User login
Cancer Data Trends 2024: Genitourinary Cancers
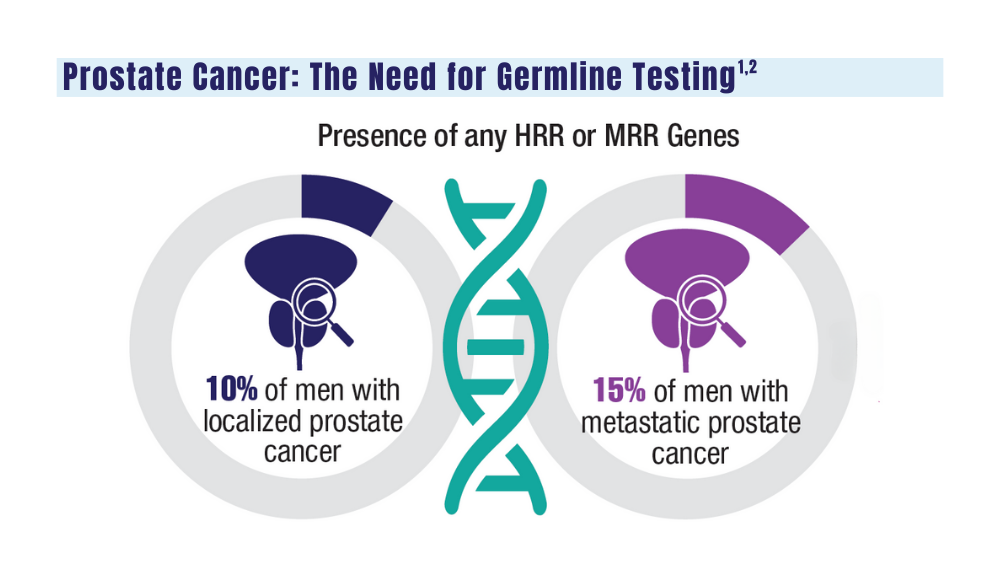
1. Sokolova A, Cheng H. Germline testing in prostate cancer: when and who to test. Oncology (Williston Park). 2021;35(10):645-653. doi:10.46883/ONC.2021.3510.0645
2. Tuffaha H, Edmunds K, Fairbairn D, et al. Guidelines for genetic testing in prostate cancer: a scoping review. Prostate Cancer Prostatic Dis. 2023 May 18. doi:10.1038/s41391-023-00676-0
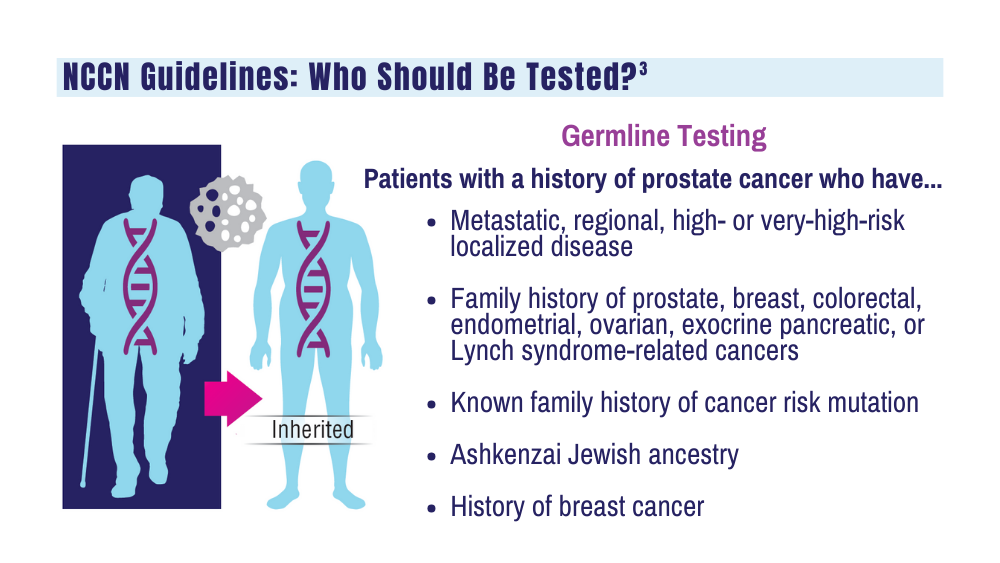
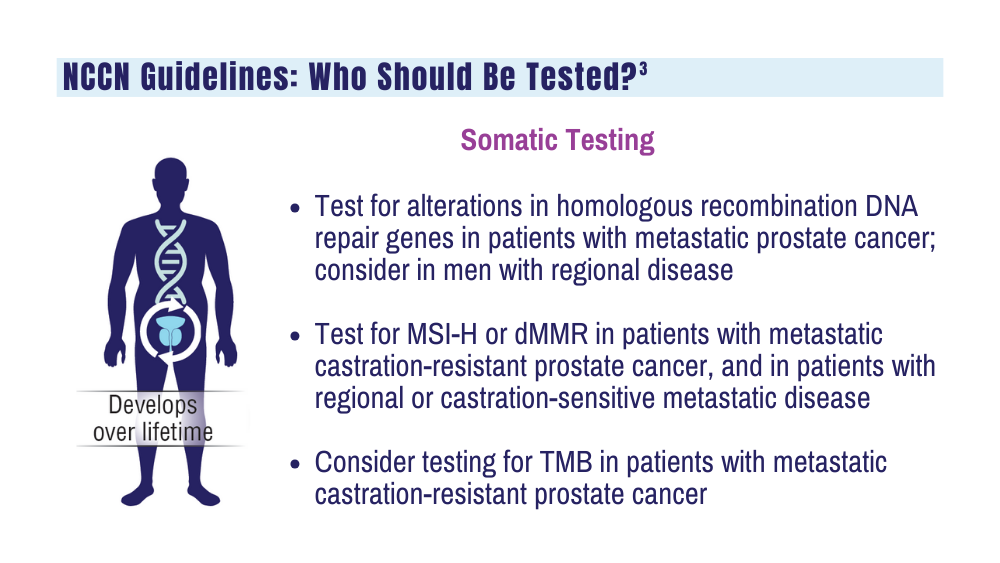
3. National Comprehensive Cancer Network. NCCN clinical practice guidelines for prostate cancer. Version 4.2023. September 7, 2023. Accessed December 20, 2023. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
