User login
Generic drugs: The benefits and risks of making the switch
• Do not authorize the pharmacy to switch patients from a brand-name antiepileptic drug to a generic without your approval. C
• Use caution when switching a patient to a generic modified-release formulation, which may not have the same pharmacokinetic profile as its brand-name counterpart. C
• Consult the FDA’s Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations, available at http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm for details on generic substitution. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Each year, Americans save an estimated $8 billion to $10 billion at retail pharmacies by purchasing generic drugs rather than brand-name medications, the US Food and Drug Administration (FDA) reports.1 The lower cost, of course, is the key advantage of generics. But the very reason for the cost savings—the fact that generic drugs do not have to undergo the large, expensive clinical trials that are required for approval of brand-name medications—gives rise to questions about the quality and safety of generics.
Are these concerns justified? Under what circumstances is it safe to prescribe generics, or to substitute a generic for a brand-name drug? Are brand-name drugs always better? To answer these questions, we conducted a thorough evidence review, which included numerous randomized controlled trials (RCTs) and case reports, as well as a single meta-analysis that assessed the benefits and risks of generics.
Generics: On the positive side
Safety and efficacy. Our literature search yielded little evidence that generic drugs are less safe or less effective than their brand-name equivalents. The meta-analysis, for example,2 included 47 studies (38 of 47 were RCTs) covering 9 subclasses of cardiovascular medications. In trials involving beta-blockers, diuretics, calcium channel blockers, antiplatelet agents, statins, angiotensin-converting enzyme inhibitors, and alpha-blockers, no evidence of superiority of brand-name drugs vs generics was found.2
Cost. Generic drugs typically cost 30% to 60% less than their brand-name counterparts,3 and widespread use of generics has the potential to reduce the price of other brand-name drugs by creating more competition.
Another plus: Patients taking generic drugs appear to be more willing to continue therapy than those taking brand-name medications.4 Lower co-pays are a key factor. In 1 recent study of patients with hypercholesterolemia or diabetes, those taking generics had greater adherence compared with patients receiving brand-name drugs.5
Quality. It is important to note that many generic medications are produced under the license of the manufacturer of the original brand-name product, with the lower-cost equivalent often introduced after the drug’s patent has expired. Even when different manufacturers produce the branded product and the generic, strict standards exist to guarantee the quality of generic drugs.
The journey to market—the similarities, the differences
Both brand-name and generic medications undergo similar new drug application (NDA) procedures. The manufacturers of both are required to submit detailed evidence of the chemistry, manufacturing, controls, labeling, and testing processes. From there, brand-name and generic products take divergent paths to market.
New nongeneric drugs must undergo rigorous animal and human studies, including large RCTs comparing the efficacy of the new product with that of a placebo and carefully tracking side effects. Bioavailability testing is required, as well. For generic drugs, the process is known as an abbreviated new drug application (ANDA), and bioequivalence studies are sufficient.1,6
The bioequivalence studies required for a new generic are based on pharmacokinetic parameters, most notably, the area under the plasma concentration curve (AUC)—a measure of overall drug exposure—and the maximal plasma concentration (Cmax). If AUC and Cmax are within an acceptance range (0.80–1.25 of the brand-name product parameters), the therapeutic equivalence of a generic drug is substantiated.7,8
Concerns about testing, formulation
Opponents of widespread use of generics point out that they are tested on only a few young, healthy individuals, compared with the large numbers of patients who participate in clinical trials of the original drug.
Bioequivalence
According to guidelines from the World Health Organization (WHO), 18 to 24 healthy adult volunteers are considered sufficient for a bioequivalence study.9 The number of participants may be greater, however, if absorption or clearance of the drug is highly variable. What’s more, the people who volunteer for generic drug studies cannot smoke or take concurrent medication. To exclude the possibility that food coadministration affects the generic medication being studied, the FDA further recommends bioequivalence testing of oral formulations on volunteers eating standardized meals.8 These criteria help minimize the magnitude of intersubject variability and reduce the possibility of bias—which could be caused by the disease process, concurrent conditions, or medication interaction, rather than by formulation differences.8
To further minimize the effects of nondrug-related variation, bioequivalence studies typically use a crossover design: Half the subjects receive the test drug first, followed by the brand-name product, with a washout period in between. The other half receive the drugs in reverse order.10 (The study format is altered, as needed, for extended-release products, topical agents, and drugs that are not absorbed systemically. A generic version of cholestyramine, for example, which acts by sequestering bile salts within the intestine, would be approved on the basis of in vitro studies that quantify the binding of the bile salts.10)
But does this testing mimic the real world? While possible confounding factors are controlled for in bioequivalence studies of generics, critics point out that this is not the case in the real world. Thus, they worry that when generics are taken by patients with actual illnesses, concurrent use of other medications, medical conditions, and the like may result in differences in treatment that did not occur in the highly controlled environment in which the equivalency studies were conducted.11
Differences in formulation
Another concern centers on formulation differences, which have the potential to affect patients taking generic drugs. A generic copy of a brand-name drug must contain the same active ingredient, in the identical quantity, as the branded product—in the same dose formulation and route of administration. It must also meet standards for strength, purity, quality, and identity.11
However, the inert ingredients in the generic version do not have to be the same as those in the brand-name drug (although the ratio of inert to active compound must be similar).12 Because drugs tested in bioequivalence studies are administered in single doses, many experts wonder whether the inert compounds used in the generics may affect the distribution, metabolism, or absorption of a drug when it is administered in multiple doses, or whether the serum concentration of the generic drug may be elevated when it is taken for long periods.
Proceed with caution in these situations
For most patients taking most medications, generic drugs pose no problems, and provide an opportunity to obtain the same therapeutic benefit at a considerably lower cost. However, making the switch with certain classes of drugs, and with drugs that have a narrow therapeutic range, poses potential problems and must be done with caution—if at all.
Antiepileptic drugs. The FDA indicates that many people who are on antiseizure medications re-experience seizures despite continued treatment,1 and that switching to a generic does not increase the risk of treatment failure.1,13 Nonetheless, there are numerous reports of differences between generic and brand-name antiseizure medications (and small studies indicating improper seizure control after switching patients from a brand-name to a generic antiepileptic drug).14
For example:
- Researchers compared the pharmacokinetic parameters of Tegretol with 3 generic formulations of carbamazepine, and found that 1 of the 3 was not bioequivalent.15
- In a crossover study of 18 healthy volunteers, 3 generic formulations of carbamazepine were all within the acceptable bioequivalence range, but were absorbed more rapidly than the brand-name drug.16
- Differences in the bioavailability of brand-name and generic products have also been reported with phenytoin, primidone, and valproic acid, but the differences were not statistically significant.17
The American Academy of Neurology has issued a set of recommendations concerning the use of generic antiepileptic drugs (TABLE).18
Narrow therapeutic ratio. The potential for complications increases in drugs with a narrow therapeutic ratio, defined by the FDA as <2-fold difference between the median lethal dose and the median effective dose, or between the minimum toxic concentration and minimum effective concentration in the blood.19 The safe and effective use of such drugs—carbamazepine, divalproex, lithium, phenytoin, and warfarin, to name a few—requires careful dosage titration and patient monitoring.
Water solubility and nonlinear pharmacokinetics may present problems in drugs with a narrow therapeutic ratio, especially phenytoin.2 The drug’s serum concentration is allowed to range from 8 to 20 mg/L. A concentration above this range increases the risk for acute cerebellar syndrome, delirium, and coma; a concentration below the range may cause seizures.12
Warfarin is also of particular concern, as there is always the possibility that a switch from Coumadin to a generic equivalent could result in under- or overcoagulation. However, studies have shown that the use of generic warfarin in patients previously receiving Coumadin did not affect the international normalized ratio more than continued use of the brand-name anticoagulant.20,21
Psychotropic agents. There has been a number of case reports of problems occurring following a switch from a brand-name antidepressant to a generic—or from 1 generic antidepressant to another. (See “Did a switch to a generic antidepressant cause relapse?” J Fam Pract. 2008;58:109-114.) In fact, the FDA cites some psychotropic drugs for which generic formulations may not be interchangeable—including amitriptyline/ perphenazine and venlafaxine—and others for which generic formulations may not be bioequivalent at all doses.22
Thyroid medication. There are also concerns about levothyroxine (LT4) administration, and major medical societies debate the use of generic substitution. According to a recent survey from the American Association of Clinical Endocrinologists, the American Thyroid Association, and The Endocrine Society, clinical use of generic LT4 continues to be associated with adverse outcomes.23 Most of the adverse events (89%) reported by survey respondents were associated with a change, either from a brand-name drug to a generic or from 1 particular generic LT4 to another.
TABLE
Generic substitution of antiepileptic agents: Where the American Academy of Neurology stands18
| The AAN opposes: |
|
| The AAN believes: |
|
| The AAN supports: |
|
| The AAN recognizes: |
|
Modified-release formulations may also pose a problem
Problems may also occur with generics in modified-release formulations, which may not have the same pharmacokinetic profiles as their brand-named counterparts. The British National Formulary has advised that prescriptions for modified-release diltiazem hydrochloride, nifedipine, and theophylline be filled with the brand-name drug only.24,25 Morever, a recent study concluded that 2 modified-release products of methylphenidate and nifedipine had concentration profiles that strongly diverged during the period of absorption, although the formulations met the regulatory criteria for bioequivalence. 26
The type of salt used to form a compound is also important. Salt-joining makes a hydrophobic molecule hydrophilic; the result, especially in psychoactive drugs, is improved kinetics, absorption, or physico-chemical properties (eg, stability, hygroscopicity, fluidity).27 This may be the reason for differences identified between generic and brand-name amitriptyline, nortriptyline, desipramine, and trimipramine.28 To avoid problems, physicians should prescribe generics containing the same salt as their brand-name counterparts.
When in doubt …
Brand-name drugs are, and always will be, the best proven therapy, because of the number and extent of clinical trials they go through. In most cases, however, there is no evidence-based reason to avoid generic substitution for patients who cannot afford the brand-name drug. When in doubt, consult the FDA’s Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations, available at http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm, before making a switch.
CORRESPONDENCE Pawel Lewek, MD, The First Department of Family Medicine, Medical University of Lodz,60 Narutowicza Street, 90-136 Lodz, Poland; [email protected]
1. US Food and Drug Administration. What are generic drugs? Available at: http://www.fda.gov/Drugs/ResourcesForYou/Consumers/BuyingUsingMedicineSafely/UnderstandingGenericDrugs/default.htm. Accessed October 19, 2010.
2. Kesselheim AS, et al. Clinical equivalence of gneric and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis. JAMA. 2008;300:2514-2526.
3. Zarowitz BJ. The generic imperative. Geriatr Nurs. 2008;29:223-226.
4. Shrank WH, Hoang T, Ettner SL, et al. The implications of choice: prescribing generic or preferred pharmaceuticals improves medication adherence for chronic conditions. Arch Intern Med. 2006;133:332-337.
5. Briesacher BA, Andrade SE, Fouayzi H, et al. Medication adherence and use of generic drug therapies. Am J Manag Care. 2009;15:450-461.
6. Peters JR, Hixon DR, Conner DP, et al. Generic drugs—safe, effective, and affordable. Dermatol Ther. 2009;22:229-240.
7. European Agency for the Evaluation of Medicinal Products. Note for guidance on the investigation of bioavailability and bioequivalence. London, England: EMEA; 2000;CPMP/EWP/ QWP/1401/98.
8. US Food and Drug Administration, Center for Research .Guidance for industry: bioavailability and bioequivalence studies for orally administered drug products—general considerations, 2002. Available at: http://www.fda.gov/cder/guidance/4964dft.pdf. Accessed January 11, 2009.
9. World Health Organization. Multi-source pharmaceutical products: WHO guideline on registration requirements to establish interchangeability. WHO Technical Support Series. Geneva, Switzerland: WHO;1996:TRS 863.
10. Meyer MC. Generic drug product equivalence: current status. Am J Manag Care. 1998;4:1183-1189.
11. Meredith P. Bioequivalence and other unresolved issues in generic drug substitution. Clin Ther. 2003;25:2875-2890.
12. Nakai K, Fujita M, Ogata H. International harmonization of bioequivalence studies and issues shared in common. Yakugaka Zasshi. 2000;120:1193-1200.
13. Randomized study of antiepileptic drug withdrawal in patients in remission Medical Research Council Antiepileptic Drug Withdrawal Study Group. Lancet. 1991;337:1175-1180.
14. Crawford P, Feely M, Guberman A, et al. Are there potential problems with generic substitution of antiepileptic drugs? A review of issues. Seizure. 2006;15:165-176.
15. Silpakit O, Amornpichetkoon M, Kaojarern S. Comparative study of bioavailability and clinical efficacy of carbamazepine in epileptic patients. Ann Pharmacother. 1997;31:548-552.
16. Wangemann M, Retzow A, Evers G, et al. Bioavailability study of two carbamazepine-containing sustained release formulations after multiple oral dose administration. Arneimittel Forschung/Drug Res. 1998;48:1131-1137.
17. Besag FM. Is generic prescribing acceptable in epilepsy? Drug Saf. 2000;23:173-182
18. Liow K, Barkley GL, Pollard JR, et al. American Academy of Neurology. Position statement on the coverage of anticonvulsant drugs for the treatment of epilepsy. Neurology. 2007;68:1249-1250.
19. US Food and Drug Administration. Bioavailability and bio-equivalence requirements. FDA Code of Federal Regulations. 21.CFR320.33.
20. Henderson JD, Esham RH. Generic substitution: issues for problematic drugs. South Med J. 2001;94:16-21.
21. Swenson CN, Fundak G. Observational cohort study of switching warfarin sodium products in a managed care organization. Am J Health Syst Pharm. 2000;57:452-455.
22. US Food and Drug Administration. Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. Available at: http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm. Accessed October 5, 2010.
23. Hennessey JV, Malabanan AO, Haugen BR, et al. Adverse event reporting in patients treated with levothyroxine: results of the Pharmacovigilance Task Force Survey of the American Thyroid Association, American Association of Clinical Endocrinologists and The Endocrine Society. Endocr Pract. 2010 Feb 11; 1-41. Epub ahead of print.
24. Calvert RT. Bioequivalence and generic prescribing: a pharmacy view. J Pharm Pharmacol. 1996;48:9-10.
25. British National Formulary: No 31. London, England: Pharmaceutical Press; 1996.
26. Endrenyi L, Tothfalusi L. Do regulatory bioequivalence requirements adequately reflect the therapeutic equivalence of modified-release drug products? J Pharm Pharmaceut Sci. 2010;13:107-113.
27. Davies G. Changing the salt, changing the drug. Pharm J. 2001;266:322-323.
28. Meredith PA. Generic drugs. Therapeutic equivalence. Drug Saf. 1996;15:233-242.
• Do not authorize the pharmacy to switch patients from a brand-name antiepileptic drug to a generic without your approval. C
• Use caution when switching a patient to a generic modified-release formulation, which may not have the same pharmacokinetic profile as its brand-name counterpart. C
• Consult the FDA’s Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations, available at http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm for details on generic substitution. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Each year, Americans save an estimated $8 billion to $10 billion at retail pharmacies by purchasing generic drugs rather than brand-name medications, the US Food and Drug Administration (FDA) reports.1 The lower cost, of course, is the key advantage of generics. But the very reason for the cost savings—the fact that generic drugs do not have to undergo the large, expensive clinical trials that are required for approval of brand-name medications—gives rise to questions about the quality and safety of generics.
Are these concerns justified? Under what circumstances is it safe to prescribe generics, or to substitute a generic for a brand-name drug? Are brand-name drugs always better? To answer these questions, we conducted a thorough evidence review, which included numerous randomized controlled trials (RCTs) and case reports, as well as a single meta-analysis that assessed the benefits and risks of generics.
Generics: On the positive side
Safety and efficacy. Our literature search yielded little evidence that generic drugs are less safe or less effective than their brand-name equivalents. The meta-analysis, for example,2 included 47 studies (38 of 47 were RCTs) covering 9 subclasses of cardiovascular medications. In trials involving beta-blockers, diuretics, calcium channel blockers, antiplatelet agents, statins, angiotensin-converting enzyme inhibitors, and alpha-blockers, no evidence of superiority of brand-name drugs vs generics was found.2
Cost. Generic drugs typically cost 30% to 60% less than their brand-name counterparts,3 and widespread use of generics has the potential to reduce the price of other brand-name drugs by creating more competition.
Another plus: Patients taking generic drugs appear to be more willing to continue therapy than those taking brand-name medications.4 Lower co-pays are a key factor. In 1 recent study of patients with hypercholesterolemia or diabetes, those taking generics had greater adherence compared with patients receiving brand-name drugs.5
Quality. It is important to note that many generic medications are produced under the license of the manufacturer of the original brand-name product, with the lower-cost equivalent often introduced after the drug’s patent has expired. Even when different manufacturers produce the branded product and the generic, strict standards exist to guarantee the quality of generic drugs.
The journey to market—the similarities, the differences
Both brand-name and generic medications undergo similar new drug application (NDA) procedures. The manufacturers of both are required to submit detailed evidence of the chemistry, manufacturing, controls, labeling, and testing processes. From there, brand-name and generic products take divergent paths to market.
New nongeneric drugs must undergo rigorous animal and human studies, including large RCTs comparing the efficacy of the new product with that of a placebo and carefully tracking side effects. Bioavailability testing is required, as well. For generic drugs, the process is known as an abbreviated new drug application (ANDA), and bioequivalence studies are sufficient.1,6
The bioequivalence studies required for a new generic are based on pharmacokinetic parameters, most notably, the area under the plasma concentration curve (AUC)—a measure of overall drug exposure—and the maximal plasma concentration (Cmax). If AUC and Cmax are within an acceptance range (0.80–1.25 of the brand-name product parameters), the therapeutic equivalence of a generic drug is substantiated.7,8
Concerns about testing, formulation
Opponents of widespread use of generics point out that they are tested on only a few young, healthy individuals, compared with the large numbers of patients who participate in clinical trials of the original drug.
Bioequivalence
According to guidelines from the World Health Organization (WHO), 18 to 24 healthy adult volunteers are considered sufficient for a bioequivalence study.9 The number of participants may be greater, however, if absorption or clearance of the drug is highly variable. What’s more, the people who volunteer for generic drug studies cannot smoke or take concurrent medication. To exclude the possibility that food coadministration affects the generic medication being studied, the FDA further recommends bioequivalence testing of oral formulations on volunteers eating standardized meals.8 These criteria help minimize the magnitude of intersubject variability and reduce the possibility of bias—which could be caused by the disease process, concurrent conditions, or medication interaction, rather than by formulation differences.8
To further minimize the effects of nondrug-related variation, bioequivalence studies typically use a crossover design: Half the subjects receive the test drug first, followed by the brand-name product, with a washout period in between. The other half receive the drugs in reverse order.10 (The study format is altered, as needed, for extended-release products, topical agents, and drugs that are not absorbed systemically. A generic version of cholestyramine, for example, which acts by sequestering bile salts within the intestine, would be approved on the basis of in vitro studies that quantify the binding of the bile salts.10)
But does this testing mimic the real world? While possible confounding factors are controlled for in bioequivalence studies of generics, critics point out that this is not the case in the real world. Thus, they worry that when generics are taken by patients with actual illnesses, concurrent use of other medications, medical conditions, and the like may result in differences in treatment that did not occur in the highly controlled environment in which the equivalency studies were conducted.11
Differences in formulation
Another concern centers on formulation differences, which have the potential to affect patients taking generic drugs. A generic copy of a brand-name drug must contain the same active ingredient, in the identical quantity, as the branded product—in the same dose formulation and route of administration. It must also meet standards for strength, purity, quality, and identity.11
However, the inert ingredients in the generic version do not have to be the same as those in the brand-name drug (although the ratio of inert to active compound must be similar).12 Because drugs tested in bioequivalence studies are administered in single doses, many experts wonder whether the inert compounds used in the generics may affect the distribution, metabolism, or absorption of a drug when it is administered in multiple doses, or whether the serum concentration of the generic drug may be elevated when it is taken for long periods.
Proceed with caution in these situations
For most patients taking most medications, generic drugs pose no problems, and provide an opportunity to obtain the same therapeutic benefit at a considerably lower cost. However, making the switch with certain classes of drugs, and with drugs that have a narrow therapeutic range, poses potential problems and must be done with caution—if at all.
Antiepileptic drugs. The FDA indicates that many people who are on antiseizure medications re-experience seizures despite continued treatment,1 and that switching to a generic does not increase the risk of treatment failure.1,13 Nonetheless, there are numerous reports of differences between generic and brand-name antiseizure medications (and small studies indicating improper seizure control after switching patients from a brand-name to a generic antiepileptic drug).14
For example:
- Researchers compared the pharmacokinetic parameters of Tegretol with 3 generic formulations of carbamazepine, and found that 1 of the 3 was not bioequivalent.15
- In a crossover study of 18 healthy volunteers, 3 generic formulations of carbamazepine were all within the acceptable bioequivalence range, but were absorbed more rapidly than the brand-name drug.16
- Differences in the bioavailability of brand-name and generic products have also been reported with phenytoin, primidone, and valproic acid, but the differences were not statistically significant.17
The American Academy of Neurology has issued a set of recommendations concerning the use of generic antiepileptic drugs (TABLE).18
Narrow therapeutic ratio. The potential for complications increases in drugs with a narrow therapeutic ratio, defined by the FDA as <2-fold difference between the median lethal dose and the median effective dose, or between the minimum toxic concentration and minimum effective concentration in the blood.19 The safe and effective use of such drugs—carbamazepine, divalproex, lithium, phenytoin, and warfarin, to name a few—requires careful dosage titration and patient monitoring.
Water solubility and nonlinear pharmacokinetics may present problems in drugs with a narrow therapeutic ratio, especially phenytoin.2 The drug’s serum concentration is allowed to range from 8 to 20 mg/L. A concentration above this range increases the risk for acute cerebellar syndrome, delirium, and coma; a concentration below the range may cause seizures.12
Warfarin is also of particular concern, as there is always the possibility that a switch from Coumadin to a generic equivalent could result in under- or overcoagulation. However, studies have shown that the use of generic warfarin in patients previously receiving Coumadin did not affect the international normalized ratio more than continued use of the brand-name anticoagulant.20,21
Psychotropic agents. There has been a number of case reports of problems occurring following a switch from a brand-name antidepressant to a generic—or from 1 generic antidepressant to another. (See “Did a switch to a generic antidepressant cause relapse?” J Fam Pract. 2008;58:109-114.) In fact, the FDA cites some psychotropic drugs for which generic formulations may not be interchangeable—including amitriptyline/ perphenazine and venlafaxine—and others for which generic formulations may not be bioequivalent at all doses.22
Thyroid medication. There are also concerns about levothyroxine (LT4) administration, and major medical societies debate the use of generic substitution. According to a recent survey from the American Association of Clinical Endocrinologists, the American Thyroid Association, and The Endocrine Society, clinical use of generic LT4 continues to be associated with adverse outcomes.23 Most of the adverse events (89%) reported by survey respondents were associated with a change, either from a brand-name drug to a generic or from 1 particular generic LT4 to another.
TABLE
Generic substitution of antiepileptic agents: Where the American Academy of Neurology stands18
| The AAN opposes: |
|
| The AAN believes: |
|
| The AAN supports: |
|
| The AAN recognizes: |
|
Modified-release formulations may also pose a problem
Problems may also occur with generics in modified-release formulations, which may not have the same pharmacokinetic profiles as their brand-named counterparts. The British National Formulary has advised that prescriptions for modified-release diltiazem hydrochloride, nifedipine, and theophylline be filled with the brand-name drug only.24,25 Morever, a recent study concluded that 2 modified-release products of methylphenidate and nifedipine had concentration profiles that strongly diverged during the period of absorption, although the formulations met the regulatory criteria for bioequivalence. 26
The type of salt used to form a compound is also important. Salt-joining makes a hydrophobic molecule hydrophilic; the result, especially in psychoactive drugs, is improved kinetics, absorption, or physico-chemical properties (eg, stability, hygroscopicity, fluidity).27 This may be the reason for differences identified between generic and brand-name amitriptyline, nortriptyline, desipramine, and trimipramine.28 To avoid problems, physicians should prescribe generics containing the same salt as their brand-name counterparts.
When in doubt …
Brand-name drugs are, and always will be, the best proven therapy, because of the number and extent of clinical trials they go through. In most cases, however, there is no evidence-based reason to avoid generic substitution for patients who cannot afford the brand-name drug. When in doubt, consult the FDA’s Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations, available at http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm, before making a switch.
CORRESPONDENCE Pawel Lewek, MD, The First Department of Family Medicine, Medical University of Lodz,60 Narutowicza Street, 90-136 Lodz, Poland; [email protected]
• Do not authorize the pharmacy to switch patients from a brand-name antiepileptic drug to a generic without your approval. C
• Use caution when switching a patient to a generic modified-release formulation, which may not have the same pharmacokinetic profile as its brand-name counterpart. C
• Consult the FDA’s Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations, available at http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm for details on generic substitution. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Each year, Americans save an estimated $8 billion to $10 billion at retail pharmacies by purchasing generic drugs rather than brand-name medications, the US Food and Drug Administration (FDA) reports.1 The lower cost, of course, is the key advantage of generics. But the very reason for the cost savings—the fact that generic drugs do not have to undergo the large, expensive clinical trials that are required for approval of brand-name medications—gives rise to questions about the quality and safety of generics.
Are these concerns justified? Under what circumstances is it safe to prescribe generics, or to substitute a generic for a brand-name drug? Are brand-name drugs always better? To answer these questions, we conducted a thorough evidence review, which included numerous randomized controlled trials (RCTs) and case reports, as well as a single meta-analysis that assessed the benefits and risks of generics.
Generics: On the positive side
Safety and efficacy. Our literature search yielded little evidence that generic drugs are less safe or less effective than their brand-name equivalents. The meta-analysis, for example,2 included 47 studies (38 of 47 were RCTs) covering 9 subclasses of cardiovascular medications. In trials involving beta-blockers, diuretics, calcium channel blockers, antiplatelet agents, statins, angiotensin-converting enzyme inhibitors, and alpha-blockers, no evidence of superiority of brand-name drugs vs generics was found.2
Cost. Generic drugs typically cost 30% to 60% less than their brand-name counterparts,3 and widespread use of generics has the potential to reduce the price of other brand-name drugs by creating more competition.
Another plus: Patients taking generic drugs appear to be more willing to continue therapy than those taking brand-name medications.4 Lower co-pays are a key factor. In 1 recent study of patients with hypercholesterolemia or diabetes, those taking generics had greater adherence compared with patients receiving brand-name drugs.5
Quality. It is important to note that many generic medications are produced under the license of the manufacturer of the original brand-name product, with the lower-cost equivalent often introduced after the drug’s patent has expired. Even when different manufacturers produce the branded product and the generic, strict standards exist to guarantee the quality of generic drugs.
The journey to market—the similarities, the differences
Both brand-name and generic medications undergo similar new drug application (NDA) procedures. The manufacturers of both are required to submit detailed evidence of the chemistry, manufacturing, controls, labeling, and testing processes. From there, brand-name and generic products take divergent paths to market.
New nongeneric drugs must undergo rigorous animal and human studies, including large RCTs comparing the efficacy of the new product with that of a placebo and carefully tracking side effects. Bioavailability testing is required, as well. For generic drugs, the process is known as an abbreviated new drug application (ANDA), and bioequivalence studies are sufficient.1,6
The bioequivalence studies required for a new generic are based on pharmacokinetic parameters, most notably, the area under the plasma concentration curve (AUC)—a measure of overall drug exposure—and the maximal plasma concentration (Cmax). If AUC and Cmax are within an acceptance range (0.80–1.25 of the brand-name product parameters), the therapeutic equivalence of a generic drug is substantiated.7,8
Concerns about testing, formulation
Opponents of widespread use of generics point out that they are tested on only a few young, healthy individuals, compared with the large numbers of patients who participate in clinical trials of the original drug.
Bioequivalence
According to guidelines from the World Health Organization (WHO), 18 to 24 healthy adult volunteers are considered sufficient for a bioequivalence study.9 The number of participants may be greater, however, if absorption or clearance of the drug is highly variable. What’s more, the people who volunteer for generic drug studies cannot smoke or take concurrent medication. To exclude the possibility that food coadministration affects the generic medication being studied, the FDA further recommends bioequivalence testing of oral formulations on volunteers eating standardized meals.8 These criteria help minimize the magnitude of intersubject variability and reduce the possibility of bias—which could be caused by the disease process, concurrent conditions, or medication interaction, rather than by formulation differences.8
To further minimize the effects of nondrug-related variation, bioequivalence studies typically use a crossover design: Half the subjects receive the test drug first, followed by the brand-name product, with a washout period in between. The other half receive the drugs in reverse order.10 (The study format is altered, as needed, for extended-release products, topical agents, and drugs that are not absorbed systemically. A generic version of cholestyramine, for example, which acts by sequestering bile salts within the intestine, would be approved on the basis of in vitro studies that quantify the binding of the bile salts.10)
But does this testing mimic the real world? While possible confounding factors are controlled for in bioequivalence studies of generics, critics point out that this is not the case in the real world. Thus, they worry that when generics are taken by patients with actual illnesses, concurrent use of other medications, medical conditions, and the like may result in differences in treatment that did not occur in the highly controlled environment in which the equivalency studies were conducted.11
Differences in formulation
Another concern centers on formulation differences, which have the potential to affect patients taking generic drugs. A generic copy of a brand-name drug must contain the same active ingredient, in the identical quantity, as the branded product—in the same dose formulation and route of administration. It must also meet standards for strength, purity, quality, and identity.11
However, the inert ingredients in the generic version do not have to be the same as those in the brand-name drug (although the ratio of inert to active compound must be similar).12 Because drugs tested in bioequivalence studies are administered in single doses, many experts wonder whether the inert compounds used in the generics may affect the distribution, metabolism, or absorption of a drug when it is administered in multiple doses, or whether the serum concentration of the generic drug may be elevated when it is taken for long periods.
Proceed with caution in these situations
For most patients taking most medications, generic drugs pose no problems, and provide an opportunity to obtain the same therapeutic benefit at a considerably lower cost. However, making the switch with certain classes of drugs, and with drugs that have a narrow therapeutic range, poses potential problems and must be done with caution—if at all.
Antiepileptic drugs. The FDA indicates that many people who are on antiseizure medications re-experience seizures despite continued treatment,1 and that switching to a generic does not increase the risk of treatment failure.1,13 Nonetheless, there are numerous reports of differences between generic and brand-name antiseizure medications (and small studies indicating improper seizure control after switching patients from a brand-name to a generic antiepileptic drug).14
For example:
- Researchers compared the pharmacokinetic parameters of Tegretol with 3 generic formulations of carbamazepine, and found that 1 of the 3 was not bioequivalent.15
- In a crossover study of 18 healthy volunteers, 3 generic formulations of carbamazepine were all within the acceptable bioequivalence range, but were absorbed more rapidly than the brand-name drug.16
- Differences in the bioavailability of brand-name and generic products have also been reported with phenytoin, primidone, and valproic acid, but the differences were not statistically significant.17
The American Academy of Neurology has issued a set of recommendations concerning the use of generic antiepileptic drugs (TABLE).18
Narrow therapeutic ratio. The potential for complications increases in drugs with a narrow therapeutic ratio, defined by the FDA as <2-fold difference between the median lethal dose and the median effective dose, or between the minimum toxic concentration and minimum effective concentration in the blood.19 The safe and effective use of such drugs—carbamazepine, divalproex, lithium, phenytoin, and warfarin, to name a few—requires careful dosage titration and patient monitoring.
Water solubility and nonlinear pharmacokinetics may present problems in drugs with a narrow therapeutic ratio, especially phenytoin.2 The drug’s serum concentration is allowed to range from 8 to 20 mg/L. A concentration above this range increases the risk for acute cerebellar syndrome, delirium, and coma; a concentration below the range may cause seizures.12
Warfarin is also of particular concern, as there is always the possibility that a switch from Coumadin to a generic equivalent could result in under- or overcoagulation. However, studies have shown that the use of generic warfarin in patients previously receiving Coumadin did not affect the international normalized ratio more than continued use of the brand-name anticoagulant.20,21
Psychotropic agents. There has been a number of case reports of problems occurring following a switch from a brand-name antidepressant to a generic—or from 1 generic antidepressant to another. (See “Did a switch to a generic antidepressant cause relapse?” J Fam Pract. 2008;58:109-114.) In fact, the FDA cites some psychotropic drugs for which generic formulations may not be interchangeable—including amitriptyline/ perphenazine and venlafaxine—and others for which generic formulations may not be bioequivalent at all doses.22
Thyroid medication. There are also concerns about levothyroxine (LT4) administration, and major medical societies debate the use of generic substitution. According to a recent survey from the American Association of Clinical Endocrinologists, the American Thyroid Association, and The Endocrine Society, clinical use of generic LT4 continues to be associated with adverse outcomes.23 Most of the adverse events (89%) reported by survey respondents were associated with a change, either from a brand-name drug to a generic or from 1 particular generic LT4 to another.
TABLE
Generic substitution of antiepileptic agents: Where the American Academy of Neurology stands18
| The AAN opposes: |
|
| The AAN believes: |
|
| The AAN supports: |
|
| The AAN recognizes: |
|
Modified-release formulations may also pose a problem
Problems may also occur with generics in modified-release formulations, which may not have the same pharmacokinetic profiles as their brand-named counterparts. The British National Formulary has advised that prescriptions for modified-release diltiazem hydrochloride, nifedipine, and theophylline be filled with the brand-name drug only.24,25 Morever, a recent study concluded that 2 modified-release products of methylphenidate and nifedipine had concentration profiles that strongly diverged during the period of absorption, although the formulations met the regulatory criteria for bioequivalence. 26
The type of salt used to form a compound is also important. Salt-joining makes a hydrophobic molecule hydrophilic; the result, especially in psychoactive drugs, is improved kinetics, absorption, or physico-chemical properties (eg, stability, hygroscopicity, fluidity).27 This may be the reason for differences identified between generic and brand-name amitriptyline, nortriptyline, desipramine, and trimipramine.28 To avoid problems, physicians should prescribe generics containing the same salt as their brand-name counterparts.
When in doubt …
Brand-name drugs are, and always will be, the best proven therapy, because of the number and extent of clinical trials they go through. In most cases, however, there is no evidence-based reason to avoid generic substitution for patients who cannot afford the brand-name drug. When in doubt, consult the FDA’s Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations, available at http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm, before making a switch.
CORRESPONDENCE Pawel Lewek, MD, The First Department of Family Medicine, Medical University of Lodz,60 Narutowicza Street, 90-136 Lodz, Poland; [email protected]
1. US Food and Drug Administration. What are generic drugs? Available at: http://www.fda.gov/Drugs/ResourcesForYou/Consumers/BuyingUsingMedicineSafely/UnderstandingGenericDrugs/default.htm. Accessed October 19, 2010.
2. Kesselheim AS, et al. Clinical equivalence of gneric and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis. JAMA. 2008;300:2514-2526.
3. Zarowitz BJ. The generic imperative. Geriatr Nurs. 2008;29:223-226.
4. Shrank WH, Hoang T, Ettner SL, et al. The implications of choice: prescribing generic or preferred pharmaceuticals improves medication adherence for chronic conditions. Arch Intern Med. 2006;133:332-337.
5. Briesacher BA, Andrade SE, Fouayzi H, et al. Medication adherence and use of generic drug therapies. Am J Manag Care. 2009;15:450-461.
6. Peters JR, Hixon DR, Conner DP, et al. Generic drugs—safe, effective, and affordable. Dermatol Ther. 2009;22:229-240.
7. European Agency for the Evaluation of Medicinal Products. Note for guidance on the investigation of bioavailability and bioequivalence. London, England: EMEA; 2000;CPMP/EWP/ QWP/1401/98.
8. US Food and Drug Administration, Center for Research .Guidance for industry: bioavailability and bioequivalence studies for orally administered drug products—general considerations, 2002. Available at: http://www.fda.gov/cder/guidance/4964dft.pdf. Accessed January 11, 2009.
9. World Health Organization. Multi-source pharmaceutical products: WHO guideline on registration requirements to establish interchangeability. WHO Technical Support Series. Geneva, Switzerland: WHO;1996:TRS 863.
10. Meyer MC. Generic drug product equivalence: current status. Am J Manag Care. 1998;4:1183-1189.
11. Meredith P. Bioequivalence and other unresolved issues in generic drug substitution. Clin Ther. 2003;25:2875-2890.
12. Nakai K, Fujita M, Ogata H. International harmonization of bioequivalence studies and issues shared in common. Yakugaka Zasshi. 2000;120:1193-1200.
13. Randomized study of antiepileptic drug withdrawal in patients in remission Medical Research Council Antiepileptic Drug Withdrawal Study Group. Lancet. 1991;337:1175-1180.
14. Crawford P, Feely M, Guberman A, et al. Are there potential problems with generic substitution of antiepileptic drugs? A review of issues. Seizure. 2006;15:165-176.
15. Silpakit O, Amornpichetkoon M, Kaojarern S. Comparative study of bioavailability and clinical efficacy of carbamazepine in epileptic patients. Ann Pharmacother. 1997;31:548-552.
16. Wangemann M, Retzow A, Evers G, et al. Bioavailability study of two carbamazepine-containing sustained release formulations after multiple oral dose administration. Arneimittel Forschung/Drug Res. 1998;48:1131-1137.
17. Besag FM. Is generic prescribing acceptable in epilepsy? Drug Saf. 2000;23:173-182
18. Liow K, Barkley GL, Pollard JR, et al. American Academy of Neurology. Position statement on the coverage of anticonvulsant drugs for the treatment of epilepsy. Neurology. 2007;68:1249-1250.
19. US Food and Drug Administration. Bioavailability and bio-equivalence requirements. FDA Code of Federal Regulations. 21.CFR320.33.
20. Henderson JD, Esham RH. Generic substitution: issues for problematic drugs. South Med J. 2001;94:16-21.
21. Swenson CN, Fundak G. Observational cohort study of switching warfarin sodium products in a managed care organization. Am J Health Syst Pharm. 2000;57:452-455.
22. US Food and Drug Administration. Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. Available at: http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm. Accessed October 5, 2010.
23. Hennessey JV, Malabanan AO, Haugen BR, et al. Adverse event reporting in patients treated with levothyroxine: results of the Pharmacovigilance Task Force Survey of the American Thyroid Association, American Association of Clinical Endocrinologists and The Endocrine Society. Endocr Pract. 2010 Feb 11; 1-41. Epub ahead of print.
24. Calvert RT. Bioequivalence and generic prescribing: a pharmacy view. J Pharm Pharmacol. 1996;48:9-10.
25. British National Formulary: No 31. London, England: Pharmaceutical Press; 1996.
26. Endrenyi L, Tothfalusi L. Do regulatory bioequivalence requirements adequately reflect the therapeutic equivalence of modified-release drug products? J Pharm Pharmaceut Sci. 2010;13:107-113.
27. Davies G. Changing the salt, changing the drug. Pharm J. 2001;266:322-323.
28. Meredith PA. Generic drugs. Therapeutic equivalence. Drug Saf. 1996;15:233-242.
1. US Food and Drug Administration. What are generic drugs? Available at: http://www.fda.gov/Drugs/ResourcesForYou/Consumers/BuyingUsingMedicineSafely/UnderstandingGenericDrugs/default.htm. Accessed October 19, 2010.
2. Kesselheim AS, et al. Clinical equivalence of gneric and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis. JAMA. 2008;300:2514-2526.
3. Zarowitz BJ. The generic imperative. Geriatr Nurs. 2008;29:223-226.
4. Shrank WH, Hoang T, Ettner SL, et al. The implications of choice: prescribing generic or preferred pharmaceuticals improves medication adherence for chronic conditions. Arch Intern Med. 2006;133:332-337.
5. Briesacher BA, Andrade SE, Fouayzi H, et al. Medication adherence and use of generic drug therapies. Am J Manag Care. 2009;15:450-461.
6. Peters JR, Hixon DR, Conner DP, et al. Generic drugs—safe, effective, and affordable. Dermatol Ther. 2009;22:229-240.
7. European Agency for the Evaluation of Medicinal Products. Note for guidance on the investigation of bioavailability and bioequivalence. London, England: EMEA; 2000;CPMP/EWP/ QWP/1401/98.
8. US Food and Drug Administration, Center for Research .Guidance for industry: bioavailability and bioequivalence studies for orally administered drug products—general considerations, 2002. Available at: http://www.fda.gov/cder/guidance/4964dft.pdf. Accessed January 11, 2009.
9. World Health Organization. Multi-source pharmaceutical products: WHO guideline on registration requirements to establish interchangeability. WHO Technical Support Series. Geneva, Switzerland: WHO;1996:TRS 863.
10. Meyer MC. Generic drug product equivalence: current status. Am J Manag Care. 1998;4:1183-1189.
11. Meredith P. Bioequivalence and other unresolved issues in generic drug substitution. Clin Ther. 2003;25:2875-2890.
12. Nakai K, Fujita M, Ogata H. International harmonization of bioequivalence studies and issues shared in common. Yakugaka Zasshi. 2000;120:1193-1200.
13. Randomized study of antiepileptic drug withdrawal in patients in remission Medical Research Council Antiepileptic Drug Withdrawal Study Group. Lancet. 1991;337:1175-1180.
14. Crawford P, Feely M, Guberman A, et al. Are there potential problems with generic substitution of antiepileptic drugs? A review of issues. Seizure. 2006;15:165-176.
15. Silpakit O, Amornpichetkoon M, Kaojarern S. Comparative study of bioavailability and clinical efficacy of carbamazepine in epileptic patients. Ann Pharmacother. 1997;31:548-552.
16. Wangemann M, Retzow A, Evers G, et al. Bioavailability study of two carbamazepine-containing sustained release formulations after multiple oral dose administration. Arneimittel Forschung/Drug Res. 1998;48:1131-1137.
17. Besag FM. Is generic prescribing acceptable in epilepsy? Drug Saf. 2000;23:173-182
18. Liow K, Barkley GL, Pollard JR, et al. American Academy of Neurology. Position statement on the coverage of anticonvulsant drugs for the treatment of epilepsy. Neurology. 2007;68:1249-1250.
19. US Food and Drug Administration. Bioavailability and bio-equivalence requirements. FDA Code of Federal Regulations. 21.CFR320.33.
20. Henderson JD, Esham RH. Generic substitution: issues for problematic drugs. South Med J. 2001;94:16-21.
21. Swenson CN, Fundak G. Observational cohort study of switching warfarin sodium products in a managed care organization. Am J Health Syst Pharm. 2000;57:452-455.
22. US Food and Drug Administration. Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. Available at: http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm. Accessed October 5, 2010.
23. Hennessey JV, Malabanan AO, Haugen BR, et al. Adverse event reporting in patients treated with levothyroxine: results of the Pharmacovigilance Task Force Survey of the American Thyroid Association, American Association of Clinical Endocrinologists and The Endocrine Society. Endocr Pract. 2010 Feb 11; 1-41. Epub ahead of print.
24. Calvert RT. Bioequivalence and generic prescribing: a pharmacy view. J Pharm Pharmacol. 1996;48:9-10.
25. British National Formulary: No 31. London, England: Pharmaceutical Press; 1996.
26. Endrenyi L, Tothfalusi L. Do regulatory bioequivalence requirements adequately reflect the therapeutic equivalence of modified-release drug products? J Pharm Pharmaceut Sci. 2010;13:107-113.
27. Davies G. Changing the salt, changing the drug. Pharm J. 2001;266:322-323.
28. Meredith PA. Generic drugs. Therapeutic equivalence. Drug Saf. 1996;15:233-242.
Is it time to drug test your chronic pain patient?
• When you initiate opioid therapy for chronic pain, inform the patient that routine monitoring includes random urine drug testing (UDT). C
• Consider UDT not only for patients at high risk for abuse of prescription opioids, but for lower-risk individuals receiving opioid therapy, as well. C
• Use caution in interpreting the results of UDT; testing cannot reliably detect some opioids, and a negative result is not necessarily an indication of noncompliance. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Marilyn H, a 54-year-old woman with multiple chronic conditions, visits a “new” primary care physician to establish care following the retirement of her previous physician. She has poorly controlled diabetes, hypertension, and a lung nodule recently noted on a chest radiograph. Marilyn requests prescriptions for hydrocodone and alprazolam, stating that she has taken both drugs for years for chronic back pain and anxiety.
CASE 2 Don F, 38, has been on oxycodone/acetaminophen (Percocet) for 3 years for back pain resulting from a car accident. He has a remote history of amphetamine abuse, but reports that he has been clean for 10 years. Since the initiation of his pain medication, there have been no problems, and no “lost” prescriptions or requests for early refills.
If you were Marilyn and Don’s physician, would you order urine drug testing (UDT)?
Management of opioid therapy is a challenge for many family physicians, particularly when treating noncancer pain. Seemingly contradictory messages from various medical associations are part of the problem. Organizations such as the Joint Commission on Accreditation of Healthcare Organizations and the American Medical Association emphasize the importance of appropriate pain management, while regulatory bodies like the US Drug Enforcement Agency and many state medical boards warn of inappropriate prescribing and diversion of controlled substances.1-4
In the realm of opioid management guidelines, however, patient monitoring is a common theme. It’s not hard to understand why. The Centers for Disease Control and Prevention reports that, between 1999 and 2005, the incidence of unintentional drug overdose more than doubled—a consequence of increasing abuse of prescription opioid analgesics.5 Prescription medications are now the second most commonly abused drug category (marijuana is first6), accounting for more cases of abuse than heroin, cocaine, and hallucinogens combined.7 In primary care and pain management settings, estimates are that more than 1 in 4 chronic pain patients misuse opioids or illicit drugs.8
Thus, physicians who prescribe controlled substances face increasing pressure to prevent opioid diversion. That pressure is reflected in the US Federation of State Medical Boards (FSMB)’s Model Policy for the Use of Controlled Substances for the Treatment of Pain, which was updated in 2004.4 This policy underscores physicians’ responsibility to closely monitor patients being treated with opioids for chronic pain.
Inexpensive and noninvasive. To this end, UDT can be a valuable tool. It is the most widely used and acceptable form of drug testing, because it is inexpensive and noninvasive, and because most drugs can be detected in urine for 1 to 3 days.9,10 But many primary care physicians are unfamiliar with the complexities of UDT, and often fail to use it.11 One study found that only 8% of family physicians employed UDT for patients on chronic opioid therapy.12
When introduced and used appropriately, UDT can not only help detect misuse of controlled substances, but may strengthen the doctor-patient relationship, as well. For that to happen, however, the physician who orders urine testing must know which patients to test, when to test, and what urine testing can (and cannot) reveal.
Consider testing all patients treated for chronic pain
The FSMB urges physicians to consider a written agreement with any patient receiving chronic opioid therapy who has a history of, or is at high risk for, substance abuse.4 (Red flags are listed in TABLE 1.13-15) The document should state that the patient is responsible for providing urine and serum specimens for drug monitoring upon request. The 2009 guidelines from the American Pain Society and the American Academy of Pain Medicine also address the role of drug monitoring, strongly recommending periodic urine screens for high-risk patients on chronic opioid therapy.16
Evidence suggests that predictors of aberrant behavior are not completely reliable, however, and that a substantial number of individuals using illicit substances will be missed if clinicians restrict urine testing to those they deem to be at high risk.17 Thus, UDT may be a valuable tool for low-risk patients on chronic opioid therapy, as well. Written agreements governing opioid therapy may also be useful for low-risk patients.
TABLE 1
Aberrant drug-related behavior: Red flags13-15
| Use of opioids for non-analgesic indications |
| Lack of control (related to drug use or to patient behavior) |
| Compulsive use of medications |
| Continued use of drugs despite harm/lack of benefit |
| Cravings |
| Escalation of drug use |
| Selling/altering prescriptions |
| Theft or diversion |
| Request for early refills |
| Claims of “lost” prescriptions |
| Reluctance to try nonpharmacologic options |
| Use of multiple prescribers or pharmacies |
| Odd stories regarding need for medication |
| Reporting vague medical history or textbook symptoms |
| Unwillingness to name regular physician |
| No interest in a physical exam, diagnostic testing, or providing past records |
| Request for specific drug(s) |
| Extensive (or very limited) understanding of medications |
| Calling or arriving after hours or when regular doctor is unavailable |
| Insistence on being seen urgently (eg, because of being late for another appointment) |
When to test, what to test for
No guidelines specify when to test, but testing upon initiation of chronic opioid treatment, followed by random testing, is the most widely used strategy. Unobserved specimen collection is generally acceptable,13 provided the specimens are requested at random rather than routinely at every visit.
Initial testing is done using an immuno-assay drug panel.13,18 TABLE 2 lists the drugs most commonly included in a standard urine test. However, the drug panel can vary from 1 laboratory to another, as can the lower limits of drug detection. No-threshold testing is mentioned in pain management literature, but is not often available in clinical practice.
Before initiating UDT, it is important to know which drugs the laboratory you use routinely tests for and what its lower limits are. The simplest way to find out is to ask lab personnel.
CASE 1 At her first visit, Marilyn H’s new physician focuses on controlling her blood sugar and blood pressure, ordering follow-up testing of the lung nodule, and refilling her hydrocodone and alprazolam prescriptions. The physician requests the patient’s medical records and orders a urine drug screen per clinic protocol, testing for benzodiazepines as well as for opioids. He gives his patient prescriptions for a 1-month supply of both drugs while the UDT results are pending.
The lab report comes in the following day, and indicates that Marilyn tested positive for cocaine but negative for other substances, including narcotics and benzodiazepines. The clinic immediately notifies the pharmacy to confiscate the patient’s new prescriptions when she presents them and calls Marilyn, advising her that she will not be given any further prescriptions for controlled substances.
The physician refers the patient to a pain clinic, gives her the number of a substance abuse treatment center, and encourages her to follow up at the clinic for other medical issues. Marilyn fails to keep her appointment at the pain clinic and does not respond to a subsequent call.
TABLE 2
A standard urine drug test panel13,18
| Amphetamines |
| Cocaine |
| Marijuana (THC) |
| Opiates (morphine and codeine) |
| Phencyclidine |
| THC, tetrahydrocannabinol. |
Talking to patients about drug testing
Physicians are often concerned about patients’ feelings about drug testing—worrying that patients may not feel trusted or respected by a doctor who asks them to submit to UDT. Others may fear that the mere mention of urine testing will encourage patients to misuse prescription opioids, that patients will view UDT as a punitive measure, or that those being tested will believe that the physician is more concerned with self-protection than with providing optimal care to the patient.
Making UDT routine. One way to circumvent such possibilities is to implement a systematic approach to drug testing. We recommend that physicians discuss the role of UDT in the initial education session with patients being started on a course of opiates. Describing UDT as simply another routine monitoring parameter—akin to the measure of microalbuminuria for patients with diabetes—can decrease or eliminate the stigma associated with drug testing.
CASE 2 A new policy encouraging UDT for all patients on chronic controlled substances has just been implemented at the clinic where Don F is being treated. His physician tells him about the policy, and a urine test is ordered at his next visit. The test comes back negative for all substances, including opioids.
When presented with the results over the phone, Don insists that he regularly takes his prescription medication, and makes a same-day appointment to discuss the results with his physician.
Interpreting test results— what UDT can (and can’t) reveal
To avoid eroding trust by falsely accusing a patient of diversion or use of an illicit substance, it’s important to familiarize yourself with testing limitations. Factors that can affect the results, and may interfere with the ability of UDT to provide a definitive picture, include:
Lab variability and technical limitations. Some urine drug panels may not have a lower limit sufficient to detect small quantities of opioids. Others may not detect certain substances, notably the semisynthetic and synthetic opioids (TABLE 3).19 Oxycodone is a prime example of a commonly prescribed semisynthetic opioid that does not appear on many urine test panels.8
In addition, individual drugs within a class may not be identified on UDT panels. When confirmation of a specific drug or metabolite is needed, serum testing must be performed.8
TABLE 3
Classifying opioids19
| Natural | Semisynthetic | Synthetic |
|---|---|---|
| Codeine | Hydrocodone | Fentanyl |
| Morphine | Hydromorphone | Meperidine |
| Oxycodone | Methadone | |
| Propoxyphene |
Differences in metabolism. Genetic differences in metabolism can also skew the results of UDT. Codeine, which relies on hepatic metabolism via cytochrome P450 2D6 for conversion to morphine, is the classic example; cytochrome P450 2D6 is a polymorphic enzyme, meaning that it manifests with different activity levels in different people. Patients who are poor metabolizers (an estimated 5%-10% of Caucasians, 1%-5% of Asians, 2%-7% of African Americans, and 2%-6% of Hispanics20) will convert very little codeine to morphine; conversely, those who are rapid metabolizers will convert extensive amounts. A rapid metabolizer taking codeine as prescribed may therefore have a negative UDT; in an average metabolizer taking the same dose, both codeine and morphine will be detected.20
Drugs’ half-lives. Opioids with a short half-life (TABLE 4)9,21 may not appear in the urine if the test is done several hours after the last dose. On the other hand, some opioids may have an extended half-life in patients with liver or kidney disease, and may appear in the urine longer than would be expected.9
False-positive results. Substances that may cause false positives for opioids on a urine test include dextromethorphan, papaverine, poppy seeds and oil, quinine, quinolones, rifampin, and verapamil.10
False-negative results. Many of the problems already discussed can lead to false-negative results, including the panel’s failure to detect semisynthetic and synthetic opioids, rapid metabolism (most notably, of codeine), the timing of the test relative to the dose, and adulteration of the specimen. Thus, a negative test result in a patient on opioid therapy does not necessarily mean that he or she is noncompliant—and certainly is not proof of diversion.
Because of the variables that affect UDT outcomes, unanticipated results should be reviewed with the patient and possibly, with the lab, and viewed within the therapeutic context. When more definitive information is needed, serum testing may be performed as follow-up. While serum testing can detect drugs and their metabolites ingested within hours, it is not widely used on initial screening because it is a more invasive procedure with higher associated costs.13
CASE 2 Upon further discussion with Don F, the physician orders a serum oxycodone test, which shows a level of 10 ng/mL. The physician notes that serum testing is more appropriate than UDT for Don because of the inconsistent detection of oxycodone in urine.
TABLE 4
Pharmacokinetics of common opioids: Time detectable in urine9,21
| Drug (half-life) | Time detectable in urine | Comment |
|---|---|---|
| Codeine (2.5-3 h) | 48 h | Pharmacogenetic-dependent effects may affect detection |
| Fentanyl Transdermal (17 h) Submucosal (7 h) | Not usually detected in urine (lack of metabolites) | Excretion of transdermal fentanyl can last days |
| Hydromorphone IR (2.3 h) ER (18.6 h) | 2-4 d | Significant interpatient variability |
| Methadone (8-59 h) | 3 d | |
| Morphine (1.5-2 h) | 48-72 h | 90% eliminated within 24 h |
| Oxycodone IR (3.2 h) ER (4.5 h) | Often not detected in urine | High-fat meals may increase serum concentrations of ER formulation |
| Propoxyphene Parent drug (6-12 h) Metabolite (30-36 h) | 6-48 h | |
| ER, extended release; IR, immediate release. | ||
CORRESPONDENCE Sarah McBane, PharmD, CDC, BCPS, University of California, San Diego, Skaggs School of Pharmacy and Pharmaceutical Sciences, 9500 Gilman Drive, La Jolla, CA 92023; [email protected]
1. Health Care Issues. Joint Commission on Accreditation of Health Care Organizations. Available at: http://www.jointcommission.org/. Accessed March 5, 2010.
2. Standards, Laws, and Regulations Addressing Pain Medications and Medical Practice: Report 6 of the Council on Science and Public Health. American Medical Association. June 2007. Available at: http://www.ama-assn.org/ama/pub/physician-resources/medical-science/council-science-public-health.shtml. Accessed July 16, 2009.
3. US Department of Justice Drug Enforcement Administration Office of Diversion Control. Available at: http://www.deadiversion.usdoj.gov/. Accessed March 5, 2010.
4. Federation of State Medical Boards. Model Policy for the Use of Controlled Substances for the Treatment of Pain. May 2004. Available at: http://www.fsmb.org/pdf/2004_grpol_Controlled_Substances.pdf. Accessed March 5, 2010.
5. Centers for Disease Control and Prevention. Prescription Drug Overdose: State Health Agencies Respond. Available at: http://www.cdc.gov/HomeandRecreationalSafety/pubs/RXReport_web-a.pdf. Accessed May 15, 2010.
6. Drug Enforcement Agency Office of Diversion Control NFLIS Special Report: Controlled Substance Prescription Drugs 2001-2005. November 2006. Available at: http://www.deadiversion.usdoj.gov/nflis/2006rx_drugs_report.pdf. Accessed May 15, 2010.
7. Department of Health and Human Services Office of Substance Abuse and Mental Health Services Administration. Results from the 2007 National Survey on Drug Use and Health: national findings. Available at: http://www.oas.samhsa.gov/nsduh/2k7nsduh/2k7Results.pdf. Accessed May 7, 2010.
8. Reisfield G, Salazar E, Bertholf R. Rational use and interpretation of urine drug testing in chronic opioid therapy. Ann Clin Lab Sci. 2007;37:301-314.
9. Clinical Pharmacology [online]. Tampa, FL: Gold Standard Inc; 2010. Accessed March 5, 2010.
10. Drug abuse urine tests: false-positive results. Pharmacist’s Letter/Prescriber’s Letter. 2005;21:210314.-
11. Reisfield GM, Webb FJ, Bertholf RL, et al. Family physicians’ proficiency in urine drug test interpretation. J Opioid Manag. 2007;3:333-337.
12. Adams N, Plane M, Fleming M, et al. Opioids and the treatment of chronic pain in a primary care sample. J Pain Symptom Manage. 2001;22:791-796.
13. Gourlay D, Caplan Y, Heit H. Urine drug testing in clinical practice: dispelling the myths and designing strategies. San Francisco, CA: California Academy of Family Physicians; 2006.
14. Cole BE. Recognizing and preventing medication diversion. Fam Pract Manag. 2001;8:37-41.
15. Jackman R, Purvis J, Mallett B. Chronic nonmalignant pain in primary care. Am Fam Physician. 2008;78:1155-1162.
16. Chou R, Fanciullo G, Fine P, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009;10:113-130.
17. Chou R, Fanciullo G, Fine P, et al. Opioids for chronic noncancer pain: prediction and identification of aberrant drug-related behaviors: a review of the evidence for an American Pain Society and American Academy of Pain Medicine Clinical Practice Guideline. J Pain. 2009;10:131-146.
18. Moeller K, Lee K, Kissack J. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83:66-76.
19. Amabile C, Bowman B. Overview of oral modified-release opioid products for the management of chronic pain. Ann Pharmaco-therapy. 2006;40:1327-1335.
20. Zhou S. Polymorphism of human cytochrome P450 2D6 and its clinical significance. Clin Pharmacokinet. 2009;48:689-723.
21. Drug Facts and Comparisons [online]. 2010. Available at: http://www.factsandcomparisons.com/. Accessed March 5, 2010.
| Drug testing conversations: Finding the right words |
Sarah McBane, PharmD, CDE, BCPS
University of California, San Diego, Skaggs School of Pharmacy and Pharmaceutical Sciences, La Jolla
[email protected]
Nancy Weigle, MD
Duke University Medical Center, Durham, NC
The authors reported no potential conflict of interest relevant to this article.
| Drug testing conversations: Finding the right words |
Sarah McBane, PharmD, CDE, BCPS
University of California, San Diego, Skaggs School of Pharmacy and Pharmaceutical Sciences, La Jolla
[email protected]
Nancy Weigle, MD
Duke University Medical Center, Durham, NC
The authors reported no potential conflict of interest relevant to this article.
| Drug testing conversations: Finding the right words |
Sarah McBane, PharmD, CDE, BCPS
University of California, San Diego, Skaggs School of Pharmacy and Pharmaceutical Sciences, La Jolla
[email protected]
Nancy Weigle, MD
Duke University Medical Center, Durham, NC
The authors reported no potential conflict of interest relevant to this article.
• When you initiate opioid therapy for chronic pain, inform the patient that routine monitoring includes random urine drug testing (UDT). C
• Consider UDT not only for patients at high risk for abuse of prescription opioids, but for lower-risk individuals receiving opioid therapy, as well. C
• Use caution in interpreting the results of UDT; testing cannot reliably detect some opioids, and a negative result is not necessarily an indication of noncompliance. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Marilyn H, a 54-year-old woman with multiple chronic conditions, visits a “new” primary care physician to establish care following the retirement of her previous physician. She has poorly controlled diabetes, hypertension, and a lung nodule recently noted on a chest radiograph. Marilyn requests prescriptions for hydrocodone and alprazolam, stating that she has taken both drugs for years for chronic back pain and anxiety.
CASE 2 Don F, 38, has been on oxycodone/acetaminophen (Percocet) for 3 years for back pain resulting from a car accident. He has a remote history of amphetamine abuse, but reports that he has been clean for 10 years. Since the initiation of his pain medication, there have been no problems, and no “lost” prescriptions or requests for early refills.
If you were Marilyn and Don’s physician, would you order urine drug testing (UDT)?
Management of opioid therapy is a challenge for many family physicians, particularly when treating noncancer pain. Seemingly contradictory messages from various medical associations are part of the problem. Organizations such as the Joint Commission on Accreditation of Healthcare Organizations and the American Medical Association emphasize the importance of appropriate pain management, while regulatory bodies like the US Drug Enforcement Agency and many state medical boards warn of inappropriate prescribing and diversion of controlled substances.1-4
In the realm of opioid management guidelines, however, patient monitoring is a common theme. It’s not hard to understand why. The Centers for Disease Control and Prevention reports that, between 1999 and 2005, the incidence of unintentional drug overdose more than doubled—a consequence of increasing abuse of prescription opioid analgesics.5 Prescription medications are now the second most commonly abused drug category (marijuana is first6), accounting for more cases of abuse than heroin, cocaine, and hallucinogens combined.7 In primary care and pain management settings, estimates are that more than 1 in 4 chronic pain patients misuse opioids or illicit drugs.8
Thus, physicians who prescribe controlled substances face increasing pressure to prevent opioid diversion. That pressure is reflected in the US Federation of State Medical Boards (FSMB)’s Model Policy for the Use of Controlled Substances for the Treatment of Pain, which was updated in 2004.4 This policy underscores physicians’ responsibility to closely monitor patients being treated with opioids for chronic pain.
Inexpensive and noninvasive. To this end, UDT can be a valuable tool. It is the most widely used and acceptable form of drug testing, because it is inexpensive and noninvasive, and because most drugs can be detected in urine for 1 to 3 days.9,10 But many primary care physicians are unfamiliar with the complexities of UDT, and often fail to use it.11 One study found that only 8% of family physicians employed UDT for patients on chronic opioid therapy.12
When introduced and used appropriately, UDT can not only help detect misuse of controlled substances, but may strengthen the doctor-patient relationship, as well. For that to happen, however, the physician who orders urine testing must know which patients to test, when to test, and what urine testing can (and cannot) reveal.
Consider testing all patients treated for chronic pain
The FSMB urges physicians to consider a written agreement with any patient receiving chronic opioid therapy who has a history of, or is at high risk for, substance abuse.4 (Red flags are listed in TABLE 1.13-15) The document should state that the patient is responsible for providing urine and serum specimens for drug monitoring upon request. The 2009 guidelines from the American Pain Society and the American Academy of Pain Medicine also address the role of drug monitoring, strongly recommending periodic urine screens for high-risk patients on chronic opioid therapy.16
Evidence suggests that predictors of aberrant behavior are not completely reliable, however, and that a substantial number of individuals using illicit substances will be missed if clinicians restrict urine testing to those they deem to be at high risk.17 Thus, UDT may be a valuable tool for low-risk patients on chronic opioid therapy, as well. Written agreements governing opioid therapy may also be useful for low-risk patients.
TABLE 1
Aberrant drug-related behavior: Red flags13-15
| Use of opioids for non-analgesic indications |
| Lack of control (related to drug use or to patient behavior) |
| Compulsive use of medications |
| Continued use of drugs despite harm/lack of benefit |
| Cravings |
| Escalation of drug use |
| Selling/altering prescriptions |
| Theft or diversion |
| Request for early refills |
| Claims of “lost” prescriptions |
| Reluctance to try nonpharmacologic options |
| Use of multiple prescribers or pharmacies |
| Odd stories regarding need for medication |
| Reporting vague medical history or textbook symptoms |
| Unwillingness to name regular physician |
| No interest in a physical exam, diagnostic testing, or providing past records |
| Request for specific drug(s) |
| Extensive (or very limited) understanding of medications |
| Calling or arriving after hours or when regular doctor is unavailable |
| Insistence on being seen urgently (eg, because of being late for another appointment) |
When to test, what to test for
No guidelines specify when to test, but testing upon initiation of chronic opioid treatment, followed by random testing, is the most widely used strategy. Unobserved specimen collection is generally acceptable,13 provided the specimens are requested at random rather than routinely at every visit.
Initial testing is done using an immuno-assay drug panel.13,18 TABLE 2 lists the drugs most commonly included in a standard urine test. However, the drug panel can vary from 1 laboratory to another, as can the lower limits of drug detection. No-threshold testing is mentioned in pain management literature, but is not often available in clinical practice.
Before initiating UDT, it is important to know which drugs the laboratory you use routinely tests for and what its lower limits are. The simplest way to find out is to ask lab personnel.
CASE 1 At her first visit, Marilyn H’s new physician focuses on controlling her blood sugar and blood pressure, ordering follow-up testing of the lung nodule, and refilling her hydrocodone and alprazolam prescriptions. The physician requests the patient’s medical records and orders a urine drug screen per clinic protocol, testing for benzodiazepines as well as for opioids. He gives his patient prescriptions for a 1-month supply of both drugs while the UDT results are pending.
The lab report comes in the following day, and indicates that Marilyn tested positive for cocaine but negative for other substances, including narcotics and benzodiazepines. The clinic immediately notifies the pharmacy to confiscate the patient’s new prescriptions when she presents them and calls Marilyn, advising her that she will not be given any further prescriptions for controlled substances.
The physician refers the patient to a pain clinic, gives her the number of a substance abuse treatment center, and encourages her to follow up at the clinic for other medical issues. Marilyn fails to keep her appointment at the pain clinic and does not respond to a subsequent call.
