User login
Telemedicine: Tuning in to teens
Times are changing! To compete in to today’s times, doctors are faced with the challenge of seeing 30-plus patients per day, keeping the wait times down, adhering to the meaningful use guidelines – all while participating in the endless maintenance of certification activities. But like it or not, medicine has changed, and you have to keep up or you likely are going to be left behind.
Pediatricians and family physicians more than other specialties are inundated with phone calls and lengthy conversations on constipation and congestion. Most of us just take the call with a smile, and chalk it up to part of the job. But what if you could provide a service that allowed you to get paid for those lengthy conversations, offered the convenience of a consultation without the patient having to come in the office – without the risk of your giving faulty advice because you haven’t actually evaluated the patient. Well, that’s what telemedicine has to offer. For a nominal monthly fee, your patients can subscribe to your “virtual” office. Whether you schedule during your office hours or set aside time before or after clinic, you now can capture a whole new clientele.

For teens, access to their doctors through their electronic devices would provide the convenience they need. Even if the issue cannot be treated without a visit, it allows for early evaluation. Acne, skin rashes, emotional issues, menstrual issues, hair issues, weight issues – all of these can be addressed via telemedicine.
The American Academy of Pediatrics’ Section on Telehealth Care (SOTC) helps guide you on how to bill for telemedicine services. It provides newsletters, educational series, and liability information. Much of the concern with telemedicine is the inconsistency of reimbursement for the service, but things are changing, and more and more of these services are being recognized for their value in meeting the needs of the patient.
There are different products on the market to assist you in setting up your virtual office. Understanding the differences in services is important. Services such as Doctor on Demand have a team of doctors available for fee-for-consult, at approximately $40. Other services, such as myowndoctor.com, set up a virtual office for you, which allows more of a concierge type service for a nominal monthly fee – approximately the amount of a copay – to allow patients access to the telemedicine service with their own physicians. This a great option that can create a cash revenue for you and broader access to patients.
There are several services provided by insurance companies – MDLIVE (Cigna), LiveHealth Online (WellPoint), and Online Care Anywhere (BC/BS Minnesota) – where providers are reimbursed at $45-$49 per visit. What is important to know when choosing a company is to be sure that the software is HIPAA (Health Insurance Portability and Accountability Act) compliant. Currently there are more than 15 companies on the market, and many more to come.
Staying up with the times is going to be key in surviving the current changes in health care. Teens in particular are a difficult group to access, but telemedicine provides that access and the comfort in continuity of care with their own physicians.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. E-mail her at [email protected].
Times are changing! To compete in to today’s times, doctors are faced with the challenge of seeing 30-plus patients per day, keeping the wait times down, adhering to the meaningful use guidelines – all while participating in the endless maintenance of certification activities. But like it or not, medicine has changed, and you have to keep up or you likely are going to be left behind.
Pediatricians and family physicians more than other specialties are inundated with phone calls and lengthy conversations on constipation and congestion. Most of us just take the call with a smile, and chalk it up to part of the job. But what if you could provide a service that allowed you to get paid for those lengthy conversations, offered the convenience of a consultation without the patient having to come in the office – without the risk of your giving faulty advice because you haven’t actually evaluated the patient. Well, that’s what telemedicine has to offer. For a nominal monthly fee, your patients can subscribe to your “virtual” office. Whether you schedule during your office hours or set aside time before or after clinic, you now can capture a whole new clientele.
For teens, access to their doctors through their electronic devices would provide the convenience they need. Even if the issue cannot be treated without a visit, it allows for early evaluation. Acne, skin rashes, emotional issues, menstrual issues, hair issues, weight issues – all of these can be addressed via telemedicine.
The American Academy of Pediatrics’ Section on Telehealth Care (SOTC) helps guide you on how to bill for telemedicine services. It provides newsletters, educational series, and liability information. Much of the concern with telemedicine is the inconsistency of reimbursement for the service, but things are changing, and more and more of these services are being recognized for their value in meeting the needs of the patient.
There are different products on the market to assist you in setting up your virtual office. Understanding the differences in services is important. Services such as Doctor on Demand have a team of doctors available for fee-for-consult, at approximately $40. Other services, such as myowndoctor.com, set up a virtual office for you, which allows more of a concierge type service for a nominal monthly fee – approximately the amount of a copay – to allow patients access to the telemedicine service with their own physicians. This a great option that can create a cash revenue for you and broader access to patients.
There are several services provided by insurance companies – MDLIVE (Cigna), LiveHealth Online (WellPoint), and Online Care Anywhere (BC/BS Minnesota) – where providers are reimbursed at $45-$49 per visit. What is important to know when choosing a company is to be sure that the software is HIPAA (Health Insurance Portability and Accountability Act) compliant. Currently there are more than 15 companies on the market, and many more to come.
Staying up with the times is going to be key in surviving the current changes in health care. Teens in particular are a difficult group to access, but telemedicine provides that access and the comfort in continuity of care with their own physicians.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. E-mail her at [email protected].
Times are changing! To compete in to today’s times, doctors are faced with the challenge of seeing 30-plus patients per day, keeping the wait times down, adhering to the meaningful use guidelines – all while participating in the endless maintenance of certification activities. But like it or not, medicine has changed, and you have to keep up or you likely are going to be left behind.
Pediatricians and family physicians more than other specialties are inundated with phone calls and lengthy conversations on constipation and congestion. Most of us just take the call with a smile, and chalk it up to part of the job. But what if you could provide a service that allowed you to get paid for those lengthy conversations, offered the convenience of a consultation without the patient having to come in the office – without the risk of your giving faulty advice because you haven’t actually evaluated the patient. Well, that’s what telemedicine has to offer. For a nominal monthly fee, your patients can subscribe to your “virtual” office. Whether you schedule during your office hours or set aside time before or after clinic, you now can capture a whole new clientele.
For teens, access to their doctors through their electronic devices would provide the convenience they need. Even if the issue cannot be treated without a visit, it allows for early evaluation. Acne, skin rashes, emotional issues, menstrual issues, hair issues, weight issues – all of these can be addressed via telemedicine.
The American Academy of Pediatrics’ Section on Telehealth Care (SOTC) helps guide you on how to bill for telemedicine services. It provides newsletters, educational series, and liability information. Much of the concern with telemedicine is the inconsistency of reimbursement for the service, but things are changing, and more and more of these services are being recognized for their value in meeting the needs of the patient.
There are different products on the market to assist you in setting up your virtual office. Understanding the differences in services is important. Services such as Doctor on Demand have a team of doctors available for fee-for-consult, at approximately $40. Other services, such as myowndoctor.com, set up a virtual office for you, which allows more of a concierge type service for a nominal monthly fee – approximately the amount of a copay – to allow patients access to the telemedicine service with their own physicians. This a great option that can create a cash revenue for you and broader access to patients.
There are several services provided by insurance companies – MDLIVE (Cigna), LiveHealth Online (WellPoint), and Online Care Anywhere (BC/BS Minnesota) – where providers are reimbursed at $45-$49 per visit. What is important to know when choosing a company is to be sure that the software is HIPAA (Health Insurance Portability and Accountability Act) compliant. Currently there are more than 15 companies on the market, and many more to come.
Staying up with the times is going to be key in surviving the current changes in health care. Teens in particular are a difficult group to access, but telemedicine provides that access and the comfort in continuity of care with their own physicians.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. E-mail her at [email protected].

Editorial: A Wintry Mix of Patients, Redux
The unconscionable extended ED boarding of acutely ill psychiatric patients in need of inpatient care was the subject of one of the most requested recent EM editorials. Tragically, in the 2 years since “A Wintry Mix of Patients” first appeared (March 2013), little has changed.
An August 7, 2014 Washington State Supreme Court decision prohibiting the use of EDs to board acutely ill psychiatric patients may be one step in the right direction. But it offers no alternatives for actually providing the care. A week after the ruling, ACEP’s president expressed concern that EPs could be caught in the middle of conflicting federal and state mandates, and medical liability risks.
Throughout the United States this winter, admitted patients and their families waited hours to days in emergency departments for inpatient beds. Few waited longer or suffered more than those waiting for a psychiatric bed. The number of patients needing hospitalization for acute psychiatric conditions and behavioral disturbances frequently exceeds the capacity of psychiatric services to admit them and increasingly exceeds the capacity of psychiatric EDs to provide continued care until beds become available. When psychiatric patients are boarded in surrounding medical EDs that were never designed for this purpose, emergency physicians, nurses, and security officers must try to provide a safe and secure environment of care for both the displaced psychiatric patients and nearby medical and surgical patients.
In a January 22, 2013, article, Washington Post reporter Olga Khazan describes the plight of a 15-year-old girl with Asperger’s syndrome and an anxiety disorder who spent 2 days on stretchers in two EDs waiting for an inpatient bed. The article attributes the nationwide bed shortage to cutbacks after “28 states and the District [of Columbia] reduced their mental health funding by a total of $1.6 billion” between 2009 and 2012.
Similarly, in a July 2012 report, “No Room at the Inn: Trends and Consequences of Closing Public Psychiatric Hospitals,” the nonprofit Treatment Advocacy Center (TAC) points out that the total number of state psychiatric beds in this country decreased by 14% from 2005 to 2010, dropping the per-capita bed ratio to the same level it was in 1850, the year that our country began to provide more humane care by hospitalizing the most severely mentally ill patients. The TAC report also notes that, in the absence of needed psychiatric treatment and care, people in acute or chronic crises gravitate to hospital EDs, jails, prisons, or the streets, and are partly responsible for higher rates of violent crimes.
At the same time that state-supported psychiatric beds are disappearing at an alarming rate, a desperate need for more med/surg beds is leading many general hospitals to convert psychiatric beds to nonpsychiatric beds. But a lack of inpatient beds is not the only factor responsible for this crisis in care. Health insurance providers are much more selective with respect to which inpatient psychiatric services they will pay for, and often will not cover an available inpatient bed nearby. Why is there a difference between psychiatric and nonpsychiatric inpatient coverage, and why do states permit the difference? This practice adds to the misery and delays the care of all patients, as emergency psychiatrists and social workers must spend hours or days arranging for covered inpatient stays.
All inpatient care, including psychiatric care, can be expensive, but how much money does the elimination of psychiatric services really save if you add in the cost of extra prison capacity, the loss of income by family members waiting in the ED with an ill relative, or the loss of productivity by victims of violent crimes committed by nonhospitalized mentally ill patients? Psychiatrists utilizing potent modern medications have made incredible strides in treatment, but treating an illness is not the same as curing it, and patients who stop taking their medications after their prescriptions run out often end up back in the ED—sometimes repeatedly. Such episodic ED care also adds to the overall costs and, more important, hurts many people in the process.
For more than 150 years, states have assumed major responsibility for providing a safe therapeutic environment for those suffering from severe mental illness. Now is not the time to abandon this responsibility. As a nation, if we cannot recognize the seriousness of this problem and if we do nothing to fix it immediately, lack of beds is not the only lack of capacity from which we suffer.
The unconscionable extended ED boarding of acutely ill psychiatric patients in need of inpatient care was the subject of one of the most requested recent EM editorials. Tragically, in the 2 years since “A Wintry Mix of Patients” first appeared (March 2013), little has changed.
An August 7, 2014 Washington State Supreme Court decision prohibiting the use of EDs to board acutely ill psychiatric patients may be one step in the right direction. But it offers no alternatives for actually providing the care. A week after the ruling, ACEP’s president expressed concern that EPs could be caught in the middle of conflicting federal and state mandates, and medical liability risks.
Throughout the United States this winter, admitted patients and their families waited hours to days in emergency departments for inpatient beds. Few waited longer or suffered more than those waiting for a psychiatric bed. The number of patients needing hospitalization for acute psychiatric conditions and behavioral disturbances frequently exceeds the capacity of psychiatric services to admit them and increasingly exceeds the capacity of psychiatric EDs to provide continued care until beds become available. When psychiatric patients are boarded in surrounding medical EDs that were never designed for this purpose, emergency physicians, nurses, and security officers must try to provide a safe and secure environment of care for both the displaced psychiatric patients and nearby medical and surgical patients.
In a January 22, 2013, article, Washington Post reporter Olga Khazan describes the plight of a 15-year-old girl with Asperger’s syndrome and an anxiety disorder who spent 2 days on stretchers in two EDs waiting for an inpatient bed. The article attributes the nationwide bed shortage to cutbacks after “28 states and the District [of Columbia] reduced their mental health funding by a total of $1.6 billion” between 2009 and 2012.
Similarly, in a July 2012 report, “No Room at the Inn: Trends and Consequences of Closing Public Psychiatric Hospitals,” the nonprofit Treatment Advocacy Center (TAC) points out that the total number of state psychiatric beds in this country decreased by 14% from 2005 to 2010, dropping the per-capita bed ratio to the same level it was in 1850, the year that our country began to provide more humane care by hospitalizing the most severely mentally ill patients. The TAC report also notes that, in the absence of needed psychiatric treatment and care, people in acute or chronic crises gravitate to hospital EDs, jails, prisons, or the streets, and are partly responsible for higher rates of violent crimes.
At the same time that state-supported psychiatric beds are disappearing at an alarming rate, a desperate need for more med/surg beds is leading many general hospitals to convert psychiatric beds to nonpsychiatric beds. But a lack of inpatient beds is not the only factor responsible for this crisis in care. Health insurance providers are much more selective with respect to which inpatient psychiatric services they will pay for, and often will not cover an available inpatient bed nearby. Why is there a difference between psychiatric and nonpsychiatric inpatient coverage, and why do states permit the difference? This practice adds to the misery and delays the care of all patients, as emergency psychiatrists and social workers must spend hours or days arranging for covered inpatient stays.
All inpatient care, including psychiatric care, can be expensive, but how much money does the elimination of psychiatric services really save if you add in the cost of extra prison capacity, the loss of income by family members waiting in the ED with an ill relative, or the loss of productivity by victims of violent crimes committed by nonhospitalized mentally ill patients? Psychiatrists utilizing potent modern medications have made incredible strides in treatment, but treating an illness is not the same as curing it, and patients who stop taking their medications after their prescriptions run out often end up back in the ED—sometimes repeatedly. Such episodic ED care also adds to the overall costs and, more important, hurts many people in the process.
For more than 150 years, states have assumed major responsibility for providing a safe therapeutic environment for those suffering from severe mental illness. Now is not the time to abandon this responsibility. As a nation, if we cannot recognize the seriousness of this problem and if we do nothing to fix it immediately, lack of beds is not the only lack of capacity from which we suffer.
The unconscionable extended ED boarding of acutely ill psychiatric patients in need of inpatient care was the subject of one of the most requested recent EM editorials. Tragically, in the 2 years since “A Wintry Mix of Patients” first appeared (March 2013), little has changed.
An August 7, 2014 Washington State Supreme Court decision prohibiting the use of EDs to board acutely ill psychiatric patients may be one step in the right direction. But it offers no alternatives for actually providing the care. A week after the ruling, ACEP’s president expressed concern that EPs could be caught in the middle of conflicting federal and state mandates, and medical liability risks.
Throughout the United States this winter, admitted patients and their families waited hours to days in emergency departments for inpatient beds. Few waited longer or suffered more than those waiting for a psychiatric bed. The number of patients needing hospitalization for acute psychiatric conditions and behavioral disturbances frequently exceeds the capacity of psychiatric services to admit them and increasingly exceeds the capacity of psychiatric EDs to provide continued care until beds become available. When psychiatric patients are boarded in surrounding medical EDs that were never designed for this purpose, emergency physicians, nurses, and security officers must try to provide a safe and secure environment of care for both the displaced psychiatric patients and nearby medical and surgical patients.
In a January 22, 2013, article, Washington Post reporter Olga Khazan describes the plight of a 15-year-old girl with Asperger’s syndrome and an anxiety disorder who spent 2 days on stretchers in two EDs waiting for an inpatient bed. The article attributes the nationwide bed shortage to cutbacks after “28 states and the District [of Columbia] reduced their mental health funding by a total of $1.6 billion” between 2009 and 2012.
Similarly, in a July 2012 report, “No Room at the Inn: Trends and Consequences of Closing Public Psychiatric Hospitals,” the nonprofit Treatment Advocacy Center (TAC) points out that the total number of state psychiatric beds in this country decreased by 14% from 2005 to 2010, dropping the per-capita bed ratio to the same level it was in 1850, the year that our country began to provide more humane care by hospitalizing the most severely mentally ill patients. The TAC report also notes that, in the absence of needed psychiatric treatment and care, people in acute or chronic crises gravitate to hospital EDs, jails, prisons, or the streets, and are partly responsible for higher rates of violent crimes.
At the same time that state-supported psychiatric beds are disappearing at an alarming rate, a desperate need for more med/surg beds is leading many general hospitals to convert psychiatric beds to nonpsychiatric beds. But a lack of inpatient beds is not the only factor responsible for this crisis in care. Health insurance providers are much more selective with respect to which inpatient psychiatric services they will pay for, and often will not cover an available inpatient bed nearby. Why is there a difference between psychiatric and nonpsychiatric inpatient coverage, and why do states permit the difference? This practice adds to the misery and delays the care of all patients, as emergency psychiatrists and social workers must spend hours or days arranging for covered inpatient stays.
All inpatient care, including psychiatric care, can be expensive, but how much money does the elimination of psychiatric services really save if you add in the cost of extra prison capacity, the loss of income by family members waiting in the ED with an ill relative, or the loss of productivity by victims of violent crimes committed by nonhospitalized mentally ill patients? Psychiatrists utilizing potent modern medications have made incredible strides in treatment, but treating an illness is not the same as curing it, and patients who stop taking their medications after their prescriptions run out often end up back in the ED—sometimes repeatedly. Such episodic ED care also adds to the overall costs and, more important, hurts many people in the process.
For more than 150 years, states have assumed major responsibility for providing a safe therapeutic environment for those suffering from severe mental illness. Now is not the time to abandon this responsibility. As a nation, if we cannot recognize the seriousness of this problem and if we do nothing to fix it immediately, lack of beds is not the only lack of capacity from which we suffer.
Better stroke treatment moves tantalizingly within reach
Stroke is one of the most feared medical conditions, with the specter of suddenly finding oneself unable to talk, eat, walk, or live independently, according to study results.
In mid-February, results from three trials reported at the International Stroke Conference in Nashville, Tenn., changed the face of ischemic stroke treatment by proving that emergency endovascular catheterization to remove the embolus blocking cerebral blood flow produced better long-term outcomes than standard treatment with intravenous thrombolysis.

It wasn’t just that patients did better with endovascular embolectomy; it was how much they did better. In the two trials run in the United States and abroad, SWIFT PRIME and ESCAPE, the percentage of patients rated as not disabled (a modified Rankin Scale score of 0-1) when assessed after 90 days was 36% and 42% for patients treated with endovascular therapy in the two studies, compared with 17% and 19% in the two control arms. Embolectomy boosted the fraction of patients having the best stroke outcomes more than twofold, a breathtaking leap in efficacy.
Dr. Jeffrey L. Saver from UCLA, lead investigator for SWIFT PRIME, called it a “once-in-a-field” result, meaning that never again will stroke clinicians see this degree of incremental improvement by adding a new intervention.
The frustrating irony is how challenging delivery of this disease-altering treatment will be on a national scale. One problem is that it didn’t result from a single change in treatment, but from a careful mix of new diagnostic techniques with sophisticated CT imaging, new systems for expediting diagnosis, triage, transport, and treatment, in combination with new technology in the form of emboli-retrieving stents.

Stroke management specialists see a daunting series of issues to tackle as they attempt to roll out emergency endovascular interventions on a routine scale throughout much of the United States. Many more centers must open, modeled on the ones that succeeded in the trials. The centers need to be rationally positioned so they are close to patients but also give each center enough case volume to foster high interventional-skill levels. Staffing must be found for fast-moving stroke response teams that can make the diagnostics and interventions available around the clock and interpret the images to select appropriate patients. Ambulance systems have to be set up that take likely stroke patients to the centers that will best meet their treatment needs.
The stroke and public health communities will need to invest a lot of time, money, and leadership to make this happen, but it’s a clear mandate, given the promise endovascular treatment now holds to blunt the impact of one of medicine’s most feared maladies.
On Twitter @mitchelzoler
Stroke is one of the most feared medical conditions, with the specter of suddenly finding oneself unable to talk, eat, walk, or live independently, according to study results.
In mid-February, results from three trials reported at the International Stroke Conference in Nashville, Tenn., changed the face of ischemic stroke treatment by proving that emergency endovascular catheterization to remove the embolus blocking cerebral blood flow produced better long-term outcomes than standard treatment with intravenous thrombolysis.
It wasn’t just that patients did better with endovascular embolectomy; it was how much they did better. In the two trials run in the United States and abroad, SWIFT PRIME and ESCAPE, the percentage of patients rated as not disabled (a modified Rankin Scale score of 0-1) when assessed after 90 days was 36% and 42% for patients treated with endovascular therapy in the two studies, compared with 17% and 19% in the two control arms. Embolectomy boosted the fraction of patients having the best stroke outcomes more than twofold, a breathtaking leap in efficacy.
Dr. Jeffrey L. Saver from UCLA, lead investigator for SWIFT PRIME, called it a “once-in-a-field” result, meaning that never again will stroke clinicians see this degree of incremental improvement by adding a new intervention.
The frustrating irony is how challenging delivery of this disease-altering treatment will be on a national scale. One problem is that it didn’t result from a single change in treatment, but from a careful mix of new diagnostic techniques with sophisticated CT imaging, new systems for expediting diagnosis, triage, transport, and treatment, in combination with new technology in the form of emboli-retrieving stents.
Stroke management specialists see a daunting series of issues to tackle as they attempt to roll out emergency endovascular interventions on a routine scale throughout much of the United States. Many more centers must open, modeled on the ones that succeeded in the trials. The centers need to be rationally positioned so they are close to patients but also give each center enough case volume to foster high interventional-skill levels. Staffing must be found for fast-moving stroke response teams that can make the diagnostics and interventions available around the clock and interpret the images to select appropriate patients. Ambulance systems have to be set up that take likely stroke patients to the centers that will best meet their treatment needs.
The stroke and public health communities will need to invest a lot of time, money, and leadership to make this happen, but it’s a clear mandate, given the promise endovascular treatment now holds to blunt the impact of one of medicine’s most feared maladies.
On Twitter @mitchelzoler
Stroke is one of the most feared medical conditions, with the specter of suddenly finding oneself unable to talk, eat, walk, or live independently, according to study results.
In mid-February, results from three trials reported at the International Stroke Conference in Nashville, Tenn., changed the face of ischemic stroke treatment by proving that emergency endovascular catheterization to remove the embolus blocking cerebral blood flow produced better long-term outcomes than standard treatment with intravenous thrombolysis.
It wasn’t just that patients did better with endovascular embolectomy; it was how much they did better. In the two trials run in the United States and abroad, SWIFT PRIME and ESCAPE, the percentage of patients rated as not disabled (a modified Rankin Scale score of 0-1) when assessed after 90 days was 36% and 42% for patients treated with endovascular therapy in the two studies, compared with 17% and 19% in the two control arms. Embolectomy boosted the fraction of patients having the best stroke outcomes more than twofold, a breathtaking leap in efficacy.
Dr. Jeffrey L. Saver from UCLA, lead investigator for SWIFT PRIME, called it a “once-in-a-field” result, meaning that never again will stroke clinicians see this degree of incremental improvement by adding a new intervention.
The frustrating irony is how challenging delivery of this disease-altering treatment will be on a national scale. One problem is that it didn’t result from a single change in treatment, but from a careful mix of new diagnostic techniques with sophisticated CT imaging, new systems for expediting diagnosis, triage, transport, and treatment, in combination with new technology in the form of emboli-retrieving stents.
Stroke management specialists see a daunting series of issues to tackle as they attempt to roll out emergency endovascular interventions on a routine scale throughout much of the United States. Many more centers must open, modeled on the ones that succeeded in the trials. The centers need to be rationally positioned so they are close to patients but also give each center enough case volume to foster high interventional-skill levels. Staffing must be found for fast-moving stroke response teams that can make the diagnostics and interventions available around the clock and interpret the images to select appropriate patients. Ambulance systems have to be set up that take likely stroke patients to the centers that will best meet their treatment needs.
The stroke and public health communities will need to invest a lot of time, money, and leadership to make this happen, but it’s a clear mandate, given the promise endovascular treatment now holds to blunt the impact of one of medicine’s most feared maladies.
On Twitter @mitchelzoler

But how many people died? Health outcomes in perspective
Before we dispense advice about staying healthy, we should know the effect of whatever we are recommending—be it diet, supplements, chemoprevention, or screening—on all meaningful outcomes, including overall mortality, quality of life, harms, inconveniences, and cost. Even though looking at all these outcomes may seem self-evidently wise, many research studies do not do it, and health care providers do not do it enough.
How would looking at all the outcomes change our opinion of health practices?
COMPARING GRAPEFRUIT AND PEACHES
A 2013 study linked eating berries with lower rates of myocardial infarction in women,1 another found that people who ate some fruits (blackberries and grapefruit) but not others (peaches and oranges) had a lower rate of incident diabetes,2 and a third linked a healthy diet to a lower incidence of pancreatic cancer.3 However, none of these studies examined all-cause mortality rates. A fourth study found that drinking green tea was associated with a lower risk of death from pneumonia in Japanese women, but not men.4
For the sake of argument, let us put aside concern about whether observational studies can reliably inform recommendations for clinical practice5 and concede that they can. The point is that studies such as those above look at some but not all meaningful outcomes, undermining the utility of their findings. If healthy people conclude that they should eat grapefruit instead of peaches, they may miss out on benefits of peaches that the study did not examine. Eating a healthy diet remains prudent, but the study linking it to a lower rate of pancreatic cancer is no tipping point, as pancreatic cancer is just one way to die. And advocating green tea to Japanese women but not men, to avoid pneumonia, would be a questionable public health strategy. Pneumonia is the sixth leading cause of death and accounts for 3.9% of disability-adjusted life-years lost,6 but what about the first five causes, which account for 96.1%?
These and many other studies of dietary habits of people who are well fail to consider end points that healthy people care about. Suppose that drinking more coffee would prevent all deaths from pancreatic cancer but would modestly increase cardiovascular deaths—say, by 5%. On a population level, recommending more coffee would be wrong, because it would result in far more deaths. Suppose that drinking tea decreased deaths from pneumonia—we should still not advise patients to drink tea, as we do not know whether tea’s net effect is beneficial.