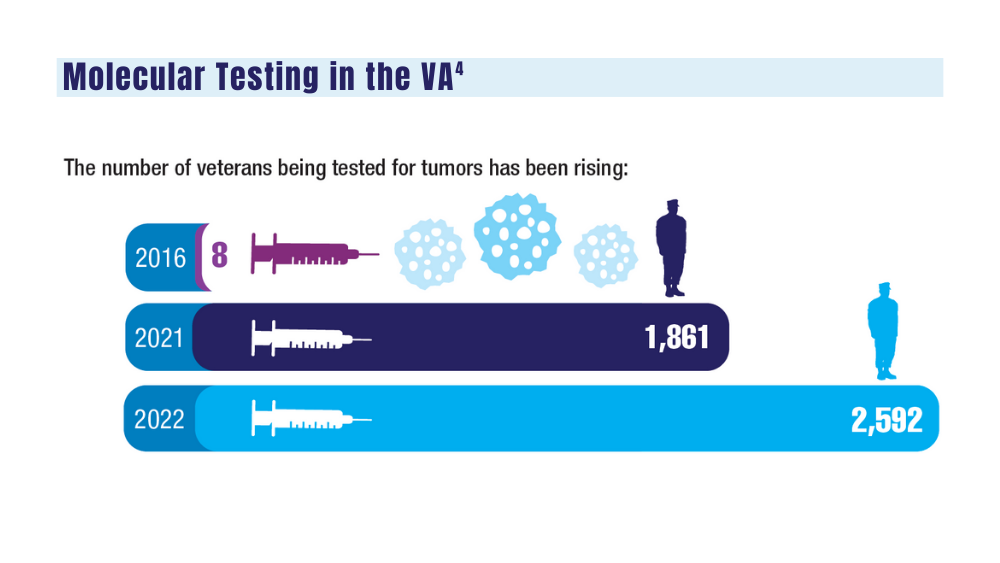
4. National Precision Oncology Program. PMID 26149669 (e-mail, December 13, 2023).
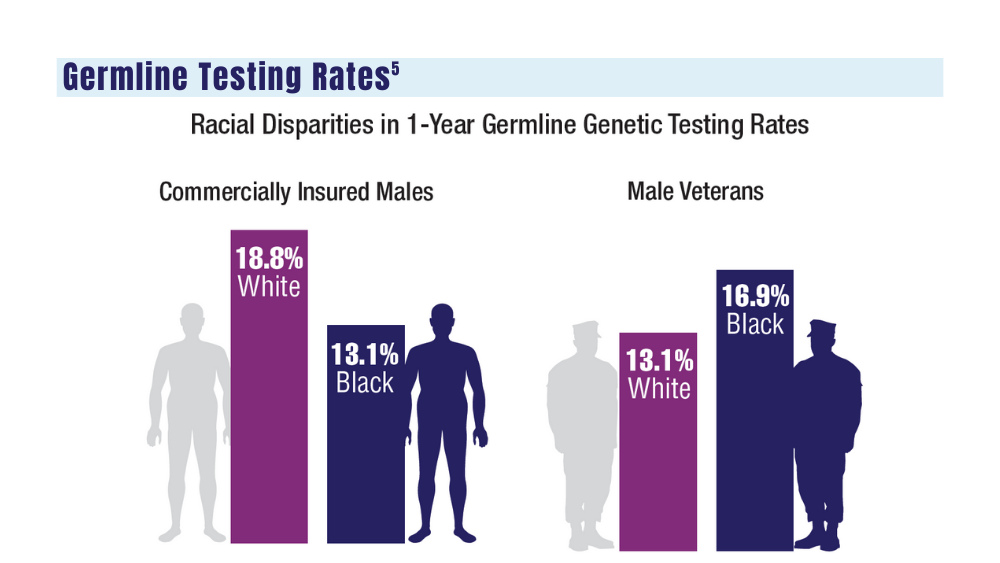
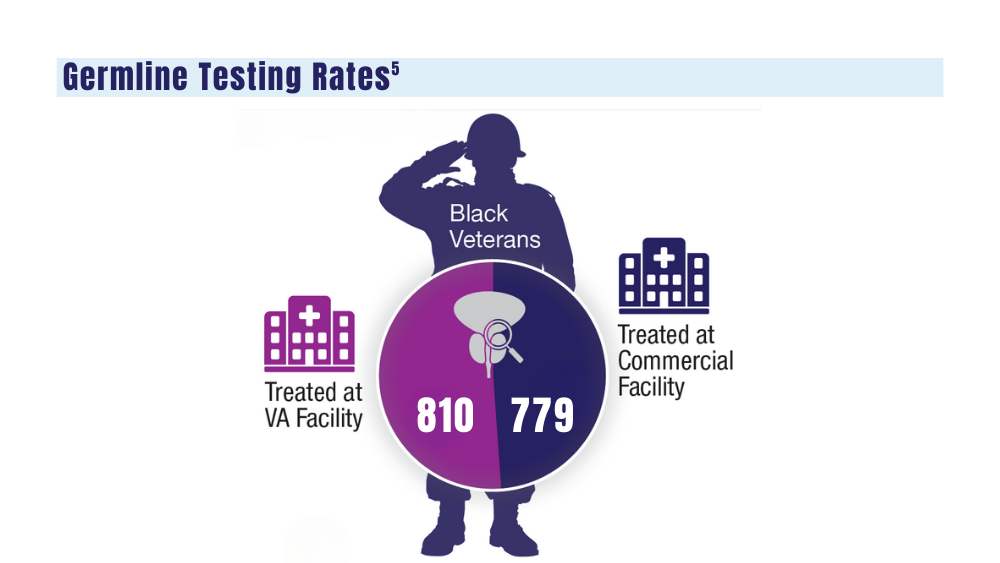
5. Shevach J, Lynch J, Candelieri-Surette D, et al. Racial disparities in germline testing among men with pancreas, breast and metastatic prostate cancers in two health systems. J Clin Oncol. 2023;41(16 suppl):abstract 10549. https://ascopubs.org/doi/abs/10.1200/JCO.2023.41.16_suppl.10549
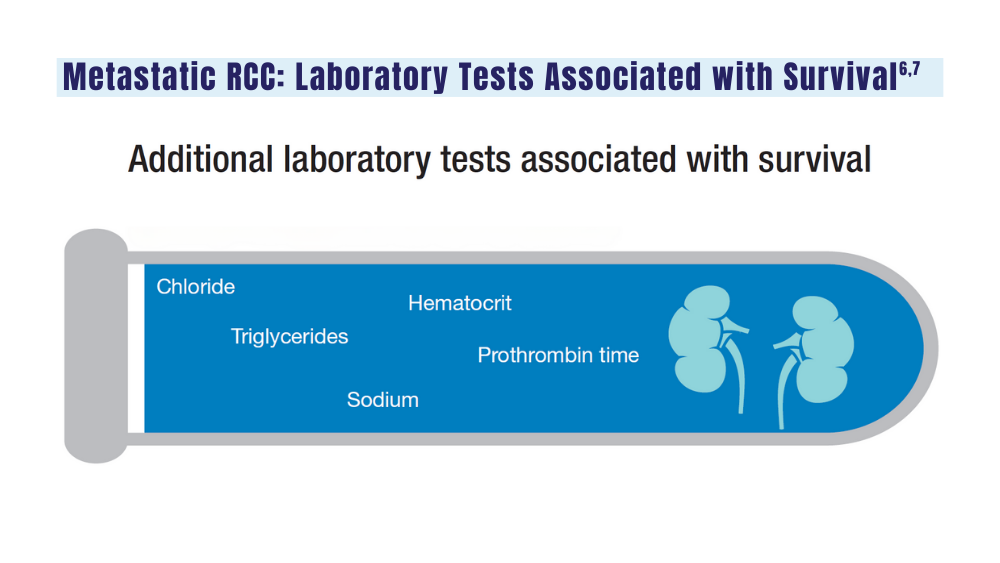
6. Velaer K, Thomas IC, Yang J, et al. Clinical laboratory tests associated with survival in patients with metastatic renal cell carcinoma: a laboratory wide association study (LWAS). Urol Oncol. 2022;40(1):12.e23-12.e30. doi:10.1016/j.urolonc.2021.08.011
7. Heng DYC, Xie W, Regan MM, et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. 2013;14(2):141-148. doi:10.1016/S1470-2045(12)70559-4
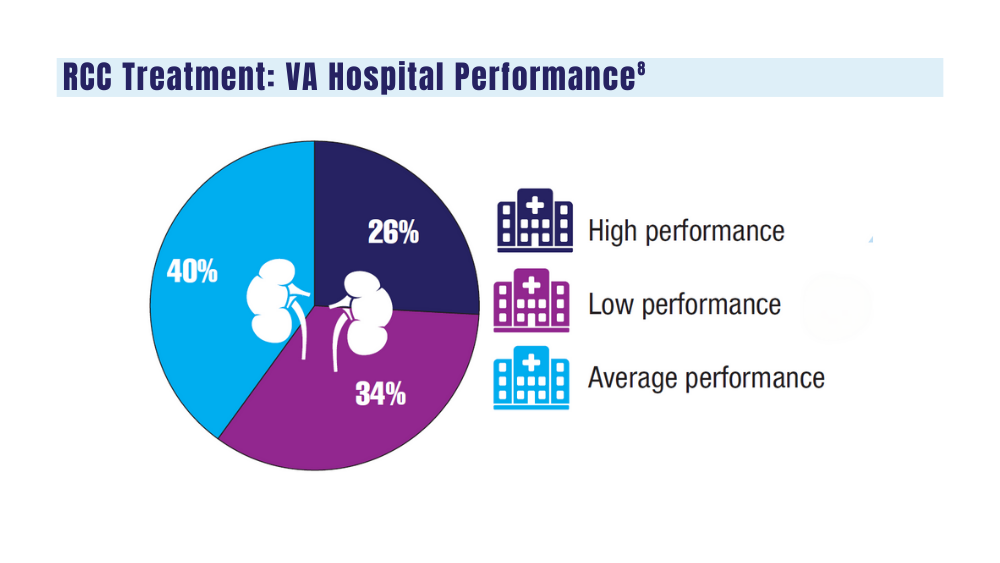
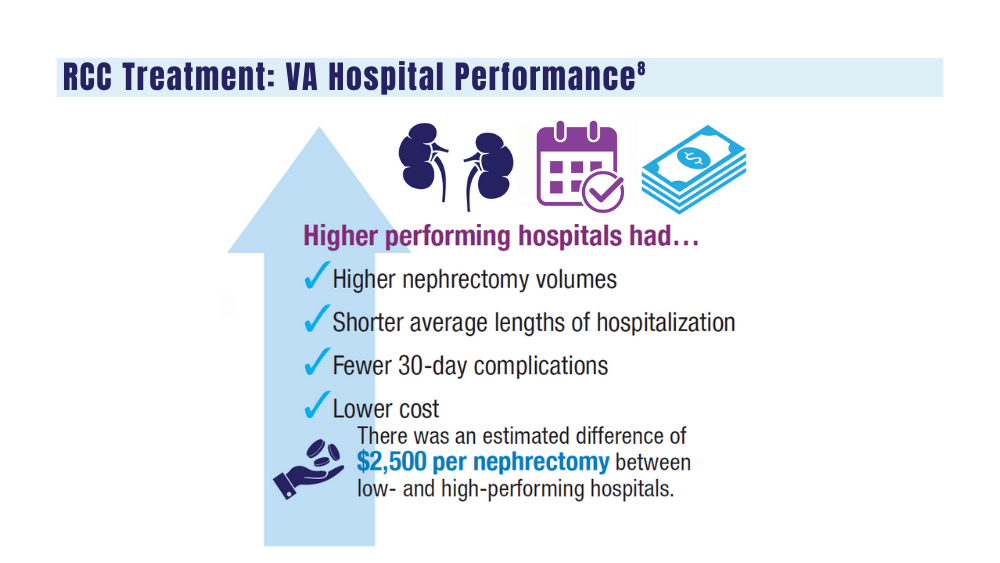
8. Aguilar Palacios D, Wilson B, Michael P, et al. A novel metric for hospital quality in kidney cancer surgery: a Veterans Affairs National Health System validation of concept. Urol Pract. 2022;9(3):237-245. doi:10.1097/UPJ.0000000000000294
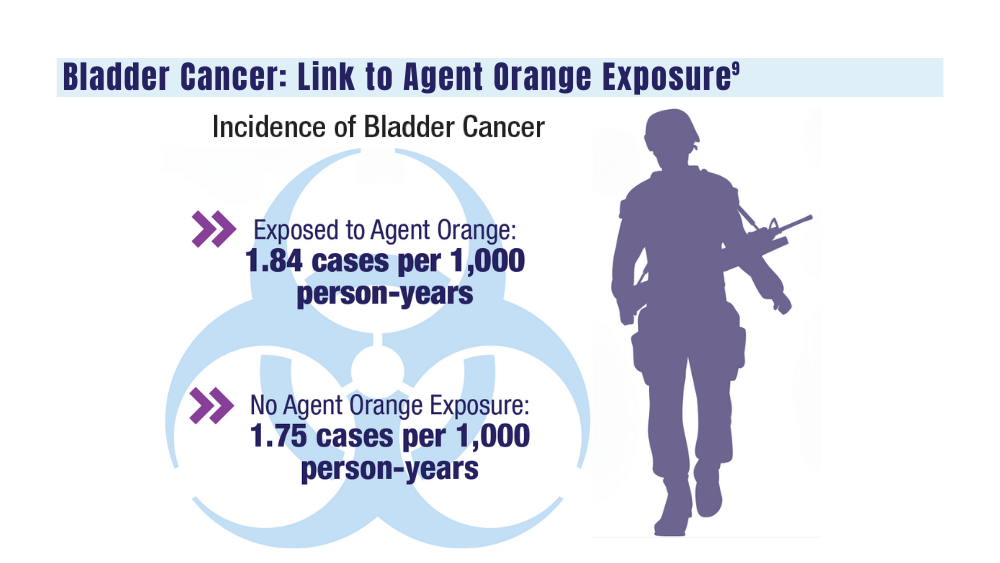
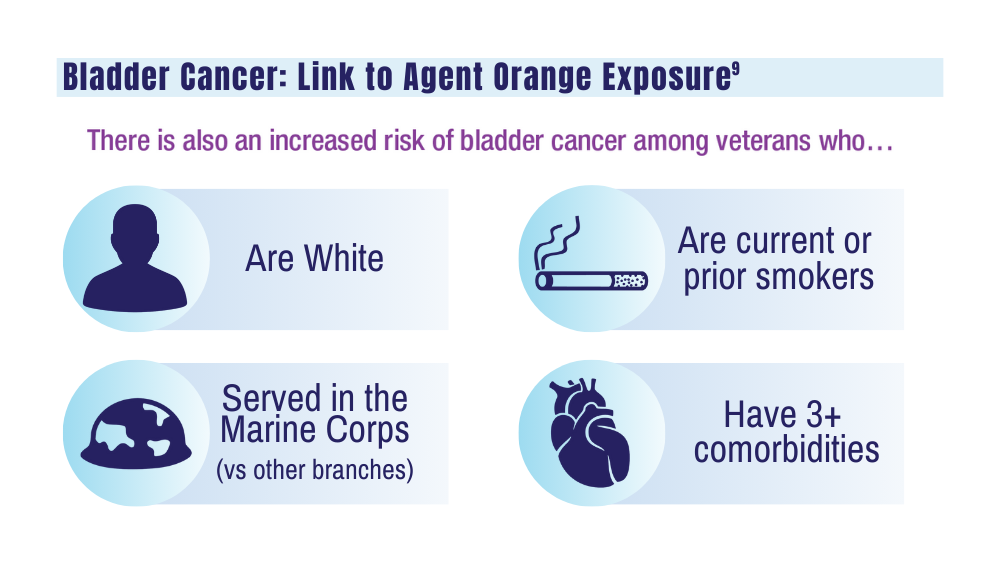
9. Williams SB, Janes JL, Howard LE, et al. Exposure to Agent Orange and risk of bladder cancer among US veterans. JAMA Netw Open. 2023;6(6):e2320593. doi:10.1001/jamanetworkopen.2023.20593
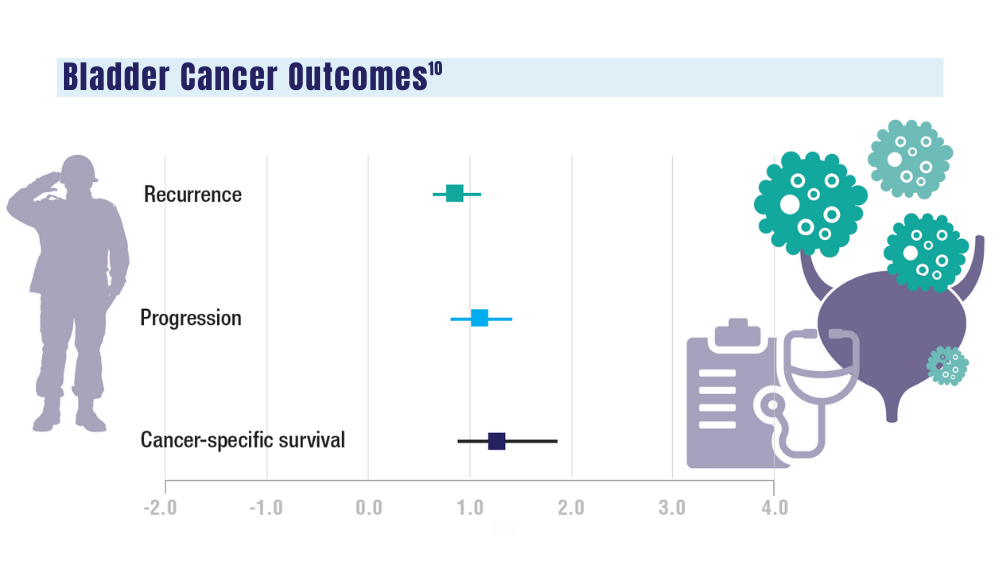
10. Penn T, Borza T, Liou JI, et al. Impact of Agent Orange exposure on non-muscle invasive bladder cancer outcomes. Urology. 2023;182:175-180. doi:10.1016/j.urology.2023.08.037
1. Sokolova A, Cheng H. Germline testing in prostate cancer: when and who to test. Oncology (Williston Park). 2021;35(10):645-653. doi:10.46883/ONC.2021.3510.0645
2. Tuffaha H, Edmunds K, Fairbairn D, et al. Guidelines for genetic testing in prostate cancer: a scoping review. Prostate Cancer Prostatic Dis. 2023 May 18. doi:10.1038/s41391-023-00676-0
