relationship of allergen-specific IgE levels and oral food challenge outcome. J Allergy Clin Immunol 2004; 114:144–149.
- Leung DY, Sampson HA, Yunginger JW, et al; Avon Longitudinal Study of Parents and Children Study Team. Effect of anti-IgE therapy in patients with peanut allergy. N Engl J Med 2003; 348:986–993.
- Sampson HA. A phase II, randomized double-blind, parallel-group, placebo-controlled, oral food challenge trial of Xolair (omalizumab) in peanut allergy (TOPS). J Allergy Clin Immunol 2007; 119 (suppl 1):S117.
- Buchanan AD, Green TD, Jones SM, et al Egg oral immunotherapy in nonanaphylactic children with egg allergy. J Allergy Clin Immunol 2007; 119:199–205.
- Burks AW, Jones SM. Egg oral immunotherapy in non-anaphylactic children with egg allergy: follow-up. J Allergy Clin Immunol 2008; 121:270–271.
- Skripak JM, Nash SD, Rowley H, et al. A randomized, double-blind, placebo-controlled study of milk oral immunotherapy for cow's milk allergy. J Allergy Clin Immunol 2008; 122:1154–1160.
- Furuta GT, Liacouras CA, Collins MH, et al; First International Gastrointestinal Eosinophil Research Symposium (FIGERS) Subcommittees. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology 2007; 133:1342–1363.
- Rodrigo S, Abboud G, Oh D, et al. High intraepithelial eosinophil counts in esophageal squamous epithelium are not specific for eosinophilic esophagitis in adults. Am J Gastroenterol 2008; 103:435–442.
- Liacouras CA, Spergel JM, Ruchelli E, et al. Eosinophilic esophagitis: a 10-year experience in 381 children. Clin Gastroenterol Hepatol 2005; 3:1198–1206.
- Simon D, Marti H, Heer P, Simon HU, Braathen LR, Straumann A. Eosinophilic esophagitis is frequently associated with IgE-mediated allergic airway diseases. J Allergy Clin Immunol 2005; 115:1090–1092.
- Rothenberg ME, Mishra A, Collins MH, Putnam PE. Pathogenesis and clinical features of eosinophilic esophagitis. J Allergy Clin Immunol 2001; 108:891–894.
- Gupta SK, Fitzgerald JF, Kondratyuk T, HogenEsch H. Cytokine expression in normal and inflamed esophageal mucosa: a study into the pathogenesis of allergic eosinophilic esophagitis. J Pediatr Gastroenterol Nutr 2006; 42:22–26.
- Straumann A, Bauer M, Fischer B, Blaser K, Simon HU. Idiopathic eosinophilic esophagitis is associated with a T(H)2-type allergic inflammatory response. J Allergy Clin Immunol 2001; 108:954–961.
- Mishra A, Rothenberg ME. Intratracheal IL-13 induces eosinophilic esophagitis by an IL-5, eotaxin-1, and STAT6-dependent mechanism. Gastroenterology 2003; 125:1419–1427.
- Akei HS, Mishra A, Blanchard C, Rothenberg ME. Epicutaneous antigen exposure primes for experimental eosinophilic esophagitis in mice. Gastroenterology 2005; 129:985–994.
- Blanchard C, Wang N, Stringer KF, et al. Eotaxin-3 and a uniquely conserved gene-expression profile in eosinophilic esophagitis. J Clin Invest 2006; 116:536–547.
- Fogg MI, Ruchelli E, Spergel JM. Pollen and eosinophilic esophagitis. J Allergy Clin Immunol 2003; 112:796–797.
- Almansa C, Krishna M, Buchner AM, et al. Seasonal distribution in newly diagnosed cases of eosinophilic esophagitis in adults. Am J Gastroenterol 2009; 104:828–833.
- Kelly KJ, Lazenby AJ, Rowe PC, Yardley JH, Perman JA, Sampson HA. Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology 1995; 109:1503–1512.
- Markowitz JE, Spergel JM, Ruchelli E, Liacouras CA. Elemental diet is an effective treatment for eosinophilic esophagitis in children and adolescents. Am J Gastroenterol 2003; 98:777–782.
- Kagalwalla AF, Sentongo TA, Ritz S, et al. Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis. Clin Gastroenterol Hepatol 2006; 4:1097–1102.
- Gonsalves N, Yang GY, Doerfler B, et al. A prospective clinical trial of six food elimination diet and reintroduction of causative agents in adults with eosinophilic esophagitis [abstract]. Gastroenterology 2008; 134( suppl 1):A104–A105.
- Simon D, Straumann A, Wenk A, Spichtin H, Simon HU, Braathen LR. Eosinophilic esophagitis in adults—no clinical relevance of wheat and rye sensitizations. Allergy 2006; 61:1480–1483.
- Antón Remirez J, Escudero R, Caceres O, Fernandez-Benitez M. Eosinophilic esophagitis. Allergol Immunopathol (Madr) 2006; 34:79–81.
- Yamazaki K, Murray JA, Arora AS, et al. Allergen-specific in vitro cytokine production in adult patients with eosinophilic esophagitis. Dig Dis Sci 2006; 51:1934–1941.
- Penfield JD, Lang DM, Goldblum JR, Lopez R, Falk GW. The role of allergy evaluation in adults with eosinophilic esophagitis. J Clin Gastroenterol 2009(Epub ahead of print)
- Spergel JM, Andrews T, Brown-Whitehorn TF, Beausoleil JL, Liacouras CA. Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch tests. Ann Allergy Asthma Immunol 2005; 95:336–343.
- Spergel JM, Brown-Whitehorn T, Beausoleil JL, Shuker M, Liacouras CA. Predictive values for skin prick test and atopy patch test for eosinophilic esophagitis. J Allergy Clin Immunol 2007; 119:509–511.
More children and even adults seem to be allergic to various foods these days than in the past. Also apparently on the rise is a linked condition, eosinophilic esophagitis.
The reason for these increases is not clear. This article confines itself to what we know about the mechanisms of food allergies and eosinophilic esophagitis, how to diagnose them, and how to treat them.
FOOD ALLERGIES ARE COMMON, AND MORE PREVALENT THAN EVER
Food allergies—abnormal immune responses to food proteins1—affect an estimated 6% to 8% of young children and 3% to 4% of adults in the United States,2,3 and their prevalence appears to be rising in developed countries. Studies in US and British children indicate that peanut allergy has doubled in the past decade. 4
Any food can provoke a reaction, but only a few foods account for most of the significant allergic reactions: cow’s milk, soy, wheat, eggs, peanuts, tree nuts, fish, and shellfish.
Approximately 80% of allergies to milk, egg, wheat, and soy resolve by the time the patient reaches early adolescence.6 Fewer cases resolve in children with tree nut allergies (approximately 9%) or peanut allergy (20%),7,8 and allergies to fish and shellfish often develop or persist in adulthood.
A family history of an atopic disease such as asthma, allergic rhinitis, eczema, or food allergy is a risk factor for developing a food allergy. 3 Considering that the rate of peanut allergy has doubled in children over the past 10 years, environmental factors may also play a role.3
How we tolerate foods or become allergic to them
The gut, the largest mucosal organ in the body, is exposed to large quantities of foreign proteins daily. Most protein is broken down by stomach acid and digestive enzymes into lessantigenic peptides or is bound by secretory immunoglobulin A (IgA), which prevents it from being absorbed. Further, the epithelial cells lining the gut do not allow large molecules to pass easily, having tight intracellular junctions and being covered with mucus.
For these reasons, less than 2% of the protein in food is absorbed in an allergenic form.9 The reason food allergies are more prevalent in children is most likely that children have an immature gut barrier, lower IgA levels, a higher gastric pH, and lower proteolytic enzyme levels.
When dietary proteins do cross the gut barrier, the immune system normally suppresses the allergic response. Regulatory T cells, dendritic cells, and local immune responses play critical roles in the development of tolerance. Several types of regulatory T cells, such as Tr1 cells (which secrete interleukin 10), TH3 cells (which secrete transforming growth factor beta), CD4+CD25+ regulatory T cells, gamma-delta T cells, and CD8+ suppressor cells can all contribute to suppressing allergic responses.10 Dendritic cells also help induce tolerance by stimulating CD4+ T cells to secrete transforming growth factor beta, which leads to the production of interleukin 10 and additional transforming growth factor beta.11
Factors that contribute to food allergy
Many factors may contribute to whether a person becomes tolerant to or sensitized to a specific food protein.
The dose of antigen. Tolerance can develop after either high or low doses of antigens, but by different mechanisms.
The antigen structure. Soluble antigens are less sensitizing than particulate antigens.12,13
Processing of foods. Dry-roasted peanuts are more allergenic than raw or boiled peanuts, partly because they are less soluble.13
The route of initial exposure. Sensitization to food proteins can occur directly through the gut or the skin. Alternatively, it can occur indirectly via the respiratory tract. Skin exposure may be especially sensitizing in children with atopic dermatitis.14,15
The gut flora. When mice are raised in a germ-free environment, they fail to develop normal tolerance.16 They are also more likely to become sensitized if they are treated with antibiotics or if they lack toll-like receptors that recognize bacterial lipopolysaccharides.17 Furthermore, human studies suggest that probiotics promote tolerance, especially in preventing atopic dermatitis, although the studies have had conflicting results.18–21
The gastric pH. Murine and human studies reveal that antacid medications increase the risk of food allergy.22,23
Genetic susceptibility. A child with a sibling who is allergic to peanuts is approximately 10 times more likely to be allergic to peanuts than predicted by the rate in the general population. Although no risk-conferring gene has been identified, a study of twins showed concordance for peanut allergy in 64.3% of identical twins vs 6.8% of fraternal twins.24
Three types of immune responses to food
Immunologic reactions to foods can be divided into three categories: mediated by immunoglobulin E (IgE), non-IgE-mediated, and mixed. Therefore, these disorders can present as an acute, potentially life-threatening reaction or as a chronic disease such as eosinophilic gastoenteropathy.
IgE-mediated reactions are immediate hypersensitivity responses. In most patients, an IgE-mediated mechanism can be confirmed by a positive skin test or a test for food-specific IgE in the serum. In this article, the term “food allergy” refers to an IgE-mediated reaction to a food, unless otherwise indicated.
Non-IgE-mediated reactions have a delayed onset and chronic symptoms. Commonly, they are confined to the gastrointestinal tract; examples are food-protein-induced enterocolitis, proctitis, and proctocolitis and celiac disease.3,26,27 However, other diseases such as contact dermatitis, dermatitis herpetiformis, and food-induced pulmonary hemosiderosis (Heiner syndrome) are also considered non-IgE-mediated allergies.
Mixed-reaction disorders are chronic and include the eosinophilic gastroenteropathies, ie, eosinophilic proctocolitis, eosinophilic gastroenteritis, and eosinophilic esophagitis.28 The pathophysiology of these diseases is poorly understood. Many patients have evidence of allergic sensitivities to food or to environmental allergens, or both, but whether these sensitivities have a causal role in these disorders is not clear.
Atopic dermatitis, another complicated disease process, may be associated with mixedreaction food allergy, as approximately 35% of young children with moderate to severe atopic dermatitis have food allergies.29
Diagnosis of IgE-mediated food allergies
A thorough history and physical examination are key to diagnosing an IgE-mediated food allergy.
The history should include potential culprit foods, the quantity eaten, the timing of the onset of symptoms, and related factors such as exercise, alcohol intake, or medication use. Symptoms of an IgE-mediated reaction are generally rapid in onset but may be delayed up to a few hours, while non-IgE mediated symptoms may present several hours to days later.
Food challenge. A double-blind, placebocontrolled oral food challenge is the gold standard for the diagnosis of food allergies. (The food to be tested is hidden in other food or in capsules.) However, this test poses significant risks, and other diagnostic methods are more practical for screening.
Skin-prick tests with commercially available extracts are a rapid and sensitive method of screening for allergy to several foods.
Negative skin-prick tests have an estimated negative predictive value of more than 95% and can therefore exclude IgE-mediated food allergies.
A positive test indicates the presence of IgE against a specific food allergen and suggests a clinical food allergy, although the specificity of the test is only about 50%, making a positive result difficult to interpret. Although the size of the skin-test response does not necessarily correlate with the potential severity of a reaction, a response larger than 3 mm does indicate a greater likelihood of clinical reactivity. A positive test is most helpful in confirming the diagnosis of IgE-mediated food allergy when combined with a clear history of food-induced symptoms.
The proteins in commercially based extracts of most fruits and vegetables are often labile; therefore, skin testing with fresh fruits and vegetables may be indicated.30
Immunoassays. Radioallergosorbent tests (RASTs) and fluorescent enzyme immunoassays are used to identity food-specific IgE antibodies in the serum. The commercially available tests do not use radioactivity, but the term “RAST” is still commonly used.
Immunoassays are generally less sensitive and more costly than skin-prick tests, and their results are not immediately available, unlike those of skin-prick testing. However, these in vitro tests are not affected by antihistamine use and are useful in patients with severe dermatologic conditions or severe anaphylaxis, for whom skin-prick testing would not be appropriate.
However, unlike a negative skin-prick test, an undetectable serum food-specific IgE level has a low negative predictive value, and an undetectable level may be associated with symptoms of an allergic reaction for 10% to 25% of patients.29 Therefore, if one suspects an allergic reaction but no food-specific IgE can be detected in the serum, confirming the absence of a clinical allergy must be done with a skin-prick test or with a physician-supervised oral challenge, or both.
Managing food allergy by avoiding the allergen
Food allergies are managed by strictly avoiding food allergens and by taking medications such as self-injectable epinephrine for anaphylactic symptoms.
Patients and caregivers must be educated about reading food labels, avoiding high-risk situations such as eating at buffets and other restaurants with high risk of cross-contamination, wearing a medical-alert bracelet, recognizing and managing early symptoms of an allergic reaction, and calling for emergency services if they are having an allergic reaction. Since January 2006, the US Food and Drug Administration has required food manufacturers to list common food allergens on food labels (cow’s milk, soy, wheat, egg, peanut, tree nuts, fish, and shellfish), and the labeling must use simple, easily understood terms, such as “milk” instead of “whey.” However, it is still prudent to read all ingredients listed on the label.
Experimental treatments for food allergies
Humanized monoclonal anti-IgE antibodies such as talizumab (also known as TNX-901) and omalizumab (Xolair) have been developed, but their use in food allergy has been limited. In a study in patients with peanut allergy, injections of talizumab increased the threshold for sensitivity to peanuts in most patients, but 25% of the patients did not have any improvement.32 A study of omalizumab in patients with peanut allergy was stopped after adverse reactions developed during oral peanut challenges.33
Oral immunotherapy. Recent studies suggest it may be possible to induce oral tolerance in patients with IgE-mediated food allergy. Pilot studies have shown that frequent, increasing doses of food allergens (egg, milk, and peanut) may raise the threshold at which symptoms occur.34–36 Though these studies suggest that oral immunotherapy may protect some patients against a reaction if they accidentally ingest a food they are allergic to, some patients could not reach the goal doses because allergic symptoms were provoked.
At this early stage, these strategies must be considered investigational, and more randomized, placebo-controlled studies are needed. Further studies will also be needed to assess whether oral immunotherapy induces only short-term desensitization (in which case the allergen needs to be ingested daily to prevent reactions) or sustained tolerance (in which case the antigenic protein can be ingested without symptoms despite periods of abstinence).
THE ROLE OF FOOD ALLERGY IN EOSINOPHILIC ESOPHAGITIS
Eosinophilic esophagitis has been recognized with increasing frequency in both children and adults over the past several years. Symptoms can include difficulty feeding, failure to thrive, vomiting, epigastric or chest pain, dysphagia, and food impaction.
Diagnostic criteria for eosinophilic esophagitis are37:
- Clinical symptoms of esophageal dysfunction
- At least 15 eosinophils per high-power field in at least one esophageal biopsy specimen
- No response to a proton-pump inhibitor in high doses (up to 2 mg/kg/day) for 1 to 2 months, or normal results on pH probe monitoring of the esophagus (the reason for this criterion is that patients with gastroesophageal reflux disease can also have large numbers of eosinophils in the esophagus—more than 100 per highpower field38)
- Exclusion of other causes.
Though the cause of eosinophilic esophagitis is not completely understood, atopy has been strongly implicated as a factor. More than 50% of patients with eosinophilic esophagitis also have an atopic condition (eg, atopic dermatitis, allergic rhinitis, asthma), as well as positive results on skin-prick testing or measurement of antigen-specific IgE in the serum.39–41 Also, since most patients improve with either dietary restriction or elemental diets, food sensitization appears to play a considerable role.
As with atopic conditions such as asthma, atopic dermatitis, allergic rhinitis, and food allergy, eosinophilic esophagitis has been linked with immune responses involving helper T cell 2 (TH2). Adults and children with eosinophilic esophagitis have been found to have elevated eosinophil counts and total IgE levels in peripheral blood.37 In the esophagus, patients have elevated levels of the TH2 cytokines often seen in atopic patients (eg, interleukins 4, 5, and 13) and mast cells.42,43 In mice, eosinophilic esophagitis can be induced by allergen exposure and overexpression of TH2 cytokines.44,45 Expression of eotaxin-3, a potent eosinophil chemoattractant, was noted to be higher in children with eosinophilic esophagitis than in controls.46
Of interest, some patients with eosinophilic esophagitis say their symptoms vary with the seasons, correlating with seasonal changes in esophageal eosinophil levels.47,48
Studies linking eosinophilic esophagitis and food allergy in children
Kelly et al49 reported that 10 children with chronic symptomatic gastroesophageal reflux and eosinophilic esophagitis all had partial or complete resolution of symptoms on an elemental diet.
Markowitz et al50 found that symptoms of chronic reflux disease and eosinophilic esophagitis improved in 49 of 51 children on an elemental diet, and the number of eosinophils in the distal esophagus decreased significantly.
Liacouras et al39 reported similar findings in a 10-year experience. Of 132 children who had eosinophilic esophagitis, 75 improved with dietary restriction based on results of skin-prick and patch testing. The 57 patients who did not respond and 115 others were started on an elemental diet. Of the 164 patients who complied with the elemental diet, 160 had significant improvement of symptoms and a significant decrease in the number of eosinophils in the esophagus. Individual foods were reintroduced approximately every 5 days, and esophagogastroduodenoscopy with biopsies was performed 4 to 8 weeks after the last was reintroduced into the diet.
In a retrospective study, Kagalwalla et al51 reported that 60 children with eosinophilic esophagitis were treated with either an elemental diet or a six-food elimination diet (no milk, soy, wheat, egg, peanut, or seafood). The two groups showed similar clinical and histologic improvements.
Collectively, these studies in pediatric patients imply that food allergy is a significant factor in the pathogenesis of eosinophilic esophagitis.
Studies in adults
Fewer studies of the link between food allergy and eosinophilic esophagitis have been done in adults.
In a preliminary study, 18 adults followed the six-food elimination diet. Symptoms improved in 17 (94%), and histologic findings improved in 14 (78%).52
On the other hand, in six adult patients with eosinophilic esophagitis, Simon et al53 found that only one had improvement in symptoms after eliminating wheat and rye from the diet, and none had significant changes in the number of eosinophils in the esophagus.
In a 37-year-old man with eosinophilic esophagitis, symptoms improved after eliminating egg from his diet.54
Yamazaki et al55 measured expression of interleukin 5 and interleukin 13 in 15 adult patients with eosinophilic esophagitis. Food and aeroallergens that included milk, soy, dust mite, ragweed, and Aspergillus induced significantly more interleukin 5 production in these patients than in atopic controls, suggesting that both foods and aeroallergens may have a role in the pathogenesis of eosinophilic esophagitis in adults.
How to identify potential food triggers of eosinophilic esophagitis
Though elemental diets have been associated with a decrease in symptoms and esophageal eosinophilia, elemental formulas are expensive and unpalatable and pose a risk of nutritional deprivation. Identifying specific food allergens to eliminate from the diet in patients with eosinophilic esophagitis may be less expensive and more desirable than a very limited or elemental diet.
However, potential food triggers have been hard to identify in eosinophilic esophagitis. A recent consensus report did not recommend in vitro food allergy testing,37 owing to a lack of positive or negative predictive values for food-specific IgE level testing in eosinophilic esophagitis. Furthermore, the absence of IgE does not eliminate a food as a potential trigger, since non-IgE mechanisms may play a role.
Skin-prick testing is one of the currently validated diagnostic methods. Several studies have used skin-prick testing of foods in patients with eosinophilic esophagitis. In these studies, approximately two-thirds of patients had positive test reactions to at least one food, most often to common food allergens such as cow’s milk, egg, soy, wheat, and peanut, but also to rye, beef, and bean.37 In a recent article,56 81% of adult patients with eosinophilic esophagitis had one or more allergens identified by skin-prick testing, and 50% of the patients tested positive for one or more food allergens.
Atopy patch testing. The combination of skin-prick testing and atopy patch testing may be more effective than skin-prick testing alone in identifying potential food triggers. Atopy patch testing has been used in the diagnosis of non-IgE cell-mediated (delayed) immune responses, in which T cells may play a significant role.
Atopy patch testing is similar to patch testing for contact dermatitis. It involves placing a small quantity of food on the skin and evaluating for a local delayed reaction after a set time.
In two studies,50,57 146 children with biopsy-proven eosinophilic esophagitis had foods eliminated from the diet on the basis of positive skin-prick tests and atopy patch tests. Approximately 77% of the children had significant reduction of esophageal eosinophils in biopsy specimens (from 20 per high-power field to 1.1). The foods most commonly implicated by skin-prick testing were cow’s milk, egg, wheat, peanut, shellfish, peas, beef, fish, rye, and tomato; those identified by atopy patch testing were cow’s milk, egg, wheat, corn, beef, milk, soy, rye, chicken, oats, and potato. The combination of both types of testing had a negative predictive value of 88% to 100% for all foods except milk, while the positive predictive value was greater than 74% for the most common foods causing eosinophilic esophagitis.58
Though atopy patch testing shows some usefulness in identifying foods that may elicit non-IgE-mediated reactions, currently these tests are not validated and have been evaluated in only a small number of studies. Currently, no standardized testing materials, methods of application, or interpretation of results exist, and no studies have included a control population to validate atopy patch testing. More studies are needed to validate atopy patch testing as a reliable diagnostic tool before it can be recommended as a component of routine diagnostic evaluation in patients with eosinophilic esophagitis.
More children and even adults seem to be allergic to various foods these days than in the past. Also apparently on the rise is a linked condition, eosinophilic esophagitis.
The reason for these increases is not clear. This article confines itself to what we know about the mechanisms of food allergies and eosinophilic esophagitis, how to diagnose them, and how to treat them.
FOOD ALLERGIES ARE COMMON, AND MORE PREVALENT THAN EVER
Food allergies—abnormal immune responses to food proteins1—affect an estimated 6% to 8% of young children and 3% to 4% of adults in the United States,2,3 and their prevalence appears to be rising in developed countries. Studies in US and British children indicate that peanut allergy has doubled in the past decade. 4
Any food can provoke a reaction, but only a few foods account for most of the significant allergic reactions: cow’s milk, soy, wheat, eggs, peanuts, tree nuts, fish, and shellfish.
