User login
COVID-19 pandemic amplifies uncertainty for immigrant hospitalists
H1-B visa program needs improvement
Statistics tell the tale of immigrants in the American health care workforce in broad strokes. In an interview, though, one hospitalist shared the particulars of his professional and personal journey since arriving in the United States from India 15 years ago.

Mihir Patel, MD, MPH, FHM, came to the United States in 2005 to complete a Master’s in Public Health. Fifteen years later, he is still waiting for the green card that signifies U.S. permanent residency status. The paperwork for the application, he said, was completed in 2012. Since then, he’s been renewing his H-1B visa every three years, and he has no expectation that anything will change soon.
“If you are from India, which has a significant backlog of green cards – up to 50 years…you just wait forever,” he said. “Many people even die waiting for their green card to arrive.”
Arriving on a student visa, Dr. Patel completed his MPH in 2008 and began an internal medicine residency that same year, holding a J-1 visa for the 3 years of his US residency program.
“Post-residency, I started working in a rural hospital in an underserved area of northeast Tennessee as a hospitalist,” thus completing the 3 years of service in a rural underserved area that’s a requirement for J-1 visa holders, said Dr. Patel. “I loved this rural community hospital so much that I ended up staying there for 6 years. During my work at this rural hospital, I was able to enjoy the autonomy of managing a small ICU, doing both critical care procedures and management of intubated critical patients while working as a hospitalist,” he said. Dr. Patel served as chief of staff at the hospital for two years, and also served on the board of directors for his 400-physician medical group.
“I was a proud member of this rural community – Rogersville,” said Dr. Patel. Although he and his wife, who was completing her hospitalist residency, lived in Johnson City, Tenn., “I did not mind driving 120 miles round trip every day to go to my small-town hospital for 6 years,” he said.
Spending this time in rural Tennessee allowed Dr. Patel to finish the requirements necessary for the Physician National Interest Waiver and submit his application for permanent residency. The waiver, though, doesn’t give him priority status in the waiting list for permanent residency status.
After a stint in northern California to be closer to extended family, the pull of “beautiful northeast Tennesse and the rural community” was too strong, so Dr. Patel and his family moved back to Johnson City in 2018.

Now, Dr. Patel is a hospitalist at Ballad Health System in Johnson City. He is the corporate director of Ballad’s telemedicine program and is now also the medical director of the COVID-19 Strike Team. He co-founded and is president of the Blue Ridge Chapter of the Society of Hospital Medicine. Under another H-1B visa, Dr. Patel works part-time from home as a telehospitalist, covering six hospitals in 4 different states.
Even in ordinary circumstances, the H-1B visa comes with constraints. Although Dr. Patel’s 6-year old daughter was born in the U.S. and is a citizen, Dr. Patel and his wife have to reapply for their visas every 3 years. “If we travel outside the U.S., we have to get our visas stamped. We cannot change jobs easily due to fear of visa denial, especially with the recent political environment,” said Dr. Patel. “It feels like we are essential health care workers but non-essential immigrants.”
Having recently completed a physician executive MBA program, Dr. Patel said he’d like to start a business of his own using Lean health care principles and telemedicine to improve rural health care. “But while on an H-1B I cannot do anything outside my sponsored employment,” he said.
Ideally, health care organizations would have high flexibility in how and where staff are deployed when a surge of COVID-19 patients hits. Dr. Patel made the point that visa restrictions can make this much harder: “During this COVID crisis, this restriction can cause significant negative impact for small rural hospitals, where local physicians are quarantined and available physicians are on a visa who cannot legally work outside their primary facilities – even though they are willing to work,” he said. “One cannot even work using telemedicine in the same health system, if that is not specifically mentioned during H-1B petition filling. More than 15,000 physicians who are struck by the green card backlog are in the same situation all over U.S.,” he added.
These constraints, though, pale before the consequences of a worst-case pandemic scenario for an immigrant family, where the physician – the primary visa-holder – becomes disabled or dies. In this case, dependent family members must self-deport. “In addition, there would not be any disability or Social Security benefits for the physician or dependents, as they are not citizens or green card holders and they cannot legally stay in the US,” noted Dr. Patel. “Any hospitalist working during the COVID-19 pandemic can have this fate due to our high exposure risk.”
Reauthorizing the H1-B visa program
SHM has been advocating to improve the H1-B visa system for years, Dr. Patel said, The Fairness for High Skilled Immigrants Act passed the U.S. House of Representatives with bipartisan support, and the Society is advocating for its passage in the Senate.

The Fairness for High-Skilled Immigrants Act (S. 386) simplifies the employment-based immigration system by removing per-country caps, converting the employment-based immigration system into a “first-come, first serve” system that does not discriminate on country of origin. The act will also help alleviate the decades-long green card and permanent residency application backlogs.
Dr. Patel emphasized the importance of action by Congress to reauthorize the physician visa waiver program and expediting physician permanent residency. “This is a crisis and we are all physicians who are ready to serve, regardless of our country of origin. Please let us help this great nation by giving us freedom from visa restrictions and providing security for our families.
“During wartime, all frontline soldiers are naturalized and given citizenship by presidential mandate; this is more than war and we are not asking for citizenship – but at least give us a green card which we have already satisfied all requirements for. If not now, then when?” he asked.
H1-B visa program needs improvement
H1-B visa program needs improvement
Statistics tell the tale of immigrants in the American health care workforce in broad strokes. In an interview, though, one hospitalist shared the particulars of his professional and personal journey since arriving in the United States from India 15 years ago.
Mihir Patel, MD, MPH, FHM, came to the United States in 2005 to complete a Master’s in Public Health. Fifteen years later, he is still waiting for the green card that signifies U.S. permanent residency status. The paperwork for the application, he said, was completed in 2012. Since then, he’s been renewing his H-1B visa every three years, and he has no expectation that anything will change soon.
“If you are from India, which has a significant backlog of green cards – up to 50 years…you just wait forever,” he said. “Many people even die waiting for their green card to arrive.”
Arriving on a student visa, Dr. Patel completed his MPH in 2008 and began an internal medicine residency that same year, holding a J-1 visa for the 3 years of his US residency program.
“Post-residency, I started working in a rural hospital in an underserved area of northeast Tennessee as a hospitalist,” thus completing the 3 years of service in a rural underserved area that’s a requirement for J-1 visa holders, said Dr. Patel. “I loved this rural community hospital so much that I ended up staying there for 6 years. During my work at this rural hospital, I was able to enjoy the autonomy of managing a small ICU, doing both critical care procedures and management of intubated critical patients while working as a hospitalist,” he said. Dr. Patel served as chief of staff at the hospital for two years, and also served on the board of directors for his 400-physician medical group.
“I was a proud member of this rural community – Rogersville,” said Dr. Patel. Although he and his wife, who was completing her hospitalist residency, lived in Johnson City, Tenn., “I did not mind driving 120 miles round trip every day to go to my small-town hospital for 6 years,” he said.
Spending this time in rural Tennessee allowed Dr. Patel to finish the requirements necessary for the Physician National Interest Waiver and submit his application for permanent residency. The waiver, though, doesn’t give him priority status in the waiting list for permanent residency status.
After a stint in northern California to be closer to extended family, the pull of “beautiful northeast Tennesse and the rural community” was too strong, so Dr. Patel and his family moved back to Johnson City in 2018.
Now, Dr. Patel is a hospitalist at Ballad Health System in Johnson City. He is the corporate director of Ballad’s telemedicine program and is now also the medical director of the COVID-19 Strike Team. He co-founded and is president of the Blue Ridge Chapter of the Society of Hospital Medicine. Under another H-1B visa, Dr. Patel works part-time from home as a telehospitalist, covering six hospitals in 4 different states.
Even in ordinary circumstances, the H-1B visa comes with constraints. Although Dr. Patel’s 6-year old daughter was born in the U.S. and is a citizen, Dr. Patel and his wife have to reapply for their visas every 3 years. “If we travel outside the U.S., we have to get our visas stamped. We cannot change jobs easily due to fear of visa denial, especially with the recent political environment,” said Dr. Patel. “It feels like we are essential health care workers but non-essential immigrants.”
Having recently completed a physician executive MBA program, Dr. Patel said he’d like to start a business of his own using Lean health care principles and telemedicine to improve rural health care. “But while on an H-1B I cannot do anything outside my sponsored employment,” he said.
Ideally, health care organizations would have high flexibility in how and where staff are deployed when a surge of COVID-19 patients hits. Dr. Patel made the point that visa restrictions can make this much harder: “During this COVID crisis, this restriction can cause significant negative impact for small rural hospitals, where local physicians are quarantined and available physicians are on a visa who cannot legally work outside their primary facilities – even though they are willing to work,” he said. “One cannot even work using telemedicine in the same health system, if that is not specifically mentioned during H-1B petition filling. More than 15,000 physicians who are struck by the green card backlog are in the same situation all over U.S.,” he added.
These constraints, though, pale before the consequences of a worst-case pandemic scenario for an immigrant family, where the physician – the primary visa-holder – becomes disabled or dies. In this case, dependent family members must self-deport. “In addition, there would not be any disability or Social Security benefits for the physician or dependents, as they are not citizens or green card holders and they cannot legally stay in the US,” noted Dr. Patel. “Any hospitalist working during the COVID-19 pandemic can have this fate due to our high exposure risk.”
Reauthorizing the H1-B visa program
SHM has been advocating to improve the H1-B visa system for years, Dr. Patel said, The Fairness for High Skilled Immigrants Act passed the U.S. House of Representatives with bipartisan support, and the Society is advocating for its passage in the Senate.
The Fairness for High-Skilled Immigrants Act (S. 386) simplifies the employment-based immigration system by removing per-country caps, converting the employment-based immigration system into a “first-come, first serve” system that does not discriminate on country of origin. The act will also help alleviate the decades-long green card and permanent residency application backlogs.
Dr. Patel emphasized the importance of action by Congress to reauthorize the physician visa waiver program and expediting physician permanent residency. “This is a crisis and we are all physicians who are ready to serve, regardless of our country of origin. Please let us help this great nation by giving us freedom from visa restrictions and providing security for our families.
“During wartime, all frontline soldiers are naturalized and given citizenship by presidential mandate; this is more than war and we are not asking for citizenship – but at least give us a green card which we have already satisfied all requirements for. If not now, then when?” he asked.
Statistics tell the tale of immigrants in the American health care workforce in broad strokes. In an interview, though, one hospitalist shared the particulars of his professional and personal journey since arriving in the United States from India 15 years ago.
Mihir Patel, MD, MPH, FHM, came to the United States in 2005 to complete a Master’s in Public Health. Fifteen years later, he is still waiting for the green card that signifies U.S. permanent residency status. The paperwork for the application, he said, was completed in 2012. Since then, he’s been renewing his H-1B visa every three years, and he has no expectation that anything will change soon.
“If you are from India, which has a significant backlog of green cards – up to 50 years…you just wait forever,” he said. “Many people even die waiting for their green card to arrive.”
Arriving on a student visa, Dr. Patel completed his MPH in 2008 and began an internal medicine residency that same year, holding a J-1 visa for the 3 years of his US residency program.
“Post-residency, I started working in a rural hospital in an underserved area of northeast Tennessee as a hospitalist,” thus completing the 3 years of service in a rural underserved area that’s a requirement for J-1 visa holders, said Dr. Patel. “I loved this rural community hospital so much that I ended up staying there for 6 years. During my work at this rural hospital, I was able to enjoy the autonomy of managing a small ICU, doing both critical care procedures and management of intubated critical patients while working as a hospitalist,” he said. Dr. Patel served as chief of staff at the hospital for two years, and also served on the board of directors for his 400-physician medical group.
“I was a proud member of this rural community – Rogersville,” said Dr. Patel. Although he and his wife, who was completing her hospitalist residency, lived in Johnson City, Tenn., “I did not mind driving 120 miles round trip every day to go to my small-town hospital for 6 years,” he said.
Spending this time in rural Tennessee allowed Dr. Patel to finish the requirements necessary for the Physician National Interest Waiver and submit his application for permanent residency. The waiver, though, doesn’t give him priority status in the waiting list for permanent residency status.
After a stint in northern California to be closer to extended family, the pull of “beautiful northeast Tennesse and the rural community” was too strong, so Dr. Patel and his family moved back to Johnson City in 2018.
Now, Dr. Patel is a hospitalist at Ballad Health System in Johnson City. He is the corporate director of Ballad’s telemedicine program and is now also the medical director of the COVID-19 Strike Team. He co-founded and is president of the Blue Ridge Chapter of the Society of Hospital Medicine. Under another H-1B visa, Dr. Patel works part-time from home as a telehospitalist, covering six hospitals in 4 different states.
Even in ordinary circumstances, the H-1B visa comes with constraints. Although Dr. Patel’s 6-year old daughter was born in the U.S. and is a citizen, Dr. Patel and his wife have to reapply for their visas every 3 years. “If we travel outside the U.S., we have to get our visas stamped. We cannot change jobs easily due to fear of visa denial, especially with the recent political environment,” said Dr. Patel. “It feels like we are essential health care workers but non-essential immigrants.”
Having recently completed a physician executive MBA program, Dr. Patel said he’d like to start a business of his own using Lean health care principles and telemedicine to improve rural health care. “But while on an H-1B I cannot do anything outside my sponsored employment,” he said.
Ideally, health care organizations would have high flexibility in how and where staff are deployed when a surge of COVID-19 patients hits. Dr. Patel made the point that visa restrictions can make this much harder: “During this COVID crisis, this restriction can cause significant negative impact for small rural hospitals, where local physicians are quarantined and available physicians are on a visa who cannot legally work outside their primary facilities – even though they are willing to work,” he said. “One cannot even work using telemedicine in the same health system, if that is not specifically mentioned during H-1B petition filling. More than 15,000 physicians who are struck by the green card backlog are in the same situation all over U.S.,” he added.
These constraints, though, pale before the consequences of a worst-case pandemic scenario for an immigrant family, where the physician – the primary visa-holder – becomes disabled or dies. In this case, dependent family members must self-deport. “In addition, there would not be any disability or Social Security benefits for the physician or dependents, as they are not citizens or green card holders and they cannot legally stay in the US,” noted Dr. Patel. “Any hospitalist working during the COVID-19 pandemic can have this fate due to our high exposure risk.”
Reauthorizing the H1-B visa program
SHM has been advocating to improve the H1-B visa system for years, Dr. Patel said, The Fairness for High Skilled Immigrants Act passed the U.S. House of Representatives with bipartisan support, and the Society is advocating for its passage in the Senate.
The Fairness for High-Skilled Immigrants Act (S. 386) simplifies the employment-based immigration system by removing per-country caps, converting the employment-based immigration system into a “first-come, first serve” system that does not discriminate on country of origin. The act will also help alleviate the decades-long green card and permanent residency application backlogs.
Dr. Patel emphasized the importance of action by Congress to reauthorize the physician visa waiver program and expediting physician permanent residency. “This is a crisis and we are all physicians who are ready to serve, regardless of our country of origin. Please let us help this great nation by giving us freedom from visa restrictions and providing security for our families.
“During wartime, all frontline soldiers are naturalized and given citizenship by presidential mandate; this is more than war and we are not asking for citizenship – but at least give us a green card which we have already satisfied all requirements for. If not now, then when?” he asked.
The socioeconomic revolving door of 30-day heart failure readmissions
Patients receiving even top-notch hospital care for heart failure (HF) are, once discharged to home, at higher short-term risk of another HF hospitalization if home is in a socioeconomically deprived neighborhood. That helps explain why Blacks in the United States have a much higher 30-day HF readmission risk than Whites, a disparity that only worsens with the level of neighborhood deprivation, a new analysis suggests.