3. National Comprehensive Cancer Network. NCCN clinical practice guidelines for prostate cancer. Version 4.2023. September 7, 2023. Accessed December 20, 2023. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
4. National Precision Oncology Program. PMID 26149669 (e-mail, December 13, 2023).
5. Shevach J, Lynch J, Candelieri-Surette D, et al. Racial disparities in germline testing among men with pancreas, breast and metastatic prostate cancers in two health systems. J Clin Oncol. 2023;41(16 suppl):abstract 10549. https://ascopubs.org/doi/abs/10.1200/JCO.2023.41.16_suppl.10549
6. Velaer K, Thomas IC, Yang J, et al. Clinical laboratory tests associated with survival in patients with metastatic renal cell carcinoma: a laboratory wide association study (LWAS). Urol Oncol. 2022;40(1):12.e23-12.e30. doi:10.1016/j.urolonc.2021.08.011
7. Heng DYC, Xie W, Regan MM, et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. 2013;14(2):141-148. doi:10.1016/S1470-2045(12)70559-4
8. Aguilar Palacios D, Wilson B, Michael P, et al. A novel metric for hospital quality in kidney cancer surgery: a Veterans Affairs National Health System validation of concept. Urol Pract. 2022;9(3):237-245. doi:10.1097/UPJ.0000000000000294
9. Williams SB, Janes JL, Howard LE, et al. Exposure to Agent Orange and risk of bladder cancer among US veterans. JAMA Netw Open. 2023;6(6):e2320593. doi:10.1001/jamanetworkopen.2023.20593
10. Penn T, Borza T, Liou JI, et al. Impact of Agent Orange exposure on non-muscle invasive bladder cancer outcomes. Urology. 2023;182:175-180. doi:10.1016/j.urology.2023.08.037
1. Sokolova A, Cheng H. Germline testing in prostate cancer: when and who to test. Oncology (Williston Park). 2021;35(10):645-653. doi:10.46883/ONC.2021.3510.0645
2. Tuffaha H, Edmunds K, Fairbairn D, et al. Guidelines for genetic testing in prostate cancer: a scoping review. Prostate Cancer Prostatic Dis. 2023 May 18. doi:10.1038/s41391-023-00676-0
3. National Comprehensive Cancer Network. NCCN clinical practice guidelines for prostate cancer. Version 4.2023. September 7, 2023. Accessed December 20, 2023. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
