User login
Large Hospital Systems, Physician Groups Most Likely to Form Accountable Care Organizations
The environment that breeds the formation of accountable care organizations (ACOs) includes large integrated hospital systems, primary care physicians (PCPs) practicing in large groups, and a greater fraction of hospital risk sharing, according to a Health Affairs report (http://content.healthaffairs.org/content/32/10/1781.abstract).
In other words, institutions and areas that have begun embracing risk-based or population-based payment models are more likely to spur the formation of ACOs, which have similar risk-reward payment structures.
For hospitalists, knowing the conditions that help foster ACOs may be an important first step in pushing for development and continued growth, says Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair and chief medical officer of Cogent HMG in Brentwood, Tenn.
It’s a shift in mindset for sure, says the report’s lead author.
“The traditional model is pretty much fill your beds with high-paying patients. An ACO is really a different kind of concept,” says David Auerbach, MS, PhD, of Boston-based RAND Corporation. “A hospital that doesn’t have any experience thinking in a different way is going to find it hard to accommodate the ACO payment model. But hospitals that do…probably have staff that have thought about this and already started to move down the path to thinking about ways to reduce their costs.”
Regional Variance
Dr. Auerbach, a policy researcher and affiliate faculty member at Pardee RAND Graduate School, says further work needs to be done to identify “key regional factors” that induce certain physicians and hospitals to launch ACOs. His paper, “Accountable Care Organization Formation Is Associated with Integrated Systems but Not High Medical Spending,” found wide disparities in ACO formation; the model is popular in the Northeast and Midwest regions but scarcely found in the Northwest.
—Ron Greeno, MD, FCCP, MHM, SHM’s Public Policy Committee chair, chief medical officer, Cogent HMG, Brentwood, Tenn.
The authors reviewed 32 Medicare Pioneer ACOs, 116 Medicare Shared Savings Program ACOs, and 77 private-market entities very similar to ACOs. The study’s multiple-regression analysis found that in the 31 regions with at least 20% of Medicare fee-for-service beneficiaries in an ACO, more than half of hospitals had a joint venture with doctors or physician groups and were affiliated with a health system. In so-called “low-ACO areas,” that percentage hovered around 30% to 40%.
And while much of the policy discussion focuses on whether ACOs can rein in healthcare spending in some of the markets where care costs the most, the study reported “no strong pattern in the relationship between ACO penetration and Medicare spending or spending growth.”
Uncertain Upside
Dr. Auerbach says that while the results of his paper did not surprise him, he hopes hospitalists and others use them educationally.
“We might think about there being demand from people in other areas that might say, ‘I want to be a part of that too. Why aren’t there any ACOs that I can be in?’” he adds. “And so a study like this says, ‘Here are some of the things that seem to be important.’ If there’s not this kind of infrastructure in your area, as a policy maker, you could go and say, ‘Let’s try and give a boost to some of these factors or proxies for these things.’”
Part of that review would include looking at those areas that saw higher rates of physician-institution consolidation and figuring out what the motivations were. Typically, the impetus of forming larger groups is partly explained by a desire to negotiate with insurers and get better deals, Dr. Auerbach says. But with more coordinated care comes a more efficient system that can offset those lower rates.
“I think right now most policymakers are not sure if the upside is better than the downside,” he adds. “I think the answer, personally, is not to try to break up providers and do a lot of anti-trust activity. We need to understand whether, and how much, integrated groups are able to use market power to charge higher prices. And, if they do, there may be other ways to combat that problem while keeping the groups intact.”
Rethinking Reimbursement
Dr. Greeno says growing pains are inevitable along the way, particularly because the move to the ACO payment model is a seismic shift for a healthcare industry that has traditionally been based on a fee-for-service model.
“How we pay for healthcare in this country is going to be completely flipped on its head,” he says. “Part of the goal, of course, is better outcomes for patients. But it’s also cost efficiency. In the meantime, the entire system for 100 years has been paying for production.”
Dr. Greeno compares it to the shift that was the managed-care movement. Moving forward, the shift will create winners and losers and most likely will result in massive consolidation of healthcare organizations—from nearly 700 today to what Dr. Greeno believes may be 50 to 70 mega-providers.
“It’s basically what happened when HMOs started paying capitated payments to physician groups,” he says. “The groups then had X amount of dollars to care for their patient population, and if they couldn’t make that work, they went out of business or were acquired by more successful groups. If they could make it work, then they survived. It’s the exact same thing. It’s not quite as dramatic, as it is not going to happen overnight, but that’s where it’s heading.
“And instead of occurring in pockets around the country like in Southern California and Minneapolis, it’s going to be nationwide, and the world’s largest insurance company, which is Medicare, is driving it.”
Dr. Auerbach notes that while the disruption already has caused some groups to drop out of the ACO programs, he does not see that as a precursor to more organizations turning away from the program, particularly as it is among the key planks of the general healthcare reform movement.
“It is part of a larger wave that really is changing the way we do healthcare,” he says. “I think that as [ACOs] grow...people are going to say that this is becoming something like the dominant form of delivering healthcare.”
Richard Quinn is a freelance writer in New Jersey.
The environment that breeds the formation of accountable care organizations (ACOs) includes large integrated hospital systems, primary care physicians (PCPs) practicing in large groups, and a greater fraction of hospital risk sharing, according to a Health Affairs report (http://content.healthaffairs.org/content/32/10/1781.abstract).
In other words, institutions and areas that have begun embracing risk-based or population-based payment models are more likely to spur the formation of ACOs, which have similar risk-reward payment structures.
For hospitalists, knowing the conditions that help foster ACOs may be an important first step in pushing for development and continued growth, says Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair and chief medical officer of Cogent HMG in Brentwood, Tenn.
It’s a shift in mindset for sure, says the report’s lead author.
“The traditional model is pretty much fill your beds with high-paying patients. An ACO is really a different kind of concept,” says David Auerbach, MS, PhD, of Boston-based RAND Corporation. “A hospital that doesn’t have any experience thinking in a different way is going to find it hard to accommodate the ACO payment model. But hospitals that do…probably have staff that have thought about this and already started to move down the path to thinking about ways to reduce their costs.”
Regional Variance
Dr. Auerbach, a policy researcher and affiliate faculty member at Pardee RAND Graduate School, says further work needs to be done to identify “key regional factors” that induce certain physicians and hospitals to launch ACOs. His paper, “Accountable Care Organization Formation Is Associated with Integrated Systems but Not High Medical Spending,” found wide disparities in ACO formation; the model is popular in the Northeast and Midwest regions but scarcely found in the Northwest.
—Ron Greeno, MD, FCCP, MHM, SHM’s Public Policy Committee chair, chief medical officer, Cogent HMG, Brentwood, Tenn.
The authors reviewed 32 Medicare Pioneer ACOs, 116 Medicare Shared Savings Program ACOs, and 77 private-market entities very similar to ACOs. The study’s multiple-regression analysis found that in the 31 regions with at least 20% of Medicare fee-for-service beneficiaries in an ACO, more than half of hospitals had a joint venture with doctors or physician groups and were affiliated with a health system. In so-called “low-ACO areas,” that percentage hovered around 30% to 40%.
And while much of the policy discussion focuses on whether ACOs can rein in healthcare spending in some of the markets where care costs the most, the study reported “no strong pattern in the relationship between ACO penetration and Medicare spending or spending growth.”
Uncertain Upside
Dr. Auerbach says that while the results of his paper did not surprise him, he hopes hospitalists and others use them educationally.
“We might think about there being demand from people in other areas that might say, ‘I want to be a part of that too. Why aren’t there any ACOs that I can be in?’” he adds. “And so a study like this says, ‘Here are some of the things that seem to be important.’ If there’s not this kind of infrastructure in your area, as a policy maker, you could go and say, ‘Let’s try and give a boost to some of these factors or proxies for these things.’”
Part of that review would include looking at those areas that saw higher rates of physician-institution consolidation and figuring out what the motivations were. Typically, the impetus of forming larger groups is partly explained by a desire to negotiate with insurers and get better deals, Dr. Auerbach says. But with more coordinated care comes a more efficient system that can offset those lower rates.
“I think right now most policymakers are not sure if the upside is better than the downside,” he adds. “I think the answer, personally, is not to try to break up providers and do a lot of anti-trust activity. We need to understand whether, and how much, integrated groups are able to use market power to charge higher prices. And, if they do, there may be other ways to combat that problem while keeping the groups intact.”
Rethinking Reimbursement
Dr. Greeno says growing pains are inevitable along the way, particularly because the move to the ACO payment model is a seismic shift for a healthcare industry that has traditionally been based on a fee-for-service model.
“How we pay for healthcare in this country is going to be completely flipped on its head,” he says. “Part of the goal, of course, is better outcomes for patients. But it’s also cost efficiency. In the meantime, the entire system for 100 years has been paying for production.”
Dr. Greeno compares it to the shift that was the managed-care movement. Moving forward, the shift will create winners and losers and most likely will result in massive consolidation of healthcare organizations—from nearly 700 today to what Dr. Greeno believes may be 50 to 70 mega-providers.
“It’s basically what happened when HMOs started paying capitated payments to physician groups,” he says. “The groups then had X amount of dollars to care for their patient population, and if they couldn’t make that work, they went out of business or were acquired by more successful groups. If they could make it work, then they survived. It’s the exact same thing. It’s not quite as dramatic, as it is not going to happen overnight, but that’s where it’s heading.
“And instead of occurring in pockets around the country like in Southern California and Minneapolis, it’s going to be nationwide, and the world’s largest insurance company, which is Medicare, is driving it.”
Dr. Auerbach notes that while the disruption already has caused some groups to drop out of the ACO programs, he does not see that as a precursor to more organizations turning away from the program, particularly as it is among the key planks of the general healthcare reform movement.
“It is part of a larger wave that really is changing the way we do healthcare,” he says. “I think that as [ACOs] grow...people are going to say that this is becoming something like the dominant form of delivering healthcare.”
Richard Quinn is a freelance writer in New Jersey.
The environment that breeds the formation of accountable care organizations (ACOs) includes large integrated hospital systems, primary care physicians (PCPs) practicing in large groups, and a greater fraction of hospital risk sharing, according to a Health Affairs report (http://content.healthaffairs.org/content/32/10/1781.abstract).
In other words, institutions and areas that have begun embracing risk-based or population-based payment models are more likely to spur the formation of ACOs, which have similar risk-reward payment structures.
For hospitalists, knowing the conditions that help foster ACOs may be an important first step in pushing for development and continued growth, says Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair and chief medical officer of Cogent HMG in Brentwood, Tenn.
It’s a shift in mindset for sure, says the report’s lead author.
“The traditional model is pretty much fill your beds with high-paying patients. An ACO is really a different kind of concept,” says David Auerbach, MS, PhD, of Boston-based RAND Corporation. “A hospital that doesn’t have any experience thinking in a different way is going to find it hard to accommodate the ACO payment model. But hospitals that do…probably have staff that have thought about this and already started to move down the path to thinking about ways to reduce their costs.”
Regional Variance
Dr. Auerbach, a policy researcher and affiliate faculty member at Pardee RAND Graduate School, says further work needs to be done to identify “key regional factors” that induce certain physicians and hospitals to launch ACOs. His paper, “Accountable Care Organization Formation Is Associated with Integrated Systems but Not High Medical Spending,” found wide disparities in ACO formation; the model is popular in the Northeast and Midwest regions but scarcely found in the Northwest.
—Ron Greeno, MD, FCCP, MHM, SHM’s Public Policy Committee chair, chief medical officer, Cogent HMG, Brentwood, Tenn.
The authors reviewed 32 Medicare Pioneer ACOs, 116 Medicare Shared Savings Program ACOs, and 77 private-market entities very similar to ACOs. The study’s multiple-regression analysis found that in the 31 regions with at least 20% of Medicare fee-for-service beneficiaries in an ACO, more than half of hospitals had a joint venture with doctors or physician groups and were affiliated with a health system. In so-called “low-ACO areas,” that percentage hovered around 30% to 40%.
And while much of the policy discussion focuses on whether ACOs can rein in healthcare spending in some of the markets where care costs the most, the study reported “no strong pattern in the relationship between ACO penetration and Medicare spending or spending growth.”
Uncertain Upside
Dr. Auerbach says that while the results of his paper did not surprise him, he hopes hospitalists and others use them educationally.
“We might think about there being demand from people in other areas that might say, ‘I want to be a part of that too. Why aren’t there any ACOs that I can be in?’” he adds. “And so a study like this says, ‘Here are some of the things that seem to be important.’ If there’s not this kind of infrastructure in your area, as a policy maker, you could go and say, ‘Let’s try and give a boost to some of these factors or proxies for these things.’”
Part of that review would include looking at those areas that saw higher rates of physician-institution consolidation and figuring out what the motivations were. Typically, the impetus of forming larger groups is partly explained by a desire to negotiate with insurers and get better deals, Dr. Auerbach says. But with more coordinated care comes a more efficient system that can offset those lower rates.
“I think right now most policymakers are not sure if the upside is better than the downside,” he adds. “I think the answer, personally, is not to try to break up providers and do a lot of anti-trust activity. We need to understand whether, and how much, integrated groups are able to use market power to charge higher prices. And, if they do, there may be other ways to combat that problem while keeping the groups intact.”
Rethinking Reimbursement
Dr. Greeno says growing pains are inevitable along the way, particularly because the move to the ACO payment model is a seismic shift for a healthcare industry that has traditionally been based on a fee-for-service model.
“How we pay for healthcare in this country is going to be completely flipped on its head,” he says. “Part of the goal, of course, is better outcomes for patients. But it’s also cost efficiency. In the meantime, the entire system for 100 years has been paying for production.”
Dr. Greeno compares it to the shift that was the managed-care movement. Moving forward, the shift will create winners and losers and most likely will result in massive consolidation of healthcare organizations—from nearly 700 today to what Dr. Greeno believes may be 50 to 70 mega-providers.
“It’s basically what happened when HMOs started paying capitated payments to physician groups,” he says. “The groups then had X amount of dollars to care for their patient population, and if they couldn’t make that work, they went out of business or were acquired by more successful groups. If they could make it work, then they survived. It’s the exact same thing. It’s not quite as dramatic, as it is not going to happen overnight, but that’s where it’s heading.
