User login
Experts call for early screening for chronic kidney disease
MADRID – A late diagnosis of chronic kidney disease is cause for concern. Scientific societies are therefore advocating for screening at younger ages to reverse this trend and slow the progression of the disease. Nearly all patients seen in primary care are candidates for screening because of their risk factors for kidney disease.
During the 29th National Conference of General and Family Medicine of the Spanish Society for General and Family Physicians, Teresa Benedito, MD, family doctor and member of the society’s cardiovascular group, and Roberto Alcázar, MD, nephrologist at the Infanta Leonor University Hospital, Madrid, presented a clinical case encountered in primary care. They used this case to frame a strong argument for the importance of early screening for chronic kidney disease, and they discussed how to properly manage such screening.
The presentation followed the guidelines in the SEMG publication regarding the management and referral of patients with type 2 diabetes. Dr. Benedito explained that the first thing to ask oneself during a patient visit is “whether they present risk factors for kidney disease. If so, we can’t let them leave before we do a kidney screening.” She then listed the factors in question: age older than 60 years, African heritage, family history of chronic kidney disease, decreased kidney mass, weight loss at birth, hypertension, diabetes, smoking, obesity, and low socioeconomic status.
For his part, Dr. Alcázar mentioned how these factors are similar to cardiovascular risk factors, because “the kidneys are a ball of vessels with double capillarization for purifying blood. They’re the organs with the most arteries per unit of weight, so anything that can damage the arteries can damage the kidneys.”
Candidates for screening
“Chronic kidney disease develops in 15% of the adult population in Spain. So, it’s worth asking how many patients have been diagnosed and who should we should be screening.” To the factors listed above, Dr. Alcázar added treatment with nephrotoxic drugs (including nonsteroidal anti-inflammatory drugs) for patients with obstructive urinary tract disease, and a history of acute kidney injury for patients with chronic autoimmune disease or neoplasms. “Thus, nearly all patients seen in primary care would need to be screened.”
Another fundamental question raised was whether patients should be screened before age 60 years. “As a nephrologist, I feel that we have been diagnosing chronic kidney disease late, even though we’ve been doing everything by the book,” said Dr. Alcázar. In his opinion, “the answer to whether we should be screening earlier ... is yes, for two reasons: first, because it’s cost-effective, and second, because it’s very inexpensive.”
Dr. Benedito explained in detail the process for diagnosing this disease. She began by defining the disease as changes in kidney structure and function that last longer than 3 months. These changes are identified by use of two criteria: glomerular filtration rate less than 60 mL/min and kidney injury or lesions with or without reduced filtration rate (renal biopsy, albumin/creatinine ratio greater than 30 mg/g, proteinuria, alterations in urinary sediment or in imaging tests). Thus, “if one of these two criteria persists for more than 3 months, the diagnosis is chronic kidney disease. Also, high creatinine levels are not diagnostic for the disease,” she emphasized.
Two related parameters
Glomerular filtration and albuminuria “are highly relevant, because screening for chronic kidney disease is based on these two parameters,” said Dr. Benedito. Glomerular filtration rate varies with age, sex, ethnicity, and body mass. It is useful for identifying the stage of the disease and for monitoring disease progression. Albuminuria, on the other hand, is an indication of the severity of the disease. It’s an early marker for kidney injury and systemic disease and is more sensitive than proteinuria. Therefore, “this factor, together with glomerular filtration rate, allows us to detect, classify, and monitor the progression of chronic kidney disease.”
On this point, Dr. Alcázar emphasized the importance of trends, since variation in glomerular filtration depends on serum creatinine, which can vary by nearly 9%. He explained that glomerular filtration rate is related to the number of nephrons remaining. A glomerular filtration rate of less than 60 mL/min implies that more than half of the nephrons in each kidney have been lost. Albuminuria informs about structural damage (that is, the condition of the remaining nephrons). It’s therefore essential to test for both parameters. “We need to be actively monitoring and then making our decisions based on trends and not on isolated results. We need to be aware of albuminuria when we make our decisions,” said Dr. Alcázar. Some studies have shown the importance of testing for albuminuria whenever creatinine level is assessed. “We need to buy into this. If we don’t do this, we’ll only ever have half the information we need.”
Reducing late diagnosis
According to the IBERICAN study, 14% of patients seen in primary care in Spain have chronic kidney disease. “This statistic should make us stop and think, own our responsibility, and ask ourselves why this screening isn’t taking place [earlier],” said Dr. Benedito. She added, “We need to head off this trend toward late diagnosis. As the disease progresses, it significantly increases cardiovascular risk and leads to higher mortality, going on dialysis, transplants, et cetera.”
Dr. Alcázar noted that 80% of nephrology cases that are referred to him come from primary care. He explained the need to understand that “these patients have a sevenfold greater risk of suffering a serious cardiovascular event within the next year than people without kidney problems.” Most of these patients will experience an event, even if they don’t undergo dialysis (stage 3 and those near stage 4).
Correct staging
Also fundamental is having a detailed understanding of how staging is performed. Dr. Benedito explained that a chart that pairs glomerular filtration rate (six categories) with the level of albuminuria (three categories) should be used during the visit. For example, a case might be classified as G3a-A2. However, the simplified form of the chart may prove more practical. It classifies chronic kidney disease as being associated with mild, moderate, and severe risk, using different colors to aid comprehension.
Dr. Alcázar noted that the latest guidelines from the European Society of Hypertension for 2023 include albuminuria as an important parameter. The guidelines indicate that for a patient with moderate or severe risk, it is not necessary to calculate their score. “It’s considered high cardiovascular risk, and steps would need to be taken for intervention.”
He then listed the tools available for reversing albuminuria. The process begins by reducing salt consumption and involves the use of medications (angiotensin-converting enzyme inhibitors/angiotensin II receptor antagonists, aldosterone receptor antagonists, glucagon-like peptide-1 analogues, and sodium-glucose cotransporter-2 inhibitors, which slow kidney damage regardless of other measures) and strict management of cardiovascular risk factors (smoking, weight management, blood glucose, hypertension, and moderate physical activity).
Reducing cardiovascular risk
Dr. Alcázar highlighted important factors to keep in mind when managing each of the cardiovascular risk factors. For hypertension, the aim is to achieve levels less than 130/80 mm Hg, although recommendations vary, depending on the guidelines consulted. “KDIGO (Kidney Disease: Improving Global Outcomes) 2021 states that there is no evidence for monitoring diastolic blood pressure, only systolic blood pressure. If we measure it according to the standardized form, SBP should be less than 120 mm Hg, and if not, we would fall back on readings of 130/80 mm Hg.”
For lipid control (specifically, low-density lipoprotein cholesterol), the staging chart indicates that for patients at mild risk, levels should be less than 100 mg/dL; for those at moderate risk, less than 70 mg/dL; and for those at severe risk, less than 55 mg/dL. Hypertriglyceridemia “should only be treated with fibrates if it comes in over 1,000 mg/dL. Also, care must be taken, because these drugs interfere with creatinine excretion, increasing it,” said Dr. Alcázar.
Guidelines from the KDIGO and the American Diabetes Association state that anyone with diabetes and chronic kidney disease should receive a sodium-glucose cotransporter-2 inhibitor if their glomerular filtration rate exceeds 20 mL/min, “which may contradict slightly what it says on the label. Also, if they have hypertension, they should take an angiotensin-converting enzyme inhibitor,” said Dr. Alcázar. He added that “oral antidiabetics, including metformin, must be adjusted based on renal function if glomerular filtration rate is under 30 mL/min.”
Act immediately
When asked whether the course of chronic kidney disease can be changed, Dr. Alcázar responded with an emphatic yes and added that cardiovascular risk can also be substantially reduced. “As nephrologists, we don’t have access to patients in early stages. But family doctors do. Hence the importance of early screening, because going on dialysis at age 60 isn’t the same as at 80.” Currently, “scientific societies are encouraging authorities to screen for chronic kidney disease at earlier ages.”
Regarding drug-based therapy, Dr. Alcázar said that “empagliflozin is not currently indicated for chronic kidney disease in adults.” This sodium-glucose cotransporter-2 inhibitor delays kidney disease and reduces morbidity. Both benefits were highlighted in two recent studies (DAPA-CKD and CREDENCE). Published in January, EMPA-KIDNEY presents a new twist on nephroprotection for patients with chronic kidney disease (diabetic or not) whose glomerular filtration rates are between 20 and 40 mL/min without albuminuria or whose glomerular filtration rates are between 45 and 90 mL/min with albuminuria. For more than 6,000 patients, empagliflozin was observed “to clearly reduce kidney disease progression, cardiovascular mortality and all-cause mortality, and the need to go on dialysis,” stated Dr. Alcázar.
What professionals expect
Dr. Benedito also explained the criteria for referral to a specialist: glomerular filtration rate less than 30 mL/min (unless the patient is older than 80 years and does not have progressively worsening renal function), albumin/creatinine ratio greater than 300 mg/g, acute worsening of renal function, progressive worsening of renal function of greater than 5 mL/min/yr, chronic kidney disease, hypertension treated with triple therapy (including a diuretic) at maximum doses, anemia of less than 10 g/dL, and nonurologic hematuria, especially in combination with albuminuria.
Dr. Benedito explained what nephrologists expect from family doctors in the management of chronic kidney disease: “screening for early detection, identifying and treating risk factors for chronic kidney disease, detecting progression and complications, adjusting drugs based on glomerular filtration rate, and ensuring that our patients are benefiting from sodium-glucose cotransporter-2 inhibitors. These are among the most important steps to be taken.”
Dr. Alcázar mentioned what family doctors expect from nephrologists: “two-way communication, accessibility, coordination of actions to be taken, and using shared and mutually agreed-upon protocols.”
This article was translated from the Medscape Spanish Edition and a version appeared on Medscape.com.
MADRID – A late diagnosis of chronic kidney disease is cause for concern. Scientific societies are therefore advocating for screening at younger ages to reverse this trend and slow the progression of the disease. Nearly all patients seen in primary care are candidates for screening because of their risk factors for kidney disease.
During the 29th National Conference of General and Family Medicine of the Spanish Society for General and Family Physicians, Teresa Benedito, MD, family doctor and member of the society’s cardiovascular group, and Roberto Alcázar, MD, nephrologist at the Infanta Leonor University Hospital, Madrid, presented a clinical case encountered in primary care. They used this case to frame a strong argument for the importance of early screening for chronic kidney disease, and they discussed how to properly manage such screening.
The presentation followed the guidelines in the SEMG publication regarding the management and referral of patients with type 2 diabetes. Dr. Benedito explained that the first thing to ask oneself during a patient visit is “whether they present risk factors for kidney disease. If so, we can’t let them leave before we do a kidney screening.” She then listed the factors in question: age older than 60 years, African heritage, family history of chronic kidney disease, decreased kidney mass, weight loss at birth, hypertension, diabetes, smoking, obesity, and low socioeconomic status.
For his part, Dr. Alcázar mentioned how these factors are similar to cardiovascular risk factors, because “the kidneys are a ball of vessels with double capillarization for purifying blood. They’re the organs with the most arteries per unit of weight, so anything that can damage the arteries can damage the kidneys.”
Candidates for screening
“Chronic kidney disease develops in 15% of the adult population in Spain. So, it’s worth asking how many patients have been diagnosed and who should we should be screening.” To the factors listed above, Dr. Alcázar added treatment with nephrotoxic drugs (including nonsteroidal anti-inflammatory drugs) for patients with obstructive urinary tract disease, and a history of acute kidney injury for patients with chronic autoimmune disease or neoplasms. “Thus, nearly all patients seen in primary care would need to be screened.”
Another fundamental question raised was whether patients should be screened before age 60 years. “As a nephrologist, I feel that we have been diagnosing chronic kidney disease late, even though we’ve been doing everything by the book,” said Dr. Alcázar. In his opinion, “the answer to whether we should be screening earlier ... is yes, for two reasons: first, because it’s cost-effective, and second, because it’s very inexpensive.”
Dr. Benedito explained in detail the process for diagnosing this disease. She began by defining the disease as changes in kidney structure and function that last longer than 3 months. These changes are identified by use of two criteria: glomerular filtration rate less than 60 mL/min and kidney injury or lesions with or without reduced filtration rate (renal biopsy, albumin/creatinine ratio greater than 30 mg/g, proteinuria, alterations in urinary sediment or in imaging tests). Thus, “if one of these two criteria persists for more than 3 months, the diagnosis is chronic kidney disease. Also, high creatinine levels are not diagnostic for the disease,” she emphasized.
Two related parameters
Glomerular filtration and albuminuria “are highly relevant, because screening for chronic kidney disease is based on these two parameters,” said Dr. Benedito. Glomerular filtration rate varies with age, sex, ethnicity, and body mass. It is useful for identifying the stage of the disease and for monitoring disease progression. Albuminuria, on the other hand, is an indication of the severity of the disease. It’s an early marker for kidney injury and systemic disease and is more sensitive than proteinuria. Therefore, “this factor, together with glomerular filtration rate, allows us to detect, classify, and monitor the progression of chronic kidney disease.”
On this point, Dr. Alcázar emphasized the importance of trends, since variation in glomerular filtration depends on serum creatinine, which can vary by nearly 9%. He explained that glomerular filtration rate is related to the number of nephrons remaining. A glomerular filtration rate of less than 60 mL/min implies that more than half of the nephrons in each kidney have been lost. Albuminuria informs about structural damage (that is, the condition of the remaining nephrons). It’s therefore essential to test for both parameters. “We need to be actively monitoring and then making our decisions based on trends and not on isolated results. We need to be aware of albuminuria when we make our decisions,” said Dr. Alcázar. Some studies have shown the importance of testing for albuminuria whenever creatinine level is assessed. “We need to buy into this. If we don’t do this, we’ll only ever have half the information we need.”
Reducing late diagnosis
According to the IBERICAN study, 14% of patients seen in primary care in Spain have chronic kidney disease. “This statistic should make us stop and think, own our responsibility, and ask ourselves why this screening isn’t taking place [earlier],” said Dr. Benedito. She added, “We need to head off this trend toward late diagnosis. As the disease progresses, it significantly increases cardiovascular risk and leads to higher mortality, going on dialysis, transplants, et cetera.”
Dr. Alcázar noted that 80% of nephrology cases that are referred to him come from primary care. He explained the need to understand that “these patients have a sevenfold greater risk of suffering a serious cardiovascular event within the next year than people without kidney problems.” Most of these patients will experience an event, even if they don’t undergo dialysis (stage 3 and those near stage 4).
Correct staging
Also fundamental is having a detailed understanding of how staging is performed. Dr. Benedito explained that a chart that pairs glomerular filtration rate (six categories) with the level of albuminuria (three categories) should be used during the visit. For example, a case might be classified as G3a-A2. However, the simplified form of the chart may prove more practical. It classifies chronic kidney disease as being associated with mild, moderate, and severe risk, using different colors to aid comprehension.
Dr. Alcázar noted that the latest guidelines from the European Society of Hypertension for 2023 include albuminuria as an important parameter. The guidelines indicate that for a patient with moderate or severe risk, it is not necessary to calculate their score. “It’s considered high cardiovascular risk, and steps would need to be taken for intervention.”
He then listed the tools available for reversing albuminuria. The process begins by reducing salt consumption and involves the use of medications (angiotensin-converting enzyme inhibitors/angiotensin II receptor antagonists, aldosterone receptor antagonists, glucagon-like peptide-1 analogues, and sodium-glucose cotransporter-2 inhibitors, which slow kidney damage regardless of other measures) and strict management of cardiovascular risk factors (smoking, weight management, blood glucose, hypertension, and moderate physical activity).
Reducing cardiovascular risk
Dr. Alcázar highlighted important factors to keep in mind when managing each of the cardiovascular risk factors. For hypertension, the aim is to achieve levels less than 130/80 mm Hg, although recommendations vary, depending on the guidelines consulted. “KDIGO (Kidney Disease: Improving Global Outcomes) 2021 states that there is no evidence for monitoring diastolic blood pressure, only systolic blood pressure. If we measure it according to the standardized form, SBP should be less than 120 mm Hg, and if not, we would fall back on readings of 130/80 mm Hg.”
For lipid control (specifically, low-density lipoprotein cholesterol), the staging chart indicates that for patients at mild risk, levels should be less than 100 mg/dL; for those at moderate risk, less than 70 mg/dL; and for those at severe risk, less than 55 mg/dL. Hypertriglyceridemia “should only be treated with fibrates if it comes in over 1,000 mg/dL. Also, care must be taken, because these drugs interfere with creatinine excretion, increasing it,” said Dr. Alcázar.
Guidelines from the KDIGO and the American Diabetes Association state that anyone with diabetes and chronic kidney disease should receive a sodium-glucose cotransporter-2 inhibitor if their glomerular filtration rate exceeds 20 mL/min, “which may contradict slightly what it says on the label. Also, if they have hypertension, they should take an angiotensin-converting enzyme inhibitor,” said Dr. Alcázar. He added that “oral antidiabetics, including metformin, must be adjusted based on renal function if glomerular filtration rate is under 30 mL/min.”
Act immediately
When asked whether the course of chronic kidney disease can be changed, Dr. Alcázar responded with an emphatic yes and added that cardiovascular risk can also be substantially reduced. “As nephrologists, we don’t have access to patients in early stages. But family doctors do. Hence the importance of early screening, because going on dialysis at age 60 isn’t the same as at 80.” Currently, “scientific societies are encouraging authorities to screen for chronic kidney disease at earlier ages.”
Regarding drug-based therapy, Dr. Alcázar said that “empagliflozin is not currently indicated for chronic kidney disease in adults.” This sodium-glucose cotransporter-2 inhibitor delays kidney disease and reduces morbidity. Both benefits were highlighted in two recent studies (DAPA-CKD and CREDENCE). Published in January, EMPA-KIDNEY presents a new twist on nephroprotection for patients with chronic kidney disease (diabetic or not) whose glomerular filtration rates are between 20 and 40 mL/min without albuminuria or whose glomerular filtration rates are between 45 and 90 mL/min with albuminuria. For more than 6,000 patients, empagliflozin was observed “to clearly reduce kidney disease progression, cardiovascular mortality and all-cause mortality, and the need to go on dialysis,” stated Dr. Alcázar.
