User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
FDA authorizes updated COVID boosters to target newest variants
The agency cited data to support the safety and efficacy of this next generation of mRNA vaccines targeted toward variants of concern.
The Pfizer EUA corresponds to the company’s combination booster shot that includes the original COVID-19 vaccine as well as a vaccine specifically designed to protect against the most recent Omicron variants, BA.4 and BA.5.
The Moderna combination vaccine will contain both the firm’s original COVID-19 vaccine and a vaccine to protect specifically against Omicron BA.4 and BA.5 subvariants.
As of Aug. 27, BA.4 and BA.4.6 account for about 11% of circulating variants and BA.5 accounts for almost all the remaining 89%, Centers for Disease Control and Prevention data show.
The next step will be review of the scientific data by the CDC’s Advisory Committee on Immunization Practices, which is set to meet Sept. 1 and 2. The final hurdle before distribution of the new vaccines will be sign-off on CDC recommendations for use by agency Director Rochelle Walensky, MD.
This is a developing story. A version of this article first appeared on WebMD.com.
The agency cited data to support the safety and efficacy of this next generation of mRNA vaccines targeted toward variants of concern.
The Pfizer EUA corresponds to the company’s combination booster shot that includes the original COVID-19 vaccine as well as a vaccine specifically designed to protect against the most recent Omicron variants, BA.4 and BA.5.
The Moderna combination vaccine will contain both the firm’s original COVID-19 vaccine and a vaccine to protect specifically against Omicron BA.4 and BA.5 subvariants.
As of Aug. 27, BA.4 and BA.4.6 account for about 11% of circulating variants and BA.5 accounts for almost all the remaining 89%, Centers for Disease Control and Prevention data show.
The next step will be review of the scientific data by the CDC’s Advisory Committee on Immunization Practices, which is set to meet Sept. 1 and 2. The final hurdle before distribution of the new vaccines will be sign-off on CDC recommendations for use by agency Director Rochelle Walensky, MD.
This is a developing story. A version of this article first appeared on WebMD.com.
The agency cited data to support the safety and efficacy of this next generation of mRNA vaccines targeted toward variants of concern.
The Pfizer EUA corresponds to the company’s combination booster shot that includes the original COVID-19 vaccine as well as a vaccine specifically designed to protect against the most recent Omicron variants, BA.4 and BA.5.
The Moderna combination vaccine will contain both the firm’s original COVID-19 vaccine and a vaccine to protect specifically against Omicron BA.4 and BA.5 subvariants.
As of Aug. 27, BA.4 and BA.4.6 account for about 11% of circulating variants and BA.5 accounts for almost all the remaining 89%, Centers for Disease Control and Prevention data show.
The next step will be review of the scientific data by the CDC’s Advisory Committee on Immunization Practices, which is set to meet Sept. 1 and 2. The final hurdle before distribution of the new vaccines will be sign-off on CDC recommendations for use by agency Director Rochelle Walensky, MD.
This is a developing story. A version of this article first appeared on WebMD.com.
Mother’s fat metabolism in early pregnancy linked to baby’s weight
A baby’s weight and neurodevelopment in the first 2 years of life could be influenced by maternal fat metabolism in the early stages of pregnancy, according to a study.
Patterns of fetal abdominal growth were associated with maternal lipid metabolites that tracked newborn growth, adiposity, and development into childhood and could be identified as early as the 5th month of pregnancy, according to researchers at the University of Oxford, working with colleagues at the University of California.
These fetal growth patterns were also associated with blood flow and nutrient transfer by the placenta, demonstrating a complex interaction between maternal and fetal nutrition early in pregnancy, with implications for postnatal weight and health in later life, they suggested.
Stephen Kennedy, MD, professor of reproductive medicine at the University of Oxford, who co-led the investigation, said it had “provided valuable new insights into the biological origins of childhood obesity, which is one of the most pressing public health issues facing governments around the world.”
International study
The prospective observational study, published in The Lancet Diabetes and Endocrinology, involved 3,598 pregnant women from six countries – Brazil, Kenya, Pakistan, South Africa, Thailand, and the United Kingdom – aged 18 and older and with a BMI of less than 35 kg/m2. The women were monitored using regular fetal ultrasound scans and metabolomic analysis of early pregnancy maternal blood and umbilical cord venous blood at the time of birth.
Their infants, who were singletons, and conceived naturally, were then followed for 2 years to assess their growth and development.
Fetal abdominal circumference growth was found to accelerate or decelerate within “a crucial 20-25 week gestational age window” that followed 4 trajectories of faltering growth, early accelerating growth, late accelerating growth, or median growth. These traits were matched by fetus-placenta blood flow patterns throughout pregnancy and different growth, adiposity, vision, and neurodevelopment outcomes in early childhood, researchers said.
Overall, 709 maternal metabolites had a positive effect for the faltering growth phenotype, and 54 for the early accelerating growth phenotype, whilst 31 had a negative effect for the faltering growth phenotype and 76 for the early accelerating growth phenotype.
The maternal metabolite signatures included 5-hydroxy-eicosatetraenoic acid and 11 phosphatidylcholines linked to oxylipin or saturated fatty acid sidechains. The fungicide, chlorothalonil, was “highly abundant” in the early accelerating growth phenotype group.
‘A unique insight’
Aris Papageorghiou, professor of Fetal Medicine at the University of Oxford, who co-led the research, said: “This study provides evidence of distinct patterns of fetal abdominal growth and placental transfer and how they relate to longer term health. The finding of an association with maternal lipid metabolism early in pregnancy also provides unique insights into how the mother’s health and diet influence her child’s adiposity.”
First author José Villar, MD, professor of perinatal medicine at Oxford, said: “The study complements our previous work that identified fetal head growth trajectories associated with different developmental, behavioral, visual, and growth outcomes at 2 years of age.” Taken together, “the growth of babies’ bodies and brain[s] track separately and early – while still within the womb,” he said.
According to Dr. Kennedy, the latest results “could contribute to earlier identification of infants at risk of obesity” and urged policymakers to “take notice of these findings in their efforts to prevent the oncoming epidemic of obesity, with all its likely adverse social and economic consequences.”
Funding for the study was provided by the Bill and Melinda Gates Foundation.
A version of this article first appeared on Medscape UK.
A baby’s weight and neurodevelopment in the first 2 years of life could be influenced by maternal fat metabolism in the early stages of pregnancy, according to a study.
Patterns of fetal abdominal growth were associated with maternal lipid metabolites that tracked newborn growth, adiposity, and development into childhood and could be identified as early as the 5th month of pregnancy, according to researchers at the University of Oxford, working with colleagues at the University of California.
These fetal growth patterns were also associated with blood flow and nutrient transfer by the placenta, demonstrating a complex interaction between maternal and fetal nutrition early in pregnancy, with implications for postnatal weight and health in later life, they suggested.
Stephen Kennedy, MD, professor of reproductive medicine at the University of Oxford, who co-led the investigation, said it had “provided valuable new insights into the biological origins of childhood obesity, which is one of the most pressing public health issues facing governments around the world.”
International study
The prospective observational study, published in The Lancet Diabetes and Endocrinology, involved 3,598 pregnant women from six countries – Brazil, Kenya, Pakistan, South Africa, Thailand, and the United Kingdom – aged 18 and older and with a BMI of less than 35 kg/m2. The women were monitored using regular fetal ultrasound scans and metabolomic analysis of early pregnancy maternal blood and umbilical cord venous blood at the time of birth.
Their infants, who were singletons, and conceived naturally, were then followed for 2 years to assess their growth and development.
Fetal abdominal circumference growth was found to accelerate or decelerate within “a crucial 20-25 week gestational age window” that followed 4 trajectories of faltering growth, early accelerating growth, late accelerating growth, or median growth. These traits were matched by fetus-placenta blood flow patterns throughout pregnancy and different growth, adiposity, vision, and neurodevelopment outcomes in early childhood, researchers said.
Overall, 709 maternal metabolites had a positive effect for the faltering growth phenotype, and 54 for the early accelerating growth phenotype, whilst 31 had a negative effect for the faltering growth phenotype and 76 for the early accelerating growth phenotype.
The maternal metabolite signatures included 5-hydroxy-eicosatetraenoic acid and 11 phosphatidylcholines linked to oxylipin or saturated fatty acid sidechains. The fungicide, chlorothalonil, was “highly abundant” in the early accelerating growth phenotype group.
‘A unique insight’
Aris Papageorghiou, professor of Fetal Medicine at the University of Oxford, who co-led the research, said: “This study provides evidence of distinct patterns of fetal abdominal growth and placental transfer and how they relate to longer term health. The finding of an association with maternal lipid metabolism early in pregnancy also provides unique insights into how the mother’s health and diet influence her child’s adiposity.”
First author José Villar, MD, professor of perinatal medicine at Oxford, said: “The study complements our previous work that identified fetal head growth trajectories associated with different developmental, behavioral, visual, and growth outcomes at 2 years of age.” Taken together, “the growth of babies’ bodies and brain[s] track separately and early – while still within the womb,” he said.
According to Dr. Kennedy, the latest results “could contribute to earlier identification of infants at risk of obesity” and urged policymakers to “take notice of these findings in their efforts to prevent the oncoming epidemic of obesity, with all its likely adverse social and economic consequences.”
Funding for the study was provided by the Bill and Melinda Gates Foundation.
A version of this article first appeared on Medscape UK.
A baby’s weight and neurodevelopment in the first 2 years of life could be influenced by maternal fat metabolism in the early stages of pregnancy, according to a study.
Patterns of fetal abdominal growth were associated with maternal lipid metabolites that tracked newborn growth, adiposity, and development into childhood and could be identified as early as the 5th month of pregnancy, according to researchers at the University of Oxford, working with colleagues at the University of California.
These fetal growth patterns were also associated with blood flow and nutrient transfer by the placenta, demonstrating a complex interaction between maternal and fetal nutrition early in pregnancy, with implications for postnatal weight and health in later life, they suggested.
