User login
Grand Rounds: Man, 30, With Traumatic Finger Amputations
A 30-year-old man sustained traumatic amputations of three of his left fingers while at work. A heavy object fell when a supporting chain snapped; although he moved quickly, three of his left distal fingers were caught under the object. He was flown to a hospital for definitive hand care.
During the preadmission history and physical, it was noted that the patient had mild right knee pain in addition to his finger injuries. He had experienced no head injury and no loss of consciousness or other complaints. He did not remember injuring his leg, although he said it might have been struck by the falling object; all he could remember was the injury to his fingers.
On physical exam, the only abnormality other than the man’s traumatic finger amputations was mild right knee edema and a small bruised area medially. Initially, he complained of mild pain on palpation and moderate pain with passive range of motion, but range of motion was intact. His pain was worse at the proximal, medial tibial area, and he had mild lateral mid-calf tenderness though no bruising. Distally, his right lower extremity motor and sensory function were intact, and he had no open wounds or skin breakdown. He had 2+ dorsalis pedis pulse and 1+ posterior tibial pulse. The toes were pink and warm with brisk capillary refill. All compartments were soft and compressible.
Upon review of his plain radiographs (three views of the right knee), the patient was noted to have a severely comminuted medial tibial plateau fracture that extended to the midline in the region of the tibial spine, with mild depression of the fracture fragments measuring about 6 mm (see Figures 1a, 1b, and 1c). This would translate into a Schatzker IV classification type1 fracture (see Figure 22,3).
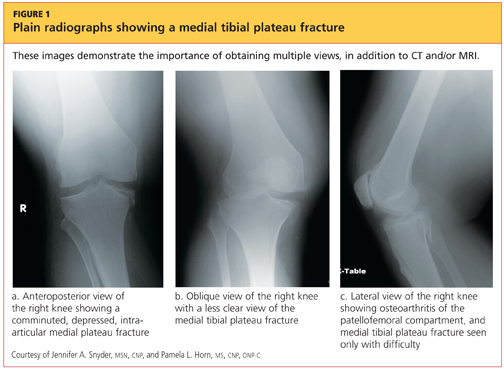
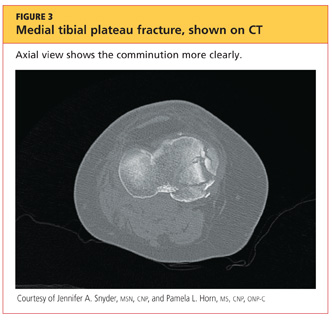
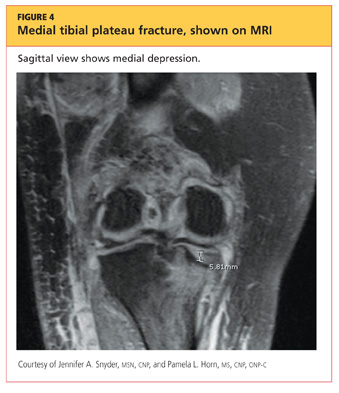
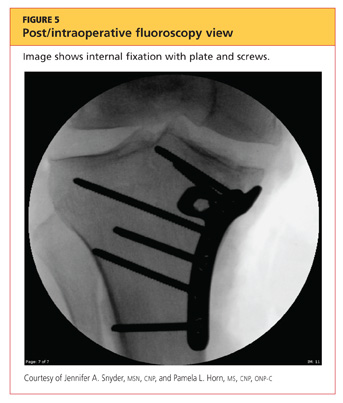
The man was admitted and underwent emergent surgery on his injured left fingers that night. Further diagnostic knee testing was performed, including CT and MRI (see Figures 3 and 4). Three days after admission, the patient underwent open reduction and internal fixation (plating) of the right medial, proximal tibia (see Figure 5). He has done very well since without issue.
DISCUSSION
Fractures of the tibial plateau occur along the articular, or joint, surface of the proximal tibia. The plateau consists of lateral and medial condylar surfaces. These concave structures function as an articulation point for the cartilaginous menisci and the femoral condyles.4 The medial plateau and condyle are stronger than those of the lateral side, and therefore are less commonly fractured. An elevated intercondylar eminence divides the lateral and medial plateaus, providing an attachment site for the cruciate ligaments.3
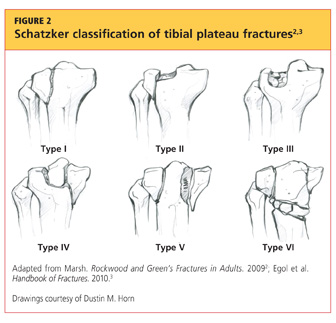
The Schatzker classification system1 is most commonly used to describe the types of tibial plateau fractures (as seen in Figure 22,3). Schatzker et al1 divided these injuries into six categories, according to the impact of increased energy exerted onto the bone; the rising classification numbers indicate an increase in complexity and severity and usually a worsening prognosis.
The type I fracture represents a split fracture of the lateral plateau. Typically, a fracture of this type has depression or displacement measuring less than 4 mm.
Type II tibial plateau fractures, the most common Schatzker injury, are lateral plateau fractures with depression noted at the split. Not always evident on plain radiographs, this depression can often be overlooked, and the injury mistaken for a type I fracture. The depression is measured vertically from the lower edge of the medial plateau to the lowest depression point of the lateral plateau.5
Type III fractures, the least common among the Schatzker injuries, are described as pure depression fractures of the lateral plateau. These fractures do not have an appreciable “split” along the plateau and are usually found in older patients with osteopenia.2
The Schatzker type IV injury is a medial fracture with displacement or depression to a portion of the plateau. The fracture may be split or comminuted and may originate in the intercondylar area.
Type V fractures, also known as “bicondylar fractures,” affect both the lateral and medial plateau. An inverted “Y” pattern is frequently seen, and there may be additional involvement of the intercondylar eminence. Type V fractures differ from type VI injuries in that there is no disturbance of the metaphyseal-diaphyseal connection. Thus, type VI fractures also include a transverse component that separates the condyles (metaphysis) of the bone from the shaft (diaphysis). Wide variation is seen among type VI fractures.5
Assessment and Diagnosis
Originally termed “fender fractures” due to their frequent association with automobile injuries, fractures of the tibial plateau account for 1% of all fractures and 8% of fractures in elderly patients.6 Tibial plateau fractures occur when varus or valgus force is combined with axial loading. The fracture itself occurs when the femoral condyle is driven into the lateral or medial plateau. Bicondylar injuries occur when rigorous axial force is sustained in a fully extended knee.
Injuries may also include those of the ligaments or menisci, resulting in joint instability. Patients may present with generalized knee pain or difficulty bearing weight after sustaining injuries, such as being struck in a motor vehicle accident, being tackled, or falling from some height.4
Evaluation of a patient with a suspected tibial plateau fracture begins with a detailed history and thorough physical examination. Details regarding the mechanism of injury help to predict the pattern of the fracture and may indicate whether a more focused neurovascular exam is warranted. Low-energy injuries (often seen with Schatzker types I to III) or twisting injuries yield low suspicion for neurovascular injury or compartment syndrome. However, high-energy injuries (seen often with Schatzker types IV through VI) have a greater likelihood of resulting in complicated injuries that must be urgently or emergently treated.5
The popliteal artery is bound posteriorly and distally to the tibial plateau, and the peroneal nerve is located laterally and positioned around the fibular head. It is essential to assess for the popliteal pulse, as well as lateral lower-extremity sensation and the patient’s ability to dorsiflex. Along with motor and neurovascular injuries, presentation with a painful, strikingly swollen knee and difficulty bearing weight may indicate a hemarthrosis. Soft tissue injuries over the knee resulting from direct trauma may require a saline arthrogram to rule out communication into the joint. Furthermore, a thorough ligamentous exam of the knee is helpful in determining the extent of the injuries.3
Compartment syndrome is a serious, emergent complication that can occur with tibial plateau fractures, especially those sustained during high-energy trauma.7 The health care provider must perform serial exams of the lower extremity to assess for classic signs of compartment syndrome. Are the compartments tense or noncompressible? Does the patient have pain with passive stretch or with range of motion of the lower extremity? Is there pallor or paresthesia to the affected limb? Is the pulse weak or absent? Presence of any of the aforementioned symptoms should prompt a high suspicion for compartment syndrome, and the patient must be sent to an emergency department for urgent evaluation.5
Treatment/Rehabilitation
For Schatzker types I through III, intervention focuses on the articular cartilage examination and repair. Type IV injuries often include corresponding damage to the popliteal artery and/or peroneal nerve, and types V and VI often have such overlying soft tissue damage that temporary placement of an external fixation device is required before definitive surgical intervention can be performed.8
However, it should be noted that conservative versus surgical treatment is often debated among surgeons for treatment of Schatzker fractures. The management of a tibial plateau fracture depends on the physical demands and health of the patient, the severity of the fracture, the stability of the joint, and the surgeon’s skill set and preferences.4 Operative intervention is generally indicated for fractures with depressions greater than 2 mm (although some surgeons allow up to 1 cm of depression), fractures with joint instability, or open fractures. Injuries with concern for vascular injury or compartment syndrome are also treated both operatively and emergently. Postoperatively, patients will remain non–weight-bearing for eight to 12 weeks after surgery, and in the interim, depending on the surgeon’s preference, may or may not engage in active or passive range of motion of the knee.
Advocates of open reduction and internal fixation (ORIF) argue that this method allows for the fracture reduction and anatomic alignment to be directly examined, but they also acknowledge that this approach compromises a great deal of soft tissue surrounding the proximal tibia.9,10
In order to reduce soft tissue damage, some surgeons favor external fixation. Initial use of this surgical technique results in minimal soft tissue swelling and allows early range of motion. While the external fixation device is in place, there is a risk for pin site infection, and proper site care must be provided.6,11
Generally, the treatment of tibial plateau fractures is considered successful when the fracture reduction is sustained, the patient’s functional capacity and axial loading are restored, and the articular surface is reconstructed. As a rule, nonoperative treatment is reserved for tibial plateau fractures that are minimally depressed or nondisplaced, or for patients with advanced osteoporosis. Under these circumstances, after a non–weight-bearing period of four to eight weeks, patients will begin to perform protected and partial weight bearing using a hinged knee brace.2 Early active range of motion, along with isometric exercises to strengthen the quadriceps, is recommended.
Whether surgical or conservative treatment is chosen, complications of tibial plateau fractures include knee stiffness, wound breakdown and infection, malunion or nonunion, vascular or neurologic injury, prominent or painful hardware, or avascular necrosis of fragmented bone pieces.4
CONCLUSION
The primary care practitioner must never overlook patients’ complaints of knee pain, especially after varus or valgus stress injuries or axial loading injuries to the knee. The patient may be able to ambulate; however, ordering a radiograph is an easy method for evaluation and for ruling out tibial plateau injuries. If there is any question regarding the presence of fracture with plain radiographs and/or the clinical exam warrants it, CT is an appropriate second diagnostic intervention.
Should a tibial plateau fracture present in a primary care or urgent care setting, thorough examination of neurovascular status and risk for compartment syndrome must be done urgently, followed by a referral to an orthopedic surgeon or emergency department.
REFERENCES
1. Schatzker J, McBroom R, Bruce D. The tibial plateau fracture: the Toronto experience, 1968–1975. Clin Orthop Relat Res. 1979;(138): 94-104.
2. Marsh JL. Tibial plateau fractures. In: Bucholz RW, Court-Brown CM, Heckman HD, Tornetta P. Rockwood and Green’s Fractures in Adults. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:1780-1831.
3. Egol K, Koval KJ, Zuckerman JD. Tibial plateau. In: Egol K, Koval KJ, Zuckerman JD. Handbook of Fractures. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010:455-463.
4. Fenton PP, Porter KK. Tibial plateau fractures: a review. Trauma. 2011;13(3):181-187.
5. Markhardt BK, Gross JM, Monu JU. Schatzker classification of tibial plateau fractures: use of CT and MR imaging improves assessment. Radiographics. 2009;29(2):585-597.
6. Lewis C. Does the mode of fixation of tibial plateau fractures, i.e. external fixation versus internal fixation, influence the time to union? A systematic review of the literature. Eur J Orthopaed Surg Traumatol. 2008;18(5):365-370.
7. Weinlein J, Schmidt A. Acute compartment syndrome in tibial plateau fractures—beware! J Knee Surg. 2010;31(1):9-16.
8. te Stroet MA, Holla M, Biert J, van Kampen A. The value of CT scan compared to plain radiographs for the classification and treatment plan in tibial plateau fractures. Emerg Radiol. 2011;18(4):279-283.
9. Musahl V, Tarkin I, Kobbe P, et al. New trends and techniques in open reduction and internal fixation of fractures of the tibial plateau. J Bone Joint Surg Br. 2009;91(4):426-433.
10. Toro-Arbelaez JB, Gardner MJ, Shindle MK, et al. Open reduction and internal fixation of intraarticular tibial plateau nonunions. Injury. 2007;38(3):378-383.
11. Marsh JL, Smith ST, Do TT. External fixation and limited internal fixation for complex fractures of the tibial plateau. J Bone Joint Surg Am. 1995;77(5):661-673.
A 30-year-old man sustained traumatic amputations of three of his left fingers while at work. A heavy object fell when a supporting chain snapped; although he moved quickly, three of his left distal fingers were caught under the object. He was flown to a hospital for definitive hand care.
During the preadmission history and physical, it was noted that the patient had mild right knee pain in addition to his finger injuries. He had experienced no head injury and no loss of consciousness or other complaints. He did not remember injuring his leg, although he said it might have been struck by the falling object; all he could remember was the injury to his fingers.
On physical exam, the only abnormality other than the man’s traumatic finger amputations was mild right knee edema and a small bruised area medially. Initially, he complained of mild pain on palpation and moderate pain with passive range of motion, but range of motion was intact. His pain was worse at the proximal, medial tibial area, and he had mild lateral mid-calf tenderness though no bruising. Distally, his right lower extremity motor and sensory function were intact, and he had no open wounds or skin breakdown. He had 2+ dorsalis pedis pulse and 1+ posterior tibial pulse. The toes were pink and warm with brisk capillary refill. All compartments were soft and compressible.
Upon review of his plain radiographs (three views of the right knee), the patient was noted to have a severely comminuted medial tibial plateau fracture that extended to the midline in the region of the tibial spine, with mild depression of the fracture fragments measuring about 6 mm (see Figures 1a, 1b, and 1c). This would translate into a Schatzker IV classification type1 fracture (see Figure 22,3).
The man was admitted and underwent emergent surgery on his injured left fingers that night. Further diagnostic knee testing was performed, including CT and MRI (see Figures 3 and 4). Three days after admission, the patient underwent open reduction and internal fixation (plating) of the right medial, proximal tibia (see Figure 5). He has done very well since without issue.
DISCUSSION
Fractures of the tibial plateau occur along the articular, or joint, surface of the proximal tibia. The plateau consists of lateral and medial condylar surfaces. These concave structures function as an articulation point for the cartilaginous menisci and the femoral condyles.4 The medial plateau and condyle are stronger than those of the lateral side, and therefore are less commonly fractured. An elevated intercondylar eminence divides the lateral and medial plateaus, providing an attachment site for the cruciate ligaments.3
The Schatzker classification system1 is most commonly used to describe the types of tibial plateau fractures (as seen in Figure 22,3). Schatzker et al1 divided these injuries into six categories, according to the impact of increased energy exerted onto the bone; the rising classification numbers indicate an increase in complexity and severity and usually a worsening prognosis.
The type I fracture represents a split fracture of the lateral plateau. Typically, a fracture of this type has depression or displacement measuring less than 4 mm.
Type II tibial plateau fractures, the most common Schatzker injury, are lateral plateau fractures with depression noted at the split. Not always evident on plain radiographs, this depression can often be overlooked, and the injury mistaken for a type I fracture. The depression is measured vertically from the lower edge of the medial plateau to the lowest depression point of the lateral plateau.5
Type III fractures, the least common among the Schatzker injuries, are described as pure depression fractures of the lateral plateau. These fractures do not have an appreciable “split” along the plateau and are usually found in older patients with osteopenia.2
The Schatzker type IV injury is a medial fracture with displacement or depression to a portion of the plateau. The fracture may be split or comminuted and may originate in the intercondylar area.
Type V fractures, also known as “bicondylar fractures,” affect both the lateral and medial plateau. An inverted “Y” pattern is frequently seen, and there may be additional involvement of the intercondylar eminence. Type V fractures differ from type VI injuries in that there is no disturbance of the metaphyseal-diaphyseal connection. Thus, type VI fractures also include a transverse component that separates the condyles (metaphysis) of the bone from the shaft (diaphysis). Wide variation is seen among type VI fractures.5
Assessment and Diagnosis
Originally termed “fender fractures” due to their frequent association with automobile injuries, fractures of the tibial plateau account for 1% of all fractures and 8% of fractures in elderly patients.6 Tibial plateau fractures occur when varus or valgus force is combined with axial loading. The fracture itself occurs when the femoral condyle is driven into the lateral or medial plateau. Bicondylar injuries occur when rigorous axial force is sustained in a fully extended knee.
Injuries may also include those of the ligaments or menisci, resulting in joint instability. Patients may present with generalized knee pain or difficulty bearing weight after sustaining injuries, such as being struck in a motor vehicle accident, being tackled, or falling from some height.4
Evaluation of a patient with a suspected tibial plateau fracture begins with a detailed history and thorough physical examination. Details regarding the mechanism of injury help to predict the pattern of the fracture and may indicate whether a more focused neurovascular exam is warranted. Low-energy injuries (often seen with Schatzker types I to III) or twisting injuries yield low suspicion for neurovascular injury or compartment syndrome. However, high-energy injuries (seen often with Schatzker types IV through VI) have a greater likelihood of resulting in complicated injuries that must be urgently or emergently treated.5
The popliteal artery is bound posteriorly and distally to the tibial plateau, and the peroneal nerve is located laterally and positioned around the fibular head. It is essential to assess for the popliteal pulse, as well as lateral lower-extremity sensation and the patient’s ability to dorsiflex. Along with motor and neurovascular injuries, presentation with a painful, strikingly swollen knee and difficulty bearing weight may indicate a hemarthrosis. Soft tissue injuries over the knee resulting from direct trauma may require a saline arthrogram to rule out communication into the joint. Furthermore, a thorough ligamentous exam of the knee is helpful in determining the extent of the injuries.3
Compartment syndrome is a serious, emergent complication that can occur with tibial plateau fractures, especially those sustained during high-energy trauma.7 The health care provider must perform serial exams of the lower extremity to assess for classic signs of compartment syndrome. Are the compartments tense or noncompressible? Does the patient have pain with passive stretch or with range of motion of the lower extremity? Is there pallor or paresthesia to the affected limb? Is the pulse weak or absent? Presence of any of the aforementioned symptoms should prompt a high suspicion for compartment syndrome, and the patient must be sent to an emergency department for urgent evaluation.5
Treatment/Rehabilitation
For Schatzker types I through III, intervention focuses on the articular cartilage examination and repair. Type IV injuries often include corresponding damage to the popliteal artery and/or peroneal nerve, and types V and VI often have such overlying soft tissue damage that temporary placement of an external fixation device is required before definitive surgical intervention can be performed.8
However, it should be noted that conservative versus surgical treatment is often debated among surgeons for treatment of Schatzker fractures. The management of a tibial plateau fracture depends on the physical demands and health of the patient, the severity of the fracture, the stability of the joint, and the surgeon’s skill set and preferences.4 Operative intervention is generally indicated for fractures with depressions greater than 2 mm (although some surgeons allow up to 1 cm of depression), fractures with joint instability, or open fractures. Injuries with concern for vascular injury or compartment syndrome are also treated both operatively and emergently. Postoperatively, patients will remain non–weight-bearing for eight to 12 weeks after surgery, and in the interim, depending on the surgeon’s preference, may or may not engage in active or passive range of motion of the knee.
Advocates of open reduction and internal fixation (ORIF) argue that this method allows for the fracture reduction and anatomic alignment to be directly examined, but they also acknowledge that this approach compromises a great deal of soft tissue surrounding the proximal tibia.9,10
In order to reduce soft tissue damage, some surgeons favor external fixation. Initial use of this surgical technique results in minimal soft tissue swelling and allows early range of motion. While the external fixation device is in place, there is a risk for pin site infection, and proper site care must be provided.6,11
Generally, the treatment of tibial plateau fractures is considered successful when the fracture reduction is sustained, the patient’s functional capacity and axial loading are restored, and the articular surface is reconstructed. As a rule, nonoperative treatment is reserved for tibial plateau fractures that are minimally depressed or nondisplaced, or for patients with advanced osteoporosis. Under these circumstances, after a non–weight-bearing period of four to eight weeks, patients will begin to perform protected and partial weight bearing using a hinged knee brace.2 Early active range of motion, along with isometric exercises to strengthen the quadriceps, is recommended.
Whether surgical or conservative treatment is chosen, complications of tibial plateau fractures include knee stiffness, wound breakdown and infection, malunion or nonunion, vascular or neurologic injury, prominent or painful hardware, or avascular necrosis of fragmented bone pieces.4
CONCLUSION
The primary care practitioner must never overlook patients’ complaints of knee pain, especially after varus or valgus stress injuries or axial loading injuries to the knee. The patient may be able to ambulate; however, ordering a radiograph is an easy method for evaluation and for ruling out tibial plateau injuries. If there is any question regarding the presence of fracture with plain radiographs and/or the clinical exam warrants it, CT is an appropriate second diagnostic intervention.
Should a tibial plateau fracture present in a primary care or urgent care setting, thorough examination of neurovascular status and risk for compartment syndrome must be done urgently, followed by a referral to an orthopedic surgeon or emergency department.
REFERENCES
1. Schatzker J, McBroom R, Bruce D. The tibial plateau fracture: the Toronto experience, 1968–1975. Clin Orthop Relat Res. 1979;(138): 94-104.
2. Marsh JL. Tibial plateau fractures. In: Bucholz RW, Court-Brown CM, Heckman HD, Tornetta P. Rockwood and Green’s Fractures in Adults. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:1780-1831.
3. Egol K, Koval KJ, Zuckerman JD. Tibial plateau. In: Egol K, Koval KJ, Zuckerman JD. Handbook of Fractures. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010:455-463.
4. Fenton PP, Porter KK. Tibial plateau fractures: a review. Trauma. 2011;13(3):181-187.
5. Markhardt BK, Gross JM, Monu JU. Schatzker classification of tibial plateau fractures: use of CT and MR imaging improves assessment. Radiographics. 2009;29(2):585-597.
6. Lewis C. Does the mode of fixation of tibial plateau fractures, i.e. external fixation versus internal fixation, influence the time to union? A systematic review of the literature. Eur J Orthopaed Surg Traumatol. 2008;18(5):365-370.
7. Weinlein J, Schmidt A. Acute compartment syndrome in tibial plateau fractures—beware! J Knee Surg. 2010;31(1):9-16.
8. te Stroet MA, Holla M, Biert J, van Kampen A. The value of CT scan compared to plain radiographs for the classification and treatment plan in tibial plateau fractures. Emerg Radiol. 2011;18(4):279-283.
9. Musahl V, Tarkin I, Kobbe P, et al. New trends and techniques in open reduction and internal fixation of fractures of the tibial plateau. J Bone Joint Surg Br. 2009;91(4):426-433.
10. Toro-Arbelaez JB, Gardner MJ, Shindle MK, et al. Open reduction and internal fixation of intraarticular tibial plateau nonunions. Injury. 2007;38(3):378-383.
11. Marsh JL, Smith ST, Do TT. External fixation and limited internal fixation for complex fractures of the tibial plateau. J Bone Joint Surg Am. 1995;77(5):661-673.
A 30-year-old man sustained traumatic amputations of three of his left fingers while at work. A heavy object fell when a supporting chain snapped; although he moved quickly, three of his left distal fingers were caught under the object. He was flown to a hospital for definitive hand care.
During the preadmission history and physical, it was noted that the patient had mild right knee pain in addition to his finger injuries. He had experienced no head injury and no loss of consciousness or other complaints. He did not remember injuring his leg, although he said it might have been struck by the falling object; all he could remember was the injury to his fingers.
On physical exam, the only abnormality other than the man’s traumatic finger amputations was mild right knee edema and a small bruised area medially. Initially, he complained of mild pain on palpation and moderate pain with passive range of motion, but range of motion was intact. His pain was worse at the proximal, medial tibial area, and he had mild lateral mid-calf tenderness though no bruising. Distally, his right lower extremity motor and sensory function were intact, and he had no open wounds or skin breakdown. He had 2+ dorsalis pedis pulse and 1+ posterior tibial pulse. The toes were pink and warm with brisk capillary refill. All compartments were soft and compressible.
