User login
U.S. measles cases up to 159 for the year
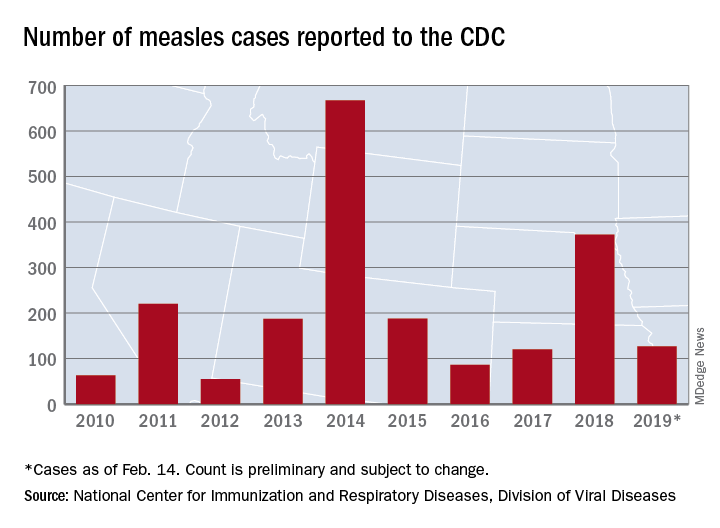
Reported measles cases are now up to 159 for the year in the United States, according to the Centers for Disease Control and Prevention.

The most recent reporting week, which ended Feb. 21, brought another 32 cases of measles and one new outbreak of 4 cases in Illinois. The total number of outbreaks – an outbreak is defined as three or more cases – is now six, and cases have been reported in 10 states, the CDC said Feb. 25.
The majority (17) of those 32 new cases occurred in Brooklyn, one of New York state’s three outbreaks this year. The largest of the 2019 outbreaks is in Washington state, primarily in Clark County, and is up to 66 cases after 4 more were reported in the last week by the state’s department of health. The outbreaks are linked to travelers who brought the disease to the United States.
There are now two measures “advancing through the [Washington] state legislature that would bar parents from using personal or philosophical exemptions to avoid immunizing their school-age children. Both have bipartisan support despite strong antivaccination sentiment in parts of the state,” the Washington Post said on Feb. 25.
Reported measles cases are now up to 159 for the year in the United States, according to the Centers for Disease Control and Prevention.
The most recent reporting week, which ended Feb. 21, brought another 32 cases of measles and one new outbreak of 4 cases in Illinois. The total number of outbreaks – an outbreak is defined as three or more cases – is now six, and cases have been reported in 10 states, the CDC said Feb. 25.
The majority (17) of those 32 new cases occurred in Brooklyn, one of New York state’s three outbreaks this year. The largest of the 2019 outbreaks is in Washington state, primarily in Clark County, and is up to 66 cases after 4 more were reported in the last week by the state’s department of health. The outbreaks are linked to travelers who brought the disease to the United States.
There are now two measures “advancing through the [Washington] state legislature that would bar parents from using personal or philosophical exemptions to avoid immunizing their school-age children. Both have bipartisan support despite strong antivaccination sentiment in parts of the state,” the Washington Post said on Feb. 25.
Reported measles cases are now up to 159 for the year in the United States, according to the Centers for Disease Control and Prevention.
The most recent reporting week, which ended Feb. 21, brought another 32 cases of measles and one new outbreak of 4 cases in Illinois. The total number of outbreaks – an outbreak is defined as three or more cases – is now six, and cases have been reported in 10 states, the CDC said Feb. 25.
The majority (17) of those 32 new cases occurred in Brooklyn, one of New York state’s three outbreaks this year. The largest of the 2019 outbreaks is in Washington state, primarily in Clark County, and is up to 66 cases after 4 more were reported in the last week by the state’s department of health. The outbreaks are linked to travelers who brought the disease to the United States.
There are now two measures “advancing through the [Washington] state legislature that would bar parents from using personal or philosophical exemptions to avoid immunizing their school-age children. Both have bipartisan support despite strong antivaccination sentiment in parts of the state,” the Washington Post said on Feb. 25.
FDA: Safety signal emerged with higher dose of tofacitinib in RA study
the Food and Drug Administration reported.

The trial’s Data Safety and Monitoring Board identified the signal in patients taking a 10-mg dose of tofacitinib twice daily, the FDA said in a safety announcement.
Pfizer, the trial’s sponsor, took “immediate action” to transition patients in the ongoing trial from the 10-mg, twice-daily dose to 5 mg twice daily, which is the approved dose for adult patients with moderate to severe rheumatoid arthritis, the agency said. The 10-mg, twice-daily dose is approved only in the dosing regimen for patients with ulcerative colitis. Xeljanz is also approved to treat psoriatic arthritis. The 11-mg, once-daily dose of Xeljanz XR that is approved to treat rheumatoid arthritis and psoriatic arthritis was not tested in the trial.
The ongoing study was designed to assess risks of cardiovascular events, cancer, and opportunistic infections with tofacitinib 10 mg twice daily or 5 mg twice daily versus the risks in a control group treated with a tumor necrosis factor (TNF) inhibitor, according to the statement.
Patients had to be 50 years of age or older and have at least one cardiovascular risk factor to be eligible for the study, which was required by the agency in 2012 when it approved tofacitinib, the statement says.
The FDA is reviewing trial data and working with Pfizer to better understand the safety signal, its effect on patients, and how tofacitinib should be used, Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in a news release. The trial will continue and is expected to be completed by the end of 2019.
