User login
9 Tips to Help Prevent Derm Biopsy Mistakes

1. CHOOSE YOUR BIOPSY TYPE WISELY
Using the appropriate type of biopsy can have the greatest effect on a proper diagnosis. The decision of which biopsy type to use is not always easy. The most common biopsy types are shave, punch, excisional, and curettage. Several reference articles detail each type of biopsy commonly used in primary care and how to perform them.1,2
Each type of biopsy has inherent advantages and disadvantages. In general, the shave biopsy is most commonly used for lesions that are solitary and elevated and give the impression that a sufficient amount of tissue can be sampled with this technique. The punch biopsy is the best choice for most “rashes” (inflammatory skin disorders).2 Excisional biopsy is used to remove melanocytic neoplasms or larger lesions. And curettage, while still used by some clinicians for melanocytic lesions because of its speed and simplicity, should almost never be used for diagnostic purposes.
Each technique is described in greater detail in the tips that follow.
Continue for tip #2 >>
2. WHEN PERFORMING A SHAVE BIOPSY, AVOID OBTAINING A SAMPLE THAT'S TOO SUPERFICIAL
The advantage of the shave biopsy is that it is minimally invasive and quick to perform. If kept small without compromising the amount of sample retrieved, the scars left by shave biopsies have the potential to blend well. The major disadvantage associated with the shave biopsy is that occasionally, if the shave is not deep enough, an insufficient amount of tissue is obtained. This can make it challenging to establish an accurate diagnosis.
Balancing the need to obtain adequate tissue with the desire to minimize scarring takes skill and experience. Taking a biopsy that is inadequate is a common occurrence. At times, the clinician’s clinical impression may be that a biopsy has obtained adequate tissue, when histologically only the superficial part of the skin surface has been sampled. This often is because of thickening of the superficial skin, whether as a manifestation of the anatomic site (eg, acral skin) or the disease process itself.
Unfortunately, this superficial skin often is nondiagnostic when unaccompanied by underlying epidermis and dermis. It is important to keep this in mind when you are obtaining a skin biopsy, especially when dealing with lesions that are very scaly or keratinized.

An equivocal biopsy wastes time, energy, and money, and it can negatively impact patient care.3 It can be difficult to balance practical aspects of the biopsy (ie, optimizing cosmetic outcomes, minimizing scarring and wound size) with the need to obtain sufficient tissue sampling (see Figure 1).
3. CHOOSE PUNCH OVER SHAVE BIOPSY FOR RASHES
In a punch biopsy, a disposable metal cylinder with a sharpened edge is used to “punch” out a piece of skin that can be examined under the microscope. Punch biopsy is the preferred technique for almost all inflammatory skin conditions (rashes) because the pathologist is able to examine both the superficial and deep portions of the dermis (see Figure 2).4
Pathologists use the pattern of inflammation, in conjunction with epidermal changes, to distinguish different types of inflammatory processes. For example, lichen planus is typically associated with superficial inflammation, while lupus is known to have prominent superficial and deep inflammation.
An inadequate punch biopsy sample can hinder histologic assessment of inflammatory skin disorders that involve both the superficial and deep portions of the dermis and can make arriving at a definitive diagnosis more challenging. The diameter of a punch cylinder ranges from 1 to 8 mm. Smaller punch biopsies often create diagnostic challenges because they provide so little sample. A punch biopsy size of 4 mm is commonly used for rashes.
An advantage of the punch biopsy is that patients are left with linear scars rather than the round, potentially dyspigmented (darker or lighter) scars that are often associated with shave biopsy. A well-sutured punch biopsy can be cosmetically elegant, particularly if closure is oriented along relaxed skin tension lines. For this reason, punch biopsies are well suited for cosmetically sensitive locations (eg, the face), although shave biopsies are also often performed on the face.

Next page: Tip #4 >>
4. CHOOSE AN EXCISIONAL BIOPSY FOR A MELANOCYTIC NEOPLASM, WHEN POSSIBLE
The purpose of an excisional biopsy (which typically includes a 1- to 3-mm rim of normal skin around the lesion) is to completely remove a lesion. Excisional biopsy generally is the preferred technique for clinically atypical melanocytic neoplasms (ie, lesions that are not definitively benign).4-8
When suspicion for melanoma is high, excisional biopsies should be performed with minimal undermining to preserve the accuracy of any future sentinel lymph node biopsy surgeries. Excisional biopsy is the most involved type of biopsy and has the largest potential for cosmetic disfigurement if not properly planned and performed. While guidelines from the American Academy of Dermatology state that “narrow excisional biopsy that encompasses [the] entire breadth of lesion with clinically negative margins to ensure that the lesion is not transected” is preferred, they also acknowledge that partial sampling (incisional biopsy) is acceptable in select clinical circumstances,9 such as when a lesion is large or on a cosmetically sensitive site (eg, the face).10
While a larger punch biopsy (6 or 8 mm) or even deep shave/saucerization may function as an excisional biopsy for very small lesions, this approach can be problematic. For one thing, these techniques are more likely than an excisional biopsy to leave a portion of the lesion in situ. Another concern is that a shave biopsy of a melanocytic lesion can lead to error or difficulty in obtaining the correct diagnosis on later biopsy.11 For pathologists, small or incomplete samples make it challenging to establish an accurate diagnosis.12 Among melanomas seen at a tertiary referral center, histopathologic misdiagnosis was more common with a punch or shave biopsy than with an excisional biopsy.9

It has been shown that partial biopsy for melanoma results in more residual disease at wide local excision and makes it more challenging to properly stage the lesion.13,14 If a shave biopsy is used to sample a suspected melanocytic neoplasm, it is imperative to document the specific site of the biopsy, indicate the size of the melanocytic lesion on the pathology requisition form, and ensure that all (or nearly all) of the clinically evident lesion is sampled. Detailing the location of the lesion in the chart is not only essential in evaluating the present lesion, but it will serve you well in the future. Without knowing the patient’s clinical history, benign nevi that recur after a prior biopsy can be difficult to histologically distinguish from melanoma (see Figure 3). For more on this, see tip #7.
5. BE CAREFUL WITH CURETTAGE
Curettage is a biopsy technique in which a curette—a surgical tool with a scoop, ring, or loop at the tip—is used in a scraping motion to retrieve tissue from the patient. This type of biopsy often produces a fragmented tissue sample. Its continued use reflects the speed and simplicity with which it can be done. However, curettage destroys the architecture of the tissue of the lesion, which can make it difficult to establish a proper diagnosis, and therefore it is best avoided when performing a biopsy of a melanocytic lesion (see Figure 4).

Continue for tip #6 >>
6. REMEMBER THE IMPORTANCE OF PROPER FIXATION AND PROCESSING
As obvious as it may sound, it is important to remember to promptly place sampled tissue in an adequate amount of formalin so that the tissue is submersed in it in the container.15 Failure to do so can result in improper fixation and will make it difficult to render an appropriate diagnosis. Conventionally, a 10:1 formalin-volume-to-tissue-volume ratio is recommended. If the “cold time”—the amount of time a tissue sample is out of formalin—is too long (> a few hours), an appropriate assessment can be impossible.
Appropriate fixation and fixation times are important because molecular testing is being increasingly used to make pathologic diagnoses.16 Additionally, aggressively manipulating a biopsy sample while extracting it or placing it in formalin can cause “crush” artifact, which can limit interpretability (see Figure 5).

7. PROPERLY PHOTOGRAPH AND DOCUMENT THE BIOPSY LOCATION
When performing a biopsy of a suspicious neoplasm, clinicians often remove all of the lesion’s superficial components, which means that at the patient’s follow-up appointment and subsequent treatments, only a well-healed biopsy site will remain. The biopsy site may be so well healed that it blends seamlessly into the surrounding skin and is nearly impossible for the clinician to identify. This problem is seen most often when patients present for surgical excision or Mohs micrographic surgery.17
To properly record the site of a biopsy for future dermatologic exams, take pictures of the lesion at the time of biopsy. The photographs should clearly document the lesion in question and should be taken far enough from the site that surrounding lesions and/or other anatomic landmarks are also visible. Biangulation or triangulation (taking a series of two or three measurements, respectively, from the site of the lesion to nearby anatomic landmarks) can be used in conjunction with photographs.
When using measurements, be as specific and accurate as possible with anatomic terms. For example, measuring the distance from the “ear” is not helpful. It would be more helpful to measure the distance from the “tragus” or the “root of the helix.” Without a properly photographed and documented biopsy site, surgical treatment may need to be delayed until the location can be confirmed.
8. GIVE THE PATHOLOGIST A PERTINENT HISTORY
Providing the pathologist with a sufficient history, including the distribution and appearance of the lesion, and how long the patient has had it, can be essential in narrowing the diagnosis or making the differential diagnoses. Things like medication use or new exposures to perfumes, lotions, or plants can be especially helpful and are often overlooked when filling out the pathology requisition form.
When warranted, phone calls are helpful. You might, for example, call the pathologist and give him or her a more detailed physical examination description or additional pertinent history that was discovered after the requisition was filled out. Providing a good history can make the difference between a specific diagnosis and a broad differential.
Tip #9: Next page >>
9. KNOW WHEN TO REFER
There is no shame in asking for a second opinion when evaluating a skin lesion, especially with melanocytic neoplasms, where the stakes can be high, or skin eruptions that do not respond to conventional therapy. Remember, many cases are difficult, even for experts, and require a careful balance of clinical and histopathologic judgment.18
REFERENCES
1. Pickett H. Shave and punch biopsy for skin lesions. Am Fam Physician. 2011;84:995-1002.
2. Alguire PC, Mathes BM. Skin biopsy techniques for the internist. J Gen Intern Med. 1998;13:46-54.
3. Fernandez EM, Helm T, Ioffreda M, et al. The vanishing biopsy: the trend toward smaller specimens. Cutis. 2005;76:335-339.
4. Hieken TJ, Hernández-Irizarry R, Boll JM, et al. Accuracy of diagnostic biopsy for cutaneous melanoma: implications for surgical oncologists. Int J Surg Oncol. 2013;2013:196493.
5. Scolyer RA, Thompson JF, McCarthy SW, et al. Incomplete biopsy of melanocytic lesions can impair the accuracy of pathological diagnosis. Australas J Dermatol. 2006;47:71-75.
6. McCarthy SW, Scolyer RA. Pitfalls and important issues in the pathologic diagnosis of melanocytic tumors. Ochsner J. 2010;10:66-74.
7. Swanson NA, Lee KK, Gorman A, et al. Biopsy techniques. Diagnosis of melanoma. Dermatol Clin. 2002;20:677-680.
8. Chang TT, Somach SC, Wagamon K, et al. The inadequacy of punch-excised melanocytic lesions: sampling through the block for the determination of “margins.” J Am Acad Dermatol. 2009;60: 990-993.
9. Bichakjian CK, Halpern AC, Johnson TM, et al; American Academy of Dermatology. Guidelines of care for the management of primary cutaneous melanoma. American Academy of Dermatology. J Am Acad Dermatol. 2011;65:1032-1047.
10. Pardasani AG, Leshin B, Hallman JR, et al. Fusiform incisional biopsy for pigmented skin lesions. Dermatol Surg. 2000;26:622-624.
11. King R, Hayzen BA, Page RN, et al. Recurrent nevus phenomenon: a clinicopathologic study of 357 cases and histologic comparison with melanoma with regression. Mod Pathol. 2009;22:611-617.
12. Mills JK, White I, Diggs B, et al. Effect of biopsy type on outcomes in the treatment of primary cutaneous melanoma. Am J Surg. 2013;205:585-590.
13. Stell VH, Norton HJ, Smith KS, et al. Method of biopsy and incidence of positive margins in primary melanoma. Ann Surg Oncol. 2007;14:
893-898.
14. Egnatios GL, Dueck AC, Macdonald JB, et al. The impact of biopsy technique on upstaging, residual disease, and outcome in cutaneous melanoma. Am J Surg. 2011;202:771-778.
15. Ackerman AB, Boer A, Bennin B, et al. Histologic Diagnosis of Inflammatory Skin Disease: An Algorithmic Method Based on Pattern Analysis. New York, NY: Ardor Scribendi; 2005.
16. Hewitt SM, Lewis FA, Cao Y, et al. Tissue handling and specimen preparation in surgical pathology: issues concerning the recovery of nucleic acids from formalin-fixed, paraffin-embedded tissue. Arch Pathol Lab Med. 2008;132:1929-1935.
17. Nemeth SA, Lawrence N. Site identification challenges in dermatologic surgery: a physician survey. J Am Acad Dermatol. 2012;67: 262-268.
18. Federman DG, Concato J, Kirsner RS. Comparison of dermatologic diagnoses by primary care practitioners and dermatologists. A review of the literature. Arch Fam Med. 1999;8:170-172.
1. CHOOSE YOUR BIOPSY TYPE WISELY
Using the appropriate type of biopsy can have the greatest effect on a proper diagnosis. The decision of which biopsy type to use is not always easy. The most common biopsy types are shave, punch, excisional, and curettage. Several reference articles detail each type of biopsy commonly used in primary care and how to perform them.1,2
Each type of biopsy has inherent advantages and disadvantages. In general, the shave biopsy is most commonly used for lesions that are solitary and elevated and give the impression that a sufficient amount of tissue can be sampled with this technique. The punch biopsy is the best choice for most “rashes” (inflammatory skin disorders).2 Excisional biopsy is used to remove melanocytic neoplasms or larger lesions. And curettage, while still used by some clinicians for melanocytic lesions because of its speed and simplicity, should almost never be used for diagnostic purposes.
Each technique is described in greater detail in the tips that follow.
Continue for tip #2 >>
2. WHEN PERFORMING A SHAVE BIOPSY, AVOID OBTAINING A SAMPLE THAT'S TOO SUPERFICIAL
The advantage of the shave biopsy is that it is minimally invasive and quick to perform. If kept small without compromising the amount of sample retrieved, the scars left by shave biopsies have the potential to blend well. The major disadvantage associated with the shave biopsy is that occasionally, if the shave is not deep enough, an insufficient amount of tissue is obtained. This can make it challenging to establish an accurate diagnosis.
Balancing the need to obtain adequate tissue with the desire to minimize scarring takes skill and experience. Taking a biopsy that is inadequate is a common occurrence. At times, the clinician’s clinical impression may be that a biopsy has obtained adequate tissue, when histologically only the superficial part of the skin surface has been sampled. This often is because of thickening of the superficial skin, whether as a manifestation of the anatomic site (eg, acral skin) or the disease process itself.
Unfortunately, this superficial skin often is nondiagnostic when unaccompanied by underlying epidermis and dermis. It is important to keep this in mind when you are obtaining a skin biopsy, especially when dealing with lesions that are very scaly or keratinized.
An equivocal biopsy wastes time, energy, and money, and it can negatively impact patient care.3 It can be difficult to balance practical aspects of the biopsy (ie, optimizing cosmetic outcomes, minimizing scarring and wound size) with the need to obtain sufficient tissue sampling (see Figure 1).
3. CHOOSE PUNCH OVER SHAVE BIOPSY FOR RASHES
In a punch biopsy, a disposable metal cylinder with a sharpened edge is used to “punch” out a piece of skin that can be examined under the microscope. Punch biopsy is the preferred technique for almost all inflammatory skin conditions (rashes) because the pathologist is able to examine both the superficial and deep portions of the dermis (see Figure 2).4
Pathologists use the pattern of inflammation, in conjunction with epidermal changes, to distinguish different types of inflammatory processes. For example, lichen planus is typically associated with superficial inflammation, while lupus is known to have prominent superficial and deep inflammation.
An inadequate punch biopsy sample can hinder histologic assessment of inflammatory skin disorders that involve both the superficial and deep portions of the dermis and can make arriving at a definitive diagnosis more challenging. The diameter of a punch cylinder ranges from 1 to 8 mm. Smaller punch biopsies often create diagnostic challenges because they provide so little sample. A punch biopsy size of 4 mm is commonly used for rashes.
An advantage of the punch biopsy is that patients are left with linear scars rather than the round, potentially dyspigmented (darker or lighter) scars that are often associated with shave biopsy. A well-sutured punch biopsy can be cosmetically elegant, particularly if closure is oriented along relaxed skin tension lines. For this reason, punch biopsies are well suited for cosmetically sensitive locations (eg, the face), although shave biopsies are also often performed on the face.
Next page: Tip #4 >>
4. CHOOSE AN EXCISIONAL BIOPSY FOR A MELANOCYTIC NEOPLASM, WHEN POSSIBLE
The purpose of an excisional biopsy (which typically includes a 1- to 3-mm rim of normal skin around the lesion) is to completely remove a lesion. Excisional biopsy generally is the preferred technique for clinically atypical melanocytic neoplasms (ie, lesions that are not definitively benign).4-8
When suspicion for melanoma is high, excisional biopsies should be performed with minimal undermining to preserve the accuracy of any future sentinel lymph node biopsy surgeries. Excisional biopsy is the most involved type of biopsy and has the largest potential for cosmetic disfigurement if not properly planned and performed. While guidelines from the American Academy of Dermatology state that “narrow excisional biopsy that encompasses [the] entire breadth of lesion with clinically negative margins to ensure that the lesion is not transected” is preferred, they also acknowledge that partial sampling (incisional biopsy) is acceptable in select clinical circumstances,9 such as when a lesion is large or on a cosmetically sensitive site (eg, the face).10
While a larger punch biopsy (6 or 8 mm) or even deep shave/saucerization may function as an excisional biopsy for very small lesions, this approach can be problematic. For one thing, these techniques are more likely than an excisional biopsy to leave a portion of the lesion in situ. Another concern is that a shave biopsy of a melanocytic lesion can lead to error or difficulty in obtaining the correct diagnosis on later biopsy.11 For pathologists, small or incomplete samples make it challenging to establish an accurate diagnosis.12 Among melanomas seen at a tertiary referral center, histopathologic misdiagnosis was more common with a punch or shave biopsy than with an excisional biopsy.9
It has been shown that partial biopsy for melanoma results in more residual disease at wide local excision and makes it more challenging to properly stage the lesion.13,14 If a shave biopsy is used to sample a suspected melanocytic neoplasm, it is imperative to document the specific site of the biopsy, indicate the size of the melanocytic lesion on the pathology requisition form, and ensure that all (or nearly all) of the clinically evident lesion is sampled. Detailing the location of the lesion in the chart is not only essential in evaluating the present lesion, but it will serve you well in the future. Without knowing the patient’s clinical history, benign nevi that recur after a prior biopsy can be difficult to histologically distinguish from melanoma (see Figure 3). For more on this, see tip #7.
5. BE CAREFUL WITH CURETTAGE
Curettage is a biopsy technique in which a curette—a surgical tool with a scoop, ring, or loop at the tip—is used in a scraping motion to retrieve tissue from the patient. This type of biopsy often produces a fragmented tissue sample. Its continued use reflects the speed and simplicity with which it can be done. However, curettage destroys the architecture of the tissue of the lesion, which can make it difficult to establish a proper diagnosis, and therefore it is best avoided when performing a biopsy of a melanocytic lesion (see Figure 4).
Continue for tip #6 >>
6. REMEMBER THE IMPORTANCE OF PROPER FIXATION AND PROCESSING
As obvious as it may sound, it is important to remember to promptly place sampled tissue in an adequate amount of formalin so that the tissue is submersed in it in the container.15 Failure to do so can result in improper fixation and will make it difficult to render an appropriate diagnosis. Conventionally, a 10:1 formalin-volume-to-tissue-volume ratio is recommended. If the “cold time”—the amount of time a tissue sample is out of formalin—is too long (> a few hours), an appropriate assessment can be impossible.
Appropriate fixation and fixation times are important because molecular testing is being increasingly used to make pathologic diagnoses.16 Additionally, aggressively manipulating a biopsy sample while extracting it or placing it in formalin can cause “crush” artifact, which can limit interpretability (see Figure 5).
7. PROPERLY PHOTOGRAPH AND DOCUMENT THE BIOPSY LOCATION
When performing a biopsy of a suspicious neoplasm, clinicians often remove all of the lesion’s superficial components, which means that at the patient’s follow-up appointment and subsequent treatments, only a well-healed biopsy site will remain. The biopsy site may be so well healed that it blends seamlessly into the surrounding skin and is nearly impossible for the clinician to identify. This problem is seen most often when patients present for surgical excision or Mohs micrographic surgery.17
To properly record the site of a biopsy for future dermatologic exams, take pictures of the lesion at the time of biopsy. The photographs should clearly document the lesion in question and should be taken far enough from the site that surrounding lesions and/or other anatomic landmarks are also visible. Biangulation or triangulation (taking a series of two or three measurements, respectively, from the site of the lesion to nearby anatomic landmarks) can be used in conjunction with photographs.
When using measurements, be as specific and accurate as possible with anatomic terms. For example, measuring the distance from the “ear” is not helpful. It would be more helpful to measure the distance from the “tragus” or the “root of the helix.” Without a properly photographed and documented biopsy site, surgical treatment may need to be delayed until the location can be confirmed.
8. GIVE THE PATHOLOGIST A PERTINENT HISTORY
Providing the pathologist with a sufficient history, including the distribution and appearance of the lesion, and how long the patient has had it, can be essential in narrowing the diagnosis or making the differential diagnoses. Things like medication use or new exposures to perfumes, lotions, or plants can be especially helpful and are often overlooked when filling out the pathology requisition form.
When warranted, phone calls are helpful. You might, for example, call the pathologist and give him or her a more detailed physical examination description or additional pertinent history that was discovered after the requisition was filled out. Providing a good history can make the difference between a specific diagnosis and a broad differential.
Tip #9: Next page >>
9. KNOW WHEN TO REFER
There is no shame in asking for a second opinion when evaluating a skin lesion, especially with melanocytic neoplasms, where the stakes can be high, or skin eruptions that do not respond to conventional therapy. Remember, many cases are difficult, even for experts, and require a careful balance of clinical and histopathologic judgment.18
REFERENCES
1. Pickett H. Shave and punch biopsy for skin lesions. Am Fam Physician. 2011;84:995-1002.
2. Alguire PC, Mathes BM. Skin biopsy techniques for the internist. J Gen Intern Med. 1998;13:46-54.
3. Fernandez EM, Helm T, Ioffreda M, et al. The vanishing biopsy: the trend toward smaller specimens. Cutis. 2005;76:335-339.
4. Hieken TJ, Hernández-Irizarry R, Boll JM, et al. Accuracy of diagnostic biopsy for cutaneous melanoma: implications for surgical oncologists. Int J Surg Oncol. 2013;2013:196493.
5. Scolyer RA, Thompson JF, McCarthy SW, et al. Incomplete biopsy of melanocytic lesions can impair the accuracy of pathological diagnosis. Australas J Dermatol. 2006;47:71-75.
6. McCarthy SW, Scolyer RA. Pitfalls and important issues in the pathologic diagnosis of melanocytic tumors. Ochsner J. 2010;10:66-74.
7. Swanson NA, Lee KK, Gorman A, et al. Biopsy techniques. Diagnosis of melanoma. Dermatol Clin. 2002;20:677-680.
8. Chang TT, Somach SC, Wagamon K, et al. The inadequacy of punch-excised melanocytic lesions: sampling through the block for the determination of “margins.” J Am Acad Dermatol. 2009;60: 990-993.
9. Bichakjian CK, Halpern AC, Johnson TM, et al; American Academy of Dermatology. Guidelines of care for the management of primary cutaneous melanoma. American Academy of Dermatology. J Am Acad Dermatol. 2011;65:1032-1047.
10. Pardasani AG, Leshin B, Hallman JR, et al. Fusiform incisional biopsy for pigmented skin lesions. Dermatol Surg. 2000;26:622-624.
11. King R, Hayzen BA, Page RN, et al. Recurrent nevus phenomenon: a clinicopathologic study of 357 cases and histologic comparison with melanoma with regression. Mod Pathol. 2009;22:611-617.
12. Mills JK, White I, Diggs B, et al. Effect of biopsy type on outcomes in the treatment of primary cutaneous melanoma. Am J Surg. 2013;205:585-590.
13. Stell VH, Norton HJ, Smith KS, et al. Method of biopsy and incidence of positive margins in primary melanoma. Ann Surg Oncol. 2007;14:
893-898.
14. Egnatios GL, Dueck AC, Macdonald JB, et al. The impact of biopsy technique on upstaging, residual disease, and outcome in cutaneous melanoma. Am J Surg. 2011;202:771-778.
15. Ackerman AB, Boer A, Bennin B, et al. Histologic Diagnosis of Inflammatory Skin Disease: An Algorithmic Method Based on Pattern Analysis. New York, NY: Ardor Scribendi; 2005.
16. Hewitt SM, Lewis FA, Cao Y, et al. Tissue handling and specimen preparation in surgical pathology: issues concerning the recovery of nucleic acids from formalin-fixed, paraffin-embedded tissue. Arch Pathol Lab Med. 2008;132:1929-1935.
17. Nemeth SA, Lawrence N. Site identification challenges in dermatologic surgery: a physician survey. J Am Acad Dermatol. 2012;67: 262-268.
18. Federman DG, Concato J, Kirsner RS. Comparison of dermatologic diagnoses by primary care practitioners and dermatologists. A review of the literature. Arch Fam Med. 1999;8:170-172.
1. CHOOSE YOUR BIOPSY TYPE WISELY
Using the appropriate type of biopsy can have the greatest effect on a proper diagnosis. The decision of which biopsy type to use is not always easy. The most common biopsy types are shave, punch, excisional, and curettage. Several reference articles detail each type of biopsy commonly used in primary care and how to perform them.1,2
Each type of biopsy has inherent advantages and disadvantages. In general, the shave biopsy is most commonly used for lesions that are solitary and elevated and give the impression that a sufficient amount of tissue can be sampled with this technique. The punch biopsy is the best choice for most “rashes” (inflammatory skin disorders).2 Excisional biopsy is used to remove melanocytic neoplasms or larger lesions. And curettage, while still used by some clinicians for melanocytic lesions because of its speed and simplicity, should almost never be used for diagnostic purposes.
Each technique is described in greater detail in the tips that follow.
Continue for tip #2 >>
2. WHEN PERFORMING A SHAVE BIOPSY, AVOID OBTAINING A SAMPLE THAT'S TOO SUPERFICIAL
The advantage of the shave biopsy is that it is minimally invasive and quick to perform. If kept small without compromising the amount of sample retrieved, the scars left by shave biopsies have the potential to blend well. The major disadvantage associated with the shave biopsy is that occasionally, if the shave is not deep enough, an insufficient amount of tissue is obtained. This can make it challenging to establish an accurate diagnosis.
Balancing the need to obtain adequate tissue with the desire to minimize scarring takes skill and experience. Taking a biopsy that is inadequate is a common occurrence. At times, the clinician’s clinical impression may be that a biopsy has obtained adequate tissue, when histologically only the superficial part of the skin surface has been sampled. This often is because of thickening of the superficial skin, whether as a manifestation of the anatomic site (eg, acral skin) or the disease process itself.
Unfortunately, this superficial skin often is nondiagnostic when unaccompanied by underlying epidermis and dermis. It is important to keep this in mind when you are obtaining a skin biopsy, especially when dealing with lesions that are very scaly or keratinized.
An equivocal biopsy wastes time, energy, and money, and it can negatively impact patient care.3 It can be difficult to balance practical aspects of the biopsy (ie, optimizing cosmetic outcomes, minimizing scarring and wound size) with the need to obtain sufficient tissue sampling (see Figure 1).
3. CHOOSE PUNCH OVER SHAVE BIOPSY FOR RASHES
In a punch biopsy, a disposable metal cylinder with a sharpened edge is used to “punch” out a piece of skin that can be examined under the microscope. Punch biopsy is the preferred technique for almost all inflammatory skin conditions (rashes) because the pathologist is able to examine both the superficial and deep portions of the dermis (see Figure 2).4
Pathologists use the pattern of inflammation, in conjunction with epidermal changes, to distinguish different types of inflammatory processes. For example, lichen planus is typically associated with superficial inflammation, while lupus is known to have prominent superficial and deep inflammation.
An inadequate punch biopsy sample can hinder histologic assessment of inflammatory skin disorders that involve both the superficial and deep portions of the dermis and can make arriving at a definitive diagnosis more challenging. The diameter of a punch cylinder ranges from 1 to 8 mm. Smaller punch biopsies often create diagnostic challenges because they provide so little sample. A punch biopsy size of 4 mm is commonly used for rashes.
An advantage of the punch biopsy is that patients are left with linear scars rather than the round, potentially dyspigmented (darker or lighter) scars that are often associated with shave biopsy. A well-sutured punch biopsy can be cosmetically elegant, particularly if closure is oriented along relaxed skin tension lines. For this reason, punch biopsies are well suited for cosmetically sensitive locations (eg, the face), although shave biopsies are also often performed on the face.
Next page: Tip #4 >>
4. CHOOSE AN EXCISIONAL BIOPSY FOR A MELANOCYTIC NEOPLASM, WHEN POSSIBLE
The purpose of an excisional biopsy (which typically includes a 1- to 3-mm rim of normal skin around the lesion) is to completely remove a lesion. Excisional biopsy generally is the preferred technique for clinically atypical melanocytic neoplasms (ie, lesions that are not definitively benign).4-8
When suspicion for melanoma is high, excisional biopsies should be performed with minimal undermining to preserve the accuracy of any future sentinel lymph node biopsy surgeries. Excisional biopsy is the most involved type of biopsy and has the largest potential for cosmetic disfigurement if not properly planned and performed. While guidelines from the American Academy of Dermatology state that “narrow excisional biopsy that encompasses [the] entire breadth of lesion with clinically negative margins to ensure that the lesion is not transected” is preferred, they also acknowledge that partial sampling (incisional biopsy) is acceptable in select clinical circumstances,9 such as when a lesion is large or on a cosmetically sensitive site (eg, the face).10
While a larger punch biopsy (6 or 8 mm) or even deep shave/saucerization may function as an excisional biopsy for very small lesions, this approach can be problematic. For one thing, these techniques are more likely than an excisional biopsy to leave a portion of the lesion in situ. Another concern is that a shave biopsy of a melanocytic lesion can lead to error or difficulty in obtaining the correct diagnosis on later biopsy.11 For pathologists, small or incomplete samples make it challenging to establish an accurate diagnosis.12 Among melanomas seen at a tertiary referral center, histopathologic misdiagnosis was more common with a punch or shave biopsy than with an excisional biopsy.9
It has been shown that partial biopsy for melanoma results in more residual disease at wide local excision and makes it more challenging to properly stage the lesion.13,14 If a shave biopsy is used to sample a suspected melanocytic neoplasm, it is imperative to document the specific site of the biopsy, indicate the size of the melanocytic lesion on the pathology requisition form, and ensure that all (or nearly all) of the clinically evident lesion is sampled. Detailing the location of the lesion in the chart is not only essential in evaluating the present lesion, but it will serve you well in the future. Without knowing the patient’s clinical history, benign nevi that recur after a prior biopsy can be difficult to histologically distinguish from melanoma (see Figure 3). For more on this, see tip #7.
5. BE CAREFUL WITH CURETTAGE
Curettage is a biopsy technique in which a curette—a surgical tool with a scoop, ring, or loop at the tip—is used in a scraping motion to retrieve tissue from the patient. This type of biopsy often produces a fragmented tissue sample. Its continued use reflects the speed and simplicity with which it can be done. However, curettage destroys the architecture of the tissue of the lesion, which can make it difficult to establish a proper diagnosis, and therefore it is best avoided when performing a biopsy of a melanocytic lesion (see Figure 4).
Continue for tip #6 >>
6. REMEMBER THE IMPORTANCE OF PROPER FIXATION AND PROCESSING
As obvious as it may sound, it is important to remember to promptly place sampled tissue in an adequate amount of formalin so that the tissue is submersed in it in the container.15 Failure to do so can result in improper fixation and will make it difficult to render an appropriate diagnosis. Conventionally, a 10:1 formalin-volume-to-tissue-volume ratio is recommended. If the “cold time”—the amount of time a tissue sample is out of formalin—is too long (> a few hours), an appropriate assessment can be impossible.
Appropriate fixation and fixation times are important because molecular testing is being increasingly used to make pathologic diagnoses.16 Additionally, aggressively manipulating a biopsy sample while extracting it or placing it in formalin can cause “crush” artifact, which can limit interpretability (see Figure 5).
7. PROPERLY PHOTOGRAPH AND DOCUMENT THE BIOPSY LOCATION
When performing a biopsy of a suspicious neoplasm, clinicians often remove all of the lesion’s superficial components, which means that at the patient’s follow-up appointment and subsequent treatments, only a well-healed biopsy site will remain. The biopsy site may be so well healed that it blends seamlessly into the surrounding skin and is nearly impossible for the clinician to identify. This problem is seen most often when patients present for surgical excision or Mohs micrographic surgery.17
To properly record the site of a biopsy for future dermatologic exams, take pictures of the lesion at the time of biopsy. The photographs should clearly document the lesion in question and should be taken far enough from the site that surrounding lesions and/or other anatomic landmarks are also visible. Biangulation or triangulation (taking a series of two or three measurements, respectively, from the site of the lesion to nearby anatomic landmarks) can be used in conjunction with photographs.
When using measurements, be as specific and accurate as possible with anatomic terms. For example, measuring the distance from the “ear” is not helpful. It would be more helpful to measure the distance from the “tragus” or the “root of the helix.” Without a properly photographed and documented biopsy site, surgical treatment may need to be delayed until the location can be confirmed.
8. GIVE THE PATHOLOGIST A PERTINENT HISTORY
Providing the pathologist with a sufficient history, including the distribution and appearance of the lesion, and how long the patient has had it, can be essential in narrowing the diagnosis or making the differential diagnoses. Things like medication use or new exposures to perfumes, lotions, or plants can be especially helpful and are often overlooked when filling out the pathology requisition form.
When warranted, phone calls are helpful. You might, for example, call the pathologist and give him or her a more detailed physical examination description or additional pertinent history that was discovered after the requisition was filled out. Providing a good history can make the difference between a specific diagnosis and a broad differential.
Tip #9: Next page >>
9. KNOW WHEN TO REFER
There is no shame in asking for a second opinion when evaluating a skin lesion, especially with melanocytic neoplasms, where the stakes can be high, or skin eruptions that do not respond to conventional therapy. Remember, many cases are difficult, even for experts, and require a careful balance of clinical and histopathologic judgment.18
REFERENCES
1. Pickett H. Shave and punch biopsy for skin lesions. Am Fam Physician. 2011;84:995-1002.
2. Alguire PC, Mathes BM. Skin biopsy techniques for the internist. J Gen Intern Med. 1998;13:46-54.
3. Fernandez EM, Helm T, Ioffreda M, et al. The vanishing biopsy: the trend toward smaller specimens. Cutis. 2005;76:335-339.
4. Hieken TJ, Hernández-Irizarry R, Boll JM, et al. Accuracy of diagnostic biopsy for cutaneous melanoma: implications for surgical oncologists. Int J Surg Oncol. 2013;2013:196493.
5. Scolyer RA, Thompson JF, McCarthy SW, et al. Incomplete biopsy of melanocytic lesions can impair the accuracy of pathological diagnosis. Australas J Dermatol. 2006;47:71-75.
6. McCarthy SW, Scolyer RA. Pitfalls and important issues in the pathologic diagnosis of melanocytic tumors. Ochsner J. 2010;10:66-74.
7. Swanson NA, Lee KK, Gorman A, et al. Biopsy techniques. Diagnosis of melanoma. Dermatol Clin. 2002;20:677-680.
8. Chang TT, Somach SC, Wagamon K, et al. The inadequacy of punch-excised melanocytic lesions: sampling through the block for the determination of “margins.” J Am Acad Dermatol. 2009;60: 990-993.
9. Bichakjian CK, Halpern AC, Johnson TM, et al; American Academy of Dermatology. Guidelines of care for the management of primary cutaneous melanoma. American Academy of Dermatology. J Am Acad Dermatol. 2011;65:1032-1047.
10. Pardasani AG, Leshin B, Hallman JR, et al. Fusiform incisional biopsy for pigmented skin lesions. Dermatol Surg. 2000;26:622-624.
11. King R, Hayzen BA, Page RN, et al. Recurrent nevus phenomenon: a clinicopathologic study of 357 cases and histologic comparison with melanoma with regression. Mod Pathol. 2009;22:611-617.
12. Mills JK, White I, Diggs B, et al. Effect of biopsy type on outcomes in the treatment of primary cutaneous melanoma. Am J Surg. 2013;205:585-590.
13. Stell VH, Norton HJ, Smith KS, et al. Method of biopsy and incidence of positive margins in primary melanoma. Ann Surg Oncol. 2007;14:
893-898.
14. Egnatios GL, Dueck AC, Macdonald JB, et al. The impact of biopsy technique on upstaging, residual disease, and outcome in cutaneous melanoma. Am J Surg. 2011;202:771-778.
15. Ackerman AB, Boer A, Bennin B, et al. Histologic Diagnosis of Inflammatory Skin Disease: An Algorithmic Method Based on Pattern Analysis. New York, NY: Ardor Scribendi; 2005.
16. Hewitt SM, Lewis FA, Cao Y, et al. Tissue handling and specimen preparation in surgical pathology: issues concerning the recovery of nucleic acids from formalin-fixed, paraffin-embedded tissue. Arch Pathol Lab Med. 2008;132:1929-1935.
17. Nemeth SA, Lawrence N. Site identification challenges in dermatologic surgery: a physician survey. J Am Acad Dermatol. 2012;67: 262-268.
18. Federman DG, Concato J, Kirsner RS. Comparison of dermatologic diagnoses by primary care practitioners and dermatologists. A review of the literature. Arch Fam Med. 1999;8:170-172.
Update on Sexual Dysfunction
Recently, three new drugs have been added to the armamentarium for menopausal symptoms and dyspareunia:
• Paroxetine 7.5 mg
• Conjugated estrogens and bazedoxifene
• Ospemifene.
In this article, I present a case-based approach to incorporating these drugs into practice and restoring sexual function in the setting of vulvovaginal atrophy and dyspareunia. As is often the case, decision-making requires sifting through multiple layers of information.
CASE: LOW DESIRE AND DISCOMFORT DURING INTERCOURSE
A 58-year-old patient mentions during her annual visit that she’s not that interested in sex anymore. Her children are grown, she’s been happily married for 28 years, and she enjoys her job and denies any symptoms of depression. She says her relationship with her husband is good and, aside from her low desire, she has no worries about the marriage. Her only medication is paroxetine 7.5 mg/d for management of her moderate hot flashes, which she initiated at her last annual visit. She reports improvement in her sleep and menopausal symptoms as a result. She has an intact uterus.
You perform a pelvic exam and find atrophic vulva and vagina with mild erythema and thinned epithelium. When you ask if she has experienced any discomfort, she reports that she needs to use lubrication for intercourse and that, even with lubrication, she has pain upon penetration and a burning sensation that continues throughout intercourse. She also reports that it seems to take her much longer to achieve arousal than in the past, and she often fails to reach orgasm.
How would you manage this patient?
Continued on next page >>
AS ALWAYS, BEGIN WITH THE HISTORY
The transition to menopause creates multiple layers of potential symptoms and problems for our patients, and sometimes medical therapy can generate additional ones.
In a patient reporting the onset of low desire and dyspareunia, you would want to first consider her medication history, despite the clear evidence of vaginal atrophy. Begin by asking whether she is taking any new medications prescribed by another provider. In some cases, antihypertensive drugs, psychotropic agents, and other medications can affect sexual function.
This patient has been taking paroxetine for one year and is happy with its effect on her sleep and hot flashes. Simon and colleagues found this nonhormonal agent for moderate to severe vasomotor symptoms produced no notable effects on weight, libido, or sleep, compared with placebo.
Nevertheless, in this case, because selective serotonin reuptake inhibitors such as paroxetine can affect arousal and orgasm, it is unclear whether the ultra-low dose of paroxetine she is taking is contributing to her problems. If you were to discontinue the drug to find out, her vasomotor symptoms and sleep disruption would likely recur.
Your decision-making is important here and should involve the patient in an extensive discussion. If there is not enough time for this discussion at the current visit, schedule a follow-up to address her concerns fully.
VULVOVAGINAL ATROPHY HAS ITS OWN TIMELINE
In many cases, vasomotor symptoms such as hot flashes occur years before the skin begins to atrophy in the vulva and vagina, particularly in women who enter menopause naturally. Among menopausal women who continue to have intercourse on a regular basis, however, these skin changes often are much less troublesome than they are for women who have sex more rarely.
In this patient, one possible scenario is that paroxetine caused a slight reduction in sexual interest, and the frequency of intercourse went down as a result. In women who have little or no intercourse, the vagina begins to shrink and the tissues lose elasticity. This patient may have been undergoing the natural process of menopause, and that process may have been compounded by a decrease in the frequency of sex.
If you were to discontinue the paroxetine, it would still be necessary to treat the vulvovaginal skin and work on manual techniques to gently dilate the introitus.
Option 1: Systemic hormone therapy >>
Option 1: Systemic hormone therapy
Systemic estrogen is the most effective treatment for menopausal vasomotor symptoms, reducing hot flashes by 50% to 100% within four weeks of initiation. However, because our patient has an intact uterus, any systemic estrogen she opts to use must be opposed by a progestin for safety reasons.
In terms of estrogen, her options are oral or nonoral formulations. Not only would estrogen manage our patient’s hot flashes but, over time, it would improve her sexual problems and atrophy, which might or might not improve her current complaint of low desire. You likely would need to add a short regimen of topical estrogen and perhaps even a dilator to restore her sexual function completely, however.
Since our patient chose the nonhormonal agent paroxetine to manage her menopausal symptoms, she may be worried about the increased risk for breast cancer associated with use of a progestin in combination with estrogen. One hormonal option now available that eliminates the need for a progestin is conjugated estrogens and bazedoxefine. Bazedoxefine is a third-generation selective estrogen receptor modulator. This drug has estrogen-like effects on bone and antiestrogen effects on the uterus.
Conjugated estrogens/bazedoxifene is indicated for use in women with a uterus for treatment of
• Moderate to severe vasomotor symptoms of menopause
• Prevention of postmenopausal osteoporosis.
Among the risks are an increased risk for venous thromboembolism (VTE) and stroke. It is not approved specifically for the treatment of dyspareunia.
Another hormonal option is ospemifene, an estrogen agonist/antagonist indicated for the treatment of moderate to severe dyspareunia in menopausal women. Among the drugs in its class, such as tamoxifen and raloxifene, ospemifene is the only agent that maintains a full estrogenic effect on vaginal tissues. Its risks include VTE and stroke.
Although the labeling includes a warning about the risk for endometrial hyperplasia associated with its use, Goldstein and colleagues found no significant difference in the rate of endometrial thickening greater than 5 mm between women taking ospemifene and those taking placebo after one year of daily oral treatment. No carcinomas were found in either group.
Option 2: Local estrogen
If our patient declines all systemic hormone therapy, the topical approach should resolve her vulvovaginal symptoms, and she could continue taking paroxetine for her menopausal symptoms. Vaginal estrogen would address the skin problems, provided the patient applies it correctly. Many women are afraid to use estrogen creams and compensate by applying them only to the vulva, thinking that, by limiting their use to external tissues, they are avoiding any associated risks.
If she opts for the local approach, this patient should be encouraged to use transvaginal estrogen in small doses to increase the elasticity of the vulvovaginal tissue, even though it may require daily use for a week or two to improve her symptoms, after which once- or twice-weekly administration should suffice.
The use of low-dose vaginal cream for a short duration is unlikely to increase her risks in any way. Local estrogen is available as a tablet, cream, or ring.
Option 3: A nonhormonal approach >>
Option 3: A nonhormonal approach
If the patient refuses any hormonal agent—even topical estrogen—I would recommend the use of silicone-based lubricants and a dilator and prescribe more frequent penetration to increase elasticity and reduce pain. Paroxetine could be continued to address her menopausal symptoms.
DON'T OVERLOOK BEHAVIORAL TECHNIQUES
Before this patient leaves your office with the option of her choice, a bit of counseling is necessary to instruct her about methods of restoring full sexual function.
Pain is a powerful aversive stimulus. This patient clearly states that she has had less frequent intercourse as a result of dyspareunia. It is not unusual for patients to develop a “habit” of avoidance in response to the behavior that causes their pain.
One recommendation is to talk to this patient about putting sex back into her life by encouraging her to increase sexual activity without penetration until she begins to arouse easily again. Arousal produces physiologic effects, increasing the caliber and length of the vagina as well as lubrication. The use of fingers or dilators may help restore caliber.
The patient can be encouraged to engage in snuggling and cuddling to regain those activities without the fear of pain associated with penetration. Follow-up after two weeks of this therapy can confirm the restoration of tissue elasticity, and the green light can be given for penetration to begin again. Couples can be encouraged to plan a “honeymoon weekend” and put some fun back into their sex lives so that this phase of healing doesn’t become an onerous task.
CASE RESOLVED
After a discussion of her options, the patient chooses to stick with paroxetine and use behavioral therapy alone to resolve her dyspareunia. At her follow-up visit two weeks later, she reports that she has enjoyed the period of pain-free “sex” and feels ready to add penetration into her activities.
You encourage her to continue sexual intercourse on a regular, relatively frequent basis to prevent a recurrence of dyspareunia. She continues to use silicone-based lubricants.
Recently, three new drugs have been added to the armamentarium for menopausal symptoms and dyspareunia:
• Paroxetine 7.5 mg
• Conjugated estrogens and bazedoxifene
• Ospemifene.
In this article, I present a case-based approach to incorporating these drugs into practice and restoring sexual function in the setting of vulvovaginal atrophy and dyspareunia. As is often the case, decision-making requires sifting through multiple layers of information.
CASE: LOW DESIRE AND DISCOMFORT DURING INTERCOURSE
A 58-year-old patient mentions during her annual visit that she’s not that interested in sex anymore. Her children are grown, she’s been happily married for 28 years, and she enjoys her job and denies any symptoms of depression. She says her relationship with her husband is good and, aside from her low desire, she has no worries about the marriage. Her only medication is paroxetine 7.5 mg/d for management of her moderate hot flashes, which she initiated at her last annual visit. She reports improvement in her sleep and menopausal symptoms as a result. She has an intact uterus.
You perform a pelvic exam and find atrophic vulva and vagina with mild erythema and thinned epithelium. When you ask if she has experienced any discomfort, she reports that she needs to use lubrication for intercourse and that, even with lubrication, she has pain upon penetration and a burning sensation that continues throughout intercourse. She also reports that it seems to take her much longer to achieve arousal than in the past, and she often fails to reach orgasm.
How would you manage this patient?
Continued on next page >>
AS ALWAYS, BEGIN WITH THE HISTORY
The transition to menopause creates multiple layers of potential symptoms and problems for our patients, and sometimes medical therapy can generate additional ones.
In a patient reporting the onset of low desire and dyspareunia, you would want to first consider her medication history, despite the clear evidence of vaginal atrophy. Begin by asking whether she is taking any new medications prescribed by another provider. In some cases, antihypertensive drugs, psychotropic agents, and other medications can affect sexual function.
This patient has been taking paroxetine for one year and is happy with its effect on her sleep and hot flashes. Simon and colleagues found this nonhormonal agent for moderate to severe vasomotor symptoms produced no notable effects on weight, libido, or sleep, compared with placebo.
Nevertheless, in this case, because selective serotonin reuptake inhibitors such as paroxetine can affect arousal and orgasm, it is unclear whether the ultra-low dose of paroxetine she is taking is contributing to her problems. If you were to discontinue the drug to find out, her vasomotor symptoms and sleep disruption would likely recur.
Your decision-making is important here and should involve the patient in an extensive discussion. If there is not enough time for this discussion at the current visit, schedule a follow-up to address her concerns fully.
VULVOVAGINAL ATROPHY HAS ITS OWN TIMELINE
In many cases, vasomotor symptoms such as hot flashes occur years before the skin begins to atrophy in the vulva and vagina, particularly in women who enter menopause naturally. Among menopausal women who continue to have intercourse on a regular basis, however, these skin changes often are much less troublesome than they are for women who have sex more rarely.
In this patient, one possible scenario is that paroxetine caused a slight reduction in sexual interest, and the frequency of intercourse went down as a result. In women who have little or no intercourse, the vagina begins to shrink and the tissues lose elasticity. This patient may have been undergoing the natural process of menopause, and that process may have been compounded by a decrease in the frequency of sex.
If you were to discontinue the paroxetine, it would still be necessary to treat the vulvovaginal skin and work on manual techniques to gently dilate the introitus.
Option 1: Systemic hormone therapy >>
Option 1: Systemic hormone therapy
Systemic estrogen is the most effective treatment for menopausal vasomotor symptoms, reducing hot flashes by 50% to 100% within four weeks of initiation. However, because our patient has an intact uterus, any systemic estrogen she opts to use must be opposed by a progestin for safety reasons.
In terms of estrogen, her options are oral or nonoral formulations. Not only would estrogen manage our patient’s hot flashes but, over time, it would improve her sexual problems and atrophy, which might or might not improve her current complaint of low desire. You likely would need to add a short regimen of topical estrogen and perhaps even a dilator to restore her sexual function completely, however.
Since our patient chose the nonhormonal agent paroxetine to manage her menopausal symptoms, she may be worried about the increased risk for breast cancer associated with use of a progestin in combination with estrogen. One hormonal option now available that eliminates the need for a progestin is conjugated estrogens and bazedoxefine. Bazedoxefine is a third-generation selective estrogen receptor modulator. This drug has estrogen-like effects on bone and antiestrogen effects on the uterus.
Conjugated estrogens/bazedoxifene is indicated for use in women with a uterus for treatment of
• Moderate to severe vasomotor symptoms of menopause
• Prevention of postmenopausal osteoporosis.
Among the risks are an increased risk for venous thromboembolism (VTE) and stroke. It is not approved specifically for the treatment of dyspareunia.
Another hormonal option is ospemifene, an estrogen agonist/antagonist indicated for the treatment of moderate to severe dyspareunia in menopausal women. Among the drugs in its class, such as tamoxifen and raloxifene, ospemifene is the only agent that maintains a full estrogenic effect on vaginal tissues. Its risks include VTE and stroke.
Although the labeling includes a warning about the risk for endometrial hyperplasia associated with its use, Goldstein and colleagues found no significant difference in the rate of endometrial thickening greater than 5 mm between women taking ospemifene and those taking placebo after one year of daily oral treatment. No carcinomas were found in either group.
Option 2: Local estrogen
If our patient declines all systemic hormone therapy, the topical approach should resolve her vulvovaginal symptoms, and she could continue taking paroxetine for her menopausal symptoms. Vaginal estrogen would address the skin problems, provided the patient applies it correctly. Many women are afraid to use estrogen creams and compensate by applying them only to the vulva, thinking that, by limiting their use to external tissues, they are avoiding any associated risks.
If she opts for the local approach, this patient should be encouraged to use transvaginal estrogen in small doses to increase the elasticity of the vulvovaginal tissue, even though it may require daily use for a week or two to improve her symptoms, after which once- or twice-weekly administration should suffice.
The use of low-dose vaginal cream for a short duration is unlikely to increase her risks in any way. Local estrogen is available as a tablet, cream, or ring.
Option 3: A nonhormonal approach >>
Option 3: A nonhormonal approach
If the patient refuses any hormonal agent—even topical estrogen—I would recommend the use of silicone-based lubricants and a dilator and prescribe more frequent penetration to increase elasticity and reduce pain. Paroxetine could be continued to address her menopausal symptoms.
DON'T OVERLOOK BEHAVIORAL TECHNIQUES
Before this patient leaves your office with the option of her choice, a bit of counseling is necessary to instruct her about methods of restoring full sexual function.
Pain is a powerful aversive stimulus. This patient clearly states that she has had less frequent intercourse as a result of dyspareunia. It is not unusual for patients to develop a “habit” of avoidance in response to the behavior that causes their pain.
One recommendation is to talk to this patient about putting sex back into her life by encouraging her to increase sexual activity without penetration until she begins to arouse easily again. Arousal produces physiologic effects, increasing the caliber and length of the vagina as well as lubrication. The use of fingers or dilators may help restore caliber.
The patient can be encouraged to engage in snuggling and cuddling to regain those activities without the fear of pain associated with penetration. Follow-up after two weeks of this therapy can confirm the restoration of tissue elasticity, and the green light can be given for penetration to begin again. Couples can be encouraged to plan a “honeymoon weekend” and put some fun back into their sex lives so that this phase of healing doesn’t become an onerous task.
CASE RESOLVED
After a discussion of her options, the patient chooses to stick with paroxetine and use behavioral therapy alone to resolve her dyspareunia. At her follow-up visit two weeks later, she reports that she has enjoyed the period of pain-free “sex” and feels ready to add penetration into her activities.
You encourage her to continue sexual intercourse on a regular, relatively frequent basis to prevent a recurrence of dyspareunia. She continues to use silicone-based lubricants.
Recently, three new drugs have been added to the armamentarium for menopausal symptoms and dyspareunia:
• Paroxetine 7.5 mg
• Conjugated estrogens and bazedoxifene
• Ospemifene.
In this article, I present a case-based approach to incorporating these drugs into practice and restoring sexual function in the setting of vulvovaginal atrophy and dyspareunia. As is often the case, decision-making requires sifting through multiple layers of information.
CASE: LOW DESIRE AND DISCOMFORT DURING INTERCOURSE
A 58-year-old patient mentions during her annual visit that she’s not that interested in sex anymore. Her children are grown, she’s been happily married for 28 years, and she enjoys her job and denies any symptoms of depression. She says her relationship with her husband is good and, aside from her low desire, she has no worries about the marriage. Her only medication is paroxetine 7.5 mg/d for management of her moderate hot flashes, which she initiated at her last annual visit. She reports improvement in her sleep and menopausal symptoms as a result. She has an intact uterus.
You perform a pelvic exam and find atrophic vulva and vagina with mild erythema and thinned epithelium. When you ask if she has experienced any discomfort, she reports that she needs to use lubrication for intercourse and that, even with lubrication, she has pain upon penetration and a burning sensation that continues throughout intercourse. She also reports that it seems to take her much longer to achieve arousal than in the past, and she often fails to reach orgasm.
How would you manage this patient?
Continued on next page >>
AS ALWAYS, BEGIN WITH THE HISTORY
The transition to menopause creates multiple layers of potential symptoms and problems for our patients, and sometimes medical therapy can generate additional ones.
In a patient reporting the onset of low desire and dyspareunia, you would want to first consider her medication history, despite the clear evidence of vaginal atrophy. Begin by asking whether she is taking any new medications prescribed by another provider. In some cases, antihypertensive drugs, psychotropic agents, and other medications can affect sexual function.
This patient has been taking paroxetine for one year and is happy with its effect on her sleep and hot flashes. Simon and colleagues found this nonhormonal agent for moderate to severe vasomotor symptoms produced no notable effects on weight, libido, or sleep, compared with placebo.
Nevertheless, in this case, because selective serotonin reuptake inhibitors such as paroxetine can affect arousal and orgasm, it is unclear whether the ultra-low dose of paroxetine she is taking is contributing to her problems. If you were to discontinue the drug to find out, her vasomotor symptoms and sleep disruption would likely recur.
Your decision-making is important here and should involve the patient in an extensive discussion. If there is not enough time for this discussion at the current visit, schedule a follow-up to address her concerns fully.
VULVOVAGINAL ATROPHY HAS ITS OWN TIMELINE
In many cases, vasomotor symptoms such as hot flashes occur years before the skin begins to atrophy in the vulva and vagina, particularly in women who enter menopause naturally. Among menopausal women who continue to have intercourse on a regular basis, however, these skin changes often are much less troublesome than they are for women who have sex more rarely.
In this patient, one possible scenario is that paroxetine caused a slight reduction in sexual interest, and the frequency of intercourse went down as a result. In women who have little or no intercourse, the vagina begins to shrink and the tissues lose elasticity. This patient may have been undergoing the natural process of menopause, and that process may have been compounded by a decrease in the frequency of sex.
If you were to discontinue the paroxetine, it would still be necessary to treat the vulvovaginal skin and work on manual techniques to gently dilate the introitus.
Option 1: Systemic hormone therapy >>
Option 1: Systemic hormone therapy
Systemic estrogen is the most effective treatment for menopausal vasomotor symptoms, reducing hot flashes by 50% to 100% within four weeks of initiation. However, because our patient has an intact uterus, any systemic estrogen she opts to use must be opposed by a progestin for safety reasons.
In terms of estrogen, her options are oral or nonoral formulations. Not only would estrogen manage our patient’s hot flashes but, over time, it would improve her sexual problems and atrophy, which might or might not improve her current complaint of low desire. You likely would need to add a short regimen of topical estrogen and perhaps even a dilator to restore her sexual function completely, however.
Since our patient chose the nonhormonal agent paroxetine to manage her menopausal symptoms, she may be worried about the increased risk for breast cancer associated with use of a progestin in combination with estrogen. One hormonal option now available that eliminates the need for a progestin is conjugated estrogens and bazedoxefine. Bazedoxefine is a third-generation selective estrogen receptor modulator. This drug has estrogen-like effects on bone and antiestrogen effects on the uterus.
Conjugated estrogens/bazedoxifene is indicated for use in women with a uterus for treatment of
• Moderate to severe vasomotor symptoms of menopause
• Prevention of postmenopausal osteoporosis.
Among the risks are an increased risk for venous thromboembolism (VTE) and stroke. It is not approved specifically for the treatment of dyspareunia.
Another hormonal option is ospemifene, an estrogen agonist/antagonist indicated for the treatment of moderate to severe dyspareunia in menopausal women. Among the drugs in its class, such as tamoxifen and raloxifene, ospemifene is the only agent that maintains a full estrogenic effect on vaginal tissues. Its risks include VTE and stroke.
