User login
Is Buprenorphine/Naloxone Safer Than Buprenorphine Alone During Pregnancy?
TOPLINE:
Buprenorphine combined with naloxone during pregnancy is associated with lower risks for neonatal abstinence syndrome and neonatal intensive care unit admission than buprenorphine alone. The study also found no significant differences in major congenital malformations between the two treatments.
METHODOLOGY:
- Researchers conducted a population-based cohort study using healthcare utilization data of people who were insured by Medicaid between 2000 and 2018.
- A total of 8695 pregnant individuals were included, with 3369 exposed to buprenorphine/naloxone and 5326 exposed to buprenorphine alone during the first trimester.
- Outcome measures included major congenital malformations, low birth weight, neonatal abstinence syndrome, neonatal intensive care unit admission, preterm birth, respiratory symptoms, small for gestational age, cesarean delivery, and maternal morbidity.
- The study excluded pregnancies with chromosomal anomalies, first-trimester exposure to known teratogens, or methadone use during baseline or the first trimester.
TAKEAWAY:
- According to the authors, buprenorphine/naloxone exposure during pregnancy was associated with a lower risk for neonatal abstinence syndrome (weighted risk ratio [RR], 0.77; 95% CI, 0.70-0.84) than buprenorphine alone.
- The researchers found a modestly lower risk for neonatal intensive care unit admission (weighted RR, 0.91; 95% CI, 0.85-0.98) and small risk for gestational age (weighted RR, 0.86; 95% CI, 0.75-0.98) in the buprenorphine/naloxone group.
- No significant differences were observed between the two groups in major congenital malformations, low birth weight, preterm birth, respiratory symptoms, or cesarean delivery.
IN PRACTICE:
“For the outcomes assessed, compared with buprenorphine alone, buprenorphine combined with naloxone during pregnancy appears to be a safe treatment option. This supports the view that both formulations are reasonable options for treatment of OUD in pregnancy, affirming flexibility in collaborative treatment decision-making,” the study authors wrote.
SOURCE:
The study was led by Loreen Straub, MD, MS, of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital and Harvard Medical School in Boston. It was published online in JAMA.
LIMITATIONS:
Some potential confounders, such as alcohol use and cigarette smoking, may not have been recorded in claims data. The findings for many of the neonatal and maternal outcomes suggest that confounding by unmeasured factors is an unlikely explanation for the associations observed. Individuals identified as exposed based on filled prescriptions might not have used the medication. The study used outcome algorithms with relatively high positive predictive values to minimize outcome misclassification. The cohort was restricted to live births to enable linkage to infants and to assess neonatal outcomes.
DISCLOSURES:
Various authors reported receiving grants and personal fees from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Drug Abuse, Roche, Moderna, Takeda, and Janssen Global, among others.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Buprenorphine combined with naloxone during pregnancy is associated with lower risks for neonatal abstinence syndrome and neonatal intensive care unit admission than buprenorphine alone. The study also found no significant differences in major congenital malformations between the two treatments.
METHODOLOGY:
- Researchers conducted a population-based cohort study using healthcare utilization data of people who were insured by Medicaid between 2000 and 2018.
- A total of 8695 pregnant individuals were included, with 3369 exposed to buprenorphine/naloxone and 5326 exposed to buprenorphine alone during the first trimester.
- Outcome measures included major congenital malformations, low birth weight, neonatal abstinence syndrome, neonatal intensive care unit admission, preterm birth, respiratory symptoms, small for gestational age, cesarean delivery, and maternal morbidity.
- The study excluded pregnancies with chromosomal anomalies, first-trimester exposure to known teratogens, or methadone use during baseline or the first trimester.
TAKEAWAY:
- According to the authors, buprenorphine/naloxone exposure during pregnancy was associated with a lower risk for neonatal abstinence syndrome (weighted risk ratio [RR], 0.77; 95% CI, 0.70-0.84) than buprenorphine alone.
- The researchers found a modestly lower risk for neonatal intensive care unit admission (weighted RR, 0.91; 95% CI, 0.85-0.98) and small risk for gestational age (weighted RR, 0.86; 95% CI, 0.75-0.98) in the buprenorphine/naloxone group.
- No significant differences were observed between the two groups in major congenital malformations, low birth weight, preterm birth, respiratory symptoms, or cesarean delivery.
IN PRACTICE:
“For the outcomes assessed, compared with buprenorphine alone, buprenorphine combined with naloxone during pregnancy appears to be a safe treatment option. This supports the view that both formulations are reasonable options for treatment of OUD in pregnancy, affirming flexibility in collaborative treatment decision-making,” the study authors wrote.
SOURCE:
The study was led by Loreen Straub, MD, MS, of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital and Harvard Medical School in Boston. It was published online in JAMA.
LIMITATIONS:
Some potential confounders, such as alcohol use and cigarette smoking, may not have been recorded in claims data. The findings for many of the neonatal and maternal outcomes suggest that confounding by unmeasured factors is an unlikely explanation for the associations observed. Individuals identified as exposed based on filled prescriptions might not have used the medication. The study used outcome algorithms with relatively high positive predictive values to minimize outcome misclassification. The cohort was restricted to live births to enable linkage to infants and to assess neonatal outcomes.
DISCLOSURES:
Various authors reported receiving grants and personal fees from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Drug Abuse, Roche, Moderna, Takeda, and Janssen Global, among others.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Buprenorphine combined with naloxone during pregnancy is associated with lower risks for neonatal abstinence syndrome and neonatal intensive care unit admission than buprenorphine alone. The study also found no significant differences in major congenital malformations between the two treatments.
METHODOLOGY:
- Researchers conducted a population-based cohort study using healthcare utilization data of people who were insured by Medicaid between 2000 and 2018.
- A total of 8695 pregnant individuals were included, with 3369 exposed to buprenorphine/naloxone and 5326 exposed to buprenorphine alone during the first trimester.
- Outcome measures included major congenital malformations, low birth weight, neonatal abstinence syndrome, neonatal intensive care unit admission, preterm birth, respiratory symptoms, small for gestational age, cesarean delivery, and maternal morbidity.
- The study excluded pregnancies with chromosomal anomalies, first-trimester exposure to known teratogens, or methadone use during baseline or the first trimester.
TAKEAWAY:
- According to the authors, buprenorphine/naloxone exposure during pregnancy was associated with a lower risk for neonatal abstinence syndrome (weighted risk ratio [RR], 0.77; 95% CI, 0.70-0.84) than buprenorphine alone.
- The researchers found a modestly lower risk for neonatal intensive care unit admission (weighted RR, 0.91; 95% CI, 0.85-0.98) and small risk for gestational age (weighted RR, 0.86; 95% CI, 0.75-0.98) in the buprenorphine/naloxone group.
- No significant differences were observed between the two groups in major congenital malformations, low birth weight, preterm birth, respiratory symptoms, or cesarean delivery.
IN PRACTICE:
“For the outcomes assessed, compared with buprenorphine alone, buprenorphine combined with naloxone during pregnancy appears to be a safe treatment option. This supports the view that both formulations are reasonable options for treatment of OUD in pregnancy, affirming flexibility in collaborative treatment decision-making,” the study authors wrote.
SOURCE:
The study was led by Loreen Straub, MD, MS, of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital and Harvard Medical School in Boston. It was published online in JAMA.
LIMITATIONS:
Some potential confounders, such as alcohol use and cigarette smoking, may not have been recorded in claims data. The findings for many of the neonatal and maternal outcomes suggest that confounding by unmeasured factors is an unlikely explanation for the associations observed. Individuals identified as exposed based on filled prescriptions might not have used the medication. The study used outcome algorithms with relatively high positive predictive values to minimize outcome misclassification. The cohort was restricted to live births to enable linkage to infants and to assess neonatal outcomes.
DISCLOSURES:
Various authors reported receiving grants and personal fees from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Drug Abuse, Roche, Moderna, Takeda, and Janssen Global, among others.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Cannabis Overuse Linked to Increased Risk for Head and Neck Cancer
TOPLINE:
The study analyzed data from over four million patients, highlighting the potential carcinogenic effects of the substance.
METHODOLOGY:
- Researchers analyzed data from a globally federated health research network TriNetX, which included over 90 million men and women from 64 health care organizations in the United States.
- More than 4.1 million patients were included in the analysis, including 116,076 individuals diagnosed with cannabis-related disorder and 3.9 million without the disorder. Cannabis-related disorders involve the excessive use of cannabis with associated psychosocial symptoms, such as impaired social and/or occupational functioning.
- Patients with cannabis-related disorder were matched with those without the disorder based on demographic characteristics, alcohol-related disorders, and tobacco use.
- The primary outcome was the diagnosis of head and neck cancer, including subsites such as oral, oropharyngeal, nasopharyngeal, laryngeal, hypopharyngeal, and salivary gland malignancies.
- Propensity score matching and Poisson regression analysis were used to compare the incidence of head and neck cancers between the groups.
TAKEAWAY:
- According to the researchers, patients with a cannabis-related disorder had a higher risk for any head and neck cancer (relative risk [RR], 3.49; 95% CI, 2.78-4.39) than those without the disorder.
- The risk for specific cancers was also higher in the group with cannabis-related disorders, including oral (RR, 2.51; 95% CI, 1.81-3.47) and oropharyngeal malignancies (RR, 4.90; 95% CI, 2.99-8.02).
- The RR for laryngeal cancer was significantly higher in the patients with a cannabis-related disorder (RR, 8.39; 95% CI, 4.72-14.90).
- The findings suggest that cannabis use disorder is associated with an increased risk for head and neck cancers, highlighting the need for further research to understand the mechanisms involved.
IN PRACTICE:
“In this cohort study, cannabis disorder diagnosis was independently associated with greater risk of subsequent development of any [head or neck cancer] as well as cancers in various subsites of the head and neck among US adults. When limited to cases of [such cancers] occurring greater than 1 year after cannabis use disorder diagnosis, many of the associations increased, demonstrating additional strength in the association,” the authors of the study wrote.
“The association of cannabis and head and neck cancer in this study spanned 2 decades during a rapid growth in use. If this association is causative, the burden of [head and neck cancers] attributable to cannabis will continue to increase, and perhaps dramatically,” said the authors of an editorial accompanying the journal article. “Given that cannabis is now a $20 billion industry in the US alone with expanding availability, use, and popularity, this may be “déjà vu, all over again” without appropriate research to understand the potential carcinogenic and salutatory effects of cannabis. Or, in the words of Yogi Berra, “If you don’t know where you are going, you might wind up someplace else.”
SOURCE:
The study was led by Tyler J. Gallagher and Niels C. Kokot, MD, at the Keck School of Medicine of the University of Southern California in Los Angeles. It was published online in JAMA Otolaryngology–Head & Neck Surgery.
LIMITATIONS:
The study had limited information about cohort composition and length of follow-up, which may affect the generalizability of the findings. The lack of direct exposure duration, intensity, and dosage information limits the ability to analyze dose-response relationships. Potential inconsistency of diagnosis and reliance on medical record codes may introduce bias. Cannabis use is likely underreported, which could decrease the relative risks discovered. The study was further limited by the lack of information on dosage and frequency of cannabis use, as well as some controls, including alcohol and tobacco use.
DISCLOSURES:
Gallagher disclosed receiving grants from the Keck School of Medicine of the University of Southern California, Los Angeles. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The study analyzed data from over four million patients, highlighting the potential carcinogenic effects of the substance.
METHODOLOGY:
- Researchers analyzed data from a globally federated health research network TriNetX, which included over 90 million men and women from 64 health care organizations in the United States.
- More than 4.1 million patients were included in the analysis, including 116,076 individuals diagnosed with cannabis-related disorder and 3.9 million without the disorder. Cannabis-related disorders involve the excessive use of cannabis with associated psychosocial symptoms, such as impaired social and/or occupational functioning.
- Patients with cannabis-related disorder were matched with those without the disorder based on demographic characteristics, alcohol-related disorders, and tobacco use.
- The primary outcome was the diagnosis of head and neck cancer, including subsites such as oral, oropharyngeal, nasopharyngeal, laryngeal, hypopharyngeal, and salivary gland malignancies.
- Propensity score matching and Poisson regression analysis were used to compare the incidence of head and neck cancers between the groups.
TAKEAWAY:
- According to the researchers, patients with a cannabis-related disorder had a higher risk for any head and neck cancer (relative risk [RR], 3.49; 95% CI, 2.78-4.39) than those without the disorder.
- The risk for specific cancers was also higher in the group with cannabis-related disorders, including oral (RR, 2.51; 95% CI, 1.81-3.47) and oropharyngeal malignancies (RR, 4.90; 95% CI, 2.99-8.02).
- The RR for laryngeal cancer was significantly higher in the patients with a cannabis-related disorder (RR, 8.39; 95% CI, 4.72-14.90).
- The findings suggest that cannabis use disorder is associated with an increased risk for head and neck cancers, highlighting the need for further research to understand the mechanisms involved.
IN PRACTICE:
“In this cohort study, cannabis disorder diagnosis was independently associated with greater risk of subsequent development of any [head or neck cancer] as well as cancers in various subsites of the head and neck among US adults. When limited to cases of [such cancers] occurring greater than 1 year after cannabis use disorder diagnosis, many of the associations increased, demonstrating additional strength in the association,” the authors of the study wrote.
“The association of cannabis and head and neck cancer in this study spanned 2 decades during a rapid growth in use. If this association is causative, the burden of [head and neck cancers] attributable to cannabis will continue to increase, and perhaps dramatically,” said the authors of an editorial accompanying the journal article. “Given that cannabis is now a $20 billion industry in the US alone with expanding availability, use, and popularity, this may be “déjà vu, all over again” without appropriate research to understand the potential carcinogenic and salutatory effects of cannabis. Or, in the words of Yogi Berra, “If you don’t know where you are going, you might wind up someplace else.”
SOURCE:
The study was led by Tyler J. Gallagher and Niels C. Kokot, MD, at the Keck School of Medicine of the University of Southern California in Los Angeles. It was published online in JAMA Otolaryngology–Head & Neck Surgery.
LIMITATIONS:
The study had limited information about cohort composition and length of follow-up, which may affect the generalizability of the findings. The lack of direct exposure duration, intensity, and dosage information limits the ability to analyze dose-response relationships. Potential inconsistency of diagnosis and reliance on medical record codes may introduce bias. Cannabis use is likely underreported, which could decrease the relative risks discovered. The study was further limited by the lack of information on dosage and frequency of cannabis use, as well as some controls, including alcohol and tobacco use.
DISCLOSURES:
Gallagher disclosed receiving grants from the Keck School of Medicine of the University of Southern California, Los Angeles. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The study analyzed data from over four million patients, highlighting the potential carcinogenic effects of the substance.
METHODOLOGY:
- Researchers analyzed data from a globally federated health research network TriNetX, which included over 90 million men and women from 64 health care organizations in the United States.
- More than 4.1 million patients were included in the analysis, including 116,076 individuals diagnosed with cannabis-related disorder and 3.9 million without the disorder. Cannabis-related disorders involve the excessive use of cannabis with associated psychosocial symptoms, such as impaired social and/or occupational functioning.
- Patients with cannabis-related disorder were matched with those without the disorder based on demographic characteristics, alcohol-related disorders, and tobacco use.
- The primary outcome was the diagnosis of head and neck cancer, including subsites such as oral, oropharyngeal, nasopharyngeal, laryngeal, hypopharyngeal, and salivary gland malignancies.
- Propensity score matching and Poisson regression analysis were used to compare the incidence of head and neck cancers between the groups.
TAKEAWAY:
- According to the researchers, patients with a cannabis-related disorder had a higher risk for any head and neck cancer (relative risk [RR], 3.49; 95% CI, 2.78-4.39) than those without the disorder.
- The risk for specific cancers was also higher in the group with cannabis-related disorders, including oral (RR, 2.51; 95% CI, 1.81-3.47) and oropharyngeal malignancies (RR, 4.90; 95% CI, 2.99-8.02).
- The RR for laryngeal cancer was significantly higher in the patients with a cannabis-related disorder (RR, 8.39; 95% CI, 4.72-14.90).
- The findings suggest that cannabis use disorder is associated with an increased risk for head and neck cancers, highlighting the need for further research to understand the mechanisms involved.
IN PRACTICE:
“In this cohort study, cannabis disorder diagnosis was independently associated with greater risk of subsequent development of any [head or neck cancer] as well as cancers in various subsites of the head and neck among US adults. When limited to cases of [such cancers] occurring greater than 1 year after cannabis use disorder diagnosis, many of the associations increased, demonstrating additional strength in the association,” the authors of the study wrote.
“The association of cannabis and head and neck cancer in this study spanned 2 decades during a rapid growth in use. If this association is causative, the burden of [head and neck cancers] attributable to cannabis will continue to increase, and perhaps dramatically,” said the authors of an editorial accompanying the journal article. “Given that cannabis is now a $20 billion industry in the US alone with expanding availability, use, and popularity, this may be “déjà vu, all over again” without appropriate research to understand the potential carcinogenic and salutatory effects of cannabis. Or, in the words of Yogi Berra, “If you don’t know where you are going, you might wind up someplace else.”
SOURCE:
The study was led by Tyler J. Gallagher and Niels C. Kokot, MD, at the Keck School of Medicine of the University of Southern California in Los Angeles. It was published online in JAMA Otolaryngology–Head & Neck Surgery.