Upon review of his plain radiographs (three views of the right knee), the patient was noted to have a severely comminuted medial tibial plateau fracture that extended to the midline in the region of the tibial spine, with mild depression of the fracture fragments measuring about 6 mm (see Figures 1a, 1b, and 1c). This would translate into a Schatzker IV classification type1 fracture (see Figure 22,3).
The man was admitted and underwent emergent surgery on his injured left fingers that night. Further diagnostic knee testing was performed, including CT and MRI (see Figures 3 and 4). Three days after admission, the patient underwent open reduction and internal fixation (plating) of the right medial, proximal tibia (see Figure 5). He has done very well since without issue.
DISCUSSION
Fractures of the tibial plateau occur along the articular, or joint, surface of the proximal tibia. The plateau consists of lateral and medial condylar surfaces. These concave structures function as an articulation point for the cartilaginous menisci and the femoral condyles.4 The medial plateau and condyle are stronger than those of the lateral side, and therefore are less commonly fractured. An elevated intercondylar eminence divides the lateral and medial plateaus, providing an attachment site for the cruciate ligaments.3
The Schatzker classification system1 is most commonly used to describe the types of tibial plateau fractures (as seen in Figure 22,3). Schatzker et al1 divided these injuries into six categories, according to the impact of increased energy exerted onto the bone; the rising classification numbers indicate an increase in complexity and severity and usually a worsening prognosis.
The type I fracture represents a split fracture of the lateral plateau. Typically, a fracture of this type has depression or displacement measuring less than 4 mm.
Type II tibial plateau fractures, the most common Schatzker injury, are lateral plateau fractures with depression noted at the split. Not always evident on plain radiographs, this depression can often be overlooked, and the injury mistaken for a type I fracture. The depression is measured vertically from the lower edge of the medial plateau to the lowest depression point of the lateral plateau.5
Type III fractures, the least common among the Schatzker injuries, are described as pure depression fractures of the lateral plateau. These fractures do not have an appreciable “split” along the plateau and are usually found in older patients with osteopenia.2
The Schatzker type IV injury is a medial fracture with displacement or depression to a portion of the plateau. The fracture may be split or comminuted and may originate in the intercondylar area.
Type V fractures, also known as “bicondylar fractures,” affect both the lateral and medial plateau. An inverted “Y” pattern is frequently seen, and there may be additional involvement of the intercondylar eminence. Type V fractures differ from type VI injuries in that there is no disturbance of the metaphyseal-diaphyseal connection. Thus, type VI fractures also include a transverse component that separates the condyles (metaphysis) of the bone from the shaft (diaphysis). Wide variation is seen among type VI fractures.5
Assessment and Diagnosis
Originally termed “fender fractures” due to their frequent association with automobile injuries, fractures of the tibial plateau account for 1% of all fractures and 8% of fractures in elderly patients.6 Tibial plateau fractures occur when varus or valgus force is combined with axial loading. The fracture itself occurs when the femoral condyle is driven into the lateral or medial plateau. Bicondylar injuries occur when rigorous axial force is sustained in a fully extended knee.
Injuries may also include those of the ligaments or menisci, resulting in joint instability. Patients may present with generalized knee pain or difficulty bearing weight after sustaining injuries, such as being struck in a motor vehicle accident, being tackled, or falling from some height.4
Evaluation of a patient with a suspected tibial plateau fracture begins with a detailed history and thorough physical examination. Details regarding the mechanism of injury help to predict the pattern of the fracture and may indicate whether a more focused neurovascular exam is warranted. Low-energy injuries (often seen with Schatzker types I to III) or twisting injuries yield low suspicion for neurovascular injury or compartment syndrome. However, high-energy injuries (seen often with Schatzker types IV through VI) have a greater likelihood of resulting in complicated injuries that must be urgently or emergently treated.5
The popliteal artery is bound posteriorly and distally to the tibial plateau, and the peroneal nerve is located laterally and positioned around the fibular head. It is essential to assess for the popliteal pulse, as well as lateral lower-extremity sensation and the patient’s ability to dorsiflex. Along with motor and neurovascular injuries, presentation with a painful, strikingly swollen knee and difficulty bearing weight may indicate a hemarthrosis. Soft tissue injuries over the knee resulting from direct trauma may require a saline arthrogram to rule out communication into the joint. Furthermore, a thorough ligamentous exam of the knee is helpful in determining the extent of the injuries.3
Compartment syndrome is a serious, emergent complication that can occur with tibial plateau fractures, especially those sustained during high-energy trauma.7 The health care provider must perform serial exams of the lower extremity to assess for classic signs of compartment syndrome. Are the compartments tense or noncompressible? Does the patient have pain with passive stretch or with range of motion of the lower extremity? Is there pallor or paresthesia to the affected limb? Is the pulse weak or absent? Presence of any of the aforementioned symptoms should prompt a high suspicion for compartment syndrome, and the patient must be sent to an emergency department for urgent evaluation.5
Treatment/Rehabilitation
For Schatzker types I through III, intervention focuses on the articular cartilage examination and repair. Type IV injuries often include corresponding damage to the popliteal artery and/or peroneal nerve, and types V and VI often have such overlying soft tissue damage that temporary placement of an external fixation device is required before definitive surgical intervention can be performed.8
However, it should be noted that conservative versus surgical treatment is often debated among surgeons for treatment of Schatzker fractures. The management of a tibial plateau fracture depends on the physical demands and health of the patient, the severity of the fracture, the stability of the joint, and the surgeon’s skill set and preferences.4 Operative intervention is generally indicated for fractures with depressions greater than 2 mm (although some surgeons allow up to 1 cm of depression), fractures with joint instability, or open fractures. Injuries with concern for vascular injury or compartment syndrome are also treated both operatively and emergently. Postoperatively, patients will remain non–weight-bearing for eight to 12 weeks after surgery, and in the interim, depending on the surgeon’s preference, may or may not engage in active or passive range of motion of the knee.
Advocates of open reduction and internal fixation (ORIF) argue that this method allows for the fracture reduction and anatomic alignment to be directly examined, but they also acknowledge that this approach compromises a great deal of soft tissue surrounding the proximal tibia.9,10
In order to reduce soft tissue damage, some surgeons favor external fixation. Initial use of this surgical technique results in minimal soft tissue swelling and allows early range of motion. While the external fixation device is in place, there is a risk for pin site infection, and proper site care must be provided.6,11
Generally, the treatment of tibial plateau fractures is considered successful when the fracture reduction is sustained, the patient’s functional capacity and axial loading are restored, and the articular surface is reconstructed. As a rule, nonoperative treatment is reserved for tibial plateau fractures that are minimally depressed or nondisplaced, or for patients with advanced osteoporosis. Under these circumstances, after a non–weight-bearing period of four to eight weeks, patients will begin to perform protected and partial weight bearing using a hinged knee brace.2 Early active range of motion, along with isometric exercises to strengthen the quadriceps, is recommended.
Whether surgical or conservative treatment is chosen, complications of tibial plateau fractures include knee stiffness, wound breakdown and infection, malunion or nonunion, vascular or neurologic injury, prominent or painful hardware, or avascular necrosis of fragmented bone pieces.4
CONCLUSION
The primary care practitioner must never overlook patients’ complaints of knee pain, especially after varus or valgus stress injuries or axial loading injuries to the knee. The patient may be able to ambulate; however, ordering a radiograph is an easy method for evaluation and for ruling out tibial plateau injuries. If there is any question regarding the presence of fracture with plain radiographs and/or the clinical exam warrants it, CT is an appropriate second diagnostic intervention.
Should a tibial plateau fracture present in a primary care or urgent care setting, thorough examination of neurovascular status and risk for compartment syndrome must be done urgently, followed by a referral to an orthopedic surgeon or emergency department.
REFERENCES
1. Schatzker J, McBroom R, Bruce D. The tibial plateau fracture: the Toronto experience, 1968–1975. Clin Orthop Relat Res. 1979;(138): 94-104.
2. Marsh JL. Tibial plateau fractures. In: Bucholz RW, Court-Brown CM, Heckman HD, Tornetta P. Rockwood and Green’s Fractures in Adults. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:1780-1831.
3. Egol K, Koval KJ, Zuckerman JD. Tibial plateau. In: Egol K, Koval KJ, Zuckerman JD. Handbook of Fractures. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010:455-463.
4. Fenton PP, Porter KK. Tibial plateau fractures: a review. Trauma. 2011;13(3):181-187.
5. Markhardt BK, Gross JM, Monu JU. Schatzker classification of tibial plateau fractures: use of CT and MR imaging improves assessment. Radiographics. 2009;29(2):585-597.
6. Lewis C. Does the mode of fixation of tibial plateau fractures, i.e. external fixation versus internal fixation, influence the time to union? A systematic review of the literature. Eur J Orthopaed Surg Traumatol. 2008;18(5):365-370.
7. Weinlein J, Schmidt A. Acute compartment syndrome in tibial plateau fractures—beware! J Knee Surg. 2010;31(1):9-16.
8. te Stroet MA, Holla M, Biert J, van Kampen A. The value of CT scan compared to plain radiographs for the classification and treatment plan in tibial plateau fractures. Emerg Radiol. 2011;18(4):279-283.
9. Musahl V, Tarkin I, Kobbe P, et al. New trends and techniques in open reduction and internal fixation of fractures of the tibial plateau. J Bone Joint Surg Br. 2009;91(4):426-433.
10. Toro-Arbelaez JB, Gardner MJ, Shindle MK, et al. Open reduction and internal fixation of intraarticular tibial plateau nonunions. Injury. 2007;38(3):378-383.
11. Marsh JL, Smith ST, Do TT. External fixation and limited internal fixation for complex fractures of the tibial plateau. J Bone Joint Surg Am. 1995;77(5):661-673.
Cover
ABCs of CCBs
5 Electrical Injuries: Risk Stratification and Treatment
electrical injuries, severe electrical exposures, minor electrical exposures, High-voltage injuries, low-voltage injuries, pediatric electrical injuries, electrical injuries in pregnancy
electrical injuries, severe electrical exposures, minor electrical exposures, High-voltage injuries, low-voltage injuries, pediatric electrical injuries, electrical injuries in pregnancy
electrical injuries, severe electrical exposures, minor electrical exposures, High-voltage injuries, low-voltage injuries, pediatric electrical injuries, electrical injuries in pregnancy
Total Joint Arthroplasty in Patients With a History of Cancer
UPDATE: MINIMALLY INVASIVE SURGERY
Dr. Garcia serves as a consultant to IOGYN, Minerva Surgical, Conceptus, Ethicon EndoSurgery, and Ethicon Women’s Health & Urology. She is a speaker for Conceptus.
Two-thirds of the almost one-half million hysterectomies performed annually in the United States for benign conditions take the abdominal route—even though less invasive transvaginal and laparoscopic approaches are available. Compared with abdominal hysterectomy, vaginal and laparoscopic hysterectomies are, on the whole, associated with less morbidity, a shorter hospital stay, and more rapid return to physical activity.
Over the past year, our understanding of the comparative advantages and risks of the various approaches to hysterectomy has been deepened by new research and by guidance from AAGL. Here is what we’ve learned, and here is how our surgical practices ought to be evolving for the long-term good of our patients.
Hysterectomy should be performed only rarely abdominally
AAGL Position Statement: Route of hysterectomy to treat benign uterine disease. J Minim Invasive Gynecol. 2011;18(1):1–3. [To link to the AAGL Position Statement, click here.]
In 2011, AAGL, which has been an international leader in promoting minimally invasive gynecologic surgery for longer than 40 years, issued a position statement on hysterectomy for the treatment of benign disease. AAGL’s position is a clear assertion that, when vaginal hysterectomy is not possible, laparoscopic hysterectomy should be performed—thus leaving few clinical indications for an abdominal hysterectomy.
Historically established contraindications to vaginal or laparoscopic hysterectomy—prior cesarean delivery, need for oophorectomy, an enlarged uterus—have been invalidated by recent studies. In competent hands, ovarian removal can be accomplished in 65% to 98.5% of vaginal hysterectomies.1 Vaginal morcellation techniques can facilitate removal of a large uterus vaginally and mechanical tissue morcellators enable laparoscopic removal.
In 2011, ACOG reaffirmed its 1999 Committee Opinion on Gynecologic Practice,1 which recommends that the vaginal approach for hysterectomy be the preferred route. ACOG asserts that, when vaginal hysterectomy is impossible, the laparoscopic and abdominal routes are alternatives.
How do these positions differ?
The difference in the AAGL Position Statement and the ACOG Committee Opinion lies in the surgeon’s ability to perform laparoscopic or vaginal hysterectomy. Although it might seem admirable for a surgeon to choose abdominal hysterectomy because he, or she, lacks the training and skills to perform the procedure laparoscopically or vaginally, AAGL does not hold this position. AAGL has established the expectation that, if a surgeon is unable to perform a hysterectomy safely vaginally or laparoscopically, he should refer the patient to a gynecologic surgeon who can.
Furthermore, AAGL recommends that abdominal hysterectomy be reserved for four broad situations, when:
- a patient has a medical condition, such as cardiopulmonary disease, in which the risk of general anesthesia or increased intraperitoneal pressure that is associated with laparoscopy is deemed unacceptable
- morcellation is known, or likely, to be required for vaginal or laparoscopic hysterectomy and uterine malignancy is either known or suspected
- hysterectomy is indicated but there is no access to surgeons or facilities required for vaginal or laparoscopic hysterectomy and referral is not feasible
- anatomy is so distorted by uterine disease or adhesions that the vaginal and laparoscopic approaches are deemed unsafe or unreasonable by a recognized expert in vaginal or laparoscopic hysterectomy techniques.
When hysterectomy is necessary, therefore, the demonstrated safety, efficacy, and cost-effectiveness of vaginal and laparoscopic approaches to surgical removal of the uterus mandate that these procedures be 1) the ones of choice and 2) presented as options to all appropriate candidates.
Whenever feasible for benign disease, perform hysterectomy vaginally or laparoscopically. Make the effort to facilitate these approaches based on the underlying principles of 1) informed patient choice and 2) preferential provision of minimally invasive options.
If you have not had the requisite training or learned the skills required to perform vaginal or laparoscopic hysterectomy, you should enlist the assistance of colleagues who do or refer your patients to those colleagues for surgical care. You should also, for the long term, seek to acquire those skills through formal training.
Nieboer T, Hendriks J, Bongers MY, Vierhout ME, Kluivers KB. Quality of life after laparoscopic and abdominal hysterectomy: a randomized controlled trial. Obstet Gynecol. 2012;119(1):85–91.
Nieboer and colleagues have presented their long-term data from a prospective, randomized evaluation of quality of life (QOL) after abdominal hysterectomy compared with QOL after laparoscopic hysterectomy. Other researchers have compared hysterectomy approaches, but most of those studies focused on such outcome measures as operation time, surgical intraoperative and postoperative complications, hospital stay, and rate of recurrence of the condition that prompted the surgery. This is the first study to address QOL parameters that are more patient-centered —using a validated questionnaire and having a median follow-up of 4.7 years (range, 188 to 303 weeks).
In 2007, investigators published the findings of a randomized comparison of QOL measures after total laparoscopic hysterectomy and total abdominal hysterectomy. Their assessment in that study utilized eight QOL measures from the RAND-36 Measure of Health-Related Quality of Life (the Dutch version of the validated QOL questionnaire, the SF-36 Health Survey)2 (TABLE).
8 key RAND-36 measures of quality of life in women who have had a hysterectomy
|
The current (Nieboer and co-workers) study evaluated 59 randomized patients from the 2007 work: 27 to laparoscopic hysterectomy and 32 to abdominal hysterectomy. The overall response rate after 4 years was 83% (N=49).
The QOL questionnaire addressed eight RAND-36 (SF-36) measures, with each measure having a possible score of 0 to 100 (maximum possible total score, 800); the higher the number, the better the QOL. The researchers considered a difference of 15 points between the two surgical approaches on any single parameter to be statistically significant.
Findings. The mean total RAND-36 (SF-36) score was 50.4 points (95% confidence interval, 1.0–99.7) higher in the laparoscopic hysterectomy group at each point of measurement in the weeks postoperatively, up to 4 years of follow-up. Higher scores at 4 years were also seen in the laparoscopy group for vitality, physical functioning, and social functioning.
From these findings, the authors surmise that QOL remains better 4 years after laparoscopic hysterectomy than it does after abdominal hysterectomy.
Why these findings? The Nieboer team offers several explanations for ongoing improvement in QOL scores among laparoscopic hysterectomy patients.
First, it is conceivable that laparoscopic patients scored higher on the Body Image Scale, benefiting from the knowledge that they underwent what, even in layman’s terms, would be called the “minimally invasive approach.”
Second, chronic abdominal or pelvic pain could affect QOL scores. It has been shown that, for other laparotomy procedures, the incidence of postop chronic pain ranges from 3% to 56%. Risk factors for postop chronic pain are female gender, younger age, and surgery for benign disease—similar to those that characterized the patient population in this study.
Some weaknesses. The authors acknowledge that the study has shortcomings, including 1) a small sample and 2) their inability to discriminate QOL that reflects subjects’ surgical outcome from QOL related to typical life events—the death of a spouse, for example.
Nieboer and colleagues conclude by saying that, given the apparent improved QOL after laparoscopic hysterectomy compared with abdominal hysterectomy, all patients in whom vaginal hysterectomy is not feasible should be able to opt for laparoscopic hysterectomy.
Vaginal and laparoscopic approaches to hysterectomy have significant short-term advantages over abdominal hysterectomy by traditionally compared measures of surgical outcome. Taking the less-invasive approach allows you to offer greater long-lasting improvement in your surgical patients’ quality of life.
Einarsson J, Suzuki Y, Vellinga T, et al. Prospective evaluation of quality of life in total versus supracervical laparoscopic hysterectomy. J Minim Invasive Gynecol. 2011;18(5):617–621.
Einarsson and colleagues sought to prospectively evaluate a cohort of patients undergoing total laparoscopic hysterectomy (TLH) or laparoscopic supracervical hysterectomy (LSH) for 1) time to recovery and 2) short-term QOL after surgery. In all, 122 women underwent surgery (TLH: N=71; LSH: N=51) for benign indications. A QOL questionnaire (again, the SF-36) was administered immediately preoperatively, as a baseline, and at 3 to 4 weeks postoperatively.
Preoperatively, patients were presented with the two surgical options, without being influenced with information about any benefit to removing or retaining the cervix at laparoscopic hysterectomy. Patients then chose which surgery they wanted, and were neither randomized nor blinded to the procedure that was performed.
Findings. The data show greater patient self-selection and more patients with endometriosis in the TLH group; other preoperative baseline characteristics were similar across groups. More operative and postoperative complications were seen in the TLH group (vaginal cuff bleeding requiring return to the operating room, 2 patients; cuff cellulitis, 1; intraoperative vaginal laceration, 1; urinary tract infection, 1), although the difference did not reach statistical significance. There were no significant differences group to group in postop nausea, pain, narcotic use, or return to daily activities.
Regarding the eight QOL parameters, however, a statistically significant difference was observed in six of them to favor laparoscopic supracervical hysterectomy: physical functioning, physical role, bodily pain, vitality, social functioning, and physical component summary.
Study has shortcomings. The authors address two limitations of their study: namely, that the participants were neither blinded nor randomized. They acknowledge that these limitations might have biased QOL measurements in a way that showed improved QOL among the supracervical hysterectomy group. They raise the possibility that not being blinded to whether the cervix was removed may have affected subjects’ bodily perception. (Patients also returned to their daily activities 5 days earlier in the supracervical group, but this finding was found to be statistically insignificant.)
It is possible, however, to look at these limitations not as shortcomings of the study but as an important insight into the validity of patient choice and the benefits of patient education and autonomy in decision-making. Perhaps patients who have chosen to keep their cervix have a discernable advantage in regard to their perception of a higher QOL after hysterectomy.
An additional critique. Although the authors addressed a return to several daily activities that are outside the SF-36 questionnaire (e.g., a return to household chores, driving, work, exercise, and normal activities) they did not address sexual activity.
It has been the generally accepted practice to instruct patients not to place anything in the vagina, and to avoid vaginal intercourse, for at least 6 weeks after the cervix has been removed—regardless of the route of removal. After supracervical hysterectomy, however, patients can resume intercourse as early as 2 weeks. I think that it would be realistic for the authors to have stated that a quicker return to sexual activity after surgery might improve QOL scores for women, but they did not specifically address this domain.
When you’ve determined that hysterectomy is indicated for treatment of a patient’s benign disease and plan a laparoscopic approach, consider that education and autonomy of choice about whether to keep the cervix might improve quality of life postoperatively.
Acknowledgment
Andrew I. Brill, MD, and William H. Parker, MD, reviewed the manuscript of this article before it was submitted for publication.
We want to hear from you! Tell us what you think.
1. American College of Obstetricians and Gynecologists. Committee Opinion No. 444: Choosing the route of hysterectomy for benign disease (reaffirmed 2011). Obstet Gynecol. 2009;114(5):1156-1158.
2. Kluivers K, Hendriks J, Mol BW, et al. Quality of life and surgical outcome after total laparoscopic hysterectomy versus total abdominal hysterectomy for benign disease: A randomized, controlled trial. J Minim Invasive Gynecol. 2007;14(2):145-152.
| Dr. Brent E. Seibel illustrates simple cystoscopy at hysterectomy |

Amy Garcia, MD
Dr. Garcia is Director of the Center for Women’s Surgery and Assistant Professor, Division of Urogynecology, at the University of New Mexico School of Medicine in Albuquerque, NM. She serves on the OBG Management Board of Editors.
| Dr. Brent E. Seibel illustrates simple cystoscopy at hysterectomy |
Amy Garcia, MD
Dr. Garcia is Director of the Center for Women’s Surgery and Assistant Professor, Division of Urogynecology, at the University of New Mexico School of Medicine in Albuquerque, NM. She serves on the OBG Management Board of Editors.
| Dr. Brent E. Seibel illustrates simple cystoscopy at hysterectomy |
Amy Garcia, MD
Dr. Garcia is Director of the Center for Women’s Surgery and Assistant Professor, Division of Urogynecology, at the University of New Mexico School of Medicine in Albuquerque, NM. She serves on the OBG Management Board of Editors.
Dr. Garcia serves as a consultant to IOGYN, Minerva Surgical, Conceptus, Ethicon EndoSurgery, and Ethicon Women’s Health & Urology. She is a speaker for Conceptus.
Two-thirds of the almost one-half million hysterectomies performed annually in the United States for benign conditions take the abdominal route—even though less invasive transvaginal and laparoscopic approaches are available. Compared with abdominal hysterectomy, vaginal and laparoscopic hysterectomies are, on the whole, associated with less morbidity, a shorter hospital stay, and more rapid return to physical activity.
Over the past year, our understanding of the comparative advantages and risks of the various approaches to hysterectomy has been deepened by new research and by guidance from AAGL. Here is what we’ve learned, and here is how our surgical practices ought to be evolving for the long-term good of our patients.
Hysterectomy should be performed only rarely abdominally
AAGL Position Statement: Route of hysterectomy to treat benign uterine disease. J Minim Invasive Gynecol. 2011;18(1):1–3. [To link to the AAGL Position Statement, click here.]
In 2011, AAGL, which has been an international leader in promoting minimally invasive gynecologic surgery for longer than 40 years, issued a position statement on hysterectomy for the treatment of benign disease. AAGL’s position is a clear assertion that, when vaginal hysterectomy is not possible, laparoscopic hysterectomy should be performed—thus leaving few clinical indications for an abdominal hysterectomy.
Historically established contraindications to vaginal or laparoscopic hysterectomy—prior cesarean delivery, need for oophorectomy, an enlarged uterus—have been invalidated by recent studies. In competent hands, ovarian removal can be accomplished in 65% to 98.5% of vaginal hysterectomies.1 Vaginal morcellation techniques can facilitate removal of a large uterus vaginally and mechanical tissue morcellators enable laparoscopic removal.
In 2011, ACOG reaffirmed its 1999 Committee Opinion on Gynecologic Practice,1 which recommends that the vaginal approach for hysterectomy be the preferred route. ACOG asserts that, when vaginal hysterectomy is impossible, the laparoscopic and abdominal routes are alternatives.
How do these positions differ?
The difference in the AAGL Position Statement and the ACOG Committee Opinion lies in the surgeon’s ability to perform laparoscopic or vaginal hysterectomy. Although it might seem admirable for a surgeon to choose abdominal hysterectomy because he, or she, lacks the training and skills to perform the procedure laparoscopically or vaginally, AAGL does not hold this position. AAGL has established the expectation that, if a surgeon is unable to perform a hysterectomy safely vaginally or laparoscopically, he should refer the patient to a gynecologic surgeon who can.
