The nexus of new technology and privacy rules springing from the Health Insurance Portability and Accountability Act of 1996 (HIPAA) leads to a lot of stress and trepidation for health care professionals. Lucia Savage, chief privacy and regulatory officer for Omada Health, and Matthew Fisher, a health law attorney based in Worcester, Mass., who specializes in compliance issues, dispel common HIPAA myths and offer advice on how to protect yourself and your practice.
Truth: Physicians are not responsible for email security flaws from patient servers, said Ms. Savage, who served as chief privacy officer for the Office of the National Coordinator for Health IT under President Obama. HIPAA requires only that health providers send emails from a secure system that protects a doctor’s message from their end, she said.
“There’s this myth out there that you cannot send an electronic message to a patient’s email box if that email is unsecured, and that’s not true,” Ms. Savage said at a recent American Bar Association meeting. “The obligation is to secure what you send, not to secure what an unregulated, private person receives.”
Just remember to warn patients that they’re responsible for the safe storage of an email message once it arrives.
Truth: An email with protected health information (PHI) accidentally sent to the wrong health provider is not likely to get doctors in trouble with the Office for Civil Rights. In the last 12 years, there have been 184,000 HIPAA-related complaints to OCR and only 55 resulted in financial settlements, according to research Ms. Savage conducted through the Department of Health & Human Services website. Of the 55 settlements, none were associated with PHI accidentally sent from one health provider to another, she said in an interview.
“[The OCR] tends to seek fines for really eye-poppingly bad behavior,” Ms. Savage said, not small-scale accidents. For example, OCR fined one hospital for including the name of a patient in a press release without patient permission. Another health professional was fined for repeated failures to encrypt their computer system.
If a document with PHI does end up in the wrong inbox, Ms. Savage advises calling the receiver and asking that they immediately delete the email.
Truth: Breaches alone are not the reason most fines are levied, nor do breach notifications mean an instant penalty, Mr. Fishersaid in an interview. Fines by OCR are more often tied to further noncompliance found when the agency begins investigating the entity after the breach report.
“Most breach reports will result in OCR conducting a follow-up investigation, usually with paper-based requests,” he said. “If responses to those requests reveal widespread or consistent noncompliance, then OCR may latch on and dig in order to impose a fine.”
For example, a breach could be the result of a lost USB drive or laptop, but OCR’s investigation might ultimately find that the practice failed to conduct an adequate risk analysis. Because a risk analysis is a fundamental component of HIPAA compliance, the inadequate risk analysis becomes the basis for a fine, Mr. Fisher said.
The best way to avoid an OCR fine is to ensure that proper HIPAA protocols are in place to assess security risks, prevent breaches, and mitigate breaches should they occur. “Part of good compliance is constant review and revision of policies as well,” Mr. Fisher said. “It is not sufficient to put the policies into place and then never revisit those policies. Circumstances change all of the time and policies need to keep up.”
Truth: Health professionals are obligated to provide copies of health information to patients and that includes electronic copies if practices have such technology. The electronic copy requirement was adopted in 2009 as part of the Health Information Technology for Economic and Clinical Health (HITECH) Act.
Despite the electronic amendment’s existence for nearly 10 years, Ms. Savage said she frequently hears from patients about the difficulty of obtaining health information and the extended time and high cost that come with requests.
“[Providing health information to patients] is an obligation,” Ms. Savage stressed. “A 21st century physician might want to be thinking about how to build on that obligation to really engage their patients in a partnership of care. If you give the patient the data, they can actually become a more valuable [participant] with you and engage in self-management.”
More information on HITECH and giving patients access to protected health information can be found here.
Truth: HIPAA is flexible and can adapt to newer technology more easily than many people think, Mr. Fisher says.
“[There is the perception] that HIPAA is archaic and does not fit with modern technology,” he said. “There are a lot of misplaced fears that digital tools cannot satisfy security requirements or will place data where they should not go.”
In actuality, many health care applications enable doctors to satisfy HIPAA requirements, while using updated technology. Secure email to send patients messages is one example, he said, as well as secure text messaging between providers.
At the same time, new technology can often assist health care privacy and advance security, Mr. Fisher noted. Technology solutions frequently automate routine tasks, such as auditing. Tools like machine learning and artificial intelligence can enhance security and catch up with attacker intelligence, he added.
“Technology should be viewed as a means of enhancing and expanding capabilities,” he said. “Using the auditing example, an individual really cannot adequately review all records or access points, but a program may be able to do so and begin to identify small trends that represent a security concern. From this perspective, the technology, as indicated, is about enhancing what can be done.”
The nexus of new technology and privacy rules springing from the Health Insurance Portability and Accountability Act of 1996 (HIPAA) leads to a lot of stress and trepidation for health care professionals. Lucia Savage, chief privacy and regulatory officer for Omada Health, and Matthew Fisher, a health law attorney based in Worcester, Mass., who specializes in compliance issues, dispel common HIPAA myths and offer advice on how to protect yourself and your practice.
Truth: Physicians are not responsible for email security flaws from patient servers, said Ms. Savage, who served as chief privacy officer for the Office of the National Coordinator for Health IT under President Obama. HIPAA requires only that health providers send emails from a secure system that protects a doctor’s message from their end, she said.
“There’s this myth out there that you cannot send an electronic message to a patient’s email box if that email is unsecured, and that’s not true,” Ms. Savage said at a recent American Bar Association meeting. “The obligation is to secure what you send, not to secure what an unregulated, private person receives.”
Just remember to warn patients that they’re responsible for the safe storage of an email message once it arrives.
Truth: An email with protected health information (PHI) accidentally sent to the wrong health provider is not likely to get doctors in trouble with the Office for Civil Rights. In the last 12 years, there have been 184,000 HIPAA-related complaints to OCR and only 55 resulted in financial settlements, according to research Ms. Savage conducted through the Department of Health & Human Services website. Of the 55 settlements, none were associated with PHI accidentally sent from one health provider to another, she said in an interview.
“[The OCR] tends to seek fines for really eye-poppingly bad behavior,” Ms. Savage said, not small-scale accidents. For example, OCR fined one hospital for including the name of a patient in a press release without patient permission. Another health professional was fined for repeated failures to encrypt their computer system.
If a document with PHI does end up in the wrong inbox, Ms. Savage advises calling the receiver and asking that they immediately delete the email.
Truth: Breaches alone are not the reason most fines are levied, nor do breach notifications mean an instant penalty, Mr. Fishersaid in an interview. Fines by OCR are more often tied to further noncompliance found when the agency begins investigating the entity after the breach report.
“Most breach reports will result in OCR conducting a follow-up investigation, usually with paper-based requests,” he said. “If responses to those requests reveal widespread or consistent noncompliance, then OCR may latch on and dig in order to impose a fine.”
For example, a breach could be the result of a lost USB drive or laptop, but OCR’s investigation might ultimately find that the practice failed to conduct an adequate risk analysis. Because a risk analysis is a fundamental component of HIPAA compliance, the inadequate risk analysis becomes the basis for a fine, Mr. Fisher said.
The best way to avoid an OCR fine is to ensure that proper HIPAA protocols are in place to assess security risks, prevent breaches, and mitigate breaches should they occur. “Part of good compliance is constant review and revision of policies as well,” Mr. Fisher said. “It is not sufficient to put the policies into place and then never revisit those policies. Circumstances change all of the time and policies need to keep up.”
Truth: Health professionals are obligated to provide copies of health information to patients and that includes electronic copies if practices have such technology. The electronic copy requirement was adopted in 2009 as part of the Health Information Technology for Economic and Clinical Health (HITECH) Act.
Despite the electronic amendment’s existence for nearly 10 years, Ms. Savage said she frequently hears from patients about the difficulty of obtaining health information and the extended time and high cost that come with requests.
“[Providing health information to patients] is an obligation,” Ms. Savage stressed. “A 21st century physician might want to be thinking about how to build on that obligation to really engage their patients in a partnership of care. If you give the patient the data, they can actually become a more valuable [participant] with you and engage in self-management.”
More information on HITECH and giving patients access to protected health information can be found here.
Truth: HIPAA is flexible and can adapt to newer technology more easily than many people think, Mr. Fisher says.
“[There is the perception] that HIPAA is archaic and does not fit with modern technology,” he said. “There are a lot of misplaced fears that digital tools cannot satisfy security requirements or will place data where they should not go.”
In actuality, many health care applications enable doctors to satisfy HIPAA requirements, while using updated technology. Secure email to send patients messages is one example, he said, as well as secure text messaging between providers.
At the same time, new technology can often assist health care privacy and advance security, Mr. Fisher noted. Technology solutions frequently automate routine tasks, such as auditing. Tools like machine learning and artificial intelligence can enhance security and catch up with attacker intelligence, he added.
“Technology should be viewed as a means of enhancing and expanding capabilities,” he said. “Using the auditing example, an individual really cannot adequately review all records or access points, but a program may be able to do so and begin to identify small trends that represent a security concern. From this perspective, the technology, as indicated, is about enhancing what can be done.”
The nexus of new technology and privacy rules springing from the Health Insurance Portability and Accountability Act of 1996 (HIPAA) leads to a lot of stress and trepidation for health care professionals. Lucia Savage, chief privacy and regulatory officer for Omada Health, and Matthew Fisher, a health law attorney based in Worcester, Mass., who specializes in compliance issues, dispel common HIPAA myths and offer advice on how to protect yourself and your practice.
Truth: Physicians are not responsible for email security flaws from patient servers, said Ms. Savage, who served as chief privacy officer for the Office of the National Coordinator for Health IT under President Obama. HIPAA requires only that health providers send emails from a secure system that protects a doctor’s message from their end, she said.
“There’s this myth out there that you cannot send an electronic message to a patient’s email box if that email is unsecured, and that’s not true,” Ms. Savage said at a recent American Bar Association meeting. “The obligation is to secure what you send, not to secure what an unregulated, private person receives.”
Just remember to warn patients that they’re responsible for the safe storage of an email message once it arrives.
Truth: An email with protected health information (PHI) accidentally sent to the wrong health provider is not likely to get doctors in trouble with the Office for Civil Rights. In the last 12 years, there have been 184,000 HIPAA-related complaints to OCR and only 55 resulted in financial settlements, according to research Ms. Savage conducted through the Department of Health & Human Services website. Of the 55 settlements, none were associated with PHI accidentally sent from one health provider to another, she said in an interview.
“[The OCR] tends to seek fines for really eye-poppingly bad behavior,” Ms. Savage said, not small-scale accidents. For example, OCR fined one hospital for including the name of a patient in a press release without patient permission. Another health professional was fined for repeated failures to encrypt their computer system.
If a document with PHI does end up in the wrong inbox, Ms. Savage advises calling the receiver and asking that they immediately delete the email.
Truth: Breaches alone are not the reason most fines are levied, nor do breach notifications mean an instant penalty, Mr. Fishersaid in an interview. Fines by OCR are more often tied to further noncompliance found when the agency begins investigating the entity after the breach report.
“Most breach reports will result in OCR conducting a follow-up investigation, usually with paper-based requests,” he said. “If responses to those requests reveal widespread or consistent noncompliance, then OCR may latch on and dig in order to impose a fine.”
For example, a breach could be the result of a lost USB drive or laptop, but OCR’s investigation might ultimately find that the practice failed to conduct an adequate risk analysis. Because a risk analysis is a fundamental component of HIPAA compliance, the inadequate risk analysis becomes the basis for a fine, Mr. Fisher said.
The best way to avoid an OCR fine is to ensure that proper HIPAA protocols are in place to assess security risks, prevent breaches, and mitigate breaches should they occur. “Part of good compliance is constant review and revision of policies as well,” Mr. Fisher said. “It is not sufficient to put the policies into place and then never revisit those policies. Circumstances change all of the time and policies need to keep up.”
Truth: Health professionals are obligated to provide copies of health information to patients and that includes electronic copies if practices have such technology. The electronic copy requirement was adopted in 2009 as part of the Health Information Technology for Economic and Clinical Health (HITECH) Act.
Despite the electronic amendment’s existence for nearly 10 years, Ms. Savage said she frequently hears from patients about the difficulty of obtaining health information and the extended time and high cost that come with requests.
“[Providing health information to patients] is an obligation,” Ms. Savage stressed. “A 21st century physician might want to be thinking about how to build on that obligation to really engage their patients in a partnership of care. If you give the patient the data, they can actually become a more valuable [participant] with you and engage in self-management.”
More information on HITECH and giving patients access to protected health information can be found here.
Truth: HIPAA is flexible and can adapt to newer technology more easily than many people think, Mr. Fisher says.
“[There is the perception] that HIPAA is archaic and does not fit with modern technology,” he said. “There are a lot of misplaced fears that digital tools cannot satisfy security requirements or will place data where they should not go.”
In actuality, many health care applications enable doctors to satisfy HIPAA requirements, while using updated technology. Secure email to send patients messages is one example, he said, as well as secure text messaging between providers.
At the same time, new technology can often assist health care privacy and advance security, Mr. Fisher noted. Technology solutions frequently automate routine tasks, such as auditing. Tools like machine learning and artificial intelligence can enhance security and catch up with attacker intelligence, he added.
“Technology should be viewed as a means of enhancing and expanding capabilities,” he said. “Using the auditing example, an individual really cannot adequately review all records or access points, but a program may be able to do so and begin to identify small trends that represent a security concern. From this perspective, the technology, as indicated, is about enhancing what can be done.”
