User login
Survey explores mental health, services use in police officers
New research shows that about a quarter of police officers in one large force report past or present mental health problems.
Responding to a survey, 26% of police officers on the Dallas police department screened positive for depression, anxiety, PTSD, or symptoms of suicide ideation or self-harm.
Mental illness rates were particularly high among female officers, those who were divorced, widowed, or separated, and those with military experience.
The study also showed that concerns over confidentiality and stigma may prevent officers with mental illness from seeking treatment.
The results underscored the need to identify police officers with psychiatric problems and to connect them to the most appropriate individualized care, author Katelyn K. Jetelina, PhD, assistant professor in the department of epidemiology, human genetics, and environmental sciences, University of Texas Health Science Center, Dallas, said in an interview.
“This is a very hard-to-reach population, and because of that, we need to be innovative in reaching them for services,” she said.
The study was published online Oct. 7 in JAMA Network Open.
Dr. Jetelina and colleagues are investigating various aspects of police officers’ well-being, including their nutritional needs and their occupational, physical, and mental health.
The current study included 434 members of the Dallas police department, the ninth largest in the United States. The mean age of the participants was 37 years, 82% were men, and about half were White. The 434 officers represented 97% of those invited to participate (n = 446) and 31% of the total patrol population of the Dallas police department (n = 1,413).
These officers completed a short survey on their smartphone that asked about lifetime diagnoses of depression, anxiety, and PTSD. They were also asked whether they experienced suicidal ideation or self-harm during the previous 2 weeks.
Overall, 12% of survey respondents reported having been diagnosed with a mental illness. This, said Jetelina, is slightly lower than the rate reported in the general population.
Study participants who had not currently been diagnosed with a mental illness completed the Patient Health Questionnaire–2 (PHQ-2), the Generalized Anxiety Disorder–2 (GAD-2), and the Primary Care–Posttraumatic Stress Disorder (PC-PTSD).
Officers were considered to have a positive result if they had a score of 3 or more (PHQ-2, sensitivity of 83% and specificity of 92%; PC-PTSD-5, sensitivity of 93% and specificity of 85%; GAD-2, sensitivity of 86% and specificity of 83%).
About 26% of respondents had a positive screening for mental illness symptoms, mainly PTSD and depression, which Dr. Jetelina noted is a higher percentage than in the general population.
This rate of mental health symptoms is “high and concerning,” but not surprising because of the work of police officers, which could include attending to sometimes violent car crashes, domestic abuse situations, and armed conflicts, said Dr. Jetelina.
“They’re constantly exposed to traumatic calls for service; they see people on their worst day, 8 hours a day, 5 days a week. That stress and exposure will have a detrimental effect on mental health, and we have to pay more attention to that,” she said.
Dr. Jetelina pointed out that the surveys were completed in January and February 2020, before COVID-19 had become a cause of stress for everyone and before the increase in calls for defunding police amid a resurgence of Black Lives Matter demonstrations.
However, she stressed that racial biases and occupational stress among police officers are “nothing new for them.” For example, in 2016, five Dallas police officers were killed during Black Lives Matter protests because of their race/ethnicity.
More at risk
The study showed that certain subgroups of officers were more at risk for mental illness. After adjustment for confounders, including demographic characteristics, marital status, and educational level, the odds of being diagnosed with a mental illness during the course of one’s life were significantly higher among female officers than male officers (adjusted odds ratio, 3.20; 95% confidence interval, 1.18-8.68).
Officers who were divorced, widowed, or separated and those who had more experience and held a higher rank were also at greater risk for mental illness.
As well, (aOR, 3.25; 95% CI, 1.38-7.67).
The study also asked participants about use of mental health care services over the past 12 months. About 35% of those who had a current mental health diagnosis and 17% of those who screened positive for mental health symptoms reported using such services.
The study also asked those who screened positive about their interest in seeking such services. After adjustments, officers with suicidal ideation or self-harm were significantly more likely to be interested in getting help, compared with officers who did not report suicidal ideation or self-harm (aOR, 7.66; 95% CI, 1.70-34.48).
Dr. Jetelina was impressed that so many officers were keen to seek help, which “is a big positive,” she said. “It’s just a matter of better detecting who needs the help and better connecting them to medical services that meet their needs.”
Mindfulness exercise
Dr. Jetelina and colleagues are conducting a pilot test of the use by police officers of smartwatches that monitor heart rate and oxygen levels. If measurements with these devices reach a predetermined threshold, the officers are “pinged” and are instructed to perform a mindfulness exercise in the field, she said.
Results so far “are really exciting,” said Dr. Jetelina. “Officers have found this extremely helpful and feasible, and so the next step is to test if this truly impacts mental illness over time.”
Routine mental health screening of officers might be beneficial, but only if it’s conducted in a manner “respectful of the officers’ needs and wants,” said Dr. Jetelina.
She pointed out that although psychological assessments are routinely carried out following an extreme traumatic call, such as one involving an officer-involved shooting, the “in-between” calls could have a more severe cumulative impact on mental health.
It’s important to provide officers with easy-to-access services tailored for their individual needs, said Dr. Jetelina.
‘Numb to it’
Eighteen patrol officers also participated in a focus group, during which several themes regarding the use of mental health care services emerged. One theme was the inability of officers to identify when they’re personally experiencing a mental health problem.
Participants said they had become “numb” to the traumatic events on the job, which is “concerning,” Dr. Jetelina said. “They think that having nightmares every week is completely normal, but it’s not, and this needs to be addressed.”
Other themes that emerged from focus groups included the belief that psychologists can’t relate to police stressors; concerns about confidentiality (one sentiment that was expressed was “you’re an idiot” if you “trust this department”); and stigma for officers who seek mental health care (participants talked about “reprisal” from seeing “a shrink,” including being labeled as “a nutter” and losing their job).
Dr. Jetelina noted that some “champion” officers revealed their mental health journey during focus groups, which tended to “open a Pandora’s box” for others to discuss their experience. She said these champions could be leveraged throughout the police department to help reduce stigma.
The study included participants from only one police department, although rigorous data collection allows for generalizability to the entire patrol department, say the authors. Although the study included only brief screens of mental illness symptoms, these short versions of screening tests have high sensitivity and specificity for mental illness in primary care, they noted.
The next step for the researchers is to study how mental illness and symptoms affect job performance, said Dr. Jetelina. “Does this impact excessive use of force? Does this impact workers’ compensation? Does this impact dispatch times, the time it takes for a police officer to respond to [a] 911 call?”
Possible underrepresentation
Anthony T. Ng, MD, regional medical director, East Region Hartford HealthCare Behavioral Health Network in Mansfield, Conn., and member of the American Psychiatric Association’s Council on Communications, found the study “helpful.”
However, the 26% who tested positive for mental illness may be an “underrepresentation” of the true picture, inasmuch as police officers might minimize or be less than truthful about their mental health status, said Dr. Ng.
Law enforcement has “never been easy,” but stressors may have escalated recently as police forces deal with shortages of staff and jails, said Dr. Ng.
He also noted that officers might face stressors at home. “Evidence shows that domestic violence is quite high – or higher than average – among law enforcement,” he said. “All these things add up.”
Psychiatrists and other mental health professionals should be “aware of the unique challenges” that police officers face and be “proactively involved” in providing guidance and education on mitigating stress, said Dr. Ng.
“You have police officers wearing body armor, so why can’t you give them some training to learn how to have psychiatric or psychological body armor?” he said. But it’s a two-way street; police forces should be open to outreach from mental health professionals. “We have to meet halfway.”
Compassion fatigue
In an accompanying commentary, John M. Violanti, PhD, of the department of epidemiology and environmental health at the State University of New York at Buffalo, said the article helps bring “to the forefront” the issue of the psychological dangers of police work.
There is conjecture as to why police experience mental distress, said Dr. Violanti, who pointed to a study of New York City police suicides during the 1930s that suggested that police have a “social license” for aggressive behavior but are restrained as part of public trust, placing them in a position of “psychological strain.”
“This situation may be reflective of the same situation police find themselves today,” said Dr. Violanti.
“Compassion fatigue,” a feeling of mental exhaustion caused by the inability to care for all persons in trouble, may also be a factor, as could the constant stress that leaves police officers feeling “cynical and isolated from others,” he wrote.
“The socialization process of becoming a police officer is associated with constrictive reasoning, viewing the world as either right or wrong, which leaves no middle ground for alternatives to deal with mental distress,” Dr. Violanti said.
He noted that police officers may abuse alcohol because of stress, peer pressure, isolation, and a culture that approves of alcohol use. “Officers tend to drink together and reinforce their own values.”.
Although no prospective studies have linked police mental health problems with childhood abuse or neglect, some mental health professionals estimate that about 25% of their police clients have a history of childhood abuse or neglect, said Dr. Violanti.
He agreed that mindfulness may help manage stress and increase cognitive flexibility in dealing with trauma and crises.
A possible way to ensure confidentiality is a peer support program that allows distressed officers to first talk privately with a trained and trusted peer officer and to then seek professional help if necessary, said Dr. Violanti.
The study was funded by a grant from the National Institute of Occupational Health and Safety. Dr. Jetelina, Dr. Ng, and Dr. Violanti disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
New research shows that about a quarter of police officers in one large force report past or present mental health problems.
Responding to a survey, 26% of police officers on the Dallas police department screened positive for depression, anxiety, PTSD, or symptoms of suicide ideation or self-harm.
Mental illness rates were particularly high among female officers, those who were divorced, widowed, or separated, and those with military experience.
The study also showed that concerns over confidentiality and stigma may prevent officers with mental illness from seeking treatment.
The results underscored the need to identify police officers with psychiatric problems and to connect them to the most appropriate individualized care, author Katelyn K. Jetelina, PhD, assistant professor in the department of epidemiology, human genetics, and environmental sciences, University of Texas Health Science Center, Dallas, said in an interview.
“This is a very hard-to-reach population, and because of that, we need to be innovative in reaching them for services,” she said.
The study was published online Oct. 7 in JAMA Network Open.
Dr. Jetelina and colleagues are investigating various aspects of police officers’ well-being, including their nutritional needs and their occupational, physical, and mental health.
The current study included 434 members of the Dallas police department, the ninth largest in the United States. The mean age of the participants was 37 years, 82% were men, and about half were White. The 434 officers represented 97% of those invited to participate (n = 446) and 31% of the total patrol population of the Dallas police department (n = 1,413).
These officers completed a short survey on their smartphone that asked about lifetime diagnoses of depression, anxiety, and PTSD. They were also asked whether they experienced suicidal ideation or self-harm during the previous 2 weeks.
Overall, 12% of survey respondents reported having been diagnosed with a mental illness. This, said Jetelina, is slightly lower than the rate reported in the general population.
Study participants who had not currently been diagnosed with a mental illness completed the Patient Health Questionnaire–2 (PHQ-2), the Generalized Anxiety Disorder–2 (GAD-2), and the Primary Care–Posttraumatic Stress Disorder (PC-PTSD).
Officers were considered to have a positive result if they had a score of 3 or more (PHQ-2, sensitivity of 83% and specificity of 92%; PC-PTSD-5, sensitivity of 93% and specificity of 85%; GAD-2, sensitivity of 86% and specificity of 83%).
About 26% of respondents had a positive screening for mental illness symptoms, mainly PTSD and depression, which Dr. Jetelina noted is a higher percentage than in the general population.
This rate of mental health symptoms is “high and concerning,” but not surprising because of the work of police officers, which could include attending to sometimes violent car crashes, domestic abuse situations, and armed conflicts, said Dr. Jetelina.
“They’re constantly exposed to traumatic calls for service; they see people on their worst day, 8 hours a day, 5 days a week. That stress and exposure will have a detrimental effect on mental health, and we have to pay more attention to that,” she said.
Dr. Jetelina pointed out that the surveys were completed in January and February 2020, before COVID-19 had become a cause of stress for everyone and before the increase in calls for defunding police amid a resurgence of Black Lives Matter demonstrations.
However, she stressed that racial biases and occupational stress among police officers are “nothing new for them.” For example, in 2016, five Dallas police officers were killed during Black Lives Matter protests because of their race/ethnicity.
More at risk
The study showed that certain subgroups of officers were more at risk for mental illness. After adjustment for confounders, including demographic characteristics, marital status, and educational level, the odds of being diagnosed with a mental illness during the course of one’s life were significantly higher among female officers than male officers (adjusted odds ratio, 3.20; 95% confidence interval, 1.18-8.68).
Officers who were divorced, widowed, or separated and those who had more experience and held a higher rank were also at greater risk for mental illness.
As well, (aOR, 3.25; 95% CI, 1.38-7.67).
The study also asked participants about use of mental health care services over the past 12 months. About 35% of those who had a current mental health diagnosis and 17% of those who screened positive for mental health symptoms reported using such services.
The study also asked those who screened positive about their interest in seeking such services. After adjustments, officers with suicidal ideation or self-harm were significantly more likely to be interested in getting help, compared with officers who did not report suicidal ideation or self-harm (aOR, 7.66; 95% CI, 1.70-34.48).
Dr. Jetelina was impressed that so many officers were keen to seek help, which “is a big positive,” she said. “It’s just a matter of better detecting who needs the help and better connecting them to medical services that meet their needs.”
Mindfulness exercise
Dr. Jetelina and colleagues are conducting a pilot test of the use by police officers of smartwatches that monitor heart rate and oxygen levels. If measurements with these devices reach a predetermined threshold, the officers are “pinged” and are instructed to perform a mindfulness exercise in the field, she said.
Results so far “are really exciting,” said Dr. Jetelina. “Officers have found this extremely helpful and feasible, and so the next step is to test if this truly impacts mental illness over time.”
Routine mental health screening of officers might be beneficial, but only if it’s conducted in a manner “respectful of the officers’ needs and wants,” said Dr. Jetelina.
She pointed out that although psychological assessments are routinely carried out following an extreme traumatic call, such as one involving an officer-involved shooting, the “in-between” calls could have a more severe cumulative impact on mental health.
It’s important to provide officers with easy-to-access services tailored for their individual needs, said Dr. Jetelina.
‘Numb to it’
Eighteen patrol officers also participated in a focus group, during which several themes regarding the use of mental health care services emerged. One theme was the inability of officers to identify when they’re personally experiencing a mental health problem.
Participants said they had become “numb” to the traumatic events on the job, which is “concerning,” Dr. Jetelina said. “They think that having nightmares every week is completely normal, but it’s not, and this needs to be addressed.”
Other themes that emerged from focus groups included the belief that psychologists can’t relate to police stressors; concerns about confidentiality (one sentiment that was expressed was “you’re an idiot” if you “trust this department”); and stigma for officers who seek mental health care (participants talked about “reprisal” from seeing “a shrink,” including being labeled as “a nutter” and losing their job).
Dr. Jetelina noted that some “champion” officers revealed their mental health journey during focus groups, which tended to “open a Pandora’s box” for others to discuss their experience. She said these champions could be leveraged throughout the police department to help reduce stigma.
The study included participants from only one police department, although rigorous data collection allows for generalizability to the entire patrol department, say the authors. Although the study included only brief screens of mental illness symptoms, these short versions of screening tests have high sensitivity and specificity for mental illness in primary care, they noted.
The next step for the researchers is to study how mental illness and symptoms affect job performance, said Dr. Jetelina. “Does this impact excessive use of force? Does this impact workers’ compensation? Does this impact dispatch times, the time it takes for a police officer to respond to [a] 911 call?”
Possible underrepresentation
Anthony T. Ng, MD, regional medical director, East Region Hartford HealthCare Behavioral Health Network in Mansfield, Conn., and member of the American Psychiatric Association’s Council on Communications, found the study “helpful.”
However, the 26% who tested positive for mental illness may be an “underrepresentation” of the true picture, inasmuch as police officers might minimize or be less than truthful about their mental health status, said Dr. Ng.
Law enforcement has “never been easy,” but stressors may have escalated recently as police forces deal with shortages of staff and jails, said Dr. Ng.
He also noted that officers might face stressors at home. “Evidence shows that domestic violence is quite high – or higher than average – among law enforcement,” he said. “All these things add up.”
Psychiatrists and other mental health professionals should be “aware of the unique challenges” that police officers face and be “proactively involved” in providing guidance and education on mitigating stress, said Dr. Ng.
“You have police officers wearing body armor, so why can’t you give them some training to learn how to have psychiatric or psychological body armor?” he said. But it’s a two-way street; police forces should be open to outreach from mental health professionals. “We have to meet halfway.”
Compassion fatigue
In an accompanying commentary, John M. Violanti, PhD, of the department of epidemiology and environmental health at the State University of New York at Buffalo, said the article helps bring “to the forefront” the issue of the psychological dangers of police work.
There is conjecture as to why police experience mental distress, said Dr. Violanti, who pointed to a study of New York City police suicides during the 1930s that suggested that police have a “social license” for aggressive behavior but are restrained as part of public trust, placing them in a position of “psychological strain.”
“This situation may be reflective of the same situation police find themselves today,” said Dr. Violanti.
“Compassion fatigue,” a feeling of mental exhaustion caused by the inability to care for all persons in trouble, may also be a factor, as could the constant stress that leaves police officers feeling “cynical and isolated from others,” he wrote.
“The socialization process of becoming a police officer is associated with constrictive reasoning, viewing the world as either right or wrong, which leaves no middle ground for alternatives to deal with mental distress,” Dr. Violanti said.
He noted that police officers may abuse alcohol because of stress, peer pressure, isolation, and a culture that approves of alcohol use. “Officers tend to drink together and reinforce their own values.”.
Although no prospective studies have linked police mental health problems with childhood abuse or neglect, some mental health professionals estimate that about 25% of their police clients have a history of childhood abuse or neglect, said Dr. Violanti.
He agreed that mindfulness may help manage stress and increase cognitive flexibility in dealing with trauma and crises.
A possible way to ensure confidentiality is a peer support program that allows distressed officers to first talk privately with a trained and trusted peer officer and to then seek professional help if necessary, said Dr. Violanti.
The study was funded by a grant from the National Institute of Occupational Health and Safety. Dr. Jetelina, Dr. Ng, and Dr. Violanti disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
New research shows that about a quarter of police officers in one large force report past or present mental health problems.
Responding to a survey, 26% of police officers on the Dallas police department screened positive for depression, anxiety, PTSD, or symptoms of suicide ideation or self-harm.
Mental illness rates were particularly high among female officers, those who were divorced, widowed, or separated, and those with military experience.
The study also showed that concerns over confidentiality and stigma may prevent officers with mental illness from seeking treatment.
The results underscored the need to identify police officers with psychiatric problems and to connect them to the most appropriate individualized care, author Katelyn K. Jetelina, PhD, assistant professor in the department of epidemiology, human genetics, and environmental sciences, University of Texas Health Science Center, Dallas, said in an interview.
“This is a very hard-to-reach population, and because of that, we need to be innovative in reaching them for services,” she said.
The study was published online Oct. 7 in JAMA Network Open.
Dr. Jetelina and colleagues are investigating various aspects of police officers’ well-being, including their nutritional needs and their occupational, physical, and mental health.
The current study included 434 members of the Dallas police department, the ninth largest in the United States. The mean age of the participants was 37 years, 82% were men, and about half were White. The 434 officers represented 97% of those invited to participate (n = 446) and 31% of the total patrol population of the Dallas police department (n = 1,413).
These officers completed a short survey on their smartphone that asked about lifetime diagnoses of depression, anxiety, and PTSD. They were also asked whether they experienced suicidal ideation or self-harm during the previous 2 weeks.
Overall, 12% of survey respondents reported having been diagnosed with a mental illness. This, said Jetelina, is slightly lower than the rate reported in the general population.
Study participants who had not currently been diagnosed with a mental illness completed the Patient Health Questionnaire–2 (PHQ-2), the Generalized Anxiety Disorder–2 (GAD-2), and the Primary Care–Posttraumatic Stress Disorder (PC-PTSD).
Officers were considered to have a positive result if they had a score of 3 or more (PHQ-2, sensitivity of 83% and specificity of 92%; PC-PTSD-5, sensitivity of 93% and specificity of 85%; GAD-2, sensitivity of 86% and specificity of 83%).
About 26% of respondents had a positive screening for mental illness symptoms, mainly PTSD and depression, which Dr. Jetelina noted is a higher percentage than in the general population.
This rate of mental health symptoms is “high and concerning,” but not surprising because of the work of police officers, which could include attending to sometimes violent car crashes, domestic abuse situations, and armed conflicts, said Dr. Jetelina.
“They’re constantly exposed to traumatic calls for service; they see people on their worst day, 8 hours a day, 5 days a week. That stress and exposure will have a detrimental effect on mental health, and we have to pay more attention to that,” she said.
Dr. Jetelina pointed out that the surveys were completed in January and February 2020, before COVID-19 had become a cause of stress for everyone and before the increase in calls for defunding police amid a resurgence of Black Lives Matter demonstrations.
However, she stressed that racial biases and occupational stress among police officers are “nothing new for them.” For example, in 2016, five Dallas police officers were killed during Black Lives Matter protests because of their race/ethnicity.
More at risk
The study showed that certain subgroups of officers were more at risk for mental illness. After adjustment for confounders, including demographic characteristics, marital status, and educational level, the odds of being diagnosed with a mental illness during the course of one’s life were significantly higher among female officers than male officers (adjusted odds ratio, 3.20; 95% confidence interval, 1.18-8.68).
Officers who were divorced, widowed, or separated and those who had more experience and held a higher rank were also at greater risk for mental illness.
As well, (aOR, 3.25; 95% CI, 1.38-7.67).
The study also asked participants about use of mental health care services over the past 12 months. About 35% of those who had a current mental health diagnosis and 17% of those who screened positive for mental health symptoms reported using such services.
The study also asked those who screened positive about their interest in seeking such services. After adjustments, officers with suicidal ideation or self-harm were significantly more likely to be interested in getting help, compared with officers who did not report suicidal ideation or self-harm (aOR, 7.66; 95% CI, 1.70-34.48).
Dr. Jetelina was impressed that so many officers were keen to seek help, which “is a big positive,” she said. “It’s just a matter of better detecting who needs the help and better connecting them to medical services that meet their needs.”
Mindfulness exercise
Dr. Jetelina and colleagues are conducting a pilot test of the use by police officers of smartwatches that monitor heart rate and oxygen levels. If measurements with these devices reach a predetermined threshold, the officers are “pinged” and are instructed to perform a mindfulness exercise in the field, she said.
Results so far “are really exciting,” said Dr. Jetelina. “Officers have found this extremely helpful and feasible, and so the next step is to test if this truly impacts mental illness over time.”
Routine mental health screening of officers might be beneficial, but only if it’s conducted in a manner “respectful of the officers’ needs and wants,” said Dr. Jetelina.
She pointed out that although psychological assessments are routinely carried out following an extreme traumatic call, such as one involving an officer-involved shooting, the “in-between” calls could have a more severe cumulative impact on mental health.
It’s important to provide officers with easy-to-access services tailored for their individual needs, said Dr. Jetelina.
‘Numb to it’
Eighteen patrol officers also participated in a focus group, during which several themes regarding the use of mental health care services emerged. One theme was the inability of officers to identify when they’re personally experiencing a mental health problem.
Participants said they had become “numb” to the traumatic events on the job, which is “concerning,” Dr. Jetelina said. “They think that having nightmares every week is completely normal, but it’s not, and this needs to be addressed.”
Other themes that emerged from focus groups included the belief that psychologists can’t relate to police stressors; concerns about confidentiality (one sentiment that was expressed was “you’re an idiot” if you “trust this department”); and stigma for officers who seek mental health care (participants talked about “reprisal” from seeing “a shrink,” including being labeled as “a nutter” and losing their job).
Dr. Jetelina noted that some “champion” officers revealed their mental health journey during focus groups, which tended to “open a Pandora’s box” for others to discuss their experience. She said these champions could be leveraged throughout the police department to help reduce stigma.
The study included participants from only one police department, although rigorous data collection allows for generalizability to the entire patrol department, say the authors. Although the study included only brief screens of mental illness symptoms, these short versions of screening tests have high sensitivity and specificity for mental illness in primary care, they noted.
The next step for the researchers is to study how mental illness and symptoms affect job performance, said Dr. Jetelina. “Does this impact excessive use of force? Does this impact workers’ compensation? Does this impact dispatch times, the time it takes for a police officer to respond to [a] 911 call?”
Possible underrepresentation
Anthony T. Ng, MD, regional medical director, East Region Hartford HealthCare Behavioral Health Network in Mansfield, Conn., and member of the American Psychiatric Association’s Council on Communications, found the study “helpful.”
However, the 26% who tested positive for mental illness may be an “underrepresentation” of the true picture, inasmuch as police officers might minimize or be less than truthful about their mental health status, said Dr. Ng.
Law enforcement has “never been easy,” but stressors may have escalated recently as police forces deal with shortages of staff and jails, said Dr. Ng.
He also noted that officers might face stressors at home. “Evidence shows that domestic violence is quite high – or higher than average – among law enforcement,” he said. “All these things add up.”
Psychiatrists and other mental health professionals should be “aware of the unique challenges” that police officers face and be “proactively involved” in providing guidance and education on mitigating stress, said Dr. Ng.
“You have police officers wearing body armor, so why can’t you give them some training to learn how to have psychiatric or psychological body armor?” he said. But it’s a two-way street; police forces should be open to outreach from mental health professionals. “We have to meet halfway.”
Compassion fatigue
In an accompanying commentary, John M. Violanti, PhD, of the department of epidemiology and environmental health at the State University of New York at Buffalo, said the article helps bring “to the forefront” the issue of the psychological dangers of police work.
There is conjecture as to why police experience mental distress, said Dr. Violanti, who pointed to a study of New York City police suicides during the 1930s that suggested that police have a “social license” for aggressive behavior but are restrained as part of public trust, placing them in a position of “psychological strain.”
“This situation may be reflective of the same situation police find themselves today,” said Dr. Violanti.
“Compassion fatigue,” a feeling of mental exhaustion caused by the inability to care for all persons in trouble, may also be a factor, as could the constant stress that leaves police officers feeling “cynical and isolated from others,” he wrote.
“The socialization process of becoming a police officer is associated with constrictive reasoning, viewing the world as either right or wrong, which leaves no middle ground for alternatives to deal with mental distress,” Dr. Violanti said.
He noted that police officers may abuse alcohol because of stress, peer pressure, isolation, and a culture that approves of alcohol use. “Officers tend to drink together and reinforce their own values.”.
Although no prospective studies have linked police mental health problems with childhood abuse or neglect, some mental health professionals estimate that about 25% of their police clients have a history of childhood abuse or neglect, said Dr. Violanti.
He agreed that mindfulness may help manage stress and increase cognitive flexibility in dealing with trauma and crises.
A possible way to ensure confidentiality is a peer support program that allows distressed officers to first talk privately with a trained and trusted peer officer and to then seek professional help if necessary, said Dr. Violanti.
The study was funded by a grant from the National Institute of Occupational Health and Safety. Dr. Jetelina, Dr. Ng, and Dr. Violanti disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Repurposing cardiovascular drugs for serious mental illness
One of the hottest topics now in psychiatry is the possibility of repurposing long-established cardiovascular medications for treatment of patients with serious mental illness, Livia De Picker, MD, PhD, said at the virtual congress of the European College of Neuropsychopharmacology.

The appeal is multifold. A huge unmet need exists in psychiatry for new and better treatments with novel mechanisms of action. Many guideline-recommended cardiovascular medications have a long track record, including a well-established safety profile with no surprises, and are available in generic versions. They can be developed for a new indication at minimal cost, noted Dr. De Picker, a psychiatrist at the University of Antwerp (Belgium).
The idea of psychiatric repurposing of drugs originally developed for nonpsychiatric indications is nothing new, she added. Examples include lithium for gout, valproate for epilepsy, and ketamine for anesthesiology.
One hitch in efforts to repurpose cardiovascular medications is that, when psychiatric patients have been included in randomized trials of the drugs’ cardiovascular effects, the psychiatric outcomes often went untallied.
Indeed, the only high-quality randomized trial evidence of psychiatric benefits for any class of cardiovascular medications is for statins, where a modest-sized meta-analysis of six placebo-controlled trials in 339 patients with schizophrenia showed the lipid-lowering agents had benefit for both positive and negative symptoms (Psychiatry Res. 2018 Apr;262:84-93). But that’s not a body of data of sufficient size to be definitive, in Dr. De Picker’s view.
Much of the recent enthusiasm for exploring the potential of cardiovascular drugs for psychiatric conditions comes from hypothesis-generating big data analyses drawn from Scandinavian national patient registries. Danish investigators scrutinized all 1.6 million Danes exposed to six classes of drugs of interest during 2005-2015 and determined that those on long-term statins, low-dose aspirin, ACE inhibitors, angiotensin receptor blockers, or allopurinol were associated with a decreased rate of new-onset depression, while high-dose aspirin and non-aspirin NSAIDs were associated with an increased rate, compared with a 30% random sample of the country’s population (Acta Psychiatr Scand. 2019 Jan;1391:68-77).
Similarly, the Danish group found that continued use of statins, angiotensin agents, or low-dose aspirin was associated with a decreased rate of new-onset bipolar disorder, while high-dose aspirin and other NSAIDs were linked to increased risk (Bipolar Disord. 2019 Aug;[15]:410-8). What these agents have in common, the investigators observed, is that they act on inflammation and potentially on the stress response system.
Meanwhile, Swedish investigators examined the course of 142,691 Swedes with a diagnosis of bipolar disorder, schizophrenia, or nonaffective psychosis during 2005-2016. They determined that, during periods when those individuals were on a statin, calcium channel blocker, or metformin, they had reduced rates of psychiatric hospitalization and self-harm (JAMA Psychiatry. 2019 Apr 1;76[4]:382-90).
Scottish researchers analyzed the health records of 144,066 patients placed on monotherapy for hypertension and determined that the lowest risk for hospitalization for a mood disorder during follow-up was in those prescribed an ACE inhibitor or angiotensin receptor blocker. The risk was significantly higher in patients on a beta-blocker or calcium channel blocker, and intermediate in those on a thiazide diuretic (Hypertension. 2016 Nov;68[5:1132-8).
“Obviously, this is all at a very macro scale and we have no idea whatsoever what this means for individual patients, number needed to treat, or which type of patients would benefit, but it does provide us with some guidance for future research,” according to Dr. De Picker.
In the meantime, while physicians await definitive evidence of any impact of cardiovascular drugs might have on psychiatric outcomes, abundant data exist underscoring what she called “shockingly high levels” of inadequate management of cardiovascular risk factors in patients with serious mental illness. That problem needs to be addressed, and Dr. De Picker offered her personal recommendations for doing so in a manner consistent with the evidence to date suggestive of potential mental health benefits of some cardiovascular medications.
She advised that, for treatment of hypertension in patients with bipolar disorder or major depression, an ACE inhibitor or angiotensin-converting enzyme inhibitor is preferred as first-line. There is some evidence to suggest lipophilic beta-blockers, which cross the blood-brain barrier, improve anxiety symptoms and panic attacks, and prevent memory consolidation in patients with posttraumatic stress disorder. But the Scottish data suggest that they may worsen mood disorders.
“I would be careful in using beta-blockers as first-line treatment for hypertension. They’re not in the guidelines for anxiety disorders. British guidelines recommend them to prevent memory consolidation in PTSD, but do not use them as first-line in patients with major depressive disorder or bipolar disorder,” she said. As for calcium channel blockers, the jury is still out, with mixed and inconsistent evidence to date as to the impact of this drug class on mental illness outcomes.
She recommended a very low threshold for prescribing statin therapy in patients with serious mental illness in light of the superb risk/benefit ratio for this drug class. In her younger patients, she turns for guidance to an online calculator of an individual’s 10-year risk of a first acute MI or stroke.
Metformin has been shown to be beneficial for addressing the weight gain and other adverse metabolic effects caused by antipsychotic agents, and there is some preliminary evidence of improved psychiatric outcomes in patients with serious mental illness.
Christian Otte, MD, who also spoke at the session, noted that not only do emerging data point to the possibility that cardiovascular drugs might have benefit in terms of psychiatric outcomes, there is also some evidence, albeit mixed, that the converse is true: that is, psychiatric drugs may have cardiovascular benefits. He pointed to a South Korean trial in which 300 patients with a recent acute coronary syndrome and major depression were randomized to 24 weeks of escitalopram or placebo. At median 8.1 years of follow-up, the group that received the SSRI had a 31% relative risk reduction in the primary composite endpoint of all-cause mortality, acute MI, or percutaneous coronary intervention (JAMA. 2018 Jul 24; 320[4]:350–7).
“Potentially independent of their antidepressant effects, some SSRIs’ antiplatelet effects could be beneficial for patients with coronary heart disease, although the jury is still open regarding this question, with evidence in both directions,” said Dr. Otte, professor of psychiatry at Charite University Medical Center in Berlin.
Dr. De Picker offered an example as well: Finnish psychiatrists recently reported that cardiovascular mortality was reduced by an adjusted 38% during periods when 62,250 Finnish schizophrenia patients were on antipsychotic agents, compared with periods of nonuse of the drugs in a national study with a median 14.1 years of follow-up (World Psychiatry. 2020 Feb;19[1]:61-8).
“What they discovered – and this is quite contrary to what we are used to hearing about antipsychotic medication and cardiovascular risk – is that while the number of cardiovascular hospitalizations was not different in periods with or without antipsychotic use, the cardiovascular mortality was quite strikingly reduced when patients were on antipsychotic medication,” she said.
Asked by an audience member whether she personally prescribes metformin, Dr. De Picker replied: “Well, yes, why not? One of the very nice things about metformin is that it is actually a very safe drug, even in the hands of nonspecialists.
“I understand that maybe psychiatrists may not feel very comfortable in starting patients on metformin due to a lack of experience. But there are really only two things you need to take into account. About one-quarter of patients will experience GI side effects – nausea, vomiting, abdominal discomfort – and this can be reduced by gradually uptitrating the dose, dosing at mealtime, and using an extended-release formulation. And the second thing is that metformin can impair vitamin B12 absorption, so I think, especially in psychiatric patients, it would be good to do an annual measurement of vitamin B12 level and, if necessary, administer intramuscular supplements,” Dr. De Picker said.
She reported having no financial conflicts regarding her presentation.
SOURCE: De Picker L. ECNP 2020. Session EDU.05.
One of the hottest topics now in psychiatry is the possibility of repurposing long-established cardiovascular medications for treatment of patients with serious mental illness, Livia De Picker, MD, PhD, said at the virtual congress of the European College of Neuropsychopharmacology.
The appeal is multifold. A huge unmet need exists in psychiatry for new and better treatments with novel mechanisms of action. Many guideline-recommended cardiovascular medications have a long track record, including a well-established safety profile with no surprises, and are available in generic versions. They can be developed for a new indication at minimal cost, noted Dr. De Picker, a psychiatrist at the University of Antwerp (Belgium).
The idea of psychiatric repurposing of drugs originally developed for nonpsychiatric indications is nothing new, she added. Examples include lithium for gout, valproate for epilepsy, and ketamine for anesthesiology.
One hitch in efforts to repurpose cardiovascular medications is that, when psychiatric patients have been included in randomized trials of the drugs’ cardiovascular effects, the psychiatric outcomes often went untallied.
Indeed, the only high-quality randomized trial evidence of psychiatric benefits for any class of cardiovascular medications is for statins, where a modest-sized meta-analysis of six placebo-controlled trials in 339 patients with schizophrenia showed the lipid-lowering agents had benefit for both positive and negative symptoms (Psychiatry Res. 2018 Apr;262:84-93). But that’s not a body of data of sufficient size to be definitive, in Dr. De Picker’s view.
Much of the recent enthusiasm for exploring the potential of cardiovascular drugs for psychiatric conditions comes from hypothesis-generating big data analyses drawn from Scandinavian national patient registries. Danish investigators scrutinized all 1.6 million Danes exposed to six classes of drugs of interest during 2005-2015 and determined that those on long-term statins, low-dose aspirin, ACE inhibitors, angiotensin receptor blockers, or allopurinol were associated with a decreased rate of new-onset depression, while high-dose aspirin and non-aspirin NSAIDs were associated with an increased rate, compared with a 30% random sample of the country’s population (Acta Psychiatr Scand. 2019 Jan;1391:68-77).
Similarly, the Danish group found that continued use of statins, angiotensin agents, or low-dose aspirin was associated with a decreased rate of new-onset bipolar disorder, while high-dose aspirin and other NSAIDs were linked to increased risk (Bipolar Disord. 2019 Aug;[15]:410-8). What these agents have in common, the investigators observed, is that they act on inflammation and potentially on the stress response system.
