User login
The Downtime Dilemma
How do you spend your time off? Do you neglect your to-do list in favor of rest and relaxation, or do you race around trying to get everything done? How you use your free time affects your energy level and on-the-job enthusiasm. Hospitalists who learn to make the most of their time off reduce their stress and master the elusive work-life balance, and are more likely to avoid burnout. It’s especially true of physicians who work long hours followed by multiple days of downtime.
“I tell hospitalists … that they have to know what a sense of ‘work-life balance’ means to them,” says Iris Grimm, creator of the Balanced Physician program and founder of Marietta, Ga.-based Master Performance Inc. (www.balanced physician.com). Understanding what you need to lead a healthy, balanced life is crucial to your happiness and well-being on and off the job.
Hospitalists who work long shifts also face extended stretches of time off that are vital to recharging one’s batteries. “One of the challenges they have is to find a routine,” Grimm says. “As human beings, we prefer to have a daily routine, which is a benefit from a health standpoint. These people have different sleep patterns when they’re off, which can throw off their bodies, which in turn has an effect on health and well-being.”
—Chad Whelan, MD, FHM, assistant professor of medicine, University of Chicago
Plan to Cope
The allure of regular, extended time off—namely, the seven-day-on, seven-day-off schedule model—can factor heavily into a physician’s decision to choose an HM career. A full week off is ideal for some, but not so ideal for others.
Many think the seven-on, seven-off schedule increases the likelihood of physician burnout. Others think the exact opposite. No matter what, the “intense shift” model is not going away anytime soon, says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine.
The first step in maximizing your personal time is to accept your schedule. “Whatever schedule you’re working, you’re going to be working when others are not,” Dr. Whelan says. “You have to recognize that, and you have to own it.”
Once you accept the fact that you’ll miss out on some activities—from dinner parties to your child’s Little League baseball games—that fall on your workdays, you can move on to a key component of maximizing your days off: the art of planning.
Planning your days off helps ensure that you don’t end up wasting them. “Your plan could include exercise, visiting with friends, and keeping up with CME,” Grimm says. Dr. Whelan agrees: “You have to do some active planning to schedule things that need to get done.” He knows from personal experience that “the mundane details are easy to drop; instead of grocery shopping, you end up ordering in. I find that if I schedule these things—even at a funky time like late at night—I’ll get them done.”
Planning works both ways. “Part of balance is using time in your off days to prepare for when you’ll be working,” Grimm says. For example, make sure you have food in your refrigerator so that you can have a healthy breakfast and occasionally prepare dinners in advance that you can quickly heat up after your shift.
Focusing your organizational skills and planning on personal “to-dos” will lighten the load of a long workday. “Automate as much as possible—such as paying bills,” Grimm advises, “and delegate what you can. The less you have to keep track of, the less stress you’ll feel and the more energy you’ll find to do what you’re paid to do.”
Time for Self
Physicians, especially those with families, need to remember to make time for themselves “so that you won’t build resentment toward others,” Grimm says. “Doing something for yourself refills your energy tank.” Whether it’s exercising, going fishing, volunteering at the community center, downloading photos from your digital camera, or reading a book, “it’s different for everyone,” Grimm points out. “You have to know what you need.”
Dr. Whelan—who is a runner—focuses on physical activity to relieve stress and re-energize his mind and body. “It’s hard, because people who are serious about exercise, however you define ‘serious,’ are told to exercise on a consistent schedule. Well, we don’t have consistent schedules,” he says. “The key is to recognize that this is a challenge and find a creative way to schedule it, just like we make other decisions creatively. You have to make an upfront commitment.”
Whatever you do to “refill your tank,” there’s a good reason to devote time to it. “The more we do for ourselves, the more we can do for others,” Grimm says. “It’s not an hour-to-hour ratio; you might just need a five-minute meditation at the end of the day. … I always challenge my clients to be aware of what gives them energy and what takes energy away from them. This is essential for work, and essential for life.”
Leave Work Behind
One of the hardest things to learn—a lesson left out of medical school texts—is how to leave the stress and responsibility of the job at the office. “These are intense jobs; they’re high-stress,” Dr. Whelan explains. “The good thing about being a hospitalist is that when you’re off, you’re off. But it’s important to be able to compartmentalize.”
Dr. Whelan learned a couple of simple strategies to help with this concept. “At the end of every work day, after you’ve signed off, dedicate some time to transition. It can be just 10 or 15 minutes. Don’t answer the phone or e-mail; just dedicate that time to transition,” he says. “Run through your day and process each part—whether that’s each patient or each administrative task—emotionally and intellectually. For each one, make a plan for what you’ll do tomorrow. Once you’ve worked through your day this way, you can allow yourself to let it go.”
He also advises hospitalists to use on-the-job time when it’s available, rather than overlapping work and personal time. “There are parts of your business that can be done when you’re not seeing patients, such as reading journals,” Dr. Whelan says. “Try to schedule those things into your [work day], so you don’t end up catching up on them at home.”
Find Your Balance
Make it a point to make the most of your time off. Plan it in advance to ensure you do what you need to do and what you want to do. Think creatively and include all types of activities. And be sure to include time for yourself.
“There are very few of us who can sustain a life made up entirely of work and still be happy,” Dr. Whelan says. “Eventually, you’ll start to resent the work, and that’s the stuff that leads to burnout. You’re also probably not doing as good a job.”
One final piece of advice: Be prepared to change.
“You need to be self-aware, and you need to realize that your definition of balance will shift with age, responsibility, and goals,” Grimm says. TH
Jane Jerrard is a freelance writer based in Chicago.
How do you spend your time off? Do you neglect your to-do list in favor of rest and relaxation, or do you race around trying to get everything done? How you use your free time affects your energy level and on-the-job enthusiasm. Hospitalists who learn to make the most of their time off reduce their stress and master the elusive work-life balance, and are more likely to avoid burnout. It’s especially true of physicians who work long hours followed by multiple days of downtime.
“I tell hospitalists … that they have to know what a sense of ‘work-life balance’ means to them,” says Iris Grimm, creator of the Balanced Physician program and founder of Marietta, Ga.-based Master Performance Inc. (www.balanced physician.com). Understanding what you need to lead a healthy, balanced life is crucial to your happiness and well-being on and off the job.
Hospitalists who work long shifts also face extended stretches of time off that are vital to recharging one’s batteries. “One of the challenges they have is to find a routine,” Grimm says. “As human beings, we prefer to have a daily routine, which is a benefit from a health standpoint. These people have different sleep patterns when they’re off, which can throw off their bodies, which in turn has an effect on health and well-being.”
—Chad Whelan, MD, FHM, assistant professor of medicine, University of Chicago
Plan to Cope
The allure of regular, extended time off—namely, the seven-day-on, seven-day-off schedule model—can factor heavily into a physician’s decision to choose an HM career. A full week off is ideal for some, but not so ideal for others.
Many think the seven-on, seven-off schedule increases the likelihood of physician burnout. Others think the exact opposite. No matter what, the “intense shift” model is not going away anytime soon, says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine.
The first step in maximizing your personal time is to accept your schedule. “Whatever schedule you’re working, you’re going to be working when others are not,” Dr. Whelan says. “You have to recognize that, and you have to own it.”
Once you accept the fact that you’ll miss out on some activities—from dinner parties to your child’s Little League baseball games—that fall on your workdays, you can move on to a key component of maximizing your days off: the art of planning.
Planning your days off helps ensure that you don’t end up wasting them. “Your plan could include exercise, visiting with friends, and keeping up with CME,” Grimm says. Dr. Whelan agrees: “You have to do some active planning to schedule things that need to get done.” He knows from personal experience that “the mundane details are easy to drop; instead of grocery shopping, you end up ordering in. I find that if I schedule these things—even at a funky time like late at night—I’ll get them done.”
Planning works both ways. “Part of balance is using time in your off days to prepare for when you’ll be working,” Grimm says. For example, make sure you have food in your refrigerator so that you can have a healthy breakfast and occasionally prepare dinners in advance that you can quickly heat up after your shift.
Focusing your organizational skills and planning on personal “to-dos” will lighten the load of a long workday. “Automate as much as possible—such as paying bills,” Grimm advises, “and delegate what you can. The less you have to keep track of, the less stress you’ll feel and the more energy you’ll find to do what you’re paid to do.”
Time for Self
Physicians, especially those with families, need to remember to make time for themselves “so that you won’t build resentment toward others,” Grimm says. “Doing something for yourself refills your energy tank.” Whether it’s exercising, going fishing, volunteering at the community center, downloading photos from your digital camera, or reading a book, “it’s different for everyone,” Grimm points out. “You have to know what you need.”
Dr. Whelan—who is a runner—focuses on physical activity to relieve stress and re-energize his mind and body. “It’s hard, because people who are serious about exercise, however you define ‘serious,’ are told to exercise on a consistent schedule. Well, we don’t have consistent schedules,” he says. “The key is to recognize that this is a challenge and find a creative way to schedule it, just like we make other decisions creatively. You have to make an upfront commitment.”
Whatever you do to “refill your tank,” there’s a good reason to devote time to it. “The more we do for ourselves, the more we can do for others,” Grimm says. “It’s not an hour-to-hour ratio; you might just need a five-minute meditation at the end of the day. … I always challenge my clients to be aware of what gives them energy and what takes energy away from them. This is essential for work, and essential for life.”
Leave Work Behind
One of the hardest things to learn—a lesson left out of medical school texts—is how to leave the stress and responsibility of the job at the office. “These are intense jobs; they’re high-stress,” Dr. Whelan explains. “The good thing about being a hospitalist is that when you’re off, you’re off. But it’s important to be able to compartmentalize.”
Dr. Whelan learned a couple of simple strategies to help with this concept. “At the end of every work day, after you’ve signed off, dedicate some time to transition. It can be just 10 or 15 minutes. Don’t answer the phone or e-mail; just dedicate that time to transition,” he says. “Run through your day and process each part—whether that’s each patient or each administrative task—emotionally and intellectually. For each one, make a plan for what you’ll do tomorrow. Once you’ve worked through your day this way, you can allow yourself to let it go.”
He also advises hospitalists to use on-the-job time when it’s available, rather than overlapping work and personal time. “There are parts of your business that can be done when you’re not seeing patients, such as reading journals,” Dr. Whelan says. “Try to schedule those things into your [work day], so you don’t end up catching up on them at home.”
Find Your Balance
Make it a point to make the most of your time off. Plan it in advance to ensure you do what you need to do and what you want to do. Think creatively and include all types of activities. And be sure to include time for yourself.
“There are very few of us who can sustain a life made up entirely of work and still be happy,” Dr. Whelan says. “Eventually, you’ll start to resent the work, and that’s the stuff that leads to burnout. You’re also probably not doing as good a job.”
One final piece of advice: Be prepared to change.
“You need to be self-aware, and you need to realize that your definition of balance will shift with age, responsibility, and goals,” Grimm says. TH
Jane Jerrard is a freelance writer based in Chicago.
How do you spend your time off? Do you neglect your to-do list in favor of rest and relaxation, or do you race around trying to get everything done? How you use your free time affects your energy level and on-the-job enthusiasm. Hospitalists who learn to make the most of their time off reduce their stress and master the elusive work-life balance, and are more likely to avoid burnout. It’s especially true of physicians who work long hours followed by multiple days of downtime.
“I tell hospitalists … that they have to know what a sense of ‘work-life balance’ means to them,” says Iris Grimm, creator of the Balanced Physician program and founder of Marietta, Ga.-based Master Performance Inc. (www.balanced physician.com). Understanding what you need to lead a healthy, balanced life is crucial to your happiness and well-being on and off the job.
Hospitalists who work long shifts also face extended stretches of time off that are vital to recharging one’s batteries. “One of the challenges they have is to find a routine,” Grimm says. “As human beings, we prefer to have a daily routine, which is a benefit from a health standpoint. These people have different sleep patterns when they’re off, which can throw off their bodies, which in turn has an effect on health and well-being.”
—Chad Whelan, MD, FHM, assistant professor of medicine, University of Chicago
Plan to Cope
The allure of regular, extended time off—namely, the seven-day-on, seven-day-off schedule model—can factor heavily into a physician’s decision to choose an HM career. A full week off is ideal for some, but not so ideal for others.
Many think the seven-on, seven-off schedule increases the likelihood of physician burnout. Others think the exact opposite. No matter what, the “intense shift” model is not going away anytime soon, says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine.
The first step in maximizing your personal time is to accept your schedule. “Whatever schedule you’re working, you’re going to be working when others are not,” Dr. Whelan says. “You have to recognize that, and you have to own it.”
Once you accept the fact that you’ll miss out on some activities—from dinner parties to your child’s Little League baseball games—that fall on your workdays, you can move on to a key component of maximizing your days off: the art of planning.
Planning your days off helps ensure that you don’t end up wasting them. “Your plan could include exercise, visiting with friends, and keeping up with CME,” Grimm says. Dr. Whelan agrees: “You have to do some active planning to schedule things that need to get done.” He knows from personal experience that “the mundane details are easy to drop; instead of grocery shopping, you end up ordering in. I find that if I schedule these things—even at a funky time like late at night—I’ll get them done.”
Planning works both ways. “Part of balance is using time in your off days to prepare for when you’ll be working,” Grimm says. For example, make sure you have food in your refrigerator so that you can have a healthy breakfast and occasionally prepare dinners in advance that you can quickly heat up after your shift.
Focusing your organizational skills and planning on personal “to-dos” will lighten the load of a long workday. “Automate as much as possible—such as paying bills,” Grimm advises, “and delegate what you can. The less you have to keep track of, the less stress you’ll feel and the more energy you’ll find to do what you’re paid to do.”
Time for Self
Physicians, especially those with families, need to remember to make time for themselves “so that you won’t build resentment toward others,” Grimm says. “Doing something for yourself refills your energy tank.” Whether it’s exercising, going fishing, volunteering at the community center, downloading photos from your digital camera, or reading a book, “it’s different for everyone,” Grimm points out. “You have to know what you need.”
Dr. Whelan—who is a runner—focuses on physical activity to relieve stress and re-energize his mind and body. “It’s hard, because people who are serious about exercise, however you define ‘serious,’ are told to exercise on a consistent schedule. Well, we don’t have consistent schedules,” he says. “The key is to recognize that this is a challenge and find a creative way to schedule it, just like we make other decisions creatively. You have to make an upfront commitment.”
Whatever you do to “refill your tank,” there’s a good reason to devote time to it. “The more we do for ourselves, the more we can do for others,” Grimm says. “It’s not an hour-to-hour ratio; you might just need a five-minute meditation at the end of the day. … I always challenge my clients to be aware of what gives them energy and what takes energy away from them. This is essential for work, and essential for life.”
Leave Work Behind
One of the hardest things to learn—a lesson left out of medical school texts—is how to leave the stress and responsibility of the job at the office. “These are intense jobs; they’re high-stress,” Dr. Whelan explains. “The good thing about being a hospitalist is that when you’re off, you’re off. But it’s important to be able to compartmentalize.”
Dr. Whelan learned a couple of simple strategies to help with this concept. “At the end of every work day, after you’ve signed off, dedicate some time to transition. It can be just 10 or 15 minutes. Don’t answer the phone or e-mail; just dedicate that time to transition,” he says. “Run through your day and process each part—whether that’s each patient or each administrative task—emotionally and intellectually. For each one, make a plan for what you’ll do tomorrow. Once you’ve worked through your day this way, you can allow yourself to let it go.”
He also advises hospitalists to use on-the-job time when it’s available, rather than overlapping work and personal time. “There are parts of your business that can be done when you’re not seeing patients, such as reading journals,” Dr. Whelan says. “Try to schedule those things into your [work day], so you don’t end up catching up on them at home.”
Find Your Balance
Make it a point to make the most of your time off. Plan it in advance to ensure you do what you need to do and what you want to do. Think creatively and include all types of activities. And be sure to include time for yourself.
“There are very few of us who can sustain a life made up entirely of work and still be happy,” Dr. Whelan says. “Eventually, you’ll start to resent the work, and that’s the stuff that leads to burnout. You’re also probably not doing as good a job.”
One final piece of advice: Be prepared to change.
“You need to be self-aware, and you need to realize that your definition of balance will shift with age, responsibility, and goals,” Grimm says. TH
Jane Jerrard is a freelance writer based in Chicago.
Simulation Sensation
To Jeffrey Barsuk, MD, FACP, FHM, the concept of simulation-based mastery learning is simplistic to the point of genius. Give a hospitalist—or any other physician—a physical task and let them practice the procedure until they master it. Take care not to fall into the decades-old mind-set that repetition alone will achieve a threshold of competence. Test the competence with a rigorous assessment schedule, which will objectively determine if the skill is truly mastered.
It’s standard operating procedure in many technical fields, such as engineering, computer programming, and aviation. For example, professional pilots undergo countless hours of simulation flying to freshen and further hone the skills they need to succeed in an airplane cockpit. But with tasks as menial as central venous catheter (CVC) insertions, the typical practice most young physicians get is the trial and error of needle passes.
More training, Dr. Barsuk argues, would make everyone involved better off—from the resident nervously seeking a line to the patient who wants the procedure completed as quickly and painlessly as possible.
“It’s very common sense,” says Dr. Barsuk, assistant professor of medicine in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago. “But no one is doing this. People don’t know that simulators are so effective. At least in the medical profession, we’re probably behind the times in it. … We’re enthusiastic about it because we believe in it so much. We want to see how far it can go. With mastery learning, the sky’s the limit. You can simulate almost anything you want.”
Dr. Barsuk and his colleagues have worked hard to translate “common sense” into empirical literature. Accordingly, the team will publish their latest work, “Use of Simulation-Based Mastery Learning to Improve the Quality of Central Venous Catheter Placement in a Medical Intensive Care Unit,” in September’s Journal of Hospital Medicine. The single-institution cohort study found simulation-based mastery learning increased internal-medicine residents’ skills in simulated CVC insertions, decreased the number of needle passes when performing actual procedures, and increased resident self-confidence.
“It’s always been assumed that experience in and of itself is a proxy for competence,” says William McGaghie, PhD, professor of medical education and preventive medicine at Feinberg, as well as director of evaluation for Northwestern University’s Clinical and Translational Science Institute (NUCATS). “We now know that is not the case … if skill acquisition is the goal. Experience on the wards isn’t enough. We have to have deliberate education interventions to practice in controlled, safe environments.”

—Jeffrey Barsuk, MD, FACP, FHM, Feinberg School of Medicine, Northwestern University, Chicago
The Northwestern study put that theory to the test. It aimed to expand mastery learning to a new skill set and assess quality indicators (number of needle passes, arterial punctures, etc.) and resident confidence before and after training modules. The team studied 41 second- and third-year residents rotating through the medical intensive-care unit (MICU) from October 2006 to February 2007. The university’s Institutional Review Board approved the study, and all of the participants gave informed consent prior to participating. Thirteen of the residents rotated through during a six-week pre-intervention phase, serving as the “traditionally-trained group,” the authors wrote. Twenty-eight residents were trained on Simulab’s CentralLineMan, a model with “ultrasound compatibility, an arterial pulse, and self-sealing veins and skins. Needles, dilators and guidewires can be inserted and realistic venous and arterial pressures demonstrated,” the authors wrote.
The residents who were trained for internal jugular (IJ) and subclavian (SC) CVC insertions received two two-hour education sessions consisting of a lecture, ultrasound training, deliberate practice, and feedback. A 27-item checklist was drafted to measure outcomes; all pre- and post-tests were graded by a single unblended instructor to ensure accuracy. According to the study:
- None of the residents met the minimum passing score (MPS) of 79.1% for CVC insertion at baseline: mean IJ=48.4%, standard deviation=23.1; mean SC=45.2%, standard deviation=26.3;
- All residents met or exceeded the MPS at testing after simulation training: mean IJ=94.8%, standard deviation=10.0; mean SC=91.1%, standard deviation=17.8 (P<0.001);
- In the MICU, simulator-trained residents required fewer needle passes to insert a CVC than traditionally trained residents: mean=1.79, standard deviation=1.0 vs. mean=2.78, standard deviation=1.77 (P=0.04);
- Simulator-trained residents displayed more self-confidence about their procedural skills: mean=81, standard deviation=11 vs. mean=68, standard deviation=20 (P=0.02).
Dr. Barsuk isn’t surprised that confidence increases with training, saying “they hammer this home.” There were several categories for which the authors found no major improvement, though, even with the addition of deliberate training and standardized didactic materials.
Notably, the authors wrote, the resident groups “did not differ in pneumothorax, arterial puncture, or mean number of CVC adjustments.” Some of the lack of disparity was attributed to the small sample size.
In interviews, the authors noted that additional study would help assess such clinical outcomes as reduced CVC-related infections after simulation-based training. Still, Dr. Barsuk says, this pilot report is an important first step to win over skeptics.
“Simulation-based training and deliberate practice in a mastery learning setting improves performance of both simulated and actual CVC insertions by internal medicine residents,” the study reads. “Procedural training remains an important component of internal medicine training although internists are performing fewer invasive procedures now than in years past. Use of a mastery model of CVC insertion requires that trainees demonstrate skill in a simulated environment before independently performing this invasive procedure on patients.”
Another advantage of the training, McGaghie says, is that it helps physicians track their own improvement. He cautions against administrators using the data for more nefarious purposes, lest the testing become unpopular and less useful to quality improvement programs.
“You don’t use these evaluations as a weapon; you use them as a tool,” McGaghie says. “No one is there to beat up the doctors; no one is there to make them look foolish. The whole idea is to be as rigorous as possible to look for improvement—constant improvement.” TH
Richard Quinn is a freelance writer based in New Jersey.
To Jeffrey Barsuk, MD, FACP, FHM, the concept of simulation-based mastery learning is simplistic to the point of genius. Give a hospitalist—or any other physician—a physical task and let them practice the procedure until they master it. Take care not to fall into the decades-old mind-set that repetition alone will achieve a threshold of competence. Test the competence with a rigorous assessment schedule, which will objectively determine if the skill is truly mastered.
It’s standard operating procedure in many technical fields, such as engineering, computer programming, and aviation. For example, professional pilots undergo countless hours of simulation flying to freshen and further hone the skills they need to succeed in an airplane cockpit. But with tasks as menial as central venous catheter (CVC) insertions, the typical practice most young physicians get is the trial and error of needle passes.
More training, Dr. Barsuk argues, would make everyone involved better off—from the resident nervously seeking a line to the patient who wants the procedure completed as quickly and painlessly as possible.
“It’s very common sense,” says Dr. Barsuk, assistant professor of medicine in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago. “But no one is doing this. People don’t know that simulators are so effective. At least in the medical profession, we’re probably behind the times in it. … We’re enthusiastic about it because we believe in it so much. We want to see how far it can go. With mastery learning, the sky’s the limit. You can simulate almost anything you want.”
Dr. Barsuk and his colleagues have worked hard to translate “common sense” into empirical literature. Accordingly, the team will publish their latest work, “Use of Simulation-Based Mastery Learning to Improve the Quality of Central Venous Catheter Placement in a Medical Intensive Care Unit,” in September’s Journal of Hospital Medicine. The single-institution cohort study found simulation-based mastery learning increased internal-medicine residents’ skills in simulated CVC insertions, decreased the number of needle passes when performing actual procedures, and increased resident self-confidence.
“It’s always been assumed that experience in and of itself is a proxy for competence,” says William McGaghie, PhD, professor of medical education and preventive medicine at Feinberg, as well as director of evaluation for Northwestern University’s Clinical and Translational Science Institute (NUCATS). “We now know that is not the case … if skill acquisition is the goal. Experience on the wards isn’t enough. We have to have deliberate education interventions to practice in controlled, safe environments.”
—Jeffrey Barsuk, MD, FACP, FHM, Feinberg School of Medicine, Northwestern University, Chicago
The Northwestern study put that theory to the test. It aimed to expand mastery learning to a new skill set and assess quality indicators (number of needle passes, arterial punctures, etc.) and resident confidence before and after training modules. The team studied 41 second- and third-year residents rotating through the medical intensive-care unit (MICU) from October 2006 to February 2007. The university’s Institutional Review Board approved the study, and all of the participants gave informed consent prior to participating. Thirteen of the residents rotated through during a six-week pre-intervention phase, serving as the “traditionally-trained group,” the authors wrote. Twenty-eight residents were trained on Simulab’s CentralLineMan, a model with “ultrasound compatibility, an arterial pulse, and self-sealing veins and skins. Needles, dilators and guidewires can be inserted and realistic venous and arterial pressures demonstrated,” the authors wrote.
The residents who were trained for internal jugular (IJ) and subclavian (SC) CVC insertions received two two-hour education sessions consisting of a lecture, ultrasound training, deliberate practice, and feedback. A 27-item checklist was drafted to measure outcomes; all pre- and post-tests were graded by a single unblended instructor to ensure accuracy. According to the study:
- None of the residents met the minimum passing score (MPS) of 79.1% for CVC insertion at baseline: mean IJ=48.4%, standard deviation=23.1; mean SC=45.2%, standard deviation=26.3;
- All residents met or exceeded the MPS at testing after simulation training: mean IJ=94.8%, standard deviation=10.0; mean SC=91.1%, standard deviation=17.8 (P<0.001);
- In the MICU, simulator-trained residents required fewer needle passes to insert a CVC than traditionally trained residents: mean=1.79, standard deviation=1.0 vs. mean=2.78, standard deviation=1.77 (P=0.04);
- Simulator-trained residents displayed more self-confidence about their procedural skills: mean=81, standard deviation=11 vs. mean=68, standard deviation=20 (P=0.02).
Dr. Barsuk isn’t surprised that confidence increases with training, saying “they hammer this home.” There were several categories for which the authors found no major improvement, though, even with the addition of deliberate training and standardized didactic materials.
Notably, the authors wrote, the resident groups “did not differ in pneumothorax, arterial puncture, or mean number of CVC adjustments.” Some of the lack of disparity was attributed to the small sample size.
In interviews, the authors noted that additional study would help assess such clinical outcomes as reduced CVC-related infections after simulation-based training. Still, Dr. Barsuk says, this pilot report is an important first step to win over skeptics.
“Simulation-based training and deliberate practice in a mastery learning setting improves performance of both simulated and actual CVC insertions by internal medicine residents,” the study reads. “Procedural training remains an important component of internal medicine training although internists are performing fewer invasive procedures now than in years past. Use of a mastery model of CVC insertion requires that trainees demonstrate skill in a simulated environment before independently performing this invasive procedure on patients.”
Another advantage of the training, McGaghie says, is that it helps physicians track their own improvement. He cautions against administrators using the data for more nefarious purposes, lest the testing become unpopular and less useful to quality improvement programs.
“You don’t use these evaluations as a weapon; you use them as a tool,” McGaghie says. “No one is there to beat up the doctors; no one is there to make them look foolish. The whole idea is to be as rigorous as possible to look for improvement—constant improvement.” TH
Richard Quinn is a freelance writer based in New Jersey.
To Jeffrey Barsuk, MD, FACP, FHM, the concept of simulation-based mastery learning is simplistic to the point of genius. Give a hospitalist—or any other physician—a physical task and let them practice the procedure until they master it. Take care not to fall into the decades-old mind-set that repetition alone will achieve a threshold of competence. Test the competence with a rigorous assessment schedule, which will objectively determine if the skill is truly mastered.
It’s standard operating procedure in many technical fields, such as engineering, computer programming, and aviation. For example, professional pilots undergo countless hours of simulation flying to freshen and further hone the skills they need to succeed in an airplane cockpit. But with tasks as menial as central venous catheter (CVC) insertions, the typical practice most young physicians get is the trial and error of needle passes.
More training, Dr. Barsuk argues, would make everyone involved better off—from the resident nervously seeking a line to the patient who wants the procedure completed as quickly and painlessly as possible.
“It’s very common sense,” says Dr. Barsuk, assistant professor of medicine in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago. “But no one is doing this. People don’t know that simulators are so effective. At least in the medical profession, we’re probably behind the times in it. … We’re enthusiastic about it because we believe in it so much. We want to see how far it can go. With mastery learning, the sky’s the limit. You can simulate almost anything you want.”
Dr. Barsuk and his colleagues have worked hard to translate “common sense” into empirical literature. Accordingly, the team will publish their latest work, “Use of Simulation-Based Mastery Learning to Improve the Quality of Central Venous Catheter Placement in a Medical Intensive Care Unit,” in September’s Journal of Hospital Medicine. The single-institution cohort study found simulation-based mastery learning increased internal-medicine residents’ skills in simulated CVC insertions, decreased the number of needle passes when performing actual procedures, and increased resident self-confidence.
“It’s always been assumed that experience in and of itself is a proxy for competence,” says William McGaghie, PhD, professor of medical education and preventive medicine at Feinberg, as well as director of evaluation for Northwestern University’s Clinical and Translational Science Institute (NUCATS). “We now know that is not the case … if skill acquisition is the goal. Experience on the wards isn’t enough. We have to have deliberate education interventions to practice in controlled, safe environments.”
—Jeffrey Barsuk, MD, FACP, FHM, Feinberg School of Medicine, Northwestern University, Chicago
The Northwestern study put that theory to the test. It aimed to expand mastery learning to a new skill set and assess quality indicators (number of needle passes, arterial punctures, etc.) and resident confidence before and after training modules. The team studied 41 second- and third-year residents rotating through the medical intensive-care unit (MICU) from October 2006 to February 2007. The university’s Institutional Review Board approved the study, and all of the participants gave informed consent prior to participating. Thirteen of the residents rotated through during a six-week pre-intervention phase, serving as the “traditionally-trained group,” the authors wrote. Twenty-eight residents were trained on Simulab’s CentralLineMan, a model with “ultrasound compatibility, an arterial pulse, and self-sealing veins and skins. Needles, dilators and guidewires can be inserted and realistic venous and arterial pressures demonstrated,” the authors wrote.