Furthermore, AAGL recommends that abdominal hysterectomy be reserved for four broad situations, when:
- a patient has a medical condition, such as cardiopulmonary disease, in which the risk of general anesthesia or increased intraperitoneal pressure that is associated with laparoscopy is deemed unacceptable
- morcellation is known, or likely, to be required for vaginal or laparoscopic hysterectomy and uterine malignancy is either known or suspected
- hysterectomy is indicated but there is no access to surgeons or facilities required for vaginal or laparoscopic hysterectomy and referral is not feasible
- anatomy is so distorted by uterine disease or adhesions that the vaginal and laparoscopic approaches are deemed unsafe or unreasonable by a recognized expert in vaginal or laparoscopic hysterectomy techniques.
When hysterectomy is necessary, therefore, the demonstrated safety, efficacy, and cost-effectiveness of vaginal and laparoscopic approaches to surgical removal of the uterus mandate that these procedures be 1) the ones of choice and 2) presented as options to all appropriate candidates.
Whenever feasible for benign disease, perform hysterectomy vaginally or laparoscopically. Make the effort to facilitate these approaches based on the underlying principles of 1) informed patient choice and 2) preferential provision of minimally invasive options.
If you have not had the requisite training or learned the skills required to perform vaginal or laparoscopic hysterectomy, you should enlist the assistance of colleagues who do or refer your patients to those colleagues for surgical care. You should also, for the long term, seek to acquire those skills through formal training.
Nieboer T, Hendriks J, Bongers MY, Vierhout ME, Kluivers KB. Quality of life after laparoscopic and abdominal hysterectomy: a randomized controlled trial. Obstet Gynecol. 2012;119(1):85–91.
Nieboer and colleagues have presented their long-term data from a prospective, randomized evaluation of quality of life (QOL) after abdominal hysterectomy compared with QOL after laparoscopic hysterectomy. Other researchers have compared hysterectomy approaches, but most of those studies focused on such outcome measures as operation time, surgical intraoperative and postoperative complications, hospital stay, and rate of recurrence of the condition that prompted the surgery. This is the first study to address QOL parameters that are more patient-centered —using a validated questionnaire and having a median follow-up of 4.7 years (range, 188 to 303 weeks).
In 2007, investigators published the findings of a randomized comparison of QOL measures after total laparoscopic hysterectomy and total abdominal hysterectomy. Their assessment in that study utilized eight QOL measures from the RAND-36 Measure of Health-Related Quality of Life (the Dutch version of the validated QOL questionnaire, the SF-36 Health Survey)2 (TABLE).
8 key RAND-36 measures of quality of life in women who have had a hysterectomy
|
The current (Nieboer and co-workers) study evaluated 59 randomized patients from the 2007 work: 27 to laparoscopic hysterectomy and 32 to abdominal hysterectomy. The overall response rate after 4 years was 83% (N=49).
The QOL questionnaire addressed eight RAND-36 (SF-36) measures, with each measure having a possible score of 0 to 100 (maximum possible total score, 800); the higher the number, the better the QOL. The researchers considered a difference of 15 points between the two surgical approaches on any single parameter to be statistically significant.
Findings. The mean total RAND-36 (SF-36) score was 50.4 points (95% confidence interval, 1.0–99.7) higher in the laparoscopic hysterectomy group at each point of measurement in the weeks postoperatively, up to 4 years of follow-up. Higher scores at 4 years were also seen in the laparoscopy group for vitality, physical functioning, and social functioning.
From these findings, the authors surmise that QOL remains better 4 years after laparoscopic hysterectomy than it does after abdominal hysterectomy.
Why these findings? The Nieboer team offers several explanations for ongoing improvement in QOL scores among laparoscopic hysterectomy patients.
First, it is conceivable that laparoscopic patients scored higher on the Body Image Scale, benefiting from the knowledge that they underwent what, even in layman’s terms, would be called the “minimally invasive approach.”
Second, chronic abdominal or pelvic pain could affect QOL scores. It has been shown that, for other laparotomy procedures, the incidence of postop chronic pain ranges from 3% to 56%. Risk factors for postop chronic pain are female gender, younger age, and surgery for benign disease—similar to those that characterized the patient population in this study.
Some weaknesses. The authors acknowledge that the study has shortcomings, including 1) a small sample and 2) their inability to discriminate QOL that reflects subjects’ surgical outcome from QOL related to typical life events—the death of a spouse, for example.
Nieboer and colleagues conclude by saying that, given the apparent improved QOL after laparoscopic hysterectomy compared with abdominal hysterectomy, all patients in whom vaginal hysterectomy is not feasible should be able to opt for laparoscopic hysterectomy.
Vaginal and laparoscopic approaches to hysterectomy have significant short-term advantages over abdominal hysterectomy by traditionally compared measures of surgical outcome. Taking the less-invasive approach allows you to offer greater long-lasting improvement in your surgical patients’ quality of life.
Einarsson J, Suzuki Y, Vellinga T, et al. Prospective evaluation of quality of life in total versus supracervical laparoscopic hysterectomy. J Minim Invasive Gynecol. 2011;18(5):617–621.
Einarsson and colleagues sought to prospectively evaluate a cohort of patients undergoing total laparoscopic hysterectomy (TLH) or laparoscopic supracervical hysterectomy (LSH) for 1) time to recovery and 2) short-term QOL after surgery. In all, 122 women underwent surgery (TLH: N=71; LSH: N=51) for benign indications. A QOL questionnaire (again, the SF-36) was administered immediately preoperatively, as a baseline, and at 3 to 4 weeks postoperatively.
Preoperatively, patients were presented with the two surgical options, without being influenced with information about any benefit to removing or retaining the cervix at laparoscopic hysterectomy. Patients then chose which surgery they wanted, and were neither randomized nor blinded to the procedure that was performed.
Findings. The data show greater patient self-selection and more patients with endometriosis in the TLH group; other preoperative baseline characteristics were similar across groups. More operative and postoperative complications were seen in the TLH group (vaginal cuff bleeding requiring return to the operating room, 2 patients; cuff cellulitis, 1; intraoperative vaginal laceration, 1; urinary tract infection, 1), although the difference did not reach statistical significance. There were no significant differences group to group in postop nausea, pain, narcotic use, or return to daily activities.
Regarding the eight QOL parameters, however, a statistically significant difference was observed in six of them to favor laparoscopic supracervical hysterectomy: physical functioning, physical role, bodily pain, vitality, social functioning, and physical component summary.
Study has shortcomings. The authors address two limitations of their study: namely, that the participants were neither blinded nor randomized. They acknowledge that these limitations might have biased QOL measurements in a way that showed improved QOL among the supracervical hysterectomy group. They raise the possibility that not being blinded to whether the cervix was removed may have affected subjects’ bodily perception. (Patients also returned to their daily activities 5 days earlier in the supracervical group, but this finding was found to be statistically insignificant.)
It is possible, however, to look at these limitations not as shortcomings of the study but as an important insight into the validity of patient choice and the benefits of patient education and autonomy in decision-making. Perhaps patients who have chosen to keep their cervix have a discernable advantage in regard to their perception of a higher QOL after hysterectomy.
An additional critique. Although the authors addressed a return to several daily activities that are outside the SF-36 questionnaire (e.g., a return to household chores, driving, work, exercise, and normal activities) they did not address sexual activity.
It has been the generally accepted practice to instruct patients not to place anything in the vagina, and to avoid vaginal intercourse, for at least 6 weeks after the cervix has been removed—regardless of the route of removal. After supracervical hysterectomy, however, patients can resume intercourse as early as 2 weeks. I think that it would be realistic for the authors to have stated that a quicker return to sexual activity after surgery might improve QOL scores for women, but they did not specifically address this domain.
When you’ve determined that hysterectomy is indicated for treatment of a patient’s benign disease and plan a laparoscopic approach, consider that education and autonomy of choice about whether to keep the cervix might improve quality of life postoperatively.
Acknowledgment
Andrew I. Brill, MD, and William H. Parker, MD, reviewed the manuscript of this article before it was submitted for publication.
We want to hear from you! Tell us what you think.
Dr. Garcia serves as a consultant to IOGYN, Minerva Surgical, Conceptus, Ethicon EndoSurgery, and Ethicon Women’s Health & Urology. She is a speaker for Conceptus.
Two-thirds of the almost one-half million hysterectomies performed annually in the United States for benign conditions take the abdominal route—even though less invasive transvaginal and laparoscopic approaches are available. Compared with abdominal hysterectomy, vaginal and laparoscopic hysterectomies are, on the whole, associated with less morbidity, a shorter hospital stay, and more rapid return to physical activity.
Over the past year, our understanding of the comparative advantages and risks of the various approaches to hysterectomy has been deepened by new research and by guidance from AAGL. Here is what we’ve learned, and here is how our surgical practices ought to be evolving for the long-term good of our patients.
Hysterectomy should be performed only rarely abdominally
AAGL Position Statement: Route of hysterectomy to treat benign uterine disease. J Minim Invasive Gynecol. 2011;18(1):1–3. [To link to the AAGL Position Statement, click here.]
In 2011, AAGL, which has been an international leader in promoting minimally invasive gynecologic surgery for longer than 40 years, issued a position statement on hysterectomy for the treatment of benign disease. AAGL’s position is a clear assertion that, when vaginal hysterectomy is not possible, laparoscopic hysterectomy should be performed—thus leaving few clinical indications for an abdominal hysterectomy.
Historically established contraindications to vaginal or laparoscopic hysterectomy—prior cesarean delivery, need for oophorectomy, an enlarged uterus—have been invalidated by recent studies. In competent hands, ovarian removal can be accomplished in 65% to 98.5% of vaginal hysterectomies.1 Vaginal morcellation techniques can facilitate removal of a large uterus vaginally and mechanical tissue morcellators enable laparoscopic removal.
In 2011, ACOG reaffirmed its 1999 Committee Opinion on Gynecologic Practice,1 which recommends that the vaginal approach for hysterectomy be the preferred route. ACOG asserts that, when vaginal hysterectomy is impossible, the laparoscopic and abdominal routes are alternatives.
How do these positions differ?
The difference in the AAGL Position Statement and the ACOG Committee Opinion lies in the surgeon’s ability to perform laparoscopic or vaginal hysterectomy. Although it might seem admirable for a surgeon to choose abdominal hysterectomy because he, or she, lacks the training and skills to perform the procedure laparoscopically or vaginally, AAGL does not hold this position. AAGL has established the expectation that, if a surgeon is unable to perform a hysterectomy safely vaginally or laparoscopically, he should refer the patient to a gynecologic surgeon who can.
Furthermore, AAGL recommends that abdominal hysterectomy be reserved for four broad situations, when:
- a patient has a medical condition, such as cardiopulmonary disease, in which the risk of general anesthesia or increased intraperitoneal pressure that is associated with laparoscopy is deemed unacceptable
- morcellation is known, or likely, to be required for vaginal or laparoscopic hysterectomy and uterine malignancy is either known or suspected
- hysterectomy is indicated but there is no access to surgeons or facilities required for vaginal or laparoscopic hysterectomy and referral is not feasible
- anatomy is so distorted by uterine disease or adhesions that the vaginal and laparoscopic approaches are deemed unsafe or unreasonable by a recognized expert in vaginal or laparoscopic hysterectomy techniques.
When hysterectomy is necessary, therefore, the demonstrated safety, efficacy, and cost-effectiveness of vaginal and laparoscopic approaches to surgical removal of the uterus mandate that these procedures be 1) the ones of choice and 2) presented as options to all appropriate candidates.
Whenever feasible for benign disease, perform hysterectomy vaginally or laparoscopically. Make the effort to facilitate these approaches based on the underlying principles of 1) informed patient choice and 2) preferential provision of minimally invasive options.
If you have not had the requisite training or learned the skills required to perform vaginal or laparoscopic hysterectomy, you should enlist the assistance of colleagues who do or refer your patients to those colleagues for surgical care. You should also, for the long term, seek to acquire those skills through formal training.
Nieboer T, Hendriks J, Bongers MY, Vierhout ME, Kluivers KB. Quality of life after laparoscopic and abdominal hysterectomy: a randomized controlled trial. Obstet Gynecol. 2012;119(1):85–91.
Nieboer and colleagues have presented their long-term data from a prospective, randomized evaluation of quality of life (QOL) after abdominal hysterectomy compared with QOL after laparoscopic hysterectomy. Other researchers have compared hysterectomy approaches, but most of those studies focused on such outcome measures as operation time, surgical intraoperative and postoperative complications, hospital stay, and rate of recurrence of the condition that prompted the surgery. This is the first study to address QOL parameters that are more patient-centered —using a validated questionnaire and having a median follow-up of 4.7 years (range, 188 to 303 weeks).
In 2007, investigators published the findings of a randomized comparison of QOL measures after total laparoscopic hysterectomy and total abdominal hysterectomy. Their assessment in that study utilized eight QOL measures from the RAND-36 Measure of Health-Related Quality of Life (the Dutch version of the validated QOL questionnaire, the SF-36 Health Survey)2 (TABLE).
8 key RAND-36 measures of quality of life in women who have had a hysterectomy
|
The current (Nieboer and co-workers) study evaluated 59 randomized patients from the 2007 work: 27 to laparoscopic hysterectomy and 32 to abdominal hysterectomy. The overall response rate after 4 years was 83% (N=49).
The QOL questionnaire addressed eight RAND-36 (SF-36) measures, with each measure having a possible score of 0 to 100 (maximum possible total score, 800); the higher the number, the better the QOL. The researchers considered a difference of 15 points between the two surgical approaches on any single parameter to be statistically significant.
Findings. The mean total RAND-36 (SF-36) score was 50.4 points (95% confidence interval, 1.0–99.7) higher in the laparoscopic hysterectomy group at each point of measurement in the weeks postoperatively, up to 4 years of follow-up. Higher scores at 4 years were also seen in the laparoscopy group for vitality, physical functioning, and social functioning.
From these findings, the authors surmise that QOL remains better 4 years after laparoscopic hysterectomy than it does after abdominal hysterectomy.
Why these findings? The Nieboer team offers several explanations for ongoing improvement in QOL scores among laparoscopic hysterectomy patients.
First, it is conceivable that laparoscopic patients scored higher on the Body Image Scale, benefiting from the knowledge that they underwent what, even in layman’s terms, would be called the “minimally invasive approach.”
Second, chronic abdominal or pelvic pain could affect QOL scores. It has been shown that, for other laparotomy procedures, the incidence of postop chronic pain ranges from 3% to 56%. Risk factors for postop chronic pain are female gender, younger age, and surgery for benign disease—similar to those that characterized the patient population in this study.
Some weaknesses. The authors acknowledge that the study has shortcomings, including 1) a small sample and 2) their inability to discriminate QOL that reflects subjects’ surgical outcome from QOL related to typical life events—the death of a spouse, for example.
Nieboer and colleagues conclude by saying that, given the apparent improved QOL after laparoscopic hysterectomy compared with abdominal hysterectomy, all patients in whom vaginal hysterectomy is not feasible should be able to opt for laparoscopic hysterectomy.
Vaginal and laparoscopic approaches to hysterectomy have significant short-term advantages over abdominal hysterectomy by traditionally compared measures of surgical outcome. Taking the less-invasive approach allows you to offer greater long-lasting improvement in your surgical patients’ quality of life.
Einarsson J, Suzuki Y, Vellinga T, et al. Prospective evaluation of quality of life in total versus supracervical laparoscopic hysterectomy. J Minim Invasive Gynecol. 2011;18(5):617–621.
Einarsson and colleagues sought to prospectively evaluate a cohort of patients undergoing total laparoscopic hysterectomy (TLH) or laparoscopic supracervical hysterectomy (LSH) for 1) time to recovery and 2) short-term QOL after surgery. In all, 122 women underwent surgery (TLH: N=71; LSH: N=51) for benign indications. A QOL questionnaire (again, the SF-36) was administered immediately preoperatively, as a baseline, and at 3 to 4 weeks postoperatively.
Preoperatively, patients were presented with the two surgical options, without being influenced with information about any benefit to removing or retaining the cervix at laparoscopic hysterectomy. Patients then chose which surgery they wanted, and were neither randomized nor blinded to the procedure that was performed.
Findings. The data show greater patient self-selection and more patients with endometriosis in the TLH group; other preoperative baseline characteristics were similar across groups. More operative and postoperative complications were seen in the TLH group (vaginal cuff bleeding requiring return to the operating room, 2 patients; cuff cellulitis, 1; intraoperative vaginal laceration, 1; urinary tract infection, 1), although the difference did not reach statistical significance. There were no significant differences group to group in postop nausea, pain, narcotic use, or return to daily activities.
Regarding the eight QOL parameters, however, a statistically significant difference was observed in six of them to favor laparoscopic supracervical hysterectomy: physical functioning, physical role, bodily pain, vitality, social functioning, and physical component summary.
Study has shortcomings. The authors address two limitations of their study: namely, that the participants were neither blinded nor randomized. They acknowledge that these limitations might have biased QOL measurements in a way that showed improved QOL among the supracervical hysterectomy group. They raise the possibility that not being blinded to whether the cervix was removed may have affected subjects’ bodily perception. (Patients also returned to their daily activities 5 days earlier in the supracervical group, but this finding was found to be statistically insignificant.)
It is possible, however, to look at these limitations not as shortcomings of the study but as an important insight into the validity of patient choice and the benefits of patient education and autonomy in decision-making. Perhaps patients who have chosen to keep their cervix have a discernable advantage in regard to their perception of a higher QOL after hysterectomy.
An additional critique. Although the authors addressed a return to several daily activities that are outside the SF-36 questionnaire (e.g., a return to household chores, driving, work, exercise, and normal activities) they did not address sexual activity.
It has been the generally accepted practice to instruct patients not to place anything in the vagina, and to avoid vaginal intercourse, for at least 6 weeks after the cervix has been removed—regardless of the route of removal. After supracervical hysterectomy, however, patients can resume intercourse as early as 2 weeks. I think that it would be realistic for the authors to have stated that a quicker return to sexual activity after surgery might improve QOL scores for women, but they did not specifically address this domain.
When you’ve determined that hysterectomy is indicated for treatment of a patient’s benign disease and plan a laparoscopic approach, consider that education and autonomy of choice about whether to keep the cervix might improve quality of life postoperatively.
Acknowledgment
Andrew I. Brill, MD, and William H. Parker, MD, reviewed the manuscript of this article before it was submitted for publication.
We want to hear from you! Tell us what you think.
1. American College of Obstetricians and Gynecologists. Committee Opinion No. 444: Choosing the route of hysterectomy for benign disease (reaffirmed 2011). Obstet Gynecol. 2009;114(5):1156-1158.
2. Kluivers K, Hendriks J, Mol BW, et al. Quality of life and surgical outcome after total laparoscopic hysterectomy versus total abdominal hysterectomy for benign disease: A randomized, controlled trial. J Minim Invasive Gynecol. 2007;14(2):145-152.
1. American College of Obstetricians and Gynecologists. Committee Opinion No. 444: Choosing the route of hysterectomy for benign disease (reaffirmed 2011). Obstet Gynecol. 2009;114(5):1156-1158.
2. Kluivers K, Hendriks J, Mol BW, et al. Quality of life and surgical outcome after total laparoscopic hysterectomy versus total abdominal hysterectomy for benign disease: A randomized, controlled trial. J Minim Invasive Gynecol. 2007;14(2):145-152.
IN THIS ARTICLE
To prep, or not? Evidence is against mechanical bowel preparation in gynecologic surgery
Think mechanical bowel preparation (MBP) is a must for gynecologic surgery?
Think again.
Although MBP has been around since the 1930s, a growing body of data suggest that, with rare exception, gynecologists can eliminate routine use of preoperative MBP from their practice.
In this article, we discuss the evidence surrounding MBP so that you can assess the benefits and risks it poses for your surgical patients.
Unproven assumptions are behind MBP
For most of the past century, MBP has been used in advance of abdominal surgery,
including gynecologic surgery. Clinicians made the rational assumption that, by decreasing the fecal load within the colon, they could lower the risk of certain surgical complications, especially during an era when antibiotics were not available to treat serious infectious morbidity. In modern times, the practice has continued when major abdominal surgery is planned. Why? Because surgeons believe it will reduce the risk of wound infection, anastomotic leakage, and bowel spillage in the event of injury, and that it will increase the ease of bowel manipulation.1
A growing body of literature challenges these assumptions and suggests that MBP is not associated with these benefits—and may even increase the incidence of some of these complications. Moreover, the induction of profuse, watery diarrhea to evacuate the colon before surgery has been associated with severe electrolyte imbalance, renal failure, and difficult intraoperative fluid management.
These risks make a thorough assessment of MBP’s effects imperative to guide optimal practice.
- Mechanical bowel prep has many side effects, ranging from mild (discomfort) to severe (renal failure).
- The risks of surgical site infection and anastomotic leakage are not lower with MBP, compared with no preparation, in patients undergoing elective colon surgery.
- MBP does not reduce the risk of intraoperative contamination of the surgical field.
- In unplanned injuries to unprepared colon (e.g., in cases involving trauma), primary anastomosis is the recommended mode of repair rather than diverting colostomy.
- MBP does not ease bowel manipulation in laparoscopy, compared with no preparation.
- The only proven value of MBP is to improve visibility during intraoperative colonoscopy.
- Gynecologists can eliminate the routine use of MBP from their surgical practice.
MBP defined
MBP is the chemical or physical process of eliminating fecal matter from the intestinal tract. There are a variety of methods, including ingestion of an oral preparation and enemas and suppositories. Historically, MBP included stimulant laxatives, such as senna extract and castor oil, and hyperosmotic solutions, such as mannitol and lactulose.
MBP is distinctly separate from antibiotic bowel preparation and preoperative prophylactic antibiotics, both of which fall beyond the scope of this article.
The most common forms of MBP prescribed today are balanced electrolyte solutions, including polyethylene glycol, and saline laxatives, such as magnesium citrate and sodium phosphate.2
Some investigators have attempted to determine which MBP formulations are most effective, based on visualization during colonoscopy, but a recent meta-analysis suggests that most formulations perform similarly.3
The risks associated with MBP are clearly documented in the literature and range in intensity from mild to severe. Overall, patients report discomfort, with symptoms such as abdominal pain and distension, nausea and vomiting, weakness, and insomnia.4 High-volume preparations, such as polyethylene glycol, are unpalatable to patients and, therefore, less likely to be ingested completely, leaving the surgeon with a partially evacuated colon.
Dehydration and electrolyte disturbances may also complicate the use of MBP, particularly with saline laxatives. Although young patients can likely tolerate electrolyte shifts without severe sequelae, elderly patients who have comorbid heart and kidney disorders may become further deconditioned during the MBP process. Seizures and esophageal tears have been reported as a result of MBP.5 Sodium phosphate, in particular, is associated with renal failure, with 171 cases reported to the US Food and Drug Administration (FDA) from 2006 to 2007—leading to an issued warning not to employ this agent in preoperative MBP in the liquid formulation.6
In addition, in one study, investigators observed an increased time to the return of bowel function and a prolonged hospital stay among patients who underwent MBP.7
Purported benefits of MBP
Reducing the risk of surgical site infection
Surgical site infection (SSI)—whether intra-abdominal or in the superficial wound—is a serious complication that can lead to severe morbidity. As colorectal surgeons began performing more aggressive colon surgery in the 1930s, 40s, and 50s, they sought a way to reduce SSI. Mortality from colon surgery was 10% to 30%, with a rate of SSI of 80% to 90%, so surgeons began to seek a method to decrease the fecal bacterial load, presuming that doing so would also reduce the rates of infection and mortality and allow for primary repair of the colon. MBP appeared to address the problem.1
The practice of MBP then spread from colorectal surgery to other areas of general and gynecologic surgery without clear evidence from randomized trials that it was necessary or beneficial.8 As surgical techniques improved over the ensuing decades, and antibiotics evolved, mortality and SSI rates dropped—although it is unclear whether this drop in infection is attributable to MBP.1
In the 1990s, researchers began to question the value of MBP in surgical practice. Multiple randomized, controlled trials in the colorectal literature have demonstrated that MBP does not reduce the rate of incisional or deep SSI, compared with no bowel preparation.9-11 The populations studied in these trials were undergoing planned bowel resection and primary re-anastomosis— procedures known to elevate the risk of contamination, unlike the majority of gynecologic surgical procedures. Even in this higher-risk population, however, MBP failed to reduce the risk of SSI, suggesting that, in less contaminated surgeries, it would have even fewer benefits.