Some systemic and entrenched socioeconomic inequities that health care providers have little sway over, and which disproportionately affect Black individuals, are independent and robust predictors of worsened HF outcomes, Alanna A. Morris, MD, MSc, Emory University, Atlanta, said during her presentation at the virtual annual scientific meeting of the Heart Failure Society of America.
In a retrospective cohort study, Blacks had a 45% higher risk of 30-day readmission than Whites (P < .001) independent of cardiovascular risk factors, clinical history, comorbidities, type and location of hospital, and type of third-party payer coverage. The analysis included more than 30,000 patients with at least one HF hospitalization at centers in a major metropolitan health system.
The racial disparity widened with worsening socioeconomic deprivation of patients’ residential neighborhoods, that is, with rising quartiles of neighborhood scores on the Social Deprivation Index (SDI).
The SDI, based on U.S. census data, incorporates seven socioeconomic criteria, including household income, education level, employment, and prevalence of rented housing and households that are without a car, single parent, or overcrowded.
There was a 4–percentage point gap in adjusted 30-day readmission rate between Blacks and Whites in the lowest quartile that widened to more than 8 points by the third quartile; the disparity in both the second and fourth quartiles was the same, at about 5.5 percentage points.
A remaining question, Dr. Morris said in an interview, is why the outcomes disparity between Blacks and Whites peaks in the third SDI quartile but drops a bit in the fourth quartile representing the most severe neighborhood deprivation.
“Our hypothesis is that when you look at patients who are the poorest, who live in the most deprived neighborhoods, race may be less of a factor,” she said. Socioeconomic deprivation may have similar consequences for everyone “regardless of race, ethnicity, gender, or other demographic characteristics if you live in a neighborhood that’s highly deprived.”

Based on the current study, “it does appear that increased heart failure incident rates are related to living in deprived neighborhoods, and it raises important clinical and public health concerns that must be addressed,” Keith C. Ferdinand, MD, Tulane University, New Orleans, said as invited discussant after the presentation from Dr. Morris.
“These findings could serve as an aid to policy makers, going forward, in terms of allocating resources for primary health care,” he said. “And it’s important looking at these data and other [data] that we target heart failure patients who reside in deprived neighborhoods before, during, and [after] hospitalization.”
Dr. Morris agreed that policy makers are in a better position to attack the racial disparity in HF readmission rates identified in the study. “This is not a problem that can be fixed within the health care system.”
If the reported interpretation is correct, it could add a twist to the public health care debate in the United States, observed session moderator Mandeep R. Mehra, MD, Brigham and Woman’s Hospital in Boston.
That debate, he noted, has often focused on insurability, access to coverage, and the merits or shortcomings of a single-payer system. Yet the study suggests outcomes disparities stemming from neighborhood deprivation will not be corrected by improved access to health insurance, a conclusion he finds “startling,” Dr. Mehra said in an interview.
Some proposed explanations for the disparities by race blame unequal access to health care and or variable health insurance coverage, Dr. Morris observed in an interview. But “that may not fully explain the increased risk that we see.”
Black patients followed at Emory University’s advanced HF clinic still have a higher risk of rehospitalization than Whites. “These are patients who have insurance, who are followed by advanced heart failure providers, who are on equal amounts of guideline-recommended medical therapy – and you still see about a 50% higher risk of rehospitalization,” Dr. Morris said, citing data that isn’t part of the current analysis.
“We can say that these patients are certainly able to access care, because they are able to access our emergency room and be taken care of within the hospital setting,” he said. The study controlled for whether health coverage was by private insurance, Medicare, or Medicaid.
Instead, the current analysis points to socioeconomic and environmental factors as a major source of the disparity in 30-day readmissions, Dr. Morris said.
“When patients are discharged from our healthcare systems, they still go back into environments where they don’t have the same resources as patients who live in higher-SDI neighborhoods,” she explained.
For example, “we tell them to eat low-sodium [foods], exercise, eat fresh fruits and vegetables, take their medicines, but the reality is that certain neighborhoods within the United States – and this is much more true for Blacks – make it very difficult to follow those self-care recommendations.”
The analysis included 16,147 Black patients and 14,483 White patients hospitalized with HF within the Emory Healthcare system at least once from 2010-2018, Dr. Morris reported. Compared with Whites, Blacks were younger (63.5 vs 69.1 years) and less likely to be 65 or older (48.9% vs. 66.5%); more likely to be women (53.5% vs. 42.2%), more likely to reside in deprived census tracts and to have diabetes, hypertension, or chronic kidney disease; and had higher comorbidity scores.
In all, 20.6% of Black and 13.5% of White patients were readmitted for HF within 30 days of discharge, for an unadjusted risk ratio of 1.52 (95% CI, 1.44-1.61).
The RR hardly budged, 1.45 (95% CI, 1.37-1.54, P < .001), after adjustment for age, sex, type of insurance, type of HF, vital signs and laboratory values, medical history (diabetes, hypertension, atrial fibrillation, coronary disease, chronic kidney disease, and chronic pulmonary disease), Charlson Comorbidity Index, discharging medical specialty, and hospital location.
The excess in 30-day HF readmissions for Black, compared with White patients climbed from the first to the third neighborhood SDI quartile, the disparity peaking at 8.2 absolute percentage points.
A major criticism of the Hospital Readmissions Reduction Program component of the Affordable Care Act, Dr. Morris said in a Q&A discussion after her presentation, is that it can hold hospitals “responsible for structural inequalities that exist beyond the health care system,” including neighborhood deprivation.
“But public policy makers have to realize that there are certain patients we take care of who don’t have the resources to carry out the therapeutic lifestyle changes that will allow them to live healthy.”
The HRRP’s 30-day HF readmission metric that steers reimbursement “is penalizing health care systems across the United States” with its premise that hospital performance can be measured by 30-day HF readmission rates, Dr. Morris said in an interview.
“The reality is that some of these patients are going to a postdischarge environment that is inherently high risk, and that many of them are going to come back to us within 30 days,” she said. “We would like to make sure that we don’t put excess penalties on health care systems that take care of disproportionate numbers of African Americans in neighborhoods that have fewer resources.”
Dr. Morris and Dr. Ferdinand have disclosed no relevant financial relationships. Dr. Mehra discloses consulting or serving on an advisory board for Abbott, Medtronic, Janssen, Leviticus, NupulseCV, FineHeart, Portola, Bayer, the Baim Institute for Clinical Research, and Mesoblast.
A version of this article originally appeared on Medscape.com.
Patients receiving even top-notch hospital care for heart failure (HF) are, once discharged to home, at higher short-term risk of another HF hospitalization if home is in a socioeconomically deprived neighborhood. That helps explain why Blacks in the United States have a much higher 30-day HF readmission risk than Whites, a disparity that only worsens with the level of neighborhood deprivation, a new analysis suggests.
Some systemic and entrenched socioeconomic inequities that health care providers have little sway over, and which disproportionately affect Black individuals, are independent and robust predictors of worsened HF outcomes, Alanna A. Morris, MD, MSc, Emory University, Atlanta, said during her presentation at the virtual annual scientific meeting of the Heart Failure Society of America.
In a retrospective cohort study, Blacks had a 45% higher risk of 30-day readmission than Whites (P < .001) independent of cardiovascular risk factors, clinical history, comorbidities, type and location of hospital, and type of third-party payer coverage. The analysis included more than 30,000 patients with at least one HF hospitalization at centers in a major metropolitan health system.
The racial disparity widened with worsening socioeconomic deprivation of patients’ residential neighborhoods, that is, with rising quartiles of neighborhood scores on the Social Deprivation Index (SDI).
The SDI, based on U.S. census data, incorporates seven socioeconomic criteria, including household income, education level, employment, and prevalence of rented housing and households that are without a car, single parent, or overcrowded.
There was a 4–percentage point gap in adjusted 30-day readmission rate between Blacks and Whites in the lowest quartile that widened to more than 8 points by the third quartile; the disparity in both the second and fourth quartiles was the same, at about 5.5 percentage points.
A remaining question, Dr. Morris said in an interview, is why the outcomes disparity between Blacks and Whites peaks in the third SDI quartile but drops a bit in the fourth quartile representing the most severe neighborhood deprivation.
“Our hypothesis is that when you look at patients who are the poorest, who live in the most deprived neighborhoods, race may be less of a factor,” she said. Socioeconomic deprivation may have similar consequences for everyone “regardless of race, ethnicity, gender, or other demographic characteristics if you live in a neighborhood that’s highly deprived.”
Based on the current study, “it does appear that increased heart failure incident rates are related to living in deprived neighborhoods, and it raises important clinical and public health concerns that must be addressed,” Keith C. Ferdinand, MD, Tulane University, New Orleans, said as invited discussant after the presentation from Dr. Morris.
“These findings could serve as an aid to policy makers, going forward, in terms of allocating resources for primary health care,” he said. “And it’s important looking at these data and other [data] that we target heart failure patients who reside in deprived neighborhoods before, during, and [after] hospitalization.”
Dr. Morris agreed that policy makers are in a better position to attack the racial disparity in HF readmission rates identified in the study. “This is not a problem that can be fixed within the health care system.”
If the reported interpretation is correct, it could add a twist to the public health care debate in the United States, observed session moderator Mandeep R. Mehra, MD, Brigham and Woman’s Hospital in Boston.
That debate, he noted, has often focused on insurability, access to coverage, and the merits or shortcomings of a single-payer system. Yet the study suggests outcomes disparities stemming from neighborhood deprivation will not be corrected by improved access to health insurance, a conclusion he finds “startling,” Dr. Mehra said in an interview.
Some proposed explanations for the disparities by race blame unequal access to health care and or variable health insurance coverage, Dr. Morris observed in an interview. But “that may not fully explain the increased risk that we see.”
Black patients followed at Emory University’s advanced HF clinic still have a higher risk of rehospitalization than Whites. “These are patients who have insurance, who are followed by advanced heart failure providers, who are on equal amounts of guideline-recommended medical therapy – and you still see about a 50% higher risk of rehospitalization,” Dr. Morris said, citing data that isn’t part of the current analysis.
“We can say that these patients are certainly able to access care, because they are able to access our emergency room and be taken care of within the hospital setting,” he said. The study controlled for whether health coverage was by private insurance, Medicare, or Medicaid.
Instead, the current analysis points to socioeconomic and environmental factors as a major source of the disparity in 30-day readmissions, Dr. Morris said.
“When patients are discharged from our healthcare systems, they still go back into environments where they don’t have the same resources as patients who live in higher-SDI neighborhoods,” she explained.
For example, “we tell them to eat low-sodium [foods], exercise, eat fresh fruits and vegetables, take their medicines, but the reality is that certain neighborhoods within the United States – and this is much more true for Blacks – make it very difficult to follow those self-care recommendations.”
The analysis included 16,147 Black patients and 14,483 White patients hospitalized with HF within the Emory Healthcare system at least once from 2010-2018, Dr. Morris reported. Compared with Whites, Blacks were younger (63.5 vs 69.1 years) and less likely to be 65 or older (48.9% vs. 66.5%); more likely to be women (53.5% vs. 42.2%), more likely to reside in deprived census tracts and to have diabetes, hypertension, or chronic kidney disease; and had higher comorbidity scores.
In all, 20.6% of Black and 13.5% of White patients were readmitted for HF within 30 days of discharge, for an unadjusted risk ratio of 1.52 (95% CI, 1.44-1.61).
The RR hardly budged, 1.45 (95% CI, 1.37-1.54, P < .001), after adjustment for age, sex, type of insurance, type of HF, vital signs and laboratory values, medical history (diabetes, hypertension, atrial fibrillation, coronary disease, chronic kidney disease, and chronic pulmonary disease), Charlson Comorbidity Index, discharging medical specialty, and hospital location.
The excess in 30-day HF readmissions for Black, compared with White patients climbed from the first to the third neighborhood SDI quartile, the disparity peaking at 8.2 absolute percentage points.
A major criticism of the Hospital Readmissions Reduction Program component of the Affordable Care Act, Dr. Morris said in a Q&A discussion after her presentation, is that it can hold hospitals “responsible for structural inequalities that exist beyond the health care system,” including neighborhood deprivation.
“But public policy makers have to realize that there are certain patients we take care of who don’t have the resources to carry out the therapeutic lifestyle changes that will allow them to live healthy.”
The HRRP’s 30-day HF readmission metric that steers reimbursement “is penalizing health care systems across the United States” with its premise that hospital performance can be measured by 30-day HF readmission rates, Dr. Morris said in an interview.
“The reality is that some of these patients are going to a postdischarge environment that is inherently high risk, and that many of them are going to come back to us within 30 days,” she said. “We would like to make sure that we don’t put excess penalties on health care systems that take care of disproportionate numbers of African Americans in neighborhoods that have fewer resources.”
Dr. Morris and Dr. Ferdinand have disclosed no relevant financial relationships. Dr. Mehra discloses consulting or serving on an advisory board for Abbott, Medtronic, Janssen, Leviticus, NupulseCV, FineHeart, Portola, Bayer, the Baim Institute for Clinical Research, and Mesoblast.
A version of this article originally appeared on Medscape.com.
Patients receiving even top-notch hospital care for heart failure (HF) are, once discharged to home, at higher short-term risk of another HF hospitalization if home is in a socioeconomically deprived neighborhood. That helps explain why Blacks in the United States have a much higher 30-day HF readmission risk than Whites, a disparity that only worsens with the level of neighborhood deprivation, a new analysis suggests.
Some systemic and entrenched socioeconomic inequities that health care providers have little sway over, and which disproportionately affect Black individuals, are independent and robust predictors of worsened HF outcomes, Alanna A. Morris, MD, MSc, Emory University, Atlanta, said during her presentation at the virtual annual scientific meeting of the Heart Failure Society of America.
In a retrospective cohort study, Blacks had a 45% higher risk of 30-day readmission than Whites (P < .001) independent of cardiovascular risk factors, clinical history, comorbidities, type and location of hospital, and type of third-party payer coverage. The analysis included more than 30,000 patients with at least one HF hospitalization at centers in a major metropolitan health system.
The racial disparity widened with worsening socioeconomic deprivation of patients’ residential neighborhoods, that is, with rising quartiles of neighborhood scores on the Social Deprivation Index (SDI).
The SDI, based on U.S. census data, incorporates seven socioeconomic criteria, including household income, education level, employment, and prevalence of rented housing and households that are without a car, single parent, or overcrowded.
There was a 4–percentage point gap in adjusted 30-day readmission rate between Blacks and Whites in the lowest quartile that widened to more than 8 points by the third quartile; the disparity in both the second and fourth quartiles was the same, at about 5.5 percentage points.
A remaining question, Dr. Morris said in an interview, is why the outcomes disparity between Blacks and Whites peaks in the third SDI quartile but drops a bit in the fourth quartile representing the most severe neighborhood deprivation.
“Our hypothesis is that when you look at patients who are the poorest, who live in the most deprived neighborhoods, race may be less of a factor,” she said. Socioeconomic deprivation may have similar consequences for everyone “regardless of race, ethnicity, gender, or other demographic characteristics if you live in a neighborhood that’s highly deprived.”
Based on the current study, “it does appear that increased heart failure incident rates are related to living in deprived neighborhoods, and it raises important clinical and public health concerns that must be addressed,” Keith C. Ferdinand, MD, Tulane University, New Orleans, said as invited discussant after the presentation from Dr. Morris.
“These findings could serve as an aid to policy makers, going forward, in terms of allocating resources for primary health care,” he said. “And it’s important looking at these data and other [data] that we target heart failure patients who reside in deprived neighborhoods before, during, and [after] hospitalization.”
