User login
A standardized approach to postop management of DOACs in AFib
Clinical question: Is it safe to adopt a standardized approach to direct oral anticoagulant (DOAC) interruption for patients with atrial fibrillation (AFib) who are undergoing elective surgeries/procedures?

Background: At present, perioperative management of DOACs for patients with AFib has significant variation, and robust data are absent. Points of controversy include: The length of time to hold DOACs before and after the procedure, whether to bridge with heparin, and whether to measure coagulation function studies prior to the procedure.
Study design: Prospective cohort study.
Setting: Conducted in Canada, the United States, and Europe.
Synopsis: The PAUSE study included adults with atrial fibrillation who were long-term users of either apixaban, dabigatran, or rivaroxaban and were scheduled for an elective procedure (n = 3,007). Patients were placed on a standardized DOAC interruption schedule based on whether their procedure had high bleeding risk (held for 2 days prior; resumed 2-3 days after) or low bleeding risk (held for 1 day prior; resumed 1 day after).
The primary clinical outcomes were major bleeding and arterial thromboembolism. Authors determined safety by comparing to expected outcome rates derived from research on perioperative warfarin management.
They found that all three drugs were associated with acceptable rates of arterial thromboembolism (apixaban 0.2%, dabigatran 0.6%, rivaroxaban 0.4%). The rates of major bleeding observed with each drug (apixaban 0.6% low-risk procedures, 3% high-risk procedures; dabigatran 0.9% both low- and high-risk procedures; and rivaroxaban 1.3% low-risk procedures, 3% high-risk procedures) were similar to those in the BRIDGE trial (patients on warfarin who were not bridged perioperatively). However, it must still be noted that only dabigatran met the authors’ predetermined definition of safety for major bleeding.
Limitations include the lack of true control rates for major bleeding and stroke, the relatively low mean CHADS2-Va2Sc of 3.3-3.5, and that greater than 95% of patients were white.
Bottom line: For patients with moderate-risk atrial fibrillation, a standardized approach to DOAC interruption in the perioperative period that omits bridging along with coagulation function testing appears safe in this preliminary study.
Citation: Douketis JD et al. Perioperative management of patients with atrial fibrillation receiving a direct oral anticoagulant. JAMA Intern Med. 2019 Aug 5. doi: 10.1001/jamainternmed.2019.2431.
Dr. Gordon is a hospitalist at Maine Medical Center in Portland.
Clinical question: Is it safe to adopt a standardized approach to direct oral anticoagulant (DOAC) interruption for patients with atrial fibrillation (AFib) who are undergoing elective surgeries/procedures?
Background: At present, perioperative management of DOACs for patients with AFib has significant variation, and robust data are absent. Points of controversy include: The length of time to hold DOACs before and after the procedure, whether to bridge with heparin, and whether to measure coagulation function studies prior to the procedure.
Study design: Prospective cohort study.
Setting: Conducted in Canada, the United States, and Europe.
Synopsis: The PAUSE study included adults with atrial fibrillation who were long-term users of either apixaban, dabigatran, or rivaroxaban and were scheduled for an elective procedure (n = 3,007). Patients were placed on a standardized DOAC interruption schedule based on whether their procedure had high bleeding risk (held for 2 days prior; resumed 2-3 days after) or low bleeding risk (held for 1 day prior; resumed 1 day after).
The primary clinical outcomes were major bleeding and arterial thromboembolism. Authors determined safety by comparing to expected outcome rates derived from research on perioperative warfarin management.
They found that all three drugs were associated with acceptable rates of arterial thromboembolism (apixaban 0.2%, dabigatran 0.6%, rivaroxaban 0.4%). The rates of major bleeding observed with each drug (apixaban 0.6% low-risk procedures, 3% high-risk procedures; dabigatran 0.9% both low- and high-risk procedures; and rivaroxaban 1.3% low-risk procedures, 3% high-risk procedures) were similar to those in the BRIDGE trial (patients on warfarin who were not bridged perioperatively). However, it must still be noted that only dabigatran met the authors’ predetermined definition of safety for major bleeding.
Limitations include the lack of true control rates for major bleeding and stroke, the relatively low mean CHADS2-Va2Sc of 3.3-3.5, and that greater than 95% of patients were white.
Bottom line: For patients with moderate-risk atrial fibrillation, a standardized approach to DOAC interruption in the perioperative period that omits bridging along with coagulation function testing appears safe in this preliminary study.
Citation: Douketis JD et al. Perioperative management of patients with atrial fibrillation receiving a direct oral anticoagulant. JAMA Intern Med. 2019 Aug 5. doi: 10.1001/jamainternmed.2019.2431.
Dr. Gordon is a hospitalist at Maine Medical Center in Portland.
Clinical question: Is it safe to adopt a standardized approach to direct oral anticoagulant (DOAC) interruption for patients with atrial fibrillation (AFib) who are undergoing elective surgeries/procedures?
Background: At present, perioperative management of DOACs for patients with AFib has significant variation, and robust data are absent. Points of controversy include: The length of time to hold DOACs before and after the procedure, whether to bridge with heparin, and whether to measure coagulation function studies prior to the procedure.
Study design: Prospective cohort study.
Setting: Conducted in Canada, the United States, and Europe.
Synopsis: The PAUSE study included adults with atrial fibrillation who were long-term users of either apixaban, dabigatran, or rivaroxaban and were scheduled for an elective procedure (n = 3,007). Patients were placed on a standardized DOAC interruption schedule based on whether their procedure had high bleeding risk (held for 2 days prior; resumed 2-3 days after) or low bleeding risk (held for 1 day prior; resumed 1 day after).
The primary clinical outcomes were major bleeding and arterial thromboembolism. Authors determined safety by comparing to expected outcome rates derived from research on perioperative warfarin management.
They found that all three drugs were associated with acceptable rates of arterial thromboembolism (apixaban 0.2%, dabigatran 0.6%, rivaroxaban 0.4%). The rates of major bleeding observed with each drug (apixaban 0.6% low-risk procedures, 3% high-risk procedures; dabigatran 0.9% both low- and high-risk procedures; and rivaroxaban 1.3% low-risk procedures, 3% high-risk procedures) were similar to those in the BRIDGE trial (patients on warfarin who were not bridged perioperatively). However, it must still be noted that only dabigatran met the authors’ predetermined definition of safety for major bleeding.
Limitations include the lack of true control rates for major bleeding and stroke, the relatively low mean CHADS2-Va2Sc of 3.3-3.5, and that greater than 95% of patients were white.
Bottom line: For patients with moderate-risk atrial fibrillation, a standardized approach to DOAC interruption in the perioperative period that omits bridging along with coagulation function testing appears safe in this preliminary study.
Citation: Douketis JD et al. Perioperative management of patients with atrial fibrillation receiving a direct oral anticoagulant. JAMA Intern Med. 2019 Aug 5. doi: 10.1001/jamainternmed.2019.2431.
Dr. Gordon is a hospitalist at Maine Medical Center in Portland.
Calcium-induced autonomic denervation linked to lower post-op AF
Intraoperative injection of calcium chloride into the four major atrial ganglionated plexi (GPs) reduced the incidence of early postoperative atrial fibrillation (POAF) in patients undergoing off-pump coronary artery bypass grafting (CABG) surgery, in a proof-of-concept study.
“[We] hypothesized that injecting [calcium chloride] into the major atrial GPs during isolated CABG can reduce the incidence of POAF by calcium-induced autonomic neurotoxicity,” wrote Huishan Wang, MD, of the General Hospital of Northern Theater Command in Shenyang, China, and colleagues. Their report was published in the Journal of the American College of Cardiology.
The single-center, sham-controlled, proof-of-concept study included 200 patients without a history of AF undergoing isolated, off-pump CABG surgery. Participants were randomized (1:1) to receive an injection of either 5% calcium chloride or 0.9% sodium chloride into the four major GPs during CABG.
Post surgery, patients were monitored for the occurrence of POAF using routine 12-lead ECG and 7-day continuous telemetry and Holter monitoring. The primary endpoint was the incidence of POAF lasting 30 seconds or longer through 7 days. Various secondary outcomes, including POAF burden and length of hospitalization, were also measured.
After analysis, the researchers found that 15 patients in the calcium chloride arm and 36 patients in the sodium chloride arm developed POAF during the first 7 days post CABG, corresponding to a POAF hazard reduction of 63% (hazard ratio, 0.37; 95% confidence interval, 0.21-0.64; P = .001) with no significant adverse effects observed among study patients.
The calcium chloride injection also resulted in reduced AF burden and lower rates of amiodarone and esmolol use to treat POAF; however, there was no difference in the length of hospitalization between the two groups. The incidences of nonsustained atrial tachyarrhythmia (less than 30 seconds) and atrial couplets were also significantly reduced in the calcium chloride group.
“We selected the 4 major atrial GPs as our targets because [of] their role in the initiation and maintenance of AF is more established than other cardiac neural plexi,” the researchers explained. “Interruption of the atrial neural network by Ca-mediated GP neurotoxicity may underlie the therapeutic effects.”
Is ‘nuisance’ arrhythmia worth targeting?
In an editorial accompanying the report, John H. Alexander, MD, MHS, wrote that intraoperative calcium chloride atrial ganglionic ablation can now be considered as an effective intervention to prevent POAF in patients undergoing cardiac surgery. “These investigators should be congratulated for studying post-operative atrial fibrillation in cardiac surgery,” he stated.

“However, this trial has two significant limitations. Firstly, it was conducted in a single center in a very homogeneous population; secondly, POAF, in and of itself, is largely a nuisance arrhythmia and hardly worth preventing, but is associated with a higher risk of other adverse outcomes,” Dr. Alexander, professor of medicine at Duke University, Durham, N.C., said in an interview.
“The unanswered question is whether preventing perioperative AF will prevent stroke, heart failure, and death,” he further explained. “Answering these questions would require a larger trial (or trials) with longer term (months to years) follow-up.”
Dr. Wang and colleagues acknowledged that the current study was underpowered for some secondary outcomes, such as length of hospitalization. They explained that a large sample size is needed to detect a difference in length of hospitalization, as well as other outcomes.
“Further studies are needed to confirm the safety and efficacy of calcium-induced atrial autonomic denervation in patients undergoing on-pump CABG and surgery for valvular heart disease,” they concluded.
The study was funded by the Provincial Key R & D Program in China. One author reported holding a U.S. patent related to the study. The remaining authors had no relevant relationships to disclose.
Intraoperative injection of calcium chloride into the four major atrial ganglionated plexi (GPs) reduced the incidence of early postoperative atrial fibrillation (POAF) in patients undergoing off-pump coronary artery bypass grafting (CABG) surgery, in a proof-of-concept study.
“[We] hypothesized that injecting [calcium chloride] into the major atrial GPs during isolated CABG can reduce the incidence of POAF by calcium-induced autonomic neurotoxicity,” wrote Huishan Wang, MD, of the General Hospital of Northern Theater Command in Shenyang, China, and colleagues. Their report was published in the Journal of the American College of Cardiology.
The single-center, sham-controlled, proof-of-concept study included 200 patients without a history of AF undergoing isolated, off-pump CABG surgery. Participants were randomized (1:1) to receive an injection of either 5% calcium chloride or 0.9% sodium chloride into the four major GPs during CABG.
Post surgery, patients were monitored for the occurrence of POAF using routine 12-lead ECG and 7-day continuous telemetry and Holter monitoring. The primary endpoint was the incidence of POAF lasting 30 seconds or longer through 7 days. Various secondary outcomes, including POAF burden and length of hospitalization, were also measured.
After analysis, the researchers found that 15 patients in the calcium chloride arm and 36 patients in the sodium chloride arm developed POAF during the first 7 days post CABG, corresponding to a POAF hazard reduction of 63% (hazard ratio, 0.37; 95% confidence interval, 0.21-0.64; P = .001) with no significant adverse effects observed among study patients.
The calcium chloride injection also resulted in reduced AF burden and lower rates of amiodarone and esmolol use to treat POAF; however, there was no difference in the length of hospitalization between the two groups. The incidences of nonsustained atrial tachyarrhythmia (less than 30 seconds) and atrial couplets were also significantly reduced in the calcium chloride group.
“We selected the 4 major atrial GPs as our targets because [of] their role in the initiation and maintenance of AF is more established than other cardiac neural plexi,” the researchers explained. “Interruption of the atrial neural network by Ca-mediated GP neurotoxicity may underlie the therapeutic effects.”
Is ‘nuisance’ arrhythmia worth targeting?
In an editorial accompanying the report, John H. Alexander, MD, MHS, wrote that intraoperative calcium chloride atrial ganglionic ablation can now be considered as an effective intervention to prevent POAF in patients undergoing cardiac surgery. “These investigators should be congratulated for studying post-operative atrial fibrillation in cardiac surgery,” he stated.
“However, this trial has two significant limitations. Firstly, it was conducted in a single center in a very homogeneous population; secondly, POAF, in and of itself, is largely a nuisance arrhythmia and hardly worth preventing, but is associated with a higher risk of other adverse outcomes,” Dr. Alexander, professor of medicine at Duke University, Durham, N.C., said in an interview.
“The unanswered question is whether preventing perioperative AF will prevent stroke, heart failure, and death,” he further explained. “Answering these questions would require a larger trial (or trials) with longer term (months to years) follow-up.”
Dr. Wang and colleagues acknowledged that the current study was underpowered for some secondary outcomes, such as length of hospitalization. They explained that a large sample size is needed to detect a difference in length of hospitalization, as well as other outcomes.
“Further studies are needed to confirm the safety and efficacy of calcium-induced atrial autonomic denervation in patients undergoing on-pump CABG and surgery for valvular heart disease,” they concluded.
The study was funded by the Provincial Key R & D Program in China. One author reported holding a U.S. patent related to the study. The remaining authors had no relevant relationships to disclose.
Intraoperative injection of calcium chloride into the four major atrial ganglionated plexi (GPs) reduced the incidence of early postoperative atrial fibrillation (POAF) in patients undergoing off-pump coronary artery bypass grafting (CABG) surgery, in a proof-of-concept study.
“[We] hypothesized that injecting [calcium chloride] into the major atrial GPs during isolated CABG can reduce the incidence of POAF by calcium-induced autonomic neurotoxicity,” wrote Huishan Wang, MD, of the General Hospital of Northern Theater Command in Shenyang, China, and colleagues. Their report was published in the Journal of the American College of Cardiology.
The single-center, sham-controlled, proof-of-concept study included 200 patients without a history of AF undergoing isolated, off-pump CABG surgery. Participants were randomized (1:1) to receive an injection of either 5% calcium chloride or 0.9% sodium chloride into the four major GPs during CABG.
Post surgery, patients were monitored for the occurrence of POAF using routine 12-lead ECG and 7-day continuous telemetry and Holter monitoring. The primary endpoint was the incidence of POAF lasting 30 seconds or longer through 7 days. Various secondary outcomes, including POAF burden and length of hospitalization, were also measured.
After analysis, the researchers found that 15 patients in the calcium chloride arm and 36 patients in the sodium chloride arm developed POAF during the first 7 days post CABG, corresponding to a POAF hazard reduction of 63% (hazard ratio, 0.37; 95% confidence interval, 0.21-0.64; P = .001) with no significant adverse effects observed among study patients.
The calcium chloride injection also resulted in reduced AF burden and lower rates of amiodarone and esmolol use to treat POAF; however, there was no difference in the length of hospitalization between the two groups. The incidences of nonsustained atrial tachyarrhythmia (less than 30 seconds) and atrial couplets were also significantly reduced in the calcium chloride group.
“We selected the 4 major atrial GPs as our targets because [of] their role in the initiation and maintenance of AF is more established than other cardiac neural plexi,” the researchers explained. “Interruption of the atrial neural network by Ca-mediated GP neurotoxicity may underlie the therapeutic effects.”