“And instead of occurring in pockets around the country like in Southern California and Minneapolis, it’s going to be nationwide, and the world’s largest insurance company, which is Medicare, is driving it.”
Dr. Auerbach notes that while the disruption already has caused some groups to drop out of the ACO programs, he does not see that as a precursor to more organizations turning away from the program, particularly as it is among the key planks of the general healthcare reform movement.
“It is part of a larger wave that really is changing the way we do healthcare,” he says. “I think that as [ACOs] grow...people are going to say that this is becoming something like the dominant form of delivering healthcare.”
Richard Quinn is a freelance writer in New Jersey.
SHM Backs Medicare Reimbursement for End-of-Life Care Counseling

Although inevitable, death is often difficult to conceptualize and even more sensitive to discuss. For hospitalists and other care providers, conversations about the end of life with families and caregivers can be fraught with emotion. The fact that something is uncomfortable does not mean it is not useful or valuable, however. Patients must be able to vocalize their end-of-life wishes and should feel confident that the healthcare system is able to respond.
To help with this effort, the Society of Hospital Medicine is supporting legislation that would encourage voluntary end-of-life conversations between patients and their healthcare providers. Sponsored by U.S. Rep. Earl Blumenauer (D-Ore.), the Personalize Your Care Act of 2013 (H.R. 1173) would make Medicare reimbursement available for advance-care planning consultations, establish grants for state-level physician orders for life-sustaining treatment (POLST) programs, and require that advance directives be honored across state lines.
Hospitalists are integral team leaders for coordinating care and, as such, are often highly involved in end-of-life care for patients. They are at the front lines of these conversations, often tasked to plan end-of-life care and then carry out those plans. Many of their patients are acutely ill and need to face these critical decisions, often in real time.
End-of-life planning, like many other cognitive medical services, is not adequately reimbursed under current Medicare payment policy. This legislation would authorize Medicare to provide coverage for voluntary advance care consultations every five years or following changes in health, health-related condition, or care setting of the patient.
SHM is strongly supportive of adequate reimbursement for the counseling these patients require in planning their end-of-life care. The bill would make these conversations a practicable addition to the care and counseling workflow for healthcare providers and would ensure that they could occur at reasonable intervals and at significant changes in health or life events. These conversations would help ensure that patient wishes are respected at the end of life and prevent the use of unwanted treatments or interventions.
As the healthcare system works toward being more coordinated and more patient-centered, voluntary advance care planning is essential. Patients often see multiple providers at the end of their lives and—particularly as questions arise—it is imperative that providers have access to the most up-to-date advance care plans. H.R. 1173 works to address this gap by moving toward electronic health record display of advance directives and POLST.
Hospitalists may be eligible for reimbursement for these consultations, particularly in cases where these discussions did not occur in the outpatient setting. SHM is actively working with Rep. Blumenauer to ensure that all providers in a position to have these important conversations would be appropriately reimbursed. Patients need to have an active mechanism to ensure that their wishes are appropriately followed; this legislation would give them better access to these important and difficult conversations.
Joshua Lapps is SHM’s government relations specialist.
Although inevitable, death is often difficult to conceptualize and even more sensitive to discuss. For hospitalists and other care providers, conversations about the end of life with families and caregivers can be fraught with emotion. The fact that something is uncomfortable does not mean it is not useful or valuable, however. Patients must be able to vocalize their end-of-life wishes and should feel confident that the healthcare system is able to respond.
To help with this effort, the Society of Hospital Medicine is supporting legislation that would encourage voluntary end-of-life conversations between patients and their healthcare providers. Sponsored by U.S. Rep. Earl Blumenauer (D-Ore.), the Personalize Your Care Act of 2013 (H.R. 1173) would make Medicare reimbursement available for advance-care planning consultations, establish grants for state-level physician orders for life-sustaining treatment (POLST) programs, and require that advance directives be honored across state lines.
Hospitalists are integral team leaders for coordinating care and, as such, are often highly involved in end-of-life care for patients. They are at the front lines of these conversations, often tasked to plan end-of-life care and then carry out those plans. Many of their patients are acutely ill and need to face these critical decisions, often in real time.
End-of-life planning, like many other cognitive medical services, is not adequately reimbursed under current Medicare payment policy. This legislation would authorize Medicare to provide coverage for voluntary advance care consultations every five years or following changes in health, health-related condition, or care setting of the patient.
SHM is strongly supportive of adequate reimbursement for the counseling these patients require in planning their end-of-life care. The bill would make these conversations a practicable addition to the care and counseling workflow for healthcare providers and would ensure that they could occur at reasonable intervals and at significant changes in health or life events. These conversations would help ensure that patient wishes are respected at the end of life and prevent the use of unwanted treatments or interventions.
As the healthcare system works toward being more coordinated and more patient-centered, voluntary advance care planning is essential. Patients often see multiple providers at the end of their lives and—particularly as questions arise—it is imperative that providers have access to the most up-to-date advance care plans. H.R. 1173 works to address this gap by moving toward electronic health record display of advance directives and POLST.
Hospitalists may be eligible for reimbursement for these consultations, particularly in cases where these discussions did not occur in the outpatient setting. SHM is actively working with Rep. Blumenauer to ensure that all providers in a position to have these important conversations would be appropriately reimbursed. Patients need to have an active mechanism to ensure that their wishes are appropriately followed; this legislation would give them better access to these important and difficult conversations.
Joshua Lapps is SHM’s government relations specialist.
Although inevitable, death is often difficult to conceptualize and even more sensitive to discuss. For hospitalists and other care providers, conversations about the end of life with families and caregivers can be fraught with emotion. The fact that something is uncomfortable does not mean it is not useful or valuable, however. Patients must be able to vocalize their end-of-life wishes and should feel confident that the healthcare system is able to respond.
To help with this effort, the Society of Hospital Medicine is supporting legislation that would encourage voluntary end-of-life conversations between patients and their healthcare providers. Sponsored by U.S. Rep. Earl Blumenauer (D-Ore.), the Personalize Your Care Act of 2013 (H.R. 1173) would make Medicare reimbursement available for advance-care planning consultations, establish grants for state-level physician orders for life-sustaining treatment (POLST) programs, and require that advance directives be honored across state lines.
Hospitalists are integral team leaders for coordinating care and, as such, are often highly involved in end-of-life care for patients. They are at the front lines of these conversations, often tasked to plan end-of-life care and then carry out those plans. Many of their patients are acutely ill and need to face these critical decisions, often in real time.
End-of-life planning, like many other cognitive medical services, is not adequately reimbursed under current Medicare payment policy. This legislation would authorize Medicare to provide coverage for voluntary advance care consultations every five years or following changes in health, health-related condition, or care setting of the patient.
SHM is strongly supportive of adequate reimbursement for the counseling these patients require in planning their end-of-life care. The bill would make these conversations a practicable addition to the care and counseling workflow for healthcare providers and would ensure that they could occur at reasonable intervals and at significant changes in health or life events. These conversations would help ensure that patient wishes are respected at the end of life and prevent the use of unwanted treatments or interventions.
As the healthcare system works toward being more coordinated and more patient-centered, voluntary advance care planning is essential. Patients often see multiple providers at the end of their lives and—particularly as questions arise—it is imperative that providers have access to the most up-to-date advance care plans. H.R. 1173 works to address this gap by moving toward electronic health record display of advance directives and POLST.
Hospitalists may be eligible for reimbursement for these consultations, particularly in cases where these discussions did not occur in the outpatient setting. SHM is actively working with Rep. Blumenauer to ensure that all providers in a position to have these important conversations would be appropriately reimbursed. Patients need to have an active mechanism to ensure that their wishes are appropriately followed; this legislation would give them better access to these important and difficult conversations.
Joshua Lapps is SHM’s government relations specialist.
In Las Vegas, HM 14 Can Include Whole Family
Enter text here
Enter text here
Enter text here
Breast biopsy delayed. $1.5M verdict

During a routine mammogram, an enlarged lymph node was found in the patient’s armpit. The patient’s primary care physician (PCP) ordered follow-up imaging and referred the patient to a surgeon for possible excisional biopsy. The surgeon suggested that the biopsy could be delayed until additional imaging studies were completed.
The patient transferred her care to another surgeon, who immediately performed the biopsy and found stage IV inoperable breast cancer. The patient underwent aggressive chemotherapy for 3 years, but died 39 months after diagnosis.
ESTATE’S CLAIM The first surgeon was negligent for not immediately performing the biopsy.
DEFENDANTS’ DEFENSE There was no negligence. An earlier biopsy would not have changed the outcome.
VERDICT A $1.5 million Massachusetts verdict was returned.
Treating bowel injury after uterine ablation
Following uterine ablation performed by a gynecologist, a 35-year-old woman suffered severe abdominal pain. Six days later, the gynecologist and a surgeon performed a hysterectomy.
Three days after discharge, the patient returned to the hospital with an abdominal infection and sepsis. During a third operation, a burn hole was found; the injured portion of bowel was resected. The patient has chronic abdominal pain.
PATIENT’S CLAIM Sepsis and infection could have been avoided if either physician had identified the injury during the second hospitalization and surgery. The patient developed psychological issues as a result of chronic pain.
DEFENDANTS’ DEFENSE A settlement was reached with the gynecologist during the trial. The surgeon denied negligence. During the second surgery, he examined her bowel for a possible injury but found none.
VERDICT A $3.5 million Illinois verdict was returned. It included
$1.5 million for past pain and suffering that was reduced by $100,000 due to the patient’s failure to report for psychological counseling. The jury found the gynecologist 65% at fault and the surgeon 35% at fault.
Mother in permanent vegetative state
When a 30-year-old woman went to a hospital in labor, she had gestational hypertension. The next morning, she suffered cardiopulmonary arrest. A healthy baby was born by emergency cesarean delivery, but the mother was left in a permanent vegetative state.
PATIENT’S CLAIM The nurses failed to ensure that the ObGyn came to the hospital and did not report blood pressure data to the ObGyn. Gestational hypertension progressed to preeclampsia. Early delivery should have been induced or magnesium sulfate should have been administered.
DEFENDANTS’ DEFENSE A confidential settlement was reached with the ObGyn before trial.
The nurses were right to rely on the ObGyn to make decisions regarding the patient’s care. They provided appropriate treatment.
VERDICT A New Jersey defense verdict was returned for the hospital.
What caused the child’s brain injuries?
After vaginal delivery, the baby was not breathing and required intubation. He had a seizure and displayed signs of oxygen deprivation, hypoxic ischemic injury, and brain damage. The child uses a special walker and can only communicate using a computer that speaks for him.
PARENTS’ CLAIM The nurses and ObGyn failed to properly assess the baby. The fetal heart-rate monitor electrode should have been placed on the fetal scalp. A cesarean delivery should have been performed.
DEFENDANTS’ DEFENSE The fetal monitor was properly placed. The child’s injury occurred 24 to 72 hours prior to birth due to an umbilical cord accident. A cesarean delivery would have not changed the outcome.
VERDICT A Georgia defense verdict was returned.

Did a woman’s vaginal infection cause her baby’s death?
At 22 weeks’ gestation, a 26-year-old woman began to leak amniotic fluid and went to the hospital. She was in premature labor. The newborn died 19 minutes after birth.
PARENTS’ CLAIM The ObGyn and nurse midwife who provided prenatal care failed to diagnose and treat a vaginal infection. The infection resulted in premature rupture of membranes, leading to premature birth and the baby’s death.
DEFENDANTS’ DEFENSE A confidential settlement was reached with the ObGyn before trial. The nurse midwife claimed the patient did not have a vaginal infection; she never reported symptoms of a foul-smelling vaginal odor or discharge. Premature rupture of membranes was not caused by a vaginal infection. The newborn’s death was related to an umbilical cord defect, the patient’s delay in coming to the hospital, and the multiple obstetric procedures the mother had undergone before this pregnancy.
VERDICT A $456,024 New Jersey verdict was returned.
Inadvertent ligation, ureteral obstruction
A 41-year-old woman suffered pelvic pain and had a history of endometriosis. In January 2007, a CT scan revealed a ruptured ovarian cyst; her ObGyn performed laparotomy for a hysterectomy and oophorectomy.
During surgery, a resident working under the supervision of the ObGyn inadvertently ligated the left ureter. The injury was close to the bladder near the ureteral vesicle junction. A few days later, cystoscopy showed ureteral obstruction. The patient underwent operative repair with nephrostomy tube placement. In May 2007, the patient had a third operation to reimplant the ureter. She has chronic flank pain.
PATIENT’S CLAIM The resident and, therefore, the ObGyn, were negligent in the performance of the procedure. Proper bladder dissection would have moved the ureter to a position where it could not have been ligated.
DEFENDANTS’ DEFENSE Ureter injury is a known risk of the procedure.
VERDICT An Illinois defense verdict was returned.
Foot drop after tubal ligatioN?
During tubal ligation, a woman in her 30s was restrained by a belt. Venodyne boots were applied to promote blood circulation.
PATIENT’S CLAIM The belt and/or boot damaged the perineal and tibial nerves in her left leg, causing foot drop. When asked to definitely identify what caused the nerve damage, the patient invoked the doctrine of res ipsa loquitur (presumed negligence during surgery).
DEFENDANTS’ DEFENSE A $400,000 settlement was reached with the hospital before the trial.
The gynecologist and anesthesiologist denied negligence. The Venodyne boots could not have caused the injury, nor could the belt, which was applied in an area that did not involve the perineal or tibial nerves. The patient did not complain of pain after surgery.
VERDICT A New York defense verdict was returned for the physicians.
Avoid surgical menopause?
After a 10-year history of endometriosis and chronic pelvic pain, a 38-year-old woman underwent bilateral salpingo-oophorectomy. Postoperatively, she suffered surgical menopause that exacerbated pre-existing anxiety and depression.
PATIENT’S CLAIM It was unnecessary to remove the healthy right ovary; having it remain would have avoided early menopause. She would not have consented to the removal of both ovaries had she been properly advised. Alternative treatment was not offered. Her marriage dissolved, her children went to live with their grandparents, and she was unable to work because of complications.
PHYSICIAN’S DEFENSE Proper consent was obtained, including alternatives to surgery. Evidence of ovarian cancer or other medical necessity was not required because full consent was obtained. Removal of the ovaries was proper due to dense pelvic and bowel adhesions, cystic adnexal masses with questionable pathology, and her chronic pelvic pain. The patient’s appendix was adhesed, causing an unreasonable risk of ovarian torsion.