Dr. Morris agreed that policy makers are in a better position to attack the racial disparity in HF readmission rates identified in the study. “This is not a problem that can be fixed within the health care system.”
If the reported interpretation is correct, it could add a twist to the public health care debate in the United States, observed session moderator Mandeep R. Mehra, MD, Brigham and Woman’s Hospital in Boston.
That debate, he noted, has often focused on insurability, access to coverage, and the merits or shortcomings of a single-payer system. Yet the study suggests outcomes disparities stemming from neighborhood deprivation will not be corrected by improved access to health insurance, a conclusion he finds “startling,” Dr. Mehra said in an interview.
Some proposed explanations for the disparities by race blame unequal access to health care and or variable health insurance coverage, Dr. Morris observed in an interview. But “that may not fully explain the increased risk that we see.”
Black patients followed at Emory University’s advanced HF clinic still have a higher risk of rehospitalization than Whites. “These are patients who have insurance, who are followed by advanced heart failure providers, who are on equal amounts of guideline-recommended medical therapy – and you still see about a 50% higher risk of rehospitalization,” Dr. Morris said, citing data that isn’t part of the current analysis.
“We can say that these patients are certainly able to access care, because they are able to access our emergency room and be taken care of within the hospital setting,” he said. The study controlled for whether health coverage was by private insurance, Medicare, or Medicaid.
Instead, the current analysis points to socioeconomic and environmental factors as a major source of the disparity in 30-day readmissions, Dr. Morris said.
“When patients are discharged from our healthcare systems, they still go back into environments where they don’t have the same resources as patients who live in higher-SDI neighborhoods,” she explained.
For example, “we tell them to eat low-sodium [foods], exercise, eat fresh fruits and vegetables, take their medicines, but the reality is that certain neighborhoods within the United States – and this is much more true for Blacks – make it very difficult to follow those self-care recommendations.”
The analysis included 16,147 Black patients and 14,483 White patients hospitalized with HF within the Emory Healthcare system at least once from 2010-2018, Dr. Morris reported. Compared with Whites, Blacks were younger (63.5 vs 69.1 years) and less likely to be 65 or older (48.9% vs. 66.5%); more likely to be women (53.5% vs. 42.2%), more likely to reside in deprived census tracts and to have diabetes, hypertension, or chronic kidney disease; and had higher comorbidity scores.
In all, 20.6% of Black and 13.5% of White patients were readmitted for HF within 30 days of discharge, for an unadjusted risk ratio of 1.52 (95% CI, 1.44-1.61).
The RR hardly budged, 1.45 (95% CI, 1.37-1.54, P < .001), after adjustment for age, sex, type of insurance, type of HF, vital signs and laboratory values, medical history (diabetes, hypertension, atrial fibrillation, coronary disease, chronic kidney disease, and chronic pulmonary disease), Charlson Comorbidity Index, discharging medical specialty, and hospital location.
The excess in 30-day HF readmissions for Black, compared with White patients climbed from the first to the third neighborhood SDI quartile, the disparity peaking at 8.2 absolute percentage points.
A major criticism of the Hospital Readmissions Reduction Program component of the Affordable Care Act, Dr. Morris said in a Q&A discussion after her presentation, is that it can hold hospitals “responsible for structural inequalities that exist beyond the health care system,” including neighborhood deprivation.
“But public policy makers have to realize that there are certain patients we take care of who don’t have the resources to carry out the therapeutic lifestyle changes that will allow them to live healthy.”
The HRRP’s 30-day HF readmission metric that steers reimbursement “is penalizing health care systems across the United States” with its premise that hospital performance can be measured by 30-day HF readmission rates, Dr. Morris said in an interview.
“The reality is that some of these patients are going to a postdischarge environment that is inherently high risk, and that many of them are going to come back to us within 30 days,” she said. “We would like to make sure that we don’t put excess penalties on health care systems that take care of disproportionate numbers of African Americans in neighborhoods that have fewer resources.”
Dr. Morris and Dr. Ferdinand have disclosed no relevant financial relationships. Dr. Mehra discloses consulting or serving on an advisory board for Abbott, Medtronic, Janssen, Leviticus, NupulseCV, FineHeart, Portola, Bayer, the Baim Institute for Clinical Research, and Mesoblast.
A version of this article originally appeared on Medscape.com.

Hospital medicine, it’s time to vote
Whether physicians or advanced practice practitioners, we are the backbone of our nation’s network of acute care facilities, and on a daily basis, we see just about everything. We have valuable insight into how to improve our nation’s health care system, especially now, as our nation continues to battle COVID-19.

Our role, squarely on the front lines during this pandemic, has given us an important perspective that needs to be heard. We spend our days managing patients with complexity, coordinating with specialists and subspecialists, and advocating – at local, state, and national levels – so that our patients can more easily transition to their lives out of the hospital.
Our current polarized political climate makes it seem that individual voices will not make a difference. It is easy to feel frustrated and powerless. However, those in our specialty are actually in a perfect position to have an educated and influential say in how we move forward, not only about the immediate health crises, but also regarding future health care issues. That voice begins with voting.
Historically, physicians have had surprisingly low rates of voting. For example, a 2007 study found significantly lower rates of voting among physicians, compared with the general public.1 While physician voter turnout may have improved in the past decade, given the substantial changes in health care and the increasing amount of physician engagement in the public sphere, our participation should be greater still. Elected officials listen to, and follow up with, constituents who make their voices heard. Each of us can ensure that the health care policy priorities of our fast-growing specialty are addressed by mobilizing to the voting booth.
Candidates we elect shape our health care system for the future, directly impacting us and our patients. Cost, coverage, access to health care, the Centers for Medicare & Medicaid Services inpatient fee schedules, the ongoing pandemic response, surprise billing, use of telehealth, observation status, and the three-midnight rule are just a few of the issues most important to hospital medicine.
Therefore, we, the SHM Public Policy Committee, urge all of our colleagues, regardless of political sway, to make your voice heard this and every election henceforth. The first step is to register to vote, if you have not done so already.2 Next, exercise that privilege. Given the pandemic, this is not as simple a process as it has been in the past. Take the time to plan your approach to early voting, mail-in voting, or election day voting. Check your County Supervisor of Elections’ website for further information, including how to register, view candidate profiles, check your precinct, and request a mail-in ballot.
In addition to casting your vote, we encourage you to share your opinions and engage in dialogue about health care issues. Clinical fact can dispel rumor and misinformation, and daily experiences can personalize our patients’ health care stories and the impact laws and rules have on our ability to practice. We are part of a trusted profession and have a unique perspective; others need and want to hear it. They can only do that if we are part of the process. Arming yourself with information and voting are the first steps on the path of advocacy. Interpersonal advocacy can also be done on social media. For example, SHM has an active grassroots advocacy network on Twitter. Tag @SHMadvocacy in your tweets to share your thoughts with their network.
Finally, as advocates for our patients in health care, we can also help ensure their safety during this election, in particular regarding COVID-19. Some patients may not wish to engage us in politics, and we must respect their decision. Others may seek our counsel and we should provide it in an unbiased fashion. We can ask our patients if they have considered a safe voting plan, help patients review the alternatives to voting in person if desired, and inform those who wish to physically cast a vote on Election Day of how to mitigate the risk of in-person voting.
Every election is important and health care is front and center for a multitude of reasons. We who practice hospital medicine are integral to our communities and need to be more politically involved. This is our chance to share our voice through our vote, not just this year, but in future elections as well.
Ann Sheehy, MD, SFHM, is division chief of the Division of Hospital Medicine at the University of Wisconsin, Madison, and chair of the SHM Public Policy Committee. Other members of the SHM PPC include Marta Almli, MD; John Biebelhausen, MD; Robert Burke, MD, MS, FHM; George Cheely, MD; Hyung (Harry) Cho, MD, SFHM; Jennifer Cowart, MD, FHM; Suparna Dutta, MD, MS, MPH; Bradley Flansbaum, DO, MPH, MHM; Alain Folefack, MD; Rick Hilger MD SFHM; Melinda Johnson, MD; Sevan Karadolian, MD; Joshua D. Lenchus, DO, FACP, SFHM; Steve Phillipson, MD; Dahlia Rizk, DO; Kendall Rogers, MD, SFHM; Brett Stauffer, MD, MHS; Amit Vashist, MD, SFHM; Robert Zipper, MD, SFHM.
References
1. Grande D et al. Do doctors vote? J Gen Int Med. 2007 May;22(5):585-9.
2. How to register to vote, confirm or change your registration and get a voter registration card. https://www.usa.gov/voter-registration/.
Whether physicians or advanced practice practitioners, we are the backbone of our nation’s network of acute care facilities, and on a daily basis, we see just about everything. We have valuable insight into how to improve our nation’s health care system, especially now, as our nation continues to battle COVID-19.
Our role, squarely on the front lines during this pandemic, has given us an important perspective that needs to be heard. We spend our days managing patients with complexity, coordinating with specialists and subspecialists, and advocating – at local, state, and national levels – so that our patients can more easily transition to their lives out of the hospital.
Our current polarized political climate makes it seem that individual voices will not make a difference. It is easy to feel frustrated and powerless. However, those in our specialty are actually in a perfect position to have an educated and influential say in how we move forward, not only about the immediate health crises, but also regarding future health care issues. That voice begins with voting.
Historically, physicians have had surprisingly low rates of voting. For example, a 2007 study found significantly lower rates of voting among physicians, compared with the general public.1 While physician voter turnout may have improved in the past decade, given the substantial changes in health care and the increasing amount of physician engagement in the public sphere, our participation should be greater still. Elected officials listen to, and follow up with, constituents who make their voices heard. Each of us can ensure that the health care policy priorities of our fast-growing specialty are addressed by mobilizing to the voting booth.
Candidates we elect shape our health care system for the future, directly impacting us and our patients. Cost, coverage, access to health care, the Centers for Medicare & Medicaid Services inpatient fee schedules, the ongoing pandemic response, surprise billing, use of telehealth, observation status, and the three-midnight rule are just a few of the issues most important to hospital medicine.
Therefore, we, the SHM Public Policy Committee, urge all of our colleagues, regardless of political sway, to make your voice heard this and every election henceforth. The first step is to register to vote, if you have not done so already.2 Next, exercise that privilege. Given the pandemic, this is not as simple a process as it has been in the past. Take the time to plan your approach to early voting, mail-in voting, or election day voting. Check your County Supervisor of Elections’ website for further information, including how to register, view candidate profiles, check your precinct, and request a mail-in ballot.
In addition to casting your vote, we encourage you to share your opinions and engage in dialogue about health care issues. Clinical fact can dispel rumor and misinformation, and daily experiences can personalize our patients’ health care stories and the impact laws and rules have on our ability to practice. We are part of a trusted profession and have a unique perspective; others need and want to hear it. They can only do that if we are part of the process. Arming yourself with information and voting are the first steps on the path of advocacy. Interpersonal advocacy can also be done on social media. For example, SHM has an active grassroots advocacy network on Twitter. Tag @SHMadvocacy in your tweets to share your thoughts with their network.
Finally, as advocates for our patients in health care, we can also help ensure their safety during this election, in particular regarding COVID-19. Some patients may not wish to engage us in politics, and we must respect their decision. Others may seek our counsel and we should provide it in an unbiased fashion. We can ask our patients if they have considered a safe voting plan, help patients review the alternatives to voting in person if desired, and inform those who wish to physically cast a vote on Election Day of how to mitigate the risk of in-person voting.
Every election is important and health care is front and center for a multitude of reasons. We who practice hospital medicine are integral to our communities and need to be more politically involved. This is our chance to share our voice through our vote, not just this year, but in future elections as well.
Ann Sheehy, MD, SFHM, is division chief of the Division of Hospital Medicine at the University of Wisconsin, Madison, and chair of the SHM Public Policy Committee. Other members of the SHM PPC include Marta Almli, MD; John Biebelhausen, MD; Robert Burke, MD, MS, FHM; George Cheely, MD; Hyung (Harry) Cho, MD, SFHM; Jennifer Cowart, MD, FHM; Suparna Dutta, MD, MS, MPH; Bradley Flansbaum, DO, MPH, MHM; Alain Folefack, MD; Rick Hilger MD SFHM; Melinda Johnson, MD; Sevan Karadolian, MD; Joshua D. Lenchus, DO, FACP, SFHM; Steve Phillipson, MD; Dahlia Rizk, DO; Kendall Rogers, MD, SFHM; Brett Stauffer, MD, MHS; Amit Vashist, MD, SFHM; Robert Zipper, MD, SFHM.
References
1. Grande D et al. Do doctors vote? J Gen Int Med. 2007 May;22(5):585-9.
2. How to register to vote, confirm or change your registration and get a voter registration card. https://www.usa.gov/voter-registration/.
Whether physicians or advanced practice practitioners, we are the backbone of our nation’s network of acute care facilities, and on a daily basis, we see just about everything. We have valuable insight into how to improve our nation’s health care system, especially now, as our nation continues to battle COVID-19.
Our role, squarely on the front lines during this pandemic, has given us an important perspective that needs to be heard. We spend our days managing patients with complexity, coordinating with specialists and subspecialists, and advocating – at local, state, and national levels – so that our patients can more easily transition to their lives out of the hospital.
Our current polarized political climate makes it seem that individual voices will not make a difference. It is easy to feel frustrated and powerless. However, those in our specialty are actually in a perfect position to have an educated and influential say in how we move forward, not only about the immediate health crises, but also regarding future health care issues. That voice begins with voting.
Historically, physicians have had surprisingly low rates of voting. For example, a 2007 study found significantly lower rates of voting among physicians, compared with the general public.1 While physician voter turnout may have improved in the past decade, given the substantial changes in health care and the increasing amount of physician engagement in the public sphere, our participation should be greater still. Elected officials listen to, and follow up with, constituents who make their voices heard. Each of us can ensure that the health care policy priorities of our fast-growing specialty are addressed by mobilizing to the voting booth.
Candidates we elect shape our health care system for the future, directly impacting us and our patients. Cost, coverage, access to health care, the Centers for Medicare & Medicaid Services inpatient fee schedules, the ongoing pandemic response, surprise billing, use of telehealth, observation status, and the three-midnight rule are just a few of the issues most important to hospital medicine.
Therefore, we, the SHM Public Policy Committee, urge all of our colleagues, regardless of political sway, to make your voice heard this and every election henceforth. The first step is to register to vote, if you have not done so already.2 Next, exercise that privilege. Given the pandemic, this is not as simple a process as it has been in the past. Take the time to plan your approach to early voting, mail-in voting, or election day voting. Check your County Supervisor of Elections’ website for further information, including how to register, view candidate profiles, check your precinct, and request a mail-in ballot.
In addition to casting your vote, we encourage you to share your opinions and engage in dialogue about health care issues. Clinical fact can dispel rumor and misinformation, and daily experiences can personalize our patients’ health care stories and the impact laws and rules have on our ability to practice. We are part of a trusted profession and have a unique perspective; others need and want to hear it. They can only do that if we are part of the process. Arming yourself with information and voting are the first steps on the path of advocacy. Interpersonal advocacy can also be done on social media. For example, SHM has an active grassroots advocacy network on Twitter. Tag @SHMadvocacy in your tweets to share your thoughts with their network.
Finally, as advocates for our patients in health care, we can also help ensure their safety during this election, in particular regarding COVID-19. Some patients may not wish to engage us in politics, and we must respect their decision. Others may seek our counsel and we should provide it in an unbiased fashion. We can ask our patients if they have considered a safe voting plan, help patients review the alternatives to voting in person if desired, and inform those who wish to physically cast a vote on Election Day of how to mitigate the risk of in-person voting.
