User login
Patient safety and tort reform
Question: Developments in medical tort reform include:
A. Continued constitutional challenges to caps on damages.
B. An emphasis on patient safety.
C. Hillary Clinton’s Senate bill.
D. Linking medical tort reform to error reduction.
E. All of the above.

Answer: E. Recent years have witnessed a stabilizing environment for medical liability, although insurance premiums continue to vary greatly by specialty and geographic location.
Recent statistics from the American Medical Association show that 2014 ob.gyn. insurance rates range from less than $50,000 in some areas of California to a high of $215,000 in Nassau and Suffolk counties in New York. The highest average expense in 2013, around a quarter of a million dollars, was for those claims that resulted in plaintiff verdicts, while defendant verdicts were substantially lower and averaged $140,000.
As in the past, most claims were dropped, dismissed, or withdrawn. About one-quarter of claims were settled, with only 2% decided by an alternative dispute resolution. Less than 8% were decided by trial verdict, with the vast majority won by the defendant.
The plaintiff bar continues to mount constitutional challenges to caps on damages. The California Supreme Court had previously ruled that reforms under California’s historic Medical Injury Compensation Reform Act (MICRA)1, which limits noneconomic recovery to $250,000, are constitutional, because they are rationally related to the legitimate legislative goal of reducing medical costs.
However, the statute has again come under challenge, only to be reaffirmed by a California state appeals court. In November 2014, California voters rejected Proposition 46, which sought to increase the cap from $250,000 to $1.1 million.
Texas, another pro-reform state, sides with California, and Mississippi also ruled that its damage cap is constitutional. However, Florida and Oklahoma recently joined jurisdictions such as Georgia, Illinois, and Missouri in ruling that damage caps are unconstitutional.
Asserting that the current health care liability system has been an inefficient and sometimes ineffective mechanism for initiating or resolving claims of medical error, medical negligence, or malpractice, then-U.S. senators Hillary Clinton (D-N.Y.) and Barack Obama (D-Ill.) in 2005 jointly sponsored legislation (S. 1784) to establish a National Medical Error Disclosure and Compensation Program (National MEDiC Act). Although the bill was killed in Senate committee, its key provisions were subsequently published in the New England Journal of Medicine (2006;354:2205-8).
The senators noted that the liability system has failed to the extent that only one medical malpractice claim is filed for every eight medical injuries, that it takes 4-8 years to resolve a claim, and that “solutions to the patient safety, litigation, and medical liability insurance problems have been elusive.”
Accordingly, the bill’s purpose was to promote the confidential disclosure to patients of medical errors in an effort to improve patient-safety systems. At the time of disclosure, there would be negotiations for compensation and proposals to prevent a recurrence of the problem that led to the patient’s injury. However, the patient would retain the right to counsel during negotiations, as well as access to the courts if no agreement were reached. The bill was entirely silent on traditional tort reform measures.
Nearly 4 decades earlier, a no-fault proposal by Professor Jeffrey O’Connell made some of these points, but with sharper focus and specificity, especially regarding damages.2
In marked contrast to the Clinton-Obama bill, his proposal gave the medical provider the exclusive option to tender payment, which would completely foreclose future tort action by the victim. Compensation benefits included net economic loss such as 100% of lost wages, replacement service loss, medical treatment expenses, and reasonable attorney’s fees. But noneconomic losses, such as pain and suffering, were not reimbursable, and payment was net of any benefits from collateral sources.
This proposal elegantly combined efficiency and fairness, and would have ameliorated the financial and emotional toll that comes with litigating injuries arising out of health care. Legislation in the House of Representatives, the Alternative Medical Liability Act (H.R. 5400), incorporated many of these features, and came before the 98th U.S. Congress in 1984. It, too, died in committee.
There may be something to the current trend toward pairing tort reform with error reduction. Thoughtful observers point to “disclosure and offer” programs such as the one at the Lexington (Ky.) Veterans Affairs Medical Center, which boasts average settlements of approximately $15,000 per claim – compared with more than $98,000 at other VA institutions. Its policy has also decreased the average duration of cases, previously 2-4 years, to 2-4 months, as well as reduced costs for legal defense.
Likewise, the program at the University of Michigan Health System has reduced both the frequency and severity of claims, duration of cases, and litigation costs. Aware of these developments, some private insurers, such as the COPIC Insurance Company in Colorado, are adopting a similar approach.
In its updated 2014 tort reform position paper, the American College of Physicians continues to endorse caps on noneconomic and punitive damages, as well as other tort reform measures.
However, it now acknowledges that “improving patient safety and preventing errors must be at the fore of the medical liability reform discussion.” The ACP correctly asserts that “emphasizing patient safety, promoting a culture of quality improvement and coordinated care, and training physicians in best practices to avoid errors and reduce risk will prevent harm and reduce the waste associated with defensive medicine.”
This hybrid approach combining traditional tort reforms with a renewed attention to patient safety through medical error reduction may yet yield additional practical benefits.
Here, the experience in anesthesiology bears recounting: Its dramatic progress in risk management has cut patient death rate from 1 in 5,000 to 1 in 200,000 to 300,000 in the space of 20 years, and this has been associated with a concurrent 37% fall in insurance premiums.
References
1. Medical Injury Compensation Reform Act of 1975, Cal. Civ. Proc. Code § 3333.2 (West 1982).
2. O’Connell, J. No-Fault Insurance for Injuries Arising from Medical Treatment: A Proposal for Elective Coverage. Emory L. J. 1975;24:21.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. Currently, he directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: Developments in medical tort reform include:
A. Continued constitutional challenges to caps on damages.
B. An emphasis on patient safety.
C. Hillary Clinton’s Senate bill.
D. Linking medical tort reform to error reduction.
E. All of the above.
Answer: E. Recent years have witnessed a stabilizing environment for medical liability, although insurance premiums continue to vary greatly by specialty and geographic location.
Recent statistics from the American Medical Association show that 2014 ob.gyn. insurance rates range from less than $50,000 in some areas of California to a high of $215,000 in Nassau and Suffolk counties in New York. The highest average expense in 2013, around a quarter of a million dollars, was for those claims that resulted in plaintiff verdicts, while defendant verdicts were substantially lower and averaged $140,000.
As in the past, most claims were dropped, dismissed, or withdrawn. About one-quarter of claims were settled, with only 2% decided by an alternative dispute resolution. Less than 8% were decided by trial verdict, with the vast majority won by the defendant.
The plaintiff bar continues to mount constitutional challenges to caps on damages. The California Supreme Court had previously ruled that reforms under California’s historic Medical Injury Compensation Reform Act (MICRA)1, which limits noneconomic recovery to $250,000, are constitutional, because they are rationally related to the legitimate legislative goal of reducing medical costs.
However, the statute has again come under challenge, only to be reaffirmed by a California state appeals court. In November 2014, California voters rejected Proposition 46, which sought to increase the cap from $250,000 to $1.1 million.
Texas, another pro-reform state, sides with California, and Mississippi also ruled that its damage cap is constitutional. However, Florida and Oklahoma recently joined jurisdictions such as Georgia, Illinois, and Missouri in ruling that damage caps are unconstitutional.
Asserting that the current health care liability system has been an inefficient and sometimes ineffective mechanism for initiating or resolving claims of medical error, medical negligence, or malpractice, then-U.S. senators Hillary Clinton (D-N.Y.) and Barack Obama (D-Ill.) in 2005 jointly sponsored legislation (S. 1784) to establish a National Medical Error Disclosure and Compensation Program (National MEDiC Act). Although the bill was killed in Senate committee, its key provisions were subsequently published in the New England Journal of Medicine (2006;354:2205-8).
The senators noted that the liability system has failed to the extent that only one medical malpractice claim is filed for every eight medical injuries, that it takes 4-8 years to resolve a claim, and that “solutions to the patient safety, litigation, and medical liability insurance problems have been elusive.”
Accordingly, the bill’s purpose was to promote the confidential disclosure to patients of medical errors in an effort to improve patient-safety systems. At the time of disclosure, there would be negotiations for compensation and proposals to prevent a recurrence of the problem that led to the patient’s injury. However, the patient would retain the right to counsel during negotiations, as well as access to the courts if no agreement were reached. The bill was entirely silent on traditional tort reform measures.
Nearly 4 decades earlier, a no-fault proposal by Professor Jeffrey O’Connell made some of these points, but with sharper focus and specificity, especially regarding damages.2
In marked contrast to the Clinton-Obama bill, his proposal gave the medical provider the exclusive option to tender payment, which would completely foreclose future tort action by the victim. Compensation benefits included net economic loss such as 100% of lost wages, replacement service loss, medical treatment expenses, and reasonable attorney’s fees. But noneconomic losses, such as pain and suffering, were not reimbursable, and payment was net of any benefits from collateral sources.
This proposal elegantly combined efficiency and fairness, and would have ameliorated the financial and emotional toll that comes with litigating injuries arising out of health care. Legislation in the House of Representatives, the Alternative Medical Liability Act (H.R. 5400), incorporated many of these features, and came before the 98th U.S. Congress in 1984. It, too, died in committee.
There may be something to the current trend toward pairing tort reform with error reduction. Thoughtful observers point to “disclosure and offer” programs such as the one at the Lexington (Ky.) Veterans Affairs Medical Center, which boasts average settlements of approximately $15,000 per claim – compared with more than $98,000 at other VA institutions. Its policy has also decreased the average duration of cases, previously 2-4 years, to 2-4 months, as well as reduced costs for legal defense.
Likewise, the program at the University of Michigan Health System has reduced both the frequency and severity of claims, duration of cases, and litigation costs. Aware of these developments, some private insurers, such as the COPIC Insurance Company in Colorado, are adopting a similar approach.
In its updated 2014 tort reform position paper, the American College of Physicians continues to endorse caps on noneconomic and punitive damages, as well as other tort reform measures.
However, it now acknowledges that “improving patient safety and preventing errors must be at the fore of the medical liability reform discussion.” The ACP correctly asserts that “emphasizing patient safety, promoting a culture of quality improvement and coordinated care, and training physicians in best practices to avoid errors and reduce risk will prevent harm and reduce the waste associated with defensive medicine.”
This hybrid approach combining traditional tort reforms with a renewed attention to patient safety through medical error reduction may yet yield additional practical benefits.
Here, the experience in anesthesiology bears recounting: Its dramatic progress in risk management has cut patient death rate from 1 in 5,000 to 1 in 200,000 to 300,000 in the space of 20 years, and this has been associated with a concurrent 37% fall in insurance premiums.
References
1. Medical Injury Compensation Reform Act of 1975, Cal. Civ. Proc. Code § 3333.2 (West 1982).
2. O’Connell, J. No-Fault Insurance for Injuries Arising from Medical Treatment: A Proposal for Elective Coverage. Emory L. J. 1975;24:21.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. Currently, he directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: Developments in medical tort reform include:
A. Continued constitutional challenges to caps on damages.
B. An emphasis on patient safety.
C. Hillary Clinton’s Senate bill.
D. Linking medical tort reform to error reduction.
E. All of the above.
Answer: E. Recent years have witnessed a stabilizing environment for medical liability, although insurance premiums continue to vary greatly by specialty and geographic location.
Recent statistics from the American Medical Association show that 2014 ob.gyn. insurance rates range from less than $50,000 in some areas of California to a high of $215,000 in Nassau and Suffolk counties in New York. The highest average expense in 2013, around a quarter of a million dollars, was for those claims that resulted in plaintiff verdicts, while defendant verdicts were substantially lower and averaged $140,000.
As in the past, most claims were dropped, dismissed, or withdrawn. About one-quarter of claims were settled, with only 2% decided by an alternative dispute resolution. Less than 8% were decided by trial verdict, with the vast majority won by the defendant.
The plaintiff bar continues to mount constitutional challenges to caps on damages. The California Supreme Court had previously ruled that reforms under California’s historic Medical Injury Compensation Reform Act (MICRA)1, which limits noneconomic recovery to $250,000, are constitutional, because they are rationally related to the legitimate legislative goal of reducing medical costs.
However, the statute has again come under challenge, only to be reaffirmed by a California state appeals court. In November 2014, California voters rejected Proposition 46, which sought to increase the cap from $250,000 to $1.1 million.
Texas, another pro-reform state, sides with California, and Mississippi also ruled that its damage cap is constitutional. However, Florida and Oklahoma recently joined jurisdictions such as Georgia, Illinois, and Missouri in ruling that damage caps are unconstitutional.
Asserting that the current health care liability system has been an inefficient and sometimes ineffective mechanism for initiating or resolving claims of medical error, medical negligence, or malpractice, then-U.S. senators Hillary Clinton (D-N.Y.) and Barack Obama (D-Ill.) in 2005 jointly sponsored legislation (S. 1784) to establish a National Medical Error Disclosure and Compensation Program (National MEDiC Act). Although the bill was killed in Senate committee, its key provisions were subsequently published in the New England Journal of Medicine (2006;354:2205-8).
The senators noted that the liability system has failed to the extent that only one medical malpractice claim is filed for every eight medical injuries, that it takes 4-8 years to resolve a claim, and that “solutions to the patient safety, litigation, and medical liability insurance problems have been elusive.”
Accordingly, the bill’s purpose was to promote the confidential disclosure to patients of medical errors in an effort to improve patient-safety systems. At the time of disclosure, there would be negotiations for compensation and proposals to prevent a recurrence of the problem that led to the patient’s injury. However, the patient would retain the right to counsel during negotiations, as well as access to the courts if no agreement were reached. The bill was entirely silent on traditional tort reform measures.
Nearly 4 decades earlier, a no-fault proposal by Professor Jeffrey O’Connell made some of these points, but with sharper focus and specificity, especially regarding damages.2
In marked contrast to the Clinton-Obama bill, his proposal gave the medical provider the exclusive option to tender payment, which would completely foreclose future tort action by the victim. Compensation benefits included net economic loss such as 100% of lost wages, replacement service loss, medical treatment expenses, and reasonable attorney’s fees. But noneconomic losses, such as pain and suffering, were not reimbursable, and payment was net of any benefits from collateral sources.
This proposal elegantly combined efficiency and fairness, and would have ameliorated the financial and emotional toll that comes with litigating injuries arising out of health care. Legislation in the House of Representatives, the Alternative Medical Liability Act (H.R. 5400), incorporated many of these features, and came before the 98th U.S. Congress in 1984. It, too, died in committee.
There may be something to the current trend toward pairing tort reform with error reduction. Thoughtful observers point to “disclosure and offer” programs such as the one at the Lexington (Ky.) Veterans Affairs Medical Center, which boasts average settlements of approximately $15,000 per claim – compared with more than $98,000 at other VA institutions. Its policy has also decreased the average duration of cases, previously 2-4 years, to 2-4 months, as well as reduced costs for legal defense.
Likewise, the program at the University of Michigan Health System has reduced both the frequency and severity of claims, duration of cases, and litigation costs. Aware of these developments, some private insurers, such as the COPIC Insurance Company in Colorado, are adopting a similar approach.
In its updated 2014 tort reform position paper, the American College of Physicians continues to endorse caps on noneconomic and punitive damages, as well as other tort reform measures.
However, it now acknowledges that “improving patient safety and preventing errors must be at the fore of the medical liability reform discussion.” The ACP correctly asserts that “emphasizing patient safety, promoting a culture of quality improvement and coordinated care, and training physicians in best practices to avoid errors and reduce risk will prevent harm and reduce the waste associated with defensive medicine.”
This hybrid approach combining traditional tort reforms with a renewed attention to patient safety through medical error reduction may yet yield additional practical benefits.
Here, the experience in anesthesiology bears recounting: Its dramatic progress in risk management has cut patient death rate from 1 in 5,000 to 1 in 200,000 to 300,000 in the space of 20 years, and this has been associated with a concurrent 37% fall in insurance premiums.
References
1. Medical Injury Compensation Reform Act of 1975, Cal. Civ. Proc. Code § 3333.2 (West 1982).
2. O’Connell, J. No-Fault Insurance for Injuries Arising from Medical Treatment: A Proposal for Elective Coverage. Emory L. J. 1975;24:21.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. Currently, he directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].

Charging doctors with homicide
Question: Charges of homicide have been successfully brought against doctors in the following situations except:
A. Withholding life-sustaining treatment.
B. Euthanasia.
C. Negligent treatment of a patient.
D. Overprescription of controlled substances.
Answer: A. Homicideis any act that causes the death of a human being with criminal intent and without legal justification. It comprises several crimes of varying severity, with murder being the most serious (requiring “malice aforethought”). Depending on the intent of the perpetrator and/or the presence of mitigating/aggravating circumstances, jurisdictions have subdivided homicide into categories such as first- and second-degree murder, voluntary and involuntary manslaughter, negligent homicide, and others.
Discontinuing futile medical treatment that ends with patient demise raises the specter of criminal prosecution for homicide. However, prosecution of doctors under such circumstances has failed. The seminal case is Barber v. Superior Court (147 Cal. App. 3d 1006 (1983)), in which the state of California brought murder charges against two doctors for discontinuing intravenous fluids and nutrition in a comatose patient.
The patient, a 55-year-old security guard, sustained a cardiopulmonary arrest following surgery for intestinal obstruction. Irreversible brain damage resulted, leaving him in a vegetative state. His family allegedly requested that life support measures and intravenous fluids be discontinued, to which the doctors complied, and the patient died 6 days later.
After a preliminary pretrial hearing, the magistrate dismissed the charges; but a trial court reinstated them. The court of appeals, however, viewed the defendant’s conduct in discontinuing intravenous fluids as an omission rather than an affirmative action, and found that a physician has no duty to continue treatment once it is proven to be ineffective.
The appeals court recognized that “a physician is authorized under the standards of medical practice to discontinue a form of therapy which in his medical judgment is useless. … If the treating physicians have determined that continued use of a respirator is useless, then they may decide to discontinue it without fear of civil or criminal liability.”
In rejecting the distinction between ordinary and extraordinary care, the court dismissed the prosecutor’s contention that unlike the respirator, fluids and nutrition represented ordinary care and therefore should never be withheld.
It concluded that “the petitioners’ omission to continue treatment under the circumstances, though intentional and with knowledge that the patient would die, was not an unlawful failure to perform a legal duty.” And because no criminal liability attaches for failure to act (i.e., an omission) unless there is a legal duty to act affirmatively, it issued a writ of prohibition restraining the lower court from taking any further action on the matter.
The U.S. Supreme Court has since validated the distinction between “letting die” and an affirmative action taken with the intention to cause death, such as the administration of a lethal injection. The former is ethical and legal, conforming to medical norms, while the latter amounts to murder (Vacco v. Quill (117 S. Ct. 2293 (1997)).
With these developments, physicians therefore need not worry about criminal prosecution for carrying out Barber-like noneuthanasia, end-of-life actions that result in the death of their patients.
On the other hand, those who act directly to end the life of a patient, even one who freely requests death, may face criminal prosecution.
The most notorious example is that of retired Michigan pathologist Dr. Jack Kevorkian, who was found guilty of the second-degree murder of Thomas Youk, a 52-year-old race-car driver with terminal Lou Gehrig’s disease. Dr. Kevorkian injected a lethal mixture of Seconal, Anectine, and potassium chloride to end the patient’s life.
At trial, Dr. Kevorkian dismissed his lawyer and served ineffectively in his own defense, never taking the witness stand. Found guilty by a jury and sentenced to 10-25 years in prison, he served just more than 8 years until 2007, when he was released for good behavior. Previous charges by the state of Michigan against Dr. Kevorkian for assisting in the suicide of some 130 patients had proven unsuccessful.
This case spawned a nationwide debate on physician-directed deaths, with a few states now legalizing physician-assisted suicide, although euthanasia remains illegal throughout the nation.
In general, the remedy sought in a medical wrongful death case lies in a malpractice civil lawsuit against the negligent doctor. Sometimes, the plaintiff may assert that there was gross negligence where the conduct was particularly blameworthy, and if proven, the jury may award punitive damages.
Rarely, however, does the level of misconduct rise to that of criminal negligence. Here, the burden of proof for a conviction requires evidence beyond reasonable doubt, rather than the lower “more probable than not” evidentiary standard required in a civil lawsuit.
However, in cases where the physician’s conduct has markedly deviated from the standard of care, doctors have been successfully prosecuted for their “criminal” conduct.
For example, in an English case, an anesthesiologist was convicted of manslaughter in the death of a patient undergoing surgery for a detached retina. During surgery, the patient’s ventilation was interrupted because of accidental disconnection of the endotracheal tube for 4 minutes, leading to a cardiac arrest. An alarm had apparently sounded but was not noticed. The injury would not have occurred had the doctor attended to the patient instead of being away from the operating room.
The tragic death of pop star Michael Jackson in 2009 is another example. Dr. Conrad Murray, a cardiologist who was Jackson’s personal physician, had used the surgical anesthetic propofol to treat Jackson’s insomnia in a bedroom setting without monitoring or resuscitation equipment. Concurrent use of the sedative lorazepam exacerbated the effect of propofol. The prosecution characterized Dr. Murray’s conduct as “egregious, unethical, and unconscionable,” which violated medical standards and amounted to criminal negligence. He was found guilty of involuntary manslaughter, and the state sentenced him to a 4-year prison term.
A new trend appears to be developing toward prosecuting doctors whose overprescription of controlled substances results in patient deaths.