TABLE 2
A standard urine drug test panel13,18
| Amphetamines |
| Cocaine |
| Marijuana (THC) |
| Opiates (morphine and codeine) |
| Phencyclidine |
| THC, tetrahydrocannabinol. |
Talking to patients about drug testing
Physicians are often concerned about patients’ feelings about drug testing—worrying that patients may not feel trusted or respected by a doctor who asks them to submit to UDT. Others may fear that the mere mention of urine testing will encourage patients to misuse prescription opioids, that patients will view UDT as a punitive measure, or that those being tested will believe that the physician is more concerned with self-protection than with providing optimal care to the patient.
Making UDT routine. One way to circumvent such possibilities is to implement a systematic approach to drug testing. We recommend that physicians discuss the role of UDT in the initial education session with patients being started on a course of opiates. Describing UDT as simply another routine monitoring parameter—akin to the measure of microalbuminuria for patients with diabetes—can decrease or eliminate the stigma associated with drug testing.
CASE 2 A new policy encouraging UDT for all patients on chronic controlled substances has just been implemented at the clinic where Don F is being treated. His physician tells him about the policy, and a urine test is ordered at his next visit. The test comes back negative for all substances, including opioids.
When presented with the results over the phone, Don insists that he regularly takes his prescription medication, and makes a same-day appointment to discuss the results with his physician.
Interpreting test results— what UDT can (and can’t) reveal
To avoid eroding trust by falsely accusing a patient of diversion or use of an illicit substance, it’s important to familiarize yourself with testing limitations. Factors that can affect the results, and may interfere with the ability of UDT to provide a definitive picture, include:
Lab variability and technical limitations. Some urine drug panels may not have a lower limit sufficient to detect small quantities of opioids. Others may not detect certain substances, notably the semisynthetic and synthetic opioids (TABLE 3).19 Oxycodone is a prime example of a commonly prescribed semisynthetic opioid that does not appear on many urine test panels.8
In addition, individual drugs within a class may not be identified on UDT panels. When confirmation of a specific drug or metabolite is needed, serum testing must be performed.8
TABLE 3
Classifying opioids19
| Natural | Semisynthetic | Synthetic |
|---|---|---|
| Codeine | Hydrocodone | Fentanyl |
| Morphine | Hydromorphone | Meperidine |
| Oxycodone | Methadone | |
| Propoxyphene |
Differences in metabolism. Genetic differences in metabolism can also skew the results of UDT. Codeine, which relies on hepatic metabolism via cytochrome P450 2D6 for conversion to morphine, is the classic example; cytochrome P450 2D6 is a polymorphic enzyme, meaning that it manifests with different activity levels in different people. Patients who are poor metabolizers (an estimated 5%-10% of Caucasians, 1%-5% of Asians, 2%-7% of African Americans, and 2%-6% of Hispanics20) will convert very little codeine to morphine; conversely, those who are rapid metabolizers will convert extensive amounts. A rapid metabolizer taking codeine as prescribed may therefore have a negative UDT; in an average metabolizer taking the same dose, both codeine and morphine will be detected.20
Drugs’ half-lives. Opioids with a short half-life (TABLE 4)9,21 may not appear in the urine if the test is done several hours after the last dose. On the other hand, some opioids may have an extended half-life in patients with liver or kidney disease, and may appear in the urine longer than would be expected.9
False-positive results. Substances that may cause false positives for opioids on a urine test include dextromethorphan, papaverine, poppy seeds and oil, quinine, quinolones, rifampin, and verapamil.10
False-negative results. Many of the problems already discussed can lead to false-negative results, including the panel’s failure to detect semisynthetic and synthetic opioids, rapid metabolism (most notably, of codeine), the timing of the test relative to the dose, and adulteration of the specimen. Thus, a negative test result in a patient on opioid therapy does not necessarily mean that he or she is noncompliant—and certainly is not proof of diversion.
Because of the variables that affect UDT outcomes, unanticipated results should be reviewed with the patient and possibly, with the lab, and viewed within the therapeutic context. When more definitive information is needed, serum testing may be performed as follow-up. While serum testing can detect drugs and their metabolites ingested within hours, it is not widely used on initial screening because it is a more invasive procedure with higher associated costs.13
CASE 2 Upon further discussion with Don F, the physician orders a serum oxycodone test, which shows a level of 10 ng/mL. The physician notes that serum testing is more appropriate than UDT for Don because of the inconsistent detection of oxycodone in urine.
TABLE 4
Pharmacokinetics of common opioids: Time detectable in urine9,21
| Drug (half-life) | Time detectable in urine | Comment |
|---|---|---|
| Codeine (2.5-3 h) | 48 h | Pharmacogenetic-dependent effects may affect detection |
| Fentanyl Transdermal (17 h) Submucosal (7 h) | Not usually detected in urine (lack of metabolites) | Excretion of transdermal fentanyl can last days |
| Hydromorphone IR (2.3 h) ER (18.6 h) | 2-4 d | Significant interpatient variability |
| Methadone (8-59 h) | 3 d | |
| Morphine (1.5-2 h) | 48-72 h | 90% eliminated within 24 h |
| Oxycodone IR (3.2 h) ER (4.5 h) | Often not detected in urine | High-fat meals may increase serum concentrations of ER formulation |
| Propoxyphene Parent drug (6-12 h) Metabolite (30-36 h) | 6-48 h | |
| ER, extended release; IR, immediate release. | ||
CORRESPONDENCE Sarah McBane, PharmD, CDC, BCPS, University of California, San Diego, Skaggs School of Pharmacy and Pharmaceutical Sciences, 9500 Gilman Drive, La Jolla, CA 92023; [email protected]
• When you initiate opioid therapy for chronic pain, inform the patient that routine monitoring includes random urine drug testing (UDT). C
• Consider UDT not only for patients at high risk for abuse of prescription opioids, but for lower-risk individuals receiving opioid therapy, as well. C
• Use caution in interpreting the results of UDT; testing cannot reliably detect some opioids, and a negative result is not necessarily an indication of noncompliance. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Marilyn H, a 54-year-old woman with multiple chronic conditions, visits a “new” primary care physician to establish care following the retirement of her previous physician. She has poorly controlled diabetes, hypertension, and a lung nodule recently noted on a chest radiograph. Marilyn requests prescriptions for hydrocodone and alprazolam, stating that she has taken both drugs for years for chronic back pain and anxiety.
CASE 2 Don F, 38, has been on oxycodone/acetaminophen (Percocet) for 3 years for back pain resulting from a car accident. He has a remote history of amphetamine abuse, but reports that he has been clean for 10 years. Since the initiation of his pain medication, there have been no problems, and no “lost” prescriptions or requests for early refills.
If you were Marilyn and Don’s physician, would you order urine drug testing (UDT)?
Management of opioid therapy is a challenge for many family physicians, particularly when treating noncancer pain. Seemingly contradictory messages from various medical associations are part of the problem. Organizations such as the Joint Commission on Accreditation of Healthcare Organizations and the American Medical Association emphasize the importance of appropriate pain management, while regulatory bodies like the US Drug Enforcement Agency and many state medical boards warn of inappropriate prescribing and diversion of controlled substances.1-4
In the realm of opioid management guidelines, however, patient monitoring is a common theme. It’s not hard to understand why. The Centers for Disease Control and Prevention reports that, between 1999 and 2005, the incidence of unintentional drug overdose more than doubled—a consequence of increasing abuse of prescription opioid analgesics.5 Prescription medications are now the second most commonly abused drug category (marijuana is first6), accounting for more cases of abuse than heroin, cocaine, and hallucinogens combined.7 In primary care and pain management settings, estimates are that more than 1 in 4 chronic pain patients misuse opioids or illicit drugs.8
Thus, physicians who prescribe controlled substances face increasing pressure to prevent opioid diversion. That pressure is reflected in the US Federation of State Medical Boards (FSMB)’s Model Policy for the Use of Controlled Substances for the Treatment of Pain, which was updated in 2004.4 This policy underscores physicians’ responsibility to closely monitor patients being treated with opioids for chronic pain.
Inexpensive and noninvasive. To this end, UDT can be a valuable tool. It is the most widely used and acceptable form of drug testing, because it is inexpensive and noninvasive, and because most drugs can be detected in urine for 1 to 3 days.9,10 But many primary care physicians are unfamiliar with the complexities of UDT, and often fail to use it.11 One study found that only 8% of family physicians employed UDT for patients on chronic opioid therapy.12
When introduced and used appropriately, UDT can not only help detect misuse of controlled substances, but may strengthen the doctor-patient relationship, as well. For that to happen, however, the physician who orders urine testing must know which patients to test, when to test, and what urine testing can (and cannot) reveal.
Consider testing all patients treated for chronic pain
The FSMB urges physicians to consider a written agreement with any patient receiving chronic opioid therapy who has a history of, or is at high risk for, substance abuse.4 (Red flags are listed in TABLE 1.13-15) The document should state that the patient is responsible for providing urine and serum specimens for drug monitoring upon request. The 2009 guidelines from the American Pain Society and the American Academy of Pain Medicine also address the role of drug monitoring, strongly recommending periodic urine screens for high-risk patients on chronic opioid therapy.16
Evidence suggests that predictors of aberrant behavior are not completely reliable, however, and that a substantial number of individuals using illicit substances will be missed if clinicians restrict urine testing to those they deem to be at high risk.17 Thus, UDT may be a valuable tool for low-risk patients on chronic opioid therapy, as well. Written agreements governing opioid therapy may also be useful for low-risk patients.
TABLE 1
Aberrant drug-related behavior: Red flags13-15
| Use of opioids for non-analgesic indications |
| Lack of control (related to drug use or to patient behavior) |
| Compulsive use of medications |
| Continued use of drugs despite harm/lack of benefit |
| Cravings |
| Escalation of drug use |
| Selling/altering prescriptions |
| Theft or diversion |
| Request for early refills |
| Claims of “lost” prescriptions |
| Reluctance to try nonpharmacologic options |
| Use of multiple prescribers or pharmacies |
| Odd stories regarding need for medication |
| Reporting vague medical history or textbook symptoms |
| Unwillingness to name regular physician |
| No interest in a physical exam, diagnostic testing, or providing past records |
| Request for specific drug(s) |
| Extensive (or very limited) understanding of medications |
| Calling or arriving after hours or when regular doctor is unavailable |
| Insistence on being seen urgently (eg, because of being late for another appointment) |
When to test, what to test for
No guidelines specify when to test, but testing upon initiation of chronic opioid treatment, followed by random testing, is the most widely used strategy. Unobserved specimen collection is generally acceptable,13 provided the specimens are requested at random rather than routinely at every visit.
Initial testing is done using an immuno-assay drug panel.13,18 TABLE 2 lists the drugs most commonly included in a standard urine test. However, the drug panel can vary from 1 laboratory to another, as can the lower limits of drug detection. No-threshold testing is mentioned in pain management literature, but is not often available in clinical practice.
Before initiating UDT, it is important to know which drugs the laboratory you use routinely tests for and what its lower limits are. The simplest way to find out is to ask lab personnel.
CASE 1 At her first visit, Marilyn H’s new physician focuses on controlling her blood sugar and blood pressure, ordering follow-up testing of the lung nodule, and refilling her hydrocodone and alprazolam prescriptions. The physician requests the patient’s medical records and orders a urine drug screen per clinic protocol, testing for benzodiazepines as well as for opioids. He gives his patient prescriptions for a 1-month supply of both drugs while the UDT results are pending.
The lab report comes in the following day, and indicates that Marilyn tested positive for cocaine but negative for other substances, including narcotics and benzodiazepines. The clinic immediately notifies the pharmacy to confiscate the patient’s new prescriptions when she presents them and calls Marilyn, advising her that she will not be given any further prescriptions for controlled substances.
The physician refers the patient to a pain clinic, gives her the number of a substance abuse treatment center, and encourages her to follow up at the clinic for other medical issues. Marilyn fails to keep her appointment at the pain clinic and does not respond to a subsequent call.
TABLE 2
A standard urine drug test panel13,18
| Amphetamines |
| Cocaine |
| Marijuana (THC) |
| Opiates (morphine and codeine) |
| Phencyclidine |
| THC, tetrahydrocannabinol. |
Talking to patients about drug testing
Physicians are often concerned about patients’ feelings about drug testing—worrying that patients may not feel trusted or respected by a doctor who asks them to submit to UDT. Others may fear that the mere mention of urine testing will encourage patients to misuse prescription opioids, that patients will view UDT as a punitive measure, or that those being tested will believe that the physician is more concerned with self-protection than with providing optimal care to the patient.
Making UDT routine. One way to circumvent such possibilities is to implement a systematic approach to drug testing. We recommend that physicians discuss the role of UDT in the initial education session with patients being started on a course of opiates. Describing UDT as simply another routine monitoring parameter—akin to the measure of microalbuminuria for patients with diabetes—can decrease or eliminate the stigma associated with drug testing.
CASE 2 A new policy encouraging UDT for all patients on chronic controlled substances has just been implemented at the clinic where Don F is being treated. His physician tells him about the policy, and a urine test is ordered at his next visit. The test comes back negative for all substances, including opioids.
When presented with the results over the phone, Don insists that he regularly takes his prescription medication, and makes a same-day appointment to discuss the results with his physician.
Interpreting test results— what UDT can (and can’t) reveal
To avoid eroding trust by falsely accusing a patient of diversion or use of an illicit substance, it’s important to familiarize yourself with testing limitations. Factors that can affect the results, and may interfere with the ability of UDT to provide a definitive picture, include:
Lab variability and technical limitations. Some urine drug panels may not have a lower limit sufficient to detect small quantities of opioids. Others may not detect certain substances, notably the semisynthetic and synthetic opioids (TABLE 3).19 Oxycodone is a prime example of a commonly prescribed semisynthetic opioid that does not appear on many urine test panels.8
In addition, individual drugs within a class may not be identified on UDT panels. When confirmation of a specific drug or metabolite is needed, serum testing must be performed.8
TABLE 3
Classifying opioids19
| Natural | Semisynthetic | Synthetic |
|---|---|---|
| Codeine | Hydrocodone | Fentanyl |
| Morphine | Hydromorphone | Meperidine |
| Oxycodone | Methadone | |
| Propoxyphene |
Differences in metabolism. Genetic differences in metabolism can also skew the results of UDT. Codeine, which relies on hepatic metabolism via cytochrome P450 2D6 for conversion to morphine, is the classic example; cytochrome P450 2D6 is a polymorphic enzyme, meaning that it manifests with different activity levels in different people. Patients who are poor metabolizers (an estimated 5%-10% of Caucasians, 1%-5% of Asians, 2%-7% of African Americans, and 2%-6% of Hispanics20) will convert very little codeine to morphine; conversely, those who are rapid metabolizers will convert extensive amounts. A rapid metabolizer taking codeine as prescribed may therefore have a negative UDT; in an average metabolizer taking the same dose, both codeine and morphine will be detected.20
Drugs’ half-lives. Opioids with a short half-life (TABLE 4)9,21 may not appear in the urine if the test is done several hours after the last dose. On the other hand, some opioids may have an extended half-life in patients with liver or kidney disease, and may appear in the urine longer than would be expected.9
False-positive results. Substances that may cause false positives for opioids on a urine test include dextromethorphan, papaverine, poppy seeds and oil, quinine, quinolones, rifampin, and verapamil.10
False-negative results. Many of the problems already discussed can lead to false-negative results, including the panel’s failure to detect semisynthetic and synthetic opioids, rapid metabolism (most notably, of codeine), the timing of the test relative to the dose, and adulteration of the specimen. Thus, a negative test result in a patient on opioid therapy does not necessarily mean that he or she is noncompliant—and certainly is not proof of diversion.
Because of the variables that affect UDT outcomes, unanticipated results should be reviewed with the patient and possibly, with the lab, and viewed within the therapeutic context. When more definitive information is needed, serum testing may be performed as follow-up. While serum testing can detect drugs and their metabolites ingested within hours, it is not widely used on initial screening because it is a more invasive procedure with higher associated costs.13
CASE 2 Upon further discussion with Don F, the physician orders a serum oxycodone test, which shows a level of 10 ng/mL. The physician notes that serum testing is more appropriate than UDT for Don because of the inconsistent detection of oxycodone in urine.
TABLE 4
Pharmacokinetics of common opioids: Time detectable in urine9,21
| Drug (half-life) | Time detectable in urine | Comment |
|---|---|---|
| Codeine (2.5-3 h) | 48 h | Pharmacogenetic-dependent effects may affect detection |
| Fentanyl Transdermal (17 h) Submucosal (7 h) | Not usually detected in urine (lack of metabolites) | Excretion of transdermal fentanyl can last days |
| Hydromorphone IR (2.3 h) ER (18.6 h) | 2-4 d | Significant interpatient variability |
| Methadone (8-59 h) | 3 d | |
| Morphine (1.5-2 h) | 48-72 h | 90% eliminated within 24 h |
| Oxycodone IR (3.2 h) ER (4.5 h) | Often not detected in urine | High-fat meals may increase serum concentrations of ER formulation |
| Propoxyphene Parent drug (6-12 h) Metabolite (30-36 h) | 6-48 h | |
| ER, extended release; IR, immediate release. | ||
CORRESPONDENCE Sarah McBane, PharmD, CDC, BCPS, University of California, San Diego, Skaggs School of Pharmacy and Pharmaceutical Sciences, 9500 Gilman Drive, La Jolla, CA 92023; [email protected]
1. Health Care Issues. Joint Commission on Accreditation of Health Care Organizations. Available at: http://www.jointcommission.org/. Accessed March 5, 2010.
2. Standards, Laws, and Regulations Addressing Pain Medications and Medical Practice: Report 6 of the Council on Science and Public Health. American Medical Association. June 2007. Available at: http://www.ama-assn.org/ama/pub/physician-resources/medical-science/council-science-public-health.shtml. Accessed July 16, 2009.
3. US Department of Justice Drug Enforcement Administration Office of Diversion Control. Available at: http://www.deadiversion.usdoj.gov/. Accessed March 5, 2010.
4. Federation of State Medical Boards. Model Policy for the Use of Controlled Substances for the Treatment of Pain. May 2004. Available at: http://www.fsmb.org/pdf/2004_grpol_Controlled_Substances.pdf. Accessed March 5, 2010.
5. Centers for Disease Control and Prevention. Prescription Drug Overdose: State Health Agencies Respond. Available at: http://www.cdc.gov/HomeandRecreationalSafety/pubs/RXReport_web-a.pdf. Accessed May 15, 2010.
6. Drug Enforcement Agency Office of Diversion Control NFLIS Special Report: Controlled Substance Prescription Drugs 2001-2005. November 2006. Available at: http://www.deadiversion.usdoj.gov/nflis/2006rx_drugs_report.pdf. Accessed May 15, 2010.
7. Department of Health and Human Services Office of Substance Abuse and Mental Health Services Administration. Results from the 2007 National Survey on Drug Use and Health: national findings. Available at: http://www.oas.samhsa.gov/nsduh/2k7nsduh/2k7Results.pdf. Accessed May 7, 2010.
8. Reisfield G, Salazar E, Bertholf R. Rational use and interpretation of urine drug testing in chronic opioid therapy. Ann Clin Lab Sci. 2007;37:301-314.
9. Clinical Pharmacology [online]. Tampa, FL: Gold Standard Inc; 2010. Accessed March 5, 2010.
10. Drug abuse urine tests: false-positive results. Pharmacist’s Letter/Prescriber’s Letter. 2005;21:210314.-
11. Reisfield GM, Webb FJ, Bertholf RL, et al. Family physicians’ proficiency in urine drug test interpretation. J Opioid Manag. 2007;3:333-337.
12. Adams N, Plane M, Fleming M, et al. Opioids and the treatment of chronic pain in a primary care sample. J Pain Symptom Manage. 2001;22:791-796.
13. Gourlay D, Caplan Y, Heit H. Urine drug testing in clinical practice: dispelling the myths and designing strategies. San Francisco, CA: California Academy of Family Physicians; 2006.
14. Cole BE. Recognizing and preventing medication diversion. Fam Pract Manag. 2001;8:37-41.
15. Jackman R, Purvis J, Mallett B. Chronic nonmalignant pain in primary care. Am Fam Physician. 2008;78:1155-1162.
16. Chou R, Fanciullo G, Fine P, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009;10:113-130.
17. Chou R, Fanciullo G, Fine P, et al. Opioids for chronic noncancer pain: prediction and identification of aberrant drug-related behaviors: a review of the evidence for an American Pain Society and American Academy of Pain Medicine Clinical Practice Guideline. J Pain. 2009;10:131-146.
18. Moeller K, Lee K, Kissack J. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83:66-76.
19. Amabile C, Bowman B. Overview of oral modified-release opioid products for the management of chronic pain. Ann Pharmaco-therapy. 2006;40:1327-1335.
20. Zhou S. Polymorphism of human cytochrome P450 2D6 and its clinical significance. Clin Pharmacokinet. 2009;48:689-723.
21. Drug Facts and Comparisons [online]. 2010. Available at: http://www.factsandcomparisons.com/. Accessed March 5, 2010.
1. Health Care Issues. Joint Commission on Accreditation of Health Care Organizations. Available at: http://www.jointcommission.org/. Accessed March 5, 2010.
2. Standards, Laws, and Regulations Addressing Pain Medications and Medical Practice: Report 6 of the Council on Science and Public Health. American Medical Association. June 2007. Available at: http://www.ama-assn.org/ama/pub/physician-resources/medical-science/council-science-public-health.shtml. Accessed July 16, 2009.
3. US Department of Justice Drug Enforcement Administration Office of Diversion Control. Available at: http://www.deadiversion.usdoj.gov/. Accessed March 5, 2010.
4. Federation of State Medical Boards. Model Policy for the Use of Controlled Substances for the Treatment of Pain. May 2004. Available at: http://www.fsmb.org/pdf/2004_grpol_Controlled_Substances.pdf. Accessed March 5, 2010.
5. Centers for Disease Control and Prevention. Prescription Drug Overdose: State Health Agencies Respond. Available at: http://www.cdc.gov/HomeandRecreationalSafety/pubs/RXReport_web-a.pdf. Accessed May 15, 2010.
6. Drug Enforcement Agency Office of Diversion Control NFLIS Special Report: Controlled Substance Prescription Drugs 2001-2005. November 2006. Available at: http://www.deadiversion.usdoj.gov/nflis/2006rx_drugs_report.pdf. Accessed May 15, 2010.
7. Department of Health and Human Services Office of Substance Abuse and Mental Health Services Administration. Results from the 2007 National Survey on Drug Use and Health: national findings. Available at: http://www.oas.samhsa.gov/nsduh/2k7nsduh/2k7Results.pdf. Accessed May 7, 2010.
8. Reisfield G, Salazar E, Bertholf R. Rational use and interpretation of urine drug testing in chronic opioid therapy. Ann Clin Lab Sci. 2007;37:301-314.
9. Clinical Pharmacology [online]. Tampa, FL: Gold Standard Inc; 2010. Accessed March 5, 2010.
10. Drug abuse urine tests: false-positive results. Pharmacist’s Letter/Prescriber’s Letter. 2005;21:210314.-
11. Reisfield GM, Webb FJ, Bertholf RL, et al. Family physicians’ proficiency in urine drug test interpretation. J Opioid Manag. 2007;3:333-337.
12. Adams N, Plane M, Fleming M, et al. Opioids and the treatment of chronic pain in a primary care sample. J Pain Symptom Manage. 2001;22:791-796.
13. Gourlay D, Caplan Y, Heit H. Urine drug testing in clinical practice: dispelling the myths and designing strategies. San Francisco, CA: California Academy of Family Physicians; 2006.
14. Cole BE. Recognizing and preventing medication diversion. Fam Pract Manag. 2001;8:37-41.
15. Jackman R, Purvis J, Mallett B. Chronic nonmalignant pain in primary care. Am Fam Physician. 2008;78:1155-1162.
16. Chou R, Fanciullo G, Fine P, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009;10:113-130.
17. Chou R, Fanciullo G, Fine P, et al. Opioids for chronic noncancer pain: prediction and identification of aberrant drug-related behaviors: a review of the evidence for an American Pain Society and American Academy of Pain Medicine Clinical Practice Guideline. J Pain. 2009;10:131-146.
18. Moeller K, Lee K, Kissack J. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83:66-76.
19. Amabile C, Bowman B. Overview of oral modified-release opioid products for the management of chronic pain. Ann Pharmaco-therapy. 2006;40:1327-1335.
20. Zhou S. Polymorphism of human cytochrome P450 2D6 and its clinical significance. Clin Pharmacokinet. 2009;48:689-723.
21. Drug Facts and Comparisons [online]. 2010. Available at: http://www.factsandcomparisons.com/. Accessed March 5, 2010.
A costly diagnostic failure
A 57-year-old man was referred by his general practitioner to our surgical team as an emergency admission. The patient had a 4-month history of post-prandial nausea and vomiting, occasional heartburn, and a change in bowel habits. (His normal bowel habit was 3 times a day, but it had changed to once every 2 to 5 days.) Over the past 2 months, he had lost 16 kg (35.3 lb).
His past medical history included esophagitis, peripheral vascular disease, and an inguinal hernia repair. He was a self-employed baker, a smoker of 8 pack-years, and his alcohol intake was 6.9 oz per week. There was nothing significant about his family history. His regular medications included omeprazole, simvastatin, and aspirin.
On examination, we noted bilateral fingernail clubbing, but no peripheral lymphadenopathy. His abdominal examination revealed mild, left upper quadrant tenderness.
His significant laboratory results were:
- hemoglobin, 11.6 g/dL
- mean corpuscular volume, 93.0 fL
- ferritin, 17 mcg/L
- serum folate, 2.3 mcg/L
- albumin, 29 g/L
- potassium, 3.3 mmol/L
- urea, 13.2 mmol/L with normal creatinine
- sodium, 141 mmol/L
A barium meal test showed a large food residue in the stomach, a markedly dilated duodenal loop, and a stricture at the duodenal-jejunal flexure. Computed tomography scan showed 2 simple liver cysts. Esophagogastroduodenoscopy showed moderate reflux esophagitis, a large residue of food and fluid in the stomach, and a stricture that appeared to be malignant at the duodenal-jejunal flexure.
Biopsies revealed severe, high-grade dysplasia and a possible invasive tumor. Incidentally, one of the biopsies also showed evidence of celiac disease (FIGURE 1A). The patient was started on total parenteral nutrition in light of his significant weight loss. He was transferred to surgical care and underwent laparotomy and resection of a proximal jejunal tumor.
Chemotherapy and a gluten-free diet
Final histopathology revealed a jejunal adenocarcinoma with extension to the serosal surface of the bowel (FIGURE 1B) and celiac lymph node involvement. Histology of the surgical specimen also confirmed the diagnosis of underlying celiac disease. The patient underwent adjuvant chemotherapy and was put on a gluten-free diet.
The patient began to gain weight. On a follow-up visit, he was 20 kg (44.1 lb) heavier than his presurgery weight. He was moving his bowel once a day with formed brown stool.
FIGURE 1
Duodenal biopsy revealed celiac disease and adenocarcinoma
One of the patient’s biopsies showed evidence of celiac disease (A). Another revealed a jejunal adenocarcinoma (B) with extension to the serosal surface of the bowel and celiac lymph node involvement.
Anemic for years, but no one dug deeper
A detailed history revealed that the patient had been anemic since the age of 20, had always had difficulty maintaining his weight, and had been having bowel movements 3 to 4 times a day throughout his life. It was unclear why his condition was never properly investigated.
Progress was short lived
Unfortunately, while receiving adjuvant chemotherapy, our patient developed a gastric outlet obstruction that required further surgery and a palliative gastroenterostomy. Despite good palliation, the patient died several months later from progressive cancer.
A valuable reminder for us all
Celiac disease is not an uncommon cause of malabsorption of 1 or more nutrients in Caucasians—especially those of European decent.1-4 Colon cancer, gastric cancer, and celiac disease are the most important gastrointestinal causes of iron deficiency anemia.5
The seroprevalence of celiac disease is as high as approximately 1% in North America and Western Europe, with a high ratio of un-diagnosed to diagnosed cases.4,6-8 The most serious complication of celiac disease is the development of a malignancy.1,9-12 Incidence of both gastrointestinal and nongastrointestinal neoplasms (as well as intestinal lymphoma) is higher in patients with celiac disease.1,9-11,13 Small-bowel lymphoma appears to be significantly associated with unrecognized celiac disease.7
Data from various studies suggest a protective role for a gluten-free diet against malignancy in celiac disease and give further support for advising all patients to adhere to a strict gluten-free diet.9,10,13,14
Follow the clues: Nutrient deficiencies, including folate and iron deficiency anemia—with all of their associated signs and symptoms—are not disease entities, but clues to diseases. We must remain vigilant in our investigative efforts.
CORRESPONDENCE Arash Assadsangabi, MD, Gastroenterology Department, Bristol Royal Infirmary, Marlborough Street, Bristol, BS2 8HW, UK; [email protected]
1. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison’s Principles of Internal Medicine. 15th ed. New York, NY: The McGraw-Hill Companies; 2001:662.
2. Menardo G, Brizzolara R, Bonassi S, et al. Population screening for coeliac disease in a low prevalence area in Italy. Scand J Gastroenterol. 2006;41:1414-1420.
3. Antunes H, Abreu I, Nogueiras A, et al. First determination of the prevalence of celiac disease in a Portuguese population. Acta Med Port. 2006;19:115-120.
4. Fruhauf P, Lojda Z, Fabianova J, et al. Changing clinical image of celiac sprue in childhood. Cas Lek Cesk. 2006;145:470-474.
5. Goddard AF, James MW, McIntyre AS, et al. Guidelines for management of iron deficiency anaemia. British Society of Gastroenterology; May 2005. Available at: www.bsg.org.uk/images/stories/docs/clinical/guidelines/sbn/iron_def.pdf. Accessed October 14, 2010.
6. Cronin CC, Feighery A, Ferriss JB, et al. High prevalence of celiac disease among patients with insulin-dependent (type 1) diabetes mellitus. Am J Gastroenterol. 1997;92:2210-2212.
7. Johnston SD, Watson RG. Small bowel lymphoma in unrecognized celiac disease: a cause for concern? Eur J Gastroenterol Hepatol. 2000;12:645-648.
8. Fowell AJ, Thomas PW, Surgenor SL, et al. The epidemiology of coeliac disease in East Dorset 1993-2002: an assessment of the ‘coeliac iceberg’, and preliminary evidence of case clustering. QJM. 2006;99:453-460.
9. Lo Russo L. Celiac disease and lymphoma: review of the literature. Clin Ther. 1997;148:267-275.
10. Holmes GK. Coeliac disease and malignancy. Dig Liver Dis. 2002;34:229-237.
11. Wright DH. The major complications of celiac disease. Baillieres Clin Gastroenterol. 1995;9:351-369.
12. Kroll MH, Jiji V, Jiji R. Microcytic hypochromic anemia associated with renal cell carcinoma. South Med J. 1984;77:635-637.
13. Green PH, Fleichauer AT, Bhagat G, et al. Risk of malignancy in patients with celiac disease. Am J Med. 2003;115:191-195.
14. Holmes GK, Prior P, Lane MR, et al. Malignancy in coeliac disease—effect of a gluten free diet. Gut. 1989;30:333-338.
A 57-year-old man was referred by his general practitioner to our surgical team as an emergency admission. The patient had a 4-month history of post-prandial nausea and vomiting, occasional heartburn, and a change in bowel habits. (His normal bowel habit was 3 times a day, but it had changed to once every 2 to 5 days.) Over the past 2 months, he had lost 16 kg (35.3 lb).
His past medical history included esophagitis, peripheral vascular disease, and an inguinal hernia repair. He was a self-employed baker, a smoker of 8 pack-years, and his alcohol intake was 6.9 oz per week. There was nothing significant about his family history. His regular medications included omeprazole, simvastatin, and aspirin.
On examination, we noted bilateral fingernail clubbing, but no peripheral lymphadenopathy. His abdominal examination revealed mild, left upper quadrant tenderness.
His significant laboratory results were:
- hemoglobin, 11.6 g/dL
- mean corpuscular volume, 93.0 fL
- ferritin, 17 mcg/L
- serum folate, 2.3 mcg/L
- albumin, 29 g/L
- potassium, 3.3 mmol/L
- urea, 13.2 mmol/L with normal creatinine
- sodium, 141 mmol/L
A barium meal test showed a large food residue in the stomach, a markedly dilated duodenal loop, and a stricture at the duodenal-jejunal flexure. Computed tomography scan showed 2 simple liver cysts. Esophagogastroduodenoscopy showed moderate reflux esophagitis, a large residue of food and fluid in the stomach, and a stricture that appeared to be malignant at the duodenal-jejunal flexure.
Biopsies revealed severe, high-grade dysplasia and a possible invasive tumor. Incidentally, one of the biopsies also showed evidence of celiac disease (FIGURE 1A). The patient was started on total parenteral nutrition in light of his significant weight loss. He was transferred to surgical care and underwent laparotomy and resection of a proximal jejunal tumor.
Chemotherapy and a gluten-free diet
Final histopathology revealed a jejunal adenocarcinoma with extension to the serosal surface of the bowel (FIGURE 1B) and celiac lymph node involvement. Histology of the surgical specimen also confirmed the diagnosis of underlying celiac disease. The patient underwent adjuvant chemotherapy and was put on a gluten-free diet.
The patient began to gain weight. On a follow-up visit, he was 20 kg (44.1 lb) heavier than his presurgery weight. He was moving his bowel once a day with formed brown stool.
FIGURE 1
Duodenal biopsy revealed celiac disease and adenocarcinoma
One of the patient’s biopsies showed evidence of celiac disease (A). Another revealed a jejunal adenocarcinoma (B) with extension to the serosal surface of the bowel and celiac lymph node involvement.
Anemic for years, but no one dug deeper
A detailed history revealed that the patient had been anemic since the age of 20, had always had difficulty maintaining his weight, and had been having bowel movements 3 to 4 times a day throughout his life. It was unclear why his condition was never properly investigated.
Progress was short lived
Unfortunately, while receiving adjuvant chemotherapy, our patient developed a gastric outlet obstruction that required further surgery and a palliative gastroenterostomy. Despite good palliation, the patient died several months later from progressive cancer.
A valuable reminder for us all
Celiac disease is not an uncommon cause of malabsorption of 1 or more nutrients in Caucasians—especially those of European decent.1-4 Colon cancer, gastric cancer, and celiac disease are the most important gastrointestinal causes of iron deficiency anemia.5
The seroprevalence of celiac disease is as high as approximately 1% in North America and Western Europe, with a high ratio of un-diagnosed to diagnosed cases.4,6-8 The most serious complication of celiac disease is the development of a malignancy.1,9-12 Incidence of both gastrointestinal and nongastrointestinal neoplasms (as well as intestinal lymphoma) is higher in patients with celiac disease.1,9-11,13 Small-bowel lymphoma appears to be significantly associated with unrecognized celiac disease.7
Data from various studies suggest a protective role for a gluten-free diet against malignancy in celiac disease and give further support for advising all patients to adhere to a strict gluten-free diet.9,10,13,14
Follow the clues: Nutrient deficiencies, including folate and iron deficiency anemia—with all of their associated signs and symptoms—are not disease entities, but clues to diseases. We must remain vigilant in our investigative efforts.
CORRESPONDENCE Arash Assadsangabi, MD, Gastroenterology Department, Bristol Royal Infirmary, Marlborough Street, Bristol, BS2 8HW, UK; [email protected]
A 57-year-old man was referred by his general practitioner to our surgical team as an emergency admission. The patient had a 4-month history of post-prandial nausea and vomiting, occasional heartburn, and a change in bowel habits. (His normal bowel habit was 3 times a day, but it had changed to once every 2 to 5 days.) Over the past 2 months, he had lost 16 kg (35.3 lb).
His past medical history included esophagitis, peripheral vascular disease, and an inguinal hernia repair. He was a self-employed baker, a smoker of 8 pack-years, and his alcohol intake was 6.9 oz per week. There was nothing significant about his family history. His regular medications included omeprazole, simvastatin, and aspirin.
On examination, we noted bilateral fingernail clubbing, but no peripheral lymphadenopathy. His abdominal examination revealed mild, left upper quadrant tenderness.
His significant laboratory results were:
- hemoglobin, 11.6 g/dL
- mean corpuscular volume, 93.0 fL
- ferritin, 17 mcg/L
- serum folate, 2.3 mcg/L
- albumin, 29 g/L
- potassium, 3.3 mmol/L
- urea, 13.2 mmol/L with normal creatinine
- sodium, 141 mmol/L
A barium meal test showed a large food residue in the stomach, a markedly dilated duodenal loop, and a stricture at the duodenal-jejunal flexure. Computed tomography scan showed 2 simple liver cysts. Esophagogastroduodenoscopy showed moderate reflux esophagitis, a large residue of food and fluid in the stomach, and a stricture that appeared to be malignant at the duodenal-jejunal flexure.
Biopsies revealed severe, high-grade dysplasia and a possible invasive tumor. Incidentally, one of the biopsies also showed evidence of celiac disease (FIGURE 1A). The patient was started on total parenteral nutrition in light of his significant weight loss. He was transferred to surgical care and underwent laparotomy and resection of a proximal jejunal tumor.
Chemotherapy and a gluten-free diet
Final histopathology revealed a jejunal adenocarcinoma with extension to the serosal surface of the bowel (FIGURE 1B) and celiac lymph node involvement. Histology of the surgical specimen also confirmed the diagnosis of underlying celiac disease. The patient underwent adjuvant chemotherapy and was put on a gluten-free diet.
The patient began to gain weight. On a follow-up visit, he was 20 kg (44.1 lb) heavier than his presurgery weight. He was moving his bowel once a day with formed brown stool.
FIGURE 1
Duodenal biopsy revealed celiac disease and adenocarcinoma
One of the patient’s biopsies showed evidence of celiac disease (A). Another revealed a jejunal adenocarcinoma (B) with extension to the serosal surface of the bowel and celiac lymph node involvement.
Anemic for years, but no one dug deeper
A detailed history revealed that the patient had been anemic since the age of 20, had always had difficulty maintaining his weight, and had been having bowel movements 3 to 4 times a day throughout his life. It was unclear why his condition was never properly investigated.
Progress was short lived
Unfortunately, while receiving adjuvant chemotherapy, our patient developed a gastric outlet obstruction that required further surgery and a palliative gastroenterostomy. Despite good palliation, the patient died several months later from progressive cancer.
A valuable reminder for us all
Celiac disease is not an uncommon cause of malabsorption of 1 or more nutrients in Caucasians—especially those of European decent.1-4 Colon cancer, gastric cancer, and celiac disease are the most important gastrointestinal causes of iron deficiency anemia.5
The seroprevalence of celiac disease is as high as approximately 1% in North America and Western Europe, with a high ratio of un-diagnosed to diagnosed cases.4,6-8 The most serious complication of celiac disease is the development of a malignancy.1,9-12 Incidence of both gastrointestinal and nongastrointestinal neoplasms (as well as intestinal lymphoma) is higher in patients with celiac disease.1,9-11,13 Small-bowel lymphoma appears to be significantly associated with unrecognized celiac disease.7
Data from various studies suggest a protective role for a gluten-free diet against malignancy in celiac disease and give further support for advising all patients to adhere to a strict gluten-free diet.9,10,13,14
Follow the clues: Nutrient deficiencies, including folate and iron deficiency anemia—with all of their associated signs and symptoms—are not disease entities, but clues to diseases. We must remain vigilant in our investigative efforts.
CORRESPONDENCE Arash Assadsangabi, MD, Gastroenterology Department, Bristol Royal Infirmary, Marlborough Street, Bristol, BS2 8HW, UK; [email protected]
1. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison’s Principles of Internal Medicine. 15th ed. New York, NY: The McGraw-Hill Companies; 2001:662.
2. Menardo G, Brizzolara R, Bonassi S, et al. Population screening for coeliac disease in a low prevalence area in Italy. Scand J Gastroenterol. 2006;41:1414-1420.
3. Antunes H, Abreu I, Nogueiras A, et al. First determination of the prevalence of celiac disease in a Portuguese population. Acta Med Port. 2006;19:115-120.
4. Fruhauf P, Lojda Z, Fabianova J, et al. Changing clinical image of celiac sprue in childhood. Cas Lek Cesk. 2006;145:470-474.
5. Goddard AF, James MW, McIntyre AS, et al. Guidelines for management of iron deficiency anaemia. British Society of Gastroenterology; May 2005. Available at: www.bsg.org.uk/images/stories/docs/clinical/guidelines/sbn/iron_def.pdf. Accessed October 14, 2010.
6. Cronin CC, Feighery A, Ferriss JB, et al. High prevalence of celiac disease among patients with insulin-dependent (type 1) diabetes mellitus. Am J Gastroenterol. 1997;92:2210-2212.
7. Johnston SD, Watson RG. Small bowel lymphoma in unrecognized celiac disease: a cause for concern? Eur J Gastroenterol Hepatol. 2000;12:645-648.
8. Fowell AJ, Thomas PW, Surgenor SL, et al. The epidemiology of coeliac disease in East Dorset 1993-2002: an assessment of the ‘coeliac iceberg’, and preliminary evidence of case clustering. QJM. 2006;99:453-460.
9. Lo Russo L. Celiac disease and lymphoma: review of the literature. Clin Ther. 1997;148:267-275.
10. Holmes GK. Coeliac disease and malignancy. Dig Liver Dis. 2002;34:229-237.
11. Wright DH. The major complications of celiac disease. Baillieres Clin Gastroenterol. 1995;9:351-369.
12. Kroll MH, Jiji V, Jiji R. Microcytic hypochromic anemia associated with renal cell carcinoma. South Med J. 1984;77:635-637.
13. Green PH, Fleichauer AT, Bhagat G, et al. Risk of malignancy in patients with celiac disease. Am J Med. 2003;115:191-195.
14. Holmes GK, Prior P, Lane MR, et al. Malignancy in coeliac disease—effect of a gluten free diet. Gut. 1989;30:333-338.
1. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison’s Principles of Internal Medicine. 15th ed. New York, NY: The McGraw-Hill Companies; 2001:662.
2. Menardo G, Brizzolara R, Bonassi S, et al. Population screening for coeliac disease in a low prevalence area in Italy. Scand J Gastroenterol. 2006;41:1414-1420.
3. Antunes H, Abreu I, Nogueiras A, et al. First determination of the prevalence of celiac disease in a Portuguese population. Acta Med Port. 2006;19:115-120.
4. Fruhauf P, Lojda Z, Fabianova J, et al. Changing clinical image of celiac sprue in childhood. Cas Lek Cesk. 2006;145:470-474.
5. Goddard AF, James MW, McIntyre AS, et al. Guidelines for management of iron deficiency anaemia. British Society of Gastroenterology; May 2005. Available at: www.bsg.org.uk/images/stories/docs/clinical/guidelines/sbn/iron_def.pdf. Accessed October 14, 2010.
6. Cronin CC, Feighery A, Ferriss JB, et al. High prevalence of celiac disease among patients with insulin-dependent (type 1) diabetes mellitus. Am J Gastroenterol. 1997;92:2210-2212.
7. Johnston SD, Watson RG. Small bowel lymphoma in unrecognized celiac disease: a cause for concern? Eur J Gastroenterol Hepatol. 2000;12:645-648.
8. Fowell AJ, Thomas PW, Surgenor SL, et al. The epidemiology of coeliac disease in East Dorset 1993-2002: an assessment of the ‘coeliac iceberg’, and preliminary evidence of case clustering. QJM. 2006;99:453-460.
9. Lo Russo L. Celiac disease and lymphoma: review of the literature. Clin Ther. 1997;148:267-275.
10. Holmes GK. Coeliac disease and malignancy. Dig Liver Dis. 2002;34:229-237.
11. Wright DH. The major complications of celiac disease. Baillieres Clin Gastroenterol. 1995;9:351-369.
12. Kroll MH, Jiji V, Jiji R. Microcytic hypochromic anemia associated with renal cell carcinoma. South Med J. 1984;77:635-637.
13. Green PH, Fleichauer AT, Bhagat G, et al. Risk of malignancy in patients with celiac disease. Am J Med. 2003;115:191-195.
14. Holmes GK, Prior P, Lane MR, et al. Malignancy in coeliac disease—effect of a gluten free diet. Gut. 1989;30:333-338.
Don’t overlook the complications of tonsillectomy
• Monitor patients for pain, nausea and vomiting, and bleeding, as they are the most common complications of tonsillectomy. A
• Effectively manage postoperative pain to prevent dehydration, which can occur when patients fail to take in enough fluids because swallowing is painful. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Although the number of patients undergoing tonsillectomy has gradually declined since the 1970s, it remains one of the most common surgical procedures performed worldwide.1 The procedure, of course, is fairly routine—but not without risk.
Mortality rates for the operation range from 1 in 10,000 to 1 in 35,000, with morbidity rates ranging from 1.5% to 14%; mortality and morbidity after tonsillectomy are usually the result of postoperative bleeding.2,3 In addition to bleeding, other common complications include pain, nausea, and vomiting.
The patient’s surgeon plays a central role in minimizing risk. But as a primary care physician, you, too, play an important role in ensuring that your patient’s tonsillectomy is uneventful. This review will help toward that end.
Refine your preop approach
Address informed consent issues. While the surgeon is responsible for obtaining informed consent, a patient may discuss the procedure with you, the family physician. (See TABLE 1 for the indications for tonsillectomy.) Although the procedure is safe and effective, the patient and his or her family need to know that bleeding will most likely occur immediately after the procedure, although it can occur at any time during the first 2 weeks postop. Advise the patient and family that postop pain is similar to that of a throat infection, but is often felt in the ears (“referred otalgia”). Because postop swallowing is painful, the patient may not drink enough fluids. If this problem because severe, he or she may need to be admitted for IV fluid replacement.
Discuss the patient’s length of stay. An increasing number of tonsillectomies are performed on an outpatient basis. However, high-risk patients—those with sleep apnea, coagulation disorders, or other underlying diseases, and anyone younger than 4 years of age or living a long distance from the hospital—should be admitted for overnight observation.4
Ask about previous surgeries. Tonsillectomies are performed under general anesthesia in most facilities. Ask about previous surgeries and conditions that may adversely affect the surgery: Does the patient have any upper airway obstruction, difficulty extending his cervical spine, or enzymatic deficiencies? A pseudocholinesterase deficiency, for instance, may cause prolonged paralysis of the respiratory muscles, requiring an extended period of time during which the patient must be mechanically ventilated.
Anesthesiologists use the Mallampati score to predict the ease of intubation.5 It’s derived by visualizing the base of the uvula, the tonsillar pillars, and the soft palate. Scoring may be done with or without phonation. A patient is considered to be in 1 of 4 classes, depending upon what can be visualized:
- Class 1: the tonsils, uvula, and soft palate
- Class 2: the hard and soft palate and upper portion of the tonsils and uvula
- Class 3: the soft and hard palate and base of the uvula
- Class 4: the hard palate.
As a general rule, patients scheduled for tonsillectomy are prone to higher scores because of underlying disease.
Order lab tests, stop certain medications. Instruct patients to discontinue aspirin 7 days before surgery, and naproxen and other nonsteroidal anti-inflammatory drugs (NSAIDs) 4 days before surgery.6 Antiplatelet aggregation drugs such as clopidogrel should also be stopped 7 days before surgery.6
While you should routinely order a complete blood count, experts disagree on the value and cost-effectiveness of routinely running prothrombin time and partial thromboplastin time.7
Assess whether the patient is anxious about the surgery. Tonsillectomy and the subsequent hospitalization can make patients anxious, bringing on sleep disturbances, behavioral problems, nightmares, enuresis, and emotional regression. Fortunately, these problems usually disappear without any intervention, but offering patients preop reassurance, demonstrations, and educational materials may help prevent them (TABLE 2).
TABLE 1
Indications for tonsillectomy
| Tonsils are infected ≥3 times a year despite adequate medical therapy |
| Peritonsillar abscess is unresponsive to medical management and drainage documented by surgeon, unless surgery is performed during acute stage |
| Chronic or recurrent tonsillitis associated with the streptococcal carrier state and not responding to beta-lactam antibiotics given with a beta-lactamase inhibitor |
| Hypertrophy causing dental malocclusion or adversely affecting orofacial growth that has been documented by orthodontist |
| Hypertrophy causing upper airway obstruction, severe dysphagia, sleep disorders, or cardiopulmonary complications |
| Persistent foul breath or bad taste in mouth due to chronic tonsillitis that has not been responsive to medical therapy |
| Unilateral tonsil hypertrophy that is presumed to be neoplastic |
| Source: Erickson BK, Larson DR, St Sauver JL, et al. Changes in incidence and indications of tonsillectomy and adenotonsillectomy, 1970-2005. Otolaryngol Head Neck Surg. 2009;140:894-901. |
TABLE 2
Patient education resources
Address postop complications
Ensure that your patient has proper pain relief. Sore throat and referred otalgia are common, but usually subside within 2 weeks. The pain typically manifests as dysphagia, which results from trauma to the pharyngeal muscles. Keep in mind that pain is not always a minor complication; if prolonged, it may be accompanied by dehydration, fever, and even bleeding. Be sure to rule out otitis media in any patient complaining of otalgia who has had both tonsillectomy and adenoidectomy.
Nearly 50% of children who have had a tonsillectomy experience severe pain, defined as a visual analog score of 8 or more.8 According to 1 large-scale study, all children will experience moderate or severe pain while at rest and when swallowing during the first 48 hours after surgery—despite an appropriate around-the-clock dose of acetaminophen with codeine.9
Although high-dose acetaminophen, with or without codeine, is the most common analgesic prescribed for children after ambulatory surgery, its analgesic effect varies widely, so it may need to be administered in conjunction with other agents.10
One meta-analysis of several prospective, randomized, double-blind trials concluded that the risk of posttonsillectomy bleeding was nearly 4 times greater when patients received nonselective NSAIDs. This prompted the recommendation that these agents be avoided.11 However, a more recent analysis that included selective cyclooxygenase-1 (COX-1) and COX-2 inhibitors found that these NSAIDs did not significantly alter perioperative bleeding.12 With that in mind, selective COX-2 inhibitors such as celecoxib may safely relieve posttonsillectomy pain.13
Because so many patients develop postop nausea and vomiting, many surgeons avoid postop opioids such as codeine or tramadol, which can aggravate nausea without significant analgesic benefit. These agents are usually prescribed only after the gastrointestinal adverse effects have subsided, or when combined with antiemetics.
Ensure that nausea and vomiting have been properly addressed. Up to 89% of children undergoing tonsillectomy have postop vomiting and nausea.14 During the surgery, intravenous dexamethasone is usually administered because of its antiemetic effect—which can last up to 48 hours—and because of its role in preventing postop oropharyngeal edema.14
Watch for postop bleeding. Bleeding, followed by hypovolemic shock, is the most common cause of morbidity and mortality among patients undergoing tonsillectomy, affecting an estimated 0.5% to 10%. Approximately 1 in 200 patients returns to the operating room (OR) so that the bleeding can be controlled. Mortality from bleeding is 2 in 10,000 tonsillectomies. Most cases of fatal postop bleeding occur within the first 24 hours after surgery.15-17
Although clinicians should attempt to estimate blood loss during active bleeding, the estimate may be too low in children because they tend to swallow blood. Despite this caveat, consider blood transfusion when the estimated blood loss is 10% or more of the blood volume in infants, 25% in children, and 20% in adults.18
If transfusion is warranted, 2 large intravenous lines will need to be inserted, blood samples will need to be sent for typing and cross-matching, and a complete blood count and coagulation studies will need to be ordered. The patient’s airway will need to be protected and hemodynamic monitoring maintained.
If the bleeding is not excessive, applying local pressure with gauze on the tonsillar bed may be effective, assuming the patient is cooperative. However, if this doesn’t work, the patient will need to be rushed to an OR to control the bleeding. Anesthetizing a patient with massive oral bleeding is among the most challenging emergencies. Always anticipate aspiration once the bleeding has been controlled.
Be ready for these complications, too
The following complications are occasionally encountered after tonsillectomy, but no large controlled studies have estimated their frequency.
Airway obstruction
Mucosal damage during intubation may cause air to enter parapharyngeal tissues, which in turn can result in laryngeal spasm and cervical emphysema after extubation. It can progress to pneumomediastinum and tension pneumothorax.19,20 Excessive pressure on the surgical blades and manipulation within the oral cavity during surgery can cause lingual and oropharyngeal edema.21 With these potential complications in mind, the primary care physician will need to monitor the patient postoperatively for dyspnea.
Acute airway obstruction can occur if blood or clots accumulate in the hypo pharynx as the patient is awakening, immediately after extubation, or later. The most important way to prevent this complication is to ensure that there are no active bleeding sites. The airway can also be compromised from residual bleeding and an evolving airway edema.
On rare occasions, a patient’s airway can become obstructed if dislodged tonsillar tissue is not fully removed during surgery, or if loose teeth and parts of surgical instrumentation find their way into the airway. Being cognizant of these possibilities will help you, the primary care physician, to make an accurate differential diagnosis postoperatively.
Children suffering from obstructive sleep apnea due to craniofacial abnormalities, hypotonia, obesity, or “kissing” tonsils are at increased risk of developing acute airway maintenance difficulties after tonsillectomy. Prolonged obstruction of the upper airway from the obstructing tonsils can increase intrathoracic pressure and decrease venous return and pulmonary blood volume. After removal of the tonsils, there is a sudden increase in venous return, pulmonary blood volume, and pulmonary hydrostatic pressure. These rapid changes cause a fluid shift from pulmonary vessels into the lungs’ interstitial spaces and alveoli. The complication is sometimes referred to as “negative-pressure pulmonary edema.”22,23
Appropriate management includes close monitoring and the use of continuous positive airway pressure ventilation, as needed. The same approach is appropriate in children with right-sided cardiac insufficiency or pulmonary hypertension.
Fever and infection
Fever may occur within 18 to 36 hours after tonsillectomy as a result of lung atelectasis, a response to anesthetic agents, or a transient bacteremia. A postop fever lasting more than 24 hours, accompanied by severe throat pain, suggests an emerging pharyngeal infection.
Some surgeons prescribe prophylactic postop antibiotics to reduce the risk of infection in the traumatized region, decrease pain, and enable the patient to return quickly to a normal oral diet.24 A meta-analysis suggests, however, that postop oral antibiotics don’t reduce infection rates, posttonsillectomy pain, or secondary hemorrhage rates; the drugs do facilitate a return to normal activity and diet about a day sooner.25,26
Pneumonia used to be a common complication due to aspirated blood during the procedure. With the advent of improved surgical and anesthetic techniques, however, this complication rarely occurs.2 Neck infection, including suppurative lymphadenitis, is also a rare complication.27
Dehydration
While postop dehydration may be uncommon in the “average” patient, the risk is more common among dysphagic children. Post-tonsillectomy vomiting worsens this situation. With that in mind, encourage patients to resume oral intake of fluids and, when necessary, provide analgesia to facilitate the process. You will need to readmit patients who are unable to drink to achieve better pain relief and restore hydration.28
Some reports suggest that severe post-tonsillectomy hyponatremia can result from excessive hypovolemia-induced antidiuretic hormone secretion, disproportionate administration of hypotonic fluids, or inadequate postop fluid intake.29,30
Encouraging patients to consume soft and cold foods after tonsillectomy will comfort patients and help restore hemostasis. Because pain is the major obstacle for a return to an oral diet, coupling analgesia and timing of oral intake is crucial for a quick recovery.
Injuries from a forceful surgical technique
Because tonsillectomy requires forceful insertion of instruments into the mouth, a loose tooth may become dislodged, or even aspirated. We don’t recommend routine pre-operative dental consultation, but do urge a watchful eye. (See TABLE 3 for details on tonsillectomy techniques.)
Temporary uvular or tongue edema can develop if the tissues were forcefully manipulated during surgery, causing the patient to feel like he or she is choking. This edema usually subsides within a few days. Additional steroid dosing can be helpful.
If the glossopharyngeal nerve is damaged during dissection or electrocautery, the patient may develop a taste disorder.31 Spontaneous healing often occurs within several weeks.
An inadvertent eye injury such as keratitis may occur from exposure or friction from surgical covers. Skin, lip, and buccal mucosa lacerations or burns may also occur, often with the use of electrocautery needles and probes.
Mandibular condyle fracture is a rare complication that can be caused by forceful opening of the mouth. Forceful opening and the use of muscular relaxants lead to dislocation or stress injury of the temporomandibular joint (TMJ).32 This TMJ disorder is treated with analgesia, soft diet, and possible surgical reduction.
Excessive hyperextension of the neck can cause muscular tension and severe neck pain after the surgery. The atlanto-axial joint is at highest risk for dislocation or subluxation, especially in patients with Down syndrome—10% of whom already have atlanto-axial joint hyperlaxity.33 With that in mind, neck radiographs should be taken prior to surgery to assess the atlanto-axial joint stability in patients with Down syndrome.
In the rare Grisel’s syndrome, patients complain of severe neck pain about a week after surgery, with limitation in neck movements and torticollis. This is due to an impaired venous drainage from the joint, local infection, and injury to the paraspinal ligaments.34 Treatment consists of rest, neck immobilization, and antibiotics.
TABLE 3
Tonsillectomy techniques
| Technique | Instrumentation | Method |
|---|---|---|
| “Cold steel” | Scalpel, dissector, guillotine | Complete blunt dissection of the tonsil from its capsule, while preserving its pillars |
| “Hot” | Diathermy, BiClamp forceps | Complete electrodissection of the tonsil from its capsule, while preserving its pillars |
| Powered intracapsular | Microdebrider | Near-complete removal of the tonsil (90%-95%) |
| Harmonic scalpel | Harmonic scalpel | Use of ultrasound energy to remove the tonsil |
| Coblation | Bipolar device | Use of radiofrequency energy to remove the tonsil in a cooler temperature |
| Laser | CO2, KTP lasers | Evaporization of tonsillar tissue |
| Source: Shah UK, Terk A. New techniques for tonsillectomy and adenoidectomy. Oper Tech Otolaryngol. 2009;20:160-166. | ||
Complications when an adenoidectomy is also done
There is an increased risk of complications when an adenoidectomy and tonsillectomy are performed together, simply because there is another operative site. The complications that may occur after adenoidectomy include velopharyngeal insufficiency and nasopharyngeal stenosis. Primary care physicians should watch for nasal or oral bleeding, crusting, halitosis, and velopharyngeal insufficiency. An ear, nose, and throat consultation is warranted when in doubt.
CORRESPONDENCE Yehudah Roth, MD, Department of Otolaryngology, Head & Neck Surgery, The Edith Wolfson Medical Center, P.O. Box 5, 58100 Holon, Israel; [email protected]
1. Vestergaard H, Wohlfahrt J, Westergaard T, et al. Incidence of tonsillectomy in Denmark, 1980 to 2001. Pediatr Infect Dis J. 2007;26:1117-1121.
2. Har-El G, Nash M. Tonsillectomy and adenoidectomy. In: Krespi Y, Ossoff R, eds. Complications in Head and Neck Surgery. Philadelphia, Pa: Saunders; 1991:75–98.
3. Cohen D, Dor M. Morbidity and mortality of post-tonsillectomy bleeding: analysis of cases. J Laryngol Otol. 2008;122:88-92.
4. Brigger MT, Brietzke SE. Outpatient tonsillectomy in children: a systematic review. Otolaryngol Head Neck Surg. 2006;135:1-7.
5. Mallampati S, Gatt S, Gugino L, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985;32:429-434.
6. Vinik R, Wanner N, Pendleton RC. Periprocedural antithrombotic management: a review of the literature and practical approach for the hospitalist physician. J Hosp Med. 2009;4:551-559.
7. Asaf T, Reuveni H, Yermiahu T, et al. The need for routine pre-operative coagulation screening tests (prothrombin time PT/ partial thromboplastin time PTT) for healthy children undergoing elective tonsillectomy and/or adenoidectomy. Int J Pediatr Otorhinolaryngol. 2001;61:217-222.
8. Marcus CL. Pathophysiology of childhood obstructive sleep apnea: current concepts. Respir Physiol. 2000;119:143-154.
9. Kotiniemi LH, Ryhänen PT, Valanne J, et al. Post-operative symptoms at home following day-case surgery in children: a multicenter survey of 551 children. Anaesthesia. 1997;52:963-969.
10. Sutters KA, Miaskowski C, Holdridge-Zeuner D, et al. A randomized clinical trial of the effectiveness of a scheduled oral analgesic dosing regimen for the management of postoperative pain in children following tonsillectomy. Pain. 2004;110:49-55.
11. Anderson BJ, Holford NH, Woollard GA, et al. Perioperative pharmacodynamics of acetaminophen analgesia in children. Anesthesiology. 1999;90:411-421.
12. Marret E, Flahault A, Samama CM, et al. Effects of post-operative, nonsteroidal, anti-inflammatory drugs on bleeding risk after tonsillectomy: meta-analysis of randomized controlled trials. Anesthesiology. 2003;98:1497-1502.
13. Cardwell M, Siviter G, Smith A. Non-steroidal anti-inflammatory drugs and perioperative bleeding in pediatric tonsillectomy. Cochrane Database Syst Rev. 2005;(2):CD003591.-
14. Bean-Lijewski JD, Kruitbosch SH, Lewis Hutchinson L, et al. Post-tonsillectomy pain management in children: Can we do better? Otolaryngol Head Neck Surg. 2007;137:545-551.
15. Windfuhr JP, Schloendorff G, Baburi D, et al. Life-threatening post-tonsillectomy hemorrhage. Laryngoscope. 2008;118:1389-1394.
16. Alexander RJ, Kukreja R, Ford GR. Secondary post-tonsillectomy hemorrhage and informed consent. J Laryngol Otol. 2004;118:937-940.
17. Carmody D, Vamadevan T, Cooper S. Post-tonsillectomy hemorrhage. J Laryngol Otol. 1982;96:635-638.
18. Practice guidelines for blood transfusions. American Red Cross, 2007, second edition. Available at: http://www.sld.cu/galerias/pdf/sitios/anestesiologia/practical_guidelines_blood_transfusion.pdf.
19. Sonne JE, Kim SB, Frank DK. Cervical necrotizing fasciitis as a complication of tonsillectomy. Otolaryngol Head Neck Surg. 2001;25:670-672.
20. Vos GD, Marres EH, Heineman E, et al. Tension pneumomediastinum as an early complication after adenotonsillectomy. J Laryngol Otol. 1995;109:440-441.
21. Shi ZP, Wang CC, Lee JC, et al. Post-tonsillectomy hematoma of the mouth floor. Eur Arch Otorhinolaryngol. 2006;263:1041-1043.
22. Feinberg A, Shabino C. Acute pulmonary edema complicating tonsillectomy and adenoidectomy. Pediatrics. 1985;75:112-114.
23. Liechti M, Feurer R, Gross D, et al. Prevention of post-operative nausea and vomiting in children following adenotonsillectomy, using tropisetron with or without low-dose dexamethasone. J Anesth. 2007;21:311-316.
24. Thomsen J, Gower V. Adjuvant therapies in children undergoing adenotonsillectomy. Laryngoscope. 2002;112:32-34.
25. Burkart CM, Steward DL. Antibiotics for reduction of post-tonsillectomy morbidity: a meta-analysis. Laryngoscope. 2005;115:997-1002.
26. Clement DM, Supriya WA, McKerrow WS. Antibiotics to reduce post-tonsillectomy morbidity. Cochrane Database Syst Rev. 2008;(2):CD005607.-
27. Tami T, Burkus J, Strom C. Cervical osteomyelitis: an unusual complication of tonsillectomy. Arch Otolaryngol Head Neck Surg. 1987;112:992-994.
28. Colclasure J, Graham S. Complications of outpatient tonsillectomy and adenoidectomy: a review of 3,340 cases. Ear Nose Throat J. 1990;69:155-160.
29. Agut Fuster MA, del Campo Biosca J, Ferrer Rodríguez A, et al. Post-tonsillectomy hyponatremia: a possible lethal complication. Acta Otorrinolaringol Esp. 2006;57:247-250.
30. McRae RG, Weissburg AJ, Chang KW. Iatrogenic hyponatremia: a cause of death following pediatric tonsillectomy. Int J Pediatr Otorhinolaryngol. 1994;30:227-232.
31. Goins MR, Pitovski DZ. Post-tonsillectomy taste disorder: a significant complication. Laryngoscope. 2004;114:1206-1213.
32. Gupta S, Sing S, Misra T, et al. Fracture of the mandibular condyle as a complication of tonsillectomy. Ear Nose Throat J. 1989;68:477-479.
33. Song D, Maher CO. Spinal disorders associated with skeletal dysplasias and syndromes. Neurosurg Clin N Am. 2007;18:499-514.
34. Wilson BC, Jarvis BL, Haydon III RC. Nontraumatic subluxation of the atlantoaxial joint: Grisel’s syndrome. Ann Otol Rhinol Laryngol. 1987;96:705-708.
• Monitor patients for pain, nausea and vomiting, and bleeding, as they are the most common complications of tonsillectomy. A
• Effectively manage postoperative pain to prevent dehydration, which can occur when patients fail to take in enough fluids because swallowing is painful. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Although the number of patients undergoing tonsillectomy has gradually declined since the 1970s, it remains one of the most common surgical procedures performed worldwide.1 The procedure, of course, is fairly routine—but not without risk.
Mortality rates for the operation range from 1 in 10,000 to 1 in 35,000, with morbidity rates ranging from 1.5% to 14%; mortality and morbidity after tonsillectomy are usually the result of postoperative bleeding.2,3 In addition to bleeding, other common complications include pain, nausea, and vomiting.
The patient’s surgeon plays a central role in minimizing risk. But as a primary care physician, you, too, play an important role in ensuring that your patient’s tonsillectomy is uneventful. This review will help toward that end.
Refine your preop approach
Address informed consent issues. While the surgeon is responsible for obtaining informed consent, a patient may discuss the procedure with you, the family physician. (See TABLE 1 for the indications for tonsillectomy.) Although the procedure is safe and effective, the patient and his or her family need to know that bleeding will most likely occur immediately after the procedure, although it can occur at any time during the first 2 weeks postop. Advise the patient and family that postop pain is similar to that of a throat infection, but is often felt in the ears (“referred otalgia”). Because postop swallowing is painful, the patient may not drink enough fluids. If this problem because severe, he or she may need to be admitted for IV fluid replacement.
Discuss the patient’s length of stay. An increasing number of tonsillectomies are performed on an outpatient basis. However, high-risk patients—those with sleep apnea, coagulation disorders, or other underlying diseases, and anyone younger than 4 years of age or living a long distance from the hospital—should be admitted for overnight observation.4
Ask about previous surgeries. Tonsillectomies are performed under general anesthesia in most facilities. Ask about previous surgeries and conditions that may adversely affect the surgery: Does the patient have any upper airway obstruction, difficulty extending his cervical spine, or enzymatic deficiencies? A pseudocholinesterase deficiency, for instance, may cause prolonged paralysis of the respiratory muscles, requiring an extended period of time during which the patient must be mechanically ventilated.