Although the labeling includes a warning about the risk for endometrial hyperplasia associated with its use, Goldstein and colleagues found no significant difference in the rate of endometrial thickening greater than 5 mm between women taking ospemifene and those taking placebo after one year of daily oral treatment. No carcinomas were found in either group.
Option 2: Local estrogen
If our patient declines all systemic hormone therapy, the topical approach should resolve her vulvovaginal symptoms, and she could continue taking paroxetine for her menopausal symptoms. Vaginal estrogen would address the skin problems, provided the patient applies it correctly. Many women are afraid to use estrogen creams and compensate by applying them only to the vulva, thinking that, by limiting their use to external tissues, they are avoiding any associated risks.
If she opts for the local approach, this patient should be encouraged to use transvaginal estrogen in small doses to increase the elasticity of the vulvovaginal tissue, even though it may require daily use for a week or two to improve her symptoms, after which once- or twice-weekly administration should suffice.
The use of low-dose vaginal cream for a short duration is unlikely to increase her risks in any way. Local estrogen is available as a tablet, cream, or ring.
Option 3: A nonhormonal approach >>
Option 3: A nonhormonal approach
If the patient refuses any hormonal agent—even topical estrogen—I would recommend the use of silicone-based lubricants and a dilator and prescribe more frequent penetration to increase elasticity and reduce pain. Paroxetine could be continued to address her menopausal symptoms.
DON'T OVERLOOK BEHAVIORAL TECHNIQUES
Before this patient leaves your office with the option of her choice, a bit of counseling is necessary to instruct her about methods of restoring full sexual function.
Pain is a powerful aversive stimulus. This patient clearly states that she has had less frequent intercourse as a result of dyspareunia. It is not unusual for patients to develop a “habit” of avoidance in response to the behavior that causes their pain.
One recommendation is to talk to this patient about putting sex back into her life by encouraging her to increase sexual activity without penetration until she begins to arouse easily again. Arousal produces physiologic effects, increasing the caliber and length of the vagina as well as lubrication. The use of fingers or dilators may help restore caliber.
The patient can be encouraged to engage in snuggling and cuddling to regain those activities without the fear of pain associated with penetration. Follow-up after two weeks of this therapy can confirm the restoration of tissue elasticity, and the green light can be given for penetration to begin again. Couples can be encouraged to plan a “honeymoon weekend” and put some fun back into their sex lives so that this phase of healing doesn’t become an onerous task.
CASE RESOLVED
After a discussion of her options, the patient chooses to stick with paroxetine and use behavioral therapy alone to resolve her dyspareunia. At her follow-up visit two weeks later, she reports that she has enjoyed the period of pain-free “sex” and feels ready to add penetration into her activities.
You encourage her to continue sexual intercourse on a regular, relatively frequent basis to prevent a recurrence of dyspareunia. She continues to use silicone-based lubricants.
Psychological Stress Interventions and Asthma: Therapeutic Considerations
From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
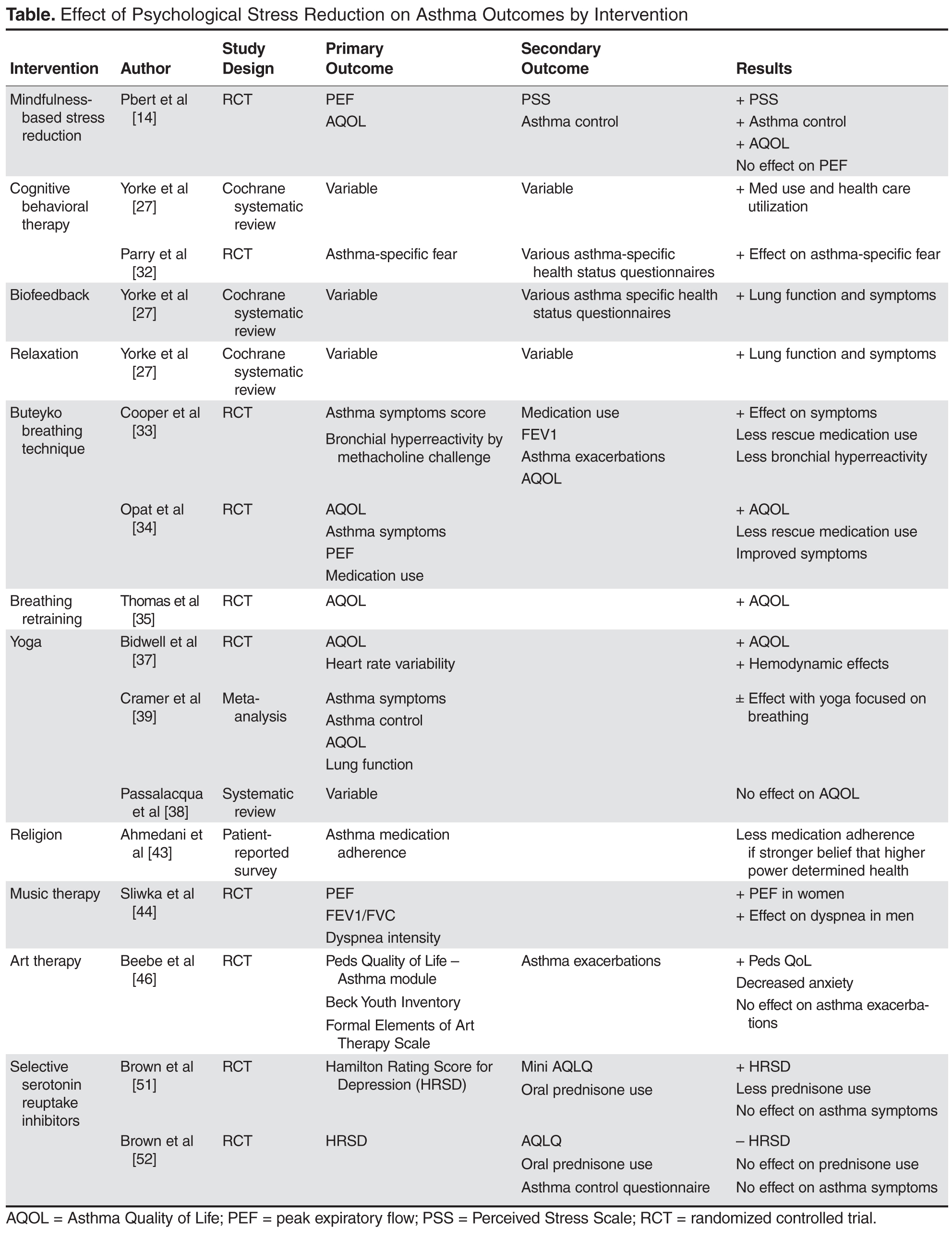
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
Psychologically Focused Interventions
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, [email protected].
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.
1. Kondo N. Socioeconomic disparities and health: impacts and pathways. J Epidemiol 2012;22:2–6.
2. Nakata A. Psychosocial job stress and immunity: a systematic review. Methods Mol Biol 2012;934:39–7.
3. Van Lieshout RJ, Macqueen GM. Relation between asthma and psychological distress: an old idea revisited. Chem Immunol Allergy 2012;98:1–13.
4. Marshall GD Jr. The adverse effects of psychological stress on immunoregulatory balance: applications to human inflammatory diseases. Immunol Allergy Clin North Am 2011;31:133–40.
5. Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005;25:1–750.
6. Harding SM. Acid reflux and asthma. Curr Opin Pulm Med 2003;9:42–5.
7. Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20.
8. Matricardi PM. Prevalence of atopy and asthma in eastern versus western Europe: why the difference? Ann Allergy Asthma Immunol 2001;87:24–7.
9. Murray CS, Woodcock A, Custovic A. The role of indoor allergen exposure in the development of sensitization and asthma. Curr Opin Allergy Clin Immunol 2001;1:407–12.
10. TePas EC, Umetsu DT. Immunotherapy of asthma and allergic diseases. Curr Opin Pediatr 2000;12:574–78.
11. Babu KS, Holgate ST. Newer therapies for asthma: a focus on anti-IgE. Indian J Chest Dis Allied Sci 2002;44:107–15.
12. Oh Y, Kim Y, Yoo S, et al. Association between stress and asthma symptoms: a population based study. Respirology 2004;9:363–8.
13. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children. Lancet 2000;356:982–7.
14. Pbert L, Madison JM, Druker S, et al. Effect of mindfulness training on asthma quality of life and lung function: a randomized controlled trial. Thorax 2012;67:769–76.
15. Wisnivesky JP, Lorenzo J, Feldman JM, et al. The relationship between perceived stress and morbidity among adult inner-city asthmatics. J Asthma 2010;47:100–4.
16. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev 2009;29:317–27.
17. Wright RJ, Cohen S, Carey V, et al. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Resp Crit Care Med 2002;165:358–65.
18. Wright RJ, Mitchell H, Visness CM, et al. Community violence and asthma morbidity in the Inner-City Asthma Study. Am J Public Health 2004;94:625–32.
19. Michel FB. Psychology of the allergic patient. Allergy 1994;49:28–30.
20. Yonas MA, Lange NE, Celedon JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol 2012;12:202–10.
21. Apter AJ, Garcia LA, Boyd RC, et al. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J Allergy Clin Immunol 2010;126:552–7.
22. Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am 2011;31:19–39.
23. Tyagi A, Cohen M. Yoga and hypertension: a systematic review. Altern Ther Health Med 2014;20:32-59.
24. Moore CJ, Cunningham SA. Social position, psychological stress, and obesity: a systematic review. J Acad Nutr Diet 2012;112:518–26.
25. Plack K, Herpertz S, Petrak F. Behavioral medicine interventions in diabetes. Curr Opin Psychiatry 2010;23:131–8.
26. Clucas C, Sibley E, Harding R, et al. A systematic review of interventions for anxiety in people with HIV. Psychol Health Med 2011;16:528–47.
27. Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med 2007;101:1–14.
28. Merkes M. Mindfulness-based stress reduction for people with chronic diseases. Aust J Prim Health 2010;16:200–10.
29. Kopf S, Oikonomou D, Hartmann M. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease- results of a randomized controlled trial (HEIDIS). Exp Clin Endocrinol Diabetes 2014;122:341–9.
30. Musial F, Bussing A, Heusser P, et al. Mindfulness-based stress reduction for integrative cancer care- a summary of evidence. Forsch Komplementmed 2011;18:192–202.
31. Shigaki CL, Glass B, Schopp LH. Mindfulness-based stress reduction in medical settings. J Clin Psychl Med Settings 2006;13:209-16.
32. Parry GD, Cooper CL, Moore JM. Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomized trial. Respir Med 2012;106;802–10.
33. Cooper S, Oborne J, Newton S, et al. Effect of two breathing exercises (Buteyko and pranayama) in asthma: a randomized controlled trial. Thorax 2003;58:674–9.
34. Opat AJ, Cohen MM, Bailey MJ, et al. A clinical trial of the Buteyko breathing technique in asthma as taught by a video. J Asthma 2000;37:557–64.
35. Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomized controlled trial. Thorax 2003;58:110–15.
36. Markham AW, Wilkinson JM. Complementary and alternative medicines (CAM) in the management of asthma: an examination of the evidence. J Asthma 2004;41:131–9.
37. Bidwell AM, Yazel B, Davin D, et al. Yoga training improves quality of life in women with asthma. J Altern Complement Med 2012;18:749–55.
38. Passalacqua G, Bousquet PJ, Carlsen KH, et al. ARIA update: I- Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–62.
39. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol 2014;112:503–10.
40. Slader CA, Reddel HK, Jenkins CR, et al. Complementary and alternative medicine use in asthma: who is using what? Respirology 2006;11:373–87.
41. Silvers WS, Bailey HK. Integrative approach to allergy and asthma using complementary and alternative medicine. Ann Allergy Asthma Immunol 2014;112;280-85.
42. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev 2005;(2):CD001002.
43. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol 2013;110:75–9.
44. Sliwka A, Nowobilski R, Polczyk R, et al. Mild asthmatics benefit from music therapy. J Asthma 2012;49:401–8.
45. Clarke SA, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life (HRQOL) amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64.
46. Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clin Immunol 2010;126:262–6.
47. Metzger LK. Assessment of use of music by patients participating in cardiac rehabilitation. J Music Ther 2004;41:55–69.
48. El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther 2009;30:718–24.
49. Thomas M, Bruton An, Moffatt M, et al. Asthma and psychological dysfunction. Prim Care Respir J 2011;20:250–6.
50. Lavoie KL, Bacon SL, Barone S, et al. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest 2006;130:1039–47.
51. Brown ES, Vigil L, Khan DA, et al. A randomized trial of citalopram versus placebo in outpatients with asthma and major depressive disorder: a proof of concept study. Biol Psychiatry 2005;58:865–70.
52. Brown ES, Howard C, Khan DA, et al. Escitalopram for severe asthma and major depressive disorder: a randomized, double-blind, placebo-controlled proof-of-concept study. Psychosomatics 2012;53:75–80.
From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
Psychologically Focused Interventions
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, [email protected].
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.
From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
Psychologically Focused Interventions
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, [email protected].
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.
1. Kondo N. Socioeconomic disparities and health: impacts and pathways. J Epidemiol 2012;22:2–6.
2. Nakata A. Psychosocial job stress and immunity: a systematic review. Methods Mol Biol 2012;934:39–7.
3. Van Lieshout RJ, Macqueen GM. Relation between asthma and psychological distress: an old idea revisited. Chem Immunol Allergy 2012;98:1–13.
4. Marshall GD Jr. The adverse effects of psychological stress on immunoregulatory balance: applications to human inflammatory diseases. Immunol Allergy Clin North Am 2011;31:133–40.
5. Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005;25:1–750.
6. Harding SM. Acid reflux and asthma. Curr Opin Pulm Med 2003;9:42–5.
7. Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20.
8. Matricardi PM. Prevalence of atopy and asthma in eastern versus western Europe: why the difference? Ann Allergy Asthma Immunol 2001;87:24–7.
9. Murray CS, Woodcock A, Custovic A. The role of indoor allergen exposure in the development of sensitization and asthma. Curr Opin Allergy Clin Immunol 2001;1:407–12.
10. TePas EC, Umetsu DT. Immunotherapy of asthma and allergic diseases. Curr Opin Pediatr 2000;12:574–78.
11. Babu KS, Holgate ST. Newer therapies for asthma: a focus on anti-IgE. Indian J Chest Dis Allied Sci 2002;44:107–15.
12. Oh Y, Kim Y, Yoo S, et al. Association between stress and asthma symptoms: a population based study. Respirology 2004;9:363–8.
13. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children. Lancet 2000;356:982–7.
14. Pbert L, Madison JM, Druker S, et al. Effect of mindfulness training on asthma quality of life and lung function: a randomized controlled trial. Thorax 2012;67:769–76.
15. Wisnivesky JP, Lorenzo J, Feldman JM, et al. The relationship between perceived stress and morbidity among adult inner-city asthmatics. J Asthma 2010;47:100–4.
16. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev 2009;29:317–27.
17. Wright RJ, Cohen S, Carey V, et al. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Resp Crit Care Med 2002;165:358–65.
18. Wright RJ, Mitchell H, Visness CM, et al. Community violence and asthma morbidity in the Inner-City Asthma Study. Am J Public Health 2004;94:625–32.
19. Michel FB. Psychology of the allergic patient. Allergy 1994;49:28–30.
20. Yonas MA, Lange NE, Celedon JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol 2012;12:202–10.
21. Apter AJ, Garcia LA, Boyd RC, et al. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J Allergy Clin Immunol 2010;126:552–7.
22. Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am 2011;31:19–39.
23. Tyagi A, Cohen M. Yoga and hypertension: a systematic review. Altern Ther Health Med 2014;20:32-59.
24. Moore CJ, Cunningham SA. Social position, psychological stress, and obesity: a systematic review. J Acad Nutr Diet 2012;112:518–26.
25. Plack K, Herpertz S, Petrak F. Behavioral medicine interventions in diabetes. Curr Opin Psychiatry 2010;23:131–8.
26. Clucas C, Sibley E, Harding R, et al. A systematic review of interventions for anxiety in people with HIV. Psychol Health Med 2011;16:528–47.
27. Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med 2007;101:1–14.
28. Merkes M. Mindfulness-based stress reduction for people with chronic diseases. Aust J Prim Health 2010;16:200–10.
29. Kopf S, Oikonomou D, Hartmann M. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease- results of a randomized controlled trial (HEIDIS). Exp Clin Endocrinol Diabetes 2014;122:341–9.
30. Musial F, Bussing A, Heusser P, et al. Mindfulness-based stress reduction for integrative cancer care- a summary of evidence. Forsch Komplementmed 2011;18:192–202.
31. Shigaki CL, Glass B, Schopp LH. Mindfulness-based stress reduction in medical settings. J Clin Psychl Med Settings 2006;13:209-16.
32. Parry GD, Cooper CL, Moore JM. Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomized trial. Respir Med 2012;106;802–10.
33. Cooper S, Oborne J, Newton S, et al. Effect of two breathing exercises (Buteyko and pranayama) in asthma: a randomized controlled trial. Thorax 2003;58:674–9.
34. Opat AJ, Cohen MM, Bailey MJ, et al. A clinical trial of the Buteyko breathing technique in asthma as taught by a video. J Asthma 2000;37:557–64.
35. Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomized controlled trial. Thorax 2003;58:110–15.
36. Markham AW, Wilkinson JM. Complementary and alternative medicines (CAM) in the management of asthma: an examination of the evidence. J Asthma 2004;41:131–9.
37. Bidwell AM, Yazel B, Davin D, et al. Yoga training improves quality of life in women with asthma. J Altern Complement Med 2012;18:749–55.
38. Passalacqua G, Bousquet PJ, Carlsen KH, et al. ARIA update: I- Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–62.
39. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol 2014;112:503–10.
40. Slader CA, Reddel HK, Jenkins CR, et al. Complementary and alternative medicine use in asthma: who is using what? Respirology 2006;11:373–87.
41. Silvers WS, Bailey HK. Integrative approach to allergy and asthma using complementary and alternative medicine. Ann Allergy Asthma Immunol 2014;112;280-85.
42. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev 2005;(2):CD001002.
43. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol 2013;110:75–9.
44. Sliwka A, Nowobilski R, Polczyk R, et al. Mild asthmatics benefit from music therapy. J Asthma 2012;49:401–8.
45. Clarke SA, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life (HRQOL) amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64.
46. Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clin Immunol 2010;126:262–6.
47. Metzger LK. Assessment of use of music by patients participating in cardiac rehabilitation. J Music Ther 2004;41:55–69.
48. El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther 2009;30:718–24.
49. Thomas M, Bruton An, Moffatt M, et al. Asthma and psychological dysfunction. Prim Care Respir J 2011;20:250–6.
50. Lavoie KL, Bacon SL, Barone S, et al. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest 2006;130:1039–47.
51. Brown ES, Vigil L, Khan DA, et al. A randomized trial of citalopram versus placebo in outpatients with asthma and major depressive disorder: a proof of concept study. Biol Psychiatry 2005;58:865–70.
52. Brown ES, Howard C, Khan DA, et al. Escitalopram for severe asthma and major depressive disorder: a randomized, double-blind, placebo-controlled proof-of-concept study. Psychosomatics 2012;53:75–80.
1. Kondo N. Socioeconomic disparities and health: impacts and pathways. J Epidemiol 2012;22:2–6.
2. Nakata A. Psychosocial job stress and immunity: a systematic review. Methods Mol Biol 2012;934:39–7.
3. Van Lieshout RJ, Macqueen GM. Relation between asthma and psychological distress: an old idea revisited. Chem Immunol Allergy 2012;98:1–13.
4. Marshall GD Jr. The adverse effects of psychological stress on immunoregulatory balance: applications to human inflammatory diseases. Immunol Allergy Clin North Am 2011;31:133–40.
5. Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005;25:1–750.
6. Harding SM. Acid reflux and asthma. Curr Opin Pulm Med 2003;9:42–5.
7. Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20.
8. Matricardi PM. Prevalence of atopy and asthma in eastern versus western Europe: why the difference? Ann Allergy Asthma Immunol 2001;87:24–7.
9. Murray CS, Woodcock A, Custovic A. The role of indoor allergen exposure in the development of sensitization and asthma. Curr Opin Allergy Clin Immunol 2001;1:407–12.
10. TePas EC, Umetsu DT. Immunotherapy of asthma and allergic diseases. Curr Opin Pediatr 2000;12:574–78.
11. Babu KS, Holgate ST. Newer therapies for asthma: a focus on anti-IgE. Indian J Chest Dis Allied Sci 2002;44:107–15.
12. Oh Y, Kim Y, Yoo S, et al. Association between stress and asthma symptoms: a population based study. Respirology 2004;9:363–8.
13. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children. Lancet 2000;356:982–7.
14. Pbert L, Madison JM, Druker S, et al. Effect of mindfulness training on asthma quality of life and lung function: a randomized controlled trial. Thorax 2012;67:769–76.
15. Wisnivesky JP, Lorenzo J, Feldman JM, et al. The relationship between perceived stress and morbidity among adult inner-city asthmatics. J Asthma 2010;47:100–4.
16. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev 2009;29:317–27.
17. Wright RJ, Cohen S, Carey V, et al. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Resp Crit Care Med 2002;165:358–65.
18. Wright RJ, Mitchell H, Visness CM, et al. Community violence and asthma morbidity in the Inner-City Asthma Study. Am J Public Health 2004;94:625–32.
19. Michel FB. Psychology of the allergic patient. Allergy 1994;49:28–30.
20. Yonas MA, Lange NE, Celedon JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol 2012;12:202–10.
21. Apter AJ, Garcia LA, Boyd RC, et al. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J Allergy Clin Immunol 2010;126:552–7.
22. Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am 2011;31:19–39.
23. Tyagi A, Cohen M. Yoga and hypertension: a systematic review. Altern Ther Health Med 2014;20:32-59.
24. Moore CJ, Cunningham SA. Social position, psychological stress, and obesity: a systematic review. J Acad Nutr Diet 2012;112:518–26.
25. Plack K, Herpertz S, Petrak F. Behavioral medicine interventions in diabetes. Curr Opin Psychiatry 2010;23:131–8.
26. Clucas C, Sibley E, Harding R, et al. A systematic review of interventions for anxiety in people with HIV. Psychol Health Med 2011;16:528–47.
27. Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med 2007;101:1–14.
28. Merkes M. Mindfulness-based stress reduction for people with chronic diseases. Aust J Prim Health 2010;16:200–10.
29. Kopf S, Oikonomou D, Hartmann M. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease- results of a randomized controlled trial (HEIDIS). Exp Clin Endocrinol Diabetes 2014;122:341–9.
30. Musial F, Bussing A, Heusser P, et al. Mindfulness-based stress reduction for integrative cancer care- a summary of evidence. Forsch Komplementmed 2011;18:192–202.
31. Shigaki CL, Glass B, Schopp LH. Mindfulness-based stress reduction in medical settings. J Clin Psychl Med Settings 2006;13:209-16.
32. Parry GD, Cooper CL, Moore JM. Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomized trial. Respir Med 2012;106;802–10.
33. Cooper S, Oborne J, Newton S, et al. Effect of two breathing exercises (Buteyko and pranayama) in asthma: a randomized controlled trial. Thorax 2003;58:674–9.
34. Opat AJ, Cohen MM, Bailey MJ, et al. A clinical trial of the Buteyko breathing technique in asthma as taught by a video. J Asthma 2000;37:557–64.
35. Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomized controlled trial. Thorax 2003;58:110–15.
36. Markham AW, Wilkinson JM. Complementary and alternative medicines (CAM) in the management of asthma: an examination of the evidence. J Asthma 2004;41:131–9.
37. Bidwell AM, Yazel B, Davin D, et al. Yoga training improves quality of life in women with asthma. J Altern Complement Med 2012;18:749–55.
38. Passalacqua G, Bousquet PJ, Carlsen KH, et al. ARIA update: I- Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–62.
39. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol 2014;112:503–10.
40. Slader CA, Reddel HK, Jenkins CR, et al. Complementary and alternative medicine use in asthma: who is using what? Respirology 2006;11:373–87.
41. Silvers WS, Bailey HK. Integrative approach to allergy and asthma using complementary and alternative medicine. Ann Allergy Asthma Immunol 2014;112;280-85.
42. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev 2005;(2):CD001002.
43. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol 2013;110:75–9.
44. Sliwka A, Nowobilski R, Polczyk R, et al. Mild asthmatics benefit from music therapy. J Asthma 2012;49:401–8.
45. Clarke SA, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life (HRQOL) amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64.
46. Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clin Immunol 2010;126:262–6.
47. Metzger LK. Assessment of use of music by patients participating in cardiac rehabilitation. J Music Ther 2004;41:55–69.
48. El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther 2009;30:718–24.
49. Thomas M, Bruton An, Moffatt M, et al. Asthma and psychological dysfunction. Prim Care Respir J 2011;20:250–6.
50. Lavoie KL, Bacon SL, Barone S, et al. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest 2006;130:1039–47.
51. Brown ES, Vigil L, Khan DA, et al. A randomized trial of citalopram versus placebo in outpatients with asthma and major depressive disorder: a proof of concept study. Biol Psychiatry 2005;58:865–70.
52. Brown ES, Howard C, Khan DA, et al. Escitalopram for severe asthma and major depressive disorder: a randomized, double-blind, placebo-controlled proof-of-concept study. Psychosomatics 2012;53:75–80.
Misuse of Prescription Stimulant Medication Among College Students: Summary of the Research Literature and Clinical Recommendations
From the University of South Carolina, Columbia, SC.
Abstract
- Objective: To provide a summary of the existing research on the characteristics of college students who report misusing prescription stimulant medications, to offer a set of clinical recommendations for practitioners, and to offer several possible prevention strategies.
- Methods: Literature review and research-based recommendations for clinical practice and prevention.
- Results: Misuse of prescription stimulant medication among college students is a prevalent and growing problem. Significant risk factors for misuse of stimulant medication include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Suggestions for preventing misuse and diversion of prescription stimulant medications, including strategies for the individual and potential policy changes on college campuses, are offered.
- Conclusions: Misuse and diversion of prescription stimulant medications is a growing concern among adolescents and young adults and should be addressed by health care practitioners. Additional research on effective intervention and prevention strategies is needed.
Prescription stimulant medications (eg, methylphenidate, amphetamines) are typically used for the treatment of attention-deficit/hyperactivity disorder (ADHD) to increase attentiveness, decrease distractibility, and improve daily functioning. Prescriptions for stimulant medications are on the rise; between 2002 and 2010, the number of prescriptions for ADHD medications for youth under 18 increased 46% [1].
A recent review of ADHD diagnosis among college students estimated a prevalence rate of 2% to 8% [2]. More individuals with ADHD are matriculating to college than in the past [3,4], as more supports have been put in place for college students diagnosed with ADHD, including improved educational/organizational treatments and accommodations [2]. Many college students with ADHD also use prescription stimulant medications as part of their treatment plan; McCabe, Teter, and Boyd reported that 2.2% of college students had prescriptions for stimulant medications annually [5].
As the number of individuals of all ages with stimulant medication prescriptions increase, more individuals without prescriptions are gaining access to stimulant medications. In a survey of college students with medication prescriptions, stimulants were the most commonly diverted medication, with 61.7% of students with these prescriptions reporting having shared or sold their medication at least once [6]. Studies report that as many as 43% of college students have misused stimulant medication in their lifetime [7], though prevalence rates vary by study. Throughout this review, “misuse of stimulant medication” refers to using prescription stimulant medications without a prescription or using more stimulant medication than prescribed (ie, a higher or more frequent dosage).
Given the ease with which college students are able to obtain stimulant medications, the alarming prevalence of stimulant medication misuse among this population, and the potentially serious health risks associated with misuse of stimulant medication (especially when combined with other substances, such as alcohol, that are commonly used by college students), there is a need to both better understand and ultimately reduce the misuse of stimulant medication among college students. Thus, the purpose of this paper is threefold. First, we provide a summary of the existing research literature on the characteristics of college students who report misusing stimulant medication. Second, we offer a set of clinical recommendations for practitioners, which includes stimulant medication indications, risks, benefits, and side effects, along with problems associated with stimulant medication diversion and misuse. Finally, we offer several prevention strategies, including strategies for the individual as well as several suggestions for changing policies on college campuses to prevent stimulant diversion and misuse. Importantly, although our literature review addresses prescription stimulant misuse among college students, our clinical recommendations are also appropriate for adolescents and young adults not enrolled in college.
Summary of the Literature
The following summary is based on a comprehensive search of the existing research literature on misuse of stimulant medication among college students, which ultimately identified 30 relevant studies using 21 unique samples. A study was included if: (1) the main focus of the study was misuse of stimulant medication, (2) it was a peer-reviewed, empirical study using quantitative data analytic techniques, (3) it was written in English, (4) only undergraduate students were included in the sample, (5) it did not focus on only one type of stimulant medication (eg, methylphenidate only), and (6) if the article discussed multiple prescription drug categories (eg, stimulants, opiates), the data must have been analyzed separately for each category. An extensive meta-analytic review of this literature will be published elsewhere (contact the corresponding author to request a reprint). The following is a brief summary of our findings.
Prevalence, Availability, and Demographic Characteristics
Among prevalence rates reported, lifetime rates of stimulant medication misuse were the most frequently reported, ranging from 8.1% [8] to 43% [7]. Rates of misuse of stimulant medications within the last year ranged from 5.3% [9] to 35.3% [10]. A number of the studies asked students how they obtained stimulant medications for misuse; peers were overwhelmingly the most common source for obtaining the medications. For example, DeSantis, Webb, and Noar [11] found that 91% of the undergraduates who were interviewed obtained stimulant medications from friends or significant others.
Perceived availability of stimulant medications was also measured in several studies. DeSantis, Webb, and Noar [11] found that 82% of students thought it was somewhat or very easy to obtain stimulant medication; however, Sharp and Rosén [12] found that only 55% of students thought it was somewhat or very easy to obtain stimulant medication. In another study that examined perceived availability, 37% of men and 29.2% of women agreed that they knew students who would provide them with stimulant medications [13].
Many of the studies reviewed examined the relation between particular demographic characteristics (eg, gender, race, socioeconomic status, religious affiliation, year in college, sorority or fraternity membership) and misuse of stimulant medication among college students. The vast majority of studies that examined gender as related to misuse of stimulant medication found that significantly more males misused stimulant medication than females. For example, one study found that 26% of males and 17.3% of females reported misusing stimulant medication [14]; another study found that 39% of males versus 30% of females reported misuse [11].
It is also clear from the existing literature that members of fraternities and sororities appear to be more at-risk for misuse of stimulant medication than non-Greek students. In multiple studies, Greek students had rates of misuse twice that of non-Greeks. For instance, 48% of Greeks misused in their lifetime compared to 22% of non-Greeks [11]; 12% of Greeks misused in the past year compared to 5% of non-Greeks [15]; and Greeks were 2.32 times more likely to initiate use than non-Greeks [9].
Unfortunately, results from studies examining other demographic characteristics (eg, race, socioeconomic status, religious affiliation, year in college) as related to misuse of stimulant medication are much less conclusive and these correlates therefore require further investigation.
Motives For Misuse and Perceived Risk
Researchers have also evaluated college students’ motives for misusing stimulant medication and the risks they associate with misuse. All of the studies that asked misusing students about their motives for misuse reported that the most commonly endorsed motives were related to academics. “To concentrate better while studying” [16], “to improve study skills” [17], “to stay awake to study longer” [11], and “to improve concentration” [18] were some of the most commonly endorsed motives in these studies. Nonacademic reasons, such as to get high, to prolong effects of alcohol and other drugs, and to lose weight, were less commonly endorsed [7,12,19]. In studies where participants were able to indicate multiple motives for misuse [16], very few students misused for only nonacademic reasons.
Several studies measured the relation between misuse of stimulant medication and perceived risk associated with misuse. Perceived risk was conceptualized as perceived harmfulness [20], perception of safety [14], concern with health risk [18], and the inverse of positive outcome expectancies [21]. These articles found that when college students perceive more risk or have less positive expectancies about stimulant medication misuse, they are less likely to misuse stimulant medication. For instance, those who associated stimulant medication misuse with low perceived harmfulness were over 10 times more likely to have used in the last year than those who associated misuse with high perceived harmfulness [20].
Academic Outcomes Associated with Misuse
Interestingly, despite academic motives being most common for college students who report misusing stimulant medication, a number of studies have found a negative association between academic outcomes and misuse of stimulant medication. For instance, nonusers reported an average grade-point average (GPA) of 3.28 compared to 3.16 for misusers [16]. Other research demonstrates that the lower the student’s GPA is, the greater the odds are of the student misusing stimulant medication [8]. Misuse is also significantly related to other detrimental academic behaviors such as skipping class and less studying [20,22].
Psychological Correlates of Misuse
Researchers have evaluated the relation between several different psychological variables and misuse of stimulant medication. The strongest association is between symptoms of ADHD and stimulant medication misuse. Studies are consistent in reporting a significant correlation between greater symptoms of ADHD and higher rates of misuse or a significant difference in rates of misuse between those who have an ADHD diagnosis and those who do not. One study found that 71.1% of stimulant medication misusers screened positive for adult ADHD symptoms [17]. Another study found that for every standard deviation increase in attention problems, the odds of becoming a stimulant misuser increased by 1.78 [9]. Two studies asked participants if they believed they had ADHD. Advokat, Guildry, and Martino found that 12% of misusers believed they had ADHD [7]. Twenty-nine percent of “self-diagnosers” reported misusing, compared to 11.4% of “non-diagnosers” in another study [18].
Although the literature base is smaller than for ADHD, several studies have suggested a significant difference in symptoms of depression between stimulant medication misusers and nonusers. Zullig and Divin [23] found that misusers were significantly more likely to feel very sad, feel depressed, and consider suicide than nonusers. More frequent misuse has also been shown to be significantly associated with depressed mood [24].
A number of studies demonstrate a clear association between high sensation-seeking and misuse of stimulant medication. These results are not surprising given the well-documented relation between sensation seeking and substance use [25–27]. One study found a significant interaction between sensation seeking and perceived harmfulness of misusing stimulant medication: those with high sensation seeking and low perceived harmfulness were most likely to misuse [20].
Other Substance Use Associated with Stimulant Misuse
Many of the reviewed studies found a positive correlation between misuse of stimulant medication and other substance use or a significant difference between stimulant misusers and nonusers in rates of other substance use. These findings held across all substances examined, including alcohol, cigarettes, marijuana, illicit stimulants (eg, ecstasy, cocaine, or amphetamines), and non-stimulant prescription medications. For instance, significant associations were found between misuse of stimulant medication and several alcohol-related constructs, such as binge drinking [28,29], problematic drinking behavior [30], or meeting the Diagnostic and Statistical Manual of Mental Disorders [21] criteria for alcohol abuse [22]. With respect to cigarettes, 50.3% of misusers were found to have smoked cigarettes in the last 6 months compared to 13.3% of nonusers [16]. Similar findings emerged for illicit drug use. One study found that 73.5% of stimulant medication misusers reported use of marijuana in the last 6 months, compared to 18.2% of nonusers [19], while another study found that 93% of misusers used marijuana in the last year compared to 34% of nonusers [5]. This same study found that 33% of stimulant medication misusers also reported cocaine use in the last year compared to 2% of stimulant nonusers [5]. Finally, many of the studies reviewed examined the association between other substance use in general and stimulant medication misuse. Results were striking; the odds of becoming a stimulant medication misuser increased by 3.81 for each standard deviation increase in the amount of other substance use [9].
Summary
The research literature reviewed in this section provides a descriptive characterization of which college students (and, by extension, adolescents and young adults not in college) may be at the greatest risk of misuse of stimulant medication. Significant risk factors include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. It is important to recognize that one, several, or many of these risk factors may be present in a given individual who is misusing stimulant medication. Moreover, there may be other risk factors not yet identified in the research literature. The following sections of this paper draw from the literature reviewed here to provide a number of clinical recommendations for reducing and preventing misuse of stimulant medications among college students, other young adults, and adolescents.
Clinical Recommendations
It is important for health care providers to be aware of the benefits and risks associated with stimulant medications, the prevalence of and risk factors for stimulant misuse, and the psychiatric, psychological, and medical comorbidities associated with the misuse of stimulant medication. Knowledge about stimulant medications, misuse of stimulant medications, and a thorough evaluation of the patient will enable health care providers to address the misuse, as well as any comorbidities or other factors that may contribute to stimulant medication misuse, either pharmacologically or through referral for more specified psychotherapeutic interventions.
Stimulant Medication Indications and Adverse Effects
Stimulant medications are efficacious for the treatment of ADHD and, when prescribed and used correctly, can improve attentiveness, decrease distractibility, and improve daily functioning in the short term [19]. When used by individuals without ADHD, patients may experience euphoria, stimulation, alertness, and are not likely to experience the cognitive benefits that those with ADHD receive [31]. Side effects can occur regardless of whether the individual is using the stimulant for ADHD, misusing, or is dependent, and include nervousness, headaches, tachycardia, poor appetite, depressed mood, and poor sleep [19,32]. Additionally, stimulant medications can cause psychosis, agitation, and hallucinations [31,33], which typically resolve after discontinuation of the stimulant within 2 to 6 days, though a longer time period to resolution has been reported [33]. Stimulant medications carry warnings about increased risk of sudden death, high blood pressure, cardiac arrest, and stroke, as well as a statement warning providers about abuse potential. Additionally, serious but rare medical complications, including seizures, tachycardia or dysrhythmias, and hyperthermia, can occur [31,34].
Physical Examination and Laboratory Data
Obtaining vital signs and performing a physical exam may reveal weight loss and an increase in heart rate or blood pressure. Methylphenidate and amphetamines are known to increase heart rate and blood pressure [35] and a recent study found an average increase in heart rate of 5.7 bpm and a 1.2–mm Hg increase in systolic and diastolic blood pressure in adults on stimulant medications compared to placebo [36]. No EKG abnormalities or changes are found with either methylphenidate or amphetamine [35]. Urine toxicology can be utilized to obtain further information if misuse is suspected. However, the clinician must be aware of the limitations of urine drug testing with stimulants [37]. The usual detection time for amphetamines is 48 hours from last use, though this may vary depending on the presence of metabolites, pharmacokinetics of the drug (eg, immediate release vs. sustained release formulations), and patient variables [37]. Additionally, a urine toxicology screen for amphetamines typically tests for amphetamines, racemic compounds such as dextroamphetamine and methamphetamine, and illicit compounds (ie, methylenedioxymethamphetamine), though there are many compounds that are structurally similar, such as weight loss agents, over-the-counter cold products, and other psychotropic medications, including methylphenidate, that can cause a false-positive result [37]. Urine toxicology should be obtained in conjunction with a thorough evaluation of patients’ alcohol and drug use patterns. These 2 components are essential to the accurate diagnosis and formulation of a comprehensive treatment plan. As noted above, stimulant medication misuse and alcohol and illicit drug use are highly comorbid and should be carefully and thoroughly assessed.
Psychiatric Comorbidity
ADHD
The prevalence of ADHD is higher among individuals with substance use disorders [38]. As noted above, patients commonly report misuse of stimulant medication to enhance academic performance. One explanation may be that individuals misusing stimulants may be self-medicating undiagnosed ADHD [39]. The prevalence of ADHD among adults is 4.1% and it is more common in men than women with a ratio of up to 6:1 [40]. Several studies have found that individuals with misuse of stimulant medications endorse symptoms of ADHD, including higher levels of inattention and hyperactivity [41]. Twelve percent of participants in one study that endorsed stimulant medication misuse also endorsed the belief they had ADHD [7]. Another study found that individuals with higher baseline self-reported ADHD symptoms were also more likely to misuse stimulants [42]. The majority of individuals with ADHD have been found to take medications appropriately, though there is a minority, often with comorbid conduct disorder or other substance use disorders, that divert or misuse stimulant medications, most often the immediate release formulations [43,44].
Accurate diagnosis of ADHD in patients with substance use disorders can be challenging given the symptom overlap between intoxication and withdrawal syndromes of substances and symptoms of ADHD. Evaluating for ADHD is an important part of a thorough assessment and can be completed in several ways. The gold standard is with a standardized diagnostic tool such as the Connors Adult ADHD Diagnostic Interview for DSM-IV (CAADID) [45], which can be time consuming for a clinician and would likely involve referral to a psychologist for completion. Other scales have been examined, and the Connors Adult ADHD Rating Scale (CAARS) has been found to closely agree with the CAADID when both are administered [45]. Other scales are available, including the Wender Utah Rating Scales (WURS) and the Adult ADHD Self-Report Scale (ASRS), and have been found to have adequate sensitivity and specificity [45]. In an international study, the ASRS, a relatively brief instrument, showed encouraging results with 84% sensitivity and 66% specificity in detecting ADHD upon entry into substance disorder treatment for treatment-seeking patients [46]. When diagnosing ADHD among adults, it is crucial not to rely only on self-reported symptoms. A thorough childhood history of ADHD symptom presentation should be collected from a parent or caregiver, and collateral concurrent report should be collected from someone who knows the patient well, such as an employer, close friend, significant other, or parent. Valid diagnosis, whether ADHD is present or not, is of utmost importance in this population as individuals with comorbid substance use disorders and ADHD tend to have worse outcomes overall [47]. It is also important to appreciate that inaccurately diagnosing ADHD in individuals misusing stimulants could potentially diminish the importance of the diagnosis [48].
If ADHD is found, there are medications available that have a lower abuse potential compared to stimulant medications. Atomoxetine is the only FDA-approved nonstimulant for ADHD; off-label or second-line treatments include antidepressants, such as bupropion, venlafaxine, or tricyclic antidepressants, for which the data is limited, and clonidine [34,49,50]. If these therapies are not effective and, after careful consideration of risks and benefits, it is determined that a trial with a stimulant is needed, longer-acting formulations appear to be less abused [34,44]. Education for both the patient and his or her family should be provided on abuse and diversion potential and appropriate use and misuse [34,43,51]. Pill counts [43], regular office visits [52], and random urine toxicology screens [34] with informed interpretation of the screens may be helpful in deterring misuse or diversion. While medications are the mainstay of treatment for ADHD, there are several psychosocial interventions available, including cognitive behavioral therapy, coaching, and behavioral modification therapies [34].
Other Comorbidities
Other psychiatric comorbidities also should be explored. Studies have found a relation between depression and misuse of stimulant medication in that there is an increased likelihood of depression and thoughts of suicide among those that misuse stimulant medication and vice versa [23,24,53]. The National Survey on Drug Use and Health in 2012 found that, of those that misused stimulants, nearly 20% had serious thoughts of suicide over the past year [54]. As noted earlier, stimulant medication can affect sleep and appetite. Among those that report misuse of stimulant medication for weight loss, these individuals are more likely to report other eating-disordered behaviors [55]. Sleep quality is worse and sleep disturbance greater in those that misuse stimulant medication [32]. Other traits and behaviors that have been described in individuals that misuse stimulant medications include impulsivity [56,57], sensation seeking [20], perfectionism [58], and poor time management skills or procrastination [59].
Appropriate treatment (which may include pharmacologic, psychological, or academic accommodation components) for individuals with these psychiatric disorders or psychological symptoms may reduce the misuse of stimulant medications among college students, especially if these students are misusing in order to reduce their symptoms (ie, a self-medication hypothesis).
Treatment
There are currently no FDA-approved medications to treat stimulant medication misuse. In fact, studies exploring pharmacotherapy for stimulant medication misuse are limited. Most trials focus on stimulants such as cocaine or methamphetamine and not stimulant medications alone. Additionally, these trials primarily include only individuals that meet criteria for stimulant dependence. Various medications and medication classes have been examined for the treatment of stimulant dependence, including naltrexone, various antipsychotics, and various antidepressants including bupropion, modafanil, baclofen, ondansetron, and dexamphetamine, with little to no effect [60]. In a review of the literature, one study examined the use of naltrexone versus placebo for stimulant dependence in 80 treatment-seeking Swedish individuals [61]. The different types of stimulants on which these individuals were dependent were not clearly delineated, though the study authors noted that the major amphetamine abused in Sweden was the racemic mixture d/l amphetamine and not methamphetamine. Naltrexone was superior to placebo in this trial, as evidenced by higher percentage of amphetamine-free urine samples. A large majority of this sample used intravenously (65%–76%) and had been using between 6 to 8 years, limiting the applicability to individuals with stimulant medication misuse. At this time, investigation into evidence-based pharmacotherapies for stimulant medication misuse remains in the early stages.
Generally speaking, efficacious behavioral treatments, such as contingency management (CM), cognitive behavioral therapy (CBT), skills training, motivational interviewing (MI), relapse prevention, couples and family treatments, and drug counseling, exist for drug abuse [62]. CBT, cognitive therapy, CM, MI, and community reinforcement approach (CRA) [63,64] have been explored for stimulant dependence and are currently the primary interventions for amphetamine-type stimulant dependence [60]. Similar to pharmacotherapy studies, most psychotherapy studies to date have examined primarily cocaine and methamphetamine dependence and not misuse of stimulant medications. In fact, no studies examining psychotherapy for stimulant medication misuse were found by our group in a search using the PubMed database. Therefore, discussion of psychotherapeutic interventions that may be efficacious for stimulant medication misuse extrapolates outcomes from studies of stimulant dependence, appreciating this is an approximation and imprecise as there are significant differences between stimulant medication misusers and those dependent upon stimulants such as methamphetamine or cocaine. As such, in a review from 2009 [63], Vocci and colleagues compared psychotherapy studies for cocaine and methamphetamine dependence and concluded that CBT and CM were moderately effective and that adding CM to standard treatment may help improve outcomes. A study of 214 amphetamine users (including methamphetamine users), with the majority (70%) enrolled in a methadone maintenance program and a large proportion (58.9%) using amphetamines intravenously, found that either 2 or 4 sessions of CBT, along with self-help material, increased rate of abstinence at 6 months post-intervention compared to the use of self-help material alone [65]. Baker and colleagues [64] recommend a practical stepped approach to treatment for stimulant dependence, including conducting a thorough assessment, offering education and self-help materials, monitoring use and consequences of use, and then transitioning to more intensive psychosocial interventions if needed, which may be applicable to those with stimulant medication misuse and is clinically reasonable. Offering a psychosocial intervention may require referral to more specialized treatment services than can be offered in a general primary care clinic. Additionally, harm reduction techniques for stimulant medication misusers to reduce the medical and social consequences can be considered as well as prevention strategies and methods, which can be utilized in any treatment setting or in high-risk populations, such as college students.
Prevention Strategies for the Individual
The research findings summarized in this review suggest several specific strategies for preventing and reducing the misuse of stimulant medication among college students, a high-risk population. First, college students with a prescription for stimulant medication play a critical role. Not only do these students have a high rate of misuse themselves [28,66], but they are also the most common source from which other students obtain stimulant medication to misuse [11,67]. It is therefore important for physicians who provide college students with prescriptions for stimulant medications to discuss the possible consequences of misusing or diverting medication, including potential negative health outcomes, legal consequences, and on-campus repercussions, for students caught diverting stimulant medications. These practitioners should also monitor their patients for signs of diversion, such as finishing a prescription early, doctor shopping, or urine drug screen which is negative for the prescribed substance. Utilizing a prescription monitoring program to access information on the prescribing and filling of controlled substances can be a valuable tool in detecting multiple concomitant prescriptions for stimulant medications, number of providers writing stimulant medication, and information on the use of other prescribed controlled medications. Providers should also discuss safe storage of stimulant medications with patients, particularly if the student is currently living in a dorm setting or another community-type setting with the potential for lots of individuals in and around their personal belongings. Additionally, providers may wish to consider dispensing a small amount at each office visit until the patient has established responsible use of the medication, particularly if there are other findings or comorbidities that perhaps increase their risk of misuse. Pill counts and frequent office visits, as noted earlier, may also help prevent diversion.
Perceived risk/harm associated with the use of stimulant medications has been negatively related to misuse [18,20]. If college students were more aware of the risks associated with stimulant medication misuse, with regards to both health and legal consequences, fewer students may choose to misuse stimulants. Educating patients and their families about the abuse potential of stimulants, as well as consequences of misuse such as psychosis and agitation, when prescriptions are given for stimulant medication, may help address the misperception that stimulant medications are benign, safe and without adverse consequences.
College Policy Changes for Prevention of Misuse
Policy changes on college campuses could also help to reduce diversion of stimulant medications. For instance, education about the risks associated with stimulant medication misuse could be incorporated into other alcohol and drug prevention programs that are already in place at colleges and universities. Many colleges/universities require all first-year students to complete an online substance use education/prevention/assessment tool. Some of these, such as AlcoholEdu and The Alcohol eCHECKUP TO GO have demonstrated some success in reducing college student alcohol use in follow-up evaluations [68]. Information about misuse of stimulant medication could be included in these existing programs. Moreover, members of certain organizations (eg, fraternities or sororities) that are known for an increased risk of substance use/abuse among members are also sometimes required by their national chapters or host colleges/universities to complete a “risk management” class, which addresses behaviors such as binge drinking and drunk driving. Since one of the demographic factors most strongly related to stimulant medication misuse is Greek organization membership [14], presenting information about stimulant medication misuse to these groups during these classes could help reduce misuse on college campuses.
Finally, the most commonly reported motives for misuse of stimulant medications among college students are academic in nature (eg, to study more, to concentrate better) [16], and many students who misuse for these reasons feel the desired effect is achieved. Colleges and universities may need to improve the identification of students who are in need of academic assistance/supports and offer these interventions earlier in students’ college careers to prevent stimulant medication misuse as a “quick fix.” Such interventions may include teaching students skills such as note-taking and academic goal setting and educating students about the link between sleep deprivation and poor concentration [69].
Summary
Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Diagnosing ADHD can be invaluable for individuals with the disorder, thus the ability to perform a thorough and accurate assessment is important; equally important is the ability to assess when ADHD is not present. Education and prevention strategies to prevent misuse and diversion should be provided if stimulant medications are indicated. College programs and policies can also utilize prevention strategies, provide education to students, and assist those with academic difficulties. Comorbidities are common and should be explored thoroughly as they may play a role in continued stimulant medication misuse and outcomes. Various treatment techniques and modalities can be explored further with each patient, based on the individual and their particular needs.
Corresponding author: Kate Flory, Univ. of South Carolina, Dept. of Psychology, Barnwell College, Columbia, SC 29208, [email protected].
Funding/support: Work on this paper was supported by a University of South Carolina Honors College Exploration Scholar Award and a University of South Carolina Magellan Fellowship, both awarded to Kari Benson.
Financial disclosures: None.
Author contributions: conception and design, KF, RAP, KB; drafting of article, KF, RAP, KB; critical revision of the article, KF, RAP, KB; literature search, KB.
1. Chai G, Governale L, Mcmahon AW, et al. Trends of outpatient prescription drug utilization in US children, 2002-2010. Pediatr 2012;130:23–31.
2. Dupaul GJ, Weyandt LL, O’dell SM, Varejao M. College students with ADHD: current status and future directions J Atten Disord 2009;13:234–50.
3. DuPaul G, Schaughency E, Weyandt L, et al. Self-report of ADHD symptoms in university students: Cross-gender and cross-national prevalence. J Learn Disabil 2001;34:370–9.
4. Wolf L. College students with ADHD and other hidden disorders: Outcomes and interventions. Ann NY Acad Arts Sci 2001;931:385–5.
5. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use, and diversion of abusable prescription drugs. J Am Coll Health 2006;54:269–78.
6. Garnier LM, Arria AM, Caldeira KM, et al. Sharing and selling of prescription medications in a college student sample. J Clin Psychiatry 2010;71:262–9.
7. Advokat CD, Guildry D, Martino L. Licit and illicit use of medications for attention-deficit hyperactivity disorder in undergraduate college students. J Am Coll Health 2008;56:601–6.
8. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use and diversion of prescription stimulant medication. J Psychoactive Drugs 2006;38:43–56.
9. Rabiner DL, Anastopoulos AD, Costello E, et al. Predictors of nonmedical ADHD medication use by college students. J Atten Disord 2010;13:640–8.
10. Graff Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
11. DeSantis AD, Webb EM, Noar SM. Illicit use of prescription ADHD medications on a college campus: A multimethodological approach. J Am Coll Health 2008;57:315–23.
12. Sharp JT, Rosén LA. Recreational stimulant use among college students. J Subst Use 2007;12:71–82.
13. Hall KM, Irwin MM, Bowman KA, et al. Illicit use of prescribed stimulant medication among college students. J Am Coll Health 2005;53:167–74.
14. Dussault CL, Weyandt LL. An examination of prescription stimulants misuse and psychological variables among sorority and fraternity college populations. J Atten Disord 2013;27:87–7.
15. McCabe SE. Misperceptions of non-medical prescription drug use: A web survey of college students. Addict Behav 2008;33:713–24.
16. Rabiner DL, Anastopoulos AD, Costello E, et al. Motives and perceived consequences of nonmedical ADHD medication use by college students: Are students treating themselves for attention problems? J Atten Disord 2009;13:259–70.
17. Peterkin AL, Crone CC, Sheridan MJ, Wise TN. Cognitive performance enhancement: Misuse or self-treatment? J Atten Disord 2011;15:263–8.
18. Judson R, Langdon SW. Illicit use of prescription stimulants among college students: Prescription status, motives, theory of planned behaviour, knowledge and self-diagnostic tendencies. Psychol Health Med 2009;14:97–104.
19. Volkow ND, Swanson JM. Adult attention deficit-hyperactivity disorder. N Engl J Med 2013;369:1935–44.
20. Arria AM, Caldeira KM, Vincent KB, et al. Perceived harmfulness predicts nonmedical use of prescription drugs among college students: Interactions with sensation-seeking. Prev Science 2008;9:191–201.
21. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. 2000.
22. Arria AM, Wilcox HC, Caldeira KM, et al. Dispelling the myth of “smart drugs”: Cannabis and alcohol use problems predict nonmedical use of prescription stimulants for studying. Addict Behav 2013;38:1643–50.
23. Zullig KJ, Divin AL. The association between non-medical prescription drug use, depressive symptoms, and suicidality among college students. Addict Behav 2012;37:890–9.
24. Teter CJ, Falone AE, Cranford JA, et al. Nonmedical use of prescription stimulants and depressed mood among college students: Frequency and routes of administration. J Subst Abuse Treat 2010;38:292–8.
25. Pedersen W. Mental health, sensation seeking and drug use patterns: a longitudinal study. Br J Addict 1991;86:195–204.
26. Jaffe LT, Archer RP. The prediction of drug use among college students from MMPI, MCMI, and sensation seeking scales. J Pers Assess 1987;51:243–53.
27. Martins SS, Storr CL, Alexandre PK, Chilcoat HD. Adolescent ecstasy and other drug use in the National Survey of Parents and Youth: The role of sensation-seeking, parental monitoring and peer’s drug use. Addict Behav 2008;33:919–33.
28. Sepúlveda DR, Thomas LM, McCabe S, et al. Misuse of prescribed stimulant medication for ADHD and associated patterns of substance use: Preliminary analysis among college students. J Pharm Pract 2011;24:551–60.
29. Teter CJ, McCabe SE, Cranford JA, et al. Prevalence and motives for illicit use of prescription stimulants in an undergraduate student sample. J Am Coll Health 2005;53:253–62.
30. Lookatch SJ, Dunne EM, Katz EC. Predictors of nonmedical use of prescription stimulants. J Psychoactive Drugs 2012;44:86–91.
31. Looby A, Kassman KT, Earlywine M. Do negative stimulant-related attitudes vary for prescription stimulants and cocaine among college students? Addict Behav 2014;39:1100–5.
32. Clegg-Kraynok MM, McBean AL, Montgomery-Downs HE. Sleep quality and characteristics of college students who use prescription psychostimulants nonmedically. Sleep Med 2011;12:598–602.
33. Ross RG. Psychotic and manic-like symptoms during stimulant treatment of attention deficit hyperactivity disorder. Am J Psychiatry 2006;163:1149–52.
34. Mariani JJ, Levin FR. Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addict 2007;16:45–56.
35. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation 2008;117:2407–23.
36. Mick E, McManus DD, Goldberg RJ. Meta-analysis of increased heart rate and blood pressure associated with CNS stimulant treatment of ADHD in adults. Eur Neuropsychopharmacol 2013;23:534–41.
37. Moeller KE, Lee KC, Kissack JC. Urine drug screening: Practical guide for clinicians. Mayo Clin Proc 2008;83:66–76.
38. Van de Glind G, Konstenius M, Koeter MWJ, et al. Variability in the prevalence of adult ADHD in treatment seeking substance use disorder patients: Results from an international multi-center study exploring DSM-IV and DSM-5 criteria. Drug Alcohol Depend 2014;134:158–66.
39. Bukstein O. Substance abuse in patients with attention-deficit/hyperactivity disorder. Medscape J Med 2008;10:24.
40. Kessler RC, Adler L, Barkley R, et al. The prevalence and comorbidity of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry 2006;163:716–23.
41. Hartung CM, Canu WH, Cleveland CS, et al. Stimulant medication use in college students: Comparison of appropriate users, misusers, and nonusers. Psychol Addict Behav 2014;27:832.
42. Upadhyaya HP. Managing attention-deficit/hyperactivity disorder in the presence of substance use disorder. J Clin Psychiatry 2007;68:23–30.
43. Wilens TE, Gignac M, Swezey A, et al. Characteristics of adolescents and young adults with ADHD who divert or misuse their prescribed medications. J Am Acad Child Adolesc Psychiatry 2006;45:408–14.
44. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: A systematic review of the literature. J Am Acad Child Adolesc Psychiatry 2008;47:21–31.
45. Dakwa E, Mahony A, Pavlicova M, et al. The utility of attention-deficit/hyperactivity disorder screening instruments in individuals seeking treatment for substance use disorders. J Clin Psychiatry 2012;73:1372–8.