Stephen Kennedy, MD, professor of reproductive medicine at the University of Oxford, who co-led the investigation, said it had “provided valuable new insights into the biological origins of childhood obesity, which is one of the most pressing public health issues facing governments around the world.”
International study
The prospective observational study, published in The Lancet Diabetes and Endocrinology, involved 3,598 pregnant women from six countries – Brazil, Kenya, Pakistan, South Africa, Thailand, and the United Kingdom – aged 18 and older and with a BMI of less than 35 kg/m2. The women were monitored using regular fetal ultrasound scans and metabolomic analysis of early pregnancy maternal blood and umbilical cord venous blood at the time of birth.
Their infants, who were singletons, and conceived naturally, were then followed for 2 years to assess their growth and development.
Fetal abdominal circumference growth was found to accelerate or decelerate within “a crucial 20-25 week gestational age window” that followed 4 trajectories of faltering growth, early accelerating growth, late accelerating growth, or median growth. These traits were matched by fetus-placenta blood flow patterns throughout pregnancy and different growth, adiposity, vision, and neurodevelopment outcomes in early childhood, researchers said.
Overall, 709 maternal metabolites had a positive effect for the faltering growth phenotype, and 54 for the early accelerating growth phenotype, whilst 31 had a negative effect for the faltering growth phenotype and 76 for the early accelerating growth phenotype.
The maternal metabolite signatures included 5-hydroxy-eicosatetraenoic acid and 11 phosphatidylcholines linked to oxylipin or saturated fatty acid sidechains. The fungicide, chlorothalonil, was “highly abundant” in the early accelerating growth phenotype group.
‘A unique insight’
Aris Papageorghiou, professor of Fetal Medicine at the University of Oxford, who co-led the research, said: “This study provides evidence of distinct patterns of fetal abdominal growth and placental transfer and how they relate to longer term health. The finding of an association with maternal lipid metabolism early in pregnancy also provides unique insights into how the mother’s health and diet influence her child’s adiposity.”
First author José Villar, MD, professor of perinatal medicine at Oxford, said: “The study complements our previous work that identified fetal head growth trajectories associated with different developmental, behavioral, visual, and growth outcomes at 2 years of age.” Taken together, “the growth of babies’ bodies and brain[s] track separately and early – while still within the womb,” he said.
According to Dr. Kennedy, the latest results “could contribute to earlier identification of infants at risk of obesity” and urged policymakers to “take notice of these findings in their efforts to prevent the oncoming epidemic of obesity, with all its likely adverse social and economic consequences.”
Funding for the study was provided by the Bill and Melinda Gates Foundation.
A version of this article first appeared on Medscape UK.
New ovulatory disorder classifications from FIGO replace 50-year-old system
The first major revision in the systematic description of ovulatory disorders in nearly 50 years has been proposed by a consensus of experts organized by the International Federation of Gynecology and Obstetrics.
“The FIGO HyPO-P system for the classification of ovulatory disorders is submitted for consideration as a worldwide standard,” according to the writing committee, who published their methodology and their proposed applications in the International Journal of Gynecology and Obstetrics.
The classification system was created to replace the much-modified World Health Organization system first described in 1973. Since that time, many modifications have been proposed to accommodate advances in imaging and new information about underlying pathologies, but there has been no subsequent authoritative reference with these modifications or any other newer organizing system.

The new consensus was developed under the aegis of FIGO, but the development group consisted of representatives from national organizations and the major subspecialty societies. Recognized experts in ovulatory disorders and representatives from lay advocacy organizations also participated.
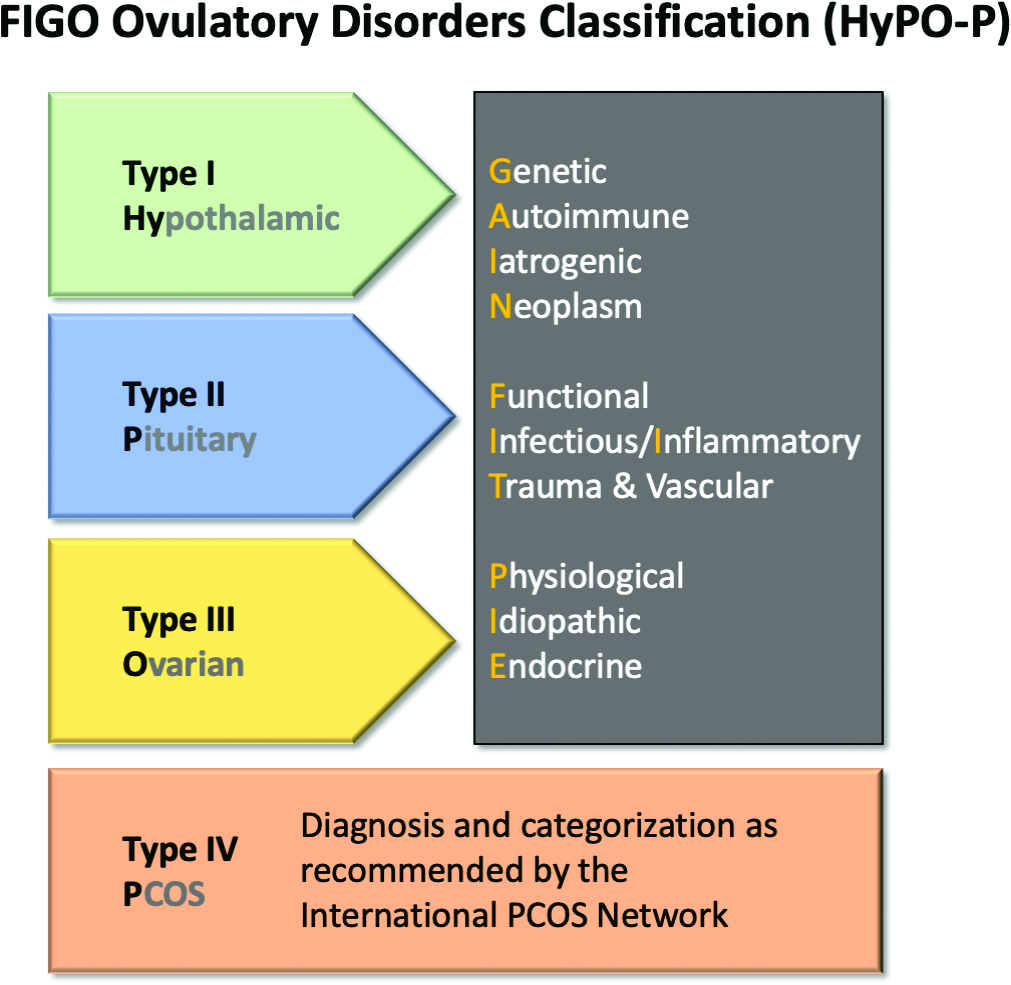
The HyPO-P system is based largely on anatomy. The acronym refers to ovulatory disorders related to the hypothalamus (type I), the pituitary (type II), and the ovary (type III).
Polycystic ovary syndrome (PCOS), one of the most common ovulatory disorders, was given a separate category (type IV) because of its complexity as well as the fact that PCOS is a heterogeneous systemic disorder with manifestations not limited to an impact on ovarian function.
As the first level of classification, three of the four primary categories (I-III) focus attention on the dominant anatomic source of the change in ovulatory function. The original WHO classification system identified as many as seven major groups, but they were based primarily on assays for gonadotropins and estradiol.

The new system “provides a different structure for determining the diagnosis. Blood tests are not a necessary first step,” explained Malcolm G. Munro, MD, clinical professor, department of obstetrics and gynecology, University of California, Los Angeles. Dr. Munro was the first author of the publication.
The classification system “is not as focused on the specific steps for investigation of ovulatory dysfunction as much as it explains how to structure an investigation of the girl or woman with an ovulatory disorder and then how to characterize the underlying cause,” Dr. Munro said in an interview. “It is designed to allow everyone, whether clinicians, researchers, or patients, to speak the same language.”
New system employs four categories
The four primary categories provide just the first level of classification. The next step is encapsulated in the GAIN-FIT-PIE acronym, which frames the presumed or documented categories of etiologies for the primary categories. GAIN stands for genetic, autoimmune, iatrogenic, or neoplasm etiologies. FIT stands for functional, infectious/inflammatory, or trauma and vascular etiologies. PIE stands for physiological, idiopathic, and endocrine etiologies.
By this methodology, a patient with irregular menses, galactorrhea, and elevated prolactin and an MRI showing a pituitary tumor would be identified a type 2-N, signifying pituitary (type 2) involvement with a neoplasm (N).
A third level of classification permits specific diagnostic entities to be named, allowing the patient in the example above to receive a diagnosis of a prolactin-secreting adenoma.
Not all etiologies can be identified with current diagnostic studies, even assuming clinicians have access to the resources, such as advanced imaging, that will increase diagnostic yield. As a result, the authors acknowledged that the classification system will be “aspirational” in at least some patients, but the structure of this system is expected to lead to greater precision in understanding the causes and defining features of ovulatory disorders, which, in turn, might facilitate new research initiatives.
In the published report, diagnostic protocols based on symptoms were described as being “beyond the spectrum” of this initial description. Rather, Dr. Munro explained that the most important contribution of this new classification system are standardization and communication. The system will be amenable for educating trainees and patients, for communicating between clinicians, and as a framework for research where investigators focus on more homogeneous populations of patients.
“There are many causes of ovulatory disorders that are not related to ovarian function. This is one message. Another is that ovulatory disorders are not binary. They occur on a spectrum. These range from transient instances of delayed or failed ovulation to chronic anovulation,” he said.
The new system is “ a welcome update,” according to Mark P. Trolice, MD, director of the IVF Center and professor of obstetrics and gynecology at the University of Central Florida, both in Orlando.
Dr. Trolice pointed to the clinical value of placing PCOS in a separate category. He noted that it affects 8%-13% of women, making it the most common single cause of ovulatory dysfunction.