Anesthesiologists use the Mallampati score to predict the ease of intubation.5 It’s derived by visualizing the base of the uvula, the tonsillar pillars, and the soft palate. Scoring may be done with or without phonation. A patient is considered to be in 1 of 4 classes, depending upon what can be visualized:
- Class 1: the tonsils, uvula, and soft palate
- Class 2: the hard and soft palate and upper portion of the tonsils and uvula
- Class 3: the soft and hard palate and base of the uvula
- Class 4: the hard palate.
As a general rule, patients scheduled for tonsillectomy are prone to higher scores because of underlying disease.
Order lab tests, stop certain medications. Instruct patients to discontinue aspirin 7 days before surgery, and naproxen and other nonsteroidal anti-inflammatory drugs (NSAIDs) 4 days before surgery.6 Antiplatelet aggregation drugs such as clopidogrel should also be stopped 7 days before surgery.6
While you should routinely order a complete blood count, experts disagree on the value and cost-effectiveness of routinely running prothrombin time and partial thromboplastin time.7
Assess whether the patient is anxious about the surgery. Tonsillectomy and the subsequent hospitalization can make patients anxious, bringing on sleep disturbances, behavioral problems, nightmares, enuresis, and emotional regression. Fortunately, these problems usually disappear without any intervention, but offering patients preop reassurance, demonstrations, and educational materials may help prevent them (TABLE 2).
TABLE 1
Indications for tonsillectomy
| Tonsils are infected ≥3 times a year despite adequate medical therapy |
| Peritonsillar abscess is unresponsive to medical management and drainage documented by surgeon, unless surgery is performed during acute stage |
| Chronic or recurrent tonsillitis associated with the streptococcal carrier state and not responding to beta-lactam antibiotics given with a beta-lactamase inhibitor |
| Hypertrophy causing dental malocclusion or adversely affecting orofacial growth that has been documented by orthodontist |
| Hypertrophy causing upper airway obstruction, severe dysphagia, sleep disorders, or cardiopulmonary complications |
| Persistent foul breath or bad taste in mouth due to chronic tonsillitis that has not been responsive to medical therapy |
| Unilateral tonsil hypertrophy that is presumed to be neoplastic |
| Source: Erickson BK, Larson DR, St Sauver JL, et al. Changes in incidence and indications of tonsillectomy and adenotonsillectomy, 1970-2005. Otolaryngol Head Neck Surg. 2009;140:894-901. |
TABLE 2
Patient education resources
Address postop complications
Ensure that your patient has proper pain relief. Sore throat and referred otalgia are common, but usually subside within 2 weeks. The pain typically manifests as dysphagia, which results from trauma to the pharyngeal muscles. Keep in mind that pain is not always a minor complication; if prolonged, it may be accompanied by dehydration, fever, and even bleeding. Be sure to rule out otitis media in any patient complaining of otalgia who has had both tonsillectomy and adenoidectomy.
Nearly 50% of children who have had a tonsillectomy experience severe pain, defined as a visual analog score of 8 or more.8 According to 1 large-scale study, all children will experience moderate or severe pain while at rest and when swallowing during the first 48 hours after surgery—despite an appropriate around-the-clock dose of acetaminophen with codeine.9
Although high-dose acetaminophen, with or without codeine, is the most common analgesic prescribed for children after ambulatory surgery, its analgesic effect varies widely, so it may need to be administered in conjunction with other agents.10
One meta-analysis of several prospective, randomized, double-blind trials concluded that the risk of posttonsillectomy bleeding was nearly 4 times greater when patients received nonselective NSAIDs. This prompted the recommendation that these agents be avoided.11 However, a more recent analysis that included selective cyclooxygenase-1 (COX-1) and COX-2 inhibitors found that these NSAIDs did not significantly alter perioperative bleeding.12 With that in mind, selective COX-2 inhibitors such as celecoxib may safely relieve posttonsillectomy pain.13
Because so many patients develop postop nausea and vomiting, many surgeons avoid postop opioids such as codeine or tramadol, which can aggravate nausea without significant analgesic benefit. These agents are usually prescribed only after the gastrointestinal adverse effects have subsided, or when combined with antiemetics.
Ensure that nausea and vomiting have been properly addressed. Up to 89% of children undergoing tonsillectomy have postop vomiting and nausea.14 During the surgery, intravenous dexamethasone is usually administered because of its antiemetic effect—which can last up to 48 hours—and because of its role in preventing postop oropharyngeal edema.14
Watch for postop bleeding. Bleeding, followed by hypovolemic shock, is the most common cause of morbidity and mortality among patients undergoing tonsillectomy, affecting an estimated 0.5% to 10%. Approximately 1 in 200 patients returns to the operating room (OR) so that the bleeding can be controlled. Mortality from bleeding is 2 in 10,000 tonsillectomies. Most cases of fatal postop bleeding occur within the first 24 hours after surgery.15-17
Although clinicians should attempt to estimate blood loss during active bleeding, the estimate may be too low in children because they tend to swallow blood. Despite this caveat, consider blood transfusion when the estimated blood loss is 10% or more of the blood volume in infants, 25% in children, and 20% in adults.18
If transfusion is warranted, 2 large intravenous lines will need to be inserted, blood samples will need to be sent for typing and cross-matching, and a complete blood count and coagulation studies will need to be ordered. The patient’s airway will need to be protected and hemodynamic monitoring maintained.
If the bleeding is not excessive, applying local pressure with gauze on the tonsillar bed may be effective, assuming the patient is cooperative. However, if this doesn’t work, the patient will need to be rushed to an OR to control the bleeding. Anesthetizing a patient with massive oral bleeding is among the most challenging emergencies. Always anticipate aspiration once the bleeding has been controlled.
Be ready for these complications, too
The following complications are occasionally encountered after tonsillectomy, but no large controlled studies have estimated their frequency.
Airway obstruction
Mucosal damage during intubation may cause air to enter parapharyngeal tissues, which in turn can result in laryngeal spasm and cervical emphysema after extubation. It can progress to pneumomediastinum and tension pneumothorax.19,20 Excessive pressure on the surgical blades and manipulation within the oral cavity during surgery can cause lingual and oropharyngeal edema.21 With these potential complications in mind, the primary care physician will need to monitor the patient postoperatively for dyspnea.
Acute airway obstruction can occur if blood or clots accumulate in the hypo pharynx as the patient is awakening, immediately after extubation, or later. The most important way to prevent this complication is to ensure that there are no active bleeding sites. The airway can also be compromised from residual bleeding and an evolving airway edema.
On rare occasions, a patient’s airway can become obstructed if dislodged tonsillar tissue is not fully removed during surgery, or if loose teeth and parts of surgical instrumentation find their way into the airway. Being cognizant of these possibilities will help you, the primary care physician, to make an accurate differential diagnosis postoperatively.
Children suffering from obstructive sleep apnea due to craniofacial abnormalities, hypotonia, obesity, or “kissing” tonsils are at increased risk of developing acute airway maintenance difficulties after tonsillectomy. Prolonged obstruction of the upper airway from the obstructing tonsils can increase intrathoracic pressure and decrease venous return and pulmonary blood volume. After removal of the tonsils, there is a sudden increase in venous return, pulmonary blood volume, and pulmonary hydrostatic pressure. These rapid changes cause a fluid shift from pulmonary vessels into the lungs’ interstitial spaces and alveoli. The complication is sometimes referred to as “negative-pressure pulmonary edema.”22,23
Appropriate management includes close monitoring and the use of continuous positive airway pressure ventilation, as needed. The same approach is appropriate in children with right-sided cardiac insufficiency or pulmonary hypertension.
Fever and infection
Fever may occur within 18 to 36 hours after tonsillectomy as a result of lung atelectasis, a response to anesthetic agents, or a transient bacteremia. A postop fever lasting more than 24 hours, accompanied by severe throat pain, suggests an emerging pharyngeal infection.
Some surgeons prescribe prophylactic postop antibiotics to reduce the risk of infection in the traumatized region, decrease pain, and enable the patient to return quickly to a normal oral diet.24 A meta-analysis suggests, however, that postop oral antibiotics don’t reduce infection rates, posttonsillectomy pain, or secondary hemorrhage rates; the drugs do facilitate a return to normal activity and diet about a day sooner.25,26
Pneumonia used to be a common complication due to aspirated blood during the procedure. With the advent of improved surgical and anesthetic techniques, however, this complication rarely occurs.2 Neck infection, including suppurative lymphadenitis, is also a rare complication.27
Dehydration
While postop dehydration may be uncommon in the “average” patient, the risk is more common among dysphagic children. Post-tonsillectomy vomiting worsens this situation. With that in mind, encourage patients to resume oral intake of fluids and, when necessary, provide analgesia to facilitate the process. You will need to readmit patients who are unable to drink to achieve better pain relief and restore hydration.28
Some reports suggest that severe post-tonsillectomy hyponatremia can result from excessive hypovolemia-induced antidiuretic hormone secretion, disproportionate administration of hypotonic fluids, or inadequate postop fluid intake.29,30
Encouraging patients to consume soft and cold foods after tonsillectomy will comfort patients and help restore hemostasis. Because pain is the major obstacle for a return to an oral diet, coupling analgesia and timing of oral intake is crucial for a quick recovery.
Injuries from a forceful surgical technique
Because tonsillectomy requires forceful insertion of instruments into the mouth, a loose tooth may become dislodged, or even aspirated. We don’t recommend routine pre-operative dental consultation, but do urge a watchful eye. (See TABLE 3 for details on tonsillectomy techniques.)
Temporary uvular or tongue edema can develop if the tissues were forcefully manipulated during surgery, causing the patient to feel like he or she is choking. This edema usually subsides within a few days. Additional steroid dosing can be helpful.
If the glossopharyngeal nerve is damaged during dissection or electrocautery, the patient may develop a taste disorder.31 Spontaneous healing often occurs within several weeks.
An inadvertent eye injury such as keratitis may occur from exposure or friction from surgical covers. Skin, lip, and buccal mucosa lacerations or burns may also occur, often with the use of electrocautery needles and probes.
Mandibular condyle fracture is a rare complication that can be caused by forceful opening of the mouth. Forceful opening and the use of muscular relaxants lead to dislocation or stress injury of the temporomandibular joint (TMJ).32 This TMJ disorder is treated with analgesia, soft diet, and possible surgical reduction.
Excessive hyperextension of the neck can cause muscular tension and severe neck pain after the surgery. The atlanto-axial joint is at highest risk for dislocation or subluxation, especially in patients with Down syndrome—10% of whom already have atlanto-axial joint hyperlaxity.33 With that in mind, neck radiographs should be taken prior to surgery to assess the atlanto-axial joint stability in patients with Down syndrome.
In the rare Grisel’s syndrome, patients complain of severe neck pain about a week after surgery, with limitation in neck movements and torticollis. This is due to an impaired venous drainage from the joint, local infection, and injury to the paraspinal ligaments.34 Treatment consists of rest, neck immobilization, and antibiotics.
TABLE 3
Tonsillectomy techniques
| Technique | Instrumentation | Method |
|---|---|---|
| “Cold steel” | Scalpel, dissector, guillotine | Complete blunt dissection of the tonsil from its capsule, while preserving its pillars |
| “Hot” | Diathermy, BiClamp forceps | Complete electrodissection of the tonsil from its capsule, while preserving its pillars |
| Powered intracapsular | Microdebrider | Near-complete removal of the tonsil (90%-95%) |
| Harmonic scalpel | Harmonic scalpel | Use of ultrasound energy to remove the tonsil |
| Coblation | Bipolar device | Use of radiofrequency energy to remove the tonsil in a cooler temperature |
| Laser | CO2, KTP lasers | Evaporization of tonsillar tissue |
| Source: Shah UK, Terk A. New techniques for tonsillectomy and adenoidectomy. Oper Tech Otolaryngol. 2009;20:160-166. | ||
Complications when an adenoidectomy is also done
There is an increased risk of complications when an adenoidectomy and tonsillectomy are performed together, simply because there is another operative site. The complications that may occur after adenoidectomy include velopharyngeal insufficiency and nasopharyngeal stenosis. Primary care physicians should watch for nasal or oral bleeding, crusting, halitosis, and velopharyngeal insufficiency. An ear, nose, and throat consultation is warranted when in doubt.
CORRESPONDENCE Yehudah Roth, MD, Department of Otolaryngology, Head & Neck Surgery, The Edith Wolfson Medical Center, P.O. Box 5, 58100 Holon, Israel; [email protected]
• Monitor patients for pain, nausea and vomiting, and bleeding, as they are the most common complications of tonsillectomy. A
• Effectively manage postoperative pain to prevent dehydration, which can occur when patients fail to take in enough fluids because swallowing is painful. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Although the number of patients undergoing tonsillectomy has gradually declined since the 1970s, it remains one of the most common surgical procedures performed worldwide.1 The procedure, of course, is fairly routine—but not without risk.
Mortality rates for the operation range from 1 in 10,000 to 1 in 35,000, with morbidity rates ranging from 1.5% to 14%; mortality and morbidity after tonsillectomy are usually the result of postoperative bleeding.2,3 In addition to bleeding, other common complications include pain, nausea, and vomiting.
The patient’s surgeon plays a central role in minimizing risk. But as a primary care physician, you, too, play an important role in ensuring that your patient’s tonsillectomy is uneventful. This review will help toward that end.
Refine your preop approach
Address informed consent issues. While the surgeon is responsible for obtaining informed consent, a patient may discuss the procedure with you, the family physician. (See TABLE 1 for the indications for tonsillectomy.) Although the procedure is safe and effective, the patient and his or her family need to know that bleeding will most likely occur immediately after the procedure, although it can occur at any time during the first 2 weeks postop. Advise the patient and family that postop pain is similar to that of a throat infection, but is often felt in the ears (“referred otalgia”). Because postop swallowing is painful, the patient may not drink enough fluids. If this problem because severe, he or she may need to be admitted for IV fluid replacement.
Discuss the patient’s length of stay. An increasing number of tonsillectomies are performed on an outpatient basis. However, high-risk patients—those with sleep apnea, coagulation disorders, or other underlying diseases, and anyone younger than 4 years of age or living a long distance from the hospital—should be admitted for overnight observation.4
Ask about previous surgeries. Tonsillectomies are performed under general anesthesia in most facilities. Ask about previous surgeries and conditions that may adversely affect the surgery: Does the patient have any upper airway obstruction, difficulty extending his cervical spine, or enzymatic deficiencies? A pseudocholinesterase deficiency, for instance, may cause prolonged paralysis of the respiratory muscles, requiring an extended period of time during which the patient must be mechanically ventilated.
Anesthesiologists use the Mallampati score to predict the ease of intubation.5 It’s derived by visualizing the base of the uvula, the tonsillar pillars, and the soft palate. Scoring may be done with or without phonation. A patient is considered to be in 1 of 4 classes, depending upon what can be visualized:
- Class 1: the tonsils, uvula, and soft palate
- Class 2: the hard and soft palate and upper portion of the tonsils and uvula
- Class 3: the soft and hard palate and base of the uvula
- Class 4: the hard palate.
As a general rule, patients scheduled for tonsillectomy are prone to higher scores because of underlying disease.
Order lab tests, stop certain medications. Instruct patients to discontinue aspirin 7 days before surgery, and naproxen and other nonsteroidal anti-inflammatory drugs (NSAIDs) 4 days before surgery.6 Antiplatelet aggregation drugs such as clopidogrel should also be stopped 7 days before surgery.6
While you should routinely order a complete blood count, experts disagree on the value and cost-effectiveness of routinely running prothrombin time and partial thromboplastin time.7
Assess whether the patient is anxious about the surgery. Tonsillectomy and the subsequent hospitalization can make patients anxious, bringing on sleep disturbances, behavioral problems, nightmares, enuresis, and emotional regression. Fortunately, these problems usually disappear without any intervention, but offering patients preop reassurance, demonstrations, and educational materials may help prevent them (TABLE 2).
TABLE 1
Indications for tonsillectomy
| Tonsils are infected ≥3 times a year despite adequate medical therapy |
| Peritonsillar abscess is unresponsive to medical management and drainage documented by surgeon, unless surgery is performed during acute stage |
| Chronic or recurrent tonsillitis associated with the streptococcal carrier state and not responding to beta-lactam antibiotics given with a beta-lactamase inhibitor |
| Hypertrophy causing dental malocclusion or adversely affecting orofacial growth that has been documented by orthodontist |
| Hypertrophy causing upper airway obstruction, severe dysphagia, sleep disorders, or cardiopulmonary complications |
| Persistent foul breath or bad taste in mouth due to chronic tonsillitis that has not been responsive to medical therapy |
| Unilateral tonsil hypertrophy that is presumed to be neoplastic |
| Source: Erickson BK, Larson DR, St Sauver JL, et al. Changes in incidence and indications of tonsillectomy and adenotonsillectomy, 1970-2005. Otolaryngol Head Neck Surg. 2009;140:894-901. |
TABLE 2
Patient education resources
Address postop complications
Ensure that your patient has proper pain relief. Sore throat and referred otalgia are common, but usually subside within 2 weeks. The pain typically manifests as dysphagia, which results from trauma to the pharyngeal muscles. Keep in mind that pain is not always a minor complication; if prolonged, it may be accompanied by dehydration, fever, and even bleeding. Be sure to rule out otitis media in any patient complaining of otalgia who has had both tonsillectomy and adenoidectomy.
Nearly 50% of children who have had a tonsillectomy experience severe pain, defined as a visual analog score of 8 or more.8 According to 1 large-scale study, all children will experience moderate or severe pain while at rest and when swallowing during the first 48 hours after surgery—despite an appropriate around-the-clock dose of acetaminophen with codeine.9
Although high-dose acetaminophen, with or without codeine, is the most common analgesic prescribed for children after ambulatory surgery, its analgesic effect varies widely, so it may need to be administered in conjunction with other agents.10
One meta-analysis of several prospective, randomized, double-blind trials concluded that the risk of posttonsillectomy bleeding was nearly 4 times greater when patients received nonselective NSAIDs. This prompted the recommendation that these agents be avoided.11 However, a more recent analysis that included selective cyclooxygenase-1 (COX-1) and COX-2 inhibitors found that these NSAIDs did not significantly alter perioperative bleeding.12 With that in mind, selective COX-2 inhibitors such as celecoxib may safely relieve posttonsillectomy pain.13
Because so many patients develop postop nausea and vomiting, many surgeons avoid postop opioids such as codeine or tramadol, which can aggravate nausea without significant analgesic benefit. These agents are usually prescribed only after the gastrointestinal adverse effects have subsided, or when combined with antiemetics.
Ensure that nausea and vomiting have been properly addressed. Up to 89% of children undergoing tonsillectomy have postop vomiting and nausea.14 During the surgery, intravenous dexamethasone is usually administered because of its antiemetic effect—which can last up to 48 hours—and because of its role in preventing postop oropharyngeal edema.14
Watch for postop bleeding. Bleeding, followed by hypovolemic shock, is the most common cause of morbidity and mortality among patients undergoing tonsillectomy, affecting an estimated 0.5% to 10%. Approximately 1 in 200 patients returns to the operating room (OR) so that the bleeding can be controlled. Mortality from bleeding is 2 in 10,000 tonsillectomies. Most cases of fatal postop bleeding occur within the first 24 hours after surgery.15-17
Although clinicians should attempt to estimate blood loss during active bleeding, the estimate may be too low in children because they tend to swallow blood. Despite this caveat, consider blood transfusion when the estimated blood loss is 10% or more of the blood volume in infants, 25% in children, and 20% in adults.18
If transfusion is warranted, 2 large intravenous lines will need to be inserted, blood samples will need to be sent for typing and cross-matching, and a complete blood count and coagulation studies will need to be ordered. The patient’s airway will need to be protected and hemodynamic monitoring maintained.
If the bleeding is not excessive, applying local pressure with gauze on the tonsillar bed may be effective, assuming the patient is cooperative. However, if this doesn’t work, the patient will need to be rushed to an OR to control the bleeding. Anesthetizing a patient with massive oral bleeding is among the most challenging emergencies. Always anticipate aspiration once the bleeding has been controlled.
Be ready for these complications, too
The following complications are occasionally encountered after tonsillectomy, but no large controlled studies have estimated their frequency.
Airway obstruction
Mucosal damage during intubation may cause air to enter parapharyngeal tissues, which in turn can result in laryngeal spasm and cervical emphysema after extubation. It can progress to pneumomediastinum and tension pneumothorax.19,20 Excessive pressure on the surgical blades and manipulation within the oral cavity during surgery can cause lingual and oropharyngeal edema.21 With these potential complications in mind, the primary care physician will need to monitor the patient postoperatively for dyspnea.
Acute airway obstruction can occur if blood or clots accumulate in the hypo pharynx as the patient is awakening, immediately after extubation, or later. The most important way to prevent this complication is to ensure that there are no active bleeding sites. The airway can also be compromised from residual bleeding and an evolving airway edema.
On rare occasions, a patient’s airway can become obstructed if dislodged tonsillar tissue is not fully removed during surgery, or if loose teeth and parts of surgical instrumentation find their way into the airway. Being cognizant of these possibilities will help you, the primary care physician, to make an accurate differential diagnosis postoperatively.
Children suffering from obstructive sleep apnea due to craniofacial abnormalities, hypotonia, obesity, or “kissing” tonsils are at increased risk of developing acute airway maintenance difficulties after tonsillectomy. Prolonged obstruction of the upper airway from the obstructing tonsils can increase intrathoracic pressure and decrease venous return and pulmonary blood volume. After removal of the tonsils, there is a sudden increase in venous return, pulmonary blood volume, and pulmonary hydrostatic pressure. These rapid changes cause a fluid shift from pulmonary vessels into the lungs’ interstitial spaces and alveoli. The complication is sometimes referred to as “negative-pressure pulmonary edema.”22,23
Appropriate management includes close monitoring and the use of continuous positive airway pressure ventilation, as needed. The same approach is appropriate in children with right-sided cardiac insufficiency or pulmonary hypertension.
Fever and infection
Fever may occur within 18 to 36 hours after tonsillectomy as a result of lung atelectasis, a response to anesthetic agents, or a transient bacteremia. A postop fever lasting more than 24 hours, accompanied by severe throat pain, suggests an emerging pharyngeal infection.
Some surgeons prescribe prophylactic postop antibiotics to reduce the risk of infection in the traumatized region, decrease pain, and enable the patient to return quickly to a normal oral diet.24 A meta-analysis suggests, however, that postop oral antibiotics don’t reduce infection rates, posttonsillectomy pain, or secondary hemorrhage rates; the drugs do facilitate a return to normal activity and diet about a day sooner.25,26
Pneumonia used to be a common complication due to aspirated blood during the procedure. With the advent of improved surgical and anesthetic techniques, however, this complication rarely occurs.2 Neck infection, including suppurative lymphadenitis, is also a rare complication.27
Dehydration
While postop dehydration may be uncommon in the “average” patient, the risk is more common among dysphagic children. Post-tonsillectomy vomiting worsens this situation. With that in mind, encourage patients to resume oral intake of fluids and, when necessary, provide analgesia to facilitate the process. You will need to readmit patients who are unable to drink to achieve better pain relief and restore hydration.28
Some reports suggest that severe post-tonsillectomy hyponatremia can result from excessive hypovolemia-induced antidiuretic hormone secretion, disproportionate administration of hypotonic fluids, or inadequate postop fluid intake.29,30
Encouraging patients to consume soft and cold foods after tonsillectomy will comfort patients and help restore hemostasis. Because pain is the major obstacle for a return to an oral diet, coupling analgesia and timing of oral intake is crucial for a quick recovery.
Injuries from a forceful surgical technique
Because tonsillectomy requires forceful insertion of instruments into the mouth, a loose tooth may become dislodged, or even aspirated. We don’t recommend routine pre-operative dental consultation, but do urge a watchful eye. (See TABLE 3 for details on tonsillectomy techniques.)
Temporary uvular or tongue edema can develop if the tissues were forcefully manipulated during surgery, causing the patient to feel like he or she is choking. This edema usually subsides within a few days. Additional steroid dosing can be helpful.
If the glossopharyngeal nerve is damaged during dissection or electrocautery, the patient may develop a taste disorder.31 Spontaneous healing often occurs within several weeks.
An inadvertent eye injury such as keratitis may occur from exposure or friction from surgical covers. Skin, lip, and buccal mucosa lacerations or burns may also occur, often with the use of electrocautery needles and probes.
Mandibular condyle fracture is a rare complication that can be caused by forceful opening of the mouth. Forceful opening and the use of muscular relaxants lead to dislocation or stress injury of the temporomandibular joint (TMJ).32 This TMJ disorder is treated with analgesia, soft diet, and possible surgical reduction.
Excessive hyperextension of the neck can cause muscular tension and severe neck pain after the surgery. The atlanto-axial joint is at highest risk for dislocation or subluxation, especially in patients with Down syndrome—10% of whom already have atlanto-axial joint hyperlaxity.33 With that in mind, neck radiographs should be taken prior to surgery to assess the atlanto-axial joint stability in patients with Down syndrome.
In the rare Grisel’s syndrome, patients complain of severe neck pain about a week after surgery, with limitation in neck movements and torticollis. This is due to an impaired venous drainage from the joint, local infection, and injury to the paraspinal ligaments.34 Treatment consists of rest, neck immobilization, and antibiotics.
TABLE 3
Tonsillectomy techniques
| Technique | Instrumentation | Method |
|---|---|---|
| “Cold steel” | Scalpel, dissector, guillotine | Complete blunt dissection of the tonsil from its capsule, while preserving its pillars |
| “Hot” | Diathermy, BiClamp forceps | Complete electrodissection of the tonsil from its capsule, while preserving its pillars |
| Powered intracapsular | Microdebrider | Near-complete removal of the tonsil (90%-95%) |
| Harmonic scalpel | Harmonic scalpel | Use of ultrasound energy to remove the tonsil |
| Coblation | Bipolar device | Use of radiofrequency energy to remove the tonsil in a cooler temperature |
| Laser | CO2, KTP lasers | Evaporization of tonsillar tissue |
| Source: Shah UK, Terk A. New techniques for tonsillectomy and adenoidectomy. Oper Tech Otolaryngol. 2009;20:160-166. | ||
Complications when an adenoidectomy is also done
There is an increased risk of complications when an adenoidectomy and tonsillectomy are performed together, simply because there is another operative site. The complications that may occur after adenoidectomy include velopharyngeal insufficiency and nasopharyngeal stenosis. Primary care physicians should watch for nasal or oral bleeding, crusting, halitosis, and velopharyngeal insufficiency. An ear, nose, and throat consultation is warranted when in doubt.
CORRESPONDENCE Yehudah Roth, MD, Department of Otolaryngology, Head & Neck Surgery, The Edith Wolfson Medical Center, P.O. Box 5, 58100 Holon, Israel; [email protected]
1. Vestergaard H, Wohlfahrt J, Westergaard T, et al. Incidence of tonsillectomy in Denmark, 1980 to 2001. Pediatr Infect Dis J. 2007;26:1117-1121.
2. Har-El G, Nash M. Tonsillectomy and adenoidectomy. In: Krespi Y, Ossoff R, eds. Complications in Head and Neck Surgery. Philadelphia, Pa: Saunders; 1991:75–98.
3. Cohen D, Dor M. Morbidity and mortality of post-tonsillectomy bleeding: analysis of cases. J Laryngol Otol. 2008;122:88-92.
4. Brigger MT, Brietzke SE. Outpatient tonsillectomy in children: a systematic review. Otolaryngol Head Neck Surg. 2006;135:1-7.
5. Mallampati S, Gatt S, Gugino L, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985;32:429-434.
6. Vinik R, Wanner N, Pendleton RC. Periprocedural antithrombotic management: a review of the literature and practical approach for the hospitalist physician. J Hosp Med. 2009;4:551-559.
7. Asaf T, Reuveni H, Yermiahu T, et al. The need for routine pre-operative coagulation screening tests (prothrombin time PT/ partial thromboplastin time PTT) for healthy children undergoing elective tonsillectomy and/or adenoidectomy. Int J Pediatr Otorhinolaryngol. 2001;61:217-222.
8. Marcus CL. Pathophysiology of childhood obstructive sleep apnea: current concepts. Respir Physiol. 2000;119:143-154.
9. Kotiniemi LH, Ryhänen PT, Valanne J, et al. Post-operative symptoms at home following day-case surgery in children: a multicenter survey of 551 children. Anaesthesia. 1997;52:963-969.
10. Sutters KA, Miaskowski C, Holdridge-Zeuner D, et al. A randomized clinical trial of the effectiveness of a scheduled oral analgesic dosing regimen for the management of postoperative pain in children following tonsillectomy. Pain. 2004;110:49-55.
11. Anderson BJ, Holford NH, Woollard GA, et al. Perioperative pharmacodynamics of acetaminophen analgesia in children. Anesthesiology. 1999;90:411-421.
12. Marret E, Flahault A, Samama CM, et al. Effects of post-operative, nonsteroidal, anti-inflammatory drugs on bleeding risk after tonsillectomy: meta-analysis of randomized controlled trials. Anesthesiology. 2003;98:1497-1502.
13. Cardwell M, Siviter G, Smith A. Non-steroidal anti-inflammatory drugs and perioperative bleeding in pediatric tonsillectomy. Cochrane Database Syst Rev. 2005;(2):CD003591.-
14. Bean-Lijewski JD, Kruitbosch SH, Lewis Hutchinson L, et al. Post-tonsillectomy pain management in children: Can we do better? Otolaryngol Head Neck Surg. 2007;137:545-551.
15. Windfuhr JP, Schloendorff G, Baburi D, et al. Life-threatening post-tonsillectomy hemorrhage. Laryngoscope. 2008;118:1389-1394.
16. Alexander RJ, Kukreja R, Ford GR. Secondary post-tonsillectomy hemorrhage and informed consent. J Laryngol Otol. 2004;118:937-940.
17. Carmody D, Vamadevan T, Cooper S. Post-tonsillectomy hemorrhage. J Laryngol Otol. 1982;96:635-638.
18. Practice guidelines for blood transfusions. American Red Cross, 2007, second edition. Available at: http://www.sld.cu/galerias/pdf/sitios/anestesiologia/practical_guidelines_blood_transfusion.pdf.
19. Sonne JE, Kim SB, Frank DK. Cervical necrotizing fasciitis as a complication of tonsillectomy. Otolaryngol Head Neck Surg. 2001;25:670-672.
20. Vos GD, Marres EH, Heineman E, et al. Tension pneumomediastinum as an early complication after adenotonsillectomy. J Laryngol Otol. 1995;109:440-441.
21. Shi ZP, Wang CC, Lee JC, et al. Post-tonsillectomy hematoma of the mouth floor. Eur Arch Otorhinolaryngol. 2006;263:1041-1043.
22. Feinberg A, Shabino C. Acute pulmonary edema complicating tonsillectomy and adenoidectomy. Pediatrics. 1985;75:112-114.
23. Liechti M, Feurer R, Gross D, et al. Prevention of post-operative nausea and vomiting in children following adenotonsillectomy, using tropisetron with or without low-dose dexamethasone. J Anesth. 2007;21:311-316.
24. Thomsen J, Gower V. Adjuvant therapies in children undergoing adenotonsillectomy. Laryngoscope. 2002;112:32-34.
25. Burkart CM, Steward DL. Antibiotics for reduction of post-tonsillectomy morbidity: a meta-analysis. Laryngoscope. 2005;115:997-1002.
26. Clement DM, Supriya WA, McKerrow WS. Antibiotics to reduce post-tonsillectomy morbidity. Cochrane Database Syst Rev. 2008;(2):CD005607.-
27. Tami T, Burkus J, Strom C. Cervical osteomyelitis: an unusual complication of tonsillectomy. Arch Otolaryngol Head Neck Surg. 1987;112:992-994.
28. Colclasure J, Graham S. Complications of outpatient tonsillectomy and adenoidectomy: a review of 3,340 cases. Ear Nose Throat J. 1990;69:155-160.
29. Agut Fuster MA, del Campo Biosca J, Ferrer Rodríguez A, et al. Post-tonsillectomy hyponatremia: a possible lethal complication. Acta Otorrinolaringol Esp. 2006;57:247-250.
30. McRae RG, Weissburg AJ, Chang KW. Iatrogenic hyponatremia: a cause of death following pediatric tonsillectomy. Int J Pediatr Otorhinolaryngol. 1994;30:227-232.
31. Goins MR, Pitovski DZ. Post-tonsillectomy taste disorder: a significant complication. Laryngoscope. 2004;114:1206-1213.
32. Gupta S, Sing S, Misra T, et al. Fracture of the mandibular condyle as a complication of tonsillectomy. Ear Nose Throat J. 1989;68:477-479.
33. Song D, Maher CO. Spinal disorders associated with skeletal dysplasias and syndromes. Neurosurg Clin N Am. 2007;18:499-514.
34. Wilson BC, Jarvis BL, Haydon III RC. Nontraumatic subluxation of the atlantoaxial joint: Grisel’s syndrome. Ann Otol Rhinol Laryngol. 1987;96:705-708.
1. Vestergaard H, Wohlfahrt J, Westergaard T, et al. Incidence of tonsillectomy in Denmark, 1980 to 2001. Pediatr Infect Dis J. 2007;26:1117-1121.
2. Har-El G, Nash M. Tonsillectomy and adenoidectomy. In: Krespi Y, Ossoff R, eds. Complications in Head and Neck Surgery. Philadelphia, Pa: Saunders; 1991:75–98.
3. Cohen D, Dor M. Morbidity and mortality of post-tonsillectomy bleeding: analysis of cases. J Laryngol Otol. 2008;122:88-92.
4. Brigger MT, Brietzke SE. Outpatient tonsillectomy in children: a systematic review. Otolaryngol Head Neck Surg. 2006;135:1-7.
5. Mallampati S, Gatt S, Gugino L, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985;32:429-434.
6. Vinik R, Wanner N, Pendleton RC. Periprocedural antithrombotic management: a review of the literature and practical approach for the hospitalist physician. J Hosp Med. 2009;4:551-559.
7. Asaf T, Reuveni H, Yermiahu T, et al. The need for routine pre-operative coagulation screening tests (prothrombin time PT/ partial thromboplastin time PTT) for healthy children undergoing elective tonsillectomy and/or adenoidectomy. Int J Pediatr Otorhinolaryngol. 2001;61:217-222.
8. Marcus CL. Pathophysiology of childhood obstructive sleep apnea: current concepts. Respir Physiol. 2000;119:143-154.
9. Kotiniemi LH, Ryhänen PT, Valanne J, et al. Post-operative symptoms at home following day-case surgery in children: a multicenter survey of 551 children. Anaesthesia. 1997;52:963-969.
10. Sutters KA, Miaskowski C, Holdridge-Zeuner D, et al. A randomized clinical trial of the effectiveness of a scheduled oral analgesic dosing regimen for the management of postoperative pain in children following tonsillectomy. Pain. 2004;110:49-55.
11. Anderson BJ, Holford NH, Woollard GA, et al. Perioperative pharmacodynamics of acetaminophen analgesia in children. Anesthesiology. 1999;90:411-421.
12. Marret E, Flahault A, Samama CM, et al. Effects of post-operative, nonsteroidal, anti-inflammatory drugs on bleeding risk after tonsillectomy: meta-analysis of randomized controlled trials. Anesthesiology. 2003;98:1497-1502.
13. Cardwell M, Siviter G, Smith A. Non-steroidal anti-inflammatory drugs and perioperative bleeding in pediatric tonsillectomy. Cochrane Database Syst Rev. 2005;(2):CD003591.-
14. Bean-Lijewski JD, Kruitbosch SH, Lewis Hutchinson L, et al. Post-tonsillectomy pain management in children: Can we do better? Otolaryngol Head Neck Surg. 2007;137:545-551.
15. Windfuhr JP, Schloendorff G, Baburi D, et al. Life-threatening post-tonsillectomy hemorrhage. Laryngoscope. 2008;118:1389-1394.
16. Alexander RJ, Kukreja R, Ford GR. Secondary post-tonsillectomy hemorrhage and informed consent. J Laryngol Otol. 2004;118:937-940.
17. Carmody D, Vamadevan T, Cooper S. Post-tonsillectomy hemorrhage. J Laryngol Otol. 1982;96:635-638.
18. Practice guidelines for blood transfusions. American Red Cross, 2007, second edition. Available at: http://www.sld.cu/galerias/pdf/sitios/anestesiologia/practical_guidelines_blood_transfusion.pdf.
19. Sonne JE, Kim SB, Frank DK. Cervical necrotizing fasciitis as a complication of tonsillectomy. Otolaryngol Head Neck Surg. 2001;25:670-672.
20. Vos GD, Marres EH, Heineman E, et al. Tension pneumomediastinum as an early complication after adenotonsillectomy. J Laryngol Otol. 1995;109:440-441.
21. Shi ZP, Wang CC, Lee JC, et al. Post-tonsillectomy hematoma of the mouth floor. Eur Arch Otorhinolaryngol. 2006;263:1041-1043.
22. Feinberg A, Shabino C. Acute pulmonary edema complicating tonsillectomy and adenoidectomy. Pediatrics. 1985;75:112-114.
23. Liechti M, Feurer R, Gross D, et al. Prevention of post-operative nausea and vomiting in children following adenotonsillectomy, using tropisetron with or without low-dose dexamethasone. J Anesth. 2007;21:311-316.
24. Thomsen J, Gower V. Adjuvant therapies in children undergoing adenotonsillectomy. Laryngoscope. 2002;112:32-34.
25. Burkart CM, Steward DL. Antibiotics for reduction of post-tonsillectomy morbidity: a meta-analysis. Laryngoscope. 2005;115:997-1002.
26. Clement DM, Supriya WA, McKerrow WS. Antibiotics to reduce post-tonsillectomy morbidity. Cochrane Database Syst Rev. 2008;(2):CD005607.-
27. Tami T, Burkus J, Strom C. Cervical osteomyelitis: an unusual complication of tonsillectomy. Arch Otolaryngol Head Neck Surg. 1987;112:992-994.
28. Colclasure J, Graham S. Complications of outpatient tonsillectomy and adenoidectomy: a review of 3,340 cases. Ear Nose Throat J. 1990;69:155-160.
29. Agut Fuster MA, del Campo Biosca J, Ferrer Rodríguez A, et al. Post-tonsillectomy hyponatremia: a possible lethal complication. Acta Otorrinolaringol Esp. 2006;57:247-250.
30. McRae RG, Weissburg AJ, Chang KW. Iatrogenic hyponatremia: a cause of death following pediatric tonsillectomy. Int J Pediatr Otorhinolaryngol. 1994;30:227-232.
31. Goins MR, Pitovski DZ. Post-tonsillectomy taste disorder: a significant complication. Laryngoscope. 2004;114:1206-1213.
32. Gupta S, Sing S, Misra T, et al. Fracture of the mandibular condyle as a complication of tonsillectomy. Ear Nose Throat J. 1989;68:477-479.
33. Song D, Maher CO. Spinal disorders associated with skeletal dysplasias and syndromes. Neurosurg Clin N Am. 2007;18:499-514.
34. Wilson BC, Jarvis BL, Haydon III RC. Nontraumatic subluxation of the atlantoaxial joint: Grisel’s syndrome. Ann Otol Rhinol Laryngol. 1987;96:705-708.
Is the thyroid to blame?
• Treat the rare case of acute suppurative thyroiditis as a medical emergency, with attention to airway protection, intravenous antibiotics, and surgical drainage. C
• Order a sedimentation rate if you suspect subacute thyroiditis. It is almost always elevated in patients with this disease. C
• Treat subacute thyroiditis with prednisone 40 mg daily in patients refractory to treatment with nonsteroidal anti-inflammatory drugs. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Sam J. is a 56-year-old man with a 2-day history of severe pain in the front of his neck. He aches all over and says he had “a bad cold” a week ago, but no fever, chills, cough, or headache. He hasn’t had a toothache or difficulty swallowing, but he does complain of a sore throat and muscle aches. His temperature is 100.7°f. He has no respiratory distress or stridor. there are no tonsillar exudates. the pharynx is not red or inflamed.
When you palpate his thyroid gland, you find diffuse tenderness. What could be causing his pain?
The patient with a painful thyroid is uncommon in clinical practice. In most cases, the culprit is a viral infection, radiation, or a traumatic injury to the gland. Bacterial, fungal, parasitic, or mycobacterial infections also occur, but these are rare, making up only 0.1% to 0.7% of all thyroid disease.1 Some thyroid infections can be devastating, necessitating quick interventions including airway protection, intravenous antibiotics, and surgical drainage in certain situations.
Subacute thyroiditis (ST), the most common source of thyroid pain, is less severe, but can be disabling if not recognized and appropriately treated.2 Occasionally, thyroid cysts can rupture, mimicking a presentation of ST.
This article will focus on how to evaluate the painful thyroid, so as to differentiate among the various conditions that can produce this uncommon presentation.
Classifying thyroiditis: Pain or no pain
Thyroiditis can be classified in several ways, but the simplest classification is in terms of pain. Conditions that can cause painless thyroiditis include Hashimoto’s disease, postpartum thyroiditis, subacute lymphocytic thyroiditis, Reidel’s thyroiditis, and thyroiditis induced by drugs such as amiodarone, interleukin-2, lithium, and interferon-alfa.3 Conditions that can cause painful thyroiditis include acute suppurative thyroiditis (AST), radiation-induced thyroiditis, trauma, ST, and ruptured cysts.1
Acute suppurative thyroiditis
AST is a rare condition most commonly caused by bacterial, mycobacterial, fungal, or parasitic infection. The thyroid is remarkably resistant to infection because the gland is encapsulated, rich in iodide content, and has an abundant blood supply and lymphatic drainage.1,2 AST usually occurs in patients with underlying thyroid disease, such as thyroid cancer, Hashimoto’s thyroiditis, multinodular goiter, congenital thyroid abnormalities such as pyriform sinus fistulas in children, and in patients who are immunocompromised.1,2
Patients with AST are acutely ill and will complain of fever, dysphagia, and severe anterior neck pain. Stridor and tracheal obstruction may occur, requiring intubation or tracheotomy. Thyroid hormone levels are sometimes increased secondary to the release of preformed hormone from the intensely inflamed gland. Computed tomography (CT) or magnetic resonance imaging (MRI) thyroid scans can identify abscesses and guide biopsies that clinch the diagnosis.
Management consists of airway support, broad-spectrum intravenous antibiotics until gram stains and cultures return (with particular attention to coverage against staphylococcal, streptococcal, and anaerobic organisms), and surgical drainage of abscesses.
Thyroiditis caused by radiation or trauma
One percent of patients develop thyroiditis after receiving radioactive iodine ablation for hyperthyroidism (Graves’ disease).4 This condition usually occurs 5 to 10 days after the treatment. Radiation triggers thyroid gland destruction, causing transient additional release of thyroid hormone. Similar damage occurs after external beam radiation for lymphomas and head and neck cancers. In such cases, use nonsteroidal anti-inflammatory drugs (NSAIDs) and prednisone to reduce inflammation and beta-blockers to control hyperthyroid symptoms.
Trauma to the thyroid—from motor vehicle accidents, falls, or physical assaults—can cause pain, tenderness, and abnormalities in thyroid hormone levels. Effects are usually self-limited, and management centers on airway protection and prevention of infection.
Subacute thyroiditis
The cause of ST is not clear. However, it typically follows an upper respiratory infection. Many viruses have been implicated in the disease, including Coxsackie, echo, adeno, and influenza viruses.5 It occurs more frequently during summer months, coinciding with the peak incidence of enterovirus.2 ST is 4 times more common in women than men, and the median age for occurrence is 45.6
Patients with ST usually seek care for such symptoms as fever, myalgias, and malaise, which suggest a viral infection.2,7-9 Neck pain is significant and may radiate to the jaw or ear.9 Patients may have pain on swallowing and a sore throat. It’s possible to confuse ST with severe pharyngitis or even epiglottitis if you fail to palpate the thyroid gland. When you examine the thyroid, the gland is exquisitely tender with ST. Patients with ST appear less ill than those with AST.
In 50% of ST patients, thyroid-stimulating hormone (TSH) is suppressed, and thyroid hormone levels are elevated.4 Patients with hyperthyroidism exhibit the usual signs and symptoms associated with high levels of the hormone: tremor, palpitations, heat intolerance, and diarrhea. After a few weeks, thyroid hormone levels normalize and then drop to below normal in the 4 to 6 months that follow. Levels return to normal in 95% of patients after 6 to 12 months. ST recurs in only 2% of patients.4
Sedimentation rates are almost always elevated in ST, reflecting the significant inflammation associated with the disease. Cytotoxic T lymphocytes damage thyroid follicles, causing release of preformed thyroid hormone, in turn suppressing TSH.4 Radioactive iodine scans show low uptake because TSH is needed for the uptake of iodine.10
Treatment of ST should focus on reducing inflammation and pain. NSAIDs may be sufficient, but patients with moderate to severe symptoms may require prednisone 40 mg daily, tapered over 4 to 6 weeks.2 If the patient is hyperthyroid, you’ll need to control symptoms with beta-blockers.
Ruptured thyroid cyst: An ST look-alike
The clinical presentation of a ruptured cyst closely mimics that of ST: thyroid pain, history of a recent cold, sore throat, aches, and pains. Laboratory and nuclear medicine evaluations, however, reveal significant differences:
- TSH is not suppressed;
- ESR is not elevated;
- Radioactive iodine uptake is normal.
Palpation may reveal a thyroid nodule. You can confirm the diagnosis by ultrasound and a needle aspiration.
CASE The right diagnosis for Sam
Sam’s initial clinical presentation suggested St, and he was started on prednisone 40 mg daily to control his pain. but when laboratory and nuclear medicine evaluations became available the next day, the St diagnosis didn’t hold up: TSH, ESR, and radioactive iodine uptake were all normal.
When Sam came in for a follow-up visit 3 days later, his thyroid pain was gone and he was feeling much better. palpation of his thyroid revealed a slightly tender nodule that went undetected in the initial exam. Subsequent thyroid ultrasound showed a 2x2 cm nodule in the right lobe. a fine needle aspiration revealed a colloid cyst. the cyst had ruptured, causing acute pain from hemorrhage and inflammation.
CORRESPONDENCE Dean Gianakos, MD, 2323 Memorial Drive, #10, Lynchburg Family Medicine Residency, Lynchburg, VA 24501; [email protected]
1. Al-Dajani N, Wooton SH. Cervical lymphadenitis, suppurative parotitis, thyroiditis, and infected cysts. Infect Dis Clin North Am. 2007;21:523-541.
2. Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003;348:2646-2655.
3. Basaria S, Cooper DS. Amiodarone and the thyroid. Am J Med. 2005;118:706-714.
4. Bindra A, Braunstein GD. Thyroiditis. Am Fam Physician. 2006;73:1769-1776.
5. Sniezek JC, Francis TB. Inflammatory thyroid disorders. Otolaryngol Clin North Am. 2003;36:55-71.
6. Fatourechi V, Aniszewski JP, Fatourechi GZ, et al. Clinical features of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, Study. J Clin Endocrinol Metab. 2003;88:2100-2105.
7. Hamburger JI. The various presentations of thyroiditis. Diagnostic considerations. Ann Int Med. 1986;104:219-224.
8. Hay ID. Thyroiditis: a clinical update. Mayo Clin Proc. 1985;60:836-843.
9. Lee SL, Ananthakrishnan S. Subacute thyroiditis. Updated April 27, 2009. Available at: http://emedicine.medscape.com/article/125648-overview. Accessed August 15, 2010.
10. Ross DS. Syndromes of thyrotoxicosis with low radioactive iodine uptake. Endocrinol Metab Clin North Am. 1998;27:169-185.
• Treat the rare case of acute suppurative thyroiditis as a medical emergency, with attention to airway protection, intravenous antibiotics, and surgical drainage. C
• Order a sedimentation rate if you suspect subacute thyroiditis. It is almost always elevated in patients with this disease. C
• Treat subacute thyroiditis with prednisone 40 mg daily in patients refractory to treatment with nonsteroidal anti-inflammatory drugs. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Sam J. is a 56-year-old man with a 2-day history of severe pain in the front of his neck. He aches all over and says he had “a bad cold” a week ago, but no fever, chills, cough, or headache. He hasn’t had a toothache or difficulty swallowing, but he does complain of a sore throat and muscle aches. His temperature is 100.7°f. He has no respiratory distress or stridor. there are no tonsillar exudates. the pharynx is not red or inflamed.
When you palpate his thyroid gland, you find diffuse tenderness. What could be causing his pain?
The patient with a painful thyroid is uncommon in clinical practice. In most cases, the culprit is a viral infection, radiation, or a traumatic injury to the gland. Bacterial, fungal, parasitic, or mycobacterial infections also occur, but these are rare, making up only 0.1% to 0.7% of all thyroid disease.1 Some thyroid infections can be devastating, necessitating quick interventions including airway protection, intravenous antibiotics, and surgical drainage in certain situations.
Subacute thyroiditis (ST), the most common source of thyroid pain, is less severe, but can be disabling if not recognized and appropriately treated.2 Occasionally, thyroid cysts can rupture, mimicking a presentation of ST.
This article will focus on how to evaluate the painful thyroid, so as to differentiate among the various conditions that can produce this uncommon presentation.
Classifying thyroiditis: Pain or no pain
Thyroiditis can be classified in several ways, but the simplest classification is in terms of pain. Conditions that can cause painless thyroiditis include Hashimoto’s disease, postpartum thyroiditis, subacute lymphocytic thyroiditis, Reidel’s thyroiditis, and thyroiditis induced by drugs such as amiodarone, interleukin-2, lithium, and interferon-alfa.3 Conditions that can cause painful thyroiditis include acute suppurative thyroiditis (AST), radiation-induced thyroiditis, trauma, ST, and ruptured cysts.1
Acute suppurative thyroiditis
AST is a rare condition most commonly caused by bacterial, mycobacterial, fungal, or parasitic infection. The thyroid is remarkably resistant to infection because the gland is encapsulated, rich in iodide content, and has an abundant blood supply and lymphatic drainage.1,2 AST usually occurs in patients with underlying thyroid disease, such as thyroid cancer, Hashimoto’s thyroiditis, multinodular goiter, congenital thyroid abnormalities such as pyriform sinus fistulas in children, and in patients who are immunocompromised.1,2
Patients with AST are acutely ill and will complain of fever, dysphagia, and severe anterior neck pain. Stridor and tracheal obstruction may occur, requiring intubation or tracheotomy. Thyroid hormone levels are sometimes increased secondary to the release of preformed hormone from the intensely inflamed gland. Computed tomography (CT) or magnetic resonance imaging (MRI) thyroid scans can identify abscesses and guide biopsies that clinch the diagnosis.
Management consists of airway support, broad-spectrum intravenous antibiotics until gram stains and cultures return (with particular attention to coverage against staphylococcal, streptococcal, and anaerobic organisms), and surgical drainage of abscesses.
Thyroiditis caused by radiation or trauma
One percent of patients develop thyroiditis after receiving radioactive iodine ablation for hyperthyroidism (Graves’ disease).4 This condition usually occurs 5 to 10 days after the treatment. Radiation triggers thyroid gland destruction, causing transient additional release of thyroid hormone. Similar damage occurs after external beam radiation for lymphomas and head and neck cancers. In such cases, use nonsteroidal anti-inflammatory drugs (NSAIDs) and prednisone to reduce inflammation and beta-blockers to control hyperthyroid symptoms.
Trauma to the thyroid—from motor vehicle accidents, falls, or physical assaults—can cause pain, tenderness, and abnormalities in thyroid hormone levels. Effects are usually self-limited, and management centers on airway protection and prevention of infection.
Subacute thyroiditis
The cause of ST is not clear. However, it typically follows an upper respiratory infection. Many viruses have been implicated in the disease, including Coxsackie, echo, adeno, and influenza viruses.5 It occurs more frequently during summer months, coinciding with the peak incidence of enterovirus.2 ST is 4 times more common in women than men, and the median age for occurrence is 45.6
Patients with ST usually seek care for such symptoms as fever, myalgias, and malaise, which suggest a viral infection.2,7-9 Neck pain is significant and may radiate to the jaw or ear.9 Patients may have pain on swallowing and a sore throat. It’s possible to confuse ST with severe pharyngitis or even epiglottitis if you fail to palpate the thyroid gland. When you examine the thyroid, the gland is exquisitely tender with ST. Patients with ST appear less ill than those with AST.
In 50% of ST patients, thyroid-stimulating hormone (TSH) is suppressed, and thyroid hormone levels are elevated.4 Patients with hyperthyroidism exhibit the usual signs and symptoms associated with high levels of the hormone: tremor, palpitations, heat intolerance, and diarrhea. After a few weeks, thyroid hormone levels normalize and then drop to below normal in the 4 to 6 months that follow. Levels return to normal in 95% of patients after 6 to 12 months. ST recurs in only 2% of patients.4
Sedimentation rates are almost always elevated in ST, reflecting the significant inflammation associated with the disease. Cytotoxic T lymphocytes damage thyroid follicles, causing release of preformed thyroid hormone, in turn suppressing TSH.4 Radioactive iodine scans show low uptake because TSH is needed for the uptake of iodine.10
Treatment of ST should focus on reducing inflammation and pain. NSAIDs may be sufficient, but patients with moderate to severe symptoms may require prednisone 40 mg daily, tapered over 4 to 6 weeks.2 If the patient is hyperthyroid, you’ll need to control symptoms with beta-blockers.
Ruptured thyroid cyst: An ST look-alike
The clinical presentation of a ruptured cyst closely mimics that of ST: thyroid pain, history of a recent cold, sore throat, aches, and pains. Laboratory and nuclear medicine evaluations, however, reveal significant differences:
- TSH is not suppressed;
- ESR is not elevated;
- Radioactive iodine uptake is normal.
Palpation may reveal a thyroid nodule. You can confirm the diagnosis by ultrasound and a needle aspiration.
CASE The right diagnosis for Sam
Sam’s initial clinical presentation suggested St, and he was started on prednisone 40 mg daily to control his pain. but when laboratory and nuclear medicine evaluations became available the next day, the St diagnosis didn’t hold up: TSH, ESR, and radioactive iodine uptake were all normal.
When Sam came in for a follow-up visit 3 days later, his thyroid pain was gone and he was feeling much better. palpation of his thyroid revealed a slightly tender nodule that went undetected in the initial exam. Subsequent thyroid ultrasound showed a 2x2 cm nodule in the right lobe. a fine needle aspiration revealed a colloid cyst. the cyst had ruptured, causing acute pain from hemorrhage and inflammation.
CORRESPONDENCE Dean Gianakos, MD, 2323 Memorial Drive, #10, Lynchburg Family Medicine Residency, Lynchburg, VA 24501; [email protected]
• Treat the rare case of acute suppurative thyroiditis as a medical emergency, with attention to airway protection, intravenous antibiotics, and surgical drainage. C
• Order a sedimentation rate if you suspect subacute thyroiditis. It is almost always elevated in patients with this disease. C
• Treat subacute thyroiditis with prednisone 40 mg daily in patients refractory to treatment with nonsteroidal anti-inflammatory drugs. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Sam J. is a 56-year-old man with a 2-day history of severe pain in the front of his neck. He aches all over and says he had “a bad cold” a week ago, but no fever, chills, cough, or headache. He hasn’t had a toothache or difficulty swallowing, but he does complain of a sore throat and muscle aches. His temperature is 100.7°f. He has no respiratory distress or stridor. there are no tonsillar exudates. the pharynx is not red or inflamed.
When you palpate his thyroid gland, you find diffuse tenderness. What could be causing his pain?
The patient with a painful thyroid is uncommon in clinical practice. In most cases, the culprit is a viral infection, radiation, or a traumatic injury to the gland. Bacterial, fungal, parasitic, or mycobacterial infections also occur, but these are rare, making up only 0.1% to 0.7% of all thyroid disease.1 Some thyroid infections can be devastating, necessitating quick interventions including airway protection, intravenous antibiotics, and surgical drainage in certain situations.
Subacute thyroiditis (ST), the most common source of thyroid pain, is less severe, but can be disabling if not recognized and appropriately treated.2 Occasionally, thyroid cysts can rupture, mimicking a presentation of ST.
This article will focus on how to evaluate the painful thyroid, so as to differentiate among the various conditions that can produce this uncommon presentation.
Classifying thyroiditis: Pain or no pain
Thyroiditis can be classified in several ways, but the simplest classification is in terms of pain. Conditions that can cause painless thyroiditis include Hashimoto’s disease, postpartum thyroiditis, subacute lymphocytic thyroiditis, Reidel’s thyroiditis, and thyroiditis induced by drugs such as amiodarone, interleukin-2, lithium, and interferon-alfa.3 Conditions that can cause painful thyroiditis include acute suppurative thyroiditis (AST), radiation-induced thyroiditis, trauma, ST, and ruptured cysts.1
Acute suppurative thyroiditis
AST is a rare condition most commonly caused by bacterial, mycobacterial, fungal, or parasitic infection. The thyroid is remarkably resistant to infection because the gland is encapsulated, rich in iodide content, and has an abundant blood supply and lymphatic drainage.1,2 AST usually occurs in patients with underlying thyroid disease, such as thyroid cancer, Hashimoto’s thyroiditis, multinodular goiter, congenital thyroid abnormalities such as pyriform sinus fistulas in children, and in patients who are immunocompromised.1,2
Patients with AST are acutely ill and will complain of fever, dysphagia, and severe anterior neck pain. Stridor and tracheal obstruction may occur, requiring intubation or tracheotomy. Thyroid hormone levels are sometimes increased secondary to the release of preformed hormone from the intensely inflamed gland. Computed tomography (CT) or magnetic resonance imaging (MRI) thyroid scans can identify abscesses and guide biopsies that clinch the diagnosis.
Management consists of airway support, broad-spectrum intravenous antibiotics until gram stains and cultures return (with particular attention to coverage against staphylococcal, streptococcal, and anaerobic organisms), and surgical drainage of abscesses.
Thyroiditis caused by radiation or trauma
One percent of patients develop thyroiditis after receiving radioactive iodine ablation for hyperthyroidism (Graves’ disease).4 This condition usually occurs 5 to 10 days after the treatment. Radiation triggers thyroid gland destruction, causing transient additional release of thyroid hormone. Similar damage occurs after external beam radiation for lymphomas and head and neck cancers. In such cases, use nonsteroidal anti-inflammatory drugs (NSAIDs) and prednisone to reduce inflammation and beta-blockers to control hyperthyroid symptoms.
Trauma to the thyroid—from motor vehicle accidents, falls, or physical assaults—can cause pain, tenderness, and abnormalities in thyroid hormone levels. Effects are usually self-limited, and management centers on airway protection and prevention of infection.
Subacute thyroiditis
The cause of ST is not clear. However, it typically follows an upper respiratory infection. Many viruses have been implicated in the disease, including Coxsackie, echo, adeno, and influenza viruses.5 It occurs more frequently during summer months, coinciding with the peak incidence of enterovirus.2 ST is 4 times more common in women than men, and the median age for occurrence is 45.6
Patients with ST usually seek care for such symptoms as fever, myalgias, and malaise, which suggest a viral infection.2,7-9 Neck pain is significant and may radiate to the jaw or ear.9 Patients may have pain on swallowing and a sore throat. It’s possible to confuse ST with severe pharyngitis or even epiglottitis if you fail to palpate the thyroid gland. When you examine the thyroid, the gland is exquisitely tender with ST. Patients with ST appear less ill than those with AST.
In 50% of ST patients, thyroid-stimulating hormone (TSH) is suppressed, and thyroid hormone levels are elevated.4 Patients with hyperthyroidism exhibit the usual signs and symptoms associated with high levels of the hormone: tremor, palpitations, heat intolerance, and diarrhea. After a few weeks, thyroid hormone levels normalize and then drop to below normal in the 4 to 6 months that follow. Levels return to normal in 95% of patients after 6 to 12 months. ST recurs in only 2% of patients.4
Sedimentation rates are almost always elevated in ST, reflecting the significant inflammation associated with the disease. Cytotoxic T lymphocytes damage thyroid follicles, causing release of preformed thyroid hormone, in turn suppressing TSH.4 Radioactive iodine scans show low uptake because TSH is needed for the uptake of iodine.10
Treatment of ST should focus on reducing inflammation and pain. NSAIDs may be sufficient, but patients with moderate to severe symptoms may require prednisone 40 mg daily, tapered over 4 to 6 weeks.2 If the patient is hyperthyroid, you’ll need to control symptoms with beta-blockers.
Ruptured thyroid cyst: An ST look-alike
The clinical presentation of a ruptured cyst closely mimics that of ST: thyroid pain, history of a recent cold, sore throat, aches, and pains. Laboratory and nuclear medicine evaluations, however, reveal significant differences:
- TSH is not suppressed;
- ESR is not elevated;
- Radioactive iodine uptake is normal.
Palpation may reveal a thyroid nodule. You can confirm the diagnosis by ultrasound and a needle aspiration.
CASE The right diagnosis for Sam
Sam’s initial clinical presentation suggested St, and he was started on prednisone 40 mg daily to control his pain. but when laboratory and nuclear medicine evaluations became available the next day, the St diagnosis didn’t hold up: TSH, ESR, and radioactive iodine uptake were all normal.
When Sam came in for a follow-up visit 3 days later, his thyroid pain was gone and he was feeling much better. palpation of his thyroid revealed a slightly tender nodule that went undetected in the initial exam. Subsequent thyroid ultrasound showed a 2x2 cm nodule in the right lobe. a fine needle aspiration revealed a colloid cyst. the cyst had ruptured, causing acute pain from hemorrhage and inflammation.
CORRESPONDENCE Dean Gianakos, MD, 2323 Memorial Drive, #10, Lynchburg Family Medicine Residency, Lynchburg, VA 24501; [email protected]
1. Al-Dajani N, Wooton SH. Cervical lymphadenitis, suppurative parotitis, thyroiditis, and infected cysts. Infect Dis Clin North Am. 2007;21:523-541.
2. Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003;348:2646-2655.
3. Basaria S, Cooper DS. Amiodarone and the thyroid. Am J Med. 2005;118:706-714.
4. Bindra A, Braunstein GD. Thyroiditis. Am Fam Physician. 2006;73:1769-1776.
5. Sniezek JC, Francis TB. Inflammatory thyroid disorders. Otolaryngol Clin North Am. 2003;36:55-71.
6. Fatourechi V, Aniszewski JP, Fatourechi GZ, et al. Clinical features of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, Study. J Clin Endocrinol Metab. 2003;88:2100-2105.
7. Hamburger JI. The various presentations of thyroiditis. Diagnostic considerations. Ann Int Med. 1986;104:219-224.
8. Hay ID. Thyroiditis: a clinical update. Mayo Clin Proc. 1985;60:836-843.
9. Lee SL, Ananthakrishnan S. Subacute thyroiditis. Updated April 27, 2009. Available at: http://emedicine.medscape.com/article/125648-overview. Accessed August 15, 2010.
10. Ross DS. Syndromes of thyrotoxicosis with low radioactive iodine uptake. Endocrinol Metab Clin North Am. 1998;27:169-185.
1. Al-Dajani N, Wooton SH. Cervical lymphadenitis, suppurative parotitis, thyroiditis, and infected cysts. Infect Dis Clin North Am. 2007;21:523-541.
2. Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003;348:2646-2655.
3. Basaria S, Cooper DS. Amiodarone and the thyroid. Am J Med. 2005;118:706-714.
4. Bindra A, Braunstein GD. Thyroiditis. Am Fam Physician. 2006;73:1769-1776.
5. Sniezek JC, Francis TB. Inflammatory thyroid disorders. Otolaryngol Clin North Am. 2003;36:55-71.
6. Fatourechi V, Aniszewski JP, Fatourechi GZ, et al. Clinical features of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, Study. J Clin Endocrinol Metab. 2003;88:2100-2105.
7. Hamburger JI. The various presentations of thyroiditis. Diagnostic considerations. Ann Int Med. 1986;104:219-224.
8. Hay ID. Thyroiditis: a clinical update. Mayo Clin Proc. 1985;60:836-843.
9. Lee SL, Ananthakrishnan S. Subacute thyroiditis. Updated April 27, 2009. Available at: http://emedicine.medscape.com/article/125648-overview. Accessed August 15, 2010.
10. Ross DS. Syndromes of thyrotoxicosis with low radioactive iodine uptake. Endocrinol Metab Clin North Am. 1998;27:169-185.
Breast cancer prevention and Tx: An evidence-based guide
• Offer screening magnetic resonance imaging (MRI) to patients with a known BRCA 1 or 2 mutation, a strong family history of breast cancer, or a lifetime risk of breast cancer >20% to 25%. B
• For early-stage breast cancer, lumpectomy and sentinel node mapping with excision is the preferred method for staging. A
• Monitor patients receiving tamoxifen for signs and symptoms of venous thromboembolism, cataracts, and uterine malignancy, and patients on aromatase inhibitors for the development of osteoporosis. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Late last year, the US Preventive Services Task Force (USPSTF) sparked a nationwide controversy when it announced that it was recommending against routine screening mammography for women younger than age 50.1 Indeed, that’s a recommendation that many other organizations, including the American Cancer Society (ACS),2 the American College of Obstetricians and Gynecologists (ACOG),3 and the National Comprehensive Cancer Network (NCCN),4 disagree with. But the age at which women should begin routine mammography isn’t the only controversial question. Experts disagree on the benefits of breast self-examination, the optimal frequency of clinical breast exams, and the use of digital mammography—among other issues. This evidence-based review can help you cut through the confusion.
CASE Carrie, a 39-year-old woman who has never been pregnant, comes in for an annual Pap smear and gynecologic exam. She has a negative past medical history, but a positive family history for breast cancer—both her mother and 1 of her sisters had the disease. How would you assess Carrie’s risk of breast cancer, and what preventive measures would you recommend?
Use this predictive model to pinpoint your patient’s risk
When making decisions regarding primary prevention of and screening for breast cancer, an accurate assessment of risk is critical. Many predictive models have been developed with that in mind. The most widely studied, the Gail model, incorporates a number of important risk factors (TABLE 1), including age; race; family history; reproductive factors such as age of menarche, menopause, and first childbirth; and previous history of breast biopsy and atypical findings, to calculate a woman’s 5-year risk.5
A risk calculator (the Breast Cancer Risk Assessment Tool) based on the Gail model is available on the National Cancer Institute’s Web site, at http://www.cancer.gov/bcrisktool. Generally, a score ≥1.66%,5 which indicates that a patient has at least a 1.66% chance of developing breast cancer over the next 5 years, is considered high risk.6,7
CASE Carrie’s 2 first-degree relatives affected by breast cancer and her nulliparous status place her at increased risk. Further questioning reveals a particularly strong family history, as both relatives were diagnosed before the age of 50 (her mom at 45 years of age and her sister, at 39). Carrie’s 5-year risk is 1.8%.