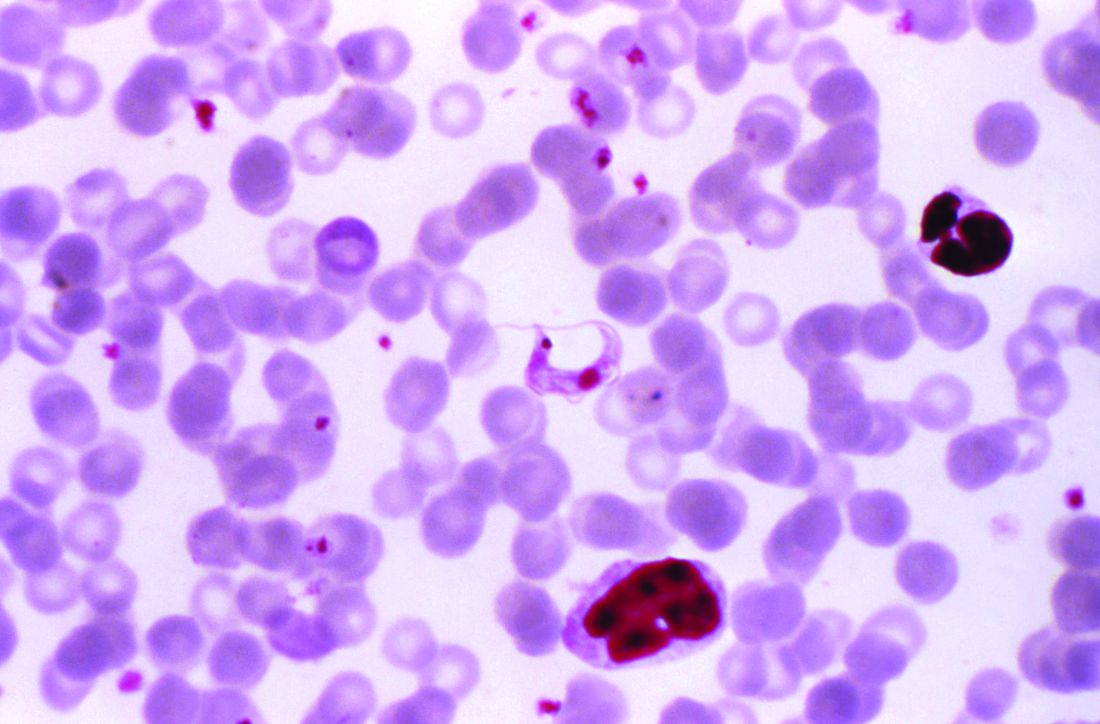
Chagas disease, a cause of serious cardiovascular problems and sudden death, was previously localized mainly in the tropics, but now affects at least 300,000 people in the United States and is growing in prevalence in other traditionally nonendemic areas, including Europe, Australia, and Japan. The American Heart Association and the Inter-American Society of Cardiology have released a statement to “increase global awareness among providers who may encounter patients with Chagas disease outside of traditionally endemic environments.”
Dr. Mae Melvin/CDC
The document summarizes the most up-to-date information on diagnosis, screening, and treatment of Trypanosoma cruzi (the protozoan cause of Chagas) infection, focusing primarily on its cardiovascular aspects, and was developed by Maria Carmo Pereira Nunes, MD, chair, and her colleagues on the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee.
Chagas disease is transmitted by a blood-sucking insect vector Triatoma infestans and, less frequently, from mother to fetus or by contaminated food or drink, and about one third of infected individuals develop chronic heart disease.
Although 60%-70% of people infected with T. cruzi never develop any symptoms, those who do can develop heart disease, including heart failure, stroke, life threatening ventricular arrhythmias, and cardiac arrest, according to the statement published in Circulation.
Chronic Chagas-related heart disease develops after several decades of the indeterminate, or subclinical, form of the disease following the initial acute infection. Potential risk factors for progression to the chronic stage include African ancestry, age, severity of acute infection, nutritional status, alcoholism, and their concomitant diseases.
In most studies, sudden death is the most common overall cause of death in patients with Chagas-related cardiomyopathy (55%-60%), followed by heart failure (25%-30%) and embolic events (10%-15%), according to the authors.
Benznidazole and nifurtimox are the only drugs with proven efficacy against Chagas disease, with benznidazole as the first-line treatment because it has better tolerance, is more widely available, and has more published data published on its efficacy. Furthermore, it is available in the United States, after the Food and Drug Administration granted fast-track approved 2017 for treatment of Chagas disease. Use of nifurtimox in the United States entails consultation with the Centers for Disease Control and prevention, according to the statement.
“More data are needed on the best practices for the treatment of Chagas cardiomyopathy. Because no specific clinical trials have been conducted, care for
patients with Chagas-induced ventricular dysfunction is extrapolated from general heart failure recommendations with unclear efficacy (and potential harm),” Dr. Pereira Nunes and her colleagues concluded.
One author disclosed receiving a research grant from Merck and speakers’ bureau and/or honoraria from Bayer; Biotronik, and Medtronic. The others had no relevant disclosures.
Chagas disease, a cause of serious cardiovascular problems and sudden death, was previously localized mainly in the tropics, but now affects at least 300,000 people in the United States and is growing in prevalence in other traditionally nonendemic areas, including Europe, Australia, and Japan. The American Heart Association and the Inter-American Society of Cardiology have released a statement to “increase global awareness among providers who may encounter patients with Chagas disease outside of traditionally endemic environments.”
Dr. Mae Melvin/CDC
The document summarizes the most up-to-date information on diagnosis, screening, and treatment of Trypanosoma cruzi (the protozoan cause of Chagas) infection, focusing primarily on its cardiovascular aspects, and was developed by Maria Carmo Pereira Nunes, MD, chair, and her colleagues on the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee.
Chagas disease is transmitted by a blood-sucking insect vector Triatoma infestans and, less frequently, from mother to fetus or by contaminated food or drink, and about one third of infected individuals develop chronic heart disease.
Although 60%-70% of people infected with T. cruzi never develop any symptoms, those who do can develop heart disease, including heart failure, stroke, life threatening ventricular arrhythmias, and cardiac arrest, according to the statement published in Circulation.
Chronic Chagas-related heart disease develops after several decades of the indeterminate, or subclinical, form of the disease following the initial acute infection. Potential risk factors for progression to the chronic stage include African ancestry, age, severity of acute infection, nutritional status, alcoholism, and their concomitant diseases.
In most studies, sudden death is the most common overall cause of death in patients with Chagas-related cardiomyopathy (55%-60%), followed by heart failure (25%-30%) and embolic events (10%-15%), according to the authors.
Benznidazole and nifurtimox are the only drugs with proven efficacy against Chagas disease, with benznidazole as the first-line treatment because it has better tolerance, is more widely available, and has more published data published on its efficacy. Furthermore, it is available in the United States, after the Food and Drug Administration granted fast-track approved 2017 for treatment of Chagas disease. Use of nifurtimox in the United States entails consultation with the Centers for Disease Control and prevention, according to the statement.
“More data are needed on the best practices for the treatment of Chagas cardiomyopathy. Because no specific clinical trials have been conducted, care for
patients with Chagas-induced ventricular dysfunction is extrapolated from general heart failure recommendations with unclear efficacy (and potential harm),” Dr. Pereira Nunes and her colleagues concluded.
One author disclosed receiving a research grant from Merck and speakers’ bureau and/or honoraria from Bayer; Biotronik, and Medtronic. The others had no relevant disclosures.
Chagas disease, a cause of serious cardiovascular problems and sudden death, was previously localized mainly in the tropics, but now affects at least 300,000 people in the United States and is growing in prevalence in other traditionally nonendemic areas, including Europe, Australia, and Japan. The American Heart Association and the Inter-American Society of Cardiology have released a statement to “increase global awareness among providers who may encounter patients with Chagas disease outside of traditionally endemic environments.”
Dr. Mae Melvin/CDC
The document summarizes the most up-to-date information on diagnosis, screening, and treatment of Trypanosoma cruzi (the protozoan cause of Chagas) infection, focusing primarily on its cardiovascular aspects, and was developed by Maria Carmo Pereira Nunes, MD, chair, and her colleagues on the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee.
Chagas disease is transmitted by a blood-sucking insect vector Triatoma infestans and, less frequently, from mother to fetus or by contaminated food or drink, and about one third of infected individuals develop chronic heart disease.
Although 60%-70% of people infected with T. cruzi never develop any symptoms, those who do can develop heart disease, including heart failure, stroke, life threatening ventricular arrhythmias, and cardiac arrest, according to the statement published in Circulation.
Chronic Chagas-related heart disease develops after several decades of the indeterminate, or subclinical, form of the disease following the initial acute infection. Potential risk factors for progression to the chronic stage include African ancestry, age, severity of acute infection, nutritional status, alcoholism, and their concomitant diseases.
In most studies, sudden death is the most common overall cause of death in patients with Chagas-related cardiomyopathy (55%-60%), followed by heart failure (25%-30%) and embolic events (10%-15%), according to the authors.
Benznidazole and nifurtimox are the only drugs with proven efficacy against Chagas disease, with benznidazole as the first-line treatment because it has better tolerance, is more widely available, and has more published data published on its efficacy. Furthermore, it is available in the United States, after the Food and Drug Administration granted fast-track approved 2017 for treatment of Chagas disease. Use of nifurtimox in the United States entails consultation with the Centers for Disease Control and prevention, according to the statement.
“More data are needed on the best practices for the treatment of Chagas cardiomyopathy. Because no specific clinical trials have been conducted, care for
patients with Chagas-induced ventricular dysfunction is extrapolated from general heart failure recommendations with unclear efficacy (and potential harm),” Dr. Pereira Nunes and her colleagues concluded.
One author disclosed receiving a research grant from Merck and speakers’ bureau and/or honoraria from Bayer; Biotronik, and Medtronic. The others had no relevant disclosures.
An estimated 72,000 drug overdose deaths occurred in 2017 in the United States, making it the worst year on record, according to preliminary data released by the Centers for Disease Control and Prevention.
The record high was driven by a sharp increase in deaths attributed to synthetic opioids, such as fentanyl and tramadol, data published on the agency’s website show.
The provisional counts are based on death records sent to the CDC’s National Center for Health Statistics from state vital registration offices in all 50 states and the District of Columbia, reported lead author Farida B. Ahmad, MPH, of the division of vital statistics at the NCHS. Overall, the predicted number of drug overdose deaths has climbed steadily, from 54,207 in November 2015 to 66,012 in November 2016, and to 72,287 in November 2017, according to an interactive chart accessible on the website.
Deaths attributable to synthetic opioids have climbed faster than any other drug class, soaring from just 9,983 in 2015 to 20,310 in 2016, and to 29,418 in 2017.
The next-largest category, heroin-related deaths, increased from 13,407 in 2015 to 16,012 in 2016, but appeared to plateau at 15,959 in 2017. However, the CDC cautioned that flat or declining numbers could be attributable to incomplete data, true decreases in deaths, or some combination of the two. “True declines or plateaus in the numbers of drug overdose deaths across the U.S. cannot be ascertained until final data become available.”
Cocaine-related deaths were fewer in number but appear to have risen substantially to the point where the number of deaths now nearly rival that of heroin. The number of deaths was 7,106 in 2015, 10,868 in 2016, and 14,614 in 2017.
The count of drug overdose deaths varied by state. Nebraska had the sharpest increase in predicted deaths between January 2017 and January 2018, coming in at 33.3%, though the absolute numbers of cases were low (114 through January 2017 and 152 through January 2018). North Carolina also showed substantial increases (from 2,053 to 2,515 cases, 22.5%), as did New Jersey (2,219 to 2,687 cases, 21.1%), the CDC data showed.
Provisional data will be updated on a monthly basis as additional records are received, the CDC said.
An estimated 72,000 drug overdose deaths occurred in 2017 in the United States, making it the worst year on record, according to preliminary data released by the Centers for Disease Control and Prevention.
The record high was driven by a sharp increase in deaths attributed to synthetic opioids, such as fentanyl and tramadol, data published on the agency’s website show.
The provisional counts are based on death records sent to the CDC’s National Center for Health Statistics from state vital registration offices in all 50 states and the District of Columbia, reported lead author Farida B. Ahmad, MPH, of the division of vital statistics at the NCHS. Overall, the predicted number of drug overdose deaths has climbed steadily, from 54,207 in November 2015 to 66,012 in November 2016, and to 72,287 in November 2017, according to an interactive chart accessible on the website.
Deaths attributable to synthetic opioids have climbed faster than any other drug class, soaring from just 9,983 in 2015 to 20,310 in 2016, and to 29,418 in 2017.
The next-largest category, heroin-related deaths, increased from 13,407 in 2015 to 16,012 in 2016, but appeared to plateau at 15,959 in 2017. However, the CDC cautioned that flat or declining numbers could be attributable to incomplete data, true decreases in deaths, or some combination of the two. “True declines or plateaus in the numbers of drug overdose deaths across the U.S. cannot be ascertained until final data become available.”
Cocaine-related deaths were fewer in number but appear to have risen substantially to the point where the number of deaths now nearly rival that of heroin. The number of deaths was 7,106 in 2015, 10,868 in 2016, and 14,614 in 2017.
The count of drug overdose deaths varied by state. Nebraska had the sharpest increase in predicted deaths between January 2017 and January 2018, coming in at 33.3%, though the absolute numbers of cases were low (114 through January 2017 and 152 through January 2018). North Carolina also showed substantial increases (from 2,053 to 2,515 cases, 22.5%), as did New Jersey (2,219 to 2,687 cases, 21.1%), the CDC data showed.
Provisional data will be updated on a monthly basis as additional records are received, the CDC said.
An estimated 72,000 drug overdose deaths occurred in 2017 in the United States, making it the worst year on record, according to preliminary data released by the Centers for Disease Control and Prevention.
The record high was driven by a sharp increase in deaths attributed to synthetic opioids, such as fentanyl and tramadol, data published on the agency’s website show.
The provisional counts are based on death records sent to the CDC’s National Center for Health Statistics from state vital registration offices in all 50 states and the District of Columbia, reported lead author Farida B. Ahmad, MPH, of the division of vital statistics at the NCHS. Overall, the predicted number of drug overdose deaths has climbed steadily, from 54,207 in November 2015 to 66,012 in November 2016, and to 72,287 in November 2017, according to an interactive chart accessible on the website.
Deaths attributable to synthetic opioids have climbed faster than any other drug class, soaring from just 9,983 in 2015 to 20,310 in 2016, and to 29,418 in 2017.
The next-largest category, heroin-related deaths, increased from 13,407 in 2015 to 16,012 in 2016, but appeared to plateau at 15,959 in 2017. However, the CDC cautioned that flat or declining numbers could be attributable to incomplete data, true decreases in deaths, or some combination of the two. “True declines or plateaus in the numbers of drug overdose deaths across the U.S. cannot be ascertained until final data become available.”
Cocaine-related deaths were fewer in number but appear to have risen substantially to the point where the number of deaths now nearly rival that of heroin. The number of deaths was 7,106 in 2015, 10,868 in 2016, and 14,614 in 2017.