46. Van de Glind G, Van den Brink W, Koeter. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend 2013;132:587–96.
47. Levin FR. Diagnosing attention-deficity/hyperactivity disorder in patients with substance use disorders. J Clin Psychiatry 2007;68:9–14.
48. Diller L. ADHD in the college student: Is anyone else worried? J Atten Disord. 2010;14:3-6.
49. Christman AK, Fermo JD, Markowitz JS. Atomoxetine, a novel treatment for attention-deficit/hyperactivity disorder. Pharmacotherapy 2004;24:1020–36.
50. Riggs P, Levin F, Green AI, Vocci F. Comorbid psychiatric and substance abuse disorders: Recent treatment research. Subst Abuse 2008;29:51–63.
51. Rabiner D L. Stimulant prescription cautions: Addressing misuse, diversion, and malingering. Curr Psychiatry Rep. 2013;15:375-383.
52. Manning JS. Strategies for managing the risks associated with ADHD medications. J Clin Psychiatry 2013;74:e19.
53. Markou A, Kosten TR, Koob GF. Neurobiological similarities in depression and drug dependence: A self-medication hypothesis. Neuropsychopharmacology 1998;18:135–74.
54. Results from the 2012 National Survey on Drug Use and Health: Mental Health Findings, NSDUH Series H-47. HHS Pub No. 13-4805. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2013.
55. Jeffers A, Benotsch EG, Koester S. Misuse of prescription stimulants for weight loss, psychosocial variables, and eating disordered behaviors. Appetite 2013;65:8–13.
56. Madden GJ, Bickel WK. Impulsivity: The behavioral and neurological science of discounting. 1st ed. Washington, DC: APA; 2010.
57. Stanford MS, Mathias CW, Dougherty DM, et al. Fifty years of the Barratt Impulsiveness Scale: An update and review. Pers Indiv Differ 2009;47:385–95.
58. Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
59. Moore DR, Burgard DA, Larson RG, Ferm M. Psychostimulant use among college students during periods of high and low stress: An interdisciplinary approach utilizing both self-report and unobtrusive chemical sample data. Addict Behav 2014;39:987–93.
60. Brensilver M, Heinzerling KG, Shoptaw S. Pharmacotherapy of amphetamine-type stimulant dependence: An update. Drug Alc Review 2013;32:449–60.
61. Jayaram-Lindstrom N, Hammarberg A, Beck O, Franck J. Naltrexone for the treatment of amphetamine dependence: A randomized, placebo-controlled trial. Am J Psychiatry 2008;165:1442–8.
62. Carroll KM, Onken LS. Behavioral therapies for drug abuse. Am J Psychiatry 2005;162:1452–60.
63. Vocci FJ, Montoya I. Psychological treatments for stimulant misuse, comparing and contrasting those for amphetamine dependence and those for cocaine dependence. Curr Opin Psychiatry 2009;22:263–8.
64. Baker A, Lee NK., Claire M, et al. Brief cognitive behavioral interventions for regular amphetamine users: a step in the right direction. Addict 2005;100:367–78.
65. Baker A, Lee NK, Claire M, et al. Drug use patterns and mental health of regular amphetamine users. Addict 2004;99:875–84.
66. Rabiner DL, Anastopoulos AD, Costello E, et al. The misuse and diversion of prescribed ADHD medications by college students. J Atten Disord 2009;13:259–70.
67. Garnier-Dykstra LM, Caldeira KM, Vincent KB, et al. Nonmedical use of prescription stimulants during college: Four year trends in exposure opportunity, use, motives, and sources. J Am Coll Health 2012;60:226–34.
68. Hustad JT, Barnett NP, Borsari B, Jackson KM. Web-based alcohol prevention for incoming college students: A randomized controlled trial. Addict Behav 2010;35:183–9.
69. Pilcher JJ, Walters AS. How sleep deprivation affects psychological variables related to college students’ cognitive performance. J Am Coll Health 1997;46:121–6.
From the University of South Carolina, Columbia, SC.
Abstract
- Objective: To provide a summary of the existing research on the characteristics of college students who report misusing prescription stimulant medications, to offer a set of clinical recommendations for practitioners, and to offer several possible prevention strategies.
- Methods: Literature review and research-based recommendations for clinical practice and prevention.
- Results: Misuse of prescription stimulant medication among college students is a prevalent and growing problem. Significant risk factors for misuse of stimulant medication include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Suggestions for preventing misuse and diversion of prescription stimulant medications, including strategies for the individual and potential policy changes on college campuses, are offered.
- Conclusions: Misuse and diversion of prescription stimulant medications is a growing concern among adolescents and young adults and should be addressed by health care practitioners. Additional research on effective intervention and prevention strategies is needed.
Prescription stimulant medications (eg, methylphenidate, amphetamines) are typically used for the treatment of attention-deficit/hyperactivity disorder (ADHD) to increase attentiveness, decrease distractibility, and improve daily functioning. Prescriptions for stimulant medications are on the rise; between 2002 and 2010, the number of prescriptions for ADHD medications for youth under 18 increased 46% [1].
A recent review of ADHD diagnosis among college students estimated a prevalence rate of 2% to 8% [2]. More individuals with ADHD are matriculating to college than in the past [3,4], as more supports have been put in place for college students diagnosed with ADHD, including improved educational/organizational treatments and accommodations [2]. Many college students with ADHD also use prescription stimulant medications as part of their treatment plan; McCabe, Teter, and Boyd reported that 2.2% of college students had prescriptions for stimulant medications annually [5].
As the number of individuals of all ages with stimulant medication prescriptions increase, more individuals without prescriptions are gaining access to stimulant medications. In a survey of college students with medication prescriptions, stimulants were the most commonly diverted medication, with 61.7% of students with these prescriptions reporting having shared or sold their medication at least once [6]. Studies report that as many as 43% of college students have misused stimulant medication in their lifetime [7], though prevalence rates vary by study. Throughout this review, “misuse of stimulant medication” refers to using prescription stimulant medications without a prescription or using more stimulant medication than prescribed (ie, a higher or more frequent dosage).
Given the ease with which college students are able to obtain stimulant medications, the alarming prevalence of stimulant medication misuse among this population, and the potentially serious health risks associated with misuse of stimulant medication (especially when combined with other substances, such as alcohol, that are commonly used by college students), there is a need to both better understand and ultimately reduce the misuse of stimulant medication among college students. Thus, the purpose of this paper is threefold. First, we provide a summary of the existing research literature on the characteristics of college students who report misusing stimulant medication. Second, we offer a set of clinical recommendations for practitioners, which includes stimulant medication indications, risks, benefits, and side effects, along with problems associated with stimulant medication diversion and misuse. Finally, we offer several prevention strategies, including strategies for the individual as well as several suggestions for changing policies on college campuses to prevent stimulant diversion and misuse. Importantly, although our literature review addresses prescription stimulant misuse among college students, our clinical recommendations are also appropriate for adolescents and young adults not enrolled in college.
Summary of the Literature
The following summary is based on a comprehensive search of the existing research literature on misuse of stimulant medication among college students, which ultimately identified 30 relevant studies using 21 unique samples. A study was included if: (1) the main focus of the study was misuse of stimulant medication, (2) it was a peer-reviewed, empirical study using quantitative data analytic techniques, (3) it was written in English, (4) only undergraduate students were included in the sample, (5) it did not focus on only one type of stimulant medication (eg, methylphenidate only), and (6) if the article discussed multiple prescription drug categories (eg, stimulants, opiates), the data must have been analyzed separately for each category. An extensive meta-analytic review of this literature will be published elsewhere (contact the corresponding author to request a reprint). The following is a brief summary of our findings.
Prevalence, Availability, and Demographic Characteristics
Among prevalence rates reported, lifetime rates of stimulant medication misuse were the most frequently reported, ranging from 8.1% [8] to 43% [7]. Rates of misuse of stimulant medications within the last year ranged from 5.3% [9] to 35.3% [10]. A number of the studies asked students how they obtained stimulant medications for misuse; peers were overwhelmingly the most common source for obtaining the medications. For example, DeSantis, Webb, and Noar [11] found that 91% of the undergraduates who were interviewed obtained stimulant medications from friends or significant others.
Perceived availability of stimulant medications was also measured in several studies. DeSantis, Webb, and Noar [11] found that 82% of students thought it was somewhat or very easy to obtain stimulant medication; however, Sharp and Rosén [12] found that only 55% of students thought it was somewhat or very easy to obtain stimulant medication. In another study that examined perceived availability, 37% of men and 29.2% of women agreed that they knew students who would provide them with stimulant medications [13].
Many of the studies reviewed examined the relation between particular demographic characteristics (eg, gender, race, socioeconomic status, religious affiliation, year in college, sorority or fraternity membership) and misuse of stimulant medication among college students. The vast majority of studies that examined gender as related to misuse of stimulant medication found that significantly more males misused stimulant medication than females. For example, one study found that 26% of males and 17.3% of females reported misusing stimulant medication [14]; another study found that 39% of males versus 30% of females reported misuse [11].
It is also clear from the existing literature that members of fraternities and sororities appear to be more at-risk for misuse of stimulant medication than non-Greek students. In multiple studies, Greek students had rates of misuse twice that of non-Greeks. For instance, 48% of Greeks misused in their lifetime compared to 22% of non-Greeks [11]; 12% of Greeks misused in the past year compared to 5% of non-Greeks [15]; and Greeks were 2.32 times more likely to initiate use than non-Greeks [9].
Unfortunately, results from studies examining other demographic characteristics (eg, race, socioeconomic status, religious affiliation, year in college) as related to misuse of stimulant medication are much less conclusive and these correlates therefore require further investigation.
Motives For Misuse and Perceived Risk
Researchers have also evaluated college students’ motives for misusing stimulant medication and the risks they associate with misuse. All of the studies that asked misusing students about their motives for misuse reported that the most commonly endorsed motives were related to academics. “To concentrate better while studying” [16], “to improve study skills” [17], “to stay awake to study longer” [11], and “to improve concentration” [18] were some of the most commonly endorsed motives in these studies. Nonacademic reasons, such as to get high, to prolong effects of alcohol and other drugs, and to lose weight, were less commonly endorsed [7,12,19]. In studies where participants were able to indicate multiple motives for misuse [16], very few students misused for only nonacademic reasons.
Several studies measured the relation between misuse of stimulant medication and perceived risk associated with misuse. Perceived risk was conceptualized as perceived harmfulness [20], perception of safety [14], concern with health risk [18], and the inverse of positive outcome expectancies [21]. These articles found that when college students perceive more risk or have less positive expectancies about stimulant medication misuse, they are less likely to misuse stimulant medication. For instance, those who associated stimulant medication misuse with low perceived harmfulness were over 10 times more likely to have used in the last year than those who associated misuse with high perceived harmfulness [20].
Academic Outcomes Associated with Misuse
Interestingly, despite academic motives being most common for college students who report misusing stimulant medication, a number of studies have found a negative association between academic outcomes and misuse of stimulant medication. For instance, nonusers reported an average grade-point average (GPA) of 3.28 compared to 3.16 for misusers [16]. Other research demonstrates that the lower the student’s GPA is, the greater the odds are of the student misusing stimulant medication [8]. Misuse is also significantly related to other detrimental academic behaviors such as skipping class and less studying [20,22].
Psychological Correlates of Misuse
Researchers have evaluated the relation between several different psychological variables and misuse of stimulant medication. The strongest association is between symptoms of ADHD and stimulant medication misuse. Studies are consistent in reporting a significant correlation between greater symptoms of ADHD and higher rates of misuse or a significant difference in rates of misuse between those who have an ADHD diagnosis and those who do not. One study found that 71.1% of stimulant medication misusers screened positive for adult ADHD symptoms [17]. Another study found that for every standard deviation increase in attention problems, the odds of becoming a stimulant misuser increased by 1.78 [9]. Two studies asked participants if they believed they had ADHD. Advokat, Guildry, and Martino found that 12% of misusers believed they had ADHD [7]. Twenty-nine percent of “self-diagnosers” reported misusing, compared to 11.4% of “non-diagnosers” in another study [18].
Although the literature base is smaller than for ADHD, several studies have suggested a significant difference in symptoms of depression between stimulant medication misusers and nonusers. Zullig and Divin [23] found that misusers were significantly more likely to feel very sad, feel depressed, and consider suicide than nonusers. More frequent misuse has also been shown to be significantly associated with depressed mood [24].
A number of studies demonstrate a clear association between high sensation-seeking and misuse of stimulant medication. These results are not surprising given the well-documented relation between sensation seeking and substance use [25–27]. One study found a significant interaction between sensation seeking and perceived harmfulness of misusing stimulant medication: those with high sensation seeking and low perceived harmfulness were most likely to misuse [20].
Other Substance Use Associated with Stimulant Misuse
Many of the reviewed studies found a positive correlation between misuse of stimulant medication and other substance use or a significant difference between stimulant misusers and nonusers in rates of other substance use. These findings held across all substances examined, including alcohol, cigarettes, marijuana, illicit stimulants (eg, ecstasy, cocaine, or amphetamines), and non-stimulant prescription medications. For instance, significant associations were found between misuse of stimulant medication and several alcohol-related constructs, such as binge drinking [28,29], problematic drinking behavior [30], or meeting the Diagnostic and Statistical Manual of Mental Disorders [21] criteria for alcohol abuse [22]. With respect to cigarettes, 50.3% of misusers were found to have smoked cigarettes in the last 6 months compared to 13.3% of nonusers [16]. Similar findings emerged for illicit drug use. One study found that 73.5% of stimulant medication misusers reported use of marijuana in the last 6 months, compared to 18.2% of nonusers [19], while another study found that 93% of misusers used marijuana in the last year compared to 34% of nonusers [5]. This same study found that 33% of stimulant medication misusers also reported cocaine use in the last year compared to 2% of stimulant nonusers [5]. Finally, many of the studies reviewed examined the association between other substance use in general and stimulant medication misuse. Results were striking; the odds of becoming a stimulant medication misuser increased by 3.81 for each standard deviation increase in the amount of other substance use [9].
Summary
The research literature reviewed in this section provides a descriptive characterization of which college students (and, by extension, adolescents and young adults not in college) may be at the greatest risk of misuse of stimulant medication. Significant risk factors include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. It is important to recognize that one, several, or many of these risk factors may be present in a given individual who is misusing stimulant medication. Moreover, there may be other risk factors not yet identified in the research literature. The following sections of this paper draw from the literature reviewed here to provide a number of clinical recommendations for reducing and preventing misuse of stimulant medications among college students, other young adults, and adolescents.
Clinical Recommendations
It is important for health care providers to be aware of the benefits and risks associated with stimulant medications, the prevalence of and risk factors for stimulant misuse, and the psychiatric, psychological, and medical comorbidities associated with the misuse of stimulant medication. Knowledge about stimulant medications, misuse of stimulant medications, and a thorough evaluation of the patient will enable health care providers to address the misuse, as well as any comorbidities or other factors that may contribute to stimulant medication misuse, either pharmacologically or through referral for more specified psychotherapeutic interventions.
Stimulant Medication Indications and Adverse Effects
Stimulant medications are efficacious for the treatment of ADHD and, when prescribed and used correctly, can improve attentiveness, decrease distractibility, and improve daily functioning in the short term [19]. When used by individuals without ADHD, patients may experience euphoria, stimulation, alertness, and are not likely to experience the cognitive benefits that those with ADHD receive [31]. Side effects can occur regardless of whether the individual is using the stimulant for ADHD, misusing, or is dependent, and include nervousness, headaches, tachycardia, poor appetite, depressed mood, and poor sleep [19,32]. Additionally, stimulant medications can cause psychosis, agitation, and hallucinations [31,33], which typically resolve after discontinuation of the stimulant within 2 to 6 days, though a longer time period to resolution has been reported [33]. Stimulant medications carry warnings about increased risk of sudden death, high blood pressure, cardiac arrest, and stroke, as well as a statement warning providers about abuse potential. Additionally, serious but rare medical complications, including seizures, tachycardia or dysrhythmias, and hyperthermia, can occur [31,34].
Physical Examination and Laboratory Data
Obtaining vital signs and performing a physical exam may reveal weight loss and an increase in heart rate or blood pressure. Methylphenidate and amphetamines are known to increase heart rate and blood pressure [35] and a recent study found an average increase in heart rate of 5.7 bpm and a 1.2–mm Hg increase in systolic and diastolic blood pressure in adults on stimulant medications compared to placebo [36]. No EKG abnormalities or changes are found with either methylphenidate or amphetamine [35]. Urine toxicology can be utilized to obtain further information if misuse is suspected. However, the clinician must be aware of the limitations of urine drug testing with stimulants [37]. The usual detection time for amphetamines is 48 hours from last use, though this may vary depending on the presence of metabolites, pharmacokinetics of the drug (eg, immediate release vs. sustained release formulations), and patient variables [37]. Additionally, a urine toxicology screen for amphetamines typically tests for amphetamines, racemic compounds such as dextroamphetamine and methamphetamine, and illicit compounds (ie, methylenedioxymethamphetamine), though there are many compounds that are structurally similar, such as weight loss agents, over-the-counter cold products, and other psychotropic medications, including methylphenidate, that can cause a false-positive result [37]. Urine toxicology should be obtained in conjunction with a thorough evaluation of patients’ alcohol and drug use patterns. These 2 components are essential to the accurate diagnosis and formulation of a comprehensive treatment plan. As noted above, stimulant medication misuse and alcohol and illicit drug use are highly comorbid and should be carefully and thoroughly assessed.
Psychiatric Comorbidity
ADHD
The prevalence of ADHD is higher among individuals with substance use disorders [38]. As noted above, patients commonly report misuse of stimulant medication to enhance academic performance. One explanation may be that individuals misusing stimulants may be self-medicating undiagnosed ADHD [39]. The prevalence of ADHD among adults is 4.1% and it is more common in men than women with a ratio of up to 6:1 [40]. Several studies have found that individuals with misuse of stimulant medications endorse symptoms of ADHD, including higher levels of inattention and hyperactivity [41]. Twelve percent of participants in one study that endorsed stimulant medication misuse also endorsed the belief they had ADHD [7]. Another study found that individuals with higher baseline self-reported ADHD symptoms were also more likely to misuse stimulants [42]. The majority of individuals with ADHD have been found to take medications appropriately, though there is a minority, often with comorbid conduct disorder or other substance use disorders, that divert or misuse stimulant medications, most often the immediate release formulations [43,44].
Accurate diagnosis of ADHD in patients with substance use disorders can be challenging given the symptom overlap between intoxication and withdrawal syndromes of substances and symptoms of ADHD. Evaluating for ADHD is an important part of a thorough assessment and can be completed in several ways. The gold standard is with a standardized diagnostic tool such as the Connors Adult ADHD Diagnostic Interview for DSM-IV (CAADID) [45], which can be time consuming for a clinician and would likely involve referral to a psychologist for completion. Other scales have been examined, and the Connors Adult ADHD Rating Scale (CAARS) has been found to closely agree with the CAADID when both are administered [45]. Other scales are available, including the Wender Utah Rating Scales (WURS) and the Adult ADHD Self-Report Scale (ASRS), and have been found to have adequate sensitivity and specificity [45]. In an international study, the ASRS, a relatively brief instrument, showed encouraging results with 84% sensitivity and 66% specificity in detecting ADHD upon entry into substance disorder treatment for treatment-seeking patients [46]. When diagnosing ADHD among adults, it is crucial not to rely only on self-reported symptoms. A thorough childhood history of ADHD symptom presentation should be collected from a parent or caregiver, and collateral concurrent report should be collected from someone who knows the patient well, such as an employer, close friend, significant other, or parent. Valid diagnosis, whether ADHD is present or not, is of utmost importance in this population as individuals with comorbid substance use disorders and ADHD tend to have worse outcomes overall [47]. It is also important to appreciate that inaccurately diagnosing ADHD in individuals misusing stimulants could potentially diminish the importance of the diagnosis [48].
If ADHD is found, there are medications available that have a lower abuse potential compared to stimulant medications. Atomoxetine is the only FDA-approved nonstimulant for ADHD; off-label or second-line treatments include antidepressants, such as bupropion, venlafaxine, or tricyclic antidepressants, for which the data is limited, and clonidine [34,49,50]. If these therapies are not effective and, after careful consideration of risks and benefits, it is determined that a trial with a stimulant is needed, longer-acting formulations appear to be less abused [34,44]. Education for both the patient and his or her family should be provided on abuse and diversion potential and appropriate use and misuse [34,43,51]. Pill counts [43], regular office visits [52], and random urine toxicology screens [34] with informed interpretation of the screens may be helpful in deterring misuse or diversion. While medications are the mainstay of treatment for ADHD, there are several psychosocial interventions available, including cognitive behavioral therapy, coaching, and behavioral modification therapies [34].
Other Comorbidities
Other psychiatric comorbidities also should be explored. Studies have found a relation between depression and misuse of stimulant medication in that there is an increased likelihood of depression and thoughts of suicide among those that misuse stimulant medication and vice versa [23,24,53]. The National Survey on Drug Use and Health in 2012 found that, of those that misused stimulants, nearly 20% had serious thoughts of suicide over the past year [54]. As noted earlier, stimulant medication can affect sleep and appetite. Among those that report misuse of stimulant medication for weight loss, these individuals are more likely to report other eating-disordered behaviors [55]. Sleep quality is worse and sleep disturbance greater in those that misuse stimulant medication [32]. Other traits and behaviors that have been described in individuals that misuse stimulant medications include impulsivity [56,57], sensation seeking [20], perfectionism [58], and poor time management skills or procrastination [59].
Appropriate treatment (which may include pharmacologic, psychological, or academic accommodation components) for individuals with these psychiatric disorders or psychological symptoms may reduce the misuse of stimulant medications among college students, especially if these students are misusing in order to reduce their symptoms (ie, a self-medication hypothesis).
Treatment
There are currently no FDA-approved medications to treat stimulant medication misuse. In fact, studies exploring pharmacotherapy for stimulant medication misuse are limited. Most trials focus on stimulants such as cocaine or methamphetamine and not stimulant medications alone. Additionally, these trials primarily include only individuals that meet criteria for stimulant dependence. Various medications and medication classes have been examined for the treatment of stimulant dependence, including naltrexone, various antipsychotics, and various antidepressants including bupropion, modafanil, baclofen, ondansetron, and dexamphetamine, with little to no effect [60]. In a review of the literature, one study examined the use of naltrexone versus placebo for stimulant dependence in 80 treatment-seeking Swedish individuals [61]. The different types of stimulants on which these individuals were dependent were not clearly delineated, though the study authors noted that the major amphetamine abused in Sweden was the racemic mixture d/l amphetamine and not methamphetamine. Naltrexone was superior to placebo in this trial, as evidenced by higher percentage of amphetamine-free urine samples. A large majority of this sample used intravenously (65%–76%) and had been using between 6 to 8 years, limiting the applicability to individuals with stimulant medication misuse. At this time, investigation into evidence-based pharmacotherapies for stimulant medication misuse remains in the early stages.
Generally speaking, efficacious behavioral treatments, such as contingency management (CM), cognitive behavioral therapy (CBT), skills training, motivational interviewing (MI), relapse prevention, couples and family treatments, and drug counseling, exist for drug abuse [62]. CBT, cognitive therapy, CM, MI, and community reinforcement approach (CRA) [63,64] have been explored for stimulant dependence and are currently the primary interventions for amphetamine-type stimulant dependence [60]. Similar to pharmacotherapy studies, most psychotherapy studies to date have examined primarily cocaine and methamphetamine dependence and not misuse of stimulant medications. In fact, no studies examining psychotherapy for stimulant medication misuse were found by our group in a search using the PubMed database. Therefore, discussion of psychotherapeutic interventions that may be efficacious for stimulant medication misuse extrapolates outcomes from studies of stimulant dependence, appreciating this is an approximation and imprecise as there are significant differences between stimulant medication misusers and those dependent upon stimulants such as methamphetamine or cocaine. As such, in a review from 2009 [63], Vocci and colleagues compared psychotherapy studies for cocaine and methamphetamine dependence and concluded that CBT and CM were moderately effective and that adding CM to standard treatment may help improve outcomes. A study of 214 amphetamine users (including methamphetamine users), with the majority (70%) enrolled in a methadone maintenance program and a large proportion (58.9%) using amphetamines intravenously, found that either 2 or 4 sessions of CBT, along with self-help material, increased rate of abstinence at 6 months post-intervention compared to the use of self-help material alone [65]. Baker and colleagues [64] recommend a practical stepped approach to treatment for stimulant dependence, including conducting a thorough assessment, offering education and self-help materials, monitoring use and consequences of use, and then transitioning to more intensive psychosocial interventions if needed, which may be applicable to those with stimulant medication misuse and is clinically reasonable. Offering a psychosocial intervention may require referral to more specialized treatment services than can be offered in a general primary care clinic. Additionally, harm reduction techniques for stimulant medication misusers to reduce the medical and social consequences can be considered as well as prevention strategies and methods, which can be utilized in any treatment setting or in high-risk populations, such as college students.
Prevention Strategies for the Individual
The research findings summarized in this review suggest several specific strategies for preventing and reducing the misuse of stimulant medication among college students, a high-risk population. First, college students with a prescription for stimulant medication play a critical role. Not only do these students have a high rate of misuse themselves [28,66], but they are also the most common source from which other students obtain stimulant medication to misuse [11,67]. It is therefore important for physicians who provide college students with prescriptions for stimulant medications to discuss the possible consequences of misusing or diverting medication, including potential negative health outcomes, legal consequences, and on-campus repercussions, for students caught diverting stimulant medications. These practitioners should also monitor their patients for signs of diversion, such as finishing a prescription early, doctor shopping, or urine drug screen which is negative for the prescribed substance. Utilizing a prescription monitoring program to access information on the prescribing and filling of controlled substances can be a valuable tool in detecting multiple concomitant prescriptions for stimulant medications, number of providers writing stimulant medication, and information on the use of other prescribed controlled medications. Providers should also discuss safe storage of stimulant medications with patients, particularly if the student is currently living in a dorm setting or another community-type setting with the potential for lots of individuals in and around their personal belongings. Additionally, providers may wish to consider dispensing a small amount at each office visit until the patient has established responsible use of the medication, particularly if there are other findings or comorbidities that perhaps increase their risk of misuse. Pill counts and frequent office visits, as noted earlier, may also help prevent diversion.
Perceived risk/harm associated with the use of stimulant medications has been negatively related to misuse [18,20]. If college students were more aware of the risks associated with stimulant medication misuse, with regards to both health and legal consequences, fewer students may choose to misuse stimulants. Educating patients and their families about the abuse potential of stimulants, as well as consequences of misuse such as psychosis and agitation, when prescriptions are given for stimulant medication, may help address the misperception that stimulant medications are benign, safe and without adverse consequences.
College Policy Changes for Prevention of Misuse
Policy changes on college campuses could also help to reduce diversion of stimulant medications. For instance, education about the risks associated with stimulant medication misuse could be incorporated into other alcohol and drug prevention programs that are already in place at colleges and universities. Many colleges/universities require all first-year students to complete an online substance use education/prevention/assessment tool. Some of these, such as AlcoholEdu and The Alcohol eCHECKUP TO GO have demonstrated some success in reducing college student alcohol use in follow-up evaluations [68]. Information about misuse of stimulant medication could be included in these existing programs. Moreover, members of certain organizations (eg, fraternities or sororities) that are known for an increased risk of substance use/abuse among members are also sometimes required by their national chapters or host colleges/universities to complete a “risk management” class, which addresses behaviors such as binge drinking and drunk driving. Since one of the demographic factors most strongly related to stimulant medication misuse is Greek organization membership [14], presenting information about stimulant medication misuse to these groups during these classes could help reduce misuse on college campuses.
Finally, the most commonly reported motives for misuse of stimulant medications among college students are academic in nature (eg, to study more, to concentrate better) [16], and many students who misuse for these reasons feel the desired effect is achieved. Colleges and universities may need to improve the identification of students who are in need of academic assistance/supports and offer these interventions earlier in students’ college careers to prevent stimulant medication misuse as a “quick fix.” Such interventions may include teaching students skills such as note-taking and academic goal setting and educating students about the link between sleep deprivation and poor concentration [69].
Summary
Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Diagnosing ADHD can be invaluable for individuals with the disorder, thus the ability to perform a thorough and accurate assessment is important; equally important is the ability to assess when ADHD is not present. Education and prevention strategies to prevent misuse and diversion should be provided if stimulant medications are indicated. College programs and policies can also utilize prevention strategies, provide education to students, and assist those with academic difficulties. Comorbidities are common and should be explored thoroughly as they may play a role in continued stimulant medication misuse and outcomes. Various treatment techniques and modalities can be explored further with each patient, based on the individual and their particular needs.
Corresponding author: Kate Flory, Univ. of South Carolina, Dept. of Psychology, Barnwell College, Columbia, SC 29208, [email protected].
Funding/support: Work on this paper was supported by a University of South Carolina Honors College Exploration Scholar Award and a University of South Carolina Magellan Fellowship, both awarded to Kari Benson.
Financial disclosures: None.
Author contributions: conception and design, KF, RAP, KB; drafting of article, KF, RAP, KB; critical revision of the article, KF, RAP, KB; literature search, KB.
From the University of South Carolina, Columbia, SC.
Abstract
- Objective: To provide a summary of the existing research on the characteristics of college students who report misusing prescription stimulant medications, to offer a set of clinical recommendations for practitioners, and to offer several possible prevention strategies.
- Methods: Literature review and research-based recommendations for clinical practice and prevention.
- Results: Misuse of prescription stimulant medication among college students is a prevalent and growing problem. Significant risk factors for misuse of stimulant medication include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Suggestions for preventing misuse and diversion of prescription stimulant medications, including strategies for the individual and potential policy changes on college campuses, are offered.
- Conclusions: Misuse and diversion of prescription stimulant medications is a growing concern among adolescents and young adults and should be addressed by health care practitioners. Additional research on effective intervention and prevention strategies is needed.
Prescription stimulant medications (eg, methylphenidate, amphetamines) are typically used for the treatment of attention-deficit/hyperactivity disorder (ADHD) to increase attentiveness, decrease distractibility, and improve daily functioning. Prescriptions for stimulant medications are on the rise; between 2002 and 2010, the number of prescriptions for ADHD medications for youth under 18 increased 46% [1].
A recent review of ADHD diagnosis among college students estimated a prevalence rate of 2% to 8% [2]. More individuals with ADHD are matriculating to college than in the past [3,4], as more supports have been put in place for college students diagnosed with ADHD, including improved educational/organizational treatments and accommodations [2]. Many college students with ADHD also use prescription stimulant medications as part of their treatment plan; McCabe, Teter, and Boyd reported that 2.2% of college students had prescriptions for stimulant medications annually [5].
As the number of individuals of all ages with stimulant medication prescriptions increase, more individuals without prescriptions are gaining access to stimulant medications. In a survey of college students with medication prescriptions, stimulants were the most commonly diverted medication, with 61.7% of students with these prescriptions reporting having shared or sold their medication at least once [6]. Studies report that as many as 43% of college students have misused stimulant medication in their lifetime [7], though prevalence rates vary by study. Throughout this review, “misuse of stimulant medication” refers to using prescription stimulant medications without a prescription or using more stimulant medication than prescribed (ie, a higher or more frequent dosage).
Given the ease with which college students are able to obtain stimulant medications, the alarming prevalence of stimulant medication misuse among this population, and the potentially serious health risks associated with misuse of stimulant medication (especially when combined with other substances, such as alcohol, that are commonly used by college students), there is a need to both better understand and ultimately reduce the misuse of stimulant medication among college students. Thus, the purpose of this paper is threefold. First, we provide a summary of the existing research literature on the characteristics of college students who report misusing stimulant medication. Second, we offer a set of clinical recommendations for practitioners, which includes stimulant medication indications, risks, benefits, and side effects, along with problems associated with stimulant medication diversion and misuse. Finally, we offer several prevention strategies, including strategies for the individual as well as several suggestions for changing policies on college campuses to prevent stimulant diversion and misuse. Importantly, although our literature review addresses prescription stimulant misuse among college students, our clinical recommendations are also appropriate for adolescents and young adults not enrolled in college.
Summary of the Literature
The following summary is based on a comprehensive search of the existing research literature on misuse of stimulant medication among college students, which ultimately identified 30 relevant studies using 21 unique samples. A study was included if: (1) the main focus of the study was misuse of stimulant medication, (2) it was a peer-reviewed, empirical study using quantitative data analytic techniques, (3) it was written in English, (4) only undergraduate students were included in the sample, (5) it did not focus on only one type of stimulant medication (eg, methylphenidate only), and (6) if the article discussed multiple prescription drug categories (eg, stimulants, opiates), the data must have been analyzed separately for each category. An extensive meta-analytic review of this literature will be published elsewhere (contact the corresponding author to request a reprint). The following is a brief summary of our findings.
Prevalence, Availability, and Demographic Characteristics
Among prevalence rates reported, lifetime rates of stimulant medication misuse were the most frequently reported, ranging from 8.1% [8] to 43% [7]. Rates of misuse of stimulant medications within the last year ranged from 5.3% [9] to 35.3% [10]. A number of the studies asked students how they obtained stimulant medications for misuse; peers were overwhelmingly the most common source for obtaining the medications. For example, DeSantis, Webb, and Noar [11] found that 91% of the undergraduates who were interviewed obtained stimulant medications from friends or significant others.
Perceived availability of stimulant medications was also measured in several studies. DeSantis, Webb, and Noar [11] found that 82% of students thought it was somewhat or very easy to obtain stimulant medication; however, Sharp and Rosén [12] found that only 55% of students thought it was somewhat or very easy to obtain stimulant medication. In another study that examined perceived availability, 37% of men and 29.2% of women agreed that they knew students who would provide them with stimulant medications [13].
Many of the studies reviewed examined the relation between particular demographic characteristics (eg, gender, race, socioeconomic status, religious affiliation, year in college, sorority or fraternity membership) and misuse of stimulant medication among college students. The vast majority of studies that examined gender as related to misuse of stimulant medication found that significantly more males misused stimulant medication than females. For example, one study found that 26% of males and 17.3% of females reported misusing stimulant medication [14]; another study found that 39% of males versus 30% of females reported misuse [11].
It is also clear from the existing literature that members of fraternities and sororities appear to be more at-risk for misuse of stimulant medication than non-Greek students. In multiple studies, Greek students had rates of misuse twice that of non-Greeks. For instance, 48% of Greeks misused in their lifetime compared to 22% of non-Greeks [11]; 12% of Greeks misused in the past year compared to 5% of non-Greeks [15]; and Greeks were 2.32 times more likely to initiate use than non-Greeks [9].
Unfortunately, results from studies examining other demographic characteristics (eg, race, socioeconomic status, religious affiliation, year in college) as related to misuse of stimulant medication are much less conclusive and these correlates therefore require further investigation.
Motives For Misuse and Perceived Risk
Researchers have also evaluated college students’ motives for misusing stimulant medication and the risks they associate with misuse. All of the studies that asked misusing students about their motives for misuse reported that the most commonly endorsed motives were related to academics. “To concentrate better while studying” [16], “to improve study skills” [17], “to stay awake to study longer” [11], and “to improve concentration” [18] were some of the most commonly endorsed motives in these studies. Nonacademic reasons, such as to get high, to prolong effects of alcohol and other drugs, and to lose weight, were less commonly endorsed [7,12,19]. In studies where participants were able to indicate multiple motives for misuse [16], very few students misused for only nonacademic reasons.
Several studies measured the relation between misuse of stimulant medication and perceived risk associated with misuse. Perceived risk was conceptualized as perceived harmfulness [20], perception of safety [14], concern with health risk [18], and the inverse of positive outcome expectancies [21]. These articles found that when college students perceive more risk or have less positive expectancies about stimulant medication misuse, they are less likely to misuse stimulant medication. For instance, those who associated stimulant medication misuse with low perceived harmfulness were over 10 times more likely to have used in the last year than those who associated misuse with high perceived harmfulness [20].
Academic Outcomes Associated with Misuse
Interestingly, despite academic motives being most common for college students who report misusing stimulant medication, a number of studies have found a negative association between academic outcomes and misuse of stimulant medication. For instance, nonusers reported an average grade-point average (GPA) of 3.28 compared to 3.16 for misusers [16]. Other research demonstrates that the lower the student’s GPA is, the greater the odds are of the student misusing stimulant medication [8]. Misuse is also significantly related to other detrimental academic behaviors such as skipping class and less studying [20,22].
Psychological Correlates of Misuse
Researchers have evaluated the relation between several different psychological variables and misuse of stimulant medication. The strongest association is between symptoms of ADHD and stimulant medication misuse. Studies are consistent in reporting a significant correlation between greater symptoms of ADHD and higher rates of misuse or a significant difference in rates of misuse between those who have an ADHD diagnosis and those who do not. One study found that 71.1% of stimulant medication misusers screened positive for adult ADHD symptoms [17]. Another study found that for every standard deviation increase in attention problems, the odds of becoming a stimulant misuser increased by 1.78 [9]. Two studies asked participants if they believed they had ADHD. Advokat, Guildry, and Martino found that 12% of misusers believed they had ADHD [7]. Twenty-nine percent of “self-diagnosers” reported misusing, compared to 11.4% of “non-diagnosers” in another study [18].
Although the literature base is smaller than for ADHD, several studies have suggested a significant difference in symptoms of depression between stimulant medication misusers and nonusers. Zullig and Divin [23] found that misusers were significantly more likely to feel very sad, feel depressed, and consider suicide than nonusers. More frequent misuse has also been shown to be significantly associated with depressed mood [24].
A number of studies demonstrate a clear association between high sensation-seeking and misuse of stimulant medication. These results are not surprising given the well-documented relation between sensation seeking and substance use [25–27]. One study found a significant interaction between sensation seeking and perceived harmfulness of misusing stimulant medication: those with high sensation seeking and low perceived harmfulness were most likely to misuse [20].
Other Substance Use Associated with Stimulant Misuse
Many of the reviewed studies found a positive correlation between misuse of stimulant medication and other substance use or a significant difference between stimulant misusers and nonusers in rates of other substance use. These findings held across all substances examined, including alcohol, cigarettes, marijuana, illicit stimulants (eg, ecstasy, cocaine, or amphetamines), and non-stimulant prescription medications. For instance, significant associations were found between misuse of stimulant medication and several alcohol-related constructs, such as binge drinking [28,29], problematic drinking behavior [30], or meeting the Diagnostic and Statistical Manual of Mental Disorders [21] criteria for alcohol abuse [22]. With respect to cigarettes, 50.3% of misusers were found to have smoked cigarettes in the last 6 months compared to 13.3% of nonusers [16]. Similar findings emerged for illicit drug use. One study found that 73.5% of stimulant medication misusers reported use of marijuana in the last 6 months, compared to 18.2% of nonusers [19], while another study found that 93% of misusers used marijuana in the last year compared to 34% of nonusers [5]. This same study found that 33% of stimulant medication misusers also reported cocaine use in the last year compared to 2% of stimulant nonusers [5]. Finally, many of the studies reviewed examined the association between other substance use in general and stimulant medication misuse. Results were striking; the odds of becoming a stimulant medication misuser increased by 3.81 for each standard deviation increase in the amount of other substance use [9].
Summary
The research literature reviewed in this section provides a descriptive characterization of which college students (and, by extension, adolescents and young adults not in college) may be at the greatest risk of misuse of stimulant medication. Significant risk factors include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. It is important to recognize that one, several, or many of these risk factors may be present in a given individual who is misusing stimulant medication. Moreover, there may be other risk factors not yet identified in the research literature. The following sections of this paper draw from the literature reviewed here to provide a number of clinical recommendations for reducing and preventing misuse of stimulant medications among college students, other young adults, and adolescents.
Clinical Recommendations
It is important for health care providers to be aware of the benefits and risks associated with stimulant medications, the prevalence of and risk factors for stimulant misuse, and the psychiatric, psychological, and medical comorbidities associated with the misuse of stimulant medication. Knowledge about stimulant medications, misuse of stimulant medications, and a thorough evaluation of the patient will enable health care providers to address the misuse, as well as any comorbidities or other factors that may contribute to stimulant medication misuse, either pharmacologically or through referral for more specified psychotherapeutic interventions.
Stimulant Medication Indications and Adverse Effects
Stimulant medications are efficacious for the treatment of ADHD and, when prescribed and used correctly, can improve attentiveness, decrease distractibility, and improve daily functioning in the short term [19]. When used by individuals without ADHD, patients may experience euphoria, stimulation, alertness, and are not likely to experience the cognitive benefits that those with ADHD receive [31]. Side effects can occur regardless of whether the individual is using the stimulant for ADHD, misusing, or is dependent, and include nervousness, headaches, tachycardia, poor appetite, depressed mood, and poor sleep [19,32]. Additionally, stimulant medications can cause psychosis, agitation, and hallucinations [31,33], which typically resolve after discontinuation of the stimulant within 2 to 6 days, though a longer time period to resolution has been reported [33]. Stimulant medications carry warnings about increased risk of sudden death, high blood pressure, cardiac arrest, and stroke, as well as a statement warning providers about abuse potential. Additionally, serious but rare medical complications, including seizures, tachycardia or dysrhythmias, and hyperthermia, can occur [31,34].
Physical Examination and Laboratory Data
Obtaining vital signs and performing a physical exam may reveal weight loss and an increase in heart rate or blood pressure. Methylphenidate and amphetamines are known to increase heart rate and blood pressure [35] and a recent study found an average increase in heart rate of 5.7 bpm and a 1.2–mm Hg increase in systolic and diastolic blood pressure in adults on stimulant medications compared to placebo [36]. No EKG abnormalities or changes are found with either methylphenidate or amphetamine [35]. Urine toxicology can be utilized to obtain further information if misuse is suspected. However, the clinician must be aware of the limitations of urine drug testing with stimulants [37]. The usual detection time for amphetamines is 48 hours from last use, though this may vary depending on the presence of metabolites, pharmacokinetics of the drug (eg, immediate release vs. sustained release formulations), and patient variables [37]. Additionally, a urine toxicology screen for amphetamines typically tests for amphetamines, racemic compounds such as dextroamphetamine and methamphetamine, and illicit compounds (ie, methylenedioxymethamphetamine), though there are many compounds that are structurally similar, such as weight loss agents, over-the-counter cold products, and other psychotropic medications, including methylphenidate, that can cause a false-positive result [37]. Urine toxicology should be obtained in conjunction with a thorough evaluation of patients’ alcohol and drug use patterns. These 2 components are essential to the accurate diagnosis and formulation of a comprehensive treatment plan. As noted above, stimulant medication misuse and alcohol and illicit drug use are highly comorbid and should be carefully and thoroughly assessed.
Psychiatric Comorbidity
ADHD
The prevalence of ADHD is higher among individuals with substance use disorders [38]. As noted above, patients commonly report misuse of stimulant medication to enhance academic performance. One explanation may be that individuals misusing stimulants may be self-medicating undiagnosed ADHD [39]. The prevalence of ADHD among adults is 4.1% and it is more common in men than women with a ratio of up to 6:1 [40]. Several studies have found that individuals with misuse of stimulant medications endorse symptoms of ADHD, including higher levels of inattention and hyperactivity [41]. Twelve percent of participants in one study that endorsed stimulant medication misuse also endorsed the belief they had ADHD [7]. Another study found that individuals with higher baseline self-reported ADHD symptoms were also more likely to misuse stimulants [42]. The majority of individuals with ADHD have been found to take medications appropriately, though there is a minority, often with comorbid conduct disorder or other substance use disorders, that divert or misuse stimulant medications, most often the immediate release formulations [43,44].
Accurate diagnosis of ADHD in patients with substance use disorders can be challenging given the symptom overlap between intoxication and withdrawal syndromes of substances and symptoms of ADHD. Evaluating for ADHD is an important part of a thorough assessment and can be completed in several ways. The gold standard is with a standardized diagnostic tool such as the Connors Adult ADHD Diagnostic Interview for DSM-IV (CAADID) [45], which can be time consuming for a clinician and would likely involve referral to a psychologist for completion. Other scales have been examined, and the Connors Adult ADHD Rating Scale (CAARS) has been found to closely agree with the CAADID when both are administered [45]. Other scales are available, including the Wender Utah Rating Scales (WURS) and the Adult ADHD Self-Report Scale (ASRS), and have been found to have adequate sensitivity and specificity [45]. In an international study, the ASRS, a relatively brief instrument, showed encouraging results with 84% sensitivity and 66% specificity in detecting ADHD upon entry into substance disorder treatment for treatment-seeking patients [46]. When diagnosing ADHD among adults, it is crucial not to rely only on self-reported symptoms. A thorough childhood history of ADHD symptom presentation should be collected from a parent or caregiver, and collateral concurrent report should be collected from someone who knows the patient well, such as an employer, close friend, significant other, or parent. Valid diagnosis, whether ADHD is present or not, is of utmost importance in this population as individuals with comorbid substance use disorders and ADHD tend to have worse outcomes overall [47]. It is also important to appreciate that inaccurately diagnosing ADHD in individuals misusing stimulants could potentially diminish the importance of the diagnosis [48].
If ADHD is found, there are medications available that have a lower abuse potential compared to stimulant medications. Atomoxetine is the only FDA-approved nonstimulant for ADHD; off-label or second-line treatments include antidepressants, such as bupropion, venlafaxine, or tricyclic antidepressants, for which the data is limited, and clonidine [34,49,50]. If these therapies are not effective and, after careful consideration of risks and benefits, it is determined that a trial with a stimulant is needed, longer-acting formulations appear to be less abused [34,44]. Education for both the patient and his or her family should be provided on abuse and diversion potential and appropriate use and misuse [34,43,51]. Pill counts [43], regular office visits [52], and random urine toxicology screens [34] with informed interpretation of the screens may be helpful in deterring misuse or diversion. While medications are the mainstay of treatment for ADHD, there are several psychosocial interventions available, including cognitive behavioral therapy, coaching, and behavioral modification therapies [34].
Other Comorbidities
Other psychiatric comorbidities also should be explored. Studies have found a relation between depression and misuse of stimulant medication in that there is an increased likelihood of depression and thoughts of suicide among those that misuse stimulant medication and vice versa [23,24,53]. The National Survey on Drug Use and Health in 2012 found that, of those that misused stimulants, nearly 20% had serious thoughts of suicide over the past year [54]. As noted earlier, stimulant medication can affect sleep and appetite. Among those that report misuse of stimulant medication for weight loss, these individuals are more likely to report other eating-disordered behaviors [55]. Sleep quality is worse and sleep disturbance greater in those that misuse stimulant medication [32]. Other traits and behaviors that have been described in individuals that misuse stimulant medications include impulsivity [56,57], sensation seeking [20], perfectionism [58], and poor time management skills or procrastination [59].
Appropriate treatment (which may include pharmacologic, psychological, or academic accommodation components) for individuals with these psychiatric disorders or psychological symptoms may reduce the misuse of stimulant medications among college students, especially if these students are misusing in order to reduce their symptoms (ie, a self-medication hypothesis).
Treatment
There are currently no FDA-approved medications to treat stimulant medication misuse. In fact, studies exploring pharmacotherapy for stimulant medication misuse are limited. Most trials focus on stimulants such as cocaine or methamphetamine and not stimulant medications alone. Additionally, these trials primarily include only individuals that meet criteria for stimulant dependence. Various medications and medication classes have been examined for the treatment of stimulant dependence, including naltrexone, various antipsychotics, and various antidepressants including bupropion, modafanil, baclofen, ondansetron, and dexamphetamine, with little to no effect [60]. In a review of the literature, one study examined the use of naltrexone versus placebo for stimulant dependence in 80 treatment-seeking Swedish individuals [61]. The different types of stimulants on which these individuals were dependent were not clearly delineated, though the study authors noted that the major amphetamine abused in Sweden was the racemic mixture d/l amphetamine and not methamphetamine. Naltrexone was superior to placebo in this trial, as evidenced by higher percentage of amphetamine-free urine samples. A large majority of this sample used intravenously (65%–76%) and had been using between 6 to 8 years, limiting the applicability to individuals with stimulant medication misuse. At this time, investigation into evidence-based pharmacotherapies for stimulant medication misuse remains in the early stages.
Generally speaking, efficacious behavioral treatments, such as contingency management (CM), cognitive behavioral therapy (CBT), skills training, motivational interviewing (MI), relapse prevention, couples and family treatments, and drug counseling, exist for drug abuse [62]. CBT, cognitive therapy, CM, MI, and community reinforcement approach (CRA) [63,64] have been explored for stimulant dependence and are currently the primary interventions for amphetamine-type stimulant dependence [60]. Similar to pharmacotherapy studies, most psychotherapy studies to date have examined primarily cocaine and methamphetamine dependence and not misuse of stimulant medications. In fact, no studies examining psychotherapy for stimulant medication misuse were found by our group in a search using the PubMed database. Therefore, discussion of psychotherapeutic interventions that may be efficacious for stimulant medication misuse extrapolates outcomes from studies of stimulant dependence, appreciating this is an approximation and imprecise as there are significant differences between stimulant medication misusers and those dependent upon stimulants such as methamphetamine or cocaine. As such, in a review from 2009 [63], Vocci and colleagues compared psychotherapy studies for cocaine and methamphetamine dependence and concluded that CBT and CM were moderately effective and that adding CM to standard treatment may help improve outcomes. A study of 214 amphetamine users (including methamphetamine users), with the majority (70%) enrolled in a methadone maintenance program and a large proportion (58.9%) using amphetamines intravenously, found that either 2 or 4 sessions of CBT, along with self-help material, increased rate of abstinence at 6 months post-intervention compared to the use of self-help material alone [65]. Baker and colleagues [64] recommend a practical stepped approach to treatment for stimulant dependence, including conducting a thorough assessment, offering education and self-help materials, monitoring use and consequences of use, and then transitioning to more intensive psychosocial interventions if needed, which may be applicable to those with stimulant medication misuse and is clinically reasonable. Offering a psychosocial intervention may require referral to more specialized treatment services than can be offered in a general primary care clinic. Additionally, harm reduction techniques for stimulant medication misusers to reduce the medical and social consequences can be considered as well as prevention strategies and methods, which can be utilized in any treatment setting or in high-risk populations, such as college students.
Prevention Strategies for the Individual
The research findings summarized in this review suggest several specific strategies for preventing and reducing the misuse of stimulant medication among college students, a high-risk population. First, college students with a prescription for stimulant medication play a critical role. Not only do these students have a high rate of misuse themselves [28,66], but they are also the most common source from which other students obtain stimulant medication to misuse [11,67]. It is therefore important for physicians who provide college students with prescriptions for stimulant medications to discuss the possible consequences of misusing or diverting medication, including potential negative health outcomes, legal consequences, and on-campus repercussions, for students caught diverting stimulant medications. These practitioners should also monitor their patients for signs of diversion, such as finishing a prescription early, doctor shopping, or urine drug screen which is negative for the prescribed substance. Utilizing a prescription monitoring program to access information on the prescribing and filling of controlled substances can be a valuable tool in detecting multiple concomitant prescriptions for stimulant medications, number of providers writing stimulant medication, and information on the use of other prescribed controlled medications. Providers should also discuss safe storage of stimulant medications with patients, particularly if the student is currently living in a dorm setting or another community-type setting with the potential for lots of individuals in and around their personal belongings. Additionally, providers may wish to consider dispensing a small amount at each office visit until the patient has established responsible use of the medication, particularly if there are other findings or comorbidities that perhaps increase their risk of misuse. Pill counts and frequent office visits, as noted earlier, may also help prevent diversion.
Perceived risk/harm associated with the use of stimulant medications has been negatively related to misuse [18,20]. If college students were more aware of the risks associated with stimulant medication misuse, with regards to both health and legal consequences, fewer students may choose to misuse stimulants. Educating patients and their families about the abuse potential of stimulants, as well as consequences of misuse such as psychosis and agitation, when prescriptions are given for stimulant medication, may help address the misperception that stimulant medications are benign, safe and without adverse consequences.
College Policy Changes for Prevention of Misuse
Policy changes on college campuses could also help to reduce diversion of stimulant medications. For instance, education about the risks associated with stimulant medication misuse could be incorporated into other alcohol and drug prevention programs that are already in place at colleges and universities. Many colleges/universities require all first-year students to complete an online substance use education/prevention/assessment tool. Some of these, such as AlcoholEdu and The Alcohol eCHECKUP TO GO have demonstrated some success in reducing college student alcohol use in follow-up evaluations [68]. Information about misuse of stimulant medication could be included in these existing programs. Moreover, members of certain organizations (eg, fraternities or sororities) that are known for an increased risk of substance use/abuse among members are also sometimes required by their national chapters or host colleges/universities to complete a “risk management” class, which addresses behaviors such as binge drinking and drunk driving. Since one of the demographic factors most strongly related to stimulant medication misuse is Greek organization membership [14], presenting information about stimulant medication misuse to these groups during these classes could help reduce misuse on college campuses.
Finally, the most commonly reported motives for misuse of stimulant medications among college students are academic in nature (eg, to study more, to concentrate better) [16], and many students who misuse for these reasons feel the desired effect is achieved. Colleges and universities may need to improve the identification of students who are in need of academic assistance/supports and offer these interventions earlier in students’ college careers to prevent stimulant medication misuse as a “quick fix.” Such interventions may include teaching students skills such as note-taking and academic goal setting and educating students about the link between sleep deprivation and poor concentration [69].
Summary
Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Diagnosing ADHD can be invaluable for individuals with the disorder, thus the ability to perform a thorough and accurate assessment is important; equally important is the ability to assess when ADHD is not present. Education and prevention strategies to prevent misuse and diversion should be provided if stimulant medications are indicated. College programs and policies can also utilize prevention strategies, provide education to students, and assist those with academic difficulties. Comorbidities are common and should be explored thoroughly as they may play a role in continued stimulant medication misuse and outcomes. Various treatment techniques and modalities can be explored further with each patient, based on the individual and their particular needs.
Corresponding author: Kate Flory, Univ. of South Carolina, Dept. of Psychology, Barnwell College, Columbia, SC 29208, [email protected].
Funding/support: Work on this paper was supported by a University of South Carolina Honors College Exploration Scholar Award and a University of South Carolina Magellan Fellowship, both awarded to Kari Benson.
Financial disclosures: None.
Author contributions: conception and design, KF, RAP, KB; drafting of article, KF, RAP, KB; critical revision of the article, KF, RAP, KB; literature search, KB.
1. Chai G, Governale L, Mcmahon AW, et al. Trends of outpatient prescription drug utilization in US children, 2002-2010. Pediatr 2012;130:23–31.
2. Dupaul GJ, Weyandt LL, O’dell SM, Varejao M. College students with ADHD: current status and future directions J Atten Disord 2009;13:234–50.
3. DuPaul G, Schaughency E, Weyandt L, et al. Self-report of ADHD symptoms in university students: Cross-gender and cross-national prevalence. J Learn Disabil 2001;34:370–9.
4. Wolf L. College students with ADHD and other hidden disorders: Outcomes and interventions. Ann NY Acad Arts Sci 2001;931:385–5.
5. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use, and diversion of abusable prescription drugs. J Am Coll Health 2006;54:269–78.
6. Garnier LM, Arria AM, Caldeira KM, et al. Sharing and selling of prescription medications in a college student sample. J Clin Psychiatry 2010;71:262–9.
7. Advokat CD, Guildry D, Martino L. Licit and illicit use of medications for attention-deficit hyperactivity disorder in undergraduate college students. J Am Coll Health 2008;56:601–6.
8. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use and diversion of prescription stimulant medication. J Psychoactive Drugs 2006;38:43–56.
9. Rabiner DL, Anastopoulos AD, Costello E, et al. Predictors of nonmedical ADHD medication use by college students. J Atten Disord 2010;13:640–8.
10. Graff Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
11. DeSantis AD, Webb EM, Noar SM. Illicit use of prescription ADHD medications on a college campus: A multimethodological approach. J Am Coll Health 2008;57:315–23.
12. Sharp JT, Rosén LA. Recreational stimulant use among college students. J Subst Use 2007;12:71–82.
13. Hall KM, Irwin MM, Bowman KA, et al. Illicit use of prescribed stimulant medication among college students. J Am Coll Health 2005;53:167–74.
14. Dussault CL, Weyandt LL. An examination of prescription stimulants misuse and psychological variables among sorority and fraternity college populations. J Atten Disord 2013;27:87–7.
15. McCabe SE. Misperceptions of non-medical prescription drug use: A web survey of college students. Addict Behav 2008;33:713–24.
16. Rabiner DL, Anastopoulos AD, Costello E, et al. Motives and perceived consequences of nonmedical ADHD medication use by college students: Are students treating themselves for attention problems? J Atten Disord 2009;13:259–70.
17. Peterkin AL, Crone CC, Sheridan MJ, Wise TN. Cognitive performance enhancement: Misuse or self-treatment? J Atten Disord 2011;15:263–8.
18. Judson R, Langdon SW. Illicit use of prescription stimulants among college students: Prescription status, motives, theory of planned behaviour, knowledge and self-diagnostic tendencies. Psychol Health Med 2009;14:97–104.
19. Volkow ND, Swanson JM. Adult attention deficit-hyperactivity disorder. N Engl J Med 2013;369:1935–44.
20. Arria AM, Caldeira KM, Vincent KB, et al. Perceived harmfulness predicts nonmedical use of prescription drugs among college students: Interactions with sensation-seeking. Prev Science 2008;9:191–201.
21. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. 2000.
22. Arria AM, Wilcox HC, Caldeira KM, et al. Dispelling the myth of “smart drugs”: Cannabis and alcohol use problems predict nonmedical use of prescription stimulants for studying. Addict Behav 2013;38:1643–50.
23. Zullig KJ, Divin AL. The association between non-medical prescription drug use, depressive symptoms, and suicidality among college students. Addict Behav 2012;37:890–9.
24. Teter CJ, Falone AE, Cranford JA, et al. Nonmedical use of prescription stimulants and depressed mood among college students: Frequency and routes of administration. J Subst Abuse Treat 2010;38:292–8.