Approximately 80% of allergies to milk, egg, wheat, and soy resolve by the time the patient reaches early adolescence.6 Fewer cases resolve in children with tree nut allergies (approximately 9%) or peanut allergy (20%),7,8 and allergies to fish and shellfish often develop or persist in adulthood.
A family history of an atopic disease such as asthma, allergic rhinitis, eczema, or food allergy is a risk factor for developing a food allergy. 3 Considering that the rate of peanut allergy has doubled in children over the past 10 years, environmental factors may also play a role.3
How we tolerate foods or become allergic to them
The gut, the largest mucosal organ in the body, is exposed to large quantities of foreign proteins daily. Most protein is broken down by stomach acid and digestive enzymes into lessantigenic peptides or is bound by secretory immunoglobulin A (IgA), which prevents it from being absorbed. Further, the epithelial cells lining the gut do not allow large molecules to pass easily, having tight intracellular junctions and being covered with mucus.
For these reasons, less than 2% of the protein in food is absorbed in an allergenic form.9 The reason food allergies are more prevalent in children is most likely that children have an immature gut barrier, lower IgA levels, a higher gastric pH, and lower proteolytic enzyme levels.
When dietary proteins do cross the gut barrier, the immune system normally suppresses the allergic response. Regulatory T cells, dendritic cells, and local immune responses play critical roles in the development of tolerance. Several types of regulatory T cells, such as Tr1 cells (which secrete interleukin 10), TH3 cells (which secrete transforming growth factor beta), CD4+CD25+ regulatory T cells, gamma-delta T cells, and CD8+ suppressor cells can all contribute to suppressing allergic responses.10 Dendritic cells also help induce tolerance by stimulating CD4+ T cells to secrete transforming growth factor beta, which leads to the production of interleukin 10 and additional transforming growth factor beta.11
Factors that contribute to food allergy
Many factors may contribute to whether a person becomes tolerant to or sensitized to a specific food protein.
The dose of antigen. Tolerance can develop after either high or low doses of antigens, but by different mechanisms.
The antigen structure. Soluble antigens are less sensitizing than particulate antigens.12,13
Processing of foods. Dry-roasted peanuts are more allergenic than raw or boiled peanuts, partly because they are less soluble.13
The route of initial exposure. Sensitization to food proteins can occur directly through the gut or the skin. Alternatively, it can occur indirectly via the respiratory tract. Skin exposure may be especially sensitizing in children with atopic dermatitis.14,15
The gut flora. When mice are raised in a germ-free environment, they fail to develop normal tolerance.16 They are also more likely to become sensitized if they are treated with antibiotics or if they lack toll-like receptors that recognize bacterial lipopolysaccharides.17 Furthermore, human studies suggest that probiotics promote tolerance, especially in preventing atopic dermatitis, although the studies have had conflicting results.18–21
The gastric pH. Murine and human studies reveal that antacid medications increase the risk of food allergy.22,23
Genetic susceptibility. A child with a sibling who is allergic to peanuts is approximately 10 times more likely to be allergic to peanuts than predicted by the rate in the general population. Although no risk-conferring gene has been identified, a study of twins showed concordance for peanut allergy in 64.3% of identical twins vs 6.8% of fraternal twins.24
Three types of immune responses to food
Immunologic reactions to foods can be divided into three categories: mediated by immunoglobulin E (IgE), non-IgE-mediated, and mixed. Therefore, these disorders can present as an acute, potentially life-threatening reaction or as a chronic disease such as eosinophilic gastoenteropathy.
IgE-mediated reactions are immediate hypersensitivity responses. In most patients, an IgE-mediated mechanism can be confirmed by a positive skin test or a test for food-specific IgE in the serum. In this article, the term “food allergy” refers to an IgE-mediated reaction to a food, unless otherwise indicated.
Non-IgE-mediated reactions have a delayed onset and chronic symptoms. Commonly, they are confined to the gastrointestinal tract; examples are food-protein-induced enterocolitis, proctitis, and proctocolitis and celiac disease.3,26,27 However, other diseases such as contact dermatitis, dermatitis herpetiformis, and food-induced pulmonary hemosiderosis (Heiner syndrome) are also considered non-IgE-mediated allergies.
Mixed-reaction disorders are chronic and include the eosinophilic gastroenteropathies, ie, eosinophilic proctocolitis, eosinophilic gastroenteritis, and eosinophilic esophagitis.28 The pathophysiology of these diseases is poorly understood. Many patients have evidence of allergic sensitivities to food or to environmental allergens, or both, but whether these sensitivities have a causal role in these disorders is not clear.
Atopic dermatitis, another complicated disease process, may be associated with mixedreaction food allergy, as approximately 35% of young children with moderate to severe atopic dermatitis have food allergies.29
Diagnosis of IgE-mediated food allergies
A thorough history and physical examination are key to diagnosing an IgE-mediated food allergy.
The history should include potential culprit foods, the quantity eaten, the timing of the onset of symptoms, and related factors such as exercise, alcohol intake, or medication use. Symptoms of an IgE-mediated reaction are generally rapid in onset but may be delayed up to a few hours, while non-IgE mediated symptoms may present several hours to days later.
Food challenge. A double-blind, placebocontrolled oral food challenge is the gold standard for the diagnosis of food allergies. (The food to be tested is hidden in other food or in capsules.) However, this test poses significant risks, and other diagnostic methods are more practical for screening.
Skin-prick tests with commercially available extracts are a rapid and sensitive method of screening for allergy to several foods.
Negative skin-prick tests have an estimated negative predictive value of more than 95% and can therefore exclude IgE-mediated food allergies.
A positive test indicates the presence of IgE against a specific food allergen and suggests a clinical food allergy, although the specificity of the test is only about 50%, making a positive result difficult to interpret. Although the size of the skin-test response does not necessarily correlate with the potential severity of a reaction, a response larger than 3 mm does indicate a greater likelihood of clinical reactivity. A positive test is most helpful in confirming the diagnosis of IgE-mediated food allergy when combined with a clear history of food-induced symptoms.
The proteins in commercially based extracts of most fruits and vegetables are often labile; therefore, skin testing with fresh fruits and vegetables may be indicated.30
Immunoassays. Radioallergosorbent tests (RASTs) and fluorescent enzyme immunoassays are used to identity food-specific IgE antibodies in the serum. The commercially available tests do not use radioactivity, but the term “RAST” is still commonly used.
Immunoassays are generally less sensitive and more costly than skin-prick tests, and their results are not immediately available, unlike those of skin-prick testing. However, these in vitro tests are not affected by antihistamine use and are useful in patients with severe dermatologic conditions or severe anaphylaxis, for whom skin-prick testing would not be appropriate.
However, unlike a negative skin-prick test, an undetectable serum food-specific IgE level has a low negative predictive value, and an undetectable level may be associated with symptoms of an allergic reaction for 10% to 25% of patients.29 Therefore, if one suspects an allergic reaction but no food-specific IgE can be detected in the serum, confirming the absence of a clinical allergy must be done with a skin-prick test or with a physician-supervised oral challenge, or both.
Managing food allergy by avoiding the allergen
Food allergies are managed by strictly avoiding food allergens and by taking medications such as self-injectable epinephrine for anaphylactic symptoms.
Patients and caregivers must be educated about reading food labels, avoiding high-risk situations such as eating at buffets and other restaurants with high risk of cross-contamination, wearing a medical-alert bracelet, recognizing and managing early symptoms of an allergic reaction, and calling for emergency services if they are having an allergic reaction. Since January 2006, the US Food and Drug Administration has required food manufacturers to list common food allergens on food labels (cow’s milk, soy, wheat, egg, peanut, tree nuts, fish, and shellfish), and the labeling must use simple, easily understood terms, such as “milk” instead of “whey.” However, it is still prudent to read all ingredients listed on the label.
Experimental treatments for food allergies
Humanized monoclonal anti-IgE antibodies such as talizumab (also known as TNX-901) and omalizumab (Xolair) have been developed, but their use in food allergy has been limited. In a study in patients with peanut allergy, injections of talizumab increased the threshold for sensitivity to peanuts in most patients, but 25% of the patients did not have any improvement.32 A study of omalizumab in patients with peanut allergy was stopped after adverse reactions developed during oral peanut challenges.33
Oral immunotherapy. Recent studies suggest it may be possible to induce oral tolerance in patients with IgE-mediated food allergy. Pilot studies have shown that frequent, increasing doses of food allergens (egg, milk, and peanut) may raise the threshold at which symptoms occur.34–36 Though these studies suggest that oral immunotherapy may protect some patients against a reaction if they accidentally ingest a food they are allergic to, some patients could not reach the goal doses because allergic symptoms were provoked.
At this early stage, these strategies must be considered investigational, and more randomized, placebo-controlled studies are needed. Further studies will also be needed to assess whether oral immunotherapy induces only short-term desensitization (in which case the allergen needs to be ingested daily to prevent reactions) or sustained tolerance (in which case the antigenic protein can be ingested without symptoms despite periods of abstinence).
THE ROLE OF FOOD ALLERGY IN EOSINOPHILIC ESOPHAGITIS
Eosinophilic esophagitis has been recognized with increasing frequency in both children and adults over the past several years. Symptoms can include difficulty feeding, failure to thrive, vomiting, epigastric or chest pain, dysphagia, and food impaction.
Diagnostic criteria for eosinophilic esophagitis are37:
- Clinical symptoms of esophageal dysfunction
- At least 15 eosinophils per high-power field in at least one esophageal biopsy specimen
- No response to a proton-pump inhibitor in high doses (up to 2 mg/kg/day) for 1 to 2 months, or normal results on pH probe monitoring of the esophagus (the reason for this criterion is that patients with gastroesophageal reflux disease can also have large numbers of eosinophils in the esophagus—more than 100 per highpower field38)
- Exclusion of other causes.
Though the cause of eosinophilic esophagitis is not completely understood, atopy has been strongly implicated as a factor. More than 50% of patients with eosinophilic esophagitis also have an atopic condition (eg, atopic dermatitis, allergic rhinitis, asthma), as well as positive results on skin-prick testing or measurement of antigen-specific IgE in the serum.39–41 Also, since most patients improve with either dietary restriction or elemental diets, food sensitization appears to play a considerable role.
As with atopic conditions such as asthma, atopic dermatitis, allergic rhinitis, and food allergy, eosinophilic esophagitis has been linked with immune responses involving helper T cell 2 (TH2). Adults and children with eosinophilic esophagitis have been found to have elevated eosinophil counts and total IgE levels in peripheral blood.37 In the esophagus, patients have elevated levels of the TH2 cytokines often seen in atopic patients (eg, interleukins 4, 5, and 13) and mast cells.42,43 In mice, eosinophilic esophagitis can be induced by allergen exposure and overexpression of TH2 cytokines.44,45 Expression of eotaxin-3, a potent eosinophil chemoattractant, was noted to be higher in children with eosinophilic esophagitis than in controls.46
Of interest, some patients with eosinophilic esophagitis say their symptoms vary with the seasons, correlating with seasonal changes in esophageal eosinophil levels.47,48
Studies linking eosinophilic esophagitis and food allergy in children
Kelly et al49 reported that 10 children with chronic symptomatic gastroesophageal reflux and eosinophilic esophagitis all had partial or complete resolution of symptoms on an elemental diet.
Markowitz et al50 found that symptoms of chronic reflux disease and eosinophilic esophagitis improved in 49 of 51 children on an elemental diet, and the number of eosinophils in the distal esophagus decreased significantly.
Liacouras et al39 reported similar findings in a 10-year experience. Of 132 children who had eosinophilic esophagitis, 75 improved with dietary restriction based on results of skin-prick and patch testing. The 57 patients who did not respond and 115 others were started on an elemental diet. Of the 164 patients who complied with the elemental diet, 160 had significant improvement of symptoms and a significant decrease in the number of eosinophils in the esophagus. Individual foods were reintroduced approximately every 5 days, and esophagogastroduodenoscopy with biopsies was performed 4 to 8 weeks after the last was reintroduced into the diet.
In a retrospective study, Kagalwalla et al51 reported that 60 children with eosinophilic esophagitis were treated with either an elemental diet or a six-food elimination diet (no milk, soy, wheat, egg, peanut, or seafood). The two groups showed similar clinical and histologic improvements.
Collectively, these studies in pediatric patients imply that food allergy is a significant factor in the pathogenesis of eosinophilic esophagitis.
Studies in adults
Fewer studies of the link between food allergy and eosinophilic esophagitis have been done in adults.
In a preliminary study, 18 adults followed the six-food elimination diet. Symptoms improved in 17 (94%), and histologic findings improved in 14 (78%).52
On the other hand, in six adult patients with eosinophilic esophagitis, Simon et al53 found that only one had improvement in symptoms after eliminating wheat and rye from the diet, and none had significant changes in the number of eosinophils in the esophagus.
In a 37-year-old man with eosinophilic esophagitis, symptoms improved after eliminating egg from his diet.54
Yamazaki et al55 measured expression of interleukin 5 and interleukin 13 in 15 adult patients with eosinophilic esophagitis. Food and aeroallergens that included milk, soy, dust mite, ragweed, and Aspergillus induced significantly more interleukin 5 production in these patients than in atopic controls, suggesting that both foods and aeroallergens may have a role in the pathogenesis of eosinophilic esophagitis in adults.
How to identify potential food triggers of eosinophilic esophagitis
Though elemental diets have been associated with a decrease in symptoms and esophageal eosinophilia, elemental formulas are expensive and unpalatable and pose a risk of nutritional deprivation. Identifying specific food allergens to eliminate from the diet in patients with eosinophilic esophagitis may be less expensive and more desirable than a very limited or elemental diet.
However, potential food triggers have been hard to identify in eosinophilic esophagitis. A recent consensus report did not recommend in vitro food allergy testing,37 owing to a lack of positive or negative predictive values for food-specific IgE level testing in eosinophilic esophagitis. Furthermore, the absence of IgE does not eliminate a food as a potential trigger, since non-IgE mechanisms may play a role.
Skin-prick testing is one of the currently validated diagnostic methods. Several studies have used skin-prick testing of foods in patients with eosinophilic esophagitis. In these studies, approximately two-thirds of patients had positive test reactions to at least one food, most often to common food allergens such as cow’s milk, egg, soy, wheat, and peanut, but also to rye, beef, and bean.37 In a recent article,56 81% of adult patients with eosinophilic esophagitis had one or more allergens identified by skin-prick testing, and 50% of the patients tested positive for one or more food allergens.
Atopy patch testing. The combination of skin-prick testing and atopy patch testing may be more effective than skin-prick testing alone in identifying potential food triggers. Atopy patch testing has been used in the diagnosis of non-IgE cell-mediated (delayed) immune responses, in which T cells may play a significant role.
Atopy patch testing is similar to patch testing for contact dermatitis. It involves placing a small quantity of food on the skin and evaluating for a local delayed reaction after a set time.
In two studies,50,57 146 children with biopsy-proven eosinophilic esophagitis had foods eliminated from the diet on the basis of positive skin-prick tests and atopy patch tests. Approximately 77% of the children had significant reduction of esophageal eosinophils in biopsy specimens (from 20 per high-power field to 1.1). The foods most commonly implicated by skin-prick testing were cow’s milk, egg, wheat, peanut, shellfish, peas, beef, fish, rye, and tomato; those identified by atopy patch testing were cow’s milk, egg, wheat, corn, beef, milk, soy, rye, chicken, oats, and potato. The combination of both types of testing had a negative predictive value of 88% to 100% for all foods except milk, while the positive predictive value was greater than 74% for the most common foods causing eosinophilic esophagitis.58
Though atopy patch testing shows some usefulness in identifying foods that may elicit non-IgE-mediated reactions, currently these tests are not validated and have been evaluated in only a small number of studies. Currently, no standardized testing materials, methods of application, or interpretation of results exist, and no studies have included a control population to validate atopy patch testing. More studies are needed to validate atopy patch testing as a reliable diagnostic tool before it can be recommended as a component of routine diagnostic evaluation in patients with eosinophilic esophagitis.
- Bruijnzeel-Koomen C, Ortolani C, Aas K, et al. Adverse reactions to food. European Academy of Allergology and Clinical Immunology Subcommittee. Allergy 1995; 50:623–635.
- Sampson HA. Update on food allergy. J Allergy Clin Immunol 2004; 113:805–819.
- Sicherer SH, Sampson HA. 9. Food allergy. J Allergy Clin Immunol 2006; 117 (suppl 2):S470–S475.
- Sicherer SH, Munoz-Furlong A, Sampson HA. Prevalence of peanut and tree nut allergy in the United States determined by means of a random digit dial telephone survey: a 5-year follow-up study. J Allergy Clin Immunol 2003; 112:1203–1207.
- American College of Allergy, Asthma, & Immunology. Food allergy: a practice parameter. Ann Allergy Asthma Immunol 2006; 96( suppl 2):S1–S68.
- Wood RA. The natural history of food allergy. Pediatrics 2003; 111:1631–1637.
- Hourihane JO, Roberts SA, Warner JO. Resolution of peanut allergy: case-control study. BMJ 1998; 316:1271–1275.
- Fleischer DM, Conover-Walker MK, Matsui EC, Wood RA. The natural history of tree nut allergy. J Allergy Clin Immunol 2005; 116:1087–1093.
- Husby S, Foged N, Host A, Svehag SE. Passage of dietary antigens into the blood of children with coeliac disease. Quantification and size distribution of absorbed antigens. Gut 1987; 28:1062–1072.
- Mowat AM. Anatomical basis of tolerance and immunity to intestinal antigens. Nat Rev Immunol 2003; 3:331–341.
- Frossard CP, Tropia L, Hauser C, Eigenmann PA. Lymphocytes in Peyer patches regulate clinical tolerance in a murine model of food allergy. J Allergy Clin Immunol 2004; 113:958–964.
- Jain SL, Barone KS, Flanagan MP, Michael JG. Activation patterns of murine B cells after oral administration of an encapsulated soluble antigen. Vaccine 1996; 14:1291–1297.
- Kopper RA, Odum NJ, Sen M, Helm RM, Stanley JS, Burks AW. Peanut protein allergens: the effect of roasting on solubility and allergenicity. Int Arch Allergy Immunol 2005; 136:16–22.
- Lack G. Epidemiologic risks for food allergy. J Allergy Clin Immunol 2008; 121:1331–1336.
- Lack G, Fox D, Northstone K, Golding J; Avon Longitudinal Study of Parents and Children Study Team. Factors associated with the development of peanut allergy in childhood. N Engl J Med 2003; 348:977–985.
- Sudo N, Sawamura S, Tanaka K, Aiba Y, Kubo C, Koga Y. The requirement of intestinal bacterial flora for the development of an IgE production system fully susceptible to oral tolerance induction. J Immunol 1997; 159:1739–1745.
- Bashir ME, Louie S, Shi HN, Nagler-Anderson C. Toll-like receptor 4 signaling by intestinal microbes influences susceptibility to food allergy. J Immunol 2004; 172:6978–6987.
- Kopp MV, Hennemuth I, Heinzmann A, Urbanek R. Randomized, double-blind, placebo-controlled trial of probiotics for primary prevention: no clinical effects of lactobacillus GG supplementation. Pediatrics 2008; 121:e850–e856.
- Kukkonen K, Savilahti E, Haahtela T, et al. Probiotics and prebiotic galacto-oligosaccharides in the prevention of allergic diseases: a randomized, double-blind, placebo-controlled trial. J Allergy Clin Immunol 2007; 119:192–198.
- Osborn DA, Sinn JK. Probiotics in infants for prevention of allergic disease and food hypersensitivity. Cochrane Database Syst Rev 2007;CD006475.
- Prescott SL, Bjorksten B. Probiotics for the prevention or treatment of allergic diseases. J Allergy Clin Immunol 2007; 120:255–262.
- Untersmayr E, Jensen-Jarolim E. The role of protein digestibility and antacids on food allergy outcomes. J Allergy Clin Immunol 2008; 121:1301–1308.
- Untersmayr E, Scholl I, Swoboda I, et al. Antacid medication inhibits digestion of dietary proteins and causes food allergy: a fish allergy model in BALB/c mice. J Allergy Clin Immunol 2003; 112:616–623.
- Sicherer SH, Furlong TJ, Maes HH, Desnick RJ, Sampson HA, Gelb BD. Genetics of peanut allergy: a twin study. J Allergy Clin Immunol 2000; 106:53–56.
- Sicherer SH, Sampson HA. Food allergy: recent advances in pathophysiology and treatment. Annu Rev Med 2009; 60:261–277.
- Sampson HA, Anderson JA. Summary and recommendations: classification of gastrointestinal manifestations due to immunologic reactions to foods in infants and young children. J Pediatr Gastroenterol Nutr 2000; 30( suppl 1):S87–S94.
- Sampson HA, Sicherer SH, Birnbaum AH. AGA technical review on the evaluation of food allergy in gastrointestinal disorders. American Gastroenterological Association. Gastroenterology 2001; 120:1026–1040.
- Spergel JM, Pawlowski NA. Food allergy. Mechanisms, diagnosis, and management in children. Pediatr Clin North Am 2002; 49:73–96.
- Sampson HA. Utility of food-specific IgE concentrations in predicting symptomatic food allergy. J Allergy Clin Immunol 2001; 107:891–896.
- Ortolani C, Ispano M, Pastorello EA, Ansaloni R, Magri GC. Comparison of results of skin prick tests (with fresh foods and commercial food extracts) and RAST in 100 patients with oral allergy syndrome. J Allergy Clin Immunol 1989; 83:683–690.
- Perry TT, Matsui EC, Kay Conover-Walker M, Wood RA. The relationship of allergen-specific IgE levels and oral food challenge outcome. J Allergy Clin Immunol 2004; 114:144–149.
- Leung DY, Sampson HA, Yunginger JW, et al; Avon Longitudinal Study of Parents and Children Study Team. Effect of anti-IgE therapy in patients with peanut allergy. N Engl J Med 2003; 348:986–993.
- Sampson HA. A phase II, randomized double-blind, parallel-group, placebo-controlled, oral food challenge trial of Xolair (omalizumab) in peanut allergy (TOPS). J Allergy Clin Immunol 2007; 119 (suppl 1):S117.
- Buchanan AD, Green TD, Jones SM, et al Egg oral immunotherapy in nonanaphylactic children with egg allergy. J Allergy Clin Immunol 2007; 119:199–205.
- Burks AW, Jones SM. Egg oral immunotherapy in non-anaphylactic children with egg allergy: follow-up. J Allergy Clin Immunol 2008; 121:270–271.
- Skripak JM, Nash SD, Rowley H, et al. A randomized, double-blind, placebo-controlled study of milk oral immunotherapy for cow's milk allergy. J Allergy Clin Immunol 2008; 122:1154–1160.