Meanwhile, Swedish investigators examined the course of 142,691 Swedes with a diagnosis of bipolar disorder, schizophrenia, or nonaffective psychosis during 2005-2016. They determined that, during periods when those individuals were on a statin, calcium channel blocker, or metformin, they had reduced rates of psychiatric hospitalization and self-harm (JAMA Psychiatry. 2019 Apr 1;76[4]:382-90).
Scottish researchers analyzed the health records of 144,066 patients placed on monotherapy for hypertension and determined that the lowest risk for hospitalization for a mood disorder during follow-up was in those prescribed an ACE inhibitor or angiotensin receptor blocker. The risk was significantly higher in patients on a beta-blocker or calcium channel blocker, and intermediate in those on a thiazide diuretic (Hypertension. 2016 Nov;68[5:1132-8).
“Obviously, this is all at a very macro scale and we have no idea whatsoever what this means for individual patients, number needed to treat, or which type of patients would benefit, but it does provide us with some guidance for future research,” according to Dr. De Picker.
In the meantime, while physicians await definitive evidence of any impact of cardiovascular drugs might have on psychiatric outcomes, abundant data exist underscoring what she called “shockingly high levels” of inadequate management of cardiovascular risk factors in patients with serious mental illness. That problem needs to be addressed, and Dr. De Picker offered her personal recommendations for doing so in a manner consistent with the evidence to date suggestive of potential mental health benefits of some cardiovascular medications.
She advised that, for treatment of hypertension in patients with bipolar disorder or major depression, an ACE inhibitor or angiotensin-converting enzyme inhibitor is preferred as first-line. There is some evidence to suggest lipophilic beta-blockers, which cross the blood-brain barrier, improve anxiety symptoms and panic attacks, and prevent memory consolidation in patients with posttraumatic stress disorder. But the Scottish data suggest that they may worsen mood disorders.
“I would be careful in using beta-blockers as first-line treatment for hypertension. They’re not in the guidelines for anxiety disorders. British guidelines recommend them to prevent memory consolidation in PTSD, but do not use them as first-line in patients with major depressive disorder or bipolar disorder,” she said. As for calcium channel blockers, the jury is still out, with mixed and inconsistent evidence to date as to the impact of this drug class on mental illness outcomes.
She recommended a very low threshold for prescribing statin therapy in patients with serious mental illness in light of the superb risk/benefit ratio for this drug class. In her younger patients, she turns for guidance to an online calculator of an individual’s 10-year risk of a first acute MI or stroke.
Metformin has been shown to be beneficial for addressing the weight gain and other adverse metabolic effects caused by antipsychotic agents, and there is some preliminary evidence of improved psychiatric outcomes in patients with serious mental illness.
Christian Otte, MD, who also spoke at the session, noted that not only do emerging data point to the possibility that cardiovascular drugs might have benefit in terms of psychiatric outcomes, there is also some evidence, albeit mixed, that the converse is true: that is, psychiatric drugs may have cardiovascular benefits. He pointed to a South Korean trial in which 300 patients with a recent acute coronary syndrome and major depression were randomized to 24 weeks of escitalopram or placebo. At median 8.1 years of follow-up, the group that received the SSRI had a 31% relative risk reduction in the primary composite endpoint of all-cause mortality, acute MI, or percutaneous coronary intervention (JAMA. 2018 Jul 24; 320[4]:350–7).
“Potentially independent of their antidepressant effects, some SSRIs’ antiplatelet effects could be beneficial for patients with coronary heart disease, although the jury is still open regarding this question, with evidence in both directions,” said Dr. Otte, professor of psychiatry at Charite University Medical Center in Berlin.
Dr. De Picker offered an example as well: Finnish psychiatrists recently reported that cardiovascular mortality was reduced by an adjusted 38% during periods when 62,250 Finnish schizophrenia patients were on antipsychotic agents, compared with periods of nonuse of the drugs in a national study with a median 14.1 years of follow-up (World Psychiatry. 2020 Feb;19[1]:61-8).
“What they discovered – and this is quite contrary to what we are used to hearing about antipsychotic medication and cardiovascular risk – is that while the number of cardiovascular hospitalizations was not different in periods with or without antipsychotic use, the cardiovascular mortality was quite strikingly reduced when patients were on antipsychotic medication,” she said.
Asked by an audience member whether she personally prescribes metformin, Dr. De Picker replied: “Well, yes, why not? One of the very nice things about metformin is that it is actually a very safe drug, even in the hands of nonspecialists.
“I understand that maybe psychiatrists may not feel very comfortable in starting patients on metformin due to a lack of experience. But there are really only two things you need to take into account. About one-quarter of patients will experience GI side effects – nausea, vomiting, abdominal discomfort – and this can be reduced by gradually uptitrating the dose, dosing at mealtime, and using an extended-release formulation. And the second thing is that metformin can impair vitamin B12 absorption, so I think, especially in psychiatric patients, it would be good to do an annual measurement of vitamin B12 level and, if necessary, administer intramuscular supplements,” Dr. De Picker said.
She reported having no financial conflicts regarding her presentation.
SOURCE: De Picker L. ECNP 2020. Session EDU.05.
One of the hottest topics now in psychiatry is the possibility of repurposing long-established cardiovascular medications for treatment of patients with serious mental illness, Livia De Picker, MD, PhD, said at the virtual congress of the European College of Neuropsychopharmacology.
The appeal is multifold. A huge unmet need exists in psychiatry for new and better treatments with novel mechanisms of action. Many guideline-recommended cardiovascular medications have a long track record, including a well-established safety profile with no surprises, and are available in generic versions. They can be developed for a new indication at minimal cost, noted Dr. De Picker, a psychiatrist at the University of Antwerp (Belgium).
The idea of psychiatric repurposing of drugs originally developed for nonpsychiatric indications is nothing new, she added. Examples include lithium for gout, valproate for epilepsy, and ketamine for anesthesiology.
One hitch in efforts to repurpose cardiovascular medications is that, when psychiatric patients have been included in randomized trials of the drugs’ cardiovascular effects, the psychiatric outcomes often went untallied.
Indeed, the only high-quality randomized trial evidence of psychiatric benefits for any class of cardiovascular medications is for statins, where a modest-sized meta-analysis of six placebo-controlled trials in 339 patients with schizophrenia showed the lipid-lowering agents had benefit for both positive and negative symptoms (Psychiatry Res. 2018 Apr;262:84-93). But that’s not a body of data of sufficient size to be definitive, in Dr. De Picker’s view.
Much of the recent enthusiasm for exploring the potential of cardiovascular drugs for psychiatric conditions comes from hypothesis-generating big data analyses drawn from Scandinavian national patient registries. Danish investigators scrutinized all 1.6 million Danes exposed to six classes of drugs of interest during 2005-2015 and determined that those on long-term statins, low-dose aspirin, ACE inhibitors, angiotensin receptor blockers, or allopurinol were associated with a decreased rate of new-onset depression, while high-dose aspirin and non-aspirin NSAIDs were associated with an increased rate, compared with a 30% random sample of the country’s population (Acta Psychiatr Scand. 2019 Jan;1391:68-77).
Similarly, the Danish group found that continued use of statins, angiotensin agents, or low-dose aspirin was associated with a decreased rate of new-onset bipolar disorder, while high-dose aspirin and other NSAIDs were linked to increased risk (Bipolar Disord. 2019 Aug;[15]:410-8). What these agents have in common, the investigators observed, is that they act on inflammation and potentially on the stress response system.
Meanwhile, Swedish investigators examined the course of 142,691 Swedes with a diagnosis of bipolar disorder, schizophrenia, or nonaffective psychosis during 2005-2016. They determined that, during periods when those individuals were on a statin, calcium channel blocker, or metformin, they had reduced rates of psychiatric hospitalization and self-harm (JAMA Psychiatry. 2019 Apr 1;76[4]:382-90).
Scottish researchers analyzed the health records of 144,066 patients placed on monotherapy for hypertension and determined that the lowest risk for hospitalization for a mood disorder during follow-up was in those prescribed an ACE inhibitor or angiotensin receptor blocker. The risk was significantly higher in patients on a beta-blocker or calcium channel blocker, and intermediate in those on a thiazide diuretic (Hypertension. 2016 Nov;68[5:1132-8).
“Obviously, this is all at a very macro scale and we have no idea whatsoever what this means for individual patients, number needed to treat, or which type of patients would benefit, but it does provide us with some guidance for future research,” according to Dr. De Picker.
In the meantime, while physicians await definitive evidence of any impact of cardiovascular drugs might have on psychiatric outcomes, abundant data exist underscoring what she called “shockingly high levels” of inadequate management of cardiovascular risk factors in patients with serious mental illness. That problem needs to be addressed, and Dr. De Picker offered her personal recommendations for doing so in a manner consistent with the evidence to date suggestive of potential mental health benefits of some cardiovascular medications.
She advised that, for treatment of hypertension in patients with bipolar disorder or major depression, an ACE inhibitor or angiotensin-converting enzyme inhibitor is preferred as first-line. There is some evidence to suggest lipophilic beta-blockers, which cross the blood-brain barrier, improve anxiety symptoms and panic attacks, and prevent memory consolidation in patients with posttraumatic stress disorder. But the Scottish data suggest that they may worsen mood disorders.
“I would be careful in using beta-blockers as first-line treatment for hypertension. They’re not in the guidelines for anxiety disorders. British guidelines recommend them to prevent memory consolidation in PTSD, but do not use them as first-line in patients with major depressive disorder or bipolar disorder,” she said. As for calcium channel blockers, the jury is still out, with mixed and inconsistent evidence to date as to the impact of this drug class on mental illness outcomes.
She recommended a very low threshold for prescribing statin therapy in patients with serious mental illness in light of the superb risk/benefit ratio for this drug class. In her younger patients, she turns for guidance to an online calculator of an individual’s 10-year risk of a first acute MI or stroke.
Metformin has been shown to be beneficial for addressing the weight gain and other adverse metabolic effects caused by antipsychotic agents, and there is some preliminary evidence of improved psychiatric outcomes in patients with serious mental illness.
Christian Otte, MD, who also spoke at the session, noted that not only do emerging data point to the possibility that cardiovascular drugs might have benefit in terms of psychiatric outcomes, there is also some evidence, albeit mixed, that the converse is true: that is, psychiatric drugs may have cardiovascular benefits. He pointed to a South Korean trial in which 300 patients with a recent acute coronary syndrome and major depression were randomized to 24 weeks of escitalopram or placebo. At median 8.1 years of follow-up, the group that received the SSRI had a 31% relative risk reduction in the primary composite endpoint of all-cause mortality, acute MI, or percutaneous coronary intervention (JAMA. 2018 Jul 24; 320[4]:350–7).
“Potentially independent of their antidepressant effects, some SSRIs’ antiplatelet effects could be beneficial for patients with coronary heart disease, although the jury is still open regarding this question, with evidence in both directions,” said Dr. Otte, professor of psychiatry at Charite University Medical Center in Berlin.
Dr. De Picker offered an example as well: Finnish psychiatrists recently reported that cardiovascular mortality was reduced by an adjusted 38% during periods when 62,250 Finnish schizophrenia patients were on antipsychotic agents, compared with periods of nonuse of the drugs in a national study with a median 14.1 years of follow-up (World Psychiatry. 2020 Feb;19[1]:61-8).
“What they discovered – and this is quite contrary to what we are used to hearing about antipsychotic medication and cardiovascular risk – is that while the number of cardiovascular hospitalizations was not different in periods with or without antipsychotic use, the cardiovascular mortality was quite strikingly reduced when patients were on antipsychotic medication,” she said.
Asked by an audience member whether she personally prescribes metformin, Dr. De Picker replied: “Well, yes, why not? One of the very nice things about metformin is that it is actually a very safe drug, even in the hands of nonspecialists.
“I understand that maybe psychiatrists may not feel very comfortable in starting patients on metformin due to a lack of experience. But there are really only two things you need to take into account. About one-quarter of patients will experience GI side effects – nausea, vomiting, abdominal discomfort – and this can be reduced by gradually uptitrating the dose, dosing at mealtime, and using an extended-release formulation. And the second thing is that metformin can impair vitamin B12 absorption, so I think, especially in psychiatric patients, it would be good to do an annual measurement of vitamin B12 level and, if necessary, administer intramuscular supplements,” Dr. De Picker said.
She reported having no financial conflicts regarding her presentation.
SOURCE: De Picker L. ECNP 2020. Session EDU.05.
FROM ECNP 2020
Mental health risks rise with age and stage for gender-incongruent youth
Gender-incongruent youth who present for gender-affirming medical care later in adolescence have higher rates of mental health problems than their younger counterparts, based on data from a review of 300 individuals.

“Puberty is a vulnerable time for youth with gender dysphoria because distress may intensify with the development of secondary sex characteristics corresponding to the assigned rather than the experienced gender,” wrote Julia C. Sorbara, MD, of the University of Toronto and the Hospital for Sick Children, also in Toronto, and colleagues.
Although gender-affirming medical care (GAMC) in the form of hormone blockers and/or gender-affirming hormones early in puberty can decrease in emotional and behavioral problems, many teens present later in puberty, and the relationship between pubertal stage at presentation for treatment and mental health has not been examined, they wrote.
In a study published in Pediatrics, the researchers reviewed data from youth with gender incongruence who were seen at a single center; 116 were younger than 15 years at presentation for GAMC and were defined as younger-presenting youth (YPY), and 184 patients aged 15 years and older were defined as older-presenting youth (OPY).
Overall, 78% of the youth reported at least one mental health problem at their initial visit. Significantly more OPY than YPY reported diagnosed depression (46% vs. 30%), self-harm (40% vs. 28%), suicidal thoughts (52% vs. 40%), suicide attempts (17% vs. 9%), and use of psychoactive medications (36% vs. 23%), all with P < .05.
In a multivariate analysis, patients in Tanner stages 4 and 5 were five times more likely to experience depressive disorders (odds ratio, 5.49) and four times as likely to experience depressive disorders (OR, 4.18) as those in earlier Tanner stages. Older age remained significantly associated with use of psychoactive medications (OR, 1.31), but not with anxiety or depression, the researchers wrote.
The YPY group were significantly younger at the age of recognizing gender incongruence, compared with the OPY group, with median ages at recognition of 5.8 years and 9 years, respectively, and younger patients came out about their gender identity at an average of 12 years, compared with 15 years for older patients.
The quantitative data are among the first to relate pubertal stage to mental health in gender-incongruent youth, “supporting clinical observations that pubertal development, menses, and erections are distressing to these youth and consistent with the beneficial role of pubertal suppression, even when used as monotherapy without gender-affirming hormones,” Dr. Sorbara and associates wrote.
The study findings were limited by several factors including the cross-sectional design and the collection of mental health data at only one time point and by the use of self-reports. However, the results suggest that “[gender-incongruent] youth who present to GAMC later in life are a particularly high-risk subset of a vulnerable population,” they noted. “Further study is required to better describe the mental health trajectories of transgender youth and determine if mental health status or age at initiation of GAMC is correlated with psychological well-being in adulthood.”
Don’t rush to puberty suppression in younger teens
To reduce the stress of puberty on gender-nonconforming youth, puberty suppression as “a reversible medical intervention” was introduced by Dutch clinicians in the early 2000s, Annelou L.C. de Vries, MD, PhD, of Amsterdam University Medical Center, wrote in an accompanying editorial.
“The aim of puberty suppression was to prevent the psychological suffering stemming from undesired physical changes when puberty starts and allowing the adolescent time to make plans regarding further transition or not,” Dr. de Vries said. “Following this rationale, younger age at the time of starting medical-affirming treatment (puberty suppression or hormones) would be expected to correlate with fewer psychological difficulties related to physical changes than older individuals,” which was confirmed in the current study.
However, clinicians should be cautious in offering puberty suppression at a younger age, in part because “despite the increased availability of gender-affirming medical interventions for younger ages in recent years, there has not been a proportional decline in older presenting youth with gender incongruence,” she said.
More data are needed on youth with postpuberty adolescent-onset transgender histories. The original Dutch studies on gender-affirming medical interventions note case histories describing “the complexities that may be associated with later-presenting transgender adolescents and describe that some eventually detransition,” Dr. de Vries explained.
Ultimately, prospective studies with longer follow-up data are needed to better inform clinicians in developing an individualized treatment plan for youth with gender incongruence, Dr. de Vries concluded.
Care barriers can include parents, access, insurance
The study authors describe the situation of gender-affirming medical care in teens perfectly, M. Brett Cooper, MD, of the University of Texas Southwestern Medical Center/Children’s Health Dallas, said in an interview.
Given a variety of factors that need further exploration, “many youth often don’t end up seeking gender-affirming medical care until puberty has progressed to near full maturity,” he said. “The findings from this study provide preliminary evidence to show that if we can identify these youth earlier in their gender journey, we might be able to impact adverse mental health outcomes in a positive way.”
Dr. Cooper said he was not surprised by the study findings. “They are similar to what I see in my clinic.
“Many of our patients often don’t present for medical care until around age 15 or older, similar to the findings of the study,” he added. “The majority of our patients have had a diagnosis of anxiety or depression at some point in their lifetime, including inpatient hospitalizations for their mental health.”
One of the most important barriers to care often can be parents or guardians, said Dr. Cooper. “Young people usually know their gender identity by about age 4-5 but parents may think that a gender-diverse identity could simply be a ‘phase.’ Other times, young people may hide their identity out of fear of a negative reaction from their parents. The distress around identity may become more pronounced once pubertal changes, such as breast and testicle development, begin to worsen their dysphoria.”
“Another barrier to care can be the inability to find a competent, gender-affirming provider,” Dr. Cooper said. “Most large United States cities have at least one gender-affirming clinic, but for those youth who grow up in smaller towns, it may be difficult to access these clinics. In addition, some clinics require a letter from a therapist stating that the young person is transgender before they can be seen for medical care. This creates an access barrier, as it may be difficult not just to find a therapist but one who has experience working with gender-diverse youth.”
Insurance coverage, including lack thereof, is yet another barrier to care for transgender youth, said Dr. Cooper. “While many insurance companies have begun to cover medications such as testosterone and estrogen for gender-affirming care, many still have exclusions on things like puberty blockers and surgical interventions.” These interventions can be lifesaving, but financially prohibitive for many families if not covered by insurance.
As for the value of early timing of gender-affirming care, Dr. Cooper agreed with the study findings that the earlier that a young person can get into medical care for their gender identity, the better chance there is to reduce the prevalence of serious mental health outcomes. “This also prevents the potential development of secondary sexual characteristics, decreasing the need for or amount of surgery in the future if desired,” he said.
“More research is needed to better understand the reasons why many youth don’t present to care until later in puberty. In addition, we need better research on interventions that are effective at reducing serious mental health events in transgender and gender diverse youth,” Dr. Cooper stated. “Another area that I would like to see researched is looking at the mental health of non-Caucasian youth. As the authors noted in their study, many clinics have a high percentage of patients presenting for care who identify as White or Caucasian, and we need to better understand why these other youth are not presenting for care.”
The study received no outside funding. Dr. Sorbara disclosed salary support from the Canadian Pediatric Endocrine Group fellowship program. Dr. de Vries had no financial conflicts to disclose. Dr. Cooper had no financial conflicts to disclose, and serves as a contributor to LGBTQ Youth Consult in Pediatric News.
SOURCES: Sorbara JC et al. Pediatrics. 2020 Sep 21. doi: 10.1542/peds.2019-3600; de Vries ALC et al. Pediatrics. 2020 Sep 21. doi: 10.1542/peds.2020-010611.
Gender-incongruent youth who present for gender-affirming medical care later in adolescence have higher rates of mental health problems than their younger counterparts, based on data from a review of 300 individuals.
“Puberty is a vulnerable time for youth with gender dysphoria because distress may intensify with the development of secondary sex characteristics corresponding to the assigned rather than the experienced gender,” wrote Julia C. Sorbara, MD, of the University of Toronto and the Hospital for Sick Children, also in Toronto, and colleagues.
Although gender-affirming medical care (GAMC) in the form of hormone blockers and/or gender-affirming hormones early in puberty can decrease in emotional and behavioral problems, many teens present later in puberty, and the relationship between pubertal stage at presentation for treatment and mental health has not been examined, they wrote.
In a study published in Pediatrics, the researchers reviewed data from youth with gender incongruence who were seen at a single center; 116 were younger than 15 years at presentation for GAMC and were defined as younger-presenting youth (YPY), and 184 patients aged 15 years and older were defined as older-presenting youth (OPY).
Overall, 78% of the youth reported at least one mental health problem at their initial visit. Significantly more OPY than YPY reported diagnosed depression (46% vs. 30%), self-harm (40% vs. 28%), suicidal thoughts (52% vs. 40%), suicide attempts (17% vs. 9%), and use of psychoactive medications (36% vs. 23%), all with P < .05.
In a multivariate analysis, patients in Tanner stages 4 and 5 were five times more likely to experience depressive disorders (odds ratio, 5.49) and four times as likely to experience depressive disorders (OR, 4.18) as those in earlier Tanner stages. Older age remained significantly associated with use of psychoactive medications (OR, 1.31), but not with anxiety or depression, the researchers wrote.
The YPY group were significantly younger at the age of recognizing gender incongruence, compared with the OPY group, with median ages at recognition of 5.8 years and 9 years, respectively, and younger patients came out about their gender identity at an average of 12 years, compared with 15 years for older patients.
The quantitative data are among the first to relate pubertal stage to mental health in gender-incongruent youth, “supporting clinical observations that pubertal development, menses, and erections are distressing to these youth and consistent with the beneficial role of pubertal suppression, even when used as monotherapy without gender-affirming hormones,” Dr. Sorbara and associates wrote.
The study findings were limited by several factors including the cross-sectional design and the collection of mental health data at only one time point and by the use of self-reports. However, the results suggest that “[gender-incongruent] youth who present to GAMC later in life are a particularly high-risk subset of a vulnerable population,” they noted. “Further study is required to better describe the mental health trajectories of transgender youth and determine if mental health status or age at initiation of GAMC is correlated with psychological well-being in adulthood.”
Don’t rush to puberty suppression in younger teens
To reduce the stress of puberty on gender-nonconforming youth, puberty suppression as “a reversible medical intervention” was introduced by Dutch clinicians in the early 2000s, Annelou L.C. de Vries, MD, PhD, of Amsterdam University Medical Center, wrote in an accompanying editorial.
“The aim of puberty suppression was to prevent the psychological suffering stemming from undesired physical changes when puberty starts and allowing the adolescent time to make plans regarding further transition or not,” Dr. de Vries said. “Following this rationale, younger age at the time of starting medical-affirming treatment (puberty suppression or hormones) would be expected to correlate with fewer psychological difficulties related to physical changes than older individuals,” which was confirmed in the current study.
However, clinicians should be cautious in offering puberty suppression at a younger age, in part because “despite the increased availability of gender-affirming medical interventions for younger ages in recent years, there has not been a proportional decline in older presenting youth with gender incongruence,” she said.
More data are needed on youth with postpuberty adolescent-onset transgender histories. The original Dutch studies on gender-affirming medical interventions note case histories describing “the complexities that may be associated with later-presenting transgender adolescents and describe that some eventually detransition,” Dr. de Vries explained.
Ultimately, prospective studies with longer follow-up data are needed to better inform clinicians in developing an individualized treatment plan for youth with gender incongruence, Dr. de Vries concluded.
Care barriers can include parents, access, insurance
The study authors describe the situation of gender-affirming medical care in teens perfectly, M. Brett Cooper, MD, of the University of Texas Southwestern Medical Center/Children’s Health Dallas, said in an interview.
Given a variety of factors that need further exploration, “many youth often don’t end up seeking gender-affirming medical care until puberty has progressed to near full maturity,” he said. “The findings from this study provide preliminary evidence to show that if we can identify these youth earlier in their gender journey, we might be able to impact adverse mental health outcomes in a positive way.”
Dr. Cooper said he was not surprised by the study findings. “They are similar to what I see in my clinic.
“Many of our patients often don’t present for medical care until around age 15 or older, similar to the findings of the study,” he added. “The majority of our patients have had a diagnosis of anxiety or depression at some point in their lifetime, including inpatient hospitalizations for their mental health.”
One of the most important barriers to care often can be parents or guardians, said Dr. Cooper. “Young people usually know their gender identity by about age 4-5 but parents may think that a gender-diverse identity could simply be a ‘phase.’ Other times, young people may hide their identity out of fear of a negative reaction from their parents. The distress around identity may become more pronounced once pubertal changes, such as breast and testicle development, begin to worsen their dysphoria.”
“Another barrier to care can be the inability to find a competent, gender-affirming provider,” Dr. Cooper said. “Most large United States cities have at least one gender-affirming clinic, but for those youth who grow up in smaller towns, it may be difficult to access these clinics. In addition, some clinics require a letter from a therapist stating that the young person is transgender before they can be seen for medical care. This creates an access barrier, as it may be difficult not just to find a therapist but one who has experience working with gender-diverse youth.”
Insurance coverage, including lack thereof, is yet another barrier to care for transgender youth, said Dr. Cooper. “While many insurance companies have begun to cover medications such as testosterone and estrogen for gender-affirming care, many still have exclusions on things like puberty blockers and surgical interventions.” These interventions can be lifesaving, but financially prohibitive for many families if not covered by insurance.
As for the value of early timing of gender-affirming care, Dr. Cooper agreed with the study findings that the earlier that a young person can get into medical care for their gender identity, the better chance there is to reduce the prevalence of serious mental health outcomes. “This also prevents the potential development of secondary sexual characteristics, decreasing the need for or amount of surgery in the future if desired,” he said.
“More research is needed to better understand the reasons why many youth don’t present to care until later in puberty. In addition, we need better research on interventions that are effective at reducing serious mental health events in transgender and gender diverse youth,” Dr. Cooper stated. “Another area that I would like to see researched is looking at the mental health of non-Caucasian youth. As the authors noted in their study, many clinics have a high percentage of patients presenting for care who identify as White or Caucasian, and we need to better understand why these other youth are not presenting for care.”
The study received no outside funding. Dr. Sorbara disclosed salary support from the Canadian Pediatric Endocrine Group fellowship program. Dr. de Vries had no financial conflicts to disclose. Dr. Cooper had no financial conflicts to disclose, and serves as a contributor to LGBTQ Youth Consult in Pediatric News.
SOURCES: Sorbara JC et al. Pediatrics. 2020 Sep 21. doi: 10.1542/peds.2019-3600; de Vries ALC et al. Pediatrics. 2020 Sep 21. doi: 10.1542/peds.2020-010611.
Gender-incongruent youth who present for gender-affirming medical care later in adolescence have higher rates of mental health problems than their younger counterparts, based on data from a review of 300 individuals.
“Puberty is a vulnerable time for youth with gender dysphoria because distress may intensify with the development of secondary sex characteristics corresponding to the assigned rather than the experienced gender,” wrote Julia C. Sorbara, MD, of the University of Toronto and the Hospital for Sick Children, also in Toronto, and colleagues.
Although gender-affirming medical care (GAMC) in the form of hormone blockers and/or gender-affirming hormones early in puberty can decrease in emotional and behavioral problems, many teens present later in puberty, and the relationship between pubertal stage at presentation for treatment and mental health has not been examined, they wrote.
In a study published in Pediatrics, the researchers reviewed data from youth with gender incongruence who were seen at a single center; 116 were younger than 15 years at presentation for GAMC and were defined as younger-presenting youth (YPY), and 184 patients aged 15 years and older were defined as older-presenting youth (OPY).
Overall, 78% of the youth reported at least one mental health problem at their initial visit. Significantly more OPY than YPY reported diagnosed depression (46% vs. 30%), self-harm (40% vs. 28%), suicidal thoughts (52% vs. 40%), suicide attempts (17% vs. 9%), and use of psychoactive medications (36% vs. 23%), all with P < .05.
In a multivariate analysis, patients in Tanner stages 4 and 5 were five times more likely to experience depressive disorders (odds ratio, 5.49) and four times as likely to experience depressive disorders (OR, 4.18) as those in earlier Tanner stages. Older age remained significantly associated with use of psychoactive medications (OR, 1.31), but not with anxiety or depression, the researchers wrote.
The YPY group were significantly younger at the age of recognizing gender incongruence, compared with the OPY group, with median ages at recognition of 5.8 years and 9 years, respectively, and younger patients came out about their gender identity at an average of 12 years, compared with 15 years for older patients.
The quantitative data are among the first to relate pubertal stage to mental health in gender-incongruent youth, “supporting clinical observations that pubertal development, menses, and erections are distressing to these youth and consistent with the beneficial role of pubertal suppression, even when used as monotherapy without gender-affirming hormones,” Dr. Sorbara and associates wrote.
The study findings were limited by several factors including the cross-sectional design and the collection of mental health data at only one time point and by the use of self-reports. However, the results suggest that “[gender-incongruent] youth who present to GAMC later in life are a particularly high-risk subset of a vulnerable population,” they noted. “Further study is required to better describe the mental health trajectories of transgender youth and determine if mental health status or age at initiation of GAMC is correlated with psychological well-being in adulthood.”
Don’t rush to puberty suppression in younger teens
To reduce the stress of puberty on gender-nonconforming youth, puberty suppression as “a reversible medical intervention” was introduced by Dutch clinicians in the early 2000s, Annelou L.C. de Vries, MD, PhD, of Amsterdam University Medical Center, wrote in an accompanying editorial.
“The aim of puberty suppression was to prevent the psychological suffering stemming from undesired physical changes when puberty starts and allowing the adolescent time to make plans regarding further transition or not,” Dr. de Vries said. “Following this rationale, younger age at the time of starting medical-affirming treatment (puberty suppression or hormones) would be expected to correlate with fewer psychological difficulties related to physical changes than older individuals,” which was confirmed in the current study.
However, clinicians should be cautious in offering puberty suppression at a younger age, in part because “despite the increased availability of gender-affirming medical interventions for younger ages in recent years, there has not been a proportional decline in older presenting youth with gender incongruence,” she said.
More data are needed on youth with postpuberty adolescent-onset transgender histories. The original Dutch studies on gender-affirming medical interventions note case histories describing “the complexities that may be associated with later-presenting transgender adolescents and describe that some eventually detransition,” Dr. de Vries explained.
Ultimately, prospective studies with longer follow-up data are needed to better inform clinicians in developing an individualized treatment plan for youth with gender incongruence, Dr. de Vries concluded.
Care barriers can include parents, access, insurance
The study authors describe the situation of gender-affirming medical care in teens perfectly, M. Brett Cooper, MD, of the University of Texas Southwestern Medical Center/Children’s Health Dallas, said in an interview.
Given a variety of factors that need further exploration, “many youth often don’t end up seeking gender-affirming medical care until puberty has progressed to near full maturity,” he said. “The findings from this study provide preliminary evidence to show that if we can identify these youth earlier in their gender journey, we might be able to impact adverse mental health outcomes in a positive way.”
Dr. Cooper said he was not surprised by the study findings. “They are similar to what I see in my clinic.
“Many of our patients often don’t present for medical care until around age 15 or older, similar to the findings of the study,” he added. “The majority of our patients have had a diagnosis of anxiety or depression at some point in their lifetime, including inpatient hospitalizations for their mental health.”
One of the most important barriers to care often can be parents or guardians, said Dr. Cooper. “Young people usually know their gender identity by about age 4-5 but parents may think that a gender-diverse identity could simply be a ‘phase.’ Other times, young people may hide their identity out of fear of a negative reaction from their parents. The distress around identity may become more pronounced once pubertal changes, such as breast and testicle development, begin to worsen their dysphoria.”
“Another barrier to care can be the inability to find a competent, gender-affirming provider,” Dr. Cooper said. “Most large United States cities have at least one gender-affirming clinic, but for those youth who grow up in smaller towns, it may be difficult to access these clinics. In addition, some clinics require a letter from a therapist stating that the young person is transgender before they can be seen for medical care. This creates an access barrier, as it may be difficult not just to find a therapist but one who has experience working with gender-diverse youth.”
Insurance coverage, including lack thereof, is yet another barrier to care for transgender youth, said Dr. Cooper. “While many insurance companies have begun to cover medications such as testosterone and estrogen for gender-affirming care, many still have exclusions on things like puberty blockers and surgical interventions.” These interventions can be lifesaving, but financially prohibitive for many families if not covered by insurance.
As for the value of early timing of gender-affirming care, Dr. Cooper agreed with the study findings that the earlier that a young person can get into medical care for their gender identity, the better chance there is to reduce the prevalence of serious mental health outcomes. “This also prevents the potential development of secondary sexual characteristics, decreasing the need for or amount of surgery in the future if desired,” he said.
“More research is needed to better understand the reasons why many youth don’t present to care until later in puberty. In addition, we need better research on interventions that are effective at reducing serious mental health events in transgender and gender diverse youth,” Dr. Cooper stated. “Another area that I would like to see researched is looking at the mental health of non-Caucasian youth. As the authors noted in their study, many clinics have a high percentage of patients presenting for care who identify as White or Caucasian, and we need to better understand why these other youth are not presenting for care.”
The study received no outside funding. Dr. Sorbara disclosed salary support from the Canadian Pediatric Endocrine Group fellowship program. Dr. de Vries had no financial conflicts to disclose. Dr. Cooper had no financial conflicts to disclose, and serves as a contributor to LGBTQ Youth Consult in Pediatric News.
SOURCES: Sorbara JC et al. Pediatrics. 2020 Sep 21. doi: 10.1542/peds.2019-3600; de Vries ALC et al. Pediatrics. 2020 Sep 21. doi: 10.1542/peds.2020-010611.
FROM PEDIATRICS
Teen affective disorders raise risk for midlife acute MI
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.

The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.
The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.
The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
FROM ESC CONGRESS 2020
A conversation on mental health and cancer
Editor’s Note: This transcript from the October 7 episode of Psychcast and the October 8 episode of Blood & Cancer has been edited for clarity.
David Henry, MD: Welcome to this episode of Blood And Cancer. I’m your host, Dr. David Henry, and I’m joined today by another host in the MDedge family, Dr. Lorenzo Norris, who is the host of MDedge Psychcast on MDedge.com or wherever you get your podcasts. He is associate dean of student affairs and administration at the George Washington School of Medicine in Washington, DC. Dr. Norris, thank you so much for taking the time to do this today.

Lorenzo Norris, MD: Dr. Henry, thank you so very much. It’s always great to participate with the MDedge family and do a collaborative podcast, so I’m really looking forward to it.
Dr. Henry: I know you wrote a really nice article on cognitive behavioral therapy (CBT) in breast cancer patients (Psychiatr Ann. 2011;41(9):439-42). So could you talk a bit about that -- what did you do, and what did you find using CBT for breast cancer patients?
Dr. Norris: CBT in a nutshell -- how you think influences greatly your emotions, which influences your behavior. Very simple and very powerful. With breast cancer, as an example, patients are dealing with a great deal of stress. They are literally fighting for their lives.

So there are going to be various thoughts associated with that...One of the uses of CBT when working with patients is to help them think about and work with adaptive thoughts that are going to help them effectively cope as well as problem solve. So for instance, in regard to breast cancer, one of the first things that you’re going to want to do is just to think about, one, helping the patient understand where they’re at, because it’s going to be a shock level type of thing.
Make sure that they don’t have unnecessary or problematic distortions, whether it’s about the treatment, the prognosis, or what they themselves are capable of. And those three areas become actually rather important. Now with a diagnosis of cancer, a number of patients are going to have a period of adjustment. One of the first things that we’re thinking about is where do our patients fit along a continuum of distress.
They could be having an adjustment disorder or none whatsoever, just normal mood or an adjustment disorder with depressed mood. They could actually be in the midst of a unipolar depression. They could have a mood disorder secondary to the effects of the cancer itself. That would be more applicable to brain cancer or pancreatic cancer. Or they could have another category of mood disorder, such as a substance abuse mood disorder. But CBT is a very useful intervention, regardless of whether a person is having a normal syndrome of distress with a very challenging diagnosis or if they’re suffering from full-on psychiatric symptomatology such as a major depressive disorder.
Dr. Henry: In my practice I see a couple of things relevant to that discussion. I’ve always felt fear of the unknown is the worst fear, and fear of the known really helps you.
Medical students say to me sometimes, you just told this patient the same thing three times. They asked you the same thing three times. Well, I say, watch their eyes. Because as their eyes drift off, they’re thinking about their family, their financials, life and death. We’ve got to bring them on back because they’re afraid and not focused. I, in my amateur way, try and bring them back to the discussion to focus on what’s going on, what’s known, and how will we address it.