What professionals expect
Dr. Benedito also explained the criteria for referral to a specialist: glomerular filtration rate less than 30 mL/min (unless the patient is older than 80 years and does not have progressively worsening renal function), albumin/creatinine ratio greater than 300 mg/g, acute worsening of renal function, progressive worsening of renal function of greater than 5 mL/min/yr, chronic kidney disease, hypertension treated with triple therapy (including a diuretic) at maximum doses, anemia of less than 10 g/dL, and nonurologic hematuria, especially in combination with albuminuria.
Dr. Benedito explained what nephrologists expect from family doctors in the management of chronic kidney disease: “screening for early detection, identifying and treating risk factors for chronic kidney disease, detecting progression and complications, adjusting drugs based on glomerular filtration rate, and ensuring that our patients are benefiting from sodium-glucose cotransporter-2 inhibitors. These are among the most important steps to be taken.”
Dr. Alcázar mentioned what family doctors expect from nephrologists: “two-way communication, accessibility, coordination of actions to be taken, and using shared and mutually agreed-upon protocols.”
This article was translated from the Medscape Spanish Edition and a version appeared on Medscape.com.
MADRID – A late diagnosis of chronic kidney disease is cause for concern. Scientific societies are therefore advocating for screening at younger ages to reverse this trend and slow the progression of the disease. Nearly all patients seen in primary care are candidates for screening because of their risk factors for kidney disease.
During the 29th National Conference of General and Family Medicine of the Spanish Society for General and Family Physicians, Teresa Benedito, MD, family doctor and member of the society’s cardiovascular group, and Roberto Alcázar, MD, nephrologist at the Infanta Leonor University Hospital, Madrid, presented a clinical case encountered in primary care. They used this case to frame a strong argument for the importance of early screening for chronic kidney disease, and they discussed how to properly manage such screening.
The presentation followed the guidelines in the SEMG publication regarding the management and referral of patients with type 2 diabetes. Dr. Benedito explained that the first thing to ask oneself during a patient visit is “whether they present risk factors for kidney disease. If so, we can’t let them leave before we do a kidney screening.” She then listed the factors in question: age older than 60 years, African heritage, family history of chronic kidney disease, decreased kidney mass, weight loss at birth, hypertension, diabetes, smoking, obesity, and low socioeconomic status.
For his part, Dr. Alcázar mentioned how these factors are similar to cardiovascular risk factors, because “the kidneys are a ball of vessels with double capillarization for purifying blood. They’re the organs with the most arteries per unit of weight, so anything that can damage the arteries can damage the kidneys.”
Candidates for screening
“Chronic kidney disease develops in 15% of the adult population in Spain. So, it’s worth asking how many patients have been diagnosed and who should we should be screening.” To the factors listed above, Dr. Alcázar added treatment with nephrotoxic drugs (including nonsteroidal anti-inflammatory drugs) for patients with obstructive urinary tract disease, and a history of acute kidney injury for patients with chronic autoimmune disease or neoplasms. “Thus, nearly all patients seen in primary care would need to be screened.”
Another fundamental question raised was whether patients should be screened before age 60 years. “As a nephrologist, I feel that we have been diagnosing chronic kidney disease late, even though we’ve been doing everything by the book,” said Dr. Alcázar. In his opinion, “the answer to whether we should be screening earlier ... is yes, for two reasons: first, because it’s cost-effective, and second, because it’s very inexpensive.”
Dr. Benedito explained in detail the process for diagnosing this disease. She began by defining the disease as changes in kidney structure and function that last longer than 3 months. These changes are identified by use of two criteria: glomerular filtration rate less than 60 mL/min and kidney injury or lesions with or without reduced filtration rate (renal biopsy, albumin/creatinine ratio greater than 30 mg/g, proteinuria, alterations in urinary sediment or in imaging tests). Thus, “if one of these two criteria persists for more than 3 months, the diagnosis is chronic kidney disease. Also, high creatinine levels are not diagnostic for the disease,” she emphasized.
Two related parameters
Glomerular filtration and albuminuria “are highly relevant, because screening for chronic kidney disease is based on these two parameters,” said Dr. Benedito. Glomerular filtration rate varies with age, sex, ethnicity, and body mass. It is useful for identifying the stage of the disease and for monitoring disease progression. Albuminuria, on the other hand, is an indication of the severity of the disease. It’s an early marker for kidney injury and systemic disease and is more sensitive than proteinuria. Therefore, “this factor, together with glomerular filtration rate, allows us to detect, classify, and monitor the progression of chronic kidney disease.”
On this point, Dr. Alcázar emphasized the importance of trends, since variation in glomerular filtration depends on serum creatinine, which can vary by nearly 9%. He explained that glomerular filtration rate is related to the number of nephrons remaining. A glomerular filtration rate of less than 60 mL/min implies that more than half of the nephrons in each kidney have been lost. Albuminuria informs about structural damage (that is, the condition of the remaining nephrons). It’s therefore essential to test for both parameters. “We need to be actively monitoring and then making our decisions based on trends and not on isolated results. We need to be aware of albuminuria when we make our decisions,” said Dr. Alcázar. Some studies have shown the importance of testing for albuminuria whenever creatinine level is assessed. “We need to buy into this. If we don’t do this, we’ll only ever have half the information we need.”
Reducing late diagnosis
According to the IBERICAN study, 14% of patients seen in primary care in Spain have chronic kidney disease. “This statistic should make us stop and think, own our responsibility, and ask ourselves why this screening isn’t taking place [earlier],” said Dr. Benedito. She added, “We need to head off this trend toward late diagnosis. As the disease progresses, it significantly increases cardiovascular risk and leads to higher mortality, going on dialysis, transplants, et cetera.”
Dr. Alcázar noted that 80% of nephrology cases that are referred to him come from primary care. He explained the need to understand that “these patients have a sevenfold greater risk of suffering a serious cardiovascular event within the next year than people without kidney problems.” Most of these patients will experience an event, even if they don’t undergo dialysis (stage 3 and those near stage 4).
Correct staging
Also fundamental is having a detailed understanding of how staging is performed. Dr. Benedito explained that a chart that pairs glomerular filtration rate (six categories) with the level of albuminuria (three categories) should be used during the visit. For example, a case might be classified as G3a-A2. However, the simplified form of the chart may prove more practical. It classifies chronic kidney disease as being associated with mild, moderate, and severe risk, using different colors to aid comprehension.
Dr. Alcázar noted that the latest guidelines from the European Society of Hypertension for 2023 include albuminuria as an important parameter. The guidelines indicate that for a patient with moderate or severe risk, it is not necessary to calculate their score. “It’s considered high cardiovascular risk, and steps would need to be taken for intervention.”
He then listed the tools available for reversing albuminuria. The process begins by reducing salt consumption and involves the use of medications (angiotensin-converting enzyme inhibitors/angiotensin II receptor antagonists, aldosterone receptor antagonists, glucagon-like peptide-1 analogues, and sodium-glucose cotransporter-2 inhibitors, which slow kidney damage regardless of other measures) and strict management of cardiovascular risk factors (smoking, weight management, blood glucose, hypertension, and moderate physical activity).
Reducing cardiovascular risk
Dr. Alcázar highlighted important factors to keep in mind when managing each of the cardiovascular risk factors. For hypertension, the aim is to achieve levels less than 130/80 mm Hg, although recommendations vary, depending on the guidelines consulted. “KDIGO (Kidney Disease: Improving Global Outcomes) 2021 states that there is no evidence for monitoring diastolic blood pressure, only systolic blood pressure. If we measure it according to the standardized form, SBP should be less than 120 mm Hg, and if not, we would fall back on readings of 130/80 mm Hg.”
For lipid control (specifically, low-density lipoprotein cholesterol), the staging chart indicates that for patients at mild risk, levels should be less than 100 mg/dL; for those at moderate risk, less than 70 mg/dL; and for those at severe risk, less than 55 mg/dL. Hypertriglyceridemia “should only be treated with fibrates if it comes in over 1,000 mg/dL. Also, care must be taken, because these drugs interfere with creatinine excretion, increasing it,” said Dr. Alcázar.
Guidelines from the KDIGO and the American Diabetes Association state that anyone with diabetes and chronic kidney disease should receive a sodium-glucose cotransporter-2 inhibitor if their glomerular filtration rate exceeds 20 mL/min, “which may contradict slightly what it says on the label. Also, if they have hypertension, they should take an angiotensin-converting enzyme inhibitor,” said Dr. Alcázar. He added that “oral antidiabetics, including metformin, must be adjusted based on renal function if glomerular filtration rate is under 30 mL/min.”
Act immediately
When asked whether the course of chronic kidney disease can be changed, Dr. Alcázar responded with an emphatic yes and added that cardiovascular risk can also be substantially reduced. “As nephrologists, we don’t have access to patients in early stages. But family doctors do. Hence the importance of early screening, because going on dialysis at age 60 isn’t the same as at 80.” Currently, “scientific societies are encouraging authorities to screen for chronic kidney disease at earlier ages.”
Regarding drug-based therapy, Dr. Alcázar said that “empagliflozin is not currently indicated for chronic kidney disease in adults.” This sodium-glucose cotransporter-2 inhibitor delays kidney disease and reduces morbidity. Both benefits were highlighted in two recent studies (DAPA-CKD and CREDENCE). Published in January, EMPA-KIDNEY presents a new twist on nephroprotection for patients with chronic kidney disease (diabetic or not) whose glomerular filtration rates are between 20 and 40 mL/min without albuminuria or whose glomerular filtration rates are between 45 and 90 mL/min with albuminuria. For more than 6,000 patients, empagliflozin was observed “to clearly reduce kidney disease progression, cardiovascular mortality and all-cause mortality, and the need to go on dialysis,” stated Dr. Alcázar.
What professionals expect
Dr. Benedito also explained the criteria for referral to a specialist: glomerular filtration rate less than 30 mL/min (unless the patient is older than 80 years and does not have progressively worsening renal function), albumin/creatinine ratio greater than 300 mg/g, acute worsening of renal function, progressive worsening of renal function of greater than 5 mL/min/yr, chronic kidney disease, hypertension treated with triple therapy (including a diuretic) at maximum doses, anemia of less than 10 g/dL, and nonurologic hematuria, especially in combination with albuminuria.
Dr. Benedito explained what nephrologists expect from family doctors in the management of chronic kidney disease: “screening for early detection, identifying and treating risk factors for chronic kidney disease, detecting progression and complications, adjusting drugs based on glomerular filtration rate, and ensuring that our patients are benefiting from sodium-glucose cotransporter-2 inhibitors. These are among the most important steps to be taken.”
Dr. Alcázar mentioned what family doctors expect from nephrologists: “two-way communication, accessibility, coordination of actions to be taken, and using shared and mutually agreed-upon protocols.”
This article was translated from the Medscape Spanish Edition and a version appeared on Medscape.com.
Aspirin not the best antiplatelet for CAD secondary prevention in meta-analysis
such as clopidogrel or ticagrelor rather than aspirin, suggests a patient-level meta-analysis of seven randomized trials.
The more than 24,000 patients in the meta-analysis, called PANTHER, had documented stable CAD, prior myocardial infarction (MI), or recent or remote surgical or percutaneous coronary revascularization.
About half of patients in each antiplatelet monotherapy trial received clopidogrel or ticagrelor, and the other half received aspirin. Follow-ups ranged from 6 months to 3 years.
Those taking a P2Y12 inhibitor showed a 12% reduction in risk (P = .012) for the primary efficacy outcome, a composite of cardiovascular (CV) death, MI, and stroke, over a median of about 1.35 years. The difference was driven primarily by a 23% reduction in risk for MI (P < .001); mortality seemed unaffected by antiplatelet treatment assignment.
Although the P2Y12 inhibitor and aspirin groups were similar with respect to risk of major bleeding, the P2Y12 inhibitor group showed significant reductions in risk for gastrointestinal (GI) bleeding, definite stent thrombosis, and hemorrhagic stroke; rates of hemorrhagic stroke were well under 1% in both groups.
The treatment effects were consistent across patient subgroups, including whether the aspirin comparison was with clopidogrel or ticagrelor.
“Taken together, our data challenge the central role of aspirin in secondary prevention and support a paradigm shift toward P2Y12 inhibitor monotherapy as long-term antiplatelet strategy in the sizable population of patients with coronary atherosclerosis,” Felice Gragnano, MD, PhD, said in an interview. “Given [their] superior efficacy and similar overall safety, P2Y12 inhibitors may be preferred [over] aspirin for the prevention of cardiovascular events in patients with CAD.”
Dr. Gragnano, of the University of Campania Luigi Vanvitelli, Caserta, Italy, who called PANTHER “the largest and most comprehensive synthesis of individual patient data from randomized trials comparing P2Y12 inhibitor monotherapy with aspirin monotherapy,” is lead author of the study, which was published online in the Journal of the American College of Cardiology.
Current guidelines recommend aspirin for antiplatelet monotherapy for patients with established CAD, Dr. Gragnano said, but “the primacy of aspirin in secondary prevention is based on historical trials conducted in the 1970s and 1980s and may not apply to contemporary practice.”
Moreover, later trials that compared P2Y12 inhibitors with aspirin for secondary prevention produced “inconsistent results,” possibly owing to their heterogeneous populations of patients with coronary, cerebrovascular, or peripheral vascular disease, he said. Study-level meta-analyses in this area “provide inconclusive evidence” because they haven’t evaluated treatment effects exclusively in patients with established CAD.
Most of the seven trials’ 24,325 participants had a history of MI, and some had peripheral artery disease (PAD); the rates were 56.2% and 9.1%, respectively. Coronary revascularization, either percutaneous or surgical, had been performed for about 70%. Most (61%) had presented with acute coronary syndromes, and the remainder had presented with chronic CAD.
About 76% of the combined cohorts were from Europe or North America; the rest were from Asia. The mean age of the patients was 64 years, and about 22% were women.
In all, 12,175 had been assigned to P2Y12 inhibitor monotherapy (62% received clopidogrel and 38% received ticagrelor); 12,147 received aspirin at dosages ranging from 75 mg to 325 mg daily.
The hazard ratio (HR) for the primary efficacy outcome, P2Y12 inhibitors vs. aspirin, was significantly reduced, at 0.88 (95% confidence interval [CI], 0.79-0.97; P = .012); the number needed to treat (NNT) to prevent one primary event over 2 years was 121, the report states.
The corresponding HR for MI was 0.77 (95% CI, 0.66-0.90; P < .001), for an NNT benefit of 136. For net adverse clinical events, the HR was 0.89 (95% CI, 0.81-0.98; P = .020), for an NNT benefit of 121.
Risk for major bleeding was not significantly different (HR, 0.87; 95% CI, 0.70-1.09; P = .23), nor were risks for stroke (HR, 0.84; 95% CI, 0.70-1.02; P = .076) or cardiovascular death (HR, 1.02; 95% CI, 0.86-1.20; P = .82).
Still, the P2Y12 inhibitor group showed significant risk reductions for the following:
- GI bleeding: HR, 0.75 (95% CI, 0.57-0.97; P = .027)
- Definite stent thrombosis: HR, 0.42 (95% CI, 0.19-0.97; P = .028)
- Hemorrhagic stroke: HR, 0.43 (95% CI, 0.23-0.83; P = .012)
The current findings are “hypothesis-generating but not definitive,” Dharam Kumbhani, MD, University of Texas Southwestern, Dallas, said in an interview.
It remains unclear “whether aspirin or P2Y12 inhibitor monotherapy is better for long-term maintenance use among patients with established CAD. Aspirin has historically been the agent of choice for this indication,” said Dr. Kumbhani, who with James A. de Lemos, MD, of the same institution, wrote an editorial accompanying the PANTHER report.
“It certainly would be appropriate to consider P2Y12 monotherapy preferentially for patients with prior or currently at high risk for GI or intracranial bleeding, for instance,” Dr. Kumbhani said. For the remainder, aspirin and P2Y12 inhibitors are both “reasonable alternatives.”
In their editorial, Dr. Kumbhani and Dr. de Lemos call the PANTHER meta-analysis “a well-done study with potentially important clinical implications.” The findings “make biological sense: P2Y12 inhibitors are more potent antiplatelet agents than aspirin and have less effect on gastrointestinal mucosal integrity.”
But for now, they wrote, “both aspirin and P2Y12 inhibitors remain viable alternatives for prevention of atherothrombotic events among patients with established CAD.”
Dr. Gragnano had no disclosures; potential conflicts for the other authors are in the report. Dr. Kumbhani reports no relevant relationships; Dr. de Lemos has received honoraria for participation in data safety monitoring boards from Eli Lilly, Novo Nordisk, AstraZeneca, and Janssen.
A version of this article first appeared on Medscape.com.
such as clopidogrel or ticagrelor rather than aspirin, suggests a patient-level meta-analysis of seven randomized trials.
The more than 24,000 patients in the meta-analysis, called PANTHER, had documented stable CAD, prior myocardial infarction (MI), or recent or remote surgical or percutaneous coronary revascularization.
About half of patients in each antiplatelet monotherapy trial received clopidogrel or ticagrelor, and the other half received aspirin. Follow-ups ranged from 6 months to 3 years.
Those taking a P2Y12 inhibitor showed a 12% reduction in risk (P = .012) for the primary efficacy outcome, a composite of cardiovascular (CV) death, MI, and stroke, over a median of about 1.35 years. The difference was driven primarily by a 23% reduction in risk for MI (P < .001); mortality seemed unaffected by antiplatelet treatment assignment.