“Another area that required clarification from prior WHO classifications was hyperprolactinemia, which is now placed in the type II category,” Dr. Trolice said in an interview.
Better terminology can help address a complex set of disorders with multiple causes and variable manifestations.
“In the evaluation of ovulation dysfunction, it is important to remember that regular menstrual intervals do not ensure ovulation,” Dr. Trolice pointed out. Even though a serum progesterone level of higher than 3 ng/mL is one of the simplest laboratory markers for ovulation, this level, he noted, “can vary through the luteal phase and even throughout the day.”
The proposed classification system, while providing a framework for describing ovulatory disorders, is designed to be adaptable, permitting advances in the understanding of the causes of ovulatory dysfunction, in the diagnosis of the causes, and in the treatments to be incorporated.
“No system should be considered permanent,” according to Dr. Munro and his coauthors. “Review and careful modification and revision should be carried out regularly.”
Dr. Munro reports financial relationships with AbbVie, American Regent, Daiichi Sankyo, Hologic, Myovant, and Pharmacosmos. Dr. Trolice reports no potential conflicts of interest.
The first major revision in the systematic description of ovulatory disorders in nearly 50 years has been proposed by a consensus of experts organized by the International Federation of Gynecology and Obstetrics.
“The FIGO HyPO-P system for the classification of ovulatory disorders is submitted for consideration as a worldwide standard,” according to the writing committee, who published their methodology and their proposed applications in the International Journal of Gynecology and Obstetrics.
The classification system was created to replace the much-modified World Health Organization system first described in 1973. Since that time, many modifications have been proposed to accommodate advances in imaging and new information about underlying pathologies, but there has been no subsequent authoritative reference with these modifications or any other newer organizing system.
The new consensus was developed under the aegis of FIGO, but the development group consisted of representatives from national organizations and the major subspecialty societies. Recognized experts in ovulatory disorders and representatives from lay advocacy organizations also participated.
The HyPO-P system is based largely on anatomy. The acronym refers to ovulatory disorders related to the hypothalamus (type I), the pituitary (type II), and the ovary (type III).
Polycystic ovary syndrome (PCOS), one of the most common ovulatory disorders, was given a separate category (type IV) because of its complexity as well as the fact that PCOS is a heterogeneous systemic disorder with manifestations not limited to an impact on ovarian function.
As the first level of classification, three of the four primary categories (I-III) focus attention on the dominant anatomic source of the change in ovulatory function. The original WHO classification system identified as many as seven major groups, but they were based primarily on assays for gonadotropins and estradiol.
The new system “provides a different structure for determining the diagnosis. Blood tests are not a necessary first step,” explained Malcolm G. Munro, MD, clinical professor, department of obstetrics and gynecology, University of California, Los Angeles. Dr. Munro was the first author of the publication.
The classification system “is not as focused on the specific steps for investigation of ovulatory dysfunction as much as it explains how to structure an investigation of the girl or woman with an ovulatory disorder and then how to characterize the underlying cause,” Dr. Munro said in an interview. “It is designed to allow everyone, whether clinicians, researchers, or patients, to speak the same language.”
New system employs four categories
The four primary categories provide just the first level of classification. The next step is encapsulated in the GAIN-FIT-PIE acronym, which frames the presumed or documented categories of etiologies for the primary categories. GAIN stands for genetic, autoimmune, iatrogenic, or neoplasm etiologies. FIT stands for functional, infectious/inflammatory, or trauma and vascular etiologies. PIE stands for physiological, idiopathic, and endocrine etiologies.
By this methodology, a patient with irregular menses, galactorrhea, and elevated prolactin and an MRI showing a pituitary tumor would be identified a type 2-N, signifying pituitary (type 2) involvement with a neoplasm (N).
A third level of classification permits specific diagnostic entities to be named, allowing the patient in the example above to receive a diagnosis of a prolactin-secreting adenoma.
Not all etiologies can be identified with current diagnostic studies, even assuming clinicians have access to the resources, such as advanced imaging, that will increase diagnostic yield. As a result, the authors acknowledged that the classification system will be “aspirational” in at least some patients, but the structure of this system is expected to lead to greater precision in understanding the causes and defining features of ovulatory disorders, which, in turn, might facilitate new research initiatives.
In the published report, diagnostic protocols based on symptoms were described as being “beyond the spectrum” of this initial description. Rather, Dr. Munro explained that the most important contribution of this new classification system are standardization and communication. The system will be amenable for educating trainees and patients, for communicating between clinicians, and as a framework for research where investigators focus on more homogeneous populations of patients.
“There are many causes of ovulatory disorders that are not related to ovarian function. This is one message. Another is that ovulatory disorders are not binary. They occur on a spectrum. These range from transient instances of delayed or failed ovulation to chronic anovulation,” he said.
The new system is “ a welcome update,” according to Mark P. Trolice, MD, director of the IVF Center and professor of obstetrics and gynecology at the University of Central Florida, both in Orlando.
Dr. Trolice pointed to the clinical value of placing PCOS in a separate category. He noted that it affects 8%-13% of women, making it the most common single cause of ovulatory dysfunction.
“Another area that required clarification from prior WHO classifications was hyperprolactinemia, which is now placed in the type II category,” Dr. Trolice said in an interview.
Better terminology can help address a complex set of disorders with multiple causes and variable manifestations.
“In the evaluation of ovulation dysfunction, it is important to remember that regular menstrual intervals do not ensure ovulation,” Dr. Trolice pointed out. Even though a serum progesterone level of higher than 3 ng/mL is one of the simplest laboratory markers for ovulation, this level, he noted, “can vary through the luteal phase and even throughout the day.”
The proposed classification system, while providing a framework for describing ovulatory disorders, is designed to be adaptable, permitting advances in the understanding of the causes of ovulatory dysfunction, in the diagnosis of the causes, and in the treatments to be incorporated.
“No system should be considered permanent,” according to Dr. Munro and his coauthors. “Review and careful modification and revision should be carried out regularly.”
Dr. Munro reports financial relationships with AbbVie, American Regent, Daiichi Sankyo, Hologic, Myovant, and Pharmacosmos. Dr. Trolice reports no potential conflicts of interest.
The first major revision in the systematic description of ovulatory disorders in nearly 50 years has been proposed by a consensus of experts organized by the International Federation of Gynecology and Obstetrics.
“The FIGO HyPO-P system for the classification of ovulatory disorders is submitted for consideration as a worldwide standard,” according to the writing committee, who published their methodology and their proposed applications in the International Journal of Gynecology and Obstetrics.
The classification system was created to replace the much-modified World Health Organization system first described in 1973. Since that time, many modifications have been proposed to accommodate advances in imaging and new information about underlying pathologies, but there has been no subsequent authoritative reference with these modifications or any other newer organizing system.
The new consensus was developed under the aegis of FIGO, but the development group consisted of representatives from national organizations and the major subspecialty societies. Recognized experts in ovulatory disorders and representatives from lay advocacy organizations also participated.
The HyPO-P system is based largely on anatomy. The acronym refers to ovulatory disorders related to the hypothalamus (type I), the pituitary (type II), and the ovary (type III).
Polycystic ovary syndrome (PCOS), one of the most common ovulatory disorders, was given a separate category (type IV) because of its complexity as well as the fact that PCOS is a heterogeneous systemic disorder with manifestations not limited to an impact on ovarian function.
As the first level of classification, three of the four primary categories (I-III) focus attention on the dominant anatomic source of the change in ovulatory function. The original WHO classification system identified as many as seven major groups, but they were based primarily on assays for gonadotropins and estradiol.
The new system “provides a different structure for determining the diagnosis. Blood tests are not a necessary first step,” explained Malcolm G. Munro, MD, clinical professor, department of obstetrics and gynecology, University of California, Los Angeles. Dr. Munro was the first author of the publication.
The classification system “is not as focused on the specific steps for investigation of ovulatory dysfunction as much as it explains how to structure an investigation of the girl or woman with an ovulatory disorder and then how to characterize the underlying cause,” Dr. Munro said in an interview. “It is designed to allow everyone, whether clinicians, researchers, or patients, to speak the same language.”
New system employs four categories
The four primary categories provide just the first level of classification. The next step is encapsulated in the GAIN-FIT-PIE acronym, which frames the presumed or documented categories of etiologies for the primary categories. GAIN stands for genetic, autoimmune, iatrogenic, or neoplasm etiologies. FIT stands for functional, infectious/inflammatory, or trauma and vascular etiologies. PIE stands for physiological, idiopathic, and endocrine etiologies.
By this methodology, a patient with irregular menses, galactorrhea, and elevated prolactin and an MRI showing a pituitary tumor would be identified a type 2-N, signifying pituitary (type 2) involvement with a neoplasm (N).
A third level of classification permits specific diagnostic entities to be named, allowing the patient in the example above to receive a diagnosis of a prolactin-secreting adenoma.
Not all etiologies can be identified with current diagnostic studies, even assuming clinicians have access to the resources, such as advanced imaging, that will increase diagnostic yield. As a result, the authors acknowledged that the classification system will be “aspirational” in at least some patients, but the structure of this system is expected to lead to greater precision in understanding the causes and defining features of ovulatory disorders, which, in turn, might facilitate new research initiatives.
In the published report, diagnostic protocols based on symptoms were described as being “beyond the spectrum” of this initial description. Rather, Dr. Munro explained that the most important contribution of this new classification system are standardization and communication. The system will be amenable for educating trainees and patients, for communicating between clinicians, and as a framework for research where investigators focus on more homogeneous populations of patients.
“There are many causes of ovulatory disorders that are not related to ovarian function. This is one message. Another is that ovulatory disorders are not binary. They occur on a spectrum. These range from transient instances of delayed or failed ovulation to chronic anovulation,” he said.
The new system is “ a welcome update,” according to Mark P. Trolice, MD, director of the IVF Center and professor of obstetrics and gynecology at the University of Central Florida, both in Orlando.