TABLE 1
Risk factors for breast cancer5,29
|
| *African American and Caucasian women are at higher risk compared with Asian, Hispanic, and Native American women. |
| †1 drink/day results in minimal increase in risk; 2-5 drinks/day result in 1.5 increased risk compared with nondrinkers. |
| HRT, hormone replacement therapy; LCIS, lobular carcinoma in situ. |
All women can benefit from these preventive measures
As primary care physicians, we have a responsibility to stress lifestyle modification as the mainstay of breast cancer prevention. Whether or not a woman is at high risk, advise her that maintaining a normal weight, exercising vigorously, limiting alcohol consumption, and breastfeeding are evidence-based methods of primary prevention. Diets low in fat and high in fiber may be associated with a lower risk of invasive breast cancer, but there is no conclusive evidence to support specific dietary interventions to reduce the risk.8-11 Nor has a link between active or passive smoking, antioxidants, or fruit and vegetable intake been firmly established.12
There is a clear association between prolonged estrogen exposure and breast cancer, however. Many reproductive factors, such as early menarche, late menopause, later age at time of first full-term pregnancy, and nulliparity, increase a woman’s exposure to endogenous estrogen—and her risk of developing breast cancer.12,13
Exposure to exogenous estrogen is also linked to the development of breast cancer. In 2002, the Women’s Health Initiative (WHI) was stopped early after a report was released stating that the risks of hormone replacement therapy (HRT)—a higher incidence of cardiovascular events, stroke, and venous thromboembolism, as well as breast cancer—outweighed the benefits.14 Subsequent analyses have found a relationship between the declining incidence of breast cancer and the marked decrease in HRT use prompted by the WHI report. While causality has not been firmly established, multiple studies strongly suggest it.15,16
The association between oral contraceptives (OCs) and breast cancer is more controversial. Some studies have found an increased breast cancer risk among OC users, but both the relative risk and absolute risk were found to be very small and to dissipate 10 years after stopping OC use. More recent studies with newer formulations containing lower doses of estrogen have failed to show an increased risk.8
Breast cancer screening: The parameters have changed
Various organizations have published guidelines for breast cancer screening (TABLE 2), and all are somewhat different. Here’s what you need to know.
Breast self-examination (BSE), which women were previously advised to perform monthly, has not been shown to improve mortality in any age group, and is no longer routinely recommended.17 While both the USPSTF and the Canadian Task Force on Preventive Health Care recommend against teaching women BSE, the ACS, ACOG, and NCCN encourage self-examination—particularly among women older than 40 years.1-4,17,18
Clinical breast examination has an average sensitivity of 50% and detects approximately 5% of mammographically occult cancers.19 It is still not clear whether clinical breast exams save lives, however—a finding that is reflected in the USPSTF’s “I” (insufficient evidence to assess the benefits and harms) recommendation.1 Other consensus guidelines still recommend clinical breast examination, albeit at varying frequencies.
Screening mammography decreases mortality rates by anywhere from 28% to 65%, depending on the statistical model used.20 The benefit is greatest in women between the ages of 50 and 69 years, however, and most groups agree that mammography every 1 to 2 years is advisable for this age group. (There is limited data on the value of mammography for women 70 years of age and older, and no consensus on the age at which to stop screening.1,21) But because the mortality benefit from screening mammography is lower for women aged 40 to 49, guidelines for this age group are more controversial.
Mammography’s sensitivity is affected by a variety of factors, including age and menopausal status, prior breast surgery or radiation, breast density, and the experience of the radiologist. Women in their 40s have denser breast tissue than older women, making mammography less sensitive for this age group. Because of that, and because the overall incidence of breast cancer is lower for women younger than 50, some argue that screening mammography for women between the ages of 40 and 49 years leads to unacceptably high false-positive rates (9.8% annually22) and that the harm associated with mammography may outweigh the benefit. Others counter that tumors in younger women tend to be more aggressive and faster growing, making early detection even more critical than for older women.
What should you advise women in this age group? You might point out that the USPSTF recommends against routine screening, but indicates that the decision to begin (or defer) routine mammography before age 50 should be individualized, based on the needs and values of each patient.1
Digital mammography. A recent study of more than 43,000 women demonstrated that digital mammography is more accurate than film—but only for certain groups: These include women <50 years of age, women with dense breasts, and pre- and perimenopausal women. 23 Because it is still not clear whether the increased accuracy will translate into a mortality benefit, more research is needed before digital mammography is widely adopted. The USPSTF maintains that there is insufficient evidence to assess the benefits and harms of using either digital mammography or magnetic resonance imaging (MRI) rather than film mammography to screen for breast cancer.1
MRI. In 2007, the ACS published guidelines on the use of MRI as an adjunct to mammography for breast cancer screening in high-risk women.24 According to ACS guidelines, screening MRI should be offered to patients with a known BRCA 1 or 2 mutation (5%-10% of all breast cancers are associated with a mutation in the BRCA 1 or BRCA 2 gene, which is transmitted in an autosomal dominant pattern6). It also should be offered to those with a strong family history, or a lifetime risk of developing breast cancer that is >20% to 25%. And finally, MRI should be offered to women who had chest wall radiation when they were between the ages of 10 and 30 years—another significant risk factor for breast cancer—and those with other genetic syndromes that increase their lifetime risk of breast cancer.24
Evidence is insufficient for or against MRI screening for women with a personal history of breast cancer, atypical hyperplasia, or lobular carcinoma in situ, however, and neither breast ultrasound (which is generally used diagnostically, not for screening purposes) nor MRI has been shown to be helpful as a screening tool in women with <15% lifetime risk of developing breast cancer.24,25
TABLE 2
Guidelines for breast cancer screening for women with average risk
| Organization | Age (years) | Breast self-exam | Clinical breast exam | Mammography |
|---|---|---|---|---|
| American Cancer Society2 | 20-40 | Optional | Every 3 y | NA |
| >40 | Encourages | Annually | Annually | |
| American College of Obstetricians and Gynecologists3 | 40-49 | Encourages | Annually | 1-2 y |
| 50-69 | Encourages | Annually | Annually | |
| Canadian Task force on Preventive Health Care18 | 40-49 | Recommends against teaching | Insufficient evidence | Insufficient evidence |
| 50-69 | Recommends against teaching | 1-2 y | 1-2 y | |
| National Comprehensive Cancer Network4 | 20-40 | Encourages | 1-3 y | NA |
| >40 | Encourages | Annually | Annually | |
| US Preventive Services Task Force1 | 40-49 | Recommends against teaching | Insufficient evidence | Not routinely recommended |
| 50-74 | Recommends against teaching | Insufficient evidence | Every 2 y | |
| NA, not addressed. | ||||
When to consider chemoprevention
For women like Carrie, who are at high risk of developing breast cancer, selective estrogen receptor modulator (SERM) therapy and surgical interventions may be options to consider. The Breast Cancer Prevention Trial demonstrated the efficacy of tamoxifen as a preventive agent. This landmark trial showed that for high-risk women older than 35, 5 years of tamoxifen therapy can reduce the incidence of invasive breast cancer by nearly 50%.26
Women with the BRCA 1 or 2 mutation—all of whom should be offered genetic counseling—were included in the study. Tamoxifen reduced the incidence of breast cancer in BRCA 2 carriers by 62%, the researchers found, but did not reduce risk in carriers of the BRCA 1 gene. This is likely due to the high prevalence of estrogen receptor-negative breast cancers among BRCA 1 carriers.26
More recently, the Study of Tamoxifen and Raloxifene (STAR) trial compared the efficacy of tamoxifen and raloxifene, a second-generation SERM, in high-risk postmenopausal women ages 35 and older. The drugs were found to be equally effective in reducing the risk of invasive breast cancer, but raloxifene had a better side effect profile, with a lower incidence of thromboembolism and cataracts. 27
What the guidelines call for. In 2003, the USPSTF recommended that clinicians discuss chemoprevention with women at high risk for breast cancer and low risk for adverse effects of SERMs.28
The most recent update to the NCCN breast cancer risk reduction guidelines recommends that clinicians offer tamoxifen to premenopausal women with a 5-year projected breast cancer risk ≥1.7% and offer tamoxifen or raloxifene to high-risk postmenopausal women.29 It is worth noting, however, that SERMs can have significant adverse effects, including venous thromboembolism, stroke, cataracts, uterine malignancy, and hot flashes, while lifestyle modifications and the avoidance of HRT have few, if any, negative effects.
CASE After consultation with a genetic counselor, Carrie underwent testing for both the BRCA 1 and BRCA 2 mutations. She tested negative for both. She declined chemoprevention and prophylactic surgery, opting for enhanced screening with yearly mammography and MRI and lifestyle modification instead.
When a mass is found
For women ages 30 or older with palpable masses or solid masses ≥2 cm found on imaging, core needle biopsy is recommended.30,31 Biopsy is indicated for women younger than 30 as well, if the mass is >2 cm or imaging is suspicious. In general, a needle biopsy read as benign is considered adequate for diagnostic purposes only if the lesion appeared benign on imaging.
For lesions shown to be cystic on imaging, recommendations for follow-up or additional testing are based on the characteristics of the cyst. For simple cysts, 2- to 4-month follow up for stability, followed by routine screening, is adequate.21 Additional evaluation of complex cysts is indicated, including aspiration for complicated cysts and biopsy for complex cysts. After aspiration, surgical excision of bloody aspirates or persistent masses is recommended.30,31
Staging using the TNM system
The TNM (tumor, node, metastases) classification system is used for the staging of breast cancer:
- T refers to the tumor type, size, and extent of local involvement
- N describes regional lymph node involvement
- M refers to distant metastases.
The TNM classifications are also grouped by stage (I through IV).,
Lumpectomy and sentinel node mapping with excision is the preferred method for staging of early-stage breast cancer without palpable lymphadenopathy—provided that the surgical team has documented experience with sentinel node biopsy.32 Sentinel node biopsy is preferred because of its safety, low (<10%) false negative rate, and decreased morbidity compared with full axillary dissection, although dissection is recommended for patients with more advanced cancer or a positive sentinel node.32 The comparative effects of sentinel node biopsy vs axillary node dissection on tumor recurrence and patient survival are not known.33
Testing for tumor markers such as estrogen and progesterone receptors and human epidermal growth factor receptor 2 (HER2) expression status in biopsy-proven breast cancer is now the standard of care. Seventy percent of breast cancers are estrogen receptor-positive, with increasing frequency associated with older age.34 Estrogen/progesterone receptor positivity is associated with a more favorable outcome, and multiple hormonal therapies can be aimed at these receptors.34 While HER2 overexpression—which occurs in 15% to 30% of newly diagnosed breast cancers35—is associated with more aggressive tumors, women with this type of tumor cell can benefit from trastuzumab, an anti-HER2 drug.36
Key factors that affect prognosis
Important factors affecting prognosis and treatment of localized breast cancer are tumor size, age and menopausal status, tumor expression of hormone receptors and/ or the HER2 protein, as well as the status of the draining axillary nodes. Factors that predict a greater chance of recurrence include the spread of disease to axillary nodes, larger tumor size, invasive histology, inflammatory pathology, lack of estrogen/progesterone receptors, and age <50 years or premenopausal status.
Treatment options include surgical resection, radiation, and systemic adjuvant therapy in the form of chemotherapy, endocrine therapy, or anti-HER2 monoclonal antibodies.37 (For more on treatment, see “Surgery, radiation, and systemic therapy: Making the most of what’s in our arsenal” at jfponline.com.)
Don’t overlook quality-of-life issues
Follow-up of breast cancer patients should go beyond treatment and work-up for recurrence and metastatic disease to focus on health and lifestyle issues, such as stress reduction, mood, smoking cessation, diet and exercise, treatment of hot flashes, sexual dysfunction, and bone health. A recent study found both reduced recurrence and increased survival in women receiving psychological interventions to improve quality-of-life measures after an 11-year follow-up.38
Refer women to targeted Web sites such as the National Breast Cancer Awareness Month organization (http://www.nbcam.org/), the National Breast Cancer Foundation (http://community.nationalbreastcancer.org/), and the Susan G. Komen Breast Cancer Foundation (http://ww5.komen.org/). Offer treatment for bothersome symptoms. Hot flashes and depression, for example, often related to endocrine therapy, can be treated with selective serotonin reuptake inhibitors (SSRIs). That said, some SSRIs decrease the active metabolite of tamoxifen by inhibiting CYP2D6 enzyme and must, therefore, be used with caution. However, venlafaxine and citalopram are less likely to alter tamoxifen metabolism than other SSRIs.39
CASE When Carrie was 47, she had an abnormal MRI of the left breast. Core needle biopsy and pathology of the lesion revealed an estrogen and progesterone receptor-positive tumor that was negative for HER2 overexpression. She underwent lumpectomy, which revealed a 1.5 cm tumor, followed by a negative sentinel node biopsy, and was diagnosed with stage I (T1N0M0) breast cancer. Carrie had radiation after surgery; she did not require chemotherapy, but was told to take tamoxifen for 5 years. This adjuvant endocrine therapy led to hot flashes and depression, both of which were successfully treated with venlafaxine. Carrie is currently cancer-free and participates in a breast cancer survivor program that includes regular visits with her primary physician and her oncologist.
CORRESPONDENCE Denise Sur, MD, 1920 Colorado Avenue, Santa Monica, CA 90404; [email protected]
Surgery, radiation, and systemic therapy: Making the most of what’s in our arsenal
Breast cancer surgery has changed dramatically over the years. Multiple studies have shown that breast-conserving therapy (lumpectomy followed by radiation) for carefully selected women is comparable to mastectomy for local recurrence and survival. While there has been much interest in determining whether a subset of patients could forego radiation after lumpectomy, a meta-analysis by the Early Breast Cancer Trialists Collaborative Group demonstrated that radiation after lumpectomy provides an absolute local recurrence risk reduction of 19%, and a 5.4% absolute reduction in 15-year breast cancer mortality rates compared with lumpectomy without radiation.1 Thus, radiation after lumpectomy remains the standard of care for all women undergoing breast-conserving therapy, regardless of tumor characteristics.
In certain women with a high risk of recurrence (≥4 positive nodes), radiation is also recommended after mastectomy. Women undergoing mastectomy have numerous options for immediate or delayed breast reconstruction. Consultation with a multidisciplinary team, including a plastic surgeon, prior to any surgical intervention is advised.2
Multiple systemic chemotherapy regimens have been shown to be beneficial in carefully selected patients with breast cancer. Systematic reviews have demonstrated that an anthracycline-based regimen can decrease annual breast cancer mortality by 38% in women <50 years old and by 20% in women ages 50 to 69 years.1 in more recent randomized controlled trials, the addition of taxanes to anthracycline-based regimens has produced promising results.3
Numerous hormonal therapies benefit women with estrogen or progesterone receptor-positive breast cancer. Tamoxifen blocks the activity of estrogen on receptors located in breast cancer tissue, for example; aromatase inhibitors block the conversion of androgens to estrogen; and gonadotropin-releasing hormone (GnRH) analogs such as leuprolide and goserelin suppress ovarian production of estrogen.
For postmenopausal women, options include an aromatase inhibitor alone or tamoxifen followed by an aromatase inhibitor.
In premenopausal women, aromatase inhibitors are not very effective, as decreasing peripheral estrogen stimulates the ovaries to produce more estrogen. Thus, for these patients, adjuvant endocrine therapy consists of tamoxifen, with ovarian ablation (via surgery or radiation) or ovarian suppression with a GnRH analog. If the patient goes through menopause as a result of this therapy, she may benefit from aromatase inhibitors at that time.4,5
Women with breast cancer that overexpresses the HER2 gene benefit from adjuvant treatment with trastuzumab, an anti-HER2 antibody.6 While current guidelines advise treatment for 1 year, multiple studies are evaluating dosing schedules and optimal duration of treatment. for now, patients should be monitored for signs of cardiotoxicity at baseline and every 3 months thereafter until completion of therapy.4
References
1. Early Breast Caner Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;265:1687-1717.
2. Codeiro P. Breast reconstruction after surgery for breast cancer. N Engl J Med. 2008;359:1590-1601.
3. DeLaurentiis M, Cancello G, D’Agostino D, et al. Taxane-based combinations as adjuvant chemotherapy of early breast cancer: a meta-analysis of randomized trials. J Clin Oncol. 2008;26:44-53.
4. National Comprehensive Cancer Network. Breast cancer risk reduction clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2003;1:280-296.
5. Baum M, Budzar AU, Cuzick J, et al. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial. Lancet. 2002;359:2131-2139.
6. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Herceptin adjuvant (HERA) Trial Study Team. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659-1672.
1. US Preventive Services Task Force Screening for breast cancer. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsbrca.htm. Accessed September 2, 2010.
2. American Cancer Society. American Cancer Society guidelines for the early detection of cancer. Available at: http://www.cancer.org/Healthy/FindCancerEarly/CancerScreeningGuidelines/american-cancer-society-guidelines-for-the-early-detection-of-cancer. Accessed September 2, 2010.
3. American College of Obstetricians and Gynecologists. Response of the American College of Obstetricians and Gynecologists to the new breast cancer screening recommendations from the US Preventive Services Task Force. Available at: http://www.acog.org/from_home/misc/uspstfresponse.cfm. Accessed September 2, 2010.
4. National Comprehensive Cancer Network. Breast cancer screening and diagnosis. Clinical Practice Guidelines in Oncology-V.1.2010. Fort Washington, Pa: National Comprehensive Cancer Network: November 3, 2009. Available at: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed September 17 , 2010.
5. National Cancer Institute. Breast cancer risk assessment tool. Available at: http://www.cancer.gov/bcrisktool/. Accessed September 2, 2010
6. Robson M, Offit K. Clinical practice. Management of an inherited predisposition to breast cancer. N Engl J Med. 2007;357:154-162.
7. Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
8. Cummings SR, Tice JA, Bauer S, et al. Prevention of breast cancer in postmenopausal women: approaches to estimating and reducing risk. J Natl Cancer Inst. 2009;18:101,-384-398.
9. Prentice RL, Caan B, Chlebowski RT, et al. Low-fat dietary pattern and risk of invasive breast cancer: the Women’s Health Initiative Randomized Controlled Dietary Modification Trial. JAMA. 2006;295:629-642.
10. Pierce JP, Natarajan L, Caan BJ, et al. Influence of a diet very high in vegetables, fruit, and fiber and low in fat on prognosis following treatment for breast cancer: the Women’s Healthy Eating and Living (WHEL) randomized trial. JAMA. 2007;298:289-298.
11. Chlebowski RT, Blackburn GL, Thomson CA, et al. Dietary fat reduction and breast cancer outcome: interim efficacy results from the Women’s Intervention Nutrition Study (WINS). J Natl Cancer Inst. 2006;98:1767-1776.
12. PDQ Cancer Information Summary. Breast Cancer Prevention (PRQ) – Health Professional. Date last modified April 30, 2009. Available at: http://www.cancer.gov/cancertopics/pdq/prevention/breast/healthprofessional. Accessed May 12, 2009.
13. Hulka BS, Moorman PG. Breast cancer: hormones and other risk factors. Maturitas. 2001;38:103-113.
14. Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288:321-333.
15. Ravdin PM, Cronin KA, Howlader N, et al. The decrease in breast-cancer incidence in 2003 in the United States. N Engl J Med. 2007;356:1670-1674.
16. Chlebowski RT, Kuller LH, Prentice RL, et al. WHI Investigators. Breast cancer after use of estrogen plus progestin in postmenopausal women. N Engl J Med. 2009;360:573-587.
17. Kosters JP, Gotzsche PC. Regular self-examination or clinical examination for early detection of breast cancer. Cochrane Database Syst Rev. 2003;(2):CD003373.-
18. Canadian Task Force on the Periodic Health Examination Ottawa, Canada: Health Canada; 1994:788-795 (reaffirmed by the Canadian Task Force on the Periodic Health Examination 1999, 2001).Available at: http://www.ctfphc.org/index/html. Accessed August 12, 2009.
19. Green BB, Taplin SH. Breast cancer screening controversies. J Am Board Fam Pract. 2003;16:233-241.
20. Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353:1784-1792.
21. Tice JA, Kerlikowske K. Screening and prevention of breast cancer in primary care. Prim Care. 2009;36:533-558.
22. US Preventive Services Task Force. Screening for breast cancer. Systematic evidence review update for the US Preventive Services Task Force. Available at: http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=es74. Accessed September 2, 2010.
23. Pisano ED, Gatsonis C, Hendrick E, et al. Digital Mammographic Imaging Screening Trial (DMIST) Investigators Group. Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med. 2005;353:1773-1783.
24. Saslow D, Boetes C, Burke W, et al. American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75-89.
25. Berg W, Blume J, Cormack J, et al. Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA. 2008;299:2151-2163.
26. King M, Wieand S, Hale K, et al. Tamoxifen and breast cancer incidence among women with inherited mutations in BRCA1 and BRCA2: National Surgical Adjuvant Breast and Bowel Project (NSABP-P1) Breast Cancer Prevention Trial. JAMA. 2001;286:2251-2256.
27. Vogel VG, Costantino JP, Wickerham DL, et al. Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes: the NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 trial. JAMA. 2006;295:2727-2741.
28. Berg AO. US Preventive Services Task Force. Chemoprevention of breast cancer: recommendations and rationale. Am J Nurs. 2003;103:107-113.
29. National Comprehensive Cancer Network. Breast cancer risk reduction. Clinical Practice Guidelines in Oncology-V.2.2010. Fort Washington, Pa: National Comprehensive Cancer Network; August 7, 2010. Available at: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed September 17, 2010.
30. Sickles EA, Filly RA, Cllen PW. Benign breast lesions: ultrasound detection and diagnosis. Radiology. 1984;151:467.-
31. Beavers TB, Anderson BO, Bonaccio E, et al. NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. J Natl Compr Canc Netw. 2009;7:1060-1096.
32. Mansel RE, Fallowfield L, Kissin M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC trial. J Natl Canc Inst. 2006;98:599-609
33. Lyman GH, Guiliano AE, Somerfield MR, et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early- stage breast cancer. J Clin Oncol. 2005;23:7703-7720.
34. Turner N, Jones A. Management of breast cancer-Part II. BMJ. 2008;337:a540.-
35. Harris L, Fritsche H, Mennel R, et al:. American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer J Clin Oncol. 2007;25:5287-5312.
36. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Herceptin adjuvant (HERA) Trial Study Team. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659-1672.
37. PDQ Cancer Information Summary Breast cancer treatment– health professional. Available at: http://www.cancer.gov/cancertopics/pdq/treatment/breast/HealthProfessional. Accessed May 12, 2009.
38. Anderson BL, Yang HC, Farrar WB, et al. Psychologic intervention improves survival for breast cancer patients: a randomized clinical trial. Cancer. 2008;113:3450-3458.
39. Jin Y, Desta Z, Stearns V, et al. CYP2D6 genotype, antidepressant use, and tamoxifen metabolism during adjuvant breast cancer treatment. J Natl Cancer Inst. 2005;97:30-39.
• Offer screening magnetic resonance imaging (MRI) to patients with a known BRCA 1 or 2 mutation, a strong family history of breast cancer, or a lifetime risk of breast cancer >20% to 25%. B
• For early-stage breast cancer, lumpectomy and sentinel node mapping with excision is the preferred method for staging. A
• Monitor patients receiving tamoxifen for signs and symptoms of venous thromboembolism, cataracts, and uterine malignancy, and patients on aromatase inhibitors for the development of osteoporosis. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Late last year, the US Preventive Services Task Force (USPSTF) sparked a nationwide controversy when it announced that it was recommending against routine screening mammography for women younger than age 50.1 Indeed, that’s a recommendation that many other organizations, including the American Cancer Society (ACS),2 the American College of Obstetricians and Gynecologists (ACOG),3 and the National Comprehensive Cancer Network (NCCN),4 disagree with. But the age at which women should begin routine mammography isn’t the only controversial question. Experts disagree on the benefits of breast self-examination, the optimal frequency of clinical breast exams, and the use of digital mammography—among other issues. This evidence-based review can help you cut through the confusion.
CASE Carrie, a 39-year-old woman who has never been pregnant, comes in for an annual Pap smear and gynecologic exam. She has a negative past medical history, but a positive family history for breast cancer—both her mother and 1 of her sisters had the disease. How would you assess Carrie’s risk of breast cancer, and what preventive measures would you recommend?
Use this predictive model to pinpoint your patient’s risk
When making decisions regarding primary prevention of and screening for breast cancer, an accurate assessment of risk is critical. Many predictive models have been developed with that in mind. The most widely studied, the Gail model, incorporates a number of important risk factors (TABLE 1), including age; race; family history; reproductive factors such as age of menarche, menopause, and first childbirth; and previous history of breast biopsy and atypical findings, to calculate a woman’s 5-year risk.5
A risk calculator (the Breast Cancer Risk Assessment Tool) based on the Gail model is available on the National Cancer Institute’s Web site, at http://www.cancer.gov/bcrisktool. Generally, a score ≥1.66%,5 which indicates that a patient has at least a 1.66% chance of developing breast cancer over the next 5 years, is considered high risk.6,7
CASE Carrie’s 2 first-degree relatives affected by breast cancer and her nulliparous status place her at increased risk. Further questioning reveals a particularly strong family history, as both relatives were diagnosed before the age of 50 (her mom at 45 years of age and her sister, at 39). Carrie’s 5-year risk is 1.8%.
TABLE 1
Risk factors for breast cancer5,29
|
| *African American and Caucasian women are at higher risk compared with Asian, Hispanic, and Native American women. |
| †1 drink/day results in minimal increase in risk; 2-5 drinks/day result in 1.5 increased risk compared with nondrinkers. |
| HRT, hormone replacement therapy; LCIS, lobular carcinoma in situ. |
All women can benefit from these preventive measures
As primary care physicians, we have a responsibility to stress lifestyle modification as the mainstay of breast cancer prevention. Whether or not a woman is at high risk, advise her that maintaining a normal weight, exercising vigorously, limiting alcohol consumption, and breastfeeding are evidence-based methods of primary prevention. Diets low in fat and high in fiber may be associated with a lower risk of invasive breast cancer, but there is no conclusive evidence to support specific dietary interventions to reduce the risk.8-11 Nor has a link between active or passive smoking, antioxidants, or fruit and vegetable intake been firmly established.12
There is a clear association between prolonged estrogen exposure and breast cancer, however. Many reproductive factors, such as early menarche, late menopause, later age at time of first full-term pregnancy, and nulliparity, increase a woman’s exposure to endogenous estrogen—and her risk of developing breast cancer.12,13
Exposure to exogenous estrogen is also linked to the development of breast cancer. In 2002, the Women’s Health Initiative (WHI) was stopped early after a report was released stating that the risks of hormone replacement therapy (HRT)—a higher incidence of cardiovascular events, stroke, and venous thromboembolism, as well as breast cancer—outweighed the benefits.14 Subsequent analyses have found a relationship between the declining incidence of breast cancer and the marked decrease in HRT use prompted by the WHI report. While causality has not been firmly established, multiple studies strongly suggest it.15,16
The association between oral contraceptives (OCs) and breast cancer is more controversial. Some studies have found an increased breast cancer risk among OC users, but both the relative risk and absolute risk were found to be very small and to dissipate 10 years after stopping OC use. More recent studies with newer formulations containing lower doses of estrogen have failed to show an increased risk.8
Breast cancer screening: The parameters have changed
Various organizations have published guidelines for breast cancer screening (TABLE 2), and all are somewhat different. Here’s what you need to know.
Breast self-examination (BSE), which women were previously advised to perform monthly, has not been shown to improve mortality in any age group, and is no longer routinely recommended.17 While both the USPSTF and the Canadian Task Force on Preventive Health Care recommend against teaching women BSE, the ACS, ACOG, and NCCN encourage self-examination—particularly among women older than 40 years.1-4,17,18
Clinical breast examination has an average sensitivity of 50% and detects approximately 5% of mammographically occult cancers.19 It is still not clear whether clinical breast exams save lives, however—a finding that is reflected in the USPSTF’s “I” (insufficient evidence to assess the benefits and harms) recommendation.1 Other consensus guidelines still recommend clinical breast examination, albeit at varying frequencies.
Screening mammography decreases mortality rates by anywhere from 28% to 65%, depending on the statistical model used.20 The benefit is greatest in women between the ages of 50 and 69 years, however, and most groups agree that mammography every 1 to 2 years is advisable for this age group. (There is limited data on the value of mammography for women 70 years of age and older, and no consensus on the age at which to stop screening.1,21) But because the mortality benefit from screening mammography is lower for women aged 40 to 49, guidelines for this age group are more controversial.
Mammography’s sensitivity is affected by a variety of factors, including age and menopausal status, prior breast surgery or radiation, breast density, and the experience of the radiologist. Women in their 40s have denser breast tissue than older women, making mammography less sensitive for this age group. Because of that, and because the overall incidence of breast cancer is lower for women younger than 50, some argue that screening mammography for women between the ages of 40 and 49 years leads to unacceptably high false-positive rates (9.8% annually22) and that the harm associated with mammography may outweigh the benefit. Others counter that tumors in younger women tend to be more aggressive and faster growing, making early detection even more critical than for older women.
What should you advise women in this age group? You might point out that the USPSTF recommends against routine screening, but indicates that the decision to begin (or defer) routine mammography before age 50 should be individualized, based on the needs and values of each patient.1
Digital mammography. A recent study of more than 43,000 women demonstrated that digital mammography is more accurate than film—but only for certain groups: These include women <50 years of age, women with dense breasts, and pre- and perimenopausal women. 23 Because it is still not clear whether the increased accuracy will translate into a mortality benefit, more research is needed before digital mammography is widely adopted. The USPSTF maintains that there is insufficient evidence to assess the benefits and harms of using either digital mammography or magnetic resonance imaging (MRI) rather than film mammography to screen for breast cancer.1
MRI. In 2007, the ACS published guidelines on the use of MRI as an adjunct to mammography for breast cancer screening in high-risk women.24 According to ACS guidelines, screening MRI should be offered to patients with a known BRCA 1 or 2 mutation (5%-10% of all breast cancers are associated with a mutation in the BRCA 1 or BRCA 2 gene, which is transmitted in an autosomal dominant pattern6). It also should be offered to those with a strong family history, or a lifetime risk of developing breast cancer that is >20% to 25%. And finally, MRI should be offered to women who had chest wall radiation when they were between the ages of 10 and 30 years—another significant risk factor for breast cancer—and those with other genetic syndromes that increase their lifetime risk of breast cancer.24
Evidence is insufficient for or against MRI screening for women with a personal history of breast cancer, atypical hyperplasia, or lobular carcinoma in situ, however, and neither breast ultrasound (which is generally used diagnostically, not for screening purposes) nor MRI has been shown to be helpful as a screening tool in women with <15% lifetime risk of developing breast cancer.24,25
TABLE 2
Guidelines for breast cancer screening for women with average risk
| Organization | Age (years) | Breast self-exam | Clinical breast exam | Mammography |
|---|---|---|---|---|
| American Cancer Society2 | 20-40 | Optional | Every 3 y | NA |
| >40 | Encourages | Annually | Annually | |
| American College of Obstetricians and Gynecologists3 | 40-49 | Encourages | Annually | 1-2 y |
| 50-69 | Encourages | Annually | Annually | |
| Canadian Task force on Preventive Health Care18 | 40-49 | Recommends against teaching | Insufficient evidence | Insufficient evidence |
| 50-69 | Recommends against teaching | 1-2 y | 1-2 y | |
| National Comprehensive Cancer Network4 | 20-40 | Encourages | 1-3 y | NA |
| >40 | Encourages | Annually | Annually | |
| US Preventive Services Task Force1 | 40-49 | Recommends against teaching | Insufficient evidence | Not routinely recommended |
| 50-74 | Recommends against teaching | Insufficient evidence | Every 2 y | |
| NA, not addressed. | ||||
When to consider chemoprevention
For women like Carrie, who are at high risk of developing breast cancer, selective estrogen receptor modulator (SERM) therapy and surgical interventions may be options to consider. The Breast Cancer Prevention Trial demonstrated the efficacy of tamoxifen as a preventive agent. This landmark trial showed that for high-risk women older than 35, 5 years of tamoxifen therapy can reduce the incidence of invasive breast cancer by nearly 50%.26
Women with the BRCA 1 or 2 mutation—all of whom should be offered genetic counseling—were included in the study. Tamoxifen reduced the incidence of breast cancer in BRCA 2 carriers by 62%, the researchers found, but did not reduce risk in carriers of the BRCA 1 gene. This is likely due to the high prevalence of estrogen receptor-negative breast cancers among BRCA 1 carriers.26
More recently, the Study of Tamoxifen and Raloxifene (STAR) trial compared the efficacy of tamoxifen and raloxifene, a second-generation SERM, in high-risk postmenopausal women ages 35 and older. The drugs were found to be equally effective in reducing the risk of invasive breast cancer, but raloxifene had a better side effect profile, with a lower incidence of thromboembolism and cataracts. 27
What the guidelines call for. In 2003, the USPSTF recommended that clinicians discuss chemoprevention with women at high risk for breast cancer and low risk for adverse effects of SERMs.28
The most recent update to the NCCN breast cancer risk reduction guidelines recommends that clinicians offer tamoxifen to premenopausal women with a 5-year projected breast cancer risk ≥1.7% and offer tamoxifen or raloxifene to high-risk postmenopausal women.29 It is worth noting, however, that SERMs can have significant adverse effects, including venous thromboembolism, stroke, cataracts, uterine malignancy, and hot flashes, while lifestyle modifications and the avoidance of HRT have few, if any, negative effects.
CASE After consultation with a genetic counselor, Carrie underwent testing for both the BRCA 1 and BRCA 2 mutations. She tested negative for both. She declined chemoprevention and prophylactic surgery, opting for enhanced screening with yearly mammography and MRI and lifestyle modification instead.
When a mass is found
For women ages 30 or older with palpable masses or solid masses ≥2 cm found on imaging, core needle biopsy is recommended.30,31 Biopsy is indicated for women younger than 30 as well, if the mass is >2 cm or imaging is suspicious. In general, a needle biopsy read as benign is considered adequate for diagnostic purposes only if the lesion appeared benign on imaging.
For lesions shown to be cystic on imaging, recommendations for follow-up or additional testing are based on the characteristics of the cyst. For simple cysts, 2- to 4-month follow up for stability, followed by routine screening, is adequate.21 Additional evaluation of complex cysts is indicated, including aspiration for complicated cysts and biopsy for complex cysts. After aspiration, surgical excision of bloody aspirates or persistent masses is recommended.30,31
Staging using the TNM system
The TNM (tumor, node, metastases) classification system is used for the staging of breast cancer:
- T refers to the tumor type, size, and extent of local involvement
- N describes regional lymph node involvement
- M refers to distant metastases.
The TNM classifications are also grouped by stage (I through IV).,
Lumpectomy and sentinel node mapping with excision is the preferred method for staging of early-stage breast cancer without palpable lymphadenopathy—provided that the surgical team has documented experience with sentinel node biopsy.32 Sentinel node biopsy is preferred because of its safety, low (<10%) false negative rate, and decreased morbidity compared with full axillary dissection, although dissection is recommended for patients with more advanced cancer or a positive sentinel node.32 The comparative effects of sentinel node biopsy vs axillary node dissection on tumor recurrence and patient survival are not known.33
Testing for tumor markers such as estrogen and progesterone receptors and human epidermal growth factor receptor 2 (HER2) expression status in biopsy-proven breast cancer is now the standard of care. Seventy percent of breast cancers are estrogen receptor-positive, with increasing frequency associated with older age.34 Estrogen/progesterone receptor positivity is associated with a more favorable outcome, and multiple hormonal therapies can be aimed at these receptors.34 While HER2 overexpression—which occurs in 15% to 30% of newly diagnosed breast cancers35—is associated with more aggressive tumors, women with this type of tumor cell can benefit from trastuzumab, an anti-HER2 drug.36
Key factors that affect prognosis
Important factors affecting prognosis and treatment of localized breast cancer are tumor size, age and menopausal status, tumor expression of hormone receptors and/ or the HER2 protein, as well as the status of the draining axillary nodes. Factors that predict a greater chance of recurrence include the spread of disease to axillary nodes, larger tumor size, invasive histology, inflammatory pathology, lack of estrogen/progesterone receptors, and age <50 years or premenopausal status.
Treatment options include surgical resection, radiation, and systemic adjuvant therapy in the form of chemotherapy, endocrine therapy, or anti-HER2 monoclonal antibodies.37 (For more on treatment, see “Surgery, radiation, and systemic therapy: Making the most of what’s in our arsenal” at jfponline.com.)
Don’t overlook quality-of-life issues
Follow-up of breast cancer patients should go beyond treatment and work-up for recurrence and metastatic disease to focus on health and lifestyle issues, such as stress reduction, mood, smoking cessation, diet and exercise, treatment of hot flashes, sexual dysfunction, and bone health. A recent study found both reduced recurrence and increased survival in women receiving psychological interventions to improve quality-of-life measures after an 11-year follow-up.38
Refer women to targeted Web sites such as the National Breast Cancer Awareness Month organization (http://www.nbcam.org/), the National Breast Cancer Foundation (http://community.nationalbreastcancer.org/), and the Susan G. Komen Breast Cancer Foundation (http://ww5.komen.org/). Offer treatment for bothersome symptoms. Hot flashes and depression, for example, often related to endocrine therapy, can be treated with selective serotonin reuptake inhibitors (SSRIs). That said, some SSRIs decrease the active metabolite of tamoxifen by inhibiting CYP2D6 enzyme and must, therefore, be used with caution. However, venlafaxine and citalopram are less likely to alter tamoxifen metabolism than other SSRIs.39
CASE When Carrie was 47, she had an abnormal MRI of the left breast. Core needle biopsy and pathology of the lesion revealed an estrogen and progesterone receptor-positive tumor that was negative for HER2 overexpression. She underwent lumpectomy, which revealed a 1.5 cm tumor, followed by a negative sentinel node biopsy, and was diagnosed with stage I (T1N0M0) breast cancer. Carrie had radiation after surgery; she did not require chemotherapy, but was told to take tamoxifen for 5 years. This adjuvant endocrine therapy led to hot flashes and depression, both of which were successfully treated with venlafaxine. Carrie is currently cancer-free and participates in a breast cancer survivor program that includes regular visits with her primary physician and her oncologist.
CORRESPONDENCE Denise Sur, MD, 1920 Colorado Avenue, Santa Monica, CA 90404; [email protected]
Surgery, radiation, and systemic therapy: Making the most of what’s in our arsenal
Breast cancer surgery has changed dramatically over the years. Multiple studies have shown that breast-conserving therapy (lumpectomy followed by radiation) for carefully selected women is comparable to mastectomy for local recurrence and survival. While there has been much interest in determining whether a subset of patients could forego radiation after lumpectomy, a meta-analysis by the Early Breast Cancer Trialists Collaborative Group demonstrated that radiation after lumpectomy provides an absolute local recurrence risk reduction of 19%, and a 5.4% absolute reduction in 15-year breast cancer mortality rates compared with lumpectomy without radiation.1 Thus, radiation after lumpectomy remains the standard of care for all women undergoing breast-conserving therapy, regardless of tumor characteristics.
In certain women with a high risk of recurrence (≥4 positive nodes), radiation is also recommended after mastectomy. Women undergoing mastectomy have numerous options for immediate or delayed breast reconstruction. Consultation with a multidisciplinary team, including a plastic surgeon, prior to any surgical intervention is advised.2
Multiple systemic chemotherapy regimens have been shown to be beneficial in carefully selected patients with breast cancer. Systematic reviews have demonstrated that an anthracycline-based regimen can decrease annual breast cancer mortality by 38% in women <50 years old and by 20% in women ages 50 to 69 years.1 in more recent randomized controlled trials, the addition of taxanes to anthracycline-based regimens has produced promising results.3
Numerous hormonal therapies benefit women with estrogen or progesterone receptor-positive breast cancer. Tamoxifen blocks the activity of estrogen on receptors located in breast cancer tissue, for example; aromatase inhibitors block the conversion of androgens to estrogen; and gonadotropin-releasing hormone (GnRH) analogs such as leuprolide and goserelin suppress ovarian production of estrogen.
For postmenopausal women, options include an aromatase inhibitor alone or tamoxifen followed by an aromatase inhibitor.
In premenopausal women, aromatase inhibitors are not very effective, as decreasing peripheral estrogen stimulates the ovaries to produce more estrogen. Thus, for these patients, adjuvant endocrine therapy consists of tamoxifen, with ovarian ablation (via surgery or radiation) or ovarian suppression with a GnRH analog. If the patient goes through menopause as a result of this therapy, she may benefit from aromatase inhibitors at that time.4,5
Women with breast cancer that overexpresses the HER2 gene benefit from adjuvant treatment with trastuzumab, an anti-HER2 antibody.6 While current guidelines advise treatment for 1 year, multiple studies are evaluating dosing schedules and optimal duration of treatment. for now, patients should be monitored for signs of cardiotoxicity at baseline and every 3 months thereafter until completion of therapy.4
References
1. Early Breast Caner Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;265:1687-1717.
2. Codeiro P. Breast reconstruction after surgery for breast cancer. N Engl J Med. 2008;359:1590-1601.
3. DeLaurentiis M, Cancello G, D’Agostino D, et al. Taxane-based combinations as adjuvant chemotherapy of early breast cancer: a meta-analysis of randomized trials. J Clin Oncol. 2008;26:44-53.
4. National Comprehensive Cancer Network. Breast cancer risk reduction clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2003;1:280-296.
5. Baum M, Budzar AU, Cuzick J, et al. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial. Lancet. 2002;359:2131-2139.
6. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Herceptin adjuvant (HERA) Trial Study Team. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659-1672.
• Offer screening magnetic resonance imaging (MRI) to patients with a known BRCA 1 or 2 mutation, a strong family history of breast cancer, or a lifetime risk of breast cancer >20% to 25%. B
• For early-stage breast cancer, lumpectomy and sentinel node mapping with excision is the preferred method for staging. A
• Monitor patients receiving tamoxifen for signs and symptoms of venous thromboembolism, cataracts, and uterine malignancy, and patients on aromatase inhibitors for the development of osteoporosis. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Late last year, the US Preventive Services Task Force (USPSTF) sparked a nationwide controversy when it announced that it was recommending against routine screening mammography for women younger than age 50.1 Indeed, that’s a recommendation that many other organizations, including the American Cancer Society (ACS),2 the American College of Obstetricians and Gynecologists (ACOG),3 and the National Comprehensive Cancer Network (NCCN),4 disagree with. But the age at which women should begin routine mammography isn’t the only controversial question. Experts disagree on the benefits of breast self-examination, the optimal frequency of clinical breast exams, and the use of digital mammography—among other issues. This evidence-based review can help you cut through the confusion.
CASE Carrie, a 39-year-old woman who has never been pregnant, comes in for an annual Pap smear and gynecologic exam. She has a negative past medical history, but a positive family history for breast cancer—both her mother and 1 of her sisters had the disease. How would you assess Carrie’s risk of breast cancer, and what preventive measures would you recommend?
Use this predictive model to pinpoint your patient’s risk
When making decisions regarding primary prevention of and screening for breast cancer, an accurate assessment of risk is critical. Many predictive models have been developed with that in mind. The most widely studied, the Gail model, incorporates a number of important risk factors (TABLE 1), including age; race; family history; reproductive factors such as age of menarche, menopause, and first childbirth; and previous history of breast biopsy and atypical findings, to calculate a woman’s 5-year risk.5
A risk calculator (the Breast Cancer Risk Assessment Tool) based on the Gail model is available on the National Cancer Institute’s Web site, at http://www.cancer.gov/bcrisktool. Generally, a score ≥1.66%,5 which indicates that a patient has at least a 1.66% chance of developing breast cancer over the next 5 years, is considered high risk.6,7
CASE Carrie’s 2 first-degree relatives affected by breast cancer and her nulliparous status place her at increased risk. Further questioning reveals a particularly strong family history, as both relatives were diagnosed before the age of 50 (her mom at 45 years of age and her sister, at 39). Carrie’s 5-year risk is 1.8%.
TABLE 1
Risk factors for breast cancer5,29
|
| *African American and Caucasian women are at higher risk compared with Asian, Hispanic, and Native American women. |
| †1 drink/day results in minimal increase in risk; 2-5 drinks/day result in 1.5 increased risk compared with nondrinkers. |
| HRT, hormone replacement therapy; LCIS, lobular carcinoma in situ. |
All women can benefit from these preventive measures
As primary care physicians, we have a responsibility to stress lifestyle modification as the mainstay of breast cancer prevention. Whether or not a woman is at high risk, advise her that maintaining a normal weight, exercising vigorously, limiting alcohol consumption, and breastfeeding are evidence-based methods of primary prevention. Diets low in fat and high in fiber may be associated with a lower risk of invasive breast cancer, but there is no conclusive evidence to support specific dietary interventions to reduce the risk.8-11 Nor has a link between active or passive smoking, antioxidants, or fruit and vegetable intake been firmly established.12
There is a clear association between prolonged estrogen exposure and breast cancer, however. Many reproductive factors, such as early menarche, late menopause, later age at time of first full-term pregnancy, and nulliparity, increase a woman’s exposure to endogenous estrogen—and her risk of developing breast cancer.12,13
Exposure to exogenous estrogen is also linked to the development of breast cancer. In 2002, the Women’s Health Initiative (WHI) was stopped early after a report was released stating that the risks of hormone replacement therapy (HRT)—a higher incidence of cardiovascular events, stroke, and venous thromboembolism, as well as breast cancer—outweighed the benefits.14 Subsequent analyses have found a relationship between the declining incidence of breast cancer and the marked decrease in HRT use prompted by the WHI report. While causality has not been firmly established, multiple studies strongly suggest it.15,16
The association between oral contraceptives (OCs) and breast cancer is more controversial. Some studies have found an increased breast cancer risk among OC users, but both the relative risk and absolute risk were found to be very small and to dissipate 10 years after stopping OC use. More recent studies with newer formulations containing lower doses of estrogen have failed to show an increased risk.8
Breast cancer screening: The parameters have changed
Various organizations have published guidelines for breast cancer screening (TABLE 2), and all are somewhat different. Here’s what you need to know.
Breast self-examination (BSE), which women were previously advised to perform monthly, has not been shown to improve mortality in any age group, and is no longer routinely recommended.17 While both the USPSTF and the Canadian Task Force on Preventive Health Care recommend against teaching women BSE, the ACS, ACOG, and NCCN encourage self-examination—particularly among women older than 40 years.1-4,17,18
Clinical breast examination has an average sensitivity of 50% and detects approximately 5% of mammographically occult cancers.19 It is still not clear whether clinical breast exams save lives, however—a finding that is reflected in the USPSTF’s “I” (insufficient evidence to assess the benefits and harms) recommendation.1 Other consensus guidelines still recommend clinical breast examination, albeit at varying frequencies.
Screening mammography decreases mortality rates by anywhere from 28% to 65%, depending on the statistical model used.20 The benefit is greatest in women between the ages of 50 and 69 years, however, and most groups agree that mammography every 1 to 2 years is advisable for this age group. (There is limited data on the value of mammography for women 70 years of age and older, and no consensus on the age at which to stop screening.1,21) But because the mortality benefit from screening mammography is lower for women aged 40 to 49, guidelines for this age group are more controversial.
Mammography’s sensitivity is affected by a variety of factors, including age and menopausal status, prior breast surgery or radiation, breast density, and the experience of the radiologist. Women in their 40s have denser breast tissue than older women, making mammography less sensitive for this age group. Because of that, and because the overall incidence of breast cancer is lower for women younger than 50, some argue that screening mammography for women between the ages of 40 and 49 years leads to unacceptably high false-positive rates (9.8% annually22) and that the harm associated with mammography may outweigh the benefit. Others counter that tumors in younger women tend to be more aggressive and faster growing, making early detection even more critical than for older women.
What should you advise women in this age group? You might point out that the USPSTF recommends against routine screening, but indicates that the decision to begin (or defer) routine mammography before age 50 should be individualized, based on the needs and values of each patient.1
Digital mammography. A recent study of more than 43,000 women demonstrated that digital mammography is more accurate than film—but only for certain groups: These include women <50 years of age, women with dense breasts, and pre- and perimenopausal women. 23 Because it is still not clear whether the increased accuracy will translate into a mortality benefit, more research is needed before digital mammography is widely adopted. The USPSTF maintains that there is insufficient evidence to assess the benefits and harms of using either digital mammography or magnetic resonance imaging (MRI) rather than film mammography to screen for breast cancer.1
MRI. In 2007, the ACS published guidelines on the use of MRI as an adjunct to mammography for breast cancer screening in high-risk women.24 According to ACS guidelines, screening MRI should be offered to patients with a known BRCA 1 or 2 mutation (5%-10% of all breast cancers are associated with a mutation in the BRCA 1 or BRCA 2 gene, which is transmitted in an autosomal dominant pattern6). It also should be offered to those with a strong family history, or a lifetime risk of developing breast cancer that is >20% to 25%. And finally, MRI should be offered to women who had chest wall radiation when they were between the ages of 10 and 30 years—another significant risk factor for breast cancer—and those with other genetic syndromes that increase their lifetime risk of breast cancer.24
Evidence is insufficient for or against MRI screening for women with a personal history of breast cancer, atypical hyperplasia, or lobular carcinoma in situ, however, and neither breast ultrasound (which is generally used diagnostically, not for screening purposes) nor MRI has been shown to be helpful as a screening tool in women with <15% lifetime risk of developing breast cancer.24,25
TABLE 2
Guidelines for breast cancer screening for women with average risk
| Organization | Age (years) | Breast self-exam | Clinical breast exam | Mammography |
|---|---|---|---|---|
| American Cancer Society2 | 20-40 | Optional | Every 3 y | NA |
| >40 | Encourages | Annually | Annually | |
| American College of Obstetricians and Gynecologists3 | 40-49 | Encourages | Annually | 1-2 y |
| 50-69 | Encourages | Annually | Annually | |
| Canadian Task force on Preventive Health Care18 | 40-49 | Recommends against teaching | Insufficient evidence | Insufficient evidence |
| 50-69 | Recommends against teaching | 1-2 y | 1-2 y | |
| National Comprehensive Cancer Network4 | 20-40 | Encourages | 1-3 y | NA |
| >40 | Encourages | Annually | Annually | |
| US Preventive Services Task Force1 | 40-49 | Recommends against teaching | Insufficient evidence | Not routinely recommended |
| 50-74 | Recommends against teaching | Insufficient evidence | Every 2 y | |
| NA, not addressed. | ||||
When to consider chemoprevention
For women like Carrie, who are at high risk of developing breast cancer, selective estrogen receptor modulator (SERM) therapy and surgical interventions may be options to consider. The Breast Cancer Prevention Trial demonstrated the efficacy of tamoxifen as a preventive agent. This landmark trial showed that for high-risk women older than 35, 5 years of tamoxifen therapy can reduce the incidence of invasive breast cancer by nearly 50%.26
Women with the BRCA 1 or 2 mutation—all of whom should be offered genetic counseling—were included in the study. Tamoxifen reduced the incidence of breast cancer in BRCA 2 carriers by 62%, the researchers found, but did not reduce risk in carriers of the BRCA 1 gene. This is likely due to the high prevalence of estrogen receptor-negative breast cancers among BRCA 1 carriers.26
More recently, the Study of Tamoxifen and Raloxifene (STAR) trial compared the efficacy of tamoxifen and raloxifene, a second-generation SERM, in high-risk postmenopausal women ages 35 and older. The drugs were found to be equally effective in reducing the risk of invasive breast cancer, but raloxifene had a better side effect profile, with a lower incidence of thromboembolism and cataracts. 27
What the guidelines call for. In 2003, the USPSTF recommended that clinicians discuss chemoprevention with women at high risk for breast cancer and low risk for adverse effects of SERMs.28
The most recent update to the NCCN breast cancer risk reduction guidelines recommends that clinicians offer tamoxifen to premenopausal women with a 5-year projected breast cancer risk ≥1.7% and offer tamoxifen or raloxifene to high-risk postmenopausal women.29 It is worth noting, however, that SERMs can have significant adverse effects, including venous thromboembolism, stroke, cataracts, uterine malignancy, and hot flashes, while lifestyle modifications and the avoidance of HRT have few, if any, negative effects.
CASE After consultation with a genetic counselor, Carrie underwent testing for both the BRCA 1 and BRCA 2 mutations. She tested negative for both. She declined chemoprevention and prophylactic surgery, opting for enhanced screening with yearly mammography and MRI and lifestyle modification instead.
When a mass is found
For women ages 30 or older with palpable masses or solid masses ≥2 cm found on imaging, core needle biopsy is recommended.30,31 Biopsy is indicated for women younger than 30 as well, if the mass is >2 cm or imaging is suspicious. In general, a needle biopsy read as benign is considered adequate for diagnostic purposes only if the lesion appeared benign on imaging.
For lesions shown to be cystic on imaging, recommendations for follow-up or additional testing are based on the characteristics of the cyst. For simple cysts, 2- to 4-month follow up for stability, followed by routine screening, is adequate.21 Additional evaluation of complex cysts is indicated, including aspiration for complicated cysts and biopsy for complex cysts. After aspiration, surgical excision of bloody aspirates or persistent masses is recommended.30,31
Staging using the TNM system
The TNM (tumor, node, metastases) classification system is used for the staging of breast cancer:
- T refers to the tumor type, size, and extent of local involvement
- N describes regional lymph node involvement
- M refers to distant metastases.
The TNM classifications are also grouped by stage (I through IV).,
Lumpectomy and sentinel node mapping with excision is the preferred method for staging of early-stage breast cancer without palpable lymphadenopathy—provided that the surgical team has documented experience with sentinel node biopsy.32 Sentinel node biopsy is preferred because of its safety, low (<10%) false negative rate, and decreased morbidity compared with full axillary dissection, although dissection is recommended for patients with more advanced cancer or a positive sentinel node.32 The comparative effects of sentinel node biopsy vs axillary node dissection on tumor recurrence and patient survival are not known.33
Testing for tumor markers such as estrogen and progesterone receptors and human epidermal growth factor receptor 2 (HER2) expression status in biopsy-proven breast cancer is now the standard of care. Seventy percent of breast cancers are estrogen receptor-positive, with increasing frequency associated with older age.34 Estrogen/progesterone receptor positivity is associated with a more favorable outcome, and multiple hormonal therapies can be aimed at these receptors.34 While HER2 overexpression—which occurs in 15% to 30% of newly diagnosed breast cancers35—is associated with more aggressive tumors, women with this type of tumor cell can benefit from trastuzumab, an anti-HER2 drug.36
Key factors that affect prognosis
Important factors affecting prognosis and treatment of localized breast cancer are tumor size, age and menopausal status, tumor expression of hormone receptors and/ or the HER2 protein, as well as the status of the draining axillary nodes. Factors that predict a greater chance of recurrence include the spread of disease to axillary nodes, larger tumor size, invasive histology, inflammatory pathology, lack of estrogen/progesterone receptors, and age <50 years or premenopausal status.
Treatment options include surgical resection, radiation, and systemic adjuvant therapy in the form of chemotherapy, endocrine therapy, or anti-HER2 monoclonal antibodies.37 (For more on treatment, see “Surgery, radiation, and systemic therapy: Making the most of what’s in our arsenal” at jfponline.com.)
Don’t overlook quality-of-life issues
Follow-up of breast cancer patients should go beyond treatment and work-up for recurrence and metastatic disease to focus on health and lifestyle issues, such as stress reduction, mood, smoking cessation, diet and exercise, treatment of hot flashes, sexual dysfunction, and bone health. A recent study found both reduced recurrence and increased survival in women receiving psychological interventions to improve quality-of-life measures after an 11-year follow-up.38
Refer women to targeted Web sites such as the National Breast Cancer Awareness Month organization (http://www.nbcam.org/), the National Breast Cancer Foundation (http://community.nationalbreastcancer.org/), and the Susan G. Komen Breast Cancer Foundation (http://ww5.komen.org/). Offer treatment for bothersome symptoms. Hot flashes and depression, for example, often related to endocrine therapy, can be treated with selective serotonin reuptake inhibitors (SSRIs). That said, some SSRIs decrease the active metabolite of tamoxifen by inhibiting CYP2D6 enzyme and must, therefore, be used with caution. However, venlafaxine and citalopram are less likely to alter tamoxifen metabolism than other SSRIs.39
CASE When Carrie was 47, she had an abnormal MRI of the left breast. Core needle biopsy and pathology of the lesion revealed an estrogen and progesterone receptor-positive tumor that was negative for HER2 overexpression. She underwent lumpectomy, which revealed a 1.5 cm tumor, followed by a negative sentinel node biopsy, and was diagnosed with stage I (T1N0M0) breast cancer. Carrie had radiation after surgery; she did not require chemotherapy, but was told to take tamoxifen for 5 years. This adjuvant endocrine therapy led to hot flashes and depression, both of which were successfully treated with venlafaxine. Carrie is currently cancer-free and participates in a breast cancer survivor program that includes regular visits with her primary physician and her oncologist.
CORRESPONDENCE Denise Sur, MD, 1920 Colorado Avenue, Santa Monica, CA 90404; [email protected]
Surgery, radiation, and systemic therapy: Making the most of what’s in our arsenal
Breast cancer surgery has changed dramatically over the years. Multiple studies have shown that breast-conserving therapy (lumpectomy followed by radiation) for carefully selected women is comparable to mastectomy for local recurrence and survival. While there has been much interest in determining whether a subset of patients could forego radiation after lumpectomy, a meta-analysis by the Early Breast Cancer Trialists Collaborative Group demonstrated that radiation after lumpectomy provides an absolute local recurrence risk reduction of 19%, and a 5.4% absolute reduction in 15-year breast cancer mortality rates compared with lumpectomy without radiation.1 Thus, radiation after lumpectomy remains the standard of care for all women undergoing breast-conserving therapy, regardless of tumor characteristics.
In certain women with a high risk of recurrence (≥4 positive nodes), radiation is also recommended after mastectomy. Women undergoing mastectomy have numerous options for immediate or delayed breast reconstruction. Consultation with a multidisciplinary team, including a plastic surgeon, prior to any surgical intervention is advised.2
Multiple systemic chemotherapy regimens have been shown to be beneficial in carefully selected patients with breast cancer. Systematic reviews have demonstrated that an anthracycline-based regimen can decrease annual breast cancer mortality by 38% in women <50 years old and by 20% in women ages 50 to 69 years.1 in more recent randomized controlled trials, the addition of taxanes to anthracycline-based regimens has produced promising results.3
Numerous hormonal therapies benefit women with estrogen or progesterone receptor-positive breast cancer. Tamoxifen blocks the activity of estrogen on receptors located in breast cancer tissue, for example; aromatase inhibitors block the conversion of androgens to estrogen; and gonadotropin-releasing hormone (GnRH) analogs such as leuprolide and goserelin suppress ovarian production of estrogen.
For postmenopausal women, options include an aromatase inhibitor alone or tamoxifen followed by an aromatase inhibitor.
In premenopausal women, aromatase inhibitors are not very effective, as decreasing peripheral estrogen stimulates the ovaries to produce more estrogen. Thus, for these patients, adjuvant endocrine therapy consists of tamoxifen, with ovarian ablation (via surgery or radiation) or ovarian suppression with a GnRH analog. If the patient goes through menopause as a result of this therapy, she may benefit from aromatase inhibitors at that time.4,5
Women with breast cancer that overexpresses the HER2 gene benefit from adjuvant treatment with trastuzumab, an anti-HER2 antibody.6 While current guidelines advise treatment for 1 year, multiple studies are evaluating dosing schedules and optimal duration of treatment. for now, patients should be monitored for signs of cardiotoxicity at baseline and every 3 months thereafter until completion of therapy.4
References
1. Early Breast Caner Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;265:1687-1717.
2. Codeiro P. Breast reconstruction after surgery for breast cancer. N Engl J Med. 2008;359:1590-1601.
3. DeLaurentiis M, Cancello G, D’Agostino D, et al. Taxane-based combinations as adjuvant chemotherapy of early breast cancer: a meta-analysis of randomized trials. J Clin Oncol. 2008;26:44-53.
4. National Comprehensive Cancer Network. Breast cancer risk reduction clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2003;1:280-296.
5. Baum M, Budzar AU, Cuzick J, et al. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial. Lancet. 2002;359:2131-2139.
6. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Herceptin adjuvant (HERA) Trial Study Team. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659-1672.
1. US Preventive Services Task Force Screening for breast cancer. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsbrca.htm. Accessed September 2, 2010.
2. American Cancer Society. American Cancer Society guidelines for the early detection of cancer. Available at: http://www.cancer.org/Healthy/FindCancerEarly/CancerScreeningGuidelines/american-cancer-society-guidelines-for-the-early-detection-of-cancer. Accessed September 2, 2010.
3. American College of Obstetricians and Gynecologists. Response of the American College of Obstetricians and Gynecologists to the new breast cancer screening recommendations from the US Preventive Services Task Force. Available at: http://www.acog.org/from_home/misc/uspstfresponse.cfm. Accessed September 2, 2010.
4. National Comprehensive Cancer Network. Breast cancer screening and diagnosis. Clinical Practice Guidelines in Oncology-V.1.2010. Fort Washington, Pa: National Comprehensive Cancer Network: November 3, 2009. Available at: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed September 17 , 2010.
5. National Cancer Institute. Breast cancer risk assessment tool. Available at: http://www.cancer.gov/bcrisktool/. Accessed September 2, 2010
6. Robson M, Offit K. Clinical practice. Management of an inherited predisposition to breast cancer. N Engl J Med. 2007;357:154-162.
7. Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
8. Cummings SR, Tice JA, Bauer S, et al. Prevention of breast cancer in postmenopausal women: approaches to estimating and reducing risk. J Natl Cancer Inst. 2009;18:101,-384-398.
9. Prentice RL, Caan B, Chlebowski RT, et al. Low-fat dietary pattern and risk of invasive breast cancer: the Women’s Health Initiative Randomized Controlled Dietary Modification Trial. JAMA. 2006;295:629-642.
10. Pierce JP, Natarajan L, Caan BJ, et al. Influence of a diet very high in vegetables, fruit, and fiber and low in fat on prognosis following treatment for breast cancer: the Women’s Healthy Eating and Living (WHEL) randomized trial. JAMA. 2007;298:289-298.
11. Chlebowski RT, Blackburn GL, Thomson CA, et al. Dietary fat reduction and breast cancer outcome: interim efficacy results from the Women’s Intervention Nutrition Study (WINS). J Natl Cancer Inst. 2006;98:1767-1776.
12. PDQ Cancer Information Summary. Breast Cancer Prevention (PRQ) – Health Professional. Date last modified April 30, 2009. Available at: http://www.cancer.gov/cancertopics/pdq/prevention/breast/healthprofessional. Accessed May 12, 2009.
13. Hulka BS, Moorman PG. Breast cancer: hormones and other risk factors. Maturitas. 2001;38:103-113.
14. Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288:321-333.
15. Ravdin PM, Cronin KA, Howlader N, et al. The decrease in breast-cancer incidence in 2003 in the United States. N Engl J Med. 2007;356:1670-1674.
16. Chlebowski RT, Kuller LH, Prentice RL, et al. WHI Investigators. Breast cancer after use of estrogen plus progestin in postmenopausal women. N Engl J Med. 2009;360:573-587.
17. Kosters JP, Gotzsche PC. Regular self-examination or clinical examination for early detection of breast cancer. Cochrane Database Syst Rev. 2003;(2):CD003373.-
18. Canadian Task Force on the Periodic Health Examination Ottawa, Canada: Health Canada; 1994:788-795 (reaffirmed by the Canadian Task Force on the Periodic Health Examination 1999, 2001).Available at: http://www.ctfphc.org/index/html. Accessed August 12, 2009.
19. Green BB, Taplin SH. Breast cancer screening controversies. J Am Board Fam Pract. 2003;16:233-241.
20. Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353:1784-1792.
21. Tice JA, Kerlikowske K. Screening and prevention of breast cancer in primary care. Prim Care. 2009;36:533-558.
22. US Preventive Services Task Force. Screening for breast cancer. Systematic evidence review update for the US Preventive Services Task Force. Available at: http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=es74. Accessed September 2, 2010.
23. Pisano ED, Gatsonis C, Hendrick E, et al. Digital Mammographic Imaging Screening Trial (DMIST) Investigators Group. Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med. 2005;353:1773-1783.
24. Saslow D, Boetes C, Burke W, et al. American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75-89.
25. Berg W, Blume J, Cormack J, et al. Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA. 2008;299:2151-2163.
26. King M, Wieand S, Hale K, et al. Tamoxifen and breast cancer incidence among women with inherited mutations in BRCA1 and BRCA2: National Surgical Adjuvant Breast and Bowel Project (NSABP-P1) Breast Cancer Prevention Trial. JAMA. 2001;286:2251-2256.
27. Vogel VG, Costantino JP, Wickerham DL, et al. Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes: the NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 trial. JAMA. 2006;295:2727-2741.
28. Berg AO. US Preventive Services Task Force. Chemoprevention of breast cancer: recommendations and rationale. Am J Nurs. 2003;103:107-113.
29. National Comprehensive Cancer Network. Breast cancer risk reduction. Clinical Practice Guidelines in Oncology-V.2.2010. Fort Washington, Pa: National Comprehensive Cancer Network; August 7, 2010. Available at: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed September 17, 2010.
30. Sickles EA, Filly RA, Cllen PW. Benign breast lesions: ultrasound detection and diagnosis. Radiology. 1984;151:467.-
31. Beavers TB, Anderson BO, Bonaccio E, et al. NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. J Natl Compr Canc Netw. 2009;7:1060-1096.
32. Mansel RE, Fallowfield L, Kissin M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC trial. J Natl Canc Inst. 2006;98:599-609
33. Lyman GH, Guiliano AE, Somerfield MR, et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early- stage breast cancer. J Clin Oncol. 2005;23:7703-7720.
34. Turner N, Jones A. Management of breast cancer-Part II. BMJ. 2008;337:a540.-
35. Harris L, Fritsche H, Mennel R, et al:. American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer J Clin Oncol. 2007;25:5287-5312.
36. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Herceptin adjuvant (HERA) Trial Study Team. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659-1672.
37. PDQ Cancer Information Summary Breast cancer treatment– health professional. Available at: http://www.cancer.gov/cancertopics/pdq/treatment/breast/HealthProfessional. Accessed May 12, 2009.