VERDICT A Michigan defense verdict was returned.
Do you enjoy reading Medical Verdicts?
Find more in the PROFESSIONAL LIABILITY Topic Collection.
Persistent voiding problems
A 52-year-old woman was given a diagnosis of stage II anterior pelvic organ prolapse, a high transverse fascial defect, stress urinary incontinence, and distal rectocele.
A gynecologist performed robotic supracervical hysterectomy and colposacropexy, with tension-free vaginal tape and perineal repair.
While in the hospital, she required a catheter to void, and was still unable to void 5 days after discharge. The gynecologist identified persistent urinary retention, released the tension-free vaginal tape, and performed a midurethral sling procedure, but the patient continued to have voiding problems.
The gynecologist suspected a neurogenic problem and referred the patient to a neuro-urologist. Continued intermittent catheterization was recommended by the neuro-urologist, but the patient had continued voiding problems and developed a urinary tract infection.
She went to her ObGyn, who performed a sling revision and cystoscopy and removed all the mesh that could be found. The patient underwent additional treatment, with some improvement.
PATIENT’S CLAIM The gynecologist was negligent for failing to offer further surgery to improve the patient’s condition.
PHYSICIAN’S DEFENSE There was no negligence. Further dissection in the presence of a neurogenic bladder carried a high risk of incontinence. The patient was told of the risk of urinary retention prior to the first procedure and signed an informed consent.
VERDICT A Virginia defense verdict was returned.
Did pathologists fail to diagnose early breast cancer?
After A 45-year-old woman underwent mammography in May 2008 at a local hospital, an oncologist noted a suspicious finding in the right breast. The patient had an incisional biopsy interpreted by Dr. A, a pathologist, and a core biopsy interpreted by Dr. B, another pathologist from the same diagnostic medical group. Both pathologists interpreted the mass as atypia, a benign abnormality.
In 2010, the patient went to a university medical center, where the mass was biopsied and the patient was found to have cancer. She underwent a right mastectomy.
PATIENT’S CLAIM The pathologists failed to diagnose her breast cancer at an early stage. Dr. A should have interpreted the 2008 incisional biopsy as malignant. A diagnosis in 2008 would have avoided the need for a mastectomy, allowing her to have a lumpectomy with chemotherapy.
DEFENDANTS’ DEFENSE The 2010 review of the 2008 data was an over-interpretation with hindsight bias; the diagnosis in 2008 was correct.
VERDICT The case against the local hospital and Dr. B were dismissed. The matter continued against Dr. A and the diagnostic medical group. A California defense verdict was returned.
Brachial plexus injury occurs after admitting physician leaves
A woman sought prenatal care from her family practitioner (FP). The FP admitted the mother to a hospital for induction of labor at 38 weeks’ gestation with concerns of increased uric acid, possible gestational hypertension, and leaking amniotic fluid. Labor progressed and the mother began pushing about 4 pm. After 30 minutes, the FP attempted vacuum extraction three times; the device popped off during one of the attempts.
The FP then left for a planned trip, and an ObGyn assumed her care. The ObGyn chose to allow the mother to rest. At 6 pm, the mother began to feel the urge to push. The ObGyn attempted vacuum extraction. Shoulder dystocia was encountered, and McRoberts and corkscrew maneuvers were used to deliver the fetus.
The child has C5–C6 brachial plexus injury with scapular winging and internal shoulder rotation.
PARENTS’ CLAIM A cesarean delivery should have been performed. The ObGyn applied excessive lateral traction, leading to the injury.
DEFENDANTS’ DEFENSE The FP and ObGyn argued that a cesarean delivery was not indicated because the fetus was not in distress. Fetal heart-rate monitoring strips were reassuring. The ObGyn denied using excessive lateral traction when freeing the shoulder dystocia.
VERDICT The hospital settled before trial for $300,000. An Illinois defense verdict was returned for the FP. The jury deadlocked as to the ObGyn’s negligence.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
During a routine mammogram, an enlarged lymph node was found in the patient’s armpit. The patient’s primary care physician (PCP) ordered follow-up imaging and referred the patient to a surgeon for possible excisional biopsy. The surgeon suggested that the biopsy could be delayed until additional imaging studies were completed.
The patient transferred her care to another surgeon, who immediately performed the biopsy and found stage IV inoperable breast cancer. The patient underwent aggressive chemotherapy for 3 years, but died 39 months after diagnosis.
ESTATE’S CLAIM The first surgeon was negligent for not immediately performing the biopsy.
DEFENDANTS’ DEFENSE There was no negligence. An earlier biopsy would not have changed the outcome.
VERDICT A $1.5 million Massachusetts verdict was returned.
Treating bowel injury after uterine ablation
Following uterine ablation performed by a gynecologist, a 35-year-old woman suffered severe abdominal pain. Six days later, the gynecologist and a surgeon performed a hysterectomy.
Three days after discharge, the patient returned to the hospital with an abdominal infection and sepsis. During a third operation, a burn hole was found; the injured portion of bowel was resected. The patient has chronic abdominal pain.
PATIENT’S CLAIM Sepsis and infection could have been avoided if either physician had identified the injury during the second hospitalization and surgery. The patient developed psychological issues as a result of chronic pain.
DEFENDANTS’ DEFENSE A settlement was reached with the gynecologist during the trial. The surgeon denied negligence. During the second surgery, he examined her bowel for a possible injury but found none.
VERDICT A $3.5 million Illinois verdict was returned. It included
$1.5 million for past pain and suffering that was reduced by $100,000 due to the patient’s failure to report for psychological counseling. The jury found the gynecologist 65% at fault and the surgeon 35% at fault.
Mother in permanent vegetative state
When a 30-year-old woman went to a hospital in labor, she had gestational hypertension. The next morning, she suffered cardiopulmonary arrest. A healthy baby was born by emergency cesarean delivery, but the mother was left in a permanent vegetative state.
PATIENT’S CLAIM The nurses failed to ensure that the ObGyn came to the hospital and did not report blood pressure data to the ObGyn. Gestational hypertension progressed to preeclampsia. Early delivery should have been induced or magnesium sulfate should have been administered.
DEFENDANTS’ DEFENSE A confidential settlement was reached with the ObGyn before trial.
The nurses were right to rely on the ObGyn to make decisions regarding the patient’s care. They provided appropriate treatment.
VERDICT A New Jersey defense verdict was returned for the hospital.
What caused the child’s brain injuries?
After vaginal delivery, the baby was not breathing and required intubation. He had a seizure and displayed signs of oxygen deprivation, hypoxic ischemic injury, and brain damage. The child uses a special walker and can only communicate using a computer that speaks for him.
PARENTS’ CLAIM The nurses and ObGyn failed to properly assess the baby. The fetal heart-rate monitor electrode should have been placed on the fetal scalp. A cesarean delivery should have been performed.
DEFENDANTS’ DEFENSE The fetal monitor was properly placed. The child’s injury occurred 24 to 72 hours prior to birth due to an umbilical cord accident. A cesarean delivery would have not changed the outcome.
VERDICT A Georgia defense verdict was returned.
Did a woman’s vaginal infection cause her baby’s death?
At 22 weeks’ gestation, a 26-year-old woman began to leak amniotic fluid and went to the hospital. She was in premature labor. The newborn died 19 minutes after birth.
PARENTS’ CLAIM The ObGyn and nurse midwife who provided prenatal care failed to diagnose and treat a vaginal infection. The infection resulted in premature rupture of membranes, leading to premature birth and the baby’s death.
DEFENDANTS’ DEFENSE A confidential settlement was reached with the ObGyn before trial. The nurse midwife claimed the patient did not have a vaginal infection; she never reported symptoms of a foul-smelling vaginal odor or discharge. Premature rupture of membranes was not caused by a vaginal infection. The newborn’s death was related to an umbilical cord defect, the patient’s delay in coming to the hospital, and the multiple obstetric procedures the mother had undergone before this pregnancy.
VERDICT A $456,024 New Jersey verdict was returned.
Inadvertent ligation, ureteral obstruction
A 41-year-old woman suffered pelvic pain and had a history of endometriosis. In January 2007, a CT scan revealed a ruptured ovarian cyst; her ObGyn performed laparotomy for a hysterectomy and oophorectomy.
During surgery, a resident working under the supervision of the ObGyn inadvertently ligated the left ureter. The injury was close to the bladder near the ureteral vesicle junction. A few days later, cystoscopy showed ureteral obstruction. The patient underwent operative repair with nephrostomy tube placement. In May 2007, the patient had a third operation to reimplant the ureter. She has chronic flank pain.
PATIENT’S CLAIM The resident and, therefore, the ObGyn, were negligent in the performance of the procedure. Proper bladder dissection would have moved the ureter to a position where it could not have been ligated.
DEFENDANTS’ DEFENSE Ureter injury is a known risk of the procedure.
VERDICT An Illinois defense verdict was returned.
Foot drop after tubal ligatioN?
During tubal ligation, a woman in her 30s was restrained by a belt. Venodyne boots were applied to promote blood circulation.
PATIENT’S CLAIM The belt and/or boot damaged the perineal and tibial nerves in her left leg, causing foot drop. When asked to definitely identify what caused the nerve damage, the patient invoked the doctrine of res ipsa loquitur (presumed negligence during surgery).
DEFENDANTS’ DEFENSE A $400,000 settlement was reached with the hospital before the trial.
The gynecologist and anesthesiologist denied negligence. The Venodyne boots could not have caused the injury, nor could the belt, which was applied in an area that did not involve the perineal or tibial nerves. The patient did not complain of pain after surgery.
VERDICT A New York defense verdict was returned for the physicians.
Avoid surgical menopause?
After a 10-year history of endometriosis and chronic pelvic pain, a 38-year-old woman underwent bilateral salpingo-oophorectomy. Postoperatively, she suffered surgical menopause that exacerbated pre-existing anxiety and depression.
PATIENT’S CLAIM It was unnecessary to remove the healthy right ovary; having it remain would have avoided early menopause. She would not have consented to the removal of both ovaries had she been properly advised. Alternative treatment was not offered. Her marriage dissolved, her children went to live with their grandparents, and she was unable to work because of complications.
PHYSICIAN’S DEFENSE Proper consent was obtained, including alternatives to surgery. Evidence of ovarian cancer or other medical necessity was not required because full consent was obtained. Removal of the ovaries was proper due to dense pelvic and bowel adhesions, cystic adnexal masses with questionable pathology, and her chronic pelvic pain. The patient’s appendix was adhesed, causing an unreasonable risk of ovarian torsion.
VERDICT A Michigan defense verdict was returned.
Do you enjoy reading Medical Verdicts?
Find more in the PROFESSIONAL LIABILITY Topic Collection.
Persistent voiding problems
A 52-year-old woman was given a diagnosis of stage II anterior pelvic organ prolapse, a high transverse fascial defect, stress urinary incontinence, and distal rectocele.
A gynecologist performed robotic supracervical hysterectomy and colposacropexy, with tension-free vaginal tape and perineal repair.
While in the hospital, she required a catheter to void, and was still unable to void 5 days after discharge. The gynecologist identified persistent urinary retention, released the tension-free vaginal tape, and performed a midurethral sling procedure, but the patient continued to have voiding problems.
The gynecologist suspected a neurogenic problem and referred the patient to a neuro-urologist. Continued intermittent catheterization was recommended by the neuro-urologist, but the patient had continued voiding problems and developed a urinary tract infection.
She went to her ObGyn, who performed a sling revision and cystoscopy and removed all the mesh that could be found. The patient underwent additional treatment, with some improvement.
PATIENT’S CLAIM The gynecologist was negligent for failing to offer further surgery to improve the patient’s condition.
PHYSICIAN’S DEFENSE There was no negligence. Further dissection in the presence of a neurogenic bladder carried a high risk of incontinence. The patient was told of the risk of urinary retention prior to the first procedure and signed an informed consent.
VERDICT A Virginia defense verdict was returned.
Did pathologists fail to diagnose early breast cancer?
After A 45-year-old woman underwent mammography in May 2008 at a local hospital, an oncologist noted a suspicious finding in the right breast. The patient had an incisional biopsy interpreted by Dr. A, a pathologist, and a core biopsy interpreted by Dr. B, another pathologist from the same diagnostic medical group. Both pathologists interpreted the mass as atypia, a benign abnormality.
In 2010, the patient went to a university medical center, where the mass was biopsied and the patient was found to have cancer. She underwent a right mastectomy.
PATIENT’S CLAIM The pathologists failed to diagnose her breast cancer at an early stage. Dr. A should have interpreted the 2008 incisional biopsy as malignant. A diagnosis in 2008 would have avoided the need for a mastectomy, allowing her to have a lumpectomy with chemotherapy.
DEFENDANTS’ DEFENSE The 2010 review of the 2008 data was an over-interpretation with hindsight bias; the diagnosis in 2008 was correct.
VERDICT The case against the local hospital and Dr. B were dismissed. The matter continued against Dr. A and the diagnostic medical group. A California defense verdict was returned.
Brachial plexus injury occurs after admitting physician leaves
A woman sought prenatal care from her family practitioner (FP). The FP admitted the mother to a hospital for induction of labor at 38 weeks’ gestation with concerns of increased uric acid, possible gestational hypertension, and leaking amniotic fluid. Labor progressed and the mother began pushing about 4 pm. After 30 minutes, the FP attempted vacuum extraction three times; the device popped off during one of the attempts.
The FP then left for a planned trip, and an ObGyn assumed her care. The ObGyn chose to allow the mother to rest. At 6 pm, the mother began to feel the urge to push. The ObGyn attempted vacuum extraction. Shoulder dystocia was encountered, and McRoberts and corkscrew maneuvers were used to deliver the fetus.
The child has C5–C6 brachial plexus injury with scapular winging and internal shoulder rotation.
PARENTS’ CLAIM A cesarean delivery should have been performed. The ObGyn applied excessive lateral traction, leading to the injury.
DEFENDANTS’ DEFENSE The FP and ObGyn argued that a cesarean delivery was not indicated because the fetus was not in distress. Fetal heart-rate monitoring strips were reassuring. The ObGyn denied using excessive lateral traction when freeing the shoulder dystocia.