The count of drug overdose deaths varied by state. Nebraska had the sharpest increase in predicted deaths between January 2017 and January 2018, coming in at 33.3%, though the absolute numbers of cases were low (114 through January 2017 and 152 through January 2018). North Carolina also showed substantial increases (from 2,053 to 2,515 cases, 22.5%), as did New Jersey (2,219 to 2,687 cases, 21.1%), the CDC data showed.
Provisional data will be updated on a monthly basis as additional records are received, the CDC said.
Society of Hospital Medicine committee participation is an exciting opportunity available to all medical students and resident physicians. Whether you are hoping to explore new facets of hospital medicine, or take the next step in shaping your career, committee involvement creates opportunities for individuals to share their insight and work collaboratively on key SHM priorities to shape the future of hospital medicine.
Dr. Christopher S. Bartlett
If you are interested, the application is short and straightforward. Requisite SHM membership is free for students and discounted for resident members. And the benefits of committee participation are far reaching.
SHM committee opportunities will cater to most interests and career paths. Our personal interest in academic hospital medicine and medical education led us to the Physicians-In-Training (PIT) committee, but seventeen committees are available (see the complete list below). Review the committee descriptions online and select the one that best aligns with your individual interests. A mentor’s insight may be valuable in determining which committee is the best opportunity.
SHM Committee Opportunities:
Academic Hospitalist Committee
Annual Meeting Committee
Awards Committee
Chapter Support Committee
Communications Strategy Committee
Digital Learning Committee
Education Committee
Hospital Quality and Patient Safety Committee
Membership Committee
Patient Experience Committee
Performance Measurement & Reporting Committee
Physicians in Training Committee
Practice Analysis Committee
Practice Management Committee
Public Policy Committee
Research Committee
Special Interest Group Support Committee
Aram A. Namavar
The most rewarding aspect of committee membership has been the opportunity to make contributions to the growth of SHM, and the advancement of hospital medicine. As members of the PIT committee, which has been charged with developing a trainee pipeline for future hospitalists, we have been fortunate to play roles in the creation of a Student and Resident Executive Council. This group of young hospital medicine leaders will seek to identify strategies to engage medical students and resident physicians in SHM. We had the opportunity to lead the first Student and Resident Interest Forum at the 2018 annual meeting, have contributed to the development of a national research study identifying qualities interviewers are looking for in hospital medicine job candidates, and are helping to craft the young hospitalist track offerings. Medical students and resident physicians are encouraged to take advantage of similar opportunities present in each of the committees.
Membership is a boon. While opportunities for personal and professional growth are less tangible than committee work products, they remain vitally important for trainees. Through their engagement, medical students and resident physicians will have the opportunity to develop new mentoring relationships beyond the confines of their training site. We believe that committee engagement offers a “leg up” on the competition for residency and fellowship applications. Moreover, networking with hospital medicine leaders from across the country has allowed us to meet and engage with current and future colleagues, as well as potential future employers. In the long term, these experiences are sure to shape our future careers. More than a line on one’s curriculum vitae, meaningful contributions will open doors to new and exciting opportunities at our home institutions and nationally through SHM.
Balancing your training requirements with committee involvement is feasible with a little foresight and flexibility. Committee participation typically requires no more than 3-5 hours per month. Monthly committee calls account for 1 hour. Time is also spent preparing for committee calls as well as working on the action items you volunteered to complete. Individual scheduling is flexible, and contributions can occur offline if one is temporarily unavailable because of training obligations. Commitments are for at least 1 year and attendance at the SHM annual conference is highly encouraged but not required. Akin to other facets of life, the degree of participation will be linked with the value derived from the experience.
SHM committees are filled by seasoned hospitalists with dizzying accomplishments. This inherent strength can lead to feelings of uncertainty among newcomers (i.e., impostor syndrome). What can I offer? Does my perspective matter? Reflecting on these fears, we are certain that we could not have been welcomed with more enthusiasm. Our committee colleagues have been 110% supportive, receptive of our viewpoints, committed to our professional growth, and genuine when reaching out to collaborate. Treated as peers, we believe that members are valued based on their commitment and not their level of training or experience.
Committees are looking for capable individuals who have a demonstrated commitment to hospital medicine, as well as specific interests and value-added skills that will enhance the objectives of the committee they are applying for. For medical students and resident physicians, selection to a committee is competitive. While not required, a letter of support from a close mentor may be beneficial. Experience has demonstrated time and again that SHM is looking to engage and cultivate future hospital medicine leaders. To that end, all should take advantage.
Ultimately, we believe that our participation has helped motivate and influence our professional paths. We encourage all medical students and resident physicians to take the next step in their hospital medicine career by applying for committee membership. Our voice as trainees is one that needs further representation within SHM. We hope this call to action will encourage you to apply to a committee. The application can be found at the following link: https://www.hospitalmedicine.org/membership/committees/#Apply_for_a_Committee.
Dr. Bartlett is a hospitalist at the University of New Mexico Hospital, Albuquerque. Mr. Namavar is a medical student at Stritch School of Medicine, Loyola University Chicago.
Opportunities to develop new mentoring relationships
Opportunities to develop new mentoring relationships
Society of Hospital Medicine committee participation is an exciting opportunity available to all medical students and resident physicians. Whether you are hoping to explore new facets of hospital medicine, or take the next step in shaping your career, committee involvement creates opportunities for individuals to share their insight and work collaboratively on key SHM priorities to shape the future of hospital medicine.
Dr. Christopher S. Bartlett
If you are interested, the application is short and straightforward. Requisite SHM membership is free for students and discounted for resident members. And the benefits of committee participation are far reaching.
SHM committee opportunities will cater to most interests and career paths. Our personal interest in academic hospital medicine and medical education led us to the Physicians-In-Training (PIT) committee, but seventeen committees are available (see the complete list below). Review the committee descriptions online and select the one that best aligns with your individual interests. A mentor’s insight may be valuable in determining which committee is the best opportunity.
SHM Committee Opportunities:
Academic Hospitalist Committee
Annual Meeting Committee
Awards Committee
Chapter Support Committee
Communications Strategy Committee
Digital Learning Committee
Education Committee
Hospital Quality and Patient Safety Committee
Membership Committee
Patient Experience Committee
Performance Measurement & Reporting Committee
Physicians in Training Committee
Practice Analysis Committee
Practice Management Committee
Public Policy Committee
Research Committee
Special Interest Group Support Committee
Aram A. Namavar
The most rewarding aspect of committee membership has been the opportunity to make contributions to the growth of SHM, and the advancement of hospital medicine. As members of the PIT committee, which has been charged with developing a trainee pipeline for future hospitalists, we have been fortunate to play roles in the creation of a Student and Resident Executive Council. This group of young hospital medicine leaders will seek to identify strategies to engage medical students and resident physicians in SHM. We had the opportunity to lead the first Student and Resident Interest Forum at the 2018 annual meeting, have contributed to the development of a national research study identifying qualities interviewers are looking for in hospital medicine job candidates, and are helping to craft the young hospitalist track offerings. Medical students and resident physicians are encouraged to take advantage of similar opportunities present in each of the committees.
Membership is a boon. While opportunities for personal and professional growth are less tangible than committee work products, they remain vitally important for trainees. Through their engagement, medical students and resident physicians will have the opportunity to develop new mentoring relationships beyond the confines of their training site. We believe that committee engagement offers a “leg up” on the competition for residency and fellowship applications. Moreover, networking with hospital medicine leaders from across the country has allowed us to meet and engage with current and future colleagues, as well as potential future employers. In the long term, these experiences are sure to shape our future careers. More than a line on one’s curriculum vitae, meaningful contributions will open doors to new and exciting opportunities at our home institutions and nationally through SHM.
Balancing your training requirements with committee involvement is feasible with a little foresight and flexibility. Committee participation typically requires no more than 3-5 hours per month. Monthly committee calls account for 1 hour. Time is also spent preparing for committee calls as well as working on the action items you volunteered to complete. Individual scheduling is flexible, and contributions can occur offline if one is temporarily unavailable because of training obligations. Commitments are for at least 1 year and attendance at the SHM annual conference is highly encouraged but not required. Akin to other facets of life, the degree of participation will be linked with the value derived from the experience.
SHM committees are filled by seasoned hospitalists with dizzying accomplishments. This inherent strength can lead to feelings of uncertainty among newcomers (i.e., impostor syndrome). What can I offer? Does my perspective matter? Reflecting on these fears, we are certain that we could not have been welcomed with more enthusiasm. Our committee colleagues have been 110% supportive, receptive of our viewpoints, committed to our professional growth, and genuine when reaching out to collaborate. Treated as peers, we believe that members are valued based on their commitment and not their level of training or experience.
Committees are looking for capable individuals who have a demonstrated commitment to hospital medicine, as well as specific interests and value-added skills that will enhance the objectives of the committee they are applying for. For medical students and resident physicians, selection to a committee is competitive. While not required, a letter of support from a close mentor may be beneficial. Experience has demonstrated time and again that SHM is looking to engage and cultivate future hospital medicine leaders. To that end, all should take advantage.
Ultimately, we believe that our participation has helped motivate and influence our professional paths. We encourage all medical students and resident physicians to take the next step in their hospital medicine career by applying for committee membership. Our voice as trainees is one that needs further representation within SHM. We hope this call to action will encourage you to apply to a committee. The application can be found at the following link: https://www.hospitalmedicine.org/membership/committees/#Apply_for_a_Committee.
Dr. Bartlett is a hospitalist at the University of New Mexico Hospital, Albuquerque. Mr. Namavar is a medical student at Stritch School of Medicine, Loyola University Chicago.
Society of Hospital Medicine committee participation is an exciting opportunity available to all medical students and resident physicians. Whether you are hoping to explore new facets of hospital medicine, or take the next step in shaping your career, committee involvement creates opportunities for individuals to share their insight and work collaboratively on key SHM priorities to shape the future of hospital medicine.
Dr. Christopher S. Bartlett
If you are interested, the application is short and straightforward. Requisite SHM membership is free for students and discounted for resident members. And the benefits of committee participation are far reaching.
SHM committee opportunities will cater to most interests and career paths. Our personal interest in academic hospital medicine and medical education led us to the Physicians-In-Training (PIT) committee, but seventeen committees are available (see the complete list below). Review the committee descriptions online and select the one that best aligns with your individual interests. A mentor’s insight may be valuable in determining which committee is the best opportunity.
SHM Committee Opportunities:
Academic Hospitalist Committee
Annual Meeting Committee
Awards Committee
Chapter Support Committee
Communications Strategy Committee
Digital Learning Committee
Education Committee
Hospital Quality and Patient Safety Committee
Membership Committee
Patient Experience Committee
Performance Measurement & Reporting Committee
Physicians in Training Committee
Practice Analysis Committee
Practice Management Committee
Public Policy Committee
Research Committee
Special Interest Group Support Committee
Aram A. Namavar
The most rewarding aspect of committee membership has been the opportunity to make contributions to the growth of SHM, and the advancement of hospital medicine. As members of the PIT committee, which has been charged with developing a trainee pipeline for future hospitalists, we have been fortunate to play roles in the creation of a Student and Resident Executive Council. This group of young hospital medicine leaders will seek to identify strategies to engage medical students and resident physicians in SHM. We had the opportunity to lead the first Student and Resident Interest Forum at the 2018 annual meeting, have contributed to the development of a national research study identifying qualities interviewers are looking for in hospital medicine job candidates, and are helping to craft the young hospitalist track offerings. Medical students and resident physicians are encouraged to take advantage of similar opportunities present in each of the committees.
Membership is a boon. While opportunities for personal and professional growth are less tangible than committee work products, they remain vitally important for trainees. Through their engagement, medical students and resident physicians will have the opportunity to develop new mentoring relationships beyond the confines of their training site. We believe that committee engagement offers a “leg up” on the competition for residency and fellowship applications. Moreover, networking with hospital medicine leaders from across the country has allowed us to meet and engage with current and future colleagues, as well as potential future employers. In the long term, these experiences are sure to shape our future careers. More than a line on one’s curriculum vitae, meaningful contributions will open doors to new and exciting opportunities at our home institutions and nationally through SHM.
Balancing your training requirements with committee involvement is feasible with a little foresight and flexibility. Committee participation typically requires no more than 3-5 hours per month. Monthly committee calls account for 1 hour. Time is also spent preparing for committee calls as well as working on the action items you volunteered to complete. Individual scheduling is flexible, and contributions can occur offline if one is temporarily unavailable because of training obligations. Commitments are for at least 1 year and attendance at the SHM annual conference is highly encouraged but not required. Akin to other facets of life, the degree of participation will be linked with the value derived from the experience.
SHM committees are filled by seasoned hospitalists with dizzying accomplishments. This inherent strength can lead to feelings of uncertainty among newcomers (i.e., impostor syndrome). What can I offer? Does my perspective matter? Reflecting on these fears, we are certain that we could not have been welcomed with more enthusiasm. Our committee colleagues have been 110% supportive, receptive of our viewpoints, committed to our professional growth, and genuine when reaching out to collaborate. Treated as peers, we believe that members are valued based on their commitment and not their level of training or experience.
Committees are looking for capable individuals who have a demonstrated commitment to hospital medicine, as well as specific interests and value-added skills that will enhance the objectives of the committee they are applying for. For medical students and resident physicians, selection to a committee is competitive. While not required, a letter of support from a close mentor may be beneficial. Experience has demonstrated time and again that SHM is looking to engage and cultivate future hospital medicine leaders. To that end, all should take advantage.
Ultimately, we believe that our participation has helped motivate and influence our professional paths. We encourage all medical students and resident physicians to take the next step in their hospital medicine career by applying for committee membership. Our voice as trainees is one that needs further representation within SHM. We hope this call to action will encourage you to apply to a committee. The application can be found at the following link: https://www.hospitalmedicine.org/membership/committees/#Apply_for_a_Committee.
Dr. Bartlett is a hospitalist at the University of New Mexico Hospital, Albuquerque. Mr. Namavar is a medical student at Stritch School of Medicine, Loyola University Chicago.
NEW ORLEANS – Nonalcoholic fatty liver disease is the 21st century epidemic in liver disease, Zobair M. Younossi, MD, declared at the annual meeting of the American College of Physicians.
Bruce Jancin/MDedge News
Dr. Zobair M. Younossi
The massive growth in nonalcoholic fatty liver disease (NAFLD) is being fueled to a great extent by the related epidemics of obesity and type 2 diabetes mellitus. While the overall prevalence of NAFLD worldwide is 24%, almost three-quarters of patients with NAFLD are obese. And the prevalence of NAFLD in individuals with T2DM was 58% in a recent meta-analysis of studies from 20 countries conducted by Dr. Younossi and his coinvestigators.