“The agency will take appropriate action, as warranted, to ensure patients enrolled in this and other trials are protected and that health care professionals and clinical trial researchers understand the risks associated with this use,” she added.
Health care professionals should follow tofacitinib prescribing information, monitor patients for the signs and symptoms of pulmonary embolism, and advise patients to seek medical attention immediately if they experience those signs and symptoms, according to the statement.
“We are communicating now, given the serious nature of the safety issue, to ensure that patients taking tofacitinib are aware that the FDA still believes the benefits of taking tofacitinib for its approved uses continue to outweigh the risks,” Dr. Woodcock said in the release.
While not approved in rheumatoid arthritis, the 10-mg, twice-daily dose of tofacitinib is approved in the dosing regimen for patients with ulcerative colitis, the release says.
the Food and Drug Administration reported.
The trial’s Data Safety and Monitoring Board identified the signal in patients taking a 10-mg dose of tofacitinib twice daily, the FDA said in a safety announcement.
Pfizer, the trial’s sponsor, took “immediate action” to transition patients in the ongoing trial from the 10-mg, twice-daily dose to 5 mg twice daily, which is the approved dose for adult patients with moderate to severe rheumatoid arthritis, the agency said. The 10-mg, twice-daily dose is approved only in the dosing regimen for patients with ulcerative colitis. Xeljanz is also approved to treat psoriatic arthritis. The 11-mg, once-daily dose of Xeljanz XR that is approved to treat rheumatoid arthritis and psoriatic arthritis was not tested in the trial.
The ongoing study was designed to assess risks of cardiovascular events, cancer, and opportunistic infections with tofacitinib 10 mg twice daily or 5 mg twice daily versus the risks in a control group treated with a tumor necrosis factor (TNF) inhibitor, according to the statement.
Patients had to be 50 years of age or older and have at least one cardiovascular risk factor to be eligible for the study, which was required by the agency in 2012 when it approved tofacitinib, the statement says.
The FDA is reviewing trial data and working with Pfizer to better understand the safety signal, its effect on patients, and how tofacitinib should be used, Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in a news release. The trial will continue and is expected to be completed by the end of 2019.
“The agency will take appropriate action, as warranted, to ensure patients enrolled in this and other trials are protected and that health care professionals and clinical trial researchers understand the risks associated with this use,” she added.
Health care professionals should follow tofacitinib prescribing information, monitor patients for the signs and symptoms of pulmonary embolism, and advise patients to seek medical attention immediately if they experience those signs and symptoms, according to the statement.
“We are communicating now, given the serious nature of the safety issue, to ensure that patients taking tofacitinib are aware that the FDA still believes the benefits of taking tofacitinib for its approved uses continue to outweigh the risks,” Dr. Woodcock said in the release.
While not approved in rheumatoid arthritis, the 10-mg, twice-daily dose of tofacitinib is approved in the dosing regimen for patients with ulcerative colitis, the release says.
the Food and Drug Administration reported.
The trial’s Data Safety and Monitoring Board identified the signal in patients taking a 10-mg dose of tofacitinib twice daily, the FDA said in a safety announcement.
Pfizer, the trial’s sponsor, took “immediate action” to transition patients in the ongoing trial from the 10-mg, twice-daily dose to 5 mg twice daily, which is the approved dose for adult patients with moderate to severe rheumatoid arthritis, the agency said. The 10-mg, twice-daily dose is approved only in the dosing regimen for patients with ulcerative colitis. Xeljanz is also approved to treat psoriatic arthritis. The 11-mg, once-daily dose of Xeljanz XR that is approved to treat rheumatoid arthritis and psoriatic arthritis was not tested in the trial.
The ongoing study was designed to assess risks of cardiovascular events, cancer, and opportunistic infections with tofacitinib 10 mg twice daily or 5 mg twice daily versus the risks in a control group treated with a tumor necrosis factor (TNF) inhibitor, according to the statement.
Patients had to be 50 years of age or older and have at least one cardiovascular risk factor to be eligible for the study, which was required by the agency in 2012 when it approved tofacitinib, the statement says.
The FDA is reviewing trial data and working with Pfizer to better understand the safety signal, its effect on patients, and how tofacitinib should be used, Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in a news release. The trial will continue and is expected to be completed by the end of 2019.
“The agency will take appropriate action, as warranted, to ensure patients enrolled in this and other trials are protected and that health care professionals and clinical trial researchers understand the risks associated with this use,” she added.
Health care professionals should follow tofacitinib prescribing information, monitor patients for the signs and symptoms of pulmonary embolism, and advise patients to seek medical attention immediately if they experience those signs and symptoms, according to the statement.
“We are communicating now, given the serious nature of the safety issue, to ensure that patients taking tofacitinib are aware that the FDA still believes the benefits of taking tofacitinib for its approved uses continue to outweigh the risks,” Dr. Woodcock said in the release.
While not approved in rheumatoid arthritis, the 10-mg, twice-daily dose of tofacitinib is approved in the dosing regimen for patients with ulcerative colitis, the release says.
Influenza activity continues to increase
The 2018-2019 flu season is showing no signs of decline as activity measures continued to increase into mid-February, according to the Centers for Disease Control and Prevention.