Interestingly, very rarely do I get, “So how long am I going to live?” You know, you see that in movies and Hollywood, and the doctor says six months, and it’s right on the button. I rarely get that question, because I think they’re afraid of the answer. If I do, I say, “Well, therapy works. You’ll do better and live on. If therapy doesn’t work, we got a problem, and it can be mortal”-- so they wouldn’t believe me if I just tiptoed around that-- but we have a second through-line. “I can always help you, win or lose.” So is that the similar way you approach those kinds of conversations?
Dr. Norris: Absolutely, Dr. Henry. I love how you described it in regard to that willingness, and I love how you described it to the medical students. A lot of being a physician or a healer is just that willingness to stay in a place with a patient and just repeat back the same thing in a different way until we make sure that they’ve heard it and we’ve heard it. And I think that’s very important.
But to get back to that “you have six months to live” type of thing. I actually find that patients actually do-- in my experience, do not immediately go there.
Dr. Henry: Agree. Agree.
Dr. Norris: There is the concept of...I wouldn’t even call that denial. But just that ability to focus on what is immediate. There are some aspects of protective denial. People intrinsically know how much information they need to focus on and deal with at the moment. Why focus on something that is outside of their control? Actually, when I see people jumping to conclusions like that, or catastrophizing, that’s a cognitive distortion. Black and white thinking is another cognitive distortion, as well as maladaptive denial, where you just kind of deny reality. Not discussing prognosis immediately--I would consider that focusing. Denying that you have cancer--that’s problematic denial to say the least.
Dr. Henry: Whole different problem.
Dr. Norris: I agree with you. I find that patients do not immediately jump to that in terms of prognosis or things of that nature. But their oncologist can do a great deal and actually level the distress just by doing what you did right there. Speaking with your patient three or four more times, repeating the same information, not using jargon, but also not sugarcoating anything, but giving what’s needed to get to the next step. And that’s probably what I think is one of the things that I focus on in therapy a lot. Let’s level the distress. Let’s focus on what’s needed to get to the next step and let’s not do anything that, if you’re not in a unipolar depression or major depression, could further exacerbate you developing it. So let’s stay focused on the treatment. And I find that a number of patients rally behind that.
Dr. Henry: Very well put, very well discussed. And we will have on our web page, the reference for the CBT article.
Dr. Norris: If you’re referring to the reference that was in an issue of “Psychiatric Annals,” that was a number of years ago. Because the actual reference you’re referring to (Psychiatr Ann. 2011;41(9):439-42) was part of a themed issue that I guest edited. It was called Cancer and Depression, and all the articles in there were focused on cancer. At that time, I was actually working with the American Cancer Society in regards to developing cancer survivorship guidelines.
Dr. Henry: So as we record this, of course, it’s the COVID era, and we’re taking care of patients with cancer who have to deal with the cancer and deal with themselves, family, and what’s happening in the world. I have found much more anxiety, much more depression than I’m used to seeing. Because they’re coming to see me, am I going to give it to them? Coming into the office, will they get it getting upstairs in our treatment area? So what are you seeing? And how are you handling taking care of patients with cancer in this time?
Dr. Norris: I hope everyone out there that’s listening is safe and well, and I hope your families are safe and well. The COVID pandemic has really unleashed something on the world as well as society that people have not seen basically since the Spanish Flu. But whether you’ve been through the AIDS epidemic or anything like that, you’ve never seen this.
So what are we seeing out there? We’re seeing that, definitively, more anxiety and depression across the board. We know that with the data now that’s been coming out that we are seeing an increase in anxiety and depression in the general population. The data in regard to cancer patients is limited, but we can start with what we know, and from that we can extrapolate and say that we would expect to see an increase in depression and anxiety.
We know that in cancer patients, depending on what study you look at, there’s going to be anywhere from a 0% to 38% prevalence of major depressive disorder and a 0% to 58% prevalence of any depressive spectrum disorder. Depending on the study, it’s going to level out somewhere around a 15% to 22% prevalence rate, regardless of cancer, of depressive symptoms. That’s usually across other medical conditions. Now the general rate of depression in a population is 6.6% with a 12-month prevalence. And the lifetime is 16.6%. So the take-home point is, with cancer, you have a two to four times greater risk of developing depression, whether you had it or not.
There’s a couple of reasons why we might be seeing an increase in depression and anxiety in this COVID era. One is isolation and lack of control. Due to quarantining and social isolation, our patients’ relationships with their oncologists can absolutely positively be disrupted. That is a very anxiety- and depression-inducing situation. One of the themes that came out of the survivorship literature when patients actually transition out of active treatment, one of the most distressing things for them, was the loss of their treatment team and their oncology provider. It almost can’t be said or overestimated the impact that the treatment team and a primary oncologist has on a patient’s life. I just wanted to make sure the audience realized that.
For your patients, you really, really, really are exceedingly important to them, as you are very much aware of that, but to levels you may or may not fully appreciate. So one of the things that COVID does, not only is it this deadly virus that our patients have to worry about in terms of it taking their life, as well as delaying treatment. It separates them from the people that have become paramount in their life, which for a number of folks is their oncology treatment team.
So when we take all of that into account, particularly isolation and loneliness, fragmentation, as well as any type of economic difficulties, that can be resulting due to the COVID-19 pandemic, you would absolutely suspect and predict that anxiety and depression in our patients would definitively increase. And a big part of that is them not being able to connect, certainly with others, but it’s [also] definitely their treatment team.
Dr. Henry: It’s been a stress on all of us, our caregivers as well as care receivers. And then back to putting on our regular oncology/hematology hats, seeing patients when COVID isn’t around. I remember a study long ago, maybe back when I was in training. I think it came out of Memorial Sloan Kettering.
It’s that fully 50% of our active advanced cancer patients are clinically depressed to the point where we should be considering intervention/medication. And if that’s still true, I’m a terrible doctor, because I am not recognizing and prescribing for that. Can you comment on how much depression and anxiety are in the average advanced cancer patient? And should we go after that in treatment?
Dr. Norris: When we’re talking about the advanced cancer patient, I definitely feel as though we should be screening as well as treating. Now as I mentioned before, in regards to the prevalence of depression or depressive spectrum disorders, it can be anywhere from 0% to 58%. In advanced stage cancer, you certainly are going to be thinking that risk is going to be high, probably anywhere from 25% to 33% or maybe even up to 50% of our patients can be suffering from symptoms of depression.
So when we’re talking about treating or referring, a big question you want to ask yourself is, what screening instrument are you using for depression? Some people argue just simply asking a patient whether they’re depressed or not would be perfectly acceptable. That is provided that you have enough time to do it, and you have enough time to follow up and you are pretty standardized with your approach.
However, clinicians just miss it. That’s well established and evidence-based. Clinicians just miss it. What I would recommend that folks consider doing is using the Patient Health Questionnaire, the two-question version called the PHQ-2 and the PHQ-9, the nine-question version. The PHQ-2 is actually a very good screening tool in regards to detecting depression. It has very good sensitivity and specificity.
And that’s going to allow you to actually think about or to screen for patients that you’re going to need to refer for treatment. So if you have a patient with advanced cancer, as an example, and you use the PHQ-2 or PHQ-9, then that’s going to give you a very evidence-based avenue in which to refer for treatment. Now you may be asking yourself, maybe I don’t want to use a PHQ-2 or 9, or I’m in a community practice or a private practice, I just don’t have the bandwidth to process this.
So I want to go off of just my own patient interaction. What are things that I can cue on?
With a patient with cancer, there’s going to be roughly four things that we’re considering in terms of depressive spectrum disorders: Adjustment disorder with depressed mood, major depression, a mood disorder due to cancer itself, or substance-induced mood disorder.
For our audience I want you to concentrate on right now on adjustment disorder with depressed mood and major depression. Now when you look at the evidence, there are roughly nine things that some people like to think about in regard to depressive symptoms to key on. For all of us as health practitioners, these are the things I would like for you to focus on in particular:
1. Non-adherence with treatment for cancer.
2. Impairment of their social or occupational function.
3. Your patient becomes demoralized when they start to lose a little bit of confidence or hope.
When you have those three things, or any one of them, in an advanced stage of cancer, with or without a PHQ screening, you need to really think about how you’re going to refer this patient for treatment. So we can break this down into three different types of interventions. One, the biggest thing, is just to ask, “How are you feeling? What is your mood? Are you suffering from a clinical depression?” You know, take a little bit of inspiration from Dr. Henry. Just give it to people straight and just ask. That’s the biggest thing people don’t do. They don’t ask.
The next thing, if you want to use an evidence-based scale, use a PHQ-2...You would have to follow up, but you-- rather you’re practicing solo or in a group practice or whether you have, your nurse or PA -- they generally assist with that.
And then the third thing is, when you’re interacting with the patient, look for those three things that I talked about: Non-adherence with treatment, impairment of social or occupational function, and then demoralization.
And then the final thing I want to focus on, because you can’t talk about depression without talking about suicide or really significant distress. Obviously, you can ask and you should ask about suicide if that is in your wheelhouse, but to be perfectly frank, most oncologists are not going to-- or most people outside of psychiatrists aren’t going to necessarily just routinely ask that question.
But here’s what I would say. It’s an old one but it’s a good one: Listen to that little voice. Listen to that little voice, all right? Depending on the evidence that you look at, a lot of detecting suicide can be aided by a clinician listening to their own gut instincts. What I mean by that is, you feel a sense of distress. You feel a sense of lack of connection. You find yourself [saying], “Wait a minute, why do I want to call that patient and checkup? Why do I want to reach out?”
When you start to feel like this, you need to listen. More importantly, you need to stop and then you need to make sure that that patient has a referral in place.
Dr. Henry: So they’re just tuning out so badly, you’re really losing the connection, and that’s when your little voice talks to you.
Dr. Norris: Exactly. Well said, Dr. Henry. Well said.
Dr. Henry: In my long career, drug abuse, narcotics, and suicide have been extremely rare. I can think of one patient who was a drug abuser with cancer, or it turned out she was a drug abuser before she had cancer. And then suicide, really quite rare. I’m sure they occur, and we have to watch for them, as you say, but fortunately I’ve not seen that so much. Thanks to your comments, I want to be sure I’m watching and looking.
And the PHQ-2 and -9, I’m sure, with so many of us having electronic medical records, you can simply Google while you’re talking to the patient for those two questionnaires and say, oh, you know, how about you answer these two questions, these nine questions, and see how many points the patient gets and worry about referral or even medication yourself if it looks like an antidepressant is in order.
Dr. Norris: Absolutely. Absolutely.
Dr. Henry: Well, I think we’ve covered an awful lot of ground. I really want to thank you. Any get-away thoughts? We worry about the cognitive behavioral therapy. We worry about it, and we should listen to it and do it.
Practicing in the COVID era is stressful for all of us. I told Dr. Norris at the outset, if I broke down and started baring my soul, he wouldn’t be surprised. Fortunately, I’ve kept it together while talking to a psychiatrist.
And finally watch for clinically significant depression, either by your own questions, which you’ve outlined, or the PHQ-2 and -9.
Really appreciate your thoughts today. Lorenzo, thanks so much for taking the time to do this today.
To hear the entire conversation, go to mdedge.com/podcasts or listen wherever you find your podcasts. David Henry, MD, is a clinical professor of medicine at the University of Pennsylvania and vice chairman of the department of medicine at Pennsylvania Hospital in Philadelphia. He is editor in chief of MDedge Hematology-Oncology and the host of the Blood & Cancer podcast. Dr. Henry reported being on the advisory board for Amgen, AMAG Pharmaceuticals, and Pharmacosmos. He reported institutional funding from the National Institutes of Health and FibroGen.
Lorenzo Norris, MD, is host of the MDedge Psychcast, editor in chief of MDedge Psychiatry, and assistant professor of psychiatry and behavioral sciences at George Washington University, Washington. He also serves as assistant dean of student affairs at the university, and medical director of psychiatric and behavioral sciences at GWU Hospital. Dr. Lorenzo Norris has no conflicts.
Editor’s Note: This transcript from the October 7 episode of Psychcast and the October 8 episode of Blood & Cancer has been edited for clarity.
David Henry, MD: Welcome to this episode of Blood And Cancer. I’m your host, Dr. David Henry, and I’m joined today by another host in the MDedge family, Dr. Lorenzo Norris, who is the host of MDedge Psychcast on MDedge.com or wherever you get your podcasts. He is associate dean of student affairs and administration at the George Washington School of Medicine in Washington, DC. Dr. Norris, thank you so much for taking the time to do this today.
Lorenzo Norris, MD: Dr. Henry, thank you so very much. It’s always great to participate with the MDedge family and do a collaborative podcast, so I’m really looking forward to it.
Dr. Henry: I know you wrote a really nice article on cognitive behavioral therapy (CBT) in breast cancer patients (Psychiatr Ann. 2011;41(9):439-42). So could you talk a bit about that -- what did you do, and what did you find using CBT for breast cancer patients?
Dr. Norris: CBT in a nutshell -- how you think influences greatly your emotions, which influences your behavior. Very simple and very powerful. With breast cancer, as an example, patients are dealing with a great deal of stress. They are literally fighting for their lives.
So there are going to be various thoughts associated with that...One of the uses of CBT when working with patients is to help them think about and work with adaptive thoughts that are going to help them effectively cope as well as problem solve. So for instance, in regard to breast cancer, one of the first things that you’re going to want to do is just to think about, one, helping the patient understand where they’re at, because it’s going to be a shock level type of thing.
Make sure that they don’t have unnecessary or problematic distortions, whether it’s about the treatment, the prognosis, or what they themselves are capable of. And those three areas become actually rather important. Now with a diagnosis of cancer, a number of patients are going to have a period of adjustment. One of the first things that we’re thinking about is where do our patients fit along a continuum of distress.
They could be having an adjustment disorder or none whatsoever, just normal mood or an adjustment disorder with depressed mood. They could actually be in the midst of a unipolar depression. They could have a mood disorder secondary to the effects of the cancer itself. That would be more applicable to brain cancer or pancreatic cancer. Or they could have another category of mood disorder, such as a substance abuse mood disorder. But CBT is a very useful intervention, regardless of whether a person is having a normal syndrome of distress with a very challenging diagnosis or if they’re suffering from full-on psychiatric symptomatology such as a major depressive disorder.
Dr. Henry: In my practice I see a couple of things relevant to that discussion. I’ve always felt fear of the unknown is the worst fear, and fear of the known really helps you.
Medical students say to me sometimes, you just told this patient the same thing three times. They asked you the same thing three times. Well, I say, watch their eyes. Because as their eyes drift off, they’re thinking about their family, their financials, life and death. We’ve got to bring them on back because they’re afraid and not focused. I, in my amateur way, try and bring them back to the discussion to focus on what’s going on, what’s known, and how will we address it.
Interestingly, very rarely do I get, “So how long am I going to live?” You know, you see that in movies and Hollywood, and the doctor says six months, and it’s right on the button. I rarely get that question, because I think they’re afraid of the answer. If I do, I say, “Well, therapy works. You’ll do better and live on. If therapy doesn’t work, we got a problem, and it can be mortal”-- so they wouldn’t believe me if I just tiptoed around that-- but we have a second through-line. “I can always help you, win or lose.” So is that the similar way you approach those kinds of conversations?
Dr. Norris: Absolutely, Dr. Henry. I love how you described it in regard to that willingness, and I love how you described it to the medical students. A lot of being a physician or a healer is just that willingness to stay in a place with a patient and just repeat back the same thing in a different way until we make sure that they’ve heard it and we’ve heard it. And I think that’s very important.
But to get back to that “you have six months to live” type of thing. I actually find that patients actually do-- in my experience, do not immediately go there.
Dr. Henry: Agree. Agree.
Dr. Norris: There is the concept of...I wouldn’t even call that denial. But just that ability to focus on what is immediate. There are some aspects of protective denial. People intrinsically know how much information they need to focus on and deal with at the moment. Why focus on something that is outside of their control? Actually, when I see people jumping to conclusions like that, or catastrophizing, that’s a cognitive distortion. Black and white thinking is another cognitive distortion, as well as maladaptive denial, where you just kind of deny reality. Not discussing prognosis immediately--I would consider that focusing. Denying that you have cancer--that’s problematic denial to say the least.
Dr. Henry: Whole different problem.
Dr. Norris: I agree with you. I find that patients do not immediately jump to that in terms of prognosis or things of that nature. But their oncologist can do a great deal and actually level the distress just by doing what you did right there. Speaking with your patient three or four more times, repeating the same information, not using jargon, but also not sugarcoating anything, but giving what’s needed to get to the next step. And that’s probably what I think is one of the things that I focus on in therapy a lot. Let’s level the distress. Let’s focus on what’s needed to get to the next step and let’s not do anything that, if you’re not in a unipolar depression or major depression, could further exacerbate you developing it. So let’s stay focused on the treatment. And I find that a number of patients rally behind that.
Dr. Henry: Very well put, very well discussed. And we will have on our web page, the reference for the CBT article.
Dr. Norris: If you’re referring to the reference that was in an issue of “Psychiatric Annals,” that was a number of years ago. Because the actual reference you’re referring to (Psychiatr Ann. 2011;41(9):439-42) was part of a themed issue that I guest edited. It was called Cancer and Depression, and all the articles in there were focused on cancer. At that time, I was actually working with the American Cancer Society in regards to developing cancer survivorship guidelines.
Dr. Henry: So as we record this, of course, it’s the COVID era, and we’re taking care of patients with cancer who have to deal with the cancer and deal with themselves, family, and what’s happening in the world. I have found much more anxiety, much more depression than I’m used to seeing. Because they’re coming to see me, am I going to give it to them? Coming into the office, will they get it getting upstairs in our treatment area? So what are you seeing? And how are you handling taking care of patients with cancer in this time?
Dr. Norris: I hope everyone out there that’s listening is safe and well, and I hope your families are safe and well. The COVID pandemic has really unleashed something on the world as well as society that people have not seen basically since the Spanish Flu. But whether you’ve been through the AIDS epidemic or anything like that, you’ve never seen this.
So what are we seeing out there? We’re seeing that, definitively, more anxiety and depression across the board. We know that with the data now that’s been coming out that we are seeing an increase in anxiety and depression in the general population. The data in regard to cancer patients is limited, but we can start with what we know, and from that we can extrapolate and say that we would expect to see an increase in depression and anxiety.
We know that in cancer patients, depending on what study you look at, there’s going to be anywhere from a 0% to 38% prevalence of major depressive disorder and a 0% to 58% prevalence of any depressive spectrum disorder. Depending on the study, it’s going to level out somewhere around a 15% to 22% prevalence rate, regardless of cancer, of depressive symptoms. That’s usually across other medical conditions. Now the general rate of depression in a population is 6.6% with a 12-month prevalence. And the lifetime is 16.6%. So the take-home point is, with cancer, you have a two to four times greater risk of developing depression, whether you had it or not.
There’s a couple of reasons why we might be seeing an increase in depression and anxiety in this COVID era. One is isolation and lack of control. Due to quarantining and social isolation, our patients’ relationships with their oncologists can absolutely positively be disrupted. That is a very anxiety- and depression-inducing situation. One of the themes that came out of the survivorship literature when patients actually transition out of active treatment, one of the most distressing things for them, was the loss of their treatment team and their oncology provider. It almost can’t be said or overestimated the impact that the treatment team and a primary oncologist has on a patient’s life. I just wanted to make sure the audience realized that.
For your patients, you really, really, really are exceedingly important to them, as you are very much aware of that, but to levels you may or may not fully appreciate. So one of the things that COVID does, not only is it this deadly virus that our patients have to worry about in terms of it taking their life, as well as delaying treatment. It separates them from the people that have become paramount in their life, which for a number of folks is their oncology treatment team.
So when we take all of that into account, particularly isolation and loneliness, fragmentation, as well as any type of economic difficulties, that can be resulting due to the COVID-19 pandemic, you would absolutely suspect and predict that anxiety and depression in our patients would definitively increase. And a big part of that is them not being able to connect, certainly with others, but it’s [also] definitely their treatment team.
Dr. Henry: It’s been a stress on all of us, our caregivers as well as care receivers. And then back to putting on our regular oncology/hematology hats, seeing patients when COVID isn’t around. I remember a study long ago, maybe back when I was in training. I think it came out of Memorial Sloan Kettering.
It’s that fully 50% of our active advanced cancer patients are clinically depressed to the point where we should be considering intervention/medication. And if that’s still true, I’m a terrible doctor, because I am not recognizing and prescribing for that. Can you comment on how much depression and anxiety are in the average advanced cancer patient? And should we go after that in treatment?
Dr. Norris: When we’re talking about the advanced cancer patient, I definitely feel as though we should be screening as well as treating. Now as I mentioned before, in regards to the prevalence of depression or depressive spectrum disorders, it can be anywhere from 0% to 58%. In advanced stage cancer, you certainly are going to be thinking that risk is going to be high, probably anywhere from 25% to 33% or maybe even up to 50% of our patients can be suffering from symptoms of depression.
So when we’re talking about treating or referring, a big question you want to ask yourself is, what screening instrument are you using for depression? Some people argue just simply asking a patient whether they’re depressed or not would be perfectly acceptable. That is provided that you have enough time to do it, and you have enough time to follow up and you are pretty standardized with your approach.
However, clinicians just miss it. That’s well established and evidence-based. Clinicians just miss it. What I would recommend that folks consider doing is using the Patient Health Questionnaire, the two-question version called the PHQ-2 and the PHQ-9, the nine-question version. The PHQ-2 is actually a very good screening tool in regards to detecting depression. It has very good sensitivity and specificity.
And that’s going to allow you to actually think about or to screen for patients that you’re going to need to refer for treatment. So if you have a patient with advanced cancer, as an example, and you use the PHQ-2 or PHQ-9, then that’s going to give you a very evidence-based avenue in which to refer for treatment. Now you may be asking yourself, maybe I don’t want to use a PHQ-2 or 9, or I’m in a community practice or a private practice, I just don’t have the bandwidth to process this.
So I want to go off of just my own patient interaction. What are things that I can cue on?
With a patient with cancer, there’s going to be roughly four things that we’re considering in terms of depressive spectrum disorders: Adjustment disorder with depressed mood, major depression, a mood disorder due to cancer itself, or substance-induced mood disorder.
For our audience I want you to concentrate on right now on adjustment disorder with depressed mood and major depression. Now when you look at the evidence, there are roughly nine things that some people like to think about in regard to depressive symptoms to key on. For all of us as health practitioners, these are the things I would like for you to focus on in particular:
1. Non-adherence with treatment for cancer.
2. Impairment of their social or occupational function.
3. Your patient becomes demoralized when they start to lose a little bit of confidence or hope.
When you have those three things, or any one of them, in an advanced stage of cancer, with or without a PHQ screening, you need to really think about how you’re going to refer this patient for treatment. So we can break this down into three different types of interventions. One, the biggest thing, is just to ask, “How are you feeling? What is your mood? Are you suffering from a clinical depression?” You know, take a little bit of inspiration from Dr. Henry. Just give it to people straight and just ask. That’s the biggest thing people don’t do. They don’t ask.
The next thing, if you want to use an evidence-based scale, use a PHQ-2...You would have to follow up, but you-- rather you’re practicing solo or in a group practice or whether you have, your nurse or PA -- they generally assist with that.
And then the third thing is, when you’re interacting with the patient, look for those three things that I talked about: Non-adherence with treatment, impairment of social or occupational function, and then demoralization.
And then the final thing I want to focus on, because you can’t talk about depression without talking about suicide or really significant distress. Obviously, you can ask and you should ask about suicide if that is in your wheelhouse, but to be perfectly frank, most oncologists are not going to-- or most people outside of psychiatrists aren’t going to necessarily just routinely ask that question.
But here’s what I would say. It’s an old one but it’s a good one: Listen to that little voice. Listen to that little voice, all right? Depending on the evidence that you look at, a lot of detecting suicide can be aided by a clinician listening to their own gut instincts. What I mean by that is, you feel a sense of distress. You feel a sense of lack of connection. You find yourself [saying], “Wait a minute, why do I want to call that patient and checkup? Why do I want to reach out?”
When you start to feel like this, you need to listen. More importantly, you need to stop and then you need to make sure that that patient has a referral in place.
Dr. Henry: So they’re just tuning out so badly, you’re really losing the connection, and that’s when your little voice talks to you.
Dr. Norris: Exactly. Well said, Dr. Henry. Well said.
Dr. Henry: In my long career, drug abuse, narcotics, and suicide have been extremely rare. I can think of one patient who was a drug abuser with cancer, or it turned out she was a drug abuser before she had cancer. And then suicide, really quite rare. I’m sure they occur, and we have to watch for them, as you say, but fortunately I’ve not seen that so much. Thanks to your comments, I want to be sure I’m watching and looking.
And the PHQ-2 and -9, I’m sure, with so many of us having electronic medical records, you can simply Google while you’re talking to the patient for those two questionnaires and say, oh, you know, how about you answer these two questions, these nine questions, and see how many points the patient gets and worry about referral or even medication yourself if it looks like an antidepressant is in order.
Dr. Norris: Absolutely. Absolutely.
Dr. Henry: Well, I think we’ve covered an awful lot of ground. I really want to thank you. Any get-away thoughts? We worry about the cognitive behavioral therapy. We worry about it, and we should listen to it and do it.
Practicing in the COVID era is stressful for all of us. I told Dr. Norris at the outset, if I broke down and started baring my soul, he wouldn’t be surprised. Fortunately, I’ve kept it together while talking to a psychiatrist.
And finally watch for clinically significant depression, either by your own questions, which you’ve outlined, or the PHQ-2 and -9.
Really appreciate your thoughts today. Lorenzo, thanks so much for taking the time to do this today.
To hear the entire conversation, go to mdedge.com/podcasts or listen wherever you find your podcasts. David Henry, MD, is a clinical professor of medicine at the University of Pennsylvania and vice chairman of the department of medicine at Pennsylvania Hospital in Philadelphia. He is editor in chief of MDedge Hematology-Oncology and the host of the Blood & Cancer podcast. Dr. Henry reported being on the advisory board for Amgen, AMAG Pharmaceuticals, and Pharmacosmos. He reported institutional funding from the National Institutes of Health and FibroGen.
Lorenzo Norris, MD, is host of the MDedge Psychcast, editor in chief of MDedge Psychiatry, and assistant professor of psychiatry and behavioral sciences at George Washington University, Washington. He also serves as assistant dean of student affairs at the university, and medical director of psychiatric and behavioral sciences at GWU Hospital. Dr. Lorenzo Norris has no conflicts.
Editor’s Note: This transcript from the October 7 episode of Psychcast and the October 8 episode of Blood & Cancer has been edited for clarity.
David Henry, MD: Welcome to this episode of Blood And Cancer. I’m your host, Dr. David Henry, and I’m joined today by another host in the MDedge family, Dr. Lorenzo Norris, who is the host of MDedge Psychcast on MDedge.com or wherever you get your podcasts. He is associate dean of student affairs and administration at the George Washington School of Medicine in Washington, DC. Dr. Norris, thank you so much for taking the time to do this today.
Lorenzo Norris, MD: Dr. Henry, thank you so very much. It’s always great to participate with the MDedge family and do a collaborative podcast, so I’m really looking forward to it.
Dr. Henry: I know you wrote a really nice article on cognitive behavioral therapy (CBT) in breast cancer patients (Psychiatr Ann. 2011;41(9):439-42). So could you talk a bit about that -- what did you do, and what did you find using CBT for breast cancer patients?
Dr. Norris: CBT in a nutshell -- how you think influences greatly your emotions, which influences your behavior. Very simple and very powerful. With breast cancer, as an example, patients are dealing with a great deal of stress. They are literally fighting for their lives.
So there are going to be various thoughts associated with that...One of the uses of CBT when working with patients is to help them think about and work with adaptive thoughts that are going to help them effectively cope as well as problem solve. So for instance, in regard to breast cancer, one of the first things that you’re going to want to do is just to think about, one, helping the patient understand where they’re at, because it’s going to be a shock level type of thing.
Make sure that they don’t have unnecessary or problematic distortions, whether it’s about the treatment, the prognosis, or what they themselves are capable of. And those three areas become actually rather important. Now with a diagnosis of cancer, a number of patients are going to have a period of adjustment. One of the first things that we’re thinking about is where do our patients fit along a continuum of distress.
They could be having an adjustment disorder or none whatsoever, just normal mood or an adjustment disorder with depressed mood. They could actually be in the midst of a unipolar depression. They could have a mood disorder secondary to the effects of the cancer itself. That would be more applicable to brain cancer or pancreatic cancer. Or they could have another category of mood disorder, such as a substance abuse mood disorder. But CBT is a very useful intervention, regardless of whether a person is having a normal syndrome of distress with a very challenging diagnosis or if they’re suffering from full-on psychiatric symptomatology such as a major depressive disorder.
Dr. Henry: In my practice I see a couple of things relevant to that discussion. I’ve always felt fear of the unknown is the worst fear, and fear of the known really helps you.
Medical students say to me sometimes, you just told this patient the same thing three times. They asked you the same thing three times. Well, I say, watch their eyes. Because as their eyes drift off, they’re thinking about their family, their financials, life and death. We’ve got to bring them on back because they’re afraid and not focused. I, in my amateur way, try and bring them back to the discussion to focus on what’s going on, what’s known, and how will we address it.
Interestingly, very rarely do I get, “So how long am I going to live?” You know, you see that in movies and Hollywood, and the doctor says six months, and it’s right on the button. I rarely get that question, because I think they’re afraid of the answer. If I do, I say, “Well, therapy works. You’ll do better and live on. If therapy doesn’t work, we got a problem, and it can be mortal”-- so they wouldn’t believe me if I just tiptoed around that-- but we have a second through-line. “I can always help you, win or lose.” So is that the similar way you approach those kinds of conversations?
Dr. Norris: Absolutely, Dr. Henry. I love how you described it in regard to that willingness, and I love how you described it to the medical students. A lot of being a physician or a healer is just that willingness to stay in a place with a patient and just repeat back the same thing in a different way until we make sure that they’ve heard it and we’ve heard it. And I think that’s very important.
But to get back to that “you have six months to live” type of thing. I actually find that patients actually do-- in my experience, do not immediately go there.
Dr. Henry: Agree. Agree.
Dr. Norris: There is the concept of...I wouldn’t even call that denial. But just that ability to focus on what is immediate. There are some aspects of protective denial. People intrinsically know how much information they need to focus on and deal with at the moment. Why focus on something that is outside of their control? Actually, when I see people jumping to conclusions like that, or catastrophizing, that’s a cognitive distortion. Black and white thinking is another cognitive distortion, as well as maladaptive denial, where you just kind of deny reality. Not discussing prognosis immediately--I would consider that focusing. Denying that you have cancer--that’s problematic denial to say the least.
Dr. Henry: Whole different problem.
Dr. Norris: I agree with you. I find that patients do not immediately jump to that in terms of prognosis or things of that nature. But their oncologist can do a great deal and actually level the distress just by doing what you did right there. Speaking with your patient three or four more times, repeating the same information, not using jargon, but also not sugarcoating anything, but giving what’s needed to get to the next step. And that’s probably what I think is one of the things that I focus on in therapy a lot. Let’s level the distress. Let’s focus on what’s needed to get to the next step and let’s not do anything that, if you’re not in a unipolar depression or major depression, could further exacerbate you developing it. So let’s stay focused on the treatment. And I find that a number of patients rally behind that.
Dr. Henry: Very well put, very well discussed. And we will have on our web page, the reference for the CBT article.
Dr. Norris: If you’re referring to the reference that was in an issue of “Psychiatric Annals,” that was a number of years ago. Because the actual reference you’re referring to (Psychiatr Ann. 2011;41(9):439-42) was part of a themed issue that I guest edited. It was called Cancer and Depression, and all the articles in there were focused on cancer. At that time, I was actually working with the American Cancer Society in regards to developing cancer survivorship guidelines.
Dr. Henry: So as we record this, of course, it’s the COVID era, and we’re taking care of patients with cancer who have to deal with the cancer and deal with themselves, family, and what’s happening in the world. I have found much more anxiety, much more depression than I’m used to seeing. Because they’re coming to see me, am I going to give it to them? Coming into the office, will they get it getting upstairs in our treatment area? So what are you seeing? And how are you handling taking care of patients with cancer in this time?
Dr. Norris: I hope everyone out there that’s listening is safe and well, and I hope your families are safe and well. The COVID pandemic has really unleashed something on the world as well as society that people have not seen basically since the Spanish Flu. But whether you’ve been through the AIDS epidemic or anything like that, you’ve never seen this.
So what are we seeing out there? We’re seeing that, definitively, more anxiety and depression across the board. We know that with the data now that’s been coming out that we are seeing an increase in anxiety and depression in the general population. The data in regard to cancer patients is limited, but we can start with what we know, and from that we can extrapolate and say that we would expect to see an increase in depression and anxiety.
We know that in cancer patients, depending on what study you look at, there’s going to be anywhere from a 0% to 38% prevalence of major depressive disorder and a 0% to 58% prevalence of any depressive spectrum disorder. Depending on the study, it’s going to level out somewhere around a 15% to 22% prevalence rate, regardless of cancer, of depressive symptoms. That’s usually across other medical conditions. Now the general rate of depression in a population is 6.6% with a 12-month prevalence. And the lifetime is 16.6%. So the take-home point is, with cancer, you have a two to four times greater risk of developing depression, whether you had it or not.
There’s a couple of reasons why we might be seeing an increase in depression and anxiety in this COVID era. One is isolation and lack of control. Due to quarantining and social isolation, our patients’ relationships with their oncologists can absolutely positively be disrupted. That is a very anxiety- and depression-inducing situation. One of the themes that came out of the survivorship literature when patients actually transition out of active treatment, one of the most distressing things for them, was the loss of their treatment team and their oncology provider. It almost can’t be said or overestimated the impact that the treatment team and a primary oncologist has on a patient’s life. I just wanted to make sure the audience realized that.
For your patients, you really, really, really are exceedingly important to them, as you are very much aware of that, but to levels you may or may not fully appreciate. So one of the things that COVID does, not only is it this deadly virus that our patients have to worry about in terms of it taking their life, as well as delaying treatment. It separates them from the people that have become paramount in their life, which for a number of folks is their oncology treatment team.
So when we take all of that into account, particularly isolation and loneliness, fragmentation, as well as any type of economic difficulties, that can be resulting due to the COVID-19 pandemic, you would absolutely suspect and predict that anxiety and depression in our patients would definitively increase. And a big part of that is them not being able to connect, certainly with others, but it’s [also] definitely their treatment team.
Dr. Henry: It’s been a stress on all of us, our caregivers as well as care receivers. And then back to putting on our regular oncology/hematology hats, seeing patients when COVID isn’t around. I remember a study long ago, maybe back when I was in training. I think it came out of Memorial Sloan Kettering.
It’s that fully 50% of our active advanced cancer patients are clinically depressed to the point where we should be considering intervention/medication. And if that’s still true, I’m a terrible doctor, because I am not recognizing and prescribing for that. Can you comment on how much depression and anxiety are in the average advanced cancer patient? And should we go after that in treatment?
Dr. Norris: When we’re talking about the advanced cancer patient, I definitely feel as though we should be screening as well as treating. Now as I mentioned before, in regards to the prevalence of depression or depressive spectrum disorders, it can be anywhere from 0% to 58%. In advanced stage cancer, you certainly are going to be thinking that risk is going to be high, probably anywhere from 25% to 33% or maybe even up to 50% of our patients can be suffering from symptoms of depression.
So when we’re talking about treating or referring, a big question you want to ask yourself is, what screening instrument are you using for depression? Some people argue just simply asking a patient whether they’re depressed or not would be perfectly acceptable. That is provided that you have enough time to do it, and you have enough time to follow up and you are pretty standardized with your approach.
However, clinicians just miss it. That’s well established and evidence-based. Clinicians just miss it. What I would recommend that folks consider doing is using the Patient Health Questionnaire, the two-question version called the PHQ-2 and the PHQ-9, the nine-question version. The PHQ-2 is actually a very good screening tool in regards to detecting depression. It has very good sensitivity and specificity.
And that’s going to allow you to actually think about or to screen for patients that you’re going to need to refer for treatment. So if you have a patient with advanced cancer, as an example, and you use the PHQ-2 or PHQ-9, then that’s going to give you a very evidence-based avenue in which to refer for treatment. Now you may be asking yourself, maybe I don’t want to use a PHQ-2 or 9, or I’m in a community practice or a private practice, I just don’t have the bandwidth to process this.