Dr. Trolice pointed to the clinical value of placing PCOS in a separate category. He noted that it affects 8%-13% of women, making it the most common single cause of ovulatory dysfunction.
“Another area that required clarification from prior WHO classifications was hyperprolactinemia, which is now placed in the type II category,” Dr. Trolice said in an interview.
Better terminology can help address a complex set of disorders with multiple causes and variable manifestations.
“In the evaluation of ovulation dysfunction, it is important to remember that regular menstrual intervals do not ensure ovulation,” Dr. Trolice pointed out. Even though a serum progesterone level of higher than 3 ng/mL is one of the simplest laboratory markers for ovulation, this level, he noted, “can vary through the luteal phase and even throughout the day.”
The proposed classification system, while providing a framework for describing ovulatory disorders, is designed to be adaptable, permitting advances in the understanding of the causes of ovulatory dysfunction, in the diagnosis of the causes, and in the treatments to be incorporated.
“No system should be considered permanent,” according to Dr. Munro and his coauthors. “Review and careful modification and revision should be carried out regularly.”
Dr. Munro reports financial relationships with AbbVie, American Regent, Daiichi Sankyo, Hologic, Myovant, and Pharmacosmos. Dr. Trolice reports no potential conflicts of interest.
FROM INTERNATIONAL JOURNAL OF GYNECOLOGY AND OBSTETRICS
Time to pull back on postsurgery radiation in breast cancer?
A new study suggests that oncologists can safely pull back on standard locoregional radiotherapy (RT) in select patients with cT1-2N1 breast cancer who are treated with primary chemotherapy prior to surgery. The key is to divide patients by risk level and treat them according to the study’s guidelines, the researchers reported.
lead study author Sabine de Wild, MD, a PhD student at Maastricht (the Netherlands) University Medical Center, said in an interview.
The study, published in The Lancet Oncology, was intended to provide insight into which breast cancer patients need adjuvant locoregional radiotherapy following postchemotherapy surgery, coauthor Liesbeth Boersma, MD, PhD, a radiation oncologist at Maastricht University Medical Center, said in an interview. “It is not yet known which of these patients would benefit from adjuvant locoregional radiotherapy and to what extent the response of the tumor to the chemotherapy should be taken into account.”
For the study, believed to be the first prospective analysis tackling this topic, researchers tracked 838 patients in The Netherlands who were treated for cT1-2N1 breast cancer with primary chemotherapy and surgery of the breast and axilla from 2011-2015. Tumors were less than 5 cm and metastases were one to three axillary nodes.
The subjects were divided into groups based on risk of locoregional recurrence, and each group underwent different therapies.
- Low-risk group: no metastases were present in the nodes (n = 291). “We omitted regional radiotherapy, and we omitted RT of the chest wall in case of a mastectomy. After breast conserving surgery, regular RT of the breast was recommended,” Dr. de Wild said.
- Intermediate-risk group, one to three metastases were still present (n = 370). “We omitted regional radiotherapy, but irradiated the chest wall or breast,” she said.
- High-risk group, three metastases were present (n = 177). “We did not de-escalate, and all patients were treated with locoregional RT,” she said.
According to the study, “the 5-year locoregional recurrence rate in all patients was 2.2% (95% confidence interval, 1.4-3.4). The 5-year locoregional recurrence rate was 2.1% (95% CI, 0.9-4.3) in the low-risk group, 2.2% (95% CI, 1.0-4.1) in the intermediate-risk group, and 2.3% (95% CI, 0.8-5.5) in the high-risk group.”
In 26% of cases, patients received more radiotherapy than the study guidelines suggested. “Remarkably,” the researchers wrote, “this did not seem to affect locoregional recurrence rate, recurrence-free interval, and overall survival in a statistically significant or clinically relevant way.”
As for limitations, the authors noted that, “in each risk group, the actual sample size treated according to the study guideline was smaller than required based on the power calculation. Nevertheless, when performing the analyses in the subset of patients treated according to the study guideline, the upper limit of 95% CI of 5-year locoregional recurrence rate did not exceed 7.8%.”
The study authors wrote that, “in the future, the results of this study might lead to more frequent omission of locoregional radiotherapy, which could result in lower morbidity and a better quality of life for patients with breast cancer who are receiving primary chemotherapy.”
However, Dr. de Wild said randomized trials are necessary “to investigate how treatment can be individualized further, i.e., by taking into account specific tumor characteristics.” Also, most patients in the study underwent axillary lymph node dissection, “while patients in daily practice may instead undergo targeted axillary dissection. Future studies are needed to determine if less radiotherapy is also safe in patients in whom axillary lymph node dissection is omitted.”
The study was funded by the Dutch Cancer Society. One coauthor reported a pending patent plus grants from AstraZeneca, Eurocept Plaza, Roche, Genentech, Gilead Sciences, Tesaro, Novartis, Dutch Cancer Society, ZonMw, and A Sister’s Hope; as well as consulting fees and other financial support from a variety of pharmaceutical companies. The other authors had no disclosures.
A new study suggests that oncologists can safely pull back on standard locoregional radiotherapy (RT) in select patients with cT1-2N1 breast cancer who are treated with primary chemotherapy prior to surgery. The key is to divide patients by risk level and treat them according to the study’s guidelines, the researchers reported.
lead study author Sabine de Wild, MD, a PhD student at Maastricht (the Netherlands) University Medical Center, said in an interview.
The study, published in The Lancet Oncology, was intended to provide insight into which breast cancer patients need adjuvant locoregional radiotherapy following postchemotherapy surgery, coauthor Liesbeth Boersma, MD, PhD, a radiation oncologist at Maastricht University Medical Center, said in an interview. “It is not yet known which of these patients would benefit from adjuvant locoregional radiotherapy and to what extent the response of the tumor to the chemotherapy should be taken into account.”
For the study, believed to be the first prospective analysis tackling this topic, researchers tracked 838 patients in The Netherlands who were treated for cT1-2N1 breast cancer with primary chemotherapy and surgery of the breast and axilla from 2011-2015. Tumors were less than 5 cm and metastases were one to three axillary nodes.
The subjects were divided into groups based on risk of locoregional recurrence, and each group underwent different therapies.
- Low-risk group: no metastases were present in the nodes (n = 291). “We omitted regional radiotherapy, and we omitted RT of the chest wall in case of a mastectomy. After breast conserving surgery, regular RT of the breast was recommended,” Dr. de Wild said.
- Intermediate-risk group, one to three metastases were still present (n = 370). “We omitted regional radiotherapy, but irradiated the chest wall or breast,” she said.
- High-risk group, three metastases were present (n = 177). “We did not de-escalate, and all patients were treated with locoregional RT,” she said.
According to the study, “the 5-year locoregional recurrence rate in all patients was 2.2% (95% confidence interval, 1.4-3.4). The 5-year locoregional recurrence rate was 2.1% (95% CI, 0.9-4.3) in the low-risk group, 2.2% (95% CI, 1.0-4.1) in the intermediate-risk group, and 2.3% (95% CI, 0.8-5.5) in the high-risk group.”
In 26% of cases, patients received more radiotherapy than the study guidelines suggested. “Remarkably,” the researchers wrote, “this did not seem to affect locoregional recurrence rate, recurrence-free interval, and overall survival in a statistically significant or clinically relevant way.”
As for limitations, the authors noted that, “in each risk group, the actual sample size treated according to the study guideline was smaller than required based on the power calculation. Nevertheless, when performing the analyses in the subset of patients treated according to the study guideline, the upper limit of 95% CI of 5-year locoregional recurrence rate did not exceed 7.8%.”
The study authors wrote that, “in the future, the results of this study might lead to more frequent omission of locoregional radiotherapy, which could result in lower morbidity and a better quality of life for patients with breast cancer who are receiving primary chemotherapy.”
However, Dr. de Wild said randomized trials are necessary “to investigate how treatment can be individualized further, i.e., by taking into account specific tumor characteristics.” Also, most patients in the study underwent axillary lymph node dissection, “while patients in daily practice may instead undergo targeted axillary dissection. Future studies are needed to determine if less radiotherapy is also safe in patients in whom axillary lymph node dissection is omitted.”
The study was funded by the Dutch Cancer Society. One coauthor reported a pending patent plus grants from AstraZeneca, Eurocept Plaza, Roche, Genentech, Gilead Sciences, Tesaro, Novartis, Dutch Cancer Society, ZonMw, and A Sister’s Hope; as well as consulting fees and other financial support from a variety of pharmaceutical companies. The other authors had no disclosures.
A new study suggests that oncologists can safely pull back on standard locoregional radiotherapy (RT) in select patients with cT1-2N1 breast cancer who are treated with primary chemotherapy prior to surgery. The key is to divide patients by risk level and treat them according to the study’s guidelines, the researchers reported.
lead study author Sabine de Wild, MD, a PhD student at Maastricht (the Netherlands) University Medical Center, said in an interview.
The study, published in The Lancet Oncology, was intended to provide insight into which breast cancer patients need adjuvant locoregional radiotherapy following postchemotherapy surgery, coauthor Liesbeth Boersma, MD, PhD, a radiation oncologist at Maastricht University Medical Center, said in an interview. “It is not yet known which of these patients would benefit from adjuvant locoregional radiotherapy and to what extent the response of the tumor to the chemotherapy should be taken into account.”
For the study, believed to be the first prospective analysis tackling this topic, researchers tracked 838 patients in The Netherlands who were treated for cT1-2N1 breast cancer with primary chemotherapy and surgery of the breast and axilla from 2011-2015. Tumors were less than 5 cm and metastases were one to three axillary nodes.
The subjects were divided into groups based on risk of locoregional recurrence, and each group underwent different therapies.
- Low-risk group: no metastases were present in the nodes (n = 291). “We omitted regional radiotherapy, and we omitted RT of the chest wall in case of a mastectomy. After breast conserving surgery, regular RT of the breast was recommended,” Dr. de Wild said.