“The prevalence of NAFLD in U.S. kids is about 10%. This is of course part of the coming tsunami because our kids are getting obese, diabetic, and they’re going to have problems with NASH [nonalcoholic steatohepatitis],” said Dr. Younossi, a gastroenterologist who is professor and chairman of the department of medicine at the Inova Fairfax (Va.) campus of Virginia Commonwealth University.
NASH is the form of NAFLD that has the strongest prognostic implications. It can progress to cirrhosis, liver failure, or hepatocellular carcinoma. As Dr. Younossi and his coworkers have shown (Hepat Commun. 2017 Jun 6;1[5]:421-8), it is associated with a significantly greater risk of both liver-related and all-cause mortality than that of non-NASH NAFLD, although NAFLD also carries an increased risk of cardiovascular disease, the leading cause of death in that population.
In addition to highlighting the enormous clinical, economic, and quality-of-life implications of the NAFLD epidemic, Dr. Younossi offered practical tips on how busy primary care physicians can identify patients in their practice who have high-risk NAFLD. They have not done a very good job of this to date. That’s possibly due to lack of incentive, since in 2018 there is no approved drug for the treatment of NASH. He cited one representative retrospective study in which only about 15% of patients identified as having NAFLD received a recommendation for lifestyle modification involving diet and exercise, which is the standard evidence-based treatment, albeit admittedly difficult to sustain. And only 3% of patients with advanced liver fibrosis were referred to a specialist for management.
“So NAFLD is common, but its recognition and doing something about it is quite a challenge,” Dr. Younossi observed.
He argued that patients who have NASH deserve to know it because of its prognostic implications and also so they can have the chance to participate in one of the roughly two dozen ongoing clinical trials of potential therapies, some of which look quite promising. All of the trials required a liver biopsy as a condition for enrollment. Plus, once a patient is known to have stage 3 fibrosis, it’s time to start screening for hepatocellular carcinoma and esophageal varices.
The scope of the epidemic
NASH is the most rapidly growing indication for liver transplantation in the United States, with most of the increase coming from the baby boomer population. NASH is now the second most common indication for placement on the wait list. Meanwhile, liver transplantation due to the consequences of hepatitis C, the No. 1 indication, is declining as a result of the spectacular advances in medical treatment introduced a few years ago. It’s likely that in coming years NASH will take over the top spot, according to Dr. Younossi.
He was coauthor of a recent study that modeled the estimated trends for the NAFLD epidemic in the United States through 2030. The forecast is that the prevalence of NAFLD among adults will climb to 33.5% and the proportion of NAFLD categorized as NASH will increase from 20% at present to 27%. Moreover, this will result in a 168% jump in the incidence of decompensated cirrhosis, a 137% increase in the incidence of hepatocellular carcinoma, and a 178% increase in liver-related mortality, which will account for an estimated 78,300 deaths in 2030 (Hepatology. 2018 Jan;67[1]:123-33).
Practical ways to identify high-risk patients
The best noninvasive means of detecting NAFLD is by ultrasound showing a fatty liver. Often the condition is detected as an incidental finding on abdominal ultrasound ordered for another reason. Elevated liver enzymes can be a tipoff as well. Of course, alcoholic liver disease and other causes must be excluded.
But what’s most important is to identify patients with NASH. It’s a diagnosis made by biopsy. However, it is unthinkable to perform liver biopsies in the entire vast population with NAFLD, so there is a great deal of interest in developing noninvasive diagnostic modalities that can help zero in on the subset of high-risk NAFLD patients who should be considered for referral for liver biopsy.
One useful clue is the presence of comorbid metabolic syndrome in patients with NAFLD. It confers a substantially higher mortality risk – especially cardiovascular mortality – than does NAFLD without metabolic syndrome. Dr. Younossi and his coinvestigators have shown in a study of 3,613 NAFLD patients followed long-term that those with one component of the metabolic syndrome – either hypertension, central obesity, increased fasting plasma glucose, or hyperlipidemia – had 8- and 16-year all-cause mortality rates of 4.7% and 11.9%, nearly double the 2.6% and 6% rates in NAFLD patients with no elements of the metabolic syndrome.
Moreover, the magnitude of risk increased with each additional metabolic syndrome condition: a 3.57-fold increased mortality risk in NAFLD patients with two components of metabolic syndrome, a 5.87-fold increase in those with three, and a 13.09-fold increase in NAFLD patients with all four elements of metabolic syndrome (Medicine [Baltimore]. 2018 Mar;97[13]:e0214. doi: 10.1097/MD.0000000000010214).
Dr. Younossi was a member of the American Association for the Study of Liver Disease expert panel that developed the latest practice guidance regarding the diagnosis and management of NAFLD (Hepatology. 2018 Jan;67[1]:328-57). He said that probably the best simple noninvasive scoring system for the detection of NASH with advanced fibrosis is the NAFLD fibrosis score, which is easily calculated using laboratory values and clinical parameters already in a patient’s chart.
A more sophisticated serum biomarker test known as ELF, or the Enhanced Liver Fibrosis test, combines serum levels of hyaluronic acid, tissue inhibitor of metalloproteinase I, and procollagen amino terminal peptide.
“ELF is a very, very good test. It’s approved in Europe and I suspect it will be in the U.S. within the next year or so,” said Dr. Younossi.
The most exciting noninvasive tests, however, involve imaging that measures liver stiffness, which provides a fairly accurate indication of the degree of scarring in the organ. There are two methods available: vibration wave transient elastography and magnetic resonance elastography.
Transient elastography using the FibroScan device is commercially available in the United States. “It’s a good test, very easy to do, noninvasive. I have a couple of these machines, and we use them all the time,” the gastroenterologist said.
MR elastography provides superior accuracy, but access is an issue.
“At our institution you sometimes have to wait for weeks to get an outpatient MRI, so if you have hundreds of patients with fatty liver disease it makes things difficult. So in our practice we use transient elastography,” he explained.
Both imaging modalities also measure the amount of fat in the liver.
Dr. Younossi uses transient elastography in patients who don’t have type 2 diabetes or frank insulin resistance. If the FibroScan score is 7 kiloPascals or more, he considers liver biopsy, since that’s the threshold for detection of earlier, potentially reversible stage 2 fibrosis. If, however, a patient has diabetes or insulin resistance along with a NAFLD fibrosis score suggesting a high possibility of fibrosis, he sends that patient for liver biopsy, since those endocrinologic disorders are known to be independent risk factors for mortality in the setting of NAFLD.
Dr. Younossi reported having no financial conflicts of interest regarding his presentation.
NEW ORLEANS – Nonalcoholic fatty liver disease is the 21st century epidemic in liver disease, Zobair M. Younossi, MD, declared at the annual meeting of the American College of Physicians.
Bruce Jancin/MDedge News
Dr. Zobair M. Younossi
The massive growth in nonalcoholic fatty liver disease (NAFLD) is being fueled to a great extent by the related epidemics of obesity and type 2 diabetes mellitus. While the overall prevalence of NAFLD worldwide is 24%, almost three-quarters of patients with NAFLD are obese. And the prevalence of NAFLD in individuals with T2DM was 58% in a recent meta-analysis of studies from 20 countries conducted by Dr. Younossi and his coinvestigators.
“The prevalence of NAFLD in U.S. kids is about 10%. This is of course part of the coming tsunami because our kids are getting obese, diabetic, and they’re going to have problems with NASH [nonalcoholic steatohepatitis],” said Dr. Younossi, a gastroenterologist who is professor and chairman of the department of medicine at the Inova Fairfax (Va.) campus of Virginia Commonwealth University.
NASH is the form of NAFLD that has the strongest prognostic implications. It can progress to cirrhosis, liver failure, or hepatocellular carcinoma. As Dr. Younossi and his coworkers have shown (Hepat Commun. 2017 Jun 6;1[5]:421-8), it is associated with a significantly greater risk of both liver-related and all-cause mortality than that of non-NASH NAFLD, although NAFLD also carries an increased risk of cardiovascular disease, the leading cause of death in that population.
In addition to highlighting the enormous clinical, economic, and quality-of-life implications of the NAFLD epidemic, Dr. Younossi offered practical tips on how busy primary care physicians can identify patients in their practice who have high-risk NAFLD. They have not done a very good job of this to date. That’s possibly due to lack of incentive, since in 2018 there is no approved drug for the treatment of NASH. He cited one representative retrospective study in which only about 15% of patients identified as having NAFLD received a recommendation for lifestyle modification involving diet and exercise, which is the standard evidence-based treatment, albeit admittedly difficult to sustain. And only 3% of patients with advanced liver fibrosis were referred to a specialist for management.
“So NAFLD is common, but its recognition and doing something about it is quite a challenge,” Dr. Younossi observed.
He argued that patients who have NASH deserve to know it because of its prognostic implications and also so they can have the chance to participate in one of the roughly two dozen ongoing clinical trials of potential therapies, some of which look quite promising. All of the trials required a liver biopsy as a condition for enrollment. Plus, once a patient is known to have stage 3 fibrosis, it’s time to start screening for hepatocellular carcinoma and esophageal varices.
The scope of the epidemic
NASH is the most rapidly growing indication for liver transplantation in the United States, with most of the increase coming from the baby boomer population. NASH is now the second most common indication for placement on the wait list. Meanwhile, liver transplantation due to the consequences of hepatitis C, the No. 1 indication, is declining as a result of the spectacular advances in medical treatment introduced a few years ago. It’s likely that in coming years NASH will take over the top spot, according to Dr. Younossi.
He was coauthor of a recent study that modeled the estimated trends for the NAFLD epidemic in the United States through 2030. The forecast is that the prevalence of NAFLD among adults will climb to 33.5% and the proportion of NAFLD categorized as NASH will increase from 20% at present to 27%. Moreover, this will result in a 168% jump in the incidence of decompensated cirrhosis, a 137% increase in the incidence of hepatocellular carcinoma, and a 178% increase in liver-related mortality, which will account for an estimated 78,300 deaths in 2030 (Hepatology. 2018 Jan;67[1]:123-33).
Practical ways to identify high-risk patients
The best noninvasive means of detecting NAFLD is by ultrasound showing a fatty liver. Often the condition is detected as an incidental finding on abdominal ultrasound ordered for another reason. Elevated liver enzymes can be a tipoff as well. Of course, alcoholic liver disease and other causes must be excluded.
But what’s most important is to identify patients with NASH. It’s a diagnosis made by biopsy. However, it is unthinkable to perform liver biopsies in the entire vast population with NAFLD, so there is a great deal of interest in developing noninvasive diagnostic modalities that can help zero in on the subset of high-risk NAFLD patients who should be considered for referral for liver biopsy.
One useful clue is the presence of comorbid metabolic syndrome in patients with NAFLD. It confers a substantially higher mortality risk – especially cardiovascular mortality – than does NAFLD without metabolic syndrome. Dr. Younossi and his coinvestigators have shown in a study of 3,613 NAFLD patients followed long-term that those with one component of the metabolic syndrome – either hypertension, central obesity, increased fasting plasma glucose, or hyperlipidemia – had 8- and 16-year all-cause mortality rates of 4.7% and 11.9%, nearly double the 2.6% and 6% rates in NAFLD patients with no elements of the metabolic syndrome.
Moreover, the magnitude of risk increased with each additional metabolic syndrome condition: a 3.57-fold increased mortality risk in NAFLD patients with two components of metabolic syndrome, a 5.87-fold increase in those with three, and a 13.09-fold increase in NAFLD patients with all four elements of metabolic syndrome (Medicine [Baltimore]. 2018 Mar;97[13]:e0214. doi: 10.1097/MD.0000000000010214).
Dr. Younossi was a member of the American Association for the Study of Liver Disease expert panel that developed the latest practice guidance regarding the diagnosis and management of NAFLD (Hepatology. 2018 Jan;67[1]:328-57). He said that probably the best simple noninvasive scoring system for the detection of NASH with advanced fibrosis is the NAFLD fibrosis score, which is easily calculated using laboratory values and clinical parameters already in a patient’s chart.
A more sophisticated serum biomarker test known as ELF, or the Enhanced Liver Fibrosis test, combines serum levels of hyaluronic acid, tissue inhibitor of metalloproteinase I, and procollagen amino terminal peptide.
“ELF is a very, very good test. It’s approved in Europe and I suspect it will be in the U.S. within the next year or so,” said Dr. Younossi.
The most exciting noninvasive tests, however, involve imaging that measures liver stiffness, which provides a fairly accurate indication of the degree of scarring in the organ. There are two methods available: vibration wave transient elastography and magnetic resonance elastography.
Transient elastography using the FibroScan device is commercially available in the United States. “It’s a good test, very easy to do, noninvasive. I have a couple of these machines, and we use them all the time,” the gastroenterologist said.
MR elastography provides superior accuracy, but access is an issue.
“At our institution you sometimes have to wait for weeks to get an outpatient MRI, so if you have hundreds of patients with fatty liver disease it makes things difficult. So in our practice we use transient elastography,” he explained.
Both imaging modalities also measure the amount of fat in the liver.
Dr. Younossi uses transient elastography in patients who don’t have type 2 diabetes or frank insulin resistance. If the FibroScan score is 7 kiloPascals or more, he considers liver biopsy, since that’s the threshold for detection of earlier, potentially reversible stage 2 fibrosis. If, however, a patient has diabetes or insulin resistance along with a NAFLD fibrosis score suggesting a high possibility of fibrosis, he sends that patient for liver biopsy, since those endocrinologic disorders are known to be independent risk factors for mortality in the setting of NAFLD.
Dr. Younossi reported having no financial conflicts of interest regarding his presentation.
NEW ORLEANS – Nonalcoholic fatty liver disease is the 21st century epidemic in liver disease, Zobair M. Younossi, MD, declared at the annual meeting of the American College of Physicians.
Bruce Jancin/MDedge News
Dr. Zobair M. Younossi
The massive growth in nonalcoholic fatty liver disease (NAFLD) is being fueled to a great extent by the related epidemics of obesity and type 2 diabetes mellitus. While the overall prevalence of NAFLD worldwide is 24%, almost three-quarters of patients with NAFLD are obese. And the prevalence of NAFLD in individuals with T2DM was 58% in a recent meta-analysis of studies from 20 countries conducted by Dr. Younossi and his coinvestigators.