So I want to go off of just my own patient interaction. What are things that I can cue on?
With a patient with cancer, there’s going to be roughly four things that we’re considering in terms of depressive spectrum disorders: Adjustment disorder with depressed mood, major depression, a mood disorder due to cancer itself, or substance-induced mood disorder.
For our audience I want you to concentrate on right now on adjustment disorder with depressed mood and major depression. Now when you look at the evidence, there are roughly nine things that some people like to think about in regard to depressive symptoms to key on. For all of us as health practitioners, these are the things I would like for you to focus on in particular:
1. Non-adherence with treatment for cancer.
2. Impairment of their social or occupational function.
3. Your patient becomes demoralized when they start to lose a little bit of confidence or hope.
When you have those three things, or any one of them, in an advanced stage of cancer, with or without a PHQ screening, you need to really think about how you’re going to refer this patient for treatment. So we can break this down into three different types of interventions. One, the biggest thing, is just to ask, “How are you feeling? What is your mood? Are you suffering from a clinical depression?” You know, take a little bit of inspiration from Dr. Henry. Just give it to people straight and just ask. That’s the biggest thing people don’t do. They don’t ask.
The next thing, if you want to use an evidence-based scale, use a PHQ-2...You would have to follow up, but you-- rather you’re practicing solo or in a group practice or whether you have, your nurse or PA -- they generally assist with that.
And then the third thing is, when you’re interacting with the patient, look for those three things that I talked about: Non-adherence with treatment, impairment of social or occupational function, and then demoralization.
And then the final thing I want to focus on, because you can’t talk about depression without talking about suicide or really significant distress. Obviously, you can ask and you should ask about suicide if that is in your wheelhouse, but to be perfectly frank, most oncologists are not going to-- or most people outside of psychiatrists aren’t going to necessarily just routinely ask that question.
But here’s what I would say. It’s an old one but it’s a good one: Listen to that little voice. Listen to that little voice, all right? Depending on the evidence that you look at, a lot of detecting suicide can be aided by a clinician listening to their own gut instincts. What I mean by that is, you feel a sense of distress. You feel a sense of lack of connection. You find yourself [saying], “Wait a minute, why do I want to call that patient and checkup? Why do I want to reach out?”
When you start to feel like this, you need to listen. More importantly, you need to stop and then you need to make sure that that patient has a referral in place.
Dr. Henry: So they’re just tuning out so badly, you’re really losing the connection, and that’s when your little voice talks to you.
Dr. Norris: Exactly. Well said, Dr. Henry. Well said.
Dr. Henry: In my long career, drug abuse, narcotics, and suicide have been extremely rare. I can think of one patient who was a drug abuser with cancer, or it turned out she was a drug abuser before she had cancer. And then suicide, really quite rare. I’m sure they occur, and we have to watch for them, as you say, but fortunately I’ve not seen that so much. Thanks to your comments, I want to be sure I’m watching and looking.
And the PHQ-2 and -9, I’m sure, with so many of us having electronic medical records, you can simply Google while you’re talking to the patient for those two questionnaires and say, oh, you know, how about you answer these two questions, these nine questions, and see how many points the patient gets and worry about referral or even medication yourself if it looks like an antidepressant is in order.
Dr. Norris: Absolutely. Absolutely.
Dr. Henry: Well, I think we’ve covered an awful lot of ground. I really want to thank you. Any get-away thoughts? We worry about the cognitive behavioral therapy. We worry about it, and we should listen to it and do it.
Practicing in the COVID era is stressful for all of us. I told Dr. Norris at the outset, if I broke down and started baring my soul, he wouldn’t be surprised. Fortunately, I’ve kept it together while talking to a psychiatrist.
And finally watch for clinically significant depression, either by your own questions, which you’ve outlined, or the PHQ-2 and -9.
Really appreciate your thoughts today. Lorenzo, thanks so much for taking the time to do this today.
To hear the entire conversation, go to mdedge.com/podcasts or listen wherever you find your podcasts. David Henry, MD, is a clinical professor of medicine at the University of Pennsylvania and vice chairman of the department of medicine at Pennsylvania Hospital in Philadelphia. He is editor in chief of MDedge Hematology-Oncology and the host of the Blood & Cancer podcast. Dr. Henry reported being on the advisory board for Amgen, AMAG Pharmaceuticals, and Pharmacosmos. He reported institutional funding from the National Institutes of Health and FibroGen.
Lorenzo Norris, MD, is host of the MDedge Psychcast, editor in chief of MDedge Psychiatry, and assistant professor of psychiatry and behavioral sciences at George Washington University, Washington. He also serves as assistant dean of student affairs at the university, and medical director of psychiatric and behavioral sciences at GWU Hospital. Dr. Lorenzo Norris has no conflicts.
Divergent COVID-19 mental health impacts seen in Spain and China
Spain and China used very different public health responses to the COVID-19 crisis, and that has had significant consequences in terms of the mental health as well as physical health of the two countries’ citizens, Roger Ho, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.

Dr. Ho, a psychiatrist at the National University of Singapore, presented a first-of-its-kind cross-cultural comparative study of the impact of the COVID-19 pandemic in two epicenters on opposite sides of the world. A total of 1,539 participants drawn from the general populations in the two countries completed the online National University of Singapore COVID-19 Questionnaire. The survey was conducted in late February/early March in China and in mid-April in Spain, times of intense disease activity in the countries.
The questionnaire assesses knowledge and concerns about COVID, precautionary measures taken in the last 14 days, contact history, and physical symptoms related to COVID in the last 14 days. The pandemic’s psychological impact was evaluated using the Impact of Event Scale–Revised (IES-R). Participants also completed the Depression, Anxiety, and Stress-21 Scale (DASS-21).
Of note, the pandemic has taken a vastly greater physical toll in Spain than China. As of May 5, there were 83,000 confirmed cases of COVID-19 in China, with a population of 1.39 billion, compared with 248,000 in Spain, with a population of 46.9 million. The Spanish case rate of 5,500 per 1 million population was 100 times greater than China’s; the Spanish mortality rate of 585 per million was 185-fold greater.
Mental health findings
Spaniards experienced significantly higher levels of stress and depression as reflected in DASS-21 subscale scores of 14.22 and 8.65, respectively, compared with 7.86 and 6.38, in Chinese respondents. Spanish subjects also reported greater anxiety levels than the Chinese on the DASS-21 anxiety subscale, although not to a statistically significant extent. Yet, counterintuitively, given the DASS-21 results, the pandemic had a greater adverse psychological impact on the Chinese subjects as reflected in their significantly higher average IES-D score of 30.76 versus 27.64 in Spain. Dr. Ho offered a hypothesis as to why: The survey documented that many Chinese respondents felt socially stigmatized, and that their nation had been discriminated against by the rest of the world because the pandemic started in China.
Satisfaction with the public health response
Spanish respondents reported less confidence in their COVID-related medical services.
“This could be due to the rising number of infected health care workers in Spain. In contrast, the Chinese had more confidence in their medical services, probably because the government quickly deployed medical personnel and treated COVID-19 patients at rapidly built hospitals,” according to Dr. Ho.
Spain and other European countries shared four shortcomings in their pandemic response, he continued: lack of personal protective equipment for health care workers, delay in developing response strategies, a shortage of hospital beds, and inability to protect vulnerable elderly individuals from infection in nursing homes.
Experiencing cough, shortness of breath, myalgia, or other physical symptoms potentially associated with COVID-19 within the past 14 days was associated with worse depression, anxiety, and stress scores in both China and Spain. This underscores from a mental health standpoint the importance of rapid and accurate testing for the infection, Dr. Ho said.
Significantly more Spanish respondents felt there was too much unnecessary worry about COVID-19, suggesting a need for better health education regarding the pandemic.
Use of face masks
Consistent use of face masks regardless of the presence or absence of symptoms was far more common in the Chinese epicenter, where, unlike in Spain, this precautionary measure was associated with significantly lower IES-R and DASS-21 scores.
but for the Spanish, wearing a face mask was associated with higher IES-R scores,” Dr. Ho said. “We understand that it is difficult for Europeans to accept the need to use masks for healthy people because mask-wearing suggests vulnerability to sickness and concealment of identity. The Chinese have a collective culture. They believe they should wear a face mask to protect their health and that of other people.”
Dr. Ho reported no financial conflicts regarding his study, conducted with coinvestigators at Huaibei (China) Normal University and Complutense University of Madrid.
SOURCE: Ho R. ECNP 2020, Session ISE01.
Spain and China used very different public health responses to the COVID-19 crisis, and that has had significant consequences in terms of the mental health as well as physical health of the two countries’ citizens, Roger Ho, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.
Dr. Ho, a psychiatrist at the National University of Singapore, presented a first-of-its-kind cross-cultural comparative study of the impact of the COVID-19 pandemic in two epicenters on opposite sides of the world. A total of 1,539 participants drawn from the general populations in the two countries completed the online National University of Singapore COVID-19 Questionnaire. The survey was conducted in late February/early March in China and in mid-April in Spain, times of intense disease activity in the countries.
The questionnaire assesses knowledge and concerns about COVID, precautionary measures taken in the last 14 days, contact history, and physical symptoms related to COVID in the last 14 days. The pandemic’s psychological impact was evaluated using the Impact of Event Scale–Revised (IES-R). Participants also completed the Depression, Anxiety, and Stress-21 Scale (DASS-21).
Of note, the pandemic has taken a vastly greater physical toll in Spain than China. As of May 5, there were 83,000 confirmed cases of COVID-19 in China, with a population of 1.39 billion, compared with 248,000 in Spain, with a population of 46.9 million. The Spanish case rate of 5,500 per 1 million population was 100 times greater than China’s; the Spanish mortality rate of 585 per million was 185-fold greater.
Mental health findings
Spaniards experienced significantly higher levels of stress and depression as reflected in DASS-21 subscale scores of 14.22 and 8.65, respectively, compared with 7.86 and 6.38, in Chinese respondents. Spanish subjects also reported greater anxiety levels than the Chinese on the DASS-21 anxiety subscale, although not to a statistically significant extent. Yet, counterintuitively, given the DASS-21 results, the pandemic had a greater adverse psychological impact on the Chinese subjects as reflected in their significantly higher average IES-D score of 30.76 versus 27.64 in Spain. Dr. Ho offered a hypothesis as to why: The survey documented that many Chinese respondents felt socially stigmatized, and that their nation had been discriminated against by the rest of the world because the pandemic started in China.
Satisfaction with the public health response
Spanish respondents reported less confidence in their COVID-related medical services.
“This could be due to the rising number of infected health care workers in Spain. In contrast, the Chinese had more confidence in their medical services, probably because the government quickly deployed medical personnel and treated COVID-19 patients at rapidly built hospitals,” according to Dr. Ho.
Spain and other European countries shared four shortcomings in their pandemic response, he continued: lack of personal protective equipment for health care workers, delay in developing response strategies, a shortage of hospital beds, and inability to protect vulnerable elderly individuals from infection in nursing homes.
Experiencing cough, shortness of breath, myalgia, or other physical symptoms potentially associated with COVID-19 within the past 14 days was associated with worse depression, anxiety, and stress scores in both China and Spain. This underscores from a mental health standpoint the importance of rapid and accurate testing for the infection, Dr. Ho said.
Significantly more Spanish respondents felt there was too much unnecessary worry about COVID-19, suggesting a need for better health education regarding the pandemic.
Use of face masks
Consistent use of face masks regardless of the presence or absence of symptoms was far more common in the Chinese epicenter, where, unlike in Spain, this precautionary measure was associated with significantly lower IES-R and DASS-21 scores.
but for the Spanish, wearing a face mask was associated with higher IES-R scores,” Dr. Ho said. “We understand that it is difficult for Europeans to accept the need to use masks for healthy people because mask-wearing suggests vulnerability to sickness and concealment of identity. The Chinese have a collective culture. They believe they should wear a face mask to protect their health and that of other people.”
Dr. Ho reported no financial conflicts regarding his study, conducted with coinvestigators at Huaibei (China) Normal University and Complutense University of Madrid.
SOURCE: Ho R. ECNP 2020, Session ISE01.
Spain and China used very different public health responses to the COVID-19 crisis, and that has had significant consequences in terms of the mental health as well as physical health of the two countries’ citizens, Roger Ho, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.
Dr. Ho, a psychiatrist at the National University of Singapore, presented a first-of-its-kind cross-cultural comparative study of the impact of the COVID-19 pandemic in two epicenters on opposite sides of the world. A total of 1,539 participants drawn from the general populations in the two countries completed the online National University of Singapore COVID-19 Questionnaire. The survey was conducted in late February/early March in China and in mid-April in Spain, times of intense disease activity in the countries.
The questionnaire assesses knowledge and concerns about COVID, precautionary measures taken in the last 14 days, contact history, and physical symptoms related to COVID in the last 14 days. The pandemic’s psychological impact was evaluated using the Impact of Event Scale–Revised (IES-R). Participants also completed the Depression, Anxiety, and Stress-21 Scale (DASS-21).
Of note, the pandemic has taken a vastly greater physical toll in Spain than China. As of May 5, there were 83,000 confirmed cases of COVID-19 in China, with a population of 1.39 billion, compared with 248,000 in Spain, with a population of 46.9 million. The Spanish case rate of 5,500 per 1 million population was 100 times greater than China’s; the Spanish mortality rate of 585 per million was 185-fold greater.
Mental health findings
Spaniards experienced significantly higher levels of stress and depression as reflected in DASS-21 subscale scores of 14.22 and 8.65, respectively, compared with 7.86 and 6.38, in Chinese respondents. Spanish subjects also reported greater anxiety levels than the Chinese on the DASS-21 anxiety subscale, although not to a statistically significant extent. Yet, counterintuitively, given the DASS-21 results, the pandemic had a greater adverse psychological impact on the Chinese subjects as reflected in their significantly higher average IES-D score of 30.76 versus 27.64 in Spain. Dr. Ho offered a hypothesis as to why: The survey documented that many Chinese respondents felt socially stigmatized, and that their nation had been discriminated against by the rest of the world because the pandemic started in China.
Satisfaction with the public health response
Spanish respondents reported less confidence in their COVID-related medical services.
“This could be due to the rising number of infected health care workers in Spain. In contrast, the Chinese had more confidence in their medical services, probably because the government quickly deployed medical personnel and treated COVID-19 patients at rapidly built hospitals,” according to Dr. Ho.
Spain and other European countries shared four shortcomings in their pandemic response, he continued: lack of personal protective equipment for health care workers, delay in developing response strategies, a shortage of hospital beds, and inability to protect vulnerable elderly individuals from infection in nursing homes.
Experiencing cough, shortness of breath, myalgia, or other physical symptoms potentially associated with COVID-19 within the past 14 days was associated with worse depression, anxiety, and stress scores in both China and Spain. This underscores from a mental health standpoint the importance of rapid and accurate testing for the infection, Dr. Ho said.
Significantly more Spanish respondents felt there was too much unnecessary worry about COVID-19, suggesting a need for better health education regarding the pandemic.
Use of face masks
Consistent use of face masks regardless of the presence or absence of symptoms was far more common in the Chinese epicenter, where, unlike in Spain, this precautionary measure was associated with significantly lower IES-R and DASS-21 scores.
but for the Spanish, wearing a face mask was associated with higher IES-R scores,” Dr. Ho said. “We understand that it is difficult for Europeans to accept the need to use masks for healthy people because mask-wearing suggests vulnerability to sickness and concealment of identity. The Chinese have a collective culture. They believe they should wear a face mask to protect their health and that of other people.”
Dr. Ho reported no financial conflicts regarding his study, conducted with coinvestigators at Huaibei (China) Normal University and Complutense University of Madrid.
SOURCE: Ho R. ECNP 2020, Session ISE01.
FROM ECNP 2020
Mental illness tied to increased mortality in COVID-19
A psychiatric diagnosis for patients hospitalized with COVID-19 is linked to a significantly increased risk for death, new research shows.

Investigators found that patients who were hospitalized with COVID-19 and who had been diagnosed with a psychiatric disorder had a 50% increased risk for a COVID-related death in comparison with COVID-19 patients who had not received a psychiatric diagnosis.
“Pay attention and potentially address/treat a prior psychiatric diagnosis if a patient is hospitalized for COVID-19, as this risk factor can impact the patient’s outcome – death – while in the hospital,” lead investigator Luming Li, MD, assistant professor of psychiatry and associate medical director of quality improvement, Yale New Haven Psychiatric Hospital, New Haven, Conn., said in an interview.
The study was published Sept. 30 in JAMA Network Open.
Negative impact
“We were interested to learn more about the impact of psychiatric diagnoses on COVID-19 mortality, as prior large cohort studies included neurological and other medical conditions but did not assess for a priori psychiatric diagnoses,” said Dr. Li.
“We know from the literature that prior psychiatric diagnoses can have a negative impact on the outcomes of medical conditions, and therefore we tested our hypothesis on a cohort of patients who were hospitalized with COVID-19,” she added.
To investigate, the researchers analyzed data on 1,685 patients hospitalized with COVID-19 between Feb. 15 and April 25, 2020, and whose cases were followed to May 27, 2020. The patients (mean age, 65.2 years; 52.6% men) were drawn from the Yale New Haven Health System.
The median follow-up period was 8 days (interquartile range, 4-16 days) .
Of these patients, 28% had received a psychiatric diagnosis prior to hospitalization. (i.e., cancer, cerebrovascular disease, heart failure, diabetes, kidney disease, liver disease, MI, and/or HIV).
Psychiatric diagnoses were defined in accordance with ICD codes that included mental and behavioral health, Alzheimer’s disease, and self-injury.
Vulnerability to stress
In the unadjusted model, the risk for COVID-19–related hospital death was greater for those who had received any psychiatric diagnosis, compared with those had not (hazard ratio, 2.3; 95% CI, 1.8-2.9; P < .001).
In the adjusted model that controlled for demographic characteristics, other medical comorbidities, and hospital location, the mortality risk somewhat decreased but still remained significantly higher (HR, 1.5; 95% CI, 1.1-1.9; P = .003).
Dr. Li noted a number of factors that might account for the higher mortality rate among psychiatric patients who had COVID-19 in comparison with COVD-19 patients who did not have a psychiatric disorder. These included “potential inflammatory and stress responses that the body experiences related to prior psychiatric conditions,” she said.
Having been previously diagnosed with a psychiatric disorder may also “reflect existing neurochemical differences, compared to those who do not have a prior psychiatric diagnosis, [and] these differences may make the population with the prior psychiatric diagnosis more vulnerable to respond to an acute stressor such as COVID-19,” she said.
Quality care
Harold Pincus, MD, professor and vice chair of the department of psychiatry at Columbia University, New York, said it “adds to the fairly well-known and well-established phenomenon that people with mental illnesses have a high risk of all sorts of morbidity and mortality for non–mental health conditions.”
The researchers “adjusted for various expected [mortality] risks that would be independent of the presence of COVID-19,” so “there was something else going on associated with mortality,” said Dr. Pincus, who is also codirector of the Irving Institute for Clinical and Translation Research. He was not involved with the study.
Beyond the possibility of “some basic immunologic process affected by the presence of a mental disorder,” it is possible that the vulnerability is “related to access to quality care for the comorbid general condition that is not being effectively treated,” he said.
“The take-home message is that people with mental disorders are at higher risk for death, and we need to make sure that, irrespective of COVID-19, they get adequate preventive and chronic-disease care, which would be the most effective way to intervene and protect the impact of a serious disease like COVID-19,” he noted. This would include being appropriately vaccinated and receiving preventive healthcare to reduce smoking and encourage weight loss.
No source of funding for the study was provided. Dr. Li reported receiving grants from a Health and Aging Policy Fellowship during the conduct of the study. Dr. Pincus reported no relevant financial relationships.
A psychiatric diagnosis for patients hospitalized with COVID-19 is linked to a significantly increased risk for death, new research shows.
Investigators found that patients who were hospitalized with COVID-19 and who had been diagnosed with a psychiatric disorder had a 50% increased risk for a COVID-related death in comparison with COVID-19 patients who had not received a psychiatric diagnosis.
“Pay attention and potentially address/treat a prior psychiatric diagnosis if a patient is hospitalized for COVID-19, as this risk factor can impact the patient’s outcome – death – while in the hospital,” lead investigator Luming Li, MD, assistant professor of psychiatry and associate medical director of quality improvement, Yale New Haven Psychiatric Hospital, New Haven, Conn., said in an interview.
The study was published Sept. 30 in JAMA Network Open.
Negative impact
“We were interested to learn more about the impact of psychiatric diagnoses on COVID-19 mortality, as prior large cohort studies included neurological and other medical conditions but did not assess for a priori psychiatric diagnoses,” said Dr. Li.
“We know from the literature that prior psychiatric diagnoses can have a negative impact on the outcomes of medical conditions, and therefore we tested our hypothesis on a cohort of patients who were hospitalized with COVID-19,” she added.
To investigate, the researchers analyzed data on 1,685 patients hospitalized with COVID-19 between Feb. 15 and April 25, 2020, and whose cases were followed to May 27, 2020. The patients (mean age, 65.2 years; 52.6% men) were drawn from the Yale New Haven Health System.
The median follow-up period was 8 days (interquartile range, 4-16 days) .
Of these patients, 28% had received a psychiatric diagnosis prior to hospitalization. (i.e., cancer, cerebrovascular disease, heart failure, diabetes, kidney disease, liver disease, MI, and/or HIV).
Psychiatric diagnoses were defined in accordance with ICD codes that included mental and behavioral health, Alzheimer’s disease, and self-injury.
Vulnerability to stress
In the unadjusted model, the risk for COVID-19–related hospital death was greater for those who had received any psychiatric diagnosis, compared with those had not (hazard ratio, 2.3; 95% CI, 1.8-2.9; P < .001).
In the adjusted model that controlled for demographic characteristics, other medical comorbidities, and hospital location, the mortality risk somewhat decreased but still remained significantly higher (HR, 1.5; 95% CI, 1.1-1.9; P = .003).
Dr. Li noted a number of factors that might account for the higher mortality rate among psychiatric patients who had COVID-19 in comparison with COVD-19 patients who did not have a psychiatric disorder. These included “potential inflammatory and stress responses that the body experiences related to prior psychiatric conditions,” she said.
Having been previously diagnosed with a psychiatric disorder may also “reflect existing neurochemical differences, compared to those who do not have a prior psychiatric diagnosis, [and] these differences may make the population with the prior psychiatric diagnosis more vulnerable to respond to an acute stressor such as COVID-19,” she said.
Quality care
Harold Pincus, MD, professor and vice chair of the department of psychiatry at Columbia University, New York, said it “adds to the fairly well-known and well-established phenomenon that people with mental illnesses have a high risk of all sorts of morbidity and mortality for non–mental health conditions.”
The researchers “adjusted for various expected [mortality] risks that would be independent of the presence of COVID-19,” so “there was something else going on associated with mortality,” said Dr. Pincus, who is also codirector of the Irving Institute for Clinical and Translation Research. He was not involved with the study.
Beyond the possibility of “some basic immunologic process affected by the presence of a mental disorder,” it is possible that the vulnerability is “related to access to quality care for the comorbid general condition that is not being effectively treated,” he said.
“The take-home message is that people with mental disorders are at higher risk for death, and we need to make sure that, irrespective of COVID-19, they get adequate preventive and chronic-disease care, which would be the most effective way to intervene and protect the impact of a serious disease like COVID-19,” he noted. This would include being appropriately vaccinated and receiving preventive healthcare to reduce smoking and encourage weight loss.
No source of funding for the study was provided. Dr. Li reported receiving grants from a Health and Aging Policy Fellowship during the conduct of the study. Dr. Pincus reported no relevant financial relationships.
A psychiatric diagnosis for patients hospitalized with COVID-19 is linked to a significantly increased risk for death, new research shows.
Investigators found that patients who were hospitalized with COVID-19 and who had been diagnosed with a psychiatric disorder had a 50% increased risk for a COVID-related death in comparison with COVID-19 patients who had not received a psychiatric diagnosis.
“Pay attention and potentially address/treat a prior psychiatric diagnosis if a patient is hospitalized for COVID-19, as this risk factor can impact the patient’s outcome – death – while in the hospital,” lead investigator Luming Li, MD, assistant professor of psychiatry and associate medical director of quality improvement, Yale New Haven Psychiatric Hospital, New Haven, Conn., said in an interview.
The study was published Sept. 30 in JAMA Network Open.
Negative impact
“We were interested to learn more about the impact of psychiatric diagnoses on COVID-19 mortality, as prior large cohort studies included neurological and other medical conditions but did not assess for a priori psychiatric diagnoses,” said Dr. Li.
“We know from the literature that prior psychiatric diagnoses can have a negative impact on the outcomes of medical conditions, and therefore we tested our hypothesis on a cohort of patients who were hospitalized with COVID-19,” she added.
To investigate, the researchers analyzed data on 1,685 patients hospitalized with COVID-19 between Feb. 15 and April 25, 2020, and whose cases were followed to May 27, 2020. The patients (mean age, 65.2 years; 52.6% men) were drawn from the Yale New Haven Health System.
The median follow-up period was 8 days (interquartile range, 4-16 days) .
Of these patients, 28% had received a psychiatric diagnosis prior to hospitalization. (i.e., cancer, cerebrovascular disease, heart failure, diabetes, kidney disease, liver disease, MI, and/or HIV).
Psychiatric diagnoses were defined in accordance with ICD codes that included mental and behavioral health, Alzheimer’s disease, and self-injury.
Vulnerability to stress
In the unadjusted model, the risk for COVID-19–related hospital death was greater for those who had received any psychiatric diagnosis, compared with those had not (hazard ratio, 2.3; 95% CI, 1.8-2.9; P < .001).
In the adjusted model that controlled for demographic characteristics, other medical comorbidities, and hospital location, the mortality risk somewhat decreased but still remained significantly higher (HR, 1.5; 95% CI, 1.1-1.9; P = .003).
Dr. Li noted a number of factors that might account for the higher mortality rate among psychiatric patients who had COVID-19 in comparison with COVD-19 patients who did not have a psychiatric disorder. These included “potential inflammatory and stress responses that the body experiences related to prior psychiatric conditions,” she said.
Having been previously diagnosed with a psychiatric disorder may also “reflect existing neurochemical differences, compared to those who do not have a prior psychiatric diagnosis, [and] these differences may make the population with the prior psychiatric diagnosis more vulnerable to respond to an acute stressor such as COVID-19,” she said.
Quality care
Harold Pincus, MD, professor and vice chair of the department of psychiatry at Columbia University, New York, said it “adds to the fairly well-known and well-established phenomenon that people with mental illnesses have a high risk of all sorts of morbidity and mortality for non–mental health conditions.”
The researchers “adjusted for various expected [mortality] risks that would be independent of the presence of COVID-19,” so “there was something else going on associated with mortality,” said Dr. Pincus, who is also codirector of the Irving Institute for Clinical and Translation Research. He was not involved with the study.
Beyond the possibility of “some basic immunologic process affected by the presence of a mental disorder,” it is possible that the vulnerability is “related to access to quality care for the comorbid general condition that is not being effectively treated,” he said.
“The take-home message is that people with mental disorders are at higher risk for death, and we need to make sure that, irrespective of COVID-19, they get adequate preventive and chronic-disease care, which would be the most effective way to intervene and protect the impact of a serious disease like COVID-19,” he noted. This would include being appropriately vaccinated and receiving preventive healthcare to reduce smoking and encourage weight loss.
No source of funding for the study was provided. Dr. Li reported receiving grants from a Health and Aging Policy Fellowship during the conduct of the study. Dr. Pincus reported no relevant financial relationships.
Validation of the Timberlawn Couple and Family Evaluation Scales–Self-Report in Veterans with PTSD
Although about 8.3% of the general adult civilian population will be diagnosed with posttraumatic stress disorder (PTSD) in their lifetime, rates of PTSD are even higher in the veteran population.1,2 PTSD is associated with a number of psychosocial consequences in veterans, including decreased intimate partner relationship functioning.3,4 For example, Cloitre and colleagues reported that PTSD is associated with difficulty with socializing, intimacy, responsibility, and control, all of which increase difficulties in intimate partner relationships.5 Similarly, researchers also have noted that traumatic experiences can affect an individual’s attachment style, resulting in progressive avoidance of interpersonal relationships, which can lead to marked difficulties in maintaining and beginning intimate partner relationships.6,7 Despite these known consequences of PTSD, as Dekel and Monson noted in a review,further research is still needed regarding the mechanisms by which trauma and PTSD result in decreased intimate partner relationship functioning among veterans.8 Nonetheless, as positive interpersonal relationships are associated with decreased PTSD symptom severity9,10 and increased engagement in PTSD treatment,11 determining methods of measuring intimate partner relationship functioning in veterans with PTSD is important to inform future research and aid the provision of care.
To date, limited research has examined the valid measurement of intimate partner relationship functioning among veterans with PTSD. Many existing measures that comprehensively assess intimate partner relationship functioning are time and resource intensive. One such measure, the Timberlawn Couple and Family Evaluation Scales (TCFES), comprehensively assesses multiple pertinent domains of intimate partner relationship functioning (ie, structure, autonomy, problem solving, affect regulation, and disagreement/conflict).12 By assessing multiple domains, the TCFES offers a method of understanding the specific components of an individual’s intimate partner relationship in need of increased clinical attention.12 However, the TCFES is a time- and labor-intensive observational measure that requires a couple to interact while a blinded, independent rater observes and rates their interactions using an intricate coding process. This survey structure precludes the ability to quickly and comprehensively assess a veteran’s intimate partner functioning in settings such as mental health outpatient clinics where mental health providers engage in brief, time-limited psychotherapy. As such, brief measures of intimate partner relationship functioning are needed to best inform clinical care among veterans with PTSD.
The primary aim of the current study was to create a psychometrically valid, yet brief, self-report version of the TCFES to assess multiple domains of intimate partner relationship functioning. The psychometric properties of this measure were assessed among a sample of US veterans with PTSD who were in an intimate partner relationship. We specifically examined factor structure, reliability, and associations to established measures of specific domains of relational functioning.
Methods
Ninety-four veterans were recruited via posted advertisements, promotion in PTSD therapy groups/staff meetings, and word of mouth at the Dallas Veterans Affairs Medical Center (VAMC). Participants were eligible if they had a documented diagnosis of PTSD as confirmed in the veteran’s electronic medical record and an affirmative response to currently being involved in an intimate partner relationship (ie, legally married, common-law spouse, involved in a relationship/partnership). There were no exclusion criteria.
Interested veterans were invited to complete several study-related self-report measures concerning their intimate partner relationships that would take about an hour. They were informed that the surveys were voluntary and confidential, and that they would be compensated for their participation. All veterans who participated provided written consent and the study was approved by the Dallas VAMC institutional review board.
Of the 94 veterans recruited, 3 veterans’ data were removed from current analyses after informed consent but before completing the surveys when they indicated they were not currently in a relationship or were divorced. After consent, the 91 participants were administered several study-related self-report measures. The measures took between 30 and 55 minutes to complete. Participants were then compensated $25 for their participation.
Intimate Partner Relationship Functioning
The 16-item TCFES self-report version (TCFES-SR) was developed to assess multiple domains of interpersonal functioning (Appendix). The observational TCFES assesses 5 intimate partner relationship characteristic domains (ie, structure, autonomy, problem solving, affect regulation, and disagreement/conflict) during a couple’s interaction by an independent trained rater.12 Each of the 16 TCFES-SR items were modeled after original constructs measured by the TCFES, including power, closeness, clarify, other’s views, responsibility, closure, negotiation, expressiveness, responsiveness, positive regard, negative regard, mood/tone, empathy, frequency, affective quality, and generalization and escalation. To maintain consistency with the TCFES, each item of the TCFES-SR was scored from 1 (severely dysfunctional) to 5 (highly functional). Additionally, all item wording for the TCFES-SR was based on wording in the TCFES manual after consultation with an expert who facilitated the development of the TCFES.12 On average, the TCFES-SR took 5 to 10 minutes to complete.
To measure concurrent validity of the modified TCFES-SR, several additional interpersonal measures were selected and administered based on prior research and established domains of the TCFES. The Positive and Negative Quality in Marriage Scale (PANQIMS) was administered to assess perceived attitudes toward a relationship.13,14 The PANQIMS generates 2 subscales: positive quality and negative quality in the relationship. Because the PANQIMS specifically assesses married relationships and our sample included married and nonmarried participants, wording was modified (eg, “spouse/partner”).
The relative power subscale of the Network Relationships Inventory–Relationship Qualities Version (NRI-RQV) measure was administered to assess the unequal/shared role romantic partners have in power equality (ie, relative power).15
The Revised Dyadic Adjustment Scale (RDAS) is a self-report measure that assesses multiple dimensions of marital adjustment and functioning.16 Six subscales of the RDAS were chosen based on items of the TCFES-SR: decision making, values, affection, conflict, activities, and discussion.
The Interpersonal Reactivity Index (IRI) empathetic concern subscale was administered to assess empathy across multiple contexts and situations17 and the Experiences in Close Relationships-Revised Questionnaire (ECR-R) was administered to assess relational functioning by determining attachment-related anxiety and avoidance.18
Sociodemographic Information
A sociodemographic questionnaire also was administered. The questionnaire assessed gender, age, education, service branch, length of interpersonal relationship, race, and ethnicity of the veteran as well as gender of the veteran’s partner.
Statistical Analysis
Factor structure of the TCFES-SR was determined by conducting an exploratory factor analysis. To allow for correlation between items, the Promax oblique rotation method was chosen.19 Number of factors was determined by agreement between number of eigenvalues ≥ 1, visual inspection of the scree plot, and a parallel analysis. Factor loadings of ≥ 0.3 were used to determine which items loaded on to which factors.
Convergent validity was assessed by conducting Pearson’s bivariate correlations between identified TCFES-SR factor(s) and other administered measures of interpersonal functioning (ie, PANQIMS positive and negative quality; NRI-RQV relative power subscale; RDAS decision making, values, affection, conflict, activities, and discussion subscales; IRI-empathetic concern subscale; and ECR-R attachment-related anxiety and avoidance subscales). Strength of relationship was determined based on the following guidelines: ± 0.3 to 0.49 = small, ± 0.5 to 0.69 = moderate, and ± 0.7 to 1.00 = large. Internal consistency was also determined for TCFES-SR factor(s) using Cronbach’s α. A standard level of significance (α=.05) was used for all statistical analyses.
Results
Eighty-six veterans provided complete data (Table 1). The Kaiser-Meyer-Olkin measure of sampling adequacy was indicative that sample size was adequate (.91), while Bartlett’s test of sphericity found the variables were suitable for structure detection, χ2 (120) = 800.00, P < .001. While 2 eigenvalues were ≥ 1, visual inspection of the scree plot and subsequent parallel analysis identified a unidimensional structure (ie, 1 factor) for the TCFES-SR. All items were found to load to this single factor, with all loadings being ≥ 0.5 (Table 2). Additionally, internal consistency was excellent for the scale (α = .93).
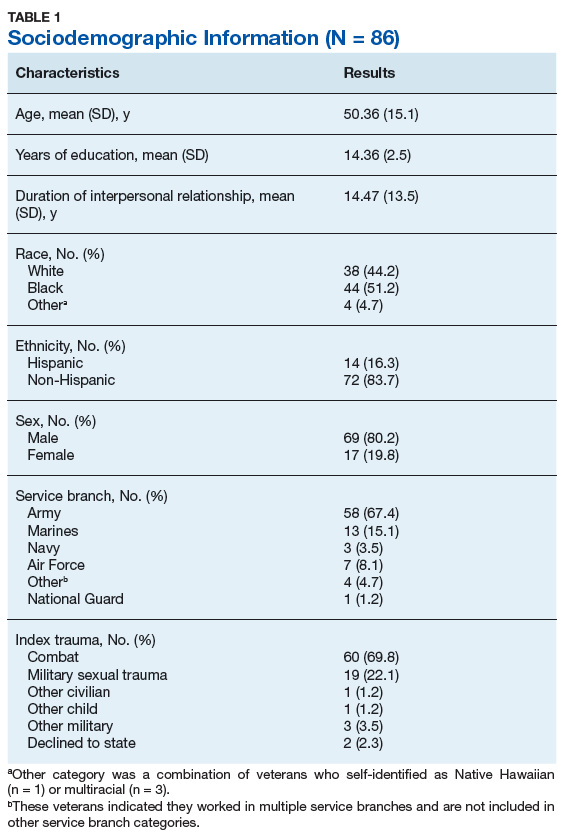
Pearson’s bivariate correlations were significant (P < .05) between TCFES-SR total score, and almost all administered interpersonal functioning measures (Table 3). Interestingly, no significant associations were found between any of the administered measures, including the TCFES-SR total score, and the IRI-empathetic concern subscale (P > .05).
