User login
In Appendicitis Case, Patient Sues Clinic, Clinic Sues NP
A 17-year-old girl with diminished appetite, abdominal pain, and vomiting presented to a pediatrics clinic in New York, where she was examined by an NP. She was found to have hematuria as well, and the NP diagnosed viral gastroenteritis.
Eight days later, the patient returned to the clinic with worsening pain. The pediatrician who examined her had her transported to a hospital, where a ruptured appendix was diagnosed. The patient underwent immediate surgery, which included resection of portions of her colon and intestines.
Despite a good recovery, the patient claimed that she suffers residual gastrointestinal dysfunction. She further claimed that the NP should have diagnosed appendicitis during her initial visit, which would have allowed for less invasive treatment.
Initially, the plaintiff brought suit against the clinic and several employees, but not the NP. She later moved to add the NP, but that motion was denied due to the statute of limitations. The clinic then impleaded the NP, arguing that it was her negligence in failing to diagnose the appendicitis.
The matter proceeded to trial against the NP and the clinic. The defendants claimed that the plaintiff’s symptoms did not suggest appendicitis at the time of the NP’s examination.
OUTCOME
A defense verdict was returned.
Continue for David M. Lang's comments >>
COMMENT
I used to tell students, “There are only two things in medicine that you need to know well: the common and the dangerous. For everything else, there is time.” I realize now that I sound like that guy from the Dos Equis commercial.
Consider this, however: If we don’t remember the difference between polymyositis and polymyalgia rheumatica, who cares? In such cases, we have time for review—and the patient will be better served by a clinician who has the intellectual curiosity to review conditions that he or she hasn’t seen in a while.
But the diseases that are both common and dangerous require our full proficiency. Basic competence requires us to be well versed in common diseases. And dangerous conditions, even if relatively rare, must be recognized and managed immediately. Entities that are common and dangerous—such as appendicitis—should enter our thoughts often.
In this case, we have a 17-year-old girl presenting to an outpatient clinic setting with abdominal pain, vomiting, and anorexia. Unfortunately, we are not given some important historical information, including duration and location of the pain and the presence or absence of pain migration. Physical exam findings are not described.
The trouble with appendicitis is that there is no single sign or symptom that can effectively diagnose it or exclude it from the differential. When evaluating a patient in a setting in which real-time laboratory testing is not generally ordered, clinicians must distinguish between self-limiting and dangerous abdominal pain. Where does that leave us in this case? Abdominal pain and vomiting are common, and ill patients frequently report anorexia.
Other clinical features associated with appendicitis may be more helpful. For example, pain migration has been described as “the most discriminating feature of the patient’s history,”1 with a sensitivity and specificity of approximately 80%.2 When present, psoas sign is fairly specific (0.95) but not sensitive (0.16).3
When evaluating patients in an outpatient setting, we have a snapshot of a disease process—a still frame of a movie. We are told what happened up to that point (with varying degrees of accuracy). But like the patient, we don’t know what will happen after he or she leaves the office: The still frame is gone, but the movie continues.
It can be helpful to inform patients of the concerning diagnoses in your differential and alert them to patterns of clinical progression that warrant return or immediate emergency department evaluation. Calling the patient to see how he or she is doing can be very useful for clinicians and generally highly valued and appreciated by patients. Here, if gastroenteritis were suspected, a phone call after a few hours of antiemetic and rehydration therapy may have been helpful to determine if the patient’s symptoms had improved. This, of course, would not be conclusive—but at least it would give the clinician additional information and the patient additional comfort.
In this case, the jury was persuaded that the NP provided good treatment and acted within the standard of care. Diagnosing appendicitis can be tricky, even under the best circumstances. The NP’s defense was probably aided by good documentation showing that appendicitis seemed less likely at the time of her evaluation. Ultimately, she performed well enough that her care withstood scrutiny from the plaintiff, the plaintiff’s expert witness, and eventually, her own practice.
This case was interesting from a legal perspective in that the plaintiff originally failed to file suit against the NP—probably resorting to liability under the theory of respondeat superior (generally, employer liability for employee actions). While the plaintiff was unsuccessful in adding the NP later, due to the statute of limitations, the NP was brought into the case by her own practice, through a procedure known as impleader. An impleader action is brought by a co-defendant. Under typical impleader rules, the defendant becomes a “third-party plaintiff” and brings suit against a “third-party defendant” (in this case, the practice and the NP, respectively).
IN SUM
Always keep important diagnoses in mind, and document well. Anticipate a changing clinical course, and instruct patients on how to respond to potential changes. In certain cases, we are well served to pick up the phone, check on the patient, and make the presentation less of a static picture and more of a dynamic movie. —DML
REFERENCES
1. Craig S, Brenner BE. Appendicitis (updated October 26, 2012). Medscape Reference. http://emedicine.medscape.com/article/773895-overview. Accessed January 16, 2015.
2. Yeh B. Evidence-based emergency medicine/rational clinical examination abstract: does this adult patient have appendicitis? Ann Emerg Med. 2008;52(3):301-303.
3. Wagner J, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276(19):1589-1594.
A 17-year-old girl with diminished appetite, abdominal pain, and vomiting presented to a pediatrics clinic in New York, where she was examined by an NP. She was found to have hematuria as well, and the NP diagnosed viral gastroenteritis.
Eight days later, the patient returned to the clinic with worsening pain. The pediatrician who examined her had her transported to a hospital, where a ruptured appendix was diagnosed. The patient underwent immediate surgery, which included resection of portions of her colon and intestines.
Despite a good recovery, the patient claimed that she suffers residual gastrointestinal dysfunction. She further claimed that the NP should have diagnosed appendicitis during her initial visit, which would have allowed for less invasive treatment.
Initially, the plaintiff brought suit against the clinic and several employees, but not the NP. She later moved to add the NP, but that motion was denied due to the statute of limitations. The clinic then impleaded the NP, arguing that it was her negligence in failing to diagnose the appendicitis.
The matter proceeded to trial against the NP and the clinic. The defendants claimed that the plaintiff’s symptoms did not suggest appendicitis at the time of the NP’s examination.
OUTCOME
A defense verdict was returned.
Continue for David M. Lang's comments >>
COMMENT
I used to tell students, “There are only two things in medicine that you need to know well: the common and the dangerous. For everything else, there is time.” I realize now that I sound like that guy from the Dos Equis commercial.
Consider this, however: If we don’t remember the difference between polymyositis and polymyalgia rheumatica, who cares? In such cases, we have time for review—and the patient will be better served by a clinician who has the intellectual curiosity to review conditions that he or she hasn’t seen in a while.
But the diseases that are both common and dangerous require our full proficiency. Basic competence requires us to be well versed in common diseases. And dangerous conditions, even if relatively rare, must be recognized and managed immediately. Entities that are common and dangerous—such as appendicitis—should enter our thoughts often.
In this case, we have a 17-year-old girl presenting to an outpatient clinic setting with abdominal pain, vomiting, and anorexia. Unfortunately, we are not given some important historical information, including duration and location of the pain and the presence or absence of pain migration. Physical exam findings are not described.
The trouble with appendicitis is that there is no single sign or symptom that can effectively diagnose it or exclude it from the differential. When evaluating a patient in a setting in which real-time laboratory testing is not generally ordered, clinicians must distinguish between self-limiting and dangerous abdominal pain. Where does that leave us in this case? Abdominal pain and vomiting are common, and ill patients frequently report anorexia.
Other clinical features associated with appendicitis may be more helpful. For example, pain migration has been described as “the most discriminating feature of the patient’s history,”1 with a sensitivity and specificity of approximately 80%.2 When present, psoas sign is fairly specific (0.95) but not sensitive (0.16).3
When evaluating patients in an outpatient setting, we have a snapshot of a disease process—a still frame of a movie. We are told what happened up to that point (with varying degrees of accuracy). But like the patient, we don’t know what will happen after he or she leaves the office: The still frame is gone, but the movie continues.
It can be helpful to inform patients of the concerning diagnoses in your differential and alert them to patterns of clinical progression that warrant return or immediate emergency department evaluation. Calling the patient to see how he or she is doing can be very useful for clinicians and generally highly valued and appreciated by patients. Here, if gastroenteritis were suspected, a phone call after a few hours of antiemetic and rehydration therapy may have been helpful to determine if the patient’s symptoms had improved. This, of course, would not be conclusive—but at least it would give the clinician additional information and the patient additional comfort.
In this case, the jury was persuaded that the NP provided good treatment and acted within the standard of care. Diagnosing appendicitis can be tricky, even under the best circumstances. The NP’s defense was probably aided by good documentation showing that appendicitis seemed less likely at the time of her evaluation. Ultimately, she performed well enough that her care withstood scrutiny from the plaintiff, the plaintiff’s expert witness, and eventually, her own practice.
This case was interesting from a legal perspective in that the plaintiff originally failed to file suit against the NP—probably resorting to liability under the theory of respondeat superior (generally, employer liability for employee actions). While the plaintiff was unsuccessful in adding the NP later, due to the statute of limitations, the NP was brought into the case by her own practice, through a procedure known as impleader. An impleader action is brought by a co-defendant. Under typical impleader rules, the defendant becomes a “third-party plaintiff” and brings suit against a “third-party defendant” (in this case, the practice and the NP, respectively).
IN SUM
Always keep important diagnoses in mind, and document well. Anticipate a changing clinical course, and instruct patients on how to respond to potential changes. In certain cases, we are well served to pick up the phone, check on the patient, and make the presentation less of a static picture and more of a dynamic movie. —DML
REFERENCES
1. Craig S, Brenner BE. Appendicitis (updated October 26, 2012). Medscape Reference. http://emedicine.medscape.com/article/773895-overview. Accessed January 16, 2015.
2. Yeh B. Evidence-based emergency medicine/rational clinical examination abstract: does this adult patient have appendicitis? Ann Emerg Med. 2008;52(3):301-303.
3. Wagner J, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276(19):1589-1594.
A 17-year-old girl with diminished appetite, abdominal pain, and vomiting presented to a pediatrics clinic in New York, where she was examined by an NP. She was found to have hematuria as well, and the NP diagnosed viral gastroenteritis.
Eight days later, the patient returned to the clinic with worsening pain. The pediatrician who examined her had her transported to a hospital, where a ruptured appendix was diagnosed. The patient underwent immediate surgery, which included resection of portions of her colon and intestines.
Despite a good recovery, the patient claimed that she suffers residual gastrointestinal dysfunction. She further claimed that the NP should have diagnosed appendicitis during her initial visit, which would have allowed for less invasive treatment.
Initially, the plaintiff brought suit against the clinic and several employees, but not the NP. She later moved to add the NP, but that motion was denied due to the statute of limitations. The clinic then impleaded the NP, arguing that it was her negligence in failing to diagnose the appendicitis.
The matter proceeded to trial against the NP and the clinic. The defendants claimed that the plaintiff’s symptoms did not suggest appendicitis at the time of the NP’s examination.
OUTCOME
A defense verdict was returned.
Continue for David M. Lang's comments >>
COMMENT
I used to tell students, “There are only two things in medicine that you need to know well: the common and the dangerous. For everything else, there is time.” I realize now that I sound like that guy from the Dos Equis commercial.
Consider this, however: If we don’t remember the difference between polymyositis and polymyalgia rheumatica, who cares? In such cases, we have time for review—and the patient will be better served by a clinician who has the intellectual curiosity to review conditions that he or she hasn’t seen in a while.
But the diseases that are both common and dangerous require our full proficiency. Basic competence requires us to be well versed in common diseases. And dangerous conditions, even if relatively rare, must be recognized and managed immediately. Entities that are common and dangerous—such as appendicitis—should enter our thoughts often.
In this case, we have a 17-year-old girl presenting to an outpatient clinic setting with abdominal pain, vomiting, and anorexia. Unfortunately, we are not given some important historical information, including duration and location of the pain and the presence or absence of pain migration. Physical exam findings are not described.
The trouble with appendicitis is that there is no single sign or symptom that can effectively diagnose it or exclude it from the differential. When evaluating a patient in a setting in which real-time laboratory testing is not generally ordered, clinicians must distinguish between self-limiting and dangerous abdominal pain. Where does that leave us in this case? Abdominal pain and vomiting are common, and ill patients frequently report anorexia.
Other clinical features associated with appendicitis may be more helpful. For example, pain migration has been described as “the most discriminating feature of the patient’s history,”1 with a sensitivity and specificity of approximately 80%.2 When present, psoas sign is fairly specific (0.95) but not sensitive (0.16).3
When evaluating patients in an outpatient setting, we have a snapshot of a disease process—a still frame of a movie. We are told what happened up to that point (with varying degrees of accuracy). But like the patient, we don’t know what will happen after he or she leaves the office: The still frame is gone, but the movie continues.
It can be helpful to inform patients of the concerning diagnoses in your differential and alert them to patterns of clinical progression that warrant return or immediate emergency department evaluation. Calling the patient to see how he or she is doing can be very useful for clinicians and generally highly valued and appreciated by patients. Here, if gastroenteritis were suspected, a phone call after a few hours of antiemetic and rehydration therapy may have been helpful to determine if the patient’s symptoms had improved. This, of course, would not be conclusive—but at least it would give the clinician additional information and the patient additional comfort.
In this case, the jury was persuaded that the NP provided good treatment and acted within the standard of care. Diagnosing appendicitis can be tricky, even under the best circumstances. The NP’s defense was probably aided by good documentation showing that appendicitis seemed less likely at the time of her evaluation. Ultimately, she performed well enough that her care withstood scrutiny from the plaintiff, the plaintiff’s expert witness, and eventually, her own practice.
This case was interesting from a legal perspective in that the plaintiff originally failed to file suit against the NP—probably resorting to liability under the theory of respondeat superior (generally, employer liability for employee actions). While the plaintiff was unsuccessful in adding the NP later, due to the statute of limitations, the NP was brought into the case by her own practice, through a procedure known as impleader. An impleader action is brought by a co-defendant. Under typical impleader rules, the defendant becomes a “third-party plaintiff” and brings suit against a “third-party defendant” (in this case, the practice and the NP, respectively).
IN SUM
Always keep important diagnoses in mind, and document well. Anticipate a changing clinical course, and instruct patients on how to respond to potential changes. In certain cases, we are well served to pick up the phone, check on the patient, and make the presentation less of a static picture and more of a dynamic movie. —DML
REFERENCES
1. Craig S, Brenner BE. Appendicitis (updated October 26, 2012). Medscape Reference. http://emedicine.medscape.com/article/773895-overview. Accessed January 16, 2015.
2. Yeh B. Evidence-based emergency medicine/rational clinical examination abstract: does this adult patient have appendicitis? Ann Emerg Med. 2008;52(3):301-303.
3. Wagner J, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276(19):1589-1594.
Vicarious liability. Second of 2 parts: When a colleague is out of line
Last month, we began consideration of the obligations of physicians and health-care organizations to take action concerning colleagues who are out of line. In part 1, we looked at a recently reported case of “The gynecologist who wore an unusual pen.” He admitted taking more than 1,000 videos and images of patients using a tiny camera embedded in a pen or key fob that he wore around his neck. This serious misconduct continued for many years without being noticed.
A class-action lawsuit against the medical center and physician resulted in a settlement of $190 million, despite the fact that the physician had not transferred the images to others. Here, we look at the obligation of the medical profession to notice and manage colleagues who are creating a risk to patients or the institution. What are the legal consequences of your relationships with your colleagues, and why is it so important for physicians and health-care centers to be alert to inappropriate conduct and deal promptly with those problems?
CASE: Well-respected clinician turns increasingly grumpy toward colleagues and patients
In your role as president of the practice, you have been asked to comment on a colleague’s behavior. You’ve known him for a long time. Dr. X has been in practice for more than 20 years, and always has been well respected in the community. Over his career he has served as residency program director for a large community hospital. He has been, in essence, a role model for physicians in training.
Over the past 6 months, a number of complaints have been brought to your attention as practice president. The primary concern is Dr. X’s temper, which he seems to be having trouble controlling. Nurses have stopped you in the hallway to discuss his change in attitude. “What’s with Dr. X?” they ask. “We are noticing a change in the way he handles patients and residents in the program.”
Now, the threat of a lawsuit because of his negative behavior has been brought to your attention.
Vicarious liability
This case scenario is becoming more frequent as time and reimbursement pressures mount. Learning to deal with it all in a meaningful manner can be a challenge.
What “checks and balances” do you have regarding colleagues’ behavior in your practice? Ethics come into play here, as we all hear about the cases, although not typical, of the clinician who has sex with his patient, sexual abuse accusations, and so forth. But there are significant legal issues even in much less extreme cases.
When the clinician is not an employee
In part 1, we discussed how and why an employer is responsible for the actions of its employees. In many circumstances, however, hospitals grant privileges to physicians who are not employees. Suppose the gynecologist in “The case of the unusual pen” had not been an employee of the hospital, but had staff privileges. Would the hospital have been liable?
Typically, a clinician with hospital privileges who is not an employee is an “independent contractor” rather than an “agent” of the hospital. As such, the vicarious liability that is a hallmark of a principal-agent arrangement is absent. However, the hospital still may be responsible for the clinician’s misconduct if that liability arises from the hospital’s own carelessness. For example, suppose the hospital had given privileges to a clinician without adequately reviewing his or her credentials, qualifications, and past conduct. Imagine that this clinician had a history of abusing patients but the hospital had failed to ascertain that fact.
A hospital that unreasonably fails to find information that would have prevented a clinician from being given privileges or that would have resulted in the limitation or removal of privileges may be liable for the harm done by the clinician, even when that person is an independent contractor. Furthermore, the failure to observe and assess the professional practice of the independent contractor may result in liability to the hospital.
Review process for hospital privileges. The National Practitioner Data Bank (NPDB) was developed to help hospitals find information about physicians who have been disciplined or had malpractice problems. A query to the NPDB may not be sufficient to discover all relevant information, however. Indeed, the NPDB itself notes that “the information from the Data Bank should be used in conjunction with, not in replacement of, information from other sources.”1 Most institutions have standard protocols for performing background checks on anyone applying for privileges; those processes must be followed carefully and reviewed on a regular basis.
The appointment procedure is the beginning, not the end, of the review process. An ongoing assessment of performance is formalized in committees in all hospitals. In addition, there are formal reappointment processes to assure continued competency and compliance with hospital standards and regulations.
And all of this is good—but still not enough.
In some cases an apology may be in order when things go wrong with patient care—and sometimes it can help defuse the tensions that arise when a bad outcome happens. For example, in an article titled, “The Last Word: The Power of Apology” a clinician’s thoughts are depicted as follows1:
Where was the right balance between sincere apology and excessive self-blame? How would this patient and the family react? Would they kick me out of the room and open up the yellow pages to find the closest malpractice attorney? Maybe.
The physician came up with a plan, reviewed it one last time right outside the door, took a deep breath and entered the room, “I’m so, so, so, sorry this happened to you.”1
The hour that followed focused on what had happened and what other physicians had told the family when they weighed in. Bottom line? There was agreement that it was a complex and tragic case. As the doctor exited, the family inquired, “You’ll still be our doctor, won’t you? We love you. You are our friend.”1
The tension left his shoulders as the physician reflected on the importance of honesty and humility and apologizing appropriately.1
Saying “I’m sorry” can be a rewarding experience.
References
- Cohen ML. The last word: the power of apology. Fam Pract Manag. 2010;17(1):40–41.
Are you responsible for reporting your colleagues’ behavior?
An important part of a hospital’s or practice’s quality assurance is the day-to-day observations of physicians, nurses, and staff members. Courts have been increasingly insistent that an institution may be liable when its physicians or nurses witness inappropriate medical practice but fail to take action to protect patients. Inappropriate practices include:
- undertaking procedures for which the clinician is not qualified or credentialed
- violating hospital or practice policy or
procedures - causing problems for patients or others.
In “The case of the unusual pen,” the plaintiffs claimed that the institution failed to “discover, stop and report” the physician because its staff was not trained to recognize and report inappropriate conduct. For example, the physician routinely may have performed gynecologic exams without a medial assistant in the room. The hospital described the physician as a “rogue” employee whose actions could not have been discovered, according to the facts we know—but the plaintiffs claimed that the hospital should have known what the physician was doing. Whatever the details of this actual case, the continued, undiscovered misconduct of a physician is, at best, bound to raise questions as to why the hospital or practice did not know about it and take action.
That brings us back to the hypothetical situation that began this article:
CASE: Next steps to confront the issue
In your role as president of the practice, you are asked to comment on a colleague’s questionable behavior.
Do you issue a statement regarding that behavior and let the matter ride, or is more action advisable?
From a legal standpoint, the suggestion that a clinician’s problem behavior is being brought to the attention of the president of the practice is positive. Identifying the problem is only the first step, however. Being asked to comment on the colleague will not be enough. Your responsibility to the practice has now been triggered and you must undertake appropriate procedures. Summarily (and inappropriately) dismissing the colleague may result in all kinds of problems, not to mention a lawsuit. Yet just observing the situation for a few months carries other legal risks. The practice or institution undoubtedly has a standard set of procedures, and you immediately should begin implementing them. These procedures usually involve informal steps—investigating the situation and giving the physician the opportunity to respond.
When the matter is outside of routine, as this case may be, we believe that it is worthwhile to consult a legal expert. Beyond the duty to patients, there are likely to be contractual obligations and complex business law issues. Ideally, the practice has an ongoing relationship with an attorney who is an expert in health matters. Knowing your practice, the attorney can be invaluable in helping you avoid problems and find a resolution to the problems that arise, and he or she should provide consultation if the matter requires formal processes.
These obligations are supported by sound legal principles. It is always important to remember that the purpose of these obligations is to avoid unnecessary harm, stress, and expense to patients who are putting their trust in your practice.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
1. US Department of Health and Human Services, Health Resources and Services Administration. The National Practitioner Data Bank: about us. HRSA Web site. http://www.npdb.hrsa.gov/topNavigation/aboutUs.jsp. Accessed December 11, 2014.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |


Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
Last month, we began consideration of the obligations of physicians and health-care organizations to take action concerning colleagues who are out of line. In part 1, we looked at a recently reported case of “The gynecologist who wore an unusual pen.” He admitted taking more than 1,000 videos and images of patients using a tiny camera embedded in a pen or key fob that he wore around his neck. This serious misconduct continued for many years without being noticed.
A class-action lawsuit against the medical center and physician resulted in a settlement of $190 million, despite the fact that the physician had not transferred the images to others. Here, we look at the obligation of the medical profession to notice and manage colleagues who are creating a risk to patients or the institution. What are the legal consequences of your relationships with your colleagues, and why is it so important for physicians and health-care centers to be alert to inappropriate conduct and deal promptly with those problems?
CASE: Well-respected clinician turns increasingly grumpy toward colleagues and patients
In your role as president of the practice, you have been asked to comment on a colleague’s behavior. You’ve known him for a long time. Dr. X has been in practice for more than 20 years, and always has been well respected in the community. Over his career he has served as residency program director for a large community hospital. He has been, in essence, a role model for physicians in training.
Over the past 6 months, a number of complaints have been brought to your attention as practice president. The primary concern is Dr. X’s temper, which he seems to be having trouble controlling. Nurses have stopped you in the hallway to discuss his change in attitude. “What’s with Dr. X?” they ask. “We are noticing a change in the way he handles patients and residents in the program.”
Now, the threat of a lawsuit because of his negative behavior has been brought to your attention.
Vicarious liability
This case scenario is becoming more frequent as time and reimbursement pressures mount. Learning to deal with it all in a meaningful manner can be a challenge.