38. Anderson BL, Yang HC, Farrar WB, et al. Psychologic intervention improves survival for breast cancer patients: a randomized clinical trial. Cancer. 2008;113:3450-3458.
39. Jin Y, Desta Z, Stearns V, et al. CYP2D6 genotype, antidepressant use, and tamoxifen metabolism during adjuvant breast cancer treatment. J Natl Cancer Inst. 2005;97:30-39.
1. US Preventive Services Task Force Screening for breast cancer. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsbrca.htm. Accessed September 2, 2010.
2. American Cancer Society. American Cancer Society guidelines for the early detection of cancer. Available at: http://www.cancer.org/Healthy/FindCancerEarly/CancerScreeningGuidelines/american-cancer-society-guidelines-for-the-early-detection-of-cancer. Accessed September 2, 2010.
3. American College of Obstetricians and Gynecologists. Response of the American College of Obstetricians and Gynecologists to the new breast cancer screening recommendations from the US Preventive Services Task Force. Available at: http://www.acog.org/from_home/misc/uspstfresponse.cfm. Accessed September 2, 2010.
4. National Comprehensive Cancer Network. Breast cancer screening and diagnosis. Clinical Practice Guidelines in Oncology-V.1.2010. Fort Washington, Pa: National Comprehensive Cancer Network: November 3, 2009. Available at: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed September 17 , 2010.
5. National Cancer Institute. Breast cancer risk assessment tool. Available at: http://www.cancer.gov/bcrisktool/. Accessed September 2, 2010
6. Robson M, Offit K. Clinical practice. Management of an inherited predisposition to breast cancer. N Engl J Med. 2007;357:154-162.
7. Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
8. Cummings SR, Tice JA, Bauer S, et al. Prevention of breast cancer in postmenopausal women: approaches to estimating and reducing risk. J Natl Cancer Inst. 2009;18:101,-384-398.
9. Prentice RL, Caan B, Chlebowski RT, et al. Low-fat dietary pattern and risk of invasive breast cancer: the Women’s Health Initiative Randomized Controlled Dietary Modification Trial. JAMA. 2006;295:629-642.
10. Pierce JP, Natarajan L, Caan BJ, et al. Influence of a diet very high in vegetables, fruit, and fiber and low in fat on prognosis following treatment for breast cancer: the Women’s Healthy Eating and Living (WHEL) randomized trial. JAMA. 2007;298:289-298.
11. Chlebowski RT, Blackburn GL, Thomson CA, et al. Dietary fat reduction and breast cancer outcome: interim efficacy results from the Women’s Intervention Nutrition Study (WINS). J Natl Cancer Inst. 2006;98:1767-1776.
12. PDQ Cancer Information Summary. Breast Cancer Prevention (PRQ) – Health Professional. Date last modified April 30, 2009. Available at: http://www.cancer.gov/cancertopics/pdq/prevention/breast/healthprofessional. Accessed May 12, 2009.
13. Hulka BS, Moorman PG. Breast cancer: hormones and other risk factors. Maturitas. 2001;38:103-113.
14. Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288:321-333.
15. Ravdin PM, Cronin KA, Howlader N, et al. The decrease in breast-cancer incidence in 2003 in the United States. N Engl J Med. 2007;356:1670-1674.
16. Chlebowski RT, Kuller LH, Prentice RL, et al. WHI Investigators. Breast cancer after use of estrogen plus progestin in postmenopausal women. N Engl J Med. 2009;360:573-587.
17. Kosters JP, Gotzsche PC. Regular self-examination or clinical examination for early detection of breast cancer. Cochrane Database Syst Rev. 2003;(2):CD003373.-
18. Canadian Task Force on the Periodic Health Examination Ottawa, Canada: Health Canada; 1994:788-795 (reaffirmed by the Canadian Task Force on the Periodic Health Examination 1999, 2001).Available at: http://www.ctfphc.org/index/html. Accessed August 12, 2009.
19. Green BB, Taplin SH. Breast cancer screening controversies. J Am Board Fam Pract. 2003;16:233-241.
20. Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353:1784-1792.
21. Tice JA, Kerlikowske K. Screening and prevention of breast cancer in primary care. Prim Care. 2009;36:533-558.
22. US Preventive Services Task Force. Screening for breast cancer. Systematic evidence review update for the US Preventive Services Task Force. Available at: http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=es74. Accessed September 2, 2010.
23. Pisano ED, Gatsonis C, Hendrick E, et al. Digital Mammographic Imaging Screening Trial (DMIST) Investigators Group. Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med. 2005;353:1773-1783.
24. Saslow D, Boetes C, Burke W, et al. American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75-89.
25. Berg W, Blume J, Cormack J, et al. Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA. 2008;299:2151-2163.
26. King M, Wieand S, Hale K, et al. Tamoxifen and breast cancer incidence among women with inherited mutations in BRCA1 and BRCA2: National Surgical Adjuvant Breast and Bowel Project (NSABP-P1) Breast Cancer Prevention Trial. JAMA. 2001;286:2251-2256.
27. Vogel VG, Costantino JP, Wickerham DL, et al. Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes: the NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 trial. JAMA. 2006;295:2727-2741.
28. Berg AO. US Preventive Services Task Force. Chemoprevention of breast cancer: recommendations and rationale. Am J Nurs. 2003;103:107-113.
29. National Comprehensive Cancer Network. Breast cancer risk reduction. Clinical Practice Guidelines in Oncology-V.2.2010. Fort Washington, Pa: National Comprehensive Cancer Network; August 7, 2010. Available at: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed September 17, 2010.
30. Sickles EA, Filly RA, Cllen PW. Benign breast lesions: ultrasound detection and diagnosis. Radiology. 1984;151:467.-
31. Beavers TB, Anderson BO, Bonaccio E, et al. NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. J Natl Compr Canc Netw. 2009;7:1060-1096.
32. Mansel RE, Fallowfield L, Kissin M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC trial. J Natl Canc Inst. 2006;98:599-609
33. Lyman GH, Guiliano AE, Somerfield MR, et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early- stage breast cancer. J Clin Oncol. 2005;23:7703-7720.
34. Turner N, Jones A. Management of breast cancer-Part II. BMJ. 2008;337:a540.-
35. Harris L, Fritsche H, Mennel R, et al:. American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer J Clin Oncol. 2007;25:5287-5312.
36. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Herceptin adjuvant (HERA) Trial Study Team. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659-1672.
37. PDQ Cancer Information Summary Breast cancer treatment– health professional. Available at: http://www.cancer.gov/cancertopics/pdq/treatment/breast/HealthProfessional. Accessed May 12, 2009.
38. Anderson BL, Yang HC, Farrar WB, et al. Psychologic intervention improves survival for breast cancer patients: a randomized clinical trial. Cancer. 2008;113:3450-3458.
39. Jin Y, Desta Z, Stearns V, et al. CYP2D6 genotype, antidepressant use, and tamoxifen metabolism during adjuvant breast cancer treatment. J Natl Cancer Inst. 2005;97:30-39.
Beneath the surface: Derm clues to underlying disorders
• When evaluating patients with suspected cutaneous lupus erythematosus, use multiple criteria—including histologic and immunofluorescent biopsy findings and American College of Rheumatology criteria—to rule out systemic disease. C
• Cancer screening with a careful history and physical examination is recommended for all adult patients whom you suspect of having dermatomyositis. C
• Suspect mixed connective tissue disease in patients with skin findings characteristic of varying auto-immune disorders appearing sequentially over several months or years. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Many systemic conditions are accompanied by skin manifestations. This is especially true for connective tissue disorders, for which dermatologic findings are often the key to diagnosis.
In this review, we describe the dermatologic findings of some well-known connective tissue disorders. The text and photographs in the pages that follow will help you hone your diagnostic skills, leading to earlier treatment and, possibly, better outcomes.
Lupus erythematosus: Cutaneous and systemic disease often overlap
Lupus erythematosus (LE), a chronic, inflammatory autoimmune condition that primarily affects women in their 20s and 30s, may initially present as a systemic disease or in a purely cutaneous form. However, most patients with systemic LE have some skin manifestations, and those with cutaneous LE often have—or subsequently develop—systemic involvement.1 Thus, recognizing the cutaneous manifestations of LE will not only aid in diagnosis, but will help you identify patients at risk for systemic disease.
Cutaneous LE has 4 subtypes
There are 4 subcategories of cutaneous LE—acute, subacute, chronic, and intermittent.2 Each is differentiated by the appearance of the lesions (TABLE 1), histology, and serological markers.1 Photosensitivity is common to all the subcategories to varying degrees.
Acute cutaneous lupus erythematosus (ACLE) is typically characterized by the classic malar “butterfly” rash, an erythematous eruption of macules or edematous papules over the bridge of the nose and cheek.3 Although this presentation is most common, there are variations—1 in which the lesions cover other exposed areas (commonly including the “V” of the chest, the extensor surface of the arms, and the hands), and a rare form in which toxic epidermal necrolysis-like blistering occurs.1,4 These skin changes—which generally last anywhere from a few hours to several weeks—typically resolve without scarring, although pigment changes can occur.5
Left: Dermatomyositis is the underlying cause of the heliotrope discoloration on this patient’s upper eyelid.
Center: Linear morphea is associated with the lesion on this patient’s face—called en coup de sabre because it resembles the mark caused by the stroke of a sword in a duel.
Right: Discoid lupus erythematosus causes hypopigmentation and scarring.Patients with ACLE have a predisposition to systemic LE; unlike those with other forms of cutaneous LE, 40% to 90% will have double-stranded DNA (dsDNA) autoantibodies.3,6
Subacute cutaneous lupus erythematosus (SCLE), which usually affects middle-aged Caucasian women, is characterized by erythematous papulosquamous (psoriasis-like) eruptions or annular lesions with raised red borders and central clearing—or both. These lesions, which are nonscarring, lack in-duration, and rarely affect the scalp or face, appear suddenly, usually after exposure to sunlight (FIGURE 1)5,7-9 or certain drugs. Hydrochlorothiazide, terbinafine, calcium channel blockers, and angiotensin-converting enzyme inhibitors are common offenders.1,6
FIGURE 1
Annular lesions in subacute cutaneous lupus erythematosus
Ring-like lesions with raised red borders and central clearing on the back of a patient with subacute cutaneous lupus erythematosus.
SCLE is often associated with extracutaneous symptoms such as arthritis and myalgias,1,8 but patients are at relatively low risk for severe systemic manifestations.5,8,10 Serology is often notable, with anti-Ro (SS-A) antibodies present in 70% to 90% of patients and anti-La (SS-B) autoantibodies found in 30% to 50%.1,11
Chronic cutaneous lupus erythematosus (CCLE) also occurs predominantly in females, at a ratio as high as 5 to 1.12 There are 3 variations of CCLE: discoid lupus erythematosus (DLE), LE profundus, and chilblain LE (TABLE 1). DLE, characterized by alopecia, skin atrophy, and dyspigmentation, is the most common and affects patients of all ages and ethnic groups.9,13,14 (See image above.)
DLE lesions typically begin as erythematous papules and plaques with scale. As the disorder progresses, the lesions spread, causing follicular plugging, peripheral hyperpigmentation and central hypopigmentation, telangiectasia, and atrophy.9,15 In some cases, patients develop thickened, scarred skin and permanent scarring alopecia.15 Prompt recognition of DLE is particularly important, as early referral and treatment may reduce the likelihood of permanent scarring alopecia and pigment changes.11
Intermittent cutaneous lupus erythematosus (ICLE), a relatively new subtype of cutaneous LE, is represented by a rare condition—lupus erythematosus tumidus (LET)—reported in <100 cases worldwide. LET is characterized by succulent, erythematous, and edematous plaques on sun-exposed parts of the body.1,16
TABLE 1
Cutaneous lupus erythematosus: Recognizing the subtypes1
| Acute cutaneous lupus erythematosus (ACLE) |
|---|
| Localized: erythematous macules or papules over the bridge of the nose and cheek, with sparing of the nasolabial folds (“butterfly rash”) |
| Generalized: similar erythematous lesions over other photodistributed parts of the body, including the neck, chest, arms, and hands |
| Toxic epidermal necrolysis-like (TEN-like): blistering and epidermal cleavage in photodistributed parts of the body |
| Subacute cutaneous lupus erythematosus (SCLE) |
| Erythematous papulosquamous (psoriasis-like) eruptions or annular (ring-like) lesions with raised red borders and central clearing, occurring symmetrically and suddenly after sunlight exposure on photo-distributed body parts; the scalp and face are rarely affected |
| Chronic cutaneous lupus erythematosus (CCLE) |
| Discoid lupus erythematosus: erythematous papules and plaques with associated scale, spreading centrifugally with follicular plugging, pigment change, telangiectasia, and atrophy; scarring alopecia can occur |
| Lupus erythematosus profundus: tender, erythematous nodules and plaques, usually involving the proximal extremities, trunk, breasts, buttocks, and face |
| Chilblain lupus erythematosus: tender, erythematous nodules and plaques, occurring in acral areas often in response to cold |
| Intermittent cutaneous lupus erythematosus (ICLE) |
| Lupus erythematosus tumidus: succulent, erythematous, and edematous plaques found on photodistributed parts of the body |
Cutaneous LE diagnosis and treatment: Start with ACR criteria
When evaluating patients with suspected cutaneous LE, it is important not only to identify the subtype, but also to rule out systemic disease using criteria established by the American College of Rheumatology (ACR).17 Notably, 4 of the 11 diagnostic criteria for systemic disease involve visual clues, including malar rash, discoid rash, photosensitivity, and oral ulcerations. Laboratory evidence of systemic disease may include a positive antinuclear antibody, anti-dsDNA, or anti-Sm autoantibody test results, as well as hematologic abnormalities described in the ACR guidelines.
Ultimately, a diagnosis of cutaneous LE should be based on the patient’s history and physical exam, autoantibody profile, and histologic and immunofluorescent biopsy findings. A rheumatologic evaluation may help to determine which patients have systemic disease, as the ACR criteria may overdiagnose systemic LE in those with predominantly skin changes.6
Treatment of cutaneous LE is based on the subtype and extent of disease, with potent topical corticosteroids, in combination with antimalarial agents, being the primary therapies. ACLE skin lesions generally respond best to systemic corticosteroids and immunosuppressive agents (such as azathioprine or cyclophosphamide) that are used to control underlying systemic disease. SCLE can be managed with topical corticosteroids; however, patients typically also require systemic treatment, often with hydroxychloroquine, for optimal control. DLE, the most common form of CCLE, is managed in a similar fashion, with a greater role for intralesional corticosteroid injections. Lesions associated with ICLE, which often resolve spontaneously, may be treated with topical corticosteroids and antimalarials.16 It is also important to advise all patients with cutaneous LE to use a broad-spectrum sunscreen, as ultraviolet (UV) exposure can induce or exacerbate the lesions.9
Dermatomyositis: Rare but serious
Dermatomyositis is an idiopathic inflammatory myopathy characterized by chronic muscle inflammation, symmetric proximal muscle weakness, and distinct cutaneous findings. In addition to possible cardiac and pulmonary complications, dysphagia, and joint contractures, dermatomyositis is associated with cancer, with up to 25% of affected adults having an underlying occult malignancy.18
Dermatomyositis is a rare condition, with a prevalence of only 1 to 10 cases per million adults and 3.2 cases per million children.19 It has a bimodal age distribution, with most juvenile cases affecting children between the ages of 5 and 14 years and most adult cases developing in the fifth and sixth decades of life. Women are affected twice as often as men.18
Suspect dermatomyositis when you see any of the following signs:
- A heliotrope rash: violaceous macules and patches, with or without edema, symmetrically on the periorbital skin, present early in the disease course in 30% to 60% of patients.19 (See image)
- Gottron’s papules: violaceous papules on the dorsal interphalangeal and metacarpophalangeal joints of the hands, elbows, and knees, occurring in as many as 70% of patients (FIGURE 2).19,20
- Gottron’s sign: nonscaling, violaceous erythematous macules and plaques occurring symmetrically in the same distribution as Gottron’s papules, but with sparing of the interphalangeal spaces.20
- Periungual erythema and telangiectasias: redness and dilation of the blood vessels in the skin surrounding the nail plate.
- The shawl and V-signs: erythematous macular eruptions occurring in a “shawl” pattern on the shoulders, arms, and upper back and in a V-shaped pattern on the anterior neck and chest.
- Mechanic’s hand: extensive scaling, fissuring, and roughening of the palmar aspect of the hand.20,21
- Poikiloderma vasculare atrophicans: circumscribed violaceous erythema with thinning of the skin, prominent telangiectasias, and a mottled pattern of hypo- and hyperpigmentation, typically occurring on the anterior neck, chest, posterior shoulders, back, and buttocks, years after onset of the disease.21-24
- Cutaneous calcification (calcinosis cutis): usually on the buttocks, elbows, knees, and traumatized areas, affecting 30% to 70% of children with dermatomyositis, but only 10% of adults with the disorder.20,25-27
FIGURE 2
Gottron’s papules in dermatomyositis
Violaceous papules on the dorsal interphalangeal and metacarpophalangeal joints of the hands are a common manifestation of dermatomyositis.
Bohan and Peter criteria help with dermatomyositis diagnosis
A diagnosis of dermatomyositis can be established using the following criteria developed by Bohan and Peter in 1975: (1) symmetric muscle weakness; (2) elevation of muscle enzymes, most notably creatinine phosphokinase; (3) evidence of inflammation on muscle biopsy; (4) electromyographic features of myositis; and (5) characteristic dermatologic signs, including a heliotrope rash and Gottron’s papules.28,29 A definitive diagnosis can be made when the patient meets 3 of the first 4 criteria, as well as the fifth.
Corticosteroids are the mainstay of treatment for dermatomyositis, although the dose and duration are subject to debate. Cutaneous manifestations of dermatomyositis are commonly treated with topical corticosteroids and oral hydroxychloroquine, as well as emollients and antipruritic agents.
Cancer screening. All adults with signs and symptoms of dermatomyositis should undergo cancer screening. The most common malignancies are ovarian cancer, gastric cancer, and lymphoma.21
Photoprotection. As with cutaneous LE, UV exposure can exacerbate dermatomyositis, and patients should use a broad-spectrum sunscreen.
Scleroderma: Localized and systemic disease
The major cutaneous manifestation of scleroderma is that of thickened, leathery, bound-down skin, seen in both localized and systemic disease. In both cases, the lesions typically evolve through 3 characteristic stages: the initial inflammatory and edematous stage; a fibrotic stage, during which the skin lesions appear hard, tight, and hidebound; and the final, atrophic stage. However, not all lesions progress to this final stage.8
Localized scleroderma (also known as morphea) affects roughly 1 in 100,000 people. It is more prevalent in females than males, with a ratio as high as 3 to 1.30-33 Cutaneous findings vary, and numerous clinical presentations are possible. The most widely used classification system, the Mayo Clinic Classification, recognizes 5 subtypes: plaque morphea (the most common), generalized morphea, linear morphea, deep morphea, and bullous morphea (TABLE 2).34 The mean age of onset depends on the subtype, and ranges from 12 years for linear morphea to 45 years for deep morphea.35
While systemic involvement is not common with localized scleroderma, extracutaneous manifestations have been reported in up to 25% of cases.31,36,37 In a 2005 multicenter study of 750 pediatric patients with localized scleroderma, the most frequently reported extracutaneous symptom was arthritis, found in 12% of patients.36 Less frequent findings included neurologic symptoms such as seizures and headaches, vascular changes such as deep vein thrombosis, and gastrointestinal, cardiac, and renal conditions. Although the precise etiology of localized scleroderma is unknown, it is thought to be associated with trauma, prior infection by Borrelia burgdorferi, chronic venous insufficiency, and irradiation for breast cancer.30,38,39
TABLE 2
Localized scleroderma: What to look for8,34
|
Systemic scleroderma is a heterogenous disorder
Commonly called systemic sclerosis (SSc), systemic scleroderma is characterized by proliferative vascular lesions; fibrosis of internal organs, including the lungs, heart, kidneys, and gastrointestinal tract; and distinct cutaneous manifestations.3 SSc affects about 240 people per million adults, mostly between the ages of 30 and 50 years, with women affected 3 times as often as men.40-42
The cause of SSc is unknown, although a genetic predisposition is likely. Environmental factors likely play a role in triggering the disease, with possible causative factors including cytomegalovirus and other viral infections and exposure to certain chemicals.43
As in localized scleroderma, cutaneous manifestations are a prominent part of SSc and typically develop early on. Raynaud’s phenomenon (RP) (FIGURE 3), which occurs in 90% to 98% of patients with SSc,44 can develop in association with other cutaneous findings or precede additional skin changes by months or years.
Other early skin changes include nonpitting edema of the fingers and toes, which creates a sausage-like appearance. This is typically followed by hardening and thickening of the skin in these areas, which can result in highly disabling sclerodactyly (FIGURE 4).45 Patients can also develop painful ulcerations on their fingertips and knuckles (rat bite necroses) due to local ischemia and vascular insufficiency. This may be complicated by secondary bacterial infection, gangrene, and acroosteolysis, leading to articular deformities and dissolution of terminal phalanges (FIGURE 5).45-48
On the face, SSc is characterized early on by periorbital edema and later by the development of a beaked nose, a reduction in the size of the mouth (microstomia) with radial furrowing, thinning of the lips, and telangiectasias.45,49 As the sclerosis worsens, patients are frequently left with expressionless, mask-like faces.48
Other common cutaneous manifestations of SSc include a “salt and pepper” appearance, with alternating areas of hypo- and hyperpigmented skin. Additionally, patients may suffer from a loss of hair follicles, severely dry skin, and pruritus.45,48
There are 2 major subsets of SSc—limited cutaneous SSc and diffuse cutaneous SSc. While they can be differentiated based on the history of symptoms, the appearance and extent of cutaneous involvement, and certain serological makers, the most important difference is the speed at which the disease progresses and its severity: Limited cutaneous SSc typically progresses slowly, while diffuse cutaneous SSc is characterized by a relatively rapid onset of disease, with skin and internal organ involvement likely to be severe.49
Scleroderma diagnosis and treatment: Vascular changes are an important clue
Skin changes seen in localized scleroderma and SSc can be clinically and histologically similar, making it difficult to arrive at a definitive diagnosis.
One clinical clue is that in localized scleroderma, vascular changes, such as RP and periungual nailfold telangiectasia, are typically absent. In addition, cutaneous changes in the hands and fingers, such as sclerodactyly, are more characteristic of systemic disease.10
SSc can be diagnosed using criteria proposed by the ACR, which have been shown to be highly sensitive (97%) and specific (98%).50 The major criterion is proximal scleroderma—symmetric thickening, tightening, and induration of the skin of the fingers and areas proximal to the metacarpophalangeal or metatarsophalangeal joints, which may include the trunk, neck, and face. Minor criteria include (1) sclerodactyly, (2) digital pitting scars of fingertips or loss of substance of the distal finger pad, and (3) bilateral basilar pulmonary fibrosis. Diagnosis is based on the presence of either the major criterion or 2 of the 3 minor criteria.50
Numerous therapies are available for localized scleroderma, including topical, intralesional, and systemic corticosteroids, topical tacrolimus, hydroxychloroquine, topical and systemic calcipotriol, penicillamine, sulfasalazine, interferon-[H9253], methotrexate, phototherapy with UV light, and imiquimod.
SSc skin manifestations, which can be severe and disabling, can be treated with a wide range of therapies. Topical or systemic corticosteroids; topical calcineurin inhibitors; systemic immunosuppressive agents such as methotrexate, cyclophosphamide, cyclosporine, and D-penicillamine; and phototherapy have all had varying success at reducing hardening of the skin.51-54 Other skin manifestations, including RP, dryness and itching, pigment changes, digital ulcerations, calcifications, and telangiectasias, should be managed as needed, with various supplemental treatment options available.45 These may include emollients, antihistamines, and topical corticosteroids for dryness and itching; laser therapy for telangiectasias; and corticosteroid injection, laser therapy, or surgery for calcifications. However, there is limited evidence of efficacy for most of these options.45
FIGURE 3
An attack of Raynaud’s phenomenon
Raynaud’s phenomenon, characterized by blanching of the distal fingertips, is shown here in a patient with systemic sclerosis.
FIGURE 4
Sclerodactyly in a patient with systemic sclerosis
Hardening and thickening of the skin can result in highly disabling sclerodactyly in patients with systemic sclerosis.
FIGURE 5
Dissolution of terminal phalanges
Bony resorption and ulceration have led to the loss of distal phalanges in this patient with systemic sclerosis.
Mixed connective tissue disease has features of several disorders
Mixed connective tissue disease (MCTD) is an apparently distinct rheumatologic condition characterized by a combination of clinical features of systemic LE, dermatomyositis, scleroderma, polymyositis, and rheumatoid arthritis. The presence of high titers of a unique autoantibody, anti-U1-RNP,54-57 aids in diagnosis.
Although precise prevalence data are lacking, MCTD is thought to occur in about 1 in 10,000 people.58 The disease is much more common in women, with a female-to-male ratio as high as 7 to 1, and generally occurs in the second or third decade of life.58-60
The clinical manifestations of MCTD typically evolve, with overlapping features of various autoimmune disorders appearing sequentially over several months to years.57 Early in the course of MCTD, patients commonly experience fatigue, polyarthritis, hand edema, and RP. In time, virtually every organ system may be involved. Pulmonary hypertension is a major cause of death.59,61
Unlike many other connective tissue disorders, MCTD lacks any distinct cutaneous findings. In addition to those mentioned earlier, prominent skin findings include swelling of the fingers, sclerodactyly, and the acute malar eruptions and discoid plaques typically associated with LE.56,57,62 Cutaneous manifestations associated with dermatomyositis and scleroderma may also be seen, particularly juxta-articular calcinosis. The mucous membranes may be involved, as well, resulting in nasal perforation, buccal and urogenital ulcerations, and sicca complex.58,63,64
MCTD diagnosis and treatment: Look for these serology and clinical findings
Diagnosing MCTD can be clinically challenging, as signs and symptoms of the disease commonly evolve over time. The Alarcon-Segovia criteria—largely regarded as the best diagnostic tool for MCTD65,66—include 1 serologic finding (elevated anti-U1-RNP [titer ≥1:1600]) and 5 clinical findings (RP, edema of the hands, synovitis, myositis, and acrosclerosis). Diagnosis requires the presence of the serologic criterion and ≥3 of the 5 clinical criteria.
Treatment of the cutaneous manifestations should be based on the effectiveness of therapies for similar skin findings seen in other disorders. In treating MCTD (or any other connective tissue disorder), a team that includes nurses, physical and occupational therapists, primary care physicians, and specialists in dermatology and rheumatology is essential for an optimal outcome.
CORRESPONDENCE Christian R. Halvorson, MD, Mercy Medical Center, Department of Medicine, 301 St. Paul Place, Baltimore, MD 21202; [email protected]
1. Renner R, Sticherling M. The different faces of cutaneous lupus erythematosus. G Ital Dermatol Venereol. 2009;144:135-147.
2. Kuhn A, Ruzicka T. Classification of cutaneous lupus erythematosus. In: Kuhn A, Lehmann P, Ruzicka T, eds. Cutaneous Lupus Erythematosus. New York: Springer; 2004:53–57.
3. Costner MI, Grau RH. Update on connective tissue diseases in dermatology. Semin Cutan Med Surg. 2006;25:207-220.
4. Ting W, Stone MS, Racila D, et al. Toxic epidermal necrolysis-like acute cutaneous lupus erythematosus and the spectrum of the acute syndrome of apoptotic pan-epidermolysis (ASAP): a case report, concept review and proposal for new classification of lupus erythematosus vesiculobullous skin lesions. Lupus. 2004;13:941-950.
5. Jorizzo JL, Carroll CL, Sangueza OP. Lupus erythematosus. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. 2nd ed. Spain: Elsevier Limited; 2008.
6. Kuhn A, Sticherling M, Bonsmann G. Clinical manifestations of cutaneous lupus erythematosus. J Dtsch Dermatol Ges. 2007;5:1124-1137.
7. Sontheimer RD, Thomas JR, Gilliam JN. Subacute cutaneous lupus erythematosus: a cutaneous marker for a distinct lupus erythematosus subset. Arch Dermatol. 1979;115:1409-1415.
8. Sontheimer RD. Skin manifestations of systemic autoimmune connective tissue disease: diagnostics and therapeutics. Best Pract Res Clin Rheumatol. 2004;18:429-462.
9. Panjwani S. Early diagnosis and treatment of discoid lupus erythematosus. J Am Board Fam Med. 2009;22:206-213.
10. Sontheimer RD, Provost TT. Lupus erythematosus. In: Sontheimer RD, Provost TT, eds. Cutaneous Manifestations of Rheumatic Diseases. Baltimore: Williams & Wilkins; 1996.
11. Mond CB, Peterson MG, Rothfield NF. Correlation of antiro antibody with photosensitivity rash in systemic lupus erythematosus patients. Arthritis Rheum. 1989;32:202-204.
12. Jacyk WK, Damisah M. Discoid lupus erythematosus in the Nigerians. Br J Dermatol. 1979;100:131-135.
13. Callen JP. Cutaneous lupus erythematosus: A personal approach to management. Australas J Dermatol. 2006;47:13-27.
14. Gilliam JN, Sontheimer RD. Distinctive cutaneous subsets in the spectrum of lupus erythematosus. J Am Acad Dermatol. 1981;4:471-475.
15. Farley-Loftus R, Mahlberg M, Merola J, et al. Generalized discoid lupus erythematosus. Dermatol Online J. 2009;15:18.-
16. Kuhn A, Richter-Hintz D, Oslislo C, et al. Lupus erythematosus tumidus—a neglected subset of cutaneous lupus erythematosus: report of 40 cases. Arch Dermatol. 2000;136:1033-1041.
17. American College of Rheumatology. The 1982 revised criteria for classification of systemic lupus erythematosus. Available at: http://www.rheumatology.org/practice/clinical/classification/SLE/sle.asp. Accessed September 21, 2010.
18. Na SJ, Kim SM, Sunwoo IN, et al. Clinical characteristics and outcomes of juvenile and adult dermatomyositis. J Korean Med Sci. 2009;24:715-721.
19. Kovacs SO, Kovacs SC. Dermatomyositis. J Am Acad Dermatol. 1998;39:899-922.
20. Koler RA, Montemarano A. Dermatomyositis. Am Fam Physician. 2001;64:1565-1572.
21. Sunkureddi P, Nguyen-Oghalai TU, Jarvis JL, et al. Signs of dermatomyositis. Hosp Physician. 2005;41:41-44.
22. Iorizzo LJ, 3rd, Jorizzo JL. The treatment and prognosis of dermatomyositis: an updated review. J Am Acad Dermatol. 2008;59:99-112.
23. Jorizzo JL, Carroll CL, Sangueza OP. Dermatomyositis. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. 2nd ed. Spain: Elsevier Limited; 2008:575–583.
24. Sontheimer RD. Dermatomyositis. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 5th ed. New York: McGraw-Hill; 1999:2009–2020.
25. Halbert AR. Juvenile dermatomyositis. Australas J Dermatol. 1996;37:106-108.
26. Orlow SJ, Watsky KL, Bolognia JL. Skin and bones II. J Am Acad Dermatol. 1991;25:447-462.
27. Bowyer SL, Blane CE, Sullivan DB, et al. Childhood dermatomyositis: factors predicting functional outcome and development of dystrophic calcification. J Pediatr. 1983;103:882-888.
28. Bohan A, Peter JB. Polymyositis and dermatomyositis (second of two parts). N Engl J Med. 1975;292:403-407.
29. Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975;292:344-347.
30. Vancheeswaran R, Black CM, David J, et al. Childhood-onset scleroderma: is it different from adult-onset disease? Arthritis Rheum. 1996;39:1041-1049.
31. Zulian F, Athreya BH, Laxer R, et al. Juvenile localized scleroderma: Clinical and epidemiological features in 750 children. An international study. Rheumatology (Oxford). 2006;45:614-620.
32. Marzano AV, Menni S, Parodi A, et al. Localized scleroderma in adults and children. clinical and laboratory investigations on 239 cases. Eur J Dermatol. 2003;13:171-176.
33. Uziel Y, Krafchik BR, Silverman ED, et al. Localized scleroderma in childhood: a report of 30 cases. Semin Arthritis Rheum. 1994;23:328-340.
34. Peterson LS, Nelson AM, Su WP. Classification of morphea (localized scleroderma). Mayo Clin Proc. 1995;70:1068-1076.
35. Peterson LS, Nelson AM, Su WP, et al. The epidemiology of morphea (localized scleroderma) in Olmsted County 1960-1993. J Rheumatol. 1997;24:73-80.
36. Zulian F, Vallongo C, Woo P, et al. Localized scleroderma in childhood is not just a skin disease. Arthritis Rheum. 2005;52:2873-2881.
37. Dehen L, Roujeau JC, Cosnes A, et al. Internal involvement in localized scleroderma. Medicine (Baltimore). 1994;73:241-245.
38. Ludwig RJ, Werner RJ, Winker W, et al. Chronic venous insufficiency - a potential trigger for localized scleroderma. J Eur Acad Dermatol Venereol. 2006;20:96-99.
39. Aberer E, Neumann R, Stanek G. Is localised scleroderma a borrelia infection? Lancet. 1985;2:278.-
40. Krishnan E, Furst DE. Systemic sclerosis mortality in the United States: 1979-1998. Eur J Epidemiol. 2005;20:855-861.
41. Silman AJ. Scleroderma—demographics and survival. J Rheumatol Suppl. 1997;48:58-61.
42. Medsger TA,, Jr, Masi AT. Epidemiology of systemic sclerosis (scleroderma). Ann Intern Med. 1971;74:714-721.
43. Charles C, Clements P, Furst DE. Systemic sclerosis: Hypothesis-driven treatment strategies. Lancet. 2006;367:1683-1691.
44. Maricq HR, Harper FE, Khan MM, et al. Microvascular abnormalities as possible predictors of disease subsets in Raynaud phenomenon and early connective tissue disease. Clin Exp Rheumatol. 1983;1:195-205.
45. Krieg T, Takehara K. Skin disease: A cardinal feature of systemic sclerosis. Rheumatology (Oxford). 2009;48 (suppl 3):S14-S18.
46. Ingraham KM, Steen VD. Morbidity of digital tip ulcerations in scleroderma. Arthritis Rheum. 2006;54(9 suppl.):F78.-
47. Ferri C, Valentini G, Cozzi F, et al. Systemic sclerosis: Demographic, clinical, and serologic features and survival in 1,012 italian patients. Medicine (Baltimore). 2002;81:139-153.
48. Haustein UF. Systemic sclerosis - scleroderma. Dermatol Online J. 2002;8.-
49. Fitzpatrick TB, Johnson RA, Klaus W, et al. In Colour Atlas and Synopsis of Clinical Dermatology. 4th ed. New York: McGraw-Hill; 2001:368–369.
50. Preliminary criteria for the classification of systemic sclerosis (scleroderma). subcommittee for scleroderma criteria of the American Rheumatism Association diagnostic and therapeutic criteria committee. Arthritis Rheum. 1980;23:581-590.
51. Valentini G, Paone C, La Montagna G, et al. Low-dose intravenous cyclophosphamide in systemic sclerosis: an open prospective efficacy study in patients with early diffuse disease. Scand J Rheumatol. 2006;35:35-38.
52. Steen VD, Medsger TA, Jr. Improvement in skin thickening in systemic sclerosis associated with improved survival. Arthritis Rheum. 2001;44:2828-2835.
53. Basso M, Filaci G, Cutolo M, et al. Long-term treatment of patients affected by systemic sclerosis with cyclosporin A. Ann Ital Med Int. 2001;16:233-239.
54. Morton SJ, Powell RJ. Cyclosporin and tacrolimus: their use in a routine clinical setting for scleroderma. Rheumatology (Oxford). 2000;39:865-869.
55. Kasukawa R. Mixed connective tissue disease. Intern Med. 1999;38:386-393.
56. Bennett RM, O’Connell DJ. Mixed connective tisssue disease: A clinicopathologic study of 20 cases. Semin Arthritis Rheum. 1980;10:25-51.
57. Sharp GC, Irvin WS, Tan EM, et al. Mixed connective tissue disease—an apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA). Am J Med. 1972;52:148-159.
58. Venables PJ. Mixed connective tissue disease. Lupus. 2006;15:132-137.
59. Farhey Y, Hess EV. Mixed connective tissue disease. Arthritis Care Res. 1997;10:333-342.
60. Alarcon-Segovia D. Mixed connective tissue disease - a decade of growing pains. J Rheumatol. 1981;8:535-540.
61. Ueda N, Mimura K, Maeda H, et al. Mixed connective tissue disease with fatal pulmonary hypertension and a review of literature. Virchows Arch A Pathol Anat Histopathol. 1984;404:335-340.
62. Bennett RM. Mixed connective tissue disease and other overlap syndromes. In: Kelley WN, Harris EDJ, Ruddy SH, et al, eds. Textbook of Rheumatology. 4th ed. Philadelphia: WB Saunders; 1993:1061.
63. Nakashima M, Suzuki K, Okada M, et al. Panniculitis in a patient with mixed connective tissue disease. Mod Rheumatol. 2004;14:250-253.
64. Magro CM, Crowson AN, Regauer S. Mixed connective tissue disease. A clinical, histologic, and immunofluorescence study of eight cases. Am J Dermatopathol. 1997;19:206-213.
65. Amigues JM, Cantagrel A, Abbal M, et al. Comparative study of 4 diagnosis criteria sets for mixed connective tissue disease in patients with anti-RNP antibodies. autoimmunity group of the hospitals of toulouse. J Rheumatol. 1996;23:2055-2062.
66. Alarcon-Segovia D, Cardiel MH. Comparison between 3 diagnostic criteria for mixed connective tissue disease. study of 593 patients. J Rheumatol. 1989;16:328-334.
• When evaluating patients with suspected cutaneous lupus erythematosus, use multiple criteria—including histologic and immunofluorescent biopsy findings and American College of Rheumatology criteria—to rule out systemic disease. C
• Cancer screening with a careful history and physical examination is recommended for all adult patients whom you suspect of having dermatomyositis. C
• Suspect mixed connective tissue disease in patients with skin findings characteristic of varying auto-immune disorders appearing sequentially over several months or years. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Many systemic conditions are accompanied by skin manifestations. This is especially true for connective tissue disorders, for which dermatologic findings are often the key to diagnosis.
In this review, we describe the dermatologic findings of some well-known connective tissue disorders. The text and photographs in the pages that follow will help you hone your diagnostic skills, leading to earlier treatment and, possibly, better outcomes.
Lupus erythematosus: Cutaneous and systemic disease often overlap
Lupus erythematosus (LE), a chronic, inflammatory autoimmune condition that primarily affects women in their 20s and 30s, may initially present as a systemic disease or in a purely cutaneous form. However, most patients with systemic LE have some skin manifestations, and those with cutaneous LE often have—or subsequently develop—systemic involvement.1 Thus, recognizing the cutaneous manifestations of LE will not only aid in diagnosis, but will help you identify patients at risk for systemic disease.
Cutaneous LE has 4 subtypes
There are 4 subcategories of cutaneous LE—acute, subacute, chronic, and intermittent.2 Each is differentiated by the appearance of the lesions (TABLE 1), histology, and serological markers.1 Photosensitivity is common to all the subcategories to varying degrees.
Acute cutaneous lupus erythematosus (ACLE) is typically characterized by the classic malar “butterfly” rash, an erythematous eruption of macules or edematous papules over the bridge of the nose and cheek.3 Although this presentation is most common, there are variations—1 in which the lesions cover other exposed areas (commonly including the “V” of the chest, the extensor surface of the arms, and the hands), and a rare form in which toxic epidermal necrolysis-like blistering occurs.1,4 These skin changes—which generally last anywhere from a few hours to several weeks—typically resolve without scarring, although pigment changes can occur.5
Left: Dermatomyositis is the underlying cause of the heliotrope discoloration on this patient’s upper eyelid.
Center: Linear morphea is associated with the lesion on this patient’s face—called en coup de sabre because it resembles the mark caused by the stroke of a sword in a duel.
Right: Discoid lupus erythematosus causes hypopigmentation and scarring.Patients with ACLE have a predisposition to systemic LE; unlike those with other forms of cutaneous LE, 40% to 90% will have double-stranded DNA (dsDNA) autoantibodies.3,6
Subacute cutaneous lupus erythematosus (SCLE), which usually affects middle-aged Caucasian women, is characterized by erythematous papulosquamous (psoriasis-like) eruptions or annular lesions with raised red borders and central clearing—or both. These lesions, which are nonscarring, lack in-duration, and rarely affect the scalp or face, appear suddenly, usually after exposure to sunlight (FIGURE 1)5,7-9 or certain drugs. Hydrochlorothiazide, terbinafine, calcium channel blockers, and angiotensin-converting enzyme inhibitors are common offenders.1,6
FIGURE 1
Annular lesions in subacute cutaneous lupus erythematosus
Ring-like lesions with raised red borders and central clearing on the back of a patient with subacute cutaneous lupus erythematosus.
SCLE is often associated with extracutaneous symptoms such as arthritis and myalgias,1,8 but patients are at relatively low risk for severe systemic manifestations.5,8,10 Serology is often notable, with anti-Ro (SS-A) antibodies present in 70% to 90% of patients and anti-La (SS-B) autoantibodies found in 30% to 50%.1,11
Chronic cutaneous lupus erythematosus (CCLE) also occurs predominantly in females, at a ratio as high as 5 to 1.12 There are 3 variations of CCLE: discoid lupus erythematosus (DLE), LE profundus, and chilblain LE (TABLE 1). DLE, characterized by alopecia, skin atrophy, and dyspigmentation, is the most common and affects patients of all ages and ethnic groups.9,13,14 (See image above.)
DLE lesions typically begin as erythematous papules and plaques with scale. As the disorder progresses, the lesions spread, causing follicular plugging, peripheral hyperpigmentation and central hypopigmentation, telangiectasia, and atrophy.9,15 In some cases, patients develop thickened, scarred skin and permanent scarring alopecia.15 Prompt recognition of DLE is particularly important, as early referral and treatment may reduce the likelihood of permanent scarring alopecia and pigment changes.11
Intermittent cutaneous lupus erythematosus (ICLE), a relatively new subtype of cutaneous LE, is represented by a rare condition—lupus erythematosus tumidus (LET)—reported in <100 cases worldwide. LET is characterized by succulent, erythematous, and edematous plaques on sun-exposed parts of the body.1,16
TABLE 1
Cutaneous lupus erythematosus: Recognizing the subtypes1
| Acute cutaneous lupus erythematosus (ACLE) |
|---|
| Localized: erythematous macules or papules over the bridge of the nose and cheek, with sparing of the nasolabial folds (“butterfly rash”) |
| Generalized: similar erythematous lesions over other photodistributed parts of the body, including the neck, chest, arms, and hands |
| Toxic epidermal necrolysis-like (TEN-like): blistering and epidermal cleavage in photodistributed parts of the body |
| Subacute cutaneous lupus erythematosus (SCLE) |
| Erythematous papulosquamous (psoriasis-like) eruptions or annular (ring-like) lesions with raised red borders and central clearing, occurring symmetrically and suddenly after sunlight exposure on photo-distributed body parts; the scalp and face are rarely affected |
| Chronic cutaneous lupus erythematosus (CCLE) |
| Discoid lupus erythematosus: erythematous papules and plaques with associated scale, spreading centrifugally with follicular plugging, pigment change, telangiectasia, and atrophy; scarring alopecia can occur |
| Lupus erythematosus profundus: tender, erythematous nodules and plaques, usually involving the proximal extremities, trunk, breasts, buttocks, and face |
| Chilblain lupus erythematosus: tender, erythematous nodules and plaques, occurring in acral areas often in response to cold |
| Intermittent cutaneous lupus erythematosus (ICLE) |
| Lupus erythematosus tumidus: succulent, erythematous, and edematous plaques found on photodistributed parts of the body |
Cutaneous LE diagnosis and treatment: Start with ACR criteria
When evaluating patients with suspected cutaneous LE, it is important not only to identify the subtype, but also to rule out systemic disease using criteria established by the American College of Rheumatology (ACR).17 Notably, 4 of the 11 diagnostic criteria for systemic disease involve visual clues, including malar rash, discoid rash, photosensitivity, and oral ulcerations. Laboratory evidence of systemic disease may include a positive antinuclear antibody, anti-dsDNA, or anti-Sm autoantibody test results, as well as hematologic abnormalities described in the ACR guidelines.
Ultimately, a diagnosis of cutaneous LE should be based on the patient’s history and physical exam, autoantibody profile, and histologic and immunofluorescent biopsy findings. A rheumatologic evaluation may help to determine which patients have systemic disease, as the ACR criteria may overdiagnose systemic LE in those with predominantly skin changes.6
Treatment of cutaneous LE is based on the subtype and extent of disease, with potent topical corticosteroids, in combination with antimalarial agents, being the primary therapies. ACLE skin lesions generally respond best to systemic corticosteroids and immunosuppressive agents (such as azathioprine or cyclophosphamide) that are used to control underlying systemic disease. SCLE can be managed with topical corticosteroids; however, patients typically also require systemic treatment, often with hydroxychloroquine, for optimal control. DLE, the most common form of CCLE, is managed in a similar fashion, with a greater role for intralesional corticosteroid injections. Lesions associated with ICLE, which often resolve spontaneously, may be treated with topical corticosteroids and antimalarials.16 It is also important to advise all patients with cutaneous LE to use a broad-spectrum sunscreen, as ultraviolet (UV) exposure can induce or exacerbate the lesions.9
Dermatomyositis: Rare but serious
Dermatomyositis is an idiopathic inflammatory myopathy characterized by chronic muscle inflammation, symmetric proximal muscle weakness, and distinct cutaneous findings. In addition to possible cardiac and pulmonary complications, dysphagia, and joint contractures, dermatomyositis is associated with cancer, with up to 25% of affected adults having an underlying occult malignancy.18
Dermatomyositis is a rare condition, with a prevalence of only 1 to 10 cases per million adults and 3.2 cases per million children.19 It has a bimodal age distribution, with most juvenile cases affecting children between the ages of 5 and 14 years and most adult cases developing in the fifth and sixth decades of life. Women are affected twice as often as men.18
Suspect dermatomyositis when you see any of the following signs:
- A heliotrope rash: violaceous macules and patches, with or without edema, symmetrically on the periorbital skin, present early in the disease course in 30% to 60% of patients.19 (See image)
- Gottron’s papules: violaceous papules on the dorsal interphalangeal and metacarpophalangeal joints of the hands, elbows, and knees, occurring in as many as 70% of patients (FIGURE 2).19,20
- Gottron’s sign: nonscaling, violaceous erythematous macules and plaques occurring symmetrically in the same distribution as Gottron’s papules, but with sparing of the interphalangeal spaces.20
- Periungual erythema and telangiectasias: redness and dilation of the blood vessels in the skin surrounding the nail plate.
- The shawl and V-signs: erythematous macular eruptions occurring in a “shawl” pattern on the shoulders, arms, and upper back and in a V-shaped pattern on the anterior neck and chest.
- Mechanic’s hand: extensive scaling, fissuring, and roughening of the palmar aspect of the hand.20,21
- Poikiloderma vasculare atrophicans: circumscribed violaceous erythema with thinning of the skin, prominent telangiectasias, and a mottled pattern of hypo- and hyperpigmentation, typically occurring on the anterior neck, chest, posterior shoulders, back, and buttocks, years after onset of the disease.21-24
- Cutaneous calcification (calcinosis cutis): usually on the buttocks, elbows, knees, and traumatized areas, affecting 30% to 70% of children with dermatomyositis, but only 10% of adults with the disorder.20,25-27
FIGURE 2
Gottron’s papules in dermatomyositis
Violaceous papules on the dorsal interphalangeal and metacarpophalangeal joints of the hands are a common manifestation of dermatomyositis.
Bohan and Peter criteria help with dermatomyositis diagnosis
A diagnosis of dermatomyositis can be established using the following criteria developed by Bohan and Peter in 1975: (1) symmetric muscle weakness; (2) elevation of muscle enzymes, most notably creatinine phosphokinase; (3) evidence of inflammation on muscle biopsy; (4) electromyographic features of myositis; and (5) characteristic dermatologic signs, including a heliotrope rash and Gottron’s papules.28,29 A definitive diagnosis can be made when the patient meets 3 of the first 4 criteria, as well as the fifth.
Corticosteroids are the mainstay of treatment for dermatomyositis, although the dose and duration are subject to debate. Cutaneous manifestations of dermatomyositis are commonly treated with topical corticosteroids and oral hydroxychloroquine, as well as emollients and antipruritic agents.
Cancer screening. All adults with signs and symptoms of dermatomyositis should undergo cancer screening. The most common malignancies are ovarian cancer, gastric cancer, and lymphoma.21
Photoprotection. As with cutaneous LE, UV exposure can exacerbate dermatomyositis, and patients should use a broad-spectrum sunscreen.
Scleroderma: Localized and systemic disease
The major cutaneous manifestation of scleroderma is that of thickened, leathery, bound-down skin, seen in both localized and systemic disease. In both cases, the lesions typically evolve through 3 characteristic stages: the initial inflammatory and edematous stage; a fibrotic stage, during which the skin lesions appear hard, tight, and hidebound; and the final, atrophic stage. However, not all lesions progress to this final stage.8
Localized scleroderma (also known as morphea) affects roughly 1 in 100,000 people. It is more prevalent in females than males, with a ratio as high as 3 to 1.30-33 Cutaneous findings vary, and numerous clinical presentations are possible. The most widely used classification system, the Mayo Clinic Classification, recognizes 5 subtypes: plaque morphea (the most common), generalized morphea, linear morphea, deep morphea, and bullous morphea (TABLE 2).34 The mean age of onset depends on the subtype, and ranges from 12 years for linear morphea to 45 years for deep morphea.35
While systemic involvement is not common with localized scleroderma, extracutaneous manifestations have been reported in up to 25% of cases.31,36,37 In a 2005 multicenter study of 750 pediatric patients with localized scleroderma, the most frequently reported extracutaneous symptom was arthritis, found in 12% of patients.36 Less frequent findings included neurologic symptoms such as seizures and headaches, vascular changes such as deep vein thrombosis, and gastrointestinal, cardiac, and renal conditions. Although the precise etiology of localized scleroderma is unknown, it is thought to be associated with trauma, prior infection by Borrelia burgdorferi, chronic venous insufficiency, and irradiation for breast cancer.30,38,39
TABLE 2
Localized scleroderma: What to look for8,34
|
Systemic scleroderma is a heterogenous disorder
Commonly called systemic sclerosis (SSc), systemic scleroderma is characterized by proliferative vascular lesions; fibrosis of internal organs, including the lungs, heart, kidneys, and gastrointestinal tract; and distinct cutaneous manifestations.3 SSc affects about 240 people per million adults, mostly between the ages of 30 and 50 years, with women affected 3 times as often as men.40-42
The cause of SSc is unknown, although a genetic predisposition is likely. Environmental factors likely play a role in triggering the disease, with possible causative factors including cytomegalovirus and other viral infections and exposure to certain chemicals.43
As in localized scleroderma, cutaneous manifestations are a prominent part of SSc and typically develop early on. Raynaud’s phenomenon (RP) (FIGURE 3), which occurs in 90% to 98% of patients with SSc,44 can develop in association with other cutaneous findings or precede additional skin changes by months or years.
Other early skin changes include nonpitting edema of the fingers and toes, which creates a sausage-like appearance. This is typically followed by hardening and thickening of the skin in these areas, which can result in highly disabling sclerodactyly (FIGURE 4).45 Patients can also develop painful ulcerations on their fingertips and knuckles (rat bite necroses) due to local ischemia and vascular insufficiency. This may be complicated by secondary bacterial infection, gangrene, and acroosteolysis, leading to articular deformities and dissolution of terminal phalanges (FIGURE 5).45-48
On the face, SSc is characterized early on by periorbital edema and later by the development of a beaked nose, a reduction in the size of the mouth (microstomia) with radial furrowing, thinning of the lips, and telangiectasias.45,49 As the sclerosis worsens, patients are frequently left with expressionless, mask-like faces.48
Other common cutaneous manifestations of SSc include a “salt and pepper” appearance, with alternating areas of hypo- and hyperpigmented skin. Additionally, patients may suffer from a loss of hair follicles, severely dry skin, and pruritus.45,48
There are 2 major subsets of SSc—limited cutaneous SSc and diffuse cutaneous SSc. While they can be differentiated based on the history of symptoms, the appearance and extent of cutaneous involvement, and certain serological makers, the most important difference is the speed at which the disease progresses and its severity: Limited cutaneous SSc typically progresses slowly, while diffuse cutaneous SSc is characterized by a relatively rapid onset of disease, with skin and internal organ involvement likely to be severe.49
Scleroderma diagnosis and treatment: Vascular changes are an important clue
Skin changes seen in localized scleroderma and SSc can be clinically and histologically similar, making it difficult to arrive at a definitive diagnosis.
One clinical clue is that in localized scleroderma, vascular changes, such as RP and periungual nailfold telangiectasia, are typically absent. In addition, cutaneous changes in the hands and fingers, such as sclerodactyly, are more characteristic of systemic disease.10
SSc can be diagnosed using criteria proposed by the ACR, which have been shown to be highly sensitive (97%) and specific (98%).50 The major criterion is proximal scleroderma—symmetric thickening, tightening, and induration of the skin of the fingers and areas proximal to the metacarpophalangeal or metatarsophalangeal joints, which may include the trunk, neck, and face. Minor criteria include (1) sclerodactyly, (2) digital pitting scars of fingertips or loss of substance of the distal finger pad, and (3) bilateral basilar pulmonary fibrosis. Diagnosis is based on the presence of either the major criterion or 2 of the 3 minor criteria.50
Numerous therapies are available for localized scleroderma, including topical, intralesional, and systemic corticosteroids, topical tacrolimus, hydroxychloroquine, topical and systemic calcipotriol, penicillamine, sulfasalazine, interferon-[H9253], methotrexate, phototherapy with UV light, and imiquimod.
SSc skin manifestations, which can be severe and disabling, can be treated with a wide range of therapies. Topical or systemic corticosteroids; topical calcineurin inhibitors; systemic immunosuppressive agents such as methotrexate, cyclophosphamide, cyclosporine, and D-penicillamine; and phototherapy have all had varying success at reducing hardening of the skin.51-54 Other skin manifestations, including RP, dryness and itching, pigment changes, digital ulcerations, calcifications, and telangiectasias, should be managed as needed, with various supplemental treatment options available.45 These may include emollients, antihistamines, and topical corticosteroids for dryness and itching; laser therapy for telangiectasias; and corticosteroid injection, laser therapy, or surgery for calcifications. However, there is limited evidence of efficacy for most of these options.45
FIGURE 3
An attack of Raynaud’s phenomenon
Raynaud’s phenomenon, characterized by blanching of the distal fingertips, is shown here in a patient with systemic sclerosis.
FIGURE 4
Sclerodactyly in a patient with systemic sclerosis
Hardening and thickening of the skin can result in highly disabling sclerodactyly in patients with systemic sclerosis.
FIGURE 5
Dissolution of terminal phalanges
Bony resorption and ulceration have led to the loss of distal phalanges in this patient with systemic sclerosis.
Mixed connective tissue disease has features of several disorders
Mixed connective tissue disease (MCTD) is an apparently distinct rheumatologic condition characterized by a combination of clinical features of systemic LE, dermatomyositis, scleroderma, polymyositis, and rheumatoid arthritis. The presence of high titers of a unique autoantibody, anti-U1-RNP,54-57 aids in diagnosis.
Although precise prevalence data are lacking, MCTD is thought to occur in about 1 in 10,000 people.58 The disease is much more common in women, with a female-to-male ratio as high as 7 to 1, and generally occurs in the second or third decade of life.58-60
The clinical manifestations of MCTD typically evolve, with overlapping features of various autoimmune disorders appearing sequentially over several months to years.57 Early in the course of MCTD, patients commonly experience fatigue, polyarthritis, hand edema, and RP. In time, virtually every organ system may be involved. Pulmonary hypertension is a major cause of death.59,61
Unlike many other connective tissue disorders, MCTD lacks any distinct cutaneous findings. In addition to those mentioned earlier, prominent skin findings include swelling of the fingers, sclerodactyly, and the acute malar eruptions and discoid plaques typically associated with LE.56,57,62 Cutaneous manifestations associated with dermatomyositis and scleroderma may also be seen, particularly juxta-articular calcinosis. The mucous membranes may be involved, as well, resulting in nasal perforation, buccal and urogenital ulcerations, and sicca complex.58,63,64
MCTD diagnosis and treatment: Look for these serology and clinical findings
Diagnosing MCTD can be clinically challenging, as signs and symptoms of the disease commonly evolve over time. The Alarcon-Segovia criteria—largely regarded as the best diagnostic tool for MCTD65,66—include 1 serologic finding (elevated anti-U1-RNP [titer ≥1:1600]) and 5 clinical findings (RP, edema of the hands, synovitis, myositis, and acrosclerosis). Diagnosis requires the presence of the serologic criterion and ≥3 of the 5 clinical criteria.
Treatment of the cutaneous manifestations should be based on the effectiveness of therapies for similar skin findings seen in other disorders. In treating MCTD (or any other connective tissue disorder), a team that includes nurses, physical and occupational therapists, primary care physicians, and specialists in dermatology and rheumatology is essential for an optimal outcome.
CORRESPONDENCE Christian R. Halvorson, MD, Mercy Medical Center, Department of Medicine, 301 St. Paul Place, Baltimore, MD 21202; [email protected]
• When evaluating patients with suspected cutaneous lupus erythematosus, use multiple criteria—including histologic and immunofluorescent biopsy findings and American College of Rheumatology criteria—to rule out systemic disease. C
• Cancer screening with a careful history and physical examination is recommended for all adult patients whom you suspect of having dermatomyositis. C
• Suspect mixed connective tissue disease in patients with skin findings characteristic of varying auto-immune disorders appearing sequentially over several months or years. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Many systemic conditions are accompanied by skin manifestations. This is especially true for connective tissue disorders, for which dermatologic findings are often the key to diagnosis.
In this review, we describe the dermatologic findings of some well-known connective tissue disorders. The text and photographs in the pages that follow will help you hone your diagnostic skills, leading to earlier treatment and, possibly, better outcomes.
Lupus erythematosus: Cutaneous and systemic disease often overlap
Lupus erythematosus (LE), a chronic, inflammatory autoimmune condition that primarily affects women in their 20s and 30s, may initially present as a systemic disease or in a purely cutaneous form. However, most patients with systemic LE have some skin manifestations, and those with cutaneous LE often have—or subsequently develop—systemic involvement.1 Thus, recognizing the cutaneous manifestations of LE will not only aid in diagnosis, but will help you identify patients at risk for systemic disease.
Cutaneous LE has 4 subtypes
There are 4 subcategories of cutaneous LE—acute, subacute, chronic, and intermittent.2 Each is differentiated by the appearance of the lesions (TABLE 1), histology, and serological markers.1 Photosensitivity is common to all the subcategories to varying degrees.
Acute cutaneous lupus erythematosus (ACLE) is typically characterized by the classic malar “butterfly” rash, an erythematous eruption of macules or edematous papules over the bridge of the nose and cheek.3 Although this presentation is most common, there are variations—1 in which the lesions cover other exposed areas (commonly including the “V” of the chest, the extensor surface of the arms, and the hands), and a rare form in which toxic epidermal necrolysis-like blistering occurs.1,4 These skin changes—which generally last anywhere from a few hours to several weeks—typically resolve without scarring, although pigment changes can occur.5
Left: Dermatomyositis is the underlying cause of the heliotrope discoloration on this patient’s upper eyelid.
Center: Linear morphea is associated with the lesion on this patient’s face—called en coup de sabre because it resembles the mark caused by the stroke of a sword in a duel.
Right: Discoid lupus erythematosus causes hypopigmentation and scarring.Patients with ACLE have a predisposition to systemic LE; unlike those with other forms of cutaneous LE, 40% to 90% will have double-stranded DNA (dsDNA) autoantibodies.3,6
Subacute cutaneous lupus erythematosus (SCLE), which usually affects middle-aged Caucasian women, is characterized by erythematous papulosquamous (psoriasis-like) eruptions or annular lesions with raised red borders and central clearing—or both. These lesions, which are nonscarring, lack in-duration, and rarely affect the scalp or face, appear suddenly, usually after exposure to sunlight (FIGURE 1)5,7-9 or certain drugs. Hydrochlorothiazide, terbinafine, calcium channel blockers, and angiotensin-converting enzyme inhibitors are common offenders.1,6
FIGURE 1
Annular lesions in subacute cutaneous lupus erythematosus
Ring-like lesions with raised red borders and central clearing on the back of a patient with subacute cutaneous lupus erythematosus.
SCLE is often associated with extracutaneous symptoms such as arthritis and myalgias,1,8 but patients are at relatively low risk for severe systemic manifestations.5,8,10 Serology is often notable, with anti-Ro (SS-A) antibodies present in 70% to 90% of patients and anti-La (SS-B) autoantibodies found in 30% to 50%.1,11
Chronic cutaneous lupus erythematosus (CCLE) also occurs predominantly in females, at a ratio as high as 5 to 1.12 There are 3 variations of CCLE: discoid lupus erythematosus (DLE), LE profundus, and chilblain LE (TABLE 1). DLE, characterized by alopecia, skin atrophy, and dyspigmentation, is the most common and affects patients of all ages and ethnic groups.9,13,14 (See image above.)
DLE lesions typically begin as erythematous papules and plaques with scale. As the disorder progresses, the lesions spread, causing follicular plugging, peripheral hyperpigmentation and central hypopigmentation, telangiectasia, and atrophy.9,15 In some cases, patients develop thickened, scarred skin and permanent scarring alopecia.15 Prompt recognition of DLE is particularly important, as early referral and treatment may reduce the likelihood of permanent scarring alopecia and pigment changes.11
Intermittent cutaneous lupus erythematosus (ICLE), a relatively new subtype of cutaneous LE, is represented by a rare condition—lupus erythematosus tumidus (LET)—reported in <100 cases worldwide. LET is characterized by succulent, erythematous, and edematous plaques on sun-exposed parts of the body.1,16
TABLE 1
Cutaneous lupus erythematosus: Recognizing the subtypes1
| Acute cutaneous lupus erythematosus (ACLE) |
|---|
| Localized: erythematous macules or papules over the bridge of the nose and cheek, with sparing of the nasolabial folds (“butterfly rash”) |
| Generalized: similar erythematous lesions over other photodistributed parts of the body, including the neck, chest, arms, and hands |
| Toxic epidermal necrolysis-like (TEN-like): blistering and epidermal cleavage in photodistributed parts of the body |
| Subacute cutaneous lupus erythematosus (SCLE) |
| Erythematous papulosquamous (psoriasis-like) eruptions or annular (ring-like) lesions with raised red borders and central clearing, occurring symmetrically and suddenly after sunlight exposure on photo-distributed body parts; the scalp and face are rarely affected |
| Chronic cutaneous lupus erythematosus (CCLE) |
| Discoid lupus erythematosus: erythematous papules and plaques with associated scale, spreading centrifugally with follicular plugging, pigment change, telangiectasia, and atrophy; scarring alopecia can occur |
| Lupus erythematosus profundus: tender, erythematous nodules and plaques, usually involving the proximal extremities, trunk, breasts, buttocks, and face |
| Chilblain lupus erythematosus: tender, erythematous nodules and plaques, occurring in acral areas often in response to cold |
| Intermittent cutaneous lupus erythematosus (ICLE) |
| Lupus erythematosus tumidus: succulent, erythematous, and edematous plaques found on photodistributed parts of the body |
Cutaneous LE diagnosis and treatment: Start with ACR criteria
When evaluating patients with suspected cutaneous LE, it is important not only to identify the subtype, but also to rule out systemic disease using criteria established by the American College of Rheumatology (ACR).17 Notably, 4 of the 11 diagnostic criteria for systemic disease involve visual clues, including malar rash, discoid rash, photosensitivity, and oral ulcerations. Laboratory evidence of systemic disease may include a positive antinuclear antibody, anti-dsDNA, or anti-Sm autoantibody test results, as well as hematologic abnormalities described in the ACR guidelines.
Ultimately, a diagnosis of cutaneous LE should be based on the patient’s history and physical exam, autoantibody profile, and histologic and immunofluorescent biopsy findings. A rheumatologic evaluation may help to determine which patients have systemic disease, as the ACR criteria may overdiagnose systemic LE in those with predominantly skin changes.6
Treatment of cutaneous LE is based on the subtype and extent of disease, with potent topical corticosteroids, in combination with antimalarial agents, being the primary therapies. ACLE skin lesions generally respond best to systemic corticosteroids and immunosuppressive agents (such as azathioprine or cyclophosphamide) that are used to control underlying systemic disease. SCLE can be managed with topical corticosteroids; however, patients typically also require systemic treatment, often with hydroxychloroquine, for optimal control. DLE, the most common form of CCLE, is managed in a similar fashion, with a greater role for intralesional corticosteroid injections. Lesions associated with ICLE, which often resolve spontaneously, may be treated with topical corticosteroids and antimalarials.16 It is also important to advise all patients with cutaneous LE to use a broad-spectrum sunscreen, as ultraviolet (UV) exposure can induce or exacerbate the lesions.9
Dermatomyositis: Rare but serious
Dermatomyositis is an idiopathic inflammatory myopathy characterized by chronic muscle inflammation, symmetric proximal muscle weakness, and distinct cutaneous findings. In addition to possible cardiac and pulmonary complications, dysphagia, and joint contractures, dermatomyositis is associated with cancer, with up to 25% of affected adults having an underlying occult malignancy.18
Dermatomyositis is a rare condition, with a prevalence of only 1 to 10 cases per million adults and 3.2 cases per million children.19 It has a bimodal age distribution, with most juvenile cases affecting children between the ages of 5 and 14 years and most adult cases developing in the fifth and sixth decades of life. Women are affected twice as often as men.18
Suspect dermatomyositis when you see any of the following signs:
- A heliotrope rash: violaceous macules and patches, with or without edema, symmetrically on the periorbital skin, present early in the disease course in 30% to 60% of patients.19 (See image)
- Gottron’s papules: violaceous papules on the dorsal interphalangeal and metacarpophalangeal joints of the hands, elbows, and knees, occurring in as many as 70% of patients (FIGURE 2).19,20
- Gottron’s sign: nonscaling, violaceous erythematous macules and plaques occurring symmetrically in the same distribution as Gottron’s papules, but with sparing of the interphalangeal spaces.20
- Periungual erythema and telangiectasias: redness and dilation of the blood vessels in the skin surrounding the nail plate.