4. National Precision Oncology Program. PMID 26149669 (e-mail, December 13, 2023).
5. Shevach J, Lynch J, Candelieri-Surette D, et al. Racial disparities in germline testing among men with pancreas, breast and metastatic prostate cancers in two health systems. J Clin Oncol. 2023;41(16 suppl):abstract 10549. https://ascopubs.org/doi/abs/10.1200/JCO.2023.41.16_suppl.10549
6. Velaer K, Thomas IC, Yang J, et al. Clinical laboratory tests associated with survival in patients with metastatic renal cell carcinoma: a laboratory wide association study (LWAS). Urol Oncol. 2022;40(1):12.e23-12.e30. doi:10.1016/j.urolonc.2021.08.011
7. Heng DYC, Xie W, Regan MM, et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. 2013;14(2):141-148. doi:10.1016/S1470-2045(12)70559-4
8. Aguilar Palacios D, Wilson B, Michael P, et al. A novel metric for hospital quality in kidney cancer surgery: a Veterans Affairs National Health System validation of concept. Urol Pract. 2022;9(3):237-245. doi:10.1097/UPJ.0000000000000294
9. Williams SB, Janes JL, Howard LE, et al. Exposure to Agent Orange and risk of bladder cancer among US veterans. JAMA Netw Open. 2023;6(6):e2320593. doi:10.1001/jamanetworkopen.2023.20593
10. Penn T, Borza T, Liou JI, et al. Impact of Agent Orange exposure on non-muscle invasive bladder cancer outcomes. Urology. 2023;182:175-180. doi:10.1016/j.urology.2023.08.037
Consider These Factors in an Academic Radiation Oncology Position
TOPLINE:
— and accept an offer if the practice is “great” in at least two of those areas and “good” in the third, experts say in a recent editorial.
METHODOLOGY:
- Many physicians choose to go into academic medicine because they want to stay involved in research and education while still treating patients.
- However, graduating radiation oncology residents often lack or have limited guidance on what to look for in a prospective job and how to assess their contract.
- This recent editorial provides guidance to radiation oncologists seeking academic positions. The authors advise prospective employees to evaluate three main factors — compensation, daily duties, and location — as well as provide tips for identifying red flags in each category.
TAKEAWAY:
- Compensation: Prospective faculty should assess both direct compensation, that is, salary, and indirect compensation, which typically includes retirement contributions and other perks. For direct compensation, what is the base salary? Is extra work compensated? How does the salary offer measure up to salary data reported by national agencies? Also: Don’t overlook uncompensated duties, such as time in tumor boards or in meetings, which may be time-consuming, and make sure compensation terms are clearly delineated in a contract and equitable among physicians in a specific rank.
- Daily duties: When it comes to daily life on the job, a prospective employee should consider many factors, including the cancer center’s excitement to hire you, the reputation of the faculty and leaders at the organization, employee turnover rates, diversity among faculty, and the time line of career advancement.
- Location: The location of the job encompasses the geography — such as distance from home to work, the number of practices covered, cost of living, and the area itself — as well as the atmosphere for conducting research and publishing.
- Finally, carefully review the job contract. All the key aspects of the job, including compensation and benefits, should be clearly stated in the contract to “improve communication of expectations.”
IN PRACTICE:
“A prospective faculty member can ask 100 questions, but they can’t make 100 demands; consideration of the three domains can help to focus negotiation efforts where the efforts are needed,” the authors noted.
SOURCE:
This editorial, led by Nicholas G. Zaorsky from the Department of Radiation Oncology, University Hospitals Seidman Cancer Center, Case Western Reserve School of Medicine, Cleveland, Ohio, was published online in Practical Radiation Oncology
DISCLOSURES:
The lead author declared being supported by the American Cancer Society and National Institutes of Health. He also reported having ties with many other sources.
A version of this article appeared on Medscape.com.
TOPLINE:
— and accept an offer if the practice is “great” in at least two of those areas and “good” in the third, experts say in a recent editorial.
METHODOLOGY:
- Many physicians choose to go into academic medicine because they want to stay involved in research and education while still treating patients.
- However, graduating radiation oncology residents often lack or have limited guidance on what to look for in a prospective job and how to assess their contract.
- This recent editorial provides guidance to radiation oncologists seeking academic positions. The authors advise prospective employees to evaluate three main factors — compensation, daily duties, and location — as well as provide tips for identifying red flags in each category.
TAKEAWAY:
- Compensation: Prospective faculty should assess both direct compensation, that is, salary, and indirect compensation, which typically includes retirement contributions and other perks. For direct compensation, what is the base salary? Is extra work compensated? How does the salary offer measure up to salary data reported by national agencies? Also: Don’t overlook uncompensated duties, such as time in tumor boards or in meetings, which may be time-consuming, and make sure compensation terms are clearly delineated in a contract and equitable among physicians in a specific rank.
- Daily duties: When it comes to daily life on the job, a prospective employee should consider many factors, including the cancer center’s excitement to hire you, the reputation of the faculty and leaders at the organization, employee turnover rates, diversity among faculty, and the time line of career advancement.
- Location: The location of the job encompasses the geography — such as distance from home to work, the number of practices covered, cost of living, and the area itself — as well as the atmosphere for conducting research and publishing.
- Finally, carefully review the job contract. All the key aspects of the job, including compensation and benefits, should be clearly stated in the contract to “improve communication of expectations.”
IN PRACTICE:
“A prospective faculty member can ask 100 questions, but they can’t make 100 demands; consideration of the three domains can help to focus negotiation efforts where the efforts are needed,” the authors noted.
SOURCE:
This editorial, led by Nicholas G. Zaorsky from the Department of Radiation Oncology, University Hospitals Seidman Cancer Center, Case Western Reserve School of Medicine, Cleveland, Ohio, was published online in Practical Radiation Oncology
DISCLOSURES:
The lead author declared being supported by the American Cancer Society and National Institutes of Health. He also reported having ties with many other sources.
A version of this article appeared on Medscape.com.
TOPLINE:
— and accept an offer if the practice is “great” in at least two of those areas and “good” in the third, experts say in a recent editorial.
METHODOLOGY:
- Many physicians choose to go into academic medicine because they want to stay involved in research and education while still treating patients.
- However, graduating radiation oncology residents often lack or have limited guidance on what to look for in a prospective job and how to assess their contract.
- This recent editorial provides guidance to radiation oncologists seeking academic positions. The authors advise prospective employees to evaluate three main factors — compensation, daily duties, and location — as well as provide tips for identifying red flags in each category.
TAKEAWAY:
- Compensation: Prospective faculty should assess both direct compensation, that is, salary, and indirect compensation, which typically includes retirement contributions and other perks. For direct compensation, what is the base salary? Is extra work compensated? How does the salary offer measure up to salary data reported by national agencies? Also: Don’t overlook uncompensated duties, such as time in tumor boards or in meetings, which may be time-consuming, and make sure compensation terms are clearly delineated in a contract and equitable among physicians in a specific rank.
- Daily duties: When it comes to daily life on the job, a prospective employee should consider many factors, including the cancer center’s excitement to hire you, the reputation of the faculty and leaders at the organization, employee turnover rates, diversity among faculty, and the time line of career advancement.
- Location: The location of the job encompasses the geography — such as distance from home to work, the number of practices covered, cost of living, and the area itself — as well as the atmosphere for conducting research and publishing.
- Finally, carefully review the job contract. All the key aspects of the job, including compensation and benefits, should be clearly stated in the contract to “improve communication of expectations.”
IN PRACTICE:
“A prospective faculty member can ask 100 questions, but they can’t make 100 demands; consideration of the three domains can help to focus negotiation efforts where the efforts are needed,” the authors noted.
SOURCE:
This editorial, led by Nicholas G. Zaorsky from the Department of Radiation Oncology, University Hospitals Seidman Cancer Center, Case Western Reserve School of Medicine, Cleveland, Ohio, was published online in Practical Radiation Oncology
DISCLOSURES:
The lead author declared being supported by the American Cancer Society and National Institutes of Health. He also reported having ties with many other sources.
A version of this article appeared on Medscape.com.
Look Beyond BMI: Metabolic Factors’ Link to Cancer Explained
The new research finds that adults with persistent metabolic syndrome that worsens over time are at increased risk for any type of cancer.
The conditions that make up metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, and colleagues.
However, a single assessment of metabolic syndrome at one point in time is inadequate to show an association with cancer risk over time, they said. In the current study, the researchers used models to examine the association between trajectory patterns of metabolic syndrome over time and the risk of overall and specific cancer types. They also examined the impact of chronic inflammation concurrent with metabolic syndrome.
What We Know About Metabolic Syndrome and Cancer Risk
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2020 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
In addition, a 2022 study by some of the current study researchers of the same Chinese cohort focused on the role of inflammation in combination with metabolic syndrome on colorectal cancer specifically, and found an increased risk for cancer when both metabolic syndrome and inflammation were present.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
“There is emerging evidence that even normal weight individuals who are metabolically unhealthy may be at an elevated cancer risk, and we need better metrics to define the underlying metabolic dysfunction in obesity,” Sheetal Hardikar, MBBS, PhD, MPH, an investigator at the Huntsman Cancer Institute, University of Utah, said in an interview.