What “checks and balances” do you have regarding colleagues’ behavior in your practice? Ethics come into play here, as we all hear about the cases, although not typical, of the clinician who has sex with his patient, sexual abuse accusations, and so forth. But there are significant legal issues even in much less extreme cases.
When the clinician is not an employee
In part 1, we discussed how and why an employer is responsible for the actions of its employees. In many circumstances, however, hospitals grant privileges to physicians who are not employees. Suppose the gynecologist in “The case of the unusual pen” had not been an employee of the hospital, but had staff privileges. Would the hospital have been liable?
Typically, a clinician with hospital privileges who is not an employee is an “independent contractor” rather than an “agent” of the hospital. As such, the vicarious liability that is a hallmark of a principal-agent arrangement is absent. However, the hospital still may be responsible for the clinician’s misconduct if that liability arises from the hospital’s own carelessness. For example, suppose the hospital had given privileges to a clinician without adequately reviewing his or her credentials, qualifications, and past conduct. Imagine that this clinician had a history of abusing patients but the hospital had failed to ascertain that fact.
A hospital that unreasonably fails to find information that would have prevented a clinician from being given privileges or that would have resulted in the limitation or removal of privileges may be liable for the harm done by the clinician, even when that person is an independent contractor. Furthermore, the failure to observe and assess the professional practice of the independent contractor may result in liability to the hospital.
Review process for hospital privileges. The National Practitioner Data Bank (NPDB) was developed to help hospitals find information about physicians who have been disciplined or had malpractice problems. A query to the NPDB may not be sufficient to discover all relevant information, however. Indeed, the NPDB itself notes that “the information from the Data Bank should be used in conjunction with, not in replacement of, information from other sources.”1 Most institutions have standard protocols for performing background checks on anyone applying for privileges; those processes must be followed carefully and reviewed on a regular basis.
The appointment procedure is the beginning, not the end, of the review process. An ongoing assessment of performance is formalized in committees in all hospitals. In addition, there are formal reappointment processes to assure continued competency and compliance with hospital standards and regulations.
And all of this is good—but still not enough.
In some cases an apology may be in order when things go wrong with patient care—and sometimes it can help defuse the tensions that arise when a bad outcome happens. For example, in an article titled, “The Last Word: The Power of Apology” a clinician’s thoughts are depicted as follows1:
Where was the right balance between sincere apology and excessive self-blame? How would this patient and the family react? Would they kick me out of the room and open up the yellow pages to find the closest malpractice attorney? Maybe.
The physician came up with a plan, reviewed it one last time right outside the door, took a deep breath and entered the room, “I’m so, so, so, sorry this happened to you.”1
The hour that followed focused on what had happened and what other physicians had told the family when they weighed in. Bottom line? There was agreement that it was a complex and tragic case. As the doctor exited, the family inquired, “You’ll still be our doctor, won’t you? We love you. You are our friend.”1
The tension left his shoulders as the physician reflected on the importance of honesty and humility and apologizing appropriately.1
Saying “I’m sorry” can be a rewarding experience.
References
- Cohen ML. The last word: the power of apology. Fam Pract Manag. 2010;17(1):40–41.
Are you responsible for reporting your colleagues’ behavior?
An important part of a hospital’s or practice’s quality assurance is the day-to-day observations of physicians, nurses, and staff members. Courts have been increasingly insistent that an institution may be liable when its physicians or nurses witness inappropriate medical practice but fail to take action to protect patients. Inappropriate practices include:
- undertaking procedures for which the clinician is not qualified or credentialed
- violating hospital or practice policy or
procedures - causing problems for patients or others.
In “The case of the unusual pen,” the plaintiffs claimed that the institution failed to “discover, stop and report” the physician because its staff was not trained to recognize and report inappropriate conduct. For example, the physician routinely may have performed gynecologic exams without a medial assistant in the room. The hospital described the physician as a “rogue” employee whose actions could not have been discovered, according to the facts we know—but the plaintiffs claimed that the hospital should have known what the physician was doing. Whatever the details of this actual case, the continued, undiscovered misconduct of a physician is, at best, bound to raise questions as to why the hospital or practice did not know about it and take action.
That brings us back to the hypothetical situation that began this article:
CASE: Next steps to confront the issue
In your role as president of the practice, you are asked to comment on a colleague’s questionable behavior.
Do you issue a statement regarding that behavior and let the matter ride, or is more action advisable?
From a legal standpoint, the suggestion that a clinician’s problem behavior is being brought to the attention of the president of the practice is positive. Identifying the problem is only the first step, however. Being asked to comment on the colleague will not be enough. Your responsibility to the practice has now been triggered and you must undertake appropriate procedures. Summarily (and inappropriately) dismissing the colleague may result in all kinds of problems, not to mention a lawsuit. Yet just observing the situation for a few months carries other legal risks. The practice or institution undoubtedly has a standard set of procedures, and you immediately should begin implementing them. These procedures usually involve informal steps—investigating the situation and giving the physician the opportunity to respond.
When the matter is outside of routine, as this case may be, we believe that it is worthwhile to consult a legal expert. Beyond the duty to patients, there are likely to be contractual obligations and complex business law issues. Ideally, the practice has an ongoing relationship with an attorney who is an expert in health matters. Knowing your practice, the attorney can be invaluable in helping you avoid problems and find a resolution to the problems that arise, and he or she should provide consultation if the matter requires formal processes.
These obligations are supported by sound legal principles. It is always important to remember that the purpose of these obligations is to avoid unnecessary harm, stress, and expense to patients who are putting their trust in your practice.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Last month, we began consideration of the obligations of physicians and health-care organizations to take action concerning colleagues who are out of line. In part 1, we looked at a recently reported case of “The gynecologist who wore an unusual pen.” He admitted taking more than 1,000 videos and images of patients using a tiny camera embedded in a pen or key fob that he wore around his neck. This serious misconduct continued for many years without being noticed.
A class-action lawsuit against the medical center and physician resulted in a settlement of $190 million, despite the fact that the physician had not transferred the images to others. Here, we look at the obligation of the medical profession to notice and manage colleagues who are creating a risk to patients or the institution. What are the legal consequences of your relationships with your colleagues, and why is it so important for physicians and health-care centers to be alert to inappropriate conduct and deal promptly with those problems?
CASE: Well-respected clinician turns increasingly grumpy toward colleagues and patients
In your role as president of the practice, you have been asked to comment on a colleague’s behavior. You’ve known him for a long time. Dr. X has been in practice for more than 20 years, and always has been well respected in the community. Over his career he has served as residency program director for a large community hospital. He has been, in essence, a role model for physicians in training.
Over the past 6 months, a number of complaints have been brought to your attention as practice president. The primary concern is Dr. X’s temper, which he seems to be having trouble controlling. Nurses have stopped you in the hallway to discuss his change in attitude. “What’s with Dr. X?” they ask. “We are noticing a change in the way he handles patients and residents in the program.”
Now, the threat of a lawsuit because of his negative behavior has been brought to your attention.
Vicarious liability
This case scenario is becoming more frequent as time and reimbursement pressures mount. Learning to deal with it all in a meaningful manner can be a challenge.
What “checks and balances” do you have regarding colleagues’ behavior in your practice? Ethics come into play here, as we all hear about the cases, although not typical, of the clinician who has sex with his patient, sexual abuse accusations, and so forth. But there are significant legal issues even in much less extreme cases.
When the clinician is not an employee
In part 1, we discussed how and why an employer is responsible for the actions of its employees. In many circumstances, however, hospitals grant privileges to physicians who are not employees. Suppose the gynecologist in “The case of the unusual pen” had not been an employee of the hospital, but had staff privileges. Would the hospital have been liable?
Typically, a clinician with hospital privileges who is not an employee is an “independent contractor” rather than an “agent” of the hospital. As such, the vicarious liability that is a hallmark of a principal-agent arrangement is absent. However, the hospital still may be responsible for the clinician’s misconduct if that liability arises from the hospital’s own carelessness. For example, suppose the hospital had given privileges to a clinician without adequately reviewing his or her credentials, qualifications, and past conduct. Imagine that this clinician had a history of abusing patients but the hospital had failed to ascertain that fact.
A hospital that unreasonably fails to find information that would have prevented a clinician from being given privileges or that would have resulted in the limitation or removal of privileges may be liable for the harm done by the clinician, even when that person is an independent contractor. Furthermore, the failure to observe and assess the professional practice of the independent contractor may result in liability to the hospital.
Review process for hospital privileges. The National Practitioner Data Bank (NPDB) was developed to help hospitals find information about physicians who have been disciplined or had malpractice problems. A query to the NPDB may not be sufficient to discover all relevant information, however. Indeed, the NPDB itself notes that “the information from the Data Bank should be used in conjunction with, not in replacement of, information from other sources.”1 Most institutions have standard protocols for performing background checks on anyone applying for privileges; those processes must be followed carefully and reviewed on a regular basis.
The appointment procedure is the beginning, not the end, of the review process. An ongoing assessment of performance is formalized in committees in all hospitals. In addition, there are formal reappointment processes to assure continued competency and compliance with hospital standards and regulations.
And all of this is good—but still not enough.
In some cases an apology may be in order when things go wrong with patient care—and sometimes it can help defuse the tensions that arise when a bad outcome happens. For example, in an article titled, “The Last Word: The Power of Apology” a clinician’s thoughts are depicted as follows1:
Where was the right balance between sincere apology and excessive self-blame? How would this patient and the family react? Would they kick me out of the room and open up the yellow pages to find the closest malpractice attorney? Maybe.
The physician came up with a plan, reviewed it one last time right outside the door, took a deep breath and entered the room, “I’m so, so, so, sorry this happened to you.”1
The hour that followed focused on what had happened and what other physicians had told the family when they weighed in. Bottom line? There was agreement that it was a complex and tragic case. As the doctor exited, the family inquired, “You’ll still be our doctor, won’t you? We love you. You are our friend.”1
The tension left his shoulders as the physician reflected on the importance of honesty and humility and apologizing appropriately.1
Saying “I’m sorry” can be a rewarding experience.
References
- Cohen ML. The last word: the power of apology. Fam Pract Manag. 2010;17(1):40–41.
Are you responsible for reporting your colleagues’ behavior?
An important part of a hospital’s or practice’s quality assurance is the day-to-day observations of physicians, nurses, and staff members. Courts have been increasingly insistent that an institution may be liable when its physicians or nurses witness inappropriate medical practice but fail to take action to protect patients. Inappropriate practices include:
- undertaking procedures for which the clinician is not qualified or credentialed
- violating hospital or practice policy or
procedures - causing problems for patients or others.
In “The case of the unusual pen,” the plaintiffs claimed that the institution failed to “discover, stop and report” the physician because its staff was not trained to recognize and report inappropriate conduct. For example, the physician routinely may have performed gynecologic exams without a medial assistant in the room. The hospital described the physician as a “rogue” employee whose actions could not have been discovered, according to the facts we know—but the plaintiffs claimed that the hospital should have known what the physician was doing. Whatever the details of this actual case, the continued, undiscovered misconduct of a physician is, at best, bound to raise questions as to why the hospital or practice did not know about it and take action.
That brings us back to the hypothetical situation that began this article:
CASE: Next steps to confront the issue
In your role as president of the practice, you are asked to comment on a colleague’s questionable behavior.
Do you issue a statement regarding that behavior and let the matter ride, or is more action advisable?
From a legal standpoint, the suggestion that a clinician’s problem behavior is being brought to the attention of the president of the practice is positive. Identifying the problem is only the first step, however. Being asked to comment on the colleague will not be enough. Your responsibility to the practice has now been triggered and you must undertake appropriate procedures. Summarily (and inappropriately) dismissing the colleague may result in all kinds of problems, not to mention a lawsuit. Yet just observing the situation for a few months carries other legal risks. The practice or institution undoubtedly has a standard set of procedures, and you immediately should begin implementing them. These procedures usually involve informal steps—investigating the situation and giving the physician the opportunity to respond.
When the matter is outside of routine, as this case may be, we believe that it is worthwhile to consult a legal expert. Beyond the duty to patients, there are likely to be contractual obligations and complex business law issues. Ideally, the practice has an ongoing relationship with an attorney who is an expert in health matters. Knowing your practice, the attorney can be invaluable in helping you avoid problems and find a resolution to the problems that arise, and he or she should provide consultation if the matter requires formal processes.
These obligations are supported by sound legal principles. It is always important to remember that the purpose of these obligations is to avoid unnecessary harm, stress, and expense to patients who are putting their trust in your practice.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
1. US Department of Health and Human Services, Health Resources and Services Administration. The National Practitioner Data Bank: about us. HRSA Web site. http://www.npdb.hrsa.gov/topNavigation/aboutUs.jsp. Accessed December 11, 2014.
Reference
1. US Department of Health and Human Services, Health Resources and Services Administration. The National Practitioner Data Bank: about us. HRSA Web site. http://www.npdb.hrsa.gov/topNavigation/aboutUs.jsp. Accessed December 11, 2014.

Blue, floppy, apneic baby: $3.25M settlement

Blue, floppy, apneic baby: $3.25M settlement
When a mother went to the hospital in labor, the fetal heart-rate monitor showed a baseline of 140–150 beats per minute (bpm). When the monitor was reapplied 3.5 hours later, the baseline heart rate had risen to 160–165 bpm and demonstrated mild but persistent decelerations. Three hours later, the mother was found to have a fever of 100.5°F; antibiotics were ordered. When persistent fetal tachycardia became evident, the mother’s membranes were artificially ruptured. Thick meconium was noted. After a direct fetal lead was applied, moderate fetal distress was apparent. The mother’s fever rose and the fetus’ late decelerations and tachycardia continued. A cesarean delivery was ordered 12 hours after the mother’s arrival.
The baby was born 45 minutes later. She was blue, floppy, and apneic, with a heart rate of 50–60 bpm. Her Apgar scores were 1, 7, and 9, at 1, 5, and 10 minutes, respectively. She was found to have hypoxic ischemic encephalopathy. The child has right-sided weakness and other cognitive impairments including speech and language delays.
PARENTS’ CLAIM The attending family physician, a second-year resident, and the attending nurse were negligent in the care of the mother during labor and delivery. Cesarean delivery should have been performed earlier when the mother developed a fever and the fetus’ tachycardia was persistent.
defendants’ DEFENSE The case was settled during trial.
VERDICT A $3.25 million Massachusetts settlement was reached.
_________________
MRSA after breast augmentation: $1M verdict
A plastic surgeon performed bilateral breast augmentation surgery on a 31-year-old woman with the help of an assistant. The operation was performed at the physician’s office. The patient was given lidocaine, diazepam (Valium), and acetaminophen and oxycodone (Percocet) as anesthetics. General anesthesia was not administered. Two 4-inch incisions were created to insert the implants.
A month later, the patient went to the emergency department (ED) reporting chest pain. She was found to have methicillin-resistant Staphylococcus aureus (MRSA) infection. She was hospitalized for 6 days.
A month later, she returned to the ED with continuing symptoms. Another surgeon removed the breast implants. A peripherally inserted central catheter (PICC) line was placed for administration of antibiotics to treat the ongoing infection. After several months, she was infection-free.
PATIENT’S CLAIM The initial breast augmentation surgery should have been conducted under sterile conditions in a surgical center under general anesthesia. The assistant was not a licensed nurse or surgical technician.
DEFENDANTS’ DEFENSE The infection is a known risk of the procedure. Sulfamethoxazole/trimethoprim (Bactrim) had been prescribed. The plastic surgeon was not given the chance to treat the infection, as the patient went to the ED instead of calling him and changed physicians.
VERDICT A $1 million Georgia verdict was returned.
_________________
Respiratory arrest after pain meds administered
A 53-year-old woman underwent gynecologic surgery. In the recovery room, a Certified Registered Nurse Anesthetist (CRNA) administered intravenous hydromorphone hydrochloride (Dilaudid HP) 2 mg for pain management. The patient went into respiratory arrest. She was resuscitated, but experienced an hypoxic brain injury. She is now legally blind and has memory deficits and confusion.
PATIENT’S CLAIM The CRNA gave an excessive dose of hydromorphone to the patient.
DEFENDANTS’ DEFENSE The dosage was appropriate. Respiratory arrest is a risk of the surgery that can occur without negligence.
VERDICT A Tennessee defense verdict was returned.
_________________

$2.97M verdict after mother and baby die from urosepsis
A 27-year-old woman was pregnant with her second child. The ObGyn had delivered her first child and provided prenatal care once again. Early in the otherwise uncomplicated second pregnancy, the mother developed pyelonephritis.
At 19 weeks’ gestation, she went to the ED with abdominal pain. The hospital nurses told her ObGyn they thought she had a urinary tract infection. He concurred without seeing her, ordered antibiotics and pain medication, and she was discharged.
When her condition worsened the next day, she returned to the ED, where she was found to have urosepsis. A urogynecologist took over her care and performed emergency surgery. The fetus died during surgery. The mother went into cardiac arrest as surgery ended. She was resuscitated but suffered significant brain damage; she died 4 days later when life support was removed.
ESTATE’S CLAIM The ObGyn was negligent in not coming to the hospital to examine the patient during her initial ED visit, knowing her history of pyelonephritis. The patient should not have been discharged; intravenous administration of antibiotics would have allowed both mother and fetus to survive.
DEFENDANTS’ DEFENSE Admission at the first ED visit was not warranted. A 19-week-old fetus is not viable.
VERDICT Claims against the hospital resulted in a confidential settlement prior to trial. A Kentucky jury found the hospital 60% at fault and the ObGyn 40% at fault. A verdict totaling $7,440,000 was returned, although no damages were awarded for the death of the fetus. The net verdict was $2,976,000.
_________________
Endometriosis surgery: oophorectomy planned but hysterectomy done
After several weeks of abdominal pain, a 44-year-old woman saw her ObGyn, Dr. A. When the pain increased 4 days later, she saw Dr. B, Dr. A’s partner. Dr. B determined that the patient had endometriosis and scheduled surgery for 3 days later. The surgical plan was to remove one ovary.
Just before surgery, the patient had an anxiety attack. After she signed the consent form, she was administered midazolam (Versed). During the operation, Dr. B decided to perform a total hysterectomy.
PATIENT’S CLAIM Dr. B was negligent in performing total hysterectomy without proper consent. The patient was incapacitated by the anxiety attack and midazolam and was incapable of giving consent. She had hoped to become pregnant.
PHYSICIAN’S DEFENSE Hysterectomy was reasonable due to severe endometriosis. All options had been discussed during the preoperative visit. The consent form the patient signed provided for performance of other procedures as needed. The patient was fully cognizant for consent purposes after administration of midazolam, based on her history of narcotic use.
VERDICT A Tennessee defense verdict was returned.
_________________
Compartment syndrome after childbirth
At 42 weeks’ gestation, a 45-year-old woman was admitted to the hospital in labor after a failed attempt at home birth. The baby was delivered 4.5 hours after her arrival. The next day, the mother reported right shin and leg pain but was able to ambulate and flex her foot. She was offered the choice of staying in the hospital for a neurologic evaluation or being discharged with outpatient follow-up if her symptoms continued. She chose to be released.
At home, her symptoms worsened: the swelling in her leg and foot increased, she could not walk or flex her foot, and there were color changes in her leg. She returned to the ED, was found to have right leg compartment syndrome, and underwent fasciotomy. She continues to have foot drop, irregular gait, and right hip pain.
PATIENT’S CLAIM The ObGyn was negligent in the care of the patient during labor and delivery.
PHYSICIAN’S DEFENSE The case was settled during trial.
VERDICT A $3,500 Washington settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Blue, floppy, apneic baby: $3.25M settlement
When a mother went to the hospital in labor, the fetal heart-rate monitor showed a baseline of 140–150 beats per minute (bpm). When the monitor was reapplied 3.5 hours later, the baseline heart rate had risen to 160–165 bpm and demonstrated mild but persistent decelerations. Three hours later, the mother was found to have a fever of 100.5°F; antibiotics were ordered. When persistent fetal tachycardia became evident, the mother’s membranes were artificially ruptured. Thick meconium was noted. After a direct fetal lead was applied, moderate fetal distress was apparent. The mother’s fever rose and the fetus’ late decelerations and tachycardia continued. A cesarean delivery was ordered 12 hours after the mother’s arrival.
The baby was born 45 minutes later. She was blue, floppy, and apneic, with a heart rate of 50–60 bpm. Her Apgar scores were 1, 7, and 9, at 1, 5, and 10 minutes, respectively. She was found to have hypoxic ischemic encephalopathy. The child has right-sided weakness and other cognitive impairments including speech and language delays.
PARENTS’ CLAIM The attending family physician, a second-year resident, and the attending nurse were negligent in the care of the mother during labor and delivery. Cesarean delivery should have been performed earlier when the mother developed a fever and the fetus’ tachycardia was persistent.
defendants’ DEFENSE The case was settled during trial.
VERDICT A $3.25 million Massachusetts settlement was reached.
_________________
MRSA after breast augmentation: $1M verdict
A plastic surgeon performed bilateral breast augmentation surgery on a 31-year-old woman with the help of an assistant. The operation was performed at the physician’s office. The patient was given lidocaine, diazepam (Valium), and acetaminophen and oxycodone (Percocet) as anesthetics. General anesthesia was not administered. Two 4-inch incisions were created to insert the implants.
A month later, the patient went to the emergency department (ED) reporting chest pain. She was found to have methicillin-resistant Staphylococcus aureus (MRSA) infection. She was hospitalized for 6 days.
A month later, she returned to the ED with continuing symptoms. Another surgeon removed the breast implants. A peripherally inserted central catheter (PICC) line was placed for administration of antibiotics to treat the ongoing infection. After several months, she was infection-free.
PATIENT’S CLAIM The initial breast augmentation surgery should have been conducted under sterile conditions in a surgical center under general anesthesia. The assistant was not a licensed nurse or surgical technician.
DEFENDANTS’ DEFENSE The infection is a known risk of the procedure. Sulfamethoxazole/trimethoprim (Bactrim) had been prescribed. The plastic surgeon was not given the chance to treat the infection, as the patient went to the ED instead of calling him and changed physicians.
VERDICT A $1 million Georgia verdict was returned.
_________________
Respiratory arrest after pain meds administered
A 53-year-old woman underwent gynecologic surgery. In the recovery room, a Certified Registered Nurse Anesthetist (CRNA) administered intravenous hydromorphone hydrochloride (Dilaudid HP) 2 mg for pain management. The patient went into respiratory arrest. She was resuscitated, but experienced an hypoxic brain injury. She is now legally blind and has memory deficits and confusion.
PATIENT’S CLAIM The CRNA gave an excessive dose of hydromorphone to the patient.
DEFENDANTS’ DEFENSE The dosage was appropriate. Respiratory arrest is a risk of the surgery that can occur without negligence.
VERDICT A Tennessee defense verdict was returned.
_________________
$2.97M verdict after mother and baby die from urosepsis
A 27-year-old woman was pregnant with her second child. The ObGyn had delivered her first child and provided prenatal care once again. Early in the otherwise uncomplicated second pregnancy, the mother developed pyelonephritis.
At 19 weeks’ gestation, she went to the ED with abdominal pain. The hospital nurses told her ObGyn they thought she had a urinary tract infection. He concurred without seeing her, ordered antibiotics and pain medication, and she was discharged.
When her condition worsened the next day, she returned to the ED, where she was found to have urosepsis. A urogynecologist took over her care and performed emergency surgery. The fetus died during surgery. The mother went into cardiac arrest as surgery ended. She was resuscitated but suffered significant brain damage; she died 4 days later when life support was removed.
ESTATE’S CLAIM The ObGyn was negligent in not coming to the hospital to examine the patient during her initial ED visit, knowing her history of pyelonephritis. The patient should not have been discharged; intravenous administration of antibiotics would have allowed both mother and fetus to survive.