The residents who were trained for internal jugular (IJ) and subclavian (SC) CVC insertions received two two-hour education sessions consisting of a lecture, ultrasound training, deliberate practice, and feedback. A 27-item checklist was drafted to measure outcomes; all pre- and post-tests were graded by a single unblended instructor to ensure accuracy. According to the study:
- None of the residents met the minimum passing score (MPS) of 79.1% for CVC insertion at baseline: mean IJ=48.4%, standard deviation=23.1; mean SC=45.2%, standard deviation=26.3;
- All residents met or exceeded the MPS at testing after simulation training: mean IJ=94.8%, standard deviation=10.0; mean SC=91.1%, standard deviation=17.8 (P<0.001);
- In the MICU, simulator-trained residents required fewer needle passes to insert a CVC than traditionally trained residents: mean=1.79, standard deviation=1.0 vs. mean=2.78, standard deviation=1.77 (P=0.04);
- Simulator-trained residents displayed more self-confidence about their procedural skills: mean=81, standard deviation=11 vs. mean=68, standard deviation=20 (P=0.02).
Dr. Barsuk isn’t surprised that confidence increases with training, saying “they hammer this home.” There were several categories for which the authors found no major improvement, though, even with the addition of deliberate training and standardized didactic materials.
Notably, the authors wrote, the resident groups “did not differ in pneumothorax, arterial puncture, or mean number of CVC adjustments.” Some of the lack of disparity was attributed to the small sample size.
In interviews, the authors noted that additional study would help assess such clinical outcomes as reduced CVC-related infections after simulation-based training. Still, Dr. Barsuk says, this pilot report is an important first step to win over skeptics.
“Simulation-based training and deliberate practice in a mastery learning setting improves performance of both simulated and actual CVC insertions by internal medicine residents,” the study reads. “Procedural training remains an important component of internal medicine training although internists are performing fewer invasive procedures now than in years past. Use of a mastery model of CVC insertion requires that trainees demonstrate skill in a simulated environment before independently performing this invasive procedure on patients.”
Another advantage of the training, McGaghie says, is that it helps physicians track their own improvement. He cautions against administrators using the data for more nefarious purposes, lest the testing become unpopular and less useful to quality improvement programs.
“You don’t use these evaluations as a weapon; you use them as a tool,” McGaghie says. “No one is there to beat up the doctors; no one is there to make them look foolish. The whole idea is to be as rigorous as possible to look for improvement—constant improvement.” TH
Richard Quinn is a freelance writer based in New Jersey.
In the Literature
In This Edition
- Pharmacists and readmission rates.
- Geriatric discharge bundles and readmission rates.
- Medication reconciliation and risk of adverse drug events.
- End-of-life discussions and care outcomes.
- Effect of case management and housing for homeless adults.
- IV esomeprazole in bleeding ulcers.
- Causes of discharge delays.
- Methods to reduce ICU medication errors.
Addition of Pharmacists to Inpatient Teams Reduces Drug-Related Readmissions, Morbidity, and Costs for Elderly Patients
Clinical question: Would a ward-based pharmacist reduce morbidity, subsequent ED visits, and readmissions for elderly patients?
Background: Adverse drug events can cause significant drug-related morbidity and mortality, and lead to unnecessary healthcare costs. Elderly patients are more vulnerable to these effects given the polypharmacy often associated with their care. The effectiveness of a ward-based pharmacist intervention for elderly patients has not yet been studied.
Study design: Randomized controlled trial.
Setting: Two acute-care, internal-medicine wards at the University Hospital of Uppsala in Uppsala, Sweden.
Synopsis: Three hundred sixty-eight hospitalized patients ages 80 or older were randomized to control or intervention groups. The latter received enhanced services from a pharmacist who was integrated into the inpatient team. This individual performed medication reconciliation, reviewed the medication list, and advised the treating physician. The pharmacist educated and monitored patients during the hospitalization, counseled them at discharge, communicated pertinent medication information to the primary-care physicians (PCPs), and called the patients two months after discharge.
The primary outcome measure was the frequency of all hospital visits (ED visits plus hospital readmissions) during 12-month follow-up. The secondary outcome measure was the cost of hospital care.
The intervention group had a 16% reduction in all hospital visits and a 47% reduction in ED visits. There were five times as many drug-related readmissions in the control group compared with the intervention group, but the study did not have enough power to show a reduction in the total number of readmissions alone. The cost of hospital care minus the cost of the intervention resulted in a net savings of $230 per patient.
Bottom line: For elderly patients, adding a pharmacist to the inpatient team could lead to significant reductions in morbidity and, on a population basis, healthcare costs.
Citation: Gillespie U, Alassaad A, Henrohn D, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894-900.
Geriatric Care Coordination at Discharge Reduces Readmission Rates at 30 Days
Clinical question: Does a discharge planning service package affect readmission rates and ED visits?
Background: Elderly patients are at high risk for readmission after a hospitalization. Coordinated care packages, although effective in congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD) management, have yielded inconsistent results in terms of decreasing readmission rates for patients with a broader range of medical issues.
Study design: Randomized controlled pilot study.
Setting: A single large academic medical center in Texas.
Synopsis: Forty-one elderly patients at high risk for readmission—because of their age and comorbidities—were enrolled within 72 hours of admission. Patients randomized to the care bundle arm received daily education about medication reconciliation, health conditions, and self-care provided by study pharmacists and nurses. The intervention required approximately 40 minutes per day: 20 to 25 minutes for the care coordinators and 20 minutes for the pharmacists. A post-discharge phone call to review medication and confirm follow-up instructions was included.
Eight patients in the control group and two patients in the intervention arm were readmitted or seen in the ED within 30 days after discharge (38% vs. 10%, P=0.004). At 60 days, the difference between the two groups was no longer significant. The intervention group had a longer time interval before its first readmission (36.2 days vs. 15.7 days). The sample was too small to determine the effect on length of hospitalization.
Limitations of the study include its small sample size and unclear costs of the intervention.
Bottom line: Geriatric discharge bundles might decrease readmission and ED visits after discharge, but larger studies are needed to confirm this finding.
Citation: Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day post-discharge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211-218.
Computer-Assisted Medication Reconciliation Might Reduce Unintentional Drug Discrepancies with Potential for Harm
Clinical question: Does a computerized medication reconciliation intervention reduce unintentional medication discrepancies?
Background: Given the high prevalence of unintentional medication discrepancies in hospitalized patients and the potential for harm, medication reconciliation is a national patient safety goal. Little data exist on the efficacy of medication reconciliation interventions for reducing medication discrepancies.
Study design: Cluster-randomized controlled trial.
Setting: Two large academic hospitals in Boston.
Synopsis: Using 14 medical teams, the study enrolled and randomized 322 patients to a floor with intervention or to a floor with traditional care. The intervention teams utilized a computerized order entry application designed to facilitate medication reconciliation, as well as a process redesign for physicians, nurses, and pharmacists.
The primary outcome was the number of unintentional medication discrepancies with the potential for causing harm (PADEs) per patient.
Patients randomized to the intervention group had a 28% reduction in relative risk compared with the control group (1.05 PADEs vs. 1.44 PADEs; absolute relative risk 0.72 (0.52-0.99)). The absolute relative risk reduction between the two arms was 0.39 PADE per patient (NNT=2.6). The intervention was associated with a significant reduction in PADEs at discharge but not at admission. The effects of the intervention were greater in patients with a higher PADE score.
Bottom line: This computerized medication reconciliation program with process redesign was associated with reduced risk of unintentional medication discrepancies with potential for causing harms (PADEs).
Citation: Schnipper JL, Hamann C, Ndumele CD, et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009;169(8):771-780.
End-of-Life Discussions Associated with Lower Healthcare Costs
Clinical question: What is the impact of patient-physician discussions of end-of-life care on healthcare costs in the final week of a patient’s life?
Background: Life-sustaining medical care of patients with advanced cancer is costly, with disproportionate spending at the end of a patient’s life. The link between discussions of end-of-life care preferences and healthcare expenditure has not been studied thoroughly.
Study design: Prospective observational study.
Setting: Seven sites in Connecticut, Texas, New Hampshire, and Massachusetts.
Synopsis: More than 600 patients with advanced cancer were recruited from September 2002 through December 2007 as part of the Coping With Cancer study. The 188 patients (31%) who reported end-of-life discussions with their physicians at baseline were less likely to undergo mechanical ventilator use or resuscitation, or to be admitted or die in an intensive-care unit in the final week of life. They were more likely to receive outpatient hospice care and had less physical distress in the last week than those who did not.
The mean aggregate cost of care in this group was $1,876, which was 36% lower than in the group that did not discuss end-of-life care ($2,917), P=0.002. In addition, higher medical costs were associated with worse quality of death, as reported by caregivers.
This study is limited by its observational design.
Bottom line: Physician communication with patients regarding end-of-life care preferences is associated with lower costs in the final week of life.
Citation: Zhang B, Wright AA, Huskamp HA, et al. Health care costs in the last week of life: associations with end-of-life conversations. Arch Intern Med. 2009;169(5):480-488.
Reduction of ED Visits and Hospitalizations for Chronically Ill and Homeless Adults
Clinical question: Can a case management and housing program reduce the utilization of ED and hospital medical services among chronically ill homeless adults?
Background: Homeless adults have high rates of chronic illness, have poor access to uninterrupted primary healthcare, and frequently use costly medical services, including those provided by EDs and inpatient hospitalizations. Studies to determine the efficacy of housing and case management services in reducing hospital and ED utilization in this population are lacking.
Study design: Randomized controlled trial.
Setting: A public teaching hospital and a private nonprofit hospital in Chicago.
Synopsis: Four hundred seven chronically ill and homeless adults were randomized to receive a case management and housing intervention or traditional care following an index hospitalization. The intervention group received assistance with stable housing on discharge and biweekly case management services throughout the study period. Traditional care consisted of routine inpatient discharge planning and transportation to a shelter.
Patients were followed for 18 months for the primary outcomes: number of hospitalizations, total hospital days, and number of ED visits.
After adjusting for differences in baseline variables, the intervention group was found to have significantly lower rates of hospitalization (relative reduction 29%), total hospital days (29%), and ED visits (24%). The authors did not find a difference in mortality or quality of life between the two groups.
Limitations of this study include a small sample size, limited geographic distribution of subjects, and the lack of a cost-benefit analysis of the intervention.
Bottom line: Case management and housing interventions can decrease hospitalizations and ED visits among chronically ill homeless adults.
Citation: Sadowski LS, Kee RA, VanderWeele TJ, Buchanan D. Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: a randomized trial. JAMA. 2009;301(17):1771-1778.
Intravenous Esomeprazole Reduces Recurrent Bleeding from Peptic Ulcers
Clinical question: Does intravenous esomeprazole prevent recurrent peptic ulcer bleeding, compared with placebo?
Background: U.S. hospitals admit more than 300,000 patients per year for peptic ulcer bleeding. Asian studies of proton pump inhibitors have demonstrated improved outcomes in patients with bleeding caused by peptic ulcers, but these results have not been consistently replicated in studies in Western Europe or North America.
Study design: Randomized, placebo-controlled, double-blind trial.
Setting: Ninety-one hospital EDs in 16 countries.
Synopsis: The study team randomized 764 adult patients with a single bleeding gastric or duodenal ulcer after successful endoscopic hemostasis. The study group received esomeprazole (80 mg bolus, given intravenously over 30 minutes, followed by an 8 mg/hour infusion for 71.5 hours). The second group received placebo. Each group subsequently received 40 mg/day of oral esomeprazole for 27 days.
Recurrent bleeding within 72 hours was reduced by nearly half in the intravenous esomeprazole arm compared with placebo (5.9% vs. 10.3%, P=0.026). This remained significant at seven and 30 days. Intravenous esomeprazole also reduced endoscopic retreatment (6.4% vs. 11.6%; P=0.012) and demonstrated a trend toward reduction in surgery (2.7% vs. 5.4%) and all-cause mortality (0.8% vs. 2.1%).
Study limitations included a lack of standardization of endoscopic therapy across institutions.
Bottom line: Given after endoscopic hemostatis, intravenous esomeprazole followed by oral esomeprazole reduced recurrent bleeding in patients with a single duodenal or gastric ulcer.
Citation: Sung JJ, Barkun A, Kuipers EJ, et al. Intravenous esomeprazole for prevention of recurrent peptic ulcer bleeding: a randomized trial. Ann Intern Med. 2009;150(7):455-464.
Discharge Time and Duration Affected by Several Factors During Hospitalization
Clinical question: What are the factors affecting late and long discharges in a general medical unit?
Background: The mismatch between admission and discharge times is a problem for many hospitals; admissions occur early in the day whereas, discharges occur later in the day. The reasons behind delays in discharge and prolongation of discharges are not fully understood.
Study design: Prospective cohort study.
Setting: A general medical unit without house staff coverage at an academic medical center in Baltimore.
Synopsis: Care providers completed surveys on 201 consecutive discharges from January to April 2005. Outcome variables included time of discharge and discharge duration.
Mean discharge time was 3:09 p.m. Delay in discharge was associated with a need for ambulance transportation (1.5 hours), need for prescriptions to be filled at the hospital (1.4 hours), and for patients whose final test was a procedure (1.2 hours) or consult (1.1 hours).
Median discharge time was 7.6 hours. Longer discharge duration was associated with discharge to a location other than home (28.9 hours), need for consultation (14.8 hours), or need for a procedure (13.4 hours) before discharge.
African-American race, gender, age, and comorbid psychiatric and substance abuse disorders were not associated with either late or prolonged discharges.
Bottom line: Final-day tests, procedures, and consults, as well as complex discharge arrangements, prolong and delay discharges more than the characteristics of patients themselves.
Citation: Chen LM, Freitag MH, Franco M, Sullivan CD, Dickson C, Brancati FL. Natural history of late discharges from a general medical ward. J Hosp Med. 2009;4(4):226-233.
Administration of Parenteral Medication a Common Point at Which Errors Occur in ICUs
Clinical question: To what extent are medication administration errors a problem across ICUs, and what are some ways to prevent them?
Background: High-acuity and complex systems increase the likelihood of medical errors in ICUs. The first multinational Sentinel Events Evaluation study reported an ICU medication error rate of 10.5 per 100 patient days at the prescription and administration stages of medication delivery.
Study design: Multinational observational, prospective, cross-sectional study.
Setting: One hundred thirteen ICUs in 27 countries on five continents.
Synopsis: This study addressed five types of medication error at the administration stage in the ICU in a 24-hour timeframe: wrong drug, wrong dose, wrong route, wrong time, and missed medication. The main outcome measures were the number and impact of administration errors, the distribution of error characteristics, and the distribution of contributing and preventive factors.
In the 1,328 critically ill patients included in the study, 861 medication errors were reported by structured questionnaire; 441 patients were affected by the errors. The prevalence was 74.5 errors per 100 patient days, and 12 patients (0.9%) suffered permanent harm or death. Most medication administration errors occurred during routine care, not during extraordinary situations. Most were omission errors.
This study is limited by its observational design and by the fact that self-reporting also carries the risk of under-reporting.
This study points out several ways to reduce medication errors. An independent predictor of decreased risk of medication errors of all types is an established incident reporting system. Routine checking of infusion pumps at every nursing shift change also reduced this risk.
Bottom line: This study confirmed that the administration of parenteral medications is a vulnerable point across many ICUs, and incident reporting systems and routine checks of infusion pumps are effective ways to reduce the risk of this type of error.
Citation: Valentin A, Capuzzo M, Guidet B, et al. Errors in administration of parenteral drugs in intensive care units: multinational prospective study. BMJ. 2009;338:b814. TH
PEDIATRIC HM LITERATURE
The Value of Pediatric Hospitalist Programs
By Mark Shen, MD

Clinical question: What is the value of pediatric hospitalist programs to hospital leaders?
Background: The growth of the HM field has resulted in an increase in both the absolute number of hospitalists and hospitalist programs in the U.S. Although the clinical impact of this model generally has been favorable, most programs still require significant financial subsidies, typically from hospitals. The perspective of hospital leaders on the reasons for giving these subsidies to pediatric hospitalist programs has not been examined.
Study design: Mailed survey to hospital leaders.
Setting: Hospitals with a pediatric hospitalist program.
Synopsis: A random sample of 213 (out of 761) American Hospital Association hospitals with an HM program and pediatric beds were selected for study. One hundred twelve pediatric hospitalist programs were confirmed at these institutions, and hospital leaders (CEOs, presidents, CFOs, CMOs, or others) were surveyed from each facility. The response rate was 69%. Almost all of the pediatric hospitalist programs (78%) were subsidized, and the vast majority of hospital leaders thought the programs increased patient satisfaction (94%) and referring physician satisfaction (90%), while decreasing length of stay (81%) and adverse events (81%). The hospital leaders also identified those four factors as the primary reasons for subsidization of the HM programs.
Although virtually all hospital leaders responding to the survey thought that pediatric hospitalist programs improved patient and referring physician satisfaction, they only reported measuring this impact 80% and 66% of the time, respectively. Thus, this survey was unable to link actual outcomes, such as increased satisfaction or decreased length of stay, to increased quantity or likelihood of funding. The literature on pediatric hospitalist programs’ impact on satisfaction, quality, and safety remains sparse; however, now there is valuable information with respect to why hospital leaders subsidize these groups.
Bottom line: Hospital leaders subsidize pediatric HM programs based on the belief that the hospitalists positively impact patient and referring physician satisfaction.
Citation: Freed GL, Dunham KM, Switalski KE, et al. Assessing the value of pediatric hospitalist programs: the perspective of hospital leaders. Acad Pediatr. 2009;9(3):192-196.
In This Edition
- Pharmacists and readmission rates.
- Geriatric discharge bundles and readmission rates.
- Medication reconciliation and risk of adverse drug events.
- End-of-life discussions and care outcomes.
- Effect of case management and housing for homeless adults.
- IV esomeprazole in bleeding ulcers.
- Causes of discharge delays.
- Methods to reduce ICU medication errors.
Addition of Pharmacists to Inpatient Teams Reduces Drug-Related Readmissions, Morbidity, and Costs for Elderly Patients
Clinical question: Would a ward-based pharmacist reduce morbidity, subsequent ED visits, and readmissions for elderly patients?
Background: Adverse drug events can cause significant drug-related morbidity and mortality, and lead to unnecessary healthcare costs. Elderly patients are more vulnerable to these effects given the polypharmacy often associated with their care. The effectiveness of a ward-based pharmacist intervention for elderly patients has not yet been studied.
Study design: Randomized controlled trial.
Setting: Two acute-care, internal-medicine wards at the University Hospital of Uppsala in Uppsala, Sweden.
Synopsis: Three hundred sixty-eight hospitalized patients ages 80 or older were randomized to control or intervention groups. The latter received enhanced services from a pharmacist who was integrated into the inpatient team. This individual performed medication reconciliation, reviewed the medication list, and advised the treating physician. The pharmacist educated and monitored patients during the hospitalization, counseled them at discharge, communicated pertinent medication information to the primary-care physicians (PCPs), and called the patients two months after discharge.
The primary outcome measure was the frequency of all hospital visits (ED visits plus hospital readmissions) during 12-month follow-up. The secondary outcome measure was the cost of hospital care.
The intervention group had a 16% reduction in all hospital visits and a 47% reduction in ED visits. There were five times as many drug-related readmissions in the control group compared with the intervention group, but the study did not have enough power to show a reduction in the total number of readmissions alone. The cost of hospital care minus the cost of the intervention resulted in a net savings of $230 per patient.
Bottom line: For elderly patients, adding a pharmacist to the inpatient team could lead to significant reductions in morbidity and, on a population basis, healthcare costs.
Citation: Gillespie U, Alassaad A, Henrohn D, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894-900.
Geriatric Care Coordination at Discharge Reduces Readmission Rates at 30 Days
Clinical question: Does a discharge planning service package affect readmission rates and ED visits?
Background: Elderly patients are at high risk for readmission after a hospitalization. Coordinated care packages, although effective in congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD) management, have yielded inconsistent results in terms of decreasing readmission rates for patients with a broader range of medical issues.
Study design: Randomized controlled pilot study.
Setting: A single large academic medical center in Texas.
Synopsis: Forty-one elderly patients at high risk for readmission—because of their age and comorbidities—were enrolled within 72 hours of admission. Patients randomized to the care bundle arm received daily education about medication reconciliation, health conditions, and self-care provided by study pharmacists and nurses. The intervention required approximately 40 minutes per day: 20 to 25 minutes for the care coordinators and 20 minutes for the pharmacists. A post-discharge phone call to review medication and confirm follow-up instructions was included.
Eight patients in the control group and two patients in the intervention arm were readmitted or seen in the ED within 30 days after discharge (38% vs. 10%, P=0.004). At 60 days, the difference between the two groups was no longer significant. The intervention group had a longer time interval before its first readmission (36.2 days vs. 15.7 days). The sample was too small to determine the effect on length of hospitalization.
Limitations of the study include its small sample size and unclear costs of the intervention.
Bottom line: Geriatric discharge bundles might decrease readmission and ED visits after discharge, but larger studies are needed to confirm this finding.
Citation: Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day post-discharge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211-218.
Computer-Assisted Medication Reconciliation Might Reduce Unintentional Drug Discrepancies with Potential for Harm
Clinical question: Does a computerized medication reconciliation intervention reduce unintentional medication discrepancies?
Background: Given the high prevalence of unintentional medication discrepancies in hospitalized patients and the potential for harm, medication reconciliation is a national patient safety goal. Little data exist on the efficacy of medication reconciliation interventions for reducing medication discrepancies.
Study design: Cluster-randomized controlled trial.
Setting: Two large academic hospitals in Boston.
Synopsis: Using 14 medical teams, the study enrolled and randomized 322 patients to a floor with intervention or to a floor with traditional care. The intervention teams utilized a computerized order entry application designed to facilitate medication reconciliation, as well as a process redesign for physicians, nurses, and pharmacists.
The primary outcome was the number of unintentional medication discrepancies with the potential for causing harm (PADEs) per patient.
Patients randomized to the intervention group had a 28% reduction in relative risk compared with the control group (1.05 PADEs vs. 1.44 PADEs; absolute relative risk 0.72 (0.52-0.99)). The absolute relative risk reduction between the two arms was 0.39 PADE per patient (NNT=2.6). The intervention was associated with a significant reduction in PADEs at discharge but not at admission. The effects of the intervention were greater in patients with a higher PADE score.
Bottom line: This computerized medication reconciliation program with process redesign was associated with reduced risk of unintentional medication discrepancies with potential for causing harms (PADEs).
Citation: Schnipper JL, Hamann C, Ndumele CD, et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009;169(8):771-780.
End-of-Life Discussions Associated with Lower Healthcare Costs
Clinical question: What is the impact of patient-physician discussions of end-of-life care on healthcare costs in the final week of a patient’s life?
Background: Life-sustaining medical care of patients with advanced cancer is costly, with disproportionate spending at the end of a patient’s life. The link between discussions of end-of-life care preferences and healthcare expenditure has not been studied thoroughly.
Study design: Prospective observational study.
Setting: Seven sites in Connecticut, Texas, New Hampshire, and Massachusetts.
Synopsis: More than 600 patients with advanced cancer were recruited from September 2002 through December 2007 as part of the Coping With Cancer study. The 188 patients (31%) who reported end-of-life discussions with their physicians at baseline were less likely to undergo mechanical ventilator use or resuscitation, or to be admitted or die in an intensive-care unit in the final week of life. They were more likely to receive outpatient hospice care and had less physical distress in the last week than those who did not.
The mean aggregate cost of care in this group was $1,876, which was 36% lower than in the group that did not discuss end-of-life care ($2,917), P=0.002. In addition, higher medical costs were associated with worse quality of death, as reported by caregivers.
This study is limited by its observational design.
Bottom line: Physician communication with patients regarding end-of-life care preferences is associated with lower costs in the final week of life.
Citation: Zhang B, Wright AA, Huskamp HA, et al. Health care costs in the last week of life: associations with end-of-life conversations. Arch Intern Med. 2009;169(5):480-488.
Reduction of ED Visits and Hospitalizations for Chronically Ill and Homeless Adults
Clinical question: Can a case management and housing program reduce the utilization of ED and hospital medical services among chronically ill homeless adults?
Background: Homeless adults have high rates of chronic illness, have poor access to uninterrupted primary healthcare, and frequently use costly medical services, including those provided by EDs and inpatient hospitalizations. Studies to determine the efficacy of housing and case management services in reducing hospital and ED utilization in this population are lacking.
Study design: Randomized controlled trial.
Setting: A public teaching hospital and a private nonprofit hospital in Chicago.
Synopsis: Four hundred seven chronically ill and homeless adults were randomized to receive a case management and housing intervention or traditional care following an index hospitalization. The intervention group received assistance with stable housing on discharge and biweekly case management services throughout the study period. Traditional care consisted of routine inpatient discharge planning and transportation to a shelter.
Patients were followed for 18 months for the primary outcomes: number of hospitalizations, total hospital days, and number of ED visits.
After adjusting for differences in baseline variables, the intervention group was found to have significantly lower rates of hospitalization (relative reduction 29%), total hospital days (29%), and ED visits (24%). The authors did not find a difference in mortality or quality of life between the two groups.
Limitations of this study include a small sample size, limited geographic distribution of subjects, and the lack of a cost-benefit analysis of the intervention.
Bottom line: Case management and housing interventions can decrease hospitalizations and ED visits among chronically ill homeless adults.
Citation: Sadowski LS, Kee RA, VanderWeele TJ, Buchanan D. Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: a randomized trial. JAMA. 2009;301(17):1771-1778.
Intravenous Esomeprazole Reduces Recurrent Bleeding from Peptic Ulcers
Clinical question: Does intravenous esomeprazole prevent recurrent peptic ulcer bleeding, compared with placebo?
Background: U.S. hospitals admit more than 300,000 patients per year for peptic ulcer bleeding. Asian studies of proton pump inhibitors have demonstrated improved outcomes in patients with bleeding caused by peptic ulcers, but these results have not been consistently replicated in studies in Western Europe or North America.
Study design: Randomized, placebo-controlled, double-blind trial.
Setting: Ninety-one hospital EDs in 16 countries.
Synopsis: The study team randomized 764 adult patients with a single bleeding gastric or duodenal ulcer after successful endoscopic hemostasis. The study group received esomeprazole (80 mg bolus, given intravenously over 30 minutes, followed by an 8 mg/hour infusion for 71.5 hours). The second group received placebo. Each group subsequently received 40 mg/day of oral esomeprazole for 27 days.
Recurrent bleeding within 72 hours was reduced by nearly half in the intravenous esomeprazole arm compared with placebo (5.9% vs. 10.3%, P=0.026). This remained significant at seven and 30 days. Intravenous esomeprazole also reduced endoscopic retreatment (6.4% vs. 11.6%; P=0.012) and demonstrated a trend toward reduction in surgery (2.7% vs. 5.4%) and all-cause mortality (0.8% vs. 2.1%).
Study limitations included a lack of standardization of endoscopic therapy across institutions.
Bottom line: Given after endoscopic hemostatis, intravenous esomeprazole followed by oral esomeprazole reduced recurrent bleeding in patients with a single duodenal or gastric ulcer.
Citation: Sung JJ, Barkun A, Kuipers EJ, et al. Intravenous esomeprazole for prevention of recurrent peptic ulcer bleeding: a randomized trial. Ann Intern Med. 2009;150(7):455-464.
Discharge Time and Duration Affected by Several Factors During Hospitalization
Clinical question: What are the factors affecting late and long discharges in a general medical unit?
Background: The mismatch between admission and discharge times is a problem for many hospitals; admissions occur early in the day whereas, discharges occur later in the day. The reasons behind delays in discharge and prolongation of discharges are not fully understood.
Study design: Prospective cohort study.
Setting: A general medical unit without house staff coverage at an academic medical center in Baltimore.
Synopsis: Care providers completed surveys on 201 consecutive discharges from January to April 2005. Outcome variables included time of discharge and discharge duration.
Mean discharge time was 3:09 p.m. Delay in discharge was associated with a need for ambulance transportation (1.5 hours), need for prescriptions to be filled at the hospital (1.4 hours), and for patients whose final test was a procedure (1.2 hours) or consult (1.1 hours).
Median discharge time was 7.6 hours. Longer discharge duration was associated with discharge to a location other than home (28.9 hours), need for consultation (14.8 hours), or need for a procedure (13.4 hours) before discharge.
African-American race, gender, age, and comorbid psychiatric and substance abuse disorders were not associated with either late or prolonged discharges.
Bottom line: Final-day tests, procedures, and consults, as well as complex discharge arrangements, prolong and delay discharges more than the characteristics of patients themselves.
Citation: Chen LM, Freitag MH, Franco M, Sullivan CD, Dickson C, Brancati FL. Natural history of late discharges from a general medical ward. J Hosp Med. 2009;4(4):226-233.
Administration of Parenteral Medication a Common Point at Which Errors Occur in ICUs
Clinical question: To what extent are medication administration errors a problem across ICUs, and what are some ways to prevent them?
Background: High-acuity and complex systems increase the likelihood of medical errors in ICUs. The first multinational Sentinel Events Evaluation study reported an ICU medication error rate of 10.5 per 100 patient days at the prescription and administration stages of medication delivery.
Study design: Multinational observational, prospective, cross-sectional study.
Setting: One hundred thirteen ICUs in 27 countries on five continents.
