User login
2019-2020 flu season starts off full throttle
For the week ending Nov. 23, there were five states, along with Puerto Rico, at the highest level of the Centers for Disease Control and Prevention’s 1-10 scale of flu activity. That’s more than any year since 2012, including the pandemic season of 2017-2018, according to CDC data, and may suggest either an early peak or the beginning of a particularly bad winter.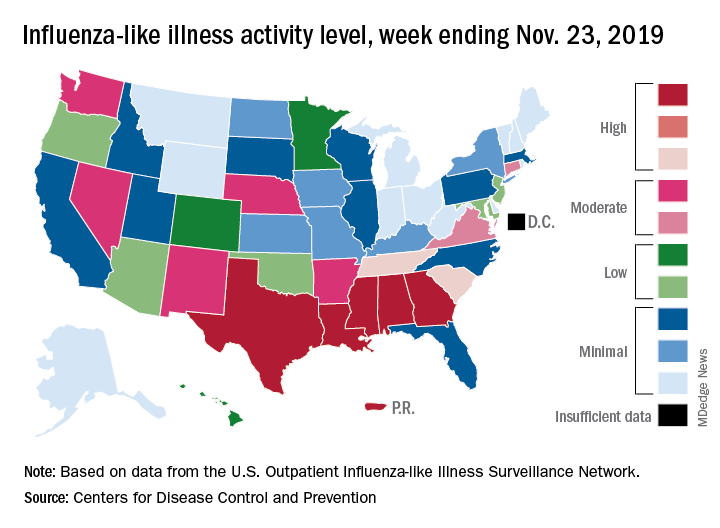
“Nationally, ILI [influenza-like illness] activity has been at or above baseline for 3 weeks; however, the amount of influenza activity across the country varies with the south and parts of the west seeing elevated activity while other parts of the country are still seeing low activity,” the CDC’s influenza division said in its weekly FluView report.
The five highest-activity states – Alabama, Georgia, Louisiana, Mississippi, and Texas – are all at level 10, and they join two others – South Carolina and Tennessee, which are at level 8 – in the “high” range from 8-10 on the ILI activity scale; Puerto Rico also is at level 10. ILI is defined as “fever (temperature of 100° F [37.8° C] or greater) and a cough and/or a sore throat without a known cause other than influenza,” the CDC said.
The activity scale is based on the percentage of outpatient visits for ILI in each state, which is reported to the CDC’s Outpatient Influenza-like Illness Surveillance Network (ILINet) each week. The national rate for the week ending Nov. 23 was 2.9%, which is above the new-for-this-season baseline rate of 2.4%. For the three previous flu seasons, the national baseline was 2.2%, having been raised from its previous level of 2.1% in 2015-2016, CDC data show.
The peak month of flu activity occurs most often in February – 15 times from 1982-1983 to 2017-2018 – but there were seven peaks in December and six each in January and March over that time period, along with one peak each in October and November, the CDC said. The October peak occurred during the H1N1 pandemic year of 2009, when the national outpatient ILI rate climbed to just over 7.7%.
For the week ending Nov. 23, there were five states, along with Puerto Rico, at the highest level of the Centers for Disease Control and Prevention’s 1-10 scale of flu activity. That’s more than any year since 2012, including the pandemic season of 2017-2018, according to CDC data, and may suggest either an early peak or the beginning of a particularly bad winter.
“Nationally, ILI [influenza-like illness] activity has been at or above baseline for 3 weeks; however, the amount of influenza activity across the country varies with the south and parts of the west seeing elevated activity while other parts of the country are still seeing low activity,” the CDC’s influenza division said in its weekly FluView report.
The five highest-activity states – Alabama, Georgia, Louisiana, Mississippi, and Texas – are all at level 10, and they join two others – South Carolina and Tennessee, which are at level 8 – in the “high” range from 8-10 on the ILI activity scale; Puerto Rico also is at level 10. ILI is defined as “fever (temperature of 100° F [37.8° C] or greater) and a cough and/or a sore throat without a known cause other than influenza,” the CDC said.
The activity scale is based on the percentage of outpatient visits for ILI in each state, which is reported to the CDC’s Outpatient Influenza-like Illness Surveillance Network (ILINet) each week. The national rate for the week ending Nov. 23 was 2.9%, which is above the new-for-this-season baseline rate of 2.4%. For the three previous flu seasons, the national baseline was 2.2%, having been raised from its previous level of 2.1% in 2015-2016, CDC data show.
The peak month of flu activity occurs most often in February – 15 times from 1982-1983 to 2017-2018 – but there were seven peaks in December and six each in January and March over that time period, along with one peak each in October and November, the CDC said. The October peak occurred during the H1N1 pandemic year of 2009, when the national outpatient ILI rate climbed to just over 7.7%.
For the week ending Nov. 23, there were five states, along with Puerto Rico, at the highest level of the Centers for Disease Control and Prevention’s 1-10 scale of flu activity. That’s more than any year since 2012, including the pandemic season of 2017-2018, according to CDC data, and may suggest either an early peak or the beginning of a particularly bad winter.
“Nationally, ILI [influenza-like illness] activity has been at or above baseline for 3 weeks; however, the amount of influenza activity across the country varies with the south and parts of the west seeing elevated activity while other parts of the country are still seeing low activity,” the CDC’s influenza division said in its weekly FluView report.
The five highest-activity states – Alabama, Georgia, Louisiana, Mississippi, and Texas – are all at level 10, and they join two others – South Carolina and Tennessee, which are at level 8 – in the “high” range from 8-10 on the ILI activity scale; Puerto Rico also is at level 10. ILI is defined as “fever (temperature of 100° F [37.8° C] or greater) and a cough and/or a sore throat without a known cause other than influenza,” the CDC said.
The activity scale is based on the percentage of outpatient visits for ILI in each state, which is reported to the CDC’s Outpatient Influenza-like Illness Surveillance Network (ILINet) each week. The national rate for the week ending Nov. 23 was 2.9%, which is above the new-for-this-season baseline rate of 2.4%. For the three previous flu seasons, the national baseline was 2.2%, having been raised from its previous level of 2.1% in 2015-2016, CDC data show.
The peak month of flu activity occurs most often in February – 15 times from 1982-1983 to 2017-2018 – but there were seven peaks in December and six each in January and March over that time period, along with one peak each in October and November, the CDC said. The October peak occurred during the H1N1 pandemic year of 2009, when the national outpatient ILI rate climbed to just over 7.7%.
Supporting quality improvement strategies
Keys to improve PDSA cycle fidelity
As many hospitalists know, a frequently deployed approach to quality improvement (QI) is the Plan-Do-Study-Act (PDSA) cycle method. But it comes with challenges, according to a recent paper in BMJ Quality & Safety.

“There is little evidence on the fidelity of PDSA cycles used by frontline teams, nor how to support and improve the method’s use,” according to the authors. They used document analysis and interviews to review 421 PDSA cycles, tracking fidelity over three annual rounds of projects.
The researchers found that modest, statistically significant improvements in PDSA fidelity occurred, but overall fidelity was low.
“Challenges to achieving greater fidelity reflected problems with understanding the PDSA methodology, intention to use and application in practice,” the authors reported. “These problems were exacerbated by assumptions made in the original QI training and support strategies: that PDSA was easy to understand, that teams would be motivated and willing to use PDSA, and that PDSA is easy to apply.”
The study describes several strategies to help improve PDSA cycle fidelity: different project selection process, redesign of training, increased hands-on support, and investment in training quality improvement support staff. “The findings suggest achieving high PDSA fidelity requires a gradual and negotiated process to explore different perspectives and encourage new ways of working,” the authors concluded.
Reference
1. McNicholas C et al. Evolving quality improvement support strategies to improve Plan-Do-Study–Act cycle fidelity: A retrospective mixed-methods study. BMJ Qual Saf. 2019 Mar 18. doi: 10.1136/bmjqs-2017-007605.
Keys to improve PDSA cycle fidelity
Keys to improve PDSA cycle fidelity
As many hospitalists know, a frequently deployed approach to quality improvement (QI) is the Plan-Do-Study-Act (PDSA) cycle method. But it comes with challenges, according to a recent paper in BMJ Quality & Safety.
“There is little evidence on the fidelity of PDSA cycles used by frontline teams, nor how to support and improve the method’s use,” according to the authors. They used document analysis and interviews to review 421 PDSA cycles, tracking fidelity over three annual rounds of projects.
The researchers found that modest, statistically significant improvements in PDSA fidelity occurred, but overall fidelity was low.
“Challenges to achieving greater fidelity reflected problems with understanding the PDSA methodology, intention to use and application in practice,” the authors reported. “These problems were exacerbated by assumptions made in the original QI training and support strategies: that PDSA was easy to understand, that teams would be motivated and willing to use PDSA, and that PDSA is easy to apply.”
The study describes several strategies to help improve PDSA cycle fidelity: different project selection process, redesign of training, increased hands-on support, and investment in training quality improvement support staff. “The findings suggest achieving high PDSA fidelity requires a gradual and negotiated process to explore different perspectives and encourage new ways of working,” the authors concluded.
Reference
1. McNicholas C et al. Evolving quality improvement support strategies to improve Plan-Do-Study–Act cycle fidelity: A retrospective mixed-methods study. BMJ Qual Saf. 2019 Mar 18. doi: 10.1136/bmjqs-2017-007605.
As many hospitalists know, a frequently deployed approach to quality improvement (QI) is the Plan-Do-Study-Act (PDSA) cycle method. But it comes with challenges, according to a recent paper in BMJ Quality & Safety.
“There is little evidence on the fidelity of PDSA cycles used by frontline teams, nor how to support and improve the method’s use,” according to the authors. They used document analysis and interviews to review 421 PDSA cycles, tracking fidelity over three annual rounds of projects.
The researchers found that modest, statistically significant improvements in PDSA fidelity occurred, but overall fidelity was low.
“Challenges to achieving greater fidelity reflected problems with understanding the PDSA methodology, intention to use and application in practice,” the authors reported. “These problems were exacerbated by assumptions made in the original QI training and support strategies: that PDSA was easy to understand, that teams would be motivated and willing to use PDSA, and that PDSA is easy to apply.”
The study describes several strategies to help improve PDSA cycle fidelity: different project selection process, redesign of training, increased hands-on support, and investment in training quality improvement support staff. “The findings suggest achieving high PDSA fidelity requires a gradual and negotiated process to explore different perspectives and encourage new ways of working,” the authors concluded.
Reference
1. McNicholas C et al. Evolving quality improvement support strategies to improve Plan-Do-Study–Act cycle fidelity: A retrospective mixed-methods study. BMJ Qual Saf. 2019 Mar 18. doi: 10.1136/bmjqs-2017-007605.
Benefiting from hospitalist-directed transfers
A ‘unique opportunity’ for hospitalists
Emergency department overcrowding is common, and it can result in both increased costs and poor clinical outcomes.

“We sought to evaluate the impact and safety of hospitalist-directed transfers on patients boarding in the ER as a means to alleviate overcrowding,” said Yihan Chen, MD, MPH, of the University of California, Los Angeles. “High inpatient census has been shown to impair ER throughput by increasing the number of ER ‘boarders,’ which creates a suboptimal care environment for practicing hospitalists. For example, some studies have shown associations with delays in medical decision making when admitted patients remain and receive care in the emergency department.”
Dr. Chen was the lead author of an abstract describing a chart review on 1,016 admissions to the hospitalist service. About half remained at the reference hospital and half were transferred to a nearby affiliate hospital.
In analyzing the data, the researchers’ top takeaway was the many benefits for the transferred patients. “Hospitalist-directed transfer and direct admission of stable ER patients to an affiliate facility with greater bed availability is associated with shorter ER lengths of stay, fewer adverse events, and lower rates of readmission within 30 days of hospitalization,” Dr. Chen said. “Having a system in place to transfer patients to an affiliate hospital with lower census is a way to improve flow.”
Hospitalists have a unique opportunity to take on a triage role in the ED to safely and effectively decrease ED overcrowding and throughput, improve resource utilization at the hospital level, and allow for other hospitalists at their institution to optimize patient care on the inpatient ward rather than in the ED, Dr. Chen said.
“Health systems privileged to have more than one facility should consider an intra–health system transfer process lead by triage hospitalists to identify stable patients who can be directly admitted to the off-site, affiliate hospital,” she said. “By improving patient throughput, hospitalists would play a critical role in relieving institutional stressors, impacting cost and quality of care, and enhancing clinical outcomes.”
Reference
1. Chen Y et al. Hospitalist-Directed Transfers Improve Emergency Room Length of Stay. Hospital Medicine 2018, Abstract 12. Accessed April 3, 2019.
A ‘unique opportunity’ for hospitalists
A ‘unique opportunity’ for hospitalists
Emergency department overcrowding is common, and it can result in both increased costs and poor clinical outcomes.
“We sought to evaluate the impact and safety of hospitalist-directed transfers on patients boarding in the ER as a means to alleviate overcrowding,” said Yihan Chen, MD, MPH, of the University of California, Los Angeles. “High inpatient census has been shown to impair ER throughput by increasing the number of ER ‘boarders,’ which creates a suboptimal care environment for practicing hospitalists. For example, some studies have shown associations with delays in medical decision making when admitted patients remain and receive care in the emergency department.”