25. Pedersen W. Mental health, sensation seeking and drug use patterns: a longitudinal study. Br J Addict 1991;86:195–204.
26. Jaffe LT, Archer RP. The prediction of drug use among college students from MMPI, MCMI, and sensation seeking scales. J Pers Assess 1987;51:243–53.
27. Martins SS, Storr CL, Alexandre PK, Chilcoat HD. Adolescent ecstasy and other drug use in the National Survey of Parents and Youth: The role of sensation-seeking, parental monitoring and peer’s drug use. Addict Behav 2008;33:919–33.
28. Sepúlveda DR, Thomas LM, McCabe S, et al. Misuse of prescribed stimulant medication for ADHD and associated patterns of substance use: Preliminary analysis among college students. J Pharm Pract 2011;24:551–60.
29. Teter CJ, McCabe SE, Cranford JA, et al. Prevalence and motives for illicit use of prescription stimulants in an undergraduate student sample. J Am Coll Health 2005;53:253–62.
30. Lookatch SJ, Dunne EM, Katz EC. Predictors of nonmedical use of prescription stimulants. J Psychoactive Drugs 2012;44:86–91.
31. Looby A, Kassman KT, Earlywine M. Do negative stimulant-related attitudes vary for prescription stimulants and cocaine among college students? Addict Behav 2014;39:1100–5.
32. Clegg-Kraynok MM, McBean AL, Montgomery-Downs HE. Sleep quality and characteristics of college students who use prescription psychostimulants nonmedically. Sleep Med 2011;12:598–602.
33. Ross RG. Psychotic and manic-like symptoms during stimulant treatment of attention deficit hyperactivity disorder. Am J Psychiatry 2006;163:1149–52.
34. Mariani JJ, Levin FR. Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addict 2007;16:45–56.
35. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation 2008;117:2407–23.
36. Mick E, McManus DD, Goldberg RJ. Meta-analysis of increased heart rate and blood pressure associated with CNS stimulant treatment of ADHD in adults. Eur Neuropsychopharmacol 2013;23:534–41.
37. Moeller KE, Lee KC, Kissack JC. Urine drug screening: Practical guide for clinicians. Mayo Clin Proc 2008;83:66–76.
38. Van de Glind G, Konstenius M, Koeter MWJ, et al. Variability in the prevalence of adult ADHD in treatment seeking substance use disorder patients: Results from an international multi-center study exploring DSM-IV and DSM-5 criteria. Drug Alcohol Depend 2014;134:158–66.
39. Bukstein O. Substance abuse in patients with attention-deficit/hyperactivity disorder. Medscape J Med 2008;10:24.
40. Kessler RC, Adler L, Barkley R, et al. The prevalence and comorbidity of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry 2006;163:716–23.
41. Hartung CM, Canu WH, Cleveland CS, et al. Stimulant medication use in college students: Comparison of appropriate users, misusers, and nonusers. Psychol Addict Behav 2014;27:832.
42. Upadhyaya HP. Managing attention-deficit/hyperactivity disorder in the presence of substance use disorder. J Clin Psychiatry 2007;68:23–30.
43. Wilens TE, Gignac M, Swezey A, et al. Characteristics of adolescents and young adults with ADHD who divert or misuse their prescribed medications. J Am Acad Child Adolesc Psychiatry 2006;45:408–14.
44. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: A systematic review of the literature. J Am Acad Child Adolesc Psychiatry 2008;47:21–31.
45. Dakwa E, Mahony A, Pavlicova M, et al. The utility of attention-deficit/hyperactivity disorder screening instruments in individuals seeking treatment for substance use disorders. J Clin Psychiatry 2012;73:1372–8.
46. Van de Glind G, Van den Brink W, Koeter. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend 2013;132:587–96.
47. Levin FR. Diagnosing attention-deficity/hyperactivity disorder in patients with substance use disorders. J Clin Psychiatry 2007;68:9–14.
48. Diller L. ADHD in the college student: Is anyone else worried? J Atten Disord. 2010;14:3-6.
49. Christman AK, Fermo JD, Markowitz JS. Atomoxetine, a novel treatment for attention-deficit/hyperactivity disorder. Pharmacotherapy 2004;24:1020–36.
50. Riggs P, Levin F, Green AI, Vocci F. Comorbid psychiatric and substance abuse disorders: Recent treatment research. Subst Abuse 2008;29:51–63.
51. Rabiner D L. Stimulant prescription cautions: Addressing misuse, diversion, and malingering. Curr Psychiatry Rep. 2013;15:375-383.
52. Manning JS. Strategies for managing the risks associated with ADHD medications. J Clin Psychiatry 2013;74:e19.
53. Markou A, Kosten TR, Koob GF. Neurobiological similarities in depression and drug dependence: A self-medication hypothesis. Neuropsychopharmacology 1998;18:135–74.
54. Results from the 2012 National Survey on Drug Use and Health: Mental Health Findings, NSDUH Series H-47. HHS Pub No. 13-4805. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2013.
55. Jeffers A, Benotsch EG, Koester S. Misuse of prescription stimulants for weight loss, psychosocial variables, and eating disordered behaviors. Appetite 2013;65:8–13.
56. Madden GJ, Bickel WK. Impulsivity: The behavioral and neurological science of discounting. 1st ed. Washington, DC: APA; 2010.
57. Stanford MS, Mathias CW, Dougherty DM, et al. Fifty years of the Barratt Impulsiveness Scale: An update and review. Pers Indiv Differ 2009;47:385–95.
58. Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
59. Moore DR, Burgard DA, Larson RG, Ferm M. Psychostimulant use among college students during periods of high and low stress: An interdisciplinary approach utilizing both self-report and unobtrusive chemical sample data. Addict Behav 2014;39:987–93.
60. Brensilver M, Heinzerling KG, Shoptaw S. Pharmacotherapy of amphetamine-type stimulant dependence: An update. Drug Alc Review 2013;32:449–60.
61. Jayaram-Lindstrom N, Hammarberg A, Beck O, Franck J. Naltrexone for the treatment of amphetamine dependence: A randomized, placebo-controlled trial. Am J Psychiatry 2008;165:1442–8.
62. Carroll KM, Onken LS. Behavioral therapies for drug abuse. Am J Psychiatry 2005;162:1452–60.
63. Vocci FJ, Montoya I. Psychological treatments for stimulant misuse, comparing and contrasting those for amphetamine dependence and those for cocaine dependence. Curr Opin Psychiatry 2009;22:263–8.
64. Baker A, Lee NK., Claire M, et al. Brief cognitive behavioral interventions for regular amphetamine users: a step in the right direction. Addict 2005;100:367–78.
65. Baker A, Lee NK, Claire M, et al. Drug use patterns and mental health of regular amphetamine users. Addict 2004;99:875–84.
66. Rabiner DL, Anastopoulos AD, Costello E, et al. The misuse and diversion of prescribed ADHD medications by college students. J Atten Disord 2009;13:259–70.
67. Garnier-Dykstra LM, Caldeira KM, Vincent KB, et al. Nonmedical use of prescription stimulants during college: Four year trends in exposure opportunity, use, motives, and sources. J Am Coll Health 2012;60:226–34.
68. Hustad JT, Barnett NP, Borsari B, Jackson KM. Web-based alcohol prevention for incoming college students: A randomized controlled trial. Addict Behav 2010;35:183–9.
69. Pilcher JJ, Walters AS. How sleep deprivation affects psychological variables related to college students’ cognitive performance. J Am Coll Health 1997;46:121–6.
1. Chai G, Governale L, Mcmahon AW, et al. Trends of outpatient prescription drug utilization in US children, 2002-2010. Pediatr 2012;130:23–31.
2. Dupaul GJ, Weyandt LL, O’dell SM, Varejao M. College students with ADHD: current status and future directions J Atten Disord 2009;13:234–50.
3. DuPaul G, Schaughency E, Weyandt L, et al. Self-report of ADHD symptoms in university students: Cross-gender and cross-national prevalence. J Learn Disabil 2001;34:370–9.
4. Wolf L. College students with ADHD and other hidden disorders: Outcomes and interventions. Ann NY Acad Arts Sci 2001;931:385–5.
5. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use, and diversion of abusable prescription drugs. J Am Coll Health 2006;54:269–78.
6. Garnier LM, Arria AM, Caldeira KM, et al. Sharing and selling of prescription medications in a college student sample. J Clin Psychiatry 2010;71:262–9.
7. Advokat CD, Guildry D, Martino L. Licit and illicit use of medications for attention-deficit hyperactivity disorder in undergraduate college students. J Am Coll Health 2008;56:601–6.
8. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use and diversion of prescription stimulant medication. J Psychoactive Drugs 2006;38:43–56.
9. Rabiner DL, Anastopoulos AD, Costello E, et al. Predictors of nonmedical ADHD medication use by college students. J Atten Disord 2010;13:640–8.
10. Graff Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
11. DeSantis AD, Webb EM, Noar SM. Illicit use of prescription ADHD medications on a college campus: A multimethodological approach. J Am Coll Health 2008;57:315–23.
12. Sharp JT, Rosén LA. Recreational stimulant use among college students. J Subst Use 2007;12:71–82.
13. Hall KM, Irwin MM, Bowman KA, et al. Illicit use of prescribed stimulant medication among college students. J Am Coll Health 2005;53:167–74.
14. Dussault CL, Weyandt LL. An examination of prescription stimulants misuse and psychological variables among sorority and fraternity college populations. J Atten Disord 2013;27:87–7.
15. McCabe SE. Misperceptions of non-medical prescription drug use: A web survey of college students. Addict Behav 2008;33:713–24.
16. Rabiner DL, Anastopoulos AD, Costello E, et al. Motives and perceived consequences of nonmedical ADHD medication use by college students: Are students treating themselves for attention problems? J Atten Disord 2009;13:259–70.
17. Peterkin AL, Crone CC, Sheridan MJ, Wise TN. Cognitive performance enhancement: Misuse or self-treatment? J Atten Disord 2011;15:263–8.
18. Judson R, Langdon SW. Illicit use of prescription stimulants among college students: Prescription status, motives, theory of planned behaviour, knowledge and self-diagnostic tendencies. Psychol Health Med 2009;14:97–104.
19. Volkow ND, Swanson JM. Adult attention deficit-hyperactivity disorder. N Engl J Med 2013;369:1935–44.
20. Arria AM, Caldeira KM, Vincent KB, et al. Perceived harmfulness predicts nonmedical use of prescription drugs among college students: Interactions with sensation-seeking. Prev Science 2008;9:191–201.
21. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. 2000.
22. Arria AM, Wilcox HC, Caldeira KM, et al. Dispelling the myth of “smart drugs”: Cannabis and alcohol use problems predict nonmedical use of prescription stimulants for studying. Addict Behav 2013;38:1643–50.
23. Zullig KJ, Divin AL. The association between non-medical prescription drug use, depressive symptoms, and suicidality among college students. Addict Behav 2012;37:890–9.
24. Teter CJ, Falone AE, Cranford JA, et al. Nonmedical use of prescription stimulants and depressed mood among college students: Frequency and routes of administration. J Subst Abuse Treat 2010;38:292–8.
25. Pedersen W. Mental health, sensation seeking and drug use patterns: a longitudinal study. Br J Addict 1991;86:195–204.
26. Jaffe LT, Archer RP. The prediction of drug use among college students from MMPI, MCMI, and sensation seeking scales. J Pers Assess 1987;51:243–53.
27. Martins SS, Storr CL, Alexandre PK, Chilcoat HD. Adolescent ecstasy and other drug use in the National Survey of Parents and Youth: The role of sensation-seeking, parental monitoring and peer’s drug use. Addict Behav 2008;33:919–33.
28. Sepúlveda DR, Thomas LM, McCabe S, et al. Misuse of prescribed stimulant medication for ADHD and associated patterns of substance use: Preliminary analysis among college students. J Pharm Pract 2011;24:551–60.
29. Teter CJ, McCabe SE, Cranford JA, et al. Prevalence and motives for illicit use of prescription stimulants in an undergraduate student sample. J Am Coll Health 2005;53:253–62.
30. Lookatch SJ, Dunne EM, Katz EC. Predictors of nonmedical use of prescription stimulants. J Psychoactive Drugs 2012;44:86–91.
31. Looby A, Kassman KT, Earlywine M. Do negative stimulant-related attitudes vary for prescription stimulants and cocaine among college students? Addict Behav 2014;39:1100–5.
32. Clegg-Kraynok MM, McBean AL, Montgomery-Downs HE. Sleep quality and characteristics of college students who use prescription psychostimulants nonmedically. Sleep Med 2011;12:598–602.
33. Ross RG. Psychotic and manic-like symptoms during stimulant treatment of attention deficit hyperactivity disorder. Am J Psychiatry 2006;163:1149–52.
34. Mariani JJ, Levin FR. Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addict 2007;16:45–56.
35. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation 2008;117:2407–23.
36. Mick E, McManus DD, Goldberg RJ. Meta-analysis of increased heart rate and blood pressure associated with CNS stimulant treatment of ADHD in adults. Eur Neuropsychopharmacol 2013;23:534–41.
37. Moeller KE, Lee KC, Kissack JC. Urine drug screening: Practical guide for clinicians. Mayo Clin Proc 2008;83:66–76.
38. Van de Glind G, Konstenius M, Koeter MWJ, et al. Variability in the prevalence of adult ADHD in treatment seeking substance use disorder patients: Results from an international multi-center study exploring DSM-IV and DSM-5 criteria. Drug Alcohol Depend 2014;134:158–66.
39. Bukstein O. Substance abuse in patients with attention-deficit/hyperactivity disorder. Medscape J Med 2008;10:24.
40. Kessler RC, Adler L, Barkley R, et al. The prevalence and comorbidity of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry 2006;163:716–23.
41. Hartung CM, Canu WH, Cleveland CS, et al. Stimulant medication use in college students: Comparison of appropriate users, misusers, and nonusers. Psychol Addict Behav 2014;27:832.
42. Upadhyaya HP. Managing attention-deficit/hyperactivity disorder in the presence of substance use disorder. J Clin Psychiatry 2007;68:23–30.
43. Wilens TE, Gignac M, Swezey A, et al. Characteristics of adolescents and young adults with ADHD who divert or misuse their prescribed medications. J Am Acad Child Adolesc Psychiatry 2006;45:408–14.
44. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: A systematic review of the literature. J Am Acad Child Adolesc Psychiatry 2008;47:21–31.
45. Dakwa E, Mahony A, Pavlicova M, et al. The utility of attention-deficit/hyperactivity disorder screening instruments in individuals seeking treatment for substance use disorders. J Clin Psychiatry 2012;73:1372–8.
46. Van de Glind G, Van den Brink W, Koeter. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend 2013;132:587–96.
47. Levin FR. Diagnosing attention-deficity/hyperactivity disorder in patients with substance use disorders. J Clin Psychiatry 2007;68:9–14.
48. Diller L. ADHD in the college student: Is anyone else worried? J Atten Disord. 2010;14:3-6.
49. Christman AK, Fermo JD, Markowitz JS. Atomoxetine, a novel treatment for attention-deficit/hyperactivity disorder. Pharmacotherapy 2004;24:1020–36.
50. Riggs P, Levin F, Green AI, Vocci F. Comorbid psychiatric and substance abuse disorders: Recent treatment research. Subst Abuse 2008;29:51–63.
51. Rabiner D L. Stimulant prescription cautions: Addressing misuse, diversion, and malingering. Curr Psychiatry Rep. 2013;15:375-383.
52. Manning JS. Strategies for managing the risks associated with ADHD medications. J Clin Psychiatry 2013;74:e19.
53. Markou A, Kosten TR, Koob GF. Neurobiological similarities in depression and drug dependence: A self-medication hypothesis. Neuropsychopharmacology 1998;18:135–74.
54. Results from the 2012 National Survey on Drug Use and Health: Mental Health Findings, NSDUH Series H-47. HHS Pub No. 13-4805. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2013.
55. Jeffers A, Benotsch EG, Koester S. Misuse of prescription stimulants for weight loss, psychosocial variables, and eating disordered behaviors. Appetite 2013;65:8–13.
56. Madden GJ, Bickel WK. Impulsivity: The behavioral and neurological science of discounting. 1st ed. Washington, DC: APA; 2010.
57. Stanford MS, Mathias CW, Dougherty DM, et al. Fifty years of the Barratt Impulsiveness Scale: An update and review. Pers Indiv Differ 2009;47:385–95.
58. Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
59. Moore DR, Burgard DA, Larson RG, Ferm M. Psychostimulant use among college students during periods of high and low stress: An interdisciplinary approach utilizing both self-report and unobtrusive chemical sample data. Addict Behav 2014;39:987–93.
60. Brensilver M, Heinzerling KG, Shoptaw S. Pharmacotherapy of amphetamine-type stimulant dependence: An update. Drug Alc Review 2013;32:449–60.
61. Jayaram-Lindstrom N, Hammarberg A, Beck O, Franck J. Naltrexone for the treatment of amphetamine dependence: A randomized, placebo-controlled trial. Am J Psychiatry 2008;165:1442–8.
62. Carroll KM, Onken LS. Behavioral therapies for drug abuse. Am J Psychiatry 2005;162:1452–60.
63. Vocci FJ, Montoya I. Psychological treatments for stimulant misuse, comparing and contrasting those for amphetamine dependence and those for cocaine dependence. Curr Opin Psychiatry 2009;22:263–8.
64. Baker A, Lee NK., Claire M, et al. Brief cognitive behavioral interventions for regular amphetamine users: a step in the right direction. Addict 2005;100:367–78.
65. Baker A, Lee NK, Claire M, et al. Drug use patterns and mental health of regular amphetamine users. Addict 2004;99:875–84.
66. Rabiner DL, Anastopoulos AD, Costello E, et al. The misuse and diversion of prescribed ADHD medications by college students. J Atten Disord 2009;13:259–70.
67. Garnier-Dykstra LM, Caldeira KM, Vincent KB, et al. Nonmedical use of prescription stimulants during college: Four year trends in exposure opportunity, use, motives, and sources. J Am Coll Health 2012;60:226–34.
68. Hustad JT, Barnett NP, Borsari B, Jackson KM. Web-based alcohol prevention for incoming college students: A randomized controlled trial. Addict Behav 2010;35:183–9.
69. Pilcher JJ, Walters AS. How sleep deprivation affects psychological variables related to college students’ cognitive performance. J Am Coll Health 1997;46:121–6.
Physical Examination of the Throwing Athlete’s Elbow
Understanding the pathomechanics of throwing and the accompanying elbow injuries is the groundwork for conducting a directed history taking and a physical examination that produce an accurate diagnosis of elbow injuries in throwing athletes. Advances in physical examination techniques have improved our ability to accurately diagnose and treat throwers’ athletic elbow disorders.
Throwing imposes an extremely high valgus stress (approaching 60-65 Nm) across the elbow. This high stress occurs during the cocking and acceleration phases of the overhead throwing motion.1-3 The valgus stress generates tension on the medial elbow, compression on the lateral elbow, and shear on the posterior aspect of the elbow. These forces cause predictable injury patterns in different parts of throwers’ elbows. Physical examination performed in a systematic anatomical fashion can enhance predictable and accurate elbow injury diagnosis. In this article, we outline 5 points in a systematic approach to physical examination of a throwing athlete’s elbow.
1. Perform a general upper extremity examination
Cervical spine and shoulder girdle
In the initial examination, the cervical spine and the entire affected upper extremity should be quickly assessed. Assessment of the cervical spine should include palpation, range of motion (ROM), and basic provocative testing, such as the Spurling test, to evaluate for radiculopathy caused by foraminal compression. Posture, asymmetry, atrophy, edema, ecchymosis, and any other deformity should be noted. For example, atrophy of the neck and shoulders suggests underlying neuropathy. In addition, fullness of the supraclavicular region and local tenderness or bruit suggest vasculopathy. Symptomatic compression of the subclavian artery and vein between the anterior and middle scalene muscles may present as weakness, fullness, heaviness, and early fatigue. Physical signs include coolness, pallor, claudication, engorgement, and edema in the arm.4 Thoracic outlet syndrome can manifest as effort-induced vague pain at the arm and elbow.5 If this syndrome is suspected, an Adson test should be performed. With the patient’s neck extended and rotated away from the affected side, the examiner, standing next to the patient, palpates the radial pulse with the patient’s elbow extended (Figure 1A). Next, the examiner abducts, extends, and externally rotates the patient’s shoulder (Figure 1B) while the patient alternates between opening and closing the fist (Figure 1C). A decrease or absence in pulse strength from the starting position is a positive test result.
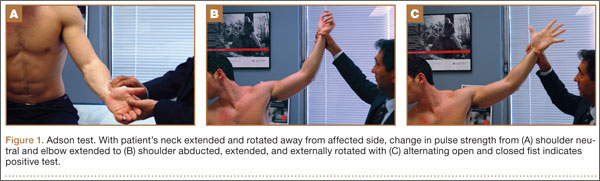
Last, the shoulder and scapulae should be assessed, as an affected shoulder or dyskinetic scapula can lead to improper mechanics of the kinetic chain at the elbow. The shoulder should be palpated, and ROM, strength, and stability should be assessed. Glenohumeral internal rotation deficit is associated with medial collateral ligament (MCL) tears; if present, this deficit should be addressed.6
Elbow
Inspection should reveal a normal carrying angle of about 11° to 14° of valgus in men and 13° to 16° in women. In immature athletes, increased valgus stresses from repetitive overhead throwing can cause medial epicondylar hypertrophy, and carrying angles of more than 15° are common.7-9
Active and passive ROM should be assessed. Normal ROM is about 0° extension and 140° flexion with 80° of supination and pronation. For determination of pathologic differences, ROM should always be compared between the affected and the contralateral sides. Painful loss of motion may be caused by soft-tissue swelling or contracture, effusion, bony impingement, or loose bodies. Crepitus, locking, catching, or another mechanical symptom may indicate loose bodies or chondral injury. Firm, mechanical blocks to ROM during flexion may indicate osteophyte formation in the coronoid fossa, and mechanical blocks to ROM during extension may indicate osteophyte formation in the olecranon fossa. Pain elicited at the end points of motion is caused by osteophytes and impingement, whereas pain elicited during the mid-arc of motion is often caused by osteochondral lesions. Terminal extension, often the first motion lost after injury, may signal intra-articular pathology, if symptomatic. However, throwing athletes may present with developmental flexion contractures of up to 20°.10
2. Examine the medial aspect of the elbow
The medial epicondyle, easy to recognize as a bony prominence on the medial side of the distal humerus, serves as an attachment site for the MCL, pronator teres, and the common flexor tendon. In throwers, assessing the MCL is crucial. The MCL should be palpated from its origin on the inferior aspect of the medial epicondyle moving distally to the sublime tubercle of the proximal ulna. Tenderness at any point along the ligament can indicate a range of ligament pathology, from attenuation to complete rupture.
The MCL is further assessed with stress tests, most commonly the valgus stress test, the milking maneuver, and the moving valgus stress test. Of these 3 procedures, the moving valgus stress test is perhaps the most sensitive and specific for MCL injury, and is the test preferred by the authors.11 This test takes into account shoulder position, simulates the position of throwing, and can account for bony structures that provide stability at more than 120° of flexion. We prefer to position the patient supine on the examining table to help stabilize the shoulder and humerus and to relax the patient. The shoulder is placed in abduction and external rotation while the examiner holds the thumb with one hand and supports the elbow with the other. The elbow is extended (Figure 2A) and flexed (Figure 2B) while valgus stress is applied. A positive test elicits pain localized to the MCL at the arc of motion between 80° to 120°.12 Pain at positions near full extension with the moving valgus stress test may also indicate chondral damage at the posteromedial trochlea.13

During pitching, the tensile demand on the MCL is reduced by the action of the flexor-pronator mass. It is common to see a flexor-pronator mass injury concurrent with MCL injury.14 Medial epicondyle tenderness that increases with resisted wrist flexion may signal flexor-pronator injury, though, classically, flexor-pronator muscle strains and tears produce pain anterior and distal to the medial epicondyle.15
Traction, compression, and friction at the medial elbow can irritate the ulnar nerve. This nerve should be inspected and palpated along its course at the cubital tunnel to determine its location and stability. Ulnar nerve hypermobility, which has been identified in 37% of elbows, can be determined by having the patient actively flex the elbow with the forearm in supination, placing a finger at the posteromedial aspect of the medial humeral epicondyle, and having the patient actively extend the elbow.16 The nerve dislocates if trapped anterior to the examiner’s finger, perches if under the examiner’s finger, or is stable if still palpable in the groove posterior to the medial epicondyle.16
The distal band of the medial triceps tendon may also sublux over the medial epicondyle with elbow flexion. This subluxation, also known as snapping triceps syndrome, may cause pain or ulnar nerve symptoms.17 Bringing the elbow from extension to flexion may produce subluxation, first of the ulnar nerve and then of the medial triceps, in 2 separate “snaps.” Tenderness can be elicited along the medial triceps muscle.
Ulnar neuritis is caused by traction injury, such as with dynamic pitching, nerve subluxation, or compression at the cubital tunnel. With MCL injury and valgus instability, the ulnar nerve can become irritated as it becomes stretched because of medial elbow laxity.18 The nerve can also be damaged during flexion as the cubital tunnel retinaculum tightens, decreasing the space available for the nerve.19 This concept is applied during the elbow flexion compression test. A positive test may elicit tingling radiating toward the small finger or pain at the elbow or medial forearm when manual pressure is directly applied over the ulnar nerve between the posteromedial olecranon and the medial humeral epicondyle as the elbow is maximally flexed.20
3. Examine the lateral aspect of the elbow
Palpation of the lateral epicondyle, the radial head, and the olecranon tip assists in defining injury to the underlying anatomy. The anconeus “soft spot” (infracondylar recess) within the triangle formed by these 3 bony landmarks should be palpated for fullness, indicating a joint effusion, hemarthrosis, or even a subluxed or dislocated radial head.
While the medial elbow endures a large tensile load, throwing imposes a tremendous compressive force at the lateral elbow, particularly at the radiocapitellar joint. This joint may be tender and produce clicking with pronation and supination in patients with radiocapitellar arthrosis, symptomatic posterolateral synovial plica, or an inflamed radial bursa. Tenderness with crepitus that can be exacerbated with forceful flexion and extension may indicate radiocapitellar overload or loose bodies.
Long-term load transmission and subsequent degeneration of the articular surface may advance to osteochondritis dissecans (OCD). Examination for capitellar OCD reveals tenderness over the radiocapitellar joint and commonly a loss of 15° to 20° of extension. The active radiocapitellar compression test is positive for OCD lesions and elicits pain in the lateral compartment of the elbow when the patient pronates (Figure 3A) and supinates (Figure 3B) the forearm with the elbow axially loaded in extension.21
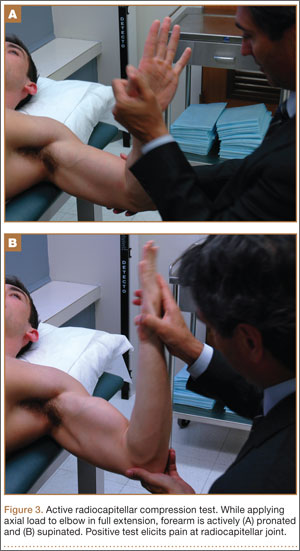
Microtrauma and inflammation may occur with repetitive eccentric overload. Although rare in throwing athletes, “tennis elbow” causes pain with gripping, and decreased grip strength. Tenderness caused by lateral epicondylitis is just anterior and distal to the epicondyle, at the origin of the extensor carpi radialis brevis. Pain is reproducible with passive wrist flexion and resisted wrist extension with the elbow extended (Cozen test).
Less commonly, athletes may complain of mechanical symptoms, such as snapping or catching with posterolateral elbow pain.22 These symptoms may be due to thickened or inflamed synovial plica causing impingement. A posterior radiocapitellar plica can be examined by bringing the elbow to full extension while applying valgus stress with the forearm in supination. Conversely, an anterior radiocapitellar plica can be examined with a valgus load on the elbow and passive flexion with the forearm in pronation.23 A palpable painful snap over the radiocapitellar joint is a positive test.
4. Examine the posterior aspect of the elbow
Posteriorly, palpation is focused on the triceps tendon and the olecranon tip. The elbow should be flexed to 30° to relax the triceps, isolate the olecranon, and allow for palpation of the olecranon fossa on either side of the triceps tendon. Tenderness at the posterolateral or posteromedial aspect of the olecranon should be noted. Warmth, fluctuance, or distension at the elbow may be caused by olecranon bursitis. The 3 heads of the triceps muscle should be palpated where they converge to form an aponeurosis, and tenderness or a palpable gap on any of the heads should be noted.
A combination of valgus force and a rapidly decelerating arm at the follow-through phase of pitching causes a shear force between the medial aspect of the olecranon tip and the olecranon fossa. This shear force can result in chondrolysis, osteophyte formation, and loose bodies, particularly in the posteromedial elbow. This valgus extension overload (VEO) syndrome often results in loss of full extension and symptoms, which may be attributed to osteophytes or fractured and nonunited fragments in the olecranon fossa or the olecranon tip. Frank crepitus may also be present with extension testing caused by loose bodies or synovial reaction over osteophytes. Assessing for VEO using the extension impingement test, the examiner places continuous valgus stress on the elbow while quickly extending from 20° to 30° of flexion (Figure 4A) to terminal extension (Figure 4B) repeatedly. The examiner repeats this without valgus load while palpating the posteromedial olecranon for tenderness to differentiate impingement caused by instability from pain over the medial olecranon without instability (Figure 4C). Particular attention should be focused posteriorly in athletes with medial instability, as MCL injuries and VEO syndrome often occur in conjunction in the throwing athlete.
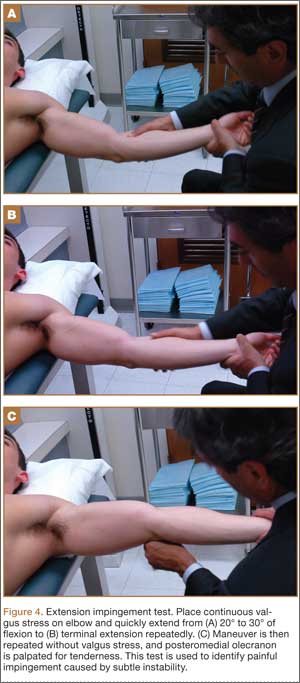
Repetitive acceleration and deceleration of the arm can also cause stress fractures. With stress fractures, pain is often noted more distal and lateral on the olecranon, but tenderness may be palpable medially from posteromedial impaction that occurs from the valgus load during the overhead throwing motion. In immature athletes, the repetitive sudden snap of full extension in the deceleration phase of throwing can cause olecranon apophysitis. Frank avulsions can occur as well but are usually preceded by chronic posterior elbow pain with possible loss of full extension.
The late cocking phase of the throwing motion (just before throwing) hyperextends the elbow and places significant strain on the elbow. Repetitive strain can cause painful posterior impingement. The arm bar test is extremely sensitive (Figure 5).13 With the patient’s elbow extended, shoulder internally rotated, and hand on the examiner’s shoulder, the examiner pulls down on the olecranon to simulate forced extension and reproduces the pain associated with posteromedial impingement.
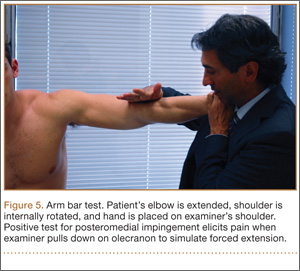
Last, though triceps tendon injuries are rare, ruptures most often occur at the origin of the lateral head of the triceps. As the initial swelling and ecchymosis subside, a palpable gap is pathognomonic for rupture. Extensor weakness can often be observed, but extension may still be possible from anconeus triceps expansion with the aid of gravity. With the elbow overhead, the athlete must extend the elbow against gravity and will exhibit weakness against resistance.
5. Examine the anterior aspect of the elbow
Anteriorly, the bulk of the flexor-pronator group restricts the extent of joint palpation, and the soft tissues are usually injured. The antecubital fossa is a triangular area on the anterior aspect of the elbow that is bounded superiorly by a horizontal line connecting the medial epicondyle to the lateral epicondyle of the humerus, medially by the lateral border of the pronator teres muscle and laterally by the medial border of the brachioradialis muscle. From lateral to medial, the antecubital fossa contains the radial nerve, the biceps brachii tendon, the brachial artery, and the median nerve. Evaluating this area is important because a visible defect, change in muscle contour, or proximal retraction of a muscle belly can indicate a muscular rupture. In particular, a distal biceps rupture (rare) may be accompanied by weakness and pain in supination and, to a lesser degree, in flexion. It is important to note that, in the case of a partial biceps rupture, ecchymosis may not appear, as the hematoma is confined by the intact lacertus fibrosis.24 The hook test can be used to evaluate for the presence of an intact distal biceps tendon (Figure 6).25 The patient abducts the shoulder, flexes the elbow to 90°, and actively supinates the forearm while the examiner attempts to hook an index finger laterally under the tendon. The test is negative if the finger can be inserted 1 cm under the tendon and positive if no cordlike structure can be hooked. Partial biceps tendon ruptures or tendinitis may exhibit tenderness of the distal biceps tendon and pain on resisted supination with a negative hook test. Often, resisted elbow flexion with the elbow at maximal extension elicits pain at the biceps insertion. Clicking with forearm rotation near the insertion of the tendon, which may be caused by an inflamed radial bursa between the distal biceps tendon and the radial tuberosity, may be associated with impending rupture.

Conclusion
Physical examination combined with thorough history taking usually provides a solid basis for a diagnosis, which in turn makes the value of surgical treatment more assured.
1. Elliott B, Fleisig G, Nicholls R, Escamilia R. Technique effects on upper limb loading in the tennis serve. J Sci Med Sport. 2003;6(1):76-87.
2. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23(2):233-239.
3. Werner SL, Fleisig GS, Dillman CJ, Andrews JR. Biomechanics of the elbow during baseball pitching. J Orthop Sports Phys Ther. 1993;17(6):274-278.
4. Aval SM, Durand P Jr, Shankwiler JA. Neurovascular injuries to the athlete’s shoulder: part II. J Am Acad Orthop Surg. 2007;15(5):281-289.
5. Strukel RJ, Garrick JG. Thoracic outlet compression in athletes: a report of four cases. Am J Sports Med. 1978;6(2):35-39.
6. Dines JS, Frank JB, Akerman M, Yocum LA. Glenohumeral internal rotation deficits in baseball players with ulnar collateral ligament insufficiency. Am J Sports Med. 2009;37(3):566-570.
7. Adams JE. Injury to the throwing arm. A study of traumatic changes in the elbow joints of boy baseball players. Calif Med. 1965;102:127-132.
8. Hang DW, Chao CM, Hang YS. A clinical and roentgenographic study of Little League elbow. Am J Sports Med. 2004;32(1):79-84.
9. King JW, Brelsford HJ, Tullos HS. Analysis of the pitching arm of the professional baseball pitcher. Clin Orthop. 1969;(67):116-123.
10. Cain EL Jr, Dugas JR, Wolf RS, Andrews JR. Elbow injuries in throwing athletes: a current concepts review. Am J Sports Med. 2003;31(4):621-635.
11. Safran M, Ahmad CS, Elattrache NS. Ulnar collateral ligament of the elbow. Arthroscopy. 2005;21(11):1381-1395.
12. O’Driscoll SW, Lawton RL, Smith AM. The “moving valgus stress test” for medial collateral ligament tears of the elbow. Am J Sports Med. 2005;33(2):231-239.
13. O’Driscoll SW. Valgus extension overload and plica. In: Levine WN, ed. The Athlete’s Elbow. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:71-83.
14. Conway JE, Jobe FW, Glousman RE, Pink M. Medial instability of the elbow in throwing athletes. Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am. 1992;74(1):67-83.
15. Andrews JR, Whiteside JA, Buettner CM. Clinical evaluation of the elbow in throwers. Oper Tech Sports Med. 1996;4(2):77-83.
16. Calfee RP, Manske PR, Gelberman RH, Van Steyn MO, Steffen J, Goldfarb CA. Clinical assessment of the ulnar nerve at the elbow: reliability of instability testing and the association of hypermobility with clinical symptoms. J Bone Joint Surg Am. 2010;92(17):2801-2808.
17. Spinner RJ, Goldner RD. Snapping of the medial head of the triceps and recurrent dislocation of the ulnar nerve. Anatomical and dynamic factors. J Bone Joint Surg Am. 1998;80(2):239-247.
18. Guerra JJ, Timmerman LA. Clinical anatomy, histology, & pathomechanics of the elbow in sports. Oper Tech Sports Med. 1996;4(2):69-76.
19. O’Driscoll SW, Horii E, Carmichael SW, Morrey BF. The cubital tunnel and ulnar neuropathy. J Bone Joint Surg Br. 1991;73(4):613-617.
20. Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg Am. 1994;19(5):817-820.
21. Andrews JR. Bony injuries about the elbow in the throwing athlete. Instr Course Lect. 1985;34:323-331.
22. Kim DH, Gambardella RA, Elattrache NS, Yocum LA, Jobe FW. Arthroscopic treatment of posterolateral elbow impingement from lateral synovial plicae in throwing athletes and golfers. Am J Sports Med. 2006;34(3):438-444.
23. Antuna SA, O’Driscoll SW. Snapping plicae associated with radiocapitellar chondromalacia. Arthroscopy. 2001;17(5):491-495.
24. Bernstein AD, Breslow MJ, Jazrawi LM. Distal biceps tendon ruptures: a historical perspective and current concepts. Am J Orthop. 2001;30(3):
193-200.
25. O’Driscoll SW, Goncalves LB, Dietz P. The hook test for distal biceps tendon avulsion. Am J Sports Med. 2007;35(11):1865-1869.
Understanding the pathomechanics of throwing and the accompanying elbow injuries is the groundwork for conducting a directed history taking and a physical examination that produce an accurate diagnosis of elbow injuries in throwing athletes. Advances in physical examination techniques have improved our ability to accurately diagnose and treat throwers’ athletic elbow disorders.
Throwing imposes an extremely high valgus stress (approaching 60-65 Nm) across the elbow. This high stress occurs during the cocking and acceleration phases of the overhead throwing motion.1-3 The valgus stress generates tension on the medial elbow, compression on the lateral elbow, and shear on the posterior aspect of the elbow. These forces cause predictable injury patterns in different parts of throwers’ elbows. Physical examination performed in a systematic anatomical fashion can enhance predictable and accurate elbow injury diagnosis. In this article, we outline 5 points in a systematic approach to physical examination of a throwing athlete’s elbow.
1. Perform a general upper extremity examination
Cervical spine and shoulder girdle
In the initial examination, the cervical spine and the entire affected upper extremity should be quickly assessed. Assessment of the cervical spine should include palpation, range of motion (ROM), and basic provocative testing, such as the Spurling test, to evaluate for radiculopathy caused by foraminal compression. Posture, asymmetry, atrophy, edema, ecchymosis, and any other deformity should be noted. For example, atrophy of the neck and shoulders suggests underlying neuropathy. In addition, fullness of the supraclavicular region and local tenderness or bruit suggest vasculopathy. Symptomatic compression of the subclavian artery and vein between the anterior and middle scalene muscles may present as weakness, fullness, heaviness, and early fatigue. Physical signs include coolness, pallor, claudication, engorgement, and edema in the arm.4 Thoracic outlet syndrome can manifest as effort-induced vague pain at the arm and elbow.5 If this syndrome is suspected, an Adson test should be performed. With the patient’s neck extended and rotated away from the affected side, the examiner, standing next to the patient, palpates the radial pulse with the patient’s elbow extended (Figure 1A). Next, the examiner abducts, extends, and externally rotates the patient’s shoulder (Figure 1B) while the patient alternates between opening and closing the fist (Figure 1C). A decrease or absence in pulse strength from the starting position is a positive test result.
Last, the shoulder and scapulae should be assessed, as an affected shoulder or dyskinetic scapula can lead to improper mechanics of the kinetic chain at the elbow. The shoulder should be palpated, and ROM, strength, and stability should be assessed. Glenohumeral internal rotation deficit is associated with medial collateral ligament (MCL) tears; if present, this deficit should be addressed.6
Elbow
Inspection should reveal a normal carrying angle of about 11° to 14° of valgus in men and 13° to 16° in women. In immature athletes, increased valgus stresses from repetitive overhead throwing can cause medial epicondylar hypertrophy, and carrying angles of more than 15° are common.7-9
Active and passive ROM should be assessed. Normal ROM is about 0° extension and 140° flexion with 80° of supination and pronation. For determination of pathologic differences, ROM should always be compared between the affected and the contralateral sides. Painful loss of motion may be caused by soft-tissue swelling or contracture, effusion, bony impingement, or loose bodies. Crepitus, locking, catching, or another mechanical symptom may indicate loose bodies or chondral injury. Firm, mechanical blocks to ROM during flexion may indicate osteophyte formation in the coronoid fossa, and mechanical blocks to ROM during extension may indicate osteophyte formation in the olecranon fossa. Pain elicited at the end points of motion is caused by osteophytes and impingement, whereas pain elicited during the mid-arc of motion is often caused by osteochondral lesions. Terminal extension, often the first motion lost after injury, may signal intra-articular pathology, if symptomatic. However, throwing athletes may present with developmental flexion contractures of up to 20°.10
2. Examine the medial aspect of the elbow
The medial epicondyle, easy to recognize as a bony prominence on the medial side of the distal humerus, serves as an attachment site for the MCL, pronator teres, and the common flexor tendon. In throwers, assessing the MCL is crucial. The MCL should be palpated from its origin on the inferior aspect of the medial epicondyle moving distally to the sublime tubercle of the proximal ulna. Tenderness at any point along the ligament can indicate a range of ligament pathology, from attenuation to complete rupture.
The MCL is further assessed with stress tests, most commonly the valgus stress test, the milking maneuver, and the moving valgus stress test. Of these 3 procedures, the moving valgus stress test is perhaps the most sensitive and specific for MCL injury, and is the test preferred by the authors.11 This test takes into account shoulder position, simulates the position of throwing, and can account for bony structures that provide stability at more than 120° of flexion. We prefer to position the patient supine on the examining table to help stabilize the shoulder and humerus and to relax the patient. The shoulder is placed in abduction and external rotation while the examiner holds the thumb with one hand and supports the elbow with the other. The elbow is extended (Figure 2A) and flexed (Figure 2B) while valgus stress is applied. A positive test elicits pain localized to the MCL at the arc of motion between 80° to 120°.12 Pain at positions near full extension with the moving valgus stress test may also indicate chondral damage at the posteromedial trochlea.13
During pitching, the tensile demand on the MCL is reduced by the action of the flexor-pronator mass. It is common to see a flexor-pronator mass injury concurrent with MCL injury.14 Medial epicondyle tenderness that increases with resisted wrist flexion may signal flexor-pronator injury, though, classically, flexor-pronator muscle strains and tears produce pain anterior and distal to the medial epicondyle.15
Traction, compression, and friction at the medial elbow can irritate the ulnar nerve. This nerve should be inspected and palpated along its course at the cubital tunnel to determine its location and stability. Ulnar nerve hypermobility, which has been identified in 37% of elbows, can be determined by having the patient actively flex the elbow with the forearm in supination, placing a finger at the posteromedial aspect of the medial humeral epicondyle, and having the patient actively extend the elbow.16 The nerve dislocates if trapped anterior to the examiner’s finger, perches if under the examiner’s finger, or is stable if still palpable in the groove posterior to the medial epicondyle.16
The distal band of the medial triceps tendon may also sublux over the medial epicondyle with elbow flexion. This subluxation, also known as snapping triceps syndrome, may cause pain or ulnar nerve symptoms.17 Bringing the elbow from extension to flexion may produce subluxation, first of the ulnar nerve and then of the medial triceps, in 2 separate “snaps.” Tenderness can be elicited along the medial triceps muscle.
Ulnar neuritis is caused by traction injury, such as with dynamic pitching, nerve subluxation, or compression at the cubital tunnel. With MCL injury and valgus instability, the ulnar nerve can become irritated as it becomes stretched because of medial elbow laxity.18 The nerve can also be damaged during flexion as the cubital tunnel retinaculum tightens, decreasing the space available for the nerve.19 This concept is applied during the elbow flexion compression test. A positive test may elicit tingling radiating toward the small finger or pain at the elbow or medial forearm when manual pressure is directly applied over the ulnar nerve between the posteromedial olecranon and the medial humeral epicondyle as the elbow is maximally flexed.20
3. Examine the lateral aspect of the elbow
Palpation of the lateral epicondyle, the radial head, and the olecranon tip assists in defining injury to the underlying anatomy. The anconeus “soft spot” (infracondylar recess) within the triangle formed by these 3 bony landmarks should be palpated for fullness, indicating a joint effusion, hemarthrosis, or even a subluxed or dislocated radial head.
While the medial elbow endures a large tensile load, throwing imposes a tremendous compressive force at the lateral elbow, particularly at the radiocapitellar joint. This joint may be tender and produce clicking with pronation and supination in patients with radiocapitellar arthrosis, symptomatic posterolateral synovial plica, or an inflamed radial bursa. Tenderness with crepitus that can be exacerbated with forceful flexion and extension may indicate radiocapitellar overload or loose bodies.
Long-term load transmission and subsequent degeneration of the articular surface may advance to osteochondritis dissecans (OCD). Examination for capitellar OCD reveals tenderness over the radiocapitellar joint and commonly a loss of 15° to 20° of extension. The active radiocapitellar compression test is positive for OCD lesions and elicits pain in the lateral compartment of the elbow when the patient pronates (Figure 3A) and supinates (Figure 3B) the forearm with the elbow axially loaded in extension.21
Microtrauma and inflammation may occur with repetitive eccentric overload. Although rare in throwing athletes, “tennis elbow” causes pain with gripping, and decreased grip strength. Tenderness caused by lateral epicondylitis is just anterior and distal to the epicondyle, at the origin of the extensor carpi radialis brevis. Pain is reproducible with passive wrist flexion and resisted wrist extension with the elbow extended (Cozen test).
Less commonly, athletes may complain of mechanical symptoms, such as snapping or catching with posterolateral elbow pain.22 These symptoms may be due to thickened or inflamed synovial plica causing impingement. A posterior radiocapitellar plica can be examined by bringing the elbow to full extension while applying valgus stress with the forearm in supination. Conversely, an anterior radiocapitellar plica can be examined with a valgus load on the elbow and passive flexion with the forearm in pronation.23 A palpable painful snap over the radiocapitellar joint is a positive test.
4. Examine the posterior aspect of the elbow
Posteriorly, palpation is focused on the triceps tendon and the olecranon tip. The elbow should be flexed to 30° to relax the triceps, isolate the olecranon, and allow for palpation of the olecranon fossa on either side of the triceps tendon. Tenderness at the posterolateral or posteromedial aspect of the olecranon should be noted. Warmth, fluctuance, or distension at the elbow may be caused by olecranon bursitis. The 3 heads of the triceps muscle should be palpated where they converge to form an aponeurosis, and tenderness or a palpable gap on any of the heads should be noted.
A combination of valgus force and a rapidly decelerating arm at the follow-through phase of pitching causes a shear force between the medial aspect of the olecranon tip and the olecranon fossa. This shear force can result in chondrolysis, osteophyte formation, and loose bodies, particularly in the posteromedial elbow. This valgus extension overload (VEO) syndrome often results in loss of full extension and symptoms, which may be attributed to osteophytes or fractured and nonunited fragments in the olecranon fossa or the olecranon tip. Frank crepitus may also be present with extension testing caused by loose bodies or synovial reaction over osteophytes. Assessing for VEO using the extension impingement test, the examiner places continuous valgus stress on the elbow while quickly extending from 20° to 30° of flexion (Figure 4A) to terminal extension (Figure 4B) repeatedly. The examiner repeats this without valgus load while palpating the posteromedial olecranon for tenderness to differentiate impingement caused by instability from pain over the medial olecranon without instability (Figure 4C). Particular attention should be focused posteriorly in athletes with medial instability, as MCL injuries and VEO syndrome often occur in conjunction in the throwing athlete.
Repetitive acceleration and deceleration of the arm can also cause stress fractures. With stress fractures, pain is often noted more distal and lateral on the olecranon, but tenderness may be palpable medially from posteromedial impaction that occurs from the valgus load during the overhead throwing motion. In immature athletes, the repetitive sudden snap of full extension in the deceleration phase of throwing can cause olecranon apophysitis. Frank avulsions can occur as well but are usually preceded by chronic posterior elbow pain with possible loss of full extension.
The late cocking phase of the throwing motion (just before throwing) hyperextends the elbow and places significant strain on the elbow. Repetitive strain can cause painful posterior impingement. The arm bar test is extremely sensitive (Figure 5).13 With the patient’s elbow extended, shoulder internally rotated, and hand on the examiner’s shoulder, the examiner pulls down on the olecranon to simulate forced extension and reproduces the pain associated with posteromedial impingement.
Last, though triceps tendon injuries are rare, ruptures most often occur at the origin of the lateral head of the triceps. As the initial swelling and ecchymosis subside, a palpable gap is pathognomonic for rupture. Extensor weakness can often be observed, but extension may still be possible from anconeus triceps expansion with the aid of gravity. With the elbow overhead, the athlete must extend the elbow against gravity and will exhibit weakness against resistance.
5. Examine the anterior aspect of the elbow
Anteriorly, the bulk of the flexor-pronator group restricts the extent of joint palpation, and the soft tissues are usually injured. The antecubital fossa is a triangular area on the anterior aspect of the elbow that is bounded superiorly by a horizontal line connecting the medial epicondyle to the lateral epicondyle of the humerus, medially by the lateral border of the pronator teres muscle and laterally by the medial border of the brachioradialis muscle. From lateral to medial, the antecubital fossa contains the radial nerve, the biceps brachii tendon, the brachial artery, and the median nerve. Evaluating this area is important because a visible defect, change in muscle contour, or proximal retraction of a muscle belly can indicate a muscular rupture. In particular, a distal biceps rupture (rare) may be accompanied by weakness and pain in supination and, to a lesser degree, in flexion. It is important to note that, in the case of a partial biceps rupture, ecchymosis may not appear, as the hematoma is confined by the intact lacertus fibrosis.24 The hook test can be used to evaluate for the presence of an intact distal biceps tendon (Figure 6).25 The patient abducts the shoulder, flexes the elbow to 90°, and actively supinates the forearm while the examiner attempts to hook an index finger laterally under the tendon. The test is negative if the finger can be inserted 1 cm under the tendon and positive if no cordlike structure can be hooked. Partial biceps tendon ruptures or tendinitis may exhibit tenderness of the distal biceps tendon and pain on resisted supination with a negative hook test. Often, resisted elbow flexion with the elbow at maximal extension elicits pain at the biceps insertion. Clicking with forearm rotation near the insertion of the tendon, which may be caused by an inflamed radial bursa between the distal biceps tendon and the radial tuberosity, may be associated with impending rupture.
Conclusion
Physical examination combined with thorough history taking usually provides a solid basis for a diagnosis, which in turn makes the value of surgical treatment more assured.
Understanding the pathomechanics of throwing and the accompanying elbow injuries is the groundwork for conducting a directed history taking and a physical examination that produce an accurate diagnosis of elbow injuries in throwing athletes. Advances in physical examination techniques have improved our ability to accurately diagnose and treat throwers’ athletic elbow disorders.
Throwing imposes an extremely high valgus stress (approaching 60-65 Nm) across the elbow. This high stress occurs during the cocking and acceleration phases of the overhead throwing motion.1-3 The valgus stress generates tension on the medial elbow, compression on the lateral elbow, and shear on the posterior aspect of the elbow. These forces cause predictable injury patterns in different parts of throwers’ elbows. Physical examination performed in a systematic anatomical fashion can enhance predictable and accurate elbow injury diagnosis. In this article, we outline 5 points in a systematic approach to physical examination of a throwing athlete’s elbow.
1. Perform a general upper extremity examination
Cervical spine and shoulder girdle
In the initial examination, the cervical spine and the entire affected upper extremity should be quickly assessed. Assessment of the cervical spine should include palpation, range of motion (ROM), and basic provocative testing, such as the Spurling test, to evaluate for radiculopathy caused by foraminal compression. Posture, asymmetry, atrophy, edema, ecchymosis, and any other deformity should be noted. For example, atrophy of the neck and shoulders suggests underlying neuropathy. In addition, fullness of the supraclavicular region and local tenderness or bruit suggest vasculopathy. Symptomatic compression of the subclavian artery and vein between the anterior and middle scalene muscles may present as weakness, fullness, heaviness, and early fatigue. Physical signs include coolness, pallor, claudication, engorgement, and edema in the arm.4 Thoracic outlet syndrome can manifest as effort-induced vague pain at the arm and elbow.5 If this syndrome is suspected, an Adson test should be performed. With the patient’s neck extended and rotated away from the affected side, the examiner, standing next to the patient, palpates the radial pulse with the patient’s elbow extended (Figure 1A). Next, the examiner abducts, extends, and externally rotates the patient’s shoulder (Figure 1B) while the patient alternates between opening and closing the fist (Figure 1C). A decrease or absence in pulse strength from the starting position is a positive test result.
Last, the shoulder and scapulae should be assessed, as an affected shoulder or dyskinetic scapula can lead to improper mechanics of the kinetic chain at the elbow. The shoulder should be palpated, and ROM, strength, and stability should be assessed. Glenohumeral internal rotation deficit is associated with medial collateral ligament (MCL) tears; if present, this deficit should be addressed.6
Elbow
Inspection should reveal a normal carrying angle of about 11° to 14° of valgus in men and 13° to 16° in women. In immature athletes, increased valgus stresses from repetitive overhead throwing can cause medial epicondylar hypertrophy, and carrying angles of more than 15° are common.7-9
Active and passive ROM should be assessed. Normal ROM is about 0° extension and 140° flexion with 80° of supination and pronation. For determination of pathologic differences, ROM should always be compared between the affected and the contralateral sides. Painful loss of motion may be caused by soft-tissue swelling or contracture, effusion, bony impingement, or loose bodies. Crepitus, locking, catching, or another mechanical symptom may indicate loose bodies or chondral injury. Firm, mechanical blocks to ROM during flexion may indicate osteophyte formation in the coronoid fossa, and mechanical blocks to ROM during extension may indicate osteophyte formation in the olecranon fossa. Pain elicited at the end points of motion is caused by osteophytes and impingement, whereas pain elicited during the mid-arc of motion is often caused by osteochondral lesions. Terminal extension, often the first motion lost after injury, may signal intra-articular pathology, if symptomatic. However, throwing athletes may present with developmental flexion contractures of up to 20°.10
2. Examine the medial aspect of the elbow
The medial epicondyle, easy to recognize as a bony prominence on the medial side of the distal humerus, serves as an attachment site for the MCL, pronator teres, and the common flexor tendon. In throwers, assessing the MCL is crucial. The MCL should be palpated from its origin on the inferior aspect of the medial epicondyle moving distally to the sublime tubercle of the proximal ulna. Tenderness at any point along the ligament can indicate a range of ligament pathology, from attenuation to complete rupture.
The MCL is further assessed with stress tests, most commonly the valgus stress test, the milking maneuver, and the moving valgus stress test. Of these 3 procedures, the moving valgus stress test is perhaps the most sensitive and specific for MCL injury, and is the test preferred by the authors.11 This test takes into account shoulder position, simulates the position of throwing, and can account for bony structures that provide stability at more than 120° of flexion. We prefer to position the patient supine on the examining table to help stabilize the shoulder and humerus and to relax the patient. The shoulder is placed in abduction and external rotation while the examiner holds the thumb with one hand and supports the elbow with the other. The elbow is extended (Figure 2A) and flexed (Figure 2B) while valgus stress is applied. A positive test elicits pain localized to the MCL at the arc of motion between 80° to 120°.12 Pain at positions near full extension with the moving valgus stress test may also indicate chondral damage at the posteromedial trochlea.13
During pitching, the tensile demand on the MCL is reduced by the action of the flexor-pronator mass. It is common to see a flexor-pronator mass injury concurrent with MCL injury.14 Medial epicondyle tenderness that increases with resisted wrist flexion may signal flexor-pronator injury, though, classically, flexor-pronator muscle strains and tears produce pain anterior and distal to the medial epicondyle.15
Traction, compression, and friction at the medial elbow can irritate the ulnar nerve. This nerve should be inspected and palpated along its course at the cubital tunnel to determine its location and stability. Ulnar nerve hypermobility, which has been identified in 37% of elbows, can be determined by having the patient actively flex the elbow with the forearm in supination, placing a finger at the posteromedial aspect of the medial humeral epicondyle, and having the patient actively extend the elbow.16 The nerve dislocates if trapped anterior to the examiner’s finger, perches if under the examiner’s finger, or is stable if still palpable in the groove posterior to the medial epicondyle.16
The distal band of the medial triceps tendon may also sublux over the medial epicondyle with elbow flexion. This subluxation, also known as snapping triceps syndrome, may cause pain or ulnar nerve symptoms.17 Bringing the elbow from extension to flexion may produce subluxation, first of the ulnar nerve and then of the medial triceps, in 2 separate “snaps.” Tenderness can be elicited along the medial triceps muscle.
Ulnar neuritis is caused by traction injury, such as with dynamic pitching, nerve subluxation, or compression at the cubital tunnel. With MCL injury and valgus instability, the ulnar nerve can become irritated as it becomes stretched because of medial elbow laxity.18 The nerve can also be damaged during flexion as the cubital tunnel retinaculum tightens, decreasing the space available for the nerve.19 This concept is applied during the elbow flexion compression test. A positive test may elicit tingling radiating toward the small finger or pain at the elbow or medial forearm when manual pressure is directly applied over the ulnar nerve between the posteromedial olecranon and the medial humeral epicondyle as the elbow is maximally flexed.20
3. Examine the lateral aspect of the elbow
Palpation of the lateral epicondyle, the radial head, and the olecranon tip assists in defining injury to the underlying anatomy. The anconeus “soft spot” (infracondylar recess) within the triangle formed by these 3 bony landmarks should be palpated for fullness, indicating a joint effusion, hemarthrosis, or even a subluxed or dislocated radial head.