LIMITATIONS:
The study had limited information about cohort composition and length of follow-up, which may affect the generalizability of the findings. The lack of direct exposure duration, intensity, and dosage information limits the ability to analyze dose-response relationships. Potential inconsistency of diagnosis and reliance on medical record codes may introduce bias. Cannabis use is likely underreported, which could decrease the relative risks discovered. The study was further limited by the lack of information on dosage and frequency of cannabis use, as well as some controls, including alcohol and tobacco use.
DISCLOSURES:
Gallagher disclosed receiving grants from the Keck School of Medicine of the University of Southern California, Los Angeles. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Few Smokers Who Want to Quit Seek Healthcare Provider Help
Approximately half of US adult smokers tried to quit in 2022, but fewer than 40% used counseling or medication, and half received assistance or advice about quitting from clinicians, based on a review in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
Previous research has shown that clinician intervention and evidence-based treatment increase the odds that smokers can quit successfully, but the extent to which these interventions are applied in practice has not been well studied, the researchers noted.
Although great progress has been made in reducing cigarette smoking in the United States, disparities remain, both in use and in cessation, with an estimated 28.8 million adults reporting cigarette smoking in 2022, lead author Brenna VanFrank, MD, MSPH, said in an interview.
“Cigarette smoking remains the leading preventable cause of death and disease in the United States,” said Dr. VanFrank, Senior Medical Officer, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion.
In a new review, the researchers examined data from the 2022 National Health Interview Survey. The study population included 27,651 adults aged 18 years and older. Current smoking was defined as currently smoking each day or some days and ever having smoked at least 100 cigarettes. The survey assessed the individuals’ interest in quitting, past-year quit attempts, recent quitting success, receipt of healthcare professional advice about quitting, use of counseling to help quit, and use of medication to help quit.
In 2022, approximately two thirds (67.7%) of the 28.8 million adult smokers in the United States wanted to quit, half (53.3%) tried to quit, but only 8.8% were successful. Of those who reported trying to quit, 38.3% used counseling or medication. Of these, 36.3% used medication, 7.3% used counseling, and 5.3% used both.
Indicators of smoking cessation varied by health characteristics and sociodemographic factors, with the highest prevalence of attempts to quit smoking in the past year among adults aged 18-24 years and the lowest among those aged 45-64 years (74.4% vs 47.5%).
Rates of successful quitting were highest among individuals with higher levels of education and income, and use of smoking cessation treatment was highest among White adults (42.7%), followed by non-Hispanic adults of another race, Black adults, and Hispanic adults (33.6%, 32.6%, and 28.8%, respectively).
Smokers of menthol cigarettes had similarly low success rates for quitting (< 10%), although they were significantly more likely than nonmenthol cigarette smokers to express interest in quitting (72.2% vs 65.4%). Smokers of menthol cigarettes also had significantly lower prevalences than smokers of nonmenthol cigarettes of receiving clinician advance to quit and using treatment strategies (both P < .05).
The study findings were limited by several factors including the use of self-reports, which may be subject to bias, and a lack of data on institutionalized adults or adults in the military, which may limit generalizability of the findings to those populations, the researchers noted.
However, the results suggest that opportunities exist to increase smoking cessation across public health and healthcare sectors by expanding access to and use of services and supports to help smokers quit, they wrote.
Ensuring Support for All Smokers Seeking to Quit
The takeaway for clinical practice remains that quitting smoking “is one of the most important actions people who smoke can take to improve their health,” Dr. VanFrank said in an interview.
“It is important to ensure everyone has an opportunity to quit smoking and has access to proven treatments to help them be successful,” she emphasized. Strategies that include behavioral counseling, cessation medications, and advice and support from healthcare professionals can increase quit success. Given that tobacco dependence is a chronic, relapsing condition driven by addiction to nicotine, quitting successfully often takes multiple tries, and those trying to quit may need long-term support and repeated treatment.
“Health systems changes, such as adoption of treatment protocols and standardized clinical work flows, can systematize clinical treatment delivery, and such changes might also serve to increase treatment access for the 75% of adults who smoke who see a healthcare professional in a given year,” said Dr. VanFrank.
As for additional research, “continued surveillance of tobacco use and cessation-related behaviors will help us monitor progress and identify continued opportunities to eliminate tobacco product use and tobacco-related disparities,” Dr. VanFrank said.
“We know a lot about what works to help people successfully quit smoking and what we can do to support people in making quit attempts,” she said. Including equitable opportunities in all commercial tobacco prevention and control efforts has the potential to reduce tobacco-related health disparities.
Overall smoking prevalence in the United States and the current study shows that most smokers would like to quit, David M. Mannino, MD, a pulmonologist and professor of medicine at the University of Kentucky, Lexington, said in an interview. The lack of success experienced by many smokers seeking to quit emphasizes the highly addictive nature of nicotine products, which cause death and disease when used as directed, added Dr. Mannino, who was not involved in the study.
The results of the review were not surprising, and reflect where tobacco treatment has been for the past 20 years, said Dr. Mannino. The good news is that smoking prevalence has continued to drop in the United States over the past 15 years. However, some bad news is that use of e-cigarettes/vaping is still increasing, especially in younger populations, and new nicotine delivery systems, such as pouches (Zyn) are addicting a new generation.
Always Ask About Smoking
In practice, “clinicians should always ask patients about cigarette smoking, as well as vaping and other nicotine use, advise them to quit, and refer them to tobacco treatment experts,” Dr. Mannino emphasized.
The bottom line is that better treatments are needed for tobacco/nicotine addiction, Dr. Mannino said. “Although we have come a long way, we have a long way to go as millions of smokers in the US and globally would like to quit.”
Tobacco-related disease continues to be the number one cause of morbidly and mortality in the United States, and although many current smokers want to quit, most are not successful, Jamie Garfield, MD, professor of thoracic medicine and surgery at the Lewis Katz School of Medicine at Temple University, Philadelphia, Pennsylvania, said in an interview.
“This review highlights the sheer number of current cigarette smokers who want to quit, how many of them attempted to quit, and how many of those were successful,” said Dr. Garfield, who was not involved in the study. Understanding the characteristics of individuals who are more or less likely to successfully quit smoking can help public health and healthcare sectors to increase smoking cessation by expanding access to and use of services and supports.
“We have to do better to control the sale of tobacco products and make tobacco cessation more accessible to everyone,” Dr. Garfield said. In addition, clinicians need to be consistent in asking patients about tobacco use. “If we don’t ask, we will not know who needs help.” Behavioral counseling helps, as does pharmacotherapy, and the two together are more effective than either alone, she added.
Cessation services need to be tailored to the many demographic groups who use tobacco products, said Dr. Garfield. “Just as marketing campaigns directed to older adults will be different from those directed to young adults, so too must cessation resources. Providers need better options to choose from with regard to cessation resources and behavioral counseling sessions. They need to be aware of what motivates one group of people to smoke and how they can be inspired to quit, including which pharmacotherapies are affordable, available, and will work; the same strategies will not work for all people”
The study was supported by the Centers for Disease Control and Prevention’s National Center for Chronic Disease Prevention and Health Promotion. The researchers had no financial conflicts to disclose. Dr. Mannino disclosed serving as an expert witness for on tobacco use and tobacco-caused disease on behalf of people suing the tobacco and vaping industries. Dr. Garfield had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Approximately half of US adult smokers tried to quit in 2022, but fewer than 40% used counseling or medication, and half received assistance or advice about quitting from clinicians, based on a review in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
Previous research has shown that clinician intervention and evidence-based treatment increase the odds that smokers can quit successfully, but the extent to which these interventions are applied in practice has not been well studied, the researchers noted.
Although great progress has been made in reducing cigarette smoking in the United States, disparities remain, both in use and in cessation, with an estimated 28.8 million adults reporting cigarette smoking in 2022, lead author Brenna VanFrank, MD, MSPH, said in an interview.
“Cigarette smoking remains the leading preventable cause of death and disease in the United States,” said Dr. VanFrank, Senior Medical Officer, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion.
In a new review, the researchers examined data from the 2022 National Health Interview Survey. The study population included 27,651 adults aged 18 years and older. Current smoking was defined as currently smoking each day or some days and ever having smoked at least 100 cigarettes. The survey assessed the individuals’ interest in quitting, past-year quit attempts, recent quitting success, receipt of healthcare professional advice about quitting, use of counseling to help quit, and use of medication to help quit.
In 2022, approximately two thirds (67.7%) of the 28.8 million adult smokers in the United States wanted to quit, half (53.3%) tried to quit, but only 8.8% were successful. Of those who reported trying to quit, 38.3% used counseling or medication. Of these, 36.3% used medication, 7.3% used counseling, and 5.3% used both.
Indicators of smoking cessation varied by health characteristics and sociodemographic factors, with the highest prevalence of attempts to quit smoking in the past year among adults aged 18-24 years and the lowest among those aged 45-64 years (74.4% vs 47.5%).
Rates of successful quitting were highest among individuals with higher levels of education and income, and use of smoking cessation treatment was highest among White adults (42.7%), followed by non-Hispanic adults of another race, Black adults, and Hispanic adults (33.6%, 32.6%, and 28.8%, respectively).
Smokers of menthol cigarettes had similarly low success rates for quitting (< 10%), although they were significantly more likely than nonmenthol cigarette smokers to express interest in quitting (72.2% vs 65.4%). Smokers of menthol cigarettes also had significantly lower prevalences than smokers of nonmenthol cigarettes of receiving clinician advance to quit and using treatment strategies (both P < .05).
The study findings were limited by several factors including the use of self-reports, which may be subject to bias, and a lack of data on institutionalized adults or adults in the military, which may limit generalizability of the findings to those populations, the researchers noted.
However, the results suggest that opportunities exist to increase smoking cessation across public health and healthcare sectors by expanding access to and use of services and supports to help smokers quit, they wrote.
Ensuring Support for All Smokers Seeking to Quit
The takeaway for clinical practice remains that quitting smoking “is one of the most important actions people who smoke can take to improve their health,” Dr. VanFrank said in an interview.
“It is important to ensure everyone has an opportunity to quit smoking and has access to proven treatments to help them be successful,” she emphasized. Strategies that include behavioral counseling, cessation medications, and advice and support from healthcare professionals can increase quit success. Given that tobacco dependence is a chronic, relapsing condition driven by addiction to nicotine, quitting successfully often takes multiple tries, and those trying to quit may need long-term support and repeated treatment.
“Health systems changes, such as adoption of treatment protocols and standardized clinical work flows, can systematize clinical treatment delivery, and such changes might also serve to increase treatment access for the 75% of adults who smoke who see a healthcare professional in a given year,” said Dr. VanFrank.
As for additional research, “continued surveillance of tobacco use and cessation-related behaviors will help us monitor progress and identify continued opportunities to eliminate tobacco product use and tobacco-related disparities,” Dr. VanFrank said.
“We know a lot about what works to help people successfully quit smoking and what we can do to support people in making quit attempts,” she said. Including equitable opportunities in all commercial tobacco prevention and control efforts has the potential to reduce tobacco-related health disparities.
Overall smoking prevalence in the United States and the current study shows that most smokers would like to quit, David M. Mannino, MD, a pulmonologist and professor of medicine at the University of Kentucky, Lexington, said in an interview. The lack of success experienced by many smokers seeking to quit emphasizes the highly addictive nature of nicotine products, which cause death and disease when used as directed, added Dr. Mannino, who was not involved in the study.
The results of the review were not surprising, and reflect where tobacco treatment has been for the past 20 years, said Dr. Mannino. The good news is that smoking prevalence has continued to drop in the United States over the past 15 years. However, some bad news is that use of e-cigarettes/vaping is still increasing, especially in younger populations, and new nicotine delivery systems, such as pouches (Zyn) are addicting a new generation.
Always Ask About Smoking
In practice, “clinicians should always ask patients about cigarette smoking, as well as vaping and other nicotine use, advise them to quit, and refer them to tobacco treatment experts,” Dr. Mannino emphasized.
The bottom line is that better treatments are needed for tobacco/nicotine addiction, Dr. Mannino said. “Although we have come a long way, we have a long way to go as millions of smokers in the US and globally would like to quit.”
Tobacco-related disease continues to be the number one cause of morbidly and mortality in the United States, and although many current smokers want to quit, most are not successful, Jamie Garfield, MD, professor of thoracic medicine and surgery at the Lewis Katz School of Medicine at Temple University, Philadelphia, Pennsylvania, said in an interview.
“This review highlights the sheer number of current cigarette smokers who want to quit, how many of them attempted to quit, and how many of those were successful,” said Dr. Garfield, who was not involved in the study. Understanding the characteristics of individuals who are more or less likely to successfully quit smoking can help public health and healthcare sectors to increase smoking cessation by expanding access to and use of services and supports.
“We have to do better to control the sale of tobacco products and make tobacco cessation more accessible to everyone,” Dr. Garfield said. In addition, clinicians need to be consistent in asking patients about tobacco use. “If we don’t ask, we will not know who needs help.” Behavioral counseling helps, as does pharmacotherapy, and the two together are more effective than either alone, she added.
Cessation services need to be tailored to the many demographic groups who use tobacco products, said Dr. Garfield. “Just as marketing campaigns directed to older adults will be different from those directed to young adults, so too must cessation resources. Providers need better options to choose from with regard to cessation resources and behavioral counseling sessions. They need to be aware of what motivates one group of people to smoke and how they can be inspired to quit, including which pharmacotherapies are affordable, available, and will work; the same strategies will not work for all people”
The study was supported by the Centers for Disease Control and Prevention’s National Center for Chronic Disease Prevention and Health Promotion. The researchers had no financial conflicts to disclose. Dr. Mannino disclosed serving as an expert witness for on tobacco use and tobacco-caused disease on behalf of people suing the tobacco and vaping industries. Dr. Garfield had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Approximately half of US adult smokers tried to quit in 2022, but fewer than 40% used counseling or medication, and half received assistance or advice about quitting from clinicians, based on a review in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
Previous research has shown that clinician intervention and evidence-based treatment increase the odds that smokers can quit successfully, but the extent to which these interventions are applied in practice has not been well studied, the researchers noted.
Although great progress has been made in reducing cigarette smoking in the United States, disparities remain, both in use and in cessation, with an estimated 28.8 million adults reporting cigarette smoking in 2022, lead author Brenna VanFrank, MD, MSPH, said in an interview.
“Cigarette smoking remains the leading preventable cause of death and disease in the United States,” said Dr. VanFrank, Senior Medical Officer, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion.
In a new review, the researchers examined data from the 2022 National Health Interview Survey. The study population included 27,651 adults aged 18 years and older. Current smoking was defined as currently smoking each day or some days and ever having smoked at least 100 cigarettes. The survey assessed the individuals’ interest in quitting, past-year quit attempts, recent quitting success, receipt of healthcare professional advice about quitting, use of counseling to help quit, and use of medication to help quit.
In 2022, approximately two thirds (67.7%) of the 28.8 million adult smokers in the United States wanted to quit, half (53.3%) tried to quit, but only 8.8% were successful. Of those who reported trying to quit, 38.3% used counseling or medication. Of these, 36.3% used medication, 7.3% used counseling, and 5.3% used both.
Indicators of smoking cessation varied by health characteristics and sociodemographic factors, with the highest prevalence of attempts to quit smoking in the past year among adults aged 18-24 years and the lowest among those aged 45-64 years (74.4% vs 47.5%).
Rates of successful quitting were highest among individuals with higher levels of education and income, and use of smoking cessation treatment was highest among White adults (42.7%), followed by non-Hispanic adults of another race, Black adults, and Hispanic adults (33.6%, 32.6%, and 28.8%, respectively).
Smokers of menthol cigarettes had similarly low success rates for quitting (< 10%), although they were significantly more likely than nonmenthol cigarette smokers to express interest in quitting (72.2% vs 65.4%). Smokers of menthol cigarettes also had significantly lower prevalences than smokers of nonmenthol cigarettes of receiving clinician advance to quit and using treatment strategies (both P < .05).
The study findings were limited by several factors including the use of self-reports, which may be subject to bias, and a lack of data on institutionalized adults or adults in the military, which may limit generalizability of the findings to those populations, the researchers noted.
However, the results suggest that opportunities exist to increase smoking cessation across public health and healthcare sectors by expanding access to and use of services and supports to help smokers quit, they wrote.
Ensuring Support for All Smokers Seeking to Quit
The takeaway for clinical practice remains that quitting smoking “is one of the most important actions people who smoke can take to improve their health,” Dr. VanFrank said in an interview.
“It is important to ensure everyone has an opportunity to quit smoking and has access to proven treatments to help them be successful,” she emphasized. Strategies that include behavioral counseling, cessation medications, and advice and support from healthcare professionals can increase quit success. Given that tobacco dependence is a chronic, relapsing condition driven by addiction to nicotine, quitting successfully often takes multiple tries, and those trying to quit may need long-term support and repeated treatment.
“Health systems changes, such as adoption of treatment protocols and standardized clinical work flows, can systematize clinical treatment delivery, and such changes might also serve to increase treatment access for the 75% of adults who smoke who see a healthcare professional in a given year,” said Dr. VanFrank.
As for additional research, “continued surveillance of tobacco use and cessation-related behaviors will help us monitor progress and identify continued opportunities to eliminate tobacco product use and tobacco-related disparities,” Dr. VanFrank said.