Although the P2Y12 inhibitor and aspirin groups were similar with respect to risk of major bleeding, the P2Y12 inhibitor group showed significant reductions in risk for gastrointestinal (GI) bleeding, definite stent thrombosis, and hemorrhagic stroke; rates of hemorrhagic stroke were well under 1% in both groups.
The treatment effects were consistent across patient subgroups, including whether the aspirin comparison was with clopidogrel or ticagrelor.
“Taken together, our data challenge the central role of aspirin in secondary prevention and support a paradigm shift toward P2Y12 inhibitor monotherapy as long-term antiplatelet strategy in the sizable population of patients with coronary atherosclerosis,” Felice Gragnano, MD, PhD, said in an interview. “Given [their] superior efficacy and similar overall safety, P2Y12 inhibitors may be preferred [over] aspirin for the prevention of cardiovascular events in patients with CAD.”
Dr. Gragnano, of the University of Campania Luigi Vanvitelli, Caserta, Italy, who called PANTHER “the largest and most comprehensive synthesis of individual patient data from randomized trials comparing P2Y12 inhibitor monotherapy with aspirin monotherapy,” is lead author of the study, which was published online in the Journal of the American College of Cardiology.
Current guidelines recommend aspirin for antiplatelet monotherapy for patients with established CAD, Dr. Gragnano said, but “the primacy of aspirin in secondary prevention is based on historical trials conducted in the 1970s and 1980s and may not apply to contemporary practice.”
Moreover, later trials that compared P2Y12 inhibitors with aspirin for secondary prevention produced “inconsistent results,” possibly owing to their heterogeneous populations of patients with coronary, cerebrovascular, or peripheral vascular disease, he said. Study-level meta-analyses in this area “provide inconclusive evidence” because they haven’t evaluated treatment effects exclusively in patients with established CAD.
Most of the seven trials’ 24,325 participants had a history of MI, and some had peripheral artery disease (PAD); the rates were 56.2% and 9.1%, respectively. Coronary revascularization, either percutaneous or surgical, had been performed for about 70%. Most (61%) had presented with acute coronary syndromes, and the remainder had presented with chronic CAD.
About 76% of the combined cohorts were from Europe or North America; the rest were from Asia. The mean age of the patients was 64 years, and about 22% were women.
In all, 12,175 had been assigned to P2Y12 inhibitor monotherapy (62% received clopidogrel and 38% received ticagrelor); 12,147 received aspirin at dosages ranging from 75 mg to 325 mg daily.
The hazard ratio (HR) for the primary efficacy outcome, P2Y12 inhibitors vs. aspirin, was significantly reduced, at 0.88 (95% confidence interval [CI], 0.79-0.97; P = .012); the number needed to treat (NNT) to prevent one primary event over 2 years was 121, the report states.
The corresponding HR for MI was 0.77 (95% CI, 0.66-0.90; P < .001), for an NNT benefit of 136. For net adverse clinical events, the HR was 0.89 (95% CI, 0.81-0.98; P = .020), for an NNT benefit of 121.
Risk for major bleeding was not significantly different (HR, 0.87; 95% CI, 0.70-1.09; P = .23), nor were risks for stroke (HR, 0.84; 95% CI, 0.70-1.02; P = .076) or cardiovascular death (HR, 1.02; 95% CI, 0.86-1.20; P = .82).
Still, the P2Y12 inhibitor group showed significant risk reductions for the following:
- GI bleeding: HR, 0.75 (95% CI, 0.57-0.97; P = .027)
- Definite stent thrombosis: HR, 0.42 (95% CI, 0.19-0.97; P = .028)
- Hemorrhagic stroke: HR, 0.43 (95% CI, 0.23-0.83; P = .012)
The current findings are “hypothesis-generating but not definitive,” Dharam Kumbhani, MD, University of Texas Southwestern, Dallas, said in an interview.
It remains unclear “whether aspirin or P2Y12 inhibitor monotherapy is better for long-term maintenance use among patients with established CAD. Aspirin has historically been the agent of choice for this indication,” said Dr. Kumbhani, who with James A. de Lemos, MD, of the same institution, wrote an editorial accompanying the PANTHER report.
“It certainly would be appropriate to consider P2Y12 monotherapy preferentially for patients with prior or currently at high risk for GI or intracranial bleeding, for instance,” Dr. Kumbhani said. For the remainder, aspirin and P2Y12 inhibitors are both “reasonable alternatives.”
In their editorial, Dr. Kumbhani and Dr. de Lemos call the PANTHER meta-analysis “a well-done study with potentially important clinical implications.” The findings “make biological sense: P2Y12 inhibitors are more potent antiplatelet agents than aspirin and have less effect on gastrointestinal mucosal integrity.”
But for now, they wrote, “both aspirin and P2Y12 inhibitors remain viable alternatives for prevention of atherothrombotic events among patients with established CAD.”
Dr. Gragnano had no disclosures; potential conflicts for the other authors are in the report. Dr. Kumbhani reports no relevant relationships; Dr. de Lemos has received honoraria for participation in data safety monitoring boards from Eli Lilly, Novo Nordisk, AstraZeneca, and Janssen.
A version of this article first appeared on Medscape.com.
such as clopidogrel or ticagrelor rather than aspirin, suggests a patient-level meta-analysis of seven randomized trials.
The more than 24,000 patients in the meta-analysis, called PANTHER, had documented stable CAD, prior myocardial infarction (MI), or recent or remote surgical or percutaneous coronary revascularization.
About half of patients in each antiplatelet monotherapy trial received clopidogrel or ticagrelor, and the other half received aspirin. Follow-ups ranged from 6 months to 3 years.
Those taking a P2Y12 inhibitor showed a 12% reduction in risk (P = .012) for the primary efficacy outcome, a composite of cardiovascular (CV) death, MI, and stroke, over a median of about 1.35 years. The difference was driven primarily by a 23% reduction in risk for MI (P < .001); mortality seemed unaffected by antiplatelet treatment assignment.
Although the P2Y12 inhibitor and aspirin groups were similar with respect to risk of major bleeding, the P2Y12 inhibitor group showed significant reductions in risk for gastrointestinal (GI) bleeding, definite stent thrombosis, and hemorrhagic stroke; rates of hemorrhagic stroke were well under 1% in both groups.
The treatment effects were consistent across patient subgroups, including whether the aspirin comparison was with clopidogrel or ticagrelor.
“Taken together, our data challenge the central role of aspirin in secondary prevention and support a paradigm shift toward P2Y12 inhibitor monotherapy as long-term antiplatelet strategy in the sizable population of patients with coronary atherosclerosis,” Felice Gragnano, MD, PhD, said in an interview. “Given [their] superior efficacy and similar overall safety, P2Y12 inhibitors may be preferred [over] aspirin for the prevention of cardiovascular events in patients with CAD.”
Dr. Gragnano, of the University of Campania Luigi Vanvitelli, Caserta, Italy, who called PANTHER “the largest and most comprehensive synthesis of individual patient data from randomized trials comparing P2Y12 inhibitor monotherapy with aspirin monotherapy,” is lead author of the study, which was published online in the Journal of the American College of Cardiology.
Current guidelines recommend aspirin for antiplatelet monotherapy for patients with established CAD, Dr. Gragnano said, but “the primacy of aspirin in secondary prevention is based on historical trials conducted in the 1970s and 1980s and may not apply to contemporary practice.”
Moreover, later trials that compared P2Y12 inhibitors with aspirin for secondary prevention produced “inconsistent results,” possibly owing to their heterogeneous populations of patients with coronary, cerebrovascular, or peripheral vascular disease, he said. Study-level meta-analyses in this area “provide inconclusive evidence” because they haven’t evaluated treatment effects exclusively in patients with established CAD.
Most of the seven trials’ 24,325 participants had a history of MI, and some had peripheral artery disease (PAD); the rates were 56.2% and 9.1%, respectively. Coronary revascularization, either percutaneous or surgical, had been performed for about 70%. Most (61%) had presented with acute coronary syndromes, and the remainder had presented with chronic CAD.
About 76% of the combined cohorts were from Europe or North America; the rest were from Asia. The mean age of the patients was 64 years, and about 22% were women.
In all, 12,175 had been assigned to P2Y12 inhibitor monotherapy (62% received clopidogrel and 38% received ticagrelor); 12,147 received aspirin at dosages ranging from 75 mg to 325 mg daily.
The hazard ratio (HR) for the primary efficacy outcome, P2Y12 inhibitors vs. aspirin, was significantly reduced, at 0.88 (95% confidence interval [CI], 0.79-0.97; P = .012); the number needed to treat (NNT) to prevent one primary event over 2 years was 121, the report states.
The corresponding HR for MI was 0.77 (95% CI, 0.66-0.90; P < .001), for an NNT benefit of 136. For net adverse clinical events, the HR was 0.89 (95% CI, 0.81-0.98; P = .020), for an NNT benefit of 121.
Risk for major bleeding was not significantly different (HR, 0.87; 95% CI, 0.70-1.09; P = .23), nor were risks for stroke (HR, 0.84; 95% CI, 0.70-1.02; P = .076) or cardiovascular death (HR, 1.02; 95% CI, 0.86-1.20; P = .82).
Still, the P2Y12 inhibitor group showed significant risk reductions for the following:
- GI bleeding: HR, 0.75 (95% CI, 0.57-0.97; P = .027)
- Definite stent thrombosis: HR, 0.42 (95% CI, 0.19-0.97; P = .028)
- Hemorrhagic stroke: HR, 0.43 (95% CI, 0.23-0.83; P = .012)
The current findings are “hypothesis-generating but not definitive,” Dharam Kumbhani, MD, University of Texas Southwestern, Dallas, said in an interview.
It remains unclear “whether aspirin or P2Y12 inhibitor monotherapy is better for long-term maintenance use among patients with established CAD. Aspirin has historically been the agent of choice for this indication,” said Dr. Kumbhani, who with James A. de Lemos, MD, of the same institution, wrote an editorial accompanying the PANTHER report.
“It certainly would be appropriate to consider P2Y12 monotherapy preferentially for patients with prior or currently at high risk for GI or intracranial bleeding, for instance,” Dr. Kumbhani said. For the remainder, aspirin and P2Y12 inhibitors are both “reasonable alternatives.”
In their editorial, Dr. Kumbhani and Dr. de Lemos call the PANTHER meta-analysis “a well-done study with potentially important clinical implications.” The findings “make biological sense: P2Y12 inhibitors are more potent antiplatelet agents than aspirin and have less effect on gastrointestinal mucosal integrity.”
But for now, they wrote, “both aspirin and P2Y12 inhibitors remain viable alternatives for prevention of atherothrombotic events among patients with established CAD.”
Dr. Gragnano had no disclosures; potential conflicts for the other authors are in the report. Dr. Kumbhani reports no relevant relationships; Dr. de Lemos has received honoraria for participation in data safety monitoring boards from Eli Lilly, Novo Nordisk, AstraZeneca, and Janssen.
A version of this article first appeared on Medscape.com.
FROM JACC
Conflicting blood pressure targets: Déjà vu all over again
Stop me if you’ve heard this before. There’s a controversy over blood pressure targets. Some argue for 140/90 mm Hg, others for 130/80 mm Hg, and some super ambitious folks think that we should aim for 120/80 mm Hg. If this sounds familiar, it should. We did it in 2017. It’s unclear what, if anything, we learned from the experience. On the upside, it’s not as bad as it was 100 years ago.
When high blood pressure was a ‘good’ thing
Back then, many believed that you needed higher blood pressure as you got older to push the blood through your progressively stiffened and hardened arteries. Hence the name “essential” hypertension. The concern was that lowering blood pressure would hypoperfuse your organs and be dangerous. In the 1930s, John Hay told an audience at a British Medical Association lecture: “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”
The 1900s were a simpler time when people had fatal strokes in their 50s, and their families were consoled by the knowledge that they had lived a good life.
If our thinking around blood pressure had evolved slightly faster, perhaps President Roosevelt wouldn’t have died of a stroke during World War II as his doctors watched his systolic blood pressure climb above 200 mm Hg and suggested massages and barbiturates to take the edge off.
The current controversy
Not that long ago, 180 mm Hg was considered mild hypertension. Now, we are arguing about a systolic blood pressure of 140 versus 130 mm Hg.
The American Academy of Family Physicians takes the view that 140/90 mm Hg is good enough for most people. Their most recent clinical practice guideline, based primarily on two 2020 Cochrane Reviews of blood pressure targets in patients with and without cardiovascular disease, did not find any mortality benefit for a lower blood pressure threshold.
This puts the AAFP guideline in conflict with the 2017 guideline issued jointly by the American College of Cardiology, American Heart Association, and nine other groups, which recommended a target of 130/80 mm Hg for pretty much everyone. Though they say greater than 140/90 mm Hg should be the threshold for low-risk patients or for starting therapy post stroke, we often forget those nuances. The main point of contention is that the AAFP guideline was looking for a mortality benefit, whereas the ACC/AHA/everyone else guideline was looking at preventing cardiovascular events. The latter guideline was driven mainly by the results of the SPRINT trial. ACC/AHA argue for more aggressive targets to prevent the things that cardiologists care about, namely heart attacks.
The AAFP guideline conceded that more aggressive control will result in fewer myocardial infarctions but warn that it comes with more adverse events. Treating 1,000 patients to this lower target would theoretically prevent four MIs, possibly prevent three strokes, but result in 30 adverse events.
In the end, what we are seeing here is not so much a debate over the evidence as a debate over priorities. Interventions that don’t improve mortality can be questioned in terms of their cost effectiveness. But you probably don’t want to have a heart attack (even a nonfatal one). And you certainly don’t want to have a stroke. However, lower blood pressure targets inevitably require more medications. Notwithstanding the economic costs, the dangers of polypharmacy, medication interactions, side effects, and syncope leading to falls cannot be ignored. Falls are not benign adverse events, especially in older adults.
The counter argument is that physicians are human and often let things slide. Set the target at 140/90 mm Hg, and many physicians won’t jump on a systolic blood pressure of 144 mm Hg. Set the target at 130 mm Hg, and maybe they’ll be more likely to react. There’s a fine line between permissiveness and complacency.
If you zoom out and look at the multitude of blood pressure guidelines, you start to notice an important fact. There is not much daylight between them. There are subtle differences in what constitutes high risk and different definitions of older (older should be defined as 10 years older than the reader’s current age). But otherwise, the blood pressure targets are not that different.
Does that final 10 mm Hg really matter when barriers to care mean that tens of millions in the United States are unaware they have hypertension? Even among those diagnosed, many are either untreated or inadequately treated.
With this context, perhaps the most insightful thing that can be said about the blood pressure guideline controversy is that it’s not all that controversial. We can likely all agree that we need to be better at treating hypertension and that creative solutions to reach underserved communities are necessary.
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating hypertension. We should acknowledge that beyond a certain point any cardiovascular benefit comes at the cost of hypotension and side effects. That tipping point will be different for different groups, and probably at a higher set point in older patients.
Individualizing care isn’t difficult. We do it all the time. We just shouldn’t be letting people walk around with untreated hypertension. It’s not the 1900s anymore.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Stop me if you’ve heard this before. There’s a controversy over blood pressure targets. Some argue for 140/90 mm Hg, others for 130/80 mm Hg, and some super ambitious folks think that we should aim for 120/80 mm Hg. If this sounds familiar, it should. We did it in 2017. It’s unclear what, if anything, we learned from the experience. On the upside, it’s not as bad as it was 100 years ago.
When high blood pressure was a ‘good’ thing
Back then, many believed that you needed higher blood pressure as you got older to push the blood through your progressively stiffened and hardened arteries. Hence the name “essential” hypertension. The concern was that lowering blood pressure would hypoperfuse your organs and be dangerous. In the 1930s, John Hay told an audience at a British Medical Association lecture: “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”
The 1900s were a simpler time when people had fatal strokes in their 50s, and their families were consoled by the knowledge that they had lived a good life.
If our thinking around blood pressure had evolved slightly faster, perhaps President Roosevelt wouldn’t have died of a stroke during World War II as his doctors watched his systolic blood pressure climb above 200 mm Hg and suggested massages and barbiturates to take the edge off.
The current controversy
Not that long ago, 180 mm Hg was considered mild hypertension. Now, we are arguing about a systolic blood pressure of 140 versus 130 mm Hg.
The American Academy of Family Physicians takes the view that 140/90 mm Hg is good enough for most people. Their most recent clinical practice guideline, based primarily on two 2020 Cochrane Reviews of blood pressure targets in patients with and without cardiovascular disease, did not find any mortality benefit for a lower blood pressure threshold.
This puts the AAFP guideline in conflict with the 2017 guideline issued jointly by the American College of Cardiology, American Heart Association, and nine other groups, which recommended a target of 130/80 mm Hg for pretty much everyone. Though they say greater than 140/90 mm Hg should be the threshold for low-risk patients or for starting therapy post stroke, we often forget those nuances. The main point of contention is that the AAFP guideline was looking for a mortality benefit, whereas the ACC/AHA/everyone else guideline was looking at preventing cardiovascular events. The latter guideline was driven mainly by the results of the SPRINT trial. ACC/AHA argue for more aggressive targets to prevent the things that cardiologists care about, namely heart attacks.
The AAFP guideline conceded that more aggressive control will result in fewer myocardial infarctions but warn that it comes with more adverse events. Treating 1,000 patients to this lower target would theoretically prevent four MIs, possibly prevent three strokes, but result in 30 adverse events.
In the end, what we are seeing here is not so much a debate over the evidence as a debate over priorities. Interventions that don’t improve mortality can be questioned in terms of their cost effectiveness. But you probably don’t want to have a heart attack (even a nonfatal one). And you certainly don’t want to have a stroke. However, lower blood pressure targets inevitably require more medications. Notwithstanding the economic costs, the dangers of polypharmacy, medication interactions, side effects, and syncope leading to falls cannot be ignored. Falls are not benign adverse events, especially in older adults.