VERDICT The hospital settled before trial for $300,000. An Illinois defense verdict was returned for the FP. The jury deadlocked as to the ObGyn’s negligence.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
During a routine mammogram, an enlarged lymph node was found in the patient’s armpit. The patient’s primary care physician (PCP) ordered follow-up imaging and referred the patient to a surgeon for possible excisional biopsy. The surgeon suggested that the biopsy could be delayed until additional imaging studies were completed.
The patient transferred her care to another surgeon, who immediately performed the biopsy and found stage IV inoperable breast cancer. The patient underwent aggressive chemotherapy for 3 years, but died 39 months after diagnosis.
ESTATE’S CLAIM The first surgeon was negligent for not immediately performing the biopsy.
DEFENDANTS’ DEFENSE There was no negligence. An earlier biopsy would not have changed the outcome.
VERDICT A $1.5 million Massachusetts verdict was returned.
Treating bowel injury after uterine ablation
Following uterine ablation performed by a gynecologist, a 35-year-old woman suffered severe abdominal pain. Six days later, the gynecologist and a surgeon performed a hysterectomy.
Three days after discharge, the patient returned to the hospital with an abdominal infection and sepsis. During a third operation, a burn hole was found; the injured portion of bowel was resected. The patient has chronic abdominal pain.
PATIENT’S CLAIM Sepsis and infection could have been avoided if either physician had identified the injury during the second hospitalization and surgery. The patient developed psychological issues as a result of chronic pain.
DEFENDANTS’ DEFENSE A settlement was reached with the gynecologist during the trial. The surgeon denied negligence. During the second surgery, he examined her bowel for a possible injury but found none.
VERDICT A $3.5 million Illinois verdict was returned. It included
$1.5 million for past pain and suffering that was reduced by $100,000 due to the patient’s failure to report for psychological counseling. The jury found the gynecologist 65% at fault and the surgeon 35% at fault.
Mother in permanent vegetative state
When a 30-year-old woman went to a hospital in labor, she had gestational hypertension. The next morning, she suffered cardiopulmonary arrest. A healthy baby was born by emergency cesarean delivery, but the mother was left in a permanent vegetative state.
PATIENT’S CLAIM The nurses failed to ensure that the ObGyn came to the hospital and did not report blood pressure data to the ObGyn. Gestational hypertension progressed to preeclampsia. Early delivery should have been induced or magnesium sulfate should have been administered.
DEFENDANTS’ DEFENSE A confidential settlement was reached with the ObGyn before trial.
The nurses were right to rely on the ObGyn to make decisions regarding the patient’s care. They provided appropriate treatment.
VERDICT A New Jersey defense verdict was returned for the hospital.
What caused the child’s brain injuries?
After vaginal delivery, the baby was not breathing and required intubation. He had a seizure and displayed signs of oxygen deprivation, hypoxic ischemic injury, and brain damage. The child uses a special walker and can only communicate using a computer that speaks for him.
PARENTS’ CLAIM The nurses and ObGyn failed to properly assess the baby. The fetal heart-rate monitor electrode should have been placed on the fetal scalp. A cesarean delivery should have been performed.
DEFENDANTS’ DEFENSE The fetal monitor was properly placed. The child’s injury occurred 24 to 72 hours prior to birth due to an umbilical cord accident. A cesarean delivery would have not changed the outcome.
VERDICT A Georgia defense verdict was returned.
Did a woman’s vaginal infection cause her baby’s death?
At 22 weeks’ gestation, a 26-year-old woman began to leak amniotic fluid and went to the hospital. She was in premature labor. The newborn died 19 minutes after birth.
PARENTS’ CLAIM The ObGyn and nurse midwife who provided prenatal care failed to diagnose and treat a vaginal infection. The infection resulted in premature rupture of membranes, leading to premature birth and the baby’s death.
DEFENDANTS’ DEFENSE A confidential settlement was reached with the ObGyn before trial. The nurse midwife claimed the patient did not have a vaginal infection; she never reported symptoms of a foul-smelling vaginal odor or discharge. Premature rupture of membranes was not caused by a vaginal infection. The newborn’s death was related to an umbilical cord defect, the patient’s delay in coming to the hospital, and the multiple obstetric procedures the mother had undergone before this pregnancy.
VERDICT A $456,024 New Jersey verdict was returned.
Inadvertent ligation, ureteral obstruction
A 41-year-old woman suffered pelvic pain and had a history of endometriosis. In January 2007, a CT scan revealed a ruptured ovarian cyst; her ObGyn performed laparotomy for a hysterectomy and oophorectomy.
During surgery, a resident working under the supervision of the ObGyn inadvertently ligated the left ureter. The injury was close to the bladder near the ureteral vesicle junction. A few days later, cystoscopy showed ureteral obstruction. The patient underwent operative repair with nephrostomy tube placement. In May 2007, the patient had a third operation to reimplant the ureter. She has chronic flank pain.
PATIENT’S CLAIM The resident and, therefore, the ObGyn, were negligent in the performance of the procedure. Proper bladder dissection would have moved the ureter to a position where it could not have been ligated.
DEFENDANTS’ DEFENSE Ureter injury is a known risk of the procedure.
VERDICT An Illinois defense verdict was returned.
Foot drop after tubal ligatioN?
During tubal ligation, a woman in her 30s was restrained by a belt. Venodyne boots were applied to promote blood circulation.
PATIENT’S CLAIM The belt and/or boot damaged the perineal and tibial nerves in her left leg, causing foot drop. When asked to definitely identify what caused the nerve damage, the patient invoked the doctrine of res ipsa loquitur (presumed negligence during surgery).
DEFENDANTS’ DEFENSE A $400,000 settlement was reached with the hospital before the trial.
The gynecologist and anesthesiologist denied negligence. The Venodyne boots could not have caused the injury, nor could the belt, which was applied in an area that did not involve the perineal or tibial nerves. The patient did not complain of pain after surgery.
VERDICT A New York defense verdict was returned for the physicians.
Avoid surgical menopause?
After a 10-year history of endometriosis and chronic pelvic pain, a 38-year-old woman underwent bilateral salpingo-oophorectomy. Postoperatively, she suffered surgical menopause that exacerbated pre-existing anxiety and depression.
PATIENT’S CLAIM It was unnecessary to remove the healthy right ovary; having it remain would have avoided early menopause. She would not have consented to the removal of both ovaries had she been properly advised. Alternative treatment was not offered. Her marriage dissolved, her children went to live with their grandparents, and she was unable to work because of complications.
PHYSICIAN’S DEFENSE Proper consent was obtained, including alternatives to surgery. Evidence of ovarian cancer or other medical necessity was not required because full consent was obtained. Removal of the ovaries was proper due to dense pelvic and bowel adhesions, cystic adnexal masses with questionable pathology, and her chronic pelvic pain. The patient’s appendix was adhesed, causing an unreasonable risk of ovarian torsion.
VERDICT A Michigan defense verdict was returned.
Do you enjoy reading Medical Verdicts?
Find more in the PROFESSIONAL LIABILITY Topic Collection.
Persistent voiding problems
A 52-year-old woman was given a diagnosis of stage II anterior pelvic organ prolapse, a high transverse fascial defect, stress urinary incontinence, and distal rectocele.
A gynecologist performed robotic supracervical hysterectomy and colposacropexy, with tension-free vaginal tape and perineal repair.
While in the hospital, she required a catheter to void, and was still unable to void 5 days after discharge. The gynecologist identified persistent urinary retention, released the tension-free vaginal tape, and performed a midurethral sling procedure, but the patient continued to have voiding problems.
The gynecologist suspected a neurogenic problem and referred the patient to a neuro-urologist. Continued intermittent catheterization was recommended by the neuro-urologist, but the patient had continued voiding problems and developed a urinary tract infection.
She went to her ObGyn, who performed a sling revision and cystoscopy and removed all the mesh that could be found. The patient underwent additional treatment, with some improvement.
PATIENT’S CLAIM The gynecologist was negligent for failing to offer further surgery to improve the patient’s condition.
PHYSICIAN’S DEFENSE There was no negligence. Further dissection in the presence of a neurogenic bladder carried a high risk of incontinence. The patient was told of the risk of urinary retention prior to the first procedure and signed an informed consent.
VERDICT A Virginia defense verdict was returned.
Did pathologists fail to diagnose early breast cancer?
After A 45-year-old woman underwent mammography in May 2008 at a local hospital, an oncologist noted a suspicious finding in the right breast. The patient had an incisional biopsy interpreted by Dr. A, a pathologist, and a core biopsy interpreted by Dr. B, another pathologist from the same diagnostic medical group. Both pathologists interpreted the mass as atypia, a benign abnormality.
In 2010, the patient went to a university medical center, where the mass was biopsied and the patient was found to have cancer. She underwent a right mastectomy.
PATIENT’S CLAIM The pathologists failed to diagnose her breast cancer at an early stage. Dr. A should have interpreted the 2008 incisional biopsy as malignant. A diagnosis in 2008 would have avoided the need for a mastectomy, allowing her to have a lumpectomy with chemotherapy.
DEFENDANTS’ DEFENSE The 2010 review of the 2008 data was an over-interpretation with hindsight bias; the diagnosis in 2008 was correct.
VERDICT The case against the local hospital and Dr. B were dismissed. The matter continued against Dr. A and the diagnostic medical group. A California defense verdict was returned.
Brachial plexus injury occurs after admitting physician leaves
A woman sought prenatal care from her family practitioner (FP). The FP admitted the mother to a hospital for induction of labor at 38 weeks’ gestation with concerns of increased uric acid, possible gestational hypertension, and leaking amniotic fluid. Labor progressed and the mother began pushing about 4 pm. After 30 minutes, the FP attempted vacuum extraction three times; the device popped off during one of the attempts.
The FP then left for a planned trip, and an ObGyn assumed her care. The ObGyn chose to allow the mother to rest. At 6 pm, the mother began to feel the urge to push. The ObGyn attempted vacuum extraction. Shoulder dystocia was encountered, and McRoberts and corkscrew maneuvers were used to deliver the fetus.
The child has C5–C6 brachial plexus injury with scapular winging and internal shoulder rotation.
PARENTS’ CLAIM A cesarean delivery should have been performed. The ObGyn applied excessive lateral traction, leading to the injury.
DEFENDANTS’ DEFENSE The FP and ObGyn argued that a cesarean delivery was not indicated because the fetus was not in distress. Fetal heart-rate monitoring strips were reassuring. The ObGyn denied using excessive lateral traction when freeing the shoulder dystocia.
VERDICT The hospital settled before trial for $300,000. An Illinois defense verdict was returned for the FP. The jury deadlocked as to the ObGyn’s negligence.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.

Was Suicide Attempt Foreseeable?
In 2009, a 14-year-old Michigan boy entered a home-based, nonhospital treatment program for at-risk teens. His family was concerned about his mental health, as he had been caught smoking marijuana. He was also being treated for depression by a psychiatrist from the program’s administrating facility.
While enrolled in the program, the patient tried to hang himself but was discovered by his mother before death occurred. He was taken to a hospital, where marijuana and lysergic acid amide (LSA) were found in his system. Since the teen kept a morning glory plant in his bedroom, it was surmised that he had sucked on its seeds to achieve an LSD-like high. It was believed that the depressant effect experienced as he came down off the drug triggered suicidal feelings.
As a result of oxygen deprivation, the patient was rendered quadriplegic. He was unable to walk, talk, or feed himself. He died in 2012, at age 17.
The plaintiffs claimed that the defendants failed to properly diagnose, monitor, and treat their son and that he had been placed in the program in order to prevent what ultimately happened. The defendants denied any negligence.
Outcome
A $5.5 million verdict was returned.
Comment
Suicide can be difficult to predict, yet we are often called upon to do just that. For clinicians working in the emergency department or urgent care settings, the likelihood of encountering at-risk patients is higher.
Liability in this case turns on whether the suicide attempt was reasonably foreseeable. We have a 14-year-old boy smoking marijuana and being treated as an outpatient for depression. There was no history of prior hospitalization, personality or thought disorder, suicidal ideation, or prior suicide attempt. Apart from the marijuana, there was no history of substance abuse (since the morning glory seed use was not discovered until after the suicide attempt).
Based on this information, would a reasonably prudent clinician detect the imminent suicide risk that ended this patient’s life? Those inclined to answer “Yes” should be prepared to state precisely what evidence was used to arrive at this conclusion. Hindsight bias may allow us to see trouble brewing in this case but will do little to form a workable standard for every depressed teenager who uses marijuana.
That being said, suicide must be taken seriously: It is the third leading cause of death among persons ages 15 to 24 and the second leading cause of death among those ages 25 to 34. Among 15- to 24-year-olds, suicide accounts for 20% of all deaths annually.1 Suicide also carries high malpractice risk, and failure to prevent suicide is the most common claim against mental health professionals.2 Non–mental health clinicians also face liability exposure, but are often less equipped to recognize and deal with imminent psychiatric events.
Psychiatry is not an exact science. For clinicians accustomed to acting on hard evidence, psychiatry can be frustratingly “squishy.” The terminology can be misused, and the diagnosis subject to interobserver differences. There are no binary tests to “rule out” conditions and no therapeutic ranges within which we can feel safe. So what can we do?
First, we can double down on the structure that is there. Be familiar with the operative Diagnostic and Statistical Manual of Mental Disorders (DSM, now in its fifth revision), or have a reference handy. Use all diagnostic terms according to the framework in the DSM; a plaintiff’s attorney will pick apart careless diagnoses, and jurors will expect clinicians to be precise.
Second, have an approach for addressing suicidality (and homocidality) forthrightly. Consider using a suicide screening tool in cases where there is a coexisting concern (eg, substance use, scholastic difficulty, traumatic life event). A screening tool may protect the patient and be helpful from a legal standpoint for the clinician. For example, the Columbia-Suicide Severity Rating Scale (C-SSRS) has been demonstrated to provide improved assessment of suicide risk.3
Use of a generally accepted screening tool may have several advantages. It demonstrates concern for the patient and a willingness to take suicidality seriously. It also prompts the uncertain clinician on how to proceed in unfamiliar waters. Furthermore, a properly executed tool will likely be respected by jurors when used in conjunction with the clinician’s demonstrated concern and judgment. Obviously, such a tool should be used as a floor, not a ceiling; where the answers on a rating scale look “good” but clinical concern remains, good clinical judgment should prevail.