“We know a lot about what works to help people successfully quit smoking and what we can do to support people in making quit attempts,” she said. Including equitable opportunities in all commercial tobacco prevention and control efforts has the potential to reduce tobacco-related health disparities.
Overall smoking prevalence in the United States and the current study shows that most smokers would like to quit, David M. Mannino, MD, a pulmonologist and professor of medicine at the University of Kentucky, Lexington, said in an interview. The lack of success experienced by many smokers seeking to quit emphasizes the highly addictive nature of nicotine products, which cause death and disease when used as directed, added Dr. Mannino, who was not involved in the study.
The results of the review were not surprising, and reflect where tobacco treatment has been for the past 20 years, said Dr. Mannino. The good news is that smoking prevalence has continued to drop in the United States over the past 15 years. However, some bad news is that use of e-cigarettes/vaping is still increasing, especially in younger populations, and new nicotine delivery systems, such as pouches (Zyn) are addicting a new generation.
Always Ask About Smoking
In practice, “clinicians should always ask patients about cigarette smoking, as well as vaping and other nicotine use, advise them to quit, and refer them to tobacco treatment experts,” Dr. Mannino emphasized.
The bottom line is that better treatments are needed for tobacco/nicotine addiction, Dr. Mannino said. “Although we have come a long way, we have a long way to go as millions of smokers in the US and globally would like to quit.”
Tobacco-related disease continues to be the number one cause of morbidly and mortality in the United States, and although many current smokers want to quit, most are not successful, Jamie Garfield, MD, professor of thoracic medicine and surgery at the Lewis Katz School of Medicine at Temple University, Philadelphia, Pennsylvania, said in an interview.
“This review highlights the sheer number of current cigarette smokers who want to quit, how many of them attempted to quit, and how many of those were successful,” said Dr. Garfield, who was not involved in the study. Understanding the characteristics of individuals who are more or less likely to successfully quit smoking can help public health and healthcare sectors to increase smoking cessation by expanding access to and use of services and supports.
“We have to do better to control the sale of tobacco products and make tobacco cessation more accessible to everyone,” Dr. Garfield said. In addition, clinicians need to be consistent in asking patients about tobacco use. “If we don’t ask, we will not know who needs help.” Behavioral counseling helps, as does pharmacotherapy, and the two together are more effective than either alone, she added.
Cessation services need to be tailored to the many demographic groups who use tobacco products, said Dr. Garfield. “Just as marketing campaigns directed to older adults will be different from those directed to young adults, so too must cessation resources. Providers need better options to choose from with regard to cessation resources and behavioral counseling sessions. They need to be aware of what motivates one group of people to smoke and how they can be inspired to quit, including which pharmacotherapies are affordable, available, and will work; the same strategies will not work for all people”
The study was supported by the Centers for Disease Control and Prevention’s National Center for Chronic Disease Prevention and Health Promotion. The researchers had no financial conflicts to disclose. Dr. Mannino disclosed serving as an expert witness for on tobacco use and tobacco-caused disease on behalf of people suing the tobacco and vaping industries. Dr. Garfield had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
FROM THE MMWR
When Is Sexual Behavior Out of Control?
A 25-year-old man comes in with a pulled muscle. You ask if he has anything else to discuss. Sheepishly, he says he is concerned about his use of pornography.
A 45-year-old woman struggling with depression finds herself persistently seeking sex outside the bounds of her long-term relationship. Her partner is threatening to leave. She is devastated and tells you she doesn’t understand her own behavior.
Do these patients have some form of sex addiction? How should a primary care clinician intervene? Is a referral to a 12-step program for sex addiction the right choice? What other options exist? Is a diagnosis — let alone treatment — possible or appropriate?
‘Who Are You Calling “Abnormal” ’?
Normal is not a meaningful concept in human sexual behavior. To quote the sex therapist Marty Klein, PhD: “Normal is just a setting on the dryer.”
The same goes among partners: What is “normal” for one person in a sexual relationship may discomfit another. In partnerships, we have differences around all sorts of issues, from finances to parenting to how to load the dishwasher. Why should sex, sexual desire, and sexual frequency be different?
Remember: Shame, fear, and secrecy often play a role in perpetuating behaviors that cause distress. Helping our patients accept and embrace their whole selves can provide important healing, relief from anxiety, and may even help them regulate their actions. Feeling less shame, fear, and secrecy may facilitate safer choices about sex, as well as testing and treatment for sexually transmitted infections.
The International Classification of Diseases-11 includes compulsive sexual behavior disorder (CSBD)as an attempt to create consensus around a complicated, and hotly debated, problem to facilitate diagnosis and research. Syndromes similar to CSBD have had many names: “hypersexual disorder,” “sexual addiction,” “sexual compulsivity,” and “out-of-control sexual behavior.” A sizable cohort of the sexuality research community casts doubt on whether CSBD is even a discrete diagnosis.
According to the ICD-11, CSBD is characterized by “intense, repetitive sexual impulses or urges that are experienced as irresistible or uncontrollable” and result in significant distress or functional impairment.
This diagnosis has several important rule-outs. First, paraphilias, defined as a set of nonconsensual sexual behaviors and interests, are excluded. Another is that distress exclusively related to moral judgment or social disapproval is not sufficient for a diagnosis of CSBD. Finally, the diagnosis hinges on distress and does not rely on frequency of any type of sexual behavior. Some people experience significant distress over behaviors in which they engage infrequently, whereas others may have no distress from activities in which they engage quite frequently.
In one study from Germany, 5% of men and 3% of women met criteria for CSBD. A small US study found the number to be 10% and 7%, respectively. The diagnosis is not simple. Compulsive sexual behavior can be secondary to other mental health or medical conditions. Behaviors sometimes confused with CSBD can result from neurologic diseases, such as frontal brain lesions or frontotemporal dementia, as well as the use of substances and medications that enhance dopaminergic activity.
Impaired control over sexual impulses occurs in manic and hypomanic episodes. Compulsive sexual behavior frequently co-occurs with mood disorders, obsessive-compulsive disorder, attention-deficit/hyperactivity disorder, and substance use disorders. Those meeting criteria for CSBD may engage in sexual behaviors as a way of coping with depression, anxiety, boredom, loneliness, or other negative affective states.
The diagnosis of CSBD may be useful for clinicians. However, many, perhaps most, patients who present with concerns about their sexual behavior will fail to meet most criteria for CSBD. Their problem is of shorter duration, related to morality, external disapproval, lack of sexual health information, and anxiety about diverse erotic interests. It may be helpful for them to understand that they are not in the grip of a lifelong disorder but are experiencing common life challenges.
Societal concerns about sexually explicit media, often called pornography, are complex, conflicting, and catastrophizing. Some studies indicate that sexually explicit media are positive for both individual and relational sexual satisfaction; other studies have found negative effects on sexual function. Concerns about pornography often are conflated with taboos about solo sexual activity. Ironically, use of pornography is associated with fear of addiction to pornography, creating a spiral of negative self-perception.
Consequences of sexual behavior may induce distress, even if a person doesn’t meet criteria for CSBD, such as potential dissolution of a marriage, loss of a job, excessive spending, sexually transmitted infections, other health concerns, and even legal problems. Sexual behavior might not be the central issue but rather an offshoot of relational distress, a mental health disorder, or a dysfunctional coping style.
Guilt and shame can act as potent contributors to maintaining the behaviors as well as promoting secrecy around them. Sexual medicine experts recommend avoiding interventions that increase the experience of discrimination and stigma and avoiding the pathologization of the behaviors of sexually diverse individuals. As in so many aspects of medical care, we must walk in our patients’ shoes and avoid imposing on them our own moral or religious values.
What Can a Primary Care Provider Do?
When a patient is concerned about sexual behavior that feels out of control, primary care providers have an important role in evaluating for neurologic disease or side effects related to the use of medication or other substances, and facilitating psychiatric assessment to evaluate for mental health comorbidities, past trauma, and associated attachment disorders.
Our patients need resources to tease out the individual and relational problems that may arise. Seek out well-trained sex therapy colleagues in your community. The American Association of Sexuality Educators, Counselors, and Therapists (AASECT) is one certifying body in the United States for sex therapy.
Because of the heterogeneity of those who present with out-of-control sexual behavior, no one treatment fits all. Twelve-step programs, especially those with a focus on sexual “abstinence,” may not be the best choice. Many psychotherapeutic modalities are effective and often focus on addressing underlying or unrecognized mental health concerns, provide training on self-regulation and urge management, and relationship skills. Most important, the therapist needs to be sexologically informed and aware of their own biases around sexuality. Medical treatments are not recommended without concurrent psychological intervention.
Relational sex therapy can help couples create clear relational agreements that work for both parties (or, in polyamorous relationships, everyone involved). Relational distress also may be a stimulus for individual psychotherapy.
Back to these two patients.
The 25-year-old could be counseled that use of sexually explicit media and solo sex are not inherently bad or damaging. When used for pleasure and enjoyment, they do not lead to problems with partnered sex or cause sexual dysfunction. Counseling him to move toward social engagement and life goals, rather than away from pornography, may be all that is necessary.
Our second patient probably will need more intensive treatment, including medication management for her mood and referral to a certified sex therapist who has expertise in working with out-of-control sexual behavior. When she returns to see you in follow-up, she ideally expresses reduced shame, more autonomy, and renewed connection to her values, and she is keeping her relational agreements without sacrificing her sexual needs.
Dr. Kranz is medical director, Rochester Center for Sexual Wellness; assistant professor of Clinical Family Medicine and Obstetrics and Gynecology, University of Rochester Medical Center, Rochester, New York. Dr. Kranz has disclosed no relevant financial relationships. Dr. Rosen is director of Behavioral Health, Rochester Center for Sexual Wellness, Rochester, New York. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
A 25-year-old man comes in with a pulled muscle. You ask if he has anything else to discuss. Sheepishly, he says he is concerned about his use of pornography.
A 45-year-old woman struggling with depression finds herself persistently seeking sex outside the bounds of her long-term relationship. Her partner is threatening to leave. She is devastated and tells you she doesn’t understand her own behavior.
Do these patients have some form of sex addiction? How should a primary care clinician intervene? Is a referral to a 12-step program for sex addiction the right choice? What other options exist? Is a diagnosis — let alone treatment — possible or appropriate?
‘Who Are You Calling “Abnormal” ’?
Normal is not a meaningful concept in human sexual behavior. To quote the sex therapist Marty Klein, PhD: “Normal is just a setting on the dryer.”
The same goes among partners: What is “normal” for one person in a sexual relationship may discomfit another. In partnerships, we have differences around all sorts of issues, from finances to parenting to how to load the dishwasher. Why should sex, sexual desire, and sexual frequency be different?
Remember: Shame, fear, and secrecy often play a role in perpetuating behaviors that cause distress. Helping our patients accept and embrace their whole selves can provide important healing, relief from anxiety, and may even help them regulate their actions. Feeling less shame, fear, and secrecy may facilitate safer choices about sex, as well as testing and treatment for sexually transmitted infections.
The International Classification of Diseases-11 includes compulsive sexual behavior disorder (CSBD)as an attempt to create consensus around a complicated, and hotly debated, problem to facilitate diagnosis and research. Syndromes similar to CSBD have had many names: “hypersexual disorder,” “sexual addiction,” “sexual compulsivity,” and “out-of-control sexual behavior.” A sizable cohort of the sexuality research community casts doubt on whether CSBD is even a discrete diagnosis.
According to the ICD-11, CSBD is characterized by “intense, repetitive sexual impulses or urges that are experienced as irresistible or uncontrollable” and result in significant distress or functional impairment.
This diagnosis has several important rule-outs. First, paraphilias, defined as a set of nonconsensual sexual behaviors and interests, are excluded. Another is that distress exclusively related to moral judgment or social disapproval is not sufficient for a diagnosis of CSBD. Finally, the diagnosis hinges on distress and does not rely on frequency of any type of sexual behavior. Some people experience significant distress over behaviors in which they engage infrequently, whereas others may have no distress from activities in which they engage quite frequently.
In one study from Germany, 5% of men and 3% of women met criteria for CSBD. A small US study found the number to be 10% and 7%, respectively. The diagnosis is not simple. Compulsive sexual behavior can be secondary to other mental health or medical conditions. Behaviors sometimes confused with CSBD can result from neurologic diseases, such as frontal brain lesions or frontotemporal dementia, as well as the use of substances and medications that enhance dopaminergic activity.
Impaired control over sexual impulses occurs in manic and hypomanic episodes. Compulsive sexual behavior frequently co-occurs with mood disorders, obsessive-compulsive disorder, attention-deficit/hyperactivity disorder, and substance use disorders. Those meeting criteria for CSBD may engage in sexual behaviors as a way of coping with depression, anxiety, boredom, loneliness, or other negative affective states.
The diagnosis of CSBD may be useful for clinicians. However, many, perhaps most, patients who present with concerns about their sexual behavior will fail to meet most criteria for CSBD. Their problem is of shorter duration, related to morality, external disapproval, lack of sexual health information, and anxiety about diverse erotic interests. It may be helpful for them to understand that they are not in the grip of a lifelong disorder but are experiencing common life challenges.
Societal concerns about sexually explicit media, often called pornography, are complex, conflicting, and catastrophizing. Some studies indicate that sexually explicit media are positive for both individual and relational sexual satisfaction; other studies have found negative effects on sexual function. Concerns about pornography often are conflated with taboos about solo sexual activity. Ironically, use of pornography is associated with fear of addiction to pornography, creating a spiral of negative self-perception.
Consequences of sexual behavior may induce distress, even if a person doesn’t meet criteria for CSBD, such as potential dissolution of a marriage, loss of a job, excessive spending, sexually transmitted infections, other health concerns, and even legal problems. Sexual behavior might not be the central issue but rather an offshoot of relational distress, a mental health disorder, or a dysfunctional coping style.
Guilt and shame can act as potent contributors to maintaining the behaviors as well as promoting secrecy around them. Sexual medicine experts recommend avoiding interventions that increase the experience of discrimination and stigma and avoiding the pathologization of the behaviors of sexually diverse individuals. As in so many aspects of medical care, we must walk in our patients’ shoes and avoid imposing on them our own moral or religious values.
What Can a Primary Care Provider Do?
When a patient is concerned about sexual behavior that feels out of control, primary care providers have an important role in evaluating for neurologic disease or side effects related to the use of medication or other substances, and facilitating psychiatric assessment to evaluate for mental health comorbidities, past trauma, and associated attachment disorders.
Our patients need resources to tease out the individual and relational problems that may arise. Seek out well-trained sex therapy colleagues in your community. The American Association of Sexuality Educators, Counselors, and Therapists (AASECT) is one certifying body in the United States for sex therapy.
Because of the heterogeneity of those who present with out-of-control sexual behavior, no one treatment fits all. Twelve-step programs, especially those with a focus on sexual “abstinence,” may not be the best choice. Many psychotherapeutic modalities are effective and often focus on addressing underlying or unrecognized mental health concerns, provide training on self-regulation and urge management, and relationship skills. Most important, the therapist needs to be sexologically informed and aware of their own biases around sexuality. Medical treatments are not recommended without concurrent psychological intervention.
Relational sex therapy can help couples create clear relational agreements that work for both parties (or, in polyamorous relationships, everyone involved). Relational distress also may be a stimulus for individual psychotherapy.
Back to these two patients.
The 25-year-old could be counseled that use of sexually explicit media and solo sex are not inherently bad or damaging. When used for pleasure and enjoyment, they do not lead to problems with partnered sex or cause sexual dysfunction. Counseling him to move toward social engagement and life goals, rather than away from pornography, may be all that is necessary.
Our second patient probably will need more intensive treatment, including medication management for her mood and referral to a certified sex therapist who has expertise in working with out-of-control sexual behavior. When she returns to see you in follow-up, she ideally expresses reduced shame, more autonomy, and renewed connection to her values, and she is keeping her relational agreements without sacrificing her sexual needs.
Dr. Kranz is medical director, Rochester Center for Sexual Wellness; assistant professor of Clinical Family Medicine and Obstetrics and Gynecology, University of Rochester Medical Center, Rochester, New York. Dr. Kranz has disclosed no relevant financial relationships. Dr. Rosen is director of Behavioral Health, Rochester Center for Sexual Wellness, Rochester, New York. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
A 25-year-old man comes in with a pulled muscle. You ask if he has anything else to discuss. Sheepishly, he says he is concerned about his use of pornography.
A 45-year-old woman struggling with depression finds herself persistently seeking sex outside the bounds of her long-term relationship. Her partner is threatening to leave. She is devastated and tells you she doesn’t understand her own behavior.
Do these patients have some form of sex addiction? How should a primary care clinician intervene? Is a referral to a 12-step program for sex addiction the right choice? What other options exist? Is a diagnosis — let alone treatment — possible or appropriate?
‘Who Are You Calling “Abnormal” ’?
Normal is not a meaningful concept in human sexual behavior. To quote the sex therapist Marty Klein, PhD: “Normal is just a setting on the dryer.”
The same goes among partners: What is “normal” for one person in a sexual relationship may discomfit another. In partnerships, we have differences around all sorts of issues, from finances to parenting to how to load the dishwasher. Why should sex, sexual desire, and sexual frequency be different?