In its practice bulletin on antibiotic prophylaxis from 2009, the American Congress of Obstetricians and Gynecologists (ACOG) noted: “There is no evidence that mechanical bowel preparation further reduces infection risk” beyond the reduction achieved with routine use of perioperative antibiotics.12
Preventing anastomotic leakage
Investigators have suggested that MBP reduces the risk of anastomotic leaks of the colon by decreasing contamination at the suture site.13 A close review of the colorectal literature, however, reveals that MBP does not affect anastomotic leakage in patients who undergo planned colon resection and primary re-anastomosis.9,10,14-17
A 2011 Cochrane review that included 5,805 patients undergoing elective colon and rectal surgery confirmed that neither oral nor rectal MBP was associated with any benefit in terms of the rates of anastomotic leakage and SSI.10 Some randomized studies have found nonstatistically significant reductions in the anastomotic leakage rate in patients who did not undergo MBP—a finding attributed to the lack of denuded mucosa and inflammation in the unprepared colon.9,15,18
However, one large, randomized, clinical trial of more than 1,000 patients found that, when anastomotic leakage did occur, the risk of infection was greater among patients who had not undergone MBP.19
Reducing the rates of intraoperative contamination and colon injury
Planned resection and inadvertent colon injury both have the potential to contaminate the surgical field, increasing the risk of morbidity. Surgeons have turned to MBP to minimize this risk in the planned surgical setting, although the practice does not appear to reduce infection or the risk of subsequent anastomotic leakage. It is largely unknown how bowel preparation affects bowel spillage during colon resection. Most investigators empirically believe that MBP will reduce bowel spillage during planned colon resection in an uncontaminated field,13 although one prospective study suggested a trend toward increased spillage of bowel contents and intraoperative contamination in patients who had undergone MBP.20
In gynecologic surgery for benign conditions, colon resection is generally unplanned, usually the result of inadvertent colon injury or unexpected findings. Traditional teaching has been that, if an unprepared colon becomes injured, the patient requires a colostomy rather than primary anastomosis, simply because there are bowel contents contaminating the surgical field.
Gynecologists may be hesitant to challenge this practice because the choice of primary anastomosis versus colostomy is often made by the consulting general surgeon. Given the low risk of bowel injury (estimated to be <2% in gynecologic surgery) and emerging data on fecal contamination and bowel resection in the trauma literature, MBP may be unnecessary on a population-wide basis.21
In fact, the trauma literature might be instructive in understanding how inadvertent colon injury in gynecologic surgery should be managed, regardless of the patient’s bowel-preparation status. Multiple randomized, controlled trials of colostomy versus primary anastomosis in trauma patients who had penetrating colon injuries demonstrated no difference in the rates of mortality and complications, including SSI and anastomotic leakage.22-24 Both colorectal and trauma surgeons performed planned and unplanned colectomy and primary re-anastomosis without MBP.
Based on these data, the recommended practice in trauma surgery is primary repair of the colon, confirming that the unprepared colon can be safely re-anastomosed, even in a grossly contaminated field. Extrapolating from this literature, it stands to reason that colon injury at the time of gynecologic surgery without preoperative MBP could also be managed primarily, eliminating the impetus for gynecologists to use MBP to avoid bowel diversion.
Although evidence-based practice is highly recommended, it is important to recognize that it is beyond the scope of most general gynecologists to perform bowel resection and anastomoses in the event of inadvertent bowel injury. Gynecologic surgeons must know the practice patterns of their local institution; if the general surgeons in that institution do not follow current recommendations, it may be prudent to continue to use MBP in cases that carry a high risk of bowel injury to avoid a potential colostomy.
Easing bowel manipulation
Some gynecologists continue to use MBP in cases at low risk for bowel injury because they are concerned about the ease of operation and want to ensure good visibility, particularly when laparoscopy is involved. Muzii and colleagues conducted a randomized, single-blinded study of MBP versus no preparation in benign cases managed by gynecologic laparoscopy. The surgeons were blinded as to whether or not the patient had undergone MBP; at the conclusion of the procedure, these surgeons rated the ease of operation and visualization based on the quality of the surgical field, evaluation of the small and large bowel, and surgical difficulty. MBP was not associated with any measured outcome, including complications, surgical time, and self-assessed ease of operation—although patients reported significantly more discomfort with MBP.4
Easing intraoperative colonoscopy
Experts agree that planned or potential intraoperative colonoscopy is a clear indication for adequate bowel preparation.10 A smaller body of evidence suggests that, when “subtle palpation of the bowel wall” is required, MBP may help the surgeon avoid mistaking a nodule for stool.5,25
Beyond these examples, routine MBP is not supported by randomized data.
We sorely need guidelines on MBP
Like many general and colorectal surgeons, many gynecologists still use MBP. A 2011 survey of Canadian gynecologic oncologists reported that 47% still routinely order MBP, although 77% of surgeons acknowledged a lack of “good evidence” to support the practice.26 Similarly, although 95% of colorectal surgeons in Michigan in 2011 believed that the data against routine use of MBP was scientifically valid, only 50% agreed that MBP was unnecessary.27 Data from Spain echo these results: 77% of surgeons viewed bowel preparation as useful or very useful.28
The striking contrast between literature and practice merits scrutiny. When the literature demonstrates no need for MBP and a risk of patient harm, why are so many surgeons still electing preoperative MBP for their patients? Reasons listed by gynecologic oncologists in a 2011 survey varied but included a reduction in anastomotic leakage (31%) and improved visualization (37%)—reasons unsupported by the randomized literature. A majority (71%) agreed that guidelines would be helpful in determining the appropriate use of MBP, if any.26 Overall, ACOG has not laid out clear guidelines on the use or avoidance of MBP to support gynecologic surgeons’ decision-making.
MBP is an antiquated practice
The colorectal literature has identified MBP as an antiquated practice without evidence to support its routine use. Therefore, mechanical bowel preparation is likely to be of minimal value for patients undergoing major gynecologic surgery, based on extensive data from randomized trials of planned bowel surgery.29 The role of MBP in laparoscopic, robotic, and vaginal surgery is less clearly defined, although there is no clear evidence to support the use of MBP in any surgical modality except intraoperative colonoscopy. Despite the lack of clear guidance from ACOG, the colorectal and gynecologic literature strongly suggests that MBP does not reduce the risk of SSI or intraoperative or postoperative complications. Nor do surgical ease and visibility appear to be improved with MBP, though the literature in this area is limited.
MBP is not without risk, particularly for elderly patients who have medical comorbidities. Without clearly established benefits, we recommend that you strongly consider these randomized data and limit—or even eliminate—the use of MBP for major abdominal procedures in your practice.
- 10 practical, evidence-based recommendations for improving maternal outcomes of cesarean delivery
Baha M. Sibai, MD (March 2012) - Step by step: Obliterating the vaginal canal to correct pelvic organ prolapse
Mickey Karram, MD; Janelle Evans, MD (February 2012) - Strategies and steps for the surgical management of endometriosis
Anthony A. Luciano, MD; Rachel LaMonica, MD; Danielle E. Luciano, MD (November 2011) - Correcting pelvic organ prolapse with robotic sacrocolpopexy
Catherine A. Matthews, MD (September 2011) - High uterosacral vaginal vault suspension to repair enterocele and apical prolapse
Mickey Karram, MD; Christine Vaccaro, DO (June 2011) - 10 practical, evidence-based suggestions to improve your minimally invasive surgical skills now
Catherine A. Matthews, MD (April 2011)
We want to hear from you! Tell us what you think.
1. Fry DE. Colon preparation and surgical site infection. Am J Surg. 2011;202(2):225-232.
2. Yang LC, Arden D, Lee TT, et al. Mechanical bowel preparation for gynecologic laparoscopy: a prospective randomized trial of oral sodium phosphate solution vs single sodium phosphate enema. J Minim Invasive Gynecol. 2011;18(2):149-156.
3. Belsey J, Crosta C, Epstein O, et al. Meta-analysis: the relative efficacy of oral bowel preparations for colonoscopy 1985-2010. Aliment Pharmacol Ther. 2012;35(2):222-237.
4. Muzii L, Bellati F, Zullo MA, Manci N, Angioli R, Panici PB. Mechanical bowel preparation before gynecologic laparoscopy: a randomized single-blind, controlled trial. Fertil Steril. 2006;85(3):689-693.
5. Botha MH. Mechanical bowel preparation in gynaecological surgery—are we doing more harm than good? S Afr Med J. 2007;97(11):1040-1043.
6. Belsey J, Epstein O, Heresbach D. Systematic review: adverse event reports for oral sodium phosphate and polyethylene glycol. Aliment Pharmacol Ther. 2009;29(1):15-28.
7. Shafii M, Murphy DM, Donovan MG, Hickey DP. Is mechanical bowel preparation necessary in patients undergoing cystectomy and urinary diversion? BJU Int. 2002;89(9):879-881.
8. Cohen SL, Einarsson JI. The role of mechanical bowel preparation in gynecologic laparoscopy. Rev Obstet Gynecol. 2011;4(1):28-31.
9. Platell C, Hall J. What is the role of mechanical bowel preparation in patients undergoing colorectal surgery? Dis Colon Rectum. 1998;41(7):875-883.
10. Güenaga KF, Matos D, Wille-Jorgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2011;9:CD001544.
11. Pena-Soria MJ, Mayol JM, Anula R, Arbeo-Escolar A, Fernandez-Represa JA. Single-blinded randomized trial of mechanical bowel preparation for colon surgery with primary intraperitoneal anastomosis. J Gastrointest Surg 2008;12(12):2103-2109.
12. Committee on Practice Bulletins—Gynecology. ACOG practice bulletin No. 104: antibiotic prophylaxis for gynecologic procedures. Obstet Gynecol. 2009;113(5):1180.-
13. Kingham TP, Pachter HL. Colonic anastomotic leak: risk factors diagnosis, and treatment. J Am Coll Surg. 2009;208(2):269-278.
14. Wille-Jorgensen P, Güenaga KF, Matos D, Castro AA. Pre-operative mechanical bowel cleansing or not? An updated meta-analysis. Colorectal Dis. 2005;7(4):304-310.
15. Miettinen RP, Laitinen ST, Makela JT, Paakkonen ME. Bowel preparation with oral polyethylene glycol electrolyte solution vs. no preparation in elective open colorectal surgery: prospective randomized study. Dis Colon Rectum. 2000;43(5):669-677.
16. Ram E, Sherman Y, Weil R, Vishne T, Kravarusic D, Dreznik Z. Is mechanical bowel preparation mandatory for elective colon surgery? A prospective randomized study. Arch Surg. 2005;140(3):285-288.
17. Mäkelä JT, Kiviniemi H, Laitinen S. Risk factors for anastomotic leakage after left-sided colorectal resection with rectal anastomosis. Dis Colon Rectum. 2003;46(5):653-660.
18. Bucher P, Gervaz P, Egger JF, Soravia C, Morel P. Morphologic alterations associated with mechanical bowel preparation before elective colorectal surgery: a randomized trial. Dis Colon Rectum. 2006;49(1):109-112.
19. Contant CM, Hop WC, van’t Sant HP, et al. Mechanical bowel preparation for elective colorectal surgery: a multicentre randomised trial. Lancet. 2007;370(9625):2112-2117.
20. Mahajna A, Krausz M, Rosin D, et al. Bowel preparation is associated with spillage of bowel contents in colorectal surgery. Dis Colon Rectum. 2005;48(8):1626-1631.
21. Brosens I, Gordon A, Campo R, Gordts S. Bowel injury in gynecologic laparoscopy. J Am Assoc Gynecol Laparosc. 2003;10(1):9-13.
22. Demetriades D, Murray JA, Chan L, et al; Committee on Multicenter Clinical Trials. American Association for the Surgery of Trauma. Penetrating colon injuries requiring resection: diversion or primary anastomosis? An AAST prospective multicenter study. J Trauma. 2001;50(5):765-775.
23. Curran TJ, Borzotta AP. Complications of primary repair of colon injury: literature review of 2,964 cases. Am J Surg. 1999;177(1):42-47.
24. Nelson R, Singer M. Primary repair for penetrating colon injuries. Cochrane Database Syst Rev. 2003;3:CD002247.
25. Rovera F, Dionigi G, Boni L, et al. Mechanical bowel preparation for colorectal surgery. Surg Infect (Larchmt). 2006;7(suppl 2):S61-S63.
26. Wells T, Plante M, McAlpine JN. Communities of Practice Groups on behalf of the Society of Gynecologic Oncologists of Canada. Preoperative bowel preparation in gynecologic oncology: a review of practice patterns and an impetus to change. Int J Gynecol Cancer. 2011;21(6):1135-1142.
27. Marchaim D, Slim J, Dhar S, et al. A regional survey of the use of mechanical bowel preparations prior to colorectal surgery. Ann Surg. 2011;253(4):839-840.
28. Roig JV, Garcia-Fadrique A, Garcia-Armengol J, et al. Mechanical bowel preparation and antibiotic prophylaxis in colorectal surgery: use by and opinions of Spanish surgeons. Colorectal Dis. 2009;11(1):44-48.
29. Fanning J, Valea FA. Perioperative bowel management for gynecologic surgery. Am J Obstet Gynecol. 2011;205(4):309-314.
Think mechanical bowel preparation (MBP) is a must for gynecologic surgery?
Think again.
Although MBP has been around since the 1930s, a growing body of data suggest that, with rare exception, gynecologists can eliminate routine use of preoperative MBP from their practice.
In this article, we discuss the evidence surrounding MBP so that you can assess the benefits and risks it poses for your surgical patients.
Unproven assumptions are behind MBP
For most of the past century, MBP has been used in advance of abdominal surgery,
including gynecologic surgery. Clinicians made the rational assumption that, by decreasing the fecal load within the colon, they could lower the risk of certain surgical complications, especially during an era when antibiotics were not available to treat serious infectious morbidity. In modern times, the practice has continued when major abdominal surgery is planned. Why? Because surgeons believe it will reduce the risk of wound infection, anastomotic leakage, and bowel spillage in the event of injury, and that it will increase the ease of bowel manipulation.1
A growing body of literature challenges these assumptions and suggests that MBP is not associated with these benefits—and may even increase the incidence of some of these complications. Moreover, the induction of profuse, watery diarrhea to evacuate the colon before surgery has been associated with severe electrolyte imbalance, renal failure, and difficult intraoperative fluid management.
These risks make a thorough assessment of MBP’s effects imperative to guide optimal practice.
- Mechanical bowel prep has many side effects, ranging from mild (discomfort) to severe (renal failure).
- The risks of surgical site infection and anastomotic leakage are not lower with MBP, compared with no preparation, in patients undergoing elective colon surgery.
- MBP does not reduce the risk of intraoperative contamination of the surgical field.
- In unplanned injuries to unprepared colon (e.g., in cases involving trauma), primary anastomosis is the recommended mode of repair rather than diverting colostomy.
- MBP does not ease bowel manipulation in laparoscopy, compared with no preparation.
- The only proven value of MBP is to improve visibility during intraoperative colonoscopy.
- Gynecologists can eliminate the routine use of MBP from their surgical practice.
MBP defined
MBP is the chemical or physical process of eliminating fecal matter from the intestinal tract. There are a variety of methods, including ingestion of an oral preparation and enemas and suppositories. Historically, MBP included stimulant laxatives, such as senna extract and castor oil, and hyperosmotic solutions, such as mannitol and lactulose.
MBP is distinctly separate from antibiotic bowel preparation and preoperative prophylactic antibiotics, both of which fall beyond the scope of this article.
The most common forms of MBP prescribed today are balanced electrolyte solutions, including polyethylene glycol, and saline laxatives, such as magnesium citrate and sodium phosphate.2
Some investigators have attempted to determine which MBP formulations are most effective, based on visualization during colonoscopy, but a recent meta-analysis suggests that most formulations perform similarly.3
The risks associated with MBP are clearly documented in the literature and range in intensity from mild to severe. Overall, patients report discomfort, with symptoms such as abdominal pain and distension, nausea and vomiting, weakness, and insomnia.4 High-volume preparations, such as polyethylene glycol, are unpalatable to patients and, therefore, less likely to be ingested completely, leaving the surgeon with a partially evacuated colon.
Dehydration and electrolyte disturbances may also complicate the use of MBP, particularly with saline laxatives. Although young patients can likely tolerate electrolyte shifts without severe sequelae, elderly patients who have comorbid heart and kidney disorders may become further deconditioned during the MBP process. Seizures and esophageal tears have been reported as a result of MBP.5 Sodium phosphate, in particular, is associated with renal failure, with 171 cases reported to the US Food and Drug Administration (FDA) from 2006 to 2007—leading to an issued warning not to employ this agent in preoperative MBP in the liquid formulation.6
In addition, in one study, investigators observed an increased time to the return of bowel function and a prolonged hospital stay among patients who underwent MBP.7
Purported benefits of MBP
Reducing the risk of surgical site infection
Surgical site infection (SSI)—whether intra-abdominal or in the superficial wound—is a serious complication that can lead to severe morbidity. As colorectal surgeons began performing more aggressive colon surgery in the 1930s, 40s, and 50s, they sought a way to reduce SSI. Mortality from colon surgery was 10% to 30%, with a rate of SSI of 80% to 90%, so surgeons began to seek a method to decrease the fecal bacterial load, presuming that doing so would also reduce the rates of infection and mortality and allow for primary repair of the colon. MBP appeared to address the problem.1
The practice of MBP then spread from colorectal surgery to other areas of general and gynecologic surgery without clear evidence from randomized trials that it was necessary or beneficial.8 As surgical techniques improved over the ensuing decades, and antibiotics evolved, mortality and SSI rates dropped—although it is unclear whether this drop in infection is attributable to MBP.1
In the 1990s, researchers began to question the value of MBP in surgical practice. Multiple randomized, controlled trials in the colorectal literature have demonstrated that MBP does not reduce the rate of incisional or deep SSI, compared with no bowel preparation.9-11 The populations studied in these trials were undergoing planned bowel resection and primary re-anastomosis— procedures known to elevate the risk of contamination, unlike the majority of gynecologic surgical procedures. Even in this higher-risk population, however, MBP failed to reduce the risk of SSI, suggesting that, in less contaminated surgeries, it would have even fewer benefits.
In its practice bulletin on antibiotic prophylaxis from 2009, the American Congress of Obstetricians and Gynecologists (ACOG) noted: “There is no evidence that mechanical bowel preparation further reduces infection risk” beyond the reduction achieved with routine use of perioperative antibiotics.12
Preventing anastomotic leakage
Investigators have suggested that MBP reduces the risk of anastomotic leaks of the colon by decreasing contamination at the suture site.13 A close review of the colorectal literature, however, reveals that MBP does not affect anastomotic leakage in patients who undergo planned colon resection and primary re-anastomosis.9,10,14-17
A 2011 Cochrane review that included 5,805 patients undergoing elective colon and rectal surgery confirmed that neither oral nor rectal MBP was associated with any benefit in terms of the rates of anastomotic leakage and SSI.10 Some randomized studies have found nonstatistically significant reductions in the anastomotic leakage rate in patients who did not undergo MBP—a finding attributed to the lack of denuded mucosa and inflammation in the unprepared colon.9,15,18
However, one large, randomized, clinical trial of more than 1,000 patients found that, when anastomotic leakage did occur, the risk of infection was greater among patients who had not undergone MBP.19
Reducing the rates of intraoperative contamination and colon injury
Planned resection and inadvertent colon injury both have the potential to contaminate the surgical field, increasing the risk of morbidity. Surgeons have turned to MBP to minimize this risk in the planned surgical setting, although the practice does not appear to reduce infection or the risk of subsequent anastomotic leakage. It is largely unknown how bowel preparation affects bowel spillage during colon resection. Most investigators empirically believe that MBP will reduce bowel spillage during planned colon resection in an uncontaminated field,13 although one prospective study suggested a trend toward increased spillage of bowel contents and intraoperative contamination in patients who had undergone MBP.20
In gynecologic surgery for benign conditions, colon resection is generally unplanned, usually the result of inadvertent colon injury or unexpected findings. Traditional teaching has been that, if an unprepared colon becomes injured, the patient requires a colostomy rather than primary anastomosis, simply because there are bowel contents contaminating the surgical field.
Gynecologists may be hesitant to challenge this practice because the choice of primary anastomosis versus colostomy is often made by the consulting general surgeon. Given the low risk of bowel injury (estimated to be <2% in gynecologic surgery) and emerging data on fecal contamination and bowel resection in the trauma literature, MBP may be unnecessary on a population-wide basis.21
In fact, the trauma literature might be instructive in understanding how inadvertent colon injury in gynecologic surgery should be managed, regardless of the patient’s bowel-preparation status. Multiple randomized, controlled trials of colostomy versus primary anastomosis in trauma patients who had penetrating colon injuries demonstrated no difference in the rates of mortality and complications, including SSI and anastomotic leakage.22-24 Both colorectal and trauma surgeons performed planned and unplanned colectomy and primary re-anastomosis without MBP.
Based on these data, the recommended practice in trauma surgery is primary repair of the colon, confirming that the unprepared colon can be safely re-anastomosed, even in a grossly contaminated field. Extrapolating from this literature, it stands to reason that colon injury at the time of gynecologic surgery without preoperative MBP could also be managed primarily, eliminating the impetus for gynecologists to use MBP to avoid bowel diversion.
Although evidence-based practice is highly recommended, it is important to recognize that it is beyond the scope of most general gynecologists to perform bowel resection and anastomoses in the event of inadvertent bowel injury. Gynecologic surgeons must know the practice patterns of their local institution; if the general surgeons in that institution do not follow current recommendations, it may be prudent to continue to use MBP in cases that carry a high risk of bowel injury to avoid a potential colostomy.
Easing bowel manipulation
Some gynecologists continue to use MBP in cases at low risk for bowel injury because they are concerned about the ease of operation and want to ensure good visibility, particularly when laparoscopy is involved. Muzii and colleagues conducted a randomized, single-blinded study of MBP versus no preparation in benign cases managed by gynecologic laparoscopy. The surgeons were blinded as to whether or not the patient had undergone MBP; at the conclusion of the procedure, these surgeons rated the ease of operation and visualization based on the quality of the surgical field, evaluation of the small and large bowel, and surgical difficulty. MBP was not associated with any measured outcome, including complications, surgical time, and self-assessed ease of operation—although patients reported significantly more discomfort with MBP.4
Easing intraoperative colonoscopy
Experts agree that planned or potential intraoperative colonoscopy is a clear indication for adequate bowel preparation.10 A smaller body of evidence suggests that, when “subtle palpation of the bowel wall” is required, MBP may help the surgeon avoid mistaking a nodule for stool.5,25
Beyond these examples, routine MBP is not supported by randomized data.
We sorely need guidelines on MBP
Like many general and colorectal surgeons, many gynecologists still use MBP. A 2011 survey of Canadian gynecologic oncologists reported that 47% still routinely order MBP, although 77% of surgeons acknowledged a lack of “good evidence” to support the practice.26 Similarly, although 95% of colorectal surgeons in Michigan in 2011 believed that the data against routine use of MBP was scientifically valid, only 50% agreed that MBP was unnecessary.27 Data from Spain echo these results: 77% of surgeons viewed bowel preparation as useful or very useful.28
The striking contrast between literature and practice merits scrutiny. When the literature demonstrates no need for MBP and a risk of patient harm, why are so many surgeons still electing preoperative MBP for their patients? Reasons listed by gynecologic oncologists in a 2011 survey varied but included a reduction in anastomotic leakage (31%) and improved visualization (37%)—reasons unsupported by the randomized literature. A majority (71%) agreed that guidelines would be helpful in determining the appropriate use of MBP, if any.26 Overall, ACOG has not laid out clear guidelines on the use or avoidance of MBP to support gynecologic surgeons’ decision-making.
MBP is an antiquated practice
The colorectal literature has identified MBP as an antiquated practice without evidence to support its routine use. Therefore, mechanical bowel preparation is likely to be of minimal value for patients undergoing major gynecologic surgery, based on extensive data from randomized trials of planned bowel surgery.29 The role of MBP in laparoscopic, robotic, and vaginal surgery is less clearly defined, although there is no clear evidence to support the use of MBP in any surgical modality except intraoperative colonoscopy. Despite the lack of clear guidance from ACOG, the colorectal and gynecologic literature strongly suggests that MBP does not reduce the risk of SSI or intraoperative or postoperative complications. Nor do surgical ease and visibility appear to be improved with MBP, though the literature in this area is limited.
MBP is not without risk, particularly for elderly patients who have medical comorbidities. Without clearly established benefits, we recommend that you strongly consider these randomized data and limit—or even eliminate—the use of MBP for major abdominal procedures in your practice.