“The prevalence of NAFLD in U.S. kids is about 10%. This is of course part of the coming tsunami because our kids are getting obese, diabetic, and they’re going to have problems with NASH [nonalcoholic steatohepatitis],” said Dr. Younossi, a gastroenterologist who is professor and chairman of the department of medicine at the Inova Fairfax (Va.) campus of Virginia Commonwealth University.
NASH is the form of NAFLD that has the strongest prognostic implications. It can progress to cirrhosis, liver failure, or hepatocellular carcinoma. As Dr. Younossi and his coworkers have shown (Hepat Commun. 2017 Jun 6;1[5]:421-8), it is associated with a significantly greater risk of both liver-related and all-cause mortality than that of non-NASH NAFLD, although NAFLD also carries an increased risk of cardiovascular disease, the leading cause of death in that population.
In addition to highlighting the enormous clinical, economic, and quality-of-life implications of the NAFLD epidemic, Dr. Younossi offered practical tips on how busy primary care physicians can identify patients in their practice who have high-risk NAFLD. They have not done a very good job of this to date. That’s possibly due to lack of incentive, since in 2018 there is no approved drug for the treatment of NASH. He cited one representative retrospective study in which only about 15% of patients identified as having NAFLD received a recommendation for lifestyle modification involving diet and exercise, which is the standard evidence-based treatment, albeit admittedly difficult to sustain. And only 3% of patients with advanced liver fibrosis were referred to a specialist for management.
“So NAFLD is common, but its recognition and doing something about it is quite a challenge,” Dr. Younossi observed.
He argued that patients who have NASH deserve to know it because of its prognostic implications and also so they can have the chance to participate in one of the roughly two dozen ongoing clinical trials of potential therapies, some of which look quite promising. All of the trials required a liver biopsy as a condition for enrollment. Plus, once a patient is known to have stage 3 fibrosis, it’s time to start screening for hepatocellular carcinoma and esophageal varices.
The scope of the epidemic
NASH is the most rapidly growing indication for liver transplantation in the United States, with most of the increase coming from the baby boomer population. NASH is now the second most common indication for placement on the wait list. Meanwhile, liver transplantation due to the consequences of hepatitis C, the No. 1 indication, is declining as a result of the spectacular advances in medical treatment introduced a few years ago. It’s likely that in coming years NASH will take over the top spot, according to Dr. Younossi.
He was coauthor of a recent study that modeled the estimated trends for the NAFLD epidemic in the United States through 2030. The forecast is that the prevalence of NAFLD among adults will climb to 33.5% and the proportion of NAFLD categorized as NASH will increase from 20% at present to 27%. Moreover, this will result in a 168% jump in the incidence of decompensated cirrhosis, a 137% increase in the incidence of hepatocellular carcinoma, and a 178% increase in liver-related mortality, which will account for an estimated 78,300 deaths in 2030 (Hepatology. 2018 Jan;67[1]:123-33).
Practical ways to identify high-risk patients
The best noninvasive means of detecting NAFLD is by ultrasound showing a fatty liver. Often the condition is detected as an incidental finding on abdominal ultrasound ordered for another reason. Elevated liver enzymes can be a tipoff as well. Of course, alcoholic liver disease and other causes must be excluded.
But what’s most important is to identify patients with NASH. It’s a diagnosis made by biopsy. However, it is unthinkable to perform liver biopsies in the entire vast population with NAFLD, so there is a great deal of interest in developing noninvasive diagnostic modalities that can help zero in on the subset of high-risk NAFLD patients who should be considered for referral for liver biopsy.
One useful clue is the presence of comorbid metabolic syndrome in patients with NAFLD. It confers a substantially higher mortality risk – especially cardiovascular mortality – than does NAFLD without metabolic syndrome. Dr. Younossi and his coinvestigators have shown in a study of 3,613 NAFLD patients followed long-term that those with one component of the metabolic syndrome – either hypertension, central obesity, increased fasting plasma glucose, or hyperlipidemia – had 8- and 16-year all-cause mortality rates of 4.7% and 11.9%, nearly double the 2.6% and 6% rates in NAFLD patients with no elements of the metabolic syndrome.
Moreover, the magnitude of risk increased with each additional metabolic syndrome condition: a 3.57-fold increased mortality risk in NAFLD patients with two components of metabolic syndrome, a 5.87-fold increase in those with three, and a 13.09-fold increase in NAFLD patients with all four elements of metabolic syndrome (Medicine [Baltimore]. 2018 Mar;97[13]:e0214. doi: 10.1097/MD.0000000000010214).
Dr. Younossi was a member of the American Association for the Study of Liver Disease expert panel that developed the latest practice guidance regarding the diagnosis and management of NAFLD (Hepatology. 2018 Jan;67[1]:328-57). He said that probably the best simple noninvasive scoring system for the detection of NASH with advanced fibrosis is the NAFLD fibrosis score, which is easily calculated using laboratory values and clinical parameters already in a patient’s chart.
A more sophisticated serum biomarker test known as ELF, or the Enhanced Liver Fibrosis test, combines serum levels of hyaluronic acid, tissue inhibitor of metalloproteinase I, and procollagen amino terminal peptide.
“ELF is a very, very good test. It’s approved in Europe and I suspect it will be in the U.S. within the next year or so,” said Dr. Younossi.
The most exciting noninvasive tests, however, involve imaging that measures liver stiffness, which provides a fairly accurate indication of the degree of scarring in the organ. There are two methods available: vibration wave transient elastography and magnetic resonance elastography.
Transient elastography using the FibroScan device is commercially available in the United States. “It’s a good test, very easy to do, noninvasive. I have a couple of these machines, and we use them all the time,” the gastroenterologist said.
MR elastography provides superior accuracy, but access is an issue.
“At our institution you sometimes have to wait for weeks to get an outpatient MRI, so if you have hundreds of patients with fatty liver disease it makes things difficult. So in our practice we use transient elastography,” he explained.
Both imaging modalities also measure the amount of fat in the liver.
Dr. Younossi uses transient elastography in patients who don’t have type 2 diabetes or frank insulin resistance. If the FibroScan score is 7 kiloPascals or more, he considers liver biopsy, since that’s the threshold for detection of earlier, potentially reversible stage 2 fibrosis. If, however, a patient has diabetes or insulin resistance along with a NAFLD fibrosis score suggesting a high possibility of fibrosis, he sends that patient for liver biopsy, since those endocrinologic disorders are known to be independent risk factors for mortality in the setting of NAFLD.
Dr. Younossi reported having no financial conflicts of interest regarding his presentation.
An update to the first-ever guideline on adult congenital heart disease, released today, provides new recommendations and a more nuanced classification system based on data and expertise accrued in the field over the past decade.
Dr. Curt J Daniels
Recommendations for more than two dozen specific lesion types are included in the 2018 American Heart Association/American College of Cardiology Guideline for the Management of Adults With Congenital Heart Disease.
The 172-page document, published online in the Journal of the American College of Cardiology and Circulation, also includes recommendations on general principles ranging from evaluation of suspected disease to palliative care and end-of-life issues.
“The original guidelines, I think everyone would agree, were just a lot more best practice and expert consensus, whereas now we have at least some data to support our recommendations,” said guideline-writing committee vice chair Curt J. Daniels, MD.
Better road map
The document is intended to provide a “better road map” for all providers who will see such patients in their practice, said Dr. Daniels, director of the adult congenital heart disease and pulmonary hypertension program at Ohio State University Heart Center and Nationwide Children’s Hospital, Columbus.
“There are not enough adult congenital heart disease cardiologists and programs in the country to care for the almost 1.5 million adults with congenital heart disease in the United States, so we know these patients are cared for by general cardiologists,” Dr. Daniels said in an interview. “Having some guidelines about when to refer to those patients was a huge part of the purpose of these updated guidelines.”
The revamped classification system underlying the new guidelines seeks to better characterize disease severity based on the complexity of its anatomy and physiology, according to Dr. Daniels.
Previous documents, including the original 2008 AHA/ACC guideline (Circulation. 2008 Nov 7;118:e714-833), focused mainly on anatomic classifications to rank severity, he said.
“Traditionally, we’ve based the severity of congenital heart disease based on the complexity of anatomy they were born with, but that goes only so far,” Dr. Daniels said in an interview.
More than just anatomy
Dr. Robert Jaquiss
In the new system, anatomy is classified as simple (I, e.g., isolated small atrial septal defect), moderately complex (II, e.g., coarctation of the aorta), or greatly complex (III, e.g., cyanotic congenital heart defect), while physiologic stages range from A to D, increasing along with the severity of physiologic variables such as New York Heart Association functional class; exercise capacity; aortic enlargement; arrhythmias; renal, hepatic, or pulmonary function; and venal or arterial stenosis.
A normotensive patient with repaired coarctation of the aorta would be classified as IIA if she had normal end-organ function and exercise capacity, whereas a similar patient with an ascending aortic diameter of 4.0 cm would be classified as IIB, and with the addition of moderate aortic stenosis, would be classified as IIIC, according to an example provided in the guidelines.
Congenital heart disease specialist Robert “Jake” Jaquiss, MD, said in an interview that consideration of physiology alongside anatomy is one of the most important features of the new guidelines.
“This is a way of thinking about patients that involves not just their anatomy, but also considering a variety of domains in which there may be physiologic dysfunction that can modify the underlying anatomy,” said Dr. Jaquiss, chief of pediatric and congenital heart surgery at Children’s Medical Center/University of Texas Southwestern Medical Center, Dallas. “I think that is a more clinically relevant way to think about patients and patient evaluation management, and I commend the authors for that focus.”
For example, one patient who has undergone a Fontan procedure may be fully functional, whereas another with nearly identical anatomy may be burdened by arrhythmias, fluid retention, and impaired exercise function. “If we don’t grasp the physiologic difference, we treat the two patients the same way, which is obviously inappropriate,” Dr. Jaquiss said.
Research directions
Much more research needs to be done, according to guideline authors, who list 60 unresolved research questions that represent evidence gaps and future directions for study.
For example, outstanding questions related to tetralogy of Fallot focus on the optimal timing for pulmonary valve replacement, the role of pulmonary valve replacement and ventricular tachycardia ablation in decreasing sudden cardiac death risk, and whether implantable cardioverter-defibrillators reduce mortality.
“These are the kinds of evolutionary sort of understandings and alterations in the intervention, both at the original operation and for assessment of care, and what we think about it and how we think about it in 2018 is quite different than how we thought in 2008, and I dare say it’ll be even more different in 2028,” Dr. Jaquiss said.
The AHA/ACC guideline was developed in association with the American Association for Thoracic Surgery, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons.
Dr. Daniels reported a relevant relationship with Actelion. Guideline coauthors reported relevant relationships in that same category with Actelion, Boehringer Ingelheim, Cormatrix, Edward Lifesciences, Gilead, Medtronic, Novartis, Sorin (LivaNova), St. Jude Medical, and United Therapeutics. No other disclosures were reported.
An update to the first-ever guideline on adult congenital heart disease, released today, provides new recommendations and a more nuanced classification system based on data and expertise accrued in the field over the past decade.
Dr. Curt J Daniels
Recommendations for more than two dozen specific lesion types are included in the 2018 American Heart Association/American College of Cardiology Guideline for the Management of Adults With Congenital Heart Disease.
The 172-page document, published online in the Journal of the American College of Cardiology and Circulation, also includes recommendations on general principles ranging from evaluation of suspected disease to palliative care and end-of-life issues.
“The original guidelines, I think everyone would agree, were just a lot more best practice and expert consensus, whereas now we have at least some data to support our recommendations,” said guideline-writing committee vice chair Curt J. Daniels, MD.
Better road map
The document is intended to provide a “better road map” for all providers who will see such patients in their practice, said Dr. Daniels, director of the adult congenital heart disease and pulmonary hypertension program at Ohio State University Heart Center and Nationwide Children’s Hospital, Columbus.
“There are not enough adult congenital heart disease cardiologists and programs in the country to care for the almost 1.5 million adults with congenital heart disease in the United States, so we know these patients are cared for by general cardiologists,” Dr. Daniels said in an interview. “Having some guidelines about when to refer to those patients was a huge part of the purpose of these updated guidelines.”
The revamped classification system underlying the new guidelines seeks to better characterize disease severity based on the complexity of its anatomy and physiology, according to Dr. Daniels.
Previous documents, including the original 2008 AHA/ACC guideline (Circulation. 2008 Nov 7;118:e714-833), focused mainly on anatomic classifications to rank severity, he said.
“Traditionally, we’ve based the severity of congenital heart disease based on the complexity of anatomy they were born with, but that goes only so far,” Dr. Daniels said in an interview.
More than just anatomy
Dr. Robert Jaquiss
In the new system, anatomy is classified as simple (I, e.g., isolated small atrial septal defect), moderately complex (II, e.g., coarctation of the aorta), or greatly complex (III, e.g., cyanotic congenital heart defect), while physiologic stages range from A to D, increasing along with the severity of physiologic variables such as New York Heart Association functional class; exercise capacity; aortic enlargement; arrhythmias; renal, hepatic, or pulmonary function; and venal or arterial stenosis.
A normotensive patient with repaired coarctation of the aorta would be classified as IIA if she had normal end-organ function and exercise capacity, whereas a similar patient with an ascending aortic diameter of 4.0 cm would be classified as IIB, and with the addition of moderate aortic stenosis, would be classified as IIIC, according to an example provided in the guidelines.
Congenital heart disease specialist Robert “Jake” Jaquiss, MD, said in an interview that consideration of physiology alongside anatomy is one of the most important features of the new guidelines.
“This is a way of thinking about patients that involves not just their anatomy, but also considering a variety of domains in which there may be physiologic dysfunction that can modify the underlying anatomy,” said Dr. Jaquiss, chief of pediatric and congenital heart surgery at Children’s Medical Center/University of Texas Southwestern Medical Center, Dallas. “I think that is a more clinically relevant way to think about patients and patient evaluation management, and I commend the authors for that focus.”
For example, one patient who has undergone a Fontan procedure may be fully functional, whereas another with nearly identical anatomy may be burdened by arrhythmias, fluid retention, and impaired exercise function. “If we don’t grasp the physiologic difference, we treat the two patients the same way, which is obviously inappropriate,” Dr. Jaquiss said.
Research directions
Much more research needs to be done, according to guideline authors, who list 60 unresolved research questions that represent evidence gaps and future directions for study.