Remember: Shame, fear, and secrecy often play a role in perpetuating behaviors that cause distress. Helping our patients accept and embrace their whole selves can provide important healing, relief from anxiety, and may even help them regulate their actions. Feeling less shame, fear, and secrecy may facilitate safer choices about sex, as well as testing and treatment for sexually transmitted infections.
The International Classification of Diseases-11 includes compulsive sexual behavior disorder (CSBD)as an attempt to create consensus around a complicated, and hotly debated, problem to facilitate diagnosis and research. Syndromes similar to CSBD have had many names: “hypersexual disorder,” “sexual addiction,” “sexual compulsivity,” and “out-of-control sexual behavior.” A sizable cohort of the sexuality research community casts doubt on whether CSBD is even a discrete diagnosis.
According to the ICD-11, CSBD is characterized by “intense, repetitive sexual impulses or urges that are experienced as irresistible or uncontrollable” and result in significant distress or functional impairment.
This diagnosis has several important rule-outs. First, paraphilias, defined as a set of nonconsensual sexual behaviors and interests, are excluded. Another is that distress exclusively related to moral judgment or social disapproval is not sufficient for a diagnosis of CSBD. Finally, the diagnosis hinges on distress and does not rely on frequency of any type of sexual behavior. Some people experience significant distress over behaviors in which they engage infrequently, whereas others may have no distress from activities in which they engage quite frequently.
In one study from Germany, 5% of men and 3% of women met criteria for CSBD. A small US study found the number to be 10% and 7%, respectively. The diagnosis is not simple. Compulsive sexual behavior can be secondary to other mental health or medical conditions. Behaviors sometimes confused with CSBD can result from neurologic diseases, such as frontal brain lesions or frontotemporal dementia, as well as the use of substances and medications that enhance dopaminergic activity.
Impaired control over sexual impulses occurs in manic and hypomanic episodes. Compulsive sexual behavior frequently co-occurs with mood disorders, obsessive-compulsive disorder, attention-deficit/hyperactivity disorder, and substance use disorders. Those meeting criteria for CSBD may engage in sexual behaviors as a way of coping with depression, anxiety, boredom, loneliness, or other negative affective states.
The diagnosis of CSBD may be useful for clinicians. However, many, perhaps most, patients who present with concerns about their sexual behavior will fail to meet most criteria for CSBD. Their problem is of shorter duration, related to morality, external disapproval, lack of sexual health information, and anxiety about diverse erotic interests. It may be helpful for them to understand that they are not in the grip of a lifelong disorder but are experiencing common life challenges.
Societal concerns about sexually explicit media, often called pornography, are complex, conflicting, and catastrophizing. Some studies indicate that sexually explicit media are positive for both individual and relational sexual satisfaction; other studies have found negative effects on sexual function. Concerns about pornography often are conflated with taboos about solo sexual activity. Ironically, use of pornography is associated with fear of addiction to pornography, creating a spiral of negative self-perception.
Consequences of sexual behavior may induce distress, even if a person doesn’t meet criteria for CSBD, such as potential dissolution of a marriage, loss of a job, excessive spending, sexually transmitted infections, other health concerns, and even legal problems. Sexual behavior might not be the central issue but rather an offshoot of relational distress, a mental health disorder, or a dysfunctional coping style.
Guilt and shame can act as potent contributors to maintaining the behaviors as well as promoting secrecy around them. Sexual medicine experts recommend avoiding interventions that increase the experience of discrimination and stigma and avoiding the pathologization of the behaviors of sexually diverse individuals. As in so many aspects of medical care, we must walk in our patients’ shoes and avoid imposing on them our own moral or religious values.
What Can a Primary Care Provider Do?
When a patient is concerned about sexual behavior that feels out of control, primary care providers have an important role in evaluating for neurologic disease or side effects related to the use of medication or other substances, and facilitating psychiatric assessment to evaluate for mental health comorbidities, past trauma, and associated attachment disorders.
Our patients need resources to tease out the individual and relational problems that may arise. Seek out well-trained sex therapy colleagues in your community. The American Association of Sexuality Educators, Counselors, and Therapists (AASECT) is one certifying body in the United States for sex therapy.
Because of the heterogeneity of those who present with out-of-control sexual behavior, no one treatment fits all. Twelve-step programs, especially those with a focus on sexual “abstinence,” may not be the best choice. Many psychotherapeutic modalities are effective and often focus on addressing underlying or unrecognized mental health concerns, provide training on self-regulation and urge management, and relationship skills. Most important, the therapist needs to be sexologically informed and aware of their own biases around sexuality. Medical treatments are not recommended without concurrent psychological intervention.
Relational sex therapy can help couples create clear relational agreements that work for both parties (or, in polyamorous relationships, everyone involved). Relational distress also may be a stimulus for individual psychotherapy.
Back to these two patients.
The 25-year-old could be counseled that use of sexually explicit media and solo sex are not inherently bad or damaging. When used for pleasure and enjoyment, they do not lead to problems with partnered sex or cause sexual dysfunction. Counseling him to move toward social engagement and life goals, rather than away from pornography, may be all that is necessary.
Our second patient probably will need more intensive treatment, including medication management for her mood and referral to a certified sex therapist who has expertise in working with out-of-control sexual behavior. When she returns to see you in follow-up, she ideally expresses reduced shame, more autonomy, and renewed connection to her values, and she is keeping her relational agreements without sacrificing her sexual needs.
Dr. Kranz is medical director, Rochester Center for Sexual Wellness; assistant professor of Clinical Family Medicine and Obstetrics and Gynecology, University of Rochester Medical Center, Rochester, New York. Dr. Kranz has disclosed no relevant financial relationships. Dr. Rosen is director of Behavioral Health, Rochester Center for Sexual Wellness, Rochester, New York. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Ozempic Curbs Hunger – And Not Just for Food
This transcript has been edited for clarity.
If you’ve been paying attention only to the headlines, when you think of “Ozempic” you’ll think of a few things: a blockbuster weight loss drug or the tip of the spear of a completely new industry — why not? A drug so popular that the people it was invented for (those with diabetes) can’t even get it.
Ozempic and other GLP-1 receptor agonists are undeniable game changers. Insofar as obesity is the number-one public health risk in the United States, antiobesity drugs hold immense promise even if all they do is reduce obesity.
In 2023, an article in Scientific Reports presented data suggesting that people on Ozempic might be reducing their alcohol intake, not just their total calories.
A 2024 article in Molecular Psychiatry found that the drug might positively impact cannabis use disorder. An article from Brain Sciences suggests that the drug reduces compulsive shopping.
A picture is starting to form, a picture that suggests these drugs curb hunger both literally and figuratively. That GLP-1 receptor agonists like Ozempic and Mounjaro are fundamentally anticonsumption drugs. In a society that — some would argue — is plagued by overconsumption, these drugs might be just what the doctor ordered.
If only they could stop people from smoking.
Oh, wait — they can.
At least it seems they can, based on a new study appearing in Annals of Internal Medicine.
Before we get too excited, this is not a randomized trial. There actually was a small randomized trial of exenatide (Byetta), which is in the same class as Ozempic but probably a bit less potent, with promising results for smoking cessation. 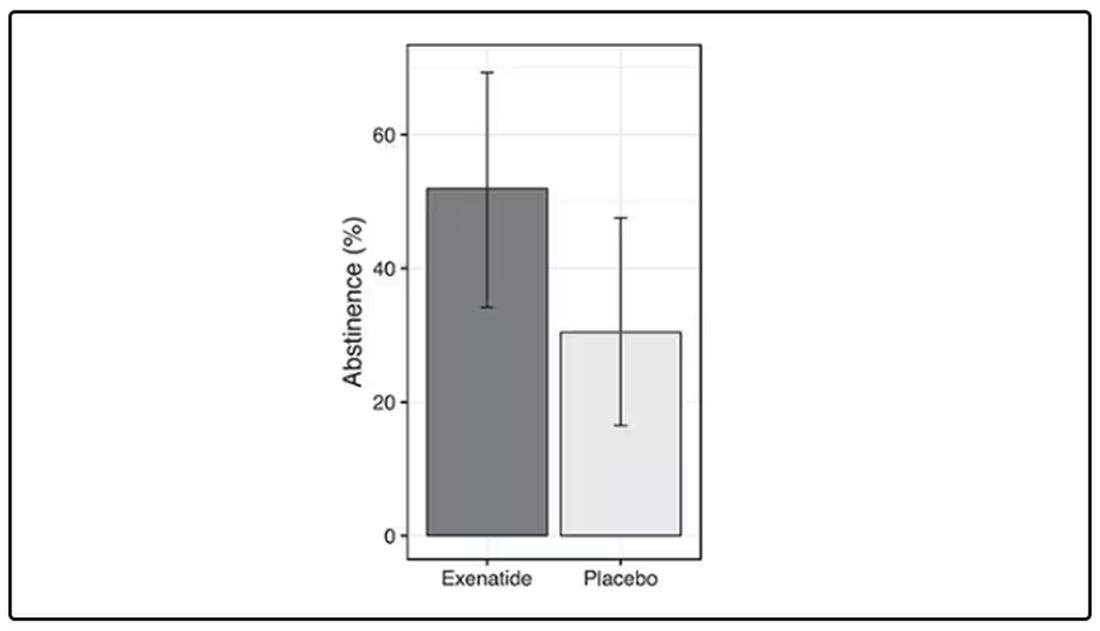
But Byetta is the weaker drug in this class; the market leader is Ozempic. So how can you figure out whether Ozempic can reduce smoking without doing a huge and expensive randomized trial? You can do what Nora Volkow and colleagues from the National Institute on Drug Abuse did: a target trial emulation study.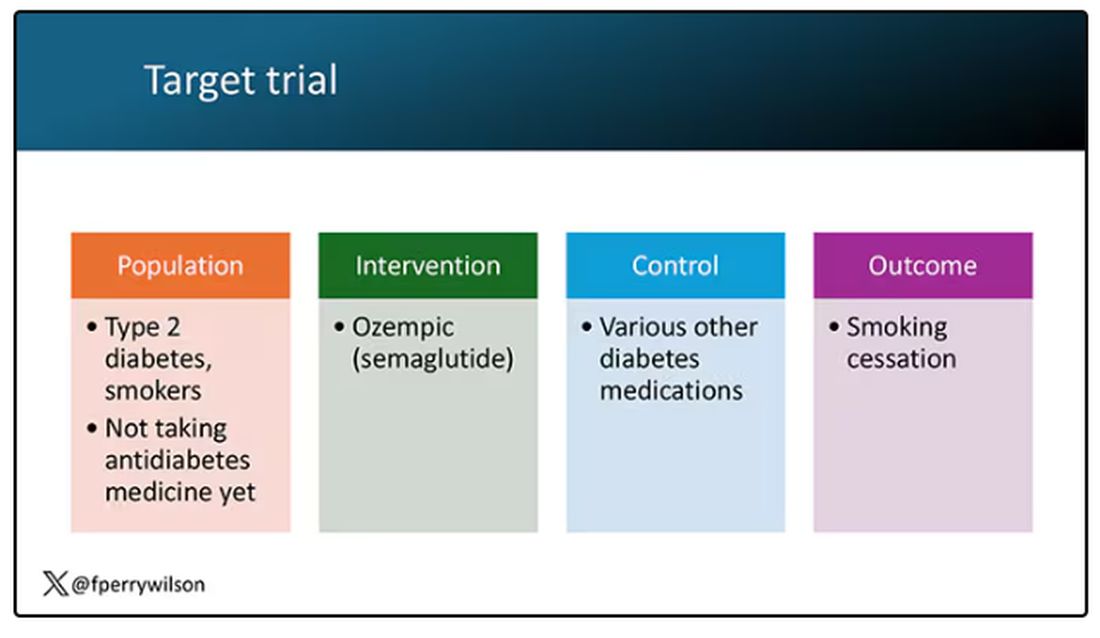
A target trial emulation study is more or less what it sounds like. First, you decide what your dream randomized controlled trial would be and you plan it all out in great detail. You define the population you would recruit, with all the relevant inclusion and exclusion criteria. You define the intervention and the control, and you define the outcome.
But you don’t actually do the trial. You could if someone would lend you $10-$50 million, but assuming you don’t have that lying around, you do the next best thing, which is to dig into a medical record database to find all the people who would be eligible for your imaginary trial. And you analyze them.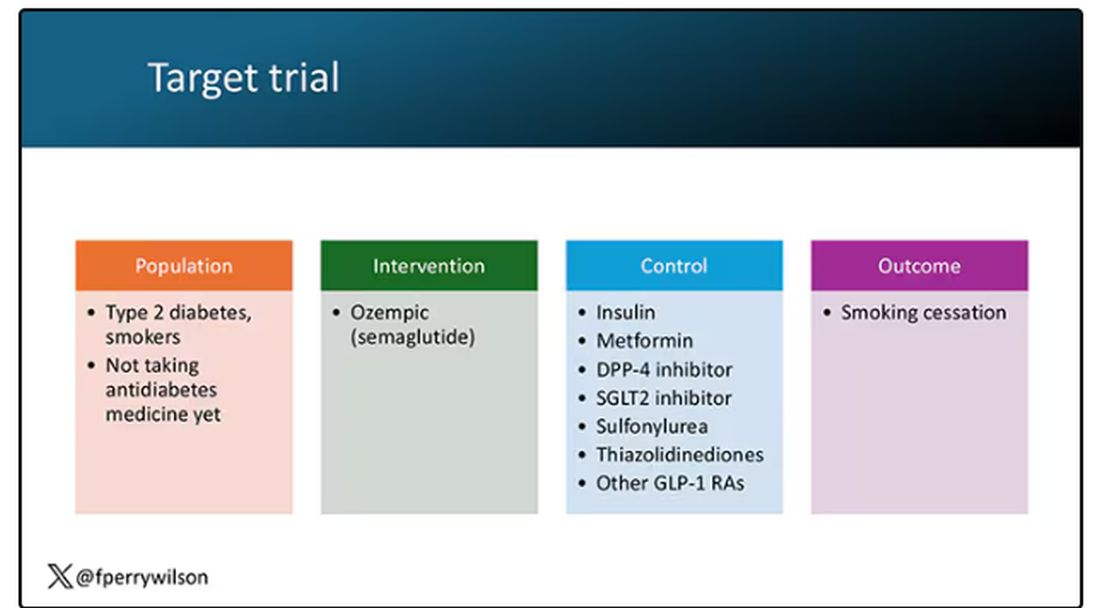
The authors wanted to study the effect of Ozempic on smoking among people with diabetes; that’s why all the comparator agents are antidiabetes drugs. They figured out whether these folks were smoking on the basis of a medical record diagnosis of tobacco use disorder before they started one of the drugs of interest. This code is fairly specific: If a patient has it, you can be pretty sure they are smoking. But it’s not very sensitive; not every smoker has this diagnostic code. This is an age-old limitation of using EHR data instead of asking patients, but it’s part of the tradeoff for not having to spend $50 million.
After applying all those inclusion and exclusion criteria, they have a defined population who could be in their dream trial. And, as luck would have it, some of those people really were treated with Ozempic and some really were treated with those other agents. Although decisions about what to prescribe were not randomized, the authors account for this confounding-by-indication using propensity-score matching. You can find a little explainer on propensity-score matching in an earlier column here. 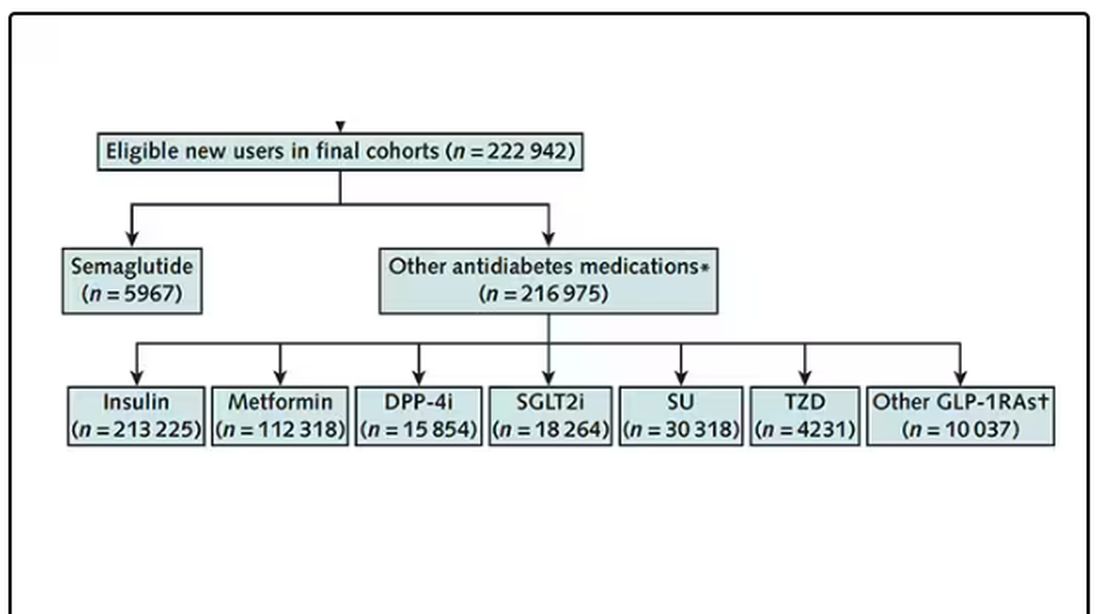
It’s easy enough, using the EHR, to figure out who has diabetes and who got which drug. But how do you know who quit smoking? Remember, everyone had a diagnosis code for tobacco use disorder prior to starting Ozempic or a comparator drug. The authors decided that if the patient had a medical visit where someone again coded tobacco-use disorder, they were still smoking. If someone prescribed smoking cessation meds like a nicotine patch or varenicline, they were obviously still smoking. If someone billed for tobacco-cessation counseling, the patient is still smoking. We’ll get back to the implications of this outcome definition in a minute.
