User login
The Medical Roundtable: The New Hypertension Guidelines: Hits and Misses
The first part of our discussion focuses on the issue of guidelines and guideline proliferation. Over the last several years, multiple professional groups and health-associated agencies have issued guidelines for the diagnosis and treatment of hypertension. It is not clear to me that these competing documents provide a rational platform for improved care. Despite some recent claims, no guideline can be fully “evidence-based” because we cannot afford clinical trials for each relevant clinical question. Furthermore, the current batch of new guidelines has yielded conflicting recommendations. For example, the definition of “elderly” as age 60 in the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) and age 80 in the recent joint guidance from the International and American Societies of Hypertension. I fear that the guideline process has essentially broken down—this benefits no one.
First, a little history. Prior JNC documents were produced under the auspices of the National High Blood Pressure Education Program, a consortium of about 3 dozen healthcare professional organizations. As a participant in JNC VI and JNC 7, I can assure you that all participants were dedicated scientists and clinicians whose common goal was to synthesize the best and most robust information into a document that provided practitioners with the most reliable guidance possible. JNC 7 was released in 2003 and was soon widely adopted; it truly stood the test of time. After that, everything changed. Dr. Basile, what has been happening since?
DR. BASILE: Thanks, Dr. Izzo. I agree with you about your concerns with guidelines. This is a very difficult issue for the practicing clinician.
With regard to JNC 8, in 2008, the National Heart, Lung, and Blood Institute (NHLBI) decided to develop its own comprehensive “evidence-based” disease prevention portfolio that included a coordinated cholesterol guideline, obesity guideline, hypertension guideline, as well as a lifestyle/risk factor modification guideline. Following the recommendations put forth by the Institute of Medicine on guidelines, the NHLBI mandated that strict rules of evidence be used for its guideline development. After the JNC 8 committee established the clinical trial criteria for use in their hypertension guideline, the NHLBI hired a professional vendor to vet the literature. The process was essentially going nowhere so a second vendor for hypertension had to be hired. In the end, few clinical trials passed the criteria used to form the basis of JNC 8. And near its completion, after the JNC 8 group toiled for over 5 years putting their report together, they learned in 2013 that the NHLBI withdrew its support for the guideline and asked the American College of Cardiology/American Heart Association to establish a joint task force (to include the JNC 8 group) to assume responsibility for the guideline process. Declining this collaborative opportunity, the JNC 8 group decided on their own to have their work submitted and it was published without organizational support in JAMA.1
Meanwhile, the Centers for Disease Control published an overall systems approach for primary care clinicians in which they released the Kaiser Permanente algorithm for effective blood pressure (BP) control.2
Of note, there are several other competing guidelines: one which is issued annually by the Canadian Hypertension Education Program. This approach is now extremely well developed and comprehensive with multiple web-based programs and information sources (www.hypertension.ca/en/chep). In addition, there is the recent effort by the European Society of Hypertension/European Society of Cardiology in 2013,3 and a newer, less formal document from the International Society of Hypertension and supported by a working group comprised of members of the American Society of Hypertension.4 Finally, there are other national guidelines around the world, perhaps most prominent among these being the British Hypertension Society National Institute for Clinical Excellence or the NICE guidelines.
DR. IZZO: That’s a good summary, Dr. Basile. What constitutes a useful guideline? Who is the audience? I don’t believe that a good guideline should be hidebound by unduly restrictive ‘evidence rules’ that ignore all but a tiny fraction of the available scientific information. A good guideline must synthesize complex data in a clear and concise way and must address the kinds of questions that real doctors need answered every day. Dr. Gradman, do you have an opinion on guidelines?
DR. GRADMAN: Part of what is going on in the revised hypertension guidelines is a worldwide shift from the treatment of individual patients to the treatment of patient populations. Such guidance for treating large groups is of great interest to governments and insurance companies but is less useful for making treatment decisions for individual patients with individual problems.
In fact, the JNC 8 guidelines specifically say that they are aimed at primary care physicians, not specialists or people who have a lot of experience with the treatment of hypertension. I think JNC 8 is to be commended for trying to make the fundamental concepts of the guidelines completely evidence-based. The guidelines delineate general targets and thresholds for treatment and also suggest the best drugs to use for most patients. Unfortunately, the exercise showed that it is not really possible to answer a lot of specific treatment questions using a strict evidence-based approach. For these we must rely on less definitive evidence and expert opinion.
I think there are different audiences; a good general guideline today should be aimed at primary care physicians but I think specialists need their own guidelines. As a cardiologist, I would want a very different set of guidelines than is presented in JNC 8.
DR. IZZO: Dr. Moser, given your long association with the highly successful parent of the JNC process, the National High Blood Pressure Education Program, I think your perspective is invaluable. Do you think any of the current guidelines hit the mark or what do you think should have been done differently?
DR. MOSER: Well, that’s a broad question. JNC 8 doesn’t differ much from JNC 7 except for one or 2 items. JNC 8 set out to answer several questions with a strict evidence-based methodology, and when they were finished, after a long period of time and substantial expenditure of money, they only ended up addressing 3 questions. The first question was when to initiate treatment, the second was related to the target or goal BPs, and the third was how to achieve goal pressures. They did address the question of whether people with comorbidities, especially diabetes and kidney disease, needed to have lower goal BPs.
On the issue of targets for BP, it was decided that 140/90 mm Hg was good enough for most people and that there was no compelling evidence that BP should be lowered below 130/80 mm Hg in diabetics or people with kidney disease. But we all know that in practice, you can’t adjust BPs to exact numbers. JNC 8 also said that the threshold for a diagnosis and target BP in people over the age of 60 was 150/90 mm Hg. This is quite different from other guidelines.
The guidelines also point out a difference in black and white patients. We’ve known for years that calcium-channel blockers (CCBs) and thiazide-type diuretics are more effective in blacks and angiotensin-converting enzyme (ACE) inhibitors or beta blockers are more effective in whites, so I don’t think JNC 8 provided any new information on this. Otherwise, you’ll find very little difference between JNC 8 and 7. What they didn’t address were possible changes in the diagnostic evaluation or nonpharmacologic therapy and they failed to discuss issues related to the delivery of care and adherence, etc. Some physicians have said that the changes are important and different, but when you look at it very carefully they’re not substantive compared to other reports.
Dr. IZZO: Is that a result of their strict rules of evidence?
Dr. MOSER: The report was supposed to be all evidence-based. They hired an outside vendor that reviewed about 6100 English-language papers. The experts on that panel could have picked up the 40 papers that they finally rated as acceptable within a few days. It took the vendors several years. As everyone has mentioned, they used the data from evidence-based trials and reached conclusions, but they also had an “out” on all of them, including the 150 mm Hg BP target in the elderly, which was arbitrarily defined as age 60. As in their other recommendations, they then said that you could rely on “expert opinion,” meaning clinical judgment. This is the basis of the major recommendation: “If you treat below 140/90 mm Hg and everybody’s happy and there are no side effects, then just continue treatment.”
Regarding their approach to the treatment of resistant patients, the proposed algorithm is almost the same as it has been for many, many years. So I’m very disappointed in what they have accomplished, especially since it took such a long period of time and cost so much money.
DR. IZZO: I echo your disappointment, especially on very fundamental grounds. First, a guideline constrained by the suffocating rules applied by the JNC 8 group is enormously biased, especially when over 99% of the potentially relevant information was ignored because it did not come from a randomized trial. Did they not understand just how biased randomized clinical trials really are? A true expert does better than that, prioritizing the value and relevance of all evidence, from bench science to randomized trials. The real test for a guideline is then in the projection of that synthesis, that is translating expert interpretation into understandable and workable recommendations. One other issue: absence of evidence should not imply a negative recommendation. If there is no definitive study proving that a lower BP target is warranted for people with kidney disease, it should also be very clear that there is existing evidence that lowering BP to 130/80 mm Hg instead of 140/90 mm Hg may be a good idea. JNC 8 chose to ignore studies of achieved (not intention-to-treat) BP values that identified better renal outcomes in diabetics5 and fewer recurrent strokes6 in trial participants with the lowest BPs. While it is true that such benefits are not achieved by all trial participants, it should be recognized that “lower is better” is probably true in at least some people.
Are there any comments or concerns that the narrow definition of evidence can actually lead us astray?
The JNC 8 tried to be an evidence-based document in that they only looked at randomized controlled hypertension trials, which in itself is a limitation. These were very strict criteria that prevented the group from including certain evidence bases. But ultimately, more than half of the guideline recommendations ended up being expert opinion. And the reason they ended up addressing only the 3 questions presented is because there just isn’t the kind of clinical trial-based evidence required to answer questions on issues such as resistant hypertension, the value of combination therapy, and contrasting differences in BP measurement techniques to detect which is best. Accordingly, we end up with a somewhat narrow perspective. In fact, JNC 8 ended up with a lot of expert opinion and failed to be as evidence-based as they would’ve liked to have been. At the end of the day, JNC 8 just doesn’t provide the clinician with the answers to many of the controversial issues that we face each and every day.
DR. IZZO: I’m with you on that last point, Dr. Basile. Speaking of evidence, although we know that systolic BP rises linearly with age, where is the study justifying that after age 60, your BP threshold should be relaxed immediately? JNC 8 said there is “no evidence of a BP benefit here”; I say there is no evidence of common sense here.
DR. BASILE: The recent American Society of Hypertension/International Society of Hypertension (ASH/ISH) guideline suggests that “elderly” means 80 years of age and older. The JNC 8 panel decided that while some trials had higher thresholds for eligibility than the BP goals tested, in an effort to simplify the message they decided that the threshold for initiating antihypertensive treatment should be made the same as the BP treatment goal. So their answer to the second question, “What should be the goal for BP reduction in patients who are 60 years of age and older?” is that it should be less than 150/90 mm Hg, the same as the threshold for starting antihypertensive therapy.
DR. MOSER: Well, the evidence doesn’t actually support this. None of the BP cutoffs were ever truly “evidence-based,” but the new guidelines do not acknowledge this. Clearly, evidence from randomized trials of any therapeutic benefit from having a systolic BP under 150 mm Hg isn’t very good, but expert opinion, clinical judgment, and epidemiologic data suggest very strongly to me that we should have kept the threshold for diagnosis and treatment at 140/90 mm Hg at any age. If a systolic pressure under 140 mm Hg is achieved in the elderly and therapy is well-tolerated, then therapy should be continued as before.
DR. GRADMAN: The targets for patients with diabetes and renal disease have been changed and that must be discussed. The revised goal of <140/90 mm Hg for diabetics was based primarily on the results of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial which compared that goal to a goal of <120/80 mm Hg and found no net advantage of very aggressive treatment. The JNC 7 goal of <130/80 mm Hg was never evaluated. It is of interest that the newest Canadian guidelines retain the <130/80 mm Hg recommendation.7 The JNC 8 document ignored individual patient differences, which might influence treatment decisions. In patients at increased risk for stroke, such as Asian populations or patients who have a history of cerebrovascular events, lower targets may be a rational treatment decision. As ACCORD demonstrated once again, stroke risk is exquisitely BP sensitive and those in the 120/80 mm Hg target group had fewer strokes; this consideration may trump others in specific patients. The JNC 8 document was certainly not for experts or specialists in the treatment of hypertension. Guidelines are also needed to address the “hard-to-treat patient” who may be defined in a number of ways.
DR. MOSER: Well, let me just embellish that, Dr. Izzo, for a second. If you ask who is going to use this document as a metric, or who is going to hold clinicians to these recommendations, at the end of the day, it may be no one. This is because JNC 8 was, unfortunately, not endorsed by any major group; it is a standalone document. It was sent out to a number of hypertension specialists who had an opportunity to give comments, but it wasn’t posted for either the professional community or the public community to see if there were any concerns before it was published.
I don’t necessarily mean this as a harsh criticism because it seems the JNC group was forced to go it alone. But there’s a possibility that not all major organizations, including the government, may actually accept the recommendations, especially the one relating to age and target BPs.
DR. GRADMAN: I wouldn’t agree with that entirely. I think people will latch onto the JNC document, in particular to the idea that patients don’t need to be treated as intensively as was recommended in the past. So these guidelines will reduce the number of people who are seen to require treatment and will lower the intensity of treatment for those who are receiving therapy. Computerized medical records will soon be almost universal and it will be easily determined if the practitioner is in compliance with a cutoff of 140/90 mm Hg in general or less than 150 mm Hg if a patient is over 60. So I think it could have more effect than you seem to think, Dr. Moser. Many people will conclude that lower really isn’t better. The cost of treatment to insurance companies and managed care organizations will go down as a lower intensity of treatment becomes the standard of care.
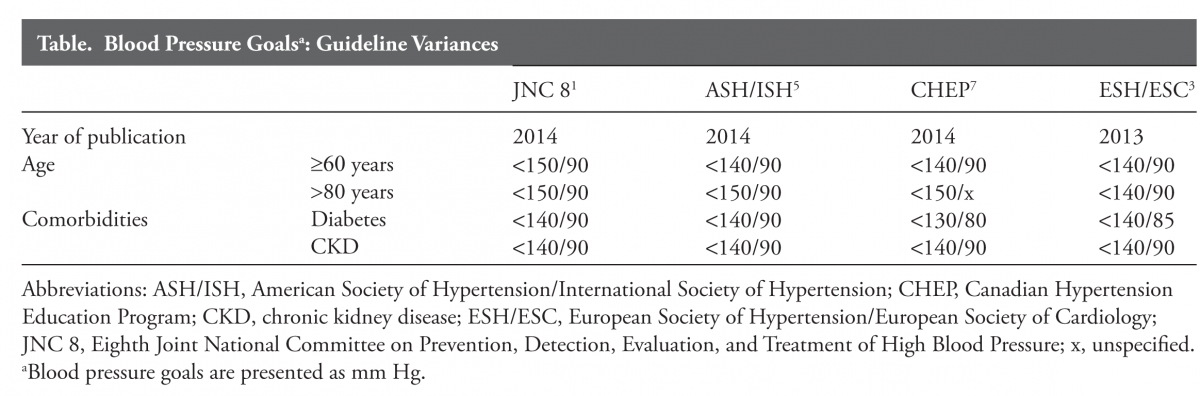
DR. BASILE: I agree with you, Dr. Gradman. The ASH/ISH and European Society documents have also abandoned the <130/80 mm Hg threshold for diabetic and chronic kidney disease (CKD) patients, in favor of a goal of <140/90 mm Hg (European Society <140/85 mm Hg in diabetes [Table]), so there is additional weight behind the new metrics in addition to JNC 8.
DR. MOSER: In response to Dr. Gradman, when you increase the target for treatment to 150 mm Hg you eliminate an enormous number of people in the “difficult-to-treat” category. Another point, some of the new guidelines are not user-friendly as Dr. Izzo pointed out. They may not be helpful for the practicing doctor. The European guidelines, for example, are too long and have too many references. I believe that JNC 8 should have been 6 or 7 pages. Physicians do not care about an A-rating, B-rating, or C-rating; they want to know what experts believe.
DR. IZZO: The European guidelines are unnecessarily complex and have other flaws, such as conflating hypertension treatment with risk scores. Interpretation and perspective are the jobs of an expert panel and those traits, labeled for what they are, need to be integral to the framework of any good guideline. That’s what JNC 7 had in greater measure and that’s what people want.
DR. IZZO: Maybe we can slightly reframe this same discussion in light of another vexing problem that seems to continue to surface. Is there a J-curve? Are there different J-curves for different organs or diseases?
DR. MOSER: The issue of J-curves has never been covered effectively.
DR. BASILE: It’s not discussed in most of the guidelines because it’s a very controversial area. In principle, there is a J-curve because when you get to a BP of 0 mm Hg, you can’t sustain life. I don’t have a problem with the JNC group or other groups not really looking into this J-curve issue but it’s a terrible problem for the clinician, never knowing what level you might put the patient in danger as you continue to lower BP.
DR. GRADMAN: I agree with you, Dr. Basile. I think the possibility that the J-curve is real underlies the changes the new guidelines made in target BPs. Higher BP targets will promote less aggressive BP-lowering, so maybe the J-curve “risk” will be diminished somewhat. Different endpoints appear to have different J-curves. You may reduce strokes, for example, but increase myocardial infarctions, and the latter seems to be related more to low diastolic BP. This risk-benefit balance of intensive treatment really underlies a lot of the changes that we’ve seen in target BPs in many guidelines, not just JNC 8. Overall attention to this equation is positive but guidance to clinicians faced with patients with specific risk factors, co morbidities, circadian BP patterns, or other clinical characteristics is completely lacking.
DR. BASILE: I totally agree with you, Dr. Gradman. Increasing the systolic BP goals will also lead to some increases in diastolic BP and perhaps less concern about J-curves, if they really exist.
One important point that I’ve been making with clinical groups is that the “ideal” BP for most patients depends on whether that patient is most at risk for stroke, heart attack, or kidney disease. These differing target organs do not all prefer to see the same amount of BP reduction. For example, the brain seems to prefer a lower target and does better with more systolic BP reduction than does the heart. Yet our antihypertensive agents are not organ specific when we use them so we have to accept a “sweet spot” that is most beneficial to the patient and causes little harm. Accordingly, I think there is a “best” BP range for most patients; the European guidelines suggest that when you keep the systolic BP for most patients between 130 and 139 mm Hg, you’re really doing the best for the patient. I agree with this. I believe this should be our “sweet spot” for most patients with hypertension except for the oldest of the old, especially those with isolated systolic hypertension, where the spot appears to be 140–149 mm Hg.
DR. MOSER: We have discussed treatment targets and it appears that we disagree generally with the change from 140 to 150 mm Hg as a target in the elderly. We seem to have decided that the target BP of 140/90 mm Hg is reasonable, and perhaps the change in targets in treating the diabetic might also be reasonable, although if you could get to 130/80 mm Hg, that’s fine. I agree with Dr. Izzo, the lower the better.
I think now we probably ought to address how to get there. If you look at the JNC 8 protocol of both the treatment of lower and the high-risk patient, it’s almost exactly the same as in JNC 7. The proposed algorithm for treatment does not contribute much that is new to the clinician’s ability to treat this disease effectively. Perhaps that is because specific therapy has not changed much in the past 5–8 years. We may have learned more about how to use certain therapies, but the actual medications haven’t changed much: the specific medications recommended are almost exactly the same as in JNC 7, except for the addition of chlorthalidone and indapamide.
DR. IZZO: Well, there is one difference: thiazide-type diuretics, dihydropyridines, and ACE inhibitors (or ARBs) are now referred to as “preferred drugs,” as was first suggested in our New York State Medicaid hypertension guideline in 2011.9 We defined a preferred agent as one with appropriate efficacy and safety that is also proven to lower cardiovascular event rates. I’d be interested in the opinions of this group with regard to treatment issues and also to the specific issue of whether beta blockers were unduly excluded.
DR. BASILE: I salute JNC 8 in leveling the playing field when they suggest that it is the amount of BP reduction achieved that is more important than the initial drug, but when you look at the outcome evidence from clinical trials for stroke as well as cardiac and renal disease, you can feel very comfortable using a renin-angiotensin system (RAS)-blocking drug, either an ACE inhibitor or an angiotensin receptor blocker (ARB), or a thiazide-type diuretic or a CCB.
I’m somewhat concerned that they lumped all CCBs together because I do think there’s more evidence of benefit for the dihydropyridines or the “pines” in hypertension than the other subclasses (diltiazem and verapamil). But I like the fact that 4 major classes are now looked at as being equal for initial therapy, even in diabetics, unless they have CKD. Unless they have CKD, JNC 8 very appropriately recommends that it’s BP reduction rather than the RAS blockade that translates into improvement in outcomes. However, for the diabetic with CKD, we would recommend an ACE or an ARB as a first drug. As for the beta blockers, they do not have the level of evidence that the thiazides have had, as most trials used once-a-day atenolol as their beta blocker. We just don’t know how some of the newer beta blockers would have stacked up to the other antihypertensive agents on clinical outcomes for those with hypertension without concomitant issues.
DR. IZZO: Dr. Gradman, as a card-carrying cardiologist, wouldn’t you be thrown out of your business if you failed to advocate for beta blockers?
DR. GRADMAN: To some extent that’s true, but the guidelines that we’re talking about are a broad-brush approach. JNC 8, based its opinion regarding the first-line use of beta blockers on one study: the Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) trial,10 which found a lower relative risk of stroke with losartan compared to atenolol. For cardiologists, beta blockers remain an essential component of treatment in the majority of patients with coronary disease, angina pectoris, and heart failure, with or without hypertension, and in patients with arrhythmias, such as atrial fibrillation. In the case of post myocardial infarction, though, it is unclear if the benefit persists, especially after 2 years.
Another criticism I have of the guidelines is that they lump all drugs from each class together. That’s especially problematic for CCBs and for beta blockers. There’s still some discussion about the variable effects of different beta blockers on glucose tolerance, side effect profile, vascular tone, and other properties.
Age may matter too, in the decision to use beta blockers. In a Canadian meta-analysis, patients under the age of 60 taking beta blockers did just as well as those taking other drugs, but beta blockers were not as effective in older patients in terms of endpoint reduction.11
In uncomplicated hypertension, though, I do agree with the broad-brush recommendations for primary care physicians that the other 4 classes of drugs (thiazide-type diuretics, ACE inhibitors, ARBs and dihydropyridine CCBs) still have more evidence of outcome benefit as first line therapy.
Again, I think these guidelines are an oversimplification and are not sufficient to guide individualized therapy.
DR. IZZO: Let’s close with some general discussion of whether the concept of the difficult-to-treat patient is useful and who might fill this definition.
DR. MOSER: It’s not necessarily related to having a comorbidity. You can have a diabetic hypertensive person with hyperlipidemia who responds very well to antihypertensive therapy. We’ve defined some patients as resistant, which may not be true. They may be difficult to treat. For example, just adding a thiazide-type diuretic to other drugs or increasing the dose of a thiazide-type diuretic will often convert a so-called “resistant patient” into a responsive patient.
That’s why I have supported JNC 7 and other guidelines that recommend starting with 2 drugs, either as 2 pills or in a single-pill combination when BP exceeds 160/100 mm Hg. One of the 2 drugs probably should be an RAS inhibitor, but the other most certainly should be a thiazide-type diuretic or perhaps a CCB.12
There are a lot of people with few other risk factors who are very difficult to control. One of the fallouts of the JNC 8 recommendations is that we may undertreat individuals over the age of 60, but that also means there will be less “resistant hypertension.”
DR. IZZO: When considering resistant hypertension, Dr. Moser suggested combination therapy. Dr. Gradman, you have had an interest in this area.
DR. GRADMAN: This is an important issue that has not really been addressed adequately in the guidelines. We know that combination therapy is required in upwards of 75% of patients using older BP targets.13 We also know that if you start people on combination therapy, you achieve target BP more rapidly and in a greater proportion of patients.
As to initial combination therapy versus the step-care type approach, either alternative is mentioned in JNC 8, but I don’t think any of the new guidelines have addressed the issue fully and no outcome studies have compared initial combination therapy versus initial monotherapy.
But the bottom line is that combination therapy is needed in the vast majority of patients although the percentage will be decreased if the newer, less aggressive BP targets are adopted. In my opinion, it should be started in almost everyone likely to eventually need more than 1 drug to achieve target BP. First-dose adverse effects, particularly hypotension, are very uncommon with 2- or 3-drug single-pill combinations that contain thiazide-type diuretics, ARBs, or CCBs. I would probably not use combinations as initial therapy in very elderly or frail patients.
DR. IZZO: I rarely use monotherapy anymore. Let me return to something that I touched on before: race as a decision point.
DR. BASILE: Well, I can understand why you’re against it, Dr. Izzo, because of the heterogeneity of how we define race. The white/black definition is certainly a simplistic approach given the way our genetics are so often mixed in today’s populations.
Both JNC 8 and the ASH/ISH document should, at least, be commended for pointing out to the clinician that if you’re looking for BP reduction, the CCB or the thiazide-type diuretic will give you more BP reduction in blacks in general than that achieved with an RAS blocker.
There are many African-American patients who are not prescribed a thiazide or a CCB as part of their cocktail. The big mistake is that these patients are considered resistant or refractory, depending on how many drugs they’re on. So I would at least point out, in line with JNC 8 and the ASH/ISH recommendations, that in the black patient, regardless of age, a CCB or a thiazide should be prescribed for BP reduction.
DR. IZZO: I think that’s a valid point. And just to summarize, the data show clearly that in an African-American population, you get about the same degree of BP reduction by using either a thiazide-type diuretic or CCB, and you do tend to have a more limited response to RAS blockers. The reverse could be stated for whites. But then again, if you use a thiazide-type diuretic and an RAS blocker together, the race issue is moot.
DR. MOSER: For years we have been studying black patients around the world, and there’s no question that there is a different response. I also want to return to something mentioned earlier: we are losing sight of the value of so-called “experts.” Simple guidelines work for the vast majority of patients. The complicated patient should probably be referred to an expert.
DR IZZO: Are there other issues when it comes to managing the hard-to-treat patient?
DR. GRADMAN: There are many reasons why a patient may be difficult to treat. Some may truly not respond to drugs but others have hypertension in the office and not at home. They may be difficult to treat because they don’t take their medications for various reasons. The other thing, of course, is to ask whether patients are taking any interfering substances like nonsteroidal antiinflammatory drugs. Most often, if you have people who are truly poorly responsive to antihypertensive therapy, it is worth reviewing whether adequate doses of preferred agents (RAS blockers, thiazide-type diuretics, and CCBs) have been used.
Most people these days also use aldosterone antagonists as the fourth drug, recognizing the danger of hyperkalemia particularly in patients receiving renin-angiotensin aldosterone system inhibitors. If patients have renal insufficiency, using a sufficient dose of thiazide-type diuretics is extremely important, and for patients with advanced renal disease, a loop diuretic is required. There may also be some intraclass differences among drugs, as between losartan and azilsartan.
DR. BASILE: I’m now running a resistant hypertension clinic, seeing only difficult-to-treat patients. As we saw in the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), there is no question that the difficult-to-treat patient may be a little more likely to be black with left ventricular hypertrophy, CKD, obese, and elderly.
But the reality is there are patients in our practices that are called resistant that really only have white-coat hypertension and may have markedly reduced BPs when they’re out of the office. These are the same patients that complain of being periodically light headed or lethargic when their pressures are low outside of the office and often have minimal target organ disease with benign eyegrounds, no left ventricular hypertrophy on electrocardiogram, and minimal if any protein in the urine.
Another major issue is the use of inadequate doses of agents such as amlodipine when started at 2.5 mg daily and never up-titrating to the standard doses of 5 or 10 mg daily because of the concern of edema. I also find that replacing hydrochlorothiazide 25 mg with chlorthalidone at the same dose can improve BP control. And we have already mentioned the important role of spironolactone.
DR. MOSER: Let me emphasize that about half of the patients referred to as “resistant” respond when you increase the thiazide-type diuretic; this also seems to be true for the addition of spironolactone to hydrochlorothiazide. Combinations have a clear advantage in terms of a meaningful response.
DR. IZZO: It still begs the question to me of whether or not we’ve given enough guidance to well-meaning practitioners in this tougher-to-treat group of patients.
DR. GRADMAN: Let me point out the paper on resistant hypertension from the American Heart Association14 as a useful comprehensive reference, but perhaps we need a relatively simple document that could be used by practicing physicians who regularly treat these patients.
DR. BASILE: I would agree with Dr. Gradman that we need to continue to provide more information on the resistant patient.
DR. IZZO: Dr. Moser, you have the last word.
DR. MOSER: If you look at the general approach in JNC 8 and the algorithm in JNC 7, you’ll find a perfectly good and reasonable approach to the management of hypertension, including for the so-called resistant or difficult-to-treat patient. It seems physicians have been afraid to lower BP, especially in the elderly. This may be one of the reasons why JNC 8 recommends a target of 150 mm Hg and not to go below that. There’s an unfounded fear of the J-curve, of causing fainting or falling in patients, especially the elderly, that does not appear to be too much of a problem if BP is reduced gradually.15
It’s unlikely that we will cause much harm and may actually reduce cardiovascular events more in the elderly if we lower the goals to what we had before. But the JNC 8 algorithm is out there and probably will be followed by many physicians.
DR. IZZO: Thank you all very much for your valuable insights. The acid test, however, is what practitioners think and what they will do. We have recent insight into this area (Table). As is readily apparent, the opinion piece we call JNC 8 does not fully resonate with the majority of primary care providers or cardiologists. What will fill the need remains to be determined.
Disclosures: Joseph Izzo has been a consultant for Novartis and Bristol-Myers Squibb, has received a research grant from Forest Laboratories, and has received speakers’ honoraria from the American Society of Hypertension. Alan Gradman is a consultant for Daiichi-Sankyo, Novartis, Forest Laboratories, and Takeda. He is a member of the Speakers Bureau for Daiichi-Sankyo, Novartis, Forest Laboratories, Takeda, and Arbor. Over the past year, he has also received honoraria for lectures sponsored by The American Society of Hypertension and The American College of Cardiology. Jan Basile is a consultant for Daiichi-Sankyo, Forest, Arbor, Eli-Lilly, and Medtronic. He has received grant/research support from NHLBI (SPRINT). He is a member of the speakers’ bureau at Daiichi-Sankyo, Forest, and Arbor.
Addendum: The concerns raised during this discussion have been echoed by clinicians in the field. Cardiologists have indicated that they are waiting for yet another hypertension guideline proposed by the American Heart Association/American Society of Cardiology for 2014–2015 (Figure). 16 Clearly the fractionation continues.
FoxP2 Media LLC is the publisher of The Medical Roundtable.
The first part of our discussion focuses on the issue of guidelines and guideline proliferation. Over the last several years, multiple professional groups and health-associated agencies have issued guidelines for the diagnosis and treatment of hypertension. It is not clear to me that these competing documents provide a rational platform for improved care. Despite some recent claims, no guideline can be fully “evidence-based” because we cannot afford clinical trials for each relevant clinical question. Furthermore, the current batch of new guidelines has yielded conflicting recommendations. For example, the definition of “elderly” as age 60 in the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) and age 80 in the recent joint guidance from the International and American Societies of Hypertension. I fear that the guideline process has essentially broken down—this benefits no one.
First, a little history. Prior JNC documents were produced under the auspices of the National High Blood Pressure Education Program, a consortium of about 3 dozen healthcare professional organizations. As a participant in JNC VI and JNC 7, I can assure you that all participants were dedicated scientists and clinicians whose common goal was to synthesize the best and most robust information into a document that provided practitioners with the most reliable guidance possible. JNC 7 was released in 2003 and was soon widely adopted; it truly stood the test of time. After that, everything changed. Dr. Basile, what has been happening since?
DR. BASILE: Thanks, Dr. Izzo. I agree with you about your concerns with guidelines. This is a very difficult issue for the practicing clinician.
With regard to JNC 8, in 2008, the National Heart, Lung, and Blood Institute (NHLBI) decided to develop its own comprehensive “evidence-based” disease prevention portfolio that included a coordinated cholesterol guideline, obesity guideline, hypertension guideline, as well as a lifestyle/risk factor modification guideline. Following the recommendations put forth by the Institute of Medicine on guidelines, the NHLBI mandated that strict rules of evidence be used for its guideline development. After the JNC 8 committee established the clinical trial criteria for use in their hypertension guideline, the NHLBI hired a professional vendor to vet the literature. The process was essentially going nowhere so a second vendor for hypertension had to be hired. In the end, few clinical trials passed the criteria used to form the basis of JNC 8. And near its completion, after the JNC 8 group toiled for over 5 years putting their report together, they learned in 2013 that the NHLBI withdrew its support for the guideline and asked the American College of Cardiology/American Heart Association to establish a joint task force (to include the JNC 8 group) to assume responsibility for the guideline process. Declining this collaborative opportunity, the JNC 8 group decided on their own to have their work submitted and it was published without organizational support in JAMA.1
Meanwhile, the Centers for Disease Control published an overall systems approach for primary care clinicians in which they released the Kaiser Permanente algorithm for effective blood pressure (BP) control.2
Of note, there are several other competing guidelines: one which is issued annually by the Canadian Hypertension Education Program. This approach is now extremely well developed and comprehensive with multiple web-based programs and information sources (www.hypertension.ca/en/chep). In addition, there is the recent effort by the European Society of Hypertension/European Society of Cardiology in 2013,3 and a newer, less formal document from the International Society of Hypertension and supported by a working group comprised of members of the American Society of Hypertension.4 Finally, there are other national guidelines around the world, perhaps most prominent among these being the British Hypertension Society National Institute for Clinical Excellence or the NICE guidelines.
DR. IZZO: That’s a good summary, Dr. Basile. What constitutes a useful guideline? Who is the audience? I don’t believe that a good guideline should be hidebound by unduly restrictive ‘evidence rules’ that ignore all but a tiny fraction of the available scientific information. A good guideline must synthesize complex data in a clear and concise way and must address the kinds of questions that real doctors need answered every day. Dr. Gradman, do you have an opinion on guidelines?
DR. GRADMAN: Part of what is going on in the revised hypertension guidelines is a worldwide shift from the treatment of individual patients to the treatment of patient populations. Such guidance for treating large groups is of great interest to governments and insurance companies but is less useful for making treatment decisions for individual patients with individual problems.
In fact, the JNC 8 guidelines specifically say that they are aimed at primary care physicians, not specialists or people who have a lot of experience with the treatment of hypertension. I think JNC 8 is to be commended for trying to make the fundamental concepts of the guidelines completely evidence-based. The guidelines delineate general targets and thresholds for treatment and also suggest the best drugs to use for most patients. Unfortunately, the exercise showed that it is not really possible to answer a lot of specific treatment questions using a strict evidence-based approach. For these we must rely on less definitive evidence and expert opinion.
I think there are different audiences; a good general guideline today should be aimed at primary care physicians but I think specialists need their own guidelines. As a cardiologist, I would want a very different set of guidelines than is presented in JNC 8.
DR. IZZO: Dr. Moser, given your long association with the highly successful parent of the JNC process, the National High Blood Pressure Education Program, I think your perspective is invaluable. Do you think any of the current guidelines hit the mark or what do you think should have been done differently?
DR. MOSER: Well, that’s a broad question. JNC 8 doesn’t differ much from JNC 7 except for one or 2 items. JNC 8 set out to answer several questions with a strict evidence-based methodology, and when they were finished, after a long period of time and substantial expenditure of money, they only ended up addressing 3 questions. The first question was when to initiate treatment, the second was related to the target or goal BPs, and the third was how to achieve goal pressures. They did address the question of whether people with comorbidities, especially diabetes and kidney disease, needed to have lower goal BPs.
On the issue of targets for BP, it was decided that 140/90 mm Hg was good enough for most people and that there was no compelling evidence that BP should be lowered below 130/80 mm Hg in diabetics or people with kidney disease. But we all know that in practice, you can’t adjust BPs to exact numbers. JNC 8 also said that the threshold for a diagnosis and target BP in people over the age of 60 was 150/90 mm Hg. This is quite different from other guidelines.
The guidelines also point out a difference in black and white patients. We’ve known for years that calcium-channel blockers (CCBs) and thiazide-type diuretics are more effective in blacks and angiotensin-converting enzyme (ACE) inhibitors or beta blockers are more effective in whites, so I don’t think JNC 8 provided any new information on this. Otherwise, you’ll find very little difference between JNC 8 and 7. What they didn’t address were possible changes in the diagnostic evaluation or nonpharmacologic therapy and they failed to discuss issues related to the delivery of care and adherence, etc. Some physicians have said that the changes are important and different, but when you look at it very carefully they’re not substantive compared to other reports.
Dr. IZZO: Is that a result of their strict rules of evidence?