Dr. Chen was the lead author of an abstract describing a chart review on 1,016 admissions to the hospitalist service. About half remained at the reference hospital and half were transferred to a nearby affiliate hospital.
In analyzing the data, the researchers’ top takeaway was the many benefits for the transferred patients. “Hospitalist-directed transfer and direct admission of stable ER patients to an affiliate facility with greater bed availability is associated with shorter ER lengths of stay, fewer adverse events, and lower rates of readmission within 30 days of hospitalization,” Dr. Chen said. “Having a system in place to transfer patients to an affiliate hospital with lower census is a way to improve flow.”
Hospitalists have a unique opportunity to take on a triage role in the ED to safely and effectively decrease ED overcrowding and throughput, improve resource utilization at the hospital level, and allow for other hospitalists at their institution to optimize patient care on the inpatient ward rather than in the ED, Dr. Chen said.
“Health systems privileged to have more than one facility should consider an intra–health system transfer process lead by triage hospitalists to identify stable patients who can be directly admitted to the off-site, affiliate hospital,” she said. “By improving patient throughput, hospitalists would play a critical role in relieving institutional stressors, impacting cost and quality of care, and enhancing clinical outcomes.”
Reference
1. Chen Y et al. Hospitalist-Directed Transfers Improve Emergency Room Length of Stay. Hospital Medicine 2018, Abstract 12. Accessed April 3, 2019.
Emergency department overcrowding is common, and it can result in both increased costs and poor clinical outcomes.
“We sought to evaluate the impact and safety of hospitalist-directed transfers on patients boarding in the ER as a means to alleviate overcrowding,” said Yihan Chen, MD, MPH, of the University of California, Los Angeles. “High inpatient census has been shown to impair ER throughput by increasing the number of ER ‘boarders,’ which creates a suboptimal care environment for practicing hospitalists. For example, some studies have shown associations with delays in medical decision making when admitted patients remain and receive care in the emergency department.”
Dr. Chen was the lead author of an abstract describing a chart review on 1,016 admissions to the hospitalist service. About half remained at the reference hospital and half were transferred to a nearby affiliate hospital.
In analyzing the data, the researchers’ top takeaway was the many benefits for the transferred patients. “Hospitalist-directed transfer and direct admission of stable ER patients to an affiliate facility with greater bed availability is associated with shorter ER lengths of stay, fewer adverse events, and lower rates of readmission within 30 days of hospitalization,” Dr. Chen said. “Having a system in place to transfer patients to an affiliate hospital with lower census is a way to improve flow.”
Hospitalists have a unique opportunity to take on a triage role in the ED to safely and effectively decrease ED overcrowding and throughput, improve resource utilization at the hospital level, and allow for other hospitalists at their institution to optimize patient care on the inpatient ward rather than in the ED, Dr. Chen said.
“Health systems privileged to have more than one facility should consider an intra–health system transfer process lead by triage hospitalists to identify stable patients who can be directly admitted to the off-site, affiliate hospital,” she said. “By improving patient throughput, hospitalists would play a critical role in relieving institutional stressors, impacting cost and quality of care, and enhancing clinical outcomes.”
Reference
1. Chen Y et al. Hospitalist-Directed Transfers Improve Emergency Room Length of Stay. Hospital Medicine 2018, Abstract 12. Accessed April 3, 2019.
PHM19: MOC Part 4 projects for community pediatric hospitalists
PHM19 session
MOC Part 4 projects for community pediatric hospitalists

Presenters
Jack M. Percelay, MD, MPH, FAAP, MHM
Nancy Chen, MD, FAAP
Elizabeth Dobler, MD, FAAP
Lindsay Fox, MD
Beth C. Natt, MD, MPH, SFHM
Clota Snow, MD, FAAP
Session summary
Dr. Jack Percelay, of Sutter Health in San Francisco, started this session at Pediatric Hospital Medicine 2019 by outlining the process of submitting a small group (n = 1-10) project for Maintenance of Certification (MOC) Part 4 credit including the basics of what is needed for the application:
- Aim statement.
- Metrics used.
- Data required (3 data points: pre, post, and sustain).
He also shared the requirement of “meaningful participation” for participants to be eligible for MOC Part 4 credit.
Examples of successful projects were shared by members of the presenting group:
- Dr. Natt: Improving the timing of the birth dose of the hepatitis B vaccination.
- Dr. Dobler: Improving the hepatitis B vaccination rate within 24 hours of birth.
- Dr. Snow: Supplementing vitamin D in the newborn nursery.
- Dr. Fox: Improving newborn discharge efficiency, improving screening for smoking exposure, and offering smoking cessation.
- Dr. Percelay: Improving hospitalist billing and coding using time as a factor.
- Dr. Chen: Improving patient satisfaction through improvement of family-centered rounds.
The workshop audience divided into groups to brainstorm/troubleshoot projects and to elicit general advice regarding the process. Sample submissions were provided.
Key takeaways
- Even small projects (i.e. single metric) can be submitted/accepted with pre- and postintervention data.
- Be creative! Think about changes you are making at your institution and gather the data to support the intervention.
- Always double-dip on QI projects to gain valuable MOC Part 4 credit!
Dr. Fox is site director, Pediatric Hospital Medicine Division at MetroWest Medical Center, Framingham, Mass.
PHM19 session
MOC Part 4 projects for community pediatric hospitalists
Presenters
Jack M. Percelay, MD, MPH, FAAP, MHM
Nancy Chen, MD, FAAP
Elizabeth Dobler, MD, FAAP
Lindsay Fox, MD
Beth C. Natt, MD, MPH, SFHM
Clota Snow, MD, FAAP
Session summary
Dr. Jack Percelay, of Sutter Health in San Francisco, started this session at Pediatric Hospital Medicine 2019 by outlining the process of submitting a small group (n = 1-10) project for Maintenance of Certification (MOC) Part 4 credit including the basics of what is needed for the application:
- Aim statement.
- Metrics used.
- Data required (3 data points: pre, post, and sustain).
He also shared the requirement of “meaningful participation” for participants to be eligible for MOC Part 4 credit.
Examples of successful projects were shared by members of the presenting group:
- Dr. Natt: Improving the timing of the birth dose of the hepatitis B vaccination.
- Dr. Dobler: Improving the hepatitis B vaccination rate within 24 hours of birth.
- Dr. Snow: Supplementing vitamin D in the newborn nursery.
- Dr. Fox: Improving newborn discharge efficiency, improving screening for smoking exposure, and offering smoking cessation.
- Dr. Percelay: Improving hospitalist billing and coding using time as a factor.
- Dr. Chen: Improving patient satisfaction through improvement of family-centered rounds.
The workshop audience divided into groups to brainstorm/troubleshoot projects and to elicit general advice regarding the process. Sample submissions were provided.
Key takeaways
- Even small projects (i.e. single metric) can be submitted/accepted with pre- and postintervention data.
- Be creative! Think about changes you are making at your institution and gather the data to support the intervention.
- Always double-dip on QI projects to gain valuable MOC Part 4 credit!
Dr. Fox is site director, Pediatric Hospital Medicine Division at MetroWest Medical Center, Framingham, Mass.
PHM19 session
MOC Part 4 projects for community pediatric hospitalists
Presenters
Jack M. Percelay, MD, MPH, FAAP, MHM
Nancy Chen, MD, FAAP
Elizabeth Dobler, MD, FAAP
Lindsay Fox, MD
Beth C. Natt, MD, MPH, SFHM
Clota Snow, MD, FAAP
Session summary
Dr. Jack Percelay, of Sutter Health in San Francisco, started this session at Pediatric Hospital Medicine 2019 by outlining the process of submitting a small group (n = 1-10) project for Maintenance of Certification (MOC) Part 4 credit including the basics of what is needed for the application:
- Aim statement.
- Metrics used.
- Data required (3 data points: pre, post, and sustain).
He also shared the requirement of “meaningful participation” for participants to be eligible for MOC Part 4 credit.
Examples of successful projects were shared by members of the presenting group:
- Dr. Natt: Improving the timing of the birth dose of the hepatitis B vaccination.
- Dr. Dobler: Improving the hepatitis B vaccination rate within 24 hours of birth.
- Dr. Snow: Supplementing vitamin D in the newborn nursery.
- Dr. Fox: Improving newborn discharge efficiency, improving screening for smoking exposure, and offering smoking cessation.
- Dr. Percelay: Improving hospitalist billing and coding using time as a factor.
- Dr. Chen: Improving patient satisfaction through improvement of family-centered rounds.
The workshop audience divided into groups to brainstorm/troubleshoot projects and to elicit general advice regarding the process. Sample submissions were provided.
Key takeaways
- Even small projects (i.e. single metric) can be submitted/accepted with pre- and postintervention data.
- Be creative! Think about changes you are making at your institution and gather the data to support the intervention.
- Always double-dip on QI projects to gain valuable MOC Part 4 credit!
Dr. Fox is site director, Pediatric Hospital Medicine Division at MetroWest Medical Center, Framingham, Mass.
ACGME deepening its commitment to physician well-being, leader says
NEW ORLEANS – When Timothy P. Brigham, MDiv, PhD, thinks about the impact of burnout and stress on the ability of physicians to practice medicine, Lewin’s equation comes to mind.

Developed by psychologist Kurt Lewin in 1936, the equation holds that behavior stems from a person’s personality and the environment that person inhabits.
Dr. Brigham, chief of staff and chief education and organizational development officer at the Chicago-based Accreditation Council for Graduate Medical Education (ACGME), said at the annual meeting of the American Academy of Pediatrics.
“It’s a toxic mine, in some ways. What we tend to do is when we detect that physicians in general are, or a particular residency program is, too stressed out or burned out, we give them resilience training. Not that that’s unimportant, but it’s like putting a canary in a toxic mine full of poison and saying, ‘We’re going to teach you to hold your breath a little bit longer.’ Our job is to detoxify the mine.”
Troubled by the rise of suicides among physicians in recent years as well as mounting evidence about the adverse impact of burnout and stress on the practice of medicine, Dr. Brigham said that the ACGME is deepening its commitment to the well-being of faculty, residents, patients, and all members of the health care team. Since launching a “call to arms” on the topic at its annual educational conference in 2015, the ACGME has added courses on well-being to its annual meeting and remolded its Clinical Learning Environmental Review program to include all clinicians, “because everybody is affected by this: nurses, coordinators, et cetera,” he said. The ACGME also has revised Common Program Requirements, disseminated tools and resources to promote well-being and new knowledge on the topic, and partnered with the National Academy of Medicine Action Collaborative on Clinician Well-Being and Resilience – all in an effort to bring about culture change.
“But we’re well aware that the ACGME can’t do this alone,” Dr. Brigham said. “We can’t ‘requirement’ our way out of this problem. It’s going to take a culture shift. Only you physicians, in collaboration with everyone in your community of learning, can create the systemic change required to improve our culture. We have a good handle on the problem at this point, but the solutions are a little bit more difficult to get a hold of. As Martin Luther King Jr. once said, ‘You don’t have to see the whole staircase, just take the first step.’ ”
The ACGME wants to work with physicians “to collect data and do joint research, to share insights, and to share tools and resources to create a better world for practicing physicians, for other members of the health care team, and for patients. After all, clinicians who care for themselves provide better care for others. They’re less likely to make errors or leave the profession,” Dr. Brigham told attendees.
He added that clinicians can gauge their risk for burnout by asking themselves three simple questions about their work environment: Does it support self-care? Does it increase and support connection with colleagues? Does it connect people to purpose and meaningful work?
“One of the problems with our resident clinical work hours is not terrible program directors saying, ‘work longer.’ It’s residents who want to take care of families for 1 more hour,” Dr. Brigham continued. “It’s residents who want to take care of patients who are going through a difficult time. You represent the top 2% in the world in terms of your intelligence and achievement, yet that’s not what makes you special. What makes you special is that the level of self-doubt in this room exceeds that of the general population by about 10 times. You also tend to run toward what everyone else runs away from: disease, despair, people who are injured and suffering. That takes a toll.”

He emphasized that positive social relationships with others are crucial to joy and well-being in the practice of medicine. “Burnout isn’t just about exhaustion; it’s about loneliness,” Dr. Brigham said. “There’s a surprising power in just asking people how they’re doing, and really wanting to know the answer.”
Negative social connections are highly correlated with burnout and depression, such as harassment, bullying, mistreatment, discrimination, “and using the power gradient to squash somebody who’s trying their best to be a physician,” he said.
Dr. Brigham acknowledged the tall task of bringing a spotlight to well-being as physicians continue to engage in tasks such as the burden and lack of standardization of prior authorization requirements, the burden of clinical documentation requirements, electronic health records and related work flow, and quality payment programs. “This is what we need to shift; this is what we need to take away so you can get back in touch with why you became a physician in the first place.”
Dr. Brigham reported having no financial disclosures.
NEW ORLEANS – When Timothy P. Brigham, MDiv, PhD, thinks about the impact of burnout and stress on the ability of physicians to practice medicine, Lewin’s equation comes to mind.
Developed by psychologist Kurt Lewin in 1936, the equation holds that behavior stems from a person’s personality and the environment that person inhabits.