- 10 practical, evidence-based recommendations for improving maternal outcomes of cesarean delivery
Baha M. Sibai, MD (March 2012) - Step by step: Obliterating the vaginal canal to correct pelvic organ prolapse
Mickey Karram, MD; Janelle Evans, MD (February 2012) - Strategies and steps for the surgical management of endometriosis
Anthony A. Luciano, MD; Rachel LaMonica, MD; Danielle E. Luciano, MD (November 2011) - Correcting pelvic organ prolapse with robotic sacrocolpopexy
Catherine A. Matthews, MD (September 2011) - High uterosacral vaginal vault suspension to repair enterocele and apical prolapse
Mickey Karram, MD; Christine Vaccaro, DO (June 2011) - 10 practical, evidence-based suggestions to improve your minimally invasive surgical skills now
Catherine A. Matthews, MD (April 2011)
We want to hear from you! Tell us what you think.
Think mechanical bowel preparation (MBP) is a must for gynecologic surgery?
Think again.
Although MBP has been around since the 1930s, a growing body of data suggest that, with rare exception, gynecologists can eliminate routine use of preoperative MBP from their practice.
In this article, we discuss the evidence surrounding MBP so that you can assess the benefits and risks it poses for your surgical patients.
Unproven assumptions are behind MBP
For most of the past century, MBP has been used in advance of abdominal surgery,
including gynecologic surgery. Clinicians made the rational assumption that, by decreasing the fecal load within the colon, they could lower the risk of certain surgical complications, especially during an era when antibiotics were not available to treat serious infectious morbidity. In modern times, the practice has continued when major abdominal surgery is planned. Why? Because surgeons believe it will reduce the risk of wound infection, anastomotic leakage, and bowel spillage in the event of injury, and that it will increase the ease of bowel manipulation.1
A growing body of literature challenges these assumptions and suggests that MBP is not associated with these benefits—and may even increase the incidence of some of these complications. Moreover, the induction of profuse, watery diarrhea to evacuate the colon before surgery has been associated with severe electrolyte imbalance, renal failure, and difficult intraoperative fluid management.
These risks make a thorough assessment of MBP’s effects imperative to guide optimal practice.
- Mechanical bowel prep has many side effects, ranging from mild (discomfort) to severe (renal failure).
- The risks of surgical site infection and anastomotic leakage are not lower with MBP, compared with no preparation, in patients undergoing elective colon surgery.
- MBP does not reduce the risk of intraoperative contamination of the surgical field.
- In unplanned injuries to unprepared colon (e.g., in cases involving trauma), primary anastomosis is the recommended mode of repair rather than diverting colostomy.
- MBP does not ease bowel manipulation in laparoscopy, compared with no preparation.
- The only proven value of MBP is to improve visibility during intraoperative colonoscopy.
- Gynecologists can eliminate the routine use of MBP from their surgical practice.
MBP defined
MBP is the chemical or physical process of eliminating fecal matter from the intestinal tract. There are a variety of methods, including ingestion of an oral preparation and enemas and suppositories. Historically, MBP included stimulant laxatives, such as senna extract and castor oil, and hyperosmotic solutions, such as mannitol and lactulose.
MBP is distinctly separate from antibiotic bowel preparation and preoperative prophylactic antibiotics, both of which fall beyond the scope of this article.
The most common forms of MBP prescribed today are balanced electrolyte solutions, including polyethylene glycol, and saline laxatives, such as magnesium citrate and sodium phosphate.2
Some investigators have attempted to determine which MBP formulations are most effective, based on visualization during colonoscopy, but a recent meta-analysis suggests that most formulations perform similarly.3
The risks associated with MBP are clearly documented in the literature and range in intensity from mild to severe. Overall, patients report discomfort, with symptoms such as abdominal pain and distension, nausea and vomiting, weakness, and insomnia.4 High-volume preparations, such as polyethylene glycol, are unpalatable to patients and, therefore, less likely to be ingested completely, leaving the surgeon with a partially evacuated colon.
Dehydration and electrolyte disturbances may also complicate the use of MBP, particularly with saline laxatives. Although young patients can likely tolerate electrolyte shifts without severe sequelae, elderly patients who have comorbid heart and kidney disorders may become further deconditioned during the MBP process. Seizures and esophageal tears have been reported as a result of MBP.5 Sodium phosphate, in particular, is associated with renal failure, with 171 cases reported to the US Food and Drug Administration (FDA) from 2006 to 2007—leading to an issued warning not to employ this agent in preoperative MBP in the liquid formulation.6
In addition, in one study, investigators observed an increased time to the return of bowel function and a prolonged hospital stay among patients who underwent MBP.7
Purported benefits of MBP
Reducing the risk of surgical site infection
Surgical site infection (SSI)—whether intra-abdominal or in the superficial wound—is a serious complication that can lead to severe morbidity. As colorectal surgeons began performing more aggressive colon surgery in the 1930s, 40s, and 50s, they sought a way to reduce SSI. Mortality from colon surgery was 10% to 30%, with a rate of SSI of 80% to 90%, so surgeons began to seek a method to decrease the fecal bacterial load, presuming that doing so would also reduce the rates of infection and mortality and allow for primary repair of the colon. MBP appeared to address the problem.1
The practice of MBP then spread from colorectal surgery to other areas of general and gynecologic surgery without clear evidence from randomized trials that it was necessary or beneficial.8 As surgical techniques improved over the ensuing decades, and antibiotics evolved, mortality and SSI rates dropped—although it is unclear whether this drop in infection is attributable to MBP.1
In the 1990s, researchers began to question the value of MBP in surgical practice. Multiple randomized, controlled trials in the colorectal literature have demonstrated that MBP does not reduce the rate of incisional or deep SSI, compared with no bowel preparation.9-11 The populations studied in these trials were undergoing planned bowel resection and primary re-anastomosis— procedures known to elevate the risk of contamination, unlike the majority of gynecologic surgical procedures. Even in this higher-risk population, however, MBP failed to reduce the risk of SSI, suggesting that, in less contaminated surgeries, it would have even fewer benefits.
In its practice bulletin on antibiotic prophylaxis from 2009, the American Congress of Obstetricians and Gynecologists (ACOG) noted: “There is no evidence that mechanical bowel preparation further reduces infection risk” beyond the reduction achieved with routine use of perioperative antibiotics.12
Preventing anastomotic leakage
Investigators have suggested that MBP reduces the risk of anastomotic leaks of the colon by decreasing contamination at the suture site.13 A close review of the colorectal literature, however, reveals that MBP does not affect anastomotic leakage in patients who undergo planned colon resection and primary re-anastomosis.9,10,14-17
A 2011 Cochrane review that included 5,805 patients undergoing elective colon and rectal surgery confirmed that neither oral nor rectal MBP was associated with any benefit in terms of the rates of anastomotic leakage and SSI.10 Some randomized studies have found nonstatistically significant reductions in the anastomotic leakage rate in patients who did not undergo MBP—a finding attributed to the lack of denuded mucosa and inflammation in the unprepared colon.9,15,18
However, one large, randomized, clinical trial of more than 1,000 patients found that, when anastomotic leakage did occur, the risk of infection was greater among patients who had not undergone MBP.19
Reducing the rates of intraoperative contamination and colon injury
Planned resection and inadvertent colon injury both have the potential to contaminate the surgical field, increasing the risk of morbidity. Surgeons have turned to MBP to minimize this risk in the planned surgical setting, although the practice does not appear to reduce infection or the risk of subsequent anastomotic leakage. It is largely unknown how bowel preparation affects bowel spillage during colon resection. Most investigators empirically believe that MBP will reduce bowel spillage during planned colon resection in an uncontaminated field,13 although one prospective study suggested a trend toward increased spillage of bowel contents and intraoperative contamination in patients who had undergone MBP.20
In gynecologic surgery for benign conditions, colon resection is generally unplanned, usually the result of inadvertent colon injury or unexpected findings. Traditional teaching has been that, if an unprepared colon becomes injured, the patient requires a colostomy rather than primary anastomosis, simply because there are bowel contents contaminating the surgical field.
Gynecologists may be hesitant to challenge this practice because the choice of primary anastomosis versus colostomy is often made by the consulting general surgeon. Given the low risk of bowel injury (estimated to be <2% in gynecologic surgery) and emerging data on fecal contamination and bowel resection in the trauma literature, MBP may be unnecessary on a population-wide basis.21
In fact, the trauma literature might be instructive in understanding how inadvertent colon injury in gynecologic surgery should be managed, regardless of the patient’s bowel-preparation status. Multiple randomized, controlled trials of colostomy versus primary anastomosis in trauma patients who had penetrating colon injuries demonstrated no difference in the rates of mortality and complications, including SSI and anastomotic leakage.22-24 Both colorectal and trauma surgeons performed planned and unplanned colectomy and primary re-anastomosis without MBP.
Based on these data, the recommended practice in trauma surgery is primary repair of the colon, confirming that the unprepared colon can be safely re-anastomosed, even in a grossly contaminated field. Extrapolating from this literature, it stands to reason that colon injury at the time of gynecologic surgery without preoperative MBP could also be managed primarily, eliminating the impetus for gynecologists to use MBP to avoid bowel diversion.
Although evidence-based practice is highly recommended, it is important to recognize that it is beyond the scope of most general gynecologists to perform bowel resection and anastomoses in the event of inadvertent bowel injury. Gynecologic surgeons must know the practice patterns of their local institution; if the general surgeons in that institution do not follow current recommendations, it may be prudent to continue to use MBP in cases that carry a high risk of bowel injury to avoid a potential colostomy.
Easing bowel manipulation
Some gynecologists continue to use MBP in cases at low risk for bowel injury because they are concerned about the ease of operation and want to ensure good visibility, particularly when laparoscopy is involved. Muzii and colleagues conducted a randomized, single-blinded study of MBP versus no preparation in benign cases managed by gynecologic laparoscopy. The surgeons were blinded as to whether or not the patient had undergone MBP; at the conclusion of the procedure, these surgeons rated the ease of operation and visualization based on the quality of the surgical field, evaluation of the small and large bowel, and surgical difficulty. MBP was not associated with any measured outcome, including complications, surgical time, and self-assessed ease of operation—although patients reported significantly more discomfort with MBP.4
Easing intraoperative colonoscopy
Experts agree that planned or potential intraoperative colonoscopy is a clear indication for adequate bowel preparation.10 A smaller body of evidence suggests that, when “subtle palpation of the bowel wall” is required, MBP may help the surgeon avoid mistaking a nodule for stool.5,25
Beyond these examples, routine MBP is not supported by randomized data.
We sorely need guidelines on MBP
Like many general and colorectal surgeons, many gynecologists still use MBP. A 2011 survey of Canadian gynecologic oncologists reported that 47% still routinely order MBP, although 77% of surgeons acknowledged a lack of “good evidence” to support the practice.26 Similarly, although 95% of colorectal surgeons in Michigan in 2011 believed that the data against routine use of MBP was scientifically valid, only 50% agreed that MBP was unnecessary.27 Data from Spain echo these results: 77% of surgeons viewed bowel preparation as useful or very useful.28
The striking contrast between literature and practice merits scrutiny. When the literature demonstrates no need for MBP and a risk of patient harm, why are so many surgeons still electing preoperative MBP for their patients? Reasons listed by gynecologic oncologists in a 2011 survey varied but included a reduction in anastomotic leakage (31%) and improved visualization (37%)—reasons unsupported by the randomized literature. A majority (71%) agreed that guidelines would be helpful in determining the appropriate use of MBP, if any.26 Overall, ACOG has not laid out clear guidelines on the use or avoidance of MBP to support gynecologic surgeons’ decision-making.
MBP is an antiquated practice
The colorectal literature has identified MBP as an antiquated practice without evidence to support its routine use. Therefore, mechanical bowel preparation is likely to be of minimal value for patients undergoing major gynecologic surgery, based on extensive data from randomized trials of planned bowel surgery.29 The role of MBP in laparoscopic, robotic, and vaginal surgery is less clearly defined, although there is no clear evidence to support the use of MBP in any surgical modality except intraoperative colonoscopy. Despite the lack of clear guidance from ACOG, the colorectal and gynecologic literature strongly suggests that MBP does not reduce the risk of SSI or intraoperative or postoperative complications. Nor do surgical ease and visibility appear to be improved with MBP, though the literature in this area is limited.
MBP is not without risk, particularly for elderly patients who have medical comorbidities. Without clearly established benefits, we recommend that you strongly consider these randomized data and limit—or even eliminate—the use of MBP for major abdominal procedures in your practice.
- 10 practical, evidence-based recommendations for improving maternal outcomes of cesarean delivery
Baha M. Sibai, MD (March 2012) - Step by step: Obliterating the vaginal canal to correct pelvic organ prolapse
Mickey Karram, MD; Janelle Evans, MD (February 2012) - Strategies and steps for the surgical management of endometriosis
Anthony A. Luciano, MD; Rachel LaMonica, MD; Danielle E. Luciano, MD (November 2011) - Correcting pelvic organ prolapse with robotic sacrocolpopexy
Catherine A. Matthews, MD (September 2011) - High uterosacral vaginal vault suspension to repair enterocele and apical prolapse
Mickey Karram, MD; Christine Vaccaro, DO (June 2011) - 10 practical, evidence-based suggestions to improve your minimally invasive surgical skills now
Catherine A. Matthews, MD (April 2011)
We want to hear from you! Tell us what you think.
1. Fry DE. Colon preparation and surgical site infection. Am J Surg. 2011;202(2):225-232.
2. Yang LC, Arden D, Lee TT, et al. Mechanical bowel preparation for gynecologic laparoscopy: a prospective randomized trial of oral sodium phosphate solution vs single sodium phosphate enema. J Minim Invasive Gynecol. 2011;18(2):149-156.
3. Belsey J, Crosta C, Epstein O, et al. Meta-analysis: the relative efficacy of oral bowel preparations for colonoscopy 1985-2010. Aliment Pharmacol Ther. 2012;35(2):222-237.
4. Muzii L, Bellati F, Zullo MA, Manci N, Angioli R, Panici PB. Mechanical bowel preparation before gynecologic laparoscopy: a randomized single-blind, controlled trial. Fertil Steril. 2006;85(3):689-693.
5. Botha MH. Mechanical bowel preparation in gynaecological surgery—are we doing more harm than good? S Afr Med J. 2007;97(11):1040-1043.
6. Belsey J, Epstein O, Heresbach D. Systematic review: adverse event reports for oral sodium phosphate and polyethylene glycol. Aliment Pharmacol Ther. 2009;29(1):15-28.
7. Shafii M, Murphy DM, Donovan MG, Hickey DP. Is mechanical bowel preparation necessary in patients undergoing cystectomy and urinary diversion? BJU Int. 2002;89(9):879-881.
8. Cohen SL, Einarsson JI. The role of mechanical bowel preparation in gynecologic laparoscopy. Rev Obstet Gynecol. 2011;4(1):28-31.
9. Platell C, Hall J. What is the role of mechanical bowel preparation in patients undergoing colorectal surgery? Dis Colon Rectum. 1998;41(7):875-883.
10. Güenaga KF, Matos D, Wille-Jorgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2011;9:CD001544.
11. Pena-Soria MJ, Mayol JM, Anula R, Arbeo-Escolar A, Fernandez-Represa JA. Single-blinded randomized trial of mechanical bowel preparation for colon surgery with primary intraperitoneal anastomosis. J Gastrointest Surg 2008;12(12):2103-2109.
12. Committee on Practice Bulletins—Gynecology. ACOG practice bulletin No. 104: antibiotic prophylaxis for gynecologic procedures. Obstet Gynecol. 2009;113(5):1180.-
13. Kingham TP, Pachter HL. Colonic anastomotic leak: risk factors diagnosis, and treatment. J Am Coll Surg. 2009;208(2):269-278.
14. Wille-Jorgensen P, Güenaga KF, Matos D, Castro AA. Pre-operative mechanical bowel cleansing or not? An updated meta-analysis. Colorectal Dis. 2005;7(4):304-310.
15. Miettinen RP, Laitinen ST, Makela JT, Paakkonen ME. Bowel preparation with oral polyethylene glycol electrolyte solution vs. no preparation in elective open colorectal surgery: prospective randomized study. Dis Colon Rectum. 2000;43(5):669-677.
16. Ram E, Sherman Y, Weil R, Vishne T, Kravarusic D, Dreznik Z. Is mechanical bowel preparation mandatory for elective colon surgery? A prospective randomized study. Arch Surg. 2005;140(3):285-288.
17. Mäkelä JT, Kiviniemi H, Laitinen S. Risk factors for anastomotic leakage after left-sided colorectal resection with rectal anastomosis. Dis Colon Rectum. 2003;46(5):653-660.
18. Bucher P, Gervaz P, Egger JF, Soravia C, Morel P. Morphologic alterations associated with mechanical bowel preparation before elective colorectal surgery: a randomized trial. Dis Colon Rectum. 2006;49(1):109-112.
19. Contant CM, Hop WC, van’t Sant HP, et al. Mechanical bowel preparation for elective colorectal surgery: a multicentre randomised trial. Lancet. 2007;370(9625):2112-2117.
20. Mahajna A, Krausz M, Rosin D, et al. Bowel preparation is associated with spillage of bowel contents in colorectal surgery. Dis Colon Rectum. 2005;48(8):1626-1631.
21. Brosens I, Gordon A, Campo R, Gordts S. Bowel injury in gynecologic laparoscopy. J Am Assoc Gynecol Laparosc. 2003;10(1):9-13.
22. Demetriades D, Murray JA, Chan L, et al; Committee on Multicenter Clinical Trials. American Association for the Surgery of Trauma. Penetrating colon injuries requiring resection: diversion or primary anastomosis? An AAST prospective multicenter study. J Trauma. 2001;50(5):765-775.
23. Curran TJ, Borzotta AP. Complications of primary repair of colon injury: literature review of 2,964 cases. Am J Surg. 1999;177(1):42-47.
24. Nelson R, Singer M. Primary repair for penetrating colon injuries. Cochrane Database Syst Rev. 2003;3:CD002247.
25. Rovera F, Dionigi G, Boni L, et al. Mechanical bowel preparation for colorectal surgery. Surg Infect (Larchmt). 2006;7(suppl 2):S61-S63.
26. Wells T, Plante M, McAlpine JN. Communities of Practice Groups on behalf of the Society of Gynecologic Oncologists of Canada. Preoperative bowel preparation in gynecologic oncology: a review of practice patterns and an impetus to change. Int J Gynecol Cancer. 2011;21(6):1135-1142.
27. Marchaim D, Slim J, Dhar S, et al. A regional survey of the use of mechanical bowel preparations prior to colorectal surgery. Ann Surg. 2011;253(4):839-840.
28. Roig JV, Garcia-Fadrique A, Garcia-Armengol J, et al. Mechanical bowel preparation and antibiotic prophylaxis in colorectal surgery: use by and opinions of Spanish surgeons. Colorectal Dis. 2009;11(1):44-48.
29. Fanning J, Valea FA. Perioperative bowel management for gynecologic surgery. Am J Obstet Gynecol. 2011;205(4):309-314.
1. Fry DE. Colon preparation and surgical site infection. Am J Surg. 2011;202(2):225-232.
2. Yang LC, Arden D, Lee TT, et al. Mechanical bowel preparation for gynecologic laparoscopy: a prospective randomized trial of oral sodium phosphate solution vs single sodium phosphate enema. J Minim Invasive Gynecol. 2011;18(2):149-156.
3. Belsey J, Crosta C, Epstein O, et al. Meta-analysis: the relative efficacy of oral bowel preparations for colonoscopy 1985-2010. Aliment Pharmacol Ther. 2012;35(2):222-237.
4. Muzii L, Bellati F, Zullo MA, Manci N, Angioli R, Panici PB. Mechanical bowel preparation before gynecologic laparoscopy: a randomized single-blind, controlled trial. Fertil Steril. 2006;85(3):689-693.
5. Botha MH. Mechanical bowel preparation in gynaecological surgery—are we doing more harm than good? S Afr Med J. 2007;97(11):1040-1043.
6. Belsey J, Epstein O, Heresbach D. Systematic review: adverse event reports for oral sodium phosphate and polyethylene glycol. Aliment Pharmacol Ther. 2009;29(1):15-28.
7. Shafii M, Murphy DM, Donovan MG, Hickey DP. Is mechanical bowel preparation necessary in patients undergoing cystectomy and urinary diversion? BJU Int. 2002;89(9):879-881.
8. Cohen SL, Einarsson JI. The role of mechanical bowel preparation in gynecologic laparoscopy. Rev Obstet Gynecol. 2011;4(1):28-31.
9. Platell C, Hall J. What is the role of mechanical bowel preparation in patients undergoing colorectal surgery? Dis Colon Rectum. 1998;41(7):875-883.
10. Güenaga KF, Matos D, Wille-Jorgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2011;9:CD001544.
11. Pena-Soria MJ, Mayol JM, Anula R, Arbeo-Escolar A, Fernandez-Represa JA. Single-blinded randomized trial of mechanical bowel preparation for colon surgery with primary intraperitoneal anastomosis. J Gastrointest Surg 2008;12(12):2103-2109.
12. Committee on Practice Bulletins—Gynecology. ACOG practice bulletin No. 104: antibiotic prophylaxis for gynecologic procedures. Obstet Gynecol. 2009;113(5):1180.-
13. Kingham TP, Pachter HL. Colonic anastomotic leak: risk factors diagnosis, and treatment. J Am Coll Surg. 2009;208(2):269-278.
14. Wille-Jorgensen P, Güenaga KF, Matos D, Castro AA. Pre-operative mechanical bowel cleansing or not? An updated meta-analysis. Colorectal Dis. 2005;7(4):304-310.
15. Miettinen RP, Laitinen ST, Makela JT, Paakkonen ME. Bowel preparation with oral polyethylene glycol electrolyte solution vs. no preparation in elective open colorectal surgery: prospective randomized study. Dis Colon Rectum. 2000;43(5):669-677.
16. Ram E, Sherman Y, Weil R, Vishne T, Kravarusic D, Dreznik Z. Is mechanical bowel preparation mandatory for elective colon surgery? A prospective randomized study. Arch Surg. 2005;140(3):285-288.
17. Mäkelä JT, Kiviniemi H, Laitinen S. Risk factors for anastomotic leakage after left-sided colorectal resection with rectal anastomosis. Dis Colon Rectum. 2003;46(5):653-660.
18. Bucher P, Gervaz P, Egger JF, Soravia C, Morel P. Morphologic alterations associated with mechanical bowel preparation before elective colorectal surgery: a randomized trial. Dis Colon Rectum. 2006;49(1):109-112.
19. Contant CM, Hop WC, van’t Sant HP, et al. Mechanical bowel preparation for elective colorectal surgery: a multicentre randomised trial. Lancet. 2007;370(9625):2112-2117.
20. Mahajna A, Krausz M, Rosin D, et al. Bowel preparation is associated with spillage of bowel contents in colorectal surgery. Dis Colon Rectum. 2005;48(8):1626-1631.
21. Brosens I, Gordon A, Campo R, Gordts S. Bowel injury in gynecologic laparoscopy. J Am Assoc Gynecol Laparosc. 2003;10(1):9-13.
22. Demetriades D, Murray JA, Chan L, et al; Committee on Multicenter Clinical Trials. American Association for the Surgery of Trauma. Penetrating colon injuries requiring resection: diversion or primary anastomosis? An AAST prospective multicenter study. J Trauma. 2001;50(5):765-775.
23. Curran TJ, Borzotta AP. Complications of primary repair of colon injury: literature review of 2,964 cases. Am J Surg. 1999;177(1):42-47.
24. Nelson R, Singer M. Primary repair for penetrating colon injuries. Cochrane Database Syst Rev. 2003;3:CD002247.
25. Rovera F, Dionigi G, Boni L, et al. Mechanical bowel preparation for colorectal surgery. Surg Infect (Larchmt). 2006;7(suppl 2):S61-S63.
26. Wells T, Plante M, McAlpine JN. Communities of Practice Groups on behalf of the Society of Gynecologic Oncologists of Canada. Preoperative bowel preparation in gynecologic oncology: a review of practice patterns and an impetus to change. Int J Gynecol Cancer. 2011;21(6):1135-1142.
27. Marchaim D, Slim J, Dhar S, et al. A regional survey of the use of mechanical bowel preparations prior to colorectal surgery. Ann Surg. 2011;253(4):839-840.
28. Roig JV, Garcia-Fadrique A, Garcia-Armengol J, et al. Mechanical bowel preparation and antibiotic prophylaxis in colorectal surgery: use by and opinions of Spanish surgeons. Colorectal Dis. 2009;11(1):44-48.