Some may argue that these epidemiologic studies are merely hypothesis-generating, but my colleagues and I analyzed all the nonrandomized studies published in several leading medical journals in 1 year and found that 59% made specific practice recommendations.5 Other studies may be misused in this fashion, even though the authors refrained from doing so.
CALCIUM PROTECTS BONES, BUT WHAT ABOUT THE HEART?
Narrow end points are not limited to dietary studies. Calcium supplementation with or without vitamin D has been vigorously promoted for decades7 to treat and prevent osteoporosis in pre- and postmenopausal women, and data confirm that these agents decrease the risk of fracture.8
But bone health is only one end point important to women, and long-term supplementation of a mineral or vitamin with the goal of strengthening bones may have unforeseen adverse effects.
In 2010, calcium supplementation without vitamin D was linked to higher rates of myocardial infarction (with some suggestion of increased rates of all-cause death) in pooled analyses of 15 trials.9 In 2011, a higher risk of cardiovascular events (stroke and myocardial infarction) was found in recipients of calcium with vitamin D in a reanalysis of the Women’s Health Initiative Calcium/Vitamin D Supplementation Study,10 adjusting for the widespread use of these supplements at baseline, and this was corroborated by a meta-analysis of eight other studies.10 A more recent study confirmed that supplemental calcium increases cardiovascular risk in men.11
Although the increase in cardiovascular risk seems to be modest, millions of people take calcium supplements; thus, many people may be harmed. Our exuberance for bone health suggests that, at times, a single outcome can distract.
DOES SCREENING IMPROVE SURVIVAL?
On the whole, the evidence for screening continues to focus only on certain outcomes. With the exception of the National Lung Cancer Screening Trial,12 to date, no cancer screening trial has shown an improvement in the overall survival rate.
In fact, a 2013 Cochrane review13 found that mammographic screening failed to lower the rate of death from all cancers, including breast cancer, after 10 years (relative risk [RR] 1.02, 95% confidence interval [CI] 0.95–1.10) and the rate of death from all causes after 13 years (RR 0.99, 95% CI 0.95–1.03). Although screening lowered the breast cancer mortality rate, the authors argued that we should not look at only some outcomes and concluded that “breast cancer mortality was an unreliable outcome” that was biased in favor of screening, mainly because of “differential misclassification of cause of death.”13
Black et al14 found that of 12 major cancer screening trials examining both disease-specific mortality and all-cause mortality, 5 had differences in mortality rates that went in opposite directions (eg, the rate of disease-specific mortality improved while overall survival was harmed, or vice-versa), suggesting paradoxical effects. In another 2 studies, differences in all-cause mortality exceeded gains in disease-specific mortality. Thus, in 7 (58%) of the 12 trials, inconsistencies existed between rates of disease-specific mortality and all-cause mortality, prompting doubt about the conclusions of the studies.14
For some cancers, data suggest that screening increases deaths from other causes, and these extra deaths are not included in the data on disease-specific mortality. For instance, men who are screened for prostate cancer have higher rates of death from cardiovascular disease and suicide,15 which might negate the tenuous benefits of screening in terms of deaths from prostate cancer.
Studies of screening for diseases other than cancer have also focused on only some outcomes. For example, the United States Preventive Services Task Force supports screening for abdominal aortic aneurysm once with ultrasonography in men ages 65 to 75 who have ever smoked,16 but the recommendation is based on improvements in the death rate from abdominal aortic aneurysm, not in all-cause mortality.17 This, along with a declining incidence of this disease and changes in how it is treated (with endovascular repair on the rise and open surgical repair declining), has led some to question if we should continue to screen for it.18
CHEMOPREVENTION: NO FREE LUNCH
Finasteride
In 2013, an analysis19 that looked at all of the outcomes laid to rest 10 years of debate over the Prostate Cancer Prevention Trial, which had randomized more than 18,000 healthy men over age 55 with no signs or symptoms of prostate cancer to receive finasteride or placebo, with the end point of prostate cancer incidence. The initial results, published in 2003,20 had found that the drug decreased the rate of incident prostate cancer but paradoxically increased the rate of high-grade (Gleason score ≥ 7) tumors. Whether these results were real or an artifact of ascertainment was debated, as was whether the adverse effects—decreases in sexual potency, libido, and ejaculation—were worth the 25% reduction in prostate cancer incidence.
Much of the debate ended with the 2013 publication, which showed that regardless of finasteride’s effect on prostate cancer, overall mortality curves at 18-year follow-up were absolutely indistinguishable.19 Healthy patients hoping that finasteride will help them live longer or better can be safely told that it does neither.
Statins as primary prevention
As for statin therapy as primary prevention, the best meta-analysis to date (which meticulously excluded secondary-prevention patients after analyzing individual patient-level data) found no improvement in overall mortality despite more than 240,000 patient-years of follow-up.21 Because of this, and because the harms of statin therapy are being increasingly (but still poorly) documented, widespread use of statins has been questioned.22
Proponents point to the ability of statins to reduce end points such as revascularization, stroke, and nonfatal myocardial infarction.23 But the main question facing healthy users is whether improvement in these end points translates to longer life or better quality of life. These questions remain unresolved.
Aspirin as primary prevention
Another example of the importance of considering all the outcomes is the issue of aspirin as primary prevention.
Enthusiasm for aspirin as primary prevention has been recently reinvigorated, with data showing it can prevent colorectal cancers that overexpress cyclooxygenase-2.24 But a meta-analysis of nine randomized trials of aspirin25 with more than 1,000 participants found that, although aspirin decreases the rate of nonfatal myocardial infarction (odds ratio [OR] 0.80, 95% CI 0.67–0.96), it does not significantly reduce cancer mortality (OR 0.93, 95% CI 0.84–1.03), and it increases the risk of nontrivial bleeding (OR 1.31; 95% CI 1.14–1.50). Its effects on overall mortality were not statistically significant but were possibly favorable (OR 0.94, 95% CI 0.88–1.00), so this requires further study.
After broad consideration of the risks and benefits of aspirin, the US Food and Drug Administration has issued a statement that aspirin is not recommended as primary prevention.26
WHY STUDIES LOOK ONLY AT SOME OUTCOMES
There are many reasons why researchers favor examining some outcomes over others, but there is no clear justification for ignoring overall mortality. Overall mortality should routinely be examined in large population studies of diet and supplements and in trials of medications27 and cancer screening.
With regard to large observational studies, it is hard to understand why some would not include survival analyses, unless the results would fail to support the study’s hypothesis. In fact, some studies do report overall survival results,28 but others do not. The omission of overall survival in large data-set research should raise concerns of multiple hypothesis testing and selective reporting. Eating peaches as opposed to grapefruit may not be associated with differences in rates of all-cause mortality, myocardial infarction, pneumonia, or lung cancer, but if you look at 20 different variables, chances are that one will have a P value less than .05, and an investigator might be tempted to report it as statistically significant and even meaningful.
Empirical studies support this claim. One group found that for 80% of ingredients randomly selected from a cookbook, there existed Medline-indexed articles assessing cancer risk, with 65% of studies finding nominally significant differences in the risk of some type of cancer.29
An excess of significant findings such as this argues that significance-chasing and selective reporting are common in this field and has led to calls for methodologic improvements, including routine falsification testing30 and up-front registration of observational studies.31
WHY ALL OUTCOMES MATTER
Healthy people do not care about some outcomes; they care about all outcomes. Some patients may truly have unique priorities (quality of life vs quantity of life), but others may overestimate their risk of death from some causes and underestimate their risk from others, and practitioners have the obligation to counsel them appropriately.
For instance, a patient who watches a brother pass away from pancreatic adenocarcinoma may wish to do everything possible to avoid that illness. But often, as in this case, fear may surpass risk. The patient’s risk of pancreatic cancer is no different than that in the general population: the best data show32 an odds ratio of 1.8, with a confidence interval spanning 1. As such, pancreatic cancer is still not among his five most likely causes of death.
Some patients may care about their bone mineral density or cholesterol level. But again, physicians have an obligation to direct patients’ attention to all of the outcomes that should be of interest to them.
OBJECTIONS TO INCLUDING ALL OUTCOMES
There are important objections to the argument I am presenting here.
First, including all outcomes is expensive. For studies involving retrospective analysis of existing data, looking at overall mortality would not incur additional costs, only an additional analysis. But for prospective trials to have statistical power to detect a difference in overall mortality, larger sample sizes or longer follow-up might be needed—either of which would add to the cost.
In chemoprevention trials, the rate of incident cancer has been called the gold standard end point.33 To design a thrifty chemoprevention study, investigators can either target a broad population and aim for incident malignancy, or target a restricted, high-risk population and aim for overall mortality. The latter is preferable because although it can inform the decisions of only some people, the former cannot inform any people, as was seen with difficulties in interpreting the Prostate Cancer Prevention Trial and trials showing reduced breast cancer incidence from tamoxifen, raloxifene, and exemestane.
In large cancer screening trials, the cost of powering the trial for overall mortality would be greater, and though a carefully selected, high-risk population can be enrolled, historically this has not been popular. In cancer screening, it is a mistake to contrast the costs of trials powered for overall mortality with those of lesser studies examining disease-specific death. Instead, we must consider the larger societal costs incurred by cancer screening that does not truly improve quantity or quality of life.34
The recent reversal of recommendations for prostate-specific antigen testing by the United States Preventive Services Task Force35 suggests that erroneous recommendations, practiced for decades, can cost society hundreds of billions of dollars but fail to improve meaningful outcomes.
The history of medicine is replete with examples of widely recommended practices and interventions that not only failed to improve the outcomes they claimed to improve, but at times increased the rate of all-cause mortality or carried harms that far outweighed benefits.36,37 The costs of conducting research to fully understand all outcomes are only a fraction of the costs of a practice that is widely disseminated.38
A second objection to my analysis is that there is more to life than survival, and outcomes besides overall mortality are important. This is a self-evident truth. That an intervention improves the rate of overall mortality is neither necessary nor sufficient for its recommendation. Practices may improve survival but worsen quality of life to such a degree that they should not be recommended. Conversely, practices that improve quality of life should be endorsed even if they fail to prolong life.
Thus, overall mortality and quality of life must be considered together, but the end points that are favored currently (disease-specific death, incident cancer, diabetes mellitus, myocardial infarction) do not do a good job of capturing either. Disease-specific death is not meaningful to any patient if deaths from other causes are increased so that overall mortality is unchanged. Furthermore, preventing a diagnosis of cancer or diabetes may offer some psychological comfort, but well-crafted quality-of-life instruments are best suited to capture just how great that benefit is and whether it justifies the cost of such interventions, particularly if the rate of survival is unchanged.
Preventing stroke or myocardial infarction is important, but we should be cautious of interpreting data when decreasing the rate of these morbid events does not lead to commensurate improvements in survival. Alternatively, if morbid events are truly avoided but survival analyses are underpowered, quality-of-life measurements should demonstrate the benefit. But the end points currently used capture neither survival nor quality of life in a meaningful way.
WHEN ADVISING HEALTHY PEOPLE
Looking at all outcomes is important when caring for patients who are sick, but even more so for patients who are well. We need to know an intervention has a net benefit before we recommend it to a healthy person. Overall mortality should be reported routinely in this population, particularly in settings where the cost to do so is trivial (ie, in observational studies). Designers of thrifty trials should try to include people at high risk and power the trial for definite end points, rather than being broadly inclusive and reaching disputed conclusions. Research and decision-making should look at all outcomes. Healthy people deserve no less.
- Cassidy A, Mukamal KJ, Liu L, Franz M, Eliassen AH, Rimm EB. High anthocyanin intake is associated with a reduced risk of myocardial infarction in young and middle-aged women. Circulation 2013; 127:188–196.
- Muraki I, Imamura F, Manson JE, et al. Fruit consumption and risk of type 2 diabetes: results from three prospective longitudinal cohort studies. BMJ 2013; 347:f5001.
- Arem H, Reedy J, Sampson J, et al. The Healthy Eating Index 2005 and risk for pancreatic cancer in the NIH-AARP study. J Natl Cancer Inst 2013; 105:1298–1305.
- Watanabe I, Kuriyama S, Kakizaki M, et al. Green tea and death from pneumonia in Japan: the Ohsaki cohort study. Am J Clin Nutr 2009; 90:672–679.
- Prasad V, Jorgenson J, Ioannidis JP, Cifu A. Observational studies often make clinical practice recommendations: an empirical evaluation of authors’ attitudes. J Clin Epidemiol 2013; 66:361–366.e4.
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380:2197–2223.
- Eastell R. Treatment of postmenopausal osteoporosis. N Engl J Med 1998; 338:736–746.
- Looker AC. Interaction of science, consumer practices and policy: calcium and bone health as a case study. J Nutr 2003; 133:1987S–1991S.
- Bolland MJ, Avenell A, Baron JA, et al. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ 2010; 341:c3691
- Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the Women’s Health Initiative limited access dataset and meta-analysis. BMJ 2011; 342:d2040.
- Xiao Q, Murphy RA, Houston DK, Harris TB, Chow WH, Park Y. Dietary and supplemental calcium intake and cardiovascular disease mortality: the National Institutes of Health-AARP diet and health study. JAMA Intern Med 2013; 173:639–646.
- The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365:395–409.
- Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2013 Jun 4;6:CD001877.
- Black WC, Haggstrom DA, Welch HG. All-cause mortality in randomized trials of cancer screening. J Natl Cancer Inst 2002; 94:167–173.
- Fall K, Fang F, Mucci LA, et al. Immediate risk for cardiovascular events and suicide following a prostate cancer diagnosis: prospective cohort study. PLoS Med 2009; 6:e1000197.
- Prasad V. An unmeasured harm of screening. Arch Intern Med 2012; 172:1442–1443.
- Guirguis-Blake JM, Beil TL, Senger CA, Whitlock EP. Ultrasonography screening for abdominal aortic aneurysms: a sytematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med 2014; 160:321–329.
- Harris R, Sheridan S, Kinsinger L. Time to rethink screening for abdominal aortic aneurysm? Arch Intern Med 2012; 172:1462–1463.
- Thompson IM Jr, Goodman PJ, Tangen CM, et al. Long-term survival of participants in the prostate cancer prevention trial. N Engl J Med 2013; 369:603–610.
- Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med 2003; 349:216–224.
- Ray KK, Seshasai SR, Erqou S, et al. Statins and all-cause mortality in high-risk primary prevention: a meta-analysis of 11 randomized controlled trials involving 65,229 participants. Arch Intern Med 2010; 170:1024–1031.
- Redberg RF, Katz MH. Healthy men should not take statins. JAMA 2012; 307:1491–1492.
- McEvoy JW, Blumenthal RS, Blaha MJ. Statin therapy for hyperlipidemia. JAMA 2013; 310:1184–1185.
- Chan AT, Ogino S, Fuchs CS. Aspirin and the risk of colorectal cancer in relation to the expression of COX-2. N Engl J Med 2007; 356:2131–2142.
- Seshasai SR, Wijesuriya S, Sivakumaran R, et al. Effect of aspirin on vascular and nonvascular outcomes: meta-analysis of randomized controlled trials. Arch Intern Med 2012; 172:209–216.
- US Food and Drug Administration. Use of aspirin for primary prevention of heart attack and stroke. www.fda.gov/Drugs/ResourcesForYou/Consumers/ucm390574.htm. Accessed February 5, 2015.
- Ioannidis JP. Mega-trials for blockbusters. JAMA 2013; 309:239–240.
- Dunkler D, Dehghan M, Teo KK, et al; ONTARGET Investigators. Diet and kidney disease in high-risk individuals with type 2 diabetes mellitus. JAMA Intern Med 2013; 173:1682–1692.
- Schoenfeld JD, Ioannidis JP. Is everything we eat associated with cancer? A systematic cookbook review. Am J Clin Nutr 2013; 97:127–134.
- Prasad V, Jena AB. Prespecified falsification end points: can they validate true observational associations? JAMA 2013; 309:241–242.
- Ioannidis JPA. The importance of potential studies that have not existed and registration of observational data sets. JAMA 2012; 308:575–576.
- Klein AP, Brune KA, Petersen GM, et al. Prospective risk of pancreatic cancer in familial pancreatic cancer kindreds. Cancer Res 2004; 64:2634–2638.
- William WN Jr, Papadimitrakopoulou VA. Optimizing biomarkers and endpoints in oral cancer chemoprevention trials. Cancer Prev Res (Phila) 2013; 6:375–378.
- Prasad V. Powering cancer screening for overall mortality. Ecancermedicalscience 2013 Oct 9; 7:ed27.
- US Preventive Services Task Force. Final recommendation statement. Prostate cancer: screening. http://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/prostate-cancer-screening. Accessed February 5, 2015.
- Prasad V, Cifu A, Ioannidis JP. Reversals of established medical practices: evidence to abandon ship. JAMA 2012; 307:37–38.
- Prasad V, Vandross A, Toomey C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc 2013; 88:790–798.
- Elshaug AG, Garber AM. How CER could pay for itself—insights from vertebral fracture treatments. N Engl J Med 2011; 364:1390–1393.
Before we dispense advice about staying healthy, we should know the effect of whatever we are recommending—be it diet, supplements, chemoprevention, or screening—on all meaningful outcomes, including overall mortality, quality of life, harms, inconveniences, and cost. Even though looking at all these outcomes may seem self-evidently wise, many research studies do not do it, and health care providers do not do it enough.
How would looking at all the outcomes change our opinion of health practices?
COMPARING GRAPEFRUIT AND PEACHES
A 2013 study linked eating berries with lower rates of myocardial infarction in women,1 another found that people who ate some fruits (blackberries and grapefruit) but not others (peaches and oranges) had a lower rate of incident diabetes,2 and a third linked a healthy diet to a lower incidence of pancreatic cancer.3 However, none of these studies examined all-cause mortality rates. A fourth study found that drinking green tea was associated with a lower risk of death from pneumonia in Japanese women, but not men.4
For the sake of argument, let us put aside concern about whether observational studies can reliably inform recommendations for clinical practice5 and concede that they can. The point is that studies such as those above look at some but not all meaningful outcomes, undermining the utility of their findings. If healthy people conclude that they should eat grapefruit instead of peaches, they may miss out on benefits of peaches that the study did not examine. Eating a healthy diet remains prudent, but the study linking it to a lower rate of pancreatic cancer is no tipping point, as pancreatic cancer is just one way to die. And advocating green tea to Japanese women but not men, to avoid pneumonia, would be a questionable public health strategy. Pneumonia is the sixth leading cause of death and accounts for 3.9% of disability-adjusted life-years lost,6 but what about the first five causes, which account for 96.1%?
These and many other studies of dietary habits of people who are well fail to consider end points that healthy people care about. Suppose that drinking more coffee would prevent all deaths from pancreatic cancer but would modestly increase cardiovascular deaths—say, by 5%. On a population level, recommending more coffee would be wrong, because it would result in far more deaths. Suppose that drinking tea decreased deaths from pneumonia—we should still not advise patients to drink tea, as we do not know whether tea’s net effect is beneficial.
Some may argue that these epidemiologic studies are merely hypothesis-generating, but my colleagues and I analyzed all the nonrandomized studies published in several leading medical journals in 1 year and found that 59% made specific practice recommendations.5 Other studies may be misused in this fashion, even though the authors refrained from doing so.
CALCIUM PROTECTS BONES, BUT WHAT ABOUT THE HEART?
Narrow end points are not limited to dietary studies. Calcium supplementation with or without vitamin D has been vigorously promoted for decades7 to treat and prevent osteoporosis in pre- and postmenopausal women, and data confirm that these agents decrease the risk of fracture.8
But bone health is only one end point important to women, and long-term supplementation of a mineral or vitamin with the goal of strengthening bones may have unforeseen adverse effects.
In 2010, calcium supplementation without vitamin D was linked to higher rates of myocardial infarction (with some suggestion of increased rates of all-cause death) in pooled analyses of 15 trials.9 In 2011, a higher risk of cardiovascular events (stroke and myocardial infarction) was found in recipients of calcium with vitamin D in a reanalysis of the Women’s Health Initiative Calcium/Vitamin D Supplementation Study,10 adjusting for the widespread use of these supplements at baseline, and this was corroborated by a meta-analysis of eight other studies.10 A more recent study confirmed that supplemental calcium increases cardiovascular risk in men.11
Although the increase in cardiovascular risk seems to be modest, millions of people take calcium supplements; thus, many people may be harmed. Our exuberance for bone health suggests that, at times, a single outcome can distract.
DOES SCREENING IMPROVE SURVIVAL?
On the whole, the evidence for screening continues to focus only on certain outcomes. With the exception of the National Lung Cancer Screening Trial,12 to date, no cancer screening trial has shown an improvement in the overall survival rate.
In fact, a 2013 Cochrane review13 found that mammographic screening failed to lower the rate of death from all cancers, including breast cancer, after 10 years (relative risk [RR] 1.02, 95% confidence interval [CI] 0.95–1.10) and the rate of death from all causes after 13 years (RR 0.99, 95% CI 0.95–1.03). Although screening lowered the breast cancer mortality rate, the authors argued that we should not look at only some outcomes and concluded that “breast cancer mortality was an unreliable outcome” that was biased in favor of screening, mainly because of “differential misclassification of cause of death.”13
Black et al14 found that of 12 major cancer screening trials examining both disease-specific mortality and all-cause mortality, 5 had differences in mortality rates that went in opposite directions (eg, the rate of disease-specific mortality improved while overall survival was harmed, or vice-versa), suggesting paradoxical effects. In another 2 studies, differences in all-cause mortality exceeded gains in disease-specific mortality. Thus, in 7 (58%) of the 12 trials, inconsistencies existed between rates of disease-specific mortality and all-cause mortality, prompting doubt about the conclusions of the studies.14
For some cancers, data suggest that screening increases deaths from other causes, and these extra deaths are not included in the data on disease-specific mortality. For instance, men who are screened for prostate cancer have higher rates of death from cardiovascular disease and suicide,15 which might negate the tenuous benefits of screening in terms of deaths from prostate cancer.
Studies of screening for diseases other than cancer have also focused on only some outcomes. For example, the United States Preventive Services Task Force supports screening for abdominal aortic aneurysm once with ultrasonography in men ages 65 to 75 who have ever smoked,16 but the recommendation is based on improvements in the death rate from abdominal aortic aneurysm, not in all-cause mortality.17 This, along with a declining incidence of this disease and changes in how it is treated (with endovascular repair on the rise and open surgical repair declining), has led some to question if we should continue to screen for it.18
CHEMOPREVENTION: NO FREE LUNCH
Finasteride
In 2013, an analysis19 that looked at all of the outcomes laid to rest 10 years of debate over the Prostate Cancer Prevention Trial, which had randomized more than 18,000 healthy men over age 55 with no signs or symptoms of prostate cancer to receive finasteride or placebo, with the end point of prostate cancer incidence. The initial results, published in 2003,20 had found that the drug decreased the rate of incident prostate cancer but paradoxically increased the rate of high-grade (Gleason score ≥ 7) tumors. Whether these results were real or an artifact of ascertainment was debated, as was whether the adverse effects—decreases in sexual potency, libido, and ejaculation—were worth the 25% reduction in prostate cancer incidence.
Much of the debate ended with the 2013 publication, which showed that regardless of finasteride’s effect on prostate cancer, overall mortality curves at 18-year follow-up were absolutely indistinguishable.19 Healthy patients hoping that finasteride will help them live longer or better can be safely told that it does neither.
Statins as primary prevention
As for statin therapy as primary prevention, the best meta-analysis to date (which meticulously excluded secondary-prevention patients after analyzing individual patient-level data) found no improvement in overall mortality despite more than 240,000 patient-years of follow-up.21 Because of this, and because the harms of statin therapy are being increasingly (but still poorly) documented, widespread use of statins has been questioned.22
Proponents point to the ability of statins to reduce end points such as revascularization, stroke, and nonfatal myocardial infarction.23 But the main question facing healthy users is whether improvement in these end points translates to longer life or better quality of life. These questions remain unresolved.
Aspirin as primary prevention
Another example of the importance of considering all the outcomes is the issue of aspirin as primary prevention.
Enthusiasm for aspirin as primary prevention has been recently reinvigorated, with data showing it can prevent colorectal cancers that overexpress cyclooxygenase-2.24 But a meta-analysis of nine randomized trials of aspirin25 with more than 1,000 participants found that, although aspirin decreases the rate of nonfatal myocardial infarction (odds ratio [OR] 0.80, 95% CI 0.67–0.96), it does not significantly reduce cancer mortality (OR 0.93, 95% CI 0.84–1.03), and it increases the risk of nontrivial bleeding (OR 1.31; 95% CI 1.14–1.50). Its effects on overall mortality were not statistically significant but were possibly favorable (OR 0.94, 95% CI 0.88–1.00), so this requires further study.
After broad consideration of the risks and benefits of aspirin, the US Food and Drug Administration has issued a statement that aspirin is not recommended as primary prevention.26
WHY STUDIES LOOK ONLY AT SOME OUTCOMES
There are many reasons why researchers favor examining some outcomes over others, but there is no clear justification for ignoring overall mortality. Overall mortality should routinely be examined in large population studies of diet and supplements and in trials of medications27 and cancer screening.
With regard to large observational studies, it is hard to understand why some would not include survival analyses, unless the results would fail to support the study’s hypothesis. In fact, some studies do report overall survival results,28 but others do not. The omission of overall survival in large data-set research should raise concerns of multiple hypothesis testing and selective reporting. Eating peaches as opposed to grapefruit may not be associated with differences in rates of all-cause mortality, myocardial infarction, pneumonia, or lung cancer, but if you look at 20 different variables, chances are that one will have a P value less than .05, and an investigator might be tempted to report it as statistically significant and even meaningful.
Empirical studies support this claim. One group found that for 80% of ingredients randomly selected from a cookbook, there existed Medline-indexed articles assessing cancer risk, with 65% of studies finding nominally significant differences in the risk of some type of cancer.29
An excess of significant findings such as this argues that significance-chasing and selective reporting are common in this field and has led to calls for methodologic improvements, including routine falsification testing30 and up-front registration of observational studies.31
WHY ALL OUTCOMES MATTER
Healthy people do not care about some outcomes; they care about all outcomes. Some patients may truly have unique priorities (quality of life vs quantity of life), but others may overestimate their risk of death from some causes and underestimate their risk from others, and practitioners have the obligation to counsel them appropriately.