According to a recent news report, New York for the first time convicted a doctor of manslaughter in the overdose deaths of patients from oxycodone and Xanax.1 Some of the patients were reportedly prescribed as many as 500-800 pills over a 5-6 week period. Dr. Stan Li, an anesthesiologist and pain management specialist, allegedly saw up to 90 patients a day in his Queens, N.Y., weekend storefront clinic, charging them on a per-prescription basis. In his defense, Dr. Li claimed that he was simply trying to help suffering people who misused medications and who misled him (“tough patients and good liars”).
Meanwhile, a similar scenario played out in Oklahoma.2 There, Dr. William Valuck, a pain management doctor, pleaded guilty to eight counts of second-degree murder in connection with several drug overdose deaths. He entered into a plea bargain with Oklahoma prosecutors and will serve 8 years in prison. Dr. Valuck had reportedly prescribed more controlled drugs than any other physician in the state of Oklahoma, which included hydrocodone, oxycodone, alprazolam, Valium, and Soma, sometimes as many as 600 pills at a time. He allegedly accepted only cash payment for the office visits, and review of his patient files revealed inadequate assessment of patient complaints or physical findings to justify the prescriptions.
Most physicians are unlikely to ever face the specter of criminal prosecution based on their medical performance. Only in the most egregious of circumstances have physicians been successfully prosecuted for homicide.
As requests for physicians to withhold or withdraw life-sustaining treatments grow, physicians may find themselves questioning what acts or omissions they may legally perform. Unless the legal landscape changes, however, it appears that the forgoing of life-sustaining treatments in the typical clinical context will not subject physicians to criminal prosecution.
References
1. “NY doctor convicted of manslaughter in 2 overdoses,” July 18, 2014 (http://bigstory.ap.org/article/ny-doctor-convicted-2-patients-overdose-deaths).
2. “Ex-doctor pleads guilty in overdose deaths,” Aug. 13, 2014 (www.usatoday.com/story/news/nation/2014/08/13/ex-doctor-guilty-deaths/14022735).
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: Charges of homicide have been successfully brought against doctors in the following situations except:
A. Withholding life-sustaining treatment.
B. Euthanasia.
C. Negligent treatment of a patient.
D. Overprescription of controlled substances.
Answer: A. Homicideis any act that causes the death of a human being with criminal intent and without legal justification. It comprises several crimes of varying severity, with murder being the most serious (requiring “malice aforethought”). Depending on the intent of the perpetrator and/or the presence of mitigating/aggravating circumstances, jurisdictions have subdivided homicide into categories such as first- and second-degree murder, voluntary and involuntary manslaughter, negligent homicide, and others.
Discontinuing futile medical treatment that ends with patient demise raises the specter of criminal prosecution for homicide. However, prosecution of doctors under such circumstances has failed. The seminal case is Barber v. Superior Court (147 Cal. App. 3d 1006 (1983)), in which the state of California brought murder charges against two doctors for discontinuing intravenous fluids and nutrition in a comatose patient.
The patient, a 55-year-old security guard, sustained a cardiopulmonary arrest following surgery for intestinal obstruction. Irreversible brain damage resulted, leaving him in a vegetative state. His family allegedly requested that life support measures and intravenous fluids be discontinued, to which the doctors complied, and the patient died 6 days later.
After a preliminary pretrial hearing, the magistrate dismissed the charges; but a trial court reinstated them. The court of appeals, however, viewed the defendant’s conduct in discontinuing intravenous fluids as an omission rather than an affirmative action, and found that a physician has no duty to continue treatment once it is proven to be ineffective.
The appeals court recognized that “a physician is authorized under the standards of medical practice to discontinue a form of therapy which in his medical judgment is useless. … If the treating physicians have determined that continued use of a respirator is useless, then they may decide to discontinue it without fear of civil or criminal liability.”
In rejecting the distinction between ordinary and extraordinary care, the court dismissed the prosecutor’s contention that unlike the respirator, fluids and nutrition represented ordinary care and therefore should never be withheld.
It concluded that “the petitioners’ omission to continue treatment under the circumstances, though intentional and with knowledge that the patient would die, was not an unlawful failure to perform a legal duty.” And because no criminal liability attaches for failure to act (i.e., an omission) unless there is a legal duty to act affirmatively, it issued a writ of prohibition restraining the lower court from taking any further action on the matter.
The U.S. Supreme Court has since validated the distinction between “letting die” and an affirmative action taken with the intention to cause death, such as the administration of a lethal injection. The former is ethical and legal, conforming to medical norms, while the latter amounts to murder (Vacco v. Quill (117 S. Ct. 2293 (1997)).
With these developments, physicians therefore need not worry about criminal prosecution for carrying out Barber-like noneuthanasia, end-of-life actions that result in the death of their patients.
On the other hand, those who act directly to end the life of a patient, even one who freely requests death, may face criminal prosecution.
The most notorious example is that of retired Michigan pathologist Dr. Jack Kevorkian, who was found guilty of the second-degree murder of Thomas Youk, a 52-year-old race-car driver with terminal Lou Gehrig’s disease. Dr. Kevorkian injected a lethal mixture of Seconal, Anectine, and potassium chloride to end the patient’s life.
At trial, Dr. Kevorkian dismissed his lawyer and served ineffectively in his own defense, never taking the witness stand. Found guilty by a jury and sentenced to 10-25 years in prison, he served just more than 8 years until 2007, when he was released for good behavior. Previous charges by the state of Michigan against Dr. Kevorkian for assisting in the suicide of some 130 patients had proven unsuccessful.
This case spawned a nationwide debate on physician-directed deaths, with a few states now legalizing physician-assisted suicide, although euthanasia remains illegal throughout the nation.
In general, the remedy sought in a medical wrongful death case lies in a malpractice civil lawsuit against the negligent doctor. Sometimes, the plaintiff may assert that there was gross negligence where the conduct was particularly blameworthy, and if proven, the jury may award punitive damages.
Rarely, however, does the level of misconduct rise to that of criminal negligence. Here, the burden of proof for a conviction requires evidence beyond reasonable doubt, rather than the lower “more probable than not” evidentiary standard required in a civil lawsuit.
However, in cases where the physician’s conduct has markedly deviated from the standard of care, doctors have been successfully prosecuted for their “criminal” conduct.
For example, in an English case, an anesthesiologist was convicted of manslaughter in the death of a patient undergoing surgery for a detached retina. During surgery, the patient’s ventilation was interrupted because of accidental disconnection of the endotracheal tube for 4 minutes, leading to a cardiac arrest. An alarm had apparently sounded but was not noticed. The injury would not have occurred had the doctor attended to the patient instead of being away from the operating room.
The tragic death of pop star Michael Jackson in 2009 is another example. Dr. Conrad Murray, a cardiologist who was Jackson’s personal physician, had used the surgical anesthetic propofol to treat Jackson’s insomnia in a bedroom setting without monitoring or resuscitation equipment. Concurrent use of the sedative lorazepam exacerbated the effect of propofol. The prosecution characterized Dr. Murray’s conduct as “egregious, unethical, and unconscionable,” which violated medical standards and amounted to criminal negligence. He was found guilty of involuntary manslaughter, and the state sentenced him to a 4-year prison term.
A new trend appears to be developing toward prosecuting doctors whose overprescription of controlled substances results in patient deaths.
According to a recent news report, New York for the first time convicted a doctor of manslaughter in the overdose deaths of patients from oxycodone and Xanax.1 Some of the patients were reportedly prescribed as many as 500-800 pills over a 5-6 week period. Dr. Stan Li, an anesthesiologist and pain management specialist, allegedly saw up to 90 patients a day in his Queens, N.Y., weekend storefront clinic, charging them on a per-prescription basis. In his defense, Dr. Li claimed that he was simply trying to help suffering people who misused medications and who misled him (“tough patients and good liars”).
Meanwhile, a similar scenario played out in Oklahoma.2 There, Dr. William Valuck, a pain management doctor, pleaded guilty to eight counts of second-degree murder in connection with several drug overdose deaths. He entered into a plea bargain with Oklahoma prosecutors and will serve 8 years in prison. Dr. Valuck had reportedly prescribed more controlled drugs than any other physician in the state of Oklahoma, which included hydrocodone, oxycodone, alprazolam, Valium, and Soma, sometimes as many as 600 pills at a time. He allegedly accepted only cash payment for the office visits, and review of his patient files revealed inadequate assessment of patient complaints or physical findings to justify the prescriptions.
Most physicians are unlikely to ever face the specter of criminal prosecution based on their medical performance. Only in the most egregious of circumstances have physicians been successfully prosecuted for homicide.
As requests for physicians to withhold or withdraw life-sustaining treatments grow, physicians may find themselves questioning what acts or omissions they may legally perform. Unless the legal landscape changes, however, it appears that the forgoing of life-sustaining treatments in the typical clinical context will not subject physicians to criminal prosecution.
References
1. “NY doctor convicted of manslaughter in 2 overdoses,” July 18, 2014 (http://bigstory.ap.org/article/ny-doctor-convicted-2-patients-overdose-deaths).
2. “Ex-doctor pleads guilty in overdose deaths,” Aug. 13, 2014 (www.usatoday.com/story/news/nation/2014/08/13/ex-doctor-guilty-deaths/14022735).
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: Charges of homicide have been successfully brought against doctors in the following situations except:
A. Withholding life-sustaining treatment.
B. Euthanasia.
C. Negligent treatment of a patient.
D. Overprescription of controlled substances.
Answer: A. Homicideis any act that causes the death of a human being with criminal intent and without legal justification. It comprises several crimes of varying severity, with murder being the most serious (requiring “malice aforethought”). Depending on the intent of the perpetrator and/or the presence of mitigating/aggravating circumstances, jurisdictions have subdivided homicide into categories such as first- and second-degree murder, voluntary and involuntary manslaughter, negligent homicide, and others.
Discontinuing futile medical treatment that ends with patient demise raises the specter of criminal prosecution for homicide. However, prosecution of doctors under such circumstances has failed. The seminal case is Barber v. Superior Court (147 Cal. App. 3d 1006 (1983)), in which the state of California brought murder charges against two doctors for discontinuing intravenous fluids and nutrition in a comatose patient.
The patient, a 55-year-old security guard, sustained a cardiopulmonary arrest following surgery for intestinal obstruction. Irreversible brain damage resulted, leaving him in a vegetative state. His family allegedly requested that life support measures and intravenous fluids be discontinued, to which the doctors complied, and the patient died 6 days later.
After a preliminary pretrial hearing, the magistrate dismissed the charges; but a trial court reinstated them. The court of appeals, however, viewed the defendant’s conduct in discontinuing intravenous fluids as an omission rather than an affirmative action, and found that a physician has no duty to continue treatment once it is proven to be ineffective.
The appeals court recognized that “a physician is authorized under the standards of medical practice to discontinue a form of therapy which in his medical judgment is useless. … If the treating physicians have determined that continued use of a respirator is useless, then they may decide to discontinue it without fear of civil or criminal liability.”
In rejecting the distinction between ordinary and extraordinary care, the court dismissed the prosecutor’s contention that unlike the respirator, fluids and nutrition represented ordinary care and therefore should never be withheld.
It concluded that “the petitioners’ omission to continue treatment under the circumstances, though intentional and with knowledge that the patient would die, was not an unlawful failure to perform a legal duty.” And because no criminal liability attaches for failure to act (i.e., an omission) unless there is a legal duty to act affirmatively, it issued a writ of prohibition restraining the lower court from taking any further action on the matter.
The U.S. Supreme Court has since validated the distinction between “letting die” and an affirmative action taken with the intention to cause death, such as the administration of a lethal injection. The former is ethical and legal, conforming to medical norms, while the latter amounts to murder (Vacco v. Quill (117 S. Ct. 2293 (1997)).
With these developments, physicians therefore need not worry about criminal prosecution for carrying out Barber-like noneuthanasia, end-of-life actions that result in the death of their patients.
On the other hand, those who act directly to end the life of a patient, even one who freely requests death, may face criminal prosecution.
The most notorious example is that of retired Michigan pathologist Dr. Jack Kevorkian, who was found guilty of the second-degree murder of Thomas Youk, a 52-year-old race-car driver with terminal Lou Gehrig’s disease. Dr. Kevorkian injected a lethal mixture of Seconal, Anectine, and potassium chloride to end the patient’s life.
At trial, Dr. Kevorkian dismissed his lawyer and served ineffectively in his own defense, never taking the witness stand. Found guilty by a jury and sentenced to 10-25 years in prison, he served just more than 8 years until 2007, when he was released for good behavior. Previous charges by the state of Michigan against Dr. Kevorkian for assisting in the suicide of some 130 patients had proven unsuccessful.
This case spawned a nationwide debate on physician-directed deaths, with a few states now legalizing physician-assisted suicide, although euthanasia remains illegal throughout the nation.
In general, the remedy sought in a medical wrongful death case lies in a malpractice civil lawsuit against the negligent doctor. Sometimes, the plaintiff may assert that there was gross negligence where the conduct was particularly blameworthy, and if proven, the jury may award punitive damages.
Rarely, however, does the level of misconduct rise to that of criminal negligence. Here, the burden of proof for a conviction requires evidence beyond reasonable doubt, rather than the lower “more probable than not” evidentiary standard required in a civil lawsuit.
However, in cases where the physician’s conduct has markedly deviated from the standard of care, doctors have been successfully prosecuted for their “criminal” conduct.
For example, in an English case, an anesthesiologist was convicted of manslaughter in the death of a patient undergoing surgery for a detached retina. During surgery, the patient’s ventilation was interrupted because of accidental disconnection of the endotracheal tube for 4 minutes, leading to a cardiac arrest. An alarm had apparently sounded but was not noticed. The injury would not have occurred had the doctor attended to the patient instead of being away from the operating room.
The tragic death of pop star Michael Jackson in 2009 is another example. Dr. Conrad Murray, a cardiologist who was Jackson’s personal physician, had used the surgical anesthetic propofol to treat Jackson’s insomnia in a bedroom setting without monitoring or resuscitation equipment. Concurrent use of the sedative lorazepam exacerbated the effect of propofol. The prosecution characterized Dr. Murray’s conduct as “egregious, unethical, and unconscionable,” which violated medical standards and amounted to criminal negligence. He was found guilty of involuntary manslaughter, and the state sentenced him to a 4-year prison term.
A new trend appears to be developing toward prosecuting doctors whose overprescription of controlled substances results in patient deaths.
According to a recent news report, New York for the first time convicted a doctor of manslaughter in the overdose deaths of patients from oxycodone and Xanax.1 Some of the patients were reportedly prescribed as many as 500-800 pills over a 5-6 week period. Dr. Stan Li, an anesthesiologist and pain management specialist, allegedly saw up to 90 patients a day in his Queens, N.Y., weekend storefront clinic, charging them on a per-prescription basis. In his defense, Dr. Li claimed that he was simply trying to help suffering people who misused medications and who misled him (“tough patients and good liars”).
Meanwhile, a similar scenario played out in Oklahoma.2 There, Dr. William Valuck, a pain management doctor, pleaded guilty to eight counts of second-degree murder in connection with several drug overdose deaths. He entered into a plea bargain with Oklahoma prosecutors and will serve 8 years in prison. Dr. Valuck had reportedly prescribed more controlled drugs than any other physician in the state of Oklahoma, which included hydrocodone, oxycodone, alprazolam, Valium, and Soma, sometimes as many as 600 pills at a time. He allegedly accepted only cash payment for the office visits, and review of his patient files revealed inadequate assessment of patient complaints or physical findings to justify the prescriptions.
Most physicians are unlikely to ever face the specter of criminal prosecution based on their medical performance. Only in the most egregious of circumstances have physicians been successfully prosecuted for homicide.
As requests for physicians to withhold or withdraw life-sustaining treatments grow, physicians may find themselves questioning what acts or omissions they may legally perform. Unless the legal landscape changes, however, it appears that the forgoing of life-sustaining treatments in the typical clinical context will not subject physicians to criminal prosecution.
References
1. “NY doctor convicted of manslaughter in 2 overdoses,” July 18, 2014 (http://bigstory.ap.org/article/ny-doctor-convicted-2-patients-overdose-deaths).
2. “Ex-doctor pleads guilty in overdose deaths,” Aug. 13, 2014 (www.usatoday.com/story/news/nation/2014/08/13/ex-doctor-guilty-deaths/14022735).
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Qualifying as an expert
Question: A patient alleges that an ophthalmologist was negligent in performing blepharoplasty. The surgical site became infected and left the patient with a disfigured eye. An infectious disease specialist was to testify as plaintiff’s expert, but the defense, relying on a state statute, objected that the expert-to-be had no specialized training in ophthalmology.
Correct statements about expert medical testimony include the following, except:
A. The federal Rules of Evidence require that an expert possess the relevant knowledge, skill, education, training, or experience.
B. Only a few states have enacted statutes specifying that an expert must be in the same or similar specialty as the defendant.
C. Advocates contend that such statutes reduce frivolous lawsuits by limiting expert shopping and the use of “hired guns.”
D. It is the sitting judge, not the jury, who interprets the statute and decides whether a witness qualifies as an expert.
E. In some cases, a nondoctor such as a nurse or pharmacist may be allowed to offer expert testimony against a doctor.
Answer: B. Lay testimony is usually insufficient to define the standard of care in a claim of medical malpractice, and “the question of negligence must be decided by reference to relevant medical standards of care for which the plaintiff carries the burden of proving through expert medical testimony” (Craft v. Peebles, 893 P.2d 138 [Haw.1995]). Court rules of evidence dictate that the expert must possess the knowledge, skill, experience, training, or education for establishing that standard.
In coming to an opinion, the expert may rely on external evidence in the form of a book, treatise, or article; and although these sources represent hearsay evidence, they are admissible to enable the expert witness to form his/her opinion.
The facts of the multiple-choice question above are taken from a recent case (Edwards v. Sunrise Ophthalmology ASC, LLC, 134 So. 3d 1056 [Fla. 4th DCA 2013]), whose appeal is yet to be heard by the Florida Supreme Court. The plaintiff alleged that the surgical site was infected with nocardia during a lower-lid blepharoplasty, which caused her to undergo additional surgery with resulting disfigurement of the eye.
A lower court disqualified the plaintiff’s expert, an infectious disease specialist, based on a Florida statute stipulating that expert medical opinion can be offered only by one in the “same or similar specialty” (Section 766.102, Florida Statutes (2009)). In the words of the court, “Simply put, the infectious disease doctor is not an eye surgeon, nor is the ophthalmologist an infectious disease doctor.”
More than half of all the states have a medical-expert law, many with language comparable to the Florida statute. The idea behind such a statute, frequently enacted as part of a state’s tort reform, is to limit expert shopping and the use of hired guns and “junk science.”
Unsurprisingly, litigation abounds over the statutory language.
For example, a Maryland court ruled that a vascular surgeon was qualified to set the standard of care when an orthopedic surgeon’s alleged negligence caused a patient to lose a leg following knee surgery. The court found the two specialties to be “related,” because the orthopedic complication was vascular in origin.
In some jurisdictions without strict statutory requirements, doctors are more likely to be allowed to testify outside their specialty.
Instances of professionals of unlike specialties qualifying as experts include a nephrologist testifying against a urologist, an infectious disease specialist offering an expert opinion in a stroke case, a pharmacist testifying on the issue of a medication side effect, and a nurse on bedsores. Georgia requires only that an expert show significant familiarity with the area of practice in which the expert opinion is to be given. Still, in a sleep apnea case (Nathans v. Diamond, 654 S.E.2d 121 [Ga. 2007]), the court held that a pulmonologist was not qualified to testify on the standard of surgical care provided by an otolaryngologist.
Besides arguing over the statutory language, litigants have also raised questions of constitutionality. For example, Arizona’s statute ARS §12-2604 (A) requires a medical expert to be a specialist who is actively practicing or teaching in that area of medicine. The state court of appeals held that this violated the separation of powers doctrine (conflicting with Arizona Rule of Evidence 702), but the Supreme Court of Arizona subsequently reversed and reinstated the law (Seisinger v. Siebel, 203 P.3d 483 [Ariz. 2009]).
More recently, the same court upheld the constitutionality of the requirement that an expert share “the same specialty” as the treating physician, and disqualified an adult hematologist from serving as an expert because the defendant was a pediatric hematologist, not an adult hematologist (Baker v. University Physicians Healthcare, 296 P.3d 42 [Ariz. 2013]).
Another issue deals with the locality rule. In an Illinois case, the court accepted an out-of-state plaintiff expert based on his qualifications, competency, and familiarity with standards in the defendant’s community. The case dealt with the development of a rectovaginal fistula that complicated an episiotomy during delivery (Purtill v. Hess, 489 N.E.2d 867 [Ill. 1986]).
The defense attempted to exclude the expert, alleging the lack of familiarity with the standards in the community (Rantoul, Ill.). However, the expert stated that he was familiar with the minimum standards of medical practice in relation to the diagnosis and treatment of rectovaginal fistulae, and those minimum standards were uniform throughout the country.
It is not necessary that the expert witness has the highest possible qualifications to testify about a particular matter. Still, in Domingo v. T.K. (289 F.3d 600 [9th Cir. 2002]), a federal court excluded the testimony of the plaintiff’s expert witness, because it lacked reliability. The plaintiff developed brain damage from fat embolism following hip surgery, and alleged that prolonged malleting of a hip prosthesis was the cause of the fat embolism syndrome (FES).
