User login
Delayed birth, intubation failure: $10M settlement

Delayed birth, intubation failure: $10M settlement
Two days shy of her due date, a woman went to an Army hospital to report bloody mucus discharge and sporadic contractions. She was 2 cm dilated and 50% effaced with the baby at –2 station. Fetal heart-rate monitor results were reassuring. She was discharged home but returned 5 hours later with increased pain and contractions. She was 5 cm dilated, 90% effaced; the baby was at –3 station. When contractions ceased, she was discharged. There had been no cervical change for 6 hours with a negative fern test. Fetal monitoring results were reassuring.
The woman returned 3 hours later with increased pain and contractions. She had a fever and high white blood cell and neutrophil counts. She was 6 cm dilated, 90% effaced, but the baby was still at –3 station. Ampicillin sodium/sulbactam sodium was administered. The ObGyn was called 4 times over the next 2.5 hours, when fetal monitoring results worsened and bradycardia developed. The nurses treated fetal distress by changing the maternal position and performing amnioinfusion. Then the ObGyn came to the bedside and ordered cesarean delivery. The baby was born severely compromised from hypoxic ischemic encephalopathy and metabolic acidosis. The pediatrician responsible for the baby’s resuscitation failed to get a response with bag ventilation after 5 minutes; 2 attempts at intubation failed. When the chief of pediatrics arrived at 15 minutes, the infant was successfully intubated. The baby was transferred to another facility. The child has profound disabilities.
Parents’ claim The hospital staff and physician did not deliver the baby in a timely manner when fetal distress was first noted. The pediatrician did not properly resuscitate the newborn.
Defendants’ defense Chorioamnionitis and funisitis caused or contributed to the infant’s injuries. Proper care was provided.
Verdict A $10 million Washington settlement was reached.
Did OCs cause this woman’s stroke?
A 40-year-old woman went to a clinic to obtain a prescription for birth control pills. A physician assistant (PA) conducted a complete physical examination. When no contraindications were found, a prescription for oral contraceptives (OCs) was provided. Two months later, the patient suffered a debilitating stroke. After the stroke, the patient was found to have a patent foramen ovale.
Patient’s claim The risks and benefits of the OC were not fully explained to the patient by the PA. She was not offered other contraceptive options. OCs are not safe for a woman her age due to a higher risk of stroke.
Defendants’ defense The patient used OCs in the past, and had received information from other physicians about their use. The stroke occurred because of the foramen ovale, not the use of OCs.
Verdict A Washington defense verdict was returned.
Ureter injury not treated until the next day
During cesarean delivery, the ObGyn identified a small ureteral injury but did not repair it. The next day, the ObGyn consulted a urologist and ordered an intravenous pyelogram (IVP). The urologist identified a ureteral obstruction and surgically repaired the injury. The patient was required to use a nephros-tomy bag for 6 months until the nephrostomy was reversed.
Patient’s claim The ObGyn was negligent in failing to immediately treat the ureter injury. The delay in repair necessitated the use of the nephrostomy bag.
Physician’s defense A ureter injury is a known complication of the procedure. The ObGyn did not cause the obstruction. Failure to perform an immediate repair was due to his concern that the patient might have lost too much blood during cesarean delivery. Bringing in the urologist the next day was appropriate. The patient completely recovered.
Verdict A $484,141 Mississippi verdict was returned.
Patient didn’t want male physician
After a woman experienced sexual assault in college, she did not want a male physician to perform a vaginal examination. When pregnant, she discussed that request with her nurse midwives. While she was in labor, a male ObGyn examined her.
Patient’s claim The nurse midwives failed to document her request not to be examined by a male clinician. The patient experienced severe emotional distress.
Defendants’ defense The midwives claimed they were never told of the patient’s aversion to having a male physician examine her. The male physician and the birthing center denied knowledge of the request.
Verdict A $270,000 Washington verdict was returned.
Symptoms attributed to anesthesia: $2M
A 62-year-old woman underwent treatment for abnormal uterine bleeding (AUB). Hysteroscopy revealed a retroverted uterus containing a 3-cm polyp. During resection of the polyp, the uterus was perforated and bowel was drawn into the uterus. The injury was not recognized. The patient was discharged home the same day.
The next day, she phoned to report vomiting, abdominal pain, and urinary retention. The gynecologist attributed the symptoms to anesthesia and told the patient to allow more time for resolution.
The patient went to an emergency department (ED) 48 hours later with a distended abdomen and severe pain. She was transferred to a regional hospital with acute sepsis. A small bowel perforation was identified, requiring extensive treatment, including hysterectomy and resection of 27 cm of small bowel.
Patient’s claim The gynecologist was negligent in failing to recognize the injury intraoperatively. He didn’t examine the patient when she first reported symptoms.
Physician’s defense The injuries are known risks of the procedure. The patient’s complaints could reasonably be associated with postanesthesia residuals.
Verdict A $5 million Virginia verdict was reduced to $2 million by the statutory cap.
Did nosebleeds cause baby’s disabilities?
After a 33-year-old woman had a nosebleed she noted decreased fetal movement. At the ED, preterm labor was ruled out, fetal monitoring results were normal, and she was discharged. She returned that afternoon with a nosebleed. After 4 hours, when fetal monitoring results were normal, she was again discharged.
The next morning, an otolaryngologist cauterized her right nostril. After another nosebleed, the physician packed the right nasal cavity. She returned with bleeding from the left nostril and remained at the ear, nose, and throat (ENT) clinic for several hours until the bleeding stopped.
The following day, she returned to the ENT clinic asking that the packing be removed, but it needed to remain. She called a covering ObGyn to request anti-anxiety medication because the packing was making her feel claustrophobic.
The next day, after additional nosebleeds, she was taken to the ED with mild contractions. Her hematocrit was 25.6% and her hemoglobin level was 8.8 g/dL. When fetal heart-rate monitoring was nonreassuring, a cesarean delivery was expedited. The child has profound physical and developmental disabilities, uses a feeding tube and ventilator, and needs 24-hour care.
Parents’ claim The mother and fetus were never properly assessed or treated.
Defendants’ defense The physicians denied negligence and disputed the severity of most of the nosebleeds. At each ED presentation, hematocrit and hemoglobin levels were normal and the mother was stable at discharge. When fetal monitoring was performed, the results were normal. When the mother left the ENT clinic after the third visit, she was told to go to the ED or call 911 if she had another nosebleed, which she did not do. When she went to the ED with contractions, staff reacted to fetal distress and performed emergency cesarean delivery.
Verdict A Texas defense verdict was returned.
Difficult neonatal resuscitation: $8.4M
A nuchal cord was discovered at delivery. The child has cerebral palsy, a seizure disorder, and developmental delays. He cannot walk or talk, uses a feeding tube, and requires 24-hour care.
Parents’ claim Monitoring showed fetal distress for 5 hours, but the staff failed to perform a cesarean delivery or have a neonatal resuscitation team ready at delivery. After delivery, the baby was deprived of oxygen for 8 minutes before intubation. A back-up team should have been available.
Medical center’s defense Proper care was given. The resuscitation team was in a surgical suite.
Verdict An $8.4 million Georgia verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Delayed birth, intubation failure: $10M settlement
Two days shy of her due date, a woman went to an Army hospital to report bloody mucus discharge and sporadic contractions. She was 2 cm dilated and 50% effaced with the baby at –2 station. Fetal heart-rate monitor results were reassuring. She was discharged home but returned 5 hours later with increased pain and contractions. She was 5 cm dilated, 90% effaced; the baby was at –3 station. When contractions ceased, she was discharged. There had been no cervical change for 6 hours with a negative fern test. Fetal monitoring results were reassuring.
The woman returned 3 hours later with increased pain and contractions. She had a fever and high white blood cell and neutrophil counts. She was 6 cm dilated, 90% effaced, but the baby was still at –3 station. Ampicillin sodium/sulbactam sodium was administered. The ObGyn was called 4 times over the next 2.5 hours, when fetal monitoring results worsened and bradycardia developed. The nurses treated fetal distress by changing the maternal position and performing amnioinfusion. Then the ObGyn came to the bedside and ordered cesarean delivery. The baby was born severely compromised from hypoxic ischemic encephalopathy and metabolic acidosis. The pediatrician responsible for the baby’s resuscitation failed to get a response with bag ventilation after 5 minutes; 2 attempts at intubation failed. When the chief of pediatrics arrived at 15 minutes, the infant was successfully intubated. The baby was transferred to another facility. The child has profound disabilities.
Parents’ claim The hospital staff and physician did not deliver the baby in a timely manner when fetal distress was first noted. The pediatrician did not properly resuscitate the newborn.
Defendants’ defense Chorioamnionitis and funisitis caused or contributed to the infant’s injuries. Proper care was provided.
Verdict A $10 million Washington settlement was reached.
Did OCs cause this woman’s stroke?
A 40-year-old woman went to a clinic to obtain a prescription for birth control pills. A physician assistant (PA) conducted a complete physical examination. When no contraindications were found, a prescription for oral contraceptives (OCs) was provided. Two months later, the patient suffered a debilitating stroke. After the stroke, the patient was found to have a patent foramen ovale.
Patient’s claim The risks and benefits of the OC were not fully explained to the patient by the PA. She was not offered other contraceptive options. OCs are not safe for a woman her age due to a higher risk of stroke.
Defendants’ defense The patient used OCs in the past, and had received information from other physicians about their use. The stroke occurred because of the foramen ovale, not the use of OCs.
Verdict A Washington defense verdict was returned.
Ureter injury not treated until the next day
During cesarean delivery, the ObGyn identified a small ureteral injury but did not repair it. The next day, the ObGyn consulted a urologist and ordered an intravenous pyelogram (IVP). The urologist identified a ureteral obstruction and surgically repaired the injury. The patient was required to use a nephros-tomy bag for 6 months until the nephrostomy was reversed.
Patient’s claim The ObGyn was negligent in failing to immediately treat the ureter injury. The delay in repair necessitated the use of the nephrostomy bag.
Physician’s defense A ureter injury is a known complication of the procedure. The ObGyn did not cause the obstruction. Failure to perform an immediate repair was due to his concern that the patient might have lost too much blood during cesarean delivery. Bringing in the urologist the next day was appropriate. The patient completely recovered.
Verdict A $484,141 Mississippi verdict was returned.
Patient didn’t want male physician
After a woman experienced sexual assault in college, she did not want a male physician to perform a vaginal examination. When pregnant, she discussed that request with her nurse midwives. While she was in labor, a male ObGyn examined her.
Patient’s claim The nurse midwives failed to document her request not to be examined by a male clinician. The patient experienced severe emotional distress.
Defendants’ defense The midwives claimed they were never told of the patient’s aversion to having a male physician examine her. The male physician and the birthing center denied knowledge of the request.
Verdict A $270,000 Washington verdict was returned.
Symptoms attributed to anesthesia: $2M
A 62-year-old woman underwent treatment for abnormal uterine bleeding (AUB). Hysteroscopy revealed a retroverted uterus containing a 3-cm polyp. During resection of the polyp, the uterus was perforated and bowel was drawn into the uterus. The injury was not recognized. The patient was discharged home the same day.
The next day, she phoned to report vomiting, abdominal pain, and urinary retention. The gynecologist attributed the symptoms to anesthesia and told the patient to allow more time for resolution.
The patient went to an emergency department (ED) 48 hours later with a distended abdomen and severe pain. She was transferred to a regional hospital with acute sepsis. A small bowel perforation was identified, requiring extensive treatment, including hysterectomy and resection of 27 cm of small bowel.
Patient’s claim The gynecologist was negligent in failing to recognize the injury intraoperatively. He didn’t examine the patient when she first reported symptoms.
Physician’s defense The injuries are known risks of the procedure. The patient’s complaints could reasonably be associated with postanesthesia residuals.
Verdict A $5 million Virginia verdict was reduced to $2 million by the statutory cap.
Did nosebleeds cause baby’s disabilities?
After a 33-year-old woman had a nosebleed she noted decreased fetal movement. At the ED, preterm labor was ruled out, fetal monitoring results were normal, and she was discharged. She returned that afternoon with a nosebleed. After 4 hours, when fetal monitoring results were normal, she was again discharged.
The next morning, an otolaryngologist cauterized her right nostril. After another nosebleed, the physician packed the right nasal cavity. She returned with bleeding from the left nostril and remained at the ear, nose, and throat (ENT) clinic for several hours until the bleeding stopped.
The following day, she returned to the ENT clinic asking that the packing be removed, but it needed to remain. She called a covering ObGyn to request anti-anxiety medication because the packing was making her feel claustrophobic.
The next day, after additional nosebleeds, she was taken to the ED with mild contractions. Her hematocrit was 25.6% and her hemoglobin level was 8.8 g/dL. When fetal heart-rate monitoring was nonreassuring, a cesarean delivery was expedited. The child has profound physical and developmental disabilities, uses a feeding tube and ventilator, and needs 24-hour care.
Parents’ claim The mother and fetus were never properly assessed or treated.
Defendants’ defense The physicians denied negligence and disputed the severity of most of the nosebleeds. At each ED presentation, hematocrit and hemoglobin levels were normal and the mother was stable at discharge. When fetal monitoring was performed, the results were normal. When the mother left the ENT clinic after the third visit, she was told to go to the ED or call 911 if she had another nosebleed, which she did not do. When she went to the ED with contractions, staff reacted to fetal distress and performed emergency cesarean delivery.
Verdict A Texas defense verdict was returned.
Difficult neonatal resuscitation: $8.4M
A nuchal cord was discovered at delivery. The child has cerebral palsy, a seizure disorder, and developmental delays. He cannot walk or talk, uses a feeding tube, and requires 24-hour care.
Parents’ claim Monitoring showed fetal distress for 5 hours, but the staff failed to perform a cesarean delivery or have a neonatal resuscitation team ready at delivery. After delivery, the baby was deprived of oxygen for 8 minutes before intubation. A back-up team should have been available.
Medical center’s defense Proper care was given. The resuscitation team was in a surgical suite.
Verdict An $8.4 million Georgia verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Delayed birth, intubation failure: $10M settlement
Two days shy of her due date, a woman went to an Army hospital to report bloody mucus discharge and sporadic contractions. She was 2 cm dilated and 50% effaced with the baby at –2 station. Fetal heart-rate monitor results were reassuring. She was discharged home but returned 5 hours later with increased pain and contractions. She was 5 cm dilated, 90% effaced; the baby was at –3 station. When contractions ceased, she was discharged. There had been no cervical change for 6 hours with a negative fern test. Fetal monitoring results were reassuring.
The woman returned 3 hours later with increased pain and contractions. She had a fever and high white blood cell and neutrophil counts. She was 6 cm dilated, 90% effaced, but the baby was still at –3 station. Ampicillin sodium/sulbactam sodium was administered. The ObGyn was called 4 times over the next 2.5 hours, when fetal monitoring results worsened and bradycardia developed. The nurses treated fetal distress by changing the maternal position and performing amnioinfusion. Then the ObGyn came to the bedside and ordered cesarean delivery. The baby was born severely compromised from hypoxic ischemic encephalopathy and metabolic acidosis. The pediatrician responsible for the baby’s resuscitation failed to get a response with bag ventilation after 5 minutes; 2 attempts at intubation failed. When the chief of pediatrics arrived at 15 minutes, the infant was successfully intubated. The baby was transferred to another facility. The child has profound disabilities.
Parents’ claim The hospital staff and physician did not deliver the baby in a timely manner when fetal distress was first noted. The pediatrician did not properly resuscitate the newborn.
Defendants’ defense Chorioamnionitis and funisitis caused or contributed to the infant’s injuries. Proper care was provided.
Verdict A $10 million Washington settlement was reached.
Did OCs cause this woman’s stroke?
A 40-year-old woman went to a clinic to obtain a prescription for birth control pills. A physician assistant (PA) conducted a complete physical examination. When no contraindications were found, a prescription for oral contraceptives (OCs) was provided. Two months later, the patient suffered a debilitating stroke. After the stroke, the patient was found to have a patent foramen ovale.
Patient’s claim The risks and benefits of the OC were not fully explained to the patient by the PA. She was not offered other contraceptive options. OCs are not safe for a woman her age due to a higher risk of stroke.
Defendants’ defense The patient used OCs in the past, and had received information from other physicians about their use. The stroke occurred because of the foramen ovale, not the use of OCs.
Verdict A Washington defense verdict was returned.
Ureter injury not treated until the next day
During cesarean delivery, the ObGyn identified a small ureteral injury but did not repair it. The next day, the ObGyn consulted a urologist and ordered an intravenous pyelogram (IVP). The urologist identified a ureteral obstruction and surgically repaired the injury. The patient was required to use a nephros-tomy bag for 6 months until the nephrostomy was reversed.
Patient’s claim The ObGyn was negligent in failing to immediately treat the ureter injury. The delay in repair necessitated the use of the nephrostomy bag.
Physician’s defense A ureter injury is a known complication of the procedure. The ObGyn did not cause the obstruction. Failure to perform an immediate repair was due to his concern that the patient might have lost too much blood during cesarean delivery. Bringing in the urologist the next day was appropriate. The patient completely recovered.
Verdict A $484,141 Mississippi verdict was returned.
Patient didn’t want male physician
After a woman experienced sexual assault in college, she did not want a male physician to perform a vaginal examination. When pregnant, she discussed that request with her nurse midwives. While she was in labor, a male ObGyn examined her.
Patient’s claim The nurse midwives failed to document her request not to be examined by a male clinician. The patient experienced severe emotional distress.
Defendants’ defense The midwives claimed they were never told of the patient’s aversion to having a male physician examine her. The male physician and the birthing center denied knowledge of the request.
Verdict A $270,000 Washington verdict was returned.
Symptoms attributed to anesthesia: $2M
A 62-year-old woman underwent treatment for abnormal uterine bleeding (AUB). Hysteroscopy revealed a retroverted uterus containing a 3-cm polyp. During resection of the polyp, the uterus was perforated and bowel was drawn into the uterus. The injury was not recognized. The patient was discharged home the same day.
The next day, she phoned to report vomiting, abdominal pain, and urinary retention. The gynecologist attributed the symptoms to anesthesia and told the patient to allow more time for resolution.
The patient went to an emergency department (ED) 48 hours later with a distended abdomen and severe pain. She was transferred to a regional hospital with acute sepsis. A small bowel perforation was identified, requiring extensive treatment, including hysterectomy and resection of 27 cm of small bowel.
Patient’s claim The gynecologist was negligent in failing to recognize the injury intraoperatively. He didn’t examine the patient when she first reported symptoms.
Physician’s defense The injuries are known risks of the procedure. The patient’s complaints could reasonably be associated with postanesthesia residuals.
Verdict A $5 million Virginia verdict was reduced to $2 million by the statutory cap.
Did nosebleeds cause baby’s disabilities?
After a 33-year-old woman had a nosebleed she noted decreased fetal movement. At the ED, preterm labor was ruled out, fetal monitoring results were normal, and she was discharged. She returned that afternoon with a nosebleed. After 4 hours, when fetal monitoring results were normal, she was again discharged.
The next morning, an otolaryngologist cauterized her right nostril. After another nosebleed, the physician packed the right nasal cavity. She returned with bleeding from the left nostril and remained at the ear, nose, and throat (ENT) clinic for several hours until the bleeding stopped.
The following day, she returned to the ENT clinic asking that the packing be removed, but it needed to remain. She called a covering ObGyn to request anti-anxiety medication because the packing was making her feel claustrophobic.
The next day, after additional nosebleeds, she was taken to the ED with mild contractions. Her hematocrit was 25.6% and her hemoglobin level was 8.8 g/dL. When fetal heart-rate monitoring was nonreassuring, a cesarean delivery was expedited. The child has profound physical and developmental disabilities, uses a feeding tube and ventilator, and needs 24-hour care.
Parents’ claim The mother and fetus were never properly assessed or treated.
Defendants’ defense The physicians denied negligence and disputed the severity of most of the nosebleeds. At each ED presentation, hematocrit and hemoglobin levels were normal and the mother was stable at discharge. When fetal monitoring was performed, the results were normal. When the mother left the ENT clinic after the third visit, she was told to go to the ED or call 911 if she had another nosebleed, which she did not do. When she went to the ED with contractions, staff reacted to fetal distress and performed emergency cesarean delivery.
Verdict A Texas defense verdict was returned.
Difficult neonatal resuscitation: $8.4M
A nuchal cord was discovered at delivery. The child has cerebral palsy, a seizure disorder, and developmental delays. He cannot walk or talk, uses a feeding tube, and requires 24-hour care.
Parents’ claim Monitoring showed fetal distress for 5 hours, but the staff failed to perform a cesarean delivery or have a neonatal resuscitation team ready at delivery. After delivery, the baby was deprived of oxygen for 8 minutes before intubation. A back-up team should have been available.
Medical center’s defense Proper care was given. The resuscitation team was in a surgical suite.
Verdict An $8.4 million Georgia verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In This Article
- Did OCs cause this woman’s stroke?
- Ureter injury not treated until the next day
- Patient didn’t want male physician
- Symptoms attributed to anesthesia: $2M
- Did nosebleeds cause baby’s disabilities?
- Difficult neonatal resuscitation: $8.4M

Mother dies after cesarean delivery: $4.5M verdict

Mother dies after cesarean delivery: $4.5M verdict
A 31-year-old woman gave birth to her first child by cesarean delivery. Over the next 3 days she reported nausea, vomiting, severe abdominal pain, and had an elevated heart rate. On day 4, she was discharged from the hospital. She went to the ObGyn’s office the next day and was told, after several hours, to return to the hospital. There she was found to have sepsis and acute renal failure. A transfer to another hospital was attempted that night, but she died during transport.
Estate's Claim: The ObGyn should have responded to her reported symptoms prior to discharge by ordering tests. The ObGyn should have called an ambulance to transport her to the hospital from his office.
Defendants’ Defense: The hospital settled for an undisclosed amount before the trial. The ObGyn claimed that there was no negligence in the patient’s treatment.
Verdict: A $4.5 million North Carolina verdict was returned.
Brain-damaged child dies at age 2
A woman was admitted to the hospital in labor. Ninety minutes later a nonreassuring fetal heart-rate tracing was noted. Two hours after that, the ObGyn decided to perform an emergency cesarean delivery.
The child was depressed at birth and required resuscitation. She was transferred to another hospital’s neonatal intensive care unit (NICU), where she was found to have had a severe and catastrophic brain injury. The child died at 2 years of age.
Parent's Claim: An emergency cesarean delivery should have been performed as soon as the fetal heart-rate tracing was found to be nonreassuring. The ObGyn failed to respond to phone calls from the nurses to report fetal distress.
Physician's Defense: The delivery was performed in a timely manner. Brain damage was due to encephalopathy that occurred prior to labor.
Verdict: A Mississippi defense verdict was returned.
Who or what was at fault for ureter injury?
A 45-year-old woman underwent hysterectomy performed by her ObGyn. During surgery, the patient’s ureter was injured. Several additional operations were needed to repair the injury.
Patient's Claim: The patient was not fully informed of the extent of the surgery or possible complications. The ObGyn was negligent in injuring the ureter.
Defendants' Defense: Three months after surgery, the physician entered notes into the patient’s chart that indicated that the ureter injuries were due to a defective monopolar device that had been provided by the hospital. Informed consent included surgical options and complications.
The hospital argued that its equipment was not defective; other surgeons had used the device without any problems. The ObGyn had not used the device before; any injuries were due to his inexperience and negligence.
Verdict: A $2 million South Carolina verdict was returned against the ObGyn. The hospital received a defense verdict.
Did excessive force cause child’s C7 injury?
During delivery, shoulder dystocia was encountered. The child has nerve root avulsion at C7 with damage to adjacent nerve trunks at C5–C6. As a result of the brachial plexus injury, the patient underwent cable grafting and muscle surgeries, but he has permanent weakness and dysfunction in his left arm.
Parent's Claim: Excessive force was used to deliver the child during manipulations for shoulder dystocia.
Physician's Defense: The ObGyn denied using excessive traction. She claimed that she had never used upward traction during a shoulder dystocia presentation. Suprapubic pressure, McRoberts’ maneuver, and delivery of the posterior arm were used. The damage occurred prior to delivery of the head.
Verdict An Illinois defense verdict was returned.

Laparoscopic sheath and coils found at exploratory surgery
In april 2007, a woman underwent a sterilization procedure (Essure) after which she reported pelvic pain. In September 2007, she consented to right salpingo-oophorectomy plus appendectomy. The ObGyn performed the surgery using a robotic device. After surgery, the pathology report indicated that the resected organs were normal and functional.
The patient moved to another state. She continued to have pain and sought treatment with another physician. A computed tomography (CT) scan more than 3 years after robotic surgery revealed foreign objects in the patient’s body. One full Essure coil, a non-fired coil, a second partial coil, and a robotic laparoscopy sheath were surgically removed.
Patient's Claim: The ObGyn was negligent in the performance of the sterilization and robotic surgery procedures. The healthy ovary and fallopian tube should not have been removed and caused her to have surgical menopause.
Physician's defense: The right ovary appeared diseased. The Essure device dropped the coils. The robot malfunctioned during the salpingo-oophorectomy.
Verdict: A $110,513 Oregon verdict was returned, including $10,500 in medical expenses and $100,000 for pain and mental anguish.
Discrepancy in fundal height; child has CP
During her second pregnancy, a 37-year-old woman saw Dr. A, her ObGyn, for regular prenatal care. At 37 weeks’ gestation, the fundal height was not consistent with the fetus’ gestational age: the measurement was higher by 2 cm. No additional testing was scheduled.