Every election is important and health care is front and center for a multitude of reasons. We who practice hospital medicine are integral to our communities and need to be more politically involved. This is our chance to share our voice through our vote, not just this year, but in future elections as well.
Ann Sheehy, MD, SFHM, is division chief of the Division of Hospital Medicine at the University of Wisconsin, Madison, and chair of the SHM Public Policy Committee. Other members of the SHM PPC include Marta Almli, MD; John Biebelhausen, MD; Robert Burke, MD, MS, FHM; George Cheely, MD; Hyung (Harry) Cho, MD, SFHM; Jennifer Cowart, MD, FHM; Suparna Dutta, MD, MS, MPH; Bradley Flansbaum, DO, MPH, MHM; Alain Folefack, MD; Rick Hilger MD SFHM; Melinda Johnson, MD; Sevan Karadolian, MD; Joshua D. Lenchus, DO, FACP, SFHM; Steve Phillipson, MD; Dahlia Rizk, DO; Kendall Rogers, MD, SFHM; Brett Stauffer, MD, MHS; Amit Vashist, MD, SFHM; Robert Zipper, MD, SFHM.
References
1. Grande D et al. Do doctors vote? J Gen Int Med. 2007 May;22(5):585-9.
2. How to register to vote, confirm or change your registration and get a voter registration card. https://www.usa.gov/voter-registration/.
‘Celebration’ will be ‘short-lived’ if COVID vaccine rushed: Experts
on Wednesday.
The career staff of the Food and Drug Administration can be counted on to appropriately weigh whether a vaccine should be cleared for use in preventing COVID-19, witnesses, including Paul A. Offit, MD, of Children’s Hospital of Philadelphia, told the House Energy and Commerce Committee’s oversight and investigations panel.
FDA staffers would object to attempts by the Trump administration to rush a vaccine to the public without proper vetting, as would veteran federal researchers, including National Institutes of Health Director Francis S. Collins, MD, PhD, and Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, Offit said.
“If COVID-19 vaccines are released before they’re ready to be released, you will hear from these people, and you will also hear from people like Dr. Francis Collins and Tony Fauci, both of whom are trusted by the American public, as well as many other academicians and researchers who wouldn’t stand for this,” he said.
“The public is already nervous about these vaccines,” said Offit, who serves on key FDA and Centers for Disease Control and Prevention committees overseeing vaccine policy. “If trusted health officials stand up and decry a premature release, the celebration by the administration will be short-lived.”
Overly optimistic estimates about a potential approval can only serve to erode the public’s trust in these crucial vaccines, said another witness, Ashish K. Jha, MD, MPH, the dean of Brown University’s School of Public Health, in Providence, Rhode Island.
“All political leaders need to stop talking about things like time lines,” Jha told the lawmakers.
President Donald Trump has several times suggested that a COVID vaccine might be approved ahead of the November 3 election, where he faces a significant challenge from his Democratic rival, former Vice President Joe Biden.
In a Tuesday night debate with Biden, Trump again raised the idea of a quick approval. “Now we’re weeks away from a vaccine,” Trump said during the debate.
Trump’s estimates, though, are not in line with those offered by most firms involved with making vaccines. The most optimistic projections have come from Pfizer Inc. The drugmaker’s chief executive, Albert Bourla, has spoken about his company possibly having data to present to the FDA as early as late October about the safety and effectiveness of a vaccine.
In a September 8 interview with the Today show, Bourla said there was a 60% chance his company would meet that goal. In response to a question, he made it clear his comments applied to a potential Pfizer application, not an approval or release of a vaccine by that time.
In response to concerns about political pressures, the FDA in June issued guidance outlining what its staff would require for approval of a COVID-19 vaccine.
Pushback on politics
Another witness at the Wednesday hearing, Mark McClellan, MD, PhD, a former FDA commissioner (2002 – 2004), pushed back on objections to a potential release of further guidance from the agency.
“Some recent statements from the White House have implied that FDA’s plan to release additional written guidance on its expectations for emergency use authorization of a vaccine is unnecessarily raising the bar on regulatory standards for authorization,” said McClellan in his testimony for the House panel. “That is not the case.”
Instead, further FDA guidance would be a welcome form of feedback for the firms trying to develop COVID-19 vaccines, according to McClellan, who also serves on the board of directors for Johnson & Johnson. Johnson & Johnson is among the firms that have advanced a COVID-19 vaccine candidate to phase 3 testing. In his role as a director, he serves on the board’s regulatory compliance committee.
Along with politics, recent stumbles at FDA with emergency use authorizations (EUAs) of treatments for COVID-19 have eroded the public’s confidence in the agency, Jha told the House panel. The FDA approved hydroxychloroquine, a medicine promoted by Trump for use in COVID, under an EUA in March and then revoked this clearance in June.
Jha said the FDA’s most serious misstep was its handling of convalescent plasma, which was approved through an EUA on August 23 “in a highly advertised and widely televised announcement including the president.
“The announcement solidified in the public conversation the impression that, increasingly with this administration, politics are taking over trusted, nonpartisan scientific institutions,” he said in his testimony.
Approving a COVID-19 vaccine on the limited evidence through an EUA would mark a serious departure from FDA policy, according to Jha.
“While we sometimes accept a certain level of potential harm in experimental treatments for those who are severely ill, vaccines are given to healthy people and therefore need to have a substantially higher measure of safety and effectiveness,” he explained.
Jha said the FDA has only once before used this EUA approach for a vaccine. That was for a vaccine against inhaled anthrax and was mostly distributed to high-risk soldiers and civilians in war zones.
COVID-19, in contrast, is an infection that has changed lives around the world. The virus has contributed to more than 1 million deaths, including more than 200,000 in the United States, according to the World Health Organization.
Scientists are hoping vaccines will help curb this infection, although much of the future success of vaccines depends on how widely they are used, witnesses told the House panel.
Debate on approaches for vaccine effectiveness
In his testimony, Jha also noted concerns about COVID-19 vaccine trials. He included a reference to a Sept. 22 opinion article titled, “These Coronavirus Trials Don›t Answer the One Question We Need to Know,” which was written by Peter Doshi, PhD, of the University of Maryland School of Pharmacy, in Baltimore, and Eric Topol, MD, a professor of molecular medicine at Scripps Research in La Jolla, Calif. Topol is also editor in chief of Medscape.
Topol and Doshi questioned why the firms Moderna, Pfizer, and AstraZeneca structured their competing trials such that “a vaccine could meet the companies’ benchmark for success if it lowered the risk of mild Covid-19, but was never shown to reduce moderate or severe forms of the disease, or the risk of hospitalization, admissions to the intensive care unit or death.”
“To say a vaccine works should mean that most people no longer run the risk of getting seriously sick,” Topol and Doshi wrote. “That’s not what these trials will determine.”
There was disagreement about this point at the hearing. U.S. Representative Morgan Griffith (R-Va.) read the section of the Doshi-Topol article quoted above and asked one witness, Offit, to weigh in.
“Do you agree with those concerns? And either way, tell me why,” Griffith asked.
“I don’t agree,” Offit responded.
“I think it’s actually much harder to prevent asymptomatic infection or mildly symptomatic infection,” he said. “If you can prevent that, you are much more likely to prevent moderate to severe disease. So I think they have it backwards.”
But other researchers also question the approaches used with the current crop of COVID-19 vaccines.
“With the current protocols, it is conceivable that a vaccine might be considered effective – and eventually approved – based primarily on its ability to prevent mild cases alone,” wrote William Haseltine, PhD, president of the nonprofit ACCESS Health International, in a September 22 opinion article in the Washington Post titled: “Beware of COVID-19 Vaccine Trials Designed to Succeed From the Start.”
In an interview with Medscape Medical News on Wednesday, Haseltine said he maintains these concerns about the tests. Earlier in his career, he was a leader in HIV research through his lab at Harvard University in Cambridge, Massachusetts, and he subsequently led a biotech company, Human Genome Sciences.
He fears consumers will not get what they might expect from the vaccines being tested.
“What people care about is if this is going to keep them out of the hospital and will it keep them alive. And that’s not even part of this protocol,” Haseltine said.
This article first appeared on Medscape.com.
on Wednesday.
The career staff of the Food and Drug Administration can be counted on to appropriately weigh whether a vaccine should be cleared for use in preventing COVID-19, witnesses, including Paul A. Offit, MD, of Children’s Hospital of Philadelphia, told the House Energy and Commerce Committee’s oversight and investigations panel.
FDA staffers would object to attempts by the Trump administration to rush a vaccine to the public without proper vetting, as would veteran federal researchers, including National Institutes of Health Director Francis S. Collins, MD, PhD, and Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, Offit said.
“If COVID-19 vaccines are released before they’re ready to be released, you will hear from these people, and you will also hear from people like Dr. Francis Collins and Tony Fauci, both of whom are trusted by the American public, as well as many other academicians and researchers who wouldn’t stand for this,” he said.
“The public is already nervous about these vaccines,” said Offit, who serves on key FDA and Centers for Disease Control and Prevention committees overseeing vaccine policy. “If trusted health officials stand up and decry a premature release, the celebration by the administration will be short-lived.”
Overly optimistic estimates about a potential approval can only serve to erode the public’s trust in these crucial vaccines, said another witness, Ashish K. Jha, MD, MPH, the dean of Brown University’s School of Public Health, in Providence, Rhode Island.
“All political leaders need to stop talking about things like time lines,” Jha told the lawmakers.
President Donald Trump has several times suggested that a COVID vaccine might be approved ahead of the November 3 election, where he faces a significant challenge from his Democratic rival, former Vice President Joe Biden.
In a Tuesday night debate with Biden, Trump again raised the idea of a quick approval. “Now we’re weeks away from a vaccine,” Trump said during the debate.
Trump’s estimates, though, are not in line with those offered by most firms involved with making vaccines. The most optimistic projections have come from Pfizer Inc. The drugmaker’s chief executive, Albert Bourla, has spoken about his company possibly having data to present to the FDA as early as late October about the safety and effectiveness of a vaccine.
In a September 8 interview with the Today show, Bourla said there was a 60% chance his company would meet that goal. In response to a question, he made it clear his comments applied to a potential Pfizer application, not an approval or release of a vaccine by that time.
In response to concerns about political pressures, the FDA in June issued guidance outlining what its staff would require for approval of a COVID-19 vaccine.
Pushback on politics
Another witness at the Wednesday hearing, Mark McClellan, MD, PhD, a former FDA commissioner (2002 – 2004), pushed back on objections to a potential release of further guidance from the agency.
“Some recent statements from the White House have implied that FDA’s plan to release additional written guidance on its expectations for emergency use authorization of a vaccine is unnecessarily raising the bar on regulatory standards for authorization,” said McClellan in his testimony for the House panel. “That is not the case.”
Instead, further FDA guidance would be a welcome form of feedback for the firms trying to develop COVID-19 vaccines, according to McClellan, who also serves on the board of directors for Johnson & Johnson. Johnson & Johnson is among the firms that have advanced a COVID-19 vaccine candidate to phase 3 testing. In his role as a director, he serves on the board’s regulatory compliance committee.
Along with politics, recent stumbles at FDA with emergency use authorizations (EUAs) of treatments for COVID-19 have eroded the public’s confidence in the agency, Jha told the House panel. The FDA approved hydroxychloroquine, a medicine promoted by Trump for use in COVID, under an EUA in March and then revoked this clearance in June.
Jha said the FDA’s most serious misstep was its handling of convalescent plasma, which was approved through an EUA on August 23 “in a highly advertised and widely televised announcement including the president.
“The announcement solidified in the public conversation the impression that, increasingly with this administration, politics are taking over trusted, nonpartisan scientific institutions,” he said in his testimony.
Approving a COVID-19 vaccine on the limited evidence through an EUA would mark a serious departure from FDA policy, according to Jha.
“While we sometimes accept a certain level of potential harm in experimental treatments for those who are severely ill, vaccines are given to healthy people and therefore need to have a substantially higher measure of safety and effectiveness,” he explained.
Jha said the FDA has only once before used this EUA approach for a vaccine. That was for a vaccine against inhaled anthrax and was mostly distributed to high-risk soldiers and civilians in war zones.
COVID-19, in contrast, is an infection that has changed lives around the world. The virus has contributed to more than 1 million deaths, including more than 200,000 in the United States, according to the World Health Organization.
Scientists are hoping vaccines will help curb this infection, although much of the future success of vaccines depends on how widely they are used, witnesses told the House panel.
Debate on approaches for vaccine effectiveness
In his testimony, Jha also noted concerns about COVID-19 vaccine trials. He included a reference to a Sept. 22 opinion article titled, “These Coronavirus Trials Don›t Answer the One Question We Need to Know,” which was written by Peter Doshi, PhD, of the University of Maryland School of Pharmacy, in Baltimore, and Eric Topol, MD, a professor of molecular medicine at Scripps Research in La Jolla, Calif. Topol is also editor in chief of Medscape.
Topol and Doshi questioned why the firms Moderna, Pfizer, and AstraZeneca structured their competing trials such that “a vaccine could meet the companies’ benchmark for success if it lowered the risk of mild Covid-19, but was never shown to reduce moderate or severe forms of the disease, or the risk of hospitalization, admissions to the intensive care unit or death.”
“To say a vaccine works should mean that most people no longer run the risk of getting seriously sick,” Topol and Doshi wrote. “That’s not what these trials will determine.”
There was disagreement about this point at the hearing. U.S. Representative Morgan Griffith (R-Va.) read the section of the Doshi-Topol article quoted above and asked one witness, Offit, to weigh in.
“Do you agree with those concerns? And either way, tell me why,” Griffith asked.
“I don’t agree,” Offit responded.
“I think it’s actually much harder to prevent asymptomatic infection or mildly symptomatic infection,” he said. “If you can prevent that, you are much more likely to prevent moderate to severe disease. So I think they have it backwards.”
But other researchers also question the approaches used with the current crop of COVID-19 vaccines.
“With the current protocols, it is conceivable that a vaccine might be considered effective – and eventually approved – based primarily on its ability to prevent mild cases alone,” wrote William Haseltine, PhD, president of the nonprofit ACCESS Health International, in a September 22 opinion article in the Washington Post titled: “Beware of COVID-19 Vaccine Trials Designed to Succeed From the Start.”
In an interview with Medscape Medical News on Wednesday, Haseltine said he maintains these concerns about the tests. Earlier in his career, he was a leader in HIV research through his lab at Harvard University in Cambridge, Massachusetts, and he subsequently led a biotech company, Human Genome Sciences.
He fears consumers will not get what they might expect from the vaccines being tested.
“What people care about is if this is going to keep them out of the hospital and will it keep them alive. And that’s not even part of this protocol,” Haseltine said.
This article first appeared on Medscape.com.
on Wednesday.
The career staff of the Food and Drug Administration can be counted on to appropriately weigh whether a vaccine should be cleared for use in preventing COVID-19, witnesses, including Paul A. Offit, MD, of Children’s Hospital of Philadelphia, told the House Energy and Commerce Committee’s oversight and investigations panel.
FDA staffers would object to attempts by the Trump administration to rush a vaccine to the public without proper vetting, as would veteran federal researchers, including National Institutes of Health Director Francis S. Collins, MD, PhD, and Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, Offit said.
“If COVID-19 vaccines are released before they’re ready to be released, you will hear from these people, and you will also hear from people like Dr. Francis Collins and Tony Fauci, both of whom are trusted by the American public, as well as many other academicians and researchers who wouldn’t stand for this,” he said.
“The public is already nervous about these vaccines,” said Offit, who serves on key FDA and Centers for Disease Control and Prevention committees overseeing vaccine policy. “If trusted health officials stand up and decry a premature release, the celebration by the administration will be short-lived.”