For example, outstanding questions related to tetralogy of Fallot focus on the optimal timing for pulmonary valve replacement, the role of pulmonary valve replacement and ventricular tachycardia ablation in decreasing sudden cardiac death risk, and whether implantable cardioverter-defibrillators reduce mortality.
“These are the kinds of evolutionary sort of understandings and alterations in the intervention, both at the original operation and for assessment of care, and what we think about it and how we think about it in 2018 is quite different than how we thought in 2008, and I dare say it’ll be even more different in 2028,” Dr. Jaquiss said.
The AHA/ACC guideline was developed in association with the American Association for Thoracic Surgery, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons.
Dr. Daniels reported a relevant relationship with Actelion. Guideline coauthors reported relevant relationships in that same category with Actelion, Boehringer Ingelheim, Cormatrix, Edward Lifesciences, Gilead, Medtronic, Novartis, Sorin (LivaNova), St. Jude Medical, and United Therapeutics. No other disclosures were reported.
An update to the first-ever guideline on adult congenital heart disease, released today, provides new recommendations and a more nuanced classification system based on data and expertise accrued in the field over the past decade.
Dr. Curt J Daniels
Recommendations for more than two dozen specific lesion types are included in the 2018 American Heart Association/American College of Cardiology Guideline for the Management of Adults With Congenital Heart Disease.
The 172-page document, published online in the Journal of the American College of Cardiology and Circulation, also includes recommendations on general principles ranging from evaluation of suspected disease to palliative care and end-of-life issues.
“The original guidelines, I think everyone would agree, were just a lot more best practice and expert consensus, whereas now we have at least some data to support our recommendations,” said guideline-writing committee vice chair Curt J. Daniels, MD.
Better road map
The document is intended to provide a “better road map” for all providers who will see such patients in their practice, said Dr. Daniels, director of the adult congenital heart disease and pulmonary hypertension program at Ohio State University Heart Center and Nationwide Children’s Hospital, Columbus.
“There are not enough adult congenital heart disease cardiologists and programs in the country to care for the almost 1.5 million adults with congenital heart disease in the United States, so we know these patients are cared for by general cardiologists,” Dr. Daniels said in an interview. “Having some guidelines about when to refer to those patients was a huge part of the purpose of these updated guidelines.”
The revamped classification system underlying the new guidelines seeks to better characterize disease severity based on the complexity of its anatomy and physiology, according to Dr. Daniels.
Previous documents, including the original 2008 AHA/ACC guideline (Circulation. 2008 Nov 7;118:e714-833), focused mainly on anatomic classifications to rank severity, he said.
“Traditionally, we’ve based the severity of congenital heart disease based on the complexity of anatomy they were born with, but that goes only so far,” Dr. Daniels said in an interview.
More than just anatomy
Dr. Robert Jaquiss
In the new system, anatomy is classified as simple (I, e.g., isolated small atrial septal defect), moderately complex (II, e.g., coarctation of the aorta), or greatly complex (III, e.g., cyanotic congenital heart defect), while physiologic stages range from A to D, increasing along with the severity of physiologic variables such as New York Heart Association functional class; exercise capacity; aortic enlargement; arrhythmias; renal, hepatic, or pulmonary function; and venal or arterial stenosis.
A normotensive patient with repaired coarctation of the aorta would be classified as IIA if she had normal end-organ function and exercise capacity, whereas a similar patient with an ascending aortic diameter of 4.0 cm would be classified as IIB, and with the addition of moderate aortic stenosis, would be classified as IIIC, according to an example provided in the guidelines.
Congenital heart disease specialist Robert “Jake” Jaquiss, MD, said in an interview that consideration of physiology alongside anatomy is one of the most important features of the new guidelines.
“This is a way of thinking about patients that involves not just their anatomy, but also considering a variety of domains in which there may be physiologic dysfunction that can modify the underlying anatomy,” said Dr. Jaquiss, chief of pediatric and congenital heart surgery at Children’s Medical Center/University of Texas Southwestern Medical Center, Dallas. “I think that is a more clinically relevant way to think about patients and patient evaluation management, and I commend the authors for that focus.”
For example, one patient who has undergone a Fontan procedure may be fully functional, whereas another with nearly identical anatomy may be burdened by arrhythmias, fluid retention, and impaired exercise function. “If we don’t grasp the physiologic difference, we treat the two patients the same way, which is obviously inappropriate,” Dr. Jaquiss said.
Research directions
Much more research needs to be done, according to guideline authors, who list 60 unresolved research questions that represent evidence gaps and future directions for study.
For example, outstanding questions related to tetralogy of Fallot focus on the optimal timing for pulmonary valve replacement, the role of pulmonary valve replacement and ventricular tachycardia ablation in decreasing sudden cardiac death risk, and whether implantable cardioverter-defibrillators reduce mortality.
“These are the kinds of evolutionary sort of understandings and alterations in the intervention, both at the original operation and for assessment of care, and what we think about it and how we think about it in 2018 is quite different than how we thought in 2008, and I dare say it’ll be even more different in 2028,” Dr. Jaquiss said.
The AHA/ACC guideline was developed in association with the American Association for Thoracic Surgery, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons.
Dr. Daniels reported a relevant relationship with Actelion. Guideline coauthors reported relevant relationships in that same category with Actelion, Boehringer Ingelheim, Cormatrix, Edward Lifesciences, Gilead, Medtronic, Novartis, Sorin (LivaNova), St. Jude Medical, and United Therapeutics. No other disclosures were reported.
Two reports in the BMJ regarding new research offer grim tidings about mortality in the United States: One study has suggested the opioid epidemic is driving down life expectancy, and another has found that midlife death rates from multiple causes are on the rise across ethnic groups.
“Death rates are increasing across the U.S. population for dozens of conditions,” according to Steven H. Woolf, MD, MPH, a professor at Virginia Commonwealth University, Richmond, and his associates, who together wrote the second study. “Of particular urgency is recognizing that the unfavorable mortality pattern that began for some groups in the 1990s is now unfolding among Hispanics and non-Hispanic blacks, a development made more consequential by their high baseline mortality rates.”
Dr. Woolf and his coinvestigators tracked midlife mortality (ages 25-64 years) from 1999-2016 across the U.S. population.
They found that all-cause mortality jumped among whites, American Indians, and Alaska Natives over that time. A trend toward decreasing all-cause mortality ended in 2009-2011 among African Americans, Hispanic American, Asian Americans, and Americans of Pacific Islander descent.
“Drug overdoses were the leading cause of increased mortality in midlife in each population, but mortality also increased for alcohol related conditions, suicides, and organ diseases involving multiple body systems,” according to the researchers.
For the life expectancy study, which was published in the BMJ, researchers led by Jessica Y. Ho, PhD, of the University of Southern California, Los Angeles, tracked all-cause and cause-specific mortality in 18 high-income nations. They focused on the years 2014-2016.
Most of the nations saw declines in life expectancy from 2014-2015, mainly caused by older people dying from physical diseases and mental disorders. From 2015-2016, most of these nations saw their life expectancy levels rebound and experienced “robust gains.”
In the United States, however, life expectancy at birth for women fell from 81.47 years in 2014 to 81.35 years in 2015, and rose to 81.40 years in 2016.
For men, life expectancy fell continuously from 76.67 years in 2014 to 76.50 years in 2015 to 76.40 years in 2016.
In 2016, these life expectancies were the lowest of 17 nations examined in the study. (Statistics from the 18th nation in the study, Canada, were not included for 2016).
The United States was an outlier in other ways. For one, deaths among people younger than 65 years were the major contributor to the life expectancy decline.
And causes of death were also different than other countries: “For American women, drug overdose and external causes, and respiratory and cardiovascular diseases, contributed roughly equally to the decline in life expectancy, but for American men, nearly all of the decline was attributable to drug overdose and external causes.”
No funding is reported for the death rates study. The study authors report no relevant disclosures.
The life expectancy study was supported by the Robert Wood Johnson Foundation. Authors variously report support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Aging, and the National Institute of Child Health and Human Development.
Life expectancy in some high-income nations has declined, at least temporarily, in recent years for apparent causes such as flu epidemics and “deaths of despair” because of drug abuse and suicide. While these newer trends may be short lived, they’re worrisome because life expectancy reflects human progress. Meanwhile, some nations and subpopulations continue to lag behind high-income nations despite the benefits of the modern era. Moving forward, we must back up policies with better scientific evidence. Improvements are needed in areas such as timely national mortality data, comparable statistics, and reliable numbers.
Domantas Jasilionis, PhD, is with the Max Planck Institute for Demographic Research, Rostock, Germany
Life expectancy in some high-income nations has declined, at least temporarily, in recent years for apparent causes such as flu epidemics and “deaths of despair” because of drug abuse and suicide. While these newer trends may be short lived, they’re worrisome because life expectancy reflects human progress. Meanwhile, some nations and subpopulations continue to lag behind high-income nations despite the benefits of the modern era. Moving forward, we must back up policies with better scientific evidence. Improvements are needed in areas such as timely national mortality data, comparable statistics, and reliable numbers.
Domantas Jasilionis, PhD, is with the Max Planck Institute for Demographic Research, Rostock, Germany
Body
Life expectancy in some high-income nations has declined, at least temporarily, in recent years for apparent causes such as flu epidemics and “deaths of despair” because of drug abuse and suicide. While these newer trends may be short lived, they’re worrisome because life expectancy reflects human progress. Meanwhile, some nations and subpopulations continue to lag behind high-income nations despite the benefits of the modern era. Moving forward, we must back up policies with better scientific evidence. Improvements are needed in areas such as timely national mortality data, comparable statistics, and reliable numbers.
Domantas Jasilionis, PhD, is with the Max Planck Institute for Demographic Research, Rostock, Germany
Title
Life expectancy fluctuations should sound alarm bells
Life expectancy fluctuations should sound alarm bells
Two reports in the BMJ regarding new research offer grim tidings about mortality in the United States: One study has suggested the opioid epidemic is driving down life expectancy, and another has found that midlife death rates from multiple causes are on the rise across ethnic groups.
“Death rates are increasing across the U.S. population for dozens of conditions,” according to Steven H. Woolf, MD, MPH, a professor at Virginia Commonwealth University, Richmond, and his associates, who together wrote the second study. “Of particular urgency is recognizing that the unfavorable mortality pattern that began for some groups in the 1990s is now unfolding among Hispanics and non-Hispanic blacks, a development made more consequential by their high baseline mortality rates.”
Dr. Woolf and his coinvestigators tracked midlife mortality (ages 25-64 years) from 1999-2016 across the U.S. population.
They found that all-cause mortality jumped among whites, American Indians, and Alaska Natives over that time. A trend toward decreasing all-cause mortality ended in 2009-2011 among African Americans, Hispanic American, Asian Americans, and Americans of Pacific Islander descent.
“Drug overdoses were the leading cause of increased mortality in midlife in each population, but mortality also increased for alcohol related conditions, suicides, and organ diseases involving multiple body systems,” according to the researchers.
For the life expectancy study, which was published in the BMJ, researchers led by Jessica Y. Ho, PhD, of the University of Southern California, Los Angeles, tracked all-cause and cause-specific mortality in 18 high-income nations. They focused on the years 2014-2016.
Most of the nations saw declines in life expectancy from 2014-2015, mainly caused by older people dying from physical diseases and mental disorders. From 2015-2016, most of these nations saw their life expectancy levels rebound and experienced “robust gains.”
In the United States, however, life expectancy at birth for women fell from 81.47 years in 2014 to 81.35 years in 2015, and rose to 81.40 years in 2016.
For men, life expectancy fell continuously from 76.67 years in 2014 to 76.50 years in 2015 to 76.40 years in 2016.
In 2016, these life expectancies were the lowest of 17 nations examined in the study. (Statistics from the 18th nation in the study, Canada, were not included for 2016).
The United States was an outlier in other ways. For one, deaths among people younger than 65 years were the major contributor to the life expectancy decline.
And causes of death were also different than other countries: “For American women, drug overdose and external causes, and respiratory and cardiovascular diseases, contributed roughly equally to the decline in life expectancy, but for American men, nearly all of the decline was attributable to drug overdose and external causes.”
No funding is reported for the death rates study. The study authors report no relevant disclosures.
The life expectancy study was supported by the Robert Wood Johnson Foundation. Authors variously report support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Aging, and the National Institute of Child Health and Human Development.
Two reports in the BMJ regarding new research offer grim tidings about mortality in the United States: One study has suggested the opioid epidemic is driving down life expectancy, and another has found that midlife death rates from multiple causes are on the rise across ethnic groups.
“Death rates are increasing across the U.S. population for dozens of conditions,” according to Steven H. Woolf, MD, MPH, a professor at Virginia Commonwealth University, Richmond, and his associates, who together wrote the second study. “Of particular urgency is recognizing that the unfavorable mortality pattern that began for some groups in the 1990s is now unfolding among Hispanics and non-Hispanic blacks, a development made more consequential by their high baseline mortality rates.”
Dr. Woolf and his coinvestigators tracked midlife mortality (ages 25-64 years) from 1999-2016 across the U.S. population.
They found that all-cause mortality jumped among whites, American Indians, and Alaska Natives over that time. A trend toward decreasing all-cause mortality ended in 2009-2011 among African Americans, Hispanic American, Asian Americans, and Americans of Pacific Islander descent.
“Drug overdoses were the leading cause of increased mortality in midlife in each population, but mortality also increased for alcohol related conditions, suicides, and organ diseases involving multiple body systems,” according to the researchers.
For the life expectancy study, which was published in the BMJ, researchers led by Jessica Y. Ho, PhD, of the University of Southern California, Los Angeles, tracked all-cause and cause-specific mortality in 18 high-income nations. They focused on the years 2014-2016.
Most of the nations saw declines in life expectancy from 2014-2015, mainly caused by older people dying from physical diseases and mental disorders. From 2015-2016, most of these nations saw their life expectancy levels rebound and experienced “robust gains.”
In the United States, however, life expectancy at birth for women fell from 81.47 years in 2014 to 81.35 years in 2015, and rose to 81.40 years in 2016.
For men, life expectancy fell continuously from 76.67 years in 2014 to 76.50 years in 2015 to 76.40 years in 2016.
In 2016, these life expectancies were the lowest of 17 nations examined in the study. (Statistics from the 18th nation in the study, Canada, were not included for 2016).