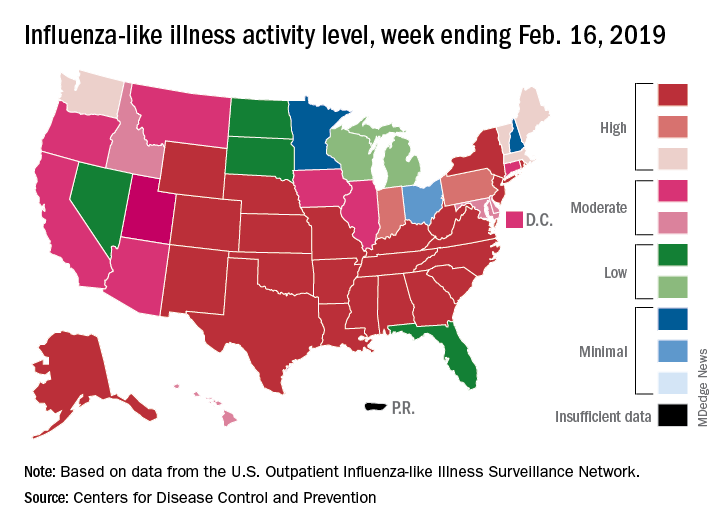
Eight of the last 10 flu seasons had already reached their peak before mid-February, but another rise brought the proportion of outpatient visits for influenza-like illness (ILI) to 5.1% for the week ending Feb. 16, compared with 4.8% the week before, the CDC’s influenza division reported Feb. 22. ILI is defined as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.
The week also brought more ILI to more states, as the number reporting an activity level of 10 on the CDC’s 1-10 scale rose from 21 to 24 and the number in the high range of 8-10 increased from 26 to 30. Another seven states – including California, which was at level 5 the previous week – and the District of Columbia were at level 7 for the current reporting week, the CDC said.
Two flu-related pediatric deaths occurred during the week ending Feb. 16 and another five were reported from previous weeks, which brings the total to 41 for the 2018-2019 season. Data for influenza deaths at all ages, which are reported a week later, show that 205 occurred in the week ending Feb. 9, with reporting 75% complete. There were 236 total deaths for the week ending Feb. 2 (94% reporting) and 218 deaths during the week ending Jan. 26 (99% reporting), the CDC said.
The 2018-2019 flu season is showing no signs of decline as activity measures continued to increase into mid-February, according to the Centers for Disease Control and Prevention.
Eight of the last 10 flu seasons had already reached their peak before mid-February, but another rise brought the proportion of outpatient visits for influenza-like illness (ILI) to 5.1% for the week ending Feb. 16, compared with 4.8% the week before, the CDC’s influenza division reported Feb. 22. ILI is defined as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.
The week also brought more ILI to more states, as the number reporting an activity level of 10 on the CDC’s 1-10 scale rose from 21 to 24 and the number in the high range of 8-10 increased from 26 to 30. Another seven states – including California, which was at level 5 the previous week – and the District of Columbia were at level 7 for the current reporting week, the CDC said.
Two flu-related pediatric deaths occurred during the week ending Feb. 16 and another five were reported from previous weeks, which brings the total to 41 for the 2018-2019 season. Data for influenza deaths at all ages, which are reported a week later, show that 205 occurred in the week ending Feb. 9, with reporting 75% complete. There were 236 total deaths for the week ending Feb. 2 (94% reporting) and 218 deaths during the week ending Jan. 26 (99% reporting), the CDC said.
The 2018-2019 flu season is showing no signs of decline as activity measures continued to increase into mid-February, according to the Centers for Disease Control and Prevention.
Eight of the last 10 flu seasons had already reached their peak before mid-February, but another rise brought the proportion of outpatient visits for influenza-like illness (ILI) to 5.1% for the week ending Feb. 16, compared with 4.8% the week before, the CDC’s influenza division reported Feb. 22. ILI is defined as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.
The week also brought more ILI to more states, as the number reporting an activity level of 10 on the CDC’s 1-10 scale rose from 21 to 24 and the number in the high range of 8-10 increased from 26 to 30. Another seven states – including California, which was at level 5 the previous week – and the District of Columbia were at level 7 for the current reporting week, the CDC said.
Two flu-related pediatric deaths occurred during the week ending Feb. 16 and another five were reported from previous weeks, which brings the total to 41 for the 2018-2019 season. Data for influenza deaths at all ages, which are reported a week later, show that 205 occurred in the week ending Feb. 9, with reporting 75% complete. There were 236 total deaths for the week ending Feb. 2 (94% reporting) and 218 deaths during the week ending Jan. 26 (99% reporting), the CDC said.
FDA clears test to monitor residual disease in CML
The Food and Drug Administration has cleared Bio-Rad’s digital polymerase chain reaction (PCR) testing solution to monitor patients’ molecular response to treatment for chronic myeloid leukemia.
The QXDx AutoDG ddPCR System combines Bio-Rad’s Droplet Digital PCR technology and the QXDx BCR-ABL %IS Kit, according to the company.
This so-called liquid biopsy test can “precisely and reproducibly” monitor the molecular response to tyrosine kinase inhibitor therapy. The current standard – reverse transcription quantitative PCR – can have variable results, especially at low levels of disease, according to Bio-Rad.
FDA clearance means that the product is “substantially equivalent” to an already-approved product and can be sold in the United States, according to the agency.
The Food and Drug Administration has cleared Bio-Rad’s digital polymerase chain reaction (PCR) testing solution to monitor patients’ molecular response to treatment for chronic myeloid leukemia.
The QXDx AutoDG ddPCR System combines Bio-Rad’s Droplet Digital PCR technology and the QXDx BCR-ABL %IS Kit, according to the company.