Discussion
These findings provide initial support for the psychometric properties of the TCFES-SR, including excellent internal consistency and the adequate association of its total score to established measures of interpersonal functioning. Contrary to the TCFES, the TCFES-SR was shown to best fit a unidimensional factor rather than a multidimensional measure of relationship functioning. However, the TCFES-SR was also shown to have strong convergent validity with multiple domains of relationship functioning, indicating that the measure of overall intimate partner relationship functioning encompasses a number of relational domains (ie, structure, autonomy, problem solving, affect regulation, and disagreement/conflict). Critically, the TCFES-SR is brief and was administered easily in our sample, providing utility as clinical tool to be used in time-sensitive outpatient settings.
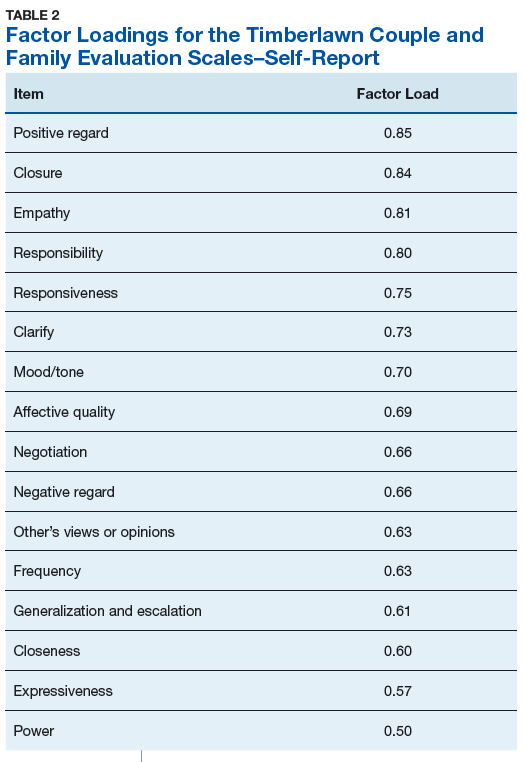
A unidimensional factor has particular strength in providing a global portrait of perceived intimate partner relationship functioning, and mental health providers can administer the TCFES-SR to assess for overall perceptions of intimate partner relationship functioning rather than administering a number of measures focusing on specific interpersonal domains (eg, decision making processes or positive/negative attitudes towards one’s relationship). This allows for the quick assessment (ie, 5-10 minutes) of overall intimate partner relationship functioning rather than administration of multiple self-report measures which can be time-intensive and expensive. However, the TCFES-SR also is limited by a lack of nuanced understanding of perceptions of functioning specific to particular domains. For example, the TCFES-SR score cannot describe intimate partner functioning in the domain of problem solving. Therefore, brief screening tools need to be developed that assess multiple intimate partner relationship domains.
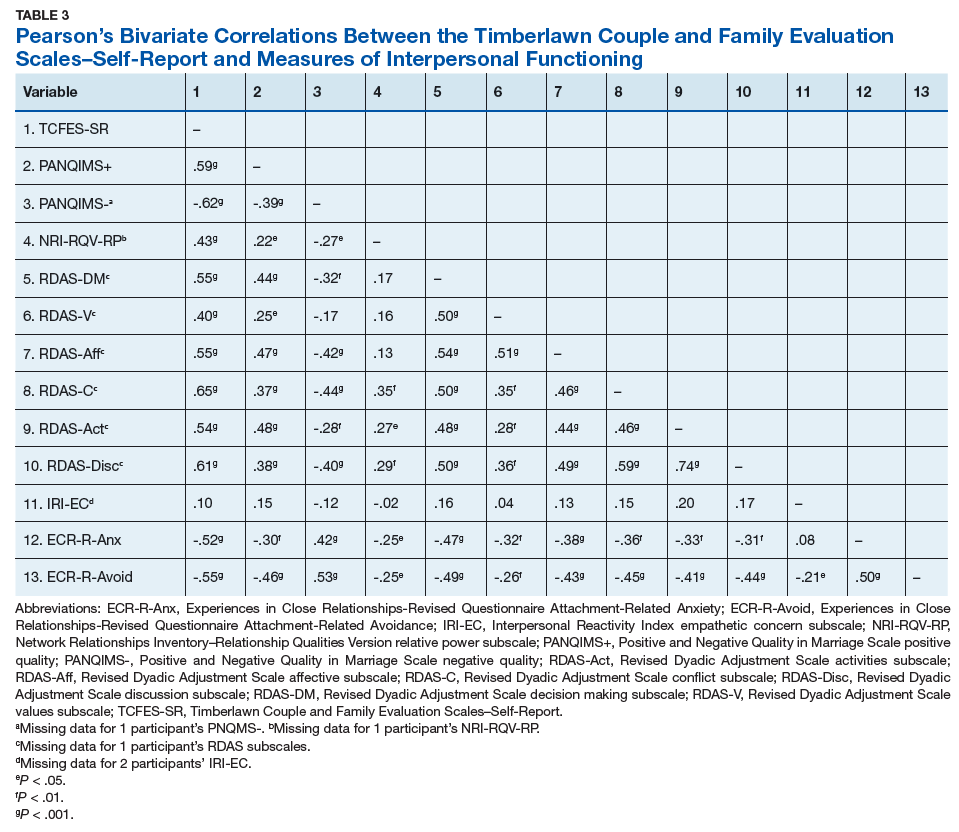
Importantly, overall intimate partner relationship functioning as measured by the TCFES-SR may not incorporate perceptions of relationship empathy, as the total score did not correlate with a measure of empathetic concern (ie, the IRI-empathetic concern subscale). As empathy was based on one item in the TCFES-SR vs 7 in the IRI-empathetic concern subscale, it is unclear if the TCFES-SR only captures a portion of the construct of empathy (ie, sensitivity to partner) vs the comprehensive assessment of trait empathy that the IRI subscale measures. Additionally, the IRI-empathetic concern subscale did not significantly correlate with any of the other administered measures of relationship functioning. Given the role of empathy in positive, healthy intimate partner relationships, future research should explore the role of empathetic concern among veterans with PTSD as it relates to overall (eg, TCFES-SR) and specific aspects of intimate partner relationship functioning.20
While the clinical applicability of the TCFES-SR requires further examination, this measure has a number of potential uses. Information captured quickly by the TCFES-SR may help to inform appropriate referral for treatment. For instance, veterans reporting low total scores on the TCFES-SR may indicate a need for a referral for intervention focused on improving overall relationship functioning (eg, Integrative Behavioral Couple Therapy).21,22 Measurement-based care (ie, tracking and discussing changes in symptoms during treatment using validated self-report measures) is now required by the Joint Commission as a standard of care,and has been shown to improve outcomes in couples therapy.23,24 As a brief self-report measure, the TCFES-SR may be able to facilitate measurement-based care and assist providers in tracking changes in overall relationship functioning over the course of treatment. However, the purpose of the current study was to validate the TCFES-SR and not to examine the utility of the TCFES-SR in clinical care; additional research is needed to determine standardized cutoff scores to indicate a need for clinical intervention.
Limitations
Several limitations should be noted. The current study only assessed perceived intimate partner relationship functioning from the perspective of the veteran, thus limiting implications as it pertains to the spouse/partner of the veteran. PTSD diagnosis was based on chart review rather than a psychodiagnostic measure (eg, Clinician Administered PTSD Scale); therefore, whether this diagnosis was current or in remission was unclear. Although our sample was adequate to conduct an exploratory factor analysis,the overall sample size was modest, and results should be considered preliminary with need for further replication.25 The sample was also primarily male, white or black, and non-Hispanic; therefore, results may not generalize to a more sociodemographically diverse population. Finally, given the focus of the study to develop a self-report measure, we did not compare the TCFES-SR to the original TCFES. Thus, further research examining the relationship between the TCFES-SR and TCFES may be needed to better understand overlap and potential incongruence in these measures, and to ascertain any differences in their factor structures.
Conclusion
This study is novel in that it adapted a comprehensive observational measure of relationship functioning to a self-report measure piloted among a sample of veterans with PTSD in an intimate partner relationship, a clinical population that remains largely understudied. Although findings are preliminary, the TCFES-SR was found to be a reliable and valid measure of overall intimate partner relationship functioning. Given the rapid administration of this self-report measure, the TCFES-SR may hold clinical utility as a screen of intimate partner relationship deficits in need of clinical intervention. Replication in a larger, more diverse sample is needed to further examine the generalizability and confirm psychometric properties of the TCFES-SR. Additionally, further understanding of the clinical utility of the TCFES-SR in treatment settings remains critical to promote the development and maintenance of healthy intimate partner relationships among veterans with PTSD. Finally, development of effective self-report measures of intimate partner relationship functioning, such as the TCFES-SR, may help to facilitate needed research to understand the effect of PTSD on establishing and maintaining healthy intimate partner relationships among veterans.
Acknowledgments
The current study was funded by the Timberlawn Psychiatric Research Foundation. This material is the result of work supported in part by the US Department of Veterans Affairs; the Rocky Mountain Mental Illness Research, Education and Clinical Center (MIRECC) for Suicide Prevention; Sierra Pacific MIRECC; and the Office of Academic Affiliations, Advanced Fellowship Program in Mental Illness Research and Treatment, Department of Veterans Affairs.
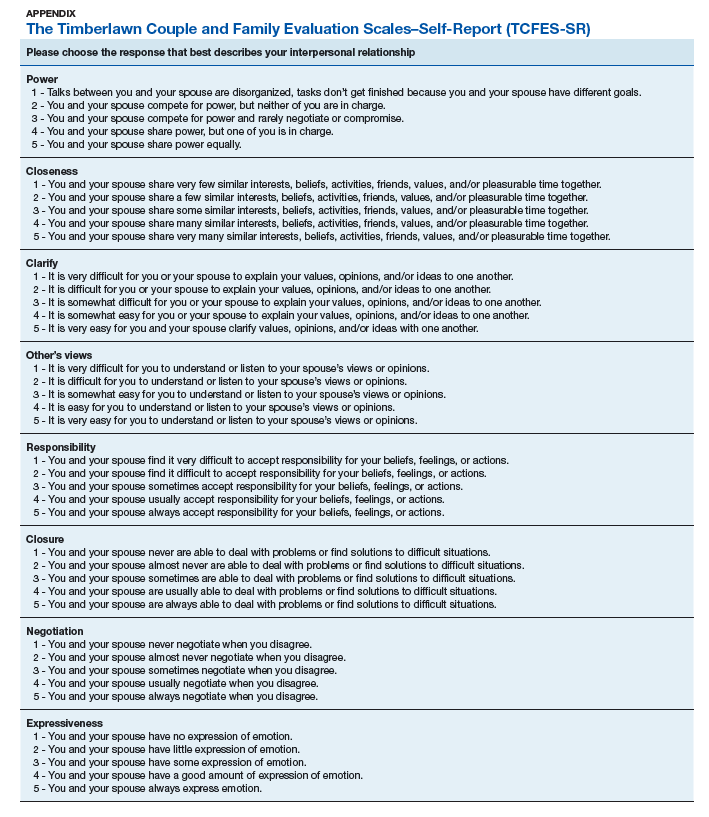
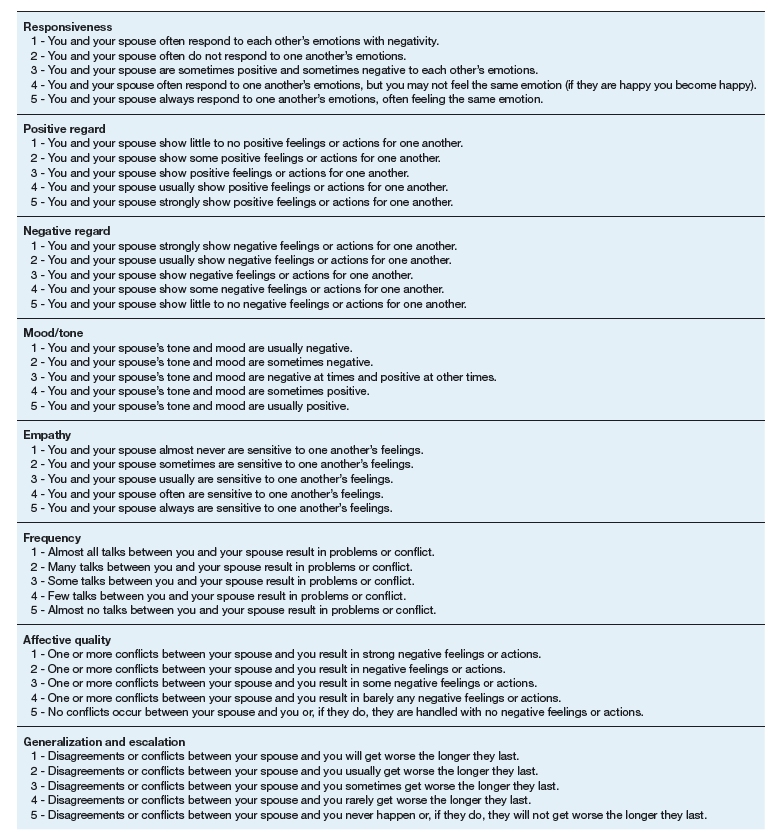
1. Kilpatrick DG, Resnick HS, Milanak ME, Miller MW, Keyes KM, Friedman MJ. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. J Trauma Stress. 2013;26(5):537-547.
2. Lehavot K, Goldberg SB, Chen JA, et al. Do trauma type, stressful life events, and social support explain women veterans’ high prevalence of PTSD? Soc Psychiatry Psychiatr Epidemiol. 2018;53(9):943-953.
3. Galovski T, Lyons JA. Psychological sequelae of combat violence: a review of the impact of PTSD on the veteran’s family and possible interventions. Aggress Violent Behav. 2004;9(5):477-501.
4. Ray SL, Vanstone M. The impact of PTSD on veterans’ family relationships: an interpretative phenomenological inquiry. Int J Nurs Stud. 2009;46(6):838-847.
5. Cloitre M, Miranda R, Stovall-McClough KC, Han H. Beyond PTSD: emotion regulation and interpersonal problems as predictors of functional impairment in survivors of childhood abuse. Behav Ther. 2005;36(2):119-124.
6. McFarlane AC, Bookless C. The effect of PTSD on interpersonal relationships: issues for emergency service works. Sex Relation Ther. 2001;16(3):261-267.
7. Itzhaky L, Stein JY, Levin Y, Solomon Z. Posttraumatic stress symptoms and marital adjustment among Israeli combat veterans: the role of loneliness and attachment. Psychol Trauma. 2017;9(6):655-662.
8. Dekel R, Monson CM. Military-related post-traumatic stress disorder and family relations: current knowledge and future directions. Aggress Violent Behav. 2010;15(4):303-309.
9. Allen ES, Rhoades GK, Stanley SM, Markman HJ. Hitting home: relationships between recent deployment, posttraumatic stress symptoms, and marital functioning for Army couples. J Fam Psychol. 2010;24(3):280-288.
10. Laffaye C, Cavella S, Drescher K, Rosen C. Relationships among PTSD symptoms, social support, and support source in veterans with chronic PTSD. J Trauma Stress. 2008;21(4):394-401.
11. Meis LA, Noorbaloochi S, Hagel Campbell EM, et al. Sticking it out in trauma-focused treatment for PTSD: it takes a village. J Consult Clin Psychol. 2019;87(3):246-256.
12. Lewis JM, Gossett JT, Housson MM, Owen MT. Timberlawn Couple and Family Evaluation Scales. Dallas, TX: Timberlawn Psychiatric Research Foundation; 1999.
13. Fincham FD, Linfield KJ. A new look at marital quality: can spouses feel positive and negative about their marriage? J Fam Psychol. 1997;11(4):489-502.
14. Kaplan KJ. On the ambivalence-indifference problem in attitude theory and measurement: a suggested modification of the semantic differential technique. Psychol Bull. 1972;77(5):361-372.
15. Buhrmester D, Furman W. The Network of Relationship Inventory: Relationship Qualities Version [unpublished measure]. University of Texas at Dallas; 2008.
16. Busby DM, Christensen C, Crane DR, Larson JH. A revision of the Dyadic Adjustment Scale for use with distressed and nondistressed couples: construct hierarchy and multidimensional scales. J Marital Fam Ther. 1995;21(3):289-308.
17. Davis MH. A multidimensional approach to individual differences in empathy. JSAS Catalog Sel Doc Psychol. 1980;10:85.
18. Fraley RC, Waller NG, Brennan KA. An item-response theory analysis of self-report measures of adult attachment. J Pers Soc Psychol. 2000;78(2):350-365.
19. Tabachnick BG, Fidell L. Using Multivariate Statistics. 6th ed. Boston, MA: Pearson; 2013.
20. Sautter FJ, Armelie AP, Glynn SM, Wielt DB. The development of a couple-based treatment for PTSD in returning veterans. Prof Psychol Res Pr. 2011;42(1):63-69.
21. Jacobson NS, Christensen A, Prince SE, Cordova J, Eldridge K. Integrative behavioral couple therapy: an acceptance-based, promising new treatment of couple discord. J Consult Clin Psychol. 2000;9(2):351-355.
22. Makin-Byrd K, Gifford E, McCutcheon S, Glynn S. Family and couples treatment for newly returning veterans. Prof Psychol Res Pr. 2011;42(1):47-55.
23. Peterson K, Anderson J, Bourne D. Evidence Brief: Use of Patient Reported Outcome Measures for Measurement Based Care in Mental Health Shared Decision Making. Washington, DC: Department of Veterans Affairs; 2018. https://www.ncbi.nlm.nih.gov/books/NBK536143. Accessed September 13, 2019.
24. Fortney JC, Unützer J, Wrenn G, et al. A tipping point for measurement-based care. Psychiatr Serv. 2017;68(2):179-188.
25. Costello AB, Osborne JW. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005;10(7):1-9.
Although about 8.3% of the general adult civilian population will be diagnosed with posttraumatic stress disorder (PTSD) in their lifetime, rates of PTSD are even higher in the veteran population.1,2 PTSD is associated with a number of psychosocial consequences in veterans, including decreased intimate partner relationship functioning.3,4 For example, Cloitre and colleagues reported that PTSD is associated with difficulty with socializing, intimacy, responsibility, and control, all of which increase difficulties in intimate partner relationships.5 Similarly, researchers also have noted that traumatic experiences can affect an individual’s attachment style, resulting in progressive avoidance of interpersonal relationships, which can lead to marked difficulties in maintaining and beginning intimate partner relationships.6,7 Despite these known consequences of PTSD, as Dekel and Monson noted in a review,further research is still needed regarding the mechanisms by which trauma and PTSD result in decreased intimate partner relationship functioning among veterans.8 Nonetheless, as positive interpersonal relationships are associated with decreased PTSD symptom severity9,10 and increased engagement in PTSD treatment,11 determining methods of measuring intimate partner relationship functioning in veterans with PTSD is important to inform future research and aid the provision of care.
To date, limited research has examined the valid measurement of intimate partner relationship functioning among veterans with PTSD. Many existing measures that comprehensively assess intimate partner relationship functioning are time and resource intensive. One such measure, the Timberlawn Couple and Family Evaluation Scales (TCFES), comprehensively assesses multiple pertinent domains of intimate partner relationship functioning (ie, structure, autonomy, problem solving, affect regulation, and disagreement/conflict).12 By assessing multiple domains, the TCFES offers a method of understanding the specific components of an individual’s intimate partner relationship in need of increased clinical attention.12 However, the TCFES is a time- and labor-intensive observational measure that requires a couple to interact while a blinded, independent rater observes and rates their interactions using an intricate coding process. This survey structure precludes the ability to quickly and comprehensively assess a veteran’s intimate partner functioning in settings such as mental health outpatient clinics where mental health providers engage in brief, time-limited psychotherapy. As such, brief measures of intimate partner relationship functioning are needed to best inform clinical care among veterans with PTSD.
The primary aim of the current study was to create a psychometrically valid, yet brief, self-report version of the TCFES to assess multiple domains of intimate partner relationship functioning. The psychometric properties of this measure were assessed among a sample of US veterans with PTSD who were in an intimate partner relationship. We specifically examined factor structure, reliability, and associations to established measures of specific domains of relational functioning.
Methods
Ninety-four veterans were recruited via posted advertisements, promotion in PTSD therapy groups/staff meetings, and word of mouth at the Dallas Veterans Affairs Medical Center (VAMC). Participants were eligible if they had a documented diagnosis of PTSD as confirmed in the veteran’s electronic medical record and an affirmative response to currently being involved in an intimate partner relationship (ie, legally married, common-law spouse, involved in a relationship/partnership). There were no exclusion criteria.
Interested veterans were invited to complete several study-related self-report measures concerning their intimate partner relationships that would take about an hour. They were informed that the surveys were voluntary and confidential, and that they would be compensated for their participation. All veterans who participated provided written consent and the study was approved by the Dallas VAMC institutional review board.
Of the 94 veterans recruited, 3 veterans’ data were removed from current analyses after informed consent but before completing the surveys when they indicated they were not currently in a relationship or were divorced. After consent, the 91 participants were administered several study-related self-report measures. The measures took between 30 and 55 minutes to complete. Participants were then compensated $25 for their participation.
Intimate Partner Relationship Functioning
The 16-item TCFES self-report version (TCFES-SR) was developed to assess multiple domains of interpersonal functioning (Appendix). The observational TCFES assesses 5 intimate partner relationship characteristic domains (ie, structure, autonomy, problem solving, affect regulation, and disagreement/conflict) during a couple’s interaction by an independent trained rater.12 Each of the 16 TCFES-SR items were modeled after original constructs measured by the TCFES, including power, closeness, clarify, other’s views, responsibility, closure, negotiation, expressiveness, responsiveness, positive regard, negative regard, mood/tone, empathy, frequency, affective quality, and generalization and escalation. To maintain consistency with the TCFES, each item of the TCFES-SR was scored from 1 (severely dysfunctional) to 5 (highly functional). Additionally, all item wording for the TCFES-SR was based on wording in the TCFES manual after consultation with an expert who facilitated the development of the TCFES.12 On average, the TCFES-SR took 5 to 10 minutes to complete.
To measure concurrent validity of the modified TCFES-SR, several additional interpersonal measures were selected and administered based on prior research and established domains of the TCFES. The Positive and Negative Quality in Marriage Scale (PANQIMS) was administered to assess perceived attitudes toward a relationship.13,14 The PANQIMS generates 2 subscales: positive quality and negative quality in the relationship. Because the PANQIMS specifically assesses married relationships and our sample included married and nonmarried participants, wording was modified (eg, “spouse/partner”).
The relative power subscale of the Network Relationships Inventory–Relationship Qualities Version (NRI-RQV) measure was administered to assess the unequal/shared role romantic partners have in power equality (ie, relative power).15
The Revised Dyadic Adjustment Scale (RDAS) is a self-report measure that assesses multiple dimensions of marital adjustment and functioning.16 Six subscales of the RDAS were chosen based on items of the TCFES-SR: decision making, values, affection, conflict, activities, and discussion.
The Interpersonal Reactivity Index (IRI) empathetic concern subscale was administered to assess empathy across multiple contexts and situations17 and the Experiences in Close Relationships-Revised Questionnaire (ECR-R) was administered to assess relational functioning by determining attachment-related anxiety and avoidance.18
Sociodemographic Information
A sociodemographic questionnaire also was administered. The questionnaire assessed gender, age, education, service branch, length of interpersonal relationship, race, and ethnicity of the veteran as well as gender of the veteran’s partner.
Statistical Analysis
Factor structure of the TCFES-SR was determined by conducting an exploratory factor analysis. To allow for correlation between items, the Promax oblique rotation method was chosen.19 Number of factors was determined by agreement between number of eigenvalues ≥ 1, visual inspection of the scree plot, and a parallel analysis. Factor loadings of ≥ 0.3 were used to determine which items loaded on to which factors.
Convergent validity was assessed by conducting Pearson’s bivariate correlations between identified TCFES-SR factor(s) and other administered measures of interpersonal functioning (ie, PANQIMS positive and negative quality; NRI-RQV relative power subscale; RDAS decision making, values, affection, conflict, activities, and discussion subscales; IRI-empathetic concern subscale; and ECR-R attachment-related anxiety and avoidance subscales). Strength of relationship was determined based on the following guidelines: ± 0.3 to 0.49 = small, ± 0.5 to 0.69 = moderate, and ± 0.7 to 1.00 = large. Internal consistency was also determined for TCFES-SR factor(s) using Cronbach’s α. A standard level of significance (α=.05) was used for all statistical analyses.
Results
Eighty-six veterans provided complete data (Table 1). The Kaiser-Meyer-Olkin measure of sampling adequacy was indicative that sample size was adequate (.91), while Bartlett’s test of sphericity found the variables were suitable for structure detection, χ2 (120) = 800.00, P < .001. While 2 eigenvalues were ≥ 1, visual inspection of the scree plot and subsequent parallel analysis identified a unidimensional structure (ie, 1 factor) for the TCFES-SR. All items were found to load to this single factor, with all loadings being ≥ 0.5 (Table 2). Additionally, internal consistency was excellent for the scale (α = .93).
Pearson’s bivariate correlations were significant (P < .05) between TCFES-SR total score, and almost all administered interpersonal functioning measures (Table 3). Interestingly, no significant associations were found between any of the administered measures, including the TCFES-SR total score, and the IRI-empathetic concern subscale (P > .05).
Discussion
These findings provide initial support for the psychometric properties of the TCFES-SR, including excellent internal consistency and the adequate association of its total score to established measures of interpersonal functioning. Contrary to the TCFES, the TCFES-SR was shown to best fit a unidimensional factor rather than a multidimensional measure of relationship functioning. However, the TCFES-SR was also shown to have strong convergent validity with multiple domains of relationship functioning, indicating that the measure of overall intimate partner relationship functioning encompasses a number of relational domains (ie, structure, autonomy, problem solving, affect regulation, and disagreement/conflict). Critically, the TCFES-SR is brief and was administered easily in our sample, providing utility as clinical tool to be used in time-sensitive outpatient settings.
A unidimensional factor has particular strength in providing a global portrait of perceived intimate partner relationship functioning, and mental health providers can administer the TCFES-SR to assess for overall perceptions of intimate partner relationship functioning rather than administering a number of measures focusing on specific interpersonal domains (eg, decision making processes or positive/negative attitudes towards one’s relationship). This allows for the quick assessment (ie, 5-10 minutes) of overall intimate partner relationship functioning rather than administration of multiple self-report measures which can be time-intensive and expensive. However, the TCFES-SR also is limited by a lack of nuanced understanding of perceptions of functioning specific to particular domains. For example, the TCFES-SR score cannot describe intimate partner functioning in the domain of problem solving. Therefore, brief screening tools need to be developed that assess multiple intimate partner relationship domains.
Importantly, overall intimate partner relationship functioning as measured by the TCFES-SR may not incorporate perceptions of relationship empathy, as the total score did not correlate with a measure of empathetic concern (ie, the IRI-empathetic concern subscale). As empathy was based on one item in the TCFES-SR vs 7 in the IRI-empathetic concern subscale, it is unclear if the TCFES-SR only captures a portion of the construct of empathy (ie, sensitivity to partner) vs the comprehensive assessment of trait empathy that the IRI subscale measures. Additionally, the IRI-empathetic concern subscale did not significantly correlate with any of the other administered measures of relationship functioning. Given the role of empathy in positive, healthy intimate partner relationships, future research should explore the role of empathetic concern among veterans with PTSD as it relates to overall (eg, TCFES-SR) and specific aspects of intimate partner relationship functioning.20
While the clinical applicability of the TCFES-SR requires further examination, this measure has a number of potential uses. Information captured quickly by the TCFES-SR may help to inform appropriate referral for treatment. For instance, veterans reporting low total scores on the TCFES-SR may indicate a need for a referral for intervention focused on improving overall relationship functioning (eg, Integrative Behavioral Couple Therapy).21,22 Measurement-based care (ie, tracking and discussing changes in symptoms during treatment using validated self-report measures) is now required by the Joint Commission as a standard of care,and has been shown to improve outcomes in couples therapy.23,24 As a brief self-report measure, the TCFES-SR may be able to facilitate measurement-based care and assist providers in tracking changes in overall relationship functioning over the course of treatment. However, the purpose of the current study was to validate the TCFES-SR and not to examine the utility of the TCFES-SR in clinical care; additional research is needed to determine standardized cutoff scores to indicate a need for clinical intervention.
Limitations
Several limitations should be noted. The current study only assessed perceived intimate partner relationship functioning from the perspective of the veteran, thus limiting implications as it pertains to the spouse/partner of the veteran. PTSD diagnosis was based on chart review rather than a psychodiagnostic measure (eg, Clinician Administered PTSD Scale); therefore, whether this diagnosis was current or in remission was unclear. Although our sample was adequate to conduct an exploratory factor analysis,the overall sample size was modest, and results should be considered preliminary with need for further replication.25 The sample was also primarily male, white or black, and non-Hispanic; therefore, results may not generalize to a more sociodemographically diverse population. Finally, given the focus of the study to develop a self-report measure, we did not compare the TCFES-SR to the original TCFES. Thus, further research examining the relationship between the TCFES-SR and TCFES may be needed to better understand overlap and potential incongruence in these measures, and to ascertain any differences in their factor structures.
Conclusion
This study is novel in that it adapted a comprehensive observational measure of relationship functioning to a self-report measure piloted among a sample of veterans with PTSD in an intimate partner relationship, a clinical population that remains largely understudied. Although findings are preliminary, the TCFES-SR was found to be a reliable and valid measure of overall intimate partner relationship functioning. Given the rapid administration of this self-report measure, the TCFES-SR may hold clinical utility as a screen of intimate partner relationship deficits in need of clinical intervention. Replication in a larger, more diverse sample is needed to further examine the generalizability and confirm psychometric properties of the TCFES-SR. Additionally, further understanding of the clinical utility of the TCFES-SR in treatment settings remains critical to promote the development and maintenance of healthy intimate partner relationships among veterans with PTSD. Finally, development of effective self-report measures of intimate partner relationship functioning, such as the TCFES-SR, may help to facilitate needed research to understand the effect of PTSD on establishing and maintaining healthy intimate partner relationships among veterans.
Acknowledgments
The current study was funded by the Timberlawn Psychiatric Research Foundation. This material is the result of work supported in part by the US Department of Veterans Affairs; the Rocky Mountain Mental Illness Research, Education and Clinical Center (MIRECC) for Suicide Prevention; Sierra Pacific MIRECC; and the Office of Academic Affiliations, Advanced Fellowship Program in Mental Illness Research and Treatment, Department of Veterans Affairs.
Although about 8.3% of the general adult civilian population will be diagnosed with posttraumatic stress disorder (PTSD) in their lifetime, rates of PTSD are even higher in the veteran population.1,2 PTSD is associated with a number of psychosocial consequences in veterans, including decreased intimate partner relationship functioning.3,4 For example, Cloitre and colleagues reported that PTSD is associated with difficulty with socializing, intimacy, responsibility, and control, all of which increase difficulties in intimate partner relationships.5 Similarly, researchers also have noted that traumatic experiences can affect an individual’s attachment style, resulting in progressive avoidance of interpersonal relationships, which can lead to marked difficulties in maintaining and beginning intimate partner relationships.6,7 Despite these known consequences of PTSD, as Dekel and Monson noted in a review,further research is still needed regarding the mechanisms by which trauma and PTSD result in decreased intimate partner relationship functioning among veterans.8 Nonetheless, as positive interpersonal relationships are associated with decreased PTSD symptom severity9,10 and increased engagement in PTSD treatment,11 determining methods of measuring intimate partner relationship functioning in veterans with PTSD is important to inform future research and aid the provision of care.
To date, limited research has examined the valid measurement of intimate partner relationship functioning among veterans with PTSD. Many existing measures that comprehensively assess intimate partner relationship functioning are time and resource intensive. One such measure, the Timberlawn Couple and Family Evaluation Scales (TCFES), comprehensively assesses multiple pertinent domains of intimate partner relationship functioning (ie, structure, autonomy, problem solving, affect regulation, and disagreement/conflict).12 By assessing multiple domains, the TCFES offers a method of understanding the specific components of an individual’s intimate partner relationship in need of increased clinical attention.12 However, the TCFES is a time- and labor-intensive observational measure that requires a couple to interact while a blinded, independent rater observes and rates their interactions using an intricate coding process. This survey structure precludes the ability to quickly and comprehensively assess a veteran’s intimate partner functioning in settings such as mental health outpatient clinics where mental health providers engage in brief, time-limited psychotherapy. As such, brief measures of intimate partner relationship functioning are needed to best inform clinical care among veterans with PTSD.
The primary aim of the current study was to create a psychometrically valid, yet brief, self-report version of the TCFES to assess multiple domains of intimate partner relationship functioning. The psychometric properties of this measure were assessed among a sample of US veterans with PTSD who were in an intimate partner relationship. We specifically examined factor structure, reliability, and associations to established measures of specific domains of relational functioning.
Methods
Ninety-four veterans were recruited via posted advertisements, promotion in PTSD therapy groups/staff meetings, and word of mouth at the Dallas Veterans Affairs Medical Center (VAMC). Participants were eligible if they had a documented diagnosis of PTSD as confirmed in the veteran’s electronic medical record and an affirmative response to currently being involved in an intimate partner relationship (ie, legally married, common-law spouse, involved in a relationship/partnership). There were no exclusion criteria.
Interested veterans were invited to complete several study-related self-report measures concerning their intimate partner relationships that would take about an hour. They were informed that the surveys were voluntary and confidential, and that they would be compensated for their participation. All veterans who participated provided written consent and the study was approved by the Dallas VAMC institutional review board.
Of the 94 veterans recruited, 3 veterans’ data were removed from current analyses after informed consent but before completing the surveys when they indicated they were not currently in a relationship or were divorced. After consent, the 91 participants were administered several study-related self-report measures. The measures took between 30 and 55 minutes to complete. Participants were then compensated $25 for their participation.
Intimate Partner Relationship Functioning
The 16-item TCFES self-report version (TCFES-SR) was developed to assess multiple domains of interpersonal functioning (Appendix). The observational TCFES assesses 5 intimate partner relationship characteristic domains (ie, structure, autonomy, problem solving, affect regulation, and disagreement/conflict) during a couple’s interaction by an independent trained rater.12 Each of the 16 TCFES-SR items were modeled after original constructs measured by the TCFES, including power, closeness, clarify, other’s views, responsibility, closure, negotiation, expressiveness, responsiveness, positive regard, negative regard, mood/tone, empathy, frequency, affective quality, and generalization and escalation. To maintain consistency with the TCFES, each item of the TCFES-SR was scored from 1 (severely dysfunctional) to 5 (highly functional). Additionally, all item wording for the TCFES-SR was based on wording in the TCFES manual after consultation with an expert who facilitated the development of the TCFES.12 On average, the TCFES-SR took 5 to 10 minutes to complete.
To measure concurrent validity of the modified TCFES-SR, several additional interpersonal measures were selected and administered based on prior research and established domains of the TCFES. The Positive and Negative Quality in Marriage Scale (PANQIMS) was administered to assess perceived attitudes toward a relationship.13,14 The PANQIMS generates 2 subscales: positive quality and negative quality in the relationship. Because the PANQIMS specifically assesses married relationships and our sample included married and nonmarried participants, wording was modified (eg, “spouse/partner”).
The relative power subscale of the Network Relationships Inventory–Relationship Qualities Version (NRI-RQV) measure was administered to assess the unequal/shared role romantic partners have in power equality (ie, relative power).15
The Revised Dyadic Adjustment Scale (RDAS) is a self-report measure that assesses multiple dimensions of marital adjustment and functioning.16 Six subscales of the RDAS were chosen based on items of the TCFES-SR: decision making, values, affection, conflict, activities, and discussion.
The Interpersonal Reactivity Index (IRI) empathetic concern subscale was administered to assess empathy across multiple contexts and situations17 and the Experiences in Close Relationships-Revised Questionnaire (ECR-R) was administered to assess relational functioning by determining attachment-related anxiety and avoidance.18
Sociodemographic Information
A sociodemographic questionnaire also was administered. The questionnaire assessed gender, age, education, service branch, length of interpersonal relationship, race, and ethnicity of the veteran as well as gender of the veteran’s partner.