Overly optimistic estimates about a potential approval can only serve to erode the public’s trust in these crucial vaccines, said another witness, Ashish K. Jha, MD, MPH, the dean of Brown University’s School of Public Health, in Providence, Rhode Island.
“All political leaders need to stop talking about things like time lines,” Jha told the lawmakers.
President Donald Trump has several times suggested that a COVID vaccine might be approved ahead of the November 3 election, where he faces a significant challenge from his Democratic rival, former Vice President Joe Biden.
In a Tuesday night debate with Biden, Trump again raised the idea of a quick approval. “Now we’re weeks away from a vaccine,” Trump said during the debate.
Trump’s estimates, though, are not in line with those offered by most firms involved with making vaccines. The most optimistic projections have come from Pfizer Inc. The drugmaker’s chief executive, Albert Bourla, has spoken about his company possibly having data to present to the FDA as early as late October about the safety and effectiveness of a vaccine.
In a September 8 interview with the Today show, Bourla said there was a 60% chance his company would meet that goal. In response to a question, he made it clear his comments applied to a potential Pfizer application, not an approval or release of a vaccine by that time.
In response to concerns about political pressures, the FDA in June issued guidance outlining what its staff would require for approval of a COVID-19 vaccine.
Pushback on politics
Another witness at the Wednesday hearing, Mark McClellan, MD, PhD, a former FDA commissioner (2002 – 2004), pushed back on objections to a potential release of further guidance from the agency.
“Some recent statements from the White House have implied that FDA’s plan to release additional written guidance on its expectations for emergency use authorization of a vaccine is unnecessarily raising the bar on regulatory standards for authorization,” said McClellan in his testimony for the House panel. “That is not the case.”
Instead, further FDA guidance would be a welcome form of feedback for the firms trying to develop COVID-19 vaccines, according to McClellan, who also serves on the board of directors for Johnson & Johnson. Johnson & Johnson is among the firms that have advanced a COVID-19 vaccine candidate to phase 3 testing. In his role as a director, he serves on the board’s regulatory compliance committee.
Along with politics, recent stumbles at FDA with emergency use authorizations (EUAs) of treatments for COVID-19 have eroded the public’s confidence in the agency, Jha told the House panel. The FDA approved hydroxychloroquine, a medicine promoted by Trump for use in COVID, under an EUA in March and then revoked this clearance in June.
Jha said the FDA’s most serious misstep was its handling of convalescent plasma, which was approved through an EUA on August 23 “in a highly advertised and widely televised announcement including the president.
“The announcement solidified in the public conversation the impression that, increasingly with this administration, politics are taking over trusted, nonpartisan scientific institutions,” he said in his testimony.
Approving a COVID-19 vaccine on the limited evidence through an EUA would mark a serious departure from FDA policy, according to Jha.
“While we sometimes accept a certain level of potential harm in experimental treatments for those who are severely ill, vaccines are given to healthy people and therefore need to have a substantially higher measure of safety and effectiveness,” he explained.
Jha said the FDA has only once before used this EUA approach for a vaccine. That was for a vaccine against inhaled anthrax and was mostly distributed to high-risk soldiers and civilians in war zones.
COVID-19, in contrast, is an infection that has changed lives around the world. The virus has contributed to more than 1 million deaths, including more than 200,000 in the United States, according to the World Health Organization.
Scientists are hoping vaccines will help curb this infection, although much of the future success of vaccines depends on how widely they are used, witnesses told the House panel.
Debate on approaches for vaccine effectiveness
In his testimony, Jha also noted concerns about COVID-19 vaccine trials. He included a reference to a Sept. 22 opinion article titled, “These Coronavirus Trials Don›t Answer the One Question We Need to Know,” which was written by Peter Doshi, PhD, of the University of Maryland School of Pharmacy, in Baltimore, and Eric Topol, MD, a professor of molecular medicine at Scripps Research in La Jolla, Calif. Topol is also editor in chief of Medscape.
Topol and Doshi questioned why the firms Moderna, Pfizer, and AstraZeneca structured their competing trials such that “a vaccine could meet the companies’ benchmark for success if it lowered the risk of mild Covid-19, but was never shown to reduce moderate or severe forms of the disease, or the risk of hospitalization, admissions to the intensive care unit or death.”
“To say a vaccine works should mean that most people no longer run the risk of getting seriously sick,” Topol and Doshi wrote. “That’s not what these trials will determine.”
There was disagreement about this point at the hearing. U.S. Representative Morgan Griffith (R-Va.) read the section of the Doshi-Topol article quoted above and asked one witness, Offit, to weigh in.
“Do you agree with those concerns? And either way, tell me why,” Griffith asked.
“I don’t agree,” Offit responded.
“I think it’s actually much harder to prevent asymptomatic infection or mildly symptomatic infection,” he said. “If you can prevent that, you are much more likely to prevent moderate to severe disease. So I think they have it backwards.”
But other researchers also question the approaches used with the current crop of COVID-19 vaccines.
“With the current protocols, it is conceivable that a vaccine might be considered effective – and eventually approved – based primarily on its ability to prevent mild cases alone,” wrote William Haseltine, PhD, president of the nonprofit ACCESS Health International, in a September 22 opinion article in the Washington Post titled: “Beware of COVID-19 Vaccine Trials Designed to Succeed From the Start.”
In an interview with Medscape Medical News on Wednesday, Haseltine said he maintains these concerns about the tests. Earlier in his career, he was a leader in HIV research through his lab at Harvard University in Cambridge, Massachusetts, and he subsequently led a biotech company, Human Genome Sciences.
He fears consumers will not get what they might expect from the vaccines being tested.
“What people care about is if this is going to keep them out of the hospital and will it keep them alive. And that’s not even part of this protocol,” Haseltine said.
This article first appeared on Medscape.com.
Physicians, make a plan to vote
In March 2020, following the announcement of the United States’ first death related to COVID-19, many physicians began using their voices to discuss the shortage of personal protective equipment (PPE). Many physicians, myself included, petitioned elected leaders at the community, state, and federal levels to address the PPE shortage.

Historically, physicians have advocated for improved public health. From seat belt laws in the 1980s and 1990s to the Affordable Care Act in the 2000s, physicians have testified at the community, state, and federal levels to advocate for the health and safety of our patients and the public. Yet while we have been making our voices heard, we are often silent at the ballot box.
In the 1996 and 2000 elections, physicians voted 9% less often than the general public, and compared with lawyers – professionals with similar educational attainment and finances – physicians voted 22% less often.1 It is unclear why physicians are less likely to vote. In a 2016 article, David Grande, MD, and Katrina Armstrong, MD, postulated that physicians may not vote because our work hours create barriers to visiting polls.2
Despite our lack of engagement at the ballot box, voting is important to improving our patients’ social determinants of health. In a recently published systematic review, the authors found several studies supporting the association between voting and social determinants of health. Their review found that, when large numbers of people from communities participated in voting, it translated into greater influence over determining who held political power in that community. Those with power introduced and supported policies responding to their constituents’ needs, ultimately influencing their constituents’ social determinants of health.3 By voting, we as physicians are helping to address the social determinants of health in our communities.
Many medical students have been doing their part to improve the social determinants of health in their communities by pledging to vote. In 2018, the American Medical Student Association launched their “Med Out the Vote” initiative prior to the election. The organization called on all health care providers and providers in training to pledge to vote in the election.4 They are continuing these efforts for the 2020 elections.
We should join our nation’s medical students by also pledging to vote. To begin, we can all Make A Plan To Vote. Each plan should include the following:
- Register to vote: In many states eligible voters can register online.
- Request an absentee ballot: Many states require registered voters to request absentee ballots online or by mail.
- Vote: Submit an absentee ballot prior to election or vote in-person on election day. Some counties allow voting early in person.
In practice, our plans will differ slightly because each state has its own election laws.
This election season let us ensure all physician voices are heard. Make A Plan To Vote for your patients and communities.
Dr. Kumar is the pediatric editor of The Hospitalist. She is clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University and a pediatric hospitalist at Cleveland Clinic Children’s.
References
1. Grande D et al. Do Doctors Vote? J Gen Intern Med. 2007 May;22(5):585-9.
2. Grande D, Armstrong K. Will Physicians Vote? Ann Intern Med. 2016;165:814-5.
3. Brown CL et al. Voting, health and interventions in healthcare settings: A scoping review. Public Health Rev. 2020 Jul. doi: 10.1186/s40985-020-00133-6.
4. American Medical Student Association. AMSA Launches Med Out the Vote Campaign, Call to Action. 2018 Jul 29. Accessed 2020 Sep 14. https://www.amsa.org/about/amsa-press-room/amsa-launches-med-out-the-vote-campaign-call-to-action/
In March 2020, following the announcement of the United States’ first death related to COVID-19, many physicians began using their voices to discuss the shortage of personal protective equipment (PPE). Many physicians, myself included, petitioned elected leaders at the community, state, and federal levels to address the PPE shortage.
Historically, physicians have advocated for improved public health. From seat belt laws in the 1980s and 1990s to the Affordable Care Act in the 2000s, physicians have testified at the community, state, and federal levels to advocate for the health and safety of our patients and the public. Yet while we have been making our voices heard, we are often silent at the ballot box.
In the 1996 and 2000 elections, physicians voted 9% less often than the general public, and compared with lawyers – professionals with similar educational attainment and finances – physicians voted 22% less often.1 It is unclear why physicians are less likely to vote. In a 2016 article, David Grande, MD, and Katrina Armstrong, MD, postulated that physicians may not vote because our work hours create barriers to visiting polls.2
Despite our lack of engagement at the ballot box, voting is important to improving our patients’ social determinants of health. In a recently published systematic review, the authors found several studies supporting the association between voting and social determinants of health. Their review found that, when large numbers of people from communities participated in voting, it translated into greater influence over determining who held political power in that community. Those with power introduced and supported policies responding to their constituents’ needs, ultimately influencing their constituents’ social determinants of health.3 By voting, we as physicians are helping to address the social determinants of health in our communities.
Many medical students have been doing their part to improve the social determinants of health in their communities by pledging to vote. In 2018, the American Medical Student Association launched their “Med Out the Vote” initiative prior to the election. The organization called on all health care providers and providers in training to pledge to vote in the election.4 They are continuing these efforts for the 2020 elections.
We should join our nation’s medical students by also pledging to vote. To begin, we can all Make A Plan To Vote. Each plan should include the following:
- Register to vote: In many states eligible voters can register online.
- Request an absentee ballot: Many states require registered voters to request absentee ballots online or by mail.
- Vote: Submit an absentee ballot prior to election or vote in-person on election day. Some counties allow voting early in person.
In practice, our plans will differ slightly because each state has its own election laws.
This election season let us ensure all physician voices are heard. Make A Plan To Vote for your patients and communities.
Dr. Kumar is the pediatric editor of The Hospitalist. She is clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University and a pediatric hospitalist at Cleveland Clinic Children’s.
References
1. Grande D et al. Do Doctors Vote? J Gen Intern Med. 2007 May;22(5):585-9.
2. Grande D, Armstrong K. Will Physicians Vote? Ann Intern Med. 2016;165:814-5.
3. Brown CL et al. Voting, health and interventions in healthcare settings: A scoping review. Public Health Rev. 2020 Jul. doi: 10.1186/s40985-020-00133-6.
4. American Medical Student Association. AMSA Launches Med Out the Vote Campaign, Call to Action. 2018 Jul 29. Accessed 2020 Sep 14. https://www.amsa.org/about/amsa-press-room/amsa-launches-med-out-the-vote-campaign-call-to-action/
In March 2020, following the announcement of the United States’ first death related to COVID-19, many physicians began using their voices to discuss the shortage of personal protective equipment (PPE). Many physicians, myself included, petitioned elected leaders at the community, state, and federal levels to address the PPE shortage.
Historically, physicians have advocated for improved public health. From seat belt laws in the 1980s and 1990s to the Affordable Care Act in the 2000s, physicians have testified at the community, state, and federal levels to advocate for the health and safety of our patients and the public. Yet while we have been making our voices heard, we are often silent at the ballot box.
In the 1996 and 2000 elections, physicians voted 9% less often than the general public, and compared with lawyers – professionals with similar educational attainment and finances – physicians voted 22% less often.1 It is unclear why physicians are less likely to vote. In a 2016 article, David Grande, MD, and Katrina Armstrong, MD, postulated that physicians may not vote because our work hours create barriers to visiting polls.2
Despite our lack of engagement at the ballot box, voting is important to improving our patients’ social determinants of health. In a recently published systematic review, the authors found several studies supporting the association between voting and social determinants of health. Their review found that, when large numbers of people from communities participated in voting, it translated into greater influence over determining who held political power in that community. Those with power introduced and supported policies responding to their constituents’ needs, ultimately influencing their constituents’ social determinants of health.3 By voting, we as physicians are helping to address the social determinants of health in our communities.
Many medical students have been doing their part to improve the social determinants of health in their communities by pledging to vote. In 2018, the American Medical Student Association launched their “Med Out the Vote” initiative prior to the election. The organization called on all health care providers and providers in training to pledge to vote in the election.4 They are continuing these efforts for the 2020 elections.
We should join our nation’s medical students by also pledging to vote. To begin, we can all Make A Plan To Vote. Each plan should include the following:
- Register to vote: In many states eligible voters can register online.
- Request an absentee ballot: Many states require registered voters to request absentee ballots online or by mail.
- Vote: Submit an absentee ballot prior to election or vote in-person on election day. Some counties allow voting early in person.
In practice, our plans will differ slightly because each state has its own election laws.
This election season let us ensure all physician voices are heard. Make A Plan To Vote for your patients and communities.
Dr. Kumar is the pediatric editor of The Hospitalist. She is clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University and a pediatric hospitalist at Cleveland Clinic Children’s.
References
1. Grande D et al. Do Doctors Vote? J Gen Intern Med. 2007 May;22(5):585-9.
2. Grande D, Armstrong K. Will Physicians Vote? Ann Intern Med. 2016;165:814-5.
3. Brown CL et al. Voting, health and interventions in healthcare settings: A scoping review. Public Health Rev. 2020 Jul. doi: 10.1186/s40985-020-00133-6.
4. American Medical Student Association. AMSA Launches Med Out the Vote Campaign, Call to Action. 2018 Jul 29. Accessed 2020 Sep 14. https://www.amsa.org/about/amsa-press-room/amsa-launches-med-out-the-vote-campaign-call-to-action/
CDC adds then retracts aerosols as main COVID-19 mode of transmission
The CDC had updated information on coronavirus spread and had acknowledged the prominence of aerosol transmission.
CDC’s new information still says that Sars-CoV-2 is commonly spread between people who are within about 6 feet of each other, which has been the agency’s stance for months now.
However, the deleted update had added it is spread “through respiratory droplets or small particles, such as those in aerosols, produced when an infected person coughs, sneezes, sings, talks, or breathes. These particles can be inhaled into the nose, mouth, airways, and lungs and cause infection. This is thought to be the main way the virus spreads.”
Responding to Medscape Medical News questions about the update, Jasmine Reed, spokesperson for the CDC, told Medscape Medical News, “A draft version of proposed changes to these recommendations was posted in error to the agency’s official website. CDC is currently updating its recommendations regarding airborne transmission of SARS-CoV-2 (the virus that causes COVID-19). Once this process has been completed, the updated language will be posted.”
Previous information
Previously, the CDC said the virus is spread mainly among people who are within about 6 feet of each another through respiratory droplets propelled when an infected person coughs, sneezes, or talks.
Previous guidance also said, “These droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs.”