At 39.5 weeks’ gestation, the mother reported decreased fetal movement. Because her regular ObGyn was on vacation, she was evaluated by another ObGyn (Dr. B). The fetal heart-rate monitor showed nonreactive results with minimal variability. Dr. B told the mother to drive herself to the emergency department (ED) for additional evaluation. At the hospital, when fetal heart-rate monitoring confirmed fetal distress, an emergency cesarean delivery was performed.
At birth, the baby was not breathing and resuscitation began. The infant was taken to a transitional care unit and then to the NICU, where he was intubated. Cord blood testing confirmed metabolic acidosis. The baby was later found to have dystonic cerebral palsy (CP). He is unable to speak, walk, eat, or care for himself, and he requires 24/7 nursing care.
Parents' Claim: Dr. A failed to order testing after the fundal height discrepancy was found. Testing could have led to an earlier delivery and avoided the injury. The pediatrician failed to ensure adequate oxygenation after delivery. The baby should have been transferred immediately to the NICU and intubated.
Physician's Defense: The fundal height discrepancy was explained by the baby’s position within the uterus. The pediatrician acted heroically to save the child’s life.
Verdict: A $3.5 million Massachusetts settlement was reached.
NT scans misread, not reported; child has Down syndrome
At 13 weeks’ gestation, a 38-year-old woman saw a maternal-fetal medicine (MFM) specialist, who interpreted a nuchal translucency (NT) scan as normal. At 20 weeks’ gestation, an ObGyn performed a second screening that indicated the fetus was at high risk for Down syndrome. However, no further testing was ordered.
At 26.5 weeks’ gestation, amniocentesis was performed after ultrasonography and an echocardiogram revealed fetal abnormalities. A diagnosis of Down syndrome was made at 29 weeks’ gestation, too late for termination of pregnancy.
Parent's Claim: The MFM specialist misread the first NT scan. The ObGyn did not inform the mother of the results of the second screening. Proper interpretation and reporting would have initiated further testing and determination that the baby had Down syndrome before the deadline for termination of pregnancy.
Defendants' Defense: The case was settled during trial.
Verdict: A $3 million New Jersey settlement was reached, including $2 million from the medical center where the second test was performed, $940,000 from the ObGyn, and $60,000 from the MFM specialist.
Uterine rupture, baby dies: $2.15M award
At 38 weeks’ gestation, a mother was admitted to a hospital for induction of labor due to pregnancy-induced hypertension. The fetus was estimated to be large for its gestational age. A uterine rupture occurred during labor. The baby was stillborn.
Parents' Claim: The uterine rupture was not immediately recognized. The ObGyn failed to come to the mother’s bedside until after the fetus had receded up the birth canal, which indicated that a rupture was occurring. The ObGyn ordered oxytocin instead of performing an immediate cesarean delivery. Eleven minutes later, the cesarean was ordered, but the baby had died.
Physician's Defense: There was no negligence; proper protocols were followed. A uterine rupture cannot be predicted.
Verdict: A $650,000 settlement was reached with the hospital before trial. Because the ObGyn was employed by a federally qualified clinic, the matter was filed in federal court. The Illinois court issued a bench decision awarding $1.5 million.
Migrated IUD causes years of pain
In september 2006, an ObGyn inserted an intrauterine device (IUD) in a patient. In February 2007, the patient had an ectopic pregnancy. The IUD was not found during dilation and curettage. The patient continued to report pain to the ObGyn. She sought treatment from another physician in November 2010 due to continuing pain. A CT scan revealed that the IUD had migrated to her abdomen. The IUD was surgically removed.
Patient's Claim: The ObGyn was unwilling to figure out why the patient had continuing pain, and told her to “just deal with it.” He should have found and removed the IUD after the ectopic pregnancy.
Physician's Defense: It was reasonable to assume that the IUD had been expelled, as 2 ultrasonographies performed after ectopic pregnancy revealed nothing. Since the IUD had not caused an abscess, infection, or inflammation, the patient suffered no injury.
Verdict: A Virginia defense verdict was returned.
Profoundly disabled child dies at age 5
A 17-year-old woman with a history of miscarriage received prenatal care from her ObGyn. A July due date was established by ultrasonography in January.
In May, the mother went to the ED with pelvic pain. She was treated for preterm labor and discharged 2 days later.
In early July, ultrasonography showed a fetus in cephalic position with a posterior-located placenta.
At a prenatal examination a week later, the patient reported vaginal discharge. Her ObGyn suspected premature rupture of membranes (PROM) and admitted her to the hospital. Oxytocin was used to induce labor. Intact membranes were artificially ruptured and an internal fetal heart-rate monitor was placed. The ObGyn recorded that the pregnancy was at term.
Hours later, the mother told the nurses that she thought the fetal monitor had become disconnected; the monitor’s placement was not confirmed. The mother was given a sedative. After a few hours, she awoke with intense pain and dizziness. She used her call button, but no one immediately responded.
When full cervical dilation was reached, the fetus was at –1, 0 station. When the fetus reached +1 station, delivery was attempted. The baby was delivered using vacuum extraction.
The child’s Apgar score was 0 at 1 minute of life. Resuscitation was started with intubation and mechanical ventilation. The child’s birth weight was 6.87 lb; arterial blood gas pH measured 6.9; and gestational age was estimated at 38 to 39 weeks.
An electro-encephalogram performed in the NICU suggested intraventricular hemorrhage. The child was found to have perinatal asphyxia, hypoxic ischemic encephalopathy, left parietal skull fracture and cephalohematoma, severe metabolic acidosis, suspected sepsis, transient oliguria, and seizure episodes. The baby was hospitalized for 3.5 months and then followed regularly.
The mother and child moved from Puerto Rico to New York City to obtain better medical care. The child was regularly hospitalized until she died at age 5.
Parent's Claim: There was a discrepancy in gestational age assessment. The nurses failed to monitor fetal heart-rate tracings at proper intervals, and they were unresponsive to the mother. Informed consent did not include vacuum extraction.
Defendants' Defense: The case was settled during trial.
Verdict: A $1.125 million Puerto Rico settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Mother dies after cesarean delivery: $4.5M verdict
A 31-year-old woman gave birth to her first child by cesarean delivery. Over the next 3 days she reported nausea, vomiting, severe abdominal pain, and had an elevated heart rate. On day 4, she was discharged from the hospital. She went to the ObGyn’s office the next day and was told, after several hours, to return to the hospital. There she was found to have sepsis and acute renal failure. A transfer to another hospital was attempted that night, but she died during transport.
Estate's Claim: The ObGyn should have responded to her reported symptoms prior to discharge by ordering tests. The ObGyn should have called an ambulance to transport her to the hospital from his office.
Defendants’ Defense: The hospital settled for an undisclosed amount before the trial. The ObGyn claimed that there was no negligence in the patient’s treatment.
Verdict: A $4.5 million North Carolina verdict was returned.
Brain-damaged child dies at age 2
A woman was admitted to the hospital in labor. Ninety minutes later a nonreassuring fetal heart-rate tracing was noted. Two hours after that, the ObGyn decided to perform an emergency cesarean delivery.
The child was depressed at birth and required resuscitation. She was transferred to another hospital’s neonatal intensive care unit (NICU), where she was found to have had a severe and catastrophic brain injury. The child died at 2 years of age.
Parent's Claim: An emergency cesarean delivery should have been performed as soon as the fetal heart-rate tracing was found to be nonreassuring. The ObGyn failed to respond to phone calls from the nurses to report fetal distress.
Physician's Defense: The delivery was performed in a timely manner. Brain damage was due to encephalopathy that occurred prior to labor.
Verdict: A Mississippi defense verdict was returned.
Who or what was at fault for ureter injury?
A 45-year-old woman underwent hysterectomy performed by her ObGyn. During surgery, the patient’s ureter was injured. Several additional operations were needed to repair the injury.
Patient's Claim: The patient was not fully informed of the extent of the surgery or possible complications. The ObGyn was negligent in injuring the ureter.
Defendants' Defense: Three months after surgery, the physician entered notes into the patient’s chart that indicated that the ureter injuries were due to a defective monopolar device that had been provided by the hospital. Informed consent included surgical options and complications.
The hospital argued that its equipment was not defective; other surgeons had used the device without any problems. The ObGyn had not used the device before; any injuries were due to his inexperience and negligence.
Verdict: A $2 million South Carolina verdict was returned against the ObGyn. The hospital received a defense verdict.
Did excessive force cause child’s C7 injury?
During delivery, shoulder dystocia was encountered. The child has nerve root avulsion at C7 with damage to adjacent nerve trunks at C5–C6. As a result of the brachial plexus injury, the patient underwent cable grafting and muscle surgeries, but he has permanent weakness and dysfunction in his left arm.
Parent's Claim: Excessive force was used to deliver the child during manipulations for shoulder dystocia.
Physician's Defense: The ObGyn denied using excessive traction. She claimed that she had never used upward traction during a shoulder dystocia presentation. Suprapubic pressure, McRoberts’ maneuver, and delivery of the posterior arm were used. The damage occurred prior to delivery of the head.
Verdict An Illinois defense verdict was returned.
Laparoscopic sheath and coils found at exploratory surgery
In april 2007, a woman underwent a sterilization procedure (Essure) after which she reported pelvic pain. In September 2007, she consented to right salpingo-oophorectomy plus appendectomy. The ObGyn performed the surgery using a robotic device. After surgery, the pathology report indicated that the resected organs were normal and functional.
The patient moved to another state. She continued to have pain and sought treatment with another physician. A computed tomography (CT) scan more than 3 years after robotic surgery revealed foreign objects in the patient’s body. One full Essure coil, a non-fired coil, a second partial coil, and a robotic laparoscopy sheath were surgically removed.
Patient's Claim: The ObGyn was negligent in the performance of the sterilization and robotic surgery procedures. The healthy ovary and fallopian tube should not have been removed and caused her to have surgical menopause.
Physician's defense: The right ovary appeared diseased. The Essure device dropped the coils. The robot malfunctioned during the salpingo-oophorectomy.
Verdict: A $110,513 Oregon verdict was returned, including $10,500 in medical expenses and $100,000 for pain and mental anguish.
Discrepancy in fundal height; child has CP
During her second pregnancy, a 37-year-old woman saw Dr. A, her ObGyn, for regular prenatal care. At 37 weeks’ gestation, the fundal height was not consistent with the fetus’ gestational age: the measurement was higher by 2 cm. No additional testing was scheduled.
At 39.5 weeks’ gestation, the mother reported decreased fetal movement. Because her regular ObGyn was on vacation, she was evaluated by another ObGyn (Dr. B). The fetal heart-rate monitor showed nonreactive results with minimal variability. Dr. B told the mother to drive herself to the emergency department (ED) for additional evaluation. At the hospital, when fetal heart-rate monitoring confirmed fetal distress, an emergency cesarean delivery was performed.
At birth, the baby was not breathing and resuscitation began. The infant was taken to a transitional care unit and then to the NICU, where he was intubated. Cord blood testing confirmed metabolic acidosis. The baby was later found to have dystonic cerebral palsy (CP). He is unable to speak, walk, eat, or care for himself, and he requires 24/7 nursing care.
Parents' Claim: Dr. A failed to order testing after the fundal height discrepancy was found. Testing could have led to an earlier delivery and avoided the injury. The pediatrician failed to ensure adequate oxygenation after delivery. The baby should have been transferred immediately to the NICU and intubated.
Physician's Defense: The fundal height discrepancy was explained by the baby’s position within the uterus. The pediatrician acted heroically to save the child’s life.
Verdict: A $3.5 million Massachusetts settlement was reached.
NT scans misread, not reported; child has Down syndrome
At 13 weeks’ gestation, a 38-year-old woman saw a maternal-fetal medicine (MFM) specialist, who interpreted a nuchal translucency (NT) scan as normal. At 20 weeks’ gestation, an ObGyn performed a second screening that indicated the fetus was at high risk for Down syndrome. However, no further testing was ordered.
At 26.5 weeks’ gestation, amniocentesis was performed after ultrasonography and an echocardiogram revealed fetal abnormalities. A diagnosis of Down syndrome was made at 29 weeks’ gestation, too late for termination of pregnancy.
Parent's Claim: The MFM specialist misread the first NT scan. The ObGyn did not inform the mother of the results of the second screening. Proper interpretation and reporting would have initiated further testing and determination that the baby had Down syndrome before the deadline for termination of pregnancy.
Defendants' Defense: The case was settled during trial.
Verdict: A $3 million New Jersey settlement was reached, including $2 million from the medical center where the second test was performed, $940,000 from the ObGyn, and $60,000 from the MFM specialist.
Uterine rupture, baby dies: $2.15M award
At 38 weeks’ gestation, a mother was admitted to a hospital for induction of labor due to pregnancy-induced hypertension. The fetus was estimated to be large for its gestational age. A uterine rupture occurred during labor. The baby was stillborn.
Parents' Claim: The uterine rupture was not immediately recognized. The ObGyn failed to come to the mother’s bedside until after the fetus had receded up the birth canal, which indicated that a rupture was occurring. The ObGyn ordered oxytocin instead of performing an immediate cesarean delivery. Eleven minutes later, the cesarean was ordered, but the baby had died.
Physician's Defense: There was no negligence; proper protocols were followed. A uterine rupture cannot be predicted.
Verdict: A $650,000 settlement was reached with the hospital before trial. Because the ObGyn was employed by a federally qualified clinic, the matter was filed in federal court. The Illinois court issued a bench decision awarding $1.5 million.
Migrated IUD causes years of pain
In september 2006, an ObGyn inserted an intrauterine device (IUD) in a patient. In February 2007, the patient had an ectopic pregnancy. The IUD was not found during dilation and curettage. The patient continued to report pain to the ObGyn. She sought treatment from another physician in November 2010 due to continuing pain. A CT scan revealed that the IUD had migrated to her abdomen. The IUD was surgically removed.
Patient's Claim: The ObGyn was unwilling to figure out why the patient had continuing pain, and told her to “just deal with it.” He should have found and removed the IUD after the ectopic pregnancy.
Physician's Defense: It was reasonable to assume that the IUD had been expelled, as 2 ultrasonographies performed after ectopic pregnancy revealed nothing. Since the IUD had not caused an abscess, infection, or inflammation, the patient suffered no injury.
Verdict: A Virginia defense verdict was returned.
Profoundly disabled child dies at age 5
A 17-year-old woman with a history of miscarriage received prenatal care from her ObGyn. A July due date was established by ultrasonography in January.
In May, the mother went to the ED with pelvic pain. She was treated for preterm labor and discharged 2 days later.
In early July, ultrasonography showed a fetus in cephalic position with a posterior-located placenta.
At a prenatal examination a week later, the patient reported vaginal discharge. Her ObGyn suspected premature rupture of membranes (PROM) and admitted her to the hospital. Oxytocin was used to induce labor. Intact membranes were artificially ruptured and an internal fetal heart-rate monitor was placed. The ObGyn recorded that the pregnancy was at term.
Hours later, the mother told the nurses that she thought the fetal monitor had become disconnected; the monitor’s placement was not confirmed. The mother was given a sedative. After a few hours, she awoke with intense pain and dizziness. She used her call button, but no one immediately responded.
When full cervical dilation was reached, the fetus was at –1, 0 station. When the fetus reached +1 station, delivery was attempted. The baby was delivered using vacuum extraction.
The child’s Apgar score was 0 at 1 minute of life. Resuscitation was started with intubation and mechanical ventilation. The child’s birth weight was 6.87 lb; arterial blood gas pH measured 6.9; and gestational age was estimated at 38 to 39 weeks.
An electro-encephalogram performed in the NICU suggested intraventricular hemorrhage. The child was found to have perinatal asphyxia, hypoxic ischemic encephalopathy, left parietal skull fracture and cephalohematoma, severe metabolic acidosis, suspected sepsis, transient oliguria, and seizure episodes. The baby was hospitalized for 3.5 months and then followed regularly.
The mother and child moved from Puerto Rico to New York City to obtain better medical care. The child was regularly hospitalized until she died at age 5.
Parent's Claim: There was a discrepancy in gestational age assessment. The nurses failed to monitor fetal heart-rate tracings at proper intervals, and they were unresponsive to the mother. Informed consent did not include vacuum extraction.
Defendants' Defense: The case was settled during trial.
Verdict: A $1.125 million Puerto Rico settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Mother dies after cesarean delivery: $4.5M verdict
A 31-year-old woman gave birth to her first child by cesarean delivery. Over the next 3 days she reported nausea, vomiting, severe abdominal pain, and had an elevated heart rate. On day 4, she was discharged from the hospital. She went to the ObGyn’s office the next day and was told, after several hours, to return to the hospital. There she was found to have sepsis and acute renal failure. A transfer to another hospital was attempted that night, but she died during transport.
Estate's Claim: The ObGyn should have responded to her reported symptoms prior to discharge by ordering tests. The ObGyn should have called an ambulance to transport her to the hospital from his office.
Defendants’ Defense: The hospital settled for an undisclosed amount before the trial. The ObGyn claimed that there was no negligence in the patient’s treatment.
Verdict: A $4.5 million North Carolina verdict was returned.
Brain-damaged child dies at age 2
A woman was admitted to the hospital in labor. Ninety minutes later a nonreassuring fetal heart-rate tracing was noted. Two hours after that, the ObGyn decided to perform an emergency cesarean delivery.
The child was depressed at birth and required resuscitation. She was transferred to another hospital’s neonatal intensive care unit (NICU), where she was found to have had a severe and catastrophic brain injury. The child died at 2 years of age.
Parent's Claim: An emergency cesarean delivery should have been performed as soon as the fetal heart-rate tracing was found to be nonreassuring. The ObGyn failed to respond to phone calls from the nurses to report fetal distress.
Physician's Defense: The delivery was performed in a timely manner. Brain damage was due to encephalopathy that occurred prior to labor.
Verdict: A Mississippi defense verdict was returned.
Who or what was at fault for ureter injury?
A 45-year-old woman underwent hysterectomy performed by her ObGyn. During surgery, the patient’s ureter was injured. Several additional operations were needed to repair the injury.
Patient's Claim: The patient was not fully informed of the extent of the surgery or possible complications. The ObGyn was negligent in injuring the ureter.
Defendants' Defense: Three months after surgery, the physician entered notes into the patient’s chart that indicated that the ureter injuries were due to a defective monopolar device that had been provided by the hospital. Informed consent included surgical options and complications.
The hospital argued that its equipment was not defective; other surgeons had used the device without any problems. The ObGyn had not used the device before; any injuries were due to his inexperience and negligence.
Verdict: A $2 million South Carolina verdict was returned against the ObGyn. The hospital received a defense verdict.
Did excessive force cause child’s C7 injury?
During delivery, shoulder dystocia was encountered. The child has nerve root avulsion at C7 with damage to adjacent nerve trunks at C5–C6. As a result of the brachial plexus injury, the patient underwent cable grafting and muscle surgeries, but he has permanent weakness and dysfunction in his left arm.
Parent's Claim: Excessive force was used to deliver the child during manipulations for shoulder dystocia.
Physician's Defense: The ObGyn denied using excessive traction. She claimed that she had never used upward traction during a shoulder dystocia presentation. Suprapubic pressure, McRoberts’ maneuver, and delivery of the posterior arm were used. The damage occurred prior to delivery of the head.
Verdict An Illinois defense verdict was returned.
Laparoscopic sheath and coils found at exploratory surgery
In april 2007, a woman underwent a sterilization procedure (Essure) after which she reported pelvic pain. In September 2007, she consented to right salpingo-oophorectomy plus appendectomy. The ObGyn performed the surgery using a robotic device. After surgery, the pathology report indicated that the resected organs were normal and functional.
The patient moved to another state. She continued to have pain and sought treatment with another physician. A computed tomography (CT) scan more than 3 years after robotic surgery revealed foreign objects in the patient’s body. One full Essure coil, a non-fired coil, a second partial coil, and a robotic laparoscopy sheath were surgically removed.
Patient's Claim: The ObGyn was negligent in the performance of the sterilization and robotic surgery procedures. The healthy ovary and fallopian tube should not have been removed and caused her to have surgical menopause.
Physician's defense: The right ovary appeared diseased. The Essure device dropped the coils. The robot malfunctioned during the salpingo-oophorectomy.
Verdict: A $110,513 Oregon verdict was returned, including $10,500 in medical expenses and $100,000 for pain and mental anguish.
Discrepancy in fundal height; child has CP
During her second pregnancy, a 37-year-old woman saw Dr. A, her ObGyn, for regular prenatal care. At 37 weeks’ gestation, the fundal height was not consistent with the fetus’ gestational age: the measurement was higher by 2 cm. No additional testing was scheduled.
At 39.5 weeks’ gestation, the mother reported decreased fetal movement. Because her regular ObGyn was on vacation, she was evaluated by another ObGyn (Dr. B). The fetal heart-rate monitor showed nonreactive results with minimal variability. Dr. B told the mother to drive herself to the emergency department (ED) for additional evaluation. At the hospital, when fetal heart-rate monitoring confirmed fetal distress, an emergency cesarean delivery was performed.
At birth, the baby was not breathing and resuscitation began. The infant was taken to a transitional care unit and then to the NICU, where he was intubated. Cord blood testing confirmed metabolic acidosis. The baby was later found to have dystonic cerebral palsy (CP). He is unable to speak, walk, eat, or care for himself, and he requires 24/7 nursing care.
Parents' Claim: Dr. A failed to order testing after the fundal height discrepancy was found. Testing could have led to an earlier delivery and avoided the injury. The pediatrician failed to ensure adequate oxygenation after delivery. The baby should have been transferred immediately to the NICU and intubated.
Physician's Defense: The fundal height discrepancy was explained by the baby’s position within the uterus. The pediatrician acted heroically to save the child’s life.
Verdict: A $3.5 million Massachusetts settlement was reached.
NT scans misread, not reported; child has Down syndrome
At 13 weeks’ gestation, a 38-year-old woman saw a maternal-fetal medicine (MFM) specialist, who interpreted a nuchal translucency (NT) scan as normal. At 20 weeks’ gestation, an ObGyn performed a second screening that indicated the fetus was at high risk for Down syndrome. However, no further testing was ordered.
At 26.5 weeks’ gestation, amniocentesis was performed after ultrasonography and an echocardiogram revealed fetal abnormalities. A diagnosis of Down syndrome was made at 29 weeks’ gestation, too late for termination of pregnancy.
Parent's Claim: The MFM specialist misread the first NT scan. The ObGyn did not inform the mother of the results of the second screening. Proper interpretation and reporting would have initiated further testing and determination that the baby had Down syndrome before the deadline for termination of pregnancy.
Defendants' Defense: The case was settled during trial.
Verdict: A $3 million New Jersey settlement was reached, including $2 million from the medical center where the second test was performed, $940,000 from the ObGyn, and $60,000 from the MFM specialist.
Uterine rupture, baby dies: $2.15M award
At 38 weeks’ gestation, a mother was admitted to a hospital for induction of labor due to pregnancy-induced hypertension. The fetus was estimated to be large for its gestational age. A uterine rupture occurred during labor. The baby was stillborn.
Parents' Claim: The uterine rupture was not immediately recognized. The ObGyn failed to come to the mother’s bedside until after the fetus had receded up the birth canal, which indicated that a rupture was occurring. The ObGyn ordered oxytocin instead of performing an immediate cesarean delivery. Eleven minutes later, the cesarean was ordered, but the baby had died.
Physician's Defense: There was no negligence; proper protocols were followed. A uterine rupture cannot be predicted.
Verdict: A $650,000 settlement was reached with the hospital before trial. Because the ObGyn was employed by a federally qualified clinic, the matter was filed in federal court. The Illinois court issued a bench decision awarding $1.5 million.
Migrated IUD causes years of pain
In september 2006, an ObGyn inserted an intrauterine device (IUD) in a patient. In February 2007, the patient had an ectopic pregnancy. The IUD was not found during dilation and curettage. The patient continued to report pain to the ObGyn. She sought treatment from another physician in November 2010 due to continuing pain. A CT scan revealed that the IUD had migrated to her abdomen. The IUD was surgically removed.
Patient's Claim: The ObGyn was unwilling to figure out why the patient had continuing pain, and told her to “just deal with it.” He should have found and removed the IUD after the ectopic pregnancy.
Physician's Defense: It was reasonable to assume that the IUD had been expelled, as 2 ultrasonographies performed after ectopic pregnancy revealed nothing. Since the IUD had not caused an abscess, infection, or inflammation, the patient suffered no injury.
Verdict: A Virginia defense verdict was returned.
Profoundly disabled child dies at age 5
A 17-year-old woman with a history of miscarriage received prenatal care from her ObGyn. A July due date was established by ultrasonography in January.
In May, the mother went to the ED with pelvic pain. She was treated for preterm labor and discharged 2 days later.
In early July, ultrasonography showed a fetus in cephalic position with a posterior-located placenta.
At a prenatal examination a week later, the patient reported vaginal discharge. Her ObGyn suspected premature rupture of membranes (PROM) and admitted her to the hospital. Oxytocin was used to induce labor. Intact membranes were artificially ruptured and an internal fetal heart-rate monitor was placed. The ObGyn recorded that the pregnancy was at term.
Hours later, the mother told the nurses that she thought the fetal monitor had become disconnected; the monitor’s placement was not confirmed. The mother was given a sedative. After a few hours, she awoke with intense pain and dizziness. She used her call button, but no one immediately responded.
When full cervical dilation was reached, the fetus was at –1, 0 station. When the fetus reached +1 station, delivery was attempted. The baby was delivered using vacuum extraction.
The child’s Apgar score was 0 at 1 minute of life. Resuscitation was started with intubation and mechanical ventilation. The child’s birth weight was 6.87 lb; arterial blood gas pH measured 6.9; and gestational age was estimated at 38 to 39 weeks.