Synopsis: This study addressed five types of medication error at the administration stage in the ICU in a 24-hour timeframe: wrong drug, wrong dose, wrong route, wrong time, and missed medication. The main outcome measures were the number and impact of administration errors, the distribution of error characteristics, and the distribution of contributing and preventive factors.
In the 1,328 critically ill patients included in the study, 861 medication errors were reported by structured questionnaire; 441 patients were affected by the errors. The prevalence was 74.5 errors per 100 patient days, and 12 patients (0.9%) suffered permanent harm or death. Most medication administration errors occurred during routine care, not during extraordinary situations. Most were omission errors.
This study is limited by its observational design and by the fact that self-reporting also carries the risk of under-reporting.
This study points out several ways to reduce medication errors. An independent predictor of decreased risk of medication errors of all types is an established incident reporting system. Routine checking of infusion pumps at every nursing shift change also reduced this risk.
Bottom line: This study confirmed that the administration of parenteral medications is a vulnerable point across many ICUs, and incident reporting systems and routine checks of infusion pumps are effective ways to reduce the risk of this type of error.
Citation: Valentin A, Capuzzo M, Guidet B, et al. Errors in administration of parenteral drugs in intensive care units: multinational prospective study. BMJ. 2009;338:b814. TH
PEDIATRIC HM LITERATURE
The Value of Pediatric Hospitalist Programs
By Mark Shen, MD
Clinical question: What is the value of pediatric hospitalist programs to hospital leaders?
Background: The growth of the HM field has resulted in an increase in both the absolute number of hospitalists and hospitalist programs in the U.S. Although the clinical impact of this model generally has been favorable, most programs still require significant financial subsidies, typically from hospitals. The perspective of hospital leaders on the reasons for giving these subsidies to pediatric hospitalist programs has not been examined.
Study design: Mailed survey to hospital leaders.
Setting: Hospitals with a pediatric hospitalist program.
Synopsis: A random sample of 213 (out of 761) American Hospital Association hospitals with an HM program and pediatric beds were selected for study. One hundred twelve pediatric hospitalist programs were confirmed at these institutions, and hospital leaders (CEOs, presidents, CFOs, CMOs, or others) were surveyed from each facility. The response rate was 69%. Almost all of the pediatric hospitalist programs (78%) were subsidized, and the vast majority of hospital leaders thought the programs increased patient satisfaction (94%) and referring physician satisfaction (90%), while decreasing length of stay (81%) and adverse events (81%). The hospital leaders also identified those four factors as the primary reasons for subsidization of the HM programs.
Although virtually all hospital leaders responding to the survey thought that pediatric hospitalist programs improved patient and referring physician satisfaction, they only reported measuring this impact 80% and 66% of the time, respectively. Thus, this survey was unable to link actual outcomes, such as increased satisfaction or decreased length of stay, to increased quantity or likelihood of funding. The literature on pediatric hospitalist programs’ impact on satisfaction, quality, and safety remains sparse; however, now there is valuable information with respect to why hospital leaders subsidize these groups.
Bottom line: Hospital leaders subsidize pediatric HM programs based on the belief that the hospitalists positively impact patient and referring physician satisfaction.
Citation: Freed GL, Dunham KM, Switalski KE, et al. Assessing the value of pediatric hospitalist programs: the perspective of hospital leaders. Acad Pediatr. 2009;9(3):192-196.
In This Edition
- Pharmacists and readmission rates.
- Geriatric discharge bundles and readmission rates.
- Medication reconciliation and risk of adverse drug events.
- End-of-life discussions and care outcomes.
- Effect of case management and housing for homeless adults.
- IV esomeprazole in bleeding ulcers.
- Causes of discharge delays.
- Methods to reduce ICU medication errors.
Addition of Pharmacists to Inpatient Teams Reduces Drug-Related Readmissions, Morbidity, and Costs for Elderly Patients
Clinical question: Would a ward-based pharmacist reduce morbidity, subsequent ED visits, and readmissions for elderly patients?
Background: Adverse drug events can cause significant drug-related morbidity and mortality, and lead to unnecessary healthcare costs. Elderly patients are more vulnerable to these effects given the polypharmacy often associated with their care. The effectiveness of a ward-based pharmacist intervention for elderly patients has not yet been studied.
Study design: Randomized controlled trial.
Setting: Two acute-care, internal-medicine wards at the University Hospital of Uppsala in Uppsala, Sweden.
Synopsis: Three hundred sixty-eight hospitalized patients ages 80 or older were randomized to control or intervention groups. The latter received enhanced services from a pharmacist who was integrated into the inpatient team. This individual performed medication reconciliation, reviewed the medication list, and advised the treating physician. The pharmacist educated and monitored patients during the hospitalization, counseled them at discharge, communicated pertinent medication information to the primary-care physicians (PCPs), and called the patients two months after discharge.
The primary outcome measure was the frequency of all hospital visits (ED visits plus hospital readmissions) during 12-month follow-up. The secondary outcome measure was the cost of hospital care.
The intervention group had a 16% reduction in all hospital visits and a 47% reduction in ED visits. There were five times as many drug-related readmissions in the control group compared with the intervention group, but the study did not have enough power to show a reduction in the total number of readmissions alone. The cost of hospital care minus the cost of the intervention resulted in a net savings of $230 per patient.
Bottom line: For elderly patients, adding a pharmacist to the inpatient team could lead to significant reductions in morbidity and, on a population basis, healthcare costs.
Citation: Gillespie U, Alassaad A, Henrohn D, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894-900.
Geriatric Care Coordination at Discharge Reduces Readmission Rates at 30 Days
Clinical question: Does a discharge planning service package affect readmission rates and ED visits?
Background: Elderly patients are at high risk for readmission after a hospitalization. Coordinated care packages, although effective in congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD) management, have yielded inconsistent results in terms of decreasing readmission rates for patients with a broader range of medical issues.
Study design: Randomized controlled pilot study.
Setting: A single large academic medical center in Texas.
Synopsis: Forty-one elderly patients at high risk for readmission—because of their age and comorbidities—were enrolled within 72 hours of admission. Patients randomized to the care bundle arm received daily education about medication reconciliation, health conditions, and self-care provided by study pharmacists and nurses. The intervention required approximately 40 minutes per day: 20 to 25 minutes for the care coordinators and 20 minutes for the pharmacists. A post-discharge phone call to review medication and confirm follow-up instructions was included.
Eight patients in the control group and two patients in the intervention arm were readmitted or seen in the ED within 30 days after discharge (38% vs. 10%, P=0.004). At 60 days, the difference between the two groups was no longer significant. The intervention group had a longer time interval before its first readmission (36.2 days vs. 15.7 days). The sample was too small to determine the effect on length of hospitalization.
Limitations of the study include its small sample size and unclear costs of the intervention.
Bottom line: Geriatric discharge bundles might decrease readmission and ED visits after discharge, but larger studies are needed to confirm this finding.
Citation: Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day post-discharge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211-218.
Computer-Assisted Medication Reconciliation Might Reduce Unintentional Drug Discrepancies with Potential for Harm
Clinical question: Does a computerized medication reconciliation intervention reduce unintentional medication discrepancies?
Background: Given the high prevalence of unintentional medication discrepancies in hospitalized patients and the potential for harm, medication reconciliation is a national patient safety goal. Little data exist on the efficacy of medication reconciliation interventions for reducing medication discrepancies.
Study design: Cluster-randomized controlled trial.
Setting: Two large academic hospitals in Boston.
Synopsis: Using 14 medical teams, the study enrolled and randomized 322 patients to a floor with intervention or to a floor with traditional care. The intervention teams utilized a computerized order entry application designed to facilitate medication reconciliation, as well as a process redesign for physicians, nurses, and pharmacists.
The primary outcome was the number of unintentional medication discrepancies with the potential for causing harm (PADEs) per patient.
Patients randomized to the intervention group had a 28% reduction in relative risk compared with the control group (1.05 PADEs vs. 1.44 PADEs; absolute relative risk 0.72 (0.52-0.99)). The absolute relative risk reduction between the two arms was 0.39 PADE per patient (NNT=2.6). The intervention was associated with a significant reduction in PADEs at discharge but not at admission. The effects of the intervention were greater in patients with a higher PADE score.
Bottom line: This computerized medication reconciliation program with process redesign was associated with reduced risk of unintentional medication discrepancies with potential for causing harms (PADEs).
Citation: Schnipper JL, Hamann C, Ndumele CD, et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009;169(8):771-780.
End-of-Life Discussions Associated with Lower Healthcare Costs
Clinical question: What is the impact of patient-physician discussions of end-of-life care on healthcare costs in the final week of a patient’s life?
Background: Life-sustaining medical care of patients with advanced cancer is costly, with disproportionate spending at the end of a patient’s life. The link between discussions of end-of-life care preferences and healthcare expenditure has not been studied thoroughly.
Study design: Prospective observational study.
Setting: Seven sites in Connecticut, Texas, New Hampshire, and Massachusetts.
Synopsis: More than 600 patients with advanced cancer were recruited from September 2002 through December 2007 as part of the Coping With Cancer study. The 188 patients (31%) who reported end-of-life discussions with their physicians at baseline were less likely to undergo mechanical ventilator use or resuscitation, or to be admitted or die in an intensive-care unit in the final week of life. They were more likely to receive outpatient hospice care and had less physical distress in the last week than those who did not.
The mean aggregate cost of care in this group was $1,876, which was 36% lower than in the group that did not discuss end-of-life care ($2,917), P=0.002. In addition, higher medical costs were associated with worse quality of death, as reported by caregivers.
This study is limited by its observational design.
Bottom line: Physician communication with patients regarding end-of-life care preferences is associated with lower costs in the final week of life.
Citation: Zhang B, Wright AA, Huskamp HA, et al. Health care costs in the last week of life: associations with end-of-life conversations. Arch Intern Med. 2009;169(5):480-488.
Reduction of ED Visits and Hospitalizations for Chronically Ill and Homeless Adults
Clinical question: Can a case management and housing program reduce the utilization of ED and hospital medical services among chronically ill homeless adults?
Background: Homeless adults have high rates of chronic illness, have poor access to uninterrupted primary healthcare, and frequently use costly medical services, including those provided by EDs and inpatient hospitalizations. Studies to determine the efficacy of housing and case management services in reducing hospital and ED utilization in this population are lacking.
Study design: Randomized controlled trial.
Setting: A public teaching hospital and a private nonprofit hospital in Chicago.
Synopsis: Four hundred seven chronically ill and homeless adults were randomized to receive a case management and housing intervention or traditional care following an index hospitalization. The intervention group received assistance with stable housing on discharge and biweekly case management services throughout the study period. Traditional care consisted of routine inpatient discharge planning and transportation to a shelter.
Patients were followed for 18 months for the primary outcomes: number of hospitalizations, total hospital days, and number of ED visits.
After adjusting for differences in baseline variables, the intervention group was found to have significantly lower rates of hospitalization (relative reduction 29%), total hospital days (29%), and ED visits (24%). The authors did not find a difference in mortality or quality of life between the two groups.
Limitations of this study include a small sample size, limited geographic distribution of subjects, and the lack of a cost-benefit analysis of the intervention.
Bottom line: Case management and housing interventions can decrease hospitalizations and ED visits among chronically ill homeless adults.
Citation: Sadowski LS, Kee RA, VanderWeele TJ, Buchanan D. Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: a randomized trial. JAMA. 2009;301(17):1771-1778.
Intravenous Esomeprazole Reduces Recurrent Bleeding from Peptic Ulcers
Clinical question: Does intravenous esomeprazole prevent recurrent peptic ulcer bleeding, compared with placebo?
Background: U.S. hospitals admit more than 300,000 patients per year for peptic ulcer bleeding. Asian studies of proton pump inhibitors have demonstrated improved outcomes in patients with bleeding caused by peptic ulcers, but these results have not been consistently replicated in studies in Western Europe or North America.
Study design: Randomized, placebo-controlled, double-blind trial.
Setting: Ninety-one hospital EDs in 16 countries.
Synopsis: The study team randomized 764 adult patients with a single bleeding gastric or duodenal ulcer after successful endoscopic hemostasis. The study group received esomeprazole (80 mg bolus, given intravenously over 30 minutes, followed by an 8 mg/hour infusion for 71.5 hours). The second group received placebo. Each group subsequently received 40 mg/day of oral esomeprazole for 27 days.
Recurrent bleeding within 72 hours was reduced by nearly half in the intravenous esomeprazole arm compared with placebo (5.9% vs. 10.3%, P=0.026). This remained significant at seven and 30 days. Intravenous esomeprazole also reduced endoscopic retreatment (6.4% vs. 11.6%; P=0.012) and demonstrated a trend toward reduction in surgery (2.7% vs. 5.4%) and all-cause mortality (0.8% vs. 2.1%).
Study limitations included a lack of standardization of endoscopic therapy across institutions.
Bottom line: Given after endoscopic hemostatis, intravenous esomeprazole followed by oral esomeprazole reduced recurrent bleeding in patients with a single duodenal or gastric ulcer.
Citation: Sung JJ, Barkun A, Kuipers EJ, et al. Intravenous esomeprazole for prevention of recurrent peptic ulcer bleeding: a randomized trial. Ann Intern Med. 2009;150(7):455-464.
Discharge Time and Duration Affected by Several Factors During Hospitalization
Clinical question: What are the factors affecting late and long discharges in a general medical unit?
Background: The mismatch between admission and discharge times is a problem for many hospitals; admissions occur early in the day whereas, discharges occur later in the day. The reasons behind delays in discharge and prolongation of discharges are not fully understood.
Study design: Prospective cohort study.
Setting: A general medical unit without house staff coverage at an academic medical center in Baltimore.
Synopsis: Care providers completed surveys on 201 consecutive discharges from January to April 2005. Outcome variables included time of discharge and discharge duration.
Mean discharge time was 3:09 p.m. Delay in discharge was associated with a need for ambulance transportation (1.5 hours), need for prescriptions to be filled at the hospital (1.4 hours), and for patients whose final test was a procedure (1.2 hours) or consult (1.1 hours).
Median discharge time was 7.6 hours. Longer discharge duration was associated with discharge to a location other than home (28.9 hours), need for consultation (14.8 hours), or need for a procedure (13.4 hours) before discharge.
African-American race, gender, age, and comorbid psychiatric and substance abuse disorders were not associated with either late or prolonged discharges.
Bottom line: Final-day tests, procedures, and consults, as well as complex discharge arrangements, prolong and delay discharges more than the characteristics of patients themselves.
Citation: Chen LM, Freitag MH, Franco M, Sullivan CD, Dickson C, Brancati FL. Natural history of late discharges from a general medical ward. J Hosp Med. 2009;4(4):226-233.
Administration of Parenteral Medication a Common Point at Which Errors Occur in ICUs
Clinical question: To what extent are medication administration errors a problem across ICUs, and what are some ways to prevent them?
Background: High-acuity and complex systems increase the likelihood of medical errors in ICUs. The first multinational Sentinel Events Evaluation study reported an ICU medication error rate of 10.5 per 100 patient days at the prescription and administration stages of medication delivery.
Study design: Multinational observational, prospective, cross-sectional study.
Setting: One hundred thirteen ICUs in 27 countries on five continents.
Synopsis: This study addressed five types of medication error at the administration stage in the ICU in a 24-hour timeframe: wrong drug, wrong dose, wrong route, wrong time, and missed medication. The main outcome measures were the number and impact of administration errors, the distribution of error characteristics, and the distribution of contributing and preventive factors.
In the 1,328 critically ill patients included in the study, 861 medication errors were reported by structured questionnaire; 441 patients were affected by the errors. The prevalence was 74.5 errors per 100 patient days, and 12 patients (0.9%) suffered permanent harm or death. Most medication administration errors occurred during routine care, not during extraordinary situations. Most were omission errors.
This study is limited by its observational design and by the fact that self-reporting also carries the risk of under-reporting.
This study points out several ways to reduce medication errors. An independent predictor of decreased risk of medication errors of all types is an established incident reporting system. Routine checking of infusion pumps at every nursing shift change also reduced this risk.
Bottom line: This study confirmed that the administration of parenteral medications is a vulnerable point across many ICUs, and incident reporting systems and routine checks of infusion pumps are effective ways to reduce the risk of this type of error.
Citation: Valentin A, Capuzzo M, Guidet B, et al. Errors in administration of parenteral drugs in intensive care units: multinational prospective study. BMJ. 2009;338:b814. TH
PEDIATRIC HM LITERATURE
The Value of Pediatric Hospitalist Programs
By Mark Shen, MD
Clinical question: What is the value of pediatric hospitalist programs to hospital leaders?
Background: The growth of the HM field has resulted in an increase in both the absolute number of hospitalists and hospitalist programs in the U.S. Although the clinical impact of this model generally has been favorable, most programs still require significant financial subsidies, typically from hospitals. The perspective of hospital leaders on the reasons for giving these subsidies to pediatric hospitalist programs has not been examined.
Study design: Mailed survey to hospital leaders.
Setting: Hospitals with a pediatric hospitalist program.
Synopsis: A random sample of 213 (out of 761) American Hospital Association hospitals with an HM program and pediatric beds were selected for study. One hundred twelve pediatric hospitalist programs were confirmed at these institutions, and hospital leaders (CEOs, presidents, CFOs, CMOs, or others) were surveyed from each facility. The response rate was 69%. Almost all of the pediatric hospitalist programs (78%) were subsidized, and the vast majority of hospital leaders thought the programs increased patient satisfaction (94%) and referring physician satisfaction (90%), while decreasing length of stay (81%) and adverse events (81%). The hospital leaders also identified those four factors as the primary reasons for subsidization of the HM programs.
Although virtually all hospital leaders responding to the survey thought that pediatric hospitalist programs improved patient and referring physician satisfaction, they only reported measuring this impact 80% and 66% of the time, respectively. Thus, this survey was unable to link actual outcomes, such as increased satisfaction or decreased length of stay, to increased quantity or likelihood of funding. The literature on pediatric hospitalist programs’ impact on satisfaction, quality, and safety remains sparse; however, now there is valuable information with respect to why hospital leaders subsidize these groups.
Bottom line: Hospital leaders subsidize pediatric HM programs based on the belief that the hospitalists positively impact patient and referring physician satisfaction.
Citation: Freed GL, Dunham KM, Switalski KE, et al. Assessing the value of pediatric hospitalist programs: the perspective of hospital leaders. Acad Pediatr. 2009;9(3):192-196.
Planned Partnerships
A day in the life of a hospitalist is not spent in a vacuum. Every day in hospitals across the country, hospitalists coordinate patient care with a host of other physicians, caregivers, and administrators. One minute, a hospitalist could be managing a patient’s treatment with a physician assistant; the next minute, the hospitalist could be reviewing a diagnosis from a cardiologist. The same hospitalist might finish the shift by reporting valuable quality-improvement (QI) data to the hospital’s management staff.
It’s that kind of collaboration that is the hallmark of HM, so it makes sense that the same level of collaboration take place between SHM and a bevy of other healthcare-related organizations.
“The delivery of hospital-based care is a team sport,” says Joe Miller, SHM’s executive advisor to the CEO. “It requires coordination across disciplines, from clinical to managerial. Hospital medicine is in the middle of a complex system, and we can’t do it ourselves. If we’re going to be successful, we need to forge partnerships.”
Chapter Updates
Indiana Chapter

The chapter met June 2 at the Tomato Pie Bistro in Indianapolis. The meeting kicked off with a welcome from chapter President Angela Corea, MD, assistant medical director at Saint Vincent Healthcare in Indianapolis, and nominations for the chapter’s 2010 officers.
Mark Bochan, MD, an infectious-disease specialist at St. Vincent’s, spoke to the group about candida and aspergillus infections. Special guest Scott Flanders, MD, FHM, president of SHM, discussed his thoughts on the growth of HM and the challenges currently facing hospitalists. He then opened up the floor for a brief question-and-answer session.
Palmetto/Eastern South Carolina Chapter
The chapter met May 28 at Victor’s Restaurant in Florence. Chapter president Beth Cardosi, DO, a hospitalist with McLeod Inpatient Services in Darlington, welcomed everyone and introduced the guest speaker, Kevin Shea, MD. Dr. Shea presented a program to the group on gram-negative infections in the hospital setting.
Milwaukee Chapter
The chapter met June 8 at Columbia Hospital. Four HM groups attended the meeting. Chapter goals for the coming months were set, including QI, advocacy, policy, and membership initiatives.
Those partnerships have been critical to SHM’s ability to create educational programs and practice management resources. It also factors into SHM’s efforts to enhance patient satisfaction and advocate for QI in healthcare. The list of SHM’s partner organizations and joint projects is an alphabet soup that includes the nation’s most influential professional societies, academies, and government entities, each of which is working to improve the delivery of care to hospitalized patients.
Small Start, Quick Growth
The relationship between SHM and the American Medical Association (AMA) began as a simple research project and has grown into a deeper collaboration. In 2007, the AMA’s Organized Medical Staff Section (OMSS), the department that advocates on behalf of physicians who are members of medical staffs and other organizations, wanted to increase understanding of how hospitalists, primary-care physicians, and other physicians work together in the hospital setting. The association collaborated with SHM to conduct a survey and obtain feedback from hospitalists.
The 2007 survey found that there was still work to be done between the organizations, namely the need for a set of guiding principles for a successful hospitalist practice. OMSS, SHM, AHA, and the Joint Commission developed the principles, which were recently endorsed by OMSS at the association’s annual conference in June.
“We feel they’re appropriate and make sense,” says Jim DeNuccio, director of AMA’s Organized Medical Staff, Group Practice, and Senior Physician Services.
The 2007 survey and the principles for a hospitalist practice have led to a new survey, conducted this year, to track how the issues and challenges within a hospital have changed. The initiatives are just the beginning of a long-term relationship between SHM and AMA.
“It’s very important for all of us to work together to continue to grow,” says DeNuccio, who cites AMA’s courses in practice management, QI, and patient safety as educational opportunities for hospitalists. “Our interest is in the patient. That’s what this is all about. The AMA and OMSS feel strongly that the profession needs to call the shots about how care is delivered in hospitals. They see that engaging the hospitalist is in the interest of the patient.”
SHM and AAPA: Educating Together
Hospitalists and physician assistants (PAs) work hand in hand to care for their patients. At the national level, SHM and the American Academy of Physician Assistants (AAPA) are coordinating educational programs to ensure PAs and hospitalists are properly informed and learning from the same page.
“It’s a very broad spectrum,” says Sharon Kulesz, AAPA director of alliance development and education. “We provide physician assistants with information about hospitalists, and we provide physicians with information about the benefit of working with physician assistants.”
Along with the American Academy of Nurse Practitioners (AANP), AAPA and SHM have coordinated educational programs at SHM’s annual meeting for hospitalists, and recently developed a stand-alone “Boot Camp” series for nurse practitioners and physician assistants to learn more about HM.
Kulesz notes, however, that not all of the education is exclusively for hospital-based workers. Some of the efforts are geared toward educating the public about hospitals’ patient-care teams. Regardless of the topic or the audience, the key is a comfortable working relationship between teams, she says.
“Our work with SHM is the model that I would like to use in all of our collaborations,” Kulesz says. “SHM gets us. They get what we can do and how a collaborative approach can be of benefit to everyone. It’s like an extended family.”
Patient-First Collaboration
The new Hospital Care Collaborative takes a team approach to hospital-based care. More than simply a partnership, the group brings together groups that represent healthcare professionals in the hospital—hospitalists, nurses, case managers, respiratory therapists, social workers—to find common approaches to QI and patient safety.
“As a group, the Hospital Care Collaborative is looking for ways to work together to improve the care of the hospitalized patient,” says Larry Wellikson, MD, FHM, CEO of SHM. “We’ve developed common principles, which have been ratified by each of our boards. At its core, the collaborative is looking for real-world ways to integrate medical professionals and help hospitals take a new approach to patient care.”
Part of the answer is in the education, development, and promotion of high-performance teams in hospital settings, Dr. Wellikson says. For instance, if a patient is admitted to the hospital with a blood clot, each team member has the opportunity to contribute his or her expertise and coordinate with others. The hospitalist might make the diagnosis, which leads to the prescription from the hospital pharmacist. With the diagnosis and list of prescriptions in hand, a nurse can then explain to the patient how the medications will affect their daily routine.
“In modern healthcare, no one professional or professional society can have all the perspectives you need,” Dr. Wellikson says. “In SHM’s approach, we’re looking at the hospital as a community, not a building. The problems we’re trying to solve are complex, and it requires an all-hands-on-deck approach. Knitting the perspectives and expertise together will be the key to treating the patient in the 21st century.” TH
Brendon Shank is a freelance writer based in Philadelphia.
A day in the life of a hospitalist is not spent in a vacuum. Every day in hospitals across the country, hospitalists coordinate patient care with a host of other physicians, caregivers, and administrators. One minute, a hospitalist could be managing a patient’s treatment with a physician assistant; the next minute, the hospitalist could be reviewing a diagnosis from a cardiologist. The same hospitalist might finish the shift by reporting valuable quality-improvement (QI) data to the hospital’s management staff.
It’s that kind of collaboration that is the hallmark of HM, so it makes sense that the same level of collaboration take place between SHM and a bevy of other healthcare-related organizations.
“The delivery of hospital-based care is a team sport,” says Joe Miller, SHM’s executive advisor to the CEO. “It requires coordination across disciplines, from clinical to managerial. Hospital medicine is in the middle of a complex system, and we can’t do it ourselves. If we’re going to be successful, we need to forge partnerships.”
Chapter Updates
Indiana Chapter
The chapter met June 2 at the Tomato Pie Bistro in Indianapolis. The meeting kicked off with a welcome from chapter President Angela Corea, MD, assistant medical director at Saint Vincent Healthcare in Indianapolis, and nominations for the chapter’s 2010 officers.
Mark Bochan, MD, an infectious-disease specialist at St. Vincent’s, spoke to the group about candida and aspergillus infections. Special guest Scott Flanders, MD, FHM, president of SHM, discussed his thoughts on the growth of HM and the challenges currently facing hospitalists. He then opened up the floor for a brief question-and-answer session.
Palmetto/Eastern South Carolina Chapter
The chapter met May 28 at Victor’s Restaurant in Florence. Chapter president Beth Cardosi, DO, a hospitalist with McLeod Inpatient Services in Darlington, welcomed everyone and introduced the guest speaker, Kevin Shea, MD. Dr. Shea presented a program to the group on gram-negative infections in the hospital setting.
Milwaukee Chapter
The chapter met June 8 at Columbia Hospital. Four HM groups attended the meeting. Chapter goals for the coming months were set, including QI, advocacy, policy, and membership initiatives.
Those partnerships have been critical to SHM’s ability to create educational programs and practice management resources. It also factors into SHM’s efforts to enhance patient satisfaction and advocate for QI in healthcare. The list of SHM’s partner organizations and joint projects is an alphabet soup that includes the nation’s most influential professional societies, academies, and government entities, each of which is working to improve the delivery of care to hospitalized patients.
Small Start, Quick Growth
The relationship between SHM and the American Medical Association (AMA) began as a simple research project and has grown into a deeper collaboration. In 2007, the AMA’s Organized Medical Staff Section (OMSS), the department that advocates on behalf of physicians who are members of medical staffs and other organizations, wanted to increase understanding of how hospitalists, primary-care physicians, and other physicians work together in the hospital setting. The association collaborated with SHM to conduct a survey and obtain feedback from hospitalists.
The 2007 survey found that there was still work to be done between the organizations, namely the need for a set of guiding principles for a successful hospitalist practice. OMSS, SHM, AHA, and the Joint Commission developed the principles, which were recently endorsed by OMSS at the association’s annual conference in June.
“We feel they’re appropriate and make sense,” says Jim DeNuccio, director of AMA’s Organized Medical Staff, Group Practice, and Senior Physician Services.
The 2007 survey and the principles for a hospitalist practice have led to a new survey, conducted this year, to track how the issues and challenges within a hospital have changed. The initiatives are just the beginning of a long-term relationship between SHM and AMA.
“It’s very important for all of us to work together to continue to grow,” says DeNuccio, who cites AMA’s courses in practice management, QI, and patient safety as educational opportunities for hospitalists. “Our interest is in the patient. That’s what this is all about. The AMA and OMSS feel strongly that the profession needs to call the shots about how care is delivered in hospitals. They see that engaging the hospitalist is in the interest of the patient.”
SHM and AAPA: Educating Together
Hospitalists and physician assistants (PAs) work hand in hand to care for their patients. At the national level, SHM and the American Academy of Physician Assistants (AAPA) are coordinating educational programs to ensure PAs and hospitalists are properly informed and learning from the same page.
“It’s a very broad spectrum,” says Sharon Kulesz, AAPA director of alliance development and education. “We provide physician assistants with information about hospitalists, and we provide physicians with information about the benefit of working with physician assistants.”
Along with the American Academy of Nurse Practitioners (AANP), AAPA and SHM have coordinated educational programs at SHM’s annual meeting for hospitalists, and recently developed a stand-alone “Boot Camp” series for nurse practitioners and physician assistants to learn more about HM.
Kulesz notes, however, that not all of the education is exclusively for hospital-based workers. Some of the efforts are geared toward educating the public about hospitals’ patient-care teams. Regardless of the topic or the audience, the key is a comfortable working relationship between teams, she says.
“Our work with SHM is the model that I would like to use in all of our collaborations,” Kulesz says. “SHM gets us. They get what we can do and how a collaborative approach can be of benefit to everyone. It’s like an extended family.”
Patient-First Collaboration
The new Hospital Care Collaborative takes a team approach to hospital-based care. More than simply a partnership, the group brings together groups that represent healthcare professionals in the hospital—hospitalists, nurses, case managers, respiratory therapists, social workers—to find common approaches to QI and patient safety.