The United States was an outlier in other ways. For one, deaths among people younger than 65 years were the major contributor to the life expectancy decline.
And causes of death were also different than other countries: “For American women, drug overdose and external causes, and respiratory and cardiovascular diseases, contributed roughly equally to the decline in life expectancy, but for American men, nearly all of the decline was attributable to drug overdose and external causes.”
No funding is reported for the death rates study. The study authors report no relevant disclosures.
The life expectancy study was supported by the Robert Wood Johnson Foundation. Authors variously report support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Aging, and the National Institute of Child Health and Human Development.
Editor’s note: SHM occasionally puts the spotlight on our most active members who are making substantial contributions to hospital medicine. Visit www.hospitalmedicine.org for more information on how you can lend your expertise to help improve the care of hospitalized patients.
This month, The Hospitalist spotlights Ramin Yazdanfar, MD, hospitalist and Harrisburg (Pa.) site medical director at UPMC Pinnacle. Dr. Ramin has been a member of SHM since 2016, has attended two annual conferences as well as Leadership Academy, and together with his team received SHM’s Award of Excellence in Teamwork.
How did you learn about SHM and why did you become a member?
I first heard about SHM during my initial job out of residency. At that time, our medical director encouraged engagement in the field of hospital medicine, and he was quite involved in local meetings and national conferences. I became a member because I felt it would be a good way to connect with other hospitalists who might have been going through similar experiences and struggles, and in the hopes of gaining something I could take back to use in my daily practice.
Dr. Ramin Yazdanfar
Which SHM conferences have you attended and why?
I have attended two national conferences thus far. The first was the 2016 SHM Annual Conference in San Diego, where our hospitalist team won the Excellence in Teamwork and Quality Improvement Awardfor our active bed management program under Mary Ellen Pfeiffer, MD, and William “Tex” Landis, MD, among others. I also attended the 2017 Leadership Academy in Scottsdale, Ariz. As a new site director for a new hospitalist group, I thought it would be a valuable learning experience, with the goal of improving my communication as a leader. I also will be attending the 2018 SHM Leadership Academy in Vancouver. I am excited to reconnect with peers I met last year and to advance my leadership skills further.
What were the main takeaways from Leadership: Mastering Teamwork, and how have you applied them in your practice?
My most vivid and actionable memory of Leadership: Mastering Teamwork was the initial session around the five dysfunctions of a team and how to build a cohesive leadership team. Allowing ourselves to be vulnerable and open creates the foundation of trust, on which we can build everything else, such as handling conflict and creating commitment, accountability, and results. I have tried to use these principles in our own practice, at UPMC Pinnacle Health in Harrisburg, Pa. We have an ever-growing health system with an expanding regional leadership team. We base our foundation on trust in one another, and in our vision, so the rest follows suit.
As a separate takeaway, I really enjoyed sessions with Leonard Marcus, PhD, on SWARM Intelligence and Meta-Leadership. He is a very engaging speaker whom I would recommend to anyone considering the Mastering Teamwork session.
What advice do you have for early-career hospitalists looking to advance their career in hospital medicine?
My advice to early-career hospitalists is to be open to opportunity. There is so much change and development in the field of hospital medicine. While the foundation of our job is in the patient care realm, many of us find a niche that interests us. My advice is pursue it and be open to what follows, without forgetting that we do this for our patients and community.
Ms. Steele is a marketing communications specialist at the Society of Hospital Medicine.
Dr. Ramin Yazdanfar grows into the role of medical director
Dr. Ramin Yazdanfar grows into the role of medical director
Editor’s note: SHM occasionally puts the spotlight on our most active members who are making substantial contributions to hospital medicine. Visit www.hospitalmedicine.org for more information on how you can lend your expertise to help improve the care of hospitalized patients.
This month, The Hospitalist spotlights Ramin Yazdanfar, MD, hospitalist and Harrisburg (Pa.) site medical director at UPMC Pinnacle. Dr. Ramin has been a member of SHM since 2016, has attended two annual conferences as well as Leadership Academy, and together with his team received SHM’s Award of Excellence in Teamwork.
How did you learn about SHM and why did you become a member?
I first heard about SHM during my initial job out of residency. At that time, our medical director encouraged engagement in the field of hospital medicine, and he was quite involved in local meetings and national conferences. I became a member because I felt it would be a good way to connect with other hospitalists who might have been going through similar experiences and struggles, and in the hopes of gaining something I could take back to use in my daily practice.
Dr. Ramin Yazdanfar
Which SHM conferences have you attended and why?
I have attended two national conferences thus far. The first was the 2016 SHM Annual Conference in San Diego, where our hospitalist team won the Excellence in Teamwork and Quality Improvement Awardfor our active bed management program under Mary Ellen Pfeiffer, MD, and William “Tex” Landis, MD, among others. I also attended the 2017 Leadership Academy in Scottsdale, Ariz. As a new site director for a new hospitalist group, I thought it would be a valuable learning experience, with the goal of improving my communication as a leader. I also will be attending the 2018 SHM Leadership Academy in Vancouver. I am excited to reconnect with peers I met last year and to advance my leadership skills further.
What were the main takeaways from Leadership: Mastering Teamwork, and how have you applied them in your practice?
My most vivid and actionable memory of Leadership: Mastering Teamwork was the initial session around the five dysfunctions of a team and how to build a cohesive leadership team. Allowing ourselves to be vulnerable and open creates the foundation of trust, on which we can build everything else, such as handling conflict and creating commitment, accountability, and results. I have tried to use these principles in our own practice, at UPMC Pinnacle Health in Harrisburg, Pa. We have an ever-growing health system with an expanding regional leadership team. We base our foundation on trust in one another, and in our vision, so the rest follows suit.
As a separate takeaway, I really enjoyed sessions with Leonard Marcus, PhD, on SWARM Intelligence and Meta-Leadership. He is a very engaging speaker whom I would recommend to anyone considering the Mastering Teamwork session.
What advice do you have for early-career hospitalists looking to advance their career in hospital medicine?
My advice to early-career hospitalists is to be open to opportunity. There is so much change and development in the field of hospital medicine. While the foundation of our job is in the patient care realm, many of us find a niche that interests us. My advice is pursue it and be open to what follows, without forgetting that we do this for our patients and community.
Ms. Steele is a marketing communications specialist at the Society of Hospital Medicine.
Editor’s note: SHM occasionally puts the spotlight on our most active members who are making substantial contributions to hospital medicine. Visit www.hospitalmedicine.org for more information on how you can lend your expertise to help improve the care of hospitalized patients.
This month, The Hospitalist spotlights Ramin Yazdanfar, MD, hospitalist and Harrisburg (Pa.) site medical director at UPMC Pinnacle. Dr. Ramin has been a member of SHM since 2016, has attended two annual conferences as well as Leadership Academy, and together with his team received SHM’s Award of Excellence in Teamwork.
How did you learn about SHM and why did you become a member?
I first heard about SHM during my initial job out of residency. At that time, our medical director encouraged engagement in the field of hospital medicine, and he was quite involved in local meetings and national conferences. I became a member because I felt it would be a good way to connect with other hospitalists who might have been going through similar experiences and struggles, and in the hopes of gaining something I could take back to use in my daily practice.
Dr. Ramin Yazdanfar
Which SHM conferences have you attended and why?
I have attended two national conferences thus far. The first was the 2016 SHM Annual Conference in San Diego, where our hospitalist team won the Excellence in Teamwork and Quality Improvement Awardfor our active bed management program under Mary Ellen Pfeiffer, MD, and William “Tex” Landis, MD, among others. I also attended the 2017 Leadership Academy in Scottsdale, Ariz. As a new site director for a new hospitalist group, I thought it would be a valuable learning experience, with the goal of improving my communication as a leader. I also will be attending the 2018 SHM Leadership Academy in Vancouver. I am excited to reconnect with peers I met last year and to advance my leadership skills further.
What were the main takeaways from Leadership: Mastering Teamwork, and how have you applied them in your practice?
My most vivid and actionable memory of Leadership: Mastering Teamwork was the initial session around the five dysfunctions of a team and how to build a cohesive leadership team. Allowing ourselves to be vulnerable and open creates the foundation of trust, on which we can build everything else, such as handling conflict and creating commitment, accountability, and results. I have tried to use these principles in our own practice, at UPMC Pinnacle Health in Harrisburg, Pa. We have an ever-growing health system with an expanding regional leadership team. We base our foundation on trust in one another, and in our vision, so the rest follows suit.
As a separate takeaway, I really enjoyed sessions with Leonard Marcus, PhD, on SWARM Intelligence and Meta-Leadership. He is a very engaging speaker whom I would recommend to anyone considering the Mastering Teamwork session.
What advice do you have for early-career hospitalists looking to advance their career in hospital medicine?
My advice to early-career hospitalists is to be open to opportunity. There is so much change and development in the field of hospital medicine. While the foundation of our job is in the patient care realm, many of us find a niche that interests us. My advice is pursue it and be open to what follows, without forgetting that we do this for our patients and community.
Ms. Steele is a marketing communications specialist at the Society of Hospital Medicine.
ATLANTA – Childhood obesity increases the risk of severe dental infections, according to a review presented at the Pediatric Hospital Medicine meeting.
M. Alexander Otto/MDedge News
Dr. Michelle Edmunds
Among 171 children admitted to Rady Children’s Hospital, San Diego, for infected cavities, obese children were almost four times more likely than others to require surgery, and five times more likely to have a tooth pulled.
The average cost for obese children was $13,000/day, versus $10,000/day for nonobese children, probably because of the greater need for surgery. Average length of stay was the same between the two groups, just under 2 days. The findings were statistically significant.
Obesity turns out to be “an important risk factor for invasive interventions for pediatric dental infections,” concluded study leader Michelle Edmunds, MD, a pediatric hospital medicine fellow at Rady.
Childhood obesity has been associated with cavities before, but it’s new information that it increases the severity of dental infections. The finding is something for pediatricians to be aware of and to use to encourage regular dental care. “Even if you are obese, if you are getting routine care, you should be able to have cavities fixed” before they get out of hand. “Unfortunately, a lot of the kids we see don’t get routine care,” Dr. Edmunds said.
The investigators couldn’t assess the role of diet because there wasn’t enough information about it in the medical records. It certainly must play a role, because soda and other junk foods increase the risk of both obesity and cavities.
Other factors also are likely at play. Obesity might affect the oral flora, and perhaps the balance of pathogens. It also seems to reduce healing and infection-fighting ability, so “there might be some immunocompromise that’s playing a role here,” Dr. Edmunds said.
The team compared 25 children up to 18 years old who were at or above the 95th percentile for body mass index – the study definition of obesity – to 146 children who were below that mark. They had all been admitted through the ED between July 2011 and June 2016 with dental abscesses, facial cellulitis, or other dental-associated infections. Eighty percent of the children were on Medicaid, which has, itself, been associated with less frequent visits to the dentist.
About 50% of the children were discharged home without a dental procedure. Among the rest, a quarter had incision and drainage, and a quarter had tooth extractions. Overall 72% (18) of obese children had surgery, usually extractions, versus 43% (62) of nonobese children.
There’s perhaps around 200,000 pediatric ED visits a year in the United States for dental problems. “We’ve had toddlers and kids who have never seen a dentist before; all of their teeth were rotten and had to be pulled out, every single tooth,” Dr. Edmunds said at the meeting sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
The mean age in the study was about 8 years. Nearly 60% of the subjects were boys, and a bit over 60% Hispanic. There were no statistical difference in demographics, prior antibiotic use, or cavity history between obese and nonobese children. Obese children were more likely to be on Medicaid, but not significantly so.
There was no industry funding for the work, and Dr. Edmunds didn’t have any disclosures.
ATLANTA – Childhood obesity increases the risk of severe dental infections, according to a review presented at the Pediatric Hospital Medicine meeting.
M. Alexander Otto/MDedge News
Dr. Michelle Edmunds
Among 171 children admitted to Rady Children’s Hospital, San Diego, for infected cavities, obese children were almost four times more likely than others to require surgery, and five times more likely to have a tooth pulled.
The average cost for obese children was $13,000/day, versus $10,000/day for nonobese children, probably because of the greater need for surgery. Average length of stay was the same between the two groups, just under 2 days. The findings were statistically significant.
Obesity turns out to be “an important risk factor for invasive interventions for pediatric dental infections,” concluded study leader Michelle Edmunds, MD, a pediatric hospital medicine fellow at Rady.
Childhood obesity has been associated with cavities before, but it’s new information that it increases the severity of dental infections. The finding is something for pediatricians to be aware of and to use to encourage regular dental care. “Even if you are obese, if you are getting routine care, you should be able to have cavities fixed” before they get out of hand. “Unfortunately, a lot of the kids we see don’t get routine care,” Dr. Edmunds said.
The investigators couldn’t assess the role of diet because there wasn’t enough information about it in the medical records. It certainly must play a role, because soda and other junk foods increase the risk of both obesity and cavities.
Other factors also are likely at play. Obesity might affect the oral flora, and perhaps the balance of pathogens. It also seems to reduce healing and infection-fighting ability, so “there might be some immunocompromise that’s playing a role here,” Dr. Edmunds said.
The team compared 25 children up to 18 years old who were at or above the 95th percentile for body mass index – the study definition of obesity – to 146 children who were below that mark. They had all been admitted through the ED between July 2011 and June 2016 with dental abscesses, facial cellulitis, or other dental-associated infections. Eighty percent of the children were on Medicaid, which has, itself, been associated with less frequent visits to the dentist.
About 50% of the children were discharged home without a dental procedure. Among the rest, a quarter had incision and drainage, and a quarter had tooth extractions. Overall 72% (18) of obese children had surgery, usually extractions, versus 43% (62) of nonobese children.
There’s perhaps around 200,000 pediatric ED visits a year in the United States for dental problems. “We’ve had toddlers and kids who have never seen a dentist before; all of their teeth were rotten and had to be pulled out, every single tooth,” Dr. Edmunds said at the meeting sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
The mean age in the study was about 8 years. Nearly 60% of the subjects were boys, and a bit over 60% Hispanic. There were no statistical difference in demographics, prior antibiotic use, or cavity history between obese and nonobese children. Obese children were more likely to be on Medicaid, but not significantly so.
There was no industry funding for the work, and Dr. Edmunds didn’t have any disclosures.
ATLANTA – Childhood obesity increases the risk of severe dental infections, according to a review presented at the Pediatric Hospital Medicine meeting.