The counter argument is that physicians are human and often let things slide. Set the target at 140/90 mm Hg, and many physicians won’t jump on a systolic blood pressure of 144 mm Hg. Set the target at 130 mm Hg, and maybe they’ll be more likely to react. There’s a fine line between permissiveness and complacency.
If you zoom out and look at the multitude of blood pressure guidelines, you start to notice an important fact. There is not much daylight between them. There are subtle differences in what constitutes high risk and different definitions of older (older should be defined as 10 years older than the reader’s current age). But otherwise, the blood pressure targets are not that different.
Does that final 10 mm Hg really matter when barriers to care mean that tens of millions in the United States are unaware they have hypertension? Even among those diagnosed, many are either untreated or inadequately treated.
With this context, perhaps the most insightful thing that can be said about the blood pressure guideline controversy is that it’s not all that controversial. We can likely all agree that we need to be better at treating hypertension and that creative solutions to reach underserved communities are necessary.
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating hypertension. We should acknowledge that beyond a certain point any cardiovascular benefit comes at the cost of hypotension and side effects. That tipping point will be different for different groups, and probably at a higher set point in older patients.
Individualizing care isn’t difficult. We do it all the time. We just shouldn’t be letting people walk around with untreated hypertension. It’s not the 1900s anymore.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Stop me if you’ve heard this before. There’s a controversy over blood pressure targets. Some argue for 140/90 mm Hg, others for 130/80 mm Hg, and some super ambitious folks think that we should aim for 120/80 mm Hg. If this sounds familiar, it should. We did it in 2017. It’s unclear what, if anything, we learned from the experience. On the upside, it’s not as bad as it was 100 years ago.
When high blood pressure was a ‘good’ thing
Back then, many believed that you needed higher blood pressure as you got older to push the blood through your progressively stiffened and hardened arteries. Hence the name “essential” hypertension. The concern was that lowering blood pressure would hypoperfuse your organs and be dangerous. In the 1930s, John Hay told an audience at a British Medical Association lecture: “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”
The 1900s were a simpler time when people had fatal strokes in their 50s, and their families were consoled by the knowledge that they had lived a good life.
If our thinking around blood pressure had evolved slightly faster, perhaps President Roosevelt wouldn’t have died of a stroke during World War II as his doctors watched his systolic blood pressure climb above 200 mm Hg and suggested massages and barbiturates to take the edge off.
The current controversy
Not that long ago, 180 mm Hg was considered mild hypertension. Now, we are arguing about a systolic blood pressure of 140 versus 130 mm Hg.
The American Academy of Family Physicians takes the view that 140/90 mm Hg is good enough for most people. Their most recent clinical practice guideline, based primarily on two 2020 Cochrane Reviews of blood pressure targets in patients with and without cardiovascular disease, did not find any mortality benefit for a lower blood pressure threshold.
This puts the AAFP guideline in conflict with the 2017 guideline issued jointly by the American College of Cardiology, American Heart Association, and nine other groups, which recommended a target of 130/80 mm Hg for pretty much everyone. Though they say greater than 140/90 mm Hg should be the threshold for low-risk patients or for starting therapy post stroke, we often forget those nuances. The main point of contention is that the AAFP guideline was looking for a mortality benefit, whereas the ACC/AHA/everyone else guideline was looking at preventing cardiovascular events. The latter guideline was driven mainly by the results of the SPRINT trial. ACC/AHA argue for more aggressive targets to prevent the things that cardiologists care about, namely heart attacks.
The AAFP guideline conceded that more aggressive control will result in fewer myocardial infarctions but warn that it comes with more adverse events. Treating 1,000 patients to this lower target would theoretically prevent four MIs, possibly prevent three strokes, but result in 30 adverse events.
In the end, what we are seeing here is not so much a debate over the evidence as a debate over priorities. Interventions that don’t improve mortality can be questioned in terms of their cost effectiveness. But you probably don’t want to have a heart attack (even a nonfatal one). And you certainly don’t want to have a stroke. However, lower blood pressure targets inevitably require more medications. Notwithstanding the economic costs, the dangers of polypharmacy, medication interactions, side effects, and syncope leading to falls cannot be ignored. Falls are not benign adverse events, especially in older adults.
The counter argument is that physicians are human and often let things slide. Set the target at 140/90 mm Hg, and many physicians won’t jump on a systolic blood pressure of 144 mm Hg. Set the target at 130 mm Hg, and maybe they’ll be more likely to react. There’s a fine line between permissiveness and complacency.
If you zoom out and look at the multitude of blood pressure guidelines, you start to notice an important fact. There is not much daylight between them. There are subtle differences in what constitutes high risk and different definitions of older (older should be defined as 10 years older than the reader’s current age). But otherwise, the blood pressure targets are not that different.
Does that final 10 mm Hg really matter when barriers to care mean that tens of millions in the United States are unaware they have hypertension? Even among those diagnosed, many are either untreated or inadequately treated.
With this context, perhaps the most insightful thing that can be said about the blood pressure guideline controversy is that it’s not all that controversial. We can likely all agree that we need to be better at treating hypertension and that creative solutions to reach underserved communities are necessary.
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating hypertension. We should acknowledge that beyond a certain point any cardiovascular benefit comes at the cost of hypotension and side effects. That tipping point will be different for different groups, and probably at a higher set point in older patients.
Individualizing care isn’t difficult. We do it all the time. We just shouldn’t be letting people walk around with untreated hypertension. It’s not the 1900s anymore.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Heart-protective diet in PURE study allows whole-fat dairy
Most of the protective food categories are in line with standard dietary guidelines for good health, but one that may be heart-protective is not usually included in such recommendations.

The food categories that were found to be protective include fruit, vegetables, nuts, legumes, and fish but also dairy, “mainly whole-fat,” in an analysis based on the international Prospective Urban and Rural Epidemiological (PURE) study and data from five other international trials that encompassed more than 240,000 people.
A healthy diet scoring system was derived from dietary patterns and clinical events observed in the PURE study and was applied to the populations of the other trials. Higher scores, corresponding to greater consumption of the six food categories, tracked with significantly reduced risks for death, myocardial infarction (MI), and stroke.
Reductions in mortality and CV-disease risk that were linked to the higher scores were especially pronounced in lower-income countries in the study published onlinein the European Heart Journal with lead author Andrew Mente, PhD, Population Health Research Institute, McMaster University, Hamilton, Ont.
The study in part refutes the frequent preference for low-fat or no-fat dairy foods over whole-fat dairy in healthy-diet recommendations. But it is consistent with earlier findings from PURE of reduced mortality risk with increased consumption of dietary fat, including saturated fat.
Whereas healthy-diet recommendations tend to emphasize reduced intake of fat, especially saturated fat, the report notes that “there are almost no national or international strategies and policies to increase a number of protective foods,” such as nuts, fish, and dairy.
“Therefore, while the findings from PURE are largely consistent with the nutrition science and modern dietary recommendations to focus on protective foods, the public’s understanding of healthy eating and relevant global policies have not yet caught up to this science,” it states.
“Guidelines and policy actions need to be updated with this newer evidence,” Dr. Mente said in an interview. “For example, the World Health Organization remains mainly focused on reducing certain nutrients, such as fat, saturated fat, added sugar, and salt,” he said. “These recommendations are echoed by government policy actions and industry, as evident by the continued focus on the usual nutrients in food labels of many countries.”
The current findings, Dr. Mente said, “can be used to ensure that the public’s understanding of healthy eating and relevant global policies are able to catch up to the science.”
Healthy diet score
PURE investigators developed their healthy diet score using data from 147,642 people from the general population in 21 countries. The investigators compared self-reported dietary intakes with long-term clinical outcomes.
The scoring system assigned a value of 1 for each of the six health-food categories when individuals’ intake exceeded the entire cohort’s median intake. It assigned a 0 when intake was below the median. The total PURE healthy diet score consisted of the sum of the six values, with higher scores corresponding to a healthier diet. The mean score for cohort was 2.95.
There were 15,707 deaths and 40,764 CV events during a median follow-up of 9.3 years. A score of at least 5 points, compared with 0 or 1 point, was associated with significantly reduced hazard ratios for mortality, MI, and stroke in multivariable analysis:
- Mortality: HR, 0.70 (95% CI, 0.63-0.77; P < .0001).
- Major CV disease: HR, 0.82 (95% CI, 0.75-0.91; P < .0001).
- MI: HR, 0.86 (95% CI, 0.75-0.99; P = .0014).
- Stroke: HR, 0.81 (95% CI, 0.71-0.93; P = .0034).
The healthy diet score’s relationship to clinical outcomes was explored in five other large independent studies, including three prospective trials of patients with CV disease that spanned 50 countries, a case-control study with MI patients in 52 countries, and a case-control study with stroke patients in 33 countries.
In the three prospective trials, higher scores were associated with reduced mortality, CV disease events, and MI:
- Mortality: HR, 0.73 (95% CI, 0.66-0.81).
- Major CV disease: HR, 0.79 (95% CI, 0.72-0.87).
- MI: HR, 0.85 (95% CI, 0.71-0.99).
In the two case-control studies, a higher diet score was associated with reduced odds ratios for first MI and for stroke:
- MI: OR, 0.72 (95% CI, 0.65-0.80).
- Stroke: OR, 0.57 (95% CI, 0.50-0.65).
In an analysis based on the PURE cohort, incorporation of unprocessed red meat or whole grains into the health diet score produced similar results, suggesting that a “modest amount” of meat or whole grains can be part of a healthy diet, the authors contend.
The results were similar in a combined analysis of all the prospective studies. In particular, improvement in diet score by one quintile was associated with significantly reduced risks for the following:
- Mortality: HR, 0.92 (95% CI, 0.90-0.93).
- Major CV disease: HR, 0.94 (95% CI, 0.93-0.95).
- MI: HR, 0.94 (95% CI, 0.92-0.96).
- Stroke: HR, 0.94 (95% CI, 0.89-0.99).
- Death or CV disease: HR, 0.93 (95% CI, 0.92-0.94).
“This strongly indicates that the take-home message for patients is the same as for general populations,” Dr. Mente said. “Eat plenty of fruits, vegetables, nuts, legumes, and a moderate amount of fish and whole-fat dairy to lower risk of CV disease and mortality.”
Dairy foods are not widely consumed in some cultures, he said, “but availability and cost are also factors in determining consumption.” Nonetheless, a high-quality diet can be achieved without including or excluding dairy foods. Context-specific policies and priorities are needed for different populations, “rather than a one-size-fits-all global policy.”
Food labels in many countries mainly focus on “reducing certain nutrients as the end-all, be-all,” Dr. Mente observed. “Our findings can be used as a basis for recommendations regarding what a healthy diet should be globally and then modified for each region based on the specific types of foods that are available and affordable in each region.”
Moreover, he said, “targeted food policies are needed to increase the availability and affordability of healthy foods, especially in lower-income countries where intakes are low.”
Common human biology
The current results from PURE “confirm prior observations from mostly Western nations that low intakes of fruits, vegetables, nuts, legumes, and fish are major risk factors for poor health,” observes Dariush Mozaffarian, MD, DrPH, MPH, Tufts University, Boston, in an accompanying editorial. “This suggests that common human biology, not merely confounding, explains these observed diet–disease relationships, strengthening causal inference on the power of nutrition.”
Moreover, “These findings provide further support that dairy foods, including whole-fat dairy, can be part of a healthy diet,” Dr. Mozaffarian writes. “The new results in PURE, in combination with prior reports, call for a re-evaluation of unrelenting guidelines to avoid whole-fat dairy products.”
Such studies “remind us of the continuing and devastating rise in diet-related chronic diseases globally, and of the power of protective foods to help address these burdens,” the editorial continues. “It is time for national nutrition guidelines, private sector innovations, government tax policy and agricultural incentives, food procurement policies, labeling and other regulatory priorities, and food-based health care interventions to catch up to the science.”
Not automatically superior
“I do not believe guidelines should be changed based on this single study,” contends Howard D. Sesso, ScD, MPH, associate director of the division of preventive medicine at Brigham and Women’s Hospital, Boston, who isn’t part of PURE. “But I welcome the scientific dialog that should come out of any study that challenges what we think we know,” he told this news organization.
“Many other dietary patterns have been identified over the years that also do a great job in predicting disease risk in observational studies,” observed Dr. Sesso. “Is PURE that much better? Maybe, maybe not. But not enough to dismiss other dietary patterns that are already the basis of dietary recommendations in the U.S., Europe, and worldwide.”
The PURE healthy diet score, he said, “appears to work well within the confines of their large pooling of studies around the world, but that doesn’t automatically make it superior to other dietary patterns.” The score “was only modestly, but not greatly, better than existing dietary patterns evaluated.”
Randomized controlled trials are needed, Dr. Sesso said, to “delve into more specific dietary components,” including unprocessed red meat, whole grains, and high-fat dairy foods. And, he said, more observational studies are needed to examine the score’s association with other cardiometabolic outcomes.
The PURE study is funded by the Population Health Research Institute, the Hamilton Health Sciences Research Institute, the Canadian Institutes of Health Research, the Heart and Stroke Foundation of Ontario; with support from Canadian Institutes of Health Research’s Strategy for Patient Oriented Research through the Ontario SPOR Support Unit, as well as the Ontario Ministry of Health and Long-Term Care; and through unrestricted grants from several pharmaceutical companies, with major contributions from AstraZeneca, Sanofi-Aventis, Boehringer Ingelheim, Servier, and GlaxoSmithKline. Additional contributions are from Novartis and King Pharma. Dr. Mente, Dr. Mozaffarian, and Dr. Sesso have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Most of the protective food categories are in line with standard dietary guidelines for good health, but one that may be heart-protective is not usually included in such recommendations.
The food categories that were found to be protective include fruit, vegetables, nuts, legumes, and fish but also dairy, “mainly whole-fat,” in an analysis based on the international Prospective Urban and Rural Epidemiological (PURE) study and data from five other international trials that encompassed more than 240,000 people.
A healthy diet scoring system was derived from dietary patterns and clinical events observed in the PURE study and was applied to the populations of the other trials. Higher scores, corresponding to greater consumption of the six food categories, tracked with significantly reduced risks for death, myocardial infarction (MI), and stroke.
Reductions in mortality and CV-disease risk that were linked to the higher scores were especially pronounced in lower-income countries in the study published onlinein the European Heart Journal with lead author Andrew Mente, PhD, Population Health Research Institute, McMaster University, Hamilton, Ont.
The study in part refutes the frequent preference for low-fat or no-fat dairy foods over whole-fat dairy in healthy-diet recommendations. But it is consistent with earlier findings from PURE of reduced mortality risk with increased consumption of dietary fat, including saturated fat.
Whereas healthy-diet recommendations tend to emphasize reduced intake of fat, especially saturated fat, the report notes that “there are almost no national or international strategies and policies to increase a number of protective foods,” such as nuts, fish, and dairy.
“Therefore, while the findings from PURE are largely consistent with the nutrition science and modern dietary recommendations to focus on protective foods, the public’s understanding of healthy eating and relevant global policies have not yet caught up to this science,” it states.
“Guidelines and policy actions need to be updated with this newer evidence,” Dr. Mente said in an interview. “For example, the World Health Organization remains mainly focused on reducing certain nutrients, such as fat, saturated fat, added sugar, and salt,” he said. “These recommendations are echoed by government policy actions and industry, as evident by the continued focus on the usual nutrients in food labels of many countries.”
The current findings, Dr. Mente said, “can be used to ensure that the public’s understanding of healthy eating and relevant global policies are able to catch up to the science.”
Healthy diet score
PURE investigators developed their healthy diet score using data from 147,642 people from the general population in 21 countries. The investigators compared self-reported dietary intakes with long-term clinical outcomes.
The scoring system assigned a value of 1 for each of the six health-food categories when individuals’ intake exceeded the entire cohort’s median intake. It assigned a 0 when intake was below the median. The total PURE healthy diet score consisted of the sum of the six values, with higher scores corresponding to a healthier diet. The mean score for cohort was 2.95.
There were 15,707 deaths and 40,764 CV events during a median follow-up of 9.3 years. A score of at least 5 points, compared with 0 or 1 point, was associated with significantly reduced hazard ratios for mortality, MI, and stroke in multivariable analysis:
- Mortality: HR, 0.70 (95% CI, 0.63-0.77; P < .0001).
- Major CV disease: HR, 0.82 (95% CI, 0.75-0.91; P < .0001).
- MI: HR, 0.86 (95% CI, 0.75-0.99; P = .0014).
- Stroke: HR, 0.81 (95% CI, 0.71-0.93; P = .0034).
The healthy diet score’s relationship to clinical outcomes was explored in five other large independent studies, including three prospective trials of patients with CV disease that spanned 50 countries, a case-control study with MI patients in 52 countries, and a case-control study with stroke patients in 33 countries.
In the three prospective trials, higher scores were associated with reduced mortality, CV disease events, and MI:
- Mortality: HR, 0.73 (95% CI, 0.66-0.81).
- Major CV disease: HR, 0.79 (95% CI, 0.72-0.87).
- MI: HR, 0.85 (95% CI, 0.71-0.99).
In the two case-control studies, a higher diet score was associated with reduced odds ratios for first MI and for stroke:
- MI: OR, 0.72 (95% CI, 0.65-0.80).
- Stroke: OR, 0.57 (95% CI, 0.50-0.65).
In an analysis based on the PURE cohort, incorporation of unprocessed red meat or whole grains into the health diet score produced similar results, suggesting that a “modest amount” of meat or whole grains can be part of a healthy diet, the authors contend.
The results were similar in a combined analysis of all the prospective studies. In particular, improvement in diet score by one quintile was associated with significantly reduced risks for the following:
- Mortality: HR, 0.92 (95% CI, 0.90-0.93).
- Major CV disease: HR, 0.94 (95% CI, 0.93-0.95).