DEFENDANTS’ DEFENSE Admission at the first ED visit was not warranted. A 19-week-old fetus is not viable.
VERDICT Claims against the hospital resulted in a confidential settlement prior to trial. A Kentucky jury found the hospital 60% at fault and the ObGyn 40% at fault. A verdict totaling $7,440,000 was returned, although no damages were awarded for the death of the fetus. The net verdict was $2,976,000.
_________________
Endometriosis surgery: oophorectomy planned but hysterectomy done
After several weeks of abdominal pain, a 44-year-old woman saw her ObGyn, Dr. A. When the pain increased 4 days later, she saw Dr. B, Dr. A’s partner. Dr. B determined that the patient had endometriosis and scheduled surgery for 3 days later. The surgical plan was to remove one ovary.
Just before surgery, the patient had an anxiety attack. After she signed the consent form, she was administered midazolam (Versed). During the operation, Dr. B decided to perform a total hysterectomy.
PATIENT’S CLAIM Dr. B was negligent in performing total hysterectomy without proper consent. The patient was incapacitated by the anxiety attack and midazolam and was incapable of giving consent. She had hoped to become pregnant.
PHYSICIAN’S DEFENSE Hysterectomy was reasonable due to severe endometriosis. All options had been discussed during the preoperative visit. The consent form the patient signed provided for performance of other procedures as needed. The patient was fully cognizant for consent purposes after administration of midazolam, based on her history of narcotic use.
VERDICT A Tennessee defense verdict was returned.
_________________
Compartment syndrome after childbirth
At 42 weeks’ gestation, a 45-year-old woman was admitted to the hospital in labor after a failed attempt at home birth. The baby was delivered 4.5 hours after her arrival. The next day, the mother reported right shin and leg pain but was able to ambulate and flex her foot. She was offered the choice of staying in the hospital for a neurologic evaluation or being discharged with outpatient follow-up if her symptoms continued. She chose to be released.
At home, her symptoms worsened: the swelling in her leg and foot increased, she could not walk or flex her foot, and there were color changes in her leg. She returned to the ED, was found to have right leg compartment syndrome, and underwent fasciotomy. She continues to have foot drop, irregular gait, and right hip pain.
PATIENT’S CLAIM The ObGyn was negligent in the care of the patient during labor and delivery.
PHYSICIAN’S DEFENSE The case was settled during trial.
VERDICT A $3,500 Washington settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Blue, floppy, apneic baby: $3.25M settlement
When a mother went to the hospital in labor, the fetal heart-rate monitor showed a baseline of 140–150 beats per minute (bpm). When the monitor was reapplied 3.5 hours later, the baseline heart rate had risen to 160–165 bpm and demonstrated mild but persistent decelerations. Three hours later, the mother was found to have a fever of 100.5°F; antibiotics were ordered. When persistent fetal tachycardia became evident, the mother’s membranes were artificially ruptured. Thick meconium was noted. After a direct fetal lead was applied, moderate fetal distress was apparent. The mother’s fever rose and the fetus’ late decelerations and tachycardia continued. A cesarean delivery was ordered 12 hours after the mother’s arrival.
The baby was born 45 minutes later. She was blue, floppy, and apneic, with a heart rate of 50–60 bpm. Her Apgar scores were 1, 7, and 9, at 1, 5, and 10 minutes, respectively. She was found to have hypoxic ischemic encephalopathy. The child has right-sided weakness and other cognitive impairments including speech and language delays.
PARENTS’ CLAIM The attending family physician, a second-year resident, and the attending nurse were negligent in the care of the mother during labor and delivery. Cesarean delivery should have been performed earlier when the mother developed a fever and the fetus’ tachycardia was persistent.
defendants’ DEFENSE The case was settled during trial.
VERDICT A $3.25 million Massachusetts settlement was reached.
_________________
MRSA after breast augmentation: $1M verdict
A plastic surgeon performed bilateral breast augmentation surgery on a 31-year-old woman with the help of an assistant. The operation was performed at the physician’s office. The patient was given lidocaine, diazepam (Valium), and acetaminophen and oxycodone (Percocet) as anesthetics. General anesthesia was not administered. Two 4-inch incisions were created to insert the implants.
A month later, the patient went to the emergency department (ED) reporting chest pain. She was found to have methicillin-resistant Staphylococcus aureus (MRSA) infection. She was hospitalized for 6 days.
A month later, she returned to the ED with continuing symptoms. Another surgeon removed the breast implants. A peripherally inserted central catheter (PICC) line was placed for administration of antibiotics to treat the ongoing infection. After several months, she was infection-free.
PATIENT’S CLAIM The initial breast augmentation surgery should have been conducted under sterile conditions in a surgical center under general anesthesia. The assistant was not a licensed nurse or surgical technician.
DEFENDANTS’ DEFENSE The infection is a known risk of the procedure. Sulfamethoxazole/trimethoprim (Bactrim) had been prescribed. The plastic surgeon was not given the chance to treat the infection, as the patient went to the ED instead of calling him and changed physicians.
VERDICT A $1 million Georgia verdict was returned.
_________________
Respiratory arrest after pain meds administered
A 53-year-old woman underwent gynecologic surgery. In the recovery room, a Certified Registered Nurse Anesthetist (CRNA) administered intravenous hydromorphone hydrochloride (Dilaudid HP) 2 mg for pain management. The patient went into respiratory arrest. She was resuscitated, but experienced an hypoxic brain injury. She is now legally blind and has memory deficits and confusion.
PATIENT’S CLAIM The CRNA gave an excessive dose of hydromorphone to the patient.
DEFENDANTS’ DEFENSE The dosage was appropriate. Respiratory arrest is a risk of the surgery that can occur without negligence.
VERDICT A Tennessee defense verdict was returned.
_________________
$2.97M verdict after mother and baby die from urosepsis
A 27-year-old woman was pregnant with her second child. The ObGyn had delivered her first child and provided prenatal care once again. Early in the otherwise uncomplicated second pregnancy, the mother developed pyelonephritis.
At 19 weeks’ gestation, she went to the ED with abdominal pain. The hospital nurses told her ObGyn they thought she had a urinary tract infection. He concurred without seeing her, ordered antibiotics and pain medication, and she was discharged.
When her condition worsened the next day, she returned to the ED, where she was found to have urosepsis. A urogynecologist took over her care and performed emergency surgery. The fetus died during surgery. The mother went into cardiac arrest as surgery ended. She was resuscitated but suffered significant brain damage; she died 4 days later when life support was removed.
ESTATE’S CLAIM The ObGyn was negligent in not coming to the hospital to examine the patient during her initial ED visit, knowing her history of pyelonephritis. The patient should not have been discharged; intravenous administration of antibiotics would have allowed both mother and fetus to survive.
DEFENDANTS’ DEFENSE Admission at the first ED visit was not warranted. A 19-week-old fetus is not viable.
VERDICT Claims against the hospital resulted in a confidential settlement prior to trial. A Kentucky jury found the hospital 60% at fault and the ObGyn 40% at fault. A verdict totaling $7,440,000 was returned, although no damages were awarded for the death of the fetus. The net verdict was $2,976,000.
_________________
Endometriosis surgery: oophorectomy planned but hysterectomy done
After several weeks of abdominal pain, a 44-year-old woman saw her ObGyn, Dr. A. When the pain increased 4 days later, she saw Dr. B, Dr. A’s partner. Dr. B determined that the patient had endometriosis and scheduled surgery for 3 days later. The surgical plan was to remove one ovary.
Just before surgery, the patient had an anxiety attack. After she signed the consent form, she was administered midazolam (Versed). During the operation, Dr. B decided to perform a total hysterectomy.
PATIENT’S CLAIM Dr. B was negligent in performing total hysterectomy without proper consent. The patient was incapacitated by the anxiety attack and midazolam and was incapable of giving consent. She had hoped to become pregnant.
PHYSICIAN’S DEFENSE Hysterectomy was reasonable due to severe endometriosis. All options had been discussed during the preoperative visit. The consent form the patient signed provided for performance of other procedures as needed. The patient was fully cognizant for consent purposes after administration of midazolam, based on her history of narcotic use.
VERDICT A Tennessee defense verdict was returned.
_________________
Compartment syndrome after childbirth
At 42 weeks’ gestation, a 45-year-old woman was admitted to the hospital in labor after a failed attempt at home birth. The baby was delivered 4.5 hours after her arrival. The next day, the mother reported right shin and leg pain but was able to ambulate and flex her foot. She was offered the choice of staying in the hospital for a neurologic evaluation or being discharged with outpatient follow-up if her symptoms continued. She chose to be released.
At home, her symptoms worsened: the swelling in her leg and foot increased, she could not walk or flex her foot, and there were color changes in her leg. She returned to the ED, was found to have right leg compartment syndrome, and underwent fasciotomy. She continues to have foot drop, irregular gait, and right hip pain.
PATIENT’S CLAIM The ObGyn was negligent in the care of the patient during labor and delivery.
PHYSICIAN’S DEFENSE The case was settled during trial.
VERDICT A $3,500 Washington settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.

Pain Out of Proportion to a Fracture
A 57-year-old woman sustained an injury to her left shoulder during a fall down stairs. She presented to the emergency department, where a physician ordered x-rays that a radiologist interpreted as depicting a simple fracture.
The patient claimed that the radiologist misread the x-rays and that the emergency medicine (EM) physician failed to realize her pain was out of proportion to a fracture. She said the EM physician should have ordered additional tests and sought a radiologic consult. The patient contended that she had actually dislocated her shoulder and that the delay in treatment caused her condition to worsen, leaving her unable to use her left hand.
In addition to the radiologist and the EM physician, two nurses were named as defendants. The plaintiff maintained that they had failed to notify the physician when her condition deteriorated.
OUTCOME
A $2.75 million settlement was reached. The hospital, the EM physician, and the nurses were responsible for $1.5 million and the radiologist, $1.25 million.
Continue for David M. Lang's comments >>
COMMENT
Although complex regional pain syndrome (CRPS, formerly known as reflex sympathetic dystrophy) is not specifically mentioned in this case synopsis, the size of the settlement suggests that it was likely claimed as the resulting injury. CRPS is frequently a source of litigation.
Relatively minor trauma can lead to CRPS; why only certain patients subsequently develop the syndrome, however, is a mystery. What is certain is that CRPS is recognized as one of the most painful conditions known to humankind. Once it develops, the syndrome can result in constant, debilitating pain, the loss of a limb, and near-total decay of a patient’s quality of life.
Plaintiffs’ attorneys are quick to claim negligence and substantial damages for these patients, with their sad, compelling stories. Because the underlying pathophysiology of CRPS is unclear, liability is often hotly debated, with cases difficult to defend.
Malpractice cases generally involve two elements: liability (the presence and magnitude of the error) and damages (the severity of the injury and impact on life). CRPS cases are often considered “damages” cases, because while liability may be uncertain, the patient’s damages are very clear. An understandingly sympathetic jury panel sees the unfortunate patient’s red, swollen, misshapen limb, hears the story of the patient’s ever-present, exquisite pain, and (based largely on human emotion) infers negligence based on the magnitude of the patient’s suffering.
In this case, the patient sustained a shoulder injury in a fall that was initially treated as a fracture (presumptively proximal) but later determined to be a dislocation. Management of the injury was not described, but we can assume that if a fracture was diagnosed, the shoulder joint was immobilized. The plaintiff did not claim that there were any diminished neurovascular findings at the time of injury. We are not told whether follow-up was arranged for the patient, what the final, full diagnosis was (eg, fracture/anterior dislocation of the proximal humerus), or when/if the shoulder was actively reduced.
Under these circumstances, what could a bedside clinician have done differently? The most prominent element is the report of “pain out of proportion to the diagnosis.” When confronted with pain that seems out of proportion to a limb injury, stop and review the case. Be sure to consider occult or evolving neurovascular injury (eg, compartment syndrome, brachial plexus injury). Seek consultation and a second opinion in cases involving pain that seems intractable and out of proportion.
One quick word about pain and drug-seeking behavior. Many of us are all too familiar with patients who overstate their symptoms to obtain narcotic pain medications. Will you encounter drug seekers who embellish their level of pain to obtain narcotics? You know the answer to that question.
But it is necessary to take an injured patient’s claim of pain as stated. Don’t view yourself as “wrong” or “fooled” if patients misstate their level of pain and you respond accordingly. In many cases, there is no way to differentiate between genuine manifestations of pain and gamesmanship. To attempt to do so is dangerous because it may lead you to dismiss a patient with genuine pain for fear of being “fooled.” Don’t. Few situations will irritate a jury more than a patient with genuine pathology who is wrongly considered a “drug seeker.” Take patients at face value and act appropriately if substance misuse is later discovered.
In this case, recognition of out-of-control pain may have resulted in an orthopedic consultation. At minimum, that would demonstrate that the patient’s pain was taken seriously and the clinicians acted with due concern for her. —DML
A 57-year-old woman sustained an injury to her left shoulder during a fall down stairs. She presented to the emergency department, where a physician ordered x-rays that a radiologist interpreted as depicting a simple fracture.
The patient claimed that the radiologist misread the x-rays and that the emergency medicine (EM) physician failed to realize her pain was out of proportion to a fracture. She said the EM physician should have ordered additional tests and sought a radiologic consult. The patient contended that she had actually dislocated her shoulder and that the delay in treatment caused her condition to worsen, leaving her unable to use her left hand.
In addition to the radiologist and the EM physician, two nurses were named as defendants. The plaintiff maintained that they had failed to notify the physician when her condition deteriorated.
OUTCOME
A $2.75 million settlement was reached. The hospital, the EM physician, and the nurses were responsible for $1.5 million and the radiologist, $1.25 million.
Continue for David M. Lang's comments >>
COMMENT
Although complex regional pain syndrome (CRPS, formerly known as reflex sympathetic dystrophy) is not specifically mentioned in this case synopsis, the size of the settlement suggests that it was likely claimed as the resulting injury. CRPS is frequently a source of litigation.
Relatively minor trauma can lead to CRPS; why only certain patients subsequently develop the syndrome, however, is a mystery. What is certain is that CRPS is recognized as one of the most painful conditions known to humankind. Once it develops, the syndrome can result in constant, debilitating pain, the loss of a limb, and near-total decay of a patient’s quality of life.
Plaintiffs’ attorneys are quick to claim negligence and substantial damages for these patients, with their sad, compelling stories. Because the underlying pathophysiology of CRPS is unclear, liability is often hotly debated, with cases difficult to defend.
Malpractice cases generally involve two elements: liability (the presence and magnitude of the error) and damages (the severity of the injury and impact on life). CRPS cases are often considered “damages” cases, because while liability may be uncertain, the patient’s damages are very clear. An understandingly sympathetic jury panel sees the unfortunate patient’s red, swollen, misshapen limb, hears the story of the patient’s ever-present, exquisite pain, and (based largely on human emotion) infers negligence based on the magnitude of the patient’s suffering.
In this case, the patient sustained a shoulder injury in a fall that was initially treated as a fracture (presumptively proximal) but later determined to be a dislocation. Management of the injury was not described, but we can assume that if a fracture was diagnosed, the shoulder joint was immobilized. The plaintiff did not claim that there were any diminished neurovascular findings at the time of injury. We are not told whether follow-up was arranged for the patient, what the final, full diagnosis was (eg, fracture/anterior dislocation of the proximal humerus), or when/if the shoulder was actively reduced.
Under these circumstances, what could a bedside clinician have done differently? The most prominent element is the report of “pain out of proportion to the diagnosis.” When confronted with pain that seems out of proportion to a limb injury, stop and review the case. Be sure to consider occult or evolving neurovascular injury (eg, compartment syndrome, brachial plexus injury). Seek consultation and a second opinion in cases involving pain that seems intractable and out of proportion.
One quick word about pain and drug-seeking behavior. Many of us are all too familiar with patients who overstate their symptoms to obtain narcotic pain medications. Will you encounter drug seekers who embellish their level of pain to obtain narcotics? You know the answer to that question.
But it is necessary to take an injured patient’s claim of pain as stated. Don’t view yourself as “wrong” or “fooled” if patients misstate their level of pain and you respond accordingly. In many cases, there is no way to differentiate between genuine manifestations of pain and gamesmanship. To attempt to do so is dangerous because it may lead you to dismiss a patient with genuine pain for fear of being “fooled.” Don’t. Few situations will irritate a jury more than a patient with genuine pathology who is wrongly considered a “drug seeker.” Take patients at face value and act appropriately if substance misuse is later discovered.
In this case, recognition of out-of-control pain may have resulted in an orthopedic consultation. At minimum, that would demonstrate that the patient’s pain was taken seriously and the clinicians acted with due concern for her. —DML
A 57-year-old woman sustained an injury to her left shoulder during a fall down stairs. She presented to the emergency department, where a physician ordered x-rays that a radiologist interpreted as depicting a simple fracture.
The patient claimed that the radiologist misread the x-rays and that the emergency medicine (EM) physician failed to realize her pain was out of proportion to a fracture. She said the EM physician should have ordered additional tests and sought a radiologic consult. The patient contended that she had actually dislocated her shoulder and that the delay in treatment caused her condition to worsen, leaving her unable to use her left hand.
In addition to the radiologist and the EM physician, two nurses were named as defendants. The plaintiff maintained that they had failed to notify the physician when her condition deteriorated.
OUTCOME
A $2.75 million settlement was reached. The hospital, the EM physician, and the nurses were responsible for $1.5 million and the radiologist, $1.25 million.
Continue for David M. Lang's comments >>
COMMENT
Although complex regional pain syndrome (CRPS, formerly known as reflex sympathetic dystrophy) is not specifically mentioned in this case synopsis, the size of the settlement suggests that it was likely claimed as the resulting injury. CRPS is frequently a source of litigation.
Relatively minor trauma can lead to CRPS; why only certain patients subsequently develop the syndrome, however, is a mystery. What is certain is that CRPS is recognized as one of the most painful conditions known to humankind. Once it develops, the syndrome can result in constant, debilitating pain, the loss of a limb, and near-total decay of a patient’s quality of life.
Plaintiffs’ attorneys are quick to claim negligence and substantial damages for these patients, with their sad, compelling stories. Because the underlying pathophysiology of CRPS is unclear, liability is often hotly debated, with cases difficult to defend.
Malpractice cases generally involve two elements: liability (the presence and magnitude of the error) and damages (the severity of the injury and impact on life). CRPS cases are often considered “damages” cases, because while liability may be uncertain, the patient’s damages are very clear. An understandingly sympathetic jury panel sees the unfortunate patient’s red, swollen, misshapen limb, hears the story of the patient’s ever-present, exquisite pain, and (based largely on human emotion) infers negligence based on the magnitude of the patient’s suffering.
In this case, the patient sustained a shoulder injury in a fall that was initially treated as a fracture (presumptively proximal) but later determined to be a dislocation. Management of the injury was not described, but we can assume that if a fracture was diagnosed, the shoulder joint was immobilized. The plaintiff did not claim that there were any diminished neurovascular findings at the time of injury. We are not told whether follow-up was arranged for the patient, what the final, full diagnosis was (eg, fracture/anterior dislocation of the proximal humerus), or when/if the shoulder was actively reduced.
Under these circumstances, what could a bedside clinician have done differently? The most prominent element is the report of “pain out of proportion to the diagnosis.” When confronted with pain that seems out of proportion to a limb injury, stop and review the case. Be sure to consider occult or evolving neurovascular injury (eg, compartment syndrome, brachial plexus injury). Seek consultation and a second opinion in cases involving pain that seems intractable and out of proportion.
One quick word about pain and drug-seeking behavior. Many of us are all too familiar with patients who overstate their symptoms to obtain narcotic pain medications. Will you encounter drug seekers who embellish their level of pain to obtain narcotics? You know the answer to that question.
But it is necessary to take an injured patient’s claim of pain as stated. Don’t view yourself as “wrong” or “fooled” if patients misstate their level of pain and you respond accordingly. In many cases, there is no way to differentiate between genuine manifestations of pain and gamesmanship. To attempt to do so is dangerous because it may lead you to dismiss a patient with genuine pain for fear of being “fooled.” Don’t. Few situations will irritate a jury more than a patient with genuine pathology who is wrongly considered a “drug seeker.” Take patients at face value and act appropriately if substance misuse is later discovered.
In this case, recognition of out-of-control pain may have resulted in an orthopedic consultation. At minimum, that would demonstrate that the patient’s pain was taken seriously and the clinicians acted with due concern for her. —DML
Vicarious liability. First of 2 Parts: The gynecologist who wore an unusual pen
What obligations do physicians and medical facilities have when it comes to dealing with troubled or troublesome clinicians? In this 2-part column, we look at a recently reported case of a gynecologist who engaged in serious misconduct without being noticed. In part 2, we will discuss the obligation of the medical profession to notice and deal with colleagues who are creating a risk to patients or the institution.
CASE: Medical center blamed for negligence when rogue physician records pelvic exams
Dr. A, a gynecologist, had been a physician at a leading academic medical center for many years. His employment was terminated in February 2013 when he admitted taking more than 1,000 videos and images using a tiny camera embedded in a pen or key fob that he wore around his neck. He stored the images on his home computer. It seems that he had been secretly recording pelvic examinations since 2005.
A class-action lawsuit initiated against the academic medical center and the physician suggested invasion of privacy, emotional distress, and negligence in oversight on the part of the academic institution. (This case was settled before trial and most of the records are not publicly available. The facts used here are based on press releases and published articles and, therefore, are incomplete and may be subject to interpretation.)
Breach of trust
Talk about a violation of the doctor-patient relationship! The suit claims, among other things, “harmful and offensive sexual contact with patients.” The hospital identified 12,700 patients that the gynecologist might have seen during his 25-year-span as an employee.
Some victims report posttraumatic stress disorder (PTSD). In addition to feeling betrayed by their physician, the victims feel the action was a breach of faith, of trust. They report being fearful of being examined by another physician, and some have refused to seek medical care. The sense of mistrust of the medical profession has resulted in some victims’ reluctance to allow their children to be seen by pediatricians.1
CASE: SETTLED
This lawsuit, possibly the largest medical malpractice case of its kind, resulted in a $190 million settlement. The academic medical center will disperse the funds to more than 7,000 possible victims.1 A special hotline Web site and a toll-free number have been established to facilitate victim reporting. A board-certified psychologist will work with victims.
Similar suits have settled
Other lawsuits involving physicians who have secretly recorded patients also have been settled:
- A Connecticut endocrinologist who took photos of patients nude settled for $50 million in 2012.1
- A pediatrician pedophile in Delaware was associated with a $123-million settlement with long-term follow-up of victims.2
WHAT ARE THE ETHICAL OBLIGATIONS?
Ethics in medicine can be discussed at great length (see “Issues of ethics in medicine”). An important question related to this case concerns the investigators’ obligations to make their findings public with the scenario that the patient/victims are not aware that a crime occurred.3 This is among the issues that will be considered in part 2 of this article that will be published next month. One concern is that publicly identifying the victims may lead to the development of PTSD and its intrinsic consequences. How can one prosecute the perpetrator and yet prevent psychological consequences of the victims?
What do ACOG and the AMA say about sexual misconduct in medicine?
ACOG. The American College of Obstetricians and Gynecologists (ACOG) is explicit about sexual misconduct. Specifically, the physician-patient relationship can be damaged when there is “confusion regarding professional roles and behavior or clear lack of integrity”1 that results in sexual exploitation and harm. ACOG further states that1:
- Mere mutual consent is rejected as a justification for sexual relations with patients because the disparity in power, status, vulnerability, and need make it difficult for a patient to give meaningful consent to sexual contact or sexual relations.