- Furuta GT, Liacouras CA, Collins MH, et al; First International Gastrointestinal Eosinophil Research Symposium (FIGERS) Subcommittees. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology 2007; 133:1342–1363.
- Rodrigo S, Abboud G, Oh D, et al. High intraepithelial eosinophil counts in esophageal squamous epithelium are not specific for eosinophilic esophagitis in adults. Am J Gastroenterol 2008; 103:435–442.
- Liacouras CA, Spergel JM, Ruchelli E, et al. Eosinophilic esophagitis: a 10-year experience in 381 children. Clin Gastroenterol Hepatol 2005; 3:1198–1206.
- Simon D, Marti H, Heer P, Simon HU, Braathen LR, Straumann A. Eosinophilic esophagitis is frequently associated with IgE-mediated allergic airway diseases. J Allergy Clin Immunol 2005; 115:1090–1092.
- Rothenberg ME, Mishra A, Collins MH, Putnam PE. Pathogenesis and clinical features of eosinophilic esophagitis. J Allergy Clin Immunol 2001; 108:891–894.
- Gupta SK, Fitzgerald JF, Kondratyuk T, HogenEsch H. Cytokine expression in normal and inflamed esophageal mucosa: a study into the pathogenesis of allergic eosinophilic esophagitis. J Pediatr Gastroenterol Nutr 2006; 42:22–26.
- Straumann A, Bauer M, Fischer B, Blaser K, Simon HU. Idiopathic eosinophilic esophagitis is associated with a T(H)2-type allergic inflammatory response. J Allergy Clin Immunol 2001; 108:954–961.
- Mishra A, Rothenberg ME. Intratracheal IL-13 induces eosinophilic esophagitis by an IL-5, eotaxin-1, and STAT6-dependent mechanism. Gastroenterology 2003; 125:1419–1427.
- Akei HS, Mishra A, Blanchard C, Rothenberg ME. Epicutaneous antigen exposure primes for experimental eosinophilic esophagitis in mice. Gastroenterology 2005; 129:985–994.
- Blanchard C, Wang N, Stringer KF, et al. Eotaxin-3 and a uniquely conserved gene-expression profile in eosinophilic esophagitis. J Clin Invest 2006; 116:536–547.
- Fogg MI, Ruchelli E, Spergel JM. Pollen and eosinophilic esophagitis. J Allergy Clin Immunol 2003; 112:796–797.
- Almansa C, Krishna M, Buchner AM, et al. Seasonal distribution in newly diagnosed cases of eosinophilic esophagitis in adults. Am J Gastroenterol 2009; 104:828–833.
- Kelly KJ, Lazenby AJ, Rowe PC, Yardley JH, Perman JA, Sampson HA. Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology 1995; 109:1503–1512.
- Markowitz JE, Spergel JM, Ruchelli E, Liacouras CA. Elemental diet is an effective treatment for eosinophilic esophagitis in children and adolescents. Am J Gastroenterol 2003; 98:777–782.
- Kagalwalla AF, Sentongo TA, Ritz S, et al. Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis. Clin Gastroenterol Hepatol 2006; 4:1097–1102.
- Gonsalves N, Yang GY, Doerfler B, et al. A prospective clinical trial of six food elimination diet and reintroduction of causative agents in adults with eosinophilic esophagitis [abstract]. Gastroenterology 2008; 134( suppl 1):A104–A105.
- Simon D, Straumann A, Wenk A, Spichtin H, Simon HU, Braathen LR. Eosinophilic esophagitis in adults—no clinical relevance of wheat and rye sensitizations. Allergy 2006; 61:1480–1483.
- Antón Remirez J, Escudero R, Caceres O, Fernandez-Benitez M. Eosinophilic esophagitis. Allergol Immunopathol (Madr) 2006; 34:79–81.
- Yamazaki K, Murray JA, Arora AS, et al. Allergen-specific in vitro cytokine production in adult patients with eosinophilic esophagitis. Dig Dis Sci 2006; 51:1934–1941.
- Penfield JD, Lang DM, Goldblum JR, Lopez R, Falk GW. The role of allergy evaluation in adults with eosinophilic esophagitis. J Clin Gastroenterol 2009(Epub ahead of print)
- Spergel JM, Andrews T, Brown-Whitehorn TF, Beausoleil JL, Liacouras CA. Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch tests. Ann Allergy Asthma Immunol 2005; 95:336–343.
- Spergel JM, Brown-Whitehorn T, Beausoleil JL, Shuker M, Liacouras CA. Predictive values for skin prick test and atopy patch test for eosinophilic esophagitis. J Allergy Clin Immunol 2007; 119:509–511.
- Bruijnzeel-Koomen C, Ortolani C, Aas K, et al. Adverse reactions to food. European Academy of Allergology and Clinical Immunology Subcommittee. Allergy 1995; 50:623–635.
- Sampson HA. Update on food allergy. J Allergy Clin Immunol 2004; 113:805–819.
- Sicherer SH, Sampson HA. 9. Food allergy. J Allergy Clin Immunol 2006; 117 (suppl 2):S470–S475.
- Sicherer SH, Munoz-Furlong A, Sampson HA. Prevalence of peanut and tree nut allergy in the United States determined by means of a random digit dial telephone survey: a 5-year follow-up study. J Allergy Clin Immunol 2003; 112:1203–1207.
- American College of Allergy, Asthma, & Immunology. Food allergy: a practice parameter. Ann Allergy Asthma Immunol 2006; 96( suppl 2):S1–S68.
- Wood RA. The natural history of food allergy. Pediatrics 2003; 111:1631–1637.
- Hourihane JO, Roberts SA, Warner JO. Resolution of peanut allergy: case-control study. BMJ 1998; 316:1271–1275.
- Fleischer DM, Conover-Walker MK, Matsui EC, Wood RA. The natural history of tree nut allergy. J Allergy Clin Immunol 2005; 116:1087–1093.
- Husby S, Foged N, Host A, Svehag SE. Passage of dietary antigens into the blood of children with coeliac disease. Quantification and size distribution of absorbed antigens. Gut 1987; 28:1062–1072.
- Mowat AM. Anatomical basis of tolerance and immunity to intestinal antigens. Nat Rev Immunol 2003; 3:331–341.
- Frossard CP, Tropia L, Hauser C, Eigenmann PA. Lymphocytes in Peyer patches regulate clinical tolerance in a murine model of food allergy. J Allergy Clin Immunol 2004; 113:958–964.
- Jain SL, Barone KS, Flanagan MP, Michael JG. Activation patterns of murine B cells after oral administration of an encapsulated soluble antigen. Vaccine 1996; 14:1291–1297.
- Kopper RA, Odum NJ, Sen M, Helm RM, Stanley JS, Burks AW. Peanut protein allergens: the effect of roasting on solubility and allergenicity. Int Arch Allergy Immunol 2005; 136:16–22.
- Lack G. Epidemiologic risks for food allergy. J Allergy Clin Immunol 2008; 121:1331–1336.
- Lack G, Fox D, Northstone K, Golding J; Avon Longitudinal Study of Parents and Children Study Team. Factors associated with the development of peanut allergy in childhood. N Engl J Med 2003; 348:977–985.
- Sudo N, Sawamura S, Tanaka K, Aiba Y, Kubo C, Koga Y. The requirement of intestinal bacterial flora for the development of an IgE production system fully susceptible to oral tolerance induction. J Immunol 1997; 159:1739–1745.
- Bashir ME, Louie S, Shi HN, Nagler-Anderson C. Toll-like receptor 4 signaling by intestinal microbes influences susceptibility to food allergy. J Immunol 2004; 172:6978–6987.
- Kopp MV, Hennemuth I, Heinzmann A, Urbanek R. Randomized, double-blind, placebo-controlled trial of probiotics for primary prevention: no clinical effects of lactobacillus GG supplementation. Pediatrics 2008; 121:e850–e856.
- Kukkonen K, Savilahti E, Haahtela T, et al. Probiotics and prebiotic galacto-oligosaccharides in the prevention of allergic diseases: a randomized, double-blind, placebo-controlled trial. J Allergy Clin Immunol 2007; 119:192–198.
- Osborn DA, Sinn JK. Probiotics in infants for prevention of allergic disease and food hypersensitivity. Cochrane Database Syst Rev 2007;CD006475.
- Prescott SL, Bjorksten B. Probiotics for the prevention or treatment of allergic diseases. J Allergy Clin Immunol 2007; 120:255–262.
- Untersmayr E, Jensen-Jarolim E. The role of protein digestibility and antacids on food allergy outcomes. J Allergy Clin Immunol 2008; 121:1301–1308.
- Untersmayr E, Scholl I, Swoboda I, et al. Antacid medication inhibits digestion of dietary proteins and causes food allergy: a fish allergy model in BALB/c mice. J Allergy Clin Immunol 2003; 112:616–623.
- Sicherer SH, Furlong TJ, Maes HH, Desnick RJ, Sampson HA, Gelb BD. Genetics of peanut allergy: a twin study. J Allergy Clin Immunol 2000; 106:53–56.
- Sicherer SH, Sampson HA. Food allergy: recent advances in pathophysiology and treatment. Annu Rev Med 2009; 60:261–277.
- Sampson HA, Anderson JA. Summary and recommendations: classification of gastrointestinal manifestations due to immunologic reactions to foods in infants and young children. J Pediatr Gastroenterol Nutr 2000; 30( suppl 1):S87–S94.
- Sampson HA, Sicherer SH, Birnbaum AH. AGA technical review on the evaluation of food allergy in gastrointestinal disorders. American Gastroenterological Association. Gastroenterology 2001; 120:1026–1040.
- Spergel JM, Pawlowski NA. Food allergy. Mechanisms, diagnosis, and management in children. Pediatr Clin North Am 2002; 49:73–96.
- Sampson HA. Utility of food-specific IgE concentrations in predicting symptomatic food allergy. J Allergy Clin Immunol 2001; 107:891–896.
- Ortolani C, Ispano M, Pastorello EA, Ansaloni R, Magri GC. Comparison of results of skin prick tests (with fresh foods and commercial food extracts) and RAST in 100 patients with oral allergy syndrome. J Allergy Clin Immunol 1989; 83:683–690.
- Perry TT, Matsui EC, Kay Conover-Walker M, Wood RA. The relationship of allergen-specific IgE levels and oral food challenge outcome. J Allergy Clin Immunol 2004; 114:144–149.
- Leung DY, Sampson HA, Yunginger JW, et al; Avon Longitudinal Study of Parents and Children Study Team. Effect of anti-IgE therapy in patients with peanut allergy. N Engl J Med 2003; 348:986–993.
- Sampson HA. A phase II, randomized double-blind, parallel-group, placebo-controlled, oral food challenge trial of Xolair (omalizumab) in peanut allergy (TOPS). J Allergy Clin Immunol 2007; 119 (suppl 1):S117.
- Buchanan AD, Green TD, Jones SM, et al Egg oral immunotherapy in nonanaphylactic children with egg allergy. J Allergy Clin Immunol 2007; 119:199–205.
- Burks AW, Jones SM. Egg oral immunotherapy in non-anaphylactic children with egg allergy: follow-up. J Allergy Clin Immunol 2008; 121:270–271.
- Skripak JM, Nash SD, Rowley H, et al. A randomized, double-blind, placebo-controlled study of milk oral immunotherapy for cow's milk allergy. J Allergy Clin Immunol 2008; 122:1154–1160.
- Furuta GT, Liacouras CA, Collins MH, et al; First International Gastrointestinal Eosinophil Research Symposium (FIGERS) Subcommittees. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology 2007; 133:1342–1363.
- Rodrigo S, Abboud G, Oh D, et al. High intraepithelial eosinophil counts in esophageal squamous epithelium are not specific for eosinophilic esophagitis in adults. Am J Gastroenterol 2008; 103:435–442.
- Liacouras CA, Spergel JM, Ruchelli E, et al. Eosinophilic esophagitis: a 10-year experience in 381 children. Clin Gastroenterol Hepatol 2005; 3:1198–1206.
- Simon D, Marti H, Heer P, Simon HU, Braathen LR, Straumann A. Eosinophilic esophagitis is frequently associated with IgE-mediated allergic airway diseases. J Allergy Clin Immunol 2005; 115:1090–1092.
- Rothenberg ME, Mishra A, Collins MH, Putnam PE. Pathogenesis and clinical features of eosinophilic esophagitis. J Allergy Clin Immunol 2001; 108:891–894.
- Gupta SK, Fitzgerald JF, Kondratyuk T, HogenEsch H. Cytokine expression in normal and inflamed esophageal mucosa: a study into the pathogenesis of allergic eosinophilic esophagitis. J Pediatr Gastroenterol Nutr 2006; 42:22–26.
- Straumann A, Bauer M, Fischer B, Blaser K, Simon HU. Idiopathic eosinophilic esophagitis is associated with a T(H)2-type allergic inflammatory response. J Allergy Clin Immunol 2001; 108:954–961.
- Mishra A, Rothenberg ME. Intratracheal IL-13 induces eosinophilic esophagitis by an IL-5, eotaxin-1, and STAT6-dependent mechanism. Gastroenterology 2003; 125:1419–1427.
- Akei HS, Mishra A, Blanchard C, Rothenberg ME. Epicutaneous antigen exposure primes for experimental eosinophilic esophagitis in mice. Gastroenterology 2005; 129:985–994.
- Blanchard C, Wang N, Stringer KF, et al. Eotaxin-3 and a uniquely conserved gene-expression profile in eosinophilic esophagitis. J Clin Invest 2006; 116:536–547.
- Fogg MI, Ruchelli E, Spergel JM. Pollen and eosinophilic esophagitis. J Allergy Clin Immunol 2003; 112:796–797.
- Almansa C, Krishna M, Buchner AM, et al. Seasonal distribution in newly diagnosed cases of eosinophilic esophagitis in adults. Am J Gastroenterol 2009; 104:828–833.
- Kelly KJ, Lazenby AJ, Rowe PC, Yardley JH, Perman JA, Sampson HA. Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology 1995; 109:1503–1512.
- Markowitz JE, Spergel JM, Ruchelli E, Liacouras CA. Elemental diet is an effective treatment for eosinophilic esophagitis in children and adolescents. Am J Gastroenterol 2003; 98:777–782.
- Kagalwalla AF, Sentongo TA, Ritz S, et al. Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis. Clin Gastroenterol Hepatol 2006; 4:1097–1102.
- Gonsalves N, Yang GY, Doerfler B, et al. A prospective clinical trial of six food elimination diet and reintroduction of causative agents in adults with eosinophilic esophagitis [abstract]. Gastroenterology 2008; 134( suppl 1):A104–A105.
- Simon D, Straumann A, Wenk A, Spichtin H, Simon HU, Braathen LR. Eosinophilic esophagitis in adults—no clinical relevance of wheat and rye sensitizations. Allergy 2006; 61:1480–1483.
- Antón Remirez J, Escudero R, Caceres O, Fernandez-Benitez M. Eosinophilic esophagitis. Allergol Immunopathol (Madr) 2006; 34:79–81.
- Yamazaki K, Murray JA, Arora AS, et al. Allergen-specific in vitro cytokine production in adult patients with eosinophilic esophagitis. Dig Dis Sci 2006; 51:1934–1941.
- Penfield JD, Lang DM, Goldblum JR, Lopez R, Falk GW. The role of allergy evaluation in adults with eosinophilic esophagitis. J Clin Gastroenterol 2009(Epub ahead of print)
- Spergel JM, Andrews T, Brown-Whitehorn TF, Beausoleil JL, Liacouras CA. Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch tests. Ann Allergy Asthma Immunol 2005; 95:336–343.
- Spergel JM, Brown-Whitehorn T, Beausoleil JL, Shuker M, Liacouras CA. Predictive values for skin prick test and atopy patch test for eosinophilic esophagitis. J Allergy Clin Immunol 2007; 119:509–511.
KEY POINTS
- Food allergies can be classified as mediated by immunoglobulin E (IgE-mediated), non-IgE-mediated, or mixed. Their clinical presentation can vary from life-threatening anaphylaxis in IgE-mediated reactions to chronic, delayed symptoms as seen in eosinophilic esophagitis (a mixed reaction).
- The diagnosis of an IgE-mediated food allergy is made by taking a complete history and performing directed testing—skin-prick testing or measurement of foodspecific IgE levels in the serum, or both.
- Despite promising developments, food allergies continue to be treated primarily by telling patients to avoid allergens and to initiate therapy if ingestion occurs.
- Because most patients with eosinophilic esophagitis have a strong history of atopic disease and respond to allergen-free diets, a complete evaluation by a specialist in allergy and immunology is recommended.
Abdominal pain in a 20-year-old woman
A 20-year-old woman presents to the emergency department with postprandial epigastric and right-upper-quadrant pain, sometimes associated with nausea. She has been having six to eight loose bowel movements every day, with no blood or mucus, and she has lost about 20 lb despite a good appetite. The diarrhea did not improve when she tried omitting milk products and carbohydrates.
Her symptoms began several months ago, but she says that 3 days ago the pain worsened steadily, radiating to the middle of her back, with associated episodes of nonbloody, nonbilious emesis. She cannot keep down liquids or solids. She says she has never had such episodes in the past.
She reports no oral ulcers, urinary symptoms, skin rashes, musculoskeletal pain, or neurologic symptoms, and she denies being anxious or depressed.
She has no history of serious illness, surgery, or hospitalization. She smokes a half pack of cigarettes a day, drinks alcohol occasionally, and smokes marijuana occasionally. She is employed as a certified nursing assistant.
She is taking ethinyl estradiol-levonorgestrel pills for birth control and takes calcium carbonate as needed for abdominal discomfort. She is taking no other medications, including nonsteroidal anti-inflammatory drugs (NSAIDs).
Her maternal uncle died of colon cancer at age 32, and her mother had colon polyps on colonoscopy. There is no family history of inflammatory bowel disease or celiac sprue. Her father committed suicide.
Her laboratory values
- White blood cell count 10.2 × 109/L (normal range 4–11)
- Red blood cell count 4.71 × 1012/L (3.9–5.5)
- Hemoglobin 14.4 g/dL (12–16)
- Hematocrit 42.4% (37%–47%)
- Mean corpuscular volume 90 fL (83–99)
- Mean corpuscular hemoglobin 30.6 pg (27–33)
- Platelet count 230 × 109/L (150–400)
- Red cell distribution width 13.3% (11.5%–14.5%)
- Sodium 140 mmol/L (132–148)
- Potassium 3.3 mmol/L (3.5–5.0)
- Chloride 104 mmol/L (98–111)
- Bicarbonate 28 mmol/L (23–32)
- Blood urea nitrogen 9 mg/dL (8–25)
- Creatinine 0.8 mg/dL (0.7–1.4)
- Glucose 87 mg/dL (65–100)
- Alanine aminotransferase 26 U/L (0–45)
- Aspartate aminotransferase 21 U/L (7–40)
- Alkaline phosphatase 101 U/L (40–150)
- Total bilirubin 0.8 mg/dL (0–1.5)
- Albumin 3.5 g/dL (3.5–5)
- Pregnancy screen negative
- Urine toxicology screen negative.
Physical examination
The patient is very thin and appears quite uncomfortable. Her temperature is 99.7°F (37.6°C), pulse rate 101, respiratory rate 18, blood pressure 111/67 mm Hg, and oxygen saturation 96% on room air. Her skin is warm and dry. Her height is 66 inches, weight 116 lb, and body mass index 18.7.
Examination of the head and neck shows normal dentition, dry mucus membranes, and no oral exudates. The thyroid is normal, and no masses or lymphadenopathy are noted.
Heart sounds and rhythm are normal, and the lungs are clear with no crackles or rubs. The abdomen is scaphoid and soft, with no distention. She has epigastric tenderness but no rebound, guarding, rigidity, palpable mass, or costovertebral angle tenderness. Bowel sounds are normal. The neurologic examination is normal.
NARROWING THE DIAGNOSIS
1. Given the history and findings so far, which is the least likely cause of her symptoms?
- Lactose intolerance
- Celiac disease
- Crohn disease
- Duodenal ulcer
- Eating disorder
This young woman’s presentation has some features found in all of these conditions. However, the least likely is lactose intolerance.
Lactose intolerance results from a shortage of the enzyme lactase, which is normally produced by the cells that line the small intestine. Close to 50 million American adults have lactose intolerance. Common symptoms include nausea, cramps, bloating, gas, and diarrhea, which begin about 30 minutes to 2 hours after eating or drinking foods containing lactose.
Since the patient’s symptoms did not improve when she tried omitting milk products, and since lactose intolerance is rarely associated with pain radiating to the back and with severe vomiting, this is the least likely cause of her symptoms.
Celiac disease presents with a myriad of symptoms—sometimes without gastrointestinal (GI) symptoms. Anemia is the most common laboratory finding, due most often to iron deficiency, but also due to deficiencies of vitamin B12 and folate as a result of malabsorption.1
Our patient’s laboratory values—especially her red cell indices—do not confirm this finding. One must also remember, however, that hemoglobin tends to be falsely elevated in patients who are dehydrated.
Crohn disease often presents with occult blood loss, low-grade fever, weight loss, and anemia. Though the condition is most often ileocolic, it can affect any part of the gastrointestinal tract. Nevertheless, most patients with gastroduodenal involvement have previously been diagnosed with ileocolic disease, and gastroduodenal involvement manifests later. Nonradiating epigastric pain is very common. Obstructive symptoms due to gastroduodenal strictures (eg, postprandial vomiting, epigastric pain, weight loss, bloating) are also common. 2
Duodenal ulcer. The most important factors responsible for duodenal ulcers are NSAID use and Helicobacter pylori infection.3 Duodenal ulcers have a variety of clinical presentations, ranging from no symptoms to severe pain. Epigastric pain can be sharp, dull, burning, or penetrating. Many patients complain of a feeling of hunger and weight gain—as opposed to gastric ulcer, in which patients experience anorexia and weight loss. Abdominal pain generally occurs several hours after meals and often awakens the patient at night. Pain is often relieved by food, but this phenomenon is present in only 20% to 60% of patients and probably is not specific for duodenal ulcer.
Our patient does not use NSAIDs, but some of her symptoms, such as postprandial pain, epigastric pain radiating to the back, and nausea and vomiting are seen with duodenal ulcer.
Eating disorders. The two main types of eating disorders—anorexia nervosa and bulimia nervosa—have a significant diagnostic overlap,4 and a third type, binge-eating disorder, is currently being investigated and defined. Girls and women are 10 times as likely as boys and men to develop an eating disorder.
People with anorexia have a distorted view of their bodies. Even when they are extremely thin, they see themselves as too fat.
Bulimia is characterized by binge-eating, purging, and overexercising to compensate for the excess calories. Patients are often close to normal weight.
Binge-eating disorder involves the consumption of very large amounts of food in a short period of time. About 2% of all young adults in the United States struggle with bingeeating. They are either overweight or obese.