Let’s talk about the results, which are pretty intriguing. 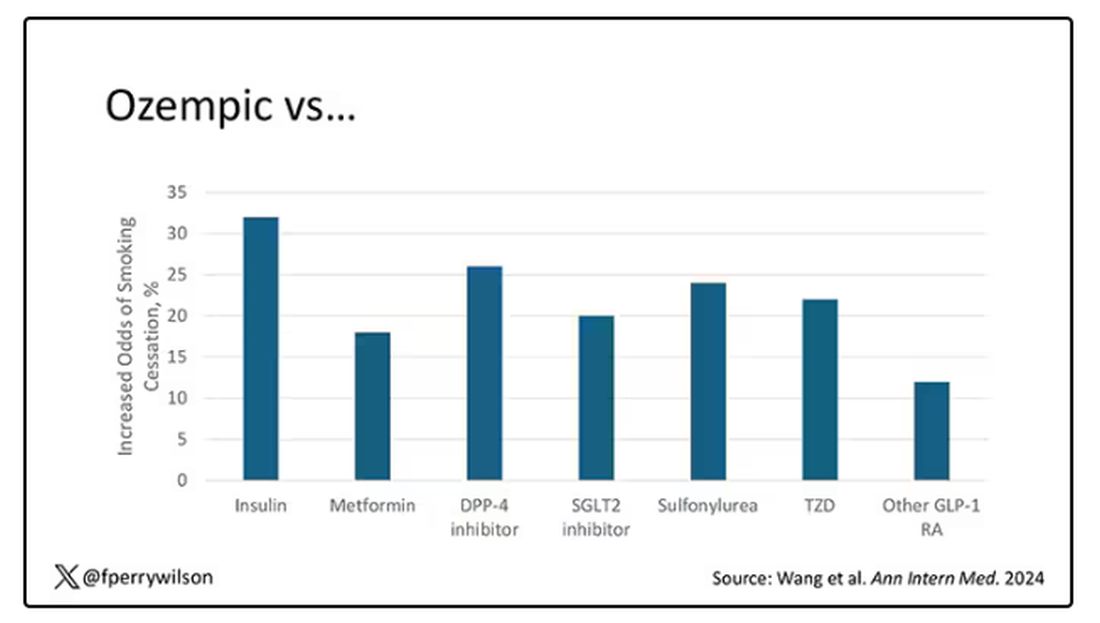
When Ozempic is compared with insulin among smokers with diabetes, those on Ozempic were about 30% more likely to quit smoking. They were about 18% more likely to quit smoking than those who took metformin. They were even slightly more likely to quit smoking than those on other GLP-1 receptor antagonists, though I should note that Mounjaro, which is probably the more potent GLP-1 drug in terms of weight loss, was not among the comparators.
This is pretty impressive for a drug that was not designed to be a smoking cessation drug. It speaks to this emerging idea that these drugs do more than curb appetite by slowing down gastric emptying or something. They work in the brain, modulating some of the reward circuitry that keeps us locked into our bad habits.
There are, of course, some caveats. As I pointed out, this study captured the idea of “still smoking” through the use of administrative codes in the EHR and prescription of smoking cessation aids. You could see similar results if taking Ozempic makes people less likely to address their smoking at all; maybe they shut down the doctor before they even talk about it, or there is too much to discuss during these visits to even get to the subject of smoking. You could also see results like this if people taking Ozempic had fewer visits overall, but the authors showed that that, at least, was not the case.
I’m inclined to believe that this effect is real, simply because we keep seeing signals from multiple sources. If that turns out to be the case, these new “weight loss” drugs may prove to be much more than that; they may turn out to be the drugs that can finally save us from ourselves.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
If you’ve been paying attention only to the headlines, when you think of “Ozempic” you’ll think of a few things: a blockbuster weight loss drug or the tip of the spear of a completely new industry — why not? A drug so popular that the people it was invented for (those with diabetes) can’t even get it.
Ozempic and other GLP-1 receptor agonists are undeniable game changers. Insofar as obesity is the number-one public health risk in the United States, antiobesity drugs hold immense promise even if all they do is reduce obesity.
In 2023, an article in Scientific Reports presented data suggesting that people on Ozempic might be reducing their alcohol intake, not just their total calories.
A 2024 article in Molecular Psychiatry found that the drug might positively impact cannabis use disorder. An article from Brain Sciences suggests that the drug reduces compulsive shopping.
A picture is starting to form, a picture that suggests these drugs curb hunger both literally and figuratively. That GLP-1 receptor agonists like Ozempic and Mounjaro are fundamentally anticonsumption drugs. In a society that — some would argue — is plagued by overconsumption, these drugs might be just what the doctor ordered.
If only they could stop people from smoking.
Oh, wait — they can.
At least it seems they can, based on a new study appearing in Annals of Internal Medicine.
Before we get too excited, this is not a randomized trial. There actually was a small randomized trial of exenatide (Byetta), which is in the same class as Ozempic but probably a bit less potent, with promising results for smoking cessation.
But Byetta is the weaker drug in this class; the market leader is Ozempic. So how can you figure out whether Ozempic can reduce smoking without doing a huge and expensive randomized trial? You can do what Nora Volkow and colleagues from the National Institute on Drug Abuse did: a target trial emulation study.
A target trial emulation study is more or less what it sounds like. First, you decide what your dream randomized controlled trial would be and you plan it all out in great detail. You define the population you would recruit, with all the relevant inclusion and exclusion criteria. You define the intervention and the control, and you define the outcome.
But you don’t actually do the trial. You could if someone would lend you $10-$50 million, but assuming you don’t have that lying around, you do the next best thing, which is to dig into a medical record database to find all the people who would be eligible for your imaginary trial. And you analyze them.
The authors wanted to study the effect of Ozempic on smoking among people with diabetes; that’s why all the comparator agents are antidiabetes drugs. They figured out whether these folks were smoking on the basis of a medical record diagnosis of tobacco use disorder before they started one of the drugs of interest. This code is fairly specific: If a patient has it, you can be pretty sure they are smoking. But it’s not very sensitive; not every smoker has this diagnostic code. This is an age-old limitation of using EHR data instead of asking patients, but it’s part of the tradeoff for not having to spend $50 million.
After applying all those inclusion and exclusion criteria, they have a defined population who could be in their dream trial. And, as luck would have it, some of those people really were treated with Ozempic and some really were treated with those other agents. Although decisions about what to prescribe were not randomized, the authors account for this confounding-by-indication using propensity-score matching. You can find a little explainer on propensity-score matching in an earlier column here.
It’s easy enough, using the EHR, to figure out who has diabetes and who got which drug. But how do you know who quit smoking? Remember, everyone had a diagnosis code for tobacco use disorder prior to starting Ozempic or a comparator drug. The authors decided that if the patient had a medical visit where someone again coded tobacco-use disorder, they were still smoking. If someone prescribed smoking cessation meds like a nicotine patch or varenicline, they were obviously still smoking. If someone billed for tobacco-cessation counseling, the patient is still smoking. We’ll get back to the implications of this outcome definition in a minute.
Let’s talk about the results, which are pretty intriguing.
When Ozempic is compared with insulin among smokers with diabetes, those on Ozempic were about 30% more likely to quit smoking. They were about 18% more likely to quit smoking than those who took metformin. They were even slightly more likely to quit smoking than those on other GLP-1 receptor antagonists, though I should note that Mounjaro, which is probably the more potent GLP-1 drug in terms of weight loss, was not among the comparators.
This is pretty impressive for a drug that was not designed to be a smoking cessation drug. It speaks to this emerging idea that these drugs do more than curb appetite by slowing down gastric emptying or something. They work in the brain, modulating some of the reward circuitry that keeps us locked into our bad habits.
There are, of course, some caveats. As I pointed out, this study captured the idea of “still smoking” through the use of administrative codes in the EHR and prescription of smoking cessation aids. You could see similar results if taking Ozempic makes people less likely to address their smoking at all; maybe they shut down the doctor before they even talk about it, or there is too much to discuss during these visits to even get to the subject of smoking. You could also see results like this if people taking Ozempic had fewer visits overall, but the authors showed that that, at least, was not the case.
I’m inclined to believe that this effect is real, simply because we keep seeing signals from multiple sources. If that turns out to be the case, these new “weight loss” drugs may prove to be much more than that; they may turn out to be the drugs that can finally save us from ourselves.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
If you’ve been paying attention only to the headlines, when you think of “Ozempic” you’ll think of a few things: a blockbuster weight loss drug or the tip of the spear of a completely new industry — why not? A drug so popular that the people it was invented for (those with diabetes) can’t even get it.
Ozempic and other GLP-1 receptor agonists are undeniable game changers. Insofar as obesity is the number-one public health risk in the United States, antiobesity drugs hold immense promise even if all they do is reduce obesity.
In 2023, an article in Scientific Reports presented data suggesting that people on Ozempic might be reducing their alcohol intake, not just their total calories.
A 2024 article in Molecular Psychiatry found that the drug might positively impact cannabis use disorder. An article from Brain Sciences suggests that the drug reduces compulsive shopping.
A picture is starting to form, a picture that suggests these drugs curb hunger both literally and figuratively. That GLP-1 receptor agonists like Ozempic and Mounjaro are fundamentally anticonsumption drugs. In a society that — some would argue — is plagued by overconsumption, these drugs might be just what the doctor ordered.
If only they could stop people from smoking.
Oh, wait — they can.
At least it seems they can, based on a new study appearing in Annals of Internal Medicine.
Before we get too excited, this is not a randomized trial. There actually was a small randomized trial of exenatide (Byetta), which is in the same class as Ozempic but probably a bit less potent, with promising results for smoking cessation.
But Byetta is the weaker drug in this class; the market leader is Ozempic. So how can you figure out whether Ozempic can reduce smoking without doing a huge and expensive randomized trial? You can do what Nora Volkow and colleagues from the National Institute on Drug Abuse did: a target trial emulation study.
A target trial emulation study is more or less what it sounds like. First, you decide what your dream randomized controlled trial would be and you plan it all out in great detail. You define the population you would recruit, with all the relevant inclusion and exclusion criteria. You define the intervention and the control, and you define the outcome.
But you don’t actually do the trial. You could if someone would lend you $10-$50 million, but assuming you don’t have that lying around, you do the next best thing, which is to dig into a medical record database to find all the people who would be eligible for your imaginary trial. And you analyze them.
The authors wanted to study the effect of Ozempic on smoking among people with diabetes; that’s why all the comparator agents are antidiabetes drugs. They figured out whether these folks were smoking on the basis of a medical record diagnosis of tobacco use disorder before they started one of the drugs of interest. This code is fairly specific: If a patient has it, you can be pretty sure they are smoking. But it’s not very sensitive; not every smoker has this diagnostic code. This is an age-old limitation of using EHR data instead of asking patients, but it’s part of the tradeoff for not having to spend $50 million.
After applying all those inclusion and exclusion criteria, they have a defined population who could be in their dream trial. And, as luck would have it, some of those people really were treated with Ozempic and some really were treated with those other agents. Although decisions about what to prescribe were not randomized, the authors account for this confounding-by-indication using propensity-score matching. You can find a little explainer on propensity-score matching in an earlier column here.
It’s easy enough, using the EHR, to figure out who has diabetes and who got which drug. But how do you know who quit smoking? Remember, everyone had a diagnosis code for tobacco use disorder prior to starting Ozempic or a comparator drug. The authors decided that if the patient had a medical visit where someone again coded tobacco-use disorder, they were still smoking. If someone prescribed smoking cessation meds like a nicotine patch or varenicline, they were obviously still smoking. If someone billed for tobacco-cessation counseling, the patient is still smoking. We’ll get back to the implications of this outcome definition in a minute.
Let’s talk about the results, which are pretty intriguing.
When Ozempic is compared with insulin among smokers with diabetes, those on Ozempic were about 30% more likely to quit smoking. They were about 18% more likely to quit smoking than those who took metformin. They were even slightly more likely to quit smoking than those on other GLP-1 receptor antagonists, though I should note that Mounjaro, which is probably the more potent GLP-1 drug in terms of weight loss, was not among the comparators.
This is pretty impressive for a drug that was not designed to be a smoking cessation drug. It speaks to this emerging idea that these drugs do more than curb appetite by slowing down gastric emptying or something. They work in the brain, modulating some of the reward circuitry that keeps us locked into our bad habits.
There are, of course, some caveats. As I pointed out, this study captured the idea of “still smoking” through the use of administrative codes in the EHR and prescription of smoking cessation aids. You could see similar results if taking Ozempic makes people less likely to address their smoking at all; maybe they shut down the doctor before they even talk about it, or there is too much to discuss during these visits to even get to the subject of smoking. You could also see results like this if people taking Ozempic had fewer visits overall, but the authors showed that that, at least, was not the case.
I’m inclined to believe that this effect is real, simply because we keep seeing signals from multiple sources. If that turns out to be the case, these new “weight loss” drugs may prove to be much more than that; they may turn out to be the drugs that can finally save us from ourselves.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Physicians Call Out Barriers in Addiction Care
Physicians who fail to help patients suffering from addiction blame their institutions and their own limitations in skill, knowledge, available brainpower, and faith that interventions will help patients, a systematic review found.
Researchers analyzed 283 international studies with data from 66,732 physicians who were asked about their reluctance to address addiction treatment and substance use. , reported Wilson M. Compton, MD, deputy director of the National Institute on Drug Abuse, Baltimore, and colleagues, in JAMA Network Open.
Lack of Priority in Addiction Care
In an interview, Sarah Wakeman, MD, senior medical director for substance use disorder at Mass General Brigham, Boston, questioned the lack of priority given to addiction care. “Many of the perceived barriers that physicians cite for why they don’t offer addiction treatment exist for many types of health conditions we routinely manage,” said Dr. Wakeman, who’s familiar with the findings but didn’t take part in the study. “Yet we as physicians would never opt out of treating diabetes or heart disease. So why is it acceptable to opt out of treating addiction?”
As the review notes, an estimate suggests that more than 46 million people in the United States were diagnosed with substance abuse disorder in the past year, and misuse of alcohol and illegal drugs costs more than $442 billion a year. However, few people with addiction get treatment — estimated at only 6.3% in 2021 — and screening rates are low.
According to its authors, the review’s goal is to summarize studies into barriers to evidence-based addiction strategies such as screening, referral to treatment, medications, and behavioral interventions.
The researchers analyzed 283 studies from 1960 to 2021, mainly (64.0%) from 2010 to 2021, with only a few (2.7%) from before 2000. Most (60.1%) were survey-based, and most (59.4%) were from the United States. The studies mainly examined alcohol, opioid, and tobacco addiction.
Challenges in Treating Addiction
The studies pinpointed various challenges in the treatment of people with addiction. On the institution front, they noted obstacles such as lack of trained staff, prior authorization hassles, lack of insurance coverage, and “acceptance of addiction interventions by staff,” according to the review. In terms of knowledge and skill, “knowledge was more deficient for treatment than for screening or diagnosis and for drug use more than for alcohol or tobacco use.”
Available brainpower “was not often characterized beyond a general sense of overwhelm with clinical tasks (eg, ‘just too busy’) and the need to prioritize patients’ competing needs,” the review stated.
The review authors wrote that “other reasons for reluctance (eg, negative social influences, negative emotions toward people who use drugs, and fear of harming the relationship with the patient by discussing substance use) could each be viewed as manifestations of stigma associated with substance use disorder and its treatment.”
The review identified limitations such as “inconsistent use of terms” across studies and lack of detail in some studies about participation by the “audience of focus.” Additionally, the authors noted that the medical treatments for addiction have evolved over the past several decades, as has the drug market.
Dr. Wakeman said the review is well done with unsurprising results. “It is helpful to understand what physicians perceive the barriers to be so that further interventions can be designed to surmount those barriers, such as skills training or educational interventions,” she said.
Going forward, she said, “we need to end substance use disorder exceptionalism and stop approaching addiction treatment as if it is something different from the rest of healthcare.”
In an interview, Michael L. Barnett, MD, associate professor of health policy and management at Harvard T.H. Chan School of Public Health, Boston, said the review is “very thorough and documents a really wide literature that is difficult to summarize, which is an impressive contribution.”
Dr. Barnett, who’s familiar with the review findings but didn’t take part in the research, also noted that the review doesn’t confirm whether the perceived obstacles actually exist or how they can be fixed. In addition, he said, “the authors spend very little time addressing the elephant in the room, which is that addiction care is poorly compensated. If physicians made 10 times the money for addiction care, I bet a lot of this ‘reluctance’ would disappear.”
Additionally, he said, “It’s easy to endorse innocuous excuses for reluctance when the real reason is that a physician just doesn’t want to treat a stigmatized population.”