While the medial elbow endures a large tensile load, throwing imposes a tremendous compressive force at the lateral elbow, particularly at the radiocapitellar joint. This joint may be tender and produce clicking with pronation and supination in patients with radiocapitellar arthrosis, symptomatic posterolateral synovial plica, or an inflamed radial bursa. Tenderness with crepitus that can be exacerbated with forceful flexion and extension may indicate radiocapitellar overload or loose bodies.
Long-term load transmission and subsequent degeneration of the articular surface may advance to osteochondritis dissecans (OCD). Examination for capitellar OCD reveals tenderness over the radiocapitellar joint and commonly a loss of 15° to 20° of extension. The active radiocapitellar compression test is positive for OCD lesions and elicits pain in the lateral compartment of the elbow when the patient pronates (Figure 3A) and supinates (Figure 3B) the forearm with the elbow axially loaded in extension.21
Microtrauma and inflammation may occur with repetitive eccentric overload. Although rare in throwing athletes, “tennis elbow” causes pain with gripping, and decreased grip strength. Tenderness caused by lateral epicondylitis is just anterior and distal to the epicondyle, at the origin of the extensor carpi radialis brevis. Pain is reproducible with passive wrist flexion and resisted wrist extension with the elbow extended (Cozen test).
Less commonly, athletes may complain of mechanical symptoms, such as snapping or catching with posterolateral elbow pain.22 These symptoms may be due to thickened or inflamed synovial plica causing impingement. A posterior radiocapitellar plica can be examined by bringing the elbow to full extension while applying valgus stress with the forearm in supination. Conversely, an anterior radiocapitellar plica can be examined with a valgus load on the elbow and passive flexion with the forearm in pronation.23 A palpable painful snap over the radiocapitellar joint is a positive test.
4. Examine the posterior aspect of the elbow
Posteriorly, palpation is focused on the triceps tendon and the olecranon tip. The elbow should be flexed to 30° to relax the triceps, isolate the olecranon, and allow for palpation of the olecranon fossa on either side of the triceps tendon. Tenderness at the posterolateral or posteromedial aspect of the olecranon should be noted. Warmth, fluctuance, or distension at the elbow may be caused by olecranon bursitis. The 3 heads of the triceps muscle should be palpated where they converge to form an aponeurosis, and tenderness or a palpable gap on any of the heads should be noted.
A combination of valgus force and a rapidly decelerating arm at the follow-through phase of pitching causes a shear force between the medial aspect of the olecranon tip and the olecranon fossa. This shear force can result in chondrolysis, osteophyte formation, and loose bodies, particularly in the posteromedial elbow. This valgus extension overload (VEO) syndrome often results in loss of full extension and symptoms, which may be attributed to osteophytes or fractured and nonunited fragments in the olecranon fossa or the olecranon tip. Frank crepitus may also be present with extension testing caused by loose bodies or synovial reaction over osteophytes. Assessing for VEO using the extension impingement test, the examiner places continuous valgus stress on the elbow while quickly extending from 20° to 30° of flexion (Figure 4A) to terminal extension (Figure 4B) repeatedly. The examiner repeats this without valgus load while palpating the posteromedial olecranon for tenderness to differentiate impingement caused by instability from pain over the medial olecranon without instability (Figure 4C). Particular attention should be focused posteriorly in athletes with medial instability, as MCL injuries and VEO syndrome often occur in conjunction in the throwing athlete.
Repetitive acceleration and deceleration of the arm can also cause stress fractures. With stress fractures, pain is often noted more distal and lateral on the olecranon, but tenderness may be palpable medially from posteromedial impaction that occurs from the valgus load during the overhead throwing motion. In immature athletes, the repetitive sudden snap of full extension in the deceleration phase of throwing can cause olecranon apophysitis. Frank avulsions can occur as well but are usually preceded by chronic posterior elbow pain with possible loss of full extension.
The late cocking phase of the throwing motion (just before throwing) hyperextends the elbow and places significant strain on the elbow. Repetitive strain can cause painful posterior impingement. The arm bar test is extremely sensitive (Figure 5).13 With the patient’s elbow extended, shoulder internally rotated, and hand on the examiner’s shoulder, the examiner pulls down on the olecranon to simulate forced extension and reproduces the pain associated with posteromedial impingement.
Last, though triceps tendon injuries are rare, ruptures most often occur at the origin of the lateral head of the triceps. As the initial swelling and ecchymosis subside, a palpable gap is pathognomonic for rupture. Extensor weakness can often be observed, but extension may still be possible from anconeus triceps expansion with the aid of gravity. With the elbow overhead, the athlete must extend the elbow against gravity and will exhibit weakness against resistance.
5. Examine the anterior aspect of the elbow
Anteriorly, the bulk of the flexor-pronator group restricts the extent of joint palpation, and the soft tissues are usually injured. The antecubital fossa is a triangular area on the anterior aspect of the elbow that is bounded superiorly by a horizontal line connecting the medial epicondyle to the lateral epicondyle of the humerus, medially by the lateral border of the pronator teres muscle and laterally by the medial border of the brachioradialis muscle. From lateral to medial, the antecubital fossa contains the radial nerve, the biceps brachii tendon, the brachial artery, and the median nerve. Evaluating this area is important because a visible defect, change in muscle contour, or proximal retraction of a muscle belly can indicate a muscular rupture. In particular, a distal biceps rupture (rare) may be accompanied by weakness and pain in supination and, to a lesser degree, in flexion. It is important to note that, in the case of a partial biceps rupture, ecchymosis may not appear, as the hematoma is confined by the intact lacertus fibrosis.24 The hook test can be used to evaluate for the presence of an intact distal biceps tendon (Figure 6).25 The patient abducts the shoulder, flexes the elbow to 90°, and actively supinates the forearm while the examiner attempts to hook an index finger laterally under the tendon. The test is negative if the finger can be inserted 1 cm under the tendon and positive if no cordlike structure can be hooked. Partial biceps tendon ruptures or tendinitis may exhibit tenderness of the distal biceps tendon and pain on resisted supination with a negative hook test. Often, resisted elbow flexion with the elbow at maximal extension elicits pain at the biceps insertion. Clicking with forearm rotation near the insertion of the tendon, which may be caused by an inflamed radial bursa between the distal biceps tendon and the radial tuberosity, may be associated with impending rupture.
Conclusion
Physical examination combined with thorough history taking usually provides a solid basis for a diagnosis, which in turn makes the value of surgical treatment more assured.
1. Elliott B, Fleisig G, Nicholls R, Escamilia R. Technique effects on upper limb loading in the tennis serve. J Sci Med Sport. 2003;6(1):76-87.
2. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23(2):233-239.
3. Werner SL, Fleisig GS, Dillman CJ, Andrews JR. Biomechanics of the elbow during baseball pitching. J Orthop Sports Phys Ther. 1993;17(6):274-278.
4. Aval SM, Durand P Jr, Shankwiler JA. Neurovascular injuries to the athlete’s shoulder: part II. J Am Acad Orthop Surg. 2007;15(5):281-289.
5. Strukel RJ, Garrick JG. Thoracic outlet compression in athletes: a report of four cases. Am J Sports Med. 1978;6(2):35-39.
6. Dines JS, Frank JB, Akerman M, Yocum LA. Glenohumeral internal rotation deficits in baseball players with ulnar collateral ligament insufficiency. Am J Sports Med. 2009;37(3):566-570.
7. Adams JE. Injury to the throwing arm. A study of traumatic changes in the elbow joints of boy baseball players. Calif Med. 1965;102:127-132.
8. Hang DW, Chao CM, Hang YS. A clinical and roentgenographic study of Little League elbow. Am J Sports Med. 2004;32(1):79-84.
9. King JW, Brelsford HJ, Tullos HS. Analysis of the pitching arm of the professional baseball pitcher. Clin Orthop. 1969;(67):116-123.
10. Cain EL Jr, Dugas JR, Wolf RS, Andrews JR. Elbow injuries in throwing athletes: a current concepts review. Am J Sports Med. 2003;31(4):621-635.
11. Safran M, Ahmad CS, Elattrache NS. Ulnar collateral ligament of the elbow. Arthroscopy. 2005;21(11):1381-1395.
12. O’Driscoll SW, Lawton RL, Smith AM. The “moving valgus stress test” for medial collateral ligament tears of the elbow. Am J Sports Med. 2005;33(2):231-239.
13. O’Driscoll SW. Valgus extension overload and plica. In: Levine WN, ed. The Athlete’s Elbow. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:71-83.
14. Conway JE, Jobe FW, Glousman RE, Pink M. Medial instability of the elbow in throwing athletes. Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am. 1992;74(1):67-83.
15. Andrews JR, Whiteside JA, Buettner CM. Clinical evaluation of the elbow in throwers. Oper Tech Sports Med. 1996;4(2):77-83.
16. Calfee RP, Manske PR, Gelberman RH, Van Steyn MO, Steffen J, Goldfarb CA. Clinical assessment of the ulnar nerve at the elbow: reliability of instability testing and the association of hypermobility with clinical symptoms. J Bone Joint Surg Am. 2010;92(17):2801-2808.
17. Spinner RJ, Goldner RD. Snapping of the medial head of the triceps and recurrent dislocation of the ulnar nerve. Anatomical and dynamic factors. J Bone Joint Surg Am. 1998;80(2):239-247.
18. Guerra JJ, Timmerman LA. Clinical anatomy, histology, & pathomechanics of the elbow in sports. Oper Tech Sports Med. 1996;4(2):69-76.
19. O’Driscoll SW, Horii E, Carmichael SW, Morrey BF. The cubital tunnel and ulnar neuropathy. J Bone Joint Surg Br. 1991;73(4):613-617.
20. Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg Am. 1994;19(5):817-820.
21. Andrews JR. Bony injuries about the elbow in the throwing athlete. Instr Course Lect. 1985;34:323-331.
22. Kim DH, Gambardella RA, Elattrache NS, Yocum LA, Jobe FW. Arthroscopic treatment of posterolateral elbow impingement from lateral synovial plicae in throwing athletes and golfers. Am J Sports Med. 2006;34(3):438-444.
23. Antuna SA, O’Driscoll SW. Snapping plicae associated with radiocapitellar chondromalacia. Arthroscopy. 2001;17(5):491-495.
24. Bernstein AD, Breslow MJ, Jazrawi LM. Distal biceps tendon ruptures: a historical perspective and current concepts. Am J Orthop. 2001;30(3):
193-200.
25. O’Driscoll SW, Goncalves LB, Dietz P. The hook test for distal biceps tendon avulsion. Am J Sports Med. 2007;35(11):1865-1869.
1. Elliott B, Fleisig G, Nicholls R, Escamilia R. Technique effects on upper limb loading in the tennis serve. J Sci Med Sport. 2003;6(1):76-87.
2. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23(2):233-239.
3. Werner SL, Fleisig GS, Dillman CJ, Andrews JR. Biomechanics of the elbow during baseball pitching. J Orthop Sports Phys Ther. 1993;17(6):274-278.
4. Aval SM, Durand P Jr, Shankwiler JA. Neurovascular injuries to the athlete’s shoulder: part II. J Am Acad Orthop Surg. 2007;15(5):281-289.
5. Strukel RJ, Garrick JG. Thoracic outlet compression in athletes: a report of four cases. Am J Sports Med. 1978;6(2):35-39.
6. Dines JS, Frank JB, Akerman M, Yocum LA. Glenohumeral internal rotation deficits in baseball players with ulnar collateral ligament insufficiency. Am J Sports Med. 2009;37(3):566-570.
7. Adams JE. Injury to the throwing arm. A study of traumatic changes in the elbow joints of boy baseball players. Calif Med. 1965;102:127-132.
8. Hang DW, Chao CM, Hang YS. A clinical and roentgenographic study of Little League elbow. Am J Sports Med. 2004;32(1):79-84.
9. King JW, Brelsford HJ, Tullos HS. Analysis of the pitching arm of the professional baseball pitcher. Clin Orthop. 1969;(67):116-123.
10. Cain EL Jr, Dugas JR, Wolf RS, Andrews JR. Elbow injuries in throwing athletes: a current concepts review. Am J Sports Med. 2003;31(4):621-635.
11. Safran M, Ahmad CS, Elattrache NS. Ulnar collateral ligament of the elbow. Arthroscopy. 2005;21(11):1381-1395.
12. O’Driscoll SW, Lawton RL, Smith AM. The “moving valgus stress test” for medial collateral ligament tears of the elbow. Am J Sports Med. 2005;33(2):231-239.
13. O’Driscoll SW. Valgus extension overload and plica. In: Levine WN, ed. The Athlete’s Elbow. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:71-83.
14. Conway JE, Jobe FW, Glousman RE, Pink M. Medial instability of the elbow in throwing athletes. Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am. 1992;74(1):67-83.
15. Andrews JR, Whiteside JA, Buettner CM. Clinical evaluation of the elbow in throwers. Oper Tech Sports Med. 1996;4(2):77-83.
16. Calfee RP, Manske PR, Gelberman RH, Van Steyn MO, Steffen J, Goldfarb CA. Clinical assessment of the ulnar nerve at the elbow: reliability of instability testing and the association of hypermobility with clinical symptoms. J Bone Joint Surg Am. 2010;92(17):2801-2808.
17. Spinner RJ, Goldner RD. Snapping of the medial head of the triceps and recurrent dislocation of the ulnar nerve. Anatomical and dynamic factors. J Bone Joint Surg Am. 1998;80(2):239-247.
18. Guerra JJ, Timmerman LA. Clinical anatomy, histology, & pathomechanics of the elbow in sports. Oper Tech Sports Med. 1996;4(2):69-76.
19. O’Driscoll SW, Horii E, Carmichael SW, Morrey BF. The cubital tunnel and ulnar neuropathy. J Bone Joint Surg Br. 1991;73(4):613-617.
20. Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg Am. 1994;19(5):817-820.
21. Andrews JR. Bony injuries about the elbow in the throwing athlete. Instr Course Lect. 1985;34:323-331.
22. Kim DH, Gambardella RA, Elattrache NS, Yocum LA, Jobe FW. Arthroscopic treatment of posterolateral elbow impingement from lateral synovial plicae in throwing athletes and golfers. Am J Sports Med. 2006;34(3):438-444.
23. Antuna SA, O’Driscoll SW. Snapping plicae associated with radiocapitellar chondromalacia. Arthroscopy. 2001;17(5):491-495.
24. Bernstein AD, Breslow MJ, Jazrawi LM. Distal biceps tendon ruptures: a historical perspective and current concepts. Am J Orthop. 2001;30(3):
193-200.
25. O’Driscoll SW, Goncalves LB, Dietz P. The hook test for distal biceps tendon avulsion. Am J Sports Med. 2007;35(11):1865-1869.

Mutual Alignment Trumps Merger for Joint VA/DoD Health Care Programs
The VA and the DoD operate completely independent health care systems. Integrated provision of health care for the populations served is a compellingly attractive goal given the obvious overlaps, but has proven deceptively difficult to implement.
Despite efforts begun in 1998 to accomplish a reliable, comprehensive, bidirectional exchange of patient-specific health care information between systems, 16 years later this has yet to be reliably available. In most locales, VHA practitioners cannot easily access details of the medical care provided to DoD personnel. Attempts to merge the 2 electronic medical record (EMR) systems have also been fraught with difficulty.1 Even at the new, joint VHA/DoD Captain James A. Lovell Federal Health Care Center in North Chicago, Illinois (which opened in October 2010 to serve a mix of active-duty servicemen, TRICARE beneficiaries, and VA enrollees under a single roof), care using a single EMR system has not been possible.
The Institute of Medicine, in an invited review, has specifically criticized the unsatisfactory, piecemeal EMR integration.2 On February 5, 2013, the Secretary of the VA and the Secretary of Defense formally abandoned efforts to construct a single VA/DoD integrated EMR system by 2017. Instead, both organizations would, in then Secretary of Defense Leon Panetta’s words, “…focus our immediate efforts on integrating VA and DoD health data as quickly as possible, by focusing on interoperability and using existing solutions.”3
Joint VA/DoD health care programs in Northern California have abandoned merged structures in favor of mutual alignment. The practical value of aligning care systems is to extract benefit from structured, economically rational, win-win collaborations, as opposed to the forced merger approach. Mutual alignment generates relatively prompt, reliable results, to the benefit of all concerned.
Related: Developing Joint VA and DoD Health Programs
This report details a consistently favorable experience with this philosophy, which has considerable relevance as federal and nonfederal systems explore future joint ventures. Specifically, this report describes the substantial multiyear savings from a combination of various DoD/VA Joint Incentive Fund (JIF) and Sharing Agreement projects conducted by the VA Northern California Health Care System (VANCHCS) and the U.S. Air Force (USAF) 60th Medical Group’s (60MDG’s) David Grant Medical Center (DGMC).
Background and Methods
VA Northern California Health Care System currently serves 92,000 unique veteran patients in a service area of 40,000 square miles through a network of facilities and clinics at 9 sites across northern California. Rapid year-over-year growth of VANCHCS continues, and in fiscal year (FY) 2013, so-called unique enrolled veterans increased by 4.7%. David Grant Medical Center is a 116-bed DoD flagship hospital at Travis Air Force Base in Fairfield, California, which is home to the 60MDG. In 2013, VANCHCS and DGMC celebrated the 20th year of collaborative projects.
Congressional mandates encompassed in sections 101, 1701, 1782, 1783, and 8111 of Title 38, United States Code, as well as sections 1074, 1079, 1086, 1104, and Chapter 61 of Title 10, United States Code, have been addressed through a variety of DoD and VA Health Care Resource Sharing Program directives. The most recent instruction covering these agreements was reissued on January 23, 2012 (DoD instruction 6010.23). Sharing Agreements and joint ventures are permitted when such arrangements “…will improve access to quality health care or increase cost-effectiveness of the health care provided … to beneficiaries of both departments.” A Joint Executive Council (JEC), co-chaired by the VA Deputy Secretary and the DoD Acting Under Secretary of Defense for Personnel and Readiness, oversees joint VA/DoD activities.
The collaborative initiatives described in this article have all blossomed into sustainable, ongoing, valuable programs. Aided by JIF grants, they transitioned to standard VHA and DoD budgetary mechanisms in the third year of operation. For the VHA, such ongoing funding is accomplished through the Veterans Equitable Resource Allocation (VERA) budgeting system. Despite overall national/regional advantages, this funding model can result in substantial fiscal pressure for rapidly growing VHA systems, such as VANCHCS. DoD facilities and deployable operational teams, such as the 60MDG, are funded through separate DoD mechanisms. TRICARE services are funded through an entirely different budget. The complexities of this process preclude easy summary in this paper.
Recognizing that new collaborative initiatives inevitably add fiscal stress to involved facilities, the JEC has periodically offered 2-year competitive grant funding on a national basis to support winning proposals. Such JIF grants offer financial support to initiate potentially value-added collaborations. The VHA and DoD equally fund the annual award pool for these JIF grants. In response to periodic solicitations, VHA facilities team with DoD partners to jointly submit concept proposals.
Proposals emerging from separate review, revision, and approval by VHA/VA and USAF/DoD leadership are subjected to a rigorous business case analysis. The JEC then competitively scores the proposals according to transparent weighted criteria. High-scoring proposals enjoy support for renovation, equipment, and personnel for a transition period of 2 years. In the third year of ongoing operation, VHA funding (ie, VERA funding) and DoD funding, sometimes modified by a specific Memoranda of Understanding, pay for the third year, based on the workload during the first year of the program. As a result of third-year reimbursement based on previous volume and care provided, productivity under any new JIF-funded program is financially incentivized from day 1.
Each JIF proposal enumerates specific workload targets and time lines. In northern California, at quarterly intervals, a local VANCHCS-DGMC Joint Venture Executive Management Team (EMT) formally reviews clinical and financial metrics. This local EMT also reports results to the national-level JEC. Clinical metrics for most programs include visit count, consult count, procedure count, and the number of individuals treated in a given year, with breakdown tallies according to patients’ VA or DoD affiliation. Financial metrics include personnel costs, equipment costs, and revenue generated or saved. Savings for VHA patients can be calculated using CPT codes, Diagnosis Related Groups (DRG), and set CHAMPUS Maximum Allowable Charge (CMAC) rates, as calculated by the TRICARE Management Calculator (TMA Calculator).
Personnel serving in joint, integrated programs remain employees of either VHA or DoD, according to the staffing plan specified in the original JIF grant. Beyond the 2-year term of the original JIF grant, VANCHCS and DGMC can jointly adjust/expand staffing to meet increasing demand and programmatic needs. Personnel in joint programs work side by side and treat patients equally regardless of VA or DoD affiliation.
By agreement, EMR orders and EMR patient care documentation are entered according to norms for the organization where the care is delivered (usually DGMC for new inpatient programs). This facilitates identical treatment of patients in JIF programs. However, specific accommodations for inadequate cross talk between VHA and DoD EMR systems have proven necessary. Such accommodations have added cost, but not to a degree that jeopardizes any particular venture.
Findings
The mutual alignment approach shows a uniformly favorable 9-year experience with 9 joint VA/DoD clinical programs initiated through JIF grants totaling $29.6 million. Formal JIF closeout reports at the 2-year mark are available for 5 programs and document positive return on investment (ROI) for all programs averaging 83%.
The Joint Neurosurgery Program, planned through a 2005 JIF grant and implemented in 2006, offers a practical example of mutual alignment at work. Pre-JIF, both organizations had limited neurosurgery capability. War-related deployments undermined DGMC service, and ongoing community care expenses beyond $1.5 million per year for DoD beneficiaries seemed inevitable. VANCHCS in 2004-2005 referred nearly all cases to either neighboring VA systems or to community hospitals, suffering both lost VERA revenue on one hand and direct cost on the other. Unreliable care, long wait times, inefficiency, and dissatisfaction plagued the arrangements, which the staff at VANCHCS considered unacceptable.
Combining forces to provide better care made sense, but reorganizing for a fully merged Neurosurgical Service revealed daunting roadblocks. Eventually, merger frustration conceived a more productive, outcome-oriented, practical philosophy: mutual alignment. We recognized that minimizing change, flexibly capitalizing on opportunity, and reinforcing areas of strength could best achieve mutual joint goals. This mind-set facilitated speedy program assembly, in a “can do” collaborative atmosphere, and with gratifyingly little disruption.
Joint Neurosurgery JIF
The joint Neurosurgery JIF fused outpatient clinics to 1 hub location (a VA clinic adjacent to DGMC), left VA and DoD EMR arrangements intact, and established a single site (DGMC) for inpatient neurosurgical procedures. Dual-trained practitioners accessed both DoD and VA EMR systems, often using side-by-side computer stations. Inpatient work, by mutual agreement, used the DoD EMR exclusively. On inpatient discharge, however, a duplicate care summary was entered into the VHA CPRS EMR system.
Using JIF grants, a sophisticated image-guided surgery system was installed at DGMC, an underused operating room (OR) at DGMC was dedicated to neurosurgery, instruments were purchased, and VA nurses were hired to augment OR/ward/intensive care unit staffing at DGMC to support neurosurgical needs. The 3-year neurosurgery JIF budget totaled $5.5 million, 90% of which was dedicated to salaries for additional personnel to expand the service at DGMC. Deliverables included volume increases of 1,100 neurosurgical consultations per year, and at least 100 major procedures per year.
At the completion of the first 3 years of operation, the final report of the JIF noted a 12% ROI. In the post-JIF sustainment years, as joint volume increased further, the program added an additional VA neurosurgeon, a physician assistant, and other staff. Volume has steadily expanded, with 318 major neurosurgical procedures completed in FY 2013. In maintenance mode, consultations remain essentially free to each organization; VANCHCS is reimbursed for salary/benefits for hospital-based VHA personnel working at DGMC; and DGMC charges VANCHCS 75% of CMAC rates for the inpatient care delivered. The arrangement remains financially desirable for both organizations. For FY 2013 the joint relationship in neurosurgery generated a 22% ROI, saving taxpayers nearly $1 million per year. Most important, patients received prompt, excellent care. Waiting times for elective consults were routinely < 14 days, emergency care was reliably available, outcomes were excellent, and satisfaction at all levels have vastly improved.
Measuring Program Success
The funded and implemented JIF programs have all been successful, with positive ROI ranging from 10% to 284% (Table 1). Newer programs lacking a final closeout report are all on track for positive ROI. One additional JIF program, for a joint hematology-oncology center, was delayed by staffing challenges but has now commenced.

Over the past 7 years, outpatient volume and services provided by DGMC have increased. Outpatient support services provided by VANCHCS for DoD personnel at remote sites, while still substantial, diminished (Figures 1 and 2). Such changes reflect intentional concentration at DGMC. Also, a VHA pharmacy service provided to USAF personnel at a site distant from DGMC was intentionally downsized to embrace a mailed-medication program.
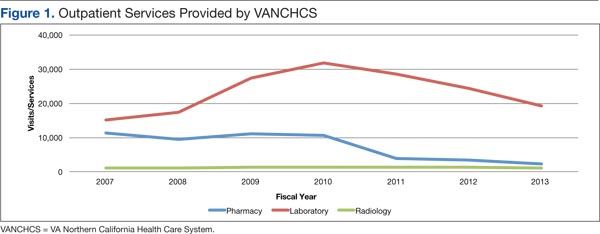
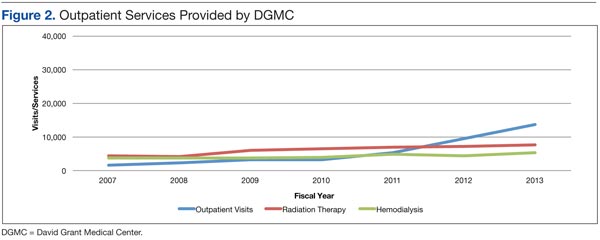
Inpatient hospital discharges for VHA enrollees and bed-days of care at DGMC have increased substantially (Figure 3). As a result of sharing programs and JIF programs, VHA enrollees currently account for about 40% of total hospital census at DGMC. About 108 professionals paid by VANCHCS currently work at DGMC. In most cases, as formalized in specific post-JIF sustainment agreements, VANCHCS is reimbursed for clinical staff salary and benefits if such staff are working at DGMC within a JIF program. For inpatient and procedural care, unless charges are specifically excluded as part of specific JIF agreements, VANCHCS pays DGMC at a rate of 75% of CMAC (ie, about 75% of Medicare rates) for every admission. Given geographic constraints, a VHA mandate to keep waits for specialty care under 14 days, and finite assistance levels from other VAMCs in VISN 21, a majority of these cases would otherwise be treated in community fee programs (at a higher cost of 100% of CMAC plus professional fees).
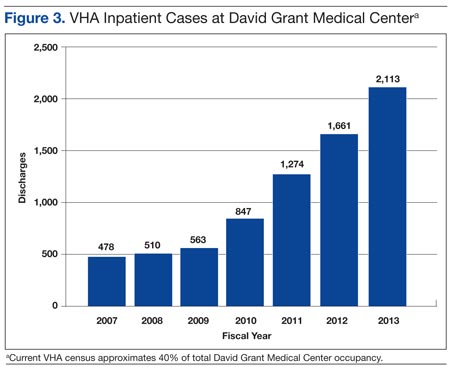
Volume has grown in all such programs (Table 2). Growth in the category of “open cardiac procedures,” however, has been intentionally limited by a VISN 21 requirement that care for VHA patients be provided only when existing VISN 21 cardiac programs cannot accommodate a particular case.
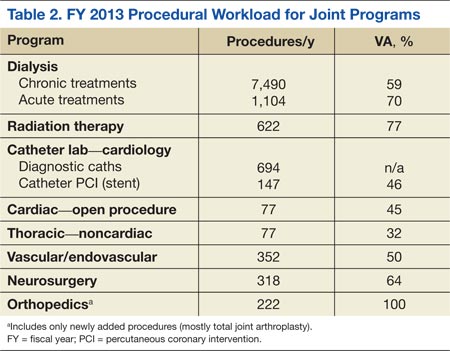
Since FY 2011, as a result of improved analytics, VANCHCS has been able to calculate its global savings (cost avoidance) stemming from all JIF and other sharing programs. Calculating the difference between community fee cost and DGMC cost as about 25% of CMAC (which offers a floor estimate of actual savings), these ongoing programs now save the VANCHCS $7.78 million per year (Table 3).

Positive overall federal ROI (ie, ROI from the taxpayer’s perspective), measured in dollars, is reported at the end of year 3 for every JIF-funded program. Substantial additional ROI could be captured by other metrics, such as timeliness of care and patient satisfaction, and would be favorable for all listed programs (data not shown).
Discussion
Had VANCHCS and DGMC attempted a merged information and management structure for the JIF programs, implementation would have been seriously delayed, if not entirely thwarted. Instead, by explicitly aligning efforts around each organization’s existing capabilities, assets and attributes, new valuable services were quickly developed. Patients now receive high-quality treatment in specialty areas not previously offered (and in some instances, not previously offered by either system).
As noted previously, the DoD and the VHA health care systems vary considerably. For DGMC and the 60MDG, during a time of war, optimal triage practices, safe/speedy transport, and the reliable delivery of appropriate trauma care for the injured warrior represent core missions. The VHA, on the other hand, is dedicated to the well-being, health, and lifetime medical-surgical care of enrolled veterans. The VHA population has relatively high numbers of elderly patients with serious chronic health conditions, such as heart disease, vascular disease, and cancer. VHA also provides subacute and rehabilitative care for younger veterans who served more recently in Iraq and Afghanistan. Overall, the VHA population stands quite distinct from that of our young active-duty forces and their dependents.
The VHA patient population (6.3 million patients receiving treatment and over 8.7 million enrolled) greatly exceeds that of the DoD. For this and other reasons, experience, current skills, and training differ considerably between VHA and DoD practitioners. For active-duty DoD practitioners, especially surgeons, the JIF projects provide avenues for development/maintenance of skills. Further, the JIF-enabled influx of VHA personnel at DGMC enhances staffing at DGMC, thereby improving the capacity of DGMC and the 60MDG’s potential surge capacity. Finally, ongoing joint programs have fostered provider relationships, academic opportunities, and training for DoD personnel between deployments.
The effort also helps personnel satisfy new, quantitative, procedural volume standards (aka currency standards) for DoD/USAF surgeons. For VANCHCS, which is seriously pressed for acute inpatient capacity, the DGMC facility space and beds supporting the joint programs represent an attractive alternative to other options, such as new hospital construction, distant transfers, or reliance on community care (Table 4).
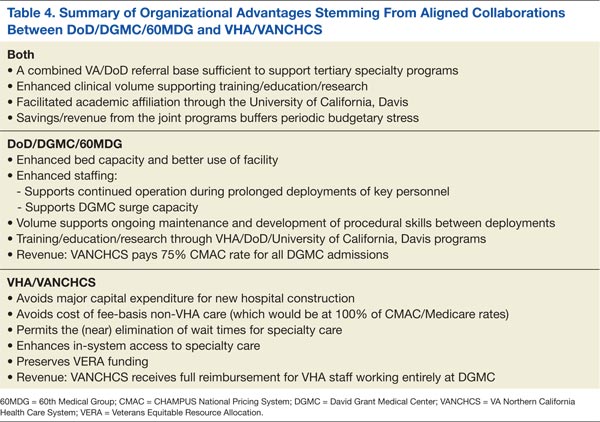
The JIF submission process encourages thoughtful planning and specific identification of resources necessary for success. The intra-and extra-organizational review process, as well as competitive national-level scoring, encourages thrift and innovation. Funded project proposals are generally compelling. Some JIF programs are constructed anew, combining space, bed capacity, and commitment with the requisite staffing, equipment, and team development to ensure safe startup. Examples include the neurosurgery and heart-lung-vascular programs. Others, like the orthopedics program, expand existing capabilities. In each instance, the new programs benefit all concerned: the federal taxpayer, each organization, and patients.
Outside Support and New Programs
The UC Davis Health System (UCDHS), through high-level education, training, and staffing, has explicitly supported these joint programs. Reliable, safe initiation, particularly for the cardiac and vascular programs, would not have been otherwise possible. Key staff members often hold academic faculty appointments, teach, write, and participate in UCDHS programs at all levels. Research in trauma care and other topics has also been facilitated. The positive relationship has supported joint program infrastructure, recruitment, and enhanced/maintained quality.
Multiple successful JIF collaborations and sharing projects, have generated a further, unforeseen benefit: The emergence of an intra-agency, financially relevant, federal market for innovative proposals. This has been coupled in the northern California setting with an emerging willingness by both organizations to potentially sustain a short-term loss for long-term financial or programmatic gain. Strict accounting between organizations, with real dollars going back and forth, has created pools of uncommitted profit, which organizational leaders can use to fund proposals not previously feasible given otherwise daunting fiscal constraints.
One recent example is a non-JIF program for patients requiring general surgery care. Under a no-load pilot program, some DoD surgeons work without additional compensation at VANCHCS facilities, and some general surgery operations are performed at DGMC. This serves to both maintain DoD practitioners’ clinical volume between deployments, and simultaneously address temporary VHA backlogs. Previous and current sharing agreement revenue, complemented by goodwill, supports the exchange. In this particular instance, previous JIF experience has cultivated innovation. Analysis and market discipline will determine its fate.
Limitations
Obstacles thwarting potential joint projects include inadequate projected case volume, logistical constraints, and inadequate ROI. Geographic challenges also limit collaboration in certain areas. The VANCHCS system covers 40,000 square miles. Emergency acute care for a patient mandates use of the nearest capable facility, often a local nonfederal facility. Inadequate communication between VHA and DoD EMR systems, exacerbated by privacy and security protections initiated by both organizations, also tends to block collaboration.
Notwithstanding the alignment over merger philosophy, merged information systems, or at least a faster, more reliable cross talk tool would certainly help. Bidirectional Healthcare Information Exchange (BHIE), if implemented more reliably, might still work. As a work-around, practitioners in joint programs usually practice with a VHA computer and a DoD computer side by side in order to obtain complete information for a given patient. Providers view this as ridiculous. However, all involved respect the need for intact DoD and VHA firewall/security systems.
These collaborative ventures have been created in a unique budgetary environment. Wars end. Congress adjusts budgets. Health care systems change. One or the other partner periodically experiences serious budgetary stress. However, the back-and-forth revenue streams described here tend to smooth the transitions. Despite budgetary and programmatic stress, we are maintaining/expanding all of the joint programs described herein. These programs deliver sustained, cost-effective care with improved access for veterans and military beneficiaries alike and continue to do so through planned, mutually aligned effort, not merger.
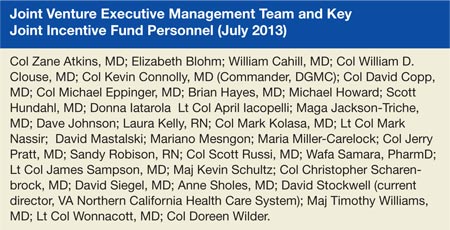
Acknowledgements
Current and former commanders of the 60th Medical Group at DGMC: Col Rawson Wood (current commander); Col Kevin Connelly, MD ; Col Brian Hayes, MD; Col Lee Payne, MD.
Current and former directors of VANCHCS: David Stockwell (current director); Brian O’Neill, MD; Lawrence Sandler; Lucille Swanson. UC Davis: Kenneth W. Kizer, MD, MPH, The Institute for Population Health Improvement, and The Center for Veterans and Military Health.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Panangala SV, Jansen DJ. Departments of Defense and Veterans Affairs: Status of the Integrated Electronic Health Record (iEHR). Federation of American Scientists Website. http://fas.org/sgp/crs/misc/R42970.pdf. Published February 26, 2013. Accessed November 11, 2014.
2. Committee on Evaluation of the Lovell Federal Health Care Center Merger; Board on the Health of Select Populations; Institute of Medicine. Evaluation of the Lovell Federal Health Care Center Merger: Findings, Conclusions and Recommendations (2012). The National Academies Press Website. http://www.iom.edu/evaluatinglovell. Released October 12, 2012. Accessed November 5, 2014.
3. U.S. Department of Defense. Remarks by Secretary Panetta and Secretary Shinseki from the Department of Veterans Affairs [News transcript]. U.S. Department of Defense Website. http://www.defense.gov/Transcripts/Transcript.aspx?TranscriptID=5187. Published February 5, 2013. Accessed November 5, 2014.
The VA and the DoD operate completely independent health care systems. Integrated provision of health care for the populations served is a compellingly attractive goal given the obvious overlaps, but has proven deceptively difficult to implement.
Despite efforts begun in 1998 to accomplish a reliable, comprehensive, bidirectional exchange of patient-specific health care information between systems, 16 years later this has yet to be reliably available. In most locales, VHA practitioners cannot easily access details of the medical care provided to DoD personnel. Attempts to merge the 2 electronic medical record (EMR) systems have also been fraught with difficulty.1 Even at the new, joint VHA/DoD Captain James A. Lovell Federal Health Care Center in North Chicago, Illinois (which opened in October 2010 to serve a mix of active-duty servicemen, TRICARE beneficiaries, and VA enrollees under a single roof), care using a single EMR system has not been possible.
The Institute of Medicine, in an invited review, has specifically criticized the unsatisfactory, piecemeal EMR integration.2 On February 5, 2013, the Secretary of the VA and the Secretary of Defense formally abandoned efforts to construct a single VA/DoD integrated EMR system by 2017. Instead, both organizations would, in then Secretary of Defense Leon Panetta’s words, “…focus our immediate efforts on integrating VA and DoD health data as quickly as possible, by focusing on interoperability and using existing solutions.”3
Joint VA/DoD health care programs in Northern California have abandoned merged structures in favor of mutual alignment. The practical value of aligning care systems is to extract benefit from structured, economically rational, win-win collaborations, as opposed to the forced merger approach. Mutual alignment generates relatively prompt, reliable results, to the benefit of all concerned.
Related: Developing Joint VA and DoD Health Programs
This report details a consistently favorable experience with this philosophy, which has considerable relevance as federal and nonfederal systems explore future joint ventures. Specifically, this report describes the substantial multiyear savings from a combination of various DoD/VA Joint Incentive Fund (JIF) and Sharing Agreement projects conducted by the VA Northern California Health Care System (VANCHCS) and the U.S. Air Force (USAF) 60th Medical Group’s (60MDG’s) David Grant Medical Center (DGMC).
Background and Methods
VA Northern California Health Care System currently serves 92,000 unique veteran patients in a service area of 40,000 square miles through a network of facilities and clinics at 9 sites across northern California. Rapid year-over-year growth of VANCHCS continues, and in fiscal year (FY) 2013, so-called unique enrolled veterans increased by 4.7%. David Grant Medical Center is a 116-bed DoD flagship hospital at Travis Air Force Base in Fairfield, California, which is home to the 60MDG. In 2013, VANCHCS and DGMC celebrated the 20th year of collaborative projects.
Congressional mandates encompassed in sections 101, 1701, 1782, 1783, and 8111 of Title 38, United States Code, as well as sections 1074, 1079, 1086, 1104, and Chapter 61 of Title 10, United States Code, have been addressed through a variety of DoD and VA Health Care Resource Sharing Program directives. The most recent instruction covering these agreements was reissued on January 23, 2012 (DoD instruction 6010.23). Sharing Agreements and joint ventures are permitted when such arrangements “…will improve access to quality health care or increase cost-effectiveness of the health care provided … to beneficiaries of both departments.” A Joint Executive Council (JEC), co-chaired by the VA Deputy Secretary and the DoD Acting Under Secretary of Defense for Personnel and Readiness, oversees joint VA/DoD activities.
The collaborative initiatives described in this article have all blossomed into sustainable, ongoing, valuable programs. Aided by JIF grants, they transitioned to standard VHA and DoD budgetary mechanisms in the third year of operation. For the VHA, such ongoing funding is accomplished through the Veterans Equitable Resource Allocation (VERA) budgeting system. Despite overall national/regional advantages, this funding model can result in substantial fiscal pressure for rapidly growing VHA systems, such as VANCHCS. DoD facilities and deployable operational teams, such as the 60MDG, are funded through separate DoD mechanisms. TRICARE services are funded through an entirely different budget. The complexities of this process preclude easy summary in this paper.
Recognizing that new collaborative initiatives inevitably add fiscal stress to involved facilities, the JEC has periodically offered 2-year competitive grant funding on a national basis to support winning proposals. Such JIF grants offer financial support to initiate potentially value-added collaborations. The VHA and DoD equally fund the annual award pool for these JIF grants. In response to periodic solicitations, VHA facilities team with DoD partners to jointly submit concept proposals.
Proposals emerging from separate review, revision, and approval by VHA/VA and USAF/DoD leadership are subjected to a rigorous business case analysis. The JEC then competitively scores the proposals according to transparent weighted criteria. High-scoring proposals enjoy support for renovation, equipment, and personnel for a transition period of 2 years. In the third year of ongoing operation, VHA funding (ie, VERA funding) and DoD funding, sometimes modified by a specific Memoranda of Understanding, pay for the third year, based on the workload during the first year of the program. As a result of third-year reimbursement based on previous volume and care provided, productivity under any new JIF-funded program is financially incentivized from day 1.
Each JIF proposal enumerates specific workload targets and time lines. In northern California, at quarterly intervals, a local VANCHCS-DGMC Joint Venture Executive Management Team (EMT) formally reviews clinical and financial metrics. This local EMT also reports results to the national-level JEC. Clinical metrics for most programs include visit count, consult count, procedure count, and the number of individuals treated in a given year, with breakdown tallies according to patients’ VA or DoD affiliation. Financial metrics include personnel costs, equipment costs, and revenue generated or saved. Savings for VHA patients can be calculated using CPT codes, Diagnosis Related Groups (DRG), and set CHAMPUS Maximum Allowable Charge (CMAC) rates, as calculated by the TRICARE Management Calculator (TMA Calculator).
Personnel serving in joint, integrated programs remain employees of either VHA or DoD, according to the staffing plan specified in the original JIF grant. Beyond the 2-year term of the original JIF grant, VANCHCS and DGMC can jointly adjust/expand staffing to meet increasing demand and programmatic needs. Personnel in joint programs work side by side and treat patients equally regardless of VA or DoD affiliation.
By agreement, EMR orders and EMR patient care documentation are entered according to norms for the organization where the care is delivered (usually DGMC for new inpatient programs). This facilitates identical treatment of patients in JIF programs. However, specific accommodations for inadequate cross talk between VHA and DoD EMR systems have proven necessary. Such accommodations have added cost, but not to a degree that jeopardizes any particular venture.
Findings
The mutual alignment approach shows a uniformly favorable 9-year experience with 9 joint VA/DoD clinical programs initiated through JIF grants totaling $29.6 million. Formal JIF closeout reports at the 2-year mark are available for 5 programs and document positive return on investment (ROI) for all programs averaging 83%.
The Joint Neurosurgery Program, planned through a 2005 JIF grant and implemented in 2006, offers a practical example of mutual alignment at work. Pre-JIF, both organizations had limited neurosurgery capability. War-related deployments undermined DGMC service, and ongoing community care expenses beyond $1.5 million per year for DoD beneficiaries seemed inevitable. VANCHCS in 2004-2005 referred nearly all cases to either neighboring VA systems or to community hospitals, suffering both lost VERA revenue on one hand and direct cost on the other. Unreliable care, long wait times, inefficiency, and dissatisfaction plagued the arrangements, which the staff at VANCHCS considered unacceptable.
Combining forces to provide better care made sense, but reorganizing for a fully merged Neurosurgical Service revealed daunting roadblocks. Eventually, merger frustration conceived a more productive, outcome-oriented, practical philosophy: mutual alignment. We recognized that minimizing change, flexibly capitalizing on opportunity, and reinforcing areas of strength could best achieve mutual joint goals. This mind-set facilitated speedy program assembly, in a “can do” collaborative atmosphere, and with gratifyingly little disruption.
Joint Neurosurgery JIF
The joint Neurosurgery JIF fused outpatient clinics to 1 hub location (a VA clinic adjacent to DGMC), left VA and DoD EMR arrangements intact, and established a single site (DGMC) for inpatient neurosurgical procedures. Dual-trained practitioners accessed both DoD and VA EMR systems, often using side-by-side computer stations. Inpatient work, by mutual agreement, used the DoD EMR exclusively. On inpatient discharge, however, a duplicate care summary was entered into the VHA CPRS EMR system.
Using JIF grants, a sophisticated image-guided surgery system was installed at DGMC, an underused operating room (OR) at DGMC was dedicated to neurosurgery, instruments were purchased, and VA nurses were hired to augment OR/ward/intensive care unit staffing at DGMC to support neurosurgical needs. The 3-year neurosurgery JIF budget totaled $5.5 million, 90% of which was dedicated to salaries for additional personnel to expand the service at DGMC. Deliverables included volume increases of 1,100 neurosurgical consultations per year, and at least 100 major procedures per year.
At the completion of the first 3 years of operation, the final report of the JIF noted a 12% ROI. In the post-JIF sustainment years, as joint volume increased further, the program added an additional VA neurosurgeon, a physician assistant, and other staff. Volume has steadily expanded, with 318 major neurosurgical procedures completed in FY 2013. In maintenance mode, consultations remain essentially free to each organization; VANCHCS is reimbursed for salary/benefits for hospital-based VHA personnel working at DGMC; and DGMC charges VANCHCS 75% of CMAC rates for the inpatient care delivered. The arrangement remains financially desirable for both organizations. For FY 2013 the joint relationship in neurosurgery generated a 22% ROI, saving taxpayers nearly $1 million per year. Most important, patients received prompt, excellent care. Waiting times for elective consults were routinely < 14 days, emergency care was reliably available, outcomes were excellent, and satisfaction at all levels have vastly improved.
Measuring Program Success
The funded and implemented JIF programs have all been successful, with positive ROI ranging from 10% to 284% (Table 1). Newer programs lacking a final closeout report are all on track for positive ROI. One additional JIF program, for a joint hematology-oncology center, was delayed by staffing challenges but has now commenced.
Over the past 7 years, outpatient volume and services provided by DGMC have increased. Outpatient support services provided by VANCHCS for DoD personnel at remote sites, while still substantial, diminished (Figures 1 and 2). Such changes reflect intentional concentration at DGMC. Also, a VHA pharmacy service provided to USAF personnel at a site distant from DGMC was intentionally downsized to embrace a mailed-medication program.
Inpatient hospital discharges for VHA enrollees and bed-days of care at DGMC have increased substantially (Figure 3). As a result of sharing programs and JIF programs, VHA enrollees currently account for about 40% of total hospital census at DGMC. About 108 professionals paid by VANCHCS currently work at DGMC. In most cases, as formalized in specific post-JIF sustainment agreements, VANCHCS is reimbursed for clinical staff salary and benefits if such staff are working at DGMC within a JIF program. For inpatient and procedural care, unless charges are specifically excluded as part of specific JIF agreements, VANCHCS pays DGMC at a rate of 75% of CMAC (ie, about 75% of Medicare rates) for every admission. Given geographic constraints, a VHA mandate to keep waits for specialty care under 14 days, and finite assistance levels from other VAMCs in VISN 21, a majority of these cases would otherwise be treated in community fee programs (at a higher cost of 100% of CMAC plus professional fees).
Volume has grown in all such programs (Table 2). Growth in the category of “open cardiac procedures,” however, has been intentionally limited by a VISN 21 requirement that care for VHA patients be provided only when existing VISN 21 cardiac programs cannot accommodate a particular case.
Since FY 2011, as a result of improved analytics, VANCHCS has been able to calculate its global savings (cost avoidance) stemming from all JIF and other sharing programs. Calculating the difference between community fee cost and DGMC cost as about 25% of CMAC (which offers a floor estimate of actual savings), these ongoing programs now save the VANCHCS $7.78 million per year (Table 3).
Positive overall federal ROI (ie, ROI from the taxpayer’s perspective), measured in dollars, is reported at the end of year 3 for every JIF-funded program. Substantial additional ROI could be captured by other metrics, such as timeliness of care and patient satisfaction, and would be favorable for all listed programs (data not shown).
Discussion
Had VANCHCS and DGMC attempted a merged information and management structure for the JIF programs, implementation would have been seriously delayed, if not entirely thwarted. Instead, by explicitly aligning efforts around each organization’s existing capabilities, assets and attributes, new valuable services were quickly developed. Patients now receive high-quality treatment in specialty areas not previously offered (and in some instances, not previously offered by either system).
As noted previously, the DoD and the VHA health care systems vary considerably. For DGMC and the 60MDG, during a time of war, optimal triage practices, safe/speedy transport, and the reliable delivery of appropriate trauma care for the injured warrior represent core missions. The VHA, on the other hand, is dedicated to the well-being, health, and lifetime medical-surgical care of enrolled veterans. The VHA population has relatively high numbers of elderly patients with serious chronic health conditions, such as heart disease, vascular disease, and cancer. VHA also provides subacute and rehabilitative care for younger veterans who served more recently in Iraq and Afghanistan. Overall, the VHA population stands quite distinct from that of our young active-duty forces and their dependents.
The VHA patient population (6.3 million patients receiving treatment and over 8.7 million enrolled) greatly exceeds that of the DoD. For this and other reasons, experience, current skills, and training differ considerably between VHA and DoD practitioners. For active-duty DoD practitioners, especially surgeons, the JIF projects provide avenues for development/maintenance of skills. Further, the JIF-enabled influx of VHA personnel at DGMC enhances staffing at DGMC, thereby improving the capacity of DGMC and the 60MDG’s potential surge capacity. Finally, ongoing joint programs have fostered provider relationships, academic opportunities, and training for DoD personnel between deployments.
The effort also helps personnel satisfy new, quantitative, procedural volume standards (aka currency standards) for DoD/USAF surgeons. For VANCHCS, which is seriously pressed for acute inpatient capacity, the DGMC facility space and beds supporting the joint programs represent an attractive alternative to other options, such as new hospital construction, distant transfers, or reliance on community care (Table 4).
The JIF submission process encourages thoughtful planning and specific identification of resources necessary for success. The intra-and extra-organizational review process, as well as competitive national-level scoring, encourages thrift and innovation. Funded project proposals are generally compelling. Some JIF programs are constructed anew, combining space, bed capacity, and commitment with the requisite staffing, equipment, and team development to ensure safe startup. Examples include the neurosurgery and heart-lung-vascular programs. Others, like the orthopedics program, expand existing capabilities. In each instance, the new programs benefit all concerned: the federal taxpayer, each organization, and patients.
Outside Support and New Programs
The UC Davis Health System (UCDHS), through high-level education, training, and staffing, has explicitly supported these joint programs. Reliable, safe initiation, particularly for the cardiac and vascular programs, would not have been otherwise possible. Key staff members often hold academic faculty appointments, teach, write, and participate in UCDHS programs at all levels. Research in trauma care and other topics has also been facilitated. The positive relationship has supported joint program infrastructure, recruitment, and enhanced/maintained quality.
Multiple successful JIF collaborations and sharing projects, have generated a further, unforeseen benefit: The emergence of an intra-agency, financially relevant, federal market for innovative proposals. This has been coupled in the northern California setting with an emerging willingness by both organizations to potentially sustain a short-term loss for long-term financial or programmatic gain. Strict accounting between organizations, with real dollars going back and forth, has created pools of uncommitted profit, which organizational leaders can use to fund proposals not previously feasible given otherwise daunting fiscal constraints.
One recent example is a non-JIF program for patients requiring general surgery care. Under a no-load pilot program, some DoD surgeons work without additional compensation at VANCHCS facilities, and some general surgery operations are performed at DGMC. This serves to both maintain DoD practitioners’ clinical volume between deployments, and simultaneously address temporary VHA backlogs. Previous and current sharing agreement revenue, complemented by goodwill, supports the exchange. In this particular instance, previous JIF experience has cultivated innovation. Analysis and market discipline will determine its fate.
Limitations
Obstacles thwarting potential joint projects include inadequate projected case volume, logistical constraints, and inadequate ROI. Geographic challenges also limit collaboration in certain areas. The VANCHCS system covers 40,000 square miles. Emergency acute care for a patient mandates use of the nearest capable facility, often a local nonfederal facility. Inadequate communication between VHA and DoD EMR systems, exacerbated by privacy and security protections initiated by both organizations, also tends to block collaboration.
Notwithstanding the alignment over merger philosophy, merged information systems, or at least a faster, more reliable cross talk tool would certainly help. Bidirectional Healthcare Information Exchange (BHIE), if implemented more reliably, might still work. As a work-around, practitioners in joint programs usually practice with a VHA computer and a DoD computer side by side in order to obtain complete information for a given patient. Providers view this as ridiculous. However, all involved respect the need for intact DoD and VHA firewall/security systems.
These collaborative ventures have been created in a unique budgetary environment. Wars end. Congress adjusts budgets. Health care systems change. One or the other partner periodically experiences serious budgetary stress. However, the back-and-forth revenue streams described here tend to smooth the transitions. Despite budgetary and programmatic stress, we are maintaining/expanding all of the joint programs described herein. These programs deliver sustained, cost-effective care with improved access for veterans and military beneficiaries alike and continue to do so through planned, mutually aligned effort, not merger.
Acknowledgements
Current and former commanders of the 60th Medical Group at DGMC: Col Rawson Wood (current commander); Col Kevin Connelly, MD ; Col Brian Hayes, MD; Col Lee Payne, MD.
Current and former directors of VANCHCS: David Stockwell (current director); Brian O’Neill, MD; Lawrence Sandler; Lucille Swanson. UC Davis: Kenneth W. Kizer, MD, MPH, The Institute for Population Health Improvement, and The Center for Veterans and Military Health.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
The VA and the DoD operate completely independent health care systems. Integrated provision of health care for the populations served is a compellingly attractive goal given the obvious overlaps, but has proven deceptively difficult to implement.
Despite efforts begun in 1998 to accomplish a reliable, comprehensive, bidirectional exchange of patient-specific health care information between systems, 16 years later this has yet to be reliably available. In most locales, VHA practitioners cannot easily access details of the medical care provided to DoD personnel. Attempts to merge the 2 electronic medical record (EMR) systems have also been fraught with difficulty.1 Even at the new, joint VHA/DoD Captain James A. Lovell Federal Health Care Center in North Chicago, Illinois (which opened in October 2010 to serve a mix of active-duty servicemen, TRICARE beneficiaries, and VA enrollees under a single roof), care using a single EMR system has not been possible.
The Institute of Medicine, in an invited review, has specifically criticized the unsatisfactory, piecemeal EMR integration.2 On February 5, 2013, the Secretary of the VA and the Secretary of Defense formally abandoned efforts to construct a single VA/DoD integrated EMR system by 2017. Instead, both organizations would, in then Secretary of Defense Leon Panetta’s words, “…focus our immediate efforts on integrating VA and DoD health data as quickly as possible, by focusing on interoperability and using existing solutions.”3
Joint VA/DoD health care programs in Northern California have abandoned merged structures in favor of mutual alignment. The practical value of aligning care systems is to extract benefit from structured, economically rational, win-win collaborations, as opposed to the forced merger approach. Mutual alignment generates relatively prompt, reliable results, to the benefit of all concerned.
Related: Developing Joint VA and DoD Health Programs
This report details a consistently favorable experience with this philosophy, which has considerable relevance as federal and nonfederal systems explore future joint ventures. Specifically, this report describes the substantial multiyear savings from a combination of various DoD/VA Joint Incentive Fund (JIF) and Sharing Agreement projects conducted by the VA Northern California Health Care System (VANCHCS) and the U.S. Air Force (USAF) 60th Medical Group’s (60MDG’s) David Grant Medical Center (DGMC).
Background and Methods
VA Northern California Health Care System currently serves 92,000 unique veteran patients in a service area of 40,000 square miles through a network of facilities and clinics at 9 sites across northern California. Rapid year-over-year growth of VANCHCS continues, and in fiscal year (FY) 2013, so-called unique enrolled veterans increased by 4.7%. David Grant Medical Center is a 116-bed DoD flagship hospital at Travis Air Force Base in Fairfield, California, which is home to the 60MDG. In 2013, VANCHCS and DGMC celebrated the 20th year of collaborative projects.
Congressional mandates encompassed in sections 101, 1701, 1782, 1783, and 8111 of Title 38, United States Code, as well as sections 1074, 1079, 1086, 1104, and Chapter 61 of Title 10, United States Code, have been addressed through a variety of DoD and VA Health Care Resource Sharing Program directives. The most recent instruction covering these agreements was reissued on January 23, 2012 (DoD instruction 6010.23). Sharing Agreements and joint ventures are permitted when such arrangements “…will improve access to quality health care or increase cost-effectiveness of the health care provided … to beneficiaries of both departments.” A Joint Executive Council (JEC), co-chaired by the VA Deputy Secretary and the DoD Acting Under Secretary of Defense for Personnel and Readiness, oversees joint VA/DoD activities.
The collaborative initiatives described in this article have all blossomed into sustainable, ongoing, valuable programs. Aided by JIF grants, they transitioned to standard VHA and DoD budgetary mechanisms in the third year of operation. For the VHA, such ongoing funding is accomplished through the Veterans Equitable Resource Allocation (VERA) budgeting system. Despite overall national/regional advantages, this funding model can result in substantial fiscal pressure for rapidly growing VHA systems, such as VANCHCS. DoD facilities and deployable operational teams, such as the 60MDG, are funded through separate DoD mechanisms. TRICARE services are funded through an entirely different budget. The complexities of this process preclude easy summary in this paper.
Recognizing that new collaborative initiatives inevitably add fiscal stress to involved facilities, the JEC has periodically offered 2-year competitive grant funding on a national basis to support winning proposals. Such JIF grants offer financial support to initiate potentially value-added collaborations. The VHA and DoD equally fund the annual award pool for these JIF grants. In response to periodic solicitations, VHA facilities team with DoD partners to jointly submit concept proposals.