In this case, there were no facts disclosed that suggested imminent suicide risk, so it seems hard to fault the psychiatrist and the treatment program for the tragic results. However, the jury expected them to do more.
Use of a screening tool in this case may have shown that the program had an organized plan to address suicide risk in these “at-risk” kids. It would have provided tangible documentation that suicide risk was considered and may have yielded an extra layer of defense against the claim that this patient’s suicide attempt was foreseeable. Most importantly, the tool may have actually saved the patient’s life by revealing his pain and suicidal thinking.
We have yet to discuss the most unusual aspect of this case: the use of morning glory flower seeds as a drug of abuse. Morning glory seeds contain LSA, which produces an effect similar to LSD. Generally, the user crushes or chews the seeds or extracts the LSA by soaking them in cold water. On consumption, the user experiences LSD-type hallucinations and may experience agitation, anxiety, and mood disturbances, including depression. Apparently, the jury was not persuaded that the morning glory seed abuse caused the patient’s suicide attempt.
In conclusion, take suicide seriously. Have a plan to manage at-risk patients. Document your concern, evaluation, and findings. Consider implementing a suicide screening tool in your practice to ensure the proper questions are asked, answered, and documented. —DML
REFERENCES
1. CDC. Suicide: facts at a glance (2012). www.cdc.gov/violenceprevention/pdf/suicide-datasheet-a.pdf. Accessed November 6, 2013.
2. Simpson S, Stacy M. Avoiding the malpractice snare: documenting suicide risk assessment. J Psychiatr Pract. 2004;10(3):185-189. www.reidpsychiatry.com/columns/Stacy%2005-04.pdf. Accessed November 15, 2013.
3. Posner K, Brown GK, Stanley B, et al. The Columbia–Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266-1277.
In 2009, a 14-year-old Michigan boy entered a home-based, nonhospital treatment program for at-risk teens. His family was concerned about his mental health, as he had been caught smoking marijuana. He was also being treated for depression by a psychiatrist from the program’s administrating facility.
While enrolled in the program, the patient tried to hang himself but was discovered by his mother before death occurred. He was taken to a hospital, where marijuana and lysergic acid amide (LSA) were found in his system. Since the teen kept a morning glory plant in his bedroom, it was surmised that he had sucked on its seeds to achieve an LSD-like high. It was believed that the depressant effect experienced as he came down off the drug triggered suicidal feelings.
As a result of oxygen deprivation, the patient was rendered quadriplegic. He was unable to walk, talk, or feed himself. He died in 2012, at age 17.
The plaintiffs claimed that the defendants failed to properly diagnose, monitor, and treat their son and that he had been placed in the program in order to prevent what ultimately happened. The defendants denied any negligence.
Outcome
A $5.5 million verdict was returned.
Comment
Suicide can be difficult to predict, yet we are often called upon to do just that. For clinicians working in the emergency department or urgent care settings, the likelihood of encountering at-risk patients is higher.
Liability in this case turns on whether the suicide attempt was reasonably foreseeable. We have a 14-year-old boy smoking marijuana and being treated as an outpatient for depression. There was no history of prior hospitalization, personality or thought disorder, suicidal ideation, or prior suicide attempt. Apart from the marijuana, there was no history of substance abuse (since the morning glory seed use was not discovered until after the suicide attempt).
Based on this information, would a reasonably prudent clinician detect the imminent suicide risk that ended this patient’s life? Those inclined to answer “Yes” should be prepared to state precisely what evidence was used to arrive at this conclusion. Hindsight bias may allow us to see trouble brewing in this case but will do little to form a workable standard for every depressed teenager who uses marijuana.
That being said, suicide must be taken seriously: It is the third leading cause of death among persons ages 15 to 24 and the second leading cause of death among those ages 25 to 34. Among 15- to 24-year-olds, suicide accounts for 20% of all deaths annually.1 Suicide also carries high malpractice risk, and failure to prevent suicide is the most common claim against mental health professionals.2 Non–mental health clinicians also face liability exposure, but are often less equipped to recognize and deal with imminent psychiatric events.
Psychiatry is not an exact science. For clinicians accustomed to acting on hard evidence, psychiatry can be frustratingly “squishy.” The terminology can be misused, and the diagnosis subject to interobserver differences. There are no binary tests to “rule out” conditions and no therapeutic ranges within which we can feel safe. So what can we do?
First, we can double down on the structure that is there. Be familiar with the operative Diagnostic and Statistical Manual of Mental Disorders (DSM, now in its fifth revision), or have a reference handy. Use all diagnostic terms according to the framework in the DSM; a plaintiff’s attorney will pick apart careless diagnoses, and jurors will expect clinicians to be precise.
Second, have an approach for addressing suicidality (and homocidality) forthrightly. Consider using a suicide screening tool in cases where there is a coexisting concern (eg, substance use, scholastic difficulty, traumatic life event). A screening tool may protect the patient and be helpful from a legal standpoint for the clinician. For example, the Columbia-Suicide Severity Rating Scale (C-SSRS) has been demonstrated to provide improved assessment of suicide risk.3
Use of a generally accepted screening tool may have several advantages. It demonstrates concern for the patient and a willingness to take suicidality seriously. It also prompts the uncertain clinician on how to proceed in unfamiliar waters. Furthermore, a properly executed tool will likely be respected by jurors when used in conjunction with the clinician’s demonstrated concern and judgment. Obviously, such a tool should be used as a floor, not a ceiling; where the answers on a rating scale look “good” but clinical concern remains, good clinical judgment should prevail.
In this case, there were no facts disclosed that suggested imminent suicide risk, so it seems hard to fault the psychiatrist and the treatment program for the tragic results. However, the jury expected them to do more.
Use of a screening tool in this case may have shown that the program had an organized plan to address suicide risk in these “at-risk” kids. It would have provided tangible documentation that suicide risk was considered and may have yielded an extra layer of defense against the claim that this patient’s suicide attempt was foreseeable. Most importantly, the tool may have actually saved the patient’s life by revealing his pain and suicidal thinking.
We have yet to discuss the most unusual aspect of this case: the use of morning glory flower seeds as a drug of abuse. Morning glory seeds contain LSA, which produces an effect similar to LSD. Generally, the user crushes or chews the seeds or extracts the LSA by soaking them in cold water. On consumption, the user experiences LSD-type hallucinations and may experience agitation, anxiety, and mood disturbances, including depression. Apparently, the jury was not persuaded that the morning glory seed abuse caused the patient’s suicide attempt.
In conclusion, take suicide seriously. Have a plan to manage at-risk patients. Document your concern, evaluation, and findings. Consider implementing a suicide screening tool in your practice to ensure the proper questions are asked, answered, and documented. —DML
REFERENCES
1. CDC. Suicide: facts at a glance (2012). www.cdc.gov/violenceprevention/pdf/suicide-datasheet-a.pdf. Accessed November 6, 2013.
2. Simpson S, Stacy M. Avoiding the malpractice snare: documenting suicide risk assessment. J Psychiatr Pract. 2004;10(3):185-189. www.reidpsychiatry.com/columns/Stacy%2005-04.pdf. Accessed November 15, 2013.
3. Posner K, Brown GK, Stanley B, et al. The Columbia–Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266-1277.
In 2009, a 14-year-old Michigan boy entered a home-based, nonhospital treatment program for at-risk teens. His family was concerned about his mental health, as he had been caught smoking marijuana. He was also being treated for depression by a psychiatrist from the program’s administrating facility.
While enrolled in the program, the patient tried to hang himself but was discovered by his mother before death occurred. He was taken to a hospital, where marijuana and lysergic acid amide (LSA) were found in his system. Since the teen kept a morning glory plant in his bedroom, it was surmised that he had sucked on its seeds to achieve an LSD-like high. It was believed that the depressant effect experienced as he came down off the drug triggered suicidal feelings.
As a result of oxygen deprivation, the patient was rendered quadriplegic. He was unable to walk, talk, or feed himself. He died in 2012, at age 17.
The plaintiffs claimed that the defendants failed to properly diagnose, monitor, and treat their son and that he had been placed in the program in order to prevent what ultimately happened. The defendants denied any negligence.
Outcome
A $5.5 million verdict was returned.
Comment
Suicide can be difficult to predict, yet we are often called upon to do just that. For clinicians working in the emergency department or urgent care settings, the likelihood of encountering at-risk patients is higher.
Liability in this case turns on whether the suicide attempt was reasonably foreseeable. We have a 14-year-old boy smoking marijuana and being treated as an outpatient for depression. There was no history of prior hospitalization, personality or thought disorder, suicidal ideation, or prior suicide attempt. Apart from the marijuana, there was no history of substance abuse (since the morning glory seed use was not discovered until after the suicide attempt).
Based on this information, would a reasonably prudent clinician detect the imminent suicide risk that ended this patient’s life? Those inclined to answer “Yes” should be prepared to state precisely what evidence was used to arrive at this conclusion. Hindsight bias may allow us to see trouble brewing in this case but will do little to form a workable standard for every depressed teenager who uses marijuana.
That being said, suicide must be taken seriously: It is the third leading cause of death among persons ages 15 to 24 and the second leading cause of death among those ages 25 to 34. Among 15- to 24-year-olds, suicide accounts for 20% of all deaths annually.1 Suicide also carries high malpractice risk, and failure to prevent suicide is the most common claim against mental health professionals.2 Non–mental health clinicians also face liability exposure, but are often less equipped to recognize and deal with imminent psychiatric events.
Psychiatry is not an exact science. For clinicians accustomed to acting on hard evidence, psychiatry can be frustratingly “squishy.” The terminology can be misused, and the diagnosis subject to interobserver differences. There are no binary tests to “rule out” conditions and no therapeutic ranges within which we can feel safe. So what can we do?
First, we can double down on the structure that is there. Be familiar with the operative Diagnostic and Statistical Manual of Mental Disorders (DSM, now in its fifth revision), or have a reference handy. Use all diagnostic terms according to the framework in the DSM; a plaintiff’s attorney will pick apart careless diagnoses, and jurors will expect clinicians to be precise.
Second, have an approach for addressing suicidality (and homocidality) forthrightly. Consider using a suicide screening tool in cases where there is a coexisting concern (eg, substance use, scholastic difficulty, traumatic life event). A screening tool may protect the patient and be helpful from a legal standpoint for the clinician. For example, the Columbia-Suicide Severity Rating Scale (C-SSRS) has been demonstrated to provide improved assessment of suicide risk.3
Use of a generally accepted screening tool may have several advantages. It demonstrates concern for the patient and a willingness to take suicidality seriously. It also prompts the uncertain clinician on how to proceed in unfamiliar waters. Furthermore, a properly executed tool will likely be respected by jurors when used in conjunction with the clinician’s demonstrated concern and judgment. Obviously, such a tool should be used as a floor, not a ceiling; where the answers on a rating scale look “good” but clinical concern remains, good clinical judgment should prevail.
In this case, there were no facts disclosed that suggested imminent suicide risk, so it seems hard to fault the psychiatrist and the treatment program for the tragic results. However, the jury expected them to do more.
Use of a screening tool in this case may have shown that the program had an organized plan to address suicide risk in these “at-risk” kids. It would have provided tangible documentation that suicide risk was considered and may have yielded an extra layer of defense against the claim that this patient’s suicide attempt was foreseeable. Most importantly, the tool may have actually saved the patient’s life by revealing his pain and suicidal thinking.
We have yet to discuss the most unusual aspect of this case: the use of morning glory flower seeds as a drug of abuse. Morning glory seeds contain LSA, which produces an effect similar to LSD. Generally, the user crushes or chews the seeds or extracts the LSA by soaking them in cold water. On consumption, the user experiences LSD-type hallucinations and may experience agitation, anxiety, and mood disturbances, including depression. Apparently, the jury was not persuaded that the morning glory seed abuse caused the patient’s suicide attempt.
In conclusion, take suicide seriously. Have a plan to manage at-risk patients. Document your concern, evaluation, and findings. Consider implementing a suicide screening tool in your practice to ensure the proper questions are asked, answered, and documented. —DML
REFERENCES
1. CDC. Suicide: facts at a glance (2012). www.cdc.gov/violenceprevention/pdf/suicide-datasheet-a.pdf. Accessed November 6, 2013.
2. Simpson S, Stacy M. Avoiding the malpractice snare: documenting suicide risk assessment. J Psychiatr Pract. 2004;10(3):185-189. www.reidpsychiatry.com/columns/Stacy%2005-04.pdf. Accessed November 15, 2013.
3. Posner K, Brown GK, Stanley B, et al. The Columbia–Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266-1277.
Are you admitting malpractice if you apologize to a patient?
Dear Dr. Mossman:
Recently, my prescribing error caused a patient to get very sick. I feel terrible. I want to tell my patient I’m sorry, but I’ve heard that a lawyer could use my “confession” to prove I’ve committed malpractice. If I apologize, could my words come back to haunt me if a lawsuit is filed?
Submitted by “Dr. E”
As several faiths have long recognized, apologies are important social acts that express our awareness of and obligations to each other. In recent years, psychologists have established how apologies confer emotional benefits on those who give and receive them.1 Offering a sincere apology can be the right thing to do and a beneficial act for both the apologizing and the injured parties.
Traditionally, physicians have avoided apologizing for errors that harmed patients. Part of the reluctance stemmed from pride or wanting to avoid shame. But as Dr. E’s question suggests, doctors also have feared—and lawyers have advised—that apologizing might compromise a malpractice defense.2
Attitudes have changed in recent years, however. Increasingly, practitioners, medical organizations, and risk management entities are telling physicians they should apologize for errors, and many states have laws that mitigate adverse legal consequences of saying “I’m sorry.”
In response to Dr. E’s questions, I’ll examine:
• ethical and professional obligations following unexpected outcomes
• physicians’ reasons for being reluctant to apologize
• the benefits of apologizing
• legal protections for apologies.
