User login
Uterine rupture, child stillborn: $3.8M net award
Uterine rupture, child stillborn: $3.8M net award
At 35 weeks' gestation, a woman went to the emergency department (ED) with abdominal pain, fast heartbeat, and irregular contractions. Her history included three cesarean deliveries, including one with a vertical incision. She was admitted, and a cesarean delivery was planned for the next day. After 8 hours, during which the patient’s condition worsened, an emergency cesarean delivery was undertaken. A full rupture of the uterus was found; the baby’s body had extruded into the mother’s abdomen. The child was stillborn.
PARENTS’ CLAIM The stillbirth could have been avoided if the nurses had communicated the mother’s worsening condition to the physicians.
DEFENDANTS’ DEFENSE After the hospital and physicians settled prior to trial, the case continued against the nurse in charge of the mother’s care and the nurse-staffing group. Negligence was denied; all protocols were followed.
VERDICT A $2.9 million Illinois verdict was returned. With a $900,000 settlement from the hospital and physicians, the net award was $3.8 million.
_______________
Where did rare strep A infection come from?
A 36-year-old woman reported heavy vaginal bleeding to her ObGyn. She underwent endometrial ablation in her physician’s office.
The next day, the woman called the office to report abdominal pain. She was told to stop the medication she was taking, and if the pain continued to the next day, to go to an ED. The next day, the patient went to the ED and was found to be in septic shock. During emergency laparotomy, 50 mL of purulent fluid were drained and an emergency hysterectomy was performed. Three days later, the patient died from pulmonary arrest caused by toxic shock syndrome. An autopsy revealed that the patient’s sepsis was caused by group A streptococci (GAS) infection.
ESTATE’S CLAIM The patient was not a proper candidate for endometrial ablation because of her history of chronic cervical infection. The ObGyn perforated the cervix during the procedure and tried to conceal it. At autopsy, bone wax was found in the rectal lumen that had been used to cover up damage to the cervix. The ObGyn introduced GAS bacteria into the patient’s system. The ObGyn’s staff failed to ask the proper questions when she called the day after the procedure. She should have been told to go directly to the ED.
DEFENDANTS’ DEFENSE The ObGyn did not perforate the cervix or uterus during the procedure. GAS infection is so rare that it would have been difficult to foresee or diagnose. Potentially, the patient had a chronic
cervical infection before ablation.
VERDICT A Texas defense verdict was returned.
_______________
DURING INSERTION, IUD PERFORATES UTERINE WALL; LATER FOUND BELOW LIVER
On July 21, a 46-year-old woman went to an ObGyn for placement of an intrauterine device (IUD). Shortly after the ObGyn inserted the levonorgestrel-releasing intrauterine system (Mirena, Bayer HealthCare), the patient reported severe pelvic and abdominal pain. On July 26, the patient underwent surgical removal of the IUD.
She was discharged on July 29 but continued to report pain. She was readmitted to the hospital the next day and treated for pain. She was bed ridden for 3 weeks after IUD-removal surgery, and had a 3-month recovery before feeling pain free.
PATIENT’S CLAIM The ObGyn was negligent in perforating the patient’s uterine wall during IUD insertion, causing the device to ultimately migrate under the patient’s liver.
DEFENDANTS’ DEFENSE Uterine perforation is a known complication of IUD insertion. The IUD escaped from the patient’s uterus at a later time and not during the insertion procedure.
VERDICT A Florida verdict of $208,839 was returned; the amount was reduced to $161,058 because the medical expenses were written off by the health-care providers.
_______________

Was travel appropriate for this pregnant woman?
A woman with a history of two premature deliveries and one miscarriage became pregnant again. She received prenatal care at an Army hospital. She traveled to Spain, where the baby was born at 31 weeks’ gestation. The baby required treatment in a neonatal intensive care unit (NICU) for 17 days. The child has cerebral palsy, with tetraplegia of all four extremities. She cannot walk without assistance and suffers severe cognitive and vision impairment.
PARENTS’ CLAIM The ObGyn at the Army hospital should not have approved the mother’s request for travel; he did so, despite knowing that the mother was at high risk for premature birth. The military medical hospital to which she was assigned in Spain could not manage a high-risk pregnancy, didn’t have a NICU, and didn’t have specialists to treat premature infants.
DEFENDANTS’ DEFENSE The ObGyn argued that he did not have access to the medical records showing the mother’s history. The patient countered that the ObGyn did indeed have the patient’s records, as he had discussed them with her.
VERDICT A $10,409,700 California verdict was returned against the ObGyn and the government facility.
_______________
Triple-negative BrCa not diagnosed until metastasized: $5.2M
After finding lumps in both breasts, a woman in her 30s saw a nurse practitioner (NP) at an Army hospital. A radiologist reported no mass in the right breast and multiple benign-appearing anechoic lesions in the left breast after bilateral mammography and ultrasonography (US) in July 2008. The Chief of Mammography Services recommended referral to a breast surgeon, but the patient never received the letter. It was placed in her mammography file, not in the treatment file.
In November 2008, the patient returned to the clinic. Bilateral diagnostic mammography and US were ordered, but for unknown reasons, cancelled. US of the left breast was interpreted as benign in January 2009.
After imaging in March 2010, followed by a needle biopsy of the right breast, a radiologist reported finding intermediate-grade infiltrating ductal carcinoma.
The patient sought care outside the military medical system at a large university hospital. In April 2010, stage 3 triple-negative invasive ductal carcinoma (IDC) was identified. The patient underwent chemotherapy, a double mastectomy, removal of 21 lymph nodes, and breast reconstruction. She was given a 60% chance of recurrence in 5–7 years.
PATIENT’S CLAIM It was negligent to not inform her of imaging results. Biopsy should have been performed in 2008, when the IDC was likely at stage 1; treatment would have been far less aggressive. Electronic medical records showed that the 2008 mammography and US results had been “signed off” by an NP at the clinic.
DEFENDANTS’ DEFENSE While unable to concede liability, the government agency did not contest the point.
VERDICT A $5.2 million Tennessee federal court bench verdict was returned, citing failures in communication, poor and improper record keeping and retention, failure to follow-up, and an unexplained cancellation of a medical order.
_______________
Woman dies from cervical cancer: $2.3M
In 2001, a 41-year-old woman had abnormal Pap smear results but her gynecologist did not order more testing. The patient was told to return in 3 months, but she did not return until 2007—reporting abnormal bleeding, vaginal discharge, and pain. Her Pap results were normal, however, and the gynecologist did not order further testing. In 2009, the patient was found to have advanced cervical cancer. She died 2 years later.
ESTATE’S CLAIM Further testing should have been ordered in 2001, which would have likely revealed dysplasia, which can lead to cancer. The laboratory incorrectly interpreted the 2007 Pap test; if the results had been properly reported, additional testing could have been ordered.
DEFENDANTS’ DEFENSE The laboratory and patient’s estate settled for a confidential amount before trial. The gynecologist denied negligence.
VERDICT A New Jersey jury found the gynecologist 40% at fault for his actions in 2007. The jury found the laboratory 50% at fault, and the patient 10% at fault. A gross verdict of $2.33 million was returned.
_______________
Bowel injury after cesarean delivery; mother dies of sepsis
At 40 4/7 weeks' gestation, a 37-year-old woman gave birth to a healthy child by cesarean delivery. The next day, the patient had an elevated white blood cell (WBC) count with a left shift, her abdomen was tympanic but soft, and she was passing flatus and belching. The ObGyn ordered a Fleet enema; only flatus was released. A covering ObGyn ordered an abdominal radiograph, which the radiologist reported as showing postoperative ileus and mild constipation. The patient was given a second Fleet enema the next day, resulting in watery stool. She vomited 300 mL of dark green fluid.
After a rectal tube was placed 2 days later, one hard brown stool and several brown, pasty, loose, and liquid stools were returned. She vomited several times that day, and was found to have hypoactive bowel sounds with continued tympanic quality in the upper quadrants. Laboratory testing revealed continued elevated WBC count with left shift. The next day, she had hypoactive bowel sounds with brown liquid stools. Later that morning, she was able to tolerate clear liquids. The ObGyn decided to discharge her home with instructions to continue on a clear liquid diet for 2 more days before advancing her diet.
The day after discharge, she was found unresponsive at home. She was taken to the hospital, but resuscitation attempts failed. She died. An autopsy revealed that the cause of death was sepsis.
ESTATE’S CLAIM The ObGyn was negligent in failing to diagnose and treat a postoperative intra-abdominal infection caused by bowel perforation. A surgical consult should have been obtained. The woman was prematurely discharged. The radiologist failed to report the presence of free air on the abdominal x-ray.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $1 million Maryland settlement was reached.
_______________
Right ureter injury detected and repaired
During laparoscopic-assisted vaginal hysterectomy, the ObGyn detected and repaired an injury to the right ureter. The patient’s recovery was delayed by the injury.
PATIENT’S CLAIM The ObGyn was negligent in using a Kleppinger bipolar cauterizing instrument to cauterize the vaginal cuff. Thermal overspray from the instrument or the instrument itself damaged the ureter. The ObGyn was also negligent in not performing diagnostic cystoscopy to confirm patency of the ureter after the repair was made.
PHYSICIAN’S DEFENSE Ureter injury is a known risk of the procedure. All procedures were performed according to protocol.
VERDICT A Florida defense verdict was returned.
_______________
Failure to detect inflammatory BrCa; woman dies
A 42-year-old woman underwent mammography in February 2002 after reporting pain, discoloration, inflammation, and swelling in her left breast. The radiologist who interpreted the mammography suggested a biopsy for a differential diagnosis of mastitis or inflammatory carcinoma. The biopsy results were negative.
The patient’s symptoms persisted, and she underwent US in late May 2002. Another radiologist interpreted the US, noting that the patient could not tolerate compression, which led to less than optimal evaluation. The radiologist suggested that mastitis was the likely cause of the patient’s symptoms.
The patient then consulted a surgeon, who ordered mammography and magnetic resonance imaging (MRI) followed by biopsy, which indicated cancer. The patient underwent a mastectomy but metastasis had already occurred. She died at age 50 prior to the trial.
ESTATE’S CLAIM If the cancer had been diagnosed earlier, the outcome would have been better. Both radiologists misinterpreted the mammographies.
DEFENDANTS’ DEFENSE The mammographies had been properly interpreted. Any missed diagnosis would not have impacted the outcome due to the type of cancer. The scans had been released to the patient, but were subsequently lost; an adverse interference instruction was given to the jury.
VERDICT A New York defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Uterine rupture, child stillborn: $3.8M net award
At 35 weeks' gestation, a woman went to the emergency department (ED) with abdominal pain, fast heartbeat, and irregular contractions. Her history included three cesarean deliveries, including one with a vertical incision. She was admitted, and a cesarean delivery was planned for the next day. After 8 hours, during which the patient’s condition worsened, an emergency cesarean delivery was undertaken. A full rupture of the uterus was found; the baby’s body had extruded into the mother’s abdomen. The child was stillborn.
PARENTS’ CLAIM The stillbirth could have been avoided if the nurses had communicated the mother’s worsening condition to the physicians.
DEFENDANTS’ DEFENSE After the hospital and physicians settled prior to trial, the case continued against the nurse in charge of the mother’s care and the nurse-staffing group. Negligence was denied; all protocols were followed.
VERDICT A $2.9 million Illinois verdict was returned. With a $900,000 settlement from the hospital and physicians, the net award was $3.8 million.
_______________
Where did rare strep A infection come from?
A 36-year-old woman reported heavy vaginal bleeding to her ObGyn. She underwent endometrial ablation in her physician’s office.
The next day, the woman called the office to report abdominal pain. She was told to stop the medication she was taking, and if the pain continued to the next day, to go to an ED. The next day, the patient went to the ED and was found to be in septic shock. During emergency laparotomy, 50 mL of purulent fluid were drained and an emergency hysterectomy was performed. Three days later, the patient died from pulmonary arrest caused by toxic shock syndrome. An autopsy revealed that the patient’s sepsis was caused by group A streptococci (GAS) infection.
ESTATE’S CLAIM The patient was not a proper candidate for endometrial ablation because of her history of chronic cervical infection. The ObGyn perforated the cervix during the procedure and tried to conceal it. At autopsy, bone wax was found in the rectal lumen that had been used to cover up damage to the cervix. The ObGyn introduced GAS bacteria into the patient’s system. The ObGyn’s staff failed to ask the proper questions when she called the day after the procedure. She should have been told to go directly to the ED.
DEFENDANTS’ DEFENSE The ObGyn did not perforate the cervix or uterus during the procedure. GAS infection is so rare that it would have been difficult to foresee or diagnose. Potentially, the patient had a chronic
cervical infection before ablation.
VERDICT A Texas defense verdict was returned.
_______________
DURING INSERTION, IUD PERFORATES UTERINE WALL; LATER FOUND BELOW LIVER
On July 21, a 46-year-old woman went to an ObGyn for placement of an intrauterine device (IUD). Shortly after the ObGyn inserted the levonorgestrel-releasing intrauterine system (Mirena, Bayer HealthCare), the patient reported severe pelvic and abdominal pain. On July 26, the patient underwent surgical removal of the IUD.
She was discharged on July 29 but continued to report pain. She was readmitted to the hospital the next day and treated for pain. She was bed ridden for 3 weeks after IUD-removal surgery, and had a 3-month recovery before feeling pain free.
PATIENT’S CLAIM The ObGyn was negligent in perforating the patient’s uterine wall during IUD insertion, causing the device to ultimately migrate under the patient’s liver.
DEFENDANTS’ DEFENSE Uterine perforation is a known complication of IUD insertion. The IUD escaped from the patient’s uterus at a later time and not during the insertion procedure.
VERDICT A Florida verdict of $208,839 was returned; the amount was reduced to $161,058 because the medical expenses were written off by the health-care providers.
_______________
Was travel appropriate for this pregnant woman?
A woman with a history of two premature deliveries and one miscarriage became pregnant again. She received prenatal care at an Army hospital. She traveled to Spain, where the baby was born at 31 weeks’ gestation. The baby required treatment in a neonatal intensive care unit (NICU) for 17 days. The child has cerebral palsy, with tetraplegia of all four extremities. She cannot walk without assistance and suffers severe cognitive and vision impairment.
PARENTS’ CLAIM The ObGyn at the Army hospital should not have approved the mother’s request for travel; he did so, despite knowing that the mother was at high risk for premature birth. The military medical hospital to which she was assigned in Spain could not manage a high-risk pregnancy, didn’t have a NICU, and didn’t have specialists to treat premature infants.
DEFENDANTS’ DEFENSE The ObGyn argued that he did not have access to the medical records showing the mother’s history. The patient countered that the ObGyn did indeed have the patient’s records, as he had discussed them with her.
VERDICT A $10,409,700 California verdict was returned against the ObGyn and the government facility.
_______________
Triple-negative BrCa not diagnosed until metastasized: $5.2M
After finding lumps in both breasts, a woman in her 30s saw a nurse practitioner (NP) at an Army hospital. A radiologist reported no mass in the right breast and multiple benign-appearing anechoic lesions in the left breast after bilateral mammography and ultrasonography (US) in July 2008. The Chief of Mammography Services recommended referral to a breast surgeon, but the patient never received the letter. It was placed in her mammography file, not in the treatment file.
In November 2008, the patient returned to the clinic. Bilateral diagnostic mammography and US were ordered, but for unknown reasons, cancelled. US of the left breast was interpreted as benign in January 2009.
After imaging in March 2010, followed by a needle biopsy of the right breast, a radiologist reported finding intermediate-grade infiltrating ductal carcinoma.
The patient sought care outside the military medical system at a large university hospital. In April 2010, stage 3 triple-negative invasive ductal carcinoma (IDC) was identified. The patient underwent chemotherapy, a double mastectomy, removal of 21 lymph nodes, and breast reconstruction. She was given a 60% chance of recurrence in 5–7 years.
PATIENT’S CLAIM It was negligent to not inform her of imaging results. Biopsy should have been performed in 2008, when the IDC was likely at stage 1; treatment would have been far less aggressive. Electronic medical records showed that the 2008 mammography and US results had been “signed off” by an NP at the clinic.
DEFENDANTS’ DEFENSE While unable to concede liability, the government agency did not contest the point.
VERDICT A $5.2 million Tennessee federal court bench verdict was returned, citing failures in communication, poor and improper record keeping and retention, failure to follow-up, and an unexplained cancellation of a medical order.
_______________
Woman dies from cervical cancer: $2.3M
In 2001, a 41-year-old woman had abnormal Pap smear results but her gynecologist did not order more testing. The patient was told to return in 3 months, but she did not return until 2007—reporting abnormal bleeding, vaginal discharge, and pain. Her Pap results were normal, however, and the gynecologist did not order further testing. In 2009, the patient was found to have advanced cervical cancer. She died 2 years later.
ESTATE’S CLAIM Further testing should have been ordered in 2001, which would have likely revealed dysplasia, which can lead to cancer. The laboratory incorrectly interpreted the 2007 Pap test; if the results had been properly reported, additional testing could have been ordered.
DEFENDANTS’ DEFENSE The laboratory and patient’s estate settled for a confidential amount before trial. The gynecologist denied negligence.
VERDICT A New Jersey jury found the gynecologist 40% at fault for his actions in 2007. The jury found the laboratory 50% at fault, and the patient 10% at fault. A gross verdict of $2.33 million was returned.
_______________
Bowel injury after cesarean delivery; mother dies of sepsis
At 40 4/7 weeks' gestation, a 37-year-old woman gave birth to a healthy child by cesarean delivery. The next day, the patient had an elevated white blood cell (WBC) count with a left shift, her abdomen was tympanic but soft, and she was passing flatus and belching. The ObGyn ordered a Fleet enema; only flatus was released. A covering ObGyn ordered an abdominal radiograph, which the radiologist reported as showing postoperative ileus and mild constipation. The patient was given a second Fleet enema the next day, resulting in watery stool. She vomited 300 mL of dark green fluid.
After a rectal tube was placed 2 days later, one hard brown stool and several brown, pasty, loose, and liquid stools were returned. She vomited several times that day, and was found to have hypoactive bowel sounds with continued tympanic quality in the upper quadrants. Laboratory testing revealed continued elevated WBC count with left shift. The next day, she had hypoactive bowel sounds with brown liquid stools. Later that morning, she was able to tolerate clear liquids. The ObGyn decided to discharge her home with instructions to continue on a clear liquid diet for 2 more days before advancing her diet.
The day after discharge, she was found unresponsive at home. She was taken to the hospital, but resuscitation attempts failed. She died. An autopsy revealed that the cause of death was sepsis.
ESTATE’S CLAIM The ObGyn was negligent in failing to diagnose and treat a postoperative intra-abdominal infection caused by bowel perforation. A surgical consult should have been obtained. The woman was prematurely discharged. The radiologist failed to report the presence of free air on the abdominal x-ray.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $1 million Maryland settlement was reached.
_______________
Right ureter injury detected and repaired
During laparoscopic-assisted vaginal hysterectomy, the ObGyn detected and repaired an injury to the right ureter. The patient’s recovery was delayed by the injury.
PATIENT’S CLAIM The ObGyn was negligent in using a Kleppinger bipolar cauterizing instrument to cauterize the vaginal cuff. Thermal overspray from the instrument or the instrument itself damaged the ureter. The ObGyn was also negligent in not performing diagnostic cystoscopy to confirm patency of the ureter after the repair was made.
PHYSICIAN’S DEFENSE Ureter injury is a known risk of the procedure. All procedures were performed according to protocol.
VERDICT A Florida defense verdict was returned.
_______________
Failure to detect inflammatory BrCa; woman dies
A 42-year-old woman underwent mammography in February 2002 after reporting pain, discoloration, inflammation, and swelling in her left breast. The radiologist who interpreted the mammography suggested a biopsy for a differential diagnosis of mastitis or inflammatory carcinoma. The biopsy results were negative.
The patient’s symptoms persisted, and she underwent US in late May 2002. Another radiologist interpreted the US, noting that the patient could not tolerate compression, which led to less than optimal evaluation. The radiologist suggested that mastitis was the likely cause of the patient’s symptoms.
The patient then consulted a surgeon, who ordered mammography and magnetic resonance imaging (MRI) followed by biopsy, which indicated cancer. The patient underwent a mastectomy but metastasis had already occurred. She died at age 50 prior to the trial.
ESTATE’S CLAIM If the cancer had been diagnosed earlier, the outcome would have been better. Both radiologists misinterpreted the mammographies.
DEFENDANTS’ DEFENSE The mammographies had been properly interpreted. Any missed diagnosis would not have impacted the outcome due to the type of cancer. The scans had been released to the patient, but were subsequently lost; an adverse interference instruction was given to the jury.
VERDICT A New York defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Uterine rupture, child stillborn: $3.8M net award
At 35 weeks' gestation, a woman went to the emergency department (ED) with abdominal pain, fast heartbeat, and irregular contractions. Her history included three cesarean deliveries, including one with a vertical incision. She was admitted, and a cesarean delivery was planned for the next day. After 8 hours, during which the patient’s condition worsened, an emergency cesarean delivery was undertaken. A full rupture of the uterus was found; the baby’s body had extruded into the mother’s abdomen. The child was stillborn.
PARENTS’ CLAIM The stillbirth could have been avoided if the nurses had communicated the mother’s worsening condition to the physicians.
DEFENDANTS’ DEFENSE After the hospital and physicians settled prior to trial, the case continued against the nurse in charge of the mother’s care and the nurse-staffing group. Negligence was denied; all protocols were followed.
VERDICT A $2.9 million Illinois verdict was returned. With a $900,000 settlement from the hospital and physicians, the net award was $3.8 million.
_______________
Where did rare strep A infection come from?
A 36-year-old woman reported heavy vaginal bleeding to her ObGyn. She underwent endometrial ablation in her physician’s office.
The next day, the woman called the office to report abdominal pain. She was told to stop the medication she was taking, and if the pain continued to the next day, to go to an ED. The next day, the patient went to the ED and was found to be in septic shock. During emergency laparotomy, 50 mL of purulent fluid were drained and an emergency hysterectomy was performed. Three days later, the patient died from pulmonary arrest caused by toxic shock syndrome. An autopsy revealed that the patient’s sepsis was caused by group A streptococci (GAS) infection.
ESTATE’S CLAIM The patient was not a proper candidate for endometrial ablation because of her history of chronic cervical infection. The ObGyn perforated the cervix during the procedure and tried to conceal it. At autopsy, bone wax was found in the rectal lumen that had been used to cover up damage to the cervix. The ObGyn introduced GAS bacteria into the patient’s system. The ObGyn’s staff failed to ask the proper questions when she called the day after the procedure. She should have been told to go directly to the ED.
DEFENDANTS’ DEFENSE The ObGyn did not perforate the cervix or uterus during the procedure. GAS infection is so rare that it would have been difficult to foresee or diagnose. Potentially, the patient had a chronic
cervical infection before ablation.
VERDICT A Texas defense verdict was returned.
_______________
DURING INSERTION, IUD PERFORATES UTERINE WALL; LATER FOUND BELOW LIVER
On July 21, a 46-year-old woman went to an ObGyn for placement of an intrauterine device (IUD). Shortly after the ObGyn inserted the levonorgestrel-releasing intrauterine system (Mirena, Bayer HealthCare), the patient reported severe pelvic and abdominal pain. On July 26, the patient underwent surgical removal of the IUD.
She was discharged on July 29 but continued to report pain. She was readmitted to the hospital the next day and treated for pain. She was bed ridden for 3 weeks after IUD-removal surgery, and had a 3-month recovery before feeling pain free.
PATIENT’S CLAIM The ObGyn was negligent in perforating the patient’s uterine wall during IUD insertion, causing the device to ultimately migrate under the patient’s liver.
DEFENDANTS’ DEFENSE Uterine perforation is a known complication of IUD insertion. The IUD escaped from the patient’s uterus at a later time and not during the insertion procedure.
VERDICT A Florida verdict of $208,839 was returned; the amount was reduced to $161,058 because the medical expenses were written off by the health-care providers.
_______________
Was travel appropriate for this pregnant woman?
A woman with a history of two premature deliveries and one miscarriage became pregnant again. She received prenatal care at an Army hospital. She traveled to Spain, where the baby was born at 31 weeks’ gestation. The baby required treatment in a neonatal intensive care unit (NICU) for 17 days. The child has cerebral palsy, with tetraplegia of all four extremities. She cannot walk without assistance and suffers severe cognitive and vision impairment.
PARENTS’ CLAIM The ObGyn at the Army hospital should not have approved the mother’s request for travel; he did so, despite knowing that the mother was at high risk for premature birth. The military medical hospital to which she was assigned in Spain could not manage a high-risk pregnancy, didn’t have a NICU, and didn’t have specialists to treat premature infants.
DEFENDANTS’ DEFENSE The ObGyn argued that he did not have access to the medical records showing the mother’s history. The patient countered that the ObGyn did indeed have the patient’s records, as he had discussed them with her.
VERDICT A $10,409,700 California verdict was returned against the ObGyn and the government facility.
_______________
Triple-negative BrCa not diagnosed until metastasized: $5.2M
After finding lumps in both breasts, a woman in her 30s saw a nurse practitioner (NP) at an Army hospital. A radiologist reported no mass in the right breast and multiple benign-appearing anechoic lesions in the left breast after bilateral mammography and ultrasonography (US) in July 2008. The Chief of Mammography Services recommended referral to a breast surgeon, but the patient never received the letter. It was placed in her mammography file, not in the treatment file.
In November 2008, the patient returned to the clinic. Bilateral diagnostic mammography and US were ordered, but for unknown reasons, cancelled. US of the left breast was interpreted as benign in January 2009.
After imaging in March 2010, followed by a needle biopsy of the right breast, a radiologist reported finding intermediate-grade infiltrating ductal carcinoma.
The patient sought care outside the military medical system at a large university hospital. In April 2010, stage 3 triple-negative invasive ductal carcinoma (IDC) was identified. The patient underwent chemotherapy, a double mastectomy, removal of 21 lymph nodes, and breast reconstruction. She was given a 60% chance of recurrence in 5–7 years.
PATIENT’S CLAIM It was negligent to not inform her of imaging results. Biopsy should have been performed in 2008, when the IDC was likely at stage 1; treatment would have been far less aggressive. Electronic medical records showed that the 2008 mammography and US results had been “signed off” by an NP at the clinic.
DEFENDANTS’ DEFENSE While unable to concede liability, the government agency did not contest the point.
VERDICT A $5.2 million Tennessee federal court bench verdict was returned, citing failures in communication, poor and improper record keeping and retention, failure to follow-up, and an unexplained cancellation of a medical order.