Dr. MOSER: The report was supposed to be all evidence-based. They hired an outside vendor that reviewed about 6100 English-language papers. The experts on that panel could have picked up the 40 papers that they finally rated as acceptable within a few days. It took the vendors several years. As everyone has mentioned, they used the data from evidence-based trials and reached conclusions, but they also had an “out” on all of them, including the 150 mm Hg BP target in the elderly, which was arbitrarily defined as age 60. As in their other recommendations, they then said that you could rely on “expert opinion,” meaning clinical judgment. This is the basis of the major recommendation: “If you treat below 140/90 mm Hg and everybody’s happy and there are no side effects, then just continue treatment.”
Regarding their approach to the treatment of resistant patients, the proposed algorithm is almost the same as it has been for many, many years. So I’m very disappointed in what they have accomplished, especially since it took such a long period of time and cost so much money.
DR. IZZO: I echo your disappointment, especially on very fundamental grounds. First, a guideline constrained by the suffocating rules applied by the JNC 8 group is enormously biased, especially when over 99% of the potentially relevant information was ignored because it did not come from a randomized trial. Did they not understand just how biased randomized clinical trials really are? A true expert does better than that, prioritizing the value and relevance of all evidence, from bench science to randomized trials. The real test for a guideline is then in the projection of that synthesis, that is translating expert interpretation into understandable and workable recommendations. One other issue: absence of evidence should not imply a negative recommendation. If there is no definitive study proving that a lower BP target is warranted for people with kidney disease, it should also be very clear that there is existing evidence that lowering BP to 130/80 mm Hg instead of 140/90 mm Hg may be a good idea. JNC 8 chose to ignore studies of achieved (not intention-to-treat) BP values that identified better renal outcomes in diabetics5 and fewer recurrent strokes6 in trial participants with the lowest BPs. While it is true that such benefits are not achieved by all trial participants, it should be recognized that “lower is better” is probably true in at least some people.
Are there any comments or concerns that the narrow definition of evidence can actually lead us astray?
The JNC 8 tried to be an evidence-based document in that they only looked at randomized controlled hypertension trials, which in itself is a limitation. These were very strict criteria that prevented the group from including certain evidence bases. But ultimately, more than half of the guideline recommendations ended up being expert opinion. And the reason they ended up addressing only the 3 questions presented is because there just isn’t the kind of clinical trial-based evidence required to answer questions on issues such as resistant hypertension, the value of combination therapy, and contrasting differences in BP measurement techniques to detect which is best. Accordingly, we end up with a somewhat narrow perspective. In fact, JNC 8 ended up with a lot of expert opinion and failed to be as evidence-based as they would’ve liked to have been. At the end of the day, JNC 8 just doesn’t provide the clinician with the answers to many of the controversial issues that we face each and every day.
DR. IZZO: I’m with you on that last point, Dr. Basile. Speaking of evidence, although we know that systolic BP rises linearly with age, where is the study justifying that after age 60, your BP threshold should be relaxed immediately? JNC 8 said there is “no evidence of a BP benefit here”; I say there is no evidence of common sense here.
DR. BASILE: The recent American Society of Hypertension/International Society of Hypertension (ASH/ISH) guideline suggests that “elderly” means 80 years of age and older. The JNC 8 panel decided that while some trials had higher thresholds for eligibility than the BP goals tested, in an effort to simplify the message they decided that the threshold for initiating antihypertensive treatment should be made the same as the BP treatment goal. So their answer to the second question, “What should be the goal for BP reduction in patients who are 60 years of age and older?” is that it should be less than 150/90 mm Hg, the same as the threshold for starting antihypertensive therapy.
DR. MOSER: Well, the evidence doesn’t actually support this. None of the BP cutoffs were ever truly “evidence-based,” but the new guidelines do not acknowledge this. Clearly, evidence from randomized trials of any therapeutic benefit from having a systolic BP under 150 mm Hg isn’t very good, but expert opinion, clinical judgment, and epidemiologic data suggest very strongly to me that we should have kept the threshold for diagnosis and treatment at 140/90 mm Hg at any age. If a systolic pressure under 140 mm Hg is achieved in the elderly and therapy is well-tolerated, then therapy should be continued as before.
DR. GRADMAN: The targets for patients with diabetes and renal disease have been changed and that must be discussed. The revised goal of <140/90 mm Hg for diabetics was based primarily on the results of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial which compared that goal to a goal of <120/80 mm Hg and found no net advantage of very aggressive treatment. The JNC 7 goal of <130/80 mm Hg was never evaluated. It is of interest that the newest Canadian guidelines retain the <130/80 mm Hg recommendation.7 The JNC 8 document ignored individual patient differences, which might influence treatment decisions. In patients at increased risk for stroke, such as Asian populations or patients who have a history of cerebrovascular events, lower targets may be a rational treatment decision. As ACCORD demonstrated once again, stroke risk is exquisitely BP sensitive and those in the 120/80 mm Hg target group had fewer strokes; this consideration may trump others in specific patients. The JNC 8 document was certainly not for experts or specialists in the treatment of hypertension. Guidelines are also needed to address the “hard-to-treat patient” who may be defined in a number of ways.
DR. MOSER: Well, let me just embellish that, Dr. Izzo, for a second. If you ask who is going to use this document as a metric, or who is going to hold clinicians to these recommendations, at the end of the day, it may be no one. This is because JNC 8 was, unfortunately, not endorsed by any major group; it is a standalone document. It was sent out to a number of hypertension specialists who had an opportunity to give comments, but it wasn’t posted for either the professional community or the public community to see if there were any concerns before it was published.
I don’t necessarily mean this as a harsh criticism because it seems the JNC group was forced to go it alone. But there’s a possibility that not all major organizations, including the government, may actually accept the recommendations, especially the one relating to age and target BPs.
DR. GRADMAN: I wouldn’t agree with that entirely. I think people will latch onto the JNC document, in particular to the idea that patients don’t need to be treated as intensively as was recommended in the past. So these guidelines will reduce the number of people who are seen to require treatment and will lower the intensity of treatment for those who are receiving therapy. Computerized medical records will soon be almost universal and it will be easily determined if the practitioner is in compliance with a cutoff of 140/90 mm Hg in general or less than 150 mm Hg if a patient is over 60. So I think it could have more effect than you seem to think, Dr. Moser. Many people will conclude that lower really isn’t better. The cost of treatment to insurance companies and managed care organizations will go down as a lower intensity of treatment becomes the standard of care.
DR. BASILE: I agree with you, Dr. Gradman. The ASH/ISH and European Society documents have also abandoned the <130/80 mm Hg threshold for diabetic and chronic kidney disease (CKD) patients, in favor of a goal of <140/90 mm Hg (European Society <140/85 mm Hg in diabetes [Table]), so there is additional weight behind the new metrics in addition to JNC 8.
DR. MOSER: In response to Dr. Gradman, when you increase the target for treatment to 150 mm Hg you eliminate an enormous number of people in the “difficult-to-treat” category. Another point, some of the new guidelines are not user-friendly as Dr. Izzo pointed out. They may not be helpful for the practicing doctor. The European guidelines, for example, are too long and have too many references. I believe that JNC 8 should have been 6 or 7 pages. Physicians do not care about an A-rating, B-rating, or C-rating; they want to know what experts believe.
DR. IZZO: The European guidelines are unnecessarily complex and have other flaws, such as conflating hypertension treatment with risk scores. Interpretation and perspective are the jobs of an expert panel and those traits, labeled for what they are, need to be integral to the framework of any good guideline. That’s what JNC 7 had in greater measure and that’s what people want.
DR. IZZO: Maybe we can slightly reframe this same discussion in light of another vexing problem that seems to continue to surface. Is there a J-curve? Are there different J-curves for different organs or diseases?
DR. MOSER: The issue of J-curves has never been covered effectively.
DR. BASILE: It’s not discussed in most of the guidelines because it’s a very controversial area. In principle, there is a J-curve because when you get to a BP of 0 mm Hg, you can’t sustain life. I don’t have a problem with the JNC group or other groups not really looking into this J-curve issue but it’s a terrible problem for the clinician, never knowing what level you might put the patient in danger as you continue to lower BP.
DR. GRADMAN: I agree with you, Dr. Basile. I think the possibility that the J-curve is real underlies the changes the new guidelines made in target BPs. Higher BP targets will promote less aggressive BP-lowering, so maybe the J-curve “risk” will be diminished somewhat. Different endpoints appear to have different J-curves. You may reduce strokes, for example, but increase myocardial infarctions, and the latter seems to be related more to low diastolic BP. This risk-benefit balance of intensive treatment really underlies a lot of the changes that we’ve seen in target BPs in many guidelines, not just JNC 8. Overall attention to this equation is positive but guidance to clinicians faced with patients with specific risk factors, co morbidities, circadian BP patterns, or other clinical characteristics is completely lacking.
DR. BASILE: I totally agree with you, Dr. Gradman. Increasing the systolic BP goals will also lead to some increases in diastolic BP and perhaps less concern about J-curves, if they really exist.
One important point that I’ve been making with clinical groups is that the “ideal” BP for most patients depends on whether that patient is most at risk for stroke, heart attack, or kidney disease. These differing target organs do not all prefer to see the same amount of BP reduction. For example, the brain seems to prefer a lower target and does better with more systolic BP reduction than does the heart. Yet our antihypertensive agents are not organ specific when we use them so we have to accept a “sweet spot” that is most beneficial to the patient and causes little harm. Accordingly, I think there is a “best” BP range for most patients; the European guidelines suggest that when you keep the systolic BP for most patients between 130 and 139 mm Hg, you’re really doing the best for the patient. I agree with this. I believe this should be our “sweet spot” for most patients with hypertension except for the oldest of the old, especially those with isolated systolic hypertension, where the spot appears to be 140–149 mm Hg.
DR. MOSER: We have discussed treatment targets and it appears that we disagree generally with the change from 140 to 150 mm Hg as a target in the elderly. We seem to have decided that the target BP of 140/90 mm Hg is reasonable, and perhaps the change in targets in treating the diabetic might also be reasonable, although if you could get to 130/80 mm Hg, that’s fine. I agree with Dr. Izzo, the lower the better.
I think now we probably ought to address how to get there. If you look at the JNC 8 protocol of both the treatment of lower and the high-risk patient, it’s almost exactly the same as in JNC 7. The proposed algorithm for treatment does not contribute much that is new to the clinician’s ability to treat this disease effectively. Perhaps that is because specific therapy has not changed much in the past 5–8 years. We may have learned more about how to use certain therapies, but the actual medications haven’t changed much: the specific medications recommended are almost exactly the same as in JNC 7, except for the addition of chlorthalidone and indapamide.
DR. IZZO: Well, there is one difference: thiazide-type diuretics, dihydropyridines, and ACE inhibitors (or ARBs) are now referred to as “preferred drugs,” as was first suggested in our New York State Medicaid hypertension guideline in 2011.9 We defined a preferred agent as one with appropriate efficacy and safety that is also proven to lower cardiovascular event rates. I’d be interested in the opinions of this group with regard to treatment issues and also to the specific issue of whether beta blockers were unduly excluded.
DR. BASILE: I salute JNC 8 in leveling the playing field when they suggest that it is the amount of BP reduction achieved that is more important than the initial drug, but when you look at the outcome evidence from clinical trials for stroke as well as cardiac and renal disease, you can feel very comfortable using a renin-angiotensin system (RAS)-blocking drug, either an ACE inhibitor or an angiotensin receptor blocker (ARB), or a thiazide-type diuretic or a CCB.
I’m somewhat concerned that they lumped all CCBs together because I do think there’s more evidence of benefit for the dihydropyridines or the “pines” in hypertension than the other subclasses (diltiazem and verapamil). But I like the fact that 4 major classes are now looked at as being equal for initial therapy, even in diabetics, unless they have CKD. Unless they have CKD, JNC 8 very appropriately recommends that it’s BP reduction rather than the RAS blockade that translates into improvement in outcomes. However, for the diabetic with CKD, we would recommend an ACE or an ARB as a first drug. As for the beta blockers, they do not have the level of evidence that the thiazides have had, as most trials used once-a-day atenolol as their beta blocker. We just don’t know how some of the newer beta blockers would have stacked up to the other antihypertensive agents on clinical outcomes for those with hypertension without concomitant issues.
DR. IZZO: Dr. Gradman, as a card-carrying cardiologist, wouldn’t you be thrown out of your business if you failed to advocate for beta blockers?
DR. GRADMAN: To some extent that’s true, but the guidelines that we’re talking about are a broad-brush approach. JNC 8, based its opinion regarding the first-line use of beta blockers on one study: the Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) trial,10 which found a lower relative risk of stroke with losartan compared to atenolol. For cardiologists, beta blockers remain an essential component of treatment in the majority of patients with coronary disease, angina pectoris, and heart failure, with or without hypertension, and in patients with arrhythmias, such as atrial fibrillation. In the case of post myocardial infarction, though, it is unclear if the benefit persists, especially after 2 years.
Another criticism I have of the guidelines is that they lump all drugs from each class together. That’s especially problematic for CCBs and for beta blockers. There’s still some discussion about the variable effects of different beta blockers on glucose tolerance, side effect profile, vascular tone, and other properties.
Age may matter too, in the decision to use beta blockers. In a Canadian meta-analysis, patients under the age of 60 taking beta blockers did just as well as those taking other drugs, but beta blockers were not as effective in older patients in terms of endpoint reduction.11
In uncomplicated hypertension, though, I do agree with the broad-brush recommendations for primary care physicians that the other 4 classes of drugs (thiazide-type diuretics, ACE inhibitors, ARBs and dihydropyridine CCBs) still have more evidence of outcome benefit as first line therapy.
Again, I think these guidelines are an oversimplification and are not sufficient to guide individualized therapy.
DR. IZZO: Let’s close with some general discussion of whether the concept of the difficult-to-treat patient is useful and who might fill this definition.
DR. MOSER: It’s not necessarily related to having a comorbidity. You can have a diabetic hypertensive person with hyperlipidemia who responds very well to antihypertensive therapy. We’ve defined some patients as resistant, which may not be true. They may be difficult to treat. For example, just adding a thiazide-type diuretic to other drugs or increasing the dose of a thiazide-type diuretic will often convert a so-called “resistant patient” into a responsive patient.
That’s why I have supported JNC 7 and other guidelines that recommend starting with 2 drugs, either as 2 pills or in a single-pill combination when BP exceeds 160/100 mm Hg. One of the 2 drugs probably should be an RAS inhibitor, but the other most certainly should be a thiazide-type diuretic or perhaps a CCB.12
There are a lot of people with few other risk factors who are very difficult to control. One of the fallouts of the JNC 8 recommendations is that we may undertreat individuals over the age of 60, but that also means there will be less “resistant hypertension.”
DR. IZZO: When considering resistant hypertension, Dr. Moser suggested combination therapy. Dr. Gradman, you have had an interest in this area.
DR. GRADMAN: This is an important issue that has not really been addressed adequately in the guidelines. We know that combination therapy is required in upwards of 75% of patients using older BP targets.13 We also know that if you start people on combination therapy, you achieve target BP more rapidly and in a greater proportion of patients.
As to initial combination therapy versus the step-care type approach, either alternative is mentioned in JNC 8, but I don’t think any of the new guidelines have addressed the issue fully and no outcome studies have compared initial combination therapy versus initial monotherapy.
But the bottom line is that combination therapy is needed in the vast majority of patients although the percentage will be decreased if the newer, less aggressive BP targets are adopted. In my opinion, it should be started in almost everyone likely to eventually need more than 1 drug to achieve target BP. First-dose adverse effects, particularly hypotension, are very uncommon with 2- or 3-drug single-pill combinations that contain thiazide-type diuretics, ARBs, or CCBs. I would probably not use combinations as initial therapy in very elderly or frail patients.
DR. IZZO: I rarely use monotherapy anymore. Let me return to something that I touched on before: race as a decision point.
DR. BASILE: Well, I can understand why you’re against it, Dr. Izzo, because of the heterogeneity of how we define race. The white/black definition is certainly a simplistic approach given the way our genetics are so often mixed in today’s populations.
Both JNC 8 and the ASH/ISH document should, at least, be commended for pointing out to the clinician that if you’re looking for BP reduction, the CCB or the thiazide-type diuretic will give you more BP reduction in blacks in general than that achieved with an RAS blocker.
There are many African-American patients who are not prescribed a thiazide or a CCB as part of their cocktail. The big mistake is that these patients are considered resistant or refractory, depending on how many drugs they’re on. So I would at least point out, in line with JNC 8 and the ASH/ISH recommendations, that in the black patient, regardless of age, a CCB or a thiazide should be prescribed for BP reduction.
DR. IZZO: I think that’s a valid point. And just to summarize, the data show clearly that in an African-American population, you get about the same degree of BP reduction by using either a thiazide-type diuretic or CCB, and you do tend to have a more limited response to RAS blockers. The reverse could be stated for whites. But then again, if you use a thiazide-type diuretic and an RAS blocker together, the race issue is moot.
DR. MOSER: For years we have been studying black patients around the world, and there’s no question that there is a different response. I also want to return to something mentioned earlier: we are losing sight of the value of so-called “experts.” Simple guidelines work for the vast majority of patients. The complicated patient should probably be referred to an expert.
DR IZZO: Are there other issues when it comes to managing the hard-to-treat patient?
DR. GRADMAN: There are many reasons why a patient may be difficult to treat. Some may truly not respond to drugs but others have hypertension in the office and not at home. They may be difficult to treat because they don’t take their medications for various reasons. The other thing, of course, is to ask whether patients are taking any interfering substances like nonsteroidal antiinflammatory drugs. Most often, if you have people who are truly poorly responsive to antihypertensive therapy, it is worth reviewing whether adequate doses of preferred agents (RAS blockers, thiazide-type diuretics, and CCBs) have been used.
Most people these days also use aldosterone antagonists as the fourth drug, recognizing the danger of hyperkalemia particularly in patients receiving renin-angiotensin aldosterone system inhibitors. If patients have renal insufficiency, using a sufficient dose of thiazide-type diuretics is extremely important, and for patients with advanced renal disease, a loop diuretic is required. There may also be some intraclass differences among drugs, as between losartan and azilsartan.
DR. BASILE: I’m now running a resistant hypertension clinic, seeing only difficult-to-treat patients. As we saw in the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), there is no question that the difficult-to-treat patient may be a little more likely to be black with left ventricular hypertrophy, CKD, obese, and elderly.
But the reality is there are patients in our practices that are called resistant that really only have white-coat hypertension and may have markedly reduced BPs when they’re out of the office. These are the same patients that complain of being periodically light headed or lethargic when their pressures are low outside of the office and often have minimal target organ disease with benign eyegrounds, no left ventricular hypertrophy on electrocardiogram, and minimal if any protein in the urine.
Another major issue is the use of inadequate doses of agents such as amlodipine when started at 2.5 mg daily and never up-titrating to the standard doses of 5 or 10 mg daily because of the concern of edema. I also find that replacing hydrochlorothiazide 25 mg with chlorthalidone at the same dose can improve BP control. And we have already mentioned the important role of spironolactone.
DR. MOSER: Let me emphasize that about half of the patients referred to as “resistant” respond when you increase the thiazide-type diuretic; this also seems to be true for the addition of spironolactone to hydrochlorothiazide. Combinations have a clear advantage in terms of a meaningful response.
DR. IZZO: It still begs the question to me of whether or not we’ve given enough guidance to well-meaning practitioners in this tougher-to-treat group of patients.
DR. GRADMAN: Let me point out the paper on resistant hypertension from the American Heart Association14 as a useful comprehensive reference, but perhaps we need a relatively simple document that could be used by practicing physicians who regularly treat these patients.
DR. BASILE: I would agree with Dr. Gradman that we need to continue to provide more information on the resistant patient.
DR. IZZO: Dr. Moser, you have the last word.
DR. MOSER: If you look at the general approach in JNC 8 and the algorithm in JNC 7, you’ll find a perfectly good and reasonable approach to the management of hypertension, including for the so-called resistant or difficult-to-treat patient. It seems physicians have been afraid to lower BP, especially in the elderly. This may be one of the reasons why JNC 8 recommends a target of 150 mm Hg and not to go below that. There’s an unfounded fear of the J-curve, of causing fainting or falling in patients, especially the elderly, that does not appear to be too much of a problem if BP is reduced gradually.15
It’s unlikely that we will cause much harm and may actually reduce cardiovascular events more in the elderly if we lower the goals to what we had before. But the JNC 8 algorithm is out there and probably will be followed by many physicians.
DR. IZZO: Thank you all very much for your valuable insights. The acid test, however, is what practitioners think and what they will do. We have recent insight into this area (Table). As is readily apparent, the opinion piece we call JNC 8 does not fully resonate with the majority of primary care providers or cardiologists. What will fill the need remains to be determined.
Disclosures: Joseph Izzo has been a consultant for Novartis and Bristol-Myers Squibb, has received a research grant from Forest Laboratories, and has received speakers’ honoraria from the American Society of Hypertension. Alan Gradman is a consultant for Daiichi-Sankyo, Novartis, Forest Laboratories, and Takeda. He is a member of the Speakers Bureau for Daiichi-Sankyo, Novartis, Forest Laboratories, Takeda, and Arbor. Over the past year, he has also received honoraria for lectures sponsored by The American Society of Hypertension and The American College of Cardiology. Jan Basile is a consultant for Daiichi-Sankyo, Forest, Arbor, Eli-Lilly, and Medtronic. He has received grant/research support from NHLBI (SPRINT). He is a member of the speakers’ bureau at Daiichi-Sankyo, Forest, and Arbor.
Addendum: The concerns raised during this discussion have been echoed by clinicians in the field. Cardiologists have indicated that they are waiting for yet another hypertension guideline proposed by the American Heart Association/American Society of Cardiology for 2014–2015 (Figure). 16 Clearly the fractionation continues.
FoxP2 Media LLC is the publisher of The Medical Roundtable.
The first part of our discussion focuses on the issue of guidelines and guideline proliferation. Over the last several years, multiple professional groups and health-associated agencies have issued guidelines for the diagnosis and treatment of hypertension. It is not clear to me that these competing documents provide a rational platform for improved care. Despite some recent claims, no guideline can be fully “evidence-based” because we cannot afford clinical trials for each relevant clinical question. Furthermore, the current batch of new guidelines has yielded conflicting recommendations. For example, the definition of “elderly” as age 60 in the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) and age 80 in the recent joint guidance from the International and American Societies of Hypertension. I fear that the guideline process has essentially broken down—this benefits no one.
First, a little history. Prior JNC documents were produced under the auspices of the National High Blood Pressure Education Program, a consortium of about 3 dozen healthcare professional organizations. As a participant in JNC VI and JNC 7, I can assure you that all participants were dedicated scientists and clinicians whose common goal was to synthesize the best and most robust information into a document that provided practitioners with the most reliable guidance possible. JNC 7 was released in 2003 and was soon widely adopted; it truly stood the test of time. After that, everything changed. Dr. Basile, what has been happening since?
DR. BASILE: Thanks, Dr. Izzo. I agree with you about your concerns with guidelines. This is a very difficult issue for the practicing clinician.
With regard to JNC 8, in 2008, the National Heart, Lung, and Blood Institute (NHLBI) decided to develop its own comprehensive “evidence-based” disease prevention portfolio that included a coordinated cholesterol guideline, obesity guideline, hypertension guideline, as well as a lifestyle/risk factor modification guideline. Following the recommendations put forth by the Institute of Medicine on guidelines, the NHLBI mandated that strict rules of evidence be used for its guideline development. After the JNC 8 committee established the clinical trial criteria for use in their hypertension guideline, the NHLBI hired a professional vendor to vet the literature. The process was essentially going nowhere so a second vendor for hypertension had to be hired. In the end, few clinical trials passed the criteria used to form the basis of JNC 8. And near its completion, after the JNC 8 group toiled for over 5 years putting their report together, they learned in 2013 that the NHLBI withdrew its support for the guideline and asked the American College of Cardiology/American Heart Association to establish a joint task force (to include the JNC 8 group) to assume responsibility for the guideline process. Declining this collaborative opportunity, the JNC 8 group decided on their own to have their work submitted and it was published without organizational support in JAMA.1
Meanwhile, the Centers for Disease Control published an overall systems approach for primary care clinicians in which they released the Kaiser Permanente algorithm for effective blood pressure (BP) control.2
Of note, there are several other competing guidelines: one which is issued annually by the Canadian Hypertension Education Program. This approach is now extremely well developed and comprehensive with multiple web-based programs and information sources (www.hypertension.ca/en/chep). In addition, there is the recent effort by the European Society of Hypertension/European Society of Cardiology in 2013,3 and a newer, less formal document from the International Society of Hypertension and supported by a working group comprised of members of the American Society of Hypertension.4 Finally, there are other national guidelines around the world, perhaps most prominent among these being the British Hypertension Society National Institute for Clinical Excellence or the NICE guidelines.
DR. IZZO: That’s a good summary, Dr. Basile. What constitutes a useful guideline? Who is the audience? I don’t believe that a good guideline should be hidebound by unduly restrictive ‘evidence rules’ that ignore all but a tiny fraction of the available scientific information. A good guideline must synthesize complex data in a clear and concise way and must address the kinds of questions that real doctors need answered every day. Dr. Gradman, do you have an opinion on guidelines?
DR. GRADMAN: Part of what is going on in the revised hypertension guidelines is a worldwide shift from the treatment of individual patients to the treatment of patient populations. Such guidance for treating large groups is of great interest to governments and insurance companies but is less useful for making treatment decisions for individual patients with individual problems.
In fact, the JNC 8 guidelines specifically say that they are aimed at primary care physicians, not specialists or people who have a lot of experience with the treatment of hypertension. I think JNC 8 is to be commended for trying to make the fundamental concepts of the guidelines completely evidence-based. The guidelines delineate general targets and thresholds for treatment and also suggest the best drugs to use for most patients. Unfortunately, the exercise showed that it is not really possible to answer a lot of specific treatment questions using a strict evidence-based approach. For these we must rely on less definitive evidence and expert opinion.
I think there are different audiences; a good general guideline today should be aimed at primary care physicians but I think specialists need their own guidelines. As a cardiologist, I would want a very different set of guidelines than is presented in JNC 8.
DR. IZZO: Dr. Moser, given your long association with the highly successful parent of the JNC process, the National High Blood Pressure Education Program, I think your perspective is invaluable. Do you think any of the current guidelines hit the mark or what do you think should have been done differently?
DR. MOSER: Well, that’s a broad question. JNC 8 doesn’t differ much from JNC 7 except for one or 2 items. JNC 8 set out to answer several questions with a strict evidence-based methodology, and when they were finished, after a long period of time and substantial expenditure of money, they only ended up addressing 3 questions. The first question was when to initiate treatment, the second was related to the target or goal BPs, and the third was how to achieve goal pressures. They did address the question of whether people with comorbidities, especially diabetes and kidney disease, needed to have lower goal BPs.
On the issue of targets for BP, it was decided that 140/90 mm Hg was good enough for most people and that there was no compelling evidence that BP should be lowered below 130/80 mm Hg in diabetics or people with kidney disease. But we all know that in practice, you can’t adjust BPs to exact numbers. JNC 8 also said that the threshold for a diagnosis and target BP in people over the age of 60 was 150/90 mm Hg. This is quite different from other guidelines.
The guidelines also point out a difference in black and white patients. We’ve known for years that calcium-channel blockers (CCBs) and thiazide-type diuretics are more effective in blacks and angiotensin-converting enzyme (ACE) inhibitors or beta blockers are more effective in whites, so I don’t think JNC 8 provided any new information on this. Otherwise, you’ll find very little difference between JNC 8 and 7. What they didn’t address were possible changes in the diagnostic evaluation or nonpharmacologic therapy and they failed to discuss issues related to the delivery of care and adherence, etc. Some physicians have said that the changes are important and different, but when you look at it very carefully they’re not substantive compared to other reports.
Dr. IZZO: Is that a result of their strict rules of evidence?
Dr. MOSER: The report was supposed to be all evidence-based. They hired an outside vendor that reviewed about 6100 English-language papers. The experts on that panel could have picked up the 40 papers that they finally rated as acceptable within a few days. It took the vendors several years. As everyone has mentioned, they used the data from evidence-based trials and reached conclusions, but they also had an “out” on all of them, including the 150 mm Hg BP target in the elderly, which was arbitrarily defined as age 60. As in their other recommendations, they then said that you could rely on “expert opinion,” meaning clinical judgment. This is the basis of the major recommendation: “If you treat below 140/90 mm Hg and everybody’s happy and there are no side effects, then just continue treatment.”
Regarding their approach to the treatment of resistant patients, the proposed algorithm is almost the same as it has been for many, many years. So I’m very disappointed in what they have accomplished, especially since it took such a long period of time and cost so much money.
DR. IZZO: I echo your disappointment, especially on very fundamental grounds. First, a guideline constrained by the suffocating rules applied by the JNC 8 group is enormously biased, especially when over 99% of the potentially relevant information was ignored because it did not come from a randomized trial. Did they not understand just how biased randomized clinical trials really are? A true expert does better than that, prioritizing the value and relevance of all evidence, from bench science to randomized trials. The real test for a guideline is then in the projection of that synthesis, that is translating expert interpretation into understandable and workable recommendations. One other issue: absence of evidence should not imply a negative recommendation. If there is no definitive study proving that a lower BP target is warranted for people with kidney disease, it should also be very clear that there is existing evidence that lowering BP to 130/80 mm Hg instead of 140/90 mm Hg may be a good idea. JNC 8 chose to ignore studies of achieved (not intention-to-treat) BP values that identified better renal outcomes in diabetics5 and fewer recurrent strokes6 in trial participants with the lowest BPs. While it is true that such benefits are not achieved by all trial participants, it should be recognized that “lower is better” is probably true in at least some people.
Are there any comments or concerns that the narrow definition of evidence can actually lead us astray?
The JNC 8 tried to be an evidence-based document in that they only looked at randomized controlled hypertension trials, which in itself is a limitation. These were very strict criteria that prevented the group from including certain evidence bases. But ultimately, more than half of the guideline recommendations ended up being expert opinion. And the reason they ended up addressing only the 3 questions presented is because there just isn’t the kind of clinical trial-based evidence required to answer questions on issues such as resistant hypertension, the value of combination therapy, and contrasting differences in BP measurement techniques to detect which is best. Accordingly, we end up with a somewhat narrow perspective. In fact, JNC 8 ended up with a lot of expert opinion and failed to be as evidence-based as they would’ve liked to have been. At the end of the day, JNC 8 just doesn’t provide the clinician with the answers to many of the controversial issues that we face each and every day.
DR. IZZO: I’m with you on that last point, Dr. Basile. Speaking of evidence, although we know that systolic BP rises linearly with age, where is the study justifying that after age 60, your BP threshold should be relaxed immediately? JNC 8 said there is “no evidence of a BP benefit here”; I say there is no evidence of common sense here.
DR. BASILE: The recent American Society of Hypertension/International Society of Hypertension (ASH/ISH) guideline suggests that “elderly” means 80 years of age and older. The JNC 8 panel decided that while some trials had higher thresholds for eligibility than the BP goals tested, in an effort to simplify the message they decided that the threshold for initiating antihypertensive treatment should be made the same as the BP treatment goal. So their answer to the second question, “What should be the goal for BP reduction in patients who are 60 years of age and older?” is that it should be less than 150/90 mm Hg, the same as the threshold for starting antihypertensive therapy.
DR. MOSER: Well, the evidence doesn’t actually support this. None of the BP cutoffs were ever truly “evidence-based,” but the new guidelines do not acknowledge this. Clearly, evidence from randomized trials of any therapeutic benefit from having a systolic BP under 150 mm Hg isn’t very good, but expert opinion, clinical judgment, and epidemiologic data suggest very strongly to me that we should have kept the threshold for diagnosis and treatment at 140/90 mm Hg at any age. If a systolic pressure under 140 mm Hg is achieved in the elderly and therapy is well-tolerated, then therapy should be continued as before.
DR. GRADMAN: The targets for patients with diabetes and renal disease have been changed and that must be discussed. The revised goal of <140/90 mm Hg for diabetics was based primarily on the results of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial which compared that goal to a goal of <120/80 mm Hg and found no net advantage of very aggressive treatment. The JNC 7 goal of <130/80 mm Hg was never evaluated. It is of interest that the newest Canadian guidelines retain the <130/80 mm Hg recommendation.7 The JNC 8 document ignored individual patient differences, which might influence treatment decisions. In patients at increased risk for stroke, such as Asian populations or patients who have a history of cerebrovascular events, lower targets may be a rational treatment decision. As ACCORD demonstrated once again, stroke risk is exquisitely BP sensitive and those in the 120/80 mm Hg target group had fewer strokes; this consideration may trump others in specific patients. The JNC 8 document was certainly not for experts or specialists in the treatment of hypertension. Guidelines are also needed to address the “hard-to-treat patient” who may be defined in a number of ways.
DR. MOSER: Well, let me just embellish that, Dr. Izzo, for a second. If you ask who is going to use this document as a metric, or who is going to hold clinicians to these recommendations, at the end of the day, it may be no one. This is because JNC 8 was, unfortunately, not endorsed by any major group; it is a standalone document. It was sent out to a number of hypertension specialists who had an opportunity to give comments, but it wasn’t posted for either the professional community or the public community to see if there were any concerns before it was published.
I don’t necessarily mean this as a harsh criticism because it seems the JNC group was forced to go it alone. But there’s a possibility that not all major organizations, including the government, may actually accept the recommendations, especially the one relating to age and target BPs.
DR. GRADMAN: I wouldn’t agree with that entirely. I think people will latch onto the JNC document, in particular to the idea that patients don’t need to be treated as intensively as was recommended in the past. So these guidelines will reduce the number of people who are seen to require treatment and will lower the intensity of treatment for those who are receiving therapy. Computerized medical records will soon be almost universal and it will be easily determined if the practitioner is in compliance with a cutoff of 140/90 mm Hg in general or less than 150 mm Hg if a patient is over 60. So I think it could have more effect than you seem to think, Dr. Moser. Many people will conclude that lower really isn’t better. The cost of treatment to insurance companies and managed care organizations will go down as a lower intensity of treatment becomes the standard of care.
DR. BASILE: I agree with you, Dr. Gradman. The ASH/ISH and European Society documents have also abandoned the <130/80 mm Hg threshold for diabetic and chronic kidney disease (CKD) patients, in favor of a goal of <140/90 mm Hg (European Society <140/85 mm Hg in diabetes [Table]), so there is additional weight behind the new metrics in addition to JNC 8.
DR. MOSER: In response to Dr. Gradman, when you increase the target for treatment to 150 mm Hg you eliminate an enormous number of people in the “difficult-to-treat” category. Another point, some of the new guidelines are not user-friendly as Dr. Izzo pointed out. They may not be helpful for the practicing doctor. The European guidelines, for example, are too long and have too many references. I believe that JNC 8 should have been 6 or 7 pages. Physicians do not care about an A-rating, B-rating, or C-rating; they want to know what experts believe.
DR. IZZO: The European guidelines are unnecessarily complex and have other flaws, such as conflating hypertension treatment with risk scores. Interpretation and perspective are the jobs of an expert panel and those traits, labeled for what they are, need to be integral to the framework of any good guideline. That’s what JNC 7 had in greater measure and that’s what people want.
DR. IZZO: Maybe we can slightly reframe this same discussion in light of another vexing problem that seems to continue to surface. Is there a J-curve? Are there different J-curves for different organs or diseases?
DR. MOSER: The issue of J-curves has never been covered effectively.
DR. BASILE: It’s not discussed in most of the guidelines because it’s a very controversial area. In principle, there is a J-curve because when you get to a BP of 0 mm Hg, you can’t sustain life. I don’t have a problem with the JNC group or other groups not really looking into this J-curve issue but it’s a terrible problem for the clinician, never knowing what level you might put the patient in danger as you continue to lower BP.