For instance, a patient who watches a brother pass away from pancreatic adenocarcinoma may wish to do everything possible to avoid that illness. But often, as in this case, fear may surpass risk. The patient’s risk of pancreatic cancer is no different than that in the general population: the best data show32 an odds ratio of 1.8, with a confidence interval spanning 1. As such, pancreatic cancer is still not among his five most likely causes of death.
Some patients may care about their bone mineral density or cholesterol level. But again, physicians have an obligation to direct patients’ attention to all of the outcomes that should be of interest to them.
OBJECTIONS TO INCLUDING ALL OUTCOMES
There are important objections to the argument I am presenting here.
First, including all outcomes is expensive. For studies involving retrospective analysis of existing data, looking at overall mortality would not incur additional costs, only an additional analysis. But for prospective trials to have statistical power to detect a difference in overall mortality, larger sample sizes or longer follow-up might be needed—either of which would add to the cost.
In chemoprevention trials, the rate of incident cancer has been called the gold standard end point.33 To design a thrifty chemoprevention study, investigators can either target a broad population and aim for incident malignancy, or target a restricted, high-risk population and aim for overall mortality. The latter is preferable because although it can inform the decisions of only some people, the former cannot inform any people, as was seen with difficulties in interpreting the Prostate Cancer Prevention Trial and trials showing reduced breast cancer incidence from tamoxifen, raloxifene, and exemestane.
In large cancer screening trials, the cost of powering the trial for overall mortality would be greater, and though a carefully selected, high-risk population can be enrolled, historically this has not been popular. In cancer screening, it is a mistake to contrast the costs of trials powered for overall mortality with those of lesser studies examining disease-specific death. Instead, we must consider the larger societal costs incurred by cancer screening that does not truly improve quantity or quality of life.34
The recent reversal of recommendations for prostate-specific antigen testing by the United States Preventive Services Task Force35 suggests that erroneous recommendations, practiced for decades, can cost society hundreds of billions of dollars but fail to improve meaningful outcomes.
The history of medicine is replete with examples of widely recommended practices and interventions that not only failed to improve the outcomes they claimed to improve, but at times increased the rate of all-cause mortality or carried harms that far outweighed benefits.36,37 The costs of conducting research to fully understand all outcomes are only a fraction of the costs of a practice that is widely disseminated.38
A second objection to my analysis is that there is more to life than survival, and outcomes besides overall mortality are important. This is a self-evident truth. That an intervention improves the rate of overall mortality is neither necessary nor sufficient for its recommendation. Practices may improve survival but worsen quality of life to such a degree that they should not be recommended. Conversely, practices that improve quality of life should be endorsed even if they fail to prolong life.
Thus, overall mortality and quality of life must be considered together, but the end points that are favored currently (disease-specific death, incident cancer, diabetes mellitus, myocardial infarction) do not do a good job of capturing either. Disease-specific death is not meaningful to any patient if deaths from other causes are increased so that overall mortality is unchanged. Furthermore, preventing a diagnosis of cancer or diabetes may offer some psychological comfort, but well-crafted quality-of-life instruments are best suited to capture just how great that benefit is and whether it justifies the cost of such interventions, particularly if the rate of survival is unchanged.
Preventing stroke or myocardial infarction is important, but we should be cautious of interpreting data when decreasing the rate of these morbid events does not lead to commensurate improvements in survival. Alternatively, if morbid events are truly avoided but survival analyses are underpowered, quality-of-life measurements should demonstrate the benefit. But the end points currently used capture neither survival nor quality of life in a meaningful way.
WHEN ADVISING HEALTHY PEOPLE
Looking at all outcomes is important when caring for patients who are sick, but even more so for patients who are well. We need to know an intervention has a net benefit before we recommend it to a healthy person. Overall mortality should be reported routinely in this population, particularly in settings where the cost to do so is trivial (ie, in observational studies). Designers of thrifty trials should try to include people at high risk and power the trial for definite end points, rather than being broadly inclusive and reaching disputed conclusions. Research and decision-making should look at all outcomes. Healthy people deserve no less.
Before we dispense advice about staying healthy, we should know the effect of whatever we are recommending—be it diet, supplements, chemoprevention, or screening—on all meaningful outcomes, including overall mortality, quality of life, harms, inconveniences, and cost. Even though looking at all these outcomes may seem self-evidently wise, many research studies do not do it, and health care providers do not do it enough.
How would looking at all the outcomes change our opinion of health practices?
COMPARING GRAPEFRUIT AND PEACHES
A 2013 study linked eating berries with lower rates of myocardial infarction in women,1 another found that people who ate some fruits (blackberries and grapefruit) but not others (peaches and oranges) had a lower rate of incident diabetes,2 and a third linked a healthy diet to a lower incidence of pancreatic cancer.3 However, none of these studies examined all-cause mortality rates. A fourth study found that drinking green tea was associated with a lower risk of death from pneumonia in Japanese women, but not men.4
For the sake of argument, let us put aside concern about whether observational studies can reliably inform recommendations for clinical practice5 and concede that they can. The point is that studies such as those above look at some but not all meaningful outcomes, undermining the utility of their findings. If healthy people conclude that they should eat grapefruit instead of peaches, they may miss out on benefits of peaches that the study did not examine. Eating a healthy diet remains prudent, but the study linking it to a lower rate of pancreatic cancer is no tipping point, as pancreatic cancer is just one way to die. And advocating green tea to Japanese women but not men, to avoid pneumonia, would be a questionable public health strategy. Pneumonia is the sixth leading cause of death and accounts for 3.9% of disability-adjusted life-years lost,6 but what about the first five causes, which account for 96.1%?
These and many other studies of dietary habits of people who are well fail to consider end points that healthy people care about. Suppose that drinking more coffee would prevent all deaths from pancreatic cancer but would modestly increase cardiovascular deaths—say, by 5%. On a population level, recommending more coffee would be wrong, because it would result in far more deaths. Suppose that drinking tea decreased deaths from pneumonia—we should still not advise patients to drink tea, as we do not know whether tea’s net effect is beneficial.
Some may argue that these epidemiologic studies are merely hypothesis-generating, but my colleagues and I analyzed all the nonrandomized studies published in several leading medical journals in 1 year and found that 59% made specific practice recommendations.5 Other studies may be misused in this fashion, even though the authors refrained from doing so.
CALCIUM PROTECTS BONES, BUT WHAT ABOUT THE HEART?
Narrow end points are not limited to dietary studies. Calcium supplementation with or without vitamin D has been vigorously promoted for decades7 to treat and prevent osteoporosis in pre- and postmenopausal women, and data confirm that these agents decrease the risk of fracture.8
But bone health is only one end point important to women, and long-term supplementation of a mineral or vitamin with the goal of strengthening bones may have unforeseen adverse effects.
In 2010, calcium supplementation without vitamin D was linked to higher rates of myocardial infarction (with some suggestion of increased rates of all-cause death) in pooled analyses of 15 trials.9 In 2011, a higher risk of cardiovascular events (stroke and myocardial infarction) was found in recipients of calcium with vitamin D in a reanalysis of the Women’s Health Initiative Calcium/Vitamin D Supplementation Study,10 adjusting for the widespread use of these supplements at baseline, and this was corroborated by a meta-analysis of eight other studies.10 A more recent study confirmed that supplemental calcium increases cardiovascular risk in men.11
Although the increase in cardiovascular risk seems to be modest, millions of people take calcium supplements; thus, many people may be harmed. Our exuberance for bone health suggests that, at times, a single outcome can distract.
DOES SCREENING IMPROVE SURVIVAL?
On the whole, the evidence for screening continues to focus only on certain outcomes. With the exception of the National Lung Cancer Screening Trial,12 to date, no cancer screening trial has shown an improvement in the overall survival rate.
In fact, a 2013 Cochrane review13 found that mammographic screening failed to lower the rate of death from all cancers, including breast cancer, after 10 years (relative risk [RR] 1.02, 95% confidence interval [CI] 0.95–1.10) and the rate of death from all causes after 13 years (RR 0.99, 95% CI 0.95–1.03). Although screening lowered the breast cancer mortality rate, the authors argued that we should not look at only some outcomes and concluded that “breast cancer mortality was an unreliable outcome” that was biased in favor of screening, mainly because of “differential misclassification of cause of death.”13
Black et al14 found that of 12 major cancer screening trials examining both disease-specific mortality and all-cause mortality, 5 had differences in mortality rates that went in opposite directions (eg, the rate of disease-specific mortality improved while overall survival was harmed, or vice-versa), suggesting paradoxical effects. In another 2 studies, differences in all-cause mortality exceeded gains in disease-specific mortality. Thus, in 7 (58%) of the 12 trials, inconsistencies existed between rates of disease-specific mortality and all-cause mortality, prompting doubt about the conclusions of the studies.14
For some cancers, data suggest that screening increases deaths from other causes, and these extra deaths are not included in the data on disease-specific mortality. For instance, men who are screened for prostate cancer have higher rates of death from cardiovascular disease and suicide,15 which might negate the tenuous benefits of screening in terms of deaths from prostate cancer.
Studies of screening for diseases other than cancer have also focused on only some outcomes. For example, the United States Preventive Services Task Force supports screening for abdominal aortic aneurysm once with ultrasonography in men ages 65 to 75 who have ever smoked,16 but the recommendation is based on improvements in the death rate from abdominal aortic aneurysm, not in all-cause mortality.17 This, along with a declining incidence of this disease and changes in how it is treated (with endovascular repair on the rise and open surgical repair declining), has led some to question if we should continue to screen for it.18
CHEMOPREVENTION: NO FREE LUNCH
Finasteride
In 2013, an analysis19 that looked at all of the outcomes laid to rest 10 years of debate over the Prostate Cancer Prevention Trial, which had randomized more than 18,000 healthy men over age 55 with no signs or symptoms of prostate cancer to receive finasteride or placebo, with the end point of prostate cancer incidence. The initial results, published in 2003,20 had found that the drug decreased the rate of incident prostate cancer but paradoxically increased the rate of high-grade (Gleason score ≥ 7) tumors. Whether these results were real or an artifact of ascertainment was debated, as was whether the adverse effects—decreases in sexual potency, libido, and ejaculation—were worth the 25% reduction in prostate cancer incidence.
Much of the debate ended with the 2013 publication, which showed that regardless of finasteride’s effect on prostate cancer, overall mortality curves at 18-year follow-up were absolutely indistinguishable.19 Healthy patients hoping that finasteride will help them live longer or better can be safely told that it does neither.
Statins as primary prevention
As for statin therapy as primary prevention, the best meta-analysis to date (which meticulously excluded secondary-prevention patients after analyzing individual patient-level data) found no improvement in overall mortality despite more than 240,000 patient-years of follow-up.21 Because of this, and because the harms of statin therapy are being increasingly (but still poorly) documented, widespread use of statins has been questioned.22
Proponents point to the ability of statins to reduce end points such as revascularization, stroke, and nonfatal myocardial infarction.23 But the main question facing healthy users is whether improvement in these end points translates to longer life or better quality of life. These questions remain unresolved.
Aspirin as primary prevention
Another example of the importance of considering all the outcomes is the issue of aspirin as primary prevention.
Enthusiasm for aspirin as primary prevention has been recently reinvigorated, with data showing it can prevent colorectal cancers that overexpress cyclooxygenase-2.24 But a meta-analysis of nine randomized trials of aspirin25 with more than 1,000 participants found that, although aspirin decreases the rate of nonfatal myocardial infarction (odds ratio [OR] 0.80, 95% CI 0.67–0.96), it does not significantly reduce cancer mortality (OR 0.93, 95% CI 0.84–1.03), and it increases the risk of nontrivial bleeding (OR 1.31; 95% CI 1.14–1.50). Its effects on overall mortality were not statistically significant but were possibly favorable (OR 0.94, 95% CI 0.88–1.00), so this requires further study.
After broad consideration of the risks and benefits of aspirin, the US Food and Drug Administration has issued a statement that aspirin is not recommended as primary prevention.26
WHY STUDIES LOOK ONLY AT SOME OUTCOMES
There are many reasons why researchers favor examining some outcomes over others, but there is no clear justification for ignoring overall mortality. Overall mortality should routinely be examined in large population studies of diet and supplements and in trials of medications27 and cancer screening.
With regard to large observational studies, it is hard to understand why some would not include survival analyses, unless the results would fail to support the study’s hypothesis. In fact, some studies do report overall survival results,28 but others do not. The omission of overall survival in large data-set research should raise concerns of multiple hypothesis testing and selective reporting. Eating peaches as opposed to grapefruit may not be associated with differences in rates of all-cause mortality, myocardial infarction, pneumonia, or lung cancer, but if you look at 20 different variables, chances are that one will have a P value less than .05, and an investigator might be tempted to report it as statistically significant and even meaningful.
Empirical studies support this claim. One group found that for 80% of ingredients randomly selected from a cookbook, there existed Medline-indexed articles assessing cancer risk, with 65% of studies finding nominally significant differences in the risk of some type of cancer.29
An excess of significant findings such as this argues that significance-chasing and selective reporting are common in this field and has led to calls for methodologic improvements, including routine falsification testing30 and up-front registration of observational studies.31
WHY ALL OUTCOMES MATTER
Healthy people do not care about some outcomes; they care about all outcomes. Some patients may truly have unique priorities (quality of life vs quantity of life), but others may overestimate their risk of death from some causes and underestimate their risk from others, and practitioners have the obligation to counsel them appropriately.
For instance, a patient who watches a brother pass away from pancreatic adenocarcinoma may wish to do everything possible to avoid that illness. But often, as in this case, fear may surpass risk. The patient’s risk of pancreatic cancer is no different than that in the general population: the best data show32 an odds ratio of 1.8, with a confidence interval spanning 1. As such, pancreatic cancer is still not among his five most likely causes of death.
Some patients may care about their bone mineral density or cholesterol level. But again, physicians have an obligation to direct patients’ attention to all of the outcomes that should be of interest to them.
OBJECTIONS TO INCLUDING ALL OUTCOMES
There are important objections to the argument I am presenting here.
First, including all outcomes is expensive. For studies involving retrospective analysis of existing data, looking at overall mortality would not incur additional costs, only an additional analysis. But for prospective trials to have statistical power to detect a difference in overall mortality, larger sample sizes or longer follow-up might be needed—either of which would add to the cost.
In chemoprevention trials, the rate of incident cancer has been called the gold standard end point.33 To design a thrifty chemoprevention study, investigators can either target a broad population and aim for incident malignancy, or target a restricted, high-risk population and aim for overall mortality. The latter is preferable because although it can inform the decisions of only some people, the former cannot inform any people, as was seen with difficulties in interpreting the Prostate Cancer Prevention Trial and trials showing reduced breast cancer incidence from tamoxifen, raloxifene, and exemestane.
In large cancer screening trials, the cost of powering the trial for overall mortality would be greater, and though a carefully selected, high-risk population can be enrolled, historically this has not been popular. In cancer screening, it is a mistake to contrast the costs of trials powered for overall mortality with those of lesser studies examining disease-specific death. Instead, we must consider the larger societal costs incurred by cancer screening that does not truly improve quantity or quality of life.34
The recent reversal of recommendations for prostate-specific antigen testing by the United States Preventive Services Task Force35 suggests that erroneous recommendations, practiced for decades, can cost society hundreds of billions of dollars but fail to improve meaningful outcomes.
The history of medicine is replete with examples of widely recommended practices and interventions that not only failed to improve the outcomes they claimed to improve, but at times increased the rate of all-cause mortality or carried harms that far outweighed benefits.36,37 The costs of conducting research to fully understand all outcomes are only a fraction of the costs of a practice that is widely disseminated.38
A second objection to my analysis is that there is more to life than survival, and outcomes besides overall mortality are important. This is a self-evident truth. That an intervention improves the rate of overall mortality is neither necessary nor sufficient for its recommendation. Practices may improve survival but worsen quality of life to such a degree that they should not be recommended. Conversely, practices that improve quality of life should be endorsed even if they fail to prolong life.
Thus, overall mortality and quality of life must be considered together, but the end points that are favored currently (disease-specific death, incident cancer, diabetes mellitus, myocardial infarction) do not do a good job of capturing either. Disease-specific death is not meaningful to any patient if deaths from other causes are increased so that overall mortality is unchanged. Furthermore, preventing a diagnosis of cancer or diabetes may offer some psychological comfort, but well-crafted quality-of-life instruments are best suited to capture just how great that benefit is and whether it justifies the cost of such interventions, particularly if the rate of survival is unchanged.
Preventing stroke or myocardial infarction is important, but we should be cautious of interpreting data when decreasing the rate of these morbid events does not lead to commensurate improvements in survival. Alternatively, if morbid events are truly avoided but survival analyses are underpowered, quality-of-life measurements should demonstrate the benefit. But the end points currently used capture neither survival nor quality of life in a meaningful way.
WHEN ADVISING HEALTHY PEOPLE
Looking at all outcomes is important when caring for patients who are sick, but even more so for patients who are well. We need to know an intervention has a net benefit before we recommend it to a healthy person. Overall mortality should be reported routinely in this population, particularly in settings where the cost to do so is trivial (ie, in observational studies). Designers of thrifty trials should try to include people at high risk and power the trial for definite end points, rather than being broadly inclusive and reaching disputed conclusions. Research and decision-making should look at all outcomes. Healthy people deserve no less.
- Cassidy A, Mukamal KJ, Liu L, Franz M, Eliassen AH, Rimm EB. High anthocyanin intake is associated with a reduced risk of myocardial infarction in young and middle-aged women. Circulation 2013; 127:188–196.
- Muraki I, Imamura F, Manson JE, et al. Fruit consumption and risk of type 2 diabetes: results from three prospective longitudinal cohort studies. BMJ 2013; 347:f5001.
- Arem H, Reedy J, Sampson J, et al. The Healthy Eating Index 2005 and risk for pancreatic cancer in the NIH-AARP study. J Natl Cancer Inst 2013; 105:1298–1305.
- Watanabe I, Kuriyama S, Kakizaki M, et al. Green tea and death from pneumonia in Japan: the Ohsaki cohort study. Am J Clin Nutr 2009; 90:672–679.
- Prasad V, Jorgenson J, Ioannidis JP, Cifu A. Observational studies often make clinical practice recommendations: an empirical evaluation of authors’ attitudes. J Clin Epidemiol 2013; 66:361–366.e4.
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380:2197–2223.
- Eastell R. Treatment of postmenopausal osteoporosis. N Engl J Med 1998; 338:736–746.
- Looker AC. Interaction of science, consumer practices and policy: calcium and bone health as a case study. J Nutr 2003; 133:1987S–1991S.
- Bolland MJ, Avenell A, Baron JA, et al. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ 2010; 341:c3691
- Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the Women’s Health Initiative limited access dataset and meta-analysis. BMJ 2011; 342:d2040.
- Xiao Q, Murphy RA, Houston DK, Harris TB, Chow WH, Park Y. Dietary and supplemental calcium intake and cardiovascular disease mortality: the National Institutes of Health-AARP diet and health study. JAMA Intern Med 2013; 173:639–646.
- The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365:395–409.
- Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2013 Jun 4;6:CD001877.
- Black WC, Haggstrom DA, Welch HG. All-cause mortality in randomized trials of cancer screening. J Natl Cancer Inst 2002; 94:167–173.
- Fall K, Fang F, Mucci LA, et al. Immediate risk for cardiovascular events and suicide following a prostate cancer diagnosis: prospective cohort study. PLoS Med 2009; 6:e1000197.
- Prasad V. An unmeasured harm of screening. Arch Intern Med 2012; 172:1442–1443.
- Guirguis-Blake JM, Beil TL, Senger CA, Whitlock EP. Ultrasonography screening for abdominal aortic aneurysms: a sytematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med 2014; 160:321–329.
- Harris R, Sheridan S, Kinsinger L. Time to rethink screening for abdominal aortic aneurysm? Arch Intern Med 2012; 172:1462–1463.
- Thompson IM Jr, Goodman PJ, Tangen CM, et al. Long-term survival of participants in the prostate cancer prevention trial. N Engl J Med 2013; 369:603–610.
- Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med 2003; 349:216–224.
- Ray KK, Seshasai SR, Erqou S, et al. Statins and all-cause mortality in high-risk primary prevention: a meta-analysis of 11 randomized controlled trials involving 65,229 participants. Arch Intern Med 2010; 170:1024–1031.
- Redberg RF, Katz MH. Healthy men should not take statins. JAMA 2012; 307:1491–1492.
- McEvoy JW, Blumenthal RS, Blaha MJ. Statin therapy for hyperlipidemia. JAMA 2013; 310:1184–1185.
- Chan AT, Ogino S, Fuchs CS. Aspirin and the risk of colorectal cancer in relation to the expression of COX-2. N Engl J Med 2007; 356:2131–2142.
- Seshasai SR, Wijesuriya S, Sivakumaran R, et al. Effect of aspirin on vascular and nonvascular outcomes: meta-analysis of randomized controlled trials. Arch Intern Med 2012; 172:209–216.
- US Food and Drug Administration. Use of aspirin for primary prevention of heart attack and stroke. www.fda.gov/Drugs/ResourcesForYou/Consumers/ucm390574.htm. Accessed February 5, 2015.
- Ioannidis JP. Mega-trials for blockbusters. JAMA 2013; 309:239–240.
- Dunkler D, Dehghan M, Teo KK, et al; ONTARGET Investigators. Diet and kidney disease in high-risk individuals with type 2 diabetes mellitus. JAMA Intern Med 2013; 173:1682–1692.
- Schoenfeld JD, Ioannidis JP. Is everything we eat associated with cancer? A systematic cookbook review. Am J Clin Nutr 2013; 97:127–134.
- Prasad V, Jena AB. Prespecified falsification end points: can they validate true observational associations? JAMA 2013; 309:241–242.
- Ioannidis JPA. The importance of potential studies that have not existed and registration of observational data sets. JAMA 2012; 308:575–576.
- Klein AP, Brune KA, Petersen GM, et al. Prospective risk of pancreatic cancer in familial pancreatic cancer kindreds. Cancer Res 2004; 64:2634–2638.
- William WN Jr, Papadimitrakopoulou VA. Optimizing biomarkers and endpoints in oral cancer chemoprevention trials. Cancer Prev Res (Phila) 2013; 6:375–378.
- Prasad V. Powering cancer screening for overall mortality. Ecancermedicalscience 2013 Oct 9; 7:ed27.
- US Preventive Services Task Force. Final recommendation statement. Prostate cancer: screening. http://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/prostate-cancer-screening. Accessed February 5, 2015.
- Prasad V, Cifu A, Ioannidis JP. Reversals of established medical practices: evidence to abandon ship. JAMA 2012; 307:37–38.
- Prasad V, Vandross A, Toomey C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc 2013; 88:790–798.
- Elshaug AG, Garber AM. How CER could pay for itself—insights from vertebral fracture treatments. N Engl J Med 2011; 364:1390–1393.
- Cassidy A, Mukamal KJ, Liu L, Franz M, Eliassen AH, Rimm EB. High anthocyanin intake is associated with a reduced risk of myocardial infarction in young and middle-aged women. Circulation 2013; 127:188–196.
- Muraki I, Imamura F, Manson JE, et al. Fruit consumption and risk of type 2 diabetes: results from three prospective longitudinal cohort studies. BMJ 2013; 347:f5001.
- Arem H, Reedy J, Sampson J, et al. The Healthy Eating Index 2005 and risk for pancreatic cancer in the NIH-AARP study. J Natl Cancer Inst 2013; 105:1298–1305.
- Watanabe I, Kuriyama S, Kakizaki M, et al. Green tea and death from pneumonia in Japan: the Ohsaki cohort study. Am J Clin Nutr 2009; 90:672–679.
- Prasad V, Jorgenson J, Ioannidis JP, Cifu A. Observational studies often make clinical practice recommendations: an empirical evaluation of authors’ attitudes. J Clin Epidemiol 2013; 66:361–366.e4.
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380:2197–2223.
- Eastell R. Treatment of postmenopausal osteoporosis. N Engl J Med 1998; 338:736–746.
- Looker AC. Interaction of science, consumer practices and policy: calcium and bone health as a case study. J Nutr 2003; 133:1987S–1991S.
- Bolland MJ, Avenell A, Baron JA, et al. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ 2010; 341:c3691
- Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the Women’s Health Initiative limited access dataset and meta-analysis. BMJ 2011; 342:d2040.
- Xiao Q, Murphy RA, Houston DK, Harris TB, Chow WH, Park Y. Dietary and supplemental calcium intake and cardiovascular disease mortality: the National Institutes of Health-AARP diet and health study. JAMA Intern Med 2013; 173:639–646.
- The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365:395–409.
- Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2013 Jun 4;6:CD001877.
- Black WC, Haggstrom DA, Welch HG. All-cause mortality in randomized trials of cancer screening. J Natl Cancer Inst 2002; 94:167–173.
- Fall K, Fang F, Mucci LA, et al. Immediate risk for cardiovascular events and suicide following a prostate cancer diagnosis: prospective cohort study. PLoS Med 2009; 6:e1000197.
- Prasad V. An unmeasured harm of screening. Arch Intern Med 2012; 172:1442–1443.
- Guirguis-Blake JM, Beil TL, Senger CA, Whitlock EP. Ultrasonography screening for abdominal aortic aneurysms: a sytematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med 2014; 160:321–329.
- Harris R, Sheridan S, Kinsinger L. Time to rethink screening for abdominal aortic aneurysm? Arch Intern Med 2012; 172:1462–1463.
- Thompson IM Jr, Goodman PJ, Tangen CM, et al. Long-term survival of participants in the prostate cancer prevention trial. N Engl J Med 2013; 369:603–610.
- Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med 2003; 349:216–224.
- Ray KK, Seshasai SR, Erqou S, et al. Statins and all-cause mortality in high-risk primary prevention: a meta-analysis of 11 randomized controlled trials involving 65,229 participants. Arch Intern Med 2010; 170:1024–1031.
- Redberg RF, Katz MH. Healthy men should not take statins. JAMA 2012; 307:1491–1492.