The now deleted update said, “There is growing evidence that droplets and airborne particles can remain suspended in the air and be breathed in by others, and travel distances beyond 6 feet (for example, during choir practice, in restaurants, or in fitness classes).”
On July 6, Clinical Infectious Diseases published the paper “It Is Time to Address Airborne Transmission of Coronavirus Disease 2019,” which was supported by 239 scientists.
The authors write, “There is significant potential for inhalation exposure to viruses in microscopic respiratory droplets (microdroplets) at short to medium distances (up to several meters, or room scale).
The World Health Organization (WHO) acknowledged after this research was published that airborne transmission of the virus may play a role in infection, especially in poorly ventilated rooms and buildings, but have yet to declare aerosols as a definitive contributor.
WHO has long stated that coronavirus is spread mainly by droplets that, once expelled by coughs and sneezes of infected people, fall quickly to the floor.
The CDC update was made Friday without announcement.
“This has been one of the problems all along,” said Leana Wen, MD, an emergency physician and public health professor at George Washington University, Washington, DC. “The guidance from CDC changes on their website, but there’s no press conference, there’s no explanation of why they’re changing this now.”
Again Monday, there was no announcement that information had changed.
Update added air purifiers for prevention
The CDC continues to recommend staying 6 feet from others, washing hands, wearing a mask and routinely disinfecting frequently touched surfaces.
The update had added, “Use air purifiers to help reduce airborne germs in indoor spaces.”
Marcia Frellick is a freelance journalist based in Chicago. She has previously written for the Chicago Tribune, Science News and Nurse.com and was an editor at the Chicago Sun-Times, the Cincinnati Enquirer, and the St. Cloud (Minnesota) Times. Follow her on Twitter at @mfrellick
This article first appeared on Medscape.com.
The CDC had updated information on coronavirus spread and had acknowledged the prominence of aerosol transmission.
CDC’s new information still says that Sars-CoV-2 is commonly spread between people who are within about 6 feet of each other, which has been the agency’s stance for months now.
However, the deleted update had added it is spread “through respiratory droplets or small particles, such as those in aerosols, produced when an infected person coughs, sneezes, sings, talks, or breathes. These particles can be inhaled into the nose, mouth, airways, and lungs and cause infection. This is thought to be the main way the virus spreads.”
Responding to Medscape Medical News questions about the update, Jasmine Reed, spokesperson for the CDC, told Medscape Medical News, “A draft version of proposed changes to these recommendations was posted in error to the agency’s official website. CDC is currently updating its recommendations regarding airborne transmission of SARS-CoV-2 (the virus that causes COVID-19). Once this process has been completed, the updated language will be posted.”
Previous information
Previously, the CDC said the virus is spread mainly among people who are within about 6 feet of each another through respiratory droplets propelled when an infected person coughs, sneezes, or talks.
Previous guidance also said, “These droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs.”
The now deleted update said, “There is growing evidence that droplets and airborne particles can remain suspended in the air and be breathed in by others, and travel distances beyond 6 feet (for example, during choir practice, in restaurants, or in fitness classes).”
On July 6, Clinical Infectious Diseases published the paper “It Is Time to Address Airborne Transmission of Coronavirus Disease 2019,” which was supported by 239 scientists.
The authors write, “There is significant potential for inhalation exposure to viruses in microscopic respiratory droplets (microdroplets) at short to medium distances (up to several meters, or room scale).
The World Health Organization (WHO) acknowledged after this research was published that airborne transmission of the virus may play a role in infection, especially in poorly ventilated rooms and buildings, but have yet to declare aerosols as a definitive contributor.
WHO has long stated that coronavirus is spread mainly by droplets that, once expelled by coughs and sneezes of infected people, fall quickly to the floor.
The CDC update was made Friday without announcement.
“This has been one of the problems all along,” said Leana Wen, MD, an emergency physician and public health professor at George Washington University, Washington, DC. “The guidance from CDC changes on their website, but there’s no press conference, there’s no explanation of why they’re changing this now.”
Again Monday, there was no announcement that information had changed.
Update added air purifiers for prevention
The CDC continues to recommend staying 6 feet from others, washing hands, wearing a mask and routinely disinfecting frequently touched surfaces.
The update had added, “Use air purifiers to help reduce airborne germs in indoor spaces.”
Marcia Frellick is a freelance journalist based in Chicago. She has previously written for the Chicago Tribune, Science News and Nurse.com and was an editor at the Chicago Sun-Times, the Cincinnati Enquirer, and the St. Cloud (Minnesota) Times. Follow her on Twitter at @mfrellick
This article first appeared on Medscape.com.
The CDC had updated information on coronavirus spread and had acknowledged the prominence of aerosol transmission.
CDC’s new information still says that Sars-CoV-2 is commonly spread between people who are within about 6 feet of each other, which has been the agency’s stance for months now.
However, the deleted update had added it is spread “through respiratory droplets or small particles, such as those in aerosols, produced when an infected person coughs, sneezes, sings, talks, or breathes. These particles can be inhaled into the nose, mouth, airways, and lungs and cause infection. This is thought to be the main way the virus spreads.”
Responding to Medscape Medical News questions about the update, Jasmine Reed, spokesperson for the CDC, told Medscape Medical News, “A draft version of proposed changes to these recommendations was posted in error to the agency’s official website. CDC is currently updating its recommendations regarding airborne transmission of SARS-CoV-2 (the virus that causes COVID-19). Once this process has been completed, the updated language will be posted.”
Previous information
Previously, the CDC said the virus is spread mainly among people who are within about 6 feet of each another through respiratory droplets propelled when an infected person coughs, sneezes, or talks.
Previous guidance also said, “These droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs.”
The now deleted update said, “There is growing evidence that droplets and airborne particles can remain suspended in the air and be breathed in by others, and travel distances beyond 6 feet (for example, during choir practice, in restaurants, or in fitness classes).”
On July 6, Clinical Infectious Diseases published the paper “It Is Time to Address Airborne Transmission of Coronavirus Disease 2019,” which was supported by 239 scientists.
The authors write, “There is significant potential for inhalation exposure to viruses in microscopic respiratory droplets (microdroplets) at short to medium distances (up to several meters, or room scale).
The World Health Organization (WHO) acknowledged after this research was published that airborne transmission of the virus may play a role in infection, especially in poorly ventilated rooms and buildings, but have yet to declare aerosols as a definitive contributor.
WHO has long stated that coronavirus is spread mainly by droplets that, once expelled by coughs and sneezes of infected people, fall quickly to the floor.
The CDC update was made Friday without announcement.
“This has been one of the problems all along,” said Leana Wen, MD, an emergency physician and public health professor at George Washington University, Washington, DC. “The guidance from CDC changes on their website, but there’s no press conference, there’s no explanation of why they’re changing this now.”
Again Monday, there was no announcement that information had changed.
Update added air purifiers for prevention
The CDC continues to recommend staying 6 feet from others, washing hands, wearing a mask and routinely disinfecting frequently touched surfaces.
The update had added, “Use air purifiers to help reduce airborne germs in indoor spaces.”
Marcia Frellick is a freelance journalist based in Chicago. She has previously written for the Chicago Tribune, Science News and Nurse.com and was an editor at the Chicago Sun-Times, the Cincinnati Enquirer, and the St. Cloud (Minnesota) Times. Follow her on Twitter at @mfrellick
This article first appeared on Medscape.com.
HHS plan to improve rural health focuses on better broadband, telehealth services
Even before the coronavirus pandemic reached into the nation’s less-populated regions, rural Americans were sicker, poorer, and older than the rest of the country. Hospitals are shuttering at record rates, and health care experts have long called for changes.
The new plan, released by the Department of Health & Human Services Secretary Alex M. Azar, II, acknowledges the gaps in health care and other problems facing rural America. It lists a litany of projects and directives, with many already underway or announced within federal agencies.
“We cannot just tinker around the edges of a rural healthcare system that has struggled for too long,” Azar said in a prepared statement.
Yet, that is exactly what experts say the administration continues to do.
“They tinker around the edges,” said Tommy Barnhart, former president of the National Rural Health Association. And he added, “there’s a lot of political hype” that has happened under President Trump, as well as previous presidents.
In the past few months, rural health care has increasingly become a focus for Mr. Trump, whose polling numbers are souring as COVID-19 kills hundreds of Americans every day, drives down restaurant demand for some farm products, and spreads through meatpacking plants. Rural states including Iowa and the Dakotas are reporting the latest surges in cases.
This announcement comes in response to Mr. Trump’s executive order last month calling for improved rural health and telehealth access. Earlier this week, three federal agencies also announced they would team up to address gaps in rural broadband service – a key need because large portions of the plan seek to expand telehealth.
The plan is more than 70 pages long and the word “telehealth” appears more than 90 times, with a focus on projects across HHS, including the Health Resources and Services Administration and the Centers for Medicare & Medicaid Services.
Mr. Barnhart said CMS has passed some public health emergency waivers since the beginning of the pandemic that helped rural facilities get more funding, including one that specifically was designed to provide additional money for telehealth services. However, those waivers are set to expire when the coronavirus emergency ends. Officials have not yet set a date for when the federal emergency will end.
Andrew Jay Schwartzman, senior counselor to the Benton Institute for Broadband & Society, a private foundation that works to ensure greater Internet access, said there are multiple challenges with implementing telehealth across the nation. Many initiatives for robust telehealth programs need fast bandwidth, yet getting the money and setting up the necessary infrastructure is very difficult, he said.
“It will be a long time before this kind of technology will be readily available to much of the country,” he said.
Ge Bai, associate professor of accounting and health policy at Johns Hopkins University in Baltimore, noted that telehealth was short on funding in the HHS initiative. However, she said, the focus on telehealth, as well as a proposed shift in payment for small rural hospitals and changing workforce licensing requirements, had good potential.
“We are so close to the election that this is probably more of a messaging issue to cater to rural residents,” Ms. Bai said. “But it doesn’t matter who will be president. This report will give the next administration useful guidance.”
The American Hospital Association, representing 5,000 hospitals nationwide, sent a letter to Mr. Trump last week recommending a host of steps the administration could take. As of late Thursday, AHA was still reviewing the HHS plan but said it was “encouraged by the increased attention on rural health care.”
Buried within the HHS announcement are technical initiatives, such as a contract to help clinics and hospitals integrate care, and detailed efforts to address gaps in care, including a proposal to increase funding for school-based mental health programs in the president’s 2021 budget.
A senior HHS official said that, while some actions have been taken in recent months to improve rural health — such as the $11 billion provided to rural hospitals through coronavirus relief funding — more is needed.
“We’re putting our stake in the ground that the time for talk is over,” he said. “We’re going to move forward.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Even before the coronavirus pandemic reached into the nation’s less-populated regions, rural Americans were sicker, poorer, and older than the rest of the country. Hospitals are shuttering at record rates, and health care experts have long called for changes.
The new plan, released by the Department of Health & Human Services Secretary Alex M. Azar, II, acknowledges the gaps in health care and other problems facing rural America. It lists a litany of projects and directives, with many already underway or announced within federal agencies.
“We cannot just tinker around the edges of a rural healthcare system that has struggled for too long,” Azar said in a prepared statement.
Yet, that is exactly what experts say the administration continues to do.
“They tinker around the edges,” said Tommy Barnhart, former president of the National Rural Health Association. And he added, “there’s a lot of political hype” that has happened under President Trump, as well as previous presidents.
In the past few months, rural health care has increasingly become a focus for Mr. Trump, whose polling numbers are souring as COVID-19 kills hundreds of Americans every day, drives down restaurant demand for some farm products, and spreads through meatpacking plants. Rural states including Iowa and the Dakotas are reporting the latest surges in cases.
This announcement comes in response to Mr. Trump’s executive order last month calling for improved rural health and telehealth access. Earlier this week, three federal agencies also announced they would team up to address gaps in rural broadband service – a key need because large portions of the plan seek to expand telehealth.
The plan is more than 70 pages long and the word “telehealth” appears more than 90 times, with a focus on projects across HHS, including the Health Resources and Services Administration and the Centers for Medicare & Medicaid Services.
Mr. Barnhart said CMS has passed some public health emergency waivers since the beginning of the pandemic that helped rural facilities get more funding, including one that specifically was designed to provide additional money for telehealth services. However, those waivers are set to expire when the coronavirus emergency ends. Officials have not yet set a date for when the federal emergency will end.
Andrew Jay Schwartzman, senior counselor to the Benton Institute for Broadband & Society, a private foundation that works to ensure greater Internet access, said there are multiple challenges with implementing telehealth across the nation. Many initiatives for robust telehealth programs need fast bandwidth, yet getting the money and setting up the necessary infrastructure is very difficult, he said.
“It will be a long time before this kind of technology will be readily available to much of the country,” he said.
Ge Bai, associate professor of accounting and health policy at Johns Hopkins University in Baltimore, noted that telehealth was short on funding in the HHS initiative. However, she said, the focus on telehealth, as well as a proposed shift in payment for small rural hospitals and changing workforce licensing requirements, had good potential.
“We are so close to the election that this is probably more of a messaging issue to cater to rural residents,” Ms. Bai said. “But it doesn’t matter who will be president. This report will give the next administration useful guidance.”
The American Hospital Association, representing 5,000 hospitals nationwide, sent a letter to Mr. Trump last week recommending a host of steps the administration could take. As of late Thursday, AHA was still reviewing the HHS plan but said it was “encouraged by the increased attention on rural health care.”
Buried within the HHS announcement are technical initiatives, such as a contract to help clinics and hospitals integrate care, and detailed efforts to address gaps in care, including a proposal to increase funding for school-based mental health programs in the president’s 2021 budget.
A senior HHS official said that, while some actions have been taken in recent months to improve rural health — such as the $11 billion provided to rural hospitals through coronavirus relief funding — more is needed.
“We’re putting our stake in the ground that the time for talk is over,” he said. “We’re going to move forward.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Even before the coronavirus pandemic reached into the nation’s less-populated regions, rural Americans were sicker, poorer, and older than the rest of the country. Hospitals are shuttering at record rates, and health care experts have long called for changes.
The new plan, released by the Department of Health & Human Services Secretary Alex M. Azar, II, acknowledges the gaps in health care and other problems facing rural America. It lists a litany of projects and directives, with many already underway or announced within federal agencies.
“We cannot just tinker around the edges of a rural healthcare system that has struggled for too long,” Azar said in a prepared statement.
Yet, that is exactly what experts say the administration continues to do.
“They tinker around the edges,” said Tommy Barnhart, former president of the National Rural Health Association. And he added, “there’s a lot of political hype” that has happened under President Trump, as well as previous presidents.
In the past few months, rural health care has increasingly become a focus for Mr. Trump, whose polling numbers are souring as COVID-19 kills hundreds of Americans every day, drives down restaurant demand for some farm products, and spreads through meatpacking plants. Rural states including Iowa and the Dakotas are reporting the latest surges in cases.
This announcement comes in response to Mr. Trump’s executive order last month calling for improved rural health and telehealth access. Earlier this week, three federal agencies also announced they would team up to address gaps in rural broadband service – a key need because large portions of the plan seek to expand telehealth.
The plan is more than 70 pages long and the word “telehealth” appears more than 90 times, with a focus on projects across HHS, including the Health Resources and Services Administration and the Centers for Medicare & Medicaid Services.
Mr. Barnhart said CMS has passed some public health emergency waivers since the beginning of the pandemic that helped rural facilities get more funding, including one that specifically was designed to provide additional money for telehealth services. However, those waivers are set to expire when the coronavirus emergency ends. Officials have not yet set a date for when the federal emergency will end.