_______________
Woman dies from cervical cancer: $2.3M
In 2001, a 41-year-old woman had abnormal Pap smear results but her gynecologist did not order more testing. The patient was told to return in 3 months, but she did not return until 2007—reporting abnormal bleeding, vaginal discharge, and pain. Her Pap results were normal, however, and the gynecologist did not order further testing. In 2009, the patient was found to have advanced cervical cancer. She died 2 years later.
ESTATE’S CLAIM Further testing should have been ordered in 2001, which would have likely revealed dysplasia, which can lead to cancer. The laboratory incorrectly interpreted the 2007 Pap test; if the results had been properly reported, additional testing could have been ordered.
DEFENDANTS’ DEFENSE The laboratory and patient’s estate settled for a confidential amount before trial. The gynecologist denied negligence.
VERDICT A New Jersey jury found the gynecologist 40% at fault for his actions in 2007. The jury found the laboratory 50% at fault, and the patient 10% at fault. A gross verdict of $2.33 million was returned.
_______________
Bowel injury after cesarean delivery; mother dies of sepsis
At 40 4/7 weeks' gestation, a 37-year-old woman gave birth to a healthy child by cesarean delivery. The next day, the patient had an elevated white blood cell (WBC) count with a left shift, her abdomen was tympanic but soft, and she was passing flatus and belching. The ObGyn ordered a Fleet enema; only flatus was released. A covering ObGyn ordered an abdominal radiograph, which the radiologist reported as showing postoperative ileus and mild constipation. The patient was given a second Fleet enema the next day, resulting in watery stool. She vomited 300 mL of dark green fluid.
After a rectal tube was placed 2 days later, one hard brown stool and several brown, pasty, loose, and liquid stools were returned. She vomited several times that day, and was found to have hypoactive bowel sounds with continued tympanic quality in the upper quadrants. Laboratory testing revealed continued elevated WBC count with left shift. The next day, she had hypoactive bowel sounds with brown liquid stools. Later that morning, she was able to tolerate clear liquids. The ObGyn decided to discharge her home with instructions to continue on a clear liquid diet for 2 more days before advancing her diet.
The day after discharge, she was found unresponsive at home. She was taken to the hospital, but resuscitation attempts failed. She died. An autopsy revealed that the cause of death was sepsis.
ESTATE’S CLAIM The ObGyn was negligent in failing to diagnose and treat a postoperative intra-abdominal infection caused by bowel perforation. A surgical consult should have been obtained. The woman was prematurely discharged. The radiologist failed to report the presence of free air on the abdominal x-ray.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $1 million Maryland settlement was reached.
_______________
Right ureter injury detected and repaired
During laparoscopic-assisted vaginal hysterectomy, the ObGyn detected and repaired an injury to the right ureter. The patient’s recovery was delayed by the injury.
PATIENT’S CLAIM The ObGyn was negligent in using a Kleppinger bipolar cauterizing instrument to cauterize the vaginal cuff. Thermal overspray from the instrument or the instrument itself damaged the ureter. The ObGyn was also negligent in not performing diagnostic cystoscopy to confirm patency of the ureter after the repair was made.
PHYSICIAN’S DEFENSE Ureter injury is a known risk of the procedure. All procedures were performed according to protocol.
VERDICT A Florida defense verdict was returned.
_______________
Failure to detect inflammatory BrCa; woman dies
A 42-year-old woman underwent mammography in February 2002 after reporting pain, discoloration, inflammation, and swelling in her left breast. The radiologist who interpreted the mammography suggested a biopsy for a differential diagnosis of mastitis or inflammatory carcinoma. The biopsy results were negative.
The patient’s symptoms persisted, and she underwent US in late May 2002. Another radiologist interpreted the US, noting that the patient could not tolerate compression, which led to less than optimal evaluation. The radiologist suggested that mastitis was the likely cause of the patient’s symptoms.
The patient then consulted a surgeon, who ordered mammography and magnetic resonance imaging (MRI) followed by biopsy, which indicated cancer. The patient underwent a mastectomy but metastasis had already occurred. She died at age 50 prior to the trial.
ESTATE’S CLAIM If the cancer had been diagnosed earlier, the outcome would have been better. Both radiologists misinterpreted the mammographies.
DEFENDANTS’ DEFENSE The mammographies had been properly interpreted. Any missed diagnosis would not have impacted the outcome due to the type of cancer. The scans had been released to the patient, but were subsequently lost; an adverse interference instruction was given to the jury.
VERDICT A New York defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
More inclusions:
- Where did rare strep A infection come from?
- During insertion, IUD perforates uterine wall; Later found below liver
- Was travel appropriate for this pregnant woman?
- Triple-negative BrCa not diagnosed until metastasized: $5.2M
- Woman dies from cervical cancer: $2.3M
- Bowel injury after cesarean delivery; mother dies of sepsis
- Right ureter injury detected and repaired
- Failure to detect inflammatory BrCa; woman dies

A Cocktail of Medications Leads to Death
Following sledding and auto accidents, a man sought treatment from Dr G. for back and shoulder strain. During this time, he was prescribed several different pain medications, including oxycodone, carisoprodol, and alprazolam.
The motor vehicle accident occurred in April 2008 and resulted in a compression fracture. In January 2009, a neurosurgeon performed a surgical alternative, and the patient was discharged the next day with a prescription for 30-mg oxycodone. This dosage was twice the amount that Dr G. had already prescribed, but Dr G. advised the patient to continue with his original prescriptions. Three days after the procedure, the man was found dead with oxycodone, carisoprodol, and alprazolam in his system.
The plaintiff alleged negligence in the prescription of this drug combination, which caused respiratory depression and arrest. The defendant claimed that the patient died from aggravation of severe chronic cardiovascular disease and that the combination of medications in his system could not have led to death in such a drug-tolerant individual.
Continue for the outcome and David Lang's comments >>
Outcome
According to a published account, a defense verdict was returned.
Comment
There are two important points here. First, medication errors are more likely when several clinicians treat a single patient. This is particularly true when the care is of short duration (ie, related to surgery). Problems arise when the consulting team does not have full knowledge of a patient’s medication list—making the obtaining of a complete and current list critical. And yes, in some cases, this may mean reviewing a dozen different medications for potential interactions with the agent you contemplate giving the patient.
Does this mean the consulting surgeon is duty-bound to optimize the patient’s regimen for diabetes and hypertension? No, but the surgeon is duty-bound to wade through all those medications to be sure there will be no interactions.
Surgeons often use a standard postoperative regime. But as clinicians, we can’t simply order “what is usually given.” Take a moment to review the patient’s active medication list—don’t put yourself on autopilot, as tempting as it may be.
Second, we live in a time when many patients do not simply take “a pill” from “their doctor.” It is far more common for patients to take a recipe of pills from an extensive medical team. Each member of the team focuses on the system of his/her specialty and directs pharmaceutical intervention at that system. But we all want the same net result: the patient’s overall condition optimized without adverse effects or drug interactions.
One way to help patients handle a medical regimen is to recommend the use of a single pharmacist. That pharmacist serves as a gatekeeper to safeguard the patient from adverse results when a consulting clinician prescribes an interacting medication. The consulting clinician may have bad information; we have all seen a patient haul a weathered medication list from the depths of her pocket, only to learn that it is not current or is incomplete. A gatekeeper pharmacist will have an up-to-date list and can help to prevent errors.
Patients are also the last line of defense against a self-administered error. Inform the patient of the general class of medication you are prescribing, as well as the impact it may have: “This is a strong pain pill. It shouldn’t be taken with any medications or anything else that can make you sleepy—including alcohol.”
Additionally, it helps to have a clear delineation of which clinician is responsible for what problem. After surgery, it helps to clearly identify for the patient who will treat pain and for how long. The primary care provider (PCP) is probably not the best source of postoperative pain control, since the surgical team has a better understanding of expected pain and the typical medications and dosages to control it and is on alert for problems heralded by prolonged or atypical pain. Of course, the PCP should be aware of the selected agent, but a clear delineation of the surgical team’s responsibility for pain control should minimize frantic calls to the PCP’s office from the patient claiming to be in pain and out of medication.
In this case, chronic pain was managed by the PCP and postoperative pain by the surgical team. It is unclear if the surgical team was aware of the carisoprodol and alprazolam and the additional prescription for oxycodone. It is also possible that the patient was milking both sources for the oxycodone and overdid it—another reason it is advisable for one clinician to manage the patient’s pain. Make sure all parties are clear as to who that clinician is.
Finally, exercise caution when the potential effects of a medication are additive, even more so if they are synergistic. As we all know, there is a synergistic effect between central nervous system (CNS) depressants. Use caution when prescribing these agents together. Patients will often add more—diphenhydramine for allergies, one of their sister’s zolpidem for insomnia, cough suppressants for a cold—and of course, ethyl alcohol for any reason (or no reason at all). A sedated patient is a distracted patient, more prone to grogginess and forgetfulness, which may lead to self-medication errors.
If for some reason the patient genuinely requires multiple strong CNS depressant agents, he should ideally be followed by a pain management specialist. The risks should be fully explained and the patient informed that any additional agents causing drowsiness will have a substantially heightened effect. Tolerance can require larger doses and multiple agents with overlapping characteristics (eg CNS depressants); however, although the patient in this case was not opiate naïve, he still died of a fatal overdose. Be wary about adding agents or increasing the dosages of medications with synergistic effects.
One last thought: Different regions of the country have different juror demographics and beliefs. While this case was tried to a defense verdict in Macomb County, Michigan, the verdict may have been different in New York City or San Francisco, where jurors might be less likely to be swayed by what were certainly suggestions that the patient was improperly self-medicating.—DML
Following sledding and auto accidents, a man sought treatment from Dr G. for back and shoulder strain. During this time, he was prescribed several different pain medications, including oxycodone, carisoprodol, and alprazolam.
The motor vehicle accident occurred in April 2008 and resulted in a compression fracture. In January 2009, a neurosurgeon performed a surgical alternative, and the patient was discharged the next day with a prescription for 30-mg oxycodone. This dosage was twice the amount that Dr G. had already prescribed, but Dr G. advised the patient to continue with his original prescriptions. Three days after the procedure, the man was found dead with oxycodone, carisoprodol, and alprazolam in his system.
The plaintiff alleged negligence in the prescription of this drug combination, which caused respiratory depression and arrest. The defendant claimed that the patient died from aggravation of severe chronic cardiovascular disease and that the combination of medications in his system could not have led to death in such a drug-tolerant individual.
Continue for the outcome and David Lang's comments >>
Outcome
According to a published account, a defense verdict was returned.
Comment
There are two important points here. First, medication errors are more likely when several clinicians treat a single patient. This is particularly true when the care is of short duration (ie, related to surgery). Problems arise when the consulting team does not have full knowledge of a patient’s medication list—making the obtaining of a complete and current list critical. And yes, in some cases, this may mean reviewing a dozen different medications for potential interactions with the agent you contemplate giving the patient.
Does this mean the consulting surgeon is duty-bound to optimize the patient’s regimen for diabetes and hypertension? No, but the surgeon is duty-bound to wade through all those medications to be sure there will be no interactions.
Surgeons often use a standard postoperative regime. But as clinicians, we can’t simply order “what is usually given.” Take a moment to review the patient’s active medication list—don’t put yourself on autopilot, as tempting as it may be.
Second, we live in a time when many patients do not simply take “a pill” from “their doctor.” It is far more common for patients to take a recipe of pills from an extensive medical team. Each member of the team focuses on the system of his/her specialty and directs pharmaceutical intervention at that system. But we all want the same net result: the patient’s overall condition optimized without adverse effects or drug interactions.
One way to help patients handle a medical regimen is to recommend the use of a single pharmacist. That pharmacist serves as a gatekeeper to safeguard the patient from adverse results when a consulting clinician prescribes an interacting medication. The consulting clinician may have bad information; we have all seen a patient haul a weathered medication list from the depths of her pocket, only to learn that it is not current or is incomplete. A gatekeeper pharmacist will have an up-to-date list and can help to prevent errors.
Patients are also the last line of defense against a self-administered error. Inform the patient of the general class of medication you are prescribing, as well as the impact it may have: “This is a strong pain pill. It shouldn’t be taken with any medications or anything else that can make you sleepy—including alcohol.”
Additionally, it helps to have a clear delineation of which clinician is responsible for what problem. After surgery, it helps to clearly identify for the patient who will treat pain and for how long. The primary care provider (PCP) is probably not the best source of postoperative pain control, since the surgical team has a better understanding of expected pain and the typical medications and dosages to control it and is on alert for problems heralded by prolonged or atypical pain. Of course, the PCP should be aware of the selected agent, but a clear delineation of the surgical team’s responsibility for pain control should minimize frantic calls to the PCP’s office from the patient claiming to be in pain and out of medication.
In this case, chronic pain was managed by the PCP and postoperative pain by the surgical team. It is unclear if the surgical team was aware of the carisoprodol and alprazolam and the additional prescription for oxycodone. It is also possible that the patient was milking both sources for the oxycodone and overdid it—another reason it is advisable for one clinician to manage the patient’s pain. Make sure all parties are clear as to who that clinician is.
Finally, exercise caution when the potential effects of a medication are additive, even more so if they are synergistic. As we all know, there is a synergistic effect between central nervous system (CNS) depressants. Use caution when prescribing these agents together. Patients will often add more—diphenhydramine for allergies, one of their sister’s zolpidem for insomnia, cough suppressants for a cold—and of course, ethyl alcohol for any reason (or no reason at all). A sedated patient is a distracted patient, more prone to grogginess and forgetfulness, which may lead to self-medication errors.
If for some reason the patient genuinely requires multiple strong CNS depressant agents, he should ideally be followed by a pain management specialist. The risks should be fully explained and the patient informed that any additional agents causing drowsiness will have a substantially heightened effect. Tolerance can require larger doses and multiple agents with overlapping characteristics (eg CNS depressants); however, although the patient in this case was not opiate naïve, he still died of a fatal overdose. Be wary about adding agents or increasing the dosages of medications with synergistic effects.
One last thought: Different regions of the country have different juror demographics and beliefs. While this case was tried to a defense verdict in Macomb County, Michigan, the verdict may have been different in New York City or San Francisco, where jurors might be less likely to be swayed by what were certainly suggestions that the patient was improperly self-medicating.—DML
Following sledding and auto accidents, a man sought treatment from Dr G. for back and shoulder strain. During this time, he was prescribed several different pain medications, including oxycodone, carisoprodol, and alprazolam.
The motor vehicle accident occurred in April 2008 and resulted in a compression fracture. In January 2009, a neurosurgeon performed a surgical alternative, and the patient was discharged the next day with a prescription for 30-mg oxycodone. This dosage was twice the amount that Dr G. had already prescribed, but Dr G. advised the patient to continue with his original prescriptions. Three days after the procedure, the man was found dead with oxycodone, carisoprodol, and alprazolam in his system.
The plaintiff alleged negligence in the prescription of this drug combination, which caused respiratory depression and arrest. The defendant claimed that the patient died from aggravation of severe chronic cardiovascular disease and that the combination of medications in his system could not have led to death in such a drug-tolerant individual.
Continue for the outcome and David Lang's comments >>
Outcome
According to a published account, a defense verdict was returned.
Comment
There are two important points here. First, medication errors are more likely when several clinicians treat a single patient. This is particularly true when the care is of short duration (ie, related to surgery). Problems arise when the consulting team does not have full knowledge of a patient’s medication list—making the obtaining of a complete and current list critical. And yes, in some cases, this may mean reviewing a dozen different medications for potential interactions with the agent you contemplate giving the patient.
Does this mean the consulting surgeon is duty-bound to optimize the patient’s regimen for diabetes and hypertension? No, but the surgeon is duty-bound to wade through all those medications to be sure there will be no interactions.
Surgeons often use a standard postoperative regime. But as clinicians, we can’t simply order “what is usually given.” Take a moment to review the patient’s active medication list—don’t put yourself on autopilot, as tempting as it may be.
Second, we live in a time when many patients do not simply take “a pill” from “their doctor.” It is far more common for patients to take a recipe of pills from an extensive medical team. Each member of the team focuses on the system of his/her specialty and directs pharmaceutical intervention at that system. But we all want the same net result: the patient’s overall condition optimized without adverse effects or drug interactions.
One way to help patients handle a medical regimen is to recommend the use of a single pharmacist. That pharmacist serves as a gatekeeper to safeguard the patient from adverse results when a consulting clinician prescribes an interacting medication. The consulting clinician may have bad information; we have all seen a patient haul a weathered medication list from the depths of her pocket, only to learn that it is not current or is incomplete. A gatekeeper pharmacist will have an up-to-date list and can help to prevent errors.
Patients are also the last line of defense against a self-administered error. Inform the patient of the general class of medication you are prescribing, as well as the impact it may have: “This is a strong pain pill. It shouldn’t be taken with any medications or anything else that can make you sleepy—including alcohol.”
Additionally, it helps to have a clear delineation of which clinician is responsible for what problem. After surgery, it helps to clearly identify for the patient who will treat pain and for how long. The primary care provider (PCP) is probably not the best source of postoperative pain control, since the surgical team has a better understanding of expected pain and the typical medications and dosages to control it and is on alert for problems heralded by prolonged or atypical pain. Of course, the PCP should be aware of the selected agent, but a clear delineation of the surgical team’s responsibility for pain control should minimize frantic calls to the PCP’s office from the patient claiming to be in pain and out of medication.
In this case, chronic pain was managed by the PCP and postoperative pain by the surgical team. It is unclear if the surgical team was aware of the carisoprodol and alprazolam and the additional prescription for oxycodone. It is also possible that the patient was milking both sources for the oxycodone and overdid it—another reason it is advisable for one clinician to manage the patient’s pain. Make sure all parties are clear as to who that clinician is.
Finally, exercise caution when the potential effects of a medication are additive, even more so if they are synergistic. As we all know, there is a synergistic effect between central nervous system (CNS) depressants. Use caution when prescribing these agents together. Patients will often add more—diphenhydramine for allergies, one of their sister’s zolpidem for insomnia, cough suppressants for a cold—and of course, ethyl alcohol for any reason (or no reason at all). A sedated patient is a distracted patient, more prone to grogginess and forgetfulness, which may lead to self-medication errors.
If for some reason the patient genuinely requires multiple strong CNS depressant agents, he should ideally be followed by a pain management specialist. The risks should be fully explained and the patient informed that any additional agents causing drowsiness will have a substantially heightened effect. Tolerance can require larger doses and multiple agents with overlapping characteristics (eg CNS depressants); however, although the patient in this case was not opiate naïve, he still died of a fatal overdose. Be wary about adding agents or increasing the dosages of medications with synergistic effects.
One last thought: Different regions of the country have different juror demographics and beliefs. While this case was tried to a defense verdict in Macomb County, Michigan, the verdict may have been different in New York City or San Francisco, where jurors might be less likely to be swayed by what were certainly suggestions that the patient was improperly self-medicating.—DML
States with higher malpractice rates have more cesarean deliveries and fewer vaginal deliveries
Over the last 20 years, litigation rates, malpractice coverage costs, and the number of cesarean deliveries have increased significantly. In fact, many ObGyns have dropped their obstetric practices because of the increased cost of malpractice insurance, say researchers from Johns Hopkins and Brown, and three states (New York, Florida, and Virginia) now have birth injury funds to help deflect the burden of malpractice insurance and litigation costs.1
What is the existing state-level relationship between malpractice rates and the mode of delivery, including cesarean delivery (CD) and vaginal delivery (VD), as well as operative vaginal delivery (OVD)? And how do the state-run injury funds affect this relationship, asked Clark T. Johnson, MD, MPH, and Erika F. Werner, MD.
To answer their question, the investigators collected 8 years of data on mode of delivery (from the Centers for Disease Control and Prevention National Vital Statistics System) and malpractice rates for ObGyns in each US state (from the 2011 Medical Liability Monitor Rate Survey). The researchers used linear regression modeling to analyze their 2003−2010 data.1
They found that states with higher malpractice rates had higher CD delivery rates and lower VD rates than states with lower malpractice rates, and that higher malpractice rates also correlated with lower rates of OVD, including the use of forceps and vacuum extraction. Overall, the change in malpractice rates between 2003 and 2010 did not correlate with the rates of OVD.1
Those states with the highest average annual malpractice insurance rate (> $120,000) to cover claims with a cap of $1 million/$3 million in 2010, were Florida, New York, and Connecticut. Illinois, Pennsylvania, New Jersey, and Maryland had an average annual rate of $100,000 to $120,000.
Those states with the lowest average annual malpractice insurance rate (0$ to $40,000) were North Dakota, South Dakota, Nebraska, Minnesota, Iowa, and Wisconsin.
In the 1980s, medical malpractice insurance rates soared and insurance companies were faced with eliminating coverage to obstetricians. In 1987, the Virginia General Assembly developed the Virginia Birth-Related Neurological Injury Compensation Program. This no-fault system ensures lifetime care to eligible participants, and has successfully stabilized the malpractice environment in the state.2 Birth-related neurologic injury funds were also created in Florida in 19883 and in New York in 2011.4
The three states with birth injury funds showed a decrease in malpractice rates, a slower rate of CD-rate increase, and an OVD-rate decrease. However, the researchers note that while developing a state birth injury fund is seen as a trend that might reduce malpractice rates, there were not enough data to demonstrate significance.1
1. Johnson CT, Werner EF. The nationwide relationship between malpractice rates and rates of vaginal and cesarean delivery. Poster presented at: American College of Obstetricians and Gynecologists 62nd Annual Clinical Meeting; April 26–30, 2014; Chicago, IL. Obstet Gynecol.
2. Medical Society of Virginia. Virginia birth injury fund (BIF) FAQs. http://www.msv.org/MainMenuCategories/MemberCenter/FAQs/Virginia-Birth-Injury-Fund-BIF-FAQs.aspx. Accessed July 30, 2014.
3. What is NICA? Florida Birth-Related Neurological Injury Compensation Association (NICA) Web site. https://www.nica.com/what-is-nica.html. Accessed July 30, 2014.
4. Medical Indemnity Fund frequently asked questions. New York State Department of Financial Services Web site. http://www.dfs.ny.gov/insurance/mif/mif_faqs.htm. Updated February 13, 2012. Accessed July 30, 2014.
Over the last 20 years, litigation rates, malpractice coverage costs, and the number of cesarean deliveries have increased significantly. In fact, many ObGyns have dropped their obstetric practices because of the increased cost of malpractice insurance, say researchers from Johns Hopkins and Brown, and three states (New York, Florida, and Virginia) now have birth injury funds to help deflect the burden of malpractice insurance and litigation costs.1
What is the existing state-level relationship between malpractice rates and the mode of delivery, including cesarean delivery (CD) and vaginal delivery (VD), as well as operative vaginal delivery (OVD)? And how do the state-run injury funds affect this relationship, asked Clark T. Johnson, MD, MPH, and Erika F. Werner, MD.
To answer their question, the investigators collected 8 years of data on mode of delivery (from the Centers for Disease Control and Prevention National Vital Statistics System) and malpractice rates for ObGyns in each US state (from the 2011 Medical Liability Monitor Rate Survey). The researchers used linear regression modeling to analyze their 2003−2010 data.1
They found that states with higher malpractice rates had higher CD delivery rates and lower VD rates than states with lower malpractice rates, and that higher malpractice rates also correlated with lower rates of OVD, including the use of forceps and vacuum extraction. Overall, the change in malpractice rates between 2003 and 2010 did not correlate with the rates of OVD.1
Those states with the highest average annual malpractice insurance rate (> $120,000) to cover claims with a cap of $1 million/$3 million in 2010, were Florida, New York, and Connecticut. Illinois, Pennsylvania, New Jersey, and Maryland had an average annual rate of $100,000 to $120,000.
Those states with the lowest average annual malpractice insurance rate (0$ to $40,000) were North Dakota, South Dakota, Nebraska, Minnesota, Iowa, and Wisconsin.
In the 1980s, medical malpractice insurance rates soared and insurance companies were faced with eliminating coverage to obstetricians. In 1987, the Virginia General Assembly developed the Virginia Birth-Related Neurological Injury Compensation Program. This no-fault system ensures lifetime care to eligible participants, and has successfully stabilized the malpractice environment in the state.2 Birth-related neurologic injury funds were also created in Florida in 19883 and in New York in 2011.4
The three states with birth injury funds showed a decrease in malpractice rates, a slower rate of CD-rate increase, and an OVD-rate decrease. However, the researchers note that while developing a state birth injury fund is seen as a trend that might reduce malpractice rates, there were not enough data to demonstrate significance.1
Over the last 20 years, litigation rates, malpractice coverage costs, and the number of cesarean deliveries have increased significantly. In fact, many ObGyns have dropped their obstetric practices because of the increased cost of malpractice insurance, say researchers from Johns Hopkins and Brown, and three states (New York, Florida, and Virginia) now have birth injury funds to help deflect the burden of malpractice insurance and litigation costs.1
What is the existing state-level relationship between malpractice rates and the mode of delivery, including cesarean delivery (CD) and vaginal delivery (VD), as well as operative vaginal delivery (OVD)? And how do the state-run injury funds affect this relationship, asked Clark T. Johnson, MD, MPH, and Erika F. Werner, MD.
To answer their question, the investigators collected 8 years of data on mode of delivery (from the Centers for Disease Control and Prevention National Vital Statistics System) and malpractice rates for ObGyns in each US state (from the 2011 Medical Liability Monitor Rate Survey). The researchers used linear regression modeling to analyze their 2003−2010 data.1
They found that states with higher malpractice rates had higher CD delivery rates and lower VD rates than states with lower malpractice rates, and that higher malpractice rates also correlated with lower rates of OVD, including the use of forceps and vacuum extraction. Overall, the change in malpractice rates between 2003 and 2010 did not correlate with the rates of OVD.1
Those states with the highest average annual malpractice insurance rate (> $120,000) to cover claims with a cap of $1 million/$3 million in 2010, were Florida, New York, and Connecticut. Illinois, Pennsylvania, New Jersey, and Maryland had an average annual rate of $100,000 to $120,000.
Those states with the lowest average annual malpractice insurance rate (0$ to $40,000) were North Dakota, South Dakota, Nebraska, Minnesota, Iowa, and Wisconsin.
