User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Study Suggests Inappropriate Use of Thyroid Ultrasounds
“The number of thyroid ultrasounds performed in the United States has increased fivefold since 2002. This substantial increase produces a significant strain on healthcare resources and leads to over-detection and overtreatment of benign thyroid nodules and small, indolent cancers with questionable clinical relevance,” wrote Elena Kennedy, MD, then a medical student in the department of surgery at the University of Wisconsin School of Medicine and Public Health, Madison, and colleagues.
The data, published online in Thyroid, come from a retrospective chart analysis of more than 1700 people who underwent dedicated (ie, specifically to look for a nodule) thyroid ultrasounds at a tertiary academic center. The rates of detecting both nodules and biopsy-recommended nodules were highest when the indication was a nodule seen incidentally on other imaging (aka “incidentaloma”) and lowest when the ultrasound was ordered because the patient had either metabolic or compressive symptoms.
And for the most commonly listed indication, a suspected palpable nodule, nearly half of the ultrasounds found no nodule, and only one in five detected a nodule that warranted a biopsy.
The principal investigator of the study David O. Francis, MD, an otolaryngologist at the University of Wisconsin, Madison, said in an interview, “Thyroid cancer has grown in incidence three to four times over the last 30 years without a good explanation for why…It seems to be that we’re detecting smaller and smaller nodules…Why are people being referred for all these ultrasounds? We looked for the upstream factors.”
One clear clinical implication of the new data, Dr. Francis noted, is that “if someone has compressive symptoms including dysphagia, swallowing problems, voice change, or globus sensation, ultrasound should not be the first way to work them up…It would be smarter to have someone evaluate their voice or their swallowing to see if there’s another reason besides the thyroid. The thyroid would have to get pretty big to cause dysphagia or swallowing problems.”
No Current Guidelines Advise When not to Order a Thyroid Ultrasound
Problematically, while there are professional society guidelines for what to do when a thyroid “incidentaloma” is found and other specific situations, there are no overall guidelines addressing when it’s appropriate to order a thyroid ultrasound, Dr. Kennedy, now an otolaryngology resident at the Indiana University of Indianapolis, and colleagues, point out.
According to Dr. Francis, “Ultrasounds are low cost and low risk. Those two factors result in people ordering more tests…The problem with that is we find things, and then we have to figure out what to do with them. That leads to incidentalomas, the surveillance, worry and anxiety, and costs…It’s tricky. We don’t want to discourage people from ever ordering ultrasounds, but there need to be some guidelines around when it’s appropriate to order.”
Asked to comment, Trevor E. Angell, MD, associate medical director of Thyroid Center at Keck School of Medicine of the University of Southern California, Los Angeles, said that the study is “clinically very important.”
Dr. Angell pointed out that the current American Thyroid Association (ATA) guidelines on thyroid nodule management, of which he is an author, recommend ultrasound for a known or suspected nodule. But he added, “there certainly should be a message that obtaining ultrasound for these other reasons are less likely to identify a nodule or anything causative. Whether it’s gastroesophageal reflux or allergic rhinitis or vocal cord dysfunction, an ultrasound isn’t a good test for those either.”
Dr. Angell said that the next ATA thyroid nodule guidelines, expected out in 2024, will address this topic more fully, but he couldn’t provide more specific information because the document is still in development. He did say, however, “Addressing when not to do an ultrasound will be an important consideration in the next guidelines.”
Low Detection Rates for Most Indications
The retrospective observational cohort study included 1739 adults (76% women; mean age, 53 years) who underwent dedicated thyroid ultrasounds between 2017 and 2019. In most cases, the recommendation for biopsy was determined using the American College of Radiology TI-RADS system, based on nodule size and TI-RADS category.
The most common indication for thyroid ultrasound, suspected palpable nodule, accounted for 40% of those performed. Follow-up for an “incidentaloma” was the indication in 28% of patients, and referral for compressive and metabolic symptoms accounted for 13% and 6% of ultrasounds, respectively.
Among all ultrasounds performed, 62% identified a thyroid nodule. Patients referred for incidental findings had the highest percentage of ultrasounds with thyroid nodules present at 94%. By contrast, in those referred for suspected palpable nodule on exam and for compressive symptoms, nodules were identified on 55% and 39% of ultrasounds, respectively. Patients with metabolic symptoms had a nodule identified on ultrasound 43% of the time. Among those referred for high risk factors, 57% had a nodule present.
Overall, only 27% of ultrasounds identified a thyroid nodule that was recommended for a biopsy. Again, those referred because of an incidental imaging finding had the highest percentage (55%), followed by those referred for a suspected palpable nodule (21%), high risk factors (20%), combined indications (16%), metabolic symptoms (10%), and compressive symptoms (6%).
Mean nodule size was largest among the patients referred for incidentalomas (2.4 cm), whereas all the other groups had mean nodule sizes between 1.2 cm and 1.8 cm, a significant difference (P < .05). The median size of nodules among those referred to ultrasound for a suspected palpable nodule was 1.4 cm.
“That’s pretty small. It would have had to be in the front of the thyroid where they could actually touch it. I would argue that the number of clinicians who actually palpated something was smaller. We’ve done several projects looking at how small a nodule a clinician can actually feel in the thyroid gland from the neck. It turns out we’re pretty bad at physical examination of the thyroid. This paper kind of reinforces that,” Dr. Francis said in an interview.
Patients with incidental nodules were over 10 times more likely to have a nodule found on an ultrasound than those referred for a suspected palpable nodule on exam (odds ratio [OR], 10.6). Conversely, those referred for compressive symptoms were half as likely to have an identifiable nodule compared with those referred for physical exam findings (OR, 0.5).
The odds of finding a nodule increased with age, especially for those aged ≥ 65 years compared with those younger than 45 years (OR, 3.6). Women were twice as likely to have a nodule found on thyroid ultrasound (OR, 2.0). Results were similar for the biopsy-recommended nodules, except that there was no difference between sexes (female vs male OR, 1.2).
Dr. Angell called the study “a very robust comprehensive evaluation,” but also noted that the single center source is a limitation. “It would be nice to have those big databases of national healthcare settings, but getting that granular level of information about why something was done is nearly impossible in that context.”
Dr. Kennedy, Dr. Francis, and Dr. Angell have no disclosures.
A version of this article appeared on Medscape.com.
“The number of thyroid ultrasounds performed in the United States has increased fivefold since 2002. This substantial increase produces a significant strain on healthcare resources and leads to over-detection and overtreatment of benign thyroid nodules and small, indolent cancers with questionable clinical relevance,” wrote Elena Kennedy, MD, then a medical student in the department of surgery at the University of Wisconsin School of Medicine and Public Health, Madison, and colleagues.
The data, published online in Thyroid, come from a retrospective chart analysis of more than 1700 people who underwent dedicated (ie, specifically to look for a nodule) thyroid ultrasounds at a tertiary academic center. The rates of detecting both nodules and biopsy-recommended nodules were highest when the indication was a nodule seen incidentally on other imaging (aka “incidentaloma”) and lowest when the ultrasound was ordered because the patient had either metabolic or compressive symptoms.
And for the most commonly listed indication, a suspected palpable nodule, nearly half of the ultrasounds found no nodule, and only one in five detected a nodule that warranted a biopsy.
The principal investigator of the study David O. Francis, MD, an otolaryngologist at the University of Wisconsin, Madison, said in an interview, “Thyroid cancer has grown in incidence three to four times over the last 30 years without a good explanation for why…It seems to be that we’re detecting smaller and smaller nodules…Why are people being referred for all these ultrasounds? We looked for the upstream factors.”
One clear clinical implication of the new data, Dr. Francis noted, is that “if someone has compressive symptoms including dysphagia, swallowing problems, voice change, or globus sensation, ultrasound should not be the first way to work them up…It would be smarter to have someone evaluate their voice or their swallowing to see if there’s another reason besides the thyroid. The thyroid would have to get pretty big to cause dysphagia or swallowing problems.”
No Current Guidelines Advise When not to Order a Thyroid Ultrasound
Problematically, while there are professional society guidelines for what to do when a thyroid “incidentaloma” is found and other specific situations, there are no overall guidelines addressing when it’s appropriate to order a thyroid ultrasound, Dr. Kennedy, now an otolaryngology resident at the Indiana University of Indianapolis, and colleagues, point out.
According to Dr. Francis, “Ultrasounds are low cost and low risk. Those two factors result in people ordering more tests…The problem with that is we find things, and then we have to figure out what to do with them. That leads to incidentalomas, the surveillance, worry and anxiety, and costs…It’s tricky. We don’t want to discourage people from ever ordering ultrasounds, but there need to be some guidelines around when it’s appropriate to order.”
Asked to comment, Trevor E. Angell, MD, associate medical director of Thyroid Center at Keck School of Medicine of the University of Southern California, Los Angeles, said that the study is “clinically very important.”
Dr. Angell pointed out that the current American Thyroid Association (ATA) guidelines on thyroid nodule management, of which he is an author, recommend ultrasound for a known or suspected nodule. But he added, “there certainly should be a message that obtaining ultrasound for these other reasons are less likely to identify a nodule or anything causative. Whether it’s gastroesophageal reflux or allergic rhinitis or vocal cord dysfunction, an ultrasound isn’t a good test for those either.”
Dr. Angell said that the next ATA thyroid nodule guidelines, expected out in 2024, will address this topic more fully, but he couldn’t provide more specific information because the document is still in development. He did say, however, “Addressing when not to do an ultrasound will be an important consideration in the next guidelines.”
Low Detection Rates for Most Indications
The retrospective observational cohort study included 1739 adults (76% women; mean age, 53 years) who underwent dedicated thyroid ultrasounds between 2017 and 2019. In most cases, the recommendation for biopsy was determined using the American College of Radiology TI-RADS system, based on nodule size and TI-RADS category.
The most common indication for thyroid ultrasound, suspected palpable nodule, accounted for 40% of those performed. Follow-up for an “incidentaloma” was the indication in 28% of patients, and referral for compressive and metabolic symptoms accounted for 13% and 6% of ultrasounds, respectively.
Among all ultrasounds performed, 62% identified a thyroid nodule. Patients referred for incidental findings had the highest percentage of ultrasounds with thyroid nodules present at 94%. By contrast, in those referred for suspected palpable nodule on exam and for compressive symptoms, nodules were identified on 55% and 39% of ultrasounds, respectively. Patients with metabolic symptoms had a nodule identified on ultrasound 43% of the time. Among those referred for high risk factors, 57% had a nodule present.
Overall, only 27% of ultrasounds identified a thyroid nodule that was recommended for a biopsy. Again, those referred because of an incidental imaging finding had the highest percentage (55%), followed by those referred for a suspected palpable nodule (21%), high risk factors (20%), combined indications (16%), metabolic symptoms (10%), and compressive symptoms (6%).
Mean nodule size was largest among the patients referred for incidentalomas (2.4 cm), whereas all the other groups had mean nodule sizes between 1.2 cm and 1.8 cm, a significant difference (P < .05). The median size of nodules among those referred to ultrasound for a suspected palpable nodule was 1.4 cm.
“That’s pretty small. It would have had to be in the front of the thyroid where they could actually touch it. I would argue that the number of clinicians who actually palpated something was smaller. We’ve done several projects looking at how small a nodule a clinician can actually feel in the thyroid gland from the neck. It turns out we’re pretty bad at physical examination of the thyroid. This paper kind of reinforces that,” Dr. Francis said in an interview.
Patients with incidental nodules were over 10 times more likely to have a nodule found on an ultrasound than those referred for a suspected palpable nodule on exam (odds ratio [OR], 10.6). Conversely, those referred for compressive symptoms were half as likely to have an identifiable nodule compared with those referred for physical exam findings (OR, 0.5).
The odds of finding a nodule increased with age, especially for those aged ≥ 65 years compared with those younger than 45 years (OR, 3.6). Women were twice as likely to have a nodule found on thyroid ultrasound (OR, 2.0). Results were similar for the biopsy-recommended nodules, except that there was no difference between sexes (female vs male OR, 1.2).
Dr. Angell called the study “a very robust comprehensive evaluation,” but also noted that the single center source is a limitation. “It would be nice to have those big databases of national healthcare settings, but getting that granular level of information about why something was done is nearly impossible in that context.”
Dr. Kennedy, Dr. Francis, and Dr. Angell have no disclosures.
A version of this article appeared on Medscape.com.
“The number of thyroid ultrasounds performed in the United States has increased fivefold since 2002. This substantial increase produces a significant strain on healthcare resources and leads to over-detection and overtreatment of benign thyroid nodules and small, indolent cancers with questionable clinical relevance,” wrote Elena Kennedy, MD, then a medical student in the department of surgery at the University of Wisconsin School of Medicine and Public Health, Madison, and colleagues.
The data, published online in Thyroid, come from a retrospective chart analysis of more than 1700 people who underwent dedicated (ie, specifically to look for a nodule) thyroid ultrasounds at a tertiary academic center. The rates of detecting both nodules and biopsy-recommended nodules were highest when the indication was a nodule seen incidentally on other imaging (aka “incidentaloma”) and lowest when the ultrasound was ordered because the patient had either metabolic or compressive symptoms.
And for the most commonly listed indication, a suspected palpable nodule, nearly half of the ultrasounds found no nodule, and only one in five detected a nodule that warranted a biopsy.
The principal investigator of the study David O. Francis, MD, an otolaryngologist at the University of Wisconsin, Madison, said in an interview, “Thyroid cancer has grown in incidence three to four times over the last 30 years without a good explanation for why…It seems to be that we’re detecting smaller and smaller nodules…Why are people being referred for all these ultrasounds? We looked for the upstream factors.”
One clear clinical implication of the new data, Dr. Francis noted, is that “if someone has compressive symptoms including dysphagia, swallowing problems, voice change, or globus sensation, ultrasound should not be the first way to work them up…It would be smarter to have someone evaluate their voice or their swallowing to see if there’s another reason besides the thyroid. The thyroid would have to get pretty big to cause dysphagia or swallowing problems.”
No Current Guidelines Advise When not to Order a Thyroid Ultrasound
Problematically, while there are professional society guidelines for what to do when a thyroid “incidentaloma” is found and other specific situations, there are no overall guidelines addressing when it’s appropriate to order a thyroid ultrasound, Dr. Kennedy, now an otolaryngology resident at the Indiana University of Indianapolis, and colleagues, point out.
According to Dr. Francis, “Ultrasounds are low cost and low risk. Those two factors result in people ordering more tests…The problem with that is we find things, and then we have to figure out what to do with them. That leads to incidentalomas, the surveillance, worry and anxiety, and costs…It’s tricky. We don’t want to discourage people from ever ordering ultrasounds, but there need to be some guidelines around when it’s appropriate to order.”
Asked to comment, Trevor E. Angell, MD, associate medical director of Thyroid Center at Keck School of Medicine of the University of Southern California, Los Angeles, said that the study is “clinically very important.”
Dr. Angell pointed out that the current American Thyroid Association (ATA) guidelines on thyroid nodule management, of which he is an author, recommend ultrasound for a known or suspected nodule. But he added, “there certainly should be a message that obtaining ultrasound for these other reasons are less likely to identify a nodule or anything causative. Whether it’s gastroesophageal reflux or allergic rhinitis or vocal cord dysfunction, an ultrasound isn’t a good test for those either.”
Dr. Angell said that the next ATA thyroid nodule guidelines, expected out in 2024, will address this topic more fully, but he couldn’t provide more specific information because the document is still in development. He did say, however, “Addressing when not to do an ultrasound will be an important consideration in the next guidelines.”
Low Detection Rates for Most Indications
The retrospective observational cohort study included 1739 adults (76% women; mean age, 53 years) who underwent dedicated thyroid ultrasounds between 2017 and 2019. In most cases, the recommendation for biopsy was determined using the American College of Radiology TI-RADS system, based on nodule size and TI-RADS category.
The most common indication for thyroid ultrasound, suspected palpable nodule, accounted for 40% of those performed. Follow-up for an “incidentaloma” was the indication in 28% of patients, and referral for compressive and metabolic symptoms accounted for 13% and 6% of ultrasounds, respectively.
Among all ultrasounds performed, 62% identified a thyroid nodule. Patients referred for incidental findings had the highest percentage of ultrasounds with thyroid nodules present at 94%. By contrast, in those referred for suspected palpable nodule on exam and for compressive symptoms, nodules were identified on 55% and 39% of ultrasounds, respectively. Patients with metabolic symptoms had a nodule identified on ultrasound 43% of the time. Among those referred for high risk factors, 57% had a nodule present.
Overall, only 27% of ultrasounds identified a thyroid nodule that was recommended for a biopsy. Again, those referred because of an incidental imaging finding had the highest percentage (55%), followed by those referred for a suspected palpable nodule (21%), high risk factors (20%), combined indications (16%), metabolic symptoms (10%), and compressive symptoms (6%).
Mean nodule size was largest among the patients referred for incidentalomas (2.4 cm), whereas all the other groups had mean nodule sizes between 1.2 cm and 1.8 cm, a significant difference (P < .05). The median size of nodules among those referred to ultrasound for a suspected palpable nodule was 1.4 cm.