29. Fanning J, Valea FA. Perioperative bowel management for gynecologic surgery. Am J Obstet Gynecol. 2011;205(4):309-314.
Can Allergy Shots Cut Asthma Risk?
Can allergen-specific immunotherapy cut the risk of asthma development in children with allergic rhinitis? Dr. Linda Cox discusses the potential implications of an ongoing retrospective review of Florida Medicaid records to determine if immunotherapy reduced asthma risk and its associated costs.
Can allergen-specific immunotherapy cut the risk of asthma development in children with allergic rhinitis? Dr. Linda Cox discusses the potential implications of an ongoing retrospective review of Florida Medicaid records to determine if immunotherapy reduced asthma risk and its associated costs.
Can allergen-specific immunotherapy cut the risk of asthma development in children with allergic rhinitis? Dr. Linda Cox discusses the potential implications of an ongoing retrospective review of Florida Medicaid records to determine if immunotherapy reduced asthma risk and its associated costs.
Identifying Child Abuse
According to data from the US Department of Health and Human Services, child protection services received more than 3.3 million reports of alleged maltreatment in 2009 that involved about six million children, and about 62% of reports required subsequent action.1 Child abuse is an ever-growing problem that affects children of both genders and in all ages, races, and socioeconomic levels. Few issues generate the concern, anger, and frustration as the abuse or neglect of children.
Primary care providers and emergency department personnel are often the child’s initial point of entry into the health care system. Clinicians who see and treat young patients can play an essential role in the recognition and reporting of child abuse. By frequently reviewing the risk factors for child abuse, its signs and symptoms, and its typical and atypical presentations, clinicians can be prepared to act when appropriate and help break the cycle of child abuse.
LEGAL MANDATES, DEFINITIONS
A relatively new concept, child abuse has been designated as a major public health issue by the United Nations Children’s Fund and the World Health Organization.2-5 In 1874, when it was decided by the American Society for the Prevention of Cruelty to Animals (ASPCA) to include children within the defined animal kingdom, the movement to protect children began in the United States.6
Both federal and state agencies have created definitions for child abuse and neglect. The key federal legislation to address child abuse and neglect, the Child Abuse Prevention and Treatment Act (CAPTA), as Amended by the Keeping Children and Families Safe Act of 2003,7,8 defines child abuse and neglect as “any recent act or failure to act on the part of a parent or caretaker, which results in death, serious physical or emotional harm, sexual abuse or exploitation, or an act or failure to act which presents an imminent risk of serious harm.”7 Although ongoing revisions of the CAPTA legislation (the most recent “reauthorization” published in 20109) become increasingly inclusive of both children’s and families’ concerns, this definition has remained consistent.
This is not the case with state definitions, however. Because these vary, it can be difficult to compare rates of reported maltreatment from state to state. Also varying among states, and among counties within some states, are recommendations for substantiation of child maltreatment. The validity of the reported data can be impaired by a lack of coordination or cooperation among different agencies and jurisdictions.
IDENTIFYING THE VICTIMS
The spectrum of child abuse includes multiple forms, which often overlap (see Table 11,9,10), and can almost always have the potential for death.11 According to findings from the National Child Abuse and Neglect Data System, despite worsening economic conditions in 2009, the child maltreatment data compiled that year showed an overall 2% decline in cases of substantiated maltreatment from the previous year.1,11

However, during that same period, child maltreatment–associated fatalities rose 3%, from 1,628 deaths in 2008 to 1,671 in 2009,1 suggesting an increase in the severity of abuse. The emotional, social, and financial ramifications of child abuse affect the local and national community, as well as each child and each family.
Children younger than 1 year, the most vulnerable to maltreatment, represent the largest proportion of substantiated abuse. One-third of all children reported as abused in 2009 were younger than 4, and children between ages 4 and 7 represented one-fifth of cases.1 Figure 1a1 categorizes the incidence of child abuse by age level, and Figure 1b1 by ethnicity/race.

Risk Factors
A number of factors, though not necessarily direct causes, have been shown to increase children’s risk for abuse or neglect. These include personal characteristics of the child and parent, and family- or environment-related factors1,12 (see Table 2,1). It is often combinations of risk factors (eg, characteristics of a parent or caregiver in addition to a specific social environment) that are most likely to increase the likelihood of abuse.
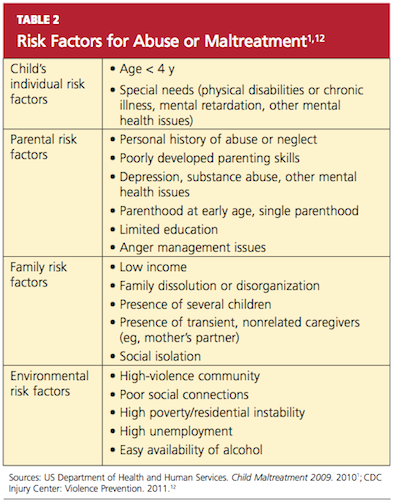
Children with special needs (physical disabilities or chronic illness, neurologic impairment, mental health issues) that increase the caregiver’s burden are at increased risk for abuse.1,12 Children with behavior disorders and mental retardation have been found at increased risk for various forms of abuse—neglect and physical or sexual maltreatment13—whereas children with speech or language disabilities are at increased risk for neglect (whether physical, emotional, or even educational14).
Children with physical limitations who experience physical abuse are reportedly subject to more serious injury than their healthier counterparts.14 Their inability to see, hear, move, or communicate, or to dress or bathe themselves independently may make them susceptible to rough, careless, or intrusive personal care, or neglect of their personal needs. Low self-esteem, whatever its cause, also appears to be a significant risk factor for intentional abuse.15
It is often the case that children with disabilities do not report abuse because they are unable to recognize an act as abusive. Depending on the severity of a child’s disability and his or her ordinarily atypical presentation, the abuse may never be discovered.15
Poverty appears to be a contributing factor. Children from families of low socioeconomic status are at least three times as likely as other children to be abused and seven times as likely to experience neglect.14 It has been conjectured that these children are more likely to have contact with social workers, law enforcement officers, and representatives of other agencies with an increased awareness of the manifestations of child abuse. Abuse within affluent families may be underreported, as such families have the wherewithal to protect themselves from detection and prosecution.16
PRESENTATION
There is no “gold standard” for making a confirmed diagnosis of child abuse,17 and no “typical” presentation of an abused child (see case study). Dress that is inappropriate for the season and consistently poor hygiene are indicative of neglect. Symptoms of abuse may be overt or silent, and signs of physical abuse are often hidden beneath clothing. Children who are physically abused often explain their injuries by saying “I fell,” or may even respond to questioning by saying, “I don’t know.” The parent or caregiver may attribute bruises or even broken bones to falls or rough play with other children. Bruises, the most common visible form of child abuse,18 may suggest the nature of injury by their location, patterns, and various stages of healing.
Fractures are the second most common presenting symptom among children experiencing physical abuse.17 According to findings from a meta-analysis by Kemp et al,19 determining whether fractures have occurred accidentally depends on three factors:
Age. Among children younger than 1 year, 25% to 56% of fractures are attributable to intentional harm. In one landmark study, one fracture in nine was found to have resulted from abuse, among children younger than 18 months—compared with one in 205 among children ages 19 months to 5 years.19,20
Site. In cases not involving a motor vehicle accident or other traumatic event, it has been determined in ongoing systematic reviews by Welsh researchers that rib fractures have a 71% probability of being inflicted, followed by humeral fractures (about 50% probability), then by femoral fractures or skull fractures (about 33% probability).19,21
Fracture type. Fracture types suggestive of abuse differ by site. Among humeral fractures, for example, a midshaft fracture is more likely to have been inflicted, whereas a supracondylar fracture is more likely the result of accidental injury. Both parietal and linear skull fractures may occur accidentally or through physical abuse.19 Epiphyseal-metaphyseal fractures, vertebral compression fractures, and lateral clavicle fractures have been associated with child abuse.22,23 Multiple or bilateral fractures have an increased association with abuse.19,20,24
Injuries that are inconsistent with the given history should raise red flags, and they should be carefully investigated, with findings documented. Minor falls cause minor injuries, not potentially life-threatening ones.
As with fractures, burns may have specific features that help the clinician distinguish between accidental and intentional. Uniform depth, well-defined edges, and multiple lesions are more likely to indicate nonaccidental contact burns, particularly when found in “protected” sites (eg, perineal and gluteal areas).18 Accidental cigarette burns are usually ovoid or irregular in shape and superficial, while those intentionally inflicted are round, deep, and well-demarcated and are often grouped on the hands, feet, or face.18,25 Burns on the chest, upper limbs, and palms of the hands are likely to be accidental; the face, the backs of the hands, the lower stomach, back, buttocks, legs, and feet are often the target of intentional burns.18,26
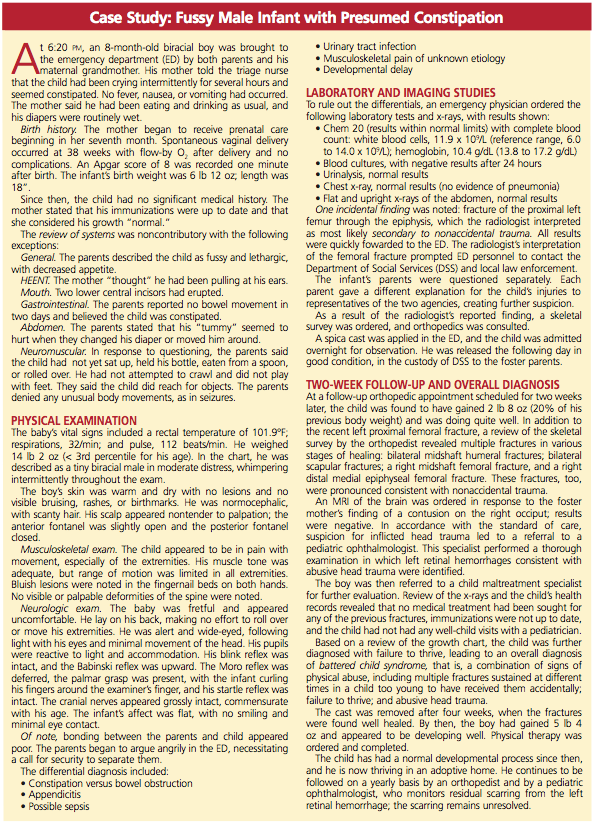
HISTORY
A key factor in suspected abuse is the child’s history. During history taking, clinicians should be alert to the evidence-based indicators of potential child abuse, as shown in Table 327-29. Not every child who exhibits these characteristics is an abused child, nor will every abused child exhibit any or all of these characteristics. Through artful, careful history taking and astute observation of the child, the clinician is usually able to distinguish between the heightened anxiety that may occur in any child during the history-taking process and the demeanor of a child who may have been coerced or threatened to maintain secrecy.
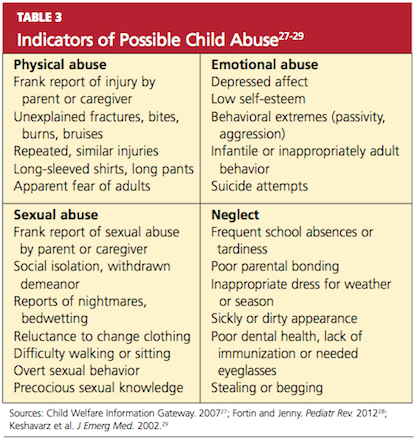
Engaging the child in a reassuring manner, the clinician can use a conversational style of questioning, such as, “Tell me how you got that bruise on your arm,” rather than a direct question: “Did [name] hit you on the arm with [his/her] fist?”
An observation of unusually sexualized behaviors or a report of excessive masturbation is more likely to be associated with sexual abuse than are genital findings (which are infrequently found).
Physical Examination
When a child presents with an acute injury or bruising is detected and the clinician’s findings are inconsistent with the given history, suspicion should be raised. The injuries inflicted by physical abuse are often hidden beneath the child’s clothing (specifically, underwear); for this reason, it is important to have children undressed during a physical exam.
The routine physical exam of an abused child may reveal defensive bruising or other wounds, trauma to the mouth, breasts, buttocks, genitalia, or anus, with possible bleeding or discharge. More commonly, the physical exam findings are normal—as is true in the majority of examinations for sexual abuse.30 In one large study, abnormal findings (eg, recent or healed genital injuries; presence of a sexually transmitted disease) were found in only about 4% of children who had been referred for an examination for suspected sexual abuse.18,31 Clearly, an appearance of “normal” does not mean “nothing happened.”32
According to CDC guidelines,33 investigation of suspected sexual abuse (for example, when a genital herpes infection is detected) should be conducted by appropriately trained, experienced clinicians—ideally, by a pediatric subspecialist in child abuse. Although the primary care clinician may examine the child briefly for visible bruises or wounds, it is essential for a specialist to perform the genital exam.33 Use of mild sedation with close monitoring may be advisable during the genital examination.30
Mimics of Child Abuse
Several conditions, including metabolic, genetic, and congenital disorders, have been reported to mimic the physical manifestations of child abuse and neglect17,22,34 (see Table 4,17,18,22,25,33-35). While health care professionals are legally and ethically bound to report abuse, conditions that may mimic abuse must be ruled out first, to avoid the mistaken removal of children from loving homes.
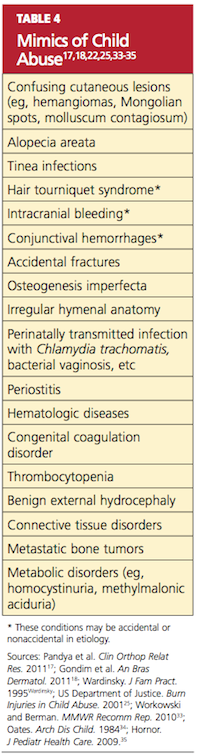
Mongolian spots, for example (see Figure 2), are frequently mistaken for bruising and reported to authorities, causing unnecessary disruption for both family and child.34,36 They typically appear as macular blue-gray pigmentation of the skin, usually on the sacrum. Resulting from entrapment of melanocytes in the dermis during fetal development, these “spots” may be present at birth or may appear during the neonatal period. Mongolian spots are most common in Native American, African-American, Asian, and Hispanic patients, are benign, and often disappear by age 4.
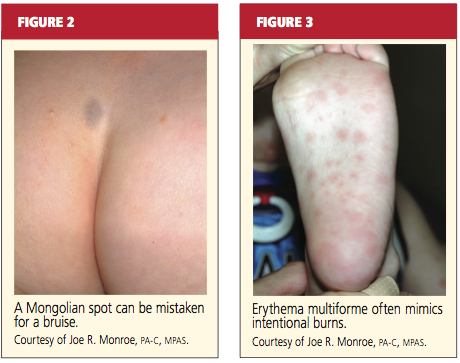
Other cutaneous manifestations that can mimic an intentional injury include molluscum contagiosum, a viral infection manifesting as a rash that may mimic the genital warts of human papillomavirus, and erythematous, edematous, and/or vesiculobullous lesions18,35 (see Figure 3). Severe diaper rash, photodermatitis, and certain allergic reactions can mimic intentional burns.25
Often mistaken for a nonaccidental injury is hair tourniquet syndrome—the circumferential strangulation of one or more appendages (eg, finger, toe, penis) by human hair or fibers.34 This uncommon condition, usually unintentional and of unknown incidence, can represent a surgical emergency; failure to recognize it in a timely fashion may lead to ischemia or necrosis, necessitating amputation of the affected appendage.37
Metabolic bone disease, such as osteogenesis imperfecta, can sometimes explain frequent fractures.17
MAKING THE DIAGNOSIS
In the primary care setting, the detection of child abuse is unexpected. However, it is often here that children are initially seen for an injury, or suspicions are raised during a routine physical.30 In the case of spontaneous disclosure of abuse, explicit, word-for-word documentation is required. The child, who may feel guilty, embarrassed, or ashamed, must be reassured that he or she is not at fault.
Either a child abuse specialist or the primary care clinician bases the ultimate diagnosis of child abuse on findings from the history and physical examination. These findings will direct the clinician’s decision to order diagnostic laboratory studies and/or diagnostic x-rays.
Diagnostic Studies
Depending on the child’s age and the type of presentation, recommended imaging studies include an x-ray skeletal survey of a child younger than 2 (see “Skeletal Survey Reading of 5-Month-Old Boy,”) or an older child with thoracoabdominal injuries that the history does not explain satisfactorily.23 For children ages 2 to 5, focused plain films of the area of suspected injury (eg, skull, chest, extremities) are considered appropriate.23,38
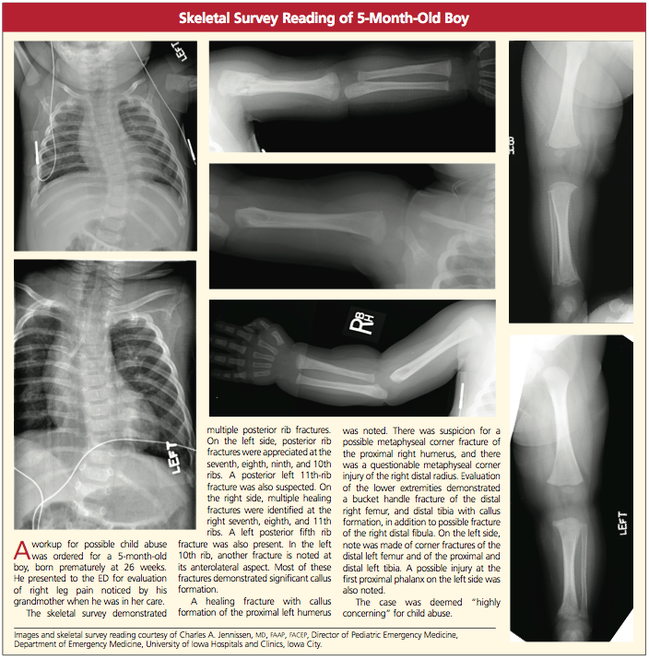
Noncontrast head CT may be appropriate in the presence of skull fractures, (as in Figures 4a and 4b) intracranial injuries, seizures, or other neurologic signs and symptoms (followed by MRI if further assessment is needed). CT with contrast may be considered when x-rays reveal certain abnormalities, the child is considered at high risk for abuse (for example, when inconsistencies are found in the history), or when soft-tissue injuries are suspected.23,39
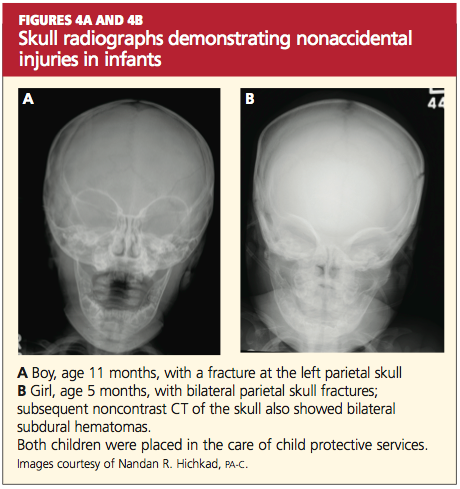
About 5% of sexually abused children contract a sexually transmitted disease.30 Appropriate laboratory tests that can be performed in the office setting include:
- Urinalysis for presence of semen
- Nucleic acid amplification testing (NAAT) for chlamydia and gonorrhea (with positive results requiring that sexual abuse be considered in children beyond neonatal age, according to CDC guidelines33); anorectal and pharyngeal infections with Neisseria gonorrhoeae are commonly found in sexually abused children
- Serologic testing for HIV33
- Urine pregnancy testing in patients of childbearing age.
As these lab specimens are collected, chain of custody must be maintained. Results may be used as evidence in the event of prosecution.
REFERRALS AND FOLLOW-UP
What referrals are made—to clinical specialists, law enforcement, social services, and other agencies—is based on the nature of the abuse, the dynamics of the family involved, the identity of the alleged perpetrator, and the perceived need to ensure the child’s safety. It is the role of these interrelated agencies to confirm the child’s diagnosis, provide for the child’s immediate safety, and ensure links within the systems involved to follow him or her into adulthood, if necessary.
Timely referral to specialized clinicians may spare the child from having to undergo multiple examinations or interviews.33 Although the burden of proof and identification of the perpetrator(s) lie with professional investigators, determination of the cause or possible causes of a child’s injury is often critical to the legal case. Specialists in child abuse, often teamed with a forensically trained interviewer to obtain a specialized history from the child who is verbal, are trained to provide the expert opinions required by the court.
Like referral options, follow-up will depend on the type of abuse that a child has experienced. Medical follow-up, as in the child in the case study, may involve orthopedists, ophthalmologists, or clinicians in other relevant specialties. A psychologist may manage counseling services for the patient and family or foster family.
A SHARED RESPONSIBILITY
Recognition of child abuse is the first step to prevent further victimization. Comprehensive education is critical for health care providers, school nurses, teachers, or anyone who comes into contact with children on a daily basis; increased awareness has been universally identified as a means to prevent child abuse. It is also imperative to educate legislators regarding the extent of this problem and to garner their support for community prevention programs.
For the primary care clinician, it is unfortunate but true that a high level of suspicion for abuse must be maintained; the best available screening tools are the astute clinician’s eyes and brain. During routine annual exams, children should be observed for any indication of abuse, and their interactions with parents should be evaluated as well. Anticipatory guidance during well-child visits has been found to help build parents’ trust in the clinician’s knowledge and compassion, increasing their adherence to effective advice and improving their parenting behavior.40
Public policies and social programs can effectively enhance family functioning, playing a key role in the protection of children.41 Existing research into the causes and effects of child abuse should be used to formulate preventive programs for schools, churches, and local health care providers.
CONCLUSION
No recipe exists for the prevention of child abuse. Health care providers must not hesitate to report suspicion of abuse. This action does not always lead to removal of children from their homes; rather, involving families and children in “the system” can give them access to services of which they might otherwise remain unaware. Home visits, anger management programs, parenting classes, counseling services, and early childhood education can instill and reinforce more positive attitudes and action, for the benefit of all involved.
1. US Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. Child Maltreatment 2009 (2010). www.acf.hhs.gov/programs/cb/pubs/cm09. Accessed February 22, 2012.
2. UNICEF Child Protection Strategy (2008). www .unrol.org/files/CP%20Strategy_English.pdf. Accessed February 22, 2012.
3. World Health Organization. Child maltreatment: Fact Sheet #150, August 2010. www.who .int/mediacentre/factsheets/fs150/en/index.html. Accessed February 22, 2012.
4. World Health Organization. Preventing Child Maltreatment: A Guide to Taking Action and Generating Evidence. http://whqlibdoc.who.int/publi cations/2006/9241594365_eng.pdf. Accessed February 22, 2012.
5. Giardino AP. Child maltreatment: is the glass half full yet? J Forensic Nurs. 2009;5(1):1-4.
6. Barriere D. Child abuse: history, laws and the ASPCA (2005). www.resourcesforattorneys.com/childabuseandtheaspcaarticle.html. Accessed February 22, 2012.
7. The Child Abuse Prevention and Treatment Act, Including Adoption Opportunities and the Abandoned Infants Assistance Act, as Amended by the Keeping Children and Families Safe Act of 2003. www.acf.hhs.gov/programs/cb/laws_policies/cblaws/capta03/capta_manual.pdf. Accessed February 22, 2012.
8. H.R. 14: Keeping Children and Families Safe Act of 2003. www.govtrack.us/congress/bill.xpd ?bill=h108-14&tab=summary. Accessed February 22, 2012.
9. S. 3817: CAPTA Reauthorization Act of 2010. www.govtrack.us/congress/bill.xpd?bill=s
111-3817. Accessed February 22, 2012.
10. National Data Archive on Child Abuse and Neglect. NCANDS State Level Data 2009: National Child Abuse and Neglect Data System. www .ndacan.cornell.edu/cmrlpostings/msg00195.html. Accessed February 22, 2012.
11. Finkelhor D, Jones L, Shattuck A; Crimes Against Children Research Center, University of New Hampshire. Updated trends in child maltreatment, 2009. http://unh.edu/ccrc/pdf/Updated_Trends_in_Child_Maltreatment_2009.pdf. Accessed February 22, 2012.
12. CDC Injury Center: Violence Prevention. Child Maltreatment: Risk and Protective Factors (2011). www.cdc.gov/violenceprevention/childmaltreat ment/riskprotectivefactors.html. Accessed February 22, 2012.
13. Sullivan P, Knutson J. Maltreatment and disabilities: a population-based epidemiological study. Child Abuse Negl. 2000;24(10):1257-1273.