- Intermediate-risk group, one to three metastases were still present (n = 370). “We omitted regional radiotherapy, but irradiated the chest wall or breast,” she said.
- High-risk group, three metastases were present (n = 177). “We did not de-escalate, and all patients were treated with locoregional RT,” she said.
According to the study, “the 5-year locoregional recurrence rate in all patients was 2.2% (95% confidence interval, 1.4-3.4). The 5-year locoregional recurrence rate was 2.1% (95% CI, 0.9-4.3) in the low-risk group, 2.2% (95% CI, 1.0-4.1) in the intermediate-risk group, and 2.3% (95% CI, 0.8-5.5) in the high-risk group.”
In 26% of cases, patients received more radiotherapy than the study guidelines suggested. “Remarkably,” the researchers wrote, “this did not seem to affect locoregional recurrence rate, recurrence-free interval, and overall survival in a statistically significant or clinically relevant way.”
As for limitations, the authors noted that, “in each risk group, the actual sample size treated according to the study guideline was smaller than required based on the power calculation. Nevertheless, when performing the analyses in the subset of patients treated according to the study guideline, the upper limit of 95% CI of 5-year locoregional recurrence rate did not exceed 7.8%.”
The study authors wrote that, “in the future, the results of this study might lead to more frequent omission of locoregional radiotherapy, which could result in lower morbidity and a better quality of life for patients with breast cancer who are receiving primary chemotherapy.”
However, Dr. de Wild said randomized trials are necessary “to investigate how treatment can be individualized further, i.e., by taking into account specific tumor characteristics.” Also, most patients in the study underwent axillary lymph node dissection, “while patients in daily practice may instead undergo targeted axillary dissection. Future studies are needed to determine if less radiotherapy is also safe in patients in whom axillary lymph node dissection is omitted.”
The study was funded by the Dutch Cancer Society. One coauthor reported a pending patent plus grants from AstraZeneca, Eurocept Plaza, Roche, Genentech, Gilead Sciences, Tesaro, Novartis, Dutch Cancer Society, ZonMw, and A Sister’s Hope; as well as consulting fees and other financial support from a variety of pharmaceutical companies. The other authors had no disclosures.
FROM THE LANCET ONCOLOGY
How do you live with COVID? One doctor’s personal experience
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”

“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
In America, cancer patients endure debt on top of disease
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Increased risk of dyspareunia following cesarean section
There is no evidence to support postulated associations between mode of delivery and subsequent maternal sexual enjoyment or frequency of intercourse, according to a new study from the University of Bristol (England). However, cesarean section was shown to be associated with a 74% increased risk of dyspareunia, and this was not necessarily due to abdominal scarring, the researchers said.
A team from the University of Bristol and the Karolinska Institutet in Sweden used data from participants in the Avon Longitudinal Study of Parents and Children, a prospective longitudinal birth cohort study also dubbed “Children of the 90s” and involving more than 14,000 women in the United Kingdom who were pregnant in 1991 and 1992. The study has been following the health and development of the parents, their children, and now their grandchildren in detail ever since.
The new study, published in BJOG, aimed to assess whether cesarean section maintains sexual well-being compared with vaginal delivery, as has been suggested to occur because of the reduced risk of genital damage – less chance of tearing – and the maintenance of vaginal tone. There is some evidence that cesarean section is associated with an increased risk of sexual problems such as dyspareunia, but few studies have looked at the postbirth period long term.
Mode of delivery was abstracted from routine obstetric records and recorded as one of either spontaneous vaginal delivery (SVD), cesarean section, assisted breech, breech extraction, forceps, or vacuum extraction. Women whose records showed “other” as mode of delivery or whose notes contained conflicting modes of delivery were excluded.
Self-reported questionnaires asking about general health and lifestyle and including questions relating to sexual enjoyment and frequency were collected at 33 months and at 5, 12, and 18 years postpartum. Women were asked if they enjoyed sexual intercourse, with possible responses of:
- Yes, very much.
- Yes, somewhat.
- No, not a lot.
- No, not at all.
- No sex at the moment.
Possible sexual frequency responses were:
- Not at all.
- Less than once a month.
- 1-3 times a month.
- About once a week.
- 2-4 times a week.
- 5 or more times a week.
First study to look at sexual frequency
The team noted that theirs is the first study investigating the association of mode of delivery with sexual frequency. “Although it may be less important for well-being than sexual enjoyment or sex-related pain, it is an important measure to observe alongside other sexual outcomes,” they said.
Separately, sex-related pain, in the vagina during sex or elsewhere after sex, was assessed once, at 11 years post partum.
The data showed that women who had a cesarean section (11% of the sample) tended to be older than those who had vaginal delivery, with a higher mean body mass index (24.2 versus 22.8 kg/m2), and were more likely to be nulliparous at the time of the index pregnancy (54% versus 44%).
There was no significant difference between cesarean section and vaginal delivery in terms of responses for sexual enjoyment or frequency at any time after childbirth, the authors said. Nor, in adjusted models, was there evidence of associations between the type of vaginal delivery and sexual enjoyment or frequency outcomes.
Pain during sex increased more than a decade after cesarean
However, while the majority of respondents reported no intercourse-related pain, those who delivered via cesarean were more likely than those who gave birth vaginally to report sex-related pain at 11 years post partum. This was specifically an elevated incidence of pain in the vagina during sex, with an odds ratio of 1.74 (95% confidence interval, 1.46-2.08) in the adjusted model. This finding was consistent for emergency and elective cesarean section separately – both types were associated with increased dyspareunia, compared with vaginal delivery.
The dataset did not include measures of individual prenatal sex-related pain and, therefore, “it is unknown from this study whether Caesarean section causes sex-related pain, as suggested by the findings, or whether prenatal sex-related pain predicts both Caesarean section and postnatal sex-related pain,” the researchers said.
“Longitudinal data on sex-related pain need to be collected both before and after parturition,” they recommend, to clarify the direction of a possible effect between cesarean section and dyspareunia.
Cesarean does not protect against sexual dysfunction
Meanwhile, “For women considering a planned Caesarean section in an uncomplicated pregnancy, evidence suggesting that Caesarean section may not protect against sexual dysfunction may help inform their decision-making in the antenatal period.”
Lead author Flo Martin, a PhD student in epidemiology at the University of Bristol, said: “Rates of Caesarean section have been rising over the last 20 years due to many contributing factors and, importantly, it has been suggested that Caesarean section maintains sexual wellbeing compared with vaginal delivery. It is crucial that a whole range of maternal and foetal outcomes following Caesarean section are investigated, including sexual wellbeing, to appropriately inform decision-making both pre- and postnatally.
“This research provides expectant mothers, as well as women who have given birth, with really important information and demonstrates that there was no difference in sexual enjoyment or sexual frequency at any time point postpartum between women who gave birth via Caesarean section and those who delivered vaginally. It also suggests that Caesarean section may not help protect against sexual dysfunction, as previously thought, where sex-related pain was higher among women who gave birth via Caesarean section more than 10 years postpartum.”
Asked to comment on the research, Dr. Leila Frodsham, consultant gynecologist and spokesperson for the Royal College of Obstetricians and Gynaecologists, told this news organization: “Sexual pain disorders affect 7.5% of women of all ages, but there are peaks: during the start of sexual activity, if subfertility is an issue, after childbirth, and in the peri/menopause. It can be up to three times more prevalent at these peak times.
“Many women with sexual pain are worried when they consider starting a family and request a Caesarean birth to reduce risk of worsening their pain. However, this study has demonstrated that a Caesarean birth is associated with increased sexual pain longer term, which is very useful for helping women to plan their births.
“While more research about postpartum sexual wellbeing is needed, the findings of this study are reassuring to those who are pregnant as it found no difference in the enjoyment or frequency of sex in the years after a vaginal or a Caesarean birth.
“Most women in the U.K. recover well whether they have a vaginal or a Caesarean birth. Women should be supported to make informed decisions about how they plan to give birth, and it is vital that health care professionals respect their preferences.”
A version of this article first appeared on Medscape UK.
There is no evidence to support postulated associations between mode of delivery and subsequent maternal sexual enjoyment or frequency of intercourse, according to a new study from the University of Bristol (England). However, cesarean section was shown to be associated with a 74% increased risk of dyspareunia, and this was not necessarily due to abdominal scarring, the researchers said.
A team from the University of Bristol and the Karolinska Institutet in Sweden used data from participants in the Avon Longitudinal Study of Parents and Children, a prospective longitudinal birth cohort study also dubbed “Children of the 90s” and involving more than 14,000 women in the United Kingdom who were pregnant in 1991 and 1992. The study has been following the health and development of the parents, their children, and now their grandchildren in detail ever since.
The new study, published in BJOG, aimed to assess whether cesarean section maintains sexual well-being compared with vaginal delivery, as has been suggested to occur because of the reduced risk of genital damage – less chance of tearing – and the maintenance of vaginal tone. There is some evidence that cesarean section is associated with an increased risk of sexual problems such as dyspareunia, but few studies have looked at the postbirth period long term.
Mode of delivery was abstracted from routine obstetric records and recorded as one of either spontaneous vaginal delivery (SVD), cesarean section, assisted breech, breech extraction, forceps, or vacuum extraction. Women whose records showed “other” as mode of delivery or whose notes contained conflicting modes of delivery were excluded.
Self-reported questionnaires asking about general health and lifestyle and including questions relating to sexual enjoyment and frequency were collected at 33 months and at 5, 12, and 18 years postpartum. Women were asked if they enjoyed sexual intercourse, with possible responses of:
- Yes, very much.
- Yes, somewhat.
- No, not a lot.
- No, not at all.
- No sex at the moment.
Possible sexual frequency responses were:
- Not at all.
- Less than once a month.
- 1-3 times a month.
- About once a week.
- 2-4 times a week.
- 5 or more times a week.