This so-called liquid biopsy test can “precisely and reproducibly” monitor the molecular response to tyrosine kinase inhibitor therapy. The current standard – reverse transcription quantitative PCR – can have variable results, especially at low levels of disease, according to Bio-Rad.
FDA clearance means that the product is “substantially equivalent” to an already-approved product and can be sold in the United States, according to the agency.
The Food and Drug Administration has cleared Bio-Rad’s digital polymerase chain reaction (PCR) testing solution to monitor patients’ molecular response to treatment for chronic myeloid leukemia.
The QXDx AutoDG ddPCR System combines Bio-Rad’s Droplet Digital PCR technology and the QXDx BCR-ABL %IS Kit, according to the company.
This so-called liquid biopsy test can “precisely and reproducibly” monitor the molecular response to tyrosine kinase inhibitor therapy. The current standard – reverse transcription quantitative PCR – can have variable results, especially at low levels of disease, according to Bio-Rad.
FDA clearance means that the product is “substantially equivalent” to an already-approved product and can be sold in the United States, according to the agency.
Death data spur black-box warning for gout drug Uloric
, the Food and Drug Administration declared on Feb. 21. The agency is now mandating a black-box warning.
![]()
“Health care professionals should reserve Uloric for use only in patients who have failed or do not tolerate allopurinol,” the FDA announced. “Counsel patients about the cardiovascular risk with Uloric,” the agency suggested, and advise them to seek medical attention at once if they have cardiac symptoms such as chest pain, shortness of breath, rapid or irregular heartbeat, or dizziness.
The FDA’s move comes a decade after it approved febuxostat as a gout treatment. As the FDA noted in its announcement, “the number of medicines to treat gout is limited, and there is an unmet need for treatments for this disease.”
Research has suggested that both febuxostat and allopurinol have similar efficacy. Some experts have recommended febuxostat as an alternative for patients who shouldn’t take allopurinol (Semin Arthritis Rheum. 2013 Dec;43[3]:367-75).
However, research has raised concerns about febuxostat’s cardiac risk. In its Feb. 21 statement, the FDA pointed to the findings of a 2010-2017 postmarket clinical trial of 6,190 patients with gout who were treated with febuxostat or allopurinol (N Engl J Med. 2018;378:1200-10).
“In patients treated with Uloric, 15 deaths from heart-related causes were observed for every 1,000 patients treated for a year compared to 11 deaths from heart-related causes per 1,000 patients treated with allopurinol for a year,” the FDA said. “In addition, there were 26 deaths from any cause per 1,000 patients treated for a year with Uloric compared to 22 deaths per 1,000 patients treated for a year with allopurinol.”
, the Food and Drug Administration declared on Feb. 21. The agency is now mandating a black-box warning.
![]()
“Health care professionals should reserve Uloric for use only in patients who have failed or do not tolerate allopurinol,” the FDA announced. “Counsel patients about the cardiovascular risk with Uloric,” the agency suggested, and advise them to seek medical attention at once if they have cardiac symptoms such as chest pain, shortness of breath, rapid or irregular heartbeat, or dizziness.
The FDA’s move comes a decade after it approved febuxostat as a gout treatment. As the FDA noted in its announcement, “the number of medicines to treat gout is limited, and there is an unmet need for treatments for this disease.”
Research has suggested that both febuxostat and allopurinol have similar efficacy. Some experts have recommended febuxostat as an alternative for patients who shouldn’t take allopurinol (Semin Arthritis Rheum. 2013 Dec;43[3]:367-75).
However, research has raised concerns about febuxostat’s cardiac risk. In its Feb. 21 statement, the FDA pointed to the findings of a 2010-2017 postmarket clinical trial of 6,190 patients with gout who were treated with febuxostat or allopurinol (N Engl J Med. 2018;378:1200-10).
“In patients treated with Uloric, 15 deaths from heart-related causes were observed for every 1,000 patients treated for a year compared to 11 deaths from heart-related causes per 1,000 patients treated with allopurinol for a year,” the FDA said. “In addition, there were 26 deaths from any cause per 1,000 patients treated for a year with Uloric compared to 22 deaths per 1,000 patients treated for a year with allopurinol.”
, the Food and Drug Administration declared on Feb. 21. The agency is now mandating a black-box warning.
![]()
“Health care professionals should reserve Uloric for use only in patients who have failed or do not tolerate allopurinol,” the FDA announced. “Counsel patients about the cardiovascular risk with Uloric,” the agency suggested, and advise them to seek medical attention at once if they have cardiac symptoms such as chest pain, shortness of breath, rapid or irregular heartbeat, or dizziness.
The FDA’s move comes a decade after it approved febuxostat as a gout treatment. As the FDA noted in its announcement, “the number of medicines to treat gout is limited, and there is an unmet need for treatments for this disease.”
Research has suggested that both febuxostat and allopurinol have similar efficacy. Some experts have recommended febuxostat as an alternative for patients who shouldn’t take allopurinol (Semin Arthritis Rheum. 2013 Dec;43[3]:367-75).
However, research has raised concerns about febuxostat’s cardiac risk. In its Feb. 21 statement, the FDA pointed to the findings of a 2010-2017 postmarket clinical trial of 6,190 patients with gout who were treated with febuxostat or allopurinol (N Engl J Med. 2018;378:1200-10).