“As a group, the Hospital Care Collaborative is looking for ways to work together to improve the care of the hospitalized patient,” says Larry Wellikson, MD, FHM, CEO of SHM. “We’ve developed common principles, which have been ratified by each of our boards. At its core, the collaborative is looking for real-world ways to integrate medical professionals and help hospitals take a new approach to patient care.”
Part of the answer is in the education, development, and promotion of high-performance teams in hospital settings, Dr. Wellikson says. For instance, if a patient is admitted to the hospital with a blood clot, each team member has the opportunity to contribute his or her expertise and coordinate with others. The hospitalist might make the diagnosis, which leads to the prescription from the hospital pharmacist. With the diagnosis and list of prescriptions in hand, a nurse can then explain to the patient how the medications will affect their daily routine.
“In modern healthcare, no one professional or professional society can have all the perspectives you need,” Dr. Wellikson says. “In SHM’s approach, we’re looking at the hospital as a community, not a building. The problems we’re trying to solve are complex, and it requires an all-hands-on-deck approach. Knitting the perspectives and expertise together will be the key to treating the patient in the 21st century.” TH
Brendon Shank is a freelance writer based in Philadelphia.
A day in the life of a hospitalist is not spent in a vacuum. Every day in hospitals across the country, hospitalists coordinate patient care with a host of other physicians, caregivers, and administrators. One minute, a hospitalist could be managing a patient’s treatment with a physician assistant; the next minute, the hospitalist could be reviewing a diagnosis from a cardiologist. The same hospitalist might finish the shift by reporting valuable quality-improvement (QI) data to the hospital’s management staff.
It’s that kind of collaboration that is the hallmark of HM, so it makes sense that the same level of collaboration take place between SHM and a bevy of other healthcare-related organizations.
“The delivery of hospital-based care is a team sport,” says Joe Miller, SHM’s executive advisor to the CEO. “It requires coordination across disciplines, from clinical to managerial. Hospital medicine is in the middle of a complex system, and we can’t do it ourselves. If we’re going to be successful, we need to forge partnerships.”
Chapter Updates
Indiana Chapter
The chapter met June 2 at the Tomato Pie Bistro in Indianapolis. The meeting kicked off with a welcome from chapter President Angela Corea, MD, assistant medical director at Saint Vincent Healthcare in Indianapolis, and nominations for the chapter’s 2010 officers.
Mark Bochan, MD, an infectious-disease specialist at St. Vincent’s, spoke to the group about candida and aspergillus infections. Special guest Scott Flanders, MD, FHM, president of SHM, discussed his thoughts on the growth of HM and the challenges currently facing hospitalists. He then opened up the floor for a brief question-and-answer session.
Palmetto/Eastern South Carolina Chapter
The chapter met May 28 at Victor’s Restaurant in Florence. Chapter president Beth Cardosi, DO, a hospitalist with McLeod Inpatient Services in Darlington, welcomed everyone and introduced the guest speaker, Kevin Shea, MD. Dr. Shea presented a program to the group on gram-negative infections in the hospital setting.
Milwaukee Chapter
The chapter met June 8 at Columbia Hospital. Four HM groups attended the meeting. Chapter goals for the coming months were set, including QI, advocacy, policy, and membership initiatives.
Those partnerships have been critical to SHM’s ability to create educational programs and practice management resources. It also factors into SHM’s efforts to enhance patient satisfaction and advocate for QI in healthcare. The list of SHM’s partner organizations and joint projects is an alphabet soup that includes the nation’s most influential professional societies, academies, and government entities, each of which is working to improve the delivery of care to hospitalized patients.
Small Start, Quick Growth
The relationship between SHM and the American Medical Association (AMA) began as a simple research project and has grown into a deeper collaboration. In 2007, the AMA’s Organized Medical Staff Section (OMSS), the department that advocates on behalf of physicians who are members of medical staffs and other organizations, wanted to increase understanding of how hospitalists, primary-care physicians, and other physicians work together in the hospital setting. The association collaborated with SHM to conduct a survey and obtain feedback from hospitalists.
The 2007 survey found that there was still work to be done between the organizations, namely the need for a set of guiding principles for a successful hospitalist practice. OMSS, SHM, AHA, and the Joint Commission developed the principles, which were recently endorsed by OMSS at the association’s annual conference in June.
“We feel they’re appropriate and make sense,” says Jim DeNuccio, director of AMA’s Organized Medical Staff, Group Practice, and Senior Physician Services.
The 2007 survey and the principles for a hospitalist practice have led to a new survey, conducted this year, to track how the issues and challenges within a hospital have changed. The initiatives are just the beginning of a long-term relationship between SHM and AMA.
“It’s very important for all of us to work together to continue to grow,” says DeNuccio, who cites AMA’s courses in practice management, QI, and patient safety as educational opportunities for hospitalists. “Our interest is in the patient. That’s what this is all about. The AMA and OMSS feel strongly that the profession needs to call the shots about how care is delivered in hospitals. They see that engaging the hospitalist is in the interest of the patient.”
SHM and AAPA: Educating Together
Hospitalists and physician assistants (PAs) work hand in hand to care for their patients. At the national level, SHM and the American Academy of Physician Assistants (AAPA) are coordinating educational programs to ensure PAs and hospitalists are properly informed and learning from the same page.
“It’s a very broad spectrum,” says Sharon Kulesz, AAPA director of alliance development and education. “We provide physician assistants with information about hospitalists, and we provide physicians with information about the benefit of working with physician assistants.”
Along with the American Academy of Nurse Practitioners (AANP), AAPA and SHM have coordinated educational programs at SHM’s annual meeting for hospitalists, and recently developed a stand-alone “Boot Camp” series for nurse practitioners and physician assistants to learn more about HM.
Kulesz notes, however, that not all of the education is exclusively for hospital-based workers. Some of the efforts are geared toward educating the public about hospitals’ patient-care teams. Regardless of the topic or the audience, the key is a comfortable working relationship between teams, she says.
“Our work with SHM is the model that I would like to use in all of our collaborations,” Kulesz says. “SHM gets us. They get what we can do and how a collaborative approach can be of benefit to everyone. It’s like an extended family.”
Patient-First Collaboration
The new Hospital Care Collaborative takes a team approach to hospital-based care. More than simply a partnership, the group brings together groups that represent healthcare professionals in the hospital—hospitalists, nurses, case managers, respiratory therapists, social workers—to find common approaches to QI and patient safety.
“As a group, the Hospital Care Collaborative is looking for ways to work together to improve the care of the hospitalized patient,” says Larry Wellikson, MD, FHM, CEO of SHM. “We’ve developed common principles, which have been ratified by each of our boards. At its core, the collaborative is looking for real-world ways to integrate medical professionals and help hospitals take a new approach to patient care.”
Part of the answer is in the education, development, and promotion of high-performance teams in hospital settings, Dr. Wellikson says. For instance, if a patient is admitted to the hospital with a blood clot, each team member has the opportunity to contribute his or her expertise and coordinate with others. The hospitalist might make the diagnosis, which leads to the prescription from the hospital pharmacist. With the diagnosis and list of prescriptions in hand, a nurse can then explain to the patient how the medications will affect their daily routine.
“In modern healthcare, no one professional or professional society can have all the perspectives you need,” Dr. Wellikson says. “In SHM’s approach, we’re looking at the hospital as a community, not a building. The problems we’re trying to solve are complex, and it requires an all-hands-on-deck approach. Knitting the perspectives and expertise together will be the key to treating the patient in the 21st century.” TH
Brendon Shank is a freelance writer based in Philadelphia.
JHM Names Baudendistel CME Editor

Some physicians have an interest in teaching; some are really good at it, and some make a career out of it. For Thomas Baudendistel, MD, FACP, teaching comes second nature and, as one of his former colleagues says, is a definition of who he is.
It’s those qualities, his experience in both academic and community hospital settings, and a passion for innovation that Dr. Baudendistel, the internal-medicine residency program director for Kaiser Permanente in Oakland, Calif., hopes to infuse as CME editor of the Journal of Hospital Medicine (JHM).
He was appointed to the new position in June. The first issue containing article-level CME, the answers to which will be submitted online, is scheduled to appear in the October issue.
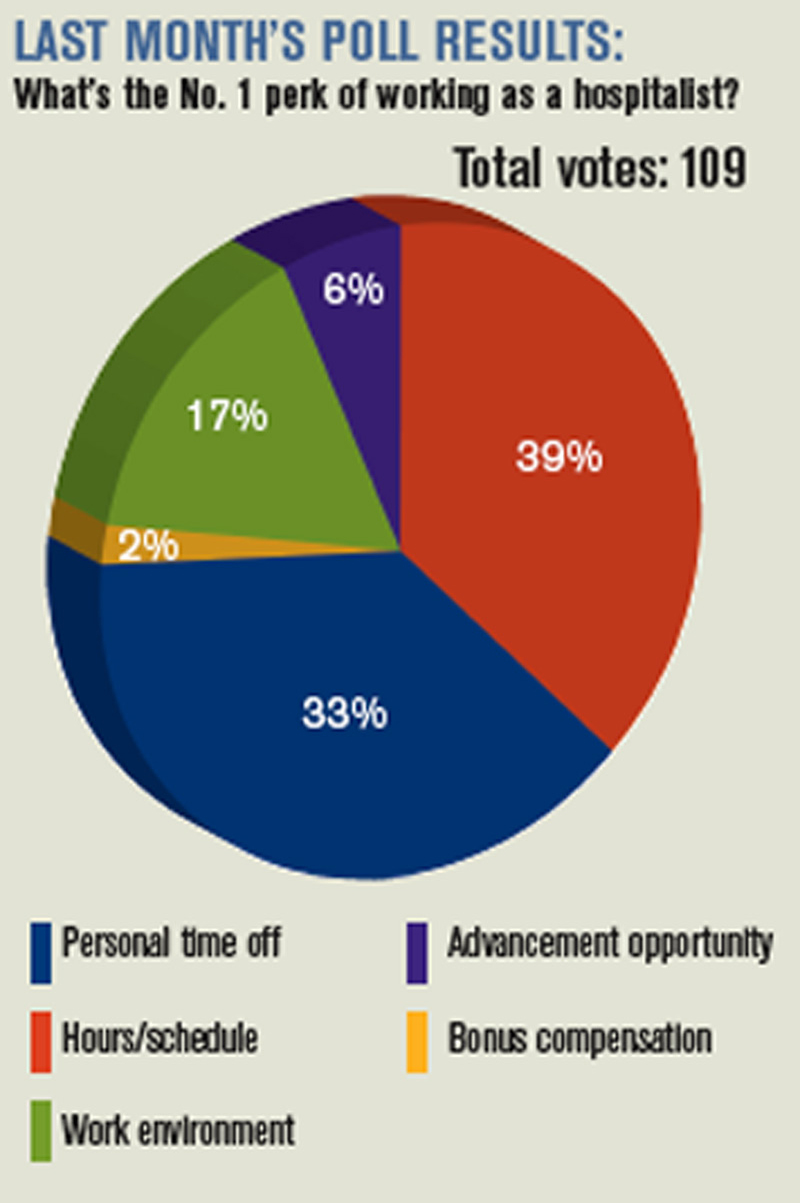
“Tom is a superlative educator. He has defined himself that way. He has a passion for it and a talent for it,” says Brian J. Harte, MD, FHM, chair of the department of hospital medicine at The Cleveland Clinic and a deputy editor of JHM.
Dr. Harte, who first met Dr. Baudendistel in 1996 during his residency at the University of California at San Francisco, says his former mentor “can take a submission, drill down to the most important teaching point, and challenge the readership.”
Dr. Baudendistel admits teaching is why he “gets out of bed in the morning.” He says he wants to take advantage of the young, tech-savvy nature of most HM physicians.
“JHM has been an innovative journal. I see the CME piece as being equally innovative,” says Dr. Baudendistel, who served four years as a JHM associate editor. “I’d like to move [CME] past the pencil-and-paper phase.” TH
Some physicians have an interest in teaching; some are really good at it, and some make a career out of it. For Thomas Baudendistel, MD, FACP, teaching comes second nature and, as one of his former colleagues says, is a definition of who he is.
It’s those qualities, his experience in both academic and community hospital settings, and a passion for innovation that Dr. Baudendistel, the internal-medicine residency program director for Kaiser Permanente in Oakland, Calif., hopes to infuse as CME editor of the Journal of Hospital Medicine (JHM).
He was appointed to the new position in June. The first issue containing article-level CME, the answers to which will be submitted online, is scheduled to appear in the October issue.
“Tom is a superlative educator. He has defined himself that way. He has a passion for it and a talent for it,” says Brian J. Harte, MD, FHM, chair of the department of hospital medicine at The Cleveland Clinic and a deputy editor of JHM.
Dr. Harte, who first met Dr. Baudendistel in 1996 during his residency at the University of California at San Francisco, says his former mentor “can take a submission, drill down to the most important teaching point, and challenge the readership.”
Dr. Baudendistel admits teaching is why he “gets out of bed in the morning.” He says he wants to take advantage of the young, tech-savvy nature of most HM physicians.
“JHM has been an innovative journal. I see the CME piece as being equally innovative,” says Dr. Baudendistel, who served four years as a JHM associate editor. “I’d like to move [CME] past the pencil-and-paper phase.” TH
Some physicians have an interest in teaching; some are really good at it, and some make a career out of it. For Thomas Baudendistel, MD, FACP, teaching comes second nature and, as one of his former colleagues says, is a definition of who he is.
It’s those qualities, his experience in both academic and community hospital settings, and a passion for innovation that Dr. Baudendistel, the internal-medicine residency program director for Kaiser Permanente in Oakland, Calif., hopes to infuse as CME editor of the Journal of Hospital Medicine (JHM).
He was appointed to the new position in June. The first issue containing article-level CME, the answers to which will be submitted online, is scheduled to appear in the October issue.
“Tom is a superlative educator. He has defined himself that way. He has a passion for it and a talent for it,” says Brian J. Harte, MD, FHM, chair of the department of hospital medicine at The Cleveland Clinic and a deputy editor of JHM.
Dr. Harte, who first met Dr. Baudendistel in 1996 during his residency at the University of California at San Francisco, says his former mentor “can take a submission, drill down to the most important teaching point, and challenge the readership.”
Dr. Baudendistel admits teaching is why he “gets out of bed in the morning.” He says he wants to take advantage of the young, tech-savvy nature of most HM physicians.
“JHM has been an innovative journal. I see the CME piece as being equally innovative,” says Dr. Baudendistel, who served four years as a JHM associate editor. “I’d like to move [CME] past the pencil-and-paper phase.” TH
Beta-blockers for hypertension: Are they going out of style?
In recent years the role of beta-blockers as a primary tool to treat hypertension has come under question. These drugs have shown disappointing results when used as antihypertensive therapy in patients without heart disease, ie, when used as primary prevention. At the same time, beta-blockers clearly reduce the risk of future cardiovascular events in patients who already have heart disease, eg, who already have had a myocardial infarction or who have congestive heart failure.
Several meta-analyses and a few clinical trials have shown that beta-blockers may have no advantage over other antihypertensive drugs, and in fact may not reduce the risk of stroke as effectively as other classes of blood pressure medications.
Why should this be? Is it that the patients in the antihypertensive trials were mostly older, and that beta-blockers do not work as well in older patients as in younger ones? Or does it have to do with the fact that atenolol (Tenormin) was the drug most often used in the trials? Would newer, different beta-blockers be better?
Hypertension experts currently disagree on how to interpret the available data, and this has led to conflict and confusion among clinicians as to the role of beta-blockers in managing hypertension. Current evidence suggests that older beta-blockers may not be the preferred first-line antihypertensive drugs for hypertensive patients who have no compelling indications for them (eg, heart failure, myocardial infarction, diabetes, high risk of coronary heart disease). However, newer beta-blockers with vasodilatory properties should be considered in cases of uncontrolled or resistant hypertension, especially in younger patients.
Further, while controversy and debate continue over the benefits and adverse effects of one class of antihypertensive drugs vs another, it is indisputable that controlling arterial blood pressure to the recommended goal offers major protection against cardiovascular and renal events in patients with hypertension.1,2
MECHANISM OF ACTION OF BETA-BLOCKERS
Beta-blockers effectively reduce blood pressure in both systolic-diastolic hypertension and isolated systolic hypertension.3–5 Exactly how is not known, but it has been proposed that they may do so by:
Reducing the heart rate and cardiac output. When catecholamines activate beta-1 receptors in the heart, the heart rate and myocardial contractility increase. By blocking beta-1 receptors, beta-blockers reduce the heart rate and myocardial contractility, thus lowering cardiac output and arterial blood pressure.6
Inhibiting renin release. Activation of the renin-angiotensin system is another major pathway that can lead to elevated arterial blood pressure. Renin release is mediated through the sympathetic nervous system via beta-1 receptors on the juxtaglomerular cells of the kidney. Beta-blockers can therefore lower blood pressure by inhibiting renin release.7
Inhibiting central nervous sympathetic outflow, thereby inducing presynaptic blockade, which in turn reduces the release of catecholamines.
Reducing venous return and plasma volume.
Generating nitric oxide, thus reducing peripheral vascular resistance (some agents).8
Reducing vasomotor tone.
Reducing vascular tone.
Improving vascular compliance.
Resetting baroreceptor levels.
Attenuating the pressor response to catecholamines with exercise and stress.
HETEROGENEITY OF BETA-BLOCKERS
Selectivity
Beta-blockers are not all the same. They can be classified into three categories.
Nonselective beta-blockers block both beta-1 and beta-2 adrenergic receptors. It is generally accepted that beta-blockers exert their primary antihypertensive effect by blocking beta-1 adrenergic receptors.6 Of interest, nonselective beta-blockers inhibit beta-2 receptors on arteries and thus cause an unopposed alpha-adrenergic effect, leading to increased peripheral vascular resistance.9 Examples of this category:
- Nadolol (Corgard)
- Pindolol (Visken)
- Propranolol (Inderal)
- Timolol (Blocadren).
Selective beta-blockers specifically block beta-1 receptors alone, although they are known to be nonselective at higher doses. Examples:
- Atenolol (Tenormin)
- Betaxolol (Kerlone)
- Bisoprolol (Zebeta)
- Esmolol (Brevibloc)
- Metoprolol (Lopressor, Toprol).
Beta-blockers with peripheral vasodilatatory effects act either via antagonism of the alpha-1 receptor, as with labetolol (Normodyne) and carvedilol (Coreg),10 or via enhanced release of nitric oxide, as with nebivolol (Bystolic).8
Lipid and water solubility
The lipid solubility and water solubility of each beta-blocker determine its bioavailability and side-effect profile.
Lipid solubility determines the degree to which a beta-blocker penetrates the blood-brain barrier and thereby leads to central nervous system side effects such as lethargy, nightmares, confusion, and depression. Propranolol is highly lipid-soluble; metoprolol and labetalol are moderately so.
Water-soluble beta-blockers such as atenolol have less tissue permeation, have a longer half-life, and cause fewer central nervous system effects and symptoms.11
Routes of elimination
Beta-blockers also differ in their route of elimination.
Atenolol and nadolol are eliminated by the kidney and require dose adjustment in patients with impaired renal function.12,13
On the other hand, propranolol, metoprolol, labetalol, carvedilol, and nebivolol are excreted primarily via hepatic metabolism.13
BETA-BLOCKERS IN THE MANAGEMENT OF HYPERTENSION
Beta-blockers were initially used to treat arrhythmias, but by the early 1970s they were also widely accepted for managing hypertension. 14 Their initial acceptance as one of the first-line classes of drugs for hypertension was based on their better side-effect profile compared with other antihypertensive drugs available at that time.
In the 1980s and 1990s, beta-blockers were listed as preferred first-line antihypertensive drugs along with diuretics in national hypertension guidelines.15 Subsequent updates of the guidelines favored diuretics as initial therapy and relegated all other classes of antihypertensive medications to be alternatives to diuretics.16 Although beta-blockers remain alternative first-line drugs in the latest guidelines (published in 2003; see reference 66), they are the preferred antihypertensive agents for patients with cardiac disease.
The current recommendations reflect the findings from hypertension trials in which patients with myocardial infarction and congestive heart failure had better cardiovascular outcomes if they received these drugs,17–19 including a lower risk of death.20,21 It was widely assumed that beta-blockers would also prevent first episodes of cardiovascular events.
However, to date, there is no evidence that beta-blockers are effective as primary prevention. Several large randomized controlled trials showed no benefit with beta-blockers compared with other antihypertensive drugs—in fact, there were more cardiovascular events with beta-blockers (see below).
Beta-blockers are well tolerated in clinical practice, although they can have side effects that include fatigue, depression, impaired exercise tolerance, sexual dysfunction, and asthma attacks.
Wiysonge et al22 analyzed how many patients withdrew from randomized trials of antihypertensive treatment because of drug-related adverse events. There was no significant difference in the incidence of fatigue, depressive symptoms, or sexual dysfunction with beta-blockers compared with placebo, and trial participants on a beta-blocker were not statistically significantly more likely to discontinue treatment than those receiving a placebo in three trials with 22,729 participants (relative risk [RR] 2.34, 95% confidence interval [CI] 0.84–6.52).
THE CONTROVERSY: WHAT THE TRIALS SHOWED
Messerli et al23 performed a meta-analysis published in 1998 that suggested that beta-blockers may not be as effective as diuretics in preventing cardiovascular events when used as first-line antihypertensive therapy in elderly patients. In 10 randomized controlled trials in 16,164 patients who were treated with either a diuretic or a beta-blocker (atenolol), blood pressure was normalized in two-thirds of diuretic-treated patients but only one-third of patients treated with atenolol as monotherapy. Diuretic therapy was superior with regard to all end points, and beta-blockers were found to be ineffective except in reducing cerebrovascular events.
The LIFE study (Losartan Intervention for Endpoint Reduction in Hypertension)24 compared the angiotensin-receptor blocker losartan (Cozaar) and atenolol in 9,193 patients with hypertension and left ventricular hypertrophy. At 4 years of follow-up, the rate of primary cardiovascular events (death, myocardial infarction, or stroke) was lower in the losartan group than in the atenolol group. The difference was mainly due to a 25% lower incidence of stroke, which was statistically significant. The rates of myocardial infarction and death from cardiovascular causes were not significantly different between the two treatment groups. The systolic blood pressure was 1 mm Hg lower in the losartan group than in the atenolol group, which was statistically significant.
Carlberg et al25 performed another important meta-analysis that questioned whether atenolol reduces rates of cardiovascular morbidity and death in hypertensive patients. The results were surprising: eight randomized controlled trials including more than 6,000 patients and comparing atenolol with placebo or no treatment showed no differences between the treatment groups with regard to the outcomes of all-cause mortality (RR 1.01, 95% CI 0.89–1.15), cardiovascular mortality (RR 0.99, 95% CI 0.83–1.18), or myocardial infarction (RR 0.99, 95% CI 0.83–1.19).
In addition, when atenolol was compared with other antihypertensives in five other randomized controlled trials that included more than 14,000 patients, those treated with atenolol had a higher risk of stroke (RR 1.30, 95% CI 1.12–1.50) and death (RR 1.13, 95% CI 1.02–1.25).
The ASCOT-BPLA trial (Anglo-Scandinavian Cardiac Outcomes Trial—Blood Pressure Lowering Arm)26 had similar results. This trial compared the combination of atenolol plus the diuretic bendroflumethiazide against the combination of the calcium channel blocker amlodipine (Norvasc) plus the angiotensin-converting enzyme (ACE) inhibitor perindopril (Aceon). Although no significant difference was seen in the primary outcome of nonfatal myocardial infarction or fatal coronary heart disease (unadjusted hazard ratio [HR] with amlodipine-perindopril 0.90, 95% CI 0.79–1.02, P = .1052), the amlodipine-plus-perindopril group had significantly fewer strokes (327 vs 422, HR 0.77, 95% CI 0.66–0.89, P = .0003), fewer total cardiovascular events (1,362 vs 1,602, HR 0.84, 95% CI 0.78–0.90, P = .0001), and fewer deaths from any cause (738 vs 820; HR 0.89, 95% CI 0.81–0.99, P = .025).
Lindholm et al27 performed a meta-analysis that included studies of selective beta-blockers (including atenolol) and nonselective beta-blockers, with a follow-up time of more than 2 years. Compared with placebo or no treatment, beta-blockers reduced the risk of stroke by 19% but had no effect on myocardial infarction or all-cause mortality. Compared with other antihypertensive drugs, beta-blockers were less than optimum, and the relative risk of stroke was 16% higher. Atenolol was the beta-blocker used in most of the randomized clinical trials included in this meta-analysis.
The Cochrane group22 found beta-blockers to be inferior to all other antihypertensive drugs with respect to the ability to lower the risk of stroke.
WHY WERE THE RESULTS SO DISAPPOINTING?
Problems with atenolol
Most of the trials in the meta-analyses discussed above used atenolol and other beta-blockers that had no vasodilatory properties.
Further, in most of the trials atenolol was used in a once-daily dosage, whereas ideally it needs to be taken more frequently, based on its pharmacokinetic and pharmacodynamic properties (a half-life of 6–9 hours).3 Neutel et al28 confirmed that atenolol, when taken once daily, leaves the patient unprotected in the last 6 hours of a 24-hour period, as demonstrated by 24-hour ambulatory blood pressure monitoring. It is possible that this short duration of action of atenolol may have contributed to the results observed in clinical trials that used atenolol to treat hypertension.
Differences between older and younger patients
Another possible reason for the disappointing results is that the trials included many elderly patients, in whom beta-blockers may not be as effective. The pathophysiology of hypertension in younger people is different from that in older patients.29 Hemodynamic characteristics of younger hypertensive patients include a high cardiac output and hyperdynamic circulation with a low pulse pressure, while older patients have lower arterial compliance with an elevated vascular resistance.
The notion of choosing antihypertensive medications on the basis of age and age-related pathophysiology is supported by several clinical studies. Randomized controlled trials appear to show that beta-blockers are effective in younger hypertensive patients.30
Conversely, the CAFE (Conduit Artery Function Evaluation) trial,31 a substudy of the main ASCOT trial,26 indicated that betablocker-based therapy was less effective in reducing central aortic pressure than were regimens based on an ACE inhibitor or a calcium channel blocker.
The CAFE researchers recruited 2,073 patients from five ASCOT centers and used radial artery applanation tonometry and pulse-wave analysis to derive central aortic pressures and hemodynamic indices during study visits up to a period of 4 years. Although the two treatment groups achieved similar brachial systolic blood pressures, the central aortic systolic pressure was 4.3 mm Hg lower in the amlodipine group (95% CI 3.3–5.4; P < .0001), and the central aortic pulse pressure was 3.0 mm Hg lower (95% CI 2.1–3.9; P < .0001).