First study to look at sexual frequency
The team noted that theirs is the first study investigating the association of mode of delivery with sexual frequency. “Although it may be less important for well-being than sexual enjoyment or sex-related pain, it is an important measure to observe alongside other sexual outcomes,” they said.
Separately, sex-related pain, in the vagina during sex or elsewhere after sex, was assessed once, at 11 years post partum.
The data showed that women who had a cesarean section (11% of the sample) tended to be older than those who had vaginal delivery, with a higher mean body mass index (24.2 versus 22.8 kg/m2), and were more likely to be nulliparous at the time of the index pregnancy (54% versus 44%).
There was no significant difference between cesarean section and vaginal delivery in terms of responses for sexual enjoyment or frequency at any time after childbirth, the authors said. Nor, in adjusted models, was there evidence of associations between the type of vaginal delivery and sexual enjoyment or frequency outcomes.
Pain during sex increased more than a decade after cesarean
However, while the majority of respondents reported no intercourse-related pain, those who delivered via cesarean were more likely than those who gave birth vaginally to report sex-related pain at 11 years post partum. This was specifically an elevated incidence of pain in the vagina during sex, with an odds ratio of 1.74 (95% confidence interval, 1.46-2.08) in the adjusted model. This finding was consistent for emergency and elective cesarean section separately – both types were associated with increased dyspareunia, compared with vaginal delivery.
The dataset did not include measures of individual prenatal sex-related pain and, therefore, “it is unknown from this study whether Caesarean section causes sex-related pain, as suggested by the findings, or whether prenatal sex-related pain predicts both Caesarean section and postnatal sex-related pain,” the researchers said.
“Longitudinal data on sex-related pain need to be collected both before and after parturition,” they recommend, to clarify the direction of a possible effect between cesarean section and dyspareunia.
Cesarean does not protect against sexual dysfunction
Meanwhile, “For women considering a planned Caesarean section in an uncomplicated pregnancy, evidence suggesting that Caesarean section may not protect against sexual dysfunction may help inform their decision-making in the antenatal period.”
Lead author Flo Martin, a PhD student in epidemiology at the University of Bristol, said: “Rates of Caesarean section have been rising over the last 20 years due to many contributing factors and, importantly, it has been suggested that Caesarean section maintains sexual wellbeing compared with vaginal delivery. It is crucial that a whole range of maternal and foetal outcomes following Caesarean section are investigated, including sexual wellbeing, to appropriately inform decision-making both pre- and postnatally.
“This research provides expectant mothers, as well as women who have given birth, with really important information and demonstrates that there was no difference in sexual enjoyment or sexual frequency at any time point postpartum between women who gave birth via Caesarean section and those who delivered vaginally. It also suggests that Caesarean section may not help protect against sexual dysfunction, as previously thought, where sex-related pain was higher among women who gave birth via Caesarean section more than 10 years postpartum.”
Asked to comment on the research, Dr. Leila Frodsham, consultant gynecologist and spokesperson for the Royal College of Obstetricians and Gynaecologists, told this news organization: “Sexual pain disorders affect 7.5% of women of all ages, but there are peaks: during the start of sexual activity, if subfertility is an issue, after childbirth, and in the peri/menopause. It can be up to three times more prevalent at these peak times.
“Many women with sexual pain are worried when they consider starting a family and request a Caesarean birth to reduce risk of worsening their pain. However, this study has demonstrated that a Caesarean birth is associated with increased sexual pain longer term, which is very useful for helping women to plan their births.
“While more research about postpartum sexual wellbeing is needed, the findings of this study are reassuring to those who are pregnant as it found no difference in the enjoyment or frequency of sex in the years after a vaginal or a Caesarean birth.
“Most women in the U.K. recover well whether they have a vaginal or a Caesarean birth. Women should be supported to make informed decisions about how they plan to give birth, and it is vital that health care professionals respect their preferences.”
A version of this article first appeared on Medscape UK.
There is no evidence to support postulated associations between mode of delivery and subsequent maternal sexual enjoyment or frequency of intercourse, according to a new study from the University of Bristol (England). However, cesarean section was shown to be associated with a 74% increased risk of dyspareunia, and this was not necessarily due to abdominal scarring, the researchers said.
A team from the University of Bristol and the Karolinska Institutet in Sweden used data from participants in the Avon Longitudinal Study of Parents and Children, a prospective longitudinal birth cohort study also dubbed “Children of the 90s” and involving more than 14,000 women in the United Kingdom who were pregnant in 1991 and 1992. The study has been following the health and development of the parents, their children, and now their grandchildren in detail ever since.
The new study, published in BJOG, aimed to assess whether cesarean section maintains sexual well-being compared with vaginal delivery, as has been suggested to occur because of the reduced risk of genital damage – less chance of tearing – and the maintenance of vaginal tone. There is some evidence that cesarean section is associated with an increased risk of sexual problems such as dyspareunia, but few studies have looked at the postbirth period long term.
Mode of delivery was abstracted from routine obstetric records and recorded as one of either spontaneous vaginal delivery (SVD), cesarean section, assisted breech, breech extraction, forceps, or vacuum extraction. Women whose records showed “other” as mode of delivery or whose notes contained conflicting modes of delivery were excluded.
Self-reported questionnaires asking about general health and lifestyle and including questions relating to sexual enjoyment and frequency were collected at 33 months and at 5, 12, and 18 years postpartum. Women were asked if they enjoyed sexual intercourse, with possible responses of:
- Yes, very much.
- Yes, somewhat.
- No, not a lot.
- No, not at all.
- No sex at the moment.
Possible sexual frequency responses were:
- Not at all.
- Less than once a month.
- 1-3 times a month.
- About once a week.
- 2-4 times a week.
- 5 or more times a week.
First study to look at sexual frequency
The team noted that theirs is the first study investigating the association of mode of delivery with sexual frequency. “Although it may be less important for well-being than sexual enjoyment or sex-related pain, it is an important measure to observe alongside other sexual outcomes,” they said.
Separately, sex-related pain, in the vagina during sex or elsewhere after sex, was assessed once, at 11 years post partum.
The data showed that women who had a cesarean section (11% of the sample) tended to be older than those who had vaginal delivery, with a higher mean body mass index (24.2 versus 22.8 kg/m2), and were more likely to be nulliparous at the time of the index pregnancy (54% versus 44%).
There was no significant difference between cesarean section and vaginal delivery in terms of responses for sexual enjoyment or frequency at any time after childbirth, the authors said. Nor, in adjusted models, was there evidence of associations between the type of vaginal delivery and sexual enjoyment or frequency outcomes.
Pain during sex increased more than a decade after cesarean
However, while the majority of respondents reported no intercourse-related pain, those who delivered via cesarean were more likely than those who gave birth vaginally to report sex-related pain at 11 years post partum. This was specifically an elevated incidence of pain in the vagina during sex, with an odds ratio of 1.74 (95% confidence interval, 1.46-2.08) in the adjusted model. This finding was consistent for emergency and elective cesarean section separately – both types were associated with increased dyspareunia, compared with vaginal delivery.
The dataset did not include measures of individual prenatal sex-related pain and, therefore, “it is unknown from this study whether Caesarean section causes sex-related pain, as suggested by the findings, or whether prenatal sex-related pain predicts both Caesarean section and postnatal sex-related pain,” the researchers said.
“Longitudinal data on sex-related pain need to be collected both before and after parturition,” they recommend, to clarify the direction of a possible effect between cesarean section and dyspareunia.
Cesarean does not protect against sexual dysfunction
Meanwhile, “For women considering a planned Caesarean section in an uncomplicated pregnancy, evidence suggesting that Caesarean section may not protect against sexual dysfunction may help inform their decision-making in the antenatal period.”
Lead author Flo Martin, a PhD student in epidemiology at the University of Bristol, said: “Rates of Caesarean section have been rising over the last 20 years due to many contributing factors and, importantly, it has been suggested that Caesarean section maintains sexual wellbeing compared with vaginal delivery. It is crucial that a whole range of maternal and foetal outcomes following Caesarean section are investigated, including sexual wellbeing, to appropriately inform decision-making both pre- and postnatally.
“This research provides expectant mothers, as well as women who have given birth, with really important information and demonstrates that there was no difference in sexual enjoyment or sexual frequency at any time point postpartum between women who gave birth via Caesarean section and those who delivered vaginally. It also suggests that Caesarean section may not help protect against sexual dysfunction, as previously thought, where sex-related pain was higher among women who gave birth via Caesarean section more than 10 years postpartum.”
Asked to comment on the research, Dr. Leila Frodsham, consultant gynecologist and spokesperson for the Royal College of Obstetricians and Gynaecologists, told this news organization: “Sexual pain disorders affect 7.5% of women of all ages, but there are peaks: during the start of sexual activity, if subfertility is an issue, after childbirth, and in the peri/menopause. It can be up to three times more prevalent at these peak times.
“Many women with sexual pain are worried when they consider starting a family and request a Caesarean birth to reduce risk of worsening their pain. However, this study has demonstrated that a Caesarean birth is associated with increased sexual pain longer term, which is very useful for helping women to plan their births.
“While more research about postpartum sexual wellbeing is needed, the findings of this study are reassuring to those who are pregnant as it found no difference in the enjoyment or frequency of sex in the years after a vaginal or a Caesarean birth.
“Most women in the U.K. recover well whether they have a vaginal or a Caesarean birth. Women should be supported to make informed decisions about how they plan to give birth, and it is vital that health care professionals respect their preferences.”
A version of this article first appeared on Medscape UK.
Tumor-bed radiotherapy boost reduces DCIS recurrence risk
Giving a boost radiation dose to the tumor bed following breast-conserving surgery and whole breast irradiation (WBI) has been shown to be effective at reducing recurrence of invasive breast cancer, and now a multinational randomized trial has shown that it can do the same for patients with non–low-risk ductal carcinoma in situ (DCIS).
“ wrote the authors, led by Boon H. Chua, PhD, from the University of New South Wales, Sydney.