- McEvoy JW, Blumenthal RS, Blaha MJ. Statin therapy for hyperlipidemia. JAMA 2013; 310:1184–1185.
- Chan AT, Ogino S, Fuchs CS. Aspirin and the risk of colorectal cancer in relation to the expression of COX-2. N Engl J Med 2007; 356:2131–2142.
- Seshasai SR, Wijesuriya S, Sivakumaran R, et al. Effect of aspirin on vascular and nonvascular outcomes: meta-analysis of randomized controlled trials. Arch Intern Med 2012; 172:209–216.
- US Food and Drug Administration. Use of aspirin for primary prevention of heart attack and stroke. www.fda.gov/Drugs/ResourcesForYou/Consumers/ucm390574.htm. Accessed February 5, 2015.
- Ioannidis JP. Mega-trials for blockbusters. JAMA 2013; 309:239–240.
- Dunkler D, Dehghan M, Teo KK, et al; ONTARGET Investigators. Diet and kidney disease in high-risk individuals with type 2 diabetes mellitus. JAMA Intern Med 2013; 173:1682–1692.
- Schoenfeld JD, Ioannidis JP. Is everything we eat associated with cancer? A systematic cookbook review. Am J Clin Nutr 2013; 97:127–134.
- Prasad V, Jena AB. Prespecified falsification end points: can they validate true observational associations? JAMA 2013; 309:241–242.
- Ioannidis JPA. The importance of potential studies that have not existed and registration of observational data sets. JAMA 2012; 308:575–576.
- Klein AP, Brune KA, Petersen GM, et al. Prospective risk of pancreatic cancer in familial pancreatic cancer kindreds. Cancer Res 2004; 64:2634–2638.
- William WN Jr, Papadimitrakopoulou VA. Optimizing biomarkers and endpoints in oral cancer chemoprevention trials. Cancer Prev Res (Phila) 2013; 6:375–378.
- Prasad V. Powering cancer screening for overall mortality. Ecancermedicalscience 2013 Oct 9; 7:ed27.
- US Preventive Services Task Force. Final recommendation statement. Prostate cancer: screening. http://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/prostate-cancer-screening. Accessed February 5, 2015.
- Prasad V, Cifu A, Ioannidis JP. Reversals of established medical practices: evidence to abandon ship. JAMA 2012; 307:37–38.
- Prasad V, Vandross A, Toomey C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc 2013; 88:790–798.
- Elshaug AG, Garber AM. How CER could pay for itself—insights from vertebral fracture treatments. N Engl J Med 2011; 364:1390–1393.

Defining “abnormal rise” is the elephant in the room

“STOP USING THE HCG DISCRIMINATORY ZONE OF 1,500 TO
2,000 mIU/mL TO GUIDE INTERVENTION DURING EARLY PREGNANCY”
ROBERT L. BARBIERI, MD (EDITORIAL; JANUARY 2015)
Defining “abnormal rise” is the elephant in the room
It was refreshing to read Dr. Barbieri’srecent editorial on the management of ectopic pregnancies based on human chorionic gonadotropin (hCG) levels. However, I feel there’s an elephant in the room. The phrase “abnormal rise” is not clearly defined, even though countless texts and review articles continue to use the phrase. In fact, many authors include a flow chart in which an abnormal rise usually is followed by a recommendation to empty the uterus in an attempt to find chorionic villi.1,2 The most recent versions of several widely used textbooks advocate this practice,3–5 and a current UpToDate article includes a flow chart suggesting that a “suboptimal rise” is sufficient for diagnosis of an abnormal pregnancy requiring treatment.6
Kadar and colleagues originally suggested that 85% of viable intrauterine pregnancies (IUPs) will have a rise in hCG levels of at least 66% every 48 hours, leading to what is commonly called the “doubling rule.”7 Barnhart and colleagues showed that the slowest recorded hCG rise for a viable pregnancy in 48 hours was 53%, demonstrating that the hCG level does not double in 48 to 72 hours as traditionally expected.8 In their final model, the authors calculated that 99% percent of normal IUPs should have an increase of at least 53% in 2 days, moving the bar for a “normal” hCG rise even lower. This also implies that 1% of viable IUPs may have a rise of less than 53% over 2 days. I have to wonder how many viable, wanted pregnancies have been interrupted by the misguided use of discriminatory zones or abnormal rises resulting in the emptying of the pregnant uterus?
Clinical assessment and ultrasonography should continue to be the mainstay of management of ectopic pregnancy. When surgical diagnosis is needed, laparoscopy should be considered. In this day and age, when we are being more cautious about emptying a uterus based on ultrasound measurements of the fetus or gestational sac, why are we still so eager to base that decision on laboratory values? Are we really willing to accept that 1% of the time we will be terminating a viable pregnancy? We should stop the continued propagation of flow charts and strategies that use hCG discriminatory zones or abnormal rises to determine viability and when to evacuate the uterus. A contemporary update to address the issue is needed.
Devin Namaky, MD
Cincinnati, Ohio
References
1. Seeber B, Barnhart K. Suspected ectopic pregnancy. Obstet Gynecol. 2006;107(2):399–413.
2. Mukul LV, Teal SB. Current management of ectopic pregnancy. Obstet Gynecol Clin North Am. 2007;34(3):403–419.
3. Ectopic pregnancy. In: Hoffman BL, Schorge JP, Schaffer JI, et al, eds. Williams Gynecology. 2nd ed. New York, NY: McGraw-Hill Professional; 2012:198–218.
4. Lobo RA. Ectopic pregnancy. In: Lentz GM, ed. Comprehensive Gynecology. 6th ed. Philadelphia, PA: Elsevier Mosby; 2012:361–382 .
5. Damario MA, Rock JA. Ectopic pregnancy. In: Rock JA, Jones HW III, eds. Te Linde’s Operative Gynecology. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:798–824.
6. Tulandi T. Ectopic pregnancy: clinical manifestations and diagnosis. UpToDate Web site. http://www.uptodate.com/contents/ectopic-pregnancy-clinical-manifestations-and-diag nosis. Updated October 22, 2014. Accessed February 18, 2015.
7. Kadar N, Caldwell BV, Romera R. A method of screening for ectopic pregnancy and its indications. Obstet Gynecol. 1981;58(2):162–166.
8. Barnhart KT, Sammel MD, Rinaudo PF, Zhou L, Hummel AC, Guo W. Symptomatic patients with an early viable intrauterine pregnancy: hCG curves redefined. Obstet Gynecol. 2004;104(1):50–55.
Why not use serum progesterone to determine early pregnancy viability?
I read with attention Dr. Barbieri’s recent editorial about evaluation of early pregnancy. My question is: Why is serum progesterone not recommended or used to assess the health of an early pregnancy?
In my practice, I always use a serum progesterone test along with hCG measurements to ascertain if an early pregnancy is healthy. I have observed, as biased as this observation can be, as I have not done any study about it, that a serum progesterone level above 12 ng/dL correlates quite well with a healthy pregnancy. I only follow more intensively with serial ultrasonography and hCG measurements in a patient whose progesterone level is below 11 ng/dL.
When a patient’s only symptom is bleeding, if the serum progesterone level is below 11 ng/dL, and her serum quantitative hCG level does not double as appropriate, I consider the pregnancy not normal and counsel the patient about continuing observation or terminating the pregnancy.
In the same laboratory scenario but with a patient who has bleeding and pain, and even moreso if the progesterone level is below 8 ng/dL, I strongly consider an ectopic pregnancy until it is proven otherwise. In this case, I offer treatment with methotrexate, as it’s my experience that the vast majority of these patients are carrying an abnormal pregnancy— either a spontaneous abortion or an ectopic pregnancy. Methotrexate therapy will prevent further complications without causing the loss of normal pregnancies.
For me, progesterone levels add one more piece to the puzzle. A patient with pain, vaginal bleeding, a quantitative hCG value of
500 mIU/mL, and a serum progesterone level of 20 ng/dL will have a normal pregnancy and is not a candidate for any intervention besides a follow-up hCG measurement to ascertain “doubling” of the analyte as expected in a normal pregnancy.
An asymptomatic patient whose quantitative hCG measurement is 1,000 mIU/mL and progesterone level is 4 ng/dL is carrying an abnormal pregnancy. If this quantitative hCG does not double appropriately in the follow-up, I counsel the patient about the greater chance of a spontaneous abortion or ectopic pregnancy.
Is this approach faulty?
Tomas Hernandez, MD
Pasco, Washington
Know the sensitivity of the HCG test
I found Dr. Barbieri’s editorial very timely. It brings some clarity to the use of the hCG discriminatory zone in symptomatic pregnant patients.
An additional important point is that it is the clinician’s obligation to know the sensitivity of the test the laboratory uses. Serum tests use the threshold for a negative result of either less than 1 mIU/mL or less than 5 mIU/mL. If possible, serial hCG measurements should be performed in the same laboratory, because the result may not represent a true change in the hCG concentration if the second test is performed at a different laboratory.1 This is especially important when the clinician is considering the use of methotrexate to treat a suspected ectopic pregnancy.
Magdalen E. Hull, MD, MPH
Great River, New York
Reference
1. Meriko Mori K, Lurain, JR. Human chorionic gonadotropin: testing in pregnancy and gestational trophoblastic disease and causes of low persistent levels. UpToDate. http://www.uptodate.com/contents/human-chorionic-gonadotropin-testing-in-pregnancy-and-gesta tional-trophoblastic-disease-and-causes-of-low-persistent-levels. Published October 23, 2013. Accessed January 29, 2015.
Further thoughts on HCG, ultrasound, and early pregnancy diagnosis
I want to thank Dr. Barbieri for his important, timely message about suspected nonviable pregnancy. I agree with virtually all of his excellent suggestions. In fact, I was part of the consensus panel that developed the findings diagnostic of and suggestive of IUP failure.1 There are a few points, however, that I believe the readership of OBG Management should know.
The endothelial heart tube, the first organ system to form, folds in on itself and begins to beat at 21 days postconception. Thus, it is present and beating prior to our ability to image it on transvaginal ultrasound. Yet new guidelines1 now say not to call an IUP failed until there is a crown-rump length of 7 mm or greater with no cardiac activity. In the past, many clinicians used 4 or 5 mm. In fact, one of the most recent studies utilizing an 8-mHz transducer found all cardiac activity was visualized by 3.1 mm embryonic size!2
So why has the number been increased to 7 mm? I’ve given this a lot of thought. Most clinical trials, from which guidelines were derived in the past, were well-designed, tightly controlled, and performed by better-trained clinicians, often with state-of-the-art equipment. In contrast, well-meaning health-care providers practicing in the field are often without the same level of quality control, equipment, or expertise but are still expected to duplicate the data from the trials used to create the guidelines. The reason this is relevant pertains to the statement that 94% of 291 cases of ectopic pregnancy had an adnexal mass.3 This is an excellent study, done at one of the nation’s most outstanding academic institutions by world-class sonologists. I do not believe that well-meaning clinicians in the field will be able to achieve this level of detection.
Dr. Barbieri also discusses an inability to see an IUP even when hCG levels are greater than 1,500 or 2,000 mIU/mL or above. He mentions obesity, fibroids, and adenomyosis as increasing the risk of an ultrasound failing to detect an early IUP. This point needs to be expanded upon. Twenty-seven years ago, we claimed a discriminatory level of 1,025 mIU/mL of hCG if the gestational sac was normal and the uterus was normal with normal echo patterns. We had three cases with markedly greater hCG levels (one, in fact, as high as 5,544 mIU/mL)with coexisting fibroids.4
I would also submit that it is the axial uterus that is a very important source of potential error. The closer the beam of sound coming off of the footprint is to a right angle with the endometrium (as it will be in a markedly anteverted or retroverted uterus), the better the resulting image. With an axial uterus, the endometrium is in the same plane as the beam of sound, and this diminishes imaging capability. Furthermore, twin pregnancies are a potential confounder in attempting to correlate hCG levels in transvaginal ultrasound findings.
I wholeheartedly agree with Dr. Barbieri: There is virtually no role to administer methotrexate based on a single hCG determination in a hemodynamically stable patient.
Steven R. Goldstein, MD
New York, New York
References
1. Doubilet PM, Benson CB, Bourne T, Blaivas M; Society of Radiologists in Ultrasound Multispecialty Panel on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
2. Abaid LN, As-Sanie S, Wolfe HM. Relationship between crown-rump length and early detection of cardiac activity. J Reprod Med. 2007;52(5):375–378.
3. Frates MC, Doubilet PM, Peters HE, Benson CR. Adnexal sonographic findings in ectopic pregnancy and their correlation with tubal rupture and human chorionic gonadotropin levels. J Ultrasound Med. 2014;33(4):697–703.
4. Goldstein SR, Snyder JR, Watson C, Danon M. Very early pregnancy detection with endovaginal ultrasound. Obstet Gynecol. 1988;72(2):200–204.
Dr. Barbieri responds
Dr. Namaky, Dr. Hernandez, Dr. Hull, and Dr. Goldstein provide great clinical advice for readers. I agree with Dr. Namaky that the mainstays of managing a pregnancy of unknown location in a stable patient are clinical assessment and ultrasonography. Dr. Hernandez recommends using the serum progesterone measurement to help guide clinical decisions in a pregnancy of unknown location. I also use serum progesterone in my practice because a very low progesterone level helps the patient to understand that she has a failed pregnancy, and facilitates her acceptance of timely intervention. Many of my colleagues do not use progesterone measurement because they prefer to rely on clinical assessment, serial hCG measurement, and ultrasound results to guide their treatment. I agree with Dr. Hull that serial hCG measurements are most useful when the same laboratory performs all the tests. Dr. Goldstein, a world class expert in the evaluation and management of early pregnancy problems, provides great advice for all readers on how to best integrate ultrasonography in their practices to optimize patient care.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“STOP USING THE HCG DISCRIMINATORY ZONE OF 1,500 TO
2,000 mIU/mL TO GUIDE INTERVENTION DURING EARLY PREGNANCY”
ROBERT L. BARBIERI, MD (EDITORIAL; JANUARY 2015)
Defining “abnormal rise” is the elephant in the room
It was refreshing to read Dr. Barbieri’srecent editorial on the management of ectopic pregnancies based on human chorionic gonadotropin (hCG) levels. However, I feel there’s an elephant in the room. The phrase “abnormal rise” is not clearly defined, even though countless texts and review articles continue to use the phrase. In fact, many authors include a flow chart in which an abnormal rise usually is followed by a recommendation to empty the uterus in an attempt to find chorionic villi.1,2 The most recent versions of several widely used textbooks advocate this practice,3–5 and a current UpToDate article includes a flow chart suggesting that a “suboptimal rise” is sufficient for diagnosis of an abnormal pregnancy requiring treatment.6
Kadar and colleagues originally suggested that 85% of viable intrauterine pregnancies (IUPs) will have a rise in hCG levels of at least 66% every 48 hours, leading to what is commonly called the “doubling rule.”7 Barnhart and colleagues showed that the slowest recorded hCG rise for a viable pregnancy in 48 hours was 53%, demonstrating that the hCG level does not double in 48 to 72 hours as traditionally expected.8 In their final model, the authors calculated that 99% percent of normal IUPs should have an increase of at least 53% in 2 days, moving the bar for a “normal” hCG rise even lower. This also implies that 1% of viable IUPs may have a rise of less than 53% over 2 days. I have to wonder how many viable, wanted pregnancies have been interrupted by the misguided use of discriminatory zones or abnormal rises resulting in the emptying of the pregnant uterus?
Clinical assessment and ultrasonography should continue to be the mainstay of management of ectopic pregnancy. When surgical diagnosis is needed, laparoscopy should be considered. In this day and age, when we are being more cautious about emptying a uterus based on ultrasound measurements of the fetus or gestational sac, why are we still so eager to base that decision on laboratory values? Are we really willing to accept that 1% of the time we will be terminating a viable pregnancy? We should stop the continued propagation of flow charts and strategies that use hCG discriminatory zones or abnormal rises to determine viability and when to evacuate the uterus. A contemporary update to address the issue is needed.
Devin Namaky, MD
Cincinnati, Ohio
References
1. Seeber B, Barnhart K. Suspected ectopic pregnancy. Obstet Gynecol. 2006;107(2):399–413.
2. Mukul LV, Teal SB. Current management of ectopic pregnancy. Obstet Gynecol Clin North Am. 2007;34(3):403–419.
3. Ectopic pregnancy. In: Hoffman BL, Schorge JP, Schaffer JI, et al, eds. Williams Gynecology. 2nd ed. New York, NY: McGraw-Hill Professional; 2012:198–218.
4. Lobo RA. Ectopic pregnancy. In: Lentz GM, ed. Comprehensive Gynecology. 6th ed. Philadelphia, PA: Elsevier Mosby; 2012:361–382 .
5. Damario MA, Rock JA. Ectopic pregnancy. In: Rock JA, Jones HW III, eds. Te Linde’s Operative Gynecology. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:798–824.
6. Tulandi T. Ectopic pregnancy: clinical manifestations and diagnosis. UpToDate Web site. http://www.uptodate.com/contents/ectopic-pregnancy-clinical-manifestations-and-diag nosis. Updated October 22, 2014. Accessed February 18, 2015.
7. Kadar N, Caldwell BV, Romera R. A method of screening for ectopic pregnancy and its indications. Obstet Gynecol. 1981;58(2):162–166.
8. Barnhart KT, Sammel MD, Rinaudo PF, Zhou L, Hummel AC, Guo W. Symptomatic patients with an early viable intrauterine pregnancy: hCG curves redefined. Obstet Gynecol. 2004;104(1):50–55.
Why not use serum progesterone to determine early pregnancy viability?
I read with attention Dr. Barbieri’s recent editorial about evaluation of early pregnancy. My question is: Why is serum progesterone not recommended or used to assess the health of an early pregnancy?
In my practice, I always use a serum progesterone test along with hCG measurements to ascertain if an early pregnancy is healthy. I have observed, as biased as this observation can be, as I have not done any study about it, that a serum progesterone level above 12 ng/dL correlates quite well with a healthy pregnancy. I only follow more intensively with serial ultrasonography and hCG measurements in a patient whose progesterone level is below 11 ng/dL.
When a patient’s only symptom is bleeding, if the serum progesterone level is below 11 ng/dL, and her serum quantitative hCG level does not double as appropriate, I consider the pregnancy not normal and counsel the patient about continuing observation or terminating the pregnancy.
In the same laboratory scenario but with a patient who has bleeding and pain, and even moreso if the progesterone level is below 8 ng/dL, I strongly consider an ectopic pregnancy until it is proven otherwise. In this case, I offer treatment with methotrexate, as it’s my experience that the vast majority of these patients are carrying an abnormal pregnancy— either a spontaneous abortion or an ectopic pregnancy. Methotrexate therapy will prevent further complications without causing the loss of normal pregnancies.
For me, progesterone levels add one more piece to the puzzle. A patient with pain, vaginal bleeding, a quantitative hCG value of
500 mIU/mL, and a serum progesterone level of 20 ng/dL will have a normal pregnancy and is not a candidate for any intervention besides a follow-up hCG measurement to ascertain “doubling” of the analyte as expected in a normal pregnancy.
An asymptomatic patient whose quantitative hCG measurement is 1,000 mIU/mL and progesterone level is 4 ng/dL is carrying an abnormal pregnancy. If this quantitative hCG does not double appropriately in the follow-up, I counsel the patient about the greater chance of a spontaneous abortion or ectopic pregnancy.
Is this approach faulty?
Tomas Hernandez, MD
Pasco, Washington
Know the sensitivity of the HCG test
I found Dr. Barbieri’s editorial very timely. It brings some clarity to the use of the hCG discriminatory zone in symptomatic pregnant patients.
An additional important point is that it is the clinician’s obligation to know the sensitivity of the test the laboratory uses. Serum tests use the threshold for a negative result of either less than 1 mIU/mL or less than 5 mIU/mL. If possible, serial hCG measurements should be performed in the same laboratory, because the result may not represent a true change in the hCG concentration if the second test is performed at a different laboratory.1 This is especially important when the clinician is considering the use of methotrexate to treat a suspected ectopic pregnancy.
Magdalen E. Hull, MD, MPH
Great River, New York
Reference
1. Meriko Mori K, Lurain, JR. Human chorionic gonadotropin: testing in pregnancy and gestational trophoblastic disease and causes of low persistent levels. UpToDate. http://www.uptodate.com/contents/human-chorionic-gonadotropin-testing-in-pregnancy-and-gesta tional-trophoblastic-disease-and-causes-of-low-persistent-levels. Published October 23, 2013. Accessed January 29, 2015.
Further thoughts on HCG, ultrasound, and early pregnancy diagnosis
I want to thank Dr. Barbieri for his important, timely message about suspected nonviable pregnancy. I agree with virtually all of his excellent suggestions. In fact, I was part of the consensus panel that developed the findings diagnostic of and suggestive of IUP failure.1 There are a few points, however, that I believe the readership of OBG Management should know.
The endothelial heart tube, the first organ system to form, folds in on itself and begins to beat at 21 days postconception. Thus, it is present and beating prior to our ability to image it on transvaginal ultrasound. Yet new guidelines1 now say not to call an IUP failed until there is a crown-rump length of 7 mm or greater with no cardiac activity. In the past, many clinicians used 4 or 5 mm. In fact, one of the most recent studies utilizing an 8-mHz transducer found all cardiac activity was visualized by 3.1 mm embryonic size!2
So why has the number been increased to 7 mm? I’ve given this a lot of thought. Most clinical trials, from which guidelines were derived in the past, were well-designed, tightly controlled, and performed by better-trained clinicians, often with state-of-the-art equipment. In contrast, well-meaning health-care providers practicing in the field are often without the same level of quality control, equipment, or expertise but are still expected to duplicate the data from the trials used to create the guidelines. The reason this is relevant pertains to the statement that 94% of 291 cases of ectopic pregnancy had an adnexal mass.3 This is an excellent study, done at one of the nation’s most outstanding academic institutions by world-class sonologists. I do not believe that well-meaning clinicians in the field will be able to achieve this level of detection.
Dr. Barbieri also discusses an inability to see an IUP even when hCG levels are greater than 1,500 or 2,000 mIU/mL or above. He mentions obesity, fibroids, and adenomyosis as increasing the risk of an ultrasound failing to detect an early IUP. This point needs to be expanded upon. Twenty-seven years ago, we claimed a discriminatory level of 1,025 mIU/mL of hCG if the gestational sac was normal and the uterus was normal with normal echo patterns. We had three cases with markedly greater hCG levels (one, in fact, as high as 5,544 mIU/mL)with coexisting fibroids.4
I would also submit that it is the axial uterus that is a very important source of potential error. The closer the beam of sound coming off of the footprint is to a right angle with the endometrium (as it will be in a markedly anteverted or retroverted uterus), the better the resulting image. With an axial uterus, the endometrium is in the same plane as the beam of sound, and this diminishes imaging capability. Furthermore, twin pregnancies are a potential confounder in attempting to correlate hCG levels in transvaginal ultrasound findings.
I wholeheartedly agree with Dr. Barbieri: There is virtually no role to administer methotrexate based on a single hCG determination in a hemodynamically stable patient.
Steven R. Goldstein, MD
New York, New York
References
1. Doubilet PM, Benson CB, Bourne T, Blaivas M; Society of Radiologists in Ultrasound Multispecialty Panel on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
2. Abaid LN, As-Sanie S, Wolfe HM. Relationship between crown-rump length and early detection of cardiac activity. J Reprod Med. 2007;52(5):375–378.
3. Frates MC, Doubilet PM, Peters HE, Benson CR. Adnexal sonographic findings in ectopic pregnancy and their correlation with tubal rupture and human chorionic gonadotropin levels. J Ultrasound Med. 2014;33(4):697–703.
4. Goldstein SR, Snyder JR, Watson C, Danon M. Very early pregnancy detection with endovaginal ultrasound. Obstet Gynecol. 1988;72(2):200–204.
Dr. Barbieri responds
Dr. Namaky, Dr. Hernandez, Dr. Hull, and Dr. Goldstein provide great clinical advice for readers. I agree with Dr. Namaky that the mainstays of managing a pregnancy of unknown location in a stable patient are clinical assessment and ultrasonography. Dr. Hernandez recommends using the serum progesterone measurement to help guide clinical decisions in a pregnancy of unknown location. I also use serum progesterone in my practice because a very low progesterone level helps the patient to understand that she has a failed pregnancy, and facilitates her acceptance of timely intervention. Many of my colleagues do not use progesterone measurement because they prefer to rely on clinical assessment, serial hCG measurement, and ultrasound results to guide their treatment. I agree with Dr. Hull that serial hCG measurements are most useful when the same laboratory performs all the tests. Dr. Goldstein, a world class expert in the evaluation and management of early pregnancy problems, provides great advice for all readers on how to best integrate ultrasonography in their practices to optimize patient care.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“STOP USING THE HCG DISCRIMINATORY ZONE OF 1,500 TO
2,000 mIU/mL TO GUIDE INTERVENTION DURING EARLY PREGNANCY”
ROBERT L. BARBIERI, MD (EDITORIAL; JANUARY 2015)
Defining “abnormal rise” is the elephant in the room
It was refreshing to read Dr. Barbieri’srecent editorial on the management of ectopic pregnancies based on human chorionic gonadotropin (hCG) levels. However, I feel there’s an elephant in the room. The phrase “abnormal rise” is not clearly defined, even though countless texts and review articles continue to use the phrase. In fact, many authors include a flow chart in which an abnormal rise usually is followed by a recommendation to empty the uterus in an attempt to find chorionic villi.1,2 The most recent versions of several widely used textbooks advocate this practice,3–5 and a current UpToDate article includes a flow chart suggesting that a “suboptimal rise” is sufficient for diagnosis of an abnormal pregnancy requiring treatment.6
Kadar and colleagues originally suggested that 85% of viable intrauterine pregnancies (IUPs) will have a rise in hCG levels of at least 66% every 48 hours, leading to what is commonly called the “doubling rule.”7 Barnhart and colleagues showed that the slowest recorded hCG rise for a viable pregnancy in 48 hours was 53%, demonstrating that the hCG level does not double in 48 to 72 hours as traditionally expected.8 In their final model, the authors calculated that 99% percent of normal IUPs should have an increase of at least 53% in 2 days, moving the bar for a “normal” hCG rise even lower. This also implies that 1% of viable IUPs may have a rise of less than 53% over 2 days. I have to wonder how many viable, wanted pregnancies have been interrupted by the misguided use of discriminatory zones or abnormal rises resulting in the emptying of the pregnant uterus?