DR. GRADMAN: I agree with you, Dr. Basile. I think the possibility that the J-curve is real underlies the changes the new guidelines made in target BPs. Higher BP targets will promote less aggressive BP-lowering, so maybe the J-curve “risk” will be diminished somewhat. Different endpoints appear to have different J-curves. You may reduce strokes, for example, but increase myocardial infarctions, and the latter seems to be related more to low diastolic BP. This risk-benefit balance of intensive treatment really underlies a lot of the changes that we’ve seen in target BPs in many guidelines, not just JNC 8. Overall attention to this equation is positive but guidance to clinicians faced with patients with specific risk factors, co morbidities, circadian BP patterns, or other clinical characteristics is completely lacking.
DR. BASILE: I totally agree with you, Dr. Gradman. Increasing the systolic BP goals will also lead to some increases in diastolic BP and perhaps less concern about J-curves, if they really exist.
One important point that I’ve been making with clinical groups is that the “ideal” BP for most patients depends on whether that patient is most at risk for stroke, heart attack, or kidney disease. These differing target organs do not all prefer to see the same amount of BP reduction. For example, the brain seems to prefer a lower target and does better with more systolic BP reduction than does the heart. Yet our antihypertensive agents are not organ specific when we use them so we have to accept a “sweet spot” that is most beneficial to the patient and causes little harm. Accordingly, I think there is a “best” BP range for most patients; the European guidelines suggest that when you keep the systolic BP for most patients between 130 and 139 mm Hg, you’re really doing the best for the patient. I agree with this. I believe this should be our “sweet spot” for most patients with hypertension except for the oldest of the old, especially those with isolated systolic hypertension, where the spot appears to be 140–149 mm Hg.
DR. MOSER: We have discussed treatment targets and it appears that we disagree generally with the change from 140 to 150 mm Hg as a target in the elderly. We seem to have decided that the target BP of 140/90 mm Hg is reasonable, and perhaps the change in targets in treating the diabetic might also be reasonable, although if you could get to 130/80 mm Hg, that’s fine. I agree with Dr. Izzo, the lower the better.
I think now we probably ought to address how to get there. If you look at the JNC 8 protocol of both the treatment of lower and the high-risk patient, it’s almost exactly the same as in JNC 7. The proposed algorithm for treatment does not contribute much that is new to the clinician’s ability to treat this disease effectively. Perhaps that is because specific therapy has not changed much in the past 5–8 years. We may have learned more about how to use certain therapies, but the actual medications haven’t changed much: the specific medications recommended are almost exactly the same as in JNC 7, except for the addition of chlorthalidone and indapamide.
DR. IZZO: Well, there is one difference: thiazide-type diuretics, dihydropyridines, and ACE inhibitors (or ARBs) are now referred to as “preferred drugs,” as was first suggested in our New York State Medicaid hypertension guideline in 2011.9 We defined a preferred agent as one with appropriate efficacy and safety that is also proven to lower cardiovascular event rates. I’d be interested in the opinions of this group with regard to treatment issues and also to the specific issue of whether beta blockers were unduly excluded.
DR. BASILE: I salute JNC 8 in leveling the playing field when they suggest that it is the amount of BP reduction achieved that is more important than the initial drug, but when you look at the outcome evidence from clinical trials for stroke as well as cardiac and renal disease, you can feel very comfortable using a renin-angiotensin system (RAS)-blocking drug, either an ACE inhibitor or an angiotensin receptor blocker (ARB), or a thiazide-type diuretic or a CCB.
I’m somewhat concerned that they lumped all CCBs together because I do think there’s more evidence of benefit for the dihydropyridines or the “pines” in hypertension than the other subclasses (diltiazem and verapamil). But I like the fact that 4 major classes are now looked at as being equal for initial therapy, even in diabetics, unless they have CKD. Unless they have CKD, JNC 8 very appropriately recommends that it’s BP reduction rather than the RAS blockade that translates into improvement in outcomes. However, for the diabetic with CKD, we would recommend an ACE or an ARB as a first drug. As for the beta blockers, they do not have the level of evidence that the thiazides have had, as most trials used once-a-day atenolol as their beta blocker. We just don’t know how some of the newer beta blockers would have stacked up to the other antihypertensive agents on clinical outcomes for those with hypertension without concomitant issues.
DR. IZZO: Dr. Gradman, as a card-carrying cardiologist, wouldn’t you be thrown out of your business if you failed to advocate for beta blockers?
DR. GRADMAN: To some extent that’s true, but the guidelines that we’re talking about are a broad-brush approach. JNC 8, based its opinion regarding the first-line use of beta blockers on one study: the Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) trial,10 which found a lower relative risk of stroke with losartan compared to atenolol. For cardiologists, beta blockers remain an essential component of treatment in the majority of patients with coronary disease, angina pectoris, and heart failure, with or without hypertension, and in patients with arrhythmias, such as atrial fibrillation. In the case of post myocardial infarction, though, it is unclear if the benefit persists, especially after 2 years.
Another criticism I have of the guidelines is that they lump all drugs from each class together. That’s especially problematic for CCBs and for beta blockers. There’s still some discussion about the variable effects of different beta blockers on glucose tolerance, side effect profile, vascular tone, and other properties.
Age may matter too, in the decision to use beta blockers. In a Canadian meta-analysis, patients under the age of 60 taking beta blockers did just as well as those taking other drugs, but beta blockers were not as effective in older patients in terms of endpoint reduction.11
In uncomplicated hypertension, though, I do agree with the broad-brush recommendations for primary care physicians that the other 4 classes of drugs (thiazide-type diuretics, ACE inhibitors, ARBs and dihydropyridine CCBs) still have more evidence of outcome benefit as first line therapy.
Again, I think these guidelines are an oversimplification and are not sufficient to guide individualized therapy.
DR. IZZO: Let’s close with some general discussion of whether the concept of the difficult-to-treat patient is useful and who might fill this definition.
DR. MOSER: It’s not necessarily related to having a comorbidity. You can have a diabetic hypertensive person with hyperlipidemia who responds very well to antihypertensive therapy. We’ve defined some patients as resistant, which may not be true. They may be difficult to treat. For example, just adding a thiazide-type diuretic to other drugs or increasing the dose of a thiazide-type diuretic will often convert a so-called “resistant patient” into a responsive patient.
That’s why I have supported JNC 7 and other guidelines that recommend starting with 2 drugs, either as 2 pills or in a single-pill combination when BP exceeds 160/100 mm Hg. One of the 2 drugs probably should be an RAS inhibitor, but the other most certainly should be a thiazide-type diuretic or perhaps a CCB.12
There are a lot of people with few other risk factors who are very difficult to control. One of the fallouts of the JNC 8 recommendations is that we may undertreat individuals over the age of 60, but that also means there will be less “resistant hypertension.”
DR. IZZO: When considering resistant hypertension, Dr. Moser suggested combination therapy. Dr. Gradman, you have had an interest in this area.
DR. GRADMAN: This is an important issue that has not really been addressed adequately in the guidelines. We know that combination therapy is required in upwards of 75% of patients using older BP targets.13 We also know that if you start people on combination therapy, you achieve target BP more rapidly and in a greater proportion of patients.
As to initial combination therapy versus the step-care type approach, either alternative is mentioned in JNC 8, but I don’t think any of the new guidelines have addressed the issue fully and no outcome studies have compared initial combination therapy versus initial monotherapy.
But the bottom line is that combination therapy is needed in the vast majority of patients although the percentage will be decreased if the newer, less aggressive BP targets are adopted. In my opinion, it should be started in almost everyone likely to eventually need more than 1 drug to achieve target BP. First-dose adverse effects, particularly hypotension, are very uncommon with 2- or 3-drug single-pill combinations that contain thiazide-type diuretics, ARBs, or CCBs. I would probably not use combinations as initial therapy in very elderly or frail patients.
DR. IZZO: I rarely use monotherapy anymore. Let me return to something that I touched on before: race as a decision point.
DR. BASILE: Well, I can understand why you’re against it, Dr. Izzo, because of the heterogeneity of how we define race. The white/black definition is certainly a simplistic approach given the way our genetics are so often mixed in today’s populations.
Both JNC 8 and the ASH/ISH document should, at least, be commended for pointing out to the clinician that if you’re looking for BP reduction, the CCB or the thiazide-type diuretic will give you more BP reduction in blacks in general than that achieved with an RAS blocker.
There are many African-American patients who are not prescribed a thiazide or a CCB as part of their cocktail. The big mistake is that these patients are considered resistant or refractory, depending on how many drugs they’re on. So I would at least point out, in line with JNC 8 and the ASH/ISH recommendations, that in the black patient, regardless of age, a CCB or a thiazide should be prescribed for BP reduction.
DR. IZZO: I think that’s a valid point. And just to summarize, the data show clearly that in an African-American population, you get about the same degree of BP reduction by using either a thiazide-type diuretic or CCB, and you do tend to have a more limited response to RAS blockers. The reverse could be stated for whites. But then again, if you use a thiazide-type diuretic and an RAS blocker together, the race issue is moot.
DR. MOSER: For years we have been studying black patients around the world, and there’s no question that there is a different response. I also want to return to something mentioned earlier: we are losing sight of the value of so-called “experts.” Simple guidelines work for the vast majority of patients. The complicated patient should probably be referred to an expert.
DR IZZO: Are there other issues when it comes to managing the hard-to-treat patient?
DR. GRADMAN: There are many reasons why a patient may be difficult to treat. Some may truly not respond to drugs but others have hypertension in the office and not at home. They may be difficult to treat because they don’t take their medications for various reasons. The other thing, of course, is to ask whether patients are taking any interfering substances like nonsteroidal antiinflammatory drugs. Most often, if you have people who are truly poorly responsive to antihypertensive therapy, it is worth reviewing whether adequate doses of preferred agents (RAS blockers, thiazide-type diuretics, and CCBs) have been used.
Most people these days also use aldosterone antagonists as the fourth drug, recognizing the danger of hyperkalemia particularly in patients receiving renin-angiotensin aldosterone system inhibitors. If patients have renal insufficiency, using a sufficient dose of thiazide-type diuretics is extremely important, and for patients with advanced renal disease, a loop diuretic is required. There may also be some intraclass differences among drugs, as between losartan and azilsartan.
DR. BASILE: I’m now running a resistant hypertension clinic, seeing only difficult-to-treat patients. As we saw in the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), there is no question that the difficult-to-treat patient may be a little more likely to be black with left ventricular hypertrophy, CKD, obese, and elderly.
But the reality is there are patients in our practices that are called resistant that really only have white-coat hypertension and may have markedly reduced BPs when they’re out of the office. These are the same patients that complain of being periodically light headed or lethargic when their pressures are low outside of the office and often have minimal target organ disease with benign eyegrounds, no left ventricular hypertrophy on electrocardiogram, and minimal if any protein in the urine.
Another major issue is the use of inadequate doses of agents such as amlodipine when started at 2.5 mg daily and never up-titrating to the standard doses of 5 or 10 mg daily because of the concern of edema. I also find that replacing hydrochlorothiazide 25 mg with chlorthalidone at the same dose can improve BP control. And we have already mentioned the important role of spironolactone.
DR. MOSER: Let me emphasize that about half of the patients referred to as “resistant” respond when you increase the thiazide-type diuretic; this also seems to be true for the addition of spironolactone to hydrochlorothiazide. Combinations have a clear advantage in terms of a meaningful response.
DR. IZZO: It still begs the question to me of whether or not we’ve given enough guidance to well-meaning practitioners in this tougher-to-treat group of patients.
DR. GRADMAN: Let me point out the paper on resistant hypertension from the American Heart Association14 as a useful comprehensive reference, but perhaps we need a relatively simple document that could be used by practicing physicians who regularly treat these patients.
DR. BASILE: I would agree with Dr. Gradman that we need to continue to provide more information on the resistant patient.
DR. IZZO: Dr. Moser, you have the last word.
DR. MOSER: If you look at the general approach in JNC 8 and the algorithm in JNC 7, you’ll find a perfectly good and reasonable approach to the management of hypertension, including for the so-called resistant or difficult-to-treat patient. It seems physicians have been afraid to lower BP, especially in the elderly. This may be one of the reasons why JNC 8 recommends a target of 150 mm Hg and not to go below that. There’s an unfounded fear of the J-curve, of causing fainting or falling in patients, especially the elderly, that does not appear to be too much of a problem if BP is reduced gradually.15
It’s unlikely that we will cause much harm and may actually reduce cardiovascular events more in the elderly if we lower the goals to what we had before. But the JNC 8 algorithm is out there and probably will be followed by many physicians.
DR. IZZO: Thank you all very much for your valuable insights. The acid test, however, is what practitioners think and what they will do. We have recent insight into this area (Table). As is readily apparent, the opinion piece we call JNC 8 does not fully resonate with the majority of primary care providers or cardiologists. What will fill the need remains to be determined.
Disclosures: Joseph Izzo has been a consultant for Novartis and Bristol-Myers Squibb, has received a research grant from Forest Laboratories, and has received speakers’ honoraria from the American Society of Hypertension. Alan Gradman is a consultant for Daiichi-Sankyo, Novartis, Forest Laboratories, and Takeda. He is a member of the Speakers Bureau for Daiichi-Sankyo, Novartis, Forest Laboratories, Takeda, and Arbor. Over the past year, he has also received honoraria for lectures sponsored by The American Society of Hypertension and The American College of Cardiology. Jan Basile is a consultant for Daiichi-Sankyo, Forest, Arbor, Eli-Lilly, and Medtronic. He has received grant/research support from NHLBI (SPRINT). He is a member of the speakers’ bureau at Daiichi-Sankyo, Forest, and Arbor.
Addendum: The concerns raised during this discussion have been echoed by clinicians in the field. Cardiologists have indicated that they are waiting for yet another hypertension guideline proposed by the American Heart Association/American Society of Cardiology for 2014–2015 (Figure). 16 Clearly the fractionation continues.
FoxP2 Media LLC is the publisher of The Medical Roundtable.
FoxP2 Media LLC

Overscheduled children
Parents want to raise their children to be happy and successful in childhood and through adulthood. For many parents, this means giving their children as many opportunities to learn, practice, and master a wide variety of skills outside of school as they possibly can. These activities often include the study of a musical instrument, a sport, an activity in the arts, religious study, and even extra academic work such as math, computer science, or a second language. Each one of these activities can mean many classes or practices outside of the home each week and additional practice time at home.

When you combine these activities with school and homework, children can be busier than most professional adults. And their parents can feel like managing their child’s schedule is another full-time job. By asking parents how many afternoons and evenings are scheduled (or how many hours of down time their children have) each week, you begin a conversation that may help parents determine the right balance for each child and the family.
Without a doubt, there can be tremendous value in making time for extracurricular activities for children. School alone usually does not offer much exposure to music education and the arts, and a daily gym class is sadly a thing of the past for most children. There is a growing body of evidence that daily vigorous exercise in childhood not only promotes good physical health and restorative sleep, and fights obesity, but that it also promotes strong cognitive development and can prevent anxiety and mood symptoms. Sustained experience with a team sport cultivates discipline, frustration tolerance, and resilience alongside friendships and fun. Likewise, there is a growing body of evidence that learning to play a musical instrument contributes in broader ways to healthy cognitive development, cultivates discipline and frustration tolerance, and improves executive function and the attention and self-regulation skills that all school-age children need to develop. Exposure to the arts, to trade skills, or to rare languages may help children discover a unique interest or passion that will draw them through their adolescence. Discovering an area of passionate interest is one of the essential goals of childhood; it can help teens feel good about themselves, and is especially meaningful in children who may not be gaining a lot of self-esteem in other areas, such as schoolwork.

But the well-meant intentions of parents (or interests of children) sometimes can lead to so many extracurricular activities that children barely have time for homework, play, or relaxation. From kindergarten through middle school, children are at the perfect age to be exploring multiple activities as they learn about their own abilities, strengths, and interests. But it is a developmental period in which there also should be plenty of open, free creative play, often with a social component. This is where children not only learn about their own talents, but also try things they might fail at, developing their curiosity, social skills, self-awareness, and resilience. While it can be wonderful to have a weekly music lesson and a team sport at this age, it is critical that there also be protected free play or down time. During this developmental period, children may switch sports, instruments, or hobbies, and it is healthy that they have the time and space to do so. Parents will say that every hour of activity is "fun." But fun with a purpose is different from "senseless fun," which is just fun without an achievement goal. Adults may have "fun" working out, but also have senseless fun playing golf, having a drink with friends, or going to a movie.
Adolescents are more likely to be "pruning" their interests as they figure out where their passions lie. Teenagers may do fewer activities overall, but spend more time on each of them. Of course, many teens will be experiencing great pressure (internal, external or both) to build the strongest possible college applications with the "right" mix of extracurricular activities, which may not line up with their actual interests. They will face the pressure also to be performing at a very high level academically. Some may have jobs, as they seek to build independence. Then add to this the fact that many will be driving themselves to each activity and wanting to spend time with friends and romantic interests, and you have a recipe for adolescents whose every moment is accounted for, to the point that they may skimp on sleep and mealtimes and feel overwhelmed. In choosing how to manage their schedules, adolescents also should be learning about the value of self-care, protecting time to relax, exercise, and sleep adequately (with a good measure of senseless fun texting as they build their identity).
So how do you help your patients and their parents reestablish some balance? You can start by figuring out if they are overscheduled. Ask if their school-age children have as many free afternoons as scheduled ones? Do they have recurring play dates as well as Russian and math classes? Do they have time for senseless fun with friends, siblings, and parents? Ask teenagers how much sleep they are getting? How often is the family able to have dinner together? When is the last time they had time to read a book for pleasure or to explore a new interest? Some children and teenagers may be very busy, but will report feeling like their battery is charged by all of their activities. Although they are busy, their schedule may be a good balance for them. But when children or teens report feeling drained by the end (or middle) of their week, they are likely overscheduled.
If parents resist some easing, you should begin to wonder if the child is the one who chose the activity or it represents a parent’s interests instead? Some parents may have strong feelings about what activities made a difference in their lives, and may not be paying attention to how their child’s temperament is different from their own. Sometimes, parents who are working might feel guilty that they are not as available as they’d like to be. They may sign their child up for many activities, hoping to make up for what they worry they are failing to directly provide their child. Parents may need a gentle reminder that a happy, calm dinner with mom and dad often is more developmentally productive than a rushed drive between two practices and a violin lesson.
Find out if specific activities are born of interest or obligation. Demanding obligatory activities should have important meaning for the child, such as Hebrew lessons prior to a Bar Mitzvah. There should be only one demanding activity that is not fun for a child at a time, though. The balance may come from fun or less-structured activities. Asking a child in front of the parents what activities are (or would be) the most fun or interesting for them can help the family to think through how to prune activities when a child is overscheduled, and remind parents of the value of play.
It also can be helpful to consider a child’s temperament when talking with a family about finding greater balance. If a child is very shy, there can be greater developmental value in activities that promote social skills, even though that child might not naturally seek those activities out. Teens who are struggling to fulfill basic responsibilities may need to have their schedules streamlined, but it is important to preserve an activity that may aid in cultivating their discipline and organization (such as a sports team or a job they value). Highly driven, ambitious adolescents sleeping only 4 hours a night to fulfill their many responsibilities would benefit from making time for relaxation and sleep, and hearing this from a pediatrician may be the critical factor in making it happen.
Finally, ask parents how drained they feel by facilitating their child’s (or children’s) schedule. When parents are so busy with their children’s activities that family time is nonexistent, or one child is receiving a greatly disproportionate share of the parents’ time, it is worth examining. Reminding parents that time spent together around the dinner table and helping with homework or in a shared activity – time that may leave them feeling more charged than drained as parents – is critical for the well-being of the whole family.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at [email protected].
Parents want to raise their children to be happy and successful in childhood and through adulthood. For many parents, this means giving their children as many opportunities to learn, practice, and master a wide variety of skills outside of school as they possibly can. These activities often include the study of a musical instrument, a sport, an activity in the arts, religious study, and even extra academic work such as math, computer science, or a second language. Each one of these activities can mean many classes or practices outside of the home each week and additional practice time at home.
When you combine these activities with school and homework, children can be busier than most professional adults. And their parents can feel like managing their child’s schedule is another full-time job. By asking parents how many afternoons and evenings are scheduled (or how many hours of down time their children have) each week, you begin a conversation that may help parents determine the right balance for each child and the family.
Without a doubt, there can be tremendous value in making time for extracurricular activities for children. School alone usually does not offer much exposure to music education and the arts, and a daily gym class is sadly a thing of the past for most children. There is a growing body of evidence that daily vigorous exercise in childhood not only promotes good physical health and restorative sleep, and fights obesity, but that it also promotes strong cognitive development and can prevent anxiety and mood symptoms. Sustained experience with a team sport cultivates discipline, frustration tolerance, and resilience alongside friendships and fun. Likewise, there is a growing body of evidence that learning to play a musical instrument contributes in broader ways to healthy cognitive development, cultivates discipline and frustration tolerance, and improves executive function and the attention and self-regulation skills that all school-age children need to develop. Exposure to the arts, to trade skills, or to rare languages may help children discover a unique interest or passion that will draw them through their adolescence. Discovering an area of passionate interest is one of the essential goals of childhood; it can help teens feel good about themselves, and is especially meaningful in children who may not be gaining a lot of self-esteem in other areas, such as schoolwork.
But the well-meant intentions of parents (or interests of children) sometimes can lead to so many extracurricular activities that children barely have time for homework, play, or relaxation. From kindergarten through middle school, children are at the perfect age to be exploring multiple activities as they learn about their own abilities, strengths, and interests. But it is a developmental period in which there also should be plenty of open, free creative play, often with a social component. This is where children not only learn about their own talents, but also try things they might fail at, developing their curiosity, social skills, self-awareness, and resilience. While it can be wonderful to have a weekly music lesson and a team sport at this age, it is critical that there also be protected free play or down time. During this developmental period, children may switch sports, instruments, or hobbies, and it is healthy that they have the time and space to do so. Parents will say that every hour of activity is "fun." But fun with a purpose is different from "senseless fun," which is just fun without an achievement goal. Adults may have "fun" working out, but also have senseless fun playing golf, having a drink with friends, or going to a movie.
Adolescents are more likely to be "pruning" their interests as they figure out where their passions lie. Teenagers may do fewer activities overall, but spend more time on each of them. Of course, many teens will be experiencing great pressure (internal, external or both) to build the strongest possible college applications with the "right" mix of extracurricular activities, which may not line up with their actual interests. They will face the pressure also to be performing at a very high level academically. Some may have jobs, as they seek to build independence. Then add to this the fact that many will be driving themselves to each activity and wanting to spend time with friends and romantic interests, and you have a recipe for adolescents whose every moment is accounted for, to the point that they may skimp on sleep and mealtimes and feel overwhelmed. In choosing how to manage their schedules, adolescents also should be learning about the value of self-care, protecting time to relax, exercise, and sleep adequately (with a good measure of senseless fun texting as they build their identity).
So how do you help your patients and their parents reestablish some balance? You can start by figuring out if they are overscheduled. Ask if their school-age children have as many free afternoons as scheduled ones? Do they have recurring play dates as well as Russian and math classes? Do they have time for senseless fun with friends, siblings, and parents? Ask teenagers how much sleep they are getting? How often is the family able to have dinner together? When is the last time they had time to read a book for pleasure or to explore a new interest? Some children and teenagers may be very busy, but will report feeling like their battery is charged by all of their activities. Although they are busy, their schedule may be a good balance for them. But when children or teens report feeling drained by the end (or middle) of their week, they are likely overscheduled.
If parents resist some easing, you should begin to wonder if the child is the one who chose the activity or it represents a parent’s interests instead? Some parents may have strong feelings about what activities made a difference in their lives, and may not be paying attention to how their child’s temperament is different from their own. Sometimes, parents who are working might feel guilty that they are not as available as they’d like to be. They may sign their child up for many activities, hoping to make up for what they worry they are failing to directly provide their child. Parents may need a gentle reminder that a happy, calm dinner with mom and dad often is more developmentally productive than a rushed drive between two practices and a violin lesson.
Find out if specific activities are born of interest or obligation. Demanding obligatory activities should have important meaning for the child, such as Hebrew lessons prior to a Bar Mitzvah. There should be only one demanding activity that is not fun for a child at a time, though. The balance may come from fun or less-structured activities. Asking a child in front of the parents what activities are (or would be) the most fun or interesting for them can help the family to think through how to prune activities when a child is overscheduled, and remind parents of the value of play.
It also can be helpful to consider a child’s temperament when talking with a family about finding greater balance. If a child is very shy, there can be greater developmental value in activities that promote social skills, even though that child might not naturally seek those activities out. Teens who are struggling to fulfill basic responsibilities may need to have their schedules streamlined, but it is important to preserve an activity that may aid in cultivating their discipline and organization (such as a sports team or a job they value). Highly driven, ambitious adolescents sleeping only 4 hours a night to fulfill their many responsibilities would benefit from making time for relaxation and sleep, and hearing this from a pediatrician may be the critical factor in making it happen.
Finally, ask parents how drained they feel by facilitating their child’s (or children’s) schedule. When parents are so busy with their children’s activities that family time is nonexistent, or one child is receiving a greatly disproportionate share of the parents’ time, it is worth examining. Reminding parents that time spent together around the dinner table and helping with homework or in a shared activity – time that may leave them feeling more charged than drained as parents – is critical for the well-being of the whole family.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at [email protected].
Parents want to raise their children to be happy and successful in childhood and through adulthood. For many parents, this means giving their children as many opportunities to learn, practice, and master a wide variety of skills outside of school as they possibly can. These activities often include the study of a musical instrument, a sport, an activity in the arts, religious study, and even extra academic work such as math, computer science, or a second language. Each one of these activities can mean many classes or practices outside of the home each week and additional practice time at home.
When you combine these activities with school and homework, children can be busier than most professional adults. And their parents can feel like managing their child’s schedule is another full-time job. By asking parents how many afternoons and evenings are scheduled (or how many hours of down time their children have) each week, you begin a conversation that may help parents determine the right balance for each child and the family.
Without a doubt, there can be tremendous value in making time for extracurricular activities for children. School alone usually does not offer much exposure to music education and the arts, and a daily gym class is sadly a thing of the past for most children. There is a growing body of evidence that daily vigorous exercise in childhood not only promotes good physical health and restorative sleep, and fights obesity, but that it also promotes strong cognitive development and can prevent anxiety and mood symptoms. Sustained experience with a team sport cultivates discipline, frustration tolerance, and resilience alongside friendships and fun. Likewise, there is a growing body of evidence that learning to play a musical instrument contributes in broader ways to healthy cognitive development, cultivates discipline and frustration tolerance, and improves executive function and the attention and self-regulation skills that all school-age children need to develop. Exposure to the arts, to trade skills, or to rare languages may help children discover a unique interest or passion that will draw them through their adolescence. Discovering an area of passionate interest is one of the essential goals of childhood; it can help teens feel good about themselves, and is especially meaningful in children who may not be gaining a lot of self-esteem in other areas, such as schoolwork.
But the well-meant intentions of parents (or interests of children) sometimes can lead to so many extracurricular activities that children barely have time for homework, play, or relaxation. From kindergarten through middle school, children are at the perfect age to be exploring multiple activities as they learn about their own abilities, strengths, and interests. But it is a developmental period in which there also should be plenty of open, free creative play, often with a social component. This is where children not only learn about their own talents, but also try things they might fail at, developing their curiosity, social skills, self-awareness, and resilience. While it can be wonderful to have a weekly music lesson and a team sport at this age, it is critical that there also be protected free play or down time. During this developmental period, children may switch sports, instruments, or hobbies, and it is healthy that they have the time and space to do so. Parents will say that every hour of activity is "fun." But fun with a purpose is different from "senseless fun," which is just fun without an achievement goal. Adults may have "fun" working out, but also have senseless fun playing golf, having a drink with friends, or going to a movie.
Adolescents are more likely to be "pruning" their interests as they figure out where their passions lie. Teenagers may do fewer activities overall, but spend more time on each of them. Of course, many teens will be experiencing great pressure (internal, external or both) to build the strongest possible college applications with the "right" mix of extracurricular activities, which may not line up with their actual interests. They will face the pressure also to be performing at a very high level academically. Some may have jobs, as they seek to build independence. Then add to this the fact that many will be driving themselves to each activity and wanting to spend time with friends and romantic interests, and you have a recipe for adolescents whose every moment is accounted for, to the point that they may skimp on sleep and mealtimes and feel overwhelmed. In choosing how to manage their schedules, adolescents also should be learning about the value of self-care, protecting time to relax, exercise, and sleep adequately (with a good measure of senseless fun texting as they build their identity).
So how do you help your patients and their parents reestablish some balance? You can start by figuring out if they are overscheduled. Ask if their school-age children have as many free afternoons as scheduled ones? Do they have recurring play dates as well as Russian and math classes? Do they have time for senseless fun with friends, siblings, and parents? Ask teenagers how much sleep they are getting? How often is the family able to have dinner together? When is the last time they had time to read a book for pleasure or to explore a new interest? Some children and teenagers may be very busy, but will report feeling like their battery is charged by all of their activities. Although they are busy, their schedule may be a good balance for them. But when children or teens report feeling drained by the end (or middle) of their week, they are likely overscheduled.
If parents resist some easing, you should begin to wonder if the child is the one who chose the activity or it represents a parent’s interests instead? Some parents may have strong feelings about what activities made a difference in their lives, and may not be paying attention to how their child’s temperament is different from their own. Sometimes, parents who are working might feel guilty that they are not as available as they’d like to be. They may sign their child up for many activities, hoping to make up for what they worry they are failing to directly provide their child. Parents may need a gentle reminder that a happy, calm dinner with mom and dad often is more developmentally productive than a rushed drive between two practices and a violin lesson.
Find out if specific activities are born of interest or obligation. Demanding obligatory activities should have important meaning for the child, such as Hebrew lessons prior to a Bar Mitzvah. There should be only one demanding activity that is not fun for a child at a time, though. The balance may come from fun or less-structured activities. Asking a child in front of the parents what activities are (or would be) the most fun or interesting for them can help the family to think through how to prune activities when a child is overscheduled, and remind parents of the value of play.
It also can be helpful to consider a child’s temperament when talking with a family about finding greater balance. If a child is very shy, there can be greater developmental value in activities that promote social skills, even though that child might not naturally seek those activities out. Teens who are struggling to fulfill basic responsibilities may need to have their schedules streamlined, but it is important to preserve an activity that may aid in cultivating their discipline and organization (such as a sports team or a job they value). Highly driven, ambitious adolescents sleeping only 4 hours a night to fulfill their many responsibilities would benefit from making time for relaxation and sleep, and hearing this from a pediatrician may be the critical factor in making it happen.
Finally, ask parents how drained they feel by facilitating their child’s (or children’s) schedule. When parents are so busy with their children’s activities that family time is nonexistent, or one child is receiving a greatly disproportionate share of the parents’ time, it is worth examining. Reminding parents that time spent together around the dinner table and helping with homework or in a shared activity – time that may leave them feeling more charged than drained as parents – is critical for the well-being of the whole family.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at [email protected].

Thoughts on the suicides of highly public figures
Suicides raise a lot of feelings in the survivors. By survivors, I mean family members, friends, coworkers, and health care providers. In the event of a public figure, such as Robin Williams, this also includes the general public.
Typically there is grief, loss, and guilt. "Why did I not know he or she was feeling so bad? Why did I not do more to prevent it?"

There is also anger, maybe or not expressed, from the family members: "How could he do this to me and/or the kids?"
From coworkers the same question, plus: "Will this reflect badly on our interactions?"
For health care workers, especially those who have taken care of the deceased: "Are my notes good enough? Will I be sued for inadequate care?"
Of course, there is always the question of "copycat" suicides, which especially trouble those in the school and correctional systems and the military.
And then we get the public reactions to the suicide of a public figure, such as Robin Williams.
So far the reactions in the media have all been laudatory about his work. Some have pointed to the need for better education about depression and addiction.
But many, including me, worry about the copycat effect. The burst of publicity and the connections to public figures who have taken their lives are concerning.
So I have my own anger about how this may contribute to other suicides, especially in younger impressionistic people.
What is the answer? No easy solutions here – other than talking about it.
Dr. Ritchie is former chief of psychiatry for the U.S. Army and current chief clinical officer in the behavioral health department for the District of Columbia.
Suicides raise a lot of feelings in the survivors. By survivors, I mean family members, friends, coworkers, and health care providers. In the event of a public figure, such as Robin Williams, this also includes the general public.
Typically there is grief, loss, and guilt. "Why did I not know he or she was feeling so bad? Why did I not do more to prevent it?"
There is also anger, maybe or not expressed, from the family members: "How could he do this to me and/or the kids?"
From coworkers the same question, plus: "Will this reflect badly on our interactions?"
For health care workers, especially those who have taken care of the deceased: "Are my notes good enough? Will I be sued for inadequate care?"
Of course, there is always the question of "copycat" suicides, which especially trouble those in the school and correctional systems and the military.
And then we get the public reactions to the suicide of a public figure, such as Robin Williams.
So far the reactions in the media have all been laudatory about his work. Some have pointed to the need for better education about depression and addiction.
But many, including me, worry about the copycat effect. The burst of publicity and the connections to public figures who have taken their lives are concerning.
So I have my own anger about how this may contribute to other suicides, especially in younger impressionistic people.
What is the answer? No easy solutions here – other than talking about it.
Dr. Ritchie is former chief of psychiatry for the U.S. Army and current chief clinical officer in the behavioral health department for the District of Columbia.
Suicides raise a lot of feelings in the survivors. By survivors, I mean family members, friends, coworkers, and health care providers. In the event of a public figure, such as Robin Williams, this also includes the general public.
Typically there is grief, loss, and guilt. "Why did I not know he or she was feeling so bad? Why did I not do more to prevent it?"
There is also anger, maybe or not expressed, from the family members: "How could he do this to me and/or the kids?"
From coworkers the same question, plus: "Will this reflect badly on our interactions?"
For health care workers, especially those who have taken care of the deceased: "Are my notes good enough? Will I be sued for inadequate care?"
Of course, there is always the question of "copycat" suicides, which especially trouble those in the school and correctional systems and the military.
And then we get the public reactions to the suicide of a public figure, such as Robin Williams.
So far the reactions in the media have all been laudatory about his work. Some have pointed to the need for better education about depression and addiction.
But many, including me, worry about the copycat effect. The burst of publicity and the connections to public figures who have taken their lives are concerning.
So I have my own anger about how this may contribute to other suicides, especially in younger impressionistic people.
What is the answer? No easy solutions here – other than talking about it.
Dr. Ritchie is former chief of psychiatry for the U.S. Army and current chief clinical officer in the behavioral health department for the District of Columbia.

Reflections on being a patient
Recently, I had an unexpected hospitalization for what ultimately proved to be ovarian torsion. I spent 4 nights in the hospital, 2 preoperatively and 2 postoperatively. While I was pleased with the care I received, I also learned a few things that will influence my future hospital-based practice. Herewith, in no particular order, are my observations:

• Emergency department wait times matter. Much has been written about inappropriate utilization of the ED and throughput. I realize that not everyone in the waiting room has a truly emergent problem, but the 75 minutes between my arrival and the time I was triaged were the longest 75 minutes of my life. I was in so much pain that I couldn’t even advocate for myself.
• When faced with equivocal diagnostic testing, return to the history and physical as Sir William Osler instructed.("Listen to your patient, he is telling you the diagnosis.") I am so fortunate to live in the 21st century and to have immediate access to diagnostic imaging, labs, and a good surgeon. It is not lost on me, however, that had CT and ultrasound not been available (and nondiagnostic), my exam and white blood cell count would have taken me to the operating room without delay, shortening both my hospital stay and my recovery time. Still, I recognize that the retrospectoscope has 100% accuracy, far exceeding that of we human physicians.
• Opioids are not the enemy. After receiving multiple doses of intravenous opioids in the ED, I asked for ketorolac. During the 2 days between onset of pain and surgery, I relied upon the ketorolac for most of my pain relief. This is in part because I felt it worked better than the opioids (but did not eliminate the need for opioids) but also in an effort to be a "good patient." When I thought I might be going home, I stopped asking for the ketorolac. In short order, the pain worsened, my vital signs worsened, and I was off to the OR for removal of what proved to be a hemorrhagic, necrotic ovary.