Is ‘nuisance’ arrhythmia worth targeting?
In an editorial accompanying the report, John H. Alexander, MD, MHS, wrote that intraoperative calcium chloride atrial ganglionic ablation can now be considered as an effective intervention to prevent POAF in patients undergoing cardiac surgery. “These investigators should be congratulated for studying post-operative atrial fibrillation in cardiac surgery,” he stated.
“However, this trial has two significant limitations. Firstly, it was conducted in a single center in a very homogeneous population; secondly, POAF, in and of itself, is largely a nuisance arrhythmia and hardly worth preventing, but is associated with a higher risk of other adverse outcomes,” Dr. Alexander, professor of medicine at Duke University, Durham, N.C., said in an interview.
“The unanswered question is whether preventing perioperative AF will prevent stroke, heart failure, and death,” he further explained. “Answering these questions would require a larger trial (or trials) with longer term (months to years) follow-up.”
Dr. Wang and colleagues acknowledged that the current study was underpowered for some secondary outcomes, such as length of hospitalization. They explained that a large sample size is needed to detect a difference in length of hospitalization, as well as other outcomes.
“Further studies are needed to confirm the safety and efficacy of calcium-induced atrial autonomic denervation in patients undergoing on-pump CABG and surgery for valvular heart disease,” they concluded.
The study was funded by the Provincial Key R & D Program in China. One author reported holding a U.S. patent related to the study. The remaining authors had no relevant relationships to disclose.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Averting COVID hospitalizations with monoclonal antibodies
The United States has allocated more than 641,000 monoclonal antibody treatments for outpatients to ease pressure on strained hospitals, but officials from Operation Warp Speed report that more than half of that reserve sits unused as clinicians grapple with best practices.
There are space and personnel limitations in hospitals right now, Janet Woodcock, MD, therapeutics lead on Operation Warp Speed, acknowledges in an interview with this news organization. “Special areas and procedures must be set up.” And the operation is in the process of broadening availability beyond hospitals, she points out.
But for frontline clinicians, questions about treatment efficacy and the logistics of administering intravenous drugs to infectious outpatients loom large.
More than 50 monoclonal antibody products that target SARS-CoV-2 are now in development. The U.S. Food and Drug Administration has already issued Emergency Use Authorization (EUA) for two such drugs on the basis of phase 2 trial data – bamlanivimab, made by Eli Lilly, and a cocktail of casirivimab plus imdevimab, made by Regeneron – and another two-antibody cocktail from AstraZeneca, AZD7442, has started phase 3 clinical trials. The Regeneron combination was used to treat President Donald Trump when he contracted COVID-19 in October.
Monoclonal antibody drugs are based on the natural antibodies that the body uses to fight infections. They work by binding to a specific target and then blocking its action or flagging it for destruction by other parts of the immune system. Both bamlanivimab and the casirivimab plus imdevimab combination target the spike protein of the virus and stop it from attaching to and entering human cells.
Targeting the spike protein out of the hospital
The antibody drugs covered by EUAs do not cure COVID-19, but they have been shown to reduce hospitalizations and visits to the emergency department for patients at high risk for disease progression. They are approved to treat patients older than 12 years with mild to moderate COVID-19 who are at high risk of progressing to severe disease or hospitalization. They are not authorized for use in patients who have been hospitalized or who are on ventilators. The hope is that antibody drugs will reduce the number of severe cases of COVID-19 and ease pressure on overstretched hospitals.
Most COVID-19 patients are outpatients, so we need something to keep them from getting worse.
This is important because it targets the greatest need in COVID-19 therapeutics, says Rajesh Gandhi, MD, an infectious disease physician at Harvard Medical School in Boston, who is a member of two panels evaluating COVID-19 treatments: one for the Infectious Disease Society of America and the other for the National Institutes of Health. “Up to now, most of the focus has been on hospitalized patients,” he says, but “most COVID-19 patients are outpatients, so we need something to keep them from getting worse.”
Both panels have said that, despite the EUAs, more evidence is needed to be sure of the efficacy of the drugs and to determine which patients will benefit the most from them.
These aren’t the mature data from drug development that guideline groups are accustomed to working with, Dr. Woodcock points out. “But this is an emergency and the data taken as a whole are pretty convincing,” she says. “As I look at the totality of the evidence, monoclonal antibodies will have a big effect in keeping people out of the hospital and helping them recover faster.”
High-risk patients are eligible for treatment, especially those older than 65 years and those with comorbidities who are younger. Access to the drugs is increasing for clinicians who are able to infuse safely or work with a site that will.
In the Boston area, several hospitals, including Massachusetts General where Dr. Gandhi works, have set up infusion centers where newly diagnosed patients can get the antibody treatment if their doctor thinks it will benefit them. And Coram, a provider of at-home infusion therapy owned by the CVS pharmacy chain, is running a pilot program offering the Eli Lilly drug to people in seven cities – including Boston, Chicago, Los Angeles, and Tampa – and their surrounding communities with a physician referral.
Getting that referral could be tricky, however, for patients without a primary care physician or for those whose doctor isn’t already connected to one of the institutions providing the infusions. The hospitals are sending out communications on how patients and physicians can get the therapy, but Dr. Gandhi says that making information about access available should be a priority. The window for the effective treatment is small – the drugs appear to work best before patients begin to make their own antibodies, says Dr. Gandhi – so it’s vital that doctors act quickly if they have a patient who is eligible.
And rolling out the new therapies to patients around the world will be a major logistical undertaking.
The first hurdle will be making enough of them to go around. Case numbers are skyrocketing around the globe, and producing the drugs is a complex time- and labor-intensive process that requires specialized facilities. Antibodies are produced by cell lines in bioreactors, so a plant that churns out generic aspirin tablets can’t simply be converted into an antibody factory.
“These types of drugs are manufactured in a sterile injectables plant, which is different from a plant where oral solids are made,” says Kim Crabtree, senior director of pharma portfolio management for Henry Schein Medical, a medical supplies distributor. “Those are not as plentiful as a standard pill factory.”
The doses required are also relatively high – 1.2 g of each antibody in Regeneron’s cocktail – which will further strain production capacity. Leah Lipsich, PhD, vice president of strategic program direction at Regeneron, says the company is prepared for high demand and has been able to respond, thanks to its rapid development and manufacturing technology, known as VelociSuite, which allows it to rapidly scale-up from discovery to productions in weeks instead of months.
“We knew supply would be a huge problem for COVID-19, but because we had such confidence in our technology, we went immediately from research-scale to our largest-scale manufacturing,” she says. “We’ve been manufacturing our cocktail for months now.”
The company has also partnered with Roche, the biggest manufacturer and vendor of monoclonal antibodies in the world, to manufacture and supply the drugs. Once full manufacturing capacity is reached in 2021, the companies expect to produce at least 2 million doses a year.
Then there is the issue of getting the drugs from the factories to the places they will be used.
Antibodies are temperature sensitive and need to be refrigerated during transport and storage, so a cold-chain-compliant supply chain is required. Fortunately, they can be kept at standard refrigerator temperatures, ranging from 2° C to 8° C, rather than the ultra-low temperatures required by some COVID-19 vaccines.
Two million doses a year
Medical logistics companies have a lot of experience dealing with products like these and are well prepared to handle the new antibody drugs. “There are quite a few products like these on the market, and the supply chain is used to shipping them,” Ms. Crabtree says.
They will be shipped to distribution centers in refrigerated trucks, repacked into smaller lots that can sustain the correct temperature for 24 hours, and then sent to their final destination, often in something as simple as a Styrofoam cooler filled with dry ice.
The expected rise in demand shouldn’t be too much of an issue for distributors either, says Ms. Crabtree; they have built systems that can deal with short-term surges in volume. The annual flu vaccine, for example, involves shipping a lot of product in a very short time, usually from August to November. “The distribution system is used to seasonal variations and peaks in demand,” she says.
The next question is how the treatments will be administered. Although most patients who will receive monoclonal antibodies will be ambulatory and not hospitalized, the administration requires intravenous infusion. Hospitals, of course, have a lot of experience with intravenous drugs, but typically give them only to inpatients. Most other monoclonal antibody drugs – such as those for cancer and autoimmune disorders – are given in specialized suites in doctor’s offices or in stand-alone infusion clinics.
That means that the places best suited to treat COVID-19 patients with antibodies are those that regularly deal with people who are immunocompromised, and such patients should not be interacting with people who have an infectious disease. “How do we protect the staff and other patients?” Dr. Gandhi asks.
Protecting staff and other patients
This is not an insurmountable obstacle, he points out, but it is one that requires careful thought and planning to accommodate COVID-19 patients without unduly disrupting life-saving treatments for other patients. It might involve, for example, treating COVID-19 patients in sequestered parts of the clinic or at different times of day, with even greater attention paid to cleaning, he explains. “We now have many months of experience with infection control, so we know how to do this; it’s just a question of logistics.”
But even once all the details around manufacturing, transporting, and administering the drugs are sorted out, there is still the issue of how they will be distributed fairly and equitably.
Despite multiple companies working to produce an array of different antibody drugs, demand is still expected to exceed supply for many months. “With more than 200,000 new cases a day in the United States, there won’t be enough antibodies to treat all of the high-risk patients,” says Dr. Gandhi. “Most of us are worried that demand will far outstrip supply. People are talking about lotteries to determine who gets them.”
The Department of Health and Human Services will continue to distribute the drugs to states on the basis of their COVID-19 burdens, and the states will then decide how much to provide to each health care facility.
Although the HHS goal is to ensure that the drugs reach as many patients as possible, no matter where they live and regardless of their income, there are still concerns that larger facilities serving more affluent areas will end up being favored, if only because they are the ones best equipped to deal with the drugs right now.
“We are all aware that this has affected certain communities more, so we need to make sure that the drugs are used equitably and made available to the communities that were hardest hit,” says Dr. Gandhi. The ability to monitor drug distribution should be built into the rollout, so that institutions and governments will have some sense of whether they are being doled out evenly, he adds.
Equity in distribution will be an issue for the rest of the world as well. Currently, 80% of monoclonal antibodies are sold in Canada, Europe, and the United States; few, if any, are available in low- and middle-income countries. The treatments are expensive: the cost of producing one g of marketed monoclonal antibodies is between $95 and $200, which does not include the cost of R&D, packaging, shipping, or administration. The median price for antibody treatment not related to COVID-19 runs from $15,000 to $200,000 per year in the United States.
Regeneron’s Dr. Lipsich says that the company has not yet set a price for its antibody cocktail. The government paid $450 million for its 300,000 doses, but that price includes the costs of research, manufacturing, and distribution, so is not a useful indicator of the eventual per-dose price. “We’re not in a position to talk about how it will be priced yet, but we will do our best to make it affordable and accessible to all,” she says.
There are some projects underway to ensure that the drugs are made available in poorer countries. In April, the COVID-19 Therapeutics Accelerator – an initiative launched by the Bill & Melinda Gates Foundation, Wellcome, and Mastercard to speed-up the response to the global pandemic – reserved manufacturing capacity with Fujifilm Diosynth Biotechnologies in Denmark for future monoclonal antibody therapies that will supply low- and middle-income countries. In October, the initiative announced that Eli Lilly would use that reserved capacity to produce its antibody drug starting in April 2021.
In the meantime, Lilly will make some of its product manufactured in other facilities available to lower-income countries. To help keep costs down, the company’s collaborators have agreed to waive their royalties on antibodies distributed in low- and middle-income countries.
“Everyone is looking carefully at how the drugs are distributed to ensure all will get access,” said Dr. Lipsich.
A version of this article first appeared on Medscape.com.
The United States has allocated more than 641,000 monoclonal antibody treatments for outpatients to ease pressure on strained hospitals, but officials from Operation Warp Speed report that more than half of that reserve sits unused as clinicians grapple with best practices.
There are space and personnel limitations in hospitals right now, Janet Woodcock, MD, therapeutics lead on Operation Warp Speed, acknowledges in an interview with this news organization. “Special areas and procedures must be set up.” And the operation is in the process of broadening availability beyond hospitals, she points out.
But for frontline clinicians, questions about treatment efficacy and the logistics of administering intravenous drugs to infectious outpatients loom large.
More than 50 monoclonal antibody products that target SARS-CoV-2 are now in development. The U.S. Food and Drug Administration has already issued Emergency Use Authorization (EUA) for two such drugs on the basis of phase 2 trial data – bamlanivimab, made by Eli Lilly, and a cocktail of casirivimab plus imdevimab, made by Regeneron – and another two-antibody cocktail from AstraZeneca, AZD7442, has started phase 3 clinical trials. The Regeneron combination was used to treat President Donald Trump when he contracted COVID-19 in October.
Monoclonal antibody drugs are based on the natural antibodies that the body uses to fight infections. They work by binding to a specific target and then blocking its action or flagging it for destruction by other parts of the immune system. Both bamlanivimab and the casirivimab plus imdevimab combination target the spike protein of the virus and stop it from attaching to and entering human cells.
Targeting the spike protein out of the hospital
The antibody drugs covered by EUAs do not cure COVID-19, but they have been shown to reduce hospitalizations and visits to the emergency department for patients at high risk for disease progression. They are approved to treat patients older than 12 years with mild to moderate COVID-19 who are at high risk of progressing to severe disease or hospitalization. They are not authorized for use in patients who have been hospitalized or who are on ventilators. The hope is that antibody drugs will reduce the number of severe cases of COVID-19 and ease pressure on overstretched hospitals.
Most COVID-19 patients are outpatients, so we need something to keep them from getting worse.
This is important because it targets the greatest need in COVID-19 therapeutics, says Rajesh Gandhi, MD, an infectious disease physician at Harvard Medical School in Boston, who is a member of two panels evaluating COVID-19 treatments: one for the Infectious Disease Society of America and the other for the National Institutes of Health. “Up to now, most of the focus has been on hospitalized patients,” he says, but “most COVID-19 patients are outpatients, so we need something to keep them from getting worse.”
Both panels have said that, despite the EUAs, more evidence is needed to be sure of the efficacy of the drugs and to determine which patients will benefit the most from them.
These aren’t the mature data from drug development that guideline groups are accustomed to working with, Dr. Woodcock points out. “But this is an emergency and the data taken as a whole are pretty convincing,” she says. “As I look at the totality of the evidence, monoclonal antibodies will have a big effect in keeping people out of the hospital and helping them recover faster.”
High-risk patients are eligible for treatment, especially those older than 65 years and those with comorbidities who are younger. Access to the drugs is increasing for clinicians who are able to infuse safely or work with a site that will.
In the Boston area, several hospitals, including Massachusetts General where Dr. Gandhi works, have set up infusion centers where newly diagnosed patients can get the antibody treatment if their doctor thinks it will benefit them. And Coram, a provider of at-home infusion therapy owned by the CVS pharmacy chain, is running a pilot program offering the Eli Lilly drug to people in seven cities – including Boston, Chicago, Los Angeles, and Tampa – and their surrounding communities with a physician referral.
Getting that referral could be tricky, however, for patients without a primary care physician or for those whose doctor isn’t already connected to one of the institutions providing the infusions. The hospitals are sending out communications on how patients and physicians can get the therapy, but Dr. Gandhi says that making information about access available should be a priority. The window for the effective treatment is small – the drugs appear to work best before patients begin to make their own antibodies, says Dr. Gandhi – so it’s vital that doctors act quickly if they have a patient who is eligible.
And rolling out the new therapies to patients around the world will be a major logistical undertaking.
The first hurdle will be making enough of them to go around. Case numbers are skyrocketing around the globe, and producing the drugs is a complex time- and labor-intensive process that requires specialized facilities. Antibodies are produced by cell lines in bioreactors, so a plant that churns out generic aspirin tablets can’t simply be converted into an antibody factory.
“These types of drugs are manufactured in a sterile injectables plant, which is different from a plant where oral solids are made,” says Kim Crabtree, senior director of pharma portfolio management for Henry Schein Medical, a medical supplies distributor. “Those are not as plentiful as a standard pill factory.”