In the 1980s, medical malpractice insurance rates soared and insurance companies were faced with eliminating coverage to obstetricians. In 1987, the Virginia General Assembly developed the Virginia Birth-Related Neurological Injury Compensation Program. This no-fault system ensures lifetime care to eligible participants, and has successfully stabilized the malpractice environment in the state.2 Birth-related neurologic injury funds were also created in Florida in 19883 and in New York in 2011.4
The three states with birth injury funds showed a decrease in malpractice rates, a slower rate of CD-rate increase, and an OVD-rate decrease. However, the researchers note that while developing a state birth injury fund is seen as a trend that might reduce malpractice rates, there were not enough data to demonstrate significance.1
1. Johnson CT, Werner EF. The nationwide relationship between malpractice rates and rates of vaginal and cesarean delivery. Poster presented at: American College of Obstetricians and Gynecologists 62nd Annual Clinical Meeting; April 26–30, 2014; Chicago, IL. Obstet Gynecol.
2. Medical Society of Virginia. Virginia birth injury fund (BIF) FAQs. http://www.msv.org/MainMenuCategories/MemberCenter/FAQs/Virginia-Birth-Injury-Fund-BIF-FAQs.aspx. Accessed July 30, 2014.
3. What is NICA? Florida Birth-Related Neurological Injury Compensation Association (NICA) Web site. https://www.nica.com/what-is-nica.html. Accessed July 30, 2014.
4. Medical Indemnity Fund frequently asked questions. New York State Department of Financial Services Web site. http://www.dfs.ny.gov/insurance/mif/mif_faqs.htm. Updated February 13, 2012. Accessed July 30, 2014.
1. Johnson CT, Werner EF. The nationwide relationship between malpractice rates and rates of vaginal and cesarean delivery. Poster presented at: American College of Obstetricians and Gynecologists 62nd Annual Clinical Meeting; April 26–30, 2014; Chicago, IL. Obstet Gynecol.
2. Medical Society of Virginia. Virginia birth injury fund (BIF) FAQs. http://www.msv.org/MainMenuCategories/MemberCenter/FAQs/Virginia-Birth-Injury-Fund-BIF-FAQs.aspx. Accessed July 30, 2014.
3. What is NICA? Florida Birth-Related Neurological Injury Compensation Association (NICA) Web site. https://www.nica.com/what-is-nica.html. Accessed July 30, 2014.
4. Medical Indemnity Fund frequently asked questions. New York State Department of Financial Services Web site. http://www.dfs.ny.gov/insurance/mif/mif_faqs.htm. Updated February 13, 2012. Accessed July 30, 2014.
Was fetus’ wrist injured during cesarean delivery?

Was fetus’ wrist injured during cesarean delivery?
At 34 weeks’ gestation, a 39-year-old woman went to the hospital in preterm labor. Her history included a prior cesarean delivery. Ultrasonography (US) showed that the fetus was in a double-footling breech position. The ObGyn decided to perform a cesarean delivery when the fetal heart-rate monitor indicated distress.
After making a midline incision through the earlier scar, the ObGyn created a low transverse uterine incision with a scalpel. The mother’s uterus was thick because labor had not progressed. When the ObGyn was unable to deliver the baby through the low transverse incision, she performed a T-extension of the incision using bandage scissors while placing her free hand inside the uterus to shield the fetus from injury. After extensive manipulation, the baby was delivered and immediately handed to a neonatologist. After surgery, the neonatologist told the mother that the baby had sustained two lacerations to the ulnar side of the right wrist. The newborn was airlifted to another hospital for treatment of sepsis. There, an orthopedic hand surgeon examined the child and determined that the lacerations were superficial and only required sutures. The orthopedist saw the infant a month later and believed there was no significant wrist injury.
When the child began preschool, she started to experience cold intolerance and difficulty writing with her right hand. The child was referred to a pediatric neurologist, who found no nerve damage and ordered occupational therapy.
The original orthopedic surgeon examined the child when she was 7 years old and determined that the flexor carpi ulnaris tendon had been completely severed with a partial injury to the ulnar nerve. He recommended a return visit at age 14 for full assessment of the wrist injury.
PARENTS’ CLAIM The ObGyn did not properly shield the fetus when performing the T-extension incision during cesarean delivery. The child’s weakness will increase with age, ruling out some occupations.
PHYSICIAN’S DEFENSE The ObGyn was not negligent; she had provided adequate protection of the fetus during both incisions.
VERDICT An Illinois defense verdict was returned.
Woman dies after tubal ligation
After a 42-year-old woman underwent tubal ligation, her surgeon was concerned about a possible bowel perforation and admitted her to the hospital. The next morning, a computed tomography (CT) scan of the abdomen did not reveal bowel injury.
That afternoon, when the patient reported shortness of breath, the surgeon called the hospitalist with concern for pulmonary embolism (PE). The hospitalist immediately ordered a CT scan of the chest, initiated PE protocol, and wrote “r/o PE” on the chart. A radiologist reminded the hospitalist of the earlier CT scan with concern for kidney damage from another dye study. The hospitalist cancelled the CT scan and PE protocol. After waiting 17 hours to run any further tests, a CT scan revealed massive bilateral PE. The patient was transferred to the ICU, but died the next day.
PATIENT’S CLAIM The 17-hour delay was negligent.
PHYSICIAN’S DEFENSE There was no negligence. The patient died of septic shock, not PE.
VERDICT A $4 million Virginia verdict was returned.
Child born without hand and forearm
During prenatal care, a mother underwent US at 20 and 36 weeks; both studies were reported as normal. The child was born missing his left hand and part of his left forearm due to a congenital amputation. The child will require prosthetics for life.
PATIENT’S CLAIM The condition should have been seen during prenatal US; an abortion was still an option at 20 weeks.
DEFENDANTS’ DEFENSE US was properly performed and evaluated. It can be difficult to differentiate the right from left extremities.
VERDICT A California defense verdict was returned.
After starting Yasmin, woman has stroke with permanent paralysis: $16.5M total award
When a 37-year-old woman reported irregular menstruation, her ObGyn prescribed drospirenone/ethinyl estradiol (Yasmin; Bayer). Thirteen days after starting the drug, the patient had a stroke. She is paralyzed on her left side, has limited ability to speak, cannot use her left arm and leg, and requires 24-hour care.
PATIENT’S CLAIM The ObGyn should have recognized that Yasmin was not appropriate for this patient because of the drug’s clotting risks. The patient’s risk factors included her age (over 35), borderline hypertension, overweight, history of smoking, and high cholesterol. The ObGyn should have offered safer alternatives, such as a progesterone-only pill. The US Food and Drug Administration (FDA) issued a safety warning that all drospirenone-containing drugs may be associated with a higher risk of venous thrombosis during the first 6 months of use.
DEFENDANTS’ DEFENSE According to Bayer, Yasmin is safe, and remains on the market. It was an appropriate drug to treat her irregular bleeding.
VERDICT Claims against the medical center that referred the patient to the ObGyn were settled for $2.5 million before trial. A $14 million Illinois verdict was returned against the ObGyn, for a total award of $16.5 million.
Who is at fault when pelvic mesh erodes?
In January 2011, an ObGyn implanted the Gynecare TVT Obturator System (TVT‑O; Ethicon) during a midurethral sling procedure to treat stress urinary incontinence (SUI) in a woman in her 60s. Shortly thereafter, the ObGyn left practice because of early-onset Alzheimer’s disease, and the patient’s care was taken over by a gynecologist.
At the 2-month postoperative visit, the gynecologist found that the mesh had eroded into the patient’s vagina. The gynecologist simply cut the mesh with a scissor, charted that a small erosion was present, and prescribed estrogen cream.
The patient continued to report pain, discomfort, pressure, difficulty voiding urine, continued incontinence, vaginal discharge, scarring, infection, odor, and bleeding.
PATIENT’S CLAIM The polypropylene mesh used during the midurethral sling procedure has been shown to be incompatible with human tissue. It promotes an immune response, which stimulates degradation of the pelvic tissue and can contribute to the development of severe adverse reactions to the mesh. Ethicon negligently designed, manufactured, marketed, labeled, and packaged the pelvic mesh products.
DEFENDANTS’ DEFENSE Proper warnings were provided about the health risks associated with polypropylene mesh products. The medical device was not properly sized.
VERDICT A Texas jury rejected the patient’s claims that Ethicon did not provide proper warnings about the sling’s health risks and declined to award punitive damages.
However, the jury decided that the mesh implant was defectively designed, and returned a $1.2 million verdict against Ethicon.
Was suspected bowel injury treated properly?
A 40-year-old woman was referred to an ObGyn after reporting abnormal uterine bleeding to her primary care physician. The patient had very light menses every few weeks. The ObGyn performed an ablation procedure, without relief. A month later, the ObGyn performed robot-assisted laparoscopic hysterectomy. The next day, the patient reported abdominal pain. Suspecting a bowel injury, the ObGyn ordered a CT scan; the bowel appeared normal, so the ObGyn referred the patient to a surgeon. During exploratory laparotomy, the surgeon found and repaired a bowel injury. The patient developed significant complications from a necrotizing infection that included respiratory distress and ongoing wound care.
PATIENT’S CLAIM Conservative treatment should have been offered before surgery. The ObGyn should have waited longer after the ablation procedure before doing the hysterectomy. The ObGyn should have checked for a possible bowel injury before closing the hysterectomy.
PHYSICIAN’S DEFENSE The bowel injury is a known complication of the procedure and was recognized and repaired in a timely manner.
VERDICT A Kentucky defense verdict was returned.

Pap smear improperly interpreted: Woman dies from cervical cancer
A 37-year-old woman underwent a pap smear in 2008 that was read by a cytotechnologist as normal. Two years later, the patient was found to have a golf-ball–sized cancerous tumor. She died from cervical cancer in 2011.
ESTATE’S CLAIM The cytotechnologist was negligent in misreading the 2008 Pap smear. If treatment had been started in 2008, the cancer could have been resolved with a simple conization biopsy.
DEFENDANTS’ DEFENSE The Pap smear interpretation was reasonable. The cancer could not have been diagnosed in 2008. The patient was at fault for failing to follow-up Pap smears during the next 2 years.
VERDICT After assigning 75% fault to the cytotechnologist and 25% fault to the patient, a Florida jury returned a $20,870,200 verdict, which was reduced to $15,816,699.
Disastrous off-label use of anticoagulation
When a pelvic abscess was found, a 50-year-old woman was admitted to the hospital for treatment. She was taking warfarin due to a history of venous thromboembolism.
Before the procedure, her physicians attempted to temporarily reverse her anticoagulation by administering Factor IX Complex (Profilnine SD, Grifols Biologicals). The dose ordered for the patient was nearly double the maximum recommended weight-based dose. Almost immediately after receiving the infusion, the patient went into cardiopulmonary arrest and died. An autopsy found the cause of death to be pulmonary emboli (PE).
ESTATE’S CLAIM An excessive dose of Profilnine caused PE. At the time of the incident, Profilnine was not FDA approved for warfarin reversal, although some off-label uses were recognized in emergent situations, such as intracranial bleeds.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $1.25 million Virginia settlement was reached.
Vesicovaginal fistula from ureteral injury
At a women’s health clinic, a patient reported continuous, heavy vaginal bleeding; pain; and shortness of breath when walking. She had a history of endometritis and multiple abdominal surgeries. Examination disclosed a profuse vaginal discharge, a normal cervix, and an enlarged uterus. The patient consented to abdominal hysterectomy and bilateral salpingo-oophorectomy performed by an ObGyn assisted by a resident.
During surgery, the ObGyn found that the patient’s uterus was at 16 to 20 weeks’ gestation size, with multiple serosal uterine fibroids and frank pus and necrosed fibroid tumors within the uterine cavity. The procedure took longer than planned because of extensive adhesions. After surgery, the patient was anemic and was given a beta-blocker for tachycardia. She was discharged 3 days later with 48 hours’ worth of intravenous antibiotics.
A month later, the patient reported urinary incontinence. She saw a urologist, who found a vesicovaginal fistula. The patient underwent nephrostomy-tube placement. Right ureterolysis and a right ureteral reimplant was performed 4 months later.
PATIENT’S CLAIM The ObGyn injured the right ureter during surgery.
DEFENDANTS’ DEFENSE The ureter injury is a known risk of the procedure. The injury was due to an infection or delayed effects of ischemia. The patient had a good recovery with no residual injury.
VERDICT A Michigan defense verdict was returned.
Why did mother die after delivering twins?
After a 35-year-old woman gave birth to twins by cesarean delivery, she died. At autopsy, 4 liters of blood were found in her abdomen.
ESTATE’S CLAIM The ObGyn failed to recognize and treat an arterial or venous bleed during surgery.
DEFENDANTS’ DEFENSE The patient died from amniotic fluid embolism. Autopsy results showed right ventricular heart failure, respiratory failure, and disseminated intravascular coagulation.
VERDICT A Florida defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Was fetus’ wrist injured during cesarean delivery?
At 34 weeks’ gestation, a 39-year-old woman went to the hospital in preterm labor. Her history included a prior cesarean delivery. Ultrasonography (US) showed that the fetus was in a double-footling breech position. The ObGyn decided to perform a cesarean delivery when the fetal heart-rate monitor indicated distress.
After making a midline incision through the earlier scar, the ObGyn created a low transverse uterine incision with a scalpel. The mother’s uterus was thick because labor had not progressed. When the ObGyn was unable to deliver the baby through the low transverse incision, she performed a T-extension of the incision using bandage scissors while placing her free hand inside the uterus to shield the fetus from injury. After extensive manipulation, the baby was delivered and immediately handed to a neonatologist. After surgery, the neonatologist told the mother that the baby had sustained two lacerations to the ulnar side of the right wrist. The newborn was airlifted to another hospital for treatment of sepsis. There, an orthopedic hand surgeon examined the child and determined that the lacerations were superficial and only required sutures. The orthopedist saw the infant a month later and believed there was no significant wrist injury.
When the child began preschool, she started to experience cold intolerance and difficulty writing with her right hand. The child was referred to a pediatric neurologist, who found no nerve damage and ordered occupational therapy.
The original orthopedic surgeon examined the child when she was 7 years old and determined that the flexor carpi ulnaris tendon had been completely severed with a partial injury to the ulnar nerve. He recommended a return visit at age 14 for full assessment of the wrist injury.
PARENTS’ CLAIM The ObGyn did not properly shield the fetus when performing the T-extension incision during cesarean delivery. The child’s weakness will increase with age, ruling out some occupations.
PHYSICIAN’S DEFENSE The ObGyn was not negligent; she had provided adequate protection of the fetus during both incisions.
VERDICT An Illinois defense verdict was returned.
Woman dies after tubal ligation
After a 42-year-old woman underwent tubal ligation, her surgeon was concerned about a possible bowel perforation and admitted her to the hospital. The next morning, a computed tomography (CT) scan of the abdomen did not reveal bowel injury.
That afternoon, when the patient reported shortness of breath, the surgeon called the hospitalist with concern for pulmonary embolism (PE). The hospitalist immediately ordered a CT scan of the chest, initiated PE protocol, and wrote “r/o PE” on the chart. A radiologist reminded the hospitalist of the earlier CT scan with concern for kidney damage from another dye study. The hospitalist cancelled the CT scan and PE protocol. After waiting 17 hours to run any further tests, a CT scan revealed massive bilateral PE. The patient was transferred to the ICU, but died the next day.
PATIENT’S CLAIM The 17-hour delay was negligent.
PHYSICIAN’S DEFENSE There was no negligence. The patient died of septic shock, not PE.
VERDICT A $4 million Virginia verdict was returned.
Child born without hand and forearm
During prenatal care, a mother underwent US at 20 and 36 weeks; both studies were reported as normal. The child was born missing his left hand and part of his left forearm due to a congenital amputation. The child will require prosthetics for life.
PATIENT’S CLAIM The condition should have been seen during prenatal US; an abortion was still an option at 20 weeks.
DEFENDANTS’ DEFENSE US was properly performed and evaluated. It can be difficult to differentiate the right from left extremities.
VERDICT A California defense verdict was returned.
After starting Yasmin, woman has stroke with permanent paralysis: $16.5M total award
When a 37-year-old woman reported irregular menstruation, her ObGyn prescribed drospirenone/ethinyl estradiol (Yasmin; Bayer). Thirteen days after starting the drug, the patient had a stroke. She is paralyzed on her left side, has limited ability to speak, cannot use her left arm and leg, and requires 24-hour care.
PATIENT’S CLAIM The ObGyn should have recognized that Yasmin was not appropriate for this patient because of the drug’s clotting risks. The patient’s risk factors included her age (over 35), borderline hypertension, overweight, history of smoking, and high cholesterol. The ObGyn should have offered safer alternatives, such as a progesterone-only pill. The US Food and Drug Administration (FDA) issued a safety warning that all drospirenone-containing drugs may be associated with a higher risk of venous thrombosis during the first 6 months of use.
DEFENDANTS’ DEFENSE According to Bayer, Yasmin is safe, and remains on the market. It was an appropriate drug to treat her irregular bleeding.
VERDICT Claims against the medical center that referred the patient to the ObGyn were settled for $2.5 million before trial. A $14 million Illinois verdict was returned against the ObGyn, for a total award of $16.5 million.
Who is at fault when pelvic mesh erodes?
In January 2011, an ObGyn implanted the Gynecare TVT Obturator System (TVT‑O; Ethicon) during a midurethral sling procedure to treat stress urinary incontinence (SUI) in a woman in her 60s. Shortly thereafter, the ObGyn left practice because of early-onset Alzheimer’s disease, and the patient’s care was taken over by a gynecologist.
At the 2-month postoperative visit, the gynecologist found that the mesh had eroded into the patient’s vagina. The gynecologist simply cut the mesh with a scissor, charted that a small erosion was present, and prescribed estrogen cream.
The patient continued to report pain, discomfort, pressure, difficulty voiding urine, continued incontinence, vaginal discharge, scarring, infection, odor, and bleeding.
PATIENT’S CLAIM The polypropylene mesh used during the midurethral sling procedure has been shown to be incompatible with human tissue. It promotes an immune response, which stimulates degradation of the pelvic tissue and can contribute to the development of severe adverse reactions to the mesh. Ethicon negligently designed, manufactured, marketed, labeled, and packaged the pelvic mesh products.
DEFENDANTS’ DEFENSE Proper warnings were provided about the health risks associated with polypropylene mesh products. The medical device was not properly sized.
VERDICT A Texas jury rejected the patient’s claims that Ethicon did not provide proper warnings about the sling’s health risks and declined to award punitive damages.
However, the jury decided that the mesh implant was defectively designed, and returned a $1.2 million verdict against Ethicon.
Was suspected bowel injury treated properly?
A 40-year-old woman was referred to an ObGyn after reporting abnormal uterine bleeding to her primary care physician. The patient had very light menses every few weeks. The ObGyn performed an ablation procedure, without relief. A month later, the ObGyn performed robot-assisted laparoscopic hysterectomy. The next day, the patient reported abdominal pain. Suspecting a bowel injury, the ObGyn ordered a CT scan; the bowel appeared normal, so the ObGyn referred the patient to a surgeon. During exploratory laparotomy, the surgeon found and repaired a bowel injury. The patient developed significant complications from a necrotizing infection that included respiratory distress and ongoing wound care.
PATIENT’S CLAIM Conservative treatment should have been offered before surgery. The ObGyn should have waited longer after the ablation procedure before doing the hysterectomy. The ObGyn should have checked for a possible bowel injury before closing the hysterectomy.
PHYSICIAN’S DEFENSE The bowel injury is a known complication of the procedure and was recognized and repaired in a timely manner.
VERDICT A Kentucky defense verdict was returned.
Pap smear improperly interpreted: Woman dies from cervical cancer
A 37-year-old woman underwent a pap smear in 2008 that was read by a cytotechnologist as normal. Two years later, the patient was found to have a golf-ball–sized cancerous tumor. She died from cervical cancer in 2011.
ESTATE’S CLAIM The cytotechnologist was negligent in misreading the 2008 Pap smear. If treatment had been started in 2008, the cancer could have been resolved with a simple conization biopsy.
DEFENDANTS’ DEFENSE The Pap smear interpretation was reasonable. The cancer could not have been diagnosed in 2008. The patient was at fault for failing to follow-up Pap smears during the next 2 years.
VERDICT After assigning 75% fault to the cytotechnologist and 25% fault to the patient, a Florida jury returned a $20,870,200 verdict, which was reduced to $15,816,699.
Disastrous off-label use of anticoagulation
When a pelvic abscess was found, a 50-year-old woman was admitted to the hospital for treatment. She was taking warfarin due to a history of venous thromboembolism.
Before the procedure, her physicians attempted to temporarily reverse her anticoagulation by administering Factor IX Complex (Profilnine SD, Grifols Biologicals). The dose ordered for the patient was nearly double the maximum recommended weight-based dose. Almost immediately after receiving the infusion, the patient went into cardiopulmonary arrest and died. An autopsy found the cause of death to be pulmonary emboli (PE).
ESTATE’S CLAIM An excessive dose of Profilnine caused PE. At the time of the incident, Profilnine was not FDA approved for warfarin reversal, although some off-label uses were recognized in emergent situations, such as intracranial bleeds.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $1.25 million Virginia settlement was reached.
Vesicovaginal fistula from ureteral injury
At a women’s health clinic, a patient reported continuous, heavy vaginal bleeding; pain; and shortness of breath when walking. She had a history of endometritis and multiple abdominal surgeries. Examination disclosed a profuse vaginal discharge, a normal cervix, and an enlarged uterus. The patient consented to abdominal hysterectomy and bilateral salpingo-oophorectomy performed by an ObGyn assisted by a resident.
During surgery, the ObGyn found that the patient’s uterus was at 16 to 20 weeks’ gestation size, with multiple serosal uterine fibroids and frank pus and necrosed fibroid tumors within the uterine cavity. The procedure took longer than planned because of extensive adhesions. After surgery, the patient was anemic and was given a beta-blocker for tachycardia. She was discharged 3 days later with 48 hours’ worth of intravenous antibiotics.
A month later, the patient reported urinary incontinence. She saw a urologist, who found a vesicovaginal fistula. The patient underwent nephrostomy-tube placement. Right ureterolysis and a right ureteral reimplant was performed 4 months later.
PATIENT’S CLAIM The ObGyn injured the right ureter during surgery.
DEFENDANTS’ DEFENSE The ureter injury is a known risk of the procedure. The injury was due to an infection or delayed effects of ischemia. The patient had a good recovery with no residual injury.
VERDICT A Michigan defense verdict was returned.
Why did mother die after delivering twins?
After a 35-year-old woman gave birth to twins by cesarean delivery, she died. At autopsy, 4 liters of blood were found in her abdomen.
ESTATE’S CLAIM The ObGyn failed to recognize and treat an arterial or venous bleed during surgery.
DEFENDANTS’ DEFENSE The patient died from amniotic fluid embolism. Autopsy results showed right ventricular heart failure, respiratory failure, and disseminated intravascular coagulation.
VERDICT A Florida defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Was fetus’ wrist injured during cesarean delivery?
At 34 weeks’ gestation, a 39-year-old woman went to the hospital in preterm labor. Her history included a prior cesarean delivery. Ultrasonography (US) showed that the fetus was in a double-footling breech position. The ObGyn decided to perform a cesarean delivery when the fetal heart-rate monitor indicated distress.
After making a midline incision through the earlier scar, the ObGyn created a low transverse uterine incision with a scalpel. The mother’s uterus was thick because labor had not progressed. When the ObGyn was unable to deliver the baby through the low transverse incision, she performed a T-extension of the incision using bandage scissors while placing her free hand inside the uterus to shield the fetus from injury. After extensive manipulation, the baby was delivered and immediately handed to a neonatologist. After surgery, the neonatologist told the mother that the baby had sustained two lacerations to the ulnar side of the right wrist. The newborn was airlifted to another hospital for treatment of sepsis. There, an orthopedic hand surgeon examined the child and determined that the lacerations were superficial and only required sutures. The orthopedist saw the infant a month later and believed there was no significant wrist injury.
When the child began preschool, she started to experience cold intolerance and difficulty writing with her right hand. The child was referred to a pediatric neurologist, who found no nerve damage and ordered occupational therapy.
The original orthopedic surgeon examined the child when she was 7 years old and determined that the flexor carpi ulnaris tendon had been completely severed with a partial injury to the ulnar nerve. He recommended a return visit at age 14 for full assessment of the wrist injury.
PARENTS’ CLAIM The ObGyn did not properly shield the fetus when performing the T-extension incision during cesarean delivery. The child’s weakness will increase with age, ruling out some occupations.
PHYSICIAN’S DEFENSE The ObGyn was not negligent; she had provided adequate protection of the fetus during both incisions.
VERDICT An Illinois defense verdict was returned.
Woman dies after tubal ligation
After a 42-year-old woman underwent tubal ligation, her surgeon was concerned about a possible bowel perforation and admitted her to the hospital. The next morning, a computed tomography (CT) scan of the abdomen did not reveal bowel injury.
That afternoon, when the patient reported shortness of breath, the surgeon called the hospitalist with concern for pulmonary embolism (PE). The hospitalist immediately ordered a CT scan of the chest, initiated PE protocol, and wrote “r/o PE” on the chart. A radiologist reminded the hospitalist of the earlier CT scan with concern for kidney damage from another dye study. The hospitalist cancelled the CT scan and PE protocol. After waiting 17 hours to run any further tests, a CT scan revealed massive bilateral PE. The patient was transferred to the ICU, but died the next day.
PATIENT’S CLAIM The 17-hour delay was negligent.
PHYSICIAN’S DEFENSE There was no negligence. The patient died of septic shock, not PE.
VERDICT A $4 million Virginia verdict was returned.
Child born without hand and forearm
During prenatal care, a mother underwent US at 20 and 36 weeks; both studies were reported as normal. The child was born missing his left hand and part of his left forearm due to a congenital amputation. The child will require prosthetics for life.
PATIENT’S CLAIM The condition should have been seen during prenatal US; an abortion was still an option at 20 weeks.
DEFENDANTS’ DEFENSE US was properly performed and evaluated. It can be difficult to differentiate the right from left extremities.
VERDICT A California defense verdict was returned.
After starting Yasmin, woman has stroke with permanent paralysis: $16.5M total award
When a 37-year-old woman reported irregular menstruation, her ObGyn prescribed drospirenone/ethinyl estradiol (Yasmin; Bayer). Thirteen days after starting the drug, the patient had a stroke. She is paralyzed on her left side, has limited ability to speak, cannot use her left arm and leg, and requires 24-hour care.