An electro-encephalogram performed in the NICU suggested intraventricular hemorrhage. The child was found to have perinatal asphyxia, hypoxic ischemic encephalopathy, left parietal skull fracture and cephalohematoma, severe metabolic acidosis, suspected sepsis, transient oliguria, and seizure episodes. The baby was hospitalized for 3.5 months and then followed regularly.
The mother and child moved from Puerto Rico to New York City to obtain better medical care. The child was regularly hospitalized until she died at age 5.
Parent's Claim: There was a discrepancy in gestational age assessment. The nurses failed to monitor fetal heart-rate tracings at proper intervals, and they were unresponsive to the mother. Informed consent did not include vacuum extraction.
Defendants' Defense: The case was settled during trial.
Verdict: A $1.125 million Puerto Rico settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
IN THIS ARTICLE
- Brain-damaged child dies at age 2
- Who or what was at fault for ureter injury?
- Did excessive force cause child’s C7 injury?
- Laparoscopic sheath and coils found at exploratory surgery
- Discrepancy in fundal height; child has CP
- NT scans misread, not reported; child has Down syndrome
- Uterine rupture, baby dies: $2.15M award
- Migrated IUD causes years of pain
- Profoundly disabled child dies at age 5
Surgical Sponge Left After Hysterectomy
In January 2009, an Alabama woman with multiple sclerosis visited Dr T., the defendant ob-gyn, for severe pelvic pain. Dr T. made a diagnosis of a fibroid uterus and ovarian cysts. The patient underwent a transvaginal hysterectomy, but her pain persisted after the surgery.
After being discharged, she discovered a long strip of packing protruding from her vagina, which Dr T. instructed her to extract herself. After doing so, however, the patient continued to have pain, bleeding, and a foul–smelling vaginal discharge. Dr T. diagnosed urinary tract infection and bacterial vaginosis. Antibiotics and pain medication were prescribed, but the patient’s pelvic pain persisted.
In April 2009, Dr T. ordered CT to rule out an abscess or a foreign body. A gauze surgical sponge, left at the conclusion of the patient’s hysterectomy, was detected. Surgery was performed to remove the sponge.
The plaintiff alleged negligence in the sponge’s retention, maintaining that not only was a second surgery required, but that her multiple sclerosis was exacerbated as a result of the entire situation.
The defendant claimed that tests had been performed to investigate the possibility of a foreign body, and that as soon as the surgical sponge was detected, it was removed.
What was the outcome? >>
OUTCOME
According to a published report, a defense verdict was returned.
COMMENT
The defense verdict here is surprising. In most cases in which surgical instruments are left in patients, plaintiffs prevail by using a legal doctrine known as res ipsa loquitur—a Latin legal term of art meaning “the thing speaks for itself.” This is generally requested as a jury charge, wherein the plaintiff asks the judge to explain to the jury that they may find negligence from a certain unusual fact that cannot have occurred without negligence (eg, a sponge left in a patient after surgery).
The history of res ipsa loquitur dates back to 1863 in the case of Byrne v Boadle, in which a barrel of flour rolled from a second-story window and struck a pedestrian below, causing serious injury. The defendants’ claim was that the plaintiff (who had no recollection of the event) was unable to show evidence of negligence. The court created the doctrine, holding that the fact of the accident itself provided ample evidence of negligence, excusing the plaintiff from the burden of proving that negligent acts (eg, inadequate harnessing of the barrels) led to the accident.
Why is this important? The concept of res ipsa loquitur is commonly invoked in medical malpractice actions. It generally requires three elements: the plaintiff suffers an unusual injury, the plaintiff was under the exclusive control of the medical defendants, and the plaintiff did not contribute to the injury.
In a leading malpractice case, Ybarra v Spangard (1944), a plaintiff awoke after undergoing an appendectomy with difficulty moving his arm as a result of reflex sympathetic dystrophy. The plaintiff alleged negligence stemming from the intraoperative positioning of his body, but he could not show the specifics of positioning during surgery. The court held that the patient’s body was under the exclusive control of the team of medical professionals, and that negligence could be inferred because loss of an arm’s function following an appendectomy is unusual and cannot occur without some negligent action involved.
When successfully used in malpractice cases, res ipsa loquitur relieves the plaintiff of the need to prove by a preponderance of the evidence the actions that led to the breach of the standard of care. In order to prevail, she must show the injury, the defendants’ exclusive control, and no contribution on her part. Practically, this permits the case to withstand defense motions for summary judgment and to be brought before a jury with scant to no evidence on the purported negligent act itself—merely the unusual injury and the defendants’ exclusive control.
Traditional application of the doctrine was limited to cases in which negligence was obvious to a layperson: for example, instruments left in patients or amputation of the wrong leg—the thing that “speaks for itself.” Newer evolution of the doctrine is problematic when extended to cases in which expert testimony should be required to demonstrate the standard of care and the defendant’s breach of it. When courts are willing to extend the doctrine, the plaintiff is awarded the presumption of negligence, which the defendant(s) must now come forward to rebut. For example, in a 2010 case in Illinois, a jury returned a $3.6 million verdict following the death of a 2-year-old who had had a seizure. The child’s seizure was reportedly controlled, but he was allegedly hypoventilated while undergoing CT and unfortunately died. The plaintiff was permitted to invoke the doctrine of res ipsa loquitur and was allowed the presumption that medical negligence was responsible for the outcome.
Unlike the surgical sponge left in a patient, matters of central nervous system status, monitoring during CT, airway and ventilation status, hypoxemia, and postictal states are not within the experience of the typical juror. The negligent “thing” is not a sponge that “speaks for itself,” but a course of actions that requires expert testimony precisely because it does not “speak for itself.” In cases in which an injury is beyond the average juror’s realm of experience, courts should require the plaintiff to prove her case. The doctrine should not “evolve” to excuse a plaintiff from the burden of producing evidence and persuading a jury. This forms the foundation of our civil law system. —DML
In January 2009, an Alabama woman with multiple sclerosis visited Dr T., the defendant ob-gyn, for severe pelvic pain. Dr T. made a diagnosis of a fibroid uterus and ovarian cysts. The patient underwent a transvaginal hysterectomy, but her pain persisted after the surgery.
After being discharged, she discovered a long strip of packing protruding from her vagina, which Dr T. instructed her to extract herself. After doing so, however, the patient continued to have pain, bleeding, and a foul–smelling vaginal discharge. Dr T. diagnosed urinary tract infection and bacterial vaginosis. Antibiotics and pain medication were prescribed, but the patient’s pelvic pain persisted.
In April 2009, Dr T. ordered CT to rule out an abscess or a foreign body. A gauze surgical sponge, left at the conclusion of the patient’s hysterectomy, was detected. Surgery was performed to remove the sponge.
The plaintiff alleged negligence in the sponge’s retention, maintaining that not only was a second surgery required, but that her multiple sclerosis was exacerbated as a result of the entire situation.
The defendant claimed that tests had been performed to investigate the possibility of a foreign body, and that as soon as the surgical sponge was detected, it was removed.
What was the outcome? >>
OUTCOME
According to a published report, a defense verdict was returned.
COMMENT
The defense verdict here is surprising. In most cases in which surgical instruments are left in patients, plaintiffs prevail by using a legal doctrine known as res ipsa loquitur—a Latin legal term of art meaning “the thing speaks for itself.” This is generally requested as a jury charge, wherein the plaintiff asks the judge to explain to the jury that they may find negligence from a certain unusual fact that cannot have occurred without negligence (eg, a sponge left in a patient after surgery).
The history of res ipsa loquitur dates back to 1863 in the case of Byrne v Boadle, in which a barrel of flour rolled from a second-story window and struck a pedestrian below, causing serious injury. The defendants’ claim was that the plaintiff (who had no recollection of the event) was unable to show evidence of negligence. The court created the doctrine, holding that the fact of the accident itself provided ample evidence of negligence, excusing the plaintiff from the burden of proving that negligent acts (eg, inadequate harnessing of the barrels) led to the accident.
Why is this important? The concept of res ipsa loquitur is commonly invoked in medical malpractice actions. It generally requires three elements: the plaintiff suffers an unusual injury, the plaintiff was under the exclusive control of the medical defendants, and the plaintiff did not contribute to the injury.
In a leading malpractice case, Ybarra v Spangard (1944), a plaintiff awoke after undergoing an appendectomy with difficulty moving his arm as a result of reflex sympathetic dystrophy. The plaintiff alleged negligence stemming from the intraoperative positioning of his body, but he could not show the specifics of positioning during surgery. The court held that the patient’s body was under the exclusive control of the team of medical professionals, and that negligence could be inferred because loss of an arm’s function following an appendectomy is unusual and cannot occur without some negligent action involved.
When successfully used in malpractice cases, res ipsa loquitur relieves the plaintiff of the need to prove by a preponderance of the evidence the actions that led to the breach of the standard of care. In order to prevail, she must show the injury, the defendants’ exclusive control, and no contribution on her part. Practically, this permits the case to withstand defense motions for summary judgment and to be brought before a jury with scant to no evidence on the purported negligent act itself—merely the unusual injury and the defendants’ exclusive control.
Traditional application of the doctrine was limited to cases in which negligence was obvious to a layperson: for example, instruments left in patients or amputation of the wrong leg—the thing that “speaks for itself.” Newer evolution of the doctrine is problematic when extended to cases in which expert testimony should be required to demonstrate the standard of care and the defendant’s breach of it. When courts are willing to extend the doctrine, the plaintiff is awarded the presumption of negligence, which the defendant(s) must now come forward to rebut. For example, in a 2010 case in Illinois, a jury returned a $3.6 million verdict following the death of a 2-year-old who had had a seizure. The child’s seizure was reportedly controlled, but he was allegedly hypoventilated while undergoing CT and unfortunately died. The plaintiff was permitted to invoke the doctrine of res ipsa loquitur and was allowed the presumption that medical negligence was responsible for the outcome.
Unlike the surgical sponge left in a patient, matters of central nervous system status, monitoring during CT, airway and ventilation status, hypoxemia, and postictal states are not within the experience of the typical juror. The negligent “thing” is not a sponge that “speaks for itself,” but a course of actions that requires expert testimony precisely because it does not “speak for itself.” In cases in which an injury is beyond the average juror’s realm of experience, courts should require the plaintiff to prove her case. The doctrine should not “evolve” to excuse a plaintiff from the burden of producing evidence and persuading a jury. This forms the foundation of our civil law system. —DML
In January 2009, an Alabama woman with multiple sclerosis visited Dr T., the defendant ob-gyn, for severe pelvic pain. Dr T. made a diagnosis of a fibroid uterus and ovarian cysts. The patient underwent a transvaginal hysterectomy, but her pain persisted after the surgery.
After being discharged, she discovered a long strip of packing protruding from her vagina, which Dr T. instructed her to extract herself. After doing so, however, the patient continued to have pain, bleeding, and a foul–smelling vaginal discharge. Dr T. diagnosed urinary tract infection and bacterial vaginosis. Antibiotics and pain medication were prescribed, but the patient’s pelvic pain persisted.
In April 2009, Dr T. ordered CT to rule out an abscess or a foreign body. A gauze surgical sponge, left at the conclusion of the patient’s hysterectomy, was detected. Surgery was performed to remove the sponge.
The plaintiff alleged negligence in the sponge’s retention, maintaining that not only was a second surgery required, but that her multiple sclerosis was exacerbated as a result of the entire situation.
The defendant claimed that tests had been performed to investigate the possibility of a foreign body, and that as soon as the surgical sponge was detected, it was removed.
What was the outcome? >>
OUTCOME
According to a published report, a defense verdict was returned.
COMMENT
The defense verdict here is surprising. In most cases in which surgical instruments are left in patients, plaintiffs prevail by using a legal doctrine known as res ipsa loquitur—a Latin legal term of art meaning “the thing speaks for itself.” This is generally requested as a jury charge, wherein the plaintiff asks the judge to explain to the jury that they may find negligence from a certain unusual fact that cannot have occurred without negligence (eg, a sponge left in a patient after surgery).
The history of res ipsa loquitur dates back to 1863 in the case of Byrne v Boadle, in which a barrel of flour rolled from a second-story window and struck a pedestrian below, causing serious injury. The defendants’ claim was that the plaintiff (who had no recollection of the event) was unable to show evidence of negligence. The court created the doctrine, holding that the fact of the accident itself provided ample evidence of negligence, excusing the plaintiff from the burden of proving that negligent acts (eg, inadequate harnessing of the barrels) led to the accident.
Why is this important? The concept of res ipsa loquitur is commonly invoked in medical malpractice actions. It generally requires three elements: the plaintiff suffers an unusual injury, the plaintiff was under the exclusive control of the medical defendants, and the plaintiff did not contribute to the injury.
In a leading malpractice case, Ybarra v Spangard (1944), a plaintiff awoke after undergoing an appendectomy with difficulty moving his arm as a result of reflex sympathetic dystrophy. The plaintiff alleged negligence stemming from the intraoperative positioning of his body, but he could not show the specifics of positioning during surgery. The court held that the patient’s body was under the exclusive control of the team of medical professionals, and that negligence could be inferred because loss of an arm’s function following an appendectomy is unusual and cannot occur without some negligent action involved.
When successfully used in malpractice cases, res ipsa loquitur relieves the plaintiff of the need to prove by a preponderance of the evidence the actions that led to the breach of the standard of care. In order to prevail, she must show the injury, the defendants’ exclusive control, and no contribution on her part. Practically, this permits the case to withstand defense motions for summary judgment and to be brought before a jury with scant to no evidence on the purported negligent act itself—merely the unusual injury and the defendants’ exclusive control.
Traditional application of the doctrine was limited to cases in which negligence was obvious to a layperson: for example, instruments left in patients or amputation of the wrong leg—the thing that “speaks for itself.” Newer evolution of the doctrine is problematic when extended to cases in which expert testimony should be required to demonstrate the standard of care and the defendant’s breach of it. When courts are willing to extend the doctrine, the plaintiff is awarded the presumption of negligence, which the defendant(s) must now come forward to rebut. For example, in a 2010 case in Illinois, a jury returned a $3.6 million verdict following the death of a 2-year-old who had had a seizure. The child’s seizure was reportedly controlled, but he was allegedly hypoventilated while undergoing CT and unfortunately died. The plaintiff was permitted to invoke the doctrine of res ipsa loquitur and was allowed the presumption that medical negligence was responsible for the outcome.
Unlike the surgical sponge left in a patient, matters of central nervous system status, monitoring during CT, airway and ventilation status, hypoxemia, and postictal states are not within the experience of the typical juror. The negligent “thing” is not a sponge that “speaks for itself,” but a course of actions that requires expert testimony precisely because it does not “speak for itself.” In cases in which an injury is beyond the average juror’s realm of experience, courts should require the plaintiff to prove her case. The doctrine should not “evolve” to excuse a plaintiff from the burden of producing evidence and persuading a jury. This forms the foundation of our civil law system. —DML
Greater Transparency for Financial Information in Healthcare Will Prompt Questions from Patients
The movement toward greater transparency of financial information in healthcare is providing patients with access to data that might affect their healthcare decisions. Not all of this information is provided in ways that give patients the full picture, and they may turn to you for some added clarity.

Financial Relationships
The Physician Payments Sunshine Act (“Sunshine Act’) was passed as a part of the Affordable Care Act and requires the public disclosure of financial relationships between physicians and the manufacturers of pharmaceuticals, devices, and supplies, as well as group purchasing organizations. The first wave of financial information was publicly disclosed in 2014 on the federal Open Payments website. When it went live, the website disclosed approximately $3.5 billion in payments made by manufacturers to physicians and teaching hospitals during the last five months of 2013. These payments include research grants, consulting fees, speaking fees, travel, and other expenses. In the future, the payments reported will span an entire year, further increasing the total dollar amount paid by industry.
The Sunshine Act is intended to expose potential conflicts of interest in healthcare so that patients are more informed consumers of healthcare services. The relationships between healthcare providers and industry have been scrutinized much more heavily over the past decade. The concern is that physicians with a financial interest, whether through a consultancy relationship with industry or through the development of new technology, might be biased in treating patients because of these relationships. On the other hand, the majority of relationships between healthcare providers and industry can be beneficial. The relationships provide education to other providers, encourage the development of new treatment options, and improve the effectiveness of existing treatments.
The Centers for Medicare and Medicaid Services (CMS) explains on its website that the disclosed financial ties are not necessarily indicators of any wrongdoing, and that the intent of publishing the information is to promote transparency and discourage inappropriate relationships. Without the proper context, these relationships could be viewed as improper by patients and the general public. Therefore, providers should be prepared to answer patients’ questions and possibly even proactively provide details, such as the scope of any relationship with industry. Many providers begin to consult with a pharmaceutical or device manufacturer because of their experience using a particular product, rather than using a particular product after forming that financial relationship. This context could shift patients’ views of what it means for their providers to have this type of connection with industry.
Providers also need to be aware that government agencies, insurers, and attorneys can track this data. Although it is still too early to know the full scope of the potential uses of this information in government investigations, insurance carrier decisions, malpractice, or other legal actions, it does provide further reason to ensure that the information posted is accurate.
During the initial launch of the Open Payments website, some data was temporarily removed due to inaccuracies, including payments linked incorrectly to physicians with the same first and last names. While these issues are being reviewed by CMS, their existence proves how important it is for all physicians (even those not affiliated with the industry) to review the data reported in order to ensure the accuracy of their information.
Procedure Costs
Another transparency requirement in the Affordable Care Act was implemented on Oct. 1, 2014, as part of the inpatient prospective payment system final rule. Hospitals are now required to make their prices for procedures public and update the list annually. The final rule is not explicit with respect to the manner of the disclosure, except that either a price list or the policy for obtaining access must be made public. Some complain that the rule is difficult to comply with because it is vague, while others point out that this fact gives hospitals necessary flexibility in the method of reporting. It is at the hospital’s discretion whether to post the information online or in a physical location.
It is important to note that patients with private payer insurance coverage have distinct rates that are set through agreements between their health plans and the hospitals, so information on the public list very likely will not be applicable to those patients and could be a source of confusion.
As patients have more access to information about the costs for procedures, providers need to be aware of where within the facility they should refer patients with questions or concerns, including information on a hospital’s financial assistance programs.
There are so many sources of information that patients and their families can obtain before ever setting foot in the hospital. An open dialogue with patients that emphasizes the context of any financial relationships with industry, including the benefits, can help to minimize the potential that the information will be treated as suspect by your patients.
Further, as patients bear more of the costs of healthcare, questions surrounding the costs of procedures relative to published data may be encountered more frequently at the bedside and in office visits. This information may have an impact on patients’ decisions about their care.

The movement toward greater transparency of financial information in healthcare is providing patients with access to data that might affect their healthcare decisions. Not all of this information is provided in ways that give patients the full picture, and they may turn to you for some added clarity.
Financial Relationships
The Physician Payments Sunshine Act (“Sunshine Act’) was passed as a part of the Affordable Care Act and requires the public disclosure of financial relationships between physicians and the manufacturers of pharmaceuticals, devices, and supplies, as well as group purchasing organizations. The first wave of financial information was publicly disclosed in 2014 on the federal Open Payments website. When it went live, the website disclosed approximately $3.5 billion in payments made by manufacturers to physicians and teaching hospitals during the last five months of 2013. These payments include research grants, consulting fees, speaking fees, travel, and other expenses. In the future, the payments reported will span an entire year, further increasing the total dollar amount paid by industry.
The Sunshine Act is intended to expose potential conflicts of interest in healthcare so that patients are more informed consumers of healthcare services. The relationships between healthcare providers and industry have been scrutinized much more heavily over the past decade. The concern is that physicians with a financial interest, whether through a consultancy relationship with industry or through the development of new technology, might be biased in treating patients because of these relationships. On the other hand, the majority of relationships between healthcare providers and industry can be beneficial. The relationships provide education to other providers, encourage the development of new treatment options, and improve the effectiveness of existing treatments.
The Centers for Medicare and Medicaid Services (CMS) explains on its website that the disclosed financial ties are not necessarily indicators of any wrongdoing, and that the intent of publishing the information is to promote transparency and discourage inappropriate relationships. Without the proper context, these relationships could be viewed as improper by patients and the general public. Therefore, providers should be prepared to answer patients’ questions and possibly even proactively provide details, such as the scope of any relationship with industry. Many providers begin to consult with a pharmaceutical or device manufacturer because of their experience using a particular product, rather than using a particular product after forming that financial relationship. This context could shift patients’ views of what it means for their providers to have this type of connection with industry.
Providers also need to be aware that government agencies, insurers, and attorneys can track this data. Although it is still too early to know the full scope of the potential uses of this information in government investigations, insurance carrier decisions, malpractice, or other legal actions, it does provide further reason to ensure that the information posted is accurate.
During the initial launch of the Open Payments website, some data was temporarily removed due to inaccuracies, including payments linked incorrectly to physicians with the same first and last names. While these issues are being reviewed by CMS, their existence proves how important it is for all physicians (even those not affiliated with the industry) to review the data reported in order to ensure the accuracy of their information.
Procedure Costs
Another transparency requirement in the Affordable Care Act was implemented on Oct. 1, 2014, as part of the inpatient prospective payment system final rule. Hospitals are now required to make their prices for procedures public and update the list annually. The final rule is not explicit with respect to the manner of the disclosure, except that either a price list or the policy for obtaining access must be made public. Some complain that the rule is difficult to comply with because it is vague, while others point out that this fact gives hospitals necessary flexibility in the method of reporting. It is at the hospital’s discretion whether to post the information online or in a physical location.
It is important to note that patients with private payer insurance coverage have distinct rates that are set through agreements between their health plans and the hospitals, so information on the public list very likely will not be applicable to those patients and could be a source of confusion.
As patients have more access to information about the costs for procedures, providers need to be aware of where within the facility they should refer patients with questions or concerns, including information on a hospital’s financial assistance programs.
There are so many sources of information that patients and their families can obtain before ever setting foot in the hospital. An open dialogue with patients that emphasizes the context of any financial relationships with industry, including the benefits, can help to minimize the potential that the information will be treated as suspect by your patients.
Further, as patients bear more of the costs of healthcare, questions surrounding the costs of procedures relative to published data may be encountered more frequently at the bedside and in office visits. This information may have an impact on patients’ decisions about their care.
The movement toward greater transparency of financial information in healthcare is providing patients with access to data that might affect their healthcare decisions. Not all of this information is provided in ways that give patients the full picture, and they may turn to you for some added clarity.
Financial Relationships
The Physician Payments Sunshine Act (“Sunshine Act’) was passed as a part of the Affordable Care Act and requires the public disclosure of financial relationships between physicians and the manufacturers of pharmaceuticals, devices, and supplies, as well as group purchasing organizations. The first wave of financial information was publicly disclosed in 2014 on the federal Open Payments website. When it went live, the website disclosed approximately $3.5 billion in payments made by manufacturers to physicians and teaching hospitals during the last five months of 2013. These payments include research grants, consulting fees, speaking fees, travel, and other expenses. In the future, the payments reported will span an entire year, further increasing the total dollar amount paid by industry.
The Sunshine Act is intended to expose potential conflicts of interest in healthcare so that patients are more informed consumers of healthcare services. The relationships between healthcare providers and industry have been scrutinized much more heavily over the past decade. The concern is that physicians with a financial interest, whether through a consultancy relationship with industry or through the development of new technology, might be biased in treating patients because of these relationships. On the other hand, the majority of relationships between healthcare providers and industry can be beneficial. The relationships provide education to other providers, encourage the development of new treatment options, and improve the effectiveness of existing treatments.
The Centers for Medicare and Medicaid Services (CMS) explains on its website that the disclosed financial ties are not necessarily indicators of any wrongdoing, and that the intent of publishing the information is to promote transparency and discourage inappropriate relationships. Without the proper context, these relationships could be viewed as improper by patients and the general public. Therefore, providers should be prepared to answer patients’ questions and possibly even proactively provide details, such as the scope of any relationship with industry. Many providers begin to consult with a pharmaceutical or device manufacturer because of their experience using a particular product, rather than using a particular product after forming that financial relationship. This context could shift patients’ views of what it means for their providers to have this type of connection with industry.
Providers also need to be aware that government agencies, insurers, and attorneys can track this data. Although it is still too early to know the full scope of the potential uses of this information in government investigations, insurance carrier decisions, malpractice, or other legal actions, it does provide further reason to ensure that the information posted is accurate.
During the initial launch of the Open Payments website, some data was temporarily removed due to inaccuracies, including payments linked incorrectly to physicians with the same first and last names. While these issues are being reviewed by CMS, their existence proves how important it is for all physicians (even those not affiliated with the industry) to review the data reported in order to ensure the accuracy of their information.
Procedure Costs
Another transparency requirement in the Affordable Care Act was implemented on Oct. 1, 2014, as part of the inpatient prospective payment system final rule. Hospitals are now required to make their prices for procedures public and update the list annually. The final rule is not explicit with respect to the manner of the disclosure, except that either a price list or the policy for obtaining access must be made public. Some complain that the rule is difficult to comply with because it is vague, while others point out that this fact gives hospitals necessary flexibility in the method of reporting. It is at the hospital’s discretion whether to post the information online or in a physical location.
It is important to note that patients with private payer insurance coverage have distinct rates that are set through agreements between their health plans and the hospitals, so information on the public list very likely will not be applicable to those patients and could be a source of confusion.
As patients have more access to information about the costs for procedures, providers need to be aware of where within the facility they should refer patients with questions or concerns, including information on a hospital’s financial assistance programs.
There are so many sources of information that patients and their families can obtain before ever setting foot in the hospital. An open dialogue with patients that emphasizes the context of any financial relationships with industry, including the benefits, can help to minimize the potential that the information will be treated as suspect by your patients.
Further, as patients bear more of the costs of healthcare, questions surrounding the costs of procedures relative to published data may be encountered more frequently at the bedside and in office visits. This information may have an impact on patients’ decisions about their care.