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances. The relevant standard is the potential for misuse of physician power and exploitation of patient emotions derived from the former relationship.
- Education on ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- Physicians have a responsibility to report offending colleagues to disciplinary boards.
The request by either a patient or a physician to have a chaperone present during a physical examination should be accommodated regardless of the physician’s sex. If a chaperone is present during the physical examination, the physician should provide a separate opportunity for private conversation.
The AMA. The American Medical Association’s Council on Ethical and Judicial Affairs developed a report titled “Sexual Misconduct in the Practice of Medicine.” The Council concluded that2:
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances.
- Education on the ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- In the case of sexual misconduct, reporting offending colleagues is especially important.
References
- Committee on Ethics. ACOG Committee Opinion No. 373. Sexual misconduct. http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Ethics/Sexual-Misconduct. Published August 2007. Accessed November 11, 2014.
- McMurray RJ, Clarke OW, Barrasso JA, et al; Council on Ethical and Judicial Affairs. Sexual misconduct in the practice of medicine. JAMA. 1991;266(19):2741–2745. http://jama.jamanetwork.com/article.aspx?articleid=393342&resultClick=3. Accessed November 11, 2014.
UNUSUAL ELEMENTS OF THIS CASE
The case of “The gynecologist who wore an unusual pen” is extraordinary in terms of the financial consequences for the medical center. Indeed, the $190 million class-action settlement is probably a record in cases of this kind. The facts (insofar as we know them, and we certainly do not know them all) are sufficiently unusual to seem more like fiction than reality.
An unusual element of the case is that the images were apparently not shared with others, but retained by the gynecologist. Thus, the $190 million settlement was not for disclosing confidential information, but for the unauthorized and inappropriate act of taking the videos and storing them at home. This case was a violation of professional obligations and clearly unethical and likely illegal. It was not associated with the distribution of images that is so often the hallmark of breach of privacy cases.
Another very unusual condition of this case was that there was no way to identify the victims. The faces of the women were not in the videos, so the subjects of the 1,200 videos and 140 images found on the physician’s home computer could have been any of more than 7,000 patients.1 The distribution of funds, therefore, may encompass all of these former patients, and the size of an individual’s recovery may depend largely on the degree of emotional upset she experiences. The victims will be asked how much time they spent with the physician, whether a nurse was present, whether there was any verbal or sexual abuse, and details about emotional harm they experienced.
VICARIOUS LIABILITY
Why was the medical center responsible?
At first blush it may seem puzzling that the medical center, rather than the gynecologist, was responsible for the damages. In fact, the gynecologist might well have been both criminally and civilly responsible, but sadly, he committed suicide after his wrongdoing was discovered.3
The hospital was civilly responsible. In this instance it appears (again, from our limited facts) that the gynecologist was an employee of the medical center. Employees are generally considered agents of their employers (“principals”). By definition, a principal has the right and obligation to oversee and control the actions of its agents. As such, the principal is generally legally liable for the actions of an employee within the course of employment. Vicarious liability essentially allows someone harmed by an agent to seek compensation from the principal because the principal selected and appointed the agent.
The vicarious responsibility of an agency relationship applies even when the employee is not following the direct instructions of the employer. For example, even if a trucking company tells its employee, “Do not drink at all and do not drive over the speed limit for any reason,” the company can still be liable when an employee becomes drunk or speeds and causes an accident. At some point, however, the employee may so deviate from tasks related to employment that the employee is off on a “lark of his own.” For example, if the driver is supposed to travel from New York City to Buffalo, but instead takes a personal side trip to Baltimore, where the truck hits a pedestrian, that side trip is probably not the responsibility of the employer.
Applying these principles to this case (assuming the physician was an employee of the medical center), the center would generally be legally responsible for the torts (wrongful acts) of the gynecologist. Now you ask, “what about the ‘lark of his own’? Wasn’t taking all those pictures and videos for his own purposes not really part of the job?” (Now you are thinking like a lawyer—that was meant as a compliment.) It is a good question. First, this involved serious misconduct, which was a violation of basic professional ethics. Second, this videotaping was not part of the job the physician was supposed to be doing. Although it may have been for his own benefit, this deviation of good practice was closely related to and entangled with the purpose of his employment. It is perhaps analogous to the truck driver who drank at lunch and then caused the accident. It made sense, therefore, for the medical center to conclude that it would likely be responsible for the actions of this employee, and settle the case.
As a side note, this vicarious liability does not just apply to medical centers. Physicians have agents in their offices (employees: nurses, interns, and even volunteers). Your medical practice is likely responsible for the actions of your staff members via the concept of vicarious liability.
In hospitals, it is common for physicians to have staff privileges without being employees. Would this case have a different result if the physician had staff privileges but was not an employee? Another good question. We are going to look at that in the next installment—and the answer has significant implications for physicians and nurses as well as for medical facilities.
We want to hear from you! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
- Gabriel T. Hospital agrees to pay $190 million over recording of pelvic exams. http://www.nytimes.com/2014/07/22/us/johns-hopkins-settlement-190-million.html?_r=0. Published July 21, 2014. Accessed November 11, 2014.
- Doe v. Bradley, 64 A.3d 379 (Del. Super. Ct. 2012). http://capegazette.villagesoup.com/media/Common/11/3A/735985/bradley-settlement-opinion.pdf. Accessed November 24, 2014.
- Klosterman C. Should unwitting victims be informed of the crime? NY Times Magazine. http://www.nytimes.com/2014/08/17/magazine/should-unwitting-victims-be-informed-of-the-crime.html. Published August 17, 2014. Accessed November 11, 2014.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
What obligations do physicians and medical facilities have when it comes to dealing with troubled or troublesome clinicians? In this 2-part column, we look at a recently reported case of a gynecologist who engaged in serious misconduct without being noticed. In part 2, we will discuss the obligation of the medical profession to notice and deal with colleagues who are creating a risk to patients or the institution.
CASE: Medical center blamed for negligence when rogue physician records pelvic exams
Dr. A, a gynecologist, had been a physician at a leading academic medical center for many years. His employment was terminated in February 2013 when he admitted taking more than 1,000 videos and images using a tiny camera embedded in a pen or key fob that he wore around his neck. He stored the images on his home computer. It seems that he had been secretly recording pelvic examinations since 2005.
A class-action lawsuit initiated against the academic medical center and the physician suggested invasion of privacy, emotional distress, and negligence in oversight on the part of the academic institution. (This case was settled before trial and most of the records are not publicly available. The facts used here are based on press releases and published articles and, therefore, are incomplete and may be subject to interpretation.)
Breach of trust
Talk about a violation of the doctor-patient relationship! The suit claims, among other things, “harmful and offensive sexual contact with patients.” The hospital identified 12,700 patients that the gynecologist might have seen during his 25-year-span as an employee.
Some victims report posttraumatic stress disorder (PTSD). In addition to feeling betrayed by their physician, the victims feel the action was a breach of faith, of trust. They report being fearful of being examined by another physician, and some have refused to seek medical care. The sense of mistrust of the medical profession has resulted in some victims’ reluctance to allow their children to be seen by pediatricians.1
CASE: SETTLED
This lawsuit, possibly the largest medical malpractice case of its kind, resulted in a $190 million settlement. The academic medical center will disperse the funds to more than 7,000 possible victims.1 A special hotline Web site and a toll-free number have been established to facilitate victim reporting. A board-certified psychologist will work with victims.
Similar suits have settled
Other lawsuits involving physicians who have secretly recorded patients also have been settled:
- A Connecticut endocrinologist who took photos of patients nude settled for $50 million in 2012.1
- A pediatrician pedophile in Delaware was associated with a $123-million settlement with long-term follow-up of victims.2
WHAT ARE THE ETHICAL OBLIGATIONS?
Ethics in medicine can be discussed at great length (see “Issues of ethics in medicine”). An important question related to this case concerns the investigators’ obligations to make their findings public with the scenario that the patient/victims are not aware that a crime occurred.3 This is among the issues that will be considered in part 2 of this article that will be published next month. One concern is that publicly identifying the victims may lead to the development of PTSD and its intrinsic consequences. How can one prosecute the perpetrator and yet prevent psychological consequences of the victims?
What do ACOG and the AMA say about sexual misconduct in medicine?
ACOG. The American College of Obstetricians and Gynecologists (ACOG) is explicit about sexual misconduct. Specifically, the physician-patient relationship can be damaged when there is “confusion regarding professional roles and behavior or clear lack of integrity”1 that results in sexual exploitation and harm. ACOG further states that1:
- Mere mutual consent is rejected as a justification for sexual relations with patients because the disparity in power, status, vulnerability, and need make it difficult for a patient to give meaningful consent to sexual contact or sexual relations.
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances. The relevant standard is the potential for misuse of physician power and exploitation of patient emotions derived from the former relationship.
- Education on ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- Physicians have a responsibility to report offending colleagues to disciplinary boards.
The request by either a patient or a physician to have a chaperone present during a physical examination should be accommodated regardless of the physician’s sex. If a chaperone is present during the physical examination, the physician should provide a separate opportunity for private conversation.
The AMA. The American Medical Association’s Council on Ethical and Judicial Affairs developed a report titled “Sexual Misconduct in the Practice of Medicine.” The Council concluded that2:
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances.
- Education on the ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- In the case of sexual misconduct, reporting offending colleagues is especially important.
References
- Committee on Ethics. ACOG Committee Opinion No. 373. Sexual misconduct. http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Ethics/Sexual-Misconduct. Published August 2007. Accessed November 11, 2014.
- McMurray RJ, Clarke OW, Barrasso JA, et al; Council on Ethical and Judicial Affairs. Sexual misconduct in the practice of medicine. JAMA. 1991;266(19):2741–2745. http://jama.jamanetwork.com/article.aspx?articleid=393342&resultClick=3. Accessed November 11, 2014.
UNUSUAL ELEMENTS OF THIS CASE
The case of “The gynecologist who wore an unusual pen” is extraordinary in terms of the financial consequences for the medical center. Indeed, the $190 million class-action settlement is probably a record in cases of this kind. The facts (insofar as we know them, and we certainly do not know them all) are sufficiently unusual to seem more like fiction than reality.
An unusual element of the case is that the images were apparently not shared with others, but retained by the gynecologist. Thus, the $190 million settlement was not for disclosing confidential information, but for the unauthorized and inappropriate act of taking the videos and storing them at home. This case was a violation of professional obligations and clearly unethical and likely illegal. It was not associated with the distribution of images that is so often the hallmark of breach of privacy cases.
Another very unusual condition of this case was that there was no way to identify the victims. The faces of the women were not in the videos, so the subjects of the 1,200 videos and 140 images found on the physician’s home computer could have been any of more than 7,000 patients.1 The distribution of funds, therefore, may encompass all of these former patients, and the size of an individual’s recovery may depend largely on the degree of emotional upset she experiences. The victims will be asked how much time they spent with the physician, whether a nurse was present, whether there was any verbal or sexual abuse, and details about emotional harm they experienced.
VICARIOUS LIABILITY
Why was the medical center responsible?
At first blush it may seem puzzling that the medical center, rather than the gynecologist, was responsible for the damages. In fact, the gynecologist might well have been both criminally and civilly responsible, but sadly, he committed suicide after his wrongdoing was discovered.3
The hospital was civilly responsible. In this instance it appears (again, from our limited facts) that the gynecologist was an employee of the medical center. Employees are generally considered agents of their employers (“principals”). By definition, a principal has the right and obligation to oversee and control the actions of its agents. As such, the principal is generally legally liable for the actions of an employee within the course of employment. Vicarious liability essentially allows someone harmed by an agent to seek compensation from the principal because the principal selected and appointed the agent.
The vicarious responsibility of an agency relationship applies even when the employee is not following the direct instructions of the employer. For example, even if a trucking company tells its employee, “Do not drink at all and do not drive over the speed limit for any reason,” the company can still be liable when an employee becomes drunk or speeds and causes an accident. At some point, however, the employee may so deviate from tasks related to employment that the employee is off on a “lark of his own.” For example, if the driver is supposed to travel from New York City to Buffalo, but instead takes a personal side trip to Baltimore, where the truck hits a pedestrian, that side trip is probably not the responsibility of the employer.
Applying these principles to this case (assuming the physician was an employee of the medical center), the center would generally be legally responsible for the torts (wrongful acts) of the gynecologist. Now you ask, “what about the ‘lark of his own’? Wasn’t taking all those pictures and videos for his own purposes not really part of the job?” (Now you are thinking like a lawyer—that was meant as a compliment.) It is a good question. First, this involved serious misconduct, which was a violation of basic professional ethics. Second, this videotaping was not part of the job the physician was supposed to be doing. Although it may have been for his own benefit, this deviation of good practice was closely related to and entangled with the purpose of his employment. It is perhaps analogous to the truck driver who drank at lunch and then caused the accident. It made sense, therefore, for the medical center to conclude that it would likely be responsible for the actions of this employee, and settle the case.
As a side note, this vicarious liability does not just apply to medical centers. Physicians have agents in their offices (employees: nurses, interns, and even volunteers). Your medical practice is likely responsible for the actions of your staff members via the concept of vicarious liability.
In hospitals, it is common for physicians to have staff privileges without being employees. Would this case have a different result if the physician had staff privileges but was not an employee? Another good question. We are going to look at that in the next installment—and the answer has significant implications for physicians and nurses as well as for medical facilities.
We want to hear from you! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
What obligations do physicians and medical facilities have when it comes to dealing with troubled or troublesome clinicians? In this 2-part column, we look at a recently reported case of a gynecologist who engaged in serious misconduct without being noticed. In part 2, we will discuss the obligation of the medical profession to notice and deal with colleagues who are creating a risk to patients or the institution.
CASE: Medical center blamed for negligence when rogue physician records pelvic exams
Dr. A, a gynecologist, had been a physician at a leading academic medical center for many years. His employment was terminated in February 2013 when he admitted taking more than 1,000 videos and images using a tiny camera embedded in a pen or key fob that he wore around his neck. He stored the images on his home computer. It seems that he had been secretly recording pelvic examinations since 2005.
A class-action lawsuit initiated against the academic medical center and the physician suggested invasion of privacy, emotional distress, and negligence in oversight on the part of the academic institution. (This case was settled before trial and most of the records are not publicly available. The facts used here are based on press releases and published articles and, therefore, are incomplete and may be subject to interpretation.)
Breach of trust
Talk about a violation of the doctor-patient relationship! The suit claims, among other things, “harmful and offensive sexual contact with patients.” The hospital identified 12,700 patients that the gynecologist might have seen during his 25-year-span as an employee.
Some victims report posttraumatic stress disorder (PTSD). In addition to feeling betrayed by their physician, the victims feel the action was a breach of faith, of trust. They report being fearful of being examined by another physician, and some have refused to seek medical care. The sense of mistrust of the medical profession has resulted in some victims’ reluctance to allow their children to be seen by pediatricians.1
CASE: SETTLED
This lawsuit, possibly the largest medical malpractice case of its kind, resulted in a $190 million settlement. The academic medical center will disperse the funds to more than 7,000 possible victims.1 A special hotline Web site and a toll-free number have been established to facilitate victim reporting. A board-certified psychologist will work with victims.
Similar suits have settled
Other lawsuits involving physicians who have secretly recorded patients also have been settled:
- A Connecticut endocrinologist who took photos of patients nude settled for $50 million in 2012.1
- A pediatrician pedophile in Delaware was associated with a $123-million settlement with long-term follow-up of victims.2
WHAT ARE THE ETHICAL OBLIGATIONS?
Ethics in medicine can be discussed at great length (see “Issues of ethics in medicine”). An important question related to this case concerns the investigators’ obligations to make their findings public with the scenario that the patient/victims are not aware that a crime occurred.3 This is among the issues that will be considered in part 2 of this article that will be published next month. One concern is that publicly identifying the victims may lead to the development of PTSD and its intrinsic consequences. How can one prosecute the perpetrator and yet prevent psychological consequences of the victims?
What do ACOG and the AMA say about sexual misconduct in medicine?
ACOG. The American College of Obstetricians and Gynecologists (ACOG) is explicit about sexual misconduct. Specifically, the physician-patient relationship can be damaged when there is “confusion regarding professional roles and behavior or clear lack of integrity”1 that results in sexual exploitation and harm. ACOG further states that1:
- Mere mutual consent is rejected as a justification for sexual relations with patients because the disparity in power, status, vulnerability, and need make it difficult for a patient to give meaningful consent to sexual contact or sexual relations.
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances. The relevant standard is the potential for misuse of physician power and exploitation of patient emotions derived from the former relationship.
- Education on ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- Physicians have a responsibility to report offending colleagues to disciplinary boards.
The request by either a patient or a physician to have a chaperone present during a physical examination should be accommodated regardless of the physician’s sex. If a chaperone is present during the physical examination, the physician should provide a separate opportunity for private conversation.
The AMA. The American Medical Association’s Council on Ethical and Judicial Affairs developed a report titled “Sexual Misconduct in the Practice of Medicine.” The Council concluded that2:
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances.
- Education on the ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- In the case of sexual misconduct, reporting offending colleagues is especially important.
References
- Committee on Ethics. ACOG Committee Opinion No. 373. Sexual misconduct. http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Ethics/Sexual-Misconduct. Published August 2007. Accessed November 11, 2014.
- McMurray RJ, Clarke OW, Barrasso JA, et al; Council on Ethical and Judicial Affairs. Sexual misconduct in the practice of medicine. JAMA. 1991;266(19):2741–2745. http://jama.jamanetwork.com/article.aspx?articleid=393342&resultClick=3. Accessed November 11, 2014.
UNUSUAL ELEMENTS OF THIS CASE
The case of “The gynecologist who wore an unusual pen” is extraordinary in terms of the financial consequences for the medical center. Indeed, the $190 million class-action settlement is probably a record in cases of this kind. The facts (insofar as we know them, and we certainly do not know them all) are sufficiently unusual to seem more like fiction than reality.
An unusual element of the case is that the images were apparently not shared with others, but retained by the gynecologist. Thus, the $190 million settlement was not for disclosing confidential information, but for the unauthorized and inappropriate act of taking the videos and storing them at home. This case was a violation of professional obligations and clearly unethical and likely illegal. It was not associated with the distribution of images that is so often the hallmark of breach of privacy cases.
Another very unusual condition of this case was that there was no way to identify the victims. The faces of the women were not in the videos, so the subjects of the 1,200 videos and 140 images found on the physician’s home computer could have been any of more than 7,000 patients.1 The distribution of funds, therefore, may encompass all of these former patients, and the size of an individual’s recovery may depend largely on the degree of emotional upset she experiences. The victims will be asked how much time they spent with the physician, whether a nurse was present, whether there was any verbal or sexual abuse, and details about emotional harm they experienced.
VICARIOUS LIABILITY
Why was the medical center responsible?
At first blush it may seem puzzling that the medical center, rather than the gynecologist, was responsible for the damages. In fact, the gynecologist might well have been both criminally and civilly responsible, but sadly, he committed suicide after his wrongdoing was discovered.3
The hospital was civilly responsible. In this instance it appears (again, from our limited facts) that the gynecologist was an employee of the medical center. Employees are generally considered agents of their employers (“principals”). By definition, a principal has the right and obligation to oversee and control the actions of its agents. As such, the principal is generally legally liable for the actions of an employee within the course of employment. Vicarious liability essentially allows someone harmed by an agent to seek compensation from the principal because the principal selected and appointed the agent.
The vicarious responsibility of an agency relationship applies even when the employee is not following the direct instructions of the employer. For example, even if a trucking company tells its employee, “Do not drink at all and do not drive over the speed limit for any reason,” the company can still be liable when an employee becomes drunk or speeds and causes an accident. At some point, however, the employee may so deviate from tasks related to employment that the employee is off on a “lark of his own.” For example, if the driver is supposed to travel from New York City to Buffalo, but instead takes a personal side trip to Baltimore, where the truck hits a pedestrian, that side trip is probably not the responsibility of the employer.
Applying these principles to this case (assuming the physician was an employee of the medical center), the center would generally be legally responsible for the torts (wrongful acts) of the gynecologist. Now you ask, “what about the ‘lark of his own’? Wasn’t taking all those pictures and videos for his own purposes not really part of the job?” (Now you are thinking like a lawyer—that was meant as a compliment.) It is a good question. First, this involved serious misconduct, which was a violation of basic professional ethics. Second, this videotaping was not part of the job the physician was supposed to be doing. Although it may have been for his own benefit, this deviation of good practice was closely related to and entangled with the purpose of his employment. It is perhaps analogous to the truck driver who drank at lunch and then caused the accident. It made sense, therefore, for the medical center to conclude that it would likely be responsible for the actions of this employee, and settle the case.
As a side note, this vicarious liability does not just apply to medical centers. Physicians have agents in their offices (employees: nurses, interns, and even volunteers). Your medical practice is likely responsible for the actions of your staff members via the concept of vicarious liability.
In hospitals, it is common for physicians to have staff privileges without being employees. Would this case have a different result if the physician had staff privileges but was not an employee? Another good question. We are going to look at that in the next installment—and the answer has significant implications for physicians and nurses as well as for medical facilities.
We want to hear from you! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
- Gabriel T. Hospital agrees to pay $190 million over recording of pelvic exams. http://www.nytimes.com/2014/07/22/us/johns-hopkins-settlement-190-million.html?_r=0. Published July 21, 2014. Accessed November 11, 2014.
- Doe v. Bradley, 64 A.3d 379 (Del. Super. Ct. 2012). http://capegazette.villagesoup.com/media/Common/11/3A/735985/bradley-settlement-opinion.pdf. Accessed November 24, 2014.
- Klosterman C. Should unwitting victims be informed of the crime? NY Times Magazine. http://www.nytimes.com/2014/08/17/magazine/should-unwitting-victims-be-informed-of-the-crime.html. Published August 17, 2014. Accessed November 11, 2014.
- Gabriel T. Hospital agrees to pay $190 million over recording of pelvic exams. http://www.nytimes.com/2014/07/22/us/johns-hopkins-settlement-190-million.html?_r=0. Published July 21, 2014. Accessed November 11, 2014.
- Doe v. Bradley, 64 A.3d 379 (Del. Super. Ct. 2012). http://capegazette.villagesoup.com/media/Common/11/3A/735985/bradley-settlement-opinion.pdf. Accessed November 24, 2014.
- Klosterman C. Should unwitting victims be informed of the crime? NY Times Magazine. http://www.nytimes.com/2014/08/17/magazine/should-unwitting-victims-be-informed-of-the-crime.html. Published August 17, 2014. Accessed November 11, 2014.
Good, bad, and ugly: Prior authorization and medicolegal risk
Dear Dr. Mossman,
Where I practice, most health care plans won’t pay for certain medications without giving prior authorization (PA). Completing PA forms and making telephone calls take up time that could be better spent treating patients. I’m tempted to set a new policy of not doing PAs. If I do, might I face legal trouble?
Submitted by “Dr. A”
If you provide clinical care, you’ve probably dealt with third-party payers who require prior authorization (PA) before they will pay for certain treatments. Dr. A is not alone in feeling exasperated about the time it takes to complete a PA.1 After spending several hours each month waiting on hold and wading through stacks of paperwork, you may feel like Dr. A and consider refusing to do any more PAs.
But is Dr. A’s proposed solution a good idea? To address this question and the frustration that lies behind it, we’ll take a cue from Italian film director Sergio Leone and discuss:
• how PAs affect psychiatric care: the good, the bad, and the ugly
• potential exposure to professional liability and ethics complaints that might result from refusing or failing to seek PA
• strategies to reduce the burden of PAs while providing efficient, effective care.
The good
Recent decades have witnessed huge increases in spending on prescription medication. Psychotropics are no exception; state Medicaid spending for anti-psychotic medication grew from <$1 billion in 1995 to >$5.5 billion in 2005.2
Requiring a PA for expensive drugs is one way that third-party payers try to rein in costs and hold down insurance premiums. Imposing financial constraints often is just one aim of a pharmacy benefit management (PBM) program. Insurers also justify PBMs by pointing out that feedback to practitioners whose prescribing falls well outside the norm—in the form of mailed warnings, physician second opinions, or pharmacist consultation—can improve patient safety and encourage appropriate treatment options for enrolled patients.3,4 Examples of such benefits include reducing overuse of prescription opioids5 and antipsychotics among children,3 misuse of buprenorphine,6 and adverse effects from potentially inappropriate prescriptions.7
The bad
The bad news for doctors: Cost savings for payers come at the expense of providers and their practices, in the form of time spent doing paperwork and talking on the phone to complete PAs or contest PA decisions.8 Addressing PA requests costs an estimated $83,000 per physician per year. The total administrative burden for all 835,000 physicians who practice in the United States therefore is 868,000,000 hours, or $69 billion annually.9
To make matters worse, PA requirements may increase the overall cost of care. After Georgia Medicaid instituted PA requirements for second-generation antipsychotics (SGAs), average monthly per member drug costs fell $19.62, but average monthly outpatient treatment costs rose $31.59 per member.10 Pharmacy savings that result from requiring PAs for SGAs can be offset quickly by small increases in the hospitalization rate or emergency department visits.9,11
The ugly
Many physicians believe that the PA process undermines patient care by decreasing time devoted to direct patient contact, incentivizing suboptimal treatment, and limiting medication access.1,12,13 But do any data support this belief? Do PAs impede treatment for vulnerable persons with severe mental illnesses?
The answer, some studies suggest, is “Yes.” A Maine Medicaid PA policy slowed initiation of treatment for bipolar disorder by reducing the rate of starting non-preferred medications, although the same policy had no impact on patients already receiving treatment.14 Another study examined the effect of PA processes for inpatient psychiatry treatment and found that patients were less likely to be admitted on weekends, probably because PA review was not available on those days.15 A third study showed that PA requirements and resulting impediments to getting refills were correlated with medication discontinuation by patients with schizophrenia or bipolar disorder, which can increase the risk of decompensation, work-related problems, and hospitalization.16
Problems with PAs
Whether they are helpful or counterproductive, PAs are a practice reality. Dr. A’s proposed solution sounds appealing, but it might create ethical and legal problems.
Among the fundamental elements of ethical medical practice is physicians’ obligation to give patients “guidance … as to the optimal course of action” and to “advocate for patients in dealing with third parties when appropriate.”17 It’s fine for psychiatrists to consider prescribing treatments that patients’ health care coverage favors, but we also have to help patients weigh and evaluate costs, particularly when patients’ circumstances and medical interests militate strongly for options that third-party payers balk at paying for. Patients’ interests—not what’s expedient—are always physicians’ foremost concern.18
Beyond purely ethical considerations, you might face legal consequences if you refuse or fail to seek PAs for what you think is the proper medication. As Table 1 shows, one key factor is whether you are under contract with the patient’s insurance carrier; if you are, failure to seek a PA when appropriate may constitute a breach of the contract (Donna Vanderpool, written communication, October 5, 2014).
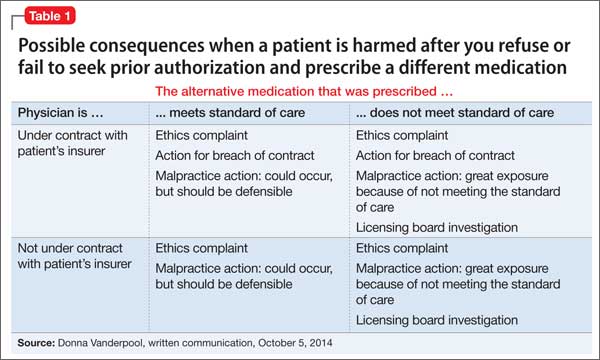
If the prescribed medication does not meet the standard of care and your patient suffers some harm, a licensing board complaint and investigation are possible. You also face exposure to a medical malpractice action. Although we do not know of any instances in which such an action has succeeded, 2 recent court decisions suggest that harm to a patient stemmed from failing to seek PA for a medication could constitute grounds for a lawsuit.19,20 Efforts to contain medical costs have been around for decades, and courts have held that physicians, third-party payers, and utilization review intermediaries are bound by “the standard of reasonable community practice”21 and should not let cost limitations “corrupt medical judgment.”22 Physicians who do not appeal limitations at odds with their medical judgment might bear responsibility for any injuries that occur.18,22
Managing PA requests
Given the inevitability of encountering PA requests and your ethical and professional obligations to help patients, what can you do (Table 29,23,27)?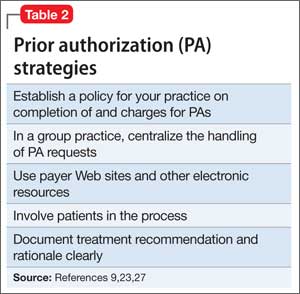
Some practitioners charge patients for time spent completing PAs.23 Although physicians should “complete without charge the appropriate ‘simplified’ insurance claim form as a part of service to the patient;” they also may consider “a charge for more complex or multiple forms … in conformity with local custom.”24 Legally, physicians’ contracts with insurance panels may preclude charging such fees, but if a patient is being seen out of network, the physician does not have a contractual obligation and may charge.9 If your practice setting lets you choose which insurances you accept, the impact and burden of seeking PAs is a factor to consider when deciding whether to participate in a particular panel.23
In an interesting twist, an Ohio physician successfully sued a medical insurance administrator for the cost of his time responding to PA inquiries.25 Reasoning that the insurance administrator “should expect to pay for the reasonable value of” the doctor’s time because the PAs “were solely intended for the benefit of the insurance administrator” or parties whom the administrator served, the judge awarded the doctor $187.50 plus 8% interest.
Considerations that are more practical relate to how to triage and address the volume of PA requests. Some large medical practices centralize PAs and try to set up pre-approved plans of care or blanket approvals for frequently encountered conditions. Centralization also allows one key administrative assistant to develop skills in processing PA requests and to build relationships with payers.26
The administrative assistant also can compile lists of preferred alternative medications, PA forms, and payer Web sites. Using and submitting requests through payer Web sites can speed up PA processing, which saves time and money.27 As electronic health records improve, they may incorporate patients’ formularies and provide automatic alerts for required PAs.23
Patients should be involved, too. They can help to obtain relevant formulary information and to weigh alternative therapies. You can help them understand your role in the PA process, the reasoning behind your treatment recommendations, and the delays in picking up prescribed medications that waiting for PA approval can create.
It’s easy to get angry about PAs
Your best response, however, is to practice prudent and—within reason— cost-effective medicine. When generic or insurer-preferred medications are clinically appropriate and meet treatment guidelines, trying them first is sensible and defensible. If your patient fails the initial low-cost treatment, or if a low-cost choice isn’t appropriate, document this clearly and seek approval for a costlier treatment.9
BOTTOM LINE
Physicians have ethical and legal obligations to advocate for their patients’ needs and best interests. This sometimes includes completing prior authorization requests. Find strategies that minimize hassle and make sense in your practice, and seek efficient ways to document the medical necessity of requested tests, procedures, or therapies.
Acknowledgment
Drs. Marett and Mossman thanks Donna Vanderpool, MBA, JD, and Annette Reynolds, MD, for their helpful input in preparing this article.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Brown CM, Richards K, Rascati KL, et al. Effects of a psychotherapeutic drug prior authorization (PA) requirement on patients and providers: a providers’ perspective. Adm Policy Ment Health. 2008;35(3):181-188.
2. Law MR, Ross-Degnan D, Soumerai SB. Effect of prior authorization of second-generation antipsychotic agents on pharmacy utilization and reimbursements. Psychiatr Serv. 2008;59(5):540-546.
3. Stein BD, Leckman-Westin E, Okeke E, et al. The effects of prior authorization policies on Medicaid-enrolled children’s use of antipsychotic medications: evidence from two Mid-Atlantic states. J Child Adolesc Psychopharmacol. 2014;24(7):374-381.
4. Adams KT. Prior authorization–still used, still an issue. Biotechnol Healthc. 2010;7(4):28.
5. Garcia MM, Angelini MC, Thomas T, et al. Implementation of an opioid management initiative by a state Medicaid program. J Manag Care Pharm. 2014;20(5):447-454.
6. Clark RE, Baxter JD, Barton BA, et al. The impact of prior authorization on buprenorphine dose, relapse rates, and cost for Massachusetts Medicaid beneficiaries with opioid dependence [published online July 9, 2014]. Health Serv Res. doi: 10.1111/1475-6773.12201.
7. Dunn RL, Harrison D, Ripley TL. The beers criteria as an outpatient screening tool for potentially inappropriate medications. Consult Pharm. 2011;26(10):754-763.
8. Lennertz MD, Wertheimer AI. Is prior authorization for prescribed drugs cost-effective? Drug Benefit Trends. 2008;20:136-139.
9. Bendix J. The prior authorization predicament. Med Econ. 2014;91(13)29-30,32,34-35.
10. Farley JF, Cline RR, Schommer JC, et al. Retrospective assessment of Medicaid step-therapy prior authorization policy for atypical antipsychotic medications. Clin Ther. 2008;30(8):1524-1539; discussion 1506-1507.
11. Abouzaid S, Jutkowitz E, Foley KA, et al. Economic impact of prior authorization policies for atypical antipsychotics in the treatment of schizophrenia. Popul Health Manag. 2010;13(5):247-254.
12. Brown CM, Nwokeji E, Rascati KL, et al. Development of the burden of prior authorization of psychotherapeutics (BoPAP) scale to assess the effects of prior authorization among Texas Medicaid providers. Adm Policy Ment Health. 2009;36(4):278-287.
13. Rascati KL, Brown CM. Prior authorization for antipsychotic medications—It’s not just about the money. Clin Ther. 2008;30(8):1506-1507.
14. Lu CY, Soumerai SB, Ross-Degnan D, et al. Unintended impacts of a Medicaid prior authorization policy on access to medications for bipolar disorder. Med Care. 2010;48(1):4-9.
15. Stephens RJ, White SE, Cudnik M, et al. Factors associated with longer lengths of stay for mental health emergency department patients. J Emerg Med. 2014; 47(4):412-419.
16. Brown JD, Barrett A, Caffery E, et al. Medication continuity among Medicaid beneficiaries with schizophrenia and bipolar disorder. Psychiatr Serv. 2013;64(9):878-885.
17. American Medical Association. Opinion 10.01– Fundamental elements of the patient-physician relationship. http://www.ama-assn.org/ama/pub/ physician-resources/medical-ethics/code-medical-ethics/opinion1001.page?. Accessed October 11, 2014.
18. Hall RC. Ethical and legal implications of managed care. Gen Hosp Psychiatry. 1997;19(3):200-208.
19. Porter v Thadani, 2010 U.S. Dist. LEXIS 35145 (NH 2010).
20. NB ex rel Peacock v District of Columbia, 682 F3d 77 (DC Cir 2012).
21. Wilson v Blue Cross of Southern California, 222 Cal App 3d 660, 271 Cal Rptr 876 (1990).
22. Wickline v State of California, 192 Cal App 3d 1630, 239 Cal Rptr 810 (1986).
23. Terry K. Prior authorization made easier. Med Econ. 2007;84(20):34,38,40.
24. American Medical Association. Ethics Opinion 6.07– Insurance forms completion charges. http://www. ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion607.page? Updated June 1994. Accessed October 11, 2014.
25. Gibson v Medco Health Solutions, 06-CVF-106 (OH 2008).
26. Bendix J. Curing the prior authorization headache. Med Econ. 2013;90(19):24,26-27,29-31.
27. American Medical Association. Electronic prior authorization toolkit. Available at http://www.ama-assn.org/ama/pub/advocacy/topics/administrative-simplification-initiatives/electronic-transactions-toolkit/ prior-authorization.page. Accessed October 11, 2014.
Dear Dr. Mossman,
Where I practice, most health care plans won’t pay for certain medications without giving prior authorization (PA). Completing PA forms and making telephone calls take up time that could be better spent treating patients. I’m tempted to set a new policy of not doing PAs. If I do, might I face legal trouble?
Submitted by “Dr. A”
If you provide clinical care, you’ve probably dealt with third-party payers who require prior authorization (PA) before they will pay for certain treatments. Dr. A is not alone in feeling exasperated about the time it takes to complete a PA.1 After spending several hours each month waiting on hold and wading through stacks of paperwork, you may feel like Dr. A and consider refusing to do any more PAs.
But is Dr. A’s proposed solution a good idea? To address this question and the frustration that lies behind it, we’ll take a cue from Italian film director Sergio Leone and discuss:
• how PAs affect psychiatric care: the good, the bad, and the ugly
• potential exposure to professional liability and ethics complaints that might result from refusing or failing to seek PA
• strategies to reduce the burden of PAs while providing efficient, effective care.
The good
Recent decades have witnessed huge increases in spending on prescription medication. Psychotropics are no exception; state Medicaid spending for anti-psychotic medication grew from <$1 billion in 1995 to >$5.5 billion in 2005.2
Requiring a PA for expensive drugs is one way that third-party payers try to rein in costs and hold down insurance premiums. Imposing financial constraints often is just one aim of a pharmacy benefit management (PBM) program. Insurers also justify PBMs by pointing out that feedback to practitioners whose prescribing falls well outside the norm—in the form of mailed warnings, physician second opinions, or pharmacist consultation—can improve patient safety and encourage appropriate treatment options for enrolled patients.3,4 Examples of such benefits include reducing overuse of prescription opioids5 and antipsychotics among children,3 misuse of buprenorphine,6 and adverse effects from potentially inappropriate prescriptions.7
The bad
The bad news for doctors: Cost savings for payers come at the expense of providers and their practices, in the form of time spent doing paperwork and talking on the phone to complete PAs or contest PA decisions.8 Addressing PA requests costs an estimated $83,000 per physician per year. The total administrative burden for all 835,000 physicians who practice in the United States therefore is 868,000,000 hours, or $69 billion annually.9
To make matters worse, PA requirements may increase the overall cost of care. After Georgia Medicaid instituted PA requirements for second-generation antipsychotics (SGAs), average monthly per member drug costs fell $19.62, but average monthly outpatient treatment costs rose $31.59 per member.10 Pharmacy savings that result from requiring PAs for SGAs can be offset quickly by small increases in the hospitalization rate or emergency department visits.9,11
The ugly
Many physicians believe that the PA process undermines patient care by decreasing time devoted to direct patient contact, incentivizing suboptimal treatment, and limiting medication access.1,12,13 But do any data support this belief? Do PAs impede treatment for vulnerable persons with severe mental illnesses?
The answer, some studies suggest, is “Yes.” A Maine Medicaid PA policy slowed initiation of treatment for bipolar disorder by reducing the rate of starting non-preferred medications, although the same policy had no impact on patients already receiving treatment.14 Another study examined the effect of PA processes for inpatient psychiatry treatment and found that patients were less likely to be admitted on weekends, probably because PA review was not available on those days.15 A third study showed that PA requirements and resulting impediments to getting refills were correlated with medication discontinuation by patients with schizophrenia or bipolar disorder, which can increase the risk of decompensation, work-related problems, and hospitalization.16
Problems with PAs
Whether they are helpful or counterproductive, PAs are a practice reality. Dr. A’s proposed solution sounds appealing, but it might create ethical and legal problems.
Among the fundamental elements of ethical medical practice is physicians’ obligation to give patients “guidance … as to the optimal course of action” and to “advocate for patients in dealing with third parties when appropriate.”17 It’s fine for psychiatrists to consider prescribing treatments that patients’ health care coverage favors, but we also have to help patients weigh and evaluate costs, particularly when patients’ circumstances and medical interests militate strongly for options that third-party payers balk at paying for. Patients’ interests—not what’s expedient—are always physicians’ foremost concern.18
Beyond purely ethical considerations, you might face legal consequences if you refuse or fail to seek PAs for what you think is the proper medication. As Table 1 shows, one key factor is whether you are under contract with the patient’s insurance carrier; if you are, failure to seek a PA when appropriate may constitute a breach of the contract (Donna Vanderpool, written communication, October 5, 2014).
If the prescribed medication does not meet the standard of care and your patient suffers some harm, a licensing board complaint and investigation are possible. You also face exposure to a medical malpractice action. Although we do not know of any instances in which such an action has succeeded, 2 recent court decisions suggest that harm to a patient stemmed from failing to seek PA for a medication could constitute grounds for a lawsuit.19,20 Efforts to contain medical costs have been around for decades, and courts have held that physicians, third-party payers, and utilization review intermediaries are bound by “the standard of reasonable community practice”21 and should not let cost limitations “corrupt medical judgment.”22 Physicians who do not appeal limitations at odds with their medical judgment might bear responsibility for any injuries that occur.18,22
Managing PA requests
Given the inevitability of encountering PA requests and your ethical and professional obligations to help patients, what can you do (Table 29,23,27)?
Some practitioners charge patients for time spent completing PAs.23 Although physicians should “complete without charge the appropriate ‘simplified’ insurance claim form as a part of service to the patient;” they also may consider “a charge for more complex or multiple forms … in conformity with local custom.”24 Legally, physicians’ contracts with insurance panels may preclude charging such fees, but if a patient is being seen out of network, the physician does not have a contractual obligation and may charge.9 If your practice setting lets you choose which insurances you accept, the impact and burden of seeking PAs is a factor to consider when deciding whether to participate in a particular panel.23
In an interesting twist, an Ohio physician successfully sued a medical insurance administrator for the cost of his time responding to PA inquiries.25 Reasoning that the insurance administrator “should expect to pay for the reasonable value of” the doctor’s time because the PAs “were solely intended for the benefit of the insurance administrator” or parties whom the administrator served, the judge awarded the doctor $187.50 plus 8% interest.
Considerations that are more practical relate to how to triage and address the volume of PA requests. Some large medical practices centralize PAs and try to set up pre-approved plans of care or blanket approvals for frequently encountered conditions. Centralization also allows one key administrative assistant to develop skills in processing PA requests and to build relationships with payers.26
The administrative assistant also can compile lists of preferred alternative medications, PA forms, and payer Web sites. Using and submitting requests through payer Web sites can speed up PA processing, which saves time and money.27 As electronic health records improve, they may incorporate patients’ formularies and provide automatic alerts for required PAs.23
Patients should be involved, too. They can help to obtain relevant formulary information and to weigh alternative therapies. You can help them understand your role in the PA process, the reasoning behind your treatment recommendations, and the delays in picking up prescribed medications that waiting for PA approval can create.
It’s easy to get angry about PAs
Your best response, however, is to practice prudent and—within reason— cost-effective medicine. When generic or insurer-preferred medications are clinically appropriate and meet treatment guidelines, trying them first is sensible and defensible. If your patient fails the initial low-cost treatment, or if a low-cost choice isn’t appropriate, document this clearly and seek approval for a costlier treatment.9
BOTTOM LINE
Physicians have ethical and legal obligations to advocate for their patients’ needs and best interests. This sometimes includes completing prior authorization requests. Find strategies that minimize hassle and make sense in your practice, and seek efficient ways to document the medical necessity of requested tests, procedures, or therapies.
Acknowledgment
Drs. Marett and Mossman thanks Donna Vanderpool, MBA, JD, and Annette Reynolds, MD, for their helpful input in preparing this article.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dear Dr. Mossman,
Where I practice, most health care plans won’t pay for certain medications without giving prior authorization (PA). Completing PA forms and making telephone calls take up time that could be better spent treating patients. I’m tempted to set a new policy of not doing PAs. If I do, might I face legal trouble?
Submitted by “Dr. A”
If you provide clinical care, you’ve probably dealt with third-party payers who require prior authorization (PA) before they will pay for certain treatments. Dr. A is not alone in feeling exasperated about the time it takes to complete a PA.1 After spending several hours each month waiting on hold and wading through stacks of paperwork, you may feel like Dr. A and consider refusing to do any more PAs.
But is Dr. A’s proposed solution a good idea? To address this question and the frustration that lies behind it, we’ll take a cue from Italian film director Sergio Leone and discuss:
• how PAs affect psychiatric care: the good, the bad, and the ugly
• potential exposure to professional liability and ethics complaints that might result from refusing or failing to seek PA
• strategies to reduce the burden of PAs while providing efficient, effective care.
The good
Recent decades have witnessed huge increases in spending on prescription medication. Psychotropics are no exception; state Medicaid spending for anti-psychotic medication grew from <$1 billion in 1995 to >$5.5 billion in 2005.2
Requiring a PA for expensive drugs is one way that third-party payers try to rein in costs and hold down insurance premiums. Imposing financial constraints often is just one aim of a pharmacy benefit management (PBM) program. Insurers also justify PBMs by pointing out that feedback to practitioners whose prescribing falls well outside the norm—in the form of mailed warnings, physician second opinions, or pharmacist consultation—can improve patient safety and encourage appropriate treatment options for enrolled patients.3,4 Examples of such benefits include reducing overuse of prescription opioids5 and antipsychotics among children,3 misuse of buprenorphine,6 and adverse effects from potentially inappropriate prescriptions.7
The bad
The bad news for doctors: Cost savings for payers come at the expense of providers and their practices, in the form of time spent doing paperwork and talking on the phone to complete PAs or contest PA decisions.8 Addressing PA requests costs an estimated $83,000 per physician per year. The total administrative burden for all 835,000 physicians who practice in the United States therefore is 868,000,000 hours, or $69 billion annually.9
To make matters worse, PA requirements may increase the overall cost of care. After Georgia Medicaid instituted PA requirements for second-generation antipsychotics (SGAs), average monthly per member drug costs fell $19.62, but average monthly outpatient treatment costs rose $31.59 per member.10 Pharmacy savings that result from requiring PAs for SGAs can be offset quickly by small increases in the hospitalization rate or emergency department visits.9,11
The ugly
Many physicians believe that the PA process undermines patient care by decreasing time devoted to direct patient contact, incentivizing suboptimal treatment, and limiting medication access.1,12,13 But do any data support this belief? Do PAs impede treatment for vulnerable persons with severe mental illnesses?
The answer, some studies suggest, is “Yes.” A Maine Medicaid PA policy slowed initiation of treatment for bipolar disorder by reducing the rate of starting non-preferred medications, although the same policy had no impact on patients already receiving treatment.14 Another study examined the effect of PA processes for inpatient psychiatry treatment and found that patients were less likely to be admitted on weekends, probably because PA review was not available on those days.15 A third study showed that PA requirements and resulting impediments to getting refills were correlated with medication discontinuation by patients with schizophrenia or bipolar disorder, which can increase the risk of decompensation, work-related problems, and hospitalization.16
Problems with PAs
Whether they are helpful or counterproductive, PAs are a practice reality. Dr. A’s proposed solution sounds appealing, but it might create ethical and legal problems.
Among the fundamental elements of ethical medical practice is physicians’ obligation to give patients “guidance … as to the optimal course of action” and to “advocate for patients in dealing with third parties when appropriate.”17 It’s fine for psychiatrists to consider prescribing treatments that patients’ health care coverage favors, but we also have to help patients weigh and evaluate costs, particularly when patients’ circumstances and medical interests militate strongly for options that third-party payers balk at paying for. Patients’ interests—not what’s expedient—are always physicians’ foremost concern.18
Beyond purely ethical considerations, you might face legal consequences if you refuse or fail to seek PAs for what you think is the proper medication. As Table 1 shows, one key factor is whether you are under contract with the patient’s insurance carrier; if you are, failure to seek a PA when appropriate may constitute a breach of the contract (Donna Vanderpool, written communication, October 5, 2014).
If the prescribed medication does not meet the standard of care and your patient suffers some harm, a licensing board complaint and investigation are possible. You also face exposure to a medical malpractice action. Although we do not know of any instances in which such an action has succeeded, 2 recent court decisions suggest that harm to a patient stemmed from failing to seek PA for a medication could constitute grounds for a lawsuit.19,20 Efforts to contain medical costs have been around for decades, and courts have held that physicians, third-party payers, and utilization review intermediaries are bound by “the standard of reasonable community practice”21 and should not let cost limitations “corrupt medical judgment.”22 Physicians who do not appeal limitations at odds with their medical judgment might bear responsibility for any injuries that occur.18,22
Managing PA requests
Given the inevitability of encountering PA requests and your ethical and professional obligations to help patients, what can you do (Table 29,23,27)?
Some practitioners charge patients for time spent completing PAs.23 Although physicians should “complete without charge the appropriate ‘simplified’ insurance claim form as a part of service to the patient;” they also may consider “a charge for more complex or multiple forms … in conformity with local custom.”24 Legally, physicians’ contracts with insurance panels may preclude charging such fees, but if a patient is being seen out of network, the physician does not have a contractual obligation and may charge.9 If your practice setting lets you choose which insurances you accept, the impact and burden of seeking PAs is a factor to consider when deciding whether to participate in a particular panel.23
In an interesting twist, an Ohio physician successfully sued a medical insurance administrator for the cost of his time responding to PA inquiries.25 Reasoning that the insurance administrator “should expect to pay for the reasonable value of” the doctor’s time because the PAs “were solely intended for the benefit of the insurance administrator” or parties whom the administrator served, the judge awarded the doctor $187.50 plus 8% interest.
Considerations that are more practical relate to how to triage and address the volume of PA requests. Some large medical practices centralize PAs and try to set up pre-approved plans of care or blanket approvals for frequently encountered conditions. Centralization also allows one key administrative assistant to develop skills in processing PA requests and to build relationships with payers.26
The administrative assistant also can compile lists of preferred alternative medications, PA forms, and payer Web sites. Using and submitting requests through payer Web sites can speed up PA processing, which saves time and money.27 As electronic health records improve, they may incorporate patients’ formularies and provide automatic alerts for required PAs.23
Patients should be involved, too. They can help to obtain relevant formulary information and to weigh alternative therapies. You can help them understand your role in the PA process, the reasoning behind your treatment recommendations, and the delays in picking up prescribed medications that waiting for PA approval can create.
It’s easy to get angry about PAs
Your best response, however, is to practice prudent and—within reason— cost-effective medicine. When generic or insurer-preferred medications are clinically appropriate and meet treatment guidelines, trying them first is sensible and defensible. If your patient fails the initial low-cost treatment, or if a low-cost choice isn’t appropriate, document this clearly and seek approval for a costlier treatment.9
BOTTOM LINE
Physicians have ethical and legal obligations to advocate for their patients’ needs and best interests. This sometimes includes completing prior authorization requests. Find strategies that minimize hassle and make sense in your practice, and seek efficient ways to document the medical necessity of requested tests, procedures, or therapies.
Acknowledgment
Drs. Marett and Mossman thanks Donna Vanderpool, MBA, JD, and Annette Reynolds, MD, for their helpful input in preparing this article.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Brown CM, Richards K, Rascati KL, et al. Effects of a psychotherapeutic drug prior authorization (PA) requirement on patients and providers: a providers’ perspective. Adm Policy Ment Health. 2008;35(3):181-188.
2. Law MR, Ross-Degnan D, Soumerai SB. Effect of prior authorization of second-generation antipsychotic agents on pharmacy utilization and reimbursements. Psychiatr Serv. 2008;59(5):540-546.
3. Stein BD, Leckman-Westin E, Okeke E, et al. The effects of prior authorization policies on Medicaid-enrolled children’s use of antipsychotic medications: evidence from two Mid-Atlantic states. J Child Adolesc Psychopharmacol. 2014;24(7):374-381.
4. Adams KT. Prior authorization–still used, still an issue. Biotechnol Healthc. 2010;7(4):28.
5. Garcia MM, Angelini MC, Thomas T, et al. Implementation of an opioid management initiative by a state Medicaid program. J Manag Care Pharm. 2014;20(5):447-454.
6. Clark RE, Baxter JD, Barton BA, et al. The impact of prior authorization on buprenorphine dose, relapse rates, and cost for Massachusetts Medicaid beneficiaries with opioid dependence [published online July 9, 2014]. Health Serv Res. doi: 10.1111/1475-6773.12201.
7. Dunn RL, Harrison D, Ripley TL. The beers criteria as an outpatient screening tool for potentially inappropriate medications. Consult Pharm. 2011;26(10):754-763.
8. Lennertz MD, Wertheimer AI. Is prior authorization for prescribed drugs cost-effective? Drug Benefit Trends. 2008;20:136-139.
9. Bendix J. The prior authorization predicament. Med Econ. 2014;91(13)29-30,32,34-35.
10. Farley JF, Cline RR, Schommer JC, et al. Retrospective assessment of Medicaid step-therapy prior authorization policy for atypical antipsychotic medications. Clin Ther. 2008;30(8):1524-1539; discussion 1506-1507.
11. Abouzaid S, Jutkowitz E, Foley KA, et al. Economic impact of prior authorization policies for atypical antipsychotics in the treatment of schizophrenia. Popul Health Manag. 2010;13(5):247-254.
12. Brown CM, Nwokeji E, Rascati KL, et al. Development of the burden of prior authorization of psychotherapeutics (BoPAP) scale to assess the effects of prior authorization among Texas Medicaid providers. Adm Policy Ment Health. 2009;36(4):278-287.
13. Rascati KL, Brown CM. Prior authorization for antipsychotic medications—It’s not just about the money. Clin Ther. 2008;30(8):1506-1507.
14. Lu CY, Soumerai SB, Ross-Degnan D, et al. Unintended impacts of a Medicaid prior authorization policy on access to medications for bipolar disorder. Med Care. 2010;48(1):4-9.
15. Stephens RJ, White SE, Cudnik M, et al. Factors associated with longer lengths of stay for mental health emergency department patients. J Emerg Med. 2014; 47(4):412-419.
16. Brown JD, Barrett A, Caffery E, et al. Medication continuity among Medicaid beneficiaries with schizophrenia and bipolar disorder. Psychiatr Serv. 2013;64(9):878-885.
17. American Medical Association. Opinion 10.01– Fundamental elements of the patient-physician relationship. http://www.ama-assn.org/ama/pub/ physician-resources/medical-ethics/code-medical-ethics/opinion1001.page?. Accessed October 11, 2014.
18. Hall RC. Ethical and legal implications of managed care. Gen Hosp Psychiatry. 1997;19(3):200-208.
19. Porter v Thadani, 2010 U.S. Dist. LEXIS 35145 (NH 2010).
20. NB ex rel Peacock v District of Columbia, 682 F3d 77 (DC Cir 2012).
21. Wilson v Blue Cross of Southern California, 222 Cal App 3d 660, 271 Cal Rptr 876 (1990).
22. Wickline v State of California, 192 Cal App 3d 1630, 239 Cal Rptr 810 (1986).
23. Terry K. Prior authorization made easier. Med Econ. 2007;84(20):34,38,40.
24. American Medical Association. Ethics Opinion 6.07– Insurance forms completion charges. http://www. ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion607.page? Updated June 1994. Accessed October 11, 2014.
25. Gibson v Medco Health Solutions, 06-CVF-106 (OH 2008).
26. Bendix J. Curing the prior authorization headache. Med Econ. 2013;90(19):24,26-27,29-31.
27. American Medical Association. Electronic prior authorization toolkit. Available at http://www.ama-assn.org/ama/pub/advocacy/topics/administrative-simplification-initiatives/electronic-transactions-toolkit/ prior-authorization.page. Accessed October 11, 2014.
1. Brown CM, Richards K, Rascati KL, et al. Effects of a psychotherapeutic drug prior authorization (PA) requirement on patients and providers: a providers’ perspective. Adm Policy Ment Health. 2008;35(3):181-188.
2. Law MR, Ross-Degnan D, Soumerai SB. Effect of prior authorization of second-generation antipsychotic agents on pharmacy utilization and reimbursements. Psychiatr Serv. 2008;59(5):540-546.
3. Stein BD, Leckman-Westin E, Okeke E, et al. The effects of prior authorization policies on Medicaid-enrolled children’s use of antipsychotic medications: evidence from two Mid-Atlantic states. J Child Adolesc Psychopharmacol. 2014;24(7):374-381.
4. Adams KT. Prior authorization–still used, still an issue. Biotechnol Healthc. 2010;7(4):28.
5. Garcia MM, Angelini MC, Thomas T, et al. Implementation of an opioid management initiative by a state Medicaid program. J Manag Care Pharm. 2014;20(5):447-454.
6. Clark RE, Baxter JD, Barton BA, et al. The impact of prior authorization on buprenorphine dose, relapse rates, and cost for Massachusetts Medicaid beneficiaries with opioid dependence [published online July 9, 2014]. Health Serv Res. doi: 10.1111/1475-6773.12201.
7. Dunn RL, Harrison D, Ripley TL. The beers criteria as an outpatient screening tool for potentially inappropriate medications. Consult Pharm. 2011;26(10):754-763.
8. Lennertz MD, Wertheimer AI. Is prior authorization for prescribed drugs cost-effective? Drug Benefit Trends. 2008;20:136-139.
9. Bendix J. The prior authorization predicament. Med Econ. 2014;91(13)29-30,32,34-35.
10. Farley JF, Cline RR, Schommer JC, et al. Retrospective assessment of Medicaid step-therapy prior authorization policy for atypical antipsychotic medications. Clin Ther. 2008;30(8):1524-1539; discussion 1506-1507.
11. Abouzaid S, Jutkowitz E, Foley KA, et al. Economic impact of prior authorization policies for atypical antipsychotics in the treatment of schizophrenia. Popul Health Manag. 2010;13(5):247-254.
12. Brown CM, Nwokeji E, Rascati KL, et al. Development of the burden of prior authorization of psychotherapeutics (BoPAP) scale to assess the effects of prior authorization among Texas Medicaid providers. Adm Policy Ment Health. 2009;36(4):278-287.
13. Rascati KL, Brown CM. Prior authorization for antipsychotic medications—It’s not just about the money. Clin Ther. 2008;30(8):1506-1507.
14. Lu CY, Soumerai SB, Ross-Degnan D, et al. Unintended impacts of a Medicaid prior authorization policy on access to medications for bipolar disorder. Med Care. 2010;48(1):4-9.
15. Stephens RJ, White SE, Cudnik M, et al. Factors associated with longer lengths of stay for mental health emergency department patients. J Emerg Med. 2014; 47(4):412-419.
16. Brown JD, Barrett A, Caffery E, et al. Medication continuity among Medicaid beneficiaries with schizophrenia and bipolar disorder. Psychiatr Serv. 2013;64(9):878-885.
17. American Medical Association. Opinion 10.01– Fundamental elements of the patient-physician relationship. http://www.ama-assn.org/ama/pub/ physician-resources/medical-ethics/code-medical-ethics/opinion1001.page?. Accessed October 11, 2014.
18. Hall RC. Ethical and legal implications of managed care. Gen Hosp Psychiatry. 1997;19(3):200-208.
19. Porter v Thadani, 2010 U.S. Dist. LEXIS 35145 (NH 2010).
20. NB ex rel Peacock v District of Columbia, 682 F3d 77 (DC Cir 2012).
21. Wilson v Blue Cross of Southern California, 222 Cal App 3d 660, 271 Cal Rptr 876 (1990).
22. Wickline v State of California, 192 Cal App 3d 1630, 239 Cal Rptr 810 (1986).
23. Terry K. Prior authorization made easier. Med Econ. 2007;84(20):34,38,40.
24. American Medical Association. Ethics Opinion 6.07– Insurance forms completion charges. http://www. ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion607.page? Updated June 1994. Accessed October 11, 2014.
25. Gibson v Medco Health Solutions, 06-CVF-106 (OH 2008).
26. Bendix J. Curing the prior authorization headache. Med Econ. 2013;90(19):24,26-27,29-31.
27. American Medical Association. Electronic prior authorization toolkit. Available at http://www.ama-assn.org/ama/pub/advocacy/topics/administrative-simplification-initiatives/electronic-transactions-toolkit/ prior-authorization.page. Accessed October 11, 2014.
Altering Record Compounds Deadly Mistake
A 17-year-old girl underwent a routine tonsillectomy without complications at a surgical center. Following the procedure, she was taken to the recovery room and administered fentanyl for pain.
The recovery room nurse assigned to monitor the patient spent 20 minutes treating another patient and then went on break, signing out to a second recovery room nurse. On receiving the signout, the second recovery room nurse discovered that the patient was in respiratory distress and began resuscitation efforts. The patient was resuscitated but died 15 days later.
The plaintiff claimed that the girl was left unmonitored by nurses assigned to the unit and that the monitoring equipment was not used, not set properly, or muted.
During her deposition, the second recovery room nurse admitted under oath that the first recovery room nurse falsified the patient’s chart; the first nurse claimed that she had assessed the patient during an important time period when she had not.
Continue for the outcome and commentary >>
OUTCOME
The case was settled for $6 million: $1 million against the surgical center’s primary policy and $5 million against its excess policy.
COMMENT
Cases such as this one are unfortunate and avoidable—and tragically, too common. On any medical malpractice lawyer’s desk is a teetering stack of potential cases; much of that stack involves narcotics. This case raises two important areas to discuss: the dangers of parenteral narcotics and the perils of falsifying medical records.
First, when parenteral narcotics are given, proper monitoring safeguards must be in place. Malpractice cases frequently involve a scenario in which patients are given parenteral narcotics and left alone, out of sight, and unmonitored. This simply can’t be done. Close supervision and monitoring—with both equipment and eyes—are required to safeguard your patients and avoid malpractice risk.
Other malpractice scenarios involve the ambulatory patient who is given parenteral narcotics in a clinic setting and discharged after a 10-minute “observation” period—a period during which peak drug effect is probably not realized. The patient is unsafely discharged before that peak is reached and suffers potentially fatal adverse effects. Even when direct fatal effects are not realized, the patient is discharged with impaired motor coordination and cognitive judgment, placing the patient at risk in his/her surroundings.
If a clinician commits to giving parenteral narcotics, he or she commits to providing “real-time” monitoring until the narcotic effects have safely diminished and the patient’s condition is thoroughly documented in the record. Generally speaking, the patient must be reasonably clear of the effects of narcotics before discharge. (Remember the special case of naloxone, administered for opiate excesses, in which naloxone is metabolized before the opiate; the patient can relapse into a coma/apnea if the naloxone fully metabolizes before the opiate.)
Here, this young woman was probably opiate naïve. While the amount she was given was certain, her response to the drug was not. She was left alone for at least 20 minutes and did not have a functioning SaO2 monitor. Close monitoring of this patient was required but not provided.
As a result of this case, the surgical center changed several policies: Nurses must be on a one-to-one ratio with patients who have received narcotics during anesthesia. Furthermore, nurses must have line-of-sight to see patients at all times and, importantly, may not mute monitors (eg, oximetry monitors).
The second salient point of this case is never, ever alter or falsify patient records! It will be discovered, and your credibility will be irretrievably damaged. Plaintiff lawyers live for this, and yet clinicians continue to do it. Don’t.
When altered medical records are discovered, the plaintiff’s theory of the case will be “cover up,” and jurors will be invited to punish the clinician for it. The jurors will do so.
Also problematic is an otherwise defensible case that becomes much more difficult to defend because a clinician has altered the records. Remember, the plaintiff must prove all aspects of negligence, including causation and damages. In some cases, the clinician knows an obvious mistake was made but does not know that the eventual damages may be minimal or attributable to another cause. By altering the medical record, the clinician may enhance the damages value of a case by introducing a punitive element. Altering records may result in a lawsuit being filed when it otherwise wouldn’t have, or maintained when it would have been dropped before trial. In sum, don’t create a case against yourself by altering the medical records.
Here, the falsification of records came to light during the deposition of the second nurse—who, being under oath, probably had little choice but to testify that the first nurse falsified the records. No doubt, this falsification made a bad case worse and gave the plaintiff leverage in securing more favorable settlement terms.
You can’t make it right by rewriting history, but you can make it right by showing concern for the patient in your actions following a problem. You can also make it right by troubleshooting problems in a closed-door, formal peer review conference. Peer review conferences are designed for full and frank communication between clinicians and staff to solve problems, and as such they are protected from plaintiff disclosure.
This is an unfortunate case and a tragic loss of life. As clinicians, we must respect the potential life-ending power of parenteral narcotics. —DML
A 17-year-old girl underwent a routine tonsillectomy without complications at a surgical center. Following the procedure, she was taken to the recovery room and administered fentanyl for pain.
The recovery room nurse assigned to monitor the patient spent 20 minutes treating another patient and then went on break, signing out to a second recovery room nurse. On receiving the signout, the second recovery room nurse discovered that the patient was in respiratory distress and began resuscitation efforts. The patient was resuscitated but died 15 days later.
The plaintiff claimed that the girl was left unmonitored by nurses assigned to the unit and that the monitoring equipment was not used, not set properly, or muted.
During her deposition, the second recovery room nurse admitted under oath that the first recovery room nurse falsified the patient’s chart; the first nurse claimed that she had assessed the patient during an important time period when she had not.
Continue for the outcome and commentary >>
OUTCOME
The case was settled for $6 million: $1 million against the surgical center’s primary policy and $5 million against its excess policy.
COMMENT
Cases such as this one are unfortunate and avoidable—and tragically, too common. On any medical malpractice lawyer’s desk is a teetering stack of potential cases; much of that stack involves narcotics. This case raises two important areas to discuss: the dangers of parenteral narcotics and the perils of falsifying medical records.
First, when parenteral narcotics are given, proper monitoring safeguards must be in place. Malpractice cases frequently involve a scenario in which patients are given parenteral narcotics and left alone, out of sight, and unmonitored. This simply can’t be done. Close supervision and monitoring—with both equipment and eyes—are required to safeguard your patients and avoid malpractice risk.
Other malpractice scenarios involve the ambulatory patient who is given parenteral narcotics in a clinic setting and discharged after a 10-minute “observation” period—a period during which peak drug effect is probably not realized. The patient is unsafely discharged before that peak is reached and suffers potentially fatal adverse effects. Even when direct fatal effects are not realized, the patient is discharged with impaired motor coordination and cognitive judgment, placing the patient at risk in his/her surroundings.
If a clinician commits to giving parenteral narcotics, he or she commits to providing “real-time” monitoring until the narcotic effects have safely diminished and the patient’s condition is thoroughly documented in the record. Generally speaking, the patient must be reasonably clear of the effects of narcotics before discharge. (Remember the special case of naloxone, administered for opiate excesses, in which naloxone is metabolized before the opiate; the patient can relapse into a coma/apnea if the naloxone fully metabolizes before the opiate.)
Here, this young woman was probably opiate naïve. While the amount she was given was certain, her response to the drug was not. She was left alone for at least 20 minutes and did not have a functioning SaO2 monitor. Close monitoring of this patient was required but not provided.
As a result of this case, the surgical center changed several policies: Nurses must be on a one-to-one ratio with patients who have received narcotics during anesthesia. Furthermore, nurses must have line-of-sight to see patients at all times and, importantly, may not mute monitors (eg, oximetry monitors).
The second salient point of this case is never, ever alter or falsify patient records! It will be discovered, and your credibility will be irretrievably damaged. Plaintiff lawyers live for this, and yet clinicians continue to do it. Don’t.
When altered medical records are discovered, the plaintiff’s theory of the case will be “cover up,” and jurors will be invited to punish the clinician for it. The jurors will do so.
Also problematic is an otherwise defensible case that becomes much more difficult to defend because a clinician has altered the records. Remember, the plaintiff must prove all aspects of negligence, including causation and damages. In some cases, the clinician knows an obvious mistake was made but does not know that the eventual damages may be minimal or attributable to another cause. By altering the medical record, the clinician may enhance the damages value of a case by introducing a punitive element. Altering records may result in a lawsuit being filed when it otherwise wouldn’t have, or maintained when it would have been dropped before trial. In sum, don’t create a case against yourself by altering the medical records.
Here, the falsification of records came to light during the deposition of the second nurse—who, being under oath, probably had little choice but to testify that the first nurse falsified the records. No doubt, this falsification made a bad case worse and gave the plaintiff leverage in securing more favorable settlement terms.
You can’t make it right by rewriting history, but you can make it right by showing concern for the patient in your actions following a problem. You can also make it right by troubleshooting problems in a closed-door, formal peer review conference. Peer review conferences are designed for full and frank communication between clinicians and staff to solve problems, and as such they are protected from plaintiff disclosure.
This is an unfortunate case and a tragic loss of life. As clinicians, we must respect the potential life-ending power of parenteral narcotics. —DML
A 17-year-old girl underwent a routine tonsillectomy without complications at a surgical center. Following the procedure, she was taken to the recovery room and administered fentanyl for pain.
The recovery room nurse assigned to monitor the patient spent 20 minutes treating another patient and then went on break, signing out to a second recovery room nurse. On receiving the signout, the second recovery room nurse discovered that the patient was in respiratory distress and began resuscitation efforts. The patient was resuscitated but died 15 days later.
The plaintiff claimed that the girl was left unmonitored by nurses assigned to the unit and that the monitoring equipment was not used, not set properly, or muted.
During her deposition, the second recovery room nurse admitted under oath that the first recovery room nurse falsified the patient’s chart; the first nurse claimed that she had assessed the patient during an important time period when she had not.
Continue for the outcome and commentary >>
OUTCOME
The case was settled for $6 million: $1 million against the surgical center’s primary policy and $5 million against its excess policy.
COMMENT
Cases such as this one are unfortunate and avoidable—and tragically, too common. On any medical malpractice lawyer’s desk is a teetering stack of potential cases; much of that stack involves narcotics. This case raises two important areas to discuss: the dangers of parenteral narcotics and the perils of falsifying medical records.
First, when parenteral narcotics are given, proper monitoring safeguards must be in place. Malpractice cases frequently involve a scenario in which patients are given parenteral narcotics and left alone, out of sight, and unmonitored. This simply can’t be done. Close supervision and monitoring—with both equipment and eyes—are required to safeguard your patients and avoid malpractice risk.
Other malpractice scenarios involve the ambulatory patient who is given parenteral narcotics in a clinic setting and discharged after a 10-minute “observation” period—a period during which peak drug effect is probably not realized. The patient is unsafely discharged before that peak is reached and suffers potentially fatal adverse effects. Even when direct fatal effects are not realized, the patient is discharged with impaired motor coordination and cognitive judgment, placing the patient at risk in his/her surroundings.
If a clinician commits to giving parenteral narcotics, he or she commits to providing “real-time” monitoring until the narcotic effects have safely diminished and the patient’s condition is thoroughly documented in the record. Generally speaking, the patient must be reasonably clear of the effects of narcotics before discharge. (Remember the special case of naloxone, administered for opiate excesses, in which naloxone is metabolized before the opiate; the patient can relapse into a coma/apnea if the naloxone fully metabolizes before the opiate.)
Here, this young woman was probably opiate naïve. While the amount she was given was certain, her response to the drug was not. She was left alone for at least 20 minutes and did not have a functioning SaO2 monitor. Close monitoring of this patient was required but not provided.
As a result of this case, the surgical center changed several policies: Nurses must be on a one-to-one ratio with patients who have received narcotics during anesthesia. Furthermore, nurses must have line-of-sight to see patients at all times and, importantly, may not mute monitors (eg, oximetry monitors).
The second salient point of this case is never, ever alter or falsify patient records! It will be discovered, and your credibility will be irretrievably damaged. Plaintiff lawyers live for this, and yet clinicians continue to do it. Don’t.
When altered medical records are discovered, the plaintiff’s theory of the case will be “cover up,” and jurors will be invited to punish the clinician for it. The jurors will do so.
Also problematic is an otherwise defensible case that becomes much more difficult to defend because a clinician has altered the records. Remember, the plaintiff must prove all aspects of negligence, including causation and damages. In some cases, the clinician knows an obvious mistake was made but does not know that the eventual damages may be minimal or attributable to another cause. By altering the medical record, the clinician may enhance the damages value of a case by introducing a punitive element. Altering records may result in a lawsuit being filed when it otherwise wouldn’t have, or maintained when it would have been dropped before trial. In sum, don’t create a case against yourself by altering the medical records.
Here, the falsification of records came to light during the deposition of the second nurse—who, being under oath, probably had little choice but to testify that the first nurse falsified the records. No doubt, this falsification made a bad case worse and gave the plaintiff leverage in securing more favorable settlement terms.
You can’t make it right by rewriting history, but you can make it right by showing concern for the patient in your actions following a problem. You can also make it right by troubleshooting problems in a closed-door, formal peer review conference. Peer review conferences are designed for full and frank communication between clinicians and staff to solve problems, and as such they are protected from plaintiff disclosure.
This is an unfortunate case and a tragic loss of life. As clinicians, we must respect the potential life-ending power of parenteral narcotics. —DML
Interplay Between Physician Employment Agreement, Hospital Medical Staff Bylaws Important

If you are a physician considering employment with a hospital or private practice in which hospital medical staff privileges will be needed or you are currently employed by a hospital or private practice and have medical staff privileges, it is imperative that you understand your rights as an employee and as a member of the hospital’s medical staff, along with the interplay between those two roles.
Employment Agreement and Hospital Medical Staff Bylaws
As an employee of a hospital or private practice, you will have an employment agreement that governs the terms of your employment. In addition, if you are on the hospital’s medical staff, you will also be subject to the hospital’s medical staff bylaws, which govern the terms of your staff membership and clinical privileges.
At the onset of an employment relationship, many physicians focus on the terms of their employment agreements, often ignoring the terms of the medical staff bylaws. This could lead to unexpected surprises, usually toward the end of the employment relationship, because both documents need to be read in conjunction with each other.
Beware of conflicting terms in your employment agreement on the one hand and the medical staff bylaws on the other. Although an employment agreement may include seemingly beneficial terms, hidden language often has the effect of negating its terms by qualifying the employment agreement with language contained in the bylaws. Examples include:
—“In the event of a conflict between the terms of the Physician’s Employment Agreement and the Medical Staff Bylaws, the Medical Staff Bylaws shall control.”
—“Subject to the Medical Staff Bylaws, Physician may …”
—“Except as otherwise stated in the Medical Staff Bylaws, Physician may …”
—“Except as permitted by the Medical Staff Bylaws, Physician may not …”
Termination of Medical Staff Privileges: Impact on Employment Agreement
Whether you are employed by a hospital or a private practice, your employment is likely at risk if your hospital medical staff privileges are suspended, revoked, or restricted. Even if your medical staff privileges are later reinstated, the initial suspension may trigger termination of your employment agreement.
Therefore, it is important to understand your due process rights, outlined in the hospital’s medical staff bylaws, as to how your privileges can be suspended, revoked, or restricted, as well as the procedure the hospital must undergo to make such a decision.
Medical staff bylaws also include a procedure for due process, including fair hearings and appeal mechanisms for medical staff decisions, such as privilege suspension, revocation, and restrictions.
Termination of Employment: Impact on Medical Staff Privileges
For hospital employees and most hospital-based physicians, termination of your employment agreement, whether for cause or without cause, may be automatic grounds for termination of your staff privileges. In such a case, your due process rights under the medical staff bylaws as they relate to your staff privileges are waived, and you will not be afforded the fair hearing and appeal procedure typically available to office-based physicians on the hospital’s medical staff.
Also, your employment agreement may contractually require you to resign from the hospital’s medical staff upon termination of the employment relationship. For example:
“Physician covenants and agrees that upon termination of Physician’s employment with Employer (whether for cause or without cause), Physician will resign from the medical staff of Hospital X, thereby relinquishing any right to due process pursuant to the medical staff bylaws.”
Some employment agreements may go even further and prohibit you from re-applying for medical staff privileges at that hospital for a stated period of time. For example:
“Physician further agrees that Physician shall not re-apply for medical staff privileges at Hospital X within two (2) years following the later of the termination of Physician’s employment or the effective date of termination of such medical staff privileges at Hospital X.”
Don’t forget about the hospital’s medical staff bylaws when entertaining an employment relationship with a hospital or private practice. The hospital’s medical staff bylaws should be reviewed in conjunction with the employment agreement.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
If you are a physician considering employment with a hospital or private practice in which hospital medical staff privileges will be needed or you are currently employed by a hospital or private practice and have medical staff privileges, it is imperative that you understand your rights as an employee and as a member of the hospital’s medical staff, along with the interplay between those two roles.
Employment Agreement and Hospital Medical Staff Bylaws
As an employee of a hospital or private practice, you will have an employment agreement that governs the terms of your employment. In addition, if you are on the hospital’s medical staff, you will also be subject to the hospital’s medical staff bylaws, which govern the terms of your staff membership and clinical privileges.
At the onset of an employment relationship, many physicians focus on the terms of their employment agreements, often ignoring the terms of the medical staff bylaws. This could lead to unexpected surprises, usually toward the end of the employment relationship, because both documents need to be read in conjunction with each other.
Beware of conflicting terms in your employment agreement on the one hand and the medical staff bylaws on the other. Although an employment agreement may include seemingly beneficial terms, hidden language often has the effect of negating its terms by qualifying the employment agreement with language contained in the bylaws. Examples include:
—“In the event of a conflict between the terms of the Physician’s Employment Agreement and the Medical Staff Bylaws, the Medical Staff Bylaws shall control.”
—“Subject to the Medical Staff Bylaws, Physician may …”
—“Except as otherwise stated in the Medical Staff Bylaws, Physician may …”
—“Except as permitted by the Medical Staff Bylaws, Physician may not …”
Termination of Medical Staff Privileges: Impact on Employment Agreement
Whether you are employed by a hospital or a private practice, your employment is likely at risk if your hospital medical staff privileges are suspended, revoked, or restricted. Even if your medical staff privileges are later reinstated, the initial suspension may trigger termination of your employment agreement.
Therefore, it is important to understand your due process rights, outlined in the hospital’s medical staff bylaws, as to how your privileges can be suspended, revoked, or restricted, as well as the procedure the hospital must undergo to make such a decision.
Medical staff bylaws also include a procedure for due process, including fair hearings and appeal mechanisms for medical staff decisions, such as privilege suspension, revocation, and restrictions.
Termination of Employment: Impact on Medical Staff Privileges
For hospital employees and most hospital-based physicians, termination of your employment agreement, whether for cause or without cause, may be automatic grounds for termination of your staff privileges. In such a case, your due process rights under the medical staff bylaws as they relate to your staff privileges are waived, and you will not be afforded the fair hearing and appeal procedure typically available to office-based physicians on the hospital’s medical staff.
Also, your employment agreement may contractually require you to resign from the hospital’s medical staff upon termination of the employment relationship. For example:
“Physician covenants and agrees that upon termination of Physician’s employment with Employer (whether for cause or without cause), Physician will resign from the medical staff of Hospital X, thereby relinquishing any right to due process pursuant to the medical staff bylaws.”
Some employment agreements may go even further and prohibit you from re-applying for medical staff privileges at that hospital for a stated period of time. For example:
“Physician further agrees that Physician shall not re-apply for medical staff privileges at Hospital X within two (2) years following the later of the termination of Physician’s employment or the effective date of termination of such medical staff privileges at Hospital X.”
Don’t forget about the hospital’s medical staff bylaws when entertaining an employment relationship with a hospital or private practice. The hospital’s medical staff bylaws should be reviewed in conjunction with the employment agreement.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
If you are a physician considering employment with a hospital or private practice in which hospital medical staff privileges will be needed or you are currently employed by a hospital or private practice and have medical staff privileges, it is imperative that you understand your rights as an employee and as a member of the hospital’s medical staff, along with the interplay between those two roles.
Employment Agreement and Hospital Medical Staff Bylaws
As an employee of a hospital or private practice, you will have an employment agreement that governs the terms of your employment. In addition, if you are on the hospital’s medical staff, you will also be subject to the hospital’s medical staff bylaws, which govern the terms of your staff membership and clinical privileges.
At the onset of an employment relationship, many physicians focus on the terms of their employment agreements, often ignoring the terms of the medical staff bylaws. This could lead to unexpected surprises, usually toward the end of the employment relationship, because both documents need to be read in conjunction with each other.
Beware of conflicting terms in your employment agreement on the one hand and the medical staff bylaws on the other. Although an employment agreement may include seemingly beneficial terms, hidden language often has the effect of negating its terms by qualifying the employment agreement with language contained in the bylaws. Examples include:
—“In the event of a conflict between the terms of the Physician’s Employment Agreement and the Medical Staff Bylaws, the Medical Staff Bylaws shall control.”
—“Subject to the Medical Staff Bylaws, Physician may …”
—“Except as otherwise stated in the Medical Staff Bylaws, Physician may …”
—“Except as permitted by the Medical Staff Bylaws, Physician may not …”
Termination of Medical Staff Privileges: Impact on Employment Agreement
Whether you are employed by a hospital or a private practice, your employment is likely at risk if your hospital medical staff privileges are suspended, revoked, or restricted. Even if your medical staff privileges are later reinstated, the initial suspension may trigger termination of your employment agreement.
Therefore, it is important to understand your due process rights, outlined in the hospital’s medical staff bylaws, as to how your privileges can be suspended, revoked, or restricted, as well as the procedure the hospital must undergo to make such a decision.
Medical staff bylaws also include a procedure for due process, including fair hearings and appeal mechanisms for medical staff decisions, such as privilege suspension, revocation, and restrictions.
Termination of Employment: Impact on Medical Staff Privileges
For hospital employees and most hospital-based physicians, termination of your employment agreement, whether for cause or without cause, may be automatic grounds for termination of your staff privileges. In such a case, your due process rights under the medical staff bylaws as they relate to your staff privileges are waived, and you will not be afforded the fair hearing and appeal procedure typically available to office-based physicians on the hospital’s medical staff.
Also, your employment agreement may contractually require you to resign from the hospital’s medical staff upon termination of the employment relationship. For example:
“Physician covenants and agrees that upon termination of Physician’s employment with Employer (whether for cause or without cause), Physician will resign from the medical staff of Hospital X, thereby relinquishing any right to due process pursuant to the medical staff bylaws.”
Some employment agreements may go even further and prohibit you from re-applying for medical staff privileges at that hospital for a stated period of time. For example:
“Physician further agrees that Physician shall not re-apply for medical staff privileges at Hospital X within two (2) years following the later of the termination of Physician’s employment or the effective date of termination of such medical staff privileges at Hospital X.”
Don’t forget about the hospital’s medical staff bylaws when entertaining an employment relationship with a hospital or private practice. The hospital’s medical staff bylaws should be reviewed in conjunction with the employment agreement.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Malpractice Counsel: Child abuse, methadone overdose
Missed Child Abuse
A 7-year-old girl was brought to the ED by her mother for discomfort with urination. The patient was otherwise healthy, up-to-date on all of her immunizations, and without any other complaints. Her vital signs were normal, and the physical examination was unremarkable. Although the chart did not reflect that a genitourinary examination was performed, the emergency physician (EP) stated that he had performed one.

A urinalysis was obtained, which was consistent with a bacterial infection. The patient was diagnosed with a urinary tract infection (UTI), prescribed an antibiotic, and discharged home with appropriate instructions.
Approximately 11 months later, it was discovered that the patient and her older sister were victims of sexual abuse by their 17-year-old stepbrother. Apparently, the abuse had started several months prior to the patient’s ED visit. The mother sued the EP and hospital for failure to recognize the signs and symptoms of sexual abuse. The plaintiff argued the child and mother should have been questioned about the possibility of sexual abuse, and that a more detailed physical examination would have shown evidence of abuse. The defense argued that the child’s presentation did not suggest sexual abuse; a defense verdict was returned.
Discussion
There are no reliable estimates of the incidence of pediatric sexual abuse in the United States. According to the most recent US Department of Health and Human Services Child Maltreatment Report, approximately 62,936 cases of child sexual abuse were reported in the United States in 2012, representing 9.3% of the total number of reported maltreatment cases that year.1 A meta-analysis of 22 US-based studies using national, local, and regional sampling found a much higher rate. This data suggest that 30% to 40% of girls and 13% of boys experienced sexual abuse during childhood.2
For EPs, sexually abused pediatric patients usually present in one of two ways: they are presented by a caregiver based on a suspicion or a disclosure of sexual abuse; or, in the more difficult presentation, they are brought in for evaluation of symptoms related to the genitourinary system or rectum. Such symptoms include vaginal discharge or anal or vaginal bleeding, and the presence of a sexually transmitted infection or UTI. While UTI is frequently listed as a potential sign of sexual abuse in children, there are no good data to demonstrate its frequency. Compounding this problem is that approximately 3% of girls and 1% of boys in the general population are diagnosed with a UTI prior to the onset of puberty.3 Interestingly, though most texts and articles discussing pediatric sexual abuse usually include UTI as a potential sign of abuse, reviews of UTIs in pediatric patients seldom include a discussion of sexual abuse as a potential etiology.
Emergency physicians must therefore maintain a high index of suspicion when evaluating a pediatric patient with a genitourinary or rectal complaint. If the child is old enough to give a history, the caregiver(s) should be asked to leave the room and the patient questioned directly about improper touching, physical activity, etc. The genital and perianal areas should be visually inspected. In general, a speculum examination is not necessary unless vaginal penetration is suspected or the patient is an older adolescent. The majority of pediatric patients can simply be examined in the supine, frog-leg position.
Physical signs of penetration include the presence of concavities (hymen notches), especially at the 6 o’clock position. In addition, irregularities in the hymen contour may be associated with prior injury. More obvious signs of sexual abuse include the presence of warts (condyloma acuminata or lata), vesicles, ulcers, bruising, or vaginal discharge.4 It is important to remember that the absence of physical findings does not exclude sexual abuse.
Laboratory testing of suspected victims of sexual abuse should include cultures of the vagina and rectum for gonorrhea and chlamydia, and throat cultures for gonorrhea.4 Additional testing should be based on the history and physical examination.
When an EP suspects child abuse, he or she must contact child protective services and/or law enforcement agencies, as required by law. It is imperative that the child be placed in a protected environment immediately; on occasion, this may require hospital admission.
This case emphasizes the need for EPs to at least consider sexual abuse in the pediatric patient with a genitourinary or rectal complaint.
Methadone Overdose: Intentional or Not
A 19-year-old woman presented to the ED via emergency medical services (EMS) unresponsive with shallow respirations. She had been found in her home by her grandmother. The paramedics brought the patient’s prescription medications to the ED, which included methadone, morphine, and naproxen. Reportedly, these medications had been prescribed by the patient’s family practitioner for chronic neck pain.

The patient was given intravenous naloxone (Narcan) and rapidly returned to her usual baseline. Her vital signs were normal and the physical examination was unremarkable. She told the EP that she had mistakenly taken the wrong dose of methadone, and vehemently denied any suicidal ideations or past attempts; she did not want to be admitted to the hospital. After several hours of observation, the patient remained in stable condition and without complaint. She was discharged home in the company of her grandmother, with instructions to continue her methadone, morphine, and naproxen, but to pay special attention to the dosage and frequency of use for each drug.
Four days later, the patient was found dead at home by her grandmother; the death was attributed to an overdose of methadone. The EP and hospital were sued by the plaintiff because of the discharge instructions to continue the same medication which had resulted in her first ED visit. The family practitioner was also sued for prescribing these medications to a patient with a history of drug abuse. At trial, it came to light that the patient had also probably ingested some illegally obtained hydrocodone/acetaminophen tablets (Vicodin). A defense verdict was returned.
Discussion
Deaths due to methadone overdose are becoming an increasing problem in the United States. In 2009 alone, more than 4 million prescriptions for methadone were written for pain patients.1 To place this figure in perspective, between 1997 and 2007 the number of grams of methadone prescribed in the United States increased more than 1,200%.2 According to US Centers for Disease Control and Prevention data from 2009, although methadone comprises approximately 2% of all analgesic prescription medications, it has been linked to more than 30% of overdose-related deaths due to prescription analgesics.1
Two factors contribute to this problem. Since methadone is so inexpensive, many states and insurance companies list it as the preferred opioid medication on their formularies. In addition, there is also the increased emphasis on physicians to adequately control pain. This helps explain, in part, for the dramatic increase in its use.
The second factor involves the toxicokinetics of methadone. This drug has a long and often unpredictable half-life, which can lead to toxic levels resulting in respiratory depression and death.1 Thus, methadone should only be prescribed by physicians well versed in its pharmacotherapy. Combined with the fact that there is very limited evidence supporting the use of methadone to treat acute or chronic pain unrelated to cancer, most experts agree there are better and safer alternatives.
This patient was treated appropriately in the ED regarding her resuscitation and observation. The real problem lies with the two narcotic medications she was prescribed for chronic pain. The combination of methadone and morphine in an otherwise healthy young woman probably should have raised a red flag. A conversation with the prescribing physician might have been helpful and resulted in a decrease in the dosage of one or both medications. Abrupt discontinuation, however, would not have been appropriate, since this would have resulted in opiate withdrawal and the associated effects of attending nausea, vomiting, diarrhea, diaphoresis, and abdominal cramping.
This patient was not a missed opportunity for psychiatric intervention and prevention of a suicide as there was no evidence she was ever depressed or suicidal. Rather, this was the case of a drug abuser accidently overdosing from multiple prescribed narcotic medications. It is going to take a multipronged effort to reverse this trend, including improved physician education regarding narcotic prescribing, additional resources to treat narcotic addiction, and improved identification of those at risk.
(Missed Child Abuse)
- U.S. Department of Health & Human Services. Administration on Children, Youth and Families, Administration for Children and Families Web site. Child maltreatment 2012. http://www.acf.hhs.gov/sites/default/files/cb/cm2012.pdf. Accessed October 23, 2014.
- Bolen RM, Scannapieco M. Presentation of child sexual abuse: a corrective meta-analysis. Social Serv Rev. 1999; 73(3): 281-313.
- Byerley JS, Steiner MJ: Urinary tract infection in infants and children. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw Hill Medical; 2011:854-860.
- Berkowitz CD, Claudius I, Tieder JS. Child abuse and neglect. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw Hill Medical; 2011:1976-1978.
(Methadone Overdose: Intentional or Not)
- Kuehn BM. Methadone overdose deaths rise with increased prescribing for pain. JAMA. 2012; 308(8):749-750.
- U.S. Department of Justice. Drug Enforcement Administration Office of Diversion Control Web site. Automation of reports and consolidation order system (ARCOS). http://www.deadiversion.usdoj.gov/arcos/index.html. Accessed October 23, 2014.
Missed Child Abuse
A 7-year-old girl was brought to the ED by her mother for discomfort with urination. The patient was otherwise healthy, up-to-date on all of her immunizations, and without any other complaints. Her vital signs were normal, and the physical examination was unremarkable. Although the chart did not reflect that a genitourinary examination was performed, the emergency physician (EP) stated that he had performed one.
A urinalysis was obtained, which was consistent with a bacterial infection. The patient was diagnosed with a urinary tract infection (UTI), prescribed an antibiotic, and discharged home with appropriate instructions.
Approximately 11 months later, it was discovered that the patient and her older sister were victims of sexual abuse by their 17-year-old stepbrother. Apparently, the abuse had started several months prior to the patient’s ED visit. The mother sued the EP and hospital for failure to recognize the signs and symptoms of sexual abuse. The plaintiff argued the child and mother should have been questioned about the possibility of sexual abuse, and that a more detailed physical examination would have shown evidence of abuse. The defense argued that the child’s presentation did not suggest sexual abuse; a defense verdict was returned.
Discussion
There are no reliable estimates of the incidence of pediatric sexual abuse in the United States. According to the most recent US Department of Health and Human Services Child Maltreatment Report, approximately 62,936 cases of child sexual abuse were reported in the United States in 2012, representing 9.3% of the total number of reported maltreatment cases that year.1 A meta-analysis of 22 US-based studies using national, local, and regional sampling found a much higher rate. This data suggest that 30% to 40% of girls and 13% of boys experienced sexual abuse during childhood.2
For EPs, sexually abused pediatric patients usually present in one of two ways: they are presented by a caregiver based on a suspicion or a disclosure of sexual abuse; or, in the more difficult presentation, they are brought in for evaluation of symptoms related to the genitourinary system or rectum. Such symptoms include vaginal discharge or anal or vaginal bleeding, and the presence of a sexually transmitted infection or UTI. While UTI is frequently listed as a potential sign of sexual abuse in children, there are no good data to demonstrate its frequency. Compounding this problem is that approximately 3% of girls and 1% of boys in the general population are diagnosed with a UTI prior to the onset of puberty.3 Interestingly, though most texts and articles discussing pediatric sexual abuse usually include UTI as a potential sign of abuse, reviews of UTIs in pediatric patients seldom include a discussion of sexual abuse as a potential etiology.
Emergency physicians must therefore maintain a high index of suspicion when evaluating a pediatric patient with a genitourinary or rectal complaint. If the child is old enough to give a history, the caregiver(s) should be asked to leave the room and the patient questioned directly about improper touching, physical activity, etc. The genital and perianal areas should be visually inspected. In general, a speculum examination is not necessary unless vaginal penetration is suspected or the patient is an older adolescent. The majority of pediatric patients can simply be examined in the supine, frog-leg position.
Physical signs of penetration include the presence of concavities (hymen notches), especially at the 6 o’clock position. In addition, irregularities in the hymen contour may be associated with prior injury. More obvious signs of sexual abuse include the presence of warts (condyloma acuminata or lata), vesicles, ulcers, bruising, or vaginal discharge.4 It is important to remember that the absence of physical findings does not exclude sexual abuse.
Laboratory testing of suspected victims of sexual abuse should include cultures of the vagina and rectum for gonorrhea and chlamydia, and throat cultures for gonorrhea.4 Additional testing should be based on the history and physical examination.
When an EP suspects child abuse, he or she must contact child protective services and/or law enforcement agencies, as required by law. It is imperative that the child be placed in a protected environment immediately; on occasion, this may require hospital admission.
This case emphasizes the need for EPs to at least consider sexual abuse in the pediatric patient with a genitourinary or rectal complaint.
Methadone Overdose: Intentional or Not
A 19-year-old woman presented to the ED via emergency medical services (EMS) unresponsive with shallow respirations. She had been found in her home by her grandmother. The paramedics brought the patient’s prescription medications to the ED, which included methadone, morphine, and naproxen. Reportedly, these medications had been prescribed by the patient’s family practitioner for chronic neck pain.
The patient was given intravenous naloxone (Narcan) and rapidly returned to her usual baseline. Her vital signs were normal and the physical examination was unremarkable. She told the EP that she had mistakenly taken the wrong dose of methadone, and vehemently denied any suicidal ideations or past attempts; she did not want to be admitted to the hospital. After several hours of observation, the patient remained in stable condition and without complaint. She was discharged home in the company of her grandmother, with instructions to continue her methadone, morphine, and naproxen, but to pay special attention to the dosage and frequency of use for each drug.
Four days later, the patient was found dead at home by her grandmother; the death was attributed to an overdose of methadone. The EP and hospital were sued by the plaintiff because of the discharge instructions to continue the same medication which had resulted in her first ED visit. The family practitioner was also sued for prescribing these medications to a patient with a history of drug abuse. At trial, it came to light that the patient had also probably ingested some illegally obtained hydrocodone/acetaminophen tablets (Vicodin). A defense verdict was returned.
Discussion
Deaths due to methadone overdose are becoming an increasing problem in the United States. In 2009 alone, more than 4 million prescriptions for methadone were written for pain patients.1 To place this figure in perspective, between 1997 and 2007 the number of grams of methadone prescribed in the United States increased more than 1,200%.2 According to US Centers for Disease Control and Prevention data from 2009, although methadone comprises approximately 2% of all analgesic prescription medications, it has been linked to more than 30% of overdose-related deaths due to prescription analgesics.1
Two factors contribute to this problem. Since methadone is so inexpensive, many states and insurance companies list it as the preferred opioid medication on their formularies. In addition, there is also the increased emphasis on physicians to adequately control pain. This helps explain, in part, for the dramatic increase in its use.
The second factor involves the toxicokinetics of methadone. This drug has a long and often unpredictable half-life, which can lead to toxic levels resulting in respiratory depression and death.1 Thus, methadone should only be prescribed by physicians well versed in its pharmacotherapy. Combined with the fact that there is very limited evidence supporting the use of methadone to treat acute or chronic pain unrelated to cancer, most experts agree there are better and safer alternatives.
This patient was treated appropriately in the ED regarding her resuscitation and observation. The real problem lies with the two narcotic medications she was prescribed for chronic pain. The combination of methadone and morphine in an otherwise healthy young woman probably should have raised a red flag. A conversation with the prescribing physician might have been helpful and resulted in a decrease in the dosage of one or both medications. Abrupt discontinuation, however, would not have been appropriate, since this would have resulted in opiate withdrawal and the associated effects of attending nausea, vomiting, diarrhea, diaphoresis, and abdominal cramping.
This patient was not a missed opportunity for psychiatric intervention and prevention of a suicide as there was no evidence she was ever depressed or suicidal. Rather, this was the case of a drug abuser accidently overdosing from multiple prescribed narcotic medications. It is going to take a multipronged effort to reverse this trend, including improved physician education regarding narcotic prescribing, additional resources to treat narcotic addiction, and improved identification of those at risk.
Missed Child Abuse
A 7-year-old girl was brought to the ED by her mother for discomfort with urination. The patient was otherwise healthy, up-to-date on all of her immunizations, and without any other complaints. Her vital signs were normal, and the physical examination was unremarkable. Although the chart did not reflect that a genitourinary examination was performed, the emergency physician (EP) stated that he had performed one.
A urinalysis was obtained, which was consistent with a bacterial infection. The patient was diagnosed with a urinary tract infection (UTI), prescribed an antibiotic, and discharged home with appropriate instructions.
Approximately 11 months later, it was discovered that the patient and her older sister were victims of sexual abuse by their 17-year-old stepbrother. Apparently, the abuse had started several months prior to the patient’s ED visit. The mother sued the EP and hospital for failure to recognize the signs and symptoms of sexual abuse. The plaintiff argued the child and mother should have been questioned about the possibility of sexual abuse, and that a more detailed physical examination would have shown evidence of abuse. The defense argued that the child’s presentation did not suggest sexual abuse; a defense verdict was returned.
Discussion
There are no reliable estimates of the incidence of pediatric sexual abuse in the United States. According to the most recent US Department of Health and Human Services Child Maltreatment Report, approximately 62,936 cases of child sexual abuse were reported in the United States in 2012, representing 9.3% of the total number of reported maltreatment cases that year.1 A meta-analysis of 22 US-based studies using national, local, and regional sampling found a much higher rate. This data suggest that 30% to 40% of girls and 13% of boys experienced sexual abuse during childhood.2
For EPs, sexually abused pediatric patients usually present in one of two ways: they are presented by a caregiver based on a suspicion or a disclosure of sexual abuse; or, in the more difficult presentation, they are brought in for evaluation of symptoms related to the genitourinary system or rectum. Such symptoms include vaginal discharge or anal or vaginal bleeding, and the presence of a sexually transmitted infection or UTI. While UTI is frequently listed as a potential sign of sexual abuse in children, there are no good data to demonstrate its frequency. Compounding this problem is that approximately 3% of girls and 1% of boys in the general population are diagnosed with a UTI prior to the onset of puberty.3 Interestingly, though most texts and articles discussing pediatric sexual abuse usually include UTI as a potential sign of abuse, reviews of UTIs in pediatric patients seldom include a discussion of sexual abuse as a potential etiology.
Emergency physicians must therefore maintain a high index of suspicion when evaluating a pediatric patient with a genitourinary or rectal complaint. If the child is old enough to give a history, the caregiver(s) should be asked to leave the room and the patient questioned directly about improper touching, physical activity, etc. The genital and perianal areas should be visually inspected. In general, a speculum examination is not necessary unless vaginal penetration is suspected or the patient is an older adolescent. The majority of pediatric patients can simply be examined in the supine, frog-leg position.
Physical signs of penetration include the presence of concavities (hymen notches), especially at the 6 o’clock position. In addition, irregularities in the hymen contour may be associated with prior injury. More obvious signs of sexual abuse include the presence of warts (condyloma acuminata or lata), vesicles, ulcers, bruising, or vaginal discharge.4 It is important to remember that the absence of physical findings does not exclude sexual abuse.
Laboratory testing of suspected victims of sexual abuse should include cultures of the vagina and rectum for gonorrhea and chlamydia, and throat cultures for gonorrhea.4 Additional testing should be based on the history and physical examination.
When an EP suspects child abuse, he or she must contact child protective services and/or law enforcement agencies, as required by law. It is imperative that the child be placed in a protected environment immediately; on occasion, this may require hospital admission.
This case emphasizes the need for EPs to at least consider sexual abuse in the pediatric patient with a genitourinary or rectal complaint.
Methadone Overdose: Intentional or Not
A 19-year-old woman presented to the ED via emergency medical services (EMS) unresponsive with shallow respirations. She had been found in her home by her grandmother. The paramedics brought the patient’s prescription medications to the ED, which included methadone, morphine, and naproxen. Reportedly, these medications had been prescribed by the patient’s family practitioner for chronic neck pain.
The patient was given intravenous naloxone (Narcan) and rapidly returned to her usual baseline. Her vital signs were normal and the physical examination was unremarkable. She told the EP that she had mistakenly taken the wrong dose of methadone, and vehemently denied any suicidal ideations or past attempts; she did not want to be admitted to the hospital. After several hours of observation, the patient remained in stable condition and without complaint. She was discharged home in the company of her grandmother, with instructions to continue her methadone, morphine, and naproxen, but to pay special attention to the dosage and frequency of use for each drug.
Four days later, the patient was found dead at home by her grandmother; the death was attributed to an overdose of methadone. The EP and hospital were sued by the plaintiff because of the discharge instructions to continue the same medication which had resulted in her first ED visit. The family practitioner was also sued for prescribing these medications to a patient with a history of drug abuse. At trial, it came to light that the patient had also probably ingested some illegally obtained hydrocodone/acetaminophen tablets (Vicodin). A defense verdict was returned.
Discussion
Deaths due to methadone overdose are becoming an increasing problem in the United States. In 2009 alone, more than 4 million prescriptions for methadone were written for pain patients.1 To place this figure in perspective, between 1997 and 2007 the number of grams of methadone prescribed in the United States increased more than 1,200%.2 According to US Centers for Disease Control and Prevention data from 2009, although methadone comprises approximately 2% of all analgesic prescription medications, it has been linked to more than 30% of overdose-related deaths due to prescription analgesics.1
Two factors contribute to this problem. Since methadone is so inexpensive, many states and insurance companies list it as the preferred opioid medication on their formularies. In addition, there is also the increased emphasis on physicians to adequately control pain. This helps explain, in part, for the dramatic increase in its use.
The second factor involves the toxicokinetics of methadone. This drug has a long and often unpredictable half-life, which can lead to toxic levels resulting in respiratory depression and death.1 Thus, methadone should only be prescribed by physicians well versed in its pharmacotherapy. Combined with the fact that there is very limited evidence supporting the use of methadone to treat acute or chronic pain unrelated to cancer, most experts agree there are better and safer alternatives.
This patient was treated appropriately in the ED regarding her resuscitation and observation. The real problem lies with the two narcotic medications she was prescribed for chronic pain. The combination of methadone and morphine in an otherwise healthy young woman probably should have raised a red flag. A conversation with the prescribing physician might have been helpful and resulted in a decrease in the dosage of one or both medications. Abrupt discontinuation, however, would not have been appropriate, since this would have resulted in opiate withdrawal and the associated effects of attending nausea, vomiting, diarrhea, diaphoresis, and abdominal cramping.
This patient was not a missed opportunity for psychiatric intervention and prevention of a suicide as there was no evidence she was ever depressed or suicidal. Rather, this was the case of a drug abuser accidently overdosing from multiple prescribed narcotic medications. It is going to take a multipronged effort to reverse this trend, including improved physician education regarding narcotic prescribing, additional resources to treat narcotic addiction, and improved identification of those at risk.
(Missed Child Abuse)
- U.S. Department of Health & Human Services. Administration on Children, Youth and Families, Administration for Children and Families Web site. Child maltreatment 2012. http://www.acf.hhs.gov/sites/default/files/cb/cm2012.pdf. Accessed October 23, 2014.
- Bolen RM, Scannapieco M. Presentation of child sexual abuse: a corrective meta-analysis. Social Serv Rev. 1999; 73(3): 281-313.
- Byerley JS, Steiner MJ: Urinary tract infection in infants and children. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw Hill Medical; 2011:854-860.
- Berkowitz CD, Claudius I, Tieder JS. Child abuse and neglect. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw Hill Medical; 2011:1976-1978.
(Methadone Overdose: Intentional or Not)
- Kuehn BM. Methadone overdose deaths rise with increased prescribing for pain. JAMA. 2012; 308(8):749-750.
- U.S. Department of Justice. Drug Enforcement Administration Office of Diversion Control Web site. Automation of reports and consolidation order system (ARCOS). http://www.deadiversion.usdoj.gov/arcos/index.html. Accessed October 23, 2014.
(Missed Child Abuse)
- U.S. Department of Health & Human Services. Administration on Children, Youth and Families, Administration for Children and Families Web site. Child maltreatment 2012. http://www.acf.hhs.gov/sites/default/files/cb/cm2012.pdf. Accessed October 23, 2014.
- Bolen RM, Scannapieco M. Presentation of child sexual abuse: a corrective meta-analysis. Social Serv Rev. 1999; 73(3): 281-313.
- Byerley JS, Steiner MJ: Urinary tract infection in infants and children. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw Hill Medical; 2011:854-860.
- Berkowitz CD, Claudius I, Tieder JS. Child abuse and neglect. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw Hill Medical; 2011:1976-1978.
(Methadone Overdose: Intentional or Not)
- Kuehn BM. Methadone overdose deaths rise with increased prescribing for pain. JAMA. 2012; 308(8):749-750.
- U.S. Department of Justice. Drug Enforcement Administration Office of Diversion Control Web site. Automation of reports and consolidation order system (ARCOS). http://www.deadiversion.usdoj.gov/arcos/index.html. Accessed October 23, 2014.

When the Biggest Mistake Yields the Smallest Impact
In February 2007, a 65-year-old man consulted an internist. A blood test showed an infection. Antibiotics were administered successfully, and the patient was declared free of infection. He was noted to have a heart murmur, however, prompting the internist to refer him to a cardiologist, Dr K., for an echocardiogram.
But the internist’s nurse practitioner provided the wrong clinical indication for the referral. As a result, Dr K., unaware of what to look for, read the echocardiogram as negative. The internist and NP did not realize the mistake, because they never requested a copy of the results.
The internist later sent the patient to an infectious disease (ID) specialist, Dr G., to rule out endocarditis. Dr G.’s opinion was that there was no infection.
The patient’s condition deteriorated, however, and he was admitted to a hospital in early May 2007. Two day later, he was diagnosed with endocarditis. He subsequently underwent open-heart surgery and received antibiotics. He died later that month.
Continue for the outcome and David Lang's comments >>
OUTCOME
A $1.2 million settlement was reached, with Dr K. paying $500,000, the internist and NP paying another $500,000, and Dr G. responsible for $200,000.
COMMENT
Here, the causal problem was a communication breakdown between the primary care provider and the cardiologist.
When ordering a test, the indication may be as important as the choice of modality. Be mindful to include the indication and patient history wherever relevant—particularly when you as the referring clinician do not directly speak to the specialist. This holds true for all diagnostic studies, but particularly for laboratory analysis and imaging studies, when the clinician and the appropriate department do not communicate verbally.
We think of studies as automated—and some are. But many more involve human decision making and interpretation.
Imaging always involves the selection of modality, which may not be chosen correctly if the technician does not know or understand what the clinician is looking for.
The same is true with laboratory analysis: While a complete blood count and electrolyte measurements are automated, other tests aren’t. When a lab technician performs a manual differential or reviews a stool specimen for ova and parasites, a human is selecting a technique and interpreting the results. When a pathologist analyzes a specimen, a human process of evaluation and interpretation is rendered based on an understanding of the issue.
Don’t order tests in a vacuum. Give your human interpreters—technicians, pathologists, radiologists—as much information about the clinical case as you reasonably can. Any unusual cases involving zebra hunting are ripe candidates for misunderstanding and require a phone call.
Clearly communicating the patient history and indication also may be helpful when the clinician has ordered an incorrect or suboptimal study. If you order a standard forearm radiograph, you will get imaging of the bones. However, if you are looking for soft-tissue foreign bodies, a soft-tissue technique is better. When the indication is communicated, it gives the technician a chance to call the unknowing clinician to discuss the better option. Keeping diagnostic staff in the dark helps no one.
Finally, when you are the evaluator, protect yourself and the patient. When asked to review a study, in your report echo back the indication for the study and what you’ve been asked to address. This ensures the ordering clinician knows how the study was undertaken and what you were looking for, and it provides an opportunity to restudy if needed. Make sure to discuss limitations in the test modality and what follow-up or repeat studies would be required to properly address the indication. Make sure the report is forwarded to the ordering clinician. If the indication is unclear or the wrong test was chosen—call the ordering clinician.
Here, the internist’s NP ordered an echocardiogram to evaluate a heart murmur. We don’t know what the stated indication for the echocardiogram was, but it was not endocarditis. The cardiologist interpreted the echocardiogram as normal. Would he have detected valvular vegetations if he knew the ordering clinician was concerned about endocarditis?
The jury was persuaded that the cardiologist’s negative interpretation of the echocardiogram breached the standard of care—even given the fact he was given the wrong indication for the study. The jury also faulted the primary care clinicians, likely in part for providing the wrong indication and in part for failing to review the report.
Interestingly, the ID specialist was held least culpable (in payment terms), despite being explicitly requested to rule out endocarditis—and failing to do so. This is probably due to a short interval between the ID physician’s evaluation and the patient’s final admission. Even given the massive breach of the standard of care in failure to diagnose endocarditis, a short delay would have a relatively modest causal role in the patient’s deterioration.
Thus, even though the ID physician arguably made the biggest mistake, it may have had the least impact on the patient’s overall condition—leaving the ID physician less legally culpable in terms of damages. —DML
In February 2007, a 65-year-old man consulted an internist. A blood test showed an infection. Antibiotics were administered successfully, and the patient was declared free of infection. He was noted to have a heart murmur, however, prompting the internist to refer him to a cardiologist, Dr K., for an echocardiogram.
But the internist’s nurse practitioner provided the wrong clinical indication for the referral. As a result, Dr K., unaware of what to look for, read the echocardiogram as negative. The internist and NP did not realize the mistake, because they never requested a copy of the results.
The internist later sent the patient to an infectious disease (ID) specialist, Dr G., to rule out endocarditis. Dr G.’s opinion was that there was no infection.
The patient’s condition deteriorated, however, and he was admitted to a hospital in early May 2007. Two day later, he was diagnosed with endocarditis. He subsequently underwent open-heart surgery and received antibiotics. He died later that month.
Continue for the outcome and David Lang's comments >>
OUTCOME
A $1.2 million settlement was reached, with Dr K. paying $500,000, the internist and NP paying another $500,000, and Dr G. responsible for $200,000.
COMMENT
Here, the causal problem was a communication breakdown between the primary care provider and the cardiologist.
When ordering a test, the indication may be as important as the choice of modality. Be mindful to include the indication and patient history wherever relevant—particularly when you as the referring clinician do not directly speak to the specialist. This holds true for all diagnostic studies, but particularly for laboratory analysis and imaging studies, when the clinician and the appropriate department do not communicate verbally.
We think of studies as automated—and some are. But many more involve human decision making and interpretation.
Imaging always involves the selection of modality, which may not be chosen correctly if the technician does not know or understand what the clinician is looking for.
The same is true with laboratory analysis: While a complete blood count and electrolyte measurements are automated, other tests aren’t. When a lab technician performs a manual differential or reviews a stool specimen for ova and parasites, a human is selecting a technique and interpreting the results. When a pathologist analyzes a specimen, a human process of evaluation and interpretation is rendered based on an understanding of the issue.
Don’t order tests in a vacuum. Give your human interpreters—technicians, pathologists, radiologists—as much information about the clinical case as you reasonably can. Any unusual cases involving zebra hunting are ripe candidates for misunderstanding and require a phone call.
Clearly communicating the patient history and indication also may be helpful when the clinician has ordered an incorrect or suboptimal study. If you order a standard forearm radiograph, you will get imaging of the bones. However, if you are looking for soft-tissue foreign bodies, a soft-tissue technique is better. When the indication is communicated, it gives the technician a chance to call the unknowing clinician to discuss the better option. Keeping diagnostic staff in the dark helps no one.
Finally, when you are the evaluator, protect yourself and the patient. When asked to review a study, in your report echo back the indication for the study and what you’ve been asked to address. This ensures the ordering clinician knows how the study was undertaken and what you were looking for, and it provides an opportunity to restudy if needed. Make sure to discuss limitations in the test modality and what follow-up or repeat studies would be required to properly address the indication. Make sure the report is forwarded to the ordering clinician. If the indication is unclear or the wrong test was chosen—call the ordering clinician.
Here, the internist’s NP ordered an echocardiogram to evaluate a heart murmur. We don’t know what the stated indication for the echocardiogram was, but it was not endocarditis. The cardiologist interpreted the echocardiogram as normal. Would he have detected valvular vegetations if he knew the ordering clinician was concerned about endocarditis?
The jury was persuaded that the cardiologist’s negative interpretation of the echocardiogram breached the standard of care—even given the fact he was given the wrong indication for the study. The jury also faulted the primary care clinicians, likely in part for providing the wrong indication and in part for failing to review the report.
Interestingly, the ID specialist was held least culpable (in payment terms), despite being explicitly requested to rule out endocarditis—and failing to do so. This is probably due to a short interval between the ID physician’s evaluation and the patient’s final admission. Even given the massive breach of the standard of care in failure to diagnose endocarditis, a short delay would have a relatively modest causal role in the patient’s deterioration.
Thus, even though the ID physician arguably made the biggest mistake, it may have had the least impact on the patient’s overall condition—leaving the ID physician less legally culpable in terms of damages. —DML
In February 2007, a 65-year-old man consulted an internist. A blood test showed an infection. Antibiotics were administered successfully, and the patient was declared free of infection. He was noted to have a heart murmur, however, prompting the internist to refer him to a cardiologist, Dr K., for an echocardiogram.
But the internist’s nurse practitioner provided the wrong clinical indication for the referral. As a result, Dr K., unaware of what to look for, read the echocardiogram as negative. The internist and NP did not realize the mistake, because they never requested a copy of the results.
The internist later sent the patient to an infectious disease (ID) specialist, Dr G., to rule out endocarditis. Dr G.’s opinion was that there was no infection.
The patient’s condition deteriorated, however, and he was admitted to a hospital in early May 2007. Two day later, he was diagnosed with endocarditis. He subsequently underwent open-heart surgery and received antibiotics. He died later that month.
Continue for the outcome and David Lang's comments >>
OUTCOME
A $1.2 million settlement was reached, with Dr K. paying $500,000, the internist and NP paying another $500,000, and Dr G. responsible for $200,000.
COMMENT
Here, the causal problem was a communication breakdown between the primary care provider and the cardiologist.
When ordering a test, the indication may be as important as the choice of modality. Be mindful to include the indication and patient history wherever relevant—particularly when you as the referring clinician do not directly speak to the specialist. This holds true for all diagnostic studies, but particularly for laboratory analysis and imaging studies, when the clinician and the appropriate department do not communicate verbally.
We think of studies as automated—and some are. But many more involve human decision making and interpretation.
Imaging always involves the selection of modality, which may not be chosen correctly if the technician does not know or understand what the clinician is looking for.
The same is true with laboratory analysis: While a complete blood count and electrolyte measurements are automated, other tests aren’t. When a lab technician performs a manual differential or reviews a stool specimen for ova and parasites, a human is selecting a technique and interpreting the results. When a pathologist analyzes a specimen, a human process of evaluation and interpretation is rendered based on an understanding of the issue.
Don’t order tests in a vacuum. Give your human interpreters—technicians, pathologists, radiologists—as much information about the clinical case as you reasonably can. Any unusual cases involving zebra hunting are ripe candidates for misunderstanding and require a phone call.
Clearly communicating the patient history and indication also may be helpful when the clinician has ordered an incorrect or suboptimal study. If you order a standard forearm radiograph, you will get imaging of the bones. However, if you are looking for soft-tissue foreign bodies, a soft-tissue technique is better. When the indication is communicated, it gives the technician a chance to call the unknowing clinician to discuss the better option. Keeping diagnostic staff in the dark helps no one.
Finally, when you are the evaluator, protect yourself and the patient. When asked to review a study, in your report echo back the indication for the study and what you’ve been asked to address. This ensures the ordering clinician knows how the study was undertaken and what you were looking for, and it provides an opportunity to restudy if needed. Make sure to discuss limitations in the test modality and what follow-up or repeat studies would be required to properly address the indication. Make sure the report is forwarded to the ordering clinician. If the indication is unclear or the wrong test was chosen—call the ordering clinician.
Here, the internist’s NP ordered an echocardiogram to evaluate a heart murmur. We don’t know what the stated indication for the echocardiogram was, but it was not endocarditis. The cardiologist interpreted the echocardiogram as normal. Would he have detected valvular vegetations if he knew the ordering clinician was concerned about endocarditis?
The jury was persuaded that the cardiologist’s negative interpretation of the echocardiogram breached the standard of care—even given the fact he was given the wrong indication for the study. The jury also faulted the primary care clinicians, likely in part for providing the wrong indication and in part for failing to review the report.
Interestingly, the ID specialist was held least culpable (in payment terms), despite being explicitly requested to rule out endocarditis—and failing to do so. This is probably due to a short interval between the ID physician’s evaluation and the patient’s final admission. Even given the massive breach of the standard of care in failure to diagnose endocarditis, a short delay would have a relatively modest causal role in the patient’s deterioration.
Thus, even though the ID physician arguably made the biggest mistake, it may have had the least impact on the patient’s overall condition—leaving the ID physician less legally culpable in terms of damages. —DML