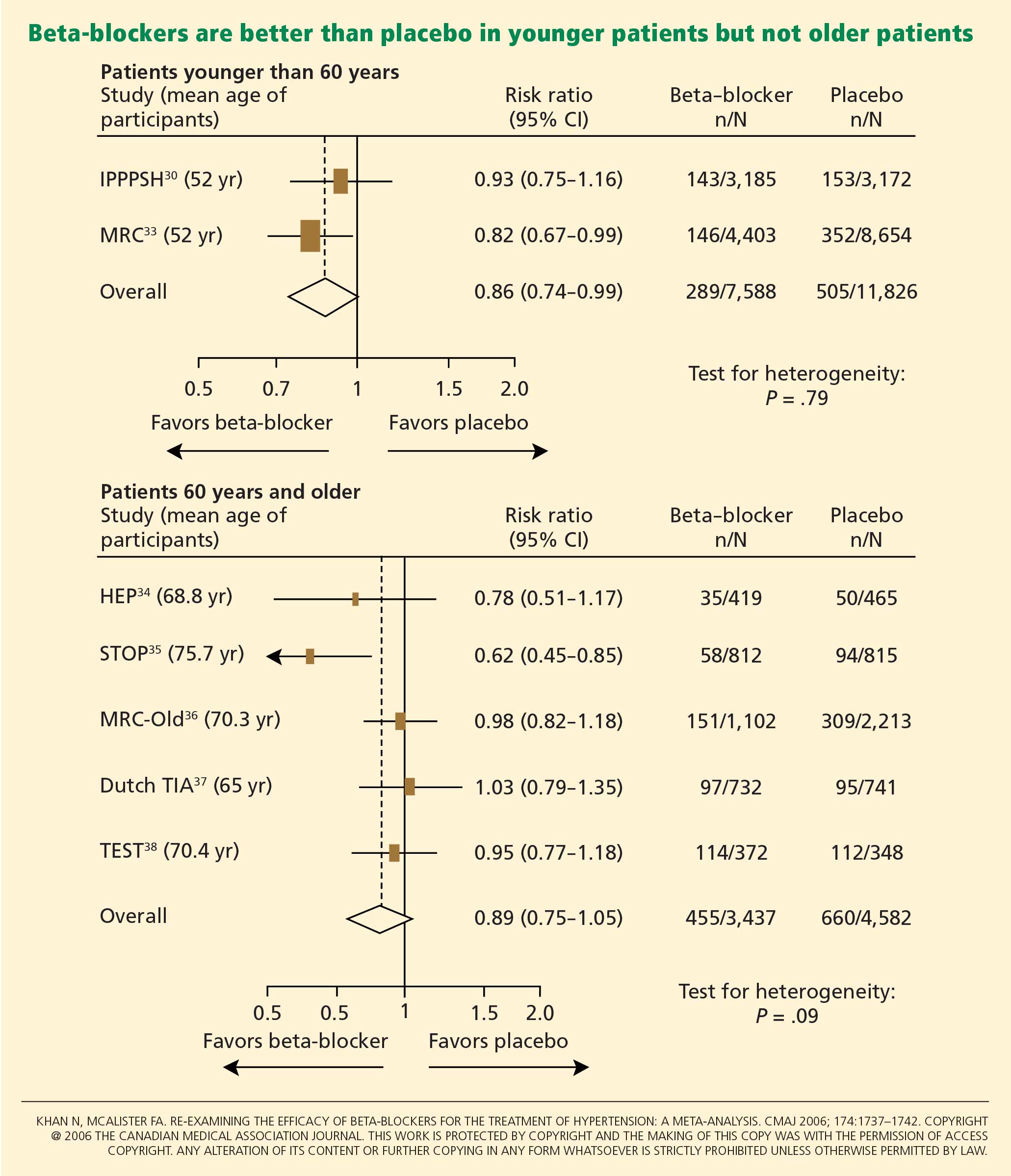
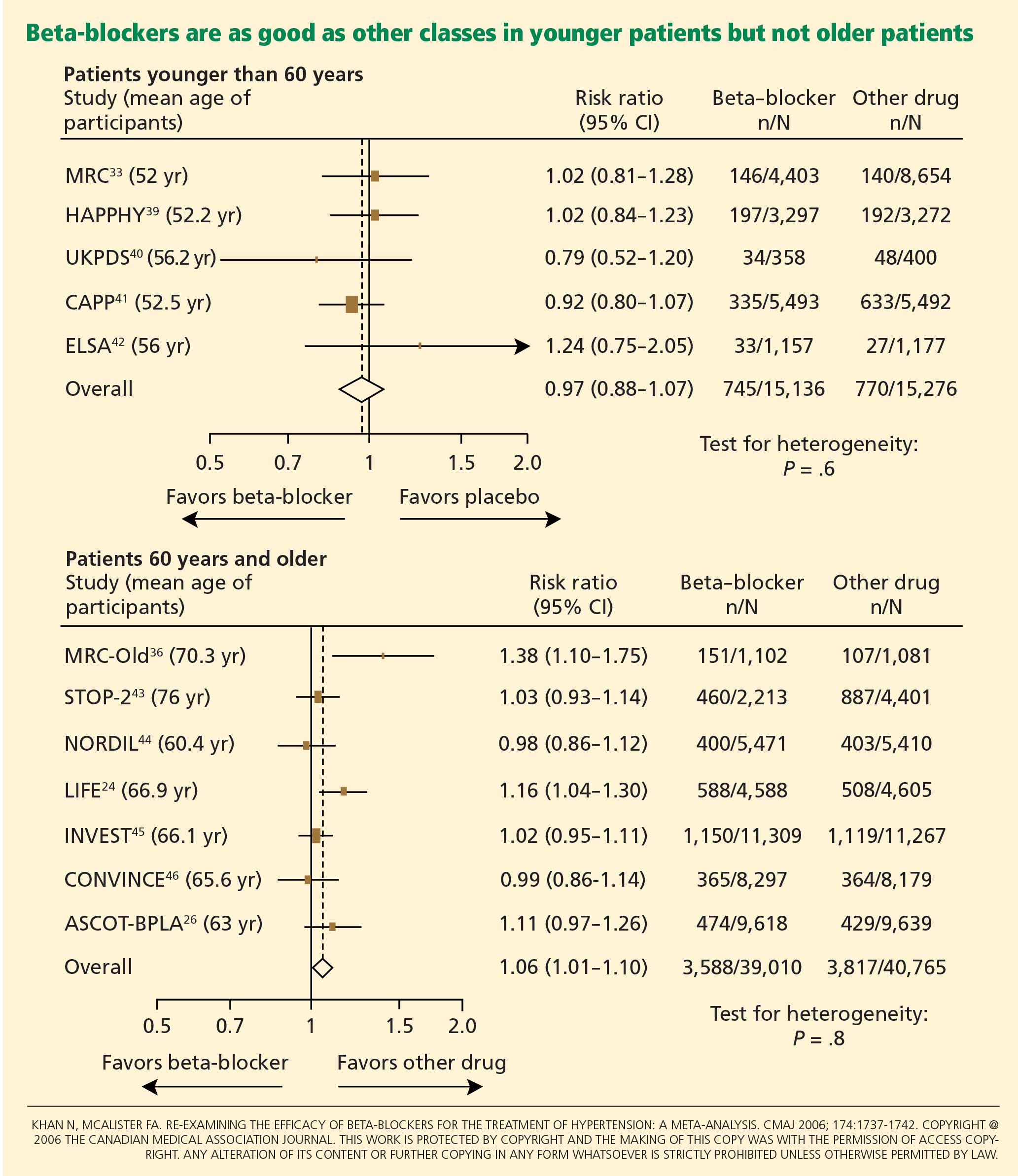
Pulse-wave dyssynchrony
Bangalore et al47 offer an interesting hypothesis to explain the probable adverse effect of beta-blockers. Their theory concerns the effect of these drugs on the arterial pulse wave.
Normally, with each contraction of the left ventricle during systole, an arterial pulse wave is generated and propagated forward to the peripheral arteries. This wave is then reflected back to the heart from the branching points of peripheral arteries. The final form of the pressure wave at the aortic root is a synchronized summation of the forward-traveling wave and the backward-reflected wave.
In healthy people with normal arteries, the reflected wave merges with the forward-traveling wave in diastole and augments coronary blood flow. In patients whose arteries are stiff due to aging or vascular comorbidities, the reflected wave returns faster and merges with the incident wave in systole, resulting in higher left ventricular afterload and less coronary perfusion.48
Bangalore et al47 propose that artificially reducing the heart rate with beta-blockers may further dyssynchronize the pulse wave, adversely affecting coronary perfusion and leading to an increased risk of cardiovascular events and death.
Metabolic side effects
Older beta-blockers, and especially atenolol, have well-known metabolic adverse effects, particularly impairment of glycemic control. This adverse effect appears to occur only with beta-blockers that do not possess vasodilatory properties and thus increase peripheral vascular resistance, which results in lower glucose availability and reduced uptake by skeletal muscles.49
Bangalore et al50 evaluated the effect of beta-blockers in a meta-analysis of 12 studies in 94,492 patients followed up for more than 1 year. Beta-blocker therapy resulted in a 22% higher risk of new-onset diabetes mellitus (RR 1.22, 95% CI 1.12–1.33) than with other nondiuretic antihypertensive agents.
Of note, however, the meta-analysis did not show a significantly higher risk of the onset of diabetes with propranolol or metoprolol than with other nondiuretic antihypertensives when studies of these beta-blockers were separated from atenolol-based studies.
Further, the United Kingdom Prospective Diabetes Study40 found that cardiovascular outcomes in patients with good blood pressure control were similar when atenolol-based therapy was compared with therapy with the ACE inhibitor captopril (Capoten).
A meta-analysis conducted by Balamuthusamy et al51 in 2009 found no higher risk of stroke in patients with hypertension and diabetes mellitus who received beta-blockers than in those who received other antihypertensive medications. However, beta-blockers were associated with a higher risk of death from cardiovascular causes (RR 1.39, 95% CI 1.07–1.804; P < .01) compared with reninangiotensin blockade.
NEWER BETA-BLOCKERS MAY BE BETTER
In the United States, more than 40 million prescriptions for atenolol are written every year, making it by far the most commonly used beta-blocker for the treatment of hypertension. 52 It is clear, however, that atenolol is not an ideal representative of this class of antihypertensive medications.
Preliminary data from studies of newer beta-blockers that possess beneficial vasodilatory properties are encouraging. Animal studies and preliminary human studies find that these new-generation beta-blockers cause fewer adverse metabolic effects and improve endothelial function, measures of arterial stiffness, and cardiovascular outcomes.
Carvedilol
Carvedilol is a nonselective beta-blocker with vasodilatory effects that are thought to be due to its ability to concurrently block alpha-1 receptors in addition to beta receptors. 53 In experiments in vitro and in trials in patients with diabetes and hypertension, carvedilol increased endothelial vasodilation and reduced inflammation and platelet aggregation. These effects may be achieved though antioxidant actions, thereby preserving nitric oxide bioactivity.54,55
In the Glycemic Effects in Diabetes Mellitus: Carvedilol-Metoprolol Comparison in Hypertensives (GEMINI) trial,56 carvedilol was associated with better maintenance of glycemic control in diabetic hypertensive patients than was metoprolol. Insulin sensitivity improved with carvedilol but not with metoprolol, and fewer patients on carvedilol progressed to microalbuminuria.
Nebivolol
Nebivolol is a novel selective beta-blocker with a much higher affinity for beta-1 adrenergic receptors than for beta-2 adrenergic receptors. Among all the beta-blockers in clinical use today, nebivolol has the highest selectivity for beta-1 receptors.8
Nebivolol causes vasodilation through activation of the l-arginine/nitric oxide pathway.57–59 Blockade of synthesis of nitric oxide leads to local arterial stiffness. Endothelial dysfunction is characterized by decreased bioavailability of nitric oxide and has been shown to be a strong predictor of cardiovascular outcomes. By generating nitric oxide, nebivolol reduces peripheral vascular resistance, overcoming a significant side effect of earlier beta-blockers that lowered blood pressure but ultimately increased peripheral vascular tone and resistance.8
In an experiment in a bovine model,60 nebivolol significantly reduced the pulse-wave velocity (a measure of arterial stiffness), while atenolol had no effect. Moreover, evidence for the role of the l-arginine/nitric oxide pathway in the vasodilatory effect of nebivolol was demonstrated by co-infusion of NG-monomethyl-L-arginine, a specific endothelial nitric oxide synthetase inhibitor that attenuated the reduction of pulse-wave velocity by nebivolol.
In studies in hypertensive patients, nebivolol was associated with a better metabolic profile than atenolol, with none of the adverse effects on insulin sensitivity that atenolol had.61 In the Study of Effects of Nebivolol Interventions on Outcomes and Rehospitalization in Seniors With Heart Failure (SENIORS) trial, significantly fewer patients receiving nebivolol died or were admitted to the hospital for cardiovascular reasons compared with those receiving placebo.62
Although these findings are encouraging, we do not yet know if these effects will translate into a significant reduction in cardiovascular outcomes in clinical trials. Large, prospective hypertension outcome trials, particularly to evaluate primary prevention of cardiovascular outcomes, are needed for an evidence-based approach to using the newer beta-blockers as preferred first-line therapy for hypertension.
WHAT RECENT GUIDELINES SAY ABOUT BETA-BLOCKERS
The British National Institute for Health and Clinical Excellence and the British Hypertension Society, in their 2004 guidelines, recommended beta-blockers as one of several first-line antihypertensive medications in young, nonblack patients.63 On the other hand, they advised clinicians to be aware of the reported increase in onset of diabetes mellitus in patients treated with these medications. After the LIFE24 and ASCOT26 study results were published, these guidelines were amended to exclude beta-blockers as preferred routine initial therapy for hypertension.64
More recently, the 2007 European Society of Hypertension and European Society of Cardiology reconsidered the role of beta-blockers, recommending them as an option in both initial and subsequent antihypertensive treatment strategies.65
The current guidelines from the National Heart, Lung, and Blood Institute,66 which were published in 2003, were highly influenced by the results of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT),2 and favor diuretics as the first-line therapy. However, they indicate that beta-blockers are a suitable alternative, particularly when a compelling cardiac indication is present.53 We hope that the next update, expected late in 2009, will re-address this issue in the light of more recent data.
- Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet 2001; 358:1305–1315.
- ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002; 288:2981–2997.
- Neutel JM, Smith DH, Ram CV, et al. Application of ambulatory blood pressure monitoring in differentiating between antihypertensive agents. Am J Med 1993; 94:181–187.
- Materson BJ, Reda DJ, Cushman WC, et al. Single-drug therapy for hypertension in men. A comparison of six antihypertensive agents with placebo. The Department of Veterans Affairs Cooperative Study Group on Antihypertensive Agents. N Engl J Med 1993; 328:914–921.
- Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associated with antihypertensive therapies used as first-line agents. A systematic review and meta-analysis. JAMA 1997; 277:739–745.
- Frishman W, Silverman R. Clinical pharmacology of the new beta-adrenergic blocking drugs. Part 2. Physiologic and metabolic effects. Am Heart J 1979; 97:797–807.
- Garrett BN, Kaplan NM. Plasma renin activity suppression: duration after withdrawal from beta-adrenergic blockade. Arch Intern Med 1980; 140:1316–1318.
- Pedersen ME, Cockcroft JR. The latest generation of beta-blockers: new pharmacologic properties. Curr Hypertens Rep 2006; 8:279–286.
- Man in’t Veld AJ, Van den Meiracker AH, Schalekamp MA. Do beta-blockers really increase peripheral vascular resistance? Review of the literature and new observations under basal conditions. Am J Hypertens 1988; 1:91–96.
- Pearce CJ, Wallin JD. Labetalol and other agents that block both alpha- and beta-adrenergic receptors. Cleve Clin J Med 1994; 61:59–69.
- Dimsdale JE, Newton RP, Joist T. Neuropsychological side effects of beta-blockers. Arch Intern Med 1989; 149:514–525.
- Agarwal R. Supervised atenolol therapy in the management of hemodialysis hypertension. Kidney Int 1999; 55:1528–1535.
- Sica DA, Black HR. Pharmacologic considerations in the positioning of beta-blockers in antihypertensive therapy. Curr Hypertens Rep 2008; 10:330–335.
- Prichard BN, Gillam GP. Use of propranolol (Inderal) in treatment of hypertension. Br Med J 1964; 19; 2:725–727.
- The fifth report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC V). Arch Intern Med 1993; 153:154–183.
- Moser M. Evolution of the treatment of hypertension from the 1940s to JNC V. Am J Hypertens 1997; 10:2S–8S.
- Houghton T, Freemantle N, Cleland JG. Are beta-blockers effective in patients who develop heart failure soon after myocardial infarction? A meta-regression analysis of randomised trials. Eur J Heart Fail 2000; 2:333–340.
- The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet 1999; 353:9–13.
- Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999; 353:2001–2007.
- Yusuf S, Peto R, Lewis J, Collins R, Sleight P. Beta blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis 1985; 27:335–371.
- Brophy JM, Joseph L, Rouleau JL. Beta-blockers in congestive heart failure. A Bayesian meta-analysis. Ann Intern Med 2001; 134:550–560.
- Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007;CD002003.
- Messerli FH, Grossman E, Goldbourt U. Are beta-blockers efficacious as first-line therapy for hypertension in the elderly? A systematic review. JAMA 1998; 279:1903–1907.
- Dahlöf B, Devereux RB, Kjeldsen SE, et al; for the LIFE study group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint Reduction in Hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359:995–1003.
- Carlberg B, Samuelsson O, Lindholm LH. Atenolol in hypertension: is it a wise choice? Lancet 2004; 364:1684–1689.
- Dahlöf B, Sever PS, Poulter NR, et al; ASCOT Investigators. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet 2005; 366:895–906.
- Lindholm LH, Carlberg B, Samuelsson O. Should beta-blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005; 366:1545–1553.
- Neutel JM, Schnaper H, Cheung DG, Graettinger WF, Weber MA. Antihypertensive effects of beta-blockers administered once daily: 24-hour measurements. Am Heart J 1990; 120:166–171.
- Franklin SS, Gustin W, Wong ND, et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation 1997; 96:308–315.
- The IPPPSH Collaborative Group. Cardiovascular risk and risk factors in a randomized trial of treatment based on the beta-blocker oxprenolol: the International Prospective Primary Prevention Study in Hypertension (IPPPSH). J Hypertens 1985; 3:379–392.
- Williams B, Lacy PS, Thom SM, et al; CAFE Investigators. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes: principal results of the Conduit Artery Function Evaluation (CAFE) study. Circulation 2006; 113:1213–1225.
- Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174:1737–1742.
- Medical Research Council Working Party. MRC trial of treatment of mild hypertension: principal results. BMJ 1985; 291:97–104.
- Coope J, Warrender TS. Randomised trial of treatment of hypertension in elderly patients in primary care. BMJ 1986; 293:1145–1151.
- Dahlöf B, Lindholm LH, Hansson L, et al. Morbidity and mortality in the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). Lancet 1991; 338:1281–1285.
- MRC Working Party. Medical Research Council trial of treatment of hypertension in older adults: principal results. BMJ 1992; 304:405–412.
- The Dutch TIA Study Group. Trial of secondary prevention with atenolol after transient ischemic attack or nondisabling ischemic stroke. Stroke 1993; 24:543–548.
- Eriksson S, Olofsson B-O, Wester P-O; for the TEST Study Group. Atenolol in secondary prevention after stroke. Cerebrovasc Dis 1995; 5:21–25.
- Wilhelmsen L, Berglund G, Elmfeldt D, et al. Beta-blockers versus diuretics in hypertensive men: main results from the HAPPHY trial. J Hypertens 1987; 5:561–572.
- UK Prospective Diabetes Study Group. Efficacy of atenolol and captopril in reducing risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 39. BMJ 1998; 317:713–720.
- Hansson L, Lindholm LH, Niskanen L, et al. Effect of angiotensin-converting enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPP) randomised trial. Lancet 1999; 353:611–616.
- Lanchetti A, Bond MG, Henning M, et al. Calcium antagonist lacidipine slow down progression of asymptomatic carotid atherosclerosis. Principal results of the European Lacidipine Study on Atherosclerosis (ELSA), a randomized, double-blind, long-term trial. Circulation 2002; 106:2422–2427.
- Hansson L, Lindholm LH, Ekbom T, et al. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity in the Swedish Trial in Old Patients with Hypertension-2 study. Lancet 1999; 354:1751–1756.
- Hansson L, Hedner T, Lund-Johansen P, et al. Randomised trial of effects of calcium antagonists compared with diuretics and ß blockers on cardiovascular morbidity and mortality in hypertension: the Nordic Diltiazem (NORDIL) study. Lancet 2000; 356:359–365.
- Pepine CJ, Handsberg EM, Cooper-DeHoff RM, et al. A calcium antagonist vs a non-calcium antagonist hypertension treatment strategy for patients with coronary artery disease. The International Verapamil-Trandolapril Study (INVEST): a randomized controlled trial. JAMA 2003; 290:2805–2816.
- Black HR, Elliott WJ, Grandits G, et al. Principal results of the Controlled Onset Verapamil Investigation of Cardiovascular End Points (CONVINCE) Trial. JAMA 2003; 289:2073–2082.
- Bangalore S, Sawhney S, Messerli FH. Relation of beta-blocker-induced heart rate lowering and cardioprotection in hypertension. J Am Coll Cardiol 2008; 52:1482–1489.
- Boutouyrie P, Vermersch S, Laurent S, Briet M. Cardiovascular risk assessment through target organ damage: role of carotid to femoral pulse wave velocity. Clin Exp Pharmacol Physiol 2008; 35:530–533.
- Kveiborg B, Christiansen B, Major-Petersen A, Torp-Pedersen C. Metabolic effects of beta-adrenoceptor antagonists with special emphasis on carvedilol. Am J Cardiovasc Drugs 2006; 6:209–217.
- Bangalore S, Parkar S, Grossman E, Messerli FH. A meta-analysis of 94,492 patients with hypertension treated with beta-blockers to determine the risk of new-onset diabetes mellitus. Am J Cardiol 2007; 100:1254–1262.
- Balamuthusamy S, Molnar J, Adigopula S, Arora R. Comparative analysis of beta-blockers with other antihypertensive agents on cardiovascular outcomes in hypertensive patients with diabetes mellitus: a systematic review and meta-analysis. Am J Ther 2009; 16:133–142.
- Berenson A. Big drug makers see sales decline with their image. New York Times 2005 Nov 14.
- Bristow MR. Beta-adrenergic receptor blockade in chronic heart failure. Circulation 2000; 101:558–569.
- Giugliano D, Marfella R, Acampora R, Giunta R, Coppola L, D’Onofrio F. Effects of perindopril and carvedilol on endothelium-dependent vascular functions in patients with diabetes and hypertension. Diabetes Care 1998; 21:631–636.
- Lopez BL, Christopher TA, Yue TL, Ruffolo R, Feuerstein GZ, Ma XL. Carvedilol, a new beta-adrenoreceptor blocker antihypertensive drug, protects against free-radical-induced endothelial dysfunction. Pharmacology 1995; 51:165–173.
- Bakris GL, Fonseca V, Katholi RE, et al; GEMINI Investigators. Metabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trial. JAMA 2004; 292:2227–2236.
- Georgescu A, Pluteanu F, Flonta ML, Badila E, Dorobantu M, Popov D. The cellular mechanisms involved in the vasodilator effect of nebivolol on the renal artery. Eur J Pharmacol 2005; 508:159–166.
- Kalinowski L, Dobrucki LW, Szczepanska-Konkel M, et al. Third-generation beta-blockers stimulate nitric oxide release from endothelial cells through ATP efflux: a novel mechanism for antihypertensive action. Circulation 2003; 107:2747–2752.
- Cockcroft JR, Chowienczyk PJ, Brett SE, et al. Nebivolol vasodilates human forearm vasculature: evidence for an L-arginine/NO-dependent mechanism. J Pharmacol Exp Ther 1995; 274:1067–1071.
- McEniery CM, Schmitt M, Qasem A, et al. Nebivolol increases arterial distensibility in vivo. Hypertension 2004; 44:305–310.
- Poirier L, Cleroux J, Nadeau A, Lacourciere Y. Effects of nebivolol and atenolol on insulin sensitivity and haemodynamics in hypertensive patients. J Hypertens 2001; 19:1429–1435.
- Flather MD, Shibata MC, Coats AJ, et al; SENIORS Investigators. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J 2005; 26:215–225.
- Williams B, Poulter NR, Brown MJ, et al; BHS guidelines working party, for the British Hypertension Society. British Hypertension Society guidelines for hypertension management 2004 (BHS-IV): summary. BMJ 2004; 328:634–640.
- Sever P. New hypertension guidelines from the National Institute for Health and Clinical Excellence and the British Hypertension Society. J Renin Angiotensin Aldosterone Syst 2006; 7:61–63.
- Mancia G, De Backer G, Dominiczak A, et al; Management of Arterial Hypertension of the European Society of Hypertension. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2007; 25:1105–1187.
- Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560–2572.
In recent years the role of beta-blockers as a primary tool to treat hypertension has come under question. These drugs have shown disappointing results when used as antihypertensive therapy in patients without heart disease, ie, when used as primary prevention. At the same time, beta-blockers clearly reduce the risk of future cardiovascular events in patients who already have heart disease, eg, who already have had a myocardial infarction or who have congestive heart failure.
Several meta-analyses and a few clinical trials have shown that beta-blockers may have no advantage over other antihypertensive drugs, and in fact may not reduce the risk of stroke as effectively as other classes of blood pressure medications.
Why should this be? Is it that the patients in the antihypertensive trials were mostly older, and that beta-blockers do not work as well in older patients as in younger ones? Or does it have to do with the fact that atenolol (Tenormin) was the drug most often used in the trials? Would newer, different beta-blockers be better?
Hypertension experts currently disagree on how to interpret the available data, and this has led to conflict and confusion among clinicians as to the role of beta-blockers in managing hypertension. Current evidence suggests that older beta-blockers may not be the preferred first-line antihypertensive drugs for hypertensive patients who have no compelling indications for them (eg, heart failure, myocardial infarction, diabetes, high risk of coronary heart disease). However, newer beta-blockers with vasodilatory properties should be considered in cases of uncontrolled or resistant hypertension, especially in younger patients.
Further, while controversy and debate continue over the benefits and adverse effects of one class of antihypertensive drugs vs another, it is indisputable that controlling arterial blood pressure to the recommended goal offers major protection against cardiovascular and renal events in patients with hypertension.1,2
MECHANISM OF ACTION OF BETA-BLOCKERS
Beta-blockers effectively reduce blood pressure in both systolic-diastolic hypertension and isolated systolic hypertension.3–5 Exactly how is not known, but it has been proposed that they may do so by:
Reducing the heart rate and cardiac output. When catecholamines activate beta-1 receptors in the heart, the heart rate and myocardial contractility increase. By blocking beta-1 receptors, beta-blockers reduce the heart rate and myocardial contractility, thus lowering cardiac output and arterial blood pressure.6
Inhibiting renin release. Activation of the renin-angiotensin system is another major pathway that can lead to elevated arterial blood pressure. Renin release is mediated through the sympathetic nervous system via beta-1 receptors on the juxtaglomerular cells of the kidney. Beta-blockers can therefore lower blood pressure by inhibiting renin release.7
Inhibiting central nervous sympathetic outflow, thereby inducing presynaptic blockade, which in turn reduces the release of catecholamines.
Reducing venous return and plasma volume.
Generating nitric oxide, thus reducing peripheral vascular resistance (some agents).8
Reducing vasomotor tone.
Reducing vascular tone.
Improving vascular compliance.
Resetting baroreceptor levels.
Attenuating the pressor response to catecholamines with exercise and stress.
HETEROGENEITY OF BETA-BLOCKERS
Selectivity
Beta-blockers are not all the same. They can be classified into three categories.
Nonselective beta-blockers block both beta-1 and beta-2 adrenergic receptors. It is generally accepted that beta-blockers exert their primary antihypertensive effect by blocking beta-1 adrenergic receptors.6 Of interest, nonselective beta-blockers inhibit beta-2 receptors on arteries and thus cause an unopposed alpha-adrenergic effect, leading to increased peripheral vascular resistance.9 Examples of this category:
- Nadolol (Corgard)
- Pindolol (Visken)
- Propranolol (Inderal)
- Timolol (Blocadren).
Selective beta-blockers specifically block beta-1 receptors alone, although they are known to be nonselective at higher doses. Examples:
- Atenolol (Tenormin)
- Betaxolol (Kerlone)
- Bisoprolol (Zebeta)
- Esmolol (Brevibloc)
- Metoprolol (Lopressor, Toprol).
Beta-blockers with peripheral vasodilatatory effects act either via antagonism of the alpha-1 receptor, as with labetolol (Normodyne) and carvedilol (Coreg),10 or via enhanced release of nitric oxide, as with nebivolol (Bystolic).8
Lipid and water solubility
The lipid solubility and water solubility of each beta-blocker determine its bioavailability and side-effect profile.
Lipid solubility determines the degree to which a beta-blocker penetrates the blood-brain barrier and thereby leads to central nervous system side effects such as lethargy, nightmares, confusion, and depression. Propranolol is highly lipid-soluble; metoprolol and labetalol are moderately so.
Water-soluble beta-blockers such as atenolol have less tissue permeation, have a longer half-life, and cause fewer central nervous system effects and symptoms.11
Routes of elimination
Beta-blockers also differ in their route of elimination.
Atenolol and nadolol are eliminated by the kidney and require dose adjustment in patients with impaired renal function.12,13
On the other hand, propranolol, metoprolol, labetalol, carvedilol, and nebivolol are excreted primarily via hepatic metabolism.13
BETA-BLOCKERS IN THE MANAGEMENT OF HYPERTENSION
Beta-blockers were initially used to treat arrhythmias, but by the early 1970s they were also widely accepted for managing hypertension. 14 Their initial acceptance as one of the first-line classes of drugs for hypertension was based on their better side-effect profile compared with other antihypertensive drugs available at that time.
In the 1980s and 1990s, beta-blockers were listed as preferred first-line antihypertensive drugs along with diuretics in national hypertension guidelines.15 Subsequent updates of the guidelines favored diuretics as initial therapy and relegated all other classes of antihypertensive medications to be alternatives to diuretics.16 Although beta-blockers remain alternative first-line drugs in the latest guidelines (published in 2003; see reference 66), they are the preferred antihypertensive agents for patients with cardiac disease.
The current recommendations reflect the findings from hypertension trials in which patients with myocardial infarction and congestive heart failure had better cardiovascular outcomes if they received these drugs,17–19 including a lower risk of death.20,21 It was widely assumed that beta-blockers would also prevent first episodes of cardiovascular events.
However, to date, there is no evidence that beta-blockers are effective as primary prevention. Several large randomized controlled trials showed no benefit with beta-blockers compared with other antihypertensive drugs—in fact, there were more cardiovascular events with beta-blockers (see below).
Beta-blockers are well tolerated in clinical practice, although they can have side effects that include fatigue, depression, impaired exercise tolerance, sexual dysfunction, and asthma attacks.
Wiysonge et al22 analyzed how many patients withdrew from randomized trials of antihypertensive treatment because of drug-related adverse events. There was no significant difference in the incidence of fatigue, depressive symptoms, or sexual dysfunction with beta-blockers compared with placebo, and trial participants on a beta-blocker were not statistically significantly more likely to discontinue treatment than those receiving a placebo in three trials with 22,729 participants (relative risk [RR] 2.34, 95% confidence interval [CI] 0.84–6.52).
THE CONTROVERSY: WHAT THE TRIALS SHOWED
Messerli et al23 performed a meta-analysis published in 1998 that suggested that beta-blockers may not be as effective as diuretics in preventing cardiovascular events when used as first-line antihypertensive therapy in elderly patients. In 10 randomized controlled trials in 16,164 patients who were treated with either a diuretic or a beta-blocker (atenolol), blood pressure was normalized in two-thirds of diuretic-treated patients but only one-third of patients treated with atenolol as monotherapy. Diuretic therapy was superior with regard to all end points, and beta-blockers were found to be ineffective except in reducing cerebrovascular events.