“That’s pretty small. It would have had to be in the front of the thyroid where they could actually touch it. I would argue that the number of clinicians who actually palpated something was smaller. We’ve done several projects looking at how small a nodule a clinician can actually feel in the thyroid gland from the neck. It turns out we’re pretty bad at physical examination of the thyroid. This paper kind of reinforces that,” Dr. Francis said in an interview.
Patients with incidental nodules were over 10 times more likely to have a nodule found on an ultrasound than those referred for a suspected palpable nodule on exam (odds ratio [OR], 10.6). Conversely, those referred for compressive symptoms were half as likely to have an identifiable nodule compared with those referred for physical exam findings (OR, 0.5).
The odds of finding a nodule increased with age, especially for those aged ≥ 65 years compared with those younger than 45 years (OR, 3.6). Women were twice as likely to have a nodule found on thyroid ultrasound (OR, 2.0). Results were similar for the biopsy-recommended nodules, except that there was no difference between sexes (female vs male OR, 1.2).
Dr. Angell called the study “a very robust comprehensive evaluation,” but also noted that the single center source is a limitation. “It would be nice to have those big databases of national healthcare settings, but getting that granular level of information about why something was done is nearly impossible in that context.”
Dr. Kennedy, Dr. Francis, and Dr. Angell have no disclosures.
A version of this article appeared on Medscape.com.
FROM THYROID
GLP-1s Face Off Against Each Other, Weight-Loss Surgery in New GI Studies
VANCOUVER — Glucagon-like peptide-1 (GLP-1) agonists, like semaglutide, liraglutide, and the newly US Food and Drug Administration–approved tirzepatide, not only are gaining popularity among the public for weight loss but also are the focus of considerable attention from gastroenterology researchers.
how they compare to bariatric surgery for weight loss or prevention of metabolic dysfunction–associated steatotic liver disease, and their potential role to prevent regain after weight-loss surgery.
Head-to-Head Comparison
Tirzepatide 15 mg emerged as superior to other GLP-1 agonists for weight loss, for example, in a network meta-analysis of randomized controlled trials looking into obesity management.
Tirzepatide 15 mg was associated with the most effective mean weight loss at just over 15% when Jena Velji-Ibrahim, MD, and colleagues combined data from 14 studies with 18,714 participants with overweight or obesity but without diabetes.
Next up in order of weight-loss efficacy was tirzepatide 10 mg with 13% mean weight loss, semaglutide 2.4 mg with just over 11% mean weight loss, and tirzepatide 5 mg with almost 10% mean weight loss. The only outlier was dulaglutide 0.75 mg, which was linked to about 8% weight gain.
“While clinical trials have been conducted to assess the weight-loss efficacy of GLP-1 agonists, there has been limited head-to-head comparisons, and the data that has been obtained has been quite inconsistent,” Dr. Velji-Ibrahim said when presenting results at the meeting.
Researchers found little difference in efficacies between tirzepatide 15 mg and 10 mg, suggesting both are a viable option for weight loss, said Dr. Velji-Ibrahim of Prisma Health Greenville Memorial Hospital and University of South Carolina School of Medicine in Greenville.
She also reported similar efficacies between oral semaglutide 50 mg and subcutaneous semaglutide 2.4 mg, “meaning that we have another option for weight management.”
Side effects among the different GLP-1 agonists, and among the same agent at different doses, were not significantly different.
Comparison With Bariatric Surgery for Reducing Major Adverse Cardiovascular Events (MACE)
For many years, bariatric surgeons have pointed to the health benefits of weight-loss surgery in the right candidates, including a reduced risk for adverse cardiovascular events.
The weight loss associated with GLP-1 agonists has likewise shown benefits in reducing MACE. However, it remains unclear if one of these weight-loss strategies is better than the other in reducing these outcomes.
To determine this, researchers compared 118,828 people who had bariatric surgery to another propensity-matched group of 118,828 others prescribed GLP-1 agonists. They included adults with a body mass index (BMI) of 35 or higher in the national TriNetX database.
The multicenter, retrospective study revealed bariatric surgery was superior in reducing the risk for heart failure, MACE, and cerebrovascular disease at 3, 5, 7, and 10 years. At 10 years, for example, bariatric surgery was associated with 31% fewer composite cardiovascular events than the GLP-1 agonists.
“Our results suggest that bariatric surgery is more effective than GLP-1 analogs in preventing adverse cardiovascular events in obese patients,” Ayowumi A. Adekolu, MD, an internal medicine resident at West Virginia School of Medicine in Morgantown, said in audio comments accompanying his ePoster at the meeting. “Although these findings highlight the benefit of bariatric surgery in mitigating adverse cardiovascular events, well-designed prospective studies are necessary to confirm these benefits in this patient population.”
Possible Role in Fatty Liver Disease Prevention
In another large multicenter study from the same institution, Ethan M. Cohen, MD, along with co-author Dr. Adekolu and others, compared the effectiveness of bariatric surgery to GLP-1 agonists for preventing nonalcoholic fatty liver disease (NAFLD). Since the study was conducted, the official name of NAFLD has changed to metabolic dysfunction–associated steatotic liver disease.
Dr. Cohen and colleagues evaluated data from the TriNetX database and included adults with a BMI of 35 or higher. They propensity matched 124,022 people who had sleeve gastrectomy or Roux-en-Y gastric bypass to another 124,022 others prescribed GLP-1 agonists. Again, they looked at outcomes at 3, 5, 7, and 10 years.
They found bariatric surgery superior to GLP-1 agonists for reducing the risk of developing NAFLD. Relative risk reduction was 25% at 3 years, 28% at 5 years, 27% at 7 years, and 26% at 10 years.
Although not to the same extent as surgery in this study, GLP-1–associated weight loss did reduce risks as well.
“An important aspect of this is that for some of these people, bariatric surgery is not even an option,” Dr. Cohen said in an interview, citing as an example those who do not meet the criteria for surgery.
Dr. Cohen and colleagues plan to continue the study with a larger number of participants.
Real-World Weight Regain
In another instance where a surgical procedure trumped GLP-1 agonists, revisional endoscopic sleeve gastroplasty (ESG) offered significantly higher weight loss than GLP-1 agonists among people who regained weight following initial weight-loss surgery, according to a case-control real-world study presented at the meeting.
“Laparoscopic sleeve gastrectomy [LSG] is a frequently performed bariatric surgery worldwide resulting in significant weight loss and improvement in obesity-related comorbidities,” said Firas Bahdi, MD, gastroenterology fellow at the David Geffen School of Medicine at University of California, Los Angeles. “Despite its success, around one third of patients, unfortunately, develop weight regain warranting intervention.”
Dr. Bahdi and colleagues retrospectively studied 68 adults prescribed subcutaneous semaglutide or tirzepatide after LSG, another 20 who had ESG for weight regain after LSG, and 87 controls with intact stomachs who also took GLP-1 agonists for weight loss.
They found that the ESG group experienced a significantly higher percentage of total body weight loss at 3 months than the GLP-1 group (10% vs 4.3%, respectively; P = .0001). Similarly, at the 6-month follow-up, the ESG group experienced 11.5% total body weight loss compared to 6.8% in the GLP-1 group (P = .03).
The GLP-1 after LSG group still fared better than the GLP-1 control group of people who never had surgery. Total body weight loss was 4.3% vs 5.7% at 3 months (P = .02), 6.8% vs 9.2% at 6 months (P = .02), and 9.2% vs 12.7% at 12 months (P = .03).
“In this real-world experience, revisional ESG offers significantly more weight loss than GLP-1 agonists for patients with weight regain, while also avoiding the challenges of medication refills, making it an attractive option,” Dr. Bahdi said.
Future multicenter studies are warranted to confirm these results and explore physiological explanations, he added.
The study received an Outstanding Research Award in the Obesity Category (Trainee).
Dr. Velji-Ibrahim, Dr. Adekolu, Dr. Cohen, and Dr. Bahdi indicated no relevant financial relationships.
A version of this article appeared on Medscape.com.
VANCOUVER — Glucagon-like peptide-1 (GLP-1) agonists, like semaglutide, liraglutide, and the newly US Food and Drug Administration–approved tirzepatide, not only are gaining popularity among the public for weight loss but also are the focus of considerable attention from gastroenterology researchers.
how they compare to bariatric surgery for weight loss or prevention of metabolic dysfunction–associated steatotic liver disease, and their potential role to prevent regain after weight-loss surgery.
Head-to-Head Comparison
Tirzepatide 15 mg emerged as superior to other GLP-1 agonists for weight loss, for example, in a network meta-analysis of randomized controlled trials looking into obesity management.
Tirzepatide 15 mg was associated with the most effective mean weight loss at just over 15% when Jena Velji-Ibrahim, MD, and colleagues combined data from 14 studies with 18,714 participants with overweight or obesity but without diabetes.
Next up in order of weight-loss efficacy was tirzepatide 10 mg with 13% mean weight loss, semaglutide 2.4 mg with just over 11% mean weight loss, and tirzepatide 5 mg with almost 10% mean weight loss. The only outlier was dulaglutide 0.75 mg, which was linked to about 8% weight gain.
“While clinical trials have been conducted to assess the weight-loss efficacy of GLP-1 agonists, there has been limited head-to-head comparisons, and the data that has been obtained has been quite inconsistent,” Dr. Velji-Ibrahim said when presenting results at the meeting.
Researchers found little difference in efficacies between tirzepatide 15 mg and 10 mg, suggesting both are a viable option for weight loss, said Dr. Velji-Ibrahim of Prisma Health Greenville Memorial Hospital and University of South Carolina School of Medicine in Greenville.
She also reported similar efficacies between oral semaglutide 50 mg and subcutaneous semaglutide 2.4 mg, “meaning that we have another option for weight management.”
Side effects among the different GLP-1 agonists, and among the same agent at different doses, were not significantly different.
Comparison With Bariatric Surgery for Reducing Major Adverse Cardiovascular Events (MACE)
For many years, bariatric surgeons have pointed to the health benefits of weight-loss surgery in the right candidates, including a reduced risk for adverse cardiovascular events.
The weight loss associated with GLP-1 agonists has likewise shown benefits in reducing MACE. However, it remains unclear if one of these weight-loss strategies is better than the other in reducing these outcomes.
To determine this, researchers compared 118,828 people who had bariatric surgery to another propensity-matched group of 118,828 others prescribed GLP-1 agonists. They included adults with a body mass index (BMI) of 35 or higher in the national TriNetX database.
The multicenter, retrospective study revealed bariatric surgery was superior in reducing the risk for heart failure, MACE, and cerebrovascular disease at 3, 5, 7, and 10 years. At 10 years, for example, bariatric surgery was associated with 31% fewer composite cardiovascular events than the GLP-1 agonists.
“Our results suggest that bariatric surgery is more effective than GLP-1 analogs in preventing adverse cardiovascular events in obese patients,” Ayowumi A. Adekolu, MD, an internal medicine resident at West Virginia School of Medicine in Morgantown, said in audio comments accompanying his ePoster at the meeting. “Although these findings highlight the benefit of bariatric surgery in mitigating adverse cardiovascular events, well-designed prospective studies are necessary to confirm these benefits in this patient population.”
Possible Role in Fatty Liver Disease Prevention
In another large multicenter study from the same institution, Ethan M. Cohen, MD, along with co-author Dr. Adekolu and others, compared the effectiveness of bariatric surgery to GLP-1 agonists for preventing nonalcoholic fatty liver disease (NAFLD). Since the study was conducted, the official name of NAFLD has changed to metabolic dysfunction–associated steatotic liver disease.
Dr. Cohen and colleagues evaluated data from the TriNetX database and included adults with a BMI of 35 or higher. They propensity matched 124,022 people who had sleeve gastrectomy or Roux-en-Y gastric bypass to another 124,022 others prescribed GLP-1 agonists. Again, they looked at outcomes at 3, 5, 7, and 10 years.
They found bariatric surgery superior to GLP-1 agonists for reducing the risk of developing NAFLD. Relative risk reduction was 25% at 3 years, 28% at 5 years, 27% at 7 years, and 26% at 10 years.
Although not to the same extent as surgery in this study, GLP-1–associated weight loss did reduce risks as well.
“An important aspect of this is that for some of these people, bariatric surgery is not even an option,” Dr. Cohen said in an interview, citing as an example those who do not meet the criteria for surgery.
Dr. Cohen and colleagues plan to continue the study with a larger number of participants.
Real-World Weight Regain
In another instance where a surgical procedure trumped GLP-1 agonists, revisional endoscopic sleeve gastroplasty (ESG) offered significantly higher weight loss than GLP-1 agonists among people who regained weight following initial weight-loss surgery, according to a case-control real-world study presented at the meeting.
“Laparoscopic sleeve gastrectomy [LSG] is a frequently performed bariatric surgery worldwide resulting in significant weight loss and improvement in obesity-related comorbidities,” said Firas Bahdi, MD, gastroenterology fellow at the David Geffen School of Medicine at University of California, Los Angeles. “Despite its success, around one third of patients, unfortunately, develop weight regain warranting intervention.”
Dr. Bahdi and colleagues retrospectively studied 68 adults prescribed subcutaneous semaglutide or tirzepatide after LSG, another 20 who had ESG for weight regain after LSG, and 87 controls with intact stomachs who also took GLP-1 agonists for weight loss.
They found that the ESG group experienced a significantly higher percentage of total body weight loss at 3 months than the GLP-1 group (10% vs 4.3%, respectively; P = .0001). Similarly, at the 6-month follow-up, the ESG group experienced 11.5% total body weight loss compared to 6.8% in the GLP-1 group (P = .03).
The GLP-1 after LSG group still fared better than the GLP-1 control group of people who never had surgery. Total body weight loss was 4.3% vs 5.7% at 3 months (P = .02), 6.8% vs 9.2% at 6 months (P = .02), and 9.2% vs 12.7% at 12 months (P = .03).
“In this real-world experience, revisional ESG offers significantly more weight loss than GLP-1 agonists for patients with weight regain, while also avoiding the challenges of medication refills, making it an attractive option,” Dr. Bahdi said.
Future multicenter studies are warranted to confirm these results and explore physiological explanations, he added.
The study received an Outstanding Research Award in the Obesity Category (Trainee).
Dr. Velji-Ibrahim, Dr. Adekolu, Dr. Cohen, and Dr. Bahdi indicated no relevant financial relationships.
A version of this article appeared on Medscape.com.
VANCOUVER — Glucagon-like peptide-1 (GLP-1) agonists, like semaglutide, liraglutide, and the newly US Food and Drug Administration–approved tirzepatide, not only are gaining popularity among the public for weight loss but also are the focus of considerable attention from gastroenterology researchers.
how they compare to bariatric surgery for weight loss or prevention of metabolic dysfunction–associated steatotic liver disease, and their potential role to prevent regain after weight-loss surgery.
Head-to-Head Comparison
Tirzepatide 15 mg emerged as superior to other GLP-1 agonists for weight loss, for example, in a network meta-analysis of randomized controlled trials looking into obesity management.
Tirzepatide 15 mg was associated with the most effective mean weight loss at just over 15% when Jena Velji-Ibrahim, MD, and colleagues combined data from 14 studies with 18,714 participants with overweight or obesity but without diabetes.
Next up in order of weight-loss efficacy was tirzepatide 10 mg with 13% mean weight loss, semaglutide 2.4 mg with just over 11% mean weight loss, and tirzepatide 5 mg with almost 10% mean weight loss. The only outlier was dulaglutide 0.75 mg, which was linked to about 8% weight gain.
“While clinical trials have been conducted to assess the weight-loss efficacy of GLP-1 agonists, there has been limited head-to-head comparisons, and the data that has been obtained has been quite inconsistent,” Dr. Velji-Ibrahim said when presenting results at the meeting.
Researchers found little difference in efficacies between tirzepatide 15 mg and 10 mg, suggesting both are a viable option for weight loss, said Dr. Velji-Ibrahim of Prisma Health Greenville Memorial Hospital and University of South Carolina School of Medicine in Greenville.
She also reported similar efficacies between oral semaglutide 50 mg and subcutaneous semaglutide 2.4 mg, “meaning that we have another option for weight management.”
Side effects among the different GLP-1 agonists, and among the same agent at different doses, were not significantly different.
Comparison With Bariatric Surgery for Reducing Major Adverse Cardiovascular Events (MACE)
For many years, bariatric surgeons have pointed to the health benefits of weight-loss surgery in the right candidates, including a reduced risk for adverse cardiovascular events.
The weight loss associated with GLP-1 agonists has likewise shown benefits in reducing MACE. However, it remains unclear if one of these weight-loss strategies is better than the other in reducing these outcomes.
To determine this, researchers compared 118,828 people who had bariatric surgery to another propensity-matched group of 118,828 others prescribed GLP-1 agonists. They included adults with a body mass index (BMI) of 35 or higher in the national TriNetX database.