Andrew Jay Schwartzman, senior counselor to the Benton Institute for Broadband & Society, a private foundation that works to ensure greater Internet access, said there are multiple challenges with implementing telehealth across the nation. Many initiatives for robust telehealth programs need fast bandwidth, yet getting the money and setting up the necessary infrastructure is very difficult, he said.
“It will be a long time before this kind of technology will be readily available to much of the country,” he said.
Ge Bai, associate professor of accounting and health policy at Johns Hopkins University in Baltimore, noted that telehealth was short on funding in the HHS initiative. However, she said, the focus on telehealth, as well as a proposed shift in payment for small rural hospitals and changing workforce licensing requirements, had good potential.
“We are so close to the election that this is probably more of a messaging issue to cater to rural residents,” Ms. Bai said. “But it doesn’t matter who will be president. This report will give the next administration useful guidance.”
The American Hospital Association, representing 5,000 hospitals nationwide, sent a letter to Mr. Trump last week recommending a host of steps the administration could take. As of late Thursday, AHA was still reviewing the HHS plan but said it was “encouraged by the increased attention on rural health care.”
Buried within the HHS announcement are technical initiatives, such as a contract to help clinics and hospitals integrate care, and detailed efforts to address gaps in care, including a proposal to increase funding for school-based mental health programs in the president’s 2021 budget.
A senior HHS official said that, while some actions have been taken in recent months to improve rural health — such as the $11 billion provided to rural hospitals through coronavirus relief funding — more is needed.
“We’re putting our stake in the ground that the time for talk is over,” he said. “We’re going to move forward.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Immigrant hospitalist dilemma takes stage at HM20 Virtual
Manpreet Malik, MD, a hospitalist at Emory University, takes care of patients with COVID-19 at Grady Memorial Hospital in downtown Atlanta. Born in India but living in the United States for more than 10 years, he is awaiting permanent resident status. At the current pace of U.S. Citizenship and Immigration Services, that may be decades away.
Dr. Malik lives and works in the United States on an H-1B visa, which is based on employment in a specialty occupation. Although he has a job that he loves, his immigrant status, social life, and geographic location in the United States is, technically, entirely dependent on doing that job.
“For single-income families with doctors on visas, the pandemic brings anxiety and uncertainty about legal status in the U.S. in case the breadwinner gets sick, disabled or unemployed,” he said.
In a presentation to be given at the HM20 Virtual, hosted by the Society of Hospital Medicine, Dr. Malik will offer perspective on the current challenges facing immigrant hospitalists and health care workers, especially in a U.S. health care system stretched thin and one in which many health professionals born outside the United States are working on the front lines. These challenges should be motivation to make legislative changes to give these health care workers more stability, flexibility, and peace of mind, he said.
The talk – to be given along with HM20 course director Benji Mathews, MD, SFHM, and called “The Immigrant Hospitalist: Navigating the Uncertain Terrain During COVID-19” – will describe a long-standing issue and outline a path forward, the two physicians said.
“The objective of this talk is to really highlight the contributions of these physicians and health care workers and also to provide a call for action for our hospitalist colleagues. This talk paints a picture of what my family and thousands of the other immigrant health care worker families are going through,” Dr. Malik said.
Dr. Mathews said that many physicians do not have benefits they can fall back on should they fall ill. And without the jobs their visas are based on, they could face deportation.
“That’s extreme – but the pathway towards that is very much there,” said Dr. Mathews, who was born in the Middle East and immigrated to the United States, received a green card, and later his citizenship. He now advocates for immigrant health and immigrant health care workers.

Dr. Malik and Dr. Mathews recently published a perspective piece in the Journal of Hospital Medicine. In it, they pointed out that 16.4% of health care workers are immigrants, and 29% of physicians are immigrants. Among practicing hospitalists, 32% are international medical graduates. They called for reform to visa regulations to allow physicians who are immigrants to travel to areas where they are most needed during the pandemic, for extensions of visa deadlines, and exemption from future immigration bans or limitations. These measures would only bolster the health care workforce that is under such strain during the pandemic, they write. (J Hosp Med. 2020 Aug;15[8]:505-506)
Dr. Malik said that, even while under added personal strain caused by the uncertainty of the past several months, he has never questioned his decision to be a physician in the United States.
“Now, more than ever, there is a sense of purpose and a passion to make a difference for our patients,” he said.
“I think most of us get into medicine and become hospitalists because we want to care for people, because we want to serve, because we want to be able to take care of sick, hospitalized patients, and that can be anywhere in the world, whether you’re in India serving a population that you grew up with or whether you’re in the U.S. serving the population that are your neighbors, your friends, your community, or people that are vulnerable. You’re serving humanity, and that is the ultimate goal.”
SHM advocacy on immigration issues
SHM has been advocating for more equitable skilled-immigration system, recognizing that from visa-backlogs to per-country caps, unfair visa restrictions have limited the United States’ ability to adequately expand its health care workforce.
The Society has consistently advocated on Capitol Hill for visa and skilled-immigration reform and has championed several significant immigration bills, including the following:
The Fairness for High Skilled Immigrants Act
- This legislation will eliminate per-country caps on green cards and convert the system into a “first-come, first-serve” system. This will help ensure certain nationalize are not disproportionally impacted by excessive green card backlogs.
- This legislation has passed the House of Representatives. Send a message to your Senator asking them to cosponsor this legislation.
The Conrad State 30 Physician Reauthorization Act
- This legislation will renew the Conrad State 30 program, which allows physicians on a J-1 visa to remain in the United States if they work in an underserved region for a minimum of three years. This legislation also included additional employment protection claims.
The Healthcare Workforce Resilience Act
- This legislation will recapture 40,000 unused immigrant visas for foreign doctors (15,000) and nurses (25,000), as well as provide visas for their spouse and children.
- This legislation will only be in effect for the duration of the COVID-19 public health emergency.
To join SHM in supporting our immigrant clinicians, you can send a message to your representatives in support of these bills by visiting hospitalmedicine.org/takeaction.
Manpreet Malik, MD, a hospitalist at Emory University, takes care of patients with COVID-19 at Grady Memorial Hospital in downtown Atlanta. Born in India but living in the United States for more than 10 years, he is awaiting permanent resident status. At the current pace of U.S. Citizenship and Immigration Services, that may be decades away.
Dr. Malik lives and works in the United States on an H-1B visa, which is based on employment in a specialty occupation. Although he has a job that he loves, his immigrant status, social life, and geographic location in the United States is, technically, entirely dependent on doing that job.
“For single-income families with doctors on visas, the pandemic brings anxiety and uncertainty about legal status in the U.S. in case the breadwinner gets sick, disabled or unemployed,” he said.
In a presentation to be given at the HM20 Virtual, hosted by the Society of Hospital Medicine, Dr. Malik will offer perspective on the current challenges facing immigrant hospitalists and health care workers, especially in a U.S. health care system stretched thin and one in which many health professionals born outside the United States are working on the front lines. These challenges should be motivation to make legislative changes to give these health care workers more stability, flexibility, and peace of mind, he said.
The talk – to be given along with HM20 course director Benji Mathews, MD, SFHM, and called “The Immigrant Hospitalist: Navigating the Uncertain Terrain During COVID-19” – will describe a long-standing issue and outline a path forward, the two physicians said.
“The objective of this talk is to really highlight the contributions of these physicians and health care workers and also to provide a call for action for our hospitalist colleagues. This talk paints a picture of what my family and thousands of the other immigrant health care worker families are going through,” Dr. Malik said.
Dr. Mathews said that many physicians do not have benefits they can fall back on should they fall ill. And without the jobs their visas are based on, they could face deportation.
“That’s extreme – but the pathway towards that is very much there,” said Dr. Mathews, who was born in the Middle East and immigrated to the United States, received a green card, and later his citizenship. He now advocates for immigrant health and immigrant health care workers.
Dr. Malik and Dr. Mathews recently published a perspective piece in the Journal of Hospital Medicine. In it, they pointed out that 16.4% of health care workers are immigrants, and 29% of physicians are immigrants. Among practicing hospitalists, 32% are international medical graduates. They called for reform to visa regulations to allow physicians who are immigrants to travel to areas where they are most needed during the pandemic, for extensions of visa deadlines, and exemption from future immigration bans or limitations. These measures would only bolster the health care workforce that is under such strain during the pandemic, they write. (J Hosp Med. 2020 Aug;15[8]:505-506)
Dr. Malik said that, even while under added personal strain caused by the uncertainty of the past several months, he has never questioned his decision to be a physician in the United States.
“Now, more than ever, there is a sense of purpose and a passion to make a difference for our patients,” he said.
“I think most of us get into medicine and become hospitalists because we want to care for people, because we want to serve, because we want to be able to take care of sick, hospitalized patients, and that can be anywhere in the world, whether you’re in India serving a population that you grew up with or whether you’re in the U.S. serving the population that are your neighbors, your friends, your community, or people that are vulnerable. You’re serving humanity, and that is the ultimate goal.”
SHM advocacy on immigration issues
SHM has been advocating for more equitable skilled-immigration system, recognizing that from visa-backlogs to per-country caps, unfair visa restrictions have limited the United States’ ability to adequately expand its health care workforce.
The Society has consistently advocated on Capitol Hill for visa and skilled-immigration reform and has championed several significant immigration bills, including the following:
The Fairness for High Skilled Immigrants Act
- This legislation will eliminate per-country caps on green cards and convert the system into a “first-come, first-serve” system. This will help ensure certain nationalize are not disproportionally impacted by excessive green card backlogs.
- This legislation has passed the House of Representatives. Send a message to your Senator asking them to cosponsor this legislation.
The Conrad State 30 Physician Reauthorization Act
- This legislation will renew the Conrad State 30 program, which allows physicians on a J-1 visa to remain in the United States if they work in an underserved region for a minimum of three years. This legislation also included additional employment protection claims.
The Healthcare Workforce Resilience Act
- This legislation will recapture 40,000 unused immigrant visas for foreign doctors (15,000) and nurses (25,000), as well as provide visas for their spouse and children.
- This legislation will only be in effect for the duration of the COVID-19 public health emergency.
To join SHM in supporting our immigrant clinicians, you can send a message to your representatives in support of these bills by visiting hospitalmedicine.org/takeaction.
Manpreet Malik, MD, a hospitalist at Emory University, takes care of patients with COVID-19 at Grady Memorial Hospital in downtown Atlanta. Born in India but living in the United States for more than 10 years, he is awaiting permanent resident status. At the current pace of U.S. Citizenship and Immigration Services, that may be decades away.
Dr. Malik lives and works in the United States on an H-1B visa, which is based on employment in a specialty occupation. Although he has a job that he loves, his immigrant status, social life, and geographic location in the United States is, technically, entirely dependent on doing that job.
“For single-income families with doctors on visas, the pandemic brings anxiety and uncertainty about legal status in the U.S. in case the breadwinner gets sick, disabled or unemployed,” he said.
In a presentation to be given at the HM20 Virtual, hosted by the Society of Hospital Medicine, Dr. Malik will offer perspective on the current challenges facing immigrant hospitalists and health care workers, especially in a U.S. health care system stretched thin and one in which many health professionals born outside the United States are working on the front lines. These challenges should be motivation to make legislative changes to give these health care workers more stability, flexibility, and peace of mind, he said.
The talk – to be given along with HM20 course director Benji Mathews, MD, SFHM, and called “The Immigrant Hospitalist: Navigating the Uncertain Terrain During COVID-19” – will describe a long-standing issue and outline a path forward, the two physicians said.
“The objective of this talk is to really highlight the contributions of these physicians and health care workers and also to provide a call for action for our hospitalist colleagues. This talk paints a picture of what my family and thousands of the other immigrant health care worker families are going through,” Dr. Malik said.
Dr. Mathews said that many physicians do not have benefits they can fall back on should they fall ill. And without the jobs their visas are based on, they could face deportation.
“That’s extreme – but the pathway towards that is very much there,” said Dr. Mathews, who was born in the Middle East and immigrated to the United States, received a green card, and later his citizenship. He now advocates for immigrant health and immigrant health care workers.
Dr. Malik and Dr. Mathews recently published a perspective piece in the Journal of Hospital Medicine. In it, they pointed out that 16.4% of health care workers are immigrants, and 29% of physicians are immigrants. Among practicing hospitalists, 32% are international medical graduates. They called for reform to visa regulations to allow physicians who are immigrants to travel to areas where they are most needed during the pandemic, for extensions of visa deadlines, and exemption from future immigration bans or limitations. These measures would only bolster the health care workforce that is under such strain during the pandemic, they write. (J Hosp Med. 2020 Aug;15[8]:505-506)
Dr. Malik said that, even while under added personal strain caused by the uncertainty of the past several months, he has never questioned his decision to be a physician in the United States.
“Now, more than ever, there is a sense of purpose and a passion to make a difference for our patients,” he said.
“I think most of us get into medicine and become hospitalists because we want to care for people, because we want to serve, because we want to be able to take care of sick, hospitalized patients, and that can be anywhere in the world, whether you’re in India serving a population that you grew up with or whether you’re in the U.S. serving the population that are your neighbors, your friends, your community, or people that are vulnerable. You’re serving humanity, and that is the ultimate goal.”
SHM advocacy on immigration issues
SHM has been advocating for more equitable skilled-immigration system, recognizing that from visa-backlogs to per-country caps, unfair visa restrictions have limited the United States’ ability to adequately expand its health care workforce.
The Society has consistently advocated on Capitol Hill for visa and skilled-immigration reform and has championed several significant immigration bills, including the following:
The Fairness for High Skilled Immigrants Act
- This legislation will eliminate per-country caps on green cards and convert the system into a “first-come, first-serve” system. This will help ensure certain nationalize are not disproportionally impacted by excessive green card backlogs.
- This legislation has passed the House of Representatives. Send a message to your Senator asking them to cosponsor this legislation.
The Conrad State 30 Physician Reauthorization Act
- This legislation will renew the Conrad State 30 program, which allows physicians on a J-1 visa to remain in the United States if they work in an underserved region for a minimum of three years. This legislation also included additional employment protection claims.
The Healthcare Workforce Resilience Act
- This legislation will recapture 40,000 unused immigrant visas for foreign doctors (15,000) and nurses (25,000), as well as provide visas for their spouse and children.
- This legislation will only be in effect for the duration of the COVID-19 public health emergency.
To join SHM in supporting our immigrant clinicians, you can send a message to your representatives in support of these bills by visiting hospitalmedicine.org/takeaction.
Schools can reopen safely with precautions, experts say
The absence of in-person school has harmed children in ways beyond loss of academic learning, according to Josh Sharfstein, MD, vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health, Baltimore. In addition to learning, school is a place where many children receive breakfast and lunch every day, as well as support services and the benefits of being in a safe and secure environment, Dr. Sharfstein said in a press briefing sponsored by Johns Hopkins University.
However, although it is an important priority for children to return to school, “we are in the midst of a pandemic that poses real risk,” he said.
In the press briefing, several experts shared ideas and considerations for safely reopening K-12 schools in the fall of 2020.
Data from other countries where schools have reopened, notably Austria and Denmark, have been reassuring about the lack of transmission of SARS-CoV-2 among children in a school setting, said Jennifer Nuzzo, DrPH, an epidemiologist at the Johns Hopkins Center for Health Security. However, other countries where schools have reopened successfully have reported low levels of viral transmission locally, and a responsible strategy for school reopening in the United States should follow a similar plan, she said. In areas where transmission and infection rates are increasing “it may not be safe to reopen,” but in areas where rates are declining or stable, schools could potentially reopen if they follow safety measures.
Dr. Nuzzo suggested that Considerations include protocols for handwashing and sanitation, and maintaining physical distance by creative use of outdoor classrooms (weather permitting) or other spaces within school buildings. Transportation to and from school also will be an issue to address, she noted.