Statistical Analysis
Factor structure of the TCFES-SR was determined by conducting an exploratory factor analysis. To allow for correlation between items, the Promax oblique rotation method was chosen.19 Number of factors was determined by agreement between number of eigenvalues ≥ 1, visual inspection of the scree plot, and a parallel analysis. Factor loadings of ≥ 0.3 were used to determine which items loaded on to which factors.
Convergent validity was assessed by conducting Pearson’s bivariate correlations between identified TCFES-SR factor(s) and other administered measures of interpersonal functioning (ie, PANQIMS positive and negative quality; NRI-RQV relative power subscale; RDAS decision making, values, affection, conflict, activities, and discussion subscales; IRI-empathetic concern subscale; and ECR-R attachment-related anxiety and avoidance subscales). Strength of relationship was determined based on the following guidelines: ± 0.3 to 0.49 = small, ± 0.5 to 0.69 = moderate, and ± 0.7 to 1.00 = large. Internal consistency was also determined for TCFES-SR factor(s) using Cronbach’s α. A standard level of significance (α=.05) was used for all statistical analyses.
Results
Eighty-six veterans provided complete data (Table 1). The Kaiser-Meyer-Olkin measure of sampling adequacy was indicative that sample size was adequate (.91), while Bartlett’s test of sphericity found the variables were suitable for structure detection, χ2 (120) = 800.00, P < .001. While 2 eigenvalues were ≥ 1, visual inspection of the scree plot and subsequent parallel analysis identified a unidimensional structure (ie, 1 factor) for the TCFES-SR. All items were found to load to this single factor, with all loadings being ≥ 0.5 (Table 2). Additionally, internal consistency was excellent for the scale (α = .93).
Pearson’s bivariate correlations were significant (P < .05) between TCFES-SR total score, and almost all administered interpersonal functioning measures (Table 3). Interestingly, no significant associations were found between any of the administered measures, including the TCFES-SR total score, and the IRI-empathetic concern subscale (P > .05).
Discussion
These findings provide initial support for the psychometric properties of the TCFES-SR, including excellent internal consistency and the adequate association of its total score to established measures of interpersonal functioning. Contrary to the TCFES, the TCFES-SR was shown to best fit a unidimensional factor rather than a multidimensional measure of relationship functioning. However, the TCFES-SR was also shown to have strong convergent validity with multiple domains of relationship functioning, indicating that the measure of overall intimate partner relationship functioning encompasses a number of relational domains (ie, structure, autonomy, problem solving, affect regulation, and disagreement/conflict). Critically, the TCFES-SR is brief and was administered easily in our sample, providing utility as clinical tool to be used in time-sensitive outpatient settings.
A unidimensional factor has particular strength in providing a global portrait of perceived intimate partner relationship functioning, and mental health providers can administer the TCFES-SR to assess for overall perceptions of intimate partner relationship functioning rather than administering a number of measures focusing on specific interpersonal domains (eg, decision making processes or positive/negative attitudes towards one’s relationship). This allows for the quick assessment (ie, 5-10 minutes) of overall intimate partner relationship functioning rather than administration of multiple self-report measures which can be time-intensive and expensive. However, the TCFES-SR also is limited by a lack of nuanced understanding of perceptions of functioning specific to particular domains. For example, the TCFES-SR score cannot describe intimate partner functioning in the domain of problem solving. Therefore, brief screening tools need to be developed that assess multiple intimate partner relationship domains.
Importantly, overall intimate partner relationship functioning as measured by the TCFES-SR may not incorporate perceptions of relationship empathy, as the total score did not correlate with a measure of empathetic concern (ie, the IRI-empathetic concern subscale). As empathy was based on one item in the TCFES-SR vs 7 in the IRI-empathetic concern subscale, it is unclear if the TCFES-SR only captures a portion of the construct of empathy (ie, sensitivity to partner) vs the comprehensive assessment of trait empathy that the IRI subscale measures. Additionally, the IRI-empathetic concern subscale did not significantly correlate with any of the other administered measures of relationship functioning. Given the role of empathy in positive, healthy intimate partner relationships, future research should explore the role of empathetic concern among veterans with PTSD as it relates to overall (eg, TCFES-SR) and specific aspects of intimate partner relationship functioning.20
While the clinical applicability of the TCFES-SR requires further examination, this measure has a number of potential uses. Information captured quickly by the TCFES-SR may help to inform appropriate referral for treatment. For instance, veterans reporting low total scores on the TCFES-SR may indicate a need for a referral for intervention focused on improving overall relationship functioning (eg, Integrative Behavioral Couple Therapy).21,22 Measurement-based care (ie, tracking and discussing changes in symptoms during treatment using validated self-report measures) is now required by the Joint Commission as a standard of care,and has been shown to improve outcomes in couples therapy.23,24 As a brief self-report measure, the TCFES-SR may be able to facilitate measurement-based care and assist providers in tracking changes in overall relationship functioning over the course of treatment. However, the purpose of the current study was to validate the TCFES-SR and not to examine the utility of the TCFES-SR in clinical care; additional research is needed to determine standardized cutoff scores to indicate a need for clinical intervention.
Limitations
Several limitations should be noted. The current study only assessed perceived intimate partner relationship functioning from the perspective of the veteran, thus limiting implications as it pertains to the spouse/partner of the veteran. PTSD diagnosis was based on chart review rather than a psychodiagnostic measure (eg, Clinician Administered PTSD Scale); therefore, whether this diagnosis was current or in remission was unclear. Although our sample was adequate to conduct an exploratory factor analysis,the overall sample size was modest, and results should be considered preliminary with need for further replication.25 The sample was also primarily male, white or black, and non-Hispanic; therefore, results may not generalize to a more sociodemographically diverse population. Finally, given the focus of the study to develop a self-report measure, we did not compare the TCFES-SR to the original TCFES. Thus, further research examining the relationship between the TCFES-SR and TCFES may be needed to better understand overlap and potential incongruence in these measures, and to ascertain any differences in their factor structures.
Conclusion
This study is novel in that it adapted a comprehensive observational measure of relationship functioning to a self-report measure piloted among a sample of veterans with PTSD in an intimate partner relationship, a clinical population that remains largely understudied. Although findings are preliminary, the TCFES-SR was found to be a reliable and valid measure of overall intimate partner relationship functioning. Given the rapid administration of this self-report measure, the TCFES-SR may hold clinical utility as a screen of intimate partner relationship deficits in need of clinical intervention. Replication in a larger, more diverse sample is needed to further examine the generalizability and confirm psychometric properties of the TCFES-SR. Additionally, further understanding of the clinical utility of the TCFES-SR in treatment settings remains critical to promote the development and maintenance of healthy intimate partner relationships among veterans with PTSD. Finally, development of effective self-report measures of intimate partner relationship functioning, such as the TCFES-SR, may help to facilitate needed research to understand the effect of PTSD on establishing and maintaining healthy intimate partner relationships among veterans.
Acknowledgments
The current study was funded by the Timberlawn Psychiatric Research Foundation. This material is the result of work supported in part by the US Department of Veterans Affairs; the Rocky Mountain Mental Illness Research, Education and Clinical Center (MIRECC) for Suicide Prevention; Sierra Pacific MIRECC; and the Office of Academic Affiliations, Advanced Fellowship Program in Mental Illness Research and Treatment, Department of Veterans Affairs.
1. Kilpatrick DG, Resnick HS, Milanak ME, Miller MW, Keyes KM, Friedman MJ. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. J Trauma Stress. 2013;26(5):537-547.
2. Lehavot K, Goldberg SB, Chen JA, et al. Do trauma type, stressful life events, and social support explain women veterans’ high prevalence of PTSD? Soc Psychiatry Psychiatr Epidemiol. 2018;53(9):943-953.
3. Galovski T, Lyons JA. Psychological sequelae of combat violence: a review of the impact of PTSD on the veteran’s family and possible interventions. Aggress Violent Behav. 2004;9(5):477-501.
4. Ray SL, Vanstone M. The impact of PTSD on veterans’ family relationships: an interpretative phenomenological inquiry. Int J Nurs Stud. 2009;46(6):838-847.
5. Cloitre M, Miranda R, Stovall-McClough KC, Han H. Beyond PTSD: emotion regulation and interpersonal problems as predictors of functional impairment in survivors of childhood abuse. Behav Ther. 2005;36(2):119-124.
6. McFarlane AC, Bookless C. The effect of PTSD on interpersonal relationships: issues for emergency service works. Sex Relation Ther. 2001;16(3):261-267.
7. Itzhaky L, Stein JY, Levin Y, Solomon Z. Posttraumatic stress symptoms and marital adjustment among Israeli combat veterans: the role of loneliness and attachment. Psychol Trauma. 2017;9(6):655-662.
8. Dekel R, Monson CM. Military-related post-traumatic stress disorder and family relations: current knowledge and future directions. Aggress Violent Behav. 2010;15(4):303-309.
9. Allen ES, Rhoades GK, Stanley SM, Markman HJ. Hitting home: relationships between recent deployment, posttraumatic stress symptoms, and marital functioning for Army couples. J Fam Psychol. 2010;24(3):280-288.
10. Laffaye C, Cavella S, Drescher K, Rosen C. Relationships among PTSD symptoms, social support, and support source in veterans with chronic PTSD. J Trauma Stress. 2008;21(4):394-401.
11. Meis LA, Noorbaloochi S, Hagel Campbell EM, et al. Sticking it out in trauma-focused treatment for PTSD: it takes a village. J Consult Clin Psychol. 2019;87(3):246-256.
12. Lewis JM, Gossett JT, Housson MM, Owen MT. Timberlawn Couple and Family Evaluation Scales. Dallas, TX: Timberlawn Psychiatric Research Foundation; 1999.
13. Fincham FD, Linfield KJ. A new look at marital quality: can spouses feel positive and negative about their marriage? J Fam Psychol. 1997;11(4):489-502.
14. Kaplan KJ. On the ambivalence-indifference problem in attitude theory and measurement: a suggested modification of the semantic differential technique. Psychol Bull. 1972;77(5):361-372.
15. Buhrmester D, Furman W. The Network of Relationship Inventory: Relationship Qualities Version [unpublished measure]. University of Texas at Dallas; 2008.
16. Busby DM, Christensen C, Crane DR, Larson JH. A revision of the Dyadic Adjustment Scale for use with distressed and nondistressed couples: construct hierarchy and multidimensional scales. J Marital Fam Ther. 1995;21(3):289-308.
17. Davis MH. A multidimensional approach to individual differences in empathy. JSAS Catalog Sel Doc Psychol. 1980;10:85.
18. Fraley RC, Waller NG, Brennan KA. An item-response theory analysis of self-report measures of adult attachment. J Pers Soc Psychol. 2000;78(2):350-365.
19. Tabachnick BG, Fidell L. Using Multivariate Statistics. 6th ed. Boston, MA: Pearson; 2013.
20. Sautter FJ, Armelie AP, Glynn SM, Wielt DB. The development of a couple-based treatment for PTSD in returning veterans. Prof Psychol Res Pr. 2011;42(1):63-69.
21. Jacobson NS, Christensen A, Prince SE, Cordova J, Eldridge K. Integrative behavioral couple therapy: an acceptance-based, promising new treatment of couple discord. J Consult Clin Psychol. 2000;9(2):351-355.
22. Makin-Byrd K, Gifford E, McCutcheon S, Glynn S. Family and couples treatment for newly returning veterans. Prof Psychol Res Pr. 2011;42(1):47-55.
23. Peterson K, Anderson J, Bourne D. Evidence Brief: Use of Patient Reported Outcome Measures for Measurement Based Care in Mental Health Shared Decision Making. Washington, DC: Department of Veterans Affairs; 2018. https://www.ncbi.nlm.nih.gov/books/NBK536143. Accessed September 13, 2019.
24. Fortney JC, Unützer J, Wrenn G, et al. A tipping point for measurement-based care. Psychiatr Serv. 2017;68(2):179-188.
25. Costello AB, Osborne JW. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005;10(7):1-9.
1. Kilpatrick DG, Resnick HS, Milanak ME, Miller MW, Keyes KM, Friedman MJ. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. J Trauma Stress. 2013;26(5):537-547.
2. Lehavot K, Goldberg SB, Chen JA, et al. Do trauma type, stressful life events, and social support explain women veterans’ high prevalence of PTSD? Soc Psychiatry Psychiatr Epidemiol. 2018;53(9):943-953.
3. Galovski T, Lyons JA. Psychological sequelae of combat violence: a review of the impact of PTSD on the veteran’s family and possible interventions. Aggress Violent Behav. 2004;9(5):477-501.
4. Ray SL, Vanstone M. The impact of PTSD on veterans’ family relationships: an interpretative phenomenological inquiry. Int J Nurs Stud. 2009;46(6):838-847.
5. Cloitre M, Miranda R, Stovall-McClough KC, Han H. Beyond PTSD: emotion regulation and interpersonal problems as predictors of functional impairment in survivors of childhood abuse. Behav Ther. 2005;36(2):119-124.
6. McFarlane AC, Bookless C. The effect of PTSD on interpersonal relationships: issues for emergency service works. Sex Relation Ther. 2001;16(3):261-267.
7. Itzhaky L, Stein JY, Levin Y, Solomon Z. Posttraumatic stress symptoms and marital adjustment among Israeli combat veterans: the role of loneliness and attachment. Psychol Trauma. 2017;9(6):655-662.
8. Dekel R, Monson CM. Military-related post-traumatic stress disorder and family relations: current knowledge and future directions. Aggress Violent Behav. 2010;15(4):303-309.
9. Allen ES, Rhoades GK, Stanley SM, Markman HJ. Hitting home: relationships between recent deployment, posttraumatic stress symptoms, and marital functioning for Army couples. J Fam Psychol. 2010;24(3):280-288.
10. Laffaye C, Cavella S, Drescher K, Rosen C. Relationships among PTSD symptoms, social support, and support source in veterans with chronic PTSD. J Trauma Stress. 2008;21(4):394-401.
11. Meis LA, Noorbaloochi S, Hagel Campbell EM, et al. Sticking it out in trauma-focused treatment for PTSD: it takes a village. J Consult Clin Psychol. 2019;87(3):246-256.
12. Lewis JM, Gossett JT, Housson MM, Owen MT. Timberlawn Couple and Family Evaluation Scales. Dallas, TX: Timberlawn Psychiatric Research Foundation; 1999.
13. Fincham FD, Linfield KJ. A new look at marital quality: can spouses feel positive and negative about their marriage? J Fam Psychol. 1997;11(4):489-502.
14. Kaplan KJ. On the ambivalence-indifference problem in attitude theory and measurement: a suggested modification of the semantic differential technique. Psychol Bull. 1972;77(5):361-372.
15. Buhrmester D, Furman W. The Network of Relationship Inventory: Relationship Qualities Version [unpublished measure]. University of Texas at Dallas; 2008.
16. Busby DM, Christensen C, Crane DR, Larson JH. A revision of the Dyadic Adjustment Scale for use with distressed and nondistressed couples: construct hierarchy and multidimensional scales. J Marital Fam Ther. 1995;21(3):289-308.
17. Davis MH. A multidimensional approach to individual differences in empathy. JSAS Catalog Sel Doc Psychol. 1980;10:85.
18. Fraley RC, Waller NG, Brennan KA. An item-response theory analysis of self-report measures of adult attachment. J Pers Soc Psychol. 2000;78(2):350-365.
19. Tabachnick BG, Fidell L. Using Multivariate Statistics. 6th ed. Boston, MA: Pearson; 2013.
20. Sautter FJ, Armelie AP, Glynn SM, Wielt DB. The development of a couple-based treatment for PTSD in returning veterans. Prof Psychol Res Pr. 2011;42(1):63-69.
21. Jacobson NS, Christensen A, Prince SE, Cordova J, Eldridge K. Integrative behavioral couple therapy: an acceptance-based, promising new treatment of couple discord. J Consult Clin Psychol. 2000;9(2):351-355.
22. Makin-Byrd K, Gifford E, McCutcheon S, Glynn S. Family and couples treatment for newly returning veterans. Prof Psychol Res Pr. 2011;42(1):47-55.
23. Peterson K, Anderson J, Bourne D. Evidence Brief: Use of Patient Reported Outcome Measures for Measurement Based Care in Mental Health Shared Decision Making. Washington, DC: Department of Veterans Affairs; 2018. https://www.ncbi.nlm.nih.gov/books/NBK536143. Accessed September 13, 2019.
24. Fortney JC, Unützer J, Wrenn G, et al. A tipping point for measurement-based care. Psychiatr Serv. 2017;68(2):179-188.
25. Costello AB, Osborne JW. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005;10(7):1-9.
Standardizing the Use of Mental Health Screening Instruments in Patients With Pain (FULL)
Chronic pain is more prevalent in the US than diabetes mellitus, cancer, and cardiovascular disease combined, impacting about 100 million adults.1 The annual cost of all that pain in the US is between $560 and $635 billion.1
The high prevalence of chronic pain among active duty service members and veterans remains a pressing concern given its negative impact on military readiness, health care utilization, productivity, quality of life, and chronic disability rates.2 Pain was found to be the leading complaint of service members returning from Operations Iraqi Freedom and Enduring Freedomand 44% of veterans returning from deployment suffered with chronic pain.3,4
Chronic pain often occurs in the presence of comorbidities. In one study for example, 45% of primary care patients with chronic pain (N = 250) screened positive for ≥ 1 of the 5 types of common anxiety disorders, and those with anxiety disorder had higher pain scores.5 Another study involving almost 6000 participants found that anxiety disorders were present in 35% of people with chronic pain compared with 18% in the general population.6
In addition, military members are prone to depression with a rate of major depressive disorder that is 5% higher than that of civilians.7 Depression often is underdiagnosed and undertreated. According to a National Center for Health Statistics, only 35% of those with symptoms of severe depression in the US saw a mental health provider in the previous year.8 Comorbid depression, anxiety, and chronic pain are strongly associated with more severe pain, greater disability, and poorer health-related quality of life.9
As a result, there was a call for system-level interventions to increase access to, and continuity of, mental health care services for active duty service members and veterans.1 It has been recommended that depression and anxiety screenings take place in primary and secondary care clinics.10 Standardized referral processes also are needed to enhance mental health diagnosis and referral techniques.11 Although various screening tools are available that have excellent reliability and construct validity (eg, General Anxiety Disorder-7 [GAD-7], Patient Health Questionnaire-9 [PHQ-9]), they are underutilized.12 I have witnessed a noticeable gap between clinical practice guidelines and current practice associated with chronic pain and screening for anxiety and depression within the Pain Management Clinic at Navy Medical Center of Camp Lejeune (NMCCL) in North Carolina.
Methods
The premise of this performance improvement (PI) project was to reduce missed opportunities of screening for anxiety and depression, and to examine the impact of the standardized use of the GAD-7 and PHQ-9 on the rate of mental health care referrals. The Theory of Unpleasant Symptoms was chosen as the underpinning of the project because it suggests that symptoms often cluster, and that the occurrence of multiple symptoms makes each of those, as well as other symptoms, worse.13 The PI model used the find, organize, clarify, understand, select (FOCUS), and plan, do, check, act (PDCA) models.14 The facility institutional review board ruled that this performance improvement project did not qualify as human research.
Inclusion and exclusion criteria
Patients were included if they were active duty service members aged 18 to 56 years at the initial patient encounter. Veterans and dependents were not part of the sample because of the high clinic volume. Patients who received mental health care services within the previous 90 days were excluded.
Registered nurses, licensed practical nurses, US Navy corpsman, medical assistants, and nurse aides were educated on the purpose of the GAD-7 and PHQ-9 and were instructed to have patients complete them upon every new patient encounter. A retrospective chart review was conducted over a 6-week time frame to collect and analyze de-identified demographic data including age, gender, prior deployment (yes or no), and branch of service. The review also examined whether the patient had received mental health care services, whether the screening instruments were completed, and whether a mental health referral was made. The clinic providers were asked to consider mental health care referrals for patients who scored ≥ 10 on either the GAD-7 or PHQ-9. The frequency of the use of the instruments and the number of mental health referrals made was calculated during the 3-week period before and after the standardized use of the instruments. The author conducted audits of the new patient charts at the end of each work day to assess whether the GAD-7 and PHQ-9 were completed.
Results
There were 117 new patient encounters during the 6-week project period. Thirty-three patients were excluded from the sample, leaving a remaining sample of 84. Thirty-two patients were included in the sample prior to the standardized use of the instruments, and 52 were included afterward (Table).
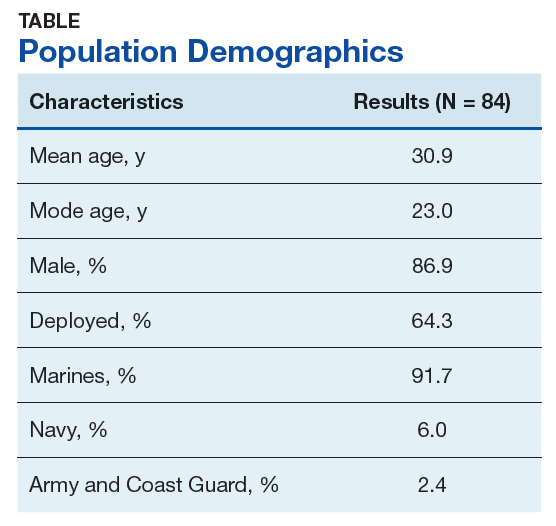
Prior to the standardized use of the screening tools, the GAD-7 was used during 75% of patient visits for pain and the PHQ-9 was used during 25%, reinforcing the premise of unpredictable utilization of the screening tools. Three mental health referrals were made during the 3-week period prior to the standardized use of the anxiety and depression instruments (3/32, 10%). After the standardized implementation of the GAD-7 and PHQ-9 tools, both instruments were used 98% of the time, and mental health referrals were made for 12 of 52 patients (23.1%). Eleven of the referrals were made based upon the trigger score of 10 on either the GAD-7 or PHQ-9. One referral was made for a patient with a score of 9 on the PHQ-9 because the provider determined a need for pain-related psychological services.
It was important to provide a link to mental health care because, as one study found, patients with a specific anxiety diagnosis are much more likely than those diagnosed with a not otherwise specified anxiety disorder to receive mental health care services (60% to 67% vs 37%).11 Similarly, patients diagnosed in specialty mental health care settings are more likely to receive mental health services than are those diagnosed in primary care.11 By the same token, experts estimate that 50% of those with severe depression symptoms are not properly diagnosed or treated in primary care.15
Strengths and Limitations
Utilization of the screening tools has led to further dialogue between patients and providers that anecdotally revealed suicidal ideation in some patients. Future studies could incorporate a qualitative component to include clinician and patient perceptions of mental health care services.
The study was limited by the lack of follow-up data to determine the effect of mental health care services on pain, function, or military readiness. Also, it is unclear whether education alone impacted the referral rate.
The author shared the outcomes of this PI project with fellow professionals at NMCCL. As a team, we explored ways for military to link with mental health care within their commands. The process of using these instruments is easily transferable to other clinics with no extraordinary cost.
Conclusion
The economic burden of major depressive disorder in the US has risen 21.5% from 2005 to 2010.16 Unfortunately, only 35% of those with symptoms of severe depression had contact with a mental health professional in the past year.8 Avoiding missing opportunities to screen for mental health conditions can decrease the disease burden. The GAD-7 and PHQ-9 are relatively cost free and are deemed reliable and valid for screening for, and determining the severity of, symptoms of anxiety and depression.12 The evidence suggests that screening for, and early recognition of, mental illness, are critical parts of evidence-based practice and provide the most cost-effective care.16
This PI project demonstrated that the standardized use of the GAD-7 and PHQ-9 during patient visits for pain did improve adherence to guidelines and resulted in a significant increase in the rate of mental health referrals from 10% to 23.1%. This information is valuable because a score of ≥ 10 on either screening instrument is considered the optimal cutoff for diagnosing and determining severity of anxiety and depression symptoms.12 The US Department of Veterans Affairs (VA) and the US Department of Defense (DoD) have jointly developed clinical practice guidelines, which recommend that interventions, such as behavioral therapies or first-line pharmacologic treatment, be offered to patients with mild to moderate symptoms of depression.17 The VA/DoD guidelines for low back pain suggest screening for mental health disorders.2 For these reasons, the standardized use of the screening instruments remains in place within the pain management clinic at NMCCL.
1. Board on Health Sciences Policy. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. The National Academies Press: Washington, DC; 2011.
2. US Department of Defense, US Department of Veterans Affairs. VA/DoD clinical practice guidelines for diagnosis and treatment of low back pain. https://www.healthquality.va.gov/guidelines/Pain/lbp/VADoDLBPCPG092917.pdf. Published October 21, 2016. Accessed September 26, 2019.
3. Gironda RJ, Clark ME, Massengale JP, Walker RL. Pain among veterans of Operations Enduring Freedom and Iraqi Freedom. Pain Med. 2006;7(4):339-343.
4. Arlotta CJ. New recommendations for pain management among active duty service military and veterans. Forbes. February 13, 2015. https://www.forbes.com/sites/cjarlotta/2015/02/13/managing-chronic-pain-in-the-active-military-and-veteran-populations/#7d7dd7d93fc3. Accessed September 26, 2019.
5. Kroenke K, Outcalt S, Krebs E, et al. Association between anxiety, health-related quality of life and functional impairment in primry care patients with chronic pain. Gen Hosp Psychiatry. 2013;35(4):359-365.
6. McWilliams LA, Cox BJ, Enns MW. Mood and anxiety disorders associated with chronic pain: an examination in a nationally representative sample. Pain. 2003;106(1-2):127-133.
7. Lazar SG. The mental health needs of active duty service members and veterans. Psychodynamic Psychiatry. 2014;42(3):459-478.
8. Pratt LA, Brody DJ. Depression in the U.S. household population, 2009-2012. NCHS Data Brief No. 172. https://www.cdc.gov/nchs/data/databriefs/db172.pdf. Published December 2014. Accessed September 26, 2019.
9. Bair MJ, Wu J, Damush TM, Sutherland JM, Kroenke K. Association of depression and anxiety alone and in combination with chronic musculoskeletal pain in primary care patients. Psychosom Med. 2008;70(8):890-897.
10. National Institute for Clinical Health and Care Excellence. Common mental health problems: identification and pathways to care. https://www.nice.org.uk/guidance/CG123/chapter/1-Guidance#step-1-identification-and-assessment. Published May 2011. Accessed September 26, 2019.
11. Barrera TL, Mott JM, Hundt NE, et al. Diagnostic specificity and mental health service utilization among veterans with newly diagnosed anxiety disorders. Gen Hosp Psychiatry. 2014;36(2):192-198.
12. Kroenke K, Spitzer RL, Williams JBW, Lowe B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. 2010;32(4):345-359.
13. Smith MJ, Liehr PR. The Theory of Unpleasant Symptoms. Middle Range Theory for Nursing. New York, NY: Springer Publishing Company, 2014:165-195.
14. Substance Abuse and Mental Health Services Administration, Health Resources and Services Administration. FOCUS PDCA: plan-do-check-act. https://www.integration.samhsa.gov/pbhci-learning-community/Cross-site_TA_slides_-_FOCUSPDCA_Final.pdf. Published September 19, 2017. Accessed September 26, 2019.
15. Bridges KW, Goldberg DP. Somatic presentation of DSM III psychiatric disorders in primary care. J Psychosom Res. 1985;29(6):563-569.
16. Greenberg PE, Fournier AA, Sisitsky T, Pike CT, Kessler RC. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J Clin Psychiatry. 2015;76(2):155-162.
17. US Department of Defense, US Department of Veterans Affairs. VA/DoD clinical practice guidelines. Management of major depressive disorder (MDD) https://www.healthquality.va.gov/guidelines/MH/mdd/. Updated October 12, 2017. Accessed September 26, 2019.
Chronic pain is more prevalent in the US than diabetes mellitus, cancer, and cardiovascular disease combined, impacting about 100 million adults.1 The annual cost of all that pain in the US is between $560 and $635 billion.1
The high prevalence of chronic pain among active duty service members and veterans remains a pressing concern given its negative impact on military readiness, health care utilization, productivity, quality of life, and chronic disability rates.2 Pain was found to be the leading complaint of service members returning from Operations Iraqi Freedom and Enduring Freedomand 44% of veterans returning from deployment suffered with chronic pain.3,4
Chronic pain often occurs in the presence of comorbidities. In one study for example, 45% of primary care patients with chronic pain (N = 250) screened positive for ≥ 1 of the 5 types of common anxiety disorders, and those with anxiety disorder had higher pain scores.5 Another study involving almost 6000 participants found that anxiety disorders were present in 35% of people with chronic pain compared with 18% in the general population.6
In addition, military members are prone to depression with a rate of major depressive disorder that is 5% higher than that of civilians.7 Depression often is underdiagnosed and undertreated. According to a National Center for Health Statistics, only 35% of those with symptoms of severe depression in the US saw a mental health provider in the previous year.8 Comorbid depression, anxiety, and chronic pain are strongly associated with more severe pain, greater disability, and poorer health-related quality of life.9
As a result, there was a call for system-level interventions to increase access to, and continuity of, mental health care services for active duty service members and veterans.1 It has been recommended that depression and anxiety screenings take place in primary and secondary care clinics.10 Standardized referral processes also are needed to enhance mental health diagnosis and referral techniques.11 Although various screening tools are available that have excellent reliability and construct validity (eg, General Anxiety Disorder-7 [GAD-7], Patient Health Questionnaire-9 [PHQ-9]), they are underutilized.12 I have witnessed a noticeable gap between clinical practice guidelines and current practice associated with chronic pain and screening for anxiety and depression within the Pain Management Clinic at Navy Medical Center of Camp Lejeune (NMCCL) in North Carolina.
Methods
The premise of this performance improvement (PI) project was to reduce missed opportunities of screening for anxiety and depression, and to examine the impact of the standardized use of the GAD-7 and PHQ-9 on the rate of mental health care referrals. The Theory of Unpleasant Symptoms was chosen as the underpinning of the project because it suggests that symptoms often cluster, and that the occurrence of multiple symptoms makes each of those, as well as other symptoms, worse.13 The PI model used the find, organize, clarify, understand, select (FOCUS), and plan, do, check, act (PDCA) models.14 The facility institutional review board ruled that this performance improvement project did not qualify as human research.
Inclusion and exclusion criteria
Patients were included if they were active duty service members aged 18 to 56 years at the initial patient encounter. Veterans and dependents were not part of the sample because of the high clinic volume. Patients who received mental health care services within the previous 90 days were excluded.
Registered nurses, licensed practical nurses, US Navy corpsman, medical assistants, and nurse aides were educated on the purpose of the GAD-7 and PHQ-9 and were instructed to have patients complete them upon every new patient encounter. A retrospective chart review was conducted over a 6-week time frame to collect and analyze de-identified demographic data including age, gender, prior deployment (yes or no), and branch of service. The review also examined whether the patient had received mental health care services, whether the screening instruments were completed, and whether a mental health referral was made. The clinic providers were asked to consider mental health care referrals for patients who scored ≥ 10 on either the GAD-7 or PHQ-9. The frequency of the use of the instruments and the number of mental health referrals made was calculated during the 3-week period before and after the standardized use of the instruments. The author conducted audits of the new patient charts at the end of each work day to assess whether the GAD-7 and PHQ-9 were completed.
Results
There were 117 new patient encounters during the 6-week project period. Thirty-three patients were excluded from the sample, leaving a remaining sample of 84. Thirty-two patients were included in the sample prior to the standardized use of the instruments, and 52 were included afterward (Table).
Prior to the standardized use of the screening tools, the GAD-7 was used during 75% of patient visits for pain and the PHQ-9 was used during 25%, reinforcing the premise of unpredictable utilization of the screening tools. Three mental health referrals were made during the 3-week period prior to the standardized use of the anxiety and depression instruments (3/32, 10%). After the standardized implementation of the GAD-7 and PHQ-9 tools, both instruments were used 98% of the time, and mental health referrals were made for 12 of 52 patients (23.1%). Eleven of the referrals were made based upon the trigger score of 10 on either the GAD-7 or PHQ-9. One referral was made for a patient with a score of 9 on the PHQ-9 because the provider determined a need for pain-related psychological services.
It was important to provide a link to mental health care because, as one study found, patients with a specific anxiety diagnosis are much more likely than those diagnosed with a not otherwise specified anxiety disorder to receive mental health care services (60% to 67% vs 37%).11 Similarly, patients diagnosed in specialty mental health care settings are more likely to receive mental health services than are those diagnosed in primary care.11 By the same token, experts estimate that 50% of those with severe depression symptoms are not properly diagnosed or treated in primary care.15
Strengths and Limitations
Utilization of the screening tools has led to further dialogue between patients and providers that anecdotally revealed suicidal ideation in some patients. Future studies could incorporate a qualitative component to include clinician and patient perceptions of mental health care services.
The study was limited by the lack of follow-up data to determine the effect of mental health care services on pain, function, or military readiness. Also, it is unclear whether education alone impacted the referral rate.
The author shared the outcomes of this PI project with fellow professionals at NMCCL. As a team, we explored ways for military to link with mental health care within their commands. The process of using these instruments is easily transferable to other clinics with no extraordinary cost.
Conclusion
The economic burden of major depressive disorder in the US has risen 21.5% from 2005 to 2010.16 Unfortunately, only 35% of those with symptoms of severe depression had contact with a mental health professional in the past year.8 Avoiding missing opportunities to screen for mental health conditions can decrease the disease burden. The GAD-7 and PHQ-9 are relatively cost free and are deemed reliable and valid for screening for, and determining the severity of, symptoms of anxiety and depression.12 The evidence suggests that screening for, and early recognition of, mental illness, are critical parts of evidence-based practice and provide the most cost-effective care.16
This PI project demonstrated that the standardized use of the GAD-7 and PHQ-9 during patient visits for pain did improve adherence to guidelines and resulted in a significant increase in the rate of mental health referrals from 10% to 23.1%. This information is valuable because a score of ≥ 10 on either screening instrument is considered the optimal cutoff for diagnosing and determining severity of anxiety and depression symptoms.12 The US Department of Veterans Affairs (VA) and the US Department of Defense (DoD) have jointly developed clinical practice guidelines, which recommend that interventions, such as behavioral therapies or first-line pharmacologic treatment, be offered to patients with mild to moderate symptoms of depression.17 The VA/DoD guidelines for low back pain suggest screening for mental health disorders.2 For these reasons, the standardized use of the screening instruments remains in place within the pain management clinic at NMCCL.
Chronic pain is more prevalent in the US than diabetes mellitus, cancer, and cardiovascular disease combined, impacting about 100 million adults.1 The annual cost of all that pain in the US is between $560 and $635 billion.1
The high prevalence of chronic pain among active duty service members and veterans remains a pressing concern given its negative impact on military readiness, health care utilization, productivity, quality of life, and chronic disability rates.2 Pain was found to be the leading complaint of service members returning from Operations Iraqi Freedom and Enduring Freedomand 44% of veterans returning from deployment suffered with chronic pain.3,4
Chronic pain often occurs in the presence of comorbidities. In one study for example, 45% of primary care patients with chronic pain (N = 250) screened positive for ≥ 1 of the 5 types of common anxiety disorders, and those with anxiety disorder had higher pain scores.5 Another study involving almost 6000 participants found that anxiety disorders were present in 35% of people with chronic pain compared with 18% in the general population.6
In addition, military members are prone to depression with a rate of major depressive disorder that is 5% higher than that of civilians.7 Depression often is underdiagnosed and undertreated. According to a National Center for Health Statistics, only 35% of those with symptoms of severe depression in the US saw a mental health provider in the previous year.8 Comorbid depression, anxiety, and chronic pain are strongly associated with more severe pain, greater disability, and poorer health-related quality of life.9
As a result, there was a call for system-level interventions to increase access to, and continuity of, mental health care services for active duty service members and veterans.1 It has been recommended that depression and anxiety screenings take place in primary and secondary care clinics.10 Standardized referral processes also are needed to enhance mental health diagnosis and referral techniques.11 Although various screening tools are available that have excellent reliability and construct validity (eg, General Anxiety Disorder-7 [GAD-7], Patient Health Questionnaire-9 [PHQ-9]), they are underutilized.12 I have witnessed a noticeable gap between clinical practice guidelines and current practice associated with chronic pain and screening for anxiety and depression within the Pain Management Clinic at Navy Medical Center of Camp Lejeune (NMCCL) in North Carolina.