The court found that “there was no evidence of widespread acceptance of Dr. Harrington’s theory linking extended malleting to FES; indeed, no theory linking extensive malleting to FES had ever been published.” It also noted the lack of any objective source, peer review, clinical tests, establishment of an error rate or other evidence to show that Dr. Harrington followed a valid, scientific method in developing his theory.
Being disqualified as an expert is one thing, but a recent case goes further. In addition to dismissing an expert’s testimony, a state judge barred the expert from ever testifying in his courtroom after it was determined that the testimony was untruthful.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected]
Question: A patient alleges that an ophthalmologist was negligent in performing blepharoplasty. The surgical site became infected and left the patient with a disfigured eye. An infectious disease specialist was to testify as plaintiff’s expert, but the defense, relying on a state statute, objected that the expert-to-be had no specialized training in ophthalmology.
Correct statements about expert medical testimony include the following, except:
A. The federal Rules of Evidence require that an expert possess the relevant knowledge, skill, education, training, or experience.
B. Only a few states have enacted statutes specifying that an expert must be in the same or similar specialty as the defendant.
C. Advocates contend that such statutes reduce frivolous lawsuits by limiting expert shopping and the use of “hired guns.”
D. It is the sitting judge, not the jury, who interprets the statute and decides whether a witness qualifies as an expert.
E. In some cases, a nondoctor such as a nurse or pharmacist may be allowed to offer expert testimony against a doctor.
Answer: B. Lay testimony is usually insufficient to define the standard of care in a claim of medical malpractice, and “the question of negligence must be decided by reference to relevant medical standards of care for which the plaintiff carries the burden of proving through expert medical testimony” (Craft v. Peebles, 893 P.2d 138 [Haw.1995]). Court rules of evidence dictate that the expert must possess the knowledge, skill, experience, training, or education for establishing that standard.
In coming to an opinion, the expert may rely on external evidence in the form of a book, treatise, or article; and although these sources represent hearsay evidence, they are admissible to enable the expert witness to form his/her opinion.
The facts of the multiple-choice question above are taken from a recent case (Edwards v. Sunrise Ophthalmology ASC, LLC, 134 So. 3d 1056 [Fla. 4th DCA 2013]), whose appeal is yet to be heard by the Florida Supreme Court. The plaintiff alleged that the surgical site was infected with nocardia during a lower-lid blepharoplasty, which caused her to undergo additional surgery with resulting disfigurement of the eye.
A lower court disqualified the plaintiff’s expert, an infectious disease specialist, based on a Florida statute stipulating that expert medical opinion can be offered only by one in the “same or similar specialty” (Section 766.102, Florida Statutes (2009)). In the words of the court, “Simply put, the infectious disease doctor is not an eye surgeon, nor is the ophthalmologist an infectious disease doctor.”
More than half of all the states have a medical-expert law, many with language comparable to the Florida statute. The idea behind such a statute, frequently enacted as part of a state’s tort reform, is to limit expert shopping and the use of hired guns and “junk science.”
Unsurprisingly, litigation abounds over the statutory language.
For example, a Maryland court ruled that a vascular surgeon was qualified to set the standard of care when an orthopedic surgeon’s alleged negligence caused a patient to lose a leg following knee surgery. The court found the two specialties to be “related,” because the orthopedic complication was vascular in origin.
In some jurisdictions without strict statutory requirements, doctors are more likely to be allowed to testify outside their specialty.
Instances of professionals of unlike specialties qualifying as experts include a nephrologist testifying against a urologist, an infectious disease specialist offering an expert opinion in a stroke case, a pharmacist testifying on the issue of a medication side effect, and a nurse on bedsores. Georgia requires only that an expert show significant familiarity with the area of practice in which the expert opinion is to be given. Still, in a sleep apnea case (Nathans v. Diamond, 654 S.E.2d 121 [Ga. 2007]), the court held that a pulmonologist was not qualified to testify on the standard of surgical care provided by an otolaryngologist.
Besides arguing over the statutory language, litigants have also raised questions of constitutionality. For example, Arizona’s statute ARS §12-2604 (A) requires a medical expert to be a specialist who is actively practicing or teaching in that area of medicine. The state court of appeals held that this violated the separation of powers doctrine (conflicting with Arizona Rule of Evidence 702), but the Supreme Court of Arizona subsequently reversed and reinstated the law (Seisinger v. Siebel, 203 P.3d 483 [Ariz. 2009]).
More recently, the same court upheld the constitutionality of the requirement that an expert share “the same specialty” as the treating physician, and disqualified an adult hematologist from serving as an expert because the defendant was a pediatric hematologist, not an adult hematologist (Baker v. University Physicians Healthcare, 296 P.3d 42 [Ariz. 2013]).
Another issue deals with the locality rule. In an Illinois case, the court accepted an out-of-state plaintiff expert based on his qualifications, competency, and familiarity with standards in the defendant’s community. The case dealt with the development of a rectovaginal fistula that complicated an episiotomy during delivery (Purtill v. Hess, 489 N.E.2d 867 [Ill. 1986]).
The defense attempted to exclude the expert, alleging the lack of familiarity with the standards in the community (Rantoul, Ill.). However, the expert stated that he was familiar with the minimum standards of medical practice in relation to the diagnosis and treatment of rectovaginal fistulae, and those minimum standards were uniform throughout the country.
It is not necessary that the expert witness has the highest possible qualifications to testify about a particular matter. Still, in Domingo v. T.K. (289 F.3d 600 [9th Cir. 2002]), a federal court excluded the testimony of the plaintiff’s expert witness, because it lacked reliability. The plaintiff developed brain damage from fat embolism following hip surgery, and alleged that prolonged malleting of a hip prosthesis was the cause of the fat embolism syndrome (FES).
The court found that “there was no evidence of widespread acceptance of Dr. Harrington’s theory linking extended malleting to FES; indeed, no theory linking extensive malleting to FES had ever been published.” It also noted the lack of any objective source, peer review, clinical tests, establishment of an error rate or other evidence to show that Dr. Harrington followed a valid, scientific method in developing his theory.
Being disqualified as an expert is one thing, but a recent case goes further. In addition to dismissing an expert’s testimony, a state judge barred the expert from ever testifying in his courtroom after it was determined that the testimony was untruthful.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected]
Question: A patient alleges that an ophthalmologist was negligent in performing blepharoplasty. The surgical site became infected and left the patient with a disfigured eye. An infectious disease specialist was to testify as plaintiff’s expert, but the defense, relying on a state statute, objected that the expert-to-be had no specialized training in ophthalmology.
Correct statements about expert medical testimony include the following, except:
A. The federal Rules of Evidence require that an expert possess the relevant knowledge, skill, education, training, or experience.
B. Only a few states have enacted statutes specifying that an expert must be in the same or similar specialty as the defendant.
C. Advocates contend that such statutes reduce frivolous lawsuits by limiting expert shopping and the use of “hired guns.”
D. It is the sitting judge, not the jury, who interprets the statute and decides whether a witness qualifies as an expert.
E. In some cases, a nondoctor such as a nurse or pharmacist may be allowed to offer expert testimony against a doctor.
Answer: B. Lay testimony is usually insufficient to define the standard of care in a claim of medical malpractice, and “the question of negligence must be decided by reference to relevant medical standards of care for which the plaintiff carries the burden of proving through expert medical testimony” (Craft v. Peebles, 893 P.2d 138 [Haw.1995]). Court rules of evidence dictate that the expert must possess the knowledge, skill, experience, training, or education for establishing that standard.
In coming to an opinion, the expert may rely on external evidence in the form of a book, treatise, or article; and although these sources represent hearsay evidence, they are admissible to enable the expert witness to form his/her opinion.
The facts of the multiple-choice question above are taken from a recent case (Edwards v. Sunrise Ophthalmology ASC, LLC, 134 So. 3d 1056 [Fla. 4th DCA 2013]), whose appeal is yet to be heard by the Florida Supreme Court. The plaintiff alleged that the surgical site was infected with nocardia during a lower-lid blepharoplasty, which caused her to undergo additional surgery with resulting disfigurement of the eye.
A lower court disqualified the plaintiff’s expert, an infectious disease specialist, based on a Florida statute stipulating that expert medical opinion can be offered only by one in the “same or similar specialty” (Section 766.102, Florida Statutes (2009)). In the words of the court, “Simply put, the infectious disease doctor is not an eye surgeon, nor is the ophthalmologist an infectious disease doctor.”
More than half of all the states have a medical-expert law, many with language comparable to the Florida statute. The idea behind such a statute, frequently enacted as part of a state’s tort reform, is to limit expert shopping and the use of hired guns and “junk science.”
Unsurprisingly, litigation abounds over the statutory language.
For example, a Maryland court ruled that a vascular surgeon was qualified to set the standard of care when an orthopedic surgeon’s alleged negligence caused a patient to lose a leg following knee surgery. The court found the two specialties to be “related,” because the orthopedic complication was vascular in origin.
In some jurisdictions without strict statutory requirements, doctors are more likely to be allowed to testify outside their specialty.
Instances of professionals of unlike specialties qualifying as experts include a nephrologist testifying against a urologist, an infectious disease specialist offering an expert opinion in a stroke case, a pharmacist testifying on the issue of a medication side effect, and a nurse on bedsores. Georgia requires only that an expert show significant familiarity with the area of practice in which the expert opinion is to be given. Still, in a sleep apnea case (Nathans v. Diamond, 654 S.E.2d 121 [Ga. 2007]), the court held that a pulmonologist was not qualified to testify on the standard of surgical care provided by an otolaryngologist.
Besides arguing over the statutory language, litigants have also raised questions of constitutionality. For example, Arizona’s statute ARS §12-2604 (A) requires a medical expert to be a specialist who is actively practicing or teaching in that area of medicine. The state court of appeals held that this violated the separation of powers doctrine (conflicting with Arizona Rule of Evidence 702), but the Supreme Court of Arizona subsequently reversed and reinstated the law (Seisinger v. Siebel, 203 P.3d 483 [Ariz. 2009]).
More recently, the same court upheld the constitutionality of the requirement that an expert share “the same specialty” as the treating physician, and disqualified an adult hematologist from serving as an expert because the defendant was a pediatric hematologist, not an adult hematologist (Baker v. University Physicians Healthcare, 296 P.3d 42 [Ariz. 2013]).
Another issue deals with the locality rule. In an Illinois case, the court accepted an out-of-state plaintiff expert based on his qualifications, competency, and familiarity with standards in the defendant’s community. The case dealt with the development of a rectovaginal fistula that complicated an episiotomy during delivery (Purtill v. Hess, 489 N.E.2d 867 [Ill. 1986]).
The defense attempted to exclude the expert, alleging the lack of familiarity with the standards in the community (Rantoul, Ill.). However, the expert stated that he was familiar with the minimum standards of medical practice in relation to the diagnosis and treatment of rectovaginal fistulae, and those minimum standards were uniform throughout the country.
It is not necessary that the expert witness has the highest possible qualifications to testify about a particular matter. Still, in Domingo v. T.K. (289 F.3d 600 [9th Cir. 2002]), a federal court excluded the testimony of the plaintiff’s expert witness, because it lacked reliability. The plaintiff developed brain damage from fat embolism following hip surgery, and alleged that prolonged malleting of a hip prosthesis was the cause of the fat embolism syndrome (FES).
The court found that “there was no evidence of widespread acceptance of Dr. Harrington’s theory linking extended malleting to FES; indeed, no theory linking extensive malleting to FES had ever been published.” It also noted the lack of any objective source, peer review, clinical tests, establishment of an error rate or other evidence to show that Dr. Harrington followed a valid, scientific method in developing his theory.
Being disqualified as an expert is one thing, but a recent case goes further. In addition to dismissing an expert’s testimony, a state judge barred the expert from ever testifying in his courtroom after it was determined that the testimony was untruthful.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected]

Inadequate evaluation of a mole has costly consequences
Inadequate evaluation of a mole has costly consequences
A 53-year-old woman went to her physician for treatment of a mole on her upper right arm, which she stated had grown and changed color. The physician burned it off without conducting a biopsy or follow-up. Fifteen months later, the patient returned to her physician because the scar was raised with small bumps. He referred her to a surgeon, who diagnosed malignant melanoma (Clark’s level V), with a satellite lesion but negative lymph nodes. The patient underwent surgery and adjuvant interferon-alpha therapy, which caused significant adverse effects.
The patient now has anxiety related to fears of recurrence or death, and must undergo regular positron emission tomography and computed tomography scans to evaluate her for recurrence.
PLAINTIFF’S CLAIM The melanoma should have been diagnosed at the patient’s initial presentation. If it had been diagnosed at that time, the patient would have had an 85% to 90% chance of survival, but because it wasn’t, her survival rate dropped to 60%.
THE DEFENSE No information about the defense is available.
VERDICT $750,000 Virginia settlement.
COMMENT When there is any doubt—by patient or physician—cut it out and send it out (for biopsy).
A higher index of suspicion for PE could have been lifesaving
A 37-year-old morbidly obese man was recovering in a rehabilitation facility from spinal surgery performed 2 weeks earlier. On the day he was to be discharged, he was transported by ambulance to the emergency department (ED) complaining of “a syncopal episode” with weakness, lightheadedness, dizziness, and sweatiness. This was followed by a second episode with similar symptoms. The patient had no wheezes or rales and his heart rhythm was normal, with no murmurs or gallop. In the ED his pulse rose from 94 to 116 and his blood pressure (BP) rose from 106/82 to 145/102. An electrocardiogram (EKG) was abnormal.
The ED physician felt that the likelihood of pulmonary embolism (PE) was low; he suspected, instead, that it was “likely vagal syncope.” The patient returned to the rehab facility, stayed overnight, and was discharged the next day. Two days later, he became short of breath, passed out, and was taken by ambulance to the hospital, where resuscitation efforts were unsuccessful. Autopsy revealed the cause of death was pulmonary thromboemboli from deep vein thrombosis.
PLAINTIFF’S CLAIM The ED physician failed to rule out PE, which should have been considered because of the patient’s obesity, recent back surgery, immobilization, syncope, tachycardia, elevated BP, and abnormal EKG.
THE DEFENSE No information about the defense is available.
VERDICT $1.25 million Massachusetts settlement.
COMMENT Why the physician decided that this patient, who died of a PE, was at low risk for one is puzzling. I count at least 4 risk factors for PE: obesity, postoperative status, abnormal EKG, and tachycardia.
Inadequate evaluation of a mole has costly consequences
A 53-year-old woman went to her physician for treatment of a mole on her upper right arm, which she stated had grown and changed color. The physician burned it off without conducting a biopsy or follow-up. Fifteen months later, the patient returned to her physician because the scar was raised with small bumps. He referred her to a surgeon, who diagnosed malignant melanoma (Clark’s level V), with a satellite lesion but negative lymph nodes. The patient underwent surgery and adjuvant interferon-alpha therapy, which caused significant adverse effects.
The patient now has anxiety related to fears of recurrence or death, and must undergo regular positron emission tomography and computed tomography scans to evaluate her for recurrence.
PLAINTIFF’S CLAIM The melanoma should have been diagnosed at the patient’s initial presentation. If it had been diagnosed at that time, the patient would have had an 85% to 90% chance of survival, but because it wasn’t, her survival rate dropped to 60%.
THE DEFENSE No information about the defense is available.
VERDICT $750,000 Virginia settlement.
COMMENT When there is any doubt—by patient or physician—cut it out and send it out (for biopsy).
A higher index of suspicion for PE could have been lifesaving
A 37-year-old morbidly obese man was recovering in a rehabilitation facility from spinal surgery performed 2 weeks earlier. On the day he was to be discharged, he was transported by ambulance to the emergency department (ED) complaining of “a syncopal episode” with weakness, lightheadedness, dizziness, and sweatiness. This was followed by a second episode with similar symptoms. The patient had no wheezes or rales and his heart rhythm was normal, with no murmurs or gallop. In the ED his pulse rose from 94 to 116 and his blood pressure (BP) rose from 106/82 to 145/102. An electrocardiogram (EKG) was abnormal.
The ED physician felt that the likelihood of pulmonary embolism (PE) was low; he suspected, instead, that it was “likely vagal syncope.” The patient returned to the rehab facility, stayed overnight, and was discharged the next day. Two days later, he became short of breath, passed out, and was taken by ambulance to the hospital, where resuscitation efforts were unsuccessful. Autopsy revealed the cause of death was pulmonary thromboemboli from deep vein thrombosis.
PLAINTIFF’S CLAIM The ED physician failed to rule out PE, which should have been considered because of the patient’s obesity, recent back surgery, immobilization, syncope, tachycardia, elevated BP, and abnormal EKG.
THE DEFENSE No information about the defense is available.
VERDICT $1.25 million Massachusetts settlement.
COMMENT Why the physician decided that this patient, who died of a PE, was at low risk for one is puzzling. I count at least 4 risk factors for PE: obesity, postoperative status, abnormal EKG, and tachycardia.
Inadequate evaluation of a mole has costly consequences
A 53-year-old woman went to her physician for treatment of a mole on her upper right arm, which she stated had grown and changed color. The physician burned it off without conducting a biopsy or follow-up. Fifteen months later, the patient returned to her physician because the scar was raised with small bumps. He referred her to a surgeon, who diagnosed malignant melanoma (Clark’s level V), with a satellite lesion but negative lymph nodes. The patient underwent surgery and adjuvant interferon-alpha therapy, which caused significant adverse effects.
The patient now has anxiety related to fears of recurrence or death, and must undergo regular positron emission tomography and computed tomography scans to evaluate her for recurrence.
PLAINTIFF’S CLAIM The melanoma should have been diagnosed at the patient’s initial presentation. If it had been diagnosed at that time, the patient would have had an 85% to 90% chance of survival, but because it wasn’t, her survival rate dropped to 60%.
THE DEFENSE No information about the defense is available.
VERDICT $750,000 Virginia settlement.
COMMENT When there is any doubt—by patient or physician—cut it out and send it out (for biopsy).
A higher index of suspicion for PE could have been lifesaving
A 37-year-old morbidly obese man was recovering in a rehabilitation facility from spinal surgery performed 2 weeks earlier. On the day he was to be discharged, he was transported by ambulance to the emergency department (ED) complaining of “a syncopal episode” with weakness, lightheadedness, dizziness, and sweatiness. This was followed by a second episode with similar symptoms. The patient had no wheezes or rales and his heart rhythm was normal, with no murmurs or gallop. In the ED his pulse rose from 94 to 116 and his blood pressure (BP) rose from 106/82 to 145/102. An electrocardiogram (EKG) was abnormal.
The ED physician felt that the likelihood of pulmonary embolism (PE) was low; he suspected, instead, that it was “likely vagal syncope.” The patient returned to the rehab facility, stayed overnight, and was discharged the next day. Two days later, he became short of breath, passed out, and was taken by ambulance to the hospital, where resuscitation efforts were unsuccessful. Autopsy revealed the cause of death was pulmonary thromboemboli from deep vein thrombosis.
PLAINTIFF’S CLAIM The ED physician failed to rule out PE, which should have been considered because of the patient’s obesity, recent back surgery, immobilization, syncope, tachycardia, elevated BP, and abnormal EKG.
THE DEFENSE No information about the defense is available.
VERDICT $1.25 million Massachusetts settlement.
COMMENT Why the physician decided that this patient, who died of a PE, was at low risk for one is puzzling. I count at least 4 risk factors for PE: obesity, postoperative status, abnormal EKG, and tachycardia.
Malpractice Counsel
Stroke in a Young Man
A 26-year-old man presented to the ED with the chief complaint of mild right-sided weakness, paresthesias, and slurred speech. He stated the onset was sudden—approximately 30 minutes prior to arrival to the ED. The patient denied any previous similar symptoms and was otherwise in good health; he denied taking any medications. He drank alcohol socially, but denied smoking or illicit drug use.
On physical examination, his vital signs and oxygen saturation were normal. Pulmonary, cardiovascular, and abdominal examinations were also normal. The patient thought his speech was somewhat slurred, but the triage nurse and treating emergency physician (EP) had difficulty detecting any altered speech. He was noted to have mild (4+/5) right upper and lower extremity weakness; no facial droop was detected. The patient did have a mild pronator drift of the right upper extremity. Gait testing revealed a mild limp of the right lower extremity.
The EP consulted the hospitalist, and the patient was admitted to a monitored bed. The following morning, a brain magnetic resonance image revealed an ischemic stroke in the distribution of the left middle cerebral artery. The patient’s hospital course was uncomplicated, but at the time of discharge, he continued to have mild right-sided weakness and required the use of a cane.
The patient sued the hospital and the EP for negligence in failing to treat his condition in a timely manner and for not consulting a neurologist. The plaintiff’s attorneys argued the patient should have been given tissue plasminogen activator (tPA), which would have avoided the residual right-sided weakness. The defense denied negligence and argued the patient’s symptoms could have been due to several things for which tPA would have been an inappropriate treatment. A defense verdict was returned.