The multicenter, retrospective study revealed bariatric surgery was superior in reducing the risk for heart failure, MACE, and cerebrovascular disease at 3, 5, 7, and 10 years. At 10 years, for example, bariatric surgery was associated with 31% fewer composite cardiovascular events than the GLP-1 agonists.
“Our results suggest that bariatric surgery is more effective than GLP-1 analogs in preventing adverse cardiovascular events in obese patients,” Ayowumi A. Adekolu, MD, an internal medicine resident at West Virginia School of Medicine in Morgantown, said in audio comments accompanying his ePoster at the meeting. “Although these findings highlight the benefit of bariatric surgery in mitigating adverse cardiovascular events, well-designed prospective studies are necessary to confirm these benefits in this patient population.”
Possible Role in Fatty Liver Disease Prevention
In another large multicenter study from the same institution, Ethan M. Cohen, MD, along with co-author Dr. Adekolu and others, compared the effectiveness of bariatric surgery to GLP-1 agonists for preventing nonalcoholic fatty liver disease (NAFLD). Since the study was conducted, the official name of NAFLD has changed to metabolic dysfunction–associated steatotic liver disease.
Dr. Cohen and colleagues evaluated data from the TriNetX database and included adults with a BMI of 35 or higher. They propensity matched 124,022 people who had sleeve gastrectomy or Roux-en-Y gastric bypass to another 124,022 others prescribed GLP-1 agonists. Again, they looked at outcomes at 3, 5, 7, and 10 years.
They found bariatric surgery superior to GLP-1 agonists for reducing the risk of developing NAFLD. Relative risk reduction was 25% at 3 years, 28% at 5 years, 27% at 7 years, and 26% at 10 years.
Although not to the same extent as surgery in this study, GLP-1–associated weight loss did reduce risks as well.
“An important aspect of this is that for some of these people, bariatric surgery is not even an option,” Dr. Cohen said in an interview, citing as an example those who do not meet the criteria for surgery.
Dr. Cohen and colleagues plan to continue the study with a larger number of participants.
Real-World Weight Regain
In another instance where a surgical procedure trumped GLP-1 agonists, revisional endoscopic sleeve gastroplasty (ESG) offered significantly higher weight loss than GLP-1 agonists among people who regained weight following initial weight-loss surgery, according to a case-control real-world study presented at the meeting.
“Laparoscopic sleeve gastrectomy [LSG] is a frequently performed bariatric surgery worldwide resulting in significant weight loss and improvement in obesity-related comorbidities,” said Firas Bahdi, MD, gastroenterology fellow at the David Geffen School of Medicine at University of California, Los Angeles. “Despite its success, around one third of patients, unfortunately, develop weight regain warranting intervention.”
Dr. Bahdi and colleagues retrospectively studied 68 adults prescribed subcutaneous semaglutide or tirzepatide after LSG, another 20 who had ESG for weight regain after LSG, and 87 controls with intact stomachs who also took GLP-1 agonists for weight loss.
They found that the ESG group experienced a significantly higher percentage of total body weight loss at 3 months than the GLP-1 group (10% vs 4.3%, respectively; P = .0001). Similarly, at the 6-month follow-up, the ESG group experienced 11.5% total body weight loss compared to 6.8% in the GLP-1 group (P = .03).
The GLP-1 after LSG group still fared better than the GLP-1 control group of people who never had surgery. Total body weight loss was 4.3% vs 5.7% at 3 months (P = .02), 6.8% vs 9.2% at 6 months (P = .02), and 9.2% vs 12.7% at 12 months (P = .03).
“In this real-world experience, revisional ESG offers significantly more weight loss than GLP-1 agonists for patients with weight regain, while also avoiding the challenges of medication refills, making it an attractive option,” Dr. Bahdi said.
Future multicenter studies are warranted to confirm these results and explore physiological explanations, he added.
The study received an Outstanding Research Award in the Obesity Category (Trainee).
Dr. Velji-Ibrahim, Dr. Adekolu, Dr. Cohen, and Dr. Bahdi indicated no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM ASG 2023
Bariatric surgery tied to less pregnancy weight gain
TOPLINE:
Pregnancy weight gain is lower in women with a history of gastric bypass or sleeve gastrectomy than in those without such a history, especially when the interval between surgery and conception is shorter, new data suggest.
METHODOLOGY:
- Using Swedish national registers, researchers investigated the association of pregnancy weight gain with history in 12,776 pregnancies — 6388 in women with a history of bariatric surgery and 6388 in women without such a history.
- Pregnancies were propensity score matched to patients’ early-pregnancy body mass index (BMI), prepregnancy diabetes, , smoking status, education, height, country of birth, and delivery year.
- Post-gastric bypass pregnancies were matched to post-sleeve gastrectomy pregnancies using the same matching strategy.
- Time from surgery to conception was also assessed.
TAKEAWAY:
- Across all early-pregnancy BMI strata, women with a history of bariatric surgery had lower pregnancy weight gain than matched controls.
- The magnitude of difference was largest for women with normal weight or overweight early-pregnancy BMI status (adjusted mean difference in z score, −0.33), which then decreased stepwise within the subclasses (−0.21, −0.16, and −0.08 for obesity classes I, II, and III, respectively).
- Pregnancy weight gain did not differ by surgery type, but lower pregnancy weight gain was associated with a shorter surgery-to-conception interval (particularly within 1 year) or lower surgery-to-conception weight loss.
IN PRACTICE:
“The highest proportion of weight gain below the recommendations was found among women with a normal weight status. Hence, clinical attention to women with history of bariatric surgery and a normal weight status in early pregnancy might be warranted,” the authors advised.
SOURCE:
The study, with the first author Huiling Xu, MD, MSc, Karolinska Institutet, Stockholm, Sweden, was published online in JAMA Network Open.
LIMITATIONS:
Despite rigorous matching, residual confounding was possible. The sample size was limited for some subgroups, possibly affecting statistical power. Although the study provides an overview of pregnancy outcomes within surgery-to-conception interval and pregnancy weight gain z scores, a more in-depth investigation is needed to understand the associations among bariatric surgery, pregnancy weight gain, and pregnancy outcomes.
DISCLOSURES:
Research for this study was supported by the Swedish Research Council for Health, Working Life and Welfare, and the Swedish Research Council. The authors have no relevant disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
Pregnancy weight gain is lower in women with a history of gastric bypass or sleeve gastrectomy than in those without such a history, especially when the interval between surgery and conception is shorter, new data suggest.
METHODOLOGY:
- Using Swedish national registers, researchers investigated the association of pregnancy weight gain with history in 12,776 pregnancies — 6388 in women with a history of bariatric surgery and 6388 in women without such a history.
- Pregnancies were propensity score matched to patients’ early-pregnancy body mass index (BMI), prepregnancy diabetes, , smoking status, education, height, country of birth, and delivery year.
- Post-gastric bypass pregnancies were matched to post-sleeve gastrectomy pregnancies using the same matching strategy.
- Time from surgery to conception was also assessed.
TAKEAWAY:
- Across all early-pregnancy BMI strata, women with a history of bariatric surgery had lower pregnancy weight gain than matched controls.
- The magnitude of difference was largest for women with normal weight or overweight early-pregnancy BMI status (adjusted mean difference in z score, −0.33), which then decreased stepwise within the subclasses (−0.21, −0.16, and −0.08 for obesity classes I, II, and III, respectively).
- Pregnancy weight gain did not differ by surgery type, but lower pregnancy weight gain was associated with a shorter surgery-to-conception interval (particularly within 1 year) or lower surgery-to-conception weight loss.
IN PRACTICE:
“The highest proportion of weight gain below the recommendations was found among women with a normal weight status. Hence, clinical attention to women with history of bariatric surgery and a normal weight status in early pregnancy might be warranted,” the authors advised.
SOURCE:
The study, with the first author Huiling Xu, MD, MSc, Karolinska Institutet, Stockholm, Sweden, was published online in JAMA Network Open.
LIMITATIONS:
Despite rigorous matching, residual confounding was possible. The sample size was limited for some subgroups, possibly affecting statistical power. Although the study provides an overview of pregnancy outcomes within surgery-to-conception interval and pregnancy weight gain z scores, a more in-depth investigation is needed to understand the associations among bariatric surgery, pregnancy weight gain, and pregnancy outcomes.
DISCLOSURES:
Research for this study was supported by the Swedish Research Council for Health, Working Life and Welfare, and the Swedish Research Council. The authors have no relevant disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
Pregnancy weight gain is lower in women with a history of gastric bypass or sleeve gastrectomy than in those without such a history, especially when the interval between surgery and conception is shorter, new data suggest.
METHODOLOGY:
- Using Swedish national registers, researchers investigated the association of pregnancy weight gain with history in 12,776 pregnancies — 6388 in women with a history of bariatric surgery and 6388 in women without such a history.
- Pregnancies were propensity score matched to patients’ early-pregnancy body mass index (BMI), prepregnancy diabetes, , smoking status, education, height, country of birth, and delivery year.
- Post-gastric bypass pregnancies were matched to post-sleeve gastrectomy pregnancies using the same matching strategy.
- Time from surgery to conception was also assessed.
TAKEAWAY:
- Across all early-pregnancy BMI strata, women with a history of bariatric surgery had lower pregnancy weight gain than matched controls.
- The magnitude of difference was largest for women with normal weight or overweight early-pregnancy BMI status (adjusted mean difference in z score, −0.33), which then decreased stepwise within the subclasses (−0.21, −0.16, and −0.08 for obesity classes I, II, and III, respectively).
- Pregnancy weight gain did not differ by surgery type, but lower pregnancy weight gain was associated with a shorter surgery-to-conception interval (particularly within 1 year) or lower surgery-to-conception weight loss.
IN PRACTICE:
“The highest proportion of weight gain below the recommendations was found among women with a normal weight status. Hence, clinical attention to women with history of bariatric surgery and a normal weight status in early pregnancy might be warranted,” the authors advised.
SOURCE:
The study, with the first author Huiling Xu, MD, MSc, Karolinska Institutet, Stockholm, Sweden, was published online in JAMA Network Open.
LIMITATIONS:
Despite rigorous matching, residual confounding was possible. The sample size was limited for some subgroups, possibly affecting statistical power. Although the study provides an overview of pregnancy outcomes within surgery-to-conception interval and pregnancy weight gain z scores, a more in-depth investigation is needed to understand the associations among bariatric surgery, pregnancy weight gain, and pregnancy outcomes.
DISCLOSURES:
Research for this study was supported by the Swedish Research Council for Health, Working Life and Welfare, and the Swedish Research Council. The authors have no relevant disclosures.
A version of this article appeared on Medscape.com.
10% of US physicians work for or under UnitedHealth. Is that a problem?
as more payers and private equity firms pursue medical practice acquisitions.
The company added 20,000 physicians in the last year alone, including a previously physician-owned multispecialty group practice of 400 doctors in New York. They join the growing web of doctors — about 90,000 of the 950,000 active US physicians — working for the UnitedHealth Group subsidiary, Optum Health, providing primary, specialty, urgent, and surgical care. Amar Desai, MD, chief executive officer of Optum Health, shared the updated workforce numbers during the health care conglomerate’s annual investor conference.
Health care mergers and consolidations have become more common as physician groups struggle to stay afloat amid dwindling payer reimbursements. Although private equity and health systems often acquire practices, payers like UHC are increasingly doing so as part of their model to advance value-based care.
Yashaswini Singh, PhD, health care economist and assistant professor of health services, policy, and practice at Brown University, says such moves mirror the broader trend in corporate consolidation of physician practices. She said in an interview that the integrated models could possibly enhance care coordination and improve outcomes, but the impact of payer-led consolidation has not been extensively studied.
Meanwhile, evidence considering private equity ownership is just emerging. In a 2022 study published in JAMA Health Forum, with Dr. Singh as lead author, findings showed that private equity involvement increased healthcare spending through higher prices and utilization.
Consolidation can also raise anti-trust concerns. “If payers incentivize referral patterns of their employed physicians to favor other physicians employed by the payer, it can reduce competition by restricting consumer choice,” said Dr. Singh.
A potential merger between Cigna and Humana that could happen by the end of the year will likely face intense scrutiny as it would create a company that rivals the size of UnitedHealth Group or CVS Health. If it goes through, the duo could streamline its insurance offerings and leverage each other’s care delivery platforms, clinics, and provider workforce.
The Biden Administration has sought to strengthen anti-trust statutes to prevent industry monopolies and consumer harm, and the US Department of Justice and Federal Trade Commission have proposed new merger guidelines that have yet to be finalized.
According to Dr. Singh, some of Optum’s medical practice purchases may bypass anti-trust statutes since most prospective mergers and acquisitions are reviewed only if they exceed a specific value ($101 million for 2023). Limited transparency in ownership structures further complicates matters. Plus, Dr. Singh said instances where physicians are hired instead of acquired through mergers would not be subject to current anti-trust laws.
The ‘corporatization’ of health care is not good for patients or physicians, said Robert McNamara, MD, chief medical officer of the American Academy of Emergency Medicine Physician Group and cofounder of Take Medicine Back, a physician group advocating to remove corporate interests from health care.
“If you ask a physician what causes them the most moral conflict, they’ll tell you it’s the insurance companies denying something they want to do for their patients,” he said. “To have the doctors now working for the insurance industry conflicts with a physician’s duty to put the patient first.”
Dr. McNamara, chair of emergency medicine at Temple University’s Katz School of Medicine, said in an interview that more than half the states in the United States have laws or court rulings that support protecting physician autonomy from corporate interests. Still, he hopes a federal prohibition on private equity’s involvement in healthcare can soon gain traction. In November, Take Medicine Back raised a resolution at the American Medical Association’s interim House of Delegates meeting, which he said was subsequently referred to a committee.
Emergency medicine was among the first specialties to succumb to private equity firms, but Dr. McNamara said that all types of health care providers and entities — from cardiology and urology to addiction treatment centers and nursing homes — are being swallowed up by larger organizations, including payers.
UHC was named in a class action suit recently for allegedly shirking doctors’ orders and relying on a flawed algorithm to determine the length of skilled nursing facility stays for Medicare Advantage policyholders.
At the investor meeting, Dr. Desai reiterated Optum’s desire to continue expanding care delivery options, especially in its pharmacy and behavioral health business lines, and focus on adopting value-based care. He credited the rapid growth to developing strong relationships with providers and standardizing technology and clinical systems.
A version of this article appeared on Medscape.com.
as more payers and private equity firms pursue medical practice acquisitions.
The company added 20,000 physicians in the last year alone, including a previously physician-owned multispecialty group practice of 400 doctors in New York. They join the growing web of doctors — about 90,000 of the 950,000 active US physicians — working for the UnitedHealth Group subsidiary, Optum Health, providing primary, specialty, urgent, and surgical care. Amar Desai, MD, chief executive officer of Optum Health, shared the updated workforce numbers during the health care conglomerate’s annual investor conference.
Health care mergers and consolidations have become more common as physician groups struggle to stay afloat amid dwindling payer reimbursements. Although private equity and health systems often acquire practices, payers like UHC are increasingly doing so as part of their model to advance value-based care.
Yashaswini Singh, PhD, health care economist and assistant professor of health services, policy, and practice at Brown University, says such moves mirror the broader trend in corporate consolidation of physician practices. She said in an interview that the integrated models could possibly enhance care coordination and improve outcomes, but the impact of payer-led consolidation has not been extensively studied.
Meanwhile, evidence considering private equity ownership is just emerging. In a 2022 study published in JAMA Health Forum, with Dr. Singh as lead author, findings showed that private equity involvement increased healthcare spending through higher prices and utilization.
Consolidation can also raise anti-trust concerns. “If payers incentivize referral patterns of their employed physicians to favor other physicians employed by the payer, it can reduce competition by restricting consumer choice,” said Dr. Singh.
A potential merger between Cigna and Humana that could happen by the end of the year will likely face intense scrutiny as it would create a company that rivals the size of UnitedHealth Group or CVS Health. If it goes through, the duo could streamline its insurance offerings and leverage each other’s care delivery platforms, clinics, and provider workforce.
The Biden Administration has sought to strengthen anti-trust statutes to prevent industry monopolies and consumer harm, and the US Department of Justice and Federal Trade Commission have proposed new merger guidelines that have yet to be finalized.
According to Dr. Singh, some of Optum’s medical practice purchases may bypass anti-trust statutes since most prospective mergers and acquisitions are reviewed only if they exceed a specific value ($101 million for 2023). Limited transparency in ownership structures further complicates matters. Plus, Dr. Singh said instances where physicians are hired instead of acquired through mergers would not be subject to current anti-trust laws.
The ‘corporatization’ of health care is not good for patients or physicians, said Robert McNamara, MD, chief medical officer of the American Academy of Emergency Medicine Physician Group and cofounder of Take Medicine Back, a physician group advocating to remove corporate interests from health care.
“If you ask a physician what causes them the most moral conflict, they’ll tell you it’s the insurance companies denying something they want to do for their patients,” he said. “To have the doctors now working for the insurance industry conflicts with a physician’s duty to put the patient first.”