The study was funded by the National Institute on Drug Abuse. Two authors disclosed receiving support from the Intramural Research Program, National Institute on Drug Abuse, and National Institutes of Health. Dr. Wakeman is an author and a textbook editor for Wolters Kluwer and Springer. Dr. Barnett had no disclosures.
A version of this article first appeared on Medscape.com.
Physicians who fail to help patients suffering from addiction blame their institutions and their own limitations in skill, knowledge, available brainpower, and faith that interventions will help patients, a systematic review found.
Researchers analyzed 283 international studies with data from 66,732 physicians who were asked about their reluctance to address addiction treatment and substance use. , reported Wilson M. Compton, MD, deputy director of the National Institute on Drug Abuse, Baltimore, and colleagues, in JAMA Network Open.
Lack of Priority in Addiction Care
In an interview, Sarah Wakeman, MD, senior medical director for substance use disorder at Mass General Brigham, Boston, questioned the lack of priority given to addiction care. “Many of the perceived barriers that physicians cite for why they don’t offer addiction treatment exist for many types of health conditions we routinely manage,” said Dr. Wakeman, who’s familiar with the findings but didn’t take part in the study. “Yet we as physicians would never opt out of treating diabetes or heart disease. So why is it acceptable to opt out of treating addiction?”
As the review notes, an estimate suggests that more than 46 million people in the United States were diagnosed with substance abuse disorder in the past year, and misuse of alcohol and illegal drugs costs more than $442 billion a year. However, few people with addiction get treatment — estimated at only 6.3% in 2021 — and screening rates are low.
According to its authors, the review’s goal is to summarize studies into barriers to evidence-based addiction strategies such as screening, referral to treatment, medications, and behavioral interventions.
The researchers analyzed 283 studies from 1960 to 2021, mainly (64.0%) from 2010 to 2021, with only a few (2.7%) from before 2000. Most (60.1%) were survey-based, and most (59.4%) were from the United States. The studies mainly examined alcohol, opioid, and tobacco addiction.
Challenges in Treating Addiction
The studies pinpointed various challenges in the treatment of people with addiction. On the institution front, they noted obstacles such as lack of trained staff, prior authorization hassles, lack of insurance coverage, and “acceptance of addiction interventions by staff,” according to the review. In terms of knowledge and skill, “knowledge was more deficient for treatment than for screening or diagnosis and for drug use more than for alcohol or tobacco use.”
Available brainpower “was not often characterized beyond a general sense of overwhelm with clinical tasks (eg, ‘just too busy’) and the need to prioritize patients’ competing needs,” the review stated.
The review authors wrote that “other reasons for reluctance (eg, negative social influences, negative emotions toward people who use drugs, and fear of harming the relationship with the patient by discussing substance use) could each be viewed as manifestations of stigma associated with substance use disorder and its treatment.”
The review identified limitations such as “inconsistent use of terms” across studies and lack of detail in some studies about participation by the “audience of focus.” Additionally, the authors noted that the medical treatments for addiction have evolved over the past several decades, as has the drug market.
Dr. Wakeman said the review is well done with unsurprising results. “It is helpful to understand what physicians perceive the barriers to be so that further interventions can be designed to surmount those barriers, such as skills training or educational interventions,” she said.
Going forward, she said, “we need to end substance use disorder exceptionalism and stop approaching addiction treatment as if it is something different from the rest of healthcare.”
In an interview, Michael L. Barnett, MD, associate professor of health policy and management at Harvard T.H. Chan School of Public Health, Boston, said the review is “very thorough and documents a really wide literature that is difficult to summarize, which is an impressive contribution.”
Dr. Barnett, who’s familiar with the review findings but didn’t take part in the research, also noted that the review doesn’t confirm whether the perceived obstacles actually exist or how they can be fixed. In addition, he said, “the authors spend very little time addressing the elephant in the room, which is that addiction care is poorly compensated. If physicians made 10 times the money for addiction care, I bet a lot of this ‘reluctance’ would disappear.”
Additionally, he said, “It’s easy to endorse innocuous excuses for reluctance when the real reason is that a physician just doesn’t want to treat a stigmatized population.”
The study was funded by the National Institute on Drug Abuse. Two authors disclosed receiving support from the Intramural Research Program, National Institute on Drug Abuse, and National Institutes of Health. Dr. Wakeman is an author and a textbook editor for Wolters Kluwer and Springer. Dr. Barnett had no disclosures.
A version of this article first appeared on Medscape.com.
Physicians who fail to help patients suffering from addiction blame their institutions and their own limitations in skill, knowledge, available brainpower, and faith that interventions will help patients, a systematic review found.
Researchers analyzed 283 international studies with data from 66,732 physicians who were asked about their reluctance to address addiction treatment and substance use. , reported Wilson M. Compton, MD, deputy director of the National Institute on Drug Abuse, Baltimore, and colleagues, in JAMA Network Open.
Lack of Priority in Addiction Care
In an interview, Sarah Wakeman, MD, senior medical director for substance use disorder at Mass General Brigham, Boston, questioned the lack of priority given to addiction care. “Many of the perceived barriers that physicians cite for why they don’t offer addiction treatment exist for many types of health conditions we routinely manage,” said Dr. Wakeman, who’s familiar with the findings but didn’t take part in the study. “Yet we as physicians would never opt out of treating diabetes or heart disease. So why is it acceptable to opt out of treating addiction?”
As the review notes, an estimate suggests that more than 46 million people in the United States were diagnosed with substance abuse disorder in the past year, and misuse of alcohol and illegal drugs costs more than $442 billion a year. However, few people with addiction get treatment — estimated at only 6.3% in 2021 — and screening rates are low.
According to its authors, the review’s goal is to summarize studies into barriers to evidence-based addiction strategies such as screening, referral to treatment, medications, and behavioral interventions.
The researchers analyzed 283 studies from 1960 to 2021, mainly (64.0%) from 2010 to 2021, with only a few (2.7%) from before 2000. Most (60.1%) were survey-based, and most (59.4%) were from the United States. The studies mainly examined alcohol, opioid, and tobacco addiction.
Challenges in Treating Addiction
The studies pinpointed various challenges in the treatment of people with addiction. On the institution front, they noted obstacles such as lack of trained staff, prior authorization hassles, lack of insurance coverage, and “acceptance of addiction interventions by staff,” according to the review. In terms of knowledge and skill, “knowledge was more deficient for treatment than for screening or diagnosis and for drug use more than for alcohol or tobacco use.”
Available brainpower “was not often characterized beyond a general sense of overwhelm with clinical tasks (eg, ‘just too busy’) and the need to prioritize patients’ competing needs,” the review stated.
The review authors wrote that “other reasons for reluctance (eg, negative social influences, negative emotions toward people who use drugs, and fear of harming the relationship with the patient by discussing substance use) could each be viewed as manifestations of stigma associated with substance use disorder and its treatment.”
The review identified limitations such as “inconsistent use of terms” across studies and lack of detail in some studies about participation by the “audience of focus.” Additionally, the authors noted that the medical treatments for addiction have evolved over the past several decades, as has the drug market.
Dr. Wakeman said the review is well done with unsurprising results. “It is helpful to understand what physicians perceive the barriers to be so that further interventions can be designed to surmount those barriers, such as skills training or educational interventions,” she said.
Going forward, she said, “we need to end substance use disorder exceptionalism and stop approaching addiction treatment as if it is something different from the rest of healthcare.”
In an interview, Michael L. Barnett, MD, associate professor of health policy and management at Harvard T.H. Chan School of Public Health, Boston, said the review is “very thorough and documents a really wide literature that is difficult to summarize, which is an impressive contribution.”
Dr. Barnett, who’s familiar with the review findings but didn’t take part in the research, also noted that the review doesn’t confirm whether the perceived obstacles actually exist or how they can be fixed. In addition, he said, “the authors spend very little time addressing the elephant in the room, which is that addiction care is poorly compensated. If physicians made 10 times the money for addiction care, I bet a lot of this ‘reluctance’ would disappear.”
Additionally, he said, “It’s easy to endorse innocuous excuses for reluctance when the real reason is that a physician just doesn’t want to treat a stigmatized population.”
The study was funded by the National Institute on Drug Abuse. Two authors disclosed receiving support from the Intramural Research Program, National Institute on Drug Abuse, and National Institutes of Health. Dr. Wakeman is an author and a textbook editor for Wolters Kluwer and Springer. Dr. Barnett had no disclosures.
A version of this article first appeared on Medscape.com.
‘Alarming’ Rise in Mental Health Hospital Admissions Involving Methamphetamine
new research showed. Investigators found that between 2008 and 2020, such admissions increased by more than 10-fold.
“Overall, our results show an alarming increase in mental health disorder–related hospitalizations with concurrent methamphetamine use from 2008 to 2020,” wrote the investigators, led by Diensn Xing, Department of Medicine, Louisiana State University Health Sciences Center, Shreveport.
“These results are especially concerning because these hospitalizations outpace hospitalizations for methamphetamine use alone or mental health disorders alone,” they added.
The study was published online in Nature Mental Health .
Action Needed
Mental illness and methamphetamine use are both growing health problems. The investigators pointed out that methamphetamine use can cause serious harm to an individual’s mental, emotional, and social well-being and can significantly alter the brain.
They added that long-term methamphetamine users can exhibit “extreme anxiety, confusion, troubled sleep, mood changes, and aggressive behavior.” In addition, use of the drug can cause psychotic side effects such as paranoia, hallucinations, delusions, and suicidality.
The investigators noted that, to date, no studies have examined the combined effects of both diseases or characterized national trends over more than 10 years.
The researchers analyzed US mental health–related trends in methamphetamine users from 2008 to 2020. In particular, they wanted to characterize which demographic and geographic groups might be affected by both of these diseases because people with mental illness and co-occurring methamphetamine use are an “intersectional group” that is “doubly vulnerable to suicide and overdose death due to the synergistic effects of methamphetamine and mental health disorders.”
The investigators evaluated US trends in mental health disorder–related hospital admissions (MHD-HAs) and compared them with mental health admissions that involved concurrent methamphetamine use (MHD-HA-MUs) between 2008 and 2020.
Using data from the largest US inpatient care database, which encompasses more than 7 million hospital stays annually, they examined close to 4 million weighted hospital admissions and found more than a 10-fold increase in MHD-HA-MUs, compared with a 1.4-fold increase in MHD-HAs.
MHD-HA-MUs increased significantly among men (13-fold), non-Hispanic Black patients (39-fold), and those aged 41-64 years (16-fold). In the southern United States, MHD-HA-MUs increased 24-fold, larger than in any other region in the United States.
“Overall, the data suggest that there are synergistic effects with methamphetamine use and mental health disorder, highlighting this patient group’s unique needs, requiring distinct action,” the researchers wrote.
They proposed several interventions, including public education about substance use disorders, mental illness, and the effects of stigma. They also suggested decreasing criminal penalties for those with substance use disorders and improving healthcare delivery for this patient population.
This work was supported by the National Institutes of Health and an award from the National Institute of General Medical Sciences. The study authors declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research showed. Investigators found that between 2008 and 2020, such admissions increased by more than 10-fold.
“Overall, our results show an alarming increase in mental health disorder–related hospitalizations with concurrent methamphetamine use from 2008 to 2020,” wrote the investigators, led by Diensn Xing, Department of Medicine, Louisiana State University Health Sciences Center, Shreveport.
“These results are especially concerning because these hospitalizations outpace hospitalizations for methamphetamine use alone or mental health disorders alone,” they added.
The study was published online in Nature Mental Health .
Action Needed
Mental illness and methamphetamine use are both growing health problems. The investigators pointed out that methamphetamine use can cause serious harm to an individual’s mental, emotional, and social well-being and can significantly alter the brain.
They added that long-term methamphetamine users can exhibit “extreme anxiety, confusion, troubled sleep, mood changes, and aggressive behavior.” In addition, use of the drug can cause psychotic side effects such as paranoia, hallucinations, delusions, and suicidality.
The investigators noted that, to date, no studies have examined the combined effects of both diseases or characterized national trends over more than 10 years.
The researchers analyzed US mental health–related trends in methamphetamine users from 2008 to 2020. In particular, they wanted to characterize which demographic and geographic groups might be affected by both of these diseases because people with mental illness and co-occurring methamphetamine use are an “intersectional group” that is “doubly vulnerable to suicide and overdose death due to the synergistic effects of methamphetamine and mental health disorders.”
The investigators evaluated US trends in mental health disorder–related hospital admissions (MHD-HAs) and compared them with mental health admissions that involved concurrent methamphetamine use (MHD-HA-MUs) between 2008 and 2020.
Using data from the largest US inpatient care database, which encompasses more than 7 million hospital stays annually, they examined close to 4 million weighted hospital admissions and found more than a 10-fold increase in MHD-HA-MUs, compared with a 1.4-fold increase in MHD-HAs.
MHD-HA-MUs increased significantly among men (13-fold), non-Hispanic Black patients (39-fold), and those aged 41-64 years (16-fold). In the southern United States, MHD-HA-MUs increased 24-fold, larger than in any other region in the United States.
“Overall, the data suggest that there are synergistic effects with methamphetamine use and mental health disorder, highlighting this patient group’s unique needs, requiring distinct action,” the researchers wrote.
They proposed several interventions, including public education about substance use disorders, mental illness, and the effects of stigma. They also suggested decreasing criminal penalties for those with substance use disorders and improving healthcare delivery for this patient population.
This work was supported by the National Institutes of Health and an award from the National Institute of General Medical Sciences. The study authors declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research showed. Investigators found that between 2008 and 2020, such admissions increased by more than 10-fold.
“Overall, our results show an alarming increase in mental health disorder–related hospitalizations with concurrent methamphetamine use from 2008 to 2020,” wrote the investigators, led by Diensn Xing, Department of Medicine, Louisiana State University Health Sciences Center, Shreveport.
“These results are especially concerning because these hospitalizations outpace hospitalizations for methamphetamine use alone or mental health disorders alone,” they added.
The study was published online in Nature Mental Health .
Action Needed
Mental illness and methamphetamine use are both growing health problems. The investigators pointed out that methamphetamine use can cause serious harm to an individual’s mental, emotional, and social well-being and can significantly alter the brain.
They added that long-term methamphetamine users can exhibit “extreme anxiety, confusion, troubled sleep, mood changes, and aggressive behavior.” In addition, use of the drug can cause psychotic side effects such as paranoia, hallucinations, delusions, and suicidality.
The investigators noted that, to date, no studies have examined the combined effects of both diseases or characterized national trends over more than 10 years.
The researchers analyzed US mental health–related trends in methamphetamine users from 2008 to 2020. In particular, they wanted to characterize which demographic and geographic groups might be affected by both of these diseases because people with mental illness and co-occurring methamphetamine use are an “intersectional group” that is “doubly vulnerable to suicide and overdose death due to the synergistic effects of methamphetamine and mental health disorders.”
The investigators evaluated US trends in mental health disorder–related hospital admissions (MHD-HAs) and compared them with mental health admissions that involved concurrent methamphetamine use (MHD-HA-MUs) between 2008 and 2020.
Using data from the largest US inpatient care database, which encompasses more than 7 million hospital stays annually, they examined close to 4 million weighted hospital admissions and found more than a 10-fold increase in MHD-HA-MUs, compared with a 1.4-fold increase in MHD-HAs.
MHD-HA-MUs increased significantly among men (13-fold), non-Hispanic Black patients (39-fold), and those aged 41-64 years (16-fold). In the southern United States, MHD-HA-MUs increased 24-fold, larger than in any other region in the United States.
“Overall, the data suggest that there are synergistic effects with methamphetamine use and mental health disorder, highlighting this patient group’s unique needs, requiring distinct action,” the researchers wrote.
They proposed several interventions, including public education about substance use disorders, mental illness, and the effects of stigma. They also suggested decreasing criminal penalties for those with substance use disorders and improving healthcare delivery for this patient population.
This work was supported by the National Institutes of Health and an award from the National Institute of General Medical Sciences. The study authors declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE MENTAL HEALTH
‘Emerging Threat’ Xylazine Use Continues to Spread Across the United States
Illicit use of the veterinary tranquilizer xylazine continues to spread across the United States. The drug, which is increasingly mixed with fentanyl, often fails to respond to the opioid overdose reversal medication naloxone and can cause severe necrotic lesions.
A report released by Millennium Health, a specialty lab that provides medication monitoring for pain management, drug treatment, and behavioral and substance use disorder treatment centers across the country, showed the number of urine specimens collected and tested at the US drug treatment centers were positive for xylazine in the most recent 6 months.
As previously reported by this news organization, in late 2022, the US Food and Drug Administration (FDA) issued a communication alerting clinicians about the special management required for opioid overdoses tainted with xylazine, which is also known as “tranq” or “tranq dope.”
Subsequently, in early 2023, The White House Office of National Drug Control Policy designated xylazine combined with fentanyl as an emerging threat to the United States.
Both the FDA and the Drug Enforcement Administration have taken steps to try to stop trafficking of the combination. However, despite these efforts, xylazine use has continued to spread.
The Millennium Health Signals report showed that the greatest increase in xylazine use was largely in the western United States. In the first 6 months of 2023, 3% of urine drug tests (UDTs) in Washington, Oregon, California, Hawaii, and Alaska were positive for xylazine. From November 2023 to April 2024, this rose to 8%, a 147% increase. In the Mountain West, xylazine-positive UDTs increased from 2% in 2023 to 4% in 2024, an increase of 94%. In addition to growth in the West, the report showed that xylazine use increased by more than 100% in New England — from 14% in 2023 to 28% in 2024.