Proposals emerging from separate review, revision, and approval by VHA/VA and USAF/DoD leadership are subjected to a rigorous business case analysis. The JEC then competitively scores the proposals according to transparent weighted criteria. High-scoring proposals enjoy support for renovation, equipment, and personnel for a transition period of 2 years. In the third year of ongoing operation, VHA funding (ie, VERA funding) and DoD funding, sometimes modified by a specific Memoranda of Understanding, pay for the third year, based on the workload during the first year of the program. As a result of third-year reimbursement based on previous volume and care provided, productivity under any new JIF-funded program is financially incentivized from day 1.
Each JIF proposal enumerates specific workload targets and time lines. In northern California, at quarterly intervals, a local VANCHCS-DGMC Joint Venture Executive Management Team (EMT) formally reviews clinical and financial metrics. This local EMT also reports results to the national-level JEC. Clinical metrics for most programs include visit count, consult count, procedure count, and the number of individuals treated in a given year, with breakdown tallies according to patients’ VA or DoD affiliation. Financial metrics include personnel costs, equipment costs, and revenue generated or saved. Savings for VHA patients can be calculated using CPT codes, Diagnosis Related Groups (DRG), and set CHAMPUS Maximum Allowable Charge (CMAC) rates, as calculated by the TRICARE Management Calculator (TMA Calculator).
Personnel serving in joint, integrated programs remain employees of either VHA or DoD, according to the staffing plan specified in the original JIF grant. Beyond the 2-year term of the original JIF grant, VANCHCS and DGMC can jointly adjust/expand staffing to meet increasing demand and programmatic needs. Personnel in joint programs work side by side and treat patients equally regardless of VA or DoD affiliation.
By agreement, EMR orders and EMR patient care documentation are entered according to norms for the organization where the care is delivered (usually DGMC for new inpatient programs). This facilitates identical treatment of patients in JIF programs. However, specific accommodations for inadequate cross talk between VHA and DoD EMR systems have proven necessary. Such accommodations have added cost, but not to a degree that jeopardizes any particular venture.
Findings
The mutual alignment approach shows a uniformly favorable 9-year experience with 9 joint VA/DoD clinical programs initiated through JIF grants totaling $29.6 million. Formal JIF closeout reports at the 2-year mark are available for 5 programs and document positive return on investment (ROI) for all programs averaging 83%.
The Joint Neurosurgery Program, planned through a 2005 JIF grant and implemented in 2006, offers a practical example of mutual alignment at work. Pre-JIF, both organizations had limited neurosurgery capability. War-related deployments undermined DGMC service, and ongoing community care expenses beyond $1.5 million per year for DoD beneficiaries seemed inevitable. VANCHCS in 2004-2005 referred nearly all cases to either neighboring VA systems or to community hospitals, suffering both lost VERA revenue on one hand and direct cost on the other. Unreliable care, long wait times, inefficiency, and dissatisfaction plagued the arrangements, which the staff at VANCHCS considered unacceptable.
Combining forces to provide better care made sense, but reorganizing for a fully merged Neurosurgical Service revealed daunting roadblocks. Eventually, merger frustration conceived a more productive, outcome-oriented, practical philosophy: mutual alignment. We recognized that minimizing change, flexibly capitalizing on opportunity, and reinforcing areas of strength could best achieve mutual joint goals. This mind-set facilitated speedy program assembly, in a “can do” collaborative atmosphere, and with gratifyingly little disruption.
Joint Neurosurgery JIF
The joint Neurosurgery JIF fused outpatient clinics to 1 hub location (a VA clinic adjacent to DGMC), left VA and DoD EMR arrangements intact, and established a single site (DGMC) for inpatient neurosurgical procedures. Dual-trained practitioners accessed both DoD and VA EMR systems, often using side-by-side computer stations. Inpatient work, by mutual agreement, used the DoD EMR exclusively. On inpatient discharge, however, a duplicate care summary was entered into the VHA CPRS EMR system.
Using JIF grants, a sophisticated image-guided surgery system was installed at DGMC, an underused operating room (OR) at DGMC was dedicated to neurosurgery, instruments were purchased, and VA nurses were hired to augment OR/ward/intensive care unit staffing at DGMC to support neurosurgical needs. The 3-year neurosurgery JIF budget totaled $5.5 million, 90% of which was dedicated to salaries for additional personnel to expand the service at DGMC. Deliverables included volume increases of 1,100 neurosurgical consultations per year, and at least 100 major procedures per year.
At the completion of the first 3 years of operation, the final report of the JIF noted a 12% ROI. In the post-JIF sustainment years, as joint volume increased further, the program added an additional VA neurosurgeon, a physician assistant, and other staff. Volume has steadily expanded, with 318 major neurosurgical procedures completed in FY 2013. In maintenance mode, consultations remain essentially free to each organization; VANCHCS is reimbursed for salary/benefits for hospital-based VHA personnel working at DGMC; and DGMC charges VANCHCS 75% of CMAC rates for the inpatient care delivered. The arrangement remains financially desirable for both organizations. For FY 2013 the joint relationship in neurosurgery generated a 22% ROI, saving taxpayers nearly $1 million per year. Most important, patients received prompt, excellent care. Waiting times for elective consults were routinely < 14 days, emergency care was reliably available, outcomes were excellent, and satisfaction at all levels have vastly improved.
Measuring Program Success
The funded and implemented JIF programs have all been successful, with positive ROI ranging from 10% to 284% (Table 1). Newer programs lacking a final closeout report are all on track for positive ROI. One additional JIF program, for a joint hematology-oncology center, was delayed by staffing challenges but has now commenced.
Over the past 7 years, outpatient volume and services provided by DGMC have increased. Outpatient support services provided by VANCHCS for DoD personnel at remote sites, while still substantial, diminished (Figures 1 and 2). Such changes reflect intentional concentration at DGMC. Also, a VHA pharmacy service provided to USAF personnel at a site distant from DGMC was intentionally downsized to embrace a mailed-medication program.
Inpatient hospital discharges for VHA enrollees and bed-days of care at DGMC have increased substantially (Figure 3). As a result of sharing programs and JIF programs, VHA enrollees currently account for about 40% of total hospital census at DGMC. About 108 professionals paid by VANCHCS currently work at DGMC. In most cases, as formalized in specific post-JIF sustainment agreements, VANCHCS is reimbursed for clinical staff salary and benefits if such staff are working at DGMC within a JIF program. For inpatient and procedural care, unless charges are specifically excluded as part of specific JIF agreements, VANCHCS pays DGMC at a rate of 75% of CMAC (ie, about 75% of Medicare rates) for every admission. Given geographic constraints, a VHA mandate to keep waits for specialty care under 14 days, and finite assistance levels from other VAMCs in VISN 21, a majority of these cases would otherwise be treated in community fee programs (at a higher cost of 100% of CMAC plus professional fees).
Volume has grown in all such programs (Table 2). Growth in the category of “open cardiac procedures,” however, has been intentionally limited by a VISN 21 requirement that care for VHA patients be provided only when existing VISN 21 cardiac programs cannot accommodate a particular case.
Since FY 2011, as a result of improved analytics, VANCHCS has been able to calculate its global savings (cost avoidance) stemming from all JIF and other sharing programs. Calculating the difference between community fee cost and DGMC cost as about 25% of CMAC (which offers a floor estimate of actual savings), these ongoing programs now save the VANCHCS $7.78 million per year (Table 3).
Positive overall federal ROI (ie, ROI from the taxpayer’s perspective), measured in dollars, is reported at the end of year 3 for every JIF-funded program. Substantial additional ROI could be captured by other metrics, such as timeliness of care and patient satisfaction, and would be favorable for all listed programs (data not shown).
Discussion
Had VANCHCS and DGMC attempted a merged information and management structure for the JIF programs, implementation would have been seriously delayed, if not entirely thwarted. Instead, by explicitly aligning efforts around each organization’s existing capabilities, assets and attributes, new valuable services were quickly developed. Patients now receive high-quality treatment in specialty areas not previously offered (and in some instances, not previously offered by either system).
As noted previously, the DoD and the VHA health care systems vary considerably. For DGMC and the 60MDG, during a time of war, optimal triage practices, safe/speedy transport, and the reliable delivery of appropriate trauma care for the injured warrior represent core missions. The VHA, on the other hand, is dedicated to the well-being, health, and lifetime medical-surgical care of enrolled veterans. The VHA population has relatively high numbers of elderly patients with serious chronic health conditions, such as heart disease, vascular disease, and cancer. VHA also provides subacute and rehabilitative care for younger veterans who served more recently in Iraq and Afghanistan. Overall, the VHA population stands quite distinct from that of our young active-duty forces and their dependents.
The VHA patient population (6.3 million patients receiving treatment and over 8.7 million enrolled) greatly exceeds that of the DoD. For this and other reasons, experience, current skills, and training differ considerably between VHA and DoD practitioners. For active-duty DoD practitioners, especially surgeons, the JIF projects provide avenues for development/maintenance of skills. Further, the JIF-enabled influx of VHA personnel at DGMC enhances staffing at DGMC, thereby improving the capacity of DGMC and the 60MDG’s potential surge capacity. Finally, ongoing joint programs have fostered provider relationships, academic opportunities, and training for DoD personnel between deployments.
The effort also helps personnel satisfy new, quantitative, procedural volume standards (aka currency standards) for DoD/USAF surgeons. For VANCHCS, which is seriously pressed for acute inpatient capacity, the DGMC facility space and beds supporting the joint programs represent an attractive alternative to other options, such as new hospital construction, distant transfers, or reliance on community care (Table 4).
The JIF submission process encourages thoughtful planning and specific identification of resources necessary for success. The intra-and extra-organizational review process, as well as competitive national-level scoring, encourages thrift and innovation. Funded project proposals are generally compelling. Some JIF programs are constructed anew, combining space, bed capacity, and commitment with the requisite staffing, equipment, and team development to ensure safe startup. Examples include the neurosurgery and heart-lung-vascular programs. Others, like the orthopedics program, expand existing capabilities. In each instance, the new programs benefit all concerned: the federal taxpayer, each organization, and patients.
Outside Support and New Programs
The UC Davis Health System (UCDHS), through high-level education, training, and staffing, has explicitly supported these joint programs. Reliable, safe initiation, particularly for the cardiac and vascular programs, would not have been otherwise possible. Key staff members often hold academic faculty appointments, teach, write, and participate in UCDHS programs at all levels. Research in trauma care and other topics has also been facilitated. The positive relationship has supported joint program infrastructure, recruitment, and enhanced/maintained quality.
Multiple successful JIF collaborations and sharing projects, have generated a further, unforeseen benefit: The emergence of an intra-agency, financially relevant, federal market for innovative proposals. This has been coupled in the northern California setting with an emerging willingness by both organizations to potentially sustain a short-term loss for long-term financial or programmatic gain. Strict accounting between organizations, with real dollars going back and forth, has created pools of uncommitted profit, which organizational leaders can use to fund proposals not previously feasible given otherwise daunting fiscal constraints.
One recent example is a non-JIF program for patients requiring general surgery care. Under a no-load pilot program, some DoD surgeons work without additional compensation at VANCHCS facilities, and some general surgery operations are performed at DGMC. This serves to both maintain DoD practitioners’ clinical volume between deployments, and simultaneously address temporary VHA backlogs. Previous and current sharing agreement revenue, complemented by goodwill, supports the exchange. In this particular instance, previous JIF experience has cultivated innovation. Analysis and market discipline will determine its fate.
Limitations
Obstacles thwarting potential joint projects include inadequate projected case volume, logistical constraints, and inadequate ROI. Geographic challenges also limit collaboration in certain areas. The VANCHCS system covers 40,000 square miles. Emergency acute care for a patient mandates use of the nearest capable facility, often a local nonfederal facility. Inadequate communication between VHA and DoD EMR systems, exacerbated by privacy and security protections initiated by both organizations, also tends to block collaboration.
Notwithstanding the alignment over merger philosophy, merged information systems, or at least a faster, more reliable cross talk tool would certainly help. Bidirectional Healthcare Information Exchange (BHIE), if implemented more reliably, might still work. As a work-around, practitioners in joint programs usually practice with a VHA computer and a DoD computer side by side in order to obtain complete information for a given patient. Providers view this as ridiculous. However, all involved respect the need for intact DoD and VHA firewall/security systems.
These collaborative ventures have been created in a unique budgetary environment. Wars end. Congress adjusts budgets. Health care systems change. One or the other partner periodically experiences serious budgetary stress. However, the back-and-forth revenue streams described here tend to smooth the transitions. Despite budgetary and programmatic stress, we are maintaining/expanding all of the joint programs described herein. These programs deliver sustained, cost-effective care with improved access for veterans and military beneficiaries alike and continue to do so through planned, mutually aligned effort, not merger.
Acknowledgements
Current and former commanders of the 60th Medical Group at DGMC: Col Rawson Wood (current commander); Col Kevin Connelly, MD ; Col Brian Hayes, MD; Col Lee Payne, MD.
Current and former directors of VANCHCS: David Stockwell (current director); Brian O’Neill, MD; Lawrence Sandler; Lucille Swanson. UC Davis: Kenneth W. Kizer, MD, MPH, The Institute for Population Health Improvement, and The Center for Veterans and Military Health.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Panangala SV, Jansen DJ. Departments of Defense and Veterans Affairs: Status of the Integrated Electronic Health Record (iEHR). Federation of American Scientists Website. http://fas.org/sgp/crs/misc/R42970.pdf. Published February 26, 2013. Accessed November 11, 2014.
2. Committee on Evaluation of the Lovell Federal Health Care Center Merger; Board on the Health of Select Populations; Institute of Medicine. Evaluation of the Lovell Federal Health Care Center Merger: Findings, Conclusions and Recommendations (2012). The National Academies Press Website. http://www.iom.edu/evaluatinglovell. Released October 12, 2012. Accessed November 5, 2014.
3. U.S. Department of Defense. Remarks by Secretary Panetta and Secretary Shinseki from the Department of Veterans Affairs [News transcript]. U.S. Department of Defense Website. http://www.defense.gov/Transcripts/Transcript.aspx?TranscriptID=5187. Published February 5, 2013. Accessed November 5, 2014.
1. Panangala SV, Jansen DJ. Departments of Defense and Veterans Affairs: Status of the Integrated Electronic Health Record (iEHR). Federation of American Scientists Website. http://fas.org/sgp/crs/misc/R42970.pdf. Published February 26, 2013. Accessed November 11, 2014.
2. Committee on Evaluation of the Lovell Federal Health Care Center Merger; Board on the Health of Select Populations; Institute of Medicine. Evaluation of the Lovell Federal Health Care Center Merger: Findings, Conclusions and Recommendations (2012). The National Academies Press Website. http://www.iom.edu/evaluatinglovell. Released October 12, 2012. Accessed November 5, 2014.
3. U.S. Department of Defense. Remarks by Secretary Panetta and Secretary Shinseki from the Department of Veterans Affairs [News transcript]. U.S. Department of Defense Website. http://www.defense.gov/Transcripts/Transcript.aspx?TranscriptID=5187. Published February 5, 2013. Accessed November 5, 2014.

Diabetes Patient-Centered Medical Home Approach
Type 2 diabetes mellitus (T2DM) is a significant, growing health problem that results in increased morbidity and mortality. In adults, T2DM accounts for about 90% to 95% of all diagnosed cases of diabetes.1 Diabetes is the leading cause of kidney failure and blindness; moreover, diabetic patients are 2 to 4 times more likely to die of complications of heart disease and/or have a stroke.2 Other complications of diabetes include nervous system damage and nontraumatic lower limb amputation. Increased morbidity and mortality not only diminishes quality of life (QOL) for patients with diabetes, but also produces a financial health care burden. The cost of diabetes in the U.S. in 2012 was more than $245 billion compared with $174 billion in 2007.1
The Centers for Disease Control and Prevention (CDC) predicts that 1 in 3 American adults will develop diabetes by 2050; thus, optimal approaches to diabetic care need to be developed and evaluated to determine best practices.3,4 Better control of blood sugar, cholesterol, and blood pressure levels in people with diabetes will help reduce the risk of complications of kidney disease, eye disease, nervous system disease, heart attack, and stroke.5 Optimal approaches to diabetes management must now be developed to prepare for the forecasted increase of T2DM.
A review of the literature confirms that lack of continuity of care often leads to patient dissatisfaction with health care, to fragmented health care, and a greater propensity to disregard a defined health care treatment plan.6,7 In addition to improved patient satisfaction and adherence to medical management, improved continuity of care is cost-effective. A longitudinal study based on claims data from 2000 to 2008, using the continuity of care index, indicated that improved continuity of care was associated with less health care waste and lower health care expenses for patients with T2DM.8 An average savings of $737 in total health care expenses per person was achieved with better continuity of care.8 These studies demonstrate that improving continuity of care improves outcomes in patients with diabetes and helps prevent excessive health care costs and waste.
Medical Center NonContinuity
Lack of continuity of care has been identified as a potential obstacle to optimal diabetic outcomes at William Beaumont Army Medical Center (WBAMC) in El Paso, Texas, based on a recent data analysis provided by TRICARE Regional Office West.9,10 As of March 2010, 56,936 patients were enrolled in TRICARE Prime. Of these patients, only 29.92% had appointments with their assigned primary care manager (PCM).9
In 2009, WBAMC developed a database to track the Healthcare Effectiveness Data and Information Set (HEDIS) measures to monitor A1c as well as other indicators of performance of health care services, such as mammography, Pap smear, bone densitometry, and colorectal screening. A recent American Diabetic Association expert committee recommendation endorsed the use of A1c value > 6.5% to confirm the diagnosis of diabetes.11 The A1c test may be confirmed with a repeat test unless clinical symptoms exist or the patient has random glucose levels > 200 mg/dL. Importantly, individuals with an A1c between 6% and 6.5% have a higher risk for developing diabetes and may be diagnosed with prediabetes.3
From 2008 to 2009, the HEDIS database tracking the progress of A1c demonstrated a 0.3% positive change and improvement in A1c ≤ 9% (normal 4%-6%). The goal for people with diabetes is A1c < 7%. Uncontrolled diabetes, (ie, A1c > 9%), is associated with greater diabetes-related complications.12 Using the HEDIS benchmark of ≥ 9%, the HEDIS A1c data for fiscal year (FY) 2008 were 71.1 (p50) and 81 (p90), and for FY 2009 were 72.2 (p50) and 81.3 (p90), reflecting p90 0.3% improvement.13 Therefore, these data reflect poor outcomes of patients with T2DM with A1c levels that were not controlled at WBAMC.
Uncontrolled diabetes accrues significant health care costs and adverse diabetic outcomes.10 Consequently, the WBAMC clinical operations division, which was tasked to monitor the HEDIS database, identified and contacted individuals to schedule health care appointments. The primary endeavor was an attempt to substantially increase benchmarks and maintain levels of A1c < 9%, demonstrate improvement in quality of care, and reduce health care costs. Unfortunately, these goals were not met for the aggregate of patients with T2DM.
Figure 1 illustrates how the diabetic population at WBAMC had experienced decreased continuity of care and the adverse effects on their diabetes management. Figure 1 also illustrates how beneficiaries of TRICARE are assigned a PCM and how this process results in a lack of continuity of care for patients with T2DM. An Army medical center (MEDCEN) typically uses PCMs who may be a physician, nurse practitioner (NP), or physician assistant. Unfortunately, the majority of these PCMs are active-duty military or civil service personnel who commonly undergo permanent change of station moves or deployments every 3 years. Additionally, military providers are often rotated through department-chief positions, thereby dissolving their patient relationships.
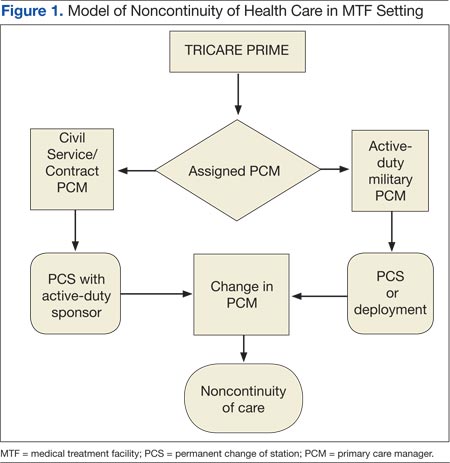
Frequent rotations offer a valid means to foster leadership skills much needed in a military conflict zone and maximize military professional development; however, rotations also contribute to the lack of continuity of patient care. This PCM instability and the distinctive military dynamic volatility are characteristic of standard military operating procedure and are unlikely to change.
New solutions are needed to promote improved continuity of care for patients with diabetes at a MEDCEN. According to Lt Gen Eric Schoomaker, former Surgeon General of the Army, “The Patient-Centered Medical Home concept is being adopted throughout the military health system.”14 The goal of the trend toward patient-centered medical home (PCMH) care delivery is to improve access to high-quality health care services.13
Patient-Centered Medical Home
The term patient-centered medical home was introduced in 1967 by the American Academy of Pediatrics (AAP).15 In 2008, PCMH principles became integral in most health care reform initiatives.16 In most PCMH models, increased continuity of care is the single common denominator of practice. Continuity of care is defined as intensified integration, coordination, and sharing of information between disciplines that result in improved patient outcomes.10,17,18
In 2007, a consensus statement was provided by the American Academy of Family Practice, the AAP, American College of Physicians, and the American Osteopathic Association stating that quality and safety are hallmarks of the PCMH and may improve outcomes for chronic disease, such as diabetes.19
Quality improvement is vital in health care organizations because of demands by government agencies, health maintenance organizations, and the public to continually improve services and to provide the highest quality health care at the best cost.20 Diabetes has become a public health crisis, as previously discussed, and a comprehensive approach to care management is essential. Developing an optimal process for diabetes health care and methods for evaluation of the delivery process is foundational for all stakeholders involved, including health care organizations, health care providers, and patients.20
Diabetic outcomes were evaluated at a recent 2-year trial PCMH approach T2DM clinic at a MEDCEN at WBAMC. The purpose of the project was to determine whether a PCMH approach improves disease management compared with routine primary care management.
Methods
The process and manner of care delivery was the focus of this analysis and evaluation, not clinician knowledge of treatment management. A comparison of care delivery approaches of PCM management and PCMH care delivery is displayed in the Table. The treatment algorithm for T2DM was not in question, because guidelines for practice are established based on scientific evidence, and medication management is based on evidence-based practice.21,22 Evaluation consisted of T2DM delivery of care process and the efficacy of outcome achieved by the specified delivery of care: (a) increased access to care; (b) intensive, repeated education; and (3) a multidisciplinary approach focused on patient empowerment. The following is a description of the specified delivery of care.
Increased Access to Care
Increased access to care addressed through frequent telecommunication provided by the registered nurse (RN) case manager who regularly called patients within 72 hours of insulin adjustment or 24 hours for insulin initiation or significant medication changes. Additionally, the diabetes team providers requested a follow-up appointment in 1 week when injectable medication was added or changes were made in insulin management. One exception was for the addition of livaglutide, in which a 2-week follow-up was made, to allow for titration of the medication. For oral medication adjustment, a 1-month follow-up was generally made, with a 2-month follow-up when a glucose histogram indicated optimal glycemic control, an average blood glucose of 7% (estimated average glucose of 154 mg/dL) or less. Time for appointments was increased by 10 minutes for a total of 30-minute appointments, compared with 20 minutes for PCM delivery.
Informational continuity was thought to be improved by use of an electronic medical record (EMR), allowing for an uninterrupted patient record. Providers were expected to document medication reconciliation with a clear explanation of medication adjustments listed in the plan. Patient teaching was documented, describing the specific patient education concerns addressed. Other data included a glucometer statistical report from the last appointment to the current appointment, to track negative or positive changes in glycemic control.
Patient Education
The management technique used in the clinic was intensive, repeated education with the goal of improving learning and retention with repeated instruction and positive reinforcement. Skinner theorized that learning is the acquisition of new behavior through conditioning (eg, repeated instruction), is in close proximity of time, and is likely to result in learning retention, which remain relevant education practice.23,24 The T2DM clinic operates on Skinner’s principles of repeated, intensive education. For example, patients must bring their glucometer to every appointment. The statistical analysis downloaded from the glucometer provides immediate reinforcement and information about patients’ glycemic control. Patients are typically excited to see an improvement from previous levels and are encouraged to continue behavior modification. Conversely, statistical analysis demonstrating poor glycemic control generally encourages the patient to make needed lifestyle changes. Thus, changes in behavior due to intensive, repeated education, followed by a reinforcing stimulus results in an increased probability of that behavior occurring in the future.23,25 The interdisciplinary team provides education during each T2DM patient encounter.
Multidisciplinary Approach
The multidisciplinary team formed at the trial T2DM clinic consisted of a medical doctor, family NP, pharmacist, RN, licensed vocational nurse, and registered dietician. The team members were each encouraged to obtain Certified Diabetes Educator (CDE) certification. For the first 6 months of developing the clinic, staff scheduled weekly team-building meetings to encourage esprit de corps. The weekly meetings were also used to discuss difficult patient cases. The RN case manager provided the patients with individualized plans to help them meet specified goals and provided easy accessibility for patient questions and concerns. The pharmacist was integral in helping patients understand the role of their medication and was also certified to make medication adjustments related to diabetes.
A recent Institute of Medicine (IOM) report encouraged the expansion of roles for nurse practitioners (NPs) in coordination and primary care delivery.26 The IOM collaborative statement is based on numerous studies showing that NPs provided equivalent quality of care compared with that of primary care physicians in routine chronic disease management.26 Nurse case managers functioned as an integral part of the intensive therapy involved in the landmark Diabetes Control and Complication Trial.27
The intended policy analysis and outcome evaluation was confined to data collected from a disease-specific (T2DM) clinic with a PCMH approach developed April 2011 at WBAMC. Data were obtained from the WBAMC database designed to track the HEDIS measures.
Enrollees of the clinic were restricted to patients diagnosed with T2DM who were TRICARE beneficiaries. Males and females, aged > 20 years with an established A1c > 6.5% comprised the patient population of the clinic. Individuals who were managed by WBAMC or were TRICARE standard beneficiaries were excluded from the study. Because patients with T1DM have a different pathology than those with T2DM, they were referred to endocrinology. Patients with gestational diabetes were referred to obstetrics for management.
Data Collection
Existing data in the Armed Forces Health Longitudinal Technology Application (AHLTA) EMR were used for this analysis. Data were accessed by a Common Access Card (CAC card) enhanced security system accessed only through secure CAC applications.
Diabetic outcomes of glycemic control as measured by the A1c value were examined prior to clinic enrollment (time 1: PCM care delivery) and subsequently (time 2: PCMH care delivery) at the health care provider’s discretion. The second time varied between 2 and 6 months, depending on (1) provider need to determine quickly (2 months) whether a downward trend was occurring because of multiple comorbidities; (2) provider discretion to wait an additional 3 months (A1c turnover x 2 = 6 months), while medication adjustments are being made; and (3) according to feasibility of follow-up based on patient’s scheduling. Low-density lipoprotein cholesterol (LDL-C) was also examined at both PCM care delivery and PCMH care delivery.
The endpoints of a reduction in A1c by 1% and an LDL-C that is ≤ 100 mg/dL determined improved diabetes outcomes. Existing data (eg, glycemic control [A1c], lipid control [LDL-C]), from April 1, 2011, to December 31, 2011, were logged in a clinic database. These data served to demonstrate the effectiveness of the T2DM PCMH approach to clinic management. The PCMH principles that were examined included the standard operating procedure for the T2DM-PCMH clinic: frequent appointments > 2 in a 3-month period), a multidisciplinary team, and intensive, repeated education.
Data analysis was conducted with descriptive statistics (frequencies, means, SDs) and t test analysis to determine relationships between variables of A1c, LDL-C, and frequency of visits. Improved diabetic outcomes, as previously defined, inferred that developing principles of a T2DM-PCMH clinic based on the principles of a PCMH provided a solution to optimal T2DM management compared with routine primary care delivery, consisting of a TRICARE-assigned PCM.
Results
A total of 638 unique patients were seen at the T2DM-PCMH clinic. Of these, 237 patient records in the database met the inclusion criteria and were acceptable for analysis and evaluation. Patients were omitted for the following reasons: 255 patients did not meet protocol of a minimum 2 visits during the evaluation period, 77 patients were omitted due to no second A1c available, 65 patients did not meet the clinic protocol of a A1c of > 6.5%, and 4 were omitted because no A1c was available for pre- or postanalysis. Data analysis and evaluation of the remaining 237 acceptable patients demonstrated that a T2DM-PCMH approach provided improved diabetic care compared with routine, PCM management.
Patients enrolled at the WBAMC T2DM clinic demonstrated clinically significant improvement (P < .001), and 80.5% achieved > 1% improvement in glycemic control. The greatest number of visits of 26 visits, an outlier not typical of the frequency of patient visits, was attributed to brittle T2DM requiring more frequent monitoring. Most patients had 3 T2DM-PCMH clinic appointments (2 were the minimum visits described in clinic protocol).
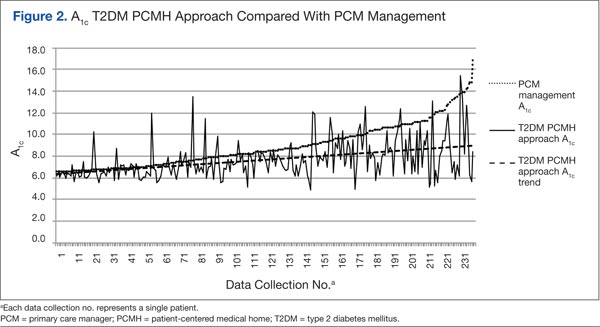
Low-density lipoprotein cholesterol levels were analyzed to determine whether patients with diabetes managed at the WBAMC T2DM clinic also had improved lipid control. A total of 638 patients had an initial LDL-C level drawn prior to clinic management. Of these patients, 282 were acceptable for analysis (Figure 2). Low-density lipoprotein cholesterol data were omitted because 93 did not have a paired pre- and postvalues, 8 values were invalid due to nonfasting laboratory status; and 255 values were omitted due to having < 2 clinic visits. Results of the data analysis demonstrated that LDL-C was well managed by the T2DM clinic, with levels ≤ 100 mg/dL (P < .001) (Figure 3).
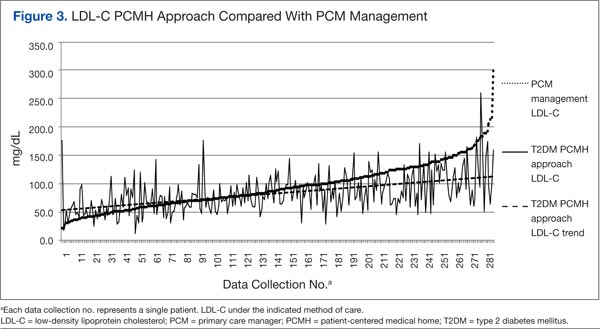
Discussion
The WBAMC T2DM clinic was formed as a trial clinic at a medical treatment facility (MTF) MEDCEN due to the failure of routine PCM care to improve outcomes in the management of the diabetes population (A1c < 7.0%). Overall, improved endpoints of A1c, LDL-C were achieved with the disease-specific PCMH approach compared with routine PCM approach. The results indicate that disease-specific management leads to improved diabetic endpoints (A1c reduction by at least 1% and LDL-C < 100 mg/dL). The clinic’s protocol (listed in the methods) was intended to improve continuity.
A review of the literature confirmed that continuity of care is integral to patient satisfaction and improved diabetes management.8,10,17,28,29 The results of the study were consistent with those in the literature. The review of the literature established that patients who develop a trusting relationship with the health care provider as the T2DM clinic promoted (eg, frequent patient appointments, telecommunication by nurse, and patient participation) are more likely to follow medical therapy and take a proactive role in disease management.6,28,30
Conclusion
This study demonstrated that PCMH-delivered care offers a solution to suboptimal management of chronic disease, such as T2DM, and that chronic disease is best managed by implementation of a disease-specific PCMH. It is recommended that a MTF develop other disease-specific PCMH and pilot-test these programs. Long-term follow-up studies and additional data collection, such as blood pressure control, abdominal circumference, body mass index, and triglyceride levels would be useful to determine effectiveness.
Based on principles of a PCMH, the efficacy of the T2DM clinic at WBAMC demonstrated that improved diabetes management was achieved by increased continuity of care; intensive, repeated patient education; and a multidisciplinary team approach. The CDC identifies self-management training as foundational to improving health outcomes and QOL for individuals with diabetes.1 Primary care providers in a MTF may improve diabetic patient outcomes by referring patients to a T2DM clinic, such as the WBAMC T2DM clinic. The multidisciplinary team facilitated patient empowerment by educating patients on the management of their disease and the problem-solving and coping skills required to manage a chronic disease.
The WBAMC T2DM-PCMH based mission of fostering patient empowerment and a team approach is a comprehensive approach to diabetes care. Currently, the PCMH model is being adapted by the military in the latest health care reform initiatives.14 However, the move toward the PCMH model does not incorporate disease-specific PCMH clinics. This study demonstrates that the disease-specific PCMH approach provides improved disease management and may be effective in other chronic disease management. A benefit of the T2DM-PCMH approach is the reduced burden of escalating health care costs related to increased morbidity and mortality, which is associated with the growing health care problem of poorly controlled T2DM.1,4,31
The disease-specific clinic evaluated at WBAMC provides an effective solution to fragmented health care for the optimal management of T2DM. The clinic’s conceptual framework of increased access to care, with consistent education at closer time intervals when compared with PCM management resulted in improved continuity and T2DM control. Future research in this area should assess measurable cost reduction. Improved disease management as demonstrated by the T2DM disease-specific clinic at WBAMC provides sufficient incentive to incorporate similar T2DM continuity clinics and changes throughout MTFs.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Centers for Disease Control and Prevention (CDC). National Diabetes Fact Sheet, 2014. CDC Website. http://www.cdc.gov/diabetes/data/statistics/2014StatisticsReport.html. Updated October 24, 2014. Accessed November 6, 2014.
2. American Diabetes Association. National Diabetes Fact Sheet. Statistics about diabetes. American Diabetes Association Website. http://www.diabetes.org/diabetes-basics/diabetes-statistics. Released June 10, 2014. Accessed November 6, 2014.
3. Centers for Disease Control and Prevention (CDC). Number of Americans with diabetes rises to nearly 26 million [press release]. CDC Website. http://www.cdc.gov/media/releases/2011/p0126_diabetes.html. Published January 26, 2011. Accessed November 6, 2014.
4. Huang ES, Basu A, O’Grady M, Capretta JC. Projecting the future diabetes population size and related costs for the U.S. Diabetes Care. 2009;32(12):2225-2229.
5. National Library of Medicine. Diabetes. PubMed Website. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002194. Reviewed May 24, 2013. Accessed November 6, 2014.
6. Chu-Weininger MY, Balkrishnan R. Consumer satisfaction with primary care provider choice and associated trust. BMC Health Serv Res. 2006;6:139.
7. Alazri MH, Neal RD, Heywood P, Leese B. Patients’ experience of continuity of care of type 2 diabetes: A focus group study in primary care. Br J Gen Prac. 2006;56(528):488-495.
8. Chen CC, Chen SH. Better continuity of care reduces costs for diabetic patients. Am J Manag Care. 2011;17(6):420-427.
9. TRICARE Regional Office-West. Military Treatment Facility (MTF) Profile of William Beaumont Army Medical Center, FY2010 Q2. El Paso, TX. Published March 2010.
10. Worrall G, Knight J. Continuity of care is good for elderly people with diabetes: Retrospective cohort study of mortality and hospitalization. Can Fam Physician. 2011;57(1):e6-e20.
11. Kerr M. ADA 2009: Expert committee recommends use of hemoglobin A1c for diagnosis. Medscape Website. http://www.medscape.com/viewarticle/704021. Published June 7, 2009. Accessed November 7, 2014.
12. Drexler AJ. Lessons learned from landmark trials of type 2 diabetes mellitus and potential applications to clinical practice. Postgrad Med. 2003;Spec No:15-26.
13. Office of Evidence-Based Practice Quality Management Division U.S. Army Medical Command. Population Health: Update of HEDIS measures. U.S. Army Medical Department Office of Quality Management Website. https://www.qmo.amedd.army.mil/HEDIS/HEDIS_MeasuresAcrossAMEDD.pdf. Published April 2010. Accessed November 2014.
14. Schoomaker E. Army medicine: Bringing value and inspiring trust. U.S. Medicine. 2011:10-13.
15. Sia C, Tonniges TF, Osterhus E, Taba S. History of the medical home concept. Pediatrics. 2004;113(5 suppl):1473-1478.
16. Kugler JP. Military Health System Patient Centered Medical Home Guide. Defense Health Agency Website. http://www.tricare.mil/tma/ocmo/download/MHSPCMHGuide.pdf. Published June 2011. Accessed November 11, 2014.
17. Naithani S, Gulliford M. Morgan M. Patients’ perceptions and experiences of ‘continuity of care’ in diabetes. Health Expect. 2006;9(2):118-129.
18. O’Malley AS, Cunningham PJ. Patient experiences with coordination of care: The benefit of continuity and primary care physician as referral source. J Gen Intern Med. 2009;24(2):170-177.
19. American Academy of Family Practice, American Academy of Pediatrics, American College of Physicians, and the American Osteopathic Association. Joint principles of the patient-centered medical home. American Academy of Family Practice Website. http://www.aafp.org/dam/AAFP/documents/practice_management/pcmh/initiatives/PCMHJoint.pdf. Published February 2007. Accessed November 7, 2014.
20. Meyer JA, Silow-Carroll S, Kutyla T, Stepnick LS, Rybowski LS. Hospital Quality: Ingredients for Success--Overview and Lessons Learned. New York, New York: The Commonwealth Fund; 2004.
21. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 8th ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2008.
22. American Association of Clinical Endocrinologists. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice. American Association of Clinical Endocrinologists Website. https://www.aace.com/files/dm-guidelines-ccp.pdf. Accessed November 7, 2014.
23. Skinner BF. The Behavior of Organisms: An Experimental Analysis. New York, NY: Appleton-Century; 1938.
24. Staddon JE, Cerutti DT. Operant conditioning. Annu Rev Psychol. 2003;54:115-144.
25. Bruner RF. Repetition Is the First Principle of All Learning. Social Science Research network Website. http://papers.ssrn.com/sol3/papers.cfm?abstract_id=224340. Posted August 26, 2001. Accessed November 7, 2014.
26. Institute of Medicine. The Future Of Nursing: Leading Change, Advancing Health. Washington, DC: National Academics Press; 2011.
27. Willens D, Cripps R, Wilson A, Wolff K, Rothman R. Interdisciplinary team care for diabetic patients by primary care physicians, advance practice nurses and clinical pharmacists. Clin Diabetes. 2011;29(2):60-68.
28. Renders CM, Valk GD, Griffin S, Wagner EH, Eijk JT, Assendelft WJ. Interventions to improve the management of diabetes mellitus in primary care, outpatient and community settings. Cochrane Database Syst Rev. 2001;(1):CD001481.
29. Health Affairs. Patient-centered medical homes. Health Affairs Website. http://www.healthaffairs.org. Dated September 14, 2010. Accessed November 7, 2014.
30. Berry LL, Parish JT, Janakiraman R, et al. Patients’ commitment to their primary physician and why it matters. Ann Fam Med. 2008;6(1):6-13.
31. Glasgow RE, Wagner EH, Kaplan RM, Vinicor F, Smith L, Norman J. If diabetes is a public health problem, why not treat it as one? A population-based approach to chronic illness. Ann Behav Med. 1999;21(2):159-170.
Type 2 diabetes mellitus (T2DM) is a significant, growing health problem that results in increased morbidity and mortality. In adults, T2DM accounts for about 90% to 95% of all diagnosed cases of diabetes.1 Diabetes is the leading cause of kidney failure and blindness; moreover, diabetic patients are 2 to 4 times more likely to die of complications of heart disease and/or have a stroke.2 Other complications of diabetes include nervous system damage and nontraumatic lower limb amputation. Increased morbidity and mortality not only diminishes quality of life (QOL) for patients with diabetes, but also produces a financial health care burden. The cost of diabetes in the U.S. in 2012 was more than $245 billion compared with $174 billion in 2007.1
The Centers for Disease Control and Prevention (CDC) predicts that 1 in 3 American adults will develop diabetes by 2050; thus, optimal approaches to diabetic care need to be developed and evaluated to determine best practices.3,4 Better control of blood sugar, cholesterol, and blood pressure levels in people with diabetes will help reduce the risk of complications of kidney disease, eye disease, nervous system disease, heart attack, and stroke.5 Optimal approaches to diabetes management must now be developed to prepare for the forecasted increase of T2DM.
A review of the literature confirms that lack of continuity of care often leads to patient dissatisfaction with health care, to fragmented health care, and a greater propensity to disregard a defined health care treatment plan.6,7 In addition to improved patient satisfaction and adherence to medical management, improved continuity of care is cost-effective. A longitudinal study based on claims data from 2000 to 2008, using the continuity of care index, indicated that improved continuity of care was associated with less health care waste and lower health care expenses for patients with T2DM.8 An average savings of $737 in total health care expenses per person was achieved with better continuity of care.8 These studies demonstrate that improving continuity of care improves outcomes in patients with diabetes and helps prevent excessive health care costs and waste.
Medical Center NonContinuity
Lack of continuity of care has been identified as a potential obstacle to optimal diabetic outcomes at William Beaumont Army Medical Center (WBAMC) in El Paso, Texas, based on a recent data analysis provided by TRICARE Regional Office West.9,10 As of March 2010, 56,936 patients were enrolled in TRICARE Prime. Of these patients, only 29.92% had appointments with their assigned primary care manager (PCM).9
In 2009, WBAMC developed a database to track the Healthcare Effectiveness Data and Information Set (HEDIS) measures to monitor A1c as well as other indicators of performance of health care services, such as mammography, Pap smear, bone densitometry, and colorectal screening. A recent American Diabetic Association expert committee recommendation endorsed the use of A1c value > 6.5% to confirm the diagnosis of diabetes.11 The A1c test may be confirmed with a repeat test unless clinical symptoms exist or the patient has random glucose levels > 200 mg/dL. Importantly, individuals with an A1c between 6% and 6.5% have a higher risk for developing diabetes and may be diagnosed with prediabetes.3
From 2008 to 2009, the HEDIS database tracking the progress of A1c demonstrated a 0.3% positive change and improvement in A1c ≤ 9% (normal 4%-6%). The goal for people with diabetes is A1c < 7%. Uncontrolled diabetes, (ie, A1c > 9%), is associated with greater diabetes-related complications.12 Using the HEDIS benchmark of ≥ 9%, the HEDIS A1c data for fiscal year (FY) 2008 were 71.1 (p50) and 81 (p90), and for FY 2009 were 72.2 (p50) and 81.3 (p90), reflecting p90 0.3% improvement.13 Therefore, these data reflect poor outcomes of patients with T2DM with A1c levels that were not controlled at WBAMC.
Uncontrolled diabetes accrues significant health care costs and adverse diabetic outcomes.10 Consequently, the WBAMC clinical operations division, which was tasked to monitor the HEDIS database, identified and contacted individuals to schedule health care appointments. The primary endeavor was an attempt to substantially increase benchmarks and maintain levels of A1c < 9%, demonstrate improvement in quality of care, and reduce health care costs. Unfortunately, these goals were not met for the aggregate of patients with T2DM.
Figure 1 illustrates how the diabetic population at WBAMC had experienced decreased continuity of care and the adverse effects on their diabetes management. Figure 1 also illustrates how beneficiaries of TRICARE are assigned a PCM and how this process results in a lack of continuity of care for patients with T2DM. An Army medical center (MEDCEN) typically uses PCMs who may be a physician, nurse practitioner (NP), or physician assistant. Unfortunately, the majority of these PCMs are active-duty military or civil service personnel who commonly undergo permanent change of station moves or deployments every 3 years. Additionally, military providers are often rotated through department-chief positions, thereby dissolving their patient relationships.
Frequent rotations offer a valid means to foster leadership skills much needed in a military conflict zone and maximize military professional development; however, rotations also contribute to the lack of continuity of patient care. This PCM instability and the distinctive military dynamic volatility are characteristic of standard military operating procedure and are unlikely to change.
New solutions are needed to promote improved continuity of care for patients with diabetes at a MEDCEN. According to Lt Gen Eric Schoomaker, former Surgeon General of the Army, “The Patient-Centered Medical Home concept is being adopted throughout the military health system.”14 The goal of the trend toward patient-centered medical home (PCMH) care delivery is to improve access to high-quality health care services.13
Patient-Centered Medical Home
The term patient-centered medical home was introduced in 1967 by the American Academy of Pediatrics (AAP).15 In 2008, PCMH principles became integral in most health care reform initiatives.16 In most PCMH models, increased continuity of care is the single common denominator of practice. Continuity of care is defined as intensified integration, coordination, and sharing of information between disciplines that result in improved patient outcomes.10,17,18
In 2007, a consensus statement was provided by the American Academy of Family Practice, the AAP, American College of Physicians, and the American Osteopathic Association stating that quality and safety are hallmarks of the PCMH and may improve outcomes for chronic disease, such as diabetes.19
Quality improvement is vital in health care organizations because of demands by government agencies, health maintenance organizations, and the public to continually improve services and to provide the highest quality health care at the best cost.20 Diabetes has become a public health crisis, as previously discussed, and a comprehensive approach to care management is essential. Developing an optimal process for diabetes health care and methods for evaluation of the delivery process is foundational for all stakeholders involved, including health care organizations, health care providers, and patients.20
Diabetic outcomes were evaluated at a recent 2-year trial PCMH approach T2DM clinic at a MEDCEN at WBAMC. The purpose of the project was to determine whether a PCMH approach improves disease management compared with routine primary care management.
Methods
The process and manner of care delivery was the focus of this analysis and evaluation, not clinician knowledge of treatment management. A comparison of care delivery approaches of PCM management and PCMH care delivery is displayed in the Table. The treatment algorithm for T2DM was not in question, because guidelines for practice are established based on scientific evidence, and medication management is based on evidence-based practice.21,22 Evaluation consisted of T2DM delivery of care process and the efficacy of outcome achieved by the specified delivery of care: (a) increased access to care; (b) intensive, repeated education; and (3) a multidisciplinary approach focused on patient empowerment. The following is a description of the specified delivery of care.
Increased Access to Care
Increased access to care addressed through frequent telecommunication provided by the registered nurse (RN) case manager who regularly called patients within 72 hours of insulin adjustment or 24 hours for insulin initiation or significant medication changes. Additionally, the diabetes team providers requested a follow-up appointment in 1 week when injectable medication was added or changes were made in insulin management. One exception was for the addition of livaglutide, in which a 2-week follow-up was made, to allow for titration of the medication. For oral medication adjustment, a 1-month follow-up was generally made, with a 2-month follow-up when a glucose histogram indicated optimal glycemic control, an average blood glucose of 7% (estimated average glucose of 154 mg/dL) or less. Time for appointments was increased by 10 minutes for a total of 30-minute appointments, compared with 20 minutes for PCM delivery.
Informational continuity was thought to be improved by use of an electronic medical record (EMR), allowing for an uninterrupted patient record. Providers were expected to document medication reconciliation with a clear explanation of medication adjustments listed in the plan. Patient teaching was documented, describing the specific patient education concerns addressed. Other data included a glucometer statistical report from the last appointment to the current appointment, to track negative or positive changes in glycemic control.
Patient Education
The management technique used in the clinic was intensive, repeated education with the goal of improving learning and retention with repeated instruction and positive reinforcement. Skinner theorized that learning is the acquisition of new behavior through conditioning (eg, repeated instruction), is in close proximity of time, and is likely to result in learning retention, which remain relevant education practice.23,24 The T2DM clinic operates on Skinner’s principles of repeated, intensive education. For example, patients must bring their glucometer to every appointment. The statistical analysis downloaded from the glucometer provides immediate reinforcement and information about patients’ glycemic control. Patients are typically excited to see an improvement from previous levels and are encouraged to continue behavior modification. Conversely, statistical analysis demonstrating poor glycemic control generally encourages the patient to make needed lifestyle changes. Thus, changes in behavior due to intensive, repeated education, followed by a reinforcing stimulus results in an increased probability of that behavior occurring in the future.23,25 The interdisciplinary team provides education during each T2DM patient encounter.
Multidisciplinary Approach
The multidisciplinary team formed at the trial T2DM clinic consisted of a medical doctor, family NP, pharmacist, RN, licensed vocational nurse, and registered dietician. The team members were each encouraged to obtain Certified Diabetes Educator (CDE) certification. For the first 6 months of developing the clinic, staff scheduled weekly team-building meetings to encourage esprit de corps. The weekly meetings were also used to discuss difficult patient cases. The RN case manager provided the patients with individualized plans to help them meet specified goals and provided easy accessibility for patient questions and concerns. The pharmacist was integral in helping patients understand the role of their medication and was also certified to make medication adjustments related to diabetes.
A recent Institute of Medicine (IOM) report encouraged the expansion of roles for nurse practitioners (NPs) in coordination and primary care delivery.26 The IOM collaborative statement is based on numerous studies showing that NPs provided equivalent quality of care compared with that of primary care physicians in routine chronic disease management.26 Nurse case managers functioned as an integral part of the intensive therapy involved in the landmark Diabetes Control and Complication Trial.27
The intended policy analysis and outcome evaluation was confined to data collected from a disease-specific (T2DM) clinic with a PCMH approach developed April 2011 at WBAMC. Data were obtained from the WBAMC database designed to track the HEDIS measures.
Enrollees of the clinic were restricted to patients diagnosed with T2DM who were TRICARE beneficiaries. Males and females, aged > 20 years with an established A1c > 6.5% comprised the patient population of the clinic. Individuals who were managed by WBAMC or were TRICARE standard beneficiaries were excluded from the study. Because patients with T1DM have a different pathology than those with T2DM, they were referred to endocrinology. Patients with gestational diabetes were referred to obstetrics for management.
Data Collection
Existing data in the Armed Forces Health Longitudinal Technology Application (AHLTA) EMR were used for this analysis. Data were accessed by a Common Access Card (CAC card) enhanced security system accessed only through secure CAC applications.
Diabetic outcomes of glycemic control as measured by the A1c value were examined prior to clinic enrollment (time 1: PCM care delivery) and subsequently (time 2: PCMH care delivery) at the health care provider’s discretion. The second time varied between 2 and 6 months, depending on (1) provider need to determine quickly (2 months) whether a downward trend was occurring because of multiple comorbidities; (2) provider discretion to wait an additional 3 months (A1c turnover x 2 = 6 months), while medication adjustments are being made; and (3) according to feasibility of follow-up based on patient’s scheduling. Low-density lipoprotein cholesterol (LDL-C) was also examined at both PCM care delivery and PCMH care delivery.
The endpoints of a reduction in A1c by 1% and an LDL-C that is ≤ 100 mg/dL determined improved diabetes outcomes. Existing data (eg, glycemic control [A1c], lipid control [LDL-C]), from April 1, 2011, to December 31, 2011, were logged in a clinic database. These data served to demonstrate the effectiveness of the T2DM PCMH approach to clinic management. The PCMH principles that were examined included the standard operating procedure for the T2DM-PCMH clinic: frequent appointments > 2 in a 3-month period), a multidisciplinary team, and intensive, repeated education.
Data analysis was conducted with descriptive statistics (frequencies, means, SDs) and t test analysis to determine relationships between variables of A1c, LDL-C, and frequency of visits. Improved diabetic outcomes, as previously defined, inferred that developing principles of a T2DM-PCMH clinic based on the principles of a PCMH provided a solution to optimal T2DM management compared with routine primary care delivery, consisting of a TRICARE-assigned PCM.
Results
A total of 638 unique patients were seen at the T2DM-PCMH clinic. Of these, 237 patient records in the database met the inclusion criteria and were acceptable for analysis and evaluation. Patients were omitted for the following reasons: 255 patients did not meet protocol of a minimum 2 visits during the evaluation period, 77 patients were omitted due to no second A1c available, 65 patients did not meet the clinic protocol of a A1c of > 6.5%, and 4 were omitted because no A1c was available for pre- or postanalysis. Data analysis and evaluation of the remaining 237 acceptable patients demonstrated that a T2DM-PCMH approach provided improved diabetic care compared with routine, PCM management.
Patients enrolled at the WBAMC T2DM clinic demonstrated clinically significant improvement (P < .001), and 80.5% achieved > 1% improvement in glycemic control. The greatest number of visits of 26 visits, an outlier not typical of the frequency of patient visits, was attributed to brittle T2DM requiring more frequent monitoring. Most patients had 3 T2DM-PCMH clinic appointments (2 were the minimum visits described in clinic protocol).
Low-density lipoprotein cholesterol levels were analyzed to determine whether patients with diabetes managed at the WBAMC T2DM clinic also had improved lipid control. A total of 638 patients had an initial LDL-C level drawn prior to clinic management. Of these patients, 282 were acceptable for analysis (Figure 2). Low-density lipoprotein cholesterol data were omitted because 93 did not have a paired pre- and postvalues, 8 values were invalid due to nonfasting laboratory status; and 255 values were omitted due to having < 2 clinic visits. Results of the data analysis demonstrated that LDL-C was well managed by the T2DM clinic, with levels ≤ 100 mg/dL (P < .001) (Figure 3).
Discussion
The WBAMC T2DM clinic was formed as a trial clinic at a medical treatment facility (MTF) MEDCEN due to the failure of routine PCM care to improve outcomes in the management of the diabetes population (A1c < 7.0%). Overall, improved endpoints of A1c, LDL-C were achieved with the disease-specific PCMH approach compared with routine PCM approach. The results indicate that disease-specific management leads to improved diabetic endpoints (A1c reduction by at least 1% and LDL-C < 100 mg/dL). The clinic’s protocol (listed in the methods) was intended to improve continuity.
A review of the literature confirmed that continuity of care is integral to patient satisfaction and improved diabetes management.8,10,17,28,29 The results of the study were consistent with those in the literature. The review of the literature established that patients who develop a trusting relationship with the health care provider as the T2DM clinic promoted (eg, frequent patient appointments, telecommunication by nurse, and patient participation) are more likely to follow medical therapy and take a proactive role in disease management.6,28,30
Conclusion
This study demonstrated that PCMH-delivered care offers a solution to suboptimal management of chronic disease, such as T2DM, and that chronic disease is best managed by implementation of a disease-specific PCMH. It is recommended that a MTF develop other disease-specific PCMH and pilot-test these programs. Long-term follow-up studies and additional data collection, such as blood pressure control, abdominal circumference, body mass index, and triglyceride levels would be useful to determine effectiveness.
Based on principles of a PCMH, the efficacy of the T2DM clinic at WBAMC demonstrated that improved diabetes management was achieved by increased continuity of care; intensive, repeated patient education; and a multidisciplinary team approach. The CDC identifies self-management training as foundational to improving health outcomes and QOL for individuals with diabetes.1 Primary care providers in a MTF may improve diabetic patient outcomes by referring patients to a T2DM clinic, such as the WBAMC T2DM clinic. The multidisciplinary team facilitated patient empowerment by educating patients on the management of their disease and the problem-solving and coping skills required to manage a chronic disease.
The WBAMC T2DM-PCMH based mission of fostering patient empowerment and a team approach is a comprehensive approach to diabetes care. Currently, the PCMH model is being adapted by the military in the latest health care reform initiatives.14 However, the move toward the PCMH model does not incorporate disease-specific PCMH clinics. This study demonstrates that the disease-specific PCMH approach provides improved disease management and may be effective in other chronic disease management. A benefit of the T2DM-PCMH approach is the reduced burden of escalating health care costs related to increased morbidity and mortality, which is associated with the growing health care problem of poorly controlled T2DM.1,4,31
The disease-specific clinic evaluated at WBAMC provides an effective solution to fragmented health care for the optimal management of T2DM. The clinic’s conceptual framework of increased access to care, with consistent education at closer time intervals when compared with PCM management resulted in improved continuity and T2DM control. Future research in this area should assess measurable cost reduction. Improved disease management as demonstrated by the T2DM disease-specific clinic at WBAMC provides sufficient incentive to incorporate similar T2DM continuity clinics and changes throughout MTFs.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Type 2 diabetes mellitus (T2DM) is a significant, growing health problem that results in increased morbidity and mortality. In adults, T2DM accounts for about 90% to 95% of all diagnosed cases of diabetes.1 Diabetes is the leading cause of kidney failure and blindness; moreover, diabetic patients are 2 to 4 times more likely to die of complications of heart disease and/or have a stroke.2 Other complications of diabetes include nervous system damage and nontraumatic lower limb amputation. Increased morbidity and mortality not only diminishes quality of life (QOL) for patients with diabetes, but also produces a financial health care burden. The cost of diabetes in the U.S. in 2012 was more than $245 billion compared with $174 billion in 2007.1
The Centers for Disease Control and Prevention (CDC) predicts that 1 in 3 American adults will develop diabetes by 2050; thus, optimal approaches to diabetic care need to be developed and evaluated to determine best practices.3,4 Better control of blood sugar, cholesterol, and blood pressure levels in people with diabetes will help reduce the risk of complications of kidney disease, eye disease, nervous system disease, heart attack, and stroke.5 Optimal approaches to diabetes management must now be developed to prepare for the forecasted increase of T2DM.
A review of the literature confirms that lack of continuity of care often leads to patient dissatisfaction with health care, to fragmented health care, and a greater propensity to disregard a defined health care treatment plan.6,7 In addition to improved patient satisfaction and adherence to medical management, improved continuity of care is cost-effective. A longitudinal study based on claims data from 2000 to 2008, using the continuity of care index, indicated that improved continuity of care was associated with less health care waste and lower health care expenses for patients with T2DM.8 An average savings of $737 in total health care expenses per person was achieved with better continuity of care.8 These studies demonstrate that improving continuity of care improves outcomes in patients with diabetes and helps prevent excessive health care costs and waste.