- MI: HR, 0.94 (95% CI, 0.92-0.96).
- Stroke: HR, 0.94 (95% CI, 0.89-0.99).
- Death or CV disease: HR, 0.93 (95% CI, 0.92-0.94).
“This strongly indicates that the take-home message for patients is the same as for general populations,” Dr. Mente said. “Eat plenty of fruits, vegetables, nuts, legumes, and a moderate amount of fish and whole-fat dairy to lower risk of CV disease and mortality.”
Dairy foods are not widely consumed in some cultures, he said, “but availability and cost are also factors in determining consumption.” Nonetheless, a high-quality diet can be achieved without including or excluding dairy foods. Context-specific policies and priorities are needed for different populations, “rather than a one-size-fits-all global policy.”
Food labels in many countries mainly focus on “reducing certain nutrients as the end-all, be-all,” Dr. Mente observed. “Our findings can be used as a basis for recommendations regarding what a healthy diet should be globally and then modified for each region based on the specific types of foods that are available and affordable in each region.”
Moreover, he said, “targeted food policies are needed to increase the availability and affordability of healthy foods, especially in lower-income countries where intakes are low.”
Common human biology
The current results from PURE “confirm prior observations from mostly Western nations that low intakes of fruits, vegetables, nuts, legumes, and fish are major risk factors for poor health,” observes Dariush Mozaffarian, MD, DrPH, MPH, Tufts University, Boston, in an accompanying editorial. “This suggests that common human biology, not merely confounding, explains these observed diet–disease relationships, strengthening causal inference on the power of nutrition.”
Moreover, “These findings provide further support that dairy foods, including whole-fat dairy, can be part of a healthy diet,” Dr. Mozaffarian writes. “The new results in PURE, in combination with prior reports, call for a re-evaluation of unrelenting guidelines to avoid whole-fat dairy products.”
Such studies “remind us of the continuing and devastating rise in diet-related chronic diseases globally, and of the power of protective foods to help address these burdens,” the editorial continues. “It is time for national nutrition guidelines, private sector innovations, government tax policy and agricultural incentives, food procurement policies, labeling and other regulatory priorities, and food-based health care interventions to catch up to the science.”
Not automatically superior
“I do not believe guidelines should be changed based on this single study,” contends Howard D. Sesso, ScD, MPH, associate director of the division of preventive medicine at Brigham and Women’s Hospital, Boston, who isn’t part of PURE. “But I welcome the scientific dialog that should come out of any study that challenges what we think we know,” he told this news organization.
“Many other dietary patterns have been identified over the years that also do a great job in predicting disease risk in observational studies,” observed Dr. Sesso. “Is PURE that much better? Maybe, maybe not. But not enough to dismiss other dietary patterns that are already the basis of dietary recommendations in the U.S., Europe, and worldwide.”
The PURE healthy diet score, he said, “appears to work well within the confines of their large pooling of studies around the world, but that doesn’t automatically make it superior to other dietary patterns.” The score “was only modestly, but not greatly, better than existing dietary patterns evaluated.”
Randomized controlled trials are needed, Dr. Sesso said, to “delve into more specific dietary components,” including unprocessed red meat, whole grains, and high-fat dairy foods. And, he said, more observational studies are needed to examine the score’s association with other cardiometabolic outcomes.
The PURE study is funded by the Population Health Research Institute, the Hamilton Health Sciences Research Institute, the Canadian Institutes of Health Research, the Heart and Stroke Foundation of Ontario; with support from Canadian Institutes of Health Research’s Strategy for Patient Oriented Research through the Ontario SPOR Support Unit, as well as the Ontario Ministry of Health and Long-Term Care; and through unrestricted grants from several pharmaceutical companies, with major contributions from AstraZeneca, Sanofi-Aventis, Boehringer Ingelheim, Servier, and GlaxoSmithKline. Additional contributions are from Novartis and King Pharma. Dr. Mente, Dr. Mozaffarian, and Dr. Sesso have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Most of the protective food categories are in line with standard dietary guidelines for good health, but one that may be heart-protective is not usually included in such recommendations.
The food categories that were found to be protective include fruit, vegetables, nuts, legumes, and fish but also dairy, “mainly whole-fat,” in an analysis based on the international Prospective Urban and Rural Epidemiological (PURE) study and data from five other international trials that encompassed more than 240,000 people.
A healthy diet scoring system was derived from dietary patterns and clinical events observed in the PURE study and was applied to the populations of the other trials. Higher scores, corresponding to greater consumption of the six food categories, tracked with significantly reduced risks for death, myocardial infarction (MI), and stroke.
Reductions in mortality and CV-disease risk that were linked to the higher scores were especially pronounced in lower-income countries in the study published onlinein the European Heart Journal with lead author Andrew Mente, PhD, Population Health Research Institute, McMaster University, Hamilton, Ont.
The study in part refutes the frequent preference for low-fat or no-fat dairy foods over whole-fat dairy in healthy-diet recommendations. But it is consistent with earlier findings from PURE of reduced mortality risk with increased consumption of dietary fat, including saturated fat.
Whereas healthy-diet recommendations tend to emphasize reduced intake of fat, especially saturated fat, the report notes that “there are almost no national or international strategies and policies to increase a number of protective foods,” such as nuts, fish, and dairy.
“Therefore, while the findings from PURE are largely consistent with the nutrition science and modern dietary recommendations to focus on protective foods, the public’s understanding of healthy eating and relevant global policies have not yet caught up to this science,” it states.
“Guidelines and policy actions need to be updated with this newer evidence,” Dr. Mente said in an interview. “For example, the World Health Organization remains mainly focused on reducing certain nutrients, such as fat, saturated fat, added sugar, and salt,” he said. “These recommendations are echoed by government policy actions and industry, as evident by the continued focus on the usual nutrients in food labels of many countries.”
The current findings, Dr. Mente said, “can be used to ensure that the public’s understanding of healthy eating and relevant global policies are able to catch up to the science.”
Healthy diet score
PURE investigators developed their healthy diet score using data from 147,642 people from the general population in 21 countries. The investigators compared self-reported dietary intakes with long-term clinical outcomes.
The scoring system assigned a value of 1 for each of the six health-food categories when individuals’ intake exceeded the entire cohort’s median intake. It assigned a 0 when intake was below the median. The total PURE healthy diet score consisted of the sum of the six values, with higher scores corresponding to a healthier diet. The mean score for cohort was 2.95.
There were 15,707 deaths and 40,764 CV events during a median follow-up of 9.3 years. A score of at least 5 points, compared with 0 or 1 point, was associated with significantly reduced hazard ratios for mortality, MI, and stroke in multivariable analysis:
- Mortality: HR, 0.70 (95% CI, 0.63-0.77; P < .0001).
- Major CV disease: HR, 0.82 (95% CI, 0.75-0.91; P < .0001).
- MI: HR, 0.86 (95% CI, 0.75-0.99; P = .0014).
- Stroke: HR, 0.81 (95% CI, 0.71-0.93; P = .0034).
The healthy diet score’s relationship to clinical outcomes was explored in five other large independent studies, including three prospective trials of patients with CV disease that spanned 50 countries, a case-control study with MI patients in 52 countries, and a case-control study with stroke patients in 33 countries.
In the three prospective trials, higher scores were associated with reduced mortality, CV disease events, and MI:
- Mortality: HR, 0.73 (95% CI, 0.66-0.81).
- Major CV disease: HR, 0.79 (95% CI, 0.72-0.87).
- MI: HR, 0.85 (95% CI, 0.71-0.99).
In the two case-control studies, a higher diet score was associated with reduced odds ratios for first MI and for stroke:
- MI: OR, 0.72 (95% CI, 0.65-0.80).
- Stroke: OR, 0.57 (95% CI, 0.50-0.65).
In an analysis based on the PURE cohort, incorporation of unprocessed red meat or whole grains into the health diet score produced similar results, suggesting that a “modest amount” of meat or whole grains can be part of a healthy diet, the authors contend.
The results were similar in a combined analysis of all the prospective studies. In particular, improvement in diet score by one quintile was associated with significantly reduced risks for the following:
- Mortality: HR, 0.92 (95% CI, 0.90-0.93).
- Major CV disease: HR, 0.94 (95% CI, 0.93-0.95).
- MI: HR, 0.94 (95% CI, 0.92-0.96).
- Stroke: HR, 0.94 (95% CI, 0.89-0.99).
- Death or CV disease: HR, 0.93 (95% CI, 0.92-0.94).
“This strongly indicates that the take-home message for patients is the same as for general populations,” Dr. Mente said. “Eat plenty of fruits, vegetables, nuts, legumes, and a moderate amount of fish and whole-fat dairy to lower risk of CV disease and mortality.”
Dairy foods are not widely consumed in some cultures, he said, “but availability and cost are also factors in determining consumption.” Nonetheless, a high-quality diet can be achieved without including or excluding dairy foods. Context-specific policies and priorities are needed for different populations, “rather than a one-size-fits-all global policy.”
Food labels in many countries mainly focus on “reducing certain nutrients as the end-all, be-all,” Dr. Mente observed. “Our findings can be used as a basis for recommendations regarding what a healthy diet should be globally and then modified for each region based on the specific types of foods that are available and affordable in each region.”
Moreover, he said, “targeted food policies are needed to increase the availability and affordability of healthy foods, especially in lower-income countries where intakes are low.”
Common human biology
The current results from PURE “confirm prior observations from mostly Western nations that low intakes of fruits, vegetables, nuts, legumes, and fish are major risk factors for poor health,” observes Dariush Mozaffarian, MD, DrPH, MPH, Tufts University, Boston, in an accompanying editorial. “This suggests that common human biology, not merely confounding, explains these observed diet–disease relationships, strengthening causal inference on the power of nutrition.”
Moreover, “These findings provide further support that dairy foods, including whole-fat dairy, can be part of a healthy diet,” Dr. Mozaffarian writes. “The new results in PURE, in combination with prior reports, call for a re-evaluation of unrelenting guidelines to avoid whole-fat dairy products.”
Such studies “remind us of the continuing and devastating rise in diet-related chronic diseases globally, and of the power of protective foods to help address these burdens,” the editorial continues. “It is time for national nutrition guidelines, private sector innovations, government tax policy and agricultural incentives, food procurement policies, labeling and other regulatory priorities, and food-based health care interventions to catch up to the science.”
Not automatically superior
“I do not believe guidelines should be changed based on this single study,” contends Howard D. Sesso, ScD, MPH, associate director of the division of preventive medicine at Brigham and Women’s Hospital, Boston, who isn’t part of PURE. “But I welcome the scientific dialog that should come out of any study that challenges what we think we know,” he told this news organization.
“Many other dietary patterns have been identified over the years that also do a great job in predicting disease risk in observational studies,” observed Dr. Sesso. “Is PURE that much better? Maybe, maybe not. But not enough to dismiss other dietary patterns that are already the basis of dietary recommendations in the U.S., Europe, and worldwide.”
The PURE healthy diet score, he said, “appears to work well within the confines of their large pooling of studies around the world, but that doesn’t automatically make it superior to other dietary patterns.” The score “was only modestly, but not greatly, better than existing dietary patterns evaluated.”
Randomized controlled trials are needed, Dr. Sesso said, to “delve into more specific dietary components,” including unprocessed red meat, whole grains, and high-fat dairy foods. And, he said, more observational studies are needed to examine the score’s association with other cardiometabolic outcomes.
The PURE study is funded by the Population Health Research Institute, the Hamilton Health Sciences Research Institute, the Canadian Institutes of Health Research, the Heart and Stroke Foundation of Ontario; with support from Canadian Institutes of Health Research’s Strategy for Patient Oriented Research through the Ontario SPOR Support Unit, as well as the Ontario Ministry of Health and Long-Term Care; and through unrestricted grants from several pharmaceutical companies, with major contributions from AstraZeneca, Sanofi-Aventis, Boehringer Ingelheim, Servier, and GlaxoSmithKline. Additional contributions are from Novartis and King Pharma. Dr. Mente, Dr. Mozaffarian, and Dr. Sesso have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EUROPEAN HEART CENTER
FDA expands inclisiran statin-adjunct indication to include primary prevention
Novartis has announced.
The first-in-class small interfering RNA (siRNA) agent was approved in 2021 as an adjunct to statins for patients with clinical cardiovascular disease or heterozygous familial hypercholesterolemia. The indications now include patients taking statins for primary dyslipidemia who have high-risk comorbidities such as diabetes but who do not have a history of cardiovascular events, the company said.
Inclisiran, with a mechanism of action unique among drugs for dyslipidemia, works by “silencing” RNA involved in the synthesis of proprotein convertase subtilisin/kexin type 9. The protein helps regulate the number of LDL cholesterol cell-surface receptors.
Novartis said it has “global rights to develop, manufacture and commercialize Leqvio under a license and collaboration agreement with Alnylam Pharmaceuticals.”
A version of this article first appeared on Medscape.com.
Novartis has announced.
The first-in-class small interfering RNA (siRNA) agent was approved in 2021 as an adjunct to statins for patients with clinical cardiovascular disease or heterozygous familial hypercholesterolemia. The indications now include patients taking statins for primary dyslipidemia who have high-risk comorbidities such as diabetes but who do not have a history of cardiovascular events, the company said.
Inclisiran, with a mechanism of action unique among drugs for dyslipidemia, works by “silencing” RNA involved in the synthesis of proprotein convertase subtilisin/kexin type 9. The protein helps regulate the number of LDL cholesterol cell-surface receptors.
Novartis said it has “global rights to develop, manufacture and commercialize Leqvio under a license and collaboration agreement with Alnylam Pharmaceuticals.”
A version of this article first appeared on Medscape.com.
Novartis has announced.
The first-in-class small interfering RNA (siRNA) agent was approved in 2021 as an adjunct to statins for patients with clinical cardiovascular disease or heterozygous familial hypercholesterolemia. The indications now include patients taking statins for primary dyslipidemia who have high-risk comorbidities such as diabetes but who do not have a history of cardiovascular events, the company said.
Inclisiran, with a mechanism of action unique among drugs for dyslipidemia, works by “silencing” RNA involved in the synthesis of proprotein convertase subtilisin/kexin type 9. The protein helps regulate the number of LDL cholesterol cell-surface receptors.
Novartis said it has “global rights to develop, manufacture and commercialize Leqvio under a license and collaboration agreement with Alnylam Pharmaceuticals.”
A version of this article first appeared on Medscape.com.
High-dose vitamin D may cut risk for new atrial fibrillation
TOPLINE:
a post hoc analysis from a randomized trial conducted in Finland suggests.

METHODOLOGY:
- Observational studies have suggested that vitamin D deficiency is associated with increased risk for AFib, but few randomized trials have looked at the effect of vitamin D supplementation on AFib incidence in healthy people.
- The study, a post hoc analysis from a trial that explored the effects of vitamin D3 supplementation on incidence of cardiovascular diseases and cancer, included 2,495 vitamin D–sufficient healthy older adults, mean age 68.2 years, of whom 43% were women.
- Participants had been randomized to one of three groups in which they received vitamin D3 at either 1,600 IU/day or 3,200 IU/day, or placebo.
- Serum 25(OH)D3 concentrations were measured and data on incident AFib were gathered from national health records.
TAKEAWAY:
- Atrial fibrillation was diagnosed in 190 participants.
- Over a follow-up averaging 4.1 years, risk for incident AFib was reduced by 27% for participants who received the 1,600 IU/day dose, compared with placebo; hazard ratio, 0.73 (95% confidence interval, 0.52-1.02; P = .07), and by 32% for those in the 3,200 IU/day arm; HR, 0.68 (95% CI, 0.48-0.96; P = .03).
- The incident-AFib risk was reduced by 30% in a comparison of the two vitamin D groups combined versus the placebo group; HR, 0.70 (95% CI, 0.53-0.94; P = .02).
- After exclusion of 122 participants who reported being on antiarrhythmic medications at baseline, the 1,600 IU/day group showed a significant 27% reduction in risk for AF (95% CI, 4%-58%; P = .03) and the 3,200 IU/day group a nonsignificant 30% (95% CI, 5%-53%; P = .08) reduction in risk.
IN PRACTICE:
High-dose vitamin D3 supplementation may reduce incidence of AFib in a generally healthy, largely vitamin D–sufficient elderly population, the authors proposed. Additional controlled trials are needed, especially in diverse populations.
STUDY DETAILS:
The study was conducted by Jyrki K. Virtanen, PhD, University of Eastern Finland, Institute of Public Health and Clinical Nutrition, Kuopio, and colleagues. It was published in the American Heart Journal.
LIMITATIONS:
Atrial fibrillation was not prespecified as a primary outcome, and the results differ from those of other randomized controlled trials. Information on type of AFib (whether paroxysmal or nonparoxysmal, for example) wasn’t available nor were participants’ history of AFib. All participants were White and from Finland, limiting generalizability of the results.
DISCLOSURES:
The study was supported by the Academy of Finland, University of Eastern Finland, the Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and the Finnish Cultural Foundation. One coauthor disclosed receiving grants from the National Institutes of Health and Mars Edge. Another coauthor disclosed receipt of a grant from Orion. The other authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
a post hoc analysis from a randomized trial conducted in Finland suggests.
METHODOLOGY:
- Observational studies have suggested that vitamin D deficiency is associated with increased risk for AFib, but few randomized trials have looked at the effect of vitamin D supplementation on AFib incidence in healthy people.
- The study, a post hoc analysis from a trial that explored the effects of vitamin D3 supplementation on incidence of cardiovascular diseases and cancer, included 2,495 vitamin D–sufficient healthy older adults, mean age 68.2 years, of whom 43% were women.
- Participants had been randomized to one of three groups in which they received vitamin D3 at either 1,600 IU/day or 3,200 IU/day, or placebo.
- Serum 25(OH)D3 concentrations were measured and data on incident AFib were gathered from national health records.
TAKEAWAY:
- Atrial fibrillation was diagnosed in 190 participants.