Lost needle tip during hysterectomy
CASE: Lost needle tip
A 36-year-old woman (G3 P2012) with stress urinary incontinence (SUI) and abnormal uterine bleeding presented to a gynecologist. She had explored medical therapy for her SUI with no symptom improvement. She had a previous tubal ligation, and the gynecologist ordered urodynamic testing, the results of which led to a discussion of vaginal hysterectomy; anterior, posterior colporrhaphy; and mesh placement. It was felt that the patient had a number of risk factors for incontinence (including pregnancy with vaginal delivery, well-controlled diabetes mellitus, and obesity). She had a long-standing history of chronic pelvic pain, with an established diagnosis of diverticulosis with episodes of diverticulitis in the past.
The gynecologist had the patient keep a bladder diary for 1 week. When asked, the patient reported no problems with sexual dysfunction, stating that her quality of life was “fine” except for the vaginal bleeding and loss of urine refractory to medical therapy. The Urogenital Distress Inventory was administered, and it identified frequent urination, leakage, and incontinence related to activities. An Incontinence Impact Questionnaire also was administered. Physical examination included cotton-tipped swab urethral, or Q-tip, test and cough stress test as part of POP-Q (Pelvic Organ Prolapse Quantification system) evaluation. Urinary tract infection was ruled out. The gynecologist counseled the patient about possible medical therapies for urinary incontinence, and she requested definitive surgery.
The gynecologist obtained informed consent for surgery that included preoperative discussion of potential surgical complications, including bleeding, infection, trauma to surrounding structures, and the possibility of additional surgical procedures secondary to complications. The gynecologist also discussed transvaginal tape versus transobturator tape (TOT) placement, including potential complications and sequelae. The final planned procedure, which was performed by the gynecologist, included vaginal hysterectomy, anterior colporrhaphy, and TOT placement.
Intraoperatively, the patient was identified (upon entering the operating room [OR]); time-out occurred, and the gynecologist proceeded with surgery. During the procedure, the tip of a needle broke off. The gynecologist noted the broken tip as he removed the needle and handed it to the surgical technician. The gynecologist palpated the sidewall in the presumed area of the needle tip and felt it easily. He attempted to remove the tip, but his effort was fruitless. He made the intraoperative decision to leave the tip in situ. A needle and sponge count was performed, reported as correct, and it was felt there was no indication for imaging of the pelvis. The circulating nurse filled out an incident report immediately following the surgery, noting the missing needle tip. The occurrence was discussed by the surgical committee at the hospital.
Postoperatively, while the patient was in the hospital, she was informed of the intra-operative incident.
Three months later, the patient reported vaginal and pelvic pain on the sidewall in the area of the lost needle tip, with radiating pain down the involved extremity. A segment of the TOT was noted to be protruding into the vagina, and this was addressed in the OR with “trimming of such.”
Postoperatively, again the patient reported pain on the involved side. She sought the opinion of another gynecologist, who subsequently performed surgical intervention to remove the needle tip. Her symptoms improved.
The patient sued the original gynecologic surgeon, alleging pain and suffering from the surgery involving the lost needle tip.
What’s the verdict?
A defense verdict was awarded.
Medical teaching points
Medical evaluation seemed appropriate. Parity is associated with SUI (but not urge incontinence). In general, urinary incontinence is more commonly associated with a history of lower urinary tract infections. The patient in this case was asked about and evaluated for:
- stress incontinence (associated with loss of urine with sneezing, coughing, and exercise)
- urge incontinence (inability to reach the bathroom in time)
- frequency of urination, especially while sleeping
- overflow incontinence
- overall loss of bladder control.
Was information on the broken needle handled appropriately? This case explores the question of what, if any, obligation the surgeon and hospital system have to the patient when informing her of a broken needle and the intraoperative decision-making process that led to its staying in place. When such a situation occurs, which is very uncommon, should an intraoperative x-ray be performed to assess the location of the needle tip? Should the patient automatically be brought back to the OR for removal?
The surgeon’s concern was a legitimate one—that additional attempts at removal could lead to complications far worse than having a small segment of a needle left in place. After all, shrapnel, bullets, etc, remain lodged in various locations throughout the body without subsequent ill effects. He did discuss with the patient the fact that a needle segment was left in the muscle wall. But how do you assess postoperative pelvic pain in a patient who had preoperative chronic pelvic pain? These are questions we as clinicians ask. Clearly, there are no black-and-white answers, and we will call upon our legal consultants for their expertise in addressing these queries.
From the gynecologic perspective, however, it is of paramount importance to address the patient’s postoperative vaginal pain and determine the best management approach. In this case the TOT, and its association with a 21.5% complication rate, including reported vaginal extrusion, introduces a whole new set of concerns.1 The TOT use in itself raises the question of liability on the part of the surgeon. This mesh has more than 150 associated complications, including obturator nerve injuries, extensive blood loss, and ischiorectal fossa abscesses.2 Once a device comes upon the radar screen of the US Food and Drug Administration for significant complications, where does that leave the clinician in regard to litigation? Let’s look to our legal colleagues for their insight and expertise.
Legal considerations
Given the facts in this case, it is not surprising that it resulted in a defense verdict. The majority of cases filed are ultimately disposed of in favor of the medical defendants, and the majority of medical malpractice cases that go to trial result in defense verdicts.
Medical malpractice, or “professional negligence,” consists of a claim that a medical professional had a duty of care to the patient, a breach of that duty, injury to the patient, and a causal connection (“causation”) between the breach of duty and the injury. It is the obligation of the plaintiff to prove the elements of negligence by a preponderance of the evidence.
Were the surgeon’s actions in line with other surgeons’ expected actions? The issue of the breach of the duty of care essentially is the question of whether the physician acted similarly to a reasonably careful practitioner of the same specialty under the same circumstances. Doctors are not held to a standard of perfection. That is, not every injury or bad outcome is negligence—only those injuries that result from actions, or inactions, that were not within the level of care acceptable in the profession.
Why would this patient file a lawsuit? The injury was not trivial (it had both pain and cost associated with it), but it was not catastrophic, and the negligence was going to be difficult to prove. Furthermore, lawsuits are expensive in terms of time, energy, and emotional commitment—few people file them for the fun of it. We can only speculate on the answer to the question but, frequently, such claims are a search for the answer to “What happened, and why?” or a reaction to feeling ignored or disrespected. There is little in the case facts that we have to work with to indicate what the communication was between the gynecologist and the patient and her family. The statement of facts, however, leaves the impression that communication deteriorated as the postoperative pain endured.
Some additional areas of potential claims for liability in this case include:
- The explanation for the needle breaking during surgery is unclear from the brief statement of case facts. There might be malpractice liability if the surgeon was unreasonable in how the needle was used, used the wrong needle, or ignored defects in the needle.
- The surgeon tried unsuccessfully to retrieve the needle during the original surgery. If the surgeon’s failure to retrieve the needle was because of inadequate training, lack of care or the like, it might be seen as the “cause” of the patient’s injuries.
- The fact that a second surgeon was able to remove the needle tip, which resolved the patient’s pain, may raise the question of whether the first surgeon’s decision not to seek to remove it in response to the continuing pain was reasonable. If the first surgeon did not want to remove the needle tip, a question might be raised about whether that surgeon should have referred the patient to another surgeon. (The patient ultimately found another surgeon on her own.)
- Regarding use of TOT: A 21.5% complication rate ordinarily would be a significant factor to consider in a decision to use the tape. Physicians are responsible for keeping up with current developments in the devices and pharmaceuticals they use. Therefore, if information on the complication rate was available, the surgeon’s documentation should reflect the basis for choosing to use the tape. More important, the surgeon should document a conversation with the patient about the risks and benefits of using the TOT and the discussion of alternatives to its use.
What factors could have tipped the case toward the defense?
The defense verdict indicates that the jury determined there was no negligence, or that the patient could not prove any of these potential bases of liability. As noted above, what may have helped the defense is the fact that the surgeon documented the details of the informed consent conversation, including that “discussion was carried out regarding” the tape. The informed consent process is an important opportunity for communication with the patient, and a chance to make sure that expectations are reasonable. Liability for the failure of informed consent is not common. When something has gone wrong, however, it can matter whether the problem was something mentioned in the informed consent process. In addition, it was positive that postoperatively the patient was informed of the broken needle—although it is not clear who informed her about it.
A couple of other legal issues are worth noting. From our fact scenario we do not know what was documented in the incident report filed by the circulating nurse and reviewed by the surgical committee. We also do not know whether the plaintiff was privy to the incident report document. The surgical committee is likely a peer-review committee, and most states provide some privilege for such committees (to avoid disclosure of committee information for discovery or at trial). The deliberations and conclusions of the committee, therefore, were likely privileged. However, incident reports are frequently used for other purposes, such as administrative reports, that are not privileged—so the incident report often is determined to be discoverable depending on the interpretation of the state’s law.
No winner in this case
Despite the defense verdict, the physician was not really the “winner” after having spent a great deal of time, energy, money, and emotion defending this suit. Ultimately, the goal is not to win malpractice cases but to avoid them—in this case, among other things, by being frank with patients about expectations, keeping an open line of communication with patients when they are concerned with an outcome that is less than ideal, and referring a patient when it may be appropriate.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Bladder sling risks, complications and side effects. DrugWatch Web site. http://www.drugwatch.com/trans vaginal-mesh/bladder-sling/. Updated January 2, 2015. Accessed February 13, 2015.
2. Boyles SH, Edwards R, Gregory W, Clark A. Complications associated with transobturator sling procedures. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(1):19–22.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |


Disclosures
The authors report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
The authors report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
The authors report no financial relationships relevant to this article.
CASE: Lost needle tip
A 36-year-old woman (G3 P2012) with stress urinary incontinence (SUI) and abnormal uterine bleeding presented to a gynecologist. She had explored medical therapy for her SUI with no symptom improvement. She had a previous tubal ligation, and the gynecologist ordered urodynamic testing, the results of which led to a discussion of vaginal hysterectomy; anterior, posterior colporrhaphy; and mesh placement. It was felt that the patient had a number of risk factors for incontinence (including pregnancy with vaginal delivery, well-controlled diabetes mellitus, and obesity). She had a long-standing history of chronic pelvic pain, with an established diagnosis of diverticulosis with episodes of diverticulitis in the past.
The gynecologist had the patient keep a bladder diary for 1 week. When asked, the patient reported no problems with sexual dysfunction, stating that her quality of life was “fine” except for the vaginal bleeding and loss of urine refractory to medical therapy. The Urogenital Distress Inventory was administered, and it identified frequent urination, leakage, and incontinence related to activities. An Incontinence Impact Questionnaire also was administered. Physical examination included cotton-tipped swab urethral, or Q-tip, test and cough stress test as part of POP-Q (Pelvic Organ Prolapse Quantification system) evaluation. Urinary tract infection was ruled out. The gynecologist counseled the patient about possible medical therapies for urinary incontinence, and she requested definitive surgery.
The gynecologist obtained informed consent for surgery that included preoperative discussion of potential surgical complications, including bleeding, infection, trauma to surrounding structures, and the possibility of additional surgical procedures secondary to complications. The gynecologist also discussed transvaginal tape versus transobturator tape (TOT) placement, including potential complications and sequelae. The final planned procedure, which was performed by the gynecologist, included vaginal hysterectomy, anterior colporrhaphy, and TOT placement.
Intraoperatively, the patient was identified (upon entering the operating room [OR]); time-out occurred, and the gynecologist proceeded with surgery. During the procedure, the tip of a needle broke off. The gynecologist noted the broken tip as he removed the needle and handed it to the surgical technician. The gynecologist palpated the sidewall in the presumed area of the needle tip and felt it easily. He attempted to remove the tip, but his effort was fruitless. He made the intraoperative decision to leave the tip in situ. A needle and sponge count was performed, reported as correct, and it was felt there was no indication for imaging of the pelvis. The circulating nurse filled out an incident report immediately following the surgery, noting the missing needle tip. The occurrence was discussed by the surgical committee at the hospital.
Postoperatively, while the patient was in the hospital, she was informed of the intra-operative incident.
Three months later, the patient reported vaginal and pelvic pain on the sidewall in the area of the lost needle tip, with radiating pain down the involved extremity. A segment of the TOT was noted to be protruding into the vagina, and this was addressed in the OR with “trimming of such.”
Postoperatively, again the patient reported pain on the involved side. She sought the opinion of another gynecologist, who subsequently performed surgical intervention to remove the needle tip. Her symptoms improved.
The patient sued the original gynecologic surgeon, alleging pain and suffering from the surgery involving the lost needle tip.
What’s the verdict?
A defense verdict was awarded.
Medical teaching points
Medical evaluation seemed appropriate. Parity is associated with SUI (but not urge incontinence). In general, urinary incontinence is more commonly associated with a history of lower urinary tract infections. The patient in this case was asked about and evaluated for:
- stress incontinence (associated with loss of urine with sneezing, coughing, and exercise)
- urge incontinence (inability to reach the bathroom in time)
- frequency of urination, especially while sleeping
- overflow incontinence
- overall loss of bladder control.
Was information on the broken needle handled appropriately? This case explores the question of what, if any, obligation the surgeon and hospital system have to the patient when informing her of a broken needle and the intraoperative decision-making process that led to its staying in place. When such a situation occurs, which is very uncommon, should an intraoperative x-ray be performed to assess the location of the needle tip? Should the patient automatically be brought back to the OR for removal?
The surgeon’s concern was a legitimate one—that additional attempts at removal could lead to complications far worse than having a small segment of a needle left in place. After all, shrapnel, bullets, etc, remain lodged in various locations throughout the body without subsequent ill effects. He did discuss with the patient the fact that a needle segment was left in the muscle wall. But how do you assess postoperative pelvic pain in a patient who had preoperative chronic pelvic pain? These are questions we as clinicians ask. Clearly, there are no black-and-white answers, and we will call upon our legal consultants for their expertise in addressing these queries.
From the gynecologic perspective, however, it is of paramount importance to address the patient’s postoperative vaginal pain and determine the best management approach. In this case the TOT, and its association with a 21.5% complication rate, including reported vaginal extrusion, introduces a whole new set of concerns.1 The TOT use in itself raises the question of liability on the part of the surgeon. This mesh has more than 150 associated complications, including obturator nerve injuries, extensive blood loss, and ischiorectal fossa abscesses.2 Once a device comes upon the radar screen of the US Food and Drug Administration for significant complications, where does that leave the clinician in regard to litigation? Let’s look to our legal colleagues for their insight and expertise.
Legal considerations
Given the facts in this case, it is not surprising that it resulted in a defense verdict. The majority of cases filed are ultimately disposed of in favor of the medical defendants, and the majority of medical malpractice cases that go to trial result in defense verdicts.
Medical malpractice, or “professional negligence,” consists of a claim that a medical professional had a duty of care to the patient, a breach of that duty, injury to the patient, and a causal connection (“causation”) between the breach of duty and the injury. It is the obligation of the plaintiff to prove the elements of negligence by a preponderance of the evidence.
Were the surgeon’s actions in line with other surgeons’ expected actions? The issue of the breach of the duty of care essentially is the question of whether the physician acted similarly to a reasonably careful practitioner of the same specialty under the same circumstances. Doctors are not held to a standard of perfection. That is, not every injury or bad outcome is negligence—only those injuries that result from actions, or inactions, that were not within the level of care acceptable in the profession.
Why would this patient file a lawsuit? The injury was not trivial (it had both pain and cost associated with it), but it was not catastrophic, and the negligence was going to be difficult to prove. Furthermore, lawsuits are expensive in terms of time, energy, and emotional commitment—few people file them for the fun of it. We can only speculate on the answer to the question but, frequently, such claims are a search for the answer to “What happened, and why?” or a reaction to feeling ignored or disrespected. There is little in the case facts that we have to work with to indicate what the communication was between the gynecologist and the patient and her family. The statement of facts, however, leaves the impression that communication deteriorated as the postoperative pain endured.
Some additional areas of potential claims for liability in this case include:
- The explanation for the needle breaking during surgery is unclear from the brief statement of case facts. There might be malpractice liability if the surgeon was unreasonable in how the needle was used, used the wrong needle, or ignored defects in the needle.
- The surgeon tried unsuccessfully to retrieve the needle during the original surgery. If the surgeon’s failure to retrieve the needle was because of inadequate training, lack of care or the like, it might be seen as the “cause” of the patient’s injuries.
- The fact that a second surgeon was able to remove the needle tip, which resolved the patient’s pain, may raise the question of whether the first surgeon’s decision not to seek to remove it in response to the continuing pain was reasonable. If the first surgeon did not want to remove the needle tip, a question might be raised about whether that surgeon should have referred the patient to another surgeon. (The patient ultimately found another surgeon on her own.)
- Regarding use of TOT: A 21.5% complication rate ordinarily would be a significant factor to consider in a decision to use the tape. Physicians are responsible for keeping up with current developments in the devices and pharmaceuticals they use. Therefore, if information on the complication rate was available, the surgeon’s documentation should reflect the basis for choosing to use the tape. More important, the surgeon should document a conversation with the patient about the risks and benefits of using the TOT and the discussion of alternatives to its use.
What factors could have tipped the case toward the defense?
The defense verdict indicates that the jury determined there was no negligence, or that the patient could not prove any of these potential bases of liability. As noted above, what may have helped the defense is the fact that the surgeon documented the details of the informed consent conversation, including that “discussion was carried out regarding” the tape. The informed consent process is an important opportunity for communication with the patient, and a chance to make sure that expectations are reasonable. Liability for the failure of informed consent is not common. When something has gone wrong, however, it can matter whether the problem was something mentioned in the informed consent process. In addition, it was positive that postoperatively the patient was informed of the broken needle—although it is not clear who informed her about it.
A couple of other legal issues are worth noting. From our fact scenario we do not know what was documented in the incident report filed by the circulating nurse and reviewed by the surgical committee. We also do not know whether the plaintiff was privy to the incident report document. The surgical committee is likely a peer-review committee, and most states provide some privilege for such committees (to avoid disclosure of committee information for discovery or at trial). The deliberations and conclusions of the committee, therefore, were likely privileged. However, incident reports are frequently used for other purposes, such as administrative reports, that are not privileged—so the incident report often is determined to be discoverable depending on the interpretation of the state’s law.
No winner in this case
Despite the defense verdict, the physician was not really the “winner” after having spent a great deal of time, energy, money, and emotion defending this suit. Ultimately, the goal is not to win malpractice cases but to avoid them—in this case, among other things, by being frank with patients about expectations, keeping an open line of communication with patients when they are concerned with an outcome that is less than ideal, and referring a patient when it may be appropriate.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
CASE: Lost needle tip
A 36-year-old woman (G3 P2012) with stress urinary incontinence (SUI) and abnormal uterine bleeding presented to a gynecologist. She had explored medical therapy for her SUI with no symptom improvement. She had a previous tubal ligation, and the gynecologist ordered urodynamic testing, the results of which led to a discussion of vaginal hysterectomy; anterior, posterior colporrhaphy; and mesh placement. It was felt that the patient had a number of risk factors for incontinence (including pregnancy with vaginal delivery, well-controlled diabetes mellitus, and obesity). She had a long-standing history of chronic pelvic pain, with an established diagnosis of diverticulosis with episodes of diverticulitis in the past.
The gynecologist had the patient keep a bladder diary for 1 week. When asked, the patient reported no problems with sexual dysfunction, stating that her quality of life was “fine” except for the vaginal bleeding and loss of urine refractory to medical therapy. The Urogenital Distress Inventory was administered, and it identified frequent urination, leakage, and incontinence related to activities. An Incontinence Impact Questionnaire also was administered. Physical examination included cotton-tipped swab urethral, or Q-tip, test and cough stress test as part of POP-Q (Pelvic Organ Prolapse Quantification system) evaluation. Urinary tract infection was ruled out. The gynecologist counseled the patient about possible medical therapies for urinary incontinence, and she requested definitive surgery.
The gynecologist obtained informed consent for surgery that included preoperative discussion of potential surgical complications, including bleeding, infection, trauma to surrounding structures, and the possibility of additional surgical procedures secondary to complications. The gynecologist also discussed transvaginal tape versus transobturator tape (TOT) placement, including potential complications and sequelae. The final planned procedure, which was performed by the gynecologist, included vaginal hysterectomy, anterior colporrhaphy, and TOT placement.
Intraoperatively, the patient was identified (upon entering the operating room [OR]); time-out occurred, and the gynecologist proceeded with surgery. During the procedure, the tip of a needle broke off. The gynecologist noted the broken tip as he removed the needle and handed it to the surgical technician. The gynecologist palpated the sidewall in the presumed area of the needle tip and felt it easily. He attempted to remove the tip, but his effort was fruitless. He made the intraoperative decision to leave the tip in situ. A needle and sponge count was performed, reported as correct, and it was felt there was no indication for imaging of the pelvis. The circulating nurse filled out an incident report immediately following the surgery, noting the missing needle tip. The occurrence was discussed by the surgical committee at the hospital.
Postoperatively, while the patient was in the hospital, she was informed of the intra-operative incident.
Three months later, the patient reported vaginal and pelvic pain on the sidewall in the area of the lost needle tip, with radiating pain down the involved extremity. A segment of the TOT was noted to be protruding into the vagina, and this was addressed in the OR with “trimming of such.”
Postoperatively, again the patient reported pain on the involved side. She sought the opinion of another gynecologist, who subsequently performed surgical intervention to remove the needle tip. Her symptoms improved.
The patient sued the original gynecologic surgeon, alleging pain and suffering from the surgery involving the lost needle tip.
What’s the verdict?
A defense verdict was awarded.
Medical teaching points
Medical evaluation seemed appropriate. Parity is associated with SUI (but not urge incontinence). In general, urinary incontinence is more commonly associated with a history of lower urinary tract infections. The patient in this case was asked about and evaluated for:
- stress incontinence (associated with loss of urine with sneezing, coughing, and exercise)
- urge incontinence (inability to reach the bathroom in time)
- frequency of urination, especially while sleeping
- overflow incontinence
- overall loss of bladder control.
Was information on the broken needle handled appropriately? This case explores the question of what, if any, obligation the surgeon and hospital system have to the patient when informing her of a broken needle and the intraoperative decision-making process that led to its staying in place. When such a situation occurs, which is very uncommon, should an intraoperative x-ray be performed to assess the location of the needle tip? Should the patient automatically be brought back to the OR for removal?
The surgeon’s concern was a legitimate one—that additional attempts at removal could lead to complications far worse than having a small segment of a needle left in place. After all, shrapnel, bullets, etc, remain lodged in various locations throughout the body without subsequent ill effects. He did discuss with the patient the fact that a needle segment was left in the muscle wall. But how do you assess postoperative pelvic pain in a patient who had preoperative chronic pelvic pain? These are questions we as clinicians ask. Clearly, there are no black-and-white answers, and we will call upon our legal consultants for their expertise in addressing these queries.
From the gynecologic perspective, however, it is of paramount importance to address the patient’s postoperative vaginal pain and determine the best management approach. In this case the TOT, and its association with a 21.5% complication rate, including reported vaginal extrusion, introduces a whole new set of concerns.1 The TOT use in itself raises the question of liability on the part of the surgeon. This mesh has more than 150 associated complications, including obturator nerve injuries, extensive blood loss, and ischiorectal fossa abscesses.2 Once a device comes upon the radar screen of the US Food and Drug Administration for significant complications, where does that leave the clinician in regard to litigation? Let’s look to our legal colleagues for their insight and expertise.
Legal considerations
Given the facts in this case, it is not surprising that it resulted in a defense verdict. The majority of cases filed are ultimately disposed of in favor of the medical defendants, and the majority of medical malpractice cases that go to trial result in defense verdicts.
Medical malpractice, or “professional negligence,” consists of a claim that a medical professional had a duty of care to the patient, a breach of that duty, injury to the patient, and a causal connection (“causation”) between the breach of duty and the injury. It is the obligation of the plaintiff to prove the elements of negligence by a preponderance of the evidence.
Were the surgeon’s actions in line with other surgeons’ expected actions? The issue of the breach of the duty of care essentially is the question of whether the physician acted similarly to a reasonably careful practitioner of the same specialty under the same circumstances. Doctors are not held to a standard of perfection. That is, not every injury or bad outcome is negligence—only those injuries that result from actions, or inactions, that were not within the level of care acceptable in the profession.
Why would this patient file a lawsuit? The injury was not trivial (it had both pain and cost associated with it), but it was not catastrophic, and the negligence was going to be difficult to prove. Furthermore, lawsuits are expensive in terms of time, energy, and emotional commitment—few people file them for the fun of it. We can only speculate on the answer to the question but, frequently, such claims are a search for the answer to “What happened, and why?” or a reaction to feeling ignored or disrespected. There is little in the case facts that we have to work with to indicate what the communication was between the gynecologist and the patient and her family. The statement of facts, however, leaves the impression that communication deteriorated as the postoperative pain endured.
Some additional areas of potential claims for liability in this case include:
- The explanation for the needle breaking during surgery is unclear from the brief statement of case facts. There might be malpractice liability if the surgeon was unreasonable in how the needle was used, used the wrong needle, or ignored defects in the needle.
- The surgeon tried unsuccessfully to retrieve the needle during the original surgery. If the surgeon’s failure to retrieve the needle was because of inadequate training, lack of care or the like, it might be seen as the “cause” of the patient’s injuries.
- The fact that a second surgeon was able to remove the needle tip, which resolved the patient’s pain, may raise the question of whether the first surgeon’s decision not to seek to remove it in response to the continuing pain was reasonable. If the first surgeon did not want to remove the needle tip, a question might be raised about whether that surgeon should have referred the patient to another surgeon. (The patient ultimately found another surgeon on her own.)