Dr. McNamara, chair of emergency medicine at Temple University’s Katz School of Medicine, said in an interview that more than half the states in the United States have laws or court rulings that support protecting physician autonomy from corporate interests. Still, he hopes a federal prohibition on private equity’s involvement in healthcare can soon gain traction. In November, Take Medicine Back raised a resolution at the American Medical Association’s interim House of Delegates meeting, which he said was subsequently referred to a committee.
Emergency medicine was among the first specialties to succumb to private equity firms, but Dr. McNamara said that all types of health care providers and entities — from cardiology and urology to addiction treatment centers and nursing homes — are being swallowed up by larger organizations, including payers.
UHC was named in a class action suit recently for allegedly shirking doctors’ orders and relying on a flawed algorithm to determine the length of skilled nursing facility stays for Medicare Advantage policyholders.
At the investor meeting, Dr. Desai reiterated Optum’s desire to continue expanding care delivery options, especially in its pharmacy and behavioral health business lines, and focus on adopting value-based care. He credited the rapid growth to developing strong relationships with providers and standardizing technology and clinical systems.
A version of this article appeared on Medscape.com.
as more payers and private equity firms pursue medical practice acquisitions.
The company added 20,000 physicians in the last year alone, including a previously physician-owned multispecialty group practice of 400 doctors in New York. They join the growing web of doctors — about 90,000 of the 950,000 active US physicians — working for the UnitedHealth Group subsidiary, Optum Health, providing primary, specialty, urgent, and surgical care. Amar Desai, MD, chief executive officer of Optum Health, shared the updated workforce numbers during the health care conglomerate’s annual investor conference.
Health care mergers and consolidations have become more common as physician groups struggle to stay afloat amid dwindling payer reimbursements. Although private equity and health systems often acquire practices, payers like UHC are increasingly doing so as part of their model to advance value-based care.
Yashaswini Singh, PhD, health care economist and assistant professor of health services, policy, and practice at Brown University, says such moves mirror the broader trend in corporate consolidation of physician practices. She said in an interview that the integrated models could possibly enhance care coordination and improve outcomes, but the impact of payer-led consolidation has not been extensively studied.
Meanwhile, evidence considering private equity ownership is just emerging. In a 2022 study published in JAMA Health Forum, with Dr. Singh as lead author, findings showed that private equity involvement increased healthcare spending through higher prices and utilization.
Consolidation can also raise anti-trust concerns. “If payers incentivize referral patterns of their employed physicians to favor other physicians employed by the payer, it can reduce competition by restricting consumer choice,” said Dr. Singh.
A potential merger between Cigna and Humana that could happen by the end of the year will likely face intense scrutiny as it would create a company that rivals the size of UnitedHealth Group or CVS Health. If it goes through, the duo could streamline its insurance offerings and leverage each other’s care delivery platforms, clinics, and provider workforce.
The Biden Administration has sought to strengthen anti-trust statutes to prevent industry monopolies and consumer harm, and the US Department of Justice and Federal Trade Commission have proposed new merger guidelines that have yet to be finalized.
According to Dr. Singh, some of Optum’s medical practice purchases may bypass anti-trust statutes since most prospective mergers and acquisitions are reviewed only if they exceed a specific value ($101 million for 2023). Limited transparency in ownership structures further complicates matters. Plus, Dr. Singh said instances where physicians are hired instead of acquired through mergers would not be subject to current anti-trust laws.
The ‘corporatization’ of health care is not good for patients or physicians, said Robert McNamara, MD, chief medical officer of the American Academy of Emergency Medicine Physician Group and cofounder of Take Medicine Back, a physician group advocating to remove corporate interests from health care.
“If you ask a physician what causes them the most moral conflict, they’ll tell you it’s the insurance companies denying something they want to do for their patients,” he said. “To have the doctors now working for the insurance industry conflicts with a physician’s duty to put the patient first.”
Dr. McNamara, chair of emergency medicine at Temple University’s Katz School of Medicine, said in an interview that more than half the states in the United States have laws or court rulings that support protecting physician autonomy from corporate interests. Still, he hopes a federal prohibition on private equity’s involvement in healthcare can soon gain traction. In November, Take Medicine Back raised a resolution at the American Medical Association’s interim House of Delegates meeting, which he said was subsequently referred to a committee.
Emergency medicine was among the first specialties to succumb to private equity firms, but Dr. McNamara said that all types of health care providers and entities — from cardiology and urology to addiction treatment centers and nursing homes — are being swallowed up by larger organizations, including payers.
UHC was named in a class action suit recently for allegedly shirking doctors’ orders and relying on a flawed algorithm to determine the length of skilled nursing facility stays for Medicare Advantage policyholders.
At the investor meeting, Dr. Desai reiterated Optum’s desire to continue expanding care delivery options, especially in its pharmacy and behavioral health business lines, and focus on adopting value-based care. He credited the rapid growth to developing strong relationships with providers and standardizing technology and clinical systems.
A version of this article appeared on Medscape.com.
Less is more for axillary surgery in early breast cancer
SAN ANTONIO — than do those who have more extensive surgery, according to findings from a large meta-analysis.
Less extensive surgery also reduced patients’ risk for lymphedema, according to research (abstract GS02-05) presented at the San Antonio Breast Cancer Symposium.
These results, which included data from more than 20,000 women, may “reassure” patients and clinicians that more extensive axillary lymph node dissection “does not improve outcomes in many women with early-stage breast cancer,” said Andrea V. Barrio, MD, a breast surgeon at Memorial Sloan Kettering Cancer Center, New York City, who was not involved in the study.
Gurdeep S. Mannu, DPhil, of the University of Oxford, United Kingdom, who presented the findings at SABCS, explained that the optimal surgical management of the axilla remains uncertain in this patient population.
To better understand the long-term risks and benefits of more vs less aggressive axillary surgery in early breast cancer, Dr. Mannu and colleagues performed a meta-analysis of 29 randomized trials conducted over six decades, which included data on 20,285 women. The trials compared more vs less extensive axillary surgery as well as axillary surgery vs axillary radiotherapy.
In trials comparing more vs less extensive axillary surgery, researchers found that 83% of locoregional recurrences occurred in the breast or in multiple sites/unspecified locations, and the remaining 17% occurred in isolated axilla or other local recurrences, such as in the supraclavicular fossa or internal mammary chain.
Those with recurrences in the breast or multiple sites/unspecified locations did not benefit from more extensive surgery, demonstrating similar recurrence rates (RR) (RR for breast, 1.13; 95% CI, 0.92-1.40; RR for other, 0.89; 95% CI, 0.67-1.18).
The group with recurrences in isolated axilla or other local recurrences tended to do better with more extensive surgery (RR, 0.43 and 0.41, respectively).
Overall though, after a median follow-up of 10 years, differences in locoregional recurrence rates at any site did not differ among patients who had more vs less extensive axillary surgery (RR, 0.91; P = .22). This finding held even when restricting the analysis to women with node-positive disease/unknown nodal status (RR, 1.00; P = .98) and for node-negative women (RR, 0.88; P = .15).
Dr. Mannu and colleagues observed similar findings for distant recurrence, breast cancer mortality, and death from any cause.
“But where there was quite a striking difference was in morbidity,” said Dr. Mannu.
To examine rates of lymphedema — the surgical complication that has been “one of the main motivations” for the deescalation trials of the past few decades — the researchers focused on more recent trials, which “are most relevant to women treated today,” Dr. Mannu explained.
These showed that more extensive axillary surgery was associated with almost 2.5-times the rate of lymphedema compared with less extensive treatment (odds ratio [OR], 2.43).
Finally, the team compared axillary dissection with axillary radiotherapy across five trials and found no significant differences in the treatment approaches in terms of locoregional occurrence, distant recurrence, breast cancer mortality, and death from any cause.
However, once again, a notable difference in rates of lymphedema occurred, with axillary dissection associated with higher rates compared with radiotherapy (OR, 1.79).
This is “probably the largest meta-analysis comparing more vs less axillary surgery,” Dr. Barrio said in an interview.
“When we have one or two positive sentinel nodes, anywhere from 30%-50% of women will have additional positive lymph nodes that we’re not removing” with less extensive surgery, she explained. This study shows that, even then, this “doesn’t seem to impact on survival.”
This is “likely related to better medical treatment and radiation techniques that can treat that disease just as well as big surgery, but with less lymphedema,” she added.
Nevertheless, Dr. Barrio believes that there are “situations where we still feel that axillary lymph node dissection is important: in women with advanced cancer, like inflammatory breast cancer, and in women who’ve received chemotherapy upfront, then had surgery, and still have positive nodes after the chemo.”
The study was funded by Cancer Research UK, British Heart Foundation, Medical Research Council.
No relevant financial relationships have been declared.
A version of this article appeared on Medscape.com.
SAN ANTONIO — than do those who have more extensive surgery, according to findings from a large meta-analysis.
Less extensive surgery also reduced patients’ risk for lymphedema, according to research (abstract GS02-05) presented at the San Antonio Breast Cancer Symposium.
These results, which included data from more than 20,000 women, may “reassure” patients and clinicians that more extensive axillary lymph node dissection “does not improve outcomes in many women with early-stage breast cancer,” said Andrea V. Barrio, MD, a breast surgeon at Memorial Sloan Kettering Cancer Center, New York City, who was not involved in the study.
Gurdeep S. Mannu, DPhil, of the University of Oxford, United Kingdom, who presented the findings at SABCS, explained that the optimal surgical management of the axilla remains uncertain in this patient population.
To better understand the long-term risks and benefits of more vs less aggressive axillary surgery in early breast cancer, Dr. Mannu and colleagues performed a meta-analysis of 29 randomized trials conducted over six decades, which included data on 20,285 women. The trials compared more vs less extensive axillary surgery as well as axillary surgery vs axillary radiotherapy.
In trials comparing more vs less extensive axillary surgery, researchers found that 83% of locoregional recurrences occurred in the breast or in multiple sites/unspecified locations, and the remaining 17% occurred in isolated axilla or other local recurrences, such as in the supraclavicular fossa or internal mammary chain.
Those with recurrences in the breast or multiple sites/unspecified locations did not benefit from more extensive surgery, demonstrating similar recurrence rates (RR) (RR for breast, 1.13; 95% CI, 0.92-1.40; RR for other, 0.89; 95% CI, 0.67-1.18).
The group with recurrences in isolated axilla or other local recurrences tended to do better with more extensive surgery (RR, 0.43 and 0.41, respectively).
Overall though, after a median follow-up of 10 years, differences in locoregional recurrence rates at any site did not differ among patients who had more vs less extensive axillary surgery (RR, 0.91; P = .22). This finding held even when restricting the analysis to women with node-positive disease/unknown nodal status (RR, 1.00; P = .98) and for node-negative women (RR, 0.88; P = .15).
Dr. Mannu and colleagues observed similar findings for distant recurrence, breast cancer mortality, and death from any cause.
“But where there was quite a striking difference was in morbidity,” said Dr. Mannu.
To examine rates of lymphedema — the surgical complication that has been “one of the main motivations” for the deescalation trials of the past few decades — the researchers focused on more recent trials, which “are most relevant to women treated today,” Dr. Mannu explained.
These showed that more extensive axillary surgery was associated with almost 2.5-times the rate of lymphedema compared with less extensive treatment (odds ratio [OR], 2.43).
Finally, the team compared axillary dissection with axillary radiotherapy across five trials and found no significant differences in the treatment approaches in terms of locoregional occurrence, distant recurrence, breast cancer mortality, and death from any cause.
However, once again, a notable difference in rates of lymphedema occurred, with axillary dissection associated with higher rates compared with radiotherapy (OR, 1.79).
This is “probably the largest meta-analysis comparing more vs less axillary surgery,” Dr. Barrio said in an interview.
“When we have one or two positive sentinel nodes, anywhere from 30%-50% of women will have additional positive lymph nodes that we’re not removing” with less extensive surgery, she explained. This study shows that, even then, this “doesn’t seem to impact on survival.”
This is “likely related to better medical treatment and radiation techniques that can treat that disease just as well as big surgery, but with less lymphedema,” she added.
Nevertheless, Dr. Barrio believes that there are “situations where we still feel that axillary lymph node dissection is important: in women with advanced cancer, like inflammatory breast cancer, and in women who’ve received chemotherapy upfront, then had surgery, and still have positive nodes after the chemo.”
The study was funded by Cancer Research UK, British Heart Foundation, Medical Research Council.
No relevant financial relationships have been declared.
A version of this article appeared on Medscape.com.
SAN ANTONIO — than do those who have more extensive surgery, according to findings from a large meta-analysis.
Less extensive surgery also reduced patients’ risk for lymphedema, according to research (abstract GS02-05) presented at the San Antonio Breast Cancer Symposium.
These results, which included data from more than 20,000 women, may “reassure” patients and clinicians that more extensive axillary lymph node dissection “does not improve outcomes in many women with early-stage breast cancer,” said Andrea V. Barrio, MD, a breast surgeon at Memorial Sloan Kettering Cancer Center, New York City, who was not involved in the study.
Gurdeep S. Mannu, DPhil, of the University of Oxford, United Kingdom, who presented the findings at SABCS, explained that the optimal surgical management of the axilla remains uncertain in this patient population.
To better understand the long-term risks and benefits of more vs less aggressive axillary surgery in early breast cancer, Dr. Mannu and colleagues performed a meta-analysis of 29 randomized trials conducted over six decades, which included data on 20,285 women. The trials compared more vs less extensive axillary surgery as well as axillary surgery vs axillary radiotherapy.
In trials comparing more vs less extensive axillary surgery, researchers found that 83% of locoregional recurrences occurred in the breast or in multiple sites/unspecified locations, and the remaining 17% occurred in isolated axilla or other local recurrences, such as in the supraclavicular fossa or internal mammary chain.
Those with recurrences in the breast or multiple sites/unspecified locations did not benefit from more extensive surgery, demonstrating similar recurrence rates (RR) (RR for breast, 1.13; 95% CI, 0.92-1.40; RR for other, 0.89; 95% CI, 0.67-1.18).
The group with recurrences in isolated axilla or other local recurrences tended to do better with more extensive surgery (RR, 0.43 and 0.41, respectively).
Overall though, after a median follow-up of 10 years, differences in locoregional recurrence rates at any site did not differ among patients who had more vs less extensive axillary surgery (RR, 0.91; P = .22). This finding held even when restricting the analysis to women with node-positive disease/unknown nodal status (RR, 1.00; P = .98) and for node-negative women (RR, 0.88; P = .15).
Dr. Mannu and colleagues observed similar findings for distant recurrence, breast cancer mortality, and death from any cause.
“But where there was quite a striking difference was in morbidity,” said Dr. Mannu.
To examine rates of lymphedema — the surgical complication that has been “one of the main motivations” for the deescalation trials of the past few decades — the researchers focused on more recent trials, which “are most relevant to women treated today,” Dr. Mannu explained.
These showed that more extensive axillary surgery was associated with almost 2.5-times the rate of lymphedema compared with less extensive treatment (odds ratio [OR], 2.43).
Finally, the team compared axillary dissection with axillary radiotherapy across five trials and found no significant differences in the treatment approaches in terms of locoregional occurrence, distant recurrence, breast cancer mortality, and death from any cause.
However, once again, a notable difference in rates of lymphedema occurred, with axillary dissection associated with higher rates compared with radiotherapy (OR, 1.79).
This is “probably the largest meta-analysis comparing more vs less axillary surgery,” Dr. Barrio said in an interview.
“When we have one or two positive sentinel nodes, anywhere from 30%-50% of women will have additional positive lymph nodes that we’re not removing” with less extensive surgery, she explained. This study shows that, even then, this “doesn’t seem to impact on survival.”
This is “likely related to better medical treatment and radiation techniques that can treat that disease just as well as big surgery, but with less lymphedema,” she added.
Nevertheless, Dr. Barrio believes that there are “situations where we still feel that axillary lymph node dissection is important: in women with advanced cancer, like inflammatory breast cancer, and in women who’ve received chemotherapy upfront, then had surgery, and still have positive nodes after the chemo.”
The study was funded by Cancer Research UK, British Heart Foundation, Medical Research Council.
No relevant financial relationships have been declared.
A version of this article appeared on Medscape.com.
FROM SABCS 2023
Supercharge your medical practice with ChatGPT: Here’s why you should upgrade
Artificial intelligence (AI) has already demonstrated its potential in various areas of healthcare, from early disease detection and drug discovery to genomics and personalized care. OpenAI’s ChatGPT, a large language model, is one AI tool that has been transforming practices across the globe, including mine.
Let me walk you through it.
ChatGPT is essentially an AI-fueled assistant, capable of interpreting and generating human-like text in response to user inputs. Imagine a well-informed and competent trainee working with you, ready to tackle tasks from handling patient inquiries to summarizing intricate medical literature.
Currently, ChatGPT works on the “freemium” pricing model; there is a free version built upon GPT-3.5 as well as a subscription “ChatGPT Plus” version based on GPT-4 which offers additional features such as the use of third-party plug-ins.
Now, you may ask, “Isn’t the free version enough?” The free version is indeed impressive, but upgrading to the paid version for $20 per month unlocks the full potential of this tool, particularly if we add plug-ins.