- Over a follow-up averaging 4.1 years, risk for incident AFib was reduced by 27% for participants who received the 1,600 IU/day dose, compared with placebo; hazard ratio, 0.73 (95% confidence interval, 0.52-1.02; P = .07), and by 32% for those in the 3,200 IU/day arm; HR, 0.68 (95% CI, 0.48-0.96; P = .03).
- The incident-AFib risk was reduced by 30% in a comparison of the two vitamin D groups combined versus the placebo group; HR, 0.70 (95% CI, 0.53-0.94; P = .02).
- After exclusion of 122 participants who reported being on antiarrhythmic medications at baseline, the 1,600 IU/day group showed a significant 27% reduction in risk for AF (95% CI, 4%-58%; P = .03) and the 3,200 IU/day group a nonsignificant 30% (95% CI, 5%-53%; P = .08) reduction in risk.
IN PRACTICE:
High-dose vitamin D3 supplementation may reduce incidence of AFib in a generally healthy, largely vitamin D–sufficient elderly population, the authors proposed. Additional controlled trials are needed, especially in diverse populations.
STUDY DETAILS:
The study was conducted by Jyrki K. Virtanen, PhD, University of Eastern Finland, Institute of Public Health and Clinical Nutrition, Kuopio, and colleagues. It was published in the American Heart Journal.
LIMITATIONS:
Atrial fibrillation was not prespecified as a primary outcome, and the results differ from those of other randomized controlled trials. Information on type of AFib (whether paroxysmal or nonparoxysmal, for example) wasn’t available nor were participants’ history of AFib. All participants were White and from Finland, limiting generalizability of the results.
DISCLOSURES:
The study was supported by the Academy of Finland, University of Eastern Finland, the Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and the Finnish Cultural Foundation. One coauthor disclosed receiving grants from the National Institutes of Health and Mars Edge. Another coauthor disclosed receipt of a grant from Orion. The other authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
a post hoc analysis from a randomized trial conducted in Finland suggests.
METHODOLOGY:
- Observational studies have suggested that vitamin D deficiency is associated with increased risk for AFib, but few randomized trials have looked at the effect of vitamin D supplementation on AFib incidence in healthy people.
- The study, a post hoc analysis from a trial that explored the effects of vitamin D3 supplementation on incidence of cardiovascular diseases and cancer, included 2,495 vitamin D–sufficient healthy older adults, mean age 68.2 years, of whom 43% were women.
- Participants had been randomized to one of three groups in which they received vitamin D3 at either 1,600 IU/day or 3,200 IU/day, or placebo.
- Serum 25(OH)D3 concentrations were measured and data on incident AFib were gathered from national health records.
TAKEAWAY:
- Atrial fibrillation was diagnosed in 190 participants.
- Over a follow-up averaging 4.1 years, risk for incident AFib was reduced by 27% for participants who received the 1,600 IU/day dose, compared with placebo; hazard ratio, 0.73 (95% confidence interval, 0.52-1.02; P = .07), and by 32% for those in the 3,200 IU/day arm; HR, 0.68 (95% CI, 0.48-0.96; P = .03).
- The incident-AFib risk was reduced by 30% in a comparison of the two vitamin D groups combined versus the placebo group; HR, 0.70 (95% CI, 0.53-0.94; P = .02).
- After exclusion of 122 participants who reported being on antiarrhythmic medications at baseline, the 1,600 IU/day group showed a significant 27% reduction in risk for AF (95% CI, 4%-58%; P = .03) and the 3,200 IU/day group a nonsignificant 30% (95% CI, 5%-53%; P = .08) reduction in risk.
IN PRACTICE:
High-dose vitamin D3 supplementation may reduce incidence of AFib in a generally healthy, largely vitamin D–sufficient elderly population, the authors proposed. Additional controlled trials are needed, especially in diverse populations.
STUDY DETAILS:
The study was conducted by Jyrki K. Virtanen, PhD, University of Eastern Finland, Institute of Public Health and Clinical Nutrition, Kuopio, and colleagues. It was published in the American Heart Journal.
LIMITATIONS:
Atrial fibrillation was not prespecified as a primary outcome, and the results differ from those of other randomized controlled trials. Information on type of AFib (whether paroxysmal or nonparoxysmal, for example) wasn’t available nor were participants’ history of AFib. All participants were White and from Finland, limiting generalizability of the results.
DISCLOSURES:
The study was supported by the Academy of Finland, University of Eastern Finland, the Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and the Finnish Cultural Foundation. One coauthor disclosed receiving grants from the National Institutes of Health and Mars Edge. Another coauthor disclosed receipt of a grant from Orion. The other authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.

PCPs key to heart failure care after discharge
Madeline Sterling, MD, knew something was wrong when she heard her patient’s voice on the phone. The patient was breathing too fast and sounded fatigued. Like many people with heart failure, this patient had several comorbidities: diabetes, high blood pressure, and cancer, which was in remission.
The patient had been in and out of the hospital several times and was afraid of going back, but Dr. Sterling, a primary care physician, advised her that it was the safe thing to do.
During the woman’s stay, the inpatient cardiology team called Dr. Sterling to provide status updates and ask for input. When the patient was discharged, Dr. Sterling received information on what medicines had been changed and scheduled follow-up care within 10 days. Dr. Sterling, who’d cared for the woman for many years, called her family, her home health aide, and another caregiver to discuss the plan.
“When you know these patients really well, it’s helpful,” Dr. Sterling, a professor of medicine at Weill Cornell Medicine, New York, said. Primary care clinicians have “an appreciation for how all these conditions fit together, how the medicines fit together, and how to put that patient’s priorities at the front of the equation.”
Research has shown that follow-up care within 7-10 days after discharge, especially for patients with heart failure, can prevent hospital readmissions. Patients’ health can change rapidly following discharge: They may start retaining fluid or may not know how to maintain a low-sodium diet, or they might have trouble obtaining medication. Primary care clinicians spot these early warning signs in follow-up visits.
Heart failure affects more than 6 million adults in the United States, according to the Centers for Disease Control and Prevention. The condition is a common cause of hospital readmissions within 30 days of discharge, according to research published by the American Heart Association.
Patients with heart failure are particularly challenging to care for because of comorbidities.
“They’re a very, very sick group of patients that are very difficult to manage,” said Noah Moss, MD, an advanced heart failure and transplant cardiologist at Mount Sinai Hospital, New York.
But patients do not always receive the follow-up care they need, some studies have found.
Right drugs at the right time
Kelly Axsom, MD, a cardiologist at the Columbia University Medical Center, New York, and director of the centralized heart failure management program at the New York–Presbyterian Hospital System, called the primary care clinician the “captain of the ship,” ensuring that medications are reconciled and providing education about what to eat after discharge.
“It’s actually pretty complicated to go from being in the hospital to being at home,” Dr. Axsom said. “There are often many medication changes, there are lots of instructions that are told to you as a patient that are hard to remember.”
A patient’s weight might fluctuate in the days following discharge because the dose of diuretics might be too low or too high and need to be adjusted, according to Ishani Ganguli, MD, MPH, an assistant professor of medicine and a general internist in the Division of General Internal Medicine and Primary Care at Harvard Medical School and Brigham and Women’s Hospital, Boston.
K. Melissa Hayes, DNP, ANP-BC, CHFN, an assistant professor in the adult gerontology primary care program at the Vanderbilt University School of Nursing, Nashville, Tenn., recalled one patient who was given a months’ worth of medications following his discharge from the hospital.
“He was given expensive medications he couldn’t afford and not any refills or how to get those medications,” Dr. Hayes said.
Sometimes patients have no way to get to the pharmacy, or their pharmacy doesn’t have the medication they need, or their insurance doesn’t cover the drugs.
“The average patient is on at least six medications for heart failure, maybe even seven, and then that’s not including all their other medications,” Dr. Hayes said. “That can be a lot for people to keep up with.”
Dr. Hayes talks to her patients with heart failure about what drugs they have been prescribed and what medications they require more of, and she deprescribes any that are duplicative.
Helping patients understand why they are taking each drug encourages them to stick to the regimen. Diuretics, for example, can lead to frequent urination. If patients are unable to take regular bathroom breaks, they may be tempted to stop using the medication – a potentially catastrophic mistake.
“Often I have patients say, ‘Nobody ever explained it to me that way,’ ” Dr. Hayes said. “Someone can have a PhD but not understand their medications.”
Clinicians also can alert patients to commonly used medications that can worsen heart failure, such as diabetes drugs and over-the-counter medications such as ibuprofen.
Patients should be prescribed a combination of four recommended medications. But several studies have found that clinicians often fail to achieve the target doses for those medications. The use of guideline-directed medications reduces mortality and hospitalization rates, according to multiple clinical trials.
Eyes and ears on the patient
Once home, patients must stick to the right diet, weigh themselves every day, and monitor their blood pressure. But changing behaviors can be a struggle.
“Being seen quickly within a couple of days of discharge, you can catch things,” said Dr. Hayes, who has edited a book on managing patients with heart failure in primary care.
“It’s an opportunity to see how they’re doing at home, make sure they have their medications, make sure there’s been no misunderstanding or miscommunication about what they’re supposed to be doing at home,” says Marc Itskowitz, MD, a primary care physician affiliated with Allegheny General Hospital, Pittsburgh.
Ideally, a record that readily integrates information from wearables – such as blood pressure and weight – would make it easier to spot abnormalities, Dr. Itskowtiz said. “I think we’re still in the infancy of the electronic health record,” he said.
Ensuring that follow-up visits are as accessible as possible for patients is also important. Telehealth makes it easier for patients after they return home from the hospital, Dr. Itskowitz said.
More infrastructure
Another challenge of providing follow-up care for patients with heart failure is completing all the tasks a clinician must do within a 20-minute visit: an examination; education on the condition and medications; counseling on diet and exercise; coordination of medical equipment, such as a blood pressure cuff for home use; and making appointments with specialists.
“In the current system, additional support for primary care is needed so we can do all this,” Dr. Sterling said.
Staff at primary care clinics should be trained to answer calls from patients when they experience changes in their weight or are worried about other potential problems. “A lot of primary care practices are bare bones,” Dr. Hayes said, meaning they might not have the staff to field those calls. Educating patients as to when they should call their physician, especially after experiencing worsening symptoms, is also important.
Dr. Hayes suggests setting aside time in the schedule each week to see patients who have been recently discharged from the hospital. In the Cardiology and Vascular Clinic at Nashville General Hospital, Tenn., where she spends half a day each week, Dr. Hayes requests 30 minutes to see patients who have recently been discharged from hospital.
Even when the process goes smoothly, some patients will return to the hospital because of the progressive nature of heart failure, according to Dr. Hayes. Improving care following their hospitalization can keep these people from rapidly declining.
“Most patients with heart failure want to be taking care of the grandchildren or be able to enjoy family dinners together,” Dr. Axsom said. “I think anything we can do to help improve their quality of life is really important.”
Take-home
- See heart failure patients early after their discharge from hospital, ideally within 7-10 days.
- Make sure patients have access to the right medications at the right dosages and that they know why they’re taking them.
- Educate patients about the diet they should be following.
- Have a system to monitor patients’ symptoms and let them know when they should call.
A version of this article first appeared on Medscape.com.
Madeline Sterling, MD, knew something was wrong when she heard her patient’s voice on the phone. The patient was breathing too fast and sounded fatigued. Like many people with heart failure, this patient had several comorbidities: diabetes, high blood pressure, and cancer, which was in remission.
The patient had been in and out of the hospital several times and was afraid of going back, but Dr. Sterling, a primary care physician, advised her that it was the safe thing to do.
During the woman’s stay, the inpatient cardiology team called Dr. Sterling to provide status updates and ask for input. When the patient was discharged, Dr. Sterling received information on what medicines had been changed and scheduled follow-up care within 10 days. Dr. Sterling, who’d cared for the woman for many years, called her family, her home health aide, and another caregiver to discuss the plan.
“When you know these patients really well, it’s helpful,” Dr. Sterling, a professor of medicine at Weill Cornell Medicine, New York, said. Primary care clinicians have “an appreciation for how all these conditions fit together, how the medicines fit together, and how to put that patient’s priorities at the front of the equation.”
Research has shown that follow-up care within 7-10 days after discharge, especially for patients with heart failure, can prevent hospital readmissions. Patients’ health can change rapidly following discharge: They may start retaining fluid or may not know how to maintain a low-sodium diet, or they might have trouble obtaining medication. Primary care clinicians spot these early warning signs in follow-up visits.
Heart failure affects more than 6 million adults in the United States, according to the Centers for Disease Control and Prevention. The condition is a common cause of hospital readmissions within 30 days of discharge, according to research published by the American Heart Association.
Patients with heart failure are particularly challenging to care for because of comorbidities.
“They’re a very, very sick group of patients that are very difficult to manage,” said Noah Moss, MD, an advanced heart failure and transplant cardiologist at Mount Sinai Hospital, New York.
But patients do not always receive the follow-up care they need, some studies have found.
Right drugs at the right time
Kelly Axsom, MD, a cardiologist at the Columbia University Medical Center, New York, and director of the centralized heart failure management program at the New York–Presbyterian Hospital System, called the primary care clinician the “captain of the ship,” ensuring that medications are reconciled and providing education about what to eat after discharge.
“It’s actually pretty complicated to go from being in the hospital to being at home,” Dr. Axsom said. “There are often many medication changes, there are lots of instructions that are told to you as a patient that are hard to remember.”
A patient’s weight might fluctuate in the days following discharge because the dose of diuretics might be too low or too high and need to be adjusted, according to Ishani Ganguli, MD, MPH, an assistant professor of medicine and a general internist in the Division of General Internal Medicine and Primary Care at Harvard Medical School and Brigham and Women’s Hospital, Boston.
K. Melissa Hayes, DNP, ANP-BC, CHFN, an assistant professor in the adult gerontology primary care program at the Vanderbilt University School of Nursing, Nashville, Tenn., recalled one patient who was given a months’ worth of medications following his discharge from the hospital.
“He was given expensive medications he couldn’t afford and not any refills or how to get those medications,” Dr. Hayes said.
Sometimes patients have no way to get to the pharmacy, or their pharmacy doesn’t have the medication they need, or their insurance doesn’t cover the drugs.
“The average patient is on at least six medications for heart failure, maybe even seven, and then that’s not including all their other medications,” Dr. Hayes said. “That can be a lot for people to keep up with.”
Dr. Hayes talks to her patients with heart failure about what drugs they have been prescribed and what medications they require more of, and she deprescribes any that are duplicative.
Helping patients understand why they are taking each drug encourages them to stick to the regimen. Diuretics, for example, can lead to frequent urination. If patients are unable to take regular bathroom breaks, they may be tempted to stop using the medication – a potentially catastrophic mistake.
“Often I have patients say, ‘Nobody ever explained it to me that way,’ ” Dr. Hayes said. “Someone can have a PhD but not understand their medications.”
Clinicians also can alert patients to commonly used medications that can worsen heart failure, such as diabetes drugs and over-the-counter medications such as ibuprofen.
Patients should be prescribed a combination of four recommended medications. But several studies have found that clinicians often fail to achieve the target doses for those medications. The use of guideline-directed medications reduces mortality and hospitalization rates, according to multiple clinical trials.
Eyes and ears on the patient
Once home, patients must stick to the right diet, weigh themselves every day, and monitor their blood pressure. But changing behaviors can be a struggle.
“Being seen quickly within a couple of days of discharge, you can catch things,” said Dr. Hayes, who has edited a book on managing patients with heart failure in primary care.
“It’s an opportunity to see how they’re doing at home, make sure they have their medications, make sure there’s been no misunderstanding or miscommunication about what they’re supposed to be doing at home,” says Marc Itskowitz, MD, a primary care physician affiliated with Allegheny General Hospital, Pittsburgh.
Ideally, a record that readily integrates information from wearables – such as blood pressure and weight – would make it easier to spot abnormalities, Dr. Itskowtiz said. “I think we’re still in the infancy of the electronic health record,” he said.
Ensuring that follow-up visits are as accessible as possible for patients is also important. Telehealth makes it easier for patients after they return home from the hospital, Dr. Itskowitz said.
More infrastructure
Another challenge of providing follow-up care for patients with heart failure is completing all the tasks a clinician must do within a 20-minute visit: an examination; education on the condition and medications; counseling on diet and exercise; coordination of medical equipment, such as a blood pressure cuff for home use; and making appointments with specialists.
“In the current system, additional support for primary care is needed so we can do all this,” Dr. Sterling said.
Staff at primary care clinics should be trained to answer calls from patients when they experience changes in their weight or are worried about other potential problems. “A lot of primary care practices are bare bones,” Dr. Hayes said, meaning they might not have the staff to field those calls. Educating patients as to when they should call their physician, especially after experiencing worsening symptoms, is also important.
Dr. Hayes suggests setting aside time in the schedule each week to see patients who have been recently discharged from the hospital. In the Cardiology and Vascular Clinic at Nashville General Hospital, Tenn., where she spends half a day each week, Dr. Hayes requests 30 minutes to see patients who have recently been discharged from hospital.
Even when the process goes smoothly, some patients will return to the hospital because of the progressive nature of heart failure, according to Dr. Hayes. Improving care following their hospitalization can keep these people from rapidly declining.
“Most patients with heart failure want to be taking care of the grandchildren or be able to enjoy family dinners together,” Dr. Axsom said. “I think anything we can do to help improve their quality of life is really important.”
Take-home
- See heart failure patients early after their discharge from hospital, ideally within 7-10 days.
- Make sure patients have access to the right medications at the right dosages and that they know why they’re taking them.
- Educate patients about the diet they should be following.
- Have a system to monitor patients’ symptoms and let them know when they should call.
A version of this article first appeared on Medscape.com.
Madeline Sterling, MD, knew something was wrong when she heard her patient’s voice on the phone. The patient was breathing too fast and sounded fatigued. Like many people with heart failure, this patient had several comorbidities: diabetes, high blood pressure, and cancer, which was in remission.