- Regarding use of TOT: A 21.5% complication rate ordinarily would be a significant factor to consider in a decision to use the tape. Physicians are responsible for keeping up with current developments in the devices and pharmaceuticals they use. Therefore, if information on the complication rate was available, the surgeon’s documentation should reflect the basis for choosing to use the tape. More important, the surgeon should document a conversation with the patient about the risks and benefits of using the TOT and the discussion of alternatives to its use.
What factors could have tipped the case toward the defense?
The defense verdict indicates that the jury determined there was no negligence, or that the patient could not prove any of these potential bases of liability. As noted above, what may have helped the defense is the fact that the surgeon documented the details of the informed consent conversation, including that “discussion was carried out regarding” the tape. The informed consent process is an important opportunity for communication with the patient, and a chance to make sure that expectations are reasonable. Liability for the failure of informed consent is not common. When something has gone wrong, however, it can matter whether the problem was something mentioned in the informed consent process. In addition, it was positive that postoperatively the patient was informed of the broken needle—although it is not clear who informed her about it.
A couple of other legal issues are worth noting. From our fact scenario we do not know what was documented in the incident report filed by the circulating nurse and reviewed by the surgical committee. We also do not know whether the plaintiff was privy to the incident report document. The surgical committee is likely a peer-review committee, and most states provide some privilege for such committees (to avoid disclosure of committee information for discovery or at trial). The deliberations and conclusions of the committee, therefore, were likely privileged. However, incident reports are frequently used for other purposes, such as administrative reports, that are not privileged—so the incident report often is determined to be discoverable depending on the interpretation of the state’s law.
No winner in this case
Despite the defense verdict, the physician was not really the “winner” after having spent a great deal of time, energy, money, and emotion defending this suit. Ultimately, the goal is not to win malpractice cases but to avoid them—in this case, among other things, by being frank with patients about expectations, keeping an open line of communication with patients when they are concerned with an outcome that is less than ideal, and referring a patient when it may be appropriate.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Bladder sling risks, complications and side effects. DrugWatch Web site. http://www.drugwatch.com/trans vaginal-mesh/bladder-sling/. Updated January 2, 2015. Accessed February 13, 2015.
2. Boyles SH, Edwards R, Gregory W, Clark A. Complications associated with transobturator sling procedures. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(1):19–22.
1. Bladder sling risks, complications and side effects. DrugWatch Web site. http://www.drugwatch.com/trans vaginal-mesh/bladder-sling/. Updated January 2, 2015. Accessed February 13, 2015.
2. Boyles SH, Edwards R, Gregory W, Clark A. Complications associated with transobturator sling procedures. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(1):19–22.
Three mesh cases: two defense verdicts; one large award
Transvaginal mesh not properly placed
In January 2007, polypropylene mesh (Gynecare Prolift Transvaginal Mesh; Ethicon) was inserted in a 57-year-old woman to treat bladder and rectal prolapse. The patient developed small-intestine obstruction, bladder contraction, and a large pelvic abscess. Surgical treatment of the complications included creation of a colostomy. She required daily self-catheterization. The patient died of unrelated causes after the suit was filed.
Estate’S CLAIM The gynecologist did not properly insert the mesh and did not fully inform the patient of possible complications.
PHYSICIAN’S DEFENSE The mesh was properly inserted. The patient developed an unpreventable adverse reaction to the mesh. Proper consent was obtained.
VERDICT A New York defense verdict was returned.
Polypropylene mesh removed due to pain
Polypropylene mesh (Obtryx Transobturator Midurethal Sling system, Boston Scientific Corporation [BSC]) was used to treat a woman’s stress urinary incontinence (SUI) in 2008. Following surgery, the patient reported pain. The mesh was partially removed in 2011. The patient has continuing pain and complications caused by remaining pieces of the mesh that the surgeon believes cannot be removed safely.
PATIENT’S CLAIM Although BSC warned that the material could oxidize and become brittle, the surgeon used it anyway. The mesh eroded through the urethra, causing permanent damage. BSC was negligent in the design, marketing, and instructions for Obtryx.
DEFENDANTS’ DEFENSE The surgeon read the instructions and felt the product was safe. BSC claimed the mesh is safe for SUI use. Directions for use clearly warn of possible erosion. A BSC engineer admitted that the tissue that surrounds the mesh can shrink, encapsulating nerves and causing chronic pain.
VERDICT A Massachusetts defense verdict was returned.
Abscesses, nerve damage: $73M
A 42-year-old woman reported SUI to her gynecologist. In January 2011, the gynecologist placed polypropylene pelvic mesh (Obtryx Trans-obturator Midurethal Sling system, BSC). Following surgery, the patient reported pain and fever; pelvic abscesses were found.
Multiple procedures partially removed the mesh and treated the infection. During one procedure, her femoral and obturator nerves were damaged; she walks with a limp. Dyspareunia and pain continue. Additional operations will be needed to remove more mesh and treat continuing infection.
PATIENT’S CLAIM BSC was negligent in the product’s design and marketing. Warnings for use were inadequate concerning the nature and extent of possible permanent injuries: groin and pelvic pain, dyspareunia, nerve damage, and chronic urinary tract infections. BSC withheld or concealed clinical trial information and did not perform and report proper post-market surveillance.
When pivotal study results were published in 2009, indicating that further research was needed to confirm that Obtryx was appropriate for treating SUI, the BSC sales department received an email telling them to not share this information with physicians.
At trial, BSC corporate executives knew little about system design and warnings regarding its use. Data that BSC provided to document the safety of Obtryx were not about that product.
MANUFACTURER’S DEFENSE Both sides agreed not to introduce discussion of the FDA and 510(k) process. BSC blamed a call-center for not passing along complaints from customers in a timely manner.
VERDICT A $73,465,000 Texas verdict was returned against BSC. The jury determined that the manufacturer displayed gross negligence; the design of the Obtryx system is faulty. The award included $50 million for exemplary damages, which the judge reduced to $11.2 million due to state caps, for a total award of $34.6 million.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Transvaginal mesh not properly placed
In January 2007, polypropylene mesh (Gynecare Prolift Transvaginal Mesh; Ethicon) was inserted in a 57-year-old woman to treat bladder and rectal prolapse. The patient developed small-intestine obstruction, bladder contraction, and a large pelvic abscess. Surgical treatment of the complications included creation of a colostomy. She required daily self-catheterization. The patient died of unrelated causes after the suit was filed.
Estate’S CLAIM The gynecologist did not properly insert the mesh and did not fully inform the patient of possible complications.
PHYSICIAN’S DEFENSE The mesh was properly inserted. The patient developed an unpreventable adverse reaction to the mesh. Proper consent was obtained.
VERDICT A New York defense verdict was returned.
Polypropylene mesh removed due to pain
Polypropylene mesh (Obtryx Transobturator Midurethal Sling system, Boston Scientific Corporation [BSC]) was used to treat a woman’s stress urinary incontinence (SUI) in 2008. Following surgery, the patient reported pain. The mesh was partially removed in 2011. The patient has continuing pain and complications caused by remaining pieces of the mesh that the surgeon believes cannot be removed safely.
PATIENT’S CLAIM Although BSC warned that the material could oxidize and become brittle, the surgeon used it anyway. The mesh eroded through the urethra, causing permanent damage. BSC was negligent in the design, marketing, and instructions for Obtryx.
DEFENDANTS’ DEFENSE The surgeon read the instructions and felt the product was safe. BSC claimed the mesh is safe for SUI use. Directions for use clearly warn of possible erosion. A BSC engineer admitted that the tissue that surrounds the mesh can shrink, encapsulating nerves and causing chronic pain.
VERDICT A Massachusetts defense verdict was returned.
Abscesses, nerve damage: $73M
A 42-year-old woman reported SUI to her gynecologist. In January 2011, the gynecologist placed polypropylene pelvic mesh (Obtryx Trans-obturator Midurethal Sling system, BSC). Following surgery, the patient reported pain and fever; pelvic abscesses were found.
Multiple procedures partially removed the mesh and treated the infection. During one procedure, her femoral and obturator nerves were damaged; she walks with a limp. Dyspareunia and pain continue. Additional operations will be needed to remove more mesh and treat continuing infection.
PATIENT’S CLAIM BSC was negligent in the product’s design and marketing. Warnings for use were inadequate concerning the nature and extent of possible permanent injuries: groin and pelvic pain, dyspareunia, nerve damage, and chronic urinary tract infections. BSC withheld or concealed clinical trial information and did not perform and report proper post-market surveillance.
When pivotal study results were published in 2009, indicating that further research was needed to confirm that Obtryx was appropriate for treating SUI, the BSC sales department received an email telling them to not share this information with physicians.
At trial, BSC corporate executives knew little about system design and warnings regarding its use. Data that BSC provided to document the safety of Obtryx were not about that product.
MANUFACTURER’S DEFENSE Both sides agreed not to introduce discussion of the FDA and 510(k) process. BSC blamed a call-center for not passing along complaints from customers in a timely manner.
VERDICT A $73,465,000 Texas verdict was returned against BSC. The jury determined that the manufacturer displayed gross negligence; the design of the Obtryx system is faulty. The award included $50 million for exemplary damages, which the judge reduced to $11.2 million due to state caps, for a total award of $34.6 million.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Transvaginal mesh not properly placed
In January 2007, polypropylene mesh (Gynecare Prolift Transvaginal Mesh; Ethicon) was inserted in a 57-year-old woman to treat bladder and rectal prolapse. The patient developed small-intestine obstruction, bladder contraction, and a large pelvic abscess. Surgical treatment of the complications included creation of a colostomy. She required daily self-catheterization. The patient died of unrelated causes after the suit was filed.
Estate’S CLAIM The gynecologist did not properly insert the mesh and did not fully inform the patient of possible complications.
PHYSICIAN’S DEFENSE The mesh was properly inserted. The patient developed an unpreventable adverse reaction to the mesh. Proper consent was obtained.
VERDICT A New York defense verdict was returned.
Polypropylene mesh removed due to pain
Polypropylene mesh (Obtryx Transobturator Midurethal Sling system, Boston Scientific Corporation [BSC]) was used to treat a woman’s stress urinary incontinence (SUI) in 2008. Following surgery, the patient reported pain. The mesh was partially removed in 2011. The patient has continuing pain and complications caused by remaining pieces of the mesh that the surgeon believes cannot be removed safely.
PATIENT’S CLAIM Although BSC warned that the material could oxidize and become brittle, the surgeon used it anyway. The mesh eroded through the urethra, causing permanent damage. BSC was negligent in the design, marketing, and instructions for Obtryx.
DEFENDANTS’ DEFENSE The surgeon read the instructions and felt the product was safe. BSC claimed the mesh is safe for SUI use. Directions for use clearly warn of possible erosion. A BSC engineer admitted that the tissue that surrounds the mesh can shrink, encapsulating nerves and causing chronic pain.
VERDICT A Massachusetts defense verdict was returned.
Abscesses, nerve damage: $73M
A 42-year-old woman reported SUI to her gynecologist. In January 2011, the gynecologist placed polypropylene pelvic mesh (Obtryx Trans-obturator Midurethal Sling system, BSC). Following surgery, the patient reported pain and fever; pelvic abscesses were found.
Multiple procedures partially removed the mesh and treated the infection. During one procedure, her femoral and obturator nerves were damaged; she walks with a limp. Dyspareunia and pain continue. Additional operations will be needed to remove more mesh and treat continuing infection.
PATIENT’S CLAIM BSC was negligent in the product’s design and marketing. Warnings for use were inadequate concerning the nature and extent of possible permanent injuries: groin and pelvic pain, dyspareunia, nerve damage, and chronic urinary tract infections. BSC withheld or concealed clinical trial information and did not perform and report proper post-market surveillance.
When pivotal study results were published in 2009, indicating that further research was needed to confirm that Obtryx was appropriate for treating SUI, the BSC sales department received an email telling them to not share this information with physicians.
At trial, BSC corporate executives knew little about system design and warnings regarding its use. Data that BSC provided to document the safety of Obtryx were not about that product.
MANUFACTURER’S DEFENSE Both sides agreed not to introduce discussion of the FDA and 510(k) process. BSC blamed a call-center for not passing along complaints from customers in a timely manner.
VERDICT A $73,465,000 Texas verdict was returned against BSC. The jury determined that the manufacturer displayed gross negligence; the design of the Obtryx system is faulty. The award included $50 million for exemplary damages, which the judge reduced to $11.2 million due to state caps, for a total award of $34.6 million.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Pulmonary Embolism Ruled Out in Error
A 28-year-old man presented to a Maryland hospital emergency department (ED) with a two-day history of low-grade fever, nonproductive cough, and dizziness. He was also tachycardic and significantly hypoxic. After an hour’s wait, the patient saw an emergency physician, who noted complaints of weakness, shortness of breath, and lightheadedness. The differential diagnosis included pneumonia, congestive heart failure, and pulmonary embolism (PE).
After an ECG, chest x-ray, and blood work, the emergency physician diagnosed pneumonia and renal insufficiency. The patient was admitted but within eight hours of arrival at the ED was transferred to another hospital. The admitting physician at the second hospital did not evaluate the patient on admission.
Almost five hours later, the patient got out of bed and collapsed in the presence of his wife. A code was called, but the man never regained consciousness and was pronounced dead about 90 minutes later. An autopsy confirmed a PE as the cause of death.
Plaintiff for the decedent alleged negligence in the clinicians’ failure to diagnose and treat the PE. The plaintiff claimed that with proper treatment, the patient would have survived.
The defendants argued that there was no negligence involved and that heparin therapy would not have prevented the patient’s death.
What was the outcome? >>
OUTCOME
According to a published account, a $6.1 million verdict was returned.
COMMENT
This is a substantial verdict, reflecting the jury’s revulsion at the loss of a 28-year-old patient. His initial presentation of low-grade fever, nonproductive cough, and dizziness with tachycardia and hypoxia could be consistent with either pneumonia or PE. The facts as presented render the chest x-ray findings and the magnitude of hypoxia unclear. We also are not told whether any specific risk factors existed to make PE more likely, nor whether there was evidence of deep vein thrombosis (DVT) during presentation or at autopsy.
Diagnosing PE can be difficult. However, jurors confronted with a case involving a fatal PE may be led to believe that the diagnosis is straightforward and should never be missed. Plaintiff’s counsel will argue that the patient “would be standing here today” in a fully functional status if the diagnosis had been made.
Here, presumptively, the chest films and chest auscultation were suggestive of pneumonia and led the clinician, who actively considered PE, to ultimately exclude the possibility. It is not clear why the patient was transferred and not formally evaluated upon arrival at the second hospital, but the facts indicate that the patient was “significantly hypoxic.” This should have entailed close monitoring by the receiving clinician, irrespective of the diagnosis.
The pathophysiology of PE is straightforward—but the presentation is often variable and nonspecific and the diagnosis tricky. Thus, for the clinician confronted with a hypoxic patient, it is important to consider this diagnosis early and thoroughly. Evaluate for risk factors: hypercoagulability, as in cases of malignancy, estrogen use, pregnancy, antiphospholipid syndrome (Hughes syndrome), or genomic mutations (eg, factor V Leiden mutation, prothrombin mutation, factor VIII mutations, protein C and protein S deficiency); venous stasis; and vascular endothelial damage, as possibly occasioned by hypertension or atherosclerotic disease.
In addition, it is important to confirm the presence or absence of a DVT. Follow evidence-based rules, such as the Wells score, to guide decision making. In Wells scoring, points are assigned for each of seven criteria, allowing the patient to be categorized by high, moderate, or low probability for PE. The Wells scoring criteria comprise
• Suspected DVT (3 points)
• PE the most likely diagnosis, or equally likely as a second diagnosis (3 points)
• Tachycardia (heart rate > 100 beats/min; 1.5 points)
• Immobilization for at least three days or surgery within the previous four weeks (1.5 points)
• History of DVT or PE (1.5 points)
• Hemoptysis (1 point)
• Malignancy with treatment within previous six months (1 point)
Patients with a total score exceeding 6 points are considered high-probability for PE and should undergo multidetector CT. Those with a score of 2 to 6 have moderate probability and should undergo high-sensitivity d-dimer testing; negative d-dimer results exclude PE and positive results warrant multidetector CT and lower-extremity ultrasound. In low-probability patients (Wells score below 2) with negative d-dimer results, PE is excluded; if d-dimer results are positive, multidetector CT should be ordered.
IN SUM
Extensive discussion of clinical predictive rules, diagnostic modalities, and treatment is beyond the scope of this comment. But clinicians should apply evidence-based decision-making rules to establish a diagnosis. And it should be apparent that hypoxic patients warrant close monitoring—particularly when a change of provider, service, or institution occurs. —DML
A 28-year-old man presented to a Maryland hospital emergency department (ED) with a two-day history of low-grade fever, nonproductive cough, and dizziness. He was also tachycardic and significantly hypoxic. After an hour’s wait, the patient saw an emergency physician, who noted complaints of weakness, shortness of breath, and lightheadedness. The differential diagnosis included pneumonia, congestive heart failure, and pulmonary embolism (PE).
After an ECG, chest x-ray, and blood work, the emergency physician diagnosed pneumonia and renal insufficiency. The patient was admitted but within eight hours of arrival at the ED was transferred to another hospital. The admitting physician at the second hospital did not evaluate the patient on admission.
Almost five hours later, the patient got out of bed and collapsed in the presence of his wife. A code was called, but the man never regained consciousness and was pronounced dead about 90 minutes later. An autopsy confirmed a PE as the cause of death.
Plaintiff for the decedent alleged negligence in the clinicians’ failure to diagnose and treat the PE. The plaintiff claimed that with proper treatment, the patient would have survived.
The defendants argued that there was no negligence involved and that heparin therapy would not have prevented the patient’s death.
What was the outcome? >>
OUTCOME
According to a published account, a $6.1 million verdict was returned.
COMMENT
This is a substantial verdict, reflecting the jury’s revulsion at the loss of a 28-year-old patient. His initial presentation of low-grade fever, nonproductive cough, and dizziness with tachycardia and hypoxia could be consistent with either pneumonia or PE. The facts as presented render the chest x-ray findings and the magnitude of hypoxia unclear. We also are not told whether any specific risk factors existed to make PE more likely, nor whether there was evidence of deep vein thrombosis (DVT) during presentation or at autopsy.
Diagnosing PE can be difficult. However, jurors confronted with a case involving a fatal PE may be led to believe that the diagnosis is straightforward and should never be missed. Plaintiff’s counsel will argue that the patient “would be standing here today” in a fully functional status if the diagnosis had been made.
Here, presumptively, the chest films and chest auscultation were suggestive of pneumonia and led the clinician, who actively considered PE, to ultimately exclude the possibility. It is not clear why the patient was transferred and not formally evaluated upon arrival at the second hospital, but the facts indicate that the patient was “significantly hypoxic.” This should have entailed close monitoring by the receiving clinician, irrespective of the diagnosis.
The pathophysiology of PE is straightforward—but the presentation is often variable and nonspecific and the diagnosis tricky. Thus, for the clinician confronted with a hypoxic patient, it is important to consider this diagnosis early and thoroughly. Evaluate for risk factors: hypercoagulability, as in cases of malignancy, estrogen use, pregnancy, antiphospholipid syndrome (Hughes syndrome), or genomic mutations (eg, factor V Leiden mutation, prothrombin mutation, factor VIII mutations, protein C and protein S deficiency); venous stasis; and vascular endothelial damage, as possibly occasioned by hypertension or atherosclerotic disease.
In addition, it is important to confirm the presence or absence of a DVT. Follow evidence-based rules, such as the Wells score, to guide decision making. In Wells scoring, points are assigned for each of seven criteria, allowing the patient to be categorized by high, moderate, or low probability for PE. The Wells scoring criteria comprise
• Suspected DVT (3 points)
• PE the most likely diagnosis, or equally likely as a second diagnosis (3 points)
• Tachycardia (heart rate > 100 beats/min; 1.5 points)
• Immobilization for at least three days or surgery within the previous four weeks (1.5 points)
• History of DVT or PE (1.5 points)
• Hemoptysis (1 point)
• Malignancy with treatment within previous six months (1 point)
Patients with a total score exceeding 6 points are considered high-probability for PE and should undergo multidetector CT. Those with a score of 2 to 6 have moderate probability and should undergo high-sensitivity d-dimer testing; negative d-dimer results exclude PE and positive results warrant multidetector CT and lower-extremity ultrasound. In low-probability patients (Wells score below 2) with negative d-dimer results, PE is excluded; if d-dimer results are positive, multidetector CT should be ordered.
IN SUM
Extensive discussion of clinical predictive rules, diagnostic modalities, and treatment is beyond the scope of this comment. But clinicians should apply evidence-based decision-making rules to establish a diagnosis. And it should be apparent that hypoxic patients warrant close monitoring—particularly when a change of provider, service, or institution occurs. —DML
A 28-year-old man presented to a Maryland hospital emergency department (ED) with a two-day history of low-grade fever, nonproductive cough, and dizziness. He was also tachycardic and significantly hypoxic. After an hour’s wait, the patient saw an emergency physician, who noted complaints of weakness, shortness of breath, and lightheadedness. The differential diagnosis included pneumonia, congestive heart failure, and pulmonary embolism (PE).
After an ECG, chest x-ray, and blood work, the emergency physician diagnosed pneumonia and renal insufficiency. The patient was admitted but within eight hours of arrival at the ED was transferred to another hospital. The admitting physician at the second hospital did not evaluate the patient on admission.
Almost five hours later, the patient got out of bed and collapsed in the presence of his wife. A code was called, but the man never regained consciousness and was pronounced dead about 90 minutes later. An autopsy confirmed a PE as the cause of death.
Plaintiff for the decedent alleged negligence in the clinicians’ failure to diagnose and treat the PE. The plaintiff claimed that with proper treatment, the patient would have survived.
The defendants argued that there was no negligence involved and that heparin therapy would not have prevented the patient’s death.
What was the outcome? >>
OUTCOME
According to a published account, a $6.1 million verdict was returned.
COMMENT
This is a substantial verdict, reflecting the jury’s revulsion at the loss of a 28-year-old patient. His initial presentation of low-grade fever, nonproductive cough, and dizziness with tachycardia and hypoxia could be consistent with either pneumonia or PE. The facts as presented render the chest x-ray findings and the magnitude of hypoxia unclear. We also are not told whether any specific risk factors existed to make PE more likely, nor whether there was evidence of deep vein thrombosis (DVT) during presentation or at autopsy.
Diagnosing PE can be difficult. However, jurors confronted with a case involving a fatal PE may be led to believe that the diagnosis is straightforward and should never be missed. Plaintiff’s counsel will argue that the patient “would be standing here today” in a fully functional status if the diagnosis had been made.
Here, presumptively, the chest films and chest auscultation were suggestive of pneumonia and led the clinician, who actively considered PE, to ultimately exclude the possibility. It is not clear why the patient was transferred and not formally evaluated upon arrival at the second hospital, but the facts indicate that the patient was “significantly hypoxic.” This should have entailed close monitoring by the receiving clinician, irrespective of the diagnosis.
The pathophysiology of PE is straightforward—but the presentation is often variable and nonspecific and the diagnosis tricky. Thus, for the clinician confronted with a hypoxic patient, it is important to consider this diagnosis early and thoroughly. Evaluate for risk factors: hypercoagulability, as in cases of malignancy, estrogen use, pregnancy, antiphospholipid syndrome (Hughes syndrome), or genomic mutations (eg, factor V Leiden mutation, prothrombin mutation, factor VIII mutations, protein C and protein S deficiency); venous stasis; and vascular endothelial damage, as possibly occasioned by hypertension or atherosclerotic disease.
In addition, it is important to confirm the presence or absence of a DVT. Follow evidence-based rules, such as the Wells score, to guide decision making. In Wells scoring, points are assigned for each of seven criteria, allowing the patient to be categorized by high, moderate, or low probability for PE. The Wells scoring criteria comprise
• Suspected DVT (3 points)
• PE the most likely diagnosis, or equally likely as a second diagnosis (3 points)
• Tachycardia (heart rate > 100 beats/min; 1.5 points)
• Immobilization for at least three days or surgery within the previous four weeks (1.5 points)
• History of DVT or PE (1.5 points)
• Hemoptysis (1 point)
• Malignancy with treatment within previous six months (1 point)
Patients with a total score exceeding 6 points are considered high-probability for PE and should undergo multidetector CT. Those with a score of 2 to 6 have moderate probability and should undergo high-sensitivity d-dimer testing; negative d-dimer results exclude PE and positive results warrant multidetector CT and lower-extremity ultrasound. In low-probability patients (Wells score below 2) with negative d-dimer results, PE is excluded; if d-dimer results are positive, multidetector CT should be ordered.
IN SUM
Extensive discussion of clinical predictive rules, diagnostic modalities, and treatment is beyond the scope of this comment. But clinicians should apply evidence-based decision-making rules to establish a diagnosis. And it should be apparent that hypoxic patients warrant close monitoring—particularly when a change of provider, service, or institution occurs. —DML
Autonomy vs abuse: Can a patient choose a new power of attorney?
Dear Dr. Mossman,
At the hospital where I serve as the psychiatric consultant, a medical team asked me to evaluate a patient’s capacity to designate a new power of attorney (POA) for health care. The patient’s relatives want the change because they think the current POA—also a relative—is stealing the patient’s funds. The contentious family situation made me wonder: What legal risks might I face after I assess the patient’s capacity to choose a new POA?
Submitted by “Dr. P”
As America’s population ages, situations like the one Dr. P has encountered will become more common. Many variables—time constraints, patients’ cognitive impairments, lack of prior relationships with patients, complex medical situations, and strained family dynamics— can make these clinical situations complex and daunting.
Dr. P realizes that feuding relatives can redirect their anger toward a well-meaning physician who might appear to take sides in a dispute. Yet staying silent isn’t a good option, either: If the patient is being mistreated or abused, Dr. P may have a duty to initiate appropriate protective action.