These disorders tend to be associated with other psychiatric disorders such as depression or obsessive-compulsive disorder. Our patient sought medical attention and was appropriately concerned about her weight loss, which make an eating disorder unlikely.
CASE CONTINUED: SHE UNDERGOES CT
2. Which of the following is the most likely diagnosis at this point?
- SMA syndrome
- Chronic mesenteric ischemia involving the SMA
- Megaduodenum due to a connective tissue disorder
SMA syndrome is the most likely diagnosis. Despite its name, this syndrome is not a vascular condition. It is an uncommon cause of proximal intestinal obstruction in which the duodenum is compressed between the SMA and the aorta. First described in 1861, it has also been known as cast syndrome, Wilkie syndrome, and arteriomesenteric duodenal obstruction.5
To date, more than 400 cases of this syndrome have been reported, twice as many in women as in men. Most patients are between 20 and 40 years of age at the time of diagnosis. Common presenting symptoms include postprandial abdominal pain, nausea, vomiting, and weight loss, which may further reduce the angle between the SMA and the aorta. Diarrhea is not generally associated with this syndrome, and in our patient’s case the diarrhea was thought to be unrelated to the SMA syndrome, since it subsided spontaneously.
Conditions and events that cause, contribute to, or worsen SMA syndrome include:
- Rapid weight loss (as in cancer or burns) or lean body habitus
- Prolonged bed rest
- Use of a body cast
- Malabsorption
- Spinal disease, deformity, or trauma
- Scoliosis surgery
- Rapid linear growth without compensatory weight gain
- Abnormally high and fixed position of the ligament of Treitz
- Abdominal surgery
- Cardiac cachexia
- Unusually low origin of the SMA.7
More common causes of mechanical smallbowel obstruction are adhesions, hernias, and tumors.8 Hyperactive, high-pitched peristalsis with rushes coinciding with cramps is typical. Abdominal cramps are centered around the umbilicus or in the epigastrium and are associated with vomiting; obstipation develops in patients with complete obstruction. Patients with partial obstruction may develop diarrhea. Paralytic ileus secondary to hypokalemia is an important consideration in partial obstruction. However, abdominal radiography and CT did not confirm an obstruction, and her symptoms persisted despite correction of the potassium level.
Chronic mesenteric ischemia can be caused by vasculitis, nonocclusive conditions that cause prolonged vasoconstriction (eg, cocaine ingestion), or reduced cardiac output.9 Symptoms are due to the gradual reduction in blood flow to the intestine that occurs during eating. Our patient’s toxicology report did not suggest cocaine abuse, and her history and the workup thus far do not suggest heart failure. A workup for vasculitis was negative.
Megaduodenum, SMA-like syndrome. In rare cases, dilation of the duodenum at the level of the SMA may be part of a generalized duodenal dilation caused by something other than obstruction due to mechanical compression. There are conditions, as described below, that cause an SMA-like syndrome.
A compression defect of the duodenum at the site where the SMA crossed the duodenum was found in a series of 11 cases of systemic sclerosis.10 These patients had definite dilation of the duodenum, but it was a result of atrophy of the muscle layers and replacement by collagenous tissue, changes that result in diminished peristalsis, loss of muscle tone, and dilation. The duodenum yields to pressure in its third portion under the SMA.
Several pathologic conditions, particularly connective tissue disorders, may predispose to the development of a megaduodenum that may result in an imprint on the duodenum at the level of the SMA. The most noteworthy of these conditions is scleroderma. Other conditions that can cause reduced duodenal peristalsis include diabetes, pancreatitis, dermatomyositis, lupus erythematosus, myxedema, and amyloidosis.11
It is important to distinguish SMA syndrome from SMA-like syndromes for several reasons.12 SMA-like syndromes result in loss of normal peristalsis. Further, the conditions have different outcomes, even though they are managed similarly initially, ie, with rehydration and parenteral nutrition. Surgery is to be avoided if possible in conditions that affect widespread areas of the intestine, such as scleroderma or diabetic neuropathy.
3. Which of the following is helpful in confirming SMA syndrome?
- CT of the abdomen
- Upper GI radiography series
- Upper GI endoscopy
All three can help confirm the diagnosis.
CT of the abdomen is a convenient, safe, rapid, readily available, and relatively noninvasive way to evaluate the aortomesenteric angle and to view retroperitoneal and mesenteric fat.13 Rehydration before injecting intravenous dye is important to avoid precipitating renal failure. In this patient, CT findings that helped make the diagnosis included a narrow aortomesenteric angle, compression of the duodenum, and a paucity of fat around the SMA.
An upper GI series can reveal dilation of the first and second portions of the duodenum and abrupt compression of the duodenal mucosal folds. Other findings can include a delay of 4 to 6 hours in gastroduodenal transit and relief of the obstruction when the patient is in the left lateral decubitus position. The Hayes maneuver refers to the disappearance of these radiologic features in the knee-chest position on cinefluoroscopy.14 The findings mentioned above are best noted in the supine position on both radiography and CT.
Endoscopy is necessary to rule out mechanical causes of duodenal obstruction. A pulsatile extrinsic compression suggests this condition but is found only occasionally.
Other imaging studies, such as ultrasonography, arteriography, and hypotonic duodenography, are used less often.
4. At this time, which of the following would be the most appropriate initial treatment in this patient?
- Conservative treatment
- Narcotics
- Duodenojejunostomy
Conservative treatment is indicated initially in all cases of SMA syndrome.15 This involves reversing precipitating factors and replacing fluid, electrolytes, and nutrition via total parenteral nutrition and nasogastric decompression.
To avoid keeping the patient on intravenous therapy for a prolonged time, it is important to start enteral feeding once the pain has subsided and the patient can tolerate it. A double-lumen nasojejunal tube is passed distal to the obstruction under fluoroscopic guidance. During feedings, the patient should be in the modified knee-chest, prone, or leftside-down position, all of which increase the aortomesenteric angle.
Delaying the treatment of SMA syndrome can increase the risk of morbidity and mortality by progressive malnutrition, dehydration, oliguria, electrolyte abnormalities (eg, hypokalemia), or intestinal perforation from prolonged ischemia.16,17
Narcotics and other drugs known to slow gut motility should be avoided.
Symptoms typically improve after restoration of normal body weight. If conservative treatment fails, or if the case is severe or chronic, surgery is required.18 Fortunately, this is not required often.
Duodenojejunostomy is the most common surgical treatment and involves creation of an alternate route between the duodenum and the jejunum, bypassing the compression between the aorta and the SMA. Other procedures include gastrojejunostomy, laparoscopic duodenojejunostomy, 19 a Roux-en-Y procedure, robotically assisted duodenojejunostomy, and anterior transposition of the third portion of the duodenum. Cleavage of the ligament of Treitz is another option, enabling the duodenum to drop away from the apex of the sharpened aortomesenteric angle.
WHEN TO CONSIDER SMA SYNDROME
The SMA syndrome is an uncommon cause of a very common presenting symptom, ie, abdominal pain. Nevertheless, it should be considered in the differential diagnosis of abdominal pain, especially in patients who have conditions that cause significant weight loss, such as anorexia nervosa, malabsorption, or hypercatabolic states such as burns, major surgery, severe injuries, or malignancies. The diagnosis is based on a thorough history and on supportive findings from CT and endoscopy.
In our patient, weight loss began with nonspecific diarrhea but perpetuated itself as SMA syndrome occurred.
Appropriate management consists of interrupting the cycle of weight loss and secondary upper gut obstruction. For patients in whom more definitive therapy is not feasible, a gastrostomy tube for decompression with a jejunal extension available for feeding appears to be a reasonable and safe treatment option. Duodenojejunostomy is considered the procedure of choice in severe cases.
CASE CONCLUDED
Fortunately, our patient responded well to conservative management. She was treated with intravenous hydration and correction of electrolytes and 10 days later was able to tolerate a soft diet. She was discharged in stable condition. At a follow-up visit 2 weeks later, she reported minimal abdominal discomfort, was able to tolerate meals, and had gained a few pounds. She continues to do well.
- Iovino P, Ciacci C, Sabbatini F, Acioli DM, D'Argenio G, Mazzacca G. Esophageal impairment in adult celiac disease with steatorrhea. Am J Gastroenterol 1998; 93:1243–1249.
- Loftus EV. Upper gastrointestinal tract Crohn’s disease. Clin Perspect Gastroenterol 2002; 5:188–191.
- Zapata-Colindres JC, Zepeda-Gómez S, Montaño-Loza A, Vázquez-Ballesteros E, de Jesús Villalobos J, Valdovinos-Andraca F. The association of Helicobacter pylori infection and nonsteroidal antiinflammatory drugs in peptic ulcer disease. Can J Gastroenterol 2006; 20:277–280.
- Milos G, Spindler A, Schnyder U, Fairburn CG. Instability of eating disorder diagnoses: prospective study. Br J Psychiatry 2005; 187:573–578.
- Wilkie DP. Chronic duodenal ileus. Br J Surg 1921; 9:204–214.
- Ozkurt H, Cenker MM, Bas N, Erturk SM, Basak M. Measurement of the distance and angle between the aorta and superior mesenteric artery: normal values in different BMI categories. Surg Radiol Anat 2007; 29:595–599.
- Lippl F, Hannig C, Weiss W, Allescher HD, Classen M, Kurjak M. Superior mesenteric artery syndrome: diagnosis and treatment from the gastroenterologist's view. J Gastroenterol 2002; 37:640–643.
- Balthazar EJ. George W. Holmes Lecture. CT of small-bowel obstruction. AJR Am J Roentgenol 1994; 162:255–261.
- Chang JB, Stein TA. Mesenteric ischemia: acute and chronic. Ann Vasc Surg 2003; 17:323–328.
- Gondos B. Duodenal compression defect and the “superior mesenteric artery syndrome” 1. Radiology 1977; 123:575–580.
- Cohen LB, Field SP, Sachar DB. The superior mesenteric artery syndrome. The disease that isn't, or is it? J Clin Gastroenterol 1985; 7:113–716.
- Ahmed AR, Taylor I. Superior mesenteric artery syndrome. Postgrad Med J 1997; 73:776–778.
- Santer R, Young C, Rossi T, Riddlesberger MM. Computed tomography in superior mesenteric artery syndrome. Pediatr Radiol 1991; 21:154–155.
- Lukes PJ, Rolny P, Nilson AE, Gamklou R, Darle N, Dotevall G. Diagnostic value of hypotonic duodenography in superior mesenteric artery syndrome. Acta Chir Scand 1978; 144:39–43.
- Dietz UA, Debus ES, Heuko-Valiati L, et al. Aorto-mesenteric artery compression syndrome. Chirurg 2000; 71:1345–1351.
- Lim JE, Duke GL, Eachempati SR. Superior mesenteric artery syndrome presenting with acute massive gastric dilatation, gastric wall pneumatosis, and portal venous gas. Surgery 2003; 134:840–843.
- Fuhrman MA, Felig DM, Tanchel ME. Superior mesenteric artery syndrome with obstructing duodenal bezoar. Gastrointest Endosc 2003; 57:387.
- Hines JR, Gore RM, Ballantyne GH. Superior mesenteric artery syndrome. Diagnostic criteria and therapeutic approaches. Am J Surg 1984; 148:630–632.
- Gersin KS, Heniford BT. Laparoscopic duodenojejunostomy for treatment of superior mesenteric artery syndrome. JSLS 1998; 2:281–284.
A 20-year-old woman presents to the emergency department with postprandial epigastric and right-upper-quadrant pain, sometimes associated with nausea. She has been having six to eight loose bowel movements every day, with no blood or mucus, and she has lost about 20 lb despite a good appetite. The diarrhea did not improve when she tried omitting milk products and carbohydrates.
Her symptoms began several months ago, but she says that 3 days ago the pain worsened steadily, radiating to the middle of her back, with associated episodes of nonbloody, nonbilious emesis. She cannot keep down liquids or solids. She says she has never had such episodes in the past.
She reports no oral ulcers, urinary symptoms, skin rashes, musculoskeletal pain, or neurologic symptoms, and she denies being anxious or depressed.
She has no history of serious illness, surgery, or hospitalization. She smokes a half pack of cigarettes a day, drinks alcohol occasionally, and smokes marijuana occasionally. She is employed as a certified nursing assistant.
She is taking ethinyl estradiol-levonorgestrel pills for birth control and takes calcium carbonate as needed for abdominal discomfort. She is taking no other medications, including nonsteroidal anti-inflammatory drugs (NSAIDs).
Her maternal uncle died of colon cancer at age 32, and her mother had colon polyps on colonoscopy. There is no family history of inflammatory bowel disease or celiac sprue. Her father committed suicide.
Her laboratory values
- White blood cell count 10.2 × 109/L (normal range 4–11)
- Red blood cell count 4.71 × 1012/L (3.9–5.5)
- Hemoglobin 14.4 g/dL (12–16)
- Hematocrit 42.4% (37%–47%)
- Mean corpuscular volume 90 fL (83–99)
- Mean corpuscular hemoglobin 30.6 pg (27–33)
- Platelet count 230 × 109/L (150–400)
- Red cell distribution width 13.3% (11.5%–14.5%)
- Sodium 140 mmol/L (132–148)
- Potassium 3.3 mmol/L (3.5–5.0)
- Chloride 104 mmol/L (98–111)
- Bicarbonate 28 mmol/L (23–32)
- Blood urea nitrogen 9 mg/dL (8–25)
- Creatinine 0.8 mg/dL (0.7–1.4)
- Glucose 87 mg/dL (65–100)
- Alanine aminotransferase 26 U/L (0–45)
- Aspartate aminotransferase 21 U/L (7–40)
- Alkaline phosphatase 101 U/L (40–150)
- Total bilirubin 0.8 mg/dL (0–1.5)
- Albumin 3.5 g/dL (3.5–5)
- Pregnancy screen negative
- Urine toxicology screen negative.
Physical examination
The patient is very thin and appears quite uncomfortable. Her temperature is 99.7°F (37.6°C), pulse rate 101, respiratory rate 18, blood pressure 111/67 mm Hg, and oxygen saturation 96% on room air. Her skin is warm and dry. Her height is 66 inches, weight 116 lb, and body mass index 18.7.
Examination of the head and neck shows normal dentition, dry mucus membranes, and no oral exudates. The thyroid is normal, and no masses or lymphadenopathy are noted.
Heart sounds and rhythm are normal, and the lungs are clear with no crackles or rubs. The abdomen is scaphoid and soft, with no distention. She has epigastric tenderness but no rebound, guarding, rigidity, palpable mass, or costovertebral angle tenderness. Bowel sounds are normal. The neurologic examination is normal.
NARROWING THE DIAGNOSIS
1. Given the history and findings so far, which is the least likely cause of her symptoms?
- Lactose intolerance
- Celiac disease
- Crohn disease
- Duodenal ulcer
- Eating disorder
This young woman’s presentation has some features found in all of these conditions. However, the least likely is lactose intolerance.
Lactose intolerance results from a shortage of the enzyme lactase, which is normally produced by the cells that line the small intestine. Close to 50 million American adults have lactose intolerance. Common symptoms include nausea, cramps, bloating, gas, and diarrhea, which begin about 30 minutes to 2 hours after eating or drinking foods containing lactose.
Since the patient’s symptoms did not improve when she tried omitting milk products, and since lactose intolerance is rarely associated with pain radiating to the back and with severe vomiting, this is the least likely cause of her symptoms.
Celiac disease presents with a myriad of symptoms—sometimes without gastrointestinal (GI) symptoms. Anemia is the most common laboratory finding, due most often to iron deficiency, but also due to deficiencies of vitamin B12 and folate as a result of malabsorption.1
Our patient’s laboratory values—especially her red cell indices—do not confirm this finding. One must also remember, however, that hemoglobin tends to be falsely elevated in patients who are dehydrated.
Crohn disease often presents with occult blood loss, low-grade fever, weight loss, and anemia. Though the condition is most often ileocolic, it can affect any part of the gastrointestinal tract. Nevertheless, most patients with gastroduodenal involvement have previously been diagnosed with ileocolic disease, and gastroduodenal involvement manifests later. Nonradiating epigastric pain is very common. Obstructive symptoms due to gastroduodenal strictures (eg, postprandial vomiting, epigastric pain, weight loss, bloating) are also common. 2
Duodenal ulcer. The most important factors responsible for duodenal ulcers are NSAID use and Helicobacter pylori infection.3 Duodenal ulcers have a variety of clinical presentations, ranging from no symptoms to severe pain. Epigastric pain can be sharp, dull, burning, or penetrating. Many patients complain of a feeling of hunger and weight gain—as opposed to gastric ulcer, in which patients experience anorexia and weight loss. Abdominal pain generally occurs several hours after meals and often awakens the patient at night. Pain is often relieved by food, but this phenomenon is present in only 20% to 60% of patients and probably is not specific for duodenal ulcer.
Our patient does not use NSAIDs, but some of her symptoms, such as postprandial pain, epigastric pain radiating to the back, and nausea and vomiting are seen with duodenal ulcer.
Eating disorders. The two main types of eating disorders—anorexia nervosa and bulimia nervosa—have a significant diagnostic overlap,4 and a third type, binge-eating disorder, is currently being investigated and defined. Girls and women are 10 times as likely as boys and men to develop an eating disorder.
People with anorexia have a distorted view of their bodies. Even when they are extremely thin, they see themselves as too fat.
Bulimia is characterized by binge-eating, purging, and overexercising to compensate for the excess calories. Patients are often close to normal weight.
Binge-eating disorder involves the consumption of very large amounts of food in a short period of time. About 2% of all young adults in the United States struggle with bingeeating. They are either overweight or obese.
These disorders tend to be associated with other psychiatric disorders such as depression or obsessive-compulsive disorder. Our patient sought medical attention and was appropriately concerned about her weight loss, which make an eating disorder unlikely.
CASE CONTINUED: SHE UNDERGOES CT
2. Which of the following is the most likely diagnosis at this point?
- SMA syndrome
- Chronic mesenteric ischemia involving the SMA
- Megaduodenum due to a connective tissue disorder
SMA syndrome is the most likely diagnosis. Despite its name, this syndrome is not a vascular condition. It is an uncommon cause of proximal intestinal obstruction in which the duodenum is compressed between the SMA and the aorta. First described in 1861, it has also been known as cast syndrome, Wilkie syndrome, and arteriomesenteric duodenal obstruction.5
To date, more than 400 cases of this syndrome have been reported, twice as many in women as in men. Most patients are between 20 and 40 years of age at the time of diagnosis. Common presenting symptoms include postprandial abdominal pain, nausea, vomiting, and weight loss, which may further reduce the angle between the SMA and the aorta. Diarrhea is not generally associated with this syndrome, and in our patient’s case the diarrhea was thought to be unrelated to the SMA syndrome, since it subsided spontaneously.
Conditions and events that cause, contribute to, or worsen SMA syndrome include:
- Rapid weight loss (as in cancer or burns) or lean body habitus
- Prolonged bed rest
- Use of a body cast
- Malabsorption
- Spinal disease, deformity, or trauma
- Scoliosis surgery
- Rapid linear growth without compensatory weight gain
- Abnormally high and fixed position of the ligament of Treitz
- Abdominal surgery
- Cardiac cachexia
- Unusually low origin of the SMA.7
More common causes of mechanical smallbowel obstruction are adhesions, hernias, and tumors.8 Hyperactive, high-pitched peristalsis with rushes coinciding with cramps is typical. Abdominal cramps are centered around the umbilicus or in the epigastrium and are associated with vomiting; obstipation develops in patients with complete obstruction. Patients with partial obstruction may develop diarrhea. Paralytic ileus secondary to hypokalemia is an important consideration in partial obstruction. However, abdominal radiography and CT did not confirm an obstruction, and her symptoms persisted despite correction of the potassium level.
Chronic mesenteric ischemia can be caused by vasculitis, nonocclusive conditions that cause prolonged vasoconstriction (eg, cocaine ingestion), or reduced cardiac output.9 Symptoms are due to the gradual reduction in blood flow to the intestine that occurs during eating. Our patient’s toxicology report did not suggest cocaine abuse, and her history and the workup thus far do not suggest heart failure. A workup for vasculitis was negative.
Megaduodenum, SMA-like syndrome. In rare cases, dilation of the duodenum at the level of the SMA may be part of a generalized duodenal dilation caused by something other than obstruction due to mechanical compression. There are conditions, as described below, that cause an SMA-like syndrome.
A compression defect of the duodenum at the site where the SMA crossed the duodenum was found in a series of 11 cases of systemic sclerosis.10 These patients had definite dilation of the duodenum, but it was a result of atrophy of the muscle layers and replacement by collagenous tissue, changes that result in diminished peristalsis, loss of muscle tone, and dilation. The duodenum yields to pressure in its third portion under the SMA.
Several pathologic conditions, particularly connective tissue disorders, may predispose to the development of a megaduodenum that may result in an imprint on the duodenum at the level of the SMA. The most noteworthy of these conditions is scleroderma. Other conditions that can cause reduced duodenal peristalsis include diabetes, pancreatitis, dermatomyositis, lupus erythematosus, myxedema, and amyloidosis.11
It is important to distinguish SMA syndrome from SMA-like syndromes for several reasons.12 SMA-like syndromes result in loss of normal peristalsis. Further, the conditions have different outcomes, even though they are managed similarly initially, ie, with rehydration and parenteral nutrition. Surgery is to be avoided if possible in conditions that affect widespread areas of the intestine, such as scleroderma or diabetic neuropathy.
3. Which of the following is helpful in confirming SMA syndrome?
- CT of the abdomen
- Upper GI radiography series
- Upper GI endoscopy
All three can help confirm the diagnosis.
CT of the abdomen is a convenient, safe, rapid, readily available, and relatively noninvasive way to evaluate the aortomesenteric angle and to view retroperitoneal and mesenteric fat.13 Rehydration before injecting intravenous dye is important to avoid precipitating renal failure. In this patient, CT findings that helped make the diagnosis included a narrow aortomesenteric angle, compression of the duodenum, and a paucity of fat around the SMA.
An upper GI series can reveal dilation of the first and second portions of the duodenum and abrupt compression of the duodenal mucosal folds. Other findings can include a delay of 4 to 6 hours in gastroduodenal transit and relief of the obstruction when the patient is in the left lateral decubitus position. The Hayes maneuver refers to the disappearance of these radiologic features in the knee-chest position on cinefluoroscopy.14 The findings mentioned above are best noted in the supine position on both radiography and CT.
Endoscopy is necessary to rule out mechanical causes of duodenal obstruction. A pulsatile extrinsic compression suggests this condition but is found only occasionally.
Other imaging studies, such as ultrasonography, arteriography, and hypotonic duodenography, are used less often.
4. At this time, which of the following would be the most appropriate initial treatment in this patient?
- Conservative treatment
- Narcotics
- Duodenojejunostomy
Conservative treatment is indicated initially in all cases of SMA syndrome.15 This involves reversing precipitating factors and replacing fluid, electrolytes, and nutrition via total parenteral nutrition and nasogastric decompression.