“In patients treated with Uloric, 15 deaths from heart-related causes were observed for every 1,000 patients treated for a year compared to 11 deaths from heart-related causes per 1,000 patients treated with allopurinol for a year,” the FDA said. “In addition, there were 26 deaths from any cause per 1,000 patients treated for a year with Uloric compared to 22 deaths per 1,000 patients treated for a year with allopurinol.”
FDA grants priority review to polatuzumab vedotin for DLBCL
With this BLA, Genentech is seeking approval for polatuzumab vedotin in combination with bendamustine and rituximab (BR) to treat patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL).
The FDA grants priority review to applications for products that are expected to provide significant improvements in the treatment, diagnosis, or prevention of serious conditions. The agency aims to take action on a priority review application within 6 months, rather than the standard 10 months.
The FDA is expected to make a decision on this BLA by Aug. 19, 2019.
The BLA is supported by a phase 1b/2 trial (NCT02257567) of patients with relapsed or refractory follicular lymphoma or DLBCL who received polatuzumab vedotin in combination with BR or obinutuzumab.
The trial’s phase 2 stage included 80 DLBCL patients who were randomized to receive BR or BR plus polatuzumab vedotin, according to Genentech.
The complete response rate was 40% in the polatuzumab vedotin arm and 18% in the BR arm. The median duration of response was 10.3 months and 4.1 months, respectively (hazard ratio [HR] = 0.44).
The median progression-free survival was 7.6 months in the polatuzumab vedotin arm and 2.0 months in the BR arm (HR = 0.34).
Among patients who were ineligible for a transplant, the median overall survival (an exploratory endpoint) was 12.4 months in the polatuzumab vedotin arm and 4.7 months in the BR arm (HR = 0.42).
Patients who received polatuzumab vedotin had higher rates of grade 3-4 cytopenias, compared with patients who received BR alone. Rates of infection and transfusion were similar between the arms.
With this BLA, Genentech is seeking approval for polatuzumab vedotin in combination with bendamustine and rituximab (BR) to treat patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL).
The FDA grants priority review to applications for products that are expected to provide significant improvements in the treatment, diagnosis, or prevention of serious conditions. The agency aims to take action on a priority review application within 6 months, rather than the standard 10 months.
The FDA is expected to make a decision on this BLA by Aug. 19, 2019.
The BLA is supported by a phase 1b/2 trial (NCT02257567) of patients with relapsed or refractory follicular lymphoma or DLBCL who received polatuzumab vedotin in combination with BR or obinutuzumab.
The trial’s phase 2 stage included 80 DLBCL patients who were randomized to receive BR or BR plus polatuzumab vedotin, according to Genentech.
The complete response rate was 40% in the polatuzumab vedotin arm and 18% in the BR arm. The median duration of response was 10.3 months and 4.1 months, respectively (hazard ratio [HR] = 0.44).
The median progression-free survival was 7.6 months in the polatuzumab vedotin arm and 2.0 months in the BR arm (HR = 0.34).
Among patients who were ineligible for a transplant, the median overall survival (an exploratory endpoint) was 12.4 months in the polatuzumab vedotin arm and 4.7 months in the BR arm (HR = 0.42).
Patients who received polatuzumab vedotin had higher rates of grade 3-4 cytopenias, compared with patients who received BR alone. Rates of infection and transfusion were similar between the arms.
With this BLA, Genentech is seeking approval for polatuzumab vedotin in combination with bendamustine and rituximab (BR) to treat patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL).
The FDA grants priority review to applications for products that are expected to provide significant improvements in the treatment, diagnosis, or prevention of serious conditions. The agency aims to take action on a priority review application within 6 months, rather than the standard 10 months.
The FDA is expected to make a decision on this BLA by Aug. 19, 2019.
The BLA is supported by a phase 1b/2 trial (NCT02257567) of patients with relapsed or refractory follicular lymphoma or DLBCL who received polatuzumab vedotin in combination with BR or obinutuzumab.
The trial’s phase 2 stage included 80 DLBCL patients who were randomized to receive BR or BR plus polatuzumab vedotin, according to Genentech.
The complete response rate was 40% in the polatuzumab vedotin arm and 18% in the BR arm. The median duration of response was 10.3 months and 4.1 months, respectively (hazard ratio [HR] = 0.44).
The median progression-free survival was 7.6 months in the polatuzumab vedotin arm and 2.0 months in the BR arm (HR = 0.34).
Among patients who were ineligible for a transplant, the median overall survival (an exploratory endpoint) was 12.4 months in the polatuzumab vedotin arm and 4.7 months in the BR arm (HR = 0.42).
Patients who received polatuzumab vedotin had higher rates of grade 3-4 cytopenias, compared with patients who received BR alone. Rates of infection and transfusion were similar between the arms.
FDA approves turoctocog alfa pegol for hemophilia A
The agency approved turoctocog alfa pegol for use as routine prophylaxis to reduce the frequency of bleeding episodes, for on-demand treatment and control of bleeding episodes, and for perioperative management of bleeding in adults and children with hemophilia A.
Turoctocog alfa pegol will not be available in the United States before 2020, according to Novo Nordisk. The company cannot yet launch the product because of third-party intellectual property agreements.
The FDA’s approval of turoctocog alfa pegol was supported by results from the pathfinder 2 (NCT01480180), pathfinder 3 (NCT01489111), and pathfinder 5 (NCT01731600) trials.
The trials included children, adolescents, and adults with previously treated, severe hemophilia A and no history of inhibitors. Turoctocog alfa pegol was considered effective and well tolerated in these trials.