In this article, we’ll respond to Dr. P’s question by examining these topics:
• what a POA is and the rationale for having one
• standards for capacity to choose a POA
• characteristics and dynamics of potential surrogates
• responding to possible elder abuse.
Surrogate decision-makers
People can lose their decision-making capacity because of dementia, acute or chronic illness, or sudden injury. Although autonomy and respecting decisions of mentally capable people are paramount American values, our legal system has several mechanisms that can be activated on behalf of people who have lost their decision-making capabilities.
When a careful evaluation suggests that a patient cannot make informed medical decisions, one solution is to turn to a surrogate decision-maker whom the patient previously has designated to act on his (her) behalf, should he (she) become incapacitated. A surrogate can make decisions based on the incapacitated person’s current utterances (eg, expressions of pain), previously expressed wishes about what should happen under certain circumstances, or the surrogate’s judgment of the person’s best interest.1
States have varied legal frameworks for establishing surrogacy and refer to a surrogate using terms such as proxy, agent, attorney-in-fact, and power of attorney.2 POA responsibilities can encompass a broad array of decision-making tasks or can be limited, for example, to handling banking transactions or managing estate planning.3,4 A POA can be “durable” and grant lasting power regardless of disability, or “springing” and operational only when the designator has lost capacity.
A health care POA designates a substitute decision-maker for medical care. The Patient Self-Determination Act and the Joint Commission obligate health care professionals to follow the decisions made by a legally valid POA. Generally, providers who follow a surrogate’s decision in good faith have legal immunity, but they must challenge a surrogate’s decision if it deviates widely from usual protocol.2
Legal standards
Dr. P received a consultation request that asked whether a patient with compromised medical decision-making powers nonetheless had the current capacity to choose a new POA.
To evaluate the patient’s capacity to designate a new POA, Dr. P must know what having this capacity means. What determines if someone has the capacity to designate a POA is a legal matter, and unless Dr. P is sure what the laws in her state say about this, she should consult a lawyer who can explain the jurisdiction’s applicable legal standards to her.5
The law generally presumes that adults are competent to make health care decisions, including decisions about appointing a POA.5 The law also recognizes that people with cognitive impairments or mental illnesses still can be competent to appoint POAs.4
Most states don’t have statutes that define the capacity to appoint a health care POA. In these jurisdictions, courts may apply standards similar to those concerning competence to enter into a contract.6Table 1 describes criteria in 4 states that do have statutory provisions concerning competence to designate a health care POA.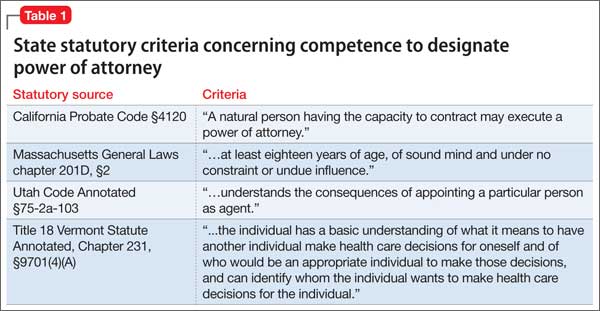
Approaching the evaluation
Before evaluating a person’s capacity to designate a POA, you should first understand the person’s medical condition and learn what powers the surrogate would have. A detailed description of the evaluation process lies beyond the scope of this article. For more information, please consult the structured interviews described by Moye et al4 and Soliman’s guide to the evaluation process.7
In addition to examining the patient’s psychological status and cognitive capacity, you also might have to consider contextual variables, such as:
• potential risks of not allowing the appointment of POA, including a delay in needed care
• the person’s relationship to the proposed POA
• possible power imbalances or evidence of coercion
• how the person would benefit from having the POA.8
People who have good marital or parent-child relationships are more likely to select loved ones as their POAs.9 Family members who have not previously served as surrogates or have not had talked with their loved ones about their preferences feel less confident exercising the duties of a POA.10 An evaluation, therefore, should consider the prior relationship between the designator and proposed surrogate, and particularly whether these parties have discussed the designator’s health care preferences. Table 2 lists potential pitfalls in POA evaluations.2,4,5,8,11-13,16
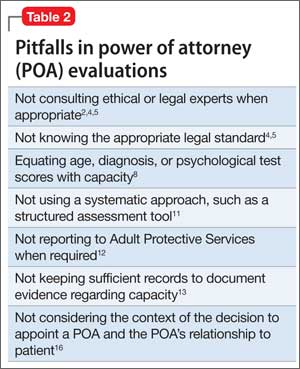
Responding to abuse
Accompanying the request for Dr. P’s evaluation were reports that the current POA had been stealing the patient’s funds. Financial exploitation of older people is not a rare phenomenon.14,15 Yet only about 1 in 25 cases is reported,16,17 and physicians discover as few as 2% of all reported cases.15
Many variables—the stress of the situation,8 pre-existing relationship dynamics,18 and caregiver psychopathology11—lead POAs to exploit their designator. Sometimes, family members believe that they are entitled to a relative’s money because of real or imagined transgressions19 or because they regard themselves as eventual heirs to their relative’s estate.16 Some designated POAs use designators’ funds simply because they need money. Kemp and Mosqueda20 have developed an evaluation framework for assessing possible financial abuse (Table 3).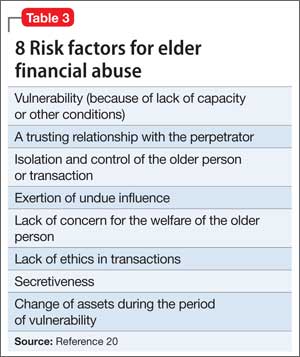
Although reporting financial abuse can strain alliances between patients and their families, psychiatrists bear a responsibility to look out for the welfare of their older patients.8 Indeed, all 50 states have elder abuse statutes, most of which mandate reporting by physicians.21
Suspicion of financial abuse could indicate the need to evaluate the susceptible person’s capacity to make financial decisions.12 Depending on the patient’s circumstances and medical problems, further steps might include:
• contacting proper authorities, such as Adult Protective Services or the Department of Human Services
• contacting local law enforcement
• instituting procedures for emergency guardianship
• arranging for more in-home services for the patient or recommending a higher level of care
• developing a treatment plan for the patient’s medical and psychiatric problems
• communicating with other trusted family members.12,18
Bottom Line
Evaluating the capacity to appoint a power of attorney (POA) often requires awareness of social systems, family dynamics, and legal requirements, combined with the psychiatric data from a systematic individual assessment. Evaluating psychiatrists should understand what type of POA is being considered and the applicable legal standards in the jurisdictions where they work.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Black PG, Derse AR, Derrington S, et al. Can a patient designate his doctor as his proxy decision maker? Pediatrics. 2013;131(5):986-990.
2. Pope TM. Legal fundamentals of surrogate decision making. Chest. 2012;141(4):1074-1081.
3. Araj V. Types of power of attorney: which POA is right for me? http://www.quickenloans.com/blog/types-power-attorney-poa#4zvT8F58fd6zVb2v.99. Published December 29, 2011. Accessed January 11, 2015.
4. Moye J, Sabatino CP, Weintraub Brendel R. Evaluation of the capacity to appoint a healthcare proxy. Am J Geriatr Psychiatry. 2013;21(4):326-336.
5. Whitman R. Capacity for lifetime and estate planning. Penn State L Rev. 2013;117(4):1061-1080.
6. Duke v Kindred Healthcare Operating, Inc., 2011 WL 864321 (Tenn. Ct. App).
7. Soliman S. Evaluating older adults’ capacity and need for guardianship. Current Psychiatry. 2012;11(4):39-42,52-53,A.
8. Katona C, Chiu E, Adelman S, et al. World psychiatric association section of old age psychiatry consensus statement on ethics and capacity in older people with mental disorders. Int J Geriatr Psychiatry. 2009;24(12):1319-1324.
9. Carr D, Moorman SM, Boerner K. End-of-life planning in a family context: does relationship quality affect whether (and with whom) older adults plan? J Gerontol B Psychol Sci Soc Sci. 2013;68(4):586-592.
10. Majesko A, Hong SY, Weissfeld L, et al. Identifying family members who may struggle in the role of surrogate decision maker. Crit Care Med. 2012;40(8):2281-2286.
11. Fulmer T, Guadagno L, Bitondo Dyer C, et al. Progress in elder abuse screening and assessment instruments. J Am Geriatr Soc. 2004;52(2):297-304.
12. Horning SM, Wilkins SS, Dhanani S, et al. A case of elder abuse and undue influence: assessment and treatment from a geriatric interdisciplinary team. Clin Case Stud. 2013;12:373-387.
13. Lui VW, Chiu CC, Ko RS, et al. The principle of assessing mental capacity for enduring power of attorney. Hong Kong Med J. 2014;20(1):59-62.
14. Acierno R, Hernandez-Tejada M, Muzzy W, et al. National Elder Mistreatment Study. Washington, DC: National Institute of Justice; 2009.
15. Wilber KH, Reynolds SL. Introducing a framework for defining financial abuse of the elderly. J Elder Abuse Negl. 1996;8(2):61-80.
16. Mukherjee D. Financial exploitation of older adults in rural settings: a family perspective. J Elder Abuse Negl. 2013; 25(5):425-437.
17. Lifespan of Greater Rochester, Inc., Weill Cornell Medical Center of Cornell University, New York City Department for the Aging. Under the Radar: New York State Elder Abuse Prevalence Study. http://nyceac.com/wp-content/ uploads/2011/05/UndertheRadar051211.pdf. Published May 16, 2011. Accessed January 10, 2015.
18. Hall RCW, Hall RCW, Chapman MJ. Exploitation of the elderly: undue influence as a form of elder abuse. Clin Geriatr. 2005;13(2):28-36.
19. Kemp B, Liao S. Elder financial abuse: tips for the medical director. J Am Med Dir Assoc. 2006;7(9):591-593.
20. Kemp BJ, Mosqueda LA. Elder financial abuse: an evaluation framework and supporting evidence. J Am Geriatr Soc. 2005;53(7):1123-1127.
21. Stiegel S, Klem E. Reporting requirements: provisions and citations in Adult Protective Services laws, by state. http:// www.americanbar.org/content/dam/aba/migrated/ aging/docs/MandatoryReportingProvisionsChart. authcheckdam.pdf. Published 2007. Accessed January 9, 2015.
Dear Dr. Mossman,
At the hospital where I serve as the psychiatric consultant, a medical team asked me to evaluate a patient’s capacity to designate a new power of attorney (POA) for health care. The patient’s relatives want the change because they think the current POA—also a relative—is stealing the patient’s funds. The contentious family situation made me wonder: What legal risks might I face after I assess the patient’s capacity to choose a new POA?
Submitted by “Dr. P”
As America’s population ages, situations like the one Dr. P has encountered will become more common. Many variables—time constraints, patients’ cognitive impairments, lack of prior relationships with patients, complex medical situations, and strained family dynamics— can make these clinical situations complex and daunting.
Dr. P realizes that feuding relatives can redirect their anger toward a well-meaning physician who might appear to take sides in a dispute. Yet staying silent isn’t a good option, either: If the patient is being mistreated or abused, Dr. P may have a duty to initiate appropriate protective action.
In this article, we’ll respond to Dr. P’s question by examining these topics:
• what a POA is and the rationale for having one
• standards for capacity to choose a POA
• characteristics and dynamics of potential surrogates
• responding to possible elder abuse.
Surrogate decision-makers
People can lose their decision-making capacity because of dementia, acute or chronic illness, or sudden injury. Although autonomy and respecting decisions of mentally capable people are paramount American values, our legal system has several mechanisms that can be activated on behalf of people who have lost their decision-making capabilities.
When a careful evaluation suggests that a patient cannot make informed medical decisions, one solution is to turn to a surrogate decision-maker whom the patient previously has designated to act on his (her) behalf, should he (she) become incapacitated. A surrogate can make decisions based on the incapacitated person’s current utterances (eg, expressions of pain), previously expressed wishes about what should happen under certain circumstances, or the surrogate’s judgment of the person’s best interest.1
States have varied legal frameworks for establishing surrogacy and refer to a surrogate using terms such as proxy, agent, attorney-in-fact, and power of attorney.2 POA responsibilities can encompass a broad array of decision-making tasks or can be limited, for example, to handling banking transactions or managing estate planning.3,4 A POA can be “durable” and grant lasting power regardless of disability, or “springing” and operational only when the designator has lost capacity.
A health care POA designates a substitute decision-maker for medical care. The Patient Self-Determination Act and the Joint Commission obligate health care professionals to follow the decisions made by a legally valid POA. Generally, providers who follow a surrogate’s decision in good faith have legal immunity, but they must challenge a surrogate’s decision if it deviates widely from usual protocol.2
Legal standards
Dr. P received a consultation request that asked whether a patient with compromised medical decision-making powers nonetheless had the current capacity to choose a new POA.
To evaluate the patient’s capacity to designate a new POA, Dr. P must know what having this capacity means. What determines if someone has the capacity to designate a POA is a legal matter, and unless Dr. P is sure what the laws in her state say about this, she should consult a lawyer who can explain the jurisdiction’s applicable legal standards to her.5
The law generally presumes that adults are competent to make health care decisions, including decisions about appointing a POA.5 The law also recognizes that people with cognitive impairments or mental illnesses still can be competent to appoint POAs.4
Most states don’t have statutes that define the capacity to appoint a health care POA. In these jurisdictions, courts may apply standards similar to those concerning competence to enter into a contract.6Table 1 describes criteria in 4 states that do have statutory provisions concerning competence to designate a health care POA.
Approaching the evaluation
Before evaluating a person’s capacity to designate a POA, you should first understand the person’s medical condition and learn what powers the surrogate would have. A detailed description of the evaluation process lies beyond the scope of this article. For more information, please consult the structured interviews described by Moye et al4 and Soliman’s guide to the evaluation process.7
In addition to examining the patient’s psychological status and cognitive capacity, you also might have to consider contextual variables, such as:
• potential risks of not allowing the appointment of POA, including a delay in needed care
• the person’s relationship to the proposed POA
• possible power imbalances or evidence of coercion
• how the person would benefit from having the POA.8
People who have good marital or parent-child relationships are more likely to select loved ones as their POAs.9 Family members who have not previously served as surrogates or have not had talked with their loved ones about their preferences feel less confident exercising the duties of a POA.10 An evaluation, therefore, should consider the prior relationship between the designator and proposed surrogate, and particularly whether these parties have discussed the designator’s health care preferences. Table 2 lists potential pitfalls in POA evaluations.2,4,5,8,11-13,16
Responding to abuse
Accompanying the request for Dr. P’s evaluation were reports that the current POA had been stealing the patient’s funds. Financial exploitation of older people is not a rare phenomenon.14,15 Yet only about 1 in 25 cases is reported,16,17 and physicians discover as few as 2% of all reported cases.15
Many variables—the stress of the situation,8 pre-existing relationship dynamics,18 and caregiver psychopathology11—lead POAs to exploit their designator. Sometimes, family members believe that they are entitled to a relative’s money because of real or imagined transgressions19 or because they regard themselves as eventual heirs to their relative’s estate.16 Some designated POAs use designators’ funds simply because they need money. Kemp and Mosqueda20 have developed an evaluation framework for assessing possible financial abuse (Table 3).
Although reporting financial abuse can strain alliances between patients and their families, psychiatrists bear a responsibility to look out for the welfare of their older patients.8 Indeed, all 50 states have elder abuse statutes, most of which mandate reporting by physicians.21
Suspicion of financial abuse could indicate the need to evaluate the susceptible person’s capacity to make financial decisions.12 Depending on the patient’s circumstances and medical problems, further steps might include:
• contacting proper authorities, such as Adult Protective Services or the Department of Human Services
• contacting local law enforcement
• instituting procedures for emergency guardianship
• arranging for more in-home services for the patient or recommending a higher level of care
• developing a treatment plan for the patient’s medical and psychiatric problems
• communicating with other trusted family members.12,18
Bottom Line
Evaluating the capacity to appoint a power of attorney (POA) often requires awareness of social systems, family dynamics, and legal requirements, combined with the psychiatric data from a systematic individual assessment. Evaluating psychiatrists should understand what type of POA is being considered and the applicable legal standards in the jurisdictions where they work.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Dear Dr. Mossman,
At the hospital where I serve as the psychiatric consultant, a medical team asked me to evaluate a patient’s capacity to designate a new power of attorney (POA) for health care. The patient’s relatives want the change because they think the current POA—also a relative—is stealing the patient’s funds. The contentious family situation made me wonder: What legal risks might I face after I assess the patient’s capacity to choose a new POA?
Submitted by “Dr. P”
As America’s population ages, situations like the one Dr. P has encountered will become more common. Many variables—time constraints, patients’ cognitive impairments, lack of prior relationships with patients, complex medical situations, and strained family dynamics— can make these clinical situations complex and daunting.
Dr. P realizes that feuding relatives can redirect their anger toward a well-meaning physician who might appear to take sides in a dispute. Yet staying silent isn’t a good option, either: If the patient is being mistreated or abused, Dr. P may have a duty to initiate appropriate protective action.
In this article, we’ll respond to Dr. P’s question by examining these topics:
• what a POA is and the rationale for having one
• standards for capacity to choose a POA
• characteristics and dynamics of potential surrogates
• responding to possible elder abuse.
Surrogate decision-makers
People can lose their decision-making capacity because of dementia, acute or chronic illness, or sudden injury. Although autonomy and respecting decisions of mentally capable people are paramount American values, our legal system has several mechanisms that can be activated on behalf of people who have lost their decision-making capabilities.
When a careful evaluation suggests that a patient cannot make informed medical decisions, one solution is to turn to a surrogate decision-maker whom the patient previously has designated to act on his (her) behalf, should he (she) become incapacitated. A surrogate can make decisions based on the incapacitated person’s current utterances (eg, expressions of pain), previously expressed wishes about what should happen under certain circumstances, or the surrogate’s judgment of the person’s best interest.1
States have varied legal frameworks for establishing surrogacy and refer to a surrogate using terms such as proxy, agent, attorney-in-fact, and power of attorney.2 POA responsibilities can encompass a broad array of decision-making tasks or can be limited, for example, to handling banking transactions or managing estate planning.3,4 A POA can be “durable” and grant lasting power regardless of disability, or “springing” and operational only when the designator has lost capacity.
A health care POA designates a substitute decision-maker for medical care. The Patient Self-Determination Act and the Joint Commission obligate health care professionals to follow the decisions made by a legally valid POA. Generally, providers who follow a surrogate’s decision in good faith have legal immunity, but they must challenge a surrogate’s decision if it deviates widely from usual protocol.2
Legal standards
Dr. P received a consultation request that asked whether a patient with compromised medical decision-making powers nonetheless had the current capacity to choose a new POA.
To evaluate the patient’s capacity to designate a new POA, Dr. P must know what having this capacity means. What determines if someone has the capacity to designate a POA is a legal matter, and unless Dr. P is sure what the laws in her state say about this, she should consult a lawyer who can explain the jurisdiction’s applicable legal standards to her.5
The law generally presumes that adults are competent to make health care decisions, including decisions about appointing a POA.5 The law also recognizes that people with cognitive impairments or mental illnesses still can be competent to appoint POAs.4
Most states don’t have statutes that define the capacity to appoint a health care POA. In these jurisdictions, courts may apply standards similar to those concerning competence to enter into a contract.6Table 1 describes criteria in 4 states that do have statutory provisions concerning competence to designate a health care POA.
Approaching the evaluation
Before evaluating a person’s capacity to designate a POA, you should first understand the person’s medical condition and learn what powers the surrogate would have. A detailed description of the evaluation process lies beyond the scope of this article. For more information, please consult the structured interviews described by Moye et al4 and Soliman’s guide to the evaluation process.7
In addition to examining the patient’s psychological status and cognitive capacity, you also might have to consider contextual variables, such as:
• potential risks of not allowing the appointment of POA, including a delay in needed care
• the person’s relationship to the proposed POA
• possible power imbalances or evidence of coercion
• how the person would benefit from having the POA.8
People who have good marital or parent-child relationships are more likely to select loved ones as their POAs.9 Family members who have not previously served as surrogates or have not had talked with their loved ones about their preferences feel less confident exercising the duties of a POA.10 An evaluation, therefore, should consider the prior relationship between the designator and proposed surrogate, and particularly whether these parties have discussed the designator’s health care preferences. Table 2 lists potential pitfalls in POA evaluations.2,4,5,8,11-13,16
Responding to abuse
Accompanying the request for Dr. P’s evaluation were reports that the current POA had been stealing the patient’s funds. Financial exploitation of older people is not a rare phenomenon.14,15 Yet only about 1 in 25 cases is reported,16,17 and physicians discover as few as 2% of all reported cases.15
Many variables—the stress of the situation,8 pre-existing relationship dynamics,18 and caregiver psychopathology11—lead POAs to exploit their designator. Sometimes, family members believe that they are entitled to a relative’s money because of real or imagined transgressions19 or because they regard themselves as eventual heirs to their relative’s estate.16 Some designated POAs use designators’ funds simply because they need money. Kemp and Mosqueda20 have developed an evaluation framework for assessing possible financial abuse (Table 3).
Although reporting financial abuse can strain alliances between patients and their families, psychiatrists bear a responsibility to look out for the welfare of their older patients.8 Indeed, all 50 states have elder abuse statutes, most of which mandate reporting by physicians.21
Suspicion of financial abuse could indicate the need to evaluate the susceptible person’s capacity to make financial decisions.12 Depending on the patient’s circumstances and medical problems, further steps might include:
• contacting proper authorities, such as Adult Protective Services or the Department of Human Services
• contacting local law enforcement
• instituting procedures for emergency guardianship
• arranging for more in-home services for the patient or recommending a higher level of care
• developing a treatment plan for the patient’s medical and psychiatric problems
• communicating with other trusted family members.12,18
Bottom Line
Evaluating the capacity to appoint a power of attorney (POA) often requires awareness of social systems, family dynamics, and legal requirements, combined with the psychiatric data from a systematic individual assessment. Evaluating psychiatrists should understand what type of POA is being considered and the applicable legal standards in the jurisdictions where they work.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Black PG, Derse AR, Derrington S, et al. Can a patient designate his doctor as his proxy decision maker? Pediatrics. 2013;131(5):986-990.
2. Pope TM. Legal fundamentals of surrogate decision making. Chest. 2012;141(4):1074-1081.
3. Araj V. Types of power of attorney: which POA is right for me? http://www.quickenloans.com/blog/types-power-attorney-poa#4zvT8F58fd6zVb2v.99. Published December 29, 2011. Accessed January 11, 2015.
4. Moye J, Sabatino CP, Weintraub Brendel R. Evaluation of the capacity to appoint a healthcare proxy. Am J Geriatr Psychiatry. 2013;21(4):326-336.
5. Whitman R. Capacity for lifetime and estate planning. Penn State L Rev. 2013;117(4):1061-1080.
6. Duke v Kindred Healthcare Operating, Inc., 2011 WL 864321 (Tenn. Ct. App).
7. Soliman S. Evaluating older adults’ capacity and need for guardianship. Current Psychiatry. 2012;11(4):39-42,52-53,A.
8. Katona C, Chiu E, Adelman S, et al. World psychiatric association section of old age psychiatry consensus statement on ethics and capacity in older people with mental disorders. Int J Geriatr Psychiatry. 2009;24(12):1319-1324.
9. Carr D, Moorman SM, Boerner K. End-of-life planning in a family context: does relationship quality affect whether (and with whom) older adults plan? J Gerontol B Psychol Sci Soc Sci. 2013;68(4):586-592.
10. Majesko A, Hong SY, Weissfeld L, et al. Identifying family members who may struggle in the role of surrogate decision maker. Crit Care Med. 2012;40(8):2281-2286.
11. Fulmer T, Guadagno L, Bitondo Dyer C, et al. Progress in elder abuse screening and assessment instruments. J Am Geriatr Soc. 2004;52(2):297-304.
12. Horning SM, Wilkins SS, Dhanani S, et al. A case of elder abuse and undue influence: assessment and treatment from a geriatric interdisciplinary team. Clin Case Stud. 2013;12:373-387.
13. Lui VW, Chiu CC, Ko RS, et al. The principle of assessing mental capacity for enduring power of attorney. Hong Kong Med J. 2014;20(1):59-62.
14. Acierno R, Hernandez-Tejada M, Muzzy W, et al. National Elder Mistreatment Study. Washington, DC: National Institute of Justice; 2009.
15. Wilber KH, Reynolds SL. Introducing a framework for defining financial abuse of the elderly. J Elder Abuse Negl. 1996;8(2):61-80.
16. Mukherjee D. Financial exploitation of older adults in rural settings: a family perspective. J Elder Abuse Negl. 2013; 25(5):425-437.
17. Lifespan of Greater Rochester, Inc., Weill Cornell Medical Center of Cornell University, New York City Department for the Aging. Under the Radar: New York State Elder Abuse Prevalence Study. http://nyceac.com/wp-content/ uploads/2011/05/UndertheRadar051211.pdf. Published May 16, 2011. Accessed January 10, 2015.
18. Hall RCW, Hall RCW, Chapman MJ. Exploitation of the elderly: undue influence as a form of elder abuse. Clin Geriatr. 2005;13(2):28-36.
19. Kemp B, Liao S. Elder financial abuse: tips for the medical director. J Am Med Dir Assoc. 2006;7(9):591-593.
20. Kemp BJ, Mosqueda LA. Elder financial abuse: an evaluation framework and supporting evidence. J Am Geriatr Soc. 2005;53(7):1123-1127.