Methods
The premise of this performance improvement (PI) project was to reduce missed opportunities of screening for anxiety and depression, and to examine the impact of the standardized use of the GAD-7 and PHQ-9 on the rate of mental health care referrals. The Theory of Unpleasant Symptoms was chosen as the underpinning of the project because it suggests that symptoms often cluster, and that the occurrence of multiple symptoms makes each of those, as well as other symptoms, worse.13 The PI model used the find, organize, clarify, understand, select (FOCUS), and plan, do, check, act (PDCA) models.14 The facility institutional review board ruled that this performance improvement project did not qualify as human research.
Inclusion and exclusion criteria
Patients were included if they were active duty service members aged 18 to 56 years at the initial patient encounter. Veterans and dependents were not part of the sample because of the high clinic volume. Patients who received mental health care services within the previous 90 days were excluded.
Registered nurses, licensed practical nurses, US Navy corpsman, medical assistants, and nurse aides were educated on the purpose of the GAD-7 and PHQ-9 and were instructed to have patients complete them upon every new patient encounter. A retrospective chart review was conducted over a 6-week time frame to collect and analyze de-identified demographic data including age, gender, prior deployment (yes or no), and branch of service. The review also examined whether the patient had received mental health care services, whether the screening instruments were completed, and whether a mental health referral was made. The clinic providers were asked to consider mental health care referrals for patients who scored ≥ 10 on either the GAD-7 or PHQ-9. The frequency of the use of the instruments and the number of mental health referrals made was calculated during the 3-week period before and after the standardized use of the instruments. The author conducted audits of the new patient charts at the end of each work day to assess whether the GAD-7 and PHQ-9 were completed.
Results
There were 117 new patient encounters during the 6-week project period. Thirty-three patients were excluded from the sample, leaving a remaining sample of 84. Thirty-two patients were included in the sample prior to the standardized use of the instruments, and 52 were included afterward (Table).
Prior to the standardized use of the screening tools, the GAD-7 was used during 75% of patient visits for pain and the PHQ-9 was used during 25%, reinforcing the premise of unpredictable utilization of the screening tools. Three mental health referrals were made during the 3-week period prior to the standardized use of the anxiety and depression instruments (3/32, 10%). After the standardized implementation of the GAD-7 and PHQ-9 tools, both instruments were used 98% of the time, and mental health referrals were made for 12 of 52 patients (23.1%). Eleven of the referrals were made based upon the trigger score of 10 on either the GAD-7 or PHQ-9. One referral was made for a patient with a score of 9 on the PHQ-9 because the provider determined a need for pain-related psychological services.
It was important to provide a link to mental health care because, as one study found, patients with a specific anxiety diagnosis are much more likely than those diagnosed with a not otherwise specified anxiety disorder to receive mental health care services (60% to 67% vs 37%).11 Similarly, patients diagnosed in specialty mental health care settings are more likely to receive mental health services than are those diagnosed in primary care.11 By the same token, experts estimate that 50% of those with severe depression symptoms are not properly diagnosed or treated in primary care.15
Strengths and Limitations
Utilization of the screening tools has led to further dialogue between patients and providers that anecdotally revealed suicidal ideation in some patients. Future studies could incorporate a qualitative component to include clinician and patient perceptions of mental health care services.
The study was limited by the lack of follow-up data to determine the effect of mental health care services on pain, function, or military readiness. Also, it is unclear whether education alone impacted the referral rate.
The author shared the outcomes of this PI project with fellow professionals at NMCCL. As a team, we explored ways for military to link with mental health care within their commands. The process of using these instruments is easily transferable to other clinics with no extraordinary cost.
Conclusion
The economic burden of major depressive disorder in the US has risen 21.5% from 2005 to 2010.16 Unfortunately, only 35% of those with symptoms of severe depression had contact with a mental health professional in the past year.8 Avoiding missing opportunities to screen for mental health conditions can decrease the disease burden. The GAD-7 and PHQ-9 are relatively cost free and are deemed reliable and valid for screening for, and determining the severity of, symptoms of anxiety and depression.12 The evidence suggests that screening for, and early recognition of, mental illness, are critical parts of evidence-based practice and provide the most cost-effective care.16
This PI project demonstrated that the standardized use of the GAD-7 and PHQ-9 during patient visits for pain did improve adherence to guidelines and resulted in a significant increase in the rate of mental health referrals from 10% to 23.1%. This information is valuable because a score of ≥ 10 on either screening instrument is considered the optimal cutoff for diagnosing and determining severity of anxiety and depression symptoms.12 The US Department of Veterans Affairs (VA) and the US Department of Defense (DoD) have jointly developed clinical practice guidelines, which recommend that interventions, such as behavioral therapies or first-line pharmacologic treatment, be offered to patients with mild to moderate symptoms of depression.17 The VA/DoD guidelines for low back pain suggest screening for mental health disorders.2 For these reasons, the standardized use of the screening instruments remains in place within the pain management clinic at NMCCL.
1. Board on Health Sciences Policy. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. The National Academies Press: Washington, DC; 2011.
2. US Department of Defense, US Department of Veterans Affairs. VA/DoD clinical practice guidelines for diagnosis and treatment of low back pain. https://www.healthquality.va.gov/guidelines/Pain/lbp/VADoDLBPCPG092917.pdf. Published October 21, 2016. Accessed September 26, 2019.
3. Gironda RJ, Clark ME, Massengale JP, Walker RL. Pain among veterans of Operations Enduring Freedom and Iraqi Freedom. Pain Med. 2006;7(4):339-343.
4. Arlotta CJ. New recommendations for pain management among active duty service military and veterans. Forbes. February 13, 2015. https://www.forbes.com/sites/cjarlotta/2015/02/13/managing-chronic-pain-in-the-active-military-and-veteran-populations/#7d7dd7d93fc3. Accessed September 26, 2019.
5. Kroenke K, Outcalt S, Krebs E, et al. Association between anxiety, health-related quality of life and functional impairment in primry care patients with chronic pain. Gen Hosp Psychiatry. 2013;35(4):359-365.
6. McWilliams LA, Cox BJ, Enns MW. Mood and anxiety disorders associated with chronic pain: an examination in a nationally representative sample. Pain. 2003;106(1-2):127-133.
7. Lazar SG. The mental health needs of active duty service members and veterans. Psychodynamic Psychiatry. 2014;42(3):459-478.
8. Pratt LA, Brody DJ. Depression in the U.S. household population, 2009-2012. NCHS Data Brief No. 172. https://www.cdc.gov/nchs/data/databriefs/db172.pdf. Published December 2014. Accessed September 26, 2019.
9. Bair MJ, Wu J, Damush TM, Sutherland JM, Kroenke K. Association of depression and anxiety alone and in combination with chronic musculoskeletal pain in primary care patients. Psychosom Med. 2008;70(8):890-897.
10. National Institute for Clinical Health and Care Excellence. Common mental health problems: identification and pathways to care. https://www.nice.org.uk/guidance/CG123/chapter/1-Guidance#step-1-identification-and-assessment. Published May 2011. Accessed September 26, 2019.
11. Barrera TL, Mott JM, Hundt NE, et al. Diagnostic specificity and mental health service utilization among veterans with newly diagnosed anxiety disorders. Gen Hosp Psychiatry. 2014;36(2):192-198.
12. Kroenke K, Spitzer RL, Williams JBW, Lowe B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. 2010;32(4):345-359.
13. Smith MJ, Liehr PR. The Theory of Unpleasant Symptoms. Middle Range Theory for Nursing. New York, NY: Springer Publishing Company, 2014:165-195.
14. Substance Abuse and Mental Health Services Administration, Health Resources and Services Administration. FOCUS PDCA: plan-do-check-act. https://www.integration.samhsa.gov/pbhci-learning-community/Cross-site_TA_slides_-_FOCUSPDCA_Final.pdf. Published September 19, 2017. Accessed September 26, 2019.
15. Bridges KW, Goldberg DP. Somatic presentation of DSM III psychiatric disorders in primary care. J Psychosom Res. 1985;29(6):563-569.
16. Greenberg PE, Fournier AA, Sisitsky T, Pike CT, Kessler RC. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J Clin Psychiatry. 2015;76(2):155-162.
17. US Department of Defense, US Department of Veterans Affairs. VA/DoD clinical practice guidelines. Management of major depressive disorder (MDD) https://www.healthquality.va.gov/guidelines/MH/mdd/. Updated October 12, 2017. Accessed September 26, 2019.
1. Board on Health Sciences Policy. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. The National Academies Press: Washington, DC; 2011.
2. US Department of Defense, US Department of Veterans Affairs. VA/DoD clinical practice guidelines for diagnosis and treatment of low back pain. https://www.healthquality.va.gov/guidelines/Pain/lbp/VADoDLBPCPG092917.pdf. Published October 21, 2016. Accessed September 26, 2019.
3. Gironda RJ, Clark ME, Massengale JP, Walker RL. Pain among veterans of Operations Enduring Freedom and Iraqi Freedom. Pain Med. 2006;7(4):339-343.
4. Arlotta CJ. New recommendations for pain management among active duty service military and veterans. Forbes. February 13, 2015. https://www.forbes.com/sites/cjarlotta/2015/02/13/managing-chronic-pain-in-the-active-military-and-veteran-populations/#7d7dd7d93fc3. Accessed September 26, 2019.
5. Kroenke K, Outcalt S, Krebs E, et al. Association between anxiety, health-related quality of life and functional impairment in primry care patients with chronic pain. Gen Hosp Psychiatry. 2013;35(4):359-365.
6. McWilliams LA, Cox BJ, Enns MW. Mood and anxiety disorders associated with chronic pain: an examination in a nationally representative sample. Pain. 2003;106(1-2):127-133.
7. Lazar SG. The mental health needs of active duty service members and veterans. Psychodynamic Psychiatry. 2014;42(3):459-478.
8. Pratt LA, Brody DJ. Depression in the U.S. household population, 2009-2012. NCHS Data Brief No. 172. https://www.cdc.gov/nchs/data/databriefs/db172.pdf. Published December 2014. Accessed September 26, 2019.
9. Bair MJ, Wu J, Damush TM, Sutherland JM, Kroenke K. Association of depression and anxiety alone and in combination with chronic musculoskeletal pain in primary care patients. Psychosom Med. 2008;70(8):890-897.
10. National Institute for Clinical Health and Care Excellence. Common mental health problems: identification and pathways to care. https://www.nice.org.uk/guidance/CG123/chapter/1-Guidance#step-1-identification-and-assessment. Published May 2011. Accessed September 26, 2019.
11. Barrera TL, Mott JM, Hundt NE, et al. Diagnostic specificity and mental health service utilization among veterans with newly diagnosed anxiety disorders. Gen Hosp Psychiatry. 2014;36(2):192-198.
12. Kroenke K, Spitzer RL, Williams JBW, Lowe B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. 2010;32(4):345-359.
13. Smith MJ, Liehr PR. The Theory of Unpleasant Symptoms. Middle Range Theory for Nursing. New York, NY: Springer Publishing Company, 2014:165-195.
14. Substance Abuse and Mental Health Services Administration, Health Resources and Services Administration. FOCUS PDCA: plan-do-check-act. https://www.integration.samhsa.gov/pbhci-learning-community/Cross-site_TA_slides_-_FOCUSPDCA_Final.pdf. Published September 19, 2017. Accessed September 26, 2019.
15. Bridges KW, Goldberg DP. Somatic presentation of DSM III psychiatric disorders in primary care. J Psychosom Res. 1985;29(6):563-569.
16. Greenberg PE, Fournier AA, Sisitsky T, Pike CT, Kessler RC. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J Clin Psychiatry. 2015;76(2):155-162.
17. US Department of Defense, US Department of Veterans Affairs. VA/DoD clinical practice guidelines. Management of major depressive disorder (MDD) https://www.healthquality.va.gov/guidelines/MH/mdd/. Updated October 12, 2017. Accessed September 26, 2019.
Assessing Refill Data Among Different Classes of Antidepressants (FULL)
Depression affects about 4.4% of the global population.1 Major depressive disorder (MDD) is currently the fourth highest cause of disability in the world and by 2030 MDD is expected to be third.2 Research has determined that 1 in 3 veterans seen in primary care shows depressive symptoms. Of these, 1 in 5 have symptoms severe enough to warrant further evaluation for MDD, and 1 in 10 require treatment.3 With this high rate of depression, optimized treatment strategies are needed, including antidepressants and psychotherapy. Antidepressants have grown in popularity since market entry in the 1950s; currently 1 in 10 US citizens aged ≥ 12 years are prescribed an antidepressant.4
Antidepressant Adherence
Antidepressant adherence is crucial for response and remission. Sansone and Sansone reported that, on average, < 50% of patients are adherent to their antidepressant treatment regimen 6 months after initiation (range, 5.4% - 87.6%).5 Fortney and colleagues found that, based on patient report, < 20% of veterans maintained at least 80% adherence at 6 months.6 Patients who are nonadherent are at an increased risk for relapse and recurrence and are more likely to seek care at an emergency department or to become hospitalized.2 In addition to the negative impact on patient outcomes, antidepressant nonadherence may also result in increased economic burden. In the US alone, the annual cost of treating MDD exceeds $210 billion, which will continue to increase if nonadherence is not mitigated.1
Patient-specific characteristics such as lack of knowledge about proper administration techniques, misguided beliefs, and negative attitudes towards treatment may affect adherence.5 In the veteran population, reasons for discontinuation also include lack of perceived benefit and adverse effects, specifically sexual difficulties.6 Sociodemographic and other patient characteristics also may be risk factors for nonadherence, including multiple medical comorbidities; substance use disorder (SUD) diagnosis; male gender; younger age; lack of health insurance or a higher medical cost burden; lack of or low involvement in psychotherapy; infrequent follow up visits; and high illness severity.1,7,8
Appreciating the adherence rates among the different antidepressant classes may help in antidepressant selection. To our knowledge, there have been no prior studies conducted in the veteran population that compared adherence rates among antidepressant classes. Studies in the nonveteran population report differing adherence rates among the antidepressant classes with generally higher adherence in patients prescribed serotonin norepinephrine reuptake inhibitors (SNRIs) and selective serotonin reuptake inhibitors (SSRIs). A retrospective review of commercial, Medicare, and Medicaid claims in > 5000 patients found that SNRIs had a significantly higher 3-month adherence rate based on the portion of days covered model (47%; P < .001) than other antidepressant classes (SSRIs, 42%; other antidepressants, 37%; tricyclic antidepressants [TCAs], 24%).7 Monoamine oxidase inhibitors (MAOIs) prescribed to 1% of the study population had the highest adherence rate at 48%.7 A study reviewing > 25 000 patient claims sourced from the IBM MarketScan research database (Armonk, NY) found that SSRIs (Odds ratio [OR], 1.26; P < .001) and norepinephrine dopamine reuptake inhibitors (NDRIs) (OR, 1.23; P = .007) had the highest ORs for adherence according to the portion of days covered model, while other serotonin modulators (OR, 0.65; P = .001) and tri/tetracyclic antidepressants (OR, 0.49; P < . 001) had the lowest ORs and were associated with lower adherence.1
VA Approaches to Adherence
To address antidepressant adherence, the US Department of Veteran Affairs (VA) adopted 2 measures from the Healthcare Effectiveness Data and Information Set: MDD43h and MDD47h. Measure MDD43h is defined as the proportion of patients with a depression diagnosis newly treated with an antidepressant medication who remained on the antidepressant medication for at least 84 out of 114 days (3 months). MDD47h is similar, but assesses patients remaining on an antidepressant medication for at least 180 out of 230 days (6 months).9 These constitute a SAIL (Strategic Analytics for Improvement and Learning) measure by which VA hospitals are compared. High performance on these measures aids in improving the comparative status of a VA facility.
To help improve performance on these measures, the VA Psychotropic Drug Safety Initiative developed the Antidepressant Nonadherence Report, which serves as a case finder for clinicians to identify veterans with low adherence and/or those overdue for a refill. The dashboard uses the medication possession ratio (MPR) to calculate adherence. While the optimal value is still widely debated, an MPR of ≥ 80% is generally accepted for many disease states.10 The dashboard defines low adherence as ≤ 60%.
As of September 2018, the Antidepressant Nonadherence Report for the Michael E. DeBakey VA Medical Center (MEDVAMC) in Houston, Texas, included > 5000 patients in both MEDVAMC and associated community-based outpatient clinics. About 30% of patients were categorized as overdue for a refill.
Study Objectives
To better understand the problem of antidepressant adherence within this population, we decided to study the relationship between antidepressant class and adherence rates, as well as how adherence relates to patient-specific characteristics. By highlighting predisposing risk factors to low adherence, we hope to provide better interventions.
The primary objective of this study was to determine whether 3-month adherence rates, measured by the MPR, differ between antidepressant classes in veterans newly initiated on antidepressant therapy. A secondary objective was to identify whether there are differences in patient characteristics between those with high MPR (≥ 80%) and low MPR (≤ 60%).
Methods
This study used a retrospective, cross-sectional chart review of MEDVAMC patients from the Antidepressant Nonadherence Report. Patients were: aged ≥ 18 years; newly initiated on an antidepressant with no previous use of the same medication; outpatient for the entire study period; and seen by a physician, physician assistant, nurse practitioner, or pharmacist mental health provider (MHP) within the 3-month study period. All patients’ charts showed a depression diagnosis—an inclusion criterion for the MDD43h and MDD47h measures. However, for this study, the indication(s) for the chosen antidepressant were determined by the MHP note in the patient electronic health record on the date that the medication was prescribed. Study patients may not have had a current depression diagnosis based upon the MHP assessment on the index date. We chose to determine the antidepressant indication(s) in this way because the MHP note would have the most detailed patient assessment.
Patients with previous use of the prescribed antidepressant were excluded because previous exposure may bias the patient and affect current adherence. Patients who were hospitalized at the VA for any reason during the 3-month study period were excluded because of a known risk during transitions of care for medications to be held or discontinued, which could impact refills and MPR. Some patients were excluded if they were taking the antidepressant for a nonmood-related indication (insomnia, neuropathy, migraine prophylaxis, etc). Patients also were excluded if the antidepressant was prescribed to take as-needed; if trazodone was the only antidepressant prescribed; if they were diagnosed with cognitive impairment including dementia or history of stroke; or if they were diagnosed with schizophrenia, schizoaffective disorder, or borderline personality disorder. Use of trazodone as the only antidepressant was excluded because of the relatively common practice to use it in the treatment of insomnia rather than depression.
Primary and Secondary Outcomes
Information collected for the primary outcome, including antidepressant class and MPR, was obtained from the Antidepressant Nonadherence Report. For the secondary outcome, the following data was collected for each patient: age, gender, race, housing status, Medication Regimen Complexity Index (MRCI), number and type of psychiatric diagnoses, number of previous antidepressants, psychotherapy involvement, and number of mental health visits during the 3-month study period. The MRCI is an objective, validated tool that determines relative medication regimen complexity by taking into consideration the number of medications, route and frequency of administration, splitting/multiple dosage units, and presence of any special instructions.11
The primary outcome was tested using a one-way analysis of variance (ANOVA). Nominal secondary outcomes were analyzed using the Fisher’s Exact. Continuous secondary outcomes were examined using an unpaired t-test.
Results
Of 320 charts, 212 patients were excluded and 108 were included (Figure). The most common reason for exclusion was a previously prescribed antidepressant. Of the included patients 49 had an MPR ≥ 80% and 24 had an MPR ≤ 60%. The characteristics of the study population are found in Table 1 and the antidepressant frequencies and MPRs are included in Table 2.
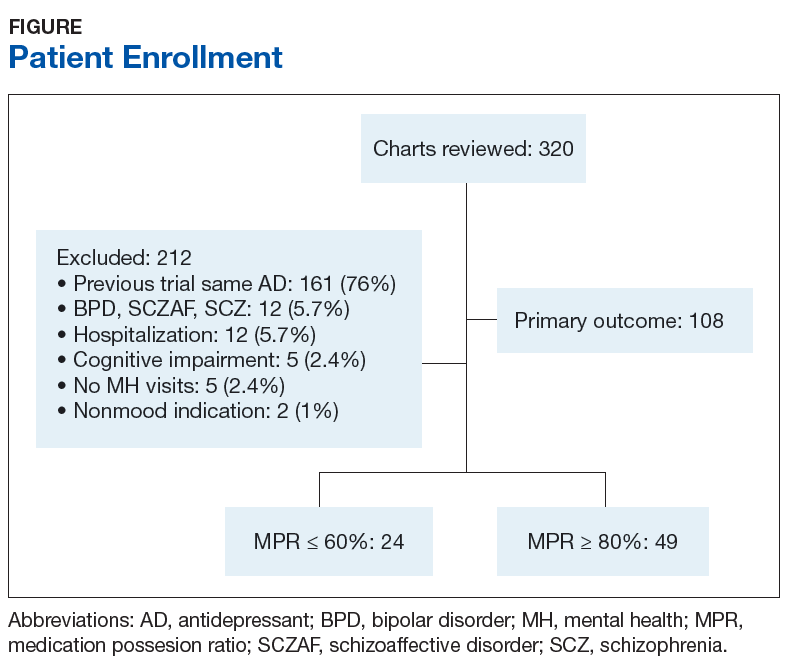
About 87% of study patients had a diagnosis of depression. Other concomitant psychiatric diagnoses include posttraumatic stress disorder (PTSD), anxiety, insomnia, and 2 cases of intermittent explosive disorder. There were no significant differences in mean MPR between the antidepressant classes (P = .31). Within each drug class, we identified the proportion of patients with high adherence (MPR ≥ 80%). Bupropion had the greatest percentage of highly adherent patients (50%) compared with SSRIs (42.5%), SNRIs (38.5%), and mirtazapine (31.3%).
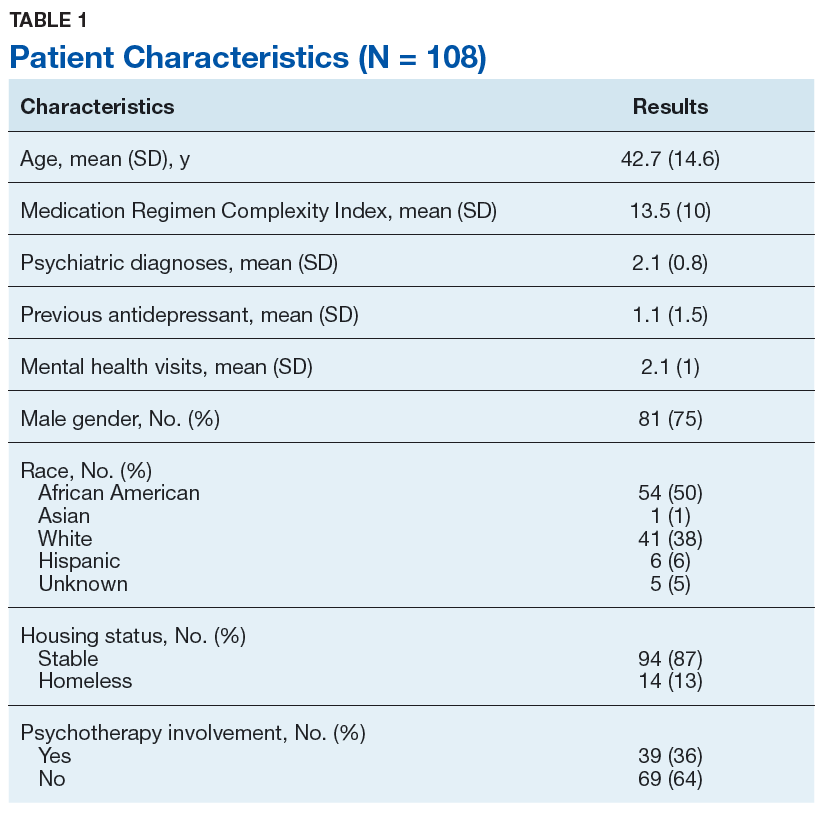
Table 3 compares the characteristics between high MPR and low MPR patients. The low MPR group showed a significantly greater proportion of patients with an SUD than the high adherence group (41.7% vs 10.2%, respectively; P = .04). The most common type of SUD was alcohol use disorder followed by cannabis use disorder. There were no other statistically significant differences identified between high and low MPR groups. There was a trend towards significance when comparing MRCI between the 2 groups (high MPR, 15.2; low MPR, 10.8; P = .06).
Discussion
In our study, there was no significant difference in 3-month adherence rates between veterans on SSRIs, SNRIs, bupropion, and mirtazapine. This result differs from a study by Keyloun and colleagues that found that SNRIs had a significantly higher adherence rate when compared with other antidepressants.7
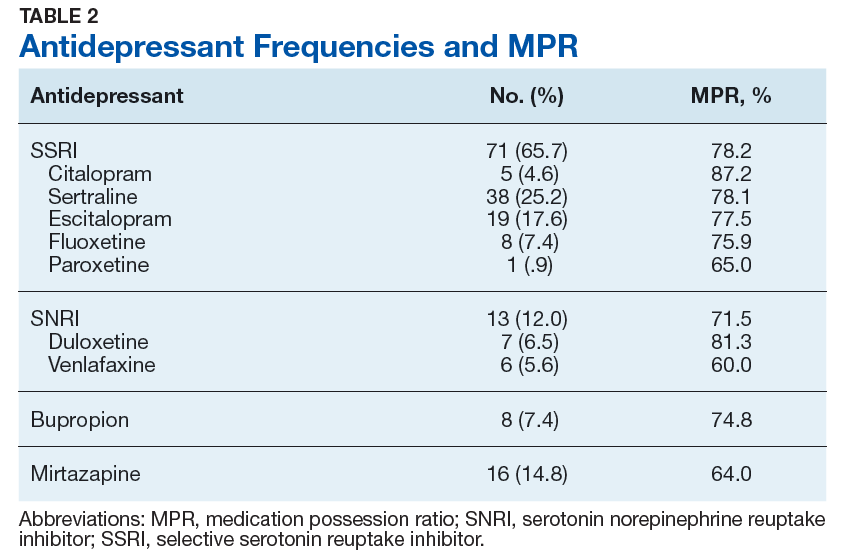
SSRIs were the most commonly prescribed antidepressant in our study, and also had the greatest mean 3-month MPR. The high use of SSRIs may be due to the greater number of SSRI choices to select from compared with other classes. SSRIs may also have been selected more frequently because nearly half (45.4%) of the patients had comorbid PTSD, for which 3 of the 4 first-line treatment options are SSRIs (sertraline, paroxetine, fluoxetine).
As previously stated, Keyloun and colleagues previously found that SNRIs had the highest 3-month adherence rate in a study of > 5000 patients.7 In our study, SNRIs had the second highest mean 3-month MPR at about 75%, but the difference was not considered significant when compared with other antidepressant classes.
Bupropion was prescribed least frequently, but had the largest proportion of adherent patients. Gaspar and colleagues demonstrated similar outcomes, reporting that patients prescribed bupropion had a high OR for adherence.1 Bupropion may have had relatively low prescribing rates in our study because 64% of patients were diagnosed with a comorbid anxiety disorder and/or PTSD. For these patients, bupropion avoidance may have been intentional so as to not exacerbate anxiety.
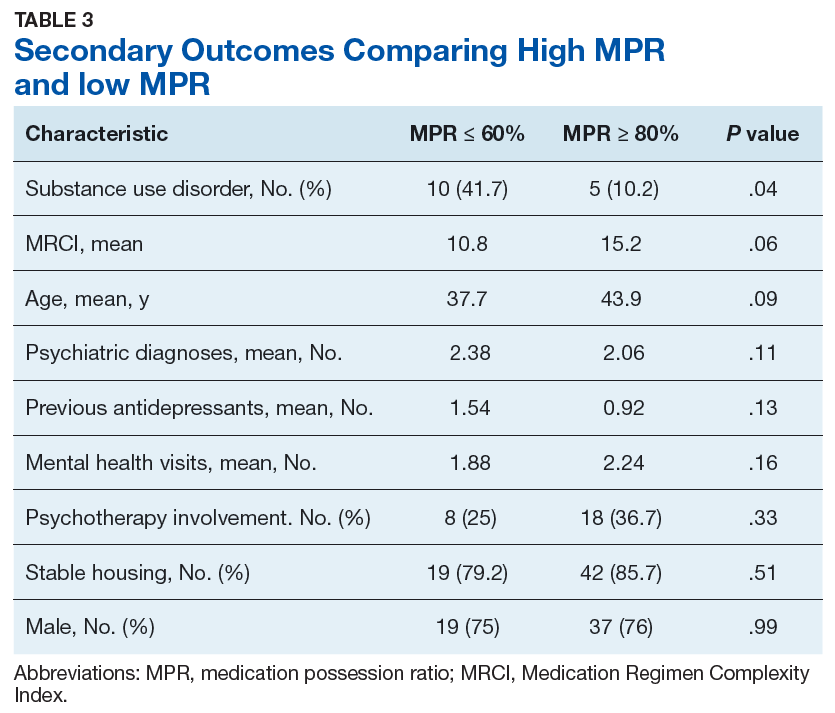
Mirtazapine had both the lowest mean MPR and the lowest proportion of adherent patients. While no significant difference between antidepressant 3-month adherence rates were found, this study’s findings were similar to previous studies that found lower adherence to mirtazapine.1,5 Adverse effects such as sedation, increased appetite, and weight gain may have contributed to low adherence with mirtazapine.4 Patients may also have been using the agent on an as needed basis to treat insomnia despite the order being written for daily use.
Substance Use Disorder Influence
A significantly greater proportion of patients had an SUD in the low MPR group, suggesting that an SUD diagnosis may be a risk factor for low adherence. This finding is consistent with previous studies that also found that an SUD was associated with poor medication adherence.1 Patients with depression and an SUD have been shown to have suboptimal outcomes compared to those without an SUD, including a lower response to antidepressant therapy and increased illness severity.11,12
In a study of 131 outpatients with dual diagnosis (26% with depression) predictors for low self-reported adherence were a medication-related variable (increased adverse effects), a cognitive variable (low self-efficacy for drug avoidance), and a social factor (low social support for recovery). This variety of predictors seems to indicate that simple memory aids may not improve adherence. “Dual focus” mutual aid groups that provide social support for patients with dual diagnosis have been shown to improve adherence.13
The MEDVAMC Substance Dependence Treatment Program (SDTP) is an outpatient program that uses group education to aid veterans, often those with comorbid psychiatric disorders, to build relapse prevention skills and provide social support. Further exploration into the relationship between involvement in SDTP groups and antidepressant adherence in patients with dual diagnosis may be warranted.
Secondary Outcomes
Trends identified in the secondary outcome were similar to outcomes of previous studies: younger age, lower therapy involvement, and more comorbid psychiatric diagnoses were associated with lower adherence.1,7,8 The presence of increased previous use of antidepressants in the low adherence group may suggest that these patients have an increased illness severity, although objective scales, such as the Patient Health Questionnaire 9 (PHQ9), were not consistently conducted and therefore not included in this analysis. It is unknown whether the previous antidepressant prescriptions were of adequate duration. These patients may have also had intolerances that led to multiple different antidepressant prescriptions and self-discontinuation.
The average MRCI of study patients was 13.5 (range 2 - 53), which was significantly lower than a previous study of geriatric patients with depression reporting an average MRCI of 25.4 (range 6 - 64).14 The positive trend between MRCI and adherence seen in this study was puzzling and counterintuitive. A more complex regimen is generally thought to be associated with poor adherence. Patients with a greater number of comorbid conditions may inherently be on more medications and thus have a more complex medication regimen. Manzano-Garcia and colleagues identified a negative relationship between adherence and the number of comorbidities (OR, 1.04-1.57; P = .021) and the MRCI (OR, 1.14-1.26; P < .001) in patients with HIV.15 Further studies are needed to clarify the relationship between medication adherence and medication regimen complexity in patients with mental health disorders. A better understanding of this relationship could possibly facilitate improved individualized prescribing practices and follow-up.
Limitations
Findings from our study should be interpreted within several limitations. Generalizability and statistical power were limited due to the small sample size, a practice site limited to 1 facility, and population type. The retrospective design of the study introduces inherent bias that would be minimized had a prospective study been conducted. The primary outcome was based upon MPR, which only accounts for refills within a specified time period and does not assess for actual or accurate use of the medication. Data collection was limited to VA and US Department of Defense records.
Geographically diverse studies with larger sample sizes need to be conducted to better understand antidepressant adherence and its barriers and facilitators in the veteran population. The exclusion of patients with previous trials of the prescribed antidepressant may have led to a possible selection bias favoring inclusion of younger patients. These patients may have a more limited period for assessment and treatment when compared with older patients, and thus may have had a smaller chance of previous exposure to the prescribed antidepressant. Neither MAOIs or TCAs were included in this study. No patients taking MAOIs were identified from the Antidepressant Nonadherence Report during the study period. Three patients on TCAs were chart reviewed, but excluded from the study because of prior use of the antidepressant or a non-mental health indication. Additionally, no newer antidepressants, including vortioxetine and vilazodone, were included, likely secondary to their nonformulary status at the VA.
Conclusion
As this study’s purpose was to improve the quality of care at our facility, we will discuss our findings with local MHPs to develop strategies to improve antidepressant adherence. While larger studies need to be conducted to confirm our findings, it is worthwhile to consider risk factors for low adherence such as SUD when prescribing antidepressant medications. Patients with SUD could be encouraged to enroll in our facility’s telephone nursing depression care management program for more frequent follow up and medication adherence counseling.
This study did not find a significant difference in 3-month adherence rates between SSRIs, SNRIs, bupropion, and mirtazapine. SUD was significantly more common in patients with low adherence than those categorized as adherent and may be a risk factor for low adherence based upon our findings and those of previous studies.
1. Gaspar FW, Zaidel CS, Dewa CS. Rates and determinants of use of pharmacotherapy and psychotherapy by patients with major depressive disorder. Psychiatr Serv. 2019;70(4):262-270.
2. Ho SC, Jacob SA, Tangiisuran B. Barriers and facilitators of adherence to antidepressants among outpatients with major depressive disorder: a qualitative study. PLoS One. 2017;12(6):e0179290.
3. US Department of Veterans Affairs, Office of Research and Development. VA research on: depression. https://www.research.va.gov/topics/depression.cfm#research1. Accessed May 30, 2019.
4. Santarsieri D, Schwartz TL. Antidepressant efficacy and side-effect burden: a quick guide for clinicians. Drugs Context. 2015;4:212290.
5. Sansone RA, Sansone LA. Antidepressant adherence: are patients taking their medications? Innov Clin Neurosci. 2012;9(5-6):41-46.
6. Fortney JC, Pyne JM, Edlund MJ, et al. Reasons for antidepressant nonadherence among veterans treated in primary care clinics. J Clin Psychiatry. 2011;72(6):827-834.
7. Keyloun KR, Hansen RN, Hepp Z, Gillard P, Thase ME, Devine EB. Adherence and persistence across antidepressant therapeutic classes: a retrospective claims analysis among insured US patients with major depressive disorder (MDD). [erratum: CNS Drugs. 2017;31(6):511.] CNS Drugs. 2017;31(5):421-432.
8. Mcinnis MG. Adherence to treatment regimens in major depression: perspectives, problems, and progress. https://www.psychiatrictimes.com/depression/adherence-treatment-regimens-major-depression-perspectives-problems-and-progress. Published September 15, 2007. Accessed September 10, 2019.
9. US Department of Veterans Affairs, Office of Mental Health Operations. Clinical support portal. User Guide – antidepressant non-adherence report (MDD43h MDD47h). https://spsites.cdw.va.gov/sites/OMHO_PsychPharm/_layouts/15/WopiFrame.aspx?sourcedoc=/sites/OMHO_PsychPharm/AnalyticsReports/UserGuideMDD43H47H.pdf. Accessed July 29, 2018. [Nonpublic site]
10. Crowe M. Do you know the difference between these adherence measures? https://www.pharmacytimes.com/contributor/michael-crowe-pharmd-mba-csp-fmpa/2015/07/do-you-know-the-difference-between-these-adherence-measures. Published July 5, 2015. Accessed September 13, 2019.
11. Watkins KE, Paddock SM, Zhang L, Wells KB. Improving care for depression in patients with comorbid substance misuse. Am J Psychiatry. 2006;163(1):125-132.
12. Magura S, Rosenblum A, Fong C. Factors associated with medication adherence among psychiatric outpatients at substance abuse risk. Open Addict J. 2011;4:58-64.
13. Magura S, Rosenblum A, Villano CL, Vogel HS, Fong C, Betzler T. Dual-focus mutual aid for co-occurring disorders: a quasi-experimental outcome evaluation study. Am J Drug Alcohol Abuse. 2008;34(1):61-74.