Medical Center NonContinuity
Lack of continuity of care has been identified as a potential obstacle to optimal diabetic outcomes at William Beaumont Army Medical Center (WBAMC) in El Paso, Texas, based on a recent data analysis provided by TRICARE Regional Office West.9,10 As of March 2010, 56,936 patients were enrolled in TRICARE Prime. Of these patients, only 29.92% had appointments with their assigned primary care manager (PCM).9
In 2009, WBAMC developed a database to track the Healthcare Effectiveness Data and Information Set (HEDIS) measures to monitor A1c as well as other indicators of performance of health care services, such as mammography, Pap smear, bone densitometry, and colorectal screening. A recent American Diabetic Association expert committee recommendation endorsed the use of A1c value > 6.5% to confirm the diagnosis of diabetes.11 The A1c test may be confirmed with a repeat test unless clinical symptoms exist or the patient has random glucose levels > 200 mg/dL. Importantly, individuals with an A1c between 6% and 6.5% have a higher risk for developing diabetes and may be diagnosed with prediabetes.3
From 2008 to 2009, the HEDIS database tracking the progress of A1c demonstrated a 0.3% positive change and improvement in A1c ≤ 9% (normal 4%-6%). The goal for people with diabetes is A1c < 7%. Uncontrolled diabetes, (ie, A1c > 9%), is associated with greater diabetes-related complications.12 Using the HEDIS benchmark of ≥ 9%, the HEDIS A1c data for fiscal year (FY) 2008 were 71.1 (p50) and 81 (p90), and for FY 2009 were 72.2 (p50) and 81.3 (p90), reflecting p90 0.3% improvement.13 Therefore, these data reflect poor outcomes of patients with T2DM with A1c levels that were not controlled at WBAMC.
Uncontrolled diabetes accrues significant health care costs and adverse diabetic outcomes.10 Consequently, the WBAMC clinical operations division, which was tasked to monitor the HEDIS database, identified and contacted individuals to schedule health care appointments. The primary endeavor was an attempt to substantially increase benchmarks and maintain levels of A1c < 9%, demonstrate improvement in quality of care, and reduce health care costs. Unfortunately, these goals were not met for the aggregate of patients with T2DM.
Figure 1 illustrates how the diabetic population at WBAMC had experienced decreased continuity of care and the adverse effects on their diabetes management. Figure 1 also illustrates how beneficiaries of TRICARE are assigned a PCM and how this process results in a lack of continuity of care for patients with T2DM. An Army medical center (MEDCEN) typically uses PCMs who may be a physician, nurse practitioner (NP), or physician assistant. Unfortunately, the majority of these PCMs are active-duty military or civil service personnel who commonly undergo permanent change of station moves or deployments every 3 years. Additionally, military providers are often rotated through department-chief positions, thereby dissolving their patient relationships.
Frequent rotations offer a valid means to foster leadership skills much needed in a military conflict zone and maximize military professional development; however, rotations also contribute to the lack of continuity of patient care. This PCM instability and the distinctive military dynamic volatility are characteristic of standard military operating procedure and are unlikely to change.
New solutions are needed to promote improved continuity of care for patients with diabetes at a MEDCEN. According to Lt Gen Eric Schoomaker, former Surgeon General of the Army, “The Patient-Centered Medical Home concept is being adopted throughout the military health system.”14 The goal of the trend toward patient-centered medical home (PCMH) care delivery is to improve access to high-quality health care services.13
Patient-Centered Medical Home
The term patient-centered medical home was introduced in 1967 by the American Academy of Pediatrics (AAP).15 In 2008, PCMH principles became integral in most health care reform initiatives.16 In most PCMH models, increased continuity of care is the single common denominator of practice. Continuity of care is defined as intensified integration, coordination, and sharing of information between disciplines that result in improved patient outcomes.10,17,18
In 2007, a consensus statement was provided by the American Academy of Family Practice, the AAP, American College of Physicians, and the American Osteopathic Association stating that quality and safety are hallmarks of the PCMH and may improve outcomes for chronic disease, such as diabetes.19
Quality improvement is vital in health care organizations because of demands by government agencies, health maintenance organizations, and the public to continually improve services and to provide the highest quality health care at the best cost.20 Diabetes has become a public health crisis, as previously discussed, and a comprehensive approach to care management is essential. Developing an optimal process for diabetes health care and methods for evaluation of the delivery process is foundational for all stakeholders involved, including health care organizations, health care providers, and patients.20
Diabetic outcomes were evaluated at a recent 2-year trial PCMH approach T2DM clinic at a MEDCEN at WBAMC. The purpose of the project was to determine whether a PCMH approach improves disease management compared with routine primary care management.
Methods
The process and manner of care delivery was the focus of this analysis and evaluation, not clinician knowledge of treatment management. A comparison of care delivery approaches of PCM management and PCMH care delivery is displayed in the Table. The treatment algorithm for T2DM was not in question, because guidelines for practice are established based on scientific evidence, and medication management is based on evidence-based practice.21,22 Evaluation consisted of T2DM delivery of care process and the efficacy of outcome achieved by the specified delivery of care: (a) increased access to care; (b) intensive, repeated education; and (3) a multidisciplinary approach focused on patient empowerment. The following is a description of the specified delivery of care.
Increased Access to Care
Increased access to care addressed through frequent telecommunication provided by the registered nurse (RN) case manager who regularly called patients within 72 hours of insulin adjustment or 24 hours for insulin initiation or significant medication changes. Additionally, the diabetes team providers requested a follow-up appointment in 1 week when injectable medication was added or changes were made in insulin management. One exception was for the addition of livaglutide, in which a 2-week follow-up was made, to allow for titration of the medication. For oral medication adjustment, a 1-month follow-up was generally made, with a 2-month follow-up when a glucose histogram indicated optimal glycemic control, an average blood glucose of 7% (estimated average glucose of 154 mg/dL) or less. Time for appointments was increased by 10 minutes for a total of 30-minute appointments, compared with 20 minutes for PCM delivery.
Informational continuity was thought to be improved by use of an electronic medical record (EMR), allowing for an uninterrupted patient record. Providers were expected to document medication reconciliation with a clear explanation of medication adjustments listed in the plan. Patient teaching was documented, describing the specific patient education concerns addressed. Other data included a glucometer statistical report from the last appointment to the current appointment, to track negative or positive changes in glycemic control.
Patient Education
The management technique used in the clinic was intensive, repeated education with the goal of improving learning and retention with repeated instruction and positive reinforcement. Skinner theorized that learning is the acquisition of new behavior through conditioning (eg, repeated instruction), is in close proximity of time, and is likely to result in learning retention, which remain relevant education practice.23,24 The T2DM clinic operates on Skinner’s principles of repeated, intensive education. For example, patients must bring their glucometer to every appointment. The statistical analysis downloaded from the glucometer provides immediate reinforcement and information about patients’ glycemic control. Patients are typically excited to see an improvement from previous levels and are encouraged to continue behavior modification. Conversely, statistical analysis demonstrating poor glycemic control generally encourages the patient to make needed lifestyle changes. Thus, changes in behavior due to intensive, repeated education, followed by a reinforcing stimulus results in an increased probability of that behavior occurring in the future.23,25 The interdisciplinary team provides education during each T2DM patient encounter.
Multidisciplinary Approach
The multidisciplinary team formed at the trial T2DM clinic consisted of a medical doctor, family NP, pharmacist, RN, licensed vocational nurse, and registered dietician. The team members were each encouraged to obtain Certified Diabetes Educator (CDE) certification. For the first 6 months of developing the clinic, staff scheduled weekly team-building meetings to encourage esprit de corps. The weekly meetings were also used to discuss difficult patient cases. The RN case manager provided the patients with individualized plans to help them meet specified goals and provided easy accessibility for patient questions and concerns. The pharmacist was integral in helping patients understand the role of their medication and was also certified to make medication adjustments related to diabetes.
A recent Institute of Medicine (IOM) report encouraged the expansion of roles for nurse practitioners (NPs) in coordination and primary care delivery.26 The IOM collaborative statement is based on numerous studies showing that NPs provided equivalent quality of care compared with that of primary care physicians in routine chronic disease management.26 Nurse case managers functioned as an integral part of the intensive therapy involved in the landmark Diabetes Control and Complication Trial.27
The intended policy analysis and outcome evaluation was confined to data collected from a disease-specific (T2DM) clinic with a PCMH approach developed April 2011 at WBAMC. Data were obtained from the WBAMC database designed to track the HEDIS measures.
Enrollees of the clinic were restricted to patients diagnosed with T2DM who were TRICARE beneficiaries. Males and females, aged > 20 years with an established A1c > 6.5% comprised the patient population of the clinic. Individuals who were managed by WBAMC or were TRICARE standard beneficiaries were excluded from the study. Because patients with T1DM have a different pathology than those with T2DM, they were referred to endocrinology. Patients with gestational diabetes were referred to obstetrics for management.
Data Collection
Existing data in the Armed Forces Health Longitudinal Technology Application (AHLTA) EMR were used for this analysis. Data were accessed by a Common Access Card (CAC card) enhanced security system accessed only through secure CAC applications.
Diabetic outcomes of glycemic control as measured by the A1c value were examined prior to clinic enrollment (time 1: PCM care delivery) and subsequently (time 2: PCMH care delivery) at the health care provider’s discretion. The second time varied between 2 and 6 months, depending on (1) provider need to determine quickly (2 months) whether a downward trend was occurring because of multiple comorbidities; (2) provider discretion to wait an additional 3 months (A1c turnover x 2 = 6 months), while medication adjustments are being made; and (3) according to feasibility of follow-up based on patient’s scheduling. Low-density lipoprotein cholesterol (LDL-C) was also examined at both PCM care delivery and PCMH care delivery.
The endpoints of a reduction in A1c by 1% and an LDL-C that is ≤ 100 mg/dL determined improved diabetes outcomes. Existing data (eg, glycemic control [A1c], lipid control [LDL-C]), from April 1, 2011, to December 31, 2011, were logged in a clinic database. These data served to demonstrate the effectiveness of the T2DM PCMH approach to clinic management. The PCMH principles that were examined included the standard operating procedure for the T2DM-PCMH clinic: frequent appointments > 2 in a 3-month period), a multidisciplinary team, and intensive, repeated education.
Data analysis was conducted with descriptive statistics (frequencies, means, SDs) and t test analysis to determine relationships between variables of A1c, LDL-C, and frequency of visits. Improved diabetic outcomes, as previously defined, inferred that developing principles of a T2DM-PCMH clinic based on the principles of a PCMH provided a solution to optimal T2DM management compared with routine primary care delivery, consisting of a TRICARE-assigned PCM.
Results
A total of 638 unique patients were seen at the T2DM-PCMH clinic. Of these, 237 patient records in the database met the inclusion criteria and were acceptable for analysis and evaluation. Patients were omitted for the following reasons: 255 patients did not meet protocol of a minimum 2 visits during the evaluation period, 77 patients were omitted due to no second A1c available, 65 patients did not meet the clinic protocol of a A1c of > 6.5%, and 4 were omitted because no A1c was available for pre- or postanalysis. Data analysis and evaluation of the remaining 237 acceptable patients demonstrated that a T2DM-PCMH approach provided improved diabetic care compared with routine, PCM management.
Patients enrolled at the WBAMC T2DM clinic demonstrated clinically significant improvement (P < .001), and 80.5% achieved > 1% improvement in glycemic control. The greatest number of visits of 26 visits, an outlier not typical of the frequency of patient visits, was attributed to brittle T2DM requiring more frequent monitoring. Most patients had 3 T2DM-PCMH clinic appointments (2 were the minimum visits described in clinic protocol).
Low-density lipoprotein cholesterol levels were analyzed to determine whether patients with diabetes managed at the WBAMC T2DM clinic also had improved lipid control. A total of 638 patients had an initial LDL-C level drawn prior to clinic management. Of these patients, 282 were acceptable for analysis (Figure 2). Low-density lipoprotein cholesterol data were omitted because 93 did not have a paired pre- and postvalues, 8 values were invalid due to nonfasting laboratory status; and 255 values were omitted due to having < 2 clinic visits. Results of the data analysis demonstrated that LDL-C was well managed by the T2DM clinic, with levels ≤ 100 mg/dL (P < .001) (Figure 3).
Discussion
The WBAMC T2DM clinic was formed as a trial clinic at a medical treatment facility (MTF) MEDCEN due to the failure of routine PCM care to improve outcomes in the management of the diabetes population (A1c < 7.0%). Overall, improved endpoints of A1c, LDL-C were achieved with the disease-specific PCMH approach compared with routine PCM approach. The results indicate that disease-specific management leads to improved diabetic endpoints (A1c reduction by at least 1% and LDL-C < 100 mg/dL). The clinic’s protocol (listed in the methods) was intended to improve continuity.
A review of the literature confirmed that continuity of care is integral to patient satisfaction and improved diabetes management.8,10,17,28,29 The results of the study were consistent with those in the literature. The review of the literature established that patients who develop a trusting relationship with the health care provider as the T2DM clinic promoted (eg, frequent patient appointments, telecommunication by nurse, and patient participation) are more likely to follow medical therapy and take a proactive role in disease management.6,28,30
Conclusion
This study demonstrated that PCMH-delivered care offers a solution to suboptimal management of chronic disease, such as T2DM, and that chronic disease is best managed by implementation of a disease-specific PCMH. It is recommended that a MTF develop other disease-specific PCMH and pilot-test these programs. Long-term follow-up studies and additional data collection, such as blood pressure control, abdominal circumference, body mass index, and triglyceride levels would be useful to determine effectiveness.
Based on principles of a PCMH, the efficacy of the T2DM clinic at WBAMC demonstrated that improved diabetes management was achieved by increased continuity of care; intensive, repeated patient education; and a multidisciplinary team approach. The CDC identifies self-management training as foundational to improving health outcomes and QOL for individuals with diabetes.1 Primary care providers in a MTF may improve diabetic patient outcomes by referring patients to a T2DM clinic, such as the WBAMC T2DM clinic. The multidisciplinary team facilitated patient empowerment by educating patients on the management of their disease and the problem-solving and coping skills required to manage a chronic disease.
The WBAMC T2DM-PCMH based mission of fostering patient empowerment and a team approach is a comprehensive approach to diabetes care. Currently, the PCMH model is being adapted by the military in the latest health care reform initiatives.14 However, the move toward the PCMH model does not incorporate disease-specific PCMH clinics. This study demonstrates that the disease-specific PCMH approach provides improved disease management and may be effective in other chronic disease management. A benefit of the T2DM-PCMH approach is the reduced burden of escalating health care costs related to increased morbidity and mortality, which is associated with the growing health care problem of poorly controlled T2DM.1,4,31
The disease-specific clinic evaluated at WBAMC provides an effective solution to fragmented health care for the optimal management of T2DM. The clinic’s conceptual framework of increased access to care, with consistent education at closer time intervals when compared with PCM management resulted in improved continuity and T2DM control. Future research in this area should assess measurable cost reduction. Improved disease management as demonstrated by the T2DM disease-specific clinic at WBAMC provides sufficient incentive to incorporate similar T2DM continuity clinics and changes throughout MTFs.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Centers for Disease Control and Prevention (CDC). National Diabetes Fact Sheet, 2014. CDC Website. http://www.cdc.gov/diabetes/data/statistics/2014StatisticsReport.html. Updated October 24, 2014. Accessed November 6, 2014.
2. American Diabetes Association. National Diabetes Fact Sheet. Statistics about diabetes. American Diabetes Association Website. http://www.diabetes.org/diabetes-basics/diabetes-statistics. Released June 10, 2014. Accessed November 6, 2014.
3. Centers for Disease Control and Prevention (CDC). Number of Americans with diabetes rises to nearly 26 million [press release]. CDC Website. http://www.cdc.gov/media/releases/2011/p0126_diabetes.html. Published January 26, 2011. Accessed November 6, 2014.
4. Huang ES, Basu A, O’Grady M, Capretta JC. Projecting the future diabetes population size and related costs for the U.S. Diabetes Care. 2009;32(12):2225-2229.
5. National Library of Medicine. Diabetes. PubMed Website. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002194. Reviewed May 24, 2013. Accessed November 6, 2014.
6. Chu-Weininger MY, Balkrishnan R. Consumer satisfaction with primary care provider choice and associated trust. BMC Health Serv Res. 2006;6:139.
7. Alazri MH, Neal RD, Heywood P, Leese B. Patients’ experience of continuity of care of type 2 diabetes: A focus group study in primary care. Br J Gen Prac. 2006;56(528):488-495.
8. Chen CC, Chen SH. Better continuity of care reduces costs for diabetic patients. Am J Manag Care. 2011;17(6):420-427.
9. TRICARE Regional Office-West. Military Treatment Facility (MTF) Profile of William Beaumont Army Medical Center, FY2010 Q2. El Paso, TX. Published March 2010.
10. Worrall G, Knight J. Continuity of care is good for elderly people with diabetes: Retrospective cohort study of mortality and hospitalization. Can Fam Physician. 2011;57(1):e6-e20.
11. Kerr M. ADA 2009: Expert committee recommends use of hemoglobin A1c for diagnosis. Medscape Website. http://www.medscape.com/viewarticle/704021. Published June 7, 2009. Accessed November 7, 2014.
12. Drexler AJ. Lessons learned from landmark trials of type 2 diabetes mellitus and potential applications to clinical practice. Postgrad Med. 2003;Spec No:15-26.
13. Office of Evidence-Based Practice Quality Management Division U.S. Army Medical Command. Population Health: Update of HEDIS measures. U.S. Army Medical Department Office of Quality Management Website. https://www.qmo.amedd.army.mil/HEDIS/HEDIS_MeasuresAcrossAMEDD.pdf. Published April 2010. Accessed November 2014.
14. Schoomaker E. Army medicine: Bringing value and inspiring trust. U.S. Medicine. 2011:10-13.
15. Sia C, Tonniges TF, Osterhus E, Taba S. History of the medical home concept. Pediatrics. 2004;113(5 suppl):1473-1478.
16. Kugler JP. Military Health System Patient Centered Medical Home Guide. Defense Health Agency Website. http://www.tricare.mil/tma/ocmo/download/MHSPCMHGuide.pdf. Published June 2011. Accessed November 11, 2014.
17. Naithani S, Gulliford M. Morgan M. Patients’ perceptions and experiences of ‘continuity of care’ in diabetes. Health Expect. 2006;9(2):118-129.
18. O’Malley AS, Cunningham PJ. Patient experiences with coordination of care: The benefit of continuity and primary care physician as referral source. J Gen Intern Med. 2009;24(2):170-177.
19. American Academy of Family Practice, American Academy of Pediatrics, American College of Physicians, and the American Osteopathic Association. Joint principles of the patient-centered medical home. American Academy of Family Practice Website. http://www.aafp.org/dam/AAFP/documents/practice_management/pcmh/initiatives/PCMHJoint.pdf. Published February 2007. Accessed November 7, 2014.
20. Meyer JA, Silow-Carroll S, Kutyla T, Stepnick LS, Rybowski LS. Hospital Quality: Ingredients for Success--Overview and Lessons Learned. New York, New York: The Commonwealth Fund; 2004.
21. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 8th ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2008.
22. American Association of Clinical Endocrinologists. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice. American Association of Clinical Endocrinologists Website. https://www.aace.com/files/dm-guidelines-ccp.pdf. Accessed November 7, 2014.
23. Skinner BF. The Behavior of Organisms: An Experimental Analysis. New York, NY: Appleton-Century; 1938.
24. Staddon JE, Cerutti DT. Operant conditioning. Annu Rev Psychol. 2003;54:115-144.
25. Bruner RF. Repetition Is the First Principle of All Learning. Social Science Research network Website. http://papers.ssrn.com/sol3/papers.cfm?abstract_id=224340. Posted August 26, 2001. Accessed November 7, 2014.
26. Institute of Medicine. The Future Of Nursing: Leading Change, Advancing Health. Washington, DC: National Academics Press; 2011.
27. Willens D, Cripps R, Wilson A, Wolff K, Rothman R. Interdisciplinary team care for diabetic patients by primary care physicians, advance practice nurses and clinical pharmacists. Clin Diabetes. 2011;29(2):60-68.
28. Renders CM, Valk GD, Griffin S, Wagner EH, Eijk JT, Assendelft WJ. Interventions to improve the management of diabetes mellitus in primary care, outpatient and community settings. Cochrane Database Syst Rev. 2001;(1):CD001481.
29. Health Affairs. Patient-centered medical homes. Health Affairs Website. http://www.healthaffairs.org. Dated September 14, 2010. Accessed November 7, 2014.
30. Berry LL, Parish JT, Janakiraman R, et al. Patients’ commitment to their primary physician and why it matters. Ann Fam Med. 2008;6(1):6-13.
31. Glasgow RE, Wagner EH, Kaplan RM, Vinicor F, Smith L, Norman J. If diabetes is a public health problem, why not treat it as one? A population-based approach to chronic illness. Ann Behav Med. 1999;21(2):159-170.
1. Centers for Disease Control and Prevention (CDC). National Diabetes Fact Sheet, 2014. CDC Website. http://www.cdc.gov/diabetes/data/statistics/2014StatisticsReport.html. Updated October 24, 2014. Accessed November 6, 2014.
2. American Diabetes Association. National Diabetes Fact Sheet. Statistics about diabetes. American Diabetes Association Website. http://www.diabetes.org/diabetes-basics/diabetes-statistics. Released June 10, 2014. Accessed November 6, 2014.
3. Centers for Disease Control and Prevention (CDC). Number of Americans with diabetes rises to nearly 26 million [press release]. CDC Website. http://www.cdc.gov/media/releases/2011/p0126_diabetes.html. Published January 26, 2011. Accessed November 6, 2014.
4. Huang ES, Basu A, O’Grady M, Capretta JC. Projecting the future diabetes population size and related costs for the U.S. Diabetes Care. 2009;32(12):2225-2229.
5. National Library of Medicine. Diabetes. PubMed Website. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002194. Reviewed May 24, 2013. Accessed November 6, 2014.
6. Chu-Weininger MY, Balkrishnan R. Consumer satisfaction with primary care provider choice and associated trust. BMC Health Serv Res. 2006;6:139.
7. Alazri MH, Neal RD, Heywood P, Leese B. Patients’ experience of continuity of care of type 2 diabetes: A focus group study in primary care. Br J Gen Prac. 2006;56(528):488-495.
8. Chen CC, Chen SH. Better continuity of care reduces costs for diabetic patients. Am J Manag Care. 2011;17(6):420-427.
9. TRICARE Regional Office-West. Military Treatment Facility (MTF) Profile of William Beaumont Army Medical Center, FY2010 Q2. El Paso, TX. Published March 2010.
10. Worrall G, Knight J. Continuity of care is good for elderly people with diabetes: Retrospective cohort study of mortality and hospitalization. Can Fam Physician. 2011;57(1):e6-e20.
11. Kerr M. ADA 2009: Expert committee recommends use of hemoglobin A1c for diagnosis. Medscape Website. http://www.medscape.com/viewarticle/704021. Published June 7, 2009. Accessed November 7, 2014.
12. Drexler AJ. Lessons learned from landmark trials of type 2 diabetes mellitus and potential applications to clinical practice. Postgrad Med. 2003;Spec No:15-26.
13. Office of Evidence-Based Practice Quality Management Division U.S. Army Medical Command. Population Health: Update of HEDIS measures. U.S. Army Medical Department Office of Quality Management Website. https://www.qmo.amedd.army.mil/HEDIS/HEDIS_MeasuresAcrossAMEDD.pdf. Published April 2010. Accessed November 2014.
14. Schoomaker E. Army medicine: Bringing value and inspiring trust. U.S. Medicine. 2011:10-13.
15. Sia C, Tonniges TF, Osterhus E, Taba S. History of the medical home concept. Pediatrics. 2004;113(5 suppl):1473-1478.
16. Kugler JP. Military Health System Patient Centered Medical Home Guide. Defense Health Agency Website. http://www.tricare.mil/tma/ocmo/download/MHSPCMHGuide.pdf. Published June 2011. Accessed November 11, 2014.
17. Naithani S, Gulliford M. Morgan M. Patients’ perceptions and experiences of ‘continuity of care’ in diabetes. Health Expect. 2006;9(2):118-129.
18. O’Malley AS, Cunningham PJ. Patient experiences with coordination of care: The benefit of continuity and primary care physician as referral source. J Gen Intern Med. 2009;24(2):170-177.
19. American Academy of Family Practice, American Academy of Pediatrics, American College of Physicians, and the American Osteopathic Association. Joint principles of the patient-centered medical home. American Academy of Family Practice Website. http://www.aafp.org/dam/AAFP/documents/practice_management/pcmh/initiatives/PCMHJoint.pdf. Published February 2007. Accessed November 7, 2014.
20. Meyer JA, Silow-Carroll S, Kutyla T, Stepnick LS, Rybowski LS. Hospital Quality: Ingredients for Success--Overview and Lessons Learned. New York, New York: The Commonwealth Fund; 2004.
21. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 8th ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2008.
22. American Association of Clinical Endocrinologists. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice. American Association of Clinical Endocrinologists Website. https://www.aace.com/files/dm-guidelines-ccp.pdf. Accessed November 7, 2014.
23. Skinner BF. The Behavior of Organisms: An Experimental Analysis. New York, NY: Appleton-Century; 1938.
24. Staddon JE, Cerutti DT. Operant conditioning. Annu Rev Psychol. 2003;54:115-144.
25. Bruner RF. Repetition Is the First Principle of All Learning. Social Science Research network Website. http://papers.ssrn.com/sol3/papers.cfm?abstract_id=224340. Posted August 26, 2001. Accessed November 7, 2014.
26. Institute of Medicine. The Future Of Nursing: Leading Change, Advancing Health. Washington, DC: National Academics Press; 2011.
27. Willens D, Cripps R, Wilson A, Wolff K, Rothman R. Interdisciplinary team care for diabetic patients by primary care physicians, advance practice nurses and clinical pharmacists. Clin Diabetes. 2011;29(2):60-68.
28. Renders CM, Valk GD, Griffin S, Wagner EH, Eijk JT, Assendelft WJ. Interventions to improve the management of diabetes mellitus in primary care, outpatient and community settings. Cochrane Database Syst Rev. 2001;(1):CD001481.
29. Health Affairs. Patient-centered medical homes. Health Affairs Website. http://www.healthaffairs.org. Dated September 14, 2010. Accessed November 7, 2014.
30. Berry LL, Parish JT, Janakiraman R, et al. Patients’ commitment to their primary physician and why it matters. Ann Fam Med. 2008;6(1):6-13.
31. Glasgow RE, Wagner EH, Kaplan RM, Vinicor F, Smith L, Norman J. If diabetes is a public health problem, why not treat it as one? A population-based approach to chronic illness. Ann Behav Med. 1999;21(2):159-170.
Acute Upper Abdominal Pain in Early Pregnancy
A 32-year-old G1P0 woman at 7 4/7 weeks’ gestation (intrauterine pregnancy confirmed by ultrasound) with a history of hypertension and anxiety presented to the emergency department reporting right upper quadrant and right flank pain. The patient did not report taking any medications. Her symptoms had begun about 6 hours prior to presentation. She did not report fever, chills, nausea, vomiting, anorexia, or urinary or bowels symptoms. She was afebrile, and her initial blood pressure was 174/84 mm Hg, but within an hour of presentation had decreased to 137/82 mm Hg.
On exam she was in moderate-to-severe discomfort. She was tender to palpation in the right flank as well as the right upper quadrant and had a positive Murphy sign. Her white blood cell (WBC) count was 18,800/μL, hemoglobin and hematocrit were normal, liver function tests were within normal limits, and sodium was 133 mmol/L; otherwise, electrolytes were normal. The urinalysis showed a specific gravity of 1.022 with 3 red blood cells per high powered field, but was otherwise normal. A right upper quadrant ultrasound showed a normal gallbladder without cholelithiasis. Subsequently, a magnetic resonance imaging (MRI) of the abdomen was obtained (Figure 1).
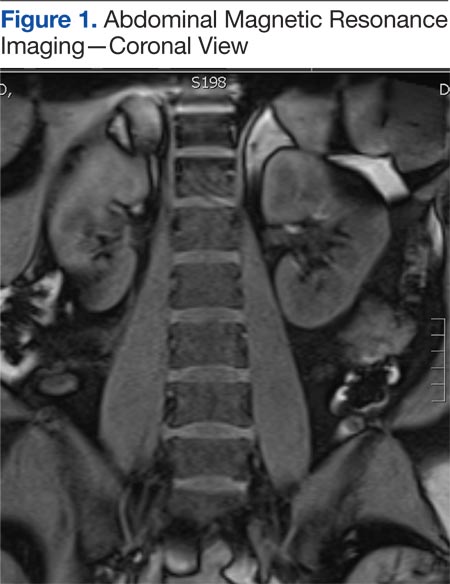
- What is your diagnosis?
- How would you treat this patient?
[Click through to the next page to see the answer.]
Our Treatment
An MRI of the abdomen revealed a right adrenal hematoma (Figure 2). This diagnosis was made after common causes of the right upper quadrant and right flank pain were excluded and was confirmed with an MRI of the abdomen.
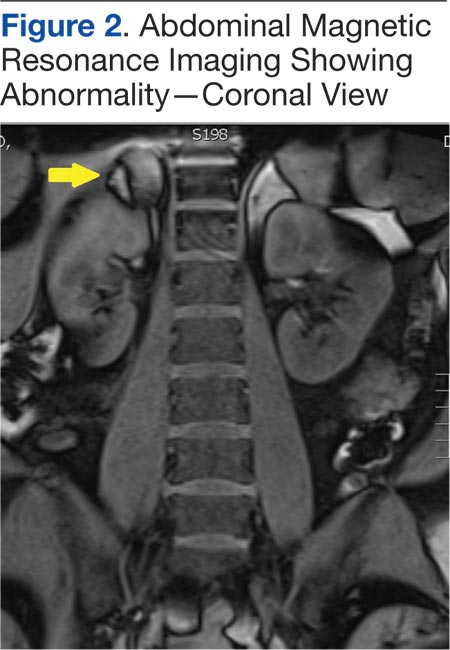
Discussion
Common causes of right flank and right upper quadrant pain include urolithiasis, pyelonephritis, and acute cholecystitis (Table). Patients with urolithiasis will typically present with sudden onset of colicky flank pain, which may radiate to the inguinal region, with or without nausea and vomiting.1,2 Microhematuria may be absent in as many as 10% to 20% of patients.2 Computed tomography is nearly 97% sensitive and 96% specific for urolithiasis.2 Although only 37% to 64% sensitive in detecting urolithiasis, abdominal ultrasound is 85% to 94% specific for detecting hydronephrosis.2
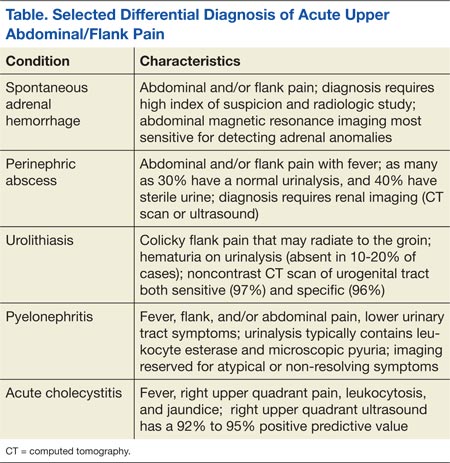
Symptoms of pyelonephritis range from mild to severe costovertebral angle pain with or without fever and/or lower urinary tract symptoms to sepsis.3 Urinalysis typically shows leukocyte esterase (72%-97% sensitive, 41%-86% specific for culture-confirmed urinary tract infection) and microscopic pyuria (90%-96% sensitive, 47%-50% specific for culture-confirmed urinary tract infection).3,4 Urine culture will reveal 105 colony-forming units in 95% of patients with acute uncomplicated pyelonephritis.3 Imaging is typically reserved for atypical presentations or in cases of nonresolution of symptoms despite treatment in order to rule out structural anomalies, an obstructive process, or abscess formation.3
Acute cholecystitis is suggested by right upper quadrant pain, often following a meal. Symptoms include fever, leukocytosis, and an elevated serum bilirubin level.5 Ultrasound findings of acute cholecystitis are gallbladder wall thickening, pericholecystic fluid, or sonographic Murphy sign.6 Ultrasound has a sensitivity of 81% and a specificity of 83% for detecting acute cholecystitis, whereas hepatobiliary iminodiacetic acid scan (cholescintigraphy) is 96% sensitive and 90% specific and is used in cases where ultrasound is indeterminate.6
Spontaneous adrenal hemorrhage (SAH) typically presents with symptoms of upper abdominal pain and/or flank pain. If hemorrhage is significant, hypotension and a drop in hematocrit may occur. Alternatively, if SAH is bilateral and results in a deficiency of adrenal hormones, hypotension may be secondary to adrenal insufficiency. Due to its ready availability, most SAHs are diagnosed by CT scan ordered for alternate reasons.7
In the pregnant patient, to avoid exposing the developing fetus to radiation, ultrasound is typically the first imaging modality to investigate right upper quadrant or flank pain. However, ultrasound is less sensitive for evaluating anomalies of the adrenal gland.8 An MRI is the most accurate imaging modality for diagnosing adrenal hemorrhage and avoids exposing the developing fetus to radiation.9 In this case, the absence of an etiology of the patient’s symptoms on right upper quadrant ultrasound led to further evaluation, with abdominal MRI revealing the diagnosis.
In a review of 141 cases of adrenal hemorrhage at the Mayo Clinic in Rochester, Minnesota, 16 patients had a spontaneous adrenal hemorrhage, which presented with severe abdominal and flank pain of sudden onset.7 Seven of these patients required surgery to control the bleeding.7 None of the 13 patients with a functioning contralateral adrenal gland required adrenal replacement therapy.7 Gavrilova-Jordan and colleagues reported a case of a spontaneous unilateral adrenal hemorrhage in the third trimester of pregnancy that was managed conservatively with favorable outcomes.10 Potential causes of spontaneous adrenal hemorrhage include:
• Antiphospholipid antibody syndrome
• Heparin-induced thrombocytopenia
• Trauma
• Physiologic stress (eg, sepsis)
• Adrenal mass (pheochromocytoma, angiomyolipoma, or metastatic cancer).6,11
Case Outcome
Initial right upper quadrant ultrasound in this patient revealed a normal gallbladder and a small amount of perinephric fluid surrounding the right kidney. On the night of admission she experienced an elevated temperature of 101.9°F. Due to the fever and leukocytosis, she was initiated on antibiotics (ampicillin-sulbactam 3 g IV every 6 hours) covering a urinary source. On hospital day 2, right lower quadrant and right upper quadrant ultrasounds were performed, revealing decreased fluid surrounding her right kidney and without evidence of appendicitis. Due to persistent leukocytosis (WBC count peaked at 26,400/μL), essentially normal urinalysis, and negative urine culture, an abdominal MRI was obtained to evaluate for a perinephric abscess. The MRI revealed the spontaneous adrenal hemorrhage.
The patient was observed as an inpatient for the following 48 hours. Her electrolytes remained normal and hemoglobin decreased to 9.5 g/dL. She remained hemodynamically stable. Serum cortisol and angiotensin levels were normal, antibiotics were discontinued, and the patient was discharged to outpatient follow-up.
A repeat MRI of the abdomen obtained 6 weeks later revealed a resolving right adrenal hematoma. At 39 weeks’ gestation, she delivered a vigorous female infant weighing 3,200 g (7 lb 1 oz) with an Apgar score at birth of 8/9.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Wasserstein AG. Nephrolithiasis. Am J Kidney Dis. 2005;45(2):422-428.
2. Ban KM, Easter JS. Selected urologic problems. In: Marx JA, Hockberger RS, Walls, RM, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia, PA: Elsevier; 2010:1297-1324.
3. Colgan R, Williams M, Johnson JR. Diagnosis and treatment of acute pyelonephritis in women. Am Fam Physician. 2011;84(5):519-526.
4. Simerville JA, Maxted WC, Pahira JJ. Urinalysis: A comprehensive review. Am Fam Physician. 2005;71(6):1153-1162.
5. Friedman LS. Liver, biliary tract & pancreas disorders. In: McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis and Treatment, 2012. 51st ed. New York, NY: Lange Medical Books/McGraw-Hill; 2012:644-698.
6. Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012;264(3):708-720.
7. Vella A, Nippoldt TB, Morris JC 3rd. Adrenal hemorrhage: A 25-year experience at the Mayo Clinic. Mayo Clin Proc. 2001;76(2):161-168.
8. Kawashima A, Sandler CM, Ernst RD, et al. Imaging of nontraumatic hemorrhage of the adrenal gland. Radiographics. 1999;19(4):949-963.
9. Hoeffel C, Legmann P, Luton JP, Chapuis Y, Fayet-Bonnin P. Spontaneous unilateral adrenal hemorrhage: Computerized tomography and magnetic resonance imaging findings in 8 cases. J Urol. 1995;154(5):1647-1651.
10. Gavrilova-Jordan L, Edmister WB, Farrell MA, Watson WJ. Spontaneous adrenal hemorrhage during pregnancy: A review of the literature and a case report of successful conservative management. Obstet Gynecol Surv. 2005;60(3):191-195.
11. Marti JL, Millet J, Sosa JA, Roman SA, Carling T, Udelsman R. Spontaneous adrenal hemorrhage with associated masses: Etiology and management in 6 cases and a review of 133 reported cases. World J Surg. 2012;36(1):75-82.
A 32-year-old G1P0 woman at 7 4/7 weeks’ gestation (intrauterine pregnancy confirmed by ultrasound) with a history of hypertension and anxiety presented to the emergency department reporting right upper quadrant and right flank pain. The patient did not report taking any medications. Her symptoms had begun about 6 hours prior to presentation. She did not report fever, chills, nausea, vomiting, anorexia, or urinary or bowels symptoms. She was afebrile, and her initial blood pressure was 174/84 mm Hg, but within an hour of presentation had decreased to 137/82 mm Hg.
On exam she was in moderate-to-severe discomfort. She was tender to palpation in the right flank as well as the right upper quadrant and had a positive Murphy sign. Her white blood cell (WBC) count was 18,800/μL, hemoglobin and hematocrit were normal, liver function tests were within normal limits, and sodium was 133 mmol/L; otherwise, electrolytes were normal. The urinalysis showed a specific gravity of 1.022 with 3 red blood cells per high powered field, but was otherwise normal. A right upper quadrant ultrasound showed a normal gallbladder without cholelithiasis. Subsequently, a magnetic resonance imaging (MRI) of the abdomen was obtained (Figure 1).
- What is your diagnosis?
- How would you treat this patient?
[Click through to the next page to see the answer.]
Our Treatment
An MRI of the abdomen revealed a right adrenal hematoma (Figure 2). This diagnosis was made after common causes of the right upper quadrant and right flank pain were excluded and was confirmed with an MRI of the abdomen.
Discussion
Common causes of right flank and right upper quadrant pain include urolithiasis, pyelonephritis, and acute cholecystitis (Table). Patients with urolithiasis will typically present with sudden onset of colicky flank pain, which may radiate to the inguinal region, with or without nausea and vomiting.1,2 Microhematuria may be absent in as many as 10% to 20% of patients.2 Computed tomography is nearly 97% sensitive and 96% specific for urolithiasis.2 Although only 37% to 64% sensitive in detecting urolithiasis, abdominal ultrasound is 85% to 94% specific for detecting hydronephrosis.2
Symptoms of pyelonephritis range from mild to severe costovertebral angle pain with or without fever and/or lower urinary tract symptoms to sepsis.3 Urinalysis typically shows leukocyte esterase (72%-97% sensitive, 41%-86% specific for culture-confirmed urinary tract infection) and microscopic pyuria (90%-96% sensitive, 47%-50% specific for culture-confirmed urinary tract infection).3,4 Urine culture will reveal 105 colony-forming units in 95% of patients with acute uncomplicated pyelonephritis.3 Imaging is typically reserved for atypical presentations or in cases of nonresolution of symptoms despite treatment in order to rule out structural anomalies, an obstructive process, or abscess formation.3
Acute cholecystitis is suggested by right upper quadrant pain, often following a meal. Symptoms include fever, leukocytosis, and an elevated serum bilirubin level.5 Ultrasound findings of acute cholecystitis are gallbladder wall thickening, pericholecystic fluid, or sonographic Murphy sign.6 Ultrasound has a sensitivity of 81% and a specificity of 83% for detecting acute cholecystitis, whereas hepatobiliary iminodiacetic acid scan (cholescintigraphy) is 96% sensitive and 90% specific and is used in cases where ultrasound is indeterminate.6
Spontaneous adrenal hemorrhage (SAH) typically presents with symptoms of upper abdominal pain and/or flank pain. If hemorrhage is significant, hypotension and a drop in hematocrit may occur. Alternatively, if SAH is bilateral and results in a deficiency of adrenal hormones, hypotension may be secondary to adrenal insufficiency. Due to its ready availability, most SAHs are diagnosed by CT scan ordered for alternate reasons.7
In the pregnant patient, to avoid exposing the developing fetus to radiation, ultrasound is typically the first imaging modality to investigate right upper quadrant or flank pain. However, ultrasound is less sensitive for evaluating anomalies of the adrenal gland.8 An MRI is the most accurate imaging modality for diagnosing adrenal hemorrhage and avoids exposing the developing fetus to radiation.9 In this case, the absence of an etiology of the patient’s symptoms on right upper quadrant ultrasound led to further evaluation, with abdominal MRI revealing the diagnosis.
In a review of 141 cases of adrenal hemorrhage at the Mayo Clinic in Rochester, Minnesota, 16 patients had a spontaneous adrenal hemorrhage, which presented with severe abdominal and flank pain of sudden onset.7 Seven of these patients required surgery to control the bleeding.7 None of the 13 patients with a functioning contralateral adrenal gland required adrenal replacement therapy.7 Gavrilova-Jordan and colleagues reported a case of a spontaneous unilateral adrenal hemorrhage in the third trimester of pregnancy that was managed conservatively with favorable outcomes.10 Potential causes of spontaneous adrenal hemorrhage include:
• Antiphospholipid antibody syndrome
• Heparin-induced thrombocytopenia
• Trauma
• Physiologic stress (eg, sepsis)
• Adrenal mass (pheochromocytoma, angiomyolipoma, or metastatic cancer).6,11
Case Outcome
Initial right upper quadrant ultrasound in this patient revealed a normal gallbladder and a small amount of perinephric fluid surrounding the right kidney. On the night of admission she experienced an elevated temperature of 101.9°F. Due to the fever and leukocytosis, she was initiated on antibiotics (ampicillin-sulbactam 3 g IV every 6 hours) covering a urinary source. On hospital day 2, right lower quadrant and right upper quadrant ultrasounds were performed, revealing decreased fluid surrounding her right kidney and without evidence of appendicitis. Due to persistent leukocytosis (WBC count peaked at 26,400/μL), essentially normal urinalysis, and negative urine culture, an abdominal MRI was obtained to evaluate for a perinephric abscess. The MRI revealed the spontaneous adrenal hemorrhage.
The patient was observed as an inpatient for the following 48 hours. Her electrolytes remained normal and hemoglobin decreased to 9.5 g/dL. She remained hemodynamically stable. Serum cortisol and angiotensin levels were normal, antibiotics were discontinued, and the patient was discharged to outpatient follow-up.
A repeat MRI of the abdomen obtained 6 weeks later revealed a resolving right adrenal hematoma. At 39 weeks’ gestation, she delivered a vigorous female infant weighing 3,200 g (7 lb 1 oz) with an Apgar score at birth of 8/9.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
A 32-year-old G1P0 woman at 7 4/7 weeks’ gestation (intrauterine pregnancy confirmed by ultrasound) with a history of hypertension and anxiety presented to the emergency department reporting right upper quadrant and right flank pain. The patient did not report taking any medications. Her symptoms had begun about 6 hours prior to presentation. She did not report fever, chills, nausea, vomiting, anorexia, or urinary or bowels symptoms. She was afebrile, and her initial blood pressure was 174/84 mm Hg, but within an hour of presentation had decreased to 137/82 mm Hg.
On exam she was in moderate-to-severe discomfort. She was tender to palpation in the right flank as well as the right upper quadrant and had a positive Murphy sign. Her white blood cell (WBC) count was 18,800/μL, hemoglobin and hematocrit were normal, liver function tests were within normal limits, and sodium was 133 mmol/L; otherwise, electrolytes were normal. The urinalysis showed a specific gravity of 1.022 with 3 red blood cells per high powered field, but was otherwise normal. A right upper quadrant ultrasound showed a normal gallbladder without cholelithiasis. Subsequently, a magnetic resonance imaging (MRI) of the abdomen was obtained (Figure 1).
- What is your diagnosis?
- How would you treat this patient?
[Click through to the next page to see the answer.]
Our Treatment
An MRI of the abdomen revealed a right adrenal hematoma (Figure 2). This diagnosis was made after common causes of the right upper quadrant and right flank pain were excluded and was confirmed with an MRI of the abdomen.
Discussion
Common causes of right flank and right upper quadrant pain include urolithiasis, pyelonephritis, and acute cholecystitis (Table). Patients with urolithiasis will typically present with sudden onset of colicky flank pain, which may radiate to the inguinal region, with or without nausea and vomiting.1,2 Microhematuria may be absent in as many as 10% to 20% of patients.2 Computed tomography is nearly 97% sensitive and 96% specific for urolithiasis.2 Although only 37% to 64% sensitive in detecting urolithiasis, abdominal ultrasound is 85% to 94% specific for detecting hydronephrosis.2
Symptoms of pyelonephritis range from mild to severe costovertebral angle pain with or without fever and/or lower urinary tract symptoms to sepsis.3 Urinalysis typically shows leukocyte esterase (72%-97% sensitive, 41%-86% specific for culture-confirmed urinary tract infection) and microscopic pyuria (90%-96% sensitive, 47%-50% specific for culture-confirmed urinary tract infection).3,4 Urine culture will reveal 105 colony-forming units in 95% of patients with acute uncomplicated pyelonephritis.3 Imaging is typically reserved for atypical presentations or in cases of nonresolution of symptoms despite treatment in order to rule out structural anomalies, an obstructive process, or abscess formation.3
Acute cholecystitis is suggested by right upper quadrant pain, often following a meal. Symptoms include fever, leukocytosis, and an elevated serum bilirubin level.5 Ultrasound findings of acute cholecystitis are gallbladder wall thickening, pericholecystic fluid, or sonographic Murphy sign.6 Ultrasound has a sensitivity of 81% and a specificity of 83% for detecting acute cholecystitis, whereas hepatobiliary iminodiacetic acid scan (cholescintigraphy) is 96% sensitive and 90% specific and is used in cases where ultrasound is indeterminate.6
Spontaneous adrenal hemorrhage (SAH) typically presents with symptoms of upper abdominal pain and/or flank pain. If hemorrhage is significant, hypotension and a drop in hematocrit may occur. Alternatively, if SAH is bilateral and results in a deficiency of adrenal hormones, hypotension may be secondary to adrenal insufficiency. Due to its ready availability, most SAHs are diagnosed by CT scan ordered for alternate reasons.7
In the pregnant patient, to avoid exposing the developing fetus to radiation, ultrasound is typically the first imaging modality to investigate right upper quadrant or flank pain. However, ultrasound is less sensitive for evaluating anomalies of the adrenal gland.8 An MRI is the most accurate imaging modality for diagnosing adrenal hemorrhage and avoids exposing the developing fetus to radiation.9 In this case, the absence of an etiology of the patient’s symptoms on right upper quadrant ultrasound led to further evaluation, with abdominal MRI revealing the diagnosis.
In a review of 141 cases of adrenal hemorrhage at the Mayo Clinic in Rochester, Minnesota, 16 patients had a spontaneous adrenal hemorrhage, which presented with severe abdominal and flank pain of sudden onset.7 Seven of these patients required surgery to control the bleeding.7 None of the 13 patients with a functioning contralateral adrenal gland required adrenal replacement therapy.7 Gavrilova-Jordan and colleagues reported a case of a spontaneous unilateral adrenal hemorrhage in the third trimester of pregnancy that was managed conservatively with favorable outcomes.10 Potential causes of spontaneous adrenal hemorrhage include:
• Antiphospholipid antibody syndrome
• Heparin-induced thrombocytopenia
• Trauma
• Physiologic stress (eg, sepsis)
• Adrenal mass (pheochromocytoma, angiomyolipoma, or metastatic cancer).6,11
Case Outcome
Initial right upper quadrant ultrasound in this patient revealed a normal gallbladder and a small amount of perinephric fluid surrounding the right kidney. On the night of admission she experienced an elevated temperature of 101.9°F. Due to the fever and leukocytosis, she was initiated on antibiotics (ampicillin-sulbactam 3 g IV every 6 hours) covering a urinary source. On hospital day 2, right lower quadrant and right upper quadrant ultrasounds were performed, revealing decreased fluid surrounding her right kidney and without evidence of appendicitis. Due to persistent leukocytosis (WBC count peaked at 26,400/μL), essentially normal urinalysis, and negative urine culture, an abdominal MRI was obtained to evaluate for a perinephric abscess. The MRI revealed the spontaneous adrenal hemorrhage.
The patient was observed as an inpatient for the following 48 hours. Her electrolytes remained normal and hemoglobin decreased to 9.5 g/dL. She remained hemodynamically stable. Serum cortisol and angiotensin levels were normal, antibiotics were discontinued, and the patient was discharged to outpatient follow-up.
A repeat MRI of the abdomen obtained 6 weeks later revealed a resolving right adrenal hematoma. At 39 weeks’ gestation, she delivered a vigorous female infant weighing 3,200 g (7 lb 1 oz) with an Apgar score at birth of 8/9.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Wasserstein AG. Nephrolithiasis. Am J Kidney Dis. 2005;45(2):422-428.
2. Ban KM, Easter JS. Selected urologic problems. In: Marx JA, Hockberger RS, Walls, RM, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia, PA: Elsevier; 2010:1297-1324.
3. Colgan R, Williams M, Johnson JR. Diagnosis and treatment of acute pyelonephritis in women. Am Fam Physician. 2011;84(5):519-526.
4. Simerville JA, Maxted WC, Pahira JJ. Urinalysis: A comprehensive review. Am Fam Physician. 2005;71(6):1153-1162.
5. Friedman LS. Liver, biliary tract & pancreas disorders. In: McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis and Treatment, 2012. 51st ed. New York, NY: Lange Medical Books/McGraw-Hill; 2012:644-698.
6. Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012;264(3):708-720.
7. Vella A, Nippoldt TB, Morris JC 3rd. Adrenal hemorrhage: A 25-year experience at the Mayo Clinic. Mayo Clin Proc. 2001;76(2):161-168.
8. Kawashima A, Sandler CM, Ernst RD, et al. Imaging of nontraumatic hemorrhage of the adrenal gland. Radiographics. 1999;19(4):949-963.
9. Hoeffel C, Legmann P, Luton JP, Chapuis Y, Fayet-Bonnin P. Spontaneous unilateral adrenal hemorrhage: Computerized tomography and magnetic resonance imaging findings in 8 cases. J Urol. 1995;154(5):1647-1651.
10. Gavrilova-Jordan L, Edmister WB, Farrell MA, Watson WJ. Spontaneous adrenal hemorrhage during pregnancy: A review of the literature and a case report of successful conservative management. Obstet Gynecol Surv. 2005;60(3):191-195.
11. Marti JL, Millet J, Sosa JA, Roman SA, Carling T, Udelsman R. Spontaneous adrenal hemorrhage with associated masses: Etiology and management in 6 cases and a review of 133 reported cases. World J Surg. 2012;36(1):75-82.
1. Wasserstein AG. Nephrolithiasis. Am J Kidney Dis. 2005;45(2):422-428.
2. Ban KM, Easter JS. Selected urologic problems. In: Marx JA, Hockberger RS, Walls, RM, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia, PA: Elsevier; 2010:1297-1324.
3. Colgan R, Williams M, Johnson JR. Diagnosis and treatment of acute pyelonephritis in women. Am Fam Physician. 2011;84(5):519-526.
4. Simerville JA, Maxted WC, Pahira JJ. Urinalysis: A comprehensive review. Am Fam Physician. 2005;71(6):1153-1162.
5. Friedman LS. Liver, biliary tract & pancreas disorders. In: McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis and Treatment, 2012. 51st ed. New York, NY: Lange Medical Books/McGraw-Hill; 2012:644-698.
6. Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012;264(3):708-720.
7. Vella A, Nippoldt TB, Morris JC 3rd. Adrenal hemorrhage: A 25-year experience at the Mayo Clinic. Mayo Clin Proc. 2001;76(2):161-168.
8. Kawashima A, Sandler CM, Ernst RD, et al. Imaging of nontraumatic hemorrhage of the adrenal gland. Radiographics. 1999;19(4):949-963.
9. Hoeffel C, Legmann P, Luton JP, Chapuis Y, Fayet-Bonnin P. Spontaneous unilateral adrenal hemorrhage: Computerized tomography and magnetic resonance imaging findings in 8 cases. J Urol. 1995;154(5):1647-1651.
10. Gavrilova-Jordan L, Edmister WB, Farrell MA, Watson WJ. Spontaneous adrenal hemorrhage during pregnancy: A review of the literature and a case report of successful conservative management. Obstet Gynecol Surv. 2005;60(3):191-195.
11. Marti JL, Millet J, Sosa JA, Roman SA, Carling T, Udelsman R. Spontaneous adrenal hemorrhage with associated masses: Etiology and management in 6 cases and a review of 133 reported cases. World J Surg. 2012;36(1):75-82.
Pulmonary Vein Thrombosis Associated With Metastatic Carcinoma
Pulmonary vein thrombosis (PVT) is rare and underdiagnosed in clinical practice. It has been described following lobectomy, lung transplant, and in association with metastatic carcinoma.1-4 Some cases have been described as idiopathic.5-7 Its exact incidence is unknown, and treatment depends on etiology. On the other hand, pulmonary artery thromboembolism is a well-known entity with identified risk factors as well as clearly defined modalities of management. The following is a case of PVT, which occurred in the setting of small cell carcinoma of the lung (SCLC) and mantle cell lymphoma of the small intestine.
CASE PRESENTATION
A 66-year-old male veteran with a past medical history of type 2 diabetes mellitus, hypertension, and chronic obstructive pulmonary disease, who had a 40 pack-year history of cigarette smoking, was admitted to the hospital for severe, sudden onset abdominal pain. The pain was localized in the right lower quadrant and then became generalized. It was sharp, aggravated by movement, and relieved by rest. The patient reported being constipated for the past couple of days.
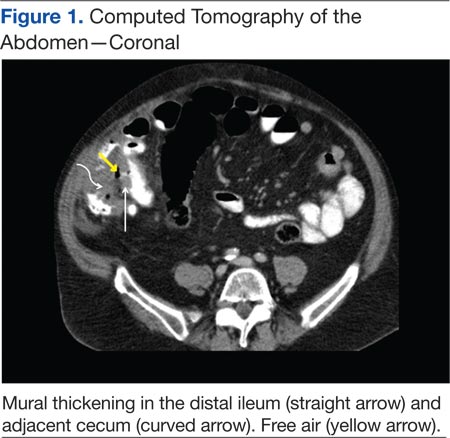
A review of systems revealed that he had been coughing for about 3 days prior to admission. A computed tomography (CT) scan of the abdomen showed pneumoperitoneum and a mass with mural thickening around the distal ileum/cecal area (Figure 1). There was also a partially visualized mass in the infrahilar area of the right lower lobe and bilateral adrenal masses seen on the scan. A chest CT with contrast was then performed, which showed a 7.5 x 6.6 x 6.6-cm mass in the right lower lobe posterior to the right hilum. The mass encased the right mainstem bronchus, and there was a low-density-filling defect in the inferior branch of the right pulmonary vein (Figure 2). An echocardiography did not show any thrombus within the atria or ventricles.
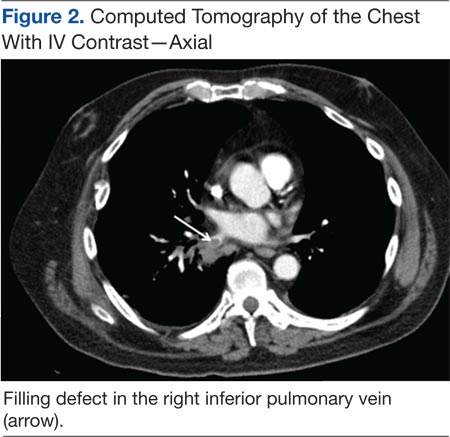
The patient underwent emergent exploratory laparotomy for bowel perforation. The operative finding was a small perforation of the small intestine with an associated mass. There were metastatic lesions throughout the abdomen. A partial small bowel resection was performed. Post exploratory laparotomy, a fiberoptic bronchoscopy was performed, which revealed a 1-cm fungating lesion at the takeoff of the superior segment of the right lower lobe. Brushings were obtained from the mass. The pathology of the lung mass was small cell carcinoma, whereas that of the bowel mass was mantle cell lymphoma. Brain magnetic resonance imaging revealed that he had metastasis to the brain with a 4-cm mass in the cerebellum. He was anticoagulated with heparin for the PVT. Based on his poor functional status and his overall clinical condition, his prognosis was poor. He received hospice care and died 3 months later.