Discussion
Stroke in young patients is relatively rare. With “young” defined as aged 18 to 45 years, this population accounts for approximately 2% to 12% of cerebral infarcts.1 In one nationwide US study of stroke in young adults, Ellis2 found that 4.9% of individuals experiencing a stroke in 2007 were between ages 18 and 44 years. Among this group, 78% experienced an ischemic stroke; 11.2% experienced a subarachnoid hemorrhage (SAH); and 10.8% had an intracerebral hemorrhage.2
While the clinical presentation of stroke in young adults is similar to that of older patients, the etiologies and risk factors are very different. In older patients, atherosclerosis is the major cause of ischemic stroke. In studies of young adults with ischemic stroke, cardioembolism was found to be the leading cause. Under this category, a patent foramen ovale (PFO) was considered a common cause, followed by atrial fibrillation, bacterial endocarditis, rheumatic heart disease, and atrial myxoma. There is, however, increasing controversy over the role of PFO as an etiology of stroke. Many investigators think its role has been overstated and is probably more of an incidental finding than a causal relationship.3 Patients with a suspected cardioembolic etiology will usually require an echocardiogram (with saline contrast or a “bubble study” for suspected PFO), cardiac monitoring, and a possible Holter monitor at the time of discharge (to detect paroxysmal arrhythmias).
Following cardioembolic etiologies, arterial dissection is the next most common category.4 In one study of patients aged 31 to 45 years old, arterial dissection was the most common cause of ischemic stroke.4 Clinical features suggesting dissection include a history of head or neck trauma (even minor trauma), headache or neck pain, and local neurological findings (eg, cranial nerve palsy or Horner syndrome).3 Unfortunately, only about 25% of patients volunteer a history of recent neck trauma. If a cervical or vertebral artery dissection is suspected, contrast enhanced magnetic resonance angiography (MRA) is the most sensitive and specific test, followed by carotid ultrasound and CT angiography.3
Traditional risk factors for stroke include hypertension and diabetes mellitus (DM). This is not true for younger adults that experience an ischemic stroke. Cigarette smoking is a very important risk factor for cerebrovascular accident in young adults; in addition, the more one smokes, the greater the risk. Other risk factors in young adults include history of migraine headaches (especially migraine with aura), pregnancy and the postpartum period, and illicit drug use.3
The defense’s argument that there are many causes of stroke in young adults that would be inappropriate for treatment with tPA, such as a PFO, carotid dissection or bacterial endocarditis, is absolutely true. Young patients need to be aggressively worked up for the etiology of their stroke, and may require additional testing, such as an MRA, echocardiogram, or Holter monitoring to determine the underlying cause of their stroke.
Obstruction Following Gastric Bypass Surgery
A 47-year-old woman presented to the ED complaining of severe back and abdominal pain. Onset had been gradual and began approximately 4 hours prior to arrival. She described the pain as crampy and constant. The patient had vomited twice; she denied diarrhea and had a normal bowel movement the previous day. She denied any vaginal or urinary complaints. Her past medical history was significant for hypertension and status post gastric bypass surgery 6 months prior. She had lost 42 pounds to date. She denied smoking or alcohol use.
The patient’s vital signs on physical examination were: blood pressure, 154/92 mm Hg; pulse, 106 beats/minute; respiratory rate, 18 breaths/minute; and temperature, 99˚F. Oxygen saturation was 96% on room air. The patient’s lungs were clear to auscultation bilaterally. The heart was mildly tachycardic, with a regular rhythm and without murmurs, rubs, or gallops. The abdominal examination revealed diffuse tenderness and involuntary guarding. There was no distention or rebound. Bowel sounds were present but hypoactive. Examination of the back revealed bilateral paraspinal muscle tenderness without costovertebral angle tenderness.
The EP ordered a CBC, BMP, serum lipase, and a urinalysis. The patient was given an intravenous (IV) bolus of 250 cc normal saline in addition to IV morphine 4 mg and IV ondansetron 4 mg. Her white blood cell (WBC) count was slightly elevated at 12.2 g/dL, with a normal differential. The remainder of the laboratory studies were normal, except for a serum bicarbonate of 22 mmol/L.
The patient stated she felt somewhat improved, but continued to have abdominal and back pain. The EP admitted her to the hospital for observation and pain control. She died the following day from a bowel obstruction. The family sued the EP for negligence in failing to order appropriate testing and for not consulting with specialists to diagnose the bowel obstruction, which is a known complication of gastric bypass surgery. The jury returned a verdict of $2.4 million against the EP.
Discussion
The frequency of bariatric surgery in the United States continues to increase, primarily due to its success with regard to weight loss, but also because of its demonstrated improvement in hypertension, obstructive sleep apnea, hyperlipidemia, and type 2 DM.1
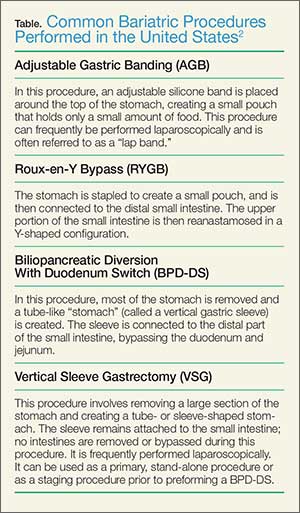
Frequently, the term “gastric bypass surgery” is used interchangeably with bariatric surgery. However, the EP must realize these terms encompass multiple different operations. The four most common types of bariatric surgery in the United Stated are (1) adjustable gastric banding (AGB); (2) the Roux-en-Y gastric bypass (RYGB); (3) biliopancreatic diversion with duodenal switch (BPD-DS); and (4) vertical sleeve gastrectomy (VSG).2 (See the Table for a brief explanation of each type of procedure.)
Since each procedure has its own respective associated complications, it is important for the EP to know which the type of gastric bypass surgery the patient had. For example, leakage is much more frequent following RYGB than in gastric banding, while slippage and obstruction are the most common complications of gastric banding.3,4 It is also very helpful to know the specific type of procedure when discussing the case with the surgical consultant.
Based on a recent review of over 800,000 bariatric surgery patients, seven serious common complications following the surgery were identified.3 These included bleeding, leakage, obstruction, stomal ulceration, pulmonary embolism and respiratory complications, blood sugar disturbances (usually hypoglycemia and/or metabolic acidosis), and nutritional disturbances. While not all-inclusive, this list represents the most common serious complications of gastric bypass surgery.
The complaint of abdominal pain in a patient that has undergone bariatric surgery should be taken very seriously. In addition to determining the specific procedure performed and date, the patient should be questioned about vomiting, bowel movements, and the presence of blood in stool or vomit. Depending upon the degree of pain present, the patient may need to be given IV opioid analgesia to facilitate a thorough abdominal examination. A rectal examination should be performed to identify occult gastrointestinal bleeding.
These patients require laboratory testing, including CBC, BMP, and other laboratory evaluation as indicated by the history and physical examination. Early consultation with the bariatric surgeon is recommended. Many, if not most, patients with abdominal pain and vomiting will require imaging, usually a CT scan with contrast of the abdomen and pelvis. Because of the difficulty in interpreting the CT scan results in these patients, the bariatric surgeon will often want to personally review the films rather than rely solely on the interpretation by radiology services.
Unfortunately, the EP in this case did not appreciate the seriousness of the situation. The presence of severe abdominal pain, tenderness, guarding, mild tachycardia with leukocytosis, and metabolic acidosis all pointed to a more serious etiology than muscle spasm. This patient required IV fluids, analgesia, and imaging, as well as consultation with the bariatric surgeon.
- Chatzikonstantinou A, Wolf ME, Hennerici MG. Ischemic stroke in young adults: classification and risk factors. J Neurol. 2012;259(4):653-659.
- Ellis C. Stroke in young adults. Disabil Health J. 2010;3(3):222-224.
- Ferro JM, Massaro AR, Mas JL. Aetiological diagnosis of ischemic stroke in young adults. Lancet Neurol. 2010;9(11):1085-1096.
- Chan MT, Nadareishvili ZG, Norris JW; Canadian Stroke Consortium. Diagnostic strategies in young patients with ischemic stroke in Canada. Can J Neurol Sci. 2000;27(2):120-124.
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724-1737.
- Livingston EH. Patient guide: Endocrine and nutritional management after bariatric surgery: A patient’s guide. Hormone Health Network Web site. http://www.hormone.org/~/media/Hormone/Files/Patient%20Guides/Mens%20Health/PGBariatricSurgery_2014.pdf. Accessed December 17, 2014.
- Hussain A, El-Hasani S. Bariatric emergencies: current evidence and strategies of management. World J Emerg Surg. 2013;8(1):58.
- Campanille FC, Boru C, Rizzello M, et al. Acute complications after laparoscopic bariatric procedures: update for the general surgeon. Langenbecks Arch Surg. 2013;398(5):669-686
Stroke in a Young Man
A 26-year-old man presented to the ED with the chief complaint of mild right-sided weakness, paresthesias, and slurred speech. He stated the onset was sudden—approximately 30 minutes prior to arrival to the ED. The patient denied any previous similar symptoms and was otherwise in good health; he denied taking any medications. He drank alcohol socially, but denied smoking or illicit drug use.
On physical examination, his vital signs and oxygen saturation were normal. Pulmonary, cardiovascular, and abdominal examinations were also normal. The patient thought his speech was somewhat slurred, but the triage nurse and treating emergency physician (EP) had difficulty detecting any altered speech. He was noted to have mild (4+/5) right upper and lower extremity weakness; no facial droop was detected. The patient did have a mild pronator drift of the right upper extremity. Gait testing revealed a mild limp of the right lower extremity.
The EP consulted the hospitalist, and the patient was admitted to a monitored bed. The following morning, a brain magnetic resonance image revealed an ischemic stroke in the distribution of the left middle cerebral artery. The patient’s hospital course was uncomplicated, but at the time of discharge, he continued to have mild right-sided weakness and required the use of a cane.
The patient sued the hospital and the EP for negligence in failing to treat his condition in a timely manner and for not consulting a neurologist. The plaintiff’s attorneys argued the patient should have been given tissue plasminogen activator (tPA), which would have avoided the residual right-sided weakness. The defense denied negligence and argued the patient’s symptoms could have been due to several things for which tPA would have been an inappropriate treatment. A defense verdict was returned.
Discussion
Stroke in young patients is relatively rare. With “young” defined as aged 18 to 45 years, this population accounts for approximately 2% to 12% of cerebral infarcts.1 In one nationwide US study of stroke in young adults, Ellis2 found that 4.9% of individuals experiencing a stroke in 2007 were between ages 18 and 44 years. Among this group, 78% experienced an ischemic stroke; 11.2% experienced a subarachnoid hemorrhage (SAH); and 10.8% had an intracerebral hemorrhage.2
While the clinical presentation of stroke in young adults is similar to that of older patients, the etiologies and risk factors are very different. In older patients, atherosclerosis is the major cause of ischemic stroke. In studies of young adults with ischemic stroke, cardioembolism was found to be the leading cause. Under this category, a patent foramen ovale (PFO) was considered a common cause, followed by atrial fibrillation, bacterial endocarditis, rheumatic heart disease, and atrial myxoma. There is, however, increasing controversy over the role of PFO as an etiology of stroke. Many investigators think its role has been overstated and is probably more of an incidental finding than a causal relationship.3 Patients with a suspected cardioembolic etiology will usually require an echocardiogram (with saline contrast or a “bubble study” for suspected PFO), cardiac monitoring, and a possible Holter monitor at the time of discharge (to detect paroxysmal arrhythmias).
Following cardioembolic etiologies, arterial dissection is the next most common category.4 In one study of patients aged 31 to 45 years old, arterial dissection was the most common cause of ischemic stroke.4 Clinical features suggesting dissection include a history of head or neck trauma (even minor trauma), headache or neck pain, and local neurological findings (eg, cranial nerve palsy or Horner syndrome).3 Unfortunately, only about 25% of patients volunteer a history of recent neck trauma. If a cervical or vertebral artery dissection is suspected, contrast enhanced magnetic resonance angiography (MRA) is the most sensitive and specific test, followed by carotid ultrasound and CT angiography.3
Traditional risk factors for stroke include hypertension and diabetes mellitus (DM). This is not true for younger adults that experience an ischemic stroke. Cigarette smoking is a very important risk factor for cerebrovascular accident in young adults; in addition, the more one smokes, the greater the risk. Other risk factors in young adults include history of migraine headaches (especially migraine with aura), pregnancy and the postpartum period, and illicit drug use.3
The defense’s argument that there are many causes of stroke in young adults that would be inappropriate for treatment with tPA, such as a PFO, carotid dissection or bacterial endocarditis, is absolutely true. Young patients need to be aggressively worked up for the etiology of their stroke, and may require additional testing, such as an MRA, echocardiogram, or Holter monitoring to determine the underlying cause of their stroke.
Obstruction Following Gastric Bypass Surgery
A 47-year-old woman presented to the ED complaining of severe back and abdominal pain. Onset had been gradual and began approximately 4 hours prior to arrival. She described the pain as crampy and constant. The patient had vomited twice; she denied diarrhea and had a normal bowel movement the previous day. She denied any vaginal or urinary complaints. Her past medical history was significant for hypertension and status post gastric bypass surgery 6 months prior. She had lost 42 pounds to date. She denied smoking or alcohol use.
The patient’s vital signs on physical examination were: blood pressure, 154/92 mm Hg; pulse, 106 beats/minute; respiratory rate, 18 breaths/minute; and temperature, 99˚F. Oxygen saturation was 96% on room air. The patient’s lungs were clear to auscultation bilaterally. The heart was mildly tachycardic, with a regular rhythm and without murmurs, rubs, or gallops. The abdominal examination revealed diffuse tenderness and involuntary guarding. There was no distention or rebound. Bowel sounds were present but hypoactive. Examination of the back revealed bilateral paraspinal muscle tenderness without costovertebral angle tenderness.
The EP ordered a CBC, BMP, serum lipase, and a urinalysis. The patient was given an intravenous (IV) bolus of 250 cc normal saline in addition to IV morphine 4 mg and IV ondansetron 4 mg. Her white blood cell (WBC) count was slightly elevated at 12.2 g/dL, with a normal differential. The remainder of the laboratory studies were normal, except for a serum bicarbonate of 22 mmol/L.
The patient stated she felt somewhat improved, but continued to have abdominal and back pain. The EP admitted her to the hospital for observation and pain control. She died the following day from a bowel obstruction. The family sued the EP for negligence in failing to order appropriate testing and for not consulting with specialists to diagnose the bowel obstruction, which is a known complication of gastric bypass surgery. The jury returned a verdict of $2.4 million against the EP.
Discussion
The frequency of bariatric surgery in the United States continues to increase, primarily due to its success with regard to weight loss, but also because of its demonstrated improvement in hypertension, obstructive sleep apnea, hyperlipidemia, and type 2 DM.1
Frequently, the term “gastric bypass surgery” is used interchangeably with bariatric surgery. However, the EP must realize these terms encompass multiple different operations. The four most common types of bariatric surgery in the United Stated are (1) adjustable gastric banding (AGB); (2) the Roux-en-Y gastric bypass (RYGB); (3) biliopancreatic diversion with duodenal switch (BPD-DS); and (4) vertical sleeve gastrectomy (VSG).2 (See the Table for a brief explanation of each type of procedure.)
Since each procedure has its own respective associated complications, it is important for the EP to know which the type of gastric bypass surgery the patient had. For example, leakage is much more frequent following RYGB than in gastric banding, while slippage and obstruction are the most common complications of gastric banding.3,4 It is also very helpful to know the specific type of procedure when discussing the case with the surgical consultant.
Based on a recent review of over 800,000 bariatric surgery patients, seven serious common complications following the surgery were identified.3 These included bleeding, leakage, obstruction, stomal ulceration, pulmonary embolism and respiratory complications, blood sugar disturbances (usually hypoglycemia and/or metabolic acidosis), and nutritional disturbances. While not all-inclusive, this list represents the most common serious complications of gastric bypass surgery.
The complaint of abdominal pain in a patient that has undergone bariatric surgery should be taken very seriously. In addition to determining the specific procedure performed and date, the patient should be questioned about vomiting, bowel movements, and the presence of blood in stool or vomit. Depending upon the degree of pain present, the patient may need to be given IV opioid analgesia to facilitate a thorough abdominal examination. A rectal examination should be performed to identify occult gastrointestinal bleeding.
These patients require laboratory testing, including CBC, BMP, and other laboratory evaluation as indicated by the history and physical examination. Early consultation with the bariatric surgeon is recommended. Many, if not most, patients with abdominal pain and vomiting will require imaging, usually a CT scan with contrast of the abdomen and pelvis. Because of the difficulty in interpreting the CT scan results in these patients, the bariatric surgeon will often want to personally review the films rather than rely solely on the interpretation by radiology services.
Unfortunately, the EP in this case did not appreciate the seriousness of the situation. The presence of severe abdominal pain, tenderness, guarding, mild tachycardia with leukocytosis, and metabolic acidosis all pointed to a more serious etiology than muscle spasm. This patient required IV fluids, analgesia, and imaging, as well as consultation with the bariatric surgeon.
Stroke in a Young Man
A 26-year-old man presented to the ED with the chief complaint of mild right-sided weakness, paresthesias, and slurred speech. He stated the onset was sudden—approximately 30 minutes prior to arrival to the ED. The patient denied any previous similar symptoms and was otherwise in good health; he denied taking any medications. He drank alcohol socially, but denied smoking or illicit drug use.
On physical examination, his vital signs and oxygen saturation were normal. Pulmonary, cardiovascular, and abdominal examinations were also normal. The patient thought his speech was somewhat slurred, but the triage nurse and treating emergency physician (EP) had difficulty detecting any altered speech. He was noted to have mild (4+/5) right upper and lower extremity weakness; no facial droop was detected. The patient did have a mild pronator drift of the right upper extremity. Gait testing revealed a mild limp of the right lower extremity.
The EP consulted the hospitalist, and the patient was admitted to a monitored bed. The following morning, a brain magnetic resonance image revealed an ischemic stroke in the distribution of the left middle cerebral artery. The patient’s hospital course was uncomplicated, but at the time of discharge, he continued to have mild right-sided weakness and required the use of a cane.
The patient sued the hospital and the EP for negligence in failing to treat his condition in a timely manner and for not consulting a neurologist. The plaintiff’s attorneys argued the patient should have been given tissue plasminogen activator (tPA), which would have avoided the residual right-sided weakness. The defense denied negligence and argued the patient’s symptoms could have been due to several things for which tPA would have been an inappropriate treatment. A defense verdict was returned.
Discussion
Stroke in young patients is relatively rare. With “young” defined as aged 18 to 45 years, this population accounts for approximately 2% to 12% of cerebral infarcts.1 In one nationwide US study of stroke in young adults, Ellis2 found that 4.9% of individuals experiencing a stroke in 2007 were between ages 18 and 44 years. Among this group, 78% experienced an ischemic stroke; 11.2% experienced a subarachnoid hemorrhage (SAH); and 10.8% had an intracerebral hemorrhage.2
While the clinical presentation of stroke in young adults is similar to that of older patients, the etiologies and risk factors are very different. In older patients, atherosclerosis is the major cause of ischemic stroke. In studies of young adults with ischemic stroke, cardioembolism was found to be the leading cause. Under this category, a patent foramen ovale (PFO) was considered a common cause, followed by atrial fibrillation, bacterial endocarditis, rheumatic heart disease, and atrial myxoma. There is, however, increasing controversy over the role of PFO as an etiology of stroke. Many investigators think its role has been overstated and is probably more of an incidental finding than a causal relationship.3 Patients with a suspected cardioembolic etiology will usually require an echocardiogram (with saline contrast or a “bubble study” for suspected PFO), cardiac monitoring, and a possible Holter monitor at the time of discharge (to detect paroxysmal arrhythmias).
Following cardioembolic etiologies, arterial dissection is the next most common category.4 In one study of patients aged 31 to 45 years old, arterial dissection was the most common cause of ischemic stroke.4 Clinical features suggesting dissection include a history of head or neck trauma (even minor trauma), headache or neck pain, and local neurological findings (eg, cranial nerve palsy or Horner syndrome).3 Unfortunately, only about 25% of patients volunteer a history of recent neck trauma. If a cervical or vertebral artery dissection is suspected, contrast enhanced magnetic resonance angiography (MRA) is the most sensitive and specific test, followed by carotid ultrasound and CT angiography.3
Traditional risk factors for stroke include hypertension and diabetes mellitus (DM). This is not true for younger adults that experience an ischemic stroke. Cigarette smoking is a very important risk factor for cerebrovascular accident in young adults; in addition, the more one smokes, the greater the risk. Other risk factors in young adults include history of migraine headaches (especially migraine with aura), pregnancy and the postpartum period, and illicit drug use.3
The defense’s argument that there are many causes of stroke in young adults that would be inappropriate for treatment with tPA, such as a PFO, carotid dissection or bacterial endocarditis, is absolutely true. Young patients need to be aggressively worked up for the etiology of their stroke, and may require additional testing, such as an MRA, echocardiogram, or Holter monitoring to determine the underlying cause of their stroke.
Obstruction Following Gastric Bypass Surgery
A 47-year-old woman presented to the ED complaining of severe back and abdominal pain. Onset had been gradual and began approximately 4 hours prior to arrival. She described the pain as crampy and constant. The patient had vomited twice; she denied diarrhea and had a normal bowel movement the previous day. She denied any vaginal or urinary complaints. Her past medical history was significant for hypertension and status post gastric bypass surgery 6 months prior. She had lost 42 pounds to date. She denied smoking or alcohol use.