Here are some of the best ways to incorporate ChatGPT Plus into your practice.
Time saver and efficiency multiplier. The paid version of ChatGPT is an extraordinary time-saving tool. It can help you sort through vast amounts of medical literature in a fraction of the time it would normally take. Imagine having to sift through hundreds of articles to find the latest research relevant to a patient’s case. With the paid version of ChatGPT, you can simply ask it to provide summaries of the most recent and relevant studies, all in seconds.
Did you forget about that PowerPoint you need to make but know the potential papers you would use? No problem. ChatGPT can create slides in a few minutes. It becomes your on-demand research assistant.
Of course, you need to provide the source you find most relevant to you. Using plug-ins such as ScholarAI and Link Reader are great.
Improved patient communication. Explaining complex medical terminology and procedures to patients can sometimes be a challenge. ChatGPT can generate simplified and personalized explanations for your patients, fostering their understanding and involvement in their care process.
Epic is currently collaborating with Nuance Communications, Microsoft’s speech recognition subsidiary, to use generative AI tools for medical note-taking in the electronic health record. However, you do not need to wait for it; it just takes a prompt in ChatGPT and then copying/pasting the results into the chart.
Smoother administrative management. The premium version of ChatGPT can automate administrative tasks such as creating letters of medical necessity, clearance to other physicians for services, or even communications to staff on specific topics. This frees you to focus more on your core work: providing patient care.
Precision medicine aid. ChatGPT can be a powerful ally in the field of precision medicine. Its capabilities for analyzing large datasets and unearthing valuable insights can help deliver more personalized and potentially effective treatment plans. For example, one can prompt ChatGPT to query the reported frequency of certain genomic variants and their implications; with the upgraded version and plug-ins, the results will have fewer hallucinations — inaccurate results — and key data references.
Unlimited accessibility. Uninterrupted access is a compelling reason to upgrade. While the free version may have usage limitations, the premium version provides unrestricted, round-the-clock access. Be it a late-night research quest or an early-morning patient query, your AI assistant will always be available.
Strengthened privacy and security. The premium version of ChatGPT includes heightened privacy and security measures. Just make sure to follow HIPAA and not include identifiers when making queries.
Embracing AI tools like ChatGPT in your practice can help you stay at the cutting edge of medical care, saving you time, enhancing patient communication, and supporting you in providing personalized care.
While the free version can serve as a good starting point (there are apps for both iOS and Android), upgrading to the paid version opens up a world of possibilities that can truly supercharge your practice.
I would love to hear your comments on this column or on future topics. Contact me at [email protected].
Arturo Loaiza-Bonilla, MD, MSEd, is the cofounder and chief medical officer at Massive Bio, a company connecting patients to clinical trials using artificial intelligence. His research and professional interests focus on precision medicine, clinical trial design, digital health, entrepreneurship, and patient advocacy. Dr. Loaiza-Bonilla is Assistant Professor of Medicine, Drexel University School of Medicine, Philadelphia, Pennsylvania, and serves as medical director of oncology research at Capital Health in New Jersey, where he maintains a connection to patient care by attending to patients 2 days a week. He has financial relationships with Verify, PSI CRO, Bayer, AstraZeneca, Cardinal Health, BrightInsight, The Lynx Group, Fresenius, Pfizer, Ipsen, Guardant, Amgen, Eisai, Natera, Merck, and Bristol Myers Squibb.
A version of this article appeared on Medscape.com.
Artificial intelligence (AI) has already demonstrated its potential in various areas of healthcare, from early disease detection and drug discovery to genomics and personalized care. OpenAI’s ChatGPT, a large language model, is one AI tool that has been transforming practices across the globe, including mine.
Let me walk you through it.
ChatGPT is essentially an AI-fueled assistant, capable of interpreting and generating human-like text in response to user inputs. Imagine a well-informed and competent trainee working with you, ready to tackle tasks from handling patient inquiries to summarizing intricate medical literature.
Currently, ChatGPT works on the “freemium” pricing model; there is a free version built upon GPT-3.5 as well as a subscription “ChatGPT Plus” version based on GPT-4 which offers additional features such as the use of third-party plug-ins.
Now, you may ask, “Isn’t the free version enough?” The free version is indeed impressive, but upgrading to the paid version for $20 per month unlocks the full potential of this tool, particularly if we add plug-ins.
Here are some of the best ways to incorporate ChatGPT Plus into your practice.
Time saver and efficiency multiplier. The paid version of ChatGPT is an extraordinary time-saving tool. It can help you sort through vast amounts of medical literature in a fraction of the time it would normally take. Imagine having to sift through hundreds of articles to find the latest research relevant to a patient’s case. With the paid version of ChatGPT, you can simply ask it to provide summaries of the most recent and relevant studies, all in seconds.
Did you forget about that PowerPoint you need to make but know the potential papers you would use? No problem. ChatGPT can create slides in a few minutes. It becomes your on-demand research assistant.
Of course, you need to provide the source you find most relevant to you. Using plug-ins such as ScholarAI and Link Reader are great.
Improved patient communication. Explaining complex medical terminology and procedures to patients can sometimes be a challenge. ChatGPT can generate simplified and personalized explanations for your patients, fostering their understanding and involvement in their care process.
Epic is currently collaborating with Nuance Communications, Microsoft’s speech recognition subsidiary, to use generative AI tools for medical note-taking in the electronic health record. However, you do not need to wait for it; it just takes a prompt in ChatGPT and then copying/pasting the results into the chart.
Smoother administrative management. The premium version of ChatGPT can automate administrative tasks such as creating letters of medical necessity, clearance to other physicians for services, or even communications to staff on specific topics. This frees you to focus more on your core work: providing patient care.
Precision medicine aid. ChatGPT can be a powerful ally in the field of precision medicine. Its capabilities for analyzing large datasets and unearthing valuable insights can help deliver more personalized and potentially effective treatment plans. For example, one can prompt ChatGPT to query the reported frequency of certain genomic variants and their implications; with the upgraded version and plug-ins, the results will have fewer hallucinations — inaccurate results — and key data references.
Unlimited accessibility. Uninterrupted access is a compelling reason to upgrade. While the free version may have usage limitations, the premium version provides unrestricted, round-the-clock access. Be it a late-night research quest or an early-morning patient query, your AI assistant will always be available.
Strengthened privacy and security. The premium version of ChatGPT includes heightened privacy and security measures. Just make sure to follow HIPAA and not include identifiers when making queries.
Embracing AI tools like ChatGPT in your practice can help you stay at the cutting edge of medical care, saving you time, enhancing patient communication, and supporting you in providing personalized care.
While the free version can serve as a good starting point (there are apps for both iOS and Android), upgrading to the paid version opens up a world of possibilities that can truly supercharge your practice.
I would love to hear your comments on this column or on future topics. Contact me at [email protected].
Arturo Loaiza-Bonilla, MD, MSEd, is the cofounder and chief medical officer at Massive Bio, a company connecting patients to clinical trials using artificial intelligence. His research and professional interests focus on precision medicine, clinical trial design, digital health, entrepreneurship, and patient advocacy. Dr. Loaiza-Bonilla is Assistant Professor of Medicine, Drexel University School of Medicine, Philadelphia, Pennsylvania, and serves as medical director of oncology research at Capital Health in New Jersey, where he maintains a connection to patient care by attending to patients 2 days a week. He has financial relationships with Verify, PSI CRO, Bayer, AstraZeneca, Cardinal Health, BrightInsight, The Lynx Group, Fresenius, Pfizer, Ipsen, Guardant, Amgen, Eisai, Natera, Merck, and Bristol Myers Squibb.
A version of this article appeared on Medscape.com.
Artificial intelligence (AI) has already demonstrated its potential in various areas of healthcare, from early disease detection and drug discovery to genomics and personalized care. OpenAI’s ChatGPT, a large language model, is one AI tool that has been transforming practices across the globe, including mine.
Let me walk you through it.
ChatGPT is essentially an AI-fueled assistant, capable of interpreting and generating human-like text in response to user inputs. Imagine a well-informed and competent trainee working with you, ready to tackle tasks from handling patient inquiries to summarizing intricate medical literature.
Currently, ChatGPT works on the “freemium” pricing model; there is a free version built upon GPT-3.5 as well as a subscription “ChatGPT Plus” version based on GPT-4 which offers additional features such as the use of third-party plug-ins.
Now, you may ask, “Isn’t the free version enough?” The free version is indeed impressive, but upgrading to the paid version for $20 per month unlocks the full potential of this tool, particularly if we add plug-ins.
Here are some of the best ways to incorporate ChatGPT Plus into your practice.
Time saver and efficiency multiplier. The paid version of ChatGPT is an extraordinary time-saving tool. It can help you sort through vast amounts of medical literature in a fraction of the time it would normally take. Imagine having to sift through hundreds of articles to find the latest research relevant to a patient’s case. With the paid version of ChatGPT, you can simply ask it to provide summaries of the most recent and relevant studies, all in seconds.
Did you forget about that PowerPoint you need to make but know the potential papers you would use? No problem. ChatGPT can create slides in a few minutes. It becomes your on-demand research assistant.
Of course, you need to provide the source you find most relevant to you. Using plug-ins such as ScholarAI and Link Reader are great.
Improved patient communication. Explaining complex medical terminology and procedures to patients can sometimes be a challenge. ChatGPT can generate simplified and personalized explanations for your patients, fostering their understanding and involvement in their care process.
Epic is currently collaborating with Nuance Communications, Microsoft’s speech recognition subsidiary, to use generative AI tools for medical note-taking in the electronic health record. However, you do not need to wait for it; it just takes a prompt in ChatGPT and then copying/pasting the results into the chart.
Smoother administrative management. The premium version of ChatGPT can automate administrative tasks such as creating letters of medical necessity, clearance to other physicians for services, or even communications to staff on specific topics. This frees you to focus more on your core work: providing patient care.
Precision medicine aid. ChatGPT can be a powerful ally in the field of precision medicine. Its capabilities for analyzing large datasets and unearthing valuable insights can help deliver more personalized and potentially effective treatment plans. For example, one can prompt ChatGPT to query the reported frequency of certain genomic variants and their implications; with the upgraded version and plug-ins, the results will have fewer hallucinations — inaccurate results — and key data references.
Unlimited accessibility. Uninterrupted access is a compelling reason to upgrade. While the free version may have usage limitations, the premium version provides unrestricted, round-the-clock access. Be it a late-night research quest or an early-morning patient query, your AI assistant will always be available.
Strengthened privacy and security. The premium version of ChatGPT includes heightened privacy and security measures. Just make sure to follow HIPAA and not include identifiers when making queries.
Embracing AI tools like ChatGPT in your practice can help you stay at the cutting edge of medical care, saving you time, enhancing patient communication, and supporting you in providing personalized care.
While the free version can serve as a good starting point (there are apps for both iOS and Android), upgrading to the paid version opens up a world of possibilities that can truly supercharge your practice.
I would love to hear your comments on this column or on future topics. Contact me at [email protected].
Arturo Loaiza-Bonilla, MD, MSEd, is the cofounder and chief medical officer at Massive Bio, a company connecting patients to clinical trials using artificial intelligence. His research and professional interests focus on precision medicine, clinical trial design, digital health, entrepreneurship, and patient advocacy. Dr. Loaiza-Bonilla is Assistant Professor of Medicine, Drexel University School of Medicine, Philadelphia, Pennsylvania, and serves as medical director of oncology research at Capital Health in New Jersey, where he maintains a connection to patient care by attending to patients 2 days a week. He has financial relationships with Verify, PSI CRO, Bayer, AstraZeneca, Cardinal Health, BrightInsight, The Lynx Group, Fresenius, Pfizer, Ipsen, Guardant, Amgen, Eisai, Natera, Merck, and Bristol Myers Squibb.
A version of this article appeared on Medscape.com.
New KDIGO guideline encourages use of HCV-positive kidneys for HCV-negative recipients
The Kidney Disease: Improving Global Outcomes (KDIGO) Work Group has updated its guideline concerning the prevention, diagnosis, evaluation, and treatment of hepatitis C virus (HCV) infection in patients with chronic kidney disease (CKD).
Of note, KDIGO now supports transplant of HCV-positive kidneys to HCV-negative recipients.
The guidance document, authored by Ahmed Arslan Yousuf Awan, MD, of Baylor College of Medicine, Houston, and colleagues, was written in light of new evidence that has emerged since the 2018 guideline was published.
“The focused update was triggered by new data on antiviral treatment in patients with advanced stages of CKD (G4, G5, or G5D), transplant of HCV-infected kidneys into uninfected recipients, and evolution of the viewpoint on the role of kidney biopsy in managing kidney disease caused by HCV,” the guideline panelists wrote in Annals of Internal Medicine. “This update is intended to assist clinicians in the care of patients with HCV infection and CKD, including patients receiving dialysis (CKD G5D) and patients with a kidney transplant (CKD G1T-G5T).”
Anjay Rastogi, MD, PhD, professor and clinical chief of nephrology at the David Geffen School of Medicine at UCLA, said the update is both “timely and relevant,” and “will really have an impact on the organ shortage that we have for kidney transplant”
The updates are outlined below.
Expanded Access to HCV-Positive Kidneys
While the 2018 guideline recommended that HCV-positive kidneys be directed to HCV-positive recipients, the new guideline suggests that these kidneys are appropriate for all patients regardless of HCV status.
In support, the panelists cited a follow-up of THINKER-1 trial, which showed that eGFR and quality of life were not negatively affected when HCV-negative patients received an HCV-positive kidney, compared with an HCV-negative kidney. Data from 525 unmatched recipients in 16 other studies support this conclusion, the panelists noted.
Jose Debes, MD, PhD, associate professor at the University of Minnesota, Minneapolis, suggested that this is the most important update to the KDIGO guidelines.
“That [change] would be the main impact of these recommendations,” Dr. Debes said in an interview. “Several centers were already doing this, since some data [were] out there, but I think the fact that they’re making this into a guideline is quite important.”
Dr. Rastogi agreed that this recommendation is the most impactful update.
“That’s a big move,” Dr. Rastogi said in an interview. He predicted that the change will “definitely increase the donor pool, which is very, very important.”
For this new recommendation to have the greatest positive effect, however, Dr. Rastogi suggested that health care providers and treatment centers need to prepare an effective implementation strategy. He emphasized the importance of early communication with patients concerning the safety of HCV-positive kidneys, which depends on early initiation of direct-acting antiviral (DAA) therapy.
In the guideline, Dr. Awan and colleagues reported three documented cases of fibrosing cholestatic hepatitis occurred in patients who did not begin DAA therapy until 30 days after transplant.
“[Patients] should start [DAA treatment] right away,” Dr. Rastogi said, “and sometimes even before the transplant.”
This will require institutional support, he noted, as centers need to ensure that patients are covered for DAA therapy and medication is readily available.
Sofosbuvir Given the Green Light
Compared with the 2018 guideline, which recommended against sofosbuvir in patients with CKD G4 and G5, including those on dialysis, because of concerns about metabolization via the kidneys, the new guideline suggests that sofosbuvir-based DAA regimens are appropriate in patients with glomerular filtration rate (GFR) less than 30 mL/min per 1.73 m2, including those receiving dialysis.
This recommendation was based on a systematic review of 106 studies including both sofosbuvir-based and non-sofosbuvir-based DAA regimens that showed high safety and efficacy for all DAA regimen types across a broad variety of patient types.
“DAAs are highly effective and well tolerated treatments for hepatitis C in patients across all stages of CKD, including those undergoing dialysis and kidney transplant recipients, with no need for dose adjustment,” Dr. Awan and colleagues wrote.
Loosened Biopsy Requirements
Unlike the 2018 guideline, which advised kidney biopsy in HCV-positive patients with clinical evidence of glomerular disease prior to initiating DAA treatment, the new guideline suggests that HCV-infected patients with a typical presentation of immune-complex proliferative glomerulonephritis do not require confirmatory kidney biopsy.
“Because almost all patients with chronic hepatitis C (with or without glomerulonephritis) should be treated with DAAs, a kidney biopsy is unlikely to change management in most patients with hepatitis C and clinical glomerulonephritis,” the panelists wrote.
If kidney disease does not stabilize or improve with achievement of sustained virologic response, or if there is evidence of rapidly progressive glomerulonephritis, then a kidney biopsy should be considered before beginning immunosuppressive therapy, according to the guideline, which includes a flow chart to guide clinicians through this decision-making process.
Individualizing Immunosuppressive Therapy
Consistent with the old guideline, the new guideline recommends DAA treatment with concurrent immunosuppressive therapy for patients with cryoglobulinemic flare or rapidly progressive kidney failure. But in contrast, the new guideline calls for an individualized approach to immunosuppression in patients with nephrotic syndrome.
Dr. Awan and colleagues suggested that “nephrotic-range proteinuria (greater than 3.5 g/d) alone does not warrant use of immunosuppressive treatment because such patients can achieve remission of proteinuria after treatment with DAAs.” Still, if other associated complications — such as anasarca, thromboembolic disease, or severe hypoalbuminemia — are present, then immunosuppressive therapy may be warranted, with rituximab remaining the preferred first-line agent.