Pooled results from pathfinder 2 and pathfinder 5 were presented at the 2018 annual meeting of the American Society of Hematology (Blood. 2018:132:1177).
Results from pathfinder 3 were previously published in Haemophilia (2017. Sep;23[5]:689-96).
The agency approved turoctocog alfa pegol for use as routine prophylaxis to reduce the frequency of bleeding episodes, for on-demand treatment and control of bleeding episodes, and for perioperative management of bleeding in adults and children with hemophilia A.
Turoctocog alfa pegol will not be available in the United States before 2020, according to Novo Nordisk. The company cannot yet launch the product because of third-party intellectual property agreements.
The FDA’s approval of turoctocog alfa pegol was supported by results from the pathfinder 2 (NCT01480180), pathfinder 3 (NCT01489111), and pathfinder 5 (NCT01731600) trials.
The trials included children, adolescents, and adults with previously treated, severe hemophilia A and no history of inhibitors. Turoctocog alfa pegol was considered effective and well tolerated in these trials.
Pooled results from pathfinder 2 and pathfinder 5 were presented at the 2018 annual meeting of the American Society of Hematology (Blood. 2018:132:1177).
Results from pathfinder 3 were previously published in Haemophilia (2017. Sep;23[5]:689-96).
The agency approved turoctocog alfa pegol for use as routine prophylaxis to reduce the frequency of bleeding episodes, for on-demand treatment and control of bleeding episodes, and for perioperative management of bleeding in adults and children with hemophilia A.
Turoctocog alfa pegol will not be available in the United States before 2020, according to Novo Nordisk. The company cannot yet launch the product because of third-party intellectual property agreements.
The FDA’s approval of turoctocog alfa pegol was supported by results from the pathfinder 2 (NCT01480180), pathfinder 3 (NCT01489111), and pathfinder 5 (NCT01731600) trials.
The trials included children, adolescents, and adults with previously treated, severe hemophilia A and no history of inhibitors. Turoctocog alfa pegol was considered effective and well tolerated in these trials.
Pooled results from pathfinder 2 and pathfinder 5 were presented at the 2018 annual meeting of the American Society of Hematology (Blood. 2018:132:1177).
Results from pathfinder 3 were previously published in Haemophilia (2017. Sep;23[5]:689-96).
Measles: 26 new cases reported last week
according to the Centers for Disease Control and Prevention.
On Jan. 31, total measles cases stood at 79, which means that the number of individuals with measles has risen by 61% in just the last 2 weeks. Of the five outbreaks (defined as three or more cases) so far in 2019, three have occurred in New York (57 cases in three counties), one in Texas (8 cases in five counties), and one in Washington (62 cases in two counties), the CDC reported Feb. 18.
The majority of the Washington cases (61 of the 62) have occurred in Clark County, which is located just across the Columbia River from Portland, Ore. Oregon, in turn, has a higher percentage of kindergartners with nonmedical exemptions from vaccination (7.5%) than any other state, the CDC reported in October 2018. Washington’s rate of 3.9% was nearly double the national median of 2.0% for the 2017-2018 school year, while Texas (1.8%) and New York (1.0%) were below it, the CDC said.
In the Pacific Northwest, however, some parents may be changing their minds about vaccinations, according to the New York Times, which reported that “about triple the number of children have been vaccinated this year, compared with the same period in 2018,” in Oregon and southwest Washington.
Individual cases of measles have been reported to the CDC by seven other states: California, Colorado, Connecticut, Georgia, Illinois, Kentucky, and Oregon.
according to the Centers for Disease Control and Prevention.
On Jan. 31, total measles cases stood at 79, which means that the number of individuals with measles has risen by 61% in just the last 2 weeks. Of the five outbreaks (defined as three or more cases) so far in 2019, three have occurred in New York (57 cases in three counties), one in Texas (8 cases in five counties), and one in Washington (62 cases in two counties), the CDC reported Feb. 18.
The majority of the Washington cases (61 of the 62) have occurred in Clark County, which is located just across the Columbia River from Portland, Ore. Oregon, in turn, has a higher percentage of kindergartners with nonmedical exemptions from vaccination (7.5%) than any other state, the CDC reported in October 2018. Washington’s rate of 3.9% was nearly double the national median of 2.0% for the 2017-2018 school year, while Texas (1.8%) and New York (1.0%) were below it, the CDC said.
In the Pacific Northwest, however, some parents may be changing their minds about vaccinations, according to the New York Times, which reported that “about triple the number of children have been vaccinated this year, compared with the same period in 2018,” in Oregon and southwest Washington.
Individual cases of measles have been reported to the CDC by seven other states: California, Colorado, Connecticut, Georgia, Illinois, Kentucky, and Oregon.
according to the Centers for Disease Control and Prevention.
On Jan. 31, total measles cases stood at 79, which means that the number of individuals with measles has risen by 61% in just the last 2 weeks. Of the five outbreaks (defined as three or more cases) so far in 2019, three have occurred in New York (57 cases in three counties), one in Texas (8 cases in five counties), and one in Washington (62 cases in two counties), the CDC reported Feb. 18.
The majority of the Washington cases (61 of the 62) have occurred in Clark County, which is located just across the Columbia River from Portland, Ore. Oregon, in turn, has a higher percentage of kindergartners with nonmedical exemptions from vaccination (7.5%) than any other state, the CDC reported in October 2018. Washington’s rate of 3.9% was nearly double the national median of 2.0% for the 2017-2018 school year, while Texas (1.8%) and New York (1.0%) were below it, the CDC said.