The LIFE study (Losartan Intervention for Endpoint Reduction in Hypertension)24 compared the angiotensin-receptor blocker losartan (Cozaar) and atenolol in 9,193 patients with hypertension and left ventricular hypertrophy. At 4 years of follow-up, the rate of primary cardiovascular events (death, myocardial infarction, or stroke) was lower in the losartan group than in the atenolol group. The difference was mainly due to a 25% lower incidence of stroke, which was statistically significant. The rates of myocardial infarction and death from cardiovascular causes were not significantly different between the two treatment groups. The systolic blood pressure was 1 mm Hg lower in the losartan group than in the atenolol group, which was statistically significant.
Carlberg et al25 performed another important meta-analysis that questioned whether atenolol reduces rates of cardiovascular morbidity and death in hypertensive patients. The results were surprising: eight randomized controlled trials including more than 6,000 patients and comparing atenolol with placebo or no treatment showed no differences between the treatment groups with regard to the outcomes of all-cause mortality (RR 1.01, 95% CI 0.89–1.15), cardiovascular mortality (RR 0.99, 95% CI 0.83–1.18), or myocardial infarction (RR 0.99, 95% CI 0.83–1.19).
In addition, when atenolol was compared with other antihypertensives in five other randomized controlled trials that included more than 14,000 patients, those treated with atenolol had a higher risk of stroke (RR 1.30, 95% CI 1.12–1.50) and death (RR 1.13, 95% CI 1.02–1.25).
The ASCOT-BPLA trial (Anglo-Scandinavian Cardiac Outcomes Trial—Blood Pressure Lowering Arm)26 had similar results. This trial compared the combination of atenolol plus the diuretic bendroflumethiazide against the combination of the calcium channel blocker amlodipine (Norvasc) plus the angiotensin-converting enzyme (ACE) inhibitor perindopril (Aceon). Although no significant difference was seen in the primary outcome of nonfatal myocardial infarction or fatal coronary heart disease (unadjusted hazard ratio [HR] with amlodipine-perindopril 0.90, 95% CI 0.79–1.02, P = .1052), the amlodipine-plus-perindopril group had significantly fewer strokes (327 vs 422, HR 0.77, 95% CI 0.66–0.89, P = .0003), fewer total cardiovascular events (1,362 vs 1,602, HR 0.84, 95% CI 0.78–0.90, P = .0001), and fewer deaths from any cause (738 vs 820; HR 0.89, 95% CI 0.81–0.99, P = .025).
Lindholm et al27 performed a meta-analysis that included studies of selective beta-blockers (including atenolol) and nonselective beta-blockers, with a follow-up time of more than 2 years. Compared with placebo or no treatment, beta-blockers reduced the risk of stroke by 19% but had no effect on myocardial infarction or all-cause mortality. Compared with other antihypertensive drugs, beta-blockers were less than optimum, and the relative risk of stroke was 16% higher. Atenolol was the beta-blocker used in most of the randomized clinical trials included in this meta-analysis.
The Cochrane group22 found beta-blockers to be inferior to all other antihypertensive drugs with respect to the ability to lower the risk of stroke.
WHY WERE THE RESULTS SO DISAPPOINTING?
Problems with atenolol
Most of the trials in the meta-analyses discussed above used atenolol and other beta-blockers that had no vasodilatory properties.
Further, in most of the trials atenolol was used in a once-daily dosage, whereas ideally it needs to be taken more frequently, based on its pharmacokinetic and pharmacodynamic properties (a half-life of 6–9 hours).3 Neutel et al28 confirmed that atenolol, when taken once daily, leaves the patient unprotected in the last 6 hours of a 24-hour period, as demonstrated by 24-hour ambulatory blood pressure monitoring. It is possible that this short duration of action of atenolol may have contributed to the results observed in clinical trials that used atenolol to treat hypertension.
Differences between older and younger patients
Another possible reason for the disappointing results is that the trials included many elderly patients, in whom beta-blockers may not be as effective. The pathophysiology of hypertension in younger people is different from that in older patients.29 Hemodynamic characteristics of younger hypertensive patients include a high cardiac output and hyperdynamic circulation with a low pulse pressure, while older patients have lower arterial compliance with an elevated vascular resistance.
The notion of choosing antihypertensive medications on the basis of age and age-related pathophysiology is supported by several clinical studies. Randomized controlled trials appear to show that beta-blockers are effective in younger hypertensive patients.30
Conversely, the CAFE (Conduit Artery Function Evaluation) trial,31 a substudy of the main ASCOT trial,26 indicated that betablocker-based therapy was less effective in reducing central aortic pressure than were regimens based on an ACE inhibitor or a calcium channel blocker.
The CAFE researchers recruited 2,073 patients from five ASCOT centers and used radial artery applanation tonometry and pulse-wave analysis to derive central aortic pressures and hemodynamic indices during study visits up to a period of 4 years. Although the two treatment groups achieved similar brachial systolic blood pressures, the central aortic systolic pressure was 4.3 mm Hg lower in the amlodipine group (95% CI 3.3–5.4; P < .0001), and the central aortic pulse pressure was 3.0 mm Hg lower (95% CI 2.1–3.9; P < .0001).
Pulse-wave dyssynchrony
Bangalore et al47 offer an interesting hypothesis to explain the probable adverse effect of beta-blockers. Their theory concerns the effect of these drugs on the arterial pulse wave.
Normally, with each contraction of the left ventricle during systole, an arterial pulse wave is generated and propagated forward to the peripheral arteries. This wave is then reflected back to the heart from the branching points of peripheral arteries. The final form of the pressure wave at the aortic root is a synchronized summation of the forward-traveling wave and the backward-reflected wave.
In healthy people with normal arteries, the reflected wave merges with the forward-traveling wave in diastole and augments coronary blood flow. In patients whose arteries are stiff due to aging or vascular comorbidities, the reflected wave returns faster and merges with the incident wave in systole, resulting in higher left ventricular afterload and less coronary perfusion.48
Bangalore et al47 propose that artificially reducing the heart rate with beta-blockers may further dyssynchronize the pulse wave, adversely affecting coronary perfusion and leading to an increased risk of cardiovascular events and death.
Metabolic side effects
Older beta-blockers, and especially atenolol, have well-known metabolic adverse effects, particularly impairment of glycemic control. This adverse effect appears to occur only with beta-blockers that do not possess vasodilatory properties and thus increase peripheral vascular resistance, which results in lower glucose availability and reduced uptake by skeletal muscles.49
Bangalore et al50 evaluated the effect of beta-blockers in a meta-analysis of 12 studies in 94,492 patients followed up for more than 1 year. Beta-blocker therapy resulted in a 22% higher risk of new-onset diabetes mellitus (RR 1.22, 95% CI 1.12–1.33) than with other nondiuretic antihypertensive agents.
Of note, however, the meta-analysis did not show a significantly higher risk of the onset of diabetes with propranolol or metoprolol than with other nondiuretic antihypertensives when studies of these beta-blockers were separated from atenolol-based studies.
Further, the United Kingdom Prospective Diabetes Study40 found that cardiovascular outcomes in patients with good blood pressure control were similar when atenolol-based therapy was compared with therapy with the ACE inhibitor captopril (Capoten).
A meta-analysis conducted by Balamuthusamy et al51 in 2009 found no higher risk of stroke in patients with hypertension and diabetes mellitus who received beta-blockers than in those who received other antihypertensive medications. However, beta-blockers were associated with a higher risk of death from cardiovascular causes (RR 1.39, 95% CI 1.07–1.804; P < .01) compared with reninangiotensin blockade.
NEWER BETA-BLOCKERS MAY BE BETTER
In the United States, more than 40 million prescriptions for atenolol are written every year, making it by far the most commonly used beta-blocker for the treatment of hypertension. 52 It is clear, however, that atenolol is not an ideal representative of this class of antihypertensive medications.
Preliminary data from studies of newer beta-blockers that possess beneficial vasodilatory properties are encouraging. Animal studies and preliminary human studies find that these new-generation beta-blockers cause fewer adverse metabolic effects and improve endothelial function, measures of arterial stiffness, and cardiovascular outcomes.
Carvedilol
Carvedilol is a nonselective beta-blocker with vasodilatory effects that are thought to be due to its ability to concurrently block alpha-1 receptors in addition to beta receptors. 53 In experiments in vitro and in trials in patients with diabetes and hypertension, carvedilol increased endothelial vasodilation and reduced inflammation and platelet aggregation. These effects may be achieved though antioxidant actions, thereby preserving nitric oxide bioactivity.54,55
In the Glycemic Effects in Diabetes Mellitus: Carvedilol-Metoprolol Comparison in Hypertensives (GEMINI) trial,56 carvedilol was associated with better maintenance of glycemic control in diabetic hypertensive patients than was metoprolol. Insulin sensitivity improved with carvedilol but not with metoprolol, and fewer patients on carvedilol progressed to microalbuminuria.
Nebivolol
Nebivolol is a novel selective beta-blocker with a much higher affinity for beta-1 adrenergic receptors than for beta-2 adrenergic receptors. Among all the beta-blockers in clinical use today, nebivolol has the highest selectivity for beta-1 receptors.8
Nebivolol causes vasodilation through activation of the l-arginine/nitric oxide pathway.57–59 Blockade of synthesis of nitric oxide leads to local arterial stiffness. Endothelial dysfunction is characterized by decreased bioavailability of nitric oxide and has been shown to be a strong predictor of cardiovascular outcomes. By generating nitric oxide, nebivolol reduces peripheral vascular resistance, overcoming a significant side effect of earlier beta-blockers that lowered blood pressure but ultimately increased peripheral vascular tone and resistance.8
In an experiment in a bovine model,60 nebivolol significantly reduced the pulse-wave velocity (a measure of arterial stiffness), while atenolol had no effect. Moreover, evidence for the role of the l-arginine/nitric oxide pathway in the vasodilatory effect of nebivolol was demonstrated by co-infusion of NG-monomethyl-L-arginine, a specific endothelial nitric oxide synthetase inhibitor that attenuated the reduction of pulse-wave velocity by nebivolol.
In studies in hypertensive patients, nebivolol was associated with a better metabolic profile than atenolol, with none of the adverse effects on insulin sensitivity that atenolol had.61 In the Study of Effects of Nebivolol Interventions on Outcomes and Rehospitalization in Seniors With Heart Failure (SENIORS) trial, significantly fewer patients receiving nebivolol died or were admitted to the hospital for cardiovascular reasons compared with those receiving placebo.62
Although these findings are encouraging, we do not yet know if these effects will translate into a significant reduction in cardiovascular outcomes in clinical trials. Large, prospective hypertension outcome trials, particularly to evaluate primary prevention of cardiovascular outcomes, are needed for an evidence-based approach to using the newer beta-blockers as preferred first-line therapy for hypertension.
WHAT RECENT GUIDELINES SAY ABOUT BETA-BLOCKERS
The British National Institute for Health and Clinical Excellence and the British Hypertension Society, in their 2004 guidelines, recommended beta-blockers as one of several first-line antihypertensive medications in young, nonblack patients.63 On the other hand, they advised clinicians to be aware of the reported increase in onset of diabetes mellitus in patients treated with these medications. After the LIFE24 and ASCOT26 study results were published, these guidelines were amended to exclude beta-blockers as preferred routine initial therapy for hypertension.64
More recently, the 2007 European Society of Hypertension and European Society of Cardiology reconsidered the role of beta-blockers, recommending them as an option in both initial and subsequent antihypertensive treatment strategies.65
The current guidelines from the National Heart, Lung, and Blood Institute,66 which were published in 2003, were highly influenced by the results of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT),2 and favor diuretics as the first-line therapy. However, they indicate that beta-blockers are a suitable alternative, particularly when a compelling cardiac indication is present.53 We hope that the next update, expected late in 2009, will re-address this issue in the light of more recent data.
In recent years the role of beta-blockers as a primary tool to treat hypertension has come under question. These drugs have shown disappointing results when used as antihypertensive therapy in patients without heart disease, ie, when used as primary prevention. At the same time, beta-blockers clearly reduce the risk of future cardiovascular events in patients who already have heart disease, eg, who already have had a myocardial infarction or who have congestive heart failure.
Several meta-analyses and a few clinical trials have shown that beta-blockers may have no advantage over other antihypertensive drugs, and in fact may not reduce the risk of stroke as effectively as other classes of blood pressure medications.
Why should this be? Is it that the patients in the antihypertensive trials were mostly older, and that beta-blockers do not work as well in older patients as in younger ones? Or does it have to do with the fact that atenolol (Tenormin) was the drug most often used in the trials? Would newer, different beta-blockers be better?
Hypertension experts currently disagree on how to interpret the available data, and this has led to conflict and confusion among clinicians as to the role of beta-blockers in managing hypertension. Current evidence suggests that older beta-blockers may not be the preferred first-line antihypertensive drugs for hypertensive patients who have no compelling indications for them (eg, heart failure, myocardial infarction, diabetes, high risk of coronary heart disease). However, newer beta-blockers with vasodilatory properties should be considered in cases of uncontrolled or resistant hypertension, especially in younger patients.
Further, while controversy and debate continue over the benefits and adverse effects of one class of antihypertensive drugs vs another, it is indisputable that controlling arterial blood pressure to the recommended goal offers major protection against cardiovascular and renal events in patients with hypertension.1,2
MECHANISM OF ACTION OF BETA-BLOCKERS
Beta-blockers effectively reduce blood pressure in both systolic-diastolic hypertension and isolated systolic hypertension.3–5 Exactly how is not known, but it has been proposed that they may do so by:
Reducing the heart rate and cardiac output. When catecholamines activate beta-1 receptors in the heart, the heart rate and myocardial contractility increase. By blocking beta-1 receptors, beta-blockers reduce the heart rate and myocardial contractility, thus lowering cardiac output and arterial blood pressure.6
Inhibiting renin release. Activation of the renin-angiotensin system is another major pathway that can lead to elevated arterial blood pressure. Renin release is mediated through the sympathetic nervous system via beta-1 receptors on the juxtaglomerular cells of the kidney. Beta-blockers can therefore lower blood pressure by inhibiting renin release.7
Inhibiting central nervous sympathetic outflow, thereby inducing presynaptic blockade, which in turn reduces the release of catecholamines.
Reducing venous return and plasma volume.
Generating nitric oxide, thus reducing peripheral vascular resistance (some agents).8
Reducing vasomotor tone.
Reducing vascular tone.
Improving vascular compliance.
Resetting baroreceptor levels.
Attenuating the pressor response to catecholamines with exercise and stress.
HETEROGENEITY OF BETA-BLOCKERS
Selectivity
Beta-blockers are not all the same. They can be classified into three categories.
Nonselective beta-blockers block both beta-1 and beta-2 adrenergic receptors. It is generally accepted that beta-blockers exert their primary antihypertensive effect by blocking beta-1 adrenergic receptors.6 Of interest, nonselective beta-blockers inhibit beta-2 receptors on arteries and thus cause an unopposed alpha-adrenergic effect, leading to increased peripheral vascular resistance.9 Examples of this category:
- Nadolol (Corgard)
- Pindolol (Visken)
- Propranolol (Inderal)
- Timolol (Blocadren).
Selective beta-blockers specifically block beta-1 receptors alone, although they are known to be nonselective at higher doses. Examples:
- Atenolol (Tenormin)
- Betaxolol (Kerlone)
- Bisoprolol (Zebeta)
- Esmolol (Brevibloc)
- Metoprolol (Lopressor, Toprol).
Beta-blockers with peripheral vasodilatatory effects act either via antagonism of the alpha-1 receptor, as with labetolol (Normodyne) and carvedilol (Coreg),10 or via enhanced release of nitric oxide, as with nebivolol (Bystolic).8
Lipid and water solubility
The lipid solubility and water solubility of each beta-blocker determine its bioavailability and side-effect profile.
Lipid solubility determines the degree to which a beta-blocker penetrates the blood-brain barrier and thereby leads to central nervous system side effects such as lethargy, nightmares, confusion, and depression. Propranolol is highly lipid-soluble; metoprolol and labetalol are moderately so.
Water-soluble beta-blockers such as atenolol have less tissue permeation, have a longer half-life, and cause fewer central nervous system effects and symptoms.11
Routes of elimination
Beta-blockers also differ in their route of elimination.
Atenolol and nadolol are eliminated by the kidney and require dose adjustment in patients with impaired renal function.12,13
On the other hand, propranolol, metoprolol, labetalol, carvedilol, and nebivolol are excreted primarily via hepatic metabolism.13
BETA-BLOCKERS IN THE MANAGEMENT OF HYPERTENSION
Beta-blockers were initially used to treat arrhythmias, but by the early 1970s they were also widely accepted for managing hypertension. 14 Their initial acceptance as one of the first-line classes of drugs for hypertension was based on their better side-effect profile compared with other antihypertensive drugs available at that time.
In the 1980s and 1990s, beta-blockers were listed as preferred first-line antihypertensive drugs along with diuretics in national hypertension guidelines.15 Subsequent updates of the guidelines favored diuretics as initial therapy and relegated all other classes of antihypertensive medications to be alternatives to diuretics.16 Although beta-blockers remain alternative first-line drugs in the latest guidelines (published in 2003; see reference 66), they are the preferred antihypertensive agents for patients with cardiac disease.
The current recommendations reflect the findings from hypertension trials in which patients with myocardial infarction and congestive heart failure had better cardiovascular outcomes if they received these drugs,17–19 including a lower risk of death.20,21 It was widely assumed that beta-blockers would also prevent first episodes of cardiovascular events.
However, to date, there is no evidence that beta-blockers are effective as primary prevention. Several large randomized controlled trials showed no benefit with beta-blockers compared with other antihypertensive drugs—in fact, there were more cardiovascular events with beta-blockers (see below).
Beta-blockers are well tolerated in clinical practice, although they can have side effects that include fatigue, depression, impaired exercise tolerance, sexual dysfunction, and asthma attacks.
Wiysonge et al22 analyzed how many patients withdrew from randomized trials of antihypertensive treatment because of drug-related adverse events. There was no significant difference in the incidence of fatigue, depressive symptoms, or sexual dysfunction with beta-blockers compared with placebo, and trial participants on a beta-blocker were not statistically significantly more likely to discontinue treatment than those receiving a placebo in three trials with 22,729 participants (relative risk [RR] 2.34, 95% confidence interval [CI] 0.84–6.52).
THE CONTROVERSY: WHAT THE TRIALS SHOWED
Messerli et al23 performed a meta-analysis published in 1998 that suggested that beta-blockers may not be as effective as diuretics in preventing cardiovascular events when used as first-line antihypertensive therapy in elderly patients. In 10 randomized controlled trials in 16,164 patients who were treated with either a diuretic or a beta-blocker (atenolol), blood pressure was normalized in two-thirds of diuretic-treated patients but only one-third of patients treated with atenolol as monotherapy. Diuretic therapy was superior with regard to all end points, and beta-blockers were found to be ineffective except in reducing cerebrovascular events.
The LIFE study (Losartan Intervention for Endpoint Reduction in Hypertension)24 compared the angiotensin-receptor blocker losartan (Cozaar) and atenolol in 9,193 patients with hypertension and left ventricular hypertrophy. At 4 years of follow-up, the rate of primary cardiovascular events (death, myocardial infarction, or stroke) was lower in the losartan group than in the atenolol group. The difference was mainly due to a 25% lower incidence of stroke, which was statistically significant. The rates of myocardial infarction and death from cardiovascular causes were not significantly different between the two treatment groups. The systolic blood pressure was 1 mm Hg lower in the losartan group than in the atenolol group, which was statistically significant.
Carlberg et al25 performed another important meta-analysis that questioned whether atenolol reduces rates of cardiovascular morbidity and death in hypertensive patients. The results were surprising: eight randomized controlled trials including more than 6,000 patients and comparing atenolol with placebo or no treatment showed no differences between the treatment groups with regard to the outcomes of all-cause mortality (RR 1.01, 95% CI 0.89–1.15), cardiovascular mortality (RR 0.99, 95% CI 0.83–1.18), or myocardial infarction (RR 0.99, 95% CI 0.83–1.19).
In addition, when atenolol was compared with other antihypertensives in five other randomized controlled trials that included more than 14,000 patients, those treated with atenolol had a higher risk of stroke (RR 1.30, 95% CI 1.12–1.50) and death (RR 1.13, 95% CI 1.02–1.25).
The ASCOT-BPLA trial (Anglo-Scandinavian Cardiac Outcomes Trial—Blood Pressure Lowering Arm)26 had similar results. This trial compared the combination of atenolol plus the diuretic bendroflumethiazide against the combination of the calcium channel blocker amlodipine (Norvasc) plus the angiotensin-converting enzyme (ACE) inhibitor perindopril (Aceon). Although no significant difference was seen in the primary outcome of nonfatal myocardial infarction or fatal coronary heart disease (unadjusted hazard ratio [HR] with amlodipine-perindopril 0.90, 95% CI 0.79–1.02, P = .1052), the amlodipine-plus-perindopril group had significantly fewer strokes (327 vs 422, HR 0.77, 95% CI 0.66–0.89, P = .0003), fewer total cardiovascular events (1,362 vs 1,602, HR 0.84, 95% CI 0.78–0.90, P = .0001), and fewer deaths from any cause (738 vs 820; HR 0.89, 95% CI 0.81–0.99, P = .025).
Lindholm et al27 performed a meta-analysis that included studies of selective beta-blockers (including atenolol) and nonselective beta-blockers, with a follow-up time of more than 2 years. Compared with placebo or no treatment, beta-blockers reduced the risk of stroke by 19% but had no effect on myocardial infarction or all-cause mortality. Compared with other antihypertensive drugs, beta-blockers were less than optimum, and the relative risk of stroke was 16% higher. Atenolol was the beta-blocker used in most of the randomized clinical trials included in this meta-analysis.
The Cochrane group22 found beta-blockers to be inferior to all other antihypertensive drugs with respect to the ability to lower the risk of stroke.
WHY WERE THE RESULTS SO DISAPPOINTING?
Problems with atenolol
Most of the trials in the meta-analyses discussed above used atenolol and other beta-blockers that had no vasodilatory properties.
Further, in most of the trials atenolol was used in a once-daily dosage, whereas ideally it needs to be taken more frequently, based on its pharmacokinetic and pharmacodynamic properties (a half-life of 6–9 hours).3 Neutel et al28 confirmed that atenolol, when taken once daily, leaves the patient unprotected in the last 6 hours of a 24-hour period, as demonstrated by 24-hour ambulatory blood pressure monitoring. It is possible that this short duration of action of atenolol may have contributed to the results observed in clinical trials that used atenolol to treat hypertension.
Differences between older and younger patients
Another possible reason for the disappointing results is that the trials included many elderly patients, in whom beta-blockers may not be as effective. The pathophysiology of hypertension in younger people is different from that in older patients.29 Hemodynamic characteristics of younger hypertensive patients include a high cardiac output and hyperdynamic circulation with a low pulse pressure, while older patients have lower arterial compliance with an elevated vascular resistance.
The notion of choosing antihypertensive medications on the basis of age and age-related pathophysiology is supported by several clinical studies. Randomized controlled trials appear to show that beta-blockers are effective in younger hypertensive patients.30
Conversely, the CAFE (Conduit Artery Function Evaluation) trial,31 a substudy of the main ASCOT trial,26 indicated that betablocker-based therapy was less effective in reducing central aortic pressure than were regimens based on an ACE inhibitor or a calcium channel blocker.
The CAFE researchers recruited 2,073 patients from five ASCOT centers and used radial artery applanation tonometry and pulse-wave analysis to derive central aortic pressures and hemodynamic indices during study visits up to a period of 4 years. Although the two treatment groups achieved similar brachial systolic blood pressures, the central aortic systolic pressure was 4.3 mm Hg lower in the amlodipine group (95% CI 3.3–5.4; P < .0001), and the central aortic pulse pressure was 3.0 mm Hg lower (95% CI 2.1–3.9; P < .0001).
Pulse-wave dyssynchrony
Bangalore et al47 offer an interesting hypothesis to explain the probable adverse effect of beta-blockers. Their theory concerns the effect of these drugs on the arterial pulse wave.
Normally, with each contraction of the left ventricle during systole, an arterial pulse wave is generated and propagated forward to the peripheral arteries. This wave is then reflected back to the heart from the branching points of peripheral arteries. The final form of the pressure wave at the aortic root is a synchronized summation of the forward-traveling wave and the backward-reflected wave.
In healthy people with normal arteries, the reflected wave merges with the forward-traveling wave in diastole and augments coronary blood flow. In patients whose arteries are stiff due to aging or vascular comorbidities, the reflected wave returns faster and merges with the incident wave in systole, resulting in higher left ventricular afterload and less coronary perfusion.48
Bangalore et al47 propose that artificially reducing the heart rate with beta-blockers may further dyssynchronize the pulse wave, adversely affecting coronary perfusion and leading to an increased risk of cardiovascular events and death.
Metabolic side effects
Older beta-blockers, and especially atenolol, have well-known metabolic adverse effects, particularly impairment of glycemic control. This adverse effect appears to occur only with beta-blockers that do not possess vasodilatory properties and thus increase peripheral vascular resistance, which results in lower glucose availability and reduced uptake by skeletal muscles.49
Bangalore et al50 evaluated the effect of beta-blockers in a meta-analysis of 12 studies in 94,492 patients followed up for more than 1 year. Beta-blocker therapy resulted in a 22% higher risk of new-onset diabetes mellitus (RR 1.22, 95% CI 1.12–1.33) than with other nondiuretic antihypertensive agents.
Of note, however, the meta-analysis did not show a significantly higher risk of the onset of diabetes with propranolol or metoprolol than with other nondiuretic antihypertensives when studies of these beta-blockers were separated from atenolol-based studies.
Further, the United Kingdom Prospective Diabetes Study40 found that cardiovascular outcomes in patients with good blood pressure control were similar when atenolol-based therapy was compared with therapy with the ACE inhibitor captopril (Capoten).
A meta-analysis conducted by Balamuthusamy et al51 in 2009 found no higher risk of stroke in patients with hypertension and diabetes mellitus who received beta-blockers than in those who received other antihypertensive medications. However, beta-blockers were associated with a higher risk of death from cardiovascular causes (RR 1.39, 95% CI 1.07–1.804; P < .01) compared with reninangiotensin blockade.
NEWER BETA-BLOCKERS MAY BE BETTER
In the United States, more than 40 million prescriptions for atenolol are written every year, making it by far the most commonly used beta-blocker for the treatment of hypertension. 52 It is clear, however, that atenolol is not an ideal representative of this class of antihypertensive medications.
Preliminary data from studies of newer beta-blockers that possess beneficial vasodilatory properties are encouraging. Animal studies and preliminary human studies find that these new-generation beta-blockers cause fewer adverse metabolic effects and improve endothelial function, measures of arterial stiffness, and cardiovascular outcomes.
Carvedilol
Carvedilol is a nonselective beta-blocker with vasodilatory effects that are thought to be due to its ability to concurrently block alpha-1 receptors in addition to beta receptors. 53 In experiments in vitro and in trials in patients with diabetes and hypertension, carvedilol increased endothelial vasodilation and reduced inflammation and platelet aggregation. These effects may be achieved though antioxidant actions, thereby preserving nitric oxide bioactivity.54,55
In the Glycemic Effects in Diabetes Mellitus: Carvedilol-Metoprolol Comparison in Hypertensives (GEMINI) trial,56 carvedilol was associated with better maintenance of glycemic control in diabetic hypertensive patients than was metoprolol. Insulin sensitivity improved with carvedilol but not with metoprolol, and fewer patients on carvedilol progressed to microalbuminuria.
Nebivolol
Nebivolol is a novel selective beta-blocker with a much higher affinity for beta-1 adrenergic receptors than for beta-2 adrenergic receptors. Among all the beta-blockers in clinical use today, nebivolol has the highest selectivity for beta-1 receptors.8
Nebivolol causes vasodilation through activation of the l-arginine/nitric oxide pathway.57–59 Blockade of synthesis of nitric oxide leads to local arterial stiffness. Endothelial dysfunction is characterized by decreased bioavailability of nitric oxide and has been shown to be a strong predictor of cardiovascular outcomes. By generating nitric oxide, nebivolol reduces peripheral vascular resistance, overcoming a significant side effect of earlier beta-blockers that lowered blood pressure but ultimately increased peripheral vascular tone and resistance.8
In an experiment in a bovine model,60 nebivolol significantly reduced the pulse-wave velocity (a measure of arterial stiffness), while atenolol had no effect. Moreover, evidence for the role of the l-arginine/nitric oxide pathway in the vasodilatory effect of nebivolol was demonstrated by co-infusion of NG-monomethyl-L-arginine, a specific endothelial nitric oxide synthetase inhibitor that attenuated the reduction of pulse-wave velocity by nebivolol.
In studies in hypertensive patients, nebivolol was associated with a better metabolic profile than atenolol, with none of the adverse effects on insulin sensitivity that atenolol had.61 In the Study of Effects of Nebivolol Interventions on Outcomes and Rehospitalization in Seniors With Heart Failure (SENIORS) trial, significantly fewer patients receiving nebivolol died or were admitted to the hospital for cardiovascular reasons compared with those receiving placebo.62
Although these findings are encouraging, we do not yet know if these effects will translate into a significant reduction in cardiovascular outcomes in clinical trials. Large, prospective hypertension outcome trials, particularly to evaluate primary prevention of cardiovascular outcomes, are needed for an evidence-based approach to using the newer beta-blockers as preferred first-line therapy for hypertension.