More Work Is Needed
Dr. Awan and colleagues concluded the guideline by highlighting areas of unmet need, and how filling these knowledge gaps could lead to additional guideline updates.
“Future studies of kidney donations from HCV-positive donors to HCV-negative recipients are needed to refine and clarify the timing of initiation and duration of DAA therapy and to assess long-term outcomes associated with this practice,” they wrote. “Also, randomized controlled trials are needed to determine which patients with HCV-associated kidney disease can be treated with DAA therapy alone versus in combination with immunosuppression and plasma exchange. KDIGO will assess the currency of its recommendations and the need to update them in the next 3 years.”
The guideline was funded by KDIGO. The investigators disclosed relationships with GSK, Gilead, Intercept, Novo Nordisk, and others. Dr. Rastogi and Dr. Debes had no conflicts of interest.
The Kidney Disease: Improving Global Outcomes (KDIGO) Work Group has updated its guideline concerning the prevention, diagnosis, evaluation, and treatment of hepatitis C virus (HCV) infection in patients with chronic kidney disease (CKD).
Of note, KDIGO now supports transplant of HCV-positive kidneys to HCV-negative recipients.
The guidance document, authored by Ahmed Arslan Yousuf Awan, MD, of Baylor College of Medicine, Houston, and colleagues, was written in light of new evidence that has emerged since the 2018 guideline was published.
“The focused update was triggered by new data on antiviral treatment in patients with advanced stages of CKD (G4, G5, or G5D), transplant of HCV-infected kidneys into uninfected recipients, and evolution of the viewpoint on the role of kidney biopsy in managing kidney disease caused by HCV,” the guideline panelists wrote in Annals of Internal Medicine. “This update is intended to assist clinicians in the care of patients with HCV infection and CKD, including patients receiving dialysis (CKD G5D) and patients with a kidney transplant (CKD G1T-G5T).”
Anjay Rastogi, MD, PhD, professor and clinical chief of nephrology at the David Geffen School of Medicine at UCLA, said the update is both “timely and relevant,” and “will really have an impact on the organ shortage that we have for kidney transplant”
The updates are outlined below.
Expanded Access to HCV-Positive Kidneys
While the 2018 guideline recommended that HCV-positive kidneys be directed to HCV-positive recipients, the new guideline suggests that these kidneys are appropriate for all patients regardless of HCV status.
In support, the panelists cited a follow-up of THINKER-1 trial, which showed that eGFR and quality of life were not negatively affected when HCV-negative patients received an HCV-positive kidney, compared with an HCV-negative kidney. Data from 525 unmatched recipients in 16 other studies support this conclusion, the panelists noted.
Jose Debes, MD, PhD, associate professor at the University of Minnesota, Minneapolis, suggested that this is the most important update to the KDIGO guidelines.
“That [change] would be the main impact of these recommendations,” Dr. Debes said in an interview. “Several centers were already doing this, since some data [were] out there, but I think the fact that they’re making this into a guideline is quite important.”
Dr. Rastogi agreed that this recommendation is the most impactful update.
“That’s a big move,” Dr. Rastogi said in an interview. He predicted that the change will “definitely increase the donor pool, which is very, very important.”
For this new recommendation to have the greatest positive effect, however, Dr. Rastogi suggested that health care providers and treatment centers need to prepare an effective implementation strategy. He emphasized the importance of early communication with patients concerning the safety of HCV-positive kidneys, which depends on early initiation of direct-acting antiviral (DAA) therapy.
In the guideline, Dr. Awan and colleagues reported three documented cases of fibrosing cholestatic hepatitis occurred in patients who did not begin DAA therapy until 30 days after transplant.
“[Patients] should start [DAA treatment] right away,” Dr. Rastogi said, “and sometimes even before the transplant.”
This will require institutional support, he noted, as centers need to ensure that patients are covered for DAA therapy and medication is readily available.
Sofosbuvir Given the Green Light
Compared with the 2018 guideline, which recommended against sofosbuvir in patients with CKD G4 and G5, including those on dialysis, because of concerns about metabolization via the kidneys, the new guideline suggests that sofosbuvir-based DAA regimens are appropriate in patients with glomerular filtration rate (GFR) less than 30 mL/min per 1.73 m2, including those receiving dialysis.
This recommendation was based on a systematic review of 106 studies including both sofosbuvir-based and non-sofosbuvir-based DAA regimens that showed high safety and efficacy for all DAA regimen types across a broad variety of patient types.
“DAAs are highly effective and well tolerated treatments for hepatitis C in patients across all stages of CKD, including those undergoing dialysis and kidney transplant recipients, with no need for dose adjustment,” Dr. Awan and colleagues wrote.
Loosened Biopsy Requirements
Unlike the 2018 guideline, which advised kidney biopsy in HCV-positive patients with clinical evidence of glomerular disease prior to initiating DAA treatment, the new guideline suggests that HCV-infected patients with a typical presentation of immune-complex proliferative glomerulonephritis do not require confirmatory kidney biopsy.
“Because almost all patients with chronic hepatitis C (with or without glomerulonephritis) should be treated with DAAs, a kidney biopsy is unlikely to change management in most patients with hepatitis C and clinical glomerulonephritis,” the panelists wrote.
If kidney disease does not stabilize or improve with achievement of sustained virologic response, or if there is evidence of rapidly progressive glomerulonephritis, then a kidney biopsy should be considered before beginning immunosuppressive therapy, according to the guideline, which includes a flow chart to guide clinicians through this decision-making process.
Individualizing Immunosuppressive Therapy
Consistent with the old guideline, the new guideline recommends DAA treatment with concurrent immunosuppressive therapy for patients with cryoglobulinemic flare or rapidly progressive kidney failure. But in contrast, the new guideline calls for an individualized approach to immunosuppression in patients with nephrotic syndrome.
Dr. Awan and colleagues suggested that “nephrotic-range proteinuria (greater than 3.5 g/d) alone does not warrant use of immunosuppressive treatment because such patients can achieve remission of proteinuria after treatment with DAAs.” Still, if other associated complications — such as anasarca, thromboembolic disease, or severe hypoalbuminemia — are present, then immunosuppressive therapy may be warranted, with rituximab remaining the preferred first-line agent.
More Work Is Needed
Dr. Awan and colleagues concluded the guideline by highlighting areas of unmet need, and how filling these knowledge gaps could lead to additional guideline updates.
“Future studies of kidney donations from HCV-positive donors to HCV-negative recipients are needed to refine and clarify the timing of initiation and duration of DAA therapy and to assess long-term outcomes associated with this practice,” they wrote. “Also, randomized controlled trials are needed to determine which patients with HCV-associated kidney disease can be treated with DAA therapy alone versus in combination with immunosuppression and plasma exchange. KDIGO will assess the currency of its recommendations and the need to update them in the next 3 years.”
The guideline was funded by KDIGO. The investigators disclosed relationships with GSK, Gilead, Intercept, Novo Nordisk, and others. Dr. Rastogi and Dr. Debes had no conflicts of interest.
The Kidney Disease: Improving Global Outcomes (KDIGO) Work Group has updated its guideline concerning the prevention, diagnosis, evaluation, and treatment of hepatitis C virus (HCV) infection in patients with chronic kidney disease (CKD).
Of note, KDIGO now supports transplant of HCV-positive kidneys to HCV-negative recipients.
The guidance document, authored by Ahmed Arslan Yousuf Awan, MD, of Baylor College of Medicine, Houston, and colleagues, was written in light of new evidence that has emerged since the 2018 guideline was published.
“The focused update was triggered by new data on antiviral treatment in patients with advanced stages of CKD (G4, G5, or G5D), transplant of HCV-infected kidneys into uninfected recipients, and evolution of the viewpoint on the role of kidney biopsy in managing kidney disease caused by HCV,” the guideline panelists wrote in Annals of Internal Medicine. “This update is intended to assist clinicians in the care of patients with HCV infection and CKD, including patients receiving dialysis (CKD G5D) and patients with a kidney transplant (CKD G1T-G5T).”
Anjay Rastogi, MD, PhD, professor and clinical chief of nephrology at the David Geffen School of Medicine at UCLA, said the update is both “timely and relevant,” and “will really have an impact on the organ shortage that we have for kidney transplant”
The updates are outlined below.
Expanded Access to HCV-Positive Kidneys
While the 2018 guideline recommended that HCV-positive kidneys be directed to HCV-positive recipients, the new guideline suggests that these kidneys are appropriate for all patients regardless of HCV status.
In support, the panelists cited a follow-up of THINKER-1 trial, which showed that eGFR and quality of life were not negatively affected when HCV-negative patients received an HCV-positive kidney, compared with an HCV-negative kidney. Data from 525 unmatched recipients in 16 other studies support this conclusion, the panelists noted.
Jose Debes, MD, PhD, associate professor at the University of Minnesota, Minneapolis, suggested that this is the most important update to the KDIGO guidelines.
“That [change] would be the main impact of these recommendations,” Dr. Debes said in an interview. “Several centers were already doing this, since some data [were] out there, but I think the fact that they’re making this into a guideline is quite important.”
Dr. Rastogi agreed that this recommendation is the most impactful update.
“That’s a big move,” Dr. Rastogi said in an interview. He predicted that the change will “definitely increase the donor pool, which is very, very important.”
For this new recommendation to have the greatest positive effect, however, Dr. Rastogi suggested that health care providers and treatment centers need to prepare an effective implementation strategy. He emphasized the importance of early communication with patients concerning the safety of HCV-positive kidneys, which depends on early initiation of direct-acting antiviral (DAA) therapy.
In the guideline, Dr. Awan and colleagues reported three documented cases of fibrosing cholestatic hepatitis occurred in patients who did not begin DAA therapy until 30 days after transplant.
“[Patients] should start [DAA treatment] right away,” Dr. Rastogi said, “and sometimes even before the transplant.”
This will require institutional support, he noted, as centers need to ensure that patients are covered for DAA therapy and medication is readily available.
Sofosbuvir Given the Green Light
Compared with the 2018 guideline, which recommended against sofosbuvir in patients with CKD G4 and G5, including those on dialysis, because of concerns about metabolization via the kidneys, the new guideline suggests that sofosbuvir-based DAA regimens are appropriate in patients with glomerular filtration rate (GFR) less than 30 mL/min per 1.73 m2, including those receiving dialysis.
This recommendation was based on a systematic review of 106 studies including both sofosbuvir-based and non-sofosbuvir-based DAA regimens that showed high safety and efficacy for all DAA regimen types across a broad variety of patient types.
“DAAs are highly effective and well tolerated treatments for hepatitis C in patients across all stages of CKD, including those undergoing dialysis and kidney transplant recipients, with no need for dose adjustment,” Dr. Awan and colleagues wrote.
Loosened Biopsy Requirements
Unlike the 2018 guideline, which advised kidney biopsy in HCV-positive patients with clinical evidence of glomerular disease prior to initiating DAA treatment, the new guideline suggests that HCV-infected patients with a typical presentation of immune-complex proliferative glomerulonephritis do not require confirmatory kidney biopsy.
“Because almost all patients with chronic hepatitis C (with or without glomerulonephritis) should be treated with DAAs, a kidney biopsy is unlikely to change management in most patients with hepatitis C and clinical glomerulonephritis,” the panelists wrote.
If kidney disease does not stabilize or improve with achievement of sustained virologic response, or if there is evidence of rapidly progressive glomerulonephritis, then a kidney biopsy should be considered before beginning immunosuppressive therapy, according to the guideline, which includes a flow chart to guide clinicians through this decision-making process.
Individualizing Immunosuppressive Therapy
Consistent with the old guideline, the new guideline recommends DAA treatment with concurrent immunosuppressive therapy for patients with cryoglobulinemic flare or rapidly progressive kidney failure. But in contrast, the new guideline calls for an individualized approach to immunosuppression in patients with nephrotic syndrome.
Dr. Awan and colleagues suggested that “nephrotic-range proteinuria (greater than 3.5 g/d) alone does not warrant use of immunosuppressive treatment because such patients can achieve remission of proteinuria after treatment with DAAs.” Still, if other associated complications — such as anasarca, thromboembolic disease, or severe hypoalbuminemia — are present, then immunosuppressive therapy may be warranted, with rituximab remaining the preferred first-line agent.
More Work Is Needed
Dr. Awan and colleagues concluded the guideline by highlighting areas of unmet need, and how filling these knowledge gaps could lead to additional guideline updates.
“Future studies of kidney donations from HCV-positive donors to HCV-negative recipients are needed to refine and clarify the timing of initiation and duration of DAA therapy and to assess long-term outcomes associated with this practice,” they wrote. “Also, randomized controlled trials are needed to determine which patients with HCV-associated kidney disease can be treated with DAA therapy alone versus in combination with immunosuppression and plasma exchange. KDIGO will assess the currency of its recommendations and the need to update them in the next 3 years.”
The guideline was funded by KDIGO. The investigators disclosed relationships with GSK, Gilead, Intercept, Novo Nordisk, and others. Dr. Rastogi and Dr. Debes had no conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Are you sure your patient is alive?
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.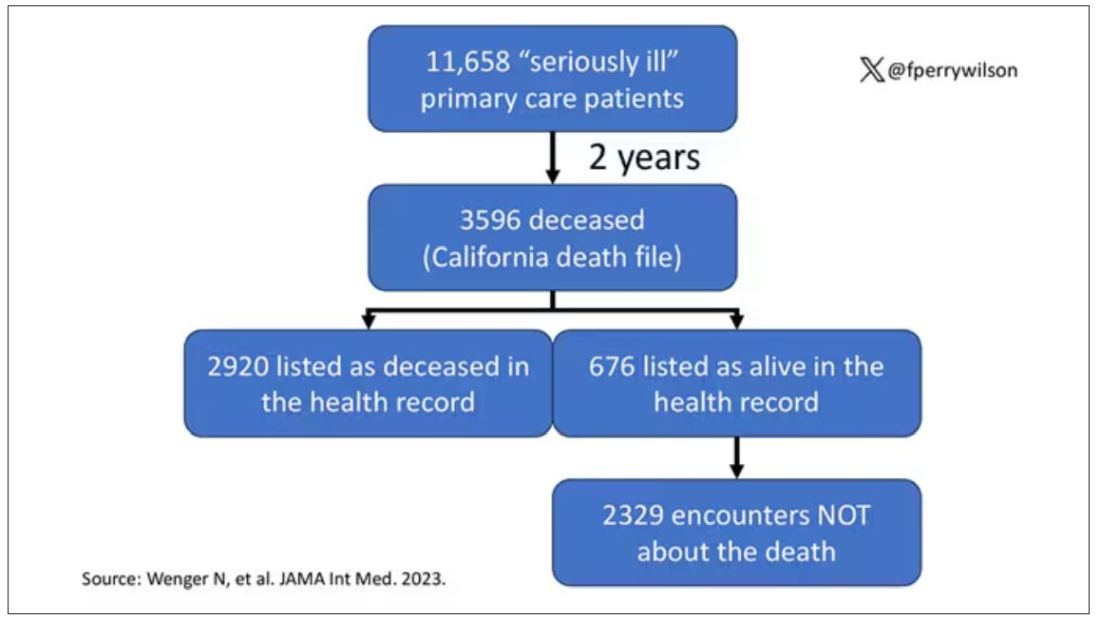
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.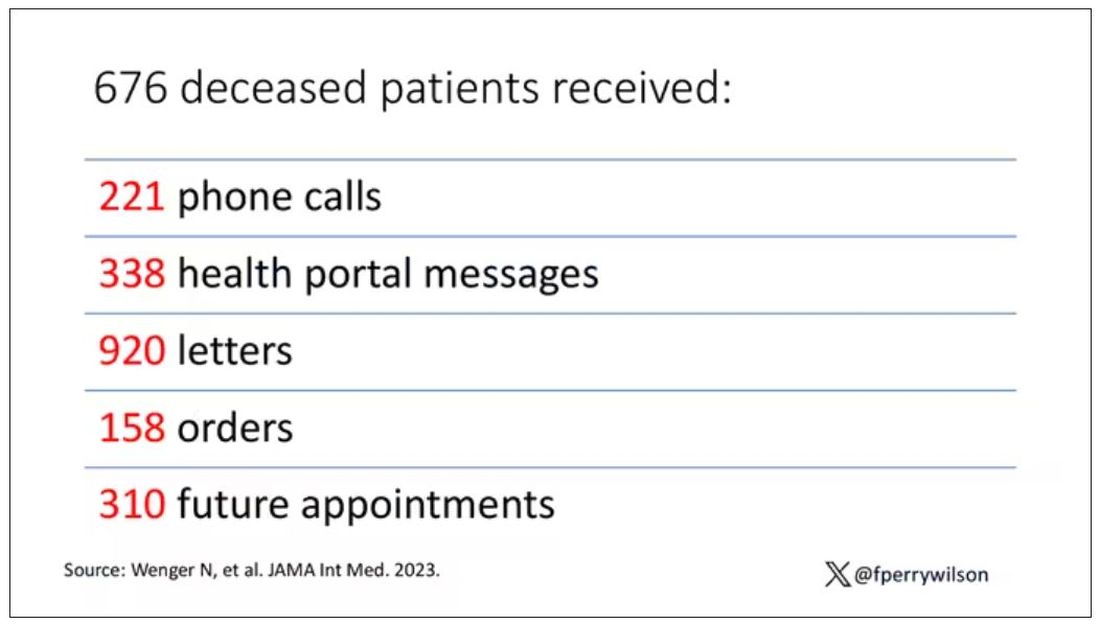
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
Experimental Therapy Restores Cognitive Function in Chronic TBI
(msTBI) and chronic sequelae.