Owning up: Ethical and professional expectations
Current codes of medical ethics say that physicians should tell patients when mistakes and misjudgments have caused harm. “It is a fundamental ethical requirement that a physician should at all times deal honestly and openly with patients,” states the American Medical Association’s Code of Ethics. When a patient suffers because of a medical error, “the physician is ethically required to inform the patient of all the facts necessary to ensure” the patient can “make informed decisions regarding future medical care.”3
The National Patient Safety Foundation,4 the American College of Physicians,5 and the Joint Commission (the agency that provides official accreditation of thousands of healthcare organizations) have voiced similar positions for years. Since 2001, the Joint Commission has required that practitioners and medical facilities tell patients and families “about the outcomes of care, treatment, and services ... including unanticipated outcomes.”6
Reluctance is understandable
Although these recommendations and policies suggest that telling patients about medical errors is an established professional expectation, physicians remain reluctant to apologize to patients for emotional and legal reasons that are easy to understand.
Apologizing is hard. On one hand, research shows that refusing to apologize sometimes increases feelings of empowerment and control, and can boost self-esteem more than apologizing does.7 On the other, apologizing often requires one to acknowledge a failure or betrayal of trust and to experience guilt, shame, embarrassment, or fear that one’s apology will be met with anger or rejection.8
Physicians historically have treated errors as personal failures. Apologizing in a medical context can feel like saying, “I am incompetent.”9,10 The law has reinforced this attitude. As the Mississippi Supreme Court put it, “Medical malpractice is legal fault by a physician or surgeon. It arises from the failure of a physician to provide the quality of care required by law” (emphasis added).11
Some lawyers continue to advise physicians not to make admissions that could be used in a malpractice case. Their reasoning: If a doctor does something that adversely affects a malpractice insurer’s ability to defend the case, the insurer might not provide liability coverage for the adverse event.12
Emotional and legal benefits
Against this no-apology stance is a growing body of theoretical, empirical, and practical arguments favoring apologies for medical errors. Case studies suggest that anger is behind much medical malpractice litigation and that physicians’ apologies—which reduce anger and increase communication—might reduce patients’ motivations to sue.13 Apologies sometimes lead to forgiveness, an emotional state that “can provide victims and offenders with many important benefits, including enhanced psychological well-being ... and greater physiological health.”14 Apologies do this by mitigating the injured party’s negative emotional states and diminishing rumination about the transgression and perceived harm severity.
The practical argument favoring apologizing is that it may defuse feelings that lead to lawsuits and reduce the size of payouts. Experimental studies suggest that apologizing leads to earlier satisfaction and closure, faster settlements, and lower damage payments. When apologies include admissions of fault, injured parties feel greater respect for and less need to punish those who have harmed them, are more willing to forgive, and are more likely to accept settlement offers.15
Hospitals in Pennsylvania, Kentucky, and Michigan have found that sincere apologies and effective error disclosure programs reduce malpractice payouts and lead to faster settlements.16 As some plaintiffs’ lawyers point out, being honest and forthright and fixing the injured parties’ problems can quickly defuse a lawsuit. One attorney explained things this way: “We never sue the nice, contrite doctors. Their patients never call our offices. But the doctors who are poor communicators and abandon their patients get sued all the time. Their patients come to our offices looking for answers.”17
Apology laws: Protection from your own words
The belief that apologies by physicians can help patients emotionally and reduce malpractice litigation has led state legislatures to enact so-called apology laws in many jurisdictions in the United States.18 The general point of these rules and statutes is to prevent later use of doctors’ words in litigation. States differ substantially in the scope and type of protection that their laws offer. Some states prohibit doctors’ apologies for adverse outcomes from being used in litigation to prove negligence, while others only exclude expressions of sympathy or offers to pay for corrective treatment. Selected language from several states’ apology laws appears in the Table.19-23
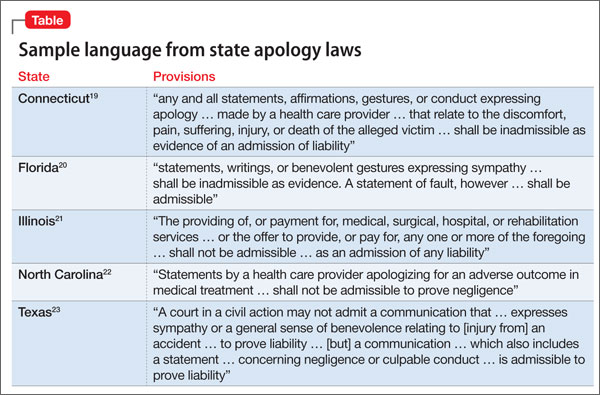
Do apology laws work? Recent research by economists Ho and Liu indicates that they do. Comparing payouts in states with and without apology laws, they conclude that “apology laws have the greatest reduction in average payment size and settlement time in cases involving more severe patient outcomes,”13 such as obstetrics and anesthesia cases, cases that involve infants, and cases in which physicians improperly manage or fail to properly diagnose an illness.24
The practical impact of apologizing for psychiatric malpractice cases is unclear, but forensic psychiatrists Marilyn Price and Patricia Recupero believe that, following some unexpected outcomes, thoughtful expressions of sympathy, regret, and—if the outcome resulted from an error—apologies may be appropriate. Price and Recupero caution that such conversations should occur as part of broader programs that investigate unanticipated adverse events and provide education and coaching about appropriate ways to make disclosures. Clinicians also should consult with legal counsel, risk management officers, and liability insurance carriers before initiating such disclosures.25
Bottom Line
Apologizing for medical errors may mitigate malpractice liability and can help injured parties and physicians feel better. Whether plaintiffs can use apologies as evidence of malpractice depends on state laws and rules of evidence. Before you apologize for an unanticipated outcome, discuss the situation with your legal counsel, risk management officers, and insurers.
Disclosure
Dr. Mossman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Featured Audio
Douglas Mossman, MD, talks about who you should consult before apologizing to a patient for a bad outcome. Dr. Mossman is Professor of Clinical Psychiatry and Director, Division of Forensic Psychiatry, University of Cincinnati College of Medicine, Cincinnati, Ohio.
1. McCullough ME, Sandage SJ, Brown SW, et al. Interpersonal forgiving in close relationships: II. Theoretical elaboration and measurement. J Pers Soc Psychol. 1998;75:1586-1603.
2. O’Reilly KB. “I’m sorry”: why is that so hard for doctors to say? http://www.amednews.com/article/20100201/profession/302019937/4. Published February 1, 2010. Accessed September 30, 2013.
3. American Medical Association. AMA Code of Medical Ethics, Opinion 8.12 – Patient information. http://www.ama-assn.org//ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion812.page. Published June 1994. Accessed September 30, 2013.
4. Hickson GB, Pichert JW. Disclosure and apology. http://www.npsf.org/wp-content/uploads/2011/10/RG_SUPS_After_Mod1_Hickson.pdf. Accessed October 4, 2013.
5. Snyder L, American College of Physicians Ethics, Professionalism, and Human Rights Committee. American College of Physicians ethics manual: sixth edition. Ann Intern Med. 2012;156(1, pt 2):73-104.
6. ECRI Institute. Disclosure of unanticipated outcomes. In: Healthcare risk control Supplement A, Risk analysis. Plymouth Meeting, PA: ECRI; 2002.
7. Okimoto TG, Wenzel M, Hedrick K. Refusing to apologize can have psychological benefits (and we issue no mea culpa for this research finding). Eur J Soc Psychol. 2013;43:22-31.
8. Lazare A. On apology. New York, NY: Oxford University Press; 2004.
9. Hilfiker D. Facing our mistakes. N Engl J Med. 1984;310:
118-122.
10. Leape LL. Error in medicine. JAMA. 1994;272:1851-1857.
11. Hall v. Hilbun, 466 So.2d 856 (Miss. 1985).
12. Kern SI. You continue to face exposure if you apologize. http://medicaleconomics.modernmedicine.com/medical-economics/news/modernmedicine/modern-medicine-now/you-continue-face-exposure-if-you-apologiz. Published September 24, 2010. Accessed October 1, 2013.
13. Ho B, Liu E. Does sorry work? The impact of apology laws on medical malpractice. J Risk Uncertain. 2011;43(2):141-167.
14. Fehr R, Gelfand MJ, Nag M. The road to forgiveness: a meta-analytic synthesis of its situational and dispositional correlates. Psychol Bull. 2010;136:894-914.
15. Robbennolt JK. Apologies and settlement. Court Review. 2009;45:90-97.
16. Saitta N, Hodge SD. Efficacy of a physician’s words of empathy: an overview of state apology laws. J Am Osteopath Assoc. 2012;112(5):302-306.
17. Wojcieszak D, Banja J, Houk C. The sorry works! coalition: making the case for full disclosure. Jt Comm J Qual Patient Saf. 2006;32(6):344-350.
18. National Conference of State Legislatures. Medical liability/Medical malpractice laws. http://www.ncsl.org/issues-research/banking/medical-liability-medical-malpractice-laws.aspx. Published August 15, 2011. Accessed October 4, 2013.
19. Conn Gen Stat Ann §52-184d(b).
20. Fla Stat §90.4026(2).
21. Ill Comp Stat §5/8-1901.
22. NC Gen Stat §8C-1, Rule 413.
23. Tex. Civ. Prac. & Rem. Code §18.061.
24. Ho B, Liu E. What’s an apology worth? Decomposing the effect of apologies on medical malpractice payments using state apology laws. J Empir Leg Stud. 2011;8:179-199.
25. Price M, Recupero PR. Risk management. In: Sharfstein SS, Dickerson FB, Oldham JM, eds. Textbook of hospital psychiatry. Arlington, VA: American Psychiatric Publishing, Inc.; 2009:411-412.
Dear Dr. Mossman:
Recently, my prescribing error caused a patient to get very sick. I feel terrible. I want to tell my patient I’m sorry, but I’ve heard that a lawyer could use my “confession” to prove I’ve committed malpractice. If I apologize, could my words come back to haunt me if a lawsuit is filed?
Submitted by “Dr. E”
As several faiths have long recognized, apologies are important social acts that express our awareness of and obligations to each other. In recent years, psychologists have established how apologies confer emotional benefits on those who give and receive them.1 Offering a sincere apology can be the right thing to do and a beneficial act for both the apologizing and the injured parties.
Traditionally, physicians have avoided apologizing for errors that harmed patients. Part of the reluctance stemmed from pride or wanting to avoid shame. But as Dr. E’s question suggests, doctors also have feared—and lawyers have advised—that apologizing might compromise a malpractice defense.2
Attitudes have changed in recent years, however. Increasingly, practitioners, medical organizations, and risk management entities are telling physicians they should apologize for errors, and many states have laws that mitigate adverse legal consequences of saying “I’m sorry.”
In response to Dr. E’s questions, I’ll examine:
• ethical and professional obligations following unexpected outcomes
• physicians’ reasons for being reluctant to apologize
• the benefits of apologizing
• legal protections for apologies.
Owning up: Ethical and professional expectations
Current codes of medical ethics say that physicians should tell patients when mistakes and misjudgments have caused harm. “It is a fundamental ethical requirement that a physician should at all times deal honestly and openly with patients,” states the American Medical Association’s Code of Ethics. When a patient suffers because of a medical error, “the physician is ethically required to inform the patient of all the facts necessary to ensure” the patient can “make informed decisions regarding future medical care.”3
The National Patient Safety Foundation,4 the American College of Physicians,5 and the Joint Commission (the agency that provides official accreditation of thousands of healthcare organizations) have voiced similar positions for years. Since 2001, the Joint Commission has required that practitioners and medical facilities tell patients and families “about the outcomes of care, treatment, and services ... including unanticipated outcomes.”6
Reluctance is understandable
Although these recommendations and policies suggest that telling patients about medical errors is an established professional expectation, physicians remain reluctant to apologize to patients for emotional and legal reasons that are easy to understand.
Apologizing is hard. On one hand, research shows that refusing to apologize sometimes increases feelings of empowerment and control, and can boost self-esteem more than apologizing does.7 On the other, apologizing often requires one to acknowledge a failure or betrayal of trust and to experience guilt, shame, embarrassment, or fear that one’s apology will be met with anger or rejection.8
Physicians historically have treated errors as personal failures. Apologizing in a medical context can feel like saying, “I am incompetent.”9,10 The law has reinforced this attitude. As the Mississippi Supreme Court put it, “Medical malpractice is legal fault by a physician or surgeon. It arises from the failure of a physician to provide the quality of care required by law” (emphasis added).11
Some lawyers continue to advise physicians not to make admissions that could be used in a malpractice case. Their reasoning: If a doctor does something that adversely affects a malpractice insurer’s ability to defend the case, the insurer might not provide liability coverage for the adverse event.12
Emotional and legal benefits
Against this no-apology stance is a growing body of theoretical, empirical, and practical arguments favoring apologies for medical errors. Case studies suggest that anger is behind much medical malpractice litigation and that physicians’ apologies—which reduce anger and increase communication—might reduce patients’ motivations to sue.13 Apologies sometimes lead to forgiveness, an emotional state that “can provide victims and offenders with many important benefits, including enhanced psychological well-being ... and greater physiological health.”14 Apologies do this by mitigating the injured party’s negative emotional states and diminishing rumination about the transgression and perceived harm severity.
The practical argument favoring apologizing is that it may defuse feelings that lead to lawsuits and reduce the size of payouts. Experimental studies suggest that apologizing leads to earlier satisfaction and closure, faster settlements, and lower damage payments. When apologies include admissions of fault, injured parties feel greater respect for and less need to punish those who have harmed them, are more willing to forgive, and are more likely to accept settlement offers.15
Hospitals in Pennsylvania, Kentucky, and Michigan have found that sincere apologies and effective error disclosure programs reduce malpractice payouts and lead to faster settlements.16 As some plaintiffs’ lawyers point out, being honest and forthright and fixing the injured parties’ problems can quickly defuse a lawsuit. One attorney explained things this way: “We never sue the nice, contrite doctors. Their patients never call our offices. But the doctors who are poor communicators and abandon their patients get sued all the time. Their patients come to our offices looking for answers.”17
Apology laws: Protection from your own words
The belief that apologies by physicians can help patients emotionally and reduce malpractice litigation has led state legislatures to enact so-called apology laws in many jurisdictions in the United States.18 The general point of these rules and statutes is to prevent later use of doctors’ words in litigation. States differ substantially in the scope and type of protection that their laws offer. Some states prohibit doctors’ apologies for adverse outcomes from being used in litigation to prove negligence, while others only exclude expressions of sympathy or offers to pay for corrective treatment. Selected language from several states’ apology laws appears in the Table.19-23
Do apology laws work? Recent research by economists Ho and Liu indicates that they do. Comparing payouts in states with and without apology laws, they conclude that “apology laws have the greatest reduction in average payment size and settlement time in cases involving more severe patient outcomes,”13 such as obstetrics and anesthesia cases, cases that involve infants, and cases in which physicians improperly manage or fail to properly diagnose an illness.24
The practical impact of apologizing for psychiatric malpractice cases is unclear, but forensic psychiatrists Marilyn Price and Patricia Recupero believe that, following some unexpected outcomes, thoughtful expressions of sympathy, regret, and—if the outcome resulted from an error—apologies may be appropriate. Price and Recupero caution that such conversations should occur as part of broader programs that investigate unanticipated adverse events and provide education and coaching about appropriate ways to make disclosures. Clinicians also should consult with legal counsel, risk management officers, and liability insurance carriers before initiating such disclosures.25
Bottom Line
Apologizing for medical errors may mitigate malpractice liability and can help injured parties and physicians feel better. Whether plaintiffs can use apologies as evidence of malpractice depends on state laws and rules of evidence. Before you apologize for an unanticipated outcome, discuss the situation with your legal counsel, risk management officers, and insurers.