21. Stiegel S, Klem E. Reporting requirements: provisions and citations in Adult Protective Services laws, by state. http:// www.americanbar.org/content/dam/aba/migrated/ aging/docs/MandatoryReportingProvisionsChart. authcheckdam.pdf. Published 2007. Accessed January 9, 2015.
1. Black PG, Derse AR, Derrington S, et al. Can a patient designate his doctor as his proxy decision maker? Pediatrics. 2013;131(5):986-990.
2. Pope TM. Legal fundamentals of surrogate decision making. Chest. 2012;141(4):1074-1081.
3. Araj V. Types of power of attorney: which POA is right for me? http://www.quickenloans.com/blog/types-power-attorney-poa#4zvT8F58fd6zVb2v.99. Published December 29, 2011. Accessed January 11, 2015.
4. Moye J, Sabatino CP, Weintraub Brendel R. Evaluation of the capacity to appoint a healthcare proxy. Am J Geriatr Psychiatry. 2013;21(4):326-336.
5. Whitman R. Capacity for lifetime and estate planning. Penn State L Rev. 2013;117(4):1061-1080.
6. Duke v Kindred Healthcare Operating, Inc., 2011 WL 864321 (Tenn. Ct. App).
7. Soliman S. Evaluating older adults’ capacity and need for guardianship. Current Psychiatry. 2012;11(4):39-42,52-53,A.
8. Katona C, Chiu E, Adelman S, et al. World psychiatric association section of old age psychiatry consensus statement on ethics and capacity in older people with mental disorders. Int J Geriatr Psychiatry. 2009;24(12):1319-1324.
9. Carr D, Moorman SM, Boerner K. End-of-life planning in a family context: does relationship quality affect whether (and with whom) older adults plan? J Gerontol B Psychol Sci Soc Sci. 2013;68(4):586-592.
10. Majesko A, Hong SY, Weissfeld L, et al. Identifying family members who may struggle in the role of surrogate decision maker. Crit Care Med. 2012;40(8):2281-2286.
11. Fulmer T, Guadagno L, Bitondo Dyer C, et al. Progress in elder abuse screening and assessment instruments. J Am Geriatr Soc. 2004;52(2):297-304.
12. Horning SM, Wilkins SS, Dhanani S, et al. A case of elder abuse and undue influence: assessment and treatment from a geriatric interdisciplinary team. Clin Case Stud. 2013;12:373-387.
13. Lui VW, Chiu CC, Ko RS, et al. The principle of assessing mental capacity for enduring power of attorney. Hong Kong Med J. 2014;20(1):59-62.
14. Acierno R, Hernandez-Tejada M, Muzzy W, et al. National Elder Mistreatment Study. Washington, DC: National Institute of Justice; 2009.
15. Wilber KH, Reynolds SL. Introducing a framework for defining financial abuse of the elderly. J Elder Abuse Negl. 1996;8(2):61-80.
16. Mukherjee D. Financial exploitation of older adults in rural settings: a family perspective. J Elder Abuse Negl. 2013; 25(5):425-437.
17. Lifespan of Greater Rochester, Inc., Weill Cornell Medical Center of Cornell University, New York City Department for the Aging. Under the Radar: New York State Elder Abuse Prevalence Study. http://nyceac.com/wp-content/ uploads/2011/05/UndertheRadar051211.pdf. Published May 16, 2011. Accessed January 10, 2015.
18. Hall RCW, Hall RCW, Chapman MJ. Exploitation of the elderly: undue influence as a form of elder abuse. Clin Geriatr. 2005;13(2):28-36.
19. Kemp B, Liao S. Elder financial abuse: tips for the medical director. J Am Med Dir Assoc. 2006;7(9):591-593.
20. Kemp BJ, Mosqueda LA. Elder financial abuse: an evaluation framework and supporting evidence. J Am Geriatr Soc. 2005;53(7):1123-1127.
21. Stiegel S, Klem E. Reporting requirements: provisions and citations in Adult Protective Services laws, by state. http:// www.americanbar.org/content/dam/aba/migrated/ aging/docs/MandatoryReportingProvisionsChart. authcheckdam.pdf. Published 2007. Accessed January 9, 2015.
Bleeding complications following femoral angiographic access
Bleeding complications following angiographic interventions have recently become an increasing cause of medical malpractice litigation. The reason for this increase is likely a result of several factors including the controversy surrounding the multiple approaches that are currently employed for the treatment of this type of bleeding, as well as the significant morbidity and mortality associated with these treatment paradigms. Allegations in these lawsuits usually include failure to diagnose, failure to treat, failure to transfuse, negligence in the use of an endovascular approach, and negligence in open surgical treatment. Physical examination, close observation, and an aggressive approach to intervention are necessary if litigation is to be avoided in this patient population.
Case 1
The patient underwent cardiac catheterization with placement of a coronary stent. The patient was placed on Integrilin. Following the catheterization, the patient had multiple episodes of hypotension. Each episode responded to fluid boluses and transfusion. No surgical consultation was obtained. The patient’s hemoglobin never fell below 8 grams. The patient was transfused approximately 8 units of blood. The patient’s Integrilin was discontinued. However, the patient progressed to multisystem organ failure and died. Autopsy revealed a massive hematoma of the retroperitoneum and a patent coronary stent. A medical malpractice suit was filed. The case was settled.
Case 2
A patient underwent cardiac catheterization and subsequently developed severe bleeding. She received approximately 10 units of blood prior to vascular surgical consultation. By the time the vascular surgeon saw the patient, the patient was intubated and on vasopressors. The vascular surgeon stated that the patient was not a candidate for surgery. The patient subsequently died. A lawsuit was filed against both the cardiologist and the vascular surgeon. This case was settled by both physicians.
Case 3
A cardiologist calls a vascular surgeon who is at home at 10 p.m. to let her know that he has a patient with a retroperitoneal hematoma following a cardiac cath. He informs the surgeon that the patient is stable. He “just wants her to be aware in case the patient’s condition deteriorates.”
During the night the patient has repeated hypotensive episodes which the cardiologist manages with transfusions. At 5 a.m. the patient arrests and is resuscitated. The surgeon is called, and she takes the patient to surgery but the patient succumbs. The surgeon is sued for not coming in to see the patient and being more involved during the night.
The jury finds in favor of the surgeon. However, the trial took 2 weeks during which time the surgeon had to attend the deliberations and so she was unable work.
Discussion
Unfortunately, the above examples represent the all too often complication of postprocedure bleeding following femoral access.

In case 1, early exploration would more likely than not, and within a reasonable degree of medical certainty, prevented the patient’s death. The presumption is that the patient died from the untreated complication of postcatheterization hemorrhage. The defendant’s claim that the patient’s hemoglobin was never lower than 8 mg did not serve as an adequate defense. Even if the patient was found at autopsy to have an occluded stent which caused an acute MI, the plaintiff’s attorney would likely argue successfully that if the bleeding had been appropriately treated, the stent would have remained patent. The cardiologist was found culpable for not consulting a vascular surgeon.
In the second example, the plaintiff’s expert explained to the jury that without surgery, the patient would continue to bleed and certainly die. He went on to opine that the only possible chance of the patient surviving was with surgical intervention, and this chance was denied to the patient by the vascular surgeon who refused to operate. In these types of cases, the surgeon incorrectly believes that he/she can avoid liability and involvement in the case by not operating on the patient. However, as this case demonstrated, the surgeon is still likely to be named as a defendant in the law suit.
The third case illustrates two common pitfalls for the vascular surgeon and perhaps represents the most dangerous situation for the vascular surgeon. The first pitfall occurs when the vascular surgeon relies on telephone information without examining the patient. Secondly, as in this case, a formal consult was never initiated by the cardiologist. The surgeon incorrectly assumed that because no formal consult was placed she had no liability. However, according to the plaintiff’s expert, since she had been informed about the patient she should have come in to see the patient.
Had she done so, he alleged she would have realized that the patient required an intervention either with a covered stent or a surgical repair of the bleeding external iliac artery. Clearly, the fact that no formal consult was placed in the chart did not prevent the vascular surgeon from being a named defendant in this case.
Several steps should be taken if a physician is to minimize the risk of being named as a defendant in a lawsuit involving postangiographic intervention bleeding. First, if the physician is a not a surgeon, surgical consultation should be obtained as soon as postprocedure bleeding is suspected. Second, surgeons should pursue an aggressive approach to the treatment of this complication. Whereas it may be reasonable to treat a single episode of hypotension with fluid or blood transfusion, unless there are mitigating circumstances, any patient who develops a second episode of hypotension in the face of ongoing bleeding should undergo intervention. Furthermore, there must be clear documentation as to why a particular approach (endovascular versus open repair) was chosen. A medical physician’s inability to perform an open approach or a surgeon’s inability to perform an endovascular approach are not sustainable defenses.
Surgeons who are consulted late in the patient’s clinical course, prior to intervention, should document the patient’s poor prognosis and make it clear that no matter what is done the patient is unlikely to survive.
However, in most situations, the defense that a patient with ongoing bleeding was too unstable to treat is likely to fail.
Access site bleeding following percutaneous interventions is often a readily treatable complication. A low threshold for intervention, cooperation among vascular specialists, and, as always, clear documentation will go a long way to keep physicians working and out of the courtroom.
Dr. Brown is associate editor of Vascular Specialist. Dr. Samson is the medical editor, Vascular Specialist. The opinions expressed by the authors neither imply nor establish a standard of care.
Bleeding complications following angiographic interventions have recently become an increasing cause of medical malpractice litigation. The reason for this increase is likely a result of several factors including the controversy surrounding the multiple approaches that are currently employed for the treatment of this type of bleeding, as well as the significant morbidity and mortality associated with these treatment paradigms. Allegations in these lawsuits usually include failure to diagnose, failure to treat, failure to transfuse, negligence in the use of an endovascular approach, and negligence in open surgical treatment. Physical examination, close observation, and an aggressive approach to intervention are necessary if litigation is to be avoided in this patient population.
Case 1
The patient underwent cardiac catheterization with placement of a coronary stent. The patient was placed on Integrilin. Following the catheterization, the patient had multiple episodes of hypotension. Each episode responded to fluid boluses and transfusion. No surgical consultation was obtained. The patient’s hemoglobin never fell below 8 grams. The patient was transfused approximately 8 units of blood. The patient’s Integrilin was discontinued. However, the patient progressed to multisystem organ failure and died. Autopsy revealed a massive hematoma of the retroperitoneum and a patent coronary stent. A medical malpractice suit was filed. The case was settled.
Case 2
A patient underwent cardiac catheterization and subsequently developed severe bleeding. She received approximately 10 units of blood prior to vascular surgical consultation. By the time the vascular surgeon saw the patient, the patient was intubated and on vasopressors. The vascular surgeon stated that the patient was not a candidate for surgery. The patient subsequently died. A lawsuit was filed against both the cardiologist and the vascular surgeon. This case was settled by both physicians.
Case 3
A cardiologist calls a vascular surgeon who is at home at 10 p.m. to let her know that he has a patient with a retroperitoneal hematoma following a cardiac cath. He informs the surgeon that the patient is stable. He “just wants her to be aware in case the patient’s condition deteriorates.”
During the night the patient has repeated hypotensive episodes which the cardiologist manages with transfusions. At 5 a.m. the patient arrests and is resuscitated. The surgeon is called, and she takes the patient to surgery but the patient succumbs. The surgeon is sued for not coming in to see the patient and being more involved during the night.
The jury finds in favor of the surgeon. However, the trial took 2 weeks during which time the surgeon had to attend the deliberations and so she was unable work.
Discussion
Unfortunately, the above examples represent the all too often complication of postprocedure bleeding following femoral access.
In case 1, early exploration would more likely than not, and within a reasonable degree of medical certainty, prevented the patient’s death. The presumption is that the patient died from the untreated complication of postcatheterization hemorrhage. The defendant’s claim that the patient’s hemoglobin was never lower than 8 mg did not serve as an adequate defense. Even if the patient was found at autopsy to have an occluded stent which caused an acute MI, the plaintiff’s attorney would likely argue successfully that if the bleeding had been appropriately treated, the stent would have remained patent. The cardiologist was found culpable for not consulting a vascular surgeon.
In the second example, the plaintiff’s expert explained to the jury that without surgery, the patient would continue to bleed and certainly die. He went on to opine that the only possible chance of the patient surviving was with surgical intervention, and this chance was denied to the patient by the vascular surgeon who refused to operate. In these types of cases, the surgeon incorrectly believes that he/she can avoid liability and involvement in the case by not operating on the patient. However, as this case demonstrated, the surgeon is still likely to be named as a defendant in the law suit.
The third case illustrates two common pitfalls for the vascular surgeon and perhaps represents the most dangerous situation for the vascular surgeon. The first pitfall occurs when the vascular surgeon relies on telephone information without examining the patient. Secondly, as in this case, a formal consult was never initiated by the cardiologist. The surgeon incorrectly assumed that because no formal consult was placed she had no liability. However, according to the plaintiff’s expert, since she had been informed about the patient she should have come in to see the patient.
Had she done so, he alleged she would have realized that the patient required an intervention either with a covered stent or a surgical repair of the bleeding external iliac artery. Clearly, the fact that no formal consult was placed in the chart did not prevent the vascular surgeon from being a named defendant in this case.
Several steps should be taken if a physician is to minimize the risk of being named as a defendant in a lawsuit involving postangiographic intervention bleeding. First, if the physician is a not a surgeon, surgical consultation should be obtained as soon as postprocedure bleeding is suspected. Second, surgeons should pursue an aggressive approach to the treatment of this complication. Whereas it may be reasonable to treat a single episode of hypotension with fluid or blood transfusion, unless there are mitigating circumstances, any patient who develops a second episode of hypotension in the face of ongoing bleeding should undergo intervention. Furthermore, there must be clear documentation as to why a particular approach (endovascular versus open repair) was chosen. A medical physician’s inability to perform an open approach or a surgeon’s inability to perform an endovascular approach are not sustainable defenses.
Surgeons who are consulted late in the patient’s clinical course, prior to intervention, should document the patient’s poor prognosis and make it clear that no matter what is done the patient is unlikely to survive.
However, in most situations, the defense that a patient with ongoing bleeding was too unstable to treat is likely to fail.
Access site bleeding following percutaneous interventions is often a readily treatable complication. A low threshold for intervention, cooperation among vascular specialists, and, as always, clear documentation will go a long way to keep physicians working and out of the courtroom.
Dr. Brown is associate editor of Vascular Specialist. Dr. Samson is the medical editor, Vascular Specialist. The opinions expressed by the authors neither imply nor establish a standard of care.
Bleeding complications following angiographic interventions have recently become an increasing cause of medical malpractice litigation. The reason for this increase is likely a result of several factors including the controversy surrounding the multiple approaches that are currently employed for the treatment of this type of bleeding, as well as the significant morbidity and mortality associated with these treatment paradigms. Allegations in these lawsuits usually include failure to diagnose, failure to treat, failure to transfuse, negligence in the use of an endovascular approach, and negligence in open surgical treatment. Physical examination, close observation, and an aggressive approach to intervention are necessary if litigation is to be avoided in this patient population.
Case 1
The patient underwent cardiac catheterization with placement of a coronary stent. The patient was placed on Integrilin. Following the catheterization, the patient had multiple episodes of hypotension. Each episode responded to fluid boluses and transfusion. No surgical consultation was obtained. The patient’s hemoglobin never fell below 8 grams. The patient was transfused approximately 8 units of blood. The patient’s Integrilin was discontinued. However, the patient progressed to multisystem organ failure and died. Autopsy revealed a massive hematoma of the retroperitoneum and a patent coronary stent. A medical malpractice suit was filed. The case was settled.
Case 2
A patient underwent cardiac catheterization and subsequently developed severe bleeding. She received approximately 10 units of blood prior to vascular surgical consultation. By the time the vascular surgeon saw the patient, the patient was intubated and on vasopressors. The vascular surgeon stated that the patient was not a candidate for surgery. The patient subsequently died. A lawsuit was filed against both the cardiologist and the vascular surgeon. This case was settled by both physicians.
Case 3
A cardiologist calls a vascular surgeon who is at home at 10 p.m. to let her know that he has a patient with a retroperitoneal hematoma following a cardiac cath. He informs the surgeon that the patient is stable. He “just wants her to be aware in case the patient’s condition deteriorates.”
During the night the patient has repeated hypotensive episodes which the cardiologist manages with transfusions. At 5 a.m. the patient arrests and is resuscitated. The surgeon is called, and she takes the patient to surgery but the patient succumbs. The surgeon is sued for not coming in to see the patient and being more involved during the night.
The jury finds in favor of the surgeon. However, the trial took 2 weeks during which time the surgeon had to attend the deliberations and so she was unable work.
Discussion
Unfortunately, the above examples represent the all too often complication of postprocedure bleeding following femoral access.
In case 1, early exploration would more likely than not, and within a reasonable degree of medical certainty, prevented the patient’s death. The presumption is that the patient died from the untreated complication of postcatheterization hemorrhage. The defendant’s claim that the patient’s hemoglobin was never lower than 8 mg did not serve as an adequate defense. Even if the patient was found at autopsy to have an occluded stent which caused an acute MI, the plaintiff’s attorney would likely argue successfully that if the bleeding had been appropriately treated, the stent would have remained patent. The cardiologist was found culpable for not consulting a vascular surgeon.
In the second example, the plaintiff’s expert explained to the jury that without surgery, the patient would continue to bleed and certainly die. He went on to opine that the only possible chance of the patient surviving was with surgical intervention, and this chance was denied to the patient by the vascular surgeon who refused to operate. In these types of cases, the surgeon incorrectly believes that he/she can avoid liability and involvement in the case by not operating on the patient. However, as this case demonstrated, the surgeon is still likely to be named as a defendant in the law suit.
The third case illustrates two common pitfalls for the vascular surgeon and perhaps represents the most dangerous situation for the vascular surgeon. The first pitfall occurs when the vascular surgeon relies on telephone information without examining the patient. Secondly, as in this case, a formal consult was never initiated by the cardiologist. The surgeon incorrectly assumed that because no formal consult was placed she had no liability. However, according to the plaintiff’s expert, since she had been informed about the patient she should have come in to see the patient.
Had she done so, he alleged she would have realized that the patient required an intervention either with a covered stent or a surgical repair of the bleeding external iliac artery. Clearly, the fact that no formal consult was placed in the chart did not prevent the vascular surgeon from being a named defendant in this case.
Several steps should be taken if a physician is to minimize the risk of being named as a defendant in a lawsuit involving postangiographic intervention bleeding. First, if the physician is a not a surgeon, surgical consultation should be obtained as soon as postprocedure bleeding is suspected. Second, surgeons should pursue an aggressive approach to the treatment of this complication. Whereas it may be reasonable to treat a single episode of hypotension with fluid or blood transfusion, unless there are mitigating circumstances, any patient who develops a second episode of hypotension in the face of ongoing bleeding should undergo intervention. Furthermore, there must be clear documentation as to why a particular approach (endovascular versus open repair) was chosen. A medical physician’s inability to perform an open approach or a surgeon’s inability to perform an endovascular approach are not sustainable defenses.
Surgeons who are consulted late in the patient’s clinical course, prior to intervention, should document the patient’s poor prognosis and make it clear that no matter what is done the patient is unlikely to survive.
However, in most situations, the defense that a patient with ongoing bleeding was too unstable to treat is likely to fail.
Access site bleeding following percutaneous interventions is often a readily treatable complication. A low threshold for intervention, cooperation among vascular specialists, and, as always, clear documentation will go a long way to keep physicians working and out of the courtroom.
Dr. Brown is associate editor of Vascular Specialist. Dr. Samson is the medical editor, Vascular Specialist. The opinions expressed by the authors neither imply nor establish a standard of care.
Negligence during cord blood sampling? Child has CP

Negligence during cord blood sampling? Child has CP
A woman’s first child was treated for neonatal alloimmune thrombocytopenia (NAIT) after birth. When prenatal testing identified NAIT in her second child, the mother received twice-weekly immunoglobulin injections to increase the fetus’ platelet count.
At 33 weeks’ gestation, percutaneous umbilical blood sampling (PUBS) was undertaken by a maternal-fetal medicine (MFM) specialist to check the baby’s platelet count and inject additional platelets. During the procedure, the mother’s blood pressure dropped from 122/80 to 80/40 mm Hg. The fetal heart rate dropped from 120–130 bpm to 65 bpm. An emergency cesarean delivery was performed.
At birth, the baby had seizures and respiratory distress secondary to perinatal asphyxia. She has severe spastic quadriplegic cerebral palsy. At age 9 years, she has been hospitalized for multiple complications, underwent tendon-release procedures on both legs, and receives occupational and physical therapy. She cannot speak, needs a feeding tube, is wheelchair bound, and requires 24-hour nursing care.
PARENTS’ CLAIM The MFM was not adequately trained to perform PUBS and did not use continuous ultrasound guidance during the procedure. She was negligent in attempting to insert the needle into the umbilical cord multiple times. She failed to recognize fetal distress. The anesthesiologist only told the MFM that the patient was hypotensive, not that the patient’s blood pressure never returned to baseline.
defendants’ DEFENSE The mother was part of a NAIT study, and the procedure was properly performed under the guidelines of that study. A sonographer constantly monitored the fetal heart rate. The anesthesiologist claimed that proper actions were taken in response to low blood pressure; there was no requirement to communicate more information to the MFM. The child’s hypoxia was due to placental abruption. The estimated cost of the life-care plan for the child is $5 to $10 million.
VERDICT A $15 million Indiana verdict was returned against the medical center that employed the anesthesiologist, but was reduced to $1,250,000 by the state cap. A defense verdict was returned for the MFM.
Woman dies from cervical cancer: $2.33M
When a woman had an abnormal Pap smear in 2001, her gynecologist did not order a repeat test, but told the patient to return in 3 months. The patient did not see the gynecologist again until 2007. At that time, her Pap smear was normal, but she was experiencing symptoms. The gynecologist did not order further testing.
In 2009, the patient was found to have advanced cervical cancer. She died 2 years later at age 48.
ESTATE’S CLAIM The second Pap smear was incorrectly interpreted. Further testing should have been ordered in 2001 and 2007.
DEFENDANTS’ DEFENSE The laboratory and patient’s estate settled for a confidential amount before the trial commenced. The gynecologist denied negligence. He claimed the patient was at fault for not returning to see him, as recommended.
VERDICT A New Jersey jury found the gynecologist 40% at fault, the laboratory 50% at fault, and the patient 10% at fault. A gross verdict of $2.33 million was returned.
Was it HELLP syndrome?
By her prenatal visit at 33 weeks’ gestation, a mother had gained 59 lb during her pregnancy. Three days later, she went to the emergency department (ED). The fetus had died.
PARENT’S CLAIM The ObGyn failed to intervene when the mother was gaining excessive weight. The mother had HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count); timely diagnosis could have avoided fetal demise.
DEFENDANTS’ DEFENSE Fetal demise could not have been diagnosed or prevented. The cause of the mother’s illness was never fully identified.
VERDICT A Tennessee defense verdict was returned.

Vesicovaginal fistula after hysterectomy
A woman underwent a hysterectomy performed by her ObGyn. A week later, during a postoperative visit, the ObGyn detected a bladder injury and related vesicovaginal fistula. He attempted a repair, but it failed. Eventually, successful repair surgery was performed by a urologist.
PATIENT’S CLAIM The ObGyn only should have used sharp dissection during the hysterectomy, as opposed to a combination of sharp and blunt dissection, due to dense adhesions that had developed after earlier abdominal surgery. Because the ObGyn had never repaired a vesicovaginal fistula before, he should have requested the assistance of a urologist or urogynecologist. A peritoneal flap should have been used during the initial repair.
PHYSICIAN’S DEFENSE Referral to a urologist or urogynecologist had been offered to the patient, but was refused (no record of this was found in the patient’s file). There was no negligence in the attempted repair.
VERDICT A $387,000 Virginia verdict was returned.
Did she really need that hysterectomy?
A 31-year-old woman went to the ED with sudden, severe abdominal pain. The radiologist noted that the patient’s appendix could not be visualized on computed tomography (CT) because it was behind the cecum. A general surgeon interpreted the report as ruling out appendicitis, made a diagnosis of pelvic inflammatory disease, and requested a gynecologic consult. An ObGyn sent his nurse practitioner to see the patient in the ED. The patient was discharged and instructed to follow up with the ObGyn.
When the patient’s condition worsened 2 days later, she returned to the ED. The ObGyn performed laparoscopic exploratory surgery. When he could not find the appendix, he called the general surgeon. The surgeon was in his car, and told the ObGyn that it was unnecessary to visualize the appendix; the ObGyn could complete the surgery. The patient was again discharged without a firm diagnosis. She was readmitted to the hospital several hours after discharge and treated for sepsis.
She was in and out of the hospital several times during the next 7 weeks until the ObGyn told her that the only way to cure her pain was to perform a partial hysterectomy. He scheduled a concurrent prophylactic appendectomy by the general surgeon. At surgery, the surgeon found and removed a burst appendix. The ObGyn then performed a hysterectomy, although he had been present during the appendectomy.
PATIENT’S CLAIM Any general surgeon could have come into the operating room during exploratory surgery to assist in ruling out appendicitis; there were other general surgeons available at the hospital. The ObGyn was negligent in performing the hysterectomy after the surgeon had performed the appendectomy.
PHYSICIAN’S DEFENSE The general surgeon died before the case could be deposed. The ObGyn admitted that the removal of the burst appendix resolved the patient’s medical problems; her uterus had not been damaged by sepsis.
VERDICT A $350,000 Michigan settlement was reached.
Erb’s palsy: $1.7M net award
At 38 weeks’ gestation, a mother went to the local ED reporting shortness of breath. She was transferred to a university medical center where a chest x-ray revealed what was thought to be pneumonia or a pulmonary embolism. The decision was made to induce labor. During vaginal delivery, shoulder dystocia was encountered.
The 3-year-old child has Erb’s palsy and, despite treatment and therapy, does not have full use of her left arm and shoulder.
PARENTS’ CLAIM Maneuvers undertaken to relieve shoulder dystocia were not properly performed, injuring the baby. A cesarean delivery should have been performed because of the mother’s condition.
DEFENDANTS’ DEFENSE Proper maneuvers were used. There was no medical necessity for emergency cesarean delivery.
VERDICT A $3 million Maryland verdict was returned. After state caps and recalculation of a lost-wages claim from the mother due to jury error, the net award was $1.7 million.
Was nonreassuring fetal heart rate ignored?
In her third trimester, a 20-year-old woman was admitted to the hospital for observation, which included fetal heart-rate monitoring.
After 2 days, the patient began to bleed vaginally, and the nurses called the ObGyn. When he came to the hospital, he performed emergency cesarean delivery. The fetus was stillborn.
PATIENT’S CLAIM The nurses failed to inform the ObGyn when nonreassuring fetal heart-rate monitoring results were first evident. The ObGyn did not come to the hospital immediately after being told about the vaginal bleeding. The surgical team was not ready when it was time for the cesarean delivery.
DEFENDANTS’ DEFENSE The case was tried against the hospital that employed the nurses and ObGyn. The hospital claimed that fetal demise was caused by a sudden placental abruption. The nurses’ actions were appropriate. The hospital faulted the ObGyn for not coming to the hospital when summoned by the nurses.
VERDICT A $100,000 Louisiana verdict was returned. The jury found the ObGyn 99% at fault and the hospital 1% at fault. The patient was awarded $100,000 from the Patient’s Compensation Fund; the hospital paid $1,000.
Patient says wrong ovary was removed
A woman saw her ObGyn (Dr. A) because of lower abdominal pain. Dr. A performed laparoscopic right salpingo-oophorectomy.
A tumor on the left ovary was found 5 months later, and a second operation was performed by another ObGyn (Dr. B) with Dr. A’s assistance. During this surgery, the patient’s sigmoid colon was injured; a fistula developed and a third operation was required to repair the colon.
PATIENT’S CLAIM The initial plan was to remove the left ovary. When Dr. Aremoved the right ovary instead of the left, the patient experienced sudden onset of menopause; the left ovary was nonfunctional. Dr. B was negligent in injuring the sigmoid colon.
PHYSICIANS’ DEFENSE Dr. B was released from the case because colon injury is a known complication of the procedure. Dr. A claimed that the radiologic film of the mass was misleading, and that the ovary he removed was diseased.
VERDICT A Virginia defense verdict was returned.
Second pregnancy ends in injury after shoulder dystocia
A mother told her new ObGyn that, during the birth of her first child a few years earlier, shoulder dystocia had been encountered. Although the baby was born unharmed, her prior ObGyn had recommended that she undergo cesarean delivery for future pregnancies. During the second pregnancy, the mother and new ObGyn discussed the possibility of a trial of labor and vaginal delivery.
When the mother went into labor at 37 weeks’ gestation, the ObGyn believed the child was of normal weight and proceeded with a vaginal delivery. When shoulder dystocia was encountered, various maneuvers were performed. Birth occurred 5 minutes later using moderate traction.
The child showed no signs of life at birth; Apgar scores were 0 for more than 14 minutes. The newborn was sent to the neonatal intensive care unit and later airlifted to another hospital. He had hypoxic ischemic encephalopathy and a C5–C6 brachial plexus injury.
Additional testing revealed that he has neurocognitive deficits including attention deficit hyperactivity disorder and executive function disabilities.
Parents’ claim The ObGyn was negligent in failing to fully explain the risks of vaginal delivery, failing to recommend cesarean delivery based on the patient’s history and prior physician’s recommendation. The ObGyn failed to perform ultrasonography when the mother was admitted to the hospital; such imaging would have revealed that the fetus was larger than her first baby, mandating cesarean delivery. The ObGyn failed to perform an episiotomy after dystocia was encountered, and he applied excessive traction during dystocial maneuvers.
PHYSICIAN’S DEFENSE The mother was extensively counseled on the risks of vaginal delivery, but the ObGyn admitted that he did not recommend a cesarean delivery. Ultrasonography would have had no benefit. The use of moderate traction was necessary to prevent severe brain damage or death. The child’s current deficits are not related to his birth.
VERDICT The hospital settled for $85,000 before the trial began. An Illinois defense verdict was returned for the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Negligence during cord blood sampling? Child has CP
A woman’s first child was treated for neonatal alloimmune thrombocytopenia (NAIT) after birth. When prenatal testing identified NAIT in her second child, the mother received twice-weekly immunoglobulin injections to increase the fetus’ platelet count.
At 33 weeks’ gestation, percutaneous umbilical blood sampling (PUBS) was undertaken by a maternal-fetal medicine (MFM) specialist to check the baby’s platelet count and inject additional platelets. During the procedure, the mother’s blood pressure dropped from 122/80 to 80/40 mm Hg. The fetal heart rate dropped from 120–130 bpm to 65 bpm. An emergency cesarean delivery was performed.
At birth, the baby had seizures and respiratory distress secondary to perinatal asphyxia. She has severe spastic quadriplegic cerebral palsy. At age 9 years, she has been hospitalized for multiple complications, underwent tendon-release procedures on both legs, and receives occupational and physical therapy. She cannot speak, needs a feeding tube, is wheelchair bound, and requires 24-hour nursing care.
PARENTS’ CLAIM The MFM was not adequately trained to perform PUBS and did not use continuous ultrasound guidance during the procedure. She was negligent in attempting to insert the needle into the umbilical cord multiple times. She failed to recognize fetal distress. The anesthesiologist only told the MFM that the patient was hypotensive, not that the patient’s blood pressure never returned to baseline.
defendants’ DEFENSE The mother was part of a NAIT study, and the procedure was properly performed under the guidelines of that study. A sonographer constantly monitored the fetal heart rate. The anesthesiologist claimed that proper actions were taken in response to low blood pressure; there was no requirement to communicate more information to the MFM. The child’s hypoxia was due to placental abruption. The estimated cost of the life-care plan for the child is $5 to $10 million.
VERDICT A $15 million Indiana verdict was returned against the medical center that employed the anesthesiologist, but was reduced to $1,250,000 by the state cap. A defense verdict was returned for the MFM.
Woman dies from cervical cancer: $2.33M
When a woman had an abnormal Pap smear in 2001, her gynecologist did not order a repeat test, but told the patient to return in 3 months. The patient did not see the gynecologist again until 2007. At that time, her Pap smear was normal, but she was experiencing symptoms. The gynecologist did not order further testing.
In 2009, the patient was found to have advanced cervical cancer. She died 2 years later at age 48.
ESTATE’S CLAIM The second Pap smear was incorrectly interpreted. Further testing should have been ordered in 2001 and 2007.
DEFENDANTS’ DEFENSE The laboratory and patient’s estate settled for a confidential amount before the trial commenced. The gynecologist denied negligence. He claimed the patient was at fault for not returning to see him, as recommended.
VERDICT A New Jersey jury found the gynecologist 40% at fault, the laboratory 50% at fault, and the patient 10% at fault. A gross verdict of $2.33 million was returned.
Was it HELLP syndrome?
By her prenatal visit at 33 weeks’ gestation, a mother had gained 59 lb during her pregnancy. Three days later, she went to the emergency department (ED). The fetus had died.
PARENT’S CLAIM The ObGyn failed to intervene when the mother was gaining excessive weight. The mother had HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count); timely diagnosis could have avoided fetal demise.
DEFENDANTS’ DEFENSE Fetal demise could not have been diagnosed or prevented. The cause of the mother’s illness was never fully identified.
VERDICT A Tennessee defense verdict was returned.
Vesicovaginal fistula after hysterectomy
A woman underwent a hysterectomy performed by her ObGyn. A week later, during a postoperative visit, the ObGyn detected a bladder injury and related vesicovaginal fistula. He attempted a repair, but it failed. Eventually, successful repair surgery was performed by a urologist.
PATIENT’S CLAIM The ObGyn only should have used sharp dissection during the hysterectomy, as opposed to a combination of sharp and blunt dissection, due to dense adhesions that had developed after earlier abdominal surgery. Because the ObGyn had never repaired a vesicovaginal fistula before, he should have requested the assistance of a urologist or urogynecologist. A peritoneal flap should have been used during the initial repair.
PHYSICIAN’S DEFENSE Referral to a urologist or urogynecologist had been offered to the patient, but was refused (no record of this was found in the patient’s file). There was no negligence in the attempted repair.
VERDICT A $387,000 Virginia verdict was returned.
Did she really need that hysterectomy?
A 31-year-old woman went to the ED with sudden, severe abdominal pain. The radiologist noted that the patient’s appendix could not be visualized on computed tomography (CT) because it was behind the cecum. A general surgeon interpreted the report as ruling out appendicitis, made a diagnosis of pelvic inflammatory disease, and requested a gynecologic consult. An ObGyn sent his nurse practitioner to see the patient in the ED. The patient was discharged and instructed to follow up with the ObGyn.
When the patient’s condition worsened 2 days later, she returned to the ED. The ObGyn performed laparoscopic exploratory surgery. When he could not find the appendix, he called the general surgeon. The surgeon was in his car, and told the ObGyn that it was unnecessary to visualize the appendix; the ObGyn could complete the surgery. The patient was again discharged without a firm diagnosis. She was readmitted to the hospital several hours after discharge and treated for sepsis.
She was in and out of the hospital several times during the next 7 weeks until the ObGyn told her that the only way to cure her pain was to perform a partial hysterectomy. He scheduled a concurrent prophylactic appendectomy by the general surgeon. At surgery, the surgeon found and removed a burst appendix. The ObGyn then performed a hysterectomy, although he had been present during the appendectomy.
PATIENT’S CLAIM Any general surgeon could have come into the operating room during exploratory surgery to assist in ruling out appendicitis; there were other general surgeons available at the hospital. The ObGyn was negligent in performing the hysterectomy after the surgeon had performed the appendectomy.
PHYSICIAN’S DEFENSE The general surgeon died before the case could be deposed. The ObGyn admitted that the removal of the burst appendix resolved the patient’s medical problems; her uterus had not been damaged by sepsis.
VERDICT A $350,000 Michigan settlement was reached.
Erb’s palsy: $1.7M net award
At 38 weeks’ gestation, a mother went to the local ED reporting shortness of breath. She was transferred to a university medical center where a chest x-ray revealed what was thought to be pneumonia or a pulmonary embolism. The decision was made to induce labor. During vaginal delivery, shoulder dystocia was encountered.
The 3-year-old child has Erb’s palsy and, despite treatment and therapy, does not have full use of her left arm and shoulder.
PARENTS’ CLAIM Maneuvers undertaken to relieve shoulder dystocia were not properly performed, injuring the baby. A cesarean delivery should have been performed because of the mother’s condition.
DEFENDANTS’ DEFENSE Proper maneuvers were used. There was no medical necessity for emergency cesarean delivery.
VERDICT A $3 million Maryland verdict was returned. After state caps and recalculation of a lost-wages claim from the mother due to jury error, the net award was $1.7 million.
Was nonreassuring fetal heart rate ignored?
In her third trimester, a 20-year-old woman was admitted to the hospital for observation, which included fetal heart-rate monitoring.
After 2 days, the patient began to bleed vaginally, and the nurses called the ObGyn. When he came to the hospital, he performed emergency cesarean delivery. The fetus was stillborn.
PATIENT’S CLAIM The nurses failed to inform the ObGyn when nonreassuring fetal heart-rate monitoring results were first evident. The ObGyn did not come to the hospital immediately after being told about the vaginal bleeding. The surgical team was not ready when it was time for the cesarean delivery.
DEFENDANTS’ DEFENSE The case was tried against the hospital that employed the nurses and ObGyn. The hospital claimed that fetal demise was caused by a sudden placental abruption. The nurses’ actions were appropriate. The hospital faulted the ObGyn for not coming to the hospital when summoned by the nurses.
VERDICT A $100,000 Louisiana verdict was returned. The jury found the ObGyn 99% at fault and the hospital 1% at fault. The patient was awarded $100,000 from the Patient’s Compensation Fund; the hospital paid $1,000.
Patient says wrong ovary was removed
A woman saw her ObGyn (Dr. A) because of lower abdominal pain. Dr. A performed laparoscopic right salpingo-oophorectomy.
A tumor on the left ovary was found 5 months later, and a second operation was performed by another ObGyn (Dr. B) with Dr. A’s assistance. During this surgery, the patient’s sigmoid colon was injured; a fistula developed and a third operation was required to repair the colon.
PATIENT’S CLAIM The initial plan was to remove the left ovary. When Dr. Aremoved the right ovary instead of the left, the patient experienced sudden onset of menopause; the left ovary was nonfunctional. Dr. B was negligent in injuring the sigmoid colon.
PHYSICIANS’ DEFENSE Dr. B was released from the case because colon injury is a known complication of the procedure. Dr. A claimed that the radiologic film of the mass was misleading, and that the ovary he removed was diseased.
VERDICT A Virginia defense verdict was returned.
Second pregnancy ends in injury after shoulder dystocia
A mother told her new ObGyn that, during the birth of her first child a few years earlier, shoulder dystocia had been encountered. Although the baby was born unharmed, her prior ObGyn had recommended that she undergo cesarean delivery for future pregnancies. During the second pregnancy, the mother and new ObGyn discussed the possibility of a trial of labor and vaginal delivery.
When the mother went into labor at 37 weeks’ gestation, the ObGyn believed the child was of normal weight and proceeded with a vaginal delivery. When shoulder dystocia was encountered, various maneuvers were performed. Birth occurred 5 minutes later using moderate traction.
The child showed no signs of life at birth; Apgar scores were 0 for more than 14 minutes. The newborn was sent to the neonatal intensive care unit and later airlifted to another hospital. He had hypoxic ischemic encephalopathy and a C5–C6 brachial plexus injury.
Additional testing revealed that he has neurocognitive deficits including attention deficit hyperactivity disorder and executive function disabilities.
Parents’ claim The ObGyn was negligent in failing to fully explain the risks of vaginal delivery, failing to recommend cesarean delivery based on the patient’s history and prior physician’s recommendation. The ObGyn failed to perform ultrasonography when the mother was admitted to the hospital; such imaging would have revealed that the fetus was larger than her first baby, mandating cesarean delivery. The ObGyn failed to perform an episiotomy after dystocia was encountered, and he applied excessive traction during dystocial maneuvers.
PHYSICIAN’S DEFENSE The mother was extensively counseled on the risks of vaginal delivery, but the ObGyn admitted that he did not recommend a cesarean delivery. Ultrasonography would have had no benefit. The use of moderate traction was necessary to prevent severe brain damage or death. The child’s current deficits are not related to his birth.
VERDICT The hospital settled for $85,000 before the trial began. An Illinois defense verdict was returned for the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Negligence during cord blood sampling? Child has CP
A woman’s first child was treated for neonatal alloimmune thrombocytopenia (NAIT) after birth. When prenatal testing identified NAIT in her second child, the mother received twice-weekly immunoglobulin injections to increase the fetus’ platelet count.
At 33 weeks’ gestation, percutaneous umbilical blood sampling (PUBS) was undertaken by a maternal-fetal medicine (MFM) specialist to check the baby’s platelet count and inject additional platelets. During the procedure, the mother’s blood pressure dropped from 122/80 to 80/40 mm Hg. The fetal heart rate dropped from 120–130 bpm to 65 bpm. An emergency cesarean delivery was performed.
At birth, the baby had seizures and respiratory distress secondary to perinatal asphyxia. She has severe spastic quadriplegic cerebral palsy. At age 9 years, she has been hospitalized for multiple complications, underwent tendon-release procedures on both legs, and receives occupational and physical therapy. She cannot speak, needs a feeding tube, is wheelchair bound, and requires 24-hour nursing care.
PARENTS’ CLAIM The MFM was not adequately trained to perform PUBS and did not use continuous ultrasound guidance during the procedure. She was negligent in attempting to insert the needle into the umbilical cord multiple times. She failed to recognize fetal distress. The anesthesiologist only told the MFM that the patient was hypotensive, not that the patient’s blood pressure never returned to baseline.
defendants’ DEFENSE The mother was part of a NAIT study, and the procedure was properly performed under the guidelines of that study. A sonographer constantly monitored the fetal heart rate. The anesthesiologist claimed that proper actions were taken in response to low blood pressure; there was no requirement to communicate more information to the MFM. The child’s hypoxia was due to placental abruption. The estimated cost of the life-care plan for the child is $5 to $10 million.
VERDICT A $15 million Indiana verdict was returned against the medical center that employed the anesthesiologist, but was reduced to $1,250,000 by the state cap. A defense verdict was returned for the MFM.
Woman dies from cervical cancer: $2.33M
When a woman had an abnormal Pap smear in 2001, her gynecologist did not order a repeat test, but told the patient to return in 3 months. The patient did not see the gynecologist again until 2007. At that time, her Pap smear was normal, but she was experiencing symptoms. The gynecologist did not order further testing.
In 2009, the patient was found to have advanced cervical cancer. She died 2 years later at age 48.
ESTATE’S CLAIM The second Pap smear was incorrectly interpreted. Further testing should have been ordered in 2001 and 2007.
DEFENDANTS’ DEFENSE The laboratory and patient’s estate settled for a confidential amount before the trial commenced. The gynecologist denied negligence. He claimed the patient was at fault for not returning to see him, as recommended.
VERDICT A New Jersey jury found the gynecologist 40% at fault, the laboratory 50% at fault, and the patient 10% at fault. A gross verdict of $2.33 million was returned.
Was it HELLP syndrome?
By her prenatal visit at 33 weeks’ gestation, a mother had gained 59 lb during her pregnancy. Three days later, she went to the emergency department (ED). The fetus had died.
PARENT’S CLAIM The ObGyn failed to intervene when the mother was gaining excessive weight. The mother had HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count); timely diagnosis could have avoided fetal demise.
DEFENDANTS’ DEFENSE Fetal demise could not have been diagnosed or prevented. The cause of the mother’s illness was never fully identified.
VERDICT A Tennessee defense verdict was returned.
Vesicovaginal fistula after hysterectomy
A woman underwent a hysterectomy performed by her ObGyn. A week later, during a postoperative visit, the ObGyn detected a bladder injury and related vesicovaginal fistula. He attempted a repair, but it failed. Eventually, successful repair surgery was performed by a urologist.
PATIENT’S CLAIM The ObGyn only should have used sharp dissection during the hysterectomy, as opposed to a combination of sharp and blunt dissection, due to dense adhesions that had developed after earlier abdominal surgery. Because the ObGyn had never repaired a vesicovaginal fistula before, he should have requested the assistance of a urologist or urogynecologist. A peritoneal flap should have been used during the initial repair.
PHYSICIAN’S DEFENSE Referral to a urologist or urogynecologist had been offered to the patient, but was refused (no record of this was found in the patient’s file). There was no negligence in the attempted repair.
VERDICT A $387,000 Virginia verdict was returned.
Did she really need that hysterectomy?
A 31-year-old woman went to the ED with sudden, severe abdominal pain. The radiologist noted that the patient’s appendix could not be visualized on computed tomography (CT) because it was behind the cecum. A general surgeon interpreted the report as ruling out appendicitis, made a diagnosis of pelvic inflammatory disease, and requested a gynecologic consult. An ObGyn sent his nurse practitioner to see the patient in the ED. The patient was discharged and instructed to follow up with the ObGyn.
When the patient’s condition worsened 2 days later, she returned to the ED. The ObGyn performed laparoscopic exploratory surgery. When he could not find the appendix, he called the general surgeon. The surgeon was in his car, and told the ObGyn that it was unnecessary to visualize the appendix; the ObGyn could complete the surgery. The patient was again discharged without a firm diagnosis. She was readmitted to the hospital several hours after discharge and treated for sepsis.
She was in and out of the hospital several times during the next 7 weeks until the ObGyn told her that the only way to cure her pain was to perform a partial hysterectomy. He scheduled a concurrent prophylactic appendectomy by the general surgeon. At surgery, the surgeon found and removed a burst appendix. The ObGyn then performed a hysterectomy, although he had been present during the appendectomy.
PATIENT’S CLAIM Any general surgeon could have come into the operating room during exploratory surgery to assist in ruling out appendicitis; there were other general surgeons available at the hospital. The ObGyn was negligent in performing the hysterectomy after the surgeon had performed the appendectomy.
PHYSICIAN’S DEFENSE The general surgeon died before the case could be deposed. The ObGyn admitted that the removal of the burst appendix resolved the patient’s medical problems; her uterus had not been damaged by sepsis.
VERDICT A $350,000 Michigan settlement was reached.
Erb’s palsy: $1.7M net award
At 38 weeks’ gestation, a mother went to the local ED reporting shortness of breath. She was transferred to a university medical center where a chest x-ray revealed what was thought to be pneumonia or a pulmonary embolism. The decision was made to induce labor. During vaginal delivery, shoulder dystocia was encountered.
The 3-year-old child has Erb’s palsy and, despite treatment and therapy, does not have full use of her left arm and shoulder.
PARENTS’ CLAIM Maneuvers undertaken to relieve shoulder dystocia were not properly performed, injuring the baby. A cesarean delivery should have been performed because of the mother’s condition.
DEFENDANTS’ DEFENSE Proper maneuvers were used. There was no medical necessity for emergency cesarean delivery.
VERDICT A $3 million Maryland verdict was returned. After state caps and recalculation of a lost-wages claim from the mother due to jury error, the net award was $1.7 million.
Was nonreassuring fetal heart rate ignored?
In her third trimester, a 20-year-old woman was admitted to the hospital for observation, which included fetal heart-rate monitoring.
After 2 days, the patient began to bleed vaginally, and the nurses called the ObGyn. When he came to the hospital, he performed emergency cesarean delivery. The fetus was stillborn.
PATIENT’S CLAIM The nurses failed to inform the ObGyn when nonreassuring fetal heart-rate monitoring results were first evident. The ObGyn did not come to the hospital immediately after being told about the vaginal bleeding. The surgical team was not ready when it was time for the cesarean delivery.
DEFENDANTS’ DEFENSE The case was tried against the hospital that employed the nurses and ObGyn. The hospital claimed that fetal demise was caused by a sudden placental abruption. The nurses’ actions were appropriate. The hospital faulted the ObGyn for not coming to the hospital when summoned by the nurses.
VERDICT A $100,000 Louisiana verdict was returned. The jury found the ObGyn 99% at fault and the hospital 1% at fault. The patient was awarded $100,000 from the Patient’s Compensation Fund; the hospital paid $1,000.
Patient says wrong ovary was removed
A woman saw her ObGyn (Dr. A) because of lower abdominal pain. Dr. A performed laparoscopic right salpingo-oophorectomy.
A tumor on the left ovary was found 5 months later, and a second operation was performed by another ObGyn (Dr. B) with Dr. A’s assistance. During this surgery, the patient’s sigmoid colon was injured; a fistula developed and a third operation was required to repair the colon.
PATIENT’S CLAIM The initial plan was to remove the left ovary. When Dr. Aremoved the right ovary instead of the left, the patient experienced sudden onset of menopause; the left ovary was nonfunctional. Dr. B was negligent in injuring the sigmoid colon.
PHYSICIANS’ DEFENSE Dr. B was released from the case because colon injury is a known complication of the procedure. Dr. A claimed that the radiologic film of the mass was misleading, and that the ovary he removed was diseased.
VERDICT A Virginia defense verdict was returned.
Second pregnancy ends in injury after shoulder dystocia
A mother told her new ObGyn that, during the birth of her first child a few years earlier, shoulder dystocia had been encountered. Although the baby was born unharmed, her prior ObGyn had recommended that she undergo cesarean delivery for future pregnancies. During the second pregnancy, the mother and new ObGyn discussed the possibility of a trial of labor and vaginal delivery.
When the mother went into labor at 37 weeks’ gestation, the ObGyn believed the child was of normal weight and proceeded with a vaginal delivery. When shoulder dystocia was encountered, various maneuvers were performed. Birth occurred 5 minutes later using moderate traction.
The child showed no signs of life at birth; Apgar scores were 0 for more than 14 minutes. The newborn was sent to the neonatal intensive care unit and later airlifted to another hospital. He had hypoxic ischemic encephalopathy and a C5–C6 brachial plexus injury.
Additional testing revealed that he has neurocognitive deficits including attention deficit hyperactivity disorder and executive function disabilities.
Parents’ claim The ObGyn was negligent in failing to fully explain the risks of vaginal delivery, failing to recommend cesarean delivery based on the patient’s history and prior physician’s recommendation. The ObGyn failed to perform ultrasonography when the mother was admitted to the hospital; such imaging would have revealed that the fetus was larger than her first baby, mandating cesarean delivery. The ObGyn failed to perform an episiotomy after dystocia was encountered, and he applied excessive traction during dystocial maneuvers.
PHYSICIAN’S DEFENSE The mother was extensively counseled on the risks of vaginal delivery, but the ObGyn admitted that he did not recommend a cesarean delivery. Ultrasonography would have had no benefit. The use of moderate traction was necessary to prevent severe brain damage or death. The child’s current deficits are not related to his birth.
VERDICT The hospital settled for $85,000 before the trial began. An Illinois defense verdict was returned for the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
IN THIS ARTICLE
-Woman dies from cervical cancer: $2.33M
-Was it HELLP syndrome?
-Vesicovaginal fistula after hysterectomy
-Did she really need that hysterectomy?
-Erb’s palsy: $1.7M net award
-Was nonreassuring fetal heart rate ignored?
-Patient says wrong ovary was removed
-Second pregnancy ends in injury after shoulder dystocia