To avoid keeping the patient on intravenous therapy for a prolonged time, it is important to start enteral feeding once the pain has subsided and the patient can tolerate it. A double-lumen nasojejunal tube is passed distal to the obstruction under fluoroscopic guidance. During feedings, the patient should be in the modified knee-chest, prone, or leftside-down position, all of which increase the aortomesenteric angle.
Delaying the treatment of SMA syndrome can increase the risk of morbidity and mortality by progressive malnutrition, dehydration, oliguria, electrolyte abnormalities (eg, hypokalemia), or intestinal perforation from prolonged ischemia.16,17
Narcotics and other drugs known to slow gut motility should be avoided.
Symptoms typically improve after restoration of normal body weight. If conservative treatment fails, or if the case is severe or chronic, surgery is required.18 Fortunately, this is not required often.
Duodenojejunostomy is the most common surgical treatment and involves creation of an alternate route between the duodenum and the jejunum, bypassing the compression between the aorta and the SMA. Other procedures include gastrojejunostomy, laparoscopic duodenojejunostomy, 19 a Roux-en-Y procedure, robotically assisted duodenojejunostomy, and anterior transposition of the third portion of the duodenum. Cleavage of the ligament of Treitz is another option, enabling the duodenum to drop away from the apex of the sharpened aortomesenteric angle.
WHEN TO CONSIDER SMA SYNDROME
The SMA syndrome is an uncommon cause of a very common presenting symptom, ie, abdominal pain. Nevertheless, it should be considered in the differential diagnosis of abdominal pain, especially in patients who have conditions that cause significant weight loss, such as anorexia nervosa, malabsorption, or hypercatabolic states such as burns, major surgery, severe injuries, or malignancies. The diagnosis is based on a thorough history and on supportive findings from CT and endoscopy.
In our patient, weight loss began with nonspecific diarrhea but perpetuated itself as SMA syndrome occurred.
Appropriate management consists of interrupting the cycle of weight loss and secondary upper gut obstruction. For patients in whom more definitive therapy is not feasible, a gastrostomy tube for decompression with a jejunal extension available for feeding appears to be a reasonable and safe treatment option. Duodenojejunostomy is considered the procedure of choice in severe cases.
CASE CONCLUDED
Fortunately, our patient responded well to conservative management. She was treated with intravenous hydration and correction of electrolytes and 10 days later was able to tolerate a soft diet. She was discharged in stable condition. At a follow-up visit 2 weeks later, she reported minimal abdominal discomfort, was able to tolerate meals, and had gained a few pounds. She continues to do well.
A 20-year-old woman presents to the emergency department with postprandial epigastric and right-upper-quadrant pain, sometimes associated with nausea. She has been having six to eight loose bowel movements every day, with no blood or mucus, and she has lost about 20 lb despite a good appetite. The diarrhea did not improve when she tried omitting milk products and carbohydrates.
Her symptoms began several months ago, but she says that 3 days ago the pain worsened steadily, radiating to the middle of her back, with associated episodes of nonbloody, nonbilious emesis. She cannot keep down liquids or solids. She says she has never had such episodes in the past.
She reports no oral ulcers, urinary symptoms, skin rashes, musculoskeletal pain, or neurologic symptoms, and she denies being anxious or depressed.
She has no history of serious illness, surgery, or hospitalization. She smokes a half pack of cigarettes a day, drinks alcohol occasionally, and smokes marijuana occasionally. She is employed as a certified nursing assistant.
She is taking ethinyl estradiol-levonorgestrel pills for birth control and takes calcium carbonate as needed for abdominal discomfort. She is taking no other medications, including nonsteroidal anti-inflammatory drugs (NSAIDs).
Her maternal uncle died of colon cancer at age 32, and her mother had colon polyps on colonoscopy. There is no family history of inflammatory bowel disease or celiac sprue. Her father committed suicide.
Her laboratory values
- White blood cell count 10.2 × 109/L (normal range 4–11)
- Red blood cell count 4.71 × 1012/L (3.9–5.5)
- Hemoglobin 14.4 g/dL (12–16)
- Hematocrit 42.4% (37%–47%)
- Mean corpuscular volume 90 fL (83–99)
- Mean corpuscular hemoglobin 30.6 pg (27–33)
- Platelet count 230 × 109/L (150–400)
- Red cell distribution width 13.3% (11.5%–14.5%)
- Sodium 140 mmol/L (132–148)
- Potassium 3.3 mmol/L (3.5–5.0)
- Chloride 104 mmol/L (98–111)
- Bicarbonate 28 mmol/L (23–32)
- Blood urea nitrogen 9 mg/dL (8–25)
- Creatinine 0.8 mg/dL (0.7–1.4)
- Glucose 87 mg/dL (65–100)
- Alanine aminotransferase 26 U/L (0–45)
- Aspartate aminotransferase 21 U/L (7–40)
- Alkaline phosphatase 101 U/L (40–150)
- Total bilirubin 0.8 mg/dL (0–1.5)
- Albumin 3.5 g/dL (3.5–5)
- Pregnancy screen negative
- Urine toxicology screen negative.
Physical examination
The patient is very thin and appears quite uncomfortable. Her temperature is 99.7°F (37.6°C), pulse rate 101, respiratory rate 18, blood pressure 111/67 mm Hg, and oxygen saturation 96% on room air. Her skin is warm and dry. Her height is 66 inches, weight 116 lb, and body mass index 18.7.
Examination of the head and neck shows normal dentition, dry mucus membranes, and no oral exudates. The thyroid is normal, and no masses or lymphadenopathy are noted.
Heart sounds and rhythm are normal, and the lungs are clear with no crackles or rubs. The abdomen is scaphoid and soft, with no distention. She has epigastric tenderness but no rebound, guarding, rigidity, palpable mass, or costovertebral angle tenderness. Bowel sounds are normal. The neurologic examination is normal.
NARROWING THE DIAGNOSIS
1. Given the history and findings so far, which is the least likely cause of her symptoms?
- Lactose intolerance
- Celiac disease
- Crohn disease
- Duodenal ulcer
- Eating disorder
This young woman’s presentation has some features found in all of these conditions. However, the least likely is lactose intolerance.
Lactose intolerance results from a shortage of the enzyme lactase, which is normally produced by the cells that line the small intestine. Close to 50 million American adults have lactose intolerance. Common symptoms include nausea, cramps, bloating, gas, and diarrhea, which begin about 30 minutes to 2 hours after eating or drinking foods containing lactose.
Since the patient’s symptoms did not improve when she tried omitting milk products, and since lactose intolerance is rarely associated with pain radiating to the back and with severe vomiting, this is the least likely cause of her symptoms.
Celiac disease presents with a myriad of symptoms—sometimes without gastrointestinal (GI) symptoms. Anemia is the most common laboratory finding, due most often to iron deficiency, but also due to deficiencies of vitamin B12 and folate as a result of malabsorption.1
Our patient’s laboratory values—especially her red cell indices—do not confirm this finding. One must also remember, however, that hemoglobin tends to be falsely elevated in patients who are dehydrated.
Crohn disease often presents with occult blood loss, low-grade fever, weight loss, and anemia. Though the condition is most often ileocolic, it can affect any part of the gastrointestinal tract. Nevertheless, most patients with gastroduodenal involvement have previously been diagnosed with ileocolic disease, and gastroduodenal involvement manifests later. Nonradiating epigastric pain is very common. Obstructive symptoms due to gastroduodenal strictures (eg, postprandial vomiting, epigastric pain, weight loss, bloating) are also common. 2
Duodenal ulcer. The most important factors responsible for duodenal ulcers are NSAID use and Helicobacter pylori infection.3 Duodenal ulcers have a variety of clinical presentations, ranging from no symptoms to severe pain. Epigastric pain can be sharp, dull, burning, or penetrating. Many patients complain of a feeling of hunger and weight gain—as opposed to gastric ulcer, in which patients experience anorexia and weight loss. Abdominal pain generally occurs several hours after meals and often awakens the patient at night. Pain is often relieved by food, but this phenomenon is present in only 20% to 60% of patients and probably is not specific for duodenal ulcer.
Our patient does not use NSAIDs, but some of her symptoms, such as postprandial pain, epigastric pain radiating to the back, and nausea and vomiting are seen with duodenal ulcer.
Eating disorders. The two main types of eating disorders—anorexia nervosa and bulimia nervosa—have a significant diagnostic overlap,4 and a third type, binge-eating disorder, is currently being investigated and defined. Girls and women are 10 times as likely as boys and men to develop an eating disorder.
People with anorexia have a distorted view of their bodies. Even when they are extremely thin, they see themselves as too fat.
Bulimia is characterized by binge-eating, purging, and overexercising to compensate for the excess calories. Patients are often close to normal weight.
Binge-eating disorder involves the consumption of very large amounts of food in a short period of time. About 2% of all young adults in the United States struggle with bingeeating. They are either overweight or obese.
These disorders tend to be associated with other psychiatric disorders such as depression or obsessive-compulsive disorder. Our patient sought medical attention and was appropriately concerned about her weight loss, which make an eating disorder unlikely.
CASE CONTINUED: SHE UNDERGOES CT
2. Which of the following is the most likely diagnosis at this point?
- SMA syndrome
- Chronic mesenteric ischemia involving the SMA
- Megaduodenum due to a connective tissue disorder
SMA syndrome is the most likely diagnosis. Despite its name, this syndrome is not a vascular condition. It is an uncommon cause of proximal intestinal obstruction in which the duodenum is compressed between the SMA and the aorta. First described in 1861, it has also been known as cast syndrome, Wilkie syndrome, and arteriomesenteric duodenal obstruction.5
To date, more than 400 cases of this syndrome have been reported, twice as many in women as in men. Most patients are between 20 and 40 years of age at the time of diagnosis. Common presenting symptoms include postprandial abdominal pain, nausea, vomiting, and weight loss, which may further reduce the angle between the SMA and the aorta. Diarrhea is not generally associated with this syndrome, and in our patient’s case the diarrhea was thought to be unrelated to the SMA syndrome, since it subsided spontaneously.
Conditions and events that cause, contribute to, or worsen SMA syndrome include:
- Rapid weight loss (as in cancer or burns) or lean body habitus
- Prolonged bed rest
- Use of a body cast
- Malabsorption
- Spinal disease, deformity, or trauma
- Scoliosis surgery
- Rapid linear growth without compensatory weight gain
- Abnormally high and fixed position of the ligament of Treitz
- Abdominal surgery
- Cardiac cachexia
- Unusually low origin of the SMA.7
More common causes of mechanical smallbowel obstruction are adhesions, hernias, and tumors.8 Hyperactive, high-pitched peristalsis with rushes coinciding with cramps is typical. Abdominal cramps are centered around the umbilicus or in the epigastrium and are associated with vomiting; obstipation develops in patients with complete obstruction. Patients with partial obstruction may develop diarrhea. Paralytic ileus secondary to hypokalemia is an important consideration in partial obstruction. However, abdominal radiography and CT did not confirm an obstruction, and her symptoms persisted despite correction of the potassium level.
Chronic mesenteric ischemia can be caused by vasculitis, nonocclusive conditions that cause prolonged vasoconstriction (eg, cocaine ingestion), or reduced cardiac output.9 Symptoms are due to the gradual reduction in blood flow to the intestine that occurs during eating. Our patient’s toxicology report did not suggest cocaine abuse, and her history and the workup thus far do not suggest heart failure. A workup for vasculitis was negative.
Megaduodenum, SMA-like syndrome. In rare cases, dilation of the duodenum at the level of the SMA may be part of a generalized duodenal dilation caused by something other than obstruction due to mechanical compression. There are conditions, as described below, that cause an SMA-like syndrome.
A compression defect of the duodenum at the site where the SMA crossed the duodenum was found in a series of 11 cases of systemic sclerosis.10 These patients had definite dilation of the duodenum, but it was a result of atrophy of the muscle layers and replacement by collagenous tissue, changes that result in diminished peristalsis, loss of muscle tone, and dilation. The duodenum yields to pressure in its third portion under the SMA.
Several pathologic conditions, particularly connective tissue disorders, may predispose to the development of a megaduodenum that may result in an imprint on the duodenum at the level of the SMA. The most noteworthy of these conditions is scleroderma. Other conditions that can cause reduced duodenal peristalsis include diabetes, pancreatitis, dermatomyositis, lupus erythematosus, myxedema, and amyloidosis.11
It is important to distinguish SMA syndrome from SMA-like syndromes for several reasons.12 SMA-like syndromes result in loss of normal peristalsis. Further, the conditions have different outcomes, even though they are managed similarly initially, ie, with rehydration and parenteral nutrition. Surgery is to be avoided if possible in conditions that affect widespread areas of the intestine, such as scleroderma or diabetic neuropathy.
3. Which of the following is helpful in confirming SMA syndrome?
- CT of the abdomen
- Upper GI radiography series
- Upper GI endoscopy
All three can help confirm the diagnosis.
CT of the abdomen is a convenient, safe, rapid, readily available, and relatively noninvasive way to evaluate the aortomesenteric angle and to view retroperitoneal and mesenteric fat.13 Rehydration before injecting intravenous dye is important to avoid precipitating renal failure. In this patient, CT findings that helped make the diagnosis included a narrow aortomesenteric angle, compression of the duodenum, and a paucity of fat around the SMA.
An upper GI series can reveal dilation of the first and second portions of the duodenum and abrupt compression of the duodenal mucosal folds. Other findings can include a delay of 4 to 6 hours in gastroduodenal transit and relief of the obstruction when the patient is in the left lateral decubitus position. The Hayes maneuver refers to the disappearance of these radiologic features in the knee-chest position on cinefluoroscopy.14 The findings mentioned above are best noted in the supine position on both radiography and CT.
Endoscopy is necessary to rule out mechanical causes of duodenal obstruction. A pulsatile extrinsic compression suggests this condition but is found only occasionally.
Other imaging studies, such as ultrasonography, arteriography, and hypotonic duodenography, are used less often.
4. At this time, which of the following would be the most appropriate initial treatment in this patient?
- Conservative treatment
- Narcotics
- Duodenojejunostomy
Conservative treatment is indicated initially in all cases of SMA syndrome.15 This involves reversing precipitating factors and replacing fluid, electrolytes, and nutrition via total parenteral nutrition and nasogastric decompression.
To avoid keeping the patient on intravenous therapy for a prolonged time, it is important to start enteral feeding once the pain has subsided and the patient can tolerate it. A double-lumen nasojejunal tube is passed distal to the obstruction under fluoroscopic guidance. During feedings, the patient should be in the modified knee-chest, prone, or leftside-down position, all of which increase the aortomesenteric angle.
Delaying the treatment of SMA syndrome can increase the risk of morbidity and mortality by progressive malnutrition, dehydration, oliguria, electrolyte abnormalities (eg, hypokalemia), or intestinal perforation from prolonged ischemia.16,17
Narcotics and other drugs known to slow gut motility should be avoided.
Symptoms typically improve after restoration of normal body weight. If conservative treatment fails, or if the case is severe or chronic, surgery is required.18 Fortunately, this is not required often.
Duodenojejunostomy is the most common surgical treatment and involves creation of an alternate route between the duodenum and the jejunum, bypassing the compression between the aorta and the SMA. Other procedures include gastrojejunostomy, laparoscopic duodenojejunostomy, 19 a Roux-en-Y procedure, robotically assisted duodenojejunostomy, and anterior transposition of the third portion of the duodenum. Cleavage of the ligament of Treitz is another option, enabling the duodenum to drop away from the apex of the sharpened aortomesenteric angle.
WHEN TO CONSIDER SMA SYNDROME
The SMA syndrome is an uncommon cause of a very common presenting symptom, ie, abdominal pain. Nevertheless, it should be considered in the differential diagnosis of abdominal pain, especially in patients who have conditions that cause significant weight loss, such as anorexia nervosa, malabsorption, or hypercatabolic states such as burns, major surgery, severe injuries, or malignancies. The diagnosis is based on a thorough history and on supportive findings from CT and endoscopy.
In our patient, weight loss began with nonspecific diarrhea but perpetuated itself as SMA syndrome occurred.
Appropriate management consists of interrupting the cycle of weight loss and secondary upper gut obstruction. For patients in whom more definitive therapy is not feasible, a gastrostomy tube for decompression with a jejunal extension available for feeding appears to be a reasonable and safe treatment option. Duodenojejunostomy is considered the procedure of choice in severe cases.
CASE CONCLUDED
Fortunately, our patient responded well to conservative management. She was treated with intravenous hydration and correction of electrolytes and 10 days later was able to tolerate a soft diet. She was discharged in stable condition. At a follow-up visit 2 weeks later, she reported minimal abdominal discomfort, was able to tolerate meals, and had gained a few pounds. She continues to do well.
- Iovino P, Ciacci C, Sabbatini F, Acioli DM, D'Argenio G, Mazzacca G. Esophageal impairment in adult celiac disease with steatorrhea. Am J Gastroenterol 1998; 93:1243–1249.
- Loftus EV. Upper gastrointestinal tract Crohn’s disease. Clin Perspect Gastroenterol 2002; 5:188–191.
- Zapata-Colindres JC, Zepeda-Gómez S, Montaño-Loza A, Vázquez-Ballesteros E, de Jesús Villalobos J, Valdovinos-Andraca F. The association of Helicobacter pylori infection and nonsteroidal antiinflammatory drugs in peptic ulcer disease. Can J Gastroenterol 2006; 20:277–280.
- Milos G, Spindler A, Schnyder U, Fairburn CG. Instability of eating disorder diagnoses: prospective study. Br J Psychiatry 2005; 187:573–578.
- Wilkie DP. Chronic duodenal ileus. Br J Surg 1921; 9:204–214.
- Ozkurt H, Cenker MM, Bas N, Erturk SM, Basak M. Measurement of the distance and angle between the aorta and superior mesenteric artery: normal values in different BMI categories. Surg Radiol Anat 2007; 29:595–599.
- Lippl F, Hannig C, Weiss W, Allescher HD, Classen M, Kurjak M. Superior mesenteric artery syndrome: diagnosis and treatment from the gastroenterologist's view. J Gastroenterol 2002; 37:640–643.
- Balthazar EJ. George W. Holmes Lecture. CT of small-bowel obstruction. AJR Am J Roentgenol 1994; 162:255–261.
- Chang JB, Stein TA. Mesenteric ischemia: acute and chronic. Ann Vasc Surg 2003; 17:323–328.
- Gondos B. Duodenal compression defect and the “superior mesenteric artery syndrome” 1. Radiology 1977; 123:575–580.
- Cohen LB, Field SP, Sachar DB. The superior mesenteric artery syndrome. The disease that isn't, or is it? J Clin Gastroenterol 1985; 7:113–716.
- Ahmed AR, Taylor I. Superior mesenteric artery syndrome. Postgrad Med J 1997; 73:776–778.
- Santer R, Young C, Rossi T, Riddlesberger MM. Computed tomography in superior mesenteric artery syndrome. Pediatr Radiol 1991; 21:154–155.
- Lukes PJ, Rolny P, Nilson AE, Gamklou R, Darle N, Dotevall G. Diagnostic value of hypotonic duodenography in superior mesenteric artery syndrome. Acta Chir Scand 1978; 144:39–43.
- Dietz UA, Debus ES, Heuko-Valiati L, et al. Aorto-mesenteric artery compression syndrome. Chirurg 2000; 71:1345–1351.
- Lim JE, Duke GL, Eachempati SR. Superior mesenteric artery syndrome presenting with acute massive gastric dilatation, gastric wall pneumatosis, and portal venous gas. Surgery 2003; 134:840–843.
- Fuhrman MA, Felig DM, Tanchel ME. Superior mesenteric artery syndrome with obstructing duodenal bezoar. Gastrointest Endosc 2003; 57:387.
- Hines JR, Gore RM, Ballantyne GH. Superior mesenteric artery syndrome. Diagnostic criteria and therapeutic approaches. Am J Surg 1984; 148:630–632.
- Gersin KS, Heniford BT. Laparoscopic duodenojejunostomy for treatment of superior mesenteric artery syndrome. JSLS 1998; 2:281–284.
- Iovino P, Ciacci C, Sabbatini F, Acioli DM, D'Argenio G, Mazzacca G. Esophageal impairment in adult celiac disease with steatorrhea. Am J Gastroenterol 1998; 93:1243–1249.
- Loftus EV. Upper gastrointestinal tract Crohn’s disease. Clin Perspect Gastroenterol 2002; 5:188–191.
- Zapata-Colindres JC, Zepeda-Gómez S, Montaño-Loza A, Vázquez-Ballesteros E, de Jesús Villalobos J, Valdovinos-Andraca F. The association of Helicobacter pylori infection and nonsteroidal antiinflammatory drugs in peptic ulcer disease. Can J Gastroenterol 2006; 20:277–280.
- Milos G, Spindler A, Schnyder U, Fairburn CG. Instability of eating disorder diagnoses: prospective study. Br J Psychiatry 2005; 187:573–578.
- Wilkie DP. Chronic duodenal ileus. Br J Surg 1921; 9:204–214.
- Ozkurt H, Cenker MM, Bas N, Erturk SM, Basak M. Measurement of the distance and angle between the aorta and superior mesenteric artery: normal values in different BMI categories. Surg Radiol Anat 2007; 29:595–599.
- Lippl F, Hannig C, Weiss W, Allescher HD, Classen M, Kurjak M. Superior mesenteric artery syndrome: diagnosis and treatment from the gastroenterologist's view. J Gastroenterol 2002; 37:640–643.
- Balthazar EJ. George W. Holmes Lecture. CT of small-bowel obstruction. AJR Am J Roentgenol 1994; 162:255–261.
- Chang JB, Stein TA. Mesenteric ischemia: acute and chronic. Ann Vasc Surg 2003; 17:323–328.
- Gondos B. Duodenal compression defect and the “superior mesenteric artery syndrome” 1. Radiology 1977; 123:575–580.
- Cohen LB, Field SP, Sachar DB. The superior mesenteric artery syndrome. The disease that isn't, or is it? J Clin Gastroenterol 1985; 7:113–716.
- Ahmed AR, Taylor I. Superior mesenteric artery syndrome. Postgrad Med J 1997; 73:776–778.
- Santer R, Young C, Rossi T, Riddlesberger MM. Computed tomography in superior mesenteric artery syndrome. Pediatr Radiol 1991; 21:154–155.
- Lukes PJ, Rolny P, Nilson AE, Gamklou R, Darle N, Dotevall G. Diagnostic value of hypotonic duodenography in superior mesenteric artery syndrome. Acta Chir Scand 1978; 144:39–43.
- Dietz UA, Debus ES, Heuko-Valiati L, et al. Aorto-mesenteric artery compression syndrome. Chirurg 2000; 71:1345–1351.
- Lim JE, Duke GL, Eachempati SR. Superior mesenteric artery syndrome presenting with acute massive gastric dilatation, gastric wall pneumatosis, and portal venous gas. Surgery 2003; 134:840–843.