Clinical assessment and ultrasonography should continue to be the mainstay of management of ectopic pregnancy. When surgical diagnosis is needed, laparoscopy should be considered. In this day and age, when we are being more cautious about emptying a uterus based on ultrasound measurements of the fetus or gestational sac, why are we still so eager to base that decision on laboratory values? Are we really willing to accept that 1% of the time we will be terminating a viable pregnancy? We should stop the continued propagation of flow charts and strategies that use hCG discriminatory zones or abnormal rises to determine viability and when to evacuate the uterus. A contemporary update to address the issue is needed.
Devin Namaky, MD
Cincinnati, Ohio
References
1. Seeber B, Barnhart K. Suspected ectopic pregnancy. Obstet Gynecol. 2006;107(2):399–413.
2. Mukul LV, Teal SB. Current management of ectopic pregnancy. Obstet Gynecol Clin North Am. 2007;34(3):403–419.
3. Ectopic pregnancy. In: Hoffman BL, Schorge JP, Schaffer JI, et al, eds. Williams Gynecology. 2nd ed. New York, NY: McGraw-Hill Professional; 2012:198–218.
4. Lobo RA. Ectopic pregnancy. In: Lentz GM, ed. Comprehensive Gynecology. 6th ed. Philadelphia, PA: Elsevier Mosby; 2012:361–382 .
5. Damario MA, Rock JA. Ectopic pregnancy. In: Rock JA, Jones HW III, eds. Te Linde’s Operative Gynecology. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:798–824.
6. Tulandi T. Ectopic pregnancy: clinical manifestations and diagnosis. UpToDate Web site. http://www.uptodate.com/contents/ectopic-pregnancy-clinical-manifestations-and-diag nosis. Updated October 22, 2014. Accessed February 18, 2015.
7. Kadar N, Caldwell BV, Romera R. A method of screening for ectopic pregnancy and its indications. Obstet Gynecol. 1981;58(2):162–166.
8. Barnhart KT, Sammel MD, Rinaudo PF, Zhou L, Hummel AC, Guo W. Symptomatic patients with an early viable intrauterine pregnancy: hCG curves redefined. Obstet Gynecol. 2004;104(1):50–55.
Why not use serum progesterone to determine early pregnancy viability?
I read with attention Dr. Barbieri’s recent editorial about evaluation of early pregnancy. My question is: Why is serum progesterone not recommended or used to assess the health of an early pregnancy?
In my practice, I always use a serum progesterone test along with hCG measurements to ascertain if an early pregnancy is healthy. I have observed, as biased as this observation can be, as I have not done any study about it, that a serum progesterone level above 12 ng/dL correlates quite well with a healthy pregnancy. I only follow more intensively with serial ultrasonography and hCG measurements in a patient whose progesterone level is below 11 ng/dL.
When a patient’s only symptom is bleeding, if the serum progesterone level is below 11 ng/dL, and her serum quantitative hCG level does not double as appropriate, I consider the pregnancy not normal and counsel the patient about continuing observation or terminating the pregnancy.
In the same laboratory scenario but with a patient who has bleeding and pain, and even moreso if the progesterone level is below 8 ng/dL, I strongly consider an ectopic pregnancy until it is proven otherwise. In this case, I offer treatment with methotrexate, as it’s my experience that the vast majority of these patients are carrying an abnormal pregnancy— either a spontaneous abortion or an ectopic pregnancy. Methotrexate therapy will prevent further complications without causing the loss of normal pregnancies.
For me, progesterone levels add one more piece to the puzzle. A patient with pain, vaginal bleeding, a quantitative hCG value of
500 mIU/mL, and a serum progesterone level of 20 ng/dL will have a normal pregnancy and is not a candidate for any intervention besides a follow-up hCG measurement to ascertain “doubling” of the analyte as expected in a normal pregnancy.
An asymptomatic patient whose quantitative hCG measurement is 1,000 mIU/mL and progesterone level is 4 ng/dL is carrying an abnormal pregnancy. If this quantitative hCG does not double appropriately in the follow-up, I counsel the patient about the greater chance of a spontaneous abortion or ectopic pregnancy.
Is this approach faulty?
Tomas Hernandez, MD
Pasco, Washington
Know the sensitivity of the HCG test
I found Dr. Barbieri’s editorial very timely. It brings some clarity to the use of the hCG discriminatory zone in symptomatic pregnant patients.
An additional important point is that it is the clinician’s obligation to know the sensitivity of the test the laboratory uses. Serum tests use the threshold for a negative result of either less than 1 mIU/mL or less than 5 mIU/mL. If possible, serial hCG measurements should be performed in the same laboratory, because the result may not represent a true change in the hCG concentration if the second test is performed at a different laboratory.1 This is especially important when the clinician is considering the use of methotrexate to treat a suspected ectopic pregnancy.
Magdalen E. Hull, MD, MPH
Great River, New York
Reference
1. Meriko Mori K, Lurain, JR. Human chorionic gonadotropin: testing in pregnancy and gestational trophoblastic disease and causes of low persistent levels. UpToDate. http://www.uptodate.com/contents/human-chorionic-gonadotropin-testing-in-pregnancy-and-gesta tional-trophoblastic-disease-and-causes-of-low-persistent-levels. Published October 23, 2013. Accessed January 29, 2015.
Further thoughts on HCG, ultrasound, and early pregnancy diagnosis
I want to thank Dr. Barbieri for his important, timely message about suspected nonviable pregnancy. I agree with virtually all of his excellent suggestions. In fact, I was part of the consensus panel that developed the findings diagnostic of and suggestive of IUP failure.1 There are a few points, however, that I believe the readership of OBG Management should know.
The endothelial heart tube, the first organ system to form, folds in on itself and begins to beat at 21 days postconception. Thus, it is present and beating prior to our ability to image it on transvaginal ultrasound. Yet new guidelines1 now say not to call an IUP failed until there is a crown-rump length of 7 mm or greater with no cardiac activity. In the past, many clinicians used 4 or 5 mm. In fact, one of the most recent studies utilizing an 8-mHz transducer found all cardiac activity was visualized by 3.1 mm embryonic size!2
So why has the number been increased to 7 mm? I’ve given this a lot of thought. Most clinical trials, from which guidelines were derived in the past, were well-designed, tightly controlled, and performed by better-trained clinicians, often with state-of-the-art equipment. In contrast, well-meaning health-care providers practicing in the field are often without the same level of quality control, equipment, or expertise but are still expected to duplicate the data from the trials used to create the guidelines. The reason this is relevant pertains to the statement that 94% of 291 cases of ectopic pregnancy had an adnexal mass.3 This is an excellent study, done at one of the nation’s most outstanding academic institutions by world-class sonologists. I do not believe that well-meaning clinicians in the field will be able to achieve this level of detection.
Dr. Barbieri also discusses an inability to see an IUP even when hCG levels are greater than 1,500 or 2,000 mIU/mL or above. He mentions obesity, fibroids, and adenomyosis as increasing the risk of an ultrasound failing to detect an early IUP. This point needs to be expanded upon. Twenty-seven years ago, we claimed a discriminatory level of 1,025 mIU/mL of hCG if the gestational sac was normal and the uterus was normal with normal echo patterns. We had three cases with markedly greater hCG levels (one, in fact, as high as 5,544 mIU/mL)with coexisting fibroids.4
I would also submit that it is the axial uterus that is a very important source of potential error. The closer the beam of sound coming off of the footprint is to a right angle with the endometrium (as it will be in a markedly anteverted or retroverted uterus), the better the resulting image. With an axial uterus, the endometrium is in the same plane as the beam of sound, and this diminishes imaging capability. Furthermore, twin pregnancies are a potential confounder in attempting to correlate hCG levels in transvaginal ultrasound findings.
I wholeheartedly agree with Dr. Barbieri: There is virtually no role to administer methotrexate based on a single hCG determination in a hemodynamically stable patient.
Steven R. Goldstein, MD
New York, New York
References
1. Doubilet PM, Benson CB, Bourne T, Blaivas M; Society of Radiologists in Ultrasound Multispecialty Panel on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
2. Abaid LN, As-Sanie S, Wolfe HM. Relationship between crown-rump length and early detection of cardiac activity. J Reprod Med. 2007;52(5):375–378.
3. Frates MC, Doubilet PM, Peters HE, Benson CR. Adnexal sonographic findings in ectopic pregnancy and their correlation with tubal rupture and human chorionic gonadotropin levels. J Ultrasound Med. 2014;33(4):697–703.
4. Goldstein SR, Snyder JR, Watson C, Danon M. Very early pregnancy detection with endovaginal ultrasound. Obstet Gynecol. 1988;72(2):200–204.
Dr. Barbieri responds
Dr. Namaky, Dr. Hernandez, Dr. Hull, and Dr. Goldstein provide great clinical advice for readers. I agree with Dr. Namaky that the mainstays of managing a pregnancy of unknown location in a stable patient are clinical assessment and ultrasonography. Dr. Hernandez recommends using the serum progesterone measurement to help guide clinical decisions in a pregnancy of unknown location. I also use serum progesterone in my practice because a very low progesterone level helps the patient to understand that she has a failed pregnancy, and facilitates her acceptance of timely intervention. Many of my colleagues do not use progesterone measurement because they prefer to rely on clinical assessment, serial hCG measurement, and ultrasound results to guide their treatment. I agree with Dr. Hull that serial hCG measurements are most useful when the same laboratory performs all the tests. Dr. Goldstein, a world class expert in the evaluation and management of early pregnancy problems, provides great advice for all readers on how to best integrate ultrasonography in their practices to optimize patient care.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Is Hemolysis a Clinical Marker of Propionibacterium acnes Orthopedic Infection or a Phylogenetic Marker?
Letter to the Editor
Is Hemolysis a Clinical Marker of Propionibacterium acnes Orthopedic Infection or a Phylogenetic Marker?
We read with great interest the study by Nodzo and colleagues in the May 2014 issue of The American Journal of Orthopedics on hemolysis as a clinical marker for Propionibacterium acnes orthopedic infection.1 We agree with the authors that determining if a P acnes culture is a true infection or a contaminant remains a challenge. Although P acnes is described as a commensal bacterium with a low pathogenicity, its involvement has been reported in many clinical entities, especially device-related infections.2P acnes is usually the cause of delayed infections occurring 3 to 24 months or more after prosthesis placement. The rate of P acnes involvement, probably underestimated, is about 10%.3 Although this bacterium was considered to be a contaminant, several virulence factors have been recently identified: putative hemolysins or cytotoxins (CAMP factors, hemolysin III) and enzymes putatively involved in degrading host tissue or molecules (GehA lipase, lysophospholipase, hyaluronate lyase, endoglycoceramidase, etc).4
Interestingly, Nodzo and colleagues revealed that 13 out of 22 P acnes strains were hemolytic and, among them, 10 were considered as definite infections, including 3 with only 1 positive sample. The authors could not identify a statistically significant trend, probably because their study was underpowered due to the size of this case series, as discussed by the authors. Nevertheless, the hemolytic activity of the strains was investigated in the 1980s by adding different concentrations of blood obtained from rabbits, sheep, or humans.5 The hemolytic activity was recorded as positive when a clear, colorless zone around the colonies appeared or weak when slight and incomplete hemolysis under the colonies was found.5 Depending on the erythrocyte origin, differences in the lytic action of hemolysin or cytotoxin may indicate the existence of various enzymes. These enzymes could have different levels of production and provide a distinct hemolytic profile. This hemolytic activity observation could also be correlated to the genetic background of the isolates.
In fact, from a genetic and epidemiological point of view, the sequence analysis of recA gene distinguished 2 distinct lineages of P acnes: types I and II.4 The association of some strains with specific clinical presentations was also demonstrated. Later, McDowell and colleagues6 reported 5 main phylogenetically distinct groups: IA, IB, IC, II, and III. It would have been interesting to know the phylogenetic groups of the strains tested in the study by Nodzo and coauthors, especially as Sampedro and colleagues7 recently reported more phylogenetic groups IA and IB among P acnes strains involved in bone and joint infections. Both of these phylotypes are hemolytic, unlike phylotypes II and III, less often encountered in this clinical entity as reported recently.8 We agree with the authors that hemolytic behavior may be one of the key factors in the variability in the pathogenicity of P acnes strains, suggesting that some strains could be more aggressive than others during deep infection. Another feature is likely the biofilm-production ability of the strains.9,10
According to our experience, the hemolysis behavior was slightly different depending on which blood agar plates were used to detect hemolytic properties. We have selected 8 isolates or reference ATCC strains from different phylotypes. Each isolate was seeded on 5 different blood agar plates with erythrocyte from various origins (Table). We can confirm that only strains belonging to IA and IB phylotypes were hemolytic, with different behavior as previously reported (Figure).8 Similarly, within IA phylotype strains, the hemolytic property could be different suggesting a difference in the genetic background. However, as the genes encoding all 5 CAMP factors are present in all P acnes groups studied by Valanne and colleagues11 (IA, IB, and II), observed differences reflected different levels of expression rather than missing genes. Moreover, when camp2 or camp4 genes were deleted, the ∆camp2 but not the ∆camp4 mutant exhibited reduced hemolytic activity with sheep erythrocytes, indicating that CAMP factor 2 seems to be the major active cohemolytic factor, but in an IA phylotype P acnes genetic background.12
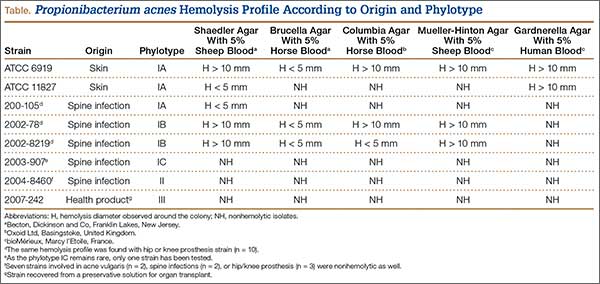
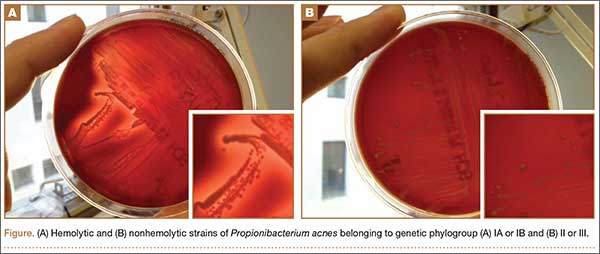
To conclude, the link between hemolysis and P acnes deep infection remains controversial and complex. The phenotypic differences observed between strains from various types reflect deeper differences in their phylogeny. The hemolytic ability raises the possibility that strains may also display a specific behavior according to their type and variation in their expression of putative virulence factors, including hemolysin, cytotoxin, or lipase. Further studies are clearly needed to better understand the virulence and phylogeny of P acnes strains in order to distinguish contamination from bone infection.
Stéphane Corvec, PharmD, PhD, Jérémy Luchetta, MSc, and Guillaume Ghislain Aubin, PharmD
Nantes University Hospital, Microbiology Laboratory, Nantes, France
Authors’ Response
Corvec and colleagues wrote an interesting summary and make excellent points about the role of hemolysis in Propionibacterium acnes. P acnes upper extremity infection has become an increasingly recognized problem, and determining whether a P acnes culture represents a true infection or a contaminant is still a challenge. We performed this study in hopes of finding an easily usable characteristic of P acnes that would assist the clinician in identifying P acnes strains as true infections rather than contaminants.
Certain pathogenic characteristics of P acnes have been identified, but the clinical implications of this bacterium are still being evaluated. We recognize that the hemolysis phenotype is a characteristic, and may not be the main pathogenic feature, of certain phylotypes of P acnes. It is possible the hemolytic strains in our study were from the IA and IB phylotypes, but, unfortunately, we did not specifically evaluate for phylogeny in our study. This would have correlated well with the work of Sampedro and colleagues,1 which suggested most deep bone and joint infections occur with type IA and IB P acnes phylotypes. Although less common in orthopedic infections, the type II and III phylotypes of P acnes are also capable of causing deep infection, and may not cause a hemolytic reaction on blood agar, which may be why we had some patients classified as a definite infection that did not have a hemolytic strain of P acnes. It is also possible a hemolytic strain may truly be a contaminant, but we did not observe this in our small case series. A larger series may help elucidate this finding, but the majority of truly infected patients in our case series had a hemolytic P acnes phenotype.
The type of blood agar used could have also influenced our results, as noted in the Table in Corvec and colleagues’ letter. We observed the most robust hemolysis on brucella blood agar, and limited hemolysis on CDC (Centers for Disease Control and Prevention) anaerobe blood agar; however, we did not evaluate multiple different blood agar preparations, which could have identified more hemolytic strains.
In our study, the presence of hemolysis was helpful in determining whether or not a true infection existed, but the absence of the hemolytic phenotype did not offer much additional information. The hemolytic phenotype may be a potential marker for those strains that are more aggressive and possibly represent the IA and IB phylotypes, which, as previously stated, are more commonly found in deep bone and joint infections.1 Hemolysis may serve as a surrogate marker for determining these phylotypes since determining phylogeny in a hospital laboratory is burdensome and not possible in most institutions.
In summary, we agree the hemolytic phenotype is commonly observed in certain P acnes phylotypes, and that not all upper extremity orthopedic P acnes infections will have a hemolytic finding. The genetic differences in P acnes strains are complex, and finding a marker of truly pathogenic strains has yet to be established. Larger studies evaluating the clinical outcomes and laboratory findings of patients with and without hemolytic strains of P acnes and evaluating which blood agar is the best at identifying the hemolytic phenotype may be beneficial. Identifying or combining multiple clinical and microbe-specific characteristics may also help guide treatment recommendations when a positive P acnes culture is identified.
Scott R. Nodzo, MD
John K. Crane, MD, PhD
Thomas R. Duquin, MD
Department of Orthopedics
University at Buffalo
Buffalo, NY
Letter to the Editor
1. Nodzo SR, Hohman DW, Crane JK, Duquin TR. Hemolysis as a clinical marker for Propionibacterium acnes orthopedic infection. Am J Orthop. 2014;43(5):E93-E97.
2. Portillo ME, Corvec S, Borens O, Trampuz A. Propionibacterium acnes: an underestimated pathogen in implant-associated infections. BioMed Res Int. 2013;2013:804391.
3. Corvec S, Portillo ME, Pasticci BM, Borens O, Trampuz A. Epidemiology and new developments in the diagnosis of prosthetic joint infection. Int J Artif Organs. 2012;35(10):923-934.
4. Aubin GG, Portillo ME, Trampuz A, Corvec S. Propionibacterium acnes, an emerging pathogen: from acne to implant-infections, from phylotype to resistance. Médecine Mal Infect. 2014;44(6):241-250.
5. Hoeffler U. Enzymatic and hemolytic properties of Propionibacterium acnes and related bacteria. J Clin Microbiol. 1977;6(6):555-558.
6. McDowell A, Perry AL, Lambert PA, Patrick S. A new phylogenetic group of Propionibacterium acnes. J Med Microbiol. 2008;57(Pt 2):218-224.
7. Sampedro MF, Piper KE, McDowell A, et al. Species of Propionibacterium and Propionibacterium acnes phylotypes associated with orthopedic implants. Diagn Microbiol Infect Dis. 2009;64(2):138-145.
8. Lomholt HB, Kilian M. Population genetic analysis of Propionibacterium acnes identifies a subpopulation and epidemic clones associated with acne. PloS One. 2010;5(8):e12277.
9. Furustrand Tafin U, Corvec S, Betrisey B, Zimmerli W, Trampuz A. Role of rifampin against Propionibacterium acnes biofilm in vitro and in an experimental foreign-body infection model. Antimicrob Agents Chemother. 2012;56(4):1885-1891.
10. Holmberg A, Lood R, Mörgelin M, et al. Biofilm formation by Propionibacterium acnes is a characteristic of invasive isolates. Clin Microbiol Infect. 2009;15(8):787-795.
11. Valanne S, McDowell A, Ramage G, et al. CAMP factor homologues in Propionibacterium acnes: a new protein family differentially expressed by types I and II. Microbiol. 2005;151(Pt 5):1369-1379.
12. Sörensen M, Mak TN, Hurwitz R, et al. Mutagenesis of Propionibacterium acnes and analysis of two CAMP factor knock-out mutants. J Microbiol Methods. 2010;83(2):211-216.
Authors' Response Reference
1. Sampedro MF, Piper KE, McDowell A, et al. Species of Propionibacterium and Propionibacterium acnes phylotypes associated with orthopedic implants. Diagn Microbiol Infect Dis. 2009;64(2):138-145.
Letter to the Editor
Is Hemolysis a Clinical Marker of Propionibacterium acnes Orthopedic Infection or a Phylogenetic Marker?
We read with great interest the study by Nodzo and colleagues in the May 2014 issue of The American Journal of Orthopedics on hemolysis as a clinical marker for Propionibacterium acnes orthopedic infection.1 We agree with the authors that determining if a P acnes culture is a true infection or a contaminant remains a challenge. Although P acnes is described as a commensal bacterium with a low pathogenicity, its involvement has been reported in many clinical entities, especially device-related infections.2P acnes is usually the cause of delayed infections occurring 3 to 24 months or more after prosthesis placement. The rate of P acnes involvement, probably underestimated, is about 10%.3 Although this bacterium was considered to be a contaminant, several virulence factors have been recently identified: putative hemolysins or cytotoxins (CAMP factors, hemolysin III) and enzymes putatively involved in degrading host tissue or molecules (GehA lipase, lysophospholipase, hyaluronate lyase, endoglycoceramidase, etc).4
Interestingly, Nodzo and colleagues revealed that 13 out of 22 P acnes strains were hemolytic and, among them, 10 were considered as definite infections, including 3 with only 1 positive sample. The authors could not identify a statistically significant trend, probably because their study was underpowered due to the size of this case series, as discussed by the authors. Nevertheless, the hemolytic activity of the strains was investigated in the 1980s by adding different concentrations of blood obtained from rabbits, sheep, or humans.5 The hemolytic activity was recorded as positive when a clear, colorless zone around the colonies appeared or weak when slight and incomplete hemolysis under the colonies was found.5 Depending on the erythrocyte origin, differences in the lytic action of hemolysin or cytotoxin may indicate the existence of various enzymes. These enzymes could have different levels of production and provide a distinct hemolytic profile. This hemolytic activity observation could also be correlated to the genetic background of the isolates.
In fact, from a genetic and epidemiological point of view, the sequence analysis of recA gene distinguished 2 distinct lineages of P acnes: types I and II.4 The association of some strains with specific clinical presentations was also demonstrated. Later, McDowell and colleagues6 reported 5 main phylogenetically distinct groups: IA, IB, IC, II, and III. It would have been interesting to know the phylogenetic groups of the strains tested in the study by Nodzo and coauthors, especially as Sampedro and colleagues7 recently reported more phylogenetic groups IA and IB among P acnes strains involved in bone and joint infections. Both of these phylotypes are hemolytic, unlike phylotypes II and III, less often encountered in this clinical entity as reported recently.8 We agree with the authors that hemolytic behavior may be one of the key factors in the variability in the pathogenicity of P acnes strains, suggesting that some strains could be more aggressive than others during deep infection. Another feature is likely the biofilm-production ability of the strains.9,10
According to our experience, the hemolysis behavior was slightly different depending on which blood agar plates were used to detect hemolytic properties. We have selected 8 isolates or reference ATCC strains from different phylotypes. Each isolate was seeded on 5 different blood agar plates with erythrocyte from various origins (Table). We can confirm that only strains belonging to IA and IB phylotypes were hemolytic, with different behavior as previously reported (Figure).8 Similarly, within IA phylotype strains, the hemolytic property could be different suggesting a difference in the genetic background. However, as the genes encoding all 5 CAMP factors are present in all P acnes groups studied by Valanne and colleagues11 (IA, IB, and II), observed differences reflected different levels of expression rather than missing genes. Moreover, when camp2 or camp4 genes were deleted, the ∆camp2 but not the ∆camp4 mutant exhibited reduced hemolytic activity with sheep erythrocytes, indicating that CAMP factor 2 seems to be the major active cohemolytic factor, but in an IA phylotype P acnes genetic background.12
To conclude, the link between hemolysis and P acnes deep infection remains controversial and complex. The phenotypic differences observed between strains from various types reflect deeper differences in their phylogeny. The hemolytic ability raises the possibility that strains may also display a specific behavior according to their type and variation in their expression of putative virulence factors, including hemolysin, cytotoxin, or lipase. Further studies are clearly needed to better understand the virulence and phylogeny of P acnes strains in order to distinguish contamination from bone infection.
Stéphane Corvec, PharmD, PhD, Jérémy Luchetta, MSc, and Guillaume Ghislain Aubin, PharmD
Nantes University Hospital, Microbiology Laboratory, Nantes, France
Authors’ Response
Corvec and colleagues wrote an interesting summary and make excellent points about the role of hemolysis in Propionibacterium acnes. P acnes upper extremity infection has become an increasingly recognized problem, and determining whether a P acnes culture represents a true infection or a contaminant is still a challenge. We performed this study in hopes of finding an easily usable characteristic of P acnes that would assist the clinician in identifying P acnes strains as true infections rather than contaminants.
Certain pathogenic characteristics of P acnes have been identified, but the clinical implications of this bacterium are still being evaluated. We recognize that the hemolysis phenotype is a characteristic, and may not be the main pathogenic feature, of certain phylotypes of P acnes. It is possible the hemolytic strains in our study were from the IA and IB phylotypes, but, unfortunately, we did not specifically evaluate for phylogeny in our study. This would have correlated well with the work of Sampedro and colleagues,1 which suggested most deep bone and joint infections occur with type IA and IB P acnes phylotypes. Although less common in orthopedic infections, the type II and III phylotypes of P acnes are also capable of causing deep infection, and may not cause a hemolytic reaction on blood agar, which may be why we had some patients classified as a definite infection that did not have a hemolytic strain of P acnes. It is also possible a hemolytic strain may truly be a contaminant, but we did not observe this in our small case series. A larger series may help elucidate this finding, but the majority of truly infected patients in our case series had a hemolytic P acnes phenotype.