Dr. Brigham, chief of staff and chief education and organizational development officer at the Chicago-based Accreditation Council for Graduate Medical Education (ACGME), said at the annual meeting of the American Academy of Pediatrics.
“It’s a toxic mine, in some ways. What we tend to do is when we detect that physicians in general are, or a particular residency program is, too stressed out or burned out, we give them resilience training. Not that that’s unimportant, but it’s like putting a canary in a toxic mine full of poison and saying, ‘We’re going to teach you to hold your breath a little bit longer.’ Our job is to detoxify the mine.”
Troubled by the rise of suicides among physicians in recent years as well as mounting evidence about the adverse impact of burnout and stress on the practice of medicine, Dr. Brigham said that the ACGME is deepening its commitment to the well-being of faculty, residents, patients, and all members of the health care team. Since launching a “call to arms” on the topic at its annual educational conference in 2015, the ACGME has added courses on well-being to its annual meeting and remolded its Clinical Learning Environmental Review program to include all clinicians, “because everybody is affected by this: nurses, coordinators, et cetera,” he said. The ACGME also has revised Common Program Requirements, disseminated tools and resources to promote well-being and new knowledge on the topic, and partnered with the National Academy of Medicine Action Collaborative on Clinician Well-Being and Resilience – all in an effort to bring about culture change.
“But we’re well aware that the ACGME can’t do this alone,” Dr. Brigham said. “We can’t ‘requirement’ our way out of this problem. It’s going to take a culture shift. Only you physicians, in collaboration with everyone in your community of learning, can create the systemic change required to improve our culture. We have a good handle on the problem at this point, but the solutions are a little bit more difficult to get a hold of. As Martin Luther King Jr. once said, ‘You don’t have to see the whole staircase, just take the first step.’ ”
The ACGME wants to work with physicians “to collect data and do joint research, to share insights, and to share tools and resources to create a better world for practicing physicians, for other members of the health care team, and for patients. After all, clinicians who care for themselves provide better care for others. They’re less likely to make errors or leave the profession,” Dr. Brigham told attendees.
He added that clinicians can gauge their risk for burnout by asking themselves three simple questions about their work environment: Does it support self-care? Does it increase and support connection with colleagues? Does it connect people to purpose and meaningful work?
“One of the problems with our resident clinical work hours is not terrible program directors saying, ‘work longer.’ It’s residents who want to take care of families for 1 more hour,” Dr. Brigham continued. “It’s residents who want to take care of patients who are going through a difficult time. You represent the top 2% in the world in terms of your intelligence and achievement, yet that’s not what makes you special. What makes you special is that the level of self-doubt in this room exceeds that of the general population by about 10 times. You also tend to run toward what everyone else runs away from: disease, despair, people who are injured and suffering. That takes a toll.”
He emphasized that positive social relationships with others are crucial to joy and well-being in the practice of medicine. “Burnout isn’t just about exhaustion; it’s about loneliness,” Dr. Brigham said. “There’s a surprising power in just asking people how they’re doing, and really wanting to know the answer.”
Negative social connections are highly correlated with burnout and depression, such as harassment, bullying, mistreatment, discrimination, “and using the power gradient to squash somebody who’s trying their best to be a physician,” he said.
Dr. Brigham acknowledged the tall task of bringing a spotlight to well-being as physicians continue to engage in tasks such as the burden and lack of standardization of prior authorization requirements, the burden of clinical documentation requirements, electronic health records and related work flow, and quality payment programs. “This is what we need to shift; this is what we need to take away so you can get back in touch with why you became a physician in the first place.”
Dr. Brigham reported having no financial disclosures.
NEW ORLEANS – When Timothy P. Brigham, MDiv, PhD, thinks about the impact of burnout and stress on the ability of physicians to practice medicine, Lewin’s equation comes to mind.
Developed by psychologist Kurt Lewin in 1936, the equation holds that behavior stems from a person’s personality and the environment that person inhabits.
Dr. Brigham, chief of staff and chief education and organizational development officer at the Chicago-based Accreditation Council for Graduate Medical Education (ACGME), said at the annual meeting of the American Academy of Pediatrics.
“It’s a toxic mine, in some ways. What we tend to do is when we detect that physicians in general are, or a particular residency program is, too stressed out or burned out, we give them resilience training. Not that that’s unimportant, but it’s like putting a canary in a toxic mine full of poison and saying, ‘We’re going to teach you to hold your breath a little bit longer.’ Our job is to detoxify the mine.”
Troubled by the rise of suicides among physicians in recent years as well as mounting evidence about the adverse impact of burnout and stress on the practice of medicine, Dr. Brigham said that the ACGME is deepening its commitment to the well-being of faculty, residents, patients, and all members of the health care team. Since launching a “call to arms” on the topic at its annual educational conference in 2015, the ACGME has added courses on well-being to its annual meeting and remolded its Clinical Learning Environmental Review program to include all clinicians, “because everybody is affected by this: nurses, coordinators, et cetera,” he said. The ACGME also has revised Common Program Requirements, disseminated tools and resources to promote well-being and new knowledge on the topic, and partnered with the National Academy of Medicine Action Collaborative on Clinician Well-Being and Resilience – all in an effort to bring about culture change.
“But we’re well aware that the ACGME can’t do this alone,” Dr. Brigham said. “We can’t ‘requirement’ our way out of this problem. It’s going to take a culture shift. Only you physicians, in collaboration with everyone in your community of learning, can create the systemic change required to improve our culture. We have a good handle on the problem at this point, but the solutions are a little bit more difficult to get a hold of. As Martin Luther King Jr. once said, ‘You don’t have to see the whole staircase, just take the first step.’ ”
The ACGME wants to work with physicians “to collect data and do joint research, to share insights, and to share tools and resources to create a better world for practicing physicians, for other members of the health care team, and for patients. After all, clinicians who care for themselves provide better care for others. They’re less likely to make errors or leave the profession,” Dr. Brigham told attendees.
He added that clinicians can gauge their risk for burnout by asking themselves three simple questions about their work environment: Does it support self-care? Does it increase and support connection with colleagues? Does it connect people to purpose and meaningful work?
“One of the problems with our resident clinical work hours is not terrible program directors saying, ‘work longer.’ It’s residents who want to take care of families for 1 more hour,” Dr. Brigham continued. “It’s residents who want to take care of patients who are going through a difficult time. You represent the top 2% in the world in terms of your intelligence and achievement, yet that’s not what makes you special. What makes you special is that the level of self-doubt in this room exceeds that of the general population by about 10 times. You also tend to run toward what everyone else runs away from: disease, despair, people who are injured and suffering. That takes a toll.”
He emphasized that positive social relationships with others are crucial to joy and well-being in the practice of medicine. “Burnout isn’t just about exhaustion; it’s about loneliness,” Dr. Brigham said. “There’s a surprising power in just asking people how they’re doing, and really wanting to know the answer.”
Negative social connections are highly correlated with burnout and depression, such as harassment, bullying, mistreatment, discrimination, “and using the power gradient to squash somebody who’s trying their best to be a physician,” he said.
Dr. Brigham acknowledged the tall task of bringing a spotlight to well-being as physicians continue to engage in tasks such as the burden and lack of standardization of prior authorization requirements, the burden of clinical documentation requirements, electronic health records and related work flow, and quality payment programs. “This is what we need to shift; this is what we need to take away so you can get back in touch with why you became a physician in the first place.”
Dr. Brigham reported having no financial disclosures.
EXPERT ANALYSIS AT AAP 2019
Anticipating the A.I. revolution
Goal is to augment human performance
Artificial intelligence (A.I.) is likely to change almost everything in medical practice, according to a new book called “Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again,” by Eric Topol, MD.
Dr. Topol told The Hospitalist that his book’s subtitle “is the paradox: the unexpected, far-reaching goal of A.I. that can, if used properly, restore the most important part of medicine – a deep patient-doctor relationship.”
That’s because A.I. can do more than enhance diagnoses; it can also help with tasks such as note-taking and reading scans, making it possible for hospitalists to spend more time connecting with their patients. “Hospitalists could have a much better handle on a patient’s dataset via algorithmic processing, providing alerts and augmented performance of hospitalists (when validated),” Dr. Topol said. “They can also expect far less keyboard use with the help of speech recognition, natural language processing, and deep learning.”In an interview with the New York Times, Dr. Topol said that by augmenting human performance, A.I. has the potential to markedly improve productivity, efficiency, work flow, accuracy and speed, both for doctors and for patients, giving more charge and control to consumers through algorithmic support of their data.
“We can’t, and will never, rely on only algorithms for interpretation of life and death matters,” he said. “That requires human expert contextualization, something machines can’t do.”Of course, there could be pitfalls. “The liabilities include breaches of privacy and security, hacking, the lack of explainability of most A.I. algorithms, the potential to worsen inequities, the embedded bias, and ethical quandaries,” he said.
Reference
1. O’Connor A. How Artificial Intelligence Could Transform Medicine. New York Times. March 11, 2019. https://www.nytimes.com/2019/03/11/well/live/how-artificial-intelligence-could-transform-medicine.html.
Goal is to augment human performance
Goal is to augment human performance
Artificial intelligence (A.I.) is likely to change almost everything in medical practice, according to a new book called “Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again,” by Eric Topol, MD.
Dr. Topol told The Hospitalist that his book’s subtitle “is the paradox: the unexpected, far-reaching goal of A.I. that can, if used properly, restore the most important part of medicine – a deep patient-doctor relationship.”
That’s because A.I. can do more than enhance diagnoses; it can also help with tasks such as note-taking and reading scans, making it possible for hospitalists to spend more time connecting with their patients. “Hospitalists could have a much better handle on a patient’s dataset via algorithmic processing, providing alerts and augmented performance of hospitalists (when validated),” Dr. Topol said. “They can also expect far less keyboard use with the help of speech recognition, natural language processing, and deep learning.”In an interview with the New York Times, Dr. Topol said that by augmenting human performance, A.I. has the potential to markedly improve productivity, efficiency, work flow, accuracy and speed, both for doctors and for patients, giving more charge and control to consumers through algorithmic support of their data.
“We can’t, and will never, rely on only algorithms for interpretation of life and death matters,” he said. “That requires human expert contextualization, something machines can’t do.”Of course, there could be pitfalls. “The liabilities include breaches of privacy and security, hacking, the lack of explainability of most A.I. algorithms, the potential to worsen inequities, the embedded bias, and ethical quandaries,” he said.
Reference
1. O’Connor A. How Artificial Intelligence Could Transform Medicine. New York Times. March 11, 2019. https://www.nytimes.com/2019/03/11/well/live/how-artificial-intelligence-could-transform-medicine.html.
Artificial intelligence (A.I.) is likely to change almost everything in medical practice, according to a new book called “Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again,” by Eric Topol, MD.
Dr. Topol told The Hospitalist that his book’s subtitle “is the paradox: the unexpected, far-reaching goal of A.I. that can, if used properly, restore the most important part of medicine – a deep patient-doctor relationship.”
That’s because A.I. can do more than enhance diagnoses; it can also help with tasks such as note-taking and reading scans, making it possible for hospitalists to spend more time connecting with their patients. “Hospitalists could have a much better handle on a patient’s dataset via algorithmic processing, providing alerts and augmented performance of hospitalists (when validated),” Dr. Topol said. “They can also expect far less keyboard use with the help of speech recognition, natural language processing, and deep learning.”In an interview with the New York Times, Dr. Topol said that by augmenting human performance, A.I. has the potential to markedly improve productivity, efficiency, work flow, accuracy and speed, both for doctors and for patients, giving more charge and control to consumers through algorithmic support of their data.
“We can’t, and will never, rely on only algorithms for interpretation of life and death matters,” he said. “That requires human expert contextualization, something machines can’t do.”Of course, there could be pitfalls. “The liabilities include breaches of privacy and security, hacking, the lack of explainability of most A.I. algorithms, the potential to worsen inequities, the embedded bias, and ethical quandaries,” he said.
Reference
1. O’Connor A. How Artificial Intelligence Could Transform Medicine. New York Times. March 11, 2019. https://www.nytimes.com/2019/03/11/well/live/how-artificial-intelligence-could-transform-medicine.html.
DAPA-HF: Dapagliflozin benefits regardless of age, HF severity
PHILADELPHIA – The substantial benefits from adding dapagliflozin to guideline-directed medical therapy for patients with heart failure with reduced ejection fraction enrolled in the DAPA-HF trial applied to patients regardless of their age or baseline health status, a pair of new post hoc analyses suggest.
These findings emerged a day after a report that more fully delineated dapagliflozin’s consistent safety and efficacy in patients with heart failure with reduced ejection fraction (HFrEF) regardless of whether they also had type 2 diabetes. One of the new, post hoc analyses reported at the American Heart Association scientific sessions suggested that even the most elderly enrolled patients, 75 years and older, had a similar cut in mortality and acute heart failure exacerbations, compared with younger patients. A second post hoc analysis indicated that patients with severe heart failure symptoms at entry into the trial received about as much benefit from the addition of dapagliflozin as did patients with mild baseline symptoms, measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ).