• Small things matter, communication. Our system has spent considerable energy improving communication between staff and patients, utilizing communication boards. The professionals caring for me performed wonderfully in this respect – without fail, I knew their names and their extensions. I never knew, though, when my doctor would be rounding.
Because of on-call responsibilities and emergencies, the times ranged between 6 a.m. and 2 p.m. I completely understand why this happens, as it has occurred in my own practice. I will remember to keep my patients informed about my own schedule as much as I can going forward.

• Small things matter, miscellaneous. Medical tape leaves adhesive residue that takes days to remove – nail polish remover is more effective than alcohol for adhesive removal. ...An improperly secured Foley catheter can wreak havoc. ... There is literally nothing on TV worth watching for days at a time, despite having 46 channels. ... Clear liquids have more sugar than should be allowed, even for those of us who are not diabetic.
Being sick is very tedious.
As a medical student (more years ago than I care to count), I participated in various activities intended to raise awareness and sensitivity to the patient experience. After my recent refresher course, I hope to be a better doctor to my patients.
Dr. Fredholm and her colleague Dr. Stephen Bekanich are codirectors of Seton Palliative Care, part of the University of Texas Southwest Residency Programs in Austin. They alternate contributions to the monthly Palliatively Speaking blog (http://tinyurl.com/Palliatively).
Recently, I had an unexpected hospitalization for what ultimately proved to be ovarian torsion. I spent 4 nights in the hospital, 2 preoperatively and 2 postoperatively. While I was pleased with the care I received, I also learned a few things that will influence my future hospital-based practice. Herewith, in no particular order, are my observations:
• Emergency department wait times matter. Much has been written about inappropriate utilization of the ED and throughput. I realize that not everyone in the waiting room has a truly emergent problem, but the 75 minutes between my arrival and the time I was triaged were the longest 75 minutes of my life. I was in so much pain that I couldn’t even advocate for myself.
• When faced with equivocal diagnostic testing, return to the history and physical as Sir William Osler instructed.("Listen to your patient, he is telling you the diagnosis.") I am so fortunate to live in the 21st century and to have immediate access to diagnostic imaging, labs, and a good surgeon. It is not lost on me, however, that had CT and ultrasound not been available (and nondiagnostic), my exam and white blood cell count would have taken me to the operating room without delay, shortening both my hospital stay and my recovery time. Still, I recognize that the retrospectoscope has 100% accuracy, far exceeding that of we human physicians.
• Opioids are not the enemy. After receiving multiple doses of intravenous opioids in the ED, I asked for ketorolac. During the 2 days between onset of pain and surgery, I relied upon the ketorolac for most of my pain relief. This is in part because I felt it worked better than the opioids (but did not eliminate the need for opioids) but also in an effort to be a "good patient." When I thought I might be going home, I stopped asking for the ketorolac. In short order, the pain worsened, my vital signs worsened, and I was off to the OR for removal of what proved to be a hemorrhagic, necrotic ovary.
• Small things matter, communication. Our system has spent considerable energy improving communication between staff and patients, utilizing communication boards. The professionals caring for me performed wonderfully in this respect – without fail, I knew their names and their extensions. I never knew, though, when my doctor would be rounding.
Because of on-call responsibilities and emergencies, the times ranged between 6 a.m. and 2 p.m. I completely understand why this happens, as it has occurred in my own practice. I will remember to keep my patients informed about my own schedule as much as I can going forward.
• Small things matter, miscellaneous. Medical tape leaves adhesive residue that takes days to remove – nail polish remover is more effective than alcohol for adhesive removal. ...An improperly secured Foley catheter can wreak havoc. ... There is literally nothing on TV worth watching for days at a time, despite having 46 channels. ... Clear liquids have more sugar than should be allowed, even for those of us who are not diabetic.
Being sick is very tedious.
As a medical student (more years ago than I care to count), I participated in various activities intended to raise awareness and sensitivity to the patient experience. After my recent refresher course, I hope to be a better doctor to my patients.
Dr. Fredholm and her colleague Dr. Stephen Bekanich are codirectors of Seton Palliative Care, part of the University of Texas Southwest Residency Programs in Austin. They alternate contributions to the monthly Palliatively Speaking blog (http://tinyurl.com/Palliatively).
Recently, I had an unexpected hospitalization for what ultimately proved to be ovarian torsion. I spent 4 nights in the hospital, 2 preoperatively and 2 postoperatively. While I was pleased with the care I received, I also learned a few things that will influence my future hospital-based practice. Herewith, in no particular order, are my observations:
• Emergency department wait times matter. Much has been written about inappropriate utilization of the ED and throughput. I realize that not everyone in the waiting room has a truly emergent problem, but the 75 minutes between my arrival and the time I was triaged were the longest 75 minutes of my life. I was in so much pain that I couldn’t even advocate for myself.
• When faced with equivocal diagnostic testing, return to the history and physical as Sir William Osler instructed.("Listen to your patient, he is telling you the diagnosis.") I am so fortunate to live in the 21st century and to have immediate access to diagnostic imaging, labs, and a good surgeon. It is not lost on me, however, that had CT and ultrasound not been available (and nondiagnostic), my exam and white blood cell count would have taken me to the operating room without delay, shortening both my hospital stay and my recovery time. Still, I recognize that the retrospectoscope has 100% accuracy, far exceeding that of we human physicians.
• Opioids are not the enemy. After receiving multiple doses of intravenous opioids in the ED, I asked for ketorolac. During the 2 days between onset of pain and surgery, I relied upon the ketorolac for most of my pain relief. This is in part because I felt it worked better than the opioids (but did not eliminate the need for opioids) but also in an effort to be a "good patient." When I thought I might be going home, I stopped asking for the ketorolac. In short order, the pain worsened, my vital signs worsened, and I was off to the OR for removal of what proved to be a hemorrhagic, necrotic ovary.
• Small things matter, communication. Our system has spent considerable energy improving communication between staff and patients, utilizing communication boards. The professionals caring for me performed wonderfully in this respect – without fail, I knew their names and their extensions. I never knew, though, when my doctor would be rounding.
Because of on-call responsibilities and emergencies, the times ranged between 6 a.m. and 2 p.m. I completely understand why this happens, as it has occurred in my own practice. I will remember to keep my patients informed about my own schedule as much as I can going forward.
• Small things matter, miscellaneous. Medical tape leaves adhesive residue that takes days to remove – nail polish remover is more effective than alcohol for adhesive removal. ...An improperly secured Foley catheter can wreak havoc. ... There is literally nothing on TV worth watching for days at a time, despite having 46 channels. ... Clear liquids have more sugar than should be allowed, even for those of us who are not diabetic.
Being sick is very tedious.
As a medical student (more years ago than I care to count), I participated in various activities intended to raise awareness and sensitivity to the patient experience. After my recent refresher course, I hope to be a better doctor to my patients.
Dr. Fredholm and her colleague Dr. Stephen Bekanich are codirectors of Seton Palliative Care, part of the University of Texas Southwest Residency Programs in Austin. They alternate contributions to the monthly Palliatively Speaking blog (http://tinyurl.com/Palliatively).

On-erous call
Being on call means different things to different people, but it is safe to say that on call is a state that most physicians would avoid if they could. On call obligations are almost always included in advertisements in search of primary care physicians because both recent graduates of training programs and older physicians with their eyes on a retirement horizon put less-taxing call rotations high on their priority lists.
What makes on call so onerous? There is the obvious fact of life that the on call person is working at times when everyone else would rather not work ... nights, weekends, holidays, etc. Being on call can mess with your mind. It smacks of martyrdom for those of us who weren’t cut out to be saints. In places like Maine where warm sunny days are a rarity, being on call can tempt even the most altruistic among us to silently harbor hopes for rain so that we won’t be missing out on as much fun.
Being on call means that you will be fielding questions and interacting with patients and families who haven’t chosen you to be their primary care physician and with whom you are unfamiliar. This mutual unfamiliarity can breed discontent. It certainly doesn’t foster confidence. As on call physicians, you may be forced to invest extra time and effort to establish a therapeutic relationship with patients to whom you are a stranger. The failure to accept this challenge makes you more vulnerable to lawsuit should there be an unexpected outcome.
The physician who has made an effort to educate his patients and families is usually rewarded with fewer calls from them after hours. But, he will be frustrated by calls from patients of physicians who haven’t been as diligent at providing anticipatory guidance.
And, of course, there is always the problem of "But, Doctor Otherguy always just calls in a prescription for eye drops." There isn’t a perfect solution to this problem because physicians don’t all pop out of the same mold. However, discussions at group or hospital meetings, even if just informal chats in front of a chafing dish of overcooked vegetables, can help create some semblance of uniformity and minimize on call friction.
In some ways, a busy on call day that involves scores of calls and patient encounters can be more tolerable than a quiet day sitting at home waiting for the occasional call or beep. When it’s busy, the time passes more quickly, and encounters may generate some income (but never enough to justify the inconvenience and discomfort of being on call). However, when it’s quiet, you can slip into denial that you are on call. You may be tempted to make plans and begin activities that if interrupted could tip you into a cauldron of anger and self-pity.
There is an art to crafting an on call lifestyle that is compatible with a quiet on call. Choosing activities that one enjoys, but can be easily interrupted is a skill that comes after years of painful trial and error. When I was carving birds, I could drop my knives and head out to the office or hospital without a whimper. However, if I was in the middle of painting a project, the process of cleaning up and preserving the mixed color was too frustrating. So I only painted when I was off call.
Choosing which social invitations to accept also can be a challenge. Backyard cookouts are usually easier to exit by disappearing into the foliage. However, a small dinner party is a bad choice when one is on call. Several years ago, I discussed the issue of drinking on call in this column, and clearly, this is a personal decision that we all must make after a period of honest introspection.
Finally, communicating to one’s family the reality of on call and the inevitability of interruptions is of critical importance. Spouses and children can learn that "it-is-what-it-is" as long as we don’t allow ourselves to dip into denial and communicate our frustrations to them. They can learn to build their own lives while we are in that onerous other world of being on call.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including "How to Say No to Your Toddler." E-mail him at [email protected].
Being on call means different things to different people, but it is safe to say that on call is a state that most physicians would avoid if they could. On call obligations are almost always included in advertisements in search of primary care physicians because both recent graduates of training programs and older physicians with their eyes on a retirement horizon put less-taxing call rotations high on their priority lists.
What makes on call so onerous? There is the obvious fact of life that the on call person is working at times when everyone else would rather not work ... nights, weekends, holidays, etc. Being on call can mess with your mind. It smacks of martyrdom for those of us who weren’t cut out to be saints. In places like Maine where warm sunny days are a rarity, being on call can tempt even the most altruistic among us to silently harbor hopes for rain so that we won’t be missing out on as much fun.
Being on call means that you will be fielding questions and interacting with patients and families who haven’t chosen you to be their primary care physician and with whom you are unfamiliar. This mutual unfamiliarity can breed discontent. It certainly doesn’t foster confidence. As on call physicians, you may be forced to invest extra time and effort to establish a therapeutic relationship with patients to whom you are a stranger. The failure to accept this challenge makes you more vulnerable to lawsuit should there be an unexpected outcome.
The physician who has made an effort to educate his patients and families is usually rewarded with fewer calls from them after hours. But, he will be frustrated by calls from patients of physicians who haven’t been as diligent at providing anticipatory guidance.
And, of course, there is always the problem of "But, Doctor Otherguy always just calls in a prescription for eye drops." There isn’t a perfect solution to this problem because physicians don’t all pop out of the same mold. However, discussions at group or hospital meetings, even if just informal chats in front of a chafing dish of overcooked vegetables, can help create some semblance of uniformity and minimize on call friction.
In some ways, a busy on call day that involves scores of calls and patient encounters can be more tolerable than a quiet day sitting at home waiting for the occasional call or beep. When it’s busy, the time passes more quickly, and encounters may generate some income (but never enough to justify the inconvenience and discomfort of being on call). However, when it’s quiet, you can slip into denial that you are on call. You may be tempted to make plans and begin activities that if interrupted could tip you into a cauldron of anger and self-pity.
There is an art to crafting an on call lifestyle that is compatible with a quiet on call. Choosing activities that one enjoys, but can be easily interrupted is a skill that comes after years of painful trial and error. When I was carving birds, I could drop my knives and head out to the office or hospital without a whimper. However, if I was in the middle of painting a project, the process of cleaning up and preserving the mixed color was too frustrating. So I only painted when I was off call.
Choosing which social invitations to accept also can be a challenge. Backyard cookouts are usually easier to exit by disappearing into the foliage. However, a small dinner party is a bad choice when one is on call. Several years ago, I discussed the issue of drinking on call in this column, and clearly, this is a personal decision that we all must make after a period of honest introspection.
Finally, communicating to one’s family the reality of on call and the inevitability of interruptions is of critical importance. Spouses and children can learn that "it-is-what-it-is" as long as we don’t allow ourselves to dip into denial and communicate our frustrations to them. They can learn to build their own lives while we are in that onerous other world of being on call.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including "How to Say No to Your Toddler." E-mail him at [email protected].
Being on call means different things to different people, but it is safe to say that on call is a state that most physicians would avoid if they could. On call obligations are almost always included in advertisements in search of primary care physicians because both recent graduates of training programs and older physicians with their eyes on a retirement horizon put less-taxing call rotations high on their priority lists.
What makes on call so onerous? There is the obvious fact of life that the on call person is working at times when everyone else would rather not work ... nights, weekends, holidays, etc. Being on call can mess with your mind. It smacks of martyrdom for those of us who weren’t cut out to be saints. In places like Maine where warm sunny days are a rarity, being on call can tempt even the most altruistic among us to silently harbor hopes for rain so that we won’t be missing out on as much fun.
Being on call means that you will be fielding questions and interacting with patients and families who haven’t chosen you to be their primary care physician and with whom you are unfamiliar. This mutual unfamiliarity can breed discontent. It certainly doesn’t foster confidence. As on call physicians, you may be forced to invest extra time and effort to establish a therapeutic relationship with patients to whom you are a stranger. The failure to accept this challenge makes you more vulnerable to lawsuit should there be an unexpected outcome.
The physician who has made an effort to educate his patients and families is usually rewarded with fewer calls from them after hours. But, he will be frustrated by calls from patients of physicians who haven’t been as diligent at providing anticipatory guidance.
And, of course, there is always the problem of "But, Doctor Otherguy always just calls in a prescription for eye drops." There isn’t a perfect solution to this problem because physicians don’t all pop out of the same mold. However, discussions at group or hospital meetings, even if just informal chats in front of a chafing dish of overcooked vegetables, can help create some semblance of uniformity and minimize on call friction.
In some ways, a busy on call day that involves scores of calls and patient encounters can be more tolerable than a quiet day sitting at home waiting for the occasional call or beep. When it’s busy, the time passes more quickly, and encounters may generate some income (but never enough to justify the inconvenience and discomfort of being on call). However, when it’s quiet, you can slip into denial that you are on call. You may be tempted to make plans and begin activities that if interrupted could tip you into a cauldron of anger and self-pity.
There is an art to crafting an on call lifestyle that is compatible with a quiet on call. Choosing activities that one enjoys, but can be easily interrupted is a skill that comes after years of painful trial and error. When I was carving birds, I could drop my knives and head out to the office or hospital without a whimper. However, if I was in the middle of painting a project, the process of cleaning up and preserving the mixed color was too frustrating. So I only painted when I was off call.
Choosing which social invitations to accept also can be a challenge. Backyard cookouts are usually easier to exit by disappearing into the foliage. However, a small dinner party is a bad choice when one is on call. Several years ago, I discussed the issue of drinking on call in this column, and clearly, this is a personal decision that we all must make after a period of honest introspection.
Finally, communicating to one’s family the reality of on call and the inevitability of interruptions is of critical importance. Spouses and children can learn that "it-is-what-it-is" as long as we don’t allow ourselves to dip into denial and communicate our frustrations to them. They can learn to build their own lives while we are in that onerous other world of being on call.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including "How to Say No to Your Toddler." E-mail him at [email protected].
The Medical Roundtable: State-of-the-Art Management of Heart Failure with Preserved Ejection Fraction
I’m Barry Massie, Professor of Medicine at the University of California in San Francisco, and I’ll be moderating the call. I’m delighted to be joined by 2 colleagues who have devoted a great deal of effort to the pathophysiology of this syndrome and potential approaches to its treatment: Michael Zile, Professor of Medicine at the Medical University of South Carolina, Principal Investigator at the Gazes Cardiac Research Institute, and Director of the Medical Intensive Care Unit at the Ralph H. Johnson Department of Veterans Affairs Medical Center, and Sanjiv Shah, Associate Professor of Medicine–Cardiology at Northwestern University.
Dr. Zile, our first presenter, will discuss the epidemiology and pathophysiology of HFpEF. I’m sure you will quickly recognize his extensive knowledge and passion for the problem. After that, Dr. Shah, a former chief resident and cardiology fellow from our program at the University of California in San Francisco, who’s established a large program devoted to the study and treatment of HFpEF patients, will discuss his approach to the diagnosis and management of these patients.
DR. ZILE: I would like to start with a very short historical perspective that puts into context some of the terminology that’s already been used by Dr. Massie. Before 2006, EF < 35% was an inclusion criterion in virtually all the HF studies conducted. Therefore, all new medical and device-based management strategies were originally applied selectively to patients with clinical HF with a reduced EF (HFrEF), which was then called systolic HF.
However, as early as the 1970s, it was recognized that there were, in fact, a group of patients who had HF but an EF substantially higher than the 35% cutoff, ie, an EF > 50%. Kenneth Kessler was the first to publish the term “diastolic heart failure” in 1988 to describe such a group of patients.1
Until 2006, almost no reports of large randomized clinical trials that had examined this group of patients were published. Fortunately, between 2006 and 2009, the results of 5 studies that had examined patients with variable EF cutoffs—35%, 40%, or 45%—were published. Therefore, the term “heart failure with preserved EF” was suggested. For symmetry, a complementary term “heart failure with reduced ejection fraction” was proposed.
The diagnostic criteria commonly used for patients with HFpEF were recently published in a comprehensive review published by the Heart Failure Society of America in Journal of Cardiac Failure.2 Diagnosis requires clinical evidence of HF, meaning evidence of both symptoms and signs of HF, often supported by findings on chest radiography, cardiopulmonary exercise testing, or assessment of natriuretic peptides.
In addition to the signs and symptoms of HF, there’s a required EF cutoff or partition value. For the sake this presentation, let’s say that cutoff value is 50%. In addition, patients should have a normal left ventricular (LV) end-diastolic volume.
Supportive evidence for the presence of this clinical syndrome is found echocardiographically in structural or functional changes. One should be cognizant of ruling out nonmyocardial disease.
Patients with HFpEF have clinical characteristics that differ from those of patients with HFrEF. Patients with HFpEF tend to be older. The average age of patients approaches 70 to 75 years. They’re typically women and more often have hypertension and less often coronary artery disease (CAD).
The prevalence of this clinical syndrome exceeds 50% and appears to be increasing over time.3,4 While the rate of HF hospitalization of HFpEF patients continues to increase, the rate of HF hospitalization for HFrEF patients is actually decreasing. Data from epidemiological studies suggest that the survival rate of both HFrEF patients and HFpEF patients at 5 years posthospitalization was approximately 60%.5 In contrast, data from randomized clinical trials suggest significant differences in both morbidity and mortality between these 2 groups of patients. In a recent study by Campbell and McMurray, the clinical trials that randomized both HFrEF and HFpEF patients found different rates of overall mortality and overall hospitalization for these 2 groups, specifically higher rates for patients with HFrEF.6 However, they found that the functional impairment experienced by HFrEF and HFpEF patients in terms of exercise intolerance is basically equivalent. One example to support this finding is that cardiopulmonary exercise data and peak oxygen consumption (VO2) values are roughly equivalent in both groups7,8 of patients and approach the peak VO2 value of ≤14 mL/kg/min, a criterion for HF transplantation.9
HFpEF is commonly associated with clear abnormalities in both structure and function at the organ and ultrastructure levels. In at least one study published in Circulation, it was demonstrated that even patients with chronic compensated HFpEF have elevated pulmonary artery diastolic pressure or pulmonary capillary wedge pressure (PCWP).10 Those who then go on to develop decompensated HFpEF have further increases in diastolic pressure. The overall relationship between LV diastolic pressure and volume in patients with HFpEF is pushed up and to the left to a steeper curve such that the LV diastolic pressure is higher in HFpEF patients as compared to normal patients at any common volume.
Echocardiographic findings demonstrate that long-term increases in diastolic pressure are evidenced by an increase in the left atrial volume. In 2 recent echocardiographic substudies of Irbesartan in Heart Failure With Preserved Systolic Function (I-PRESERVE) and Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity (CHARM-Preserved), 60% to 70% of these patients experienced increase in left atrial volume.11,12 This increase in left atrial volume predicted a marked increase in cumulative event rates in terms of primary both end points and HF end points in both studies.
HFpEF patients have significant increases in fibrillar collagen, which are under the control of the cardiac fibroblast. Abnormalities can be seen in at least 4 specific mechanisms controlling collagen homeostasis, including synthesis, postsynthetic processing, posttranslational modification, and degradation.
In one exemplary study by Westermann and colleagues published in 2011, LV biopsy of patients with HFpEF revealed a 3-fold increase in collagen volume fraction and a 4-fold increase in collagen type 1 volume fraction compared to that in the control subjects.13
If you look at the evidence of abnormalities and extracellular matrix homeostasis in the plasma, you will find changes in collagen pro-peptides such as the N-terminal pro-peptide of collagen 3; in matrix metalloproteinases (MMPs), specifically MMP2 and MMP8; and in the tissue inhibitors of MMP (TIMPs), specifically TIMP4. Abnormalities in these 4 plasma biomarkers taken in aggregate as a biomarker panel are evidence of abnormalities in extracellular matrix homeostasis and can be used diagnostically to detect the presence of HFpEF.
There are, however, some issues that have been raised regarding the natural history and the underlying pathophysiologic mechanisms in HFpEF. I’ll give you 2 examples.
Some scientists and clinicians have argued that HFpEF is not a clinical syndrome, but rather a group of symptoms and signs caused by comorbidities and associated with specific epidemiologic factors such as advanced age, female sex, CAD, diabetes, and hypertension. However, if this were true, then the morbidity and mortality rates should be comparable between patients who have only these underlying comorbidities and patients who have these comorbidities and HFpEF.
Campbell and McMurray compared the overall mortality and HF hospitalization rates of studies that examined patients with underlying comorbidities such as diabetes, hypertension, or CAD and no HFpEF, versus those patients studied in trials with HFpEF.14 For example, in studies patients with hypertension, diabetes, or CAD but no HF, the HF hospitalization rate was <12/100 patient-years, whereas in patients with these comorbidities and HFpEF, the rate was >40/100 patient-years.
The second challenge put forth by some scientists and clinicians is that HF is a continuum and HFpEF and HFrEF are, in fact, expressions of one disease process.15 However, there are clear structural and functional differences between these 2 clinical syndromes and that patients with HFpEF do not, in fact, progress to become patients with HFrEF. I’ll give you 2 sets of evidence to support that.
Patients with HFpEF, in general, have a normal ventricular volume but experience increases in LV mass, which supports the existence of a type of structural abnormality summarized by the term “concentric remodeling” or “concentric hypertrophy.” In contrast, patients with HFrEF experience marked increases in volumes without a proportional increase in LV mass, and thus experience eccentric remodeling or eccentric hypertrophy. These chamber abnormalities are mirrored by ultrastructural abnormalities such as those seen in the cardiomyocyte length, width, and area in animal models of eccentric versus concentric hypertrophy. In addition, there are significant differences in extracellular matrix remodeling.16
Finally, at least 4 studies demonstrate that over variable periods of time and in the absence of an intercurrent myocardial infarction, patients with concentric remodeling, a common structural manifestation of HFpEF, do not frequently progress to eccentric remodeling, a common structural manifestation of HFrEF. This conversion rate is less than 1% per year.17–20
I think I’ll stop my comments there and let Dr. Massie talk about the clinical trials that have been performed over the past 5 years.
DR. MASSIE: In terms of treating these patients, I think Dr. Zile already alluded to the fact that it’s challenging, but we’re learning more and getting better at it. Compared with HFrEF, the most commonly studied variety of HF, we have fewer data for HFpEF, but our knowledge is growing. This subject is currently gaining importance.
Among the relatively few randomized trials, I’ll review and comment on 4 of them. Guidelines don’t have much to say because, frankly, we haven’t found much for them to say. Treatment remains relatively empiric, and different clinicians have different biases that affect the treatment that they provide; some, for instance, simply treat HFpEF patients with diuretics when they become edematous.
Several small studies have shown that some agents seem to work. Certainly, diuretics, while not truly addressing the underlying mechanism of HFpEF, make patients feel better when they are volume overloaded. Some have tried calcium blockers, although I don’t think they have much clinical benefit. Beta blockers, angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers, and now aldosterone blockers. Most recent trials have focused on inhibitors of the renin angiotensin system. Frankly, there hasn’t been a lot of beneficial evidence.
It’s sort of paradoxical, but the first trial of HFpEF ever conducted on a moderate scale was with digoxin in the Digitalis Investigation Group (DIG) trial.21 Given digoxin’s utility as an inotropic agent, studying it in patients with HFpEF is, of course, somewhat counterintuitive. Nevertheless, I think studying these patients was a wonderful idea by Richard Gorlin, who was running the large DIG trial of HFrEF and thought it was about time to look at HFpEF as well.
The DIG study enrolled patients aged 67 years and older and included a larger proportion of women than you’d generally see in trials of HFrEF. The criterion for enrollment was an EF > 45%. The average EF was 55%, but 27% of patients had an EF < 50%. I will talk about that in more detail further, but this is where the 2 types of HF sometimes overlap in these trials.
Only half of the patients had a history of myocardial infarction, which is not surprising given the physiology and pathophysiology that Dr. Zile talked about, but hypertension was the dominant finding. When asked to speculate on the cause, the investigators stated hypertension for 23% of the patients, but we’ll see in other trials that hypertension is much more prevalent. In the Digitalis Investigation Group-Preserved Ejection Fraction (DIG-PEF), 56% of the patients were deemed to have an ischemic etiology.
The CHARM study,22 an angiotensin receptor blocker trial, that also conducted parallel examination of groups of HFrEF and HFpEF patients, observed the same phenomenon observed in the DIG trial: When you examine heterogeneous populations, you ultimately examine people who are more likely to reflect a dominant population, which in this case were HFrEF patients.
The Perindopril in Elderly Persons (PEP) trial,23 in which the mean age was 75 years and included more women than men, reported a higher mean EF than the previous 2 trials. We don’t know how many patients had EF < 50% because the PEP trial used a wall motion score index rather than the more typical EF value. As in the previous trials, relatively low rates of prior myocardial infarction were observed, and hypertension was thought to be the major player for a very large number of patients.
The last of the 4 investigations is the I-PRESERVE trial,24 the largest of these trials. As in the previous studies, the trial included patients of advanced age with a normal EF and a high percentage of women. Among the 88% of patients who had hypertension, the investigators indicated that the hypertension was responsible for the HFpEF in about two-thirds of the population, although it’s not entirely clear how they could make that judgment. Ischemic etiology was less common.
In the DIG-Preserved trial, there was early separation in the event-free survival curves for digoxin and placebo, which is perhaps a little difficult to explain, but probably one of the few positive findings at any point in any of these trials.
I wanted to elaborate a little more on I-PRESERVE, a trial that included 360 centers in 29 countries, for several reasons. One is that many of us were involved in it, and we believe that it probably provided more data than any other single trial. It used an angiotensin receptor blocker like CHARM did, but clearly separated the HFrEF and HFpEF patients. Over 4000 HFpEF patients developed 140 events.
The inclusion criteria for I-PRESERVE were EF < 45% with symptomatic HF and either recent hospitalization for HF or findings that fit the profile of diastolic HF or HFpEF. Use of an ACE inhibitor was not a contraindication, largely because ACE inhibitors were becoming the standard therapy for diabetics who comprised a fair number of these patients. We also didn’t feel that we could ethically withhold an ACE inhibitor from them.
The primary end point was a composite outcome of all-cause mortality or cardiovascular hospitalization. An echocardiography substudy that Dr. Zile published gives much insight, more than we had in the past, on the pathophysiology of HFpEF.25
There were no patients in whom EF was <45%. In the 2 trials that did not allow patients with EF < 45% (PEP and I-PRESERVE), the Kaplan–Meier event curves did not separate much (ie, there were no major differences in outcomes).
Those are the trials that have been completed, and from which we’ve derived most of our current data. Trial of Aldosterone Antagonist Therapy in Adults With Preserved Ejection Fraction Congestive Heart Failure (TOPCAT), a National Institute of Health-sponsored randomized controlled trial of spironolactone versus placebo in HFpEF,26 has clearly finished enrollment, but the results are not yet available. TOPCAT was originally designed to enroll 4500 patients, but could not reach that total because of challenges in the identification and recruitment of patients with HFpEF. The criteria for TOPCAT enrollment were age ≥50 years; EF ≥45%, as measured within 6 months of enrollment; signs and symptoms of HF; control of blood pressure at the time of study enrollment, despite the fact that the vast majority of patients had a history of hypertension and most other trials did not share this inclusion criterion; and, to ensure adequate event rates, at least one other high-risk HF feature, including hospitalization for HF within the past year and/or elevated levels of brain natriuretic peptides, either B-type natriuretic peptide (BNP) or N-terminal BNP.
Many of us thought that spironolactone might be an ideal drug because fibrosis, which spironolactone can at least reduce, if not prevent, is a major problem in some HFpEF patients.27 The composite primary end point in TOPCAT was cardiovascular death, aborted cardiac arrest, and hospitalization for HF management. The TOPCAT results are projected to be available in mid-2013.
So, what’s the conclusion? Do we know how to treat this entity? The answer in my mind is not yet, but we can prevent it, which would be my approach until we come up with a magic bullet to treat it. Most of these patients have hypertension, and many binge on salt, which is one of the reasons they have hypertension; obesity and diabetes seem to play a role to some degree as well. At this point, we don’t have any definitive answers about therapy.
In HYVET, indapamide, a thiazide-like diuretic, either with or without perindopril was found to be very effective in preventing HF hospitalization in patients aged >80 years. Although EF was not documented in HYVET, HFpEF is the predominant form of HF in the elderly; thus, it is likely that indapamide reduced hospitalization for HFpEF in that trial.29
Both ALLHAT and HYVET are important because they show that HFpEF can be prevented in hypertensive individuals. Some may argue that diuretics had an unfair advantage in both trials; namely, that HF hospitalization diagnosis was in part due to fluid overload, which diuretics treat and prevent. However, regardless of the mechanism of benefit, the results of these trials clearly show that HFpEF hospitalization can be prevented. Given the high rates of morbidity and mortality after HFpEF hospitalization, prevention by any means is critical.3,30
Although HFpEF can be prevented, we still have the challenge of managing the millions of patients suffering from HFpEF syndrome. In 2007, we founded a dedicated HFpEF program here at Northwestern University. Our reasons for doing so included the heterogeneity and diverse etiology and pathophysiology of the patient population; the lack of both a classification system and treatments for HFpEF; and as Dr. Zile mentioned, the difficulty in diagnosing HFpEF. Unlike HFrEF, we can’t use a simple EF indicator (ie, low EF) to make a diagnosis. Therefore, we need to be more systematic about identifying these patients and recruiting them into our clinical and research HFpEF program.
Between 2007 and 2012 we enrolled >750 patients into our program and have since been able to collect comprehensive data on 430 of these patients. We created a systematic algorithm for patient identification, focusing on inpatients because, as stated earlier, these are the patients at highest risk. We perform a daily query of the inpatient electronic medical records using one or more of the following criteria: the word “heart failure” in the hospital notes, or BNP > 100 pg/mL, or administration of 2 or more doses of intravenous diuretics. This gives us a long list of patients on a daily basis that we trim down by excluding all those with EF < 50%. We then have a study coordinator review all the remaining charts to identify patients who meet the Framingham criteria for HF and then offer these patients postdischarge follow-up in the HFpEF clinic.
For those who decide to come to our clinic after hospitalization, we confirm the HFpEF diagnosis based on much of the criteria that Dr. Zile mentioned. We also exclude some patients, such as those with a prior history of reduced EF (<40%), severe valvular disease, or prior history of cardiac transplant. We then enroll the remaining patients into our registry. We perform physical examination, electrocardiography, laboratory testing, and echocardiography in all patients, and arterial tonometry, pulmonary function testing, and cardiopulmonary exercise testing, as well as overnight polysomnography in a subset of patients. We try to have all patients undergo cardiac catheterization because we want to exclude CAD and invasively confirm elevated LV filling pressures. This is especially important in patients who have signs and symptoms of HF but whose echocardiography results are equivocal for diastolic dysfunction and BNP < 100 pg/mL.
Importantly, we try to enroll every patient in a clinical trial. We were quite successful with that regard with the current TOPCAT, for which, as the leading enroller in the United States, we enrolled 77 patients. Clinical trial enrollment for HFpEF has been very challenging, and we believe that dedicated HFpEF programs will be critical for enhancing enrollment in HFpEF studies. Finally, after conducting initial confirmation of HFpEF diagnosis, baseline testing, and consideration for clinical trial enrollment, we follow patients every 3 to 6 months (or sooner as needed) to manage their HFpEF.
Our patients are younger by about 10 years as compared to those who have participated in the observational studies and clinical trials, such as I-PRESERVE, likely because elderly patients tend to not want to change doctors or have to see a new cardiologist, so elect not to enroll in our program. However, I also think that we identify patients at a younger age. We’re seeing younger patients with morbid obesity and diabetes and/or metabolic syndrome who are developing HFpEF. In our urban Chicago area, we have a diverse mix of ethnicity and races, and approximately 40% of the patient population is African-American, which is much higher than that in prior observational studies and clinical trials. Finally, as expected, comorbidities are quite common in patients in our HFpEF program, and the body mass index of our patients is much higher than that of patients in prior studies (mean body mass index, 33 kg/m2).
Analysis of data collected from patients enrolled in our HFpEF program confirmed that they met the objective criteria for HFpEF syndrome.31 Despite enrolling after HF hospitalization, during which they underwent intensive diuresis, they have remained quite symptomatic, with 49% continuing to have New York Heart Association Functional Classification (NYHA) Class III or IV symptoms. Furthermore, EF in our cohort is preserved (mean EF 61±7%), LV end-diastolic volume index is normal (41±12 mL/m2), and the majority have evidence of moderate or greater diastolic dysfunction (72% with grade 2 or 3 diastolic dysfunction and 79% with echocardiographic evidence of elevated LV end-diastolic pressure or PCWP). On invasive hemodynamic testing, mean PCWP was 23 mm Hg, which is quite high, considering that they had already undergone intravenous diuresis in the hospital. Thus, patients enrolled in our HFpEF program meet the objective criteria for HFpEF and despite treatment, remain quite symptomatic and fluid overloaded.
Drs. Zile and Massie described how we diagnose these patients and the lack of clinical trial data that we can refer to when treating these patients. These facts are important to know, but clinicians who treat these patients still need a roadmap for the major steps in diagnosis and treatment of HFpEF. The first step is to accurately diagnose the HFpEF syndrome (given its high prevalence, clinicians should have a low threshold to suspect the diagnosis in the dyspneic patient). Despite the limited data regarding BNP levels in diagnosis of HFpEF, clinicians often use levels of natriuretic peptides in diagnosis. When we systematically analyzed BNP levels in the patients in our program, we found that in up to 30% with confirmed HFpEF (ie, elevated PCWP and preserved EF), BNP level was normal (<100 pg/mL).32 Thus, a normal BNP level does not exclude a diagnosis of HFpEF syndrome.