The type of blood agar used could have also influenced our results, as noted in the Table in Corvec and colleagues’ letter. We observed the most robust hemolysis on brucella blood agar, and limited hemolysis on CDC (Centers for Disease Control and Prevention) anaerobe blood agar; however, we did not evaluate multiple different blood agar preparations, which could have identified more hemolytic strains.
In our study, the presence of hemolysis was helpful in determining whether or not a true infection existed, but the absence of the hemolytic phenotype did not offer much additional information. The hemolytic phenotype may be a potential marker for those strains that are more aggressive and possibly represent the IA and IB phylotypes, which, as previously stated, are more commonly found in deep bone and joint infections.1 Hemolysis may serve as a surrogate marker for determining these phylotypes since determining phylogeny in a hospital laboratory is burdensome and not possible in most institutions.
In summary, we agree the hemolytic phenotype is commonly observed in certain P acnes phylotypes, and that not all upper extremity orthopedic P acnes infections will have a hemolytic finding. The genetic differences in P acnes strains are complex, and finding a marker of truly pathogenic strains has yet to be established. Larger studies evaluating the clinical outcomes and laboratory findings of patients with and without hemolytic strains of P acnes and evaluating which blood agar is the best at identifying the hemolytic phenotype may be beneficial. Identifying or combining multiple clinical and microbe-specific characteristics may also help guide treatment recommendations when a positive P acnes culture is identified.
Scott R. Nodzo, MD
John K. Crane, MD, PhD
Thomas R. Duquin, MD
Department of Orthopedics
University at Buffalo
Buffalo, NY
Letter to the Editor
Is Hemolysis a Clinical Marker of Propionibacterium acnes Orthopedic Infection or a Phylogenetic Marker?
We read with great interest the study by Nodzo and colleagues in the May 2014 issue of The American Journal of Orthopedics on hemolysis as a clinical marker for Propionibacterium acnes orthopedic infection.1 We agree with the authors that determining if a P acnes culture is a true infection or a contaminant remains a challenge. Although P acnes is described as a commensal bacterium with a low pathogenicity, its involvement has been reported in many clinical entities, especially device-related infections.2P acnes is usually the cause of delayed infections occurring 3 to 24 months or more after prosthesis placement. The rate of P acnes involvement, probably underestimated, is about 10%.3 Although this bacterium was considered to be a contaminant, several virulence factors have been recently identified: putative hemolysins or cytotoxins (CAMP factors, hemolysin III) and enzymes putatively involved in degrading host tissue or molecules (GehA lipase, lysophospholipase, hyaluronate lyase, endoglycoceramidase, etc).4
Interestingly, Nodzo and colleagues revealed that 13 out of 22 P acnes strains were hemolytic and, among them, 10 were considered as definite infections, including 3 with only 1 positive sample. The authors could not identify a statistically significant trend, probably because their study was underpowered due to the size of this case series, as discussed by the authors. Nevertheless, the hemolytic activity of the strains was investigated in the 1980s by adding different concentrations of blood obtained from rabbits, sheep, or humans.5 The hemolytic activity was recorded as positive when a clear, colorless zone around the colonies appeared or weak when slight and incomplete hemolysis under the colonies was found.5 Depending on the erythrocyte origin, differences in the lytic action of hemolysin or cytotoxin may indicate the existence of various enzymes. These enzymes could have different levels of production and provide a distinct hemolytic profile. This hemolytic activity observation could also be correlated to the genetic background of the isolates.
In fact, from a genetic and epidemiological point of view, the sequence analysis of recA gene distinguished 2 distinct lineages of P acnes: types I and II.4 The association of some strains with specific clinical presentations was also demonstrated. Later, McDowell and colleagues6 reported 5 main phylogenetically distinct groups: IA, IB, IC, II, and III. It would have been interesting to know the phylogenetic groups of the strains tested in the study by Nodzo and coauthors, especially as Sampedro and colleagues7 recently reported more phylogenetic groups IA and IB among P acnes strains involved in bone and joint infections. Both of these phylotypes are hemolytic, unlike phylotypes II and III, less often encountered in this clinical entity as reported recently.8 We agree with the authors that hemolytic behavior may be one of the key factors in the variability in the pathogenicity of P acnes strains, suggesting that some strains could be more aggressive than others during deep infection. Another feature is likely the biofilm-production ability of the strains.9,10
According to our experience, the hemolysis behavior was slightly different depending on which blood agar plates were used to detect hemolytic properties. We have selected 8 isolates or reference ATCC strains from different phylotypes. Each isolate was seeded on 5 different blood agar plates with erythrocyte from various origins (Table). We can confirm that only strains belonging to IA and IB phylotypes were hemolytic, with different behavior as previously reported (Figure).8 Similarly, within IA phylotype strains, the hemolytic property could be different suggesting a difference in the genetic background. However, as the genes encoding all 5 CAMP factors are present in all P acnes groups studied by Valanne and colleagues11 (IA, IB, and II), observed differences reflected different levels of expression rather than missing genes. Moreover, when camp2 or camp4 genes were deleted, the ∆camp2 but not the ∆camp4 mutant exhibited reduced hemolytic activity with sheep erythrocytes, indicating that CAMP factor 2 seems to be the major active cohemolytic factor, but in an IA phylotype P acnes genetic background.12
To conclude, the link between hemolysis and P acnes deep infection remains controversial and complex. The phenotypic differences observed between strains from various types reflect deeper differences in their phylogeny. The hemolytic ability raises the possibility that strains may also display a specific behavior according to their type and variation in their expression of putative virulence factors, including hemolysin, cytotoxin, or lipase. Further studies are clearly needed to better understand the virulence and phylogeny of P acnes strains in order to distinguish contamination from bone infection.
Stéphane Corvec, PharmD, PhD, Jérémy Luchetta, MSc, and Guillaume Ghislain Aubin, PharmD
Nantes University Hospital, Microbiology Laboratory, Nantes, France
Authors’ Response
Corvec and colleagues wrote an interesting summary and make excellent points about the role of hemolysis in Propionibacterium acnes. P acnes upper extremity infection has become an increasingly recognized problem, and determining whether a P acnes culture represents a true infection or a contaminant is still a challenge. We performed this study in hopes of finding an easily usable characteristic of P acnes that would assist the clinician in identifying P acnes strains as true infections rather than contaminants.
Certain pathogenic characteristics of P acnes have been identified, but the clinical implications of this bacterium are still being evaluated. We recognize that the hemolysis phenotype is a characteristic, and may not be the main pathogenic feature, of certain phylotypes of P acnes. It is possible the hemolytic strains in our study were from the IA and IB phylotypes, but, unfortunately, we did not specifically evaluate for phylogeny in our study. This would have correlated well with the work of Sampedro and colleagues,1 which suggested most deep bone and joint infections occur with type IA and IB P acnes phylotypes. Although less common in orthopedic infections, the type II and III phylotypes of P acnes are also capable of causing deep infection, and may not cause a hemolytic reaction on blood agar, which may be why we had some patients classified as a definite infection that did not have a hemolytic strain of P acnes. It is also possible a hemolytic strain may truly be a contaminant, but we did not observe this in our small case series. A larger series may help elucidate this finding, but the majority of truly infected patients in our case series had a hemolytic P acnes phenotype.
The type of blood agar used could have also influenced our results, as noted in the Table in Corvec and colleagues’ letter. We observed the most robust hemolysis on brucella blood agar, and limited hemolysis on CDC (Centers for Disease Control and Prevention) anaerobe blood agar; however, we did not evaluate multiple different blood agar preparations, which could have identified more hemolytic strains.
In our study, the presence of hemolysis was helpful in determining whether or not a true infection existed, but the absence of the hemolytic phenotype did not offer much additional information. The hemolytic phenotype may be a potential marker for those strains that are more aggressive and possibly represent the IA and IB phylotypes, which, as previously stated, are more commonly found in deep bone and joint infections.1 Hemolysis may serve as a surrogate marker for determining these phylotypes since determining phylogeny in a hospital laboratory is burdensome and not possible in most institutions.
In summary, we agree the hemolytic phenotype is commonly observed in certain P acnes phylotypes, and that not all upper extremity orthopedic P acnes infections will have a hemolytic finding. The genetic differences in P acnes strains are complex, and finding a marker of truly pathogenic strains has yet to be established. Larger studies evaluating the clinical outcomes and laboratory findings of patients with and without hemolytic strains of P acnes and evaluating which blood agar is the best at identifying the hemolytic phenotype may be beneficial. Identifying or combining multiple clinical and microbe-specific characteristics may also help guide treatment recommendations when a positive P acnes culture is identified.
Scott R. Nodzo, MD
John K. Crane, MD, PhD
Thomas R. Duquin, MD
Department of Orthopedics
University at Buffalo
Buffalo, NY
Letter to the Editor
1. Nodzo SR, Hohman DW, Crane JK, Duquin TR. Hemolysis as a clinical marker for Propionibacterium acnes orthopedic infection. Am J Orthop. 2014;43(5):E93-E97.
2. Portillo ME, Corvec S, Borens O, Trampuz A. Propionibacterium acnes: an underestimated pathogen in implant-associated infections. BioMed Res Int. 2013;2013:804391.
3. Corvec S, Portillo ME, Pasticci BM, Borens O, Trampuz A. Epidemiology and new developments in the diagnosis of prosthetic joint infection. Int J Artif Organs. 2012;35(10):923-934.
4. Aubin GG, Portillo ME, Trampuz A, Corvec S. Propionibacterium acnes, an emerging pathogen: from acne to implant-infections, from phylotype to resistance. Médecine Mal Infect. 2014;44(6):241-250.
5. Hoeffler U. Enzymatic and hemolytic properties of Propionibacterium acnes and related bacteria. J Clin Microbiol. 1977;6(6):555-558.
6. McDowell A, Perry AL, Lambert PA, Patrick S. A new phylogenetic group of Propionibacterium acnes. J Med Microbiol. 2008;57(Pt 2):218-224.
7. Sampedro MF, Piper KE, McDowell A, et al. Species of Propionibacterium and Propionibacterium acnes phylotypes associated with orthopedic implants. Diagn Microbiol Infect Dis. 2009;64(2):138-145.
8. Lomholt HB, Kilian M. Population genetic analysis of Propionibacterium acnes identifies a subpopulation and epidemic clones associated with acne. PloS One. 2010;5(8):e12277.
9. Furustrand Tafin U, Corvec S, Betrisey B, Zimmerli W, Trampuz A. Role of rifampin against Propionibacterium acnes biofilm in vitro and in an experimental foreign-body infection model. Antimicrob Agents Chemother. 2012;56(4):1885-1891.
10. Holmberg A, Lood R, Mörgelin M, et al. Biofilm formation by Propionibacterium acnes is a characteristic of invasive isolates. Clin Microbiol Infect. 2009;15(8):787-795.
11. Valanne S, McDowell A, Ramage G, et al. CAMP factor homologues in Propionibacterium acnes: a new protein family differentially expressed by types I and II. Microbiol. 2005;151(Pt 5):1369-1379.
12. Sörensen M, Mak TN, Hurwitz R, et al. Mutagenesis of Propionibacterium acnes and analysis of two CAMP factor knock-out mutants. J Microbiol Methods. 2010;83(2):211-216.
Authors' Response Reference
1. Sampedro MF, Piper KE, McDowell A, et al. Species of Propionibacterium and Propionibacterium acnes phylotypes associated with orthopedic implants. Diagn Microbiol Infect Dis. 2009;64(2):138-145.
Letter to the Editor
1. Nodzo SR, Hohman DW, Crane JK, Duquin TR. Hemolysis as a clinical marker for Propionibacterium acnes orthopedic infection. Am J Orthop. 2014;43(5):E93-E97.
2. Portillo ME, Corvec S, Borens O, Trampuz A. Propionibacterium acnes: an underestimated pathogen in implant-associated infections. BioMed Res Int. 2013;2013:804391.
3. Corvec S, Portillo ME, Pasticci BM, Borens O, Trampuz A. Epidemiology and new developments in the diagnosis of prosthetic joint infection. Int J Artif Organs. 2012;35(10):923-934.
4. Aubin GG, Portillo ME, Trampuz A, Corvec S. Propionibacterium acnes, an emerging pathogen: from acne to implant-infections, from phylotype to resistance. Médecine Mal Infect. 2014;44(6):241-250.
5. Hoeffler U. Enzymatic and hemolytic properties of Propionibacterium acnes and related bacteria. J Clin Microbiol. 1977;6(6):555-558.
6. McDowell A, Perry AL, Lambert PA, Patrick S. A new phylogenetic group of Propionibacterium acnes. J Med Microbiol. 2008;57(Pt 2):218-224.
7. Sampedro MF, Piper KE, McDowell A, et al. Species of Propionibacterium and Propionibacterium acnes phylotypes associated with orthopedic implants. Diagn Microbiol Infect Dis. 2009;64(2):138-145.
8. Lomholt HB, Kilian M. Population genetic analysis of Propionibacterium acnes identifies a subpopulation and epidemic clones associated with acne. PloS One. 2010;5(8):e12277.
9. Furustrand Tafin U, Corvec S, Betrisey B, Zimmerli W, Trampuz A. Role of rifampin against Propionibacterium acnes biofilm in vitro and in an experimental foreign-body infection model. Antimicrob Agents Chemother. 2012;56(4):1885-1891.
10. Holmberg A, Lood R, Mörgelin M, et al. Biofilm formation by Propionibacterium acnes is a characteristic of invasive isolates. Clin Microbiol Infect. 2009;15(8):787-795.
11. Valanne S, McDowell A, Ramage G, et al. CAMP factor homologues in Propionibacterium acnes: a new protein family differentially expressed by types I and II. Microbiol. 2005;151(Pt 5):1369-1379.
12. Sörensen M, Mak TN, Hurwitz R, et al. Mutagenesis of Propionibacterium acnes and analysis of two CAMP factor knock-out mutants. J Microbiol Methods. 2010;83(2):211-216.
Authors' Response Reference
1. Sampedro MF, Piper KE, McDowell A, et al. Species of Propionibacterium and Propionibacterium acnes phylotypes associated with orthopedic implants. Diagn Microbiol Infect Dis. 2009;64(2):138-145.
Nanotechnology: Why Should We Care?
The orthopedic community is increasingly deluged with advancements in the basic sciences. With each step, we must evaluate the necessity of new information and the relevance of these topics for clinical practice. Since the late 1990s, the promise of nanotechnology to effect significant changes in the medical field has been heralded. However, in this coming decade, we as a profession will see unprecedented advances in the movement of this technology “from the bench to the bedside.” Not unlike many other basic science advancements in our field, nanotechnology is poorly understood among clinicians and residents. As the use of biologics and drug delivery systems expands in orthopedics, nanoparticle-based devices will become more prevalent and have a momentous impact on the way we treat and diagnose orthopedic patients.
A nanoparticle is generally defined as a particle in which at least 1 dimension is between 1 to 100 nanometers and has material properties consistent with quantum mechanics.1 Nanomaterials can be composed of organic and inorganic chemical elements that enable basic chemical processes to create more complex systems. Individual nanoparticle units can be synthesized to form nanostructures, including nanotubes, nanoscaffolds, nanofibers, and even nanodiamonds.2-4 Nanoparticles at this scale display unique optical, chemical, and physical properties that can be manipulated to create specific end-use applications. Such uses may include glass fabrication, optical probes, television screens, drug delivery, gene delivery, and multiplex diagnostic assays.5-7 By crossing disciplines of physics, engineering, and medical sciences, we can create novel technology that includes nanomanufacturing, targeted drug delivery, nanorobotics in conjunction with artificial intelligence, and point-of-care diagnostics.7-9
The field of orthopedics has benefited from nanotechnologic advances, such as new therapeutics and implant-related technology. Nanotubes are hollow nanosized cylinders that are commonly created from titania, silica, or carbon-based substrates. They have garnered significant interest for their high tensile and shear strength, favorable microstructure for bony ingrowth, and their capacity to hold antibiotics or growth factors, such as bone morphogenic proteins (BMPs).10 The current local delivery limitations of BMPs via a collagen sponge have the potential to be maximized and better controlled with a nanotechnology-based approach. The size, internal structure, and shape of the nanoparticle can be manipulated to control the release of these growth factors, and certain nanoparticles can be dual-layered, allowing for release of multiple growth factors at once or in succession.11,12 A more powerful and targeted delivery system of these types of growth factors may result in improved or more robust outcomes, and further research is warranted.
It is possible that carbon-based nanotubes can be categorized as a biomedical implant secondary to their mechanical properties.13 Their strength and ability to be augmented with osteogenic materials has made them an attractive area of research as alternative implant surfaces and stand-alone implants. Nanotubes are capable of acting as a scaffold for antibiotic-loaded, carbon-based nanodiamonds for localized treatment of periprosthetic infection, and research has been directed toward controlled release of the nanodiamond-antibiotic construct from these scaffolds or hydrogels.4,14 Technologies like this may allow the clinician to treat periprosthetic infections locally and minimize the use of systemic antibiotics. The perfection of this type of delivery system may augment the role of antibiotic-laden cement and improve our treatment success rates, even in traditionally hard-to-treat organisms.
Nanoscaffolds and nanofibers are created from nanosized polymers and rendered into a 3-dimensional structure that can be loaded with biologic particles or acting as a scaffold/template for tissue or bone ingrowth. Nanofibers created using biodegradable substrates such as poly(lactic-co-glycolic acid) (PLGA) and chitosan have been extensively studied for their delayed-release properties and biocompatibility.15 These scaffolds are often soaked or loaded with chondrogenic, osteogenic, or antibacterial agents, and have been evaluated in both in vitro and in vivo studies with promising results.15,16 They have been an exciting area of research in tissue engineering, and have been accepted as an adjunct in tendon-repair treatments and local bone regeneration.3,17 As this technology is perfected, the potential to treat more effectively massive rotator cuff tears or tears with poor tissue integrity will dramatically improve and expand the indications for rotator cuff repair.
Augmentation of implant surfaces with nanomaterials that improve osseointegration, or that act as antimicrobial agents have also been a focus of research in hopes of decreasing the rates of aseptic failure and periprosthetic infection in arthroplasty procedures. Nanocrystalline surfaces made of hydroxyapatite and cobalt chromium have been evaluated for their enhanced osteoconductive properties, and may replace standard surfaces.18-20 Recent work evaluating nanoparticle-antibiotic constructs that have been covalently bound to implant surfaces for delayed release of antibiotics during the perioperative period has shown promise, and may allow a more targeted and localized treatment strategy for periprosthetic infection.21,22
Major limitations regarding successful clinical implementation of nanotechnology include both cost and regulatory processes. Currently, pharmaceutical companies estimate that, on average, successful clinical trials from phase 1 to completion for new drugs can cost hundreds of millions of dollars.23 Such high costs result partially from the laborious and capital-intensive process of conducting clinical trials that meet US Food and Drug Administration (FDA) requirements. These regulations would apply to both surface-coated implants and nanoparticle-based drug delivery systems. These types of implants would not be expedited into the market secondary to their drug delivery component and would likely require lengthy clinical studies. Implant companies may be reluctant to invest millions of dollars in multiple FDA trials when they have lucrative implants on the market.
Other limitations include the particles’ complex 3-dimensional structure, which can present challenges for mass production. Producing large quantities of nanoparticles at a consistent quality may be a major limitation to the more unique and target-based nanotherapies. Recent concerns with the toxicity profile of nanotechnology-based medicines have resulted in more intense scrutiny of the nanotechnology safety profile.24,25 Currently, nanoparticle technology is evaluated case by case with each technology requiring its own toxicology and safety profile testing if it is intended for human use. These tests can be cost-prohibitive and require extensive private and government capital for successful market entry. Despite these limitations, nanotechnology will impact the next generation of orthopedic surgeons. Current estimates project the nanomedicine market to be worth $177.6 billion by 2019.26
Advances in nanobased orthopedic technologies have expanded dramatically in the past decade, and we, as the treating physicians, must make educated decisions on how and when to use nanoparticle-based therapies and treatment options. Nanotechnology’s basic science is confusing and often burdensome, but contemporary review articles may be helpful in keeping the orthopedic resident and clinician current with advancements.10,27,28 The more we educate ourselves about evolving nanotechnologies, the less reluctance we will have when evaluating new diagnostic and therapeutic treatment modalities.
1. Hewakuruppu YL, Dombrovsky LA, Chen C, et al. Plasmonic “pump-probe” method to study semi-transparent nanofluids. Appl Opt. 2013;52(24):6041-6050.
2. Balasundaram G, Webster TJ. An overview of nano-polymers for orthopedic applications. Macromol Biosci. 2007;7(5):635-642.
3. Zhang Z, Hu J, Ma PX. Nanofiber-based delivery of bioactive agents and stem cells to bone sites. Adv Drug Deliv Rev. 2012;64(12):1129-1141.
4. Mochalin VN, Shenderova O, Ho D, Gogotsi Y. The properties and applications of nanodiamonds. Nat Nanotechnol. 2012;7(1):11-23.
5. Kneipp J, Kneipp H, Rice WL, Kneipp K. Optical probes for biological applications based on surface-enhanced Raman scattering from indocyanine green on gold nanoparticles. Anal Chem. 2005;77(8):2381-2385.
6. Wang L, O’Donoghue MB, Tan W. Nanoparticles for multiplex diagnostics and imaging. Nanomedicine (Lond). 2006;1(4):413-426.
7. Krebs MD, Salter E, Chen E, Sutter KA, Alsberg E. Calcium phosphate-DNA nanoparticle gene delivery from alginate hydrogels induces in vivo osteogenesis. J Biomed Mater Res A. 2010;92(3):1131-1138.
8. Myers FB, Lee LP. Innovations in optical microfluidic technologies for point-of-care diagnostics. Lab Chip. 2008;8(12):2015-2031.
9. Sacha GM, Varona P. Artificial intelligence in nanotechnology. Nanotechnology. 2013;24(45):452002.
10. Ganguly DY, Shahbazian R, Shokuhfar T. Recent advances in nanotubes for orthopedic implants. J Nanotech Smart Mater. 2014;1:1-10.
11. Srivastava S, Kotov NA. Composite Layer-by-Layer (LBL) assembly with inorganic nanoparticles and nanowires. Acc Chem Res. 2008;41(12):1831-1841.
12. Panda HS, Srivastava R, Bahadur D. Shape and size control of nano dispersed Mg/Al layered double hydroxide. J Nanosci Nanotechnol. 2008;8(8):4218-4223.
13. Wang X, Li Q, Xie J, et al. Fabrication of ultralong and electrically uniform single-walled carbon nanotubes on clean substrates. Nano Lett. 2009;9(9):3137-3141.
14. Zhu Y, Li J, Li W, et al. The biocompatibility of nanodiamonds and their application in drug delivery systems. Theranostics. 2012;2(3):302-312.
15. Wu L, Ding J. In vitro degradation of three-dimensional porous poly(D,L-lactide-co-glycolide) scaffolds for tissue engineering. Biomaterials. 2004;25(2):5821-5830.
16. Wu X, Rabkin-Aikawa E, Guleserian KJ, et al. Tissue-engineered microvessels on three-dimensional biodegradable scaffolds using human endothelial progenitor cells. Am J Physiol Heart Circ Physiol. 2004;287(2):H480-H487.
17. Xia W, Liu W, Cui L, et al. Tissue engineering of cartilage with the use of chitosan-gelatin complex scaffolds. J Biomed Mater Res B Appl Biomater. 2004;71(2):373-380.
18. Laurencin CT, Kumbar SG, Nukavarapu SP. Nanotechnology and orthopedics: a personal perspective. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2009;1(1):6-10.
19. Webster TJ, Ejiofor JU. Increased osteoblast adhesion on nanophase metals: Ti, Ti6Al4V, and CoCrMo. Biomaterials. 2004;25(19):4731-4739.
20. Webster TJ, Ergun C, Doremus RH, Siegel RW, Bizios R. Enhanced functions of osteoblasts on nanophase ceramics. Biomaterials. 2000;21(17):1803-1810.
21. Stewart S, Barr S, Engiles J, et al. Vancomycin-modified implant surface inhibits biofilm formation and supports bone-healing in an infected osteotomy model in sheep: a proof-of-concept study. J Bone Joint Surg Am. 2012;94(15):1406-1415.
22. Hickok NJ, Shapiro IM. Immobilized antibiotics to prevent orthopaedic implant infections. Adv Drug Deliv Rev. 2012;64(12):1165-1176.
23. DiMasi JA, Hansen RW, Grabowski HG. The price of innovation: new estimates of drug development costs. J Health Econ. 2003;22(2):151-185.
24. Vines T, Faunce T. Assessing the safety and cost-effectiveness of early nanodrugs. J Law Med. 2009;16(5):822-845.
25. Nel A, Xia T, Mädler L, Li N. Toxic potential of materials at the nanolevel. Science. 2006;311(5761):622-627.
26. Nanomedicine Market (Neurology, Cardiovascular, Anti-Inflammatory, Anti-Infective, and Oncology Applications): Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013-2019. Transparency Market Research website. http://www.transparencymarketresearch.com/nanomedicine-market.html. Published August 1, 2014. Accessed January 20, 2015.
27. Sullivan MP, McHale KJ, Parvizi J, Mehta S. Nanotechnology: current concepts in orthopaedic surgery and future directions. Bone Joint J. 2014;96-B(5):569-573.
28. Pleshko N, Grande DA, Myers KR. Nanotechnology in orthopaedics. J Am Acad Orthop Surg. 2012;20(1):60-62.
The orthopedic community is increasingly deluged with advancements in the basic sciences. With each step, we must evaluate the necessity of new information and the relevance of these topics for clinical practice. Since the late 1990s, the promise of nanotechnology to effect significant changes in the medical field has been heralded. However, in this coming decade, we as a profession will see unprecedented advances in the movement of this technology “from the bench to the bedside.” Not unlike many other basic science advancements in our field, nanotechnology is poorly understood among clinicians and residents. As the use of biologics and drug delivery systems expands in orthopedics, nanoparticle-based devices will become more prevalent and have a momentous impact on the way we treat and diagnose orthopedic patients.