Participants in this first-in-humans trial experienced brain injuries between 3-18 years before the study that left them with persistent neuropsychological impairment and a range of functional disabilities.
This is the first time a DBS device has been implanted in the central thalamus in humans, an area of the brain measuring only a few millimeters wide that helps regulate consciousness.
Placing the electrodes required a novel surgical technique developed by the investigators that included virtual models of each participant’s brain, microelectrode recording, and neuroimaging to identify neuronal circuits affected by the TBI.
After 3 months of 12-hour daily DBS treatments, participants’ performance on cognitive tests improved by an average of 32% from baseline. Participants were able to read books, watch TV shows, play video games, complete schoolwork, and felt significantly less fatigued during the day.
Although the small trial only included five patients, the work is already being hailed by other experts as significant.“We were looking for partial restoration of executive attention and expected [the treatment] would have an effect, but I wouldn’t have anticipated the effect size we saw,” co-lead investigator Nicholas Schiff, MD, professor of neuroscience at Weill Cornell Medical College, New York City, said in an interview.
The findings were published online Dec. 4 in Nature Medicine.
“No Trivial Feat”
An estimated 5.3 million children and adults are living with a permanent TBI-related disability in the US today. There currently is no effective therapy for impaired attention, executive function, working memory or information-processing speed caused by the initial injury.
Previous research suggests that a loss of activity in key brain circuits in the thalamus may be associated with a loss of cognitive function.
The investigators recruited six adults (four men and two women) between the ages of 22 and 60 years with a history of msTBI and chronic neuropsychological impairment and functional disability. One participant was later withdrawn from the trial for protocol noncompliance.
Participants completed a range of questionnaires and tests to establish baseline cognitive, psychological, and quality-of-life status.
To restore lost executive functioning in the brain, investigators had to target not only the central lateral nucleus, but also the neuronal network connected to the region that reaches other parts of the brain.
“To do both of those things we had to develop a whole toolset in order to model both the target and trajectory, which had to be right to make it work properly,” co-lead investigator Jaimie Henderson, MD, professor of neurosurgery at Stanford University College of Medicine, Stanford, California, said in an interview. “That gave us a pretty narrow window in which to work and getting an electrode accurately to this target is not a trivial feat.”
“A Moving Target”
Each participant’s brain physiology was slightly different, meaning the path that worked for one individual might not work for another. The surgery was further complicated by shifting in the brain that occurred as individual electrodes were placed.
“It was a literal moving target,” Dr. Henderson said.
In the beginning, investigators used microelectrode recording to “listen” to individual neurons to see which ones weren’t firing correctly.
When that method failed to offer the precise information needed for electrode placement, the investigators switched to neuroimaging, which allowed them to complete the surgery more quickly and accurately.
Participants remained in the hospital 1-2 days after surgery. They returned for postoperative imaging 30 days after surgery and were randomly assigned to different schedules for a 14-day titration period to optimize DBS stimulation.
The primary outcome was a 10% improvement on part B of the trail-making test, a neuropsychological test that measures executive functioning.
After 90 days of 12-hour daily DBS treatments, participants’ scores increased 15%–52% (average 32%) from baseline. Participants also reported an average of 33% decline in fatigue, one of the most common side effects of msTBI, and an average 80% improvement in attention.
The main safety risk during the 3- to-4-hour procedure is bleeding, which didn’t affect any of the participants in this study. One participant developed a surgical site infection, but all other side effects were mild.
After the 90-day treatment period, the study plan called for patients to be randomly assigned to a blinded withdrawal of treatment, with the DBS turned off for 21 days. Two of the patients declined to be randomized. DBS was turned off in one participant while the other two continued as normal.
After 3 weeks, the patient whose DBS was turned off showed a 34% decline on cognitive tests. The device was reactivated after the study and that participant has since reported improvements.
The DBS devices continue to function in all participants. Although their performance is not being measured as part of the study, anecdotal reports indicate sustained improvement in executive functioning.
“The brain injury causes this global down-regulation of brain function and what we think that this is doing is turning that back up again,” Dr. Henderson said. “At a very simplistic level, what we’re trying to do is turn the lights back up after the dimmer switch is switched down from the injury.”
New Hope
TBI patients are usually treated aggressively during the first year, when significant improvements are most likely, but there are few therapeutic options beyond that time, said neurologist Javier Cardenas, MD, who commented on the findings for this article.
“Many providers throw their hands up after a year in terms of intervention and then we’re always looking at potential declines over time,” said Dr. Cardenas, director of the Concussion and Brain Injury Center at the Rockefeller Neuroscience Institution, West Virginia University, Morgantown. “Most people plateau and don’t decline but we’re always worried about a secondary decline in traumatic brain injury.”Surgery is usually only employed immediately following the brain injury. The notion of surgery as a therapeutic option years after the initial assault on the brain is novel, said Jimmy Yang, MD, assistant professor of neurologic surgery at Ohio State University College of Medicine, Columbus, who commented on the findings for this article.
“While deep brain stimulation surgery in clinical practice is specifically tailored to each patient we treat, this study goes a step further by integrating research tools that have not yet made it to the clinical realm,” Dr. Yang said. “As a result, while these methods are not commonly used in clinical care, the overall strategy highlights how research advances are linked to clinical advances.”
Investigators are working to secure funding for a larger phase 2 trial.
“With millions of people affected by traumatic brain injury but without effective therapies, this study brings hope that options are on the horizon to help these patients,” Dr. Yang said.
The study was supported by funding from the National Institute of Health BRAIN Initiative and a grant from the Translational Science Center at Weill Cornell Medical College. Surgical implants were provided by Medtronic. Dr. Henderson and Dr. Schiff are listed as inventors on several patent applications for the experimental DBS therapy described in the study. Dr. Cardenas and Dr. Yang report no relevant financial relationships.
A version of this article first appeared on Medscape.com .
(msTBI) and chronic sequelae.
Participants in this first-in-humans trial experienced brain injuries between 3-18 years before the study that left them with persistent neuropsychological impairment and a range of functional disabilities.
This is the first time a DBS device has been implanted in the central thalamus in humans, an area of the brain measuring only a few millimeters wide that helps regulate consciousness.
Placing the electrodes required a novel surgical technique developed by the investigators that included virtual models of each participant’s brain, microelectrode recording, and neuroimaging to identify neuronal circuits affected by the TBI.
After 3 months of 12-hour daily DBS treatments, participants’ performance on cognitive tests improved by an average of 32% from baseline. Participants were able to read books, watch TV shows, play video games, complete schoolwork, and felt significantly less fatigued during the day.
Although the small trial only included five patients, the work is already being hailed by other experts as significant.“We were looking for partial restoration of executive attention and expected [the treatment] would have an effect, but I wouldn’t have anticipated the effect size we saw,” co-lead investigator Nicholas Schiff, MD, professor of neuroscience at Weill Cornell Medical College, New York City, said in an interview.
The findings were published online Dec. 4 in Nature Medicine.
“No Trivial Feat”
An estimated 5.3 million children and adults are living with a permanent TBI-related disability in the US today. There currently is no effective therapy for impaired attention, executive function, working memory or information-processing speed caused by the initial injury.
Previous research suggests that a loss of activity in key brain circuits in the thalamus may be associated with a loss of cognitive function.
The investigators recruited six adults (four men and two women) between the ages of 22 and 60 years with a history of msTBI and chronic neuropsychological impairment and functional disability. One participant was later withdrawn from the trial for protocol noncompliance.
Participants completed a range of questionnaires and tests to establish baseline cognitive, psychological, and quality-of-life status.
To restore lost executive functioning in the brain, investigators had to target not only the central lateral nucleus, but also the neuronal network connected to the region that reaches other parts of the brain.
“To do both of those things we had to develop a whole toolset in order to model both the target and trajectory, which had to be right to make it work properly,” co-lead investigator Jaimie Henderson, MD, professor of neurosurgery at Stanford University College of Medicine, Stanford, California, said in an interview. “That gave us a pretty narrow window in which to work and getting an electrode accurately to this target is not a trivial feat.”
“A Moving Target”
Each participant’s brain physiology was slightly different, meaning the path that worked for one individual might not work for another. The surgery was further complicated by shifting in the brain that occurred as individual electrodes were placed.
“It was a literal moving target,” Dr. Henderson said.
In the beginning, investigators used microelectrode recording to “listen” to individual neurons to see which ones weren’t firing correctly.
When that method failed to offer the precise information needed for electrode placement, the investigators switched to neuroimaging, which allowed them to complete the surgery more quickly and accurately.
Participants remained in the hospital 1-2 days after surgery. They returned for postoperative imaging 30 days after surgery and were randomly assigned to different schedules for a 14-day titration period to optimize DBS stimulation.
The primary outcome was a 10% improvement on part B of the trail-making test, a neuropsychological test that measures executive functioning.
After 90 days of 12-hour daily DBS treatments, participants’ scores increased 15%–52% (average 32%) from baseline. Participants also reported an average of 33% decline in fatigue, one of the most common side effects of msTBI, and an average 80% improvement in attention.
The main safety risk during the 3- to-4-hour procedure is bleeding, which didn’t affect any of the participants in this study. One participant developed a surgical site infection, but all other side effects were mild.
After the 90-day treatment period, the study plan called for patients to be randomly assigned to a blinded withdrawal of treatment, with the DBS turned off for 21 days. Two of the patients declined to be randomized. DBS was turned off in one participant while the other two continued as normal.
After 3 weeks, the patient whose DBS was turned off showed a 34% decline on cognitive tests. The device was reactivated after the study and that participant has since reported improvements.
The DBS devices continue to function in all participants. Although their performance is not being measured as part of the study, anecdotal reports indicate sustained improvement in executive functioning.
“The brain injury causes this global down-regulation of brain function and what we think that this is doing is turning that back up again,” Dr. Henderson said. “At a very simplistic level, what we’re trying to do is turn the lights back up after the dimmer switch is switched down from the injury.”
New Hope
TBI patients are usually treated aggressively during the first year, when significant improvements are most likely, but there are few therapeutic options beyond that time, said neurologist Javier Cardenas, MD, who commented on the findings for this article.
“Many providers throw their hands up after a year in terms of intervention and then we’re always looking at potential declines over time,” said Dr. Cardenas, director of the Concussion and Brain Injury Center at the Rockefeller Neuroscience Institution, West Virginia University, Morgantown. “Most people plateau and don’t decline but we’re always worried about a secondary decline in traumatic brain injury.”Surgery is usually only employed immediately following the brain injury. The notion of surgery as a therapeutic option years after the initial assault on the brain is novel, said Jimmy Yang, MD, assistant professor of neurologic surgery at Ohio State University College of Medicine, Columbus, who commented on the findings for this article.
“While deep brain stimulation surgery in clinical practice is specifically tailored to each patient we treat, this study goes a step further by integrating research tools that have not yet made it to the clinical realm,” Dr. Yang said. “As a result, while these methods are not commonly used in clinical care, the overall strategy highlights how research advances are linked to clinical advances.”
Investigators are working to secure funding for a larger phase 2 trial.
“With millions of people affected by traumatic brain injury but without effective therapies, this study brings hope that options are on the horizon to help these patients,” Dr. Yang said.
The study was supported by funding from the National Institute of Health BRAIN Initiative and a grant from the Translational Science Center at Weill Cornell Medical College. Surgical implants were provided by Medtronic. Dr. Henderson and Dr. Schiff are listed as inventors on several patent applications for the experimental DBS therapy described in the study. Dr. Cardenas and Dr. Yang report no relevant financial relationships.
A version of this article first appeared on Medscape.com .
(msTBI) and chronic sequelae.
Participants in this first-in-humans trial experienced brain injuries between 3-18 years before the study that left them with persistent neuropsychological impairment and a range of functional disabilities.
This is the first time a DBS device has been implanted in the central thalamus in humans, an area of the brain measuring only a few millimeters wide that helps regulate consciousness.
Placing the electrodes required a novel surgical technique developed by the investigators that included virtual models of each participant’s brain, microelectrode recording, and neuroimaging to identify neuronal circuits affected by the TBI.
After 3 months of 12-hour daily DBS treatments, participants’ performance on cognitive tests improved by an average of 32% from baseline. Participants were able to read books, watch TV shows, play video games, complete schoolwork, and felt significantly less fatigued during the day.
Although the small trial only included five patients, the work is already being hailed by other experts as significant.“We were looking for partial restoration of executive attention and expected [the treatment] would have an effect, but I wouldn’t have anticipated the effect size we saw,” co-lead investigator Nicholas Schiff, MD, professor of neuroscience at Weill Cornell Medical College, New York City, said in an interview.
The findings were published online Dec. 4 in Nature Medicine.
“No Trivial Feat”
An estimated 5.3 million children and adults are living with a permanent TBI-related disability in the US today. There currently is no effective therapy for impaired attention, executive function, working memory or information-processing speed caused by the initial injury.
Previous research suggests that a loss of activity in key brain circuits in the thalamus may be associated with a loss of cognitive function.
The investigators recruited six adults (four men and two women) between the ages of 22 and 60 years with a history of msTBI and chronic neuropsychological impairment and functional disability. One participant was later withdrawn from the trial for protocol noncompliance.
Participants completed a range of questionnaires and tests to establish baseline cognitive, psychological, and quality-of-life status.
To restore lost executive functioning in the brain, investigators had to target not only the central lateral nucleus, but also the neuronal network connected to the region that reaches other parts of the brain.
“To do both of those things we had to develop a whole toolset in order to model both the target and trajectory, which had to be right to make it work properly,” co-lead investigator Jaimie Henderson, MD, professor of neurosurgery at Stanford University College of Medicine, Stanford, California, said in an interview. “That gave us a pretty narrow window in which to work and getting an electrode accurately to this target is not a trivial feat.”
“A Moving Target”
Each participant’s brain physiology was slightly different, meaning the path that worked for one individual might not work for another. The surgery was further complicated by shifting in the brain that occurred as individual electrodes were placed.
“It was a literal moving target,” Dr. Henderson said.
In the beginning, investigators used microelectrode recording to “listen” to individual neurons to see which ones weren’t firing correctly.
When that method failed to offer the precise information needed for electrode placement, the investigators switched to neuroimaging, which allowed them to complete the surgery more quickly and accurately.
Participants remained in the hospital 1-2 days after surgery. They returned for postoperative imaging 30 days after surgery and were randomly assigned to different schedules for a 14-day titration period to optimize DBS stimulation.
The primary outcome was a 10% improvement on part B of the trail-making test, a neuropsychological test that measures executive functioning.
After 90 days of 12-hour daily DBS treatments, participants’ scores increased 15%–52% (average 32%) from baseline. Participants also reported an average of 33% decline in fatigue, one of the most common side effects of msTBI, and an average 80% improvement in attention.
The main safety risk during the 3- to-4-hour procedure is bleeding, which didn’t affect any of the participants in this study. One participant developed a surgical site infection, but all other side effects were mild.
After the 90-day treatment period, the study plan called for patients to be randomly assigned to a blinded withdrawal of treatment, with the DBS turned off for 21 days. Two of the patients declined to be randomized. DBS was turned off in one participant while the other two continued as normal.
After 3 weeks, the patient whose DBS was turned off showed a 34% decline on cognitive tests. The device was reactivated after the study and that participant has since reported improvements.
The DBS devices continue to function in all participants. Although their performance is not being measured as part of the study, anecdotal reports indicate sustained improvement in executive functioning.
“The brain injury causes this global down-regulation of brain function and what we think that this is doing is turning that back up again,” Dr. Henderson said. “At a very simplistic level, what we’re trying to do is turn the lights back up after the dimmer switch is switched down from the injury.”
New Hope
TBI patients are usually treated aggressively during the first year, when significant improvements are most likely, but there are few therapeutic options beyond that time, said neurologist Javier Cardenas, MD, who commented on the findings for this article.
“Many providers throw their hands up after a year in terms of intervention and then we’re always looking at potential declines over time,” said Dr. Cardenas, director of the Concussion and Brain Injury Center at the Rockefeller Neuroscience Institution, West Virginia University, Morgantown. “Most people plateau and don’t decline but we’re always worried about a secondary decline in traumatic brain injury.”Surgery is usually only employed immediately following the brain injury. The notion of surgery as a therapeutic option years after the initial assault on the brain is novel, said Jimmy Yang, MD, assistant professor of neurologic surgery at Ohio State University College of Medicine, Columbus, who commented on the findings for this article.