Disclosure
Dr. Mossman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Featured Audio
Douglas Mossman, MD, talks about who you should consult before apologizing to a patient for a bad outcome. Dr. Mossman is Professor of Clinical Psychiatry and Director, Division of Forensic Psychiatry, University of Cincinnati College of Medicine, Cincinnati, Ohio.
Dear Dr. Mossman:
Recently, my prescribing error caused a patient to get very sick. I feel terrible. I want to tell my patient I’m sorry, but I’ve heard that a lawyer could use my “confession” to prove I’ve committed malpractice. If I apologize, could my words come back to haunt me if a lawsuit is filed?
Submitted by “Dr. E”
As several faiths have long recognized, apologies are important social acts that express our awareness of and obligations to each other. In recent years, psychologists have established how apologies confer emotional benefits on those who give and receive them.1 Offering a sincere apology can be the right thing to do and a beneficial act for both the apologizing and the injured parties.
Traditionally, physicians have avoided apologizing for errors that harmed patients. Part of the reluctance stemmed from pride or wanting to avoid shame. But as Dr. E’s question suggests, doctors also have feared—and lawyers have advised—that apologizing might compromise a malpractice defense.2
Attitudes have changed in recent years, however. Increasingly, practitioners, medical organizations, and risk management entities are telling physicians they should apologize for errors, and many states have laws that mitigate adverse legal consequences of saying “I’m sorry.”
In response to Dr. E’s questions, I’ll examine:
• ethical and professional obligations following unexpected outcomes
• physicians’ reasons for being reluctant to apologize
• the benefits of apologizing
• legal protections for apologies.
Owning up: Ethical and professional expectations
Current codes of medical ethics say that physicians should tell patients when mistakes and misjudgments have caused harm. “It is a fundamental ethical requirement that a physician should at all times deal honestly and openly with patients,” states the American Medical Association’s Code of Ethics. When a patient suffers because of a medical error, “the physician is ethically required to inform the patient of all the facts necessary to ensure” the patient can “make informed decisions regarding future medical care.”3
The National Patient Safety Foundation,4 the American College of Physicians,5 and the Joint Commission (the agency that provides official accreditation of thousands of healthcare organizations) have voiced similar positions for years. Since 2001, the Joint Commission has required that practitioners and medical facilities tell patients and families “about the outcomes of care, treatment, and services ... including unanticipated outcomes.”6
Reluctance is understandable
Although these recommendations and policies suggest that telling patients about medical errors is an established professional expectation, physicians remain reluctant to apologize to patients for emotional and legal reasons that are easy to understand.
Apologizing is hard. On one hand, research shows that refusing to apologize sometimes increases feelings of empowerment and control, and can boost self-esteem more than apologizing does.7 On the other, apologizing often requires one to acknowledge a failure or betrayal of trust and to experience guilt, shame, embarrassment, or fear that one’s apology will be met with anger or rejection.8
Physicians historically have treated errors as personal failures. Apologizing in a medical context can feel like saying, “I am incompetent.”9,10 The law has reinforced this attitude. As the Mississippi Supreme Court put it, “Medical malpractice is legal fault by a physician or surgeon. It arises from the failure of a physician to provide the quality of care required by law” (emphasis added).11
Some lawyers continue to advise physicians not to make admissions that could be used in a malpractice case. Their reasoning: If a doctor does something that adversely affects a malpractice insurer’s ability to defend the case, the insurer might not provide liability coverage for the adverse event.12
Emotional and legal benefits
Against this no-apology stance is a growing body of theoretical, empirical, and practical arguments favoring apologies for medical errors. Case studies suggest that anger is behind much medical malpractice litigation and that physicians’ apologies—which reduce anger and increase communication—might reduce patients’ motivations to sue.13 Apologies sometimes lead to forgiveness, an emotional state that “can provide victims and offenders with many important benefits, including enhanced psychological well-being ... and greater physiological health.”14 Apologies do this by mitigating the injured party’s negative emotional states and diminishing rumination about the transgression and perceived harm severity.
The practical argument favoring apologizing is that it may defuse feelings that lead to lawsuits and reduce the size of payouts. Experimental studies suggest that apologizing leads to earlier satisfaction and closure, faster settlements, and lower damage payments. When apologies include admissions of fault, injured parties feel greater respect for and less need to punish those who have harmed them, are more willing to forgive, and are more likely to accept settlement offers.15
Hospitals in Pennsylvania, Kentucky, and Michigan have found that sincere apologies and effective error disclosure programs reduce malpractice payouts and lead to faster settlements.16 As some plaintiffs’ lawyers point out, being honest and forthright and fixing the injured parties’ problems can quickly defuse a lawsuit. One attorney explained things this way: “We never sue the nice, contrite doctors. Their patients never call our offices. But the doctors who are poor communicators and abandon their patients get sued all the time. Their patients come to our offices looking for answers.”17
Apology laws: Protection from your own words
The belief that apologies by physicians can help patients emotionally and reduce malpractice litigation has led state legislatures to enact so-called apology laws in many jurisdictions in the United States.18 The general point of these rules and statutes is to prevent later use of doctors’ words in litigation. States differ substantially in the scope and type of protection that their laws offer. Some states prohibit doctors’ apologies for adverse outcomes from being used in litigation to prove negligence, while others only exclude expressions of sympathy or offers to pay for corrective treatment. Selected language from several states’ apology laws appears in the Table.19-23
Do apology laws work? Recent research by economists Ho and Liu indicates that they do. Comparing payouts in states with and without apology laws, they conclude that “apology laws have the greatest reduction in average payment size and settlement time in cases involving more severe patient outcomes,”13 such as obstetrics and anesthesia cases, cases that involve infants, and cases in which physicians improperly manage or fail to properly diagnose an illness.24
The practical impact of apologizing for psychiatric malpractice cases is unclear, but forensic psychiatrists Marilyn Price and Patricia Recupero believe that, following some unexpected outcomes, thoughtful expressions of sympathy, regret, and—if the outcome resulted from an error—apologies may be appropriate. Price and Recupero caution that such conversations should occur as part of broader programs that investigate unanticipated adverse events and provide education and coaching about appropriate ways to make disclosures. Clinicians also should consult with legal counsel, risk management officers, and liability insurance carriers before initiating such disclosures.25
Bottom Line
Apologizing for medical errors may mitigate malpractice liability and can help injured parties and physicians feel better. Whether plaintiffs can use apologies as evidence of malpractice depends on state laws and rules of evidence. Before you apologize for an unanticipated outcome, discuss the situation with your legal counsel, risk management officers, and insurers.
Disclosure
Dr. Mossman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Featured Audio
Douglas Mossman, MD, talks about who you should consult before apologizing to a patient for a bad outcome. Dr. Mossman is Professor of Clinical Psychiatry and Director, Division of Forensic Psychiatry, University of Cincinnati College of Medicine, Cincinnati, Ohio.
1. McCullough ME, Sandage SJ, Brown SW, et al. Interpersonal forgiving in close relationships: II. Theoretical elaboration and measurement. J Pers Soc Psychol. 1998;75:1586-1603.
2. O’Reilly KB. “I’m sorry”: why is that so hard for doctors to say? http://www.amednews.com/article/20100201/profession/302019937/4. Published February 1, 2010. Accessed September 30, 2013.
3. American Medical Association. AMA Code of Medical Ethics, Opinion 8.12 – Patient information. http://www.ama-assn.org//ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion812.page. Published June 1994. Accessed September 30, 2013.
4. Hickson GB, Pichert JW. Disclosure and apology. http://www.npsf.org/wp-content/uploads/2011/10/RG_SUPS_After_Mod1_Hickson.pdf. Accessed October 4, 2013.
5. Snyder L, American College of Physicians Ethics, Professionalism, and Human Rights Committee. American College of Physicians ethics manual: sixth edition. Ann Intern Med. 2012;156(1, pt 2):73-104.
6. ECRI Institute. Disclosure of unanticipated outcomes. In: Healthcare risk control Supplement A, Risk analysis. Plymouth Meeting, PA: ECRI; 2002.
7. Okimoto TG, Wenzel M, Hedrick K. Refusing to apologize can have psychological benefits (and we issue no mea culpa for this research finding). Eur J Soc Psychol. 2013;43:22-31.
8. Lazare A. On apology. New York, NY: Oxford University Press; 2004.
9. Hilfiker D. Facing our mistakes. N Engl J Med. 1984;310:
118-122.
10. Leape LL. Error in medicine. JAMA. 1994;272:1851-1857.
11. Hall v. Hilbun, 466 So.2d 856 (Miss. 1985).
12. Kern SI. You continue to face exposure if you apologize. http://medicaleconomics.modernmedicine.com/medical-economics/news/modernmedicine/modern-medicine-now/you-continue-face-exposure-if-you-apologiz. Published September 24, 2010. Accessed October 1, 2013.
13. Ho B, Liu E. Does sorry work? The impact of apology laws on medical malpractice. J Risk Uncertain. 2011;43(2):141-167.
14. Fehr R, Gelfand MJ, Nag M. The road to forgiveness: a meta-analytic synthesis of its situational and dispositional correlates. Psychol Bull. 2010;136:894-914.
15. Robbennolt JK. Apologies and settlement. Court Review. 2009;45:90-97.
16. Saitta N, Hodge SD. Efficacy of a physician’s words of empathy: an overview of state apology laws. J Am Osteopath Assoc. 2012;112(5):302-306.
17. Wojcieszak D, Banja J, Houk C. The sorry works! coalition: making the case for full disclosure. Jt Comm J Qual Patient Saf. 2006;32(6):344-350.
18. National Conference of State Legislatures. Medical liability/Medical malpractice laws. http://www.ncsl.org/issues-research/banking/medical-liability-medical-malpractice-laws.aspx. Published August 15, 2011. Accessed October 4, 2013.
19. Conn Gen Stat Ann §52-184d(b).
20. Fla Stat §90.4026(2).
21. Ill Comp Stat §5/8-1901.
22. NC Gen Stat §8C-1, Rule 413.
23. Tex. Civ. Prac. & Rem. Code §18.061.
24. Ho B, Liu E. What’s an apology worth? Decomposing the effect of apologies on medical malpractice payments using state apology laws. J Empir Leg Stud. 2011;8:179-199.
25. Price M, Recupero PR. Risk management. In: Sharfstein SS, Dickerson FB, Oldham JM, eds. Textbook of hospital psychiatry. Arlington, VA: American Psychiatric Publishing, Inc.; 2009:411-412.
1. McCullough ME, Sandage SJ, Brown SW, et al. Interpersonal forgiving in close relationships: II. Theoretical elaboration and measurement. J Pers Soc Psychol. 1998;75:1586-1603.
2. O’Reilly KB. “I’m sorry”: why is that so hard for doctors to say? http://www.amednews.com/article/20100201/profession/302019937/4. Published February 1, 2010. Accessed September 30, 2013.
3. American Medical Association. AMA Code of Medical Ethics, Opinion 8.12 – Patient information. http://www.ama-assn.org//ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion812.page. Published June 1994. Accessed September 30, 2013.
4. Hickson GB, Pichert JW. Disclosure and apology. http://www.npsf.org/wp-content/uploads/2011/10/RG_SUPS_After_Mod1_Hickson.pdf. Accessed October 4, 2013.
5. Snyder L, American College of Physicians Ethics, Professionalism, and Human Rights Committee. American College of Physicians ethics manual: sixth edition. Ann Intern Med. 2012;156(1, pt 2):73-104.
6. ECRI Institute. Disclosure of unanticipated outcomes. In: Healthcare risk control Supplement A, Risk analysis. Plymouth Meeting, PA: ECRI; 2002.
7. Okimoto TG, Wenzel M, Hedrick K. Refusing to apologize can have psychological benefits (and we issue no mea culpa for this research finding). Eur J Soc Psychol. 2013;43:22-31.
8. Lazare A. On apology. New York, NY: Oxford University Press; 2004.
9. Hilfiker D. Facing our mistakes. N Engl J Med. 1984;310:
118-122.
10. Leape LL. Error in medicine. JAMA. 1994;272:1851-1857.
11. Hall v. Hilbun, 466 So.2d 856 (Miss. 1985).
12. Kern SI. You continue to face exposure if you apologize. http://medicaleconomics.modernmedicine.com/medical-economics/news/modernmedicine/modern-medicine-now/you-continue-face-exposure-if-you-apologiz. Published September 24, 2010. Accessed October 1, 2013.
13. Ho B, Liu E. Does sorry work? The impact of apology laws on medical malpractice. J Risk Uncertain. 2011;43(2):141-167.
14. Fehr R, Gelfand MJ, Nag M. The road to forgiveness: a meta-analytic synthesis of its situational and dispositional correlates. Psychol Bull. 2010;136:894-914.
15. Robbennolt JK. Apologies and settlement. Court Review. 2009;45:90-97.
16. Saitta N, Hodge SD. Efficacy of a physician’s words of empathy: an overview of state apology laws. J Am Osteopath Assoc. 2012;112(5):302-306.