PATIENT’S CLAIM The ObGyn should have recognized that Yasmin was not appropriate for this patient because of the drug’s clotting risks. The patient’s risk factors included her age (over 35), borderline hypertension, overweight, history of smoking, and high cholesterol. The ObGyn should have offered safer alternatives, such as a progesterone-only pill. The US Food and Drug Administration (FDA) issued a safety warning that all drospirenone-containing drugs may be associated with a higher risk of venous thrombosis during the first 6 months of use.
DEFENDANTS’ DEFENSE According to Bayer, Yasmin is safe, and remains on the market. It was an appropriate drug to treat her irregular bleeding.
VERDICT Claims against the medical center that referred the patient to the ObGyn were settled for $2.5 million before trial. A $14 million Illinois verdict was returned against the ObGyn, for a total award of $16.5 million.
Who is at fault when pelvic mesh erodes?
In January 2011, an ObGyn implanted the Gynecare TVT Obturator System (TVT‑O; Ethicon) during a midurethral sling procedure to treat stress urinary incontinence (SUI) in a woman in her 60s. Shortly thereafter, the ObGyn left practice because of early-onset Alzheimer’s disease, and the patient’s care was taken over by a gynecologist.
At the 2-month postoperative visit, the gynecologist found that the mesh had eroded into the patient’s vagina. The gynecologist simply cut the mesh with a scissor, charted that a small erosion was present, and prescribed estrogen cream.
The patient continued to report pain, discomfort, pressure, difficulty voiding urine, continued incontinence, vaginal discharge, scarring, infection, odor, and bleeding.
PATIENT’S CLAIM The polypropylene mesh used during the midurethral sling procedure has been shown to be incompatible with human tissue. It promotes an immune response, which stimulates degradation of the pelvic tissue and can contribute to the development of severe adverse reactions to the mesh. Ethicon negligently designed, manufactured, marketed, labeled, and packaged the pelvic mesh products.
DEFENDANTS’ DEFENSE Proper warnings were provided about the health risks associated with polypropylene mesh products. The medical device was not properly sized.
VERDICT A Texas jury rejected the patient’s claims that Ethicon did not provide proper warnings about the sling’s health risks and declined to award punitive damages.
However, the jury decided that the mesh implant was defectively designed, and returned a $1.2 million verdict against Ethicon.
Was suspected bowel injury treated properly?
A 40-year-old woman was referred to an ObGyn after reporting abnormal uterine bleeding to her primary care physician. The patient had very light menses every few weeks. The ObGyn performed an ablation procedure, without relief. A month later, the ObGyn performed robot-assisted laparoscopic hysterectomy. The next day, the patient reported abdominal pain. Suspecting a bowel injury, the ObGyn ordered a CT scan; the bowel appeared normal, so the ObGyn referred the patient to a surgeon. During exploratory laparotomy, the surgeon found and repaired a bowel injury. The patient developed significant complications from a necrotizing infection that included respiratory distress and ongoing wound care.
PATIENT’S CLAIM Conservative treatment should have been offered before surgery. The ObGyn should have waited longer after the ablation procedure before doing the hysterectomy. The ObGyn should have checked for a possible bowel injury before closing the hysterectomy.
PHYSICIAN’S DEFENSE The bowel injury is a known complication of the procedure and was recognized and repaired in a timely manner.
VERDICT A Kentucky defense verdict was returned.
Pap smear improperly interpreted: Woman dies from cervical cancer
A 37-year-old woman underwent a pap smear in 2008 that was read by a cytotechnologist as normal. Two years later, the patient was found to have a golf-ball–sized cancerous tumor. She died from cervical cancer in 2011.
ESTATE’S CLAIM The cytotechnologist was negligent in misreading the 2008 Pap smear. If treatment had been started in 2008, the cancer could have been resolved with a simple conization biopsy.
DEFENDANTS’ DEFENSE The Pap smear interpretation was reasonable. The cancer could not have been diagnosed in 2008. The patient was at fault for failing to follow-up Pap smears during the next 2 years.
VERDICT After assigning 75% fault to the cytotechnologist and 25% fault to the patient, a Florida jury returned a $20,870,200 verdict, which was reduced to $15,816,699.
Disastrous off-label use of anticoagulation
When a pelvic abscess was found, a 50-year-old woman was admitted to the hospital for treatment. She was taking warfarin due to a history of venous thromboembolism.
Before the procedure, her physicians attempted to temporarily reverse her anticoagulation by administering Factor IX Complex (Profilnine SD, Grifols Biologicals). The dose ordered for the patient was nearly double the maximum recommended weight-based dose. Almost immediately after receiving the infusion, the patient went into cardiopulmonary arrest and died. An autopsy found the cause of death to be pulmonary emboli (PE).
ESTATE’S CLAIM An excessive dose of Profilnine caused PE. At the time of the incident, Profilnine was not FDA approved for warfarin reversal, although some off-label uses were recognized in emergent situations, such as intracranial bleeds.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $1.25 million Virginia settlement was reached.
Vesicovaginal fistula from ureteral injury
At a women’s health clinic, a patient reported continuous, heavy vaginal bleeding; pain; and shortness of breath when walking. She had a history of endometritis and multiple abdominal surgeries. Examination disclosed a profuse vaginal discharge, a normal cervix, and an enlarged uterus. The patient consented to abdominal hysterectomy and bilateral salpingo-oophorectomy performed by an ObGyn assisted by a resident.
During surgery, the ObGyn found that the patient’s uterus was at 16 to 20 weeks’ gestation size, with multiple serosal uterine fibroids and frank pus and necrosed fibroid tumors within the uterine cavity. The procedure took longer than planned because of extensive adhesions. After surgery, the patient was anemic and was given a beta-blocker for tachycardia. She was discharged 3 days later with 48 hours’ worth of intravenous antibiotics.
A month later, the patient reported urinary incontinence. She saw a urologist, who found a vesicovaginal fistula. The patient underwent nephrostomy-tube placement. Right ureterolysis and a right ureteral reimplant was performed 4 months later.
PATIENT’S CLAIM The ObGyn injured the right ureter during surgery.
DEFENDANTS’ DEFENSE The ureter injury is a known risk of the procedure. The injury was due to an infection or delayed effects of ischemia. The patient had a good recovery with no residual injury.
VERDICT A Michigan defense verdict was returned.
Why did mother die after delivering twins?
After a 35-year-old woman gave birth to twins by cesarean delivery, she died. At autopsy, 4 liters of blood were found in her abdomen.
ESTATE’S CLAIM The ObGyn failed to recognize and treat an arterial or venous bleed during surgery.
DEFENDANTS’ DEFENSE The patient died from amniotic fluid embolism. Autopsy results showed right ventricular heart failure, respiratory failure, and disseminated intravascular coagulation.
VERDICT A Florida defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

In Child Abuse Case, Everyone Fails
In May 2009, an employee of the New Jersey Division of Youth and Family Services brought a child to an urban medical center for evaluation of possible child abuse that had been reported by the child’s maternal grandmother. The infant, who was two-and-a-half months old at the time, was bleeding from the blood vessels of both eyes and had bruises on both sides of his face.
The treating physician, Dr A., ordered a series of x-rays of the entire body and CT of the head. The CT findings were initially read as negative, and the baby was discharged on the same day with a diagnosis of “suspected child abuse.” Two radiologists who reviewed the CT results identified fluid on the brain.
Three weeks later, the infant’s parents brought him to another medical center. He was bleeding from the mouth, and a lacerated frenum was diagnosed. Attending physician Dr K. discharged the infant with a notation that the injury had been sustained when the baby’s father “tried to put a bottle in the child’s mouth.”
In mid-July 2009, at the age of 4 months, the child was severely beaten by his father and sustained brain damage. The child was removed from his parents’ custody and placed with his grandmother. The father was later convicted of aggravated assault and child cruelty.
The child’s grandmother alleged negligence by the defendants in failing to recognize child abuse, which would have resulted in the infant being removed from his home earlier, before the brain damage could occur.
Continue for the outcome and David Lang's comments >>
OUTCOME
A $7.4 million settlement was reached. Dr A. and his facility were responsible for $4.5 million; one of the radiologists and her employer, $475,000; the other radiologist and his employer, $750,000; Dr K. and his employer, $1.19 million; and the second medical center and several of its nurses, $560,000.
COMMENT
In this horrible case, there was no failure to diagnose. Dr A. diagnosed “suspected child abuse” during the May 2009 visit. The issue was the management of the case after abuse was suspected.
Suspected child abuse is a “hot potato,” and the cases are difficult to manage. Clinicians are trained to spot and treat illness. We are not well equipped to identify short-term safe housing, file court papers to terminate parental rights, conduct home visits, or interview family, friends, and neighbors to determine the best living arrangement for an at-risk patient.
Many clinicians feel that issues of abuse are outside medicine and are more appropriately dealt with by social workers, the courts, and law enforcement. Candidly, managing these cases is taxing. But manage them we must to adequately protect those who cannot protect themselves.
This case proves clinicians will be held accountable for child abuse. The defense attorneys realized the enormous malpractice exposure and consented to the substantial $7.4 million settlement. (This, it should be noted, is in addition to the largest verdict against the State of New Jersey in history: $166 million awarded against the Division of Youth and Family Services. As for the abusive father in this case, he received a paltry jail term of six years.)
So what do we do when evidence of abuse is discovered? How do we proceed? First, in cases when abuse is suspected, it is a bedrock principle that a child can’t be returned to the hands of the abuser. But how do we secure the patient’s safety after making a diagnosis of “likely child abuse”? As clinicians, we are duty bound to report abuse. Yet, under most circumstances, we do not have an automatic mechanism to emergently remove a child from a dangerous situation under our own authority: With great responsibility comes limited power. Sarcasm aside, there are steps we can take to safeguard children at risk.
Continue to learn how to safeguard children at risk >>
Consider emergency removal through your state’s child protection agency. In most cases, a child is removed from an unfit home by a court order. However, when the child is in imminent danger and there is insufficient time to follow this procedure, the child may be removed from the home by the state’s child protection agency without parental consent. (New Jersey, where this case occurred, is one such example; see NJSA 9:6-8.29[a].)
Know your state’s rules for emergency removal, and have the child abuse hotline number handy. If evidence of child abuse is present, contact the appropriate agency in your state and insist that emergency removal is warranted.
The local police department may be another option. Many states’ emergency removal procedures authorize and require local authorities to remove a child who is in imminent danger. Explain your evidence of abuse and the need for emergency action.
Lastly, if your state’s protective agency or your local police will not remove the child from the dangerous situation, another option is inpatient admission. Yes, beds are limited and costs are high. But far higher is the cost of a seriously injured child when we fail to act.
In this case, the New Jersey Division of Youth and Family Services was involved. The social workers only performed a background check and missed some 20 arrests on charges of assault and other crimes that the father had logged in Florida.
The first emergency physician who identified abuse faced liability exposure for returning the child to the abuser. He pursued a work-up for child abuse and made a diagnosis of child abuse, yet he did not adopt a disposition consistent with his work-up and diagnosis.
The second physician failed to recognize the significance of a lacerated labial frenum in a 2-month-old. This type of injury is particularly suggestive in children who are not independently mobile and thus incapable of accidental injury. Force sufficient to rip a 2-month-old’s lip away from his mouth should have been recognized as abusive force. There is no evidence in the case report that the second physician identified the abuse or acted to stop it.
IN SUM
Recognize and report abuse. Know your state’s emergency removal law, and marshal your evidence of abuse to impel state agency workers to act on their power to remove a child from an abusive situation. Above all, do not return a child to his or her abuser. —DML
In May 2009, an employee of the New Jersey Division of Youth and Family Services brought a child to an urban medical center for evaluation of possible child abuse that had been reported by the child’s maternal grandmother. The infant, who was two-and-a-half months old at the time, was bleeding from the blood vessels of both eyes and had bruises on both sides of his face.
The treating physician, Dr A., ordered a series of x-rays of the entire body and CT of the head. The CT findings were initially read as negative, and the baby was discharged on the same day with a diagnosis of “suspected child abuse.” Two radiologists who reviewed the CT results identified fluid on the brain.
Three weeks later, the infant’s parents brought him to another medical center. He was bleeding from the mouth, and a lacerated frenum was diagnosed. Attending physician Dr K. discharged the infant with a notation that the injury had been sustained when the baby’s father “tried to put a bottle in the child’s mouth.”
In mid-July 2009, at the age of 4 months, the child was severely beaten by his father and sustained brain damage. The child was removed from his parents’ custody and placed with his grandmother. The father was later convicted of aggravated assault and child cruelty.
The child’s grandmother alleged negligence by the defendants in failing to recognize child abuse, which would have resulted in the infant being removed from his home earlier, before the brain damage could occur.
Continue for the outcome and David Lang's comments >>
OUTCOME
A $7.4 million settlement was reached. Dr A. and his facility were responsible for $4.5 million; one of the radiologists and her employer, $475,000; the other radiologist and his employer, $750,000; Dr K. and his employer, $1.19 million; and the second medical center and several of its nurses, $560,000.
COMMENT
In this horrible case, there was no failure to diagnose. Dr A. diagnosed “suspected child abuse” during the May 2009 visit. The issue was the management of the case after abuse was suspected.
Suspected child abuse is a “hot potato,” and the cases are difficult to manage. Clinicians are trained to spot and treat illness. We are not well equipped to identify short-term safe housing, file court papers to terminate parental rights, conduct home visits, or interview family, friends, and neighbors to determine the best living arrangement for an at-risk patient.
Many clinicians feel that issues of abuse are outside medicine and are more appropriately dealt with by social workers, the courts, and law enforcement. Candidly, managing these cases is taxing. But manage them we must to adequately protect those who cannot protect themselves.
This case proves clinicians will be held accountable for child abuse. The defense attorneys realized the enormous malpractice exposure and consented to the substantial $7.4 million settlement. (This, it should be noted, is in addition to the largest verdict against the State of New Jersey in history: $166 million awarded against the Division of Youth and Family Services. As for the abusive father in this case, he received a paltry jail term of six years.)
So what do we do when evidence of abuse is discovered? How do we proceed? First, in cases when abuse is suspected, it is a bedrock principle that a child can’t be returned to the hands of the abuser. But how do we secure the patient’s safety after making a diagnosis of “likely child abuse”? As clinicians, we are duty bound to report abuse. Yet, under most circumstances, we do not have an automatic mechanism to emergently remove a child from a dangerous situation under our own authority: With great responsibility comes limited power. Sarcasm aside, there are steps we can take to safeguard children at risk.
Continue to learn how to safeguard children at risk >>
Consider emergency removal through your state’s child protection agency. In most cases, a child is removed from an unfit home by a court order. However, when the child is in imminent danger and there is insufficient time to follow this procedure, the child may be removed from the home by the state’s child protection agency without parental consent. (New Jersey, where this case occurred, is one such example; see NJSA 9:6-8.29[a].)
Know your state’s rules for emergency removal, and have the child abuse hotline number handy. If evidence of child abuse is present, contact the appropriate agency in your state and insist that emergency removal is warranted.
The local police department may be another option. Many states’ emergency removal procedures authorize and require local authorities to remove a child who is in imminent danger. Explain your evidence of abuse and the need for emergency action.
Lastly, if your state’s protective agency or your local police will not remove the child from the dangerous situation, another option is inpatient admission. Yes, beds are limited and costs are high. But far higher is the cost of a seriously injured child when we fail to act.
In this case, the New Jersey Division of Youth and Family Services was involved. The social workers only performed a background check and missed some 20 arrests on charges of assault and other crimes that the father had logged in Florida.
The first emergency physician who identified abuse faced liability exposure for returning the child to the abuser. He pursued a work-up for child abuse and made a diagnosis of child abuse, yet he did not adopt a disposition consistent with his work-up and diagnosis.
The second physician failed to recognize the significance of a lacerated labial frenum in a 2-month-old. This type of injury is particularly suggestive in children who are not independently mobile and thus incapable of accidental injury. Force sufficient to rip a 2-month-old’s lip away from his mouth should have been recognized as abusive force. There is no evidence in the case report that the second physician identified the abuse or acted to stop it.
IN SUM
Recognize and report abuse. Know your state’s emergency removal law, and marshal your evidence of abuse to impel state agency workers to act on their power to remove a child from an abusive situation. Above all, do not return a child to his or her abuser. —DML
In May 2009, an employee of the New Jersey Division of Youth and Family Services brought a child to an urban medical center for evaluation of possible child abuse that had been reported by the child’s maternal grandmother. The infant, who was two-and-a-half months old at the time, was bleeding from the blood vessels of both eyes and had bruises on both sides of his face.
The treating physician, Dr A., ordered a series of x-rays of the entire body and CT of the head. The CT findings were initially read as negative, and the baby was discharged on the same day with a diagnosis of “suspected child abuse.” Two radiologists who reviewed the CT results identified fluid on the brain.
Three weeks later, the infant’s parents brought him to another medical center. He was bleeding from the mouth, and a lacerated frenum was diagnosed. Attending physician Dr K. discharged the infant with a notation that the injury had been sustained when the baby’s father “tried to put a bottle in the child’s mouth.”
In mid-July 2009, at the age of 4 months, the child was severely beaten by his father and sustained brain damage. The child was removed from his parents’ custody and placed with his grandmother. The father was later convicted of aggravated assault and child cruelty.
The child’s grandmother alleged negligence by the defendants in failing to recognize child abuse, which would have resulted in the infant being removed from his home earlier, before the brain damage could occur.
Continue for the outcome and David Lang's comments >>
OUTCOME
A $7.4 million settlement was reached. Dr A. and his facility were responsible for $4.5 million; one of the radiologists and her employer, $475,000; the other radiologist and his employer, $750,000; Dr K. and his employer, $1.19 million; and the second medical center and several of its nurses, $560,000.
COMMENT
In this horrible case, there was no failure to diagnose. Dr A. diagnosed “suspected child abuse” during the May 2009 visit. The issue was the management of the case after abuse was suspected.
Suspected child abuse is a “hot potato,” and the cases are difficult to manage. Clinicians are trained to spot and treat illness. We are not well equipped to identify short-term safe housing, file court papers to terminate parental rights, conduct home visits, or interview family, friends, and neighbors to determine the best living arrangement for an at-risk patient.
Many clinicians feel that issues of abuse are outside medicine and are more appropriately dealt with by social workers, the courts, and law enforcement. Candidly, managing these cases is taxing. But manage them we must to adequately protect those who cannot protect themselves.
This case proves clinicians will be held accountable for child abuse. The defense attorneys realized the enormous malpractice exposure and consented to the substantial $7.4 million settlement. (This, it should be noted, is in addition to the largest verdict against the State of New Jersey in history: $166 million awarded against the Division of Youth and Family Services. As for the abusive father in this case, he received a paltry jail term of six years.)
So what do we do when evidence of abuse is discovered? How do we proceed? First, in cases when abuse is suspected, it is a bedrock principle that a child can’t be returned to the hands of the abuser. But how do we secure the patient’s safety after making a diagnosis of “likely child abuse”? As clinicians, we are duty bound to report abuse. Yet, under most circumstances, we do not have an automatic mechanism to emergently remove a child from a dangerous situation under our own authority: With great responsibility comes limited power. Sarcasm aside, there are steps we can take to safeguard children at risk.
Continue to learn how to safeguard children at risk >>
Consider emergency removal through your state’s child protection agency. In most cases, a child is removed from an unfit home by a court order. However, when the child is in imminent danger and there is insufficient time to follow this procedure, the child may be removed from the home by the state’s child protection agency without parental consent. (New Jersey, where this case occurred, is one such example; see NJSA 9:6-8.29[a].)
Know your state’s rules for emergency removal, and have the child abuse hotline number handy. If evidence of child abuse is present, contact the appropriate agency in your state and insist that emergency removal is warranted.
The local police department may be another option. Many states’ emergency removal procedures authorize and require local authorities to remove a child who is in imminent danger. Explain your evidence of abuse and the need for emergency action.
Lastly, if your state’s protective agency or your local police will not remove the child from the dangerous situation, another option is inpatient admission. Yes, beds are limited and costs are high. But far higher is the cost of a seriously injured child when we fail to act.
In this case, the New Jersey Division of Youth and Family Services was involved. The social workers only performed a background check and missed some 20 arrests on charges of assault and other crimes that the father had logged in Florida.
The first emergency physician who identified abuse faced liability exposure for returning the child to the abuser. He pursued a work-up for child abuse and made a diagnosis of child abuse, yet he did not adopt a disposition consistent with his work-up and diagnosis.
The second physician failed to recognize the significance of a lacerated labial frenum in a 2-month-old. This type of injury is particularly suggestive in children who are not independently mobile and thus incapable of accidental injury. Force sufficient to rip a 2-month-old’s lip away from his mouth should have been recognized as abusive force. There is no evidence in the case report that the second physician identified the abuse or acted to stop it.
IN SUM
Recognize and report abuse. Know your state’s emergency removal law, and marshal your evidence of abuse to impel state agency workers to act on their power to remove a child from an abusive situation. Above all, do not return a child to his or her abuser. —DML
What are your responsibilities after a screening call?
Dear Dr. Mossman,
When I take a call from a treatment-seeker at our outpatient clinic, I ask brief screening questions to determine whether our services would be appropriate. Shortly after I screened one caller, Ms. C, she called back requesting a medication refill and asking about her diagnosis.
What obligation do I have to Ms. C? Is she my patient? Would I be liable if I didn’t help her out and something bad happened to her?
Submitted by “Dr. S”
Office and hospital Web sites, LinkedIn profiles, and Facebook pages are just a few of the ways that people find physicians and learn about their services. But most 21st century doctor-patient relationships still start with 19th century technology: a telephone call.
Talking with prospective patients before setting up an appointment makes sense. A short conversation can clarify whether you offer the services that a caller needs and increases the show-up rate for initial appointments.1
But if you ask for some personal history and information about symptoms in a screening interview, does that make the caller your patient? Ms. C seemed to have thought so. To find out whether Ms. C was right and to learn how Dr. S should handle initial telephone calls, we’ll look at:
• the rationale for screening callers before initiating treatment
• features of screening that can create a doctor-patient relationship
• how to fulfill duties that result from screening.
Why screen prospective patients?
Mental health treatment has become more diversified and specialized over the past 30 years. No psychiatrist nowadays has all the therapeutic skills that all potential patients might need.
Before speaking to you, a treatment-seeker often won’t know whether your practice style will fit his (her) needs. You might prefer not to provide medication management for another clinician’s psychotherapy patient or, if you’re like most psychiatrists, you might not offer psychotherapy.
In the absence of prior obligation (eg, agreeing to provide coverage for an emergency room), physicians may structure their practices and contract for their services as they see fit2—but this leaves you with some obligation to screen potential patients for appropriate mutual fit. In years past, some psychiatrists saw potential patients for an in-office evaluation to decide whether to provide treatment—a practicethat remains acceptable if the person is told, when the appointment is made, that the first meeting is “to meet each other and see if you want to establish a treatment relationship.”3
Good treatment plans take into account patients’ temperament, emotional state, cognitive capacity, culture, family circumstances, substance use, and medical history.4 Common mental conditions often can be identified in a telephone call.5,6 Although the diagnostic accuracy of such efforts is uncertain,7 such calls can help practitioners determine whether they offer the right services for callers. Good decisions about initiating care always take financial pressures and constraints into account,8 and a pre-appointment telephone call can address those issues, too.
For all these reasons, talking to a prospective patient before he comes to see you makes sense. Screening lets you decide:
• whether you’re the right clinician for his needs
• who the right clinician is if you are not
• whether he should seek emergency evaluation when the situation sounds urgent.
Do phone calls start treatment?
As Dr. S’s questions show, telephone screenings might leave some callers thinking that treatment has started, even before their first office appointment. Having a treatment relationship is a prerequisite to malpractice liability,9 and courts have concluded that, under the right circumstances, telephone assessments do create physician-patient relationships.
Creating a physician-patient relationship
How or when might telephone screening make someone your patient? This question doesn’t have a precise answer, but how courts decided similar questions has depended on the questions the physician asked and whether the physician offered what sounded like medical advice.10,11 A physician-patient relationship forms when the physician takes some implied or affirmative action to treat, see, examine, care for, or offer a diagnosis to the patient,9,12,13 such as:
• knowingly accepting someone as a patient14
• explicitly agreeing to treat a person
• “acting in some other way such that the patient might reasonably be led to assume a doctor-patient relationship has been established.”15
Also, the “fact that a physician does not deal directly with a patient does not necessarily preclude the existence of a physician-patient relationship,”12 so a telephone conversation can create such a relationship if it contains the right elements. Table 116 highlights actions that, during the course of screening, might constitute initiation of a physician-patient relationship. Table 2 offers suggestions for managing initial telephone contacts to reduce the chance of inadvertently creating a physician-patient relationship.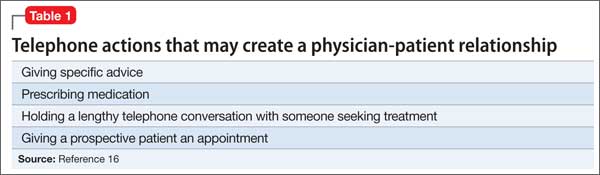
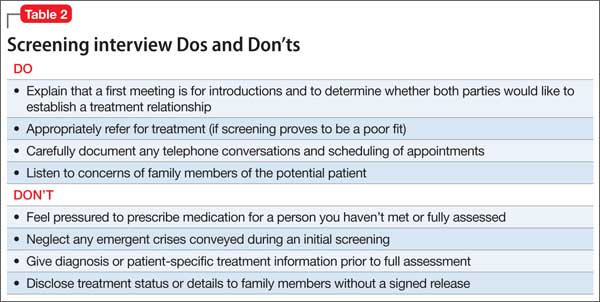
In the eyes of the law, whether a physician-patient relationship was formed depends on specific facts of the situation and may be decided by a jury.13,14 In the case of Ms. C, Dr. S might avoid premature creation of a physician-patient relationship by refraining from offering a diagnosis at the conclusion of the screening call.17
Prescribing
Although features of the original screening interview indicated that Ms. C was not yet Dr. S’s patient, prescribing certainly would commence a physician-patient relationship.18 But even if the screening had made Ms. C a patient, refilling her prescription now probably is a bad idea.
Assuming that a physician-patient relationship exists, it is unlikely that a short telephone interview gave Dr. S enough information about Ms. C’s medical history and present mental status to ensure that his diagnostic reasoning would not be faulty. It also is unlikely that telephone screening allowed Dr. S to meet the standard of care for prescribing—a process that involves choosing medications suitable to the patient’s clinical needs, checking the results of any necessary lab tests, and obtaining appropriate informed consent.19
Satisfying duties
Outpatient facilities can instruct telephone screeners to conduct interviews in ways that reduce inadvertent establishment of a treatment relationship, but establishing such a relationship cannot be avoided in all cases. If a caller is distraught or in crisis, for example, compassion dictates helping him, and some callers (eg, Ms. C) may feel they have a firmer treatment relationship than actually exists.
Once you have created a physician-patient relationship, you must continue that relationship until you end it appropriately.3 That does not mean you have to provide definitive treatment; you simply need to exercise “reasonable care according to the standards of the profession.”16,20 If a caller telephones in an emergency situation, for example, the screening clinician should take appropriate steps to ensure safety, which might include calling law enforcement or facilitating hospitalization.3
One way to fulfill the duties of a physician-patient relationship inadvertently established during initial screening is through explicit discharge (if medically appropriate) or transfer of care to another physician.15 A prudent clinic or practitioner will describe other mental health resources in the community and sometimes assist with referral if the inquiring potential patient needs services that the provider does not offer.
In many communities, finding appropriate mental health resources is difficult. Creative approaches to this problem include transitional psychiatry or crisis support clinics that serve as a “bridge” to longer-term services,21,22 preliminary process groups,23 and telepsychiatry transitional clinics.24 When a clinic does not accept a person as a patient, the clinic should clearly document 1) key features of the contact and 2) the rationale for that decision
Bottom Line
You have a right and a responsibility to screen prospective patients for good fit to your treatment services. In doing so, however, you might inadvertently create a physician-patient relationship. If this happens, you should fulfill your clinical responsibilities, as you would for any patient, by helping the patient get appropriate care from you or another provider.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Shoffner J, Staudt M, Marcus S, et al. Using telephone reminders to increase attendance at psychiatric appointments: findings of a pilot study in rural Appalachia. Psychiatr Serv. 2007;58(6):872-875.
2. Hiser v Randolph, 1980 617 P2d 774 (Ariz App).
3. American Psychiatric Association. Practice management for early career psychiatrists: a reference guide, 6th edition. http://www.psych.org/practice/managing-a-practice/ starting-a-practice. Published October 16, 2006. Accessed July 8, 2014.
4. Delgado SV, Strawn JR. Difficult psychiatric consultations: an integrated approach. New York, NY: Springer; 2014.
5. Aziz MA, Kenford S. Comparability of telephone and face-to-face interviews in assessing patients with posttraumatic stress disorder. J Psychiatric Pract. 2004;10(5): 307-313.
6. Michel C, Schimmelmann BG, Kupferschmid S, et al. Reliability of telephone assessments of at-risk criteria of psychosis: a comparison to face-to-face interviews. Schizophr Res. 2014;153(1-3):251-253.
7. Muskens EM, Lucassen P, Groenleer W, et al. Psychiatric diagnosis by telephone: is it an opportunity [published online March 15, 2014]? Soc Psychiatry Psychiatr Epidemiol. doi: 10.1007/s00127-014-0861-9.
8. Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care. JAMA. 2012;307(17):1801-1802.
9. Roberts v Sankey, 2004 813 NE2d 1195 (Ind App).
10. O’Neill v Montefiore Hospital, 1960 202 NYS 2d 436 (NY App).
11. McKinney v Schlatter, 1997 692 NE2d 1045 (Ohio App).
12. Dehn v Edgecombe, 865 A2d 603 (Md 2005).
13. Kelley v Middle Tennessee Emergency Physicians, 133 SW3d 587 (Tenn 2004).
14. Oliver v Brock, 342 So2d 1 (Ala 1976).
15. Appelbaum PS, Gutheil TG. Malpractice and other forms of liability. In: Appelbaum PS, Gutheil TG, eds. Clinical Handbook of Psychiatry and the Law, 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007:115-116.
16. Simon RI, Shuman DW. The doctor-patient relationship. Focus. 2007;5(4):423-431.
17. Torres A, Wagner R. Establishing the physician-patient relationship. J Dermatol Surg Oncol. 1993;19(2):147-149.
18. Aboff BM, Collier VU, Farber NJ, et al. Residents’ prescription writing for nonpatients. JAMA. 2002;288(3):381-385.
19. Edersheim JG, Stern TA. Liability associated with prescribing medications. Prim Care Companion J Clin Psychiatry. 2009;11(3):115-119.
20. Brown v Koulizakis, 331 SE2d 440 (Va 1985).
21. University of Michigan Department of Psychiatry. Crisis support clinic. http://www.psych.med.umich.edu/patient-care/crisis-support-clinic. Accessed July 9, 2014.
22. UAB Department of Psychiatry. http://www.uab.edu/ medicine/psychiatry. Accessed July 9, 2014.
23. Stone WN, Klein EB. The waiting-list group. Int J Group Psychother. 1999;49(4):417-428.
24. Detweiler MB, Arif S, Candelario J, et al. A telepsychiatry transition clinic: the first 12 months experience. J Telemed Telecare. 2011;17(6):293-297.
Dear Dr. Mossman,
When I take a call from a treatment-seeker at our outpatient clinic, I ask brief screening questions to determine whether our services would be appropriate. Shortly after I screened one caller, Ms. C, she called back requesting a medication refill and asking about her diagnosis.
What obligation do I have to Ms. C? Is she my patient? Would I be liable if I didn’t help her out and something bad happened to her?
Submitted by “Dr. S”
Office and hospital Web sites, LinkedIn profiles, and Facebook pages are just a few of the ways that people find physicians and learn about their services. But most 21st century doctor-patient relationships still start with 19th century technology: a telephone call.
Talking with prospective patients before setting up an appointment makes sense. A short conversation can clarify whether you offer the services that a caller needs and increases the show-up rate for initial appointments.1
But if you ask for some personal history and information about symptoms in a screening interview, does that make the caller your patient? Ms. C seemed to have thought so. To find out whether Ms. C was right and to learn how Dr. S should handle initial telephone calls, we’ll look at:
• the rationale for screening callers before initiating treatment
• features of screening that can create a doctor-patient relationship
• how to fulfill duties that result from screening.
Why screen prospective patients?
Mental health treatment has become more diversified and specialized over the past 30 years. No psychiatrist nowadays has all the therapeutic skills that all potential patients might need.
Before speaking to you, a treatment-seeker often won’t know whether your practice style will fit his (her) needs. You might prefer not to provide medication management for another clinician’s psychotherapy patient or, if you’re like most psychiatrists, you might not offer psychotherapy.
In the absence of prior obligation (eg, agreeing to provide coverage for an emergency room), physicians may structure their practices and contract for their services as they see fit2—but this leaves you with some obligation to screen potential patients for appropriate mutual fit. In years past, some psychiatrists saw potential patients for an in-office evaluation to decide whether to provide treatment—a practicethat remains acceptable if the person is told, when the appointment is made, that the first meeting is “to meet each other and see if you want to establish a treatment relationship.”3
Good treatment plans take into account patients’ temperament, emotional state, cognitive capacity, culture, family circumstances, substance use, and medical history.4 Common mental conditions often can be identified in a telephone call.5,6 Although the diagnostic accuracy of such efforts is uncertain,7 such calls can help practitioners determine whether they offer the right services for callers. Good decisions about initiating care always take financial pressures and constraints into account,8 and a pre-appointment telephone call can address those issues, too.
For all these reasons, talking to a prospective patient before he comes to see you makes sense. Screening lets you decide:
• whether you’re the right clinician for his needs
• who the right clinician is if you are not
• whether he should seek emergency evaluation when the situation sounds urgent.
Do phone calls start treatment?
As Dr. S’s questions show, telephone screenings might leave some callers thinking that treatment has started, even before their first office appointment. Having a treatment relationship is a prerequisite to malpractice liability,9 and courts have concluded that, under the right circumstances, telephone assessments do create physician-patient relationships.
Creating a physician-patient relationship
How or when might telephone screening make someone your patient? This question doesn’t have a precise answer, but how courts decided similar questions has depended on the questions the physician asked and whether the physician offered what sounded like medical advice.10,11 A physician-patient relationship forms when the physician takes some implied or affirmative action to treat, see, examine, care for, or offer a diagnosis to the patient,9,12,13 such as:
• knowingly accepting someone as a patient14
• explicitly agreeing to treat a person
• “acting in some other way such that the patient might reasonably be led to assume a doctor-patient relationship has been established.”15
Also, the “fact that a physician does not deal directly with a patient does not necessarily preclude the existence of a physician-patient relationship,”12 so a telephone conversation can create such a relationship if it contains the right elements. Table 116 highlights actions that, during the course of screening, might constitute initiation of a physician-patient relationship. Table 2 offers suggestions for managing initial telephone contacts to reduce the chance of inadvertently creating a physician-patient relationship.
In the eyes of the law, whether a physician-patient relationship was formed depends on specific facts of the situation and may be decided by a jury.13,14 In the case of Ms. C, Dr. S might avoid premature creation of a physician-patient relationship by refraining from offering a diagnosis at the conclusion of the screening call.17
Prescribing
Although features of the original screening interview indicated that Ms. C was not yet Dr. S’s patient, prescribing certainly would commence a physician-patient relationship.18 But even if the screening had made Ms. C a patient, refilling her prescription now probably is a bad idea.
Assuming that a physician-patient relationship exists, it is unlikely that a short telephone interview gave Dr. S enough information about Ms. C’s medical history and present mental status to ensure that his diagnostic reasoning would not be faulty. It also is unlikely that telephone screening allowed Dr. S to meet the standard of care for prescribing—a process that involves choosing medications suitable to the patient’s clinical needs, checking the results of any necessary lab tests, and obtaining appropriate informed consent.19
Satisfying duties
Outpatient facilities can instruct telephone screeners to conduct interviews in ways that reduce inadvertent establishment of a treatment relationship, but establishing such a relationship cannot be avoided in all cases. If a caller is distraught or in crisis, for example, compassion dictates helping him, and some callers (eg, Ms. C) may feel they have a firmer treatment relationship than actually exists.
Once you have created a physician-patient relationship, you must continue that relationship until you end it appropriately.3 That does not mean you have to provide definitive treatment; you simply need to exercise “reasonable care according to the standards of the profession.”16,20 If a caller telephones in an emergency situation, for example, the screening clinician should take appropriate steps to ensure safety, which might include calling law enforcement or facilitating hospitalization.3
One way to fulfill the duties of a physician-patient relationship inadvertently established during initial screening is through explicit discharge (if medically appropriate) or transfer of care to another physician.15 A prudent clinic or practitioner will describe other mental health resources in the community and sometimes assist with referral if the inquiring potential patient needs services that the provider does not offer.
In many communities, finding appropriate mental health resources is difficult. Creative approaches to this problem include transitional psychiatry or crisis support clinics that serve as a “bridge” to longer-term services,21,22 preliminary process groups,23 and telepsychiatry transitional clinics.24 When a clinic does not accept a person as a patient, the clinic should clearly document 1) key features of the contact and 2) the rationale for that decision
Bottom Line
You have a right and a responsibility to screen prospective patients for good fit to your treatment services. In doing so, however, you might inadvertently create a physician-patient relationship. If this happens, you should fulfill your clinical responsibilities, as you would for any patient, by helping the patient get appropriate care from you or another provider.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dear Dr. Mossman,
When I take a call from a treatment-seeker at our outpatient clinic, I ask brief screening questions to determine whether our services would be appropriate. Shortly after I screened one caller, Ms. C, she called back requesting a medication refill and asking about her diagnosis.
What obligation do I have to Ms. C? Is she my patient? Would I be liable if I didn’t help her out and something bad happened to her?
Submitted by “Dr. S”
Office and hospital Web sites, LinkedIn profiles, and Facebook pages are just a few of the ways that people find physicians and learn about their services. But most 21st century doctor-patient relationships still start with 19th century technology: a telephone call.
Talking with prospective patients before setting up an appointment makes sense. A short conversation can clarify whether you offer the services that a caller needs and increases the show-up rate for initial appointments.1
But if you ask for some personal history and information about symptoms in a screening interview, does that make the caller your patient? Ms. C seemed to have thought so. To find out whether Ms. C was right and to learn how Dr. S should handle initial telephone calls, we’ll look at:
• the rationale for screening callers before initiating treatment
• features of screening that can create a doctor-patient relationship
• how to fulfill duties that result from screening.
Why screen prospective patients?
Mental health treatment has become more diversified and specialized over the past 30 years. No psychiatrist nowadays has all the therapeutic skills that all potential patients might need.
Before speaking to you, a treatment-seeker often won’t know whether your practice style will fit his (her) needs. You might prefer not to provide medication management for another clinician’s psychotherapy patient or, if you’re like most psychiatrists, you might not offer psychotherapy.
In the absence of prior obligation (eg, agreeing to provide coverage for an emergency room), physicians may structure their practices and contract for their services as they see fit2—but this leaves you with some obligation to screen potential patients for appropriate mutual fit. In years past, some psychiatrists saw potential patients for an in-office evaluation to decide whether to provide treatment—a practicethat remains acceptable if the person is told, when the appointment is made, that the first meeting is “to meet each other and see if you want to establish a treatment relationship.”3
Good treatment plans take into account patients’ temperament, emotional state, cognitive capacity, culture, family circumstances, substance use, and medical history.4 Common mental conditions often can be identified in a telephone call.5,6 Although the diagnostic accuracy of such efforts is uncertain,7 such calls can help practitioners determine whether they offer the right services for callers. Good decisions about initiating care always take financial pressures and constraints into account,8 and a pre-appointment telephone call can address those issues, too.
For all these reasons, talking to a prospective patient before he comes to see you makes sense. Screening lets you decide:
• whether you’re the right clinician for his needs
• who the right clinician is if you are not
• whether he should seek emergency evaluation when the situation sounds urgent.
Do phone calls start treatment?
As Dr. S’s questions show, telephone screenings might leave some callers thinking that treatment has started, even before their first office appointment. Having a treatment relationship is a prerequisite to malpractice liability,9 and courts have concluded that, under the right circumstances, telephone assessments do create physician-patient relationships.
Creating a physician-patient relationship
How or when might telephone screening make someone your patient? This question doesn’t have a precise answer, but how courts decided similar questions has depended on the questions the physician asked and whether the physician offered what sounded like medical advice.10,11 A physician-patient relationship forms when the physician takes some implied or affirmative action to treat, see, examine, care for, or offer a diagnosis to the patient,9,12,13 such as:
• knowingly accepting someone as a patient14
• explicitly agreeing to treat a person
• “acting in some other way such that the patient might reasonably be led to assume a doctor-patient relationship has been established.”15
Also, the “fact that a physician does not deal directly with a patient does not necessarily preclude the existence of a physician-patient relationship,”12 so a telephone conversation can create such a relationship if it contains the right elements. Table 116 highlights actions that, during the course of screening, might constitute initiation of a physician-patient relationship. Table 2 offers suggestions for managing initial telephone contacts to reduce the chance of inadvertently creating a physician-patient relationship.
In the eyes of the law, whether a physician-patient relationship was formed depends on specific facts of the situation and may be decided by a jury.13,14 In the case of Ms. C, Dr. S might avoid premature creation of a physician-patient relationship by refraining from offering a diagnosis at the conclusion of the screening call.17
Prescribing
Although features of the original screening interview indicated that Ms. C was not yet Dr. S’s patient, prescribing certainly would commence a physician-patient relationship.18 But even if the screening had made Ms. C a patient, refilling her prescription now probably is a bad idea.
Assuming that a physician-patient relationship exists, it is unlikely that a short telephone interview gave Dr. S enough information about Ms. C’s medical history and present mental status to ensure that his diagnostic reasoning would not be faulty. It also is unlikely that telephone screening allowed Dr. S to meet the standard of care for prescribing—a process that involves choosing medications suitable to the patient’s clinical needs, checking the results of any necessary lab tests, and obtaining appropriate informed consent.19
Satisfying duties
Outpatient facilities can instruct telephone screeners to conduct interviews in ways that reduce inadvertent establishment of a treatment relationship, but establishing such a relationship cannot be avoided in all cases. If a caller is distraught or in crisis, for example, compassion dictates helping him, and some callers (eg, Ms. C) may feel they have a firmer treatment relationship than actually exists.
Once you have created a physician-patient relationship, you must continue that relationship until you end it appropriately.3 That does not mean you have to provide definitive treatment; you simply need to exercise “reasonable care according to the standards of the profession.”16,20 If a caller telephones in an emergency situation, for example, the screening clinician should take appropriate steps to ensure safety, which might include calling law enforcement or facilitating hospitalization.3
One way to fulfill the duties of a physician-patient relationship inadvertently established during initial screening is through explicit discharge (if medically appropriate) or transfer of care to another physician.15 A prudent clinic or practitioner will describe other mental health resources in the community and sometimes assist with referral if the inquiring potential patient needs services that the provider does not offer.
In many communities, finding appropriate mental health resources is difficult. Creative approaches to this problem include transitional psychiatry or crisis support clinics that serve as a “bridge” to longer-term services,21,22 preliminary process groups,23 and telepsychiatry transitional clinics.24 When a clinic does not accept a person as a patient, the clinic should clearly document 1) key features of the contact and 2) the rationale for that decision
Bottom Line
You have a right and a responsibility to screen prospective patients for good fit to your treatment services. In doing so, however, you might inadvertently create a physician-patient relationship. If this happens, you should fulfill your clinical responsibilities, as you would for any patient, by helping the patient get appropriate care from you or another provider.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Shoffner J, Staudt M, Marcus S, et al. Using telephone reminders to increase attendance at psychiatric appointments: findings of a pilot study in rural Appalachia. Psychiatr Serv. 2007;58(6):872-875.
2. Hiser v Randolph, 1980 617 P2d 774 (Ariz App).
3. American Psychiatric Association. Practice management for early career psychiatrists: a reference guide, 6th edition. http://www.psych.org/practice/managing-a-practice/ starting-a-practice. Published October 16, 2006. Accessed July 8, 2014.
4. Delgado SV, Strawn JR. Difficult psychiatric consultations: an integrated approach. New York, NY: Springer; 2014.
5. Aziz MA, Kenford S. Comparability of telephone and face-to-face interviews in assessing patients with posttraumatic stress disorder. J Psychiatric Pract. 2004;10(5): 307-313.
6. Michel C, Schimmelmann BG, Kupferschmid S, et al. Reliability of telephone assessments of at-risk criteria of psychosis: a comparison to face-to-face interviews. Schizophr Res. 2014;153(1-3):251-253.
7. Muskens EM, Lucassen P, Groenleer W, et al. Psychiatric diagnosis by telephone: is it an opportunity [published online March 15, 2014]? Soc Psychiatry Psychiatr Epidemiol. doi: 10.1007/s00127-014-0861-9.
8. Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care. JAMA. 2012;307(17):1801-1802.
9. Roberts v Sankey, 2004 813 NE2d 1195 (Ind App).
10. O’Neill v Montefiore Hospital, 1960 202 NYS 2d 436 (NY App).
11. McKinney v Schlatter, 1997 692 NE2d 1045 (Ohio App).
12. Dehn v Edgecombe, 865 A2d 603 (Md 2005).
13. Kelley v Middle Tennessee Emergency Physicians, 133 SW3d 587 (Tenn 2004).
14. Oliver v Brock, 342 So2d 1 (Ala 1976).
15. Appelbaum PS, Gutheil TG. Malpractice and other forms of liability. In: Appelbaum PS, Gutheil TG, eds. Clinical Handbook of Psychiatry and the Law, 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007:115-116.
16. Simon RI, Shuman DW. The doctor-patient relationship. Focus. 2007;5(4):423-431.
17. Torres A, Wagner R. Establishing the physician-patient relationship. J Dermatol Surg Oncol. 1993;19(2):147-149.
18. Aboff BM, Collier VU, Farber NJ, et al. Residents’ prescription writing for nonpatients. JAMA. 2002;288(3):381-385.
19. Edersheim JG, Stern TA. Liability associated with prescribing medications. Prim Care Companion J Clin Psychiatry. 2009;11(3):115-119.
20. Brown v Koulizakis, 331 SE2d 440 (Va 1985).
21. University of Michigan Department of Psychiatry. Crisis support clinic. http://www.psych.med.umich.edu/patient-care/crisis-support-clinic. Accessed July 9, 2014.
22. UAB Department of Psychiatry. http://www.uab.edu/ medicine/psychiatry. Accessed July 9, 2014.
23. Stone WN, Klein EB. The waiting-list group. Int J Group Psychother. 1999;49(4):417-428.
24. Detweiler MB, Arif S, Candelario J, et al. A telepsychiatry transition clinic: the first 12 months experience. J Telemed Telecare. 2011;17(6):293-297.
1. Shoffner J, Staudt M, Marcus S, et al. Using telephone reminders to increase attendance at psychiatric appointments: findings of a pilot study in rural Appalachia. Psychiatr Serv. 2007;58(6):872-875.
2. Hiser v Randolph, 1980 617 P2d 774 (Ariz App).
3. American Psychiatric Association. Practice management for early career psychiatrists: a reference guide, 6th edition. http://www.psych.org/practice/managing-a-practice/ starting-a-practice. Published October 16, 2006. Accessed July 8, 2014.
4. Delgado SV, Strawn JR. Difficult psychiatric consultations: an integrated approach. New York, NY: Springer; 2014.
5. Aziz MA, Kenford S. Comparability of telephone and face-to-face interviews in assessing patients with posttraumatic stress disorder. J Psychiatric Pract. 2004;10(5): 307-313.
6. Michel C, Schimmelmann BG, Kupferschmid S, et al. Reliability of telephone assessments of at-risk criteria of psychosis: a comparison to face-to-face interviews. Schizophr Res. 2014;153(1-3):251-253.
7. Muskens EM, Lucassen P, Groenleer W, et al. Psychiatric diagnosis by telephone: is it an opportunity [published online March 15, 2014]? Soc Psychiatry Psychiatr Epidemiol. doi: 10.1007/s00127-014-0861-9.
8. Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care. JAMA. 2012;307(17):1801-1802.
9. Roberts v Sankey, 2004 813 NE2d 1195 (Ind App).
10. O’Neill v Montefiore Hospital, 1960 202 NYS 2d 436 (NY App).
11. McKinney v Schlatter, 1997 692 NE2d 1045 (Ohio App).
12. Dehn v Edgecombe, 865 A2d 603 (Md 2005).
13. Kelley v Middle Tennessee Emergency Physicians, 133 SW3d 587 (Tenn 2004).
14. Oliver v Brock, 342 So2d 1 (Ala 1976).
15. Appelbaum PS, Gutheil TG. Malpractice and other forms of liability. In: Appelbaum PS, Gutheil TG, eds. Clinical Handbook of Psychiatry and the Law, 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007:115-116.
16. Simon RI, Shuman DW. The doctor-patient relationship. Focus. 2007;5(4):423-431.
17. Torres A, Wagner R. Establishing the physician-patient relationship. J Dermatol Surg Oncol. 1993;19(2):147-149.
18. Aboff BM, Collier VU, Farber NJ, et al. Residents’ prescription writing for nonpatients. JAMA. 2002;288(3):381-385.
19. Edersheim JG, Stern TA. Liability associated with prescribing medications. Prim Care Companion J Clin Psychiatry. 2009;11(3):115-119.
20. Brown v Koulizakis, 331 SE2d 440 (Va 1985).
21. University of Michigan Department of Psychiatry. Crisis support clinic. http://www.psych.med.umich.edu/patient-care/crisis-support-clinic. Accessed July 9, 2014.
22. UAB Department of Psychiatry. http://www.uab.edu/ medicine/psychiatry. Accessed July 9, 2014.
23. Stone WN, Klein EB. The waiting-list group. Int J Group Psychother. 1999;49(4):417-428.
24. Detweiler MB, Arif S, Candelario J, et al. A telepsychiatry transition clinic: the first 12 months experience. J Telemed Telecare. 2011;17(6):293-297.
The High Cost of “Free Advice”
A couple had their first child in May 1998. The boy exhibited developmental delays and had chronic problems with eating and weight gain. In August 1999, he collapsed with uncontrollable seizures. He was placed in a drug-induced coma. A month later, when he emerged from the coma, he was neurologically compromised. He recovered somewhat but then regressed, experiencing another seizure episode. He died in January 2000. MRI of his brain showed a lesion on his thalamus.
The couple’s second child was born in April 2002. This child also had delays and developed seizures, was placed in a coma, and emerged neurologically impaired. She too was found to have an abnormality in her thalamus. She died in July 2004.
The couple was referred to Dr. S, a geneticist. They consulted Dr. S both before and after the second child’s death. After their daughter’s death, the couple asked Dr. S whether it was possible to have biological children who would not have the same problems. Dr. S told them that he could not identify the specific gene causing the defect but advised that it would be safe to conceive a child with a donor egg from the general population and the husband’s sperm through in vitro fertilization.
Dr. S allegedly advised the couple that a child conceived this way would have essentially the same risk for the unidentified disease as anyone in the general population. The couple asked in writing if it would be safer to use both a donor sperm and a donor egg to further reduce the risk, and Dr. S replied by letter that the difference was “negligible.”
In June 2007, the couple had a child who was conceived with a donated egg and the husband’s sperm. This child suffered the same fate as the two previous children, dying in September 2008. MRI of the child’s brain, like the others, showed an abnormality of the thalamus. The child was diagnosed with Alpers syndrome postmortem.
The plaintiffs claimed that the chances of having a child with Alpers syndrome are about 1:200,000 in the general population, but that the chances if one parent is a known carrier are about 1:1,000. The plaintiffs claimed that if they had known of this risk, they would have used a donor egg and donor sperm to conceive a child or would have adopted. The plaintiffs alleged negligence by Dr. S in failing to give them this information.
Continue for the outcome and David Lang's comment >>
OUTCOME
A $1,086,612 verdict was returned, with the jury finding Dr. S 25% at fault and the plaintiffs 75% at fault.
COMMENT
A skilled tax accountant will provide guidance on how to claim deductions. Many lawyers listen and advise but do little else. These people sit at a desk and provide advice—that is what they do. Dispensing advice from a seated position is their only stock in store.
By contrast, clinicians are kinetic people. They are on their feet, up and about. They perform workups and surgeries, procedures and treatments. Clinicians are people in motion accustomed to action.
Yet clinicians often forget: Dispensing advice is practicing medicine. They are conditioned to dispense this advice freely, and by freely I mean both casually and without compensation. As a result, clinicians often fail to realize the value and potential liability of the spoken word. Make no mistake: Giving medical advice incurs legal risk. Lawyers know this; how many give free advice while absorbing the risk for that advice? Yeah, I thought so ....
Clinicians can be held legally liable for misinformation as easily as they can for misdiagnosis. The key is detrimental reliance. When a clinician gives a patient incorrect information, there is no legal case. The patient has a legal case if, and only if, he or she relies on that information and is injured (detriment) based on that reliance.
Here, the standard of care required the geneticist to be familiar with Alpers syndrome and accurately convey the risk associated with different courses of action. Like an accountant or attorney, the service sought and tendered is advice. The plaintiff was told that the risk for having another child with Alpers syndrome was “negligible” and made a decision based on that risk assessment.
The risk, however, was not negligible; it was 200 times greater than that in the general population. Relying on the geneticist’s information, the plaintiffs decided to use the father’s sperm and suffered legally compensable injury when their third child was born with the same condition. There was clearly clinician error.
Nevertheless, the jurors found the parents 75% at fault (for attempting to have another child) and the physician 25% at fault. Some states only allow a plaintiff to recover damages if they have no fault at all (pure contributory negligence), while others permit recovery if the plaintiff is 50% or less at fault. A handful of states—including Florida, where this case occurred—allow a plaintiff to recover even if they are 99% at fault (pure comparative negligence). In those cases, the jury determines the damages and the parties’ respective fault percentages, and the plaintiff’s recovery is reduced by that percentage. Here, the physician was responsible for 25% of the $1,086,612 award and thus had to pay $271,653.
In sum: Don’t give “free advice” too freely. >>
IN SUM
Don’t give “free advice” too freely. Document advice and options, and make sure the patient understands them. Understand that providing advice establishes a clinician–patient relationship and that you are legally responsible for advice given.
Beware of dispensing advice electronically or over the phone, where you are off your turf and lack the usual preconditions to high quality care (eg, a chart, vital signs, a medication/allergy/problem list). Never provide advice in situations where you cannot do so (my recurring favorite: a request for telephone diagnosis of a rash you’ve never seen). Dispense advice as you would medication: cautiously and with documentation. —DML
A couple had their first child in May 1998. The boy exhibited developmental delays and had chronic problems with eating and weight gain. In August 1999, he collapsed with uncontrollable seizures. He was placed in a drug-induced coma. A month later, when he emerged from the coma, he was neurologically compromised. He recovered somewhat but then regressed, experiencing another seizure episode. He died in January 2000. MRI of his brain showed a lesion on his thalamus.
The couple’s second child was born in April 2002. This child also had delays and developed seizures, was placed in a coma, and emerged neurologically impaired. She too was found to have an abnormality in her thalamus. She died in July 2004.
The couple was referred to Dr. S, a geneticist. They consulted Dr. S both before and after the second child’s death. After their daughter’s death, the couple asked Dr. S whether it was possible to have biological children who would not have the same problems. Dr. S told them that he could not identify the specific gene causing the defect but advised that it would be safe to conceive a child with a donor egg from the general population and the husband’s sperm through in vitro fertilization.
Dr. S allegedly advised the couple that a child conceived this way would have essentially the same risk for the unidentified disease as anyone in the general population. The couple asked in writing if it would be safer to use both a donor sperm and a donor egg to further reduce the risk, and Dr. S replied by letter that the difference was “negligible.”
In June 2007, the couple had a child who was conceived with a donated egg and the husband’s sperm. This child suffered the same fate as the two previous children, dying in September 2008. MRI of the child’s brain, like the others, showed an abnormality of the thalamus. The child was diagnosed with Alpers syndrome postmortem.
The plaintiffs claimed that the chances of having a child with Alpers syndrome are about 1:200,000 in the general population, but that the chances if one parent is a known carrier are about 1:1,000. The plaintiffs claimed that if they had known of this risk, they would have used a donor egg and donor sperm to conceive a child or would have adopted. The plaintiffs alleged negligence by Dr. S in failing to give them this information.
Continue for the outcome and David Lang's comment >>
OUTCOME
A $1,086,612 verdict was returned, with the jury finding Dr. S 25% at fault and the plaintiffs 75% at fault.
COMMENT
A skilled tax accountant will provide guidance on how to claim deductions. Many lawyers listen and advise but do little else. These people sit at a desk and provide advice—that is what they do. Dispensing advice from a seated position is their only stock in store.
By contrast, clinicians are kinetic people. They are on their feet, up and about. They perform workups and surgeries, procedures and treatments. Clinicians are people in motion accustomed to action.
Yet clinicians often forget: Dispensing advice is practicing medicine. They are conditioned to dispense this advice freely, and by freely I mean both casually and without compensation. As a result, clinicians often fail to realize the value and potential liability of the spoken word. Make no mistake: Giving medical advice incurs legal risk. Lawyers know this; how many give free advice while absorbing the risk for that advice? Yeah, I thought so ....
Clinicians can be held legally liable for misinformation as easily as they can for misdiagnosis. The key is detrimental reliance. When a clinician gives a patient incorrect information, there is no legal case. The patient has a legal case if, and only if, he or she relies on that information and is injured (detriment) based on that reliance.
Here, the standard of care required the geneticist to be familiar with Alpers syndrome and accurately convey the risk associated with different courses of action. Like an accountant or attorney, the service sought and tendered is advice. The plaintiff was told that the risk for having another child with Alpers syndrome was “negligible” and made a decision based on that risk assessment.
The risk, however, was not negligible; it was 200 times greater than that in the general population. Relying on the geneticist’s information, the plaintiffs decided to use the father’s sperm and suffered legally compensable injury when their third child was born with the same condition. There was clearly clinician error.
Nevertheless, the jurors found the parents 75% at fault (for attempting to have another child) and the physician 25% at fault. Some states only allow a plaintiff to recover damages if they have no fault at all (pure contributory negligence), while others permit recovery if the plaintiff is 50% or less at fault. A handful of states—including Florida, where this case occurred—allow a plaintiff to recover even if they are 99% at fault (pure comparative negligence). In those cases, the jury determines the damages and the parties’ respective fault percentages, and the plaintiff’s recovery is reduced by that percentage. Here, the physician was responsible for 25% of the $1,086,612 award and thus had to pay $271,653.
In sum: Don’t give “free advice” too freely. >>
IN SUM
Don’t give “free advice” too freely. Document advice and options, and make sure the patient understands them. Understand that providing advice establishes a clinician–patient relationship and that you are legally responsible for advice given.
Beware of dispensing advice electronically or over the phone, where you are off your turf and lack the usual preconditions to high quality care (eg, a chart, vital signs, a medication/allergy/problem list). Never provide advice in situations where you cannot do so (my recurring favorite: a request for telephone diagnosis of a rash you’ve never seen). Dispense advice as you would medication: cautiously and with documentation. —DML
A couple had their first child in May 1998. The boy exhibited developmental delays and had chronic problems with eating and weight gain. In August 1999, he collapsed with uncontrollable seizures. He was placed in a drug-induced coma. A month later, when he emerged from the coma, he was neurologically compromised. He recovered somewhat but then regressed, experiencing another seizure episode. He died in January 2000. MRI of his brain showed a lesion on his thalamus.
The couple’s second child was born in April 2002. This child also had delays and developed seizures, was placed in a coma, and emerged neurologically impaired. She too was found to have an abnormality in her thalamus. She died in July 2004.
The couple was referred to Dr. S, a geneticist. They consulted Dr. S both before and after the second child’s death. After their daughter’s death, the couple asked Dr. S whether it was possible to have biological children who would not have the same problems. Dr. S told them that he could not identify the specific gene causing the defect but advised that it would be safe to conceive a child with a donor egg from the general population and the husband’s sperm through in vitro fertilization.
Dr. S allegedly advised the couple that a child conceived this way would have essentially the same risk for the unidentified disease as anyone in the general population. The couple asked in writing if it would be safer to use both a donor sperm and a donor egg to further reduce the risk, and Dr. S replied by letter that the difference was “negligible.”
In June 2007, the couple had a child who was conceived with a donated egg and the husband’s sperm. This child suffered the same fate as the two previous children, dying in September 2008. MRI of the child’s brain, like the others, showed an abnormality of the thalamus. The child was diagnosed with Alpers syndrome postmortem.
The plaintiffs claimed that the chances of having a child with Alpers syndrome are about 1:200,000 in the general population, but that the chances if one parent is a known carrier are about 1:1,000. The plaintiffs claimed that if they had known of this risk, they would have used a donor egg and donor sperm to conceive a child or would have adopted. The plaintiffs alleged negligence by Dr. S in failing to give them this information.
Continue for the outcome and David Lang's comment >>
OUTCOME
A $1,086,612 verdict was returned, with the jury finding Dr. S 25% at fault and the plaintiffs 75% at fault.
COMMENT
A skilled tax accountant will provide guidance on how to claim deductions. Many lawyers listen and advise but do little else. These people sit at a desk and provide advice—that is what they do. Dispensing advice from a seated position is their only stock in store.
By contrast, clinicians are kinetic people. They are on their feet, up and about. They perform workups and surgeries, procedures and treatments. Clinicians are people in motion accustomed to action.
Yet clinicians often forget: Dispensing advice is practicing medicine. They are conditioned to dispense this advice freely, and by freely I mean both casually and without compensation. As a result, clinicians often fail to realize the value and potential liability of the spoken word. Make no mistake: Giving medical advice incurs legal risk. Lawyers know this; how many give free advice while absorbing the risk for that advice? Yeah, I thought so ....
Clinicians can be held legally liable for misinformation as easily as they can for misdiagnosis. The key is detrimental reliance. When a clinician gives a patient incorrect information, there is no legal case. The patient has a legal case if, and only if, he or she relies on that information and is injured (detriment) based on that reliance.
Here, the standard of care required the geneticist to be familiar with Alpers syndrome and accurately convey the risk associated with different courses of action. Like an accountant or attorney, the service sought and tendered is advice. The plaintiff was told that the risk for having another child with Alpers syndrome was “negligible” and made a decision based on that risk assessment.
The risk, however, was not negligible; it was 200 times greater than that in the general population. Relying on the geneticist’s information, the plaintiffs decided to use the father’s sperm and suffered legally compensable injury when their third child was born with the same condition. There was clearly clinician error.
Nevertheless, the jurors found the parents 75% at fault (for attempting to have another child) and the physician 25% at fault. Some states only allow a plaintiff to recover damages if they have no fault at all (pure contributory negligence), while others permit recovery if the plaintiff is 50% or less at fault. A handful of states—including Florida, where this case occurred—allow a plaintiff to recover even if they are 99% at fault (pure comparative negligence). In those cases, the jury determines the damages and the parties’ respective fault percentages, and the plaintiff’s recovery is reduced by that percentage. Here, the physician was responsible for 25% of the $1,086,612 award and thus had to pay $271,653.
In sum: Don’t give “free advice” too freely. >>
IN SUM
Don’t give “free advice” too freely. Document advice and options, and make sure the patient understands them. Understand that providing advice establishes a clinician–patient relationship and that you are legally responsible for advice given.
Beware of dispensing advice electronically or over the phone, where you are off your turf and lack the usual preconditions to high quality care (eg, a chart, vital signs, a medication/allergy/problem list). Never provide advice in situations where you cannot do so (my recurring favorite: a request for telephone diagnosis of a rash you’ve never seen). Dispense advice as you would medication: cautiously and with documentation. —DML
Could thorough documentation have changed the outcome of this trial?
Case: Did the gynecologist have the right to not remove the ovaries?
A 36-year-old woman (G3 P3003) presented to her gynecologist with dysmenorrhea and abnormal uterine bleeding. She reported a family history of ovarian cancer for two generations. She was evaluated and underwent physical examination and preoperative ultrasound examination of pelvic organs. All findings were unremarkable. The gynecologist prescribed oral contraceptives (OCs). After an initial excellent response, the patient reported a reoccurrence of pelvic pain and abnormal bleeding 6 years later. The gynecologist suggested options including operative hysteroscopy, dilatation and curettage (D&C), endometrial ablation, off-label use of an intrauterine contraceptive system, or hysterectomy performed via a minimally invasive, vaginal, or abdominal approach. The patient opted for hysteroscopy, D&C, and endometrial ablation and operative laparoscopy. The patient received a diagnosis of stage I endometriosis, which was treated with fulguration.
Two years later, she reported menorrhagia and pelvic pain. The gynecologist suggested trying an OC again, and the patient was given a prescription for a low-dose estrogen/desogestrel combination pill. The patient then changed her mind within 72 hours, never took the OC, and contacted her gynecologist to schedule surgery with him. Upon a return visit to the office, the patient and gynecologist decided to proceed with laparoscopic-assisted vaginal hysterectomy (LAVH) with bilateral salpingo-oophorectomy (BSO). The written consent included laparoscopic hysterectomy with removal of ovary or ovaries and bilateral fallopian tubes, with a possibility of abdominal hysterectomy.
The gynecologist met with the patient preoperatively to update the history, which was unchanged from her prior office visit. In the operating room, “time out” occurred and was documented appropriately—concerns were to be provided to the gynecologist; none were noted.
Intraoperatively, the ovaries were normal in appearance and no endometriosis was noted. The gynecologist proceeded with LAVH and, because the ovaries were normal, did not remove them or the fallopian tubes.
The patient sued the gynecologist on the grounds that, because the originally planned BSO was not performed, she was fearful of developing ovarian cancer in the future.
Preoperative documentation was “sketchy”at best and did not reflect the preoperative discussion and options presented to the patient. There was no documentation of anyone accompanying the patient at the preoperative office visit.
The case went to trial.
What’s the verdict?
CASE: Final verdict was for the patient
The jury awarded damages to the patient based on the absence of adequate consent and failure to perform what was preoperatively agreed to in the consent form.
Legal takeaways from this case
This is an unusual case. Absent something else, it is unusual for there to be liability for not doing a procedure, where the procedure seemed medically unnecessary based on observations during surgery and where language of the signed written consent form created ambiguity about the plan for the removal of the ovaries. Here the patient alleged that her consent was not “informed.” Although informed consent claims are fairly common in malpractice litigation, they are generally appended to an underlying count (or counts) of negligent care; it is uncommon for there to be recovery of damages based solely on the absence of informed consent.
A signed consent form may not be sufficient. In general, a patient’s signature on a consent form alone is not sufficient evidence of informed consent. Whether the patient was truly informed will be judged by the circumstances during which the patient’s consent was obtained.
State laws vary on the specifics of informed consent. Many states have specific statutes or regulations dealing with informed consent. The “informed” part of informed consent generally requires that the patient be informed of:
- the nature of the procedure proposed
- the risks and benefits of the procedure
- the alternative forms of treatment
- the consequences of not undertaking the proposed procedure or an alternative.
In this case, the lawsuit alleges damages based on the fear of future ovarian cancer. It is likely that the patient offered credible testimony that she decided to proceed with surgery specifically because of her fear of ovarian cancer. The patient may have offered testimony about her specific request for her ovaries to be removed because of this fear, or she may have offered testimony about her belief or understanding that the ovaries were going to be removed based on her preoperative discussion with the gynecologist.
Related article: Sound strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Written consent must reflect the actual preoperative discussion
The written consent stated: “hysterectomy with removal of ovary or ovaries,” creating some ambiguity regarding whether the gynecologist had latitude in deciding whether or not to remove the ovaries. However, certain “facts” in this case scenario support the claim that the written consent form was meant to have reflected a decision and agreement between the doctor and patient that the ovaries were to be removed, including:
- the patient had a significant family history of ovarian cancer, making the fear of future ovarian cancer reasonable
- the patient opted out of a conservative treatment plan within 3 days and asked instead to schedule major surgery.
The gynecologist may have testified that the preoperative discussion included only the possibility of removing the ovaries, to be determined based upon what was observed in the course of the surgery. However, in the case description, we are told that the “preoperative documentation was ‘sketchy’ at best.” The jury may have concluded that the gynecologist did not know the wishes of the patient in the event that the ovaries appeared normal during the surgery.
We also know that when the patient returned to the gynecologist’s office after requesting surgery, a “discussion occurred to ‘proceed with LAVH with BSO.’” If this precise language was noted in the patient’s chart, the jury may have concluded that the gynecologist ignored the patient’s wishes!
A claim that the patient was adequately informed prior to treatment can be difficult to address if the informed consent process has not been adequately documented. Often in litigation the decisive question is not whether the right thing was done but whether that can be demonstrated. This case emphasizes the need for good documentation reflecting the specific discussions with the patient.
Litigation prevention rule #1: Thorough documentationVital elements to document | |
| Preoperative office-visit records
Written consent form
| Operative report
Postoperative office-visit records
|
*In the event of an adverse outcome, your actions will be judged on whether you were acting reasonably and using your best judgment. Your documentation needs to explain in detail what you did and why you did it that way. If what you did was a “variance,” explain why. | |
Clinical takeaways
The importance of a good rapport with patients as well as clear discussion of clinical findings, test results, and options for treatment remains paramount. This includes documentation of discussions, recording of who is present during the discussion (including witnesses), as well as the patient’s response to various treatment offerings.
The informed consent process from the clinician’s perspective should reflect discussion of risks, benefits, alternatives, sequelae of complications, and an appropriate risk of refusal. It is most important to pay attention to detail, and record that detail which will reflect your effort to be thorough. Make sure that the surgical consent form includes the operating physician’s name, the name(s) of the assisting physician(s), and no blank spaces.
Related article: More strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Open communication plus complete documentation are key
A well-designed history form—without blanks but with documentation of the physical examination and reflection of the impression and plan—can serve to avert litigation. Ideally, the operative report will reflect not only what was done but also the intraoperative decision-making process on the part of the gynecologist. Documentation of the physician’s thoroughness with intraoperative assessment may well avoid acceptance of a case by a patient’s attorney. Most importantly, transparent postoperative discussions with the patient and family detailing what occurred and the intraoperative decision-making process may convince the patient and family that the clinician has nothing to hide and has the patient’s best interest in mind.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Please include the city and state in which you practice.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |


Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith and Ms. Pruitt report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith and Ms. Pruitt report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith and Ms. Pruitt report no financial relationships relevant to this article.
Case: Did the gynecologist have the right to not remove the ovaries?
A 36-year-old woman (G3 P3003) presented to her gynecologist with dysmenorrhea and abnormal uterine bleeding. She reported a family history of ovarian cancer for two generations. She was evaluated and underwent physical examination and preoperative ultrasound examination of pelvic organs. All findings were unremarkable. The gynecologist prescribed oral contraceptives (OCs). After an initial excellent response, the patient reported a reoccurrence of pelvic pain and abnormal bleeding 6 years later. The gynecologist suggested options including operative hysteroscopy, dilatation and curettage (D&C), endometrial ablation, off-label use of an intrauterine contraceptive system, or hysterectomy performed via a minimally invasive, vaginal, or abdominal approach. The patient opted for hysteroscopy, D&C, and endometrial ablation and operative laparoscopy. The patient received a diagnosis of stage I endometriosis, which was treated with fulguration.
Two years later, she reported menorrhagia and pelvic pain. The gynecologist suggested trying an OC again, and the patient was given a prescription for a low-dose estrogen/desogestrel combination pill. The patient then changed her mind within 72 hours, never took the OC, and contacted her gynecologist to schedule surgery with him. Upon a return visit to the office, the patient and gynecologist decided to proceed with laparoscopic-assisted vaginal hysterectomy (LAVH) with bilateral salpingo-oophorectomy (BSO). The written consent included laparoscopic hysterectomy with removal of ovary or ovaries and bilateral fallopian tubes, with a possibility of abdominal hysterectomy.
The gynecologist met with the patient preoperatively to update the history, which was unchanged from her prior office visit. In the operating room, “time out” occurred and was documented appropriately—concerns were to be provided to the gynecologist; none were noted.
Intraoperatively, the ovaries were normal in appearance and no endometriosis was noted. The gynecologist proceeded with LAVH and, because the ovaries were normal, did not remove them or the fallopian tubes.
The patient sued the gynecologist on the grounds that, because the originally planned BSO was not performed, she was fearful of developing ovarian cancer in the future.
Preoperative documentation was “sketchy”at best and did not reflect the preoperative discussion and options presented to the patient. There was no documentation of anyone accompanying the patient at the preoperative office visit.
The case went to trial.
What’s the verdict?
CASE: Final verdict was for the patient
The jury awarded damages to the patient based on the absence of adequate consent and failure to perform what was preoperatively agreed to in the consent form.
Legal takeaways from this case
This is an unusual case. Absent something else, it is unusual for there to be liability for not doing a procedure, where the procedure seemed medically unnecessary based on observations during surgery and where language of the signed written consent form created ambiguity about the plan for the removal of the ovaries. Here the patient alleged that her consent was not “informed.” Although informed consent claims are fairly common in malpractice litigation, they are generally appended to an underlying count (or counts) of negligent care; it is uncommon for there to be recovery of damages based solely on the absence of informed consent.
A signed consent form may not be sufficient. In general, a patient’s signature on a consent form alone is not sufficient evidence of informed consent. Whether the patient was truly informed will be judged by the circumstances during which the patient’s consent was obtained.
State laws vary on the specifics of informed consent. Many states have specific statutes or regulations dealing with informed consent. The “informed” part of informed consent generally requires that the patient be informed of:
- the nature of the procedure proposed
- the risks and benefits of the procedure
- the alternative forms of treatment
- the consequences of not undertaking the proposed procedure or an alternative.
In this case, the lawsuit alleges damages based on the fear of future ovarian cancer. It is likely that the patient offered credible testimony that she decided to proceed with surgery specifically because of her fear of ovarian cancer. The patient may have offered testimony about her specific request for her ovaries to be removed because of this fear, or she may have offered testimony about her belief or understanding that the ovaries were going to be removed based on her preoperative discussion with the gynecologist.
Related article: Sound strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Written consent must reflect the actual preoperative discussion
The written consent stated: “hysterectomy with removal of ovary or ovaries,” creating some ambiguity regarding whether the gynecologist had latitude in deciding whether or not to remove the ovaries. However, certain “facts” in this case scenario support the claim that the written consent form was meant to have reflected a decision and agreement between the doctor and patient that the ovaries were to be removed, including:
- the patient had a significant family history of ovarian cancer, making the fear of future ovarian cancer reasonable
- the patient opted out of a conservative treatment plan within 3 days and asked instead to schedule major surgery.
The gynecologist may have testified that the preoperative discussion included only the possibility of removing the ovaries, to be determined based upon what was observed in the course of the surgery. However, in the case description, we are told that the “preoperative documentation was ‘sketchy’ at best.” The jury may have concluded that the gynecologist did not know the wishes of the patient in the event that the ovaries appeared normal during the surgery.
We also know that when the patient returned to the gynecologist’s office after requesting surgery, a “discussion occurred to ‘proceed with LAVH with BSO.’” If this precise language was noted in the patient’s chart, the jury may have concluded that the gynecologist ignored the patient’s wishes!
A claim that the patient was adequately informed prior to treatment can be difficult to address if the informed consent process has not been adequately documented. Often in litigation the decisive question is not whether the right thing was done but whether that can be demonstrated. This case emphasizes the need for good documentation reflecting the specific discussions with the patient.
Litigation prevention rule #1: Thorough documentationVital elements to document | |
| Preoperative office-visit records
Written consent form
| Operative report
Postoperative office-visit records
|
*In the event of an adverse outcome, your actions will be judged on whether you were acting reasonably and using your best judgment. Your documentation needs to explain in detail what you did and why you did it that way. If what you did was a “variance,” explain why. | |
Clinical takeaways
The importance of a good rapport with patients as well as clear discussion of clinical findings, test results, and options for treatment remains paramount. This includes documentation of discussions, recording of who is present during the discussion (including witnesses), as well as the patient’s response to various treatment offerings.
The informed consent process from the clinician’s perspective should reflect discussion of risks, benefits, alternatives, sequelae of complications, and an appropriate risk of refusal. It is most important to pay attention to detail, and record that detail which will reflect your effort to be thorough. Make sure that the surgical consent form includes the operating physician’s name, the name(s) of the assisting physician(s), and no blank spaces.
Related article: More strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Open communication plus complete documentation are key
A well-designed history form—without blanks but with documentation of the physical examination and reflection of the impression and plan—can serve to avert litigation. Ideally, the operative report will reflect not only what was done but also the intraoperative decision-making process on the part of the gynecologist. Documentation of the physician’s thoroughness with intraoperative assessment may well avoid acceptance of a case by a patient’s attorney. Most importantly, transparent postoperative discussions with the patient and family detailing what occurred and the intraoperative decision-making process may convince the patient and family that the clinician has nothing to hide and has the patient’s best interest in mind.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Please include the city and state in which you practice.
Case: Did the gynecologist have the right to not remove the ovaries?
A 36-year-old woman (G3 P3003) presented to her gynecologist with dysmenorrhea and abnormal uterine bleeding. She reported a family history of ovarian cancer for two generations. She was evaluated and underwent physical examination and preoperative ultrasound examination of pelvic organs. All findings were unremarkable. The gynecologist prescribed oral contraceptives (OCs). After an initial excellent response, the patient reported a reoccurrence of pelvic pain and abnormal bleeding 6 years later. The gynecologist suggested options including operative hysteroscopy, dilatation and curettage (D&C), endometrial ablation, off-label use of an intrauterine contraceptive system, or hysterectomy performed via a minimally invasive, vaginal, or abdominal approach. The patient opted for hysteroscopy, D&C, and endometrial ablation and operative laparoscopy. The patient received a diagnosis of stage I endometriosis, which was treated with fulguration.
Two years later, she reported menorrhagia and pelvic pain. The gynecologist suggested trying an OC again, and the patient was given a prescription for a low-dose estrogen/desogestrel combination pill. The patient then changed her mind within 72 hours, never took the OC, and contacted her gynecologist to schedule surgery with him. Upon a return visit to the office, the patient and gynecologist decided to proceed with laparoscopic-assisted vaginal hysterectomy (LAVH) with bilateral salpingo-oophorectomy (BSO). The written consent included laparoscopic hysterectomy with removal of ovary or ovaries and bilateral fallopian tubes, with a possibility of abdominal hysterectomy.
The gynecologist met with the patient preoperatively to update the history, which was unchanged from her prior office visit. In the operating room, “time out” occurred and was documented appropriately—concerns were to be provided to the gynecologist; none were noted.
Intraoperatively, the ovaries were normal in appearance and no endometriosis was noted. The gynecologist proceeded with LAVH and, because the ovaries were normal, did not remove them or the fallopian tubes.
The patient sued the gynecologist on the grounds that, because the originally planned BSO was not performed, she was fearful of developing ovarian cancer in the future.
Preoperative documentation was “sketchy”at best and did not reflect the preoperative discussion and options presented to the patient. There was no documentation of anyone accompanying the patient at the preoperative office visit.
The case went to trial.
What’s the verdict?
CASE: Final verdict was for the patient
The jury awarded damages to the patient based on the absence of adequate consent and failure to perform what was preoperatively agreed to in the consent form.
Legal takeaways from this case
This is an unusual case. Absent something else, it is unusual for there to be liability for not doing a procedure, where the procedure seemed medically unnecessary based on observations during surgery and where language of the signed written consent form created ambiguity about the plan for the removal of the ovaries. Here the patient alleged that her consent was not “informed.” Although informed consent claims are fairly common in malpractice litigation, they are generally appended to an underlying count (or counts) of negligent care; it is uncommon for there to be recovery of damages based solely on the absence of informed consent.
A signed consent form may not be sufficient. In general, a patient’s signature on a consent form alone is not sufficient evidence of informed consent. Whether the patient was truly informed will be judged by the circumstances during which the patient’s consent was obtained.
State laws vary on the specifics of informed consent. Many states have specific statutes or regulations dealing with informed consent. The “informed” part of informed consent generally requires that the patient be informed of:
- the nature of the procedure proposed
- the risks and benefits of the procedure
- the alternative forms of treatment
- the consequences of not undertaking the proposed procedure or an alternative.
In this case, the lawsuit alleges damages based on the fear of future ovarian cancer. It is likely that the patient offered credible testimony that she decided to proceed with surgery specifically because of her fear of ovarian cancer. The patient may have offered testimony about her specific request for her ovaries to be removed because of this fear, or she may have offered testimony about her belief or understanding that the ovaries were going to be removed based on her preoperative discussion with the gynecologist.
Related article: Sound strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Written consent must reflect the actual preoperative discussion
The written consent stated: “hysterectomy with removal of ovary or ovaries,” creating some ambiguity regarding whether the gynecologist had latitude in deciding whether or not to remove the ovaries. However, certain “facts” in this case scenario support the claim that the written consent form was meant to have reflected a decision and agreement between the doctor and patient that the ovaries were to be removed, including:
- the patient had a significant family history of ovarian cancer, making the fear of future ovarian cancer reasonable
- the patient opted out of a conservative treatment plan within 3 days and asked instead to schedule major surgery.
The gynecologist may have testified that the preoperative discussion included only the possibility of removing the ovaries, to be determined based upon what was observed in the course of the surgery. However, in the case description, we are told that the “preoperative documentation was ‘sketchy’ at best.” The jury may have concluded that the gynecologist did not know the wishes of the patient in the event that the ovaries appeared normal during the surgery.
We also know that when the patient returned to the gynecologist’s office after requesting surgery, a “discussion occurred to ‘proceed with LAVH with BSO.’” If this precise language was noted in the patient’s chart, the jury may have concluded that the gynecologist ignored the patient’s wishes!
A claim that the patient was adequately informed prior to treatment can be difficult to address if the informed consent process has not been adequately documented. Often in litigation the decisive question is not whether the right thing was done but whether that can be demonstrated. This case emphasizes the need for good documentation reflecting the specific discussions with the patient.
Litigation prevention rule #1: Thorough documentationVital elements to document | |
| Preoperative office-visit records
Written consent form
| Operative report
Postoperative office-visit records
|
*In the event of an adverse outcome, your actions will be judged on whether you were acting reasonably and using your best judgment. Your documentation needs to explain in detail what you did and why you did it that way. If what you did was a “variance,” explain why. | |
Clinical takeaways
The importance of a good rapport with patients as well as clear discussion of clinical findings, test results, and options for treatment remains paramount. This includes documentation of discussions, recording of who is present during the discussion (including witnesses), as well as the patient’s response to various treatment offerings.
The informed consent process from the clinician’s perspective should reflect discussion of risks, benefits, alternatives, sequelae of complications, and an appropriate risk of refusal. It is most important to pay attention to detail, and record that detail which will reflect your effort to be thorough. Make sure that the surgical consent form includes the operating physician’s name, the name(s) of the assisting physician(s), and no blank spaces.
Related article: More strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Open communication plus complete documentation are key
A well-designed history form—without blanks but with documentation of the physical examination and reflection of the impression and plan—can serve to avert litigation. Ideally, the operative report will reflect not only what was done but also the intraoperative decision-making process on the part of the gynecologist. Documentation of the physician’s thoroughness with intraoperative assessment may well avoid acceptance of a case by a patient’s attorney. Most importantly, transparent postoperative discussions with the patient and family detailing what occurred and the intraoperative decision-making process may convince the patient and family that the clinician has nothing to hide and has the patient’s best interest in mind.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Please include the city and state in which you practice.

Blue towel left in abdomen: $7.2M verdict

Blue towel left in abdomen: $7.2M verdict
When a 61-year-old woman underwent laparoscopic hysterectomy, her gynecologist, Dr. A, was assisted by another gynecologist (Dr. B), a nurse, and a technician. When Dr. A noted that the uterine artery had been injured, he converted to an open procedure, retracted the bowel, repaired the artery, and completed the operation.
Postdischarge, the patient was febrile and developed abdominal pain and an odorous vaginal discharge. A month later, exploratory surgery revealed a retained blue towel that had been used for bowel retraction. The patient required open healing of the surgical wound and a temporary colostomy. She developed an incisional hernia after colostomy reversal, and hernia repair required resection of a small portion of the bowel.
PATIENT’S CLAIM It was negligent to use a blue towel to retract the bowel. The towel should have been removed from her abdomen before closure.
DEFENDANTS’ DEFENSE The technician claimed that she did not provide the towel, did not see the towel used, and that she was not told that the towel had to be tracked. She noted that its color indicated that it lacked a radiopaque tag, and that hospital policy forbade use of untagged towels in an open wound.
Dr. A claimed that he specifically requested a blue towel because it was absorbent, that the technician provided the towel, and that the towel’s use prevented the patient from bleeding to death.
VERDICT A $7.2 million New York verdict was returned against both gynecologists and the hospital as the technician’s employer.
MISCARRIAGE AFTER D&C
A few days after a woman thought she miscarried, her family practi-tioner (FP) performed a dilation and curettage (D&C).
The patient was at work 12 days later when she expelled a fully formed 14-week fetus into a toilet. She was taken to the emergency department (ED), where the cord was cut. Later that day, she passed placental tissue; a repeat D&C was performed the next day.
PATIENT'S CLAIM The FP did not properly perform the first D&C. Although the pathology report was available to the FP prior to the patient’s postoperative visit, the FP failed to inform the patient that no fetal parts had been extracted.
PHYSICIAN’S DEFENSE Because the FP thought that the fetus had been passed prior to the D&C, she believed the pathology report was appropriate.
The patient had been informed of the possibility of retained products of conception after the D&C. The FP had ordered a blood pregnancy test that would have revealed the presence of retained products of conception, but the patient did not have the test. The patient did not contact the FP to report symptoms that felt like labor pains on the day that she passed the fetus.
VERDICT A bench trial resulted in a $51,000 California verdict.
PREGNANT WOMAN COMPLAINS OF LEG PAIN; DIES OF DVT
A 23-year-old woman went to the ED with pain and swelling in her lower left leg and calf. The symptoms were reported to her ObGyn, who examined and then discharged her within a few hours, with instructions to come for her regularly scheduled prenatal visit.
The patient died 2 weeks later. The cause of death was determined to be a pulmonary embolus from a thrombus of the left popliteal vein.
ESTATE’S CLAIM The ObGyn was negligent in failing to test the patient for thrombosis in her left leg when she was in the ED or several days later at the office, when she continued to report leg pain.
PHYSICIAN’S DEFENSE The patient did not have signs of thrombosis at the ED or at the subsequent office visit. The pathologist reported that the clot that caused the embolus appeared fresh. The ObGyn surmised that it had formed after the patient’s last appointment.
VERDICT A Texas defense verdict was returned.

Mother took topiramate; child born with cleft lip and palate: $3M verdict
When a woman learned she was pregnant in December 2007, she was taking topiramate (Topamax) to treat migraine headaches. She discussed tapering off but not discontinuing topiramate usage with her neurologist. The patient’s ObGyn told her that topiramate was safe to take during pregnancy. The child was born with a cleft lip and palate.
PARENTS’ CLAIM Janssen Pharmaceuticals, manufacturer of Topamax, failed to provide adequate warnings about the potential risks associated with Topamax until labeling was changed in March 2011. Janssen knew of potential birth defects associated with Topamax use during pregnancy more than a decade before the labeling change; Janssen’s associate director of regulatory affairs had testified in an earlier hearing that there was knowledge of related birth defects as early as 1996.
DEFENDANTS’ DEFENSE There is uncertainty as to whether exposure to Topamax during pregnancy causes birth defects. The neurologist had warned the patient of possible risks associated with taking Topamax during pregnancy, but the patient had refused to discontinue the drug.
VERDICT A $3 million Pennsylvania verdict was returned.
Related articles:
• Is it time to rethink the use of oral contraceptives in premenopausal women with migraine? Anne H. Calhoun, MD (Audiocast; October 2013)
• How to choose a contraceptive for a patient who has headaches. Kristina M. Tocce, MD; Stephanie B. Teal, MD, MPH (February 2011)
• The gynecologist’s role in managing menstrual migraine. Anne H. Calhoun, MD (April 2010)
WAS MOTHER’S HISTORY OF INCOMPETENT CERVIX IGNORED?
Early in her second pregnancy, a woman told her ObGyn that she had previously miscarried due to an incompetent cervix.
At 24 weeks’ gestation, the patient was admitted to the hospital with back and pelvic pain and vaginal bleeding. Shortly after admission, the ObGyn performed a vaginal examination and ordered ultrasonography (US), which showed that the fetus was in the transverse position and the membranes were bulging.
The ObGyn performed an emergency cesarean delivery, but the premature infant died within 2 hours.
PARENTS’ CLAIM The ObGyn should have performed a cervical cerclage because of the mother’s history of an incompetent cervix. The mother should have been placed on bed rest and monitored every 2 weeks for cervical dilation.
PHYSICIAN’S DEFENSE The patient underwent regular prenatal evaluations for an incompetent cervix, and the findings were always normal.
VERDICT A Florida defense verdict was returned.
Related article:
A stepwise approach to cervical cerclage. Katrin Karl, MD; Michael Katz, MD (Surgical Technique; June 2012)
ObGyn unresponsive to patient’s postsurgical phone calls
In 2009, a 50-year-old woman reported occasional right lower quadrant pain to her ObGyn. US results were normal. The menopausal patient’s history included three cesarean deliveries, a total abdominal hysterectomy, and a laparoscopic ovarian cystectomy.
When the patient saw her ObGyn in December 2010, she reported intermittent, progressive right lower quadrant pain that radiated down her right leg. She also reported urine loss with coughing or sneezing, and slight pain on intercourse. The ObGyn prescribed oxybutynin chloride (Ditropan) to treat the patient’s incontinence.
Three weeks later, the patient reported bilateral lower quadrant pain to her ObGyn, with minor improvement in incontinence.
The ObGyn performed bilateral salpingo-oophorectomy (BSO) in January 2011. Surgery took 3.5 hours due to extensive adhesiolysis.
After discharge, the patient felt ill and vomited. She attempted to reach the ObGyn by phone several times. That evening, the ObGyn prescribed a suppository to treat nausea and vomiting.
The patient went to the ED later that night and was found to have a perforated colon. Emergency surgery to repair the injury included creation of a colostomy, which was repaired 20 months later.
PATIENT’S CLAIM A proper workup of her symptoms was not performed; BSO was unnecessary. The ObGyn was negligent for failing to respond in a timely manner to her post-discharge phone calls, and did not properly evaluate her postoperative symptoms.
PHYSICIAN’S DEFENSE BSO was warranted. Colon injury is a known complication of the procedure.
VERDICT A $716,976 California verdict was returned, but was reduced to $591,967 under the state cap.

Who delayed delivery? $32.8M verdict for child with CP
An 18-year-old woman at 38 weeks’ gestation went to the hospital in labor. After 3.5 hours, the fetal heart rate dropped to 60 bpm. A nurse repositioned the patient, administered oxygen, and increased intravenous fluids. When the nurse rang the emergency call bell, a second nurse responded. Eighteen minutes after the fetal heart rate first dropped, a nurse rang the call bell again and the on-call ObGyn appeared.
The ObGyn performed a vaginal examination and repositioned the patient. She noted that the fetal heart-rate monitor was not working correctly, and called for an emergency cesarean delivery. The baby was born 42 minutes after the fetal heart rate initially dropped.
The child received a diagnosis of spastic-quadriplegia cerebral palsy (CP). She requires a wheelchair and has severe speech deficits and developmental delays.
PARENT’S CLAIM Cesarean delivery was not performed in a timely manner; the delivery delay was responsible for the injury that caused CP. The ObGyn was negligent in not responding to the initial emergency call. The nurses should have summoned the ObGyn earlier.
DEFENDANTS’ DEFENSE The hospital argued that the nurses followed proper protocol. Furthermore, the hospital noted that the ObGyn did not respond to the first call, and did not request a cesarean delivery for 17 minutes.
The ObGyn claimed that she made the decision to perform cesarean delivery within 5 minutes of her arrival, but it took another 15 minutes to gather the surgical team.
VERDICT A $32,882,860 Pennsylvania verdict was returned against the hospital. The ObGyn was vindicated.
DIFFICULT DELIVERY: ZAVANELLI MANEUVER
At 38 5/7 weeks’ gestation, a woman went to the hospital for induction of labor. Twenty-four hours later, she began to push. After an hour of pushing, the mother was exhausted and had a low-grade fever, and the fetal heart rate was slowing. Her ObGyn, Dr. A, attempted vacuum extraction and performed a midline episiotomy. Shoulder dystocia was encountered and maneuvers were used, but without success. Another ObGyn, Dr. B, arrived to assist and also attempted the maneuvers.
The physicians agreed to try the Zavanelli maneuver, which involves pushing the baby’s head back inside the vagina and performing a cesarean delivery.
The baby was sent to the neonatal intensive care unit, where her breathing quickly normalized without supplemental oxygen. The child has a brachial plexus injury.
PARENTS’ CLAIM Dr. A should have performed an earlier cesarean delivery. Excessive traction was used when shoulder dystocia maneuvers were attempted.
PHYSICIANS’ DEFENSE The ObGyns’ actions saved the baby’s life and prevented serious injury to both mother and baby.
VERDICT An Alabama defense verdict was returned.
Related article:
You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial; May 2013)
PLACENTA PREVIA FOUND EARLY, BUT FETUS DIES
A woman's first pregnancy was complicated by complete placenta previa. A cesarean delivery was scheduled at 36 weeks’ gestation. However, before that date, the mother developed vaginal bleeding and was taken to the ED. The covering ObGyn was notified of the mother’s arrival within 15 minutes, but did not come to the hospital for 2.5 hours. After examining her, the ObGyn ordered US evaluation and transferred the mother to the obstetric floor. Nursing notes indicate that the fetal heart rate was 120 bpm at that time.
There are no notes from the ObGyn between 5:30 am and mid-afternoon. There is no record of the fetal heart rate when the mother was taken for US in the afternoon, which revealed fetal demise and a large extraovular hematoma. A cesarean delivery was performed. It was determined that the fetus died from placental abruption.
PARENTS’ CLAIM The mother was not adequately evaluated and monitored, which led to fetal demise. Delivery could have proceeded while the fetus was still alive.
PHYSICIAN’S DEFENSE The case was settled during the trial.
VERDICT A $495,000 Massachusetts settlement was reached.
Related articles:
• What is the optimal time to deliver a woman who has placenta previa? John T. Repke, MD (Examining the Evidence; April 2011)
• Act fast when confronted by a coagulopathy postpartum. Robert L. Barbieri, MD (Editorial; March 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK! Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state. Stay in touch! Your feedback is important to us!
Blue towel left in abdomen: $7.2M verdict
When a 61-year-old woman underwent laparoscopic hysterectomy, her gynecologist, Dr. A, was assisted by another gynecologist (Dr. B), a nurse, and a technician. When Dr. A noted that the uterine artery had been injured, he converted to an open procedure, retracted the bowel, repaired the artery, and completed the operation.
Postdischarge, the patient was febrile and developed abdominal pain and an odorous vaginal discharge. A month later, exploratory surgery revealed a retained blue towel that had been used for bowel retraction. The patient required open healing of the surgical wound and a temporary colostomy. She developed an incisional hernia after colostomy reversal, and hernia repair required resection of a small portion of the bowel.
PATIENT’S CLAIM It was negligent to use a blue towel to retract the bowel. The towel should have been removed from her abdomen before closure.
DEFENDANTS’ DEFENSE The technician claimed that she did not provide the towel, did not see the towel used, and that she was not told that the towel had to be tracked. She noted that its color indicated that it lacked a radiopaque tag, and that hospital policy forbade use of untagged towels in an open wound.
Dr. A claimed that he specifically requested a blue towel because it was absorbent, that the technician provided the towel, and that the towel’s use prevented the patient from bleeding to death.
VERDICT A $7.2 million New York verdict was returned against both gynecologists and the hospital as the technician’s employer.
MISCARRIAGE AFTER D&C
A few days after a woman thought she miscarried, her family practi-tioner (FP) performed a dilation and curettage (D&C).
The patient was at work 12 days later when she expelled a fully formed 14-week fetus into a toilet. She was taken to the emergency department (ED), where the cord was cut. Later that day, she passed placental tissue; a repeat D&C was performed the next day.
PATIENT'S CLAIM The FP did not properly perform the first D&C. Although the pathology report was available to the FP prior to the patient’s postoperative visit, the FP failed to inform the patient that no fetal parts had been extracted.
PHYSICIAN’S DEFENSE Because the FP thought that the fetus had been passed prior to the D&C, she believed the pathology report was appropriate.
The patient had been informed of the possibility of retained products of conception after the D&C. The FP had ordered a blood pregnancy test that would have revealed the presence of retained products of conception, but the patient did not have the test. The patient did not contact the FP to report symptoms that felt like labor pains on the day that she passed the fetus.
VERDICT A bench trial resulted in a $51,000 California verdict.
PREGNANT WOMAN COMPLAINS OF LEG PAIN; DIES OF DVT
A 23-year-old woman went to the ED with pain and swelling in her lower left leg and calf. The symptoms were reported to her ObGyn, who examined and then discharged her within a few hours, with instructions to come for her regularly scheduled prenatal visit.
The patient died 2 weeks later. The cause of death was determined to be a pulmonary embolus from a thrombus of the left popliteal vein.
ESTATE’S CLAIM The ObGyn was negligent in failing to test the patient for thrombosis in her left leg when she was in the ED or several days later at the office, when she continued to report leg pain.
PHYSICIAN’S DEFENSE The patient did not have signs of thrombosis at the ED or at the subsequent office visit. The pathologist reported that the clot that caused the embolus appeared fresh. The ObGyn surmised that it had formed after the patient’s last appointment.
VERDICT A Texas defense verdict was returned.
Mother took topiramate; child born with cleft lip and palate: $3M verdict
When a woman learned she was pregnant in December 2007, she was taking topiramate (Topamax) to treat migraine headaches. She discussed tapering off but not discontinuing topiramate usage with her neurologist. The patient’s ObGyn told her that topiramate was safe to take during pregnancy. The child was born with a cleft lip and palate.
PARENTS’ CLAIM Janssen Pharmaceuticals, manufacturer of Topamax, failed to provide adequate warnings about the potential risks associated with Topamax until labeling was changed in March 2011. Janssen knew of potential birth defects associated with Topamax use during pregnancy more than a decade before the labeling change; Janssen’s associate director of regulatory affairs had testified in an earlier hearing that there was knowledge of related birth defects as early as 1996.
DEFENDANTS’ DEFENSE There is uncertainty as to whether exposure to Topamax during pregnancy causes birth defects. The neurologist had warned the patient of possible risks associated with taking Topamax during pregnancy, but the patient had refused to discontinue the drug.
VERDICT A $3 million Pennsylvania verdict was returned.
Related articles:
• Is it time to rethink the use of oral contraceptives in premenopausal women with migraine? Anne H. Calhoun, MD (Audiocast; October 2013)
• How to choose a contraceptive for a patient who has headaches. Kristina M. Tocce, MD; Stephanie B. Teal, MD, MPH (February 2011)
• The gynecologist’s role in managing menstrual migraine. Anne H. Calhoun, MD (April 2010)
WAS MOTHER’S HISTORY OF INCOMPETENT CERVIX IGNORED?
Early in her second pregnancy, a woman told her ObGyn that she had previously miscarried due to an incompetent cervix.
At 24 weeks’ gestation, the patient was admitted to the hospital with back and pelvic pain and vaginal bleeding. Shortly after admission, the ObGyn performed a vaginal examination and ordered ultrasonography (US), which showed that the fetus was in the transverse position and the membranes were bulging.
The ObGyn performed an emergency cesarean delivery, but the premature infant died within 2 hours.
PARENTS’ CLAIM The ObGyn should have performed a cervical cerclage because of the mother’s history of an incompetent cervix. The mother should have been placed on bed rest and monitored every 2 weeks for cervical dilation.
PHYSICIAN’S DEFENSE The patient underwent regular prenatal evaluations for an incompetent cervix, and the findings were always normal.
VERDICT A Florida defense verdict was returned.
Related article:
A stepwise approach to cervical cerclage. Katrin Karl, MD; Michael Katz, MD (Surgical Technique; June 2012)
ObGyn unresponsive to patient’s postsurgical phone calls
In 2009, a 50-year-old woman reported occasional right lower quadrant pain to her ObGyn. US results were normal. The menopausal patient’s history included three cesarean deliveries, a total abdominal hysterectomy, and a laparoscopic ovarian cystectomy.
When the patient saw her ObGyn in December 2010, she reported intermittent, progressive right lower quadrant pain that radiated down her right leg. She also reported urine loss with coughing or sneezing, and slight pain on intercourse. The ObGyn prescribed oxybutynin chloride (Ditropan) to treat the patient’s incontinence.
Three weeks later, the patient reported bilateral lower quadrant pain to her ObGyn, with minor improvement in incontinence.
The ObGyn performed bilateral salpingo-oophorectomy (BSO) in January 2011. Surgery took 3.5 hours due to extensive adhesiolysis.
After discharge, the patient felt ill and vomited. She attempted to reach the ObGyn by phone several times. That evening, the ObGyn prescribed a suppository to treat nausea and vomiting.
The patient went to the ED later that night and was found to have a perforated colon. Emergency surgery to repair the injury included creation of a colostomy, which was repaired 20 months later.
PATIENT’S CLAIM A proper workup of her symptoms was not performed; BSO was unnecessary. The ObGyn was negligent for failing to respond in a timely manner to her post-discharge phone calls, and did not properly evaluate her postoperative symptoms.
PHYSICIAN’S DEFENSE BSO was warranted. Colon injury is a known complication of the procedure.
VERDICT A $716,976 California verdict was returned, but was reduced to $591,967 under the state cap.
Who delayed delivery? $32.8M verdict for child with CP
An 18-year-old woman at 38 weeks’ gestation went to the hospital in labor. After 3.5 hours, the fetal heart rate dropped to 60 bpm. A nurse repositioned the patient, administered oxygen, and increased intravenous fluids. When the nurse rang the emergency call bell, a second nurse responded. Eighteen minutes after the fetal heart rate first dropped, a nurse rang the call bell again and the on-call ObGyn appeared.
The ObGyn performed a vaginal examination and repositioned the patient. She noted that the fetal heart-rate monitor was not working correctly, and called for an emergency cesarean delivery. The baby was born 42 minutes after the fetal heart rate initially dropped.
The child received a diagnosis of spastic-quadriplegia cerebral palsy (CP). She requires a wheelchair and has severe speech deficits and developmental delays.
PARENT’S CLAIM Cesarean delivery was not performed in a timely manner; the delivery delay was responsible for the injury that caused CP. The ObGyn was negligent in not responding to the initial emergency call. The nurses should have summoned the ObGyn earlier.
DEFENDANTS’ DEFENSE The hospital argued that the nurses followed proper protocol. Furthermore, the hospital noted that the ObGyn did not respond to the first call, and did not request a cesarean delivery for 17 minutes.
The ObGyn claimed that she made the decision to perform cesarean delivery within 5 minutes of her arrival, but it took another 15 minutes to gather the surgical team.
VERDICT A $32,882,860 Pennsylvania verdict was returned against the hospital. The ObGyn was vindicated.
DIFFICULT DELIVERY: ZAVANELLI MANEUVER
At 38 5/7 weeks’ gestation, a woman went to the hospital for induction of labor. Twenty-four hours later, she began to push. After an hour of pushing, the mother was exhausted and had a low-grade fever, and the fetal heart rate was slowing. Her ObGyn, Dr. A, attempted vacuum extraction and performed a midline episiotomy. Shoulder dystocia was encountered and maneuvers were used, but without success. Another ObGyn, Dr. B, arrived to assist and also attempted the maneuvers.
The physicians agreed to try the Zavanelli maneuver, which involves pushing the baby’s head back inside the vagina and performing a cesarean delivery.
The baby was sent to the neonatal intensive care unit, where her breathing quickly normalized without supplemental oxygen. The child has a brachial plexus injury.
PARENTS’ CLAIM Dr. A should have performed an earlier cesarean delivery. Excessive traction was used when shoulder dystocia maneuvers were attempted.
PHYSICIANS’ DEFENSE The ObGyns’ actions saved the baby’s life and prevented serious injury to both mother and baby.
VERDICT An Alabama defense verdict was returned.
Related article:
You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial; May 2013)
PLACENTA PREVIA FOUND EARLY, BUT FETUS DIES
A woman's first pregnancy was complicated by complete placenta previa. A cesarean delivery was scheduled at 36 weeks’ gestation. However, before that date, the mother developed vaginal bleeding and was taken to the ED. The covering ObGyn was notified of the mother’s arrival within 15 minutes, but did not come to the hospital for 2.5 hours. After examining her, the ObGyn ordered US evaluation and transferred the mother to the obstetric floor. Nursing notes indicate that the fetal heart rate was 120 bpm at that time.
There are no notes from the ObGyn between 5:30 am and mid-afternoon. There is no record of the fetal heart rate when the mother was taken for US in the afternoon, which revealed fetal demise and a large extraovular hematoma. A cesarean delivery was performed. It was determined that the fetus died from placental abruption.
PARENTS’ CLAIM The mother was not adequately evaluated and monitored, which led to fetal demise. Delivery could have proceeded while the fetus was still alive.
PHYSICIAN’S DEFENSE The case was settled during the trial.
VERDICT A $495,000 Massachusetts settlement was reached.
Related articles:
• What is the optimal time to deliver a woman who has placenta previa? John T. Repke, MD (Examining the Evidence; April 2011)
• Act fast when confronted by a coagulopathy postpartum. Robert L. Barbieri, MD (Editorial; March 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK! Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state. Stay in touch! Your feedback is important to us!
Blue towel left in abdomen: $7.2M verdict
When a 61-year-old woman underwent laparoscopic hysterectomy, her gynecologist, Dr. A, was assisted by another gynecologist (Dr. B), a nurse, and a technician. When Dr. A noted that the uterine artery had been injured, he converted to an open procedure, retracted the bowel, repaired the artery, and completed the operation.
Postdischarge, the patient was febrile and developed abdominal pain and an odorous vaginal discharge. A month later, exploratory surgery revealed a retained blue towel that had been used for bowel retraction. The patient required open healing of the surgical wound and a temporary colostomy. She developed an incisional hernia after colostomy reversal, and hernia repair required resection of a small portion of the bowel.
PATIENT’S CLAIM It was negligent to use a blue towel to retract the bowel. The towel should have been removed from her abdomen before closure.
DEFENDANTS’ DEFENSE The technician claimed that she did not provide the towel, did not see the towel used, and that she was not told that the towel had to be tracked. She noted that its color indicated that it lacked a radiopaque tag, and that hospital policy forbade use of untagged towels in an open wound.
Dr. A claimed that he specifically requested a blue towel because it was absorbent, that the technician provided the towel, and that the towel’s use prevented the patient from bleeding to death.
VERDICT A $7.2 million New York verdict was returned against both gynecologists and the hospital as the technician’s employer.
MISCARRIAGE AFTER D&C
A few days after a woman thought she miscarried, her family practi-tioner (FP) performed a dilation and curettage (D&C).
The patient was at work 12 days later when she expelled a fully formed 14-week fetus into a toilet. She was taken to the emergency department (ED), where the cord was cut. Later that day, she passed placental tissue; a repeat D&C was performed the next day.
PATIENT'S CLAIM The FP did not properly perform the first D&C. Although the pathology report was available to the FP prior to the patient’s postoperative visit, the FP failed to inform the patient that no fetal parts had been extracted.
PHYSICIAN’S DEFENSE Because the FP thought that the fetus had been passed prior to the D&C, she believed the pathology report was appropriate.
The patient had been informed of the possibility of retained products of conception after the D&C. The FP had ordered a blood pregnancy test that would have revealed the presence of retained products of conception, but the patient did not have the test. The patient did not contact the FP to report symptoms that felt like labor pains on the day that she passed the fetus.
VERDICT A bench trial resulted in a $51,000 California verdict.
PREGNANT WOMAN COMPLAINS OF LEG PAIN; DIES OF DVT
A 23-year-old woman went to the ED with pain and swelling in her lower left leg and calf. The symptoms were reported to her ObGyn, who examined and then discharged her within a few hours, with instructions to come for her regularly scheduled prenatal visit.
The patient died 2 weeks later. The cause of death was determined to be a pulmonary embolus from a thrombus of the left popliteal vein.
ESTATE’S CLAIM The ObGyn was negligent in failing to test the patient for thrombosis in her left leg when she was in the ED or several days later at the office, when she continued to report leg pain.
PHYSICIAN’S DEFENSE The patient did not have signs of thrombosis at the ED or at the subsequent office visit. The pathologist reported that the clot that caused the embolus appeared fresh. The ObGyn surmised that it had formed after the patient’s last appointment.
VERDICT A Texas defense verdict was returned.
Mother took topiramate; child born with cleft lip and palate: $3M verdict
When a woman learned she was pregnant in December 2007, she was taking topiramate (Topamax) to treat migraine headaches. She discussed tapering off but not discontinuing topiramate usage with her neurologist. The patient’s ObGyn told her that topiramate was safe to take during pregnancy. The child was born with a cleft lip and palate.
PARENTS’ CLAIM Janssen Pharmaceuticals, manufacturer of Topamax, failed to provide adequate warnings about the potential risks associated with Topamax until labeling was changed in March 2011. Janssen knew of potential birth defects associated with Topamax use during pregnancy more than a decade before the labeling change; Janssen’s associate director of regulatory affairs had testified in an earlier hearing that there was knowledge of related birth defects as early as 1996.
DEFENDANTS’ DEFENSE There is uncertainty as to whether exposure to Topamax during pregnancy causes birth defects. The neurologist had warned the patient of possible risks associated with taking Topamax during pregnancy, but the patient had refused to discontinue the drug.
VERDICT A $3 million Pennsylvania verdict was returned.
Related articles:
• Is it time to rethink the use of oral contraceptives in premenopausal women with migraine? Anne H. Calhoun, MD (Audiocast; October 2013)
• How to choose a contraceptive for a patient who has headaches. Kristina M. Tocce, MD; Stephanie B. Teal, MD, MPH (February 2011)
• The gynecologist’s role in managing menstrual migraine. Anne H. Calhoun, MD (April 2010)
WAS MOTHER’S HISTORY OF INCOMPETENT CERVIX IGNORED?
Early in her second pregnancy, a woman told her ObGyn that she had previously miscarried due to an incompetent cervix.
At 24 weeks’ gestation, the patient was admitted to the hospital with back and pelvic pain and vaginal bleeding. Shortly after admission, the ObGyn performed a vaginal examination and ordered ultrasonography (US), which showed that the fetus was in the transverse position and the membranes were bulging.
The ObGyn performed an emergency cesarean delivery, but the premature infant died within 2 hours.
PARENTS’ CLAIM The ObGyn should have performed a cervical cerclage because of the mother’s history of an incompetent cervix. The mother should have been placed on bed rest and monitored every 2 weeks for cervical dilation.
PHYSICIAN’S DEFENSE The patient underwent regular prenatal evaluations for an incompetent cervix, and the findings were always normal.
VERDICT A Florida defense verdict was returned.
Related article:
A stepwise approach to cervical cerclage. Katrin Karl, MD; Michael Katz, MD (Surgical Technique; June 2012)
ObGyn unresponsive to patient’s postsurgical phone calls
In 2009, a 50-year-old woman reported occasional right lower quadrant pain to her ObGyn. US results were normal. The menopausal patient’s history included three cesarean deliveries, a total abdominal hysterectomy, and a laparoscopic ovarian cystectomy.
When the patient saw her ObGyn in December 2010, she reported intermittent, progressive right lower quadrant pain that radiated down her right leg. She also reported urine loss with coughing or sneezing, and slight pain on intercourse. The ObGyn prescribed oxybutynin chloride (Ditropan) to treat the patient’s incontinence.
Three weeks later, the patient reported bilateral lower quadrant pain to her ObGyn, with minor improvement in incontinence.
The ObGyn performed bilateral salpingo-oophorectomy (BSO) in January 2011. Surgery took 3.5 hours due to extensive adhesiolysis.
After discharge, the patient felt ill and vomited. She attempted to reach the ObGyn by phone several times. That evening, the ObGyn prescribed a suppository to treat nausea and vomiting.
The patient went to the ED later that night and was found to have a perforated colon. Emergency surgery to repair the injury included creation of a colostomy, which was repaired 20 months later.
PATIENT’S CLAIM A proper workup of her symptoms was not performed; BSO was unnecessary. The ObGyn was negligent for failing to respond in a timely manner to her post-discharge phone calls, and did not properly evaluate her postoperative symptoms.
PHYSICIAN’S DEFENSE BSO was warranted. Colon injury is a known complication of the procedure.
VERDICT A $716,976 California verdict was returned, but was reduced to $591,967 under the state cap.
Who delayed delivery? $32.8M verdict for child with CP
An 18-year-old woman at 38 weeks’ gestation went to the hospital in labor. After 3.5 hours, the fetal heart rate dropped to 60 bpm. A nurse repositioned the patient, administered oxygen, and increased intravenous fluids. When the nurse rang the emergency call bell, a second nurse responded. Eighteen minutes after the fetal heart rate first dropped, a nurse rang the call bell again and the on-call ObGyn appeared.
The ObGyn performed a vaginal examination and repositioned the patient. She noted that the fetal heart-rate monitor was not working correctly, and called for an emergency cesarean delivery. The baby was born 42 minutes after the fetal heart rate initially dropped.
The child received a diagnosis of spastic-quadriplegia cerebral palsy (CP). She requires a wheelchair and has severe speech deficits and developmental delays.
PARENT’S CLAIM Cesarean delivery was not performed in a timely manner; the delivery delay was responsible for the injury that caused CP. The ObGyn was negligent in not responding to the initial emergency call. The nurses should have summoned the ObGyn earlier.
DEFENDANTS’ DEFENSE The hospital argued that the nurses followed proper protocol. Furthermore, the hospital noted that the ObGyn did not respond to the first call, and did not request a cesarean delivery for 17 minutes.
The ObGyn claimed that she made the decision to perform cesarean delivery within 5 minutes of her arrival, but it took another 15 minutes to gather the surgical team.
VERDICT A $32,882,860 Pennsylvania verdict was returned against the hospital. The ObGyn was vindicated.
DIFFICULT DELIVERY: ZAVANELLI MANEUVER
At 38 5/7 weeks’ gestation, a woman went to the hospital for induction of labor. Twenty-four hours later, she began to push. After an hour of pushing, the mother was exhausted and had a low-grade fever, and the fetal heart rate was slowing. Her ObGyn, Dr. A, attempted vacuum extraction and performed a midline episiotomy. Shoulder dystocia was encountered and maneuvers were used, but without success. Another ObGyn, Dr. B, arrived to assist and also attempted the maneuvers.
The physicians agreed to try the Zavanelli maneuver, which involves pushing the baby’s head back inside the vagina and performing a cesarean delivery.
The baby was sent to the neonatal intensive care unit, where her breathing quickly normalized without supplemental oxygen. The child has a brachial plexus injury.
PARENTS’ CLAIM Dr. A should have performed an earlier cesarean delivery. Excessive traction was used when shoulder dystocia maneuvers were attempted.
PHYSICIANS’ DEFENSE The ObGyns’ actions saved the baby’s life and prevented serious injury to both mother and baby.
VERDICT An Alabama defense verdict was returned.
Related article:
You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial; May 2013)
PLACENTA PREVIA FOUND EARLY, BUT FETUS DIES
A woman's first pregnancy was complicated by complete placenta previa. A cesarean delivery was scheduled at 36 weeks’ gestation. However, before that date, the mother developed vaginal bleeding and was taken to the ED. The covering ObGyn was notified of the mother’s arrival within 15 minutes, but did not come to the hospital for 2.5 hours. After examining her, the ObGyn ordered US evaluation and transferred the mother to the obstetric floor. Nursing notes indicate that the fetal heart rate was 120 bpm at that time.
There are no notes from the ObGyn between 5:30 am and mid-afternoon. There is no record of the fetal heart rate when the mother was taken for US in the afternoon, which revealed fetal demise and a large extraovular hematoma. A cesarean delivery was performed. It was determined that the fetus died from placental abruption.
PARENTS’ CLAIM The mother was not adequately evaluated and monitored, which led to fetal demise. Delivery could have proceeded while the fetus was still alive.
PHYSICIAN’S DEFENSE The case was settled during the trial.
VERDICT A $495,000 Massachusetts settlement was reached.
Related articles:
• What is the optimal time to deliver a woman who has placenta previa? John T. Repke, MD (Examining the Evidence; April 2011)
• Act fast when confronted by a coagulopathy postpartum. Robert L. Barbieri, MD (Editorial; March 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK! Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state. Stay in touch! Your feedback is important to us!

Keep Calm & Provide Good Care
In July 2010, a 67-year-old woman underwent a laparoscopic cholecystectomy performed by Dr. P at a Georgia hospital. When extensive scar tissue was found, the procedure was converted to an open surgery.
In the process, Dr. P encountered excessive bleeding and discovered a tear in the portal vein (which carries blood from the spleen, pancreas, and gallbladder to the liver). Dr. P called in a vascular surgeon, Dr. L, to repair the vein. But the woman had already experienced catastrophic blood loss, and she died in the ICU shortly after surgery.
The plaintiffs argued that Dr. P was behind schedule and rushed through the surgery, inserting a trocar tube without proper visualization and causing the portal vein injury. Dr. P claimed that the scar tissue had caused complications but admitted that he had not inserted a Veress needle into the abdominal cavity to create space around the organs before inserting the trocar tube. Dr. P claimed that this was not negligence, just a departure from his own usual practice.
Continue for the outcome and discussion >>
OUTCOME
A $1,050,000 settlement was reached during jury deliberations. This included $1 million from the insurer and $50,000 from Dr. P personally.
COMMENT
Here, the surgeon injured the portal vein during insertion of a trocar. Often, a Veress needle is first inserted and carbon dioxide insufflated into the peritoneum to establish a pneumoperitoneum that provides space between injury-prone structures. However, trocars can also be inserted directly, without a pneumoperitoneum (this is known as direct trocar insertion). It has been estimated that 40% of surgeons use Veress needle insufflation prior to primary trocar insertion, 30% use direct trocar insertion, and another 30% use the Hasson (direct visualization) technique.1
The plaintiff’s expert witness attempted to convince the jury that the standard of care required a pneumoperitoneum and proper visualization. The defense expert likely offered a compelling defense that the direct trocar insertion technique was an acceptable alternative. But did this case ultimately hinge on two competing methods of trocar placement, or something else? I would suggest the latter.
First, be cautious about letting scheduling drive any aspect of patient care. In this case, the plaintiffs were able to show that the surgeon was behind schedule and that he departed from his usual practices by foregoing the pneumoperitoneum. This was aided by the defendant’s own admission. While lay jurors may have difficulty understanding complication rate data on the Veress needle insufflation technique versus direct trocar insertion technique or the location of the portal vein, they can easily understand rushing through a job and will use the physician’s own haste-based departure from usual practice against him. In sum, do not depart from usual practices because of scheduling matters or patient backlogs.
Furthermore, while it is tempting to let patients know the emergency department is busy, or that you are swamped or backlogged in the clinic—don’t. Just don’t. Never give patients the perception that you are too busy. At best, it will be interpreted as an admission that you are overtaxed; at worst, an admission that you are shortchanging the patient.
I have seen the bursting waiting room; the inbox overflowing with charts; patients and family members wandering in and out of treatment areas asking “How long?”; the single patient who requires nearly all resources; and of course, the wait for a callback from the on-call consultant who never responds. As clinicians, we can only do our best on these shifts, despite being tired, overwhelmed, and besieged.
But I have also seen the other side, where the plaintiff’s attorney’s theory of the case centers around the idea that his client received substandard treatment because of taxed system resources—with you taking the fall. What would they like to prove? That you were tired, overwhelmed, and besieged.
Don’t hang yourself with your own words. Nothing furthers the plaintiff’s case like statements from the clinician such as “Things are crazy here tonight,” “We are just trying to get by,” “We are two people short,” etc. While such statements are fine for KFC or the DMV, they have no place in clinical practice. Even when invited—perhaps the patient says, “You guys are hopping tonight”—the best response is, “We just want to provide the best care for everyone here.”
Why this paranoia about the spoken word? It’s simple: Should any outcome be unfavorable, patients will have the perception that they were “rushed through.” Under evidence law, your statements to the patient and family about the “crazy shift” may be directly admissible as evidence against you, being classified either as nonhearsay or as an exception to the hearsay rule.
You want the jurors to judge you on the merits of the care provided, not on collateral matters out of your control. In a close case, a “rushed out the door” narrative may tip the balance in the plaintiff’s favor. Avoid setting this table for the plaintiff.
If you become dangerously busy, your system is broken and must be fixed. It must be fixed for burnout reasons, for patient satisfaction reasons, and most importantly, for patient safety reasons. Have this discussion, but have it with the right people in your practice—not the patient or patient’s family at bedside.
This surgeon paid part of the settlement out of his own pocket. His malpractice insurance policy was likely capped at $1 million. After the close of final arguments, the parties, believing the case could go either way, reached a settlement of $1 million plus a sizable contribution of $50,000 from the surgeon’s personal assets. This may have been preferable to the prospect of a runaway verdict with the potential to bankrupt the surgeon and his family.
What about your malpractice policy? It’s no romance novel or bestseller, but you should be familiar with the general terms: the policy limits, who has settlement authority (the clinician or insurance company), and any important exclusions/limitations. Furthermore, NPs and PAs should know whether they are covered as an insured party in their own right or if coverage is shared with a physician. The difference could be an important one. —DML
REFERENCE
1. Emergency Care Research Institute. Trocars: safety and selection. Health Devices. 1998;27(11):376-399.
In July 2010, a 67-year-old woman underwent a laparoscopic cholecystectomy performed by Dr. P at a Georgia hospital. When extensive scar tissue was found, the procedure was converted to an open surgery.
In the process, Dr. P encountered excessive bleeding and discovered a tear in the portal vein (which carries blood from the spleen, pancreas, and gallbladder to the liver). Dr. P called in a vascular surgeon, Dr. L, to repair the vein. But the woman had already experienced catastrophic blood loss, and she died in the ICU shortly after surgery.
The plaintiffs argued that Dr. P was behind schedule and rushed through the surgery, inserting a trocar tube without proper visualization and causing the portal vein injury. Dr. P claimed that the scar tissue had caused complications but admitted that he had not inserted a Veress needle into the abdominal cavity to create space around the organs before inserting the trocar tube. Dr. P claimed that this was not negligence, just a departure from his own usual practice.
Continue for the outcome and discussion >>
OUTCOME
A $1,050,000 settlement was reached during jury deliberations. This included $1 million from the insurer and $50,000 from Dr. P personally.
COMMENT
Here, the surgeon injured the portal vein during insertion of a trocar. Often, a Veress needle is first inserted and carbon dioxide insufflated into the peritoneum to establish a pneumoperitoneum that provides space between injury-prone structures. However, trocars can also be inserted directly, without a pneumoperitoneum (this is known as direct trocar insertion). It has been estimated that 40% of surgeons use Veress needle insufflation prior to primary trocar insertion, 30% use direct trocar insertion, and another 30% use the Hasson (direct visualization) technique.1
The plaintiff’s expert witness attempted to convince the jury that the standard of care required a pneumoperitoneum and proper visualization. The defense expert likely offered a compelling defense that the direct trocar insertion technique was an acceptable alternative. But did this case ultimately hinge on two competing methods of trocar placement, or something else? I would suggest the latter.
First, be cautious about letting scheduling drive any aspect of patient care. In this case, the plaintiffs were able to show that the surgeon was behind schedule and that he departed from his usual practices by foregoing the pneumoperitoneum. This was aided by the defendant’s own admission. While lay jurors may have difficulty understanding complication rate data on the Veress needle insufflation technique versus direct trocar insertion technique or the location of the portal vein, they can easily understand rushing through a job and will use the physician’s own haste-based departure from usual practice against him. In sum, do not depart from usual practices because of scheduling matters or patient backlogs.
Furthermore, while it is tempting to let patients know the emergency department is busy, or that you are swamped or backlogged in the clinic—don’t. Just don’t. Never give patients the perception that you are too busy. At best, it will be interpreted as an admission that you are overtaxed; at worst, an admission that you are shortchanging the patient.
I have seen the bursting waiting room; the inbox overflowing with charts; patients and family members wandering in and out of treatment areas asking “How long?”; the single patient who requires nearly all resources; and of course, the wait for a callback from the on-call consultant who never responds. As clinicians, we can only do our best on these shifts, despite being tired, overwhelmed, and besieged.
But I have also seen the other side, where the plaintiff’s attorney’s theory of the case centers around the idea that his client received substandard treatment because of taxed system resources—with you taking the fall. What would they like to prove? That you were tired, overwhelmed, and besieged.
Don’t hang yourself with your own words. Nothing furthers the plaintiff’s case like statements from the clinician such as “Things are crazy here tonight,” “We are just trying to get by,” “We are two people short,” etc. While such statements are fine for KFC or the DMV, they have no place in clinical practice. Even when invited—perhaps the patient says, “You guys are hopping tonight”—the best response is, “We just want to provide the best care for everyone here.”
Why this paranoia about the spoken word? It’s simple: Should any outcome be unfavorable, patients will have the perception that they were “rushed through.” Under evidence law, your statements to the patient and family about the “crazy shift” may be directly admissible as evidence against you, being classified either as nonhearsay or as an exception to the hearsay rule.
You want the jurors to judge you on the merits of the care provided, not on collateral matters out of your control. In a close case, a “rushed out the door” narrative may tip the balance in the plaintiff’s favor. Avoid setting this table for the plaintiff.
If you become dangerously busy, your system is broken and must be fixed. It must be fixed for burnout reasons, for patient satisfaction reasons, and most importantly, for patient safety reasons. Have this discussion, but have it with the right people in your practice—not the patient or patient’s family at bedside.
This surgeon paid part of the settlement out of his own pocket. His malpractice insurance policy was likely capped at $1 million. After the close of final arguments, the parties, believing the case could go either way, reached a settlement of $1 million plus a sizable contribution of $50,000 from the surgeon’s personal assets. This may have been preferable to the prospect of a runaway verdict with the potential to bankrupt the surgeon and his family.
What about your malpractice policy? It’s no romance novel or bestseller, but you should be familiar with the general terms: the policy limits, who has settlement authority (the clinician or insurance company), and any important exclusions/limitations. Furthermore, NPs and PAs should know whether they are covered as an insured party in their own right or if coverage is shared with a physician. The difference could be an important one. —DML
REFERENCE
1. Emergency Care Research Institute. Trocars: safety and selection. Health Devices. 1998;27(11):376-399.
In July 2010, a 67-year-old woman underwent a laparoscopic cholecystectomy performed by Dr. P at a Georgia hospital. When extensive scar tissue was found, the procedure was converted to an open surgery.
In the process, Dr. P encountered excessive bleeding and discovered a tear in the portal vein (which carries blood from the spleen, pancreas, and gallbladder to the liver). Dr. P called in a vascular surgeon, Dr. L, to repair the vein. But the woman had already experienced catastrophic blood loss, and she died in the ICU shortly after surgery.
The plaintiffs argued that Dr. P was behind schedule and rushed through the surgery, inserting a trocar tube without proper visualization and causing the portal vein injury. Dr. P claimed that the scar tissue had caused complications but admitted that he had not inserted a Veress needle into the abdominal cavity to create space around the organs before inserting the trocar tube. Dr. P claimed that this was not negligence, just a departure from his own usual practice.
Continue for the outcome and discussion >>
OUTCOME
A $1,050,000 settlement was reached during jury deliberations. This included $1 million from the insurer and $50,000 from Dr. P personally.
COMMENT
Here, the surgeon injured the portal vein during insertion of a trocar. Often, a Veress needle is first inserted and carbon dioxide insufflated into the peritoneum to establish a pneumoperitoneum that provides space between injury-prone structures. However, trocars can also be inserted directly, without a pneumoperitoneum (this is known as direct trocar insertion). It has been estimated that 40% of surgeons use Veress needle insufflation prior to primary trocar insertion, 30% use direct trocar insertion, and another 30% use the Hasson (direct visualization) technique.1
The plaintiff’s expert witness attempted to convince the jury that the standard of care required a pneumoperitoneum and proper visualization. The defense expert likely offered a compelling defense that the direct trocar insertion technique was an acceptable alternative. But did this case ultimately hinge on two competing methods of trocar placement, or something else? I would suggest the latter.
First, be cautious about letting scheduling drive any aspect of patient care. In this case, the plaintiffs were able to show that the surgeon was behind schedule and that he departed from his usual practices by foregoing the pneumoperitoneum. This was aided by the defendant’s own admission. While lay jurors may have difficulty understanding complication rate data on the Veress needle insufflation technique versus direct trocar insertion technique or the location of the portal vein, they can easily understand rushing through a job and will use the physician’s own haste-based departure from usual practice against him. In sum, do not depart from usual practices because of scheduling matters or patient backlogs.
Furthermore, while it is tempting to let patients know the emergency department is busy, or that you are swamped or backlogged in the clinic—don’t. Just don’t. Never give patients the perception that you are too busy. At best, it will be interpreted as an admission that you are overtaxed; at worst, an admission that you are shortchanging the patient.
I have seen the bursting waiting room; the inbox overflowing with charts; patients and family members wandering in and out of treatment areas asking “How long?”; the single patient who requires nearly all resources; and of course, the wait for a callback from the on-call consultant who never responds. As clinicians, we can only do our best on these shifts, despite being tired, overwhelmed, and besieged.
But I have also seen the other side, where the plaintiff’s attorney’s theory of the case centers around the idea that his client received substandard treatment because of taxed system resources—with you taking the fall. What would they like to prove? That you were tired, overwhelmed, and besieged.
Don’t hang yourself with your own words. Nothing furthers the plaintiff’s case like statements from the clinician such as “Things are crazy here tonight,” “We are just trying to get by,” “We are two people short,” etc. While such statements are fine for KFC or the DMV, they have no place in clinical practice. Even when invited—perhaps the patient says, “You guys are hopping tonight”—the best response is, “We just want to provide the best care for everyone here.”
Why this paranoia about the spoken word? It’s simple: Should any outcome be unfavorable, patients will have the perception that they were “rushed through.” Under evidence law, your statements to the patient and family about the “crazy shift” may be directly admissible as evidence against you, being classified either as nonhearsay or as an exception to the hearsay rule.
You want the jurors to judge you on the merits of the care provided, not on collateral matters out of your control. In a close case, a “rushed out the door” narrative may tip the balance in the plaintiff’s favor. Avoid setting this table for the plaintiff.
If you become dangerously busy, your system is broken and must be fixed. It must be fixed for burnout reasons, for patient satisfaction reasons, and most importantly, for patient safety reasons. Have this discussion, but have it with the right people in your practice—not the patient or patient’s family at bedside.
This surgeon paid part of the settlement out of his own pocket. His malpractice insurance policy was likely capped at $1 million. After the close of final arguments, the parties, believing the case could go either way, reached a settlement of $1 million plus a sizable contribution of $50,000 from the surgeon’s personal assets. This may have been preferable to the prospect of a runaway verdict with the potential to bankrupt the surgeon and his family.
What about your malpractice policy? It’s no romance novel or bestseller, but you should be familiar with the general terms: the policy limits, who has settlement authority (the clinician or insurance company), and any important exclusions/limitations. Furthermore, NPs and PAs should know whether they are covered as an insured party in their own right or if coverage is shared with a physician. The difference could be an important one. —DML
REFERENCE
1. Emergency Care Research Institute. Trocars: safety and selection. Health Devices. 1998;27(11):376-399.