The patient’s vital signs on physical examination were: blood pressure, 154/92 mm Hg; pulse, 106 beats/minute; respiratory rate, 18 breaths/minute; and temperature, 99˚F. Oxygen saturation was 96% on room air. The patient’s lungs were clear to auscultation bilaterally. The heart was mildly tachycardic, with a regular rhythm and without murmurs, rubs, or gallops. The abdominal examination revealed diffuse tenderness and involuntary guarding. There was no distention or rebound. Bowel sounds were present but hypoactive. Examination of the back revealed bilateral paraspinal muscle tenderness without costovertebral angle tenderness.
The EP ordered a CBC, BMP, serum lipase, and a urinalysis. The patient was given an intravenous (IV) bolus of 250 cc normal saline in addition to IV morphine 4 mg and IV ondansetron 4 mg. Her white blood cell (WBC) count was slightly elevated at 12.2 g/dL, with a normal differential. The remainder of the laboratory studies were normal, except for a serum bicarbonate of 22 mmol/L.
The patient stated she felt somewhat improved, but continued to have abdominal and back pain. The EP admitted her to the hospital for observation and pain control. She died the following day from a bowel obstruction. The family sued the EP for negligence in failing to order appropriate testing and for not consulting with specialists to diagnose the bowel obstruction, which is a known complication of gastric bypass surgery. The jury returned a verdict of $2.4 million against the EP.
Discussion
The frequency of bariatric surgery in the United States continues to increase, primarily due to its success with regard to weight loss, but also because of its demonstrated improvement in hypertension, obstructive sleep apnea, hyperlipidemia, and type 2 DM.1
Frequently, the term “gastric bypass surgery” is used interchangeably with bariatric surgery. However, the EP must realize these terms encompass multiple different operations. The four most common types of bariatric surgery in the United Stated are (1) adjustable gastric banding (AGB); (2) the Roux-en-Y gastric bypass (RYGB); (3) biliopancreatic diversion with duodenal switch (BPD-DS); and (4) vertical sleeve gastrectomy (VSG).2 (See the Table for a brief explanation of each type of procedure.)
Since each procedure has its own respective associated complications, it is important for the EP to know which the type of gastric bypass surgery the patient had. For example, leakage is much more frequent following RYGB than in gastric banding, while slippage and obstruction are the most common complications of gastric banding.3,4 It is also very helpful to know the specific type of procedure when discussing the case with the surgical consultant.
Based on a recent review of over 800,000 bariatric surgery patients, seven serious common complications following the surgery were identified.3 These included bleeding, leakage, obstruction, stomal ulceration, pulmonary embolism and respiratory complications, blood sugar disturbances (usually hypoglycemia and/or metabolic acidosis), and nutritional disturbances. While not all-inclusive, this list represents the most common serious complications of gastric bypass surgery.
The complaint of abdominal pain in a patient that has undergone bariatric surgery should be taken very seriously. In addition to determining the specific procedure performed and date, the patient should be questioned about vomiting, bowel movements, and the presence of blood in stool or vomit. Depending upon the degree of pain present, the patient may need to be given IV opioid analgesia to facilitate a thorough abdominal examination. A rectal examination should be performed to identify occult gastrointestinal bleeding.
These patients require laboratory testing, including CBC, BMP, and other laboratory evaluation as indicated by the history and physical examination. Early consultation with the bariatric surgeon is recommended. Many, if not most, patients with abdominal pain and vomiting will require imaging, usually a CT scan with contrast of the abdomen and pelvis. Because of the difficulty in interpreting the CT scan results in these patients, the bariatric surgeon will often want to personally review the films rather than rely solely on the interpretation by radiology services.
Unfortunately, the EP in this case did not appreciate the seriousness of the situation. The presence of severe abdominal pain, tenderness, guarding, mild tachycardia with leukocytosis, and metabolic acidosis all pointed to a more serious etiology than muscle spasm. This patient required IV fluids, analgesia, and imaging, as well as consultation with the bariatric surgeon.
- Chatzikonstantinou A, Wolf ME, Hennerici MG. Ischemic stroke in young adults: classification and risk factors. J Neurol. 2012;259(4):653-659.
- Ellis C. Stroke in young adults. Disabil Health J. 2010;3(3):222-224.
- Ferro JM, Massaro AR, Mas JL. Aetiological diagnosis of ischemic stroke in young adults. Lancet Neurol. 2010;9(11):1085-1096.
- Chan MT, Nadareishvili ZG, Norris JW; Canadian Stroke Consortium. Diagnostic strategies in young patients with ischemic stroke in Canada. Can J Neurol Sci. 2000;27(2):120-124.
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724-1737.
- Livingston EH. Patient guide: Endocrine and nutritional management after bariatric surgery: A patient’s guide. Hormone Health Network Web site. http://www.hormone.org/~/media/Hormone/Files/Patient%20Guides/Mens%20Health/PGBariatricSurgery_2014.pdf. Accessed December 17, 2014.
- Hussain A, El-Hasani S. Bariatric emergencies: current evidence and strategies of management. World J Emerg Surg. 2013;8(1):58.
- Campanille FC, Boru C, Rizzello M, et al. Acute complications after laparoscopic bariatric procedures: update for the general surgeon. Langenbecks Arch Surg. 2013;398(5):669-686
- Chatzikonstantinou A, Wolf ME, Hennerici MG. Ischemic stroke in young adults: classification and risk factors. J Neurol. 2012;259(4):653-659.
- Ellis C. Stroke in young adults. Disabil Health J. 2010;3(3):222-224.
- Ferro JM, Massaro AR, Mas JL. Aetiological diagnosis of ischemic stroke in young adults. Lancet Neurol. 2010;9(11):1085-1096.
- Chan MT, Nadareishvili ZG, Norris JW; Canadian Stroke Consortium. Diagnostic strategies in young patients with ischemic stroke in Canada. Can J Neurol Sci. 2000;27(2):120-124.
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724-1737.
- Livingston EH. Patient guide: Endocrine and nutritional management after bariatric surgery: A patient’s guide. Hormone Health Network Web site. http://www.hormone.org/~/media/Hormone/Files/Patient%20Guides/Mens%20Health/PGBariatricSurgery_2014.pdf. Accessed December 17, 2014.
- Hussain A, El-Hasani S. Bariatric emergencies: current evidence and strategies of management. World J Emerg Surg. 2013;8(1):58.
- Campanille FC, Boru C, Rizzello M, et al. Acute complications after laparoscopic bariatric procedures: update for the general surgeon. Langenbecks Arch Surg. 2013;398(5):669-686
An overlooked laboratory report
Question: Your office assistant misfiled a critical laboratory report showing dangerous hyperkalemia of 6.5 mEq/L. Unaware of the abnormality, you failed to notify the end-stage renal patient to return for treatment. In the meantime, the patient collapsed and died, and an autopsy revealed a fresh transmural myocardial infarct.
Which of the following statements is best?
A. You are negligent, because the standard of care is to promptly contact the patient.
B. Your office assistant is negligent, because she was the one who misfiled the report.
C. Liability rests with the laboratory, because it should have called the office immediately with the critical value.
D. Your lawyer will defend you on the legal theory that hyperkalemia was not the proximate cause of death.
E. All of the above.
Answer: E. In any negligence action, the plaintiff bears the burden of proof, on a balance of probabilities, that the defendant owes him/her a duty of care, the breach of which proximately caused the plaintiff’s injuries.
One begins with an inquiry into whether a duty exists and whether a breach has occurred. Generally, doctors owe a legal duty of due care to their patients arising out of the doctor-patient relationship. By “missing” the laboratory report, especially one of urgency, and not immediately notifying the patient, the doctor has likely breached his/her duty. Another way of putting it is to ask whether the conduct has fallen below what is ordinarily expected of a practitioner in a similar situation.
The doctor will likely blame the office assistant for misfiling the report, and the assistant is indeed liable, as he/she also owes a direct legal duty to the patient. However, such liability will then fall upon the doctor under “respondeat superior” or “let the master answer,” which is the legal doctrine underpinning vicarious liability. This is characteristically seen in an employer-employee situation, where liability is imputed to the employer despite the tortious act being committed only by the employee.
The idea behind this rule is to ensure that the employer, as supervisor, will enforce proper work conditions to avoid risk of harm. The employer also is better able to shoulder the cost of compensating the victim.
For vicarious liability to arise, the employee’s act must have occurred during and within the scope of employment, and the risk of harm must be foreseeable. Under the facts of this hypothetical scenario, it is easy to see that the doctor will be vicariously liable for the negligent act of the assistant.
The clinical laboratory also owes an independent duty to the patient, which includes, among other things, assuring the proper standards in specimen collection and test performance. The duty extends to timely and accurate reporting of the results, including calling the physician when there is a critically high or low value if that is the standard of care in the community, as it generally is.
Thus, the laboratory in this case will likely be named as a codefendant. This is called joint and several liability, where more than one defendant has concurrently or successively caused a plaintiff’s indivisible injury, and the latter can recover all damages from any of the wrongdoers irrespective of degree of fault, as long as causation is proven. However, the plaintiff is not entitled to double recovery, and a defendant can proceed against the other liable parties for contribution.
Proving existence and breach of duty are necessary but insufficient steps toward winning the lawsuit. The plaintiff must also establish causation, i.e., that the substandard care caused the injury.
Causation inquires into both cause-in-fact and cause-in-law, and the term “proximate cause” is used to cover both of these aspects of causation. Cause-in-fact is established with the “but for” test – whether it can be said that had it not been for the defendant’s actions, the plaintiff would not have suffered the injury.
In this scenario, the doctor’s attorney will argue that the cause of death, a myocardial infarct, was preexisting atherosclerotic heart disease, rather than hyperkalemia. Besides, the chronic renal patient typically adapts to hyperkalemia and can tolerate elevated levels better than nonrenal patients. Of course, the counterargument is that the patient’s cardiac injury was a likely consequence of hyperkalemia-induced ventricular arrhythmia.
The doctor, the nurse, and the laboratory will all be named as codefendants. However, the laboratory will attempt to escape liability by arguing that its negligence, if any, was superseded by the doctor’s own negligent failure to read the report. Cause-in-law analysis examines whether a new independent event has intervened between the negligent act and the outcome, which may have been aggravated by the new event.
It naturally raises the question whether the original wrongdoer – in this case, the laboratory – continues to be liable, or whether the chain of causation has been broken by the intervening cause (the doctor’s negligence).
In a federal case, the Florida District Court of Appeals found several doctors liable for missing the diagnosis of tuberculous meningitis (Hadley v. Terwilleger, 873 So.2d 378 (Fl. 2004)). The doctors had seen the patient at various times in a sequential manner. The court held that the plaintiff was entitled to concurring-cause, rather than superseding-cause, jury instructions. The purpose of such instruction was to negate the idea that a defendant is excused from the consequences of his or her negligence by reason of some other cause concurring in time and contributing to the same injury.
Overlooked, misfiled, or otherwise “missed” laboratory or x-ray reports are commonly encountered in medical practice, and may lead in some instances to serious patient injury. They are typically systems errors rather than the fault of any single individual, and like most medical errors, largely preventable.
Physicians and health care institutions should put in place tested protocols that protect patients from risk of harm, and, as the Institute of Medicine stated in its 2000 report, “To Err Is Human: Building a Safer Health System,” move away from “a culture of blame to a culture of safety.”
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at s[email protected].
Question: Your office assistant misfiled a critical laboratory report showing dangerous hyperkalemia of 6.5 mEq/L. Unaware of the abnormality, you failed to notify the end-stage renal patient to return for treatment. In the meantime, the patient collapsed and died, and an autopsy revealed a fresh transmural myocardial infarct.
Which of the following statements is best?
A. You are negligent, because the standard of care is to promptly contact the patient.
B. Your office assistant is negligent, because she was the one who misfiled the report.
C. Liability rests with the laboratory, because it should have called the office immediately with the critical value.
D. Your lawyer will defend you on the legal theory that hyperkalemia was not the proximate cause of death.
E. All of the above.
Answer: E. In any negligence action, the plaintiff bears the burden of proof, on a balance of probabilities, that the defendant owes him/her a duty of care, the breach of which proximately caused the plaintiff’s injuries.
One begins with an inquiry into whether a duty exists and whether a breach has occurred. Generally, doctors owe a legal duty of due care to their patients arising out of the doctor-patient relationship. By “missing” the laboratory report, especially one of urgency, and not immediately notifying the patient, the doctor has likely breached his/her duty. Another way of putting it is to ask whether the conduct has fallen below what is ordinarily expected of a practitioner in a similar situation.
The doctor will likely blame the office assistant for misfiling the report, and the assistant is indeed liable, as he/she also owes a direct legal duty to the patient. However, such liability will then fall upon the doctor under “respondeat superior” or “let the master answer,” which is the legal doctrine underpinning vicarious liability. This is characteristically seen in an employer-employee situation, where liability is imputed to the employer despite the tortious act being committed only by the employee.
The idea behind this rule is to ensure that the employer, as supervisor, will enforce proper work conditions to avoid risk of harm. The employer also is better able to shoulder the cost of compensating the victim.
For vicarious liability to arise, the employee’s act must have occurred during and within the scope of employment, and the risk of harm must be foreseeable. Under the facts of this hypothetical scenario, it is easy to see that the doctor will be vicariously liable for the negligent act of the assistant.
The clinical laboratory also owes an independent duty to the patient, which includes, among other things, assuring the proper standards in specimen collection and test performance. The duty extends to timely and accurate reporting of the results, including calling the physician when there is a critically high or low value if that is the standard of care in the community, as it generally is.
Thus, the laboratory in this case will likely be named as a codefendant. This is called joint and several liability, where more than one defendant has concurrently or successively caused a plaintiff’s indivisible injury, and the latter can recover all damages from any of the wrongdoers irrespective of degree of fault, as long as causation is proven. However, the plaintiff is not entitled to double recovery, and a defendant can proceed against the other liable parties for contribution.
Proving existence and breach of duty are necessary but insufficient steps toward winning the lawsuit. The plaintiff must also establish causation, i.e., that the substandard care caused the injury.
Causation inquires into both cause-in-fact and cause-in-law, and the term “proximate cause” is used to cover both of these aspects of causation. Cause-in-fact is established with the “but for” test – whether it can be said that had it not been for the defendant’s actions, the plaintiff would not have suffered the injury.
In this scenario, the doctor’s attorney will argue that the cause of death, a myocardial infarct, was preexisting atherosclerotic heart disease, rather than hyperkalemia. Besides, the chronic renal patient typically adapts to hyperkalemia and can tolerate elevated levels better than nonrenal patients. Of course, the counterargument is that the patient’s cardiac injury was a likely consequence of hyperkalemia-induced ventricular arrhythmia.
The doctor, the nurse, and the laboratory will all be named as codefendants. However, the laboratory will attempt to escape liability by arguing that its negligence, if any, was superseded by the doctor’s own negligent failure to read the report. Cause-in-law analysis examines whether a new independent event has intervened between the negligent act and the outcome, which may have been aggravated by the new event.
It naturally raises the question whether the original wrongdoer – in this case, the laboratory – continues to be liable, or whether the chain of causation has been broken by the intervening cause (the doctor’s negligence).
In a federal case, the Florida District Court of Appeals found several doctors liable for missing the diagnosis of tuberculous meningitis (Hadley v. Terwilleger, 873 So.2d 378 (Fl. 2004)). The doctors had seen the patient at various times in a sequential manner. The court held that the plaintiff was entitled to concurring-cause, rather than superseding-cause, jury instructions. The purpose of such instruction was to negate the idea that a defendant is excused from the consequences of his or her negligence by reason of some other cause concurring in time and contributing to the same injury.
Overlooked, misfiled, or otherwise “missed” laboratory or x-ray reports are commonly encountered in medical practice, and may lead in some instances to serious patient injury. They are typically systems errors rather than the fault of any single individual, and like most medical errors, largely preventable.
Physicians and health care institutions should put in place tested protocols that protect patients from risk of harm, and, as the Institute of Medicine stated in its 2000 report, “To Err Is Human: Building a Safer Health System,” move away from “a culture of blame to a culture of safety.”
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at s[email protected].
Question: Your office assistant misfiled a critical laboratory report showing dangerous hyperkalemia of 6.5 mEq/L. Unaware of the abnormality, you failed to notify the end-stage renal patient to return for treatment. In the meantime, the patient collapsed and died, and an autopsy revealed a fresh transmural myocardial infarct.
Which of the following statements is best?
A. You are negligent, because the standard of care is to promptly contact the patient.
B. Your office assistant is negligent, because she was the one who misfiled the report.
C. Liability rests with the laboratory, because it should have called the office immediately with the critical value.
D. Your lawyer will defend you on the legal theory that hyperkalemia was not the proximate cause of death.
E. All of the above.
Answer: E. In any negligence action, the plaintiff bears the burden of proof, on a balance of probabilities, that the defendant owes him/her a duty of care, the breach of which proximately caused the plaintiff’s injuries.
One begins with an inquiry into whether a duty exists and whether a breach has occurred. Generally, doctors owe a legal duty of due care to their patients arising out of the doctor-patient relationship. By “missing” the laboratory report, especially one of urgency, and not immediately notifying the patient, the doctor has likely breached his/her duty. Another way of putting it is to ask whether the conduct has fallen below what is ordinarily expected of a practitioner in a similar situation.
The doctor will likely blame the office assistant for misfiling the report, and the assistant is indeed liable, as he/she also owes a direct legal duty to the patient. However, such liability will then fall upon the doctor under “respondeat superior” or “let the master answer,” which is the legal doctrine underpinning vicarious liability. This is characteristically seen in an employer-employee situation, where liability is imputed to the employer despite the tortious act being committed only by the employee.
The idea behind this rule is to ensure that the employer, as supervisor, will enforce proper work conditions to avoid risk of harm. The employer also is better able to shoulder the cost of compensating the victim.
For vicarious liability to arise, the employee’s act must have occurred during and within the scope of employment, and the risk of harm must be foreseeable. Under the facts of this hypothetical scenario, it is easy to see that the doctor will be vicariously liable for the negligent act of the assistant.
The clinical laboratory also owes an independent duty to the patient, which includes, among other things, assuring the proper standards in specimen collection and test performance. The duty extends to timely and accurate reporting of the results, including calling the physician when there is a critically high or low value if that is the standard of care in the community, as it generally is.
Thus, the laboratory in this case will likely be named as a codefendant. This is called joint and several liability, where more than one defendant has concurrently or successively caused a plaintiff’s indivisible injury, and the latter can recover all damages from any of the wrongdoers irrespective of degree of fault, as long as causation is proven. However, the plaintiff is not entitled to double recovery, and a defendant can proceed against the other liable parties for contribution.
Proving existence and breach of duty are necessary but insufficient steps toward winning the lawsuit. The plaintiff must also establish causation, i.e., that the substandard care caused the injury.
Causation inquires into both cause-in-fact and cause-in-law, and the term “proximate cause” is used to cover both of these aspects of causation. Cause-in-fact is established with the “but for” test – whether it can be said that had it not been for the defendant’s actions, the plaintiff would not have suffered the injury.
In this scenario, the doctor’s attorney will argue that the cause of death, a myocardial infarct, was preexisting atherosclerotic heart disease, rather than hyperkalemia. Besides, the chronic renal patient typically adapts to hyperkalemia and can tolerate elevated levels better than nonrenal patients. Of course, the counterargument is that the patient’s cardiac injury was a likely consequence of hyperkalemia-induced ventricular arrhythmia.
The doctor, the nurse, and the laboratory will all be named as codefendants. However, the laboratory will attempt to escape liability by arguing that its negligence, if any, was superseded by the doctor’s own negligent failure to read the report. Cause-in-law analysis examines whether a new independent event has intervened between the negligent act and the outcome, which may have been aggravated by the new event.
It naturally raises the question whether the original wrongdoer – in this case, the laboratory – continues to be liable, or whether the chain of causation has been broken by the intervening cause (the doctor’s negligence).
In a federal case, the Florida District Court of Appeals found several doctors liable for missing the diagnosis of tuberculous meningitis (Hadley v. Terwilleger, 873 So.2d 378 (Fl. 2004)). The doctors had seen the patient at various times in a sequential manner. The court held that the plaintiff was entitled to concurring-cause, rather than superseding-cause, jury instructions. The purpose of such instruction was to negate the idea that a defendant is excused from the consequences of his or her negligence by reason of some other cause concurring in time and contributing to the same injury.
Overlooked, misfiled, or otherwise “missed” laboratory or x-ray reports are commonly encountered in medical practice, and may lead in some instances to serious patient injury. They are typically systems errors rather than the fault of any single individual, and like most medical errors, largely preventable.
Physicians and health care institutions should put in place tested protocols that protect patients from risk of harm, and, as the Institute of Medicine stated in its 2000 report, “To Err Is Human: Building a Safer Health System,” move away from “a culture of blame to a culture of safety.”
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at s[email protected].