None of the strategies being considered will completely eliminate risk of SARS-CoV-2 infection in school settings, so allowing parents and students to opt out and choose distance learning will be important as well, said Dr. Nuzzo. In addition, schools may need to consider alternative roles for teachers and staff who don’t feel comfortable being in contact with students and fellow staff members. “All of these things are going to be hard,” Dr. Nuzzo acknowledged. “Hard should not be a deterrent,” to reopening schools, but “we acknowledge the resources that schools will need in order to do this.”
At present, all 50 states and the District of Columbia have released some type of plan for reopening schools, said Megan Collins, MD, MPH, codirector the Johns Hopkins Consortium for School-Based Health Solutions.
Dr. Collins and colleagues have developed a school reopening tracker, which is “a national snapshot of current reopening plans that have been released,” she said. The tracker is being updated continuously as plans evolve. The eSchool+ K-12 School Reopening Tracker identifies 12 reopening categories that states could potentially address in the plans. These categories are divided into Operational and Ethics/Equity. The operational categories include:
- Core academics
- SARS-CoV-2 protection
- Before and after school programs
- School access and transportation
- Student health services
- Food and nutrition.
Ethics/equity categories include the following:
- Parent choice
- Teacher and staff choice
- Children of poverty and systemic disadvantage
- Children with special needs/English as second language/gifted and twice exceptional
- Privacy
- Engagement and transparency.
As of July 15, 2020, 16 states (Arizona, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, North Carolina, North Dakota, Ohio, Rhode Island, Tennessee, Texas, Virginia, Washington, and Wisconsin) had addressed all 12 categories in their reopening plans, Dr. Collins said.
School reopening plans must take equity issues into account, said Annette Anderson, PhD, of the Johns Hopkins University School of Education.
Specifically, developing learning plans for special education students and others at the most risk for learning loss will be essential. “The digital divide has become a digital canyon” in some areas, Dr. Anderson noted, and schools need to rethink eligibility and work to provide access to devices for online learning for all students.
In addition, schools need to convince parents that schools are safe. She recommended that schools consider inviting parents and families to visit buildings in advance of reopening so they can see the safety measures, such as space between desks, cleaning stations, and other protective strategies.
The message to pediatricians and health care professionals when counseling families about returning individual children to school is to consider the risk to the child and the family directly in the context of the local plans, Dr. Sharfstein said during a question and answer session. “One school system’s plan is one school system’s plan,” he said, and added that families who are concerned about the risk should have an online option. However, “if you see a thoughtful approach” to reopening, with safety steps taken and parents informed, with protocols such as keeping small groups of children together to reduce transmission, “it is a pretty good trade-off,” and that is why the American Academy of Pediatrics currently favors children returning to school, he said.
The briefing participants had no relevant financial conflicts to disclose.
The absence of in-person school has harmed children in ways beyond loss of academic learning, according to Josh Sharfstein, MD, vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health, Baltimore. In addition to learning, school is a place where many children receive breakfast and lunch every day, as well as support services and the benefits of being in a safe and secure environment, Dr. Sharfstein said in a press briefing sponsored by Johns Hopkins University.
However, although it is an important priority for children to return to school, “we are in the midst of a pandemic that poses real risk,” he said.
In the press briefing, several experts shared ideas and considerations for safely reopening K-12 schools in the fall of 2020.
Data from other countries where schools have reopened, notably Austria and Denmark, have been reassuring about the lack of transmission of SARS-CoV-2 among children in a school setting, said Jennifer Nuzzo, DrPH, an epidemiologist at the Johns Hopkins Center for Health Security. However, other countries where schools have reopened successfully have reported low levels of viral transmission locally, and a responsible strategy for school reopening in the United States should follow a similar plan, she said. In areas where transmission and infection rates are increasing “it may not be safe to reopen,” but in areas where rates are declining or stable, schools could potentially reopen if they follow safety measures.
Dr. Nuzzo suggested that Considerations include protocols for handwashing and sanitation, and maintaining physical distance by creative use of outdoor classrooms (weather permitting) or other spaces within school buildings. Transportation to and from school also will be an issue to address, she noted.
None of the strategies being considered will completely eliminate risk of SARS-CoV-2 infection in school settings, so allowing parents and students to opt out and choose distance learning will be important as well, said Dr. Nuzzo. In addition, schools may need to consider alternative roles for teachers and staff who don’t feel comfortable being in contact with students and fellow staff members. “All of these things are going to be hard,” Dr. Nuzzo acknowledged. “Hard should not be a deterrent,” to reopening schools, but “we acknowledge the resources that schools will need in order to do this.”
At present, all 50 states and the District of Columbia have released some type of plan for reopening schools, said Megan Collins, MD, MPH, codirector the Johns Hopkins Consortium for School-Based Health Solutions.
Dr. Collins and colleagues have developed a school reopening tracker, which is “a national snapshot of current reopening plans that have been released,” she said. The tracker is being updated continuously as plans evolve. The eSchool+ K-12 School Reopening Tracker identifies 12 reopening categories that states could potentially address in the plans. These categories are divided into Operational and Ethics/Equity. The operational categories include:
- Core academics
- SARS-CoV-2 protection
- Before and after school programs
- School access and transportation
- Student health services
- Food and nutrition.
Ethics/equity categories include the following:
- Parent choice
- Teacher and staff choice
- Children of poverty and systemic disadvantage
- Children with special needs/English as second language/gifted and twice exceptional
- Privacy
- Engagement and transparency.
As of July 15, 2020, 16 states (Arizona, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, North Carolina, North Dakota, Ohio, Rhode Island, Tennessee, Texas, Virginia, Washington, and Wisconsin) had addressed all 12 categories in their reopening plans, Dr. Collins said.
School reopening plans must take equity issues into account, said Annette Anderson, PhD, of the Johns Hopkins University School of Education.
Specifically, developing learning plans for special education students and others at the most risk for learning loss will be essential. “The digital divide has become a digital canyon” in some areas, Dr. Anderson noted, and schools need to rethink eligibility and work to provide access to devices for online learning for all students.
In addition, schools need to convince parents that schools are safe. She recommended that schools consider inviting parents and families to visit buildings in advance of reopening so they can see the safety measures, such as space between desks, cleaning stations, and other protective strategies.
The message to pediatricians and health care professionals when counseling families about returning individual children to school is to consider the risk to the child and the family directly in the context of the local plans, Dr. Sharfstein said during a question and answer session. “One school system’s plan is one school system’s plan,” he said, and added that families who are concerned about the risk should have an online option. However, “if you see a thoughtful approach” to reopening, with safety steps taken and parents informed, with protocols such as keeping small groups of children together to reduce transmission, “it is a pretty good trade-off,” and that is why the American Academy of Pediatrics currently favors children returning to school, he said.
The briefing participants had no relevant financial conflicts to disclose.
The absence of in-person school has harmed children in ways beyond loss of academic learning, according to Josh Sharfstein, MD, vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health, Baltimore. In addition to learning, school is a place where many children receive breakfast and lunch every day, as well as support services and the benefits of being in a safe and secure environment, Dr. Sharfstein said in a press briefing sponsored by Johns Hopkins University.
However, although it is an important priority for children to return to school, “we are in the midst of a pandemic that poses real risk,” he said.
In the press briefing, several experts shared ideas and considerations for safely reopening K-12 schools in the fall of 2020.
Data from other countries where schools have reopened, notably Austria and Denmark, have been reassuring about the lack of transmission of SARS-CoV-2 among children in a school setting, said Jennifer Nuzzo, DrPH, an epidemiologist at the Johns Hopkins Center for Health Security. However, other countries where schools have reopened successfully have reported low levels of viral transmission locally, and a responsible strategy for school reopening in the United States should follow a similar plan, she said. In areas where transmission and infection rates are increasing “it may not be safe to reopen,” but in areas where rates are declining or stable, schools could potentially reopen if they follow safety measures.
Dr. Nuzzo suggested that Considerations include protocols for handwashing and sanitation, and maintaining physical distance by creative use of outdoor classrooms (weather permitting) or other spaces within school buildings. Transportation to and from school also will be an issue to address, she noted.
None of the strategies being considered will completely eliminate risk of SARS-CoV-2 infection in school settings, so allowing parents and students to opt out and choose distance learning will be important as well, said Dr. Nuzzo. In addition, schools may need to consider alternative roles for teachers and staff who don’t feel comfortable being in contact with students and fellow staff members. “All of these things are going to be hard,” Dr. Nuzzo acknowledged. “Hard should not be a deterrent,” to reopening schools, but “we acknowledge the resources that schools will need in order to do this.”
At present, all 50 states and the District of Columbia have released some type of plan for reopening schools, said Megan Collins, MD, MPH, codirector the Johns Hopkins Consortium for School-Based Health Solutions.
Dr. Collins and colleagues have developed a school reopening tracker, which is “a national snapshot of current reopening plans that have been released,” she said. The tracker is being updated continuously as plans evolve. The eSchool+ K-12 School Reopening Tracker identifies 12 reopening categories that states could potentially address in the plans. These categories are divided into Operational and Ethics/Equity. The operational categories include:
- Core academics
- SARS-CoV-2 protection
- Before and after school programs
- School access and transportation
- Student health services
- Food and nutrition.
Ethics/equity categories include the following:
- Parent choice
- Teacher and staff choice
- Children of poverty and systemic disadvantage
- Children with special needs/English as second language/gifted and twice exceptional
- Privacy
- Engagement and transparency.
As of July 15, 2020, 16 states (Arizona, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, North Carolina, North Dakota, Ohio, Rhode Island, Tennessee, Texas, Virginia, Washington, and Wisconsin) had addressed all 12 categories in their reopening plans, Dr. Collins said.
School reopening plans must take equity issues into account, said Annette Anderson, PhD, of the Johns Hopkins University School of Education.
Specifically, developing learning plans for special education students and others at the most risk for learning loss will be essential. “The digital divide has become a digital canyon” in some areas, Dr. Anderson noted, and schools need to rethink eligibility and work to provide access to devices for online learning for all students.
In addition, schools need to convince parents that schools are safe. She recommended that schools consider inviting parents and families to visit buildings in advance of reopening so they can see the safety measures, such as space between desks, cleaning stations, and other protective strategies.
The message to pediatricians and health care professionals when counseling families about returning individual children to school is to consider the risk to the child and the family directly in the context of the local plans, Dr. Sharfstein said during a question and answer session. “One school system’s plan is one school system’s plan,” he said, and added that families who are concerned about the risk should have an online option. However, “if you see a thoughtful approach” to reopening, with safety steps taken and parents informed, with protocols such as keeping small groups of children together to reduce transmission, “it is a pretty good trade-off,” and that is why the American Academy of Pediatrics currently favors children returning to school, he said.
The briefing participants had no relevant financial conflicts to disclose.
COVID-19: Medicare data show long hospital stays, disparities
according to a new analysis by the Centers for Medicare & Medicaid Services.
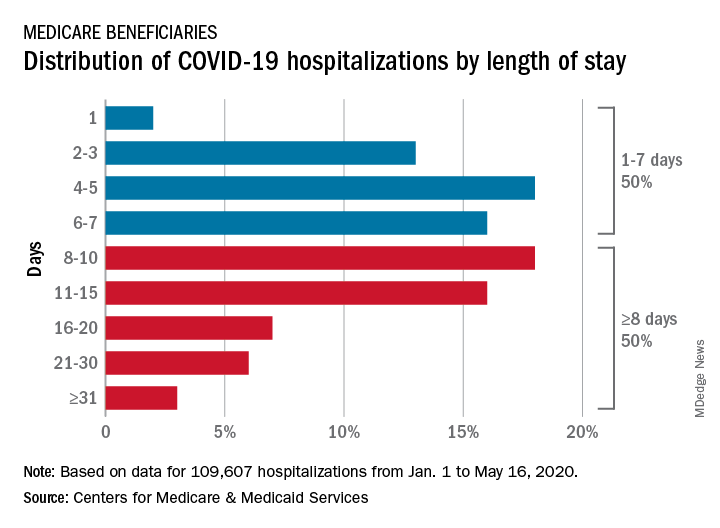
CMS encounter and claims data show almost 110,000 hospital stays for COVID-19 from Jan. 1 to May 16, 2020. Of the longer admissions, 18% were 8-10 days, 16% were 11-15 days, and another 16% were 16 days or longer, the CMS reported in a preliminary data snapshot released June 22.
The hospitalization rate for the Medicare population was 175 per 100,000 as of May 16, but the CMS data show a number of disparities involving race/ethnicity and other demographic characteristics were uncovered, such as the following:
- Black patients were hospitalized for COVID-19 at a much higher rate, at 465 per 100,000 beneficiaries, than were Hispanics (258), Asians (187), and whites (123).
- Residents of urban/suburban areas had a much higher hospitalization rate than did those living in rural areas: 205 versus 57 per 100,000.
- Beneficiaries enrolled in both Medicare and Medicaid had 473 hospitalizations per 100,000, but the rate for those with Medicare only was 112.
“The disparities in the data reflect longstanding challenges facing minority communities and low-income older adults, many of whom face structural challenges to their health that go far beyond what is traditionally considered ‘medical,’ ” CMS Administrator Seema Verma said in a separate statement.
according to a new analysis by the Centers for Medicare & Medicaid Services.
CMS encounter and claims data show almost 110,000 hospital stays for COVID-19 from Jan. 1 to May 16, 2020. Of the longer admissions, 18% were 8-10 days, 16% were 11-15 days, and another 16% were 16 days or longer, the CMS reported in a preliminary data snapshot released June 22.
The hospitalization rate for the Medicare population was 175 per 100,000 as of May 16, but the CMS data show a number of disparities involving race/ethnicity and other demographic characteristics were uncovered, such as the following:
- Black patients were hospitalized for COVID-19 at a much higher rate, at 465 per 100,000 beneficiaries, than were Hispanics (258), Asians (187), and whites (123).
- Residents of urban/suburban areas had a much higher hospitalization rate than did those living in rural areas: 205 versus 57 per 100,000.
- Beneficiaries enrolled in both Medicare and Medicaid had 473 hospitalizations per 100,000, but the rate for those with Medicare only was 112.
“The disparities in the data reflect longstanding challenges facing minority communities and low-income older adults, many of whom face structural challenges to their health that go far beyond what is traditionally considered ‘medical,’ ” CMS Administrator Seema Verma said in a separate statement.
according to a new analysis by the Centers for Medicare & Medicaid Services.
CMS encounter and claims data show almost 110,000 hospital stays for COVID-19 from Jan. 1 to May 16, 2020. Of the longer admissions, 18% were 8-10 days, 16% were 11-15 days, and another 16% were 16 days or longer, the CMS reported in a preliminary data snapshot released June 22.
The hospitalization rate for the Medicare population was 175 per 100,000 as of May 16, but the CMS data show a number of disparities involving race/ethnicity and other demographic characteristics were uncovered, such as the following:
- Black patients were hospitalized for COVID-19 at a much higher rate, at 465 per 100,000 beneficiaries, than were Hispanics (258), Asians (187), and whites (123).
- Residents of urban/suburban areas had a much higher hospitalization rate than did those living in rural areas: 205 versus 57 per 100,000.
- Beneficiaries enrolled in both Medicare and Medicaid had 473 hospitalizations per 100,000, but the rate for those with Medicare only was 112.
“The disparities in the data reflect longstanding challenges facing minority communities and low-income older adults, many of whom face structural challenges to their health that go far beyond what is traditionally considered ‘medical,’ ” CMS Administrator Seema Verma said in a separate statement.