“While deep brain stimulation surgery in clinical practice is specifically tailored to each patient we treat, this study goes a step further by integrating research tools that have not yet made it to the clinical realm,” Dr. Yang said. “As a result, while these methods are not commonly used in clinical care, the overall strategy highlights how research advances are linked to clinical advances.”
Investigators are working to secure funding for a larger phase 2 trial.
“With millions of people affected by traumatic brain injury but without effective therapies, this study brings hope that options are on the horizon to help these patients,” Dr. Yang said.
The study was supported by funding from the National Institute of Health BRAIN Initiative and a grant from the Translational Science Center at Weill Cornell Medical College. Surgical implants were provided by Medtronic. Dr. Henderson and Dr. Schiff are listed as inventors on several patent applications for the experimental DBS therapy described in the study. Dr. Cardenas and Dr. Yang report no relevant financial relationships.
A version of this article first appeared on Medscape.com .
Antireflux surgery may not reduce cancer risk in Barrett’s esophagus
, according to a Nordic retrospective study.
Risk of EAC was higher among patients who underwent surgery, and risk appeared to increase over time, suggesting that postoperative patients should continue to participate in surveillance programs, reported lead author Jesper Lagergren, MD, PhD, of the Karolinska Institutet, Stockholm, and colleagues.
“Antireflux surgery with fundoplication increases the ability of the gastroesophageal anatomic and physiological barrier to prevent reflux, and can thus prevent any carcinogenic gastric content from reaching the esophagus, including both acid and bile,” the investigators wrote in Gastroenterology, noting that surgery reduces esophageal acid exposure to a greater degree than medication. “Antireflux surgery may thus prevent esophageal adenocarcinoma better than antireflux medication.”
Three meta-analyses to date, however, have failed to provide consistent support for this hypothesis.
“Most of the studies included in these meta-analyses came from single centers, were of small sample size, examined only one treatment arm, and had a short or incomplete follow-up, and ... were hampered by heterogeneity among the included studies,” they noted.
For the present study, Dr. Lagergren and colleagues analyzed national registry data from 33,939 patients with Barrett’s esophagus in Denmark, Finland, Norway, and Sweden. Out of this group, 542 patients (1.6%) had undergone antireflux surgery, while the remainder were managed with antireflux medication.
In both groups, approximately two-thirds of the patients were men. The median age at enrollment was about a decade higher in the medication group (66 vs. 54 years), and this group also tended to have more comorbidities.
After a follow-up period as long as 32 years, the absolute rates of EAC were 1.3% and 2.6% in the medication and surgery groups, respectively. Multivariate analysis, with adjustments for sex, age, year, comorbidities, and age, revealed that postsurgical patients had a 90% increased risk of EAC (hazard ratio [HR], 1.9; 95% CI, 1.1-3.5), versus patients treated with antireflux medication alone.
The relatively higher risk of EAC appeared to increase over time, based on a nonsignificant hazard ratio of 1.8 during the 1- to 4-year follow-up period (HR, 1.8; 95% CI, 0.6-5.0), versus a significant, fourfold risk elevation during the 10- to 32-year follow-up period (HR, 4.4; 95% CI, 1.4-13.5).
“In this cohort of patients with Barrett’s esophagus, the risk of esophageal adenocarcinoma did not decrease after antireflux surgery compared with antireflux medication,” the investigators wrote. “Instead, the risk was increased throughout the follow-up among patients having undergone antireflux surgery.”
Dr. Lagergren and colleagues suggested that the reason for relatively higher cancer risk in the group that underwent surgery likely stems from early and prolonged acid exposure.
“[P]erforming antireflux surgery after years of GERD may be too late to enable a cancer-preventative effect, and most of the patients first diagnosed with Barrett’s esophagus reported a history of many years of GERD symptoms,” they wrote, suggesting that carcinogenic processes had already been set in motion by the time surgery was performed.
“[P]atients with Barrett’s esophagus who undergo antireflux surgery remain at an increased risk of esophageal adenocarcinoma and should continue taking part in surveillance programs,” the investigators concluded.
The study was funded by the Swedish Cancer Society, Swedish Research Council, and Stockholm County Council. The investigators disclosed no conflicts of interest.
Esophageal adenocarcinoma (EAC) has been increasing in frequency for decades. EAC’s only known precursor is Barrett’s esophagus (BE), a complication of GERD with chronic esophageal inflammation (reflux esophagitis). Chronic inflammation can predispose to cancer and refluxed acid itself can cause potentially carcinogenic double-strand DNA breaks in Barrett’s metaplasia. PPIs, which block secretion of the gastric acid that causes reflux esophagitis and DNA damage, are recommended to BE patients for cancer prevention. Logical as that practice may seem, meta-analyses have reached contradictory conclusions regarding the cancer-preventive benefits of PPIs. PPIs do not stop the reflux of other potential carcinogens such as bile salts, and thus it has been argued that fundoplication, which blocks the reflux of all gastric material, should be superior to PPIs for cancer prevention. Plausible as that argument sounds, meta-analyses of the generally small and heterogeneous studies on this issue have not found consistently that antireflux surgery is superior to medical therapy for cancer prevention in BE.
Now, a large, population-based cohort study by Åkerström et al. of Nordic BE patients followed for up to 32 years has found that the overall risk of EAC was higher for patients treated with fundoplication than for those treated with medication (adjusted HR 1.9, 95%CI 1.1-3.5). Furthermore, the EAC risk increased over time in the surgical patients. Well done as this study was, it has important limitations. The overall BE population was large (n=33,939), but only 1.6% (542 patients) had antireflux surgery, and only 14 of those developed EAC during follow-up. Those small numbers limit statistical power. Moreover, important residual confounding cannot be excluded. The surgical patients might have had more severe GERD than medical patients, and it is difficult to make a plausible argument for why fundoplication should increase EAC risk. Nevertheless, this study provides a good lesson on why a plausible argument needs supportive evidence before acting on it in clinical practice. While there may be some excellent reasons for recommending antireflux surgery over medication for patients with severe GERD, better esophageal cancer prevention does not appear to be one of them.
Stuart Jon Spechler, MD, is chief of the division of gastroenterology and codirector of the Center for Esophageal Diseases at Baylor University Medical Center, and codirector of the Center for Esophageal Research at Baylor Scott & White Research Institute, Dallas, Texas. Dr. Spechler is a consultant for Phathom Pharmaceuticals and ISOThrive, LLC.
Esophageal adenocarcinoma (EAC) has been increasing in frequency for decades. EAC’s only known precursor is Barrett’s esophagus (BE), a complication of GERD with chronic esophageal inflammation (reflux esophagitis). Chronic inflammation can predispose to cancer and refluxed acid itself can cause potentially carcinogenic double-strand DNA breaks in Barrett’s metaplasia. PPIs, which block secretion of the gastric acid that causes reflux esophagitis and DNA damage, are recommended to BE patients for cancer prevention. Logical as that practice may seem, meta-analyses have reached contradictory conclusions regarding the cancer-preventive benefits of PPIs. PPIs do not stop the reflux of other potential carcinogens such as bile salts, and thus it has been argued that fundoplication, which blocks the reflux of all gastric material, should be superior to PPIs for cancer prevention. Plausible as that argument sounds, meta-analyses of the generally small and heterogeneous studies on this issue have not found consistently that antireflux surgery is superior to medical therapy for cancer prevention in BE.
Now, a large, population-based cohort study by Åkerström et al. of Nordic BE patients followed for up to 32 years has found that the overall risk of EAC was higher for patients treated with fundoplication than for those treated with medication (adjusted HR 1.9, 95%CI 1.1-3.5). Furthermore, the EAC risk increased over time in the surgical patients. Well done as this study was, it has important limitations. The overall BE population was large (n=33,939), but only 1.6% (542 patients) had antireflux surgery, and only 14 of those developed EAC during follow-up. Those small numbers limit statistical power. Moreover, important residual confounding cannot be excluded. The surgical patients might have had more severe GERD than medical patients, and it is difficult to make a plausible argument for why fundoplication should increase EAC risk. Nevertheless, this study provides a good lesson on why a plausible argument needs supportive evidence before acting on it in clinical practice. While there may be some excellent reasons for recommending antireflux surgery over medication for patients with severe GERD, better esophageal cancer prevention does not appear to be one of them.
Stuart Jon Spechler, MD, is chief of the division of gastroenterology and codirector of the Center for Esophageal Diseases at Baylor University Medical Center, and codirector of the Center for Esophageal Research at Baylor Scott & White Research Institute, Dallas, Texas. Dr. Spechler is a consultant for Phathom Pharmaceuticals and ISOThrive, LLC.
Esophageal adenocarcinoma (EAC) has been increasing in frequency for decades. EAC’s only known precursor is Barrett’s esophagus (BE), a complication of GERD with chronic esophageal inflammation (reflux esophagitis). Chronic inflammation can predispose to cancer and refluxed acid itself can cause potentially carcinogenic double-strand DNA breaks in Barrett’s metaplasia. PPIs, which block secretion of the gastric acid that causes reflux esophagitis and DNA damage, are recommended to BE patients for cancer prevention. Logical as that practice may seem, meta-analyses have reached contradictory conclusions regarding the cancer-preventive benefits of PPIs. PPIs do not stop the reflux of other potential carcinogens such as bile salts, and thus it has been argued that fundoplication, which blocks the reflux of all gastric material, should be superior to PPIs for cancer prevention. Plausible as that argument sounds, meta-analyses of the generally small and heterogeneous studies on this issue have not found consistently that antireflux surgery is superior to medical therapy for cancer prevention in BE.
Now, a large, population-based cohort study by Åkerström et al. of Nordic BE patients followed for up to 32 years has found that the overall risk of EAC was higher for patients treated with fundoplication than for those treated with medication (adjusted HR 1.9, 95%CI 1.1-3.5). Furthermore, the EAC risk increased over time in the surgical patients. Well done as this study was, it has important limitations. The overall BE population was large (n=33,939), but only 1.6% (542 patients) had antireflux surgery, and only 14 of those developed EAC during follow-up. Those small numbers limit statistical power. Moreover, important residual confounding cannot be excluded. The surgical patients might have had more severe GERD than medical patients, and it is difficult to make a plausible argument for why fundoplication should increase EAC risk. Nevertheless, this study provides a good lesson on why a plausible argument needs supportive evidence before acting on it in clinical practice. While there may be some excellent reasons for recommending antireflux surgery over medication for patients with severe GERD, better esophageal cancer prevention does not appear to be one of them.
Stuart Jon Spechler, MD, is chief of the division of gastroenterology and codirector of the Center for Esophageal Diseases at Baylor University Medical Center, and codirector of the Center for Esophageal Research at Baylor Scott & White Research Institute, Dallas, Texas. Dr. Spechler is a consultant for Phathom Pharmaceuticals and ISOThrive, LLC.
, according to a Nordic retrospective study.
Risk of EAC was higher among patients who underwent surgery, and risk appeared to increase over time, suggesting that postoperative patients should continue to participate in surveillance programs, reported lead author Jesper Lagergren, MD, PhD, of the Karolinska Institutet, Stockholm, and colleagues.
“Antireflux surgery with fundoplication increases the ability of the gastroesophageal anatomic and physiological barrier to prevent reflux, and can thus prevent any carcinogenic gastric content from reaching the esophagus, including both acid and bile,” the investigators wrote in Gastroenterology, noting that surgery reduces esophageal acid exposure to a greater degree than medication. “Antireflux surgery may thus prevent esophageal adenocarcinoma better than antireflux medication.”
Three meta-analyses to date, however, have failed to provide consistent support for this hypothesis.
“Most of the studies included in these meta-analyses came from single centers, were of small sample size, examined only one treatment arm, and had a short or incomplete follow-up, and ... were hampered by heterogeneity among the included studies,” they noted.
For the present study, Dr. Lagergren and colleagues analyzed national registry data from 33,939 patients with Barrett’s esophagus in Denmark, Finland, Norway, and Sweden. Out of this group, 542 patients (1.6%) had undergone antireflux surgery, while the remainder were managed with antireflux medication.
In both groups, approximately two-thirds of the patients were men. The median age at enrollment was about a decade higher in the medication group (66 vs. 54 years), and this group also tended to have more comorbidities.
After a follow-up period as long as 32 years, the absolute rates of EAC were 1.3% and 2.6% in the medication and surgery groups, respectively. Multivariate analysis, with adjustments for sex, age, year, comorbidities, and age, revealed that postsurgical patients had a 90% increased risk of EAC (hazard ratio [HR], 1.9; 95% CI, 1.1-3.5), versus patients treated with antireflux medication alone.
The relatively higher risk of EAC appeared to increase over time, based on a nonsignificant hazard ratio of 1.8 during the 1- to 4-year follow-up period (HR, 1.8; 95% CI, 0.6-5.0), versus a significant, fourfold risk elevation during the 10- to 32-year follow-up period (HR, 4.4; 95% CI, 1.4-13.5).
“In this cohort of patients with Barrett’s esophagus, the risk of esophageal adenocarcinoma did not decrease after antireflux surgery compared with antireflux medication,” the investigators wrote. “Instead, the risk was increased throughout the follow-up among patients having undergone antireflux surgery.”
Dr. Lagergren and colleagues suggested that the reason for relatively higher cancer risk in the group that underwent surgery likely stems from early and prolonged acid exposure.
“[P]erforming antireflux surgery after years of GERD may be too late to enable a cancer-preventative effect, and most of the patients first diagnosed with Barrett’s esophagus reported a history of many years of GERD symptoms,” they wrote, suggesting that carcinogenic processes had already been set in motion by the time surgery was performed.
“[P]atients with Barrett’s esophagus who undergo antireflux surgery remain at an increased risk of esophageal adenocarcinoma and should continue taking part in surveillance programs,” the investigators concluded.
The study was funded by the Swedish Cancer Society, Swedish Research Council, and Stockholm County Council. The investigators disclosed no conflicts of interest.
, according to a Nordic retrospective study.
Risk of EAC was higher among patients who underwent surgery, and risk appeared to increase over time, suggesting that postoperative patients should continue to participate in surveillance programs, reported lead author Jesper Lagergren, MD, PhD, of the Karolinska Institutet, Stockholm, and colleagues.
“Antireflux surgery with fundoplication increases the ability of the gastroesophageal anatomic and physiological barrier to prevent reflux, and can thus prevent any carcinogenic gastric content from reaching the esophagus, including both acid and bile,” the investigators wrote in Gastroenterology, noting that surgery reduces esophageal acid exposure to a greater degree than medication. “Antireflux surgery may thus prevent esophageal adenocarcinoma better than antireflux medication.”
Three meta-analyses to date, however, have failed to provide consistent support for this hypothesis.
“Most of the studies included in these meta-analyses came from single centers, were of small sample size, examined only one treatment arm, and had a short or incomplete follow-up, and ... were hampered by heterogeneity among the included studies,” they noted.
For the present study, Dr. Lagergren and colleagues analyzed national registry data from 33,939 patients with Barrett’s esophagus in Denmark, Finland, Norway, and Sweden. Out of this group, 542 patients (1.6%) had undergone antireflux surgery, while the remainder were managed with antireflux medication.
In both groups, approximately two-thirds of the patients were men. The median age at enrollment was about a decade higher in the medication group (66 vs. 54 years), and this group also tended to have more comorbidities.
After a follow-up period as long as 32 years, the absolute rates of EAC were 1.3% and 2.6% in the medication and surgery groups, respectively. Multivariate analysis, with adjustments for sex, age, year, comorbidities, and age, revealed that postsurgical patients had a 90% increased risk of EAC (hazard ratio [HR], 1.9; 95% CI, 1.1-3.5), versus patients treated with antireflux medication alone.
The relatively higher risk of EAC appeared to increase over time, based on a nonsignificant hazard ratio of 1.8 during the 1- to 4-year follow-up period (HR, 1.8; 95% CI, 0.6-5.0), versus a significant, fourfold risk elevation during the 10- to 32-year follow-up period (HR, 4.4; 95% CI, 1.4-13.5).
“In this cohort of patients with Barrett’s esophagus, the risk of esophageal adenocarcinoma did not decrease after antireflux surgery compared with antireflux medication,” the investigators wrote. “Instead, the risk was increased throughout the follow-up among patients having undergone antireflux surgery.”
Dr. Lagergren and colleagues suggested that the reason for relatively higher cancer risk in the group that underwent surgery likely stems from early and prolonged acid exposure.
“[P]erforming antireflux surgery after years of GERD may be too late to enable a cancer-preventative effect, and most of the patients first diagnosed with Barrett’s esophagus reported a history of many years of GERD symptoms,” they wrote, suggesting that carcinogenic processes had already been set in motion by the time surgery was performed.
“[P]atients with Barrett’s esophagus who undergo antireflux surgery remain at an increased risk of esophageal adenocarcinoma and should continue taking part in surveillance programs,” the investigators concluded.
The study was funded by the Swedish Cancer Society, Swedish Research Council, and Stockholm County Council. The investigators disclosed no conflicts of interest.
FROM GASTROENTEROLOGY