The primary results from the DAPA-HF (Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure) trial, first reported in August 2019, showed that among more than 4,700 patients with HFrEF randomized to receive the sodium-glucose cotransporter 2 (SGLT2) inhibitor dapagliflozin (Farxiga) on top of standard HFrEF medications or placebo, those who received dapagliflozin had a statistically significant, 26% decrease in their incidence of the primary study endpoint over a median 18 months, regardless of diabetes status (N Engl J Med. 2019 Nov 21;381[21]:1995-2008).
“These benefits were entirely consistent across the range of ages studied,” extending from patients younger than 55 years to those older than 75 years, John McMurray, MD, said at the meeting. “In many parts of the world, particularly North America and Western Europe, we have an increasingly elderly population. Many patients with heart failure are much older than in clinical trials,” he said.

“The thing of concern is whether elderly patients get as much benefit and tolerate treatment as well as younger patients,” said Dr. McMurray, professor of medical cardiology at the University of Glasgow.
“Dapagliflozin worked across all ages, including some very elderly patients enrolled in the trial,” said Mary Norine Walsh, MD, medical director of the heart failure and transplant program at St. Vincent Heart Center of Indiana in Indianapolis. “Many trials have not looked at age like this. I hope this is a new way to analyze trials to produce more information that can help patients,” she said in an interview.

Quality-of-life outcomes
The other new, post hoc analysis showed that patients with severe HF symptoms at entry into the trial received about as much benefit from the addition of dapagliflozin as did patients with milder baseline symptoms and less impaired function, measured by the KCCQ. Dapagliflozin treatment “improved cardiovascular death and worsening heart failure to a similar extent across the entire range of KCCQ at baseline,” Mikhail N. Kosiborod, MD, said in a separate talk at the meeting. In addition, dapagliflozin treatment increased the rate of small, moderate, and large clinically meaningful improvements in patients’ KCCQ scores across all key domains of the metric, which scores symptom frequency and severity, physical and social limitations, and quality of life, said Dr. Kosiborod, a cardiologist and professor of medicine at the University of Missouri–Kansas City.

After the first 8 months of treatment in the DAPA-HF trial, 58% of the 2,373 patients who received dapagliflozin had a clinically meaningful improvement in their total KCCQ symptom score of at least 5 points, compared with a 51% rate in the 2,371 patients in the control arm, a statistically significant difference. This meant that the number needed to treat with dapagliflozin was 14 patients to produce one additional patient with at least a 5-point KCCQ improvement compared with controls, a “very small” number needed to treat, Dr. Kosiborod said in an interview.
Addition of the KCCQ to the panel of assessments that patients underwent during DAPA-HF reflected an evolved approach to measuring efficacy outcomes in clinical trials by including patient-reported outcomes. Earlier in 2019, the Food and Drug Administration released draft guidance for heart failure drug development that explicitly called for efficacy endpoints in pivotal studies that measure how patients feel and function, and stating that these endpoints can be the basis for new drug approvals.
“To many patients, how they feel matters as much if not more than how long they live,” Dr. Kosiborod noted. The goals of heart failure treatments are not only to extend survival and reduced hospitalizations, but also to improve symptoms, function, and quality of life, he said.
“There is a lot of interest now in having outcomes in heart failure trials that are more meaningful to patients, like feeling better and being able to do more,” noted Dr. Walsh.
The DAPA-HF results also showed that patients had similar rates of reduction in death, heart failure hospitalization, or urgent clinical visits, regardless of how severely they were affected by their heart failure when they began dapagliflozin treatment. The researchers ran an analysis that divided the entire trial population into tertiles based on their KCCQ score on entering the study. Patients in the most severely-affected tertile had a 30% cut in their rate of death or acute heart failure exacerbation on dapagliflozin compared with placebo, while patients in the tertile with the mildest symptoms at baseline had a 38% reduction in their primary outcome incidence compared with controls who received placebo. Concurrently with Dr. Kosiborod’s report, the results appeared in an article online (Circulation. 2019 Nov 17. doi: 10.1161/CIRCULATIONAHA.119.044138).
Outcomes by age
Not surprisingly in DAPA-HF, the older patients were, the sicker, Dr. McMurray observed. Of the study’s 1,149 patients (24% of the study cohort) who were at least 75 years old, 62% had chronic kidney disease, compared with a 14% prevalence among the 636 patients younger than age 55. The 75-and-older group showed a steeper, 32% decline in incidence of the primary endpoint – a composite of cardiovascular (CV) death, HF hospitalization, or urgent HF visit requiring intravenous therapy – than in the other studied age groups: a 24% decline in those 65-74 years old, a 29% cut in those 55-64 years old, and a 13% drop in patients younger than 55 years old.
In addition, patients aged 75 years or greater were just as likely as the overall group to show at least a 5-point improvement in their KCCQ Total Symptom Score on dapagliflozin, as well as about the same reduced rate of deterioration compared with placebo as tracked with the KCCQ.
Patients “got as much benefit in terms of symptoms as well as morbidity and mortality,” Dr. McMurray concluded. Concurrently with the meeting report the results appeared in an article online (Circulation. 2019 Nov 17. doi: 10.1161/CIRCULATIONAHA.119.044133).
“These data are of critical importance, as improving patient-reported outcomes in heart failure, especially in highly symptomatic patients, is an important goal in drug development,” G. Michael Felker, MD, wrote in an editorial accompanying the two published analyses (Circulation. 2019 Nov 17. doi: 10.1161/CIRCULATIONAHA.119.044578). These new analyses also highlight another attractive feature of dapagliflozin and, apparently, the entire class of SGLT2 inhibitors: They “ ‘play well with others’ when it comes to overlapping intolerances that often limit (either in reality or in perception) optimization of GDMT [guideline-directed medical therapy]. Although SGLT2 inhibitor therapy may lead to volume depletion and require adjustment of diuretics, the SGLT2 inhibitors generally lack some of the other dose-limiting adverse effects (such as renal dysfunction, hyperkalemia, and hypotension) that can make aggressive up-titration of GDMT problematic, particularly in older patients or those with more advanced disease,“ wrote Dr. Felker, professor of medicine at Duke University in Durham, N.C. “We stand at the beginning of a new era of ‘quadruple therapy’ for HFrEF with beta-blockers, an angiotensin receptor neprilysin inhibitor, mineralocorticoid receptor antagonists, and SGLT2 inhibitors,” he concluded.
A version of this article also appears on Medscape.com
In DAPA-HF, treatment with dapagliflozin met the three critical goals of heart failure management. When used on top of current guideline-directed medical therapy, the treatment reduced mortality, cut hospitalizations, and improved heart failure–related health status – all to a similar extent regardless of patients’ age or symptom severity at entry. These new, post hoc findings provide important, additional data supporting inhibition of sodium-glucose cotransporter (SGLT) 2 with dapagliflozin as the newest foundational pillar of treatment for heart failure with reduced ejection fraction (HFrEF).

The results of the analysis by baseline symptoms severity as measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ) showed similar treatment effects from dapagliflozin regardless of a patient’s baseline KCCQ score, suggesting that the prior report of a blunted effect of dapagliflozin in patients classified at baseline as being in New York Heart Association functional class III or IV compared with class I and II patients was likely a chance finding.
Both the analyses by age and by KCCQ scores were limited by their post hoc status using data collected in a single study. No evidence addresses whether these are class effects for all drugs in the SGLT2-inhibitor class, whether these findings from DAPA-HF are generalizable to real world practice, or whether treatment with dapagliflozin would have similar effects on outcomes if it had been used more often in combination with sacubitril/valsartan. In DAPA-HF, 11% of patients also received sacubitril/valsartan even though existing management guidelines recommend sacubitril/valsartan as the preferred agent for inhibiting the renin-angiotensin system.
It’s also unclear whether patient-reported outcomes such as those measured by the KCCQ will help in sequencing the introduction of drugs for HFrEF patients, or drug selection by patients, providers, payers, and in guidelines.
Carolyn S.P. Lam, MD, is professor of medicine at Duke-National University of Singapore. She has been a consultant to and has received research funding from AstraZeneca and several other companies. She made these comments as designated discussant for the two reports.
In DAPA-HF, treatment with dapagliflozin met the three critical goals of heart failure management. When used on top of current guideline-directed medical therapy, the treatment reduced mortality, cut hospitalizations, and improved heart failure–related health status – all to a similar extent regardless of patients’ age or symptom severity at entry. These new, post hoc findings provide important, additional data supporting inhibition of sodium-glucose cotransporter (SGLT) 2 with dapagliflozin as the newest foundational pillar of treatment for heart failure with reduced ejection fraction (HFrEF).
The results of the analysis by baseline symptoms severity as measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ) showed similar treatment effects from dapagliflozin regardless of a patient’s baseline KCCQ score, suggesting that the prior report of a blunted effect of dapagliflozin in patients classified at baseline as being in New York Heart Association functional class III or IV compared with class I and II patients was likely a chance finding.
Both the analyses by age and by KCCQ scores were limited by their post hoc status using data collected in a single study. No evidence addresses whether these are class effects for all drugs in the SGLT2-inhibitor class, whether these findings from DAPA-HF are generalizable to real world practice, or whether treatment with dapagliflozin would have similar effects on outcomes if it had been used more often in combination with sacubitril/valsartan. In DAPA-HF, 11% of patients also received sacubitril/valsartan even though existing management guidelines recommend sacubitril/valsartan as the preferred agent for inhibiting the renin-angiotensin system.
It’s also unclear whether patient-reported outcomes such as those measured by the KCCQ will help in sequencing the introduction of drugs for HFrEF patients, or drug selection by patients, providers, payers, and in guidelines.
Carolyn S.P. Lam, MD, is professor of medicine at Duke-National University of Singapore. She has been a consultant to and has received research funding from AstraZeneca and several other companies. She made these comments as designated discussant for the two reports.
In DAPA-HF, treatment with dapagliflozin met the three critical goals of heart failure management. When used on top of current guideline-directed medical therapy, the treatment reduced mortality, cut hospitalizations, and improved heart failure–related health status – all to a similar extent regardless of patients’ age or symptom severity at entry. These new, post hoc findings provide important, additional data supporting inhibition of sodium-glucose cotransporter (SGLT) 2 with dapagliflozin as the newest foundational pillar of treatment for heart failure with reduced ejection fraction (HFrEF).
The results of the analysis by baseline symptoms severity as measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ) showed similar treatment effects from dapagliflozin regardless of a patient’s baseline KCCQ score, suggesting that the prior report of a blunted effect of dapagliflozin in patients classified at baseline as being in New York Heart Association functional class III or IV compared with class I and II patients was likely a chance finding.
Both the analyses by age and by KCCQ scores were limited by their post hoc status using data collected in a single study. No evidence addresses whether these are class effects for all drugs in the SGLT2-inhibitor class, whether these findings from DAPA-HF are generalizable to real world practice, or whether treatment with dapagliflozin would have similar effects on outcomes if it had been used more often in combination with sacubitril/valsartan. In DAPA-HF, 11% of patients also received sacubitril/valsartan even though existing management guidelines recommend sacubitril/valsartan as the preferred agent for inhibiting the renin-angiotensin system.
It’s also unclear whether patient-reported outcomes such as those measured by the KCCQ will help in sequencing the introduction of drugs for HFrEF patients, or drug selection by patients, providers, payers, and in guidelines.
Carolyn S.P. Lam, MD, is professor of medicine at Duke-National University of Singapore. She has been a consultant to and has received research funding from AstraZeneca and several other companies. She made these comments as designated discussant for the two reports.
PHILADELPHIA – The substantial benefits from adding dapagliflozin to guideline-directed medical therapy for patients with heart failure with reduced ejection fraction enrolled in the DAPA-HF trial applied to patients regardless of their age or baseline health status, a pair of new post hoc analyses suggest.
These findings emerged a day after a report that more fully delineated dapagliflozin’s consistent safety and efficacy in patients with heart failure with reduced ejection fraction (HFrEF) regardless of whether they also had type 2 diabetes. One of the new, post hoc analyses reported at the American Heart Association scientific sessions suggested that even the most elderly enrolled patients, 75 years and older, had a similar cut in mortality and acute heart failure exacerbations, compared with younger patients. A second post hoc analysis indicated that patients with severe heart failure symptoms at entry into the trial received about as much benefit from the addition of dapagliflozin as did patients with mild baseline symptoms, measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ).
The primary results from the DAPA-HF (Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure) trial, first reported in August 2019, showed that among more than 4,700 patients with HFrEF randomized to receive the sodium-glucose cotransporter 2 (SGLT2) inhibitor dapagliflozin (Farxiga) on top of standard HFrEF medications or placebo, those who received dapagliflozin had a statistically significant, 26% decrease in their incidence of the primary study endpoint over a median 18 months, regardless of diabetes status (N Engl J Med. 2019 Nov 21;381[21]:1995-2008).
“These benefits were entirely consistent across the range of ages studied,” extending from patients younger than 55 years to those older than 75 years, John McMurray, MD, said at the meeting. “In many parts of the world, particularly North America and Western Europe, we have an increasingly elderly population. Many patients with heart failure are much older than in clinical trials,” he said.
“The thing of concern is whether elderly patients get as much benefit and tolerate treatment as well as younger patients,” said Dr. McMurray, professor of medical cardiology at the University of Glasgow.