17. Wojcieszak D, Banja J, Houk C. The sorry works! coalition: making the case for full disclosure. Jt Comm J Qual Patient Saf. 2006;32(6):344-350.
18. National Conference of State Legislatures. Medical liability/Medical malpractice laws. http://www.ncsl.org/issues-research/banking/medical-liability-medical-malpractice-laws.aspx. Published August 15, 2011. Accessed October 4, 2013.
19. Conn Gen Stat Ann §52-184d(b).
20. Fla Stat §90.4026(2).
21. Ill Comp Stat §5/8-1901.
22. NC Gen Stat §8C-1, Rule 413.
23. Tex. Civ. Prac. & Rem. Code §18.061.
24. Ho B, Liu E. What’s an apology worth? Decomposing the effect of apologies on medical malpractice payments using state apology laws. J Empir Leg Stud. 2011;8:179-199.
25. Price M, Recupero PR. Risk management. In: Sharfstein SS, Dickerson FB, Oldham JM, eds. Textbook of hospital psychiatry. Arlington, VA: American Psychiatric Publishing, Inc.; 2009:411-412.
Report on England’s Health System Mirrors Need for Improvement in U.S.

Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
CDC Expert Discusses MRSA Infections and Monitoring for Anti-Microbial Resistance
Click here to listen to more of our interview with Dr. Patel
Click here to listen to more of our interview with Dr. Patel
Click here to listen to more of our interview with Dr. Patel
Hospitalist Greg Harlan Embraces Everything Hospital Medicine Career Offers

If he wasn’t a physician administrator working for one of the largest physician management companies in the country, or a clinical instructor at a medical school, or a pediatric hospitalist picking up shifts at a children’s hospital, Greg Harlan, MD, MPH, would have a very different life.
He says he’d “promote vegetable gardens to kindergartners, hike the West Coast Trail, fight the obesity epidemic, and play lots of golf.”
Oh, yeah, one more: “Give every kid a bicycle.”
It’s quite the altruistic—some might say enviable—list. Instead, Dr. Harlan is hard at work as director of medical affairs at North Hollywood, Calif.-based IPC The Hospitalist Company. He is also a clinical instructor at the University of Southern California Medical School and moonlights as a pediatric hospitalist in Los Angeles.
He says he chose to focus on hospital medicine as a career while working as a young faculty member at the University of Utah.
“I noticed that lots of innovation, experimentation, and energy was coming from the newly formed hospitalist division,” says Dr. Harlan, one of nine new members of Team Hospitalist, The Hospitalist’s volunteer editorial advisory group. “I tried it out and loved it, especially getting to teach the students and residents for intense periods of time.”
At IPC, Dr. Harlan leads company-wide quality improvement (QI) initiatives, coordinates risk reduction activities, and directs the IPC-University of California San Francisco Fellowship for Hospitalist Leaders. He says he has a growing interest in “physician leadership, high-functioning teams, and physician groups’ well-being.”

“I am using my QI background to apply these principles to better understanding how teams and leaders can thrive,” he says.
Question: Why did you choose a career in medicine?
A: Medicine is a cool combination of hard science, psychology, counseling, and teaching. It’s an amazing way to combine multiple passions and get to be involved on a very intimate level with many people.
Q: What do you like most about working as a hospitalist?
A: The focus on improving the system as a whole. Ultimately, the patients benefit, but so do many of the other stakeholders in the processes we touch.
Q: What do you dislike most?
A: It’s tough to take in-house call at night. It’s also hard to step in to many sick patients’ care for a short period of time, especially midway through their hospitalization.
Q: What’s the best advice you ever received?
A: Find the people who actually do the work. This is the concept of going to the front line, to see where the real work is being done. It never ceases to amaze me to find out the difference between what we think is going on and what is actually going on.
Q: What’s the biggest change you’ve seen in HM in your career?
A: Providers are getting squeezed a little more each year. There are growing pressures from many sides, and the providers are feeling “crunched.”
Q: Why is it important for you to continue seeing patients?
A: Feeling the joy and pain of actually providing care for patients is integral to leading the hospitalist movement. By acutely experiencing an electronic health record, or dealing with medication authorizations or handoffs, one stays in the real world of hospital medicine.
Q: What is your biggest professional challenge?
A: Balancing my multiple passions. I love being a teacher and still teach young med students at USC med school (my alma mater). I still enjoy seeing patients, too. I am most excited by a growing interest in leadership and teamwork, but it’s still in its development stage as a career path.
Q: What is your biggest professional reward?
A: Being able to see others flourish. Whether it’s beginning med students, professional colleagues, or administrative staff, I truly beam when someone I’ve helped succeeds.
Q: When you aren’t working, what is important to you?
A: My family, my health, and staying balanced. I am learning the importance of listening to my body, trusting my intuition, and finding true “balance.” It’s not easy, but it’s imperative.
Q: What’s next professionally?
A: I am really excited to put some science behind “leadership in medicine” and “optimal teamwork in medicine.” I think there is so much more we can learn and implement.
Q: What’s the best book you’ve read recently? Why?
A: A few come to mind: “18 Minutes” by Peter Bregman offers some really easy steps to getting organized and focused; “Six Thinking Hats” by Edward de Bono is a great framework for approaching problems and innovations; “The Inner Game of Golf” by W. Timothy Gallwey makes me realize how amazing our bodies and minds truly are.
Q: How many Apple products do you interface with in a given week?
A: I only have an iPhone. Amazing little gadget, but I don’t want to become wedded to it. Maybe I’ll get a MacBook soon.
Q: What’s next in your Netflix queue?
A: We use Netflix mainly for their drama series. I prefer foreign films and documentaries. My wife and I love “Breaking Bad.” My kids and I are working our way through the “Star Wars” episodes.
Richard Quinn is a freelance writer in New Jersey.
If he wasn’t a physician administrator working for one of the largest physician management companies in the country, or a clinical instructor at a medical school, or a pediatric hospitalist picking up shifts at a children’s hospital, Greg Harlan, MD, MPH, would have a very different life.
He says he’d “promote vegetable gardens to kindergartners, hike the West Coast Trail, fight the obesity epidemic, and play lots of golf.”
Oh, yeah, one more: “Give every kid a bicycle.”
It’s quite the altruistic—some might say enviable—list. Instead, Dr. Harlan is hard at work as director of medical affairs at North Hollywood, Calif.-based IPC The Hospitalist Company. He is also a clinical instructor at the University of Southern California Medical School and moonlights as a pediatric hospitalist in Los Angeles.
He says he chose to focus on hospital medicine as a career while working as a young faculty member at the University of Utah.
“I noticed that lots of innovation, experimentation, and energy was coming from the newly formed hospitalist division,” says Dr. Harlan, one of nine new members of Team Hospitalist, The Hospitalist’s volunteer editorial advisory group. “I tried it out and loved it, especially getting to teach the students and residents for intense periods of time.”
At IPC, Dr. Harlan leads company-wide quality improvement (QI) initiatives, coordinates risk reduction activities, and directs the IPC-University of California San Francisco Fellowship for Hospitalist Leaders. He says he has a growing interest in “physician leadership, high-functioning teams, and physician groups’ well-being.”
“I am using my QI background to apply these principles to better understanding how teams and leaders can thrive,” he says.
Question: Why did you choose a career in medicine?
A: Medicine is a cool combination of hard science, psychology, counseling, and teaching. It’s an amazing way to combine multiple passions and get to be involved on a very intimate level with many people.
Q: What do you like most about working as a hospitalist?
A: The focus on improving the system as a whole. Ultimately, the patients benefit, but so do many of the other stakeholders in the processes we touch.
Q: What do you dislike most?
A: It’s tough to take in-house call at night. It’s also hard to step in to many sick patients’ care for a short period of time, especially midway through their hospitalization.
Q: What’s the best advice you ever received?
A: Find the people who actually do the work. This is the concept of going to the front line, to see where the real work is being done. It never ceases to amaze me to find out the difference between what we think is going on and what is actually going on.
Q: What’s the biggest change you’ve seen in HM in your career?
A: Providers are getting squeezed a little more each year. There are growing pressures from many sides, and the providers are feeling “crunched.”
Q: Why is it important for you to continue seeing patients?
A: Feeling the joy and pain of actually providing care for patients is integral to leading the hospitalist movement. By acutely experiencing an electronic health record, or dealing with medication authorizations or handoffs, one stays in the real world of hospital medicine.
Q: What is your biggest professional challenge?
A: Balancing my multiple passions. I love being a teacher and still teach young med students at USC med school (my alma mater). I still enjoy seeing patients, too. I am most excited by a growing interest in leadership and teamwork, but it’s still in its development stage as a career path.
Q: What is your biggest professional reward?
A: Being able to see others flourish. Whether it’s beginning med students, professional colleagues, or administrative staff, I truly beam when someone I’ve helped succeeds.
Q: When you aren’t working, what is important to you?
A: My family, my health, and staying balanced. I am learning the importance of listening to my body, trusting my intuition, and finding true “balance.” It’s not easy, but it’s imperative.
Q: What’s next professionally?
A: I am really excited to put some science behind “leadership in medicine” and “optimal teamwork in medicine.” I think there is so much more we can learn and implement.
Q: What’s the best book you’ve read recently? Why?
A: A few come to mind: “18 Minutes” by Peter Bregman offers some really easy steps to getting organized and focused; “Six Thinking Hats” by Edward de Bono is a great framework for approaching problems and innovations; “The Inner Game of Golf” by W. Timothy Gallwey makes me realize how amazing our bodies and minds truly are.
Q: How many Apple products do you interface with in a given week?
A: I only have an iPhone. Amazing little gadget, but I don’t want to become wedded to it. Maybe I’ll get a MacBook soon.
Q: What’s next in your Netflix queue?
A: We use Netflix mainly for their drama series. I prefer foreign films and documentaries. My wife and I love “Breaking Bad.” My kids and I are working our way through the “Star Wars” episodes.
Richard Quinn is a freelance writer in New Jersey.
If he wasn’t a physician administrator working for one of the largest physician management companies in the country, or a clinical instructor at a medical school, or a pediatric hospitalist picking up shifts at a children’s hospital, Greg Harlan, MD, MPH, would have a very different life.
He says he’d “promote vegetable gardens to kindergartners, hike the West Coast Trail, fight the obesity epidemic, and play lots of golf.”
Oh, yeah, one more: “Give every kid a bicycle.”
It’s quite the altruistic—some might say enviable—list. Instead, Dr. Harlan is hard at work as director of medical affairs at North Hollywood, Calif.-based IPC The Hospitalist Company. He is also a clinical instructor at the University of Southern California Medical School and moonlights as a pediatric hospitalist in Los Angeles.
He says he chose to focus on hospital medicine as a career while working as a young faculty member at the University of Utah.
“I noticed that lots of innovation, experimentation, and energy was coming from the newly formed hospitalist division,” says Dr. Harlan, one of nine new members of Team Hospitalist, The Hospitalist’s volunteer editorial advisory group. “I tried it out and loved it, especially getting to teach the students and residents for intense periods of time.”
At IPC, Dr. Harlan leads company-wide quality improvement (QI) initiatives, coordinates risk reduction activities, and directs the IPC-University of California San Francisco Fellowship for Hospitalist Leaders. He says he has a growing interest in “physician leadership, high-functioning teams, and physician groups’ well-being.”
“I am using my QI background to apply these principles to better understanding how teams and leaders can thrive,” he says.
Question: Why did you choose a career in medicine?
A: Medicine is a cool combination of hard science, psychology, counseling, and teaching. It’s an amazing way to combine multiple passions and get to be involved on a very intimate level with many people.
Q: What do you like most about working as a hospitalist?
A: The focus on improving the system as a whole. Ultimately, the patients benefit, but so do many of the other stakeholders in the processes we touch.
Q: What do you dislike most?
A: It’s tough to take in-house call at night. It’s also hard to step in to many sick patients’ care for a short period of time, especially midway through their hospitalization.
Q: What’s the best advice you ever received?
A: Find the people who actually do the work. This is the concept of going to the front line, to see where the real work is being done. It never ceases to amaze me to find out the difference between what we think is going on and what is actually going on.
Q: What’s the biggest change you’ve seen in HM in your career?
A: Providers are getting squeezed a little more each year. There are growing pressures from many sides, and the providers are feeling “crunched.”
Q: Why is it important for you to continue seeing patients?
A: Feeling the joy and pain of actually providing care for patients is integral to leading the hospitalist movement. By acutely experiencing an electronic health record, or dealing with medication authorizations or handoffs, one stays in the real world of hospital medicine.
Q: What is your biggest professional challenge?
A: Balancing my multiple passions. I love being a teacher and still teach young med students at USC med school (my alma mater). I still enjoy seeing patients, too. I am most excited by a growing interest in leadership and teamwork, but it’s still in its development stage as a career path.
Q: What is your biggest professional reward?
A: Being able to see others flourish. Whether it’s beginning med students, professional colleagues, or administrative staff, I truly beam when someone I’ve helped succeeds.
Q: When you aren’t working, what is important to you?
A: My family, my health, and staying balanced. I am learning the importance of listening to my body, trusting my intuition, and finding true “balance.” It’s not easy, but it’s imperative.
Q: What’s next professionally?
A: I am really excited to put some science behind “leadership in medicine” and “optimal teamwork in medicine.” I think there is so much more we can learn and implement.
Q: What’s the best book you’ve read recently? Why?
A: A few come to mind: “18 Minutes” by Peter Bregman offers some really easy steps to getting organized and focused; “Six Thinking Hats” by Edward de Bono is a great framework for approaching problems and innovations; “The Inner Game of Golf” by W. Timothy Gallwey makes me realize how amazing our bodies and minds truly are.
Q: How many Apple products do you interface with in a given week?
A: I only have an iPhone. Amazing little gadget, but I don’t want to become wedded to it. Maybe I’ll get a MacBook soon.
Q: What’s next in your Netflix queue?
A: We use Netflix mainly for their drama series. I prefer foreign films and documentaries. My wife and I love “Breaking Bad.” My kids and I are working our way through the “Star Wars” episodes.
Richard Quinn is a freelance writer in New Jersey.
Industry Insider Explains the State of Medical Liability Insurance
Click here to listen to more of our interview with Mike Matray
Click here to listen to more of our interview with Mike Matray
Click here to listen to more of our interview with Mike Matray