The doses required are also relatively high – 1.2 g of each antibody in Regeneron’s cocktail – which will further strain production capacity. Leah Lipsich, PhD, vice president of strategic program direction at Regeneron, says the company is prepared for high demand and has been able to respond, thanks to its rapid development and manufacturing technology, known as VelociSuite, which allows it to rapidly scale-up from discovery to productions in weeks instead of months.
“We knew supply would be a huge problem for COVID-19, but because we had such confidence in our technology, we went immediately from research-scale to our largest-scale manufacturing,” she says. “We’ve been manufacturing our cocktail for months now.”
The company has also partnered with Roche, the biggest manufacturer and vendor of monoclonal antibodies in the world, to manufacture and supply the drugs. Once full manufacturing capacity is reached in 2021, the companies expect to produce at least 2 million doses a year.
Then there is the issue of getting the drugs from the factories to the places they will be used.
Antibodies are temperature sensitive and need to be refrigerated during transport and storage, so a cold-chain-compliant supply chain is required. Fortunately, they can be kept at standard refrigerator temperatures, ranging from 2° C to 8° C, rather than the ultra-low temperatures required by some COVID-19 vaccines.
Two million doses a year
Medical logistics companies have a lot of experience dealing with products like these and are well prepared to handle the new antibody drugs. “There are quite a few products like these on the market, and the supply chain is used to shipping them,” Ms. Crabtree says.
They will be shipped to distribution centers in refrigerated trucks, repacked into smaller lots that can sustain the correct temperature for 24 hours, and then sent to their final destination, often in something as simple as a Styrofoam cooler filled with dry ice.
The expected rise in demand shouldn’t be too much of an issue for distributors either, says Ms. Crabtree; they have built systems that can deal with short-term surges in volume. The annual flu vaccine, for example, involves shipping a lot of product in a very short time, usually from August to November. “The distribution system is used to seasonal variations and peaks in demand,” she says.
The next question is how the treatments will be administered. Although most patients who will receive monoclonal antibodies will be ambulatory and not hospitalized, the administration requires intravenous infusion. Hospitals, of course, have a lot of experience with intravenous drugs, but typically give them only to inpatients. Most other monoclonal antibody drugs – such as those for cancer and autoimmune disorders – are given in specialized suites in doctor’s offices or in stand-alone infusion clinics.
That means that the places best suited to treat COVID-19 patients with antibodies are those that regularly deal with people who are immunocompromised, and such patients should not be interacting with people who have an infectious disease. “How do we protect the staff and other patients?” Dr. Gandhi asks.
Protecting staff and other patients
This is not an insurmountable obstacle, he points out, but it is one that requires careful thought and planning to accommodate COVID-19 patients without unduly disrupting life-saving treatments for other patients. It might involve, for example, treating COVID-19 patients in sequestered parts of the clinic or at different times of day, with even greater attention paid to cleaning, he explains. “We now have many months of experience with infection control, so we know how to do this; it’s just a question of logistics.”
But even once all the details around manufacturing, transporting, and administering the drugs are sorted out, there is still the issue of how they will be distributed fairly and equitably.
Despite multiple companies working to produce an array of different antibody drugs, demand is still expected to exceed supply for many months. “With more than 200,000 new cases a day in the United States, there won’t be enough antibodies to treat all of the high-risk patients,” says Dr. Gandhi. “Most of us are worried that demand will far outstrip supply. People are talking about lotteries to determine who gets them.”
The Department of Health and Human Services will continue to distribute the drugs to states on the basis of their COVID-19 burdens, and the states will then decide how much to provide to each health care facility.
Although the HHS goal is to ensure that the drugs reach as many patients as possible, no matter where they live and regardless of their income, there are still concerns that larger facilities serving more affluent areas will end up being favored, if only because they are the ones best equipped to deal with the drugs right now.
“We are all aware that this has affected certain communities more, so we need to make sure that the drugs are used equitably and made available to the communities that were hardest hit,” says Dr. Gandhi. The ability to monitor drug distribution should be built into the rollout, so that institutions and governments will have some sense of whether they are being doled out evenly, he adds.
Equity in distribution will be an issue for the rest of the world as well. Currently, 80% of monoclonal antibodies are sold in Canada, Europe, and the United States; few, if any, are available in low- and middle-income countries. The treatments are expensive: the cost of producing one g of marketed monoclonal antibodies is between $95 and $200, which does not include the cost of R&D, packaging, shipping, or administration. The median price for antibody treatment not related to COVID-19 runs from $15,000 to $200,000 per year in the United States.
Regeneron’s Dr. Lipsich says that the company has not yet set a price for its antibody cocktail. The government paid $450 million for its 300,000 doses, but that price includes the costs of research, manufacturing, and distribution, so is not a useful indicator of the eventual per-dose price. “We’re not in a position to talk about how it will be priced yet, but we will do our best to make it affordable and accessible to all,” she says.
There are some projects underway to ensure that the drugs are made available in poorer countries. In April, the COVID-19 Therapeutics Accelerator – an initiative launched by the Bill & Melinda Gates Foundation, Wellcome, and Mastercard to speed-up the response to the global pandemic – reserved manufacturing capacity with Fujifilm Diosynth Biotechnologies in Denmark for future monoclonal antibody therapies that will supply low- and middle-income countries. In October, the initiative announced that Eli Lilly would use that reserved capacity to produce its antibody drug starting in April 2021.
In the meantime, Lilly will make some of its product manufactured in other facilities available to lower-income countries. To help keep costs down, the company’s collaborators have agreed to waive their royalties on antibodies distributed in low- and middle-income countries.
“Everyone is looking carefully at how the drugs are distributed to ensure all will get access,” said Dr. Lipsich.
A version of this article first appeared on Medscape.com.
The United States has allocated more than 641,000 monoclonal antibody treatments for outpatients to ease pressure on strained hospitals, but officials from Operation Warp Speed report that more than half of that reserve sits unused as clinicians grapple with best practices.
There are space and personnel limitations in hospitals right now, Janet Woodcock, MD, therapeutics lead on Operation Warp Speed, acknowledges in an interview with this news organization. “Special areas and procedures must be set up.” And the operation is in the process of broadening availability beyond hospitals, she points out.
But for frontline clinicians, questions about treatment efficacy and the logistics of administering intravenous drugs to infectious outpatients loom large.
More than 50 monoclonal antibody products that target SARS-CoV-2 are now in development. The U.S. Food and Drug Administration has already issued Emergency Use Authorization (EUA) for two such drugs on the basis of phase 2 trial data – bamlanivimab, made by Eli Lilly, and a cocktail of casirivimab plus imdevimab, made by Regeneron – and another two-antibody cocktail from AstraZeneca, AZD7442, has started phase 3 clinical trials. The Regeneron combination was used to treat President Donald Trump when he contracted COVID-19 in October.
Monoclonal antibody drugs are based on the natural antibodies that the body uses to fight infections. They work by binding to a specific target and then blocking its action or flagging it for destruction by other parts of the immune system. Both bamlanivimab and the casirivimab plus imdevimab combination target the spike protein of the virus and stop it from attaching to and entering human cells.
Targeting the spike protein out of the hospital
The antibody drugs covered by EUAs do not cure COVID-19, but they have been shown to reduce hospitalizations and visits to the emergency department for patients at high risk for disease progression. They are approved to treat patients older than 12 years with mild to moderate COVID-19 who are at high risk of progressing to severe disease or hospitalization. They are not authorized for use in patients who have been hospitalized or who are on ventilators. The hope is that antibody drugs will reduce the number of severe cases of COVID-19 and ease pressure on overstretched hospitals.
Most COVID-19 patients are outpatients, so we need something to keep them from getting worse.
This is important because it targets the greatest need in COVID-19 therapeutics, says Rajesh Gandhi, MD, an infectious disease physician at Harvard Medical School in Boston, who is a member of two panels evaluating COVID-19 treatments: one for the Infectious Disease Society of America and the other for the National Institutes of Health. “Up to now, most of the focus has been on hospitalized patients,” he says, but “most COVID-19 patients are outpatients, so we need something to keep them from getting worse.”
Both panels have said that, despite the EUAs, more evidence is needed to be sure of the efficacy of the drugs and to determine which patients will benefit the most from them.
These aren’t the mature data from drug development that guideline groups are accustomed to working with, Dr. Woodcock points out. “But this is an emergency and the data taken as a whole are pretty convincing,” she says. “As I look at the totality of the evidence, monoclonal antibodies will have a big effect in keeping people out of the hospital and helping them recover faster.”
High-risk patients are eligible for treatment, especially those older than 65 years and those with comorbidities who are younger. Access to the drugs is increasing for clinicians who are able to infuse safely or work with a site that will.
In the Boston area, several hospitals, including Massachusetts General where Dr. Gandhi works, have set up infusion centers where newly diagnosed patients can get the antibody treatment if their doctor thinks it will benefit them. And Coram, a provider of at-home infusion therapy owned by the CVS pharmacy chain, is running a pilot program offering the Eli Lilly drug to people in seven cities – including Boston, Chicago, Los Angeles, and Tampa – and their surrounding communities with a physician referral.
Getting that referral could be tricky, however, for patients without a primary care physician or for those whose doctor isn’t already connected to one of the institutions providing the infusions. The hospitals are sending out communications on how patients and physicians can get the therapy, but Dr. Gandhi says that making information about access available should be a priority. The window for the effective treatment is small – the drugs appear to work best before patients begin to make their own antibodies, says Dr. Gandhi – so it’s vital that doctors act quickly if they have a patient who is eligible.
And rolling out the new therapies to patients around the world will be a major logistical undertaking.
The first hurdle will be making enough of them to go around. Case numbers are skyrocketing around the globe, and producing the drugs is a complex time- and labor-intensive process that requires specialized facilities. Antibodies are produced by cell lines in bioreactors, so a plant that churns out generic aspirin tablets can’t simply be converted into an antibody factory.
“These types of drugs are manufactured in a sterile injectables plant, which is different from a plant where oral solids are made,” says Kim Crabtree, senior director of pharma portfolio management for Henry Schein Medical, a medical supplies distributor. “Those are not as plentiful as a standard pill factory.”
The doses required are also relatively high – 1.2 g of each antibody in Regeneron’s cocktail – which will further strain production capacity. Leah Lipsich, PhD, vice president of strategic program direction at Regeneron, says the company is prepared for high demand and has been able to respond, thanks to its rapid development and manufacturing technology, known as VelociSuite, which allows it to rapidly scale-up from discovery to productions in weeks instead of months.
“We knew supply would be a huge problem for COVID-19, but because we had such confidence in our technology, we went immediately from research-scale to our largest-scale manufacturing,” she says. “We’ve been manufacturing our cocktail for months now.”
The company has also partnered with Roche, the biggest manufacturer and vendor of monoclonal antibodies in the world, to manufacture and supply the drugs. Once full manufacturing capacity is reached in 2021, the companies expect to produce at least 2 million doses a year.
Then there is the issue of getting the drugs from the factories to the places they will be used.
Antibodies are temperature sensitive and need to be refrigerated during transport and storage, so a cold-chain-compliant supply chain is required. Fortunately, they can be kept at standard refrigerator temperatures, ranging from 2° C to 8° C, rather than the ultra-low temperatures required by some COVID-19 vaccines.
Two million doses a year
Medical logistics companies have a lot of experience dealing with products like these and are well prepared to handle the new antibody drugs. “There are quite a few products like these on the market, and the supply chain is used to shipping them,” Ms. Crabtree says.
They will be shipped to distribution centers in refrigerated trucks, repacked into smaller lots that can sustain the correct temperature for 24 hours, and then sent to their final destination, often in something as simple as a Styrofoam cooler filled with dry ice.
The expected rise in demand shouldn’t be too much of an issue for distributors either, says Ms. Crabtree; they have built systems that can deal with short-term surges in volume. The annual flu vaccine, for example, involves shipping a lot of product in a very short time, usually from August to November. “The distribution system is used to seasonal variations and peaks in demand,” she says.
The next question is how the treatments will be administered. Although most patients who will receive monoclonal antibodies will be ambulatory and not hospitalized, the administration requires intravenous infusion. Hospitals, of course, have a lot of experience with intravenous drugs, but typically give them only to inpatients. Most other monoclonal antibody drugs – such as those for cancer and autoimmune disorders – are given in specialized suites in doctor’s offices or in stand-alone infusion clinics.
That means that the places best suited to treat COVID-19 patients with antibodies are those that regularly deal with people who are immunocompromised, and such patients should not be interacting with people who have an infectious disease. “How do we protect the staff and other patients?” Dr. Gandhi asks.
Protecting staff and other patients
This is not an insurmountable obstacle, he points out, but it is one that requires careful thought and planning to accommodate COVID-19 patients without unduly disrupting life-saving treatments for other patients. It might involve, for example, treating COVID-19 patients in sequestered parts of the clinic or at different times of day, with even greater attention paid to cleaning, he explains. “We now have many months of experience with infection control, so we know how to do this; it’s just a question of logistics.”
But even once all the details around manufacturing, transporting, and administering the drugs are sorted out, there is still the issue of how they will be distributed fairly and equitably.
Despite multiple companies working to produce an array of different antibody drugs, demand is still expected to exceed supply for many months. “With more than 200,000 new cases a day in the United States, there won’t be enough antibodies to treat all of the high-risk patients,” says Dr. Gandhi. “Most of us are worried that demand will far outstrip supply. People are talking about lotteries to determine who gets them.”
The Department of Health and Human Services will continue to distribute the drugs to states on the basis of their COVID-19 burdens, and the states will then decide how much to provide to each health care facility.
Although the HHS goal is to ensure that the drugs reach as many patients as possible, no matter where they live and regardless of their income, there are still concerns that larger facilities serving more affluent areas will end up being favored, if only because they are the ones best equipped to deal with the drugs right now.
“We are all aware that this has affected certain communities more, so we need to make sure that the drugs are used equitably and made available to the communities that were hardest hit,” says Dr. Gandhi. The ability to monitor drug distribution should be built into the rollout, so that institutions and governments will have some sense of whether they are being doled out evenly, he adds.
Equity in distribution will be an issue for the rest of the world as well. Currently, 80% of monoclonal antibodies are sold in Canada, Europe, and the United States; few, if any, are available in low- and middle-income countries. The treatments are expensive: the cost of producing one g of marketed monoclonal antibodies is between $95 and $200, which does not include the cost of R&D, packaging, shipping, or administration. The median price for antibody treatment not related to COVID-19 runs from $15,000 to $200,000 per year in the United States.
Regeneron’s Dr. Lipsich says that the company has not yet set a price for its antibody cocktail. The government paid $450 million for its 300,000 doses, but that price includes the costs of research, manufacturing, and distribution, so is not a useful indicator of the eventual per-dose price. “We’re not in a position to talk about how it will be priced yet, but we will do our best to make it affordable and accessible to all,” she says.
There are some projects underway to ensure that the drugs are made available in poorer countries. In April, the COVID-19 Therapeutics Accelerator – an initiative launched by the Bill & Melinda Gates Foundation, Wellcome, and Mastercard to speed-up the response to the global pandemic – reserved manufacturing capacity with Fujifilm Diosynth Biotechnologies in Denmark for future monoclonal antibody therapies that will supply low- and middle-income countries. In October, the initiative announced that Eli Lilly would use that reserved capacity to produce its antibody drug starting in April 2021.
In the meantime, Lilly will make some of its product manufactured in other facilities available to lower-income countries. To help keep costs down, the company’s collaborators have agreed to waive their royalties on antibodies distributed in low- and middle-income countries.
“Everyone is looking carefully at how the drugs are distributed to ensure all will get access,” said Dr. Lipsich.
A version of this article first appeared on Medscape.com.