A nanoparticle is generally defined as a particle in which at least 1 dimension is between 1 to 100 nanometers and has material properties consistent with quantum mechanics.1 Nanomaterials can be composed of organic and inorganic chemical elements that enable basic chemical processes to create more complex systems. Individual nanoparticle units can be synthesized to form nanostructures, including nanotubes, nanoscaffolds, nanofibers, and even nanodiamonds.2-4 Nanoparticles at this scale display unique optical, chemical, and physical properties that can be manipulated to create specific end-use applications. Such uses may include glass fabrication, optical probes, television screens, drug delivery, gene delivery, and multiplex diagnostic assays.5-7 By crossing disciplines of physics, engineering, and medical sciences, we can create novel technology that includes nanomanufacturing, targeted drug delivery, nanorobotics in conjunction with artificial intelligence, and point-of-care diagnostics.7-9
The field of orthopedics has benefited from nanotechnologic advances, such as new therapeutics and implant-related technology. Nanotubes are hollow nanosized cylinders that are commonly created from titania, silica, or carbon-based substrates. They have garnered significant interest for their high tensile and shear strength, favorable microstructure for bony ingrowth, and their capacity to hold antibiotics or growth factors, such as bone morphogenic proteins (BMPs).10 The current local delivery limitations of BMPs via a collagen sponge have the potential to be maximized and better controlled with a nanotechnology-based approach. The size, internal structure, and shape of the nanoparticle can be manipulated to control the release of these growth factors, and certain nanoparticles can be dual-layered, allowing for release of multiple growth factors at once or in succession.11,12 A more powerful and targeted delivery system of these types of growth factors may result in improved or more robust outcomes, and further research is warranted.
It is possible that carbon-based nanotubes can be categorized as a biomedical implant secondary to their mechanical properties.13 Their strength and ability to be augmented with osteogenic materials has made them an attractive area of research as alternative implant surfaces and stand-alone implants. Nanotubes are capable of acting as a scaffold for antibiotic-loaded, carbon-based nanodiamonds for localized treatment of periprosthetic infection, and research has been directed toward controlled release of the nanodiamond-antibiotic construct from these scaffolds or hydrogels.4,14 Technologies like this may allow the clinician to treat periprosthetic infections locally and minimize the use of systemic antibiotics. The perfection of this type of delivery system may augment the role of antibiotic-laden cement and improve our treatment success rates, even in traditionally hard-to-treat organisms.
Nanoscaffolds and nanofibers are created from nanosized polymers and rendered into a 3-dimensional structure that can be loaded with biologic particles or acting as a scaffold/template for tissue or bone ingrowth. Nanofibers created using biodegradable substrates such as poly(lactic-co-glycolic acid) (PLGA) and chitosan have been extensively studied for their delayed-release properties and biocompatibility.15 These scaffolds are often soaked or loaded with chondrogenic, osteogenic, or antibacterial agents, and have been evaluated in both in vitro and in vivo studies with promising results.15,16 They have been an exciting area of research in tissue engineering, and have been accepted as an adjunct in tendon-repair treatments and local bone regeneration.3,17 As this technology is perfected, the potential to treat more effectively massive rotator cuff tears or tears with poor tissue integrity will dramatically improve and expand the indications for rotator cuff repair.
Augmentation of implant surfaces with nanomaterials that improve osseointegration, or that act as antimicrobial agents have also been a focus of research in hopes of decreasing the rates of aseptic failure and periprosthetic infection in arthroplasty procedures. Nanocrystalline surfaces made of hydroxyapatite and cobalt chromium have been evaluated for their enhanced osteoconductive properties, and may replace standard surfaces.18-20 Recent work evaluating nanoparticle-antibiotic constructs that have been covalently bound to implant surfaces for delayed release of antibiotics during the perioperative period has shown promise, and may allow a more targeted and localized treatment strategy for periprosthetic infection.21,22
Major limitations regarding successful clinical implementation of nanotechnology include both cost and regulatory processes. Currently, pharmaceutical companies estimate that, on average, successful clinical trials from phase 1 to completion for new drugs can cost hundreds of millions of dollars.23 Such high costs result partially from the laborious and capital-intensive process of conducting clinical trials that meet US Food and Drug Administration (FDA) requirements. These regulations would apply to both surface-coated implants and nanoparticle-based drug delivery systems. These types of implants would not be expedited into the market secondary to their drug delivery component and would likely require lengthy clinical studies. Implant companies may be reluctant to invest millions of dollars in multiple FDA trials when they have lucrative implants on the market.
Other limitations include the particles’ complex 3-dimensional structure, which can present challenges for mass production. Producing large quantities of nanoparticles at a consistent quality may be a major limitation to the more unique and target-based nanotherapies. Recent concerns with the toxicity profile of nanotechnology-based medicines have resulted in more intense scrutiny of the nanotechnology safety profile.24,25 Currently, nanoparticle technology is evaluated case by case with each technology requiring its own toxicology and safety profile testing if it is intended for human use. These tests can be cost-prohibitive and require extensive private and government capital for successful market entry. Despite these limitations, nanotechnology will impact the next generation of orthopedic surgeons. Current estimates project the nanomedicine market to be worth $177.6 billion by 2019.26
Advances in nanobased orthopedic technologies have expanded dramatically in the past decade, and we, as the treating physicians, must make educated decisions on how and when to use nanoparticle-based therapies and treatment options. Nanotechnology’s basic science is confusing and often burdensome, but contemporary review articles may be helpful in keeping the orthopedic resident and clinician current with advancements.10,27,28 The more we educate ourselves about evolving nanotechnologies, the less reluctance we will have when evaluating new diagnostic and therapeutic treatment modalities.
The orthopedic community is increasingly deluged with advancements in the basic sciences. With each step, we must evaluate the necessity of new information and the relevance of these topics for clinical practice. Since the late 1990s, the promise of nanotechnology to effect significant changes in the medical field has been heralded. However, in this coming decade, we as a profession will see unprecedented advances in the movement of this technology “from the bench to the bedside.” Not unlike many other basic science advancements in our field, nanotechnology is poorly understood among clinicians and residents. As the use of biologics and drug delivery systems expands in orthopedics, nanoparticle-based devices will become more prevalent and have a momentous impact on the way we treat and diagnose orthopedic patients.
A nanoparticle is generally defined as a particle in which at least 1 dimension is between 1 to 100 nanometers and has material properties consistent with quantum mechanics.1 Nanomaterials can be composed of organic and inorganic chemical elements that enable basic chemical processes to create more complex systems. Individual nanoparticle units can be synthesized to form nanostructures, including nanotubes, nanoscaffolds, nanofibers, and even nanodiamonds.2-4 Nanoparticles at this scale display unique optical, chemical, and physical properties that can be manipulated to create specific end-use applications. Such uses may include glass fabrication, optical probes, television screens, drug delivery, gene delivery, and multiplex diagnostic assays.5-7 By crossing disciplines of physics, engineering, and medical sciences, we can create novel technology that includes nanomanufacturing, targeted drug delivery, nanorobotics in conjunction with artificial intelligence, and point-of-care diagnostics.7-9
The field of orthopedics has benefited from nanotechnologic advances, such as new therapeutics and implant-related technology. Nanotubes are hollow nanosized cylinders that are commonly created from titania, silica, or carbon-based substrates. They have garnered significant interest for their high tensile and shear strength, favorable microstructure for bony ingrowth, and their capacity to hold antibiotics or growth factors, such as bone morphogenic proteins (BMPs).10 The current local delivery limitations of BMPs via a collagen sponge have the potential to be maximized and better controlled with a nanotechnology-based approach. The size, internal structure, and shape of the nanoparticle can be manipulated to control the release of these growth factors, and certain nanoparticles can be dual-layered, allowing for release of multiple growth factors at once or in succession.11,12 A more powerful and targeted delivery system of these types of growth factors may result in improved or more robust outcomes, and further research is warranted.
It is possible that carbon-based nanotubes can be categorized as a biomedical implant secondary to their mechanical properties.13 Their strength and ability to be augmented with osteogenic materials has made them an attractive area of research as alternative implant surfaces and stand-alone implants. Nanotubes are capable of acting as a scaffold for antibiotic-loaded, carbon-based nanodiamonds for localized treatment of periprosthetic infection, and research has been directed toward controlled release of the nanodiamond-antibiotic construct from these scaffolds or hydrogels.4,14 Technologies like this may allow the clinician to treat periprosthetic infections locally and minimize the use of systemic antibiotics. The perfection of this type of delivery system may augment the role of antibiotic-laden cement and improve our treatment success rates, even in traditionally hard-to-treat organisms.
Nanoscaffolds and nanofibers are created from nanosized polymers and rendered into a 3-dimensional structure that can be loaded with biologic particles or acting as a scaffold/template for tissue or bone ingrowth. Nanofibers created using biodegradable substrates such as poly(lactic-co-glycolic acid) (PLGA) and chitosan have been extensively studied for their delayed-release properties and biocompatibility.15 These scaffolds are often soaked or loaded with chondrogenic, osteogenic, or antibacterial agents, and have been evaluated in both in vitro and in vivo studies with promising results.15,16 They have been an exciting area of research in tissue engineering, and have been accepted as an adjunct in tendon-repair treatments and local bone regeneration.3,17 As this technology is perfected, the potential to treat more effectively massive rotator cuff tears or tears with poor tissue integrity will dramatically improve and expand the indications for rotator cuff repair.
Augmentation of implant surfaces with nanomaterials that improve osseointegration, or that act as antimicrobial agents have also been a focus of research in hopes of decreasing the rates of aseptic failure and periprosthetic infection in arthroplasty procedures. Nanocrystalline surfaces made of hydroxyapatite and cobalt chromium have been evaluated for their enhanced osteoconductive properties, and may replace standard surfaces.18-20 Recent work evaluating nanoparticle-antibiotic constructs that have been covalently bound to implant surfaces for delayed release of antibiotics during the perioperative period has shown promise, and may allow a more targeted and localized treatment strategy for periprosthetic infection.21,22
Major limitations regarding successful clinical implementation of nanotechnology include both cost and regulatory processes. Currently, pharmaceutical companies estimate that, on average, successful clinical trials from phase 1 to completion for new drugs can cost hundreds of millions of dollars.23 Such high costs result partially from the laborious and capital-intensive process of conducting clinical trials that meet US Food and Drug Administration (FDA) requirements. These regulations would apply to both surface-coated implants and nanoparticle-based drug delivery systems. These types of implants would not be expedited into the market secondary to their drug delivery component and would likely require lengthy clinical studies. Implant companies may be reluctant to invest millions of dollars in multiple FDA trials when they have lucrative implants on the market.
Other limitations include the particles’ complex 3-dimensional structure, which can present challenges for mass production. Producing large quantities of nanoparticles at a consistent quality may be a major limitation to the more unique and target-based nanotherapies. Recent concerns with the toxicity profile of nanotechnology-based medicines have resulted in more intense scrutiny of the nanotechnology safety profile.24,25 Currently, nanoparticle technology is evaluated case by case with each technology requiring its own toxicology and safety profile testing if it is intended for human use. These tests can be cost-prohibitive and require extensive private and government capital for successful market entry. Despite these limitations, nanotechnology will impact the next generation of orthopedic surgeons. Current estimates project the nanomedicine market to be worth $177.6 billion by 2019.26
Advances in nanobased orthopedic technologies have expanded dramatically in the past decade, and we, as the treating physicians, must make educated decisions on how and when to use nanoparticle-based therapies and treatment options. Nanotechnology’s basic science is confusing and often burdensome, but contemporary review articles may be helpful in keeping the orthopedic resident and clinician current with advancements.10,27,28 The more we educate ourselves about evolving nanotechnologies, the less reluctance we will have when evaluating new diagnostic and therapeutic treatment modalities.
1. Hewakuruppu YL, Dombrovsky LA, Chen C, et al. Plasmonic “pump-probe” method to study semi-transparent nanofluids. Appl Opt. 2013;52(24):6041-6050.
2. Balasundaram G, Webster TJ. An overview of nano-polymers for orthopedic applications. Macromol Biosci. 2007;7(5):635-642.
3. Zhang Z, Hu J, Ma PX. Nanofiber-based delivery of bioactive agents and stem cells to bone sites. Adv Drug Deliv Rev. 2012;64(12):1129-1141.
4. Mochalin VN, Shenderova O, Ho D, Gogotsi Y. The properties and applications of nanodiamonds. Nat Nanotechnol. 2012;7(1):11-23.
5. Kneipp J, Kneipp H, Rice WL, Kneipp K. Optical probes for biological applications based on surface-enhanced Raman scattering from indocyanine green on gold nanoparticles. Anal Chem. 2005;77(8):2381-2385.
6. Wang L, O’Donoghue MB, Tan W. Nanoparticles for multiplex diagnostics and imaging. Nanomedicine (Lond). 2006;1(4):413-426.
7. Krebs MD, Salter E, Chen E, Sutter KA, Alsberg E. Calcium phosphate-DNA nanoparticle gene delivery from alginate hydrogels induces in vivo osteogenesis. J Biomed Mater Res A. 2010;92(3):1131-1138.
8. Myers FB, Lee LP. Innovations in optical microfluidic technologies for point-of-care diagnostics. Lab Chip. 2008;8(12):2015-2031.
9. Sacha GM, Varona P. Artificial intelligence in nanotechnology. Nanotechnology. 2013;24(45):452002.
10. Ganguly DY, Shahbazian R, Shokuhfar T. Recent advances in nanotubes for orthopedic implants. J Nanotech Smart Mater. 2014;1:1-10.
11. Srivastava S, Kotov NA. Composite Layer-by-Layer (LBL) assembly with inorganic nanoparticles and nanowires. Acc Chem Res. 2008;41(12):1831-1841.
12. Panda HS, Srivastava R, Bahadur D. Shape and size control of nano dispersed Mg/Al layered double hydroxide. J Nanosci Nanotechnol. 2008;8(8):4218-4223.
13. Wang X, Li Q, Xie J, et al. Fabrication of ultralong and electrically uniform single-walled carbon nanotubes on clean substrates. Nano Lett. 2009;9(9):3137-3141.
14. Zhu Y, Li J, Li W, et al. The biocompatibility of nanodiamonds and their application in drug delivery systems. Theranostics. 2012;2(3):302-312.
15. Wu L, Ding J. In vitro degradation of three-dimensional porous poly(D,L-lactide-co-glycolide) scaffolds for tissue engineering. Biomaterials. 2004;25(2):5821-5830.
16. Wu X, Rabkin-Aikawa E, Guleserian KJ, et al. Tissue-engineered microvessels on three-dimensional biodegradable scaffolds using human endothelial progenitor cells. Am J Physiol Heart Circ Physiol. 2004;287(2):H480-H487.
17. Xia W, Liu W, Cui L, et al. Tissue engineering of cartilage with the use of chitosan-gelatin complex scaffolds. J Biomed Mater Res B Appl Biomater. 2004;71(2):373-380.
18. Laurencin CT, Kumbar SG, Nukavarapu SP. Nanotechnology and orthopedics: a personal perspective. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2009;1(1):6-10.
19. Webster TJ, Ejiofor JU. Increased osteoblast adhesion on nanophase metals: Ti, Ti6Al4V, and CoCrMo. Biomaterials. 2004;25(19):4731-4739.
20. Webster TJ, Ergun C, Doremus RH, Siegel RW, Bizios R. Enhanced functions of osteoblasts on nanophase ceramics. Biomaterials. 2000;21(17):1803-1810.
21. Stewart S, Barr S, Engiles J, et al. Vancomycin-modified implant surface inhibits biofilm formation and supports bone-healing in an infected osteotomy model in sheep: a proof-of-concept study. J Bone Joint Surg Am. 2012;94(15):1406-1415.
22. Hickok NJ, Shapiro IM. Immobilized antibiotics to prevent orthopaedic implant infections. Adv Drug Deliv Rev. 2012;64(12):1165-1176.
23. DiMasi JA, Hansen RW, Grabowski HG. The price of innovation: new estimates of drug development costs. J Health Econ. 2003;22(2):151-185.
24. Vines T, Faunce T. Assessing the safety and cost-effectiveness of early nanodrugs. J Law Med. 2009;16(5):822-845.
25. Nel A, Xia T, Mädler L, Li N. Toxic potential of materials at the nanolevel. Science. 2006;311(5761):622-627.
26. Nanomedicine Market (Neurology, Cardiovascular, Anti-Inflammatory, Anti-Infective, and Oncology Applications): Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013-2019. Transparency Market Research website. http://www.transparencymarketresearch.com/nanomedicine-market.html. Published August 1, 2014. Accessed January 20, 2015.
27. Sullivan MP, McHale KJ, Parvizi J, Mehta S. Nanotechnology: current concepts in orthopaedic surgery and future directions. Bone Joint J. 2014;96-B(5):569-573.
28. Pleshko N, Grande DA, Myers KR. Nanotechnology in orthopaedics. J Am Acad Orthop Surg. 2012;20(1):60-62.
1. Hewakuruppu YL, Dombrovsky LA, Chen C, et al. Plasmonic “pump-probe” method to study semi-transparent nanofluids. Appl Opt. 2013;52(24):6041-6050.
2. Balasundaram G, Webster TJ. An overview of nano-polymers for orthopedic applications. Macromol Biosci. 2007;7(5):635-642.
3. Zhang Z, Hu J, Ma PX. Nanofiber-based delivery of bioactive agents and stem cells to bone sites. Adv Drug Deliv Rev. 2012;64(12):1129-1141.
4. Mochalin VN, Shenderova O, Ho D, Gogotsi Y. The properties and applications of nanodiamonds. Nat Nanotechnol. 2012;7(1):11-23.
5. Kneipp J, Kneipp H, Rice WL, Kneipp K. Optical probes for biological applications based on surface-enhanced Raman scattering from indocyanine green on gold nanoparticles. Anal Chem. 2005;77(8):2381-2385.
6. Wang L, O’Donoghue MB, Tan W. Nanoparticles for multiplex diagnostics and imaging. Nanomedicine (Lond). 2006;1(4):413-426.
7. Krebs MD, Salter E, Chen E, Sutter KA, Alsberg E. Calcium phosphate-DNA nanoparticle gene delivery from alginate hydrogels induces in vivo osteogenesis. J Biomed Mater Res A. 2010;92(3):1131-1138.
8. Myers FB, Lee LP. Innovations in optical microfluidic technologies for point-of-care diagnostics. Lab Chip. 2008;8(12):2015-2031.
9. Sacha GM, Varona P. Artificial intelligence in nanotechnology. Nanotechnology. 2013;24(45):452002.
10. Ganguly DY, Shahbazian R, Shokuhfar T. Recent advances in nanotubes for orthopedic implants. J Nanotech Smart Mater. 2014;1:1-10.
11. Srivastava S, Kotov NA. Composite Layer-by-Layer (LBL) assembly with inorganic nanoparticles and nanowires. Acc Chem Res. 2008;41(12):1831-1841.
12. Panda HS, Srivastava R, Bahadur D. Shape and size control of nano dispersed Mg/Al layered double hydroxide. J Nanosci Nanotechnol. 2008;8(8):4218-4223.
13. Wang X, Li Q, Xie J, et al. Fabrication of ultralong and electrically uniform single-walled carbon nanotubes on clean substrates. Nano Lett. 2009;9(9):3137-3141.
14. Zhu Y, Li J, Li W, et al. The biocompatibility of nanodiamonds and their application in drug delivery systems. Theranostics. 2012;2(3):302-312.
15. Wu L, Ding J. In vitro degradation of three-dimensional porous poly(D,L-lactide-co-glycolide) scaffolds for tissue engineering. Biomaterials. 2004;25(2):5821-5830.
16. Wu X, Rabkin-Aikawa E, Guleserian KJ, et al. Tissue-engineered microvessels on three-dimensional biodegradable scaffolds using human endothelial progenitor cells. Am J Physiol Heart Circ Physiol. 2004;287(2):H480-H487.
17. Xia W, Liu W, Cui L, et al. Tissue engineering of cartilage with the use of chitosan-gelatin complex scaffolds. J Biomed Mater Res B Appl Biomater. 2004;71(2):373-380.
18. Laurencin CT, Kumbar SG, Nukavarapu SP. Nanotechnology and orthopedics: a personal perspective. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2009;1(1):6-10.
19. Webster TJ, Ejiofor JU. Increased osteoblast adhesion on nanophase metals: Ti, Ti6Al4V, and CoCrMo. Biomaterials. 2004;25(19):4731-4739.
20. Webster TJ, Ergun C, Doremus RH, Siegel RW, Bizios R. Enhanced functions of osteoblasts on nanophase ceramics. Biomaterials. 2000;21(17):1803-1810.
21. Stewart S, Barr S, Engiles J, et al. Vancomycin-modified implant surface inhibits biofilm formation and supports bone-healing in an infected osteotomy model in sheep: a proof-of-concept study. J Bone Joint Surg Am. 2012;94(15):1406-1415.
22. Hickok NJ, Shapiro IM. Immobilized antibiotics to prevent orthopaedic implant infections. Adv Drug Deliv Rev. 2012;64(12):1165-1176.
23. DiMasi JA, Hansen RW, Grabowski HG. The price of innovation: new estimates of drug development costs. J Health Econ. 2003;22(2):151-185.
24. Vines T, Faunce T. Assessing the safety and cost-effectiveness of early nanodrugs. J Law Med. 2009;16(5):822-845.
25. Nel A, Xia T, Mädler L, Li N. Toxic potential of materials at the nanolevel. Science. 2006;311(5761):622-627.
26. Nanomedicine Market (Neurology, Cardiovascular, Anti-Inflammatory, Anti-Infective, and Oncology Applications): Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013-2019. Transparency Market Research website. http://www.transparencymarketresearch.com/nanomedicine-market.html. Published August 1, 2014. Accessed January 20, 2015.
27. Sullivan MP, McHale KJ, Parvizi J, Mehta S. Nanotechnology: current concepts in orthopaedic surgery and future directions. Bone Joint J. 2014;96-B(5):569-573.
28. Pleshko N, Grande DA, Myers KR. Nanotechnology in orthopaedics. J Am Acad Orthop Surg. 2012;20(1):60-62.
Team-based care: Worth a second look

Team care is not a new idea. For many years, our office teams have included physicians, nurse practitioners, physician assistants, nurses, medical assistants, front office staff, and administrative staff who functioned quite well in caring for our patients.
But primary care changed drastically after the publication of 2 landmark Institute of Medicine reports: To Err is Human: Building a Safer Health System1 (in 1999) and Crossing the Quality Chasm: A New Health System for the 21st Century2 (in 2001). These scathing reports told us we were providing inadequate care to our patients, and they contained plenty of truth. What followed is that expectations increased exponentially, and we found our offices were not prepared to deal with the new mandates for computerized medical records, high performance on quality and patient satisfaction measures, and population management.
Addressing these expanded expectations requires redefining roles and adding new players to our office teams, including nurse care coordinators, “navigators,” clinical pharmacists, psychologists, information technologists, and who knows what else. One innovative role that has seen limited testing is what some call practice facilitators.3 These are trained agents who do some of the heavy lifting required to change things like office systems and work flow.
I think that expanding the role of nurses and medical assistants is one of best ways to ensure that all of our patients get the care they deserve. Each office is unique, however, and physicians need to do the hard work of selecting the best team configuration to care for their patients. One of the more successful team-based practices is the Nuka System of Care in Alaska, which was crafted in collaboration with the tribal council. Read this fascinating story at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3752290 and then create your own story of a successful, high-quality primary care office.
1. Kohn LT, Corrigan JM, Donaldson MS (eds); Committee on Quality of Health Care in America, Institute of Medicine. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
2. Committee on Quality of Health Care in America; Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
3. Nagykaldi Z, Mold JW, Aspy CB. Practice facilitators: a review of the literature. Fam Med. 2005;37:581-588.
Team care is not a new idea. For many years, our office teams have included physicians, nurse practitioners, physician assistants, nurses, medical assistants, front office staff, and administrative staff who functioned quite well in caring for our patients.
But primary care changed drastically after the publication of 2 landmark Institute of Medicine reports: To Err is Human: Building a Safer Health System1 (in 1999) and Crossing the Quality Chasm: A New Health System for the 21st Century2 (in 2001). These scathing reports told us we were providing inadequate care to our patients, and they contained plenty of truth. What followed is that expectations increased exponentially, and we found our offices were not prepared to deal with the new mandates for computerized medical records, high performance on quality and patient satisfaction measures, and population management.
Addressing these expanded expectations requires redefining roles and adding new players to our office teams, including nurse care coordinators, “navigators,” clinical pharmacists, psychologists, information technologists, and who knows what else. One innovative role that has seen limited testing is what some call practice facilitators.3 These are trained agents who do some of the heavy lifting required to change things like office systems and work flow.
I think that expanding the role of nurses and medical assistants is one of best ways to ensure that all of our patients get the care they deserve. Each office is unique, however, and physicians need to do the hard work of selecting the best team configuration to care for their patients. One of the more successful team-based practices is the Nuka System of Care in Alaska, which was crafted in collaboration with the tribal council. Read this fascinating story at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3752290 and then create your own story of a successful, high-quality primary care office.
Team care is not a new idea. For many years, our office teams have included physicians, nurse practitioners, physician assistants, nurses, medical assistants, front office staff, and administrative staff who functioned quite well in caring for our patients.
But primary care changed drastically after the publication of 2 landmark Institute of Medicine reports: To Err is Human: Building a Safer Health System1 (in 1999) and Crossing the Quality Chasm: A New Health System for the 21st Century2 (in 2001). These scathing reports told us we were providing inadequate care to our patients, and they contained plenty of truth. What followed is that expectations increased exponentially, and we found our offices were not prepared to deal with the new mandates for computerized medical records, high performance on quality and patient satisfaction measures, and population management.
Addressing these expanded expectations requires redefining roles and adding new players to our office teams, including nurse care coordinators, “navigators,” clinical pharmacists, psychologists, information technologists, and who knows what else. One innovative role that has seen limited testing is what some call practice facilitators.3 These are trained agents who do some of the heavy lifting required to change things like office systems and work flow.
I think that expanding the role of nurses and medical assistants is one of best ways to ensure that all of our patients get the care they deserve. Each office is unique, however, and physicians need to do the hard work of selecting the best team configuration to care for their patients. One of the more successful team-based practices is the Nuka System of Care in Alaska, which was crafted in collaboration with the tribal council. Read this fascinating story at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3752290 and then create your own story of a successful, high-quality primary care office.