Among 1,608 patients with DCIS with at least one clinical or pathological marker for increased risk of local recurrence, 5-year rates of freedom from local recurrence were 97.1% for patients assigned to received a tumor bed boost versus 92.7% for patients who did not receive a boost dose. This difference translated into a hazard ratio for recurrence with radiation boost of 0.47 (P < .001).
“Our results support the use of tumor-bed boost radiation after postoperative WBI in patients with non–low-risk DCIS to optimize local control, and the adoption of moderately hypofractionated whole breast irradiation in practice to improve the balance of local control, toxicity, and socioeconomic burdens of treatment,” the authors wrote in a study published in The Lancet.
The investigators, from cancer centers in Australia, Europe, and Canada, noted that the advent of screening mammography was followed by a substantial increase in the diagnosis of DCIS. They also noted that patients who undergo breast-conserving surgery for DCIS are at risk for local recurrence, and half of recurrences present as invasive disease.
In addition, they said, there were high recurrence rates in randomized clinical for patients with DCIS who received conventionally fractionated WBI without a tumor boost following surgery.
“Further, the inconvenience of a 5- to 6-week course of conventionally fractionated WBI decreased the quality of life of patients. Thus, tailoring radiation dose fractionation according to recurrence risk is a prominent controversy in the radiation treatment of DCIS,” they wrote.
Four-way trial
To see whether a tumor-bed boost following WBI and alternative WBI fractionation schedules could improve outcomes for patients with non–low-risk DCIS, the researchers enrolled patients and assigned them on an equal basis to one of four groups, in which they would receive either conventional or hypofractionated WBI with or without a tumor-bed boost.
The conventional WBI regimen consisted of a total of 50 Gy delivered over 25 fractions. The hypofractionated regimen consisted of a total dose of 42.5 Gy delivered in 16 fractions. Patients assigned to get a boost dose to the tumor bed received an additional 16 Gy in eight fractions after WBI.
Of the 1,608 patients enrolled who eligible for randomization, 803 received a boost dose and 805 did not. As noted before, the risk of recurrence at 5 years was significantly lower with boosting, with 5-year free-from-local-recurrence rates of 97.1%, compared with 92.7% for patients who did not get a tumor-bed boost.
There were no significant differences according to fractionation schedule, however: among all randomly assigned patients the rate of 5-year freedom from recurrence was 94.9% for both the conventionally fractionated and hypofractionated WBI groups.
Not surprisingly, patients who received the boost dose had higher rates of grade 2 or greater toxicities, including breast pain (14% vs. 10%; P = .03) and induration (14% vs. 6%; P < .001).
The study was supported by the National Health and Medical Research Council of Australia, Susan G. Komen for the Cure, Breast Cancer Now, OncoSuisse, Dutch Cancer Society, and Canadian Cancer Trials Group. Dr. Chua disclosed grant support from the organizations and others.
Giving a boost radiation dose to the tumor bed following breast-conserving surgery and whole breast irradiation (WBI) has been shown to be effective at reducing recurrence of invasive breast cancer, and now a multinational randomized trial has shown that it can do the same for patients with non–low-risk ductal carcinoma in situ (DCIS).
“ wrote the authors, led by Boon H. Chua, PhD, from the University of New South Wales, Sydney.
Among 1,608 patients with DCIS with at least one clinical or pathological marker for increased risk of local recurrence, 5-year rates of freedom from local recurrence were 97.1% for patients assigned to received a tumor bed boost versus 92.7% for patients who did not receive a boost dose. This difference translated into a hazard ratio for recurrence with radiation boost of 0.47 (P < .001).
“Our results support the use of tumor-bed boost radiation after postoperative WBI in patients with non–low-risk DCIS to optimize local control, and the adoption of moderately hypofractionated whole breast irradiation in practice to improve the balance of local control, toxicity, and socioeconomic burdens of treatment,” the authors wrote in a study published in The Lancet.
The investigators, from cancer centers in Australia, Europe, and Canada, noted that the advent of screening mammography was followed by a substantial increase in the diagnosis of DCIS. They also noted that patients who undergo breast-conserving surgery for DCIS are at risk for local recurrence, and half of recurrences present as invasive disease.
In addition, they said, there were high recurrence rates in randomized clinical for patients with DCIS who received conventionally fractionated WBI without a tumor boost following surgery.
“Further, the inconvenience of a 5- to 6-week course of conventionally fractionated WBI decreased the quality of life of patients. Thus, tailoring radiation dose fractionation according to recurrence risk is a prominent controversy in the radiation treatment of DCIS,” they wrote.
Four-way trial
To see whether a tumor-bed boost following WBI and alternative WBI fractionation schedules could improve outcomes for patients with non–low-risk DCIS, the researchers enrolled patients and assigned them on an equal basis to one of four groups, in which they would receive either conventional or hypofractionated WBI with or without a tumor-bed boost.
The conventional WBI regimen consisted of a total of 50 Gy delivered over 25 fractions. The hypofractionated regimen consisted of a total dose of 42.5 Gy delivered in 16 fractions. Patients assigned to get a boost dose to the tumor bed received an additional 16 Gy in eight fractions after WBI.
Of the 1,608 patients enrolled who eligible for randomization, 803 received a boost dose and 805 did not. As noted before, the risk of recurrence at 5 years was significantly lower with boosting, with 5-year free-from-local-recurrence rates of 97.1%, compared with 92.7% for patients who did not get a tumor-bed boost.
There were no significant differences according to fractionation schedule, however: among all randomly assigned patients the rate of 5-year freedom from recurrence was 94.9% for both the conventionally fractionated and hypofractionated WBI groups.
Not surprisingly, patients who received the boost dose had higher rates of grade 2 or greater toxicities, including breast pain (14% vs. 10%; P = .03) and induration (14% vs. 6%; P < .001).
The study was supported by the National Health and Medical Research Council of Australia, Susan G. Komen for the Cure, Breast Cancer Now, OncoSuisse, Dutch Cancer Society, and Canadian Cancer Trials Group. Dr. Chua disclosed grant support from the organizations and others.
Giving a boost radiation dose to the tumor bed following breast-conserving surgery and whole breast irradiation (WBI) has been shown to be effective at reducing recurrence of invasive breast cancer, and now a multinational randomized trial has shown that it can do the same for patients with non–low-risk ductal carcinoma in situ (DCIS).
“ wrote the authors, led by Boon H. Chua, PhD, from the University of New South Wales, Sydney.
Among 1,608 patients with DCIS with at least one clinical or pathological marker for increased risk of local recurrence, 5-year rates of freedom from local recurrence were 97.1% for patients assigned to received a tumor bed boost versus 92.7% for patients who did not receive a boost dose. This difference translated into a hazard ratio for recurrence with radiation boost of 0.47 (P < .001).
“Our results support the use of tumor-bed boost radiation after postoperative WBI in patients with non–low-risk DCIS to optimize local control, and the adoption of moderately hypofractionated whole breast irradiation in practice to improve the balance of local control, toxicity, and socioeconomic burdens of treatment,” the authors wrote in a study published in The Lancet.
The investigators, from cancer centers in Australia, Europe, and Canada, noted that the advent of screening mammography was followed by a substantial increase in the diagnosis of DCIS. They also noted that patients who undergo breast-conserving surgery for DCIS are at risk for local recurrence, and half of recurrences present as invasive disease.
In addition, they said, there were high recurrence rates in randomized clinical for patients with DCIS who received conventionally fractionated WBI without a tumor boost following surgery.
“Further, the inconvenience of a 5- to 6-week course of conventionally fractionated WBI decreased the quality of life of patients. Thus, tailoring radiation dose fractionation according to recurrence risk is a prominent controversy in the radiation treatment of DCIS,” they wrote.
Four-way trial
To see whether a tumor-bed boost following WBI and alternative WBI fractionation schedules could improve outcomes for patients with non–low-risk DCIS, the researchers enrolled patients and assigned them on an equal basis to one of four groups, in which they would receive either conventional or hypofractionated WBI with or without a tumor-bed boost.
The conventional WBI regimen consisted of a total of 50 Gy delivered over 25 fractions. The hypofractionated regimen consisted of a total dose of 42.5 Gy delivered in 16 fractions. Patients assigned to get a boost dose to the tumor bed received an additional 16 Gy in eight fractions after WBI.
Of the 1,608 patients enrolled who eligible for randomization, 803 received a boost dose and 805 did not. As noted before, the risk of recurrence at 5 years was significantly lower with boosting, with 5-year free-from-local-recurrence rates of 97.1%, compared with 92.7% for patients who did not get a tumor-bed boost.
There were no significant differences according to fractionation schedule, however: among all randomly assigned patients the rate of 5-year freedom from recurrence was 94.9% for both the conventionally fractionated and hypofractionated WBI groups.
Not surprisingly, patients who received the boost dose had higher rates of grade 2 or greater toxicities, including breast pain (14% vs. 10%; P = .03) and induration (14% vs. 6%; P < .001).
The study was supported by the National Health and Medical Research Council of Australia, Susan G. Komen for the Cure, Breast Cancer Now, OncoSuisse, Dutch Cancer Society, and Canadian Cancer Trials Group. Dr. Chua disclosed grant support from the organizations and others.
FROM THE LANCET
Infographic: Is physician behavior on social media really so bad?