COVID-19 in children: Weekly cases trending downward
The United States added over 171,000 new COVID-19 cases in children during the week ending Jan. 7, but that figure is lower than 3 of the previous 4 weeks, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
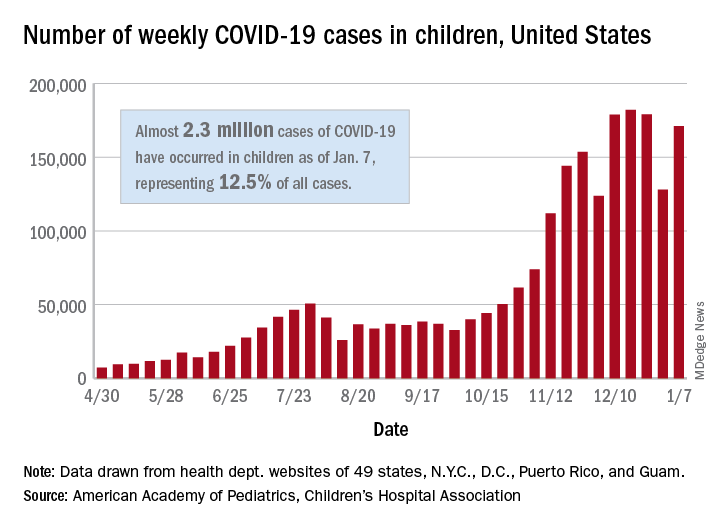
Despite an increase compared with the week ending Dec. 31, the most recent weekly total is down from the high of 182,000 cases reported for the week ending Dec. 17, based on data collected from the health department websites of 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Those jurisdictions have recorded a total of almost 2.3 million COVID-19 cases in children since the beginning of the pandemic, which amounts to 12.5% of reported cases among all ages. The 171,000 child cases for the most recent week represented 12.9% of the more than 1.3 million cases nationwide, the AAP and CHA said in their latest weekly update.
The United States now has a rate of 3,055 COVID-19 cases per 100,000 children in the population, the report shows, with 31 states above that figure and 14 states reporting rates above 4,500 per 100,000 children.
Severe illness, however, continues to be rare among children. So far, children represent 1.8% of all hospitalizations in the jurisdictions reporting such data (24 states and New York City), and just 0.9% of infected children have been hospitalized. There have been 188 deaths among children in 42 states and New York City, which makes up just 0.06% of the total for all ages in those jurisdictions, the AAP and CHA reported.
There are 13 states that have reported no coronavirus-related deaths in children, while Texas (34), New York City (21), Arizona (17), and Illinois (11) are the only jurisdictions with 10 or more. Nevada has the highest proportion of child deaths to all deaths at 0.2%, with Arizona and Nebraska next at 0.18%, according to the AAP/CHA report.
The United States added over 171,000 new COVID-19 cases in children during the week ending Jan. 7, but that figure is lower than 3 of the previous 4 weeks, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
Despite an increase compared with the week ending Dec. 31, the most recent weekly total is down from the high of 182,000 cases reported for the week ending Dec. 17, based on data collected from the health department websites of 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Those jurisdictions have recorded a total of almost 2.3 million COVID-19 cases in children since the beginning of the pandemic, which amounts to 12.5% of reported cases among all ages. The 171,000 child cases for the most recent week represented 12.9% of the more than 1.3 million cases nationwide, the AAP and CHA said in their latest weekly update.
The United States now has a rate of 3,055 COVID-19 cases per 100,000 children in the population, the report shows, with 31 states above that figure and 14 states reporting rates above 4,500 per 100,000 children.
Severe illness, however, continues to be rare among children. So far, children represent 1.8% of all hospitalizations in the jurisdictions reporting such data (24 states and New York City), and just 0.9% of infected children have been hospitalized. There have been 188 deaths among children in 42 states and New York City, which makes up just 0.06% of the total for all ages in those jurisdictions, the AAP and CHA reported.
There are 13 states that have reported no coronavirus-related deaths in children, while Texas (34), New York City (21), Arizona (17), and Illinois (11) are the only jurisdictions with 10 or more. Nevada has the highest proportion of child deaths to all deaths at 0.2%, with Arizona and Nebraska next at 0.18%, according to the AAP/CHA report.
The United States added over 171,000 new COVID-19 cases in children during the week ending Jan. 7, but that figure is lower than 3 of the previous 4 weeks, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
Despite an increase compared with the week ending Dec. 31, the most recent weekly total is down from the high of 182,000 cases reported for the week ending Dec. 17, based on data collected from the health department websites of 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Those jurisdictions have recorded a total of almost 2.3 million COVID-19 cases in children since the beginning of the pandemic, which amounts to 12.5% of reported cases among all ages. The 171,000 child cases for the most recent week represented 12.9% of the more than 1.3 million cases nationwide, the AAP and CHA said in their latest weekly update.
The United States now has a rate of 3,055 COVID-19 cases per 100,000 children in the population, the report shows, with 31 states above that figure and 14 states reporting rates above 4,500 per 100,000 children.
Severe illness, however, continues to be rare among children. So far, children represent 1.8% of all hospitalizations in the jurisdictions reporting such data (24 states and New York City), and just 0.9% of infected children have been hospitalized. There have been 188 deaths among children in 42 states and New York City, which makes up just 0.06% of the total for all ages in those jurisdictions, the AAP and CHA reported.
There are 13 states that have reported no coronavirus-related deaths in children, while Texas (34), New York City (21), Arizona (17), and Illinois (11) are the only jurisdictions with 10 or more. Nevada has the highest proportion of child deaths to all deaths at 0.2%, with Arizona and Nebraska next at 0.18%, according to the AAP/CHA report.
Eosinophilia-guided treatment cuts corticosteroid exposure in COPD exacerbations
Background: Corticosteroids in the setting of an acute exacerbation of improve COPD symptoms but do not affect the decline in lung function, rate of repeat exacerbations after a month, or mortality. There is concern regarding the cumulative adverse effects over time. Limited prior research suggests that a patient’s blood eosinophil count may be useful for determining the necessity of steroids for treatment of exacerbation.
Study design: Randomized, controlled, open-label trial.
Setting: Respiratory departments of three university hospitals in Denmark.
Synopsis: A total of 318 patients admitted for COPD exacerbation were randomized to standard or eosinophilia-guided therapy. On day 1, all patients received 80 mg of IV methylprednisolone. The standard-therapy group then received 37.5 mg of oral prednisolone for 4 more days. In contrast, the eosinophilia-guided group received prednisolone only if their blood eosinophil count was 300 cells/mcL or greater.
The primary outcome of days alive and out of the hospital within 14 days after recruitment was similar between groups (9 days; P = .34), along with the secondary outcome of treatment failure (26%; P = .90). Importantly, the cumulative steroid dose in the eosinophilia-guided group was lower than that of the control group at days 5, 30, and 90 (P less than or equal to .0002). Additionally, the control arm had worsening of baseline diabetes within 30 days and was more likely to require antibiotics for infections within 90 days.
Although not statistically significant, a trend was noted toward increased readmission for COPD exacerbations or death at 30 days in the eosinophilia-guided group (25% vs. 17% of control; P = .10). Future work will need to further study this trend.
Bottom line: Eosinophilia-guided treatment of COPD exacerbations reduced the cumulative exposure of steroid therapy, thereby decreasing side effects, although further study of safety profile is warranted.
Citation: Sivapalan P et al. Eosinophil-guided corticosteroid therapy in patients admitted to hospital with COPD exacerbation (CORTICO-COP): A multicenter, randomized, controlled, open-label, non-inferiority trial. Lancet Respir Med. 2019 Aug;7(8): 699-709.
Dr. Dupuis is a hospitalist at Maine Medical Center in Portland.
Background: Corticosteroids in the setting of an acute exacerbation of improve COPD symptoms but do not affect the decline in lung function, rate of repeat exacerbations after a month, or mortality. There is concern regarding the cumulative adverse effects over time. Limited prior research suggests that a patient’s blood eosinophil count may be useful for determining the necessity of steroids for treatment of exacerbation.
Study design: Randomized, controlled, open-label trial.
Setting: Respiratory departments of three university hospitals in Denmark.
Synopsis: A total of 318 patients admitted for COPD exacerbation were randomized to standard or eosinophilia-guided therapy. On day 1, all patients received 80 mg of IV methylprednisolone. The standard-therapy group then received 37.5 mg of oral prednisolone for 4 more days. In contrast, the eosinophilia-guided group received prednisolone only if their blood eosinophil count was 300 cells/mcL or greater.
The primary outcome of days alive and out of the hospital within 14 days after recruitment was similar between groups (9 days; P = .34), along with the secondary outcome of treatment failure (26%; P = .90). Importantly, the cumulative steroid dose in the eosinophilia-guided group was lower than that of the control group at days 5, 30, and 90 (P less than or equal to .0002). Additionally, the control arm had worsening of baseline diabetes within 30 days and was more likely to require antibiotics for infections within 90 days.
Although not statistically significant, a trend was noted toward increased readmission for COPD exacerbations or death at 30 days in the eosinophilia-guided group (25% vs. 17% of control; P = .10). Future work will need to further study this trend.
Bottom line: Eosinophilia-guided treatment of COPD exacerbations reduced the cumulative exposure of steroid therapy, thereby decreasing side effects, although further study of safety profile is warranted.
Citation: Sivapalan P et al. Eosinophil-guided corticosteroid therapy in patients admitted to hospital with COPD exacerbation (CORTICO-COP): A multicenter, randomized, controlled, open-label, non-inferiority trial. Lancet Respir Med. 2019 Aug;7(8): 699-709.
Dr. Dupuis is a hospitalist at Maine Medical Center in Portland.
Background: Corticosteroids in the setting of an acute exacerbation of improve COPD symptoms but do not affect the decline in lung function, rate of repeat exacerbations after a month, or mortality. There is concern regarding the cumulative adverse effects over time. Limited prior research suggests that a patient’s blood eosinophil count may be useful for determining the necessity of steroids for treatment of exacerbation.
Study design: Randomized, controlled, open-label trial.
Setting: Respiratory departments of three university hospitals in Denmark.
Synopsis: A total of 318 patients admitted for COPD exacerbation were randomized to standard or eosinophilia-guided therapy. On day 1, all patients received 80 mg of IV methylprednisolone. The standard-therapy group then received 37.5 mg of oral prednisolone for 4 more days. In contrast, the eosinophilia-guided group received prednisolone only if their blood eosinophil count was 300 cells/mcL or greater.
The primary outcome of days alive and out of the hospital within 14 days after recruitment was similar between groups (9 days; P = .34), along with the secondary outcome of treatment failure (26%; P = .90). Importantly, the cumulative steroid dose in the eosinophilia-guided group was lower than that of the control group at days 5, 30, and 90 (P less than or equal to .0002). Additionally, the control arm had worsening of baseline diabetes within 30 days and was more likely to require antibiotics for infections within 90 days.
Although not statistically significant, a trend was noted toward increased readmission for COPD exacerbations or death at 30 days in the eosinophilia-guided group (25% vs. 17% of control; P = .10). Future work will need to further study this trend.
Bottom line: Eosinophilia-guided treatment of COPD exacerbations reduced the cumulative exposure of steroid therapy, thereby decreasing side effects, although further study of safety profile is warranted.
Citation: Sivapalan P et al. Eosinophil-guided corticosteroid therapy in patients admitted to hospital with COPD exacerbation (CORTICO-COP): A multicenter, randomized, controlled, open-label, non-inferiority trial. Lancet Respir Med. 2019 Aug;7(8): 699-709.
Dr. Dupuis is a hospitalist at Maine Medical Center in Portland.
Updated USPSTF HBV screening recommendation may be a ‘lost opportunity’
An update of the U.S. Preventive Services Task Force recommendation for hepatitis B screening shows little change from the 2014 version, but some wonder if it should have gone farther than a risk-based approach.
The recommendation, which was published in JAMA, reinforces that screening should be conducted among adolescents and adults who are at increased risk of hepatitis B virus (HBV) infection. The USPSTF named six categories of individuals at increased risk of infection: Persons born in countries with a 2% or higher prevalence of hepatitis B, such as Asia, Africa, the Pacific Islands, and some areas of South America; unvaccinated individuals born in the United States to parents from regions with a very high prevalence of HBV (≥8%); HIV-positive individuals; those who use injected drugs; men who have sex with men; and people who live with people who have HBV or who have HBV-infected sexual partners. It also recommended that pregnant women be screened for HBV infection during their first prenatal visit.
“I view the updated recommendations as an important document because it validates the importance of HBV screening, and the Grade B recommendation supports mandated insurance coverage for the screening test,” said Joseph Lim, MD, who is a professor of medicine at Yale University and director of the Yale Viral Hepatitis Program, both in New Haven, Conn.
Still, the recommendation could have gone further. Notably absent from the USPSTF document, yet featured in recommendations from the Centers for Disease Control and Prevention and the American Association for the Study of Liver Disease, are patients who have diabetes, are on immunosuppressive therapy, or have elevated liver enzymes or liver disease. Furthermore, a single-center study found that, among physicians administering immunosuppressive therapy, a setting in which HBV reactivation is a concern, there were low rates of screening for HBV infection, and the physicians did not reliably identify high-risk patients.
“This may also be viewed as a lost opportunity. Evidence suggests that risk factor–based screening is ineffective for the identification of chronic conditions such as hepatitis B. Risk factor–based screening is difficult to implement across health systems and exacerbates the burden on community-based organizations that are motivated to address viral hepatitis. It may further exacerbate labeling, stigma, and discrimination within already marginalized communities that are deemed to be at high risk,” said Dr. Lim.
A similar view was expressed by Avegail Flores, MD, medical director of liver transplantation at the Michael E. DeBakey Veterans Affairs Medical Center and assistant professor of medicine at Baylor College of Medicine, both in Houston. “This is a good launching point, and with further evidence provided, hopefully it will also bring in a broader conversation about other persons who are at risk but not included in these criteria.” Neither Dr. Lim nor Dr. Flores were involved in the study.
She noted that resistance to universal screening may be caused by the relatively low prevalence of hepatitis B infection in the United States. However, the CDC estimates that only about 61% of people infected with HBV are aware of it. “I don’t think we have done a good job screening those who are at risk,” said Dr. Flores.
Universal screening could help, but would have a low yield. Dr. Flores suggested expansion into other at-risk groups, such as Baby Boomers. With respect to other risk groups that could be stigmatized or discriminated against, Dr. Flores recalled her medical school days when some students went directly into underserved communities to provide information and screening services. “We have to think of creative ways of how to reach out to people, not just relying on the usual physician-patient relationship.”
The issue is especially timely because the World Health Organization has declared a target to reduce new hepatitis B infections by 90% by 2030, and that will require addressing gaps in diagnosis. “That’s why these recommendations are so consequential. We are at a critical juncture in terms of global hepatitis elimination efforts. There is a time sensitive need to have multistakeholder engagement in ensuring that all aspects of the care cascade are addressed. Because of the central role of screening and diagnosis, it’s of critical importance that organizations such as USPSTF are in alignment with other organizations that have already issued clear guidance on who should be screened. It is (my) hope that further examination of the evidence-base will further support broadening USPSTF guidance to include a larger group of at-risk individuals, or ideally a universal screening strategy,” said Dr. Lim.
The recommendation’s authors received travel reimbursement for their involvement, and one author reported receiving grants and personal fees from Healthwise. Dr. Flores has no relevant financial disclosures. Dr. Lim is a member of the American Association for the Study of Liver Disease’s Viral Hepatitis Elimination Task Force.
SOURCE: U.S. Preventive Services Task Force. JAMA. 2020 Dec 15. doi: 10.1001/jama.2020.22980.
Updated Jan. 20, 2021
An update of the U.S. Preventive Services Task Force recommendation for hepatitis B screening shows little change from the 2014 version, but some wonder if it should have gone farther than a risk-based approach.