LAW & MEDICINE: ‘Defective and unreasonably dangerous’
Question: After statins had been in use for several years, data began to accumulate purporting to show that they increase the risk of diabetes. When Mrs. Smith learned that her recent diagnosis of diabetes might have something to do with the drug, she consulted a lawyer who began advertising for similar cases to consolidate them into a class action lawsuit. The legal theory (theories) seeking to prove product liability will be based on:
A. Contract law and breach of warranty.
B. Negligence in tort law.
C. Strict liability without requiring proof of fault.
D. A defective product that is unreasonably dangerous.
E. All of the above.
Answer:E. Should a prescription drug lead to harm, an injured party can sue the manufacturer who had placed it into the stream of commerce. The law of products liability governs this cause of action, wherein recovery is based on a number of legal theories, specifically negligence, breach of warranty, and strict liability. The latter is the most favored, as there is no need to prove fault or warranty. Products liability law also covers defective medical devices. The recent multimillion-dollar settlements and jury verdicts with Endo, Johnson & Johnson, Bard, and other manufacturers over their vaginal mesh devices are good examples.
In products liability, injured plaintiffs frequently claim a failure to warn of known risks, such as cardiovascular deaths caused by Vioxx, a nonsteroidal anti-inflammatory drug that was withdrawn in 2004. Merck, its manufacturer, has thus far won 11 and lost 3 of the cases that have gone to trial. Some of these judgments are under appeal; most notably, a Texas Court of Appeals recently reversed a $253 million award initially won by plaintiff Robert Ernst in the very first trial. However, the company has proposed $4.85 billion to settle tens of thousands of similar pending lawsuits. Other recent examples alleging failure to warn are heart attacks linked to the diabetes drug rosiglitazone and bladder cancer associated with the diabetes drug pioglitazone.
In 1963, the California Supreme Court bypassed the law of contracts and warranty in a seminal case of product-related injury, and introduced the notion of strict liability, which goes beyond simple negligence (Greenman v Yuba Power Products Inc., 377 P.2d 897 [Cal. 1963]). The strict liability approach centers on whether a product is defective and unreasonably dangerous, and it has now been adopted in virtually all jurisdictions.
The theory holds that a professional supplier who sells a product that is both defective and unreasonably dangerous is strictly liable to foreseeable plaintiffs. “Defective” is usually defined as product quality that is less than what a reasonable consumer expects. “Unreasonably dangerous” is a conclusion that the risks that result from its condition outweigh the product’s advantages.
Strict liability is not about negligence or fault, but about a social policy that shifts to the manufacturer the cost of compensating the injured consumer. To prevail, the plaintiff must show proximate cause, and assumption of risk is still a valid defense.
Statins, which are powerful HMG-CoA reductase inhibitors widely used to treat hypercholesterolemia, are currently at the center of pharmaceutical products litigation.
Pfizer, the manufacturer of Lipitor (atorvastatin) has become the target of numerous lawsuits alleging that the drug causes diabetes. Lipitor is the best-selling prescription drug ever, with sales reaching $130 billion since it was approved in 1996. In the United States alone, more than 29 million people have been prescribed this medication. The drug is highly effective in lowering serum cholesterol and is proven to reduce cardiovascular deaths.
A meta-analysis in 2010 revealed an increased risk of diabetes in patients taking statins (Lancet 2010;375:735-42). Statin therapy was associated with a 9% increased risk for incident diabetes; it was calculated that treatment of 255 patients with statins for 4 years resulted in 1 extra case of diabetes. An earlier smaller study had rejected this conclusion, but other studies were in support.
In 2012, the Food and Drug Administration (FDA) required the revision of the package insert of Lipitor and other statins to warn that their use had been linked to a small increased risk of diabetes.
In 2013, a large Canadian study confirmed the increased incidence of new-onset diabetes in patients taking atorvastatin (hazard ratio, 1.22) and simvastatin (hazard ratio, 1.10). This population-based cohort study involved nondiabetic patients age 66 years or older who started statins between 1997 and 2010 (BMJ 2013;346:f2610).
These and other results, coupled with the FDA-mandated revised labeling, have spawned the filing of nearly 1,000 lawsuits by patients who developed diabetes while taking statins, especially postmenopausal women. The rapid increase in the number of lawsuits may be related to the recent decision of a federal judicial panel on multidistrict litigation to consolidate all Lipitor diabetes lawsuits into a single federal courtroom in Charleston, S.C., as a class-action suit. The first case has yet to go to trial, but is expected to do so in 2015.
Previous products liability cases implicating statins have famously involved cerivastatin (Baycol), a one-time rival to Lipitor, for causing rhabdomyolysis. The drug was pulled from the market in 2001 after it reportedly caused 31 deaths. Bayer, its manufacturer, paid about $1 billion in 2005 to settle some 3,000 cases. An example of a medication causing diabetes is quetiapine (Seroquel), an antipsychotic drug manufactured by AstraZeneca, which in 2011 agreed to pay $647 million to settle more than 28,000 lawsuits.
However, the upcoming Lipitor litigation may be more difficult for the plaintiffs to win. Among some of the medico-legal questions to be addressed are:
1) Was there prior company knowledge of the risk and a failure to warn?
2) Were the patients harmed by the drug, given that diabetes is a very common disease and may be linked more to genetics and/or an underlying metabolic syndrome in those who are hyperlipidemic, hypertensive, or obese – the very same patients likely to be on a statin?
3) Is Lipitor a defective product, and is it unreasonably dangerous?
Despite the FDA-directed change in labeling, a number of scientists and the FDA itself have emphasized that the cardiac benefits of a statin drug are greater than any small increased risk of developing diabetes.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: After statins had been in use for several years, data began to accumulate purporting to show that they increase the risk of diabetes. When Mrs. Smith learned that her recent diagnosis of diabetes might have something to do with the drug, she consulted a lawyer who began advertising for similar cases to consolidate them into a class action lawsuit. The legal theory (theories) seeking to prove product liability will be based on:
A. Contract law and breach of warranty.
B. Negligence in tort law.
C. Strict liability without requiring proof of fault.
D. A defective product that is unreasonably dangerous.
E. All of the above.
Answer:E. Should a prescription drug lead to harm, an injured party can sue the manufacturer who had placed it into the stream of commerce. The law of products liability governs this cause of action, wherein recovery is based on a number of legal theories, specifically negligence, breach of warranty, and strict liability. The latter is the most favored, as there is no need to prove fault or warranty. Products liability law also covers defective medical devices. The recent multimillion-dollar settlements and jury verdicts with Endo, Johnson & Johnson, Bard, and other manufacturers over their vaginal mesh devices are good examples.
In products liability, injured plaintiffs frequently claim a failure to warn of known risks, such as cardiovascular deaths caused by Vioxx, a nonsteroidal anti-inflammatory drug that was withdrawn in 2004. Merck, its manufacturer, has thus far won 11 and lost 3 of the cases that have gone to trial. Some of these judgments are under appeal; most notably, a Texas Court of Appeals recently reversed a $253 million award initially won by plaintiff Robert Ernst in the very first trial. However, the company has proposed $4.85 billion to settle tens of thousands of similar pending lawsuits. Other recent examples alleging failure to warn are heart attacks linked to the diabetes drug rosiglitazone and bladder cancer associated with the diabetes drug pioglitazone.
In 1963, the California Supreme Court bypassed the law of contracts and warranty in a seminal case of product-related injury, and introduced the notion of strict liability, which goes beyond simple negligence (Greenman v Yuba Power Products Inc., 377 P.2d 897 [Cal. 1963]). The strict liability approach centers on whether a product is defective and unreasonably dangerous, and it has now been adopted in virtually all jurisdictions.
The theory holds that a professional supplier who sells a product that is both defective and unreasonably dangerous is strictly liable to foreseeable plaintiffs. “Defective” is usually defined as product quality that is less than what a reasonable consumer expects. “Unreasonably dangerous” is a conclusion that the risks that result from its condition outweigh the product’s advantages.
Strict liability is not about negligence or fault, but about a social policy that shifts to the manufacturer the cost of compensating the injured consumer. To prevail, the plaintiff must show proximate cause, and assumption of risk is still a valid defense.
Statins, which are powerful HMG-CoA reductase inhibitors widely used to treat hypercholesterolemia, are currently at the center of pharmaceutical products litigation.
Pfizer, the manufacturer of Lipitor (atorvastatin) has become the target of numerous lawsuits alleging that the drug causes diabetes. Lipitor is the best-selling prescription drug ever, with sales reaching $130 billion since it was approved in 1996. In the United States alone, more than 29 million people have been prescribed this medication. The drug is highly effective in lowering serum cholesterol and is proven to reduce cardiovascular deaths.
A meta-analysis in 2010 revealed an increased risk of diabetes in patients taking statins (Lancet 2010;375:735-42). Statin therapy was associated with a 9% increased risk for incident diabetes; it was calculated that treatment of 255 patients with statins for 4 years resulted in 1 extra case of diabetes. An earlier smaller study had rejected this conclusion, but other studies were in support.
In 2012, the Food and Drug Administration (FDA) required the revision of the package insert of Lipitor and other statins to warn that their use had been linked to a small increased risk of diabetes.
In 2013, a large Canadian study confirmed the increased incidence of new-onset diabetes in patients taking atorvastatin (hazard ratio, 1.22) and simvastatin (hazard ratio, 1.10). This population-based cohort study involved nondiabetic patients age 66 years or older who started statins between 1997 and 2010 (BMJ 2013;346:f2610).
These and other results, coupled with the FDA-mandated revised labeling, have spawned the filing of nearly 1,000 lawsuits by patients who developed diabetes while taking statins, especially postmenopausal women. The rapid increase in the number of lawsuits may be related to the recent decision of a federal judicial panel on multidistrict litigation to consolidate all Lipitor diabetes lawsuits into a single federal courtroom in Charleston, S.C., as a class-action suit. The first case has yet to go to trial, but is expected to do so in 2015.
Previous products liability cases implicating statins have famously involved cerivastatin (Baycol), a one-time rival to Lipitor, for causing rhabdomyolysis. The drug was pulled from the market in 2001 after it reportedly caused 31 deaths. Bayer, its manufacturer, paid about $1 billion in 2005 to settle some 3,000 cases. An example of a medication causing diabetes is quetiapine (Seroquel), an antipsychotic drug manufactured by AstraZeneca, which in 2011 agreed to pay $647 million to settle more than 28,000 lawsuits.
However, the upcoming Lipitor litigation may be more difficult for the plaintiffs to win. Among some of the medico-legal questions to be addressed are:
1) Was there prior company knowledge of the risk and a failure to warn?
2) Were the patients harmed by the drug, given that diabetes is a very common disease and may be linked more to genetics and/or an underlying metabolic syndrome in those who are hyperlipidemic, hypertensive, or obese – the very same patients likely to be on a statin?
3) Is Lipitor a defective product, and is it unreasonably dangerous?
Despite the FDA-directed change in labeling, a number of scientists and the FDA itself have emphasized that the cardiac benefits of a statin drug are greater than any small increased risk of developing diabetes.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: After statins had been in use for several years, data began to accumulate purporting to show that they increase the risk of diabetes. When Mrs. Smith learned that her recent diagnosis of diabetes might have something to do with the drug, she consulted a lawyer who began advertising for similar cases to consolidate them into a class action lawsuit. The legal theory (theories) seeking to prove product liability will be based on:
A. Contract law and breach of warranty.
B. Negligence in tort law.
C. Strict liability without requiring proof of fault.
D. A defective product that is unreasonably dangerous.
E. All of the above.
Answer:E. Should a prescription drug lead to harm, an injured party can sue the manufacturer who had placed it into the stream of commerce. The law of products liability governs this cause of action, wherein recovery is based on a number of legal theories, specifically negligence, breach of warranty, and strict liability. The latter is the most favored, as there is no need to prove fault or warranty. Products liability law also covers defective medical devices. The recent multimillion-dollar settlements and jury verdicts with Endo, Johnson & Johnson, Bard, and other manufacturers over their vaginal mesh devices are good examples.
In products liability, injured plaintiffs frequently claim a failure to warn of known risks, such as cardiovascular deaths caused by Vioxx, a nonsteroidal anti-inflammatory drug that was withdrawn in 2004. Merck, its manufacturer, has thus far won 11 and lost 3 of the cases that have gone to trial. Some of these judgments are under appeal; most notably, a Texas Court of Appeals recently reversed a $253 million award initially won by plaintiff Robert Ernst in the very first trial. However, the company has proposed $4.85 billion to settle tens of thousands of similar pending lawsuits. Other recent examples alleging failure to warn are heart attacks linked to the diabetes drug rosiglitazone and bladder cancer associated with the diabetes drug pioglitazone.
In 1963, the California Supreme Court bypassed the law of contracts and warranty in a seminal case of product-related injury, and introduced the notion of strict liability, which goes beyond simple negligence (Greenman v Yuba Power Products Inc., 377 P.2d 897 [Cal. 1963]). The strict liability approach centers on whether a product is defective and unreasonably dangerous, and it has now been adopted in virtually all jurisdictions.
The theory holds that a professional supplier who sells a product that is both defective and unreasonably dangerous is strictly liable to foreseeable plaintiffs. “Defective” is usually defined as product quality that is less than what a reasonable consumer expects. “Unreasonably dangerous” is a conclusion that the risks that result from its condition outweigh the product’s advantages.
Strict liability is not about negligence or fault, but about a social policy that shifts to the manufacturer the cost of compensating the injured consumer. To prevail, the plaintiff must show proximate cause, and assumption of risk is still a valid defense.
Statins, which are powerful HMG-CoA reductase inhibitors widely used to treat hypercholesterolemia, are currently at the center of pharmaceutical products litigation.
Pfizer, the manufacturer of Lipitor (atorvastatin) has become the target of numerous lawsuits alleging that the drug causes diabetes. Lipitor is the best-selling prescription drug ever, with sales reaching $130 billion since it was approved in 1996. In the United States alone, more than 29 million people have been prescribed this medication. The drug is highly effective in lowering serum cholesterol and is proven to reduce cardiovascular deaths.
A meta-analysis in 2010 revealed an increased risk of diabetes in patients taking statins (Lancet 2010;375:735-42). Statin therapy was associated with a 9% increased risk for incident diabetes; it was calculated that treatment of 255 patients with statins for 4 years resulted in 1 extra case of diabetes. An earlier smaller study had rejected this conclusion, but other studies were in support.
In 2012, the Food and Drug Administration (FDA) required the revision of the package insert of Lipitor and other statins to warn that their use had been linked to a small increased risk of diabetes.
In 2013, a large Canadian study confirmed the increased incidence of new-onset diabetes in patients taking atorvastatin (hazard ratio, 1.22) and simvastatin (hazard ratio, 1.10). This population-based cohort study involved nondiabetic patients age 66 years or older who started statins between 1997 and 2010 (BMJ 2013;346:f2610).
These and other results, coupled with the FDA-mandated revised labeling, have spawned the filing of nearly 1,000 lawsuits by patients who developed diabetes while taking statins, especially postmenopausal women. The rapid increase in the number of lawsuits may be related to the recent decision of a federal judicial panel on multidistrict litigation to consolidate all Lipitor diabetes lawsuits into a single federal courtroom in Charleston, S.C., as a class-action suit. The first case has yet to go to trial, but is expected to do so in 2015.
Previous products liability cases implicating statins have famously involved cerivastatin (Baycol), a one-time rival to Lipitor, for causing rhabdomyolysis. The drug was pulled from the market in 2001 after it reportedly caused 31 deaths. Bayer, its manufacturer, paid about $1 billion in 2005 to settle some 3,000 cases. An example of a medication causing diabetes is quetiapine (Seroquel), an antipsychotic drug manufactured by AstraZeneca, which in 2011 agreed to pay $647 million to settle more than 28,000 lawsuits.
However, the upcoming Lipitor litigation may be more difficult for the plaintiffs to win. Among some of the medico-legal questions to be addressed are:
1) Was there prior company knowledge of the risk and a failure to warn?
2) Were the patients harmed by the drug, given that diabetes is a very common disease and may be linked more to genetics and/or an underlying metabolic syndrome in those who are hyperlipidemic, hypertensive, or obese – the very same patients likely to be on a statin?
3) Is Lipitor a defective product, and is it unreasonably dangerous?
Despite the FDA-directed change in labeling, a number of scientists and the FDA itself have emphasized that the cardiac benefits of a statin drug are greater than any small increased risk of developing diabetes.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].

Failure to properly manage a patient’s hypertension
Failure to properly manage a patient’s hypertension
A 44-YEAR-OLD MAN WHO WEIGHED >450 POUNDS went to his internist for treatment of hypertension. At a work-related physical the previous day, his blood pressure had been 160/110 mm Hg. After examination, the internist wrote a 30-day prescription for amlodipine, 5 mg/d, with 3 refills. The patient saw the physician 2 weeks later but not again until 3 months later. At that visit, the internist prescribed amlodipine, 5 mg/d, for 90 days with 2 refills. The patient missed his next appointment, which was set for 4 months later, but when his medication was about to run out, he was able to get a prescription for 10 months’ worth of amlodipine by phone. The patient died 2 months before the prescription ran out.
PLAINTIFF’S CLAIM The physician failed to properly manage and monitor the patient’s hypertension. The dosage of amlodipine was insufficient.
THE DEFENSE The patient was noncompliant and failed to show for follow-up appointments. The dosage of amlodipine was sufficient. The cause of death was unknown because no autopsy was performed.
VERDICT $136,000 New Jersey verdict.
COMMENT If we accept a patient into our practice, we need to have reasonable policies for patients to show up for follow-up, and to consider having them find another physician if they do not.
Did the patient’s age discourage proper evaluation?
THREE MONTHS AFTER NOTICING BLOOD IN HER STOOL, a 19-year-old woman went to see her physician. Without ordering a flexible sigmoidoscopy or colonoscopy, the physician diagnosed a healing anal fissure. Approximately 4 years later, the patient developed bloody diarrhea and went to a gastroenterologist, who found a 2.6 cm lesion in her rectum during a flexible sigmoidoscopy. Biopsy confirmed a low-grade adenocarcinoma. Imaging studies revealed that the cancer had spread to her lungs and liver, and she was diagnosed with Stage IV rectal cancer. After 2 years of extensive treatment that included surgical resection, conventional and experimental chemotherapy, and radiation therapy, the patient died.
PLAINTIFF’S CLAIM If the physician had ordered endoscopy exams when the patient first presented for treatment, testing could have identified a polyp or early-stage cancer.
THE DEFENSE No information about the defense is available.
VERDICT $2.5 million Maryland verdict.
COMMENT Colon cancer in a 19-year-old is extraordinarily rare. I doubt that the patient didn’t experience any more rectal bleeding until 4 years after she first sought treatment. A lesson in this tragic case is to be sure to document when you tell patients to “come back to see me right away if this happens again.”
23-year-old dies when myocarditis is mistaken for bronchitis
A 23-YEAR-OLD MAN PRESENTED TO THE EMERGENCY DEPARTMENT (ED) with chest tightness, cough, and fever. After a chest x-ray, the ED physician diagnosed bronchitis and sent the patient home with prescriptions for hydrocodone/acetaminophen and antibiotics. He was found dead in his bed less than 24 hours later. An autopsy determined the cause of death was myocarditis.
PLAINTIFF’S CLAIM The physician didn’t perform an electrocardiogram (EKG), which is a routine evaluation for a patient with chest pain. The EKG would have detected myocarditis.
THE DEFENSE The patient was evaluated properly. An EKG was not necessary.
VERDICT $2.9 million Massachusetts verdict.
COMMENT I think the jury got this one wrong. I don’t think an EKG is necessary for every case of acute bronchitis. However, I do wonder if the chest x-ray showed a large heart shadow.
Failure to properly manage a patient’s hypertension
A 44-YEAR-OLD MAN WHO WEIGHED >450 POUNDS went to his internist for treatment of hypertension. At a work-related physical the previous day, his blood pressure had been 160/110 mm Hg. After examination, the internist wrote a 30-day prescription for amlodipine, 5 mg/d, with 3 refills. The patient saw the physician 2 weeks later but not again until 3 months later. At that visit, the internist prescribed amlodipine, 5 mg/d, for 90 days with 2 refills. The patient missed his next appointment, which was set for 4 months later, but when his medication was about to run out, he was able to get a prescription for 10 months’ worth of amlodipine by phone. The patient died 2 months before the prescription ran out.
PLAINTIFF’S CLAIM The physician failed to properly manage and monitor the patient’s hypertension. The dosage of amlodipine was insufficient.
THE DEFENSE The patient was noncompliant and failed to show for follow-up appointments. The dosage of amlodipine was sufficient. The cause of death was unknown because no autopsy was performed.
VERDICT $136,000 New Jersey verdict.
COMMENT If we accept a patient into our practice, we need to have reasonable policies for patients to show up for follow-up, and to consider having them find another physician if they do not.
Did the patient’s age discourage proper evaluation?
THREE MONTHS AFTER NOTICING BLOOD IN HER STOOL, a 19-year-old woman went to see her physician. Without ordering a flexible sigmoidoscopy or colonoscopy, the physician diagnosed a healing anal fissure. Approximately 4 years later, the patient developed bloody diarrhea and went to a gastroenterologist, who found a 2.6 cm lesion in her rectum during a flexible sigmoidoscopy. Biopsy confirmed a low-grade adenocarcinoma. Imaging studies revealed that the cancer had spread to her lungs and liver, and she was diagnosed with Stage IV rectal cancer. After 2 years of extensive treatment that included surgical resection, conventional and experimental chemotherapy, and radiation therapy, the patient died.