When in doubt about HFpEF diagnosis, we perform cardiac catheterization for confirmation. While invasive hemodynamic testing is not necessary for all patients, it’s preferable to identify and diagnose HFpEF than miss it. We also routinely and systematically evaluate patients for CAD through stress testing and coronary angiography when possible, because multi-vessel CAD can mimic HFpEF, and treatment of CAD can provide symptomatic benefit.
The second step is to identify, target, and treat the underlying cause of HFpEF, an important part of our therapeutic strategy for the individual patient. Although HFpEF is very common and most commonly caused by standard comorbidities like hypertension, obesity, diabetes, CAD, and chronic kidney disease, we approach each patient as a unique case until proven otherwise. We must ensure that we don’t fail to detect constrictive pericarditis or infiltrative cardiomyopathy, which, although rarely causes HFpEF, requires treatment that differs significantly from that provided for HFpEF caused by more common conditions. Here, close examination of the echocardiogram can be very helpful. For example, on tissue Doppler imaging of the lateral mitral annulus, severe reduction in longitudinal systolic velocity (s′) and early diastolic velocity (e′) with preserved global EF suggests the possibility of infiltrative cardiomyopathy, especially in the setting of increased wall thickness and a low voltage electrocardiogram. On the other hand, a normal or exaggerated e′ velocity, despite a mitral inflow pattern, suggestive of significant diastolic dysfunction, can be a sign of constrictive pericarditis, especially if there are additional echocardiographic signs such as increased respiratory variation in the mitral inflow, diastolic septal bounce, or increased hepatic vein diastolic flow reversal during expiration.
Step 3 is, as stated in the HF guidelines, to treat HF by controlling blood pressure and treat fluid overload using diuretics. In terms of pharmacotherapy, I like to prescribe carvedilol, bumetanide, chlorthalidone, lisinopril, and spironolactone. As Dr. Massie just mentioned, we don’t have great data for any of these medications, but given the wide availability of generic forms of these agents and the use of many in the treatment of comorbidities common in HFpEF patients, they are affordable and effective options for the treatment of hypertension and fluid overload in these patients.
Step 4 is to aggressively treat comorbidities, which is a major reason for the high rate of morbidity of mortality in HFpEF patients. More than 90% of patients with HFpEF have hypertension, CAD, diabetes, and/or chronic kidney disease, and many have sleep-disordered breathing and chronic pulmonary obstructive disease.33,34 Thus, HFpEF patients are not treated just by treating their HF; we really need to treat the whole patient and work with our colleagues in internal medicine, geriatrics, and other subspecialties to provide holistic care.
Step 5 is to provide a structured program of exercise training. A recent meta-analysis on and several high-quality smaller studies have found that exercise training is beneficial in HFpEF.35–39
Step 6 is to provide HF education to our patients. In an analysis of data from the Mid-Michigan Guidelines Applied in Practice–Heart Failure (GAP-HF) trial, Hummel and colleagues found that HFpEF patients are less likely to receive appropriate discharge instructions than patients with HFrEF.40 Although the Get with the Guidelines–Heart Failure (GWTG-HF) study found that while discharge instructions for HFpEF patients have improved over time, they are still inadequate.4 Thus, HFpEF patients need better education at discharge regarding salt restriction and fluid management.
Step 7 is to group HFpEF patients into categories, given the heterogeneity of HFpEF syndrome. The first category is what we call "garden-variety" HFpEF patients, who are typically hypertensive and obese, may or may not have diabetes, and often have chronic kidney disease. In these patients, we treat the underlying hypertension and focus on weight loss and control of diabetes, if present.
The next subgroup is HFpEF patients in whom CAD is the primary driver of HFpEF. While we need better data on how to treat these patients, based on their pathophysiology (worse biventricular longitudinal systolic function) and my anecdotal experience, I treat them like HFrEF patients, with beta blockers, renin-angiotensin-aldosterone system (RAAS) antagonists, statins, and revascularization, which are often indicated for the treatment of CAD.
The next subgroup is HFpEF patients with atrial arrhythmia and few other comorbidities. These patients, who often have normal or easily controlled blood pressure and experience episodes of tachyarrhythmia that exacerbate HF, appear to be suffering from HFpEF due to the underlying atrial arrhythmia. In these patients, I attempt to maintain normal sinus rhythm, especially if they are less symptomatic and less fluid overloaded when in a normal sinus rhythm.
Some patients with HFpEF have predominantly right ventricular (RV) HF symptoms. These are patients with high pulmonary artery pressure and RV dysfunction on echocardiography in the setting of elevated LV end-diastolic pressure and clear LV diastolic dysfunction. The management of these patients is often challenging. As RV dysfunction worsens, significant tricuspid regurgitation occurs often, cardiac output decreases, and systemic pressures decline. The resultant severe central venous congestion can lead to “congestive nephropathy,” while renal function worsens, leading to even more fluid overload. In these patients, intensive diuresis (or ultrafiltration when needed), spironolactone, and digoxin can be helpful. If systemic hypotension limits adequate diuresis, we treat patients with midodrine. In patients with HFpEF with significant RV dysfunction and elevated pulmonary artery pressure, especially those with pulmonary arterial hypertension superimposed on pulmonary venous hypertension (defined as a PA diastolic pressure-PCWP gradient > 5 mmHg), sildenafil may be beneficial.41
Another group of patients includes those with HFpEF in the setting of cardiac structural and functional changes that mimic hypertrophic cardiomyopathy. These are elderly patients with long-standing hypertension whose echocardiographic findings are indistinguishable from hypertrophic cardiomyopathy. I therefore treat them by focusing on negative inotropes such as long-acting metoprolol, diltiazem, or verapamil and avoiding aggressive diuresis, which can result in LV outflow tract or intracavitary obstruction.
There are a few additional subgroups of HFpEF patients. Some patients have HFpEF associated with a high-output state, such as those with end-stage liver disease, hyperthyroidism, arteriovenous fistulas, or severe anemia. Enlargement of all 4 cardiac chambers is a clue to this diagnosis. In these cases, we treat the underlying cause and use diuretics as a mainstay. Some patients have multivalvular HFpEF, and in such patients, having moderate disease of multiple valves presents a treatment challenge. These patients often do not meet the criteria for valve replacement or repair, but develop moderate valvular lesions, which, combined with other risk factors for HFpEF, lead to symptomatic HF. Finally, there are patients with HFpEF caused by rare conditions such as infiltrative cardiomyopathies and constrictive pericarditis. I treat the underlying cause in these patients and enroll them in a clinical trial, if possible.
I’ll conclude by touching on beta-blocker therapy in HFpEF. There have been multiple observational studies and some clinical trials of this topic, including the Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors with Heart Failure (SENIORS),42 which studied nebivolol, a vasodilating beta blocker. When considering beta-blocker use in HFpEF, there are several key points to remember. We know that some patients with HFpEF have chronotropic incompetence, which underlies their inability to increase cardiac output with exercise.43,44 In these patients, beta-blocker therapy could be harmful. However, observational studies of HFpEF have shown that beta blockers are associated with better outcomes in HFpEF patients.
What’s key here is that if a beta blocker is going to be used, it should be a vasodilating beta blocker, and that’s why I like carvedilol; it acts as a potent blood pressure-lowering agent due to its vasodilating properties. In the Coreg Heart Failure Registry (COHERE), registry led by Dr. Massie, carvedilol was found to be associated with better outcomes in HF, regardless of the underlying EF.45 This study was limited by its observational design, but nevertheless indicates some potential benefit.
The last point I’ll mention on beta blockers in HFpEF is that it is important to differentiate not only the patients with chronotropic incompetence but also those with severe diastolic dysfunction and restricted filling on echocardiography—patients who have evidence of a restrictive cardiomyopathy. These patients are typically very sensitive to any rate-controlling agents because stroke volume is fixed, and they rely on increasing heart rate with exercise in order to augment cardiac output. In these patients, in particular, I am very hesitant about using beta blockers unless they have an atrial arrhythmia that results in high heart rates and worsening HF. In patients with a hypertrophic cardiomyopathy-like phenotype, on the other hand, who need adequate diastolic filling time and atrial kick, I find beta blockers very helpful. These are just anecdotal observations, but I’ve found them to be helpful.
I’ll conclude by stating that right now I agree with Dr. Massie that we don’t have good clinical trial data, but it’s clear that the next 5 to 10 years will be an exciting time in which we’re likely to reinvent our knowledge about HFpEF and the clinical management of this syndrome.
DR. MASSIE: Dr. Shah, have you had to send anybody with HFpEF for transplantation?
DR. SHAH: In my practice, we have considered cardiac transplantation in cases of severe restrictive cardiomyopathy.
DR. MASSIE: What about patients with amyloid-type cardiomyopathy?
DR. SHAH: Yes, cardiac amyloidosis, and those with idiopathic restrictive cardiomyopathy. Typically, these are the patients with restrictive cardiomyopathy that develop end-stage HF. Patients with “garden-variety” HFpEF typically don’t develop severe enough end-stage HF to warrant cardiac transplantation, and their advanced age and multiple comorbidities often preclude consideration for transplant. Patients with restrictive cardiomyopathy represent a difficult challenge in the current era of cardiac transplantation. These patients typically have small ventricular volumes and are therefore not good candidates for mechanical circulatory support. However, because of a preserved EF, inotropes are not helpful in most of these patients. Thus, they often wait on the transplant list for quite some time and get bypassed by HFrEF patients who have a 1B or 1A status in the setting of ventricular assist devices. Finally, in patients with primary (AL) cardiac amyloidosis some advocate cardiac transplant,46 but it has been our practice to use chemotherapy followed by autologous stem-cell transplantation for these types of patients, provided that we can get patients close to euvolemia and control their HF symptoms.
DR. ZILE: I have had patients with hypertrophic cardiomyopathy with a normal EF who have had very low myocardial peak VO2 values, ie, myocardial VO2 values significantly less than 14 mL/kg/min, who have gone in for transplantation. I suppose that there are some patients with valvular heart disease for whom, if they’re young enough, one could consider transplantation as well, if they’re not candidates for surgical replacement.
I’d like to talk about a couple of other issues that Dr. Shah’s comments have raised. One is the use of implantable hemodynamic monitors in this group of patients. The second is the use of device therapy for the treatment of hypertension, particularly resistant hypertension. Dr. Shah’s comment regarding the variety of diuretics that he uses in his incredibly well-developed clinic brings to mind 2 concepts. One is that the reason why diuretics reduce HF hospitalization is, in fact, the judicious use of small changes in dose. Small but judicious increases and decreases can not only acutely but chronically lower filling pressure. This has been demonstrated in at least 3 studies—Chronicle Offers Management to Patients With Advanced Signs and Symptoms of Heart Failure (COMPASS-HF),47 CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Patients (CHAMPION),48 and Home Self-Therapy in Severe Heart Failure Patients (HOMEOSTASIS).49
In addition, HOMEOSTASIS and its ongoing follow-up study, Left Atrial Pressure Monitoring to Optimize Heart Failure Therapy (LAPTOP-HF),50 not only demonstrated that it is important to lower pressure by making small and judicious changes in diuretic dose but also showed that every time we increase diuretic dose, we also increase activation of the sympathetic nervous system or the RAAS. When the diuretic dosage is increased, it should be accompanied by uptitration of sympathetic antagonist beta blockers and RAAS antagonists, if possible.
The only clinical trial that I know that demonstrated a clear statistically significant reduction in HF hospitalizations in this group of patients is CHAMPION, which achieved a very large reduction in HF hospitalization—one virtually unheard of in any other trial—by maintaining low filling pressures by the therapeutic interventions that I’ve just mentioned.
DR. SHAH: I was very impressed by CHAMPION—it’s exactly what we see clinically with these patients. For example, I’m continually amazed at the close relationship between dietary indiscretion and worsening HF. Another such example is that fact that around the Thanksgiving holiday, many of my patients with HFpEF will develop significant volume overload, often necessitating hospitalization for HF exacerbation. Dietary indiscretion and medication noncompliance inevitably lead to a sudden rise in filling pressures. If we could implant an implantable monitor in these patients, we would have the ability to preemptively strike and give them an increased dose, thereby improving their outcomes.
I also agree with being judicious, especially with loop diuretics, so that we don’t trigger the intense sympathetic response. I teach our cardiology fellows that while we treat with diuretics because they’re very effective in controlling symptoms, we try to find the minimal dose to keep patients euvolemic and thereby limit the degree of sympathetic discharge.
DR. ZILE: To follow-up on your comments, in CHAMPION and HOMEOSTASIS, in an average 7-day week, changes in medications for diuretics—and I should also mention long-acting nitrates—were made on about 5 of the 7 days, but the changes were very small. For example, small changes were made in furosemide dose, from 20 to 30 mg or from 30 to 40 mg (eg, ±10 mg/day), but produced significant long-term falls in filling pressure.
The other topic that I think we should mention is that new devices that are being used to treat resistant hypertension, which is important from the point of view of prevention and the treatment of hypertension. There’s no question that if you could achieve regression of LV hypertrophy in hypertensive HFpEF patients with LV hypertrophy, you could markedly decrease both morbidity and mortality.
This can be accomplished with renal artery denervation (RAD) through a transcatheter approach. The Renal Denervation in Patients With Uncontrolled Hypertension (Symplicity HTN-2) study showed that RAD could markedly decrease LV mass, as evidenced by a 13% reduction in LV mass 1 month and a 17% decrease in LV mass 6 months after RAD,51 and significantly increase percentages higher than those obtained with the pharmacologic interventions we’ve used in hypertension trials to cause regression of LV hypertrophy.
In addition to RAD, there’s also carotid sinus stimulation, vagal nerve stimulation, and spinal cord stimulation, which are being examined.
DR. MASSIE: I’m certainly impressed with the renal sympathetic nerve ablation data, which I think a group in London is acting upon by doing a trial on HFpEF patients. I think hypertension is at the core of this. Frankly, it’s people’s behavioral patterns that make that the case. So, if you ablate the renal sympathetic nerves, the patient probably can’t overcome that and consequently benefit from it.
I think renal sympathetic nerve ablation is something that’s probably here to stay. I haven’t been as impressed with carotid sinus stimulation, compared with the renal sympathetic nerve denervation. I think it’s time to have a laboratory to gather a working group to study HFpEF and probably take on some further trials with some of the promising therapies.
Data from Olmsted County, Minnesota, indicate that pulmonary hypertension, defined as elevated pulmonary artery systolic pressure on echocardiography, is very common in HFpEF.52 In addition, elevated pulmonary artery systolic pressure was found to be the best echocardiographic sign differentiating patients with HFpEF from patients with hypertension without HF.52 The high prevalence of pulmonary hypertension in HFpEF makes sense—high left atrial pressure at rest or with exercise, which is nearly universal in HFpEF, leads to passive elevation of pulmonary venous pressures and thus, pulmonary hypertension. In addition, akin to systolic systemic hypertension of the elderly, patients with HFpEF have systolic pulmonary hypertension, ie, they have disproportionate elevation of pulmonary artery systolic pressure and high pulmonary artery pulse pressure.
What’s not clear, as I stated earlier, is why some patients with HFpEF further develop an elevated pulmonary vascular resistance or a more reactive form of pulmonary hypertension. Whether the presence of superimposed pulmonary arterial hypertension or pulmonary arterial remodeling is due to comorbidities that cause pulmonary arterial hypertension, HF duration and severity of left atrial pressure elevation, or genetic factors is also unknown.
Regardless of the cause of superimposed (reactive) pulmonary arterial hypertension in HFpEF, it seems to be relatively uncommon in this patient population. RV dysfunction, however, is relatively common,53 and PDE5 inhibitors may have a role in either reactive pulmonary arterial hypertension or RV dysfunction in HFpEF, as demonstrated by Guazzi et al. in the aforementioned small clinical trial of sildenafil in such patients.41
The Evaluating the Effectiveness of Sildenafil at Improving Health Outcomes and Exercise Ability in People With Diastolic Heart Failure (RELAX) trial is a National Heart, Lung, and Blood Institute study that did not look at pulmonary hypertension specifically in HFpEF but rather, a broad spectrum of HFpEF patients. The idea behind RELAX was that PDE5 inhibitors have lusitropic myocardial effects that may improve diastolic function and are therefore useful simply on the basis of their action as vasodilators in HFpEF. However, the RELAX trial did not show any benefit to PDE5 inhibition in HFpEF patients without superimposed pulmonary arterial hypertension.54
Along with the PDE5 inhibitors, ranolazine, a late inward sodium channel (I[Na+]) inhibitor that seems to exert anti-ischemic effects in chronic stable angina by increasing myocardial relaxation, may be beneficial in patients with HFpEF. By blocking the late I[Na+] current, which is augmented in HF, there is less sodium in the myocyte, which results in less calcium in the myocyte during systole. Therefore, there is less postsystolic contraction of the myocyte, improved calcium handling, and better myocyte relaxation. Unfortunately, ranolazine did not demonstrate significant benefit in the Ranolazine for the Treatment of Diastolic Heart Failure (RALI-DHF) study, which was a small proof-of-concept HFpEF trial.55,56
DR. MASSIE: I think this has been a great discussion. The two of you come at HFpEF from somewhat different perspectives, but the consensus is that it’s a big problem and remains one of the most challenging problems in clinical cardiology. We need to continue to work to identify HFpEF patients and enroll them in clinical trials so that we can advance our knowledge in this patient population and find new targeted therapies for this patient population. Let’s hope some of these things that people are beginning to work with are successful.
UPDATE
The baseline clinical and echocardiographic characteristics of the TOPCAT trial have been published,57,58 providing insight into the 3445 patients with symptomatic heart failure with preserved ejection fraction (HFpEF) who were enrolled. Patients enrolled in the TOPCAT trial were similar to those in other HFpEF clinical trials and registries: the patients were older, more often female, and had a high prevalence of hypertension (91%). Baseline blood pressure, however, was well controlled (129/76 mm Hg; 7–16 mm Hg lower than that in other HFpEF clinical trials). Comorbidities were common, and quality life was poor (similar to end-stage renal disease). Structural heart disease was common in the TOPCAT trial, with a high prevalence of concentric left ventricular remodeling or hypertrophy and frequent left atrial enlargement. In November 2013, the results of the TOPCAT trial were presented at the American Heart Association Scientific Sessions. The TOPCAT trial failed to meet the primary combined endpoint of reducing cardiovascular mortality, aborted cardiac arrest, or HF hospitalization (hazard ratio [HR], 0.89; 95% confidence interval [CI], 0.77–1.04]; P = 0.14). Although spironolactone treatment did decrease HF hospitalization (HR, 0.83; 95% CI, 0.69–0.99; P = 0.042), all-cause hospitalizations did not differ among the treatment groups.
In a prespecified subgroup analysis based on the enrollment criteria, there was a statistically significant reduction in the primary endpoint in patients who entered the trial based on elevated natriuretic peptide levels (brain natriuretic peptide or N-terminal pro-brain natriuretic peptide). There was no difference in the primary endpoint for those patients who entered the trial based on prior history of HF hospitalization. Further exploration into the apparent dichotomy in the results, based on the enrollment criteria, revealed that there were major differences in the event rates in the Americas (United States, Canada, Brazil, and Argentina, where event rates were high [31.8%], similar to prior epidemiologic and observational studies) compared to Eastern Europe (Russia and the Republic of Georgia, where event rates were very low [8.4%]). A post-hoc analysis demonstrated that spironolactone treatment was beneficial in the Americas (HR, 0.82; 95% CI, 0.69–0.98 for the primary endpoint), but not in Eastern Europe. Furthermore, the majority of patients who entered the study based on the more objective natriuretic peptide criteria were from the Americas. These data demonstrate the importance of diagnosing HFpEF accurately (patients in Eastern Europe may not have had the HFpEF syndrome), and show that there may be patients with HFpEF, especially those with elevated natriuretic peptide levels, who would truly benefit from mineralocorticoid receptor antagonism.
Importantly, while hyperkalemia was more common in the TOPCAT trial patients treated with spironolactone (18.7% vs. 9.1%, respectively; P < 0.001), hypokalemia was less common in the spironolactone arm (16.2% vs. 22.9%, respectively), and there were no hyperkalemia-related deaths. Thus, if clinicians choose to use spironolactone to treat HFpEF, they should follow the TOPCAT trial guidelines for checking potassium levels and renal function at 1 week as well as at 30 days after starting spironolactone treatment, to prevent adverse events due to hyperkalemia. —Sanjiv J. Shah, MD, Northwestern University Feinberg School of Medicine, Chicago, IL
FoxP2 Media LLC is the publisher of The Medical Roundtable.
I’m Barry Massie, Professor of Medicine at the University of California in San Francisco, and I’ll be moderating the call. I’m delighted to be joined by 2 colleagues who have devoted a great deal of effort to the pathophysiology of this syndrome and potential approaches to its treatment: Michael Zile, Professor of Medicine at the Medical University of South Carolina, Principal Investigator at the Gazes Cardiac Research Institute, and Director of the Medical Intensive Care Unit at the Ralph H. Johnson Department of Veterans Affairs Medical Center, and Sanjiv Shah, Associate Professor of Medicine–Cardiology at Northwestern University.
Dr. Zile, our first presenter, will discuss the epidemiology and pathophysiology of HFpEF. I’m sure you will quickly recognize his extensive knowledge and passion for the problem. After that, Dr. Shah, a former chief resident and cardiology fellow from our program at the University of California in San Francisco, who’s established a large program devoted to the study and treatment of HFpEF patients, will discuss his approach to the diagnosis and management of these patients.
DR. ZILE: I would like to start with a very short historical perspective that puts into context some of the terminology that’s already been used by Dr. Massie. Before 2006, EF < 35% was an inclusion criterion in virtually all the HF studies conducted. Therefore, all new medical and device-based management strategies were originally applied selectively to patients with clinical HF with a reduced EF (HFrEF), which was then called systolic HF.
However, as early as the 1970s, it was recognized that there were, in fact, a group of patients who had HF but an EF substantially higher than the 35% cutoff, ie, an EF > 50%. Kenneth Kessler was the first to publish the term “diastolic heart failure” in 1988 to describe such a group of patients.1
Until 2006, almost no reports of large randomized clinical trials that had examined this group of patients were published. Fortunately, between 2006 and 2009, the results of 5 studies that had examined patients with variable EF cutoffs—35%, 40%, or 45%—were published. Therefore, the term “heart failure with preserved EF” was suggested. For symmetry, a complementary term “heart failure with reduced ejection fraction” was proposed.
The diagnostic criteria commonly used for patients with HFpEF were recently published in a comprehensive review published by the Heart Failure Society of America in Journal of Cardiac Failure.2 Diagnosis requires clinical evidence of HF, meaning evidence of both symptoms and signs of HF, often supported by findings on chest radiography, cardiopulmonary exercise testing, or assessment of natriuretic peptides.
In addition to the signs and symptoms of HF, there’s a required EF cutoff or partition value. For the sake this presentation, let’s say that cutoff value is 50%. In addition, patients should have a normal left ventricular (LV) end-diastolic volume.
Supportive evidence for the presence of this clinical syndrome is found echocardiographically in structural or functional changes. One should be cognizant of ruling out nonmyocardial disease.
Patients with HFpEF have clinical characteristics that differ from those of patients with HFrEF. Patients with HFpEF tend to be older. The average age of patients approaches 70 to 75 years. They’re typically women and more often have hypertension and less often coronary artery disease (CAD).
The prevalence of this clinical syndrome exceeds 50% and appears to be increasing over time.3,4 While the rate of HF hospitalization of HFpEF patients continues to increase, the rate of HF hospitalization for HFrEF patients is actually decreasing. Data from epidemiological studies suggest that the survival rate of both HFrEF patients and HFpEF patients at 5 years posthospitalization was approximately 60%.5 In contrast, data from randomized clinical trials suggest significant differences in both morbidity and mortality between these 2 groups of patients. In a recent study by Campbell and McMurray, the clinical trials that randomized both HFrEF and HFpEF patients found different rates of overall mortality and overall hospitalization for these 2 groups, specifically higher rates for patients with HFrEF.6 However, they found that the functional impairment experienced by HFrEF and HFpEF patients in terms of exercise intolerance is basically equivalent. One example to support this finding is that cardiopulmonary exercise data and peak oxygen consumption (VO2) values are roughly equivalent in both groups7,8 of patients and approach the peak VO2 value of ≤14 mL/kg/min, a criterion for HF transplantation.9
HFpEF is commonly associated with clear abnormalities in both structure and function at the organ and ultrastructure levels. In at least one study published in Circulation, it was demonstrated that even patients with chronic compensated HFpEF have elevated pulmonary artery diastolic pressure or pulmonary capillary wedge pressure (PCWP).10 Those who then go on to develop decompensated HFpEF have further increases in diastolic pressure. The overall relationship between LV diastolic pressure and volume in patients with HFpEF is pushed up and to the left to a steeper curve such that the LV diastolic pressure is higher in HFpEF patients as compared to normal patients at any common volume.
Echocardiographic findings demonstrate that long-term increases in diastolic pressure are evidenced by an increase in the left atrial volume. In 2 recent echocardiographic substudies of Irbesartan in Heart Failure With Preserved Systolic Function (I-PRESERVE) and Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity (CHARM-Preserved), 60% to 70% of these patients experienced increase in left atrial volume.11,12 This increase in left atrial volume predicted a marked increase in cumulative event rates in terms of primary both end points and HF end points in both studies.
HFpEF patients have significant increases in fibrillar collagen, which are under the control of the cardiac fibroblast. Abnormalities can be seen in at least 4 specific mechanisms controlling collagen homeostasis, including synthesis, postsynthetic processing, posttranslational modification, and degradation.
In one exemplary study by Westermann and colleagues published in 2011, LV biopsy of patients with HFpEF revealed a 3-fold increase in collagen volume fraction and a 4-fold increase in collagen type 1 volume fraction compared to that in the control subjects.13
If you look at the evidence of abnormalities and extracellular matrix homeostasis in the plasma, you will find changes in collagen pro-peptides such as the N-terminal pro-peptide of collagen 3; in matrix metalloproteinases (MMPs), specifically MMP2 and MMP8; and in the tissue inhibitors of MMP (TIMPs), specifically TIMP4. Abnormalities in these 4 plasma biomarkers taken in aggregate as a biomarker panel are evidence of abnormalities in extracellular matrix homeostasis and can be used diagnostically to detect the presence of HFpEF.
There are, however, some issues that have been raised regarding the natural history and the underlying pathophysiologic mechanisms in HFpEF. I’ll give you 2 examples.
Some scientists and clinicians have argued that HFpEF is not a clinical syndrome, but rather a group of symptoms and signs caused by comorbidities and associated with specific epidemiologic factors such as advanced age, female sex, CAD, diabetes, and hypertension. However, if this were true, then the morbidity and mortality rates should be comparable between patients who have only these underlying comorbidities and patients who have these comorbidities and HFpEF.
Campbell and McMurray compared the overall mortality and HF hospitalization rates of studies that examined patients with underlying comorbidities such as diabetes, hypertension, or CAD and no HFpEF, versus those patients studied in trials with HFpEF.14 For example, in studies patients with hypertension, diabetes, or CAD but no HF, the HF hospitalization rate was <12/100 patient-years, whereas in patients with these comorbidities and HFpEF, the rate was >40/100 patient-years.
The second challenge put forth by some scientists and clinicians is that HF is a continuum and HFpEF and HFrEF are, in fact, expressions of one disease process.15 However, there are clear structural and functional differences between these 2 clinical syndromes and that patients with HFpEF do not, in fact, progress to become patients with HFrEF. I’ll give you 2 sets of evidence to support that.
Patients with HFpEF, in general, have a normal ventricular volume but experience increases in LV mass, which supports the existence of a type of structural abnormality summarized by the term “concentric remodeling” or “concentric hypertrophy.” In contrast, patients with HFrEF experience marked increases in volumes without a proportional increase in LV mass, and thus experience eccentric remodeling or eccentric hypertrophy. These chamber abnormalities are mirrored by ultrastructural abnormalities such as those seen in the cardiomyocyte length, width, and area in animal models of eccentric versus concentric hypertrophy. In addition, there are significant differences in extracellular matrix remodeling.16
Finally, at least 4 studies demonstrate that over variable periods of time and in the absence of an intercurrent myocardial infarction, patients with concentric remodeling, a common structural manifestation of HFpEF, do not frequently progress to eccentric remodeling, a common structural manifestation of HFrEF. This conversion rate is less than 1% per year.17–20
I think I’ll stop my comments there and let Dr. Massie talk about the clinical trials that have been performed over the past 5 years.
DR. MASSIE: In terms of treating these patients, I think Dr. Zile already alluded to the fact that it’s challenging, but we’re learning more and getting better at it. Compared with HFrEF, the most commonly studied variety of HF, we have fewer data for HFpEF, but our knowledge is growing. This subject is currently gaining importance.
Among the relatively few randomized trials, I’ll review and comment on 4 of them. Guidelines don’t have much to say because, frankly, we haven’t found much for them to say. Treatment remains relatively empiric, and different clinicians have different biases that affect the treatment that they provide; some, for instance, simply treat HFpEF patients with diuretics when they become edematous.
Several small studies have shown that some agents seem to work. Certainly, diuretics, while not truly addressing the underlying mechanism of HFpEF, make patients feel better when they are volume overloaded. Some have tried calcium blockers, although I don’t think they have much clinical benefit. Beta blockers, angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers, and now aldosterone blockers. Most recent trials have focused on inhibitors of the renin angiotensin system. Frankly, there hasn’t been a lot of beneficial evidence.
It’s sort of paradoxical, but the first trial of HFpEF ever conducted on a moderate scale was with digoxin in the Digitalis Investigation Group (DIG) trial.21 Given digoxin’s utility as an inotropic agent, studying it in patients with HFpEF is, of course, somewhat counterintuitive. Nevertheless, I think studying these patients was a wonderful idea by Richard Gorlin, who was running the large DIG trial of HFrEF and thought it was about time to look at HFpEF as well.
The DIG study enrolled patients aged 67 years and older and included a larger proportion of women than you’d generally see in trials of HFrEF. The criterion for enrollment was an EF > 45%. The average EF was 55%, but 27% of patients had an EF < 50%. I will talk about that in more detail further, but this is where the 2 types of HF sometimes overlap in these trials.
Only half of the patients had a history of myocardial infarction, which is not surprising given the physiology and pathophysiology that Dr. Zile talked about, but hypertension was the dominant finding. When asked to speculate on the cause, the investigators stated hypertension for 23% of the patients, but we’ll see in other trials that hypertension is much more prevalent. In the Digitalis Investigation Group-Preserved Ejection Fraction (DIG-PEF), 56% of the patients were deemed to have an ischemic etiology.
The CHARM study,22 an angiotensin receptor blocker trial, that also conducted parallel examination of groups of HFrEF and HFpEF patients, observed the same phenomenon observed in the DIG trial: When you examine heterogeneous populations, you ultimately examine people who are more likely to reflect a dominant population, which in this case were HFrEF patients.
The Perindopril in Elderly Persons (PEP) trial,23 in which the mean age was 75 years and included more women than men, reported a higher mean EF than the previous 2 trials. We don’t know how many patients had EF < 50% because the PEP trial used a wall motion score index rather than the more typical EF value. As in the previous trials, relatively low rates of prior myocardial infarction were observed, and hypertension was thought to be the major player for a very large number of patients.
The last of the 4 investigations is the I-PRESERVE trial,24 the largest of these trials. As in the previous studies, the trial included patients of advanced age with a normal EF and a high percentage of women. Among the 88% of patients who had hypertension, the investigators indicated that the hypertension was responsible for the HFpEF in about two-thirds of the population, although it’s not entirely clear how they could make that judgment. Ischemic etiology was less common.
In the DIG-Preserved trial, there was early separation in the event-free survival curves for digoxin and placebo, which is perhaps a little difficult to explain, but probably one of the few positive findings at any point in any of these trials.
I wanted to elaborate a little more on I-PRESERVE, a trial that included 360 centers in 29 countries, for several reasons. One is that many of us were involved in it, and we believe that it probably provided more data than any other single trial. It used an angiotensin receptor blocker like CHARM did, but clearly separated the HFrEF and HFpEF patients. Over 4000 HFpEF patients developed 140 events.
The inclusion criteria for I-PRESERVE were EF < 45% with symptomatic HF and either recent hospitalization for HF or findings that fit the profile of diastolic HF or HFpEF. Use of an ACE inhibitor was not a contraindication, largely because ACE inhibitors were becoming the standard therapy for diabetics who comprised a fair number of these patients. We also didn’t feel that we could ethically withhold an ACE inhibitor from them.
The primary end point was a composite outcome of all-cause mortality or cardiovascular hospitalization. An echocardiography substudy that Dr. Zile published gives much insight, more than we had in the past, on the pathophysiology of HFpEF.25
There were no patients in whom EF was <45%. In the 2 trials that did not allow patients with EF < 45% (PEP and I-PRESERVE), the Kaplan–Meier event curves did not separate much (ie, there were no major differences in outcomes).
Those are the trials that have been completed, and from which we’ve derived most of our current data. Trial of Aldosterone Antagonist Therapy in Adults With Preserved Ejection Fraction Congestive Heart Failure (TOPCAT), a National Institute of Health-sponsored randomized controlled trial of spironolactone versus placebo in HFpEF,26 has clearly finished enrollment, but the results are not yet available. TOPCAT was originally designed to enroll 4500 patients, but could not reach that total because of challenges in the identification and recruitment of patients with HFpEF. The criteria for TOPCAT enrollment were age ≥50 years; EF ≥45%, as measured within 6 months of enrollment; signs and symptoms of HF; control of blood pressure at the time of study enrollment, despite the fact that the vast majority of patients had a history of hypertension and most other trials did not share this inclusion criterion; and, to ensure adequate event rates, at least one other high-risk HF feature, including hospitalization for HF within the past year and/or elevated levels of brain natriuretic peptides, either B-type natriuretic peptide (BNP) or N-terminal BNP.
Many of us thought that spironolactone might be an ideal drug because fibrosis, which spironolactone can at least reduce, if not prevent, is a major problem in some HFpEF patients.27 The composite primary end point in TOPCAT was cardiovascular death, aborted cardiac arrest, and hospitalization for HF management. The TOPCAT results are projected to be available in mid-2013.
So, what’s the conclusion? Do we know how to treat this entity? The answer in my mind is not yet, but we can prevent it, which would be my approach until we come up with a magic bullet to treat it. Most of these patients have hypertension, and many binge on salt, which is one of the reasons they have hypertension; obesity and diabetes seem to play a role to some degree as well. At this point, we don’t have any definitive answers about therapy.
In HYVET, indapamide, a thiazide-like diuretic, either with or without perindopril was found to be very effective in preventing HF hospitalization in patients aged >80 years. Although EF was not documented in HYVET, HFpEF is the predominant form of HF in the elderly; thus, it is likely that indapamide reduced hospitalization for HFpEF in that trial.29
Both ALLHAT and HYVET are important because they show that HFpEF can be prevented in hypertensive individuals. Some may argue that diuretics had an unfair advantage in both trials; namely, that HF hospitalization diagnosis was in part due to fluid overload, which diuretics treat and prevent. However, regardless of the mechanism of benefit, the results of these trials clearly show that HFpEF hospitalization can be prevented. Given the high rates of morbidity and mortality after HFpEF hospitalization, prevention by any means is critical.3,30
Although HFpEF can be prevented, we still have the challenge of managing the millions of patients suffering from HFpEF syndrome. In 2007, we founded a dedicated HFpEF program here at Northwestern University. Our reasons for doing so included the heterogeneity and diverse etiology and pathophysiology of the patient population; the lack of both a classification system and treatments for HFpEF; and as Dr. Zile mentioned, the difficulty in diagnosing HFpEF. Unlike HFrEF, we can’t use a simple EF indicator (ie, low EF) to make a diagnosis. Therefore, we need to be more systematic about identifying these patients and recruiting them into our clinical and research HFpEF program.