The recommendation, which was published in JAMA, reinforces that screening should be conducted among adolescents and adults who are at increased risk of hepatitis B virus (HBV) infection. The USPSTF named six categories of individuals at increased risk of infection: Persons born in countries with a 2% or higher prevalence of hepatitis B, such as Asia, Africa, the Pacific Islands, and some areas of South America; unvaccinated individuals born in the United States to parents from regions with a very high prevalence of HBV (≥8%); HIV-positive individuals; those who use injected drugs; men who have sex with men; and people who live with people who have HBV or who have HBV-infected sexual partners. It also recommended that pregnant women be screened for HBV infection during their first prenatal visit.
“I view the updated recommendations as an important document because it validates the importance of HBV screening, and the Grade B recommendation supports mandated insurance coverage for the screening test,” said Joseph Lim, MD, who is a professor of medicine at Yale University and director of the Yale Viral Hepatitis Program, both in New Haven, Conn.
Still, the recommendation could have gone further. Notably absent from the USPSTF document, yet featured in recommendations from the Centers for Disease Control and Prevention and the American Association for the Study of Liver Disease, are patients who have diabetes, are on immunosuppressive therapy, or have elevated liver enzymes or liver disease. Furthermore, a single-center study found that, among physicians administering immunosuppressive therapy, a setting in which HBV reactivation is a concern, there were low rates of screening for HBV infection, and the physicians did not reliably identify high-risk patients.
“This may also be viewed as a lost opportunity. Evidence suggests that risk factor–based screening is ineffective for the identification of chronic conditions such as hepatitis B. Risk factor–based screening is difficult to implement across health systems and exacerbates the burden on community-based organizations that are motivated to address viral hepatitis. It may further exacerbate labeling, stigma, and discrimination within already marginalized communities that are deemed to be at high risk,” said Dr. Lim.
A similar view was expressed by Avegail Flores, MD, medical director of liver transplantation at the Michael E. DeBakey Veterans Affairs Medical Center and assistant professor of medicine at Baylor College of Medicine, both in Houston. “This is a good launching point, and with further evidence provided, hopefully it will also bring in a broader conversation about other persons who are at risk but not included in these criteria.” Neither Dr. Lim nor Dr. Flores were involved in the study.
She noted that resistance to universal screening may be caused by the relatively low prevalence of hepatitis B infection in the United States. However, the CDC estimates that only about 61% of people infected with HBV are aware of it. “I don’t think we have done a good job screening those who are at risk,” said Dr. Flores.
Universal screening could help, but would have a low yield. Dr. Flores suggested expansion into other at-risk groups, such as Baby Boomers. With respect to other risk groups that could be stigmatized or discriminated against, Dr. Flores recalled her medical school days when some students went directly into underserved communities to provide information and screening services. “We have to think of creative ways of how to reach out to people, not just relying on the usual physician-patient relationship.”
The issue is especially timely because the World Health Organization has declared a target to reduce new hepatitis B infections by 90% by 2030, and that will require addressing gaps in diagnosis. “That’s why these recommendations are so consequential. We are at a critical juncture in terms of global hepatitis elimination efforts. There is a time sensitive need to have multistakeholder engagement in ensuring that all aspects of the care cascade are addressed. Because of the central role of screening and diagnosis, it’s of critical importance that organizations such as USPSTF are in alignment with other organizations that have already issued clear guidance on who should be screened. It is (my) hope that further examination of the evidence-base will further support broadening USPSTF guidance to include a larger group of at-risk individuals, or ideally a universal screening strategy,” said Dr. Lim.
The recommendation’s authors received travel reimbursement for their involvement, and one author reported receiving grants and personal fees from Healthwise. Dr. Flores has no relevant financial disclosures. Dr. Lim is a member of the American Association for the Study of Liver Disease’s Viral Hepatitis Elimination Task Force.
SOURCE: U.S. Preventive Services Task Force. JAMA. 2020 Dec 15. doi: 10.1001/jama.2020.22980.
Updated Jan. 20, 2021
An update of the U.S. Preventive Services Task Force recommendation for hepatitis B screening shows little change from the 2014 version, but some wonder if it should have gone farther than a risk-based approach.
The recommendation, which was published in JAMA, reinforces that screening should be conducted among adolescents and adults who are at increased risk of hepatitis B virus (HBV) infection. The USPSTF named six categories of individuals at increased risk of infection: Persons born in countries with a 2% or higher prevalence of hepatitis B, such as Asia, Africa, the Pacific Islands, and some areas of South America; unvaccinated individuals born in the United States to parents from regions with a very high prevalence of HBV (≥8%); HIV-positive individuals; those who use injected drugs; men who have sex with men; and people who live with people who have HBV or who have HBV-infected sexual partners. It also recommended that pregnant women be screened for HBV infection during their first prenatal visit.
“I view the updated recommendations as an important document because it validates the importance of HBV screening, and the Grade B recommendation supports mandated insurance coverage for the screening test,” said Joseph Lim, MD, who is a professor of medicine at Yale University and director of the Yale Viral Hepatitis Program, both in New Haven, Conn.
Still, the recommendation could have gone further. Notably absent from the USPSTF document, yet featured in recommendations from the Centers for Disease Control and Prevention and the American Association for the Study of Liver Disease, are patients who have diabetes, are on immunosuppressive therapy, or have elevated liver enzymes or liver disease. Furthermore, a single-center study found that, among physicians administering immunosuppressive therapy, a setting in which HBV reactivation is a concern, there were low rates of screening for HBV infection, and the physicians did not reliably identify high-risk patients.
“This may also be viewed as a lost opportunity. Evidence suggests that risk factor–based screening is ineffective for the identification of chronic conditions such as hepatitis B. Risk factor–based screening is difficult to implement across health systems and exacerbates the burden on community-based organizations that are motivated to address viral hepatitis. It may further exacerbate labeling, stigma, and discrimination within already marginalized communities that are deemed to be at high risk,” said Dr. Lim.
A similar view was expressed by Avegail Flores, MD, medical director of liver transplantation at the Michael E. DeBakey Veterans Affairs Medical Center and assistant professor of medicine at Baylor College of Medicine, both in Houston. “This is a good launching point, and with further evidence provided, hopefully it will also bring in a broader conversation about other persons who are at risk but not included in these criteria.” Neither Dr. Lim nor Dr. Flores were involved in the study.
She noted that resistance to universal screening may be caused by the relatively low prevalence of hepatitis B infection in the United States. However, the CDC estimates that only about 61% of people infected with HBV are aware of it. “I don’t think we have done a good job screening those who are at risk,” said Dr. Flores.
Universal screening could help, but would have a low yield. Dr. Flores suggested expansion into other at-risk groups, such as Baby Boomers. With respect to other risk groups that could be stigmatized or discriminated against, Dr. Flores recalled her medical school days when some students went directly into underserved communities to provide information and screening services. “We have to think of creative ways of how to reach out to people, not just relying on the usual physician-patient relationship.”
The issue is especially timely because the World Health Organization has declared a target to reduce new hepatitis B infections by 90% by 2030, and that will require addressing gaps in diagnosis. “That’s why these recommendations are so consequential. We are at a critical juncture in terms of global hepatitis elimination efforts. There is a time sensitive need to have multistakeholder engagement in ensuring that all aspects of the care cascade are addressed. Because of the central role of screening and diagnosis, it’s of critical importance that organizations such as USPSTF are in alignment with other organizations that have already issued clear guidance on who should be screened. It is (my) hope that further examination of the evidence-base will further support broadening USPSTF guidance to include a larger group of at-risk individuals, or ideally a universal screening strategy,” said Dr. Lim.
The recommendation’s authors received travel reimbursement for their involvement, and one author reported receiving grants and personal fees from Healthwise. Dr. Flores has no relevant financial disclosures. Dr. Lim is a member of the American Association for the Study of Liver Disease’s Viral Hepatitis Elimination Task Force.
SOURCE: U.S. Preventive Services Task Force. JAMA. 2020 Dec 15. doi: 10.1001/jama.2020.22980.
Updated Jan. 20, 2021
FROM JAMA
In COVID-19 patients, risk of bleeding rivals risk of thromboembolism
There is no question that COVID-19 infection increases the risks of serious thromboembolic events, including pulmonary embolism (PE), but it also increases the risk of bleeding, complicating the benefit-to-risk calculations for anticoagulation, according to a review of data at the virtual Going Back to the Heart of Cardiology meeting.
“Bleeding is a significant cause of morbidity in patients with COVID-19, and this is an important concept to appreciate,” reported Rachel P. Rosovsky, MD, director of thrombosis research, Massachusetts General Hospital, Boston.
At least five guidelines, including those issued by the American College of Cardiology, International Society on Thrombosis and Haemostasis (ISTH), and the American College of Chest Physicians, have recently addressed anticoagulation in patients infected with COVID-19, but there are “substantive differences” between them, according to Dr. Rosovsky. The reason is that they are essentially no high quality trials to guide practice. Rather, the recommendations are based primarily on retrospective studies and expert opinion.
The single most common theme from the guidelines is that anticoagulation must be individualized to balance patient-specific risks of venous thromboembolism (VTE) and bleeding, said Dr. Rosovsky, whose group published a recent comparison of these guidelines (Flaczyk A et al. Crit Care 2020;24:559).
Although there is general consensus that all hospitalized patients with COVID-19 should receive anticoagulation unless there are contraindications, there are differences in the recommended intensity of the anticoagulation for different risk groups and there is even less is less consensus on the need to anticoagulate outpatients or patients after discharge, according to Dr. Rosovsky
In her own center, the standard is a prophylactic dose of low molecular weight heparin (LMWH) in an algorithm that calls for dose adjustments for some groups such as those with renal impairment or obesity. Alternative forms of anticoagulation are recommended for patients with a history of thrombocytopenia or are at high risk for hemorrhage. Full dose LMWH is recommended in patients already on an oral anticoagulant at time of hospitalization.
“The biggest question right now is when to consider increasing from a prophylactic dose to intermediate or full dose anticoagulation in high risk patients, especially those in the ICU patients,” Dr. Rosovsky said.
Current practices are diverse, according to a recently published survey led by Dr. Rosovsky (Rosovsky RP et al. Res Pract Thromb Haemost. 2020;4:969-83). According to the survey, which had responses from more than 500 physicians in 41 countries, 30% of centers escalate from a prophylactic dose of anticoagulation to an intermediate dose when patients move to the ICU. Although not all answered this question, 25% reported that they do not escalate at ICU transfer. For 15% of respondents, dose escalation is being offered to patients with a D-dimer exceeding six-times the upper limit of normal.
These practices have developed in the absence of prospective clinical trials, which are urgently needed, according to Dr. Rosovsky. The reason that trials specific to COVID-19 are particularly important is that this infection also engenders a high risk of major bleeding.
For example, in a multicenter retrospective study of 400 hospital-admitted COVID-19 patients the rates of major bleeding was 4.8% or exactly the same as the rate of radiographically confirmed VTE. At 7.6%, the rates of VTE and major bleeding were also exactly the same for ICU patients (Al-Samkari H et al. Blood 2020;136:489-500).
“An elevated D-dimer was a marker for both VTE and major bleeding,” reported Dr. Rosovsky, who was the senior author of this study. On the basis of odds ratio (OR), the risk of VTE was increased more than six-fold (OR, 6.79) and the risk of major bleeding by more than three-fold (OR, 3.56) when the D-dimer exceeded 2,500 ng/mL.
The risk of VTE from COVID-19 infection is well documented. For example, autopsy studies have shown widespread thrombosis, including PE, in patients who have died from COVID-19 infection, according to Dr. Rosovsky.
There is also evidence of benefit from anticoagulation. In an retrospective study from China undertaken early in the pandemic, there was no overall mortality benefit at 28 days among those who did receive LMWH when compared to those who did not, but there was a 20% absolute mortality benefit (52.4% vs. 32.8%; P = .017) in those with a D-dimer six-fold ULN (Tang N et al. J Thromb Haemost 2020;18:1094-9).
These types of data support the use of anticoagulation to manage VTE risk in at least some patients, but the reported rates of VTE across institutions and across inpatient and outpatient settings have varied “dramatically,” according to Dr. Rosovsky. The balance of VTE and major bleeding is delicate. In one retrospective study, the mortality advantage for therapeutic versus prophylactic dose of LMWH did not reach statistical significance, but the rate of major bleeding was nearly doubled (3.0% vs. 1.7%) (Nadkarni GN et al J Am Coll Cardiol 2020;76:1815-26).
Because of the many variables that might affect risk of VTE and risk of major bleeding in any individual patient, the benefit-to-risk calculation of anticoagulation is “complex,” according to Dr. Rosovsky. It is for this reason she urged clinicians to consider entering patients into clinical trials designed to generate evidence-based answers.
There is large and growing body of retrospective data that have helped characterize the risk of VTE and bleeding in patients with COVID-19, but “there is no substitute for a well-controlled clinical trial,” agreed Robert A. Harrington, MD, chairman of the department of medicine, Stanford (Calif.) University.
He and the comoderator of the session in which these data were presented agreed that anticoagulation must be administered within a narrow therapeutic window that will be best defined through controlled trial designs.
“There is a significant risk of doing harm,” said Fatima Rodriguez, MD, assistant professor of cardiology at Stanford University. She seconded the critical role of trial participation when possible and the need for clinical trials to better guide treatment decisions.
The meeting was sponsored by MedscapeLive. MedscapeLive and this news organization are owned by the same parent company.
There is no question that COVID-19 infection increases the risks of serious thromboembolic events, including pulmonary embolism (PE), but it also increases the risk of bleeding, complicating the benefit-to-risk calculations for anticoagulation, according to a review of data at the virtual Going Back to the Heart of Cardiology meeting.
“Bleeding is a significant cause of morbidity in patients with COVID-19, and this is an important concept to appreciate,” reported Rachel P. Rosovsky, MD, director of thrombosis research, Massachusetts General Hospital, Boston.
At least five guidelines, including those issued by the American College of Cardiology, International Society on Thrombosis and Haemostasis (ISTH), and the American College of Chest Physicians, have recently addressed anticoagulation in patients infected with COVID-19, but there are “substantive differences” between them, according to Dr. Rosovsky. The reason is that they are essentially no high quality trials to guide practice. Rather, the recommendations are based primarily on retrospective studies and expert opinion.
The single most common theme from the guidelines is that anticoagulation must be individualized to balance patient-specific risks of venous thromboembolism (VTE) and bleeding, said Dr. Rosovsky, whose group published a recent comparison of these guidelines (Flaczyk A et al. Crit Care 2020;24:559).
Although there is general consensus that all hospitalized patients with COVID-19 should receive anticoagulation unless there are contraindications, there are differences in the recommended intensity of the anticoagulation for different risk groups and there is even less is less consensus on the need to anticoagulate outpatients or patients after discharge, according to Dr. Rosovsky
In her own center, the standard is a prophylactic dose of low molecular weight heparin (LMWH) in an algorithm that calls for dose adjustments for some groups such as those with renal impairment or obesity. Alternative forms of anticoagulation are recommended for patients with a history of thrombocytopenia or are at high risk for hemorrhage. Full dose LMWH is recommended in patients already on an oral anticoagulant at time of hospitalization.
“The biggest question right now is when to consider increasing from a prophylactic dose to intermediate or full dose anticoagulation in high risk patients, especially those in the ICU patients,” Dr. Rosovsky said.
Current practices are diverse, according to a recently published survey led by Dr. Rosovsky (Rosovsky RP et al. Res Pract Thromb Haemost. 2020;4:969-83). According to the survey, which had responses from more than 500 physicians in 41 countries, 30% of centers escalate from a prophylactic dose of anticoagulation to an intermediate dose when patients move to the ICU. Although not all answered this question, 25% reported that they do not escalate at ICU transfer. For 15% of respondents, dose escalation is being offered to patients with a D-dimer exceeding six-times the upper limit of normal.