“Dapagliflozin worked across all ages, including some very elderly patients enrolled in the trial,” said Mary Norine Walsh, MD, medical director of the heart failure and transplant program at St. Vincent Heart Center of Indiana in Indianapolis. “Many trials have not looked at age like this. I hope this is a new way to analyze trials to produce more information that can help patients,” she said in an interview.
Quality-of-life outcomes
The other new, post hoc analysis showed that patients with severe HF symptoms at entry into the trial received about as much benefit from the addition of dapagliflozin as did patients with milder baseline symptoms and less impaired function, measured by the KCCQ. Dapagliflozin treatment “improved cardiovascular death and worsening heart failure to a similar extent across the entire range of KCCQ at baseline,” Mikhail N. Kosiborod, MD, said in a separate talk at the meeting. In addition, dapagliflozin treatment increased the rate of small, moderate, and large clinically meaningful improvements in patients’ KCCQ scores across all key domains of the metric, which scores symptom frequency and severity, physical and social limitations, and quality of life, said Dr. Kosiborod, a cardiologist and professor of medicine at the University of Missouri–Kansas City.
After the first 8 months of treatment in the DAPA-HF trial, 58% of the 2,373 patients who received dapagliflozin had a clinically meaningful improvement in their total KCCQ symptom score of at least 5 points, compared with a 51% rate in the 2,371 patients in the control arm, a statistically significant difference. This meant that the number needed to treat with dapagliflozin was 14 patients to produce one additional patient with at least a 5-point KCCQ improvement compared with controls, a “very small” number needed to treat, Dr. Kosiborod said in an interview.
Addition of the KCCQ to the panel of assessments that patients underwent during DAPA-HF reflected an evolved approach to measuring efficacy outcomes in clinical trials by including patient-reported outcomes. Earlier in 2019, the Food and Drug Administration released draft guidance for heart failure drug development that explicitly called for efficacy endpoints in pivotal studies that measure how patients feel and function, and stating that these endpoints can be the basis for new drug approvals.
“To many patients, how they feel matters as much if not more than how long they live,” Dr. Kosiborod noted. The goals of heart failure treatments are not only to extend survival and reduced hospitalizations, but also to improve symptoms, function, and quality of life, he said.
“There is a lot of interest now in having outcomes in heart failure trials that are more meaningful to patients, like feeling better and being able to do more,” noted Dr. Walsh.
The DAPA-HF results also showed that patients had similar rates of reduction in death, heart failure hospitalization, or urgent clinical visits, regardless of how severely they were affected by their heart failure when they began dapagliflozin treatment. The researchers ran an analysis that divided the entire trial population into tertiles based on their KCCQ score on entering the study. Patients in the most severely-affected tertile had a 30% cut in their rate of death or acute heart failure exacerbation on dapagliflozin compared with placebo, while patients in the tertile with the mildest symptoms at baseline had a 38% reduction in their primary outcome incidence compared with controls who received placebo. Concurrently with Dr. Kosiborod’s report, the results appeared in an article online (Circulation. 2019 Nov 17. doi: 10.1161/CIRCULATIONAHA.119.044138).
Outcomes by age
Not surprisingly in DAPA-HF, the older patients were, the sicker, Dr. McMurray observed. Of the study’s 1,149 patients (24% of the study cohort) who were at least 75 years old, 62% had chronic kidney disease, compared with a 14% prevalence among the 636 patients younger than age 55. The 75-and-older group showed a steeper, 32% decline in incidence of the primary endpoint – a composite of cardiovascular (CV) death, HF hospitalization, or urgent HF visit requiring intravenous therapy – than in the other studied age groups: a 24% decline in those 65-74 years old, a 29% cut in those 55-64 years old, and a 13% drop in patients younger than 55 years old.
In addition, patients aged 75 years or greater were just as likely as the overall group to show at least a 5-point improvement in their KCCQ Total Symptom Score on dapagliflozin, as well as about the same reduced rate of deterioration compared with placebo as tracked with the KCCQ.
Patients “got as much benefit in terms of symptoms as well as morbidity and mortality,” Dr. McMurray concluded. Concurrently with the meeting report the results appeared in an article online (Circulation. 2019 Nov 17. doi: 10.1161/CIRCULATIONAHA.119.044133).
“These data are of critical importance, as improving patient-reported outcomes in heart failure, especially in highly symptomatic patients, is an important goal in drug development,” G. Michael Felker, MD, wrote in an editorial accompanying the two published analyses (Circulation. 2019 Nov 17. doi: 10.1161/CIRCULATIONAHA.119.044578). These new analyses also highlight another attractive feature of dapagliflozin and, apparently, the entire class of SGLT2 inhibitors: They “ ‘play well with others’ when it comes to overlapping intolerances that often limit (either in reality or in perception) optimization of GDMT [guideline-directed medical therapy]. Although SGLT2 inhibitor therapy may lead to volume depletion and require adjustment of diuretics, the SGLT2 inhibitors generally lack some of the other dose-limiting adverse effects (such as renal dysfunction, hyperkalemia, and hypotension) that can make aggressive up-titration of GDMT problematic, particularly in older patients or those with more advanced disease,“ wrote Dr. Felker, professor of medicine at Duke University in Durham, N.C. “We stand at the beginning of a new era of ‘quadruple therapy’ for HFrEF with beta-blockers, an angiotensin receptor neprilysin inhibitor, mineralocorticoid receptor antagonists, and SGLT2 inhibitors,” he concluded.
A version of this article also appears on Medscape.com
PHILADELPHIA – The substantial benefits from adding dapagliflozin to guideline-directed medical therapy for patients with heart failure with reduced ejection fraction enrolled in the DAPA-HF trial applied to patients regardless of their age or baseline health status, a pair of new post hoc analyses suggest.
These findings emerged a day after a report that more fully delineated dapagliflozin’s consistent safety and efficacy in patients with heart failure with reduced ejection fraction (HFrEF) regardless of whether they also had type 2 diabetes. One of the new, post hoc analyses reported at the American Heart Association scientific sessions suggested that even the most elderly enrolled patients, 75 years and older, had a similar cut in mortality and acute heart failure exacerbations, compared with younger patients. A second post hoc analysis indicated that patients with severe heart failure symptoms at entry into the trial received about as much benefit from the addition of dapagliflozin as did patients with mild baseline symptoms, measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ).
The primary results from the DAPA-HF (Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure) trial, first reported in August 2019, showed that among more than 4,700 patients with HFrEF randomized to receive the sodium-glucose cotransporter 2 (SGLT2) inhibitor dapagliflozin (Farxiga) on top of standard HFrEF medications or placebo, those who received dapagliflozin had a statistically significant, 26% decrease in their incidence of the primary study endpoint over a median 18 months, regardless of diabetes status (N Engl J Med. 2019 Nov 21;381[21]:1995-2008).
“These benefits were entirely consistent across the range of ages studied,” extending from patients younger than 55 years to those older than 75 years, John McMurray, MD, said at the meeting. “In many parts of the world, particularly North America and Western Europe, we have an increasingly elderly population. Many patients with heart failure are much older than in clinical trials,” he said.
“The thing of concern is whether elderly patients get as much benefit and tolerate treatment as well as younger patients,” said Dr. McMurray, professor of medical cardiology at the University of Glasgow.
“Dapagliflozin worked across all ages, including some very elderly patients enrolled in the trial,” said Mary Norine Walsh, MD, medical director of the heart failure and transplant program at St. Vincent Heart Center of Indiana in Indianapolis. “Many trials have not looked at age like this. I hope this is a new way to analyze trials to produce more information that can help patients,” she said in an interview.
Quality-of-life outcomes
The other new, post hoc analysis showed that patients with severe HF symptoms at entry into the trial received about as much benefit from the addition of dapagliflozin as did patients with milder baseline symptoms and less impaired function, measured by the KCCQ. Dapagliflozin treatment “improved cardiovascular death and worsening heart failure to a similar extent across the entire range of KCCQ at baseline,” Mikhail N. Kosiborod, MD, said in a separate talk at the meeting. In addition, dapagliflozin treatment increased the rate of small, moderate, and large clinically meaningful improvements in patients’ KCCQ scores across all key domains of the metric, which scores symptom frequency and severity, physical and social limitations, and quality of life, said Dr. Kosiborod, a cardiologist and professor of medicine at the University of Missouri–Kansas City.
After the first 8 months of treatment in the DAPA-HF trial, 58% of the 2,373 patients who received dapagliflozin had a clinically meaningful improvement in their total KCCQ symptom score of at least 5 points, compared with a 51% rate in the 2,371 patients in the control arm, a statistically significant difference. This meant that the number needed to treat with dapagliflozin was 14 patients to produce one additional patient with at least a 5-point KCCQ improvement compared with controls, a “very small” number needed to treat, Dr. Kosiborod said in an interview.
Addition of the KCCQ to the panel of assessments that patients underwent during DAPA-HF reflected an evolved approach to measuring efficacy outcomes in clinical trials by including patient-reported outcomes. Earlier in 2019, the Food and Drug Administration released draft guidance for heart failure drug development that explicitly called for efficacy endpoints in pivotal studies that measure how patients feel and function, and stating that these endpoints can be the basis for new drug approvals.
“To many patients, how they feel matters as much if not more than how long they live,” Dr. Kosiborod noted. The goals of heart failure treatments are not only to extend survival and reduced hospitalizations, but also to improve symptoms, function, and quality of life, he said.
“There is a lot of interest now in having outcomes in heart failure trials that are more meaningful to patients, like feeling better and being able to do more,” noted Dr. Walsh.
The DAPA-HF results also showed that patients had similar rates of reduction in death, heart failure hospitalization, or urgent clinical visits, regardless of how severely they were affected by their heart failure when they began dapagliflozin treatment. The researchers ran an analysis that divided the entire trial population into tertiles based on their KCCQ score on entering the study. Patients in the most severely-affected tertile had a 30% cut in their rate of death or acute heart failure exacerbation on dapagliflozin compared with placebo, while patients in the tertile with the mildest symptoms at baseline had a 38% reduction in their primary outcome incidence compared with controls who received placebo. Concurrently with Dr. Kosiborod’s report, the results appeared in an article online (Circulation. 2019 Nov 17. doi: 10.1161/CIRCULATIONAHA.119.044138).
Outcomes by age
Not surprisingly in DAPA-HF, the older patients were, the sicker, Dr. McMurray observed. Of the study’s 1,149 patients (24% of the study cohort) who were at least 75 years old, 62% had chronic kidney disease, compared with a 14% prevalence among the 636 patients younger than age 55. The 75-and-older group showed a steeper, 32% decline in incidence of the primary endpoint – a composite of cardiovascular (CV) death, HF hospitalization, or urgent HF visit requiring intravenous therapy – than in the other studied age groups: a 24% decline in those 65-74 years old, a 29% cut in those 55-64 years old, and a 13% drop in patients younger than 55 years old.
In addition, patients aged 75 years or greater were just as likely as the overall group to show at least a 5-point improvement in their KCCQ Total Symptom Score on dapagliflozin, as well as about the same reduced rate of deterioration compared with placebo as tracked with the KCCQ.
Patients “got as much benefit in terms of symptoms as well as morbidity and mortality,” Dr. McMurray concluded. Concurrently with the meeting report the results appeared in an article online (Circulation. 2019 Nov 17. doi: 10.1161/CIRCULATIONAHA.119.044133).
“These data are of critical importance, as improving patient-reported outcomes in heart failure, especially in highly symptomatic patients, is an important goal in drug development,” G. Michael Felker, MD, wrote in an editorial accompanying the two published analyses (Circulation. 2019 Nov 17. doi: 10.1161/CIRCULATIONAHA.119.044578). These new analyses also highlight another attractive feature of dapagliflozin and, apparently, the entire class of SGLT2 inhibitors: They “ ‘play well with others’ when it comes to overlapping intolerances that often limit (either in reality or in perception) optimization of GDMT [guideline-directed medical therapy]. Although SGLT2 inhibitor therapy may lead to volume depletion and require adjustment of diuretics, the SGLT2 inhibitors generally lack some of the other dose-limiting adverse effects (such as renal dysfunction, hyperkalemia, and hypotension) that can make aggressive up-titration of GDMT problematic, particularly in older patients or those with more advanced disease,“ wrote Dr. Felker, professor of medicine at Duke University in Durham, N.C. “We stand at the beginning of a new era of ‘quadruple therapy’ for HFrEF with beta-blockers, an angiotensin receptor neprilysin inhibitor, mineralocorticoid receptor antagonists, and SGLT2 inhibitors,” he concluded.
A version of this article also appears on Medscape.com
REPORTING FROM THE AHA SCIENTIFIC SESSIONS
Hospitalist movers and shakers – November 2019
Amith Skandhan, MD, SFHM, has been announced as Southeast Health Statera Network’s (Dothan, Ala.) director of physician integration, and chairman of the network’s Physicians Participation Committee. Dr. Skandhan is senior lead hospitalist with Southeast Health, where he has worked for nearly a decade. He also champions the medical group’s clinical documentation improvement faction.