Between 2007 and 2012 we enrolled >750 patients into our program and have since been able to collect comprehensive data on 430 of these patients. We created a systematic algorithm for patient identification, focusing on inpatients because, as stated earlier, these are the patients at highest risk. We perform a daily query of the inpatient electronic medical records using one or more of the following criteria: the word “heart failure” in the hospital notes, or BNP > 100 pg/mL, or administration of 2 or more doses of intravenous diuretics. This gives us a long list of patients on a daily basis that we trim down by excluding all those with EF < 50%. We then have a study coordinator review all the remaining charts to identify patients who meet the Framingham criteria for HF and then offer these patients postdischarge follow-up in the HFpEF clinic.
For those who decide to come to our clinic after hospitalization, we confirm the HFpEF diagnosis based on much of the criteria that Dr. Zile mentioned. We also exclude some patients, such as those with a prior history of reduced EF (<40%), severe valvular disease, or prior history of cardiac transplant. We then enroll the remaining patients into our registry. We perform physical examination, electrocardiography, laboratory testing, and echocardiography in all patients, and arterial tonometry, pulmonary function testing, and cardiopulmonary exercise testing, as well as overnight polysomnography in a subset of patients. We try to have all patients undergo cardiac catheterization because we want to exclude CAD and invasively confirm elevated LV filling pressures. This is especially important in patients who have signs and symptoms of HF but whose echocardiography results are equivocal for diastolic dysfunction and BNP < 100 pg/mL.
Importantly, we try to enroll every patient in a clinical trial. We were quite successful with that regard with the current TOPCAT, for which, as the leading enroller in the United States, we enrolled 77 patients. Clinical trial enrollment for HFpEF has been very challenging, and we believe that dedicated HFpEF programs will be critical for enhancing enrollment in HFpEF studies. Finally, after conducting initial confirmation of HFpEF diagnosis, baseline testing, and consideration for clinical trial enrollment, we follow patients every 3 to 6 months (or sooner as needed) to manage their HFpEF.
Our patients are younger by about 10 years as compared to those who have participated in the observational studies and clinical trials, such as I-PRESERVE, likely because elderly patients tend to not want to change doctors or have to see a new cardiologist, so elect not to enroll in our program. However, I also think that we identify patients at a younger age. We’re seeing younger patients with morbid obesity and diabetes and/or metabolic syndrome who are developing HFpEF. In our urban Chicago area, we have a diverse mix of ethnicity and races, and approximately 40% of the patient population is African-American, which is much higher than that in prior observational studies and clinical trials. Finally, as expected, comorbidities are quite common in patients in our HFpEF program, and the body mass index of our patients is much higher than that of patients in prior studies (mean body mass index, 33 kg/m2).
Analysis of data collected from patients enrolled in our HFpEF program confirmed that they met the objective criteria for HFpEF syndrome.31 Despite enrolling after HF hospitalization, during which they underwent intensive diuresis, they have remained quite symptomatic, with 49% continuing to have New York Heart Association Functional Classification (NYHA) Class III or IV symptoms. Furthermore, EF in our cohort is preserved (mean EF 61±7%), LV end-diastolic volume index is normal (41±12 mL/m2), and the majority have evidence of moderate or greater diastolic dysfunction (72% with grade 2 or 3 diastolic dysfunction and 79% with echocardiographic evidence of elevated LV end-diastolic pressure or PCWP). On invasive hemodynamic testing, mean PCWP was 23 mm Hg, which is quite high, considering that they had already undergone intravenous diuresis in the hospital. Thus, patients enrolled in our HFpEF program meet the objective criteria for HFpEF and despite treatment, remain quite symptomatic and fluid overloaded.
Drs. Zile and Massie described how we diagnose these patients and the lack of clinical trial data that we can refer to when treating these patients. These facts are important to know, but clinicians who treat these patients still need a roadmap for the major steps in diagnosis and treatment of HFpEF. The first step is to accurately diagnose the HFpEF syndrome (given its high prevalence, clinicians should have a low threshold to suspect the diagnosis in the dyspneic patient). Despite the limited data regarding BNP levels in diagnosis of HFpEF, clinicians often use levels of natriuretic peptides in diagnosis. When we systematically analyzed BNP levels in the patients in our program, we found that in up to 30% with confirmed HFpEF (ie, elevated PCWP and preserved EF), BNP level was normal (<100 pg/mL).32 Thus, a normal BNP level does not exclude a diagnosis of HFpEF syndrome.
When in doubt about HFpEF diagnosis, we perform cardiac catheterization for confirmation. While invasive hemodynamic testing is not necessary for all patients, it’s preferable to identify and diagnose HFpEF than miss it. We also routinely and systematically evaluate patients for CAD through stress testing and coronary angiography when possible, because multi-vessel CAD can mimic HFpEF, and treatment of CAD can provide symptomatic benefit.
The second step is to identify, target, and treat the underlying cause of HFpEF, an important part of our therapeutic strategy for the individual patient. Although HFpEF is very common and most commonly caused by standard comorbidities like hypertension, obesity, diabetes, CAD, and chronic kidney disease, we approach each patient as a unique case until proven otherwise. We must ensure that we don’t fail to detect constrictive pericarditis or infiltrative cardiomyopathy, which, although rarely causes HFpEF, requires treatment that differs significantly from that provided for HFpEF caused by more common conditions. Here, close examination of the echocardiogram can be very helpful. For example, on tissue Doppler imaging of the lateral mitral annulus, severe reduction in longitudinal systolic velocity (s′) and early diastolic velocity (e′) with preserved global EF suggests the possibility of infiltrative cardiomyopathy, especially in the setting of increased wall thickness and a low voltage electrocardiogram. On the other hand, a normal or exaggerated e′ velocity, despite a mitral inflow pattern, suggestive of significant diastolic dysfunction, can be a sign of constrictive pericarditis, especially if there are additional echocardiographic signs such as increased respiratory variation in the mitral inflow, diastolic septal bounce, or increased hepatic vein diastolic flow reversal during expiration.
Step 3 is, as stated in the HF guidelines, to treat HF by controlling blood pressure and treat fluid overload using diuretics. In terms of pharmacotherapy, I like to prescribe carvedilol, bumetanide, chlorthalidone, lisinopril, and spironolactone. As Dr. Massie just mentioned, we don’t have great data for any of these medications, but given the wide availability of generic forms of these agents and the use of many in the treatment of comorbidities common in HFpEF patients, they are affordable and effective options for the treatment of hypertension and fluid overload in these patients.
Step 4 is to aggressively treat comorbidities, which is a major reason for the high rate of morbidity of mortality in HFpEF patients. More than 90% of patients with HFpEF have hypertension, CAD, diabetes, and/or chronic kidney disease, and many have sleep-disordered breathing and chronic pulmonary obstructive disease.33,34 Thus, HFpEF patients are not treated just by treating their HF; we really need to treat the whole patient and work with our colleagues in internal medicine, geriatrics, and other subspecialties to provide holistic care.
Step 5 is to provide a structured program of exercise training. A recent meta-analysis on and several high-quality smaller studies have found that exercise training is beneficial in HFpEF.35–39
Step 6 is to provide HF education to our patients. In an analysis of data from the Mid-Michigan Guidelines Applied in Practice–Heart Failure (GAP-HF) trial, Hummel and colleagues found that HFpEF patients are less likely to receive appropriate discharge instructions than patients with HFrEF.40 Although the Get with the Guidelines–Heart Failure (GWTG-HF) study found that while discharge instructions for HFpEF patients have improved over time, they are still inadequate.4 Thus, HFpEF patients need better education at discharge regarding salt restriction and fluid management.
Step 7 is to group HFpEF patients into categories, given the heterogeneity of HFpEF syndrome. The first category is what we call "garden-variety" HFpEF patients, who are typically hypertensive and obese, may or may not have diabetes, and often have chronic kidney disease. In these patients, we treat the underlying hypertension and focus on weight loss and control of diabetes, if present.
The next subgroup is HFpEF patients in whom CAD is the primary driver of HFpEF. While we need better data on how to treat these patients, based on their pathophysiology (worse biventricular longitudinal systolic function) and my anecdotal experience, I treat them like HFrEF patients, with beta blockers, renin-angiotensin-aldosterone system (RAAS) antagonists, statins, and revascularization, which are often indicated for the treatment of CAD.
The next subgroup is HFpEF patients with atrial arrhythmia and few other comorbidities. These patients, who often have normal or easily controlled blood pressure and experience episodes of tachyarrhythmia that exacerbate HF, appear to be suffering from HFpEF due to the underlying atrial arrhythmia. In these patients, I attempt to maintain normal sinus rhythm, especially if they are less symptomatic and less fluid overloaded when in a normal sinus rhythm.
Some patients with HFpEF have predominantly right ventricular (RV) HF symptoms. These are patients with high pulmonary artery pressure and RV dysfunction on echocardiography in the setting of elevated LV end-diastolic pressure and clear LV diastolic dysfunction. The management of these patients is often challenging. As RV dysfunction worsens, significant tricuspid regurgitation occurs often, cardiac output decreases, and systemic pressures decline. The resultant severe central venous congestion can lead to “congestive nephropathy,” while renal function worsens, leading to even more fluid overload. In these patients, intensive diuresis (or ultrafiltration when needed), spironolactone, and digoxin can be helpful. If systemic hypotension limits adequate diuresis, we treat patients with midodrine. In patients with HFpEF with significant RV dysfunction and elevated pulmonary artery pressure, especially those with pulmonary arterial hypertension superimposed on pulmonary venous hypertension (defined as a PA diastolic pressure-PCWP gradient > 5 mmHg), sildenafil may be beneficial.41
Another group of patients includes those with HFpEF in the setting of cardiac structural and functional changes that mimic hypertrophic cardiomyopathy. These are elderly patients with long-standing hypertension whose echocardiographic findings are indistinguishable from hypertrophic cardiomyopathy. I therefore treat them by focusing on negative inotropes such as long-acting metoprolol, diltiazem, or verapamil and avoiding aggressive diuresis, which can result in LV outflow tract or intracavitary obstruction.
There are a few additional subgroups of HFpEF patients. Some patients have HFpEF associated with a high-output state, such as those with end-stage liver disease, hyperthyroidism, arteriovenous fistulas, or severe anemia. Enlargement of all 4 cardiac chambers is a clue to this diagnosis. In these cases, we treat the underlying cause and use diuretics as a mainstay. Some patients have multivalvular HFpEF, and in such patients, having moderate disease of multiple valves presents a treatment challenge. These patients often do not meet the criteria for valve replacement or repair, but develop moderate valvular lesions, which, combined with other risk factors for HFpEF, lead to symptomatic HF. Finally, there are patients with HFpEF caused by rare conditions such as infiltrative cardiomyopathies and constrictive pericarditis. I treat the underlying cause in these patients and enroll them in a clinical trial, if possible.
I’ll conclude by touching on beta-blocker therapy in HFpEF. There have been multiple observational studies and some clinical trials of this topic, including the Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors with Heart Failure (SENIORS),42 which studied nebivolol, a vasodilating beta blocker. When considering beta-blocker use in HFpEF, there are several key points to remember. We know that some patients with HFpEF have chronotropic incompetence, which underlies their inability to increase cardiac output with exercise.43,44 In these patients, beta-blocker therapy could be harmful. However, observational studies of HFpEF have shown that beta blockers are associated with better outcomes in HFpEF patients.
What’s key here is that if a beta blocker is going to be used, it should be a vasodilating beta blocker, and that’s why I like carvedilol; it acts as a potent blood pressure-lowering agent due to its vasodilating properties. In the Coreg Heart Failure Registry (COHERE), registry led by Dr. Massie, carvedilol was found to be associated with better outcomes in HF, regardless of the underlying EF.45 This study was limited by its observational design, but nevertheless indicates some potential benefit.
The last point I’ll mention on beta blockers in HFpEF is that it is important to differentiate not only the patients with chronotropic incompetence but also those with severe diastolic dysfunction and restricted filling on echocardiography—patients who have evidence of a restrictive cardiomyopathy. These patients are typically very sensitive to any rate-controlling agents because stroke volume is fixed, and they rely on increasing heart rate with exercise in order to augment cardiac output. In these patients, in particular, I am very hesitant about using beta blockers unless they have an atrial arrhythmia that results in high heart rates and worsening HF. In patients with a hypertrophic cardiomyopathy-like phenotype, on the other hand, who need adequate diastolic filling time and atrial kick, I find beta blockers very helpful. These are just anecdotal observations, but I’ve found them to be helpful.
I’ll conclude by stating that right now I agree with Dr. Massie that we don’t have good clinical trial data, but it’s clear that the next 5 to 10 years will be an exciting time in which we’re likely to reinvent our knowledge about HFpEF and the clinical management of this syndrome.
DR. MASSIE: Dr. Shah, have you had to send anybody with HFpEF for transplantation?
DR. SHAH: In my practice, we have considered cardiac transplantation in cases of severe restrictive cardiomyopathy.
DR. MASSIE: What about patients with amyloid-type cardiomyopathy?
DR. SHAH: Yes, cardiac amyloidosis, and those with idiopathic restrictive cardiomyopathy. Typically, these are the patients with restrictive cardiomyopathy that develop end-stage HF. Patients with “garden-variety” HFpEF typically don’t develop severe enough end-stage HF to warrant cardiac transplantation, and their advanced age and multiple comorbidities often preclude consideration for transplant. Patients with restrictive cardiomyopathy represent a difficult challenge in the current era of cardiac transplantation. These patients typically have small ventricular volumes and are therefore not good candidates for mechanical circulatory support. However, because of a preserved EF, inotropes are not helpful in most of these patients. Thus, they often wait on the transplant list for quite some time and get bypassed by HFrEF patients who have a 1B or 1A status in the setting of ventricular assist devices. Finally, in patients with primary (AL) cardiac amyloidosis some advocate cardiac transplant,46 but it has been our practice to use chemotherapy followed by autologous stem-cell transplantation for these types of patients, provided that we can get patients close to euvolemia and control their HF symptoms.
DR. ZILE: I have had patients with hypertrophic cardiomyopathy with a normal EF who have had very low myocardial peak VO2 values, ie, myocardial VO2 values significantly less than 14 mL/kg/min, who have gone in for transplantation. I suppose that there are some patients with valvular heart disease for whom, if they’re young enough, one could consider transplantation as well, if they’re not candidates for surgical replacement.
I’d like to talk about a couple of other issues that Dr. Shah’s comments have raised. One is the use of implantable hemodynamic monitors in this group of patients. The second is the use of device therapy for the treatment of hypertension, particularly resistant hypertension. Dr. Shah’s comment regarding the variety of diuretics that he uses in his incredibly well-developed clinic brings to mind 2 concepts. One is that the reason why diuretics reduce HF hospitalization is, in fact, the judicious use of small changes in dose. Small but judicious increases and decreases can not only acutely but chronically lower filling pressure. This has been demonstrated in at least 3 studies—Chronicle Offers Management to Patients With Advanced Signs and Symptoms of Heart Failure (COMPASS-HF),47 CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Patients (CHAMPION),48 and Home Self-Therapy in Severe Heart Failure Patients (HOMEOSTASIS).49
In addition, HOMEOSTASIS and its ongoing follow-up study, Left Atrial Pressure Monitoring to Optimize Heart Failure Therapy (LAPTOP-HF),50 not only demonstrated that it is important to lower pressure by making small and judicious changes in diuretic dose but also showed that every time we increase diuretic dose, we also increase activation of the sympathetic nervous system or the RAAS. When the diuretic dosage is increased, it should be accompanied by uptitration of sympathetic antagonist beta blockers and RAAS antagonists, if possible.
The only clinical trial that I know that demonstrated a clear statistically significant reduction in HF hospitalizations in this group of patients is CHAMPION, which achieved a very large reduction in HF hospitalization—one virtually unheard of in any other trial—by maintaining low filling pressures by the therapeutic interventions that I’ve just mentioned.
DR. SHAH: I was very impressed by CHAMPION—it’s exactly what we see clinically with these patients. For example, I’m continually amazed at the close relationship between dietary indiscretion and worsening HF. Another such example is that fact that around the Thanksgiving holiday, many of my patients with HFpEF will develop significant volume overload, often necessitating hospitalization for HF exacerbation. Dietary indiscretion and medication noncompliance inevitably lead to a sudden rise in filling pressures. If we could implant an implantable monitor in these patients, we would have the ability to preemptively strike and give them an increased dose, thereby improving their outcomes.
I also agree with being judicious, especially with loop diuretics, so that we don’t trigger the intense sympathetic response. I teach our cardiology fellows that while we treat with diuretics because they’re very effective in controlling symptoms, we try to find the minimal dose to keep patients euvolemic and thereby limit the degree of sympathetic discharge.
DR. ZILE: To follow-up on your comments, in CHAMPION and HOMEOSTASIS, in an average 7-day week, changes in medications for diuretics—and I should also mention long-acting nitrates—were made on about 5 of the 7 days, but the changes were very small. For example, small changes were made in furosemide dose, from 20 to 30 mg or from 30 to 40 mg (eg, ±10 mg/day), but produced significant long-term falls in filling pressure.
The other topic that I think we should mention is that new devices that are being used to treat resistant hypertension, which is important from the point of view of prevention and the treatment of hypertension. There’s no question that if you could achieve regression of LV hypertrophy in hypertensive HFpEF patients with LV hypertrophy, you could markedly decrease both morbidity and mortality.
This can be accomplished with renal artery denervation (RAD) through a transcatheter approach. The Renal Denervation in Patients With Uncontrolled Hypertension (Symplicity HTN-2) study showed that RAD could markedly decrease LV mass, as evidenced by a 13% reduction in LV mass 1 month and a 17% decrease in LV mass 6 months after RAD,51 and significantly increase percentages higher than those obtained with the pharmacologic interventions we’ve used in hypertension trials to cause regression of LV hypertrophy.
In addition to RAD, there’s also carotid sinus stimulation, vagal nerve stimulation, and spinal cord stimulation, which are being examined.
DR. MASSIE: I’m certainly impressed with the renal sympathetic nerve ablation data, which I think a group in London is acting upon by doing a trial on HFpEF patients. I think hypertension is at the core of this. Frankly, it’s people’s behavioral patterns that make that the case. So, if you ablate the renal sympathetic nerves, the patient probably can’t overcome that and consequently benefit from it.
I think renal sympathetic nerve ablation is something that’s probably here to stay. I haven’t been as impressed with carotid sinus stimulation, compared with the renal sympathetic nerve denervation. I think it’s time to have a laboratory to gather a working group to study HFpEF and probably take on some further trials with some of the promising therapies.
Data from Olmsted County, Minnesota, indicate that pulmonary hypertension, defined as elevated pulmonary artery systolic pressure on echocardiography, is very common in HFpEF.52 In addition, elevated pulmonary artery systolic pressure was found to be the best echocardiographic sign differentiating patients with HFpEF from patients with hypertension without HF.52 The high prevalence of pulmonary hypertension in HFpEF makes sense—high left atrial pressure at rest or with exercise, which is nearly universal in HFpEF, leads to passive elevation of pulmonary venous pressures and thus, pulmonary hypertension. In addition, akin to systolic systemic hypertension of the elderly, patients with HFpEF have systolic pulmonary hypertension, ie, they have disproportionate elevation of pulmonary artery systolic pressure and high pulmonary artery pulse pressure.
What’s not clear, as I stated earlier, is why some patients with HFpEF further develop an elevated pulmonary vascular resistance or a more reactive form of pulmonary hypertension. Whether the presence of superimposed pulmonary arterial hypertension or pulmonary arterial remodeling is due to comorbidities that cause pulmonary arterial hypertension, HF duration and severity of left atrial pressure elevation, or genetic factors is also unknown.
Regardless of the cause of superimposed (reactive) pulmonary arterial hypertension in HFpEF, it seems to be relatively uncommon in this patient population. RV dysfunction, however, is relatively common,53 and PDE5 inhibitors may have a role in either reactive pulmonary arterial hypertension or RV dysfunction in HFpEF, as demonstrated by Guazzi et al. in the aforementioned small clinical trial of sildenafil in such patients.41
The Evaluating the Effectiveness of Sildenafil at Improving Health Outcomes and Exercise Ability in People With Diastolic Heart Failure (RELAX) trial is a National Heart, Lung, and Blood Institute study that did not look at pulmonary hypertension specifically in HFpEF but rather, a broad spectrum of HFpEF patients. The idea behind RELAX was that PDE5 inhibitors have lusitropic myocardial effects that may improve diastolic function and are therefore useful simply on the basis of their action as vasodilators in HFpEF. However, the RELAX trial did not show any benefit to PDE5 inhibition in HFpEF patients without superimposed pulmonary arterial hypertension.54
Along with the PDE5 inhibitors, ranolazine, a late inward sodium channel (I[Na+]) inhibitor that seems to exert anti-ischemic effects in chronic stable angina by increasing myocardial relaxation, may be beneficial in patients with HFpEF. By blocking the late I[Na+] current, which is augmented in HF, there is less sodium in the myocyte, which results in less calcium in the myocyte during systole. Therefore, there is less postsystolic contraction of the myocyte, improved calcium handling, and better myocyte relaxation. Unfortunately, ranolazine did not demonstrate significant benefit in the Ranolazine for the Treatment of Diastolic Heart Failure (RALI-DHF) study, which was a small proof-of-concept HFpEF trial.55,56
DR. MASSIE: I think this has been a great discussion. The two of you come at HFpEF from somewhat different perspectives, but the consensus is that it’s a big problem and remains one of the most challenging problems in clinical cardiology. We need to continue to work to identify HFpEF patients and enroll them in clinical trials so that we can advance our knowledge in this patient population and find new targeted therapies for this patient population. Let’s hope some of these things that people are beginning to work with are successful.
UPDATE
The baseline clinical and echocardiographic characteristics of the TOPCAT trial have been published,57,58 providing insight into the 3445 patients with symptomatic heart failure with preserved ejection fraction (HFpEF) who were enrolled. Patients enrolled in the TOPCAT trial were similar to those in other HFpEF clinical trials and registries: the patients were older, more often female, and had a high prevalence of hypertension (91%). Baseline blood pressure, however, was well controlled (129/76 mm Hg; 7–16 mm Hg lower than that in other HFpEF clinical trials). Comorbidities were common, and quality life was poor (similar to end-stage renal disease). Structural heart disease was common in the TOPCAT trial, with a high prevalence of concentric left ventricular remodeling or hypertrophy and frequent left atrial enlargement. In November 2013, the results of the TOPCAT trial were presented at the American Heart Association Scientific Sessions. The TOPCAT trial failed to meet the primary combined endpoint of reducing cardiovascular mortality, aborted cardiac arrest, or HF hospitalization (hazard ratio [HR], 0.89; 95% confidence interval [CI], 0.77–1.04]; P = 0.14). Although spironolactone treatment did decrease HF hospitalization (HR, 0.83; 95% CI, 0.69–0.99; P = 0.042), all-cause hospitalizations did not differ among the treatment groups.
In a prespecified subgroup analysis based on the enrollment criteria, there was a statistically significant reduction in the primary endpoint in patients who entered the trial based on elevated natriuretic peptide levels (brain natriuretic peptide or N-terminal pro-brain natriuretic peptide). There was no difference in the primary endpoint for those patients who entered the trial based on prior history of HF hospitalization. Further exploration into the apparent dichotomy in the results, based on the enrollment criteria, revealed that there were major differences in the event rates in the Americas (United States, Canada, Brazil, and Argentina, where event rates were high [31.8%], similar to prior epidemiologic and observational studies) compared to Eastern Europe (Russia and the Republic of Georgia, where event rates were very low [8.4%]). A post-hoc analysis demonstrated that spironolactone treatment was beneficial in the Americas (HR, 0.82; 95% CI, 0.69–0.98 for the primary endpoint), but not in Eastern Europe. Furthermore, the majority of patients who entered the study based on the more objective natriuretic peptide criteria were from the Americas. These data demonstrate the importance of diagnosing HFpEF accurately (patients in Eastern Europe may not have had the HFpEF syndrome), and show that there may be patients with HFpEF, especially those with elevated natriuretic peptide levels, who would truly benefit from mineralocorticoid receptor antagonism.
Importantly, while hyperkalemia was more common in the TOPCAT trial patients treated with spironolactone (18.7% vs. 9.1%, respectively; P < 0.001), hypokalemia was less common in the spironolactone arm (16.2% vs. 22.9%, respectively), and there were no hyperkalemia-related deaths. Thus, if clinicians choose to use spironolactone to treat HFpEF, they should follow the TOPCAT trial guidelines for checking potassium levels and renal function at 1 week as well as at 30 days after starting spironolactone treatment, to prevent adverse events due to hyperkalemia. —Sanjiv J. Shah, MD, Northwestern University Feinberg School of Medicine, Chicago, IL
FoxP2 Media LLC is the publisher of The Medical Roundtable.
I’m Barry Massie, Professor of Medicine at the University of California in San Francisco, and I’ll be moderating the call. I’m delighted to be joined by 2 colleagues who have devoted a great deal of effort to the pathophysiology of this syndrome and potential approaches to its treatment: Michael Zile, Professor of Medicine at the Medical University of South Carolina, Principal Investigator at the Gazes Cardiac Research Institute, and Director of the Medical Intensive Care Unit at the Ralph H. Johnson Department of Veterans Affairs Medical Center, and Sanjiv Shah, Associate Professor of Medicine–Cardiology at Northwestern University.
Dr. Zile, our first presenter, will discuss the epidemiology and pathophysiology of HFpEF. I’m sure you will quickly recognize his extensive knowledge and passion for the problem. After that, Dr. Shah, a former chief resident and cardiology fellow from our program at the University of California in San Francisco, who’s established a large program devoted to the study and treatment of HFpEF patients, will discuss his approach to the diagnosis and management of these patients.
DR. ZILE: I would like to start with a very short historical perspective that puts into context some of the terminology that’s already been used by Dr. Massie. Before 2006, EF < 35% was an inclusion criterion in virtually all the HF studies conducted. Therefore, all new medical and device-based management strategies were originally applied selectively to patients with clinical HF with a reduced EF (HFrEF), which was then called systolic HF.
However, as early as the 1970s, it was recognized that there were, in fact, a group of patients who had HF but an EF substantially higher than the 35% cutoff, ie, an EF > 50%. Kenneth Kessler was the first to publish the term “diastolic heart failure” in 1988 to describe such a group of patients.1
Until 2006, almost no reports of large randomized clinical trials that had examined this group of patients were published. Fortunately, between 2006 and 2009, the results of 5 studies that had examined patients with variable EF cutoffs—35%, 40%, or 45%—were published. Therefore, the term “heart failure with preserved EF” was suggested. For symmetry, a complementary term “heart failure with reduced ejection fraction” was proposed.
The diagnostic criteria commonly used for patients with HFpEF were recently published in a comprehensive review published by the Heart Failure Society of America in Journal of Cardiac Failure.2 Diagnosis requires clinical evidence of HF, meaning evidence of both symptoms and signs of HF, often supported by findings on chest radiography, cardiopulmonary exercise testing, or assessment of natriuretic peptides.
In addition to the signs and symptoms of HF, there’s a required EF cutoff or partition value. For the sake this presentation, let’s say that cutoff value is 50%. In addition, patients should have a normal left ventricular (LV) end-diastolic volume.
Supportive evidence for the presence of this clinical syndrome is found echocardiographically in structural or functional changes. One should be cognizant of ruling out nonmyocardial disease.
Patients with HFpEF have clinical characteristics that differ from those of patients with HFrEF. Patients with HFpEF tend to be older. The average age of patients approaches 70 to 75 years. They’re typically women and more often have hypertension and less often coronary artery disease (CAD).
The prevalence of this clinical syndrome exceeds 50% and appears to be increasing over time.3,4 While the rate of HF hospitalization of HFpEF patients continues to increase, the rate of HF hospitalization for HFrEF patients is actually decreasing. Data from epidemiological studies suggest that the survival rate of both HFrEF patients and HFpEF patients at 5 years posthospitalization was approximately 60%.5 In contrast, data from randomized clinical trials suggest significant differences in both morbidity and mortality between these 2 groups of patients. In a recent study by Campbell and McMurray, the clinical trials that randomized both HFrEF and HFpEF patients found different rates of overall mortality and overall hospitalization for these 2 groups, specifically higher rates for patients with HFrEF.6 However, they found that the functional impairment experienced by HFrEF and HFpEF patients in terms of exercise intolerance is basically equivalent. One example to support this finding is that cardiopulmonary exercise data and peak oxygen consumption (VO2) values are roughly equivalent in both groups7,8 of patients and approach the peak VO2 value of ≤14 mL/kg/min, a criterion for HF transplantation.9
HFpEF is commonly associated with clear abnormalities in both structure and function at the organ and ultrastructure levels. In at least one study published in Circulation, it was demonstrated that even patients with chronic compensated HFpEF have elevated pulmonary artery diastolic pressure or pulmonary capillary wedge pressure (PCWP).10 Those who then go on to develop decompensated HFpEF have further increases in diastolic pressure. The overall relationship between LV diastolic pressure and volume in patients with HFpEF is pushed up and to the left to a steeper curve such that the LV diastolic pressure is higher in HFpEF patients as compared to normal patients at any common volume.
Echocardiographic findings demonstrate that long-term increases in diastolic pressure are evidenced by an increase in the left atrial volume. In 2 recent echocardiographic substudies of Irbesartan in Heart Failure With Preserved Systolic Function (I-PRESERVE) and Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity (CHARM-Preserved), 60% to 70% of these patients experienced increase in left atrial volume.11,12 This increase in left atrial volume predicted a marked increase in cumulative event rates in terms of primary both end points and HF end points in both studies.
HFpEF patients have significant increases in fibrillar collagen, which are under the control of the cardiac fibroblast. Abnormalities can be seen in at least 4 specific mechanisms controlling collagen homeostasis, including synthesis, postsynthetic processing, posttranslational modification, and degradation.
In one exemplary study by Westermann and colleagues published in 2011, LV biopsy of patients with HFpEF revealed a 3-fold increase in collagen volume fraction and a 4-fold increase in collagen type 1 volume fraction compared to that in the control subjects.13
If you look at the evidence of abnormalities and extracellular matrix homeostasis in the plasma, you will find changes in collagen pro-peptides such as the N-terminal pro-peptide of collagen 3; in matrix metalloproteinases (MMPs), specifically MMP2 and MMP8; and in the tissue inhibitors of MMP (TIMPs), specifically TIMP4. Abnormalities in these 4 plasma biomarkers taken in aggregate as a biomarker panel are evidence of abnormalities in extracellular matrix homeostasis and can be used diagnostically to detect the presence of HFpEF.
There are, however, some issues that have been raised regarding the natural history and the underlying pathophysiologic mechanisms in HFpEF. I’ll give you 2 examples.
Some scientists and clinicians have argued that HFpEF is not a clinical syndrome, but rather a group of symptoms and signs caused by comorbidities and associated with specific epidemiologic factors such as advanced age, female sex, CAD, diabetes, and hypertension. However, if this were true, then the morbidity and mortality rates should be comparable between patients who have only these underlying comorbidities and patients who have these comorbidities and HFpEF.
Campbell and McMurray compared the overall mortality and HF hospitalization rates of studies that examined patients with underlying comorbidities such as diabetes, hypertension, or CAD and no HFpEF, versus those patients studied in trials with HFpEF.14 For example, in studies patients with hypertension, diabetes, or CAD but no HF, the HF hospitalization rate was <12/100 patient-years, whereas in patients with these comorbidities and HFpEF, the rate was >40/100 patient-years.
The second challenge put forth by some scientists and clinicians is that HF is a continuum and HFpEF and HFrEF are, in fact, expressions of one disease process.15 However, there are clear structural and functional differences between these 2 clinical syndromes and that patients with HFpEF do not, in fact, progress to become patients with HFrEF. I’ll give you 2 sets of evidence to support that.
Patients with HFpEF, in general, have a normal ventricular volume but experience increases in LV mass, which supports the existence of a type of structural abnormality summarized by the term “concentric remodeling” or “concentric hypertrophy.” In contrast, patients with HFrEF experience marked increases in volumes without a proportional increase in LV mass, and thus experience eccentric remodeling or eccentric hypertrophy. These chamber abnormalities are mirrored by ultrastructural abnormalities such as those seen in the cardiomyocyte length, width, and area in animal models of eccentric versus concentric hypertrophy. In addition, there are significant differences in extracellular matrix remodeling.16
Finally, at least 4 studies demonstrate that over variable periods of time and in the absence of an intercurrent myocardial infarction, patients with concentric remodeling, a common structural manifestation of HFpEF, do not frequently progress to eccentric remodeling, a common structural manifestation of HFrEF. This conversion rate is less than 1% per year.17–20
I think I’ll stop my comments there and let Dr. Massie talk about the clinical trials that have been performed over the past 5 years.
DR. MASSIE: In terms of treating these patients, I think Dr. Zile already alluded to the fact that it’s challenging, but we’re learning more and getting better at it. Compared with HFrEF, the most commonly studied variety of HF, we have fewer data for HFpEF, but our knowledge is growing. This subject is currently gaining importance.
Among the relatively few randomized trials, I’ll review and comment on 4 of them. Guidelines don’t have much to say because, frankly, we haven’t found much for them to say. Treatment remains relatively empiric, and different clinicians have different biases that affect the treatment that they provide; some, for instance, simply treat HFpEF patients with diuretics when they become edematous.
Several small studies have shown that some agents seem to work. Certainly, diuretics, while not truly addressing the underlying mechanism of HFpEF, make patients feel better when they are volume overloaded. Some have tried calcium blockers, although I don’t think they have much clinical benefit. Beta blockers, angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers, and now aldosterone blockers. Most recent trials have focused on inhibitors of the renin angiotensin system. Frankly, there hasn’t been a lot of beneficial evidence.
It’s sort of paradoxical, but the first trial of HFpEF ever conducted on a moderate scale was with digoxin in the Digitalis Investigation Group (DIG) trial.21 Given digoxin’s utility as an inotropic agent, studying it in patients with HFpEF is, of course, somewhat counterintuitive. Nevertheless, I think studying these patients was a wonderful idea by Richard Gorlin, who was running the large DIG trial of HFrEF and thought it was about time to look at HFpEF as well.
The DIG study enrolled patients aged 67 years and older and included a larger proportion of women than you’d generally see in trials of HFrEF. The criterion for enrollment was an EF > 45%. The average EF was 55%, but 27% of patients had an EF < 50%. I will talk about that in more detail further, but this is where the 2 types of HF sometimes overlap in these trials.
Only half of the patients had a history of myocardial infarction, which is not surprising given the physiology and pathophysiology that Dr. Zile talked about, but hypertension was the dominant finding. When asked to speculate on the cause, the investigators stated hypertension for 23% of the patients, but we’ll see in other trials that hypertension is much more prevalent. In the Digitalis Investigation Group-Preserved Ejection Fraction (DIG-PEF), 56% of the patients were deemed to have an ischemic etiology.
The CHARM study,22 an angiotensin receptor blocker trial, that also conducted parallel examination of groups of HFrEF and HFpEF patients, observed the same phenomenon observed in the DIG trial: When you examine heterogeneous populations, you ultimately examine people who are more likely to reflect a dominant population, which in this case were HFrEF patients.
The Perindopril in Elderly Persons (PEP) trial,23 in which the mean age was 75 years and included more women than men, reported a higher mean EF than the previous 2 trials. We don’t know how many patients had EF < 50% because the PEP trial used a wall motion score index rather than the more typical EF value. As in the previous trials, relatively low rates of prior myocardial infarction were observed, and hypertension was thought to be the major player for a very large number of patients.
The last of the 4 investigations is the I-PRESERVE trial,24 the largest of these trials. As in the previous studies, the trial included patients of advanced age with a normal EF and a high percentage of women. Among the 88% of patients who had hypertension, the investigators indicated that the hypertension was responsible for the HFpEF in about two-thirds of the population, although it’s not entirely clear how they could make that judgment. Ischemic etiology was less common.