DISCUSSION
Pulmonary vein thrombosis is a rare condition. The incidence is unclear, as most of the literature includes case reports. The majority of PVT cases are reported following lobectomy for malignancy and lung transplantation.1-3 The incidence following lung transplant was reported in the early postoperative period to be 15% in a center during the first 2 years of the study.3 Pulmonary vein thrombosis has also been described following metastatic cancer, such as liposarcoma.4
This patient’s case was discovered in the setting of SCLC and mantle cell lymphoma of the small intestine. Small cell carcinoma of the lung was reported to invade the pulmonary vein into the left atrium.8 In this patient, the left atrium was not invaded. There have been cases of spontaneous or idiopathic PVT described, presenting as abdominal pain, hemoptysis, and chest pain.5-7 No precipitating causes were detected in these patients.
The pathogenesis of PVT from a tumor is unclear, although several theories have been postulated: It could result from direct extension of the tumor into the vein, from compression of the vein by the tumor, or from epithelial damage as a result of tumor invasion. The tumor thrombus has been described to extend into the right atrium.6,8 The mechanism of thrombosis remains unclear in the patient postlobectomy or postlung transplantation, although intraoperative torsion and injury of vessels are implicated. Similar to deep vein thrombosis, PVT could also result from intimal damage or sluggish flow in the pulmonary stump in the postoperative patient.2,9,10
The presentation of PVT is usually nonspecific, including dyspnea, cough, pleuritic chest pain, and hemoptysis. It has been reported as causing massive hemoptysis due to acute pulmonary infarction.7 Acute PVT occurring postoperatively in the lung transplant patient may be disastrous and lead to early postoperative allograft failure.11 Pulmonary vein thrombosis may also present more insidiously with recurrent pulmonary edema and pulmonary fibrosis.12 This patient presented with abdominal pain; further workup led to the finding of a lung mass. Pulmonary vein thrombosis has been reported to result in systemic emboli, resulting in cerebrovascular accidents, or it can manifest as aseptic and tumor emboli.2,5,10,13,14
Newer CT techniques have made identifying PVT possible in a similar manner to which pulmonary arterial emboli are detected by using the pulmonary venous phase of a contrast CT of the chest.5 Echocardiography may demonstrate the extension of the thrombus into the atrium; a transesophageal echocardiogram would be preferable over a transthoracic echocardiogram. Magnetic resonance imaging of the chest is another useful modality for diagnosis, because it is able to distinguish between a bland thrombus and a tumor thrombus in the pulmonary vein.15
Treatment of PVT depends on the overall clinical condition of the patient. Irrespective of the etiology, a review of the literature does not indicate the preferred duration of anticoagulation or preference for modality of anticoagulation between oral vitamin K antagonists or heparin—low molecular or unfractionated.1,3-6 Patients who develop PVT following malignancy are usually anticoagulated with therapy for the cancer. The treatment of PVT in the setting of lung transplant is more challenging and includes systemic heparinization, thrombolytics, and surgical thrombectomy.3,11,16 The majority of the literature includes case reports with varying morbidity and mortality, depending on the etiology. Ninety-day mortality of 38% was reported following lung transplant.3
CONCLUSION
Pulmonary vein thrombosis presents in a nonspecific manner. The diagnosis is now more readily made with the advent of a variety of diagnostic modalities, especially with transesophageal echocardiography, which may be performed at the bedside in the intensive care unit. The treatment remains challenging with mortality dependent on the etiology. A diagnosis of PVT needs to be considered in patients with appropriate risk factors. A high index of suspicion will enable the diagnosis in the proper clinical scenario.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Genta PR, Ho N, Beyruti R, Takagaki TY, Terra-Filho M. Pulmonary vein thrombosis after bilobectomy and development of collateral circulation. Thorax. 2003;58(6):550-551.
2. Ohtaka K, Hida Y, Kaga K, et al. Pulmonary vein thrombosis after video-assisted thoracoscopic left upper lobectomy. J Thorac Cardiovasc Surg. 2012;143(1):e3-e5.
3. Schulman LL, Anandarangam T, Leibowitz DW, et al. Four-year prospective study of pulmonary venous thrombosis after lung transplantation. J Am Soc Echocardiogr. 2001;14(8):806-812.
4. Tamizifar B, Zadeh MR, Foroghi E. Pulmonary vein thrombosis after metastatic liposarcoma. Med Arh. 2012;66(1):68-69.
5. Selvidge SD, Gavant ML. Idiopathic pulmonary vein thrombosis: Detection by CT and MR imaging. AJR Am J Roentgenol. 1999;172(6):1639-1641.
6. Wu JP, Wu Q, Yang Y, DU ZZ, Sun HF. Idiopathic pulmonary vein thrombosis extending to left atrium: A case report with a literature review. Chin Med J (Engl). 2012;125(6):1197-1200.
7. Alexander GR, Reddi A, Reddy D. Idiopathic pulmonary vein thrombosis: A rare cause of massive hemoptysis. Ann Thorac Surg. 2009;88(1):281-283.
8. Chan V, Neumann D. Small cell lung carcinoma invading the pulmonary vein and left atrium as imaged by PET/CT. Eur J Nucl Med Mol Imaging. 2005;32(12):1493.
9. Burri E, Duwe J, Kull C, Glaser C, Maurer CA. Pulmonary vein thrombosis after lower lobectomy of the left lung. J Cardiovasc Surg (Torino). 2006;47(5):609-612.
10. Schwalm S, Ward RP, Spencer KT. Transient ischemic attack in a patient with pulmonary vein thrombosis after left upper lobectomy for squamous cell lung cancer. J Am Soc Echocardiogr. 2004;17(5):487-488.
11. Cywinski JB, Wallace L, Parker BM. Pulmonary vein thrombosis after sequential double-lung transplantation. J Cardiothorac Vasc Anesth. 2005;19(2):225-227.
12. Cavaco RA, Kaul S, Chapman T, et al. Idiopathic pulmonary fibrosis associated with pulmonary vein thrombosis: A case report. Cases J. 2009;2:9156.
13. Kim NH, Roldan CA, Shively BK. Pulmonary vein thrombosis. Chest. 1993;104(2):624-626.
14. Uhlmann EJ, Dunitz JM, Fiol ME. Pulmonary vein thrombosis after lung transplantation presenting as stroke. J Heart Lung Transplant. 2009;28(2):209-210.
15. Hricak H, Amparo E, Fisher MR, Crooks L, Higgins CB. Abdominal venous system: Assessment using MR. Radiology. 1985;156(2):415-422.
16. Nagahiro I, Horton M, Wilson M, Bennetts J, Spratt P, Glanville AR. Pulmonary vein thrombosis treated successfully by thrombectomy after bilateral sequential lung transplantation: Report of a case. Surg Today. 2003;33(4):282-284.
Pulmonary vein thrombosis (PVT) is rare and underdiagnosed in clinical practice. It has been described following lobectomy, lung transplant, and in association with metastatic carcinoma.1-4 Some cases have been described as idiopathic.5-7 Its exact incidence is unknown, and treatment depends on etiology. On the other hand, pulmonary artery thromboembolism is a well-known entity with identified risk factors as well as clearly defined modalities of management. The following is a case of PVT, which occurred in the setting of small cell carcinoma of the lung (SCLC) and mantle cell lymphoma of the small intestine.
CASE PRESENTATION
A 66-year-old male veteran with a past medical history of type 2 diabetes mellitus, hypertension, and chronic obstructive pulmonary disease, who had a 40 pack-year history of cigarette smoking, was admitted to the hospital for severe, sudden onset abdominal pain. The pain was localized in the right lower quadrant and then became generalized. It was sharp, aggravated by movement, and relieved by rest. The patient reported being constipated for the past couple of days.
A review of systems revealed that he had been coughing for about 3 days prior to admission. A computed tomography (CT) scan of the abdomen showed pneumoperitoneum and a mass with mural thickening around the distal ileum/cecal area (Figure 1). There was also a partially visualized mass in the infrahilar area of the right lower lobe and bilateral adrenal masses seen on the scan. A chest CT with contrast was then performed, which showed a 7.5 x 6.6 x 6.6-cm mass in the right lower lobe posterior to the right hilum. The mass encased the right mainstem bronchus, and there was a low-density-filling defect in the inferior branch of the right pulmonary vein (Figure 2). An echocardiography did not show any thrombus within the atria or ventricles.
The patient underwent emergent exploratory laparotomy for bowel perforation. The operative finding was a small perforation of the small intestine with an associated mass. There were metastatic lesions throughout the abdomen. A partial small bowel resection was performed. Post exploratory laparotomy, a fiberoptic bronchoscopy was performed, which revealed a 1-cm fungating lesion at the takeoff of the superior segment of the right lower lobe. Brushings were obtained from the mass. The pathology of the lung mass was small cell carcinoma, whereas that of the bowel mass was mantle cell lymphoma. Brain magnetic resonance imaging revealed that he had metastasis to the brain with a 4-cm mass in the cerebellum. He was anticoagulated with heparin for the PVT. Based on his poor functional status and his overall clinical condition, his prognosis was poor. He received hospice care and died 3 months later.
DISCUSSION
Pulmonary vein thrombosis is a rare condition. The incidence is unclear, as most of the literature includes case reports. The majority of PVT cases are reported following lobectomy for malignancy and lung transplantation.1-3 The incidence following lung transplant was reported in the early postoperative period to be 15% in a center during the first 2 years of the study.3 Pulmonary vein thrombosis has also been described following metastatic cancer, such as liposarcoma.4
This patient’s case was discovered in the setting of SCLC and mantle cell lymphoma of the small intestine. Small cell carcinoma of the lung was reported to invade the pulmonary vein into the left atrium.8 In this patient, the left atrium was not invaded. There have been cases of spontaneous or idiopathic PVT described, presenting as abdominal pain, hemoptysis, and chest pain.5-7 No precipitating causes were detected in these patients.
The pathogenesis of PVT from a tumor is unclear, although several theories have been postulated: It could result from direct extension of the tumor into the vein, from compression of the vein by the tumor, or from epithelial damage as a result of tumor invasion. The tumor thrombus has been described to extend into the right atrium.6,8 The mechanism of thrombosis remains unclear in the patient postlobectomy or postlung transplantation, although intraoperative torsion and injury of vessels are implicated. Similar to deep vein thrombosis, PVT could also result from intimal damage or sluggish flow in the pulmonary stump in the postoperative patient.2,9,10
The presentation of PVT is usually nonspecific, including dyspnea, cough, pleuritic chest pain, and hemoptysis. It has been reported as causing massive hemoptysis due to acute pulmonary infarction.7 Acute PVT occurring postoperatively in the lung transplant patient may be disastrous and lead to early postoperative allograft failure.11 Pulmonary vein thrombosis may also present more insidiously with recurrent pulmonary edema and pulmonary fibrosis.12 This patient presented with abdominal pain; further workup led to the finding of a lung mass. Pulmonary vein thrombosis has been reported to result in systemic emboli, resulting in cerebrovascular accidents, or it can manifest as aseptic and tumor emboli.2,5,10,13,14
Newer CT techniques have made identifying PVT possible in a similar manner to which pulmonary arterial emboli are detected by using the pulmonary venous phase of a contrast CT of the chest.5 Echocardiography may demonstrate the extension of the thrombus into the atrium; a transesophageal echocardiogram would be preferable over a transthoracic echocardiogram. Magnetic resonance imaging of the chest is another useful modality for diagnosis, because it is able to distinguish between a bland thrombus and a tumor thrombus in the pulmonary vein.15
Treatment of PVT depends on the overall clinical condition of the patient. Irrespective of the etiology, a review of the literature does not indicate the preferred duration of anticoagulation or preference for modality of anticoagulation between oral vitamin K antagonists or heparin—low molecular or unfractionated.1,3-6 Patients who develop PVT following malignancy are usually anticoagulated with therapy for the cancer. The treatment of PVT in the setting of lung transplant is more challenging and includes systemic heparinization, thrombolytics, and surgical thrombectomy.3,11,16 The majority of the literature includes case reports with varying morbidity and mortality, depending on the etiology. Ninety-day mortality of 38% was reported following lung transplant.3
CONCLUSION
Pulmonary vein thrombosis presents in a nonspecific manner. The diagnosis is now more readily made with the advent of a variety of diagnostic modalities, especially with transesophageal echocardiography, which may be performed at the bedside in the intensive care unit. The treatment remains challenging with mortality dependent on the etiology. A diagnosis of PVT needs to be considered in patients with appropriate risk factors. A high index of suspicion will enable the diagnosis in the proper clinical scenario.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Pulmonary vein thrombosis (PVT) is rare and underdiagnosed in clinical practice. It has been described following lobectomy, lung transplant, and in association with metastatic carcinoma.1-4 Some cases have been described as idiopathic.5-7 Its exact incidence is unknown, and treatment depends on etiology. On the other hand, pulmonary artery thromboembolism is a well-known entity with identified risk factors as well as clearly defined modalities of management. The following is a case of PVT, which occurred in the setting of small cell carcinoma of the lung (SCLC) and mantle cell lymphoma of the small intestine.
CASE PRESENTATION
A 66-year-old male veteran with a past medical history of type 2 diabetes mellitus, hypertension, and chronic obstructive pulmonary disease, who had a 40 pack-year history of cigarette smoking, was admitted to the hospital for severe, sudden onset abdominal pain. The pain was localized in the right lower quadrant and then became generalized. It was sharp, aggravated by movement, and relieved by rest. The patient reported being constipated for the past couple of days.
A review of systems revealed that he had been coughing for about 3 days prior to admission. A computed tomography (CT) scan of the abdomen showed pneumoperitoneum and a mass with mural thickening around the distal ileum/cecal area (Figure 1). There was also a partially visualized mass in the infrahilar area of the right lower lobe and bilateral adrenal masses seen on the scan. A chest CT with contrast was then performed, which showed a 7.5 x 6.6 x 6.6-cm mass in the right lower lobe posterior to the right hilum. The mass encased the right mainstem bronchus, and there was a low-density-filling defect in the inferior branch of the right pulmonary vein (Figure 2). An echocardiography did not show any thrombus within the atria or ventricles.
The patient underwent emergent exploratory laparotomy for bowel perforation. The operative finding was a small perforation of the small intestine with an associated mass. There were metastatic lesions throughout the abdomen. A partial small bowel resection was performed. Post exploratory laparotomy, a fiberoptic bronchoscopy was performed, which revealed a 1-cm fungating lesion at the takeoff of the superior segment of the right lower lobe. Brushings were obtained from the mass. The pathology of the lung mass was small cell carcinoma, whereas that of the bowel mass was mantle cell lymphoma. Brain magnetic resonance imaging revealed that he had metastasis to the brain with a 4-cm mass in the cerebellum. He was anticoagulated with heparin for the PVT. Based on his poor functional status and his overall clinical condition, his prognosis was poor. He received hospice care and died 3 months later.
DISCUSSION
Pulmonary vein thrombosis is a rare condition. The incidence is unclear, as most of the literature includes case reports. The majority of PVT cases are reported following lobectomy for malignancy and lung transplantation.1-3 The incidence following lung transplant was reported in the early postoperative period to be 15% in a center during the first 2 years of the study.3 Pulmonary vein thrombosis has also been described following metastatic cancer, such as liposarcoma.4
This patient’s case was discovered in the setting of SCLC and mantle cell lymphoma of the small intestine. Small cell carcinoma of the lung was reported to invade the pulmonary vein into the left atrium.8 In this patient, the left atrium was not invaded. There have been cases of spontaneous or idiopathic PVT described, presenting as abdominal pain, hemoptysis, and chest pain.5-7 No precipitating causes were detected in these patients.
The pathogenesis of PVT from a tumor is unclear, although several theories have been postulated: It could result from direct extension of the tumor into the vein, from compression of the vein by the tumor, or from epithelial damage as a result of tumor invasion. The tumor thrombus has been described to extend into the right atrium.6,8 The mechanism of thrombosis remains unclear in the patient postlobectomy or postlung transplantation, although intraoperative torsion and injury of vessels are implicated. Similar to deep vein thrombosis, PVT could also result from intimal damage or sluggish flow in the pulmonary stump in the postoperative patient.2,9,10
The presentation of PVT is usually nonspecific, including dyspnea, cough, pleuritic chest pain, and hemoptysis. It has been reported as causing massive hemoptysis due to acute pulmonary infarction.7 Acute PVT occurring postoperatively in the lung transplant patient may be disastrous and lead to early postoperative allograft failure.11 Pulmonary vein thrombosis may also present more insidiously with recurrent pulmonary edema and pulmonary fibrosis.12 This patient presented with abdominal pain; further workup led to the finding of a lung mass. Pulmonary vein thrombosis has been reported to result in systemic emboli, resulting in cerebrovascular accidents, or it can manifest as aseptic and tumor emboli.2,5,10,13,14
Newer CT techniques have made identifying PVT possible in a similar manner to which pulmonary arterial emboli are detected by using the pulmonary venous phase of a contrast CT of the chest.5 Echocardiography may demonstrate the extension of the thrombus into the atrium; a transesophageal echocardiogram would be preferable over a transthoracic echocardiogram. Magnetic resonance imaging of the chest is another useful modality for diagnosis, because it is able to distinguish between a bland thrombus and a tumor thrombus in the pulmonary vein.15
Treatment of PVT depends on the overall clinical condition of the patient. Irrespective of the etiology, a review of the literature does not indicate the preferred duration of anticoagulation or preference for modality of anticoagulation between oral vitamin K antagonists or heparin—low molecular or unfractionated.1,3-6 Patients who develop PVT following malignancy are usually anticoagulated with therapy for the cancer. The treatment of PVT in the setting of lung transplant is more challenging and includes systemic heparinization, thrombolytics, and surgical thrombectomy.3,11,16 The majority of the literature includes case reports with varying morbidity and mortality, depending on the etiology. Ninety-day mortality of 38% was reported following lung transplant.3
CONCLUSION
Pulmonary vein thrombosis presents in a nonspecific manner. The diagnosis is now more readily made with the advent of a variety of diagnostic modalities, especially with transesophageal echocardiography, which may be performed at the bedside in the intensive care unit. The treatment remains challenging with mortality dependent on the etiology. A diagnosis of PVT needs to be considered in patients with appropriate risk factors. A high index of suspicion will enable the diagnosis in the proper clinical scenario.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Genta PR, Ho N, Beyruti R, Takagaki TY, Terra-Filho M. Pulmonary vein thrombosis after bilobectomy and development of collateral circulation. Thorax. 2003;58(6):550-551.
2. Ohtaka K, Hida Y, Kaga K, et al. Pulmonary vein thrombosis after video-assisted thoracoscopic left upper lobectomy. J Thorac Cardiovasc Surg. 2012;143(1):e3-e5.
3. Schulman LL, Anandarangam T, Leibowitz DW, et al. Four-year prospective study of pulmonary venous thrombosis after lung transplantation. J Am Soc Echocardiogr. 2001;14(8):806-812.
4. Tamizifar B, Zadeh MR, Foroghi E. Pulmonary vein thrombosis after metastatic liposarcoma. Med Arh. 2012;66(1):68-69.
5. Selvidge SD, Gavant ML. Idiopathic pulmonary vein thrombosis: Detection by CT and MR imaging. AJR Am J Roentgenol. 1999;172(6):1639-1641.
6. Wu JP, Wu Q, Yang Y, DU ZZ, Sun HF. Idiopathic pulmonary vein thrombosis extending to left atrium: A case report with a literature review. Chin Med J (Engl). 2012;125(6):1197-1200.
7. Alexander GR, Reddi A, Reddy D. Idiopathic pulmonary vein thrombosis: A rare cause of massive hemoptysis. Ann Thorac Surg. 2009;88(1):281-283.
8. Chan V, Neumann D. Small cell lung carcinoma invading the pulmonary vein and left atrium as imaged by PET/CT. Eur J Nucl Med Mol Imaging. 2005;32(12):1493.
9. Burri E, Duwe J, Kull C, Glaser C, Maurer CA. Pulmonary vein thrombosis after lower lobectomy of the left lung. J Cardiovasc Surg (Torino). 2006;47(5):609-612.
10. Schwalm S, Ward RP, Spencer KT. Transient ischemic attack in a patient with pulmonary vein thrombosis after left upper lobectomy for squamous cell lung cancer. J Am Soc Echocardiogr. 2004;17(5):487-488.
11. Cywinski JB, Wallace L, Parker BM. Pulmonary vein thrombosis after sequential double-lung transplantation. J Cardiothorac Vasc Anesth. 2005;19(2):225-227.
12. Cavaco RA, Kaul S, Chapman T, et al. Idiopathic pulmonary fibrosis associated with pulmonary vein thrombosis: A case report. Cases J. 2009;2:9156.
13. Kim NH, Roldan CA, Shively BK. Pulmonary vein thrombosis. Chest. 1993;104(2):624-626.
14. Uhlmann EJ, Dunitz JM, Fiol ME. Pulmonary vein thrombosis after lung transplantation presenting as stroke. J Heart Lung Transplant. 2009;28(2):209-210.
15. Hricak H, Amparo E, Fisher MR, Crooks L, Higgins CB. Abdominal venous system: Assessment using MR. Radiology. 1985;156(2):415-422.
16. Nagahiro I, Horton M, Wilson M, Bennetts J, Spratt P, Glanville AR. Pulmonary vein thrombosis treated successfully by thrombectomy after bilateral sequential lung transplantation: Report of a case. Surg Today. 2003;33(4):282-284.
1. Genta PR, Ho N, Beyruti R, Takagaki TY, Terra-Filho M. Pulmonary vein thrombosis after bilobectomy and development of collateral circulation. Thorax. 2003;58(6):550-551.
2. Ohtaka K, Hida Y, Kaga K, et al. Pulmonary vein thrombosis after video-assisted thoracoscopic left upper lobectomy. J Thorac Cardiovasc Surg. 2012;143(1):e3-e5.
3. Schulman LL, Anandarangam T, Leibowitz DW, et al. Four-year prospective study of pulmonary venous thrombosis after lung transplantation. J Am Soc Echocardiogr. 2001;14(8):806-812.
4. Tamizifar B, Zadeh MR, Foroghi E. Pulmonary vein thrombosis after metastatic liposarcoma. Med Arh. 2012;66(1):68-69.
5. Selvidge SD, Gavant ML. Idiopathic pulmonary vein thrombosis: Detection by CT and MR imaging. AJR Am J Roentgenol. 1999;172(6):1639-1641.
6. Wu JP, Wu Q, Yang Y, DU ZZ, Sun HF. Idiopathic pulmonary vein thrombosis extending to left atrium: A case report with a literature review. Chin Med J (Engl). 2012;125(6):1197-1200.
7. Alexander GR, Reddi A, Reddy D. Idiopathic pulmonary vein thrombosis: A rare cause of massive hemoptysis. Ann Thorac Surg. 2009;88(1):281-283.
8. Chan V, Neumann D. Small cell lung carcinoma invading the pulmonary vein and left atrium as imaged by PET/CT. Eur J Nucl Med Mol Imaging. 2005;32(12):1493.
9. Burri E, Duwe J, Kull C, Glaser C, Maurer CA. Pulmonary vein thrombosis after lower lobectomy of the left lung. J Cardiovasc Surg (Torino). 2006;47(5):609-612.
10. Schwalm S, Ward RP, Spencer KT. Transient ischemic attack in a patient with pulmonary vein thrombosis after left upper lobectomy for squamous cell lung cancer. J Am Soc Echocardiogr. 2004;17(5):487-488.
11. Cywinski JB, Wallace L, Parker BM. Pulmonary vein thrombosis after sequential double-lung transplantation. J Cardiothorac Vasc Anesth. 2005;19(2):225-227.
12. Cavaco RA, Kaul S, Chapman T, et al. Idiopathic pulmonary fibrosis associated with pulmonary vein thrombosis: A case report. Cases J. 2009;2:9156.
13. Kim NH, Roldan CA, Shively BK. Pulmonary vein thrombosis. Chest. 1993;104(2):624-626.
14. Uhlmann EJ, Dunitz JM, Fiol ME. Pulmonary vein thrombosis after lung transplantation presenting as stroke. J Heart Lung Transplant. 2009;28(2):209-210.
15. Hricak H, Amparo E, Fisher MR, Crooks L, Higgins CB. Abdominal venous system: Assessment using MR. Radiology. 1985;156(2):415-422.
16. Nagahiro I, Horton M, Wilson M, Bennetts J, Spratt P, Glanville AR. Pulmonary vein thrombosis treated successfully by thrombectomy after bilateral sequential lung transplantation: Report of a case. Surg Today. 2003;33(4):282-284.
Bronchogenic Squamous Cell Carcinoma With Soft-Tissue Metastasis to the Hand: An Unusual Case Presentation and Review of the Literature
Carcinoma of the lung is the most common lethal form of cancer in both men and women worldwide.1 It accounts for more deaths than the next 3 most common cancers combined. In 2012, 160,000 Americans are estimated to have died from lung cancer.1 Lung cancer is known to have a high metastatic potential for the brain, bones, adrenal glands, lungs, and liver.2 Orthopedic manifestations frequently include bony metastasis, most commonly the vertebrae (42%), ribs (20%), and pelvis (18%).3 Acral metastatic disease is defined as metastasis distal to the elbow or the knee. Bony acral metastases from lung carcinoma to the upper and lower extremities are extremely uncommon, accounting for only 1% each of total bone metastases from carcinoma of the lung.3 Metastases to the bones of the hand are even rarer. Only 0.1% of metastatic disease from any type of carcinoma or sarcoma manifests as metastasis in the hand.4 There are only a few reports in the literature of soft-tissue or muscular metastasis to the hand from a carcinoma. Of these cases, the majority are caused by metastatic lung carcinoma.5-9 There are no reports in the literature of metastatic disease of squamous cell origin affecting the soft tissues of the hand.
We present a case of a man with known metastatic squamous cell carcinoma of the lung who presented with acral soft-tissue metastatic disease. This report highlights a rare clinical scenario that has not been reported in the literature. The report also emphasizes a rare but important consideration for clinicians who encounter acral soft-tissue lesions in patients with a history of a primary carcinoma. The patient provided written informed consent for print and electronic publication of this case report.
Continue for case report >>
Case Report
A 56-year-old man presented with right-sided pleuritic flank pain, along with a 30-lb weight loss over a 6-month period. A computed tomographic scan revealed a 5.58×3.7-cm cavitary lesion in the right lower lobe with abutment of the posterior chest wall (Figure 1). He underwent biopsy and staging, and was found to be T3N1, with biopsy-proven well-differentiated bronchogenic squamous cell carcinoma. The patient then underwent right lower and middle lobectomy with concomitant en-bloc resection of the posterior portion of ribs 7 to 11, along with mediastinal lymph-node dissection with negative margins. After surgery, he was treated with 4 cycles of adjuvant chemotherapy with cisplatin and docetaxel.
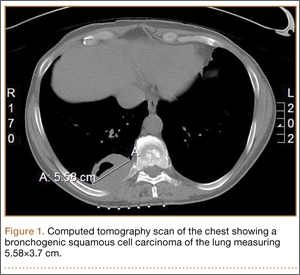
Six months after surgery, the patient began to complain of right-hand pain isolated to the thenar eminence. He also described swelling and significant pain with active or passive movement of the thumb and with relatively mild-to-moderate palpation of the area. The patient reported that the functioning of his thumb deteriorated rapidly over the course of about 1 month. On physical examination, he was neurovascularly intact with no apparent deficit in sensation of his right hand. There was no erythema or overlying skin changes. His right thenar eminence was mildly enlarged as compared with the left, and a firm, focal mass was readily palpated. Range of motion at the metacarpophalangeal joint of the thumb and index finger was limited because of pain. Thumb opposition was markedly limited. After a detailed history and physical examination, we were concerned about possible deep space infection, old hematoma, or possible metastatic disease. Magnetic resonance imaging (MRI) was ordered to evaluate the palpable mass.
Radiographically, localized soft-tissue swelling was present on the palmar surface of the hand obliquely overlying the index finger metacarpal (Figures 2, 3). On MRI, the lesion measured approximately 1.8×3.3 cm and was isointense to slightly hyperintense diffusely with central hyperintensity on T1 images (Figure 4). On T2 and short tau inversion recovery images, the lesion was more strikingly hyperintense and infiltrative in appearance (Figure 5). Postcontrast images showed avid enhancement peripherally, with central nonenhancement consistent with necrosis in the adductor pollicis.

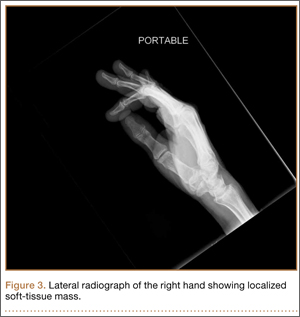
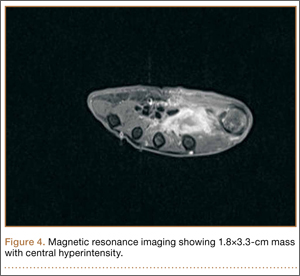
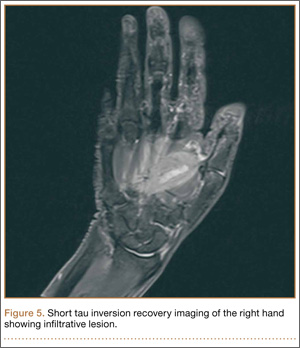
Continue for biopsy results and discussion >>
We performed a biopsy of the lesion with the aid of immediate adequacy by fine needle aspiration cytology. We saw mitotically active malignant cells with large nuclei, high nuclear-to-cytoplasmic ratios, nucleoli, and dense cytoplasm, suggesting a metastatic squamous cell carcinoma. Because infection was part of the differential, it is pertinent to note that there was no significant inflammatory infiltrate. The core biopsy was consistent with metastatic lung cancer (Figure 6).
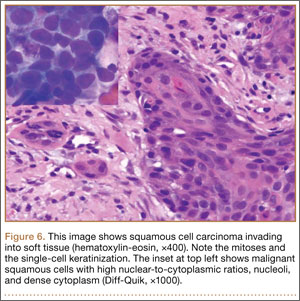
Discussion
This patient presented an interesting diagnostic challenge, particularly because of his previous malignancy. The differential diagnosis of acute onset thenar pain without history of trauma would include encompassing soft-tissue abscess, osteomyelitis, and infectious myositis. Soft-tissue hematoma is also in the differential for this patient, especially given the malignancy. Bony metastasis should be considered in this patient given the propensity of lung carcinoma to metastasize to bone. The location would certainly be atypical, with metastasis to the bones of the forearm or hand representing only 0.1% of all metastasis of any type of primary carcinoma or sarcoma.4 Primary bone or soft-tissue sarcoma should also be considered. Some authors have also suggested that necrosis, peritumoral edema-like signal, and lobulation are more common with skeletal muscle metastasis than with a primary sarcoma.10 In this case, the degree of surrounding postcontrast enhancement made simple muscle tear with hematoma unlikely, despite the presence of increased T1 signal. The lack of evidence for localized infection and the presence of a firm focal mass on physical examination made tumor more likely than infection.
Acrometastasis
Metastatic disease distal to the elbow and knee is very rare; specifically, metastatic disease of the hands or feet accounts for approximately 0.1% of all metastases.4 Carcinoma of the lung accounts for 44% to 47% of all acrometastasis.11,12 When hand acrometastasis is considered, the right hand accounts for 55% of bony cases, likely because of hand dominance, although approximately 10% of patients had bilateral acral metastatic disease.12 The underlying mechanism of acrometastasis remains unclear; however, some authors have postulated that it may result from an increase in vascularity or a trauma to the affected extremity.12,13 Flynn and colleagues12 reviewed the literature and reported a total of 257 cases of acral metastasis to the hand; they found that the median age at presentation was 58 years. Men were more than twice as likely to be affected when compared with women. Most commonly, the primary malignancies were in the lung (44%), kidney (12%), and breast (10%). The authors also reported less common cases of acral metastasis with primary malignancies located in the stomach, liver, rectum, prostate, and colon. Most commonly, these metastases were found in the distal phalynx, followed by the metacarpals, proximal phalynx, and middle phalynx.12
Soft-Tissue Metastasis
Skeletal muscle metastasis occurs in 0.8% to 17.5% of metastatic neoplasms.14-17 Studies in lung cancer patients have also revealed a low prevalence of muscular metastasis (0% to 0.8%).16 The rarity of muscular metastatic disease has been attributed to local inhibition of tumor survival secondary to muscle contraction, increased diffusing capacity of enzymes and immune cells, and extreme variability in blood flow and pH, lactate, and oxygen concentration. Skeletal muscular metastases most commonly arise from the lung, kidneys, colon, or melanoma.16 In a recent large series of more than 1400 patients imaged for soft-tissue masses, 2.5% were metastatic.18 There are only 2 reports of soft-tissue metastatic disease involving the hand: one from a patient with a thyroid carcinoma and the other from a patient with a lung adenocarcinoma.18 Soft-tissue metastatic disease from squamous cell carcinoma distal to the wrist has never been reported in the literature.
Acral Soft-Tissue Metastasis
A review from 2012 found 264 cases of skeletal muscle metastasis from 151 articles.6 Only 2 (0.75%) of these patients, as reported above, had a soft-tissue metastasis distal to the wrist.6,17
Continue for conclusion >>
Conclusion
We report the first known case of a soft-tissue metastasis distal to the wrist from a primary bronchogenic squamous cell carcinoma. This report highlights the extremely uncommon presentation of soft-tissue acral metastatic disease of a bronchogenic squamous cell carcinoma of the lung. Although exceedingly rare, oncologists and physicians who manage pathology of the hand should consider metastatic disease when evaluating a patient with complaints of hand pain and a soft-tissue mass, especially in a patient with a known primary malignancy.
1. American Cancer Society. Lung Cancer (Non-Small Cell). http://www.cancer.org/acs/groups/cid/documents/webcontent/003115-pdf.pdf. Revised April 30, 2014. Accessed July 22, 2014.
2. Willis RA. Pathology of Tumors. London, England: Butterworth; 1960.
3. Sugiura H, Yamada K, Sugiura T, Hida T, Mitsudomi T. Predictors of survival in patients with bone metastasis of lung cancer. Clin Orthop. 2008;466(3):729-736.
4. Kerin R. Metastatic tumors of the hand. A review of the literature. J Bone Joint Surg Am. 1983;65(9):1331-1335.
5. Alpar S. Muscle metastasis in a patient with squamous cell lung cancer. Turkish Respiratory Journal. 2002;3(2):75-78.
6. Haygood TM, Wong J, Lin JC, et al. Skeletal muscle metastases: a three-part study of a not-so-rare entity. Skeletal Radiol. 2012;41(8):899-909.
7. Tuoheti Y, Okada K, Osanai T, et al. Skeletal muscle metastases of carcinoma: a clinicopathological study of 12 cases. Jpn J Clin Oncol. 2004;34(4):210-214.
8. Chan NP, Yeo W, Ahuja AT, King AD. Multiple skeletal muscle metastases. Hong Kong Med J. 1999;5(4):410.
9. Molina-Garrido MJ, Guillen-Ponce C. Muscle metastasis of carcinoma. Clin Transl Oncol. 2011;13(2):98-101.
10. Williams JB, Youngberg RA, Bui-Mansfield LT, Pitcher JD. MR imaging of skeletal muscle metastases. AJR Am J Roentgenol. 1997;168(2):555-557.
11. Libson E, Bloom RA, Husband JE, Stoker DJ. Metastatic tumours of bones of the hand and foot. A comparative review and report of 43 additional cases. Skeletal Radiol. 1987;16(5):387-392.
12. Flynn CJ, Danjoux C, Wong J, et al. Two cases of acrometastasis to the hands and review of the literature. Curr Oncol. 2008;15(5):51-58.
13. Healey JH, Turnbull AD, Miedema B, Lane JM. Acrometastases. A study of twenty-nine patients with osseous involvement of the hands and feet. J Bone Joint Surg Am. 1986;68(5):743-746.
14. Sudo A, Ogihara Y, Shiokawa Y, Fujinami S, Sekiguchi S. Intramuscular metastasis of carcinoma. Clin Orthop. 1993(296):213-217.
15. Surov A, Hainz M, Holzhausen HJ, et al. Skeletal muscle metastases: primary tumours, prevalence, and radiological features. Eur Radiol. 2010;20(3):649-658.
16. Pearson CM. Incidence and type of pathologic alterations observed in muscle in a routine autopsy survey. Neurology. 1959;9:757-766.
17. Acinas Garcia O, Fernández FA, Satué EG, Beulta L, Val-Bernal JF. Metastasis of malignant neoplasms to skeletal muscle. Rev Esp Oncol. 1984;31(1):57-67.
18. Glockner JF, White LM, Sundaram M, McDonald DJ. Unsuspected metastases presenting as solitary soft tissue lesions: a fourteen-year review. Skeletal Radiol. 2000;29(5):270-274.
Carcinoma of the lung is the most common lethal form of cancer in both men and women worldwide.1 It accounts for more deaths than the next 3 most common cancers combined. In 2012, 160,000 Americans are estimated to have died from lung cancer.1 Lung cancer is known to have a high metastatic potential for the brain, bones, adrenal glands, lungs, and liver.2 Orthopedic manifestations frequently include bony metastasis, most commonly the vertebrae (42%), ribs (20%), and pelvis (18%).3 Acral metastatic disease is defined as metastasis distal to the elbow or the knee. Bony acral metastases from lung carcinoma to the upper and lower extremities are extremely uncommon, accounting for only 1% each of total bone metastases from carcinoma of the lung.3 Metastases to the bones of the hand are even rarer. Only 0.1% of metastatic disease from any type of carcinoma or sarcoma manifests as metastasis in the hand.4 There are only a few reports in the literature of soft-tissue or muscular metastasis to the hand from a carcinoma. Of these cases, the majority are caused by metastatic lung carcinoma.5-9 There are no reports in the literature of metastatic disease of squamous cell origin affecting the soft tissues of the hand.
We present a case of a man with known metastatic squamous cell carcinoma of the lung who presented with acral soft-tissue metastatic disease. This report highlights a rare clinical scenario that has not been reported in the literature. The report also emphasizes a rare but important consideration for clinicians who encounter acral soft-tissue lesions in patients with a history of a primary carcinoma. The patient provided written informed consent for print and electronic publication of this case report.
Continue for case report >>
Case Report
A 56-year-old man presented with right-sided pleuritic flank pain, along with a 30-lb weight loss over a 6-month period. A computed tomographic scan revealed a 5.58×3.7-cm cavitary lesion in the right lower lobe with abutment of the posterior chest wall (Figure 1). He underwent biopsy and staging, and was found to be T3N1, with biopsy-proven well-differentiated bronchogenic squamous cell carcinoma. The patient then underwent right lower and middle lobectomy with concomitant en-bloc resection of the posterior portion of ribs 7 to 11, along with mediastinal lymph-node dissection with negative margins. After surgery, he was treated with 4 cycles of adjuvant chemotherapy with cisplatin and docetaxel.
Six months after surgery, the patient began to complain of right-hand pain isolated to the thenar eminence. He also described swelling and significant pain with active or passive movement of the thumb and with relatively mild-to-moderate palpation of the area. The patient reported that the functioning of his thumb deteriorated rapidly over the course of about 1 month. On physical examination, he was neurovascularly intact with no apparent deficit in sensation of his right hand. There was no erythema or overlying skin changes. His right thenar eminence was mildly enlarged as compared with the left, and a firm, focal mass was readily palpated. Range of motion at the metacarpophalangeal joint of the thumb and index finger was limited because of pain. Thumb opposition was markedly limited. After a detailed history and physical examination, we were concerned about possible deep space infection, old hematoma, or possible metastatic disease. Magnetic resonance imaging (MRI) was ordered to evaluate the palpable mass.
Radiographically, localized soft-tissue swelling was present on the palmar surface of the hand obliquely overlying the index finger metacarpal (Figures 2, 3). On MRI, the lesion measured approximately 1.8×3.3 cm and was isointense to slightly hyperintense diffusely with central hyperintensity on T1 images (Figure 4). On T2 and short tau inversion recovery images, the lesion was more strikingly hyperintense and infiltrative in appearance (Figure 5). Postcontrast images showed avid enhancement peripherally, with central nonenhancement consistent with necrosis in the adductor pollicis.
Continue for biopsy results and discussion >>
We performed a biopsy of the lesion with the aid of immediate adequacy by fine needle aspiration cytology. We saw mitotically active malignant cells with large nuclei, high nuclear-to-cytoplasmic ratios, nucleoli, and dense cytoplasm, suggesting a metastatic squamous cell carcinoma. Because infection was part of the differential, it is pertinent to note that there was no significant inflammatory infiltrate. The core biopsy was consistent with metastatic lung cancer (Figure 6).
Discussion
This patient presented an interesting diagnostic challenge, particularly because of his previous malignancy. The differential diagnosis of acute onset thenar pain without history of trauma would include encompassing soft-tissue abscess, osteomyelitis, and infectious myositis. Soft-tissue hematoma is also in the differential for this patient, especially given the malignancy. Bony metastasis should be considered in this patient given the propensity of lung carcinoma to metastasize to bone. The location would certainly be atypical, with metastasis to the bones of the forearm or hand representing only 0.1% of all metastasis of any type of primary carcinoma or sarcoma.4 Primary bone or soft-tissue sarcoma should also be considered. Some authors have also suggested that necrosis, peritumoral edema-like signal, and lobulation are more common with skeletal muscle metastasis than with a primary sarcoma.10 In this case, the degree of surrounding postcontrast enhancement made simple muscle tear with hematoma unlikely, despite the presence of increased T1 signal. The lack of evidence for localized infection and the presence of a firm focal mass on physical examination made tumor more likely than infection.
Acrometastasis
Metastatic disease distal to the elbow and knee is very rare; specifically, metastatic disease of the hands or feet accounts for approximately 0.1% of all metastases.4 Carcinoma of the lung accounts for 44% to 47% of all acrometastasis.11,12 When hand acrometastasis is considered, the right hand accounts for 55% of bony cases, likely because of hand dominance, although approximately 10% of patients had bilateral acral metastatic disease.12 The underlying mechanism of acrometastasis remains unclear; however, some authors have postulated that it may result from an increase in vascularity or a trauma to the affected extremity.12,13 Flynn and colleagues12 reviewed the literature and reported a total of 257 cases of acral metastasis to the hand; they found that the median age at presentation was 58 years. Men were more than twice as likely to be affected when compared with women. Most commonly, the primary malignancies were in the lung (44%), kidney (12%), and breast (10%). The authors also reported less common cases of acral metastasis with primary malignancies located in the stomach, liver, rectum, prostate, and colon. Most commonly, these metastases were found in the distal phalynx, followed by the metacarpals, proximal phalynx, and middle phalynx.12
Soft-Tissue Metastasis
Skeletal muscle metastasis occurs in 0.8% to 17.5% of metastatic neoplasms.14-17 Studies in lung cancer patients have also revealed a low prevalence of muscular metastasis (0% to 0.8%).16 The rarity of muscular metastatic disease has been attributed to local inhibition of tumor survival secondary to muscle contraction, increased diffusing capacity of enzymes and immune cells, and extreme variability in blood flow and pH, lactate, and oxygen concentration. Skeletal muscular metastases most commonly arise from the lung, kidneys, colon, or melanoma.16 In a recent large series of more than 1400 patients imaged for soft-tissue masses, 2.5% were metastatic.18 There are only 2 reports of soft-tissue metastatic disease involving the hand: one from a patient with a thyroid carcinoma and the other from a patient with a lung adenocarcinoma.18 Soft-tissue metastatic disease from squamous cell carcinoma distal to the wrist has never been reported in the literature.
Acral Soft-Tissue Metastasis
A review from 2012 found 264 cases of skeletal muscle metastasis from 151 articles.6 Only 2 (0.75%) of these patients, as reported above, had a soft-tissue metastasis distal to the wrist.6,17
Continue for conclusion >>
Conclusion
We report the first known case of a soft-tissue metastasis distal to the wrist from a primary bronchogenic squamous cell carcinoma. This report highlights the extremely uncommon presentation of soft-tissue acral metastatic disease of a bronchogenic squamous cell carcinoma of the lung. Although exceedingly rare, oncologists and physicians who manage pathology of the hand should consider metastatic disease when evaluating a patient with complaints of hand pain and a soft-tissue mass, especially in a patient with a known primary malignancy.
Carcinoma of the lung is the most common lethal form of cancer in both men and women worldwide.1 It accounts for more deaths than the next 3 most common cancers combined. In 2012, 160,000 Americans are estimated to have died from lung cancer.1 Lung cancer is known to have a high metastatic potential for the brain, bones, adrenal glands, lungs, and liver.2 Orthopedic manifestations frequently include bony metastasis, most commonly the vertebrae (42%), ribs (20%), and pelvis (18%).3 Acral metastatic disease is defined as metastasis distal to the elbow or the knee. Bony acral metastases from lung carcinoma to the upper and lower extremities are extremely uncommon, accounting for only 1% each of total bone metastases from carcinoma of the lung.3 Metastases to the bones of the hand are even rarer. Only 0.1% of metastatic disease from any type of carcinoma or sarcoma manifests as metastasis in the hand.4 There are only a few reports in the literature of soft-tissue or muscular metastasis to the hand from a carcinoma. Of these cases, the majority are caused by metastatic lung carcinoma.5-9 There are no reports in the literature of metastatic disease of squamous cell origin affecting the soft tissues of the hand.
We present a case of a man with known metastatic squamous cell carcinoma of the lung who presented with acral soft-tissue metastatic disease. This report highlights a rare clinical scenario that has not been reported in the literature. The report also emphasizes a rare but important consideration for clinicians who encounter acral soft-tissue lesions in patients with a history of a primary carcinoma. The patient provided written informed consent for print and electronic publication of this case report.
Continue for case report >>
Case Report
A 56-year-old man presented with right-sided pleuritic flank pain, along with a 30-lb weight loss over a 6-month period. A computed tomographic scan revealed a 5.58×3.7-cm cavitary lesion in the right lower lobe with abutment of the posterior chest wall (Figure 1). He underwent biopsy and staging, and was found to be T3N1, with biopsy-proven well-differentiated bronchogenic squamous cell carcinoma. The patient then underwent right lower and middle lobectomy with concomitant en-bloc resection of the posterior portion of ribs 7 to 11, along with mediastinal lymph-node dissection with negative margins. After surgery, he was treated with 4 cycles of adjuvant chemotherapy with cisplatin and docetaxel.
Six months after surgery, the patient began to complain of right-hand pain isolated to the thenar eminence. He also described swelling and significant pain with active or passive movement of the thumb and with relatively mild-to-moderate palpation of the area. The patient reported that the functioning of his thumb deteriorated rapidly over the course of about 1 month. On physical examination, he was neurovascularly intact with no apparent deficit in sensation of his right hand. There was no erythema or overlying skin changes. His right thenar eminence was mildly enlarged as compared with the left, and a firm, focal mass was readily palpated. Range of motion at the metacarpophalangeal joint of the thumb and index finger was limited because of pain. Thumb opposition was markedly limited. After a detailed history and physical examination, we were concerned about possible deep space infection, old hematoma, or possible metastatic disease. Magnetic resonance imaging (MRI) was ordered to evaluate the palpable mass.
Radiographically, localized soft-tissue swelling was present on the palmar surface of the hand obliquely overlying the index finger metacarpal (Figures 2, 3). On MRI, the lesion measured approximately 1.8×3.3 cm and was isointense to slightly hyperintense diffusely with central hyperintensity on T1 images (Figure 4). On T2 and short tau inversion recovery images, the lesion was more strikingly hyperintense and infiltrative in appearance (Figure 5). Postcontrast images showed avid enhancement peripherally, with central nonenhancement consistent with necrosis in the adductor pollicis.
Continue for biopsy results and discussion >>
We performed a biopsy of the lesion with the aid of immediate adequacy by fine needle aspiration cytology. We saw mitotically active malignant cells with large nuclei, high nuclear-to-cytoplasmic ratios, nucleoli, and dense cytoplasm, suggesting a metastatic squamous cell carcinoma. Because infection was part of the differential, it is pertinent to note that there was no significant inflammatory infiltrate. The core biopsy was consistent with metastatic lung cancer (Figure 6).
Discussion
This patient presented an interesting diagnostic challenge, particularly because of his previous malignancy. The differential diagnosis of acute onset thenar pain without history of trauma would include encompassing soft-tissue abscess, osteomyelitis, and infectious myositis. Soft-tissue hematoma is also in the differential for this patient, especially given the malignancy. Bony metastasis should be considered in this patient given the propensity of lung carcinoma to metastasize to bone. The location would certainly be atypical, with metastasis to the bones of the forearm or hand representing only 0.1% of all metastasis of any type of primary carcinoma or sarcoma.4 Primary bone or soft-tissue sarcoma should also be considered. Some authors have also suggested that necrosis, peritumoral edema-like signal, and lobulation are more common with skeletal muscle metastasis than with a primary sarcoma.10 In this case, the degree of surrounding postcontrast enhancement made simple muscle tear with hematoma unlikely, despite the presence of increased T1 signal. The lack of evidence for localized infection and the presence of a firm focal mass on physical examination made tumor more likely than infection.
Acrometastasis
Metastatic disease distal to the elbow and knee is very rare; specifically, metastatic disease of the hands or feet accounts for approximately 0.1% of all metastases.4 Carcinoma of the lung accounts for 44% to 47% of all acrometastasis.11,12 When hand acrometastasis is considered, the right hand accounts for 55% of bony cases, likely because of hand dominance, although approximately 10% of patients had bilateral acral metastatic disease.12 The underlying mechanism of acrometastasis remains unclear; however, some authors have postulated that it may result from an increase in vascularity or a trauma to the affected extremity.12,13 Flynn and colleagues12 reviewed the literature and reported a total of 257 cases of acral metastasis to the hand; they found that the median age at presentation was 58 years. Men were more than twice as likely to be affected when compared with women. Most commonly, the primary malignancies were in the lung (44%), kidney (12%), and breast (10%). The authors also reported less common cases of acral metastasis with primary malignancies located in the stomach, liver, rectum, prostate, and colon. Most commonly, these metastases were found in the distal phalynx, followed by the metacarpals, proximal phalynx, and middle phalynx.12
Soft-Tissue Metastasis
Skeletal muscle metastasis occurs in 0.8% to 17.5% of metastatic neoplasms.14-17 Studies in lung cancer patients have also revealed a low prevalence of muscular metastasis (0% to 0.8%).16 The rarity of muscular metastatic disease has been attributed to local inhibition of tumor survival secondary to muscle contraction, increased diffusing capacity of enzymes and immune cells, and extreme variability in blood flow and pH, lactate, and oxygen concentration. Skeletal muscular metastases most commonly arise from the lung, kidneys, colon, or melanoma.16 In a recent large series of more than 1400 patients imaged for soft-tissue masses, 2.5% were metastatic.18 There are only 2 reports of soft-tissue metastatic disease involving the hand: one from a patient with a thyroid carcinoma and the other from a patient with a lung adenocarcinoma.18 Soft-tissue metastatic disease from squamous cell carcinoma distal to the wrist has never been reported in the literature.
Acral Soft-Tissue Metastasis
A review from 2012 found 264 cases of skeletal muscle metastasis from 151 articles.6 Only 2 (0.75%) of these patients, as reported above, had a soft-tissue metastasis distal to the wrist.6,17
Continue for conclusion >>
Conclusion
We report the first known case of a soft-tissue metastasis distal to the wrist from a primary bronchogenic squamous cell carcinoma. This report highlights the extremely uncommon presentation of soft-tissue acral metastatic disease of a bronchogenic squamous cell carcinoma of the lung. Although exceedingly rare, oncologists and physicians who manage pathology of the hand should consider metastatic disease when evaluating a patient with complaints of hand pain and a soft-tissue mass, especially in a patient with a known primary malignancy.
1. American Cancer Society. Lung Cancer (Non-Small Cell). http://www.cancer.org/acs/groups/cid/documents/webcontent/003115-pdf.pdf. Revised April 30, 2014. Accessed July 22, 2014.
2. Willis RA. Pathology of Tumors. London, England: Butterworth; 1960.
3. Sugiura H, Yamada K, Sugiura T, Hida T, Mitsudomi T. Predictors of survival in patients with bone metastasis of lung cancer. Clin Orthop. 2008;466(3):729-736.
4. Kerin R. Metastatic tumors of the hand. A review of the literature. J Bone Joint Surg Am. 1983;65(9):1331-1335.
5. Alpar S. Muscle metastasis in a patient with squamous cell lung cancer. Turkish Respiratory Journal. 2002;3(2):75-78.
6. Haygood TM, Wong J, Lin JC, et al. Skeletal muscle metastases: a three-part study of a not-so-rare entity. Skeletal Radiol. 2012;41(8):899-909.
7. Tuoheti Y, Okada K, Osanai T, et al. Skeletal muscle metastases of carcinoma: a clinicopathological study of 12 cases. Jpn J Clin Oncol. 2004;34(4):210-214.
8. Chan NP, Yeo W, Ahuja AT, King AD. Multiple skeletal muscle metastases. Hong Kong Med J. 1999;5(4):410.
9. Molina-Garrido MJ, Guillen-Ponce C. Muscle metastasis of carcinoma. Clin Transl Oncol. 2011;13(2):98-101.
10. Williams JB, Youngberg RA, Bui-Mansfield LT, Pitcher JD. MR imaging of skeletal muscle metastases. AJR Am J Roentgenol. 1997;168(2):555-557.
11. Libson E, Bloom RA, Husband JE, Stoker DJ. Metastatic tumours of bones of the hand and foot. A comparative review and report of 43 additional cases. Skeletal Radiol. 1987;16(5):387-392.
12. Flynn CJ, Danjoux C, Wong J, et al. Two cases of acrometastasis to the hands and review of the literature. Curr Oncol. 2008;15(5):51-58.
13. Healey JH, Turnbull AD, Miedema B, Lane JM. Acrometastases. A study of twenty-nine patients with osseous involvement of the hands and feet. J Bone Joint Surg Am. 1986;68(5):743-746.
14. Sudo A, Ogihara Y, Shiokawa Y, Fujinami S, Sekiguchi S. Intramuscular metastasis of carcinoma. Clin Orthop. 1993(296):213-217.
15. Surov A, Hainz M, Holzhausen HJ, et al. Skeletal muscle metastases: primary tumours, prevalence, and radiological features. Eur Radiol. 2010;20(3):649-658.
16. Pearson CM. Incidence and type of pathologic alterations observed in muscle in a routine autopsy survey. Neurology. 1959;9:757-766.
17. Acinas Garcia O, Fernández FA, Satué EG, Beulta L, Val-Bernal JF. Metastasis of malignant neoplasms to skeletal muscle. Rev Esp Oncol. 1984;31(1):57-67.
18. Glockner JF, White LM, Sundaram M, McDonald DJ. Unsuspected metastases presenting as solitary soft tissue lesions: a fourteen-year review. Skeletal Radiol. 2000;29(5):270-274.
1. American Cancer Society. Lung Cancer (Non-Small Cell). http://www.cancer.org/acs/groups/cid/documents/webcontent/003115-pdf.pdf. Revised April 30, 2014. Accessed July 22, 2014.
2. Willis RA. Pathology of Tumors. London, England: Butterworth; 1960.
3. Sugiura H, Yamada K, Sugiura T, Hida T, Mitsudomi T. Predictors of survival in patients with bone metastasis of lung cancer. Clin Orthop. 2008;466(3):729-736.
4. Kerin R. Metastatic tumors of the hand. A review of the literature. J Bone Joint Surg Am. 1983;65(9):1331-1335.
5. Alpar S. Muscle metastasis in a patient with squamous cell lung cancer. Turkish Respiratory Journal. 2002;3(2):75-78.
6. Haygood TM, Wong J, Lin JC, et al. Skeletal muscle metastases: a three-part study of a not-so-rare entity. Skeletal Radiol. 2012;41(8):899-909.
7. Tuoheti Y, Okada K, Osanai T, et al. Skeletal muscle metastases of carcinoma: a clinicopathological study of 12 cases. Jpn J Clin Oncol. 2004;34(4):210-214.
8. Chan NP, Yeo W, Ahuja AT, King AD. Multiple skeletal muscle metastases. Hong Kong Med J. 1999;5(4):410.
9. Molina-Garrido MJ, Guillen-Ponce C. Muscle metastasis of carcinoma. Clin Transl Oncol. 2011;13(2):98-101.
10. Williams JB, Youngberg RA, Bui-Mansfield LT, Pitcher JD. MR imaging of skeletal muscle metastases. AJR Am J Roentgenol. 1997;168(2):555-557.
11. Libson E, Bloom RA, Husband JE, Stoker DJ. Metastatic tumours of bones of the hand and foot. A comparative review and report of 43 additional cases. Skeletal Radiol. 1987;16(5):387-392.
12. Flynn CJ, Danjoux C, Wong J, et al. Two cases of acrometastasis to the hands and review of the literature. Curr Oncol. 2008;15(5):51-58.
13. Healey JH, Turnbull AD, Miedema B, Lane JM. Acrometastases. A study of twenty-nine patients with osseous involvement of the hands and feet. J Bone Joint Surg Am. 1986;68(5):743-746.
14. Sudo A, Ogihara Y, Shiokawa Y, Fujinami S, Sekiguchi S. Intramuscular metastasis of carcinoma. Clin Orthop. 1993(296):213-217.
15. Surov A, Hainz M, Holzhausen HJ, et al. Skeletal muscle metastases: primary tumours, prevalence, and radiological features. Eur Radiol. 2010;20(3):649-658.
16. Pearson CM. Incidence and type of pathologic alterations observed in muscle in a routine autopsy survey. Neurology. 1959;9:757-766.
17. Acinas Garcia O, Fernández FA, Satué EG, Beulta L, Val-Bernal JF. Metastasis of malignant neoplasms to skeletal muscle. Rev Esp Oncol. 1984;31(1):57-67.
18. Glockner JF, White LM, Sundaram M, McDonald DJ. Unsuspected metastases presenting as solitary soft tissue lesions: a fourteen-year review. Skeletal Radiol. 2000;29(5):270-274.