- The shawl and V-signs: erythematous macular eruptions occurring in a “shawl” pattern on the shoulders, arms, and upper back and in a V-shaped pattern on the anterior neck and chest.
- Mechanic’s hand: extensive scaling, fissuring, and roughening of the palmar aspect of the hand.20,21
- Poikiloderma vasculare atrophicans: circumscribed violaceous erythema with thinning of the skin, prominent telangiectasias, and a mottled pattern of hypo- and hyperpigmentation, typically occurring on the anterior neck, chest, posterior shoulders, back, and buttocks, years after onset of the disease.21-24
- Cutaneous calcification (calcinosis cutis): usually on the buttocks, elbows, knees, and traumatized areas, affecting 30% to 70% of children with dermatomyositis, but only 10% of adults with the disorder.20,25-27
FIGURE 2
Gottron’s papules in dermatomyositis
Violaceous papules on the dorsal interphalangeal and metacarpophalangeal joints of the hands are a common manifestation of dermatomyositis.
Bohan and Peter criteria help with dermatomyositis diagnosis
A diagnosis of dermatomyositis can be established using the following criteria developed by Bohan and Peter in 1975: (1) symmetric muscle weakness; (2) elevation of muscle enzymes, most notably creatinine phosphokinase; (3) evidence of inflammation on muscle biopsy; (4) electromyographic features of myositis; and (5) characteristic dermatologic signs, including a heliotrope rash and Gottron’s papules.28,29 A definitive diagnosis can be made when the patient meets 3 of the first 4 criteria, as well as the fifth.
Corticosteroids are the mainstay of treatment for dermatomyositis, although the dose and duration are subject to debate. Cutaneous manifestations of dermatomyositis are commonly treated with topical corticosteroids and oral hydroxychloroquine, as well as emollients and antipruritic agents.
Cancer screening. All adults with signs and symptoms of dermatomyositis should undergo cancer screening. The most common malignancies are ovarian cancer, gastric cancer, and lymphoma.21
Photoprotection. As with cutaneous LE, UV exposure can exacerbate dermatomyositis, and patients should use a broad-spectrum sunscreen.
Scleroderma: Localized and systemic disease
The major cutaneous manifestation of scleroderma is that of thickened, leathery, bound-down skin, seen in both localized and systemic disease. In both cases, the lesions typically evolve through 3 characteristic stages: the initial inflammatory and edematous stage; a fibrotic stage, during which the skin lesions appear hard, tight, and hidebound; and the final, atrophic stage. However, not all lesions progress to this final stage.8
Localized scleroderma (also known as morphea) affects roughly 1 in 100,000 people. It is more prevalent in females than males, with a ratio as high as 3 to 1.30-33 Cutaneous findings vary, and numerous clinical presentations are possible. The most widely used classification system, the Mayo Clinic Classification, recognizes 5 subtypes: plaque morphea (the most common), generalized morphea, linear morphea, deep morphea, and bullous morphea (TABLE 2).34 The mean age of onset depends on the subtype, and ranges from 12 years for linear morphea to 45 years for deep morphea.35
While systemic involvement is not common with localized scleroderma, extracutaneous manifestations have been reported in up to 25% of cases.31,36,37 In a 2005 multicenter study of 750 pediatric patients with localized scleroderma, the most frequently reported extracutaneous symptom was arthritis, found in 12% of patients.36 Less frequent findings included neurologic symptoms such as seizures and headaches, vascular changes such as deep vein thrombosis, and gastrointestinal, cardiac, and renal conditions. Although the precise etiology of localized scleroderma is unknown, it is thought to be associated with trauma, prior infection by Borrelia burgdorferi, chronic venous insufficiency, and irradiation for breast cancer.30,38,39
TABLE 2
Localized scleroderma: What to look for8,34
|
Systemic scleroderma is a heterogenous disorder
Commonly called systemic sclerosis (SSc), systemic scleroderma is characterized by proliferative vascular lesions; fibrosis of internal organs, including the lungs, heart, kidneys, and gastrointestinal tract; and distinct cutaneous manifestations.3 SSc affects about 240 people per million adults, mostly between the ages of 30 and 50 years, with women affected 3 times as often as men.40-42
The cause of SSc is unknown, although a genetic predisposition is likely. Environmental factors likely play a role in triggering the disease, with possible causative factors including cytomegalovirus and other viral infections and exposure to certain chemicals.43
As in localized scleroderma, cutaneous manifestations are a prominent part of SSc and typically develop early on. Raynaud’s phenomenon (RP) (FIGURE 3), which occurs in 90% to 98% of patients with SSc,44 can develop in association with other cutaneous findings or precede additional skin changes by months or years.
Other early skin changes include nonpitting edema of the fingers and toes, which creates a sausage-like appearance. This is typically followed by hardening and thickening of the skin in these areas, which can result in highly disabling sclerodactyly (FIGURE 4).45 Patients can also develop painful ulcerations on their fingertips and knuckles (rat bite necroses) due to local ischemia and vascular insufficiency. This may be complicated by secondary bacterial infection, gangrene, and acroosteolysis, leading to articular deformities and dissolution of terminal phalanges (FIGURE 5).45-48
On the face, SSc is characterized early on by periorbital edema and later by the development of a beaked nose, a reduction in the size of the mouth (microstomia) with radial furrowing, thinning of the lips, and telangiectasias.45,49 As the sclerosis worsens, patients are frequently left with expressionless, mask-like faces.48
Other common cutaneous manifestations of SSc include a “salt and pepper” appearance, with alternating areas of hypo- and hyperpigmented skin. Additionally, patients may suffer from a loss of hair follicles, severely dry skin, and pruritus.45,48
There are 2 major subsets of SSc—limited cutaneous SSc and diffuse cutaneous SSc. While they can be differentiated based on the history of symptoms, the appearance and extent of cutaneous involvement, and certain serological makers, the most important difference is the speed at which the disease progresses and its severity: Limited cutaneous SSc typically progresses slowly, while diffuse cutaneous SSc is characterized by a relatively rapid onset of disease, with skin and internal organ involvement likely to be severe.49
Scleroderma diagnosis and treatment: Vascular changes are an important clue
Skin changes seen in localized scleroderma and SSc can be clinically and histologically similar, making it difficult to arrive at a definitive diagnosis.
One clinical clue is that in localized scleroderma, vascular changes, such as RP and periungual nailfold telangiectasia, are typically absent. In addition, cutaneous changes in the hands and fingers, such as sclerodactyly, are more characteristic of systemic disease.10
SSc can be diagnosed using criteria proposed by the ACR, which have been shown to be highly sensitive (97%) and specific (98%).50 The major criterion is proximal scleroderma—symmetric thickening, tightening, and induration of the skin of the fingers and areas proximal to the metacarpophalangeal or metatarsophalangeal joints, which may include the trunk, neck, and face. Minor criteria include (1) sclerodactyly, (2) digital pitting scars of fingertips or loss of substance of the distal finger pad, and (3) bilateral basilar pulmonary fibrosis. Diagnosis is based on the presence of either the major criterion or 2 of the 3 minor criteria.50
Numerous therapies are available for localized scleroderma, including topical, intralesional, and systemic corticosteroids, topical tacrolimus, hydroxychloroquine, topical and systemic calcipotriol, penicillamine, sulfasalazine, interferon-[H9253], methotrexate, phototherapy with UV light, and imiquimod.
SSc skin manifestations, which can be severe and disabling, can be treated with a wide range of therapies. Topical or systemic corticosteroids; topical calcineurin inhibitors; systemic immunosuppressive agents such as methotrexate, cyclophosphamide, cyclosporine, and D-penicillamine; and phototherapy have all had varying success at reducing hardening of the skin.51-54 Other skin manifestations, including RP, dryness and itching, pigment changes, digital ulcerations, calcifications, and telangiectasias, should be managed as needed, with various supplemental treatment options available.45 These may include emollients, antihistamines, and topical corticosteroids for dryness and itching; laser therapy for telangiectasias; and corticosteroid injection, laser therapy, or surgery for calcifications. However, there is limited evidence of efficacy for most of these options.45
FIGURE 3
An attack of Raynaud’s phenomenon
Raynaud’s phenomenon, characterized by blanching of the distal fingertips, is shown here in a patient with systemic sclerosis.
FIGURE 4
Sclerodactyly in a patient with systemic sclerosis
Hardening and thickening of the skin can result in highly disabling sclerodactyly in patients with systemic sclerosis.
FIGURE 5
Dissolution of terminal phalanges
Bony resorption and ulceration have led to the loss of distal phalanges in this patient with systemic sclerosis.
Mixed connective tissue disease has features of several disorders
Mixed connective tissue disease (MCTD) is an apparently distinct rheumatologic condition characterized by a combination of clinical features of systemic LE, dermatomyositis, scleroderma, polymyositis, and rheumatoid arthritis. The presence of high titers of a unique autoantibody, anti-U1-RNP,54-57 aids in diagnosis.
Although precise prevalence data are lacking, MCTD is thought to occur in about 1 in 10,000 people.58 The disease is much more common in women, with a female-to-male ratio as high as 7 to 1, and generally occurs in the second or third decade of life.58-60
The clinical manifestations of MCTD typically evolve, with overlapping features of various autoimmune disorders appearing sequentially over several months to years.57 Early in the course of MCTD, patients commonly experience fatigue, polyarthritis, hand edema, and RP. In time, virtually every organ system may be involved. Pulmonary hypertension is a major cause of death.59,61
Unlike many other connective tissue disorders, MCTD lacks any distinct cutaneous findings. In addition to those mentioned earlier, prominent skin findings include swelling of the fingers, sclerodactyly, and the acute malar eruptions and discoid plaques typically associated with LE.56,57,62 Cutaneous manifestations associated with dermatomyositis and scleroderma may also be seen, particularly juxta-articular calcinosis. The mucous membranes may be involved, as well, resulting in nasal perforation, buccal and urogenital ulcerations, and sicca complex.58,63,64
MCTD diagnosis and treatment: Look for these serology and clinical findings
Diagnosing MCTD can be clinically challenging, as signs and symptoms of the disease commonly evolve over time. The Alarcon-Segovia criteria—largely regarded as the best diagnostic tool for MCTD65,66—include 1 serologic finding (elevated anti-U1-RNP [titer ≥1:1600]) and 5 clinical findings (RP, edema of the hands, synovitis, myositis, and acrosclerosis). Diagnosis requires the presence of the serologic criterion and ≥3 of the 5 clinical criteria.
Treatment of the cutaneous manifestations should be based on the effectiveness of therapies for similar skin findings seen in other disorders. In treating MCTD (or any other connective tissue disorder), a team that includes nurses, physical and occupational therapists, primary care physicians, and specialists in dermatology and rheumatology is essential for an optimal outcome.
CORRESPONDENCE Christian R. Halvorson, MD, Mercy Medical Center, Department of Medicine, 301 St. Paul Place, Baltimore, MD 21202; [email protected]
1. Renner R, Sticherling M. The different faces of cutaneous lupus erythematosus. G Ital Dermatol Venereol. 2009;144:135-147.
2. Kuhn A, Ruzicka T. Classification of cutaneous lupus erythematosus. In: Kuhn A, Lehmann P, Ruzicka T, eds. Cutaneous Lupus Erythematosus. New York: Springer; 2004:53–57.
3. Costner MI, Grau RH. Update on connective tissue diseases in dermatology. Semin Cutan Med Surg. 2006;25:207-220.
4. Ting W, Stone MS, Racila D, et al. Toxic epidermal necrolysis-like acute cutaneous lupus erythematosus and the spectrum of the acute syndrome of apoptotic pan-epidermolysis (ASAP): a case report, concept review and proposal for new classification of lupus erythematosus vesiculobullous skin lesions. Lupus. 2004;13:941-950.
5. Jorizzo JL, Carroll CL, Sangueza OP. Lupus erythematosus. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. 2nd ed. Spain: Elsevier Limited; 2008.
6. Kuhn A, Sticherling M, Bonsmann G. Clinical manifestations of cutaneous lupus erythematosus. J Dtsch Dermatol Ges. 2007;5:1124-1137.
7. Sontheimer RD, Thomas JR, Gilliam JN. Subacute cutaneous lupus erythematosus: a cutaneous marker for a distinct lupus erythematosus subset. Arch Dermatol. 1979;115:1409-1415.
8. Sontheimer RD. Skin manifestations of systemic autoimmune connective tissue disease: diagnostics and therapeutics. Best Pract Res Clin Rheumatol. 2004;18:429-462.
9. Panjwani S. Early diagnosis and treatment of discoid lupus erythematosus. J Am Board Fam Med. 2009;22:206-213.
10. Sontheimer RD, Provost TT. Lupus erythematosus. In: Sontheimer RD, Provost TT, eds. Cutaneous Manifestations of Rheumatic Diseases. Baltimore: Williams & Wilkins; 1996.
11. Mond CB, Peterson MG, Rothfield NF. Correlation of antiro antibody with photosensitivity rash in systemic lupus erythematosus patients. Arthritis Rheum. 1989;32:202-204.
12. Jacyk WK, Damisah M. Discoid lupus erythematosus in the Nigerians. Br J Dermatol. 1979;100:131-135.
13. Callen JP. Cutaneous lupus erythematosus: A personal approach to management. Australas J Dermatol. 2006;47:13-27.
14. Gilliam JN, Sontheimer RD. Distinctive cutaneous subsets in the spectrum of lupus erythematosus. J Am Acad Dermatol. 1981;4:471-475.
15. Farley-Loftus R, Mahlberg M, Merola J, et al. Generalized discoid lupus erythematosus. Dermatol Online J. 2009;15:18.-
16. Kuhn A, Richter-Hintz D, Oslislo C, et al. Lupus erythematosus tumidus—a neglected subset of cutaneous lupus erythematosus: report of 40 cases. Arch Dermatol. 2000;136:1033-1041.
17. American College of Rheumatology. The 1982 revised criteria for classification of systemic lupus erythematosus. Available at: http://www.rheumatology.org/practice/clinical/classification/SLE/sle.asp. Accessed September 21, 2010.
18. Na SJ, Kim SM, Sunwoo IN, et al. Clinical characteristics and outcomes of juvenile and adult dermatomyositis. J Korean Med Sci. 2009;24:715-721.
19. Kovacs SO, Kovacs SC. Dermatomyositis. J Am Acad Dermatol. 1998;39:899-922.
20. Koler RA, Montemarano A. Dermatomyositis. Am Fam Physician. 2001;64:1565-1572.
21. Sunkureddi P, Nguyen-Oghalai TU, Jarvis JL, et al. Signs of dermatomyositis. Hosp Physician. 2005;41:41-44.
22. Iorizzo LJ, 3rd, Jorizzo JL. The treatment and prognosis of dermatomyositis: an updated review. J Am Acad Dermatol. 2008;59:99-112.
23. Jorizzo JL, Carroll CL, Sangueza OP. Dermatomyositis. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. 2nd ed. Spain: Elsevier Limited; 2008:575–583.
24. Sontheimer RD. Dermatomyositis. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 5th ed. New York: McGraw-Hill; 1999:2009–2020.
25. Halbert AR. Juvenile dermatomyositis. Australas J Dermatol. 1996;37:106-108.
26. Orlow SJ, Watsky KL, Bolognia JL. Skin and bones II. J Am Acad Dermatol. 1991;25:447-462.
27. Bowyer SL, Blane CE, Sullivan DB, et al. Childhood dermatomyositis: factors predicting functional outcome and development of dystrophic calcification. J Pediatr. 1983;103:882-888.
28. Bohan A, Peter JB. Polymyositis and dermatomyositis (second of two parts). N Engl J Med. 1975;292:403-407.
29. Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975;292:344-347.
30. Vancheeswaran R, Black CM, David J, et al. Childhood-onset scleroderma: is it different from adult-onset disease? Arthritis Rheum. 1996;39:1041-1049.
31. Zulian F, Athreya BH, Laxer R, et al. Juvenile localized scleroderma: Clinical and epidemiological features in 750 children. An international study. Rheumatology (Oxford). 2006;45:614-620.
32. Marzano AV, Menni S, Parodi A, et al. Localized scleroderma in adults and children. clinical and laboratory investigations on 239 cases. Eur J Dermatol. 2003;13:171-176.
33. Uziel Y, Krafchik BR, Silverman ED, et al. Localized scleroderma in childhood: a report of 30 cases. Semin Arthritis Rheum. 1994;23:328-340.
34. Peterson LS, Nelson AM, Su WP. Classification of morphea (localized scleroderma). Mayo Clin Proc. 1995;70:1068-1076.
35. Peterson LS, Nelson AM, Su WP, et al. The epidemiology of morphea (localized scleroderma) in Olmsted County 1960-1993. J Rheumatol. 1997;24:73-80.
36. Zulian F, Vallongo C, Woo P, et al. Localized scleroderma in childhood is not just a skin disease. Arthritis Rheum. 2005;52:2873-2881.
37. Dehen L, Roujeau JC, Cosnes A, et al. Internal involvement in localized scleroderma. Medicine (Baltimore). 1994;73:241-245.
38. Ludwig RJ, Werner RJ, Winker W, et al. Chronic venous insufficiency - a potential trigger for localized scleroderma. J Eur Acad Dermatol Venereol. 2006;20:96-99.
39. Aberer E, Neumann R, Stanek G. Is localised scleroderma a borrelia infection? Lancet. 1985;2:278.-
40. Krishnan E, Furst DE. Systemic sclerosis mortality in the United States: 1979-1998. Eur J Epidemiol. 2005;20:855-861.
41. Silman AJ. Scleroderma—demographics and survival. J Rheumatol Suppl. 1997;48:58-61.
42. Medsger TA,, Jr, Masi AT. Epidemiology of systemic sclerosis (scleroderma). Ann Intern Med. 1971;74:714-721.
43. Charles C, Clements P, Furst DE. Systemic sclerosis: Hypothesis-driven treatment strategies. Lancet. 2006;367:1683-1691.
44. Maricq HR, Harper FE, Khan MM, et al. Microvascular abnormalities as possible predictors of disease subsets in Raynaud phenomenon and early connective tissue disease. Clin Exp Rheumatol. 1983;1:195-205.
45. Krieg T, Takehara K. Skin disease: A cardinal feature of systemic sclerosis. Rheumatology (Oxford). 2009;48 (suppl 3):S14-S18.
46. Ingraham KM, Steen VD. Morbidity of digital tip ulcerations in scleroderma. Arthritis Rheum. 2006;54(9 suppl.):F78.-
47. Ferri C, Valentini G, Cozzi F, et al. Systemic sclerosis: Demographic, clinical, and serologic features and survival in 1,012 italian patients. Medicine (Baltimore). 2002;81:139-153.
48. Haustein UF. Systemic sclerosis - scleroderma. Dermatol Online J. 2002;8.-
49. Fitzpatrick TB, Johnson RA, Klaus W, et al. In Colour Atlas and Synopsis of Clinical Dermatology. 4th ed. New York: McGraw-Hill; 2001:368–369.
50. Preliminary criteria for the classification of systemic sclerosis (scleroderma). subcommittee for scleroderma criteria of the American Rheumatism Association diagnostic and therapeutic criteria committee. Arthritis Rheum. 1980;23:581-590.
51. Valentini G, Paone C, La Montagna G, et al. Low-dose intravenous cyclophosphamide in systemic sclerosis: an open prospective efficacy study in patients with early diffuse disease. Scand J Rheumatol. 2006;35:35-38.
52. Steen VD, Medsger TA, Jr. Improvement in skin thickening in systemic sclerosis associated with improved survival. Arthritis Rheum. 2001;44:2828-2835.
53. Basso M, Filaci G, Cutolo M, et al. Long-term treatment of patients affected by systemic sclerosis with cyclosporin A. Ann Ital Med Int. 2001;16:233-239.
54. Morton SJ, Powell RJ. Cyclosporin and tacrolimus: their use in a routine clinical setting for scleroderma. Rheumatology (Oxford). 2000;39:865-869.
55. Kasukawa R. Mixed connective tissue disease. Intern Med. 1999;38:386-393.
56. Bennett RM, O’Connell DJ. Mixed connective tisssue disease: A clinicopathologic study of 20 cases. Semin Arthritis Rheum. 1980;10:25-51.
57. Sharp GC, Irvin WS, Tan EM, et al. Mixed connective tissue disease—an apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA). Am J Med. 1972;52:148-159.
58. Venables PJ. Mixed connective tissue disease. Lupus. 2006;15:132-137.
59. Farhey Y, Hess EV. Mixed connective tissue disease. Arthritis Care Res. 1997;10:333-342.
60. Alarcon-Segovia D. Mixed connective tissue disease - a decade of growing pains. J Rheumatol. 1981;8:535-540.
61. Ueda N, Mimura K, Maeda H, et al. Mixed connective tissue disease with fatal pulmonary hypertension and a review of literature. Virchows Arch A Pathol Anat Histopathol. 1984;404:335-340.
62. Bennett RM. Mixed connective tissue disease and other overlap syndromes. In: Kelley WN, Harris EDJ, Ruddy SH, et al, eds. Textbook of Rheumatology. 4th ed. Philadelphia: WB Saunders; 1993:1061.
63. Nakashima M, Suzuki K, Okada M, et al. Panniculitis in a patient with mixed connective tissue disease. Mod Rheumatol. 2004;14:250-253.
64. Magro CM, Crowson AN, Regauer S. Mixed connective tissue disease. A clinical, histologic, and immunofluorescence study of eight cases. Am J Dermatopathol. 1997;19:206-213.
65. Amigues JM, Cantagrel A, Abbal M, et al. Comparative study of 4 diagnosis criteria sets for mixed connective tissue disease in patients with anti-RNP antibodies. autoimmunity group of the hospitals of toulouse. J Rheumatol. 1996;23:2055-2062.
66. Alarcon-Segovia D, Cardiel MH. Comparison between 3 diagnostic criteria for mixed connective tissue disease. study of 593 patients. J Rheumatol. 1989;16:328-334.
1. Renner R, Sticherling M. The different faces of cutaneous lupus erythematosus. G Ital Dermatol Venereol. 2009;144:135-147.
2. Kuhn A, Ruzicka T. Classification of cutaneous lupus erythematosus. In: Kuhn A, Lehmann P, Ruzicka T, eds. Cutaneous Lupus Erythematosus. New York: Springer; 2004:53–57.
3. Costner MI, Grau RH. Update on connective tissue diseases in dermatology. Semin Cutan Med Surg. 2006;25:207-220.
4. Ting W, Stone MS, Racila D, et al. Toxic epidermal necrolysis-like acute cutaneous lupus erythematosus and the spectrum of the acute syndrome of apoptotic pan-epidermolysis (ASAP): a case report, concept review and proposal for new classification of lupus erythematosus vesiculobullous skin lesions. Lupus. 2004;13:941-950.
5. Jorizzo JL, Carroll CL, Sangueza OP. Lupus erythematosus. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. 2nd ed. Spain: Elsevier Limited; 2008.
6. Kuhn A, Sticherling M, Bonsmann G. Clinical manifestations of cutaneous lupus erythematosus. J Dtsch Dermatol Ges. 2007;5:1124-1137.
7. Sontheimer RD, Thomas JR, Gilliam JN. Subacute cutaneous lupus erythematosus: a cutaneous marker for a distinct lupus erythematosus subset. Arch Dermatol. 1979;115:1409-1415.
8. Sontheimer RD. Skin manifestations of systemic autoimmune connective tissue disease: diagnostics and therapeutics. Best Pract Res Clin Rheumatol. 2004;18:429-462.
9. Panjwani S. Early diagnosis and treatment of discoid lupus erythematosus. J Am Board Fam Med. 2009;22:206-213.
10. Sontheimer RD, Provost TT. Lupus erythematosus. In: Sontheimer RD, Provost TT, eds. Cutaneous Manifestations of Rheumatic Diseases. Baltimore: Williams & Wilkins; 1996.
11. Mond CB, Peterson MG, Rothfield NF. Correlation of antiro antibody with photosensitivity rash in systemic lupus erythematosus patients. Arthritis Rheum. 1989;32:202-204.
12. Jacyk WK, Damisah M. Discoid lupus erythematosus in the Nigerians. Br J Dermatol. 1979;100:131-135.
13. Callen JP. Cutaneous lupus erythematosus: A personal approach to management. Australas J Dermatol. 2006;47:13-27.
14. Gilliam JN, Sontheimer RD. Distinctive cutaneous subsets in the spectrum of lupus erythematosus. J Am Acad Dermatol. 1981;4:471-475.
15. Farley-Loftus R, Mahlberg M, Merola J, et al. Generalized discoid lupus erythematosus. Dermatol Online J. 2009;15:18.-
16. Kuhn A, Richter-Hintz D, Oslislo C, et al. Lupus erythematosus tumidus—a neglected subset of cutaneous lupus erythematosus: report of 40 cases. Arch Dermatol. 2000;136:1033-1041.
17. American College of Rheumatology. The 1982 revised criteria for classification of systemic lupus erythematosus. Available at: http://www.rheumatology.org/practice/clinical/classification/SLE/sle.asp. Accessed September 21, 2010.
18. Na SJ, Kim SM, Sunwoo IN, et al. Clinical characteristics and outcomes of juvenile and adult dermatomyositis. J Korean Med Sci. 2009;24:715-721.
19. Kovacs SO, Kovacs SC. Dermatomyositis. J Am Acad Dermatol. 1998;39:899-922.
20. Koler RA, Montemarano A. Dermatomyositis. Am Fam Physician. 2001;64:1565-1572.
21. Sunkureddi P, Nguyen-Oghalai TU, Jarvis JL, et al. Signs of dermatomyositis. Hosp Physician. 2005;41:41-44.
22. Iorizzo LJ, 3rd, Jorizzo JL. The treatment and prognosis of dermatomyositis: an updated review. J Am Acad Dermatol. 2008;59:99-112.
23. Jorizzo JL, Carroll CL, Sangueza OP. Dermatomyositis. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. 2nd ed. Spain: Elsevier Limited; 2008:575–583.
24. Sontheimer RD. Dermatomyositis. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 5th ed. New York: McGraw-Hill; 1999:2009–2020.
25. Halbert AR. Juvenile dermatomyositis. Australas J Dermatol. 1996;37:106-108.
26. Orlow SJ, Watsky KL, Bolognia JL. Skin and bones II. J Am Acad Dermatol. 1991;25:447-462.
27. Bowyer SL, Blane CE, Sullivan DB, et al. Childhood dermatomyositis: factors predicting functional outcome and development of dystrophic calcification. J Pediatr. 1983;103:882-888.
28. Bohan A, Peter JB. Polymyositis and dermatomyositis (second of two parts). N Engl J Med. 1975;292:403-407.
29. Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975;292:344-347.
30. Vancheeswaran R, Black CM, David J, et al. Childhood-onset scleroderma: is it different from adult-onset disease? Arthritis Rheum. 1996;39:1041-1049.
31. Zulian F, Athreya BH, Laxer R, et al. Juvenile localized scleroderma: Clinical and epidemiological features in 750 children. An international study. Rheumatology (Oxford). 2006;45:614-620.
32. Marzano AV, Menni S, Parodi A, et al. Localized scleroderma in adults and children. clinical and laboratory investigations on 239 cases. Eur J Dermatol. 2003;13:171-176.
33. Uziel Y, Krafchik BR, Silverman ED, et al. Localized scleroderma in childhood: a report of 30 cases. Semin Arthritis Rheum. 1994;23:328-340.
34. Peterson LS, Nelson AM, Su WP. Classification of morphea (localized scleroderma). Mayo Clin Proc. 1995;70:1068-1076.
35. Peterson LS, Nelson AM, Su WP, et al. The epidemiology of morphea (localized scleroderma) in Olmsted County 1960-1993. J Rheumatol. 1997;24:73-80.
36. Zulian F, Vallongo C, Woo P, et al. Localized scleroderma in childhood is not just a skin disease. Arthritis Rheum. 2005;52:2873-2881.
37. Dehen L, Roujeau JC, Cosnes A, et al. Internal involvement in localized scleroderma. Medicine (Baltimore). 1994;73:241-245.
38. Ludwig RJ, Werner RJ, Winker W, et al. Chronic venous insufficiency - a potential trigger for localized scleroderma. J Eur Acad Dermatol Venereol. 2006;20:96-99.
39. Aberer E, Neumann R, Stanek G. Is localised scleroderma a borrelia infection? Lancet. 1985;2:278.-
40. Krishnan E, Furst DE. Systemic sclerosis mortality in the United States: 1979-1998. Eur J Epidemiol. 2005;20:855-861.
41. Silman AJ. Scleroderma—demographics and survival. J Rheumatol Suppl. 1997;48:58-61.
42. Medsger TA,, Jr, Masi AT. Epidemiology of systemic sclerosis (scleroderma). Ann Intern Med. 1971;74:714-721.
43. Charles C, Clements P, Furst DE. Systemic sclerosis: Hypothesis-driven treatment strategies. Lancet. 2006;367:1683-1691.
44. Maricq HR, Harper FE, Khan MM, et al. Microvascular abnormalities as possible predictors of disease subsets in Raynaud phenomenon and early connective tissue disease. Clin Exp Rheumatol. 1983;1:195-205.
45. Krieg T, Takehara K. Skin disease: A cardinal feature of systemic sclerosis. Rheumatology (Oxford). 2009;48 (suppl 3):S14-S18.
46. Ingraham KM, Steen VD. Morbidity of digital tip ulcerations in scleroderma. Arthritis Rheum. 2006;54(9 suppl.):F78.-
47. Ferri C, Valentini G, Cozzi F, et al. Systemic sclerosis: Demographic, clinical, and serologic features and survival in 1,012 italian patients. Medicine (Baltimore). 2002;81:139-153.
48. Haustein UF. Systemic sclerosis - scleroderma. Dermatol Online J. 2002;8.-
49. Fitzpatrick TB, Johnson RA, Klaus W, et al. In Colour Atlas and Synopsis of Clinical Dermatology. 4th ed. New York: McGraw-Hill; 2001:368–369.
50. Preliminary criteria for the classification of systemic sclerosis (scleroderma). subcommittee for scleroderma criteria of the American Rheumatism Association diagnostic and therapeutic criteria committee. Arthritis Rheum. 1980;23:581-590.
51. Valentini G, Paone C, La Montagna G, et al. Low-dose intravenous cyclophosphamide in systemic sclerosis: an open prospective efficacy study in patients with early diffuse disease. Scand J Rheumatol. 2006;35:35-38.
52. Steen VD, Medsger TA, Jr. Improvement in skin thickening in systemic sclerosis associated with improved survival. Arthritis Rheum. 2001;44:2828-2835.
53. Basso M, Filaci G, Cutolo M, et al. Long-term treatment of patients affected by systemic sclerosis with cyclosporin A. Ann Ital Med Int. 2001;16:233-239.
54. Morton SJ, Powell RJ. Cyclosporin and tacrolimus: their use in a routine clinical setting for scleroderma. Rheumatology (Oxford). 2000;39:865-869.
55. Kasukawa R. Mixed connective tissue disease. Intern Med. 1999;38:386-393.
56. Bennett RM, O’Connell DJ. Mixed connective tisssue disease: A clinicopathologic study of 20 cases. Semin Arthritis Rheum. 1980;10:25-51.
57. Sharp GC, Irvin WS, Tan EM, et al. Mixed connective tissue disease—an apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA). Am J Med. 1972;52:148-159.
58. Venables PJ. Mixed connective tissue disease. Lupus. 2006;15:132-137.
59. Farhey Y, Hess EV. Mixed connective tissue disease. Arthritis Care Res. 1997;10:333-342.
60. Alarcon-Segovia D. Mixed connective tissue disease - a decade of growing pains. J Rheumatol. 1981;8:535-540.
61. Ueda N, Mimura K, Maeda H, et al. Mixed connective tissue disease with fatal pulmonary hypertension and a review of literature. Virchows Arch A Pathol Anat Histopathol. 1984;404:335-340.
62. Bennett RM. Mixed connective tissue disease and other overlap syndromes. In: Kelley WN, Harris EDJ, Ruddy SH, et al, eds. Textbook of Rheumatology. 4th ed. Philadelphia: WB Saunders; 1993:1061.
63. Nakashima M, Suzuki K, Okada M, et al. Panniculitis in a patient with mixed connective tissue disease. Mod Rheumatol. 2004;14:250-253.
64. Magro CM, Crowson AN, Regauer S. Mixed connective tissue disease. A clinical, histologic, and immunofluorescence study of eight cases. Am J Dermatopathol. 1997;19:206-213.
65. Amigues JM, Cantagrel A, Abbal M, et al. Comparative study of 4 diagnosis criteria sets for mixed connective tissue disease in patients with anti-RNP antibodies. autoimmunity group of the hospitals of toulouse. J Rheumatol. 1996;23:2055-2062.
66. Alarcon-Segovia D, Cardiel MH. Comparison between 3 diagnostic criteria for mixed connective tissue disease. study of 593 patients. J Rheumatol. 1989;16:328-334.
What’s causing your young patient’s hip pain?
• When you suspect an infectious cause of hip pain, immediately order laboratory studies, blood cultures, and hip radiographs to rule out septic arthritis. A
• When you suspect avascular necrosis of the femoral head, instruct the patient to remain non-weight bearing and provide a referral to an orthopedist. A
• Stabilization with in situ pinning is the gold standard treatment for slipped capital femoral epiphysis, whether the slip is stable or unstable. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Sean L, a 12-year-old middle school student in the 90th percentile for weight, limps into your office and reports that it hurts to put his full weight down on his right leg. The pain just started, Sean says, but he began limping a day or 2 earlier. Sean plays on his school’s football team, and he wants to know what you can give him to relieve the pain so he won’t have to miss any games. What can you tell him?
Family physicians are increasingly likely to see children and adolescents with hip pain, the combined result of greater sports participation and a surge in childhood obesity. Diagnosing pediatric hip pain can be a daunting task, not only because of the complexity of the hip joint, but because of the need to consider bone, joint, tendon, muscle, bursa, and referred pain in the differential diagnosis.
But it doesn’t have to be. Being familiar with the major causes of pediatric hip pain, the diagnostic tests and maneuvers that are part of a comprehensive work-up, and the conditions that require rapid referral to an orthopedist makes it possible to adopt a straightforward approach. We’ve developed this review with that goal in mind.
Assess pain and movement with these maneuvers and tests
Begin with a pain history, determining the location of the hip pain—anterior, lateral, or posterior. Ask the patient to describe the pain and its quality: Is it diffuse, localized, or radiating? Identify any aggravating or relieving factors, and question the patient (or parents) about the onset, reproducibility, and timing of the pain, including the presence or absence of nighttime pain.
Find out, too, whether the pain is causing a limp; what effect, if any, the pain has had on the patient’s ability to bear weight; and to what extent the patient’s activity level has been affected. Then move on to the physical examination.
Begin with the patient standing up. Observe his or her gait, posture, and alignment. Check for Trendelenburg’s sign, in which the ipsilateral hip drops when the patient raises the unaffected leg. Its presence indicates a weakness of the opposite hip abductor.
With the patient in a supine position, inspect the hip for swelling, erythema, and warmth. Palpate the affected area, but keep in mind that palpation may not always reveal much because of the depth of the hip joint. If the patient is overweight, palpation of the muscles, tendons, or bones may be particularly difficult.
Test active and passive range of motion (ROM) and muscle strength of the hip in all directions. (Patients who are unable to tolerate lying down can undergo most of the ROM and strength tests in a seated position.) Check for a discrepancy in leg length, not only by visual inspection, but by measuring from the anterior superior iliac spine (ASIS) to the lateral malleoli.
Perform more focused maneuvers, as needed. If lumbar radiculopathy is a possibility, for example, do a straight leg raise, lifting the leg on the affected side in full extension with the ankle dorsiflexed, and repeat with the leg on the unaffected side. The test is positive if radiating pain down the affected leg and buttock is reproduced at ≤60° of leg elevation (or leg extension if the patient is seated). Conduct Ober’s test (FIGURE 1) to check for iliotibial band syndrome.
Follow with a system review, asking about recent conditions, including fever and infection, trauma, and constitutional, abdominal, and genitourinary symptoms. Perform an abdominal exam, and, if indicated, a pelvic or hernia exam. Check reflexes and sensation, as warranted, and examine the spine and knee.
CASE Sean is a healthy boy with no known medical problems. He has not been ill recently, and has not had any unexplained weight loss. His vital signs are normal, and he does not appear ill. He walks with a limp.
On examination, Sean has no palpable area of tenderness, swelling, or ecchymosis. His right hip has limited and painful internal rotation and, when flexed, it falls out to the side in external rotation.
FIGURE 1
Ober’s test for iliotibial band syndrome

With the patient lying on the unaffected side, passively extend the affected leg and allow the knee to drop. The test is positive if the patient experiences pain along the lateral side of the thigh or the knee does not drop down to the table.
Hip pain and infection? Consider septic arthritis
Is your patient febrile or recovering from an infection? When you suspect an acute infectious cause of hip pain, there are 2 disorders to consider in the differential diagnosis: transient synovitis (TS) and septic arthritis. Both are associated with an acute onset of pain and limping or non-weight bearing, and generally affect young children: Septic arthritis is most common in children between the age of 3 and 6 years, while the typical age range for TS is 3 through 8.1-4
There are other important differences. TS is a benign, self-limited, and common cause of hip pain in young children,5 which may be preceded by a viral infection.1 Septic arthritis is a serious condition that requires rapid identification; a delay in treatment can cause significant long-term morbidity. Complications may include early arthritis, shortened limb, dislocation, and osteonecrosis.
Because it can be difficult to distinguish between septic arthritis and TS, multiple studies have looked at the best way to make that determination. 1-7
The criteria most commonly used to identify septic arthritis are:
- fever
- refusal to bear weight
- erythrocyte sedimentation rate (ESR) >40 mm/h
- white blood cell count >12,000 mm3.
One study showed a predictive probability of 97% for septic arthritis when 3 of the 4 above criteria were present, and 99% if the patient had all 4.2,4 Other studies added 2 additional criteria—C-reactive protein (CRP) >1 mg/dL and medial joint space widening of >2 mm—with similar predictive probabilities (93% and 99%, respectively, if 3 or 4 of the 6 criteria were positive).2,4,6
Order lab work (ESR, CRP, complete blood count, and blood cultures) for any young patient whose hip pain is thought to be associated with an infectious process. Obtain hip anterior/posterior (AP) and frog lateral radiographs to look for joint space widening, as well.1-4
In addition to the above criteria, suspect septic arthritis in a child who presents with acute onset of hip pain, looks ill, and has limited ROM—particularly with internal rotation. In contrast, children with TS do not look sick and, while they often have limited ROM, it is primarily just at extremes. A modified log roll test can be used to assess the rotation of the hip.
An ultrasound-guided aspiration of fluid is the gold standard for septic arthritis diagnosis. Treatment is emergent surgical drainage and parenteral antibiotics, which should be withheld until fluid is aspirated or the joint is surgically drained. The most common causative organism is Staphylococcus aureus.3,7
It is reasonable to withhold joint aspiration for patients who don’t look sick and have normal labs and reliable follow-up, and to watch closely, with conservative management including nonsteroidal anti-inflammatory drugs (NSAIDs) and activity, as tolerated, instead.
There is some concern that TS may lead to Legg-Calves-Perthe’s disease, also known as avascular necrosis of the femoral head, although there is no strong evidence to support it. To be safe, however, obtain radiographs 2 to 18 months after TS resolves to check for further damage or complications.1,8
Femoral head disorders: When x-rays help, when they don’t
There are 2 femoral head disorders that commonly affect children and adolescents: Avascular necrosis of the femoral head and slipped capital femoral epiphysis (SCFE). Age alone is a clue to detection; children with avascular necrosis tend to be younger than those with SCFE.
Avascular necrosis of the femoral head is most commonly seen in children between the ages of 4 and 8 years, and occurs more frequently in boys than in girls. Although there is disagreement about the etiology of avascular necrosis, the condition is thought to result from a disruption in femoral blood supply, leading to osteonecrosis and flattening of the weight-bearing surface of the femoral head. One study found that structural abnormalities in the epiphyseal cartilage may lead to collapse.9
The condition often begins with a painless limp that develops—typically in 1 to 3 months—into groin, thigh, or knee pain; worsens with activity; and is relieved with rest.5 Abduction and internal rotation are limited on exam.
In patients with avascular necrosis, hip AP and frog lateral radiographs are diagnostic, with evidence of increased density of 1 epiphysis and flattening or fragmentation of the femoral head.7 When you suspect avascular necrosis, advise the patient to avoid weight bearing—and provide a referral to a pediatric orthopedist.
Treatment has consisted of containment of the femoral head with the use of splints, although there is little evidence that this treatment alters outcomes.9,10 One study found conflicting evidence that it improved results and does not support its use.9 This is why having a pediatric orthopedist involved in these cases is important.
Long-term prognosis is closely related to the degree of involvement of the femoral head and to the age at onset. Those who are younger than 6 to 8 years typically have the best outcomes, with less hip pain and dysfunction later in life.9,10
SCFE, the most common hip disorder in adolescents, can be easily missed. SCFE has a strong correlation with obesity and is especially common in obese males between the ages of 10 and 16 years who have delayed secondary sex characteristics.2,11 SCFE is generally a mechanical disorder, but in children who are younger than 10 or have low weight or height for their age, an endocrine work-up is indicated.
Symptoms include a painful limp and nonspecific knee, anterior thigh, or groin pain. A delay in diagnosis has a significant effect on complications. Prognosis is also related to the stability of the slip.11,12 An unstable slip is defined as the inability to bear weight.13 The risk of osteonecrosis, a complication of SCFE, is negligible if the slip is stable, but may be as high as 50% when the slip is unstable.2
On examination, internal rotation is painful and limited, and flexion of the hip will lead to simultaneous external rotation. Leg length discrepancy or a positive Trendelenburg’s sign may be present. Diagnosis may be made with bilateral AP (FIGURES 2A AND 2B) and frog lateral radiographic views, looking for growth plate widening.12 Klein’s line—the line that would intersect the epiphysis when drawn along the anterior neck of the femur of an AP view of a normal hip13—is abnormal in a hip with SCFE.
CT or MRI can be performed in patients who have clinical evidence of SCFE but normal radiographs. Treatment is the same regardless of whether the slip is stable or unstable—patients are told to avoid weight bearing and are sent to an orthopedist. Stabilization with in situ pinning is the gold standard, regardless of severity.9,10,12
CASE AP x-rays of Sean’s right hip are abnormal, showing that the femoral epiphysis is not aligned with the femoral neck correctly when compared with the opposite side. You advise the patient and his parents that he has a serious condition called SCFE, which can lead to long-term problems if not treated surgically. You recommend that he start using crutches and remain fully non-weight bearing on his right leg, and refer him to a pediatric orthopedist.
FIGURE 2
Bilateral AP views reveal slipped capital femoral epiphysis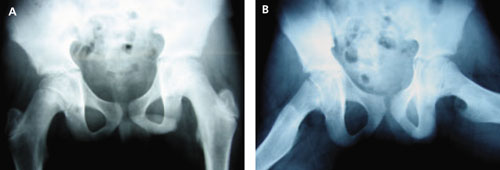
X-rays show the pelvic widening of the physis on the right (A) and the epiphysis slipping posteriorly and inferiorly (B).
Suspect these hip disorders in young athletes
Femoral stress fractures are particularly common in adolescents who are runners or endurance athletes. The classic history is gradual onset of anterior thigh pain, beginning during physical activity and progressing to pain at rest. Risk factors for femoral stress fractures include the female athlete triad (amenorrhea, eating disorder, and osteoporosis), a recent change in training, poor biomechanics, and underlying bone or metabolic disease.14
A positive hop test. The physical exam in a patient with a femoral stress fracture is likely to be normal, with the possible exception of limitation in hip ROM at the extremes. Pain may be reproduced with hopping (a positive result) on the affected leg; 1 study noted that 70% of patients with femoral stress fractures had a positive hop test.15
Hip radiographs should be done, but may not be helpful. In initial x-rays, sensitivity may be as low as 15%; delayed x-rays, taken 2 to 4 weeks later, have a sensitivity of about 50% for findings suggestive of a stress fracture.16
Although bone scan and MRI have approximately equal sensitivity, bone scan is less specific for detecting early stress fractures, so MRI has become the gold standard for diagnosing femoral stress fractures.14 Treatment depends on the location of the fracture. A compression stress fracture on the inferior surface of the femoral neck has a good prognosis when the patient remains non-weight bearing for 6 to 8 weeks, then gradually returns to activity.14
Tension stress fractures are on the superior surface, and patients need to be sent to an orthopedist for internal fixation.14,16 A tension-sided fracture can progress to non-union or avascular necrosis. Training and diet should be modified as indicated to promote healing and prevent recurrence.
Does the patient’s hip make a snapping sound?
Patients with snapping of the hip can be categorized into those whose injuries are painful, and those whose injuries are not. Reassure patients with pain-free snapping that there is no reason to be concerned.
External snapping is usually related to the iliotibial band moving over the greater trochanteric bursa, which can lead to a painful bursa.17 The key symptom, in addition to the snapping, is lateral hip pain of gradual onset. Examination reproduces the pain with the snapping hip maneuver (FIGURES 3A AND 3B).
Internal snapping is related to the iliopsoas tendon passing over the femoral head and hip capsule or over the iliopectineal eminence and bony ridge of the lesser trochanter.17 Inflammation of the iliopsoas bursa may lead to painful snapping. This pain is anterior in location, and the snap can be reproduced with the patient lying on the unaffected side, bringing the affected hip passively from flexed, abducted, and externally rotated to a medial position of extension, adduction, and internal rotation.
Internal and external snapping usually occurs in patients whose activities involve the repetitive motions done in the exam maneuvers. Intra-articular snapping is due to loose bodies or acetabular labral tears.
Imaging for the patient with painful hip snapping consists of hip radiographs—usually negative—and ultrasound. MRI is done if intra-articular pathology is suspected.17 Treatment of snapping hips includes activity modification, NSAIDs, physical therapy, and possible steroid injection. Rarely is the condition surgically treated.
FIGURE 3
Snapping maneuver can help identify source of pain
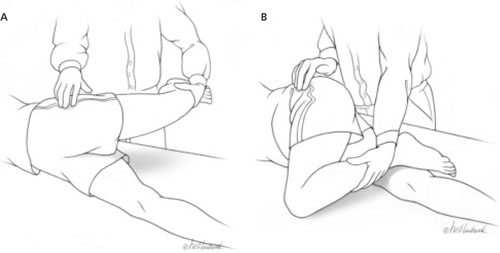
With the patient lying with the unaffected side down, passively abduct the affected hip (A), then move from full extension to 90° of flexion (B). External snapping is usually related to the iliotibial band moving over the greater trochanter, which can lead to a painful bursa.
Avulsion fractures, acetabular tears, and bursitis
Avulsion fractures are a separation of the secondary growth center, the apophyses, from the underlying bone in skeletally immature athletes. They occur because the athlete’s tendons are stronger than the cartilaginous growth centers,10,11,16,18 and are produced by sudden forceful contraction of the muscle. The patient will complain of acute pain and swelling. The exam will be positive for palpable tenderness at the bony site and for muscle weakness. The most common sites of avulsion fractures causing hip pain are the sartorius attachment at the ASIS, the rectus femoris attachment at the anterior inferior iliac spine, and the hamstring attachment onto the ischial tuberosity.10 Radiographs are diagnostic.16,18
Treatment is conservative, including rest, ice, analgesics, and ROM exercises. Advise the patient to refrain from stretching the injured muscle attachment for 6 weeks, then gradually return to activity. Surgery is needed only if there is a large separation (>2 cm).
Acetabular labral tears are seen in athletes of all ages. Pain may be acute from a traumatic event or insidious from repetitive trauma.10 Structural or developmental abnormalities may also predispose certain athletes to injury.10 Patients will complain of pain, snapping, or a “giving way” sensation in the anteromedial area of the hip. On examination, the impingement test—forced flexion/adduction and internal rotation— may reproduce the groin pain, or the snapping maneuver may produce an audible sound.10,16,19
Radiographs are obtained initially to rule out other causes of hip pain and to assess for predisposing abnormalities, such as femoroacetabular impingement. Magnetic resonance arthrogram is a highly sensitive test for labral tears and is usually diagnostic.10 Labral tears are rarely an isolated event, however, and are usually seen in combination with a chondral injury, ligamentum teres tear, synovitis, or loose bodies.10
After diagnosis, a trial of activity modification, NSAIDs, and physical therapy is acceptable. If there is no improvement after 4 to 6 weeks, patients should be referred to an orthopedist for hip arthroscopy. A few studies have found that arthroscopy provides excellent symptom relief in 70% to 90% of patients,10,19 with a return to full activity in 6 to 12 weeks.
Trochanteric bursitis is commonly seen in older adults, but can occur in children. It has been associated with leg length discrepancy and obesity—and, in younger athletes, it is often linked to running and climbing.
The condition is caused by repetitive trauma from contraction of the muscles inserting on the greater trochanter. Patients develop chronic, intermittent lateral hip pain, which may be worse with direct pressure. The predominant physical exam finding is pain with direct pressure over the greater trochanter. One study reported that >50% of patients with trochanteric bursitis had a positive Patrick’s test—the presence of pain with Flexion, ABduction, and External Rotation (FABER) of the affected hip.20
ROM and hip radiographs are typically normal. Diagnosis is clinical, although there is a spectrum of disorders that present with lateral hip pain. The exact source of pain is often unknown and can be from bone, tendon, or bursa. In patients with trochanteric bursitis, gluteus medius tendinopathy or syndrome should also be considered.
Treatment begins with conservative management—starting with heat and NSAIDs for the first 4 weeks, restriction of repetitive motion, correction of any underlying gait disturbance, and performance of passive stretching exercises. If no improvement occurs, a local corticosteroid injection into the point of maximum tenderness can be therapeutic. It can also be diagnostic for trochanteric bursitis if symptom relief is achieved. One study showed a 90% improvement rate with 1 to 3 injections.21,22 More recent studies show the average improvement in symptom relief is in the range of 70% to 100%, but long-term follow-up varies.20
Is an osteoid osteoma to blame?
Osteoid osteomas are common benign skeletal lesions seen in young adults with hip pain, but may be an incidental finding. The average patient age is 10 to 20 years, with males affected more than females. Pain is the predominant symptom, starting as mild and intermittent and progressing to constant and severe. Night pain is common.23 Other symptoms are swelling, deformity, or limp.
Dramatic relief of pain with aspirin or NSAIDs is a diagnostic sign of osteoid osteoma. Diagnosis is made by radiographs. Treatment is surgical excision of the osteoid osteoma nidus, resulting in a good long-term prognosis.23
CORRESPONDENCE Janna Johanns, MD, Montana Family Medicine Residency, 123 South 27th Street, Billings, MT 59101; [email protected]
1. Haueisen DC, Weiner DS, Weiner SD. The characterization of “transient synovitis of the hip” in children. J Pediatr Orthop. 1986;6:11-17.
2. Frick S. Evaluation of the child who has hip pain. Orthop Clin North Am. 2006;37:133-140.
3. Bennett OM, Namnyak SS. Acute septic arthritis of the hip joint in infancy and childhood. Clin Orthop Relat Res. 1992;281:123-132.
4. Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction alogrithm. J Bone Joint. 1999;81:1662-1670.
5. Adkins SB, III, Figler RA. Hip pain in athletes. Am Fam Physician. 2000;61:2109-2118.
6. Liu RW, Abaza H, Gilmore A. The limping child in the urgent care center. J Urgent Care Med. 2007;2:11-22.
7. Leet AI, Skaggs DL. Evaluation of the acutely limping child. Am Fam Physician. 2000;61:1011-1018.
8. Landin LA, Danielson LG, Wattsgard CW. Transient synovitis of the hip. Its incidence, epidemiology, and relation to Perthes’ disease. J Bone Joint Surg. 1987;69:238-242.
9. Weinstein SL. Bristol-Myers Squibb/Zimmer award for distinguished achievement in orthopaedic research. Long term follow-up of pediatric orthopedic conditions. J Bone Joint Surg. 2000;82-A:980-990.
10. Kocher MS, Tucker R. Pediatric athlete hip disorders. Clin Sports Med. 2006;25:241-253.
11. Lacroix VJ. A complete approach to groin pain. Phys Sportsmed. 2000;28:66-86.
12. Tokmakova KP, Stanton RP, Mason DE. Factors influencing the development of osteonecrosis in patients treated for slipped capital femoral epiphysis. J Bone Joint Surg Am. 2003;85:798-801.
13. Reynolds R. Diagnosis and treatment of slipped capital femoral epiphysis. Curr Opin Pediatr. 1999;11:80-83.
14. Heyworth BE, Green DW. Lower extremity stress fractures in pediatric and adolescent athletes. Curr Opin Pediatr. 2008;20:58-61.
15. Clement DB, Ammann W, Taunton JE, et al. Exercise-induced stress injuries to the femur. Int J Sports Med. 1993;14:347-352.
16. Ecklund K. Magnetic resonance imaging of pediatric musculoskeletal trauma. Top Magn Reson Imaging. 2002;13:203-217.
17. Idjadi J, Meislin R. Symptomatic snapping hip. Phys Sportsmed. 2004;32:25-31.
18. Paluska SA. An overview of hip injuries in running. Sports Med. 2005;35:991-1014.
19. Larson C, Swaringen J, Morrison G. Evaluation and management of hip pain. The emerging role of hip arthroscopy. Phys Sportsmed. 2005;33:26-32.
20. Shbeeb MI, Matteson EL. Trochanteric bursitis (greater trochanteric pain syndrome). Mayo Clin Proc. 1996;71:565-569.
21. Schapira D, Nahir M, Scharf Y. Trochanteric bursitis: a common clinical problem. Arch Phys Med Rehab. 1986;67:815-817.
22. Ege Rasmussen KJ, Fano N. Trochanteric bursitis. Treatment by corticosteroid injection. Scand J Rheumatol. 1985;14:417-420.
23. Kransdorf MJ, Stull MA, Gilkey FW, et al. Osteoid osteoma. Radiographics. 1991;11:671-696.
• When you suspect an infectious cause of hip pain, immediately order laboratory studies, blood cultures, and hip radiographs to rule out septic arthritis. A
• When you suspect avascular necrosis of the femoral head, instruct the patient to remain non-weight bearing and provide a referral to an orthopedist. A
• Stabilization with in situ pinning is the gold standard treatment for slipped capital femoral epiphysis, whether the slip is stable or unstable. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Sean L, a 12-year-old middle school student in the 90th percentile for weight, limps into your office and reports that it hurts to put his full weight down on his right leg. The pain just started, Sean says, but he began limping a day or 2 earlier. Sean plays on his school’s football team, and he wants to know what you can give him to relieve the pain so he won’t have to miss any games. What can you tell him?
Family physicians are increasingly likely to see children and adolescents with hip pain, the combined result of greater sports participation and a surge in childhood obesity. Diagnosing pediatric hip pain can be a daunting task, not only because of the complexity of the hip joint, but because of the need to consider bone, joint, tendon, muscle, bursa, and referred pain in the differential diagnosis.
But it doesn’t have to be. Being familiar with the major causes of pediatric hip pain, the diagnostic tests and maneuvers that are part of a comprehensive work-up, and the conditions that require rapid referral to an orthopedist makes it possible to adopt a straightforward approach. We’ve developed this review with that goal in mind.
Assess pain and movement with these maneuvers and tests
Begin with a pain history, determining the location of the hip pain—anterior, lateral, or posterior. Ask the patient to describe the pain and its quality: Is it diffuse, localized, or radiating? Identify any aggravating or relieving factors, and question the patient (or parents) about the onset, reproducibility, and timing of the pain, including the presence or absence of nighttime pain.
Find out, too, whether the pain is causing a limp; what effect, if any, the pain has had on the patient’s ability to bear weight; and to what extent the patient’s activity level has been affected. Then move on to the physical examination.
Begin with the patient standing up. Observe his or her gait, posture, and alignment. Check for Trendelenburg’s sign, in which the ipsilateral hip drops when the patient raises the unaffected leg. Its presence indicates a weakness of the opposite hip abductor.
With the patient in a supine position, inspect the hip for swelling, erythema, and warmth. Palpate the affected area, but keep in mind that palpation may not always reveal much because of the depth of the hip joint. If the patient is overweight, palpation of the muscles, tendons, or bones may be particularly difficult.
Test active and passive range of motion (ROM) and muscle strength of the hip in all directions. (Patients who are unable to tolerate lying down can undergo most of the ROM and strength tests in a seated position.) Check for a discrepancy in leg length, not only by visual inspection, but by measuring from the anterior superior iliac spine (ASIS) to the lateral malleoli.
Perform more focused maneuvers, as needed. If lumbar radiculopathy is a possibility, for example, do a straight leg raise, lifting the leg on the affected side in full extension with the ankle dorsiflexed, and repeat with the leg on the unaffected side. The test is positive if radiating pain down the affected leg and buttock is reproduced at ≤60° of leg elevation (or leg extension if the patient is seated). Conduct Ober’s test (FIGURE 1) to check for iliotibial band syndrome.
Follow with a system review, asking about recent conditions, including fever and infection, trauma, and constitutional, abdominal, and genitourinary symptoms. Perform an abdominal exam, and, if indicated, a pelvic or hernia exam. Check reflexes and sensation, as warranted, and examine the spine and knee.
CASE Sean is a healthy boy with no known medical problems. He has not been ill recently, and has not had any unexplained weight loss. His vital signs are normal, and he does not appear ill. He walks with a limp.
On examination, Sean has no palpable area of tenderness, swelling, or ecchymosis. His right hip has limited and painful internal rotation and, when flexed, it falls out to the side in external rotation.
FIGURE 1
Ober’s test for iliotibial band syndrome
With the patient lying on the unaffected side, passively extend the affected leg and allow the knee to drop. The test is positive if the patient experiences pain along the lateral side of the thigh or the knee does not drop down to the table.
Hip pain and infection? Consider septic arthritis
Is your patient febrile or recovering from an infection? When you suspect an acute infectious cause of hip pain, there are 2 disorders to consider in the differential diagnosis: transient synovitis (TS) and septic arthritis. Both are associated with an acute onset of pain and limping or non-weight bearing, and generally affect young children: Septic arthritis is most common in children between the age of 3 and 6 years, while the typical age range for TS is 3 through 8.1-4
There are other important differences. TS is a benign, self-limited, and common cause of hip pain in young children,5 which may be preceded by a viral infection.1 Septic arthritis is a serious condition that requires rapid identification; a delay in treatment can cause significant long-term morbidity. Complications may include early arthritis, shortened limb, dislocation, and osteonecrosis.
Because it can be difficult to distinguish between septic arthritis and TS, multiple studies have looked at the best way to make that determination. 1-7
The criteria most commonly used to identify septic arthritis are:
- fever
- refusal to bear weight
- erythrocyte sedimentation rate (ESR) >40 mm/h
- white blood cell count >12,000 mm3.
One study showed a predictive probability of 97% for septic arthritis when 3 of the 4 above criteria were present, and 99% if the patient had all 4.2,4 Other studies added 2 additional criteria—C-reactive protein (CRP) >1 mg/dL and medial joint space widening of >2 mm—with similar predictive probabilities (93% and 99%, respectively, if 3 or 4 of the 6 criteria were positive).2,4,6
Order lab work (ESR, CRP, complete blood count, and blood cultures) for any young patient whose hip pain is thought to be associated with an infectious process. Obtain hip anterior/posterior (AP) and frog lateral radiographs to look for joint space widening, as well.1-4
In addition to the above criteria, suspect septic arthritis in a child who presents with acute onset of hip pain, looks ill, and has limited ROM—particularly with internal rotation. In contrast, children with TS do not look sick and, while they often have limited ROM, it is primarily just at extremes. A modified log roll test can be used to assess the rotation of the hip.
An ultrasound-guided aspiration of fluid is the gold standard for septic arthritis diagnosis. Treatment is emergent surgical drainage and parenteral antibiotics, which should be withheld until fluid is aspirated or the joint is surgically drained. The most common causative organism is Staphylococcus aureus.3,7
It is reasonable to withhold joint aspiration for patients who don’t look sick and have normal labs and reliable follow-up, and to watch closely, with conservative management including nonsteroidal anti-inflammatory drugs (NSAIDs) and activity, as tolerated, instead.
There is some concern that TS may lead to Legg-Calves-Perthe’s disease, also known as avascular necrosis of the femoral head, although there is no strong evidence to support it. To be safe, however, obtain radiographs 2 to 18 months after TS resolves to check for further damage or complications.1,8
Femoral head disorders: When x-rays help, when they don’t
There are 2 femoral head disorders that commonly affect children and adolescents: Avascular necrosis of the femoral head and slipped capital femoral epiphysis (SCFE). Age alone is a clue to detection; children with avascular necrosis tend to be younger than those with SCFE.
Avascular necrosis of the femoral head is most commonly seen in children between the ages of 4 and 8 years, and occurs more frequently in boys than in girls. Although there is disagreement about the etiology of avascular necrosis, the condition is thought to result from a disruption in femoral blood supply, leading to osteonecrosis and flattening of the weight-bearing surface of the femoral head. One study found that structural abnormalities in the epiphyseal cartilage may lead to collapse.9
The condition often begins with a painless limp that develops—typically in 1 to 3 months—into groin, thigh, or knee pain; worsens with activity; and is relieved with rest.5 Abduction and internal rotation are limited on exam.
In patients with avascular necrosis, hip AP and frog lateral radiographs are diagnostic, with evidence of increased density of 1 epiphysis and flattening or fragmentation of the femoral head.7 When you suspect avascular necrosis, advise the patient to avoid weight bearing—and provide a referral to a pediatric orthopedist.
Treatment has consisted of containment of the femoral head with the use of splints, although there is little evidence that this treatment alters outcomes.9,10 One study found conflicting evidence that it improved results and does not support its use.9 This is why having a pediatric orthopedist involved in these cases is important.
Long-term prognosis is closely related to the degree of involvement of the femoral head and to the age at onset. Those who are younger than 6 to 8 years typically have the best outcomes, with less hip pain and dysfunction later in life.9,10
SCFE, the most common hip disorder in adolescents, can be easily missed. SCFE has a strong correlation with obesity and is especially common in obese males between the ages of 10 and 16 years who have delayed secondary sex characteristics.2,11 SCFE is generally a mechanical disorder, but in children who are younger than 10 or have low weight or height for their age, an endocrine work-up is indicated.
Symptoms include a painful limp and nonspecific knee, anterior thigh, or groin pain. A delay in diagnosis has a significant effect on complications. Prognosis is also related to the stability of the slip.11,12 An unstable slip is defined as the inability to bear weight.13 The risk of osteonecrosis, a complication of SCFE, is negligible if the slip is stable, but may be as high as 50% when the slip is unstable.2
On examination, internal rotation is painful and limited, and flexion of the hip will lead to simultaneous external rotation. Leg length discrepancy or a positive Trendelenburg’s sign may be present. Diagnosis may be made with bilateral AP (FIGURES 2A AND 2B) and frog lateral radiographic views, looking for growth plate widening.12 Klein’s line—the line that would intersect the epiphysis when drawn along the anterior neck of the femur of an AP view of a normal hip13—is abnormal in a hip with SCFE.
CT or MRI can be performed in patients who have clinical evidence of SCFE but normal radiographs. Treatment is the same regardless of whether the slip is stable or unstable—patients are told to avoid weight bearing and are sent to an orthopedist. Stabilization with in situ pinning is the gold standard, regardless of severity.9,10,12
CASE AP x-rays of Sean’s right hip are abnormal, showing that the femoral epiphysis is not aligned with the femoral neck correctly when compared with the opposite side. You advise the patient and his parents that he has a serious condition called SCFE, which can lead to long-term problems if not treated surgically. You recommend that he start using crutches and remain fully non-weight bearing on his right leg, and refer him to a pediatric orthopedist.
FIGURE 2
Bilateral AP views reveal slipped capital femoral epiphysis
X-rays show the pelvic widening of the physis on the right (A) and the epiphysis slipping posteriorly and inferiorly (B).
Suspect these hip disorders in young athletes
Femoral stress fractures are particularly common in adolescents who are runners or endurance athletes. The classic history is gradual onset of anterior thigh pain, beginning during physical activity and progressing to pain at rest. Risk factors for femoral stress fractures include the female athlete triad (amenorrhea, eating disorder, and osteoporosis), a recent change in training, poor biomechanics, and underlying bone or metabolic disease.14
A positive hop test. The physical exam in a patient with a femoral stress fracture is likely to be normal, with the possible exception of limitation in hip ROM at the extremes. Pain may be reproduced with hopping (a positive result) on the affected leg; 1 study noted that 70% of patients with femoral stress fractures had a positive hop test.15
Hip radiographs should be done, but may not be helpful. In initial x-rays, sensitivity may be as low as 15%; delayed x-rays, taken 2 to 4 weeks later, have a sensitivity of about 50% for findings suggestive of a stress fracture.16
Although bone scan and MRI have approximately equal sensitivity, bone scan is less specific for detecting early stress fractures, so MRI has become the gold standard for diagnosing femoral stress fractures.14 Treatment depends on the location of the fracture. A compression stress fracture on the inferior surface of the femoral neck has a good prognosis when the patient remains non-weight bearing for 6 to 8 weeks, then gradually returns to activity.14
Tension stress fractures are on the superior surface, and patients need to be sent to an orthopedist for internal fixation.14,16 A tension-sided fracture can progress to non-union or avascular necrosis. Training and diet should be modified as indicated to promote healing and prevent recurrence.
Does the patient’s hip make a snapping sound?
Patients with snapping of the hip can be categorized into those whose injuries are painful, and those whose injuries are not. Reassure patients with pain-free snapping that there is no reason to be concerned.
External snapping is usually related to the iliotibial band moving over the greater trochanteric bursa, which can lead to a painful bursa.17 The key symptom, in addition to the snapping, is lateral hip pain of gradual onset. Examination reproduces the pain with the snapping hip maneuver (FIGURES 3A AND 3B).
Internal snapping is related to the iliopsoas tendon passing over the femoral head and hip capsule or over the iliopectineal eminence and bony ridge of the lesser trochanter.17 Inflammation of the iliopsoas bursa may lead to painful snapping. This pain is anterior in location, and the snap can be reproduced with the patient lying on the unaffected side, bringing the affected hip passively from flexed, abducted, and externally rotated to a medial position of extension, adduction, and internal rotation.
Internal and external snapping usually occurs in patients whose activities involve the repetitive motions done in the exam maneuvers. Intra-articular snapping is due to loose bodies or acetabular labral tears.