Dr. Hardikar, who serves as assistant professor in the department of population health sciences at the University of Utah, was not involved in the current study. She and her colleagues published a research paper on data from the National Health and Nutrition Examination Survey in 2023 that showed an increased risk of obesity-related cancer.
What New Study Adds to Related Research
Previous studies have consistently reported an approximately 30% increased risk of cancer with metabolic syndrome, Dr. Hardikar said. “What is unique about this study is the examination of metabolic syndrome trajectories over four years, and not just the presence of metabolic syndrome at one point in time,” she said.
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years; the mean body mass index ranged from approximately 22 kg/m2 in the low-stable group to approximately 28 kg/m2 in the elevated-increasing group.
The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
Using the International Diabetes Federation criteria was another limitation, because it prevented the assessment of cancer risk in normal weight individuals with metabolic dysfunction, Dr. Hardikar noted.
Does Metabolic Syndrome Cause Cancer?
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, noted in a statement on the study.
More research is needed to assess the impact of these interventions on cancer risk. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he continued.
“Current evidence based on this study and many other reports strongly suggests an increased risk for cancer associated with metabolic syndrome,” Dr. Hardikar said in an interview. The data serve as a reminder to clinicians to look beyond BMI as the only measure of obesity, and to consider metabolic factors together to identify individuals at increased risk for cancer, she said.
“We must continue to educate patients about obesity and all the chronic conditions it may lead to, but we cannot ignore this emerging phenotype of being of normal weight but metabolically unhealthy,” Dr. Hardikar emphasized.
What Additional Research is Needed?
Looking ahead, “we need well-designed interventions to test causality for metabolic syndrome and cancer risk, though the evidence from the observational studies is very strong,” Dr. Hardikar said.
In addition, a consensus is needed to better define metabolic dysfunction,and to explore cancer risk in normal weight but metabolically unhealthy individuals, she said.
The study was supported by the National Key Research and Development Program of China. The researchers and Dr. Hardikar had no financial conflicts to disclose.
The new research finds that adults with persistent metabolic syndrome that worsens over time are at increased risk for any type of cancer.
The conditions that make up metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, and colleagues.
However, a single assessment of metabolic syndrome at one point in time is inadequate to show an association with cancer risk over time, they said. In the current study, the researchers used models to examine the association between trajectory patterns of metabolic syndrome over time and the risk of overall and specific cancer types. They also examined the impact of chronic inflammation concurrent with metabolic syndrome.
What We Know About Metabolic Syndrome and Cancer Risk
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2020 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
In addition, a 2022 study by some of the current study researchers of the same Chinese cohort focused on the role of inflammation in combination with metabolic syndrome on colorectal cancer specifically, and found an increased risk for cancer when both metabolic syndrome and inflammation were present.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
“There is emerging evidence that even normal weight individuals who are metabolically unhealthy may be at an elevated cancer risk, and we need better metrics to define the underlying metabolic dysfunction in obesity,” Sheetal Hardikar, MBBS, PhD, MPH, an investigator at the Huntsman Cancer Institute, University of Utah, said in an interview.
Dr. Hardikar, who serves as assistant professor in the department of population health sciences at the University of Utah, was not involved in the current study. She and her colleagues published a research paper on data from the National Health and Nutrition Examination Survey in 2023 that showed an increased risk of obesity-related cancer.
What New Study Adds to Related Research
Previous studies have consistently reported an approximately 30% increased risk of cancer with metabolic syndrome, Dr. Hardikar said. “What is unique about this study is the examination of metabolic syndrome trajectories over four years, and not just the presence of metabolic syndrome at one point in time,” she said.
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years; the mean body mass index ranged from approximately 22 kg/m2 in the low-stable group to approximately 28 kg/m2 in the elevated-increasing group.
The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
Using the International Diabetes Federation criteria was another limitation, because it prevented the assessment of cancer risk in normal weight individuals with metabolic dysfunction, Dr. Hardikar noted.
Does Metabolic Syndrome Cause Cancer?
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, noted in a statement on the study.
More research is needed to assess the impact of these interventions on cancer risk. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he continued.
“Current evidence based on this study and many other reports strongly suggests an increased risk for cancer associated with metabolic syndrome,” Dr. Hardikar said in an interview. The data serve as a reminder to clinicians to look beyond BMI as the only measure of obesity, and to consider metabolic factors together to identify individuals at increased risk for cancer, she said.
“We must continue to educate patients about obesity and all the chronic conditions it may lead to, but we cannot ignore this emerging phenotype of being of normal weight but metabolically unhealthy,” Dr. Hardikar emphasized.
What Additional Research is Needed?
Looking ahead, “we need well-designed interventions to test causality for metabolic syndrome and cancer risk, though the evidence from the observational studies is very strong,” Dr. Hardikar said.
In addition, a consensus is needed to better define metabolic dysfunction,and to explore cancer risk in normal weight but metabolically unhealthy individuals, she said.
The study was supported by the National Key Research and Development Program of China. The researchers and Dr. Hardikar had no financial conflicts to disclose.
The new research finds that adults with persistent metabolic syndrome that worsens over time are at increased risk for any type of cancer.
The conditions that make up metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, and colleagues.
However, a single assessment of metabolic syndrome at one point in time is inadequate to show an association with cancer risk over time, they said. In the current study, the researchers used models to examine the association between trajectory patterns of metabolic syndrome over time and the risk of overall and specific cancer types. They also examined the impact of chronic inflammation concurrent with metabolic syndrome.
What We Know About Metabolic Syndrome and Cancer Risk
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2020 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
In addition, a 2022 study by some of the current study researchers of the same Chinese cohort focused on the role of inflammation in combination with metabolic syndrome on colorectal cancer specifically, and found an increased risk for cancer when both metabolic syndrome and inflammation were present.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
“There is emerging evidence that even normal weight individuals who are metabolically unhealthy may be at an elevated cancer risk, and we need better metrics to define the underlying metabolic dysfunction in obesity,” Sheetal Hardikar, MBBS, PhD, MPH, an investigator at the Huntsman Cancer Institute, University of Utah, said in an interview.
Dr. Hardikar, who serves as assistant professor in the department of population health sciences at the University of Utah, was not involved in the current study. She and her colleagues published a research paper on data from the National Health and Nutrition Examination Survey in 2023 that showed an increased risk of obesity-related cancer.
What New Study Adds to Related Research
Previous studies have consistently reported an approximately 30% increased risk of cancer with metabolic syndrome, Dr. Hardikar said. “What is unique about this study is the examination of metabolic syndrome trajectories over four years, and not just the presence of metabolic syndrome at one point in time,” she said.
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years; the mean body mass index ranged from approximately 22 kg/m2 in the low-stable group to approximately 28 kg/m2 in the elevated-increasing group.
The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
Using the International Diabetes Federation criteria was another limitation, because it prevented the assessment of cancer risk in normal weight individuals with metabolic dysfunction, Dr. Hardikar noted.
Does Metabolic Syndrome Cause Cancer?
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, noted in a statement on the study.
More research is needed to assess the impact of these interventions on cancer risk. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he continued.
“Current evidence based on this study and many other reports strongly suggests an increased risk for cancer associated with metabolic syndrome,” Dr. Hardikar said in an interview. The data serve as a reminder to clinicians to look beyond BMI as the only measure of obesity, and to consider metabolic factors together to identify individuals at increased risk for cancer, she said.
“We must continue to educate patients about obesity and all the chronic conditions it may lead to, but we cannot ignore this emerging phenotype of being of normal weight but metabolically unhealthy,” Dr. Hardikar emphasized.
What Additional Research is Needed?
Looking ahead, “we need well-designed interventions to test causality for metabolic syndrome and cancer risk, though the evidence from the observational studies is very strong,” Dr. Hardikar said.
In addition, a consensus is needed to better define metabolic dysfunction,and to explore cancer risk in normal weight but metabolically unhealthy individuals, she said.
The study was supported by the National Key Research and Development Program of China. The researchers and Dr. Hardikar had no financial conflicts to disclose.
FROM CANCER
ASTRO Pushes Return to Direct Supervision in RT: Needed or ‘Babysitting’?
Although serious errors during virtual supervision are rare, ASTRO said radiation treatments (RT) should be done with a radiation oncologist on site to ensure high-quality care. But some radiation oncologists do not agree with the proposal to move back to direct in-person supervision only.
Changes to Direct Supervision
Most radiation oncology treatments are delivered in an outpatient setting under a physician’s direction and control.
During the COVID-19 pandemic when social distancing mandates were in place, CMS temporarily changed the definition of “direct supervision” to include telehealth, specifying that a physician must be immediately available to assist and direct a procedure virtually using real-time audio and video. In other words, a physician did not need to be physically present in the room when the treatment was being performed.
CMS has extended this rule until the end of 2024 and is considering making it a permanent change. In the Calendar Year (CY) 2024 Medicare Physician Fee Schedule (PFS) Final Rule, CMS asked for comments on whether to extend the rule.