These practices have developed in the absence of prospective clinical trials, which are urgently needed, according to Dr. Rosovsky. The reason that trials specific to COVID-19 are particularly important is that this infection also engenders a high risk of major bleeding.
For example, in a multicenter retrospective study of 400 hospital-admitted COVID-19 patients the rates of major bleeding was 4.8% or exactly the same as the rate of radiographically confirmed VTE. At 7.6%, the rates of VTE and major bleeding were also exactly the same for ICU patients (Al-Samkari H et al. Blood 2020;136:489-500).
“An elevated D-dimer was a marker for both VTE and major bleeding,” reported Dr. Rosovsky, who was the senior author of this study. On the basis of odds ratio (OR), the risk of VTE was increased more than six-fold (OR, 6.79) and the risk of major bleeding by more than three-fold (OR, 3.56) when the D-dimer exceeded 2,500 ng/mL.
The risk of VTE from COVID-19 infection is well documented. For example, autopsy studies have shown widespread thrombosis, including PE, in patients who have died from COVID-19 infection, according to Dr. Rosovsky.
There is also evidence of benefit from anticoagulation. In an retrospective study from China undertaken early in the pandemic, there was no overall mortality benefit at 28 days among those who did receive LMWH when compared to those who did not, but there was a 20% absolute mortality benefit (52.4% vs. 32.8%; P = .017) in those with a D-dimer six-fold ULN (Tang N et al. J Thromb Haemost 2020;18:1094-9).
These types of data support the use of anticoagulation to manage VTE risk in at least some patients, but the reported rates of VTE across institutions and across inpatient and outpatient settings have varied “dramatically,” according to Dr. Rosovsky. The balance of VTE and major bleeding is delicate. In one retrospective study, the mortality advantage for therapeutic versus prophylactic dose of LMWH did not reach statistical significance, but the rate of major bleeding was nearly doubled (3.0% vs. 1.7%) (Nadkarni GN et al J Am Coll Cardiol 2020;76:1815-26).
Because of the many variables that might affect risk of VTE and risk of major bleeding in any individual patient, the benefit-to-risk calculation of anticoagulation is “complex,” according to Dr. Rosovsky. It is for this reason she urged clinicians to consider entering patients into clinical trials designed to generate evidence-based answers.
There is large and growing body of retrospective data that have helped characterize the risk of VTE and bleeding in patients with COVID-19, but “there is no substitute for a well-controlled clinical trial,” agreed Robert A. Harrington, MD, chairman of the department of medicine, Stanford (Calif.) University.
He and the comoderator of the session in which these data were presented agreed that anticoagulation must be administered within a narrow therapeutic window that will be best defined through controlled trial designs.
“There is a significant risk of doing harm,” said Fatima Rodriguez, MD, assistant professor of cardiology at Stanford University. She seconded the critical role of trial participation when possible and the need for clinical trials to better guide treatment decisions.
The meeting was sponsored by MedscapeLive. MedscapeLive and this news organization are owned by the same parent company.
There is no question that COVID-19 infection increases the risks of serious thromboembolic events, including pulmonary embolism (PE), but it also increases the risk of bleeding, complicating the benefit-to-risk calculations for anticoagulation, according to a review of data at the virtual Going Back to the Heart of Cardiology meeting.
“Bleeding is a significant cause of morbidity in patients with COVID-19, and this is an important concept to appreciate,” reported Rachel P. Rosovsky, MD, director of thrombosis research, Massachusetts General Hospital, Boston.
At least five guidelines, including those issued by the American College of Cardiology, International Society on Thrombosis and Haemostasis (ISTH), and the American College of Chest Physicians, have recently addressed anticoagulation in patients infected with COVID-19, but there are “substantive differences” between them, according to Dr. Rosovsky. The reason is that they are essentially no high quality trials to guide practice. Rather, the recommendations are based primarily on retrospective studies and expert opinion.
The single most common theme from the guidelines is that anticoagulation must be individualized to balance patient-specific risks of venous thromboembolism (VTE) and bleeding, said Dr. Rosovsky, whose group published a recent comparison of these guidelines (Flaczyk A et al. Crit Care 2020;24:559).
Although there is general consensus that all hospitalized patients with COVID-19 should receive anticoagulation unless there are contraindications, there are differences in the recommended intensity of the anticoagulation for different risk groups and there is even less is less consensus on the need to anticoagulate outpatients or patients after discharge, according to Dr. Rosovsky
In her own center, the standard is a prophylactic dose of low molecular weight heparin (LMWH) in an algorithm that calls for dose adjustments for some groups such as those with renal impairment or obesity. Alternative forms of anticoagulation are recommended for patients with a history of thrombocytopenia or are at high risk for hemorrhage. Full dose LMWH is recommended in patients already on an oral anticoagulant at time of hospitalization.
“The biggest question right now is when to consider increasing from a prophylactic dose to intermediate or full dose anticoagulation in high risk patients, especially those in the ICU patients,” Dr. Rosovsky said.
Current practices are diverse, according to a recently published survey led by Dr. Rosovsky (Rosovsky RP et al. Res Pract Thromb Haemost. 2020;4:969-83). According to the survey, which had responses from more than 500 physicians in 41 countries, 30% of centers escalate from a prophylactic dose of anticoagulation to an intermediate dose when patients move to the ICU. Although not all answered this question, 25% reported that they do not escalate at ICU transfer. For 15% of respondents, dose escalation is being offered to patients with a D-dimer exceeding six-times the upper limit of normal.
These practices have developed in the absence of prospective clinical trials, which are urgently needed, according to Dr. Rosovsky. The reason that trials specific to COVID-19 are particularly important is that this infection also engenders a high risk of major bleeding.
For example, in a multicenter retrospective study of 400 hospital-admitted COVID-19 patients the rates of major bleeding was 4.8% or exactly the same as the rate of radiographically confirmed VTE. At 7.6%, the rates of VTE and major bleeding were also exactly the same for ICU patients (Al-Samkari H et al. Blood 2020;136:489-500).
“An elevated D-dimer was a marker for both VTE and major bleeding,” reported Dr. Rosovsky, who was the senior author of this study. On the basis of odds ratio (OR), the risk of VTE was increased more than six-fold (OR, 6.79) and the risk of major bleeding by more than three-fold (OR, 3.56) when the D-dimer exceeded 2,500 ng/mL.
The risk of VTE from COVID-19 infection is well documented. For example, autopsy studies have shown widespread thrombosis, including PE, in patients who have died from COVID-19 infection, according to Dr. Rosovsky.
There is also evidence of benefit from anticoagulation. In an retrospective study from China undertaken early in the pandemic, there was no overall mortality benefit at 28 days among those who did receive LMWH when compared to those who did not, but there was a 20% absolute mortality benefit (52.4% vs. 32.8%; P = .017) in those with a D-dimer six-fold ULN (Tang N et al. J Thromb Haemost 2020;18:1094-9).
These types of data support the use of anticoagulation to manage VTE risk in at least some patients, but the reported rates of VTE across institutions and across inpatient and outpatient settings have varied “dramatically,” according to Dr. Rosovsky. The balance of VTE and major bleeding is delicate. In one retrospective study, the mortality advantage for therapeutic versus prophylactic dose of LMWH did not reach statistical significance, but the rate of major bleeding was nearly doubled (3.0% vs. 1.7%) (Nadkarni GN et al J Am Coll Cardiol 2020;76:1815-26).
Because of the many variables that might affect risk of VTE and risk of major bleeding in any individual patient, the benefit-to-risk calculation of anticoagulation is “complex,” according to Dr. Rosovsky. It is for this reason she urged clinicians to consider entering patients into clinical trials designed to generate evidence-based answers.
There is large and growing body of retrospective data that have helped characterize the risk of VTE and bleeding in patients with COVID-19, but “there is no substitute for a well-controlled clinical trial,” agreed Robert A. Harrington, MD, chairman of the department of medicine, Stanford (Calif.) University.
He and the comoderator of the session in which these data were presented agreed that anticoagulation must be administered within a narrow therapeutic window that will be best defined through controlled trial designs.
“There is a significant risk of doing harm,” said Fatima Rodriguez, MD, assistant professor of cardiology at Stanford University. She seconded the critical role of trial participation when possible and the need for clinical trials to better guide treatment decisions.
The meeting was sponsored by MedscapeLive. MedscapeLive and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM THE GOING BACK TO THE HEART OF CARDIOLOGY MEETING
Cloth masks provide inferior protection vs. medical masks, suggests evidence review
according to an evidence review published Jan. 11 in Annals of Family Medicine.
Nevertheless, cloth masks may provide some degree of protection, filtration studies indicate. If clinicians use cloth masks, they should take into account the fit, material, and number of layers, the review authors wrote.
And if cloth masks are used as a last resort, such as during shortages of personal protective equipment (PPE), additional measures may help, such as pairing cloth masks with plastic face shields.
“We recommend frequent cloth mask changes to reduce the risk of moisture retention and washing according to hospital laundry standards to decrease the risk of ineffective cleaning,” review author Ariel Kiyomi Daoud, a researcher at the University of Colorado at Denver, Aurora, and colleagues wrote.
The investigators identified and analyzed nine studies related to cloth masks’ ability to prevent respiratory viral infections among health care clinicians. The studies generally were not specific to SARS-CoV-2. They focused on four nonrandomized trials, three laboratory efficacy studies, one single-case experiment, and one randomized controlled trial.
Filtration and fit
“Seven publications addressed the filtration efficacy of commercial cloth masks or materials used to create homemade masks ... in a laboratory setting,” the researchers wrote. These studies found that cloth materials prevent some level of penetration, but generally have “lesser filtration efficiency and greater variability than medical masks” do.
One study found that the materials with the greatest filtration efficacy – vacuum bags and tea towels – had low airflow, which limits their use.
Two studies found that additional layers may increase the viral filtration efficacy of cloth masks.
Several studies that assessed mask fit and airflow found that cloth masks “have worse fit and a greater level of particle leakage, compared to medical masks,” the authors reported. Most studies did not examine cloth masks’ ability to protect wearers from respiratory droplets or contact, which the World Health Organization consider the primary means of SARS-CoV-2 spread, with aerosols playing a smaller role. “Thus, we must interpret these results with caution in the context of COVID-19,” the authors wrote. “For a primary care clinician without access to medical masks, our qualitative synthesis of the literature suggests that it is better to wear a cloth mask than no mask,” as long as other protective measures are considered along with cloth mask use.
Generally consistent guidance
Agencies and researchers have shared similar recommendations about the use of cloth masks in health care settings.
“Health care workers are at the frontline and they need to be protected,” said Abrar Ahmad Chughtai, MBBS, MPH, PhD, an epidemiologist at University of New South Wales, Sydney, in an interview. “Many studies show that respirators are more effective, compared to medical masks, and medical masks are more effective, compared to cloth masks. So ideally, all frontline health care workers should use respirators. If respirators are not available, then medical masks should be used. Cloth masks are not as effective as medical masks and ideally should not be used in health care settings.”
Dr. Chughtai has written about cloth masks for protection against SARS-CoV-2 and was an investigator for a 2015 randomized trial that compared medical masks and cloth masks in health care workers.
In that trial, which was considered in the review, greater rates of influenza-like illness occurred in the cloth mask arm, compared with the medical mask arm.
“Studies show that three or more layers of cloth may reduce the spread of droplets and aerosols from the wearers,” Dr. Chughtai said. “So, cloth masks may be used in community settings to prevent spread of infections from the sick, particularly asymptomatic, people.”
In addition, cloth masks “may be used by health care workers as a last resort, if no other option is available,” he said. In that case, they should have at least three layers, fit to the face, and be washed regularly.
Not considered PPE
According to routine infection prevention and control recommendations for health care personnel from the Centers for Disease Control and Prevention, face masks – often referred to as surgical masks or procedure masks – should be worn by workers “at all times while they are in the healthcare facility, including in break rooms or other spaces where they might encounter coworkers.”
Unlike cloth masks, face masks offer “protection for the wearer against exposure to splashes and sprays of infectious material from others,” as well as source control, the agency says. Health care personnel “should remove their respirator or face mask, perform hand hygiene, and put on their cloth mask when leaving the facility at the end of their shift,” according to the CDC.
“Cloth masks are NOT PPE and should not be worn for the care of patients with suspected or confirmed COVID-19 or other situations where use of a respirator or face mask is recommended,” the agency notes.
When respirators or face masks are unavailable, health care personnel “might use cloth masks as a last resort for care of patients with suspected or confirmed diagnosis for which face mask or respirator use is normally recommended,” according to CDC guidance.
In that scenario, cloth masks “should ideally be used in combination with a face shield that covers the entire front (that extends to the chin or below) and sides of the face,” the CDC says.
Limited data for comparisons
A Dec. 29, 2020, update in Annals of Internal Medicine about masks for prevention of respiratory virus infections highlighted two recent studies in the United States that reported on mask use in health care settings. A study of more than 16,000 health care workers and first responders found that those who used an N95 or surgical mask all of the time were less likely to have SARS-CoV-2 antibodies, compared with workers who did not wear masks all the time. The adjusted odds ratio with consistent N95 use was 0.83, and the aOR with consistent surgical mask use was 0.86.
In the second study, which included more than 20,000 asymptomatic health care workers, risk for infection was reduced with any mask use versus no mask use (OR, 0.58). An N95 mask was associated with decreased risk versus a surgical mask (OR, 0.76). The studies had methodological limitations, however, and “evidence for various comparisons about mask use in health care settings and risk for SARS-CoV-2 remains insufficient,” the authors of the update wrote.
The Annals of Family Medicine review authors had no relevant disclosures. Dr. Chughtai has tested filtration of 3M masks and worked with CleanSpace Technology to research fit testing of respirators, and the 2015 randomized trial was funded by an Australian Research Council Linkage Grant with 3M as a partner on the grant. The Dec. 29, 2020, update was of a review that originally was supported by grants from the Agency for Healthcare Research Quality.
SOURCE: Daoud AK et al. Ann Fam Med. 2020 Jan 11. doi: 10.1370/afm.2640.
according to an evidence review published Jan. 11 in Annals of Family Medicine.
Nevertheless, cloth masks may provide some degree of protection, filtration studies indicate. If clinicians use cloth masks, they should take into account the fit, material, and number of layers, the review authors wrote.
And if cloth masks are used as a last resort, such as during shortages of personal protective equipment (PPE), additional measures may help, such as pairing cloth masks with plastic face shields.
“We recommend frequent cloth mask changes to reduce the risk of moisture retention and washing according to hospital laundry standards to decrease the risk of ineffective cleaning,” review author Ariel Kiyomi Daoud, a researcher at the University of Colorado at Denver, Aurora, and colleagues wrote.
The investigators identified and analyzed nine studies related to cloth masks’ ability to prevent respiratory viral infections among health care clinicians. The studies generally were not specific to SARS-CoV-2. They focused on four nonrandomized trials, three laboratory efficacy studies, one single-case experiment, and one randomized controlled trial.
Filtration and fit
“Seven publications addressed the filtration efficacy of commercial cloth masks or materials used to create homemade masks ... in a laboratory setting,” the researchers wrote. These studies found that cloth materials prevent some level of penetration, but generally have “lesser filtration efficiency and greater variability than medical masks” do.
One study found that the materials with the greatest filtration efficacy – vacuum bags and tea towels – had low airflow, which limits their use.
Two studies found that additional layers may increase the viral filtration efficacy of cloth masks.
Several studies that assessed mask fit and airflow found that cloth masks “have worse fit and a greater level of particle leakage, compared to medical masks,” the authors reported. Most studies did not examine cloth masks’ ability to protect wearers from respiratory droplets or contact, which the World Health Organization consider the primary means of SARS-CoV-2 spread, with aerosols playing a smaller role. “Thus, we must interpret these results with caution in the context of COVID-19,” the authors wrote. “For a primary care clinician without access to medical masks, our qualitative synthesis of the literature suggests that it is better to wear a cloth mask than no mask,” as long as other protective measures are considered along with cloth mask use.