The patient had been in and out of the hospital several times and was afraid of going back, but Dr. Sterling, a primary care physician, advised her that it was the safe thing to do.
During the woman’s stay, the inpatient cardiology team called Dr. Sterling to provide status updates and ask for input. When the patient was discharged, Dr. Sterling received information on what medicines had been changed and scheduled follow-up care within 10 days. Dr. Sterling, who’d cared for the woman for many years, called her family, her home health aide, and another caregiver to discuss the plan.
“When you know these patients really well, it’s helpful,” Dr. Sterling, a professor of medicine at Weill Cornell Medicine, New York, said. Primary care clinicians have “an appreciation for how all these conditions fit together, how the medicines fit together, and how to put that patient’s priorities at the front of the equation.”
Research has shown that follow-up care within 7-10 days after discharge, especially for patients with heart failure, can prevent hospital readmissions. Patients’ health can change rapidly following discharge: They may start retaining fluid or may not know how to maintain a low-sodium diet, or they might have trouble obtaining medication. Primary care clinicians spot these early warning signs in follow-up visits.
Heart failure affects more than 6 million adults in the United States, according to the Centers for Disease Control and Prevention. The condition is a common cause of hospital readmissions within 30 days of discharge, according to research published by the American Heart Association.
Patients with heart failure are particularly challenging to care for because of comorbidities.
“They’re a very, very sick group of patients that are very difficult to manage,” said Noah Moss, MD, an advanced heart failure and transplant cardiologist at Mount Sinai Hospital, New York.
But patients do not always receive the follow-up care they need, some studies have found.
Right drugs at the right time
Kelly Axsom, MD, a cardiologist at the Columbia University Medical Center, New York, and director of the centralized heart failure management program at the New York–Presbyterian Hospital System, called the primary care clinician the “captain of the ship,” ensuring that medications are reconciled and providing education about what to eat after discharge.
“It’s actually pretty complicated to go from being in the hospital to being at home,” Dr. Axsom said. “There are often many medication changes, there are lots of instructions that are told to you as a patient that are hard to remember.”
A patient’s weight might fluctuate in the days following discharge because the dose of diuretics might be too low or too high and need to be adjusted, according to Ishani Ganguli, MD, MPH, an assistant professor of medicine and a general internist in the Division of General Internal Medicine and Primary Care at Harvard Medical School and Brigham and Women’s Hospital, Boston.
K. Melissa Hayes, DNP, ANP-BC, CHFN, an assistant professor in the adult gerontology primary care program at the Vanderbilt University School of Nursing, Nashville, Tenn., recalled one patient who was given a months’ worth of medications following his discharge from the hospital.
“He was given expensive medications he couldn’t afford and not any refills or how to get those medications,” Dr. Hayes said.
Sometimes patients have no way to get to the pharmacy, or their pharmacy doesn’t have the medication they need, or their insurance doesn’t cover the drugs.
“The average patient is on at least six medications for heart failure, maybe even seven, and then that’s not including all their other medications,” Dr. Hayes said. “That can be a lot for people to keep up with.”
Dr. Hayes talks to her patients with heart failure about what drugs they have been prescribed and what medications they require more of, and she deprescribes any that are duplicative.
Helping patients understand why they are taking each drug encourages them to stick to the regimen. Diuretics, for example, can lead to frequent urination. If patients are unable to take regular bathroom breaks, they may be tempted to stop using the medication – a potentially catastrophic mistake.
“Often I have patients say, ‘Nobody ever explained it to me that way,’ ” Dr. Hayes said. “Someone can have a PhD but not understand their medications.”
Clinicians also can alert patients to commonly used medications that can worsen heart failure, such as diabetes drugs and over-the-counter medications such as ibuprofen.
Patients should be prescribed a combination of four recommended medications. But several studies have found that clinicians often fail to achieve the target doses for those medications. The use of guideline-directed medications reduces mortality and hospitalization rates, according to multiple clinical trials.
Eyes and ears on the patient
Once home, patients must stick to the right diet, weigh themselves every day, and monitor their blood pressure. But changing behaviors can be a struggle.
“Being seen quickly within a couple of days of discharge, you can catch things,” said Dr. Hayes, who has edited a book on managing patients with heart failure in primary care.
“It’s an opportunity to see how they’re doing at home, make sure they have their medications, make sure there’s been no misunderstanding or miscommunication about what they’re supposed to be doing at home,” says Marc Itskowitz, MD, a primary care physician affiliated with Allegheny General Hospital, Pittsburgh.
Ideally, a record that readily integrates information from wearables – such as blood pressure and weight – would make it easier to spot abnormalities, Dr. Itskowtiz said. “I think we’re still in the infancy of the electronic health record,” he said.
Ensuring that follow-up visits are as accessible as possible for patients is also important. Telehealth makes it easier for patients after they return home from the hospital, Dr. Itskowitz said.
More infrastructure
Another challenge of providing follow-up care for patients with heart failure is completing all the tasks a clinician must do within a 20-minute visit: an examination; education on the condition and medications; counseling on diet and exercise; coordination of medical equipment, such as a blood pressure cuff for home use; and making appointments with specialists.
“In the current system, additional support for primary care is needed so we can do all this,” Dr. Sterling said.
Staff at primary care clinics should be trained to answer calls from patients when they experience changes in their weight or are worried about other potential problems. “A lot of primary care practices are bare bones,” Dr. Hayes said, meaning they might not have the staff to field those calls. Educating patients as to when they should call their physician, especially after experiencing worsening symptoms, is also important.
Dr. Hayes suggests setting aside time in the schedule each week to see patients who have been recently discharged from the hospital. In the Cardiology and Vascular Clinic at Nashville General Hospital, Tenn., where she spends half a day each week, Dr. Hayes requests 30 minutes to see patients who have recently been discharged from hospital.
Even when the process goes smoothly, some patients will return to the hospital because of the progressive nature of heart failure, according to Dr. Hayes. Improving care following their hospitalization can keep these people from rapidly declining.
“Most patients with heart failure want to be taking care of the grandchildren or be able to enjoy family dinners together,” Dr. Axsom said. “I think anything we can do to help improve their quality of life is really important.”
Take-home
- See heart failure patients early after their discharge from hospital, ideally within 7-10 days.
- Make sure patients have access to the right medications at the right dosages and that they know why they’re taking them.
- Educate patients about the diet they should be following.
- Have a system to monitor patients’ symptoms and let them know when they should call.
A version of this article first appeared on Medscape.com.
FDA approves first leadless dual-chamber pacing system
, one based in part on an already-approved leadless single-chamber device, Abbott has announced.

The company’s AVEIR DR leadless pacing system consists of two percutaneously implanted devices, the single-chamber AVEIR VR leadless pacemaker, implanted within the right ventricle, and the novel AVEIR AR single-chamber pacemaker for implantation in the right atrium.
The AVEIR DR system relies on proprietary wireless technology to provide bidirectional, beat-to-beat communication between its two components to achieve dual-chamber synchronization, the company stated in a press release on the approval.
The system also provides real-time pacing analysis, Abbott said, allowing clinicians to assess proper device placement during the procedure and before implantation. The system is designed to be easily removed if the patient’s pacing needs evolve or its battery needs replacing.
Experienced operators achieved a 98% implantation success rate using the AVIER DR system in a 300-patient study conducted at 55 sites in Canada, Europe, and the United States. In that study, 63% of the patients had sinus-node dysfunction and 33% had AV block as their primary dual-chamber pacing indication.
The system exceeded its predefined safety and performance goals, providing AV-synchronous pacing in 97% of patients for at least 3 months, it was reported in May at the annual scientific sessions of the Heart Rhythm Society and in a simultaneous publication in The New England Journal of Medicine.
“Modern medicine has been filled with technological achievements that fundamentally changed how doctors approach patient care, and now we can officially add dual-chamber leadless pacing to that list of achievements,” coauthor Vivek Reddy, MD, director of cardiac arrhythmia services for Mount Sinai Hospital and the Mount Sinai Health System, New York, said in the press release.
A version of this article first appeared on Medscape.com.
, one based in part on an already-approved leadless single-chamber device, Abbott has announced.
The company’s AVEIR DR leadless pacing system consists of two percutaneously implanted devices, the single-chamber AVEIR VR leadless pacemaker, implanted within the right ventricle, and the novel AVEIR AR single-chamber pacemaker for implantation in the right atrium.
The AVEIR DR system relies on proprietary wireless technology to provide bidirectional, beat-to-beat communication between its two components to achieve dual-chamber synchronization, the company stated in a press release on the approval.
The system also provides real-time pacing analysis, Abbott said, allowing clinicians to assess proper device placement during the procedure and before implantation. The system is designed to be easily removed if the patient’s pacing needs evolve or its battery needs replacing.
Experienced operators achieved a 98% implantation success rate using the AVIER DR system in a 300-patient study conducted at 55 sites in Canada, Europe, and the United States. In that study, 63% of the patients had sinus-node dysfunction and 33% had AV block as their primary dual-chamber pacing indication.
The system exceeded its predefined safety and performance goals, providing AV-synchronous pacing in 97% of patients for at least 3 months, it was reported in May at the annual scientific sessions of the Heart Rhythm Society and in a simultaneous publication in The New England Journal of Medicine.
“Modern medicine has been filled with technological achievements that fundamentally changed how doctors approach patient care, and now we can officially add dual-chamber leadless pacing to that list of achievements,” coauthor Vivek Reddy, MD, director of cardiac arrhythmia services for Mount Sinai Hospital and the Mount Sinai Health System, New York, said in the press release.
A version of this article first appeared on Medscape.com.
, one based in part on an already-approved leadless single-chamber device, Abbott has announced.
The company’s AVEIR DR leadless pacing system consists of two percutaneously implanted devices, the single-chamber AVEIR VR leadless pacemaker, implanted within the right ventricle, and the novel AVEIR AR single-chamber pacemaker for implantation in the right atrium.
The AVEIR DR system relies on proprietary wireless technology to provide bidirectional, beat-to-beat communication between its two components to achieve dual-chamber synchronization, the company stated in a press release on the approval.
The system also provides real-time pacing analysis, Abbott said, allowing clinicians to assess proper device placement during the procedure and before implantation. The system is designed to be easily removed if the patient’s pacing needs evolve or its battery needs replacing.
Experienced operators achieved a 98% implantation success rate using the AVIER DR system in a 300-patient study conducted at 55 sites in Canada, Europe, and the United States. In that study, 63% of the patients had sinus-node dysfunction and 33% had AV block as their primary dual-chamber pacing indication.
The system exceeded its predefined safety and performance goals, providing AV-synchronous pacing in 97% of patients for at least 3 months, it was reported in May at the annual scientific sessions of the Heart Rhythm Society and in a simultaneous publication in The New England Journal of Medicine.
“Modern medicine has been filled with technological achievements that fundamentally changed how doctors approach patient care, and now we can officially add dual-chamber leadless pacing to that list of achievements,” coauthor Vivek Reddy, MD, director of cardiac arrhythmia services for Mount Sinai Hospital and the Mount Sinai Health System, New York, said in the press release.
A version of this article first appeared on Medscape.com.
Peripartum cardiomyopathy raises risks at future pregnancy despite LV recovery
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
New definition for iron deficiency in CV disease proposed
with implications that may extend to cardiovascular disease in general.
In the study involving more than 900 patients with PH, investigators at seven U.S. centers determined the prevalence of iron deficiency by two separate definitions and assessed its associations with functional measures and quality of life (QoL) scores.
An iron deficiency definition used conventionally in heart failure (HF) – ferritin less than 100 g/mL or 100-299 ng/mL with transferrin saturation (TSAT) less than 20% – failed to discriminate patients with reduced peak oxygen consumption (peakVO2), 6-minute walk test (6MWT) results, and QoL scores on the 36-item Short Form Survey (SF-36).
But an alternative definition for iron deficiency, simply a TSAT less than 21%, did predict such patients with reduced peakVO2, 6MWT, and QoL. It was also associated with an increased mortality risk. The study was published in the European Heart Journal.
“A low TSAT, less than 21%, is key in the pathophysiology of iron deficiency in pulmonary hypertension” and is associated with those important clinical and functional characteristics, lead author Pieter Martens MD, PhD, said in an interview. The study “underscores the importance of these criteria in future intervention studies in the field of pulmonary hypertension testing iron therapies.”
A broader implication is that “we should revise how we define iron deficiency in heart failure and cardiovascular disease in general and how we select patients for iron therapies,” said Dr. Martens, of the Heart, Vascular & Thoracic Institute of the Cleveland Clinic.
Iron’s role in pulmonary vascular disease
“Iron deficiency is associated with an energetic deficit, especially in high energy–demanding tissue, leading to early skeletal muscle acidification and diminished left and right ventricular (RV) contractile reserve during exercise,” the published report states. It can lead to “maladaptive RV remodeling,” which is a “hallmark feature” predictive of morbidity and mortality in patients with pulmonary vascular disease (PVD).
Some studies have suggested that iron deficiency is a common comorbidity in patients with PVD, their estimates of its prevalence ranging widely due in part to the “absence of a uniform definition,” write the authors.
Dr. Martens said the current study was conducted partly in response to the increasingly common observation that the HF-associated definition of iron deficiency “has limitations.” Yet, “without validation in the field of pulmonary hypertension, the 2022 pulmonary hypertension guidelines endorse this definition.”
As iron deficiency is a causal risk factor for HF progression, Dr. Martens added, the HF field has “taught us the importance of using validated definitions for iron deficiency when selecting patients for iron treatment in randomized controlled trials.”
Moreover, some evidence suggests that iron deficiency by some definitions may be associated with diminished exercise capacity and QoL in patients with PVD, which are associations that have not been confirmed in large studies, the report notes.
Therefore, it continues, the study sought to “determine and validate” the optimal definition of iron deficiency in patients with PVD; document its prevalence; and explore associations between iron deficiency and exercise capacity, QoL, and cardiac and pulmonary vascular remodeling.
Evaluating definitions of iron deficiency
The prospective study, called PVDOMICS, entered 1,195 subjects with available iron levels. After exclusion of 38 patients with sarcoidosis, myeloproliferative disease, or hemoglobinopathy, there remained 693 patients with “overt” PH, 225 with a milder form of PH who served as PVD comparators, and 90 age-, sex-, race/ethnicity- matched “healthy” adults who served as controls.
According to the conventional HF definition of iron deficiency – that is, ferritin 100-299 ng/mL and TSAT less than 20% – the prevalences were 74% in patients with overt PH and 72% of those “across the PVD spectrum.”
But by that definition, iron deficient and non-iron deficient patients didn’t differ significantly in peakVO2, 6MWT distance, or SF-36 physical component scores.
In contrast, patients meeting the alternative definition of iron deficiency of TSAT less than 21% showed significantly reduced functional and QoL measures, compared with those with TSAT greater than or equal to 21%.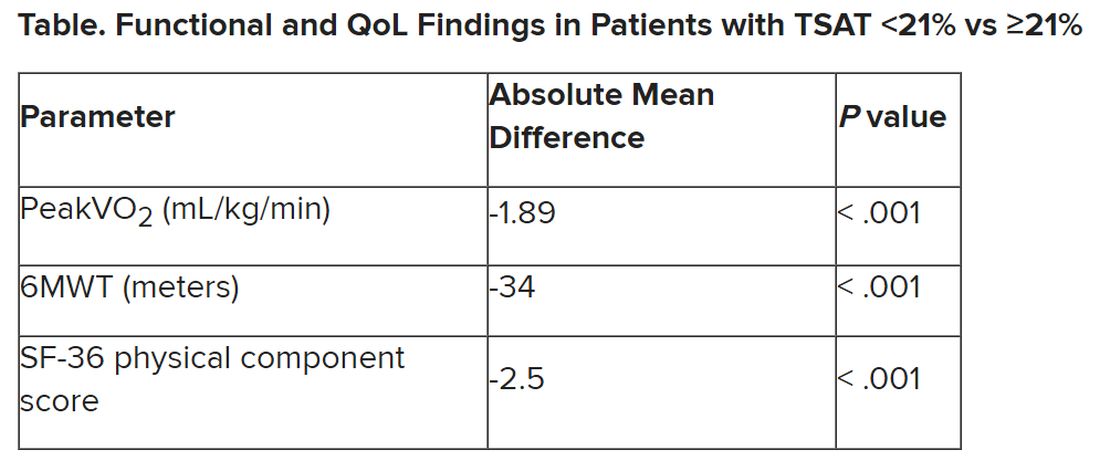
The group with TSAT less than 21% also showed significantly more RV remodeling at cardiac MRI, compared with those who had TSAT greater than or equal to 21%, but their invasively measured pulmonary vascular resistance was comparable.
Of note, those with TSAT less than 21% also showed significantly increased all-cause mortality (hazard ratio, 1.63; 95% confidence interval, 1.13-2.34; P = .009) after adjustment for age, sex, hemoglobin, and natriuretic peptide levels.
“Proper validation of the definition of iron deficiency is important for prognostication,” the published report states, “but also for providing a working definition that can be used to identify suitable patients for inclusion in randomized controlled trials” of drugs for iron deficiency.
Additionally, the finding that TSAT less than 21% points to patients with diminished functional and exercise capacity is “consistent with more recent studies in the field of heart failure” that suggest “functional abnormalities and adverse cardiac remodeling are worse in patients with a low TSAT.” Indeed, the report states, such treatment effects have been “the most convincing” in HF trials.
Broader implications
An accompanying editorial agrees that the study’s implications apply well beyond PH. It highlights that iron deficiency is common in PH, while such PH is “not substantially different from the problem in patients with heart failure, chronic kidney disease, and cardiovascular disease in general,” lead editorialist John G.F. Cleland, MD, PhD, University of Glasgow, said in an interview. “It’s also common as people get older, even in those without these diseases.”