In the Pacific Northwest, however, some parents may be changing their minds about vaccinations, according to the New York Times, which reported that “about triple the number of children have been vaccinated this year, compared with the same period in 2018,” in Oregon and southwest Washington.
Individual cases of measles have been reported to the CDC by seven other states: California, Colorado, Connecticut, Georgia, Illinois, Kentucky, and Oregon.
Flu season showing its staying power
Like an unwelcome guest, the 2018-2019 flu season seems to be settling in for a lengthy stay as three more states have reached the highest level of influenza-like illness (ILI) activity, according to the Centers for Disease Control and Prevention.
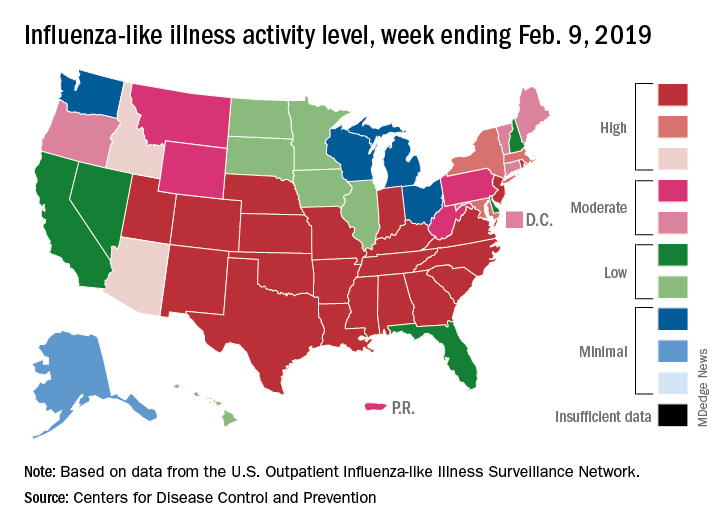
There are now 21 states at level 10 on the CDC’s 1-10 scale, with the South showing up almost solidly red on the flu activity map for the week ending Feb. 9. Another five states are at levels 8 and 9, bringing the total in the high range to 26 for the week, compared with 24 the previous week, the CDC’s influenza division reported Feb. 15.
National activity, reflected in the proportion of outpatient visits involving ILI, took a step up from 4.3% the week before to 4.8% for the week ending Feb. 9. The national baseline rate is 2.2% for ILI, which the CDC defines “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Two flu-related pediatric deaths occurred during the week ending Feb. 9, and another four were reported from earlier weeks, which brings the total for the 2018-2019 season to 34, the CDC said. At the same point in last year’s flu season, there had been 84 flu-related deaths in children.
In a separate report, the CDC said that, based on data collected from Nov. 23, 2018 to Feb. 2, 2019, “the influenza vaccine has been 47% effective in preventing medically attended acute respiratory virus infection across all age groups and specifically was 46% effective in preventing medical visits associated with influenza A(H1N1)pdm09.” The effectiveness of the vaccine was 61% for children aged 6 months to 17 years, the CDC said (MMWR. 2019 Feb 15;68[6];135-9).
Flu vaccination during the 2017-2018 season prevented 7.1 million illnesses, 3.7 million medical visits, 109,000 hospitalizations, and 8,000 flu-related deaths, the CDC said, adding that “vaccination has been found to reduce deaths, intensive care unit admissions and length of stay, and overall duration of hospitalization among hospitalized influenza patients.”
Forecasts for the rest of the 2018-2019 season “predict that elevated influenza activity in parts of the United States will continue for several more weeks,” the CDC said.
Like an unwelcome guest, the 2018-2019 flu season seems to be settling in for a lengthy stay as three more states have reached the highest level of influenza-like illness (ILI) activity, according to the Centers for Disease Control and Prevention.
There are now 21 states at level 10 on the CDC’s 1-10 scale, with the South showing up almost solidly red on the flu activity map for the week ending Feb. 9. Another five states are at levels 8 and 9, bringing the total in the high range to 26 for the week, compared with 24 the previous week, the CDC’s influenza division reported Feb. 15.
National activity, reflected in the proportion of outpatient visits involving ILI, took a step up from 4.3% the week before to 4.8% for the week ending Feb. 9. The national baseline rate is 2.2% for ILI, which the CDC defines “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Two flu-related pediatric deaths occurred during the week ending Feb. 9, and another four were reported from earlier weeks, which brings the total for the 2018-2019 season to 34, the CDC said. At the same point in last year’s flu season, there had been 84 flu-related deaths in children.
In a separate report, the CDC said that, based on data collected from Nov. 23, 2018 to Feb. 2, 2019, “the influenza vaccine has been 47% effective in preventing medically attended acute respiratory virus infection across all age groups and specifically was 46% effective in preventing medical visits associated with influenza A(H1N1)pdm09.” The effectiveness of the vaccine was 61% for children aged 6 months to 17 years, the CDC said (MMWR. 2019 Feb 15;68[6];135-9).
Flu vaccination during the 2017-2018 season prevented 7.1 million illnesses, 3.7 million medical visits, 109,000 hospitalizations, and 8,000 flu-related deaths, the CDC said, adding that “vaccination has been found to reduce deaths, intensive care unit admissions and length of stay, and overall duration of hospitalization among hospitalized influenza patients.”
Forecasts for the rest of the 2018-2019 season “predict that elevated influenza activity in parts of the United States will continue for several more weeks,” the CDC said.