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
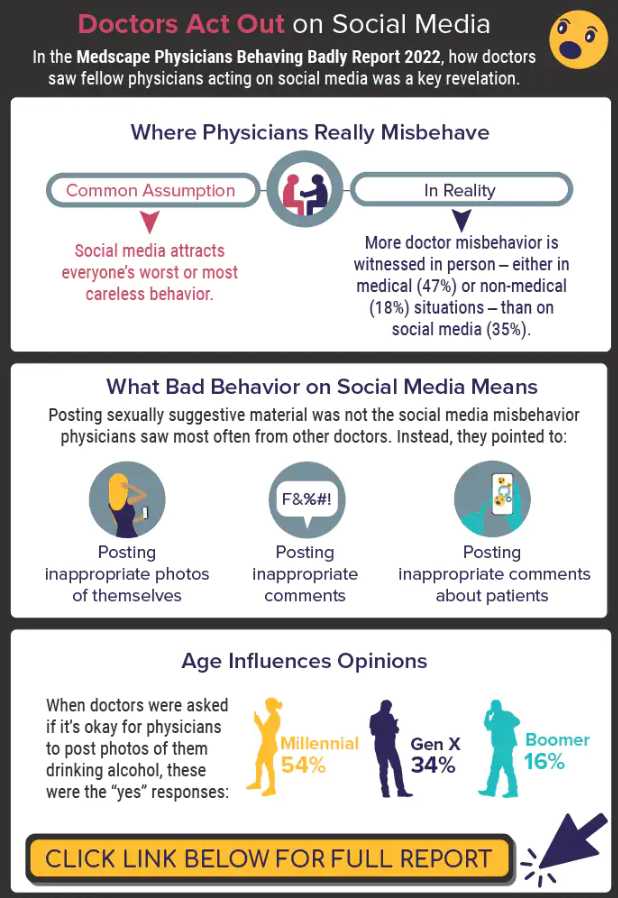
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.
Paxlovid reduces risk of COVID death by 79% in older adults
The antiviral drug Paxlovid appears to reduce the risk of dying from COVID-19 by 79% and decrease hospitalizations by 73% in at-risk patients who are ages 65 and older, according to a new study published in The New England Journal of Medicine.
The pill, which is a combination of the drugs nirmatrelvir and ritonavir, received FDA emergency use authorization in December 2021 to treat mild to moderate disease in ages 12 and older who face high risks for having severe COVID-19, hospitalization, and death.
“The results of the study show unequivocally that treatment with Paxlovid significantly reduces the risk of hospitalization and death from COVID-19,” Doron Netzer, MD, the senior study author and a researcher with Clalit Health Services, Tel Aviv, told The Jerusalem Post.
“We are the country’s leader in the provision of giving Paxlovid to relevant patients,” he said. “It was given to patients all over the country, with medical teams monitoring the patients who took the pills.”
, the news outlet reported. The research team analyzed information from Clalit’s electronic medical records. The health care organization covers about 52% of the Israeli population and almost two-thirds of older adults. More than 30,000 COVID-19 patients in Israel have been treated with the drug so far.
Dr. Netzer and colleagues looked at hospitalization and death data for at-risk COVID-19 patients ages 40 and older between Jan. 9 and March 31, when the original Omicron variant was the dominant strain in Israel. During that time, more than 1.1 million Clalit patients were infected with COVID-19, 109,000 patients were considered at-risk, and 3,900 patients received the drug.
The average age of the patients was 60, and 39% of the patients were 65 and older. Overall, 78% of the patients had previous COVID-19 immunity due to vaccination, prior infection, or both.
Among ages 65 and older, the rate of COVID-19 hospitalization was 14.7 cases per 100,000 person-days among treated patients, compared with 58.9 cases per 100,000 person-days among untreated patients. This represented a 73% lower chance of being hospitalized.
Among ages 40-64, the rate of hospitalization due to COVID-19 was 15.2 cases per 100,000 person-days among treated patients, compared with 15.8 cases per 100,000 person-days among untreated patients. The risk of hospitalization wasn’t significantly lower for this age group.
Among ages 65 and older, there were two deaths from COVID-19 in 2,484 treated patients, compared with 158 in the 40,337 untreated patients. This represented a 79% lower chance of dying from COVID-19.
Among ages 40-64, there was one death from COVID-19 in 1,418 treated patients, compared with 16 in the 65,015 untreated patients. The risk of death wasn’t significantly lower for this age group.
For both age groups, a lack of previous COVID-19 immunity and a previous hospitalization were most strongly linked to high rates of hospitalization during the Omicron wave.
The researchers noted that they didn’t break down the data on ages 40-64 who had cancer and other severe conditions that weaken the immune system. These patients may be more likely to benefit from Paxlovid, they said, though future studies will need to analyze the data.
The study didn’t receive any financial or in-kind support, the authors said.
A version of this article first appeared on WebMD.com.
The antiviral drug Paxlovid appears to reduce the risk of dying from COVID-19 by 79% and decrease hospitalizations by 73% in at-risk patients who are ages 65 and older, according to a new study published in The New England Journal of Medicine.
The pill, which is a combination of the drugs nirmatrelvir and ritonavir, received FDA emergency use authorization in December 2021 to treat mild to moderate disease in ages 12 and older who face high risks for having severe COVID-19, hospitalization, and death.
“The results of the study show unequivocally that treatment with Paxlovid significantly reduces the risk of hospitalization and death from COVID-19,” Doron Netzer, MD, the senior study author and a researcher with Clalit Health Services, Tel Aviv, told The Jerusalem Post.
“We are the country’s leader in the provision of giving Paxlovid to relevant patients,” he said. “It was given to patients all over the country, with medical teams monitoring the patients who took the pills.”
, the news outlet reported. The research team analyzed information from Clalit’s electronic medical records. The health care organization covers about 52% of the Israeli population and almost two-thirds of older adults. More than 30,000 COVID-19 patients in Israel have been treated with the drug so far.
Dr. Netzer and colleagues looked at hospitalization and death data for at-risk COVID-19 patients ages 40 and older between Jan. 9 and March 31, when the original Omicron variant was the dominant strain in Israel. During that time, more than 1.1 million Clalit patients were infected with COVID-19, 109,000 patients were considered at-risk, and 3,900 patients received the drug.
The average age of the patients was 60, and 39% of the patients were 65 and older. Overall, 78% of the patients had previous COVID-19 immunity due to vaccination, prior infection, or both.
Among ages 65 and older, the rate of COVID-19 hospitalization was 14.7 cases per 100,000 person-days among treated patients, compared with 58.9 cases per 100,000 person-days among untreated patients. This represented a 73% lower chance of being hospitalized.
Among ages 40-64, the rate of hospitalization due to COVID-19 was 15.2 cases per 100,000 person-days among treated patients, compared with 15.8 cases per 100,000 person-days among untreated patients. The risk of hospitalization wasn’t significantly lower for this age group.
Among ages 65 and older, there were two deaths from COVID-19 in 2,484 treated patients, compared with 158 in the 40,337 untreated patients. This represented a 79% lower chance of dying from COVID-19.
Among ages 40-64, there was one death from COVID-19 in 1,418 treated patients, compared with 16 in the 65,015 untreated patients. The risk of death wasn’t significantly lower for this age group.
For both age groups, a lack of previous COVID-19 immunity and a previous hospitalization were most strongly linked to high rates of hospitalization during the Omicron wave.
The researchers noted that they didn’t break down the data on ages 40-64 who had cancer and other severe conditions that weaken the immune system. These patients may be more likely to benefit from Paxlovid, they said, though future studies will need to analyze the data.
The study didn’t receive any financial or in-kind support, the authors said.
A version of this article first appeared on WebMD.com.
The antiviral drug Paxlovid appears to reduce the risk of dying from COVID-19 by 79% and decrease hospitalizations by 73% in at-risk patients who are ages 65 and older, according to a new study published in The New England Journal of Medicine.
The pill, which is a combination of the drugs nirmatrelvir and ritonavir, received FDA emergency use authorization in December 2021 to treat mild to moderate disease in ages 12 and older who face high risks for having severe COVID-19, hospitalization, and death.
“The results of the study show unequivocally that treatment with Paxlovid significantly reduces the risk of hospitalization and death from COVID-19,” Doron Netzer, MD, the senior study author and a researcher with Clalit Health Services, Tel Aviv, told The Jerusalem Post.
“We are the country’s leader in the provision of giving Paxlovid to relevant patients,” he said. “It was given to patients all over the country, with medical teams monitoring the patients who took the pills.”
, the news outlet reported. The research team analyzed information from Clalit’s electronic medical records. The health care organization covers about 52% of the Israeli population and almost two-thirds of older adults. More than 30,000 COVID-19 patients in Israel have been treated with the drug so far.
Dr. Netzer and colleagues looked at hospitalization and death data for at-risk COVID-19 patients ages 40 and older between Jan. 9 and March 31, when the original Omicron variant was the dominant strain in Israel. During that time, more than 1.1 million Clalit patients were infected with COVID-19, 109,000 patients were considered at-risk, and 3,900 patients received the drug.
The average age of the patients was 60, and 39% of the patients were 65 and older. Overall, 78% of the patients had previous COVID-19 immunity due to vaccination, prior infection, or both.
Among ages 65 and older, the rate of COVID-19 hospitalization was 14.7 cases per 100,000 person-days among treated patients, compared with 58.9 cases per 100,000 person-days among untreated patients. This represented a 73% lower chance of being hospitalized.
Among ages 40-64, the rate of hospitalization due to COVID-19 was 15.2 cases per 100,000 person-days among treated patients, compared with 15.8 cases per 100,000 person-days among untreated patients. The risk of hospitalization wasn’t significantly lower for this age group.
Among ages 65 and older, there were two deaths from COVID-19 in 2,484 treated patients, compared with 158 in the 40,337 untreated patients. This represented a 79% lower chance of dying from COVID-19.
Among ages 40-64, there was one death from COVID-19 in 1,418 treated patients, compared with 16 in the 65,015 untreated patients. The risk of death wasn’t significantly lower for this age group.
For both age groups, a lack of previous COVID-19 immunity and a previous hospitalization were most strongly linked to high rates of hospitalization during the Omicron wave.
The researchers noted that they didn’t break down the data on ages 40-64 who had cancer and other severe conditions that weaken the immune system. These patients may be more likely to benefit from Paxlovid, they said, though future studies will need to analyze the data.
The study didn’t receive any financial or in-kind support, the authors said.
A version of this article first appeared on WebMD.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE