User login
Are the people we serve ‘patients’ or ‘customers’?
Dear Dr. Mossman,
At the multispecialty hospital where I work, administrators refer to patients as “customers” and tell us that, by improving “the customer experience,” we can reduce complaints and avoid malpractice suits. This business lingo offends me. Doesn’t providing good care do more to prevent malpractice claims than calling sick patients “customers”?
Submitted by “Dr. H”
“All words are pegs to hang ideas on.” As was true when Reverend Henry Ward Beecher uttered this phrase in the 19th century,1 names affect how we relate to and feel about people. Many doctors don’t think of themselves as “selling” services, and they find calling patients “customers” distasteful.
But for at least 4 decades, mental health professionals themselves have used a “customer approach” to think about certain aspects of psychiatrist–patient encounters.2 More pertinent to Dr. H’s questions, many attorneys who advise physicians are convinced that giving patients a satisfying “customer experience” is a sound strategy for reducing the risk of malpractice litigation.3
If the attorneys are right, taking a customer service perspective can lower the likelihood that psychiatrists will be sued. To understand why, this article looks at:
• terms for referring to health care recipients
• the feelings those terms generate
• how the “customer service” perspective has become a malpractice prevention
strategy.
Off-putting connotations
All the currently used ways of referring to persons served by doctors have off-putting features.
The word “patient” dates back to the 14th century and comes from Latin present
participles of pati, “to suffer.” Although Alpha Omega Alpha’s motto—“be worthy
to serve the suffering”4—expresses doctors’ commitment to help others, “patient”
carries emotional baggage. A “patient” is “a sick individual” who seeks treatment
from a physician,5 a circumstance that most people (including doctors) find unpleasant and hope is only temporary. The adjective “patient” means “bearing pains or trials calmly or without complaint” and “manifesting forbearance under provocation or strain,”5 phrases associated with passivity, deference, and a long wait to see the doctor.
Because “patient” evokes notions of helplessness and need for direction, non-medical psychotherapists often use “client” to designate care recipients. “Client” has the same Latin root as “to lean” and refers to someone “under the protection of another.” More pertinent to discussions of mental health care, a “client” also is “a person who pays a professional person or organization for services” or “a customer.”5 The latter definition explains what makes “client” feel wrong to medical practitioners, who regard those they treat as deserving more compassion and sacrifice than someone who simply purchases professional services.
“Consumer,” a word of French origin derived from the Latin consumere (“to take
up”), refers to “a person who buys goods and services.”5 If “consumers” are buyers, then those from whom they make purchases are merchants or sellers. Western marketplace concepts often regard consumers as sovereign judges of their needs, and the role of commodity producers is to try to satisfy those needs.6
The problem with viewing health care recipients this way is that sellers don’t caution customers about buying things when only principles of supply-and-demand govern exchange relationships.7 Quite the contrary: producers sometimes promote their products through “advertising [that] distorts reality and creates artificial needs to make profit for a firm.”8 If physicians behave this way, however, they get criticism and deserve it.
A “customer” in 15th-century Middle English was a tax collector, but in modern
usage, a customer is someone who, like a consumer, “purchases some commodity or service.”5 By the early 20th century, “customer” became associated with notions of empowerment embodied in the merchants’ credo, “The customer is always right.”9 Chronic illnesses often require self-management and collaboration with those labeled the “givers” and “recipients” of medical care. Research shows that “patients are more trusting of, and committed to, physicians who adopt an empowering communication style with them,” which suggests “that empowering
patients presents a means to improve the patient–physician relationship.”10
Feelings about names
People have strong feelings about what they are called. In opposing calling patients “consumers,” Nobel Prize-winning economist Paul Krugman explains: “Medical care is an area in which crucial decisions—life and death decisions—must be made; yet making those decisions intelligently requires a vast amount of specialized knowledge; and often those decisions must also be made under conditions in which the patient …needs action immediately, with no time for discussion, let alone comparison shopping. …That’s why doctors have traditionally…been expected to behave according to higher standards than the average professional…The idea that all this can be reduced to money—that doctors are just people selling services to consumers of health care—is, well, sickening.”11
Less famous recipients of nonpsychiatric medical services also prefer being called
“patients” over “clients” or “consumers.”12-14 Recipients of mental health services have a different view, however. In some surveys, “patient” gets a plurality or majority of service recipients’ votes,15,16 but in others, recipients prefer to be called “clients” or other terms.17,18 Of note, people who prefer being called “patients” tend to strongly dislike being called “clients.”19 On the professional
side, psychiatrists—along with other physicians—prefer to speak of treating “patients” and to criticize letting economic phrases infect medical discourse.20-22
Names: A practical difference?
Does what psychiatrists call those they serve make any practical difference? Perhaps not, but evidence suggests that the attitudes that doctors take toward patients affects economic success and malpractice risk.
When they have choices about where they can seek health care, medical patients value physicians’ competence, but they also consider nonclinical factors such as family members’ opinions and convenience.23 Knowing this, the federal government’s Centers for Medicare & Medicaid Services publishes results from its Hospital Consumer Assessment of Healthcare Providers and Systems to “create incentives for hospitals to improve their quality of care.”24
Nonclinical factors play a big part in patients’ decisions about suing their doctors, too. Many malpractice claims turn out to be groundless in the sense that they do not involve medical errors,25 and most errors that result in injury do not lead to malpractice suits.26
What explains this disparity? Often when a lawsuit is filed, whatever injury may have occurred is coupled with an aggravating factor, such as a communication gaffe,27 a physician’s domineering tone of voice,28 or failure to acknowledge error.29 The lower a physician’s patient satisfaction ratings, the higher the physician’s likelihood of receiving complaints and getting sued for malpractice.30,31
These kinds of considerations probably lie behind the recommendation of one hospital manager to doctors: “Continue to call them patients but treat them like
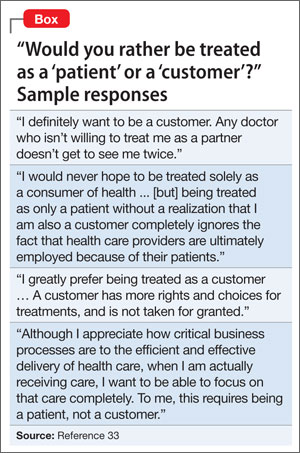
customers.”32 More insights into this view come from responses solicited from Yale
students, staff members, and alumni about whether it seems preferable to be a “patient” or a “customer” (Box).33
Bottom Line
When patients get injured during medical care, evidence suggests that how they feel about their doctors makes a big difference in whether they decide to file suit. If you’re like most psychiatrists, you prefer to call persons whom you treat “patients.” But watching and improving the things that affect your patients’ “customer experience” may help you avoid malpractice litigation.
Related Resource
• Goldhill D. To fix healthcare, turn patients into customers. Bloomberg Personal Finance. www.bloomberg.com/news/2013-01-03/to-fix-health-care-turn-patients-intocustomers.html.
Disclosure
Dr. Mossman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Beecher HW, Drysdale W. Proverbs from Plymouth pulpit. New York, NY: D. Appleton & Co.;1887.
2. Lazare A, Eisenthal S, Wasserman L. The customer approach to patienthood: attending to patient requests in a walk-in clinic. Arch Gen Psychiatry. 1975;32:553-558.
3. Schleiter KE. Difficult patient-physician relationships and the risk of medical malpractice litigation. Virtual Mentor. 2009;11:242-246.
4. Alpha Omega Alpha Honor Medical Society. Alpha Omega Alpha constitution. http://www.alphaomegaalpha.org/constitution.html. Accessed December 13, 2013. Accessed December 13, 2013.
5. Merriam-Webster. Dictionary. http://www.merriamwebster.com. Accessed December 9, 2013.
6. Kotler P, Burton S, Deans K, et al. Marketing, 9th ed. Frenchs Forest, Australia: Pearson Education Australia; 2013.
7. Deber RB. Getting what we pay for: myths and realities about financing Canada’s health care system. Health Law Can. 2000;21(2):9-56.
8. Takala T, Uusitalo O. An alternative view of relationship marketing: a framework for ethical analysis. Eur J Mark. 1996;30:45-60.
9. Van Vuren FS. The Yankee who taught Britishers that ‘the customer is always right.’ Milwaukee Journal. http://www.wisconsinhistory.org/wlhba/articleView.
asp?pg=1&id=11176. Published September 9, 1932. Accessed December 20, 2013.
10. Ouschan T, Sweeney J, Johnson L. Customer empowerment and relationship outcomes in healthcare consultations. Eur J Mark. 2006;40:1068-1086.
11. Krugman P. Patients are not consumers. The New York Times. http://krugman.blogs.nytimes.com/2011/04/20/patients-are-not-consumers. Published April 20, 2011. Accessed December 13, 2013.
12. Nair BR. Patient, client or customer? Med J Aust. 1998;169:593.
13. Wing PC. Patient or client? If in doubt, ask. CMAJ. 1997;157:287-289.
14. Deber RB, Kraetschmer N, Urowitz S, et al. Patient, consumer, client, or customer: what do people want to be called? Health Expect. 2005;8(4):345-351.
15. Sharma V, Whitney D, Kazarian SS, et al. Preferred terms for users of mental health services among service providers and recipients. Psychiatr Serv. 2000;51(2): 203-209.
16. Simmons P, Hawley CJ, Gale TM, et al. Service user, patient, client, user or survivor: describing recipients of mental health services. Psychiatrist. 2010;34:20-23.
17. Lloyd C, King R, Bassett H, et al. Patient, client or consumer? A survey of preferred terms. Australas Psychiatry. 2001; 9(4):321-324.
18. Covell NH, McCorkle BH, Weissman EM, et al. What’s in a name? Terms preferred by service recipients. Adm Policy Ment Health. 2007;34(5):443-447.
19. Ritchie CW, Hayes D, Ames DJ. Patient or client? The opinions of people attending a psychiatric clinic. Psychiatrist. 2000;24(12):447-450.
20. Andreasen NC. Clients, consumers, providers, and products: where will it all end? Am J Psychiatry. 1995;152:1107-1109.
21. Editorial. What’s in a name? Lancet. 2000;356(9248):2111.
22. Torrey EF. Patients, clients, consumers, survivors et al: what’s in a name? Schizophr Bull. 2011;37(3):466-468.
23. Wilson CT, Woloshin S, Schwartz L. Choosing where to have major surgery: who makes the decision? Arch Surg. 2007;142(3):242-246.
24. Centers for Medicare & Medicaid Services. Hospital consumer assessment of healthcare providers and systems. http://www.hcahpsonline.org. Accessed
January 26, 2014.
25. Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006;354:2024-2033.
26. Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence—results of the Harvard Medical Practice Study III. N Engl J Med. 1991;325:245-251.
27. Huntington B, Kuhn N. Communication gaffes: a root cause of malpractice claims. Bayl Univ Med Cent. 2003;16(2):157-161.
28. Ambady N, Laplante D, Nguyen T, et al. Surgeons’ tone of voice: a clue to malpractice history. Surgery. 2002;132(1):5-9.
29. Witman AB, Park DM, Hardin SB. How do patients want physicians to handle mistakes? A survey of internal medicine patients in an academic setting. Arch Intern Med. 1996;156(22):2565-2569.
30. Stelfox HT, Gandhi TK, Orav EJ, et al. The relation of patient satisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005;118(10):
1126-1133.
31. Hickson GB, Federspiel CF, Pichert JW, et al. Patient complaints and malpractice risk. JAMA. 2002;287(22):2951-2957.
32. Bain W. Do we need a new word for patients? Continue to call them patients but treat them like customers. BMJ. 1999;319(7222):1436.
33. Johnson R, Moskowitz E, Thomas J, et al. Would you rather be treated as a patient or a customer? Yale Insights. http://insights.som.yale.edu/insights/would-you-rather-betreated-patient-or-customer. Accessed December 13, 2013.
Dear Dr. Mossman,
At the multispecialty hospital where I work, administrators refer to patients as “customers” and tell us that, by improving “the customer experience,” we can reduce complaints and avoid malpractice suits. This business lingo offends me. Doesn’t providing good care do more to prevent malpractice claims than calling sick patients “customers”?
Submitted by “Dr. H”
“All words are pegs to hang ideas on.” As was true when Reverend Henry Ward Beecher uttered this phrase in the 19th century,1 names affect how we relate to and feel about people. Many doctors don’t think of themselves as “selling” services, and they find calling patients “customers” distasteful.
But for at least 4 decades, mental health professionals themselves have used a “customer approach” to think about certain aspects of psychiatrist–patient encounters.2 More pertinent to Dr. H’s questions, many attorneys who advise physicians are convinced that giving patients a satisfying “customer experience” is a sound strategy for reducing the risk of malpractice litigation.3
If the attorneys are right, taking a customer service perspective can lower the likelihood that psychiatrists will be sued. To understand why, this article looks at:
• terms for referring to health care recipients
• the feelings those terms generate
• how the “customer service” perspective has become a malpractice prevention
strategy.
Off-putting connotations
All the currently used ways of referring to persons served by doctors have off-putting features.
The word “patient” dates back to the 14th century and comes from Latin present
participles of pati, “to suffer.” Although Alpha Omega Alpha’s motto—“be worthy
to serve the suffering”4—expresses doctors’ commitment to help others, “patient”
carries emotional baggage. A “patient” is “a sick individual” who seeks treatment
from a physician,5 a circumstance that most people (including doctors) find unpleasant and hope is only temporary. The adjective “patient” means “bearing pains or trials calmly or without complaint” and “manifesting forbearance under provocation or strain,”5 phrases associated with passivity, deference, and a long wait to see the doctor.
Because “patient” evokes notions of helplessness and need for direction, non-medical psychotherapists often use “client” to designate care recipients. “Client” has the same Latin root as “to lean” and refers to someone “under the protection of another.” More pertinent to discussions of mental health care, a “client” also is “a person who pays a professional person or organization for services” or “a customer.”5 The latter definition explains what makes “client” feel wrong to medical practitioners, who regard those they treat as deserving more compassion and sacrifice than someone who simply purchases professional services.
“Consumer,” a word of French origin derived from the Latin consumere (“to take
up”), refers to “a person who buys goods and services.”5 If “consumers” are buyers, then those from whom they make purchases are merchants or sellers. Western marketplace concepts often regard consumers as sovereign judges of their needs, and the role of commodity producers is to try to satisfy those needs.6
The problem with viewing health care recipients this way is that sellers don’t caution customers about buying things when only principles of supply-and-demand govern exchange relationships.7 Quite the contrary: producers sometimes promote their products through “advertising [that] distorts reality and creates artificial needs to make profit for a firm.”8 If physicians behave this way, however, they get criticism and deserve it.
A “customer” in 15th-century Middle English was a tax collector, but in modern
usage, a customer is someone who, like a consumer, “purchases some commodity or service.”5 By the early 20th century, “customer” became associated with notions of empowerment embodied in the merchants’ credo, “The customer is always right.”9 Chronic illnesses often require self-management and collaboration with those labeled the “givers” and “recipients” of medical care. Research shows that “patients are more trusting of, and committed to, physicians who adopt an empowering communication style with them,” which suggests “that empowering
patients presents a means to improve the patient–physician relationship.”10
Feelings about names
People have strong feelings about what they are called. In opposing calling patients “consumers,” Nobel Prize-winning economist Paul Krugman explains: “Medical care is an area in which crucial decisions—life and death decisions—must be made; yet making those decisions intelligently requires a vast amount of specialized knowledge; and often those decisions must also be made under conditions in which the patient …needs action immediately, with no time for discussion, let alone comparison shopping. …That’s why doctors have traditionally…been expected to behave according to higher standards than the average professional…The idea that all this can be reduced to money—that doctors are just people selling services to consumers of health care—is, well, sickening.”11
Less famous recipients of nonpsychiatric medical services also prefer being called
“patients” over “clients” or “consumers.”12-14 Recipients of mental health services have a different view, however. In some surveys, “patient” gets a plurality or majority of service recipients’ votes,15,16 but in others, recipients prefer to be called “clients” or other terms.17,18 Of note, people who prefer being called “patients” tend to strongly dislike being called “clients.”19 On the professional
side, psychiatrists—along with other physicians—prefer to speak of treating “patients” and to criticize letting economic phrases infect medical discourse.20-22
Names: A practical difference?
Does what psychiatrists call those they serve make any practical difference? Perhaps not, but evidence suggests that the attitudes that doctors take toward patients affects economic success and malpractice risk.
When they have choices about where they can seek health care, medical patients value physicians’ competence, but they also consider nonclinical factors such as family members’ opinions and convenience.23 Knowing this, the federal government’s Centers for Medicare & Medicaid Services publishes results from its Hospital Consumer Assessment of Healthcare Providers and Systems to “create incentives for hospitals to improve their quality of care.”24
Nonclinical factors play a big part in patients’ decisions about suing their doctors, too. Many malpractice claims turn out to be groundless in the sense that they do not involve medical errors,25 and most errors that result in injury do not lead to malpractice suits.26
What explains this disparity? Often when a lawsuit is filed, whatever injury may have occurred is coupled with an aggravating factor, such as a communication gaffe,27 a physician’s domineering tone of voice,28 or failure to acknowledge error.29 The lower a physician’s patient satisfaction ratings, the higher the physician’s likelihood of receiving complaints and getting sued for malpractice.30,31
These kinds of considerations probably lie behind the recommendation of one hospital manager to doctors: “Continue to call them patients but treat them like
customers.”32 More insights into this view come from responses solicited from Yale
students, staff members, and alumni about whether it seems preferable to be a “patient” or a “customer” (Box).33
Bottom Line
When patients get injured during medical care, evidence suggests that how they feel about their doctors makes a big difference in whether they decide to file suit. If you’re like most psychiatrists, you prefer to call persons whom you treat “patients.” But watching and improving the things that affect your patients’ “customer experience” may help you avoid malpractice litigation.
Related Resource
• Goldhill D. To fix healthcare, turn patients into customers. Bloomberg Personal Finance. www.bloomberg.com/news/2013-01-03/to-fix-health-care-turn-patients-intocustomers.html.
Disclosure
Dr. Mossman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dear Dr. Mossman,
At the multispecialty hospital where I work, administrators refer to patients as “customers” and tell us that, by improving “the customer experience,” we can reduce complaints and avoid malpractice suits. This business lingo offends me. Doesn’t providing good care do more to prevent malpractice claims than calling sick patients “customers”?
Submitted by “Dr. H”
“All words are pegs to hang ideas on.” As was true when Reverend Henry Ward Beecher uttered this phrase in the 19th century,1 names affect how we relate to and feel about people. Many doctors don’t think of themselves as “selling” services, and they find calling patients “customers” distasteful.
But for at least 4 decades, mental health professionals themselves have used a “customer approach” to think about certain aspects of psychiatrist–patient encounters.2 More pertinent to Dr. H’s questions, many attorneys who advise physicians are convinced that giving patients a satisfying “customer experience” is a sound strategy for reducing the risk of malpractice litigation.3
If the attorneys are right, taking a customer service perspective can lower the likelihood that psychiatrists will be sued. To understand why, this article looks at:
• terms for referring to health care recipients
• the feelings those terms generate
• how the “customer service” perspective has become a malpractice prevention
strategy.
Off-putting connotations
All the currently used ways of referring to persons served by doctors have off-putting features.
The word “patient” dates back to the 14th century and comes from Latin present
participles of pati, “to suffer.” Although Alpha Omega Alpha’s motto—“be worthy
to serve the suffering”4—expresses doctors’ commitment to help others, “patient”
carries emotional baggage. A “patient” is “a sick individual” who seeks treatment
from a physician,5 a circumstance that most people (including doctors) find unpleasant and hope is only temporary. The adjective “patient” means “bearing pains or trials calmly or without complaint” and “manifesting forbearance under provocation or strain,”5 phrases associated with passivity, deference, and a long wait to see the doctor.
Because “patient” evokes notions of helplessness and need for direction, non-medical psychotherapists often use “client” to designate care recipients. “Client” has the same Latin root as “to lean” and refers to someone “under the protection of another.” More pertinent to discussions of mental health care, a “client” also is “a person who pays a professional person or organization for services” or “a customer.”5 The latter definition explains what makes “client” feel wrong to medical practitioners, who regard those they treat as deserving more compassion and sacrifice than someone who simply purchases professional services.
“Consumer,” a word of French origin derived from the Latin consumere (“to take
up”), refers to “a person who buys goods and services.”5 If “consumers” are buyers, then those from whom they make purchases are merchants or sellers. Western marketplace concepts often regard consumers as sovereign judges of their needs, and the role of commodity producers is to try to satisfy those needs.6
The problem with viewing health care recipients this way is that sellers don’t caution customers about buying things when only principles of supply-and-demand govern exchange relationships.7 Quite the contrary: producers sometimes promote their products through “advertising [that] distorts reality and creates artificial needs to make profit for a firm.”8 If physicians behave this way, however, they get criticism and deserve it.
A “customer” in 15th-century Middle English was a tax collector, but in modern
usage, a customer is someone who, like a consumer, “purchases some commodity or service.”5 By the early 20th century, “customer” became associated with notions of empowerment embodied in the merchants’ credo, “The customer is always right.”9 Chronic illnesses often require self-management and collaboration with those labeled the “givers” and “recipients” of medical care. Research shows that “patients are more trusting of, and committed to, physicians who adopt an empowering communication style with them,” which suggests “that empowering
patients presents a means to improve the patient–physician relationship.”10
Feelings about names
People have strong feelings about what they are called. In opposing calling patients “consumers,” Nobel Prize-winning economist Paul Krugman explains: “Medical care is an area in which crucial decisions—life and death decisions—must be made; yet making those decisions intelligently requires a vast amount of specialized knowledge; and often those decisions must also be made under conditions in which the patient …needs action immediately, with no time for discussion, let alone comparison shopping. …That’s why doctors have traditionally…been expected to behave according to higher standards than the average professional…The idea that all this can be reduced to money—that doctors are just people selling services to consumers of health care—is, well, sickening.”11
Less famous recipients of nonpsychiatric medical services also prefer being called
“patients” over “clients” or “consumers.”12-14 Recipients of mental health services have a different view, however. In some surveys, “patient” gets a plurality or majority of service recipients’ votes,15,16 but in others, recipients prefer to be called “clients” or other terms.17,18 Of note, people who prefer being called “patients” tend to strongly dislike being called “clients.”19 On the professional
side, psychiatrists—along with other physicians—prefer to speak of treating “patients” and to criticize letting economic phrases infect medical discourse.20-22
Names: A practical difference?
Does what psychiatrists call those they serve make any practical difference? Perhaps not, but evidence suggests that the attitudes that doctors take toward patients affects economic success and malpractice risk.
When they have choices about where they can seek health care, medical patients value physicians’ competence, but they also consider nonclinical factors such as family members’ opinions and convenience.23 Knowing this, the federal government’s Centers for Medicare & Medicaid Services publishes results from its Hospital Consumer Assessment of Healthcare Providers and Systems to “create incentives for hospitals to improve their quality of care.”24
Nonclinical factors play a big part in patients’ decisions about suing their doctors, too. Many malpractice claims turn out to be groundless in the sense that they do not involve medical errors,25 and most errors that result in injury do not lead to malpractice suits.26
What explains this disparity? Often when a lawsuit is filed, whatever injury may have occurred is coupled with an aggravating factor, such as a communication gaffe,27 a physician’s domineering tone of voice,28 or failure to acknowledge error.29 The lower a physician’s patient satisfaction ratings, the higher the physician’s likelihood of receiving complaints and getting sued for malpractice.30,31
These kinds of considerations probably lie behind the recommendation of one hospital manager to doctors: “Continue to call them patients but treat them like
customers.”32 More insights into this view come from responses solicited from Yale
students, staff members, and alumni about whether it seems preferable to be a “patient” or a “customer” (Box).33
Bottom Line
When patients get injured during medical care, evidence suggests that how they feel about their doctors makes a big difference in whether they decide to file suit. If you’re like most psychiatrists, you prefer to call persons whom you treat “patients.” But watching and improving the things that affect your patients’ “customer experience” may help you avoid malpractice litigation.
Related Resource
• Goldhill D. To fix healthcare, turn patients into customers. Bloomberg Personal Finance. www.bloomberg.com/news/2013-01-03/to-fix-health-care-turn-patients-intocustomers.html.
Disclosure
Dr. Mossman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Beecher HW, Drysdale W. Proverbs from Plymouth pulpit. New York, NY: D. Appleton & Co.;1887.
2. Lazare A, Eisenthal S, Wasserman L. The customer approach to patienthood: attending to patient requests in a walk-in clinic. Arch Gen Psychiatry. 1975;32:553-558.
3. Schleiter KE. Difficult patient-physician relationships and the risk of medical malpractice litigation. Virtual Mentor. 2009;11:242-246.
4. Alpha Omega Alpha Honor Medical Society. Alpha Omega Alpha constitution. http://www.alphaomegaalpha.org/constitution.html. Accessed December 13, 2013. Accessed December 13, 2013.
5. Merriam-Webster. Dictionary. http://www.merriamwebster.com. Accessed December 9, 2013.
6. Kotler P, Burton S, Deans K, et al. Marketing, 9th ed. Frenchs Forest, Australia: Pearson Education Australia; 2013.
7. Deber RB. Getting what we pay for: myths and realities about financing Canada’s health care system. Health Law Can. 2000;21(2):9-56.
8. Takala T, Uusitalo O. An alternative view of relationship marketing: a framework for ethical analysis. Eur J Mark. 1996;30:45-60.
9. Van Vuren FS. The Yankee who taught Britishers that ‘the customer is always right.’ Milwaukee Journal. http://www.wisconsinhistory.org/wlhba/articleView.
asp?pg=1&id=11176. Published September 9, 1932. Accessed December 20, 2013.
10. Ouschan T, Sweeney J, Johnson L. Customer empowerment and relationship outcomes in healthcare consultations. Eur J Mark. 2006;40:1068-1086.
11. Krugman P. Patients are not consumers. The New York Times. http://krugman.blogs.nytimes.com/2011/04/20/patients-are-not-consumers. Published April 20, 2011. Accessed December 13, 2013.
12. Nair BR. Patient, client or customer? Med J Aust. 1998;169:593.
13. Wing PC. Patient or client? If in doubt, ask. CMAJ. 1997;157:287-289.
14. Deber RB, Kraetschmer N, Urowitz S, et al. Patient, consumer, client, or customer: what do people want to be called? Health Expect. 2005;8(4):345-351.
15. Sharma V, Whitney D, Kazarian SS, et al. Preferred terms for users of mental health services among service providers and recipients. Psychiatr Serv. 2000;51(2): 203-209.
16. Simmons P, Hawley CJ, Gale TM, et al. Service user, patient, client, user or survivor: describing recipients of mental health services. Psychiatrist. 2010;34:20-23.
17. Lloyd C, King R, Bassett H, et al. Patient, client or consumer? A survey of preferred terms. Australas Psychiatry. 2001; 9(4):321-324.
18. Covell NH, McCorkle BH, Weissman EM, et al. What’s in a name? Terms preferred by service recipients. Adm Policy Ment Health. 2007;34(5):443-447.
19. Ritchie CW, Hayes D, Ames DJ. Patient or client? The opinions of people attending a psychiatric clinic. Psychiatrist. 2000;24(12):447-450.
20. Andreasen NC. Clients, consumers, providers, and products: where will it all end? Am J Psychiatry. 1995;152:1107-1109.
21. Editorial. What’s in a name? Lancet. 2000;356(9248):2111.
22. Torrey EF. Patients, clients, consumers, survivors et al: what’s in a name? Schizophr Bull. 2011;37(3):466-468.
23. Wilson CT, Woloshin S, Schwartz L. Choosing where to have major surgery: who makes the decision? Arch Surg. 2007;142(3):242-246.
24. Centers for Medicare & Medicaid Services. Hospital consumer assessment of healthcare providers and systems. http://www.hcahpsonline.org. Accessed
January 26, 2014.
25. Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006;354:2024-2033.
26. Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence—results of the Harvard Medical Practice Study III. N Engl J Med. 1991;325:245-251.
27. Huntington B, Kuhn N. Communication gaffes: a root cause of malpractice claims. Bayl Univ Med Cent. 2003;16(2):157-161.
28. Ambady N, Laplante D, Nguyen T, et al. Surgeons’ tone of voice: a clue to malpractice history. Surgery. 2002;132(1):5-9.
29. Witman AB, Park DM, Hardin SB. How do patients want physicians to handle mistakes? A survey of internal medicine patients in an academic setting. Arch Intern Med. 1996;156(22):2565-2569.
30. Stelfox HT, Gandhi TK, Orav EJ, et al. The relation of patient satisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005;118(10):
1126-1133.
31. Hickson GB, Federspiel CF, Pichert JW, et al. Patient complaints and malpractice risk. JAMA. 2002;287(22):2951-2957.
32. Bain W. Do we need a new word for patients? Continue to call them patients but treat them like customers. BMJ. 1999;319(7222):1436.
33. Johnson R, Moskowitz E, Thomas J, et al. Would you rather be treated as a patient or a customer? Yale Insights. http://insights.som.yale.edu/insights/would-you-rather-betreated-patient-or-customer. Accessed December 13, 2013.
1. Beecher HW, Drysdale W. Proverbs from Plymouth pulpit. New York, NY: D. Appleton & Co.;1887.
2. Lazare A, Eisenthal S, Wasserman L. The customer approach to patienthood: attending to patient requests in a walk-in clinic. Arch Gen Psychiatry. 1975;32:553-558.
3. Schleiter KE. Difficult patient-physician relationships and the risk of medical malpractice litigation. Virtual Mentor. 2009;11:242-246.
4. Alpha Omega Alpha Honor Medical Society. Alpha Omega Alpha constitution. http://www.alphaomegaalpha.org/constitution.html. Accessed December 13, 2013. Accessed December 13, 2013.
5. Merriam-Webster. Dictionary. http://www.merriamwebster.com. Accessed December 9, 2013.
6. Kotler P, Burton S, Deans K, et al. Marketing, 9th ed. Frenchs Forest, Australia: Pearson Education Australia; 2013.
7. Deber RB. Getting what we pay for: myths and realities about financing Canada’s health care system. Health Law Can. 2000;21(2):9-56.
8. Takala T, Uusitalo O. An alternative view of relationship marketing: a framework for ethical analysis. Eur J Mark. 1996;30:45-60.
9. Van Vuren FS. The Yankee who taught Britishers that ‘the customer is always right.’ Milwaukee Journal. http://www.wisconsinhistory.org/wlhba/articleView.
asp?pg=1&id=11176. Published September 9, 1932. Accessed December 20, 2013.
10. Ouschan T, Sweeney J, Johnson L. Customer empowerment and relationship outcomes in healthcare consultations. Eur J Mark. 2006;40:1068-1086.
11. Krugman P. Patients are not consumers. The New York Times. http://krugman.blogs.nytimes.com/2011/04/20/patients-are-not-consumers. Published April 20, 2011. Accessed December 13, 2013.
12. Nair BR. Patient, client or customer? Med J Aust. 1998;169:593.
13. Wing PC. Patient or client? If in doubt, ask. CMAJ. 1997;157:287-289.
14. Deber RB, Kraetschmer N, Urowitz S, et al. Patient, consumer, client, or customer: what do people want to be called? Health Expect. 2005;8(4):345-351.
15. Sharma V, Whitney D, Kazarian SS, et al. Preferred terms for users of mental health services among service providers and recipients. Psychiatr Serv. 2000;51(2): 203-209.
16. Simmons P, Hawley CJ, Gale TM, et al. Service user, patient, client, user or survivor: describing recipients of mental health services. Psychiatrist. 2010;34:20-23.
17. Lloyd C, King R, Bassett H, et al. Patient, client or consumer? A survey of preferred terms. Australas Psychiatry. 2001; 9(4):321-324.
18. Covell NH, McCorkle BH, Weissman EM, et al. What’s in a name? Terms preferred by service recipients. Adm Policy Ment Health. 2007;34(5):443-447.
19. Ritchie CW, Hayes D, Ames DJ. Patient or client? The opinions of people attending a psychiatric clinic. Psychiatrist. 2000;24(12):447-450.
20. Andreasen NC. Clients, consumers, providers, and products: where will it all end? Am J Psychiatry. 1995;152:1107-1109.
21. Editorial. What’s in a name? Lancet. 2000;356(9248):2111.
22. Torrey EF. Patients, clients, consumers, survivors et al: what’s in a name? Schizophr Bull. 2011;37(3):466-468.
23. Wilson CT, Woloshin S, Schwartz L. Choosing where to have major surgery: who makes the decision? Arch Surg. 2007;142(3):242-246.
24. Centers for Medicare & Medicaid Services. Hospital consumer assessment of healthcare providers and systems. http://www.hcahpsonline.org. Accessed
January 26, 2014.
25. Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006;354:2024-2033.
26. Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence—results of the Harvard Medical Practice Study III. N Engl J Med. 1991;325:245-251.
27. Huntington B, Kuhn N. Communication gaffes: a root cause of malpractice claims. Bayl Univ Med Cent. 2003;16(2):157-161.
28. Ambady N, Laplante D, Nguyen T, et al. Surgeons’ tone of voice: a clue to malpractice history. Surgery. 2002;132(1):5-9.
29. Witman AB, Park DM, Hardin SB. How do patients want physicians to handle mistakes? A survey of internal medicine patients in an academic setting. Arch Intern Med. 1996;156(22):2565-2569.
30. Stelfox HT, Gandhi TK, Orav EJ, et al. The relation of patient satisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005;118(10):
1126-1133.
31. Hickson GB, Federspiel CF, Pichert JW, et al. Patient complaints and malpractice risk. JAMA. 2002;287(22):2951-2957.
32. Bain W. Do we need a new word for patients? Continue to call them patients but treat them like customers. BMJ. 1999;319(7222):1436.
33. Johnson R, Moskowitz E, Thomas J, et al. Would you rather be treated as a patient or a customer? Yale Insights. http://insights.som.yale.edu/insights/would-you-rather-betreated-patient-or-customer. Accessed December 13, 2013.
Why Punching a Window Is Never a Good Idea
In September 2007, a 23-year-old man drank a six-pack of beer, had an argument with his girlfriend, and punched a plate-glass window with both fists. He sustained lacerations to his right arm. The man removed a large piece of glass from his arm, resulting in significant bleeding. He then wrapped a belt around his arm to stop the blood flow and went to the emergency department of the local hospital, where he was treated by Dr. S.
Dr. S. removed glass fragments from the patient’s arm, sutured it, and instructed him to follow up with his family physician in one to two weeks. When the patient saw another clinician, Dr. A., for suture removal, he reported worsening neurologic symptoms in his right arm. An appointment with an orthopedist was made, which the patient subsequently canceled.
About two months later, a retained glass fragment was removed by orthopedist Dr. R. The plaintiff alleged negligence by Dr. S. for his failure to remove all the glass fragments at the initial presentation. The plaintiff claimed that as a result he suffered a median nerve injury.
The defendant claimed that the nerve injury was most likely inflicted when the plaintiff removed the piece of glass himself before going to the hospital. The defendant also claimed that the plaintiff had been negligent in his failure to seek follow-up treatment as recommended. The defendant further maintained that the physician who removed the retained glass fragment had not determined it to be in the proximity of the median nerve.
Continue for the outcome...
OUTCOME
A jury returned a verdict for the plaintiff that totaled $460,595. The defendant filed a motion for judgment notwithstanding the verdict and for a new trial. A confidential settlement was reached prior to a hearing on the motion.
Continue for David Lang's comments...
COMMENT
Patients and jurors expect foreign bodies to be discovered and removed with 100% precision. However, any clinician who has removed a foreign body knows that trying to locate one can be difficult under the best of circumstances.
Further, in cases in which a foreign body is not near a sensitive structure and is not likely to cause additional injury, removal may not be indicated (eg, retained bullet fragments not near a joint). In this case, the foreign body is glass and the location is described as the “arm,” which in all likelihood means the proximal forearm. So we have a potentially sharp item contained within a small space holding many sensitive structures.
Apparently, radiographs were not obtained. While some foreign bodies are radiolucent and generally considered “invisible,” glass is not necessarily one of them. There is a myth that glass is never visible on x-ray and another that glass is visible on x-ray only if there is sufficient “lead content” in it to make it so. Contrary to these beliefs, glass may be visible on standard x-ray, whether or not there is lead in it.
Here, it would have been reasonable to obtain radiographs to identify foreign bodies prior to closing the wound. The glass may have been visible and if detected, the emergency physician could have made a decision either to remove the glass or refer the patient if it was located deeply, next to a sensitive structure. Despite radiographic and physical exam findings, it is always important to remind patients that retained foreign bodies are possible and that follow-up is required. Schedule follow-up and document what the patient was told.
But what about foreign bodies that are almost always radiolucent on a standard film? Wood can be maddening: invisible on x-ray and hard to remove because unlike glass, metal, or stone, there is no confirming “scratch” or “clink” when wood is contacted with a localizing needle. Wood is also virtually guaranteed to suppurate if not removed.
Radiolucent or radiopaque is often considered an inherent quality of an object. But what is visible and what is invisible depends on radiographic technique. For foreign bodies generally considered radiolucent (eg, wood), consider a “soft-tissue technique,” which may demonstrate the foreign body, particularly if it is relatively large. While a positive image can be helpful, a negative one cannot rule out the presence of a foreign body. If available, ultrasound is also useful in detecting radiolucent foreign bodies and should be exploited by those skilled in its use.
In sum, jurors hate foreign bodies left in patients, be they items left in after surgery or not removed following an injury. Do your best, while explaining the limitations of removal efforts and the need for follow-up in complicated cases and self-monitoring in all cases. Instruct patients to return promptly for worsening signs and symptoms. Document that you informed the patient that 100% removal is never guaranteed and that they have agreed to return as scheduled or as needed. —DML
In September 2007, a 23-year-old man drank a six-pack of beer, had an argument with his girlfriend, and punched a plate-glass window with both fists. He sustained lacerations to his right arm. The man removed a large piece of glass from his arm, resulting in significant bleeding. He then wrapped a belt around his arm to stop the blood flow and went to the emergency department of the local hospital, where he was treated by Dr. S.
Dr. S. removed glass fragments from the patient’s arm, sutured it, and instructed him to follow up with his family physician in one to two weeks. When the patient saw another clinician, Dr. A., for suture removal, he reported worsening neurologic symptoms in his right arm. An appointment with an orthopedist was made, which the patient subsequently canceled.
About two months later, a retained glass fragment was removed by orthopedist Dr. R. The plaintiff alleged negligence by Dr. S. for his failure to remove all the glass fragments at the initial presentation. The plaintiff claimed that as a result he suffered a median nerve injury.
The defendant claimed that the nerve injury was most likely inflicted when the plaintiff removed the piece of glass himself before going to the hospital. The defendant also claimed that the plaintiff had been negligent in his failure to seek follow-up treatment as recommended. The defendant further maintained that the physician who removed the retained glass fragment had not determined it to be in the proximity of the median nerve.
Continue for the outcome...
OUTCOME
A jury returned a verdict for the plaintiff that totaled $460,595. The defendant filed a motion for judgment notwithstanding the verdict and for a new trial. A confidential settlement was reached prior to a hearing on the motion.
Continue for David Lang's comments...
COMMENT
Patients and jurors expect foreign bodies to be discovered and removed with 100% precision. However, any clinician who has removed a foreign body knows that trying to locate one can be difficult under the best of circumstances.
Further, in cases in which a foreign body is not near a sensitive structure and is not likely to cause additional injury, removal may not be indicated (eg, retained bullet fragments not near a joint). In this case, the foreign body is glass and the location is described as the “arm,” which in all likelihood means the proximal forearm. So we have a potentially sharp item contained within a small space holding many sensitive structures.
Apparently, radiographs were not obtained. While some foreign bodies are radiolucent and generally considered “invisible,” glass is not necessarily one of them. There is a myth that glass is never visible on x-ray and another that glass is visible on x-ray only if there is sufficient “lead content” in it to make it so. Contrary to these beliefs, glass may be visible on standard x-ray, whether or not there is lead in it.
Here, it would have been reasonable to obtain radiographs to identify foreign bodies prior to closing the wound. The glass may have been visible and if detected, the emergency physician could have made a decision either to remove the glass or refer the patient if it was located deeply, next to a sensitive structure. Despite radiographic and physical exam findings, it is always important to remind patients that retained foreign bodies are possible and that follow-up is required. Schedule follow-up and document what the patient was told.
But what about foreign bodies that are almost always radiolucent on a standard film? Wood can be maddening: invisible on x-ray and hard to remove because unlike glass, metal, or stone, there is no confirming “scratch” or “clink” when wood is contacted with a localizing needle. Wood is also virtually guaranteed to suppurate if not removed.
Radiolucent or radiopaque is often considered an inherent quality of an object. But what is visible and what is invisible depends on radiographic technique. For foreign bodies generally considered radiolucent (eg, wood), consider a “soft-tissue technique,” which may demonstrate the foreign body, particularly if it is relatively large. While a positive image can be helpful, a negative one cannot rule out the presence of a foreign body. If available, ultrasound is also useful in detecting radiolucent foreign bodies and should be exploited by those skilled in its use.
In sum, jurors hate foreign bodies left in patients, be they items left in after surgery or not removed following an injury. Do your best, while explaining the limitations of removal efforts and the need for follow-up in complicated cases and self-monitoring in all cases. Instruct patients to return promptly for worsening signs and symptoms. Document that you informed the patient that 100% removal is never guaranteed and that they have agreed to return as scheduled or as needed. —DML
In September 2007, a 23-year-old man drank a six-pack of beer, had an argument with his girlfriend, and punched a plate-glass window with both fists. He sustained lacerations to his right arm. The man removed a large piece of glass from his arm, resulting in significant bleeding. He then wrapped a belt around his arm to stop the blood flow and went to the emergency department of the local hospital, where he was treated by Dr. S.
Dr. S. removed glass fragments from the patient’s arm, sutured it, and instructed him to follow up with his family physician in one to two weeks. When the patient saw another clinician, Dr. A., for suture removal, he reported worsening neurologic symptoms in his right arm. An appointment with an orthopedist was made, which the patient subsequently canceled.
About two months later, a retained glass fragment was removed by orthopedist Dr. R. The plaintiff alleged negligence by Dr. S. for his failure to remove all the glass fragments at the initial presentation. The plaintiff claimed that as a result he suffered a median nerve injury.
The defendant claimed that the nerve injury was most likely inflicted when the plaintiff removed the piece of glass himself before going to the hospital. The defendant also claimed that the plaintiff had been negligent in his failure to seek follow-up treatment as recommended. The defendant further maintained that the physician who removed the retained glass fragment had not determined it to be in the proximity of the median nerve.
Continue for the outcome...
OUTCOME
A jury returned a verdict for the plaintiff that totaled $460,595. The defendant filed a motion for judgment notwithstanding the verdict and for a new trial. A confidential settlement was reached prior to a hearing on the motion.
Continue for David Lang's comments...
COMMENT
Patients and jurors expect foreign bodies to be discovered and removed with 100% precision. However, any clinician who has removed a foreign body knows that trying to locate one can be difficult under the best of circumstances.
Further, in cases in which a foreign body is not near a sensitive structure and is not likely to cause additional injury, removal may not be indicated (eg, retained bullet fragments not near a joint). In this case, the foreign body is glass and the location is described as the “arm,” which in all likelihood means the proximal forearm. So we have a potentially sharp item contained within a small space holding many sensitive structures.
Apparently, radiographs were not obtained. While some foreign bodies are radiolucent and generally considered “invisible,” glass is not necessarily one of them. There is a myth that glass is never visible on x-ray and another that glass is visible on x-ray only if there is sufficient “lead content” in it to make it so. Contrary to these beliefs, glass may be visible on standard x-ray, whether or not there is lead in it.
Here, it would have been reasonable to obtain radiographs to identify foreign bodies prior to closing the wound. The glass may have been visible and if detected, the emergency physician could have made a decision either to remove the glass or refer the patient if it was located deeply, next to a sensitive structure. Despite radiographic and physical exam findings, it is always important to remind patients that retained foreign bodies are possible and that follow-up is required. Schedule follow-up and document what the patient was told.
But what about foreign bodies that are almost always radiolucent on a standard film? Wood can be maddening: invisible on x-ray and hard to remove because unlike glass, metal, or stone, there is no confirming “scratch” or “clink” when wood is contacted with a localizing needle. Wood is also virtually guaranteed to suppurate if not removed.
Radiolucent or radiopaque is often considered an inherent quality of an object. But what is visible and what is invisible depends on radiographic technique. For foreign bodies generally considered radiolucent (eg, wood), consider a “soft-tissue technique,” which may demonstrate the foreign body, particularly if it is relatively large. While a positive image can be helpful, a negative one cannot rule out the presence of a foreign body. If available, ultrasound is also useful in detecting radiolucent foreign bodies and should be exploited by those skilled in its use.
In sum, jurors hate foreign bodies left in patients, be they items left in after surgery or not removed following an injury. Do your best, while explaining the limitations of removal efforts and the need for follow-up in complicated cases and self-monitoring in all cases. Instruct patients to return promptly for worsening signs and symptoms. Document that you informed the patient that 100% removal is never guaranteed and that they have agreed to return as scheduled or as needed. —DML
Eight tools for improving obstetric patient safety and unit performance
Obstetricians, obstetric nurses, nurse managers, and obstetric department heads are almost always well-trained, hard working, highly motivated individuals dedicated to providing the best possible care for their patients. Nevertheless, errors in the provision of care are all too common.1–3 Even though these errors are confined to a small percentage of patient interactions, they engender profound consequences: injuries to mothers or their babies, higher costs to treat associated complications, and medical-legal suits that can entangle both clinicians and plaintiffs for years.
Why do such errors occur when it is the goal of well-trained and dedicated practi-tioners to provide error-free care? There are several reasons:
- The provision of medical care in the early 21st Century is an enormously complex endeavor.
- Physicians and nurses are human beings and, therefore, do not—and never will—perform perfectly all the time, in every situation, with every patient.
- The systems within which care providers work and the tools with which they work are often suboptimal and inefficient and are not designed to maximize patient safety.
- Financial constraints on hospital systems and physician practices dictate that obstetricians and obstetric nurses care for as many patients as possible in limited periods of time.
How then can obstetrics professionals seek to eradicate or at least decrease the number of medical errors that occur during the provision of maternity care?
To accomplish this, we must address the core issues at the root of these medical errors. Solutions must be implemented to 1) simplify the often unnecessary complexity of delivering medical care and 2) create systems and tools that minimize errors and catch those that do occur before they can cause harm.
Yet, how is this to be accomplished? In this article, I describe eight tools developed over time by clinicians who have worked in the field of obstetric patient safety. These tools provide some answers and concrete starting points.
TOOL 1: CONTINUING EDUCATION
William Osler once said, “It is astonishing with how little reading a doctor can practice medicine, but it is not astonishing how badly he may do it.”
As the years out of residency and nursing school accumulate, clinicians—both obstetricians and obstetric nurses—find it all too easy to continue to practice pretty much the way they did during training. However, medical science changes, new protocols improve on the old, and new techniques and medications are introduced yearly into the practice arena. If a clinician is to deliver the best possible care, he or she has to keep abreast of these developments in obstetrics and refresh his or her memory from time to time about things learned long ago. Such acquisition of new and review of old obstetric knowledge can be achieved only through ongoing study.
There are many ways continuing education can be accomplished. You can read new editions of textbooks when they are published or follow an obstetric journal through its yearly cycle. Cutting-edge, clinically oriented, interactive courses in all major areas of obstetrics are available to clinicians online. The recertification criteria of the American College of Obstetricians and Gynecologists (ACOG), state licensing requirements, and individual obstetric department recredentialing requirements often mandate such continuing education.
TOOL 2: SIMULATION PROGRAMS
Most obstetric emergencies, especially the most dangerous ones, occur infrequently, making it difficult for the many members of any labor and delivery unit to have their skills sharply honed to best deal with them. This is less of a problem at busy institutions where, simply due to the numbers of patients cared for, such emergencies are encountered on a regular basis. But at smaller facilities they are, fortunately, rare. The only way a unit can maintain its competency to handle such situations when they do arise—and they will—is to practice them in simulation mode.
There is now an increasing amount of literature demonstrating that simulation programs are effective not only at improving the knowledge base of obstetrics providers but also at improving Apgar scores, reducing admissions to neonatal intensive care units (NICUs), and preventing brachial plexus injuries.4
An effective simulation program should contain the following features:
- a thorough, didactic review of the clinical aspects of emergency care for all of the major obstetric emergencies (postpartum hemorrhage, shoulder dystocia, eclamptic seizure, maternal collapse, and urgent cesarean section)
- practice drills for the above
- training in teamwork and communication skills
- frequent repetition, ideally with each major obstetric emergency being covered twice per year.
Many institutions have developed simulation training centers. While these can be excellent teaching facilities, something is lost if simulation training is not done on the actual unit where obstetricians and obstetric nurses will encounter emergencies. Simulation programs also should be time-efficient and should be scheduled to make it easy for obstetrics personnel to participate. For greater convenience and knowledge retention, it is better to have short simulation programs at frequent intervals than day-long programs once per year or every other year.
Related Article: How simulation can train, and refresh, physicians for critical OB events Robert Gherman, MD; Andrew Satin, MD; Roxane Gardner, MD, MPH
TOOL 3: INTERNAL AUDITS
It is a mantra in business that you can’t fix what you can’t measure. And while obstetric units usually keep track of such things as rates of cesarean section, elective induction at less than 39 weeks, and admission to the NICU, it is rare that data are kept on other extremely important information. For instance, how often is an induction started with no indication for it written in the admission note? How often is the vacuum or forceps applied with no note documenting the reason or the discussion of risks and benefits with the patient? How often does estimated fetal weight go unnoted in the medical record of a mother with gestational diabetes?
An audit program, either in computer format or with manual collection on paper, is a vital tool for each labor and delivery unit to use in assessing the quality of the care it provides. Such an audit, by covering a sufficiently large number of clinical data points, can give tremendous insight into the specifics of the unit’s performance over the range of obstetric care situations. It will show where things are being done well and where they are not. The audit becomes even more valuable if it is designed so that each of the measured data points can be evaluated for individual clinician performance as well as for the labor and delivery unit as a whole.
Similar audits also should be conducted in individual physician offices and obstetric clinics. Many of the errors that occur in providing obstetric care occur prenatally: tests not performed, lack of follow-up of known problems, or poor communication with patients or with the labor and delivery unit.
One of the major benefits of audit programs that are conducted on a regular basis—every 6 months or annually are common intervals—is that trends in performance in each area of care can be evaluated. As deficiencies are pointed out to providers, their compliance with best care practices should improve from cycle to cycle.
TOOL 4: BEST PRACTICE PROTOCOLS
Medicine is now well past the point where protocols are seen as “restrictive” or “advocating cookbook medicine.” Well-designed protocols summarize best practices derived from evidence-based studies and the consensus of obstetric experts. They serve as convenient reminders to physicians in various clinical situations so that these clinicians do not have to rely solely on what they happen to remember about caring for a given condition. Protocols also provide a certain uniformity of care, which in itself decreases the likelihood of errors being made.
Each obstetric department should have a set of protocols to cover the most common obstetric situations, such as:
- premature rupture of membranes
- instrumental vaginal deliveries
- oxytocin administration.
Each unit does not have to devise its own protocols; ACOG and nearby academic institutions are excellent sources for protocols that can be replicated and implemented so that they do not have to be created de novo.
Related Article: More strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD; Alexis C. Gimovsky, MD (January 2011)
TOOL 5: SAFETY CHECKLISTS
Just as well-designed protocols can serve as convenient reminders of best practices, low-tech physical checklists can be kept at nursing stations and in labor and delivery rooms to serve as reminders of best practices during obstetric emergencies. For instance, having a laminated set of easy-to-read protocols for postpartum hemorrhage, eclamptic seizure, maternal collapse, and shoulder dystocia in a delivery room can allow a charge nurse or other supervisor to check to make sure all proper procedures are being performed by the team actually administering care to a patient in crisis, with nothing important overlooked.
Related Article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
TOOL 6: COMPLETE DOCUMENTATION
Almost as many lawsuits are lost because of poor documentation as are lost because of inappropriate medical care. The obstetric literature,1 and my own experience with the medical-legal system, clearly demonstrate the need for appropriate, careful documentation of the events that transpire during patient care. Notes do not have to be especially long or verbose—but they must contain all relevant information and describe the obstetrician’s thinking at various decision points.
Documentation can be inadequate because of time constraints, poor understanding of the events that transpired, or simply a lack of remembering to include salient points that should be covered in a clinical note.
Clinicians can be prompted to include key aspects of care in the medical record by using prepared templates. Such templates are easy to fill out, remind clinicians to document information that would otherwise not get recorded, and result in a much more complete patient chart. By using a template, a clinician would never forget to record the head-to-body delivery interval after a shoulder dystocia or whether a fetal heart rate was obtained in the operating room just prior to starting a cesarean section.
Related Article: Sound strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010)
TOOL 7: SMART MEDICAL RECORDS
In obstetrics we are fortunate that there is a limited range of issues that recur repeatedly, such as gestational hypertension, placental abruption, and fetal distress. One soon gains experience in managing these conditions and, with the help of best-practice protocols, optimal care almost always can be provided.
Still, many clinical presentations can pose diagnostic challenges, especially in atypical cases. Moreover, clinicians managing a patient’s care may not immediately remember the best means of evaluating and treating a certain condition in specific circumstances. For example, at 3:00 am it may be difficult to recall whether it is nifedipine or labetalol that should be avoided with asthmatic patients or which antibiotic formulation is currently recommended for prophylaxis in a patient with premature rupture of membranes at 30 weeks’ gestation who is allergic to penicillin.
Smart medical records, already widely used in other fields of medicine, are an antidote to this problem. When certain diagnoses, physical findings, clinical details, or laboratory data are entered into specific fields in an electronic medical record, templates that have been added to the record automatically appear to show relevant information, such as tests that should be performed, treatments that should be administered, and alternative diagnoses that should be considered. Such reminders are not presented as obligations or “hard stops”; they are usually displayed in the form of easily dismissible pop-ups or “reminder bubbles” that appear on the screen and serve solely to jog memory and provide information.
Such smart electronic medical record features can be provided either by the main electronic medical record vendor or added as subprograms by other providers.
Related Article: EHRs and medicolegal risk: How they help, when they could hurt Martin L. Gimovsky, MD; Baohuong N. Trans, DO (March 2013)
TOOL 8: MATERNITY UNIT ON-SITE CONSULTATIONS
Every labor and delivery unit has its own culture, a combination of institutional history and the personality of the doctors and nurses working there. Some units function efficiently, have the most modern equipment, and provide superb medical care. Other units have less than adequate facilities, remain entrenched in older practices, and have disruptive or uncooperative personnel that interfere with the smooth running of the unit. Moreover, each maternity unit, based on its resources, patient population, and staff skills, devises its own solutions to the same sorts of problems that all other obstetric units share. Unfortunately, there is little collaboration between units to discuss common problems and trade best practices. The result is that all too often each unit invents its own “wheel” when many excellent “wheels” already have been developed for the same issues around the country.
An on-site visit by an outside consultant—an obstetrician, an obstetric nurse, or both—can identify ongoing institutional problems, point out care deficiencies the unit may not be aware of, and provide resources and ideas to help solve the issues identified. Moreover, an outside consultant can offer unbiased and authoritative opinions to help move initiatives that may be stalled by local personalities or institutional politics.
Some features that a well-conducted on-site consultation will evaluate are:
- adequacy of obstetric triage
- capacity to perform stat cesarean sections 24/7
- 24-hour availability of obstetricians, anesthesiologists, pediatricians, and operating room teams
- preparation for handling various obstetric emergencies
- oxytocin administration protocols and compliance
- adequacy of physician and nurse charting
- ongoing skills assessment of fetal heart-rate monitor interpretation
- presence of practitioners whose disruptive behavior compromises the safety of the unit
- preparation for nonmedical emergencies, such as infant abduction, natural disaster; fire; shooter; or disruptive patients, visitors, or staff.
IMPLEMENTATION CAN EQUAL SAFER CARE
As long as people have babies, less than desirable outcomes will occasionally occur. As long as care providers are human beings, the provision of obstetric care will continue to be imperfect.
It is up to those entrusted with the responsibility of caring for mothers and their babies to provide as much support and backup as possible to obstetricians and obstetric nurses, all of whom sincerely desire to do everything possible to deliver safe care to their patients.
Tools for providing such support and backup are available and can be implemented fairly easily on most obstetric units. They do involve an expenditure of both time and money. However, the most important requirement for success is an institutional willingness to 1) acknowledge that the care a given unit provides can be improved, 2) perform an in-depth evaluation of the quality of care currently being administered, and 3) move ahead with the sorts of tools discussed in this article that will enable clinicians to provide optimal care for mothers and babies.
SHARE YOUR EXPERIENCE!
Did implementation of a tool described in this article solve a problem or improve performance for your obstetric unit? Tell us about it by emailing to: [email protected] Please include your name, city, and state.
- Clark SL, Belfort MA, Dildy GA, Meyers JA. Reducing obstetric litigation through alterations in practice patterns. Obstet Gynecol. 2008;112(6):1279–1283.
- Gluck PA. Medical error theory. Obstet Gynecol Clin North Am. 2008;35(1):11–17, vii.
- Anakiraman V, Ecker J. Quality in obstetric care: measuring what matters. Obstet Gynecol. 2010;116(3):728–732.
- Draycott T, Sibanda T, Owen L, et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113(2):177–182.

Henry M. Lerner, MD, is Assistant Clinical Professor of Obstetrics & Gynecology at Harvard Medical School in Boston, Massachusetts. He has been in private practice of obstetrics and gynecology for 35 years, has served on the board of a major medical malpractice carrier for 14 years, and has helped defend more than 300 obstetricians in medical malpractice cases across the country.
Dr. Lerner reports that he is a consultant to The Sullivan Group, a patient safety education provider.
Henry M. Lerner, MD, is Assistant Clinical Professor of Obstetrics & Gynecology at Harvard Medical School in Boston, Massachusetts. He has been in private practice of obstetrics and gynecology for 35 years, has served on the board of a major medical malpractice carrier for 14 years, and has helped defend more than 300 obstetricians in medical malpractice cases across the country.
Dr. Lerner reports that he is a consultant to The Sullivan Group, a patient safety education provider.
Henry M. Lerner, MD, is Assistant Clinical Professor of Obstetrics & Gynecology at Harvard Medical School in Boston, Massachusetts. He has been in private practice of obstetrics and gynecology for 35 years, has served on the board of a major medical malpractice carrier for 14 years, and has helped defend more than 300 obstetricians in medical malpractice cases across the country.
Dr. Lerner reports that he is a consultant to The Sullivan Group, a patient safety education provider.
Obstetricians, obstetric nurses, nurse managers, and obstetric department heads are almost always well-trained, hard working, highly motivated individuals dedicated to providing the best possible care for their patients. Nevertheless, errors in the provision of care are all too common.1–3 Even though these errors are confined to a small percentage of patient interactions, they engender profound consequences: injuries to mothers or their babies, higher costs to treat associated complications, and medical-legal suits that can entangle both clinicians and plaintiffs for years.
Why do such errors occur when it is the goal of well-trained and dedicated practi-tioners to provide error-free care? There are several reasons:
- The provision of medical care in the early 21st Century is an enormously complex endeavor.
- Physicians and nurses are human beings and, therefore, do not—and never will—perform perfectly all the time, in every situation, with every patient.
- The systems within which care providers work and the tools with which they work are often suboptimal and inefficient and are not designed to maximize patient safety.
- Financial constraints on hospital systems and physician practices dictate that obstetricians and obstetric nurses care for as many patients as possible in limited periods of time.
How then can obstetrics professionals seek to eradicate or at least decrease the number of medical errors that occur during the provision of maternity care?
To accomplish this, we must address the core issues at the root of these medical errors. Solutions must be implemented to 1) simplify the often unnecessary complexity of delivering medical care and 2) create systems and tools that minimize errors and catch those that do occur before they can cause harm.
Yet, how is this to be accomplished? In this article, I describe eight tools developed over time by clinicians who have worked in the field of obstetric patient safety. These tools provide some answers and concrete starting points.
TOOL 1: CONTINUING EDUCATION
William Osler once said, “It is astonishing with how little reading a doctor can practice medicine, but it is not astonishing how badly he may do it.”
As the years out of residency and nursing school accumulate, clinicians—both obstetricians and obstetric nurses—find it all too easy to continue to practice pretty much the way they did during training. However, medical science changes, new protocols improve on the old, and new techniques and medications are introduced yearly into the practice arena. If a clinician is to deliver the best possible care, he or she has to keep abreast of these developments in obstetrics and refresh his or her memory from time to time about things learned long ago. Such acquisition of new and review of old obstetric knowledge can be achieved only through ongoing study.
There are many ways continuing education can be accomplished. You can read new editions of textbooks when they are published or follow an obstetric journal through its yearly cycle. Cutting-edge, clinically oriented, interactive courses in all major areas of obstetrics are available to clinicians online. The recertification criteria of the American College of Obstetricians and Gynecologists (ACOG), state licensing requirements, and individual obstetric department recredentialing requirements often mandate such continuing education.
TOOL 2: SIMULATION PROGRAMS
Most obstetric emergencies, especially the most dangerous ones, occur infrequently, making it difficult for the many members of any labor and delivery unit to have their skills sharply honed to best deal with them. This is less of a problem at busy institutions where, simply due to the numbers of patients cared for, such emergencies are encountered on a regular basis. But at smaller facilities they are, fortunately, rare. The only way a unit can maintain its competency to handle such situations when they do arise—and they will—is to practice them in simulation mode.
There is now an increasing amount of literature demonstrating that simulation programs are effective not only at improving the knowledge base of obstetrics providers but also at improving Apgar scores, reducing admissions to neonatal intensive care units (NICUs), and preventing brachial plexus injuries.4
An effective simulation program should contain the following features:
- a thorough, didactic review of the clinical aspects of emergency care for all of the major obstetric emergencies (postpartum hemorrhage, shoulder dystocia, eclamptic seizure, maternal collapse, and urgent cesarean section)
- practice drills for the above
- training in teamwork and communication skills
- frequent repetition, ideally with each major obstetric emergency being covered twice per year.
Many institutions have developed simulation training centers. While these can be excellent teaching facilities, something is lost if simulation training is not done on the actual unit where obstetricians and obstetric nurses will encounter emergencies. Simulation programs also should be time-efficient and should be scheduled to make it easy for obstetrics personnel to participate. For greater convenience and knowledge retention, it is better to have short simulation programs at frequent intervals than day-long programs once per year or every other year.
Related Article: How simulation can train, and refresh, physicians for critical OB events Robert Gherman, MD; Andrew Satin, MD; Roxane Gardner, MD, MPH
TOOL 3: INTERNAL AUDITS
It is a mantra in business that you can’t fix what you can’t measure. And while obstetric units usually keep track of such things as rates of cesarean section, elective induction at less than 39 weeks, and admission to the NICU, it is rare that data are kept on other extremely important information. For instance, how often is an induction started with no indication for it written in the admission note? How often is the vacuum or forceps applied with no note documenting the reason or the discussion of risks and benefits with the patient? How often does estimated fetal weight go unnoted in the medical record of a mother with gestational diabetes?
An audit program, either in computer format or with manual collection on paper, is a vital tool for each labor and delivery unit to use in assessing the quality of the care it provides. Such an audit, by covering a sufficiently large number of clinical data points, can give tremendous insight into the specifics of the unit’s performance over the range of obstetric care situations. It will show where things are being done well and where they are not. The audit becomes even more valuable if it is designed so that each of the measured data points can be evaluated for individual clinician performance as well as for the labor and delivery unit as a whole.
Similar audits also should be conducted in individual physician offices and obstetric clinics. Many of the errors that occur in providing obstetric care occur prenatally: tests not performed, lack of follow-up of known problems, or poor communication with patients or with the labor and delivery unit.
One of the major benefits of audit programs that are conducted on a regular basis—every 6 months or annually are common intervals—is that trends in performance in each area of care can be evaluated. As deficiencies are pointed out to providers, their compliance with best care practices should improve from cycle to cycle.
TOOL 4: BEST PRACTICE PROTOCOLS
Medicine is now well past the point where protocols are seen as “restrictive” or “advocating cookbook medicine.” Well-designed protocols summarize best practices derived from evidence-based studies and the consensus of obstetric experts. They serve as convenient reminders to physicians in various clinical situations so that these clinicians do not have to rely solely on what they happen to remember about caring for a given condition. Protocols also provide a certain uniformity of care, which in itself decreases the likelihood of errors being made.
Each obstetric department should have a set of protocols to cover the most common obstetric situations, such as:
- premature rupture of membranes
- instrumental vaginal deliveries
- oxytocin administration.
Each unit does not have to devise its own protocols; ACOG and nearby academic institutions are excellent sources for protocols that can be replicated and implemented so that they do not have to be created de novo.
Related Article: More strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD; Alexis C. Gimovsky, MD (January 2011)
TOOL 5: SAFETY CHECKLISTS
Just as well-designed protocols can serve as convenient reminders of best practices, low-tech physical checklists can be kept at nursing stations and in labor and delivery rooms to serve as reminders of best practices during obstetric emergencies. For instance, having a laminated set of easy-to-read protocols for postpartum hemorrhage, eclamptic seizure, maternal collapse, and shoulder dystocia in a delivery room can allow a charge nurse or other supervisor to check to make sure all proper procedures are being performed by the team actually administering care to a patient in crisis, with nothing important overlooked.
Related Article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
TOOL 6: COMPLETE DOCUMENTATION
Almost as many lawsuits are lost because of poor documentation as are lost because of inappropriate medical care. The obstetric literature,1 and my own experience with the medical-legal system, clearly demonstrate the need for appropriate, careful documentation of the events that transpire during patient care. Notes do not have to be especially long or verbose—but they must contain all relevant information and describe the obstetrician’s thinking at various decision points.
Documentation can be inadequate because of time constraints, poor understanding of the events that transpired, or simply a lack of remembering to include salient points that should be covered in a clinical note.
Clinicians can be prompted to include key aspects of care in the medical record by using prepared templates. Such templates are easy to fill out, remind clinicians to document information that would otherwise not get recorded, and result in a much more complete patient chart. By using a template, a clinician would never forget to record the head-to-body delivery interval after a shoulder dystocia or whether a fetal heart rate was obtained in the operating room just prior to starting a cesarean section.
Related Article: Sound strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010)
TOOL 7: SMART MEDICAL RECORDS
In obstetrics we are fortunate that there is a limited range of issues that recur repeatedly, such as gestational hypertension, placental abruption, and fetal distress. One soon gains experience in managing these conditions and, with the help of best-practice protocols, optimal care almost always can be provided.
Still, many clinical presentations can pose diagnostic challenges, especially in atypical cases. Moreover, clinicians managing a patient’s care may not immediately remember the best means of evaluating and treating a certain condition in specific circumstances. For example, at 3:00 am it may be difficult to recall whether it is nifedipine or labetalol that should be avoided with asthmatic patients or which antibiotic formulation is currently recommended for prophylaxis in a patient with premature rupture of membranes at 30 weeks’ gestation who is allergic to penicillin.
Smart medical records, already widely used in other fields of medicine, are an antidote to this problem. When certain diagnoses, physical findings, clinical details, or laboratory data are entered into specific fields in an electronic medical record, templates that have been added to the record automatically appear to show relevant information, such as tests that should be performed, treatments that should be administered, and alternative diagnoses that should be considered. Such reminders are not presented as obligations or “hard stops”; they are usually displayed in the form of easily dismissible pop-ups or “reminder bubbles” that appear on the screen and serve solely to jog memory and provide information.
Such smart electronic medical record features can be provided either by the main electronic medical record vendor or added as subprograms by other providers.
Related Article: EHRs and medicolegal risk: How they help, when they could hurt Martin L. Gimovsky, MD; Baohuong N. Trans, DO (March 2013)
TOOL 8: MATERNITY UNIT ON-SITE CONSULTATIONS
Every labor and delivery unit has its own culture, a combination of institutional history and the personality of the doctors and nurses working there. Some units function efficiently, have the most modern equipment, and provide superb medical care. Other units have less than adequate facilities, remain entrenched in older practices, and have disruptive or uncooperative personnel that interfere with the smooth running of the unit. Moreover, each maternity unit, based on its resources, patient population, and staff skills, devises its own solutions to the same sorts of problems that all other obstetric units share. Unfortunately, there is little collaboration between units to discuss common problems and trade best practices. The result is that all too often each unit invents its own “wheel” when many excellent “wheels” already have been developed for the same issues around the country.
An on-site visit by an outside consultant—an obstetrician, an obstetric nurse, or both—can identify ongoing institutional problems, point out care deficiencies the unit may not be aware of, and provide resources and ideas to help solve the issues identified. Moreover, an outside consultant can offer unbiased and authoritative opinions to help move initiatives that may be stalled by local personalities or institutional politics.
Some features that a well-conducted on-site consultation will evaluate are:
- adequacy of obstetric triage
- capacity to perform stat cesarean sections 24/7
- 24-hour availability of obstetricians, anesthesiologists, pediatricians, and operating room teams
- preparation for handling various obstetric emergencies
- oxytocin administration protocols and compliance
- adequacy of physician and nurse charting
- ongoing skills assessment of fetal heart-rate monitor interpretation
- presence of practitioners whose disruptive behavior compromises the safety of the unit
- preparation for nonmedical emergencies, such as infant abduction, natural disaster; fire; shooter; or disruptive patients, visitors, or staff.
IMPLEMENTATION CAN EQUAL SAFER CARE
As long as people have babies, less than desirable outcomes will occasionally occur. As long as care providers are human beings, the provision of obstetric care will continue to be imperfect.
It is up to those entrusted with the responsibility of caring for mothers and their babies to provide as much support and backup as possible to obstetricians and obstetric nurses, all of whom sincerely desire to do everything possible to deliver safe care to their patients.
Tools for providing such support and backup are available and can be implemented fairly easily on most obstetric units. They do involve an expenditure of both time and money. However, the most important requirement for success is an institutional willingness to 1) acknowledge that the care a given unit provides can be improved, 2) perform an in-depth evaluation of the quality of care currently being administered, and 3) move ahead with the sorts of tools discussed in this article that will enable clinicians to provide optimal care for mothers and babies.
SHARE YOUR EXPERIENCE!
Did implementation of a tool described in this article solve a problem or improve performance for your obstetric unit? Tell us about it by emailing to: [email protected] Please include your name, city, and state.
Obstetricians, obstetric nurses, nurse managers, and obstetric department heads are almost always well-trained, hard working, highly motivated individuals dedicated to providing the best possible care for their patients. Nevertheless, errors in the provision of care are all too common.1–3 Even though these errors are confined to a small percentage of patient interactions, they engender profound consequences: injuries to mothers or their babies, higher costs to treat associated complications, and medical-legal suits that can entangle both clinicians and plaintiffs for years.
Why do such errors occur when it is the goal of well-trained and dedicated practi-tioners to provide error-free care? There are several reasons:
- The provision of medical care in the early 21st Century is an enormously complex endeavor.
- Physicians and nurses are human beings and, therefore, do not—and never will—perform perfectly all the time, in every situation, with every patient.
- The systems within which care providers work and the tools with which they work are often suboptimal and inefficient and are not designed to maximize patient safety.
- Financial constraints on hospital systems and physician practices dictate that obstetricians and obstetric nurses care for as many patients as possible in limited periods of time.
How then can obstetrics professionals seek to eradicate or at least decrease the number of medical errors that occur during the provision of maternity care?
To accomplish this, we must address the core issues at the root of these medical errors. Solutions must be implemented to 1) simplify the often unnecessary complexity of delivering medical care and 2) create systems and tools that minimize errors and catch those that do occur before they can cause harm.
Yet, how is this to be accomplished? In this article, I describe eight tools developed over time by clinicians who have worked in the field of obstetric patient safety. These tools provide some answers and concrete starting points.
TOOL 1: CONTINUING EDUCATION
William Osler once said, “It is astonishing with how little reading a doctor can practice medicine, but it is not astonishing how badly he may do it.”
As the years out of residency and nursing school accumulate, clinicians—both obstetricians and obstetric nurses—find it all too easy to continue to practice pretty much the way they did during training. However, medical science changes, new protocols improve on the old, and new techniques and medications are introduced yearly into the practice arena. If a clinician is to deliver the best possible care, he or she has to keep abreast of these developments in obstetrics and refresh his or her memory from time to time about things learned long ago. Such acquisition of new and review of old obstetric knowledge can be achieved only through ongoing study.
There are many ways continuing education can be accomplished. You can read new editions of textbooks when they are published or follow an obstetric journal through its yearly cycle. Cutting-edge, clinically oriented, interactive courses in all major areas of obstetrics are available to clinicians online. The recertification criteria of the American College of Obstetricians and Gynecologists (ACOG), state licensing requirements, and individual obstetric department recredentialing requirements often mandate such continuing education.
TOOL 2: SIMULATION PROGRAMS
Most obstetric emergencies, especially the most dangerous ones, occur infrequently, making it difficult for the many members of any labor and delivery unit to have their skills sharply honed to best deal with them. This is less of a problem at busy institutions where, simply due to the numbers of patients cared for, such emergencies are encountered on a regular basis. But at smaller facilities they are, fortunately, rare. The only way a unit can maintain its competency to handle such situations when they do arise—and they will—is to practice them in simulation mode.
There is now an increasing amount of literature demonstrating that simulation programs are effective not only at improving the knowledge base of obstetrics providers but also at improving Apgar scores, reducing admissions to neonatal intensive care units (NICUs), and preventing brachial plexus injuries.4
An effective simulation program should contain the following features:
- a thorough, didactic review of the clinical aspects of emergency care for all of the major obstetric emergencies (postpartum hemorrhage, shoulder dystocia, eclamptic seizure, maternal collapse, and urgent cesarean section)
- practice drills for the above
- training in teamwork and communication skills
- frequent repetition, ideally with each major obstetric emergency being covered twice per year.
Many institutions have developed simulation training centers. While these can be excellent teaching facilities, something is lost if simulation training is not done on the actual unit where obstetricians and obstetric nurses will encounter emergencies. Simulation programs also should be time-efficient and should be scheduled to make it easy for obstetrics personnel to participate. For greater convenience and knowledge retention, it is better to have short simulation programs at frequent intervals than day-long programs once per year or every other year.
Related Article: How simulation can train, and refresh, physicians for critical OB events Robert Gherman, MD; Andrew Satin, MD; Roxane Gardner, MD, MPH
TOOL 3: INTERNAL AUDITS
It is a mantra in business that you can’t fix what you can’t measure. And while obstetric units usually keep track of such things as rates of cesarean section, elective induction at less than 39 weeks, and admission to the NICU, it is rare that data are kept on other extremely important information. For instance, how often is an induction started with no indication for it written in the admission note? How often is the vacuum or forceps applied with no note documenting the reason or the discussion of risks and benefits with the patient? How often does estimated fetal weight go unnoted in the medical record of a mother with gestational diabetes?
An audit program, either in computer format or with manual collection on paper, is a vital tool for each labor and delivery unit to use in assessing the quality of the care it provides. Such an audit, by covering a sufficiently large number of clinical data points, can give tremendous insight into the specifics of the unit’s performance over the range of obstetric care situations. It will show where things are being done well and where they are not. The audit becomes even more valuable if it is designed so that each of the measured data points can be evaluated for individual clinician performance as well as for the labor and delivery unit as a whole.
Similar audits also should be conducted in individual physician offices and obstetric clinics. Many of the errors that occur in providing obstetric care occur prenatally: tests not performed, lack of follow-up of known problems, or poor communication with patients or with the labor and delivery unit.
One of the major benefits of audit programs that are conducted on a regular basis—every 6 months or annually are common intervals—is that trends in performance in each area of care can be evaluated. As deficiencies are pointed out to providers, their compliance with best care practices should improve from cycle to cycle.
TOOL 4: BEST PRACTICE PROTOCOLS
Medicine is now well past the point where protocols are seen as “restrictive” or “advocating cookbook medicine.” Well-designed protocols summarize best practices derived from evidence-based studies and the consensus of obstetric experts. They serve as convenient reminders to physicians in various clinical situations so that these clinicians do not have to rely solely on what they happen to remember about caring for a given condition. Protocols also provide a certain uniformity of care, which in itself decreases the likelihood of errors being made.
Each obstetric department should have a set of protocols to cover the most common obstetric situations, such as:
- premature rupture of membranes
- instrumental vaginal deliveries
- oxytocin administration.
Each unit does not have to devise its own protocols; ACOG and nearby academic institutions are excellent sources for protocols that can be replicated and implemented so that they do not have to be created de novo.
Related Article: More strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD; Alexis C. Gimovsky, MD (January 2011)
TOOL 5: SAFETY CHECKLISTS
Just as well-designed protocols can serve as convenient reminders of best practices, low-tech physical checklists can be kept at nursing stations and in labor and delivery rooms to serve as reminders of best practices during obstetric emergencies. For instance, having a laminated set of easy-to-read protocols for postpartum hemorrhage, eclamptic seizure, maternal collapse, and shoulder dystocia in a delivery room can allow a charge nurse or other supervisor to check to make sure all proper procedures are being performed by the team actually administering care to a patient in crisis, with nothing important overlooked.
Related Article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
TOOL 6: COMPLETE DOCUMENTATION
Almost as many lawsuits are lost because of poor documentation as are lost because of inappropriate medical care. The obstetric literature,1 and my own experience with the medical-legal system, clearly demonstrate the need for appropriate, careful documentation of the events that transpire during patient care. Notes do not have to be especially long or verbose—but they must contain all relevant information and describe the obstetrician’s thinking at various decision points.
Documentation can be inadequate because of time constraints, poor understanding of the events that transpired, or simply a lack of remembering to include salient points that should be covered in a clinical note.
Clinicians can be prompted to include key aspects of care in the medical record by using prepared templates. Such templates are easy to fill out, remind clinicians to document information that would otherwise not get recorded, and result in a much more complete patient chart. By using a template, a clinician would never forget to record the head-to-body delivery interval after a shoulder dystocia or whether a fetal heart rate was obtained in the operating room just prior to starting a cesarean section.
Related Article: Sound strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010)
TOOL 7: SMART MEDICAL RECORDS
In obstetrics we are fortunate that there is a limited range of issues that recur repeatedly, such as gestational hypertension, placental abruption, and fetal distress. One soon gains experience in managing these conditions and, with the help of best-practice protocols, optimal care almost always can be provided.
Still, many clinical presentations can pose diagnostic challenges, especially in atypical cases. Moreover, clinicians managing a patient’s care may not immediately remember the best means of evaluating and treating a certain condition in specific circumstances. For example, at 3:00 am it may be difficult to recall whether it is nifedipine or labetalol that should be avoided with asthmatic patients or which antibiotic formulation is currently recommended for prophylaxis in a patient with premature rupture of membranes at 30 weeks’ gestation who is allergic to penicillin.
Smart medical records, already widely used in other fields of medicine, are an antidote to this problem. When certain diagnoses, physical findings, clinical details, or laboratory data are entered into specific fields in an electronic medical record, templates that have been added to the record automatically appear to show relevant information, such as tests that should be performed, treatments that should be administered, and alternative diagnoses that should be considered. Such reminders are not presented as obligations or “hard stops”; they are usually displayed in the form of easily dismissible pop-ups or “reminder bubbles” that appear on the screen and serve solely to jog memory and provide information.
Such smart electronic medical record features can be provided either by the main electronic medical record vendor or added as subprograms by other providers.
Related Article: EHRs and medicolegal risk: How they help, when they could hurt Martin L. Gimovsky, MD; Baohuong N. Trans, DO (March 2013)
TOOL 8: MATERNITY UNIT ON-SITE CONSULTATIONS
Every labor and delivery unit has its own culture, a combination of institutional history and the personality of the doctors and nurses working there. Some units function efficiently, have the most modern equipment, and provide superb medical care. Other units have less than adequate facilities, remain entrenched in older practices, and have disruptive or uncooperative personnel that interfere with the smooth running of the unit. Moreover, each maternity unit, based on its resources, patient population, and staff skills, devises its own solutions to the same sorts of problems that all other obstetric units share. Unfortunately, there is little collaboration between units to discuss common problems and trade best practices. The result is that all too often each unit invents its own “wheel” when many excellent “wheels” already have been developed for the same issues around the country.
An on-site visit by an outside consultant—an obstetrician, an obstetric nurse, or both—can identify ongoing institutional problems, point out care deficiencies the unit may not be aware of, and provide resources and ideas to help solve the issues identified. Moreover, an outside consultant can offer unbiased and authoritative opinions to help move initiatives that may be stalled by local personalities or institutional politics.
Some features that a well-conducted on-site consultation will evaluate are:
- adequacy of obstetric triage
- capacity to perform stat cesarean sections 24/7
- 24-hour availability of obstetricians, anesthesiologists, pediatricians, and operating room teams
- preparation for handling various obstetric emergencies
- oxytocin administration protocols and compliance
- adequacy of physician and nurse charting
- ongoing skills assessment of fetal heart-rate monitor interpretation
- presence of practitioners whose disruptive behavior compromises the safety of the unit
- preparation for nonmedical emergencies, such as infant abduction, natural disaster; fire; shooter; or disruptive patients, visitors, or staff.
IMPLEMENTATION CAN EQUAL SAFER CARE
As long as people have babies, less than desirable outcomes will occasionally occur. As long as care providers are human beings, the provision of obstetric care will continue to be imperfect.
It is up to those entrusted with the responsibility of caring for mothers and their babies to provide as much support and backup as possible to obstetricians and obstetric nurses, all of whom sincerely desire to do everything possible to deliver safe care to their patients.
Tools for providing such support and backup are available and can be implemented fairly easily on most obstetric units. They do involve an expenditure of both time and money. However, the most important requirement for success is an institutional willingness to 1) acknowledge that the care a given unit provides can be improved, 2) perform an in-depth evaluation of the quality of care currently being administered, and 3) move ahead with the sorts of tools discussed in this article that will enable clinicians to provide optimal care for mothers and babies.
SHARE YOUR EXPERIENCE!
Did implementation of a tool described in this article solve a problem or improve performance for your obstetric unit? Tell us about it by emailing to: [email protected] Please include your name, city, and state.
- Clark SL, Belfort MA, Dildy GA, Meyers JA. Reducing obstetric litigation through alterations in practice patterns. Obstet Gynecol. 2008;112(6):1279–1283.
- Gluck PA. Medical error theory. Obstet Gynecol Clin North Am. 2008;35(1):11–17, vii.
- Anakiraman V, Ecker J. Quality in obstetric care: measuring what matters. Obstet Gynecol. 2010;116(3):728–732.
- Draycott T, Sibanda T, Owen L, et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113(2):177–182.
- Clark SL, Belfort MA, Dildy GA, Meyers JA. Reducing obstetric litigation through alterations in practice patterns. Obstet Gynecol. 2008;112(6):1279–1283.
- Gluck PA. Medical error theory. Obstet Gynecol Clin North Am. 2008;35(1):11–17, vii.
- Anakiraman V, Ecker J. Quality in obstetric care: measuring what matters. Obstet Gynecol. 2010;116(3):728–732.
- Draycott T, Sibanda T, Owen L, et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113(2):177–182.

Placenta fails to deliver: Mother dies of hemorrhage
PLACENTA FAILS TO DELIVER: MOTHER DIES OF HEMORRHAGE
After a 38-year-old woman gave birth, the placenta did not deliver. The ObGyn was unable remove the entire placenta and the mother began to hemorrhage. After an hour, the patient was given a blood transfusion. She could not be stabilized and died.
ESTATE’S CLAIM The ObGyn was negligent. He failed to remove the entire placenta and did not treat the hemorrhage in a timely manner. The hospital staff was negligent in failing to properly address the massive hemorrhage. A prompt transfusion would have saved the woman’s life, but the anesthesiologist who had to approve the procedure could not be located. Other procedures, including a hysterectomy, could have saved the mother’s life.
DEFENDANTS’ DEFENSE The ObGyn claimed that incomplete delivery of the placenta and postpartum hemorrhage are known complications of a delivery. The hospital claimed that the staff had acted appropriately and that it was not responsible for the actions of the anesthesiologist, an independent contractor. The anesthesiologist denied negligence.
VERDICT A $2 million New York settlement was reached that included $200,000 from the hospital and $1.8 million from the physicians’ insurers.
Related Article: Postpartum hemorrhage: 11 critical questions, answered by an expert Haywood L. Brown, MD (January 2011)
DECREASED FETAL MOVEMENT OVERLOOKED; SEVERE INJURY TO BABY
At her 39th-week prenatal visit at a clinic, the mother reported decreased fetal movement. Acoustic stimulation of the fetus was attempted twice without response. The fetal heart-rate monitor identified a normal heart rate without variability or accelerations. The mother was taken by wheelchair to the hospital next door. A note explaining the nonreassuring findings allegedly accompanied her.
The mother waited to be admitted. When a fetal heart-rate monitor was connected 30 minutes after admission, results were still nonreassuring.
A resident examined the mother 45 minutes later. He called the attending ObGyn, and they decided to postpone cesarean delivery because the mother had eaten breakfast.
When the fetal heart rate crashed 4 hours later, a second-year resident began emergency cesarean delivery. The ObGyn, who had never examined the patient, observed some of the procedure in the OR.
The baby was born with catastrophic brain damage, and has spastic quadriplegia cerebral palsy, feeding problems, and significant cognitive and developmental delays.
PARENTS’ CLAIM A cesarean delivery should have been performed immediately after the mother’s admission. Even if the cesarean had been begun 15 to 20 minutes earlier, the injury could have been avoided. The ObGyn never examined the mother nor did he participate in the cesarean delivery.
DEFENDANTS’ DEFENSE The ObGyn and hospital denied negligence. The note was not attached to the patient’s chart. At trial, the ObGyn admitted that a delivery 15 to 20 minutes earlier might have avoided the injury.
VERDICT A $33,591,900 Tennessee verdict was returned.
WOMAN BECOMES PREGNANT AFTER TUBAL LIGATION
A 32-year-old woman requested sterilization after the birth of her third child. A Falope ring tubal ligation procedure was performed by a gynecologist in April 2006. During surgery, the device used by the gynecologist ejected 2 silastic bands on the right side instead of one.
The patient learned she was pregnant in March 2007. Her high-risk pregnancy ended with cesarean delivery in September 2007. The delivering ObGyn found the patient’s right fallopian tube in its natural, unscarred state. A silastic band was applied to the right ovarian ligament, not the right fallopian tube.
PATIENT’S CLAIM The gynecologist banded the ovarian ligament instead of the fallopian tube.
PHYSICIAN’S DEFENSE The procedure was properly performed. The rings initially enclosed the fallopian tube and ovarian ligament, but the top ring subsequently migrated off the structures, allowing the fallopian tube to slip out of the attachment. Failure to sterilize is a known risk of the procedure.
VERDICT An Illinois defense verdict was returned.
ABORTION ATTEMPTED BUT PREGNANCY IS ECTOPIC
A 14-year-old patient went to a clinic for elective abortion at 8 weeks’ gestation. Ultrasonography (US) prior to the procedure showed an intrauterine pregnancy. After dilating the cervix, the ObGyn inserted a semi-rigid vacuum aspiration curette to suction the uterine contents, but received nothing. A second US confirmed an intrauterine pregnancy. The ObGyn was able to locate the pregnancy and indent the gestational sac with 3 different dilators and the curette. The pregnancy decreased in size on US after the suction was applied. However, the patient’s vital signs dropped dramatically, and she was rushed to the hospital. During emergency surgery, severe pelvic adhesive disease complicated the ability to stop the hemorrhage. Four physicians concurred that supracervical hysterectomy was needed to save the patient’s life. Postoperative pathology identified a cornual or interstitial ectopic pregnancy.
PATIENT’S CLAIM The ObGyn failed to heed several warning signs of ectopic pregnancy. Further testing should have been done before the second round of vacuum. If ectopic pregnancy had been discovered earlier, the patient could have undergone surgery that would have preserved her uterus and allowed her to bear children. The ObGyn tore the uterus multiple times when he turned on the suction, causing massive hemorrhage.
PHYSICIAN’S DEFENSE Ultrasonography clearly showed an intrauterine pregnancy. There was nothing to cause suspicion that the pregnancy was ectopic. She might be able to have a child through surrogacy.
VERDICT A $950,000 Illinois verdict was returned.
Related Article: Is the hCG discriminatory zone a reliable indicator of intrauterine or ectopic pregnancy? Andrew M. Kaunitz, MD (Examining the Evidence, February 2012)
MACROSOMIC FETUS: MOTHER AND BABY BOTH INJURED
When prenatal ultrasonography indicated the fetal weight was 10 lbs, the patient and her mother expressed concern over delivery of such a large baby. The ObGyn reassured them that it would not be a problem.
Four days later, the mother went into labor. She was 9-cm dilated 4.5 hours later, but only progressed to 9.5 cm over the next 7 hours. She was told to begin to push, but, after 2 hours, birth had not occurred. The ObGyn used forceps to deliver the head 45 minutes later. Shoulder dystocia was encountered and there was a 3.5-minute delivery delay. The baby suffered oxygen deprivation and the mother experienced a 4th-degree perineal tear.
After the NICU team resuscitated the baby, she was transferred to another hospital, where she underwent “head cooling” in an attempt to mitigate her injuries. The child has mild cerebral palsy, with right hemiparesis, speech delay, and additional neurologic injuries.
PARENTS' CLAIM Cesarean delivery was unnecessarily delayed. The ObGyn was negligent in not performing an emergency cesarean delivery after 2 hours of pushing was not effective. The ObGyn never suggested a cesarean delivery, it was not noted in the chart, and no one else present at the time remembered the option being offered.
PHYSICIAN’S DEFENSE There was nothing during labor to contraindicate a vaginal birth. The ObGyn claimed that he offered a cesarean delivery after 2 hours of pushing. The baby’s blood gas reading at delivery was normal. Any brain injuries to the baby were from resuscitation.
VERDICT A $4,080,500 Pennsylvania verdict was returned.
Related Articles:
When macrosomia is suspected at term, does induction of labor lower the risk of cesarean delivery? Jennifer T. Ahn, MD (Examining the Evidence, May 2012)
Develop and use a checklist for 3rd- and 4th-degree perinatal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
BOWEL INJURY DURING CESAREAN DELIVERY
During cesarean delivery, the mother suffered a bowel injury that led to infection and several abdominal abscesses. She required two procedures for drain placement plus two additional operations.
PATIENT’S CLAIM The ObGyn was negligent in how he performed the cesarean delivery and for not treating the injury and subsequent infection in a timely manner. The abscesses took 3 years to resolve; additional procedures left scarring and aggravated a spinal injury.
PHYSICIAN’S DEFENSE Bowel perforation is a known complication of cesarean delivery. It probably occurred during manipulation of the uterus in an area that was not visible.
VERDICT A $750,000 New Jersey verdict was returned.
Related Article: How to avoid intestinal and urinary tract injuries during gynecologic laparoscopy Michael Baggish, MD (Surgical Technique, October 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue.
Send your letter to: [email protected] Please include the city and state in which you practice.
Stay in touch! Your feedback is important to us!
PLACENTA FAILS TO DELIVER: MOTHER DIES OF HEMORRHAGE
After a 38-year-old woman gave birth, the placenta did not deliver. The ObGyn was unable remove the entire placenta and the mother began to hemorrhage. After an hour, the patient was given a blood transfusion. She could not be stabilized and died.
ESTATE’S CLAIM The ObGyn was negligent. He failed to remove the entire placenta and did not treat the hemorrhage in a timely manner. The hospital staff was negligent in failing to properly address the massive hemorrhage. A prompt transfusion would have saved the woman’s life, but the anesthesiologist who had to approve the procedure could not be located. Other procedures, including a hysterectomy, could have saved the mother’s life.
DEFENDANTS’ DEFENSE The ObGyn claimed that incomplete delivery of the placenta and postpartum hemorrhage are known complications of a delivery. The hospital claimed that the staff had acted appropriately and that it was not responsible for the actions of the anesthesiologist, an independent contractor. The anesthesiologist denied negligence.
VERDICT A $2 million New York settlement was reached that included $200,000 from the hospital and $1.8 million from the physicians’ insurers.
Related Article: Postpartum hemorrhage: 11 critical questions, answered by an expert Haywood L. Brown, MD (January 2011)
DECREASED FETAL MOVEMENT OVERLOOKED; SEVERE INJURY TO BABY
At her 39th-week prenatal visit at a clinic, the mother reported decreased fetal movement. Acoustic stimulation of the fetus was attempted twice without response. The fetal heart-rate monitor identified a normal heart rate without variability or accelerations. The mother was taken by wheelchair to the hospital next door. A note explaining the nonreassuring findings allegedly accompanied her.
The mother waited to be admitted. When a fetal heart-rate monitor was connected 30 minutes after admission, results were still nonreassuring.
A resident examined the mother 45 minutes later. He called the attending ObGyn, and they decided to postpone cesarean delivery because the mother had eaten breakfast.
When the fetal heart rate crashed 4 hours later, a second-year resident began emergency cesarean delivery. The ObGyn, who had never examined the patient, observed some of the procedure in the OR.
The baby was born with catastrophic brain damage, and has spastic quadriplegia cerebral palsy, feeding problems, and significant cognitive and developmental delays.
PARENTS’ CLAIM A cesarean delivery should have been performed immediately after the mother’s admission. Even if the cesarean had been begun 15 to 20 minutes earlier, the injury could have been avoided. The ObGyn never examined the mother nor did he participate in the cesarean delivery.
DEFENDANTS’ DEFENSE The ObGyn and hospital denied negligence. The note was not attached to the patient’s chart. At trial, the ObGyn admitted that a delivery 15 to 20 minutes earlier might have avoided the injury.
VERDICT A $33,591,900 Tennessee verdict was returned.
WOMAN BECOMES PREGNANT AFTER TUBAL LIGATION
A 32-year-old woman requested sterilization after the birth of her third child. A Falope ring tubal ligation procedure was performed by a gynecologist in April 2006. During surgery, the device used by the gynecologist ejected 2 silastic bands on the right side instead of one.
The patient learned she was pregnant in March 2007. Her high-risk pregnancy ended with cesarean delivery in September 2007. The delivering ObGyn found the patient’s right fallopian tube in its natural, unscarred state. A silastic band was applied to the right ovarian ligament, not the right fallopian tube.
PATIENT’S CLAIM The gynecologist banded the ovarian ligament instead of the fallopian tube.
PHYSICIAN’S DEFENSE The procedure was properly performed. The rings initially enclosed the fallopian tube and ovarian ligament, but the top ring subsequently migrated off the structures, allowing the fallopian tube to slip out of the attachment. Failure to sterilize is a known risk of the procedure.
VERDICT An Illinois defense verdict was returned.
ABORTION ATTEMPTED BUT PREGNANCY IS ECTOPIC
A 14-year-old patient went to a clinic for elective abortion at 8 weeks’ gestation. Ultrasonography (US) prior to the procedure showed an intrauterine pregnancy. After dilating the cervix, the ObGyn inserted a semi-rigid vacuum aspiration curette to suction the uterine contents, but received nothing. A second US confirmed an intrauterine pregnancy. The ObGyn was able to locate the pregnancy and indent the gestational sac with 3 different dilators and the curette. The pregnancy decreased in size on US after the suction was applied. However, the patient’s vital signs dropped dramatically, and she was rushed to the hospital. During emergency surgery, severe pelvic adhesive disease complicated the ability to stop the hemorrhage. Four physicians concurred that supracervical hysterectomy was needed to save the patient’s life. Postoperative pathology identified a cornual or interstitial ectopic pregnancy.
PATIENT’S CLAIM The ObGyn failed to heed several warning signs of ectopic pregnancy. Further testing should have been done before the second round of vacuum. If ectopic pregnancy had been discovered earlier, the patient could have undergone surgery that would have preserved her uterus and allowed her to bear children. The ObGyn tore the uterus multiple times when he turned on the suction, causing massive hemorrhage.
PHYSICIAN’S DEFENSE Ultrasonography clearly showed an intrauterine pregnancy. There was nothing to cause suspicion that the pregnancy was ectopic. She might be able to have a child through surrogacy.
VERDICT A $950,000 Illinois verdict was returned.
Related Article: Is the hCG discriminatory zone a reliable indicator of intrauterine or ectopic pregnancy? Andrew M. Kaunitz, MD (Examining the Evidence, February 2012)
MACROSOMIC FETUS: MOTHER AND BABY BOTH INJURED
When prenatal ultrasonography indicated the fetal weight was 10 lbs, the patient and her mother expressed concern over delivery of such a large baby. The ObGyn reassured them that it would not be a problem.
Four days later, the mother went into labor. She was 9-cm dilated 4.5 hours later, but only progressed to 9.5 cm over the next 7 hours. She was told to begin to push, but, after 2 hours, birth had not occurred. The ObGyn used forceps to deliver the head 45 minutes later. Shoulder dystocia was encountered and there was a 3.5-minute delivery delay. The baby suffered oxygen deprivation and the mother experienced a 4th-degree perineal tear.
After the NICU team resuscitated the baby, she was transferred to another hospital, where she underwent “head cooling” in an attempt to mitigate her injuries. The child has mild cerebral palsy, with right hemiparesis, speech delay, and additional neurologic injuries.
PARENTS' CLAIM Cesarean delivery was unnecessarily delayed. The ObGyn was negligent in not performing an emergency cesarean delivery after 2 hours of pushing was not effective. The ObGyn never suggested a cesarean delivery, it was not noted in the chart, and no one else present at the time remembered the option being offered.
PHYSICIAN’S DEFENSE There was nothing during labor to contraindicate a vaginal birth. The ObGyn claimed that he offered a cesarean delivery after 2 hours of pushing. The baby’s blood gas reading at delivery was normal. Any brain injuries to the baby were from resuscitation.
VERDICT A $4,080,500 Pennsylvania verdict was returned.
Related Articles:
When macrosomia is suspected at term, does induction of labor lower the risk of cesarean delivery? Jennifer T. Ahn, MD (Examining the Evidence, May 2012)
Develop and use a checklist for 3rd- and 4th-degree perinatal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
BOWEL INJURY DURING CESAREAN DELIVERY
During cesarean delivery, the mother suffered a bowel injury that led to infection and several abdominal abscesses. She required two procedures for drain placement plus two additional operations.
PATIENT’S CLAIM The ObGyn was negligent in how he performed the cesarean delivery and for not treating the injury and subsequent infection in a timely manner. The abscesses took 3 years to resolve; additional procedures left scarring and aggravated a spinal injury.
PHYSICIAN’S DEFENSE Bowel perforation is a known complication of cesarean delivery. It probably occurred during manipulation of the uterus in an area that was not visible.
VERDICT A $750,000 New Jersey verdict was returned.
Related Article: How to avoid intestinal and urinary tract injuries during gynecologic laparoscopy Michael Baggish, MD (Surgical Technique, October 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue.
Send your letter to: [email protected] Please include the city and state in which you practice.
Stay in touch! Your feedback is important to us!
PLACENTA FAILS TO DELIVER: MOTHER DIES OF HEMORRHAGE
After a 38-year-old woman gave birth, the placenta did not deliver. The ObGyn was unable remove the entire placenta and the mother began to hemorrhage. After an hour, the patient was given a blood transfusion. She could not be stabilized and died.
ESTATE’S CLAIM The ObGyn was negligent. He failed to remove the entire placenta and did not treat the hemorrhage in a timely manner. The hospital staff was negligent in failing to properly address the massive hemorrhage. A prompt transfusion would have saved the woman’s life, but the anesthesiologist who had to approve the procedure could not be located. Other procedures, including a hysterectomy, could have saved the mother’s life.
DEFENDANTS’ DEFENSE The ObGyn claimed that incomplete delivery of the placenta and postpartum hemorrhage are known complications of a delivery. The hospital claimed that the staff had acted appropriately and that it was not responsible for the actions of the anesthesiologist, an independent contractor. The anesthesiologist denied negligence.
VERDICT A $2 million New York settlement was reached that included $200,000 from the hospital and $1.8 million from the physicians’ insurers.
Related Article: Postpartum hemorrhage: 11 critical questions, answered by an expert Haywood L. Brown, MD (January 2011)
DECREASED FETAL MOVEMENT OVERLOOKED; SEVERE INJURY TO BABY
At her 39th-week prenatal visit at a clinic, the mother reported decreased fetal movement. Acoustic stimulation of the fetus was attempted twice without response. The fetal heart-rate monitor identified a normal heart rate without variability or accelerations. The mother was taken by wheelchair to the hospital next door. A note explaining the nonreassuring findings allegedly accompanied her.
The mother waited to be admitted. When a fetal heart-rate monitor was connected 30 minutes after admission, results were still nonreassuring.
A resident examined the mother 45 minutes later. He called the attending ObGyn, and they decided to postpone cesarean delivery because the mother had eaten breakfast.
When the fetal heart rate crashed 4 hours later, a second-year resident began emergency cesarean delivery. The ObGyn, who had never examined the patient, observed some of the procedure in the OR.
The baby was born with catastrophic brain damage, and has spastic quadriplegia cerebral palsy, feeding problems, and significant cognitive and developmental delays.
PARENTS’ CLAIM A cesarean delivery should have been performed immediately after the mother’s admission. Even if the cesarean had been begun 15 to 20 minutes earlier, the injury could have been avoided. The ObGyn never examined the mother nor did he participate in the cesarean delivery.
DEFENDANTS’ DEFENSE The ObGyn and hospital denied negligence. The note was not attached to the patient’s chart. At trial, the ObGyn admitted that a delivery 15 to 20 minutes earlier might have avoided the injury.
VERDICT A $33,591,900 Tennessee verdict was returned.
WOMAN BECOMES PREGNANT AFTER TUBAL LIGATION
A 32-year-old woman requested sterilization after the birth of her third child. A Falope ring tubal ligation procedure was performed by a gynecologist in April 2006. During surgery, the device used by the gynecologist ejected 2 silastic bands on the right side instead of one.
The patient learned she was pregnant in March 2007. Her high-risk pregnancy ended with cesarean delivery in September 2007. The delivering ObGyn found the patient’s right fallopian tube in its natural, unscarred state. A silastic band was applied to the right ovarian ligament, not the right fallopian tube.
PATIENT’S CLAIM The gynecologist banded the ovarian ligament instead of the fallopian tube.
PHYSICIAN’S DEFENSE The procedure was properly performed. The rings initially enclosed the fallopian tube and ovarian ligament, but the top ring subsequently migrated off the structures, allowing the fallopian tube to slip out of the attachment. Failure to sterilize is a known risk of the procedure.
VERDICT An Illinois defense verdict was returned.
ABORTION ATTEMPTED BUT PREGNANCY IS ECTOPIC
A 14-year-old patient went to a clinic for elective abortion at 8 weeks’ gestation. Ultrasonography (US) prior to the procedure showed an intrauterine pregnancy. After dilating the cervix, the ObGyn inserted a semi-rigid vacuum aspiration curette to suction the uterine contents, but received nothing. A second US confirmed an intrauterine pregnancy. The ObGyn was able to locate the pregnancy and indent the gestational sac with 3 different dilators and the curette. The pregnancy decreased in size on US after the suction was applied. However, the patient’s vital signs dropped dramatically, and she was rushed to the hospital. During emergency surgery, severe pelvic adhesive disease complicated the ability to stop the hemorrhage. Four physicians concurred that supracervical hysterectomy was needed to save the patient’s life. Postoperative pathology identified a cornual or interstitial ectopic pregnancy.
PATIENT’S CLAIM The ObGyn failed to heed several warning signs of ectopic pregnancy. Further testing should have been done before the second round of vacuum. If ectopic pregnancy had been discovered earlier, the patient could have undergone surgery that would have preserved her uterus and allowed her to bear children. The ObGyn tore the uterus multiple times when he turned on the suction, causing massive hemorrhage.
PHYSICIAN’S DEFENSE Ultrasonography clearly showed an intrauterine pregnancy. There was nothing to cause suspicion that the pregnancy was ectopic. She might be able to have a child through surrogacy.
VERDICT A $950,000 Illinois verdict was returned.
Related Article: Is the hCG discriminatory zone a reliable indicator of intrauterine or ectopic pregnancy? Andrew M. Kaunitz, MD (Examining the Evidence, February 2012)
MACROSOMIC FETUS: MOTHER AND BABY BOTH INJURED
When prenatal ultrasonography indicated the fetal weight was 10 lbs, the patient and her mother expressed concern over delivery of such a large baby. The ObGyn reassured them that it would not be a problem.
Four days later, the mother went into labor. She was 9-cm dilated 4.5 hours later, but only progressed to 9.5 cm over the next 7 hours. She was told to begin to push, but, after 2 hours, birth had not occurred. The ObGyn used forceps to deliver the head 45 minutes later. Shoulder dystocia was encountered and there was a 3.5-minute delivery delay. The baby suffered oxygen deprivation and the mother experienced a 4th-degree perineal tear.
After the NICU team resuscitated the baby, she was transferred to another hospital, where she underwent “head cooling” in an attempt to mitigate her injuries. The child has mild cerebral palsy, with right hemiparesis, speech delay, and additional neurologic injuries.
PARENTS' CLAIM Cesarean delivery was unnecessarily delayed. The ObGyn was negligent in not performing an emergency cesarean delivery after 2 hours of pushing was not effective. The ObGyn never suggested a cesarean delivery, it was not noted in the chart, and no one else present at the time remembered the option being offered.
PHYSICIAN’S DEFENSE There was nothing during labor to contraindicate a vaginal birth. The ObGyn claimed that he offered a cesarean delivery after 2 hours of pushing. The baby’s blood gas reading at delivery was normal. Any brain injuries to the baby were from resuscitation.
VERDICT A $4,080,500 Pennsylvania verdict was returned.
Related Articles:
When macrosomia is suspected at term, does induction of labor lower the risk of cesarean delivery? Jennifer T. Ahn, MD (Examining the Evidence, May 2012)
Develop and use a checklist for 3rd- and 4th-degree perinatal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
BOWEL INJURY DURING CESAREAN DELIVERY
During cesarean delivery, the mother suffered a bowel injury that led to infection and several abdominal abscesses. She required two procedures for drain placement plus two additional operations.
PATIENT’S CLAIM The ObGyn was negligent in how he performed the cesarean delivery and for not treating the injury and subsequent infection in a timely manner. The abscesses took 3 years to resolve; additional procedures left scarring and aggravated a spinal injury.
PHYSICIAN’S DEFENSE Bowel perforation is a known complication of cesarean delivery. It probably occurred during manipulation of the uterus in an area that was not visible.
VERDICT A $750,000 New Jersey verdict was returned.
Related Article: How to avoid intestinal and urinary tract injuries during gynecologic laparoscopy Michael Baggish, MD (Surgical Technique, October 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue.
Send your letter to: [email protected] Please include the city and state in which you practice.
Stay in touch! Your feedback is important to us!
What Physicians Should Know About Buying into Hospitalist Practice
Physicians who join a hospitalist practice often have the opportunity to purchase an equity interest after some period of employment. The future possibility of the physician-employee becoming an owner of the practice is sometimes addressed in the physician’s employment agreement. The amount of detail in the employment agreement regarding potential ownership will vary depending on the practice and the negotiating power of the individual physician. Clearly, the more specificity found in the contract, the better the hospitalist is served.
Because the circumstances of the individual parties will govern the terms of the buy-in, there is no standard contract language universally used in physician employment agreements. Specific aspects exist in many buy-in provisions contained in physician employment agreements, however. Such issues include: (i) the opportunity to purchase an ownership interest; (ii) performance reviews; (iii) how the interest will be valued; and (iv) payment terms.
Ownership Interest
The employment agreement should specify whether and when the employee-physician will be eligible to acquire an interest in the practice. The idea of remaining an employee may be attractive to some physicians who prefer to have less involvement in the business and financial aspects of the hospitalist practice. Sometimes cost becomes a critical issue.
However, if the parties do intend for the physician to have the right to purchase an ownership interest, the timeframe and conditions for exercising that right should be specified in writing. The following is an example of a provision addressing the opportunity to purchase an equity interest:
“The parties agree that it is their intent that upon X years of continuous employment pursuant to the terms and conditions of this Agreement, Hospitalist shall be given the opportunity to purchase [a partnership interest or stock] in Practice.”
Performance Reviews
One condition precedent to the right to purchase an equity interest may be satisfactory performance reviews by senior physicians. Although these reviews frequently are based on subjective standards, the employee-physician should seek a contractual commitment describing the criteria to be evaluated in order to make the reviews as objective as possible. Standard criteria include statistical analysis (e.g. number of patients seen a day), the quality of patient care rendered, and contributions to the practice’s operations (e.g. marketing, community outreach).
In addition, the physician’s employment agreement should specify the frequency of performance reviews. Physician reviews commonly occur on an annual, and sometimes semi-annual, basis, especially during the initial years of employment. Regardless of how often the reviews are conducted, it is highly beneficial to both the practice and the physician-employee that the time periods for evaluations be strictly enforced. Consistent, formal performance reviews promote improvement and synergy between the physician and the practice.
Equity Interest
Typically, an employment agreement will either provide an exact purchase price or, more often, state the future method to be used for calculating the buy-in price. Ordinarily, the buy-in price will be a function of the valuation of the total equity of the practice and the percentage of that equity, which is represented by the interests to be acquired by the purchasing physician. While there are a few formulas for valuing the equity of a hospitalist practice, the most common method is discounted present value of net revenue stream.
The appropriate valuation method will depend on a number of factors unique to the individual practice. Therefore, the practice should seek the assistance of an accountant or practice valuation specialist when determining the value. Stating an agreed-upon valuation method in the employment agreement will limit surprises and “sticker shock” to the buy-in price when the ownership decision is made down the road.
Payment Terms
In the event that the physician-employee exercises the opportunity to buy in, the employment or purchase agreement should provide terms governing how the purchase price will be paid. Often, the practice will be flexible in negotiating payment terms that meet the physician’s individual financial needs; however, the parties frequently agree that the physician will either pay the owners in full up front or make installment payments over a specified number of years.
If the physician is required to pay the total purchase price up front, he or she will be personally responsible for obtaining the necessary funding through bank loans or other sources. If the purchasing physician is permitted to make installment payments, he or she will be required to sign a promissory note in which the payee is the practice and the note is secured by a security interest in the equity granted to the physician. There are important tax strategies that can be implemented when installment payments are agreed upon. In the event that the physician fails to make the installment payments, the practice may be able to recover the equity interest.
In Sum
Both parties should review and understand the terms and conditions of the buy-in so that all parties enter the employment relationship with the same expectations for future ownership.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Physicians who join a hospitalist practice often have the opportunity to purchase an equity interest after some period of employment. The future possibility of the physician-employee becoming an owner of the practice is sometimes addressed in the physician’s employment agreement. The amount of detail in the employment agreement regarding potential ownership will vary depending on the practice and the negotiating power of the individual physician. Clearly, the more specificity found in the contract, the better the hospitalist is served.
Because the circumstances of the individual parties will govern the terms of the buy-in, there is no standard contract language universally used in physician employment agreements. Specific aspects exist in many buy-in provisions contained in physician employment agreements, however. Such issues include: (i) the opportunity to purchase an ownership interest; (ii) performance reviews; (iii) how the interest will be valued; and (iv) payment terms.
Ownership Interest
The employment agreement should specify whether and when the employee-physician will be eligible to acquire an interest in the practice. The idea of remaining an employee may be attractive to some physicians who prefer to have less involvement in the business and financial aspects of the hospitalist practice. Sometimes cost becomes a critical issue.
However, if the parties do intend for the physician to have the right to purchase an ownership interest, the timeframe and conditions for exercising that right should be specified in writing. The following is an example of a provision addressing the opportunity to purchase an equity interest:
“The parties agree that it is their intent that upon X years of continuous employment pursuant to the terms and conditions of this Agreement, Hospitalist shall be given the opportunity to purchase [a partnership interest or stock] in Practice.”
Performance Reviews
One condition precedent to the right to purchase an equity interest may be satisfactory performance reviews by senior physicians. Although these reviews frequently are based on subjective standards, the employee-physician should seek a contractual commitment describing the criteria to be evaluated in order to make the reviews as objective as possible. Standard criteria include statistical analysis (e.g. number of patients seen a day), the quality of patient care rendered, and contributions to the practice’s operations (e.g. marketing, community outreach).
In addition, the physician’s employment agreement should specify the frequency of performance reviews. Physician reviews commonly occur on an annual, and sometimes semi-annual, basis, especially during the initial years of employment. Regardless of how often the reviews are conducted, it is highly beneficial to both the practice and the physician-employee that the time periods for evaluations be strictly enforced. Consistent, formal performance reviews promote improvement and synergy between the physician and the practice.
Equity Interest
Typically, an employment agreement will either provide an exact purchase price or, more often, state the future method to be used for calculating the buy-in price. Ordinarily, the buy-in price will be a function of the valuation of the total equity of the practice and the percentage of that equity, which is represented by the interests to be acquired by the purchasing physician. While there are a few formulas for valuing the equity of a hospitalist practice, the most common method is discounted present value of net revenue stream.
The appropriate valuation method will depend on a number of factors unique to the individual practice. Therefore, the practice should seek the assistance of an accountant or practice valuation specialist when determining the value. Stating an agreed-upon valuation method in the employment agreement will limit surprises and “sticker shock” to the buy-in price when the ownership decision is made down the road.
Payment Terms
In the event that the physician-employee exercises the opportunity to buy in, the employment or purchase agreement should provide terms governing how the purchase price will be paid. Often, the practice will be flexible in negotiating payment terms that meet the physician’s individual financial needs; however, the parties frequently agree that the physician will either pay the owners in full up front or make installment payments over a specified number of years.
If the physician is required to pay the total purchase price up front, he or she will be personally responsible for obtaining the necessary funding through bank loans or other sources. If the purchasing physician is permitted to make installment payments, he or she will be required to sign a promissory note in which the payee is the practice and the note is secured by a security interest in the equity granted to the physician. There are important tax strategies that can be implemented when installment payments are agreed upon. In the event that the physician fails to make the installment payments, the practice may be able to recover the equity interest.
In Sum
Both parties should review and understand the terms and conditions of the buy-in so that all parties enter the employment relationship with the same expectations for future ownership.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Physicians who join a hospitalist practice often have the opportunity to purchase an equity interest after some period of employment. The future possibility of the physician-employee becoming an owner of the practice is sometimes addressed in the physician’s employment agreement. The amount of detail in the employment agreement regarding potential ownership will vary depending on the practice and the negotiating power of the individual physician. Clearly, the more specificity found in the contract, the better the hospitalist is served.
Because the circumstances of the individual parties will govern the terms of the buy-in, there is no standard contract language universally used in physician employment agreements. Specific aspects exist in many buy-in provisions contained in physician employment agreements, however. Such issues include: (i) the opportunity to purchase an ownership interest; (ii) performance reviews; (iii) how the interest will be valued; and (iv) payment terms.
Ownership Interest
The employment agreement should specify whether and when the employee-physician will be eligible to acquire an interest in the practice. The idea of remaining an employee may be attractive to some physicians who prefer to have less involvement in the business and financial aspects of the hospitalist practice. Sometimes cost becomes a critical issue.
However, if the parties do intend for the physician to have the right to purchase an ownership interest, the timeframe and conditions for exercising that right should be specified in writing. The following is an example of a provision addressing the opportunity to purchase an equity interest:
“The parties agree that it is their intent that upon X years of continuous employment pursuant to the terms and conditions of this Agreement, Hospitalist shall be given the opportunity to purchase [a partnership interest or stock] in Practice.”
Performance Reviews
One condition precedent to the right to purchase an equity interest may be satisfactory performance reviews by senior physicians. Although these reviews frequently are based on subjective standards, the employee-physician should seek a contractual commitment describing the criteria to be evaluated in order to make the reviews as objective as possible. Standard criteria include statistical analysis (e.g. number of patients seen a day), the quality of patient care rendered, and contributions to the practice’s operations (e.g. marketing, community outreach).
In addition, the physician’s employment agreement should specify the frequency of performance reviews. Physician reviews commonly occur on an annual, and sometimes semi-annual, basis, especially during the initial years of employment. Regardless of how often the reviews are conducted, it is highly beneficial to both the practice and the physician-employee that the time periods for evaluations be strictly enforced. Consistent, formal performance reviews promote improvement and synergy between the physician and the practice.
Equity Interest
Typically, an employment agreement will either provide an exact purchase price or, more often, state the future method to be used for calculating the buy-in price. Ordinarily, the buy-in price will be a function of the valuation of the total equity of the practice and the percentage of that equity, which is represented by the interests to be acquired by the purchasing physician. While there are a few formulas for valuing the equity of a hospitalist practice, the most common method is discounted present value of net revenue stream.
The appropriate valuation method will depend on a number of factors unique to the individual practice. Therefore, the practice should seek the assistance of an accountant or practice valuation specialist when determining the value. Stating an agreed-upon valuation method in the employment agreement will limit surprises and “sticker shock” to the buy-in price when the ownership decision is made down the road.
Payment Terms
In the event that the physician-employee exercises the opportunity to buy in, the employment or purchase agreement should provide terms governing how the purchase price will be paid. Often, the practice will be flexible in negotiating payment terms that meet the physician’s individual financial needs; however, the parties frequently agree that the physician will either pay the owners in full up front or make installment payments over a specified number of years.
If the physician is required to pay the total purchase price up front, he or she will be personally responsible for obtaining the necessary funding through bank loans or other sources. If the purchasing physician is permitted to make installment payments, he or she will be required to sign a promissory note in which the payee is the practice and the note is secured by a security interest in the equity granted to the physician. There are important tax strategies that can be implemented when installment payments are agreed upon. In the event that the physician fails to make the installment payments, the practice may be able to recover the equity interest.
In Sum
Both parties should review and understand the terms and conditions of the buy-in so that all parties enter the employment relationship with the same expectations for future ownership.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Tips for Landing Your First Job in Hospital Medicine
Finding the right hospitalist position can help make the transition from resident to attending enjoyable as you adjust to a new level of responsibility. But the wrong job can leave you feeling overwhelmed and unsupported. So what is a busy senior resident to do? Here we offer selected pearls and pitfalls to help you find a great position.
Initial Steps and Things to Consider
Start applying in the fall of your PGY-3 year. The process of interviewing applicants, finalizing contracts, arranging for hospital privileges, and enrolling a new hire in insurance plans can take many months. Many employers start looking early.
Meet with your residency program director and your hospitalist group director to discuss your plans. They can help you clarify your goals, serving as coaches throughout the process, and they may know people at the places you are interested in. Recruiters can be helpful, but remember—many are incentivized to find you a position. Advertisements in the back of journals and professional society publications are useful resources.
Obtain your medical license as early as possible. Getting licensed in the state you will be working in can be much faster if you already have a license from another state. Applicants have lost positions because they didn’t have their medical license in time.
Don’t shop for a job based on schedule and salary alone. There are reasons some jobs pay better than most, and they aren’t always good (home call, for example). A seven-on, seven-off schedule affords a lot of free time, but while you are on service, family life often takes a back seat. Conversely, working every Monday to Friday offers less free time for travel or moonlighting.
Think about the care model you prefer. Do you want to work with residents, physician assistants, nurse practitioners, or in a “direct care” model where it’s just you and the nurses caring for patients? Salaries often are inversely related to the number of providers between you and the patients. Positions without resident support might require procedural competence. Demonstrating academic productivity, especially in the area of quality improvement or patient safety, can help you secure a position working with residents. Some programs first place new hires on the non-teaching service to earn the chance to work with residents and medical students.
Think about what type of career you want. Do you only want to see patients, or do you want a career that includes a non-clinical role for which you will be paid? Some hospitalists find that becoming a patient safety officer or residency program director, trying out a medical student clerkship, or growing into another administrative role is a great complement to their clinical time and prevents burnout.
How to Stand Out
Start off by getting the basics right. Make sure your e-mail address sounds professional. A well-formatted CV, with no spelling errors or unexplained time gaps, is a must. A cover letter that succinctly describes the type of position you are looking for, highlights your strengths, and does not wax on about why you wanted to become a doctor—that was your personal statement for med school—is helpful. Don’t correspond with employers using your smartphone if you’re prone to autocorrect or spelling errors, or if you tend to write too casually from a mobile device. Before you shoot off that immediate e-mail response, make sure you’re addressing people properly and not mixing up employers.
Join SHM (they have trainee rates!), and attend an SHM conference or local chapter meeting if you can (www.hospitalmedicine.org/events). SHM membership reflects your commitment to the specialty. Membership in other professional societies is a plus as well.
Quality improvement (QI), patient safety, and patient satisfaction are central to hospital medicine. Medication reconciliation, infection control, handoff, transitions of care, listening carefully to patients, and explaining things to them are likely things you’ve done throughout residency. Communicate to employers your experience in and appreciation of these areas. Completing a QI or patient safety project and participating on a hospital committee will help make you a competitive applicant.
Interview Do’s and Don’ts
The advice most were given when applying to residency still holds. Be on time, dress professionally, research the program, and be prepared to speak about why you want to work at a particular place. Speak to hospitalists in the group, and be very courteous to everyone.
Don’t start off by asking about salary—if you move along in the process, compensation will be discussed. Get a clear picture of the schedule and how time off/non-clinical time occurs, but don’t come off as inflexible or too needy.
Ask why hospitalists have left a group. Frequent turnover without good reason could be a red flag. If the hospitalist director and/or department chair are new or will be leaving, you should ask how that might affect the group. If the current leadership has been stable, ask what growth has occurred for the group overall and among individuals during their tenure.
Find out whether hospitalists have been promoted academically and if there are career growth opportunities in areas you are interested in. Try to determine if the group has a “voice” with administration by asking for examples of how hospitalist concerns have been positively addressed.
Having a clear picture of how much nursing, social work, case management, subspecialist, and intensivist support is available is critical. Whether billing is done electronically or on paper is important, as is the degree of instruction and support for billing.
Take the opportunity to meet the current hospitalists—and note that their input often is solicited as to whether or not to hire a candidate—and ask them questions away from the ears of the program leadership; most hospitalists like to meet potential colleagues.
Closing the Deal
If you make it past the interview stage, be sure additional deliverables, such as letters of recommendation, are on time. Now is the time to ask about salary. Don’t be afraid to inquire about relocation or sign-on bonuses. At this point, the employer likes you and has invested time in recruiting you. You can gently leverage this in your negotiations. Consult your program director or other mentors at this point—they can provide guidance.
If you are uncertain about accepting an offer, be open about this with the employer. Your honesty in the process is essential, will be viewed positively, and can trigger additional dialogue that may help you decide. Juggling multiple offers dishonestly is not ethical and can backfire, as many hospitalist directors know each other.
Have an attorney familiar with physician contracts review yours. Look at whether “tail coverage,” which insures legal actions brought against you after you have left, is provided. Take note of “non-compete” clauses; they may limit your ability to practice in the area if you leave a practice. Find out if moonlighting is allowed and if the hospital requires you to give them a percentage of your outside earnings.
If you secure a position, whether as a career hospitalist or just for a year or two before fellowship, you should be excited. HM is a wonderful field with tremendous and varied opportunities. Dive in, enjoy, and explore everything it has to offer!
Dr. Bryson is medical director of teaching services, associate program director of internal medicine residency, and assistant professor at Tufts University, and a hospitalist at Baystate Medical Center in Springfield, Mass. Dr. Steinberg is residency program director in the Department of Medicine at Beth Israel Medical Center, and associate professor of medicine at the Icahn School of Medicine at Mount Sinai in New York City. Both are members of SHM’s Physicians in Training Committee.
Finding the right hospitalist position can help make the transition from resident to attending enjoyable as you adjust to a new level of responsibility. But the wrong job can leave you feeling overwhelmed and unsupported. So what is a busy senior resident to do? Here we offer selected pearls and pitfalls to help you find a great position.
Initial Steps and Things to Consider
Start applying in the fall of your PGY-3 year. The process of interviewing applicants, finalizing contracts, arranging for hospital privileges, and enrolling a new hire in insurance plans can take many months. Many employers start looking early.
Meet with your residency program director and your hospitalist group director to discuss your plans. They can help you clarify your goals, serving as coaches throughout the process, and they may know people at the places you are interested in. Recruiters can be helpful, but remember—many are incentivized to find you a position. Advertisements in the back of journals and professional society publications are useful resources.
Obtain your medical license as early as possible. Getting licensed in the state you will be working in can be much faster if you already have a license from another state. Applicants have lost positions because they didn’t have their medical license in time.
Don’t shop for a job based on schedule and salary alone. There are reasons some jobs pay better than most, and they aren’t always good (home call, for example). A seven-on, seven-off schedule affords a lot of free time, but while you are on service, family life often takes a back seat. Conversely, working every Monday to Friday offers less free time for travel or moonlighting.
Think about the care model you prefer. Do you want to work with residents, physician assistants, nurse practitioners, or in a “direct care” model where it’s just you and the nurses caring for patients? Salaries often are inversely related to the number of providers between you and the patients. Positions without resident support might require procedural competence. Demonstrating academic productivity, especially in the area of quality improvement or patient safety, can help you secure a position working with residents. Some programs first place new hires on the non-teaching service to earn the chance to work with residents and medical students.
Think about what type of career you want. Do you only want to see patients, or do you want a career that includes a non-clinical role for which you will be paid? Some hospitalists find that becoming a patient safety officer or residency program director, trying out a medical student clerkship, or growing into another administrative role is a great complement to their clinical time and prevents burnout.
How to Stand Out
Start off by getting the basics right. Make sure your e-mail address sounds professional. A well-formatted CV, with no spelling errors or unexplained time gaps, is a must. A cover letter that succinctly describes the type of position you are looking for, highlights your strengths, and does not wax on about why you wanted to become a doctor—that was your personal statement for med school—is helpful. Don’t correspond with employers using your smartphone if you’re prone to autocorrect or spelling errors, or if you tend to write too casually from a mobile device. Before you shoot off that immediate e-mail response, make sure you’re addressing people properly and not mixing up employers.
Join SHM (they have trainee rates!), and attend an SHM conference or local chapter meeting if you can (www.hospitalmedicine.org/events). SHM membership reflects your commitment to the specialty. Membership in other professional societies is a plus as well.
Quality improvement (QI), patient safety, and patient satisfaction are central to hospital medicine. Medication reconciliation, infection control, handoff, transitions of care, listening carefully to patients, and explaining things to them are likely things you’ve done throughout residency. Communicate to employers your experience in and appreciation of these areas. Completing a QI or patient safety project and participating on a hospital committee will help make you a competitive applicant.
Interview Do’s and Don’ts
The advice most were given when applying to residency still holds. Be on time, dress professionally, research the program, and be prepared to speak about why you want to work at a particular place. Speak to hospitalists in the group, and be very courteous to everyone.
Don’t start off by asking about salary—if you move along in the process, compensation will be discussed. Get a clear picture of the schedule and how time off/non-clinical time occurs, but don’t come off as inflexible or too needy.
Ask why hospitalists have left a group. Frequent turnover without good reason could be a red flag. If the hospitalist director and/or department chair are new or will be leaving, you should ask how that might affect the group. If the current leadership has been stable, ask what growth has occurred for the group overall and among individuals during their tenure.
Find out whether hospitalists have been promoted academically and if there are career growth opportunities in areas you are interested in. Try to determine if the group has a “voice” with administration by asking for examples of how hospitalist concerns have been positively addressed.
Having a clear picture of how much nursing, social work, case management, subspecialist, and intensivist support is available is critical. Whether billing is done electronically or on paper is important, as is the degree of instruction and support for billing.
Take the opportunity to meet the current hospitalists—and note that their input often is solicited as to whether or not to hire a candidate—and ask them questions away from the ears of the program leadership; most hospitalists like to meet potential colleagues.
Closing the Deal
If you make it past the interview stage, be sure additional deliverables, such as letters of recommendation, are on time. Now is the time to ask about salary. Don’t be afraid to inquire about relocation or sign-on bonuses. At this point, the employer likes you and has invested time in recruiting you. You can gently leverage this in your negotiations. Consult your program director or other mentors at this point—they can provide guidance.
If you are uncertain about accepting an offer, be open about this with the employer. Your honesty in the process is essential, will be viewed positively, and can trigger additional dialogue that may help you decide. Juggling multiple offers dishonestly is not ethical and can backfire, as many hospitalist directors know each other.
Have an attorney familiar with physician contracts review yours. Look at whether “tail coverage,” which insures legal actions brought against you after you have left, is provided. Take note of “non-compete” clauses; they may limit your ability to practice in the area if you leave a practice. Find out if moonlighting is allowed and if the hospital requires you to give them a percentage of your outside earnings.
If you secure a position, whether as a career hospitalist or just for a year or two before fellowship, you should be excited. HM is a wonderful field with tremendous and varied opportunities. Dive in, enjoy, and explore everything it has to offer!
Dr. Bryson is medical director of teaching services, associate program director of internal medicine residency, and assistant professor at Tufts University, and a hospitalist at Baystate Medical Center in Springfield, Mass. Dr. Steinberg is residency program director in the Department of Medicine at Beth Israel Medical Center, and associate professor of medicine at the Icahn School of Medicine at Mount Sinai in New York City. Both are members of SHM’s Physicians in Training Committee.
Finding the right hospitalist position can help make the transition from resident to attending enjoyable as you adjust to a new level of responsibility. But the wrong job can leave you feeling overwhelmed and unsupported. So what is a busy senior resident to do? Here we offer selected pearls and pitfalls to help you find a great position.
Initial Steps and Things to Consider
Start applying in the fall of your PGY-3 year. The process of interviewing applicants, finalizing contracts, arranging for hospital privileges, and enrolling a new hire in insurance plans can take many months. Many employers start looking early.
Meet with your residency program director and your hospitalist group director to discuss your plans. They can help you clarify your goals, serving as coaches throughout the process, and they may know people at the places you are interested in. Recruiters can be helpful, but remember—many are incentivized to find you a position. Advertisements in the back of journals and professional society publications are useful resources.
Obtain your medical license as early as possible. Getting licensed in the state you will be working in can be much faster if you already have a license from another state. Applicants have lost positions because they didn’t have their medical license in time.
Don’t shop for a job based on schedule and salary alone. There are reasons some jobs pay better than most, and they aren’t always good (home call, for example). A seven-on, seven-off schedule affords a lot of free time, but while you are on service, family life often takes a back seat. Conversely, working every Monday to Friday offers less free time for travel or moonlighting.
Think about the care model you prefer. Do you want to work with residents, physician assistants, nurse practitioners, or in a “direct care” model where it’s just you and the nurses caring for patients? Salaries often are inversely related to the number of providers between you and the patients. Positions without resident support might require procedural competence. Demonstrating academic productivity, especially in the area of quality improvement or patient safety, can help you secure a position working with residents. Some programs first place new hires on the non-teaching service to earn the chance to work with residents and medical students.
Think about what type of career you want. Do you only want to see patients, or do you want a career that includes a non-clinical role for which you will be paid? Some hospitalists find that becoming a patient safety officer or residency program director, trying out a medical student clerkship, or growing into another administrative role is a great complement to their clinical time and prevents burnout.
How to Stand Out
Start off by getting the basics right. Make sure your e-mail address sounds professional. A well-formatted CV, with no spelling errors or unexplained time gaps, is a must. A cover letter that succinctly describes the type of position you are looking for, highlights your strengths, and does not wax on about why you wanted to become a doctor—that was your personal statement for med school—is helpful. Don’t correspond with employers using your smartphone if you’re prone to autocorrect or spelling errors, or if you tend to write too casually from a mobile device. Before you shoot off that immediate e-mail response, make sure you’re addressing people properly and not mixing up employers.
Join SHM (they have trainee rates!), and attend an SHM conference or local chapter meeting if you can (www.hospitalmedicine.org/events). SHM membership reflects your commitment to the specialty. Membership in other professional societies is a plus as well.
Quality improvement (QI), patient safety, and patient satisfaction are central to hospital medicine. Medication reconciliation, infection control, handoff, transitions of care, listening carefully to patients, and explaining things to them are likely things you’ve done throughout residency. Communicate to employers your experience in and appreciation of these areas. Completing a QI or patient safety project and participating on a hospital committee will help make you a competitive applicant.
Interview Do’s and Don’ts
The advice most were given when applying to residency still holds. Be on time, dress professionally, research the program, and be prepared to speak about why you want to work at a particular place. Speak to hospitalists in the group, and be very courteous to everyone.
Don’t start off by asking about salary—if you move along in the process, compensation will be discussed. Get a clear picture of the schedule and how time off/non-clinical time occurs, but don’t come off as inflexible or too needy.
Ask why hospitalists have left a group. Frequent turnover without good reason could be a red flag. If the hospitalist director and/or department chair are new or will be leaving, you should ask how that might affect the group. If the current leadership has been stable, ask what growth has occurred for the group overall and among individuals during their tenure.
Find out whether hospitalists have been promoted academically and if there are career growth opportunities in areas you are interested in. Try to determine if the group has a “voice” with administration by asking for examples of how hospitalist concerns have been positively addressed.
Having a clear picture of how much nursing, social work, case management, subspecialist, and intensivist support is available is critical. Whether billing is done electronically or on paper is important, as is the degree of instruction and support for billing.
Take the opportunity to meet the current hospitalists—and note that their input often is solicited as to whether or not to hire a candidate—and ask them questions away from the ears of the program leadership; most hospitalists like to meet potential colleagues.
Closing the Deal
If you make it past the interview stage, be sure additional deliverables, such as letters of recommendation, are on time. Now is the time to ask about salary. Don’t be afraid to inquire about relocation or sign-on bonuses. At this point, the employer likes you and has invested time in recruiting you. You can gently leverage this in your negotiations. Consult your program director or other mentors at this point—they can provide guidance.
If you are uncertain about accepting an offer, be open about this with the employer. Your honesty in the process is essential, will be viewed positively, and can trigger additional dialogue that may help you decide. Juggling multiple offers dishonestly is not ethical and can backfire, as many hospitalist directors know each other.
Have an attorney familiar with physician contracts review yours. Look at whether “tail coverage,” which insures legal actions brought against you after you have left, is provided. Take note of “non-compete” clauses; they may limit your ability to practice in the area if you leave a practice. Find out if moonlighting is allowed and if the hospital requires you to give them a percentage of your outside earnings.
If you secure a position, whether as a career hospitalist or just for a year or two before fellowship, you should be excited. HM is a wonderful field with tremendous and varied opportunities. Dive in, enjoy, and explore everything it has to offer!
Dr. Bryson is medical director of teaching services, associate program director of internal medicine residency, and assistant professor at Tufts University, and a hospitalist at Baystate Medical Center in Springfield, Mass. Dr. Steinberg is residency program director in the Department of Medicine at Beth Israel Medical Center, and associate professor of medicine at the Icahn School of Medicine at Mount Sinai in New York City. Both are members of SHM’s Physicians in Training Committee.
Failure to Manage Hand Infection Results in Disability
A 50-year-old man sustained a rope-burn injury to his left hand during a fishing trip in early August 2004. He subsequently presented to an orthopedic facility with complaints of a hand infection and was eventually referred to orthopedic surgeon Dr. W.
One week later, Dr. W administered a steroid injection, which caused the infection to worsen. The patient claimed that the steroid injection was contraindicated by the underlying infection. Dr. W referred the patient to Dr. C for infectious disease management.
In November 2004, Dr. W performed an incision and drainage procedure, and specimens were sent for pathology study and cultures. The pathology results were sent to both Dr. W and Dr. C, but the culture results were sent only to Dr. W. Other specimens were sent for culture in November 2004 and January 2005.
The results from the first culture, received by Dr. W in three reports, indicated “Mycobacterium,” “rare presumptive Mycobacterium marinum,” and “Myocbacterium marinum.” Dr. W did not forward these results to Dr. C and allegedly did not review the last report. Dr. C treated the plaintiff for a fungal infection based on the results of the second culture. After the third specimen in January 2005 grew acid-fast bacilli, Dr. C was informed that the patient likely had an infection caused by M. marinum.
The patient alleged that the 44-day delay in diagnosis and treatment of the M. marinum infection allowed the infection to worsen. The patient was hospitalized for one week at a major clinic and underwent three debridement surgeries to his left hand. He subsequently underwent five months of physical therapy and received long-term intravenous antibiotics for the infection.
The patient lacks full range of motion in his hand and is unable to fully open the fingers or make a tight fist. He has a trigger finger, surgical scars, and painful nodules. The hand is also extremely intolerant to temperature. The plaintiff claimed that the debridement surgeries would have been unnecessary if the initial culture reports had been acted upon in a timely manner.
The defendants claimed Dr. W saw no evidence of infection at the first office visit and that there was no sign of infection when the steroid injection was administered. The defendants claimed that the hand’s condition did not worsen after the injection and that the plaintiff was referred to Dr. C when a second fishing trip led to a flare-up that eluded diagnosis. Dr. W maintained that, during the procedure that produced the first cultures, he instructed the circulating nurse to have all lab results sent to both himself and Dr. C. Dr. W believed that Dr. C had been sent the results when he saw both their names on the pathology reports.
Continue reading to see the outcome...
OUTCOME
A $215,000 verdict was returned. The surgical center at which the procedure was performed that produced the first culture settled prior to trial for $200,000.
Continue reading for David M. Lang's commentary...
COMMENT
This case raises three issues:
First, hand infections can be problematic and are often trivialized by the initially consulted clinician. The presentation of certain hand infections, such as paronychiae and felons, generally will be straightforward. Paronychiae are usually managed by the clinician who first sees the patient. Felon management is more difficult, but it still may be drained in ambulatory settings by experienced clinicians. Deeper and more troublesome infections of the hand should raise immediate concern; these include tendon sheath infection, septic arthritis, and deep space hand infections. Hand cases can become complicated, and prompt referral to a specialist is usually warranted for all but the most basic infections.
Second, clinicians must always be on the lookout for important clues pointing to an oddball cause. Here, the overlooked clue was the significance of the patient’s fishing trip. While M. marinum seems obscure, the specific bacteria is known to cause tendon sheath infections when a patient’s hand is punctured by fish spines or when a simple wound is contaminated with stagnant water in nature or from an aquarium.1 Many of us are familiar with the fungal infection sporotrichosis, which can occur after a gardener is stuck by a rose thorn. Asking about a patient’s hobbies and activities may provide a context for an injury.
Third, communication breakdown is something clinicians often just don’t “get.” After receiving the culture report, the orthopedist should have called the infectious diseases physician to discuss the unusual case. This is particularly true in light of the fact that the orthopedic surgeon injected the hand with steroids, which may have worsened the patient’s condition. Jurors would have the expectation that the case would be followed closely. Everyone is busy, but unusual cases such as this one require a quick call to help the patient and avert liability. Pick up the phone.
Furthermore, the defense strategy here seems misplaced. The defense argued that the orthopedic surgeon saw no evidence of infection but administered a steroid injection for inflammation. But how can you tell the difference from external observation alone? We’ve all been trained in the classic signs and symptoms of calor (heat), dolor (pain), rubor (redness), and tumor (swelling). But both infectious and noninfectious inflammation will produce these, so the cause would not be readily distinguishable without further investigation.
In sum, take hand infections seriously. Thanks to television shows such as House, lay jurors expect clinicians to puzzle together facts to arrive at an obscure diagnosis. So, before we discharge a patient with a common condition, it is useful to ask about the patient’s job and hobbies. We might also ask the generic question “Were you doing anything unusual?” You may just save a patient and solve a puzzle at the same time.
Finally, communication with other clinicians in complicated cases is required and expected by jurors. —DML
Reference
1. American Society for Surgery of the Hand. Hand infections. www.assh.org/Public/HandConditions/Pages/HandInfections.aspx. Accessed January 9, 2014.
A 50-year-old man sustained a rope-burn injury to his left hand during a fishing trip in early August 2004. He subsequently presented to an orthopedic facility with complaints of a hand infection and was eventually referred to orthopedic surgeon Dr. W.
One week later, Dr. W administered a steroid injection, which caused the infection to worsen. The patient claimed that the steroid injection was contraindicated by the underlying infection. Dr. W referred the patient to Dr. C for infectious disease management.
In November 2004, Dr. W performed an incision and drainage procedure, and specimens were sent for pathology study and cultures. The pathology results were sent to both Dr. W and Dr. C, but the culture results were sent only to Dr. W. Other specimens were sent for culture in November 2004 and January 2005.
The results from the first culture, received by Dr. W in three reports, indicated “Mycobacterium,” “rare presumptive Mycobacterium marinum,” and “Myocbacterium marinum.” Dr. W did not forward these results to Dr. C and allegedly did not review the last report. Dr. C treated the plaintiff for a fungal infection based on the results of the second culture. After the third specimen in January 2005 grew acid-fast bacilli, Dr. C was informed that the patient likely had an infection caused by M. marinum.
The patient alleged that the 44-day delay in diagnosis and treatment of the M. marinum infection allowed the infection to worsen. The patient was hospitalized for one week at a major clinic and underwent three debridement surgeries to his left hand. He subsequently underwent five months of physical therapy and received long-term intravenous antibiotics for the infection.
The patient lacks full range of motion in his hand and is unable to fully open the fingers or make a tight fist. He has a trigger finger, surgical scars, and painful nodules. The hand is also extremely intolerant to temperature. The plaintiff claimed that the debridement surgeries would have been unnecessary if the initial culture reports had been acted upon in a timely manner.
The defendants claimed Dr. W saw no evidence of infection at the first office visit and that there was no sign of infection when the steroid injection was administered. The defendants claimed that the hand’s condition did not worsen after the injection and that the plaintiff was referred to Dr. C when a second fishing trip led to a flare-up that eluded diagnosis. Dr. W maintained that, during the procedure that produced the first cultures, he instructed the circulating nurse to have all lab results sent to both himself and Dr. C. Dr. W believed that Dr. C had been sent the results when he saw both their names on the pathology reports.
Continue reading to see the outcome...
OUTCOME
A $215,000 verdict was returned. The surgical center at which the procedure was performed that produced the first culture settled prior to trial for $200,000.
Continue reading for David M. Lang's commentary...
COMMENT
This case raises three issues:
First, hand infections can be problematic and are often trivialized by the initially consulted clinician. The presentation of certain hand infections, such as paronychiae and felons, generally will be straightforward. Paronychiae are usually managed by the clinician who first sees the patient. Felon management is more difficult, but it still may be drained in ambulatory settings by experienced clinicians. Deeper and more troublesome infections of the hand should raise immediate concern; these include tendon sheath infection, septic arthritis, and deep space hand infections. Hand cases can become complicated, and prompt referral to a specialist is usually warranted for all but the most basic infections.
Second, clinicians must always be on the lookout for important clues pointing to an oddball cause. Here, the overlooked clue was the significance of the patient’s fishing trip. While M. marinum seems obscure, the specific bacteria is known to cause tendon sheath infections when a patient’s hand is punctured by fish spines or when a simple wound is contaminated with stagnant water in nature or from an aquarium.1 Many of us are familiar with the fungal infection sporotrichosis, which can occur after a gardener is stuck by a rose thorn. Asking about a patient’s hobbies and activities may provide a context for an injury.
Third, communication breakdown is something clinicians often just don’t “get.” After receiving the culture report, the orthopedist should have called the infectious diseases physician to discuss the unusual case. This is particularly true in light of the fact that the orthopedic surgeon injected the hand with steroids, which may have worsened the patient’s condition. Jurors would have the expectation that the case would be followed closely. Everyone is busy, but unusual cases such as this one require a quick call to help the patient and avert liability. Pick up the phone.
Furthermore, the defense strategy here seems misplaced. The defense argued that the orthopedic surgeon saw no evidence of infection but administered a steroid injection for inflammation. But how can you tell the difference from external observation alone? We’ve all been trained in the classic signs and symptoms of calor (heat), dolor (pain), rubor (redness), and tumor (swelling). But both infectious and noninfectious inflammation will produce these, so the cause would not be readily distinguishable without further investigation.
In sum, take hand infections seriously. Thanks to television shows such as House, lay jurors expect clinicians to puzzle together facts to arrive at an obscure diagnosis. So, before we discharge a patient with a common condition, it is useful to ask about the patient’s job and hobbies. We might also ask the generic question “Were you doing anything unusual?” You may just save a patient and solve a puzzle at the same time.
Finally, communication with other clinicians in complicated cases is required and expected by jurors. —DML
Reference
1. American Society for Surgery of the Hand. Hand infections. www.assh.org/Public/HandConditions/Pages/HandInfections.aspx. Accessed January 9, 2014.
A 50-year-old man sustained a rope-burn injury to his left hand during a fishing trip in early August 2004. He subsequently presented to an orthopedic facility with complaints of a hand infection and was eventually referred to orthopedic surgeon Dr. W.
One week later, Dr. W administered a steroid injection, which caused the infection to worsen. The patient claimed that the steroid injection was contraindicated by the underlying infection. Dr. W referred the patient to Dr. C for infectious disease management.
In November 2004, Dr. W performed an incision and drainage procedure, and specimens were sent for pathology study and cultures. The pathology results were sent to both Dr. W and Dr. C, but the culture results were sent only to Dr. W. Other specimens were sent for culture in November 2004 and January 2005.
The results from the first culture, received by Dr. W in three reports, indicated “Mycobacterium,” “rare presumptive Mycobacterium marinum,” and “Myocbacterium marinum.” Dr. W did not forward these results to Dr. C and allegedly did not review the last report. Dr. C treated the plaintiff for a fungal infection based on the results of the second culture. After the third specimen in January 2005 grew acid-fast bacilli, Dr. C was informed that the patient likely had an infection caused by M. marinum.
The patient alleged that the 44-day delay in diagnosis and treatment of the M. marinum infection allowed the infection to worsen. The patient was hospitalized for one week at a major clinic and underwent three debridement surgeries to his left hand. He subsequently underwent five months of physical therapy and received long-term intravenous antibiotics for the infection.
The patient lacks full range of motion in his hand and is unable to fully open the fingers or make a tight fist. He has a trigger finger, surgical scars, and painful nodules. The hand is also extremely intolerant to temperature. The plaintiff claimed that the debridement surgeries would have been unnecessary if the initial culture reports had been acted upon in a timely manner.
The defendants claimed Dr. W saw no evidence of infection at the first office visit and that there was no sign of infection when the steroid injection was administered. The defendants claimed that the hand’s condition did not worsen after the injection and that the plaintiff was referred to Dr. C when a second fishing trip led to a flare-up that eluded diagnosis. Dr. W maintained that, during the procedure that produced the first cultures, he instructed the circulating nurse to have all lab results sent to both himself and Dr. C. Dr. W believed that Dr. C had been sent the results when he saw both their names on the pathology reports.
Continue reading to see the outcome...
OUTCOME
A $215,000 verdict was returned. The surgical center at which the procedure was performed that produced the first culture settled prior to trial for $200,000.
Continue reading for David M. Lang's commentary...
COMMENT
This case raises three issues:
First, hand infections can be problematic and are often trivialized by the initially consulted clinician. The presentation of certain hand infections, such as paronychiae and felons, generally will be straightforward. Paronychiae are usually managed by the clinician who first sees the patient. Felon management is more difficult, but it still may be drained in ambulatory settings by experienced clinicians. Deeper and more troublesome infections of the hand should raise immediate concern; these include tendon sheath infection, septic arthritis, and deep space hand infections. Hand cases can become complicated, and prompt referral to a specialist is usually warranted for all but the most basic infections.
Second, clinicians must always be on the lookout for important clues pointing to an oddball cause. Here, the overlooked clue was the significance of the patient’s fishing trip. While M. marinum seems obscure, the specific bacteria is known to cause tendon sheath infections when a patient’s hand is punctured by fish spines or when a simple wound is contaminated with stagnant water in nature or from an aquarium.1 Many of us are familiar with the fungal infection sporotrichosis, which can occur after a gardener is stuck by a rose thorn. Asking about a patient’s hobbies and activities may provide a context for an injury.
Third, communication breakdown is something clinicians often just don’t “get.” After receiving the culture report, the orthopedist should have called the infectious diseases physician to discuss the unusual case. This is particularly true in light of the fact that the orthopedic surgeon injected the hand with steroids, which may have worsened the patient’s condition. Jurors would have the expectation that the case would be followed closely. Everyone is busy, but unusual cases such as this one require a quick call to help the patient and avert liability. Pick up the phone.
Furthermore, the defense strategy here seems misplaced. The defense argued that the orthopedic surgeon saw no evidence of infection but administered a steroid injection for inflammation. But how can you tell the difference from external observation alone? We’ve all been trained in the classic signs and symptoms of calor (heat), dolor (pain), rubor (redness), and tumor (swelling). But both infectious and noninfectious inflammation will produce these, so the cause would not be readily distinguishable without further investigation.
In sum, take hand infections seriously. Thanks to television shows such as House, lay jurors expect clinicians to puzzle together facts to arrive at an obscure diagnosis. So, before we discharge a patient with a common condition, it is useful to ask about the patient’s job and hobbies. We might also ask the generic question “Were you doing anything unusual?” You may just save a patient and solve a puzzle at the same time.
Finally, communication with other clinicians in complicated cases is required and expected by jurors. —DML
Reference
1. American Society for Surgery of the Hand. Hand infections. www.assh.org/Public/HandConditions/Pages/HandInfections.aspx. Accessed January 9, 2014.
Circumcision accident: $1.3M verdict

CIRCUMCISION ACCIDENT: $1.3M VERDICT
A newborn underwent circumcision when 12 hours old. The ObGyn removed adhesions present between the foreskin and glans. After locking the Mogen clamp, the ObGyn amputated a 9-mm by 8-mm portion of the top of the penis along with the foreskin. The newborn was rushed to a children’s hospital where a pediatric urologist surgically reattached the amputated glans. The child’s penis is not cosmetically normal, with permanent scars and disfigurement. He has altered nerve sensation at and above the area of the amputation.
PARENTS’ CLAIM The ObGyn improperly performed the circumcision. He failed to remove a sufficient amount of adhesions, pulled too much into the clamp, and amputated 30% of the distal portion of the glans.
PHYSICIAN’S DEFENSE The ObGyn circumcised this child the same way he had performed more than 1,000 circumcisions. Multiple dense adhesions between the glans and foreskin caused the top of the penis to be inadvertently pulled through the clamp. Amputation is a known risk of the procedure.
VERDICT A $1,357,901 Illinois verdict was returned.
WHAT CAUSED CHILD’S KIDNEY DISEASE?
At 36 weeks’ gestation, a mother came to the emergency department (ED) with abdominal pain. She had proteinuria, elevated liver enzymes, and a low-normal platelet count. An ObGyn determined that the fetus was normal, and discharged her.
The patient returned 2 days later with internal bleeding and placental abruption. She was diagnosed with hemolysis, elevated liver enzymes, and low platelet count (HELLP syndrome). The child, born by cesarean delivery, had kidney failure that caused growth retardation. The child has received a kidney transplant.
PARENTS’ CLAIM The mother should not have been discharged from the hospital with abnormal findings.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $1 million New Jersey settlement was reached, of which $100,000 was provided to the mother.
Related Article: A stepwise approach to managing eclampsia and other hypertensive emergencies Baha M. Sibai, MD (October 2013)
EXCESSIVE FORCE BLAMED FOR ERB’S PALSY
Shoulder dystocia was encountered during delivery. The child suffered a brachial plexus injury with Erb’s palsy. She received botulinum toxin injections and underwent nerve-graft surgery to restore some function. She has limited use of her right arm and a protruding right elbow.
PARENTS’ CLAIM The ObGyn used excessive force in response to shoulder dystocia.
PHYSICIAN’S DEFENSE The case was settled at trial.
VERDICT A $1 million New Jersey settlement was placed in a structured payment fund to provide a net $1.78 million over the child’s lifetime.
Related Article: You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial, May 2013)
WAS WOMAN UNLAWFULLY SEEKING DRUGS?
A 30-year-old woman went to an ED with pelvic pain and vaginal discharge. An ED physician conducted a physical exam. Blood tests indicated the patient had taken barbiturates, but the patient could not explain the findings. Determining no cause for her symptoms, the ED physician discharged the patient.
Just after she left, the ED physician found that the patient had several narcotics prescriptions and called the police. The patient was arrested and charged with unlawfully seeking drugs at the hospital. Criminal charges were later dismissed.
PATIENT’S CLAIM The ED physician did not properly examine her; she was found to have endometriosis and underwent surgery a few weeks later. The ED physician was negligent for divulging her personal information to police.
The ED physician had had his physician’s license suspended due to substance abuse and had also been arrested for driving under the influence after his license was restored.
PHYSICIAN’S DEFENSE The ED physician’s examination and treatment were proper. The phone call to police was not part of treatment. The patient had a malicious prosecution basis for any claims.
VERDICT A $125,000 Kentucky verdict was returned.

CASCADING PROBLEMS: MOTHER AND BABY DIE
A pregnant woman was admitted to an ED, where the on-call physician determined that she had pneumonia. The patient’s ObGyn, 45 miles away, refused to come to the hospital or arrange for another ObGyn to take the case.
Several hours later, after the mother was found to have fulminant preeclampsia, the ObGyn demanded the patient be moved to the hospital’s internal medicine (IM) service. However, the IM service refused to admit the patient because she needed obstetric care. The ObGyn tried to transfer the patient to a maternal-fetal medicine (MFM) specialist at a tertiary care center; transfer was refused because the patient was too unstable and needed an emergency cesarean delivery. The ObGyn continued to refuse to relinquish care to another ObGyn.
The ED physician decided to transfer the patient to another hospital 50 miles away even though she was now in active labor. An MFM specialist accepted transfer. After 5 hours in the ED, the mother left by ambulance, but, during transport, she suffered placental abruption and internal hemorrhaging. She was in critical condition upon arrival. An emergency cesarean delivery was performed, but the mother died. The baby, born with severe brain damage, also died.
ESTATES’ CLAIM The ED physician failed to properly and timely determine that the mother had preeclampsia; no treatment for hypertension was provided. The ED physician withheld critical information, including the patient’s severe hypertension, proteinurea, and edema, when speaking to the MFM specialist who accepted transfer. The ED physician did not evaluate the mother before departure and certified the transfer although the patient was highly unstable.
The ObGyn was negligent in not transferring care to another ObGyn and not coming to the hospital. The ObGyn did not inform the ED physician of the rejected attempt to transfer the patient or of the first MFM specialist’s recommendation for emergency cesarean. Both mother and baby could have survived with proper treatment.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $900,000 Michigan settlement was reached.
FECAL INCONTINENCE AFTER EPISIOTOMY
A 26-year-old woman gave birth after her ObGyn created an episiotomy to facilitate delivery. The incision was repaired and the ObGyn prescribed docusate (Colace) to soften her stools.
A month later, the patient report-ed fecal incontinence. The ObGyn determined that the incontinence was related to the episiotomy, but did not feel that immediate attention was needed. When the condition did not improve, the patient saw a colorectal surgeon, who diagnosed a significant sphincter defect. The patient underwent a sphincteroplasty, with minor improvement.
PATIENT’S CLAIM The ObGyn failed to properly manage episiotomy healing. The patient remembers being told to stop docusate after she had passed one stool after delivery. A 10-day regimen of docusate and a diet to reduce defecation frequency should have been prescribed. Incontinence should have prompted an immediate referral to a colorectal surgeon.
PHYSICIAN’S DEFENSE Prompt surgical intervention was not necessary. Sphincteroplasty can be delayed until conservative methods have been tried. Episiotomy healing was properly addressed. Permanent incontinence is a known risk of the procedure.
VERDICT A $6 million New York verdict was returned.
Related Article: Does mediolateral episiotomy reduce the risk of anal sphincter injury in operative vaginal delivery? Errol R. Norwitz, MD, PhD (Examining the Evidence, August 2012)
MECONIUM ASPIRATION SYNDROME
A baby stayed in hospital for 3 weeks postdelivery due to meconium aspiration syndrome.
PARENTS’ CLAIM The resident who followed the mother during her pregnancy was negligent in allowing the pregnancy to progress to 46 weeks’ gestation before delivery.
DEFENDANTS’ DEFENSE The estimated date of conception was disputed. The resident claimed that the baby was born at 42 weeks’ gestation. An attending physician reviewed all prenatal visits with the resident. The mother’s cervix was never ripe before induction of labor. Aspiration occurred despite aggressive suctioning. The child has had no further respiratory issues since her neonatal discharge.
VERDICT An Illinois defense verdict was returned.
BOWEL INJURY AFTER HYSTERECTOMY
A woman underwent laparoscopic-assisted vaginal hysterectomy and was discharged the following day. Two days later, she went to an ED in acute distress. A bowel perforation was found during emergency surgery, and her colon was repaired. She made a full recovery.
PATIENT’S CLAIM The ObGyn was negligent in failing to properly evaluate the patient after surgery. The ObGyn also failed to explain the signs of a possible perforation to the patient before she left the hospital.
PHYSICIAN’S DEFENSE The patient’s postoperative course was normal while she was hospitalized. Bowel perforation is a known complication of the procedure. The patient had been informed of all the signs and symptoms of a bowel perforation and had been instructed to call the ObGyn or return to the hospital if she began to have any symptoms.
VERDICT A South Carolina defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
CIRCUMCISION ACCIDENT: $1.3M VERDICT
A newborn underwent circumcision when 12 hours old. The ObGyn removed adhesions present between the foreskin and glans. After locking the Mogen clamp, the ObGyn amputated a 9-mm by 8-mm portion of the top of the penis along with the foreskin. The newborn was rushed to a children’s hospital where a pediatric urologist surgically reattached the amputated glans. The child’s penis is not cosmetically normal, with permanent scars and disfigurement. He has altered nerve sensation at and above the area of the amputation.
PARENTS’ CLAIM The ObGyn improperly performed the circumcision. He failed to remove a sufficient amount of adhesions, pulled too much into the clamp, and amputated 30% of the distal portion of the glans.
PHYSICIAN’S DEFENSE The ObGyn circumcised this child the same way he had performed more than 1,000 circumcisions. Multiple dense adhesions between the glans and foreskin caused the top of the penis to be inadvertently pulled through the clamp. Amputation is a known risk of the procedure.
VERDICT A $1,357,901 Illinois verdict was returned.
WHAT CAUSED CHILD’S KIDNEY DISEASE?
At 36 weeks’ gestation, a mother came to the emergency department (ED) with abdominal pain. She had proteinuria, elevated liver enzymes, and a low-normal platelet count. An ObGyn determined that the fetus was normal, and discharged her.
The patient returned 2 days later with internal bleeding and placental abruption. She was diagnosed with hemolysis, elevated liver enzymes, and low platelet count (HELLP syndrome). The child, born by cesarean delivery, had kidney failure that caused growth retardation. The child has received a kidney transplant.
PARENTS’ CLAIM The mother should not have been discharged from the hospital with abnormal findings.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $1 million New Jersey settlement was reached, of which $100,000 was provided to the mother.
Related Article: A stepwise approach to managing eclampsia and other hypertensive emergencies Baha M. Sibai, MD (October 2013)
EXCESSIVE FORCE BLAMED FOR ERB’S PALSY
Shoulder dystocia was encountered during delivery. The child suffered a brachial plexus injury with Erb’s palsy. She received botulinum toxin injections and underwent nerve-graft surgery to restore some function. She has limited use of her right arm and a protruding right elbow.
PARENTS’ CLAIM The ObGyn used excessive force in response to shoulder dystocia.
PHYSICIAN’S DEFENSE The case was settled at trial.
VERDICT A $1 million New Jersey settlement was placed in a structured payment fund to provide a net $1.78 million over the child’s lifetime.
Related Article: You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial, May 2013)
WAS WOMAN UNLAWFULLY SEEKING DRUGS?
A 30-year-old woman went to an ED with pelvic pain and vaginal discharge. An ED physician conducted a physical exam. Blood tests indicated the patient had taken barbiturates, but the patient could not explain the findings. Determining no cause for her symptoms, the ED physician discharged the patient.
Just after she left, the ED physician found that the patient had several narcotics prescriptions and called the police. The patient was arrested and charged with unlawfully seeking drugs at the hospital. Criminal charges were later dismissed.
PATIENT’S CLAIM The ED physician did not properly examine her; she was found to have endometriosis and underwent surgery a few weeks later. The ED physician was negligent for divulging her personal information to police.
The ED physician had had his physician’s license suspended due to substance abuse and had also been arrested for driving under the influence after his license was restored.
PHYSICIAN’S DEFENSE The ED physician’s examination and treatment were proper. The phone call to police was not part of treatment. The patient had a malicious prosecution basis for any claims.
VERDICT A $125,000 Kentucky verdict was returned.
CASCADING PROBLEMS: MOTHER AND BABY DIE
A pregnant woman was admitted to an ED, where the on-call physician determined that she had pneumonia. The patient’s ObGyn, 45 miles away, refused to come to the hospital or arrange for another ObGyn to take the case.
Several hours later, after the mother was found to have fulminant preeclampsia, the ObGyn demanded the patient be moved to the hospital’s internal medicine (IM) service. However, the IM service refused to admit the patient because she needed obstetric care. The ObGyn tried to transfer the patient to a maternal-fetal medicine (MFM) specialist at a tertiary care center; transfer was refused because the patient was too unstable and needed an emergency cesarean delivery. The ObGyn continued to refuse to relinquish care to another ObGyn.
The ED physician decided to transfer the patient to another hospital 50 miles away even though she was now in active labor. An MFM specialist accepted transfer. After 5 hours in the ED, the mother left by ambulance, but, during transport, she suffered placental abruption and internal hemorrhaging. She was in critical condition upon arrival. An emergency cesarean delivery was performed, but the mother died. The baby, born with severe brain damage, also died.
ESTATES’ CLAIM The ED physician failed to properly and timely determine that the mother had preeclampsia; no treatment for hypertension was provided. The ED physician withheld critical information, including the patient’s severe hypertension, proteinurea, and edema, when speaking to the MFM specialist who accepted transfer. The ED physician did not evaluate the mother before departure and certified the transfer although the patient was highly unstable.
The ObGyn was negligent in not transferring care to another ObGyn and not coming to the hospital. The ObGyn did not inform the ED physician of the rejected attempt to transfer the patient or of the first MFM specialist’s recommendation for emergency cesarean. Both mother and baby could have survived with proper treatment.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $900,000 Michigan settlement was reached.
FECAL INCONTINENCE AFTER EPISIOTOMY
A 26-year-old woman gave birth after her ObGyn created an episiotomy to facilitate delivery. The incision was repaired and the ObGyn prescribed docusate (Colace) to soften her stools.
A month later, the patient report-ed fecal incontinence. The ObGyn determined that the incontinence was related to the episiotomy, but did not feel that immediate attention was needed. When the condition did not improve, the patient saw a colorectal surgeon, who diagnosed a significant sphincter defect. The patient underwent a sphincteroplasty, with minor improvement.
PATIENT’S CLAIM The ObGyn failed to properly manage episiotomy healing. The patient remembers being told to stop docusate after she had passed one stool after delivery. A 10-day regimen of docusate and a diet to reduce defecation frequency should have been prescribed. Incontinence should have prompted an immediate referral to a colorectal surgeon.
PHYSICIAN’S DEFENSE Prompt surgical intervention was not necessary. Sphincteroplasty can be delayed until conservative methods have been tried. Episiotomy healing was properly addressed. Permanent incontinence is a known risk of the procedure.
VERDICT A $6 million New York verdict was returned.
Related Article: Does mediolateral episiotomy reduce the risk of anal sphincter injury in operative vaginal delivery? Errol R. Norwitz, MD, PhD (Examining the Evidence, August 2012)
MECONIUM ASPIRATION SYNDROME
A baby stayed in hospital for 3 weeks postdelivery due to meconium aspiration syndrome.
PARENTS’ CLAIM The resident who followed the mother during her pregnancy was negligent in allowing the pregnancy to progress to 46 weeks’ gestation before delivery.
DEFENDANTS’ DEFENSE The estimated date of conception was disputed. The resident claimed that the baby was born at 42 weeks’ gestation. An attending physician reviewed all prenatal visits with the resident. The mother’s cervix was never ripe before induction of labor. Aspiration occurred despite aggressive suctioning. The child has had no further respiratory issues since her neonatal discharge.
VERDICT An Illinois defense verdict was returned.
BOWEL INJURY AFTER HYSTERECTOMY
A woman underwent laparoscopic-assisted vaginal hysterectomy and was discharged the following day. Two days later, she went to an ED in acute distress. A bowel perforation was found during emergency surgery, and her colon was repaired. She made a full recovery.
PATIENT’S CLAIM The ObGyn was negligent in failing to properly evaluate the patient after surgery. The ObGyn also failed to explain the signs of a possible perforation to the patient before she left the hospital.
PHYSICIAN’S DEFENSE The patient’s postoperative course was normal while she was hospitalized. Bowel perforation is a known complication of the procedure. The patient had been informed of all the signs and symptoms of a bowel perforation and had been instructed to call the ObGyn or return to the hospital if she began to have any symptoms.
VERDICT A South Carolina defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
CIRCUMCISION ACCIDENT: $1.3M VERDICT
A newborn underwent circumcision when 12 hours old. The ObGyn removed adhesions present between the foreskin and glans. After locking the Mogen clamp, the ObGyn amputated a 9-mm by 8-mm portion of the top of the penis along with the foreskin. The newborn was rushed to a children’s hospital where a pediatric urologist surgically reattached the amputated glans. The child’s penis is not cosmetically normal, with permanent scars and disfigurement. He has altered nerve sensation at and above the area of the amputation.
PARENTS’ CLAIM The ObGyn improperly performed the circumcision. He failed to remove a sufficient amount of adhesions, pulled too much into the clamp, and amputated 30% of the distal portion of the glans.
PHYSICIAN’S DEFENSE The ObGyn circumcised this child the same way he had performed more than 1,000 circumcisions. Multiple dense adhesions between the glans and foreskin caused the top of the penis to be inadvertently pulled through the clamp. Amputation is a known risk of the procedure.
VERDICT A $1,357,901 Illinois verdict was returned.
WHAT CAUSED CHILD’S KIDNEY DISEASE?
At 36 weeks’ gestation, a mother came to the emergency department (ED) with abdominal pain. She had proteinuria, elevated liver enzymes, and a low-normal platelet count. An ObGyn determined that the fetus was normal, and discharged her.
The patient returned 2 days later with internal bleeding and placental abruption. She was diagnosed with hemolysis, elevated liver enzymes, and low platelet count (HELLP syndrome). The child, born by cesarean delivery, had kidney failure that caused growth retardation. The child has received a kidney transplant.
PARENTS’ CLAIM The mother should not have been discharged from the hospital with abnormal findings.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $1 million New Jersey settlement was reached, of which $100,000 was provided to the mother.
Related Article: A stepwise approach to managing eclampsia and other hypertensive emergencies Baha M. Sibai, MD (October 2013)
EXCESSIVE FORCE BLAMED FOR ERB’S PALSY
Shoulder dystocia was encountered during delivery. The child suffered a brachial plexus injury with Erb’s palsy. She received botulinum toxin injections and underwent nerve-graft surgery to restore some function. She has limited use of her right arm and a protruding right elbow.
PARENTS’ CLAIM The ObGyn used excessive force in response to shoulder dystocia.
PHYSICIAN’S DEFENSE The case was settled at trial.
VERDICT A $1 million New Jersey settlement was placed in a structured payment fund to provide a net $1.78 million over the child’s lifetime.
Related Article: You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial, May 2013)
WAS WOMAN UNLAWFULLY SEEKING DRUGS?
A 30-year-old woman went to an ED with pelvic pain and vaginal discharge. An ED physician conducted a physical exam. Blood tests indicated the patient had taken barbiturates, but the patient could not explain the findings. Determining no cause for her symptoms, the ED physician discharged the patient.
Just after she left, the ED physician found that the patient had several narcotics prescriptions and called the police. The patient was arrested and charged with unlawfully seeking drugs at the hospital. Criminal charges were later dismissed.
PATIENT’S CLAIM The ED physician did not properly examine her; she was found to have endometriosis and underwent surgery a few weeks later. The ED physician was negligent for divulging her personal information to police.
The ED physician had had his physician’s license suspended due to substance abuse and had also been arrested for driving under the influence after his license was restored.
PHYSICIAN’S DEFENSE The ED physician’s examination and treatment were proper. The phone call to police was not part of treatment. The patient had a malicious prosecution basis for any claims.
VERDICT A $125,000 Kentucky verdict was returned.
CASCADING PROBLEMS: MOTHER AND BABY DIE
A pregnant woman was admitted to an ED, where the on-call physician determined that she had pneumonia. The patient’s ObGyn, 45 miles away, refused to come to the hospital or arrange for another ObGyn to take the case.
Several hours later, after the mother was found to have fulminant preeclampsia, the ObGyn demanded the patient be moved to the hospital’s internal medicine (IM) service. However, the IM service refused to admit the patient because she needed obstetric care. The ObGyn tried to transfer the patient to a maternal-fetal medicine (MFM) specialist at a tertiary care center; transfer was refused because the patient was too unstable and needed an emergency cesarean delivery. The ObGyn continued to refuse to relinquish care to another ObGyn.
The ED physician decided to transfer the patient to another hospital 50 miles away even though she was now in active labor. An MFM specialist accepted transfer. After 5 hours in the ED, the mother left by ambulance, but, during transport, she suffered placental abruption and internal hemorrhaging. She was in critical condition upon arrival. An emergency cesarean delivery was performed, but the mother died. The baby, born with severe brain damage, also died.
ESTATES’ CLAIM The ED physician failed to properly and timely determine that the mother had preeclampsia; no treatment for hypertension was provided. The ED physician withheld critical information, including the patient’s severe hypertension, proteinurea, and edema, when speaking to the MFM specialist who accepted transfer. The ED physician did not evaluate the mother before departure and certified the transfer although the patient was highly unstable.
The ObGyn was negligent in not transferring care to another ObGyn and not coming to the hospital. The ObGyn did not inform the ED physician of the rejected attempt to transfer the patient or of the first MFM specialist’s recommendation for emergency cesarean. Both mother and baby could have survived with proper treatment.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $900,000 Michigan settlement was reached.
FECAL INCONTINENCE AFTER EPISIOTOMY
A 26-year-old woman gave birth after her ObGyn created an episiotomy to facilitate delivery. The incision was repaired and the ObGyn prescribed docusate (Colace) to soften her stools.
A month later, the patient report-ed fecal incontinence. The ObGyn determined that the incontinence was related to the episiotomy, but did not feel that immediate attention was needed. When the condition did not improve, the patient saw a colorectal surgeon, who diagnosed a significant sphincter defect. The patient underwent a sphincteroplasty, with minor improvement.
PATIENT’S CLAIM The ObGyn failed to properly manage episiotomy healing. The patient remembers being told to stop docusate after she had passed one stool after delivery. A 10-day regimen of docusate and a diet to reduce defecation frequency should have been prescribed. Incontinence should have prompted an immediate referral to a colorectal surgeon.
PHYSICIAN’S DEFENSE Prompt surgical intervention was not necessary. Sphincteroplasty can be delayed until conservative methods have been tried. Episiotomy healing was properly addressed. Permanent incontinence is a known risk of the procedure.
VERDICT A $6 million New York verdict was returned.
Related Article: Does mediolateral episiotomy reduce the risk of anal sphincter injury in operative vaginal delivery? Errol R. Norwitz, MD, PhD (Examining the Evidence, August 2012)
MECONIUM ASPIRATION SYNDROME
A baby stayed in hospital for 3 weeks postdelivery due to meconium aspiration syndrome.
PARENTS’ CLAIM The resident who followed the mother during her pregnancy was negligent in allowing the pregnancy to progress to 46 weeks’ gestation before delivery.
DEFENDANTS’ DEFENSE The estimated date of conception was disputed. The resident claimed that the baby was born at 42 weeks’ gestation. An attending physician reviewed all prenatal visits with the resident. The mother’s cervix was never ripe before induction of labor. Aspiration occurred despite aggressive suctioning. The child has had no further respiratory issues since her neonatal discharge.
VERDICT An Illinois defense verdict was returned.
BOWEL INJURY AFTER HYSTERECTOMY
A woman underwent laparoscopic-assisted vaginal hysterectomy and was discharged the following day. Two days later, she went to an ED in acute distress. A bowel perforation was found during emergency surgery, and her colon was repaired. She made a full recovery.
PATIENT’S CLAIM The ObGyn was negligent in failing to properly evaluate the patient after surgery. The ObGyn also failed to explain the signs of a possible perforation to the patient before she left the hospital.
PHYSICIAN’S DEFENSE The patient’s postoperative course was normal while she was hospitalized. Bowel perforation is a known complication of the procedure. The patient had been informed of all the signs and symptoms of a bowel perforation and had been instructed to call the ObGyn or return to the hospital if she began to have any symptoms.
VERDICT A South Carolina defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]

Was Surgery Justified?
In March 2005, a 59-year-old woman underwent cataract surgery performed by an ophthalmologist. After the procedure, a chronic detached retina was found. The patient’s pain persisted, and she underwent three subsequent retinal surgeries. Her left eye is still painful.
The plaintiff alleged negligence in the ophthalmologist’s failure to refer her either for a B-scan ocular ultrasound or to a retinal specialist prior to determining whether cataract surgery would be appropriate. Since the plaintiff was not a good candidate for retinal surgery, she claimed the cataract surgery was unnecessary.
The defendant argued that the patient eventually underwent surgery to repair her detached retina, and the cataract surgery (in addition to the retinal surgery) was required to restore any meaningful vision.
OUTCOME
A $678,483 verdict was returned.
COMMENT
This is an interesting case: The plaintiff did not allege that the cataract surgery itself was negligent, but rather inappropriate because she had a chronic detached retina and couldn’t benefit from the procedure. The jury agreed, concluding that the standard of care required the ophthalmologist to confirm that the retina was viable prior to the surgery.
The lesson here? For surgical services, take reasonable efforts to ensure the patient will receive the benefit of those services.
Nationally, there is growing media attention on “unnecessary surgeries.” For example, last summer, a 22-year-old semiprofessional baseball player, Jonathan Stelly, made headlines after a Louisiana cardiologist implanted a pacemaker in him following a single syncopal episode. Several cardiologists who subsequently reviewed the case determined that placement of the pacemaker was grossly inappropriate. The offending cardiologist is now in prison, serving a sentence for Medicare fraud after billing for dozens of similar unnecessary procedures.
As the federal government becomes more involved in health care, we can expect aggressive auditing that seeks to ferret out “unnecessary” or “inappropriate” surgeries. The question is, who makes that determination?
Do your part to protect yourself, your practice, and most importantly, your patient. Communicate all surgical procedure risks, expectations, and limitations to the patient. Discuss and document all options, especially nonsurgical ones. Be particularly cautious in “borderline” cases in which either the indication for surgery is a close call or the benefit is uncertain or minimal.
Should you find yourself trapped in a practice in which surgeries are performed that are clearly fraudulently inappropriate, it is your ethical duty to get out of the practice and make reasonable efforts to stop the fraudulent activity. —DML
In March 2005, a 59-year-old woman underwent cataract surgery performed by an ophthalmologist. After the procedure, a chronic detached retina was found. The patient’s pain persisted, and she underwent three subsequent retinal surgeries. Her left eye is still painful.
The plaintiff alleged negligence in the ophthalmologist’s failure to refer her either for a B-scan ocular ultrasound or to a retinal specialist prior to determining whether cataract surgery would be appropriate. Since the plaintiff was not a good candidate for retinal surgery, she claimed the cataract surgery was unnecessary.
The defendant argued that the patient eventually underwent surgery to repair her detached retina, and the cataract surgery (in addition to the retinal surgery) was required to restore any meaningful vision.
OUTCOME
A $678,483 verdict was returned.
COMMENT
This is an interesting case: The plaintiff did not allege that the cataract surgery itself was negligent, but rather inappropriate because she had a chronic detached retina and couldn’t benefit from the procedure. The jury agreed, concluding that the standard of care required the ophthalmologist to confirm that the retina was viable prior to the surgery.
The lesson here? For surgical services, take reasonable efforts to ensure the patient will receive the benefit of those services.
Nationally, there is growing media attention on “unnecessary surgeries.” For example, last summer, a 22-year-old semiprofessional baseball player, Jonathan Stelly, made headlines after a Louisiana cardiologist implanted a pacemaker in him following a single syncopal episode. Several cardiologists who subsequently reviewed the case determined that placement of the pacemaker was grossly inappropriate. The offending cardiologist is now in prison, serving a sentence for Medicare fraud after billing for dozens of similar unnecessary procedures.
As the federal government becomes more involved in health care, we can expect aggressive auditing that seeks to ferret out “unnecessary” or “inappropriate” surgeries. The question is, who makes that determination?
Do your part to protect yourself, your practice, and most importantly, your patient. Communicate all surgical procedure risks, expectations, and limitations to the patient. Discuss and document all options, especially nonsurgical ones. Be particularly cautious in “borderline” cases in which either the indication for surgery is a close call or the benefit is uncertain or minimal.
Should you find yourself trapped in a practice in which surgeries are performed that are clearly fraudulently inappropriate, it is your ethical duty to get out of the practice and make reasonable efforts to stop the fraudulent activity. —DML
In March 2005, a 59-year-old woman underwent cataract surgery performed by an ophthalmologist. After the procedure, a chronic detached retina was found. The patient’s pain persisted, and she underwent three subsequent retinal surgeries. Her left eye is still painful.
The plaintiff alleged negligence in the ophthalmologist’s failure to refer her either for a B-scan ocular ultrasound or to a retinal specialist prior to determining whether cataract surgery would be appropriate. Since the plaintiff was not a good candidate for retinal surgery, she claimed the cataract surgery was unnecessary.
The defendant argued that the patient eventually underwent surgery to repair her detached retina, and the cataract surgery (in addition to the retinal surgery) was required to restore any meaningful vision.
OUTCOME
A $678,483 verdict was returned.
COMMENT
This is an interesting case: The plaintiff did not allege that the cataract surgery itself was negligent, but rather inappropriate because she had a chronic detached retina and couldn’t benefit from the procedure. The jury agreed, concluding that the standard of care required the ophthalmologist to confirm that the retina was viable prior to the surgery.
The lesson here? For surgical services, take reasonable efforts to ensure the patient will receive the benefit of those services.
Nationally, there is growing media attention on “unnecessary surgeries.” For example, last summer, a 22-year-old semiprofessional baseball player, Jonathan Stelly, made headlines after a Louisiana cardiologist implanted a pacemaker in him following a single syncopal episode. Several cardiologists who subsequently reviewed the case determined that placement of the pacemaker was grossly inappropriate. The offending cardiologist is now in prison, serving a sentence for Medicare fraud after billing for dozens of similar unnecessary procedures.
As the federal government becomes more involved in health care, we can expect aggressive auditing that seeks to ferret out “unnecessary” or “inappropriate” surgeries. The question is, who makes that determination?
Do your part to protect yourself, your practice, and most importantly, your patient. Communicate all surgical procedure risks, expectations, and limitations to the patient. Discuss and document all options, especially nonsurgical ones. Be particularly cautious in “borderline” cases in which either the indication for surgery is a close call or the benefit is uncertain or minimal.
Should you find yourself trapped in a practice in which surgeries are performed that are clearly fraudulently inappropriate, it is your ethical duty to get out of the practice and make reasonable efforts to stop the fraudulent activity. —DML
Uterine rupture after unplanned VBAC

Uterine rupture after unplanned VBAC
A 34-year-old woman went into labor 9 days before a scheduled repeat cesarean. She gave birth vaginally to a healthy baby.
After delivery, the mother complained of sharp abdominal pain that she rated 10/10 on the pain scale; pain was unrelieved by morphine. Moderate bleeding was noted. After the ObGyn performed a manual exploration and curette procedure, uterine scar rupture was ruled out and the patient was treated for uterine atony. For 90 minutes, the patient was hypotensive and tachycardic with moderate bleeding. Her hemoglobin and hematocrit levels dropped lower than before delivery, and she went into cardiac arrest. After resuscitation, she received a blood transfusion. A second ObGyn took over her care.
Although the patient received 7 U each of packed red blood cells (PRBC) and fresh frozen plasma (FFP) over the next 5 hours, she continued to have low hemoglobin and hematocrit values. Bleeding was noted as sporadic. Shortly after a decision was made to perform a hysterectomy, the patient experienced cardiac arrest and was successfully resuscitated. At surgery, a uterine rupture was noted. She received 14 U each of PRBC and FFP during surgery. Bleeding stopped after the hysterectomy, but the patient remained on a ventilator for 9 days, suffered renal failure and adrenal insufficiency, and went into cardiac arrest twice more.
The patient suffered brain damage and has poor memory function. She had to relearn to walk, talk, and perform normal life tasks. She underwent a kidney transplant because of permanent kidney damage and will require additional kidney transplants during her lifetime.
PATIENT’S CLAIM The ObGyn failed to recognize uterine scar rupture and perform an immediate hysterectomy. The operative report from the hysterectomy used the words uterine scar “rupture” and “dehiscence” interchangeably as the source of bleeding and hemorrhagic shock.
DEFENDANTS’ DEFENSE The patient’s injury was a prior uterine scar “dehiscence” and not a complete rupture; conservative measures were appropriate.
VERDICT A $4 million Virginia verdict was returned that was reduced to $2 million under the state cap.
Woman in vegetative state after cystectomy
Two days after ovarian cystectomy, a 55-year-old woman was returned to the operating room for primary repair of a colon injury. Postoperatively, a colovesical fistula developed. During a third operation, the patient suffered cardiac arrest and sustained brain damage due to lack of oxygen. She remains in a vegetative state.
PATIENT’S CLAIM The colon injury was not detected or treated in a timely manner. A temporary colostomy should have been performed. Metoprolol tartrate, given after the third operation, caused cardiac arrest.
DEFENDANTS’ DEFENSE A settlement was reached during trial.
VERDICT A $2.725 million New Jersey settlement was reached with two physicians, a nurse, and the hospital. A third physician was released from liability.
Breast surgery leaves triangular areola
Cosmetic breast surgery on a 37-year-old woman included insertion of implants, a mastopexy, and reduction of the areolae. After surgery, one areola appeared triangularly shaped. After several months, the patient saw another plastic surgeon who surgically removed the undesirable tissue to reshape the areola.
PATIENT’S CLAIM Postoperatively, the plastic surgeon explained that the patient’s nipples were surrounded by hyperpigmented tissue that had to be removed during a second operation. The patient signed a consent to surgery, but the document did not explain that additional procedures could be necessary.
PHYSICIAN’S DEFENSE The signed consent form included language that additional procedures could be necessary. The plastic surgeon would have performed a free correction of the areola, but the procedure could not occur until the patient’s breasts had healed. In the meantime, the patient went to another surgeon.
VERDICT A New York defense verdict was returned.
Operative report contested
A gynecologist performed a hysterectomy on a 43-year-old woman. Two days after surgery, she was found to have an obstruction of the left ureter and a bladder injury. Extensive treatment was required to treat the injury.
PATIENT’S CLAIM Surgery was performed in a negligent manner. The surgical report states that the arteries were clamped and sutured before the ureters had been identified. The ureter injury was caused by the improper use of a clamp.
DEFENDANTS’ DEFENSE The gynecologist claimed that the proper sequence was used during surgery; an assisting physician may have erroneously documented the sequence of events. Surgery was complicated by fibroids that distorted the patient’s anatomy. The injury was a known risk of the procedure. Damage to the ureter could have been caused by a kink in the ureter or by treatment given later by a urologist.
VERDICT A $526,088 verdict was returned.
Was CP a result of poor communication?
The on-call ObGyn was notified that a woman was about to deliver at the hospital. The attending resident monitored labor and delivery until the ObGyn arrived. A cesarean delivery was performed. The child suffered hypoxic ischemic encephalopathy with brain damage and cerebral palsy.
PARENTS’ CLAIM A delay in performing cesarean delivery caused the child’s injuries. The ObGyn, who was not present during labor, failed to properly instruct the resident.
DEFENDANTS’ DEFENSE The ObGyn claimed the resident’s interpretation of the fetal monitoring strips misled her to believe that there was no emergency. Cesarean delivery was immediately performed upon the ObGyn’s arrival.
VERDICT The hospital and resident settled for an undisclosed amount before trial. An Ohio defense verdict was returned for the ObGyn.
Was excessive electrocautery used?
A 52-year-old woman underwent supracervical hysterectomy with bilateral salpingo-oophorectomy. She developed a vaginal-peritoneal fistula and a chronic abscess with pain; additional operations were required.
PATIENT’S CLAIM The ObGyn used excessive electrocauterization during the first operation, leading to fistula development. An adhesive barrier prevented fistula healing. The patient would not have had her ovaries removed had she known the consequences, including hot flashes and painful sexual intercourse.
PHYSICIAN’S DEFENSE Surgery was properly performed; excessive electrocautery was not used. The adhesive barrier was correctly applied and did not cause injury. Fistula development is a known complication of the procedure. Appropriate consent was obtained.
VERDICT An Illinois defense verdict was returned.
Why did child have brain damage?
At 25 weeks’ gestation, a mother was found to have genital herpes and received medication. Gestational diabetes was diagnosed at 29 weeks’ gestation and treated with diet. At 38 weeks’ gestation, the patient came to her prenatal visit with scabies on her abdomen, hands, and feet; a scabicide was prescribed. The resident in charge of her care planned to induce labor between 39 and 40 weeks’ gestation.
Meconium was present when the membranes were broken. When fetal heart-rate monitors showed nonreassuring heart tones, an emergency cesarean delivery was performed.
The baby required resuscitation due to a low heart rate. She experienced a seizure at 4 hours of life. Head imaging was consistent with a herpes infection or an hypoxic ischemic event. The child has cerebral palsy with speech and motor deficits.
PATIENT’S CLAIM The resident failed to respond to signs of fetal distress and call in the attending physician. Cesarean delivery should have been performed earlier.
DEFENDANTS’ DEFENSE The baby recovered well after being slightly depressed at birth; umbilical cord blood gases were in the normal range. There was no hypoxic ischemic event during labor. The baby’s injuries were due to infection.
VERDICT A New York defense verdict was returned.
Diaphragmatic hernia missed on fetal US
At 19 weeks’ gestation, a 25-year-old woman underwent fetal ultrasonography at a radiology clinic. The radiologist’s report indicated that the standard fetal structural survey was “unremarkable.” When the child was born, catastrophic impairment and deformity were present due to a diaphragmatic hernia.
PARENTS’ CLAIM The parents claimed wrongful birth. The radiologist missed a diaphragmatic hernia that was evident on the ultrasound.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $333,664 net Florida settlement was reached after deduction of attorney’s fees.
Was breast cancer missed on screening mammogram?
Screening mammography conducted in July 2009 was reported by a radiologist as being unchanged when compared to studies from the previous 2 years. Several months later, the patient discovered a lump in her right breast that was diagnosed as cancer. She underwent a lumpectomy in July 2010, followed by chemotherapy. The patient’s cancer metastasized and she developed lymphedema.
PATIENT’S CLAIM The 2009 mammography showed an abnormality in the right breast that was not present on earlier films. Further testing and treatment in 2009 would have prevented metastasis.
PHYSICIAN’S DEFENSE There was no negligence; the 2009 mammogram was properly read. Treatment and outcome would have been the same regardless of the timing of diagnosis.
VERDICT A $140,919 Michigan verdict was returned.
Premature twin has CP
Born at 26 weeks’ gestation, one twin was in critical condition. She was taken to the pediatric intensive care unit, where she remained for 46 days, and was then transferred to a long-term care center. She suffers from cerebral palsy.
PARENTS’ CLAIM Prompt treatment would have reduced or eliminated some of the effects of cerebral palsy. The birth hospital did not have pulmonary surfactant or nitric oxide with high-frequency jet-ventilation therapy that would have improved the newborn’s respiration. The baby should have been immediately transferred to a facility where this treatment was available. The parents requested a transfer, but it was denied.
DEFENDANTS’ DEFENSE The child was given every appropriate method of treatment; she was adequately oxygenated. Nitric oxide was not FDA-approved for use in this case. The child’s disabilities were a result of her prematurity.
VERDICT A New York defense verdict was returned.
Benign findings after radiation had started
After a 45-year-old woman found a lump in her right breast in October 2006, a pathologist interpreted biopsy results as ductal carcinoma in situ. A general surgeon and an oncologist both recommended partial mastectomy and lymphadenectomy with radiotherapy and possible tamoxifen treatment. Surgery was performed in November 2006, and radiation treatment began in early December.
The oncologist required that slides be reviewed by pathologists at her cancer center before determining if tamoxifen was appropriate. The pathology report indicated that the patient did not have breast cancer, but had atypical ductal hyperplasia. When the patient learned she did not have cancer, she immediately halted radiation therapy, but had already suffered radiation burns on her breast.
PATIENT’S CLAIM The oncologist was notified that the patient did not have cancer in mid-December, but did not tell the patient until January, when they met to discuss tamoxifen therapy. The patient is now at risk for sarcoma, changes in breast tissue, and rib fractures because of radiation therapy. Partial mastectomy and lymphadenectomy are proper treatment for atypical ductal hyperplasia, but radiation therapy is not. The patient is depressed and anxious.
DEFENDANTS’ DEFENSE The oncologist claimed the patient was not informed of the change in diagnosis because radiation treatment is acceptable treatment for atypical ductal hyperplasia; there was no reason for treatment to be stopped.
The pathologist stated that cell variation between ductal carcinoma and atypical ductal hyperplasia is so slight that two pathologists could reach different conclusions reading the same slide. His interpretation was appropriate. The patient was not clinically depressed; she never sought treatment.
VERDICT A $150,000 Pennsylvania verdict was returned against the oncologist. A defense verdict was returned for the pathologist.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WE WANT TO HEAR FROM YOU. Tell us what you think.
Uterine rupture after unplanned VBAC
A 34-year-old woman went into labor 9 days before a scheduled repeat cesarean. She gave birth vaginally to a healthy baby.
After delivery, the mother complained of sharp abdominal pain that she rated 10/10 on the pain scale; pain was unrelieved by morphine. Moderate bleeding was noted. After the ObGyn performed a manual exploration and curette procedure, uterine scar rupture was ruled out and the patient was treated for uterine atony. For 90 minutes, the patient was hypotensive and tachycardic with moderate bleeding. Her hemoglobin and hematocrit levels dropped lower than before delivery, and she went into cardiac arrest. After resuscitation, she received a blood transfusion. A second ObGyn took over her care.
Although the patient received 7 U each of packed red blood cells (PRBC) and fresh frozen plasma (FFP) over the next 5 hours, she continued to have low hemoglobin and hematocrit values. Bleeding was noted as sporadic. Shortly after a decision was made to perform a hysterectomy, the patient experienced cardiac arrest and was successfully resuscitated. At surgery, a uterine rupture was noted. She received 14 U each of PRBC and FFP during surgery. Bleeding stopped after the hysterectomy, but the patient remained on a ventilator for 9 days, suffered renal failure and adrenal insufficiency, and went into cardiac arrest twice more.
The patient suffered brain damage and has poor memory function. She had to relearn to walk, talk, and perform normal life tasks. She underwent a kidney transplant because of permanent kidney damage and will require additional kidney transplants during her lifetime.
PATIENT’S CLAIM The ObGyn failed to recognize uterine scar rupture and perform an immediate hysterectomy. The operative report from the hysterectomy used the words uterine scar “rupture” and “dehiscence” interchangeably as the source of bleeding and hemorrhagic shock.
DEFENDANTS’ DEFENSE The patient’s injury was a prior uterine scar “dehiscence” and not a complete rupture; conservative measures were appropriate.
VERDICT A $4 million Virginia verdict was returned that was reduced to $2 million under the state cap.
Woman in vegetative state after cystectomy
Two days after ovarian cystectomy, a 55-year-old woman was returned to the operating room for primary repair of a colon injury. Postoperatively, a colovesical fistula developed. During a third operation, the patient suffered cardiac arrest and sustained brain damage due to lack of oxygen. She remains in a vegetative state.
PATIENT’S CLAIM The colon injury was not detected or treated in a timely manner. A temporary colostomy should have been performed. Metoprolol tartrate, given after the third operation, caused cardiac arrest.
DEFENDANTS’ DEFENSE A settlement was reached during trial.
VERDICT A $2.725 million New Jersey settlement was reached with two physicians, a nurse, and the hospital. A third physician was released from liability.
Breast surgery leaves triangular areola
Cosmetic breast surgery on a 37-year-old woman included insertion of implants, a mastopexy, and reduction of the areolae. After surgery, one areola appeared triangularly shaped. After several months, the patient saw another plastic surgeon who surgically removed the undesirable tissue to reshape the areola.
PATIENT’S CLAIM Postoperatively, the plastic surgeon explained that the patient’s nipples were surrounded by hyperpigmented tissue that had to be removed during a second operation. The patient signed a consent to surgery, but the document did not explain that additional procedures could be necessary.
PHYSICIAN’S DEFENSE The signed consent form included language that additional procedures could be necessary. The plastic surgeon would have performed a free correction of the areola, but the procedure could not occur until the patient’s breasts had healed. In the meantime, the patient went to another surgeon.
VERDICT A New York defense verdict was returned.
Operative report contested
A gynecologist performed a hysterectomy on a 43-year-old woman. Two days after surgery, she was found to have an obstruction of the left ureter and a bladder injury. Extensive treatment was required to treat the injury.
PATIENT’S CLAIM Surgery was performed in a negligent manner. The surgical report states that the arteries were clamped and sutured before the ureters had been identified. The ureter injury was caused by the improper use of a clamp.
DEFENDANTS’ DEFENSE The gynecologist claimed that the proper sequence was used during surgery; an assisting physician may have erroneously documented the sequence of events. Surgery was complicated by fibroids that distorted the patient’s anatomy. The injury was a known risk of the procedure. Damage to the ureter could have been caused by a kink in the ureter or by treatment given later by a urologist.
VERDICT A $526,088 verdict was returned.
Was CP a result of poor communication?
The on-call ObGyn was notified that a woman was about to deliver at the hospital. The attending resident monitored labor and delivery until the ObGyn arrived. A cesarean delivery was performed. The child suffered hypoxic ischemic encephalopathy with brain damage and cerebral palsy.
PARENTS’ CLAIM A delay in performing cesarean delivery caused the child’s injuries. The ObGyn, who was not present during labor, failed to properly instruct the resident.
DEFENDANTS’ DEFENSE The ObGyn claimed the resident’s interpretation of the fetal monitoring strips misled her to believe that there was no emergency. Cesarean delivery was immediately performed upon the ObGyn’s arrival.
VERDICT The hospital and resident settled for an undisclosed amount before trial. An Ohio defense verdict was returned for the ObGyn.
Was excessive electrocautery used?
A 52-year-old woman underwent supracervical hysterectomy with bilateral salpingo-oophorectomy. She developed a vaginal-peritoneal fistula and a chronic abscess with pain; additional operations were required.
PATIENT’S CLAIM The ObGyn used excessive electrocauterization during the first operation, leading to fistula development. An adhesive barrier prevented fistula healing. The patient would not have had her ovaries removed had she known the consequences, including hot flashes and painful sexual intercourse.
PHYSICIAN’S DEFENSE Surgery was properly performed; excessive electrocautery was not used. The adhesive barrier was correctly applied and did not cause injury. Fistula development is a known complication of the procedure. Appropriate consent was obtained.
VERDICT An Illinois defense verdict was returned.
Why did child have brain damage?
At 25 weeks’ gestation, a mother was found to have genital herpes and received medication. Gestational diabetes was diagnosed at 29 weeks’ gestation and treated with diet. At 38 weeks’ gestation, the patient came to her prenatal visit with scabies on her abdomen, hands, and feet; a scabicide was prescribed. The resident in charge of her care planned to induce labor between 39 and 40 weeks’ gestation.
Meconium was present when the membranes were broken. When fetal heart-rate monitors showed nonreassuring heart tones, an emergency cesarean delivery was performed.
The baby required resuscitation due to a low heart rate. She experienced a seizure at 4 hours of life. Head imaging was consistent with a herpes infection or an hypoxic ischemic event. The child has cerebral palsy with speech and motor deficits.
PATIENT’S CLAIM The resident failed to respond to signs of fetal distress and call in the attending physician. Cesarean delivery should have been performed earlier.
DEFENDANTS’ DEFENSE The baby recovered well after being slightly depressed at birth; umbilical cord blood gases were in the normal range. There was no hypoxic ischemic event during labor. The baby’s injuries were due to infection.
VERDICT A New York defense verdict was returned.
Diaphragmatic hernia missed on fetal US
At 19 weeks’ gestation, a 25-year-old woman underwent fetal ultrasonography at a radiology clinic. The radiologist’s report indicated that the standard fetal structural survey was “unremarkable.” When the child was born, catastrophic impairment and deformity were present due to a diaphragmatic hernia.
PARENTS’ CLAIM The parents claimed wrongful birth. The radiologist missed a diaphragmatic hernia that was evident on the ultrasound.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $333,664 net Florida settlement was reached after deduction of attorney’s fees.
Was breast cancer missed on screening mammogram?
Screening mammography conducted in July 2009 was reported by a radiologist as being unchanged when compared to studies from the previous 2 years. Several months later, the patient discovered a lump in her right breast that was diagnosed as cancer. She underwent a lumpectomy in July 2010, followed by chemotherapy. The patient’s cancer metastasized and she developed lymphedema.
PATIENT’S CLAIM The 2009 mammography showed an abnormality in the right breast that was not present on earlier films. Further testing and treatment in 2009 would have prevented metastasis.
PHYSICIAN’S DEFENSE There was no negligence; the 2009 mammogram was properly read. Treatment and outcome would have been the same regardless of the timing of diagnosis.
VERDICT A $140,919 Michigan verdict was returned.
Premature twin has CP
Born at 26 weeks’ gestation, one twin was in critical condition. She was taken to the pediatric intensive care unit, where she remained for 46 days, and was then transferred to a long-term care center. She suffers from cerebral palsy.
PARENTS’ CLAIM Prompt treatment would have reduced or eliminated some of the effects of cerebral palsy. The birth hospital did not have pulmonary surfactant or nitric oxide with high-frequency jet-ventilation therapy that would have improved the newborn’s respiration. The baby should have been immediately transferred to a facility where this treatment was available. The parents requested a transfer, but it was denied.
DEFENDANTS’ DEFENSE The child was given every appropriate method of treatment; she was adequately oxygenated. Nitric oxide was not FDA-approved for use in this case. The child’s disabilities were a result of her prematurity.
VERDICT A New York defense verdict was returned.
Benign findings after radiation had started
After a 45-year-old woman found a lump in her right breast in October 2006, a pathologist interpreted biopsy results as ductal carcinoma in situ. A general surgeon and an oncologist both recommended partial mastectomy and lymphadenectomy with radiotherapy and possible tamoxifen treatment. Surgery was performed in November 2006, and radiation treatment began in early December.
The oncologist required that slides be reviewed by pathologists at her cancer center before determining if tamoxifen was appropriate. The pathology report indicated that the patient did not have breast cancer, but had atypical ductal hyperplasia. When the patient learned she did not have cancer, she immediately halted radiation therapy, but had already suffered radiation burns on her breast.
PATIENT’S CLAIM The oncologist was notified that the patient did not have cancer in mid-December, but did not tell the patient until January, when they met to discuss tamoxifen therapy. The patient is now at risk for sarcoma, changes in breast tissue, and rib fractures because of radiation therapy. Partial mastectomy and lymphadenectomy are proper treatment for atypical ductal hyperplasia, but radiation therapy is not. The patient is depressed and anxious.
DEFENDANTS’ DEFENSE The oncologist claimed the patient was not informed of the change in diagnosis because radiation treatment is acceptable treatment for atypical ductal hyperplasia; there was no reason for treatment to be stopped.
The pathologist stated that cell variation between ductal carcinoma and atypical ductal hyperplasia is so slight that two pathologists could reach different conclusions reading the same slide. His interpretation was appropriate. The patient was not clinically depressed; she never sought treatment.
VERDICT A $150,000 Pennsylvania verdict was returned against the oncologist. A defense verdict was returned for the pathologist.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WE WANT TO HEAR FROM YOU. Tell us what you think.
Uterine rupture after unplanned VBAC
A 34-year-old woman went into labor 9 days before a scheduled repeat cesarean. She gave birth vaginally to a healthy baby.
After delivery, the mother complained of sharp abdominal pain that she rated 10/10 on the pain scale; pain was unrelieved by morphine. Moderate bleeding was noted. After the ObGyn performed a manual exploration and curette procedure, uterine scar rupture was ruled out and the patient was treated for uterine atony. For 90 minutes, the patient was hypotensive and tachycardic with moderate bleeding. Her hemoglobin and hematocrit levels dropped lower than before delivery, and she went into cardiac arrest. After resuscitation, she received a blood transfusion. A second ObGyn took over her care.
Although the patient received 7 U each of packed red blood cells (PRBC) and fresh frozen plasma (FFP) over the next 5 hours, she continued to have low hemoglobin and hematocrit values. Bleeding was noted as sporadic. Shortly after a decision was made to perform a hysterectomy, the patient experienced cardiac arrest and was successfully resuscitated. At surgery, a uterine rupture was noted. She received 14 U each of PRBC and FFP during surgery. Bleeding stopped after the hysterectomy, but the patient remained on a ventilator for 9 days, suffered renal failure and adrenal insufficiency, and went into cardiac arrest twice more.
The patient suffered brain damage and has poor memory function. She had to relearn to walk, talk, and perform normal life tasks. She underwent a kidney transplant because of permanent kidney damage and will require additional kidney transplants during her lifetime.
PATIENT’S CLAIM The ObGyn failed to recognize uterine scar rupture and perform an immediate hysterectomy. The operative report from the hysterectomy used the words uterine scar “rupture” and “dehiscence” interchangeably as the source of bleeding and hemorrhagic shock.
DEFENDANTS’ DEFENSE The patient’s injury was a prior uterine scar “dehiscence” and not a complete rupture; conservative measures were appropriate.
VERDICT A $4 million Virginia verdict was returned that was reduced to $2 million under the state cap.
Woman in vegetative state after cystectomy
Two days after ovarian cystectomy, a 55-year-old woman was returned to the operating room for primary repair of a colon injury. Postoperatively, a colovesical fistula developed. During a third operation, the patient suffered cardiac arrest and sustained brain damage due to lack of oxygen. She remains in a vegetative state.
PATIENT’S CLAIM The colon injury was not detected or treated in a timely manner. A temporary colostomy should have been performed. Metoprolol tartrate, given after the third operation, caused cardiac arrest.
DEFENDANTS’ DEFENSE A settlement was reached during trial.
VERDICT A $2.725 million New Jersey settlement was reached with two physicians, a nurse, and the hospital. A third physician was released from liability.
Breast surgery leaves triangular areola
Cosmetic breast surgery on a 37-year-old woman included insertion of implants, a mastopexy, and reduction of the areolae. After surgery, one areola appeared triangularly shaped. After several months, the patient saw another plastic surgeon who surgically removed the undesirable tissue to reshape the areola.
PATIENT’S CLAIM Postoperatively, the plastic surgeon explained that the patient’s nipples were surrounded by hyperpigmented tissue that had to be removed during a second operation. The patient signed a consent to surgery, but the document did not explain that additional procedures could be necessary.
PHYSICIAN’S DEFENSE The signed consent form included language that additional procedures could be necessary. The plastic surgeon would have performed a free correction of the areola, but the procedure could not occur until the patient’s breasts had healed. In the meantime, the patient went to another surgeon.
VERDICT A New York defense verdict was returned.
Operative report contested
A gynecologist performed a hysterectomy on a 43-year-old woman. Two days after surgery, she was found to have an obstruction of the left ureter and a bladder injury. Extensive treatment was required to treat the injury.
PATIENT’S CLAIM Surgery was performed in a negligent manner. The surgical report states that the arteries were clamped and sutured before the ureters had been identified. The ureter injury was caused by the improper use of a clamp.
DEFENDANTS’ DEFENSE The gynecologist claimed that the proper sequence was used during surgery; an assisting physician may have erroneously documented the sequence of events. Surgery was complicated by fibroids that distorted the patient’s anatomy. The injury was a known risk of the procedure. Damage to the ureter could have been caused by a kink in the ureter or by treatment given later by a urologist.
VERDICT A $526,088 verdict was returned.
Was CP a result of poor communication?
The on-call ObGyn was notified that a woman was about to deliver at the hospital. The attending resident monitored labor and delivery until the ObGyn arrived. A cesarean delivery was performed. The child suffered hypoxic ischemic encephalopathy with brain damage and cerebral palsy.
PARENTS’ CLAIM A delay in performing cesarean delivery caused the child’s injuries. The ObGyn, who was not present during labor, failed to properly instruct the resident.
DEFENDANTS’ DEFENSE The ObGyn claimed the resident’s interpretation of the fetal monitoring strips misled her to believe that there was no emergency. Cesarean delivery was immediately performed upon the ObGyn’s arrival.
VERDICT The hospital and resident settled for an undisclosed amount before trial. An Ohio defense verdict was returned for the ObGyn.
Was excessive electrocautery used?
A 52-year-old woman underwent supracervical hysterectomy with bilateral salpingo-oophorectomy. She developed a vaginal-peritoneal fistula and a chronic abscess with pain; additional operations were required.
PATIENT’S CLAIM The ObGyn used excessive electrocauterization during the first operation, leading to fistula development. An adhesive barrier prevented fistula healing. The patient would not have had her ovaries removed had she known the consequences, including hot flashes and painful sexual intercourse.
PHYSICIAN’S DEFENSE Surgery was properly performed; excessive electrocautery was not used. The adhesive barrier was correctly applied and did not cause injury. Fistula development is a known complication of the procedure. Appropriate consent was obtained.
VERDICT An Illinois defense verdict was returned.
Why did child have brain damage?
At 25 weeks’ gestation, a mother was found to have genital herpes and received medication. Gestational diabetes was diagnosed at 29 weeks’ gestation and treated with diet. At 38 weeks’ gestation, the patient came to her prenatal visit with scabies on her abdomen, hands, and feet; a scabicide was prescribed. The resident in charge of her care planned to induce labor between 39 and 40 weeks’ gestation.
Meconium was present when the membranes were broken. When fetal heart-rate monitors showed nonreassuring heart tones, an emergency cesarean delivery was performed.
The baby required resuscitation due to a low heart rate. She experienced a seizure at 4 hours of life. Head imaging was consistent with a herpes infection or an hypoxic ischemic event. The child has cerebral palsy with speech and motor deficits.
PATIENT’S CLAIM The resident failed to respond to signs of fetal distress and call in the attending physician. Cesarean delivery should have been performed earlier.
DEFENDANTS’ DEFENSE The baby recovered well after being slightly depressed at birth; umbilical cord blood gases were in the normal range. There was no hypoxic ischemic event during labor. The baby’s injuries were due to infection.
VERDICT A New York defense verdict was returned.
Diaphragmatic hernia missed on fetal US
At 19 weeks’ gestation, a 25-year-old woman underwent fetal ultrasonography at a radiology clinic. The radiologist’s report indicated that the standard fetal structural survey was “unremarkable.” When the child was born, catastrophic impairment and deformity were present due to a diaphragmatic hernia.
PARENTS’ CLAIM The parents claimed wrongful birth. The radiologist missed a diaphragmatic hernia that was evident on the ultrasound.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $333,664 net Florida settlement was reached after deduction of attorney’s fees.
Was breast cancer missed on screening mammogram?
Screening mammography conducted in July 2009 was reported by a radiologist as being unchanged when compared to studies from the previous 2 years. Several months later, the patient discovered a lump in her right breast that was diagnosed as cancer. She underwent a lumpectomy in July 2010, followed by chemotherapy. The patient’s cancer metastasized and she developed lymphedema.
PATIENT’S CLAIM The 2009 mammography showed an abnormality in the right breast that was not present on earlier films. Further testing and treatment in 2009 would have prevented metastasis.
PHYSICIAN’S DEFENSE There was no negligence; the 2009 mammogram was properly read. Treatment and outcome would have been the same regardless of the timing of diagnosis.
VERDICT A $140,919 Michigan verdict was returned.
Premature twin has CP
Born at 26 weeks’ gestation, one twin was in critical condition. She was taken to the pediatric intensive care unit, where she remained for 46 days, and was then transferred to a long-term care center. She suffers from cerebral palsy.
PARENTS’ CLAIM Prompt treatment would have reduced or eliminated some of the effects of cerebral palsy. The birth hospital did not have pulmonary surfactant or nitric oxide with high-frequency jet-ventilation therapy that would have improved the newborn’s respiration. The baby should have been immediately transferred to a facility where this treatment was available. The parents requested a transfer, but it was denied.
DEFENDANTS’ DEFENSE The child was given every appropriate method of treatment; she was adequately oxygenated. Nitric oxide was not FDA-approved for use in this case. The child’s disabilities were a result of her prematurity.
VERDICT A New York defense verdict was returned.
Benign findings after radiation had started
After a 45-year-old woman found a lump in her right breast in October 2006, a pathologist interpreted biopsy results as ductal carcinoma in situ. A general surgeon and an oncologist both recommended partial mastectomy and lymphadenectomy with radiotherapy and possible tamoxifen treatment. Surgery was performed in November 2006, and radiation treatment began in early December.
The oncologist required that slides be reviewed by pathologists at her cancer center before determining if tamoxifen was appropriate. The pathology report indicated that the patient did not have breast cancer, but had atypical ductal hyperplasia. When the patient learned she did not have cancer, she immediately halted radiation therapy, but had already suffered radiation burns on her breast.
PATIENT’S CLAIM The oncologist was notified that the patient did not have cancer in mid-December, but did not tell the patient until January, when they met to discuss tamoxifen therapy. The patient is now at risk for sarcoma, changes in breast tissue, and rib fractures because of radiation therapy. Partial mastectomy and lymphadenectomy are proper treatment for atypical ductal hyperplasia, but radiation therapy is not. The patient is depressed and anxious.
DEFENDANTS’ DEFENSE The oncologist claimed the patient was not informed of the change in diagnosis because radiation treatment is acceptable treatment for atypical ductal hyperplasia; there was no reason for treatment to be stopped.
The pathologist stated that cell variation between ductal carcinoma and atypical ductal hyperplasia is so slight that two pathologists could reach different conclusions reading the same slide. His interpretation was appropriate. The patient was not clinically depressed; she never sought treatment.
VERDICT A $150,000 Pennsylvania verdict was returned against the oncologist. A defense verdict was returned for the pathologist.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WE WANT TO HEAR FROM YOU. Tell us what you think.