Generally consistent guidance
Agencies and researchers have shared similar recommendations about the use of cloth masks in health care settings.
“Health care workers are at the frontline and they need to be protected,” said Abrar Ahmad Chughtai, MBBS, MPH, PhD, an epidemiologist at University of New South Wales, Sydney, in an interview. “Many studies show that respirators are more effective, compared to medical masks, and medical masks are more effective, compared to cloth masks. So ideally, all frontline health care workers should use respirators. If respirators are not available, then medical masks should be used. Cloth masks are not as effective as medical masks and ideally should not be used in health care settings.”
Dr. Chughtai has written about cloth masks for protection against SARS-CoV-2 and was an investigator for a 2015 randomized trial that compared medical masks and cloth masks in health care workers.
In that trial, which was considered in the review, greater rates of influenza-like illness occurred in the cloth mask arm, compared with the medical mask arm.
“Studies show that three or more layers of cloth may reduce the spread of droplets and aerosols from the wearers,” Dr. Chughtai said. “So, cloth masks may be used in community settings to prevent spread of infections from the sick, particularly asymptomatic, people.”
In addition, cloth masks “may be used by health care workers as a last resort, if no other option is available,” he said. In that case, they should have at least three layers, fit to the face, and be washed regularly.
Not considered PPE
According to routine infection prevention and control recommendations for health care personnel from the Centers for Disease Control and Prevention, face masks – often referred to as surgical masks or procedure masks – should be worn by workers “at all times while they are in the healthcare facility, including in break rooms or other spaces where they might encounter coworkers.”
Unlike cloth masks, face masks offer “protection for the wearer against exposure to splashes and sprays of infectious material from others,” as well as source control, the agency says. Health care personnel “should remove their respirator or face mask, perform hand hygiene, and put on their cloth mask when leaving the facility at the end of their shift,” according to the CDC.
“Cloth masks are NOT PPE and should not be worn for the care of patients with suspected or confirmed COVID-19 or other situations where use of a respirator or face mask is recommended,” the agency notes.
When respirators or face masks are unavailable, health care personnel “might use cloth masks as a last resort for care of patients with suspected or confirmed diagnosis for which face mask or respirator use is normally recommended,” according to CDC guidance.
In that scenario, cloth masks “should ideally be used in combination with a face shield that covers the entire front (that extends to the chin or below) and sides of the face,” the CDC says.
Limited data for comparisons
A Dec. 29, 2020, update in Annals of Internal Medicine about masks for prevention of respiratory virus infections highlighted two recent studies in the United States that reported on mask use in health care settings. A study of more than 16,000 health care workers and first responders found that those who used an N95 or surgical mask all of the time were less likely to have SARS-CoV-2 antibodies, compared with workers who did not wear masks all the time. The adjusted odds ratio with consistent N95 use was 0.83, and the aOR with consistent surgical mask use was 0.86.
In the second study, which included more than 20,000 asymptomatic health care workers, risk for infection was reduced with any mask use versus no mask use (OR, 0.58). An N95 mask was associated with decreased risk versus a surgical mask (OR, 0.76). The studies had methodological limitations, however, and “evidence for various comparisons about mask use in health care settings and risk for SARS-CoV-2 remains insufficient,” the authors of the update wrote.
The Annals of Family Medicine review authors had no relevant disclosures. Dr. Chughtai has tested filtration of 3M masks and worked with CleanSpace Technology to research fit testing of respirators, and the 2015 randomized trial was funded by an Australian Research Council Linkage Grant with 3M as a partner on the grant. The Dec. 29, 2020, update was of a review that originally was supported by grants from the Agency for Healthcare Research Quality.
SOURCE: Daoud AK et al. Ann Fam Med. 2020 Jan 11. doi: 10.1370/afm.2640.
according to an evidence review published Jan. 11 in Annals of Family Medicine.
Nevertheless, cloth masks may provide some degree of protection, filtration studies indicate. If clinicians use cloth masks, they should take into account the fit, material, and number of layers, the review authors wrote.
And if cloth masks are used as a last resort, such as during shortages of personal protective equipment (PPE), additional measures may help, such as pairing cloth masks with plastic face shields.
“We recommend frequent cloth mask changes to reduce the risk of moisture retention and washing according to hospital laundry standards to decrease the risk of ineffective cleaning,” review author Ariel Kiyomi Daoud, a researcher at the University of Colorado at Denver, Aurora, and colleagues wrote.
The investigators identified and analyzed nine studies related to cloth masks’ ability to prevent respiratory viral infections among health care clinicians. The studies generally were not specific to SARS-CoV-2. They focused on four nonrandomized trials, three laboratory efficacy studies, one single-case experiment, and one randomized controlled trial.
Filtration and fit
“Seven publications addressed the filtration efficacy of commercial cloth masks or materials used to create homemade masks ... in a laboratory setting,” the researchers wrote. These studies found that cloth materials prevent some level of penetration, but generally have “lesser filtration efficiency and greater variability than medical masks” do.
One study found that the materials with the greatest filtration efficacy – vacuum bags and tea towels – had low airflow, which limits their use.
Two studies found that additional layers may increase the viral filtration efficacy of cloth masks.
Several studies that assessed mask fit and airflow found that cloth masks “have worse fit and a greater level of particle leakage, compared to medical masks,” the authors reported. Most studies did not examine cloth masks’ ability to protect wearers from respiratory droplets or contact, which the World Health Organization consider the primary means of SARS-CoV-2 spread, with aerosols playing a smaller role. “Thus, we must interpret these results with caution in the context of COVID-19,” the authors wrote. “For a primary care clinician without access to medical masks, our qualitative synthesis of the literature suggests that it is better to wear a cloth mask than no mask,” as long as other protective measures are considered along with cloth mask use.
Generally consistent guidance
Agencies and researchers have shared similar recommendations about the use of cloth masks in health care settings.
“Health care workers are at the frontline and they need to be protected,” said Abrar Ahmad Chughtai, MBBS, MPH, PhD, an epidemiologist at University of New South Wales, Sydney, in an interview. “Many studies show that respirators are more effective, compared to medical masks, and medical masks are more effective, compared to cloth masks. So ideally, all frontline health care workers should use respirators. If respirators are not available, then medical masks should be used. Cloth masks are not as effective as medical masks and ideally should not be used in health care settings.”
Dr. Chughtai has written about cloth masks for protection against SARS-CoV-2 and was an investigator for a 2015 randomized trial that compared medical masks and cloth masks in health care workers.
In that trial, which was considered in the review, greater rates of influenza-like illness occurred in the cloth mask arm, compared with the medical mask arm.
“Studies show that three or more layers of cloth may reduce the spread of droplets and aerosols from the wearers,” Dr. Chughtai said. “So, cloth masks may be used in community settings to prevent spread of infections from the sick, particularly asymptomatic, people.”
In addition, cloth masks “may be used by health care workers as a last resort, if no other option is available,” he said. In that case, they should have at least three layers, fit to the face, and be washed regularly.
Not considered PPE
According to routine infection prevention and control recommendations for health care personnel from the Centers for Disease Control and Prevention, face masks – often referred to as surgical masks or procedure masks – should be worn by workers “at all times while they are in the healthcare facility, including in break rooms or other spaces where they might encounter coworkers.”
Unlike cloth masks, face masks offer “protection for the wearer against exposure to splashes and sprays of infectious material from others,” as well as source control, the agency says. Health care personnel “should remove their respirator or face mask, perform hand hygiene, and put on their cloth mask when leaving the facility at the end of their shift,” according to the CDC.
“Cloth masks are NOT PPE and should not be worn for the care of patients with suspected or confirmed COVID-19 or other situations where use of a respirator or face mask is recommended,” the agency notes.
When respirators or face masks are unavailable, health care personnel “might use cloth masks as a last resort for care of patients with suspected or confirmed diagnosis for which face mask or respirator use is normally recommended,” according to CDC guidance.
In that scenario, cloth masks “should ideally be used in combination with a face shield that covers the entire front (that extends to the chin or below) and sides of the face,” the CDC says.
Limited data for comparisons
A Dec. 29, 2020, update in Annals of Internal Medicine about masks for prevention of respiratory virus infections highlighted two recent studies in the United States that reported on mask use in health care settings. A study of more than 16,000 health care workers and first responders found that those who used an N95 or surgical mask all of the time were less likely to have SARS-CoV-2 antibodies, compared with workers who did not wear masks all the time. The adjusted odds ratio with consistent N95 use was 0.83, and the aOR with consistent surgical mask use was 0.86.
In the second study, which included more than 20,000 asymptomatic health care workers, risk for infection was reduced with any mask use versus no mask use (OR, 0.58). An N95 mask was associated with decreased risk versus a surgical mask (OR, 0.76). The studies had methodological limitations, however, and “evidence for various comparisons about mask use in health care settings and risk for SARS-CoV-2 remains insufficient,” the authors of the update wrote.
The Annals of Family Medicine review authors had no relevant disclosures. Dr. Chughtai has tested filtration of 3M masks and worked with CleanSpace Technology to research fit testing of respirators, and the 2015 randomized trial was funded by an Australian Research Council Linkage Grant with 3M as a partner on the grant. The Dec. 29, 2020, update was of a review that originally was supported by grants from the Agency for Healthcare Research Quality.
SOURCE: Daoud AK et al. Ann Fam Med. 2020 Jan 11. doi: 10.1370/afm.2640.
FROM ANNALS OF FAMILY MEDICINE
A 4-point thrombocytopenia score was found able to rule out suspected HIT
The real strength of the 4T score for heparin-induced thrombocytopenia (HIT) is its negative predictive value, according to hematologist Adam Cuker, MD, of the department of medicine at the University of Pennsylvania, Philadelphia.
The score assigns patients points based on degree of thrombocytopenia, timing of platelet count fall in relation to heparin exposure, presence of thrombosis and other sequelae, and the likelihood of other causes of thrombocytopenia.
A low score – 3 points or less – has a negative predictive value of 99.8%, “so HIT is basically ruled out; you do not need to order lab testing for HIT or manage the patient empirically for HIT,” and should look for other causes of thrombocytopenia, said Dr. Cuker, lead author of the American Society of Hematology’s most recent HIT guidelines.
Intermediate scores of 4 or 5 points, and high scores of 6-8 points, are a different story. The positive predictive value of an intermediate score is only 14%, and of a high score, 64%, so although they don’t confirm the diagnosis, “you have to take the possibility of HIT seriously.” Discontinue heparin, start a nonheparin anticoagulant, and order a HIT immunoassay. If it’s positive, order a functional assay to confirm the diagnosis, he said.
Suspicion of HIT “is perhaps the most common consult that we get on the hematology service. These are tough consults because it is a high-stakes decision.” There is about a 6% risk of thromboembolism, amputation, and death for every day treatment is delayed. “On the other hand, the nonheparin anticoagulants are expensive, and they carry about a 1% daily risk of major bleeding,” Dr. Cuker explained during his presentation at the 2020 Update in Nonneoplastic Hematology virtual conference.
ELISA immunoassay detects antiplatelet factor 4 heparin antibodies but doesn’t tell whether or not they are able to activate platelets and cause HIT. Functional tests such as the serotonin-release assay detect only those antibodies able to do so, but the assays are difficult to perform, and often require samples to be sent out to a reference lab.
ASH did not specify a particular nonheparin anticoagulant in its 2018 guidelines because “the best choice for your patient” depends on which drugs you have available, your familiarity with them, and patient factors, Dr. Cuker said at the conference sponsored by MedscapeLive.
It makes sense, for instance, to use a short-acting agent such as argatroban or bivalirudin in patients who are critically ill, at high risk of bleeding, or likely to need an urgent unplanned procedure. Fondaparinux or direct oral anticoagulants (DOACs) make sense if patients are clinically stable with good organ function and no more than average bleeding risk, because they are easier to administer and facilitate transition to the outpatient setting.
DOACs are newcomers to ASH’s guidelines. Just 81 patients had been reported in the literature when they were being drafted, but only 2 patients had recurrence or progression of thromboembolic events, and there were no major bleeds. The results compared favorably with other options.
The studies were subject to selection and reporting biases, “but, nonetheless, the panel felt the results were positive enough that DOACs ought to be listed as an option,” Dr. Cuker said.
The guidelines note that parenteral options may be the best choice for life- or limb-threatening thrombosis “because few such patients have been treated with a DOAC.” Anticoagulation must continue until platelet counts recover.
Dr. Cuker is a consultant for Synergy and has institutional research support from Alexion, Bayer, Sanofi, and other companies. MedscapeLive and this news organization are owned by the same parent company.
The real strength of the 4T score for heparin-induced thrombocytopenia (HIT) is its negative predictive value, according to hematologist Adam Cuker, MD, of the department of medicine at the University of Pennsylvania, Philadelphia.
The score assigns patients points based on degree of thrombocytopenia, timing of platelet count fall in relation to heparin exposure, presence of thrombosis and other sequelae, and the likelihood of other causes of thrombocytopenia.
A low score – 3 points or less – has a negative predictive value of 99.8%, “so HIT is basically ruled out; you do not need to order lab testing for HIT or manage the patient empirically for HIT,” and should look for other causes of thrombocytopenia, said Dr. Cuker, lead author of the American Society of Hematology’s most recent HIT guidelines.
Intermediate scores of 4 or 5 points, and high scores of 6-8 points, are a different story. The positive predictive value of an intermediate score is only 14%, and of a high score, 64%, so although they don’t confirm the diagnosis, “you have to take the possibility of HIT seriously.” Discontinue heparin, start a nonheparin anticoagulant, and order a HIT immunoassay. If it’s positive, order a functional assay to confirm the diagnosis, he said.
Suspicion of HIT “is perhaps the most common consult that we get on the hematology service. These are tough consults because it is a high-stakes decision.” There is about a 6% risk of thromboembolism, amputation, and death for every day treatment is delayed. “On the other hand, the nonheparin anticoagulants are expensive, and they carry about a 1% daily risk of major bleeding,” Dr. Cuker explained during his presentation at the 2020 Update in Nonneoplastic Hematology virtual conference.
ELISA immunoassay detects antiplatelet factor 4 heparin antibodies but doesn’t tell whether or not they are able to activate platelets and cause HIT. Functional tests such as the serotonin-release assay detect only those antibodies able to do so, but the assays are difficult to perform, and often require samples to be sent out to a reference lab.
ASH did not specify a particular nonheparin anticoagulant in its 2018 guidelines because “the best choice for your patient” depends on which drugs you have available, your familiarity with them, and patient factors, Dr. Cuker said at the conference sponsored by MedscapeLive.
It makes sense, for instance, to use a short-acting agent such as argatroban or bivalirudin in patients who are critically ill, at high risk of bleeding, or likely to need an urgent unplanned procedure. Fondaparinux or direct oral anticoagulants (DOACs) make sense if patients are clinically stable with good organ function and no more than average bleeding risk, because they are easier to administer and facilitate transition to the outpatient setting.
DOACs are newcomers to ASH’s guidelines. Just 81 patients had been reported in the literature when they were being drafted, but only 2 patients had recurrence or progression of thromboembolic events, and there were no major bleeds. The results compared favorably with other options.
The studies were subject to selection and reporting biases, “but, nonetheless, the panel felt the results were positive enough that DOACs ought to be listed as an option,” Dr. Cuker said.
The guidelines note that parenteral options may be the best choice for life- or limb-threatening thrombosis “because few such patients have been treated with a DOAC.” Anticoagulation must continue until platelet counts recover.
Dr. Cuker is a consultant for Synergy and has institutional research support from Alexion, Bayer, Sanofi, and other companies. MedscapeLive and this news organization are owned by the same parent company.