- Fuhrman MA, Felig DM, Tanchel ME. Superior mesenteric artery syndrome with obstructing duodenal bezoar. Gastrointest Endosc 2003; 57:387.
- Hines JR, Gore RM, Ballantyne GH. Superior mesenteric artery syndrome. Diagnostic criteria and therapeutic approaches. Am J Surg 1984; 148:630–632.
- Gersin KS, Heniford BT. Laparoscopic duodenojejunostomy for treatment of superior mesenteric artery syndrome. JSLS 1998; 2:281–284.
Myelodysplastic syndromes: A practical approach to diagnosis and treatment
Myelodysplastic syndromes (MDS) are a heterogeneous group of disorders of blood cell production in the bone marrow that can transform into acute myeloid leukemia (AML).1,2 They are diagnosed most often in the elderly.
Primary care physicians and geriatricians tend to be the first to identify the problem, as they recognize that cytopenias are not simply a normal consequence of aging.
MDS are considered to be cancers, akin to chronic leukemia or acute leukemia, with epidemiologic data tracked by national cancer registries and the US Centers for Disease Control and Prevention, under the auspices of the Surveillance, Epidemiology, and End Results (SEER) program.3
In this article, we briefly review the classification of MDS, current epidemiologic data, key diagnostic features, and current management options.
WHEN TO SUSPECT MDS
In many patients, MDS are asymptomatic and appear as an abnormality on a routine complete blood cell count (CBC) or as part of a workup for anemia. Symptoms develop as the bone marrow’s ability to produce normal-functioning blood cells is more and more compromised. The range of symptoms depends on the bone marrow cell type affected.
Patients with MDS typically have some degree of anemia, often detected incidentally on a routine CBC, or they have symptoms stemming from anemia or thrombocytopenia, or have recurrent infections.
Subtypes of MDS have different pathologic and clinical presentations and different prognoses. They are often categorized as lower-risk or higher-risk, depending on the likelihood of transforming to AML. Patients with lower-risk MDS survive a median of 3 to 7 years. Higher-risk types are pathobiologically similar to AML in older adults, and patients either develop AML or die of complications of MDS, on average within 1.5 years.
Several classification schemes and prognostic models guide the selection of the most appropriate therapy.
Older age and comorbidities such as coronary artery disease, chronic obstructive pulmonary disease, and chronic kidney disease make MDS more difficult to manage and worsen the prognosis.4
MOST PATIENTS ARE OLDER
Only since 2001, when MDS became reportable to SEER,3,5 has the epidemiology of MDS been reported in the United States.
MDS are currently diagnosed in an estimated 3.4 per 100,000 US citizens yearly.
The incidence rate increased from 3.28 per 100,000 per year in 2001 to 3.56 per 100,000 in 2004.5 The increase has been attributed to enhanced awareness of the disease and to the aging of the population, with the number of people age 65 or older in the United States expected to double from the year 2000 to 2030. Another factor is that effective therapies are now available, possibly making hematologists and oncologists more likely to pursue the diagnosis.
These numbers translate to 10,000 to 15,000 new cases annually, and given the life expectancy of patients affected by this disease (and the life-extending treatments for it), an estimated 30,000 to 60,000 Americans living with MDS.6,7
Even though MDS can occur at any age, most patients are older. The median age at diagnosis is 71 years,3,5,8 and 72% of patients are age 70 or older.3 The prevalence increases with age, to a rate of 36 per 100,000 in those age 80 and older.9 However, in areas of East Asia, it occurs at ages almost 2 decades younger than in the rest of the world.5
MDS are more common in men than in women and in whites than in blacks. Smoking appears to increase the risk, but alcohol consumption does not.10
About 10% of cases of MDS are secondary, most often due to radiation treatment or chemotherapy (particularly with alkylating agents and topoisomerase inhibitors) for cancer. The time from treatment of a primary malignancy (most often prostate, breast, bladder, lung, or non-Hodgkin lymphoma) to the development of MDS is about 5 years.5 A small number of cases are due to occupational exposure to radiation or benzene or other organic solvents, as might occur in the rubber industry (see below). Secondary MDS have a worse prognosis than primary (de novo) MDS.
GENETIC AND ENVIRONMENTAL FACTORS
The cause of de novo MDS is not known. Genetic and environmental factors probably both play a role. The lower median age at diagnosis in Eastern countries such as Japan than in the United States suggests that environmental factors11 such as smoking, ionizing radiation, and benzene exposure play a role.12,13 Some epidemiologic evidence suggests a higher incidence of MDS after exposure to solvents, hair dyes, and pesticides.13
Congenital conditions such as Down syndrome, Fanconi anemia, and Bloom syndrome are associated with MDS. Those affected usually present at an earlier age,13 suggesting a “multiple-hit” mechanism of cancer development with genetic and environmental factors. MDS rarely run in families.
SYMPTOMS ARE OFTEN NONSPECIFIC
Symptoms of MDS are often vague and nonspecific, and the diagnosis is often made during a workup for anemia, thrombocytopenia, or neutropenia discovered on a CBC. If present, signs and symptoms depend on the blood and bone marrow cell types that are affected.
When erythrocytes are affected (the most common situation), patients present with signs of anemia, including pallor, pale conjunctiva, tachycardia, hypotension, fatigue, headache, and exercise intolerance, or with signs and symptoms of a worsening underlying condition such as angina pectoris, heart failure, or emphysema.
When platelets or neutrophils are affected. Fewer than 20% of patients present with symptoms of isolated thrombocytopenia such as minor bleeding (eg, mucosal bleeding, petechiae, easy bruising, epistaxis) or major bleeding (eg, gastrointestinal bleeding, intracranial hemorrhage) or of isolated neutropenia (eg, fatigue, frequent bacterial infections of different organs systems).
Splenomegaly and lymphadenopathy are uncommon in MDS and, if detected, should raise suspicion of a myeloproliferative or lymphoproliferative neoplasm.
LABORATORY TESTS NEEDED
Complete blood cell count
Once the common causes of patient’s symptoms are evaluated, a CBC is needed to look for a hematologic cause. If a patient is ultimately determined to have MDS, anemia is the most common finding on the CBC: about 80% of patients with MDS are anemic at presentation. 6
Anemia associated with MDS can be microcytic, normocytic, or, most commonly, macrocytic. 14 Thrombocytopenia and neutropenia can be solitary or associated with anemia, and they are seen in about 40% of patients at the time of diagnosis.6 As the disease progresses, the degree of cytopenia worsens and, in most cases, preserved cell lineages are eventually affected.
Once cytopenia is discovered, a workup for the cause is needed. We emphasize a workup first for anemia, as it is the most common form of cytopenia in MDS. A workup for isolated thrombocytopenia or neutropenia usually requires a bone marrow examination earlier in the course, and we will discuss it only briefly here. Multilineage cytopenia almost always suggests abnormal bone marrow function and can be the basis for referral to a hematologist or oncologist.
Evaluation of anemia
If anemia is detected, it is reasonable to look for nonhematologic causes such as gastrointestinal bleeding, a cardiac cause, or a nutritional deficiency.
Anemia has a variety of possible hematologic causes, as shown in a study in the United States.15 When blood samples were collected from more than 2,000 people age 65 and older, 10.6% were found to have anemia, categorized as follows:
- Nutrient-deficiency anemia, related to low levels of vitamin B12, folate, or more commonly iron
- Anemia of chronic inflammation (formerly anemia of chronic disease, associated with a major medical disorder)
- Unexplained anemia (of those with unexplained anemia, 17.4% had blood findings compatible with MDS).15
- Tests for nutrient deficiencies such as iron, vitamin B12, and folate levels. Subsequent tests can include assessment for copper deficiencies. Vitamin B12 and copper deficiency can mimic MDS.
- Fecal occult blood testing, and, if positive, further evaluation for a source of gastrointestinal bleeding.
- Liver function tests, renal function tests, and tests for endocrine disorders, such as thyroid function tests.
- Review of drugs that can cause megaloblastoid erythropoiesis, such as methotrexate (Trexall), valproic acid (Depakote), phenytoin (Dilantin), phenobarbital (Luminal), sulfasalazine (Sulfazine), and zidovudine (Retrovir).
- Assesment of the responsiveness of the bone marrow to anemia, via a reticulocyte count or an erythropoietin level, or both, prior to any blood transfusion.
- Screening for relevant infections, including human immunodeficiency virus (HIV), hepatitis, or, in rare cases, parvovirus.
- Screening for lifestyle factors that may result in bone marrow suppression, such as excessive alcohol intake.
Evaluation of other cytopenias
In cases of isolated thrombocytopenia or combined bicytopenia (eg, anemia and thrombocytopenia), abdominal ultrasonography should be done to evaluate for splenomegaly.
Blood tests to evaluate for immune-mediated cytopenias, including idiopathic thrombocytopenic purpura and hemolytic anemia, include the direct and indirect Coombs antiglobulin tests, the lactate dehydrogenase level, the reticulocyte count, and the haptoglobin level. Other immune-mediated causes of cytopenia include connective tissue disorders and vasculitides, and an antinuclear antibody titer and rheumatoid factor level can also be considered.
Referral if tests are negative
If all these tests are negative, the next step is referral to a hematologist-oncologist for further workup, which may include a review of the peripheral blood smear; bone marrow aspiration and biopsy for evaluation of iron stores and bone marrow cellularity; and specialized tests such as assessment of antiplatelet antibodies, protein electrophoresis, or fluorescence in situ hybridization to evaluate for specific clonal disorders. The purpose of bone marrow aspiration and biopsy in MDS is to evaluate the morphology of the bone marrow and the patient’s cytogenetic profile. Each has its prognostic and therapeutic implications.
SCORING SYSTEMS FOR MDS, RATHER THAN STAGING SYSTEMS
The purpose of classification systems for any medical condition is to uniformly evaluate and group patients with a disease subtype to compare patient populations similarly throughout the world, to predict prognosis, and to dictate therapeutic directions.
MDS have two main classification systems, the FAB (French-American-British) and the WHO (World Health Organization). Revised in 2008,16 the WHO classification (Table 2, not available online)17 is widely accepted because it incorporates morphologic and cytogenetic factors and correlates with prognosis.18 The categories are distinguished by specific characteristics of peripheral blood and bone marrow.
Unlike many other cancers, MDS are not “staged.” Rather, prognostic systems have been devised to predict the risk of transformation to AML and to predict overall survival. These systems are based on:
- The number of myeloblasts in the bone marrow (the higher the count, the worse the prognosis)
- The number or degree of cytopenias
- Cytogenetic abnormalities (acquired genetic abnormalities in the neoplastic clone), found in about half of patients with MDS.19
The most widely used prognostic systems are the International Prognostic Scoring System (Table 3, not available online)2 and the WPSS (WHO Classification-based Prognostic Scoring System1). The latter system encorporates transfusion burden.
SUPPORTIVE CARE
Supportive care includes transfusion of blood products to minimize complications of cytopenias and to improve quality of life, as well as antibiotics to treat active infections.
Transfusions
Almost all patients with MDS need red cell transfusions at some point, while fewer need platelets. The frequency of transfusion depends on the extent of the disease and on comorbidities.
Red blood cells typically are given when the hemoglobin level falls below 8.5 g/dL, and platelets are given when the platelet count is below 100 × 109/L, in the absence of symptoms. Patients with symptomatic anemia should receive transfusion to relieve their symptoms. Some patients need transfusions occasionally, while others are transfusion-dependent.
Iron chelation
Blood product transfusions can lead to iron overload, particularly with a lifetime administration of more than 20 units, or with a year of continuous transfusions, and this is associated with diminished survival.20
However, considering the short survival of patients with MDS, the benefit of iron chelation is debatable. This intervention should be reserved for patients with lower-risk disease who are expected to survive more than 1 year and who have received more than 25 units of packed red blood cells.21
Antibiotics
Neutropenia is defined as an absolute neutrophil count less than 1.5 × 109/L. The risk of infection, particularly bacterial infection, is significantly increased when the neutrophil count is below 0.5 × 109/L. Fever (temperature > 100.4°F or 38.0°C) in neutropenic patients is an emergency, requiring hospitalization and immediate initiation of broad-spectrum antibiotics along with a workup for the cause of the fever.22 Prophylactic antibiotics have no proven role in MDS patients with neutropenia.
TREATMENT OF LOWER-RISK DISEASE
Erythropoiesis-stimulating agents
Once a patient starts to require red blood cell transfusions, an erythropoiesis-stimulating agent (EPA) can be considered.23,24 These include recombinant agents such as erythropoietin (Procrit) and darbepoetin alfa (Aranesp).
Response is measured as an improvement in hemoglobin or as independence from transfusions in those previously dependent on them. Patients most likely to respond are those whose pretransfusion erythropoietin level is below 100 IU/L and who have minimal transfusion needs.25,26 Addition of a colony-stimulating factor can be considered for patients with neutropenia. On average, about 40% of patients ultimately respond to an EPA, but those who respond eventually develop resistance to the agent. Retrospective data indicate that use of EPAs may improve survival in MDS.23,24
The recommended threshold hemoglobin level for starting an EPA is less than 10 g/dL. Patients need to be monitored with a CBC every time they receive treatment. The agent should be stopped once the hemoglobin level reaches 12 g/dL. A number of studies have shown lower survival rates when ESAs are used in nonhematologic malignancies, particularly if the malignancy is advanced and when the ESA is used to achieve a goal hemoglobin above 12 g/dL. There are no data to suggest a higher death rate in patients with hematologic malignancies who take ESAs. The use of ESAs in MDS patients should be judicious, however, and titrated to a goal hemoglobin level no higher than 12 g/dL.27
Other treatments
If ESA treatment is ineffective, other treatments may be considered, usually initiated by a hematologist or medical oncologist.
Immunosuppressive therapy with antithymocyte globulin (Thymoglobulin)28 is an option for patients with hypocellular or immune-mediated MDS. This treatment may decrease the need for transfusion and may improve the blood count.
Lenalidomide (Revlimid) for MDS with isolated chromosome 5q deletion29 can decrease the need for blood transfusion in approximately two-thirds of these patients.
Azacitidine (Vidaza) or decitabine (Dacogen), in patients with more advanced subtypes of MDS (eg, those with excess blasts) or with pancytopenia unresponsive to other therapies, can induce hematologic improvement and decrease transfusion dependence, as well as prolong survival.
Stem cell transplantation, for patients with more advanced subtypes of MDS and who have an appropriately matched donor, has the potential of being curative.
Experimental treatments are available in clinical trials.
TREATMENT OF HIGHER-RISK DISEASE
About 25% of patients with newly diagnosed MDS and 15% to 20% of patients with established MDS have higher-risk disease.30 These patients should almost always be followed by a hematologist or medical oncologist, with therapy initiated immediately, regardless of blood counts, given the high likelihood of transformation to AML or death within 1.5 years.
The treatment options for higher-risk disease include:
- Methyltransferase inhibitors such as azacitidine and decitabine31–34
- Cytotoxic chemotherapy (similar to treatment of acute myeloid leukemia)
- Bone marrow-hematopoeitic stem cell transplantation35,36
- Experimental treatments in clinical trials.
As mentioned earlier, outside of transplantation, only azacitidine has been shown to improve overall survival (with a doubling of survival at 2 years, to 50%), and no drug therapy is curative. Managing patient expectations for treatment outcome is thus crucial in higher-risk disease, and ongoing assessments of quality of life, both on or off therapy, should be considered obligatory.
Stem cell transplantation cures MDS
MDS are complex and heterogeneous, so treatment options range from supportive care to chemotherapy and allogeneic stem cell transplantation.6 The choice depends on the severity of disease, ie, lower-risk or higherrisk (Table 3, not available online), as well as on the prognosis, the availability of therapeutic options, and the patient’s expectations.
Hematopoietic stem cell transplantation is the only curative treatment for MDS. However, it is performed in fewer than 5% of patients,30 usually younger patients with few comorbidities, because the rate of transplantrelated death is high. Therefore, most treatments are palliative, aimed at improving the quality of life and prolonging survival.
The balance between risks and benefits of these treatments must be justifiable.30 Further, patients who have no symptoms or who have lower-risk disease need no treatment and may not for years. However, they do need close follow-up, because their symptoms will worsen and will eventually require treatment.
TAKE-HOME POINTS
- Myelodysplastic syndromes are more prevalent than previously realized. Mainly a disease of older adults, they should be suspected in any patient with unexplained cytopenia.
- Life expectancy at the time of diagnosis depends on the types of cells affected.
- Supportive and disease-altering options are available.
- Prompt referral to a hematologist or oncologist is important for confirmation of the diagnosis and initiation of an appropriate treatment plan. Patients with lower-risk disease can continue follow-up with their primary care provider once treatment goals and plans are established.
ACKNOWLEDGMENT
We thank Dr. Karl Theil of the Cleveland Clinic Department of Clinical Pathology for the photomicrographs used on the cover.
- Malcovati L, Nimer SD. Myelodysplastic syndromes: diagnosis and staging. Cancer Control 2008; 15 (suppl 4):4–13.
- Greenberg P, Cox C, LeBeau MM, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood 1997; 89:2079–2088.
- Rollison DE, Howlader N, Smith MT, et al. Epidemiology of myelodysplastic syndromes and chronic myeloproliferative disorders in the United States, 2001–2004, using data from the NAACCR and SEER programs. Blood 2008; 112:45–52.
- Lichtman MA, Rowe JM. The relationship of patient age to the pathobiology of the clonal myeloid diseases. Semin Oncol 2004; 31:185–197.
- Ma X, Does M, Raza A, Mayne ST. Myelodysplastic syndromes: incidence and survival in the United States. Cancer 2007; 109:1536–1542.
- Steensma DP, Bennett JM. The myelodysplastic syndromes: diagnosis and treatment. Mayo Clin Proc 2006; 81:104–130.
- The MDS Foundation. http://www.mds-foundation.org/. Accessed August 27, 2009.
- Sekeres M, Cosgrove D, Falco A. Managing patients with low-risk MDS. Clin Adv Hematol Oncol 2006; 4( 7 suppl 16):1–10.
- Sandhu SK, Sekeres MA. Myelodysplastic syndromes: more prevalent than we know. Geriatrics 2008; 63:10–17.
- Strom SS, Gu Y, Gruschkus SK, Pierce SA, Estey EH. Risk factors of myelodysplastic syndromes: a case-control study. Leukemia 2005; 19:1912–1918.
- Kuendgen A, Matsuda A, Germing U. Differences in epidemiology of MDS between Western and Eastern countries: Ethnic differences or environmental influence? Leuk Res 2007; 31:103–104.
- Bjork J, Johansson B, Broberg K, Albin M. Smoking as a risk factor for myelodysplastic syndromes and acute myeloid leukemia and its relation to cytogenetic findings: a case-control study. Leuk Res 2009; 33:788–791.
- Germing U, Aul C, Niemeyer CM, Haas R, Bennett JM. Epidemiology, classification and prognosis of adults and children with myelodysplastic syndromes. Ann Hematol 2008; 87:691–699.
- Juneja SK, Imbert M, Jouault H, Scoazec JY, Sigaux F, Sultan C. Haematological features of primary myelodysplastic syndromes (PMDS) at initial presentation: a study of 118 cases. J Clin Pathol 1983; 36:1129–1135.
- Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC. Prevalence of anemia in persons 65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood 2004; 104:2263–2268.
- Swerdlow SH, Campo E, Harris NL, et al. International Agency for Research on Cancer, World Health Organization. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed. International Agency for Research on Cancer: Lyon, France; 2008.
- Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood 2009; 114:937–951.
- Bennett JM. A comparative review of classification systems in myelodysplastic syndromes (MDS). Semin Oncol 2005; 32( 4 suppl 5):S3–S10.
- Haase D. Cytogenetic features in myelodysplastic syndromes. Ann Hematol 2008; 87:515–526.
- Malcovati L, Della Porta MG, Cazzola M. Predicting survival and leukemic evolution in patients with myelodysplastic syndrome. Haematologica 2006; 91:1588–1590.
- Bowen D, Culligan D, Jowitt S, et al. Guidelines for the diagnosis and therapy of adult myelodysplastic syndromes. Br J Haematol 2003; 120:187–200.
- Segal BH, Freifeld AG, Baden LR, et al. Prevention and treatment of cancer-related infections. J Natl Compr Canc Netw 2008; 6:122–174.
- Golshayan AR, Jin T, Maciejewski J, et al. Efficacy of growth factors compared to other therapies for low-risk myelodysplastic syndromes. Br J Haematol 2007; 137:125–132.
- Jadersten M, Malcovati L, Dybedal I, et al. Erythropoietin and granulocyte-colony stimulating factor treatment associated with improved survival in myelodysplastic syndrome. J Clin Oncol 2008; 26:3607–3613.
- Hellstrom-Lindberg E, Gulbrandsen N, Lindberg G, et al; Scandinavian MDS Group. A validated decision model for treating the anaemia of myelodysplastic syndromes with erythropoietin + granulocyte colony-stimulating factor: significant effects on quality of life. Br J Haematol 2003; 120:1037–1046.
- Cheson BD, Greenberg PL, Bennett JM, et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood 2006; 108:419–425.
- ARANESP Prescribing Information. http://pi.amgen.com/united_states/aranesp/ckd/aranesp_pi_hcp_english.pdf. Accessed August 28, 2009.
- Molldrem JJ, Leifer E, Bahceci E, et al. Antithymocyte globulin for treatment of the bone marrow failure associated with myelodysplastic syndromes. Ann Intern Med 2002; 137:156–163.
- List A, Dewald G, Bennett J, et al; Myelodysplastic Syndrome-003 Study Investigators. Lenalidomide in the myelodysplastic syndrome with chromosome 5q deletion. N Engl J Med 2006; 355:1456–1465.
- Sekeres MA, Schoonen WM, Kantarjian H, et al. Characteristics of US patients with myelodysplastic syndromes: results of six crosssectional physician surveys. J Natl Cancer Inst 2008; 100:1542–1551.
- Stone R, Sekeres M, Garcia-Manero G, Lyons RM. Recent advances in low-and intermediate-1-risk myelodysplastic syndrome: developing a consensus for optimal therapy. Clin Adv Hematol Oncol 2008; 6:1–15.
- Kantarjian H, Issa JP, Rosenfeld CS, et al. Decitabine improves patient outcomes in myelodysplastic syndromes: results of a phase III randomized study. Cancer 2006; 106:1794–1803.
- Fenaux P, Mufti GJ, Hellstrom-Lindberg E, et al; International Vidaza High-Risk MDS Survival Study Group. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: a randomised, open-label, phase III study. Lancet Oncol 2009; 10:223–232.
- Silverman LR, Demakos EP, Peterson BL, et al. Randomized controlled trial of azacitidine in patients with the myelodysplastic syndrome: a study of the cancer and leukemia group B. J Clin Oncol 2002; 20:2429–2440.
- Giralt S. Bone marrow transplant in myelodysplastic syndromes: new technologies, same questions. Curr Hematol Rep 2005; 4:200–207.