“We received input from interested parties on potential patient safety or quality concerns when direct supervision occurs virtually, which we will consider for future rulemaking,” a CMS spokesperson told this news organization. “CMS is currently considering the best approach that will protect patient access and safety as well as quality of care and program integrity concerns following CY 2024.”
CMS also noted its concerns that an abrupt transition back to requiring a physician’s physical presence could interrupt care from practitioners who have established new patterns of practice with telehealth.
What Are ASTRO’s Concerns?
Late last month, ASTRO sent CMS a letter, asking the agency to change the rules back to direct in-person supervision for all radiation services, citing that virtual supervision jeopardizes patient safety and quality of care.
Jeff Michalski, MD, MBA, chair of the ASTRO Board of Directors, said in an interview that radiation oncologists should be physically present to supervise the treatments.
“ASTRO is concerned that blanket policies of general or virtual supervision could lead to patients not having direct, in-person access to their doctors’ care,” he said. “While serious errors are rare, real-world experiences of radiation oncologists across practice settings demonstrate how an in-person radiation oncology physician is best suited to ensure high-quality care.”
What Do Radiation Oncologists Think?
According to ASTRO, most radiation oncologists would agree that in-person supervision is best for patients.
But that might not be the case.
Radiation oncologists took to X (formerly Twitter) to voice their opinions about ASTRO’s letter.
Jason Beckta, MD, PhD, of Rutland Regional’s Foley Cancer Center, Vermont, said “the February 26th ASTRO letter reads like an Onion article.”
“I’m struggling to understand the Luddite-level myopia around this topic,” he said in another tweet. “Virtual direct/outpatient general supervision has done nothing but boost my productivity and in particular, face-to-face patient contact.”
Join Y. Luh, MD, with the Providence Medical Network in Eureka, California, said he understands the challenges faced by clinicians working in more isolated rural settings. “For them, it’s either having virtual supervision or closing the center,” Dr. Luh said.
“Virtual care is definitely at my clinic and is not only an option but is critical to my patients who are 2+ snowy, mountainous hours away,” Dr. Luh wrote. “But I’m still in the clinic directly supervising treatments.”
Sidney Roberts, MD, with the CHI St. Luke’s Health-Memorial, Texas, tweeted that supervision does require some face-to-face care but contended that “babysitting trained therapists for every routine treatment is a farce.”
Another issue Dr. Luh brought up is reimbursement for virtual supervision, noting that “the elephant in the room is whether that level of service should be reimbursed at the same rate. Reimbursement has not changed — but will it stay that way?”
ASTRO has acknowledged that radiation oncologists will have varying opinions and says it is working to balance these challenges.
CMS has not reached a decision on whether the change will be implemented permanently. The organization will assess concern, patient safety, and quality of care at the end of the year.
A version of this article first appeared on Medscape.com
Although serious errors during virtual supervision are rare, ASTRO said radiation treatments (RT) should be done with a radiation oncologist on site to ensure high-quality care. But some radiation oncologists do not agree with the proposal to move back to direct in-person supervision only.
Changes to Direct Supervision
Most radiation oncology treatments are delivered in an outpatient setting under a physician’s direction and control.
During the COVID-19 pandemic when social distancing mandates were in place, CMS temporarily changed the definition of “direct supervision” to include telehealth, specifying that a physician must be immediately available to assist and direct a procedure virtually using real-time audio and video. In other words, a physician did not need to be physically present in the room when the treatment was being performed.
CMS has extended this rule until the end of 2024 and is considering making it a permanent change. In the Calendar Year (CY) 2024 Medicare Physician Fee Schedule (PFS) Final Rule, CMS asked for comments on whether to extend the rule.
“We received input from interested parties on potential patient safety or quality concerns when direct supervision occurs virtually, which we will consider for future rulemaking,” a CMS spokesperson told this news organization. “CMS is currently considering the best approach that will protect patient access and safety as well as quality of care and program integrity concerns following CY 2024.”
CMS also noted its concerns that an abrupt transition back to requiring a physician’s physical presence could interrupt care from practitioners who have established new patterns of practice with telehealth.
What Are ASTRO’s Concerns?
Late last month, ASTRO sent CMS a letter, asking the agency to change the rules back to direct in-person supervision for all radiation services, citing that virtual supervision jeopardizes patient safety and quality of care.
Jeff Michalski, MD, MBA, chair of the ASTRO Board of Directors, said in an interview that radiation oncologists should be physically present to supervise the treatments.
“ASTRO is concerned that blanket policies of general or virtual supervision could lead to patients not having direct, in-person access to their doctors’ care,” he said. “While serious errors are rare, real-world experiences of radiation oncologists across practice settings demonstrate how an in-person radiation oncology physician is best suited to ensure high-quality care.”
What Do Radiation Oncologists Think?
According to ASTRO, most radiation oncologists would agree that in-person supervision is best for patients.
But that might not be the case.
Radiation oncologists took to X (formerly Twitter) to voice their opinions about ASTRO’s letter.
Jason Beckta, MD, PhD, of Rutland Regional’s Foley Cancer Center, Vermont, said “the February 26th ASTRO letter reads like an Onion article.”
“I’m struggling to understand the Luddite-level myopia around this topic,” he said in another tweet. “Virtual direct/outpatient general supervision has done nothing but boost my productivity and in particular, face-to-face patient contact.”
Join Y. Luh, MD, with the Providence Medical Network in Eureka, California, said he understands the challenges faced by clinicians working in more isolated rural settings. “For them, it’s either having virtual supervision or closing the center,” Dr. Luh said.
“Virtual care is definitely at my clinic and is not only an option but is critical to my patients who are 2+ snowy, mountainous hours away,” Dr. Luh wrote. “But I’m still in the clinic directly supervising treatments.”
Sidney Roberts, MD, with the CHI St. Luke’s Health-Memorial, Texas, tweeted that supervision does require some face-to-face care but contended that “babysitting trained therapists for every routine treatment is a farce.”
Another issue Dr. Luh brought up is reimbursement for virtual supervision, noting that “the elephant in the room is whether that level of service should be reimbursed at the same rate. Reimbursement has not changed — but will it stay that way?”
ASTRO has acknowledged that radiation oncologists will have varying opinions and says it is working to balance these challenges.
CMS has not reached a decision on whether the change will be implemented permanently. The organization will assess concern, patient safety, and quality of care at the end of the year.
A version of this article first appeared on Medscape.com
Although serious errors during virtual supervision are rare, ASTRO said radiation treatments (RT) should be done with a radiation oncologist on site to ensure high-quality care. But some radiation oncologists do not agree with the proposal to move back to direct in-person supervision only.
Changes to Direct Supervision
Most radiation oncology treatments are delivered in an outpatient setting under a physician’s direction and control.
During the COVID-19 pandemic when social distancing mandates were in place, CMS temporarily changed the definition of “direct supervision” to include telehealth, specifying that a physician must be immediately available to assist and direct a procedure virtually using real-time audio and video. In other words, a physician did not need to be physically present in the room when the treatment was being performed.
CMS has extended this rule until the end of 2024 and is considering making it a permanent change. In the Calendar Year (CY) 2024 Medicare Physician Fee Schedule (PFS) Final Rule, CMS asked for comments on whether to extend the rule.
“We received input from interested parties on potential patient safety or quality concerns when direct supervision occurs virtually, which we will consider for future rulemaking,” a CMS spokesperson told this news organization. “CMS is currently considering the best approach that will protect patient access and safety as well as quality of care and program integrity concerns following CY 2024.”
CMS also noted its concerns that an abrupt transition back to requiring a physician’s physical presence could interrupt care from practitioners who have established new patterns of practice with telehealth.
What Are ASTRO’s Concerns?
Late last month, ASTRO sent CMS a letter, asking the agency to change the rules back to direct in-person supervision for all radiation services, citing that virtual supervision jeopardizes patient safety and quality of care.
Jeff Michalski, MD, MBA, chair of the ASTRO Board of Directors, said in an interview that radiation oncologists should be physically present to supervise the treatments.
“ASTRO is concerned that blanket policies of general or virtual supervision could lead to patients not having direct, in-person access to their doctors’ care,” he said. “While serious errors are rare, real-world experiences of radiation oncologists across practice settings demonstrate how an in-person radiation oncology physician is best suited to ensure high-quality care.”
What Do Radiation Oncologists Think?
According to ASTRO, most radiation oncologists would agree that in-person supervision is best for patients.
But that might not be the case.
Radiation oncologists took to X (formerly Twitter) to voice their opinions about ASTRO’s letter.
Jason Beckta, MD, PhD, of Rutland Regional’s Foley Cancer Center, Vermont, said “the February 26th ASTRO letter reads like an Onion article.”
“I’m struggling to understand the Luddite-level myopia around this topic,” he said in another tweet. “Virtual direct/outpatient general supervision has done nothing but boost my productivity and in particular, face-to-face patient contact.”
Join Y. Luh, MD, with the Providence Medical Network in Eureka, California, said he understands the challenges faced by clinicians working in more isolated rural settings. “For them, it’s either having virtual supervision or closing the center,” Dr. Luh said.