Dr. Cleland said the anemia definition currently used in cardiovascular research and practice is based on a hemoglobin concentration below the 5th percentile of age and sex in primarily young, healthy people, and not on its association with clinical outcomes.
“We recently analyzed data on a large population in the United Kingdom with a broad range of cardiovascular diseases and found that unless anemia is severe, [other] markers of iron deficiency are usually not measured,” he said. A low hemoglobin and TSAT, but not low ferritin levels, are associated with worse prognosis.
Dr. Cleland agreed that the HF-oriented definition is “poor,” with profound implications for the conduct of clinical trials. “If the definition of iron deficiency lacks specificity, then clinical trials will include many patients without iron deficiency who are unlikely to benefit from and might be harmed by IV iron.” Inclusion of such patients may also “dilute” any benefit that might emerge and render the outcome inaccurate.
But if the definition of iron deficiency lacks sensitivity, “then in clinical practice, many patients with iron deficiency may be denied a simple and effective treatment.”
Measuring serum iron could potentially be useful, but it’s usually not done in randomized trials “especially since taking an iron tablet can give a temporary ‘blip’ in serum iron,” Dr. Cleland said. “So TSAT is a reasonable compromise.” He said he “looks forward” to any further data on serum iron as a way of assessing iron deficiency and anemia.
Half full vs. half empty
Dr. Cleland likened the question of whom to treat with iron supplementation as a “glass half full versus half empty” clinical dilemma. “One approach is to give iron to everyone unless there’s evidence that they’re overloaded,” he said, “while the other is to withhold iron from everyone unless there’s evidence that they’re iron depleted.”
Recent evidence from the IRONMAN trial suggested that its patients with HF who received intravenous iron were less likely to be hospitalized for infections, particularly COVID-19, than a usual-care group. The treatment may also help reduce frailty.
“So should we be offering IV iron specifically to people considered iron deficient, or should we be ensuring that everyone over age 70 get iron supplements?” Dr. Cleland mused rhetorically. On a cautionary note, he added, perhaps iron supplementation will be harmful if it’s not necessary.
Dr. Cleland proposed “focusing for the moment on people who are iron deficient but investigating the possibility that we are being overly restrictive and should be giving iron to a much broader population.” That course, however, would require large population-based studies.
“We need more experience,” Dr. Cleland said, “to make sure that the benefits outweigh any risks before we can just give iron to everyone.”
Dr. Martens has received consultancy fees from AstraZeneca, Abbott, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Novartis, Novo Nordisk, and Vifor Pharma. Dr. Cleland declares grant support, support for travel, and personal honoraria from Pharmacosmos and Vifor. Disclosures for other authors are in the published report and editorial.
A version of this article first appeared on Medscape.com.
with implications that may extend to cardiovascular disease in general.
In the study involving more than 900 patients with PH, investigators at seven U.S. centers determined the prevalence of iron deficiency by two separate definitions and assessed its associations with functional measures and quality of life (QoL) scores.
An iron deficiency definition used conventionally in heart failure (HF) – ferritin less than 100 g/mL or 100-299 ng/mL with transferrin saturation (TSAT) less than 20% – failed to discriminate patients with reduced peak oxygen consumption (peakVO2), 6-minute walk test (6MWT) results, and QoL scores on the 36-item Short Form Survey (SF-36).
But an alternative definition for iron deficiency, simply a TSAT less than 21%, did predict such patients with reduced peakVO2, 6MWT, and QoL. It was also associated with an increased mortality risk. The study was published in the European Heart Journal.
“A low TSAT, less than 21%, is key in the pathophysiology of iron deficiency in pulmonary hypertension” and is associated with those important clinical and functional characteristics, lead author Pieter Martens MD, PhD, said in an interview. The study “underscores the importance of these criteria in future intervention studies in the field of pulmonary hypertension testing iron therapies.”
A broader implication is that “we should revise how we define iron deficiency in heart failure and cardiovascular disease in general and how we select patients for iron therapies,” said Dr. Martens, of the Heart, Vascular & Thoracic Institute of the Cleveland Clinic.
Iron’s role in pulmonary vascular disease
“Iron deficiency is associated with an energetic deficit, especially in high energy–demanding tissue, leading to early skeletal muscle acidification and diminished left and right ventricular (RV) contractile reserve during exercise,” the published report states. It can lead to “maladaptive RV remodeling,” which is a “hallmark feature” predictive of morbidity and mortality in patients with pulmonary vascular disease (PVD).
Some studies have suggested that iron deficiency is a common comorbidity in patients with PVD, their estimates of its prevalence ranging widely due in part to the “absence of a uniform definition,” write the authors.
Dr. Martens said the current study was conducted partly in response to the increasingly common observation that the HF-associated definition of iron deficiency “has limitations.” Yet, “without validation in the field of pulmonary hypertension, the 2022 pulmonary hypertension guidelines endorse this definition.”
As iron deficiency is a causal risk factor for HF progression, Dr. Martens added, the HF field has “taught us the importance of using validated definitions for iron deficiency when selecting patients for iron treatment in randomized controlled trials.”
Moreover, some evidence suggests that iron deficiency by some definitions may be associated with diminished exercise capacity and QoL in patients with PVD, which are associations that have not been confirmed in large studies, the report notes.
Therefore, it continues, the study sought to “determine and validate” the optimal definition of iron deficiency in patients with PVD; document its prevalence; and explore associations between iron deficiency and exercise capacity, QoL, and cardiac and pulmonary vascular remodeling.
Evaluating definitions of iron deficiency
The prospective study, called PVDOMICS, entered 1,195 subjects with available iron levels. After exclusion of 38 patients with sarcoidosis, myeloproliferative disease, or hemoglobinopathy, there remained 693 patients with “overt” PH, 225 with a milder form of PH who served as PVD comparators, and 90 age-, sex-, race/ethnicity- matched “healthy” adults who served as controls.
According to the conventional HF definition of iron deficiency – that is, ferritin 100-299 ng/mL and TSAT less than 20% – the prevalences were 74% in patients with overt PH and 72% of those “across the PVD spectrum.”
But by that definition, iron deficient and non-iron deficient patients didn’t differ significantly in peakVO2, 6MWT distance, or SF-36 physical component scores.
In contrast, patients meeting the alternative definition of iron deficiency of TSAT less than 21% showed significantly reduced functional and QoL measures, compared with those with TSAT greater than or equal to 21%.
The group with TSAT less than 21% also showed significantly more RV remodeling at cardiac MRI, compared with those who had TSAT greater than or equal to 21%, but their invasively measured pulmonary vascular resistance was comparable.
Of note, those with TSAT less than 21% also showed significantly increased all-cause mortality (hazard ratio, 1.63; 95% confidence interval, 1.13-2.34; P = .009) after adjustment for age, sex, hemoglobin, and natriuretic peptide levels.
“Proper validation of the definition of iron deficiency is important for prognostication,” the published report states, “but also for providing a working definition that can be used to identify suitable patients for inclusion in randomized controlled trials” of drugs for iron deficiency.
Additionally, the finding that TSAT less than 21% points to patients with diminished functional and exercise capacity is “consistent with more recent studies in the field of heart failure” that suggest “functional abnormalities and adverse cardiac remodeling are worse in patients with a low TSAT.” Indeed, the report states, such treatment effects have been “the most convincing” in HF trials.
Broader implications
An accompanying editorial agrees that the study’s implications apply well beyond PH. It highlights that iron deficiency is common in PH, while such PH is “not substantially different from the problem in patients with heart failure, chronic kidney disease, and cardiovascular disease in general,” lead editorialist John G.F. Cleland, MD, PhD, University of Glasgow, said in an interview. “It’s also common as people get older, even in those without these diseases.”
Dr. Cleland said the anemia definition currently used in cardiovascular research and practice is based on a hemoglobin concentration below the 5th percentile of age and sex in primarily young, healthy people, and not on its association with clinical outcomes.
“We recently analyzed data on a large population in the United Kingdom with a broad range of cardiovascular diseases and found that unless anemia is severe, [other] markers of iron deficiency are usually not measured,” he said. A low hemoglobin and TSAT, but not low ferritin levels, are associated with worse prognosis.
Dr. Cleland agreed that the HF-oriented definition is “poor,” with profound implications for the conduct of clinical trials. “If the definition of iron deficiency lacks specificity, then clinical trials will include many patients without iron deficiency who are unlikely to benefit from and might be harmed by IV iron.” Inclusion of such patients may also “dilute” any benefit that might emerge and render the outcome inaccurate.
But if the definition of iron deficiency lacks sensitivity, “then in clinical practice, many patients with iron deficiency may be denied a simple and effective treatment.”
Measuring serum iron could potentially be useful, but it’s usually not done in randomized trials “especially since taking an iron tablet can give a temporary ‘blip’ in serum iron,” Dr. Cleland said. “So TSAT is a reasonable compromise.” He said he “looks forward” to any further data on serum iron as a way of assessing iron deficiency and anemia.
Half full vs. half empty
Dr. Cleland likened the question of whom to treat with iron supplementation as a “glass half full versus half empty” clinical dilemma. “One approach is to give iron to everyone unless there’s evidence that they’re overloaded,” he said, “while the other is to withhold iron from everyone unless there’s evidence that they’re iron depleted.”
Recent evidence from the IRONMAN trial suggested that its patients with HF who received intravenous iron were less likely to be hospitalized for infections, particularly COVID-19, than a usual-care group. The treatment may also help reduce frailty.
“So should we be offering IV iron specifically to people considered iron deficient, or should we be ensuring that everyone over age 70 get iron supplements?” Dr. Cleland mused rhetorically. On a cautionary note, he added, perhaps iron supplementation will be harmful if it’s not necessary.
Dr. Cleland proposed “focusing for the moment on people who are iron deficient but investigating the possibility that we are being overly restrictive and should be giving iron to a much broader population.” That course, however, would require large population-based studies.
“We need more experience,” Dr. Cleland said, “to make sure that the benefits outweigh any risks before we can just give iron to everyone.”
Dr. Martens has received consultancy fees from AstraZeneca, Abbott, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Novartis, Novo Nordisk, and Vifor Pharma. Dr. Cleland declares grant support, support for travel, and personal honoraria from Pharmacosmos and Vifor. Disclosures for other authors are in the published report and editorial.
A version of this article first appeared on Medscape.com.
with implications that may extend to cardiovascular disease in general.
In the study involving more than 900 patients with PH, investigators at seven U.S. centers determined the prevalence of iron deficiency by two separate definitions and assessed its associations with functional measures and quality of life (QoL) scores.
An iron deficiency definition used conventionally in heart failure (HF) – ferritin less than 100 g/mL or 100-299 ng/mL with transferrin saturation (TSAT) less than 20% – failed to discriminate patients with reduced peak oxygen consumption (peakVO2), 6-minute walk test (6MWT) results, and QoL scores on the 36-item Short Form Survey (SF-36).
But an alternative definition for iron deficiency, simply a TSAT less than 21%, did predict such patients with reduced peakVO2, 6MWT, and QoL. It was also associated with an increased mortality risk. The study was published in the European Heart Journal.
“A low TSAT, less than 21%, is key in the pathophysiology of iron deficiency in pulmonary hypertension” and is associated with those important clinical and functional characteristics, lead author Pieter Martens MD, PhD, said in an interview. The study “underscores the importance of these criteria in future intervention studies in the field of pulmonary hypertension testing iron therapies.”
A broader implication is that “we should revise how we define iron deficiency in heart failure and cardiovascular disease in general and how we select patients for iron therapies,” said Dr. Martens, of the Heart, Vascular & Thoracic Institute of the Cleveland Clinic.
Iron’s role in pulmonary vascular disease
“Iron deficiency is associated with an energetic deficit, especially in high energy–demanding tissue, leading to early skeletal muscle acidification and diminished left and right ventricular (RV) contractile reserve during exercise,” the published report states. It can lead to “maladaptive RV remodeling,” which is a “hallmark feature” predictive of morbidity and mortality in patients with pulmonary vascular disease (PVD).
Some studies have suggested that iron deficiency is a common comorbidity in patients with PVD, their estimates of its prevalence ranging widely due in part to the “absence of a uniform definition,” write the authors.
Dr. Martens said the current study was conducted partly in response to the increasingly common observation that the HF-associated definition of iron deficiency “has limitations.” Yet, “without validation in the field of pulmonary hypertension, the 2022 pulmonary hypertension guidelines endorse this definition.”
As iron deficiency is a causal risk factor for HF progression, Dr. Martens added, the HF field has “taught us the importance of using validated definitions for iron deficiency when selecting patients for iron treatment in randomized controlled trials.”
Moreover, some evidence suggests that iron deficiency by some definitions may be associated with diminished exercise capacity and QoL in patients with PVD, which are associations that have not been confirmed in large studies, the report notes.
Therefore, it continues, the study sought to “determine and validate” the optimal definition of iron deficiency in patients with PVD; document its prevalence; and explore associations between iron deficiency and exercise capacity, QoL, and cardiac and pulmonary vascular remodeling.
Evaluating definitions of iron deficiency
The prospective study, called PVDOMICS, entered 1,195 subjects with available iron levels. After exclusion of 38 patients with sarcoidosis, myeloproliferative disease, or hemoglobinopathy, there remained 693 patients with “overt” PH, 225 with a milder form of PH who served as PVD comparators, and 90 age-, sex-, race/ethnicity- matched “healthy” adults who served as controls.
According to the conventional HF definition of iron deficiency – that is, ferritin 100-299 ng/mL and TSAT less than 20% – the prevalences were 74% in patients with overt PH and 72% of those “across the PVD spectrum.”
But by that definition, iron deficient and non-iron deficient patients didn’t differ significantly in peakVO2, 6MWT distance, or SF-36 physical component scores.
In contrast, patients meeting the alternative definition of iron deficiency of TSAT less than 21% showed significantly reduced functional and QoL measures, compared with those with TSAT greater than or equal to 21%.
The group with TSAT less than 21% also showed significantly more RV remodeling at cardiac MRI, compared with those who had TSAT greater than or equal to 21%, but their invasively measured pulmonary vascular resistance was comparable.
Of note, those with TSAT less than 21% also showed significantly increased all-cause mortality (hazard ratio, 1.63; 95% confidence interval, 1.13-2.34; P = .009) after adjustment for age, sex, hemoglobin, and natriuretic peptide levels.
“Proper validation of the definition of iron deficiency is important for prognostication,” the published report states, “but also for providing a working definition that can be used to identify suitable patients for inclusion in randomized controlled trials” of drugs for iron deficiency.
Additionally, the finding that TSAT less than 21% points to patients with diminished functional and exercise capacity is “consistent with more recent studies in the field of heart failure” that suggest “functional abnormalities and adverse cardiac remodeling are worse in patients with a low TSAT.” Indeed, the report states, such treatment effects have been “the most convincing” in HF trials.
Broader implications
An accompanying editorial agrees that the study’s implications apply well beyond PH. It highlights that iron deficiency is common in PH, while such PH is “not substantially different from the problem in patients with heart failure, chronic kidney disease, and cardiovascular disease in general,” lead editorialist John G.F. Cleland, MD, PhD, University of Glasgow, said in an interview. “It’s also common as people get older, even in those without these diseases.”
Dr. Cleland said the anemia definition currently used in cardiovascular research and practice is based on a hemoglobin concentration below the 5th percentile of age and sex in primarily young, healthy people, and not on its association with clinical outcomes.
“We recently analyzed data on a large population in the United Kingdom with a broad range of cardiovascular diseases and found that unless anemia is severe, [other] markers of iron deficiency are usually not measured,” he said. A low hemoglobin and TSAT, but not low ferritin levels, are associated with worse prognosis.
Dr. Cleland agreed that the HF-oriented definition is “poor,” with profound implications for the conduct of clinical trials. “If the definition of iron deficiency lacks specificity, then clinical trials will include many patients without iron deficiency who are unlikely to benefit from and might be harmed by IV iron.” Inclusion of such patients may also “dilute” any benefit that might emerge and render the outcome inaccurate.
But if the definition of iron deficiency lacks sensitivity, “then in clinical practice, many patients with iron deficiency may be denied a simple and effective treatment.”
Measuring serum iron could potentially be useful, but it’s usually not done in randomized trials “especially since taking an iron tablet can give a temporary ‘blip’ in serum iron,” Dr. Cleland said. “So TSAT is a reasonable compromise.” He said he “looks forward” to any further data on serum iron as a way of assessing iron deficiency and anemia.
Half full vs. half empty
Dr. Cleland likened the question of whom to treat with iron supplementation as a “glass half full versus half empty” clinical dilemma. “One approach is to give iron to everyone unless there’s evidence that they’re overloaded,” he said, “while the other is to withhold iron from everyone unless there’s evidence that they’re iron depleted.”
Recent evidence from the IRONMAN trial suggested that its patients with HF who received intravenous iron were less likely to be hospitalized for infections, particularly COVID-19, than a usual-care group. The treatment may also help reduce frailty.
“So should we be offering IV iron specifically to people considered iron deficient, or should we be ensuring that everyone over age 70 get iron supplements?” Dr. Cleland mused rhetorically. On a cautionary note, he added, perhaps iron supplementation will be harmful if it’s not necessary.
Dr. Cleland proposed “focusing for the moment on people who are iron deficient but investigating the possibility that we are being overly restrictive and should be giving iron to a much broader population.” That course, however, would require large population-based studies.
“We need more experience,” Dr. Cleland said, “to make sure that the benefits outweigh any risks before we can just give iron to everyone.”
Dr. Martens has received consultancy fees from AstraZeneca, Abbott, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Novartis, Novo Nordisk, and Vifor Pharma. Dr. Cleland declares grant support, support for travel, and personal honoraria from Pharmacosmos and Vifor. Disclosures for other authors are in the published report and editorial.
A version of this article first appeared on Medscape.com.
FROM EUROPEAN HEART JOURNAL