- Cutler CS, Lee SJ, Greenberg P, et al. A decision analysis of allogeneic bone marrow transplantation for the myelodysplastic syndromes: delayed transplantation for low-risk myelodysplasia is associated with improved outcome. Blood 2004; 104:579–585.
Myelodysplastic syndromes (MDS) are a heterogeneous group of disorders of blood cell production in the bone marrow that can transform into acute myeloid leukemia (AML).1,2 They are diagnosed most often in the elderly.
Primary care physicians and geriatricians tend to be the first to identify the problem, as they recognize that cytopenias are not simply a normal consequence of aging.
MDS are considered to be cancers, akin to chronic leukemia or acute leukemia, with epidemiologic data tracked by national cancer registries and the US Centers for Disease Control and Prevention, under the auspices of the Surveillance, Epidemiology, and End Results (SEER) program.3
In this article, we briefly review the classification of MDS, current epidemiologic data, key diagnostic features, and current management options.
WHEN TO SUSPECT MDS
In many patients, MDS are asymptomatic and appear as an abnormality on a routine complete blood cell count (CBC) or as part of a workup for anemia. Symptoms develop as the bone marrow’s ability to produce normal-functioning blood cells is more and more compromised. The range of symptoms depends on the bone marrow cell type affected.
Patients with MDS typically have some degree of anemia, often detected incidentally on a routine CBC, or they have symptoms stemming from anemia or thrombocytopenia, or have recurrent infections.
Subtypes of MDS have different pathologic and clinical presentations and different prognoses. They are often categorized as lower-risk or higher-risk, depending on the likelihood of transforming to AML. Patients with lower-risk MDS survive a median of 3 to 7 years. Higher-risk types are pathobiologically similar to AML in older adults, and patients either develop AML or die of complications of MDS, on average within 1.5 years.
Several classification schemes and prognostic models guide the selection of the most appropriate therapy.
Older age and comorbidities such as coronary artery disease, chronic obstructive pulmonary disease, and chronic kidney disease make MDS more difficult to manage and worsen the prognosis.4
MOST PATIENTS ARE OLDER
Only since 2001, when MDS became reportable to SEER,3,5 has the epidemiology of MDS been reported in the United States.
MDS are currently diagnosed in an estimated 3.4 per 100,000 US citizens yearly.
The incidence rate increased from 3.28 per 100,000 per year in 2001 to 3.56 per 100,000 in 2004.5 The increase has been attributed to enhanced awareness of the disease and to the aging of the population, with the number of people age 65 or older in the United States expected to double from the year 2000 to 2030. Another factor is that effective therapies are now available, possibly making hematologists and oncologists more likely to pursue the diagnosis.
These numbers translate to 10,000 to 15,000 new cases annually, and given the life expectancy of patients affected by this disease (and the life-extending treatments for it), an estimated 30,000 to 60,000 Americans living with MDS.6,7
Even though MDS can occur at any age, most patients are older. The median age at diagnosis is 71 years,3,5,8 and 72% of patients are age 70 or older.3 The prevalence increases with age, to a rate of 36 per 100,000 in those age 80 and older.9 However, in areas of East Asia, it occurs at ages almost 2 decades younger than in the rest of the world.5
MDS are more common in men than in women and in whites than in blacks. Smoking appears to increase the risk, but alcohol consumption does not.10
About 10% of cases of MDS are secondary, most often due to radiation treatment or chemotherapy (particularly with alkylating agents and topoisomerase inhibitors) for cancer. The time from treatment of a primary malignancy (most often prostate, breast, bladder, lung, or non-Hodgkin lymphoma) to the development of MDS is about 5 years.5 A small number of cases are due to occupational exposure to radiation or benzene or other organic solvents, as might occur in the rubber industry (see below). Secondary MDS have a worse prognosis than primary (de novo) MDS.
GENETIC AND ENVIRONMENTAL FACTORS
The cause of de novo MDS is not known. Genetic and environmental factors probably both play a role. The lower median age at diagnosis in Eastern countries such as Japan than in the United States suggests that environmental factors11 such as smoking, ionizing radiation, and benzene exposure play a role.12,13 Some epidemiologic evidence suggests a higher incidence of MDS after exposure to solvents, hair dyes, and pesticides.13
Congenital conditions such as Down syndrome, Fanconi anemia, and Bloom syndrome are associated with MDS. Those affected usually present at an earlier age,13 suggesting a “multiple-hit” mechanism of cancer development with genetic and environmental factors. MDS rarely run in families.
SYMPTOMS ARE OFTEN NONSPECIFIC
Symptoms of MDS are often vague and nonspecific, and the diagnosis is often made during a workup for anemia, thrombocytopenia, or neutropenia discovered on a CBC. If present, signs and symptoms depend on the blood and bone marrow cell types that are affected.
When erythrocytes are affected (the most common situation), patients present with signs of anemia, including pallor, pale conjunctiva, tachycardia, hypotension, fatigue, headache, and exercise intolerance, or with signs and symptoms of a worsening underlying condition such as angina pectoris, heart failure, or emphysema.
When platelets or neutrophils are affected. Fewer than 20% of patients present with symptoms of isolated thrombocytopenia such as minor bleeding (eg, mucosal bleeding, petechiae, easy bruising, epistaxis) or major bleeding (eg, gastrointestinal bleeding, intracranial hemorrhage) or of isolated neutropenia (eg, fatigue, frequent bacterial infections of different organs systems).
Splenomegaly and lymphadenopathy are uncommon in MDS and, if detected, should raise suspicion of a myeloproliferative or lymphoproliferative neoplasm.
LABORATORY TESTS NEEDED
Complete blood cell count
Once the common causes of patient’s symptoms are evaluated, a CBC is needed to look for a hematologic cause. If a patient is ultimately determined to have MDS, anemia is the most common finding on the CBC: about 80% of patients with MDS are anemic at presentation. 6
Anemia associated with MDS can be microcytic, normocytic, or, most commonly, macrocytic. 14 Thrombocytopenia and neutropenia can be solitary or associated with anemia, and they are seen in about 40% of patients at the time of diagnosis.6 As the disease progresses, the degree of cytopenia worsens and, in most cases, preserved cell lineages are eventually affected.
Once cytopenia is discovered, a workup for the cause is needed. We emphasize a workup first for anemia, as it is the most common form of cytopenia in MDS. A workup for isolated thrombocytopenia or neutropenia usually requires a bone marrow examination earlier in the course, and we will discuss it only briefly here. Multilineage cytopenia almost always suggests abnormal bone marrow function and can be the basis for referral to a hematologist or oncologist.
Evaluation of anemia
If anemia is detected, it is reasonable to look for nonhematologic causes such as gastrointestinal bleeding, a cardiac cause, or a nutritional deficiency.
Anemia has a variety of possible hematologic causes, as shown in a study in the United States.15 When blood samples were collected from more than 2,000 people age 65 and older, 10.6% were found to have anemia, categorized as follows:
- Nutrient-deficiency anemia, related to low levels of vitamin B12, folate, or more commonly iron
- Anemia of chronic inflammation (formerly anemia of chronic disease, associated with a major medical disorder)
- Unexplained anemia (of those with unexplained anemia, 17.4% had blood findings compatible with MDS).15
- Tests for nutrient deficiencies such as iron, vitamin B12, and folate levels. Subsequent tests can include assessment for copper deficiencies. Vitamin B12 and copper deficiency can mimic MDS.
- Fecal occult blood testing, and, if positive, further evaluation for a source of gastrointestinal bleeding.
- Liver function tests, renal function tests, and tests for endocrine disorders, such as thyroid function tests.
- Review of drugs that can cause megaloblastoid erythropoiesis, such as methotrexate (Trexall), valproic acid (Depakote), phenytoin (Dilantin), phenobarbital (Luminal), sulfasalazine (Sulfazine), and zidovudine (Retrovir).
- Assesment of the responsiveness of the bone marrow to anemia, via a reticulocyte count or an erythropoietin level, or both, prior to any blood transfusion.
- Screening for relevant infections, including human immunodeficiency virus (HIV), hepatitis, or, in rare cases, parvovirus.
- Screening for lifestyle factors that may result in bone marrow suppression, such as excessive alcohol intake.
Evaluation of other cytopenias
In cases of isolated thrombocytopenia or combined bicytopenia (eg, anemia and thrombocytopenia), abdominal ultrasonography should be done to evaluate for splenomegaly.
Blood tests to evaluate for immune-mediated cytopenias, including idiopathic thrombocytopenic purpura and hemolytic anemia, include the direct and indirect Coombs antiglobulin tests, the lactate dehydrogenase level, the reticulocyte count, and the haptoglobin level. Other immune-mediated causes of cytopenia include connective tissue disorders and vasculitides, and an antinuclear antibody titer and rheumatoid factor level can also be considered.
Referral if tests are negative
If all these tests are negative, the next step is referral to a hematologist-oncologist for further workup, which may include a review of the peripheral blood smear; bone marrow aspiration and biopsy for evaluation of iron stores and bone marrow cellularity; and specialized tests such as assessment of antiplatelet antibodies, protein electrophoresis, or fluorescence in situ hybridization to evaluate for specific clonal disorders. The purpose of bone marrow aspiration and biopsy in MDS is to evaluate the morphology of the bone marrow and the patient’s cytogenetic profile. Each has its prognostic and therapeutic implications.
SCORING SYSTEMS FOR MDS, RATHER THAN STAGING SYSTEMS
The purpose of classification systems for any medical condition is to uniformly evaluate and group patients with a disease subtype to compare patient populations similarly throughout the world, to predict prognosis, and to dictate therapeutic directions.
MDS have two main classification systems, the FAB (French-American-British) and the WHO (World Health Organization). Revised in 2008,16 the WHO classification (Table 2, not available online)17 is widely accepted because it incorporates morphologic and cytogenetic factors and correlates with prognosis.18 The categories are distinguished by specific characteristics of peripheral blood and bone marrow.
Unlike many other cancers, MDS are not “staged.” Rather, prognostic systems have been devised to predict the risk of transformation to AML and to predict overall survival. These systems are based on:
- The number of myeloblasts in the bone marrow (the higher the count, the worse the prognosis)
- The number or degree of cytopenias
- Cytogenetic abnormalities (acquired genetic abnormalities in the neoplastic clone), found in about half of patients with MDS.19
The most widely used prognostic systems are the International Prognostic Scoring System (Table 3, not available online)2 and the WPSS (WHO Classification-based Prognostic Scoring System1). The latter system encorporates transfusion burden.
SUPPORTIVE CARE
Supportive care includes transfusion of blood products to minimize complications of cytopenias and to improve quality of life, as well as antibiotics to treat active infections.
Transfusions
Almost all patients with MDS need red cell transfusions at some point, while fewer need platelets. The frequency of transfusion depends on the extent of the disease and on comorbidities.
Red blood cells typically are given when the hemoglobin level falls below 8.5 g/dL, and platelets are given when the platelet count is below 100 × 109/L, in the absence of symptoms. Patients with symptomatic anemia should receive transfusion to relieve their symptoms. Some patients need transfusions occasionally, while others are transfusion-dependent.
Iron chelation
Blood product transfusions can lead to iron overload, particularly with a lifetime administration of more than 20 units, or with a year of continuous transfusions, and this is associated with diminished survival.20
However, considering the short survival of patients with MDS, the benefit of iron chelation is debatable. This intervention should be reserved for patients with lower-risk disease who are expected to survive more than 1 year and who have received more than 25 units of packed red blood cells.21
Antibiotics
Neutropenia is defined as an absolute neutrophil count less than 1.5 × 109/L. The risk of infection, particularly bacterial infection, is significantly increased when the neutrophil count is below 0.5 × 109/L. Fever (temperature > 100.4°F or 38.0°C) in neutropenic patients is an emergency, requiring hospitalization and immediate initiation of broad-spectrum antibiotics along with a workup for the cause of the fever.22 Prophylactic antibiotics have no proven role in MDS patients with neutropenia.
TREATMENT OF LOWER-RISK DISEASE
Erythropoiesis-stimulating agents
Once a patient starts to require red blood cell transfusions, an erythropoiesis-stimulating agent (EPA) can be considered.23,24 These include recombinant agents such as erythropoietin (Procrit) and darbepoetin alfa (Aranesp).
Response is measured as an improvement in hemoglobin or as independence from transfusions in those previously dependent on them. Patients most likely to respond are those whose pretransfusion erythropoietin level is below 100 IU/L and who have minimal transfusion needs.25,26 Addition of a colony-stimulating factor can be considered for patients with neutropenia. On average, about 40% of patients ultimately respond to an EPA, but those who respond eventually develop resistance to the agent. Retrospective data indicate that use of EPAs may improve survival in MDS.23,24
The recommended threshold hemoglobin level for starting an EPA is less than 10 g/dL. Patients need to be monitored with a CBC every time they receive treatment. The agent should be stopped once the hemoglobin level reaches 12 g/dL. A number of studies have shown lower survival rates when ESAs are used in nonhematologic malignancies, particularly if the malignancy is advanced and when the ESA is used to achieve a goal hemoglobin above 12 g/dL. There are no data to suggest a higher death rate in patients with hematologic malignancies who take ESAs. The use of ESAs in MDS patients should be judicious, however, and titrated to a goal hemoglobin level no higher than 12 g/dL.27
Other treatments
If ESA treatment is ineffective, other treatments may be considered, usually initiated by a hematologist or medical oncologist.
Immunosuppressive therapy with antithymocyte globulin (Thymoglobulin)28 is an option for patients with hypocellular or immune-mediated MDS. This treatment may decrease the need for transfusion and may improve the blood count.
Lenalidomide (Revlimid) for MDS with isolated chromosome 5q deletion29 can decrease the need for blood transfusion in approximately two-thirds of these patients.
Azacitidine (Vidaza) or decitabine (Dacogen), in patients with more advanced subtypes of MDS (eg, those with excess blasts) or with pancytopenia unresponsive to other therapies, can induce hematologic improvement and decrease transfusion dependence, as well as prolong survival.
Stem cell transplantation, for patients with more advanced subtypes of MDS and who have an appropriately matched donor, has the potential of being curative.
Experimental treatments are available in clinical trials.
TREATMENT OF HIGHER-RISK DISEASE
About 25% of patients with newly diagnosed MDS and 15% to 20% of patients with established MDS have higher-risk disease.30 These patients should almost always be followed by a hematologist or medical oncologist, with therapy initiated immediately, regardless of blood counts, given the high likelihood of transformation to AML or death within 1.5 years.
The treatment options for higher-risk disease include:
- Methyltransferase inhibitors such as azacitidine and decitabine31–34
- Cytotoxic chemotherapy (similar to treatment of acute myeloid leukemia)
- Bone marrow-hematopoeitic stem cell transplantation35,36
- Experimental treatments in clinical trials.
As mentioned earlier, outside of transplantation, only azacitidine has been shown to improve overall survival (with a doubling of survival at 2 years, to 50%), and no drug therapy is curative. Managing patient expectations for treatment outcome is thus crucial in higher-risk disease, and ongoing assessments of quality of life, both on or off therapy, should be considered obligatory.
Stem cell transplantation cures MDS
MDS are complex and heterogeneous, so treatment options range from supportive care to chemotherapy and allogeneic stem cell transplantation.6 The choice depends on the severity of disease, ie, lower-risk or higherrisk (Table 3, not available online), as well as on the prognosis, the availability of therapeutic options, and the patient’s expectations.
Hematopoietic stem cell transplantation is the only curative treatment for MDS. However, it is performed in fewer than 5% of patients,30 usually younger patients with few comorbidities, because the rate of transplantrelated death is high. Therefore, most treatments are palliative, aimed at improving the quality of life and prolonging survival.
The balance between risks and benefits of these treatments must be justifiable.30 Further, patients who have no symptoms or who have lower-risk disease need no treatment and may not for years. However, they do need close follow-up, because their symptoms will worsen and will eventually require treatment.
TAKE-HOME POINTS
- Myelodysplastic syndromes are more prevalent than previously realized. Mainly a disease of older adults, they should be suspected in any patient with unexplained cytopenia.
- Life expectancy at the time of diagnosis depends on the types of cells affected.
- Supportive and disease-altering options are available.
- Prompt referral to a hematologist or oncologist is important for confirmation of the diagnosis and initiation of an appropriate treatment plan. Patients with lower-risk disease can continue follow-up with their primary care provider once treatment goals and plans are established.
ACKNOWLEDGMENT
We thank Dr. Karl Theil of the Cleveland Clinic Department of Clinical Pathology for the photomicrographs used on the cover.
Myelodysplastic syndromes (MDS) are a heterogeneous group of disorders of blood cell production in the bone marrow that can transform into acute myeloid leukemia (AML).1,2 They are diagnosed most often in the elderly.
Primary care physicians and geriatricians tend to be the first to identify the problem, as they recognize that cytopenias are not simply a normal consequence of aging.
MDS are considered to be cancers, akin to chronic leukemia or acute leukemia, with epidemiologic data tracked by national cancer registries and the US Centers for Disease Control and Prevention, under the auspices of the Surveillance, Epidemiology, and End Results (SEER) program.3
In this article, we briefly review the classification of MDS, current epidemiologic data, key diagnostic features, and current management options.
WHEN TO SUSPECT MDS
In many patients, MDS are asymptomatic and appear as an abnormality on a routine complete blood cell count (CBC) or as part of a workup for anemia. Symptoms develop as the bone marrow’s ability to produce normal-functioning blood cells is more and more compromised. The range of symptoms depends on the bone marrow cell type affected.
Patients with MDS typically have some degree of anemia, often detected incidentally on a routine CBC, or they have symptoms stemming from anemia or thrombocytopenia, or have recurrent infections.
Subtypes of MDS have different pathologic and clinical presentations and different prognoses. They are often categorized as lower-risk or higher-risk, depending on the likelihood of transforming to AML. Patients with lower-risk MDS survive a median of 3 to 7 years. Higher-risk types are pathobiologically similar to AML in older adults, and patients either develop AML or die of complications of MDS, on average within 1.5 years.
Several classification schemes and prognostic models guide the selection of the most appropriate therapy.
Older age and comorbidities such as coronary artery disease, chronic obstructive pulmonary disease, and chronic kidney disease make MDS more difficult to manage and worsen the prognosis.4
MOST PATIENTS ARE OLDER
Only since 2001, when MDS became reportable to SEER,3,5 has the epidemiology of MDS been reported in the United States.
MDS are currently diagnosed in an estimated 3.4 per 100,000 US citizens yearly.
The incidence rate increased from 3.28 per 100,000 per year in 2001 to 3.56 per 100,000 in 2004.5 The increase has been attributed to enhanced awareness of the disease and to the aging of the population, with the number of people age 65 or older in the United States expected to double from the year 2000 to 2030. Another factor is that effective therapies are now available, possibly making hematologists and oncologists more likely to pursue the diagnosis.
These numbers translate to 10,000 to 15,000 new cases annually, and given the life expectancy of patients affected by this disease (and the life-extending treatments for it), an estimated 30,000 to 60,000 Americans living with MDS.6,7
Even though MDS can occur at any age, most patients are older. The median age at diagnosis is 71 years,3,5,8 and 72% of patients are age 70 or older.3 The prevalence increases with age, to a rate of 36 per 100,000 in those age 80 and older.9 However, in areas of East Asia, it occurs at ages almost 2 decades younger than in the rest of the world.5
MDS are more common in men than in women and in whites than in blacks. Smoking appears to increase the risk, but alcohol consumption does not.10
About 10% of cases of MDS are secondary, most often due to radiation treatment or chemotherapy (particularly with alkylating agents and topoisomerase inhibitors) for cancer. The time from treatment of a primary malignancy (most often prostate, breast, bladder, lung, or non-Hodgkin lymphoma) to the development of MDS is about 5 years.5 A small number of cases are due to occupational exposure to radiation or benzene or other organic solvents, as might occur in the rubber industry (see below). Secondary MDS have a worse prognosis than primary (de novo) MDS.
GENETIC AND ENVIRONMENTAL FACTORS
The cause of de novo MDS is not known. Genetic and environmental factors probably both play a role. The lower median age at diagnosis in Eastern countries such as Japan than in the United States suggests that environmental factors11 such as smoking, ionizing radiation, and benzene exposure play a role.12,13 Some epidemiologic evidence suggests a higher incidence of MDS after exposure to solvents, hair dyes, and pesticides.13
Congenital conditions such as Down syndrome, Fanconi anemia, and Bloom syndrome are associated with MDS. Those affected usually present at an earlier age,13 suggesting a “multiple-hit” mechanism of cancer development with genetic and environmental factors. MDS rarely run in families.
SYMPTOMS ARE OFTEN NONSPECIFIC
Symptoms of MDS are often vague and nonspecific, and the diagnosis is often made during a workup for anemia, thrombocytopenia, or neutropenia discovered on a CBC. If present, signs and symptoms depend on the blood and bone marrow cell types that are affected.
When erythrocytes are affected (the most common situation), patients present with signs of anemia, including pallor, pale conjunctiva, tachycardia, hypotension, fatigue, headache, and exercise intolerance, or with signs and symptoms of a worsening underlying condition such as angina pectoris, heart failure, or emphysema.
When platelets or neutrophils are affected. Fewer than 20% of patients present with symptoms of isolated thrombocytopenia such as minor bleeding (eg, mucosal bleeding, petechiae, easy bruising, epistaxis) or major bleeding (eg, gastrointestinal bleeding, intracranial hemorrhage) or of isolated neutropenia (eg, fatigue, frequent bacterial infections of different organs systems).
Splenomegaly and lymphadenopathy are uncommon in MDS and, if detected, should raise suspicion of a myeloproliferative or lymphoproliferative neoplasm.
LABORATORY TESTS NEEDED
Complete blood cell count
Once the common causes of patient’s symptoms are evaluated, a CBC is needed to look for a hematologic cause. If a patient is ultimately determined to have MDS, anemia is the most common finding on the CBC: about 80% of patients with MDS are anemic at presentation. 6
Anemia associated with MDS can be microcytic, normocytic, or, most commonly, macrocytic. 14 Thrombocytopenia and neutropenia can be solitary or associated with anemia, and they are seen in about 40% of patients at the time of diagnosis.6 As the disease progresses, the degree of cytopenia worsens and, in most cases, preserved cell lineages are eventually affected.
Once cytopenia is discovered, a workup for the cause is needed. We emphasize a workup first for anemia, as it is the most common form of cytopenia in MDS. A workup for isolated thrombocytopenia or neutropenia usually requires a bone marrow examination earlier in the course, and we will discuss it only briefly here. Multilineage cytopenia almost always suggests abnormal bone marrow function and can be the basis for referral to a hematologist or oncologist.
Evaluation of anemia
If anemia is detected, it is reasonable to look for nonhematologic causes such as gastrointestinal bleeding, a cardiac cause, or a nutritional deficiency.