Imaging for the patient with painful hip snapping consists of hip radiographs—usually negative—and ultrasound. MRI is done if intra-articular pathology is suspected.17 Treatment of snapping hips includes activity modification, NSAIDs, physical therapy, and possible steroid injection. Rarely is the condition surgically treated.
FIGURE 3
Snapping maneuver can help identify source of pain
With the patient lying with the unaffected side down, passively abduct the affected hip (A), then move from full extension to 90° of flexion (B). External snapping is usually related to the iliotibial band moving over the greater trochanter, which can lead to a painful bursa.
Avulsion fractures, acetabular tears, and bursitis
Avulsion fractures are a separation of the secondary growth center, the apophyses, from the underlying bone in skeletally immature athletes. They occur because the athlete’s tendons are stronger than the cartilaginous growth centers,10,11,16,18 and are produced by sudden forceful contraction of the muscle. The patient will complain of acute pain and swelling. The exam will be positive for palpable tenderness at the bony site and for muscle weakness. The most common sites of avulsion fractures causing hip pain are the sartorius attachment at the ASIS, the rectus femoris attachment at the anterior inferior iliac spine, and the hamstring attachment onto the ischial tuberosity.10 Radiographs are diagnostic.16,18
Treatment is conservative, including rest, ice, analgesics, and ROM exercises. Advise the patient to refrain from stretching the injured muscle attachment for 6 weeks, then gradually return to activity. Surgery is needed only if there is a large separation (>2 cm).
Acetabular labral tears are seen in athletes of all ages. Pain may be acute from a traumatic event or insidious from repetitive trauma.10 Structural or developmental abnormalities may also predispose certain athletes to injury.10 Patients will complain of pain, snapping, or a “giving way” sensation in the anteromedial area of the hip. On examination, the impingement test—forced flexion/adduction and internal rotation— may reproduce the groin pain, or the snapping maneuver may produce an audible sound.10,16,19
Radiographs are obtained initially to rule out other causes of hip pain and to assess for predisposing abnormalities, such as femoroacetabular impingement. Magnetic resonance arthrogram is a highly sensitive test for labral tears and is usually diagnostic.10 Labral tears are rarely an isolated event, however, and are usually seen in combination with a chondral injury, ligamentum teres tear, synovitis, or loose bodies.10
After diagnosis, a trial of activity modification, NSAIDs, and physical therapy is acceptable. If there is no improvement after 4 to 6 weeks, patients should be referred to an orthopedist for hip arthroscopy. A few studies have found that arthroscopy provides excellent symptom relief in 70% to 90% of patients,10,19 with a return to full activity in 6 to 12 weeks.
Trochanteric bursitis is commonly seen in older adults, but can occur in children. It has been associated with leg length discrepancy and obesity—and, in younger athletes, it is often linked to running and climbing.
The condition is caused by repetitive trauma from contraction of the muscles inserting on the greater trochanter. Patients develop chronic, intermittent lateral hip pain, which may be worse with direct pressure. The predominant physical exam finding is pain with direct pressure over the greater trochanter. One study reported that >50% of patients with trochanteric bursitis had a positive Patrick’s test—the presence of pain with Flexion, ABduction, and External Rotation (FABER) of the affected hip.20
ROM and hip radiographs are typically normal. Diagnosis is clinical, although there is a spectrum of disorders that present with lateral hip pain. The exact source of pain is often unknown and can be from bone, tendon, or bursa. In patients with trochanteric bursitis, gluteus medius tendinopathy or syndrome should also be considered.
Treatment begins with conservative management—starting with heat and NSAIDs for the first 4 weeks, restriction of repetitive motion, correction of any underlying gait disturbance, and performance of passive stretching exercises. If no improvement occurs, a local corticosteroid injection into the point of maximum tenderness can be therapeutic. It can also be diagnostic for trochanteric bursitis if symptom relief is achieved. One study showed a 90% improvement rate with 1 to 3 injections.21,22 More recent studies show the average improvement in symptom relief is in the range of 70% to 100%, but long-term follow-up varies.20
Is an osteoid osteoma to blame?
Osteoid osteomas are common benign skeletal lesions seen in young adults with hip pain, but may be an incidental finding. The average patient age is 10 to 20 years, with males affected more than females. Pain is the predominant symptom, starting as mild and intermittent and progressing to constant and severe. Night pain is common.23 Other symptoms are swelling, deformity, or limp.
Dramatic relief of pain with aspirin or NSAIDs is a diagnostic sign of osteoid osteoma. Diagnosis is made by radiographs. Treatment is surgical excision of the osteoid osteoma nidus, resulting in a good long-term prognosis.23
CORRESPONDENCE Janna Johanns, MD, Montana Family Medicine Residency, 123 South 27th Street, Billings, MT 59101; [email protected]
• When you suspect an infectious cause of hip pain, immediately order laboratory studies, blood cultures, and hip radiographs to rule out septic arthritis. A
• When you suspect avascular necrosis of the femoral head, instruct the patient to remain non-weight bearing and provide a referral to an orthopedist. A
• Stabilization with in situ pinning is the gold standard treatment for slipped capital femoral epiphysis, whether the slip is stable or unstable. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Sean L, a 12-year-old middle school student in the 90th percentile for weight, limps into your office and reports that it hurts to put his full weight down on his right leg. The pain just started, Sean says, but he began limping a day or 2 earlier. Sean plays on his school’s football team, and he wants to know what you can give him to relieve the pain so he won’t have to miss any games. What can you tell him?
Family physicians are increasingly likely to see children and adolescents with hip pain, the combined result of greater sports participation and a surge in childhood obesity. Diagnosing pediatric hip pain can be a daunting task, not only because of the complexity of the hip joint, but because of the need to consider bone, joint, tendon, muscle, bursa, and referred pain in the differential diagnosis.
But it doesn’t have to be. Being familiar with the major causes of pediatric hip pain, the diagnostic tests and maneuvers that are part of a comprehensive work-up, and the conditions that require rapid referral to an orthopedist makes it possible to adopt a straightforward approach. We’ve developed this review with that goal in mind.
Assess pain and movement with these maneuvers and tests
Begin with a pain history, determining the location of the hip pain—anterior, lateral, or posterior. Ask the patient to describe the pain and its quality: Is it diffuse, localized, or radiating? Identify any aggravating or relieving factors, and question the patient (or parents) about the onset, reproducibility, and timing of the pain, including the presence or absence of nighttime pain.
Find out, too, whether the pain is causing a limp; what effect, if any, the pain has had on the patient’s ability to bear weight; and to what extent the patient’s activity level has been affected. Then move on to the physical examination.
Begin with the patient standing up. Observe his or her gait, posture, and alignment. Check for Trendelenburg’s sign, in which the ipsilateral hip drops when the patient raises the unaffected leg. Its presence indicates a weakness of the opposite hip abductor.
With the patient in a supine position, inspect the hip for swelling, erythema, and warmth. Palpate the affected area, but keep in mind that palpation may not always reveal much because of the depth of the hip joint. If the patient is overweight, palpation of the muscles, tendons, or bones may be particularly difficult.
Test active and passive range of motion (ROM) and muscle strength of the hip in all directions. (Patients who are unable to tolerate lying down can undergo most of the ROM and strength tests in a seated position.) Check for a discrepancy in leg length, not only by visual inspection, but by measuring from the anterior superior iliac spine (ASIS) to the lateral malleoli.
Perform more focused maneuvers, as needed. If lumbar radiculopathy is a possibility, for example, do a straight leg raise, lifting the leg on the affected side in full extension with the ankle dorsiflexed, and repeat with the leg on the unaffected side. The test is positive if radiating pain down the affected leg and buttock is reproduced at ≤60° of leg elevation (or leg extension if the patient is seated). Conduct Ober’s test (FIGURE 1) to check for iliotibial band syndrome.
Follow with a system review, asking about recent conditions, including fever and infection, trauma, and constitutional, abdominal, and genitourinary symptoms. Perform an abdominal exam, and, if indicated, a pelvic or hernia exam. Check reflexes and sensation, as warranted, and examine the spine and knee.
CASE Sean is a healthy boy with no known medical problems. He has not been ill recently, and has not had any unexplained weight loss. His vital signs are normal, and he does not appear ill. He walks with a limp.
On examination, Sean has no palpable area of tenderness, swelling, or ecchymosis. His right hip has limited and painful internal rotation and, when flexed, it falls out to the side in external rotation.
FIGURE 1
Ober’s test for iliotibial band syndrome
With the patient lying on the unaffected side, passively extend the affected leg and allow the knee to drop. The test is positive if the patient experiences pain along the lateral side of the thigh or the knee does not drop down to the table.
Hip pain and infection? Consider septic arthritis
Is your patient febrile or recovering from an infection? When you suspect an acute infectious cause of hip pain, there are 2 disorders to consider in the differential diagnosis: transient synovitis (TS) and septic arthritis. Both are associated with an acute onset of pain and limping or non-weight bearing, and generally affect young children: Septic arthritis is most common in children between the age of 3 and 6 years, while the typical age range for TS is 3 through 8.1-4
There are other important differences. TS is a benign, self-limited, and common cause of hip pain in young children,5 which may be preceded by a viral infection.1 Septic arthritis is a serious condition that requires rapid identification; a delay in treatment can cause significant long-term morbidity. Complications may include early arthritis, shortened limb, dislocation, and osteonecrosis.
Because it can be difficult to distinguish between septic arthritis and TS, multiple studies have looked at the best way to make that determination. 1-7
The criteria most commonly used to identify septic arthritis are:
- fever
- refusal to bear weight
- erythrocyte sedimentation rate (ESR) >40 mm/h
- white blood cell count >12,000 mm3.
One study showed a predictive probability of 97% for septic arthritis when 3 of the 4 above criteria were present, and 99% if the patient had all 4.2,4 Other studies added 2 additional criteria—C-reactive protein (CRP) >1 mg/dL and medial joint space widening of >2 mm—with similar predictive probabilities (93% and 99%, respectively, if 3 or 4 of the 6 criteria were positive).2,4,6
Order lab work (ESR, CRP, complete blood count, and blood cultures) for any young patient whose hip pain is thought to be associated with an infectious process. Obtain hip anterior/posterior (AP) and frog lateral radiographs to look for joint space widening, as well.1-4
In addition to the above criteria, suspect septic arthritis in a child who presents with acute onset of hip pain, looks ill, and has limited ROM—particularly with internal rotation. In contrast, children with TS do not look sick and, while they often have limited ROM, it is primarily just at extremes. A modified log roll test can be used to assess the rotation of the hip.
An ultrasound-guided aspiration of fluid is the gold standard for septic arthritis diagnosis. Treatment is emergent surgical drainage and parenteral antibiotics, which should be withheld until fluid is aspirated or the joint is surgically drained. The most common causative organism is Staphylococcus aureus.3,7
It is reasonable to withhold joint aspiration for patients who don’t look sick and have normal labs and reliable follow-up, and to watch closely, with conservative management including nonsteroidal anti-inflammatory drugs (NSAIDs) and activity, as tolerated, instead.
There is some concern that TS may lead to Legg-Calves-Perthe’s disease, also known as avascular necrosis of the femoral head, although there is no strong evidence to support it. To be safe, however, obtain radiographs 2 to 18 months after TS resolves to check for further damage or complications.1,8
Femoral head disorders: When x-rays help, when they don’t
There are 2 femoral head disorders that commonly affect children and adolescents: Avascular necrosis of the femoral head and slipped capital femoral epiphysis (SCFE). Age alone is a clue to detection; children with avascular necrosis tend to be younger than those with SCFE.
Avascular necrosis of the femoral head is most commonly seen in children between the ages of 4 and 8 years, and occurs more frequently in boys than in girls. Although there is disagreement about the etiology of avascular necrosis, the condition is thought to result from a disruption in femoral blood supply, leading to osteonecrosis and flattening of the weight-bearing surface of the femoral head. One study found that structural abnormalities in the epiphyseal cartilage may lead to collapse.9
The condition often begins with a painless limp that develops—typically in 1 to 3 months—into groin, thigh, or knee pain; worsens with activity; and is relieved with rest.5 Abduction and internal rotation are limited on exam.
In patients with avascular necrosis, hip AP and frog lateral radiographs are diagnostic, with evidence of increased density of 1 epiphysis and flattening or fragmentation of the femoral head.7 When you suspect avascular necrosis, advise the patient to avoid weight bearing—and provide a referral to a pediatric orthopedist.
Treatment has consisted of containment of the femoral head with the use of splints, although there is little evidence that this treatment alters outcomes.9,10 One study found conflicting evidence that it improved results and does not support its use.9 This is why having a pediatric orthopedist involved in these cases is important.
Long-term prognosis is closely related to the degree of involvement of the femoral head and to the age at onset. Those who are younger than 6 to 8 years typically have the best outcomes, with less hip pain and dysfunction later in life.9,10
SCFE, the most common hip disorder in adolescents, can be easily missed. SCFE has a strong correlation with obesity and is especially common in obese males between the ages of 10 and 16 years who have delayed secondary sex characteristics.2,11 SCFE is generally a mechanical disorder, but in children who are younger than 10 or have low weight or height for their age, an endocrine work-up is indicated.
Symptoms include a painful limp and nonspecific knee, anterior thigh, or groin pain. A delay in diagnosis has a significant effect on complications. Prognosis is also related to the stability of the slip.11,12 An unstable slip is defined as the inability to bear weight.13 The risk of osteonecrosis, a complication of SCFE, is negligible if the slip is stable, but may be as high as 50% when the slip is unstable.2
On examination, internal rotation is painful and limited, and flexion of the hip will lead to simultaneous external rotation. Leg length discrepancy or a positive Trendelenburg’s sign may be present. Diagnosis may be made with bilateral AP (FIGURES 2A AND 2B) and frog lateral radiographic views, looking for growth plate widening.12 Klein’s line—the line that would intersect the epiphysis when drawn along the anterior neck of the femur of an AP view of a normal hip13—is abnormal in a hip with SCFE.
CT or MRI can be performed in patients who have clinical evidence of SCFE but normal radiographs. Treatment is the same regardless of whether the slip is stable or unstable—patients are told to avoid weight bearing and are sent to an orthopedist. Stabilization with in situ pinning is the gold standard, regardless of severity.9,10,12
CASE AP x-rays of Sean’s right hip are abnormal, showing that the femoral epiphysis is not aligned with the femoral neck correctly when compared with the opposite side. You advise the patient and his parents that he has a serious condition called SCFE, which can lead to long-term problems if not treated surgically. You recommend that he start using crutches and remain fully non-weight bearing on his right leg, and refer him to a pediatric orthopedist.
FIGURE 2
Bilateral AP views reveal slipped capital femoral epiphysis
X-rays show the pelvic widening of the physis on the right (A) and the epiphysis slipping posteriorly and inferiorly (B).
Suspect these hip disorders in young athletes
Femoral stress fractures are particularly common in adolescents who are runners or endurance athletes. The classic history is gradual onset of anterior thigh pain, beginning during physical activity and progressing to pain at rest. Risk factors for femoral stress fractures include the female athlete triad (amenorrhea, eating disorder, and osteoporosis), a recent change in training, poor biomechanics, and underlying bone or metabolic disease.14
A positive hop test. The physical exam in a patient with a femoral stress fracture is likely to be normal, with the possible exception of limitation in hip ROM at the extremes. Pain may be reproduced with hopping (a positive result) on the affected leg; 1 study noted that 70% of patients with femoral stress fractures had a positive hop test.15
Hip radiographs should be done, but may not be helpful. In initial x-rays, sensitivity may be as low as 15%; delayed x-rays, taken 2 to 4 weeks later, have a sensitivity of about 50% for findings suggestive of a stress fracture.16
Although bone scan and MRI have approximately equal sensitivity, bone scan is less specific for detecting early stress fractures, so MRI has become the gold standard for diagnosing femoral stress fractures.14 Treatment depends on the location of the fracture. A compression stress fracture on the inferior surface of the femoral neck has a good prognosis when the patient remains non-weight bearing for 6 to 8 weeks, then gradually returns to activity.14
Tension stress fractures are on the superior surface, and patients need to be sent to an orthopedist for internal fixation.14,16 A tension-sided fracture can progress to non-union or avascular necrosis. Training and diet should be modified as indicated to promote healing and prevent recurrence.
Does the patient’s hip make a snapping sound?
Patients with snapping of the hip can be categorized into those whose injuries are painful, and those whose injuries are not. Reassure patients with pain-free snapping that there is no reason to be concerned.
External snapping is usually related to the iliotibial band moving over the greater trochanteric bursa, which can lead to a painful bursa.17 The key symptom, in addition to the snapping, is lateral hip pain of gradual onset. Examination reproduces the pain with the snapping hip maneuver (FIGURES 3A AND 3B).
Internal snapping is related to the iliopsoas tendon passing over the femoral head and hip capsule or over the iliopectineal eminence and bony ridge of the lesser trochanter.17 Inflammation of the iliopsoas bursa may lead to painful snapping. This pain is anterior in location, and the snap can be reproduced with the patient lying on the unaffected side, bringing the affected hip passively from flexed, abducted, and externally rotated to a medial position of extension, adduction, and internal rotation.
Internal and external snapping usually occurs in patients whose activities involve the repetitive motions done in the exam maneuvers. Intra-articular snapping is due to loose bodies or acetabular labral tears.
Imaging for the patient with painful hip snapping consists of hip radiographs—usually negative—and ultrasound. MRI is done if intra-articular pathology is suspected.17 Treatment of snapping hips includes activity modification, NSAIDs, physical therapy, and possible steroid injection. Rarely is the condition surgically treated.
FIGURE 3
Snapping maneuver can help identify source of pain
With the patient lying with the unaffected side down, passively abduct the affected hip (A), then move from full extension to 90° of flexion (B). External snapping is usually related to the iliotibial band moving over the greater trochanter, which can lead to a painful bursa.
Avulsion fractures, acetabular tears, and bursitis
Avulsion fractures are a separation of the secondary growth center, the apophyses, from the underlying bone in skeletally immature athletes. They occur because the athlete’s tendons are stronger than the cartilaginous growth centers,10,11,16,18 and are produced by sudden forceful contraction of the muscle. The patient will complain of acute pain and swelling. The exam will be positive for palpable tenderness at the bony site and for muscle weakness. The most common sites of avulsion fractures causing hip pain are the sartorius attachment at the ASIS, the rectus femoris attachment at the anterior inferior iliac spine, and the hamstring attachment onto the ischial tuberosity.10 Radiographs are diagnostic.16,18
Treatment is conservative, including rest, ice, analgesics, and ROM exercises. Advise the patient to refrain from stretching the injured muscle attachment for 6 weeks, then gradually return to activity. Surgery is needed only if there is a large separation (>2 cm).
Acetabular labral tears are seen in athletes of all ages. Pain may be acute from a traumatic event or insidious from repetitive trauma.10 Structural or developmental abnormalities may also predispose certain athletes to injury.10 Patients will complain of pain, snapping, or a “giving way” sensation in the anteromedial area of the hip. On examination, the impingement test—forced flexion/adduction and internal rotation— may reproduce the groin pain, or the snapping maneuver may produce an audible sound.10,16,19
Radiographs are obtained initially to rule out other causes of hip pain and to assess for predisposing abnormalities, such as femoroacetabular impingement. Magnetic resonance arthrogram is a highly sensitive test for labral tears and is usually diagnostic.10 Labral tears are rarely an isolated event, however, and are usually seen in combination with a chondral injury, ligamentum teres tear, synovitis, or loose bodies.10
After diagnosis, a trial of activity modification, NSAIDs, and physical therapy is acceptable. If there is no improvement after 4 to 6 weeks, patients should be referred to an orthopedist for hip arthroscopy. A few studies have found that arthroscopy provides excellent symptom relief in 70% to 90% of patients,10,19 with a return to full activity in 6 to 12 weeks.
Trochanteric bursitis is commonly seen in older adults, but can occur in children. It has been associated with leg length discrepancy and obesity—and, in younger athletes, it is often linked to running and climbing.
The condition is caused by repetitive trauma from contraction of the muscles inserting on the greater trochanter. Patients develop chronic, intermittent lateral hip pain, which may be worse with direct pressure. The predominant physical exam finding is pain with direct pressure over the greater trochanter. One study reported that >50% of patients with trochanteric bursitis had a positive Patrick’s test—the presence of pain with Flexion, ABduction, and External Rotation (FABER) of the affected hip.20
ROM and hip radiographs are typically normal. Diagnosis is clinical, although there is a spectrum of disorders that present with lateral hip pain. The exact source of pain is often unknown and can be from bone, tendon, or bursa. In patients with trochanteric bursitis, gluteus medius tendinopathy or syndrome should also be considered.
Treatment begins with conservative management—starting with heat and NSAIDs for the first 4 weeks, restriction of repetitive motion, correction of any underlying gait disturbance, and performance of passive stretching exercises. If no improvement occurs, a local corticosteroid injection into the point of maximum tenderness can be therapeutic. It can also be diagnostic for trochanteric bursitis if symptom relief is achieved. One study showed a 90% improvement rate with 1 to 3 injections.21,22 More recent studies show the average improvement in symptom relief is in the range of 70% to 100%, but long-term follow-up varies.20
Is an osteoid osteoma to blame?
Osteoid osteomas are common benign skeletal lesions seen in young adults with hip pain, but may be an incidental finding. The average patient age is 10 to 20 years, with males affected more than females. Pain is the predominant symptom, starting as mild and intermittent and progressing to constant and severe. Night pain is common.23 Other symptoms are swelling, deformity, or limp.
Dramatic relief of pain with aspirin or NSAIDs is a diagnostic sign of osteoid osteoma. Diagnosis is made by radiographs. Treatment is surgical excision of the osteoid osteoma nidus, resulting in a good long-term prognosis.23
CORRESPONDENCE Janna Johanns, MD, Montana Family Medicine Residency, 123 South 27th Street, Billings, MT 59101; [email protected]
1. Haueisen DC, Weiner DS, Weiner SD. The characterization of “transient synovitis of the hip” in children. J Pediatr Orthop. 1986;6:11-17.
2. Frick S. Evaluation of the child who has hip pain. Orthop Clin North Am. 2006;37:133-140.
3. Bennett OM, Namnyak SS. Acute septic arthritis of the hip joint in infancy and childhood. Clin Orthop Relat Res. 1992;281:123-132.
4. Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction alogrithm. J Bone Joint. 1999;81:1662-1670.
5. Adkins SB, III, Figler RA. Hip pain in athletes. Am Fam Physician. 2000;61:2109-2118.
6. Liu RW, Abaza H, Gilmore A. The limping child in the urgent care center. J Urgent Care Med. 2007;2:11-22.
7. Leet AI, Skaggs DL. Evaluation of the acutely limping child. Am Fam Physician. 2000;61:1011-1018.
8. Landin LA, Danielson LG, Wattsgard CW. Transient synovitis of the hip. Its incidence, epidemiology, and relation to Perthes’ disease. J Bone Joint Surg. 1987;69:238-242.
9. Weinstein SL. Bristol-Myers Squibb/Zimmer award for distinguished achievement in orthopaedic research. Long term follow-up of pediatric orthopedic conditions. J Bone Joint Surg. 2000;82-A:980-990.
10. Kocher MS, Tucker R. Pediatric athlete hip disorders. Clin Sports Med. 2006;25:241-253.
11. Lacroix VJ. A complete approach to groin pain. Phys Sportsmed. 2000;28:66-86.
12. Tokmakova KP, Stanton RP, Mason DE. Factors influencing the development of osteonecrosis in patients treated for slipped capital femoral epiphysis. J Bone Joint Surg Am. 2003;85:798-801.
13. Reynolds R. Diagnosis and treatment of slipped capital femoral epiphysis. Curr Opin Pediatr. 1999;11:80-83.
14. Heyworth BE, Green DW. Lower extremity stress fractures in pediatric and adolescent athletes. Curr Opin Pediatr. 2008;20:58-61.
15. Clement DB, Ammann W, Taunton JE, et al. Exercise-induced stress injuries to the femur. Int J Sports Med. 1993;14:347-352.
16. Ecklund K. Magnetic resonance imaging of pediatric musculoskeletal trauma. Top Magn Reson Imaging. 2002;13:203-217.
17. Idjadi J, Meislin R. Symptomatic snapping hip. Phys Sportsmed. 2004;32:25-31.
18. Paluska SA. An overview of hip injuries in running. Sports Med. 2005;35:991-1014.
19. Larson C, Swaringen J, Morrison G. Evaluation and management of hip pain. The emerging role of hip arthroscopy. Phys Sportsmed. 2005;33:26-32.
20. Shbeeb MI, Matteson EL. Trochanteric bursitis (greater trochanteric pain syndrome). Mayo Clin Proc. 1996;71:565-569.
21. Schapira D, Nahir M, Scharf Y. Trochanteric bursitis: a common clinical problem. Arch Phys Med Rehab. 1986;67:815-817.
22. Ege Rasmussen KJ, Fano N. Trochanteric bursitis. Treatment by corticosteroid injection. Scand J Rheumatol. 1985;14:417-420.
23. Kransdorf MJ, Stull MA, Gilkey FW, et al. Osteoid osteoma. Radiographics. 1991;11:671-696.
1. Haueisen DC, Weiner DS, Weiner SD. The characterization of “transient synovitis of the hip” in children. J Pediatr Orthop. 1986;6:11-17.
2. Frick S. Evaluation of the child who has hip pain. Orthop Clin North Am. 2006;37:133-140.
3. Bennett OM, Namnyak SS. Acute septic arthritis of the hip joint in infancy and childhood. Clin Orthop Relat Res. 1992;281:123-132.
4. Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction alogrithm. J Bone Joint. 1999;81:1662-1670.
5. Adkins SB, III, Figler RA. Hip pain in athletes. Am Fam Physician. 2000;61:2109-2118.
6. Liu RW, Abaza H, Gilmore A. The limping child in the urgent care center. J Urgent Care Med. 2007;2:11-22.
7. Leet AI, Skaggs DL. Evaluation of the acutely limping child. Am Fam Physician. 2000;61:1011-1018.
8. Landin LA, Danielson LG, Wattsgard CW. Transient synovitis of the hip. Its incidence, epidemiology, and relation to Perthes’ disease. J Bone Joint Surg. 1987;69:238-242.
9. Weinstein SL. Bristol-Myers Squibb/Zimmer award for distinguished achievement in orthopaedic research. Long term follow-up of pediatric orthopedic conditions. J Bone Joint Surg. 2000;82-A:980-990.
10. Kocher MS, Tucker R. Pediatric athlete hip disorders. Clin Sports Med. 2006;25:241-253.
11. Lacroix VJ. A complete approach to groin pain. Phys Sportsmed. 2000;28:66-86.
12. Tokmakova KP, Stanton RP, Mason DE. Factors influencing the development of osteonecrosis in patients treated for slipped capital femoral epiphysis. J Bone Joint Surg Am. 2003;85:798-801.
13. Reynolds R. Diagnosis and treatment of slipped capital femoral epiphysis. Curr Opin Pediatr. 1999;11:80-83.
14. Heyworth BE, Green DW. Lower extremity stress fractures in pediatric and adolescent athletes. Curr Opin Pediatr. 2008;20:58-61.
15. Clement DB, Ammann W, Taunton JE, et al. Exercise-induced stress injuries to the femur. Int J Sports Med. 1993;14:347-352.
16. Ecklund K. Magnetic resonance imaging of pediatric musculoskeletal trauma. Top Magn Reson Imaging. 2002;13:203-217.
17. Idjadi J, Meislin R. Symptomatic snapping hip. Phys Sportsmed. 2004;32:25-31.
18. Paluska SA. An overview of hip injuries in running. Sports Med. 2005;35:991-1014.
19. Larson C, Swaringen J, Morrison G. Evaluation and management of hip pain. The emerging role of hip arthroscopy. Phys Sportsmed. 2005;33:26-32.
20. Shbeeb MI, Matteson EL. Trochanteric bursitis (greater trochanteric pain syndrome). Mayo Clin Proc. 1996;71:565-569.
21. Schapira D, Nahir M, Scharf Y. Trochanteric bursitis: a common clinical problem. Arch Phys Med Rehab. 1986;67:815-817.
22. Ege Rasmussen KJ, Fano N. Trochanteric bursitis. Treatment by corticosteroid injection. Scand J Rheumatol. 1985;14:417-420.
23. Kransdorf MJ, Stull MA, Gilkey FW, et al. Osteoid osteoma. Radiographics. 1991;11:671-696.
When to suspect atypical cystic fibrosis
• Don’t dismiss a cystic fibrosis diagnosis just because a patient’s sweat chloride levels are <60 mmol/L. A
• Suspect atypical cystic fibrosis in adults with single organ involvement, including mild lung disease, nasal polyposis, recurrent pancreatitis, biliary cirrhosis, portal hypertension, or obstructive azoospermia. A
• Consider respiratory therapies such as tobramycin, hypertonic saline, and recombinant human DNase in cystic fibrosis patients with relatively mild or atypical disease. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1: Lauren W*
Two years ago, Lauren W, a 57-year-old Caucasian woman, sought care at our medical center after learning that her pregnant daughter tested positive during a prenatal cystic fibrosis mutation genetic screen. Lauren had clinical symptoms of malodorous and greasy bowel movements, dyspepsia, early satiety, and a history of recurrent bronchitis since childhood.
According to her history, she did not suffer from failure to thrive as a child. She’d had 5 episodes of adult-onset acute pancreatitis and had 2 surgeries for sinusitis.
On physical exam, we heard no crackles during lung auscultation. Lauren also had mild digital clubbing.
Testing: We ordered a chest x-ray, which revealed left upper lobe atelectasis, but there was no bronchiectasis.
Pulmonary function tests indicated mild obstructive lung disease with forced vital capacity (FVC) 2.39 L or 84% predicted; forced expiratory volume in 1 second (FEV1) 1.59 L or 68% predicted; and an FEV1/FVC of 0.66.
A sweat chloride test was positive on both arms: 77 and 83 mmol/L. Genetic testing revealed compound heterozygosity for cystic fibrosis transmembrane conductance regulator (CFTR) gene mutations Δ F508 and R117H with a 5T allele. To test for pancreatic insufficiency, we performed a 72-hour fecal fat testing while she was on a low-fat diet; it revealed 5.5 g of fat per 24-hour period, suggesting fat malabsorption. Based on positive quantitative sweat test ≥60 mmol/L and the presence of 2 cystic fibrosis–causing mutations, we made the diagnosis of cystic fibrosis.
Treatment: We put Lauren on albuterol and recombinant human DNase respiratory treatments, pancreatic enzymes, and multivitamins with extra lipid-soluble vitamins and calcium supplements. We also continued her low-fat diet of 1500 to 1800 calories per day due to a diagnosis of coronary artery disease.
*Patients’ names have been changed to protect their privacy.
CASE 2: Zack P*
Zack P, a 6-year-old Caucasian boy, was admitted to the hospital with what we suspected was acute gastroenteritis. Serum testing revealed elevated pancreatic enzymes. He had recently sustained an injury to the mid-abdomen during a soccer game and also had a history of chronic sinusitis. One month after his release from the hospital, his symptoms resolved, but his pancreatic enzymes remained elevated (amylase 130 U/L, lipase 177 U/L).
Testing: He underwent 2 sweat chloride tests, which were borderline elevated at 49 mmol/L on the right arm and 40 mmol/L on the left arm; repeat testing was 49 mmol/L on the left arm, 43 mmol/L on the right arm. Genetic testing revealed heterozygosity for CFTR gene mutation Δ F508 with the presence of 7T and 9T allele variants. Over an 8-month period, Zack remained asymptomatic, but his pancreatic enzymes were persistently elevated.
Zack’s physical exam showed that his weight had dropped from the 75th to the 50th percentile. A magnetic resonance cholangiopancreatography indicated homogeneous parenchyma and normal enhancement throughout his pancreas. Similarly, we could not find evidence of acute pancreatitis or biliary or pancreatic duct dilation, and a 72-hour fecal fat study was normal. Given Zack’s borderline sweat chloride, compound heterozygosity of cystic fibrosis mutations, and his phenotype of recurrent pancreatitis, he was given a diagnosis of atypical cystic fibrosis.
Treatment: Based on our diagnostic workup, pancreatic enzyme therapy was not warranted.
*Patients’ names have been changed to protect their privacy.
These 2 cases illustrate how clinically diverse cystic fibrosis can be. The cystic fibrosis phenotype can range from a patient with 2 disease-causing cystic fibrosis mutations with significant sweat gland dysfunction and childhood onset of mild cystic fibrosis symptomatology with normal growth—Lauren—to a patient who is CFTR heterozygous with pancreatitis and a borderline sweat chloride concentration—Zack. Both cases emphasize the need to think “outside the box” and not expect all patients with cystic fibrosis to come in with typical signs and symptoms.
What does the “nonclassic” cystic fibrosis patient look like?
Patients with cystic fibrosis are usually diagnosed during childhood with pulmonary disease, pancreatic insufficiency, malabsorption, malnutrition, elevated sweat chloride, and male infertility. But more recently, patients have been diagnosed in adulthood because either they lacked significant clinical symptoms in childhood or they came in with atypical signs or symptoms (pancreatic sufficiency and sweat chloride <60 mmol/L).
In the past, cystic fibrosis patients rarely lived past their second decade, but those with atypical cystic fibrosis tend to have milder disease, including less severe respiratory signs and symptoms. The good news is that often translates into a long lifespan.1 As recently as 2005, the Cystic Fibrosis Foundation had listed a median survival age of 37.2 Advances in respiratory, gastrointestinal, and nutritional therapies have significantly contributed to the increased survival of these patients. Unfortunately, such milder cases can easily go undetected.
Sweat chloride testing remains a gold standard for the diagnosis of cystic fibrosis. As previously mentioned, classic cystic fibrosis patients are typically diagnosed during childhood and have a sweat chloride concentration ≥60 mmol/L and more severe multiorgan involvement (sinopulmonary and gastrointestinal disease with failure to thrive).
There are 5 classes of CFTR mutations that result in compromised CFTR function: The presence of 2 severe CFTR mutations (classes I-III) completely abolishes CFTR function. It is diagnosed in childhood and usually results in the classic clinical features of pancreatic insufficiency and failure to thrive. However, patients who are compound heterozygous for the milder CFTR mutations (classes IV and V) experience partial CFTR function, which in turn results in atypical features such as pancreatic sufficiency and normal or borderline sweat chloride concentrations. That makes the diagnosis more elusive during early childhood.1,3
The severity of sweat gland and exocrine pancreatic dysfunction produced by a cystic fibrosis mutation depends on the class of CFTR gene mutation and the level of CFTR gene and protein expression.4,5 In certain genetic backgrounds, the 5T allele associated with a high number of TG (thymine/guanine) repeats found in compound heterozygosity with a disease-causing CFTR mutation acts as a “mild CFTR mutation,” resulting in the nonclassic cystic fibrosis phenotype.3 Individuals with atypical cystic fibrosis diagnosed later in life may have single organ involvement, such as mild lung disease, nasal polyposis, recurrent pancreatitis, biliary cirrhosis, portal hypertension, or obstructive azoospermia.1
Lauren had several classic cystic fibrosis features, including recurrent lung disease, pancreatic insufficiency, and sweat gland dysfunction, but it’s likely that her relatively mild pulmonary presentation, normal body mass index, and lack of failure to thrive led to a delay in her diagnosis.
Some patients with atypical cystic fibrosis seek care for idiopathic chronic pancreatitis (ICP), and researchers have found a link between ICP and CFTR gene mutations. For instance, recent studies of ICP patients compared with geographically and ethnically matched controls revealed a higher frequency of abnormal CFTR alleles in the ICP population.6,7 Milder CFTR mutations resulting in partial CFTR function have also been associated with ICP.7,8
Zack was heterozygous for Δ F508, a common CFTR mutation in the Caucasian population. Cohn et al found a higher frequency of this mutation in ICP patients from Europe (mostly English, Italian, and Czech).9 Poly T allele variants such as 5T, 7T, and 9T have not been associated with a higher frequency of ICP.6,7
Early detection may translate into better treatment
Although patients diagnosed with cystic fibrosis as adults are less likely to present with classic clinical features, they may develop bronchiectasis and advanced lung disease.10,11 Those who are identified early on—including those who are asymptomatic and have normal lung function—may benefit from respiratory therapy to prevent or delay lung disease.12 Several studies have shown that patients with mild cystic fibrosis disease and stable spirometry results have evidence of bronchiectasis on their x-rays and advanced lung disease that appears on high-resolution CT.13,14
Judge et al have suggested that mucus plugging occurs early in cystic fibrosis lung disease and at a milder stage of lung function impairment, and that bronchiectasis may be an end result of such abnormalities.14 Nonclassic cystic fibrosis patients often have episodes of “bronchitis,” and once the practitioner becomes concerned, the radiographic image may already show evidence of bronchiectasis. Once again, this emphasizes the importance of early detection and prompt treatment.15
CASE 1: Lauren
Unfortunately, Lauren was unable to benefit from early use of respiratory therapies like tobramycin, hypertonic saline, and recombinant human DNase. She began these treatments after developing advanced lung disease. Studies have shown that tobramycin, long-term inhaled hypertonic saline, and recombinant human DNase can reduce the number of pulmonary exacerbations and increase both FVC and FEV1 values in previously stable cystic fibrosis patients.16-18
Similarly, because Lauren’s pancreatitis was due to pancreatic insufficiency, early recognition of pancreatic insufficiency and enzyme therapy may have greatly reduced the number and severity of her pancreatic episodes.19
Unfortunately, over the last few years, Lauren’s lung function has declined and she has been hospitalized for cystic fibrosis exacerbations and sinusitis; she has had 3 additional episodes of acute pancreatitis. Although her FEV1 is lower than on initial evaluation, she is clinically stable.
CASE 2: Zack
Clinically, Zack is stable and his recent amylase and lipase are elevated at 92 U/L and 71 U/L, respectively. He has had no acute exacerbations.
Patients like Lauren and Zack serve to remind us of the need to recognize and closely monitor patients with nonclassic cystic fibrosis. These patients may come to the office with “asthma-like” symptoms, bronchitis, polyps, pancreatitis, cholelithiasis, constipation, abdominal bloating/flatus, and infertility. Because their symptoms may not be severe enough to be referred to a subspecialist, family physicians play a critical role in recognizing these overlooked cases early on.
CORRESPONDENCE Anupama Chawla, MD, Director, Division of Pediatric Gastroenterology and Nutrition, Stony Brook University Hospital, Stony Brook, NY 11794; [email protected]
1. Kerem E. Atypical CF and CF related diseases. Paediatr Respir Rev. 2006;7(suppl 1):S144-S146.
2. Cystic Fibrosis Foundation. Cystic Fibrosis Foundation Annual Patient Registry Data Report 2005. Bethesda, Md; 2006.
3. Castellani C, Cuppens H, Macek M, Jr, et al. Consensus on the use and interpretation of cystic fibrosis mutation analysis in clinical practice. J Cyst Fibros. 2008;7:179-196.
4. Wilchanski M, Zielenski J, Markiewicz D. Correlation of sweat chloride concentration with classes of the cystic fibrosis trans-membrane conductance regulator gene mutation, J Pediatr. 1995;127:705-710.
5. Mickle JE, Cutting GR. Genotype-phenotype relationships in cystic fibrosis. Med Clin North Am. 2000;84:597-607.
6. Weiss FU, Simon P, Bogdanova MJ, et al. Complete cystic fibrosis transmembrane conductance regulator gene sequencing in patients with idiopathic pancreatitis and controls. Gut. 2005;54:1456-1460.
7. Chang MC, Chang YT, Wei S, et al. Spectrum of mutations and variants/haplotypes of CFTR and genotype-phenotype correlation in idiopathic chronic pancreatitis and controls in Chinese by complete analysis. Clin Genet. 2007;71:530-539.
8. Noone PG, Knowles MR. “CFTR-opathies”: disease phenotypes associated with cystic fibrosis transmembrane regulator gene mutations. Respir Res. 2001;2:328-332.
9. Cohn JA, Neoptolemos JP, Feng J, et al. Increased risk of idiopathic pancreatitis in cystic fibrosis carriers. Hum Mutat. 2005;26:303-307.
10. Nick JA, Rodman DM. Manifestations of cystic fibrosis diagnosed in adulthood. Curr Opin Pulm Med 2005;11:513-518.
11. Poller W, Farber JP, Scholz S, et al. Sequence analysis of the cystic fibrosis gene in patients with disseminated bronchiectatic lung disease. Application in the identification of a cystic fibrosis patient with atypical clinical course. Klin Wochenschr. 1991;69:657-663.
12. Quan JM, Tiddens HA, Sy JP, et al. A two-year randomized, placebo-controlled trial of dornase alfa in young patients with cystic fibrosis with mild lung function abnormalities. J Pediatr. 2001;139:813-820.
13. Tiddens HA. Detecting early structural lung damage in cystic fibrosis. Pediatr Pulmonol. 2002;34:228-231.
14. Judge EP, Dodd JD, Masterson JB, et al. Pulmonary abnormalities on high-resolution CT demonstrate more rapid decline than FEV1 in adults with cystic fibrosis. Chest. 2006;130:1424-1432.
15. Robinson TE, Goris ML, Zhu HJ, et al. Dornase alfa reduces air trapping in children with mild cystic fibrosis lung disease. Chest. 2005;128:2327-2335.
16. Fuchs HJ, Borowitz DS, Christiansen DH, et al. The Pulmozyme Study Group. Effect of aerosolized recombinant human DNase on exacerbations of respiratory symptoms and on pulmonary function in patients with cystic fibrosis. N Engl J Med. 1994;331:637-642.
17. Ramsey BW, Pepe MS, Quan JM, et al. Cystic Fibrosis Inhaled Tobramycin Study Group. Intermittent administration of inhaled tobramycin in patients with cystic fibrosis. N Engl J Med. 1999;340:23-30.
18. Elkins MR, Robinson M, Rose BR, et al. The National Hyper-tonic Saline in Cystic Fibrosis Study Group. A controlled trial of long-term inhaled hypertonic saline in patients with cystic fibrosis. N Engl J Med. 2006;354:229-240.
19. Witt H. Chronic pancreatitis and cystic fibrosis. Gut. 2003;52(suppl 2):ii31-ii41.
• Don’t dismiss a cystic fibrosis diagnosis just because a patient’s sweat chloride levels are <60 mmol/L. A
• Suspect atypical cystic fibrosis in adults with single organ involvement, including mild lung disease, nasal polyposis, recurrent pancreatitis, biliary cirrhosis, portal hypertension, or obstructive azoospermia. A
• Consider respiratory therapies such as tobramycin, hypertonic saline, and recombinant human DNase in cystic fibrosis patients with relatively mild or atypical disease. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1: Lauren W*
Two years ago, Lauren W, a 57-year-old Caucasian woman, sought care at our medical center after learning that her pregnant daughter tested positive during a prenatal cystic fibrosis mutation genetic screen. Lauren had clinical symptoms of malodorous and greasy bowel movements, dyspepsia, early satiety, and a history of recurrent bronchitis since childhood.
According to her history, she did not suffer from failure to thrive as a child. She’d had 5 episodes of adult-onset acute pancreatitis and had 2 surgeries for sinusitis.
On physical exam, we heard no crackles during lung auscultation. Lauren also had mild digital clubbing.
Testing: We ordered a chest x-ray, which revealed left upper lobe atelectasis, but there was no bronchiectasis.
Pulmonary function tests indicated mild obstructive lung disease with forced vital capacity (FVC) 2.39 L or 84% predicted; forced expiratory volume in 1 second (FEV1) 1.59 L or 68% predicted; and an FEV1/FVC of 0.66.
A sweat chloride test was positive on both arms: 77 and 83 mmol/L. Genetic testing revealed compound heterozygosity for cystic fibrosis transmembrane conductance regulator (CFTR) gene mutations Δ F508 and R117H with a 5T allele. To test for pancreatic insufficiency, we performed a 72-hour fecal fat testing while she was on a low-fat diet; it revealed 5.5 g of fat per 24-hour period, suggesting fat malabsorption. Based on positive quantitative sweat test ≥60 mmol/L and the presence of 2 cystic fibrosis–causing mutations, we made the diagnosis of cystic fibrosis.
Treatment: We put Lauren on albuterol and recombinant human DNase respiratory treatments, pancreatic enzymes, and multivitamins with extra lipid-soluble vitamins and calcium supplements. We also continued her low-fat diet of 1500 to 1800 calories per day due to a diagnosis of coronary artery disease.
*Patients’ names have been changed to protect their privacy.
CASE 2: Zack P*
Zack P, a 6-year-old Caucasian boy, was admitted to the hospital with what we suspected was acute gastroenteritis. Serum testing revealed elevated pancreatic enzymes. He had recently sustained an injury to the mid-abdomen during a soccer game and also had a history of chronic sinusitis. One month after his release from the hospital, his symptoms resolved, but his pancreatic enzymes remained elevated (amylase 130 U/L, lipase 177 U/L).
Testing: He underwent 2 sweat chloride tests, which were borderline elevated at 49 mmol/L on the right arm and 40 mmol/L on the left arm; repeat testing was 49 mmol/L on the left arm, 43 mmol/L on the right arm. Genetic testing revealed heterozygosity for CFTR gene mutation Δ F508 with the presence of 7T and 9T allele variants. Over an 8-month period, Zack remained asymptomatic, but his pancreatic enzymes were persistently elevated.
Zack’s physical exam showed that his weight had dropped from the 75th to the 50th percentile. A magnetic resonance cholangiopancreatography indicated homogeneous parenchyma and normal enhancement throughout his pancreas. Similarly, we could not find evidence of acute pancreatitis or biliary or pancreatic duct dilation, and a 72-hour fecal fat study was normal. Given Zack’s borderline sweat chloride, compound heterozygosity of cystic fibrosis mutations, and his phenotype of recurrent pancreatitis, he was given a diagnosis of atypical cystic fibrosis.
Treatment: Based on our diagnostic workup, pancreatic enzyme therapy was not warranted.
*Patients’ names have been changed to protect their privacy.
These 2 cases illustrate how clinically diverse cystic fibrosis can be. The cystic fibrosis phenotype can range from a patient with 2 disease-causing cystic fibrosis mutations with significant sweat gland dysfunction and childhood onset of mild cystic fibrosis symptomatology with normal growth—Lauren—to a patient who is CFTR heterozygous with pancreatitis and a borderline sweat chloride concentration—Zack. Both cases emphasize the need to think “outside the box” and not expect all patients with cystic fibrosis to come in with typical signs and symptoms.
What does the “nonclassic” cystic fibrosis patient look like?
Patients with cystic fibrosis are usually diagnosed during childhood with pulmonary disease, pancreatic insufficiency, malabsorption, malnutrition, elevated sweat chloride, and male infertility. But more recently, patients have been diagnosed in adulthood because either they lacked significant clinical symptoms in childhood or they came in with atypical signs or symptoms (pancreatic sufficiency and sweat chloride <60 mmol/L).
In the past, cystic fibrosis patients rarely lived past their second decade, but those with atypical cystic fibrosis tend to have milder disease, including less severe respiratory signs and symptoms. The good news is that often translates into a long lifespan.1 As recently as 2005, the Cystic Fibrosis Foundation had listed a median survival age of 37.2 Advances in respiratory, gastrointestinal, and nutritional therapies have significantly contributed to the increased survival of these patients. Unfortunately, such milder cases can easily go undetected.
Sweat chloride testing remains a gold standard for the diagnosis of cystic fibrosis. As previously mentioned, classic cystic fibrosis patients are typically diagnosed during childhood and have a sweat chloride concentration ≥60 mmol/L and more severe multiorgan involvement (sinopulmonary and gastrointestinal disease with failure to thrive).
There are 5 classes of CFTR mutations that result in compromised CFTR function: The presence of 2 severe CFTR mutations (classes I-III) completely abolishes CFTR function. It is diagnosed in childhood and usually results in the classic clinical features of pancreatic insufficiency and failure to thrive. However, patients who are compound heterozygous for the milder CFTR mutations (classes IV and V) experience partial CFTR function, which in turn results in atypical features such as pancreatic sufficiency and normal or borderline sweat chloride concentrations. That makes the diagnosis more elusive during early childhood.1,3
The severity of sweat gland and exocrine pancreatic dysfunction produced by a cystic fibrosis mutation depends on the class of CFTR gene mutation and the level of CFTR gene and protein expression.4,5 In certain genetic backgrounds, the 5T allele associated with a high number of TG (thymine/guanine) repeats found in compound heterozygosity with a disease-causing CFTR mutation acts as a “mild CFTR mutation,” resulting in the nonclassic cystic fibrosis phenotype.3 Individuals with atypical cystic fibrosis diagnosed later in life may have single organ involvement, such as mild lung disease, nasal polyposis, recurrent pancreatitis, biliary cirrhosis, portal hypertension, or obstructive azoospermia.1
Lauren had several classic cystic fibrosis features, including recurrent lung disease, pancreatic insufficiency, and sweat gland dysfunction, but it’s likely that her relatively mild pulmonary presentation, normal body mass index, and lack of failure to thrive led to a delay in her diagnosis.
Some patients with atypical cystic fibrosis seek care for idiopathic chronic pancreatitis (ICP), and researchers have found a link between ICP and CFTR gene mutations. For instance, recent studies of ICP patients compared with geographically and ethnically matched controls revealed a higher frequency of abnormal CFTR alleles in the ICP population.6,7 Milder CFTR mutations resulting in partial CFTR function have also been associated with ICP.7,8
Zack was heterozygous for Δ F508, a common CFTR mutation in the Caucasian population. Cohn et al found a higher frequency of this mutation in ICP patients from Europe (mostly English, Italian, and Czech).9 Poly T allele variants such as 5T, 7T, and 9T have not been associated with a higher frequency of ICP.6,7
Early detection may translate into better treatment
Although patients diagnosed with cystic fibrosis as adults are less likely to present with classic clinical features, they may develop bronchiectasis and advanced lung disease.10,11 Those who are identified early on—including those who are asymptomatic and have normal lung function—may benefit from respiratory therapy to prevent or delay lung disease.12 Several studies have shown that patients with mild cystic fibrosis disease and stable spirometry results have evidence of bronchiectasis on their x-rays and advanced lung disease that appears on high-resolution CT.13,14
Judge et al have suggested that mucus plugging occurs early in cystic fibrosis lung disease and at a milder stage of lung function impairment, and that bronchiectasis may be an end result of such abnormalities.14 Nonclassic cystic fibrosis patients often have episodes of “bronchitis,” and once the practitioner becomes concerned, the radiographic image may already show evidence of bronchiectasis. Once again, this emphasizes the importance of early detection and prompt treatment.15
CASE 1: Lauren
Unfortunately, Lauren was unable to benefit from early use of respiratory therapies like tobramycin, hypertonic saline, and recombinant human DNase. She began these treatments after developing advanced lung disease. Studies have shown that tobramycin, long-term inhaled hypertonic saline, and recombinant human DNase can reduce the number of pulmonary exacerbations and increase both FVC and FEV1 values in previously stable cystic fibrosis patients.16-18
Similarly, because Lauren’s pancreatitis was due to pancreatic insufficiency, early recognition of pancreatic insufficiency and enzyme therapy may have greatly reduced the number and severity of her pancreatic episodes.19
Unfortunately, over the last few years, Lauren’s lung function has declined and she has been hospitalized for cystic fibrosis exacerbations and sinusitis; she has had 3 additional episodes of acute pancreatitis. Although her FEV1 is lower than on initial evaluation, she is clinically stable.
CASE 2: Zack
Clinically, Zack is stable and his recent amylase and lipase are elevated at 92 U/L and 71 U/L, respectively. He has had no acute exacerbations.
Patients like Lauren and Zack serve to remind us of the need to recognize and closely monitor patients with nonclassic cystic fibrosis. These patients may come to the office with “asthma-like” symptoms, bronchitis, polyps, pancreatitis, cholelithiasis, constipation, abdominal bloating/flatus, and infertility. Because their symptoms may not be severe enough to be referred to a subspecialist, family physicians play a critical role in recognizing these overlooked cases early on.
CORRESPONDENCE Anupama Chawla, MD, Director, Division of Pediatric Gastroenterology and Nutrition, Stony Brook University Hospital, Stony Brook, NY 11794; [email protected]
• Don’t dismiss a cystic fibrosis diagnosis just because a patient’s sweat chloride levels are <60 mmol/L. A
• Suspect atypical cystic fibrosis in adults with single organ involvement, including mild lung disease, nasal polyposis, recurrent pancreatitis, biliary cirrhosis, portal hypertension, or obstructive azoospermia. A
• Consider respiratory therapies such as tobramycin, hypertonic saline, and recombinant human DNase in cystic fibrosis patients with relatively mild or atypical disease. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1: Lauren W*
Two years ago, Lauren W, a 57-year-old Caucasian woman, sought care at our medical center after learning that her pregnant daughter tested positive during a prenatal cystic fibrosis mutation genetic screen. Lauren had clinical symptoms of malodorous and greasy bowel movements, dyspepsia, early satiety, and a history of recurrent bronchitis since childhood.
According to her history, she did not suffer from failure to thrive as a child. She’d had 5 episodes of adult-onset acute pancreatitis and had 2 surgeries for sinusitis.
On physical exam, we heard no crackles during lung auscultation. Lauren also had mild digital clubbing.
Testing: We ordered a chest x-ray, which revealed left upper lobe atelectasis, but there was no bronchiectasis.
Pulmonary function tests indicated mild obstructive lung disease with forced vital capacity (FVC) 2.39 L or 84% predicted; forced expiratory volume in 1 second (FEV1) 1.59 L or 68% predicted; and an FEV1/FVC of 0.66.
A sweat chloride test was positive on both arms: 77 and 83 mmol/L. Genetic testing revealed compound heterozygosity for cystic fibrosis transmembrane conductance regulator (CFTR) gene mutations Δ F508 and R117H with a 5T allele. To test for pancreatic insufficiency, we performed a 72-hour fecal fat testing while she was on a low-fat diet; it revealed 5.5 g of fat per 24-hour period, suggesting fat malabsorption. Based on positive quantitative sweat test ≥60 mmol/L and the presence of 2 cystic fibrosis–causing mutations, we made the diagnosis of cystic fibrosis.
Treatment: We put Lauren on albuterol and recombinant human DNase respiratory treatments, pancreatic enzymes, and multivitamins with extra lipid-soluble vitamins and calcium supplements. We also continued her low-fat diet of 1500 to 1800 calories per day due to a diagnosis of coronary artery disease.
*Patients’ names have been changed to protect their privacy.
CASE 2: Zack P*
Zack P, a 6-year-old Caucasian boy, was admitted to the hospital with what we suspected was acute gastroenteritis. Serum testing revealed elevated pancreatic enzymes. He had recently sustained an injury to the mid-abdomen during a soccer game and also had a history of chronic sinusitis. One month after his release from the hospital, his symptoms resolved, but his pancreatic enzymes remained elevated (amylase 130 U/L, lipase 177 U/L).
Testing: He underwent 2 sweat chloride tests, which were borderline elevated at 49 mmol/L on the right arm and 40 mmol/L on the left arm; repeat testing was 49 mmol/L on the left arm, 43 mmol/L on the right arm. Genetic testing revealed heterozygosity for CFTR gene mutation Δ F508 with the presence of 7T and 9T allele variants. Over an 8-month period, Zack remained asymptomatic, but his pancreatic enzymes were persistently elevated.
Zack’s physical exam showed that his weight had dropped from the 75th to the 50th percentile. A magnetic resonance cholangiopancreatography indicated homogeneous parenchyma and normal enhancement throughout his pancreas. Similarly, we could not find evidence of acute pancreatitis or biliary or pancreatic duct dilation, and a 72-hour fecal fat study was normal. Given Zack’s borderline sweat chloride, compound heterozygosity of cystic fibrosis mutations, and his phenotype of recurrent pancreatitis, he was given a diagnosis of atypical cystic fibrosis.
Treatment: Based on our diagnostic workup, pancreatic enzyme therapy was not warranted.
*Patients’ names have been changed to protect their privacy.
These 2 cases illustrate how clinically diverse cystic fibrosis can be. The cystic fibrosis phenotype can range from a patient with 2 disease-causing cystic fibrosis mutations with significant sweat gland dysfunction and childhood onset of mild cystic fibrosis symptomatology with normal growth—Lauren—to a patient who is CFTR heterozygous with pancreatitis and a borderline sweat chloride concentration—Zack. Both cases emphasize the need to think “outside the box” and not expect all patients with cystic fibrosis to come in with typical signs and symptoms.
What does the “nonclassic” cystic fibrosis patient look like?
Patients with cystic fibrosis are usually diagnosed during childhood with pulmonary disease, pancreatic insufficiency, malabsorption, malnutrition, elevated sweat chloride, and male infertility. But more recently, patients have been diagnosed in adulthood because either they lacked significant clinical symptoms in childhood or they came in with atypical signs or symptoms (pancreatic sufficiency and sweat chloride <60 mmol/L).
In the past, cystic fibrosis patients rarely lived past their second decade, but those with atypical cystic fibrosis tend to have milder disease, including less severe respiratory signs and symptoms. The good news is that often translates into a long lifespan.1 As recently as 2005, the Cystic Fibrosis Foundation had listed a median survival age of 37.2 Advances in respiratory, gastrointestinal, and nutritional therapies have significantly contributed to the increased survival of these patients. Unfortunately, such milder cases can easily go undetected.
Sweat chloride testing remains a gold standard for the diagnosis of cystic fibrosis. As previously mentioned, classic cystic fibrosis patients are typically diagnosed during childhood and have a sweat chloride concentration ≥60 mmol/L and more severe multiorgan involvement (sinopulmonary and gastrointestinal disease with failure to thrive).
There are 5 classes of CFTR mutations that result in compromised CFTR function: The presence of 2 severe CFTR mutations (classes I-III) completely abolishes CFTR function. It is diagnosed in childhood and usually results in the classic clinical features of pancreatic insufficiency and failure to thrive. However, patients who are compound heterozygous for the milder CFTR mutations (classes IV and V) experience partial CFTR function, which in turn results in atypical features such as pancreatic sufficiency and normal or borderline sweat chloride concentrations. That makes the diagnosis more elusive during early childhood.1,3
The severity of sweat gland and exocrine pancreatic dysfunction produced by a cystic fibrosis mutation depends on the class of CFTR gene mutation and the level of CFTR gene and protein expression.4,5 In certain genetic backgrounds, the 5T allele associated with a high number of TG (thymine/guanine) repeats found in compound heterozygosity with a disease-causing CFTR mutation acts as a “mild CFTR mutation,” resulting in the nonclassic cystic fibrosis phenotype.3 Individuals with atypical cystic fibrosis diagnosed later in life may have single organ involvement, such as mild lung disease, nasal polyposis, recurrent pancreatitis, biliary cirrhosis, portal hypertension, or obstructive azoospermia.1
Lauren had several classic cystic fibrosis features, including recurrent lung disease, pancreatic insufficiency, and sweat gland dysfunction, but it’s likely that her relatively mild pulmonary presentation, normal body mass index, and lack of failure to thrive led to a delay in her diagnosis.
Some patients with atypical cystic fibrosis seek care for idiopathic chronic pancreatitis (ICP), and researchers have found a link between ICP and CFTR gene mutations. For instance, recent studies of ICP patients compared with geographically and ethnically matched controls revealed a higher frequency of abnormal CFTR alleles in the ICP population.6,7 Milder CFTR mutations resulting in partial CFTR function have also been associated with ICP.7,8
Zack was heterozygous for Δ F508, a common CFTR mutation in the Caucasian population. Cohn et al found a higher frequency of this mutation in ICP patients from Europe (mostly English, Italian, and Czech).9 Poly T allele variants such as 5T, 7T, and 9T have not been associated with a higher frequency of ICP.6,7
Early detection may translate into better treatment
Although patients diagnosed with cystic fibrosis as adults are less likely to present with classic clinical features, they may develop bronchiectasis and advanced lung disease.10,11 Those who are identified early on—including those who are asymptomatic and have normal lung function—may benefit from respiratory therapy to prevent or delay lung disease.12 Several studies have shown that patients with mild cystic fibrosis disease and stable spirometry results have evidence of bronchiectasis on their x-rays and advanced lung disease that appears on high-resolution CT.13,14
Judge et al have suggested that mucus plugging occurs early in cystic fibrosis lung disease and at a milder stage of lung function impairment, and that bronchiectasis may be an end result of such abnormalities.14 Nonclassic cystic fibrosis patients often have episodes of “bronchitis,” and once the practitioner becomes concerned, the radiographic image may already show evidence of bronchiectasis. Once again, this emphasizes the importance of early detection and prompt treatment.15
CASE 1: Lauren
Unfortunately, Lauren was unable to benefit from early use of respiratory therapies like tobramycin, hypertonic saline, and recombinant human DNase. She began these treatments after developing advanced lung disease. Studies have shown that tobramycin, long-term inhaled hypertonic saline, and recombinant human DNase can reduce the number of pulmonary exacerbations and increase both FVC and FEV1 values in previously stable cystic fibrosis patients.16-18
Similarly, because Lauren’s pancreatitis was due to pancreatic insufficiency, early recognition of pancreatic insufficiency and enzyme therapy may have greatly reduced the number and severity of her pancreatic episodes.19
Unfortunately, over the last few years, Lauren’s lung function has declined and she has been hospitalized for cystic fibrosis exacerbations and sinusitis; she has had 3 additional episodes of acute pancreatitis. Although her FEV1 is lower than on initial evaluation, she is clinically stable.
CASE 2: Zack
Clinically, Zack is stable and his recent amylase and lipase are elevated at 92 U/L and 71 U/L, respectively. He has had no acute exacerbations.
Patients like Lauren and Zack serve to remind us of the need to recognize and closely monitor patients with nonclassic cystic fibrosis. These patients may come to the office with “asthma-like” symptoms, bronchitis, polyps, pancreatitis, cholelithiasis, constipation, abdominal bloating/flatus, and infertility. Because their symptoms may not be severe enough to be referred to a subspecialist, family physicians play a critical role in recognizing these overlooked cases early on.
CORRESPONDENCE Anupama Chawla, MD, Director, Division of Pediatric Gastroenterology and Nutrition, Stony Brook University Hospital, Stony Brook, NY 11794; [email protected]
1. Kerem E. Atypical CF and CF related diseases. Paediatr Respir Rev. 2006;7(suppl 1):S144-S146.
2. Cystic Fibrosis Foundation. Cystic Fibrosis Foundation Annual Patient Registry Data Report 2005. Bethesda, Md; 2006.
3. Castellani C, Cuppens H, Macek M, Jr, et al. Consensus on the use and interpretation of cystic fibrosis mutation analysis in clinical practice. J Cyst Fibros. 2008;7:179-196.
4. Wilchanski M, Zielenski J, Markiewicz D. Correlation of sweat chloride concentration with classes of the cystic fibrosis trans-membrane conductance regulator gene mutation, J Pediatr. 1995;127:705-710.
5. Mickle JE, Cutting GR. Genotype-phenotype relationships in cystic fibrosis. Med Clin North Am. 2000;84:597-607.
6. Weiss FU, Simon P, Bogdanova MJ, et al. Complete cystic fibrosis transmembrane conductance regulator gene sequencing in patients with idiopathic pancreatitis and controls. Gut. 2005;54:1456-1460.
7. Chang MC, Chang YT, Wei S, et al. Spectrum of mutations and variants/haplotypes of CFTR and genotype-phenotype correlation in idiopathic chronic pancreatitis and controls in Chinese by complete analysis. Clin Genet. 2007;71:530-539.
8. Noone PG, Knowles MR. “CFTR-opathies”: disease phenotypes associated with cystic fibrosis transmembrane regulator gene mutations. Respir Res. 2001;2:328-332.
9. Cohn JA, Neoptolemos JP, Feng J, et al. Increased risk of idiopathic pancreatitis in cystic fibrosis carriers. Hum Mutat. 2005;26:303-307.
10. Nick JA, Rodman DM. Manifestations of cystic fibrosis diagnosed in adulthood. Curr Opin Pulm Med 2005;11:513-518.
11. Poller W, Farber JP, Scholz S, et al. Sequence analysis of the cystic fibrosis gene in patients with disseminated bronchiectatic lung disease. Application in the identification of a cystic fibrosis patient with atypical clinical course. Klin Wochenschr. 1991;69:657-663.
12. Quan JM, Tiddens HA, Sy JP, et al. A two-year randomized, placebo-controlled trial of dornase alfa in young patients with cystic fibrosis with mild lung function abnormalities. J Pediatr. 2001;139:813-820.
13. Tiddens HA. Detecting early structural lung damage in cystic fibrosis. Pediatr Pulmonol. 2002;34:228-231.
14. Judge EP, Dodd JD, Masterson JB, et al. Pulmonary abnormalities on high-resolution CT demonstrate more rapid decline than FEV1 in adults with cystic fibrosis. Chest. 2006;130:1424-1432.
15. Robinson TE, Goris ML, Zhu HJ, et al. Dornase alfa reduces air trapping in children with mild cystic fibrosis lung disease. Chest. 2005;128:2327-2335.
16. Fuchs HJ, Borowitz DS, Christiansen DH, et al. The Pulmozyme Study Group. Effect of aerosolized recombinant human DNase on exacerbations of respiratory symptoms and on pulmonary function in patients with cystic fibrosis. N Engl J Med. 1994;331:637-642.
17. Ramsey BW, Pepe MS, Quan JM, et al. Cystic Fibrosis Inhaled Tobramycin Study Group. Intermittent administration of inhaled tobramycin in patients with cystic fibrosis. N Engl J Med. 1999;340:23-30.
18. Elkins MR, Robinson M, Rose BR, et al. The National Hyper-tonic Saline in Cystic Fibrosis Study Group. A controlled trial of long-term inhaled hypertonic saline in patients with cystic fibrosis. N Engl J Med. 2006;354:229-240.
19. Witt H. Chronic pancreatitis and cystic fibrosis. Gut. 2003;52(suppl 2):ii31-ii41.
1. Kerem E. Atypical CF and CF related diseases. Paediatr Respir Rev. 2006;7(suppl 1):S144-S146.
2. Cystic Fibrosis Foundation. Cystic Fibrosis Foundation Annual Patient Registry Data Report 2005. Bethesda, Md; 2006.
3. Castellani C, Cuppens H, Macek M, Jr, et al. Consensus on the use and interpretation of cystic fibrosis mutation analysis in clinical practice. J Cyst Fibros. 2008;7:179-196.
4. Wilchanski M, Zielenski J, Markiewicz D. Correlation of sweat chloride concentration with classes of the cystic fibrosis trans-membrane conductance regulator gene mutation, J Pediatr. 1995;127:705-710.