One of just 10 hospitalists in the nation to receive Top Hospitalist recognition by the American College of Physicians in 2018, Dr. Skandhan is also an assistant professor at Alabama College of Osteopathic Medicine and is one of Southeast Health’s Internal Medicine Residency Program’s core faculty members.
Ruby Sahoo, DO, has been promoted by Team Health (Knoxville, Tenn.) as regional performance director of its hospitalist services performance improvement team. Dr. Sahoo joined Team Health in 2016 and has most recently served as medical director and chief of staff at Grand Strand Medical Center (Myrtle Beach, S.C.).

Dr. Sahoo is a highly decorated internist and hospitalist. She was Team Health’s Medical Director of the Year for Hospital Medicine 2018, and a Frist Humanitarian Award winner in 2017. Additionally, Dr. Sahoo is a member of the Society of Hospital Medicine, the American College of Physicians, and the American Association of Physician Leadership.

David Vandenberg, MD, SFHM, recently was elevated to chief medical officer at St. Joseph Mercy Hospital (Ann Arbor and Livingston, Mich.). The hospitalist and senior fellow of hospital medicine previously has been St. Joseph’s vice chair of internal medicine and medical director of care management and documentation integrity. Dr. Vandenberg has spent 20 years as an employee at St. Joseph’s.
Cristian Andrade, MD, has been elevated to vice president of medical affairs with St. Joseph’s Health (Syracuse, N.Y.). A 16-year veteran with St. Joseph’s, Dr. Andrade has been a hospitalist with the system since 2006, and most recently has served as chief of hospitalist services.
Dr. Andrade now will provide guidance focusing on improving length of stay, as well as staff governance, utilization review, and the hospitalist program in general.
Paul DeJac, MD, has received a promotion to chief of hospitalist medicine at Roswell Park Comprehensive Cancer Center (Buffalo, N.Y.). Dr. DeJac was hired at Roswell Park in 2016, becoming lead hospitalist in 2017. He will look to boost professional development on the hospitalist team with a focus on improving patient care.
Independent Emergency Physicians (Farmington, Mich.), which provides hospitalist physicians, ED physicians, scribes, and more at a handful of hospitals in Michigan, has added urgent care facilities in Southfield, Mich., and Novi, Mich., to its portfolio. In addition, IEP has joined with Healthy Urgent Care to create a network of up to 15 urgent care centers in Southeast Michigan.
This is IEP’s first foray into urgent care. The company was founded in 1997 and practices at Ascension Health, Trinity Health, and Henry Ford Health System, covering four different hospitals.
Private hospitalist management provider Sound Physicians (Tacoma, Wash.) has grown once again, acquiring Indigo Health Partners (Traverse City, Mich.), one of Michigan’s largest private hospitalist groups. The new company will be known as Indigo, a division of Sound Inpatient Physicians.
Indigo’s approximately 150 providers are included in the transaction, which includes professionals in hospitals, skilled nursing facilities, and assisted living facilities. Indigo was previously known as Hospitalists of Northwest Michigan, based out of Munson Medical Center.
Amith Skandhan, MD, SFHM, has been announced as Southeast Health Statera Network’s (Dothan, Ala.) director of physician integration, and chairman of the network’s Physicians Participation Committee. Dr. Skandhan is senior lead hospitalist with Southeast Health, where he has worked for nearly a decade. He also champions the medical group’s clinical documentation improvement faction.
One of just 10 hospitalists in the nation to receive Top Hospitalist recognition by the American College of Physicians in 2018, Dr. Skandhan is also an assistant professor at Alabama College of Osteopathic Medicine and is one of Southeast Health’s Internal Medicine Residency Program’s core faculty members.
Ruby Sahoo, DO, has been promoted by Team Health (Knoxville, Tenn.) as regional performance director of its hospitalist services performance improvement team. Dr. Sahoo joined Team Health in 2016 and has most recently served as medical director and chief of staff at Grand Strand Medical Center (Myrtle Beach, S.C.).
Dr. Sahoo is a highly decorated internist and hospitalist. She was Team Health’s Medical Director of the Year for Hospital Medicine 2018, and a Frist Humanitarian Award winner in 2017. Additionally, Dr. Sahoo is a member of the Society of Hospital Medicine, the American College of Physicians, and the American Association of Physician Leadership.
David Vandenberg, MD, SFHM, recently was elevated to chief medical officer at St. Joseph Mercy Hospital (Ann Arbor and Livingston, Mich.). The hospitalist and senior fellow of hospital medicine previously has been St. Joseph’s vice chair of internal medicine and medical director of care management and documentation integrity. Dr. Vandenberg has spent 20 years as an employee at St. Joseph’s.
Cristian Andrade, MD, has been elevated to vice president of medical affairs with St. Joseph’s Health (Syracuse, N.Y.). A 16-year veteran with St. Joseph’s, Dr. Andrade has been a hospitalist with the system since 2006, and most recently has served as chief of hospitalist services.
Dr. Andrade now will provide guidance focusing on improving length of stay, as well as staff governance, utilization review, and the hospitalist program in general.
Paul DeJac, MD, has received a promotion to chief of hospitalist medicine at Roswell Park Comprehensive Cancer Center (Buffalo, N.Y.). Dr. DeJac was hired at Roswell Park in 2016, becoming lead hospitalist in 2017. He will look to boost professional development on the hospitalist team with a focus on improving patient care.
Independent Emergency Physicians (Farmington, Mich.), which provides hospitalist physicians, ED physicians, scribes, and more at a handful of hospitals in Michigan, has added urgent care facilities in Southfield, Mich., and Novi, Mich., to its portfolio. In addition, IEP has joined with Healthy Urgent Care to create a network of up to 15 urgent care centers in Southeast Michigan.
This is IEP’s first foray into urgent care. The company was founded in 1997 and practices at Ascension Health, Trinity Health, and Henry Ford Health System, covering four different hospitals.
Private hospitalist management provider Sound Physicians (Tacoma, Wash.) has grown once again, acquiring Indigo Health Partners (Traverse City, Mich.), one of Michigan’s largest private hospitalist groups. The new company will be known as Indigo, a division of Sound Inpatient Physicians.
Indigo’s approximately 150 providers are included in the transaction, which includes professionals in hospitals, skilled nursing facilities, and assisted living facilities. Indigo was previously known as Hospitalists of Northwest Michigan, based out of Munson Medical Center.
Amith Skandhan, MD, SFHM, has been announced as Southeast Health Statera Network’s (Dothan, Ala.) director of physician integration, and chairman of the network’s Physicians Participation Committee. Dr. Skandhan is senior lead hospitalist with Southeast Health, where he has worked for nearly a decade. He also champions the medical group’s clinical documentation improvement faction.
One of just 10 hospitalists in the nation to receive Top Hospitalist recognition by the American College of Physicians in 2018, Dr. Skandhan is also an assistant professor at Alabama College of Osteopathic Medicine and is one of Southeast Health’s Internal Medicine Residency Program’s core faculty members.
Ruby Sahoo, DO, has been promoted by Team Health (Knoxville, Tenn.) as regional performance director of its hospitalist services performance improvement team. Dr. Sahoo joined Team Health in 2016 and has most recently served as medical director and chief of staff at Grand Strand Medical Center (Myrtle Beach, S.C.).
Dr. Sahoo is a highly decorated internist and hospitalist. She was Team Health’s Medical Director of the Year for Hospital Medicine 2018, and a Frist Humanitarian Award winner in 2017. Additionally, Dr. Sahoo is a member of the Society of Hospital Medicine, the American College of Physicians, and the American Association of Physician Leadership.
David Vandenberg, MD, SFHM, recently was elevated to chief medical officer at St. Joseph Mercy Hospital (Ann Arbor and Livingston, Mich.). The hospitalist and senior fellow of hospital medicine previously has been St. Joseph’s vice chair of internal medicine and medical director of care management and documentation integrity. Dr. Vandenberg has spent 20 years as an employee at St. Joseph’s.
Cristian Andrade, MD, has been elevated to vice president of medical affairs with St. Joseph’s Health (Syracuse, N.Y.). A 16-year veteran with St. Joseph’s, Dr. Andrade has been a hospitalist with the system since 2006, and most recently has served as chief of hospitalist services.
Dr. Andrade now will provide guidance focusing on improving length of stay, as well as staff governance, utilization review, and the hospitalist program in general.
Paul DeJac, MD, has received a promotion to chief of hospitalist medicine at Roswell Park Comprehensive Cancer Center (Buffalo, N.Y.). Dr. DeJac was hired at Roswell Park in 2016, becoming lead hospitalist in 2017. He will look to boost professional development on the hospitalist team with a focus on improving patient care.
Independent Emergency Physicians (Farmington, Mich.), which provides hospitalist physicians, ED physicians, scribes, and more at a handful of hospitals in Michigan, has added urgent care facilities in Southfield, Mich., and Novi, Mich., to its portfolio. In addition, IEP has joined with Healthy Urgent Care to create a network of up to 15 urgent care centers in Southeast Michigan.
This is IEP’s first foray into urgent care. The company was founded in 1997 and practices at Ascension Health, Trinity Health, and Henry Ford Health System, covering four different hospitals.
Private hospitalist management provider Sound Physicians (Tacoma, Wash.) has grown once again, acquiring Indigo Health Partners (Traverse City, Mich.), one of Michigan’s largest private hospitalist groups. The new company will be known as Indigo, a division of Sound Inpatient Physicians.
Indigo’s approximately 150 providers are included in the transaction, which includes professionals in hospitals, skilled nursing facilities, and assisted living facilities. Indigo was previously known as Hospitalists of Northwest Michigan, based out of Munson Medical Center.
Large population-based study underscores link between gout, CVD event risk
ATLANTA – Gout is associated with an increased risk of both fatal and nonfatal cardiovascular disease events, according to a large population-based health data linkage study in New Zealand.

“Overall, the survival was quite good within both cohorts, but ... there is a clear and statistically significant difference in the survival between the people with gout and those without gout,” Ken Cai, MBBS, reported at the annual meeting of the American College of Rheumatology, noting that a similarly “significant and clear” difference was seen in nonfatal CVD events between the groups.
Of 968,387 individuals included in the analysis, 34,056 had gout, said Dr. Cai, a rheumatology clinical fellow at the University of Auckland (New Zealand). After adjusting for population-level estimated 5-year CVD risk for cardiovascular death, nonfatal myocardial infarction, stroke, or other vascular event, the adjusted hazard ratios were 1.20 for fatal and 1.32 for nonfatal first CVD events in patients with gout. The CVD risk score used in the analysis accounted for age, gender, ethnicity, level of social deprivation, diabetes status, previous hospitalization for atrial fibrillation, and baseline dispensing of blood pressure–lowering, lipid-lowering, and antiplatelet/anticoagulant medications.
“To allow for any other differences between the gout and nongout cohorts with respect to gender, age, ethnicity, and social deprivation, we further adjusted for these factors again, even though they had been accounted for within our CVD risk score,” he said, noting that “gout continued to demonstrate an increased adjusted hazard ratio” for fatal and nonfatal events after that adjustment (HRs, 1.40 and 1.35, respectively)
Additional analysis in the gout patients showed that CVD risk was similarly increased both in those who had been dispensed allopurinol at least once in the prior 5 years and those who had not (adjusted HRs for fatal events, 1.41 and 1.33; and for nonfatal, first CVD events, 1.34 and 1.38, respectively), and “there was no significant difference between these two groups, compared to people without gout,” he said.
Adjustment for serum urate levels in gout patients also showed similarly increased risk for fatal and nonfatal events for those with levels less than 6 mg/dL and those with levels of 6 mg/dL or greater (adjusted HRs of 1.32 and 1.42 for fatal events, and 1.27 and 1.43 for nonfatal first CVD events, respectively).
Again, no significant difference was seen in the risk of events between these two groups and those without gout, Dr. Cai said, noting that patients with no serum urate monitoring also had an increased risk of events (adjusted HR of 1.41 for fatal events and 1.29 for nonfatal, first CVD events).
Gout and hyperuricemia have previously been reported to be independent risk factors for CVD and CVD events, and urate-lowering therapy such as allopurinol have been thought to potentially be associated with reduced risk of CVD, he said, noting that the relationships are of particular concern in New Zealand, where gout affects more than 4% of the adult population.
“Maori, who are the indigenous people of New Zealand, and Pasifika people are disproportionately affected by gout; 8.5% of Maori, and 13.9% of Pasifika adults have gout,” he said, adding that an estimated one-third of Maori and Pasifika adults over age 65 years have gout.
To further assess the relationships between gout and CVD risk, he and his colleagues used validated population-level risk-prediction equations and linked National Health Identifier (NHI) data, he said.
National registries of medicines dispensing data, hospitalization, and death were linked to the Auckland/Northland regional repository of laboratory results from Jan. 1, 2012 to Dec. 31, 2016.
“We included all New Zealand residents aged 20 years or older who were in contact with publicly funded services in 2011 and were alive at the end of December, 2011,” he said, adding that those with a previous hospitalization for CVD or heart failure prior to the end of December 2011 were excluded, as were those with primary residence outside of the region for the prior 3 years and those missing predictor variable data.
Although the findings are limited by an inability to adjust for smoking status, body mass index, and blood pressure – as such data are not collected at the national level, and by the population-based nature of the study, which does not allow determination about causation, they nevertheless reinforce the association between gout and an increased estimated risk of CVD events, Dr. Cai said.