WHAT RECENT GUIDELINES SAY ABOUT BETA-BLOCKERS
The British National Institute for Health and Clinical Excellence and the British Hypertension Society, in their 2004 guidelines, recommended beta-blockers as one of several first-line antihypertensive medications in young, nonblack patients.63 On the other hand, they advised clinicians to be aware of the reported increase in onset of diabetes mellitus in patients treated with these medications. After the LIFE24 and ASCOT26 study results were published, these guidelines were amended to exclude beta-blockers as preferred routine initial therapy for hypertension.64
More recently, the 2007 European Society of Hypertension and European Society of Cardiology reconsidered the role of beta-blockers, recommending them as an option in both initial and subsequent antihypertensive treatment strategies.65
The current guidelines from the National Heart, Lung, and Blood Institute,66 which were published in 2003, were highly influenced by the results of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT),2 and favor diuretics as the first-line therapy. However, they indicate that beta-blockers are a suitable alternative, particularly when a compelling cardiac indication is present.53 We hope that the next update, expected late in 2009, will re-address this issue in the light of more recent data.
- Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet 2001; 358:1305–1315.
- ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002; 288:2981–2997.
- Neutel JM, Smith DH, Ram CV, et al. Application of ambulatory blood pressure monitoring in differentiating between antihypertensive agents. Am J Med 1993; 94:181–187.
- Materson BJ, Reda DJ, Cushman WC, et al. Single-drug therapy for hypertension in men. A comparison of six antihypertensive agents with placebo. The Department of Veterans Affairs Cooperative Study Group on Antihypertensive Agents. N Engl J Med 1993; 328:914–921.
- Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associated with antihypertensive therapies used as first-line agents. A systematic review and meta-analysis. JAMA 1997; 277:739–745.
- Frishman W, Silverman R. Clinical pharmacology of the new beta-adrenergic blocking drugs. Part 2. Physiologic and metabolic effects. Am Heart J 1979; 97:797–807.
- Garrett BN, Kaplan NM. Plasma renin activity suppression: duration after withdrawal from beta-adrenergic blockade. Arch Intern Med 1980; 140:1316–1318.
- Pedersen ME, Cockcroft JR. The latest generation of beta-blockers: new pharmacologic properties. Curr Hypertens Rep 2006; 8:279–286.
- Man in’t Veld AJ, Van den Meiracker AH, Schalekamp MA. Do beta-blockers really increase peripheral vascular resistance? Review of the literature and new observations under basal conditions. Am J Hypertens 1988; 1:91–96.
- Pearce CJ, Wallin JD. Labetalol and other agents that block both alpha- and beta-adrenergic receptors. Cleve Clin J Med 1994; 61:59–69.
- Dimsdale JE, Newton RP, Joist T. Neuropsychological side effects of beta-blockers. Arch Intern Med 1989; 149:514–525.
- Agarwal R. Supervised atenolol therapy in the management of hemodialysis hypertension. Kidney Int 1999; 55:1528–1535.
- Sica DA, Black HR. Pharmacologic considerations in the positioning of beta-blockers in antihypertensive therapy. Curr Hypertens Rep 2008; 10:330–335.
- Prichard BN, Gillam GP. Use of propranolol (Inderal) in treatment of hypertension. Br Med J 1964; 19; 2:725–727.
- The fifth report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC V). Arch Intern Med 1993; 153:154–183.
- Moser M. Evolution of the treatment of hypertension from the 1940s to JNC V. Am J Hypertens 1997; 10:2S–8S.
- Houghton T, Freemantle N, Cleland JG. Are beta-blockers effective in patients who develop heart failure soon after myocardial infarction? A meta-regression analysis of randomised trials. Eur J Heart Fail 2000; 2:333–340.
- The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet 1999; 353:9–13.
- Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999; 353:2001–2007.
- Yusuf S, Peto R, Lewis J, Collins R, Sleight P. Beta blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis 1985; 27:335–371.
- Brophy JM, Joseph L, Rouleau JL. Beta-blockers in congestive heart failure. A Bayesian meta-analysis. Ann Intern Med 2001; 134:550–560.
- Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007;CD002003.
- Messerli FH, Grossman E, Goldbourt U. Are beta-blockers efficacious as first-line therapy for hypertension in the elderly? A systematic review. JAMA 1998; 279:1903–1907.
- Dahlöf B, Devereux RB, Kjeldsen SE, et al; for the LIFE study group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint Reduction in Hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359:995–1003.
- Carlberg B, Samuelsson O, Lindholm LH. Atenolol in hypertension: is it a wise choice? Lancet 2004; 364:1684–1689.
- Dahlöf B, Sever PS, Poulter NR, et al; ASCOT Investigators. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet 2005; 366:895–906.
- Lindholm LH, Carlberg B, Samuelsson O. Should beta-blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005; 366:1545–1553.
- Neutel JM, Schnaper H, Cheung DG, Graettinger WF, Weber MA. Antihypertensive effects of beta-blockers administered once daily: 24-hour measurements. Am Heart J 1990; 120:166–171.
- Franklin SS, Gustin W, Wong ND, et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation 1997; 96:308–315.
- The IPPPSH Collaborative Group. Cardiovascular risk and risk factors in a randomized trial of treatment based on the beta-blocker oxprenolol: the International Prospective Primary Prevention Study in Hypertension (IPPPSH). J Hypertens 1985; 3:379–392.
- Williams B, Lacy PS, Thom SM, et al; CAFE Investigators. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes: principal results of the Conduit Artery Function Evaluation (CAFE) study. Circulation 2006; 113:1213–1225.
- Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174:1737–1742.
- Medical Research Council Working Party. MRC trial of treatment of mild hypertension: principal results. BMJ 1985; 291:97–104.
- Coope J, Warrender TS. Randomised trial of treatment of hypertension in elderly patients in primary care. BMJ 1986; 293:1145–1151.
- Dahlöf B, Lindholm LH, Hansson L, et al. Morbidity and mortality in the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). Lancet 1991; 338:1281–1285.
- MRC Working Party. Medical Research Council trial of treatment of hypertension in older adults: principal results. BMJ 1992; 304:405–412.
- The Dutch TIA Study Group. Trial of secondary prevention with atenolol after transient ischemic attack or nondisabling ischemic stroke. Stroke 1993; 24:543–548.
- Eriksson S, Olofsson B-O, Wester P-O; for the TEST Study Group. Atenolol in secondary prevention after stroke. Cerebrovasc Dis 1995; 5:21–25.
- Wilhelmsen L, Berglund G, Elmfeldt D, et al. Beta-blockers versus diuretics in hypertensive men: main results from the HAPPHY trial. J Hypertens 1987; 5:561–572.
- UK Prospective Diabetes Study Group. Efficacy of atenolol and captopril in reducing risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 39. BMJ 1998; 317:713–720.
- Hansson L, Lindholm LH, Niskanen L, et al. Effect of angiotensin-converting enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPP) randomised trial. Lancet 1999; 353:611–616.
- Lanchetti A, Bond MG, Henning M, et al. Calcium antagonist lacidipine slow down progression of asymptomatic carotid atherosclerosis. Principal results of the European Lacidipine Study on Atherosclerosis (ELSA), a randomized, double-blind, long-term trial. Circulation 2002; 106:2422–2427.
- Hansson L, Lindholm LH, Ekbom T, et al. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity in the Swedish Trial in Old Patients with Hypertension-2 study. Lancet 1999; 354:1751–1756.
- Hansson L, Hedner T, Lund-Johansen P, et al. Randomised trial of effects of calcium antagonists compared with diuretics and ß blockers on cardiovascular morbidity and mortality in hypertension: the Nordic Diltiazem (NORDIL) study. Lancet 2000; 356:359–365.
- Pepine CJ, Handsberg EM, Cooper-DeHoff RM, et al. A calcium antagonist vs a non-calcium antagonist hypertension treatment strategy for patients with coronary artery disease. The International Verapamil-Trandolapril Study (INVEST): a randomized controlled trial. JAMA 2003; 290:2805–2816.
- Black HR, Elliott WJ, Grandits G, et al. Principal results of the Controlled Onset Verapamil Investigation of Cardiovascular End Points (CONVINCE) Trial. JAMA 2003; 289:2073–2082.
- Bangalore S, Sawhney S, Messerli FH. Relation of beta-blocker-induced heart rate lowering and cardioprotection in hypertension. J Am Coll Cardiol 2008; 52:1482–1489.
- Boutouyrie P, Vermersch S, Laurent S, Briet M. Cardiovascular risk assessment through target organ damage: role of carotid to femoral pulse wave velocity. Clin Exp Pharmacol Physiol 2008; 35:530–533.
- Kveiborg B, Christiansen B, Major-Petersen A, Torp-Pedersen C. Metabolic effects of beta-adrenoceptor antagonists with special emphasis on carvedilol. Am J Cardiovasc Drugs 2006; 6:209–217.
- Bangalore S, Parkar S, Grossman E, Messerli FH. A meta-analysis of 94,492 patients with hypertension treated with beta-blockers to determine the risk of new-onset diabetes mellitus. Am J Cardiol 2007; 100:1254–1262.
- Balamuthusamy S, Molnar J, Adigopula S, Arora R. Comparative analysis of beta-blockers with other antihypertensive agents on cardiovascular outcomes in hypertensive patients with diabetes mellitus: a systematic review and meta-analysis. Am J Ther 2009; 16:133–142.
- Berenson A. Big drug makers see sales decline with their image. New York Times 2005 Nov 14.
- Bristow MR. Beta-adrenergic receptor blockade in chronic heart failure. Circulation 2000; 101:558–569.
- Giugliano D, Marfella R, Acampora R, Giunta R, Coppola L, D’Onofrio F. Effects of perindopril and carvedilol on endothelium-dependent vascular functions in patients with diabetes and hypertension. Diabetes Care 1998; 21:631–636.
- Lopez BL, Christopher TA, Yue TL, Ruffolo R, Feuerstein GZ, Ma XL. Carvedilol, a new beta-adrenoreceptor blocker antihypertensive drug, protects against free-radical-induced endothelial dysfunction. Pharmacology 1995; 51:165–173.
- Bakris GL, Fonseca V, Katholi RE, et al; GEMINI Investigators. Metabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trial. JAMA 2004; 292:2227–2236.
- Georgescu A, Pluteanu F, Flonta ML, Badila E, Dorobantu M, Popov D. The cellular mechanisms involved in the vasodilator effect of nebivolol on the renal artery. Eur J Pharmacol 2005; 508:159–166.
- Kalinowski L, Dobrucki LW, Szczepanska-Konkel M, et al. Third-generation beta-blockers stimulate nitric oxide release from endothelial cells through ATP efflux: a novel mechanism for antihypertensive action. Circulation 2003; 107:2747–2752.
- Cockcroft JR, Chowienczyk PJ, Brett SE, et al. Nebivolol vasodilates human forearm vasculature: evidence for an L-arginine/NO-dependent mechanism. J Pharmacol Exp Ther 1995; 274:1067–1071.
- McEniery CM, Schmitt M, Qasem A, et al. Nebivolol increases arterial distensibility in vivo. Hypertension 2004; 44:305–310.
- Poirier L, Cleroux J, Nadeau A, Lacourciere Y. Effects of nebivolol and atenolol on insulin sensitivity and haemodynamics in hypertensive patients. J Hypertens 2001; 19:1429–1435.
- Flather MD, Shibata MC, Coats AJ, et al; SENIORS Investigators. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J 2005; 26:215–225.
- Williams B, Poulter NR, Brown MJ, et al; BHS guidelines working party, for the British Hypertension Society. British Hypertension Society guidelines for hypertension management 2004 (BHS-IV): summary. BMJ 2004; 328:634–640.
- Sever P. New hypertension guidelines from the National Institute for Health and Clinical Excellence and the British Hypertension Society. J Renin Angiotensin Aldosterone Syst 2006; 7:61–63.
- Mancia G, De Backer G, Dominiczak A, et al; Management of Arterial Hypertension of the European Society of Hypertension. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2007; 25:1105–1187.
- Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560–2572.
- Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet 2001; 358:1305–1315.
- ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002; 288:2981–2997.
- Neutel JM, Smith DH, Ram CV, et al. Application of ambulatory blood pressure monitoring in differentiating between antihypertensive agents. Am J Med 1993; 94:181–187.
- Materson BJ, Reda DJ, Cushman WC, et al. Single-drug therapy for hypertension in men. A comparison of six antihypertensive agents with placebo. The Department of Veterans Affairs Cooperative Study Group on Antihypertensive Agents. N Engl J Med 1993; 328:914–921.
- Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associated with antihypertensive therapies used as first-line agents. A systematic review and meta-analysis. JAMA 1997; 277:739–745.
- Frishman W, Silverman R. Clinical pharmacology of the new beta-adrenergic blocking drugs. Part 2. Physiologic and metabolic effects. Am Heart J 1979; 97:797–807.
- Garrett BN, Kaplan NM. Plasma renin activity suppression: duration after withdrawal from beta-adrenergic blockade. Arch Intern Med 1980; 140:1316–1318.
- Pedersen ME, Cockcroft JR. The latest generation of beta-blockers: new pharmacologic properties. Curr Hypertens Rep 2006; 8:279–286.
- Man in’t Veld AJ, Van den Meiracker AH, Schalekamp MA. Do beta-blockers really increase peripheral vascular resistance? Review of the literature and new observations under basal conditions. Am J Hypertens 1988; 1:91–96.
- Pearce CJ, Wallin JD. Labetalol and other agents that block both alpha- and beta-adrenergic receptors. Cleve Clin J Med 1994; 61:59–69.
- Dimsdale JE, Newton RP, Joist T. Neuropsychological side effects of beta-blockers. Arch Intern Med 1989; 149:514–525.
- Agarwal R. Supervised atenolol therapy in the management of hemodialysis hypertension. Kidney Int 1999; 55:1528–1535.
- Sica DA, Black HR. Pharmacologic considerations in the positioning of beta-blockers in antihypertensive therapy. Curr Hypertens Rep 2008; 10:330–335.
- Prichard BN, Gillam GP. Use of propranolol (Inderal) in treatment of hypertension. Br Med J 1964; 19; 2:725–727.
- The fifth report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC V). Arch Intern Med 1993; 153:154–183.
- Moser M. Evolution of the treatment of hypertension from the 1940s to JNC V. Am J Hypertens 1997; 10:2S–8S.
- Houghton T, Freemantle N, Cleland JG. Are beta-blockers effective in patients who develop heart failure soon after myocardial infarction? A meta-regression analysis of randomised trials. Eur J Heart Fail 2000; 2:333–340.
- The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet 1999; 353:9–13.
- Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999; 353:2001–2007.
- Yusuf S, Peto R, Lewis J, Collins R, Sleight P. Beta blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis 1985; 27:335–371.
- Brophy JM, Joseph L, Rouleau JL. Beta-blockers in congestive heart failure. A Bayesian meta-analysis. Ann Intern Med 2001; 134:550–560.
- Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007;CD002003.
- Messerli FH, Grossman E, Goldbourt U. Are beta-blockers efficacious as first-line therapy for hypertension in the elderly? A systematic review. JAMA 1998; 279:1903–1907.
- Dahlöf B, Devereux RB, Kjeldsen SE, et al; for the LIFE study group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint Reduction in Hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359:995–1003.
- Carlberg B, Samuelsson O, Lindholm LH. Atenolol in hypertension: is it a wise choice? Lancet 2004; 364:1684–1689.
- Dahlöf B, Sever PS, Poulter NR, et al; ASCOT Investigators. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet 2005; 366:895–906.
- Lindholm LH, Carlberg B, Samuelsson O. Should beta-blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005; 366:1545–1553.
- Neutel JM, Schnaper H, Cheung DG, Graettinger WF, Weber MA. Antihypertensive effects of beta-blockers administered once daily: 24-hour measurements. Am Heart J 1990; 120:166–171.
- Franklin SS, Gustin W, Wong ND, et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation 1997; 96:308–315.
- The IPPPSH Collaborative Group. Cardiovascular risk and risk factors in a randomized trial of treatment based on the beta-blocker oxprenolol: the International Prospective Primary Prevention Study in Hypertension (IPPPSH). J Hypertens 1985; 3:379–392.
- Williams B, Lacy PS, Thom SM, et al; CAFE Investigators. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes: principal results of the Conduit Artery Function Evaluation (CAFE) study. Circulation 2006; 113:1213–1225.
- Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174:1737–1742.
- Medical Research Council Working Party. MRC trial of treatment of mild hypertension: principal results. BMJ 1985; 291:97–104.
- Coope J, Warrender TS. Randomised trial of treatment of hypertension in elderly patients in primary care. BMJ 1986; 293:1145–1151.
- Dahlöf B, Lindholm LH, Hansson L, et al. Morbidity and mortality in the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). Lancet 1991; 338:1281–1285.
- MRC Working Party. Medical Research Council trial of treatment of hypertension in older adults: principal results. BMJ 1992; 304:405–412.
- The Dutch TIA Study Group. Trial of secondary prevention with atenolol after transient ischemic attack or nondisabling ischemic stroke. Stroke 1993; 24:543–548.
- Eriksson S, Olofsson B-O, Wester P-O; for the TEST Study Group. Atenolol in secondary prevention after stroke. Cerebrovasc Dis 1995; 5:21–25.
- Wilhelmsen L, Berglund G, Elmfeldt D, et al. Beta-blockers versus diuretics in hypertensive men: main results from the HAPPHY trial. J Hypertens 1987; 5:561–572.
- UK Prospective Diabetes Study Group. Efficacy of atenolol and captopril in reducing risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 39. BMJ 1998; 317:713–720.
- Hansson L, Lindholm LH, Niskanen L, et al. Effect of angiotensin-converting enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPP) randomised trial. Lancet 1999; 353:611–616.
- Lanchetti A, Bond MG, Henning M, et al. Calcium antagonist lacidipine slow down progression of asymptomatic carotid atherosclerosis. Principal results of the European Lacidipine Study on Atherosclerosis (ELSA), a randomized, double-blind, long-term trial. Circulation 2002; 106:2422–2427.
- Hansson L, Lindholm LH, Ekbom T, et al. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity in the Swedish Trial in Old Patients with Hypertension-2 study. Lancet 1999; 354:1751–1756.
- Hansson L, Hedner T, Lund-Johansen P, et al. Randomised trial of effects of calcium antagonists compared with diuretics and ß blockers on cardiovascular morbidity and mortality in hypertension: the Nordic Diltiazem (NORDIL) study. Lancet 2000; 356:359–365.
- Pepine CJ, Handsberg EM, Cooper-DeHoff RM, et al. A calcium antagonist vs a non-calcium antagonist hypertension treatment strategy for patients with coronary artery disease. The International Verapamil-Trandolapril Study (INVEST): a randomized controlled trial. JAMA 2003; 290:2805–2816.
- Black HR, Elliott WJ, Grandits G, et al. Principal results of the Controlled Onset Verapamil Investigation of Cardiovascular End Points (CONVINCE) Trial. JAMA 2003; 289:2073–2082.
- Bangalore S, Sawhney S, Messerli FH. Relation of beta-blocker-induced heart rate lowering and cardioprotection in hypertension. J Am Coll Cardiol 2008; 52:1482–1489.
- Boutouyrie P, Vermersch S, Laurent S, Briet M. Cardiovascular risk assessment through target organ damage: role of carotid to femoral pulse wave velocity. Clin Exp Pharmacol Physiol 2008; 35:530–533.
- Kveiborg B, Christiansen B, Major-Petersen A, Torp-Pedersen C. Metabolic effects of beta-adrenoceptor antagonists with special emphasis on carvedilol. Am J Cardiovasc Drugs 2006; 6:209–217.
- Bangalore S, Parkar S, Grossman E, Messerli FH. A meta-analysis of 94,492 patients with hypertension treated with beta-blockers to determine the risk of new-onset diabetes mellitus. Am J Cardiol 2007; 100:1254–1262.
- Balamuthusamy S, Molnar J, Adigopula S, Arora R. Comparative analysis of beta-blockers with other antihypertensive agents on cardiovascular outcomes in hypertensive patients with diabetes mellitus: a systematic review and meta-analysis. Am J Ther 2009; 16:133–142.
- Berenson A. Big drug makers see sales decline with their image. New York Times 2005 Nov 14.
- Bristow MR. Beta-adrenergic receptor blockade in chronic heart failure. Circulation 2000; 101:558–569.
- Giugliano D, Marfella R, Acampora R, Giunta R, Coppola L, D’Onofrio F. Effects of perindopril and carvedilol on endothelium-dependent vascular functions in patients with diabetes and hypertension. Diabetes Care 1998; 21:631–636.
- Lopez BL, Christopher TA, Yue TL, Ruffolo R, Feuerstein GZ, Ma XL. Carvedilol, a new beta-adrenoreceptor blocker antihypertensive drug, protects against free-radical-induced endothelial dysfunction. Pharmacology 1995; 51:165–173.
- Bakris GL, Fonseca V, Katholi RE, et al; GEMINI Investigators. Metabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trial. JAMA 2004; 292:2227–2236.
- Georgescu A, Pluteanu F, Flonta ML, Badila E, Dorobantu M, Popov D. The cellular mechanisms involved in the vasodilator effect of nebivolol on the renal artery. Eur J Pharmacol 2005; 508:159–166.
- Kalinowski L, Dobrucki LW, Szczepanska-Konkel M, et al. Third-generation beta-blockers stimulate nitric oxide release from endothelial cells through ATP efflux: a novel mechanism for antihypertensive action. Circulation 2003; 107:2747–2752.
- Cockcroft JR, Chowienczyk PJ, Brett SE, et al. Nebivolol vasodilates human forearm vasculature: evidence for an L-arginine/NO-dependent mechanism. J Pharmacol Exp Ther 1995; 274:1067–1071.
- McEniery CM, Schmitt M, Qasem A, et al. Nebivolol increases arterial distensibility in vivo. Hypertension 2004; 44:305–310.
- Poirier L, Cleroux J, Nadeau A, Lacourciere Y. Effects of nebivolol and atenolol on insulin sensitivity and haemodynamics in hypertensive patients. J Hypertens 2001; 19:1429–1435.
- Flather MD, Shibata MC, Coats AJ, et al; SENIORS Investigators. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J 2005; 26:215–225.
- Williams B, Poulter NR, Brown MJ, et al; BHS guidelines working party, for the British Hypertension Society. British Hypertension Society guidelines for hypertension management 2004 (BHS-IV): summary. BMJ 2004; 328:634–640.
- Sever P. New hypertension guidelines from the National Institute for Health and Clinical Excellence and the British Hypertension Society. J Renin Angiotensin Aldosterone Syst 2006; 7:61–63.
- Mancia G, De Backer G, Dominiczak A, et al; Management of Arterial Hypertension of the European Society of Hypertension. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2007; 25:1105–1187.
- Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560–2572.
KEY POINTS
- No evidence exists that beta-blockers prevent first episodes of cardiovascular events in patients with hypertension, and in some trials, outcomes were worse with beta-blockers than with antihypertensive drugs of other classes.
- Younger hypertensive patients have hemodynamic characteristics that would seem to be amenable to beta-blocker therapy. However, most clinical trials of beta blockers did not stratify patients by age.
- Most trials of the antihypertensive effects of beta-blockers used atenolol (Tenormin), which is not an ideal representative of this class of drugs.
- Newer beta-blockers with vasodilatory properties may overcome the adverse effect of increased peripheral vascular resistance that occurs with older agents such as atenolol.
Vertebroplasty, evidence, and health care reform: What is quality care?

Should only evidence-based medicine be reimbursed?
In this time of intense discussion about ways to reduce health costs, and of President Obama’s desire to include efficacy and safety outcome data in the dialogue of how to deliver health services to everyone (although perhaps not every possible health service to everyone), the practical and philosophical implications of studies like these are worth pondering. Like it or not, the concept that all health care services will be paid for on demand by third-party payers is not a sustainable model of health care.
Randomized placebo-controlled trials are the cornerstone of evidence-based medicine. But at their best they provide only an approximation of the truth. Sample size is always a limitation. Patients and physicians in the office or operating suite do not always behave exactly like those in clinical trials. Yet, well-designed clinical trials are often considered to be the best we can do. Practice guidelines and US Food and Drug Administration approvals are based more on the results of randomized clinical trials and less on information from clinical registries and real-world observational outcome studies (which have technical foibles of their own). Approval for devices and procedures does not historically get the same type of regulatory scrutiny, but health care payers in the future may be less likely to cover the cost of procedures that lack proof of efficacy from rigorously conducted outcome studies. The development of quality care measures also depends on appropriate conduct and application of these trials.
The deadly sins and decision-making
We physicians generally take umbrage with external oversight of our decision-making. It is our job and our responsibility to balance the science (evidence-based medicine) and the art (experience and gestalt) of clinical care for the benefit of our patients. But as I thought about the impact these new studies may exert on vertebroplasty utilization, I also wondered about the factors that influence our decision-making process. For example, we have long had solid data on the value of treating systolic hypertension (we undertreat), and of treating uncomplicated urinary tract infections with only 3 days of antibiotics (we overtreat). Performance indicators suggest that this solid evidence has only a modest influence on practice patterns. Why?
I recently heard Dr. Louis B. Rice, Professor of Medicine at Case Western Reserve University and Chief of the Medical Service at the Louis Stokes Cleveland VA Medical Center, discuss the possible impact of some of the seven deadly sins on clinical decision-making. A similar analysis applies when thinking about why some treatments continue to be offered despite good evidence of only limited efficacy.
Pride plays a role. We believe that our own clinical skills will permit us to select the ideal patient to undergo a procedure or therapy, whereas such cherry-picking of patients does not generally occur in large clinical trials. This argument (and others of “external validity,” in the lingo of evidence-based medicine) has been put forth to defend the continued use of some procedures that may not have fared well against sham controls in clinical trials, and these procedures continue to flourish.
Pride may also apply to the feeling we physicians have for doing something right for our patients. This feeling may push us to believe we can succeed where an impersonal clinical trial failed. I suspect this is most keenly felt when the therapy is a procedure that depends on our own individual skills. I suspect that internists and subspecialists with special interest in osteoporosis will interpret these trials differently than surgeons and interventional radiologists who are routinely performing these procedures.
Avarice must be considered, and regulatory controls in the future may limit financial gain from these therapies. But I am not convinced that monetary greed drives all clinical decisions that go against the grain of evidence-based medicine.
And then there is gluttony: we and our patients want it all. We do not want to hear that our patient cannot be provided the most recent therapeutic advance—it might work.
Placebo effect, other issues in ‘negative’ studies
A number of factors in these trials of vertebroplasty need to be dissected and discussed. Not the least is the apparent salubrious effect of the sham procedure. This was documented previously with intra-articular injections of saline (placebo) in studies of hyaluronate joint injections for the pain of knee osteoarthritis,3 in which either type of injection provided significant pain relief. Are these truly markedly positive effects of the sham but invasive maneuvers in the vertebroplasty studies, or are we witnessing the natural history of pain resolution in these disorders (in the absence of a true nonintervention control group that could help make this distinction)?
Crossover issues in one of the vertebroplasty papers will certainly generate letters to the editor. Were patients really blinded to their procedure throughout? Which subsets of patients might have responded better or worse? What about balloon kyphoplasty?
We plan to publish commentaries from proceduralists and medical experts in osteoporosis to critique these key clinical trials for us and to put these issues into clinical perspective.
What role for evidence-based medicine?
In the meantime, I urge you to peruse these papers along with the op-ed pieces in your local newspapers as catalysts to reconsider the role evidence-based medicine should play in our daily one-on-one routine with patients, as well as in the redesign of our health care delivery and reimbursement systems. I don’t think that clinical conundrums can be resolved with a simple look at P values and confidence intervals; clinical trials are not the total story. As physicians, we always need to put the trial results into a clinical perspective. Nonetheless, our personal belief of efficacy (or lack of efficacy) also should not be the total story as we make decisions with individual patients and allocate resources within the health care system.
In the end, it should be all about giving high-quality care to the patient sitting in front of us. A question to be addressed is how well we can assess the quality of a given treatment prior to its administration.
- Kallmes DF, Comstock BA, Heagerty PJ, et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med 2009; 361:569–579.
- Buchbinder R, Osborne RH, Ebeling PR, et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med 2009; 361:557–568.
- Lundsgaard C, Dufour N, Fallentin E, Winkel P, Gluud C. Intra-articular sodium hyaluronate 2 mL versus physiological saline 20 mL versus physiological saline 2 mL for painful knee osteoarthritis: a randomized clinical trial. Scand J Rheumatol 2008; 37:142–150.
Should only evidence-based medicine be reimbursed?
In this time of intense discussion about ways to reduce health costs, and of President Obama’s desire to include efficacy and safety outcome data in the dialogue of how to deliver health services to everyone (although perhaps not every possible health service to everyone), the practical and philosophical implications of studies like these are worth pondering. Like it or not, the concept that all health care services will be paid for on demand by third-party payers is not a sustainable model of health care.
Randomized placebo-controlled trials are the cornerstone of evidence-based medicine. But at their best they provide only an approximation of the truth. Sample size is always a limitation. Patients and physicians in the office or operating suite do not always behave exactly like those in clinical trials. Yet, well-designed clinical trials are often considered to be the best we can do. Practice guidelines and US Food and Drug Administration approvals are based more on the results of randomized clinical trials and less on information from clinical registries and real-world observational outcome studies (which have technical foibles of their own). Approval for devices and procedures does not historically get the same type of regulatory scrutiny, but health care payers in the future may be less likely to cover the cost of procedures that lack proof of efficacy from rigorously conducted outcome studies. The development of quality care measures also depends on appropriate conduct and application of these trials.
The deadly sins and decision-making
We physicians generally take umbrage with external oversight of our decision-making. It is our job and our responsibility to balance the science (evidence-based medicine) and the art (experience and gestalt) of clinical care for the benefit of our patients. But as I thought about the impact these new studies may exert on vertebroplasty utilization, I also wondered about the factors that influence our decision-making process. For example, we have long had solid data on the value of treating systolic hypertension (we undertreat), and of treating uncomplicated urinary tract infections with only 3 days of antibiotics (we overtreat). Performance indicators suggest that this solid evidence has only a modest influence on practice patterns. Why?