M. Alexander Otto/MDedge News
Dr. Michelle Edmunds
Among 171 children admitted to Rady Children’s Hospital, San Diego, for infected cavities, obese children were almost four times more likely than others to require surgery, and five times more likely to have a tooth pulled.
The average cost for obese children was $13,000/day, versus $10,000/day for nonobese children, probably because of the greater need for surgery. Average length of stay was the same between the two groups, just under 2 days. The findings were statistically significant.
Obesity turns out to be “an important risk factor for invasive interventions for pediatric dental infections,” concluded study leader Michelle Edmunds, MD, a pediatric hospital medicine fellow at Rady.
Childhood obesity has been associated with cavities before, but it’s new information that it increases the severity of dental infections. The finding is something for pediatricians to be aware of and to use to encourage regular dental care. “Even if you are obese, if you are getting routine care, you should be able to have cavities fixed” before they get out of hand. “Unfortunately, a lot of the kids we see don’t get routine care,” Dr. Edmunds said.
The investigators couldn’t assess the role of diet because there wasn’t enough information about it in the medical records. It certainly must play a role, because soda and other junk foods increase the risk of both obesity and cavities.
Other factors also are likely at play. Obesity might affect the oral flora, and perhaps the balance of pathogens. It also seems to reduce healing and infection-fighting ability, so “there might be some immunocompromise that’s playing a role here,” Dr. Edmunds said.
The team compared 25 children up to 18 years old who were at or above the 95th percentile for body mass index – the study definition of obesity – to 146 children who were below that mark. They had all been admitted through the ED between July 2011 and June 2016 with dental abscesses, facial cellulitis, or other dental-associated infections. Eighty percent of the children were on Medicaid, which has, itself, been associated with less frequent visits to the dentist.
About 50% of the children were discharged home without a dental procedure. Among the rest, a quarter had incision and drainage, and a quarter had tooth extractions. Overall 72% (18) of obese children had surgery, usually extractions, versus 43% (62) of nonobese children.
There’s perhaps around 200,000 pediatric ED visits a year in the United States for dental problems. “We’ve had toddlers and kids who have never seen a dentist before; all of their teeth were rotten and had to be pulled out, every single tooth,” Dr. Edmunds said at the meeting sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
The mean age in the study was about 8 years. Nearly 60% of the subjects were boys, and a bit over 60% Hispanic. There were no statistical difference in demographics, prior antibiotic use, or cavity history between obese and nonobese children. Obese children were more likely to be on Medicaid, but not significantly so.
There was no industry funding for the work, and Dr. Edmunds didn’t have any disclosures.
At HM18 in Orlando, the Society of Hospital Medicine’s CEO Larry Wellikson, MD, MHM, challenged our thinking by sharing a slide with the attendees that effectively and accurately captured the current environment. Today’s largest retailer, Amazon, owns no inventory; today’s largest taxi company, Uber, owns no cars; and today’s largest provider of accommodations, Airbnb, owns no real estate.
Dr. Nasim Afsar
This powerful statement captures a transformative way of thinking, functioning, and thriving that has rapidly evolved over the past decade in the United States. And yet, health care fundamentally functions very similarly to how it did 10 years ago. I think we can all acknowledge that this is not a sustainable way to advance.
With megamergers dominating the health care landscape in 2017, the industry has become consolidated to weather the economic challenges ahead. Hospital contribution margins have been declining, forcing systems to critically evaluate how they deliver value-based care. In addition, the joining of forces between Amazon, Berkshire Hathaway, and JPMorgan further illustrates the pressures employers are experiencing with costs in the market.
What can we in hospital medicine do to proactively respond to, and shape, the evolving U.S. health care landscape?
If I had a crystal ball and could predict the future, I would say hospital medicine will be functioning very differently in 10 years to respond to today’s challenges.
The acute becomes more acute
When I started working as a hospitalist more than a decade ago, in a tertiary/quaternary academic medical center, the patients were severely ill with multiple comorbidities. Yet, in the span of 10 years, we care for many of those diagnoses in the ambulatory setting.
Reflecting on the severity of illness in my patients when I was recently on the medicine wards, I have to admit the patients now have a significantly higher burden of disease with twice as many comorbidities. As medicine has advanced and we have become more skilled at caring for patients, the acuity of patients has exponentially increased.
As this trend continues, hospitalists will need greater training in critical care components of hospital-based care. While we may comanage some of these patients with critical care, our skill sets need to intensify to address the growing needs of our patient population.
“Bread and butter” moves to lower-acuity settings and home
As our ability to manage patients advances, and the existing inpatient beds are occupied by sicker patients, the common hospital medicine diagnoses will move to skilled nursing facilities, long-term acute care settings, and ultimately home.
Delivery systems will have to create robust networks of home health and home services to actively manage patients with accountability. This provides an opportunity for hospitalists to manage acutely ill patients in less intense settings of care, and the emergence of telehealth will help facilitate this.
In a Feb. 6, 2018 article in JAMA – “Is it Time for a New Medical Specialty?” – Dr. Michael Nochomovitz and Dr. Rahul Sharma argue that, with rapid advances in technology and the establishment of telemedicine, a new specialty – the virtualist – will need to formally emerge (JAMA. 2018;319[5]:437-8. While telehealth has been successfully utilized for the delivery of acute care in remote regions, as well as the delivery of basic services for common diagnoses, it is not robustly and broadly integrated into all aspects of care delivery.
As we move from the hospital setting to less acute settings of care and home-based care, providers need specific training and skill sets in how to manage and deliver care without the patient in front of them. This includes knowledge of how to remotely manage acutely ill patients who are stable and do not require a hospitalization, as well as effectively managing day-to-day issues that arise with patients.
Translating our role in population health management
I have written previously about the expanding role of hospitalists in population health management. In addition to the transitions of care work that we are all involved in, hospitalists must actively partner with our ambulatory colleagues to identify and communicate key barriers to care.
Hospitalists are already instrumental in a number of institutions providing inpatient and ambulatory care for a select group of patients with high utilization. We have the ability to care for high utilizers and partner with ambulatory providers who can ensure we care for patients with high burdens of disease in the most appropriate settings of care. In the fall of 2018, SHM is convening a group of experts in population health to discuss the role of hospitalists in this area.
While I don’t have a crystal ball to predict the future, sadly, SHM is committed to proactively defining and advancing our specialty. I am confident that together we can find the solutions that will successfully advance us towards the future.
Dr. Afsar is president of the Society of Hospital Medicine, and chief ambulatory officer and chief medical officer for accountable care organizations at UC Irvine Health.
At HM18 in Orlando, the Society of Hospital Medicine’s CEO Larry Wellikson, MD, MHM, challenged our thinking by sharing a slide with the attendees that effectively and accurately captured the current environment. Today’s largest retailer, Amazon, owns no inventory; today’s largest taxi company, Uber, owns no cars; and today’s largest provider of accommodations, Airbnb, owns no real estate.
Dr. Nasim Afsar
This powerful statement captures a transformative way of thinking, functioning, and thriving that has rapidly evolved over the past decade in the United States. And yet, health care fundamentally functions very similarly to how it did 10 years ago. I think we can all acknowledge that this is not a sustainable way to advance.
With megamergers dominating the health care landscape in 2017, the industry has become consolidated to weather the economic challenges ahead. Hospital contribution margins have been declining, forcing systems to critically evaluate how they deliver value-based care. In addition, the joining of forces between Amazon, Berkshire Hathaway, and JPMorgan further illustrates the pressures employers are experiencing with costs in the market.
What can we in hospital medicine do to proactively respond to, and shape, the evolving U.S. health care landscape?
If I had a crystal ball and could predict the future, I would say hospital medicine will be functioning very differently in 10 years to respond to today’s challenges.
The acute becomes more acute
When I started working as a hospitalist more than a decade ago, in a tertiary/quaternary academic medical center, the patients were severely ill with multiple comorbidities. Yet, in the span of 10 years, we care for many of those diagnoses in the ambulatory setting.
Reflecting on the severity of illness in my patients when I was recently on the medicine wards, I have to admit the patients now have a significantly higher burden of disease with twice as many comorbidities. As medicine has advanced and we have become more skilled at caring for patients, the acuity of patients has exponentially increased.
As this trend continues, hospitalists will need greater training in critical care components of hospital-based care. While we may comanage some of these patients with critical care, our skill sets need to intensify to address the growing needs of our patient population.
“Bread and butter” moves to lower-acuity settings and home
As our ability to manage patients advances, and the existing inpatient beds are occupied by sicker patients, the common hospital medicine diagnoses will move to skilled nursing facilities, long-term acute care settings, and ultimately home.
Delivery systems will have to create robust networks of home health and home services to actively manage patients with accountability. This provides an opportunity for hospitalists to manage acutely ill patients in less intense settings of care, and the emergence of telehealth will help facilitate this.
In a Feb. 6, 2018 article in JAMA – “Is it Time for a New Medical Specialty?” – Dr. Michael Nochomovitz and Dr. Rahul Sharma argue that, with rapid advances in technology and the establishment of telemedicine, a new specialty – the virtualist – will need to formally emerge (JAMA. 2018;319[5]:437-8. While telehealth has been successfully utilized for the delivery of acute care in remote regions, as well as the delivery of basic services for common diagnoses, it is not robustly and broadly integrated into all aspects of care delivery.
As we move from the hospital setting to less acute settings of care and home-based care, providers need specific training and skill sets in how to manage and deliver care without the patient in front of them. This includes knowledge of how to remotely manage acutely ill patients who are stable and do not require a hospitalization, as well as effectively managing day-to-day issues that arise with patients.
Translating our role in population health management
I have written previously about the expanding role of hospitalists in population health management. In addition to the transitions of care work that we are all involved in, hospitalists must actively partner with our ambulatory colleagues to identify and communicate key barriers to care.
Hospitalists are already instrumental in a number of institutions providing inpatient and ambulatory care for a select group of patients with high utilization. We have the ability to care for high utilizers and partner with ambulatory providers who can ensure we care for patients with high burdens of disease in the most appropriate settings of care. In the fall of 2018, SHM is convening a group of experts in population health to discuss the role of hospitalists in this area.
While I don’t have a crystal ball to predict the future, sadly, SHM is committed to proactively defining and advancing our specialty. I am confident that together we can find the solutions that will successfully advance us towards the future.
Dr. Afsar is president of the Society of Hospital Medicine, and chief ambulatory officer and chief medical officer for accountable care organizations at UC Irvine Health.
At HM18 in Orlando, the Society of Hospital Medicine’s CEO Larry Wellikson, MD, MHM, challenged our thinking by sharing a slide with the attendees that effectively and accurately captured the current environment. Today’s largest retailer, Amazon, owns no inventory; today’s largest taxi company, Uber, owns no cars; and today’s largest provider of accommodations, Airbnb, owns no real estate.
Dr. Nasim Afsar
This powerful statement captures a transformative way of thinking, functioning, and thriving that has rapidly evolved over the past decade in the United States. And yet, health care fundamentally functions very similarly to how it did 10 years ago. I think we can all acknowledge that this is not a sustainable way to advance.
With megamergers dominating the health care landscape in 2017, the industry has become consolidated to weather the economic challenges ahead. Hospital contribution margins have been declining, forcing systems to critically evaluate how they deliver value-based care. In addition, the joining of forces between Amazon, Berkshire Hathaway, and JPMorgan further illustrates the pressures employers are experiencing with costs in the market.
What can we in hospital medicine do to proactively respond to, and shape, the evolving U.S. health care landscape?
If I had a crystal ball and could predict the future, I would say hospital medicine will be functioning very differently in 10 years to respond to today’s challenges.
The acute becomes more acute
When I started working as a hospitalist more than a decade ago, in a tertiary/quaternary academic medical center, the patients were severely ill with multiple comorbidities. Yet, in the span of 10 years, we care for many of those diagnoses in the ambulatory setting.
Reflecting on the severity of illness in my patients when I was recently on the medicine wards, I have to admit the patients now have a significantly higher burden of disease with twice as many comorbidities. As medicine has advanced and we have become more skilled at caring for patients, the acuity of patients has exponentially increased.
As this trend continues, hospitalists will need greater training in critical care components of hospital-based care. While we may comanage some of these patients with critical care, our skill sets need to intensify to address the growing needs of our patient population.
“Bread and butter” moves to lower-acuity settings and home
As our ability to manage patients advances, and the existing inpatient beds are occupied by sicker patients, the common hospital medicine diagnoses will move to skilled nursing facilities, long-term acute care settings, and ultimately home.
Delivery systems will have to create robust networks of home health and home services to actively manage patients with accountability. This provides an opportunity for hospitalists to manage acutely ill patients in less intense settings of care, and the emergence of telehealth will help facilitate this.
In a Feb. 6, 2018 article in JAMA – “Is it Time for a New Medical Specialty?” – Dr. Michael Nochomovitz and Dr. Rahul Sharma argue that, with rapid advances in technology and the establishment of telemedicine, a new specialty – the virtualist – will need to formally emerge (JAMA. 2018;319[5]:437-8. While telehealth has been successfully utilized for the delivery of acute care in remote regions, as well as the delivery of basic services for common diagnoses, it is not robustly and broadly integrated into all aspects of care delivery.
As we move from the hospital setting to less acute settings of care and home-based care, providers need specific training and skill sets in how to manage and deliver care without the patient in front of them. This includes knowledge of how to remotely manage acutely ill patients who are stable and do not require a hospitalization, as well as effectively managing day-to-day issues that arise with patients.
Translating our role in population health management
I have written previously about the expanding role of hospitalists in population health management. In addition to the transitions of care work that we are all involved in, hospitalists must actively partner with our ambulatory colleagues to identify and communicate key barriers to care.
Hospitalists are already instrumental in a number of institutions providing inpatient and ambulatory care for a select group of patients with high utilization. We have the ability to care for high utilizers and partner with ambulatory providers who can ensure we care for patients with high burdens of disease in the most appropriate settings of care. In the fall of 2018, SHM is convening a group of experts in population health to discuss the role of hospitalists in this area.
While I don’t have a crystal ball to predict the future, sadly, SHM is committed to proactively defining and advancing our specialty. I am confident that together we can find the solutions that will successfully advance us towards the future.
Dr. Afsar is president of the Society of Hospital Medicine, and chief ambulatory officer and chief medical officer for accountable care organizations at UC Irvine Health.