“Even after adjustment for estimated 5-year CVD risk and the additional weighting of risk factors within it, gout independently increased the hazard ratio for fatal and nonfatal events,” he said. “In our study, this effect was not ameliorated by allopurinol use or serum urate lowering to treatment target.”
Similar studies are needed in other populations, he said.
Dr. Cai reported grant support from Arthritis Australia.
SOURCE: Cai K et al. Arthritis Rheumatol. 2019;71(suppl 10), Abstract 2732.
ATLANTA – Gout is associated with an increased risk of both fatal and nonfatal cardiovascular disease events, according to a large population-based health data linkage study in New Zealand.
“Overall, the survival was quite good within both cohorts, but ... there is a clear and statistically significant difference in the survival between the people with gout and those without gout,” Ken Cai, MBBS, reported at the annual meeting of the American College of Rheumatology, noting that a similarly “significant and clear” difference was seen in nonfatal CVD events between the groups.
Of 968,387 individuals included in the analysis, 34,056 had gout, said Dr. Cai, a rheumatology clinical fellow at the University of Auckland (New Zealand). After adjusting for population-level estimated 5-year CVD risk for cardiovascular death, nonfatal myocardial infarction, stroke, or other vascular event, the adjusted hazard ratios were 1.20 for fatal and 1.32 for nonfatal first CVD events in patients with gout. The CVD risk score used in the analysis accounted for age, gender, ethnicity, level of social deprivation, diabetes status, previous hospitalization for atrial fibrillation, and baseline dispensing of blood pressure–lowering, lipid-lowering, and antiplatelet/anticoagulant medications.
“To allow for any other differences between the gout and nongout cohorts with respect to gender, age, ethnicity, and social deprivation, we further adjusted for these factors again, even though they had been accounted for within our CVD risk score,” he said, noting that “gout continued to demonstrate an increased adjusted hazard ratio” for fatal and nonfatal events after that adjustment (HRs, 1.40 and 1.35, respectively)
Additional analysis in the gout patients showed that CVD risk was similarly increased both in those who had been dispensed allopurinol at least once in the prior 5 years and those who had not (adjusted HRs for fatal events, 1.41 and 1.33; and for nonfatal, first CVD events, 1.34 and 1.38, respectively), and “there was no significant difference between these two groups, compared to people without gout,” he said.
Adjustment for serum urate levels in gout patients also showed similarly increased risk for fatal and nonfatal events for those with levels less than 6 mg/dL and those with levels of 6 mg/dL or greater (adjusted HRs of 1.32 and 1.42 for fatal events, and 1.27 and 1.43 for nonfatal first CVD events, respectively).
Again, no significant difference was seen in the risk of events between these two groups and those without gout, Dr. Cai said, noting that patients with no serum urate monitoring also had an increased risk of events (adjusted HR of 1.41 for fatal events and 1.29 for nonfatal, first CVD events).
Gout and hyperuricemia have previously been reported to be independent risk factors for CVD and CVD events, and urate-lowering therapy such as allopurinol have been thought to potentially be associated with reduced risk of CVD, he said, noting that the relationships are of particular concern in New Zealand, where gout affects more than 4% of the adult population.
“Maori, who are the indigenous people of New Zealand, and Pasifika people are disproportionately affected by gout; 8.5% of Maori, and 13.9% of Pasifika adults have gout,” he said, adding that an estimated one-third of Maori and Pasifika adults over age 65 years have gout.
To further assess the relationships between gout and CVD risk, he and his colleagues used validated population-level risk-prediction equations and linked National Health Identifier (NHI) data, he said.
National registries of medicines dispensing data, hospitalization, and death were linked to the Auckland/Northland regional repository of laboratory results from Jan. 1, 2012 to Dec. 31, 2016.
“We included all New Zealand residents aged 20 years or older who were in contact with publicly funded services in 2011 and were alive at the end of December, 2011,” he said, adding that those with a previous hospitalization for CVD or heart failure prior to the end of December 2011 were excluded, as were those with primary residence outside of the region for the prior 3 years and those missing predictor variable data.
Although the findings are limited by an inability to adjust for smoking status, body mass index, and blood pressure – as such data are not collected at the national level, and by the population-based nature of the study, which does not allow determination about causation, they nevertheless reinforce the association between gout and an increased estimated risk of CVD events, Dr. Cai said.
“Even after adjustment for estimated 5-year CVD risk and the additional weighting of risk factors within it, gout independently increased the hazard ratio for fatal and nonfatal events,” he said. “In our study, this effect was not ameliorated by allopurinol use or serum urate lowering to treatment target.”
Similar studies are needed in other populations, he said.
Dr. Cai reported grant support from Arthritis Australia.
SOURCE: Cai K et al. Arthritis Rheumatol. 2019;71(suppl 10), Abstract 2732.
ATLANTA – Gout is associated with an increased risk of both fatal and nonfatal cardiovascular disease events, according to a large population-based health data linkage study in New Zealand.
“Overall, the survival was quite good within both cohorts, but ... there is a clear and statistically significant difference in the survival between the people with gout and those without gout,” Ken Cai, MBBS, reported at the annual meeting of the American College of Rheumatology, noting that a similarly “significant and clear” difference was seen in nonfatal CVD events between the groups.
Of 968,387 individuals included in the analysis, 34,056 had gout, said Dr. Cai, a rheumatology clinical fellow at the University of Auckland (New Zealand). After adjusting for population-level estimated 5-year CVD risk for cardiovascular death, nonfatal myocardial infarction, stroke, or other vascular event, the adjusted hazard ratios were 1.20 for fatal and 1.32 for nonfatal first CVD events in patients with gout. The CVD risk score used in the analysis accounted for age, gender, ethnicity, level of social deprivation, diabetes status, previous hospitalization for atrial fibrillation, and baseline dispensing of blood pressure–lowering, lipid-lowering, and antiplatelet/anticoagulant medications.
“To allow for any other differences between the gout and nongout cohorts with respect to gender, age, ethnicity, and social deprivation, we further adjusted for these factors again, even though they had been accounted for within our CVD risk score,” he said, noting that “gout continued to demonstrate an increased adjusted hazard ratio” for fatal and nonfatal events after that adjustment (HRs, 1.40 and 1.35, respectively)
Additional analysis in the gout patients showed that CVD risk was similarly increased both in those who had been dispensed allopurinol at least once in the prior 5 years and those who had not (adjusted HRs for fatal events, 1.41 and 1.33; and for nonfatal, first CVD events, 1.34 and 1.38, respectively), and “there was no significant difference between these two groups, compared to people without gout,” he said.
Adjustment for serum urate levels in gout patients also showed similarly increased risk for fatal and nonfatal events for those with levels less than 6 mg/dL and those with levels of 6 mg/dL or greater (adjusted HRs of 1.32 and 1.42 for fatal events, and 1.27 and 1.43 for nonfatal first CVD events, respectively).
Again, no significant difference was seen in the risk of events between these two groups and those without gout, Dr. Cai said, noting that patients with no serum urate monitoring also had an increased risk of events (adjusted HR of 1.41 for fatal events and 1.29 for nonfatal, first CVD events).
Gout and hyperuricemia have previously been reported to be independent risk factors for CVD and CVD events, and urate-lowering therapy such as allopurinol have been thought to potentially be associated with reduced risk of CVD, he said, noting that the relationships are of particular concern in New Zealand, where gout affects more than 4% of the adult population.
“Maori, who are the indigenous people of New Zealand, and Pasifika people are disproportionately affected by gout; 8.5% of Maori, and 13.9% of Pasifika adults have gout,” he said, adding that an estimated one-third of Maori and Pasifika adults over age 65 years have gout.
To further assess the relationships between gout and CVD risk, he and his colleagues used validated population-level risk-prediction equations and linked National Health Identifier (NHI) data, he said.
National registries of medicines dispensing data, hospitalization, and death were linked to the Auckland/Northland regional repository of laboratory results from Jan. 1, 2012 to Dec. 31, 2016.
“We included all New Zealand residents aged 20 years or older who were in contact with publicly funded services in 2011 and were alive at the end of December, 2011,” he said, adding that those with a previous hospitalization for CVD or heart failure prior to the end of December 2011 were excluded, as were those with primary residence outside of the region for the prior 3 years and those missing predictor variable data.
Although the findings are limited by an inability to adjust for smoking status, body mass index, and blood pressure – as such data are not collected at the national level, and by the population-based nature of the study, which does not allow determination about causation, they nevertheless reinforce the association between gout and an increased estimated risk of CVD events, Dr. Cai said.
“Even after adjustment for estimated 5-year CVD risk and the additional weighting of risk factors within it, gout independently increased the hazard ratio for fatal and nonfatal events,” he said. “In our study, this effect was not ameliorated by allopurinol use or serum urate lowering to treatment target.”
Similar studies are needed in other populations, he said.
Dr. Cai reported grant support from Arthritis Australia.
SOURCE: Cai K et al. Arthritis Rheumatol. 2019;71(suppl 10), Abstract 2732.
REPORTING FROM ACR 2019
The 2018 SoHM Report: Takeaways for pediatric hospitalists
Increased complexity in workforce staffing
In November 2019, more than 1,500 pediatric hospitalists will be first to take the subspecialty exam approved by the American Board of Pediatrics (ABP) for certification in pediatric hospital medicine (PHM). This landmark signifies the recognition of hospital medicine as an essential component of the health care landscape and further acknowledges the importance of our expanding field.

But recent controversy over the requirements set by the ABP to sit for the exam has highlighted the new considerations for practice management that will be associated with this change. The need to analyze and understand how PHM programs function has never been more important for hospital medicine groups that care for children. This information is essential if they are to remain nimble in their approach to the changes that will occur in the years ahead.
To understand the impact that the new subspecialty board exam will have on groups that care for children, we need to first understand the criteria for eligibility. As for all ABP subspecialty boards, applicants must be Pediatric Board certified. The ABP has established three pathways by which practitioners can attain eligibility to sit for the PHM exam.1 Most currently practicing hospitalists have applied to take the exam under the “practice pathway,” which will be available temporarily to allow candidates to apply for the certifying exam based on experience rather than fellowship training. This temporary period will span the first three examination cycles (2019, 2021, 2023). The requirements for inclusion via this pathway, recently modified by the ABP in response to concerns voiced by the PHM community at large,2 consist of the following:
1. Practice period of 4 years (with a start date of July 2015 to be eligible for the November 2019 exam.
2. Work hours for all PHM professional activities of more than 900-1000 hours/year.
3. Patient care hours in PHM of more than 450-500 hours per year, every year for the preceding 4 years.
4. Scope of practice covering the full range of hospitalized children.
5. Practice experience and hours acquired in the United States or Canada.
This set of criteria raises several questions about the eligibility of the physicians currently caring for children in the hospital setting. The State of Hospital Medicine Report is an excellent source of information about hospital medicine trends in staffing and much more. While the response to the survey is more robust from practices that care for adults only, important information can be gleaned from the participant groups that care for children.
Question 1: How many clinicians that care for children in the hospital are trained in pediatrics, thereby meeting the first criteria to sit for the boards?
Based on the 2018 State of Hospital Medicine Report, 100% of groups that treat only children had physicians trained in pediatrics, 41.7% employed physicians trained in med/peds, and 5.6% had clinicians trained in internal medicine.
In groups that treat both children and adults the variation in practitioner type was much broader. While 85.7% of groups reported employing physicians trained in internal medicine and 64.3% employed family medicine practitioners, only 35.7% reported employing physicians trained in pediatrics and 46.4% with training in med/peds. A smattering of other clinician types was also noted, most of which were not likely to be pediatrics trained.
If information based on this relatively small number of respondents is generalizable, it means that a large number of the practitioners currently caring for hospitalized children are not pediatrics board-certified and therefore will not be eligible to sit for the subspecialty exam.
Question 2: What portion of the current PHM new hires are fellowship trained?
The 2018 State of Hospital Medicine Report notes that over 50% of new physicians joining a group treating only children come directly from residency, while only 5.1% come from a hospital medicine fellowship. For groups that treat adults and children, this percentage is even more significant, with 63% coming directly from residency and only 2.2% coming from a fellowship program.
The residents who recently graduated in 2019 are the last to be eligible to meet the practice duration criteria (4 years) during the “practice pathway” temporary period, thereby allowing them to sit for the subspecialty board exam without completing a fellowship. Recent surveys have shown that over 10% of graduating residents in pediatrics plan to pursue a career in PHM (over 280 respondents), however only under 75 fellows graduate from PHM fellowships each year.3 As the current number of fellowship positions in PHM are not adequate to meet the demand of the rapidly expanding workforce, groups treating children will need to continue to fill staff vacancies with variably trained clinicians.
In the years to come, information from the State of Hospital Medicine Report will be increasingly important, as programs that care for children meet the challenge of blending their workforce to include members with variable board certification and eligibility.
Question 3: How do the “patient care hours” and “work hours for all PHM activities” requirements affect currently practicing hospitalists in terms of their board eligibility?