14. Sedlak AJ, Mettenburg J, Basena M, et al. Fourth National Incidence Study of Child Abuse and Neglect (NIS–4): Report to Congress, Executive Summary. January 2010. Washington, DC: US Department of Health and Human Services, Administration for Children and Families.
15. National Clearinghouse on Family Violence, Public Health Agency of Canada. Abuse of children with disabilities (2000). www.phac-aspc
.gc.ca/ncfv-cnivf/pdfs/nfnts-disabl-eng.pdf. Accessed February 22, 2012.
16. Endorm EE. (2011, June 7, 2011). Physical abuse in children: epidemiology and clinical manifestations. www.uptodate.com/contents/physical-abuse-in-children-epidemiology-and-clinical-manifestations?source=search_result&
search=Phsical+abuse+i+children%3A+Epidemiology+and+clinical+manifestations&selectedTi
tle=1~150. Accessed February 22, 2012.
17. Pandya NK, Baldwin K, Kamath AF, et al. Unexplained fractures: child abuse or bone disease? A systematic review. Clin Orthop Relat Res. 2011; 469(3):805-812.
18. Gondim RM, Muñoz DR, Petri V. Child abuse: skin markers and differential diagnosis. An Bras Dermatol. 2011;86(3):527-536.
19. Kemp AM, Dunstan F, Harrison S, et al. Patterns of skeletal fractures in child abuse: systematic review. BMJ. 2008;337:a1518.
20. Worlock P, Stower M, Barbor P. Patterns of fractures in accidental and non-accidental injury in children: a comparative study. Br Med J (Clin Res Ed). 1986;293(6539):100-102.
21. Welsh Child Protection Systematic Review Group. www.core-info.cf.ac.uk. Accessed February 22, 2012.
22. Wardinsky TD. Genetic and congenital defect conditions that mimic child abuse. J Fam Pract. 1995;41(4):377-383.
23. American College of Radiology. ACR appropriateness criteria (2009). www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria/pdf/ExpertPanelonPediatricImaging/Suspected PhysicalAbuseChildDoc9.aspx. Accessed February 22, 2012.
24. Meservy CJ, Towbin R, McLaurin RL, et al. Radiographic characteristics of skull fractures resulting from child abuse. AJR Am J Roentgenol. 1987;149(1):173-175.
25. US Department of Justice, Office of Justice Programs, Office of Juvenile Justice and Delinquency Prevention. Burn Injuries in Child Abuse (2001). www.ncjrs.gov/pdffiles/91190-6.pdf. Accessed February 22, 2012.
26. Lane WG, Dubowitz H. Primary care pediatricians’ experience, comfort and competence in the evaluation and management of child maltreatment: do we need child abuse experts? Child Abuse Negl. 2009;33(2):76-83.
27. Child Welfare Information Gateway, US Department of Health and Human Services, Administration for Children and Families. Recognizing child abuse and neglect: signs and symptoms (2007). www.childwelfare.gov/pubs/factsheets/signs.cfm. Accessed February 22, 2012.
28. Fortin K, Jenny C. Sexual abuse. Pediatr Rev. 2012;33(1):19–32.
29. Keshavarz R, Kawashima R, Low C. Child abuse and neglect presentations to a pediatric emergency department. J Emerg Med. 2002;23(4): 341-345.
30. Kellogg N; American Academy of Pediatrics Committee on Child Abuse and Neglect. The evaluation of sexual abuse in children. Pediatrics. 2005;116(2):506-512.
31. Heger A, Ticson L, Velasquez O, Bernier R. Children referred for possible sexual abuse: medical findings in 2384 children. Child Abuse Negl. 2002;26(6-7):645-659.
32. Kellogg ND, Menard SW, Santos A. Genital anatomy in pregnant adolescents: “normal” does not mean “nothing happened.” Pediatrics. 2004; 113(1):e67-e69.
33. Workowski KA, Berman S; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
34. Oates RK. Overturning the diagnosis of child abuse. Arch Dis Child. 1984;59(7):665-666.
35. Hornor G. Common conditions that mimic findings of sexual abuse. J Pediatr Health Care. 2009;23(5):283-288.
36. Asnes RS. Buttock bruises: Mongolian spot. Pediatrics. 1984;74(2):321.
37. Klusmann A, Lenard HG. Tourniquet syndrome: accident or abuse? Eur J Pediatr. 2004; 163(8):495-498.
38. Merten DF, Carpenter BL. Radiologic imaging of inflicted injury in the child abuse syndrome. Pediatr Clin North Am. 1990;37(4):815-837.
39. Mok JY. Non-accidental injury in children: an update. Injury. 2008;39(9):978-985.
40. Nelson CS, Higman SM, Sia C, et al. Medical homes for at-risk children: parental reports of clinician-parent relationships, anticipatory guidance, and behavior changes. Pediatrics. 2005; 115(1):48-56.
41. Dubowitz H. Prevention of child maltreatment: what is known. Pediatrics. 1989;83(4):570-577.
According to data from the US Department of Health and Human Services, child protection services received more than 3.3 million reports of alleged maltreatment in 2009 that involved about six million children, and about 62% of reports required subsequent action.1 Child abuse is an ever-growing problem that affects children of both genders and in all ages, races, and socioeconomic levels. Few issues generate the concern, anger, and frustration as the abuse or neglect of children.
Primary care providers and emergency department personnel are often the child’s initial point of entry into the health care system. Clinicians who see and treat young patients can play an essential role in the recognition and reporting of child abuse. By frequently reviewing the risk factors for child abuse, its signs and symptoms, and its typical and atypical presentations, clinicians can be prepared to act when appropriate and help break the cycle of child abuse.
LEGAL MANDATES, DEFINITIONS
A relatively new concept, child abuse has been designated as a major public health issue by the United Nations Children’s Fund and the World Health Organization.2-5 In 1874, when it was decided by the American Society for the Prevention of Cruelty to Animals (ASPCA) to include children within the defined animal kingdom, the movement to protect children began in the United States.6
Both federal and state agencies have created definitions for child abuse and neglect. The key federal legislation to address child abuse and neglect, the Child Abuse Prevention and Treatment Act (CAPTA), as Amended by the Keeping Children and Families Safe Act of 2003,7,8 defines child abuse and neglect as “any recent act or failure to act on the part of a parent or caretaker, which results in death, serious physical or emotional harm, sexual abuse or exploitation, or an act or failure to act which presents an imminent risk of serious harm.”7 Although ongoing revisions of the CAPTA legislation (the most recent “reauthorization” published in 20109) become increasingly inclusive of both children’s and families’ concerns, this definition has remained consistent.
This is not the case with state definitions, however. Because these vary, it can be difficult to compare rates of reported maltreatment from state to state. Also varying among states, and among counties within some states, are recommendations for substantiation of child maltreatment. The validity of the reported data can be impaired by a lack of coordination or cooperation among different agencies and jurisdictions.
IDENTIFYING THE VICTIMS
The spectrum of child abuse includes multiple forms, which often overlap (see Table 11,9,10), and can almost always have the potential for death.11 According to findings from the National Child Abuse and Neglect Data System, despite worsening economic conditions in 2009, the child maltreatment data compiled that year showed an overall 2% decline in cases of substantiated maltreatment from the previous year.1,11
However, during that same period, child maltreatment–associated fatalities rose 3%, from 1,628 deaths in 2008 to 1,671 in 2009,1 suggesting an increase in the severity of abuse. The emotional, social, and financial ramifications of child abuse affect the local and national community, as well as each child and each family.
Children younger than 1 year, the most vulnerable to maltreatment, represent the largest proportion of substantiated abuse. One-third of all children reported as abused in 2009 were younger than 4, and children between ages 4 and 7 represented one-fifth of cases.1 Figure 1a1 categorizes the incidence of child abuse by age level, and Figure 1b1 by ethnicity/race.
Risk Factors
A number of factors, though not necessarily direct causes, have been shown to increase children’s risk for abuse or neglect. These include personal characteristics of the child and parent, and family- or environment-related factors1,12 (see Table 2,1). It is often combinations of risk factors (eg, characteristics of a parent or caregiver in addition to a specific social environment) that are most likely to increase the likelihood of abuse.
Children with special needs (physical disabilities or chronic illness, neurologic impairment, mental health issues) that increase the caregiver’s burden are at increased risk for abuse.1,12 Children with behavior disorders and mental retardation have been found at increased risk for various forms of abuse—neglect and physical or sexual maltreatment13—whereas children with speech or language disabilities are at increased risk for neglect (whether physical, emotional, or even educational14).
Children with physical limitations who experience physical abuse are reportedly subject to more serious injury than their healthier counterparts.14 Their inability to see, hear, move, or communicate, or to dress or bathe themselves independently may make them susceptible to rough, careless, or intrusive personal care, or neglect of their personal needs. Low self-esteem, whatever its cause, also appears to be a significant risk factor for intentional abuse.15
It is often the case that children with disabilities do not report abuse because they are unable to recognize an act as abusive. Depending on the severity of a child’s disability and his or her ordinarily atypical presentation, the abuse may never be discovered.15
Poverty appears to be a contributing factor. Children from families of low socioeconomic status are at least three times as likely as other children to be abused and seven times as likely to experience neglect.14 It has been conjectured that these children are more likely to have contact with social workers, law enforcement officers, and representatives of other agencies with an increased awareness of the manifestations of child abuse. Abuse within affluent families may be underreported, as such families have the wherewithal to protect themselves from detection and prosecution.16
PRESENTATION
There is no “gold standard” for making a confirmed diagnosis of child abuse,17 and no “typical” presentation of an abused child (see case study). Dress that is inappropriate for the season and consistently poor hygiene are indicative of neglect. Symptoms of abuse may be overt or silent, and signs of physical abuse are often hidden beneath clothing. Children who are physically abused often explain their injuries by saying “I fell,” or may even respond to questioning by saying, “I don’t know.” The parent or caregiver may attribute bruises or even broken bones to falls or rough play with other children. Bruises, the most common visible form of child abuse,18 may suggest the nature of injury by their location, patterns, and various stages of healing.
Fractures are the second most common presenting symptom among children experiencing physical abuse.17 According to findings from a meta-analysis by Kemp et al,19 determining whether fractures have occurred accidentally depends on three factors:
Age. Among children younger than 1 year, 25% to 56% of fractures are attributable to intentional harm. In one landmark study, one fracture in nine was found to have resulted from abuse, among children younger than 18 months—compared with one in 205 among children ages 19 months to 5 years.19,20
Site. In cases not involving a motor vehicle accident or other traumatic event, it has been determined in ongoing systematic reviews by Welsh researchers that rib fractures have a 71% probability of being inflicted, followed by humeral fractures (about 50% probability), then by femoral fractures or skull fractures (about 33% probability).19,21
Fracture type. Fracture types suggestive of abuse differ by site. Among humeral fractures, for example, a midshaft fracture is more likely to have been inflicted, whereas a supracondylar fracture is more likely the result of accidental injury. Both parietal and linear skull fractures may occur accidentally or through physical abuse.19 Epiphyseal-metaphyseal fractures, vertebral compression fractures, and lateral clavicle fractures have been associated with child abuse.22,23 Multiple or bilateral fractures have an increased association with abuse.19,20,24
Injuries that are inconsistent with the given history should raise red flags, and they should be carefully investigated, with findings documented. Minor falls cause minor injuries, not potentially life-threatening ones.
As with fractures, burns may have specific features that help the clinician distinguish between accidental and intentional. Uniform depth, well-defined edges, and multiple lesions are more likely to indicate nonaccidental contact burns, particularly when found in “protected” sites (eg, perineal and gluteal areas).18 Accidental cigarette burns are usually ovoid or irregular in shape and superficial, while those intentionally inflicted are round, deep, and well-demarcated and are often grouped on the hands, feet, or face.18,25 Burns on the chest, upper limbs, and palms of the hands are likely to be accidental; the face, the backs of the hands, the lower stomach, back, buttocks, legs, and feet are often the target of intentional burns.18,26
HISTORY
A key factor in suspected abuse is the child’s history. During history taking, clinicians should be alert to the evidence-based indicators of potential child abuse, as shown in Table 327-29. Not every child who exhibits these characteristics is an abused child, nor will every abused child exhibit any or all of these characteristics. Through artful, careful history taking and astute observation of the child, the clinician is usually able to distinguish between the heightened anxiety that may occur in any child during the history-taking process and the demeanor of a child who may have been coerced or threatened to maintain secrecy.
Engaging the child in a reassuring manner, the clinician can use a conversational style of questioning, such as, “Tell me how you got that bruise on your arm,” rather than a direct question: “Did [name] hit you on the arm with [his/her] fist?”
An observation of unusually sexualized behaviors or a report of excessive masturbation is more likely to be associated with sexual abuse than are genital findings (which are infrequently found).
Physical Examination
When a child presents with an acute injury or bruising is detected and the clinician’s findings are inconsistent with the given history, suspicion should be raised. The injuries inflicted by physical abuse are often hidden beneath the child’s clothing (specifically, underwear); for this reason, it is important to have children undressed during a physical exam.
The routine physical exam of an abused child may reveal defensive bruising or other wounds, trauma to the mouth, breasts, buttocks, genitalia, or anus, with possible bleeding or discharge. More commonly, the physical exam findings are normal—as is true in the majority of examinations for sexual abuse.30 In one large study, abnormal findings (eg, recent or healed genital injuries; presence of a sexually transmitted disease) were found in only about 4% of children who had been referred for an examination for suspected sexual abuse.18,31 Clearly, an appearance of “normal” does not mean “nothing happened.”32
According to CDC guidelines,33 investigation of suspected sexual abuse (for example, when a genital herpes infection is detected) should be conducted by appropriately trained, experienced clinicians—ideally, by a pediatric subspecialist in child abuse. Although the primary care clinician may examine the child briefly for visible bruises or wounds, it is essential for a specialist to perform the genital exam.33 Use of mild sedation with close monitoring may be advisable during the genital examination.30
Mimics of Child Abuse
Several conditions, including metabolic, genetic, and congenital disorders, have been reported to mimic the physical manifestations of child abuse and neglect17,22,34 (see Table 4,17,18,22,25,33-35). While health care professionals are legally and ethically bound to report abuse, conditions that may mimic abuse must be ruled out first, to avoid the mistaken removal of children from loving homes.
Mongolian spots, for example (see Figure 2), are frequently mistaken for bruising and reported to authorities, causing unnecessary disruption for both family and child.34,36 They typically appear as macular blue-gray pigmentation of the skin, usually on the sacrum. Resulting from entrapment of melanocytes in the dermis during fetal development, these “spots” may be present at birth or may appear during the neonatal period. Mongolian spots are most common in Native American, African-American, Asian, and Hispanic patients, are benign, and often disappear by age 4.
Other cutaneous manifestations that can mimic an intentional injury include molluscum contagiosum, a viral infection manifesting as a rash that may mimic the genital warts of human papillomavirus, and erythematous, edematous, and/or vesiculobullous lesions18,35 (see Figure 3). Severe diaper rash, photodermatitis, and certain allergic reactions can mimic intentional burns.25
Often mistaken for a nonaccidental injury is hair tourniquet syndrome—the circumferential strangulation of one or more appendages (eg, finger, toe, penis) by human hair or fibers.34 This uncommon condition, usually unintentional and of unknown incidence, can represent a surgical emergency; failure to recognize it in a timely fashion may lead to ischemia or necrosis, necessitating amputation of the affected appendage.37
Metabolic bone disease, such as osteogenesis imperfecta, can sometimes explain frequent fractures.17
MAKING THE DIAGNOSIS
In the primary care setting, the detection of child abuse is unexpected. However, it is often here that children are initially seen for an injury, or suspicions are raised during a routine physical.30 In the case of spontaneous disclosure of abuse, explicit, word-for-word documentation is required. The child, who may feel guilty, embarrassed, or ashamed, must be reassured that he or she is not at fault.
Either a child abuse specialist or the primary care clinician bases the ultimate diagnosis of child abuse on findings from the history and physical examination. These findings will direct the clinician’s decision to order diagnostic laboratory studies and/or diagnostic x-rays.
Diagnostic Studies
Depending on the child’s age and the type of presentation, recommended imaging studies include an x-ray skeletal survey of a child younger than 2 (see “Skeletal Survey Reading of 5-Month-Old Boy,”) or an older child with thoracoabdominal injuries that the history does not explain satisfactorily.23 For children ages 2 to 5, focused plain films of the area of suspected injury (eg, skull, chest, extremities) are considered appropriate.23,38
Noncontrast head CT may be appropriate in the presence of skull fractures, (as in Figures 4a and 4b) intracranial injuries, seizures, or other neurologic signs and symptoms (followed by MRI if further assessment is needed). CT with contrast may be considered when x-rays reveal certain abnormalities, the child is considered at high risk for abuse (for example, when inconsistencies are found in the history), or when soft-tissue injuries are suspected.23,39
About 5% of sexually abused children contract a sexually transmitted disease.30 Appropriate laboratory tests that can be performed in the office setting include:
- Urinalysis for presence of semen
- Nucleic acid amplification testing (NAAT) for chlamydia and gonorrhea (with positive results requiring that sexual abuse be considered in children beyond neonatal age, according to CDC guidelines33); anorectal and pharyngeal infections with Neisseria gonorrhoeae are commonly found in sexually abused children
- Serologic testing for HIV33
- Urine pregnancy testing in patients of childbearing age.
As these lab specimens are collected, chain of custody must be maintained. Results may be used as evidence in the event of prosecution.
REFERRALS AND FOLLOW-UP
What referrals are made—to clinical specialists, law enforcement, social services, and other agencies—is based on the nature of the abuse, the dynamics of the family involved, the identity of the alleged perpetrator, and the perceived need to ensure the child’s safety. It is the role of these interrelated agencies to confirm the child’s diagnosis, provide for the child’s immediate safety, and ensure links within the systems involved to follow him or her into adulthood, if necessary.
Timely referral to specialized clinicians may spare the child from having to undergo multiple examinations or interviews.33 Although the burden of proof and identification of the perpetrator(s) lie with professional investigators, determination of the cause or possible causes of a child’s injury is often critical to the legal case. Specialists in child abuse, often teamed with a forensically trained interviewer to obtain a specialized history from the child who is verbal, are trained to provide the expert opinions required by the court.
Like referral options, follow-up will depend on the type of abuse that a child has experienced. Medical follow-up, as in the child in the case study, may involve orthopedists, ophthalmologists, or clinicians in other relevant specialties. A psychologist may manage counseling services for the patient and family or foster family.
A SHARED RESPONSIBILITY
Recognition of child abuse is the first step to prevent further victimization. Comprehensive education is critical for health care providers, school nurses, teachers, or anyone who comes into contact with children on a daily basis; increased awareness has been universally identified as a means to prevent child abuse. It is also imperative to educate legislators regarding the extent of this problem and to garner their support for community prevention programs.
For the primary care clinician, it is unfortunate but true that a high level of suspicion for abuse must be maintained; the best available screening tools are the astute clinician’s eyes and brain. During routine annual exams, children should be observed for any indication of abuse, and their interactions with parents should be evaluated as well. Anticipatory guidance during well-child visits has been found to help build parents’ trust in the clinician’s knowledge and compassion, increasing their adherence to effective advice and improving their parenting behavior.40
Public policies and social programs can effectively enhance family functioning, playing a key role in the protection of children.41 Existing research into the causes and effects of child abuse should be used to formulate preventive programs for schools, churches, and local health care providers.
CONCLUSION
No recipe exists for the prevention of child abuse. Health care providers must not hesitate to report suspicion of abuse. This action does not always lead to removal of children from their homes; rather, involving families and children in “the system” can give them access to services of which they might otherwise remain unaware. Home visits, anger management programs, parenting classes, counseling services, and early childhood education can instill and reinforce more positive attitudes and action, for the benefit of all involved.
According to data from the US Department of Health and Human Services, child protection services received more than 3.3 million reports of alleged maltreatment in 2009 that involved about six million children, and about 62% of reports required subsequent action.1 Child abuse is an ever-growing problem that affects children of both genders and in all ages, races, and socioeconomic levels. Few issues generate the concern, anger, and frustration as the abuse or neglect of children.
Primary care providers and emergency department personnel are often the child’s initial point of entry into the health care system. Clinicians who see and treat young patients can play an essential role in the recognition and reporting of child abuse. By frequently reviewing the risk factors for child abuse, its signs and symptoms, and its typical and atypical presentations, clinicians can be prepared to act when appropriate and help break the cycle of child abuse.
LEGAL MANDATES, DEFINITIONS
A relatively new concept, child abuse has been designated as a major public health issue by the United Nations Children’s Fund and the World Health Organization.2-5 In 1874, when it was decided by the American Society for the Prevention of Cruelty to Animals (ASPCA) to include children within the defined animal kingdom, the movement to protect children began in the United States.6
Both federal and state agencies have created definitions for child abuse and neglect. The key federal legislation to address child abuse and neglect, the Child Abuse Prevention and Treatment Act (CAPTA), as Amended by the Keeping Children and Families Safe Act of 2003,7,8 defines child abuse and neglect as “any recent act or failure to act on the part of a parent or caretaker, which results in death, serious physical or emotional harm, sexual abuse or exploitation, or an act or failure to act which presents an imminent risk of serious harm.”7 Although ongoing revisions of the CAPTA legislation (the most recent “reauthorization” published in 20109) become increasingly inclusive of both children’s and families’ concerns, this definition has remained consistent.
This is not the case with state definitions, however. Because these vary, it can be difficult to compare rates of reported maltreatment from state to state. Also varying among states, and among counties within some states, are recommendations for substantiation of child maltreatment. The validity of the reported data can be impaired by a lack of coordination or cooperation among different agencies and jurisdictions.
IDENTIFYING THE VICTIMS
The spectrum of child abuse includes multiple forms, which often overlap (see Table 11,9,10), and can almost always have the potential for death.11 According to findings from the National Child Abuse and Neglect Data System, despite worsening economic conditions in 2009, the child maltreatment data compiled that year showed an overall 2% decline in cases of substantiated maltreatment from the previous year.1,11
However, during that same period, child maltreatment–associated fatalities rose 3%, from 1,628 deaths in 2008 to 1,671 in 2009,1 suggesting an increase in the severity of abuse. The emotional, social, and financial ramifications of child abuse affect the local and national community, as well as each child and each family.
Children younger than 1 year, the most vulnerable to maltreatment, represent the largest proportion of substantiated abuse. One-third of all children reported as abused in 2009 were younger than 4, and children between ages 4 and 7 represented one-fifth of cases.1 Figure 1a1 categorizes the incidence of child abuse by age level, and Figure 1b1 by ethnicity/race.
Risk Factors
A number of factors, though not necessarily direct causes, have been shown to increase children’s risk for abuse or neglect. These include personal characteristics of the child and parent, and family- or environment-related factors1,12 (see Table 2,1). It is often combinations of risk factors (eg, characteristics of a parent or caregiver in addition to a specific social environment) that are most likely to increase the likelihood of abuse.
Children with special needs (physical disabilities or chronic illness, neurologic impairment, mental health issues) that increase the caregiver’s burden are at increased risk for abuse.1,12 Children with behavior disorders and mental retardation have been found at increased risk for various forms of abuse—neglect and physical or sexual maltreatment13—whereas children with speech or language disabilities are at increased risk for neglect (whether physical, emotional, or even educational14).
Children with physical limitations who experience physical abuse are reportedly subject to more serious injury than their healthier counterparts.14 Their inability to see, hear, move, or communicate, or to dress or bathe themselves independently may make them susceptible to rough, careless, or intrusive personal care, or neglect of their personal needs. Low self-esteem, whatever its cause, also appears to be a significant risk factor for intentional abuse.15
It is often the case that children with disabilities do not report abuse because they are unable to recognize an act as abusive. Depending on the severity of a child’s disability and his or her ordinarily atypical presentation, the abuse may never be discovered.15
Poverty appears to be a contributing factor. Children from families of low socioeconomic status are at least three times as likely as other children to be abused and seven times as likely to experience neglect.14 It has been conjectured that these children are more likely to have contact with social workers, law enforcement officers, and representatives of other agencies with an increased awareness of the manifestations of child abuse. Abuse within affluent families may be underreported, as such families have the wherewithal to protect themselves from detection and prosecution.16
PRESENTATION
There is no “gold standard” for making a confirmed diagnosis of child abuse,17 and no “typical” presentation of an abused child (see case study). Dress that is inappropriate for the season and consistently poor hygiene are indicative of neglect. Symptoms of abuse may be overt or silent, and signs of physical abuse are often hidden beneath clothing. Children who are physically abused often explain their injuries by saying “I fell,” or may even respond to questioning by saying, “I don’t know.” The parent or caregiver may attribute bruises or even broken bones to falls or rough play with other children. Bruises, the most common visible form of child abuse,18 may suggest the nature of injury by their location, patterns, and various stages of healing.