1. Kohn LT, Corrigan JM, Donaldson MS (eds); Committee on Quality of Health Care in America, Institute of Medicine. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
2. Committee on Quality of Health Care in America; Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
3. Nagykaldi Z, Mold JW, Aspy CB. Practice facilitators: a review of the literature. Fam Med. 2005;37:581-588.
1. Kohn LT, Corrigan JM, Donaldson MS (eds); Committee on Quality of Health Care in America, Institute of Medicine. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
2. Committee on Quality of Health Care in America; Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
3. Nagykaldi Z, Mold JW, Aspy CB. Practice facilitators: a review of the literature. Fam Med. 2005;37:581-588.
Patient Satisfaction as a Metric for Quality
As orthopedic surgeons, we typically equate a quality outcome with the patient’s end result—resolved or diminished functional disability, fracture union, and/or pain relief, to name a few metrics. Although research has not identified a clear link between quality outcomes and patient satisfaction scores, patient satisfaction is increasingly used as a proxy for quality of care. It’s speculated that more personal care may result in better communication, more reasonable expectations, and more patient involvement, all of which may result in better quality of care. Regardless, it’s unclear whether satisfaction is an attribute of quality care or an indicator.
In a recent article in Modern Healthcare, Irwin Press,1 cofounder of Press Ganey, challenges any campaign to cast doubt on satisfaction as a relevant indicator of quality care: “It can be argued that diagnostic procedures, surgeries and therapies constitute treatment, but not care. Treatment alone isn’t care…. One is objective, involving highly standardized technical, mechanical or chemical interventions. The other is subjective, composed of behaviors, decisions and interactions of humans with idiosyncratic personalities, stresses, agendas and sensitivities.”
As surgeons, we understandably focus on objective treatment and outcome and may underappreciate the importance of the process—the experience of care. Wellness probably requires mastery of both. Indeed, just as a patient’s poor coping skills, depression, anxiety, and proclivity to catastrophize may compromise their recovery and self-reported assessments of outcome,2-5 so too do the qualitative components of our interaction with patients undoubtedly impact, not only their experience, but also their recovery. Patient self-efficacy (the feeling that they can do it), engagement (“activation”), compliance, and expectations all derive in part from the “Art” of our practice. Our “Heart” is as important to that Art, if not more so, than our “Head” (our intellect and knowledge). Whether we buy into this or not is a matter of personal opinion and experience, I suppose, but the reality is that the important singular metric of patient satisfaction is here to stay—patient satisfaction has become an important component of pay-for-performance metrics which expressly intend to reward quality over volume.
What does this mean for us? First, we need to adapt to the reality that the patient’s perception of their interaction with us impacts their experience and their level of satisfaction, and accept our role in their overall perception of quality. Being rewarded with a high satisfaction score is within our sphere of influence and requires more than just providing a good objective outcome. We might not revisit a restaurant with great food but lousy service and an underwhelming environment. We might also never eat at a place that was really nice inside and had great service, but which provided horrible food. So we must aspire to provide both objective quality outcomes and stellar patient care. As third-party payers increasingly follow the lead of the Centers for Medicare and Medicaid Services (CMS), the patient will not be at our table unless we both ask for feedback and respond to it. We all aspire to be great technicians and have a command of the knowledge base in our respective areas of practice. Some of us are privileged to have earned regional, national, or international reputations among our peers, but we all will be increasingly judged based on patient satisfaction with our care. This means that we must care about their experience and how they perceive our care: Do we spend enough time, listen attentively, answer questions, and explain the diagnosis and plan?
Just as we may hold our breath unknowingly during stressful situations when we are not mindful, so too might our “Heart” not be clearly evident in the complex health care environment today—too little time, too much paperwork, increasing patient demands. But practicing with heightened self-awareness, empathy, and unambiguous intention, and modeling our values during our interaction with our patients—“mindful practice”—is increasingly advocated as a necessary component to “best practice.” For truly rewarding practice, during which we can attain not only great results but also satisfied patients, we need to revisit why we do what we do, and rebalance our emphasis on what we do and how we do it. Mindful practice is both an objective and a strategy. It may require making structural adjustments to our practice, such as seeing fewer patients per hour, for, perhaps, an hour or two more in a day, completing some of our electronic medical record notes at day’s end, and maybe adding an extra clinic day every other week. We must also deliberately solicit feedback from our patients so that we can respond to any perceived room for improvement.
Thirteen years ago when I received my Master of Business Administration (MBA) degree, I felt that improving operational efficiency would enable me to do more in a day—and it did. But when patient satisfaction becomes the proxy for quality, sound business practice may not translate into sound clinical practice. After 21 years of practice, and deliberate attentiveness to patient feedback, I am increasingly aware that the Art of practice is as important as the Science—our Heart is as important as our Head. In this light, patient satisfaction is a very sound metric for quality.
1. Press I. Don’t downplay patient satisfaction. Modern Healthcare. http://www.modernhealthcare.com/article/20140322/MAGAZINE/303229940. Published March 22, 2014. Accessed January 7, 2015.
2. Cho CH, Seo HJ, Bae KC, Lee KJ, Hwang I, Warner JJ. The impact of depression and anxiety on self-assessed pain, disability, and quality of life in patients scheduled for rotator cuff repair. J Shoulder Elbow Surg. 2013;22(9):1160-1166.
3. Blackburn J, Qureshi A, Amirfeyz R, Bannister G. Does preoperative anxiety and depression predict satisfaction after total knee replacement? Knee. 2012;19(5):522-524.
4. Rosenberger PH, Jokl P, Ickovics J. Psychosocial factors and surgical outcomes: an evidence-based literature review. J Am Acad Orthop Surg. 2006;14(7):397-405.
5. Keefe FJ, Brown GK, Wallston KA, Caldwell DS. Coping with rheumatoid arthritis pain: catastrophizing as a maladaptive strategy. Pain. 1989;37(1):51-56.
As orthopedic surgeons, we typically equate a quality outcome with the patient’s end result—resolved or diminished functional disability, fracture union, and/or pain relief, to name a few metrics. Although research has not identified a clear link between quality outcomes and patient satisfaction scores, patient satisfaction is increasingly used as a proxy for quality of care. It’s speculated that more personal care may result in better communication, more reasonable expectations, and more patient involvement, all of which may result in better quality of care. Regardless, it’s unclear whether satisfaction is an attribute of quality care or an indicator.
In a recent article in Modern Healthcare, Irwin Press,1 cofounder of Press Ganey, challenges any campaign to cast doubt on satisfaction as a relevant indicator of quality care: “It can be argued that diagnostic procedures, surgeries and therapies constitute treatment, but not care. Treatment alone isn’t care…. One is objective, involving highly standardized technical, mechanical or chemical interventions. The other is subjective, composed of behaviors, decisions and interactions of humans with idiosyncratic personalities, stresses, agendas and sensitivities.”
As surgeons, we understandably focus on objective treatment and outcome and may underappreciate the importance of the process—the experience of care. Wellness probably requires mastery of both. Indeed, just as a patient’s poor coping skills, depression, anxiety, and proclivity to catastrophize may compromise their recovery and self-reported assessments of outcome,2-5 so too do the qualitative components of our interaction with patients undoubtedly impact, not only their experience, but also their recovery. Patient self-efficacy (the feeling that they can do it), engagement (“activation”), compliance, and expectations all derive in part from the “Art” of our practice. Our “Heart” is as important to that Art, if not more so, than our “Head” (our intellect and knowledge). Whether we buy into this or not is a matter of personal opinion and experience, I suppose, but the reality is that the important singular metric of patient satisfaction is here to stay—patient satisfaction has become an important component of pay-for-performance metrics which expressly intend to reward quality over volume.
What does this mean for us? First, we need to adapt to the reality that the patient’s perception of their interaction with us impacts their experience and their level of satisfaction, and accept our role in their overall perception of quality. Being rewarded with a high satisfaction score is within our sphere of influence and requires more than just providing a good objective outcome. We might not revisit a restaurant with great food but lousy service and an underwhelming environment. We might also never eat at a place that was really nice inside and had great service, but which provided horrible food. So we must aspire to provide both objective quality outcomes and stellar patient care. As third-party payers increasingly follow the lead of the Centers for Medicare and Medicaid Services (CMS), the patient will not be at our table unless we both ask for feedback and respond to it. We all aspire to be great technicians and have a command of the knowledge base in our respective areas of practice. Some of us are privileged to have earned regional, national, or international reputations among our peers, but we all will be increasingly judged based on patient satisfaction with our care. This means that we must care about their experience and how they perceive our care: Do we spend enough time, listen attentively, answer questions, and explain the diagnosis and plan?
Just as we may hold our breath unknowingly during stressful situations when we are not mindful, so too might our “Heart” not be clearly evident in the complex health care environment today—too little time, too much paperwork, increasing patient demands. But practicing with heightened self-awareness, empathy, and unambiguous intention, and modeling our values during our interaction with our patients—“mindful practice”—is increasingly advocated as a necessary component to “best practice.” For truly rewarding practice, during which we can attain not only great results but also satisfied patients, we need to revisit why we do what we do, and rebalance our emphasis on what we do and how we do it. Mindful practice is both an objective and a strategy. It may require making structural adjustments to our practice, such as seeing fewer patients per hour, for, perhaps, an hour or two more in a day, completing some of our electronic medical record notes at day’s end, and maybe adding an extra clinic day every other week. We must also deliberately solicit feedback from our patients so that we can respond to any perceived room for improvement.
Thirteen years ago when I received my Master of Business Administration (MBA) degree, I felt that improving operational efficiency would enable me to do more in a day—and it did. But when patient satisfaction becomes the proxy for quality, sound business practice may not translate into sound clinical practice. After 21 years of practice, and deliberate attentiveness to patient feedback, I am increasingly aware that the Art of practice is as important as the Science—our Heart is as important as our Head. In this light, patient satisfaction is a very sound metric for quality.
As orthopedic surgeons, we typically equate a quality outcome with the patient’s end result—resolved or diminished functional disability, fracture union, and/or pain relief, to name a few metrics. Although research has not identified a clear link between quality outcomes and patient satisfaction scores, patient satisfaction is increasingly used as a proxy for quality of care. It’s speculated that more personal care may result in better communication, more reasonable expectations, and more patient involvement, all of which may result in better quality of care. Regardless, it’s unclear whether satisfaction is an attribute of quality care or an indicator.
In a recent article in Modern Healthcare, Irwin Press,1 cofounder of Press Ganey, challenges any campaign to cast doubt on satisfaction as a relevant indicator of quality care: “It can be argued that diagnostic procedures, surgeries and therapies constitute treatment, but not care. Treatment alone isn’t care…. One is objective, involving highly standardized technical, mechanical or chemical interventions. The other is subjective, composed of behaviors, decisions and interactions of humans with idiosyncratic personalities, stresses, agendas and sensitivities.”
As surgeons, we understandably focus on objective treatment and outcome and may underappreciate the importance of the process—the experience of care. Wellness probably requires mastery of both. Indeed, just as a patient’s poor coping skills, depression, anxiety, and proclivity to catastrophize may compromise their recovery and self-reported assessments of outcome,2-5 so too do the qualitative components of our interaction with patients undoubtedly impact, not only their experience, but also their recovery. Patient self-efficacy (the feeling that they can do it), engagement (“activation”), compliance, and expectations all derive in part from the “Art” of our practice. Our “Heart” is as important to that Art, if not more so, than our “Head” (our intellect and knowledge). Whether we buy into this or not is a matter of personal opinion and experience, I suppose, but the reality is that the important singular metric of patient satisfaction is here to stay—patient satisfaction has become an important component of pay-for-performance metrics which expressly intend to reward quality over volume.
What does this mean for us? First, we need to adapt to the reality that the patient’s perception of their interaction with us impacts their experience and their level of satisfaction, and accept our role in their overall perception of quality. Being rewarded with a high satisfaction score is within our sphere of influence and requires more than just providing a good objective outcome. We might not revisit a restaurant with great food but lousy service and an underwhelming environment. We might also never eat at a place that was really nice inside and had great service, but which provided horrible food. So we must aspire to provide both objective quality outcomes and stellar patient care. As third-party payers increasingly follow the lead of the Centers for Medicare and Medicaid Services (CMS), the patient will not be at our table unless we both ask for feedback and respond to it. We all aspire to be great technicians and have a command of the knowledge base in our respective areas of practice. Some of us are privileged to have earned regional, national, or international reputations among our peers, but we all will be increasingly judged based on patient satisfaction with our care. This means that we must care about their experience and how they perceive our care: Do we spend enough time, listen attentively, answer questions, and explain the diagnosis and plan?
Just as we may hold our breath unknowingly during stressful situations when we are not mindful, so too might our “Heart” not be clearly evident in the complex health care environment today—too little time, too much paperwork, increasing patient demands. But practicing with heightened self-awareness, empathy, and unambiguous intention, and modeling our values during our interaction with our patients—“mindful practice”—is increasingly advocated as a necessary component to “best practice.” For truly rewarding practice, during which we can attain not only great results but also satisfied patients, we need to revisit why we do what we do, and rebalance our emphasis on what we do and how we do it. Mindful practice is both an objective and a strategy. It may require making structural adjustments to our practice, such as seeing fewer patients per hour, for, perhaps, an hour or two more in a day, completing some of our electronic medical record notes at day’s end, and maybe adding an extra clinic day every other week. We must also deliberately solicit feedback from our patients so that we can respond to any perceived room for improvement.
Thirteen years ago when I received my Master of Business Administration (MBA) degree, I felt that improving operational efficiency would enable me to do more in a day—and it did. But when patient satisfaction becomes the proxy for quality, sound business practice may not translate into sound clinical practice. After 21 years of practice, and deliberate attentiveness to patient feedback, I am increasingly aware that the Art of practice is as important as the Science—our Heart is as important as our Head. In this light, patient satisfaction is a very sound metric for quality.
1. Press I. Don’t downplay patient satisfaction. Modern Healthcare. http://www.modernhealthcare.com/article/20140322/MAGAZINE/303229940. Published March 22, 2014. Accessed January 7, 2015.
2. Cho CH, Seo HJ, Bae KC, Lee KJ, Hwang I, Warner JJ. The impact of depression and anxiety on self-assessed pain, disability, and quality of life in patients scheduled for rotator cuff repair. J Shoulder Elbow Surg. 2013;22(9):1160-1166.
3. Blackburn J, Qureshi A, Amirfeyz R, Bannister G. Does preoperative anxiety and depression predict satisfaction after total knee replacement? Knee. 2012;19(5):522-524.
4. Rosenberger PH, Jokl P, Ickovics J. Psychosocial factors and surgical outcomes: an evidence-based literature review. J Am Acad Orthop Surg. 2006;14(7):397-405.
5. Keefe FJ, Brown GK, Wallston KA, Caldwell DS. Coping with rheumatoid arthritis pain: catastrophizing as a maladaptive strategy. Pain. 1989;37(1):51-56.
1. Press I. Don’t downplay patient satisfaction. Modern Healthcare. http://www.modernhealthcare.com/article/20140322/MAGAZINE/303229940. Published March 22, 2014. Accessed January 7, 2015.
2. Cho CH, Seo HJ, Bae KC, Lee KJ, Hwang I, Warner JJ. The impact of depression and anxiety on self-assessed pain, disability, and quality of life in patients scheduled for rotator cuff repair. J Shoulder Elbow Surg. 2013;22(9):1160-1166.
3. Blackburn J, Qureshi A, Amirfeyz R, Bannister G. Does preoperative anxiety and depression predict satisfaction after total knee replacement? Knee. 2012;19(5):522-524.
4. Rosenberger PH, Jokl P, Ickovics J. Psychosocial factors and surgical outcomes: an evidence-based literature review. J Am Acad Orthop Surg. 2006;14(7):397-405.
5. Keefe FJ, Brown GK, Wallston KA, Caldwell DS. Coping with rheumatoid arthritis pain: catastrophizing as a maladaptive strategy. Pain. 1989;37(1):51-56.

Playing with fire
Hoping to learn a bit more about the apparently healthy 8-year-old who has been deposited in your exam room for his biannual checkup, you take the opportunity to ask him a few questions with his mother in the waiting room. “So, Jason, what do you like to do for fun?”
“Well, yesterday I started a fire with my buddy Rudy, and we burned a whole bunch of sticks and stuff.”
“Does your mother know about this?”
“She wasn’t around, but I think so. We’ve done it a bunch of times before.”
Okay, here you are with an 8-year-old pyromaniac whose parents are clearly under-supervising him. Who do you call first? The folks at Child Protective Services or the State Fire Marshall’s Office? Clearly, he and your community are at significant risk.
If you were practicing in Wrexham, a town in North Wales, you would continue your questioning with, “So you like to go to The Land after school? I’ve heard it’s a fun place?”
The Land is 3-year-old adventure playground that I learned about in a thought-provoking article in The Atlantic (The Overprotected Kid, by Hanna Rosin, April 2014). The nearly acre-sized site would look like a junkyard to any adult whose imagination has atrophied with age. Strewn with used tires, wooden palettes, dirty old mattresses, and decrepit lawn furniture, it provides endless opportunities for children to create their own places for play and adventure. By stacking, rolling, hammering together, and rearranging the loose detritus of society, children can transform the junk into an ever-changing landscape for fun. A fire pit and an old oil drum – among the most popular items – are often smoldering with fires the children have started. The filthy mattresses become trampolines. The children are observed by professionally trained “playworkers” who are continually updating the risk assessments of the activities that were begun prior to the opening of the facility. The observers seldom have to intervene. Other than a few scraped knees, no children have been injured.
Although adventure playgrounds were relatively common in the U.K. during the 1940’s, their popularity faded until the last few years when they have enjoyed a modest resurgence. In the article in The Atlantic, author Hanna Rosin chronicles the de-riskification of playgrounds in America that began in the 1970’s. The process was fueled by an unfortunate incident in which a toddler supervised by his mother fell off a 12-foot playground slide in a Chicago playground. The child sustained a significant and permanent brain injury and received a multimillion dollar award in the suit that followed.
A commentary in Pediatrics entitled “X-rated playgrounds?” (Pediatrics 1979;64:961) and a crusade by its author, Theodora Briggs Sweeney culminated in the release of the Handbook for Public Playground Safety (U.S. Consumer Product Safety Commission, 1981) which listed in minute detail guidelines for dimensions and materials for playground equipment and play surfaces. Although these were only “guidelines,” only the most foolish manufacturer would ignore them. Little thought was given to the validity of the alarming statistics that had prompted these changes. What were the denominators? Can you compare 1970’s hospital data with those from the 1950’s when injured children were managed at home or in their doctors’ offices?
Regardless of the validity of the data, the result was that these redesigned playgrounds offered so little sense of risk that they were abandoned by all but the youngest children. Numerous studies suggest that by eliminating risk or at least the appearance of risk, we are robbing children of important learning experiences on which they can build fuller, more creative, successful, and less anxiety-dominated lives. I urge you to look at that Atlantic article for a more robust description of the evidence.
I suspect that you may be a bit uncomfortable with 8-year-old boys playing with fire, but do you agree that we need to seriously rethink our attempts to protect children from the ordinary risks of an active life? Or do you think those of us who believe children will benefit from more perceived risk are just a bunch of fogys who begin every other sentence, “When I was your age ... .”
Do you encourage parents to allow their children to walk to school unattended? Do you caution parents about being overprotective? Have I ignited a spark of concern in you, or am I just playing with fire?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].
Hoping to learn a bit more about the apparently healthy 8-year-old who has been deposited in your exam room for his biannual checkup, you take the opportunity to ask him a few questions with his mother in the waiting room. “So, Jason, what do you like to do for fun?”
“Well, yesterday I started a fire with my buddy Rudy, and we burned a whole bunch of sticks and stuff.”
“Does your mother know about this?”
“She wasn’t around, but I think so. We’ve done it a bunch of times before.”
Okay, here you are with an 8-year-old pyromaniac whose parents are clearly under-supervising him. Who do you call first? The folks at Child Protective Services or the State Fire Marshall’s Office? Clearly, he and your community are at significant risk.
If you were practicing in Wrexham, a town in North Wales, you would continue your questioning with, “So you like to go to The Land after school? I’ve heard it’s a fun place?”
The Land is 3-year-old adventure playground that I learned about in a thought-provoking article in The Atlantic (The Overprotected Kid, by Hanna Rosin, April 2014). The nearly acre-sized site would look like a junkyard to any adult whose imagination has atrophied with age. Strewn with used tires, wooden palettes, dirty old mattresses, and decrepit lawn furniture, it provides endless opportunities for children to create their own places for play and adventure. By stacking, rolling, hammering together, and rearranging the loose detritus of society, children can transform the junk into an ever-changing landscape for fun. A fire pit and an old oil drum – among the most popular items – are often smoldering with fires the children have started. The filthy mattresses become trampolines. The children are observed by professionally trained “playworkers” who are continually updating the risk assessments of the activities that were begun prior to the opening of the facility. The observers seldom have to intervene. Other than a few scraped knees, no children have been injured.
Although adventure playgrounds were relatively common in the U.K. during the 1940’s, their popularity faded until the last few years when they have enjoyed a modest resurgence. In the article in The Atlantic, author Hanna Rosin chronicles the de-riskification of playgrounds in America that began in the 1970’s. The process was fueled by an unfortunate incident in which a toddler supervised by his mother fell off a 12-foot playground slide in a Chicago playground. The child sustained a significant and permanent brain injury and received a multimillion dollar award in the suit that followed.
A commentary in Pediatrics entitled “X-rated playgrounds?” (Pediatrics 1979;64:961) and a crusade by its author, Theodora Briggs Sweeney culminated in the release of the Handbook for Public Playground Safety (U.S. Consumer Product Safety Commission, 1981) which listed in minute detail guidelines for dimensions and materials for playground equipment and play surfaces. Although these were only “guidelines,” only the most foolish manufacturer would ignore them. Little thought was given to the validity of the alarming statistics that had prompted these changes. What were the denominators? Can you compare 1970’s hospital data with those from the 1950’s when injured children were managed at home or in their doctors’ offices?
Regardless of the validity of the data, the result was that these redesigned playgrounds offered so little sense of risk that they were abandoned by all but the youngest children. Numerous studies suggest that by eliminating risk or at least the appearance of risk, we are robbing children of important learning experiences on which they can build fuller, more creative, successful, and less anxiety-dominated lives. I urge you to look at that Atlantic article for a more robust description of the evidence.
I suspect that you may be a bit uncomfortable with 8-year-old boys playing with fire, but do you agree that we need to seriously rethink our attempts to protect children from the ordinary risks of an active life? Or do you think those of us who believe children will benefit from more perceived risk are just a bunch of fogys who begin every other sentence, “When I was your age ... .”
Do you encourage parents to allow their children to walk to school unattended? Do you caution parents about being overprotective? Have I ignited a spark of concern in you, or am I just playing with fire?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].
Hoping to learn a bit more about the apparently healthy 8-year-old who has been deposited in your exam room for his biannual checkup, you take the opportunity to ask him a few questions with his mother in the waiting room. “So, Jason, what do you like to do for fun?”
“Well, yesterday I started a fire with my buddy Rudy, and we burned a whole bunch of sticks and stuff.”
“Does your mother know about this?”
“She wasn’t around, but I think so. We’ve done it a bunch of times before.”
Okay, here you are with an 8-year-old pyromaniac whose parents are clearly under-supervising him. Who do you call first? The folks at Child Protective Services or the State Fire Marshall’s Office? Clearly, he and your community are at significant risk.
If you were practicing in Wrexham, a town in North Wales, you would continue your questioning with, “So you like to go to The Land after school? I’ve heard it’s a fun place?”
The Land is 3-year-old adventure playground that I learned about in a thought-provoking article in The Atlantic (The Overprotected Kid, by Hanna Rosin, April 2014). The nearly acre-sized site would look like a junkyard to any adult whose imagination has atrophied with age. Strewn with used tires, wooden palettes, dirty old mattresses, and decrepit lawn furniture, it provides endless opportunities for children to create their own places for play and adventure. By stacking, rolling, hammering together, and rearranging the loose detritus of society, children can transform the junk into an ever-changing landscape for fun. A fire pit and an old oil drum – among the most popular items – are often smoldering with fires the children have started. The filthy mattresses become trampolines. The children are observed by professionally trained “playworkers” who are continually updating the risk assessments of the activities that were begun prior to the opening of the facility. The observers seldom have to intervene. Other than a few scraped knees, no children have been injured.
Although adventure playgrounds were relatively common in the U.K. during the 1940’s, their popularity faded until the last few years when they have enjoyed a modest resurgence. In the article in The Atlantic, author Hanna Rosin chronicles the de-riskification of playgrounds in America that began in the 1970’s. The process was fueled by an unfortunate incident in which a toddler supervised by his mother fell off a 12-foot playground slide in a Chicago playground. The child sustained a significant and permanent brain injury and received a multimillion dollar award in the suit that followed.
A commentary in Pediatrics entitled “X-rated playgrounds?” (Pediatrics 1979;64:961) and a crusade by its author, Theodora Briggs Sweeney culminated in the release of the Handbook for Public Playground Safety (U.S. Consumer Product Safety Commission, 1981) which listed in minute detail guidelines for dimensions and materials for playground equipment and play surfaces. Although these were only “guidelines,” only the most foolish manufacturer would ignore them. Little thought was given to the validity of the alarming statistics that had prompted these changes. What were the denominators? Can you compare 1970’s hospital data with those from the 1950’s when injured children were managed at home or in their doctors’ offices?
Regardless of the validity of the data, the result was that these redesigned playgrounds offered so little sense of risk that they were abandoned by all but the youngest children. Numerous studies suggest that by eliminating risk or at least the appearance of risk, we are robbing children of important learning experiences on which they can build fuller, more creative, successful, and less anxiety-dominated lives. I urge you to look at that Atlantic article for a more robust description of the evidence.
I suspect that you may be a bit uncomfortable with 8-year-old boys playing with fire, but do you agree that we need to seriously rethink our attempts to protect children from the ordinary risks of an active life? Or do you think those of us who believe children will benefit from more perceived risk are just a bunch of fogys who begin every other sentence, “When I was your age ... .”
Do you encourage parents to allow their children to walk to school unattended? Do you caution parents about being overprotective? Have I ignited a spark of concern in you, or am I just playing with fire?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].