Like an unwelcome guest, the 2018-2019 flu season seems to be settling in for a lengthy stay as three more states have reached the highest level of influenza-like illness (ILI) activity, according to the Centers for Disease Control and Prevention.
There are now 21 states at level 10 on the CDC’s 1-10 scale, with the South showing up almost solidly red on the flu activity map for the week ending Feb. 9. Another five states are at levels 8 and 9, bringing the total in the high range to 26 for the week, compared with 24 the previous week, the CDC’s influenza division reported Feb. 15.
National activity, reflected in the proportion of outpatient visits involving ILI, took a step up from 4.3% the week before to 4.8% for the week ending Feb. 9. The national baseline rate is 2.2% for ILI, which the CDC defines “as fever (temperature of 100°F [37.8°C] or greater) and cough and/or sore throat.”
Two flu-related pediatric deaths occurred during the week ending Feb. 9, and another four were reported from earlier weeks, which brings the total for the 2018-2019 season to 34, the CDC said. At the same point in last year’s flu season, there had been 84 flu-related deaths in children.
In a separate report, the CDC said that, based on data collected from Nov. 23, 2018 to Feb. 2, 2019, “the influenza vaccine has been 47% effective in preventing medically attended acute respiratory virus infection across all age groups and specifically was 46% effective in preventing medical visits associated with influenza A(H1N1)pdm09.” The effectiveness of the vaccine was 61% for children aged 6 months to 17 years, the CDC said (MMWR. 2019 Feb 15;68[6];135-9).
Flu vaccination during the 2017-2018 season prevented 7.1 million illnesses, 3.7 million medical visits, 109,000 hospitalizations, and 8,000 flu-related deaths, the CDC said, adding that “vaccination has been found to reduce deaths, intensive care unit admissions and length of stay, and overall duration of hospitalization among hospitalized influenza patients.”
Forecasts for the rest of the 2018-2019 season “predict that elevated influenza activity in parts of the United States will continue for several more weeks,” the CDC said.
FDA approves daratumumab split-dosing regimen in MM
The Food and Drug Administration has approved a split-dosing regimen for daratumumab (Darzalex) in patients with multiple myeloma, allowing the first infusion to be split over 2 days.
FDA approval is based on results from the global, multi-arm, phase 1b EQUULEUS (MMY1001) trial, which evaluated daratumumab in combination with a variety of treatment regimens. Splitting the first infusion over 2 consecutive days reduced the duration of the infusion and resulted in a similar rate of infusion site reactions; concentrations were similar at the end of weekly dosing in patients who received the first infusion at once or over a 2-day period.
The adverse events reported in EQUULEUS (MMY1001) were largely similar to those seen in previous trials; the most common adverse events include infusion reactions, neutropenia, thrombocytopenia, fatigue, nausea, diarrhea, constipation, vomiting, muscle spasms, arthralgia, back pain, pyrexia, chills, dizziness, insomnia, cough, dyspnea, peripheral edema, peripheral sensory neuropathy, and upper respiratory tract infection.
The approval providers “added flexibility for how patients may receive initial treatment,” Craig Tendler, MD, vice president of clinical development and global medical affairs at Janssen Research & Development, said in a statement.
The Food and Drug Administration has approved a split-dosing regimen for daratumumab (Darzalex) in patients with multiple myeloma, allowing the first infusion to be split over 2 days.
FDA approval is based on results from the global, multi-arm, phase 1b EQUULEUS (MMY1001) trial, which evaluated daratumumab in combination with a variety of treatment regimens. Splitting the first infusion over 2 consecutive days reduced the duration of the infusion and resulted in a similar rate of infusion site reactions; concentrations were similar at the end of weekly dosing in patients who received the first infusion at once or over a 2-day period.
The adverse events reported in EQUULEUS (MMY1001) were largely similar to those seen in previous trials; the most common adverse events include infusion reactions, neutropenia, thrombocytopenia, fatigue, nausea, diarrhea, constipation, vomiting, muscle spasms, arthralgia, back pain, pyrexia, chills, dizziness, insomnia, cough, dyspnea, peripheral edema, peripheral sensory neuropathy, and upper respiratory tract infection.
The approval providers “added flexibility for how patients may receive initial treatment,” Craig Tendler, MD, vice president of clinical development and global medical affairs at Janssen Research & Development, said in a statement.
The Food and Drug Administration has approved a split-dosing regimen for daratumumab (Darzalex) in patients with multiple myeloma, allowing the first infusion to be split over 2 days.
FDA approval is based on results from the global, multi-arm, phase 1b EQUULEUS (MMY1001) trial, which evaluated daratumumab in combination with a variety of treatment regimens. Splitting the first infusion over 2 consecutive days reduced the duration of the infusion and resulted in a similar rate of infusion site reactions; concentrations were similar at the end of weekly dosing in patients who received the first infusion at once or over a 2-day period.
The adverse events reported in EQUULEUS (MMY1001) were largely similar to those seen in previous trials; the most common adverse events include infusion reactions, neutropenia, thrombocytopenia, fatigue, nausea, diarrhea, constipation, vomiting, muscle spasms, arthralgia, back pain, pyrexia, chills, dizziness, insomnia, cough, dyspnea, peripheral edema, peripheral sensory neuropathy, and upper respiratory tract infection.
The approval providers “added flexibility for how patients may receive initial treatment,” Craig Tendler, MD, vice president of clinical development and global medical affairs at Janssen Research & Development, said in a statement.