Nationally, 16% of all urine specimens were positive for xylazine from late 2023 to April 2024, up slightly from 14% from April to October 2023.
Xylazine use was highest in the East and in the mid-Atlantic United States. Still, positivity rates in the mid-Atlantic dropped from 44% to 33%. The states included in that group were New York, Pennsylvania, Delaware, and New Jersey. East North Central states (Ohio, Michigan, Wisconsin, Indiana, and Illinois) also experienced a decline in positive tests from 32% to 30%.
The South Atlantic states, which include Maryland, Virginia, West Virginia, North and South Carolina, Georgia, and Florida, had a 17% increase in positivity — from 22% to 26%.
From April 2023 to April 2024 state-level UDT positivity rates were 40% in Pennsylvania, 37% in New York, and 35% in Ohio. But rates vary by locality. In Clermont and Hamilton counties in Ohio — both in the Cincinnati area — about 70% of specimens were positive for xylazine.
About one third of specimens in Maryland and South Carolina contained xylazine.
“Because xylazine exposure remains a significant challenge in the East and is a growing concern in the West, clinicians across the US need to be prepared to recognize and address the consequences of xylazine use — like diminished responses to naloxone and severe skin wounds that may lead to amputation — among people who use fentanyl,” Millennium Health Chief Clinical Officer Angela Huskey, PharmD, said in a press release.
The Health Signals Alert analyzed more than 50,000 fentanyl-positive UDT specimens collected between April 12, 2023, and April 11, 2024. Millennium Health researchers analyzed xylazine positivity rates in fentanyl-positive UDT specimens by the US Census Division and state.
A version of this article first appeared on Medscape.com.
Illicit use of the veterinary tranquilizer xylazine continues to spread across the United States. The drug, which is increasingly mixed with fentanyl, often fails to respond to the opioid overdose reversal medication naloxone and can cause severe necrotic lesions.
A report released by Millennium Health, a specialty lab that provides medication monitoring for pain management, drug treatment, and behavioral and substance use disorder treatment centers across the country, showed the number of urine specimens collected and tested at the US drug treatment centers were positive for xylazine in the most recent 6 months.
As previously reported by this news organization, in late 2022, the US Food and Drug Administration (FDA) issued a communication alerting clinicians about the special management required for opioid overdoses tainted with xylazine, which is also known as “tranq” or “tranq dope.”
Subsequently, in early 2023, The White House Office of National Drug Control Policy designated xylazine combined with fentanyl as an emerging threat to the United States.
Both the FDA and the Drug Enforcement Administration have taken steps to try to stop trafficking of the combination. However, despite these efforts, xylazine use has continued to spread.
The Millennium Health Signals report showed that the greatest increase in xylazine use was largely in the western United States. In the first 6 months of 2023, 3% of urine drug tests (UDTs) in Washington, Oregon, California, Hawaii, and Alaska were positive for xylazine. From November 2023 to April 2024, this rose to 8%, a 147% increase. In the Mountain West, xylazine-positive UDTs increased from 2% in 2023 to 4% in 2024, an increase of 94%. In addition to growth in the West, the report showed that xylazine use increased by more than 100% in New England — from 14% in 2023 to 28% in 2024.
Nationally, 16% of all urine specimens were positive for xylazine from late 2023 to April 2024, up slightly from 14% from April to October 2023.
Xylazine use was highest in the East and in the mid-Atlantic United States. Still, positivity rates in the mid-Atlantic dropped from 44% to 33%. The states included in that group were New York, Pennsylvania, Delaware, and New Jersey. East North Central states (Ohio, Michigan, Wisconsin, Indiana, and Illinois) also experienced a decline in positive tests from 32% to 30%.
The South Atlantic states, which include Maryland, Virginia, West Virginia, North and South Carolina, Georgia, and Florida, had a 17% increase in positivity — from 22% to 26%.
From April 2023 to April 2024 state-level UDT positivity rates were 40% in Pennsylvania, 37% in New York, and 35% in Ohio. But rates vary by locality. In Clermont and Hamilton counties in Ohio — both in the Cincinnati area — about 70% of specimens were positive for xylazine.
About one third of specimens in Maryland and South Carolina contained xylazine.
“Because xylazine exposure remains a significant challenge in the East and is a growing concern in the West, clinicians across the US need to be prepared to recognize and address the consequences of xylazine use — like diminished responses to naloxone and severe skin wounds that may lead to amputation — among people who use fentanyl,” Millennium Health Chief Clinical Officer Angela Huskey, PharmD, said in a press release.
The Health Signals Alert analyzed more than 50,000 fentanyl-positive UDT specimens collected between April 12, 2023, and April 11, 2024. Millennium Health researchers analyzed xylazine positivity rates in fentanyl-positive UDT specimens by the US Census Division and state.
A version of this article first appeared on Medscape.com.
Illicit use of the veterinary tranquilizer xylazine continues to spread across the United States. The drug, which is increasingly mixed with fentanyl, often fails to respond to the opioid overdose reversal medication naloxone and can cause severe necrotic lesions.
A report released by Millennium Health, a specialty lab that provides medication monitoring for pain management, drug treatment, and behavioral and substance use disorder treatment centers across the country, showed the number of urine specimens collected and tested at the US drug treatment centers were positive for xylazine in the most recent 6 months.
As previously reported by this news organization, in late 2022, the US Food and Drug Administration (FDA) issued a communication alerting clinicians about the special management required for opioid overdoses tainted with xylazine, which is also known as “tranq” or “tranq dope.”
Subsequently, in early 2023, The White House Office of National Drug Control Policy designated xylazine combined with fentanyl as an emerging threat to the United States.
Both the FDA and the Drug Enforcement Administration have taken steps to try to stop trafficking of the combination. However, despite these efforts, xylazine use has continued to spread.
The Millennium Health Signals report showed that the greatest increase in xylazine use was largely in the western United States. In the first 6 months of 2023, 3% of urine drug tests (UDTs) in Washington, Oregon, California, Hawaii, and Alaska were positive for xylazine. From November 2023 to April 2024, this rose to 8%, a 147% increase. In the Mountain West, xylazine-positive UDTs increased from 2% in 2023 to 4% in 2024, an increase of 94%. In addition to growth in the West, the report showed that xylazine use increased by more than 100% in New England — from 14% in 2023 to 28% in 2024.
Nationally, 16% of all urine specimens were positive for xylazine from late 2023 to April 2024, up slightly from 14% from April to October 2023.
Xylazine use was highest in the East and in the mid-Atlantic United States. Still, positivity rates in the mid-Atlantic dropped from 44% to 33%. The states included in that group were New York, Pennsylvania, Delaware, and New Jersey. East North Central states (Ohio, Michigan, Wisconsin, Indiana, and Illinois) also experienced a decline in positive tests from 32% to 30%.
The South Atlantic states, which include Maryland, Virginia, West Virginia, North and South Carolina, Georgia, and Florida, had a 17% increase in positivity — from 22% to 26%.
From April 2023 to April 2024 state-level UDT positivity rates were 40% in Pennsylvania, 37% in New York, and 35% in Ohio. But rates vary by locality. In Clermont and Hamilton counties in Ohio — both in the Cincinnati area — about 70% of specimens were positive for xylazine.
About one third of specimens in Maryland and South Carolina contained xylazine.
“Because xylazine exposure remains a significant challenge in the East and is a growing concern in the West, clinicians across the US need to be prepared to recognize and address the consequences of xylazine use — like diminished responses to naloxone and severe skin wounds that may lead to amputation — among people who use fentanyl,” Millennium Health Chief Clinical Officer Angela Huskey, PharmD, said in a press release.
The Health Signals Alert analyzed more than 50,000 fentanyl-positive UDT specimens collected between April 12, 2023, and April 11, 2024. Millennium Health researchers analyzed xylazine positivity rates in fentanyl-positive UDT specimens by the US Census Division and state.
A version of this article first appeared on Medscape.com.
Guidance on How Best to Manage Opioid Risks in Older Adults
Polypharmacy and slow metabolism of drugs create a high risk among older adults for substance use disorder, raising the odds of intentional and unintentional overdoses. However, screening, assessment, and treatment for substance use disorder occurs less often in younger adults.
Rates of overdose from opioids increased the most among people aged 65 years and older from 2021 to 2022, compared with among younger age groups. Meanwhile, recent data show less than half older adults with opioid use disorder (OUD) receive care for the condition.
“Nobody is immune to developing some kind of use disorder, so don’t just assume that because someone’s 80 years old that there’s no way that they have a problem,” said Sara Meyer, PharmD, a medication safety pharmacist at Novant Health in Winston-Salem, North Carolina. “You never know who’s going to potentially have an issue.”
in an effort to reduce addiction and overdoses.
Older Adults Have Unique Needs
A major challenge of treating older adults is their high incidence of chronic pain and multiple complex chronic conditions. As a result, some of the nonopioid medications clinicians might otherwise prescribe, like nonsteroidal anti-inflammatory drugs, cannot be used, according to Caroline Goldzweig, MD, chief medical officer of the Cedars-Sinai Medical Network in Los Angeles, California.
“Before you know it, the only thing left is an opiate, so you can sometimes be between a rock and a hard place,” she said.
But for adults older than 65 years, opioids can carry problematic side effects, including sedation, cognitive impairment, falls, and fractures.
With those factors in mind, part of a yearly checkup or wellness visit should include time to discuss how a patient is managing their chronic pain, according to Timothy Anderson, MD, an assistant professor of medicine at the University of Pittsburgh, Pittsburgh, Pennsylvania, and codirector of the Prescribing Wisely Lab, a research collaboration between that institution and Beth Israel Deaconess Medical Center in Boston.
When considering a prescription for pain medication, Dr. Anderson said he evaluates the potential worst, best, and average outcomes for a patient. Nonopioid options should always be considered first-line treatment. Patients and physicians often struggle with balancing an option that meets a patient’s goals for pain relief but does not put them at a risk for adverse outcomes, he said.
Greater Risk
Older adults experience neurophysiologic effects different from younger people, said Benjamin Han, MD, a geriatrician and addiction medicine specialist at the University of California, San Diego.
Seniors also absorb, metabolize, and excrete drugs differently, sometimes affected by decreased production of gastric acid, lean body mass, and renal function. Coupled with complications of other chronic conditions or medications, diagnosing problematic opioid use or OUD can be one of the most challenging experiences in geriatrics, Dr. Han said.
As a result, OUD is often underdiagnosed in these patients, he said. Single-item screening tools like the TAPS and OWLS can be used to assess if the benefits of an opioid outweigh a patient’s risk for addiction.
Dr. Han finds medications like buprenorphine to be relatively safe and effective, along with nonpharmacologic interventions like physical therapy. He also advised clinicians to provide patients with opioid-overdose reversal agents.
“Naloxone is only used for reversing opioid withdrawal, but it is important to ensure that any patient at risk for an overdose, including being on chronic opioids, is provided naloxone and educated on preventing opioid overdoses,” he said.
Steroid injections and medications that target specific pathways, such as neuropathic pain, can be helpful in primary care for these older patients, according to Pooja Lagisetty, MD, an internal medicine physician at Michigan Medicine and a research scientist at VA Ann Arbor Health Care, Ann Arbor, Michigan.
She often recommends to her patients online programs that help them maintain strength and mobility, as well as low-impact exercises like tai chi, for pain management.
“This will ensure a much more balanced, patient-centered conversation with whatever decisions you and your patient come to,” Dr. Lagisetty said.
New Protocols for Pain Management in Older Adults
At the health system level, clinicians can use treatment agreements for patients taking opioids. At Novant, patients must attest they agree to take the medications only as prescribed and from a specified pharmacy. They promise not to seek opioids from other sources, to submit to random drug screenings, and to communicate regularly with their clinician about any health issues.
If a patient violates any part of this agreement, their clinician can stop the treatment. The system encourages clinicians to help patients find additional care for substance abuse disorder or pain management if it occurs.
Over the past 2 years, Novant also developed an AI prediction model, which generates a score for the risk a patient has in developing substance use disorder or experiencing an overdose within a year of initial opioid prescription. The model was validated by an internal team at the system but has not been independently certified.
If a patient has a high-risk score, their clinician considers additional risk mitigation strategies, such as seeing the patient more frequently or using an abuse deterrent formulation of an opioid. They also have the option of referring the patient to specialists in addiction medicine or neurology. Opioids are not necessarily withheld, according to Dr. Meyer. The tool is now used by clinicians during Medicare annual wellness visits.
And coming later this year are new protocols for pain management in patients aged 80 years and older. Clinicians will target a 50% dose reduction, compared with what a younger patient might receive to account for physiologic differences.
“We know that especially with some opioids like morphine, they’re not going to metabolize that the same way a young person with a young kidney will, so we’re trying to set the clinician up to select a lower starting dose for patients that are older,” Dr. Meyer said.
In 2017, the system implemented a program to reduce prescription of opioids to less than 350 morphine milligram equivalents (MME) per order following any kind of surgery. The health system compared numbers of prescriptions written among surgical colleagues and met with them to discuss alternative approaches. Novant said it continues to monitor the data and follow-up with surgeons who are not in alignment with the goal.
Between 2017 and 2019, patients switching to lower doses after surgeries rose by 20%.
Across the country at Cedars-Sinai Medical Network, leadership in 2016 made the move to deprescribe opioids or lower doses of the drugs to less than 90 MME per day, in accordance with Centers for Disease Control and Prevention guidelines established that year. Patients were referred to their pain program for support and for nonopioid interventions. Pharmacists worked closely with clinicians on safely tapering these medications in patients taking high doses.
The program worked, according to Dr. Goldzweig. Dr. Goldzweig could only find two patients currently taking high-dose opioids in the system’s database out of more than 7000 patients with Medicare Advantage insurance coverage.
“There will always be some patients who have no alternative than opioids, but we established some discipline with urine tox screens and pain agreements, and over time, we’ve been able to reduce the number of high-risk opioid prescriptions,” she said.
A version of this article first appeared on Medscape.com.
Polypharmacy and slow metabolism of drugs create a high risk among older adults for substance use disorder, raising the odds of intentional and unintentional overdoses. However, screening, assessment, and treatment for substance use disorder occurs less often in younger adults.
Rates of overdose from opioids increased the most among people aged 65 years and older from 2021 to 2022, compared with among younger age groups. Meanwhile, recent data show less than half older adults with opioid use disorder (OUD) receive care for the condition.
“Nobody is immune to developing some kind of use disorder, so don’t just assume that because someone’s 80 years old that there’s no way that they have a problem,” said Sara Meyer, PharmD, a medication safety pharmacist at Novant Health in Winston-Salem, North Carolina. “You never know who’s going to potentially have an issue.”
in an effort to reduce addiction and overdoses.
Older Adults Have Unique Needs
A major challenge of treating older adults is their high incidence of chronic pain and multiple complex chronic conditions. As a result, some of the nonopioid medications clinicians might otherwise prescribe, like nonsteroidal anti-inflammatory drugs, cannot be used, according to Caroline Goldzweig, MD, chief medical officer of the Cedars-Sinai Medical Network in Los Angeles, California.
“Before you know it, the only thing left is an opiate, so you can sometimes be between a rock and a hard place,” she said.
But for adults older than 65 years, opioids can carry problematic side effects, including sedation, cognitive impairment, falls, and fractures.
With those factors in mind, part of a yearly checkup or wellness visit should include time to discuss how a patient is managing their chronic pain, according to Timothy Anderson, MD, an assistant professor of medicine at the University of Pittsburgh, Pittsburgh, Pennsylvania, and codirector of the Prescribing Wisely Lab, a research collaboration between that institution and Beth Israel Deaconess Medical Center in Boston.
When considering a prescription for pain medication, Dr. Anderson said he evaluates the potential worst, best, and average outcomes for a patient. Nonopioid options should always be considered first-line treatment. Patients and physicians often struggle with balancing an option that meets a patient’s goals for pain relief but does not put them at a risk for adverse outcomes, he said.
Greater Risk
Older adults experience neurophysiologic effects different from younger people, said Benjamin Han, MD, a geriatrician and addiction medicine specialist at the University of California, San Diego.
Seniors also absorb, metabolize, and excrete drugs differently, sometimes affected by decreased production of gastric acid, lean body mass, and renal function. Coupled with complications of other chronic conditions or medications, diagnosing problematic opioid use or OUD can be one of the most challenging experiences in geriatrics, Dr. Han said.
As a result, OUD is often underdiagnosed in these patients, he said. Single-item screening tools like the TAPS and OWLS can be used to assess if the benefits of an opioid outweigh a patient’s risk for addiction.
Dr. Han finds medications like buprenorphine to be relatively safe and effective, along with nonpharmacologic interventions like physical therapy. He also advised clinicians to provide patients with opioid-overdose reversal agents.
“Naloxone is only used for reversing opioid withdrawal, but it is important to ensure that any patient at risk for an overdose, including being on chronic opioids, is provided naloxone and educated on preventing opioid overdoses,” he said.
Steroid injections and medications that target specific pathways, such as neuropathic pain, can be helpful in primary care for these older patients, according to Pooja Lagisetty, MD, an internal medicine physician at Michigan Medicine and a research scientist at VA Ann Arbor Health Care, Ann Arbor, Michigan.