I recently heard Dr. Louis B. Rice, Professor of Medicine at Case Western Reserve University and Chief of the Medical Service at the Louis Stokes Cleveland VA Medical Center, discuss the possible impact of some of the seven deadly sins on clinical decision-making. A similar analysis applies when thinking about why some treatments continue to be offered despite good evidence of only limited efficacy.
Pride plays a role. We believe that our own clinical skills will permit us to select the ideal patient to undergo a procedure or therapy, whereas such cherry-picking of patients does not generally occur in large clinical trials. This argument (and others of “external validity,” in the lingo of evidence-based medicine) has been put forth to defend the continued use of some procedures that may not have fared well against sham controls in clinical trials, and these procedures continue to flourish.
Pride may also apply to the feeling we physicians have for doing something right for our patients. This feeling may push us to believe we can succeed where an impersonal clinical trial failed. I suspect this is most keenly felt when the therapy is a procedure that depends on our own individual skills. I suspect that internists and subspecialists with special interest in osteoporosis will interpret these trials differently than surgeons and interventional radiologists who are routinely performing these procedures.
Avarice must be considered, and regulatory controls in the future may limit financial gain from these therapies. But I am not convinced that monetary greed drives all clinical decisions that go against the grain of evidence-based medicine.
And then there is gluttony: we and our patients want it all. We do not want to hear that our patient cannot be provided the most recent therapeutic advance—it might work.
Placebo effect, other issues in ‘negative’ studies
A number of factors in these trials of vertebroplasty need to be dissected and discussed. Not the least is the apparent salubrious effect of the sham procedure. This was documented previously with intra-articular injections of saline (placebo) in studies of hyaluronate joint injections for the pain of knee osteoarthritis,3 in which either type of injection provided significant pain relief. Are these truly markedly positive effects of the sham but invasive maneuvers in the vertebroplasty studies, or are we witnessing the natural history of pain resolution in these disorders (in the absence of a true nonintervention control group that could help make this distinction)?
Crossover issues in one of the vertebroplasty papers will certainly generate letters to the editor. Were patients really blinded to their procedure throughout? Which subsets of patients might have responded better or worse? What about balloon kyphoplasty?
We plan to publish commentaries from proceduralists and medical experts in osteoporosis to critique these key clinical trials for us and to put these issues into clinical perspective.
What role for evidence-based medicine?
In the meantime, I urge you to peruse these papers along with the op-ed pieces in your local newspapers as catalysts to reconsider the role evidence-based medicine should play in our daily one-on-one routine with patients, as well as in the redesign of our health care delivery and reimbursement systems. I don’t think that clinical conundrums can be resolved with a simple look at P values and confidence intervals; clinical trials are not the total story. As physicians, we always need to put the trial results into a clinical perspective. Nonetheless, our personal belief of efficacy (or lack of efficacy) also should not be the total story as we make decisions with individual patients and allocate resources within the health care system.
In the end, it should be all about giving high-quality care to the patient sitting in front of us. A question to be addressed is how well we can assess the quality of a given treatment prior to its administration.
Should only evidence-based medicine be reimbursed?
In this time of intense discussion about ways to reduce health costs, and of President Obama’s desire to include efficacy and safety outcome data in the dialogue of how to deliver health services to everyone (although perhaps not every possible health service to everyone), the practical and philosophical implications of studies like these are worth pondering. Like it or not, the concept that all health care services will be paid for on demand by third-party payers is not a sustainable model of health care.
Randomized placebo-controlled trials are the cornerstone of evidence-based medicine. But at their best they provide only an approximation of the truth. Sample size is always a limitation. Patients and physicians in the office or operating suite do not always behave exactly like those in clinical trials. Yet, well-designed clinical trials are often considered to be the best we can do. Practice guidelines and US Food and Drug Administration approvals are based more on the results of randomized clinical trials and less on information from clinical registries and real-world observational outcome studies (which have technical foibles of their own). Approval for devices and procedures does not historically get the same type of regulatory scrutiny, but health care payers in the future may be less likely to cover the cost of procedures that lack proof of efficacy from rigorously conducted outcome studies. The development of quality care measures also depends on appropriate conduct and application of these trials.
The deadly sins and decision-making
We physicians generally take umbrage with external oversight of our decision-making. It is our job and our responsibility to balance the science (evidence-based medicine) and the art (experience and gestalt) of clinical care for the benefit of our patients. But as I thought about the impact these new studies may exert on vertebroplasty utilization, I also wondered about the factors that influence our decision-making process. For example, we have long had solid data on the value of treating systolic hypertension (we undertreat), and of treating uncomplicated urinary tract infections with only 3 days of antibiotics (we overtreat). Performance indicators suggest that this solid evidence has only a modest influence on practice patterns. Why?
I recently heard Dr. Louis B. Rice, Professor of Medicine at Case Western Reserve University and Chief of the Medical Service at the Louis Stokes Cleveland VA Medical Center, discuss the possible impact of some of the seven deadly sins on clinical decision-making. A similar analysis applies when thinking about why some treatments continue to be offered despite good evidence of only limited efficacy.
Pride plays a role. We believe that our own clinical skills will permit us to select the ideal patient to undergo a procedure or therapy, whereas such cherry-picking of patients does not generally occur in large clinical trials. This argument (and others of “external validity,” in the lingo of evidence-based medicine) has been put forth to defend the continued use of some procedures that may not have fared well against sham controls in clinical trials, and these procedures continue to flourish.
Pride may also apply to the feeling we physicians have for doing something right for our patients. This feeling may push us to believe we can succeed where an impersonal clinical trial failed. I suspect this is most keenly felt when the therapy is a procedure that depends on our own individual skills. I suspect that internists and subspecialists with special interest in osteoporosis will interpret these trials differently than surgeons and interventional radiologists who are routinely performing these procedures.
Avarice must be considered, and regulatory controls in the future may limit financial gain from these therapies. But I am not convinced that monetary greed drives all clinical decisions that go against the grain of evidence-based medicine.
And then there is gluttony: we and our patients want it all. We do not want to hear that our patient cannot be provided the most recent therapeutic advance—it might work.
Placebo effect, other issues in ‘negative’ studies
A number of factors in these trials of vertebroplasty need to be dissected and discussed. Not the least is the apparent salubrious effect of the sham procedure. This was documented previously with intra-articular injections of saline (placebo) in studies of hyaluronate joint injections for the pain of knee osteoarthritis,3 in which either type of injection provided significant pain relief. Are these truly markedly positive effects of the sham but invasive maneuvers in the vertebroplasty studies, or are we witnessing the natural history of pain resolution in these disorders (in the absence of a true nonintervention control group that could help make this distinction)?
Crossover issues in one of the vertebroplasty papers will certainly generate letters to the editor. Were patients really blinded to their procedure throughout? Which subsets of patients might have responded better or worse? What about balloon kyphoplasty?
We plan to publish commentaries from proceduralists and medical experts in osteoporosis to critique these key clinical trials for us and to put these issues into clinical perspective.
What role for evidence-based medicine?
In the meantime, I urge you to peruse these papers along with the op-ed pieces in your local newspapers as catalysts to reconsider the role evidence-based medicine should play in our daily one-on-one routine with patients, as well as in the redesign of our health care delivery and reimbursement systems. I don’t think that clinical conundrums can be resolved with a simple look at P values and confidence intervals; clinical trials are not the total story. As physicians, we always need to put the trial results into a clinical perspective. Nonetheless, our personal belief of efficacy (or lack of efficacy) also should not be the total story as we make decisions with individual patients and allocate resources within the health care system.
In the end, it should be all about giving high-quality care to the patient sitting in front of us. A question to be addressed is how well we can assess the quality of a given treatment prior to its administration.
- Kallmes DF, Comstock BA, Heagerty PJ, et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med 2009; 361:569–579.
- Buchbinder R, Osborne RH, Ebeling PR, et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med 2009; 361:557–568.
- Lundsgaard C, Dufour N, Fallentin E, Winkel P, Gluud C. Intra-articular sodium hyaluronate 2 mL versus physiological saline 20 mL versus physiological saline 2 mL for painful knee osteoarthritis: a randomized clinical trial. Scand J Rheumatol 2008; 37:142–150.
- Kallmes DF, Comstock BA, Heagerty PJ, et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med 2009; 361:569–579.
- Buchbinder R, Osborne RH, Ebeling PR, et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med 2009; 361:557–568.
- Lundsgaard C, Dufour N, Fallentin E, Winkel P, Gluud C. Intra-articular sodium hyaluronate 2 mL versus physiological saline 20 mL versus physiological saline 2 mL for painful knee osteoarthritis: a randomized clinical trial. Scand J Rheumatol 2008; 37:142–150.
Tinea Cruris in Children
Fungal Foes: Rhinosporidium seeberi
That time of year: Turn back the clock, watch H1N1 flu return, and adopt a new ICD-9 code set
Additions and revision to this year’s International Classification of Diseases, Clinical Modification (ICD-9-CM)—which go into effect on October 1—reflect tinkering with existing codes and expansion of others to boost granularity and clarity in your reporting of diagnostic work. To that add a number of new codes—including one that acknowledges the arrival of the H1N1 (swine flu) virus nationwide.
In obstetrics, there are now specific codes for different types of puerperal infection and a requirement for more diagnostic information when a patient has venous complications during pregnancy and intrapartum.
On the gynecology side, changes include the way you report a finding of endometrial intraepithelial neoplasia. New codes have been created to report:
- visits and procedures for fertility preservation
- inconclusive mammography
- preprocedural laboratory testing.
Remember: On October 1, 2009, the new and revised codes discussed here, plus others, will be added to the national ICD-9-CM code set. Be cautioned that, as in past years, there is no grace period!
Changes to obstetric codes
PUERPERAL INFECTIONS
Before October 1, 2009, all puerperal infections were lumped into one code: 670.0 (Major puerperal infection). This changes now: You’ll be required to document, more specifically, the type of infection that your patient has.
Continue to report code 670.0 for an unspecified puerperal infection; but, if you admit the patient to the hospital, using that unspecified code may lead to a first-submission denial of claim. A fifth digit is also required for the unspecified and new more specific codes: 0 (unspecified as to episode of care or not applicable), 2 (delivered with mention of postpartum complication), or 4 (postpartum condition or complication) (to be reported only once the patient is discharged after delivery).
670.1x [0,2,4] Puerperal endometritis
670.2x [0,2,4] Puerperal sepsis
670.3x [0,2,4] Puerperal septic thrombophlebitis
670.8x [0,2,4] Other major puerperal infection
VENOUS COMPLICATIONS IN PREGNANCY AND PUERPERIUM
Code category 671 (venous complications in pregnancy and the puerperium) retains its current codes, but ICD-9 has added notes to clarify that additional information is required.
For example: When a patient has deep-vein thrombosis, either antepartum (671.3x) or postpartum (671.4x), assign a secondary diagnosis from code category 453 (Other venous embolism and thrombosis). If, in addition, the patient has been taking an anticoagulant for a long time and is currently taking it, report code V56.81, as well, to indicate this.
Gyn code changes
HYPERPLASIA
Over time, codes for hyperplasia have evolved from a system that described mild, moderate, severe, or atypical, to one in which hyperplasia was subdivided by architectural complexity, such as simple versus complex and whether or not atypia were present. Even this terminology fails, however, to adequately identify patients’ risk of cancer to improve therapeutic triaging.
In more recent years, physicians and pathologists have begun to distinguish benign hormonal effects of unopposed estrogen, classified as benign hyperplasia, from pre-cancerous lesions classified as endometrial intraepithelial neoplasia (EIN). To capture this newer terminology, ICD-9 has added two new codes.
ICD-9 has elected to retain existing codes in this area of diagnosis and assessment because the old terminology is still used by many older practicing physicians. The hope, however, is that, over time, more accurate distinctions between the types of hyperplasia will replace the older distinctions.
A note in ICD-9 will instruct providers that older codes may not be reported if one of the newer codes is assigned.
An additional note that accompanies the EIN diagnosis indicates that, if a patient is given a diagnosis of malignant neoplasm of the endometrium with endometrial intraepithelial neoplasia, the code for the malignancy (182.0, Malignant neoplasm of body of uterus; corpus uteri, except isthmus) would be reported instead of the EIN code.
621.34 Benign endometrial hyperplasia
621.35 Endometrial intraepithelial neoplasia
Routine mammograms are, as you know, sometimes labeled “inconclusive” because of what are termed “dense breasts.” This finding isn’t considered to represent an abnormal condition, but it does require further testing to confirm that no malignant condition exists that cannot be seen on mammogram.
Because many payers cover a repeat mammogram only when an abnormal finding is reported, a new code has been needed—and has now been added—to explain the reason for a second mammogram.
Because of the added code, ICD-9 also decided to revise wording for the 793 code category (until now, it’s been Nonspecific abnormal findings on radiological and other examination of body structure) to a more general heading of Nonspecific findings, which covers inconclusive and abnormal findings.
793.82 Inconclusive mammogram
FERTILITY PRESERVATION PRIOR TO ANTINEOPLASTIC THERAPY
Two new codes have been added to this area of practice at the request of the American Society for Reproductive Medicine (ASRM) and ACOG. They allow you to report visits and procedures aimed at preserving fertility in women who must undergo chemotherapy, surgery, or radiation therapy that might otherwise leave them sterile.
The codes reflect that, before a patient is treated, you may discuss a range of options that can increase her chances of becoming pregnant, including:
- conception before cancer treatment
- banking of sperm, eggs, ovarian tissue, and embryos
- protecting the ovaries during radiation therapy
- modifying surgery to spare the uterus.
V26.42 Encounter for fertility preservation counseling
V26.82 Encounter for fertility preservation procedure
PREPROCEDURAL EVALUATIONS
Code category V72.6 has been expanded from four to five digits to better capture reasons for ordering or performing laboratory tests that are not specifically linked to a medical diagnosis.
For example: If you order routine tests as part of a routine, general medical or gyn annual examination, report code V72.62. For routine preoperative lab tests, report V72.63 instead.
ICD-9 has clarified that V72.61 can be reported for testing of immune status, and that current code V72.83 (Other specified pre-operative examination) is the one to report when an exam precedes chemotherapy.
Note: ICD-9 rules require that you list the preprocedural examination code as the primary diagnosis, followed by the code that represents the reason for the surgery or procedure.
V72.60 Laboratory examination, unspecified
V72.61 Antibody response examination
V72.62 Laboratory examination ordered as part of a routine general medical examination
V72.63 Preprocedural laboratory examination
V72.69 Other laboratory examination
PERSONAL HISTORY CODES
A history of drug therapy can affect the care that you are giving a patient now, and may require testing from time to time to assess the consequences of such therapy.
Two examples are long-term estrogen therapy, which may increase a woman’s risk of developing breast cancer, and inhaled steroids, which can decrease bone density. In the absence of a known problem with these (or other) therapies in a given patient, new history codes listed below may be useful in communicating with a payer about ongoing follow-up care or testing that you are providing.
V87.43 Personal history of estrogen therapy
V87.44 Personal history of inhaled steroid therapy
V87.45 Personal history of systemic steroid therapy
V87.46 Personal history of immunosuppressive therapy
Plus a number of miscellaneous additions and changes
Here are few more new codes that may better explain why you saw a patient, provided:
- the new code for swine flu is reported only for a confirmed case, per ICD-9 rules
- the new V codes are reported only if the personal history or family circumstance affected treatment at the time of the visit, or if the patient was receiving counseling concerning only those issues.
995.24 Failed moderate sedation during procedure
V10.90 Personal history of unspecified type of malignant neoplasm
V15.80 Personal history of failed moderate sedation
V61.07 Family disruption due to death of family member
V61.08 Family disruption due to other extended absence of a family member
V61.42 Substance abuse in family
Additions and revision to this year’s International Classification of Diseases, Clinical Modification (ICD-9-CM)—which go into effect on October 1—reflect tinkering with existing codes and expansion of others to boost granularity and clarity in your reporting of diagnostic work. To that add a number of new codes—including one that acknowledges the arrival of the H1N1 (swine flu) virus nationwide.
In obstetrics, there are now specific codes for different types of puerperal infection and a requirement for more diagnostic information when a patient has venous complications during pregnancy and intrapartum.
On the gynecology side, changes include the way you report a finding of endometrial intraepithelial neoplasia. New codes have been created to report:
- visits and procedures for fertility preservation
- inconclusive mammography
- preprocedural laboratory testing.
Remember: On October 1, 2009, the new and revised codes discussed here, plus others, will be added to the national ICD-9-CM code set. Be cautioned that, as in past years, there is no grace period!
Changes to obstetric codes
PUERPERAL INFECTIONS
Before October 1, 2009, all puerperal infections were lumped into one code: 670.0 (Major puerperal infection). This changes now: You’ll be required to document, more specifically, the type of infection that your patient has.
Continue to report code 670.0 for an unspecified puerperal infection; but, if you admit the patient to the hospital, using that unspecified code may lead to a first-submission denial of claim. A fifth digit is also required for the unspecified and new more specific codes: 0 (unspecified as to episode of care or not applicable), 2 (delivered with mention of postpartum complication), or 4 (postpartum condition or complication) (to be reported only once the patient is discharged after delivery).
670.1x [0,2,4] Puerperal endometritis
670.2x [0,2,4] Puerperal sepsis
670.3x [0,2,4] Puerperal septic thrombophlebitis
670.8x [0,2,4] Other major puerperal infection
VENOUS COMPLICATIONS IN PREGNANCY AND PUERPERIUM
Code category 671 (venous complications in pregnancy and the puerperium) retains its current codes, but ICD-9 has added notes to clarify that additional information is required.
For example: When a patient has deep-vein thrombosis, either antepartum (671.3x) or postpartum (671.4x), assign a secondary diagnosis from code category 453 (Other venous embolism and thrombosis). If, in addition, the patient has been taking an anticoagulant for a long time and is currently taking it, report code V56.81, as well, to indicate this.
Gyn code changes
HYPERPLASIA
Over time, codes for hyperplasia have evolved from a system that described mild, moderate, severe, or atypical, to one in which hyperplasia was subdivided by architectural complexity, such as simple versus complex and whether or not atypia were present. Even this terminology fails, however, to adequately identify patients’ risk of cancer to improve therapeutic triaging.
In more recent years, physicians and pathologists have begun to distinguish benign hormonal effects of unopposed estrogen, classified as benign hyperplasia, from pre-cancerous lesions classified as endometrial intraepithelial neoplasia (EIN). To capture this newer terminology, ICD-9 has added two new codes.
ICD-9 has elected to retain existing codes in this area of diagnosis and assessment because the old terminology is still used by many older practicing physicians. The hope, however, is that, over time, more accurate distinctions between the types of hyperplasia will replace the older distinctions.
A note in ICD-9 will instruct providers that older codes may not be reported if one of the newer codes is assigned.
An additional note that accompanies the EIN diagnosis indicates that, if a patient is given a diagnosis of malignant neoplasm of the endometrium with endometrial intraepithelial neoplasia, the code for the malignancy (182.0, Malignant neoplasm of body of uterus; corpus uteri, except isthmus) would be reported instead of the EIN code.
621.34 Benign endometrial hyperplasia
621.35 Endometrial intraepithelial neoplasia
Routine mammograms are, as you know, sometimes labeled “inconclusive” because of what are termed “dense breasts.” This finding isn’t considered to represent an abnormal condition, but it does require further testing to confirm that no malignant condition exists that cannot be seen on mammogram.
Because many payers cover a repeat mammogram only when an abnormal finding is reported, a new code has been needed—and has now been added—to explain the reason for a second mammogram.
Because of the added code, ICD-9 also decided to revise wording for the 793 code category (until now, it’s been Nonspecific abnormal findings on radiological and other examination of body structure) to a more general heading of Nonspecific findings, which covers inconclusive and abnormal findings.
793.82 Inconclusive mammogram
FERTILITY PRESERVATION PRIOR TO ANTINEOPLASTIC THERAPY
Two new codes have been added to this area of practice at the request of the American Society for Reproductive Medicine (ASRM) and ACOG. They allow you to report visits and procedures aimed at preserving fertility in women who must undergo chemotherapy, surgery, or radiation therapy that might otherwise leave them sterile.
The codes reflect that, before a patient is treated, you may discuss a range of options that can increase her chances of becoming pregnant, including:
- conception before cancer treatment
- banking of sperm, eggs, ovarian tissue, and embryos
- protecting the ovaries during radiation therapy
- modifying surgery to spare the uterus.
V26.42 Encounter for fertility preservation counseling
V26.82 Encounter for fertility preservation procedure
PREPROCEDURAL EVALUATIONS
Code category V72.6 has been expanded from four to five digits to better capture reasons for ordering or performing laboratory tests that are not specifically linked to a medical diagnosis.
For example: If you order routine tests as part of a routine, general medical or gyn annual examination, report code V72.62. For routine preoperative lab tests, report V72.63 instead.
ICD-9 has clarified that V72.61 can be reported for testing of immune status, and that current code V72.83 (Other specified pre-operative examination) is the one to report when an exam precedes chemotherapy.
Note: ICD-9 rules require that you list the preprocedural examination code as the primary diagnosis, followed by the code that represents the reason for the surgery or procedure.
V72.60 Laboratory examination, unspecified
V72.61 Antibody response examination
V72.62 Laboratory examination ordered as part of a routine general medical examination
V72.63 Preprocedural laboratory examination
V72.69 Other laboratory examination
PERSONAL HISTORY CODES
A history of drug therapy can affect the care that you are giving a patient now, and may require testing from time to time to assess the consequences of such therapy.
Two examples are long-term estrogen therapy, which may increase a woman’s risk of developing breast cancer, and inhaled steroids, which can decrease bone density. In the absence of a known problem with these (or other) therapies in a given patient, new history codes listed below may be useful in communicating with a payer about ongoing follow-up care or testing that you are providing.
V87.43 Personal history of estrogen therapy
V87.44 Personal history of inhaled steroid therapy
V87.45 Personal history of systemic steroid therapy
V87.46 Personal history of immunosuppressive therapy
Plus a number of miscellaneous additions and changes
Here are few more new codes that may better explain why you saw a patient, provided:
- the new code for swine flu is reported only for a confirmed case, per ICD-9 rules
- the new V codes are reported only if the personal history or family circumstance affected treatment at the time of the visit, or if the patient was receiving counseling concerning only those issues.
995.24 Failed moderate sedation during procedure
V10.90 Personal history of unspecified type of malignant neoplasm
V15.80 Personal history of failed moderate sedation
V61.07 Family disruption due to death of family member
V61.08 Family disruption due to other extended absence of a family member
V61.42 Substance abuse in family
Additions and revision to this year’s International Classification of Diseases, Clinical Modification (ICD-9-CM)—which go into effect on October 1—reflect tinkering with existing codes and expansion of others to boost granularity and clarity in your reporting of diagnostic work. To that add a number of new codes—including one that acknowledges the arrival of the H1N1 (swine flu) virus nationwide.
In obstetrics, there are now specific codes for different types of puerperal infection and a requirement for more diagnostic information when a patient has venous complications during pregnancy and intrapartum.
On the gynecology side, changes include the way you report a finding of endometrial intraepithelial neoplasia. New codes have been created to report:
- visits and procedures for fertility preservation
- inconclusive mammography
- preprocedural laboratory testing.
Remember: On October 1, 2009, the new and revised codes discussed here, plus others, will be added to the national ICD-9-CM code set. Be cautioned that, as in past years, there is no grace period!
Changes to obstetric codes
PUERPERAL INFECTIONS
Before October 1, 2009, all puerperal infections were lumped into one code: 670.0 (Major puerperal infection). This changes now: You’ll be required to document, more specifically, the type of infection that your patient has.
Continue to report code 670.0 for an unspecified puerperal infection; but, if you admit the patient to the hospital, using that unspecified code may lead to a first-submission denial of claim. A fifth digit is also required for the unspecified and new more specific codes: 0 (unspecified as to episode of care or not applicable), 2 (delivered with mention of postpartum complication), or 4 (postpartum condition or complication) (to be reported only once the patient is discharged after delivery).
670.1x [0,2,4] Puerperal endometritis
670.2x [0,2,4] Puerperal sepsis
670.3x [0,2,4] Puerperal septic thrombophlebitis
670.8x [0,2,4] Other major puerperal infection
VENOUS COMPLICATIONS IN PREGNANCY AND PUERPERIUM
Code category 671 (venous complications in pregnancy and the puerperium) retains its current codes, but ICD-9 has added notes to clarify that additional information is required.
For example: When a patient has deep-vein thrombosis, either antepartum (671.3x) or postpartum (671.4x), assign a secondary diagnosis from code category 453 (Other venous embolism and thrombosis). If, in addition, the patient has been taking an anticoagulant for a long time and is currently taking it, report code V56.81, as well, to indicate this.
Gyn code changes
HYPERPLASIA
Over time, codes for hyperplasia have evolved from a system that described mild, moderate, severe, or atypical, to one in which hyperplasia was subdivided by architectural complexity, such as simple versus complex and whether or not atypia were present. Even this terminology fails, however, to adequately identify patients’ risk of cancer to improve therapeutic triaging.
In more recent years, physicians and pathologists have begun to distinguish benign hormonal effects of unopposed estrogen, classified as benign hyperplasia, from pre-cancerous lesions classified as endometrial intraepithelial neoplasia (EIN). To capture this newer terminology, ICD-9 has added two new codes.
ICD-9 has elected to retain existing codes in this area of diagnosis and assessment because the old terminology is still used by many older practicing physicians. The hope, however, is that, over time, more accurate distinctions between the types of hyperplasia will replace the older distinctions.
A note in ICD-9 will instruct providers that older codes may not be reported if one of the newer codes is assigned.
An additional note that accompanies the EIN diagnosis indicates that, if a patient is given a diagnosis of malignant neoplasm of the endometrium with endometrial intraepithelial neoplasia, the code for the malignancy (182.0, Malignant neoplasm of body of uterus; corpus uteri, except isthmus) would be reported instead of the EIN code.
621.34 Benign endometrial hyperplasia
621.35 Endometrial intraepithelial neoplasia
Routine mammograms are, as you know, sometimes labeled “inconclusive” because of what are termed “dense breasts.” This finding isn’t considered to represent an abnormal condition, but it does require further testing to confirm that no malignant condition exists that cannot be seen on mammogram.
Because many payers cover a repeat mammogram only when an abnormal finding is reported, a new code has been needed—and has now been added—to explain the reason for a second mammogram.
Because of the added code, ICD-9 also decided to revise wording for the 793 code category (until now, it’s been Nonspecific abnormal findings on radiological and other examination of body structure) to a more general heading of Nonspecific findings, which covers inconclusive and abnormal findings.
793.82 Inconclusive mammogram
FERTILITY PRESERVATION PRIOR TO ANTINEOPLASTIC THERAPY
Two new codes have been added to this area of practice at the request of the American Society for Reproductive Medicine (ASRM) and ACOG. They allow you to report visits and procedures aimed at preserving fertility in women who must undergo chemotherapy, surgery, or radiation therapy that might otherwise leave them sterile.
The codes reflect that, before a patient is treated, you may discuss a range of options that can increase her chances of becoming pregnant, including:
- conception before cancer treatment
- banking of sperm, eggs, ovarian tissue, and embryos
- protecting the ovaries during radiation therapy
- modifying surgery to spare the uterus.
V26.42 Encounter for fertility preservation counseling
V26.82 Encounter for fertility preservation procedure
PREPROCEDURAL EVALUATIONS
Code category V72.6 has been expanded from four to five digits to better capture reasons for ordering or performing laboratory tests that are not specifically linked to a medical diagnosis.
For example: If you order routine tests as part of a routine, general medical or gyn annual examination, report code V72.62. For routine preoperative lab tests, report V72.63 instead.
ICD-9 has clarified that V72.61 can be reported for testing of immune status, and that current code V72.83 (Other specified pre-operative examination) is the one to report when an exam precedes chemotherapy.
Note: ICD-9 rules require that you list the preprocedural examination code as the primary diagnosis, followed by the code that represents the reason for the surgery or procedure.
V72.60 Laboratory examination, unspecified
V72.61 Antibody response examination
V72.62 Laboratory examination ordered as part of a routine general medical examination
V72.63 Preprocedural laboratory examination
V72.69 Other laboratory examination
PERSONAL HISTORY CODES
A history of drug therapy can affect the care that you are giving a patient now, and may require testing from time to time to assess the consequences of such therapy.
Two examples are long-term estrogen therapy, which may increase a woman’s risk of developing breast cancer, and inhaled steroids, which can decrease bone density. In the absence of a known problem with these (or other) therapies in a given patient, new history codes listed below may be useful in communicating with a payer about ongoing follow-up care or testing that you are providing.
V87.43 Personal history of estrogen therapy
V87.44 Personal history of inhaled steroid therapy
V87.45 Personal history of systemic steroid therapy
V87.46 Personal history of immunosuppressive therapy
Plus a number of miscellaneous additions and changes
Here are few more new codes that may better explain why you saw a patient, provided:
- the new code for swine flu is reported only for a confirmed case, per ICD-9 rules
- the new V codes are reported only if the personal history or family circumstance affected treatment at the time of the visit, or if the patient was receiving counseling concerning only those issues.
995.24 Failed moderate sedation during procedure
V10.90 Personal history of unspecified type of malignant neoplasm
V15.80 Personal history of failed moderate sedation
V61.07 Family disruption due to death of family member
V61.08 Family disruption due to other extended absence of a family member
V61.42 Substance abuse in family