Fractures are the second most common presenting symptom among children experiencing physical abuse.17 According to findings from a meta-analysis by Kemp et al,19 determining whether fractures have occurred accidentally depends on three factors:
Age. Among children younger than 1 year, 25% to 56% of fractures are attributable to intentional harm. In one landmark study, one fracture in nine was found to have resulted from abuse, among children younger than 18 months—compared with one in 205 among children ages 19 months to 5 years.19,20
Site. In cases not involving a motor vehicle accident or other traumatic event, it has been determined in ongoing systematic reviews by Welsh researchers that rib fractures have a 71% probability of being inflicted, followed by humeral fractures (about 50% probability), then by femoral fractures or skull fractures (about 33% probability).19,21
Fracture type. Fracture types suggestive of abuse differ by site. Among humeral fractures, for example, a midshaft fracture is more likely to have been inflicted, whereas a supracondylar fracture is more likely the result of accidental injury. Both parietal and linear skull fractures may occur accidentally or through physical abuse.19 Epiphyseal-metaphyseal fractures, vertebral compression fractures, and lateral clavicle fractures have been associated with child abuse.22,23 Multiple or bilateral fractures have an increased association with abuse.19,20,24
Injuries that are inconsistent with the given history should raise red flags, and they should be carefully investigated, with findings documented. Minor falls cause minor injuries, not potentially life-threatening ones.
As with fractures, burns may have specific features that help the clinician distinguish between accidental and intentional. Uniform depth, well-defined edges, and multiple lesions are more likely to indicate nonaccidental contact burns, particularly when found in “protected” sites (eg, perineal and gluteal areas).18 Accidental cigarette burns are usually ovoid or irregular in shape and superficial, while those intentionally inflicted are round, deep, and well-demarcated and are often grouped on the hands, feet, or face.18,25 Burns on the chest, upper limbs, and palms of the hands are likely to be accidental; the face, the backs of the hands, the lower stomach, back, buttocks, legs, and feet are often the target of intentional burns.18,26
HISTORY
A key factor in suspected abuse is the child’s history. During history taking, clinicians should be alert to the evidence-based indicators of potential child abuse, as shown in Table 327-29. Not every child who exhibits these characteristics is an abused child, nor will every abused child exhibit any or all of these characteristics. Through artful, careful history taking and astute observation of the child, the clinician is usually able to distinguish between the heightened anxiety that may occur in any child during the history-taking process and the demeanor of a child who may have been coerced or threatened to maintain secrecy.
Engaging the child in a reassuring manner, the clinician can use a conversational style of questioning, such as, “Tell me how you got that bruise on your arm,” rather than a direct question: “Did [name] hit you on the arm with [his/her] fist?”
An observation of unusually sexualized behaviors or a report of excessive masturbation is more likely to be associated with sexual abuse than are genital findings (which are infrequently found).
Physical Examination
When a child presents with an acute injury or bruising is detected and the clinician’s findings are inconsistent with the given history, suspicion should be raised. The injuries inflicted by physical abuse are often hidden beneath the child’s clothing (specifically, underwear); for this reason, it is important to have children undressed during a physical exam.
The routine physical exam of an abused child may reveal defensive bruising or other wounds, trauma to the mouth, breasts, buttocks, genitalia, or anus, with possible bleeding or discharge. More commonly, the physical exam findings are normal—as is true in the majority of examinations for sexual abuse.30 In one large study, abnormal findings (eg, recent or healed genital injuries; presence of a sexually transmitted disease) were found in only about 4% of children who had been referred for an examination for suspected sexual abuse.18,31 Clearly, an appearance of “normal” does not mean “nothing happened.”32
According to CDC guidelines,33 investigation of suspected sexual abuse (for example, when a genital herpes infection is detected) should be conducted by appropriately trained, experienced clinicians—ideally, by a pediatric subspecialist in child abuse. Although the primary care clinician may examine the child briefly for visible bruises or wounds, it is essential for a specialist to perform the genital exam.33 Use of mild sedation with close monitoring may be advisable during the genital examination.30
Mimics of Child Abuse
Several conditions, including metabolic, genetic, and congenital disorders, have been reported to mimic the physical manifestations of child abuse and neglect17,22,34 (see Table 4,17,18,22,25,33-35). While health care professionals are legally and ethically bound to report abuse, conditions that may mimic abuse must be ruled out first, to avoid the mistaken removal of children from loving homes.
Mongolian spots, for example (see Figure 2), are frequently mistaken for bruising and reported to authorities, causing unnecessary disruption for both family and child.34,36 They typically appear as macular blue-gray pigmentation of the skin, usually on the sacrum. Resulting from entrapment of melanocytes in the dermis during fetal development, these “spots” may be present at birth or may appear during the neonatal period. Mongolian spots are most common in Native American, African-American, Asian, and Hispanic patients, are benign, and often disappear by age 4.
Other cutaneous manifestations that can mimic an intentional injury include molluscum contagiosum, a viral infection manifesting as a rash that may mimic the genital warts of human papillomavirus, and erythematous, edematous, and/or vesiculobullous lesions18,35 (see Figure 3). Severe diaper rash, photodermatitis, and certain allergic reactions can mimic intentional burns.25
Often mistaken for a nonaccidental injury is hair tourniquet syndrome—the circumferential strangulation of one or more appendages (eg, finger, toe, penis) by human hair or fibers.34 This uncommon condition, usually unintentional and of unknown incidence, can represent a surgical emergency; failure to recognize it in a timely fashion may lead to ischemia or necrosis, necessitating amputation of the affected appendage.37
Metabolic bone disease, such as osteogenesis imperfecta, can sometimes explain frequent fractures.17
MAKING THE DIAGNOSIS
In the primary care setting, the detection of child abuse is unexpected. However, it is often here that children are initially seen for an injury, or suspicions are raised during a routine physical.30 In the case of spontaneous disclosure of abuse, explicit, word-for-word documentation is required. The child, who may feel guilty, embarrassed, or ashamed, must be reassured that he or she is not at fault.
Either a child abuse specialist or the primary care clinician bases the ultimate diagnosis of child abuse on findings from the history and physical examination. These findings will direct the clinician’s decision to order diagnostic laboratory studies and/or diagnostic x-rays.
Diagnostic Studies
Depending on the child’s age and the type of presentation, recommended imaging studies include an x-ray skeletal survey of a child younger than 2 (see “Skeletal Survey Reading of 5-Month-Old Boy,”) or an older child with thoracoabdominal injuries that the history does not explain satisfactorily.23 For children ages 2 to 5, focused plain films of the area of suspected injury (eg, skull, chest, extremities) are considered appropriate.23,38
Noncontrast head CT may be appropriate in the presence of skull fractures, (as in Figures 4a and 4b) intracranial injuries, seizures, or other neurologic signs and symptoms (followed by MRI if further assessment is needed). CT with contrast may be considered when x-rays reveal certain abnormalities, the child is considered at high risk for abuse (for example, when inconsistencies are found in the history), or when soft-tissue injuries are suspected.23,39
About 5% of sexually abused children contract a sexually transmitted disease.30 Appropriate laboratory tests that can be performed in the office setting include:
- Urinalysis for presence of semen
- Nucleic acid amplification testing (NAAT) for chlamydia and gonorrhea (with positive results requiring that sexual abuse be considered in children beyond neonatal age, according to CDC guidelines33); anorectal and pharyngeal infections with Neisseria gonorrhoeae are commonly found in sexually abused children
- Serologic testing for HIV33
- Urine pregnancy testing in patients of childbearing age.
As these lab specimens are collected, chain of custody must be maintained. Results may be used as evidence in the event of prosecution.
REFERRALS AND FOLLOW-UP
What referrals are made—to clinical specialists, law enforcement, social services, and other agencies—is based on the nature of the abuse, the dynamics of the family involved, the identity of the alleged perpetrator, and the perceived need to ensure the child’s safety. It is the role of these interrelated agencies to confirm the child’s diagnosis, provide for the child’s immediate safety, and ensure links within the systems involved to follow him or her into adulthood, if necessary.
Timely referral to specialized clinicians may spare the child from having to undergo multiple examinations or interviews.33 Although the burden of proof and identification of the perpetrator(s) lie with professional investigators, determination of the cause or possible causes of a child’s injury is often critical to the legal case. Specialists in child abuse, often teamed with a forensically trained interviewer to obtain a specialized history from the child who is verbal, are trained to provide the expert opinions required by the court.
Like referral options, follow-up will depend on the type of abuse that a child has experienced. Medical follow-up, as in the child in the case study, may involve orthopedists, ophthalmologists, or clinicians in other relevant specialties. A psychologist may manage counseling services for the patient and family or foster family.
A SHARED RESPONSIBILITY
Recognition of child abuse is the first step to prevent further victimization. Comprehensive education is critical for health care providers, school nurses, teachers, or anyone who comes into contact with children on a daily basis; increased awareness has been universally identified as a means to prevent child abuse. It is also imperative to educate legislators regarding the extent of this problem and to garner their support for community prevention programs.
For the primary care clinician, it is unfortunate but true that a high level of suspicion for abuse must be maintained; the best available screening tools are the astute clinician’s eyes and brain. During routine annual exams, children should be observed for any indication of abuse, and their interactions with parents should be evaluated as well. Anticipatory guidance during well-child visits has been found to help build parents’ trust in the clinician’s knowledge and compassion, increasing their adherence to effective advice and improving their parenting behavior.40
Public policies and social programs can effectively enhance family functioning, playing a key role in the protection of children.41 Existing research into the causes and effects of child abuse should be used to formulate preventive programs for schools, churches, and local health care providers.
CONCLUSION
No recipe exists for the prevention of child abuse. Health care providers must not hesitate to report suspicion of abuse. This action does not always lead to removal of children from their homes; rather, involving families and children in “the system” can give them access to services of which they might otherwise remain unaware. Home visits, anger management programs, parenting classes, counseling services, and early childhood education can instill and reinforce more positive attitudes and action, for the benefit of all involved.
1. US Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. Child Maltreatment 2009 (2010). www.acf.hhs.gov/programs/cb/pubs/cm09. Accessed February 22, 2012.
2. UNICEF Child Protection Strategy (2008). www .unrol.org/files/CP%20Strategy_English.pdf. Accessed February 22, 2012.
3. World Health Organization. Child maltreatment: Fact Sheet #150, August 2010. www.who .int/mediacentre/factsheets/fs150/en/index.html. Accessed February 22, 2012.
4. World Health Organization. Preventing Child Maltreatment: A Guide to Taking Action and Generating Evidence. http://whqlibdoc.who.int/publi cations/2006/9241594365_eng.pdf. Accessed February 22, 2012.
5. Giardino AP. Child maltreatment: is the glass half full yet? J Forensic Nurs. 2009;5(1):1-4.
6. Barriere D. Child abuse: history, laws and the ASPCA (2005). www.resourcesforattorneys.com/childabuseandtheaspcaarticle.html. Accessed February 22, 2012.
7. The Child Abuse Prevention and Treatment Act, Including Adoption Opportunities and the Abandoned Infants Assistance Act, as Amended by the Keeping Children and Families Safe Act of 2003. www.acf.hhs.gov/programs/cb/laws_policies/cblaws/capta03/capta_manual.pdf. Accessed February 22, 2012.
8. H.R. 14: Keeping Children and Families Safe Act of 2003. www.govtrack.us/congress/bill.xpd ?bill=h108-14&tab=summary. Accessed February 22, 2012.
9. S. 3817: CAPTA Reauthorization Act of 2010. www.govtrack.us/congress/bill.xpd?bill=s
111-3817. Accessed February 22, 2012.
10. National Data Archive on Child Abuse and Neglect. NCANDS State Level Data 2009: National Child Abuse and Neglect Data System. www .ndacan.cornell.edu/cmrlpostings/msg00195.html. Accessed February 22, 2012.
11. Finkelhor D, Jones L, Shattuck A; Crimes Against Children Research Center, University of New Hampshire. Updated trends in child maltreatment, 2009. http://unh.edu/ccrc/pdf/Updated_Trends_in_Child_Maltreatment_2009.pdf. Accessed February 22, 2012.
12. CDC Injury Center: Violence Prevention. Child Maltreatment: Risk and Protective Factors (2011). www.cdc.gov/violenceprevention/childmaltreat ment/riskprotectivefactors.html. Accessed February 22, 2012.
13. Sullivan P, Knutson J. Maltreatment and disabilities: a population-based epidemiological study. Child Abuse Negl. 2000;24(10):1257-1273.
14. Sedlak AJ, Mettenburg J, Basena M, et al. Fourth National Incidence Study of Child Abuse and Neglect (NIS–4): Report to Congress, Executive Summary. January 2010. Washington, DC: US Department of Health and Human Services, Administration for Children and Families.
15. National Clearinghouse on Family Violence, Public Health Agency of Canada. Abuse of children with disabilities (2000). www.phac-aspc
.gc.ca/ncfv-cnivf/pdfs/nfnts-disabl-eng.pdf. Accessed February 22, 2012.
16. Endorm EE. (2011, June 7, 2011). Physical abuse in children: epidemiology and clinical manifestations. www.uptodate.com/contents/physical-abuse-in-children-epidemiology-and-clinical-manifestations?source=search_result&
search=Phsical+abuse+i+children%3A+Epidemiology+and+clinical+manifestations&selectedTi
tle=1~150. Accessed February 22, 2012.
17. Pandya NK, Baldwin K, Kamath AF, et al. Unexplained fractures: child abuse or bone disease? A systematic review. Clin Orthop Relat Res. 2011; 469(3):805-812.
18. Gondim RM, Muñoz DR, Petri V. Child abuse: skin markers and differential diagnosis. An Bras Dermatol. 2011;86(3):527-536.
19. Kemp AM, Dunstan F, Harrison S, et al. Patterns of skeletal fractures in child abuse: systematic review. BMJ. 2008;337:a1518.
20. Worlock P, Stower M, Barbor P. Patterns of fractures in accidental and non-accidental injury in children: a comparative study. Br Med J (Clin Res Ed). 1986;293(6539):100-102.
21. Welsh Child Protection Systematic Review Group. www.core-info.cf.ac.uk. Accessed February 22, 2012.
22. Wardinsky TD. Genetic and congenital defect conditions that mimic child abuse. J Fam Pract. 1995;41(4):377-383.
23. American College of Radiology. ACR appropriateness criteria (2009). www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria/pdf/ExpertPanelonPediatricImaging/Suspected PhysicalAbuseChildDoc9.aspx. Accessed February 22, 2012.
24. Meservy CJ, Towbin R, McLaurin RL, et al. Radiographic characteristics of skull fractures resulting from child abuse. AJR Am J Roentgenol. 1987;149(1):173-175.
25. US Department of Justice, Office of Justice Programs, Office of Juvenile Justice and Delinquency Prevention. Burn Injuries in Child Abuse (2001). www.ncjrs.gov/pdffiles/91190-6.pdf. Accessed February 22, 2012.
26. Lane WG, Dubowitz H. Primary care pediatricians’ experience, comfort and competence in the evaluation and management of child maltreatment: do we need child abuse experts? Child Abuse Negl. 2009;33(2):76-83.
27. Child Welfare Information Gateway, US Department of Health and Human Services, Administration for Children and Families. Recognizing child abuse and neglect: signs and symptoms (2007). www.childwelfare.gov/pubs/factsheets/signs.cfm. Accessed February 22, 2012.
28. Fortin K, Jenny C. Sexual abuse. Pediatr Rev. 2012;33(1):19–32.
29. Keshavarz R, Kawashima R, Low C. Child abuse and neglect presentations to a pediatric emergency department. J Emerg Med. 2002;23(4): 341-345.
30. Kellogg N; American Academy of Pediatrics Committee on Child Abuse and Neglect. The evaluation of sexual abuse in children. Pediatrics. 2005;116(2):506-512.
31. Heger A, Ticson L, Velasquez O, Bernier R. Children referred for possible sexual abuse: medical findings in 2384 children. Child Abuse Negl. 2002;26(6-7):645-659.
32. Kellogg ND, Menard SW, Santos A. Genital anatomy in pregnant adolescents: “normal” does not mean “nothing happened.” Pediatrics. 2004; 113(1):e67-e69.
33. Workowski KA, Berman S; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
34. Oates RK. Overturning the diagnosis of child abuse. Arch Dis Child. 1984;59(7):665-666.
35. Hornor G. Common conditions that mimic findings of sexual abuse. J Pediatr Health Care. 2009;23(5):283-288.
36. Asnes RS. Buttock bruises: Mongolian spot. Pediatrics. 1984;74(2):321.
37. Klusmann A, Lenard HG. Tourniquet syndrome: accident or abuse? Eur J Pediatr. 2004; 163(8):495-498.
38. Merten DF, Carpenter BL. Radiologic imaging of inflicted injury in the child abuse syndrome. Pediatr Clin North Am. 1990;37(4):815-837.
39. Mok JY. Non-accidental injury in children: an update. Injury. 2008;39(9):978-985.
40. Nelson CS, Higman SM, Sia C, et al. Medical homes for at-risk children: parental reports of clinician-parent relationships, anticipatory guidance, and behavior changes. Pediatrics. 2005; 115(1):48-56.
41. Dubowitz H. Prevention of child maltreatment: what is known. Pediatrics. 1989;83(4):570-577.
1. US Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. Child Maltreatment 2009 (2010). www.acf.hhs.gov/programs/cb/pubs/cm09. Accessed February 22, 2012.
2. UNICEF Child Protection Strategy (2008). www .unrol.org/files/CP%20Strategy_English.pdf. Accessed February 22, 2012.
3. World Health Organization. Child maltreatment: Fact Sheet #150, August 2010. www.who .int/mediacentre/factsheets/fs150/en/index.html. Accessed February 22, 2012.
4. World Health Organization. Preventing Child Maltreatment: A Guide to Taking Action and Generating Evidence. http://whqlibdoc.who.int/publi cations/2006/9241594365_eng.pdf. Accessed February 22, 2012.
5. Giardino AP. Child maltreatment: is the glass half full yet? J Forensic Nurs. 2009;5(1):1-4.
6. Barriere D. Child abuse: history, laws and the ASPCA (2005). www.resourcesforattorneys.com/childabuseandtheaspcaarticle.html. Accessed February 22, 2012.
7. The Child Abuse Prevention and Treatment Act, Including Adoption Opportunities and the Abandoned Infants Assistance Act, as Amended by the Keeping Children and Families Safe Act of 2003. www.acf.hhs.gov/programs/cb/laws_policies/cblaws/capta03/capta_manual.pdf. Accessed February 22, 2012.
8. H.R. 14: Keeping Children and Families Safe Act of 2003. www.govtrack.us/congress/bill.xpd ?bill=h108-14&tab=summary. Accessed February 22, 2012.
9. S. 3817: CAPTA Reauthorization Act of 2010. www.govtrack.us/congress/bill.xpd?bill=s
111-3817. Accessed February 22, 2012.
10. National Data Archive on Child Abuse and Neglect. NCANDS State Level Data 2009: National Child Abuse and Neglect Data System. www .ndacan.cornell.edu/cmrlpostings/msg00195.html. Accessed February 22, 2012.
11. Finkelhor D, Jones L, Shattuck A; Crimes Against Children Research Center, University of New Hampshire. Updated trends in child maltreatment, 2009. http://unh.edu/ccrc/pdf/Updated_Trends_in_Child_Maltreatment_2009.pdf. Accessed February 22, 2012.
12. CDC Injury Center: Violence Prevention. Child Maltreatment: Risk and Protective Factors (2011). www.cdc.gov/violenceprevention/childmaltreat ment/riskprotectivefactors.html. Accessed February 22, 2012.
13. Sullivan P, Knutson J. Maltreatment and disabilities: a population-based epidemiological study. Child Abuse Negl. 2000;24(10):1257-1273.
14. Sedlak AJ, Mettenburg J, Basena M, et al. Fourth National Incidence Study of Child Abuse and Neglect (NIS–4): Report to Congress, Executive Summary. January 2010. Washington, DC: US Department of Health and Human Services, Administration for Children and Families.
15. National Clearinghouse on Family Violence, Public Health Agency of Canada. Abuse of children with disabilities (2000). www.phac-aspc
.gc.ca/ncfv-cnivf/pdfs/nfnts-disabl-eng.pdf. Accessed February 22, 2012.
16. Endorm EE. (2011, June 7, 2011). Physical abuse in children: epidemiology and clinical manifestations. www.uptodate.com/contents/physical-abuse-in-children-epidemiology-and-clinical-manifestations?source=search_result&
search=Phsical+abuse+i+children%3A+Epidemiology+and+clinical+manifestations&selectedTi
tle=1~150. Accessed February 22, 2012.
17. Pandya NK, Baldwin K, Kamath AF, et al. Unexplained fractures: child abuse or bone disease? A systematic review. Clin Orthop Relat Res. 2011; 469(3):805-812.
18. Gondim RM, Muñoz DR, Petri V. Child abuse: skin markers and differential diagnosis. An Bras Dermatol. 2011;86(3):527-536.
19. Kemp AM, Dunstan F, Harrison S, et al. Patterns of skeletal fractures in child abuse: systematic review. BMJ. 2008;337:a1518.
20. Worlock P, Stower M, Barbor P. Patterns of fractures in accidental and non-accidental injury in children: a comparative study. Br Med J (Clin Res Ed). 1986;293(6539):100-102.
21. Welsh Child Protection Systematic Review Group. www.core-info.cf.ac.uk. Accessed February 22, 2012.
22. Wardinsky TD. Genetic and congenital defect conditions that mimic child abuse. J Fam Pract. 1995;41(4):377-383.
23. American College of Radiology. ACR appropriateness criteria (2009). www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria/pdf/ExpertPanelonPediatricImaging/Suspected PhysicalAbuseChildDoc9.aspx. Accessed February 22, 2012.
24. Meservy CJ, Towbin R, McLaurin RL, et al. Radiographic characteristics of skull fractures resulting from child abuse. AJR Am J Roentgenol. 1987;149(1):173-175.
25. US Department of Justice, Office of Justice Programs, Office of Juvenile Justice and Delinquency Prevention. Burn Injuries in Child Abuse (2001). www.ncjrs.gov/pdffiles/91190-6.pdf. Accessed February 22, 2012.
26. Lane WG, Dubowitz H. Primary care pediatricians’ experience, comfort and competence in the evaluation and management of child maltreatment: do we need child abuse experts? Child Abuse Negl. 2009;33(2):76-83.
27. Child Welfare Information Gateway, US Department of Health and Human Services, Administration for Children and Families. Recognizing child abuse and neglect: signs and symptoms (2007). www.childwelfare.gov/pubs/factsheets/signs.cfm. Accessed February 22, 2012.
28. Fortin K, Jenny C. Sexual abuse. Pediatr Rev. 2012;33(1):19–32.
29. Keshavarz R, Kawashima R, Low C. Child abuse and neglect presentations to a pediatric emergency department. J Emerg Med. 2002;23(4): 341-345.
30. Kellogg N; American Academy of Pediatrics Committee on Child Abuse and Neglect. The evaluation of sexual abuse in children. Pediatrics. 2005;116(2):506-512.
31. Heger A, Ticson L, Velasquez O, Bernier R. Children referred for possible sexual abuse: medical findings in 2384 children. Child Abuse Negl. 2002;26(6-7):645-659.
32. Kellogg ND, Menard SW, Santos A. Genital anatomy in pregnant adolescents: “normal” does not mean “nothing happened.” Pediatrics. 2004; 113(1):e67-e69.
33. Workowski KA, Berman S; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
34. Oates RK. Overturning the diagnosis of child abuse. Arch Dis Child. 1984;59(7):665-666.
35. Hornor G. Common conditions that mimic findings of sexual abuse. J Pediatr Health Care. 2009;23(5):283-288.
36. Asnes RS. Buttock bruises: Mongolian spot. Pediatrics. 1984;74(2):321.
37. Klusmann A, Lenard HG. Tourniquet syndrome: accident or abuse? Eur J Pediatr. 2004; 163(8):495-498.
38. Merten DF, Carpenter BL. Radiologic imaging of inflicted injury in the child abuse syndrome. Pediatr Clin North Am. 1990;37(4):815-837.
39. Mok JY. Non-accidental injury in children: an update. Injury. 2008;39(9):978-985.
40. Nelson CS, Higman SM, Sia C, et al. Medical homes for at-risk children: parental reports of clinician-parent relationships, anticipatory guidance, and behavior changes. Pediatrics. 2005; 115(1):48-56.
41. Dubowitz H. Prevention of child maltreatment: what is known. Pediatrics. 1989;83(4):570-577.