PLAINTIFF’S CLAIM If the physician had ordered endoscopy exams when the patient first presented for treatment, testing could have identified a polyp or early-stage cancer.
THE DEFENSE No information about the defense is available.
VERDICT $2.5 million Maryland verdict.
COMMENT Colon cancer in a 19-year-old is extraordinarily rare. I doubt that the patient didn’t experience any more rectal bleeding until 4 years after she first sought treatment. A lesson in this tragic case is to be sure to document when you tell patients to “come back to see me right away if this happens again.”
23-year-old dies when myocarditis is mistaken for bronchitis
A 23-YEAR-OLD MAN PRESENTED TO THE EMERGENCY DEPARTMENT (ED) with chest tightness, cough, and fever. After a chest x-ray, the ED physician diagnosed bronchitis and sent the patient home with prescriptions for hydrocodone/acetaminophen and antibiotics. He was found dead in his bed less than 24 hours later. An autopsy determined the cause of death was myocarditis.
PLAINTIFF’S CLAIM The physician didn’t perform an electrocardiogram (EKG), which is a routine evaluation for a patient with chest pain. The EKG would have detected myocarditis.
THE DEFENSE The patient was evaluated properly. An EKG was not necessary.
VERDICT $2.9 million Massachusetts verdict.
COMMENT I think the jury got this one wrong. I don’t think an EKG is necessary for every case of acute bronchitis. However, I do wonder if the chest x-ray showed a large heart shadow.
Failure to properly manage a patient’s hypertension
A 44-YEAR-OLD MAN WHO WEIGHED >450 POUNDS went to his internist for treatment of hypertension. At a work-related physical the previous day, his blood pressure had been 160/110 mm Hg. After examination, the internist wrote a 30-day prescription for amlodipine, 5 mg/d, with 3 refills. The patient saw the physician 2 weeks later but not again until 3 months later. At that visit, the internist prescribed amlodipine, 5 mg/d, for 90 days with 2 refills. The patient missed his next appointment, which was set for 4 months later, but when his medication was about to run out, he was able to get a prescription for 10 months’ worth of amlodipine by phone. The patient died 2 months before the prescription ran out.
PLAINTIFF’S CLAIM The physician failed to properly manage and monitor the patient’s hypertension. The dosage of amlodipine was insufficient.
THE DEFENSE The patient was noncompliant and failed to show for follow-up appointments. The dosage of amlodipine was sufficient. The cause of death was unknown because no autopsy was performed.
VERDICT $136,000 New Jersey verdict.
COMMENT If we accept a patient into our practice, we need to have reasonable policies for patients to show up for follow-up, and to consider having them find another physician if they do not.
Did the patient’s age discourage proper evaluation?
THREE MONTHS AFTER NOTICING BLOOD IN HER STOOL, a 19-year-old woman went to see her physician. Without ordering a flexible sigmoidoscopy or colonoscopy, the physician diagnosed a healing anal fissure. Approximately 4 years later, the patient developed bloody diarrhea and went to a gastroenterologist, who found a 2.6 cm lesion in her rectum during a flexible sigmoidoscopy. Biopsy confirmed a low-grade adenocarcinoma. Imaging studies revealed that the cancer had spread to her lungs and liver, and she was diagnosed with Stage IV rectal cancer. After 2 years of extensive treatment that included surgical resection, conventional and experimental chemotherapy, and radiation therapy, the patient died.
PLAINTIFF’S CLAIM If the physician had ordered endoscopy exams when the patient first presented for treatment, testing could have identified a polyp or early-stage cancer.
THE DEFENSE No information about the defense is available.
VERDICT $2.5 million Maryland verdict.
COMMENT Colon cancer in a 19-year-old is extraordinarily rare. I doubt that the patient didn’t experience any more rectal bleeding until 4 years after she first sought treatment. A lesson in this tragic case is to be sure to document when you tell patients to “come back to see me right away if this happens again.”
23-year-old dies when myocarditis is mistaken for bronchitis
A 23-YEAR-OLD MAN PRESENTED TO THE EMERGENCY DEPARTMENT (ED) with chest tightness, cough, and fever. After a chest x-ray, the ED physician diagnosed bronchitis and sent the patient home with prescriptions for hydrocodone/acetaminophen and antibiotics. He was found dead in his bed less than 24 hours later. An autopsy determined the cause of death was myocarditis.
PLAINTIFF’S CLAIM The physician didn’t perform an electrocardiogram (EKG), which is a routine evaluation for a patient with chest pain. The EKG would have detected myocarditis.
THE DEFENSE The patient was evaluated properly. An EKG was not necessary.
VERDICT $2.9 million Massachusetts verdict.
COMMENT I think the jury got this one wrong. I don’t think an EKG is necessary for every case of acute bronchitis. However, I do wonder if the chest x-ray showed a large heart shadow.
Malpractice Counsel
Aortic Rupture
A 59-year-old woman involved in a motor vehicle crash presented to the ED via emergency medical services. The patient had been the front-seat passenger and was wearing a seat belt. She complained of chest wall pain, but denied head injury, loss of consciousness, neck pain, abdominal pain, or shortness of breath. Her past medical history was unremarkable.

A chest X-ray was performed and interpreted as normal by the attending radiologist. Laboratory studies were normal except for mild anemia. The patient was discharged from the hospital with a diagnosis of chest wall contusion. She died 36 hours later from a ruptured thoracic aorta. The family of the patient brought a malpractice suit against the emergency physician (EP) for failing to diagnose and treat acute aortic rupture. At trial, a defense verdict was returned.
Discussion
Aortic rupture from blunt trauma is a devastating injury. More than 90% of patients who have sustained this type of injury in a motor vehicle crash die at the scene.1 For the remaining 10%, 50% die within the following 24 hours.1 The injury occurs in the proximal descending aorta, secondary to the fixation of the vessels between the left subclavian artery and the ligamentum arteriosum; the cause in approximately 80% to 90% of cases is due to blunt trauma. Involvement of the ascending aorta is much less common. Many patients, such as the one in this case, exhibit no external physical findings of injury. Chest pain is the most frequent complaint, followed by dyspnea—both fairly nonspecific symptoms. Physical findings that should raise a suspicion for a thoracic aortic injury include hypotension, hypertension in the upper extremity and hypotension in the lower extremity, unequal BPs in the extremities, external evidence of chest wall trauma, and palpable fractures of the sternum and ribs.2 While it is unclear if this patient had unequal extremity BPs, she did not have any of the other classic findings of aortic rupture. Associated neurological, abdominal, or orthopedic injuries are frequently present as well, and can mask the subtle signs of aortic rupture.
A chest radiograph is often the initial screening test used to evaluate for possible thoracic aortic injury. Suspicious findings include a widened mediastinum (greater than 8 cm), right-sided deviation of the esophagus, depression of the left mainstem bronchus, loss of the aortic knob, and an apical pleural cap. Unfortunately, chest X-ray can be normal, and a normal mediastinum on the radiograph does not exclude the diagnosis.
For patients with suspected thoracic aortic injury, helical computed tomography with angiography is the study of choice. It can accurately identify operative and nonoperative lesions, as well as associated injuries (eg, small pneumothorax, rib fractures). Magnetic resonance angiography provides similar sensitivity and specificity, but is not practical for the majority of trauma patients. Occasionally, aortography can be considered when the CT scan results are indeterminate and when thought to be needed to plan operative intervention. Finally, transesophageal echocardiography can be considered in hemodynamically unstable patients unable to be transferred to the radiology suite.
For most patients, immediate operative intervention is the definitive treatment. For patients with suspected thoracic aortic injury and hypertension, shear forces need to be decreased just as they are for patients with aortic dissection. A short-acting β-blocker like intravenous (IV) esmolol can be used initially to slow HR. Then, an IV arterial vasodilator can be given to decrease BP. To prevent rebound tachycardia and increased shear forces, the β-blocker should always be initiated before the vasodilator is given. Vital-sign targets include an HR of 60 beats/minute and a systolic BP in the range of 100 to 120 mm Hg.
This was a very atypical presentation of a devastating injury. Given the benign presentation, lack of associated injuries, and the normal chest X-ray, a defense verdict appears to be the correct one in this very unfortunate case.

Foot Drop
A 20-year-old woman presented to the ED complaining of severe numbness, tingling, and pain in her left calf. According to the patient, she had attended a New Year’s Eve party, where she spent much of the time dancing. She was awakened by calf pain on the following morning and sought treatment at the ED.
On physical examination, the patient’s vital signs were normal. Examination of the left calf revealed tenderness to palpation; no swelling was noted. The patient was unable to lift her left foot or bear weight on the left leg. She had normal dorsalis pedis and posterior tibial pulses in the affected leg. The remainder of her examination was normal and no testing was performed. The patient was diagnosed with “floppy foot syndrome” and discharged home with a prescription for a nonsteroidal anti-inflammatory drug.
The next day, the patient presented to a different ED because of worsening pain and swelling of the calf. She was admitted to the hospital and the orthopedic service was consulted. The patient was diagnosed with compartment syndrome; however, by that time her condition was complicated by rhabdomyolysis, resulting in acute renal failure.
The patient underwent a fasciotomy. After surgery, she required hemodialysis until her kidney function returned. She had damage to the nerves in her left calf and leg resulting in a permanent foot drop that required prolonged physical therapy following her hospitalization.
The patient sued the initial EP for failure to diagnose compartment syndrome, which resulted in permanent nerve damage and foot drop. A $750,000 settlement was reached.
Discussion
The EP did not appear to have taken this case seriously, as “floppy foot syndrome” is not a recognized diagnosis. No significance was attached to the presence of the foot drop, which is an objective and concerning physical finding.
The differential diagnoses of foot drop are relatively small: a nerve injury, which is the most common cause; a central nervous system event, such as a stroke; or a muscular disorder.3 An injury or problem with the peroneal nerve is the most common cause of foot drop.
While the patient’s history was not typical for the development of compartment syndrome, she potentially participated in strenuous physical activity, which can result in muscle swelling and subsequent compartment syndrome.4 The pain from compartment syndrome is typically described as out of proportion to physical findings; this seems to have been the case for this patient.
The symptoms and findings of compartment syndrome are classically taught as the five “Ps”: pain, paresthesias, paralysis, pallor, and pulselessness, with the symptoms typically presenting in this order. The patient had the first three symptoms, but they were not appreciated in the initial evaluation. Pulselessness is usually the last finding to develop, and tissue damage is frequently present at that point.
Interestingly, approximately 40% of compartment syndromes occur at the level of the tibia and fibula. The lower leg has four compartments: the anterior, which contains the anterior tibial artery and deep peroneal nerve; the lateral, which contains the superficial peroneal nerve; the superficial posterior, which contains the sural nerve; and the deep posterior, which contains the posterior tibial artery and nerve.
As pressure within the enclosed space increases due to swelling, hemorrhage, fracture, etc, the blood supply as well as nerve and muscle functions become compromised. Left untreated, the increased pressure can result in permanent tissue and nerve damage.
Compartment syndrome is a time sensitive diagnosis because of the need for surgical intervention to open the compartment. The EP can measure compartment pressures if he or she has the right equipment and training. A normal compartment pressure is less than 10 mm Hg. When the compartment pressure begins to exceed 30 mm Hg, tissue damage can occur. If unable to measure compartment pressure, an emergent orthopedic consult is indicated.
- Chiesa R, de Moura MR, Lucci C, et al. Traumatic rupture of the thoracic aorta. Acta Chir Belq. 2003;103(4):364-374.
- Ross C, Schwab TM. Cardiac trauma. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD. Ross C. In: Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw Hill Medical; 2011:1758-1765.
- Ricarte IF, Figueiredo MM, Fukuda TG, Pedroso JL, Silva GS. Acute foot drop syndrome mimicking peroneal nerve injury: an atypical presentation of ischemic stroke. J Stroke Cerebrovasc Dis. 2014:23(5):1229-1231.
- Aliano K, Gulati S, Stavrides S, Davenport T, Hines G. Low-impact trauma causing acute compartment syndrome of the lower extremities. Am J Emerg Med. 2013;31(5):890.e3-e4.
Aortic Rupture
A 59-year-old woman involved in a motor vehicle crash presented to the ED via emergency medical services. The patient had been the front-seat passenger and was wearing a seat belt. She complained of chest wall pain, but denied head injury, loss of consciousness, neck pain, abdominal pain, or shortness of breath. Her past medical history was unremarkable.
A chest X-ray was performed and interpreted as normal by the attending radiologist. Laboratory studies were normal except for mild anemia. The patient was discharged from the hospital with a diagnosis of chest wall contusion. She died 36 hours later from a ruptured thoracic aorta. The family of the patient brought a malpractice suit against the emergency physician (EP) for failing to diagnose and treat acute aortic rupture. At trial, a defense verdict was returned.
Discussion
Aortic rupture from blunt trauma is a devastating injury. More than 90% of patients who have sustained this type of injury in a motor vehicle crash die at the scene.1 For the remaining 10%, 50% die within the following 24 hours.1 The injury occurs in the proximal descending aorta, secondary to the fixation of the vessels between the left subclavian artery and the ligamentum arteriosum; the cause in approximately 80% to 90% of cases is due to blunt trauma. Involvement of the ascending aorta is much less common. Many patients, such as the one in this case, exhibit no external physical findings of injury. Chest pain is the most frequent complaint, followed by dyspnea—both fairly nonspecific symptoms. Physical findings that should raise a suspicion for a thoracic aortic injury include hypotension, hypertension in the upper extremity and hypotension in the lower extremity, unequal BPs in the extremities, external evidence of chest wall trauma, and palpable fractures of the sternum and ribs.2 While it is unclear if this patient had unequal extremity BPs, she did not have any of the other classic findings of aortic rupture. Associated neurological, abdominal, or orthopedic injuries are frequently present as well, and can mask the subtle signs of aortic rupture.
A chest radiograph is often the initial screening test used to evaluate for possible thoracic aortic injury. Suspicious findings include a widened mediastinum (greater than 8 cm), right-sided deviation of the esophagus, depression of the left mainstem bronchus, loss of the aortic knob, and an apical pleural cap. Unfortunately, chest X-ray can be normal, and a normal mediastinum on the radiograph does not exclude the diagnosis.
For patients with suspected thoracic aortic injury, helical computed tomography with angiography is the study of choice. It can accurately identify operative and nonoperative lesions, as well as associated injuries (eg, small pneumothorax, rib fractures). Magnetic resonance angiography provides similar sensitivity and specificity, but is not practical for the majority of trauma patients. Occasionally, aortography can be considered when the CT scan results are indeterminate and when thought to be needed to plan operative intervention. Finally, transesophageal echocardiography can be considered in hemodynamically unstable patients unable to be transferred to the radiology suite.
For most patients, immediate operative intervention is the definitive treatment. For patients with suspected thoracic aortic injury and hypertension, shear forces need to be decreased just as they are for patients with aortic dissection. A short-acting β-blocker like intravenous (IV) esmolol can be used initially to slow HR. Then, an IV arterial vasodilator can be given to decrease BP. To prevent rebound tachycardia and increased shear forces, the β-blocker should always be initiated before the vasodilator is given. Vital-sign targets include an HR of 60 beats/minute and a systolic BP in the range of 100 to 120 mm Hg.
This was a very atypical presentation of a devastating injury. Given the benign presentation, lack of associated injuries, and the normal chest X-ray, a defense verdict appears to be the correct one in this very unfortunate case.
Foot Drop
A 20-year-old woman presented to the ED complaining of severe numbness, tingling, and pain in her left calf. According to the patient, she had attended a New Year’s Eve party, where she spent much of the time dancing. She was awakened by calf pain on the following morning and sought treatment at the ED.
On physical examination, the patient’s vital signs were normal. Examination of the left calf revealed tenderness to palpation; no swelling was noted. The patient was unable to lift her left foot or bear weight on the left leg. She had normal dorsalis pedis and posterior tibial pulses in the affected leg. The remainder of her examination was normal and no testing was performed. The patient was diagnosed with “floppy foot syndrome” and discharged home with a prescription for a nonsteroidal anti-inflammatory drug.
The next day, the patient presented to a different ED because of worsening pain and swelling of the calf. She was admitted to the hospital and the orthopedic service was consulted. The patient was diagnosed with compartment syndrome; however, by that time her condition was complicated by rhabdomyolysis, resulting in acute renal failure.
The patient underwent a fasciotomy. After surgery, she required hemodialysis until her kidney function returned. She had damage to the nerves in her left calf and leg resulting in a permanent foot drop that required prolonged physical therapy following her hospitalization.
The patient sued the initial EP for failure to diagnose compartment syndrome, which resulted in permanent nerve damage and foot drop. A $750,000 settlement was reached.
Discussion
The EP did not appear to have taken this case seriously, as “floppy foot syndrome” is not a recognized diagnosis. No significance was attached to the presence of the foot drop, which is an objective and concerning physical finding.
The differential diagnoses of foot drop are relatively small: a nerve injury, which is the most common cause; a central nervous system event, such as a stroke; or a muscular disorder.3 An injury or problem with the peroneal nerve is the most common cause of foot drop.
While the patient’s history was not typical for the development of compartment syndrome, she potentially participated in strenuous physical activity, which can result in muscle swelling and subsequent compartment syndrome.4 The pain from compartment syndrome is typically described as out of proportion to physical findings; this seems to have been the case for this patient.
The symptoms and findings of compartment syndrome are classically taught as the five “Ps”: pain, paresthesias, paralysis, pallor, and pulselessness, with the symptoms typically presenting in this order. The patient had the first three symptoms, but they were not appreciated in the initial evaluation. Pulselessness is usually the last finding to develop, and tissue damage is frequently present at that point.
Interestingly, approximately 40% of compartment syndromes occur at the level of the tibia and fibula. The lower leg has four compartments: the anterior, which contains the anterior tibial artery and deep peroneal nerve; the lateral, which contains the superficial peroneal nerve; the superficial posterior, which contains the sural nerve; and the deep posterior, which contains the posterior tibial artery and nerve.
As pressure within the enclosed space increases due to swelling, hemorrhage, fracture, etc, the blood supply as well as nerve and muscle functions become compromised. Left untreated, the increased pressure can result in permanent tissue and nerve damage.
Compartment syndrome is a time sensitive diagnosis because of the need for surgical intervention to open the compartment. The EP can measure compartment pressures if he or she has the right equipment and training. A normal compartment pressure is less than 10 mm Hg. When the compartment pressure begins to exceed 30 mm Hg, tissue damage can occur. If unable to measure compartment pressure, an emergent orthopedic consult is indicated.
Aortic Rupture
A 59-year-old woman involved in a motor vehicle crash presented to the ED via emergency medical services. The patient had been the front-seat passenger and was wearing a seat belt. She complained of chest wall pain, but denied head injury, loss of consciousness, neck pain, abdominal pain, or shortness of breath. Her past medical history was unremarkable.
A chest X-ray was performed and interpreted as normal by the attending radiologist. Laboratory studies were normal except for mild anemia. The patient was discharged from the hospital with a diagnosis of chest wall contusion. She died 36 hours later from a ruptured thoracic aorta. The family of the patient brought a malpractice suit against the emergency physician (EP) for failing to diagnose and treat acute aortic rupture. At trial, a defense verdict was returned.
Discussion
Aortic rupture from blunt trauma is a devastating injury. More than 90% of patients who have sustained this type of injury in a motor vehicle crash die at the scene.1 For the remaining 10%, 50% die within the following 24 hours.1 The injury occurs in the proximal descending aorta, secondary to the fixation of the vessels between the left subclavian artery and the ligamentum arteriosum; the cause in approximately 80% to 90% of cases is due to blunt trauma. Involvement of the ascending aorta is much less common. Many patients, such as the one in this case, exhibit no external physical findings of injury. Chest pain is the most frequent complaint, followed by dyspnea—both fairly nonspecific symptoms. Physical findings that should raise a suspicion for a thoracic aortic injury include hypotension, hypertension in the upper extremity and hypotension in the lower extremity, unequal BPs in the extremities, external evidence of chest wall trauma, and palpable fractures of the sternum and ribs.2 While it is unclear if this patient had unequal extremity BPs, she did not have any of the other classic findings of aortic rupture. Associated neurological, abdominal, or orthopedic injuries are frequently present as well, and can mask the subtle signs of aortic rupture.
A chest radiograph is often the initial screening test used to evaluate for possible thoracic aortic injury. Suspicious findings include a widened mediastinum (greater than 8 cm), right-sided deviation of the esophagus, depression of the left mainstem bronchus, loss of the aortic knob, and an apical pleural cap. Unfortunately, chest X-ray can be normal, and a normal mediastinum on the radiograph does not exclude the diagnosis.
For patients with suspected thoracic aortic injury, helical computed tomography with angiography is the study of choice. It can accurately identify operative and nonoperative lesions, as well as associated injuries (eg, small pneumothorax, rib fractures). Magnetic resonance angiography provides similar sensitivity and specificity, but is not practical for the majority of trauma patients. Occasionally, aortography can be considered when the CT scan results are indeterminate and when thought to be needed to plan operative intervention. Finally, transesophageal echocardiography can be considered in hemodynamically unstable patients unable to be transferred to the radiology suite.