14. Libby AM, Fish DN, Hosokawa PW, et al. Patient-level medication regimen complexity across populations with chronic disease. Clin Ther. 2013;35(4):385-398.e1.
15. Manzano-García M, Pérez-Guerrero C, Álvarez de Sotomayor Paz M, Robustillo-Cortés MLA, Almeida-González CV, Morillo-Verdugo R. Identification of the medication regimen complexity index as an associated factor of nonadherence to antiretroviral treatment in HIV positive patients. Ann Pharmacother. 2018;52(9):862-867.
Depression affects about 4.4% of the global population.1 Major depressive disorder (MDD) is currently the fourth highest cause of disability in the world and by 2030 MDD is expected to be third.2 Research has determined that 1 in 3 veterans seen in primary care shows depressive symptoms. Of these, 1 in 5 have symptoms severe enough to warrant further evaluation for MDD, and 1 in 10 require treatment.3 With this high rate of depression, optimized treatment strategies are needed, including antidepressants and psychotherapy. Antidepressants have grown in popularity since market entry in the 1950s; currently 1 in 10 US citizens aged ≥ 12 years are prescribed an antidepressant.4
Antidepressant Adherence
Antidepressant adherence is crucial for response and remission. Sansone and Sansone reported that, on average, < 50% of patients are adherent to their antidepressant treatment regimen 6 months after initiation (range, 5.4% - 87.6%).5 Fortney and colleagues found that, based on patient report, < 20% of veterans maintained at least 80% adherence at 6 months.6 Patients who are nonadherent are at an increased risk for relapse and recurrence and are more likely to seek care at an emergency department or to become hospitalized.2 In addition to the negative impact on patient outcomes, antidepressant nonadherence may also result in increased economic burden. In the US alone, the annual cost of treating MDD exceeds $210 billion, which will continue to increase if nonadherence is not mitigated.1
Patient-specific characteristics such as lack of knowledge about proper administration techniques, misguided beliefs, and negative attitudes towards treatment may affect adherence.5 In the veteran population, reasons for discontinuation also include lack of perceived benefit and adverse effects, specifically sexual difficulties.6 Sociodemographic and other patient characteristics also may be risk factors for nonadherence, including multiple medical comorbidities; substance use disorder (SUD) diagnosis; male gender; younger age; lack of health insurance or a higher medical cost burden; lack of or low involvement in psychotherapy; infrequent follow up visits; and high illness severity.1,7,8
Appreciating the adherence rates among the different antidepressant classes may help in antidepressant selection. To our knowledge, there have been no prior studies conducted in the veteran population that compared adherence rates among antidepressant classes. Studies in the nonveteran population report differing adherence rates among the antidepressant classes with generally higher adherence in patients prescribed serotonin norepinephrine reuptake inhibitors (SNRIs) and selective serotonin reuptake inhibitors (SSRIs). A retrospective review of commercial, Medicare, and Medicaid claims in > 5000 patients found that SNRIs had a significantly higher 3-month adherence rate based on the portion of days covered model (47%; P < .001) than other antidepressant classes (SSRIs, 42%; other antidepressants, 37%; tricyclic antidepressants [TCAs], 24%).7 Monoamine oxidase inhibitors (MAOIs) prescribed to 1% of the study population had the highest adherence rate at 48%.7 A study reviewing > 25 000 patient claims sourced from the IBM MarketScan research database (Armonk, NY) found that SSRIs (Odds ratio [OR], 1.26; P < .001) and norepinephrine dopamine reuptake inhibitors (NDRIs) (OR, 1.23; P = .007) had the highest ORs for adherence according to the portion of days covered model, while other serotonin modulators (OR, 0.65; P = .001) and tri/tetracyclic antidepressants (OR, 0.49; P < . 001) had the lowest ORs and were associated with lower adherence.1
VA Approaches to Adherence
To address antidepressant adherence, the US Department of Veteran Affairs (VA) adopted 2 measures from the Healthcare Effectiveness Data and Information Set: MDD43h and MDD47h. Measure MDD43h is defined as the proportion of patients with a depression diagnosis newly treated with an antidepressant medication who remained on the antidepressant medication for at least 84 out of 114 days (3 months). MDD47h is similar, but assesses patients remaining on an antidepressant medication for at least 180 out of 230 days (6 months).9 These constitute a SAIL (Strategic Analytics for Improvement and Learning) measure by which VA hospitals are compared. High performance on these measures aids in improving the comparative status of a VA facility.
To help improve performance on these measures, the VA Psychotropic Drug Safety Initiative developed the Antidepressant Nonadherence Report, which serves as a case finder for clinicians to identify veterans with low adherence and/or those overdue for a refill. The dashboard uses the medication possession ratio (MPR) to calculate adherence. While the optimal value is still widely debated, an MPR of ≥ 80% is generally accepted for many disease states.10 The dashboard defines low adherence as ≤ 60%.
As of September 2018, the Antidepressant Nonadherence Report for the Michael E. DeBakey VA Medical Center (MEDVAMC) in Houston, Texas, included > 5000 patients in both MEDVAMC and associated community-based outpatient clinics. About 30% of patients were categorized as overdue for a refill.
Study Objectives
To better understand the problem of antidepressant adherence within this population, we decided to study the relationship between antidepressant class and adherence rates, as well as how adherence relates to patient-specific characteristics. By highlighting predisposing risk factors to low adherence, we hope to provide better interventions.
The primary objective of this study was to determine whether 3-month adherence rates, measured by the MPR, differ between antidepressant classes in veterans newly initiated on antidepressant therapy. A secondary objective was to identify whether there are differences in patient characteristics between those with high MPR (≥ 80%) and low MPR (≤ 60%).
Methods
This study used a retrospective, cross-sectional chart review of MEDVAMC patients from the Antidepressant Nonadherence Report. Patients were: aged ≥ 18 years; newly initiated on an antidepressant with no previous use of the same medication; outpatient for the entire study period; and seen by a physician, physician assistant, nurse practitioner, or pharmacist mental health provider (MHP) within the 3-month study period. All patients’ charts showed a depression diagnosis—an inclusion criterion for the MDD43h and MDD47h measures. However, for this study, the indication(s) for the chosen antidepressant were determined by the MHP note in the patient electronic health record on the date that the medication was prescribed. Study patients may not have had a current depression diagnosis based upon the MHP assessment on the index date. We chose to determine the antidepressant indication(s) in this way because the MHP note would have the most detailed patient assessment.
Patients with previous use of the prescribed antidepressant were excluded because previous exposure may bias the patient and affect current adherence. Patients who were hospitalized at the VA for any reason during the 3-month study period were excluded because of a known risk during transitions of care for medications to be held or discontinued, which could impact refills and MPR. Some patients were excluded if they were taking the antidepressant for a nonmood-related indication (insomnia, neuropathy, migraine prophylaxis, etc). Patients also were excluded if the antidepressant was prescribed to take as-needed; if trazodone was the only antidepressant prescribed; if they were diagnosed with cognitive impairment including dementia or history of stroke; or if they were diagnosed with schizophrenia, schizoaffective disorder, or borderline personality disorder. Use of trazodone as the only antidepressant was excluded because of the relatively common practice to use it in the treatment of insomnia rather than depression.
Primary and Secondary Outcomes
Information collected for the primary outcome, including antidepressant class and MPR, was obtained from the Antidepressant Nonadherence Report. For the secondary outcome, the following data was collected for each patient: age, gender, race, housing status, Medication Regimen Complexity Index (MRCI), number and type of psychiatric diagnoses, number of previous antidepressants, psychotherapy involvement, and number of mental health visits during the 3-month study period. The MRCI is an objective, validated tool that determines relative medication regimen complexity by taking into consideration the number of medications, route and frequency of administration, splitting/multiple dosage units, and presence of any special instructions.11
The primary outcome was tested using a one-way analysis of variance (ANOVA). Nominal secondary outcomes were analyzed using the Fisher’s Exact. Continuous secondary outcomes were examined using an unpaired t-test.
Results
Of 320 charts, 212 patients were excluded and 108 were included (Figure). The most common reason for exclusion was a previously prescribed antidepressant. Of the included patients 49 had an MPR ≥ 80% and 24 had an MPR ≤ 60%. The characteristics of the study population are found in Table 1 and the antidepressant frequencies and MPRs are included in Table 2.
About 87% of study patients had a diagnosis of depression. Other concomitant psychiatric diagnoses include posttraumatic stress disorder (PTSD), anxiety, insomnia, and 2 cases of intermittent explosive disorder. There were no significant differences in mean MPR between the antidepressant classes (P = .31). Within each drug class, we identified the proportion of patients with high adherence (MPR ≥ 80%). Bupropion had the greatest percentage of highly adherent patients (50%) compared with SSRIs (42.5%), SNRIs (38.5%), and mirtazapine (31.3%).
Table 3 compares the characteristics between high MPR and low MPR patients. The low MPR group showed a significantly greater proportion of patients with an SUD than the high adherence group (41.7% vs 10.2%, respectively; P = .04). The most common type of SUD was alcohol use disorder followed by cannabis use disorder. There were no other statistically significant differences identified between high and low MPR groups. There was a trend towards significance when comparing MRCI between the 2 groups (high MPR, 15.2; low MPR, 10.8; P = .06).
Discussion
In our study, there was no significant difference in 3-month adherence rates between veterans on SSRIs, SNRIs, bupropion, and mirtazapine. This result differs from a study by Keyloun and colleagues that found that SNRIs had a significantly higher adherence rate when compared with other antidepressants.7
SSRIs were the most commonly prescribed antidepressant in our study, and also had the greatest mean 3-month MPR. The high use of SSRIs may be due to the greater number of SSRI choices to select from compared with other classes. SSRIs may also have been selected more frequently because nearly half (45.4%) of the patients had comorbid PTSD, for which 3 of the 4 first-line treatment options are SSRIs (sertraline, paroxetine, fluoxetine).
As previously stated, Keyloun and colleagues previously found that SNRIs had the highest 3-month adherence rate in a study of > 5000 patients.7 In our study, SNRIs had the second highest mean 3-month MPR at about 75%, but the difference was not considered significant when compared with other antidepressant classes.
Bupropion was prescribed least frequently, but had the largest proportion of adherent patients. Gaspar and colleagues demonstrated similar outcomes, reporting that patients prescribed bupropion had a high OR for adherence.1 Bupropion may have had relatively low prescribing rates in our study because 64% of patients were diagnosed with a comorbid anxiety disorder and/or PTSD. For these patients, bupropion avoidance may have been intentional so as to not exacerbate anxiety.
Mirtazapine had both the lowest mean MPR and the lowest proportion of adherent patients. While no significant difference between antidepressant 3-month adherence rates were found, this study’s findings were similar to previous studies that found lower adherence to mirtazapine.1,5 Adverse effects such as sedation, increased appetite, and weight gain may have contributed to low adherence with mirtazapine.4 Patients may also have been using the agent on an as needed basis to treat insomnia despite the order being written for daily use.
Substance Use Disorder Influence
A significantly greater proportion of patients had an SUD in the low MPR group, suggesting that an SUD diagnosis may be a risk factor for low adherence. This finding is consistent with previous studies that also found that an SUD was associated with poor medication adherence.1 Patients with depression and an SUD have been shown to have suboptimal outcomes compared to those without an SUD, including a lower response to antidepressant therapy and increased illness severity.11,12
In a study of 131 outpatients with dual diagnosis (26% with depression) predictors for low self-reported adherence were a medication-related variable (increased adverse effects), a cognitive variable (low self-efficacy for drug avoidance), and a social factor (low social support for recovery). This variety of predictors seems to indicate that simple memory aids may not improve adherence. “Dual focus” mutual aid groups that provide social support for patients with dual diagnosis have been shown to improve adherence.13
The MEDVAMC Substance Dependence Treatment Program (SDTP) is an outpatient program that uses group education to aid veterans, often those with comorbid psychiatric disorders, to build relapse prevention skills and provide social support. Further exploration into the relationship between involvement in SDTP groups and antidepressant adherence in patients with dual diagnosis may be warranted.
Secondary Outcomes
Trends identified in the secondary outcome were similar to outcomes of previous studies: younger age, lower therapy involvement, and more comorbid psychiatric diagnoses were associated with lower adherence.1,7,8 The presence of increased previous use of antidepressants in the low adherence group may suggest that these patients have an increased illness severity, although objective scales, such as the Patient Health Questionnaire 9 (PHQ9), were not consistently conducted and therefore not included in this analysis. It is unknown whether the previous antidepressant prescriptions were of adequate duration. These patients may have also had intolerances that led to multiple different antidepressant prescriptions and self-discontinuation.
The average MRCI of study patients was 13.5 (range 2 - 53), which was significantly lower than a previous study of geriatric patients with depression reporting an average MRCI of 25.4 (range 6 - 64).14 The positive trend between MRCI and adherence seen in this study was puzzling and counterintuitive. A more complex regimen is generally thought to be associated with poor adherence. Patients with a greater number of comorbid conditions may inherently be on more medications and thus have a more complex medication regimen. Manzano-Garcia and colleagues identified a negative relationship between adherence and the number of comorbidities (OR, 1.04-1.57; P = .021) and the MRCI (OR, 1.14-1.26; P < .001) in patients with HIV.15 Further studies are needed to clarify the relationship between medication adherence and medication regimen complexity in patients with mental health disorders. A better understanding of this relationship could possibly facilitate improved individualized prescribing practices and follow-up.
Limitations
Findings from our study should be interpreted within several limitations. Generalizability and statistical power were limited due to the small sample size, a practice site limited to 1 facility, and population type. The retrospective design of the study introduces inherent bias that would be minimized had a prospective study been conducted. The primary outcome was based upon MPR, which only accounts for refills within a specified time period and does not assess for actual or accurate use of the medication. Data collection was limited to VA and US Department of Defense records.
Geographically diverse studies with larger sample sizes need to be conducted to better understand antidepressant adherence and its barriers and facilitators in the veteran population. The exclusion of patients with previous trials of the prescribed antidepressant may have led to a possible selection bias favoring inclusion of younger patients. These patients may have a more limited period for assessment and treatment when compared with older patients, and thus may have had a smaller chance of previous exposure to the prescribed antidepressant. Neither MAOIs or TCAs were included in this study. No patients taking MAOIs were identified from the Antidepressant Nonadherence Report during the study period. Three patients on TCAs were chart reviewed, but excluded from the study because of prior use of the antidepressant or a non-mental health indication. Additionally, no newer antidepressants, including vortioxetine and vilazodone, were included, likely secondary to their nonformulary status at the VA.
Conclusion
As this study’s purpose was to improve the quality of care at our facility, we will discuss our findings with local MHPs to develop strategies to improve antidepressant adherence. While larger studies need to be conducted to confirm our findings, it is worthwhile to consider risk factors for low adherence such as SUD when prescribing antidepressant medications. Patients with SUD could be encouraged to enroll in our facility’s telephone nursing depression care management program for more frequent follow up and medication adherence counseling.
This study did not find a significant difference in 3-month adherence rates between SSRIs, SNRIs, bupropion, and mirtazapine. SUD was significantly more common in patients with low adherence than those categorized as adherent and may be a risk factor for low adherence based upon our findings and those of previous studies.
Depression affects about 4.4% of the global population.1 Major depressive disorder (MDD) is currently the fourth highest cause of disability in the world and by 2030 MDD is expected to be third.2 Research has determined that 1 in 3 veterans seen in primary care shows depressive symptoms. Of these, 1 in 5 have symptoms severe enough to warrant further evaluation for MDD, and 1 in 10 require treatment.3 With this high rate of depression, optimized treatment strategies are needed, including antidepressants and psychotherapy. Antidepressants have grown in popularity since market entry in the 1950s; currently 1 in 10 US citizens aged ≥ 12 years are prescribed an antidepressant.4
Antidepressant Adherence
Antidepressant adherence is crucial for response and remission. Sansone and Sansone reported that, on average, < 50% of patients are adherent to their antidepressant treatment regimen 6 months after initiation (range, 5.4% - 87.6%).5 Fortney and colleagues found that, based on patient report, < 20% of veterans maintained at least 80% adherence at 6 months.6 Patients who are nonadherent are at an increased risk for relapse and recurrence and are more likely to seek care at an emergency department or to become hospitalized.2 In addition to the negative impact on patient outcomes, antidepressant nonadherence may also result in increased economic burden. In the US alone, the annual cost of treating MDD exceeds $210 billion, which will continue to increase if nonadherence is not mitigated.1
Patient-specific characteristics such as lack of knowledge about proper administration techniques, misguided beliefs, and negative attitudes towards treatment may affect adherence.5 In the veteran population, reasons for discontinuation also include lack of perceived benefit and adverse effects, specifically sexual difficulties.6 Sociodemographic and other patient characteristics also may be risk factors for nonadherence, including multiple medical comorbidities; substance use disorder (SUD) diagnosis; male gender; younger age; lack of health insurance or a higher medical cost burden; lack of or low involvement in psychotherapy; infrequent follow up visits; and high illness severity.1,7,8
Appreciating the adherence rates among the different antidepressant classes may help in antidepressant selection. To our knowledge, there have been no prior studies conducted in the veteran population that compared adherence rates among antidepressant classes. Studies in the nonveteran population report differing adherence rates among the antidepressant classes with generally higher adherence in patients prescribed serotonin norepinephrine reuptake inhibitors (SNRIs) and selective serotonin reuptake inhibitors (SSRIs). A retrospective review of commercial, Medicare, and Medicaid claims in > 5000 patients found that SNRIs had a significantly higher 3-month adherence rate based on the portion of days covered model (47%; P < .001) than other antidepressant classes (SSRIs, 42%; other antidepressants, 37%; tricyclic antidepressants [TCAs], 24%).7 Monoamine oxidase inhibitors (MAOIs) prescribed to 1% of the study population had the highest adherence rate at 48%.7 A study reviewing > 25 000 patient claims sourced from the IBM MarketScan research database (Armonk, NY) found that SSRIs (Odds ratio [OR], 1.26; P < .001) and norepinephrine dopamine reuptake inhibitors (NDRIs) (OR, 1.23; P = .007) had the highest ORs for adherence according to the portion of days covered model, while other serotonin modulators (OR, 0.65; P = .001) and tri/tetracyclic antidepressants (OR, 0.49; P < . 001) had the lowest ORs and were associated with lower adherence.1
VA Approaches to Adherence
To address antidepressant adherence, the US Department of Veteran Affairs (VA) adopted 2 measures from the Healthcare Effectiveness Data and Information Set: MDD43h and MDD47h. Measure MDD43h is defined as the proportion of patients with a depression diagnosis newly treated with an antidepressant medication who remained on the antidepressant medication for at least 84 out of 114 days (3 months). MDD47h is similar, but assesses patients remaining on an antidepressant medication for at least 180 out of 230 days (6 months).9 These constitute a SAIL (Strategic Analytics for Improvement and Learning) measure by which VA hospitals are compared. High performance on these measures aids in improving the comparative status of a VA facility.
To help improve performance on these measures, the VA Psychotropic Drug Safety Initiative developed the Antidepressant Nonadherence Report, which serves as a case finder for clinicians to identify veterans with low adherence and/or those overdue for a refill. The dashboard uses the medication possession ratio (MPR) to calculate adherence. While the optimal value is still widely debated, an MPR of ≥ 80% is generally accepted for many disease states.10 The dashboard defines low adherence as ≤ 60%.
As of September 2018, the Antidepressant Nonadherence Report for the Michael E. DeBakey VA Medical Center (MEDVAMC) in Houston, Texas, included > 5000 patients in both MEDVAMC and associated community-based outpatient clinics. About 30% of patients were categorized as overdue for a refill.
Study Objectives
To better understand the problem of antidepressant adherence within this population, we decided to study the relationship between antidepressant class and adherence rates, as well as how adherence relates to patient-specific characteristics. By highlighting predisposing risk factors to low adherence, we hope to provide better interventions.
The primary objective of this study was to determine whether 3-month adherence rates, measured by the MPR, differ between antidepressant classes in veterans newly initiated on antidepressant therapy. A secondary objective was to identify whether there are differences in patient characteristics between those with high MPR (≥ 80%) and low MPR (≤ 60%).
Methods
This study used a retrospective, cross-sectional chart review of MEDVAMC patients from the Antidepressant Nonadherence Report. Patients were: aged ≥ 18 years; newly initiated on an antidepressant with no previous use of the same medication; outpatient for the entire study period; and seen by a physician, physician assistant, nurse practitioner, or pharmacist mental health provider (MHP) within the 3-month study period. All patients’ charts showed a depression diagnosis—an inclusion criterion for the MDD43h and MDD47h measures. However, for this study, the indication(s) for the chosen antidepressant were determined by the MHP note in the patient electronic health record on the date that the medication was prescribed. Study patients may not have had a current depression diagnosis based upon the MHP assessment on the index date. We chose to determine the antidepressant indication(s) in this way because the MHP note would have the most detailed patient assessment.
Patients with previous use of the prescribed antidepressant were excluded because previous exposure may bias the patient and affect current adherence. Patients who were hospitalized at the VA for any reason during the 3-month study period were excluded because of a known risk during transitions of care for medications to be held or discontinued, which could impact refills and MPR. Some patients were excluded if they were taking the antidepressant for a nonmood-related indication (insomnia, neuropathy, migraine prophylaxis, etc). Patients also were excluded if the antidepressant was prescribed to take as-needed; if trazodone was the only antidepressant prescribed; if they were diagnosed with cognitive impairment including dementia or history of stroke; or if they were diagnosed with schizophrenia, schizoaffective disorder, or borderline personality disorder. Use of trazodone as the only antidepressant was excluded because of the relatively common practice to use it in the treatment of insomnia rather than depression.
Primary and Secondary Outcomes
Information collected for the primary outcome, including antidepressant class and MPR, was obtained from the Antidepressant Nonadherence Report. For the secondary outcome, the following data was collected for each patient: age, gender, race, housing status, Medication Regimen Complexity Index (MRCI), number and type of psychiatric diagnoses, number of previous antidepressants, psychotherapy involvement, and number of mental health visits during the 3-month study period. The MRCI is an objective, validated tool that determines relative medication regimen complexity by taking into consideration the number of medications, route and frequency of administration, splitting/multiple dosage units, and presence of any special instructions.11
The primary outcome was tested using a one-way analysis of variance (ANOVA). Nominal secondary outcomes were analyzed using the Fisher’s Exact. Continuous secondary outcomes were examined using an unpaired t-test.
Results
Of 320 charts, 212 patients were excluded and 108 were included (Figure). The most common reason for exclusion was a previously prescribed antidepressant. Of the included patients 49 had an MPR ≥ 80% and 24 had an MPR ≤ 60%. The characteristics of the study population are found in Table 1 and the antidepressant frequencies and MPRs are included in Table 2.
About 87% of study patients had a diagnosis of depression. Other concomitant psychiatric diagnoses include posttraumatic stress disorder (PTSD), anxiety, insomnia, and 2 cases of intermittent explosive disorder. There were no significant differences in mean MPR between the antidepressant classes (P = .31). Within each drug class, we identified the proportion of patients with high adherence (MPR ≥ 80%). Bupropion had the greatest percentage of highly adherent patients (50%) compared with SSRIs (42.5%), SNRIs (38.5%), and mirtazapine (31.3%).
Table 3 compares the characteristics between high MPR and low MPR patients. The low MPR group showed a significantly greater proportion of patients with an SUD than the high adherence group (41.7% vs 10.2%, respectively; P = .04). The most common type of SUD was alcohol use disorder followed by cannabis use disorder. There were no other statistically significant differences identified between high and low MPR groups. There was a trend towards significance when comparing MRCI between the 2 groups (high MPR, 15.2; low MPR, 10.8; P = .06).
Discussion
In our study, there was no significant difference in 3-month adherence rates between veterans on SSRIs, SNRIs, bupropion, and mirtazapine. This result differs from a study by Keyloun and colleagues that found that SNRIs had a significantly higher adherence rate when compared with other antidepressants.7
SSRIs were the most commonly prescribed antidepressant in our study, and also had the greatest mean 3-month MPR. The high use of SSRIs may be due to the greater number of SSRI choices to select from compared with other classes. SSRIs may also have been selected more frequently because nearly half (45.4%) of the patients had comorbid PTSD, for which 3 of the 4 first-line treatment options are SSRIs (sertraline, paroxetine, fluoxetine).
As previously stated, Keyloun and colleagues previously found that SNRIs had the highest 3-month adherence rate in a study of > 5000 patients.7 In our study, SNRIs had the second highest mean 3-month MPR at about 75%, but the difference was not considered significant when compared with other antidepressant classes.
Bupropion was prescribed least frequently, but had the largest proportion of adherent patients. Gaspar and colleagues demonstrated similar outcomes, reporting that patients prescribed bupropion had a high OR for adherence.1 Bupropion may have had relatively low prescribing rates in our study because 64% of patients were diagnosed with a comorbid anxiety disorder and/or PTSD. For these patients, bupropion avoidance may have been intentional so as to not exacerbate anxiety.
Mirtazapine had both the lowest mean MPR and the lowest proportion of adherent patients. While no significant difference between antidepressant 3-month adherence rates were found, this study’s findings were similar to previous studies that found lower adherence to mirtazapine.1,5 Adverse effects such as sedation, increased appetite, and weight gain may have contributed to low adherence with mirtazapine.4 Patients may also have been using the agent on an as needed basis to treat insomnia despite the order being written for daily use.
Substance Use Disorder Influence
A significantly greater proportion of patients had an SUD in the low MPR group, suggesting that an SUD diagnosis may be a risk factor for low adherence. This finding is consistent with previous studies that also found that an SUD was associated with poor medication adherence.1 Patients with depression and an SUD have been shown to have suboptimal outcomes compared to those without an SUD, including a lower response to antidepressant therapy and increased illness severity.11,12
In a study of 131 outpatients with dual diagnosis (26% with depression) predictors for low self-reported adherence were a medication-related variable (increased adverse effects), a cognitive variable (low self-efficacy for drug avoidance), and a social factor (low social support for recovery). This variety of predictors seems to indicate that simple memory aids may not improve adherence. “Dual focus” mutual aid groups that provide social support for patients with dual diagnosis have been shown to improve adherence.13
The MEDVAMC Substance Dependence Treatment Program (SDTP) is an outpatient program that uses group education to aid veterans, often those with comorbid psychiatric disorders, to build relapse prevention skills and provide social support. Further exploration into the relationship between involvement in SDTP groups and antidepressant adherence in patients with dual diagnosis may be warranted.
Secondary Outcomes
Trends identified in the secondary outcome were similar to outcomes of previous studies: younger age, lower therapy involvement, and more comorbid psychiatric diagnoses were associated with lower adherence.1,7,8 The presence of increased previous use of antidepressants in the low adherence group may suggest that these patients have an increased illness severity, although objective scales, such as the Patient Health Questionnaire 9 (PHQ9), were not consistently conducted and therefore not included in this analysis. It is unknown whether the previous antidepressant prescriptions were of adequate duration. These patients may have also had intolerances that led to multiple different antidepressant prescriptions and self-discontinuation.
The average MRCI of study patients was 13.5 (range 2 - 53), which was significantly lower than a previous study of geriatric patients with depression reporting an average MRCI of 25.4 (range 6 - 64).14 The positive trend between MRCI and adherence seen in this study was puzzling and counterintuitive. A more complex regimen is generally thought to be associated with poor adherence. Patients with a greater number of comorbid conditions may inherently be on more medications and thus have a more complex medication regimen. Manzano-Garcia and colleagues identified a negative relationship between adherence and the number of comorbidities (OR, 1.04-1.57; P = .021) and the MRCI (OR, 1.14-1.26; P < .001) in patients with HIV.15 Further studies are needed to clarify the relationship between medication adherence and medication regimen complexity in patients with mental health disorders. A better understanding of this relationship could possibly facilitate improved individualized prescribing practices and follow-up.
Limitations
Findings from our study should be interpreted within several limitations. Generalizability and statistical power were limited due to the small sample size, a practice site limited to 1 facility, and population type. The retrospective design of the study introduces inherent bias that would be minimized had a prospective study been conducted. The primary outcome was based upon MPR, which only accounts for refills within a specified time period and does not assess for actual or accurate use of the medication. Data collection was limited to VA and US Department of Defense records.
Geographically diverse studies with larger sample sizes need to be conducted to better understand antidepressant adherence and its barriers and facilitators in the veteran population. The exclusion of patients with previous trials of the prescribed antidepressant may have led to a possible selection bias favoring inclusion of younger patients. These patients may have a more limited period for assessment and treatment when compared with older patients, and thus may have had a smaller chance of previous exposure to the prescribed antidepressant. Neither MAOIs or TCAs were included in this study. No patients taking MAOIs were identified from the Antidepressant Nonadherence Report during the study period. Three patients on TCAs were chart reviewed, but excluded from the study because of prior use of the antidepressant or a non-mental health indication. Additionally, no newer antidepressants, including vortioxetine and vilazodone, were included, likely secondary to their nonformulary status at the VA.
Conclusion
As this study’s purpose was to improve the quality of care at our facility, we will discuss our findings with local MHPs to develop strategies to improve antidepressant adherence. While larger studies need to be conducted to confirm our findings, it is worthwhile to consider risk factors for low adherence such as SUD when prescribing antidepressant medications. Patients with SUD could be encouraged to enroll in our facility’s telephone nursing depression care management program for more frequent follow up and medication adherence counseling.
This study did not find a significant difference in 3-month adherence rates between SSRIs, SNRIs, bupropion, and mirtazapine. SUD was significantly more common in patients with low adherence than those categorized as adherent and may be a risk factor for low adherence based upon our findings and those of previous studies.
1. Gaspar FW, Zaidel CS, Dewa CS. Rates and determinants of use of pharmacotherapy and psychotherapy by patients with major depressive disorder. Psychiatr Serv. 2019;70(4):262-270.
2. Ho SC, Jacob SA, Tangiisuran B. Barriers and facilitators of adherence to antidepressants among outpatients with major depressive disorder: a qualitative study. PLoS One. 2017;12(6):e0179290.
3. US Department of Veterans Affairs, Office of Research and Development. VA research on: depression. https://www.research.va.gov/topics/depression.cfm#research1. Accessed May 30, 2019.
4. Santarsieri D, Schwartz TL. Antidepressant efficacy and side-effect burden: a quick guide for clinicians. Drugs Context. 2015;4:212290.
5. Sansone RA, Sansone LA. Antidepressant adherence: are patients taking their medications? Innov Clin Neurosci. 2012;9(5-6):41-46.
6. Fortney JC, Pyne JM, Edlund MJ, et al. Reasons for antidepressant nonadherence among veterans treated in primary care clinics. J Clin Psychiatry. 2011;72(6):827-834.
7. Keyloun KR, Hansen RN, Hepp Z, Gillard P, Thase ME, Devine EB. Adherence and persistence across antidepressant therapeutic classes: a retrospective claims analysis among insured US patients with major depressive disorder (MDD). [erratum: CNS Drugs. 2017;31(6):511.] CNS Drugs. 2017;31(5):421-432.
8. Mcinnis MG. Adherence to treatment regimens in major depression: perspectives, problems, and progress. https://www.psychiatrictimes.com/depression/adherence-treatment-regimens-major-depression-perspectives-problems-and-progress. Published September 15, 2007. Accessed September 10, 2019.
9. US Department of Veterans Affairs, Office of Mental Health Operations. Clinical support portal. User Guide – antidepressant non-adherence report (MDD43h MDD47h). https://spsites.cdw.va.gov/sites/OMHO_PsychPharm/_layouts/15/WopiFrame.aspx?sourcedoc=/sites/OMHO_PsychPharm/AnalyticsReports/UserGuideMDD43H47H.pdf. Accessed July 29, 2018. [Nonpublic site]
10. Crowe M. Do you know the difference between these adherence measures? https://www.pharmacytimes.com/contributor/michael-crowe-pharmd-mba-csp-fmpa/2015/07/do-you-know-the-difference-between-these-adherence-measures. Published July 5, 2015. Accessed September 13, 2019.
11. Watkins KE, Paddock SM, Zhang L, Wells KB. Improving care for depression in patients with comorbid substance misuse. Am J Psychiatry. 2006;163(1):125-132.
12. Magura S, Rosenblum A, Fong C. Factors associated with medication adherence among psychiatric outpatients at substance abuse risk. Open Addict J. 2011;4:58-64.
13. Magura S, Rosenblum A, Villano CL, Vogel HS, Fong C, Betzler T. Dual-focus mutual aid for co-occurring disorders: a quasi-experimental outcome evaluation study. Am J Drug Alcohol Abuse. 2008;34(1):61-74.
14. Libby AM, Fish DN, Hosokawa PW, et al. Patient-level medication regimen complexity across populations with chronic disease. Clin Ther. 2013;35(4):385-398.e1.
15. Manzano-García M, Pérez-Guerrero C, Álvarez de Sotomayor Paz M, Robustillo-Cortés MLA, Almeida-González CV, Morillo-Verdugo R. Identification of the medication regimen complexity index as an associated factor of nonadherence to antiretroviral treatment in HIV positive patients. Ann Pharmacother. 2018;52(9):862-867.
1. Gaspar FW, Zaidel CS, Dewa CS. Rates and determinants of use of pharmacotherapy and psychotherapy by patients with major depressive disorder. Psychiatr Serv. 2019;70(4):262-270.
2. Ho SC, Jacob SA, Tangiisuran B. Barriers and facilitators of adherence to antidepressants among outpatients with major depressive disorder: a qualitative study. PLoS One. 2017;12(6):e0179290.
3. US Department of Veterans Affairs, Office of Research and Development. VA research on: depression. https://www.research.va.gov/topics/depression.cfm#research1. Accessed May 30, 2019.
4. Santarsieri D, Schwartz TL. Antidepressant efficacy and side-effect burden: a quick guide for clinicians. Drugs Context. 2015;4:212290.
5. Sansone RA, Sansone LA. Antidepressant adherence: are patients taking their medications? Innov Clin Neurosci. 2012;9(5-6):41-46.
6. Fortney JC, Pyne JM, Edlund MJ, et al. Reasons for antidepressant nonadherence among veterans treated in primary care clinics. J Clin Psychiatry. 2011;72(6):827-834.
7. Keyloun KR, Hansen RN, Hepp Z, Gillard P, Thase ME, Devine EB. Adherence and persistence across antidepressant therapeutic classes: a retrospective claims analysis among insured US patients with major depressive disorder (MDD). [erratum: CNS Drugs. 2017;31(6):511.] CNS Drugs. 2017;31(5):421-432.
8. Mcinnis MG. Adherence to treatment regimens in major depression: perspectives, problems, and progress. https://www.psychiatrictimes.com/depression/adherence-treatment-regimens-major-depression-perspectives-problems-and-progress. Published September 15, 2007. Accessed September 10, 2019.
9. US Department of Veterans Affairs, Office of Mental Health Operations. Clinical support portal. User Guide – antidepressant non-adherence report (MDD43h MDD47h). https://spsites.cdw.va.gov/sites/OMHO_PsychPharm/_layouts/15/WopiFrame.aspx?sourcedoc=/sites/OMHO_PsychPharm/AnalyticsReports/UserGuideMDD43H47H.pdf. Accessed July 29, 2018. [Nonpublic site]
10. Crowe M. Do you know the difference between these adherence measures? https://www.pharmacytimes.com/contributor/michael-crowe-pharmd-mba-csp-fmpa/2015/07/do-you-know-the-difference-between-these-adherence-measures. Published July 5, 2015. Accessed September 13, 2019.
11. Watkins KE, Paddock SM, Zhang L, Wells KB. Improving care for depression in patients with comorbid substance misuse. Am J Psychiatry. 2006;163(1):125-132.
12. Magura S, Rosenblum A, Fong C. Factors associated with medication adherence among psychiatric outpatients at substance abuse risk. Open Addict J. 2011;4:58-64.
13. Magura S, Rosenblum A, Villano CL, Vogel HS, Fong C, Betzler T. Dual-focus mutual aid for co-occurring disorders: a quasi-experimental outcome evaluation study. Am J Drug Alcohol Abuse. 2008;34(1):61-74.
14. Libby AM, Fish DN, Hosokawa PW, et al. Patient-level medication regimen complexity across populations with chronic disease. Clin Ther. 2013;35(4):385-398.e1.
15. Manzano-García M, Pérez-Guerrero C, Álvarez de Sotomayor Paz M, Robustillo-Cortés MLA, Almeida-González CV, Morillo-Verdugo R. Identification of the medication regimen complexity index as an associated factor of nonadherence to antiretroviral treatment in HIV positive patients. Ann Pharmacother. 2018;52(9):862-867.