In the DIG-Preserved trial, there was early separation in the event-free survival curves for digoxin and placebo, which is perhaps a little difficult to explain, but probably one of the few positive findings at any point in any of these trials.
I wanted to elaborate a little more on I-PRESERVE, a trial that included 360 centers in 29 countries, for several reasons. One is that many of us were involved in it, and we believe that it probably provided more data than any other single trial. It used an angiotensin receptor blocker like CHARM did, but clearly separated the HFrEF and HFpEF patients. Over 4000 HFpEF patients developed 140 events.
The inclusion criteria for I-PRESERVE were EF < 45% with symptomatic HF and either recent hospitalization for HF or findings that fit the profile of diastolic HF or HFpEF. Use of an ACE inhibitor was not a contraindication, largely because ACE inhibitors were becoming the standard therapy for diabetics who comprised a fair number of these patients. We also didn’t feel that we could ethically withhold an ACE inhibitor from them.
The primary end point was a composite outcome of all-cause mortality or cardiovascular hospitalization. An echocardiography substudy that Dr. Zile published gives much insight, more than we had in the past, on the pathophysiology of HFpEF.25
There were no patients in whom EF was <45%. In the 2 trials that did not allow patients with EF < 45% (PEP and I-PRESERVE), the Kaplan–Meier event curves did not separate much (ie, there were no major differences in outcomes).
Those are the trials that have been completed, and from which we’ve derived most of our current data. Trial of Aldosterone Antagonist Therapy in Adults With Preserved Ejection Fraction Congestive Heart Failure (TOPCAT), a National Institute of Health-sponsored randomized controlled trial of spironolactone versus placebo in HFpEF,26 has clearly finished enrollment, but the results are not yet available. TOPCAT was originally designed to enroll 4500 patients, but could not reach that total because of challenges in the identification and recruitment of patients with HFpEF. The criteria for TOPCAT enrollment were age ≥50 years; EF ≥45%, as measured within 6 months of enrollment; signs and symptoms of HF; control of blood pressure at the time of study enrollment, despite the fact that the vast majority of patients had a history of hypertension and most other trials did not share this inclusion criterion; and, to ensure adequate event rates, at least one other high-risk HF feature, including hospitalization for HF within the past year and/or elevated levels of brain natriuretic peptides, either B-type natriuretic peptide (BNP) or N-terminal BNP.
Many of us thought that spironolactone might be an ideal drug because fibrosis, which spironolactone can at least reduce, if not prevent, is a major problem in some HFpEF patients.27 The composite primary end point in TOPCAT was cardiovascular death, aborted cardiac arrest, and hospitalization for HF management. The TOPCAT results are projected to be available in mid-2013.
So, what’s the conclusion? Do we know how to treat this entity? The answer in my mind is not yet, but we can prevent it, which would be my approach until we come up with a magic bullet to treat it. Most of these patients have hypertension, and many binge on salt, which is one of the reasons they have hypertension; obesity and diabetes seem to play a role to some degree as well. At this point, we don’t have any definitive answers about therapy.
In HYVET, indapamide, a thiazide-like diuretic, either with or without perindopril was found to be very effective in preventing HF hospitalization in patients aged >80 years. Although EF was not documented in HYVET, HFpEF is the predominant form of HF in the elderly; thus, it is likely that indapamide reduced hospitalization for HFpEF in that trial.29
Both ALLHAT and HYVET are important because they show that HFpEF can be prevented in hypertensive individuals. Some may argue that diuretics had an unfair advantage in both trials; namely, that HF hospitalization diagnosis was in part due to fluid overload, which diuretics treat and prevent. However, regardless of the mechanism of benefit, the results of these trials clearly show that HFpEF hospitalization can be prevented. Given the high rates of morbidity and mortality after HFpEF hospitalization, prevention by any means is critical.3,30
Although HFpEF can be prevented, we still have the challenge of managing the millions of patients suffering from HFpEF syndrome. In 2007, we founded a dedicated HFpEF program here at Northwestern University. Our reasons for doing so included the heterogeneity and diverse etiology and pathophysiology of the patient population; the lack of both a classification system and treatments for HFpEF; and as Dr. Zile mentioned, the difficulty in diagnosing HFpEF. Unlike HFrEF, we can’t use a simple EF indicator (ie, low EF) to make a diagnosis. Therefore, we need to be more systematic about identifying these patients and recruiting them into our clinical and research HFpEF program.
Between 2007 and 2012 we enrolled >750 patients into our program and have since been able to collect comprehensive data on 430 of these patients. We created a systematic algorithm for patient identification, focusing on inpatients because, as stated earlier, these are the patients at highest risk. We perform a daily query of the inpatient electronic medical records using one or more of the following criteria: the word “heart failure” in the hospital notes, or BNP > 100 pg/mL, or administration of 2 or more doses of intravenous diuretics. This gives us a long list of patients on a daily basis that we trim down by excluding all those with EF < 50%. We then have a study coordinator review all the remaining charts to identify patients who meet the Framingham criteria for HF and then offer these patients postdischarge follow-up in the HFpEF clinic.
For those who decide to come to our clinic after hospitalization, we confirm the HFpEF diagnosis based on much of the criteria that Dr. Zile mentioned. We also exclude some patients, such as those with a prior history of reduced EF (<40%), severe valvular disease, or prior history of cardiac transplant. We then enroll the remaining patients into our registry. We perform physical examination, electrocardiography, laboratory testing, and echocardiography in all patients, and arterial tonometry, pulmonary function testing, and cardiopulmonary exercise testing, as well as overnight polysomnography in a subset of patients. We try to have all patients undergo cardiac catheterization because we want to exclude CAD and invasively confirm elevated LV filling pressures. This is especially important in patients who have signs and symptoms of HF but whose echocardiography results are equivocal for diastolic dysfunction and BNP < 100 pg/mL.
Importantly, we try to enroll every patient in a clinical trial. We were quite successful with that regard with the current TOPCAT, for which, as the leading enroller in the United States, we enrolled 77 patients. Clinical trial enrollment for HFpEF has been very challenging, and we believe that dedicated HFpEF programs will be critical for enhancing enrollment in HFpEF studies. Finally, after conducting initial confirmation of HFpEF diagnosis, baseline testing, and consideration for clinical trial enrollment, we follow patients every 3 to 6 months (or sooner as needed) to manage their HFpEF.
Our patients are younger by about 10 years as compared to those who have participated in the observational studies and clinical trials, such as I-PRESERVE, likely because elderly patients tend to not want to change doctors or have to see a new cardiologist, so elect not to enroll in our program. However, I also think that we identify patients at a younger age. We’re seeing younger patients with morbid obesity and diabetes and/or metabolic syndrome who are developing HFpEF. In our urban Chicago area, we have a diverse mix of ethnicity and races, and approximately 40% of the patient population is African-American, which is much higher than that in prior observational studies and clinical trials. Finally, as expected, comorbidities are quite common in patients in our HFpEF program, and the body mass index of our patients is much higher than that of patients in prior studies (mean body mass index, 33 kg/m2).
Analysis of data collected from patients enrolled in our HFpEF program confirmed that they met the objective criteria for HFpEF syndrome.31 Despite enrolling after HF hospitalization, during which they underwent intensive diuresis, they have remained quite symptomatic, with 49% continuing to have New York Heart Association Functional Classification (NYHA) Class III or IV symptoms. Furthermore, EF in our cohort is preserved (mean EF 61±7%), LV end-diastolic volume index is normal (41±12 mL/m2), and the majority have evidence of moderate or greater diastolic dysfunction (72% with grade 2 or 3 diastolic dysfunction and 79% with echocardiographic evidence of elevated LV end-diastolic pressure or PCWP). On invasive hemodynamic testing, mean PCWP was 23 mm Hg, which is quite high, considering that they had already undergone intravenous diuresis in the hospital. Thus, patients enrolled in our HFpEF program meet the objective criteria for HFpEF and despite treatment, remain quite symptomatic and fluid overloaded.
Drs. Zile and Massie described how we diagnose these patients and the lack of clinical trial data that we can refer to when treating these patients. These facts are important to know, but clinicians who treat these patients still need a roadmap for the major steps in diagnosis and treatment of HFpEF. The first step is to accurately diagnose the HFpEF syndrome (given its high prevalence, clinicians should have a low threshold to suspect the diagnosis in the dyspneic patient). Despite the limited data regarding BNP levels in diagnosis of HFpEF, clinicians often use levels of natriuretic peptides in diagnosis. When we systematically analyzed BNP levels in the patients in our program, we found that in up to 30% with confirmed HFpEF (ie, elevated PCWP and preserved EF), BNP level was normal (<100 pg/mL).32 Thus, a normal BNP level does not exclude a diagnosis of HFpEF syndrome.
When in doubt about HFpEF diagnosis, we perform cardiac catheterization for confirmation. While invasive hemodynamic testing is not necessary for all patients, it’s preferable to identify and diagnose HFpEF than miss it. We also routinely and systematically evaluate patients for CAD through stress testing and coronary angiography when possible, because multi-vessel CAD can mimic HFpEF, and treatment of CAD can provide symptomatic benefit.
The second step is to identify, target, and treat the underlying cause of HFpEF, an important part of our therapeutic strategy for the individual patient. Although HFpEF is very common and most commonly caused by standard comorbidities like hypertension, obesity, diabetes, CAD, and chronic kidney disease, we approach each patient as a unique case until proven otherwise. We must ensure that we don’t fail to detect constrictive pericarditis or infiltrative cardiomyopathy, which, although rarely causes HFpEF, requires treatment that differs significantly from that provided for HFpEF caused by more common conditions. Here, close examination of the echocardiogram can be very helpful. For example, on tissue Doppler imaging of the lateral mitral annulus, severe reduction in longitudinal systolic velocity (s′) and early diastolic velocity (e′) with preserved global EF suggests the possibility of infiltrative cardiomyopathy, especially in the setting of increased wall thickness and a low voltage electrocardiogram. On the other hand, a normal or exaggerated e′ velocity, despite a mitral inflow pattern, suggestive of significant diastolic dysfunction, can be a sign of constrictive pericarditis, especially if there are additional echocardiographic signs such as increased respiratory variation in the mitral inflow, diastolic septal bounce, or increased hepatic vein diastolic flow reversal during expiration.
Step 3 is, as stated in the HF guidelines, to treat HF by controlling blood pressure and treat fluid overload using diuretics. In terms of pharmacotherapy, I like to prescribe carvedilol, bumetanide, chlorthalidone, lisinopril, and spironolactone. As Dr. Massie just mentioned, we don’t have great data for any of these medications, but given the wide availability of generic forms of these agents and the use of many in the treatment of comorbidities common in HFpEF patients, they are affordable and effective options for the treatment of hypertension and fluid overload in these patients.
Step 4 is to aggressively treat comorbidities, which is a major reason for the high rate of morbidity of mortality in HFpEF patients. More than 90% of patients with HFpEF have hypertension, CAD, diabetes, and/or chronic kidney disease, and many have sleep-disordered breathing and chronic pulmonary obstructive disease.33,34 Thus, HFpEF patients are not treated just by treating their HF; we really need to treat the whole patient and work with our colleagues in internal medicine, geriatrics, and other subspecialties to provide holistic care.
Step 5 is to provide a structured program of exercise training. A recent meta-analysis on and several high-quality smaller studies have found that exercise training is beneficial in HFpEF.35–39
Step 6 is to provide HF education to our patients. In an analysis of data from the Mid-Michigan Guidelines Applied in Practice–Heart Failure (GAP-HF) trial, Hummel and colleagues found that HFpEF patients are less likely to receive appropriate discharge instructions than patients with HFrEF.40 Although the Get with the Guidelines–Heart Failure (GWTG-HF) study found that while discharge instructions for HFpEF patients have improved over time, they are still inadequate.4 Thus, HFpEF patients need better education at discharge regarding salt restriction and fluid management.
Step 7 is to group HFpEF patients into categories, given the heterogeneity of HFpEF syndrome. The first category is what we call "garden-variety" HFpEF patients, who are typically hypertensive and obese, may or may not have diabetes, and often have chronic kidney disease. In these patients, we treat the underlying hypertension and focus on weight loss and control of diabetes, if present.
The next subgroup is HFpEF patients in whom CAD is the primary driver of HFpEF. While we need better data on how to treat these patients, based on their pathophysiology (worse biventricular longitudinal systolic function) and my anecdotal experience, I treat them like HFrEF patients, with beta blockers, renin-angiotensin-aldosterone system (RAAS) antagonists, statins, and revascularization, which are often indicated for the treatment of CAD.
The next subgroup is HFpEF patients with atrial arrhythmia and few other comorbidities. These patients, who often have normal or easily controlled blood pressure and experience episodes of tachyarrhythmia that exacerbate HF, appear to be suffering from HFpEF due to the underlying atrial arrhythmia. In these patients, I attempt to maintain normal sinus rhythm, especially if they are less symptomatic and less fluid overloaded when in a normal sinus rhythm.
Some patients with HFpEF have predominantly right ventricular (RV) HF symptoms. These are patients with high pulmonary artery pressure and RV dysfunction on echocardiography in the setting of elevated LV end-diastolic pressure and clear LV diastolic dysfunction. The management of these patients is often challenging. As RV dysfunction worsens, significant tricuspid regurgitation occurs often, cardiac output decreases, and systemic pressures decline. The resultant severe central venous congestion can lead to “congestive nephropathy,” while renal function worsens, leading to even more fluid overload. In these patients, intensive diuresis (or ultrafiltration when needed), spironolactone, and digoxin can be helpful. If systemic hypotension limits adequate diuresis, we treat patients with midodrine. In patients with HFpEF with significant RV dysfunction and elevated pulmonary artery pressure, especially those with pulmonary arterial hypertension superimposed on pulmonary venous hypertension (defined as a PA diastolic pressure-PCWP gradient > 5 mmHg), sildenafil may be beneficial.41
Another group of patients includes those with HFpEF in the setting of cardiac structural and functional changes that mimic hypertrophic cardiomyopathy. These are elderly patients with long-standing hypertension whose echocardiographic findings are indistinguishable from hypertrophic cardiomyopathy. I therefore treat them by focusing on negative inotropes such as long-acting metoprolol, diltiazem, or verapamil and avoiding aggressive diuresis, which can result in LV outflow tract or intracavitary obstruction.
There are a few additional subgroups of HFpEF patients. Some patients have HFpEF associated with a high-output state, such as those with end-stage liver disease, hyperthyroidism, arteriovenous fistulas, or severe anemia. Enlargement of all 4 cardiac chambers is a clue to this diagnosis. In these cases, we treat the underlying cause and use diuretics as a mainstay. Some patients have multivalvular HFpEF, and in such patients, having moderate disease of multiple valves presents a treatment challenge. These patients often do not meet the criteria for valve replacement or repair, but develop moderate valvular lesions, which, combined with other risk factors for HFpEF, lead to symptomatic HF. Finally, there are patients with HFpEF caused by rare conditions such as infiltrative cardiomyopathies and constrictive pericarditis. I treat the underlying cause in these patients and enroll them in a clinical trial, if possible.
I’ll conclude by touching on beta-blocker therapy in HFpEF. There have been multiple observational studies and some clinical trials of this topic, including the Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors with Heart Failure (SENIORS),42 which studied nebivolol, a vasodilating beta blocker. When considering beta-blocker use in HFpEF, there are several key points to remember. We know that some patients with HFpEF have chronotropic incompetence, which underlies their inability to increase cardiac output with exercise.43,44 In these patients, beta-blocker therapy could be harmful. However, observational studies of HFpEF have shown that beta blockers are associated with better outcomes in HFpEF patients.
What’s key here is that if a beta blocker is going to be used, it should be a vasodilating beta blocker, and that’s why I like carvedilol; it acts as a potent blood pressure-lowering agent due to its vasodilating properties. In the Coreg Heart Failure Registry (COHERE), registry led by Dr. Massie, carvedilol was found to be associated with better outcomes in HF, regardless of the underlying EF.45 This study was limited by its observational design, but nevertheless indicates some potential benefit.
The last point I’ll mention on beta blockers in HFpEF is that it is important to differentiate not only the patients with chronotropic incompetence but also those with severe diastolic dysfunction and restricted filling on echocardiography—patients who have evidence of a restrictive cardiomyopathy. These patients are typically very sensitive to any rate-controlling agents because stroke volume is fixed, and they rely on increasing heart rate with exercise in order to augment cardiac output. In these patients, in particular, I am very hesitant about using beta blockers unless they have an atrial arrhythmia that results in high heart rates and worsening HF. In patients with a hypertrophic cardiomyopathy-like phenotype, on the other hand, who need adequate diastolic filling time and atrial kick, I find beta blockers very helpful. These are just anecdotal observations, but I’ve found them to be helpful.
I’ll conclude by stating that right now I agree with Dr. Massie that we don’t have good clinical trial data, but it’s clear that the next 5 to 10 years will be an exciting time in which we’re likely to reinvent our knowledge about HFpEF and the clinical management of this syndrome.
DR. MASSIE: Dr. Shah, have you had to send anybody with HFpEF for transplantation?
DR. SHAH: In my practice, we have considered cardiac transplantation in cases of severe restrictive cardiomyopathy.
DR. MASSIE: What about patients with amyloid-type cardiomyopathy?
DR. SHAH: Yes, cardiac amyloidosis, and those with idiopathic restrictive cardiomyopathy. Typically, these are the patients with restrictive cardiomyopathy that develop end-stage HF. Patients with “garden-variety” HFpEF typically don’t develop severe enough end-stage HF to warrant cardiac transplantation, and their advanced age and multiple comorbidities often preclude consideration for transplant. Patients with restrictive cardiomyopathy represent a difficult challenge in the current era of cardiac transplantation. These patients typically have small ventricular volumes and are therefore not good candidates for mechanical circulatory support. However, because of a preserved EF, inotropes are not helpful in most of these patients. Thus, they often wait on the transplant list for quite some time and get bypassed by HFrEF patients who have a 1B or 1A status in the setting of ventricular assist devices. Finally, in patients with primary (AL) cardiac amyloidosis some advocate cardiac transplant,46 but it has been our practice to use chemotherapy followed by autologous stem-cell transplantation for these types of patients, provided that we can get patients close to euvolemia and control their HF symptoms.
DR. ZILE: I have had patients with hypertrophic cardiomyopathy with a normal EF who have had very low myocardial peak VO2 values, ie, myocardial VO2 values significantly less than 14 mL/kg/min, who have gone in for transplantation. I suppose that there are some patients with valvular heart disease for whom, if they’re young enough, one could consider transplantation as well, if they’re not candidates for surgical replacement.
I’d like to talk about a couple of other issues that Dr. Shah’s comments have raised. One is the use of implantable hemodynamic monitors in this group of patients. The second is the use of device therapy for the treatment of hypertension, particularly resistant hypertension. Dr. Shah’s comment regarding the variety of diuretics that he uses in his incredibly well-developed clinic brings to mind 2 concepts. One is that the reason why diuretics reduce HF hospitalization is, in fact, the judicious use of small changes in dose. Small but judicious increases and decreases can not only acutely but chronically lower filling pressure. This has been demonstrated in at least 3 studies—Chronicle Offers Management to Patients With Advanced Signs and Symptoms of Heart Failure (COMPASS-HF),47 CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Patients (CHAMPION),48 and Home Self-Therapy in Severe Heart Failure Patients (HOMEOSTASIS).49
In addition, HOMEOSTASIS and its ongoing follow-up study, Left Atrial Pressure Monitoring to Optimize Heart Failure Therapy (LAPTOP-HF),50 not only demonstrated that it is important to lower pressure by making small and judicious changes in diuretic dose but also showed that every time we increase diuretic dose, we also increase activation of the sympathetic nervous system or the RAAS. When the diuretic dosage is increased, it should be accompanied by uptitration of sympathetic antagonist beta blockers and RAAS antagonists, if possible.
The only clinical trial that I know that demonstrated a clear statistically significant reduction in HF hospitalizations in this group of patients is CHAMPION, which achieved a very large reduction in HF hospitalization—one virtually unheard of in any other trial—by maintaining low filling pressures by the therapeutic interventions that I’ve just mentioned.
DR. SHAH: I was very impressed by CHAMPION—it’s exactly what we see clinically with these patients. For example, I’m continually amazed at the close relationship between dietary indiscretion and worsening HF. Another such example is that fact that around the Thanksgiving holiday, many of my patients with HFpEF will develop significant volume overload, often necessitating hospitalization for HF exacerbation. Dietary indiscretion and medication noncompliance inevitably lead to a sudden rise in filling pressures. If we could implant an implantable monitor in these patients, we would have the ability to preemptively strike and give them an increased dose, thereby improving their outcomes.
I also agree with being judicious, especially with loop diuretics, so that we don’t trigger the intense sympathetic response. I teach our cardiology fellows that while we treat with diuretics because they’re very effective in controlling symptoms, we try to find the minimal dose to keep patients euvolemic and thereby limit the degree of sympathetic discharge.
DR. ZILE: To follow-up on your comments, in CHAMPION and HOMEOSTASIS, in an average 7-day week, changes in medications for diuretics—and I should also mention long-acting nitrates—were made on about 5 of the 7 days, but the changes were very small. For example, small changes were made in furosemide dose, from 20 to 30 mg or from 30 to 40 mg (eg, ±10 mg/day), but produced significant long-term falls in filling pressure.
The other topic that I think we should mention is that new devices that are being used to treat resistant hypertension, which is important from the point of view of prevention and the treatment of hypertension. There’s no question that if you could achieve regression of LV hypertrophy in hypertensive HFpEF patients with LV hypertrophy, you could markedly decrease both morbidity and mortality.
This can be accomplished with renal artery denervation (RAD) through a transcatheter approach. The Renal Denervation in Patients With Uncontrolled Hypertension (Symplicity HTN-2) study showed that RAD could markedly decrease LV mass, as evidenced by a 13% reduction in LV mass 1 month and a 17% decrease in LV mass 6 months after RAD,51 and significantly increase percentages higher than those obtained with the pharmacologic interventions we’ve used in hypertension trials to cause regression of LV hypertrophy.
In addition to RAD, there’s also carotid sinus stimulation, vagal nerve stimulation, and spinal cord stimulation, which are being examined.
DR. MASSIE: I’m certainly impressed with the renal sympathetic nerve ablation data, which I think a group in London is acting upon by doing a trial on HFpEF patients. I think hypertension is at the core of this. Frankly, it’s people’s behavioral patterns that make that the case. So, if you ablate the renal sympathetic nerves, the patient probably can’t overcome that and consequently benefit from it.
I think renal sympathetic nerve ablation is something that’s probably here to stay. I haven’t been as impressed with carotid sinus stimulation, compared with the renal sympathetic nerve denervation. I think it’s time to have a laboratory to gather a working group to study HFpEF and probably take on some further trials with some of the promising therapies.
Data from Olmsted County, Minnesota, indicate that pulmonary hypertension, defined as elevated pulmonary artery systolic pressure on echocardiography, is very common in HFpEF.52 In addition, elevated pulmonary artery systolic pressure was found to be the best echocardiographic sign differentiating patients with HFpEF from patients with hypertension without HF.52 The high prevalence of pulmonary hypertension in HFpEF makes sense—high left atrial pressure at rest or with exercise, which is nearly universal in HFpEF, leads to passive elevation of pulmonary venous pressures and thus, pulmonary hypertension. In addition, akin to systolic systemic hypertension of the elderly, patients with HFpEF have systolic pulmonary hypertension, ie, they have disproportionate elevation of pulmonary artery systolic pressure and high pulmonary artery pulse pressure.
What’s not clear, as I stated earlier, is why some patients with HFpEF further develop an elevated pulmonary vascular resistance or a more reactive form of pulmonary hypertension. Whether the presence of superimposed pulmonary arterial hypertension or pulmonary arterial remodeling is due to comorbidities that cause pulmonary arterial hypertension, HF duration and severity of left atrial pressure elevation, or genetic factors is also unknown.
Regardless of the cause of superimposed (reactive) pulmonary arterial hypertension in HFpEF, it seems to be relatively uncommon in this patient population. RV dysfunction, however, is relatively common,53 and PDE5 inhibitors may have a role in either reactive pulmonary arterial hypertension or RV dysfunction in HFpEF, as demonstrated by Guazzi et al. in the aforementioned small clinical trial of sildenafil in such patients.41
The Evaluating the Effectiveness of Sildenafil at Improving Health Outcomes and Exercise Ability in People With Diastolic Heart Failure (RELAX) trial is a National Heart, Lung, and Blood Institute study that did not look at pulmonary hypertension specifically in HFpEF but rather, a broad spectrum of HFpEF patients. The idea behind RELAX was that PDE5 inhibitors have lusitropic myocardial effects that may improve diastolic function and are therefore useful simply on the basis of their action as vasodilators in HFpEF. However, the RELAX trial did not show any benefit to PDE5 inhibition in HFpEF patients without superimposed pulmonary arterial hypertension.54
Along with the PDE5 inhibitors, ranolazine, a late inward sodium channel (I[Na+]) inhibitor that seems to exert anti-ischemic effects in chronic stable angina by increasing myocardial relaxation, may be beneficial in patients with HFpEF. By blocking the late I[Na+] current, which is augmented in HF, there is less sodium in the myocyte, which results in less calcium in the myocyte during systole. Therefore, there is less postsystolic contraction of the myocyte, improved calcium handling, and better myocyte relaxation. Unfortunately, ranolazine did not demonstrate significant benefit in the Ranolazine for the Treatment of Diastolic Heart Failure (RALI-DHF) study, which was a small proof-of-concept HFpEF trial.55,56
DR. MASSIE: I think this has been a great discussion. The two of you come at HFpEF from somewhat different perspectives, but the consensus is that it’s a big problem and remains one of the most challenging problems in clinical cardiology. We need to continue to work to identify HFpEF patients and enroll them in clinical trials so that we can advance our knowledge in this patient population and find new targeted therapies for this patient population. Let’s hope some of these things that people are beginning to work with are successful.
UPDATE
The baseline clinical and echocardiographic characteristics of the TOPCAT trial have been published,57,58 providing insight into the 3445 patients with symptomatic heart failure with preserved ejection fraction (HFpEF) who were enrolled. Patients enrolled in the TOPCAT trial were similar to those in other HFpEF clinical trials and registries: the patients were older, more often female, and had a high prevalence of hypertension (91%). Baseline blood pressure, however, was well controlled (129/76 mm Hg; 7–16 mm Hg lower than that in other HFpEF clinical trials). Comorbidities were common, and quality life was poor (similar to end-stage renal disease). Structural heart disease was common in the TOPCAT trial, with a high prevalence of concentric left ventricular remodeling or hypertrophy and frequent left atrial enlargement. In November 2013, the results of the TOPCAT trial were presented at the American Heart Association Scientific Sessions. The TOPCAT trial failed to meet the primary combined endpoint of reducing cardiovascular mortality, aborted cardiac arrest, or HF hospitalization (hazard ratio [HR], 0.89; 95% confidence interval [CI], 0.77–1.04]; P = 0.14). Although spironolactone treatment did decrease HF hospitalization (HR, 0.83; 95% CI, 0.69–0.99; P = 0.042), all-cause hospitalizations did not differ among the treatment groups.
In a prespecified subgroup analysis based on the enrollment criteria, there was a statistically significant reduction in the primary endpoint in patients who entered the trial based on elevated natriuretic peptide levels (brain natriuretic peptide or N-terminal pro-brain natriuretic peptide). There was no difference in the primary endpoint for those patients who entered the trial based on prior history of HF hospitalization. Further exploration into the apparent dichotomy in the results, based on the enrollment criteria, revealed that there were major differences in the event rates in the Americas (United States, Canada, Brazil, and Argentina, where event rates were high [31.8%], similar to prior epidemiologic and observational studies) compared to Eastern Europe (Russia and the Republic of Georgia, where event rates were very low [8.4%]). A post-hoc analysis demonstrated that spironolactone treatment was beneficial in the Americas (HR, 0.82; 95% CI, 0.69–0.98 for the primary endpoint), but not in Eastern Europe. Furthermore, the majority of patients who entered the study based on the more objective natriuretic peptide criteria were from the Americas. These data demonstrate the importance of diagnosing HFpEF accurately (patients in Eastern Europe may not have had the HFpEF syndrome), and show that there may be patients with HFpEF, especially those with elevated natriuretic peptide levels, who would truly benefit from mineralocorticoid receptor antagonism.
Importantly, while hyperkalemia was more common in the TOPCAT trial patients treated with spironolactone (18.7% vs. 9.1%, respectively; P < 0.001), hypokalemia was less common in the spironolactone arm (16.2% vs. 22.9%, respectively), and there were no hyperkalemia-related deaths. Thus, if clinicians choose to use spironolactone to treat HFpEF, they should follow the TOPCAT trial guidelines for checking potassium levels and renal function at 1 week as well as at 30 days after starting spironolactone treatment, to prevent adverse events due to hyperkalemia. —Sanjiv J. Shah, MD, Northwestern University Feinberg School of Medicine, Chicago, IL
FoxP2 Media LLC is the publisher of The Medical Roundtable.
FoxP2 Media LLC

A Very Special Issue
Since 2011, Federal Practitioner and the Association of VA Hematology/Oncology have teamed up to create the “Advances in Hematology and Oncology” special issues. The collaboration has been a rewarding one for everyone involved, and we trust it will continue for years to come.
The issues have showcased the broad experience and expertise of VA hematology and oncology care providers. Over the years, we’ve highlighted the important research often coming out of the VA and have brought that knowledge to an audience that goes well beyond the 900 or so AVAHO members.
Still, that doesn’t seem like enough. More often than not, primary care providers are the first line of defense for patients. More important, as survivorship expands and new therapies continue to increase overall survival, all providers across the federal health care systems are treating patients after their diagnosis. There have been significant developments recently in hematology and oncology, and primary care providers are caring for more patients than ever who have cancer and leukemia, not only at the VA, but also at the PHS and DoD. This research is relevant to the entire Federal Practitioner audience, and we felt it was important to share as widely as possible.
The 7 articles included in this special issue are broad and diverse, illustrating the high degree of specialization that is occurring in the fields of hematology and oncology. These features cover breast cancer, chronic myelogenous leukemia, prostate cancer, mantle cell lymphoma, chronic lymphocytic leukemia, pancreatic cancer, and melanoma. Sometimes, the articles focus on highly specific topics for specialists, such as the role of autologous hematopoietic stem cell transplantation in mantle cell lymphoma. Other times, the articles are aimed at a primary care audience, providing an essential update on prostate cancer survivorship care. In either case, we hope you will find these articles valuable and worthwhile.
To compliment the features, we added a new Patient Information handout on hospice care as well as some recent news updates in our Clinical Digest department. We also wanted to echo these important research updates with audio interviews, blogs, and other online exclusive features.
We would like to thank the Association of VA Hematology/Oncology (AVAHO) for their cooperation and help in putting together this series. The AVAHO mission is to facilitate interaction and cooperation among VA hematology and oncology health care providers and to enhance professional careers and improve patient care, and we are honored to be able to help carry out that mission. The AVAHO Annual Meeting will be September 12-14, 2014, in Portland, Oregon. For more information visit avaho.org.
We would also like to thank Paulette Mehta, MD, MPH, and Peter Silberstein, MD, for their significant efforts and the time they put into making this special issue possible. Their commitment to creating this issue and to ensuring that Federal Practitioner remains on top of the latest advances in trends and practices in these quickly changing fields cannot be understated.
Since 2011, Federal Practitioner and the Association of VA Hematology/Oncology have teamed up to create the “Advances in Hematology and Oncology” special issues. The collaboration has been a rewarding one for everyone involved, and we trust it will continue for years to come.
The issues have showcased the broad experience and expertise of VA hematology and oncology care providers. Over the years, we’ve highlighted the important research often coming out of the VA and have brought that knowledge to an audience that goes well beyond the 900 or so AVAHO members.
Still, that doesn’t seem like enough. More often than not, primary care providers are the first line of defense for patients. More important, as survivorship expands and new therapies continue to increase overall survival, all providers across the federal health care systems are treating patients after their diagnosis. There have been significant developments recently in hematology and oncology, and primary care providers are caring for more patients than ever who have cancer and leukemia, not only at the VA, but also at the PHS and DoD. This research is relevant to the entire Federal Practitioner audience, and we felt it was important to share as widely as possible.
The 7 articles included in this special issue are broad and diverse, illustrating the high degree of specialization that is occurring in the fields of hematology and oncology. These features cover breast cancer, chronic myelogenous leukemia, prostate cancer, mantle cell lymphoma, chronic lymphocytic leukemia, pancreatic cancer, and melanoma. Sometimes, the articles focus on highly specific topics for specialists, such as the role of autologous hematopoietic stem cell transplantation in mantle cell lymphoma. Other times, the articles are aimed at a primary care audience, providing an essential update on prostate cancer survivorship care. In either case, we hope you will find these articles valuable and worthwhile.
To compliment the features, we added a new Patient Information handout on hospice care as well as some recent news updates in our Clinical Digest department. We also wanted to echo these important research updates with audio interviews, blogs, and other online exclusive features.
We would like to thank the Association of VA Hematology/Oncology (AVAHO) for their cooperation and help in putting together this series. The AVAHO mission is to facilitate interaction and cooperation among VA hematology and oncology health care providers and to enhance professional careers and improve patient care, and we are honored to be able to help carry out that mission. The AVAHO Annual Meeting will be September 12-14, 2014, in Portland, Oregon. For more information visit avaho.org.
We would also like to thank Paulette Mehta, MD, MPH, and Peter Silberstein, MD, for their significant efforts and the time they put into making this special issue possible. Their commitment to creating this issue and to ensuring that Federal Practitioner remains on top of the latest advances in trends and practices in these quickly changing fields cannot be understated.
Since 2011, Federal Practitioner and the Association of VA Hematology/Oncology have teamed up to create the “Advances in Hematology and Oncology” special issues. The collaboration has been a rewarding one for everyone involved, and we trust it will continue for years to come.
The issues have showcased the broad experience and expertise of VA hematology and oncology care providers. Over the years, we’ve highlighted the important research often coming out of the VA and have brought that knowledge to an audience that goes well beyond the 900 or so AVAHO members.
Still, that doesn’t seem like enough. More often than not, primary care providers are the first line of defense for patients. More important, as survivorship expands and new therapies continue to increase overall survival, all providers across the federal health care systems are treating patients after their diagnosis. There have been significant developments recently in hematology and oncology, and primary care providers are caring for more patients than ever who have cancer and leukemia, not only at the VA, but also at the PHS and DoD. This research is relevant to the entire Federal Practitioner audience, and we felt it was important to share as widely as possible.
The 7 articles included in this special issue are broad and diverse, illustrating the high degree of specialization that is occurring in the fields of hematology and oncology. These features cover breast cancer, chronic myelogenous leukemia, prostate cancer, mantle cell lymphoma, chronic lymphocytic leukemia, pancreatic cancer, and melanoma. Sometimes, the articles focus on highly specific topics for specialists, such as the role of autologous hematopoietic stem cell transplantation in mantle cell lymphoma. Other times, the articles are aimed at a primary care audience, providing an essential update on prostate cancer survivorship care. In either case, we hope you will find these articles valuable and worthwhile.
To compliment the features, we added a new Patient Information handout on hospice care as well as some recent news updates in our Clinical Digest department. We also wanted to echo these important research updates with audio interviews, blogs, and other online exclusive features.
We would like to thank the Association of VA Hematology/Oncology (AVAHO) for their cooperation and help in putting together this series. The AVAHO mission is to facilitate interaction and cooperation among VA hematology and oncology health care providers and to enhance professional careers and improve patient care, and we are honored to be able to help carry out that mission. The AVAHO Annual Meeting will be September 12-14, 2014, in Portland, Oregon. For more information visit avaho.org.
We would also like to thank Paulette Mehta, MD, MPH, and Peter Silberstein, MD, for their significant efforts and the time they put into making this special issue possible. Their commitment to creating this issue and to ensuring that Federal Practitioner remains on top of the latest advances in trends and practices in these quickly changing fields cannot be understated.