For most patients, immediate operative intervention is the definitive treatment. For patients with suspected thoracic aortic injury and hypertension, shear forces need to be decreased just as they are for patients with aortic dissection. A short-acting β-blocker like intravenous (IV) esmolol can be used initially to slow HR. Then, an IV arterial vasodilator can be given to decrease BP. To prevent rebound tachycardia and increased shear forces, the β-blocker should always be initiated before the vasodilator is given. Vital-sign targets include an HR of 60 beats/minute and a systolic BP in the range of 100 to 120 mm Hg.
This was a very atypical presentation of a devastating injury. Given the benign presentation, lack of associated injuries, and the normal chest X-ray, a defense verdict appears to be the correct one in this very unfortunate case.
Foot Drop
A 20-year-old woman presented to the ED complaining of severe numbness, tingling, and pain in her left calf. According to the patient, she had attended a New Year’s Eve party, where she spent much of the time dancing. She was awakened by calf pain on the following morning and sought treatment at the ED.
On physical examination, the patient’s vital signs were normal. Examination of the left calf revealed tenderness to palpation; no swelling was noted. The patient was unable to lift her left foot or bear weight on the left leg. She had normal dorsalis pedis and posterior tibial pulses in the affected leg. The remainder of her examination was normal and no testing was performed. The patient was diagnosed with “floppy foot syndrome” and discharged home with a prescription for a nonsteroidal anti-inflammatory drug.
The next day, the patient presented to a different ED because of worsening pain and swelling of the calf. She was admitted to the hospital and the orthopedic service was consulted. The patient was diagnosed with compartment syndrome; however, by that time her condition was complicated by rhabdomyolysis, resulting in acute renal failure.
The patient underwent a fasciotomy. After surgery, she required hemodialysis until her kidney function returned. She had damage to the nerves in her left calf and leg resulting in a permanent foot drop that required prolonged physical therapy following her hospitalization.
The patient sued the initial EP for failure to diagnose compartment syndrome, which resulted in permanent nerve damage and foot drop. A $750,000 settlement was reached.
Discussion
The EP did not appear to have taken this case seriously, as “floppy foot syndrome” is not a recognized diagnosis. No significance was attached to the presence of the foot drop, which is an objective and concerning physical finding.
The differential diagnoses of foot drop are relatively small: a nerve injury, which is the most common cause; a central nervous system event, such as a stroke; or a muscular disorder.3 An injury or problem with the peroneal nerve is the most common cause of foot drop.
While the patient’s history was not typical for the development of compartment syndrome, she potentially participated in strenuous physical activity, which can result in muscle swelling and subsequent compartment syndrome.4 The pain from compartment syndrome is typically described as out of proportion to physical findings; this seems to have been the case for this patient.
The symptoms and findings of compartment syndrome are classically taught as the five “Ps”: pain, paresthesias, paralysis, pallor, and pulselessness, with the symptoms typically presenting in this order. The patient had the first three symptoms, but they were not appreciated in the initial evaluation. Pulselessness is usually the last finding to develop, and tissue damage is frequently present at that point.
Interestingly, approximately 40% of compartment syndromes occur at the level of the tibia and fibula. The lower leg has four compartments: the anterior, which contains the anterior tibial artery and deep peroneal nerve; the lateral, which contains the superficial peroneal nerve; the superficial posterior, which contains the sural nerve; and the deep posterior, which contains the posterior tibial artery and nerve.
As pressure within the enclosed space increases due to swelling, hemorrhage, fracture, etc, the blood supply as well as nerve and muscle functions become compromised. Left untreated, the increased pressure can result in permanent tissue and nerve damage.
Compartment syndrome is a time sensitive diagnosis because of the need for surgical intervention to open the compartment. The EP can measure compartment pressures if he or she has the right equipment and training. A normal compartment pressure is less than 10 mm Hg. When the compartment pressure begins to exceed 30 mm Hg, tissue damage can occur. If unable to measure compartment pressure, an emergent orthopedic consult is indicated.
- Chiesa R, de Moura MR, Lucci C, et al. Traumatic rupture of the thoracic aorta. Acta Chir Belq. 2003;103(4):364-374.
- Ross C, Schwab TM. Cardiac trauma. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD. Ross C. In: Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw Hill Medical; 2011:1758-1765.
- Ricarte IF, Figueiredo MM, Fukuda TG, Pedroso JL, Silva GS. Acute foot drop syndrome mimicking peroneal nerve injury: an atypical presentation of ischemic stroke. J Stroke Cerebrovasc Dis. 2014:23(5):1229-1231.
- Aliano K, Gulati S, Stavrides S, Davenport T, Hines G. Low-impact trauma causing acute compartment syndrome of the lower extremities. Am J Emerg Med. 2013;31(5):890.e3-e4.
- Chiesa R, de Moura MR, Lucci C, et al. Traumatic rupture of the thoracic aorta. Acta Chir Belq. 2003;103(4):364-374.
- Ross C, Schwab TM. Cardiac trauma. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD. Ross C. In: Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw Hill Medical; 2011:1758-1765.
- Ricarte IF, Figueiredo MM, Fukuda TG, Pedroso JL, Silva GS. Acute foot drop syndrome mimicking peroneal nerve injury: an atypical presentation of ischemic stroke. J Stroke Cerebrovasc Dis. 2014:23(5):1229-1231.
- Aliano K, Gulati S, Stavrides S, Davenport T, Hines G. Low-impact trauma causing acute compartment syndrome of the lower extremities. Am J Emerg Med. 2013;31(5):890.e3-e4.

Dermatology: The Last Refuge for Private Practice?
The unprecedented challenges that I have been discussing in this column over the last several months—the Patient Protection and Affordable Care Act, drastic revisions in confidentiality rules and diagnosis codes, and the movement toward electronic health records, among others—have triggered widespread predictions that the independent private physician practice model will largely be replaced in the not too distant future.1
Although I am skeptical of such bleak blanket projections, there is no question that the ongoing sea change in medicine has already led to substantial erosion of physician autonomy and ever-increasing administrative burdens that hit small practices the hardest. More changes are on the way, and physicians in solo offices and small groups will need to explore their options, which include cooperative arrangements with other small offices, joining a large group or independent practice association (IPA), and others that are yet to be defined.
It will be years before the fate of private practice is clear. In the meantime, private practice physicians need a strategy tailored to the current situation and long-term goals. Small practices that offer unique services or fill an unmet niche may not need to modify their practice models at all. Concierge medicine is also worth considering if you are committed to remaining private and independent. Most small practices, however, will be compelled to consider a larger alternative.
Cooperative Groups
One attractive and relatively straightforward strategy is the formation of a cooperative group. In most geographic areas, there are likely several small practice physicians in similar predicaments who might be receptive to discussing collaboration on billing and purchasing. This arrangement allows each participant to maintain independence as a private practice while pooling resources toward the goal of easing the administrative burdens for all physicians involved. Once the arrangement is in place, the group can consider more ambitious projects, such as purchasing an electronic health records system jointly, sharing personnel to decrease staffing costs, and implementing an integrated scheduling system. The latter will be particularly attractive to participants who are considering an intermediate option somewhere between full-time work and complete retirement.
After a time, when the structure is stabilized and everyone agrees that his/her individual and shared interests and goals are being met, an outright merger can be contemplated. Obviously, projects of this scope require careful planning and implementation, and they should not be undertaken without the help of competent legal counsel and an experienced business consultant.
Independent Practice Associations
A more complex but increasingly popular option is to join other small practices and providers to create an IPA. A growing number of IPAs have already formed around the country, according to recent reports from the American Medical Association.2 An IPA is a legal entity organized and directed by physicians for the purpose of negotiating contracts with insurance companies on their behalf. Because of its structure, an IPA is better positioned than individual practices to enter into such financial arrangements and to counterbalance the leverage of insurers; however, there are legal issues to consider. Many IPAs are vulnerable to antitrust charges because they are comprised of competing health care providers. You should check with legal counsel before signing on to an IPA to make sure it abides by all applicable antitrust and price-fixing laws. Independent practice associations also have been known to fail, particularly in states where they are not adequately regulated.
Accountable Care Organizations
A number of IPAs are converting to accountable care organizations (ACOs), a move that requires a more formal management structure. Although the official definition of the structure remains somewhat nebulous, an ACO basically is a network of physicians and hospitals that share financial and medical responsibility for providing coordinated and efficient care to patients. The goal of ACO participants is to limit unnecessary spending, both individually and collectively, according to criteria established by the Centers for Medicare & Medicaid Services (CMS), without compromising quality of care in the process. More than 600 ACOs had been approved by the CMS as of the beginning of 2014.3
It is important to remember that the ACO model remains very much a work in progress. Accountable care organizations make providers jointly accountable for the health of their patients; they offer financial incentives to cooperate with each other and to save money by avoiding unnecessary tests and procedures. A key component is sharing information. Providers who save money while also meeting quality targets are theoretically entitled to a portion of the savings.3
As with IPAs, ACO ventures involve a measure of risk. Accountable care organizations that fail to meet the CMS performance and savings benchmarks can be stuck with the bill for investments made to improve care (eg, equipment, computer purchases) and for the hire of mid-level providers and managers. They also may be assessed monetary penalties. Accountable care organizations sponsored by physicians or rural providers, however, can apply to receive payments in advance to help them build the infrastructure necessary for coordinated care, a concession the Obama administration made because of concerns from rural hospitals.4
Final Thoughts
Clearly the price of remaining autonomous will not be insignificant, and many private practitioners will be unwilling to pay it. Only 36% of physicians remained in independent practice at the end of 2013, a decrease from 57% in 2000.2 Does that mean that private practice is doomed, as the “experts” predict? Absolutely not. Those of us who remain committed to it will find a new strategy. As always, we will adjust and adapt as the playing field changes. In medicine, as in life, those who are the most responsive to change will survive and flourish.
1. Health Reform and the Decline of Physician Private Practice. The Physicians’ Foundation Web site. http://www.physiciansfoundation.org/uploads/default/Health_Reform_and_the_Decline_of_Physician_Private_Practice.pdf. Published October 2010. Accessed August 15, 2014.
2. Elliott VS. Doctors describe pressures driving them from independent practice. American Medical News. November 19, 2013. http://www.amednews.com/article/20121119/business/311199971/2/. Accessed August 15, 2014.
3. Muhlestein D. Accountable care growth in 2014: a look ahead. Health Affairs Web site. http://healthaffairs.org/blog/2014/01/29/accountable-care-growth-in-2014-a-look-ahead. Published January 29, 2014. Accessed August 15, 2014.
4. Gold J. FAQ on ACOs: accountable care organizations, explained. Kaiser Health News. April 16, 2014.
The unprecedented challenges that I have been discussing in this column over the last several months—the Patient Protection and Affordable Care Act, drastic revisions in confidentiality rules and diagnosis codes, and the movement toward electronic health records, among others—have triggered widespread predictions that the independent private physician practice model will largely be replaced in the not too distant future.1
Although I am skeptical of such bleak blanket projections, there is no question that the ongoing sea change in medicine has already led to substantial erosion of physician autonomy and ever-increasing administrative burdens that hit small practices the hardest. More changes are on the way, and physicians in solo offices and small groups will need to explore their options, which include cooperative arrangements with other small offices, joining a large group or independent practice association (IPA), and others that are yet to be defined.
It will be years before the fate of private practice is clear. In the meantime, private practice physicians need a strategy tailored to the current situation and long-term goals. Small practices that offer unique services or fill an unmet niche may not need to modify their practice models at all. Concierge medicine is also worth considering if you are committed to remaining private and independent. Most small practices, however, will be compelled to consider a larger alternative.
Cooperative Groups
One attractive and relatively straightforward strategy is the formation of a cooperative group. In most geographic areas, there are likely several small practice physicians in similar predicaments who might be receptive to discussing collaboration on billing and purchasing. This arrangement allows each participant to maintain independence as a private practice while pooling resources toward the goal of easing the administrative burdens for all physicians involved. Once the arrangement is in place, the group can consider more ambitious projects, such as purchasing an electronic health records system jointly, sharing personnel to decrease staffing costs, and implementing an integrated scheduling system. The latter will be particularly attractive to participants who are considering an intermediate option somewhere between full-time work and complete retirement.
After a time, when the structure is stabilized and everyone agrees that his/her individual and shared interests and goals are being met, an outright merger can be contemplated. Obviously, projects of this scope require careful planning and implementation, and they should not be undertaken without the help of competent legal counsel and an experienced business consultant.
Independent Practice Associations
A more complex but increasingly popular option is to join other small practices and providers to create an IPA. A growing number of IPAs have already formed around the country, according to recent reports from the American Medical Association.2 An IPA is a legal entity organized and directed by physicians for the purpose of negotiating contracts with insurance companies on their behalf. Because of its structure, an IPA is better positioned than individual practices to enter into such financial arrangements and to counterbalance the leverage of insurers; however, there are legal issues to consider. Many IPAs are vulnerable to antitrust charges because they are comprised of competing health care providers. You should check with legal counsel before signing on to an IPA to make sure it abides by all applicable antitrust and price-fixing laws. Independent practice associations also have been known to fail, particularly in states where they are not adequately regulated.
Accountable Care Organizations
A number of IPAs are converting to accountable care organizations (ACOs), a move that requires a more formal management structure. Although the official definition of the structure remains somewhat nebulous, an ACO basically is a network of physicians and hospitals that share financial and medical responsibility for providing coordinated and efficient care to patients. The goal of ACO participants is to limit unnecessary spending, both individually and collectively, according to criteria established by the Centers for Medicare & Medicaid Services (CMS), without compromising quality of care in the process. More than 600 ACOs had been approved by the CMS as of the beginning of 2014.3
It is important to remember that the ACO model remains very much a work in progress. Accountable care organizations make providers jointly accountable for the health of their patients; they offer financial incentives to cooperate with each other and to save money by avoiding unnecessary tests and procedures. A key component is sharing information. Providers who save money while also meeting quality targets are theoretically entitled to a portion of the savings.3
As with IPAs, ACO ventures involve a measure of risk. Accountable care organizations that fail to meet the CMS performance and savings benchmarks can be stuck with the bill for investments made to improve care (eg, equipment, computer purchases) and for the hire of mid-level providers and managers. They also may be assessed monetary penalties. Accountable care organizations sponsored by physicians or rural providers, however, can apply to receive payments in advance to help them build the infrastructure necessary for coordinated care, a concession the Obama administration made because of concerns from rural hospitals.4
Final Thoughts
Clearly the price of remaining autonomous will not be insignificant, and many private practitioners will be unwilling to pay it. Only 36% of physicians remained in independent practice at the end of 2013, a decrease from 57% in 2000.2 Does that mean that private practice is doomed, as the “experts” predict? Absolutely not. Those of us who remain committed to it will find a new strategy. As always, we will adjust and adapt as the playing field changes. In medicine, as in life, those who are the most responsive to change will survive and flourish.
The unprecedented challenges that I have been discussing in this column over the last several months—the Patient Protection and Affordable Care Act, drastic revisions in confidentiality rules and diagnosis codes, and the movement toward electronic health records, among others—have triggered widespread predictions that the independent private physician practice model will largely be replaced in the not too distant future.1
Although I am skeptical of such bleak blanket projections, there is no question that the ongoing sea change in medicine has already led to substantial erosion of physician autonomy and ever-increasing administrative burdens that hit small practices the hardest. More changes are on the way, and physicians in solo offices and small groups will need to explore their options, which include cooperative arrangements with other small offices, joining a large group or independent practice association (IPA), and others that are yet to be defined.
It will be years before the fate of private practice is clear. In the meantime, private practice physicians need a strategy tailored to the current situation and long-term goals. Small practices that offer unique services or fill an unmet niche may not need to modify their practice models at all. Concierge medicine is also worth considering if you are committed to remaining private and independent. Most small practices, however, will be compelled to consider a larger alternative.
Cooperative Groups
One attractive and relatively straightforward strategy is the formation of a cooperative group. In most geographic areas, there are likely several small practice physicians in similar predicaments who might be receptive to discussing collaboration on billing and purchasing. This arrangement allows each participant to maintain independence as a private practice while pooling resources toward the goal of easing the administrative burdens for all physicians involved. Once the arrangement is in place, the group can consider more ambitious projects, such as purchasing an electronic health records system jointly, sharing personnel to decrease staffing costs, and implementing an integrated scheduling system. The latter will be particularly attractive to participants who are considering an intermediate option somewhere between full-time work and complete retirement.
After a time, when the structure is stabilized and everyone agrees that his/her individual and shared interests and goals are being met, an outright merger can be contemplated. Obviously, projects of this scope require careful planning and implementation, and they should not be undertaken without the help of competent legal counsel and an experienced business consultant.
Independent Practice Associations
A more complex but increasingly popular option is to join other small practices and providers to create an IPA. A growing number of IPAs have already formed around the country, according to recent reports from the American Medical Association.2 An IPA is a legal entity organized and directed by physicians for the purpose of negotiating contracts with insurance companies on their behalf. Because of its structure, an IPA is better positioned than individual practices to enter into such financial arrangements and to counterbalance the leverage of insurers; however, there are legal issues to consider. Many IPAs are vulnerable to antitrust charges because they are comprised of competing health care providers. You should check with legal counsel before signing on to an IPA to make sure it abides by all applicable antitrust and price-fixing laws. Independent practice associations also have been known to fail, particularly in states where they are not adequately regulated.
Accountable Care Organizations
A number of IPAs are converting to accountable care organizations (ACOs), a move that requires a more formal management structure. Although the official definition of the structure remains somewhat nebulous, an ACO basically is a network of physicians and hospitals that share financial and medical responsibility for providing coordinated and efficient care to patients. The goal of ACO participants is to limit unnecessary spending, both individually and collectively, according to criteria established by the Centers for Medicare & Medicaid Services (CMS), without compromising quality of care in the process. More than 600 ACOs had been approved by the CMS as of the beginning of 2014.3
It is important to remember that the ACO model remains very much a work in progress. Accountable care organizations make providers jointly accountable for the health of their patients; they offer financial incentives to cooperate with each other and to save money by avoiding unnecessary tests and procedures. A key component is sharing information. Providers who save money while also meeting quality targets are theoretically entitled to a portion of the savings.3
As with IPAs, ACO ventures involve a measure of risk. Accountable care organizations that fail to meet the CMS performance and savings benchmarks can be stuck with the bill for investments made to improve care (eg, equipment, computer purchases) and for the hire of mid-level providers and managers. They also may be assessed monetary penalties. Accountable care organizations sponsored by physicians or rural providers, however, can apply to receive payments in advance to help them build the infrastructure necessary for coordinated care, a concession the Obama administration made because of concerns from rural hospitals.4
Final Thoughts
Clearly the price of remaining autonomous will not be insignificant, and many private practitioners will be unwilling to pay it. Only 36% of physicians remained in independent practice at the end of 2013, a decrease from 57% in 2000.2 Does that mean that private practice is doomed, as the “experts” predict? Absolutely not. Those of us who remain committed to it will find a new strategy. As always, we will adjust and adapt as the playing field changes. In medicine, as in life, those who are the most responsive to change will survive and flourish.
1. Health Reform and the Decline of Physician Private Practice. The Physicians’ Foundation Web site. http://www.physiciansfoundation.org/uploads/default/Health_Reform_and_the_Decline_of_Physician_Private_Practice.pdf. Published October 2010. Accessed August 15, 2014.
2. Elliott VS. Doctors describe pressures driving them from independent practice. American Medical News. November 19, 2013. http://www.amednews.com/article/20121119/business/311199971/2/. Accessed August 15, 2014.
3. Muhlestein D. Accountable care growth in 2014: a look ahead. Health Affairs Web site. http://healthaffairs.org/blog/2014/01/29/accountable-care-growth-in-2014-a-look-ahead. Published January 29, 2014. Accessed August 15, 2014.
4. Gold J. FAQ on ACOs: accountable care organizations, explained. Kaiser Health News. April 16, 2014.
1. Health Reform and the Decline of Physician Private Practice. The Physicians’ Foundation Web site. http://www.physiciansfoundation.org/uploads/default/Health_Reform_and_the_Decline_of_Physician_Private_Practice.pdf. Published October 2010. Accessed August 15, 2014.
2. Elliott VS. Doctors describe pressures driving them from independent practice. American Medical News. November 19, 2013. http://www.amednews.com/article/20121119/business/311199971/2/. Accessed August 15, 2014.
3. Muhlestein D. Accountable care growth in 2014: a look ahead. Health Affairs Web site. http://healthaffairs.org/blog/2014/01/29/accountable-care-growth-in-2014-a-look-ahead. Published January 29, 2014. Accessed August 15, 2014.
4. Gold J. FAQ on ACOs: accountable care organizations, explained. Kaiser Health News. April 16, 2014.
Practice Points
- Private practices that can adapt to changes brought on by health care reform will survive and even flourish. Private practice physicians must weigh their options to find a strategy that is tailored to their current situation and long-term goals.
- Cooperative groups allow small practice physicians to pool resources while maintaining independence as a private practice.
- The number of independent practice associations has grown, but there are risks.
- Accountable care organizations allow a network of physicians and hospitals to share financial and medical responsibility for providing coordinated and efficient care to patients.