“Virtual care is definitely at my clinic and is not only an option but is critical to my patients who are 2+ snowy, mountainous hours away,” Dr. Luh wrote. “But I’m still in the clinic directly supervising treatments.”
Sidney Roberts, MD, with the CHI St. Luke’s Health-Memorial, Texas, tweeted that supervision does require some face-to-face care but contended that “babysitting trained therapists for every routine treatment is a farce.”
Another issue Dr. Luh brought up is reimbursement for virtual supervision, noting that “the elephant in the room is whether that level of service should be reimbursed at the same rate. Reimbursement has not changed — but will it stay that way?”
ASTRO has acknowledged that radiation oncologists will have varying opinions and says it is working to balance these challenges.
CMS has not reached a decision on whether the change will be implemented permanently. The organization will assess concern, patient safety, and quality of care at the end of the year.
A version of this article first appeared on Medscape.com
The Urethra Is a Sex Organ; Why This Matters in Incontinence
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, urologist and sexual medicine specialist in the Washington, DC, area. We are coming to you live from the Mayo Clinic Urology Conference in Maui, Hawaii, with the world’s leading experts in men’s health, sexual health, and quality of life. I’m bringing in Dr. Allen Morey from the North Dallas area, one of the world’s leading experts in reconstructive urology. He deals with all things urinary incontinence, penile curvature, and sexual health.
Dr. Morey said something at this conference that really put my chin on the floor. He said, So, Dr. Morey, tell us more about why you made that comment and about the incontinence in men that you deal with all the time.
Allen F. Morey, MD: For many years, I’ve worked at cancer centers where, through the various treatments for prostate cancer, the men suffered from urinary incontinence and we put a lot of artificial urinary sphincters in those patients. I had one patient who asked, “Why do I keep having this erosion?” Of course, the erosion is where the cuff compresses the tissue surrounding the urethra, and the tissue gives way, leaving a hole in the urethra. I looked at him and noticed that he was pale. And I thought, Let me check his testosterone level. We started checking it on everybody who had this problem, and sure enough, the ones who had the cup erosion — who had the atrophic tissue around the urethra — most of them had low testosterone levels. Some of this was due to the cancer treatment, but in other men, it was just due to old age.
We started thinking that this is a causal relationship. And we tested it. I had a fellow who was a board-certified pathologist before becoming a urologist. He obtained some specimens from the urethra and did very sophisticated, elegant stains on that tissue. We found that it’s just erectile tissue surrounding the urethra. That’s why I call it a sex organ. I tell my patients, “When you are a teenager, this tissue is thin, like on your pinky finger. As you get older, it becomes thicker. And then as you get even older, and you may be having cancer treatment, that tissue is gone.” You can show them your little finger; it’s about that size. All the meat is off the bone. There’s nothing left protecting the urinary mucosa from the device.
That’s why it’s important to maintain the optimal health of those tissues and for them to remain dry. Because let’s face it: Urinary incontinence is a horrible quality of life. These are my happiest patients when we fix it. Before that, when they go on vacation, they have a separate suitcase filled with diapers. They can’t go anywhere. They can’t do anything. When they become incontinent after the prostatectomy, they gain weight. And when you put in the device to treat it, they lose weight and you can track it. The urinary incontinence patients really suffer. And we need to consider the medical optimization of those patients.
Dr. Rubin: It’s so important, and I love how analogous this is to our female patients. We know that incontinence is devastating to our female patients as well, and there’s a lot of hope. As we get older we start to pee every time we cough, laugh, or sneeze. Men are a little more bothered by it when it happens; they don’t expect it. Among women, it’s thought of as normal, but it’s not normal. There is so much we can do to help these patients, ranging from conservative treatment to surgical therapies.
The connection between hormones and urethral health is true on the female side as well. As you go through menopause, the urethral tissue thins out, gets dry, gets irritated, and can cause worsening incontinence, pain with sex, and genital urinary syndrome of menopause. It’s really important.
For our primary care doctors, how should we talk about stress incontinence in men? How do we diagnose it?
Dr. Morey: It’s easy to diagnose. Just do a quick history. Find out how many pads a day they are using. You have to ask the question, and then you have them stand up and look inside their underwear. You’ll see what kind of pad they are wearing. Is it just a shield or are they actually wearing full diapers? Then I have them do a standing cough test. I stand off to the side, holding a couple of towels, and have the patient cough four times. I can tell if it’s a full stream or just a couple of drops. Is it nothing but they are wearing a pad? You match up what you see with their experience, and in an instant it tells you how severe their problem is and it helps you direct them on to further treatment, because many patients have treatment fatigue. They’ve already been through the system. They have really suffered and they don’t know which way to go. They don’t know what’s available.
Dr. Rubin: On the female side, we have pelvic floor physical therapy. We have pads and devices that you can wear, and pessaries. We have surgical options, like bulking agents into the urethra as well as urethral slings, which can be quite helpful for women. So there’s a lot of hope out there for women, and from what I learned from you at this conference, there’s a lot of hope for men as well. So talk us through treatment, from conservative to surgical options.
Dr. Morey: There hasn’t been much innovation in male incontinence treatment over the past few decades, but we’re starting to see signs of new products appearing on the horizon, so I’m very optimistic that in the next 5 or 10 years, we’ll have more. But right now it comes down to slings and artificial sphincters, which are devices with little pumps and hydraulics, and they’re very good. But they’ve been around for 50 years, and they have this other potential risk factor of the erosion of the tissue.
We don’t have a pill that we can give the patient to tighten up those muscles. We can help them with overactive bladder. But maybe the hormonal influence is a way to optimize the health of the tissue so that these surgical treatments can really deliver the best outcomes. And as I always say, and having treated so many of these patients, it’s really a game of millimeters — how much coaptation you get. If you’re off by the slightest amount, that’s an unhappy patient. So it doesn’t take much to make it a lot better.
Dr. Rubin: There’s so much hope for our patients, and this can really have an effect on sexual health. You know the benefits you see in their quality of life and sexual health when you can stop leakage.
Dr. Morey: I always take care of the waterworks first. Many of the men have both urinary problems and erectile problems. Nobody feels sexy when they’re leaking urine all over their partner. So first we take care of that. And then, in the motivated younger patients, we bring them back and talk to them about potentially having a second operation.
Dr. Rubin: And so similarly, in women with urinary incontinence, it can have a major impact on sexual health — how they show up and how they talk to their partner. So, it is really important for our primary care docs to talk to patients about urinary incontinence and not just say, “Oh, well, you’re getting older. There’s nothing that you can do.” There’s actually no age at which there is nothing that we can do. And it’s really important to refer patients to those urologists who have extra training in incontinence and sexual health, because we do care about these quality-of-life measures and there is a lot we can do, ranging from conservative to more invasive treatments. But patients really should have options.
Dr. Morey: I heard during this meeting that urinary incontinence was the number-one source of treatment regret among patients who had their prostate treated for cancer. So, this is a really big deal for our patients. And it impacts wellness, quality of life, and overall well-being.
Dr. Rubin: When we are counseling patients for cancer surgeries or cancer treatments such as radiation therapy, it’s really hard for the patients who have never had urinary incontinence to imagine what that might be like. When you’re telling them they could have a stroke or a heart attack, or they could have erectile dysfunction or urinary incontinence, it all sounds similar to them. It could happen to someone else. It’s very hard to truly counsel patients on these quality-of-life issues that they’ve never encountered before.
Dr. Morey: We have found that it takes a long time for patients to get into our office for treatment, and it’s unbelievable — often 5 years in diapers before they find us.
Dr. Rubin: Hopefully videos like this will teach our docs and our patients that there is hope out there, that you don’t need to wait through years of suffering from incontinence. So, how does somebody find a reconstructive urologist or a sexual medicine urologist?
Dr. Morey: There are a couple of good websites out there, such as fixincontinence.com and edcure.org. The device manufacturers have pretty good information for patients.
Dr. Rubin: The Sexual Medicine Society of North America (SMSNA) has a great find-a-provider website, which provides a list of urologists who are trained in both sexual health and urinary incontinence, because they both matter. Our patients deeply care about these issues.
Rachel S. Rubin, MD, has disclosed the following relevant financial relationships: Serve(d) as a speaker for Sprout; received research grant from Maternal Medical; received income in an amount equal to or greater than $250 from Absorption Pharmaceuticals, GSK, Endo.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, urologist and sexual medicine specialist in the Washington, DC, area. We are coming to you live from the Mayo Clinic Urology Conference in Maui, Hawaii, with the world’s leading experts in men’s health, sexual health, and quality of life. I’m bringing in Dr. Allen Morey from the North Dallas area, one of the world’s leading experts in reconstructive urology. He deals with all things urinary incontinence, penile curvature, and sexual health.
Dr. Morey said something at this conference that really put my chin on the floor. He said, So, Dr. Morey, tell us more about why you made that comment and about the incontinence in men that you deal with all the time.
Allen F. Morey, MD: For many years, I’ve worked at cancer centers where, through the various treatments for prostate cancer, the men suffered from urinary incontinence and we put a lot of artificial urinary sphincters in those patients. I had one patient who asked, “Why do I keep having this erosion?” Of course, the erosion is where the cuff compresses the tissue surrounding the urethra, and the tissue gives way, leaving a hole in the urethra. I looked at him and noticed that he was pale. And I thought, Let me check his testosterone level. We started checking it on everybody who had this problem, and sure enough, the ones who had the cup erosion — who had the atrophic tissue around the urethra — most of them had low testosterone levels. Some of this was due to the cancer treatment, but in other men, it was just due to old age.