Caring for an expectant mother
"Mrs. Jones in ED room 12? Septic with severe multilobar pneumonia and hypoxemic respiratory failure? Got it. I’m on my way down to the ED now." The heart races in anticipation of caring for this critically ill patient near death’s door. But it’s okay. You know exactly what you have to do. You have done it many times before. No problem. Just as you are about to hang up the phone you learn more ...
"What’s that? She is 22 weeks pregnant? Uh, all right."

Suddenly, what initially seemed to be a routine case takes a complicated twist. You are no longer caring for one life, you are caring for two (or more), and one of those is extremely frail and vulnerable. The bugs, the drugs, maintaining adequate perfusion of vital organs – both hers and her baby’s – the questions of "What if ... ?" and "Should I ... ?" race through your mind. Should you get infectious disease and pulmonary consultations for an added layer of protection or should you treat her as you have treated so many others before her, the caveat, of course, being the need to check every single drug for its teratogenicity.
If you have ever felt at least a little queasiness in the pit of your stomach when called upon to care for an expectant mother, you are notalone. I think it is natural to feel a bit uneasy when we care for pregnant patients because most of us do it rather infrequently and there may not be room for a do-over even if you make the tiniest mistake. Each drug we order has the potential to do harm and any missed or delayed diagnosis may be tolerated well by mom, but maybe not much by the tiny baby growing inside her. Get it right and the family may live a storybook fantasy. Yet, a single miscalculation, an honest mistake, and that innocent child’s future may be compromised or destroyed.
Fortunately, these days, horror stories seem to be less frequent than in the past. But we must remain vigilant to not only optimally treat our patient (mommy), but also to protect our patients (mommy and baby) from future complications of treatment. If there is any doubt, go ahead and call an infectious disease and pulmonary consultation. Sometimes, everyone sleeps better when we do.
Dr. A. Maria Hester is a hospitalist with Baltimore-Washington Medical Center, Glen Burnie, Md., who has a passion for empowering patients to partner in their health care. She is the creator of the Patient Whiz, a patient-engagement app for iOS.
"Mrs. Jones in ED room 12? Septic with severe multilobar pneumonia and hypoxemic respiratory failure? Got it. I’m on my way down to the ED now." The heart races in anticipation of caring for this critically ill patient near death’s door. But it’s okay. You know exactly what you have to do. You have done it many times before. No problem. Just as you are about to hang up the phone you learn more ...
"What’s that? She is 22 weeks pregnant? Uh, all right."
Suddenly, what initially seemed to be a routine case takes a complicated twist. You are no longer caring for one life, you are caring for two (or more), and one of those is extremely frail and vulnerable. The bugs, the drugs, maintaining adequate perfusion of vital organs – both hers and her baby’s – the questions of "What if ... ?" and "Should I ... ?" race through your mind. Should you get infectious disease and pulmonary consultations for an added layer of protection or should you treat her as you have treated so many others before her, the caveat, of course, being the need to check every single drug for its teratogenicity.
If you have ever felt at least a little queasiness in the pit of your stomach when called upon to care for an expectant mother, you are notalone. I think it is natural to feel a bit uneasy when we care for pregnant patients because most of us do it rather infrequently and there may not be room for a do-over even if you make the tiniest mistake. Each drug we order has the potential to do harm and any missed or delayed diagnosis may be tolerated well by mom, but maybe not much by the tiny baby growing inside her. Get it right and the family may live a storybook fantasy. Yet, a single miscalculation, an honest mistake, and that innocent child’s future may be compromised or destroyed.
Fortunately, these days, horror stories seem to be less frequent than in the past. But we must remain vigilant to not only optimally treat our patient (mommy), but also to protect our patients (mommy and baby) from future complications of treatment. If there is any doubt, go ahead and call an infectious disease and pulmonary consultation. Sometimes, everyone sleeps better when we do.
Dr. A. Maria Hester is a hospitalist with Baltimore-Washington Medical Center, Glen Burnie, Md., who has a passion for empowering patients to partner in their health care. She is the creator of the Patient Whiz, a patient-engagement app for iOS.
"Mrs. Jones in ED room 12? Septic with severe multilobar pneumonia and hypoxemic respiratory failure? Got it. I’m on my way down to the ED now." The heart races in anticipation of caring for this critically ill patient near death’s door. But it’s okay. You know exactly what you have to do. You have done it many times before. No problem. Just as you are about to hang up the phone you learn more ...
"What’s that? She is 22 weeks pregnant? Uh, all right."
Suddenly, what initially seemed to be a routine case takes a complicated twist. You are no longer caring for one life, you are caring for two (or more), and one of those is extremely frail and vulnerable. The bugs, the drugs, maintaining adequate perfusion of vital organs – both hers and her baby’s – the questions of "What if ... ?" and "Should I ... ?" race through your mind. Should you get infectious disease and pulmonary consultations for an added layer of protection or should you treat her as you have treated so many others before her, the caveat, of course, being the need to check every single drug for its teratogenicity.
If you have ever felt at least a little queasiness in the pit of your stomach when called upon to care for an expectant mother, you are notalone. I think it is natural to feel a bit uneasy when we care for pregnant patients because most of us do it rather infrequently and there may not be room for a do-over even if you make the tiniest mistake. Each drug we order has the potential to do harm and any missed or delayed diagnosis may be tolerated well by mom, but maybe not much by the tiny baby growing inside her. Get it right and the family may live a storybook fantasy. Yet, a single miscalculation, an honest mistake, and that innocent child’s future may be compromised or destroyed.
Fortunately, these days, horror stories seem to be less frequent than in the past. But we must remain vigilant to not only optimally treat our patient (mommy), but also to protect our patients (mommy and baby) from future complications of treatment. If there is any doubt, go ahead and call an infectious disease and pulmonary consultation. Sometimes, everyone sleeps better when we do.
Dr. A. Maria Hester is a hospitalist with Baltimore-Washington Medical Center, Glen Burnie, Md., who has a passion for empowering patients to partner in their health care. She is the creator of the Patient Whiz, a patient-engagement app for iOS.

File it under fiction
Doctors once received a free pass when it came to penmanship. We wrote our prescriptions in Latin. So, it was okay that everything else we scribbled looked like Greek. Referrals and consultations occurred in hospital corridors or doctors’ lounges. Documentation was spotty if it happened at all. Our handwriting was a joke. As long as we could sort of decipher our own scribbling, that was okay. But, the laughing stopped when third-party payers began to ask for proof that they were getting their money’s worth for our services – a proof that they could read.
Dictation with transcription was the obvious solution. It was efficient and produced a legible result. Whatever was lost in transcription resulted in humorous and usually harmless errors. As a card-carrying cheapskate, I typed my own letters. My typos added a kind of homey touch to my communications, and they were certainly more readable than my scrawl.
Dictated and transcribed reports seemed to be a relatively accurate reflection of what had occurred at an office visit, and it kept the payers happy for a while. Most physicians continued to handwrite their office notes. But, it was clear that handwriting was coming off the walls. Insurance companies, the government, quality control folks, and risk assessment managers all wanted more documentation. Computerization seemed to offer a reasonable compromise. The payers got the data, and physicians could take advantage of the efficiencies that electronic records promised.
The software vendors’ sales pitch went like this, "Doc, aren’t most of your visits pretty much the same? History, physical, lab, diagnosis, plan? And, you do pretty much the same exam on everyone? And most of the stuff is normal, right? We’ll show you how to make some templates that will save you a ton of time without all that repetition – done in just a couple of mouse clicks."
So, the templates were made, sometimes with the physician’s help, but often without. And accuracy was sacrificed in the name of legibility and efficiency. The problem is that patients with the same diagnosis aren’t all the same. Their examinations are as different as snowflakes.
What makes a normal ENT exam normal? Is the absence of tonsils worth noting? A bifid uvula? It depends. What does the template include in its definition of normal? More importantly, does the physician remember or did he ever know what his computer considers normal? With a single mouse click, he can create a crisp, laser-printable document that because of its legibility and level of detail appears to be the gospel truth.
But of course, sometimes and certainly too often, it’s not the truth. I recently received an e-mail from a pediatrician who said that he files the EHR records from specialists, emergency departments, and urgent care centers in the "fiction section." He cited an example of a report from a neurologist about a 10-month-old that included a "normal sense of smell" and a warning against driving while taking the medicine prescribed. I can’t top that; maybe you can. But I certainly have received numerous reports that clearly bore little relationship to what had transpired in the clinic or specialist’s office – complete neurologic exams that would have taken 30 minutes to perform, normal tympanic membranes in children with PE (pressure equalization) tubes or cavernous perforations.
Although I frequently complain about the sad state of the physical examination, a bigger problem may be the reliance on the EHR to document the result of the exam. I fear there is little incentive to correct the problem because of the malpractice lawyers’ mantra, "if you didn’t document it, it wasn’t done." Unfortunately, that has come to mean that if it’s legible and detailed, it must be the truth. I would enjoy hearing from you some examples in which you know this clearly wasn’t the case.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including "How to Say No to Your Toddler." E-mail him at [email protected].
Doctors once received a free pass when it came to penmanship. We wrote our prescriptions in Latin. So, it was okay that everything else we scribbled looked like Greek. Referrals and consultations occurred in hospital corridors or doctors’ lounges. Documentation was spotty if it happened at all. Our handwriting was a joke. As long as we could sort of decipher our own scribbling, that was okay. But, the laughing stopped when third-party payers began to ask for proof that they were getting their money’s worth for our services – a proof that they could read.
Dictation with transcription was the obvious solution. It was efficient and produced a legible result. Whatever was lost in transcription resulted in humorous and usually harmless errors. As a card-carrying cheapskate, I typed my own letters. My typos added a kind of homey touch to my communications, and they were certainly more readable than my scrawl.
Dictated and transcribed reports seemed to be a relatively accurate reflection of what had occurred at an office visit, and it kept the payers happy for a while. Most physicians continued to handwrite their office notes. But, it was clear that handwriting was coming off the walls. Insurance companies, the government, quality control folks, and risk assessment managers all wanted more documentation. Computerization seemed to offer a reasonable compromise. The payers got the data, and physicians could take advantage of the efficiencies that electronic records promised.
The software vendors’ sales pitch went like this, "Doc, aren’t most of your visits pretty much the same? History, physical, lab, diagnosis, plan? And, you do pretty much the same exam on everyone? And most of the stuff is normal, right? We’ll show you how to make some templates that will save you a ton of time without all that repetition – done in just a couple of mouse clicks."
So, the templates were made, sometimes with the physician’s help, but often without. And accuracy was sacrificed in the name of legibility and efficiency. The problem is that patients with the same diagnosis aren’t all the same. Their examinations are as different as snowflakes.
What makes a normal ENT exam normal? Is the absence of tonsils worth noting? A bifid uvula? It depends. What does the template include in its definition of normal? More importantly, does the physician remember or did he ever know what his computer considers normal? With a single mouse click, he can create a crisp, laser-printable document that because of its legibility and level of detail appears to be the gospel truth.
But of course, sometimes and certainly too often, it’s not the truth. I recently received an e-mail from a pediatrician who said that he files the EHR records from specialists, emergency departments, and urgent care centers in the "fiction section." He cited an example of a report from a neurologist about a 10-month-old that included a "normal sense of smell" and a warning against driving while taking the medicine prescribed. I can’t top that; maybe you can. But I certainly have received numerous reports that clearly bore little relationship to what had transpired in the clinic or specialist’s office – complete neurologic exams that would have taken 30 minutes to perform, normal tympanic membranes in children with PE (pressure equalization) tubes or cavernous perforations.
Although I frequently complain about the sad state of the physical examination, a bigger problem may be the reliance on the EHR to document the result of the exam. I fear there is little incentive to correct the problem because of the malpractice lawyers’ mantra, "if you didn’t document it, it wasn’t done." Unfortunately, that has come to mean that if it’s legible and detailed, it must be the truth. I would enjoy hearing from you some examples in which you know this clearly wasn’t the case.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including "How to Say No to Your Toddler." E-mail him at [email protected].
Doctors once received a free pass when it came to penmanship. We wrote our prescriptions in Latin. So, it was okay that everything else we scribbled looked like Greek. Referrals and consultations occurred in hospital corridors or doctors’ lounges. Documentation was spotty if it happened at all. Our handwriting was a joke. As long as we could sort of decipher our own scribbling, that was okay. But, the laughing stopped when third-party payers began to ask for proof that they were getting their money’s worth for our services – a proof that they could read.
Dictation with transcription was the obvious solution. It was efficient and produced a legible result. Whatever was lost in transcription resulted in humorous and usually harmless errors. As a card-carrying cheapskate, I typed my own letters. My typos added a kind of homey touch to my communications, and they were certainly more readable than my scrawl.
Dictated and transcribed reports seemed to be a relatively accurate reflection of what had occurred at an office visit, and it kept the payers happy for a while. Most physicians continued to handwrite their office notes. But, it was clear that handwriting was coming off the walls. Insurance companies, the government, quality control folks, and risk assessment managers all wanted more documentation. Computerization seemed to offer a reasonable compromise. The payers got the data, and physicians could take advantage of the efficiencies that electronic records promised.
The software vendors’ sales pitch went like this, "Doc, aren’t most of your visits pretty much the same? History, physical, lab, diagnosis, plan? And, you do pretty much the same exam on everyone? And most of the stuff is normal, right? We’ll show you how to make some templates that will save you a ton of time without all that repetition – done in just a couple of mouse clicks."
So, the templates were made, sometimes with the physician’s help, but often without. And accuracy was sacrificed in the name of legibility and efficiency. The problem is that patients with the same diagnosis aren’t all the same. Their examinations are as different as snowflakes.
What makes a normal ENT exam normal? Is the absence of tonsils worth noting? A bifid uvula? It depends. What does the template include in its definition of normal? More importantly, does the physician remember or did he ever know what his computer considers normal? With a single mouse click, he can create a crisp, laser-printable document that because of its legibility and level of detail appears to be the gospel truth.
But of course, sometimes and certainly too often, it’s not the truth. I recently received an e-mail from a pediatrician who said that he files the EHR records from specialists, emergency departments, and urgent care centers in the "fiction section." He cited an example of a report from a neurologist about a 10-month-old that included a "normal sense of smell" and a warning against driving while taking the medicine prescribed. I can’t top that; maybe you can. But I certainly have received numerous reports that clearly bore little relationship to what had transpired in the clinic or specialist’s office – complete neurologic exams that would have taken 30 minutes to perform, normal tympanic membranes in children with PE (pressure equalization) tubes or cavernous perforations.
Although I frequently complain about the sad state of the physical examination, a bigger problem may be the reliance on the EHR to document the result of the exam. I fear there is little incentive to correct the problem because of the malpractice lawyers’ mantra, "if you didn’t document it, it wasn’t done." Unfortunately, that has come to mean that if it’s legible and detailed, it must be the truth. I would enjoy hearing from you some examples in which you know this clearly wasn’t the case.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including "How to Say No to Your Toddler." E-mail him at [email protected].
Almonds
A tree species belonging to the Rosaceae family and native to the Middle East and South Asia, Prunus dulcis (also called Prunus amygdalus), popularly known as almond, is cultivated widely in warm, arid locations and used primarily for its edible seeds (J. Agric. Food Chem. 2007;55:8498-507; J. Agric. Food Chem. 2006;54:312-8). Almonds and almond skins are rich in polyphenols and are an important source of these phytonutrients, particularly flavan-3-ols and flavonols (J. Proteome Res. 2010;9:5859-67). Almonds also are known to contain an abundance of fiber (Anaerobe 2014;26:1-6). Almond extracts are used in cosmetic formulations because of their high concentration of polyphenols, particularly flavonoids and phenolic acids (Int. J. Curr. Pharm. Res. 2011;3:57-9).
Key components
In 2006, Milbury et al. determined that the main flavonoids and phenolic acids in Prunus dulcis skins and kernels are isorhamnetin-3-O-rutinoside and isorhamnetin-3-O-glucoside (in combination), catechin, kaempferol-3-O-rutinoside, epicatechin, quercetin-3-O-galactoside, and isorhamnetin-3-O-galactoside (J. Agric. Food Chem. 2006;54:5027-33).

In a separate study that year, Wijeratne et al. identified quercetin, isorhamnetin, quercitrin, kaempferol 3-O-rutinoside, isorhamnetin 3-O-glucoside, and morin as the primary flavonoids in various whole-seed, brown, skin, and green-shell-cover almond extracts (J. Agric. Food Chem. 2006;54:312-8). Almond seed skin also has been shown to contain highly polymerized polyphenols that exhibit potent alpha-amylase inhibitory activity, thus slowing the absorption of carbohydrate (J. Agric. Food Chem. 2013;61:4570-6).
In 2010, Bartolomé et al. identified A- and B-type procyanidin, propelargonidin, and prodelphinidin polymers in almond skins. In human plasma and urine samples taken after consumption of almond skin polyphenols, the investigators detected O-methyl glucuronide sulfate and O-methyl sulfate derivatives of (epi)catechin; the glucuronide conjugates of naringenin and isorhamnetin; and sulfate conjugates of isorhamnetin, together with conjugates of hydroxyphenylvalerolactones. They also identified various microbial-derived metabolites, including hydroxyphenylpropionic, hydroxyphenylacetic, hydroxycinnamic, hydroxybenzoic, and hydroxyhippuric acids (Arch. Biochem. Biophys. 2010;501:124-33).
A functional food: Antioxidant constituents and activity
In a study of two human subjects conducted in 2009, Urpi-Sarda et al. profiled microbial-derived phenolic metabolites in plasma and urine samples before and after the consumption of almond skins. They detected glucuronide, O-methyl glucuronide sulfate, and O-methyl sulfate derivatives of epicatechin, the glucuronide conjugates of naringenin and glucuronide, and sulfate conjugates of isorhamnetin. The researchers also detected, in their glucuronide and sulfate forms, microbial-derived metabolites of flavanols, including 5-(dihydroxyphenyl)-gamma-valerolactone and 5-(hydroxymethoxyphenyl)-gamma-valerolactone (J. Agric. Food Chem. 2009;57:10134-42).
A 2010 study with 24 volunteers conducted by Llorach et al. investigated urinary metabolome changes during the 24-hour period following ingestion of a single dose of almond skin extract. The participants, who were following a polyphenol-free diet for 48 hours, were divided into two groups: the almond skin group or a placebo group. Thirty-four metabolites were linked to the consumption of the almond extract (J. Proteome Res. 2010;9:5859-67).

Monagas et al. previously led a comprehensive investigation of the phenolic composition of almond skins to elucidate its potential as a functional food. They identified 33 compounds, including flavanols, flavonols, dihydroflavonols, and flavanones, as well as nonflavonoid substances. The most abundant phenols were flavanols (38%-57%) and flavonol glycosides (14%-35%). Further, the researchers measured the oxygen radical absorbance capacity of almond skins at 0.398-0.500 mmol Trolox/g, a range that suggests its antioxidant potency (J. Agric. Food Chem. 2007;55:8498-507).
In 2008, Garrido et al. investigated the phenolic composition and antioxidant activity of almond skins (Prunus dulcis) obtained from three almond varieties and through various industrial processes, including blanching, blanching and drying, as well as roasting. Identified were 31 phenolic compounds, including flavan-3-ols, flavonol glycosides, hydroxybenzoic acids and aldehydes, flavonol aglycones, flavanone glycosides, flavanone aglycones, hydroxycinnamic acids, and dihydroflavonol aglycones. Phenolic content as well as antioxidant activity were significantly higher in the roasted samples (J. Food Sci. 2008;73:C106-15).
In 2014, Liu et al. conducted a study in healthy humans of the potential prebiotic effects of consuming almonds and almond skins. For 6 weeks, 48 adult volunteers ingested a daily dose of roasted almonds, almond skins, or a positive control (commercial fructo-oligosaccharides). The investigators collected fecal samples and analyzed them for microbiota composition. They observed significant increases in populations of Bifidobacterium spp. and Lactobacillus spp. in fecal samples after almond or almond skin supplementation; substantial inhibition of the growth of the pathogen Clostridium perfringens; and favorable changes in bacterial enzyme activities. They concluded that almonds and almond skins appear to exhibit potential prebiotic qualities (Anaerobe 2014;26:1-6).
Topical antiaging potential
In 2011, Sachdeva and Katyal assessed the antioxidant and antiwrinkle effects of almond skin extracts in UV-induced photoaging in mice. Twenty-five mice were used as an unirradiated control, receiving neither UV exposure nor almond skin treatment. A second group of 24 mice received only UV exposure of 5 minutes twice a day, and served as an irradiated control. Further groups of 24 mice received both UV radiation and treatment with prepared formulation. The treatment groups received various topical almond skin extract doses 2 hours prior to the same level of UV exposure. Significant decreases in malondialdehyde and increases in glutathione levels, respectively, suggested to the investigators that the almond skin extracts effectively scavenged free radicals while also enhancing moisturization. They concluded that almond skin extracts display potential as antiaging ingredients in topical cosmetic formulations (Int. J. Curr. Pharm. Res. 2011;3:57-9).
Conclusion
Almonds are believed to be a healthy addition to the human diet, with their regular consumption thought to confer cardiovascular benefits. The healthful effects of dietary intake of almonds are often attributed to the presence of several polyphenolic constituents. While it is speculated that such ingredients also play a role in imparting cutaneous benefits, the body of evidence supporting such claims remains sparse to date. Nevertheless, P. dulcis is incorporated in various cosmetic formulations. More research is necessary to ascertain whether such inclusion is warranted.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in Miami Beach. She founded the cosmetic dermatology center at the University of Miami in 1997. Dr. Baumann wrote the textbook "Cosmetic Dermatology: Principles and Practice" (McGraw-Hill, April 2002), and a book for consumers, "The Skin Type Solution" (Bantam, 2006). She has contributed to the Cosmeceutical Critique column in Skin & Allergy News since January 2001. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Galderma, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Stiefel, Topix Pharmaceuticals, and Unilever.
A tree species belonging to the Rosaceae family and native to the Middle East and South Asia, Prunus dulcis (also called Prunus amygdalus), popularly known as almond, is cultivated widely in warm, arid locations and used primarily for its edible seeds (J. Agric. Food Chem. 2007;55:8498-507; J. Agric. Food Chem. 2006;54:312-8). Almonds and almond skins are rich in polyphenols and are an important source of these phytonutrients, particularly flavan-3-ols and flavonols (J. Proteome Res. 2010;9:5859-67). Almonds also are known to contain an abundance of fiber (Anaerobe 2014;26:1-6). Almond extracts are used in cosmetic formulations because of their high concentration of polyphenols, particularly flavonoids and phenolic acids (Int. J. Curr. Pharm. Res. 2011;3:57-9).
Key components
In 2006, Milbury et al. determined that the main flavonoids and phenolic acids in Prunus dulcis skins and kernels are isorhamnetin-3-O-rutinoside and isorhamnetin-3-O-glucoside (in combination), catechin, kaempferol-3-O-rutinoside, epicatechin, quercetin-3-O-galactoside, and isorhamnetin-3-O-galactoside (J. Agric. Food Chem. 2006;54:5027-33).
In a separate study that year, Wijeratne et al. identified quercetin, isorhamnetin, quercitrin, kaempferol 3-O-rutinoside, isorhamnetin 3-O-glucoside, and morin as the primary flavonoids in various whole-seed, brown, skin, and green-shell-cover almond extracts (J. Agric. Food Chem. 2006;54:312-8). Almond seed skin also has been shown to contain highly polymerized polyphenols that exhibit potent alpha-amylase inhibitory activity, thus slowing the absorption of carbohydrate (J. Agric. Food Chem. 2013;61:4570-6).
In 2010, Bartolomé et al. identified A- and B-type procyanidin, propelargonidin, and prodelphinidin polymers in almond skins. In human plasma and urine samples taken after consumption of almond skin polyphenols, the investigators detected O-methyl glucuronide sulfate and O-methyl sulfate derivatives of (epi)catechin; the glucuronide conjugates of naringenin and isorhamnetin; and sulfate conjugates of isorhamnetin, together with conjugates of hydroxyphenylvalerolactones. They also identified various microbial-derived metabolites, including hydroxyphenylpropionic, hydroxyphenylacetic, hydroxycinnamic, hydroxybenzoic, and hydroxyhippuric acids (Arch. Biochem. Biophys. 2010;501:124-33).
A functional food: Antioxidant constituents and activity
In a study of two human subjects conducted in 2009, Urpi-Sarda et al. profiled microbial-derived phenolic metabolites in plasma and urine samples before and after the consumption of almond skins. They detected glucuronide, O-methyl glucuronide sulfate, and O-methyl sulfate derivatives of epicatechin, the glucuronide conjugates of naringenin and glucuronide, and sulfate conjugates of isorhamnetin. The researchers also detected, in their glucuronide and sulfate forms, microbial-derived metabolites of flavanols, including 5-(dihydroxyphenyl)-gamma-valerolactone and 5-(hydroxymethoxyphenyl)-gamma-valerolactone (J. Agric. Food Chem. 2009;57:10134-42).
A 2010 study with 24 volunteers conducted by Llorach et al. investigated urinary metabolome changes during the 24-hour period following ingestion of a single dose of almond skin extract. The participants, who were following a polyphenol-free diet for 48 hours, were divided into two groups: the almond skin group or a placebo group. Thirty-four metabolites were linked to the consumption of the almond extract (J. Proteome Res. 2010;9:5859-67).
Monagas et al. previously led a comprehensive investigation of the phenolic composition of almond skins to elucidate its potential as a functional food. They identified 33 compounds, including flavanols, flavonols, dihydroflavonols, and flavanones, as well as nonflavonoid substances. The most abundant phenols were flavanols (38%-57%) and flavonol glycosides (14%-35%). Further, the researchers measured the oxygen radical absorbance capacity of almond skins at 0.398-0.500 mmol Trolox/g, a range that suggests its antioxidant potency (J. Agric. Food Chem. 2007;55:8498-507).
In 2008, Garrido et al. investigated the phenolic composition and antioxidant activity of almond skins (Prunus dulcis) obtained from three almond varieties and through various industrial processes, including blanching, blanching and drying, as well as roasting. Identified were 31 phenolic compounds, including flavan-3-ols, flavonol glycosides, hydroxybenzoic acids and aldehydes, flavonol aglycones, flavanone glycosides, flavanone aglycones, hydroxycinnamic acids, and dihydroflavonol aglycones. Phenolic content as well as antioxidant activity were significantly higher in the roasted samples (J. Food Sci. 2008;73:C106-15).
In 2014, Liu et al. conducted a study in healthy humans of the potential prebiotic effects of consuming almonds and almond skins. For 6 weeks, 48 adult volunteers ingested a daily dose of roasted almonds, almond skins, or a positive control (commercial fructo-oligosaccharides). The investigators collected fecal samples and analyzed them for microbiota composition. They observed significant increases in populations of Bifidobacterium spp. and Lactobacillus spp. in fecal samples after almond or almond skin supplementation; substantial inhibition of the growth of the pathogen Clostridium perfringens; and favorable changes in bacterial enzyme activities. They concluded that almonds and almond skins appear to exhibit potential prebiotic qualities (Anaerobe 2014;26:1-6).
Topical antiaging potential
In 2011, Sachdeva and Katyal assessed the antioxidant and antiwrinkle effects of almond skin extracts in UV-induced photoaging in mice. Twenty-five mice were used as an unirradiated control, receiving neither UV exposure nor almond skin treatment. A second group of 24 mice received only UV exposure of 5 minutes twice a day, and served as an irradiated control. Further groups of 24 mice received both UV radiation and treatment with prepared formulation. The treatment groups received various topical almond skin extract doses 2 hours prior to the same level of UV exposure. Significant decreases in malondialdehyde and increases in glutathione levels, respectively, suggested to the investigators that the almond skin extracts effectively scavenged free radicals while also enhancing moisturization. They concluded that almond skin extracts display potential as antiaging ingredients in topical cosmetic formulations (Int. J. Curr. Pharm. Res. 2011;3:57-9).
Conclusion
Almonds are believed to be a healthy addition to the human diet, with their regular consumption thought to confer cardiovascular benefits. The healthful effects of dietary intake of almonds are often attributed to the presence of several polyphenolic constituents. While it is speculated that such ingredients also play a role in imparting cutaneous benefits, the body of evidence supporting such claims remains sparse to date. Nevertheless, P. dulcis is incorporated in various cosmetic formulations. More research is necessary to ascertain whether such inclusion is warranted.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in Miami Beach. She founded the cosmetic dermatology center at the University of Miami in 1997. Dr. Baumann wrote the textbook "Cosmetic Dermatology: Principles and Practice" (McGraw-Hill, April 2002), and a book for consumers, "The Skin Type Solution" (Bantam, 2006). She has contributed to the Cosmeceutical Critique column in Skin & Allergy News since January 2001. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Galderma, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Stiefel, Topix Pharmaceuticals, and Unilever.
A tree species belonging to the Rosaceae family and native to the Middle East and South Asia, Prunus dulcis (also called Prunus amygdalus), popularly known as almond, is cultivated widely in warm, arid locations and used primarily for its edible seeds (J. Agric. Food Chem. 2007;55:8498-507; J. Agric. Food Chem. 2006;54:312-8). Almonds and almond skins are rich in polyphenols and are an important source of these phytonutrients, particularly flavan-3-ols and flavonols (J. Proteome Res. 2010;9:5859-67). Almonds also are known to contain an abundance of fiber (Anaerobe 2014;26:1-6). Almond extracts are used in cosmetic formulations because of their high concentration of polyphenols, particularly flavonoids and phenolic acids (Int. J. Curr. Pharm. Res. 2011;3:57-9).
Key components
In 2006, Milbury et al. determined that the main flavonoids and phenolic acids in Prunus dulcis skins and kernels are isorhamnetin-3-O-rutinoside and isorhamnetin-3-O-glucoside (in combination), catechin, kaempferol-3-O-rutinoside, epicatechin, quercetin-3-O-galactoside, and isorhamnetin-3-O-galactoside (J. Agric. Food Chem. 2006;54:5027-33).
In a separate study that year, Wijeratne et al. identified quercetin, isorhamnetin, quercitrin, kaempferol 3-O-rutinoside, isorhamnetin 3-O-glucoside, and morin as the primary flavonoids in various whole-seed, brown, skin, and green-shell-cover almond extracts (J. Agric. Food Chem. 2006;54:312-8). Almond seed skin also has been shown to contain highly polymerized polyphenols that exhibit potent alpha-amylase inhibitory activity, thus slowing the absorption of carbohydrate (J. Agric. Food Chem. 2013;61:4570-6).
In 2010, Bartolomé et al. identified A- and B-type procyanidin, propelargonidin, and prodelphinidin polymers in almond skins. In human plasma and urine samples taken after consumption of almond skin polyphenols, the investigators detected O-methyl glucuronide sulfate and O-methyl sulfate derivatives of (epi)catechin; the glucuronide conjugates of naringenin and isorhamnetin; and sulfate conjugates of isorhamnetin, together with conjugates of hydroxyphenylvalerolactones. They also identified various microbial-derived metabolites, including hydroxyphenylpropionic, hydroxyphenylacetic, hydroxycinnamic, hydroxybenzoic, and hydroxyhippuric acids (Arch. Biochem. Biophys. 2010;501:124-33).
A functional food: Antioxidant constituents and activity
In a study of two human subjects conducted in 2009, Urpi-Sarda et al. profiled microbial-derived phenolic metabolites in plasma and urine samples before and after the consumption of almond skins. They detected glucuronide, O-methyl glucuronide sulfate, and O-methyl sulfate derivatives of epicatechin, the glucuronide conjugates of naringenin and glucuronide, and sulfate conjugates of isorhamnetin. The researchers also detected, in their glucuronide and sulfate forms, microbial-derived metabolites of flavanols, including 5-(dihydroxyphenyl)-gamma-valerolactone and 5-(hydroxymethoxyphenyl)-gamma-valerolactone (J. Agric. Food Chem. 2009;57:10134-42).
A 2010 study with 24 volunteers conducted by Llorach et al. investigated urinary metabolome changes during the 24-hour period following ingestion of a single dose of almond skin extract. The participants, who were following a polyphenol-free diet for 48 hours, were divided into two groups: the almond skin group or a placebo group. Thirty-four metabolites were linked to the consumption of the almond extract (J. Proteome Res. 2010;9:5859-67).
Monagas et al. previously led a comprehensive investigation of the phenolic composition of almond skins to elucidate its potential as a functional food. They identified 33 compounds, including flavanols, flavonols, dihydroflavonols, and flavanones, as well as nonflavonoid substances. The most abundant phenols were flavanols (38%-57%) and flavonol glycosides (14%-35%). Further, the researchers measured the oxygen radical absorbance capacity of almond skins at 0.398-0.500 mmol Trolox/g, a range that suggests its antioxidant potency (J. Agric. Food Chem. 2007;55:8498-507).
In 2008, Garrido et al. investigated the phenolic composition and antioxidant activity of almond skins (Prunus dulcis) obtained from three almond varieties and through various industrial processes, including blanching, blanching and drying, as well as roasting. Identified were 31 phenolic compounds, including flavan-3-ols, flavonol glycosides, hydroxybenzoic acids and aldehydes, flavonol aglycones, flavanone glycosides, flavanone aglycones, hydroxycinnamic acids, and dihydroflavonol aglycones. Phenolic content as well as antioxidant activity were significantly higher in the roasted samples (J. Food Sci. 2008;73:C106-15).
In 2014, Liu et al. conducted a study in healthy humans of the potential prebiotic effects of consuming almonds and almond skins. For 6 weeks, 48 adult volunteers ingested a daily dose of roasted almonds, almond skins, or a positive control (commercial fructo-oligosaccharides). The investigators collected fecal samples and analyzed them for microbiota composition. They observed significant increases in populations of Bifidobacterium spp. and Lactobacillus spp. in fecal samples after almond or almond skin supplementation; substantial inhibition of the growth of the pathogen Clostridium perfringens; and favorable changes in bacterial enzyme activities. They concluded that almonds and almond skins appear to exhibit potential prebiotic qualities (Anaerobe 2014;26:1-6).
Topical antiaging potential
In 2011, Sachdeva and Katyal assessed the antioxidant and antiwrinkle effects of almond skin extracts in UV-induced photoaging in mice. Twenty-five mice were used as an unirradiated control, receiving neither UV exposure nor almond skin treatment. A second group of 24 mice received only UV exposure of 5 minutes twice a day, and served as an irradiated control. Further groups of 24 mice received both UV radiation and treatment with prepared formulation. The treatment groups received various topical almond skin extract doses 2 hours prior to the same level of UV exposure. Significant decreases in malondialdehyde and increases in glutathione levels, respectively, suggested to the investigators that the almond skin extracts effectively scavenged free radicals while also enhancing moisturization. They concluded that almond skin extracts display potential as antiaging ingredients in topical cosmetic formulations (Int. J. Curr. Pharm. Res. 2011;3:57-9).
Conclusion
Almonds are believed to be a healthy addition to the human diet, with their regular consumption thought to confer cardiovascular benefits. The healthful effects of dietary intake of almonds are often attributed to the presence of several polyphenolic constituents. While it is speculated that such ingredients also play a role in imparting cutaneous benefits, the body of evidence supporting such claims remains sparse to date. Nevertheless, P. dulcis is incorporated in various cosmetic formulations. More research is necessary to ascertain whether such inclusion is warranted.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in Miami Beach. She founded the cosmetic dermatology center at the University of Miami in 1997. Dr. Baumann wrote the textbook "Cosmetic Dermatology: Principles and Practice" (McGraw-Hill, April 2002), and a book for consumers, "The Skin Type Solution" (Bantam, 2006). She has contributed to the Cosmeceutical Critique column in Skin & Allergy News since January 2001. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Galderma, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Stiefel, Topix Pharmaceuticals, and Unilever.