Anemia has a variety of possible hematologic causes, as shown in a study in the United States.15 When blood samples were collected from more than 2,000 people age 65 and older, 10.6% were found to have anemia, categorized as follows:
- Nutrient-deficiency anemia, related to low levels of vitamin B12, folate, or more commonly iron
- Anemia of chronic inflammation (formerly anemia of chronic disease, associated with a major medical disorder)
- Unexplained anemia (of those with unexplained anemia, 17.4% had blood findings compatible with MDS).15
- Tests for nutrient deficiencies such as iron, vitamin B12, and folate levels. Subsequent tests can include assessment for copper deficiencies. Vitamin B12 and copper deficiency can mimic MDS.
- Fecal occult blood testing, and, if positive, further evaluation for a source of gastrointestinal bleeding.
- Liver function tests, renal function tests, and tests for endocrine disorders, such as thyroid function tests.
- Review of drugs that can cause megaloblastoid erythropoiesis, such as methotrexate (Trexall), valproic acid (Depakote), phenytoin (Dilantin), phenobarbital (Luminal), sulfasalazine (Sulfazine), and zidovudine (Retrovir).
- Assesment of the responsiveness of the bone marrow to anemia, via a reticulocyte count or an erythropoietin level, or both, prior to any blood transfusion.
- Screening for relevant infections, including human immunodeficiency virus (HIV), hepatitis, or, in rare cases, parvovirus.
- Screening for lifestyle factors that may result in bone marrow suppression, such as excessive alcohol intake.
Evaluation of other cytopenias
In cases of isolated thrombocytopenia or combined bicytopenia (eg, anemia and thrombocytopenia), abdominal ultrasonography should be done to evaluate for splenomegaly.
Blood tests to evaluate for immune-mediated cytopenias, including idiopathic thrombocytopenic purpura and hemolytic anemia, include the direct and indirect Coombs antiglobulin tests, the lactate dehydrogenase level, the reticulocyte count, and the haptoglobin level. Other immune-mediated causes of cytopenia include connective tissue disorders and vasculitides, and an antinuclear antibody titer and rheumatoid factor level can also be considered.
Referral if tests are negative
If all these tests are negative, the next step is referral to a hematologist-oncologist for further workup, which may include a review of the peripheral blood smear; bone marrow aspiration and biopsy for evaluation of iron stores and bone marrow cellularity; and specialized tests such as assessment of antiplatelet antibodies, protein electrophoresis, or fluorescence in situ hybridization to evaluate for specific clonal disorders. The purpose of bone marrow aspiration and biopsy in MDS is to evaluate the morphology of the bone marrow and the patient’s cytogenetic profile. Each has its prognostic and therapeutic implications.
SCORING SYSTEMS FOR MDS, RATHER THAN STAGING SYSTEMS
The purpose of classification systems for any medical condition is to uniformly evaluate and group patients with a disease subtype to compare patient populations similarly throughout the world, to predict prognosis, and to dictate therapeutic directions.
MDS have two main classification systems, the FAB (French-American-British) and the WHO (World Health Organization). Revised in 2008,16 the WHO classification (Table 2, not available online)17 is widely accepted because it incorporates morphologic and cytogenetic factors and correlates with prognosis.18 The categories are distinguished by specific characteristics of peripheral blood and bone marrow.
Unlike many other cancers, MDS are not “staged.” Rather, prognostic systems have been devised to predict the risk of transformation to AML and to predict overall survival. These systems are based on:
- The number of myeloblasts in the bone marrow (the higher the count, the worse the prognosis)
- The number or degree of cytopenias
- Cytogenetic abnormalities (acquired genetic abnormalities in the neoplastic clone), found in about half of patients with MDS.19
The most widely used prognostic systems are the International Prognostic Scoring System (Table 3, not available online)2 and the WPSS (WHO Classification-based Prognostic Scoring System1). The latter system encorporates transfusion burden.
SUPPORTIVE CARE
Supportive care includes transfusion of blood products to minimize complications of cytopenias and to improve quality of life, as well as antibiotics to treat active infections.
Transfusions
Almost all patients with MDS need red cell transfusions at some point, while fewer need platelets. The frequency of transfusion depends on the extent of the disease and on comorbidities.
Red blood cells typically are given when the hemoglobin level falls below 8.5 g/dL, and platelets are given when the platelet count is below 100 × 109/L, in the absence of symptoms. Patients with symptomatic anemia should receive transfusion to relieve their symptoms. Some patients need transfusions occasionally, while others are transfusion-dependent.
Iron chelation
Blood product transfusions can lead to iron overload, particularly with a lifetime administration of more than 20 units, or with a year of continuous transfusions, and this is associated with diminished survival.20
However, considering the short survival of patients with MDS, the benefit of iron chelation is debatable. This intervention should be reserved for patients with lower-risk disease who are expected to survive more than 1 year and who have received more than 25 units of packed red blood cells.21
Antibiotics
Neutropenia is defined as an absolute neutrophil count less than 1.5 × 109/L. The risk of infection, particularly bacterial infection, is significantly increased when the neutrophil count is below 0.5 × 109/L. Fever (temperature > 100.4°F or 38.0°C) in neutropenic patients is an emergency, requiring hospitalization and immediate initiation of broad-spectrum antibiotics along with a workup for the cause of the fever.22 Prophylactic antibiotics have no proven role in MDS patients with neutropenia.
TREATMENT OF LOWER-RISK DISEASE
Erythropoiesis-stimulating agents
Once a patient starts to require red blood cell transfusions, an erythropoiesis-stimulating agent (EPA) can be considered.23,24 These include recombinant agents such as erythropoietin (Procrit) and darbepoetin alfa (Aranesp).
Response is measured as an improvement in hemoglobin or as independence from transfusions in those previously dependent on them. Patients most likely to respond are those whose pretransfusion erythropoietin level is below 100 IU/L and who have minimal transfusion needs.25,26 Addition of a colony-stimulating factor can be considered for patients with neutropenia. On average, about 40% of patients ultimately respond to an EPA, but those who respond eventually develop resistance to the agent. Retrospective data indicate that use of EPAs may improve survival in MDS.23,24
The recommended threshold hemoglobin level for starting an EPA is less than 10 g/dL. Patients need to be monitored with a CBC every time they receive treatment. The agent should be stopped once the hemoglobin level reaches 12 g/dL. A number of studies have shown lower survival rates when ESAs are used in nonhematologic malignancies, particularly if the malignancy is advanced and when the ESA is used to achieve a goal hemoglobin above 12 g/dL. There are no data to suggest a higher death rate in patients with hematologic malignancies who take ESAs. The use of ESAs in MDS patients should be judicious, however, and titrated to a goal hemoglobin level no higher than 12 g/dL.27
Other treatments
If ESA treatment is ineffective, other treatments may be considered, usually initiated by a hematologist or medical oncologist.
Immunosuppressive therapy with antithymocyte globulin (Thymoglobulin)28 is an option for patients with hypocellular or immune-mediated MDS. This treatment may decrease the need for transfusion and may improve the blood count.
Lenalidomide (Revlimid) for MDS with isolated chromosome 5q deletion29 can decrease the need for blood transfusion in approximately two-thirds of these patients.
Azacitidine (Vidaza) or decitabine (Dacogen), in patients with more advanced subtypes of MDS (eg, those with excess blasts) or with pancytopenia unresponsive to other therapies, can induce hematologic improvement and decrease transfusion dependence, as well as prolong survival.
Stem cell transplantation, for patients with more advanced subtypes of MDS and who have an appropriately matched donor, has the potential of being curative.
Experimental treatments are available in clinical trials.
TREATMENT OF HIGHER-RISK DISEASE
About 25% of patients with newly diagnosed MDS and 15% to 20% of patients with established MDS have higher-risk disease.30 These patients should almost always be followed by a hematologist or medical oncologist, with therapy initiated immediately, regardless of blood counts, given the high likelihood of transformation to AML or death within 1.5 years.
The treatment options for higher-risk disease include:
- Methyltransferase inhibitors such as azacitidine and decitabine31–34
- Cytotoxic chemotherapy (similar to treatment of acute myeloid leukemia)
- Bone marrow-hematopoeitic stem cell transplantation35,36
- Experimental treatments in clinical trials.
As mentioned earlier, outside of transplantation, only azacitidine has been shown to improve overall survival (with a doubling of survival at 2 years, to 50%), and no drug therapy is curative. Managing patient expectations for treatment outcome is thus crucial in higher-risk disease, and ongoing assessments of quality of life, both on or off therapy, should be considered obligatory.
Stem cell transplantation cures MDS
MDS are complex and heterogeneous, so treatment options range from supportive care to chemotherapy and allogeneic stem cell transplantation.6 The choice depends on the severity of disease, ie, lower-risk or higherrisk (Table 3, not available online), as well as on the prognosis, the availability of therapeutic options, and the patient’s expectations.
Hematopoietic stem cell transplantation is the only curative treatment for MDS. However, it is performed in fewer than 5% of patients,30 usually younger patients with few comorbidities, because the rate of transplantrelated death is high. Therefore, most treatments are palliative, aimed at improving the quality of life and prolonging survival.
The balance between risks and benefits of these treatments must be justifiable.30 Further, patients who have no symptoms or who have lower-risk disease need no treatment and may not for years. However, they do need close follow-up, because their symptoms will worsen and will eventually require treatment.
TAKE-HOME POINTS
- Myelodysplastic syndromes are more prevalent than previously realized. Mainly a disease of older adults, they should be suspected in any patient with unexplained cytopenia.
- Life expectancy at the time of diagnosis depends on the types of cells affected.
- Supportive and disease-altering options are available.
- Prompt referral to a hematologist or oncologist is important for confirmation of the diagnosis and initiation of an appropriate treatment plan. Patients with lower-risk disease can continue follow-up with their primary care provider once treatment goals and plans are established.
ACKNOWLEDGMENT
We thank Dr. Karl Theil of the Cleveland Clinic Department of Clinical Pathology for the photomicrographs used on the cover.
- Malcovati L, Nimer SD. Myelodysplastic syndromes: diagnosis and staging. Cancer Control 2008; 15 (suppl 4):4–13.
- Greenberg P, Cox C, LeBeau MM, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood 1997; 89:2079–2088.
- Rollison DE, Howlader N, Smith MT, et al. Epidemiology of myelodysplastic syndromes and chronic myeloproliferative disorders in the United States, 2001–2004, using data from the NAACCR and SEER programs. Blood 2008; 112:45–52.
- Lichtman MA, Rowe JM. The relationship of patient age to the pathobiology of the clonal myeloid diseases. Semin Oncol 2004; 31:185–197.
- Ma X, Does M, Raza A, Mayne ST. Myelodysplastic syndromes: incidence and survival in the United States. Cancer 2007; 109:1536–1542.
- Steensma DP, Bennett JM. The myelodysplastic syndromes: diagnosis and treatment. Mayo Clin Proc 2006; 81:104–130.
- The MDS Foundation. http://www.mds-foundation.org/. Accessed August 27, 2009.
- Sekeres M, Cosgrove D, Falco A. Managing patients with low-risk MDS. Clin Adv Hematol Oncol 2006; 4( 7 suppl 16):1–10.
- Sandhu SK, Sekeres MA. Myelodysplastic syndromes: more prevalent than we know. Geriatrics 2008; 63:10–17.
- Strom SS, Gu Y, Gruschkus SK, Pierce SA, Estey EH. Risk factors of myelodysplastic syndromes: a case-control study. Leukemia 2005; 19:1912–1918.
- Kuendgen A, Matsuda A, Germing U. Differences in epidemiology of MDS between Western and Eastern countries: Ethnic differences or environmental influence? Leuk Res 2007; 31:103–104.
- Bjork J, Johansson B, Broberg K, Albin M. Smoking as a risk factor for myelodysplastic syndromes and acute myeloid leukemia and its relation to cytogenetic findings: a case-control study. Leuk Res 2009; 33:788–791.
- Germing U, Aul C, Niemeyer CM, Haas R, Bennett JM. Epidemiology, classification and prognosis of adults and children with myelodysplastic syndromes. Ann Hematol 2008; 87:691–699.
- Juneja SK, Imbert M, Jouault H, Scoazec JY, Sigaux F, Sultan C. Haematological features of primary myelodysplastic syndromes (PMDS) at initial presentation: a study of 118 cases. J Clin Pathol 1983; 36:1129–1135.
- Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC. Prevalence of anemia in persons 65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood 2004; 104:2263–2268.
- Swerdlow SH, Campo E, Harris NL, et al. International Agency for Research on Cancer, World Health Organization. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed. International Agency for Research on Cancer: Lyon, France; 2008.
- Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood 2009; 114:937–951.
- Bennett JM. A comparative review of classification systems in myelodysplastic syndromes (MDS). Semin Oncol 2005; 32( 4 suppl 5):S3–S10.
- Haase D. Cytogenetic features in myelodysplastic syndromes. Ann Hematol 2008; 87:515–526.
- Malcovati L, Della Porta MG, Cazzola M. Predicting survival and leukemic evolution in patients with myelodysplastic syndrome. Haematologica 2006; 91:1588–1590.
- Bowen D, Culligan D, Jowitt S, et al. Guidelines for the diagnosis and therapy of adult myelodysplastic syndromes. Br J Haematol 2003; 120:187–200.
- Segal BH, Freifeld AG, Baden LR, et al. Prevention and treatment of cancer-related infections. J Natl Compr Canc Netw 2008; 6:122–174.
- Golshayan AR, Jin T, Maciejewski J, et al. Efficacy of growth factors compared to other therapies for low-risk myelodysplastic syndromes. Br J Haematol 2007; 137:125–132.
- Jadersten M, Malcovati L, Dybedal I, et al. Erythropoietin and granulocyte-colony stimulating factor treatment associated with improved survival in myelodysplastic syndrome. J Clin Oncol 2008; 26:3607–3613.
- Hellstrom-Lindberg E, Gulbrandsen N, Lindberg G, et al; Scandinavian MDS Group. A validated decision model for treating the anaemia of myelodysplastic syndromes with erythropoietin + granulocyte colony-stimulating factor: significant effects on quality of life. Br J Haematol 2003; 120:1037–1046.
- Cheson BD, Greenberg PL, Bennett JM, et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood 2006; 108:419–425.
- ARANESP Prescribing Information. http://pi.amgen.com/united_states/aranesp/ckd/aranesp_pi_hcp_english.pdf. Accessed August 28, 2009.
- Molldrem JJ, Leifer E, Bahceci E, et al. Antithymocyte globulin for treatment of the bone marrow failure associated with myelodysplastic syndromes. Ann Intern Med 2002; 137:156–163.
- List A, Dewald G, Bennett J, et al; Myelodysplastic Syndrome-003 Study Investigators. Lenalidomide in the myelodysplastic syndrome with chromosome 5q deletion. N Engl J Med 2006; 355:1456–1465.
- Sekeres MA, Schoonen WM, Kantarjian H, et al. Characteristics of US patients with myelodysplastic syndromes: results of six crosssectional physician surveys. J Natl Cancer Inst 2008; 100:1542–1551.
- Stone R, Sekeres M, Garcia-Manero G, Lyons RM. Recent advances in low-and intermediate-1-risk myelodysplastic syndrome: developing a consensus for optimal therapy. Clin Adv Hematol Oncol 2008; 6:1–15.
- Kantarjian H, Issa JP, Rosenfeld CS, et al. Decitabine improves patient outcomes in myelodysplastic syndromes: results of a phase III randomized study. Cancer 2006; 106:1794–1803.
- Fenaux P, Mufti GJ, Hellstrom-Lindberg E, et al; International Vidaza High-Risk MDS Survival Study Group. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: a randomised, open-label, phase III study. Lancet Oncol 2009; 10:223–232.
- Silverman LR, Demakos EP, Peterson BL, et al. Randomized controlled trial of azacitidine in patients with the myelodysplastic syndrome: a study of the cancer and leukemia group B. J Clin Oncol 2002; 20:2429–2440.
- Giralt S. Bone marrow transplant in myelodysplastic syndromes: new technologies, same questions. Curr Hematol Rep 2005; 4:200–207.
- Cutler CS, Lee SJ, Greenberg P, et al. A decision analysis of allogeneic bone marrow transplantation for the myelodysplastic syndromes: delayed transplantation for low-risk myelodysplasia is associated with improved outcome. Blood 2004; 104:579–585.
- Malcovati L, Nimer SD. Myelodysplastic syndromes: diagnosis and staging. Cancer Control 2008; 15 (suppl 4):4–13.
- Greenberg P, Cox C, LeBeau MM, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood 1997; 89:2079–2088.
- Rollison DE, Howlader N, Smith MT, et al. Epidemiology of myelodysplastic syndromes and chronic myeloproliferative disorders in the United States, 2001–2004, using data from the NAACCR and SEER programs. Blood 2008; 112:45–52.
- Lichtman MA, Rowe JM. The relationship of patient age to the pathobiology of the clonal myeloid diseases. Semin Oncol 2004; 31:185–197.
- Ma X, Does M, Raza A, Mayne ST. Myelodysplastic syndromes: incidence and survival in the United States. Cancer 2007; 109:1536–1542.
- Steensma DP, Bennett JM. The myelodysplastic syndromes: diagnosis and treatment. Mayo Clin Proc 2006; 81:104–130.
- The MDS Foundation. http://www.mds-foundation.org/. Accessed August 27, 2009.
- Sekeres M, Cosgrove D, Falco A. Managing patients with low-risk MDS. Clin Adv Hematol Oncol 2006; 4( 7 suppl 16):1–10.
- Sandhu SK, Sekeres MA. Myelodysplastic syndromes: more prevalent than we know. Geriatrics 2008; 63:10–17.
- Strom SS, Gu Y, Gruschkus SK, Pierce SA, Estey EH. Risk factors of myelodysplastic syndromes: a case-control study. Leukemia 2005; 19:1912–1918.
- Kuendgen A, Matsuda A, Germing U. Differences in epidemiology of MDS between Western and Eastern countries: Ethnic differences or environmental influence? Leuk Res 2007; 31:103–104.
- Bjork J, Johansson B, Broberg K, Albin M. Smoking as a risk factor for myelodysplastic syndromes and acute myeloid leukemia and its relation to cytogenetic findings: a case-control study. Leuk Res 2009; 33:788–791.
- Germing U, Aul C, Niemeyer CM, Haas R, Bennett JM. Epidemiology, classification and prognosis of adults and children with myelodysplastic syndromes. Ann Hematol 2008; 87:691–699.
- Juneja SK, Imbert M, Jouault H, Scoazec JY, Sigaux F, Sultan C. Haematological features of primary myelodysplastic syndromes (PMDS) at initial presentation: a study of 118 cases. J Clin Pathol 1983; 36:1129–1135.
- Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC. Prevalence of anemia in persons 65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood 2004; 104:2263–2268.
- Swerdlow SH, Campo E, Harris NL, et al. International Agency for Research on Cancer, World Health Organization. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed. International Agency for Research on Cancer: Lyon, France; 2008.
- Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood 2009; 114:937–951.
- Bennett JM. A comparative review of classification systems in myelodysplastic syndromes (MDS). Semin Oncol 2005; 32( 4 suppl 5):S3–S10.
- Haase D. Cytogenetic features in myelodysplastic syndromes. Ann Hematol 2008; 87:515–526.
- Malcovati L, Della Porta MG, Cazzola M. Predicting survival and leukemic evolution in patients with myelodysplastic syndrome. Haematologica 2006; 91:1588–1590.
- Bowen D, Culligan D, Jowitt S, et al. Guidelines for the diagnosis and therapy of adult myelodysplastic syndromes. Br J Haematol 2003; 120:187–200.
- Segal BH, Freifeld AG, Baden LR, et al. Prevention and treatment of cancer-related infections. J Natl Compr Canc Netw 2008; 6:122–174.
- Golshayan AR, Jin T, Maciejewski J, et al. Efficacy of growth factors compared to other therapies for low-risk myelodysplastic syndromes. Br J Haematol 2007; 137:125–132.
- Jadersten M, Malcovati L, Dybedal I, et al. Erythropoietin and granulocyte-colony stimulating factor treatment associated with improved survival in myelodysplastic syndrome. J Clin Oncol 2008; 26:3607–3613.
- Hellstrom-Lindberg E, Gulbrandsen N, Lindberg G, et al; Scandinavian MDS Group. A validated decision model for treating the anaemia of myelodysplastic syndromes with erythropoietin + granulocyte colony-stimulating factor: significant effects on quality of life. Br J Haematol 2003; 120:1037–1046.
- Cheson BD, Greenberg PL, Bennett JM, et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood 2006; 108:419–425.
- ARANESP Prescribing Information. http://pi.amgen.com/united_states/aranesp/ckd/aranesp_pi_hcp_english.pdf. Accessed August 28, 2009.
- Molldrem JJ, Leifer E, Bahceci E, et al. Antithymocyte globulin for treatment of the bone marrow failure associated with myelodysplastic syndromes. Ann Intern Med 2002; 137:156–163.
- List A, Dewald G, Bennett J, et al; Myelodysplastic Syndrome-003 Study Investigators. Lenalidomide in the myelodysplastic syndrome with chromosome 5q deletion. N Engl J Med 2006; 355:1456–1465.
- Sekeres MA, Schoonen WM, Kantarjian H, et al. Characteristics of US patients with myelodysplastic syndromes: results of six crosssectional physician surveys. J Natl Cancer Inst 2008; 100:1542–1551.
- Stone R, Sekeres M, Garcia-Manero G, Lyons RM. Recent advances in low-and intermediate-1-risk myelodysplastic syndrome: developing a consensus for optimal therapy. Clin Adv Hematol Oncol 2008; 6:1–15.
- Kantarjian H, Issa JP, Rosenfeld CS, et al. Decitabine improves patient outcomes in myelodysplastic syndromes: results of a phase III randomized study. Cancer 2006; 106:1794–1803.
- Fenaux P, Mufti GJ, Hellstrom-Lindberg E, et al; International Vidaza High-Risk MDS Survival Study Group. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: a randomised, open-label, phase III study. Lancet Oncol 2009; 10:223–232.
- Silverman LR, Demakos EP, Peterson BL, et al. Randomized controlled trial of azacitidine in patients with the myelodysplastic syndrome: a study of the cancer and leukemia group B. J Clin Oncol 2002; 20:2429–2440.
- Giralt S. Bone marrow transplant in myelodysplastic syndromes: new technologies, same questions. Curr Hematol Rep 2005; 4:200–207.
- Cutler CS, Lee SJ, Greenberg P, et al. A decision analysis of allogeneic bone marrow transplantation for the myelodysplastic syndromes: delayed transplantation for low-risk myelodysplasia is associated with improved outcome. Blood 2004; 104:579–585.
KEY POINTS
- Multilineage cytopenia almost always suggests abnormal bone marrow function and can be the reason for referral to a hematologist-oncologist.
- Factors that make MDS more difficult to manage and that worsen the prognosis are older age at diagnosis and comorbidities such as coronary artery disease, chronic obstructive pulmonary disease, and chronic kidney disease.
- Patients with lower-risk disease can continue followup with their primary care provider once the treatment goals and plans are established.