The real strength of the 4T score for heparin-induced thrombocytopenia (HIT) is its negative predictive value, according to hematologist Adam Cuker, MD, of the department of medicine at the University of Pennsylvania, Philadelphia.
The score assigns patients points based on degree of thrombocytopenia, timing of platelet count fall in relation to heparin exposure, presence of thrombosis and other sequelae, and the likelihood of other causes of thrombocytopenia.
A low score – 3 points or less – has a negative predictive value of 99.8%, “so HIT is basically ruled out; you do not need to order lab testing for HIT or manage the patient empirically for HIT,” and should look for other causes of thrombocytopenia, said Dr. Cuker, lead author of the American Society of Hematology’s most recent HIT guidelines.
Intermediate scores of 4 or 5 points, and high scores of 6-8 points, are a different story. The positive predictive value of an intermediate score is only 14%, and of a high score, 64%, so although they don’t confirm the diagnosis, “you have to take the possibility of HIT seriously.” Discontinue heparin, start a nonheparin anticoagulant, and order a HIT immunoassay. If it’s positive, order a functional assay to confirm the diagnosis, he said.
Suspicion of HIT “is perhaps the most common consult that we get on the hematology service. These are tough consults because it is a high-stakes decision.” There is about a 6% risk of thromboembolism, amputation, and death for every day treatment is delayed. “On the other hand, the nonheparin anticoagulants are expensive, and they carry about a 1% daily risk of major bleeding,” Dr. Cuker explained during his presentation at the 2020 Update in Nonneoplastic Hematology virtual conference.
ELISA immunoassay detects antiplatelet factor 4 heparin antibodies but doesn’t tell whether or not they are able to activate platelets and cause HIT. Functional tests such as the serotonin-release assay detect only those antibodies able to do so, but the assays are difficult to perform, and often require samples to be sent out to a reference lab.
ASH did not specify a particular nonheparin anticoagulant in its 2018 guidelines because “the best choice for your patient” depends on which drugs you have available, your familiarity with them, and patient factors, Dr. Cuker said at the conference sponsored by MedscapeLive.
It makes sense, for instance, to use a short-acting agent such as argatroban or bivalirudin in patients who are critically ill, at high risk of bleeding, or likely to need an urgent unplanned procedure. Fondaparinux or direct oral anticoagulants (DOACs) make sense if patients are clinically stable with good organ function and no more than average bleeding risk, because they are easier to administer and facilitate transition to the outpatient setting.
DOACs are newcomers to ASH’s guidelines. Just 81 patients had been reported in the literature when they were being drafted, but only 2 patients had recurrence or progression of thromboembolic events, and there were no major bleeds. The results compared favorably with other options.
The studies were subject to selection and reporting biases, “but, nonetheless, the panel felt the results were positive enough that DOACs ought to be listed as an option,” Dr. Cuker said.
The guidelines note that parenteral options may be the best choice for life- or limb-threatening thrombosis “because few such patients have been treated with a DOAC.” Anticoagulation must continue until platelet counts recover.
Dr. Cuker is a consultant for Synergy and has institutional research support from Alexion, Bayer, Sanofi, and other companies. MedscapeLive and this news organization are owned by the same parent company.
FROM 2020 UNNH
Updated ACC decision pathway embraces new heart failure treatment strategies
A newly updated expert consensus from the American College of Cardiology for management of heart failure with reduced ejection fraction includes several new guideline-directed medical therapies among other substantial changes relative to its 2017 predecessor.

The advances in treatment of heart failure with reduced ejection fraction (HFrEF) have resulted in a substantial increase in complexity in reaching treatment goals, according to the authors of the new guidance. Structured similarly to the 2017 ACC Expert Consensus Decision Pathway, the update accommodates a series of practical tips to bring all patients on board with the newer as well as the established therapies with lifesaving potential.
The potential return from implementing these recommendations is not trivial. Relative to an ACE inhibitor and a beta-blocker alone, optimal implementation of the current guideline-directed medical therapies (GDMT) “can extend medical survival by more than 6 years,” according to Gregg C. Fonarow, MD, chief of cardiology at the University of California, Los Angeles.
A member of the writing committee for the 2021 update, Dr. Fonarow explained that the consensus pathway is more than a list of therapies and recommended doses. The detailed advice on how to overcome the barriers to GDMT is meant to close the substantial gap between current practice and unmet opportunities for inhibiting HFrEF progression.
“Optimal GDMT among HFrEF patients is distressingly low, due in part to the number and complexity of medications that now constitute GDMT,” said the chair of the writing committee, Thomas M. Maddox, MD, executive director, Healthcare Innovation Lab, BJC HealthCare/Washington University, St. Louis. Like Dr. Fonarow, Dr. Maddox emphasized that the importance of the update for the practical strategies it offers to place patients on optimal care.

In the 2017 guidance, 10 pivotal issues were tackled, ranging from advice of how to put HFrEF patients on the multiple drugs that now constitute optimal therapy to when to transition patients to hospice care. The 2021 update covers the same ground but incorporates new information that has changed the definition of optimal care.
Perhaps most importantly, sacubitril/valsartan, an angiotensin receptor neprilysin inhibitor (ARNi), and SGLT2 inhibitors represent major new additions in HFrEF GDMT. Dr. Maddox called the practical information about how these should be incorporated into HFrEF management represents one of the “major highlights” of the update.
Two algorithms outline the expert consensus recommendations of the order and the dose of the multiple drugs that now constitute the current GDMT. With the goal of explaining exactly how to place patients on all the HFrEF therapies associated with improved outcome, “I think these figures can really help us in guiding our patients to optimal medication regimens and dosages,” Dr. Maddox said. If successful, clinicians “can make a significant difference in these patients’ length and quality of life.”
Most cardiologists and others who treat HFrEF are likely aware of the major improvements in outcome documented in large trials when an ARNi and a SGLT2 inhibitor were added to previously established GDMT, but the update like the 2017 document is focused on the practical strategies of implementation, according to Larry A. Allen, MD, medical director of advanced heart failure at the University of Colorado at Denver, Aurora.
“The 2017 Expert Consensus Decision Pathway got a lot of attention because it takes a very practical approach to questions that clinicians and their patients have to tackle everyday but for which there was not always clean answers from the data,” said Dr. Allen, a member of the writing committee for both the 2017 expert consensus and the 2021 update. He noted that the earlier document was one of the most downloaded articles from the ACC’s journal in the year it appeared.
“There is excellent data on the benefits of beta-blockers, ARNi, mineralocorticoid antagonists, and SGLT2 inhibitors, but how does one decide what order to use them in?” Dr. Allen asked in outlining goals of the expert consensus.
While the new update “focuses on the newer drug classes, particularly SGLT2 inhibitors,” it traces care from first-line therapies to end-of-life management, according to Dr. Allen. This includes information on when to consider advanced therapies, such as left ventricular assist devices or transplant in order to get patients to these treatments before the opportunity for benefit is missed.
Both the 2017 version and the update offer a table to summarize triggers for referral. The complexity of individualizing care in a group of patients likely to have variable manifestations of disease and multiple comorbidities was a theme of the 2017 document that has been reprised in the 2021 update,
“Good communication and team-based care” is one of common management gaps that the update addresses, Dr. Allen said. He indicated that the checklists and algorithms in the update would help with complex decision-making and encourage the multidisciplinary care that ensures optimal management.
SOURCE: Maddox TM et al. J Am Coll Cardiol. 2021 Jan 11. doi: 10.1016/j.jacc.2020.11.022.
A newly updated expert consensus from the American College of Cardiology for management of heart failure with reduced ejection fraction includes several new guideline-directed medical therapies among other substantial changes relative to its 2017 predecessor.
The advances in treatment of heart failure with reduced ejection fraction (HFrEF) have resulted in a substantial increase in complexity in reaching treatment goals, according to the authors of the new guidance. Structured similarly to the 2017 ACC Expert Consensus Decision Pathway, the update accommodates a series of practical tips to bring all patients on board with the newer as well as the established therapies with lifesaving potential.
The potential return from implementing these recommendations is not trivial. Relative to an ACE inhibitor and a beta-blocker alone, optimal implementation of the current guideline-directed medical therapies (GDMT) “can extend medical survival by more than 6 years,” according to Gregg C. Fonarow, MD, chief of cardiology at the University of California, Los Angeles.
A member of the writing committee for the 2021 update, Dr. Fonarow explained that the consensus pathway is more than a list of therapies and recommended doses. The detailed advice on how to overcome the barriers to GDMT is meant to close the substantial gap between current practice and unmet opportunities for inhibiting HFrEF progression.
“Optimal GDMT among HFrEF patients is distressingly low, due in part to the number and complexity of medications that now constitute GDMT,” said the chair of the writing committee, Thomas M. Maddox, MD, executive director, Healthcare Innovation Lab, BJC HealthCare/Washington University, St. Louis. Like Dr. Fonarow, Dr. Maddox emphasized that the importance of the update for the practical strategies it offers to place patients on optimal care.
In the 2017 guidance, 10 pivotal issues were tackled, ranging from advice of how to put HFrEF patients on the multiple drugs that now constitute optimal therapy to when to transition patients to hospice care. The 2021 update covers the same ground but incorporates new information that has changed the definition of optimal care.
Perhaps most importantly, sacubitril/valsartan, an angiotensin receptor neprilysin inhibitor (ARNi), and SGLT2 inhibitors represent major new additions in HFrEF GDMT. Dr. Maddox called the practical information about how these should be incorporated into HFrEF management represents one of the “major highlights” of the update.
Two algorithms outline the expert consensus recommendations of the order and the dose of the multiple drugs that now constitute the current GDMT. With the goal of explaining exactly how to place patients on all the HFrEF therapies associated with improved outcome, “I think these figures can really help us in guiding our patients to optimal medication regimens and dosages,” Dr. Maddox said. If successful, clinicians “can make a significant difference in these patients’ length and quality of life.”
Most cardiologists and others who treat HFrEF are likely aware of the major improvements in outcome documented in large trials when an ARNi and a SGLT2 inhibitor were added to previously established GDMT, but the update like the 2017 document is focused on the practical strategies of implementation, according to Larry A. Allen, MD, medical director of advanced heart failure at the University of Colorado at Denver, Aurora.
“The 2017 Expert Consensus Decision Pathway got a lot of attention because it takes a very practical approach to questions that clinicians and their patients have to tackle everyday but for which there was not always clean answers from the data,” said Dr. Allen, a member of the writing committee for both the 2017 expert consensus and the 2021 update. He noted that the earlier document was one of the most downloaded articles from the ACC’s journal in the year it appeared.
“There is excellent data on the benefits of beta-blockers, ARNi, mineralocorticoid antagonists, and SGLT2 inhibitors, but how does one decide what order to use them in?” Dr. Allen asked in outlining goals of the expert consensus.
While the new update “focuses on the newer drug classes, particularly SGLT2 inhibitors,” it traces care from first-line therapies to end-of-life management, according to Dr. Allen. This includes information on when to consider advanced therapies, such as left ventricular assist devices or transplant in order to get patients to these treatments before the opportunity for benefit is missed.
Both the 2017 version and the update offer a table to summarize triggers for referral. The complexity of individualizing care in a group of patients likely to have variable manifestations of disease and multiple comorbidities was a theme of the 2017 document that has been reprised in the 2021 update,
“Good communication and team-based care” is one of common management gaps that the update addresses, Dr. Allen said. He indicated that the checklists and algorithms in the update would help with complex decision-making and encourage the multidisciplinary care that ensures optimal management.
SOURCE: Maddox TM et al. J Am Coll Cardiol. 2021 Jan 11. doi: 10.1016/j.jacc.2020.11.022.
A newly updated expert consensus from the American College of Cardiology for management of heart failure with reduced ejection fraction includes several new guideline-directed medical therapies among other substantial changes relative to its 2017 predecessor.
The advances in treatment of heart failure with reduced ejection fraction (HFrEF) have resulted in a substantial increase in complexity in reaching treatment goals, according to the authors of the new guidance. Structured similarly to the 2017 ACC Expert Consensus Decision Pathway, the update accommodates a series of practical tips to bring all patients on board with the newer as well as the established therapies with lifesaving potential.
The potential return from implementing these recommendations is not trivial. Relative to an ACE inhibitor and a beta-blocker alone, optimal implementation of the current guideline-directed medical therapies (GDMT) “can extend medical survival by more than 6 years,” according to Gregg C. Fonarow, MD, chief of cardiology at the University of California, Los Angeles.
A member of the writing committee for the 2021 update, Dr. Fonarow explained that the consensus pathway is more than a list of therapies and recommended doses. The detailed advice on how to overcome the barriers to GDMT is meant to close the substantial gap between current practice and unmet opportunities for inhibiting HFrEF progression.
“Optimal GDMT among HFrEF patients is distressingly low, due in part to the number and complexity of medications that now constitute GDMT,” said the chair of the writing committee, Thomas M. Maddox, MD, executive director, Healthcare Innovation Lab, BJC HealthCare/Washington University, St. Louis. Like Dr. Fonarow, Dr. Maddox emphasized that the importance of the update for the practical strategies it offers to place patients on optimal care.
In the 2017 guidance, 10 pivotal issues were tackled, ranging from advice of how to put HFrEF patients on the multiple drugs that now constitute optimal therapy to when to transition patients to hospice care. The 2021 update covers the same ground but incorporates new information that has changed the definition of optimal care.
Perhaps most importantly, sacubitril/valsartan, an angiotensin receptor neprilysin inhibitor (ARNi), and SGLT2 inhibitors represent major new additions in HFrEF GDMT. Dr. Maddox called the practical information about how these should be incorporated into HFrEF management represents one of the “major highlights” of the update.
Two algorithms outline the expert consensus recommendations of the order and the dose of the multiple drugs that now constitute the current GDMT. With the goal of explaining exactly how to place patients on all the HFrEF therapies associated with improved outcome, “I think these figures can really help us in guiding our patients to optimal medication regimens and dosages,” Dr. Maddox said. If successful, clinicians “can make a significant difference in these patients’ length and quality of life.”
Most cardiologists and others who treat HFrEF are likely aware of the major improvements in outcome documented in large trials when an ARNi and a SGLT2 inhibitor were added to previously established GDMT, but the update like the 2017 document is focused on the practical strategies of implementation, according to Larry A. Allen, MD, medical director of advanced heart failure at the University of Colorado at Denver, Aurora.
“The 2017 Expert Consensus Decision Pathway got a lot of attention because it takes a very practical approach to questions that clinicians and their patients have to tackle everyday but for which there was not always clean answers from the data,” said Dr. Allen, a member of the writing committee for both the 2017 expert consensus and the 2021 update. He noted that the earlier document was one of the most downloaded articles from the ACC’s journal in the year it appeared.
“There is excellent data on the benefits of beta-blockers, ARNi, mineralocorticoid antagonists, and SGLT2 inhibitors, but how does one decide what order to use them in?” Dr. Allen asked in outlining goals of the expert consensus.
While the new update “focuses on the newer drug classes, particularly SGLT2 inhibitors,” it traces care from first-line therapies to end-of-life management, according to Dr. Allen. This includes information on when to consider advanced therapies, such as left ventricular assist devices or transplant in order to get patients to these treatments before the opportunity for benefit is missed.
Both the 2017 version and the update offer a table to summarize triggers for referral. The complexity of individualizing care in a group of patients likely to have variable manifestations of disease and multiple comorbidities was a theme of the 2017 document that has been reprised in the 2021 update,
“Good communication and team-based care” is one of common management gaps that the update addresses, Dr. Allen said. He indicated that the checklists and algorithms in the update would help with complex decision-making and encourage the multidisciplinary care that ensures optimal management.
SOURCE: Maddox TM et al. J Am Coll Cardiol. 2021 Jan 11. doi: 10.1016/j.jacc.2020.11.022.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY