User login
The Failure to Deliver as Promised
In March 2009, a 63-year-old man was diagnosed with stage IV gastric carcinoma with metastasis to the liver. His treating oncologist gave him a prognosis of about 10 months’ life expectancy with chemotherapy. The patient’s family searched for alternative treatment options and found a natural alternative treatment center claiming the ability to cure the patient.
The patient and his family decided to defer chemotherapy, and he was admitted to the alternative treatment center for three to four weeks of inpatient care. The treatment consisted of “colonic hydrotherapy,” supplements designed to cleanse the body, and a diet restricted to seed milk, vegetable juice, and spinach soup.
After six days, the patient developed severe diarrhea, confusion, and profound weakness. He was taken to a local hospital and admitted with a diagnosis of acute renal failure. Dialysis attempts were unsuccessful, and the man died of respiratory distress secondary to acute renal failure a week later.
The plaintiff claimed that the treatment provided by the defendants was contraindicated and caused acute renal failure, noting that the patient’s kidney function had been relatively normal when he entered the treatment facility. The plaintiff claimed that defendant Dr N., a chiropractor, never reviewed any of the decedent’s medical records, did not discuss the proposed treatment plan with his treating physicians, and failed to properly monitor the patient’s condition, notice his deterioration, and provide timely transfer to a hospital.
The defendant claimed that the treatment given had no adverse effects on the decedent and that the acute renal failure was due to hepatorenal syndrome due to his advanced metastatic liver cancer.
What was the outcome? >>
OUTCOME
A $2.5 million verdict was returned. An appeal was pending.
COMMENT
This is a case against a chiropractor, so why discuss it in a journal dedicated to NP and PA practice? Because it involves scope of practice, alternative medicine, the safety of “natural” treatments, and the ethical and legal problems of making unsupportable promises to patients.
Know your scope of practice, and don’t overextend. Clinicians trained as specialists (eg, in pediatrics, midwifery, or anesthesia) should use caution departing from that area. Those trained as “generalists” need to be careful as well; even if you were trained in a family practice program, if you are a PA who has worked in dermatology for the past 10 years, think twice about giving treatment or advice to your friend with a neurologic complaint. In the event of a lawsuit, the plaintiff will spend a great deal of time building your resume as an expert in your discipline, only to attack you as inexperienced and unqualified in the case in which you extended yourself.
Here a chiropractor, without ever examining the patient, directed the treatment of a very sick man in an area in which he was not qualified. While chiropractors may claim the ability to treat outside their traditional scope, the jury’s verdict in this case proves that they were not persuaded he was right to do so. The chiropractor, Dr N., eventually lost his license, based in part on the false promises he made about his ability to cure patients of “any and all diseases, including cancer, by restoring the body to its natural state ….” This opportunistic preying upon the most ill and vulnerable in our society likely irked the jurors, who returned a substantial award, considering that the patient’s short life expectancy was uncontested.
Handle alternative medicine with particular care, because an alternative treatment may not qualify as “medicine” at all. If we define medicine as the application of scientific principles to health care, an alternative that is unproven, unstudied, and unknown does not qualify. Rather, it is guesswork—with potentially devastating consequences.
In this case, through his company, the chiropractor based his treatment plan on guesswork that colonic hydrotherapy and severe dietary restrictions would help a patient with stage IV metastatic gastric carcinoma. He was wrong, and the jury concluded that these alternatives injured the patient and hastened his death.
Certainly, Western medicine has been rightly and fairly criticized for failing to promote wellness through a healthy lifestyle, including diet, exercise, safety, emotional well-being, and stress management. However, when venturing from generally accepted health promotion strategies to a specific recommendation that an alternative agent “is good for” a specific problem, be careful. You may believe lavender oil is an effective antibiotic—but can you prove it?
If you choose lavender oil over a demonstrably effective antibiotic to treat pneumonia, and the patient deteriorates, you will be held accountable. The plaintiff will demand answers, and the jury will await your explanation. Reliance on vague concepts, not generally accepted in the literature (eg, “energy management,” detoxifying, unblocking “clogged” nervous systems), will be ridiculed by the plaintiff’s experts, and you will be skewered on cross-examination. It is not enough to personally “believe” in the alternative; you must be able to support your treatment decisions through the best evidence possible.
To be fair, this cuts both ways: Some Western medical practices are based on anecdotal evidence with minimal scientific support. There was a time when a corneal abrasion was patched, a fractured clavicle was stabilized with a figure-of-eight dressing, and narcotics were withheld from a suffering patient with acute abdomen because it would “mask signs.” Our “Western” system is not immune from the impact of poor research, group-think, dogmas leading to inappropriate practice, and other sources of logical fallacy.
As NPs and PAs, we will be held to a scientific evidentiary standard. The standard of care will be based upon the care a reasonably prudent clinician would deliver in a similar situation. At trial, you will be confronted with a PA or NP on the stand testifying against you regarding what is reasonably prudent, acceptable care. Make sure your actions are scientifically defensible.
Interestingly, the standard for admitting a scientific opinion as expert testimony has changed. In 1923, Frye v United States1 established that, for an expert opinion to be admissible, the testimony had to be based on what is “generally accepted in the scientific community.” In 1993, the Supreme Court case Daubert v Merrell Dow Pharmaceuticals2 determined that the opinion need not be “generally accepted” but must be based on scientific method and must be relevant to the case; the judge serves as a “gatekeeper” to be sure the opinions flow from “scientific knowledge.”
Medical malpractice cases are based on state law. Some follow Frye, some Daubert. The latter is a more relaxed standard, but even in states following Daubert, an expert witness who purports to testify on an alternative treatment must follow the scientific method. For example, the webpage of the defendant chiropractor’s institute (still in business) currently claims that “Heart/Brain Entrainment Therapy balances frequencies of organs/glands/tissues. Everything in the universe resonates at a particular frequency—light, sound, and every cell, organ, gland, and tissue in you.”3
So, whatever Heart/Brain Entrainment Therapy is, for that theory to be admissible in a Frye jurisdiction it would likely have to be “generally accepted” in the medical community. To be admissible in a Daubert jurisdiction, proponents of the testimony would have to show evidence of a scientific methodology supporting the theory before the jury could hear any testimony about it. In either case, strategically, the defense attorney would likely file a motion to block either certain parts of the testimony or the testimony entirely.
IN SUM
Jurors expect sound scientific methodology supporting medical decisions; use care when selecting treatment for patients. Robustly adopt health promotion and general wellness strategies. However, if you use alternatives directed toward a specific therapy solving a specific problem, use them cautiously and with an awareness that the indication for the therapy should be scientifically defensible. —DML
REFERENCES
1. Frye v United States, 293 F. 1013 (D.C. Cir. 1923).
2. Daubert v Merrell Dow Pharmaceuticals, 509 U.S. 579 (1993).
3. Total Health Institute. Bioelectrical Energy, Quantum Frequency Resonance. www.totalhealthinstitute.com/about. Accessed July 14, 2015.
In March 2009, a 63-year-old man was diagnosed with stage IV gastric carcinoma with metastasis to the liver. His treating oncologist gave him a prognosis of about 10 months’ life expectancy with chemotherapy. The patient’s family searched for alternative treatment options and found a natural alternative treatment center claiming the ability to cure the patient.
The patient and his family decided to defer chemotherapy, and he was admitted to the alternative treatment center for three to four weeks of inpatient care. The treatment consisted of “colonic hydrotherapy,” supplements designed to cleanse the body, and a diet restricted to seed milk, vegetable juice, and spinach soup.
After six days, the patient developed severe diarrhea, confusion, and profound weakness. He was taken to a local hospital and admitted with a diagnosis of acute renal failure. Dialysis attempts were unsuccessful, and the man died of respiratory distress secondary to acute renal failure a week later.
The plaintiff claimed that the treatment provided by the defendants was contraindicated and caused acute renal failure, noting that the patient’s kidney function had been relatively normal when he entered the treatment facility. The plaintiff claimed that defendant Dr N., a chiropractor, never reviewed any of the decedent’s medical records, did not discuss the proposed treatment plan with his treating physicians, and failed to properly monitor the patient’s condition, notice his deterioration, and provide timely transfer to a hospital.
The defendant claimed that the treatment given had no adverse effects on the decedent and that the acute renal failure was due to hepatorenal syndrome due to his advanced metastatic liver cancer.
What was the outcome? >>
OUTCOME
A $2.5 million verdict was returned. An appeal was pending.
COMMENT
This is a case against a chiropractor, so why discuss it in a journal dedicated to NP and PA practice? Because it involves scope of practice, alternative medicine, the safety of “natural” treatments, and the ethical and legal problems of making unsupportable promises to patients.
Know your scope of practice, and don’t overextend. Clinicians trained as specialists (eg, in pediatrics, midwifery, or anesthesia) should use caution departing from that area. Those trained as “generalists” need to be careful as well; even if you were trained in a family practice program, if you are a PA who has worked in dermatology for the past 10 years, think twice about giving treatment or advice to your friend with a neurologic complaint. In the event of a lawsuit, the plaintiff will spend a great deal of time building your resume as an expert in your discipline, only to attack you as inexperienced and unqualified in the case in which you extended yourself.
Here a chiropractor, without ever examining the patient, directed the treatment of a very sick man in an area in which he was not qualified. While chiropractors may claim the ability to treat outside their traditional scope, the jury’s verdict in this case proves that they were not persuaded he was right to do so. The chiropractor, Dr N., eventually lost his license, based in part on the false promises he made about his ability to cure patients of “any and all diseases, including cancer, by restoring the body to its natural state ….” This opportunistic preying upon the most ill and vulnerable in our society likely irked the jurors, who returned a substantial award, considering that the patient’s short life expectancy was uncontested.
Handle alternative medicine with particular care, because an alternative treatment may not qualify as “medicine” at all. If we define medicine as the application of scientific principles to health care, an alternative that is unproven, unstudied, and unknown does not qualify. Rather, it is guesswork—with potentially devastating consequences.
In this case, through his company, the chiropractor based his treatment plan on guesswork that colonic hydrotherapy and severe dietary restrictions would help a patient with stage IV metastatic gastric carcinoma. He was wrong, and the jury concluded that these alternatives injured the patient and hastened his death.
Certainly, Western medicine has been rightly and fairly criticized for failing to promote wellness through a healthy lifestyle, including diet, exercise, safety, emotional well-being, and stress management. However, when venturing from generally accepted health promotion strategies to a specific recommendation that an alternative agent “is good for” a specific problem, be careful. You may believe lavender oil is an effective antibiotic—but can you prove it?
If you choose lavender oil over a demonstrably effective antibiotic to treat pneumonia, and the patient deteriorates, you will be held accountable. The plaintiff will demand answers, and the jury will await your explanation. Reliance on vague concepts, not generally accepted in the literature (eg, “energy management,” detoxifying, unblocking “clogged” nervous systems), will be ridiculed by the plaintiff’s experts, and you will be skewered on cross-examination. It is not enough to personally “believe” in the alternative; you must be able to support your treatment decisions through the best evidence possible.
To be fair, this cuts both ways: Some Western medical practices are based on anecdotal evidence with minimal scientific support. There was a time when a corneal abrasion was patched, a fractured clavicle was stabilized with a figure-of-eight dressing, and narcotics were withheld from a suffering patient with acute abdomen because it would “mask signs.” Our “Western” system is not immune from the impact of poor research, group-think, dogmas leading to inappropriate practice, and other sources of logical fallacy.
As NPs and PAs, we will be held to a scientific evidentiary standard. The standard of care will be based upon the care a reasonably prudent clinician would deliver in a similar situation. At trial, you will be confronted with a PA or NP on the stand testifying against you regarding what is reasonably prudent, acceptable care. Make sure your actions are scientifically defensible.
Interestingly, the standard for admitting a scientific opinion as expert testimony has changed. In 1923, Frye v United States1 established that, for an expert opinion to be admissible, the testimony had to be based on what is “generally accepted in the scientific community.” In 1993, the Supreme Court case Daubert v Merrell Dow Pharmaceuticals2 determined that the opinion need not be “generally accepted” but must be based on scientific method and must be relevant to the case; the judge serves as a “gatekeeper” to be sure the opinions flow from “scientific knowledge.”
Medical malpractice cases are based on state law. Some follow Frye, some Daubert. The latter is a more relaxed standard, but even in states following Daubert, an expert witness who purports to testify on an alternative treatment must follow the scientific method. For example, the webpage of the defendant chiropractor’s institute (still in business) currently claims that “Heart/Brain Entrainment Therapy balances frequencies of organs/glands/tissues. Everything in the universe resonates at a particular frequency—light, sound, and every cell, organ, gland, and tissue in you.”3
So, whatever Heart/Brain Entrainment Therapy is, for that theory to be admissible in a Frye jurisdiction it would likely have to be “generally accepted” in the medical community. To be admissible in a Daubert jurisdiction, proponents of the testimony would have to show evidence of a scientific methodology supporting the theory before the jury could hear any testimony about it. In either case, strategically, the defense attorney would likely file a motion to block either certain parts of the testimony or the testimony entirely.
IN SUM
Jurors expect sound scientific methodology supporting medical decisions; use care when selecting treatment for patients. Robustly adopt health promotion and general wellness strategies. However, if you use alternatives directed toward a specific therapy solving a specific problem, use them cautiously and with an awareness that the indication for the therapy should be scientifically defensible. —DML
REFERENCES
1. Frye v United States, 293 F. 1013 (D.C. Cir. 1923).
2. Daubert v Merrell Dow Pharmaceuticals, 509 U.S. 579 (1993).
3. Total Health Institute. Bioelectrical Energy, Quantum Frequency Resonance. www.totalhealthinstitute.com/about. Accessed July 14, 2015.
In March 2009, a 63-year-old man was diagnosed with stage IV gastric carcinoma with metastasis to the liver. His treating oncologist gave him a prognosis of about 10 months’ life expectancy with chemotherapy. The patient’s family searched for alternative treatment options and found a natural alternative treatment center claiming the ability to cure the patient.
The patient and his family decided to defer chemotherapy, and he was admitted to the alternative treatment center for three to four weeks of inpatient care. The treatment consisted of “colonic hydrotherapy,” supplements designed to cleanse the body, and a diet restricted to seed milk, vegetable juice, and spinach soup.
After six days, the patient developed severe diarrhea, confusion, and profound weakness. He was taken to a local hospital and admitted with a diagnosis of acute renal failure. Dialysis attempts were unsuccessful, and the man died of respiratory distress secondary to acute renal failure a week later.
The plaintiff claimed that the treatment provided by the defendants was contraindicated and caused acute renal failure, noting that the patient’s kidney function had been relatively normal when he entered the treatment facility. The plaintiff claimed that defendant Dr N., a chiropractor, never reviewed any of the decedent’s medical records, did not discuss the proposed treatment plan with his treating physicians, and failed to properly monitor the patient’s condition, notice his deterioration, and provide timely transfer to a hospital.
The defendant claimed that the treatment given had no adverse effects on the decedent and that the acute renal failure was due to hepatorenal syndrome due to his advanced metastatic liver cancer.
What was the outcome? >>
OUTCOME
A $2.5 million verdict was returned. An appeal was pending.
COMMENT
This is a case against a chiropractor, so why discuss it in a journal dedicated to NP and PA practice? Because it involves scope of practice, alternative medicine, the safety of “natural” treatments, and the ethical and legal problems of making unsupportable promises to patients.
Know your scope of practice, and don’t overextend. Clinicians trained as specialists (eg, in pediatrics, midwifery, or anesthesia) should use caution departing from that area. Those trained as “generalists” need to be careful as well; even if you were trained in a family practice program, if you are a PA who has worked in dermatology for the past 10 years, think twice about giving treatment or advice to your friend with a neurologic complaint. In the event of a lawsuit, the plaintiff will spend a great deal of time building your resume as an expert in your discipline, only to attack you as inexperienced and unqualified in the case in which you extended yourself.
Here a chiropractor, without ever examining the patient, directed the treatment of a very sick man in an area in which he was not qualified. While chiropractors may claim the ability to treat outside their traditional scope, the jury’s verdict in this case proves that they were not persuaded he was right to do so. The chiropractor, Dr N., eventually lost his license, based in part on the false promises he made about his ability to cure patients of “any and all diseases, including cancer, by restoring the body to its natural state ….” This opportunistic preying upon the most ill and vulnerable in our society likely irked the jurors, who returned a substantial award, considering that the patient’s short life expectancy was uncontested.
Handle alternative medicine with particular care, because an alternative treatment may not qualify as “medicine” at all. If we define medicine as the application of scientific principles to health care, an alternative that is unproven, unstudied, and unknown does not qualify. Rather, it is guesswork—with potentially devastating consequences.
In this case, through his company, the chiropractor based his treatment plan on guesswork that colonic hydrotherapy and severe dietary restrictions would help a patient with stage IV metastatic gastric carcinoma. He was wrong, and the jury concluded that these alternatives injured the patient and hastened his death.
Certainly, Western medicine has been rightly and fairly criticized for failing to promote wellness through a healthy lifestyle, including diet, exercise, safety, emotional well-being, and stress management. However, when venturing from generally accepted health promotion strategies to a specific recommendation that an alternative agent “is good for” a specific problem, be careful. You may believe lavender oil is an effective antibiotic—but can you prove it?
If you choose lavender oil over a demonstrably effective antibiotic to treat pneumonia, and the patient deteriorates, you will be held accountable. The plaintiff will demand answers, and the jury will await your explanation. Reliance on vague concepts, not generally accepted in the literature (eg, “energy management,” detoxifying, unblocking “clogged” nervous systems), will be ridiculed by the plaintiff’s experts, and you will be skewered on cross-examination. It is not enough to personally “believe” in the alternative; you must be able to support your treatment decisions through the best evidence possible.
To be fair, this cuts both ways: Some Western medical practices are based on anecdotal evidence with minimal scientific support. There was a time when a corneal abrasion was patched, a fractured clavicle was stabilized with a figure-of-eight dressing, and narcotics were withheld from a suffering patient with acute abdomen because it would “mask signs.” Our “Western” system is not immune from the impact of poor research, group-think, dogmas leading to inappropriate practice, and other sources of logical fallacy.
As NPs and PAs, we will be held to a scientific evidentiary standard. The standard of care will be based upon the care a reasonably prudent clinician would deliver in a similar situation. At trial, you will be confronted with a PA or NP on the stand testifying against you regarding what is reasonably prudent, acceptable care. Make sure your actions are scientifically defensible.
Interestingly, the standard for admitting a scientific opinion as expert testimony has changed. In 1923, Frye v United States1 established that, for an expert opinion to be admissible, the testimony had to be based on what is “generally accepted in the scientific community.” In 1993, the Supreme Court case Daubert v Merrell Dow Pharmaceuticals2 determined that the opinion need not be “generally accepted” but must be based on scientific method and must be relevant to the case; the judge serves as a “gatekeeper” to be sure the opinions flow from “scientific knowledge.”
Medical malpractice cases are based on state law. Some follow Frye, some Daubert. The latter is a more relaxed standard, but even in states following Daubert, an expert witness who purports to testify on an alternative treatment must follow the scientific method. For example, the webpage of the defendant chiropractor’s institute (still in business) currently claims that “Heart/Brain Entrainment Therapy balances frequencies of organs/glands/tissues. Everything in the universe resonates at a particular frequency—light, sound, and every cell, organ, gland, and tissue in you.”3
So, whatever Heart/Brain Entrainment Therapy is, for that theory to be admissible in a Frye jurisdiction it would likely have to be “generally accepted” in the medical community. To be admissible in a Daubert jurisdiction, proponents of the testimony would have to show evidence of a scientific methodology supporting the theory before the jury could hear any testimony about it. In either case, strategically, the defense attorney would likely file a motion to block either certain parts of the testimony or the testimony entirely.
IN SUM
Jurors expect sound scientific methodology supporting medical decisions; use care when selecting treatment for patients. Robustly adopt health promotion and general wellness strategies. However, if you use alternatives directed toward a specific therapy solving a specific problem, use them cautiously and with an awareness that the indication for the therapy should be scientifically defensible. —DML
REFERENCES
1. Frye v United States, 293 F. 1013 (D.C. Cir. 1923).
2. Daubert v Merrell Dow Pharmaceuticals, 509 U.S. 579 (1993).
3. Total Health Institute. Bioelectrical Energy, Quantum Frequency Resonance. www.totalhealthinstitute.com/about. Accessed July 14, 2015.
Was the ObGyn’s dexterity compromised?

Was the ObGyn’s dexterity compromised?
A woman underwent a hysterectomy. During surgery, the patient’s bladder was injured; the ObGyn called in a urologist to make the repair.
Patient’s claim The ObGyn failed to inform the patient about the possible complications from hysterectomy. The patient also claimed fraudulent concealment because the ObGyn had suffered a serious injury 3 years earlier that affected his dexterity. At the time of surgery, the ObGyn had a pending lawsuit against the owner of the premises where he fell in which he claimed that he was unable to continue his surgical practice because of the injury. The ObGyn never informed the patient of the extent of his injury or any associated risks related to his injury.
Defendants’ defense The patient was fully informed that bladder injury is a known risk of the procedure. The ObGyn maintained that his injury only affected his ability to stand for many hours while operating. The hospital settled during trial.
Verdict A $12,000 Louisiana settlement was reached with the hospital. Summary judgment was granted to the ObGyn on the informed consent claim. A $30,000 verdict was returned on the fraud count.
Placental abruption: Was child dead?
At 32 weeks’ gestation, a woman was found to have placental abruption. At the hospital, her ObGyn could not find a fetal heartbeat or detectable fetal movement on ultrasonography. A radiologist performed another ultrasound 30 minutes later and detected a fetal heart rate of 47 bpm. An emergency cesarean delivery was performed. Soon after birth, the child had seizures and was found to have hypoxic ischemic encephalopathy and diffuse brain injury. The child is profoundly disabled.
Parents’ claim The ObGyn was negligent for failing to detect the fetal heart rate and in failing to respond properly to placental abruption. Cesarean delivery should have been performed immediately after placental abruption was identified.
Defendant’s defense The case was settled at trial.
Verdict A $13 million Illinois settlement was reached, including $5 million in cash and $8 million placed in trust for the child.
Large fetus, shoulder dystocia: Erb’s palsy
Labor was induced at 39 weeks’ gestation because the fetus was anticipated to be large. During vaginal delivery, shoulder dystocia was encountered. At birth, the baby weighed 9 lb 2 oz. She sustained a brachial plexus injury to the posterior shoulder with permanent nerve root damage and Erb’s palsy. The child continues to have limited use of her left arm and hand even after 3 corrective operations.
Parents’ claim While performing maneuvers to relieve shoulder dystocia, the ObGyn exerted excessive traction on the baby’s head, causing a C-5 nerve root injury and complete avulsion at C-8. A cesarean delivery should have been performed.
Physician’s defense There was no negligence. The nerve injury was caused by the natural forces of labor and the mother’s pushing while the posterior shoulder was wedged behind the mother’s sa-
cral promontory.
Verdict A $1 million Illinois verdict was returned.
Woman dies from toxemia
A 22-year-old woman was seen by her ObGyn 4 days after vaginal delivery. Early the next day, the patient had a seizure at home and was transported by ambulance to the hospital. She could not be resuscitated and died. At autopsy, the cause of death was determined to be toxemia from pregnancy.
Estate’s claim The ObGyn failed to properly diagnose and treat the patient’s hypertension.
Defendant’s defense The case was settled during trial.
Verdict A $775,000 New York settlement was reached.

Blood transfusion delayed for hours: $14.75M net award
After emergency cesarean delivery, the baby was extremely anemic. The physicians determined that a fetal-maternal hemorrhage had started days before, causing the fetus to lose most of her blood.
An hour after birth, the attending neonatologist ordered blood from the hospital’s blood bank and arranged for emergency transport to a neonatal intensive care unit (NICU). Blood transfusion did not occur prior to transport. The child has severe cerebral palsy (CP) and cannot walk or talk at age 8 years.
Parents’ claim The neonatologist ordered cross-matched blood, which, because it is tested for compatibility, takes longer to supply. Universal donor blood could have been delivered in 20 minutes or less because it is readily available. The ambulance from the receiving hospital took an hour to drive 9 miles between the facilities, a trip that should have taken 12 minutes. The ambulance staff did not call ahead to the medical center to have blood ready for the baby. It took 4.5 hours before the newborn received a blood transfusion, a delay that caused severe injury to the child.
Defendants’ defense The matter went to trial against the neonatologist and his employer after the other defendants settled.
Verdict Before trial, an ObGyn and the hospital settled for a combined $750,000, and the county agreed to a $12 million settlement. During trial, a $2 million Illinois settlement was reached.
Pregnant woman has a massive stroke: $10.9M
Pregnant with her third child and at 26 weeks’ gestation, a 35-year-old woman had a massive intracerebral hemorrhage at home.
The day before, she had contacted her ObGyn’s office to report severe headache and abdominal pain. The call was taken by an associate of her ObGyn, who told her there was no need to go to the hospital and suggested that she had a gastrointestinal virus.
The stroke caused severe cognitive impairment, loss of memory, partial vision loss, dysphasia, and partial paralysis on her right side. At trial, she was still undergoing therapy to regain mobility, speech, and memory. She uses a wheelchair.
Patient’s claim The covering ObGyn was negligent for not sending the patient to the hospital when she reported severe headache.
Defendants’ defense The ObGyn and medical practice denied negligence, contending that the patient’s pregnancy was normal and that there was no indication that she was at risk for a stroke.
Verdict A $10,928,188 Ohio verdict was returned.
Was the fetus properly monitored?
One month before her due date, a woman was found to have premature rupture of membranes. She had gestational diabetes controlled by diet. She was admitted for induction of labor.
For more than 12 hours, external fetal monitor heart-rate tracings were reassuring. Then tracings began to show variable decelerations. For a period of 90 minutes, it was impossible to evaluate the fetal heart rate because the monitor was not working. An internal monitor was not placed. Just prior to birth, the tracings showed a 15-minute period of fetal tachycardia with the heart rate at 180 bpm. The physician’s notes indicated that the baby’s head had crowned for a prolonged period of time.
The baby was floppy at birth with Apgar scores of 2, 4, and 6 at 1, 5, and 10 minutes, respectively. The child was resuscitated and transferred to the NICU. She was found to have perinatal asphyxia, severe metabolic acidosis, multiorgan injury, hypoxic ischemic encephalopathy, and seizures. She stayed in the NICU for 1 month. At age 9 years, she has developmental delays and memory problems, but no motor injuries.
Parents’ claim During the 90 minutes in which the fetal heart-rate monitor was not working properly, the fetus was in distress. An emergency cesarean delivery should have been performed when variable decelerations were seen on tracings.
Physician’s defense The lack of motor injury indicates that the injury was not related to birth.
Verdict A $2 million Michigan settlement was reached.
Rectal tear after vacuum extraction
Vacuum extraction was used to deliver a 47-year-old woman’s child. Later, the mother developed a rectovaginal fistula that became inflamed and involved vaginal passage of stool. The patient required 2 operations and still has residual complications.
Patient’s claim The ObGyn should have found and repaired the rectal tear at delivery. Vacuum extraction was used after only 2 pushes. The mother did not consent to the use of the vacuum extractor.
Physician’s defense The ObGyn admitted that he did not specifically remember this delivery. He claimed that there was informed consent and that the rectal injury was small and easy to overlook.
Verdict A $1.02 million New York verdict was returned.
Preeclamptic mother dies after giving birth
A 24-year-old woman developed preeclampsia when under prenatal care at a hospital clinic. At 36 weeks’ gestation, she presented to the clinic with a headache, “seeing spots,” and feeling ill; her blood pressure (BP) was 169/89 mm Hg. She was admitted for induction of labor and treated for preeclampsia with magnesium sulfate. A healthy baby was born 2 days later. The mother continued to have high BP and was prescribed nifedipine.
Her BP was 148/88 mm Hg at discharge. No antihypertensive medications were prescribed. She was given standard postpartum instructions and told to schedule a follow-up appointment in 6 to 8 weeks.
Five days after discharge, she experienced shortness of breath and swelling in her extremities, but did not seek medical attention until the next day, when breathing became labored. When emergency medical services arrived, she was in cardiac arrest. Prolonged resuscitation was required with intubation and artificial respiration. A computed tomog-raphy (CT) scan revealed cerebral edema from prolonged hypoxia. She was transferred to another hospital where a neurologist determined that she had suffered a profound anoxic brain injury. She died 3 days later.
Estate’s claim The hospital staff was negligent for failing to inform the patient of the signs and symptoms of continuing preeclampsia and for not prescribing antihypertensive medication at discharge. Her follow-up appointment should have been scheduled for 1 week.
Defendant’s defense The patient was given oral instructions regarding postpartum preeclampsia. The case was settled during trial.
Verdict A $50,000 North Carolina settlement was reached.
Was delivery properly managed?
When a 16-year-old woman was found to have preeclampsia, she was admitted and labor was induced using oxytocin. An external fetal heart-rate monitor was placed.
Three hours later, her ObGyn took over her care from the attending physician. He saw the patient once in the evening, then left to deliver a baby at another hospital. He maintained telephone contact with labor and delivery nurses, who told him that the mother’s labor was progressing as planned. Early the next morning, the nurse called the ObGyn to report that the mother was fully dilated and ready to deliver. The ObGyn was at the patient’s bedside within 30 minutes. After the mother pushed once, the ObGyn determined that a cesarean delivery was necessary.
After birth, the child suffered seizures in the NICU and was transferred to another facility. With CP and microcephaly, he cannot speak, is incontinent, has motor difficulties, and will require 24-hour care for life.
Parent’s claim Labor was not properly monitored. Oxytocin doses were too large and continued for too long.
Defendants’ defense The mother’s treatment was appropriate and timely. There was no negligence.
Verdict A confidential Kansas settlement was reached with another defendant during the trial. A defense verdict was returned for the ObGyn.
Evidence of CMV on ultrasonography
During her pregnancy in 2012, a woman contracted congenital cytomegalovirus (CMV), although she did not have any symptoms. The child has CP, a hearing deficiency, and other complications caused by the virus.
Parents’ claim The ObGyn failed to identify CMV, despite ultrasound evidence that the virus was affecting the fetus. Studies available at the time of the pregnancy show considerable success in treating the condition in utero with hyperimmune globulin antiviral agents.
Defendant’s defense The case was settled during trial.
Verdict A confidential Idaho settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Was the ObGyn’s dexterity compromised?
A woman underwent a hysterectomy. During surgery, the patient’s bladder was injured; the ObGyn called in a urologist to make the repair.
Patient’s claim The ObGyn failed to inform the patient about the possible complications from hysterectomy. The patient also claimed fraudulent concealment because the ObGyn had suffered a serious injury 3 years earlier that affected his dexterity. At the time of surgery, the ObGyn had a pending lawsuit against the owner of the premises where he fell in which he claimed that he was unable to continue his surgical practice because of the injury. The ObGyn never informed the patient of the extent of his injury or any associated risks related to his injury.
Defendants’ defense The patient was fully informed that bladder injury is a known risk of the procedure. The ObGyn maintained that his injury only affected his ability to stand for many hours while operating. The hospital settled during trial.
Verdict A $12,000 Louisiana settlement was reached with the hospital. Summary judgment was granted to the ObGyn on the informed consent claim. A $30,000 verdict was returned on the fraud count.
Placental abruption: Was child dead?
At 32 weeks’ gestation, a woman was found to have placental abruption. At the hospital, her ObGyn could not find a fetal heartbeat or detectable fetal movement on ultrasonography. A radiologist performed another ultrasound 30 minutes later and detected a fetal heart rate of 47 bpm. An emergency cesarean delivery was performed. Soon after birth, the child had seizures and was found to have hypoxic ischemic encephalopathy and diffuse brain injury. The child is profoundly disabled.
Parents’ claim The ObGyn was negligent for failing to detect the fetal heart rate and in failing to respond properly to placental abruption. Cesarean delivery should have been performed immediately after placental abruption was identified.
Defendant’s defense The case was settled at trial.
Verdict A $13 million Illinois settlement was reached, including $5 million in cash and $8 million placed in trust for the child.
Large fetus, shoulder dystocia: Erb’s palsy
Labor was induced at 39 weeks’ gestation because the fetus was anticipated to be large. During vaginal delivery, shoulder dystocia was encountered. At birth, the baby weighed 9 lb 2 oz. She sustained a brachial plexus injury to the posterior shoulder with permanent nerve root damage and Erb’s palsy. The child continues to have limited use of her left arm and hand even after 3 corrective operations.
Parents’ claim While performing maneuvers to relieve shoulder dystocia, the ObGyn exerted excessive traction on the baby’s head, causing a C-5 nerve root injury and complete avulsion at C-8. A cesarean delivery should have been performed.
Physician’s defense There was no negligence. The nerve injury was caused by the natural forces of labor and the mother’s pushing while the posterior shoulder was wedged behind the mother’s sa-
cral promontory.
Verdict A $1 million Illinois verdict was returned.
Woman dies from toxemia
A 22-year-old woman was seen by her ObGyn 4 days after vaginal delivery. Early the next day, the patient had a seizure at home and was transported by ambulance to the hospital. She could not be resuscitated and died. At autopsy, the cause of death was determined to be toxemia from pregnancy.
Estate’s claim The ObGyn failed to properly diagnose and treat the patient’s hypertension.
Defendant’s defense The case was settled during trial.
Verdict A $775,000 New York settlement was reached.
Blood transfusion delayed for hours: $14.75M net award
After emergency cesarean delivery, the baby was extremely anemic. The physicians determined that a fetal-maternal hemorrhage had started days before, causing the fetus to lose most of her blood.
An hour after birth, the attending neonatologist ordered blood from the hospital’s blood bank and arranged for emergency transport to a neonatal intensive care unit (NICU). Blood transfusion did not occur prior to transport. The child has severe cerebral palsy (CP) and cannot walk or talk at age 8 years.
Parents’ claim The neonatologist ordered cross-matched blood, which, because it is tested for compatibility, takes longer to supply. Universal donor blood could have been delivered in 20 minutes or less because it is readily available. The ambulance from the receiving hospital took an hour to drive 9 miles between the facilities, a trip that should have taken 12 minutes. The ambulance staff did not call ahead to the medical center to have blood ready for the baby. It took 4.5 hours before the newborn received a blood transfusion, a delay that caused severe injury to the child.
Defendants’ defense The matter went to trial against the neonatologist and his employer after the other defendants settled.
Verdict Before trial, an ObGyn and the hospital settled for a combined $750,000, and the county agreed to a $12 million settlement. During trial, a $2 million Illinois settlement was reached.
Pregnant woman has a massive stroke: $10.9M
Pregnant with her third child and at 26 weeks’ gestation, a 35-year-old woman had a massive intracerebral hemorrhage at home.
The day before, she had contacted her ObGyn’s office to report severe headache and abdominal pain. The call was taken by an associate of her ObGyn, who told her there was no need to go to the hospital and suggested that she had a gastrointestinal virus.
The stroke caused severe cognitive impairment, loss of memory, partial vision loss, dysphasia, and partial paralysis on her right side. At trial, she was still undergoing therapy to regain mobility, speech, and memory. She uses a wheelchair.
Patient’s claim The covering ObGyn was negligent for not sending the patient to the hospital when she reported severe headache.
Defendants’ defense The ObGyn and medical practice denied negligence, contending that the patient’s pregnancy was normal and that there was no indication that she was at risk for a stroke.
Verdict A $10,928,188 Ohio verdict was returned.
Was the fetus properly monitored?
One month before her due date, a woman was found to have premature rupture of membranes. She had gestational diabetes controlled by diet. She was admitted for induction of labor.
For more than 12 hours, external fetal monitor heart-rate tracings were reassuring. Then tracings began to show variable decelerations. For a period of 90 minutes, it was impossible to evaluate the fetal heart rate because the monitor was not working. An internal monitor was not placed. Just prior to birth, the tracings showed a 15-minute period of fetal tachycardia with the heart rate at 180 bpm. The physician’s notes indicated that the baby’s head had crowned for a prolonged period of time.
The baby was floppy at birth with Apgar scores of 2, 4, and 6 at 1, 5, and 10 minutes, respectively. The child was resuscitated and transferred to the NICU. She was found to have perinatal asphyxia, severe metabolic acidosis, multiorgan injury, hypoxic ischemic encephalopathy, and seizures. She stayed in the NICU for 1 month. At age 9 years, she has developmental delays and memory problems, but no motor injuries.
Parents’ claim During the 90 minutes in which the fetal heart-rate monitor was not working properly, the fetus was in distress. An emergency cesarean delivery should have been performed when variable decelerations were seen on tracings.
Physician’s defense The lack of motor injury indicates that the injury was not related to birth.
Verdict A $2 million Michigan settlement was reached.
Rectal tear after vacuum extraction
Vacuum extraction was used to deliver a 47-year-old woman’s child. Later, the mother developed a rectovaginal fistula that became inflamed and involved vaginal passage of stool. The patient required 2 operations and still has residual complications.
Patient’s claim The ObGyn should have found and repaired the rectal tear at delivery. Vacuum extraction was used after only 2 pushes. The mother did not consent to the use of the vacuum extractor.
Physician’s defense The ObGyn admitted that he did not specifically remember this delivery. He claimed that there was informed consent and that the rectal injury was small and easy to overlook.
Verdict A $1.02 million New York verdict was returned.
Preeclamptic mother dies after giving birth
A 24-year-old woman developed preeclampsia when under prenatal care at a hospital clinic. At 36 weeks’ gestation, she presented to the clinic with a headache, “seeing spots,” and feeling ill; her blood pressure (BP) was 169/89 mm Hg. She was admitted for induction of labor and treated for preeclampsia with magnesium sulfate. A healthy baby was born 2 days later. The mother continued to have high BP and was prescribed nifedipine.
Her BP was 148/88 mm Hg at discharge. No antihypertensive medications were prescribed. She was given standard postpartum instructions and told to schedule a follow-up appointment in 6 to 8 weeks.
Five days after discharge, she experienced shortness of breath and swelling in her extremities, but did not seek medical attention until the next day, when breathing became labored. When emergency medical services arrived, she was in cardiac arrest. Prolonged resuscitation was required with intubation and artificial respiration. A computed tomog-raphy (CT) scan revealed cerebral edema from prolonged hypoxia. She was transferred to another hospital where a neurologist determined that she had suffered a profound anoxic brain injury. She died 3 days later.
Estate’s claim The hospital staff was negligent for failing to inform the patient of the signs and symptoms of continuing preeclampsia and for not prescribing antihypertensive medication at discharge. Her follow-up appointment should have been scheduled for 1 week.
Defendant’s defense The patient was given oral instructions regarding postpartum preeclampsia. The case was settled during trial.
Verdict A $50,000 North Carolina settlement was reached.
Was delivery properly managed?
When a 16-year-old woman was found to have preeclampsia, she was admitted and labor was induced using oxytocin. An external fetal heart-rate monitor was placed.
Three hours later, her ObGyn took over her care from the attending physician. He saw the patient once in the evening, then left to deliver a baby at another hospital. He maintained telephone contact with labor and delivery nurses, who told him that the mother’s labor was progressing as planned. Early the next morning, the nurse called the ObGyn to report that the mother was fully dilated and ready to deliver. The ObGyn was at the patient’s bedside within 30 minutes. After the mother pushed once, the ObGyn determined that a cesarean delivery was necessary.
After birth, the child suffered seizures in the NICU and was transferred to another facility. With CP and microcephaly, he cannot speak, is incontinent, has motor difficulties, and will require 24-hour care for life.
Parent’s claim Labor was not properly monitored. Oxytocin doses were too large and continued for too long.
Defendants’ defense The mother’s treatment was appropriate and timely. There was no negligence.
Verdict A confidential Kansas settlement was reached with another defendant during the trial. A defense verdict was returned for the ObGyn.
Evidence of CMV on ultrasonography
During her pregnancy in 2012, a woman contracted congenital cytomegalovirus (CMV), although she did not have any symptoms. The child has CP, a hearing deficiency, and other complications caused by the virus.
Parents’ claim The ObGyn failed to identify CMV, despite ultrasound evidence that the virus was affecting the fetus. Studies available at the time of the pregnancy show considerable success in treating the condition in utero with hyperimmune globulin antiviral agents.
Defendant’s defense The case was settled during trial.
Verdict A confidential Idaho settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Was the ObGyn’s dexterity compromised?
A woman underwent a hysterectomy. During surgery, the patient’s bladder was injured; the ObGyn called in a urologist to make the repair.
Patient’s claim The ObGyn failed to inform the patient about the possible complications from hysterectomy. The patient also claimed fraudulent concealment because the ObGyn had suffered a serious injury 3 years earlier that affected his dexterity. At the time of surgery, the ObGyn had a pending lawsuit against the owner of the premises where he fell in which he claimed that he was unable to continue his surgical practice because of the injury. The ObGyn never informed the patient of the extent of his injury or any associated risks related to his injury.
Defendants’ defense The patient was fully informed that bladder injury is a known risk of the procedure. The ObGyn maintained that his injury only affected his ability to stand for many hours while operating. The hospital settled during trial.
Verdict A $12,000 Louisiana settlement was reached with the hospital. Summary judgment was granted to the ObGyn on the informed consent claim. A $30,000 verdict was returned on the fraud count.
Placental abruption: Was child dead?
At 32 weeks’ gestation, a woman was found to have placental abruption. At the hospital, her ObGyn could not find a fetal heartbeat or detectable fetal movement on ultrasonography. A radiologist performed another ultrasound 30 minutes later and detected a fetal heart rate of 47 bpm. An emergency cesarean delivery was performed. Soon after birth, the child had seizures and was found to have hypoxic ischemic encephalopathy and diffuse brain injury. The child is profoundly disabled.
Parents’ claim The ObGyn was negligent for failing to detect the fetal heart rate and in failing to respond properly to placental abruption. Cesarean delivery should have been performed immediately after placental abruption was identified.
Defendant’s defense The case was settled at trial.
Verdict A $13 million Illinois settlement was reached, including $5 million in cash and $8 million placed in trust for the child.
Large fetus, shoulder dystocia: Erb’s palsy
Labor was induced at 39 weeks’ gestation because the fetus was anticipated to be large. During vaginal delivery, shoulder dystocia was encountered. At birth, the baby weighed 9 lb 2 oz. She sustained a brachial plexus injury to the posterior shoulder with permanent nerve root damage and Erb’s palsy. The child continues to have limited use of her left arm and hand even after 3 corrective operations.
Parents’ claim While performing maneuvers to relieve shoulder dystocia, the ObGyn exerted excessive traction on the baby’s head, causing a C-5 nerve root injury and complete avulsion at C-8. A cesarean delivery should have been performed.
Physician’s defense There was no negligence. The nerve injury was caused by the natural forces of labor and the mother’s pushing while the posterior shoulder was wedged behind the mother’s sa-
cral promontory.
Verdict A $1 million Illinois verdict was returned.
Woman dies from toxemia
A 22-year-old woman was seen by her ObGyn 4 days after vaginal delivery. Early the next day, the patient had a seizure at home and was transported by ambulance to the hospital. She could not be resuscitated and died. At autopsy, the cause of death was determined to be toxemia from pregnancy.
Estate’s claim The ObGyn failed to properly diagnose and treat the patient’s hypertension.
Defendant’s defense The case was settled during trial.
Verdict A $775,000 New York settlement was reached.
Blood transfusion delayed for hours: $14.75M net award
After emergency cesarean delivery, the baby was extremely anemic. The physicians determined that a fetal-maternal hemorrhage had started days before, causing the fetus to lose most of her blood.
An hour after birth, the attending neonatologist ordered blood from the hospital’s blood bank and arranged for emergency transport to a neonatal intensive care unit (NICU). Blood transfusion did not occur prior to transport. The child has severe cerebral palsy (CP) and cannot walk or talk at age 8 years.
Parents’ claim The neonatologist ordered cross-matched blood, which, because it is tested for compatibility, takes longer to supply. Universal donor blood could have been delivered in 20 minutes or less because it is readily available. The ambulance from the receiving hospital took an hour to drive 9 miles between the facilities, a trip that should have taken 12 minutes. The ambulance staff did not call ahead to the medical center to have blood ready for the baby. It took 4.5 hours before the newborn received a blood transfusion, a delay that caused severe injury to the child.
Defendants’ defense The matter went to trial against the neonatologist and his employer after the other defendants settled.
Verdict Before trial, an ObGyn and the hospital settled for a combined $750,000, and the county agreed to a $12 million settlement. During trial, a $2 million Illinois settlement was reached.
Pregnant woman has a massive stroke: $10.9M
Pregnant with her third child and at 26 weeks’ gestation, a 35-year-old woman had a massive intracerebral hemorrhage at home.
The day before, she had contacted her ObGyn’s office to report severe headache and abdominal pain. The call was taken by an associate of her ObGyn, who told her there was no need to go to the hospital and suggested that she had a gastrointestinal virus.
The stroke caused severe cognitive impairment, loss of memory, partial vision loss, dysphasia, and partial paralysis on her right side. At trial, she was still undergoing therapy to regain mobility, speech, and memory. She uses a wheelchair.
Patient’s claim The covering ObGyn was negligent for not sending the patient to the hospital when she reported severe headache.
Defendants’ defense The ObGyn and medical practice denied negligence, contending that the patient’s pregnancy was normal and that there was no indication that she was at risk for a stroke.
Verdict A $10,928,188 Ohio verdict was returned.
Was the fetus properly monitored?
One month before her due date, a woman was found to have premature rupture of membranes. She had gestational diabetes controlled by diet. She was admitted for induction of labor.
For more than 12 hours, external fetal monitor heart-rate tracings were reassuring. Then tracings began to show variable decelerations. For a period of 90 minutes, it was impossible to evaluate the fetal heart rate because the monitor was not working. An internal monitor was not placed. Just prior to birth, the tracings showed a 15-minute period of fetal tachycardia with the heart rate at 180 bpm. The physician’s notes indicated that the baby’s head had crowned for a prolonged period of time.
The baby was floppy at birth with Apgar scores of 2, 4, and 6 at 1, 5, and 10 minutes, respectively. The child was resuscitated and transferred to the NICU. She was found to have perinatal asphyxia, severe metabolic acidosis, multiorgan injury, hypoxic ischemic encephalopathy, and seizures. She stayed in the NICU for 1 month. At age 9 years, she has developmental delays and memory problems, but no motor injuries.
Parents’ claim During the 90 minutes in which the fetal heart-rate monitor was not working properly, the fetus was in distress. An emergency cesarean delivery should have been performed when variable decelerations were seen on tracings.
Physician’s defense The lack of motor injury indicates that the injury was not related to birth.
Verdict A $2 million Michigan settlement was reached.
Rectal tear after vacuum extraction
Vacuum extraction was used to deliver a 47-year-old woman’s child. Later, the mother developed a rectovaginal fistula that became inflamed and involved vaginal passage of stool. The patient required 2 operations and still has residual complications.
Patient’s claim The ObGyn should have found and repaired the rectal tear at delivery. Vacuum extraction was used after only 2 pushes. The mother did not consent to the use of the vacuum extractor.
Physician’s defense The ObGyn admitted that he did not specifically remember this delivery. He claimed that there was informed consent and that the rectal injury was small and easy to overlook.
Verdict A $1.02 million New York verdict was returned.
Preeclamptic mother dies after giving birth
A 24-year-old woman developed preeclampsia when under prenatal care at a hospital clinic. At 36 weeks’ gestation, she presented to the clinic with a headache, “seeing spots,” and feeling ill; her blood pressure (BP) was 169/89 mm Hg. She was admitted for induction of labor and treated for preeclampsia with magnesium sulfate. A healthy baby was born 2 days later. The mother continued to have high BP and was prescribed nifedipine.
Her BP was 148/88 mm Hg at discharge. No antihypertensive medications were prescribed. She was given standard postpartum instructions and told to schedule a follow-up appointment in 6 to 8 weeks.
Five days after discharge, she experienced shortness of breath and swelling in her extremities, but did not seek medical attention until the next day, when breathing became labored. When emergency medical services arrived, she was in cardiac arrest. Prolonged resuscitation was required with intubation and artificial respiration. A computed tomog-raphy (CT) scan revealed cerebral edema from prolonged hypoxia. She was transferred to another hospital where a neurologist determined that she had suffered a profound anoxic brain injury. She died 3 days later.
Estate’s claim The hospital staff was negligent for failing to inform the patient of the signs and symptoms of continuing preeclampsia and for not prescribing antihypertensive medication at discharge. Her follow-up appointment should have been scheduled for 1 week.
Defendant’s defense The patient was given oral instructions regarding postpartum preeclampsia. The case was settled during trial.
Verdict A $50,000 North Carolina settlement was reached.
Was delivery properly managed?
When a 16-year-old woman was found to have preeclampsia, she was admitted and labor was induced using oxytocin. An external fetal heart-rate monitor was placed.
Three hours later, her ObGyn took over her care from the attending physician. He saw the patient once in the evening, then left to deliver a baby at another hospital. He maintained telephone contact with labor and delivery nurses, who told him that the mother’s labor was progressing as planned. Early the next morning, the nurse called the ObGyn to report that the mother was fully dilated and ready to deliver. The ObGyn was at the patient’s bedside within 30 minutes. After the mother pushed once, the ObGyn determined that a cesarean delivery was necessary.
After birth, the child suffered seizures in the NICU and was transferred to another facility. With CP and microcephaly, he cannot speak, is incontinent, has motor difficulties, and will require 24-hour care for life.
Parent’s claim Labor was not properly monitored. Oxytocin doses were too large and continued for too long.
Defendants’ defense The mother’s treatment was appropriate and timely. There was no negligence.
Verdict A confidential Kansas settlement was reached with another defendant during the trial. A defense verdict was returned for the ObGyn.
Evidence of CMV on ultrasonography
During her pregnancy in 2012, a woman contracted congenital cytomegalovirus (CMV), although she did not have any symptoms. The child has CP, a hearing deficiency, and other complications caused by the virus.
Parents’ claim The ObGyn failed to identify CMV, despite ultrasound evidence that the virus was affecting the fetus. Studies available at the time of the pregnancy show considerable success in treating the condition in utero with hyperimmune globulin antiviral agents.
Defendant’s defense The case was settled during trial.
Verdict A confidential Idaho settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In this Article
- Placental abruption: Was child dead?
- Large fetus, shoulder dystocia: Erb’s palsy
- Woman dies from toxemia
- Blood transfusion delayed for hours: $14.75M net award
- Pregnant woman has a massive stroke: $10.9M
- Was the fetus properly monitored?
- Rectal tear after vacuum extraction
- Preeclamptic mother dies after giving birth
- Was delivery properly managed?
- Evidence of CMV on ultrasonography

A survey of liability claims against obstetric providers highlights major areas of contention
An analysis of 882 obstetric claims closed between 2007 and 2014 highlighted 3 common allegationsby patients1:
- a delay in the treatment of fetal distress (22%). The term “fetal distress” remains a common allegation in malpractice claims. Cases in this category most often reflected a delay or failure to act in the face of Category II or III fetal heart-rate tracings.
- improper performance of vaginal delivery (20%). Almost half of the cases in this category involved brachial plexus injuries linked to shoulder dystocia. Patients alleged that improper maneuvers were used to resolve the dystocia. The remainder of cases in this category involved forceps and vacuum extraction deliveries.
- improper management of pregnancy (17%). Among the allegations were a failure to test for fetal abnormalities, failure to recognize complications of pregnancy, and failure to address abnormal findings.
Together, these 3 allegations accounted for 59% of claims. Other allegations included diagnosis-related claims, delay in delivery, improper performance of operative delivery, retained foreign bodies, and improper choice of delivery method.1
Where are the really big malpractice awards?
Everything may be bigger in Texas, but New York is the biggest in at least 1 area: large medical malpractice payments. New York had more than 3 times as many $1 million-plus malpractice awards as any other state in 2014, according to data from the National Practitioner Data Bank (NPDB).1
New York physicians had 210 malpractice payments of $1 million or more reported to the NPDB last year, compared with 61 for Illinois, the next-highest state. Rounding out the top 5 were Massachusetts with 49, followed by California with 43, and New Jersey with 41, the NPDB data show.
After taking population into account, New York was still the leader with 10.66 large awards per million residents. Next in this category was the New England trio of Rhode Island, which had 9.42 such payments per 1 million population; Massachusetts (7.26); and Connecticut (6.39).
In 2014, there were 4 states that had no malpractice payments of at least $1 million reported to the NPDB: Alaska, Kansas, North Dakota, and Nebraska, with Kansas having the largest population. In states with at least one $1 million-plus malpractice payment, Texas physicians had the lowest rate per million population, 0.22—just 6 awards from a population of 27 million.
Reference
1. NPDB Research Statistics. National Practitioner Data Bank. http://www.npdb.hrsa.gov/resources/npdbstats/npdbStatistics.jsp. Accessed
July 17, 2015.
Copyright © 2015 Ob.Gyn. News Digital Network, Frontline Medical Communications. Available at: http://www.obgynews.com/?id=11146&tx_ttnews[tt_news]=417377&cHash=5cc8cd69fa7c8a1186aaeec0e814e4e4
The Obstetrics Closed Claims Study findings were released earlier this spring by the Napa, California−based Doctors Company, the nation’s largest physician-owned medical malpractice insurer.1 Susan Mann, MD,a spokesperson for the company, provided expert commentary on the study at the 2015 Annual Clinical Meeting of the American College of Obstetricians and Gynecologists in San Francisco (see “Frequent sources of malpractice claims” below).
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel |
Frequent sources of malpractice claims
Communication breakdowns and treatment delays are frequent sources of malpractice claims. Susan Mann, MD, spokesperson for The Doctors Company, the nation’s largest physician-owned medical malpractice insurer, discusses the underlying practice vulnerabilities revealed by the Obstetrics Closed Claims Study.
Dr. Mann practices obstetrics and gynecology in Brookline, Massachusetts, and at Beth Israel Deaconess Medical Center in Boston. She is president of the QualBridge Institute, a consulting firm focused on issues of quality and safety.
Top 7 factors contributing to patient injury
The Doctors Company identified specific factors that contributed to patient injury in the closed claims1:
- Selection and management of therapy(34%). Among the issues here were decisions involving augmentation of labor, route of delivery, and the timing of interventions. This factor also related to medications—for example, a failure to order antibiotics for Group A and Group B strep, a failure to order Rho(D) immune globulin for Rh-negative mothers, and a failure to provide magnesium sulfate for women with eclampsia.
- Patient-assessment issues (32%). The Doctors Company reviewers found that physicians frequently failed to consider information that was available, or overlooked abnormal findings.
- Technical performance (18%). This factor involved problems associated with known risks of various procedures, such as postpartum hemorrhage and brachial plexus injuries. It also included poor technique.
- Communication problems among providers (17%).
- Patient factors (16%). These factors included a failure to comply with therapy or to show up for appointments.
- Insufficient notes or a lack of documentation (14%).
- Communication problems between patient/family and provider (14%).
“Studying obstetrical medical malpractice claims sheds light on the wide array of problems that may arise during pregnancy and in labor and delivery,” the study authors conclude. “Many of these cases reflect unusual maternal or neonatal conditions that can be diagnosed only with vigilance. Examples include protein deficiencies, clotting abnormalities, placental abruptions, infections, and genetic abnormalities. More common conditions should be identified with close attention to vital signs, laboratory studies, changes to maternal and neonatal conditions, and patient complaints.”1 See “Tips for reducing malpractice claims in obstetrics” below.
Tips for reducing malpractice claims in obstetrics1
The Obstetrics Closed Claim Study identified a number of “underlying vulnerabilities” that place patients at risk and increase liability for clinicians. The Doctors Company offers the following tips to help reduce these claims:
Require periodic training and certification for physicians and nurses to maintain competency and facilitate conversations about fetal heart-rate (FHR) tracing interpretation. Both parties should use the same terminology when discussing the strips.
Use technology that allows physicians to review FHR patterns from remote locations so that physicians and nurses are able to see the same information when discussing next steps.
When operative vaginal delivery is attempted in the face of a Category III FHR tracing, a contingency team should be available for possible emergent cesarean delivery.
Foster a culture in which caregivers feel comfortable speaking up if they have a concern. Ensure that the organization has a well-defined escalation guideline.
“Obstetric departments must plan for clinical emergencies by developing and maintaining physician and staff competencies through mock drills and simulations that reduce the likelihood of injuries to mothers and their infants,” the study authors conclude.1
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
1. The Doctors Company. Obstetrics Closed Claim Study. http://www.thedoctors.com/KnowledgeCenter/Pa tient Safety/articles/CON_ID_011803. Published April 2015. Accessed May 6, 2015.
An analysis of 882 obstetric claims closed between 2007 and 2014 highlighted 3 common allegationsby patients1:
- a delay in the treatment of fetal distress (22%). The term “fetal distress” remains a common allegation in malpractice claims. Cases in this category most often reflected a delay or failure to act in the face of Category II or III fetal heart-rate tracings.
- improper performance of vaginal delivery (20%). Almost half of the cases in this category involved brachial plexus injuries linked to shoulder dystocia. Patients alleged that improper maneuvers were used to resolve the dystocia. The remainder of cases in this category involved forceps and vacuum extraction deliveries.
- improper management of pregnancy (17%). Among the allegations were a failure to test for fetal abnormalities, failure to recognize complications of pregnancy, and failure to address abnormal findings.
Together, these 3 allegations accounted for 59% of claims. Other allegations included diagnosis-related claims, delay in delivery, improper performance of operative delivery, retained foreign bodies, and improper choice of delivery method.1
Where are the really big malpractice awards?
Everything may be bigger in Texas, but New York is the biggest in at least 1 area: large medical malpractice payments. New York had more than 3 times as many $1 million-plus malpractice awards as any other state in 2014, according to data from the National Practitioner Data Bank (NPDB).1
New York physicians had 210 malpractice payments of $1 million or more reported to the NPDB last year, compared with 61 for Illinois, the next-highest state. Rounding out the top 5 were Massachusetts with 49, followed by California with 43, and New Jersey with 41, the NPDB data show.
After taking population into account, New York was still the leader with 10.66 large awards per million residents. Next in this category was the New England trio of Rhode Island, which had 9.42 such payments per 1 million population; Massachusetts (7.26); and Connecticut (6.39).
In 2014, there were 4 states that had no malpractice payments of at least $1 million reported to the NPDB: Alaska, Kansas, North Dakota, and Nebraska, with Kansas having the largest population. In states with at least one $1 million-plus malpractice payment, Texas physicians had the lowest rate per million population, 0.22—just 6 awards from a population of 27 million.
Reference
1. NPDB Research Statistics. National Practitioner Data Bank. http://www.npdb.hrsa.gov/resources/npdbstats/npdbStatistics.jsp. Accessed
July 17, 2015.
Copyright © 2015 Ob.Gyn. News Digital Network, Frontline Medical Communications. Available at: http://www.obgynews.com/?id=11146&tx_ttnews[tt_news]=417377&cHash=5cc8cd69fa7c8a1186aaeec0e814e4e4
The Obstetrics Closed Claims Study findings were released earlier this spring by the Napa, California−based Doctors Company, the nation’s largest physician-owned medical malpractice insurer.1 Susan Mann, MD,a spokesperson for the company, provided expert commentary on the study at the 2015 Annual Clinical Meeting of the American College of Obstetricians and Gynecologists in San Francisco (see “Frequent sources of malpractice claims” below).
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel |
Frequent sources of malpractice claims
Communication breakdowns and treatment delays are frequent sources of malpractice claims. Susan Mann, MD, spokesperson for The Doctors Company, the nation’s largest physician-owned medical malpractice insurer, discusses the underlying practice vulnerabilities revealed by the Obstetrics Closed Claims Study.
Dr. Mann practices obstetrics and gynecology in Brookline, Massachusetts, and at Beth Israel Deaconess Medical Center in Boston. She is president of the QualBridge Institute, a consulting firm focused on issues of quality and safety.
Top 7 factors contributing to patient injury
The Doctors Company identified specific factors that contributed to patient injury in the closed claims1:
- Selection and management of therapy(34%). Among the issues here were decisions involving augmentation of labor, route of delivery, and the timing of interventions. This factor also related to medications—for example, a failure to order antibiotics for Group A and Group B strep, a failure to order Rho(D) immune globulin for Rh-negative mothers, and a failure to provide magnesium sulfate for women with eclampsia.
- Patient-assessment issues (32%). The Doctors Company reviewers found that physicians frequently failed to consider information that was available, or overlooked abnormal findings.
- Technical performance (18%). This factor involved problems associated with known risks of various procedures, such as postpartum hemorrhage and brachial plexus injuries. It also included poor technique.
- Communication problems among providers (17%).
- Patient factors (16%). These factors included a failure to comply with therapy or to show up for appointments.
- Insufficient notes or a lack of documentation (14%).
- Communication problems between patient/family and provider (14%).
“Studying obstetrical medical malpractice claims sheds light on the wide array of problems that may arise during pregnancy and in labor and delivery,” the study authors conclude. “Many of these cases reflect unusual maternal or neonatal conditions that can be diagnosed only with vigilance. Examples include protein deficiencies, clotting abnormalities, placental abruptions, infections, and genetic abnormalities. More common conditions should be identified with close attention to vital signs, laboratory studies, changes to maternal and neonatal conditions, and patient complaints.”1 See “Tips for reducing malpractice claims in obstetrics” below.
Tips for reducing malpractice claims in obstetrics1
The Obstetrics Closed Claim Study identified a number of “underlying vulnerabilities” that place patients at risk and increase liability for clinicians. The Doctors Company offers the following tips to help reduce these claims:
Require periodic training and certification for physicians and nurses to maintain competency and facilitate conversations about fetal heart-rate (FHR) tracing interpretation. Both parties should use the same terminology when discussing the strips.
Use technology that allows physicians to review FHR patterns from remote locations so that physicians and nurses are able to see the same information when discussing next steps.
When operative vaginal delivery is attempted in the face of a Category III FHR tracing, a contingency team should be available for possible emergent cesarean delivery.
Foster a culture in which caregivers feel comfortable speaking up if they have a concern. Ensure that the organization has a well-defined escalation guideline.
“Obstetric departments must plan for clinical emergencies by developing and maintaining physician and staff competencies through mock drills and simulations that reduce the likelihood of injuries to mothers and their infants,” the study authors conclude.1
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
An analysis of 882 obstetric claims closed between 2007 and 2014 highlighted 3 common allegationsby patients1:
- a delay in the treatment of fetal distress (22%). The term “fetal distress” remains a common allegation in malpractice claims. Cases in this category most often reflected a delay or failure to act in the face of Category II or III fetal heart-rate tracings.
- improper performance of vaginal delivery (20%). Almost half of the cases in this category involved brachial plexus injuries linked to shoulder dystocia. Patients alleged that improper maneuvers were used to resolve the dystocia. The remainder of cases in this category involved forceps and vacuum extraction deliveries.
- improper management of pregnancy (17%). Among the allegations were a failure to test for fetal abnormalities, failure to recognize complications of pregnancy, and failure to address abnormal findings.
Together, these 3 allegations accounted for 59% of claims. Other allegations included diagnosis-related claims, delay in delivery, improper performance of operative delivery, retained foreign bodies, and improper choice of delivery method.1
Where are the really big malpractice awards?
Everything may be bigger in Texas, but New York is the biggest in at least 1 area: large medical malpractice payments. New York had more than 3 times as many $1 million-plus malpractice awards as any other state in 2014, according to data from the National Practitioner Data Bank (NPDB).1
New York physicians had 210 malpractice payments of $1 million or more reported to the NPDB last year, compared with 61 for Illinois, the next-highest state. Rounding out the top 5 were Massachusetts with 49, followed by California with 43, and New Jersey with 41, the NPDB data show.
After taking population into account, New York was still the leader with 10.66 large awards per million residents. Next in this category was the New England trio of Rhode Island, which had 9.42 such payments per 1 million population; Massachusetts (7.26); and Connecticut (6.39).
In 2014, there were 4 states that had no malpractice payments of at least $1 million reported to the NPDB: Alaska, Kansas, North Dakota, and Nebraska, with Kansas having the largest population. In states with at least one $1 million-plus malpractice payment, Texas physicians had the lowest rate per million population, 0.22—just 6 awards from a population of 27 million.
Reference
1. NPDB Research Statistics. National Practitioner Data Bank. http://www.npdb.hrsa.gov/resources/npdbstats/npdbStatistics.jsp. Accessed
July 17, 2015.
Copyright © 2015 Ob.Gyn. News Digital Network, Frontline Medical Communications. Available at: http://www.obgynews.com/?id=11146&tx_ttnews[tt_news]=417377&cHash=5cc8cd69fa7c8a1186aaeec0e814e4e4
The Obstetrics Closed Claims Study findings were released earlier this spring by the Napa, California−based Doctors Company, the nation’s largest physician-owned medical malpractice insurer.1 Susan Mann, MD,a spokesperson for the company, provided expert commentary on the study at the 2015 Annual Clinical Meeting of the American College of Obstetricians and Gynecologists in San Francisco (see “Frequent sources of malpractice claims” below).
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel |
Frequent sources of malpractice claims
Communication breakdowns and treatment delays are frequent sources of malpractice claims. Susan Mann, MD, spokesperson for The Doctors Company, the nation’s largest physician-owned medical malpractice insurer, discusses the underlying practice vulnerabilities revealed by the Obstetrics Closed Claims Study.
Dr. Mann practices obstetrics and gynecology in Brookline, Massachusetts, and at Beth Israel Deaconess Medical Center in Boston. She is president of the QualBridge Institute, a consulting firm focused on issues of quality and safety.
Top 7 factors contributing to patient injury
The Doctors Company identified specific factors that contributed to patient injury in the closed claims1:
- Selection and management of therapy(34%). Among the issues here were decisions involving augmentation of labor, route of delivery, and the timing of interventions. This factor also related to medications—for example, a failure to order antibiotics for Group A and Group B strep, a failure to order Rho(D) immune globulin for Rh-negative mothers, and a failure to provide magnesium sulfate for women with eclampsia.
- Patient-assessment issues (32%). The Doctors Company reviewers found that physicians frequently failed to consider information that was available, or overlooked abnormal findings.
- Technical performance (18%). This factor involved problems associated with known risks of various procedures, such as postpartum hemorrhage and brachial plexus injuries. It also included poor technique.
- Communication problems among providers (17%).
- Patient factors (16%). These factors included a failure to comply with therapy or to show up for appointments.
- Insufficient notes or a lack of documentation (14%).
- Communication problems between patient/family and provider (14%).
“Studying obstetrical medical malpractice claims sheds light on the wide array of problems that may arise during pregnancy and in labor and delivery,” the study authors conclude. “Many of these cases reflect unusual maternal or neonatal conditions that can be diagnosed only with vigilance. Examples include protein deficiencies, clotting abnormalities, placental abruptions, infections, and genetic abnormalities. More common conditions should be identified with close attention to vital signs, laboratory studies, changes to maternal and neonatal conditions, and patient complaints.”1 See “Tips for reducing malpractice claims in obstetrics” below.
Tips for reducing malpractice claims in obstetrics1
The Obstetrics Closed Claim Study identified a number of “underlying vulnerabilities” that place patients at risk and increase liability for clinicians. The Doctors Company offers the following tips to help reduce these claims:
Require periodic training and certification for physicians and nurses to maintain competency and facilitate conversations about fetal heart-rate (FHR) tracing interpretation. Both parties should use the same terminology when discussing the strips.
Use technology that allows physicians to review FHR patterns from remote locations so that physicians and nurses are able to see the same information when discussing next steps.
When operative vaginal delivery is attempted in the face of a Category III FHR tracing, a contingency team should be available for possible emergent cesarean delivery.
Foster a culture in which caregivers feel comfortable speaking up if they have a concern. Ensure that the organization has a well-defined escalation guideline.
“Obstetric departments must plan for clinical emergencies by developing and maintaining physician and staff competencies through mock drills and simulations that reduce the likelihood of injuries to mothers and their infants,” the study authors conclude.1
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
1. The Doctors Company. Obstetrics Closed Claim Study. http://www.thedoctors.com/KnowledgeCenter/Pa tient Safety/articles/CON_ID_011803. Published April 2015. Accessed May 6, 2015.
Reference
1. The Doctors Company. Obstetrics Closed Claim Study. http://www.thedoctors.com/KnowledgeCenter/Pa tient Safety/articles/CON_ID_011803. Published April 2015. Accessed May 6, 2015.
In this Article
- Tips for reducing malpractice claims in obstetrics
- Where are the really big malpractice awards?
- Top 7 factors contributing topatient injury
Value-based care poses new legal risks for doctors
The government’s push toward value-based care aims to fix a broken reimbursement system and improve quality of care for patients. But the new payment models also bring new legal risks for physicians, experts and anti-fraud officials warn.
“Novel payment methodologies may present new program integrity vulnerabilities,” Dr. Shantanu Agrawal, director of the Center for Program Integrity at the Centers for Medicare & Medicaid Services, said at a recent American Bar Association meeting. “As they assume financial risk, providers are also assuming program integrity risk. Without adequate controls, provider-run systems may be relatively vulnerable.”

The Department of Health and Human Services plans to have 30% of Medicare payments in value-based payment structures by the end of 2016, and 50% by the end of 2018. The transition will be driven through investments in alternative payment models such as Accountable Care Organizations (ACOs), advanced primary care medical home models, bundled payments models, and integrated care demonstrations for Medicare and Medicaid patients.
At the end of 2014, value-based payments represented 20% of Medicare fee-for-service payments to providers, according to CMS data. The rate was fueled by government programs such as the Medicare Shared Savings Program (MSSP), Pioneer ACOs, the Bundled Payments for Care Improvement Initiative, and the Comprehensive Primary Care Initiative. Meanwhile, HHS is encouraging private payers, marketplace plans, Medicare Advantage plans, and state Medicaid programs to move in the same value-based direction.
With so many new regulations, mandates, and programs coming down the pipeline, physicians are likely not thinking about the legal dangers that may arise with alternative payment structures, said Mark S. Kopson, a health law attorney in Bloomfield Hills, Mich., and chair of the American Health Lawyers Association’s Payers, Plans and Managed Care Practice Group.

Fee-for-service models can involve claims “about excess treatments and unnecessary services to drive up reimbursement,” Mr. Kopson said in an interview. “When you get into these [value-based] types of programs, it’s the exact opposite. The real threat is the withholding of necessary care in order to reduce expenses and therefore drive up those margins for the providers.”
To avoid such claims, physicians should ensure that their charts include the reasoning behind treatment decisions and a thorough record of why certain treatments were chosen and diagnoses were made, Mr. Kopson advised.
“Going forward, your charting better be completely accurate and detailed so that you don’t leave room for the government to make an argument that you should have provided this or that additional treatment,” he said.
Inaccurate reporting of enrollment data or financial information within new payment models could also land doctors in legal trouble, according to CMS officials.
Problematic reports, enrollee data, or other information physicians are required to submit to the government could be considered falsification and lead to False Claims Act violations.
“Providers are responsible for the information reported and should ensure that the appropriate checks and balances are in place that verify data is reported timely and accurately,” Tony A. Salters, a CMS spokesman, said in an interview. “For some models, providers must attest to the accuracy of this data. [To] report inaccurately could result in violations of federal laws.”
Physician-run payment models, such as doctor-led ACOs, may also draw legal scrutiny if physicians fail to prevent bad behavior by de facto partners. Physicians must ensure that all costs claimed by subcontractors, other providers, and suppliers who are paid from or authorized by the provider-run system, have been validated, Mr. Salters said.
“Doctors need to be aware that other entities who become new partners should hold themselves to the same high standards,” he said. “Providers should have basic financial mechanisms in place, with more sophisticated systems requiring more sophisticated methods,” to ensure validation.
CMS officials recommend doctors conduct independent audits of their accounts, manual validation of record system accuracy, and periodic verification of subcontractor claims to confirm the accuracy of claims and costs within new payment models.
These are “all routine steps that practitioners can take in their own offices but which are even more important when the doctor assumes responsibility for a larger scope of services,” Mr. Salters said.
Gaps in documentation surrounding bundled payments can be another legal land mine, Mr. Kopson noted. Adequate records of the care spectrum are essential to prevent accusations that care was not provided during a single episode of care, or over a specific period of time.
“You have to capture and document all the services you are delivering, and have accurate tracking in place for the entire continuum of care,” Mr. Kopson said.
CMS recommends that physicians establish a strong compliance program to assist with anti-fraud controls of new payment systems. When creating or updating a compliance program, government officials said providers should consider the unique characteristics of the model in which they participate.
On Twitter @legal_med
The government’s push toward value-based care aims to fix a broken reimbursement system and improve quality of care for patients. But the new payment models also bring new legal risks for physicians, experts and anti-fraud officials warn.
“Novel payment methodologies may present new program integrity vulnerabilities,” Dr. Shantanu Agrawal, director of the Center for Program Integrity at the Centers for Medicare & Medicaid Services, said at a recent American Bar Association meeting. “As they assume financial risk, providers are also assuming program integrity risk. Without adequate controls, provider-run systems may be relatively vulnerable.”
The Department of Health and Human Services plans to have 30% of Medicare payments in value-based payment structures by the end of 2016, and 50% by the end of 2018. The transition will be driven through investments in alternative payment models such as Accountable Care Organizations (ACOs), advanced primary care medical home models, bundled payments models, and integrated care demonstrations for Medicare and Medicaid patients.
At the end of 2014, value-based payments represented 20% of Medicare fee-for-service payments to providers, according to CMS data. The rate was fueled by government programs such as the Medicare Shared Savings Program (MSSP), Pioneer ACOs, the Bundled Payments for Care Improvement Initiative, and the Comprehensive Primary Care Initiative. Meanwhile, HHS is encouraging private payers, marketplace plans, Medicare Advantage plans, and state Medicaid programs to move in the same value-based direction.
With so many new regulations, mandates, and programs coming down the pipeline, physicians are likely not thinking about the legal dangers that may arise with alternative payment structures, said Mark S. Kopson, a health law attorney in Bloomfield Hills, Mich., and chair of the American Health Lawyers Association’s Payers, Plans and Managed Care Practice Group.
Fee-for-service models can involve claims “about excess treatments and unnecessary services to drive up reimbursement,” Mr. Kopson said in an interview. “When you get into these [value-based] types of programs, it’s the exact opposite. The real threat is the withholding of necessary care in order to reduce expenses and therefore drive up those margins for the providers.”
To avoid such claims, physicians should ensure that their charts include the reasoning behind treatment decisions and a thorough record of why certain treatments were chosen and diagnoses were made, Mr. Kopson advised.
“Going forward, your charting better be completely accurate and detailed so that you don’t leave room for the government to make an argument that you should have provided this or that additional treatment,” he said.
Inaccurate reporting of enrollment data or financial information within new payment models could also land doctors in legal trouble, according to CMS officials.
Problematic reports, enrollee data, or other information physicians are required to submit to the government could be considered falsification and lead to False Claims Act violations.
“Providers are responsible for the information reported and should ensure that the appropriate checks and balances are in place that verify data is reported timely and accurately,” Tony A. Salters, a CMS spokesman, said in an interview. “For some models, providers must attest to the accuracy of this data. [To] report inaccurately could result in violations of federal laws.”
Physician-run payment models, such as doctor-led ACOs, may also draw legal scrutiny if physicians fail to prevent bad behavior by de facto partners. Physicians must ensure that all costs claimed by subcontractors, other providers, and suppliers who are paid from or authorized by the provider-run system, have been validated, Mr. Salters said.
“Doctors need to be aware that other entities who become new partners should hold themselves to the same high standards,” he said. “Providers should have basic financial mechanisms in place, with more sophisticated systems requiring more sophisticated methods,” to ensure validation.
CMS officials recommend doctors conduct independent audits of their accounts, manual validation of record system accuracy, and periodic verification of subcontractor claims to confirm the accuracy of claims and costs within new payment models.
These are “all routine steps that practitioners can take in their own offices but which are even more important when the doctor assumes responsibility for a larger scope of services,” Mr. Salters said.
Gaps in documentation surrounding bundled payments can be another legal land mine, Mr. Kopson noted. Adequate records of the care spectrum are essential to prevent accusations that care was not provided during a single episode of care, or over a specific period of time.
“You have to capture and document all the services you are delivering, and have accurate tracking in place for the entire continuum of care,” Mr. Kopson said.
CMS recommends that physicians establish a strong compliance program to assist with anti-fraud controls of new payment systems. When creating or updating a compliance program, government officials said providers should consider the unique characteristics of the model in which they participate.
On Twitter @legal_med
The government’s push toward value-based care aims to fix a broken reimbursement system and improve quality of care for patients. But the new payment models also bring new legal risks for physicians, experts and anti-fraud officials warn.
“Novel payment methodologies may present new program integrity vulnerabilities,” Dr. Shantanu Agrawal, director of the Center for Program Integrity at the Centers for Medicare & Medicaid Services, said at a recent American Bar Association meeting. “As they assume financial risk, providers are also assuming program integrity risk. Without adequate controls, provider-run systems may be relatively vulnerable.”
The Department of Health and Human Services plans to have 30% of Medicare payments in value-based payment structures by the end of 2016, and 50% by the end of 2018. The transition will be driven through investments in alternative payment models such as Accountable Care Organizations (ACOs), advanced primary care medical home models, bundled payments models, and integrated care demonstrations for Medicare and Medicaid patients.
At the end of 2014, value-based payments represented 20% of Medicare fee-for-service payments to providers, according to CMS data. The rate was fueled by government programs such as the Medicare Shared Savings Program (MSSP), Pioneer ACOs, the Bundled Payments for Care Improvement Initiative, and the Comprehensive Primary Care Initiative. Meanwhile, HHS is encouraging private payers, marketplace plans, Medicare Advantage plans, and state Medicaid programs to move in the same value-based direction.
With so many new regulations, mandates, and programs coming down the pipeline, physicians are likely not thinking about the legal dangers that may arise with alternative payment structures, said Mark S. Kopson, a health law attorney in Bloomfield Hills, Mich., and chair of the American Health Lawyers Association’s Payers, Plans and Managed Care Practice Group.
Fee-for-service models can involve claims “about excess treatments and unnecessary services to drive up reimbursement,” Mr. Kopson said in an interview. “When you get into these [value-based] types of programs, it’s the exact opposite. The real threat is the withholding of necessary care in order to reduce expenses and therefore drive up those margins for the providers.”
To avoid such claims, physicians should ensure that their charts include the reasoning behind treatment decisions and a thorough record of why certain treatments were chosen and diagnoses were made, Mr. Kopson advised.
“Going forward, your charting better be completely accurate and detailed so that you don’t leave room for the government to make an argument that you should have provided this or that additional treatment,” he said.
Inaccurate reporting of enrollment data or financial information within new payment models could also land doctors in legal trouble, according to CMS officials.
Problematic reports, enrollee data, or other information physicians are required to submit to the government could be considered falsification and lead to False Claims Act violations.
“Providers are responsible for the information reported and should ensure that the appropriate checks and balances are in place that verify data is reported timely and accurately,” Tony A. Salters, a CMS spokesman, said in an interview. “For some models, providers must attest to the accuracy of this data. [To] report inaccurately could result in violations of federal laws.”
Physician-run payment models, such as doctor-led ACOs, may also draw legal scrutiny if physicians fail to prevent bad behavior by de facto partners. Physicians must ensure that all costs claimed by subcontractors, other providers, and suppliers who are paid from or authorized by the provider-run system, have been validated, Mr. Salters said.
“Doctors need to be aware that other entities who become new partners should hold themselves to the same high standards,” he said. “Providers should have basic financial mechanisms in place, with more sophisticated systems requiring more sophisticated methods,” to ensure validation.
CMS officials recommend doctors conduct independent audits of their accounts, manual validation of record system accuracy, and periodic verification of subcontractor claims to confirm the accuracy of claims and costs within new payment models.
These are “all routine steps that practitioners can take in their own offices but which are even more important when the doctor assumes responsibility for a larger scope of services,” Mr. Salters said.
Gaps in documentation surrounding bundled payments can be another legal land mine, Mr. Kopson noted. Adequate records of the care spectrum are essential to prevent accusations that care was not provided during a single episode of care, or over a specific period of time.
“You have to capture and document all the services you are delivering, and have accurate tracking in place for the entire continuum of care,” Mr. Kopson said.
CMS recommends that physicians establish a strong compliance program to assist with anti-fraud controls of new payment systems. When creating or updating a compliance program, government officials said providers should consider the unique characteristics of the model in which they participate.
On Twitter @legal_med

Why Diabetic Patients Need a “Sick Day” Plan
In October 2010, a 33-year-old woman with type 1 diabetes presented to a medical center in Cook County, Illinois, with shortness of breath. She was diagnosed with excessive fluid around her lungs, for which she received treatment. When her pain persisted, she was placed on hydromorphone. A long-acting form of insulin was also prescribed.
Two days later, the woman experienced respiratory arrest—presumed to be a reaction to the medication. She was resuscitated and remained in the ICU. Although she was not eating food by mouth, no order for a diet change was received or documented. She continued to be administered insulin and went into a diabetic coma, dying about a week after admission.
The plaintiff claimed that the internal medicine physician employed by the hospital failed to review the decedent’s medical chart and discuss the decedent’s risk for low blood sugar levels with the attending physician. The defendants argued that the decedent was receiving regular dialysis due to end-stage renal failure and had a short life expectancy.
What was the outcome? >>
OUTCOME
A $2 million settlement was reached.
COMMENT
This patient’s admission to the ICU and continued monitoring were obviously stressful and ensured that her serum glucose would be high. Systems should have been in place to prevent a fatal outcome—yet the system failed in this case.
The clinicians failed to recognize the need for closer monitoring and management in a sick, acutely stressed patient. The internist did not revisit the prescribed diet and did not appreciate the impact an acute illness can have on glycemic control—and thus did not order closer serum glucose monitoring.
Because diabetes is common, jurors expect competent management; as a result, this case was likely difficult to defend. The case report tells us that the defense did not challenge a breach of the standard of care (liability) but instead focused on the ultimate impact of the mistake, given the patient’s end-stage renal failure and short life expectancy (damages).
The $2 million settlement is relatively restrained, given the patient’s young age and the location of the case. This suggests the defense had some success arguing that the patient, at baseline, was gravely ill with a diminished lifespan.
As clinicians, we would all agree that an acutely stressed, hospitalized diabetic patient should be managed closely. But how often do we see diabetic patients in an ambulatory setting who are moderately stressed, ill, vomiting, and not eating? How often do we consider the possibility that these patients could slip out of control if not monitored more closely?
While we can’t revamp our diabetic patients’ regimens for every cold, we can encourage them to develop a “sick day” plan and remind them to be vigilant about managing their diabetes during illness. Consider the “sick day” advice given to patients by the Joslin Diabetes Center:
• Always take your diabetes medication. If you have difficulty keeping the medicine down due to vomiting, call your clinician.
• Check your blood glucose level at least 4 times a day. If you are too sick to test it yourself, have someone else do it. Record your levels in case you need to contact your clinician.
• Check for ketones if your blood glucose is 250 or higher. Again, write down your levels for reference.
• Stick to your normal meal plan, if possible.
• Drink lots of sugar-free liquids to prevent dehydration.1
Patients are also advised to contact their health care provider if they have any of the following symptoms: a fever of more than 100.5°F; vomiting or diarrhea of more than two hours’ duration; blood glucose levels higher than 250 mg after two checks, or levels that do not decrease after extra insulin is taken; and moderate or large ketones.1
The instruction to call the office for any fever higher than 100.5°F may seem abundantly cautious. But the discussion that ensues would serve as an opportunity to reinforce the need for closer monitoring—perhaps preventing a patient with a modest illness from spiraling out of glycemic control. —DML
REFERENCE
1. Joslin Diabetes Center. Sick Days. www.joslin.org/info/Sick_Days.html. Accessed June 10, 2015.
In October 2010, a 33-year-old woman with type 1 diabetes presented to a medical center in Cook County, Illinois, with shortness of breath. She was diagnosed with excessive fluid around her lungs, for which she received treatment. When her pain persisted, she was placed on hydromorphone. A long-acting form of insulin was also prescribed.
Two days later, the woman experienced respiratory arrest—presumed to be a reaction to the medication. She was resuscitated and remained in the ICU. Although she was not eating food by mouth, no order for a diet change was received or documented. She continued to be administered insulin and went into a diabetic coma, dying about a week after admission.
The plaintiff claimed that the internal medicine physician employed by the hospital failed to review the decedent’s medical chart and discuss the decedent’s risk for low blood sugar levels with the attending physician. The defendants argued that the decedent was receiving regular dialysis due to end-stage renal failure and had a short life expectancy.
What was the outcome? >>
OUTCOME
A $2 million settlement was reached.
COMMENT
This patient’s admission to the ICU and continued monitoring were obviously stressful and ensured that her serum glucose would be high. Systems should have been in place to prevent a fatal outcome—yet the system failed in this case.
The clinicians failed to recognize the need for closer monitoring and management in a sick, acutely stressed patient. The internist did not revisit the prescribed diet and did not appreciate the impact an acute illness can have on glycemic control—and thus did not order closer serum glucose monitoring.
Because diabetes is common, jurors expect competent management; as a result, this case was likely difficult to defend. The case report tells us that the defense did not challenge a breach of the standard of care (liability) but instead focused on the ultimate impact of the mistake, given the patient’s end-stage renal failure and short life expectancy (damages).
The $2 million settlement is relatively restrained, given the patient’s young age and the location of the case. This suggests the defense had some success arguing that the patient, at baseline, was gravely ill with a diminished lifespan.
As clinicians, we would all agree that an acutely stressed, hospitalized diabetic patient should be managed closely. But how often do we see diabetic patients in an ambulatory setting who are moderately stressed, ill, vomiting, and not eating? How often do we consider the possibility that these patients could slip out of control if not monitored more closely?
While we can’t revamp our diabetic patients’ regimens for every cold, we can encourage them to develop a “sick day” plan and remind them to be vigilant about managing their diabetes during illness. Consider the “sick day” advice given to patients by the Joslin Diabetes Center:
• Always take your diabetes medication. If you have difficulty keeping the medicine down due to vomiting, call your clinician.
• Check your blood glucose level at least 4 times a day. If you are too sick to test it yourself, have someone else do it. Record your levels in case you need to contact your clinician.
• Check for ketones if your blood glucose is 250 or higher. Again, write down your levels for reference.
• Stick to your normal meal plan, if possible.
• Drink lots of sugar-free liquids to prevent dehydration.1
Patients are also advised to contact their health care provider if they have any of the following symptoms: a fever of more than 100.5°F; vomiting or diarrhea of more than two hours’ duration; blood glucose levels higher than 250 mg after two checks, or levels that do not decrease after extra insulin is taken; and moderate or large ketones.1
The instruction to call the office for any fever higher than 100.5°F may seem abundantly cautious. But the discussion that ensues would serve as an opportunity to reinforce the need for closer monitoring—perhaps preventing a patient with a modest illness from spiraling out of glycemic control. —DML
REFERENCE
1. Joslin Diabetes Center. Sick Days. www.joslin.org/info/Sick_Days.html. Accessed June 10, 2015.
In October 2010, a 33-year-old woman with type 1 diabetes presented to a medical center in Cook County, Illinois, with shortness of breath. She was diagnosed with excessive fluid around her lungs, for which she received treatment. When her pain persisted, she was placed on hydromorphone. A long-acting form of insulin was also prescribed.
Two days later, the woman experienced respiratory arrest—presumed to be a reaction to the medication. She was resuscitated and remained in the ICU. Although she was not eating food by mouth, no order for a diet change was received or documented. She continued to be administered insulin and went into a diabetic coma, dying about a week after admission.
The plaintiff claimed that the internal medicine physician employed by the hospital failed to review the decedent’s medical chart and discuss the decedent’s risk for low blood sugar levels with the attending physician. The defendants argued that the decedent was receiving regular dialysis due to end-stage renal failure and had a short life expectancy.
What was the outcome? >>
OUTCOME
A $2 million settlement was reached.
COMMENT
This patient’s admission to the ICU and continued monitoring were obviously stressful and ensured that her serum glucose would be high. Systems should have been in place to prevent a fatal outcome—yet the system failed in this case.
The clinicians failed to recognize the need for closer monitoring and management in a sick, acutely stressed patient. The internist did not revisit the prescribed diet and did not appreciate the impact an acute illness can have on glycemic control—and thus did not order closer serum glucose monitoring.
Because diabetes is common, jurors expect competent management; as a result, this case was likely difficult to defend. The case report tells us that the defense did not challenge a breach of the standard of care (liability) but instead focused on the ultimate impact of the mistake, given the patient’s end-stage renal failure and short life expectancy (damages).
The $2 million settlement is relatively restrained, given the patient’s young age and the location of the case. This suggests the defense had some success arguing that the patient, at baseline, was gravely ill with a diminished lifespan.
As clinicians, we would all agree that an acutely stressed, hospitalized diabetic patient should be managed closely. But how often do we see diabetic patients in an ambulatory setting who are moderately stressed, ill, vomiting, and not eating? How often do we consider the possibility that these patients could slip out of control if not monitored more closely?
While we can’t revamp our diabetic patients’ regimens for every cold, we can encourage them to develop a “sick day” plan and remind them to be vigilant about managing their diabetes during illness. Consider the “sick day” advice given to patients by the Joslin Diabetes Center:
• Always take your diabetes medication. If you have difficulty keeping the medicine down due to vomiting, call your clinician.
• Check your blood glucose level at least 4 times a day. If you are too sick to test it yourself, have someone else do it. Record your levels in case you need to contact your clinician.
• Check for ketones if your blood glucose is 250 or higher. Again, write down your levels for reference.
• Stick to your normal meal plan, if possible.
• Drink lots of sugar-free liquids to prevent dehydration.1
Patients are also advised to contact their health care provider if they have any of the following symptoms: a fever of more than 100.5°F; vomiting or diarrhea of more than two hours’ duration; blood glucose levels higher than 250 mg after two checks, or levels that do not decrease after extra insulin is taken; and moderate or large ketones.1
The instruction to call the office for any fever higher than 100.5°F may seem abundantly cautious. But the discussion that ensues would serve as an opportunity to reinforce the need for closer monitoring—perhaps preventing a patient with a modest illness from spiraling out of glycemic control. —DML
REFERENCE
1. Joslin Diabetes Center. Sick Days. www.joslin.org/info/Sick_Days.html. Accessed June 10, 2015.
Who was responsible for excessive oxytocin doses? $18.2M verdict

Who was responsible for excessive oxytocin doses? $18.2M verdict
Early in the morning, a woman at 40 weeks’ gestation presented to the hospital for induction of labor managed by her ObGyn. Labor was lengthy, and the mother was given increasing doses of 22, 24, and 26 mIU/min of oxytocin to stimulate labor. The baby was delivered in the evening. The child suffered a hypoxic birth injury and has cerebral palsy.
Parents’ claim Excessive oxytocin was administered, causing uterine hyperstimulation and excessive contractions. Nurses failed to inform the ObGyn of an abnormal fetal heart rate during the afternoon.
Defendants’ defense The parties disputed the oxytocin orders. The ObGyn claimed she has a standing order against oxytocin doses over 20 mIU/min. The nurses claimed that the dosage was based on the ObGyn’s verbal orders, which the ObGyn denied. The ObGyn denied negligence and maintained that if she’d known of the oxytocin administration greater than 20 mIU/min and the abnormal fetal heart rate, she immediately would have called for cesarean delivery. The hospital denied negligence and maintained that the oxytocin was administered 10 hours before delivery and played no role in fetal distress.
Verdict At trial, the ObGyn did not call expert witnesses and, in closing arguments, the physician’s attorney asked for exoneration of the ObGyn and a finding of fault solely against the hospital. An $18.2 million Washington verdict was returned against the hospital.
What caused the child’s Erb’s palsy?
A mother presented to the hospital for induction of labor. Oxytocin was administered and the first stage of labor progressed normally. When the mother began pushing, the ObGyn noted a turtle sign at crowning and called for assistance. The ObGyn attempted to deliver the fetus with downward guidance of the fetal head but encountered shoulder dystocia and a nuchal cord. He unwrapped the cord and instructed the nursing staff to place the mother in the McRobert’s position to help dislodge the right shoulder. When that did not work, the ObGyn performed a first-degree episiotomy and completed delivery. The child was found to have Erb’s palsy of the right arm. She underwent decompression and neurolysis of the brachial plexus using sural nerve grafts but still has reduced use of her right arm.
Parents’ claim Shoulder dystocia was improperly managed, causing the brachial plexus injury.
Defendants’ defense The ObGyn and hospital system denied negligence. The child’s injury occurred in utero due to natural forces of the mother’s uterine contractions.
Verdict An Ohio defense verdict was returned.
Woman claims lack of proper consent
A 47-year-old woman underwent endometrial ablation performed by her ObGyn. During the procedure, the uterus was perforated and the ObGyn performed a hysterectomy. Six days later, the patient was found to have peritonitis and underwent bowel repair surgery. The patient developed untreatable bowel adhesions that cause chronic pain.
Patient’s claim There were less expensive and invasive alternatives to the ablation that the ObGyn did not offer. The patient claimed lack of informed consent for the ablation and hysterectomy and negligence in perforating the bowel. The ObGyn was also negligent in failing to recognize the perforation and to diagnose peritonitis in a timely manner.
Texas state law requires consent for hysterectomies without documented evidence of immediate danger to life. Her husband did not have the authority to consent on her behalf.
Physician’s defense The husband gave informed consent. Failure to recognize the perforation was not negligent; it is a known risk of the surgery. The patient’s care was transferred to another physician after the second postoperative day.
Verdict A $200,000 Texas settlement was reached.
Bowel obstruction in pregnant woman
A 29-year-old woman at 27 weeks’ gestation had abdominal pain. She went to a community hospital where a hospitalist was assigned to her care. After a day, the patient was found to have a small bowel obstruction and necrosis of the bowel. The baby was delivered preterm. The mother underwent 12 operations; half of her intestines were resected. The mother is being treated for posttraumatic stress syndrome. The child is autistic.
Parents’ claim The hospitalist did not diagnose the mother’s intestinal blockage in a timely manner and did not obtain an obstetric consult or notify the patient’s ObGyn. The hospital staff did not follow protocol to notify the mother’s ObGyn. The child’s autism is a result of preterm delivery.
Defendants’ defense The hospital denied any duty to notify the ObGyn if the patient was admitted to the hospital for nonobstetric reasons. The case was settled during trial.
Verdict A $4.2 million Washington settlement was reached including $3 million from the hospital.
Fourth-degree perineal tear and continuing pain after delivery
A woman in her 30s went to the hospital for induction of labor. After many hours, the ObGyn used vacuum extraction due to maternal fatigue. The baby emerged in compound presentation, with her hand at the side of her head. She weighed 9 lb 12 oz at birth. A fourth-degree perineal tear occurred at birth. Postpartum, a rectovaginal fistula developed that required several repair operations. The mother is unable to have intercourse due to continuing vaginal pain and discomfort.
Patient’s Claim Knowing that the father’s head was overly large, the ObGyn should have better estimated the fetus’ size, and should have performed cesarean delivery.
Physician’s defense The ObGyn admitted that he knew the baby was large but maintained that a large fetus does not mandate a cesarean delivery. There were no indications that the baby’s head or body was too large to fit through the mother’s pelvis, so a vaginal delivery was appropriate. A perineal tear is a known complication of childbirth and could not be prevented. The patient’s current pain is unrelated to the perineal tear.
Verdict A Pennsylvania defense verdict was returned.
Breast cancer missed in woman with dense breasts
In 2003, a 44-year-old woman was told she had dense fibrocystic breasts. From 2003 through 2009 she regularly saw a breast surgeon due to concern that breast cancer might be difficult to detect.
In August 2009, her ObGyn identified a questionable mass in her left breast after ultrasonography and mammography. The patient saw the surgeon in late September 2009; no further imaging was ordered and she was told to return in a year.
The patient, concerned about the mass, returned to the surgeon in May 2010. Testing revealed cancer, and she underwent radical mastectomy and other treatment.
Patient’s claim Because the mass had not been treated in a timely manner, her 5-year survival rate in May 2010 was less than 50%. The surgeon was negligent in failing to order additional testing in September 2009. Magnetic resonance imaging (MRI) would have detected the cancer at a time when her survival rate could have been 80%.
Physician’s defense The cancer was diagnosed in a timely manner. An earlier diagnosis would not have changed the outcome.
Verdict A Tennessee defense verdict was returned.
Child stillborn, mother injured after vacuum extraction
When the mother’s labor slowed at a birthing center, she received several medications including castor oil, blue cohosh, and black cohosh to induce labor. The mother was later transferred by ambulance to a hospital. Ninety minutes after admission, the ObGyn used vacuum extraction to deliver a stillborn child. The mother sustained damage to her rectum, uterus, and vagina, had repair surgery, and has been unable to get pregnant again.
Parents’ claim While in labor at the birthing center, the castor oil, blue cohosh, and black cohosh caused the patient’s uterus to contract excessively and contributed to fetal death. The patient should have been transferred to the hospital earlier. Cesarean delivery should have been performed immediately upon her arrival at the hospital but the ObGyn did not arrive at the hospital for an hour after the patient’s admission.
Defendants’ defense The head midwife at the birthing center conceded negligence. The hospital claimed that the fetus was already dead before the mother arrived. The ObGyn denied negligence, arguing that he had no supervisory role or ownership in the birthing center and was not present during the mother’s labor. He also claimed that the fetus was dead in utero 12 or more hours before delivery and that an infectious process had developed in the mother during the 17 hours that she was at the birthing center.
Verdict A $4,095,000 Florida verdict was returned against the ObGyn. A directed verdict was granted for the hospital.
Patient still in pain after labia reduction
A 44-year-old woman underwent surgical reduction of her labia minora performed by a gynecologist. The procedure was intended to relieve discomfort during sexual activity. The patient continues to have pain.
Patient’s claim An excessive amount of the right labia minora was removed because proper presurgical demarcation of the operative area was not performed. Her pain during intercourse has worsened and she cannot properly urinate.
Physician’s defense Presurgical demarcation was correctly completed using clamps. Surgery was properly performed. The asymmetry is due to poor healing of the surgical wound. The patient’s clitoris was not scarred. The patient never reported complications related to urination to her gynecologist. Her ongoing pain is due to an estrogen deficiency.
Verdict A New York defense verdict was returned.
Uterine rupture after version for breech presentation: $7M
A woman went to the hospital for delivery of her baby. The fetus was in breech position, but the mother requested vaginal delivery. When the ObGyn attempted an external cephalic version to turn the baby, the uterus ruptured and the placenta was damaged. The baby sustained hypoxic-ischemic encephalopathy resulting in cerebral palsy (CP). He requires constant nursing care.
Parents’ claim The ObGyn failed to recognize fetal distress during the breech version. The ObGyn improperly performed the version, causing the uterine rupture. There was lack of informed consent for the version.
Defendants’ defense The case was settled during trial.
Verdict A $7 million New Jersey settlement was reached.
Sepsis following hysterectomy
An ObGyn performed total abdominal hysterectomy to treat uterine fibroids in a 26-year-old woman. Despite reporting abdominal pain, the patient was discharged on postsurgical day 4.
Three days later, she went to a different hospital with moderate diffuse abdominal pain, constipation, nausea, emesis, tachycardia, and low-grade fever. An abdominal radiograph was taken, the patient was given morphine and ketorolac, and she was sent home.
She returned to the first hospital 3 days later reporting fever, nausea, emesis, diarrhea, and severe abdominal pain. After an abdominal computed tomography (CT) scan revealed numerous fluid- and gas-filled collections, indicative of abscess, intravenous antibiotics were ordered and administered.
Six days later, an infectious disease physician was consulted. He made a diagnosis of sepsis secondary to abdominal infection.
The next day, an abdominal CT scan revealed enlargement of multiple abdominal and pelvic fluid collections.
At exploratory laparotomy, purulent fluid was found in the anterior fascial compartment, with gross pus in the abdomen. The entire bowel was dilated, inflamed, and matted. Necrotic rind and infection were noted on multiple surfaces of the colon and small intestine and the transverse colon was gangrenous and sealed to the right lower quadrant. The patient’s intestines were resected and an ileostomy was placed, which was reversed several months later.
Patient’s claim The ObGyn did not offer an alternative to hysterectomy. The ObGyn was negligent in injuring the small intestine during surgery and failing to recognize and treat it intraoperatively. The patient should not have been discharged based on her reported symptoms. Failure to recognize and treat the injury led to sepsis with severe complications and months of recuperation.
Physician’s defense There was no negligence; small bowel injury is a known risk of hysterectomy. Other caregivers at both hospitals were at fault for not properly diagnosing and treating the infection.
Verdict A $901,420 Nevada verdict was returned; the ObGyn was found 85% at fault and other parties 15% at fault. The court granted the physician’s motion to reduce the verdict to $436,954, which included $371,411 from the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Who was responsible for excessive oxytocin doses? $18.2M verdict
Early in the morning, a woman at 40 weeks’ gestation presented to the hospital for induction of labor managed by her ObGyn. Labor was lengthy, and the mother was given increasing doses of 22, 24, and 26 mIU/min of oxytocin to stimulate labor. The baby was delivered in the evening. The child suffered a hypoxic birth injury and has cerebral palsy.
Parents’ claim Excessive oxytocin was administered, causing uterine hyperstimulation and excessive contractions. Nurses failed to inform the ObGyn of an abnormal fetal heart rate during the afternoon.
Defendants’ defense The parties disputed the oxytocin orders. The ObGyn claimed she has a standing order against oxytocin doses over 20 mIU/min. The nurses claimed that the dosage was based on the ObGyn’s verbal orders, which the ObGyn denied. The ObGyn denied negligence and maintained that if she’d known of the oxytocin administration greater than 20 mIU/min and the abnormal fetal heart rate, she immediately would have called for cesarean delivery. The hospital denied negligence and maintained that the oxytocin was administered 10 hours before delivery and played no role in fetal distress.
Verdict At trial, the ObGyn did not call expert witnesses and, in closing arguments, the physician’s attorney asked for exoneration of the ObGyn and a finding of fault solely against the hospital. An $18.2 million Washington verdict was returned against the hospital.
What caused the child’s Erb’s palsy?
A mother presented to the hospital for induction of labor. Oxytocin was administered and the first stage of labor progressed normally. When the mother began pushing, the ObGyn noted a turtle sign at crowning and called for assistance. The ObGyn attempted to deliver the fetus with downward guidance of the fetal head but encountered shoulder dystocia and a nuchal cord. He unwrapped the cord and instructed the nursing staff to place the mother in the McRobert’s position to help dislodge the right shoulder. When that did not work, the ObGyn performed a first-degree episiotomy and completed delivery. The child was found to have Erb’s palsy of the right arm. She underwent decompression and neurolysis of the brachial plexus using sural nerve grafts but still has reduced use of her right arm.
Parents’ claim Shoulder dystocia was improperly managed, causing the brachial plexus injury.
Defendants’ defense The ObGyn and hospital system denied negligence. The child’s injury occurred in utero due to natural forces of the mother’s uterine contractions.
Verdict An Ohio defense verdict was returned.
Woman claims lack of proper consent
A 47-year-old woman underwent endometrial ablation performed by her ObGyn. During the procedure, the uterus was perforated and the ObGyn performed a hysterectomy. Six days later, the patient was found to have peritonitis and underwent bowel repair surgery. The patient developed untreatable bowel adhesions that cause chronic pain.
Patient’s claim There were less expensive and invasive alternatives to the ablation that the ObGyn did not offer. The patient claimed lack of informed consent for the ablation and hysterectomy and negligence in perforating the bowel. The ObGyn was also negligent in failing to recognize the perforation and to diagnose peritonitis in a timely manner.
Texas state law requires consent for hysterectomies without documented evidence of immediate danger to life. Her husband did not have the authority to consent on her behalf.
Physician’s defense The husband gave informed consent. Failure to recognize the perforation was not negligent; it is a known risk of the surgery. The patient’s care was transferred to another physician after the second postoperative day.
Verdict A $200,000 Texas settlement was reached.
Bowel obstruction in pregnant woman
A 29-year-old woman at 27 weeks’ gestation had abdominal pain. She went to a community hospital where a hospitalist was assigned to her care. After a day, the patient was found to have a small bowel obstruction and necrosis of the bowel. The baby was delivered preterm. The mother underwent 12 operations; half of her intestines were resected. The mother is being treated for posttraumatic stress syndrome. The child is autistic.
Parents’ claim The hospitalist did not diagnose the mother’s intestinal blockage in a timely manner and did not obtain an obstetric consult or notify the patient’s ObGyn. The hospital staff did not follow protocol to notify the mother’s ObGyn. The child’s autism is a result of preterm delivery.
Defendants’ defense The hospital denied any duty to notify the ObGyn if the patient was admitted to the hospital for nonobstetric reasons. The case was settled during trial.
Verdict A $4.2 million Washington settlement was reached including $3 million from the hospital.
Fourth-degree perineal tear and continuing pain after delivery
A woman in her 30s went to the hospital for induction of labor. After many hours, the ObGyn used vacuum extraction due to maternal fatigue. The baby emerged in compound presentation, with her hand at the side of her head. She weighed 9 lb 12 oz at birth. A fourth-degree perineal tear occurred at birth. Postpartum, a rectovaginal fistula developed that required several repair operations. The mother is unable to have intercourse due to continuing vaginal pain and discomfort.
Patient’s Claim Knowing that the father’s head was overly large, the ObGyn should have better estimated the fetus’ size, and should have performed cesarean delivery.
Physician’s defense The ObGyn admitted that he knew the baby was large but maintained that a large fetus does not mandate a cesarean delivery. There were no indications that the baby’s head or body was too large to fit through the mother’s pelvis, so a vaginal delivery was appropriate. A perineal tear is a known complication of childbirth and could not be prevented. The patient’s current pain is unrelated to the perineal tear.
Verdict A Pennsylvania defense verdict was returned.
Breast cancer missed in woman with dense breasts
In 2003, a 44-year-old woman was told she had dense fibrocystic breasts. From 2003 through 2009 she regularly saw a breast surgeon due to concern that breast cancer might be difficult to detect.
In August 2009, her ObGyn identified a questionable mass in her left breast after ultrasonography and mammography. The patient saw the surgeon in late September 2009; no further imaging was ordered and she was told to return in a year.
The patient, concerned about the mass, returned to the surgeon in May 2010. Testing revealed cancer, and she underwent radical mastectomy and other treatment.
Patient’s claim Because the mass had not been treated in a timely manner, her 5-year survival rate in May 2010 was less than 50%. The surgeon was negligent in failing to order additional testing in September 2009. Magnetic resonance imaging (MRI) would have detected the cancer at a time when her survival rate could have been 80%.
Physician’s defense The cancer was diagnosed in a timely manner. An earlier diagnosis would not have changed the outcome.
Verdict A Tennessee defense verdict was returned.
Child stillborn, mother injured after vacuum extraction
When the mother’s labor slowed at a birthing center, she received several medications including castor oil, blue cohosh, and black cohosh to induce labor. The mother was later transferred by ambulance to a hospital. Ninety minutes after admission, the ObGyn used vacuum extraction to deliver a stillborn child. The mother sustained damage to her rectum, uterus, and vagina, had repair surgery, and has been unable to get pregnant again.
Parents’ claim While in labor at the birthing center, the castor oil, blue cohosh, and black cohosh caused the patient’s uterus to contract excessively and contributed to fetal death. The patient should have been transferred to the hospital earlier. Cesarean delivery should have been performed immediately upon her arrival at the hospital but the ObGyn did not arrive at the hospital for an hour after the patient’s admission.
Defendants’ defense The head midwife at the birthing center conceded negligence. The hospital claimed that the fetus was already dead before the mother arrived. The ObGyn denied negligence, arguing that he had no supervisory role or ownership in the birthing center and was not present during the mother’s labor. He also claimed that the fetus was dead in utero 12 or more hours before delivery and that an infectious process had developed in the mother during the 17 hours that she was at the birthing center.
Verdict A $4,095,000 Florida verdict was returned against the ObGyn. A directed verdict was granted for the hospital.
Patient still in pain after labia reduction
A 44-year-old woman underwent surgical reduction of her labia minora performed by a gynecologist. The procedure was intended to relieve discomfort during sexual activity. The patient continues to have pain.
Patient’s claim An excessive amount of the right labia minora was removed because proper presurgical demarcation of the operative area was not performed. Her pain during intercourse has worsened and she cannot properly urinate.
Physician’s defense Presurgical demarcation was correctly completed using clamps. Surgery was properly performed. The asymmetry is due to poor healing of the surgical wound. The patient’s clitoris was not scarred. The patient never reported complications related to urination to her gynecologist. Her ongoing pain is due to an estrogen deficiency.
Verdict A New York defense verdict was returned.
Uterine rupture after version for breech presentation: $7M
A woman went to the hospital for delivery of her baby. The fetus was in breech position, but the mother requested vaginal delivery. When the ObGyn attempted an external cephalic version to turn the baby, the uterus ruptured and the placenta was damaged. The baby sustained hypoxic-ischemic encephalopathy resulting in cerebral palsy (CP). He requires constant nursing care.
Parents’ claim The ObGyn failed to recognize fetal distress during the breech version. The ObGyn improperly performed the version, causing the uterine rupture. There was lack of informed consent for the version.
Defendants’ defense The case was settled during trial.
Verdict A $7 million New Jersey settlement was reached.
Sepsis following hysterectomy
An ObGyn performed total abdominal hysterectomy to treat uterine fibroids in a 26-year-old woman. Despite reporting abdominal pain, the patient was discharged on postsurgical day 4.
Three days later, she went to a different hospital with moderate diffuse abdominal pain, constipation, nausea, emesis, tachycardia, and low-grade fever. An abdominal radiograph was taken, the patient was given morphine and ketorolac, and she was sent home.
She returned to the first hospital 3 days later reporting fever, nausea, emesis, diarrhea, and severe abdominal pain. After an abdominal computed tomography (CT) scan revealed numerous fluid- and gas-filled collections, indicative of abscess, intravenous antibiotics were ordered and administered.
Six days later, an infectious disease physician was consulted. He made a diagnosis of sepsis secondary to abdominal infection.
The next day, an abdominal CT scan revealed enlargement of multiple abdominal and pelvic fluid collections.
At exploratory laparotomy, purulent fluid was found in the anterior fascial compartment, with gross pus in the abdomen. The entire bowel was dilated, inflamed, and matted. Necrotic rind and infection were noted on multiple surfaces of the colon and small intestine and the transverse colon was gangrenous and sealed to the right lower quadrant. The patient’s intestines were resected and an ileostomy was placed, which was reversed several months later.
Patient’s claim The ObGyn did not offer an alternative to hysterectomy. The ObGyn was negligent in injuring the small intestine during surgery and failing to recognize and treat it intraoperatively. The patient should not have been discharged based on her reported symptoms. Failure to recognize and treat the injury led to sepsis with severe complications and months of recuperation.
Physician’s defense There was no negligence; small bowel injury is a known risk of hysterectomy. Other caregivers at both hospitals were at fault for not properly diagnosing and treating the infection.
Verdict A $901,420 Nevada verdict was returned; the ObGyn was found 85% at fault and other parties 15% at fault. The court granted the physician’s motion to reduce the verdict to $436,954, which included $371,411 from the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Who was responsible for excessive oxytocin doses? $18.2M verdict
Early in the morning, a woman at 40 weeks’ gestation presented to the hospital for induction of labor managed by her ObGyn. Labor was lengthy, and the mother was given increasing doses of 22, 24, and 26 mIU/min of oxytocin to stimulate labor. The baby was delivered in the evening. The child suffered a hypoxic birth injury and has cerebral palsy.
Parents’ claim Excessive oxytocin was administered, causing uterine hyperstimulation and excessive contractions. Nurses failed to inform the ObGyn of an abnormal fetal heart rate during the afternoon.
Defendants’ defense The parties disputed the oxytocin orders. The ObGyn claimed she has a standing order against oxytocin doses over 20 mIU/min. The nurses claimed that the dosage was based on the ObGyn’s verbal orders, which the ObGyn denied. The ObGyn denied negligence and maintained that if she’d known of the oxytocin administration greater than 20 mIU/min and the abnormal fetal heart rate, she immediately would have called for cesarean delivery. The hospital denied negligence and maintained that the oxytocin was administered 10 hours before delivery and played no role in fetal distress.
Verdict At trial, the ObGyn did not call expert witnesses and, in closing arguments, the physician’s attorney asked for exoneration of the ObGyn and a finding of fault solely against the hospital. An $18.2 million Washington verdict was returned against the hospital.
What caused the child’s Erb’s palsy?
A mother presented to the hospital for induction of labor. Oxytocin was administered and the first stage of labor progressed normally. When the mother began pushing, the ObGyn noted a turtle sign at crowning and called for assistance. The ObGyn attempted to deliver the fetus with downward guidance of the fetal head but encountered shoulder dystocia and a nuchal cord. He unwrapped the cord and instructed the nursing staff to place the mother in the McRobert’s position to help dislodge the right shoulder. When that did not work, the ObGyn performed a first-degree episiotomy and completed delivery. The child was found to have Erb’s palsy of the right arm. She underwent decompression and neurolysis of the brachial plexus using sural nerve grafts but still has reduced use of her right arm.
Parents’ claim Shoulder dystocia was improperly managed, causing the brachial plexus injury.
Defendants’ defense The ObGyn and hospital system denied negligence. The child’s injury occurred in utero due to natural forces of the mother’s uterine contractions.
Verdict An Ohio defense verdict was returned.
Woman claims lack of proper consent
A 47-year-old woman underwent endometrial ablation performed by her ObGyn. During the procedure, the uterus was perforated and the ObGyn performed a hysterectomy. Six days later, the patient was found to have peritonitis and underwent bowel repair surgery. The patient developed untreatable bowel adhesions that cause chronic pain.
Patient’s claim There were less expensive and invasive alternatives to the ablation that the ObGyn did not offer. The patient claimed lack of informed consent for the ablation and hysterectomy and negligence in perforating the bowel. The ObGyn was also negligent in failing to recognize the perforation and to diagnose peritonitis in a timely manner.
Texas state law requires consent for hysterectomies without documented evidence of immediate danger to life. Her husband did not have the authority to consent on her behalf.
Physician’s defense The husband gave informed consent. Failure to recognize the perforation was not negligent; it is a known risk of the surgery. The patient’s care was transferred to another physician after the second postoperative day.
Verdict A $200,000 Texas settlement was reached.
Bowel obstruction in pregnant woman
A 29-year-old woman at 27 weeks’ gestation had abdominal pain. She went to a community hospital where a hospitalist was assigned to her care. After a day, the patient was found to have a small bowel obstruction and necrosis of the bowel. The baby was delivered preterm. The mother underwent 12 operations; half of her intestines were resected. The mother is being treated for posttraumatic stress syndrome. The child is autistic.
Parents’ claim The hospitalist did not diagnose the mother’s intestinal blockage in a timely manner and did not obtain an obstetric consult or notify the patient’s ObGyn. The hospital staff did not follow protocol to notify the mother’s ObGyn. The child’s autism is a result of preterm delivery.
Defendants’ defense The hospital denied any duty to notify the ObGyn if the patient was admitted to the hospital for nonobstetric reasons. The case was settled during trial.
Verdict A $4.2 million Washington settlement was reached including $3 million from the hospital.
Fourth-degree perineal tear and continuing pain after delivery
A woman in her 30s went to the hospital for induction of labor. After many hours, the ObGyn used vacuum extraction due to maternal fatigue. The baby emerged in compound presentation, with her hand at the side of her head. She weighed 9 lb 12 oz at birth. A fourth-degree perineal tear occurred at birth. Postpartum, a rectovaginal fistula developed that required several repair operations. The mother is unable to have intercourse due to continuing vaginal pain and discomfort.
Patient’s Claim Knowing that the father’s head was overly large, the ObGyn should have better estimated the fetus’ size, and should have performed cesarean delivery.
Physician’s defense The ObGyn admitted that he knew the baby was large but maintained that a large fetus does not mandate a cesarean delivery. There were no indications that the baby’s head or body was too large to fit through the mother’s pelvis, so a vaginal delivery was appropriate. A perineal tear is a known complication of childbirth and could not be prevented. The patient’s current pain is unrelated to the perineal tear.
Verdict A Pennsylvania defense verdict was returned.
Breast cancer missed in woman with dense breasts
In 2003, a 44-year-old woman was told she had dense fibrocystic breasts. From 2003 through 2009 she regularly saw a breast surgeon due to concern that breast cancer might be difficult to detect.
In August 2009, her ObGyn identified a questionable mass in her left breast after ultrasonography and mammography. The patient saw the surgeon in late September 2009; no further imaging was ordered and she was told to return in a year.
The patient, concerned about the mass, returned to the surgeon in May 2010. Testing revealed cancer, and she underwent radical mastectomy and other treatment.
Patient’s claim Because the mass had not been treated in a timely manner, her 5-year survival rate in May 2010 was less than 50%. The surgeon was negligent in failing to order additional testing in September 2009. Magnetic resonance imaging (MRI) would have detected the cancer at a time when her survival rate could have been 80%.
Physician’s defense The cancer was diagnosed in a timely manner. An earlier diagnosis would not have changed the outcome.
Verdict A Tennessee defense verdict was returned.
Child stillborn, mother injured after vacuum extraction
When the mother’s labor slowed at a birthing center, she received several medications including castor oil, blue cohosh, and black cohosh to induce labor. The mother was later transferred by ambulance to a hospital. Ninety minutes after admission, the ObGyn used vacuum extraction to deliver a stillborn child. The mother sustained damage to her rectum, uterus, and vagina, had repair surgery, and has been unable to get pregnant again.
Parents’ claim While in labor at the birthing center, the castor oil, blue cohosh, and black cohosh caused the patient’s uterus to contract excessively and contributed to fetal death. The patient should have been transferred to the hospital earlier. Cesarean delivery should have been performed immediately upon her arrival at the hospital but the ObGyn did not arrive at the hospital for an hour after the patient’s admission.
Defendants’ defense The head midwife at the birthing center conceded negligence. The hospital claimed that the fetus was already dead before the mother arrived. The ObGyn denied negligence, arguing that he had no supervisory role or ownership in the birthing center and was not present during the mother’s labor. He also claimed that the fetus was dead in utero 12 or more hours before delivery and that an infectious process had developed in the mother during the 17 hours that she was at the birthing center.
Verdict A $4,095,000 Florida verdict was returned against the ObGyn. A directed verdict was granted for the hospital.
Patient still in pain after labia reduction
A 44-year-old woman underwent surgical reduction of her labia minora performed by a gynecologist. The procedure was intended to relieve discomfort during sexual activity. The patient continues to have pain.
Patient’s claim An excessive amount of the right labia minora was removed because proper presurgical demarcation of the operative area was not performed. Her pain during intercourse has worsened and she cannot properly urinate.
Physician’s defense Presurgical demarcation was correctly completed using clamps. Surgery was properly performed. The asymmetry is due to poor healing of the surgical wound. The patient’s clitoris was not scarred. The patient never reported complications related to urination to her gynecologist. Her ongoing pain is due to an estrogen deficiency.
Verdict A New York defense verdict was returned.
Uterine rupture after version for breech presentation: $7M
A woman went to the hospital for delivery of her baby. The fetus was in breech position, but the mother requested vaginal delivery. When the ObGyn attempted an external cephalic version to turn the baby, the uterus ruptured and the placenta was damaged. The baby sustained hypoxic-ischemic encephalopathy resulting in cerebral palsy (CP). He requires constant nursing care.
Parents’ claim The ObGyn failed to recognize fetal distress during the breech version. The ObGyn improperly performed the version, causing the uterine rupture. There was lack of informed consent for the version.
Defendants’ defense The case was settled during trial.
Verdict A $7 million New Jersey settlement was reached.
Sepsis following hysterectomy
An ObGyn performed total abdominal hysterectomy to treat uterine fibroids in a 26-year-old woman. Despite reporting abdominal pain, the patient was discharged on postsurgical day 4.
Three days later, she went to a different hospital with moderate diffuse abdominal pain, constipation, nausea, emesis, tachycardia, and low-grade fever. An abdominal radiograph was taken, the patient was given morphine and ketorolac, and she was sent home.
She returned to the first hospital 3 days later reporting fever, nausea, emesis, diarrhea, and severe abdominal pain. After an abdominal computed tomography (CT) scan revealed numerous fluid- and gas-filled collections, indicative of abscess, intravenous antibiotics were ordered and administered.
Six days later, an infectious disease physician was consulted. He made a diagnosis of sepsis secondary to abdominal infection.
The next day, an abdominal CT scan revealed enlargement of multiple abdominal and pelvic fluid collections.
At exploratory laparotomy, purulent fluid was found in the anterior fascial compartment, with gross pus in the abdomen. The entire bowel was dilated, inflamed, and matted. Necrotic rind and infection were noted on multiple surfaces of the colon and small intestine and the transverse colon was gangrenous and sealed to the right lower quadrant. The patient’s intestines were resected and an ileostomy was placed, which was reversed several months later.
Patient’s claim The ObGyn did not offer an alternative to hysterectomy. The ObGyn was negligent in injuring the small intestine during surgery and failing to recognize and treat it intraoperatively. The patient should not have been discharged based on her reported symptoms. Failure to recognize and treat the injury led to sepsis with severe complications and months of recuperation.
Physician’s defense There was no negligence; small bowel injury is a known risk of hysterectomy. Other caregivers at both hospitals were at fault for not properly diagnosing and treating the infection.
Verdict A $901,420 Nevada verdict was returned; the ObGyn was found 85% at fault and other parties 15% at fault. The court granted the physician’s motion to reduce the verdict to $436,954, which included $371,411 from the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In this article
- What caused the child’s Erb’s palsy?
- Woman claims lack of proper consent
- Bowel obstruction in pregnant woman
- Fourth-degree perineal tear and continuing pain after delivery
- Breast cancer missed in woman with dense breasts
- Child stillborn, mother injured after vacuum extraction
- Patient still in pain after labia reduction
- Uterine rupture after version for breech presentation: $7M
- Sepsis following hysterectomy

Medicolegal issues: The consequences of AAA repair
Dr. Risley together with associate editor Dr. O. William Brown describe a case involving failure to document, a common complaint in malpractice litigation.
A 63-year-old white male, actively working, presented with a 5.3-cm infra-renal abdominal aortic aneurysm (AAA). His anatomy was deemed appropriate for endovascular AAA repair and was cleared by his cardiologist for that procedure. The patient underwent a thorough informed consent regarding endovascular and open options as well as the option for continued AAA surveillance. Of note, the patient never had his family with him at any time during the decision-making process, nor with him in the preoperative holding area.
He underwent an aorto- bi- iliac unibody endovascular graft placement. During delivery of the main body, the right common iliac artery ruptured. Initial attempts at endovascular control and subsequent right retroperitoneal exposure and repair of the iliac rupture were unsuccessful, ultimately requiring laparotomy, explant of the device, and aorto- bi-femoral bypass graft. The first time the surgeon met the large family was at the completion of the procedure to explain the complications that were encountered. The patient had a very “rocky” ICU course with complications of ARDS (acute respiratory distress syndrome), acute renal insufficiency, anemia, encephalopathy, and thrombocytopenia. He was initially started on Lovenox on POD # 2 in addition to SCDs (sequential compression devices) for DVT prophylaxis.
Lovenox was stopped because of thrombocytopenia, and mechanical SCD prophylaxis was maintained. As his platelet count recovered and his HIT (heparin-induced thrombocytopenia) screen came back negative, discussion was undertaken to resume his chemical thromboprophylaxis.
It was elected to leave him on only the SCDs because of potential bleeding complications. He continued to improve, but developed a swollen left lower extremity as a result of a DVT. He was placed on heparin drip and converted to Coumadin. Despite an INR of 2.7 on the day he was to be discharged to the rehabilitation center, and shortly after a walk with the therapists and his family, he suffered a fatal pulmonary embolism.
Ultimately, the hospital, the intensivist and the surgeon were sued for failure to adequately provide prophylaxis and treat the DVT. The case was settled. The criticisms were that the physicians failed to provide both mechanical and chemical thromboprophylaxis, particularly after the HIT panel was negative. No criticisms of the intra-operative complications were levied.
The plaintiff’s expert in this case was a physician who was board certified in internal medicine, anesthesiology, and critical care. He had no training in general surgery or vascular surgery. Accordingly, although he may have made suggestions regarding post operative surgical care he had no experience in being the responsible physician for making a postoperative surgical decision. In addition, assertions regarding the incidence of DVT in specific patient populations were exaggerated. Yet the case still settled.
This case emphasizes several important issues. First, communication is paramount in potentially avoiding medical malpractice litigation. The surgeon never met anyone from the patient’s large and involved family until he had to explain the reason his 2-hour planned procedure took 8 hours. The patient had clearly minimized to his family any of the risks discussed with him preoperatively. Prior to proceeding with any surgical intervention it is important that, if possible, a family member be informed of the risks and benefits of the planned procedure and that this conversation be documented in the chart.
Documentation remains very important not only during the informed consent process prior to surgery, but also in decision making regarding postoperative care. Although the physicians discussed the options of resuming the patient’s chemothromboprophylaxis, nothing was documented in the chart. If the discussion was documented, they may have been able to refute the allegation of failure to prevent the DVT.
Finally, in certain instances even when the facts support the judgments that were made regarding the care given, it may be the best “business decision” to settle a case. This is perhaps the most difficult concept for practicing surgeons to grasp. Whether physicians like it or not, medicine is a business and decisions made regarding defending or settling a law suit should not be based on emotion. We don’t do that in the operating room, and we should not do it in the courtroom.
Dr. Risley is the medical director of the Jacksonville Vein Center, Fla.
The opinions expressed by the author neither imply nor establish a standard of care. Cases have been modified and may be fictional in order to maintain HIPPA and confidentiality regulations.
Dr. Risley together with associate editor Dr. O. William Brown describe a case involving failure to document, a common complaint in malpractice litigation.
A 63-year-old white male, actively working, presented with a 5.3-cm infra-renal abdominal aortic aneurysm (AAA). His anatomy was deemed appropriate for endovascular AAA repair and was cleared by his cardiologist for that procedure. The patient underwent a thorough informed consent regarding endovascular and open options as well as the option for continued AAA surveillance. Of note, the patient never had his family with him at any time during the decision-making process, nor with him in the preoperative holding area.
He underwent an aorto- bi- iliac unibody endovascular graft placement. During delivery of the main body, the right common iliac artery ruptured. Initial attempts at endovascular control and subsequent right retroperitoneal exposure and repair of the iliac rupture were unsuccessful, ultimately requiring laparotomy, explant of the device, and aorto- bi-femoral bypass graft. The first time the surgeon met the large family was at the completion of the procedure to explain the complications that were encountered. The patient had a very “rocky” ICU course with complications of ARDS (acute respiratory distress syndrome), acute renal insufficiency, anemia, encephalopathy, and thrombocytopenia. He was initially started on Lovenox on POD # 2 in addition to SCDs (sequential compression devices) for DVT prophylaxis.
Lovenox was stopped because of thrombocytopenia, and mechanical SCD prophylaxis was maintained. As his platelet count recovered and his HIT (heparin-induced thrombocytopenia) screen came back negative, discussion was undertaken to resume his chemical thromboprophylaxis.
It was elected to leave him on only the SCDs because of potential bleeding complications. He continued to improve, but developed a swollen left lower extremity as a result of a DVT. He was placed on heparin drip and converted to Coumadin. Despite an INR of 2.7 on the day he was to be discharged to the rehabilitation center, and shortly after a walk with the therapists and his family, he suffered a fatal pulmonary embolism.
Ultimately, the hospital, the intensivist and the surgeon were sued for failure to adequately provide prophylaxis and treat the DVT. The case was settled. The criticisms were that the physicians failed to provide both mechanical and chemical thromboprophylaxis, particularly after the HIT panel was negative. No criticisms of the intra-operative complications were levied.
The plaintiff’s expert in this case was a physician who was board certified in internal medicine, anesthesiology, and critical care. He had no training in general surgery or vascular surgery. Accordingly, although he may have made suggestions regarding post operative surgical care he had no experience in being the responsible physician for making a postoperative surgical decision. In addition, assertions regarding the incidence of DVT in specific patient populations were exaggerated. Yet the case still settled.
This case emphasizes several important issues. First, communication is paramount in potentially avoiding medical malpractice litigation. The surgeon never met anyone from the patient’s large and involved family until he had to explain the reason his 2-hour planned procedure took 8 hours. The patient had clearly minimized to his family any of the risks discussed with him preoperatively. Prior to proceeding with any surgical intervention it is important that, if possible, a family member be informed of the risks and benefits of the planned procedure and that this conversation be documented in the chart.
Documentation remains very important not only during the informed consent process prior to surgery, but also in decision making regarding postoperative care. Although the physicians discussed the options of resuming the patient’s chemothromboprophylaxis, nothing was documented in the chart. If the discussion was documented, they may have been able to refute the allegation of failure to prevent the DVT.
Finally, in certain instances even when the facts support the judgments that were made regarding the care given, it may be the best “business decision” to settle a case. This is perhaps the most difficult concept for practicing surgeons to grasp. Whether physicians like it or not, medicine is a business and decisions made regarding defending or settling a law suit should not be based on emotion. We don’t do that in the operating room, and we should not do it in the courtroom.
Dr. Risley is the medical director of the Jacksonville Vein Center, Fla.
The opinions expressed by the author neither imply nor establish a standard of care. Cases have been modified and may be fictional in order to maintain HIPPA and confidentiality regulations.
Dr. Risley together with associate editor Dr. O. William Brown describe a case involving failure to document, a common complaint in malpractice litigation.
A 63-year-old white male, actively working, presented with a 5.3-cm infra-renal abdominal aortic aneurysm (AAA). His anatomy was deemed appropriate for endovascular AAA repair and was cleared by his cardiologist for that procedure. The patient underwent a thorough informed consent regarding endovascular and open options as well as the option for continued AAA surveillance. Of note, the patient never had his family with him at any time during the decision-making process, nor with him in the preoperative holding area.
He underwent an aorto- bi- iliac unibody endovascular graft placement. During delivery of the main body, the right common iliac artery ruptured. Initial attempts at endovascular control and subsequent right retroperitoneal exposure and repair of the iliac rupture were unsuccessful, ultimately requiring laparotomy, explant of the device, and aorto- bi-femoral bypass graft. The first time the surgeon met the large family was at the completion of the procedure to explain the complications that were encountered. The patient had a very “rocky” ICU course with complications of ARDS (acute respiratory distress syndrome), acute renal insufficiency, anemia, encephalopathy, and thrombocytopenia. He was initially started on Lovenox on POD # 2 in addition to SCDs (sequential compression devices) for DVT prophylaxis.
Lovenox was stopped because of thrombocytopenia, and mechanical SCD prophylaxis was maintained. As his platelet count recovered and his HIT (heparin-induced thrombocytopenia) screen came back negative, discussion was undertaken to resume his chemical thromboprophylaxis.
It was elected to leave him on only the SCDs because of potential bleeding complications. He continued to improve, but developed a swollen left lower extremity as a result of a DVT. He was placed on heparin drip and converted to Coumadin. Despite an INR of 2.7 on the day he was to be discharged to the rehabilitation center, and shortly after a walk with the therapists and his family, he suffered a fatal pulmonary embolism.
Ultimately, the hospital, the intensivist and the surgeon were sued for failure to adequately provide prophylaxis and treat the DVT. The case was settled. The criticisms were that the physicians failed to provide both mechanical and chemical thromboprophylaxis, particularly after the HIT panel was negative. No criticisms of the intra-operative complications were levied.
The plaintiff’s expert in this case was a physician who was board certified in internal medicine, anesthesiology, and critical care. He had no training in general surgery or vascular surgery. Accordingly, although he may have made suggestions regarding post operative surgical care he had no experience in being the responsible physician for making a postoperative surgical decision. In addition, assertions regarding the incidence of DVT in specific patient populations were exaggerated. Yet the case still settled.
This case emphasizes several important issues. First, communication is paramount in potentially avoiding medical malpractice litigation. The surgeon never met anyone from the patient’s large and involved family until he had to explain the reason his 2-hour planned procedure took 8 hours. The patient had clearly minimized to his family any of the risks discussed with him preoperatively. Prior to proceeding with any surgical intervention it is important that, if possible, a family member be informed of the risks and benefits of the planned procedure and that this conversation be documented in the chart.
Documentation remains very important not only during the informed consent process prior to surgery, but also in decision making regarding postoperative care. Although the physicians discussed the options of resuming the patient’s chemothromboprophylaxis, nothing was documented in the chart. If the discussion was documented, they may have been able to refute the allegation of failure to prevent the DVT.
Finally, in certain instances even when the facts support the judgments that were made regarding the care given, it may be the best “business decision” to settle a case. This is perhaps the most difficult concept for practicing surgeons to grasp. Whether physicians like it or not, medicine is a business and decisions made regarding defending or settling a law suit should not be based on emotion. We don’t do that in the operating room, and we should not do it in the courtroom.
Dr. Risley is the medical director of the Jacksonville Vein Center, Fla.
The opinions expressed by the author neither imply nor establish a standard of care. Cases have been modified and may be fictional in order to maintain HIPPA and confidentiality regulations.

How do you dismiss a patient from your practice’s care?
Case: Patient becomes a liability when nonadherant to prescribed tests
MC, a 42-year-old woman (G1P1001), presents for an office visit. As the medical assistant hands you the chart, she says, “Good luck with this one. She yelled at me because you were 20 minutes behind schedule. She didn’t like sitting in the waiting room.” You greet the patient, obtain her medical history, proceed with a physical examination, and outline a management plan. You recall from the chart that you operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the operating room (OR) for a laparotomy to control bleeding. The patient has not brought this up since being discharged from the hospital.
During the current office visit, the esprit de corps in the consultation room is a bit uncomfortable, and you sense the patient is not happy. You leave the examination room and discuss the management plan with the nurse, who then returns to the patient to review the plan. The patient is unhappy with the battery of tests you have ordered but tells the nurse that she will comply.
One week later the nurse follows up with the patient by phone because she has not obtained the requested lab tests. The nurse reports to you, “She read me the riot act: ‘Why do I need all these tests? They are expensive.’ The patient indicated that she has no understanding as to why the tests were ordered in the first place.” After a discussion with you, the nurse calls the patient back in an effort to clarify her understanding of the need for the tests. The patient hangs up on her in the middle of the conversation.
The office manager tracks you down to discuss this patient. “Enough is enough,” she exclaims. “This patient is harassing the staff. She told the nurse what tests she herself believes are best and that those are the only ones she will comply with.” Your office manager states that this patient is “a liability.”
What are your choices at this point? You have thought about picking up the phone and calling her. You have considered ending her relationship with your practice. You ask yourself again, what is the best approach?
Patients have the legal right to “dismiss” or change health care providers at any time and for almost any reason without notice. But that right is not reciprocal—clinicians have a legal duty not to abandon a patient and an ethical duty to promote continuity of patient care. A clinician may dismiss a patient from his or her practice (other than for a discriminatory reason that violates ethical or legal limitations), but it must be done in the proper way.
We examine the legal, practical, and ethical issues in dismissing a patient, and how to do it without unnecessary risk. In addition, we will look at a new issue that sometimes arises in these circumstances—managed care limitations.
Physicians’ ethical obligations
The American Medical Association suggests the following ethical consideration:
Reference
- American Medical Association Council on Ethical and Judicial Affairs. Opinion 10.015. The Patient-Physician Relationship. Code of Medical Ethics. American Medical Association. http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion10015.page. Issued December 2001. Accessed May 8, 2015.
Legal and medical issues
Why would you end a clinician−patient relationship?
There are a number of reasons for dismissing a patient, including1,2:
- the patient’s failure to comply with a treatment plan (probably the most frequent reason)
- persistent, inappropriate, rude, or disruptive behavior
- falsifying medical history
- seductive behavior toward health care professionals or staff
- Sentinel incident (verbal threat, violence, or criminal activity—as when a patient threatens or inappropriately touches or hits your staff)
- failure to pay billed charges (this can raise special legal issues).
The legal details vary from state to state, but fortunately there is sufficient similarity that best practices can be determined. The law starts with the proposition that ordinarily professionals may choose their patients or clients. There are limits, however, in state and federal law. A clinician may not discriminate based, for example, on ethnicity, religion, gender, or sexual orientation. In addition, the Americans with Disabilities Act limits the basis for not providing care to a patient.3
Limiting factors when dismissing a patient
Once a patient has been accepted and a professional relationship has begun, the clinician has a duty of continued care and must act reasonably to end the relationship in a way that protects the patient’s well-being.
Other recognized limitations to the ending of a treatment relationship exist. These are:
- In an emergency situation or during ongoing care in which it proves unfeasible to find another physician. At the extreme, a surgeon may not leave in the middle of surgery. Less clear, but still problematic, is the obstetrician who wants to dismiss a patient 1 or 2 weeks before an expected delivery. In any event, a clinician should not leave a patient at a critical stage without giving reasonable notice or making suitable arrangements for the attendance of another equally competent substitute.
- When there is no other health care provider available who could provide the continuity of care the clinician has begun. This limitation probably arises from the frontier days (when it was much more common for no other health care professional to be available who could provide the continuity of care the clinician began). A modern version of this might be a patient in an HMO who does not have other physicians of the same subspecialty available who are taking patients. This, of course, requires consultation with the managed care organization.
Abandonment
The legal and ethical issues are essentially related to “abandonment”—dismissing a patient improperly. Technically, abandonment is a form of negligence (the clinician does not act reasonably to protect the patient’s interests). The Oklahoma Supreme Court put it clearly: “When further medical and/or surgical attention is needed, a physician may terminate the doctor−patient relationship only after giving reasonable notice and affording an ample opportunity for the patient to secure other medical attention from other physicians” (emphasis added).4–6
How to end a patient relationship
Always send a letter
Two elements must be taken into account when dismissing a patient:
- reasonable notice
- reasonable opportunity to find another clinician.
Together, these elements mean that the intention of ending the clinician−patient relationship and the importance of finding an alternative care provider must be clearly communicated to the patient. That communication needs to be in writing—both to get the patient’s attention and as clear proof of what was said.
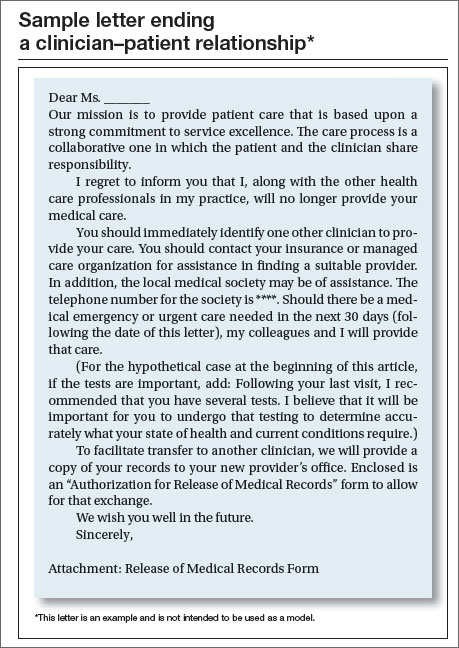
Some experts suggest that the best process is to have a face-to-face meeting with the patient followed by a letter. A goal of such a meeting is to make the parting as amicable as possible. It may seem more professional for a clinician to communicate such an important matter in person. The risk is that it may become a confrontation that exacerbates the situation because one or both parties may have some built-up emotion. It, therefore, depends on the circumstances as to whether such a meeting is desirable. Even if there is an oral conversation, it must be followed up with a letter to the patient.
A reasonable time frame to give the patient to find another clinician is commonly a maximum of 30 days of follow-up and emergency care. A set period of time may be a legitimate starting point but it needs to be adjusted in lieu of special circumstances, such as the availability of other similar specialists in the vicinity who are taking new patients or managed care complications. A specific time period should be indicated, along with an agreement to provide care during that time period in “emergency” or “urgent” circumstances. Of course, ongoing care also should be continued for a reasonable time (30 days is often reasonable, as mentioned). It may be best to also discuss any specific ongoing issues that should be attended to (such as the recommended tests in our opening case).
There is disagreement among experts as to whether a general statement of the reasons for ending the care relationship should be included in the letter. The argument for doing so is that, without a stated reason, the patient may call to ask why. The other side of the argument is that it adds an element of accusation; the patient undoubtedly knows what the problem is. Not writing down the reasons seems the better part of valor, especially if there has been an oral conversation.7,8
The box above provides an example of a letter to a patient (but not a model). Experts agree that the letter should be sent by certified mail with return receipt. Should the patient reject the letter, a regular delivery letter should be sent with full documentation kept in the file of the time and place it was mailed.
Managed care considerations
A consideration of increasing importance is managed care. Before taking any action, ensure that the managed care contract(s) (including federal or state government programs) have provisions concerning patient dismissals. These may be as simple as notifying the organization as to any time limits for care or of the process of dismissal.
Make sure your staff knows
Your scheduling staff needs to know with clarity the rules for scheduling (or not scheduling) this patient in the future. As a general matter, the better course of action is to allow an appointment if the patient reports that it is an emergency, whether the staff believes it is or not. In such cases it may be good to document to the patient that the emergency care does not constitute reestablishing a regular clinician−patient relationship.
Document everything
The patient’s record, at a minimum, should contain a copy of the letter sent to the patient and a log of any conversations with her about ending the relationship. Keep your own notes concerning the disruption or problems with the patient over time.
Are there risks of a malpractice lawsuit?
The abandonment claim is, of course, one possibility for a malpractice lawsuit. That is why documentation and careful communication are so important. This is one area in which having legal advice when developing a letter template should be part of the ongoing relationship with a health law attorney.
There is another malpractice risk illustrated in our hypothetical case. The physician “operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the OR and laparotomy to control bleeding.” Malpractice claims (as opposed to actual malpractice occurrences) most often arise because of bad communication with patients or when patients feel ignored. The clinician is thus between a rock and a hard place. On one hand, by ending this relationship, the clinician could well precipitate a claim based primarily on the earlier “maloccurrence.” On the other hand, continuing to treat a patient who is resisting care and creating problems with the staff has its own difficulties. It may be time for the health care professional to discuss the matter with an attorney.
Although not present in this hypothetical case, ending a patient relationship because of nonpayment of professional fees is also a touchy situation. It can be one of the other precipitating events for malpractice claims, and calls for special care.
Tread with care
Having to dismiss a patient is almost always a difficult process. The decision neither can be made lightly nor implemented sloppily. Because it is difficult, it calls on professionals to be particularly careful to not cut essential corners.9
Case: Resolved
You ask the nurse to note the details of her follow-up phone conversation with the patient in the chart. You then call MC to explain the importance of the tests. She says she is unavailable to talk right now, so you ask her to come in for an appointment, free of charge. The patient makes an appointment but does not show.
You send a letter by certified mail describing the medical necessity for the tests and that her lack of adherence and refusal to come to the office have compelled you to end your clinician−patient relationship. You write that she should immediately identify another health care professional and suggest that she contact her managed care organization for assistance. You note that, should there be a medical emergency or urgent care needed in the next 30 days, you will provide that care. You enclose a release of medical records form in the letter.
In the patient’s record you note the details of the phone conversation and ask the office manager to add that the patient was a no show for her appointment. You include a copy of the certified letter and proof of mailing in the chart.
Two weeks later, the office manager reports that she is sending the patient’s records to another physician upon receipt of the release of medical records form from the patient.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Kodner C. Challenging physician-patient interactions. FP Essentials. ed 354. AAFP home study. Leawood, KS: American Academy of Family Physicians; November 2008.
2. Harris SM. Take care when firing a patient. Am Med News. http://www.ama-assn.org/amed- news/2008/02/04/bica0204 .htm. Published February 4, 2008. Accessed May 8, 2015.
3. Lynch HF. Discrimination at the doctor’s office. N Engl J Med. 2013;386(18):1668–1670.
4. Jackson v Oklahoma Memorial Hospital, 909 P.2d 765 (OK 1995). http://law.justia.com/cases/oklahoma/supreme-court/1995/4226-1.html. Accessed May 8, 2015.
5. Randolph DS, Burkett TM. When physicians fire patients: avoiding patient “abandonment” lawsuits. J Okla State Med Assoc. 2009;102(11):356–358.
6. Crauman R, Baruch J. Abandonment in the physician-patient relationship. Med Health R I. 2004;87(5):154–156.
7. Cepelewicz BB. Firing a patient: when its needed and how to handle it correctly. Med Econ. 2014;91(2):42–43.
8. Santalucia C, Michota F. When and how is it appropriate to terminate the physician-patient relationship? Cleve Clin J Med. 2004;71(3):179–183.
9. Lippman H, Davenport J. Patient dismissal: the right way to do it. J Fam Pract. 2011;60(3):135–140. http://www.jfponline.com/specialty-focus/practice-management/article/patient-dismissal-the-right-way-to-do-it/30f9501e8b3eb6ddaf6dd67ce88e0d16.html. Accessed May 8, 2015.
Joseph S. Sanfilippo, MD, MBA, and Steven R. Smith, JD
| Joseph S. Sanfilippo, MD, MBA is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
|
Steven R. Smith, JD, is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California. |
|
Shirley M. Pruitt, BSN, JD, is a Partner in the firm of Yates, McLamb & Weyher, LLP, in Raleigh, North Carolina. She is an OBG Management Contributing Editor. |


The authors report no financial relationships relevant to this article.
*The “facts” of this case are based on actual cases but are a composite of several events and do not reflect a specific case.
Joseph S. Sanfilippo, MD, MBA, and Steven R. Smith, JD
|
| Joseph S. Sanfilippo, MD, MBA is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
|
Steven R. Smith, JD, is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California. |
|
Shirley M. Pruitt, BSN, JD, is a Partner in the firm of Yates, McLamb & Weyher, LLP, in Raleigh, North Carolina. She is an OBG Management Contributing Editor. |
The authors report no financial relationships relevant to this article.
*The “facts” of this case are based on actual cases but are a composite of several events and do not reflect a specific case.
Joseph S. Sanfilippo, MD, MBA, and Steven R. Smith, JD
|
| Joseph S. Sanfilippo, MD, MBA is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
|
Steven R. Smith, JD, is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California. |
|
Shirley M. Pruitt, BSN, JD, is a Partner in the firm of Yates, McLamb & Weyher, LLP, in Raleigh, North Carolina. She is an OBG Management Contributing Editor. |
The authors report no financial relationships relevant to this article.
*The “facts” of this case are based on actual cases but are a composite of several events and do not reflect a specific case.
Case: Patient becomes a liability when nonadherant to prescribed tests
MC, a 42-year-old woman (G1P1001), presents for an office visit. As the medical assistant hands you the chart, she says, “Good luck with this one. She yelled at me because you were 20 minutes behind schedule. She didn’t like sitting in the waiting room.” You greet the patient, obtain her medical history, proceed with a physical examination, and outline a management plan. You recall from the chart that you operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the operating room (OR) for a laparotomy to control bleeding. The patient has not brought this up since being discharged from the hospital.
During the current office visit, the esprit de corps in the consultation room is a bit uncomfortable, and you sense the patient is not happy. You leave the examination room and discuss the management plan with the nurse, who then returns to the patient to review the plan. The patient is unhappy with the battery of tests you have ordered but tells the nurse that she will comply.
One week later the nurse follows up with the patient by phone because she has not obtained the requested lab tests. The nurse reports to you, “She read me the riot act: ‘Why do I need all these tests? They are expensive.’ The patient indicated that she has no understanding as to why the tests were ordered in the first place.” After a discussion with you, the nurse calls the patient back in an effort to clarify her understanding of the need for the tests. The patient hangs up on her in the middle of the conversation.
The office manager tracks you down to discuss this patient. “Enough is enough,” she exclaims. “This patient is harassing the staff. She told the nurse what tests she herself believes are best and that those are the only ones she will comply with.” Your office manager states that this patient is “a liability.”
What are your choices at this point? You have thought about picking up the phone and calling her. You have considered ending her relationship with your practice. You ask yourself again, what is the best approach?
Patients have the legal right to “dismiss” or change health care providers at any time and for almost any reason without notice. But that right is not reciprocal—clinicians have a legal duty not to abandon a patient and an ethical duty to promote continuity of patient care. A clinician may dismiss a patient from his or her practice (other than for a discriminatory reason that violates ethical or legal limitations), but it must be done in the proper way.
We examine the legal, practical, and ethical issues in dismissing a patient, and how to do it without unnecessary risk. In addition, we will look at a new issue that sometimes arises in these circumstances—managed care limitations.
Physicians’ ethical obligations
The American Medical Association suggests the following ethical consideration:
Reference
- American Medical Association Council on Ethical and Judicial Affairs. Opinion 10.015. The Patient-Physician Relationship. Code of Medical Ethics. American Medical Association. http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion10015.page. Issued December 2001. Accessed May 8, 2015.
Legal and medical issues
Why would you end a clinician−patient relationship?
There are a number of reasons for dismissing a patient, including1,2:
- the patient’s failure to comply with a treatment plan (probably the most frequent reason)
- persistent, inappropriate, rude, or disruptive behavior
- falsifying medical history
- seductive behavior toward health care professionals or staff
- Sentinel incident (verbal threat, violence, or criminal activity—as when a patient threatens or inappropriately touches or hits your staff)
- failure to pay billed charges (this can raise special legal issues).
The legal details vary from state to state, but fortunately there is sufficient similarity that best practices can be determined. The law starts with the proposition that ordinarily professionals may choose their patients or clients. There are limits, however, in state and federal law. A clinician may not discriminate based, for example, on ethnicity, religion, gender, or sexual orientation. In addition, the Americans with Disabilities Act limits the basis for not providing care to a patient.3
Limiting factors when dismissing a patient
Once a patient has been accepted and a professional relationship has begun, the clinician has a duty of continued care and must act reasonably to end the relationship in a way that protects the patient’s well-being.
Other recognized limitations to the ending of a treatment relationship exist. These are:
- In an emergency situation or during ongoing care in which it proves unfeasible to find another physician. At the extreme, a surgeon may not leave in the middle of surgery. Less clear, but still problematic, is the obstetrician who wants to dismiss a patient 1 or 2 weeks before an expected delivery. In any event, a clinician should not leave a patient at a critical stage without giving reasonable notice or making suitable arrangements for the attendance of another equally competent substitute.
- When there is no other health care provider available who could provide the continuity of care the clinician has begun. This limitation probably arises from the frontier days (when it was much more common for no other health care professional to be available who could provide the continuity of care the clinician began). A modern version of this might be a patient in an HMO who does not have other physicians of the same subspecialty available who are taking patients. This, of course, requires consultation with the managed care organization.
Abandonment
The legal and ethical issues are essentially related to “abandonment”—dismissing a patient improperly. Technically, abandonment is a form of negligence (the clinician does not act reasonably to protect the patient’s interests). The Oklahoma Supreme Court put it clearly: “When further medical and/or surgical attention is needed, a physician may terminate the doctor−patient relationship only after giving reasonable notice and affording an ample opportunity for the patient to secure other medical attention from other physicians” (emphasis added).4–6
How to end a patient relationship
Always send a letter
Two elements must be taken into account when dismissing a patient:
- reasonable notice
- reasonable opportunity to find another clinician.
Together, these elements mean that the intention of ending the clinician−patient relationship and the importance of finding an alternative care provider must be clearly communicated to the patient. That communication needs to be in writing—both to get the patient’s attention and as clear proof of what was said.
Some experts suggest that the best process is to have a face-to-face meeting with the patient followed by a letter. A goal of such a meeting is to make the parting as amicable as possible. It may seem more professional for a clinician to communicate such an important matter in person. The risk is that it may become a confrontation that exacerbates the situation because one or both parties may have some built-up emotion. It, therefore, depends on the circumstances as to whether such a meeting is desirable. Even if there is an oral conversation, it must be followed up with a letter to the patient.
A reasonable time frame to give the patient to find another clinician is commonly a maximum of 30 days of follow-up and emergency care. A set period of time may be a legitimate starting point but it needs to be adjusted in lieu of special circumstances, such as the availability of other similar specialists in the vicinity who are taking new patients or managed care complications. A specific time period should be indicated, along with an agreement to provide care during that time period in “emergency” or “urgent” circumstances. Of course, ongoing care also should be continued for a reasonable time (30 days is often reasonable, as mentioned). It may be best to also discuss any specific ongoing issues that should be attended to (such as the recommended tests in our opening case).
There is disagreement among experts as to whether a general statement of the reasons for ending the care relationship should be included in the letter. The argument for doing so is that, without a stated reason, the patient may call to ask why. The other side of the argument is that it adds an element of accusation; the patient undoubtedly knows what the problem is. Not writing down the reasons seems the better part of valor, especially if there has been an oral conversation.7,8
The box above provides an example of a letter to a patient (but not a model). Experts agree that the letter should be sent by certified mail with return receipt. Should the patient reject the letter, a regular delivery letter should be sent with full documentation kept in the file of the time and place it was mailed.
Managed care considerations
A consideration of increasing importance is managed care. Before taking any action, ensure that the managed care contract(s) (including federal or state government programs) have provisions concerning patient dismissals. These may be as simple as notifying the organization as to any time limits for care or of the process of dismissal.
Make sure your staff knows
Your scheduling staff needs to know with clarity the rules for scheduling (or not scheduling) this patient in the future. As a general matter, the better course of action is to allow an appointment if the patient reports that it is an emergency, whether the staff believes it is or not. In such cases it may be good to document to the patient that the emergency care does not constitute reestablishing a regular clinician−patient relationship.
Document everything
The patient’s record, at a minimum, should contain a copy of the letter sent to the patient and a log of any conversations with her about ending the relationship. Keep your own notes concerning the disruption or problems with the patient over time.
Are there risks of a malpractice lawsuit?
The abandonment claim is, of course, one possibility for a malpractice lawsuit. That is why documentation and careful communication are so important. This is one area in which having legal advice when developing a letter template should be part of the ongoing relationship with a health law attorney.
There is another malpractice risk illustrated in our hypothetical case. The physician “operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the OR and laparotomy to control bleeding.” Malpractice claims (as opposed to actual malpractice occurrences) most often arise because of bad communication with patients or when patients feel ignored. The clinician is thus between a rock and a hard place. On one hand, by ending this relationship, the clinician could well precipitate a claim based primarily on the earlier “maloccurrence.” On the other hand, continuing to treat a patient who is resisting care and creating problems with the staff has its own difficulties. It may be time for the health care professional to discuss the matter with an attorney.
Although not present in this hypothetical case, ending a patient relationship because of nonpayment of professional fees is also a touchy situation. It can be one of the other precipitating events for malpractice claims, and calls for special care.
Tread with care
Having to dismiss a patient is almost always a difficult process. The decision neither can be made lightly nor implemented sloppily. Because it is difficult, it calls on professionals to be particularly careful to not cut essential corners.9
Case: Resolved
You ask the nurse to note the details of her follow-up phone conversation with the patient in the chart. You then call MC to explain the importance of the tests. She says she is unavailable to talk right now, so you ask her to come in for an appointment, free of charge. The patient makes an appointment but does not show.
You send a letter by certified mail describing the medical necessity for the tests and that her lack of adherence and refusal to come to the office have compelled you to end your clinician−patient relationship. You write that she should immediately identify another health care professional and suggest that she contact her managed care organization for assistance. You note that, should there be a medical emergency or urgent care needed in the next 30 days, you will provide that care. You enclose a release of medical records form in the letter.
In the patient’s record you note the details of the phone conversation and ask the office manager to add that the patient was a no show for her appointment. You include a copy of the certified letter and proof of mailing in the chart.
Two weeks later, the office manager reports that she is sending the patient’s records to another physician upon receipt of the release of medical records form from the patient.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Case: Patient becomes a liability when nonadherant to prescribed tests
MC, a 42-year-old woman (G1P1001), presents for an office visit. As the medical assistant hands you the chart, she says, “Good luck with this one. She yelled at me because you were 20 minutes behind schedule. She didn’t like sitting in the waiting room.” You greet the patient, obtain her medical history, proceed with a physical examination, and outline a management plan. You recall from the chart that you operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the operating room (OR) for a laparotomy to control bleeding. The patient has not brought this up since being discharged from the hospital.
During the current office visit, the esprit de corps in the consultation room is a bit uncomfortable, and you sense the patient is not happy. You leave the examination room and discuss the management plan with the nurse, who then returns to the patient to review the plan. The patient is unhappy with the battery of tests you have ordered but tells the nurse that she will comply.
One week later the nurse follows up with the patient by phone because she has not obtained the requested lab tests. The nurse reports to you, “She read me the riot act: ‘Why do I need all these tests? They are expensive.’ The patient indicated that she has no understanding as to why the tests were ordered in the first place.” After a discussion with you, the nurse calls the patient back in an effort to clarify her understanding of the need for the tests. The patient hangs up on her in the middle of the conversation.
The office manager tracks you down to discuss this patient. “Enough is enough,” she exclaims. “This patient is harassing the staff. She told the nurse what tests she herself believes are best and that those are the only ones she will comply with.” Your office manager states that this patient is “a liability.”
What are your choices at this point? You have thought about picking up the phone and calling her. You have considered ending her relationship with your practice. You ask yourself again, what is the best approach?
Patients have the legal right to “dismiss” or change health care providers at any time and for almost any reason without notice. But that right is not reciprocal—clinicians have a legal duty not to abandon a patient and an ethical duty to promote continuity of patient care. A clinician may dismiss a patient from his or her practice (other than for a discriminatory reason that violates ethical or legal limitations), but it must be done in the proper way.
We examine the legal, practical, and ethical issues in dismissing a patient, and how to do it without unnecessary risk. In addition, we will look at a new issue that sometimes arises in these circumstances—managed care limitations.
Physicians’ ethical obligations
The American Medical Association suggests the following ethical consideration:
Reference
- American Medical Association Council on Ethical and Judicial Affairs. Opinion 10.015. The Patient-Physician Relationship. Code of Medical Ethics. American Medical Association. http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion10015.page. Issued December 2001. Accessed May 8, 2015.
Legal and medical issues
Why would you end a clinician−patient relationship?
There are a number of reasons for dismissing a patient, including1,2:
- the patient’s failure to comply with a treatment plan (probably the most frequent reason)
- persistent, inappropriate, rude, or disruptive behavior
- falsifying medical history
- seductive behavior toward health care professionals or staff
- Sentinel incident (verbal threat, violence, or criminal activity—as when a patient threatens or inappropriately touches or hits your staff)
- failure to pay billed charges (this can raise special legal issues).
The legal details vary from state to state, but fortunately there is sufficient similarity that best practices can be determined. The law starts with the proposition that ordinarily professionals may choose their patients or clients. There are limits, however, in state and federal law. A clinician may not discriminate based, for example, on ethnicity, religion, gender, or sexual orientation. In addition, the Americans with Disabilities Act limits the basis for not providing care to a patient.3
Limiting factors when dismissing a patient
Once a patient has been accepted and a professional relationship has begun, the clinician has a duty of continued care and must act reasonably to end the relationship in a way that protects the patient’s well-being.
Other recognized limitations to the ending of a treatment relationship exist. These are:
- In an emergency situation or during ongoing care in which it proves unfeasible to find another physician. At the extreme, a surgeon may not leave in the middle of surgery. Less clear, but still problematic, is the obstetrician who wants to dismiss a patient 1 or 2 weeks before an expected delivery. In any event, a clinician should not leave a patient at a critical stage without giving reasonable notice or making suitable arrangements for the attendance of another equally competent substitute.
- When there is no other health care provider available who could provide the continuity of care the clinician has begun. This limitation probably arises from the frontier days (when it was much more common for no other health care professional to be available who could provide the continuity of care the clinician began). A modern version of this might be a patient in an HMO who does not have other physicians of the same subspecialty available who are taking patients. This, of course, requires consultation with the managed care organization.
Abandonment
The legal and ethical issues are essentially related to “abandonment”—dismissing a patient improperly. Technically, abandonment is a form of negligence (the clinician does not act reasonably to protect the patient’s interests). The Oklahoma Supreme Court put it clearly: “When further medical and/or surgical attention is needed, a physician may terminate the doctor−patient relationship only after giving reasonable notice and affording an ample opportunity for the patient to secure other medical attention from other physicians” (emphasis added).4–6
How to end a patient relationship
Always send a letter
Two elements must be taken into account when dismissing a patient:
- reasonable notice
- reasonable opportunity to find another clinician.
Together, these elements mean that the intention of ending the clinician−patient relationship and the importance of finding an alternative care provider must be clearly communicated to the patient. That communication needs to be in writing—both to get the patient’s attention and as clear proof of what was said.
Some experts suggest that the best process is to have a face-to-face meeting with the patient followed by a letter. A goal of such a meeting is to make the parting as amicable as possible. It may seem more professional for a clinician to communicate such an important matter in person. The risk is that it may become a confrontation that exacerbates the situation because one or both parties may have some built-up emotion. It, therefore, depends on the circumstances as to whether such a meeting is desirable. Even if there is an oral conversation, it must be followed up with a letter to the patient.
A reasonable time frame to give the patient to find another clinician is commonly a maximum of 30 days of follow-up and emergency care. A set period of time may be a legitimate starting point but it needs to be adjusted in lieu of special circumstances, such as the availability of other similar specialists in the vicinity who are taking new patients or managed care complications. A specific time period should be indicated, along with an agreement to provide care during that time period in “emergency” or “urgent” circumstances. Of course, ongoing care also should be continued for a reasonable time (30 days is often reasonable, as mentioned). It may be best to also discuss any specific ongoing issues that should be attended to (such as the recommended tests in our opening case).
There is disagreement among experts as to whether a general statement of the reasons for ending the care relationship should be included in the letter. The argument for doing so is that, without a stated reason, the patient may call to ask why. The other side of the argument is that it adds an element of accusation; the patient undoubtedly knows what the problem is. Not writing down the reasons seems the better part of valor, especially if there has been an oral conversation.7,8
The box above provides an example of a letter to a patient (but not a model). Experts agree that the letter should be sent by certified mail with return receipt. Should the patient reject the letter, a regular delivery letter should be sent with full documentation kept in the file of the time and place it was mailed.
Managed care considerations
A consideration of increasing importance is managed care. Before taking any action, ensure that the managed care contract(s) (including federal or state government programs) have provisions concerning patient dismissals. These may be as simple as notifying the organization as to any time limits for care or of the process of dismissal.
Make sure your staff knows
Your scheduling staff needs to know with clarity the rules for scheduling (or not scheduling) this patient in the future. As a general matter, the better course of action is to allow an appointment if the patient reports that it is an emergency, whether the staff believes it is or not. In such cases it may be good to document to the patient that the emergency care does not constitute reestablishing a regular clinician−patient relationship.
Document everything
The patient’s record, at a minimum, should contain a copy of the letter sent to the patient and a log of any conversations with her about ending the relationship. Keep your own notes concerning the disruption or problems with the patient over time.
Are there risks of a malpractice lawsuit?
The abandonment claim is, of course, one possibility for a malpractice lawsuit. That is why documentation and careful communication are so important. This is one area in which having legal advice when developing a letter template should be part of the ongoing relationship with a health law attorney.
There is another malpractice risk illustrated in our hypothetical case. The physician “operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the OR and laparotomy to control bleeding.” Malpractice claims (as opposed to actual malpractice occurrences) most often arise because of bad communication with patients or when patients feel ignored. The clinician is thus between a rock and a hard place. On one hand, by ending this relationship, the clinician could well precipitate a claim based primarily on the earlier “maloccurrence.” On the other hand, continuing to treat a patient who is resisting care and creating problems with the staff has its own difficulties. It may be time for the health care professional to discuss the matter with an attorney.
Although not present in this hypothetical case, ending a patient relationship because of nonpayment of professional fees is also a touchy situation. It can be one of the other precipitating events for malpractice claims, and calls for special care.
Tread with care
Having to dismiss a patient is almost always a difficult process. The decision neither can be made lightly nor implemented sloppily. Because it is difficult, it calls on professionals to be particularly careful to not cut essential corners.9
Case: Resolved
You ask the nurse to note the details of her follow-up phone conversation with the patient in the chart. You then call MC to explain the importance of the tests. She says she is unavailable to talk right now, so you ask her to come in for an appointment, free of charge. The patient makes an appointment but does not show.
You send a letter by certified mail describing the medical necessity for the tests and that her lack of adherence and refusal to come to the office have compelled you to end your clinician−patient relationship. You write that she should immediately identify another health care professional and suggest that she contact her managed care organization for assistance. You note that, should there be a medical emergency or urgent care needed in the next 30 days, you will provide that care. You enclose a release of medical records form in the letter.
In the patient’s record you note the details of the phone conversation and ask the office manager to add that the patient was a no show for her appointment. You include a copy of the certified letter and proof of mailing in the chart.
Two weeks later, the office manager reports that she is sending the patient’s records to another physician upon receipt of the release of medical records form from the patient.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Kodner C. Challenging physician-patient interactions. FP Essentials. ed 354. AAFP home study. Leawood, KS: American Academy of Family Physicians; November 2008.
2. Harris SM. Take care when firing a patient. Am Med News. http://www.ama-assn.org/amed- news/2008/02/04/bica0204 .htm. Published February 4, 2008. Accessed May 8, 2015.
3. Lynch HF. Discrimination at the doctor’s office. N Engl J Med. 2013;386(18):1668–1670.
4. Jackson v Oklahoma Memorial Hospital, 909 P.2d 765 (OK 1995). http://law.justia.com/cases/oklahoma/supreme-court/1995/4226-1.html. Accessed May 8, 2015.
5. Randolph DS, Burkett TM. When physicians fire patients: avoiding patient “abandonment” lawsuits. J Okla State Med Assoc. 2009;102(11):356–358.
6. Crauman R, Baruch J. Abandonment in the physician-patient relationship. Med Health R I. 2004;87(5):154–156.
7. Cepelewicz BB. Firing a patient: when its needed and how to handle it correctly. Med Econ. 2014;91(2):42–43.
8. Santalucia C, Michota F. When and how is it appropriate to terminate the physician-patient relationship? Cleve Clin J Med. 2004;71(3):179–183.
9. Lippman H, Davenport J. Patient dismissal: the right way to do it. J Fam Pract. 2011;60(3):135–140. http://www.jfponline.com/specialty-focus/practice-management/article/patient-dismissal-the-right-way-to-do-it/30f9501e8b3eb6ddaf6dd67ce88e0d16.html. Accessed May 8, 2015.
1. Kodner C. Challenging physician-patient interactions. FP Essentials. ed 354. AAFP home study. Leawood, KS: American Academy of Family Physicians; November 2008.
2. Harris SM. Take care when firing a patient. Am Med News. http://www.ama-assn.org/amed- news/2008/02/04/bica0204 .htm. Published February 4, 2008. Accessed May 8, 2015.
3. Lynch HF. Discrimination at the doctor’s office. N Engl J Med. 2013;386(18):1668–1670.
4. Jackson v Oklahoma Memorial Hospital, 909 P.2d 765 (OK 1995). http://law.justia.com/cases/oklahoma/supreme-court/1995/4226-1.html. Accessed May 8, 2015.
5. Randolph DS, Burkett TM. When physicians fire patients: avoiding patient “abandonment” lawsuits. J Okla State Med Assoc. 2009;102(11):356–358.
6. Crauman R, Baruch J. Abandonment in the physician-patient relationship. Med Health R I. 2004;87(5):154–156.
7. Cepelewicz BB. Firing a patient: when its needed and how to handle it correctly. Med Econ. 2014;91(2):42–43.
8. Santalucia C, Michota F. When and how is it appropriate to terminate the physician-patient relationship? Cleve Clin J Med. 2004;71(3):179–183.
9. Lippman H, Davenport J. Patient dismissal: the right way to do it. J Fam Pract. 2011;60(3):135–140. http://www.jfponline.com/specialty-focus/practice-management/article/patient-dismissal-the-right-way-to-do-it/30f9501e8b3eb6ddaf6dd67ce88e0d16.html. Accessed May 8, 2015.
In this article
- Physicians’ ethical obligations
- Sample letter ending a clinician–patient relationship

Before you hit 'send': Will an e-mail to your patient put you at legal risk?
Dear Dr. Mossman,
Some of my patients e-mail me questions about their prescriptions, test results, treatment, appointments, etc. I’m often unsure about the best way to respond. If I use e-mail to communicate with patients, what step(s) should I take to minimize medicolegal risks?
Submitted by “Dr. V”
Medicine adopts new communication technologies cautiously. Calling patients seems unremarkable to us now, but it took decades after the invention of the telephone for doctors to feel comfortable talking to patients other than in face-to-face meetings.1,2
Patients want to communicate with their physicians via electronic mail,3 but concerns about security, confidentiality, and liability stop many physicians from using e-mail in their practice. Yet many medical organizations, including the Institute of Medicine,4 the American Medical Association,5 and the American Psychiatric Association,6 recognize that e-mail can facilitate care, if used properly.
Although e-mailing patients may feel awkward, a growing minority of clinicians regularly use e-mail for patient communication.2,7 In this article, we discuss ways to help safeguard your patients and their communications and to protect yourself from legal headaches.8
As you’re reading, please remember that we’re discussing communications to patients through standard e-mail, not secure portals (such as MyChart) that allow patients to contact physicians confidentially through their electronic medical records.
Privacy and security
Doctor-patient e-mails implicate the same professional, ethical, and legal responsibilities that govern any communication with patients.2,9,10 If handled improperly, outside-the-office doctor-patient communication can breach traditional duties to protect confidentiality, or they can violate provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA).11 Confidentiality breaches can lead to malpractice litigation, and HIPAA infractions can result in civil and criminal penalties levied by federal agencies.12 Further, e-mails that breach ethical standards (Table 15) can generate complaints to your state’s medical licensure board.
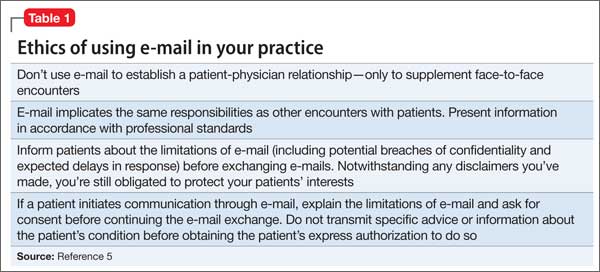
E-mail appeals to many patients, if for no other reason than to save time or avoid the inconvenience of playing “phone tag” with the doctor’s office. But e-mail has drawbacks. Patients may think or behave as though online communications are intimate and confidential, but they usually aren’t. If e-mail programs are left open or aren’t password protected, friends and family members might look at messages and even act upon them. For this reason, doctors often cannot be sure whether they are communicating with the patient or with someone else who has gained access to the patient’s e-mail account.
Parties outside the treatment relationship could have access to e-mail data stored on servers.6 Also, it’s easy to misread or mistype an e-mail address and send confidential information to the wrong person. A truly “secure” e-mail exchange uses encryption software that protects messages during transmission and storage and requires users to authenticate who they are through actions that link their identity to the e-mail address.13 But some patients and physicians do not know about the availability of such security measures, and implementing them can feel cumbersome to those who are not computer savvy. Not surprisingly, then, recent studies have shown that such measures are used infrequently by physicians and patients.14
Topics for e-mail communication
One way to minimize potential privacy problems is to limit the topics and types of communication dealt with by e-mail. Several experts and organizations have published suggestions, recommendations, and resources for doing this with common practices (Table 2).6,7,15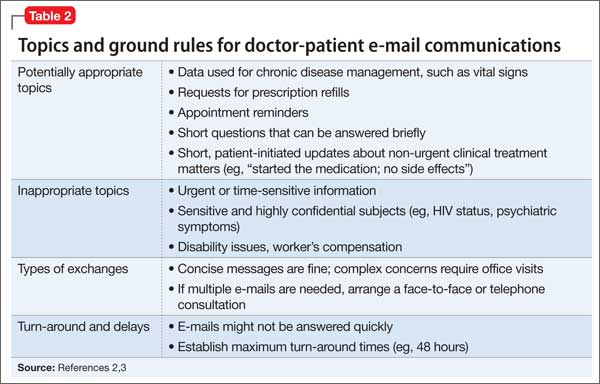
Receiving e-mail permission
Many patients e-mail their physicians without the physicians’ prior agreement. But physicians who plan to use e-mail in their practice should get patients’ explicit consent. This can be done verbally, with the content of the discussion documented in the medical record. But it’s better to have patients authorize e-mail communications in writing by means of a permission form that also sets out your office’s e-mail policies, expected response times, and privacy limitations.
Commonly recommended contents of such forms5-7,9,15,16 include:
• discussing security mechanisms and limits of security
• e-mail encryption requirements (or waiving them, if the patient prefers)
• providing an expected response time
• indemnifying you or your institution for information loss caused by technical failure
• identifying who reads e-mails (eg, office staff members, a nurse, physician [only])
• asking patients to put their name and other identifying information in the body of the message, not the subject line
• asking patients to put the type of question in the subject line (eg, “prescription,” “appointment,” “billing”)
• asking patients to use the “auto reply” feature to acknowledge receipt of your messages.
In addition to using patient consent forms, other suggestions and recommendations for physicians include:
• Do not use e-mail to establish patient-physician relationships, only to supplement personal encounters.
• If you work for an agency or institution, know and follow its guidelines and policies.
• If a rule or “boundary” is breached (eg, a patient sends you a detailed e-mail on a topic beyond the scope of your previous agreement), address this directly in a treatment session.
• File e-mail correspondence, including your reply, in the patient’s medical record.
• Use encryption technology if it is available, practical, and user-friendly.
• Use a practice-dedicated e-mail address with an automatic response that explains when e-mail will be answered and reminds patients to seek immediate help for urgent matters.
Real legal risk
Earlier, we described conceivable legal risks that e-mail might create. But has e-mail caused legal problems for physicians? At least 3 recent published decisions answer: “Yes.” And, remember, only a fraction of legal cases lead to published decisions.
• Huffine v Department of Health17 concerns a psychiatrist who was censured by the Washington state medical quality assurance commission for several boundary crossings, including sending his adolescent patient overly intimate e-mails.
• Wheeler v Kron18 lists a variety of legal claims—intentional infliction of emotional distress, negligent infliction of emotional distress, general negligence, and medical malpractice—that arose from a psychiatrist’s e-mailed concerns about visitation arrangements in a divorcing couple’s custody dispute. Although the court dismissed the last 3 claims, it allowed the intentional infliction of emotional distress claim to proceed.
• Ortegoza v Kho19 includes excerpts of e-mails between a primary care physician and his married patient, with whom the physician had affair that led to a medical malpractice lawsuit.
Bottom Line
Most patients want to e-mail their physicians, and many psychiatrists find e-mail helpful in caring for patients. If you are using e-mail in your practice or are contemplating doing so, get the patient’s permission (preferably in writing), and follow the recommendations and guidelines cited in this article’s references.
Related Resources
• Kane B, Sands DZ. Guidelines for the clinical use of electronic mail with patients. http://jamia.oxfordjournals.org/content/5/1/104.long.
• Professional Risk Management Services, Inc. Sample email consent and guide to email use. www.psychprogram.com/currentpsychiatry.html.
1. Wieczorek SM. From telegraph to e-mail: preserving the doctor-patient relationship in a high-tech environment. ETC: A Review of General Semantics. 2010;67(3):311-327.
2. Spielberg AR. Online without a net: physician-patient communication by electronic mail. Am J Law Med. 1999;25(2-3):267-295.
3. Pelletier AL, Sutton GR, Walker RR. Are your patients ready for electronic communication? Fam Pract Manag. 2007;14(9):25-26.
4. Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academies Press; 2001.
5. American Medical Association. AMA Code of Medical Ethics. Opinion 5.026 - the use of electronic mail. http:// www.ama-assn.org/ama/pub/physician-resources/ medical-ethics/code-medical-ethics/opinion5026.page. Published June 2013. Accessed March 8, 2015.
6. American Psychiatric Association, Council on Psychiatry & Law. Resource document on telepsychiatry and related technologies in clinical psychiatry. http://www.psychiatry. org/learn/library--archives/resource-documents. Published January 2014. Accessed March 25, 2015.
7. Koh S, Cattell GM, Cochran DM, et al. Psychiatrists’ use of electronic communication and social media and a proposed framework for future guidelines. J Psychiatr Pract. 2013;19(3):254-263.
8. Sands DZ. Help for physicians contemplating use of e-mail with patients. J Am Med Inform Assoc. 2004;11(4):268-269.
9. Bovi AM; Council on Ethical and Judicial Affairs of the American Medical Association. Ethical guidelines for use of electronic mail between patients and physicians. Am J Bioeth. 2003;3(3):W-IF2.
10. Kuszler PC. A question of duty: common law legal issues resulting from physician response to unsolicited patient email inquiries. J Med Internet Res. 2000;2(3):E17.
11. 45 CFR Parts 160 and 164.
12. Vanderpool D. Hippa-should I be worried? Innov Clin Neurosci. 2012;9(11-12):51-55.
13. Tjora A, Tran T, Faxvaag A. Privacy vs. usability: a qualitative exploration of patients’ experiences with secure internet communication with their general practitioner. J Med Internet Res. 2005;7(2):e15.
14. Menachemi N, Prickett CT, Brooks RG. The use of physician-patient email: a follow-up examination of adoption and best-practice adherence 2005-2008. J Med Internet Res. 2011;13(1):e23.
15. Kane B, Sands DZ. Guidelines for the clinical use of electronic mail with patients. The AMIA Internet Working Group, Task Force on guidelines for the use of clinic-patient electronic mail. J Am Med Inform Assoc. 1998;5(1):104-111.
16. Car J, Sheikh A. Email consultations in health care: 2–acceptability and safe application. BMJ. 2004; 329(7463):439-442.
17. Huffine v Department of Health, 148 Wn App 1015 (Wash Ct App 2009).
18. Wheeler v Akron (NY Misc LEXIS 942, 2011) NY Slip Op 30530(U) (NY Misc 2011).
19. Ortegoza v Kho, 2013 U.S. Dist .LEXIS 69999 (SD Cal 2013).
Dear Dr. Mossman,
Some of my patients e-mail me questions about their prescriptions, test results, treatment, appointments, etc. I’m often unsure about the best way to respond. If I use e-mail to communicate with patients, what step(s) should I take to minimize medicolegal risks?
Submitted by “Dr. V”
Medicine adopts new communication technologies cautiously. Calling patients seems unremarkable to us now, but it took decades after the invention of the telephone for doctors to feel comfortable talking to patients other than in face-to-face meetings.1,2
Patients want to communicate with their physicians via electronic mail,3 but concerns about security, confidentiality, and liability stop many physicians from using e-mail in their practice. Yet many medical organizations, including the Institute of Medicine,4 the American Medical Association,5 and the American Psychiatric Association,6 recognize that e-mail can facilitate care, if used properly.
Although e-mailing patients may feel awkward, a growing minority of clinicians regularly use e-mail for patient communication.2,7 In this article, we discuss ways to help safeguard your patients and their communications and to protect yourself from legal headaches.8
As you’re reading, please remember that we’re discussing communications to patients through standard e-mail, not secure portals (such as MyChart) that allow patients to contact physicians confidentially through their electronic medical records.
Privacy and security
Doctor-patient e-mails implicate the same professional, ethical, and legal responsibilities that govern any communication with patients.2,9,10 If handled improperly, outside-the-office doctor-patient communication can breach traditional duties to protect confidentiality, or they can violate provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA).11 Confidentiality breaches can lead to malpractice litigation, and HIPAA infractions can result in civil and criminal penalties levied by federal agencies.12 Further, e-mails that breach ethical standards (Table 15) can generate complaints to your state’s medical licensure board.
E-mail appeals to many patients, if for no other reason than to save time or avoid the inconvenience of playing “phone tag” with the doctor’s office. But e-mail has drawbacks. Patients may think or behave as though online communications are intimate and confidential, but they usually aren’t. If e-mail programs are left open or aren’t password protected, friends and family members might look at messages and even act upon them. For this reason, doctors often cannot be sure whether they are communicating with the patient or with someone else who has gained access to the patient’s e-mail account.
Parties outside the treatment relationship could have access to e-mail data stored on servers.6 Also, it’s easy to misread or mistype an e-mail address and send confidential information to the wrong person. A truly “secure” e-mail exchange uses encryption software that protects messages during transmission and storage and requires users to authenticate who they are through actions that link their identity to the e-mail address.13 But some patients and physicians do not know about the availability of such security measures, and implementing them can feel cumbersome to those who are not computer savvy. Not surprisingly, then, recent studies have shown that such measures are used infrequently by physicians and patients.14
Topics for e-mail communication
One way to minimize potential privacy problems is to limit the topics and types of communication dealt with by e-mail. Several experts and organizations have published suggestions, recommendations, and resources for doing this with common practices (Table 2).6,7,15
Receiving e-mail permission
Many patients e-mail their physicians without the physicians’ prior agreement. But physicians who plan to use e-mail in their practice should get patients’ explicit consent. This can be done verbally, with the content of the discussion documented in the medical record. But it’s better to have patients authorize e-mail communications in writing by means of a permission form that also sets out your office’s e-mail policies, expected response times, and privacy limitations.
Commonly recommended contents of such forms5-7,9,15,16 include:
• discussing security mechanisms and limits of security
• e-mail encryption requirements (or waiving them, if the patient prefers)
• providing an expected response time
• indemnifying you or your institution for information loss caused by technical failure
• identifying who reads e-mails (eg, office staff members, a nurse, physician [only])
• asking patients to put their name and other identifying information in the body of the message, not the subject line
• asking patients to put the type of question in the subject line (eg, “prescription,” “appointment,” “billing”)
• asking patients to use the “auto reply” feature to acknowledge receipt of your messages.
In addition to using patient consent forms, other suggestions and recommendations for physicians include:
• Do not use e-mail to establish patient-physician relationships, only to supplement personal encounters.
• If you work for an agency or institution, know and follow its guidelines and policies.
• If a rule or “boundary” is breached (eg, a patient sends you a detailed e-mail on a topic beyond the scope of your previous agreement), address this directly in a treatment session.
• File e-mail correspondence, including your reply, in the patient’s medical record.
• Use encryption technology if it is available, practical, and user-friendly.
• Use a practice-dedicated e-mail address with an automatic response that explains when e-mail will be answered and reminds patients to seek immediate help for urgent matters.
Real legal risk
Earlier, we described conceivable legal risks that e-mail might create. But has e-mail caused legal problems for physicians? At least 3 recent published decisions answer: “Yes.” And, remember, only a fraction of legal cases lead to published decisions.
• Huffine v Department of Health17 concerns a psychiatrist who was censured by the Washington state medical quality assurance commission for several boundary crossings, including sending his adolescent patient overly intimate e-mails.
• Wheeler v Kron18 lists a variety of legal claims—intentional infliction of emotional distress, negligent infliction of emotional distress, general negligence, and medical malpractice—that arose from a psychiatrist’s e-mailed concerns about visitation arrangements in a divorcing couple’s custody dispute. Although the court dismissed the last 3 claims, it allowed the intentional infliction of emotional distress claim to proceed.
• Ortegoza v Kho19 includes excerpts of e-mails between a primary care physician and his married patient, with whom the physician had affair that led to a medical malpractice lawsuit.
Bottom Line
Most patients want to e-mail their physicians, and many psychiatrists find e-mail helpful in caring for patients. If you are using e-mail in your practice or are contemplating doing so, get the patient’s permission (preferably in writing), and follow the recommendations and guidelines cited in this article’s references.
Related Resources
• Kane B, Sands DZ. Guidelines for the clinical use of electronic mail with patients. http://jamia.oxfordjournals.org/content/5/1/104.long.
• Professional Risk Management Services, Inc. Sample email consent and guide to email use. www.psychprogram.com/currentpsychiatry.html.
Dear Dr. Mossman,
Some of my patients e-mail me questions about their prescriptions, test results, treatment, appointments, etc. I’m often unsure about the best way to respond. If I use e-mail to communicate with patients, what step(s) should I take to minimize medicolegal risks?
Submitted by “Dr. V”
Medicine adopts new communication technologies cautiously. Calling patients seems unremarkable to us now, but it took decades after the invention of the telephone for doctors to feel comfortable talking to patients other than in face-to-face meetings.1,2
Patients want to communicate with their physicians via electronic mail,3 but concerns about security, confidentiality, and liability stop many physicians from using e-mail in their practice. Yet many medical organizations, including the Institute of Medicine,4 the American Medical Association,5 and the American Psychiatric Association,6 recognize that e-mail can facilitate care, if used properly.
Although e-mailing patients may feel awkward, a growing minority of clinicians regularly use e-mail for patient communication.2,7 In this article, we discuss ways to help safeguard your patients and their communications and to protect yourself from legal headaches.8
As you’re reading, please remember that we’re discussing communications to patients through standard e-mail, not secure portals (such as MyChart) that allow patients to contact physicians confidentially through their electronic medical records.
Privacy and security
Doctor-patient e-mails implicate the same professional, ethical, and legal responsibilities that govern any communication with patients.2,9,10 If handled improperly, outside-the-office doctor-patient communication can breach traditional duties to protect confidentiality, or they can violate provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA).11 Confidentiality breaches can lead to malpractice litigation, and HIPAA infractions can result in civil and criminal penalties levied by federal agencies.12 Further, e-mails that breach ethical standards (Table 15) can generate complaints to your state’s medical licensure board.
E-mail appeals to many patients, if for no other reason than to save time or avoid the inconvenience of playing “phone tag” with the doctor’s office. But e-mail has drawbacks. Patients may think or behave as though online communications are intimate and confidential, but they usually aren’t. If e-mail programs are left open or aren’t password protected, friends and family members might look at messages and even act upon them. For this reason, doctors often cannot be sure whether they are communicating with the patient or with someone else who has gained access to the patient’s e-mail account.
Parties outside the treatment relationship could have access to e-mail data stored on servers.6 Also, it’s easy to misread or mistype an e-mail address and send confidential information to the wrong person. A truly “secure” e-mail exchange uses encryption software that protects messages during transmission and storage and requires users to authenticate who they are through actions that link their identity to the e-mail address.13 But some patients and physicians do not know about the availability of such security measures, and implementing them can feel cumbersome to those who are not computer savvy. Not surprisingly, then, recent studies have shown that such measures are used infrequently by physicians and patients.14
Topics for e-mail communication
One way to minimize potential privacy problems is to limit the topics and types of communication dealt with by e-mail. Several experts and organizations have published suggestions, recommendations, and resources for doing this with common practices (Table 2).6,7,15
Receiving e-mail permission
Many patients e-mail their physicians without the physicians’ prior agreement. But physicians who plan to use e-mail in their practice should get patients’ explicit consent. This can be done verbally, with the content of the discussion documented in the medical record. But it’s better to have patients authorize e-mail communications in writing by means of a permission form that also sets out your office’s e-mail policies, expected response times, and privacy limitations.
Commonly recommended contents of such forms5-7,9,15,16 include:
• discussing security mechanisms and limits of security
• e-mail encryption requirements (or waiving them, if the patient prefers)
• providing an expected response time
• indemnifying you or your institution for information loss caused by technical failure
• identifying who reads e-mails (eg, office staff members, a nurse, physician [only])
• asking patients to put their name and other identifying information in the body of the message, not the subject line
• asking patients to put the type of question in the subject line (eg, “prescription,” “appointment,” “billing”)
• asking patients to use the “auto reply” feature to acknowledge receipt of your messages.
In addition to using patient consent forms, other suggestions and recommendations for physicians include:
• Do not use e-mail to establish patient-physician relationships, only to supplement personal encounters.
• If you work for an agency or institution, know and follow its guidelines and policies.
• If a rule or “boundary” is breached (eg, a patient sends you a detailed e-mail on a topic beyond the scope of your previous agreement), address this directly in a treatment session.
• File e-mail correspondence, including your reply, in the patient’s medical record.
• Use encryption technology if it is available, practical, and user-friendly.
• Use a practice-dedicated e-mail address with an automatic response that explains when e-mail will be answered and reminds patients to seek immediate help for urgent matters.
Real legal risk
Earlier, we described conceivable legal risks that e-mail might create. But has e-mail caused legal problems for physicians? At least 3 recent published decisions answer: “Yes.” And, remember, only a fraction of legal cases lead to published decisions.
• Huffine v Department of Health17 concerns a psychiatrist who was censured by the Washington state medical quality assurance commission for several boundary crossings, including sending his adolescent patient overly intimate e-mails.
• Wheeler v Kron18 lists a variety of legal claims—intentional infliction of emotional distress, negligent infliction of emotional distress, general negligence, and medical malpractice—that arose from a psychiatrist’s e-mailed concerns about visitation arrangements in a divorcing couple’s custody dispute. Although the court dismissed the last 3 claims, it allowed the intentional infliction of emotional distress claim to proceed.
• Ortegoza v Kho19 includes excerpts of e-mails between a primary care physician and his married patient, with whom the physician had affair that led to a medical malpractice lawsuit.
Bottom Line
Most patients want to e-mail their physicians, and many psychiatrists find e-mail helpful in caring for patients. If you are using e-mail in your practice or are contemplating doing so, get the patient’s permission (preferably in writing), and follow the recommendations and guidelines cited in this article’s references.
Related Resources
• Kane B, Sands DZ. Guidelines for the clinical use of electronic mail with patients. http://jamia.oxfordjournals.org/content/5/1/104.long.
• Professional Risk Management Services, Inc. Sample email consent and guide to email use. www.psychprogram.com/currentpsychiatry.html.
1. Wieczorek SM. From telegraph to e-mail: preserving the doctor-patient relationship in a high-tech environment. ETC: A Review of General Semantics. 2010;67(3):311-327.
2. Spielberg AR. Online without a net: physician-patient communication by electronic mail. Am J Law Med. 1999;25(2-3):267-295.
3. Pelletier AL, Sutton GR, Walker RR. Are your patients ready for electronic communication? Fam Pract Manag. 2007;14(9):25-26.
4. Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academies Press; 2001.
5. American Medical Association. AMA Code of Medical Ethics. Opinion 5.026 - the use of electronic mail. http:// www.ama-assn.org/ama/pub/physician-resources/ medical-ethics/code-medical-ethics/opinion5026.page. Published June 2013. Accessed March 8, 2015.
6. American Psychiatric Association, Council on Psychiatry & Law. Resource document on telepsychiatry and related technologies in clinical psychiatry. http://www.psychiatry. org/learn/library--archives/resource-documents. Published January 2014. Accessed March 25, 2015.
7. Koh S, Cattell GM, Cochran DM, et al. Psychiatrists’ use of electronic communication and social media and a proposed framework for future guidelines. J Psychiatr Pract. 2013;19(3):254-263.
8. Sands DZ. Help for physicians contemplating use of e-mail with patients. J Am Med Inform Assoc. 2004;11(4):268-269.
9. Bovi AM; Council on Ethical and Judicial Affairs of the American Medical Association. Ethical guidelines for use of electronic mail between patients and physicians. Am J Bioeth. 2003;3(3):W-IF2.
10. Kuszler PC. A question of duty: common law legal issues resulting from physician response to unsolicited patient email inquiries. J Med Internet Res. 2000;2(3):E17.
11. 45 CFR Parts 160 and 164.
12. Vanderpool D. Hippa-should I be worried? Innov Clin Neurosci. 2012;9(11-12):51-55.
13. Tjora A, Tran T, Faxvaag A. Privacy vs. usability: a qualitative exploration of patients’ experiences with secure internet communication with their general practitioner. J Med Internet Res. 2005;7(2):e15.
14. Menachemi N, Prickett CT, Brooks RG. The use of physician-patient email: a follow-up examination of adoption and best-practice adherence 2005-2008. J Med Internet Res. 2011;13(1):e23.
15. Kane B, Sands DZ. Guidelines for the clinical use of electronic mail with patients. The AMIA Internet Working Group, Task Force on guidelines for the use of clinic-patient electronic mail. J Am Med Inform Assoc. 1998;5(1):104-111.
16. Car J, Sheikh A. Email consultations in health care: 2–acceptability and safe application. BMJ. 2004; 329(7463):439-442.
17. Huffine v Department of Health, 148 Wn App 1015 (Wash Ct App 2009).
18. Wheeler v Akron (NY Misc LEXIS 942, 2011) NY Slip Op 30530(U) (NY Misc 2011).
19. Ortegoza v Kho, 2013 U.S. Dist .LEXIS 69999 (SD Cal 2013).
1. Wieczorek SM. From telegraph to e-mail: preserving the doctor-patient relationship in a high-tech environment. ETC: A Review of General Semantics. 2010;67(3):311-327.
2. Spielberg AR. Online without a net: physician-patient communication by electronic mail. Am J Law Med. 1999;25(2-3):267-295.
3. Pelletier AL, Sutton GR, Walker RR. Are your patients ready for electronic communication? Fam Pract Manag. 2007;14(9):25-26.
4. Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academies Press; 2001.
5. American Medical Association. AMA Code of Medical Ethics. Opinion 5.026 - the use of electronic mail. http:// www.ama-assn.org/ama/pub/physician-resources/ medical-ethics/code-medical-ethics/opinion5026.page. Published June 2013. Accessed March 8, 2015.
6. American Psychiatric Association, Council on Psychiatry & Law. Resource document on telepsychiatry and related technologies in clinical psychiatry. http://www.psychiatry. org/learn/library--archives/resource-documents. Published January 2014. Accessed March 25, 2015.
7. Koh S, Cattell GM, Cochran DM, et al. Psychiatrists’ use of electronic communication and social media and a proposed framework for future guidelines. J Psychiatr Pract. 2013;19(3):254-263.
8. Sands DZ. Help for physicians contemplating use of e-mail with patients. J Am Med Inform Assoc. 2004;11(4):268-269.
9. Bovi AM; Council on Ethical and Judicial Affairs of the American Medical Association. Ethical guidelines for use of electronic mail between patients and physicians. Am J Bioeth. 2003;3(3):W-IF2.
10. Kuszler PC. A question of duty: common law legal issues resulting from physician response to unsolicited patient email inquiries. J Med Internet Res. 2000;2(3):E17.
11. 45 CFR Parts 160 and 164.
12. Vanderpool D. Hippa-should I be worried? Innov Clin Neurosci. 2012;9(11-12):51-55.
13. Tjora A, Tran T, Faxvaag A. Privacy vs. usability: a qualitative exploration of patients’ experiences with secure internet communication with their general practitioner. J Med Internet Res. 2005;7(2):e15.
14. Menachemi N, Prickett CT, Brooks RG. The use of physician-patient email: a follow-up examination of adoption and best-practice adherence 2005-2008. J Med Internet Res. 2011;13(1):e23.
15. Kane B, Sands DZ. Guidelines for the clinical use of electronic mail with patients. The AMIA Internet Working Group, Task Force on guidelines for the use of clinic-patient electronic mail. J Am Med Inform Assoc. 1998;5(1):104-111.
16. Car J, Sheikh A. Email consultations in health care: 2–acceptability and safe application. BMJ. 2004; 329(7463):439-442.
17. Huffine v Department of Health, 148 Wn App 1015 (Wash Ct App 2009).
18. Wheeler v Akron (NY Misc LEXIS 942, 2011) NY Slip Op 30530(U) (NY Misc 2011).
19. Ortegoza v Kho, 2013 U.S. Dist .LEXIS 69999 (SD Cal 2013).
When Wrong Test Is Ordered, “Wrongful Birth” Results
At a New Jersey hospital, a pregnant woman underwent an ultrasound examination with results suggesting a possible fetal abnormality. In response, DNA testing of the patient and her husband was ordered to investigate for a suspected hormonal disorder. But the wrong test was ordered, and the results of that test were negative.
A baby girl was born with congenital adrenal hyperplasia, a condition causing ambiguous genitalia due to exposure to high concentrations of androgens in utero. She underwent genital reconstructive surgery at age 4 months and is expected to require additional surgery, lifelong hormone replacement therapy, and lifelong monitoring.
The parents claimed that they would have elected to terminate the pregnancy if they had been properly informed of the child’s condition.
What was the outcome? >>
OUTCOME
A jury returned a ruling of 75% liability to the hospital and 25% liability to a hospital lab technician. The verdict was for $1 million, comprising $625,000 for the child and $375,000 for her parents.
COMMENT
The controversial legal theory of recovery in this case is known as “wrongful life” or “wrongful birth.” To prevail on these tort actions, one must prove that the defendant’s negligence led to the birth of an infant following a pregnancy that would have been terminated, had the parents been given all the prenatal screening information required by the standard of care.
The goal of any prenatal screening program should be to provide parents with information that is adequate, accurate, and timely. In this case, after the suspicious sonographic findings were encountered, the wrong test was ordered and the diagnosis was missed. Each practice providing prenatal screening should have a checklist to confirm that the correct test was ordered, completed, and documented—not to mention discussed with the patient in a timely manner.
In this case, the clinician ordered the wrong test, which left the patient with inadequate information. From the facts given, it is unclear if the ordering clinician became aware of this fact and what information, if any, the patient was given regarding the error. Importantly, information must also be given in a timely manner, leaving the patient adequate time to make an informed decision regarding termination—before fetal viability. But how is viability defined?
Although a detailed discussion of the constitutional principles of fetal viability is beyond the scope of this commentary, three US Supreme Court cases paved the way for successful wrongful life/wrongful birth actions. In Griswold v Connecticut (1965), the court held that decisions regarding birth control were protected by the right to privacy. In Roe v Wade (1973), the court held that a constitutionally protected right to privacy exists with regard to pregnancy terminations until the point of “viability,” originally defined as between 24 and 28 gestational weeks. Planned Parenthood v Casey (1991) held that advances in neonatal care required a revised definition of viability to a point “somewhat earlier,” without establishing a specific bright-line rule for viability.
To complicate matters, in recent years, at least 14 states (Alabama, Arizona, Arkansas, Georgia, Idaho, Indiana, Kansas, Louisiana, Mississippi, Nebraska, North Carolina, North Dakota, Oklahoma, and Texas) have redefined viability and passed laws banning therapeutic abortion beyond week 20 (although some of these bans have been judicially blocked). In states with this type of legislation, whether a clinician could be held legally responsible for failing to provide information necessary to permit an informed decision prior to the 20-week mark is unclear.
Questions as to whether these state laws were in conflict with Roe v Wade led to a constitutional challenge. In 2013, the US Court of Appeals for the Ninth Circuit (the highest level before the Supreme Court) ruled that a 20-week cutoff was unconstitutional because it violated the “viability rule” established by Roe and Casey. The Supreme Court declined to review that decision.1
Damage awards in wrongful life/wrongful birth cases are often substantial. The verdict in this case was relatively restrained.
Without doubt, this is a sensitive issue, and respect for our fellow clinicians’ opinions is warranted. However, from a liability standpoint, the safest course of action is to provide patients with all the necessary information—including prenatal testing results—as soon as possible, allowing them to make an informed decision before viability (however that is defined in your state). —DML
REFERENCE
1. Isaacson v. Horne, 716 F.3d 1213, 1225 (9th Cir. 2013), cert denied, 134 S. Ct. 905 (2014).
At a New Jersey hospital, a pregnant woman underwent an ultrasound examination with results suggesting a possible fetal abnormality. In response, DNA testing of the patient and her husband was ordered to investigate for a suspected hormonal disorder. But the wrong test was ordered, and the results of that test were negative.
A baby girl was born with congenital adrenal hyperplasia, a condition causing ambiguous genitalia due to exposure to high concentrations of androgens in utero. She underwent genital reconstructive surgery at age 4 months and is expected to require additional surgery, lifelong hormone replacement therapy, and lifelong monitoring.
The parents claimed that they would have elected to terminate the pregnancy if they had been properly informed of the child’s condition.
What was the outcome? >>
OUTCOME
A jury returned a ruling of 75% liability to the hospital and 25% liability to a hospital lab technician. The verdict was for $1 million, comprising $625,000 for the child and $375,000 for her parents.
COMMENT
The controversial legal theory of recovery in this case is known as “wrongful life” or “wrongful birth.” To prevail on these tort actions, one must prove that the defendant’s negligence led to the birth of an infant following a pregnancy that would have been terminated, had the parents been given all the prenatal screening information required by the standard of care.
The goal of any prenatal screening program should be to provide parents with information that is adequate, accurate, and timely. In this case, after the suspicious sonographic findings were encountered, the wrong test was ordered and the diagnosis was missed. Each practice providing prenatal screening should have a checklist to confirm that the correct test was ordered, completed, and documented—not to mention discussed with the patient in a timely manner.
In this case, the clinician ordered the wrong test, which left the patient with inadequate information. From the facts given, it is unclear if the ordering clinician became aware of this fact and what information, if any, the patient was given regarding the error. Importantly, information must also be given in a timely manner, leaving the patient adequate time to make an informed decision regarding termination—before fetal viability. But how is viability defined?
Although a detailed discussion of the constitutional principles of fetal viability is beyond the scope of this commentary, three US Supreme Court cases paved the way for successful wrongful life/wrongful birth actions. In Griswold v Connecticut (1965), the court held that decisions regarding birth control were protected by the right to privacy. In Roe v Wade (1973), the court held that a constitutionally protected right to privacy exists with regard to pregnancy terminations until the point of “viability,” originally defined as between 24 and 28 gestational weeks. Planned Parenthood v Casey (1991) held that advances in neonatal care required a revised definition of viability to a point “somewhat earlier,” without establishing a specific bright-line rule for viability.
To complicate matters, in recent years, at least 14 states (Alabama, Arizona, Arkansas, Georgia, Idaho, Indiana, Kansas, Louisiana, Mississippi, Nebraska, North Carolina, North Dakota, Oklahoma, and Texas) have redefined viability and passed laws banning therapeutic abortion beyond week 20 (although some of these bans have been judicially blocked). In states with this type of legislation, whether a clinician could be held legally responsible for failing to provide information necessary to permit an informed decision prior to the 20-week mark is unclear.
Questions as to whether these state laws were in conflict with Roe v Wade led to a constitutional challenge. In 2013, the US Court of Appeals for the Ninth Circuit (the highest level before the Supreme Court) ruled that a 20-week cutoff was unconstitutional because it violated the “viability rule” established by Roe and Casey. The Supreme Court declined to review that decision.1
Damage awards in wrongful life/wrongful birth cases are often substantial. The verdict in this case was relatively restrained.
Without doubt, this is a sensitive issue, and respect for our fellow clinicians’ opinions is warranted. However, from a liability standpoint, the safest course of action is to provide patients with all the necessary information—including prenatal testing results—as soon as possible, allowing them to make an informed decision before viability (however that is defined in your state). —DML
REFERENCE
1. Isaacson v. Horne, 716 F.3d 1213, 1225 (9th Cir. 2013), cert denied, 134 S. Ct. 905 (2014).
At a New Jersey hospital, a pregnant woman underwent an ultrasound examination with results suggesting a possible fetal abnormality. In response, DNA testing of the patient and her husband was ordered to investigate for a suspected hormonal disorder. But the wrong test was ordered, and the results of that test were negative.
A baby girl was born with congenital adrenal hyperplasia, a condition causing ambiguous genitalia due to exposure to high concentrations of androgens in utero. She underwent genital reconstructive surgery at age 4 months and is expected to require additional surgery, lifelong hormone replacement therapy, and lifelong monitoring.
The parents claimed that they would have elected to terminate the pregnancy if they had been properly informed of the child’s condition.
What was the outcome? >>
OUTCOME
A jury returned a ruling of 75% liability to the hospital and 25% liability to a hospital lab technician. The verdict was for $1 million, comprising $625,000 for the child and $375,000 for her parents.
COMMENT
The controversial legal theory of recovery in this case is known as “wrongful life” or “wrongful birth.” To prevail on these tort actions, one must prove that the defendant’s negligence led to the birth of an infant following a pregnancy that would have been terminated, had the parents been given all the prenatal screening information required by the standard of care.
The goal of any prenatal screening program should be to provide parents with information that is adequate, accurate, and timely. In this case, after the suspicious sonographic findings were encountered, the wrong test was ordered and the diagnosis was missed. Each practice providing prenatal screening should have a checklist to confirm that the correct test was ordered, completed, and documented—not to mention discussed with the patient in a timely manner.
In this case, the clinician ordered the wrong test, which left the patient with inadequate information. From the facts given, it is unclear if the ordering clinician became aware of this fact and what information, if any, the patient was given regarding the error. Importantly, information must also be given in a timely manner, leaving the patient adequate time to make an informed decision regarding termination—before fetal viability. But how is viability defined?
Although a detailed discussion of the constitutional principles of fetal viability is beyond the scope of this commentary, three US Supreme Court cases paved the way for successful wrongful life/wrongful birth actions. In Griswold v Connecticut (1965), the court held that decisions regarding birth control were protected by the right to privacy. In Roe v Wade (1973), the court held that a constitutionally protected right to privacy exists with regard to pregnancy terminations until the point of “viability,” originally defined as between 24 and 28 gestational weeks. Planned Parenthood v Casey (1991) held that advances in neonatal care required a revised definition of viability to a point “somewhat earlier,” without establishing a specific bright-line rule for viability.
To complicate matters, in recent years, at least 14 states (Alabama, Arizona, Arkansas, Georgia, Idaho, Indiana, Kansas, Louisiana, Mississippi, Nebraska, North Carolina, North Dakota, Oklahoma, and Texas) have redefined viability and passed laws banning therapeutic abortion beyond week 20 (although some of these bans have been judicially blocked). In states with this type of legislation, whether a clinician could be held legally responsible for failing to provide information necessary to permit an informed decision prior to the 20-week mark is unclear.
Questions as to whether these state laws were in conflict with Roe v Wade led to a constitutional challenge. In 2013, the US Court of Appeals for the Ninth Circuit (the highest level before the Supreme Court) ruled that a 20-week cutoff was unconstitutional because it violated the “viability rule” established by Roe and Casey. The Supreme Court declined to review that decision.1
Damage awards in wrongful life/wrongful birth cases are often substantial. The verdict in this case was relatively restrained.
Without doubt, this is a sensitive issue, and respect for our fellow clinicians’ opinions is warranted. However, from a liability standpoint, the safest course of action is to provide patients with all the necessary information—including prenatal testing results—as soon as possible, allowing them to make an informed decision before viability (however that is defined in your state). —DML
REFERENCE
1. Isaacson v. Horne, 716 F.3d 1213, 1225 (9th Cir. 2013), cert denied, 134 S. Ct. 905 (2014).