Because of rigorous ABP criteria to sit for the PHM subspecialty exam, especially those regarding the minimum clinical and overall work hours in the care of children, many part time and med-peds practitioners may find that they are not board eligible. Variations in clinical coverage needs at individual sites, as well as competing nonclinical tasks in the adult setting, may limit pediatric-specific work hours for med/peds trained hospitalists.
As noted above, in groups that treat only children and groups that treat both adults and children, the 2018 State of Hospital Medicine Report shows that over 40% had physicians trained in med-peds. These highly trained and capable physicians will continue to be assets to their group; however, they may wish to find other ways to achieve merit-based distinction. For these physicians, the Fellow designation through SHM may provide an alternate means of recognition.
With the increasing complexity of staffing a workforce for the treatment of children that the PHM board subspecialty exam brings, the SHM Practice Analysis Committee developed a task force of pediatric leaders from across the country to aid in the development of additional pediatric-specific questions for the 2020 version of the State of Hospital Medicine Report. The questions to be included in the 2020 version will request information about the number of clinical hours (rather than shifts) per year required for full-time faculty, the percentage of the workforce that is part time, and the percentage of personnel in each group that is board certified in pediatric hospital medicine.
It is our hope that all groups treating children will respond to the 2020 State of Hospital Medicine survey, as a robust response will provide meaningful information to direct the leaders of these groups in the changing days ahead.
Dr. Gage is associate division chief, department of hospital medicine, at Phoenix Children’s Hospital and clinical associate professor, University of Arizona, Phoenix. She is a member of the SHM Practice Analysis Committee.
References
1. American Board of Pediatrics. Pediatric Hospital Medicine Certification. 2019 Edition.
2. American Board of Pediatrics. ABP responds to pediatric hospital medicine petition. 2019 Aug 29.
3. Pediatric Hospital Medicine Fellows. 2019 Edition.
Increased complexity in workforce staffing
Increased complexity in workforce staffing
In November 2019, more than 1,500 pediatric hospitalists will be first to take the subspecialty exam approved by the American Board of Pediatrics (ABP) for certification in pediatric hospital medicine (PHM). This landmark signifies the recognition of hospital medicine as an essential component of the health care landscape and further acknowledges the importance of our expanding field.
But recent controversy over the requirements set by the ABP to sit for the exam has highlighted the new considerations for practice management that will be associated with this change. The need to analyze and understand how PHM programs function has never been more important for hospital medicine groups that care for children. This information is essential if they are to remain nimble in their approach to the changes that will occur in the years ahead.
To understand the impact that the new subspecialty board exam will have on groups that care for children, we need to first understand the criteria for eligibility. As for all ABP subspecialty boards, applicants must be Pediatric Board certified. The ABP has established three pathways by which practitioners can attain eligibility to sit for the PHM exam.1 Most currently practicing hospitalists have applied to take the exam under the “practice pathway,” which will be available temporarily to allow candidates to apply for the certifying exam based on experience rather than fellowship training. This temporary period will span the first three examination cycles (2019, 2021, 2023). The requirements for inclusion via this pathway, recently modified by the ABP in response to concerns voiced by the PHM community at large,2 consist of the following:
1. Practice period of 4 years (with a start date of July 2015 to be eligible for the November 2019 exam.
2. Work hours for all PHM professional activities of more than 900-1000 hours/year.
3. Patient care hours in PHM of more than 450-500 hours per year, every year for the preceding 4 years.
4. Scope of practice covering the full range of hospitalized children.
5. Practice experience and hours acquired in the United States or Canada.
This set of criteria raises several questions about the eligibility of the physicians currently caring for children in the hospital setting. The State of Hospital Medicine Report is an excellent source of information about hospital medicine trends in staffing and much more. While the response to the survey is more robust from practices that care for adults only, important information can be gleaned from the participant groups that care for children.
Question 1: How many clinicians that care for children in the hospital are trained in pediatrics, thereby meeting the first criteria to sit for the boards?
Based on the 2018 State of Hospital Medicine Report, 100% of groups that treat only children had physicians trained in pediatrics, 41.7% employed physicians trained in med/peds, and 5.6% had clinicians trained in internal medicine.
In groups that treat both children and adults the variation in practitioner type was much broader. While 85.7% of groups reported employing physicians trained in internal medicine and 64.3% employed family medicine practitioners, only 35.7% reported employing physicians trained in pediatrics and 46.4% with training in med/peds. A smattering of other clinician types was also noted, most of which were not likely to be pediatrics trained.
If information based on this relatively small number of respondents is generalizable, it means that a large number of the practitioners currently caring for hospitalized children are not pediatrics board-certified and therefore will not be eligible to sit for the subspecialty exam.
Question 2: What portion of the current PHM new hires are fellowship trained?
The 2018 State of Hospital Medicine Report notes that over 50% of new physicians joining a group treating only children come directly from residency, while only 5.1% come from a hospital medicine fellowship. For groups that treat adults and children, this percentage is even more significant, with 63% coming directly from residency and only 2.2% coming from a fellowship program.
The residents who recently graduated in 2019 are the last to be eligible to meet the practice duration criteria (4 years) during the “practice pathway” temporary period, thereby allowing them to sit for the subspecialty board exam without completing a fellowship. Recent surveys have shown that over 10% of graduating residents in pediatrics plan to pursue a career in PHM (over 280 respondents), however only under 75 fellows graduate from PHM fellowships each year.3 As the current number of fellowship positions in PHM are not adequate to meet the demand of the rapidly expanding workforce, groups treating children will need to continue to fill staff vacancies with variably trained clinicians.
In the years to come, information from the State of Hospital Medicine Report will be increasingly important, as programs that care for children meet the challenge of blending their workforce to include members with variable board certification and eligibility.
Question 3: How do the “patient care hours” and “work hours for all PHM activities” requirements affect currently practicing hospitalists in terms of their board eligibility?
Because of rigorous ABP criteria to sit for the PHM subspecialty exam, especially those regarding the minimum clinical and overall work hours in the care of children, many part time and med-peds practitioners may find that they are not board eligible. Variations in clinical coverage needs at individual sites, as well as competing nonclinical tasks in the adult setting, may limit pediatric-specific work hours for med/peds trained hospitalists.
As noted above, in groups that treat only children and groups that treat both adults and children, the 2018 State of Hospital Medicine Report shows that over 40% had physicians trained in med-peds. These highly trained and capable physicians will continue to be assets to their group; however, they may wish to find other ways to achieve merit-based distinction. For these physicians, the Fellow designation through SHM may provide an alternate means of recognition.
With the increasing complexity of staffing a workforce for the treatment of children that the PHM board subspecialty exam brings, the SHM Practice Analysis Committee developed a task force of pediatric leaders from across the country to aid in the development of additional pediatric-specific questions for the 2020 version of the State of Hospital Medicine Report. The questions to be included in the 2020 version will request information about the number of clinical hours (rather than shifts) per year required for full-time faculty, the percentage of the workforce that is part time, and the percentage of personnel in each group that is board certified in pediatric hospital medicine.
It is our hope that all groups treating children will respond to the 2020 State of Hospital Medicine survey, as a robust response will provide meaningful information to direct the leaders of these groups in the changing days ahead.
Dr. Gage is associate division chief, department of hospital medicine, at Phoenix Children’s Hospital and clinical associate professor, University of Arizona, Phoenix. She is a member of the SHM Practice Analysis Committee.
References
1. American Board of Pediatrics. Pediatric Hospital Medicine Certification. 2019 Edition.
2. American Board of Pediatrics. ABP responds to pediatric hospital medicine petition. 2019 Aug 29.
3. Pediatric Hospital Medicine Fellows. 2019 Edition.
In November 2019, more than 1,500 pediatric hospitalists will be first to take the subspecialty exam approved by the American Board of Pediatrics (ABP) for certification in pediatric hospital medicine (PHM). This landmark signifies the recognition of hospital medicine as an essential component of the health care landscape and further acknowledges the importance of our expanding field.
But recent controversy over the requirements set by the ABP to sit for the exam has highlighted the new considerations for practice management that will be associated with this change. The need to analyze and understand how PHM programs function has never been more important for hospital medicine groups that care for children. This information is essential if they are to remain nimble in their approach to the changes that will occur in the years ahead.
To understand the impact that the new subspecialty board exam will have on groups that care for children, we need to first understand the criteria for eligibility. As for all ABP subspecialty boards, applicants must be Pediatric Board certified. The ABP has established three pathways by which practitioners can attain eligibility to sit for the PHM exam.1 Most currently practicing hospitalists have applied to take the exam under the “practice pathway,” which will be available temporarily to allow candidates to apply for the certifying exam based on experience rather than fellowship training. This temporary period will span the first three examination cycles (2019, 2021, 2023). The requirements for inclusion via this pathway, recently modified by the ABP in response to concerns voiced by the PHM community at large,2 consist of the following:
1. Practice period of 4 years (with a start date of July 2015 to be eligible for the November 2019 exam.
2. Work hours for all PHM professional activities of more than 900-1000 hours/year.
3. Patient care hours in PHM of more than 450-500 hours per year, every year for the preceding 4 years.
4. Scope of practice covering the full range of hospitalized children.
5. Practice experience and hours acquired in the United States or Canada.
This set of criteria raises several questions about the eligibility of the physicians currently caring for children in the hospital setting. The State of Hospital Medicine Report is an excellent source of information about hospital medicine trends in staffing and much more. While the response to the survey is more robust from practices that care for adults only, important information can be gleaned from the participant groups that care for children.
Question 1: How many clinicians that care for children in the hospital are trained in pediatrics, thereby meeting the first criteria to sit for the boards?
Based on the 2018 State of Hospital Medicine Report, 100% of groups that treat only children had physicians trained in pediatrics, 41.7% employed physicians trained in med/peds, and 5.6% had clinicians trained in internal medicine.
In groups that treat both children and adults the variation in practitioner type was much broader. While 85.7% of groups reported employing physicians trained in internal medicine and 64.3% employed family medicine practitioners, only 35.7% reported employing physicians trained in pediatrics and 46.4% with training in med/peds. A smattering of other clinician types was also noted, most of which were not likely to be pediatrics trained.
If information based on this relatively small number of respondents is generalizable, it means that a large number of the practitioners currently caring for hospitalized children are not pediatrics board-certified and therefore will not be eligible to sit for the subspecialty exam.
Question 2: What portion of the current PHM new hires are fellowship trained?
The 2018 State of Hospital Medicine Report notes that over 50% of new physicians joining a group treating only children come directly from residency, while only 5.1% come from a hospital medicine fellowship. For groups that treat adults and children, this percentage is even more significant, with 63% coming directly from residency and only 2.2% coming from a fellowship program.
The residents who recently graduated in 2019 are the last to be eligible to meet the practice duration criteria (4 years) during the “practice pathway” temporary period, thereby allowing them to sit for the subspecialty board exam without completing a fellowship. Recent surveys have shown that over 10% of graduating residents in pediatrics plan to pursue a career in PHM (over 280 respondents), however only under 75 fellows graduate from PHM fellowships each year.3 As the current number of fellowship positions in PHM are not adequate to meet the demand of the rapidly expanding workforce, groups treating children will need to continue to fill staff vacancies with variably trained clinicians.
In the years to come, information from the State of Hospital Medicine Report will be increasingly important, as programs that care for children meet the challenge of blending their workforce to include members with variable board certification and eligibility.
Question 3: How do the “patient care hours” and “work hours for all PHM activities” requirements affect currently practicing hospitalists in terms of their board eligibility?
Because of rigorous ABP criteria to sit for the PHM subspecialty exam, especially those regarding the minimum clinical and overall work hours in the care of children, many part time and med-peds practitioners may find that they are not board eligible. Variations in clinical coverage needs at individual sites, as well as competing nonclinical tasks in the adult setting, may limit pediatric-specific work hours for med/peds trained hospitalists.
As noted above, in groups that treat only children and groups that treat both adults and children, the 2018 State of Hospital Medicine Report shows that over 40% had physicians trained in med-peds. These highly trained and capable physicians will continue to be assets to their group; however, they may wish to find other ways to achieve merit-based distinction. For these physicians, the Fellow designation through SHM may provide an alternate means of recognition.
With the increasing complexity of staffing a workforce for the treatment of children that the PHM board subspecialty exam brings, the SHM Practice Analysis Committee developed a task force of pediatric leaders from across the country to aid in the development of additional pediatric-specific questions for the 2020 version of the State of Hospital Medicine Report. The questions to be included in the 2020 version will request information about the number of clinical hours (rather than shifts) per year required for full-time faculty, the percentage of the workforce that is part time, and the percentage of personnel in each group that is board certified in pediatric hospital medicine.
It is our hope that all groups treating children will respond to the 2020 State of Hospital Medicine survey, as a robust response will provide meaningful information to direct the leaders of these groups in the changing days ahead.
Dr. Gage is associate division chief, department of hospital medicine, at Phoenix Children’s Hospital and clinical associate professor, University of Arizona, Phoenix. She is a member of the SHM Practice Analysis Committee.
References
1. American Board of Pediatrics. Pediatric Hospital Medicine Certification. 2019 Edition.
2. American Board of Pediatrics. ABP responds to pediatric hospital medicine petition. 2019 Aug 29.
3. Pediatric Hospital Medicine Fellows. 2019 Edition.