5. Mickle JE, Cutting GR. Genotype-phenotype relationships in cystic fibrosis. Med Clin North Am. 2000;84:597-607.
6. Weiss FU, Simon P, Bogdanova MJ, et al. Complete cystic fibrosis transmembrane conductance regulator gene sequencing in patients with idiopathic pancreatitis and controls. Gut. 2005;54:1456-1460.
7. Chang MC, Chang YT, Wei S, et al. Spectrum of mutations and variants/haplotypes of CFTR and genotype-phenotype correlation in idiopathic chronic pancreatitis and controls in Chinese by complete analysis. Clin Genet. 2007;71:530-539.
8. Noone PG, Knowles MR. “CFTR-opathies”: disease phenotypes associated with cystic fibrosis transmembrane regulator gene mutations. Respir Res. 2001;2:328-332.
9. Cohn JA, Neoptolemos JP, Feng J, et al. Increased risk of idiopathic pancreatitis in cystic fibrosis carriers. Hum Mutat. 2005;26:303-307.
10. Nick JA, Rodman DM. Manifestations of cystic fibrosis diagnosed in adulthood. Curr Opin Pulm Med 2005;11:513-518.
11. Poller W, Farber JP, Scholz S, et al. Sequence analysis of the cystic fibrosis gene in patients with disseminated bronchiectatic lung disease. Application in the identification of a cystic fibrosis patient with atypical clinical course. Klin Wochenschr. 1991;69:657-663.
12. Quan JM, Tiddens HA, Sy JP, et al. A two-year randomized, placebo-controlled trial of dornase alfa in young patients with cystic fibrosis with mild lung function abnormalities. J Pediatr. 2001;139:813-820.
13. Tiddens HA. Detecting early structural lung damage in cystic fibrosis. Pediatr Pulmonol. 2002;34:228-231.
14. Judge EP, Dodd JD, Masterson JB, et al. Pulmonary abnormalities on high-resolution CT demonstrate more rapid decline than FEV1 in adults with cystic fibrosis. Chest. 2006;130:1424-1432.
15. Robinson TE, Goris ML, Zhu HJ, et al. Dornase alfa reduces air trapping in children with mild cystic fibrosis lung disease. Chest. 2005;128:2327-2335.
16. Fuchs HJ, Borowitz DS, Christiansen DH, et al. The Pulmozyme Study Group. Effect of aerosolized recombinant human DNase on exacerbations of respiratory symptoms and on pulmonary function in patients with cystic fibrosis. N Engl J Med. 1994;331:637-642.
17. Ramsey BW, Pepe MS, Quan JM, et al. Cystic Fibrosis Inhaled Tobramycin Study Group. Intermittent administration of inhaled tobramycin in patients with cystic fibrosis. N Engl J Med. 1999;340:23-30.
18. Elkins MR, Robinson M, Rose BR, et al. The National Hyper-tonic Saline in Cystic Fibrosis Study Group. A controlled trial of long-term inhaled hypertonic saline in patients with cystic fibrosis. N Engl J Med. 2006;354:229-240.
19. Witt H. Chronic pancreatitis and cystic fibrosis. Gut. 2003;52(suppl 2):ii31-ii41.
Sued for misdiagnosis? It could happen to you
• Create a problem list for each patient, including chronic and acute conditions, unexplained signs and symptoms, medications, and allergies. C
• Avoid attributing every new symptom to the patient’s documented medical conditions. C
• Develop and adhere to “don’t-miss” lists of signs and symptoms that warrant rapid action. C
• Establish a fail-safe system to ensure that you receive notification whenever a final imaging or lab report differs from the preliminary report and document your response to each abnormal result. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series

Misdiagnosis accounts for more malpractice claims than medication errors—indeed, for more lawsuits than any other medical misstep.1-5 Yet until recently, diagnostic errors garnered little attention from patient safety advocates.
That’s no longer the case. In 2007, the Agency for Healthcare Research and Quality (AHRQ) identified diagnostic errors (a catchall category encompassing delayed, incorrect, and missed diagnoses) as a problem that warranted closer study.6 The inaugural conference on Diagnostic Error in Medicine, cosponsored by AHRQ and the American Medical Informatics Association, took place in 2008. The third annual Diagnostic Error in Medicine conference will be held in Canada in October, reflecting the expanding focus on uncovering root causes of diagnostic error and developing preventive measures aimed at safeguarding patients and avoiding lawsuits.
Because diagnostic errors have long been underemphasized and understudied—and remain difficult to track—it is hard to know just how often they occur. Estimates of their frequency fluctuate widely from 1 study to another, but are generally in the range of 10% to 15%.7 Fatal illnesses appear to be misdiagnosed more frequently than less severe conditions: A review of more than 50 autopsy studies found that, on average, about 1 in 4 (23.5%) major diagnoses were missed.1
Whatever the numbers, diagnostic missteps are clearly common enough to be on patients’ radar screen. In a recent survey of US adults, 55% of respondents cited misdiagnosis as their greatest concern when they see a doctor in an outpatient setting.8 In a Harris Poll commissioned by the National Patient Safety Foundation9 several years earlier, 1 in 6 adults reported having had a condition that was misdiagnosed.
Evidence suggests that while years of experience and strong diagnostic skills help prevent diagnostic errors, they do not afford full protection against the cascade of events that can result in a serious diagnostic error. In fact, overconfidence may contribute to the problem.10,11
Check out the 3 legal cases in the pages that follow from the files of John Davenport, MD, JD. Dr. Davenport, a medical malpractice attorney, provided legal representation in each of these cases.
The take-away message: No physician is immune to misdiagnosis or to a subsequent lawsuit. There are, however, steps you can take to safeguard your patients and yourself, but first you need to know where the pitfalls lie.
Misdiagnosis in primary care: What malpractice claims reveal
Diagnostic errors that result in malpractice claims undergo extensive legal review. Thus, they provide an excellent opportunity for analysis, as the authors of a study of 181 “closed,” or completed, claims from 4 malpractice insurers found.12 The errors all occurred in ambulatory settings, with primary care physicians most frequently involved.
Nearly 6 in 10 of the lawsuits were for missed or delayed cancer diagnoses, followed by misdiagnosis of infection, fracture, and myocardial infarction. Overall, 24% of the cases involved breast cancer. No other disorder came close.
The most common problems, or “breakdowns,” in the diagnostic process were:
- failure to order the appropriate diagnostic test (which occurred in 55% of the cases)
- failure to create a proper follow-up plan (45%)
- failure to obtain a thorough medical history or to perform a thorough physical examination (42%).12
Notably, however, diagnostic errors rarely had a single cause. A median of 3 breakdowns per case was identified, and more than 4 in 10 cases involved more than 1 clinician.
Additional sources of breakdowns ran the gamut from patient factors (eg, non-compliance, atypical presentation, or a delay in seeking care) to system errors (eg, delay in seeing a test result, referral delay, or a mishandled handoff). Rarely was misdiagnosis attributed to a physician’s cognitive error alone. Most diagnostic errors, the authors reported, involved “a potent combination of individual and system factors.” 12
Is it cancer? Failure to test or follow up
Cancer may not be the most frequently misdiagnosed condition, but because of the dire consequences often associated with a delay in detection, cancer is No. 1 in frequency of diagnostic error lawsuits13—with breast cancer typically at or near the top of the list. Evidence suggests that clinician preconception plays a role.
Most women who develop breast cancer are over the age of 50, but plaintiffs in breast cancer suits tend to be younger.14,15 This may be partly because of overreliance on age as a predictive factor, causing some physicians to offer a younger woman what may be unwarranted reassurance that a breast lump is due to fibrocystic tissue rather than malignancy (CASE 1).
Ordering a test is not enough. Even when physicians order the correct test, follow-up may fall short. In the closed claims study, physicians incorrectly interpreted test results in 37% of the cases.12 Other evidence suggests that about a third of women with abnormal mammograms do not receive follow-up care that’s consistent with established guidelines.16
What’s more, physicians sometimes overlook the fact that diagnostic tests are rarely 100% accurate. Mammography misses approximately 20% of breast cancer cases,17 for example, and a woman with a palpable lump should be closely watched, not dismissed on the basis of a negative mammogram result.1,15
What happens to test results? In other cases, the problem is not that a test result doesn’t match the clinical findings, but that the result is not reviewed by the physician or conveyed to the patient in a timely manner. Indeed, the title of a published report of a survey of internists starts with the quote, “I wish I had seen this test result earlier!” 18 Of the 262 internists surveyed, only 41% expressed satisfaction with their method of handling test results.
What would satisfy these physicians? Respondents said what they wanted in a test result management system were tools that would help them generate letters to patients detailing the results, prioritize their workflow, and track orders for tests to completion.
A 32-year-old woman sought care for “sore breasts” 4 months postpartum. Her primary care physician found “bilateral lumpy and tender breasts,” diagnosed fibrocystic breast disease, and prescribed a nonsteroidal anti-inflammatory drug. There was no follow-up plan documented.
She returned in 4 months, stating her symptoms were better but she still had soreness in her left breast. The physician did not examine her, but changed her medication to a different anti-inflammatory. Follow-up was to “return to clinic PRN.”
On her next visit she complained of a lump in the left breast. The physician found a “spongy irregular 2 cm lump” in the upper outer quadrant of the breast, diagnosed a fibrocystic lesion, and reassured the patient. Follow-up again was to return PRN.
Several months later, the patient saw another physician, for back pain and a painful and enlarging breast lump. The physician suspected fibrocystic disease but was unable to obtain fluid by fine needle aspiration. The patient was referred to a surgeon, who obtained a nondiagnostic needle biopsy and an excisional biopsy, which revealed breast cancer. The patient’s back pain turned out to be from metastatic breast cancer. She sued for failure to diagnose breast cancer. The case was settled for an undisclosed large sum.
Commentary: Failure to diagnose breast cancer is a leading cause of malpractice lawsuits, many of them in younger women. Plaintiff recoveries correlate with the length of the delay in diagnosis.
In this case, experts identified a series of missteps in the care of this patient which, when combined with a young, very sick, and sympathetic plaintiff, led to a large recovery. Although it may have been reasonable to diagnose fibrocystic disease on the first visit, experts cited the failure to take a family history (the patient’s aunt and maternal grandmother had had breast cancer) and the failure to document a follow-up plan as damaging to the doctor’s case. They also faulted the physician for failing to examine the breast on the second visit and failing to do fine needle aspiration or refer on the third visit, and for the nonspecific follow-up plans.
Diagnostic lesson: Although breast cancer is less common in women younger than 40, it does occur, and the same diligence in examination, charting, and follow up is required regardless of the patient’s age.
By the way, doc… Harried physician, hurried response
What physician isn’t familiar with the patient who comes in for care of 1, or several, chronic conditions, but mentions another problem as he or she is getting ready to walk out the door (CASE 2)? If that problem appears to be a transient and treatable condition, the temptation is to make a hasty diagnosis and write a prescription, without the usual degree of history taking, patient examination, contemplation, or documentation. Doing so, however, poses considerable risk, to both patient and physician.
If the condition or symptom is serious enough to address in the course of the visit, it requires the same level of attention as any other presenting problem. When time constraints prevent you from addressing the complaint with the proper diligence, it would be appropriate—assuming the symptom in question is nonurgent—to ask the patient to make another appointment. But be sure to document that you did so.
A 62-year-old man saw his family physician for routine care of hypertension, diabetes, and hyperlipidemia. During the visit, the patient mentioned that he had back pain, insomnia, and a sore tongue, which the physician diagnosed as aphthous stomatitis and for which a steroidal oral cream was prescribed.
The patient was scheduled to return for a routine visit in 4 months, but did not come in until 7 months had passed—at which time the physician noted a >1 cm nodular bleeding tongue lesion. Biopsy showed squamous cell cancer, and the patient required extensive surgery, chemotherapy, and radiation. He sued for misdiagnosis and delayed diagnosis.
The physician’s defense was that given the symptoms and findings, aphthous stomatitis was a reasonable diagnosis and that he had instructed the patient to return to the office if he didn’t feel better in a few weeks. The patient disputed this. His attorney noted that the patient had multiple risk factors for tongue cancer that were not in the medical record; nor was there documentation of a tongue examination or the claimed instructions for the return visit, indicating that the patient received substandard care. The case was settled at trial for $300,000.
Commentary: The contrast between the thorough documentation for the patient’s chronic disease history and physical exam and the absence of documentation for the sore tongue suggests that this was an instance of a “by the way, doc” conversation—and a reminder of the risk that physicians assume when managing patients with multiple conditions.
Diagnostic lesson: The law does not give physicians a pass on the standard of care, regardless of how many conditions are treated in a single visit. To avoid a diagnostic error—and a potential lawsuit—a symptom-specific history, physical, and clear instructions with a follow-up plan are necessary for every condition that’s addressed.
How sure are you of the diagnosis?
It’s human nature to see things in terms of what you’re familiar with. A doctor who has been treating a patient with migraine headaches for years, for example, is apt to assume that “the worst migraine I’ve ever had” is more of the same (CASE 3). Similarly, a clinician who has identified a disorder that matches several of a patient’s symptoms may dismiss or overlook signs and symptoms that do not fit that explanation or diagnosis. Safety advocates refer to this phenomenon as “premature closure.” It may also be a function of overconfidence.
One example of physician overconfidence comes from a study in which experienced dermatologists were asked to examine lesions and diagnose melanoma. Although the specialists confidently diagnosed melanoma in more than 50% of the test cases, 30% of their decisions were later found to be incorrect.19
A 47-year-old man with a history of migraines walked into his physician’s clinic with a complaint of a severe headache. His physician was fully booked but he was given an appointment with a per diem physician. According to the patient and a friend who accompanied him, the patient told the doctor, “This is the worst migraine of my life.” The physician simply documented, “flare of migraine.” The chart indicated that the physical revealed normal vital signs and noted that the patient was “photophobic,” but that his neurological exam was “intact.”
Over the next several hours, the patient received sumatriptan and several doses of opioid analgesics. He stated that he still had a headache but felt better and was sent home with instructions to call or come in if the headache returned.
The next morning a neighbor, unable to reach the patient on the phone, went to his house and found him in a stupor, with slurred speech. The patient was taken by ambulance to a local hospital and found to have a subarachnoid hemorrhage. After weeks in the hospital and a rehabilitation center, he was left with significant cognitive and neurological impairments. He sued for failure to diagnose and won a multimillion dollar award at trial.
Commentary: Expert testimony clearly pointed to the history and physical as being substandard. Specifically, the physical should have included, among other things, a test for nuchal rigidity. Had the patient not had a history of migraines, he might have undergone a more complete medical history and physical evaluation and his symptoms would likely have been evaluated more thoroughly.
Diagnostic lesson: Be wary of “diagnostic inertia”—the tendency to depend too much on a past diagnosis when symptoms arise. Don’t be trapped into attributing all new symptoms to an old disease.
Build a no-fault, fail-safe system
The purpose of analyzing diagnostic errors is not to assign blame or point a finger at physicians, but rather to find and fix flaws in the medical system.20 That approach has been used by patient safety advocates to address other types of errors following the publication of the Institute of Medicine’s landmark report on medical error 11 years ago.21
Since then, many physician leaders have looked to the airline industry—a field in which the consequences for not strictly adhering to a fail-safe system are likely to be fatal. That reality has led to the development of vital checklists, forcing functions (in which the user is prevented from moving to the next step until the current step is completed), and computerized reminders in an attempt to eliminate, to the extent possible, the chance of human error.
The same principle can be applied to misdiagnosis. Recommended steps—ordering diagnostic tests or referring to a specialist, for example—should be put into motion whenever a set of predetermined parameters are met, rather than relying on physician memory or choice.20
Similarly, checklists should specify questions to ask or criteria to be met under specified circumstances to prevent physicians from prematurely settling on a (possibly incorrect) diagnosis. To avoid a rush to judgment, some patient safety advocates1 stress the importance of assessing the urgency of a patient’s condition, rather than trying to arrive at a definitive diagnosis the first time he or she presents with a perplexing set of signs and symptoms. Other recommendations follow:
Mandate a second look. Develop and adhere to a set of criteria to determine when a referral to a specialist or a physician consultation is needed, rather than deciding on a case-by-case basis.
Plug the holes in your follow-up system. Develop a fail-safe system for reviewing diagnostic tests or laboratory findings and reporting them to patients without delay. This can be done with an electronic health record (EHR) system or by developing and adhering to parameters requiring, for instance, that no test result get filed until there are 2 signatures on it—that of the physician who ordered the test, indicating that he or she has seen it, and that of a staff member, indicating that the patient has been notified of the results. As an additional back-up, tell patients undergoing tests when to expect to get results, and stress the importance of calling the office if they do not receive such notification within a specified time frame.
Partner with patients. Engage patients in the pursuit of a definitive diagnosis. Discuss your preliminary findings, describe your treatment decision and what you expect to occur, and urge patients to contact you with evidence that confirms or refutes that expectation. Elicit additional feedback at each visit until either the symptoms have fully resolved or you have gathered enough information to arrive at a definitive diagnosis.
Develop “don’t-miss” checklists. One list should cover diagnostic red flags to be considered anytime you see a symptomatic patient to ensure that you don’t overlook important signs and symptoms, and include findings that warrant hospital admission, specified diagnostic tests, and immediate referral. (A patient who comes in with a “common pink eye,” but has consensual photophobia, is at risk for iritis and needs an urgent ophthalmology evaluation, for instance.) Another list you should develop is a “must-do” list for well visits, featuring clinical scenarios to address and screening tests to remember, such as an eye exam for patients with diabetes.
Question your initial diagnosis. Beware of “premature closure”—the tendency to stop looking for other signs and symptoms once you find a presumptive diagnosis—and “diagnostic inertia”—evaluating new signs and symptoms almost exclusively on the basis of past medical history. If aspects of a patient presentation do not fit your presumed diagnosis, use a decision support system, if available, to review other possibilities.
Head off hand-off errors. Develop a problem list for each patient to reduce the likelihood that crucial information will be overlooked when more than 1 clinician is involved in his or her care. Include chronic and acute conditions, unexplained signs and symptoms, medications, and allergies. Create a fail-safe system for other potential hand-off problems, as well—requiring confirmation that the findings in a preliminary radiology report are the same as those in the final report before you take action based on the preliminary report, for example, and ensuring that you receive prompt notification whenever that is not the case.
EHRs and decision support: Isn’t it time?
In 2009, 44% of office-based physicians had EHRs, according to a Centers for Disease Control and Prevention preliminary report.22 Federal funding to promote the adoption of EHRs is expected to accelerate their use. Among the benefits of EHRs are clinical reminders, system alerts, and documentation tools that can help reduce the risk of diagnostic missteps and avert misdiagnosis lawsuits.
The Department of Veterans Affairs uses a notification system called View Alert, for example, that tracks acknowledgement of abnormal radiology test results and flags those that remain unacknowledged. 23 EHR systems can also be programmed to issue automated appointment reminders that make it easier to track patients who do not show up for critical follow-up visits.
Diagnostic decision support software adds another critical element. When a clinician inputs a set of symptoms and patient-specific data, such systems produce lists of possible diagnoses, often divided by bodily system.
While many safety advocates believe that the use of such systems will increase the likelihood of accurate diagnosis, critics point out that the software is only as good as the clinician using it. One concern is that computerized systems typically come with a “macro” ability—that is, the ability to enter large amounts of information with the click of a key. This raises the possibility that an overload of patient data, some of which may be incorrect, will be added to the medical record—or that the system will generate so many possibilities that clinicians will cease to pay attention. Both can lead to inferences of inattention or raise doubts about a physician’s credibility in a legal setting.
Electronic prescribing software systems that flag potential drug interactions are a case in point. Forty-five percent of family physicians responding to a Journal of Family Practice Instant Poll about their use of such systems reported that they override them frequently. The problem, according to 1 respondent: The system gives “so many red flags that I routinely ignore them all—like the little boy who cried wolf.”
CORRESPONDENCE John Davenport, MD, JD, 13 Redonda, Irvine, CA 92620; [email protected]
1. Schiff GD, Kim S, Abrams R, et al. Diagnosing diagnosis errors: lessons from a multi-institutional collaborative project. Adv Patient Safety. 2005;255:255-278.
2. Sato L. Evidence-based patient safety and risk management technology. J Qual Improv. 2001;27:435.-
3. Phillips R, Bartholomew L, Dovey S, et al. Learning from malpractice claims about negligent, adverse events in primary care in the United States. Qual Saf Health Care. 2004;13:121-126.
4. Fitzgerald N. Top five causes of malpractice claims. American Physicians Assurance Corporation. 2004. Available at: http://www.apassurance.com/RiskMgt/Articles_RM/5%20Causes%20of%20Claims_RMArticle.pdf. Accessed August 2, 2010.
5. Chandra A, Nundy S, Seabury SA. The growth of physician medical malpractice payments: evidence from the National Practitioner Data Bank. Health Aff (Millwood). 2005;W5(suppl):240-249.
6. Agency for Healthcare Research and Quality Special emphasis notice (SEN): AHRQ announces interest in research on diagnostic errors in ambulatory care settings. Available at: http://grants.nih.gv/grants/guide/notice-files-NOT-HS-08-002.html. Accessed July 30, 2010.
7. Berner ES, Graber ML. Overconfidence as a cause of diagnostic error in medicine. Am J Med. 2008;121(suppl 5A):S2-S23.
8. Isabel Healthcare. Misdiagnosis is an overlooked and growing patient safety issue and core mission of Isabel Healthcare. March 20, 2006. Available at http://www.isabelhealthcare.com/pdf/USsurveyrelease-Final.pdf. Accessed August 4, 2010.
9. Golodner L. How the public perceives patient safety. Newsletter of the National Patient Safety Foundation. 2004;1997:1-6.
10. Berner ES. Diagnostic error in medicine: introduction. Adv Health Sci Educ Theory Pract. 2009;14(suppl 1):1-5.
11. Friedman CP, Gatti GG, Franz TM, et al. Do physicians know when their diagnoses are correct? Implications for decision support and error reduction. J Gen Intern Med. 2005;20:334-339.
12. Ghandi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med. 2006;145:488-496.
13. McDonald C, Hernandez MB, Gofman Y, et al. The five most common misdiagnoses: a meta-analysis of autopsy and malpractice data. Internet J Fam Pract. 2009;7(2). Available at http://www.ispub.com/journal/the_internet_journal_of_family_practice/volume_7_number_2_19/article/the-five-most-common-misdiagnosesa-meta-analysis-of-autopsy-and-malpractice-data.html. Accessed July 23, 2010.
14. Mitnick JS, Vasquez MF, Kronovet SZ, et al. Malpractice litigation involving patients with carcinoma of the breast. J Am Coll Surg. 1995;181:315-321.
15. Failure to diagnose breast cancer. Medical Malpractice Lawyers and Attorneys Online. http://www.medical-malpractice-attorneys-lawsuits.com/pages/breast-cancer.html. Accessed August 2, 2010.
16. Poon EG, Haas JS, Puopolo AL, et al. Communication factors in the follow-up of abnormal mammograms. J Gen Intern Med. 2004;19:316-323.
17. National Cancer Institute. Fact sheet. Mammograms. Available at: http://www.cancer.gov/cancertopics/factsheet/Detection/mammograms. Accessed August 3, 2010.
18. Poon EG, Gandhi TK, Sequist TD, et al. “I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care. Arch Intern Med. 2004;164:2223-2228.
19. Dreistl S, Binder M. Do physicians value decision support? A look at the effect of decision support on physician opinion. Artif Intell Med. 2005;33:25-30.
20. Newman-Toker DE, Pronovost PJ. Diagnostic errors: the new frontier for patient safety. JAMA. 2009;301:1060-1062.
21. Institute of Medicine. To err is human: building a safer health system. Washington, DC: November 1, 1999.
22. Centers for Disease Control and Prevention. NCHS Health E-Stat. Electronic medical record/electronic health record use by office-based physicians: United States, 2008 and preliminary 2009. Available at: http://www.cdc.gov/nchs/data/hestat/emr_ehr/emr_ehr.htm. Accessed July 30, 2010.
23. Singh H, Arora HS, Vij MS, et al. Communication outcomes of critical imaging results in a computerized notification system. J Am Med Inform Assoc. 2007;14:459-466.
| Made a medical error? What to say to the patient |
Helen Lippman, MA
The Journal of Family Practice, Parsippany, NJ
John Davenport, MD, JD
Kaiser Permanente Orange County, Irvine, Calif
[email protected]
The authors reported no potential conflict of interest relevant to this article.
| Made a medical error? What to say to the patient |
Helen Lippman, MA
The Journal of Family Practice, Parsippany, NJ
John Davenport, MD, JD
Kaiser Permanente Orange County, Irvine, Calif
[email protected]
The authors reported no potential conflict of interest relevant to this article.
| Made a medical error? What to say to the patient |
Helen Lippman, MA
The Journal of Family Practice, Parsippany, NJ
John Davenport, MD, JD
Kaiser Permanente Orange County, Irvine, Calif
[email protected]
The authors reported no potential conflict of interest relevant to this article.
• Create a problem list for each patient, including chronic and acute conditions, unexplained signs and symptoms, medications, and allergies. C
• Avoid attributing every new symptom to the patient’s documented medical conditions. C
• Develop and adhere to “don’t-miss” lists of signs and symptoms that warrant rapid action. C
• Establish a fail-safe system to ensure that you receive notification whenever a final imaging or lab report differs from the preliminary report and document your response to each abnormal result. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Misdiagnosis accounts for more malpractice claims than medication errors—indeed, for more lawsuits than any other medical misstep.1-5 Yet until recently, diagnostic errors garnered little attention from patient safety advocates.
That’s no longer the case. In 2007, the Agency for Healthcare Research and Quality (AHRQ) identified diagnostic errors (a catchall category encompassing delayed, incorrect, and missed diagnoses) as a problem that warranted closer study.6 The inaugural conference on Diagnostic Error in Medicine, cosponsored by AHRQ and the American Medical Informatics Association, took place in 2008. The third annual Diagnostic Error in Medicine conference will be held in Canada in October, reflecting the expanding focus on uncovering root causes of diagnostic error and developing preventive measures aimed at safeguarding patients and avoiding lawsuits.
Because diagnostic errors have long been underemphasized and understudied—and remain difficult to track—it is hard to know just how often they occur. Estimates of their frequency fluctuate widely from 1 study to another, but are generally in the range of 10% to 15%.7 Fatal illnesses appear to be misdiagnosed more frequently than less severe conditions: A review of more than 50 autopsy studies found that, on average, about 1 in 4 (23.5%) major diagnoses were missed.1
Whatever the numbers, diagnostic missteps are clearly common enough to be on patients’ radar screen. In a recent survey of US adults, 55% of respondents cited misdiagnosis as their greatest concern when they see a doctor in an outpatient setting.8 In a Harris Poll commissioned by the National Patient Safety Foundation9 several years earlier, 1 in 6 adults reported having had a condition that was misdiagnosed.
Evidence suggests that while years of experience and strong diagnostic skills help prevent diagnostic errors, they do not afford full protection against the cascade of events that can result in a serious diagnostic error. In fact, overconfidence may contribute to the problem.10,11
Check out the 3 legal cases in the pages that follow from the files of John Davenport, MD, JD. Dr. Davenport, a medical malpractice attorney, provided legal representation in each of these cases.
The take-away message: No physician is immune to misdiagnosis or to a subsequent lawsuit. There are, however, steps you can take to safeguard your patients and yourself, but first you need to know where the pitfalls lie.
Misdiagnosis in primary care: What malpractice claims reveal
Diagnostic errors that result in malpractice claims undergo extensive legal review. Thus, they provide an excellent opportunity for analysis, as the authors of a study of 181 “closed,” or completed, claims from 4 malpractice insurers found.12 The errors all occurred in ambulatory settings, with primary care physicians most frequently involved.
Nearly 6 in 10 of the lawsuits were for missed or delayed cancer diagnoses, followed by misdiagnosis of infection, fracture, and myocardial infarction. Overall, 24% of the cases involved breast cancer. No other disorder came close.
The most common problems, or “breakdowns,” in the diagnostic process were:
- failure to order the appropriate diagnostic test (which occurred in 55% of the cases)
- failure to create a proper follow-up plan (45%)
- failure to obtain a thorough medical history or to perform a thorough physical examination (42%).12
Notably, however, diagnostic errors rarely had a single cause. A median of 3 breakdowns per case was identified, and more than 4 in 10 cases involved more than 1 clinician.
Additional sources of breakdowns ran the gamut from patient factors (eg, non-compliance, atypical presentation, or a delay in seeking care) to system errors (eg, delay in seeing a test result, referral delay, or a mishandled handoff). Rarely was misdiagnosis attributed to a physician’s cognitive error alone. Most diagnostic errors, the authors reported, involved “a potent combination of individual and system factors.” 12
Is it cancer? Failure to test or follow up
Cancer may not be the most frequently misdiagnosed condition, but because of the dire consequences often associated with a delay in detection, cancer is No. 1 in frequency of diagnostic error lawsuits13—with breast cancer typically at or near the top of the list. Evidence suggests that clinician preconception plays a role.
Most women who develop breast cancer are over the age of 50, but plaintiffs in breast cancer suits tend to be younger.14,15 This may be partly because of overreliance on age as a predictive factor, causing some physicians to offer a younger woman what may be unwarranted reassurance that a breast lump is due to fibrocystic tissue rather than malignancy (CASE 1).
Ordering a test is not enough. Even when physicians order the correct test, follow-up may fall short. In the closed claims study, physicians incorrectly interpreted test results in 37% of the cases.12 Other evidence suggests that about a third of women with abnormal mammograms do not receive follow-up care that’s consistent with established guidelines.16
What’s more, physicians sometimes overlook the fact that diagnostic tests are rarely 100% accurate. Mammography misses approximately 20% of breast cancer cases,17 for example, and a woman with a palpable lump should be closely watched, not dismissed on the basis of a negative mammogram result.1,15
What happens to test results? In other cases, the problem is not that a test result doesn’t match the clinical findings, but that the result is not reviewed by the physician or conveyed to the patient in a timely manner. Indeed, the title of a published report of a survey of internists starts with the quote, “I wish I had seen this test result earlier!” 18 Of the 262 internists surveyed, only 41% expressed satisfaction with their method of handling test results.
What would satisfy these physicians? Respondents said what they wanted in a test result management system were tools that would help them generate letters to patients detailing the results, prioritize their workflow, and track orders for tests to completion.
A 32-year-old woman sought care for “sore breasts” 4 months postpartum. Her primary care physician found “bilateral lumpy and tender breasts,” diagnosed fibrocystic breast disease, and prescribed a nonsteroidal anti-inflammatory drug. There was no follow-up plan documented.
She returned in 4 months, stating her symptoms were better but she still had soreness in her left breast. The physician did not examine her, but changed her medication to a different anti-inflammatory. Follow-up was to “return to clinic PRN.”
On her next visit she complained of a lump in the left breast. The physician found a “spongy irregular 2 cm lump” in the upper outer quadrant of the breast, diagnosed a fibrocystic lesion, and reassured the patient. Follow-up again was to return PRN.
Several months later, the patient saw another physician, for back pain and a painful and enlarging breast lump. The physician suspected fibrocystic disease but was unable to obtain fluid by fine needle aspiration. The patient was referred to a surgeon, who obtained a nondiagnostic needle biopsy and an excisional biopsy, which revealed breast cancer. The patient’s back pain turned out to be from metastatic breast cancer. She sued for failure to diagnose breast cancer. The case was settled for an undisclosed large sum.
Commentary: Failure to diagnose breast cancer is a leading cause of malpractice lawsuits, many of them in younger women. Plaintiff recoveries correlate with the length of the delay in diagnosis.
In this case, experts identified a series of missteps in the care of this patient which, when combined with a young, very sick, and sympathetic plaintiff, led to a large recovery. Although it may have been reasonable to diagnose fibrocystic disease on the first visit, experts cited the failure to take a family history (the patient’s aunt and maternal grandmother had had breast cancer) and the failure to document a follow-up plan as damaging to the doctor’s case. They also faulted the physician for failing to examine the breast on the second visit and failing to do fine needle aspiration or refer on the third visit, and for the nonspecific follow-up plans.
Diagnostic lesson: Although breast cancer is less common in women younger than 40, it does occur, and the same diligence in examination, charting, and follow up is required regardless of the patient’s age.
By the way, doc… Harried physician, hurried response
What physician isn’t familiar with the patient who comes in for care of 1, or several, chronic conditions, but mentions another problem as he or she is getting ready to walk out the door (CASE 2)? If that problem appears to be a transient and treatable condition, the temptation is to make a hasty diagnosis and write a prescription, without the usual degree of history taking, patient examination, contemplation, or documentation. Doing so, however, poses considerable risk, to both patient and physician.
If the condition or symptom is serious enough to address in the course of the visit, it requires the same level of attention as any other presenting problem. When time constraints prevent you from addressing the complaint with the proper diligence, it would be appropriate—assuming the symptom in question is nonurgent—to ask the patient to make another appointment. But be sure to document that you did so.
A 62-year-old man saw his family physician for routine care of hypertension, diabetes, and hyperlipidemia. During the visit, the patient mentioned that he had back pain, insomnia, and a sore tongue, which the physician diagnosed as aphthous stomatitis and for which a steroidal oral cream was prescribed.
The patient was scheduled to return for a routine visit in 4 months, but did not come in until 7 months had passed—at which time the physician noted a >1 cm nodular bleeding tongue lesion. Biopsy showed squamous cell cancer, and the patient required extensive surgery, chemotherapy, and radiation. He sued for misdiagnosis and delayed diagnosis.
The physician’s defense was that given the symptoms and findings, aphthous stomatitis was a reasonable diagnosis and that he had instructed the patient to return to the office if he didn’t feel better in a few weeks. The patient disputed this. His attorney noted that the patient had multiple risk factors for tongue cancer that were not in the medical record; nor was there documentation of a tongue examination or the claimed instructions for the return visit, indicating that the patient received substandard care. The case was settled at trial for $300,000.
Commentary: The contrast between the thorough documentation for the patient’s chronic disease history and physical exam and the absence of documentation for the sore tongue suggests that this was an instance of a “by the way, doc” conversation—and a reminder of the risk that physicians assume when managing patients with multiple conditions.
Diagnostic lesson: The law does not give physicians a pass on the standard of care, regardless of how many conditions are treated in a single visit. To avoid a diagnostic error—and a potential lawsuit—a symptom-specific history, physical, and clear instructions with a follow-up plan are necessary for every condition that’s addressed.
How sure are you of the diagnosis?
It’s human nature to see things in terms of what you’re familiar with. A doctor who has been treating a patient with migraine headaches for years, for example, is apt to assume that “the worst migraine I’ve ever had” is more of the same (CASE 3). Similarly, a clinician who has identified a disorder that matches several of a patient’s symptoms may dismiss or overlook signs and symptoms that do not fit that explanation or diagnosis. Safety advocates refer to this phenomenon as “premature closure.” It may also be a function of overconfidence.
One example of physician overconfidence comes from a study in which experienced dermatologists were asked to examine lesions and diagnose melanoma. Although the specialists confidently diagnosed melanoma in more than 50% of the test cases, 30% of their decisions were later found to be incorrect.19
A 47-year-old man with a history of migraines walked into his physician’s clinic with a complaint of a severe headache. His physician was fully booked but he was given an appointment with a per diem physician. According to the patient and a friend who accompanied him, the patient told the doctor, “This is the worst migraine of my life.” The physician simply documented, “flare of migraine.” The chart indicated that the physical revealed normal vital signs and noted that the patient was “photophobic,” but that his neurological exam was “intact.”
Over the next several hours, the patient received sumatriptan and several doses of opioid analgesics. He stated that he still had a headache but felt better and was sent home with instructions to call or come in if the headache returned.
The next morning a neighbor, unable to reach the patient on the phone, went to his house and found him in a stupor, with slurred speech. The patient was taken by ambulance to a local hospital and found to have a subarachnoid hemorrhage. After weeks in the hospital and a rehabilitation center, he was left with significant cognitive and neurological impairments. He sued for failure to diagnose and won a multimillion dollar award at trial.
Commentary: Expert testimony clearly pointed to the history and physical as being substandard. Specifically, the physical should have included, among other things, a test for nuchal rigidity. Had the patient not had a history of migraines, he might have undergone a more complete medical history and physical evaluation and his symptoms would likely have been evaluated more thoroughly.
Diagnostic lesson: Be wary of “diagnostic inertia”—the tendency to depend too much on a past diagnosis when symptoms arise. Don’t be trapped into attributing all new symptoms to an old disease.
Build a no-fault, fail-safe system
The purpose of analyzing diagnostic errors is not to assign blame or point a finger at physicians, but rather to find and fix flaws in the medical system.20 That approach has been used by patient safety advocates to address other types of errors following the publication of the Institute of Medicine’s landmark report on medical error 11 years ago.21
Since then, many physician leaders have looked to the airline industry—a field in which the consequences for not strictly adhering to a fail-safe system are likely to be fatal. That reality has led to the development of vital checklists, forcing functions (in which the user is prevented from moving to the next step until the current step is completed), and computerized reminders in an attempt to eliminate, to the extent possible, the chance of human error.
The same principle can be applied to misdiagnosis. Recommended steps—ordering diagnostic tests or referring to a specialist, for example—should be put into motion whenever a set of predetermined parameters are met, rather than relying on physician memory or choice.20
Similarly, checklists should specify questions to ask or criteria to be met under specified circumstances to prevent physicians from prematurely settling on a (possibly incorrect) diagnosis. To avoid a rush to judgment, some patient safety advocates1 stress the importance of assessing the urgency of a patient’s condition, rather than trying to arrive at a definitive diagnosis the first time he or she presents with a perplexing set of signs and symptoms. Other recommendations follow:
Mandate a second look. Develop and adhere to a set of criteria to determine when a referral to a specialist or a physician consultation is needed, rather than deciding on a case-by-case basis.
Plug the holes in your follow-up system. Develop a fail-safe system for reviewing diagnostic tests or laboratory findings and reporting them to patients without delay. This can be done with an electronic health record (EHR) system or by developing and adhering to parameters requiring, for instance, that no test result get filed until there are 2 signatures on it—that of the physician who ordered the test, indicating that he or she has seen it, and that of a staff member, indicating that the patient has been notified of the results. As an additional back-up, tell patients undergoing tests when to expect to get results, and stress the importance of calling the office if they do not receive such notification within a specified time frame.
Partner with patients. Engage patients in the pursuit of a definitive diagnosis. Discuss your preliminary findings, describe your treatment decision and what you expect to occur, and urge patients to contact you with evidence that confirms or refutes that expectation. Elicit additional feedback at each visit until either the symptoms have fully resolved or you have gathered enough information to arrive at a definitive diagnosis.
Develop “don’t-miss” checklists. One list should cover diagnostic red flags to be considered anytime you see a symptomatic patient to ensure that you don’t overlook important signs and symptoms, and include findings that warrant hospital admission, specified diagnostic tests, and immediate referral. (A patient who comes in with a “common pink eye,” but has consensual photophobia, is at risk for iritis and needs an urgent ophthalmology evaluation, for instance.) Another list you should develop is a “must-do” list for well visits, featuring clinical scenarios to address and screening tests to remember, such as an eye exam for patients with diabetes.
Question your initial diagnosis. Beware of “premature closure”—the tendency to stop looking for other signs and symptoms once you find a presumptive diagnosis—and “diagnostic inertia”—evaluating new signs and symptoms almost exclusively on the basis of past medical history. If aspects of a patient presentation do not fit your presumed diagnosis, use a decision support system, if available, to review other possibilities.
Head off hand-off errors. Develop a problem list for each patient to reduce the likelihood that crucial information will be overlooked when more than 1 clinician is involved in his or her care. Include chronic and acute conditions, unexplained signs and symptoms, medications, and allergies. Create a fail-safe system for other potential hand-off problems, as well—requiring confirmation that the findings in a preliminary radiology report are the same as those in the final report before you take action based on the preliminary report, for example, and ensuring that you receive prompt notification whenever that is not the case.
EHRs and decision support: Isn’t it time?
In 2009, 44% of office-based physicians had EHRs, according to a Centers for Disease Control and Prevention preliminary report.22 Federal funding to promote the adoption of EHRs is expected to accelerate their use. Among the benefits of EHRs are clinical reminders, system alerts, and documentation tools that can help reduce the risk of diagnostic missteps and avert misdiagnosis lawsuits.
The Department of Veterans Affairs uses a notification system called View Alert, for example, that tracks acknowledgement of abnormal radiology test results and flags those that remain unacknowledged. 23 EHR systems can also be programmed to issue automated appointment reminders that make it easier to track patients who do not show up for critical follow-up visits.
Diagnostic decision support software adds another critical element. When a clinician inputs a set of symptoms and patient-specific data, such systems produce lists of possible diagnoses, often divided by bodily system.
While many safety advocates believe that the use of such systems will increase the likelihood of accurate diagnosis, critics point out that the software is only as good as the clinician using it. One concern is that computerized systems typically come with a “macro” ability—that is, the ability to enter large amounts of information with the click of a key. This raises the possibility that an overload of patient data, some of which may be incorrect, will be added to the medical record—or that the system will generate so many possibilities that clinicians will cease to pay attention. Both can lead to inferences of inattention or raise doubts about a physician’s credibility in a legal setting.
Electronic prescribing software systems that flag potential drug interactions are a case in point. Forty-five percent of family physicians responding to a Journal of Family Practice Instant Poll about their use of such systems reported that they override them frequently. The problem, according to 1 respondent: The system gives “so many red flags that I routinely ignore them all—like the little boy who cried wolf.”
CORRESPONDENCE John Davenport, MD, JD, 13 Redonda, Irvine, CA 92620; [email protected]
• Create a problem list for each patient, including chronic and acute conditions, unexplained signs and symptoms, medications, and allergies. C
• Avoid attributing every new symptom to the patient’s documented medical conditions. C
• Develop and adhere to “don’t-miss” lists of signs and symptoms that warrant rapid action. C
• Establish a fail-safe system to ensure that you receive notification whenever a final imaging or lab report differs from the preliminary report and document your response to each abnormal result. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Misdiagnosis accounts for more malpractice claims than medication errors—indeed, for more lawsuits than any other medical misstep.1-5 Yet until recently, diagnostic errors garnered little attention from patient safety advocates.
That’s no longer the case. In 2007, the Agency for Healthcare Research and Quality (AHRQ) identified diagnostic errors (a catchall category encompassing delayed, incorrect, and missed diagnoses) as a problem that warranted closer study.6 The inaugural conference on Diagnostic Error in Medicine, cosponsored by AHRQ and the American Medical Informatics Association, took place in 2008. The third annual Diagnostic Error in Medicine conference will be held in Canada in October, reflecting the expanding focus on uncovering root causes of diagnostic error and developing preventive measures aimed at safeguarding patients and avoiding lawsuits.
Because diagnostic errors have long been underemphasized and understudied—and remain difficult to track—it is hard to know just how often they occur. Estimates of their frequency fluctuate widely from 1 study to another, but are generally in the range of 10% to 15%.7 Fatal illnesses appear to be misdiagnosed more frequently than less severe conditions: A review of more than 50 autopsy studies found that, on average, about 1 in 4 (23.5%) major diagnoses were missed.1
Whatever the numbers, diagnostic missteps are clearly common enough to be on patients’ radar screen. In a recent survey of US adults, 55% of respondents cited misdiagnosis as their greatest concern when they see a doctor in an outpatient setting.8 In a Harris Poll commissioned by the National Patient Safety Foundation9 several years earlier, 1 in 6 adults reported having had a condition that was misdiagnosed.
Evidence suggests that while years of experience and strong diagnostic skills help prevent diagnostic errors, they do not afford full protection against the cascade of events that can result in a serious diagnostic error. In fact, overconfidence may contribute to the problem.10,11
Check out the 3 legal cases in the pages that follow from the files of John Davenport, MD, JD. Dr. Davenport, a medical malpractice attorney, provided legal representation in each of these cases.
The take-away message: No physician is immune to misdiagnosis or to a subsequent lawsuit. There are, however, steps you can take to safeguard your patients and yourself, but first you need to know where the pitfalls lie.
Misdiagnosis in primary care: What malpractice claims reveal
Diagnostic errors that result in malpractice claims undergo extensive legal review. Thus, they provide an excellent opportunity for analysis, as the authors of a study of 181 “closed,” or completed, claims from 4 malpractice insurers found.12 The errors all occurred in ambulatory settings, with primary care physicians most frequently involved.
Nearly 6 in 10 of the lawsuits were for missed or delayed cancer diagnoses, followed by misdiagnosis of infection, fracture, and myocardial infarction. Overall, 24% of the cases involved breast cancer. No other disorder came close.
The most common problems, or “breakdowns,” in the diagnostic process were:
- failure to order the appropriate diagnostic test (which occurred in 55% of the cases)
- failure to create a proper follow-up plan (45%)
- failure to obtain a thorough medical history or to perform a thorough physical examination (42%).12
Notably, however, diagnostic errors rarely had a single cause. A median of 3 breakdowns per case was identified, and more than 4 in 10 cases involved more than 1 clinician.
Additional sources of breakdowns ran the gamut from patient factors (eg, non-compliance, atypical presentation, or a delay in seeking care) to system errors (eg, delay in seeing a test result, referral delay, or a mishandled handoff). Rarely was misdiagnosis attributed to a physician’s cognitive error alone. Most diagnostic errors, the authors reported, involved “a potent combination of individual and system factors.” 12
Is it cancer? Failure to test or follow up
Cancer may not be the most frequently misdiagnosed condition, but because of the dire consequences often associated with a delay in detection, cancer is No. 1 in frequency of diagnostic error lawsuits13—with breast cancer typically at or near the top of the list. Evidence suggests that clinician preconception plays a role.
Most women who develop breast cancer are over the age of 50, but plaintiffs in breast cancer suits tend to be younger.14,15 This may be partly because of overreliance on age as a predictive factor, causing some physicians to offer a younger woman what may be unwarranted reassurance that a breast lump is due to fibrocystic tissue rather than malignancy (CASE 1).
Ordering a test is not enough. Even when physicians order the correct test, follow-up may fall short. In the closed claims study, physicians incorrectly interpreted test results in 37% of the cases.12 Other evidence suggests that about a third of women with abnormal mammograms do not receive follow-up care that’s consistent with established guidelines.16
What’s more, physicians sometimes overlook the fact that diagnostic tests are rarely 100% accurate. Mammography misses approximately 20% of breast cancer cases,17 for example, and a woman with a palpable lump should be closely watched, not dismissed on the basis of a negative mammogram result.1,15
What happens to test results? In other cases, the problem is not that a test result doesn’t match the clinical findings, but that the result is not reviewed by the physician or conveyed to the patient in a timely manner. Indeed, the title of a published report of a survey of internists starts with the quote, “I wish I had seen this test result earlier!” 18 Of the 262 internists surveyed, only 41% expressed satisfaction with their method of handling test results.
What would satisfy these physicians? Respondents said what they wanted in a test result management system were tools that would help them generate letters to patients detailing the results, prioritize their workflow, and track orders for tests to completion.
A 32-year-old woman sought care for “sore breasts” 4 months postpartum. Her primary care physician found “bilateral lumpy and tender breasts,” diagnosed fibrocystic breast disease, and prescribed a nonsteroidal anti-inflammatory drug. There was no follow-up plan documented.
She returned in 4 months, stating her symptoms were better but she still had soreness in her left breast. The physician did not examine her, but changed her medication to a different anti-inflammatory. Follow-up was to “return to clinic PRN.”
On her next visit she complained of a lump in the left breast. The physician found a “spongy irregular 2 cm lump” in the upper outer quadrant of the breast, diagnosed a fibrocystic lesion, and reassured the patient. Follow-up again was to return PRN.
Several months later, the patient saw another physician, for back pain and a painful and enlarging breast lump. The physician suspected fibrocystic disease but was unable to obtain fluid by fine needle aspiration. The patient was referred to a surgeon, who obtained a nondiagnostic needle biopsy and an excisional biopsy, which revealed breast cancer. The patient’s back pain turned out to be from metastatic breast cancer. She sued for failure to diagnose breast cancer. The case was settled for an undisclosed large sum.
Commentary: Failure to diagnose breast cancer is a leading cause of malpractice lawsuits, many of them in younger women. Plaintiff recoveries correlate with the length of the delay in diagnosis.
In this case, experts identified a series of missteps in the care of this patient which, when combined with a young, very sick, and sympathetic plaintiff, led to a large recovery. Although it may have been reasonable to diagnose fibrocystic disease on the first visit, experts cited the failure to take a family history (the patient’s aunt and maternal grandmother had had breast cancer) and the failure to document a follow-up plan as damaging to the doctor’s case. They also faulted the physician for failing to examine the breast on the second visit and failing to do fine needle aspiration or refer on the third visit, and for the nonspecific follow-up plans.
Diagnostic lesson: Although breast cancer is less common in women younger than 40, it does occur, and the same diligence in examination, charting, and follow up is required regardless of the patient’s age.
By the way, doc… Harried physician, hurried response
What physician isn’t familiar with the patient who comes in for care of 1, or several, chronic conditions, but mentions another problem as he or she is getting ready to walk out the door (CASE 2)? If that problem appears to be a transient and treatable condition, the temptation is to make a hasty diagnosis and write a prescription, without the usual degree of history taking, patient examination, contemplation, or documentation. Doing so, however, poses considerable risk, to both patient and physician.
If the condition or symptom is serious enough to address in the course of the visit, it requires the same level of attention as any other presenting problem. When time constraints prevent you from addressing the complaint with the proper diligence, it would be appropriate—assuming the symptom in question is nonurgent—to ask the patient to make another appointment. But be sure to document that you did so.
A 62-year-old man saw his family physician for routine care of hypertension, diabetes, and hyperlipidemia. During the visit, the patient mentioned that he had back pain, insomnia, and a sore tongue, which the physician diagnosed as aphthous stomatitis and for which a steroidal oral cream was prescribed.
The patient was scheduled to return for a routine visit in 4 months, but did not come in until 7 months had passed—at which time the physician noted a >1 cm nodular bleeding tongue lesion. Biopsy showed squamous cell cancer, and the patient required extensive surgery, chemotherapy, and radiation. He sued for misdiagnosis and delayed diagnosis.
The physician’s defense was that given the symptoms and findings, aphthous stomatitis was a reasonable diagnosis and that he had instructed the patient to return to the office if he didn’t feel better in a few weeks. The patient disputed this. His attorney noted that the patient had multiple risk factors for tongue cancer that were not in the medical record; nor was there documentation of a tongue examination or the claimed instructions for the return visit, indicating that the patient received substandard care. The case was settled at trial for $300,000.
Commentary: The contrast between the thorough documentation for the patient’s chronic disease history and physical exam and the absence of documentation for the sore tongue suggests that this was an instance of a “by the way, doc” conversation—and a reminder of the risk that physicians assume when managing patients with multiple conditions.
Diagnostic lesson: The law does not give physicians a pass on the standard of care, regardless of how many conditions are treated in a single visit. To avoid a diagnostic error—and a potential lawsuit—a symptom-specific history, physical, and clear instructions with a follow-up plan are necessary for every condition that’s addressed.
How sure are you of the diagnosis?
It’s human nature to see things in terms of what you’re familiar with. A doctor who has been treating a patient with migraine headaches for years, for example, is apt to assume that “the worst migraine I’ve ever had” is more of the same (CASE 3). Similarly, a clinician who has identified a disorder that matches several of a patient’s symptoms may dismiss or overlook signs and symptoms that do not fit that explanation or diagnosis. Safety advocates refer to this phenomenon as “premature closure.” It may also be a function of overconfidence.
One example of physician overconfidence comes from a study in which experienced dermatologists were asked to examine lesions and diagnose melanoma. Although the specialists confidently diagnosed melanoma in more than 50% of the test cases, 30% of their decisions were later found to be incorrect.19
A 47-year-old man with a history of migraines walked into his physician’s clinic with a complaint of a severe headache. His physician was fully booked but he was given an appointment with a per diem physician. According to the patient and a friend who accompanied him, the patient told the doctor, “This is the worst migraine of my life.” The physician simply documented, “flare of migraine.” The chart indicated that the physical revealed normal vital signs and noted that the patient was “photophobic,” but that his neurological exam was “intact.”
Over the next several hours, the patient received sumatriptan and several doses of opioid analgesics. He stated that he still had a headache but felt better and was sent home with instructions to call or come in if the headache returned.
The next morning a neighbor, unable to reach the patient on the phone, went to his house and found him in a stupor, with slurred speech. The patient was taken by ambulance to a local hospital and found to have a subarachnoid hemorrhage. After weeks in the hospital and a rehabilitation center, he was left with significant cognitive and neurological impairments. He sued for failure to diagnose and won a multimillion dollar award at trial.
Commentary: Expert testimony clearly pointed to the history and physical as being substandard. Specifically, the physical should have included, among other things, a test for nuchal rigidity. Had the patient not had a history of migraines, he might have undergone a more complete medical history and physical evaluation and his symptoms would likely have been evaluated more thoroughly.
Diagnostic lesson: Be wary of “diagnostic inertia”—the tendency to depend too much on a past diagnosis when symptoms arise. Don’t be trapped into attributing all new symptoms to an old disease.
Build a no-fault, fail-safe system
The purpose of analyzing diagnostic errors is not to assign blame or point a finger at physicians, but rather to find and fix flaws in the medical system.20 That approach has been used by patient safety advocates to address other types of errors following the publication of the Institute of Medicine’s landmark report on medical error 11 years ago.21
Since then, many physician leaders have looked to the airline industry—a field in which the consequences for not strictly adhering to a fail-safe system are likely to be fatal. That reality has led to the development of vital checklists, forcing functions (in which the user is prevented from moving to the next step until the current step is completed), and computerized reminders in an attempt to eliminate, to the extent possible, the chance of human error.
The same principle can be applied to misdiagnosis. Recommended steps—ordering diagnostic tests or referring to a specialist, for example—should be put into motion whenever a set of predetermined parameters are met, rather than relying on physician memory or choice.20
Similarly, checklists should specify questions to ask or criteria to be met under specified circumstances to prevent physicians from prematurely settling on a (possibly incorrect) diagnosis. To avoid a rush to judgment, some patient safety advocates1 stress the importance of assessing the urgency of a patient’s condition, rather than trying to arrive at a definitive diagnosis the first time he or she presents with a perplexing set of signs and symptoms. Other recommendations follow:
Mandate a second look. Develop and adhere to a set of criteria to determine when a referral to a specialist or a physician consultation is needed, rather than deciding on a case-by-case basis.
Plug the holes in your follow-up system. Develop a fail-safe system for reviewing diagnostic tests or laboratory findings and reporting them to patients without delay. This can be done with an electronic health record (EHR) system or by developing and adhering to parameters requiring, for instance, that no test result get filed until there are 2 signatures on it—that of the physician who ordered the test, indicating that he or she has seen it, and that of a staff member, indicating that the patient has been notified of the results. As an additional back-up, tell patients undergoing tests when to expect to get results, and stress the importance of calling the office if they do not receive such notification within a specified time frame.
Partner with patients. Engage patients in the pursuit of a definitive diagnosis. Discuss your preliminary findings, describe your treatment decision and what you expect to occur, and urge patients to contact you with evidence that confirms or refutes that expectation. Elicit additional feedback at each visit until either the symptoms have fully resolved or you have gathered enough information to arrive at a definitive diagnosis.
Develop “don’t-miss” checklists. One list should cover diagnostic red flags to be considered anytime you see a symptomatic patient to ensure that you don’t overlook important signs and symptoms, and include findings that warrant hospital admission, specified diagnostic tests, and immediate referral. (A patient who comes in with a “common pink eye,” but has consensual photophobia, is at risk for iritis and needs an urgent ophthalmology evaluation, for instance.) Another list you should develop is a “must-do” list for well visits, featuring clinical scenarios to address and screening tests to remember, such as an eye exam for patients with diabetes.
Question your initial diagnosis. Beware of “premature closure”—the tendency to stop looking for other signs and symptoms once you find a presumptive diagnosis—and “diagnostic inertia”—evaluating new signs and symptoms almost exclusively on the basis of past medical history. If aspects of a patient presentation do not fit your presumed diagnosis, use a decision support system, if available, to review other possibilities.
Head off hand-off errors. Develop a problem list for each patient to reduce the likelihood that crucial information will be overlooked when more than 1 clinician is involved in his or her care. Include chronic and acute conditions, unexplained signs and symptoms, medications, and allergies. Create a fail-safe system for other potential hand-off problems, as well—requiring confirmation that the findings in a preliminary radiology report are the same as those in the final report before you take action based on the preliminary report, for example, and ensuring that you receive prompt notification whenever that is not the case.
EHRs and decision support: Isn’t it time?
In 2009, 44% of office-based physicians had EHRs, according to a Centers for Disease Control and Prevention preliminary report.22 Federal funding to promote the adoption of EHRs is expected to accelerate their use. Among the benefits of EHRs are clinical reminders, system alerts, and documentation tools that can help reduce the risk of diagnostic missteps and avert misdiagnosis lawsuits.
The Department of Veterans Affairs uses a notification system called View Alert, for example, that tracks acknowledgement of abnormal radiology test results and flags those that remain unacknowledged. 23 EHR systems can also be programmed to issue automated appointment reminders that make it easier to track patients who do not show up for critical follow-up visits.
Diagnostic decision support software adds another critical element. When a clinician inputs a set of symptoms and patient-specific data, such systems produce lists of possible diagnoses, often divided by bodily system.
While many safety advocates believe that the use of such systems will increase the likelihood of accurate diagnosis, critics point out that the software is only as good as the clinician using it. One concern is that computerized systems typically come with a “macro” ability—that is, the ability to enter large amounts of information with the click of a key. This raises the possibility that an overload of patient data, some of which may be incorrect, will be added to the medical record—or that the system will generate so many possibilities that clinicians will cease to pay attention. Both can lead to inferences of inattention or raise doubts about a physician’s credibility in a legal setting.
Electronic prescribing software systems that flag potential drug interactions are a case in point. Forty-five percent of family physicians responding to a Journal of Family Practice Instant Poll about their use of such systems reported that they override them frequently. The problem, according to 1 respondent: The system gives “so many red flags that I routinely ignore them all—like the little boy who cried wolf.”
CORRESPONDENCE John Davenport, MD, JD, 13 Redonda, Irvine, CA 92620; [email protected]
1. Schiff GD, Kim S, Abrams R, et al. Diagnosing diagnosis errors: lessons from a multi-institutional collaborative project. Adv Patient Safety. 2005;255:255-278.
2. Sato L. Evidence-based patient safety and risk management technology. J Qual Improv. 2001;27:435.-
3. Phillips R, Bartholomew L, Dovey S, et al. Learning from malpractice claims about negligent, adverse events in primary care in the United States. Qual Saf Health Care. 2004;13:121-126.
4. Fitzgerald N. Top five causes of malpractice claims. American Physicians Assurance Corporation. 2004. Available at: http://www.apassurance.com/RiskMgt/Articles_RM/5%20Causes%20of%20Claims_RMArticle.pdf. Accessed August 2, 2010.
5. Chandra A, Nundy S, Seabury SA. The growth of physician medical malpractice payments: evidence from the National Practitioner Data Bank. Health Aff (Millwood). 2005;W5(suppl):240-249.
6. Agency for Healthcare Research and Quality Special emphasis notice (SEN): AHRQ announces interest in research on diagnostic errors in ambulatory care settings. Available at: http://grants.nih.gv/grants/guide/notice-files-NOT-HS-08-002.html. Accessed July 30, 2010.
7. Berner ES, Graber ML. Overconfidence as a cause of diagnostic error in medicine. Am J Med. 2008;121(suppl 5A):S2-S23.
8. Isabel Healthcare. Misdiagnosis is an overlooked and growing patient safety issue and core mission of Isabel Healthcare. March 20, 2006. Available at http://www.isabelhealthcare.com/pdf/USsurveyrelease-Final.pdf. Accessed August 4, 2010.
9. Golodner L. How the public perceives patient safety. Newsletter of the National Patient Safety Foundation. 2004;1997:1-6.
10. Berner ES. Diagnostic error in medicine: introduction. Adv Health Sci Educ Theory Pract. 2009;14(suppl 1):1-5.
11. Friedman CP, Gatti GG, Franz TM, et al. Do physicians know when their diagnoses are correct? Implications for decision support and error reduction. J Gen Intern Med. 2005;20:334-339.
12. Ghandi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med. 2006;145:488-496.
13. McDonald C, Hernandez MB, Gofman Y, et al. The five most common misdiagnoses: a meta-analysis of autopsy and malpractice data. Internet J Fam Pract. 2009;7(2). Available at http://www.ispub.com/journal/the_internet_journal_of_family_practice/volume_7_number_2_19/article/the-five-most-common-misdiagnosesa-meta-analysis-of-autopsy-and-malpractice-data.html. Accessed July 23, 2010.
14. Mitnick JS, Vasquez MF, Kronovet SZ, et al. Malpractice litigation involving patients with carcinoma of the breast. J Am Coll Surg. 1995;181:315-321.
15. Failure to diagnose breast cancer. Medical Malpractice Lawyers and Attorneys Online. http://www.medical-malpractice-attorneys-lawsuits.com/pages/breast-cancer.html. Accessed August 2, 2010.
16. Poon EG, Haas JS, Puopolo AL, et al. Communication factors in the follow-up of abnormal mammograms. J Gen Intern Med. 2004;19:316-323.
17. National Cancer Institute. Fact sheet. Mammograms. Available at: http://www.cancer.gov/cancertopics/factsheet/Detection/mammograms. Accessed August 3, 2010.
18. Poon EG, Gandhi TK, Sequist TD, et al. “I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care. Arch Intern Med. 2004;164:2223-2228.
19. Dreistl S, Binder M. Do physicians value decision support? A look at the effect of decision support on physician opinion. Artif Intell Med. 2005;33:25-30.
20. Newman-Toker DE, Pronovost PJ. Diagnostic errors: the new frontier for patient safety. JAMA. 2009;301:1060-1062.
21. Institute of Medicine. To err is human: building a safer health system. Washington, DC: November 1, 1999.
22. Centers for Disease Control and Prevention. NCHS Health E-Stat. Electronic medical record/electronic health record use by office-based physicians: United States, 2008 and preliminary 2009. Available at: http://www.cdc.gov/nchs/data/hestat/emr_ehr/emr_ehr.htm. Accessed July 30, 2010.
23. Singh H, Arora HS, Vij MS, et al. Communication outcomes of critical imaging results in a computerized notification system. J Am Med Inform Assoc. 2007;14:459-466.
1. Schiff GD, Kim S, Abrams R, et al. Diagnosing diagnosis errors: lessons from a multi-institutional collaborative project. Adv Patient Safety. 2005;255:255-278.
2. Sato L. Evidence-based patient safety and risk management technology. J Qual Improv. 2001;27:435.-
3. Phillips R, Bartholomew L, Dovey S, et al. Learning from malpractice claims about negligent, adverse events in primary care in the United States. Qual Saf Health Care. 2004;13:121-126.
4. Fitzgerald N. Top five causes of malpractice claims. American Physicians Assurance Corporation. 2004. Available at: http://www.apassurance.com/RiskMgt/Articles_RM/5%20Causes%20of%20Claims_RMArticle.pdf. Accessed August 2, 2010.
5. Chandra A, Nundy S, Seabury SA. The growth of physician medical malpractice payments: evidence from the National Practitioner Data Bank. Health Aff (Millwood). 2005;W5(suppl):240-249.
6. Agency for Healthcare Research and Quality Special emphasis notice (SEN): AHRQ announces interest in research on diagnostic errors in ambulatory care settings. Available at: http://grants.nih.gv/grants/guide/notice-files-NOT-HS-08-002.html. Accessed July 30, 2010.
7. Berner ES, Graber ML. Overconfidence as a cause of diagnostic error in medicine. Am J Med. 2008;121(suppl 5A):S2-S23.
8. Isabel Healthcare. Misdiagnosis is an overlooked and growing patient safety issue and core mission of Isabel Healthcare. March 20, 2006. Available at http://www.isabelhealthcare.com/pdf/USsurveyrelease-Final.pdf. Accessed August 4, 2010.
9. Golodner L. How the public perceives patient safety. Newsletter of the National Patient Safety Foundation. 2004;1997:1-6.
10. Berner ES. Diagnostic error in medicine: introduction. Adv Health Sci Educ Theory Pract. 2009;14(suppl 1):1-5.
11. Friedman CP, Gatti GG, Franz TM, et al. Do physicians know when their diagnoses are correct? Implications for decision support and error reduction. J Gen Intern Med. 2005;20:334-339.
12. Ghandi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med. 2006;145:488-496.
13. McDonald C, Hernandez MB, Gofman Y, et al. The five most common misdiagnoses: a meta-analysis of autopsy and malpractice data. Internet J Fam Pract. 2009;7(2). Available at http://www.ispub.com/journal/the_internet_journal_of_family_practice/volume_7_number_2_19/article/the-five-most-common-misdiagnosesa-meta-analysis-of-autopsy-and-malpractice-data.html. Accessed July 23, 2010.
14. Mitnick JS, Vasquez MF, Kronovet SZ, et al. Malpractice litigation involving patients with carcinoma of the breast. J Am Coll Surg. 1995;181:315-321.
15. Failure to diagnose breast cancer. Medical Malpractice Lawyers and Attorneys Online. http://www.medical-malpractice-attorneys-lawsuits.com/pages/breast-cancer.html. Accessed August 2, 2010.
16. Poon EG, Haas JS, Puopolo AL, et al. Communication factors in the follow-up of abnormal mammograms. J Gen Intern Med. 2004;19:316-323.
17. National Cancer Institute. Fact sheet. Mammograms. Available at: http://www.cancer.gov/cancertopics/factsheet/Detection/mammograms. Accessed August 3, 2010.
18. Poon EG, Gandhi TK, Sequist TD, et al. “I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care. Arch Intern Med. 2004;164:2223-2228.
19. Dreistl S, Binder M. Do physicians value decision support? A look at the effect of decision support on physician opinion. Artif Intell Med. 2005;33:25-30.
20. Newman-Toker DE, Pronovost PJ. Diagnostic errors: the new frontier for patient safety. JAMA. 2009;301:1060-1062.
21. Institute of Medicine. To err is human: building a safer health system. Washington, DC: November 1, 1999.
22. Centers for Disease Control and Prevention. NCHS Health E-Stat. Electronic medical record/electronic health record use by office-based physicians: United States, 2008 and preliminary 2009. Available at: http://www.cdc.gov/nchs/data/hestat/emr_ehr/emr_ehr.htm. Accessed July 30, 2010.
23. Singh H, Arora HS, Vij MS, et al. Communication outcomes of critical imaging results in a computerized notification system. J Am Med Inform Assoc. 2007;14:459-466.