She often recommends to her patients online programs that help them maintain strength and mobility, as well as low-impact exercises like tai chi, for pain management.
“This will ensure a much more balanced, patient-centered conversation with whatever decisions you and your patient come to,” Dr. Lagisetty said.
New Protocols for Pain Management in Older Adults
At the health system level, clinicians can use treatment agreements for patients taking opioids. At Novant, patients must attest they agree to take the medications only as prescribed and from a specified pharmacy. They promise not to seek opioids from other sources, to submit to random drug screenings, and to communicate regularly with their clinician about any health issues.
If a patient violates any part of this agreement, their clinician can stop the treatment. The system encourages clinicians to help patients find additional care for substance abuse disorder or pain management if it occurs.
Over the past 2 years, Novant also developed an AI prediction model, which generates a score for the risk a patient has in developing substance use disorder or experiencing an overdose within a year of initial opioid prescription. The model was validated by an internal team at the system but has not been independently certified.
If a patient has a high-risk score, their clinician considers additional risk mitigation strategies, such as seeing the patient more frequently or using an abuse deterrent formulation of an opioid. They also have the option of referring the patient to specialists in addiction medicine or neurology. Opioids are not necessarily withheld, according to Dr. Meyer. The tool is now used by clinicians during Medicare annual wellness visits.
And coming later this year are new protocols for pain management in patients aged 80 years and older. Clinicians will target a 50% dose reduction, compared with what a younger patient might receive to account for physiologic differences.
“We know that especially with some opioids like morphine, they’re not going to metabolize that the same way a young person with a young kidney will, so we’re trying to set the clinician up to select a lower starting dose for patients that are older,” Dr. Meyer said.
In 2017, the system implemented a program to reduce prescription of opioids to less than 350 morphine milligram equivalents (MME) per order following any kind of surgery. The health system compared numbers of prescriptions written among surgical colleagues and met with them to discuss alternative approaches. Novant said it continues to monitor the data and follow-up with surgeons who are not in alignment with the goal.
Between 2017 and 2019, patients switching to lower doses after surgeries rose by 20%.
Across the country at Cedars-Sinai Medical Network, leadership in 2016 made the move to deprescribe opioids or lower doses of the drugs to less than 90 MME per day, in accordance with Centers for Disease Control and Prevention guidelines established that year. Patients were referred to their pain program for support and for nonopioid interventions. Pharmacists worked closely with clinicians on safely tapering these medications in patients taking high doses.
The program worked, according to Dr. Goldzweig. Dr. Goldzweig could only find two patients currently taking high-dose opioids in the system’s database out of more than 7000 patients with Medicare Advantage insurance coverage.
“There will always be some patients who have no alternative than opioids, but we established some discipline with urine tox screens and pain agreements, and over time, we’ve been able to reduce the number of high-risk opioid prescriptions,” she said.
A version of this article first appeared on Medscape.com.
Polypharmacy and slow metabolism of drugs create a high risk among older adults for substance use disorder, raising the odds of intentional and unintentional overdoses. However, screening, assessment, and treatment for substance use disorder occurs less often in younger adults.
Rates of overdose from opioids increased the most among people aged 65 years and older from 2021 to 2022, compared with among younger age groups. Meanwhile, recent data show less than half older adults with opioid use disorder (OUD) receive care for the condition.
“Nobody is immune to developing some kind of use disorder, so don’t just assume that because someone’s 80 years old that there’s no way that they have a problem,” said Sara Meyer, PharmD, a medication safety pharmacist at Novant Health in Winston-Salem, North Carolina. “You never know who’s going to potentially have an issue.”
in an effort to reduce addiction and overdoses.
Older Adults Have Unique Needs
A major challenge of treating older adults is their high incidence of chronic pain and multiple complex chronic conditions. As a result, some of the nonopioid medications clinicians might otherwise prescribe, like nonsteroidal anti-inflammatory drugs, cannot be used, according to Caroline Goldzweig, MD, chief medical officer of the Cedars-Sinai Medical Network in Los Angeles, California.
“Before you know it, the only thing left is an opiate, so you can sometimes be between a rock and a hard place,” she said.
But for adults older than 65 years, opioids can carry problematic side effects, including sedation, cognitive impairment, falls, and fractures.
With those factors in mind, part of a yearly checkup or wellness visit should include time to discuss how a patient is managing their chronic pain, according to Timothy Anderson, MD, an assistant professor of medicine at the University of Pittsburgh, Pittsburgh, Pennsylvania, and codirector of the Prescribing Wisely Lab, a research collaboration between that institution and Beth Israel Deaconess Medical Center in Boston.
When considering a prescription for pain medication, Dr. Anderson said he evaluates the potential worst, best, and average outcomes for a patient. Nonopioid options should always be considered first-line treatment. Patients and physicians often struggle with balancing an option that meets a patient’s goals for pain relief but does not put them at a risk for adverse outcomes, he said.
Greater Risk
Older adults experience neurophysiologic effects different from younger people, said Benjamin Han, MD, a geriatrician and addiction medicine specialist at the University of California, San Diego.
Seniors also absorb, metabolize, and excrete drugs differently, sometimes affected by decreased production of gastric acid, lean body mass, and renal function. Coupled with complications of other chronic conditions or medications, diagnosing problematic opioid use or OUD can be one of the most challenging experiences in geriatrics, Dr. Han said.
As a result, OUD is often underdiagnosed in these patients, he said. Single-item screening tools like the TAPS and OWLS can be used to assess if the benefits of an opioid outweigh a patient’s risk for addiction.
Dr. Han finds medications like buprenorphine to be relatively safe and effective, along with nonpharmacologic interventions like physical therapy. He also advised clinicians to provide patients with opioid-overdose reversal agents.
“Naloxone is only used for reversing opioid withdrawal, but it is important to ensure that any patient at risk for an overdose, including being on chronic opioids, is provided naloxone and educated on preventing opioid overdoses,” he said.
Steroid injections and medications that target specific pathways, such as neuropathic pain, can be helpful in primary care for these older patients, according to Pooja Lagisetty, MD, an internal medicine physician at Michigan Medicine and a research scientist at VA Ann Arbor Health Care, Ann Arbor, Michigan.
She often recommends to her patients online programs that help them maintain strength and mobility, as well as low-impact exercises like tai chi, for pain management.
“This will ensure a much more balanced, patient-centered conversation with whatever decisions you and your patient come to,” Dr. Lagisetty said.
New Protocols for Pain Management in Older Adults
At the health system level, clinicians can use treatment agreements for patients taking opioids. At Novant, patients must attest they agree to take the medications only as prescribed and from a specified pharmacy. They promise not to seek opioids from other sources, to submit to random drug screenings, and to communicate regularly with their clinician about any health issues.
If a patient violates any part of this agreement, their clinician can stop the treatment. The system encourages clinicians to help patients find additional care for substance abuse disorder or pain management if it occurs.
Over the past 2 years, Novant also developed an AI prediction model, which generates a score for the risk a patient has in developing substance use disorder or experiencing an overdose within a year of initial opioid prescription. The model was validated by an internal team at the system but has not been independently certified.
If a patient has a high-risk score, their clinician considers additional risk mitigation strategies, such as seeing the patient more frequently or using an abuse deterrent formulation of an opioid. They also have the option of referring the patient to specialists in addiction medicine or neurology. Opioids are not necessarily withheld, according to Dr. Meyer. The tool is now used by clinicians during Medicare annual wellness visits.
And coming later this year are new protocols for pain management in patients aged 80 years and older. Clinicians will target a 50% dose reduction, compared with what a younger patient might receive to account for physiologic differences.
“We know that especially with some opioids like morphine, they’re not going to metabolize that the same way a young person with a young kidney will, so we’re trying to set the clinician up to select a lower starting dose for patients that are older,” Dr. Meyer said.
In 2017, the system implemented a program to reduce prescription of opioids to less than 350 morphine milligram equivalents (MME) per order following any kind of surgery. The health system compared numbers of prescriptions written among surgical colleagues and met with them to discuss alternative approaches. Novant said it continues to monitor the data and follow-up with surgeons who are not in alignment with the goal.
Between 2017 and 2019, patients switching to lower doses after surgeries rose by 20%.
Across the country at Cedars-Sinai Medical Network, leadership in 2016 made the move to deprescribe opioids or lower doses of the drugs to less than 90 MME per day, in accordance with Centers for Disease Control and Prevention guidelines established that year. Patients were referred to their pain program for support and for nonopioid interventions. Pharmacists worked closely with clinicians on safely tapering these medications in patients taking high doses.
The program worked, according to Dr. Goldzweig. Dr. Goldzweig could only find two patients currently taking high-dose opioids in the system’s database out of more than 7000 patients with Medicare Advantage insurance coverage.
“There will always be some patients who have no alternative than opioids, but we established some discipline with urine tox screens and pain agreements, and over time, we’ve been able to reduce the number of high-risk opioid prescriptions,” she said.
A version of this article first appeared on Medscape.com.
Opioids Post T&A
I recently encountered a study that reviewed return visits of pediatric patients after undergoing adenotonsillectomy. The investigators discovered that pain-related visits were higher for patients who had received prescriptions for opioids. After the Food and Drug Administration (FDA) issued a boxed warning about the use of codeine in postoperative pediatric tonsillectomy with adenoidectomy (T&A), patients pain-related return visits declined and steroid prescriptions increased.

On the surface, this inverse relationship between opioid prescriptions and pain-related visits seems counterintuitive. This is particularly true if you believe that opioids are effective pain medications. The relationship between pain-related visits, steroid use, and the boxed warning is a bit easier to understand and most likely points to the effectiveness of the steroids.
Keeping in mind this was a single-institution study that included more than 5000 patients and more than 700 return visits, we should be careful in reading too much into these results. However, I can’t resist the temptation to use it as a springboard from which to launch a short dissertation on pain management.
First, let’s consider whether there was something about the opioids that was causing more pain for the patients. I’m not aware of any studies that suggest pain as a side effect of codeine. Nausea and vomiting, yes. And, although the investigators were focusing on pain, it may have been that the general discomfort associated with the gastrointestinal effects of the drug were lowering the patients’ pain threshold. I certainly know of many adults who have said that they now avoid opioids postoperatively because of the general sense of unwellness they have experienced during previous surgical adventures.
However, my bias leads me to focus on this question: If the patients didn’t receive opioids postoperatively, were they receiving something else that was making them less likely to arrive at the hospital or clinic complaining of pain? I assume the researchers would have told us about some new alternative miracle painkiller that was being prescribed.
As a card-carrying nihilist in good standing, I am tempted to claim that this is another example of nothing is better than most well-intentioned somethings. However, I am going to posit that these patients were receiving something that lessened their need to seek help with their pain.
Most likely that something was a thoughtful preemptive dialogue postoperatively about what they (and in most cases their parents) might expect in the way of symptoms. And ... an easy-to-reach contact point preferably with a person with whom they were familiar. And ... were scheduled to receive follow up phone calls at intervals relevant to the details of their surgery.
I know many of you are going to say, “We are already doing those things.” And, if so, you are to be commended. And, I’m sure that every outpatient postoperative manual includes all of those common-sense ingredients of good follow-up care. However, you know as well as I do that not all postoperative instructions are delivered with same degree of thoroughness nor with sufficient pauses thoughtfully delivered to make it a real dialogue. Nor is the follow-up contact person as easy to reach as promised.
I’m not sure how much we can thank the FDA boxed warning about codeine for the decrease in postoperative pain-generated visits. However, it could be that when physicians were discouraged from prescribing postoperative opioids, they may have felt the need to lean more heavily on good old-fashioned postoperative follow-up care. Instructions presented more as a dialogue and preemptive follow-up calls made with an aura of caring are well known deterrents of middle-of-the-night calls for help.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I recently encountered a study that reviewed return visits of pediatric patients after undergoing adenotonsillectomy. The investigators discovered that pain-related visits were higher for patients who had received prescriptions for opioids. After the Food and Drug Administration (FDA) issued a boxed warning about the use of codeine in postoperative pediatric tonsillectomy with adenoidectomy (T&A), patients pain-related return visits declined and steroid prescriptions increased.
On the surface, this inverse relationship between opioid prescriptions and pain-related visits seems counterintuitive. This is particularly true if you believe that opioids are effective pain medications. The relationship between pain-related visits, steroid use, and the boxed warning is a bit easier to understand and most likely points to the effectiveness of the steroids.
Keeping in mind this was a single-institution study that included more than 5000 patients and more than 700 return visits, we should be careful in reading too much into these results. However, I can’t resist the temptation to use it as a springboard from which to launch a short dissertation on pain management.
First, let’s consider whether there was something about the opioids that was causing more pain for the patients. I’m not aware of any studies that suggest pain as a side effect of codeine. Nausea and vomiting, yes. And, although the investigators were focusing on pain, it may have been that the general discomfort associated with the gastrointestinal effects of the drug were lowering the patients’ pain threshold. I certainly know of many adults who have said that they now avoid opioids postoperatively because of the general sense of unwellness they have experienced during previous surgical adventures.
However, my bias leads me to focus on this question: If the patients didn’t receive opioids postoperatively, were they receiving something else that was making them less likely to arrive at the hospital or clinic complaining of pain? I assume the researchers would have told us about some new alternative miracle painkiller that was being prescribed.
As a card-carrying nihilist in good standing, I am tempted to claim that this is another example of nothing is better than most well-intentioned somethings. However, I am going to posit that these patients were receiving something that lessened their need to seek help with their pain.
Most likely that something was a thoughtful preemptive dialogue postoperatively about what they (and in most cases their parents) might expect in the way of symptoms. And ... an easy-to-reach contact point preferably with a person with whom they were familiar. And ... were scheduled to receive follow up phone calls at intervals relevant to the details of their surgery.
I know many of you are going to say, “We are already doing those things.” And, if so, you are to be commended. And, I’m sure that every outpatient postoperative manual includes all of those common-sense ingredients of good follow-up care. However, you know as well as I do that not all postoperative instructions are delivered with same degree of thoroughness nor with sufficient pauses thoughtfully delivered to make it a real dialogue. Nor is the follow-up contact person as easy to reach as promised.
I’m not sure how much we can thank the FDA boxed warning about codeine for the decrease in postoperative pain-generated visits. However, it could be that when physicians were discouraged from prescribing postoperative opioids, they may have felt the need to lean more heavily on good old-fashioned postoperative follow-up care. Instructions presented more as a dialogue and preemptive follow-up calls made with an aura of caring are well known deterrents of middle-of-the-night calls for help.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I recently encountered a study that reviewed return visits of pediatric patients after undergoing adenotonsillectomy. The investigators discovered that pain-related visits were higher for patients who had received prescriptions for opioids. After the Food and Drug Administration (FDA) issued a boxed warning about the use of codeine in postoperative pediatric tonsillectomy with adenoidectomy (T&A), patients pain-related return visits declined and steroid prescriptions increased.
On the surface, this inverse relationship between opioid prescriptions and pain-related visits seems counterintuitive. This is particularly true if you believe that opioids are effective pain medications. The relationship between pain-related visits, steroid use, and the boxed warning is a bit easier to understand and most likely points to the effectiveness of the steroids.
Keeping in mind this was a single-institution study that included more than 5000 patients and more than 700 return visits, we should be careful in reading too much into these results. However, I can’t resist the temptation to use it as a springboard from which to launch a short dissertation on pain management.
First, let’s consider whether there was something about the opioids that was causing more pain for the patients. I’m not aware of any studies that suggest pain as a side effect of codeine. Nausea and vomiting, yes. And, although the investigators were focusing on pain, it may have been that the general discomfort associated with the gastrointestinal effects of the drug were lowering the patients’ pain threshold. I certainly know of many adults who have said that they now avoid opioids postoperatively because of the general sense of unwellness they have experienced during previous surgical adventures.
However, my bias leads me to focus on this question: If the patients didn’t receive opioids postoperatively, were they receiving something else that was making them less likely to arrive at the hospital or clinic complaining of pain? I assume the researchers would have told us about some new alternative miracle painkiller that was being prescribed.
As a card-carrying nihilist in good standing, I am tempted to claim that this is another example of nothing is better than most well-intentioned somethings. However, I am going to posit that these patients were receiving something that lessened their need to seek help with their pain.
Most likely that something was a thoughtful preemptive dialogue postoperatively about what they (and in most cases their parents) might expect in the way of symptoms. And ... an easy-to-reach contact point preferably with a person with whom they were familiar. And ... were scheduled to receive follow up phone calls at intervals relevant to the details of their surgery.
I know many of you are going to say, “We are already doing those things.” And, if so, you are to be commended. And, I’m sure that every outpatient postoperative manual includes all of those common-sense ingredients of good follow-up care. However, you know as well as I do that not all postoperative instructions are delivered with same degree of thoroughness nor with sufficient pauses thoughtfully delivered to make it a real dialogue. Nor is the follow-up contact person as easy to reach as promised.
I’m not sure how much we can thank the FDA boxed warning about codeine for the decrease in postoperative pain-generated visits. However, it could be that when physicians were discouraged from prescribing postoperative opioids, they may have felt the need to lean more heavily on good old-fashioned postoperative follow-up care. Instructions presented more as a dialogue and preemptive follow-up calls made with an aura of caring are well known deterrents of middle-of-the-night calls for help.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].