We started thinking that this is a causal relationship. And we tested it. I had a fellow who was a board-certified pathologist before becoming a urologist. He obtained some specimens from the urethra and did very sophisticated, elegant stains on that tissue. We found that it’s just erectile tissue surrounding the urethra. That’s why I call it a sex organ. I tell my patients, “When you are a teenager, this tissue is thin, like on your pinky finger. As you get older, it becomes thicker. And then as you get even older, and you may be having cancer treatment, that tissue is gone.” You can show them your little finger; it’s about that size. All the meat is off the bone. There’s nothing left protecting the urinary mucosa from the device.
That’s why it’s important to maintain the optimal health of those tissues and for them to remain dry. Because let’s face it: Urinary incontinence is a horrible quality of life. These are my happiest patients when we fix it. Before that, when they go on vacation, they have a separate suitcase filled with diapers. They can’t go anywhere. They can’t do anything. When they become incontinent after the prostatectomy, they gain weight. And when you put in the device to treat it, they lose weight and you can track it. The urinary incontinence patients really suffer. And we need to consider the medical optimization of those patients.
Dr. Rubin: It’s so important, and I love how analogous this is to our female patients. We know that incontinence is devastating to our female patients as well, and there’s a lot of hope. As we get older we start to pee every time we cough, laugh, or sneeze. Men are a little more bothered by it when it happens; they don’t expect it. Among women, it’s thought of as normal, but it’s not normal. There is so much we can do to help these patients, ranging from conservative treatment to surgical therapies.
The connection between hormones and urethral health is true on the female side as well. As you go through menopause, the urethral tissue thins out, gets dry, gets irritated, and can cause worsening incontinence, pain with sex, and genital urinary syndrome of menopause. It’s really important.
For our primary care doctors, how should we talk about stress incontinence in men? How do we diagnose it?
Dr. Morey: It’s easy to diagnose. Just do a quick history. Find out how many pads a day they are using. You have to ask the question, and then you have them stand up and look inside their underwear. You’ll see what kind of pad they are wearing. Is it just a shield or are they actually wearing full diapers? Then I have them do a standing cough test. I stand off to the side, holding a couple of towels, and have the patient cough four times. I can tell if it’s a full stream or just a couple of drops. Is it nothing but they are wearing a pad? You match up what you see with their experience, and in an instant it tells you how severe their problem is and it helps you direct them on to further treatment, because many patients have treatment fatigue. They’ve already been through the system. They have really suffered and they don’t know which way to go. They don’t know what’s available.
Dr. Rubin: On the female side, we have pelvic floor physical therapy. We have pads and devices that you can wear, and pessaries. We have surgical options, like bulking agents into the urethra as well as urethral slings, which can be quite helpful for women. So there’s a lot of hope out there for women, and from what I learned from you at this conference, there’s a lot of hope for men as well. So talk us through treatment, from conservative to surgical options.
Dr. Morey: There hasn’t been much innovation in male incontinence treatment over the past few decades, but we’re starting to see signs of new products appearing on the horizon, so I’m very optimistic that in the next 5 or 10 years, we’ll have more. But right now it comes down to slings and artificial sphincters, which are devices with little pumps and hydraulics, and they’re very good. But they’ve been around for 50 years, and they have this other potential risk factor of the erosion of the tissue.
We don’t have a pill that we can give the patient to tighten up those muscles. We can help them with overactive bladder. But maybe the hormonal influence is a way to optimize the health of the tissue so that these surgical treatments can really deliver the best outcomes. And as I always say, and having treated so many of these patients, it’s really a game of millimeters — how much coaptation you get. If you’re off by the slightest amount, that’s an unhappy patient. So it doesn’t take much to make it a lot better.
Dr. Rubin: There’s so much hope for our patients, and this can really have an effect on sexual health. You know the benefits you see in their quality of life and sexual health when you can stop leakage.
Dr. Morey: I always take care of the waterworks first. Many of the men have both urinary problems and erectile problems. Nobody feels sexy when they’re leaking urine all over their partner. So first we take care of that. And then, in the motivated younger patients, we bring them back and talk to them about potentially having a second operation.
Dr. Rubin: And so similarly, in women with urinary incontinence, it can have a major impact on sexual health — how they show up and how they talk to their partner. So, it is really important for our primary care docs to talk to patients about urinary incontinence and not just say, “Oh, well, you’re getting older. There’s nothing that you can do.” There’s actually no age at which there is nothing that we can do. And it’s really important to refer patients to those urologists who have extra training in incontinence and sexual health, because we do care about these quality-of-life measures and there is a lot we can do, ranging from conservative to more invasive treatments. But patients really should have options.
Dr. Morey: I heard during this meeting that urinary incontinence was the number-one source of treatment regret among patients who had their prostate treated for cancer. So, this is a really big deal for our patients. And it impacts wellness, quality of life, and overall well-being.
Dr. Rubin: When we are counseling patients for cancer surgeries or cancer treatments such as radiation therapy, it’s really hard for the patients who have never had urinary incontinence to imagine what that might be like. When you’re telling them they could have a stroke or a heart attack, or they could have erectile dysfunction or urinary incontinence, it all sounds similar to them. It could happen to someone else. It’s very hard to truly counsel patients on these quality-of-life issues that they’ve never encountered before.
Dr. Morey: We have found that it takes a long time for patients to get into our office for treatment, and it’s unbelievable — often 5 years in diapers before they find us.
Dr. Rubin: Hopefully videos like this will teach our docs and our patients that there is hope out there, that you don’t need to wait through years of suffering from incontinence. So, how does somebody find a reconstructive urologist or a sexual medicine urologist?
Dr. Morey: There are a couple of good websites out there, such as fixincontinence.com and edcure.org. The device manufacturers have pretty good information for patients.
Dr. Rubin: The Sexual Medicine Society of North America (SMSNA) has a great find-a-provider website, which provides a list of urologists who are trained in both sexual health and urinary incontinence, because they both matter. Our patients deeply care about these issues.
Rachel S. Rubin, MD, has disclosed the following relevant financial relationships: Serve(d) as a speaker for Sprout; received research grant from Maternal Medical; received income in an amount equal to or greater than $250 from Absorption Pharmaceuticals, GSK, Endo.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Rachel S. Rubin, MD: I’m Dr. Rachel Rubin, urologist and sexual medicine specialist in the Washington, DC, area. We are coming to you live from the Mayo Clinic Urology Conference in Maui, Hawaii, with the world’s leading experts in men’s health, sexual health, and quality of life. I’m bringing in Dr. Allen Morey from the North Dallas area, one of the world’s leading experts in reconstructive urology. He deals with all things urinary incontinence, penile curvature, and sexual health.
Dr. Morey said something at this conference that really put my chin on the floor. He said, So, Dr. Morey, tell us more about why you made that comment and about the incontinence in men that you deal with all the time.
Allen F. Morey, MD: For many years, I’ve worked at cancer centers where, through the various treatments for prostate cancer, the men suffered from urinary incontinence and we put a lot of artificial urinary sphincters in those patients. I had one patient who asked, “Why do I keep having this erosion?” Of course, the erosion is where the cuff compresses the tissue surrounding the urethra, and the tissue gives way, leaving a hole in the urethra. I looked at him and noticed that he was pale. And I thought, Let me check his testosterone level. We started checking it on everybody who had this problem, and sure enough, the ones who had the cup erosion — who had the atrophic tissue around the urethra — most of them had low testosterone levels. Some of this was due to the cancer treatment, but in other men, it was just due to old age.
We started thinking that this is a causal relationship. And we tested it. I had a fellow who was a board-certified pathologist before becoming a urologist. He obtained some specimens from the urethra and did very sophisticated, elegant stains on that tissue. We found that it’s just erectile tissue surrounding the urethra. That’s why I call it a sex organ. I tell my patients, “When you are a teenager, this tissue is thin, like on your pinky finger. As you get older, it becomes thicker. And then as you get even older, and you may be having cancer treatment, that tissue is gone.” You can show them your little finger; it’s about that size. All the meat is off the bone. There’s nothing left protecting the urinary mucosa from the device.
That’s why it’s important to maintain the optimal health of those tissues and for them to remain dry. Because let’s face it: Urinary incontinence is a horrible quality of life. These are my happiest patients when we fix it. Before that, when they go on vacation, they have a separate suitcase filled with diapers. They can’t go anywhere. They can’t do anything. When they become incontinent after the prostatectomy, they gain weight. And when you put in the device to treat it, they lose weight and you can track it. The urinary incontinence patients really suffer. And we need to consider the medical optimization of those patients.
Dr. Rubin: It’s so important, and I love how analogous this is to our female patients. We know that incontinence is devastating to our female patients as well, and there’s a lot of hope. As we get older we start to pee every time we cough, laugh, or sneeze. Men are a little more bothered by it when it happens; they don’t expect it. Among women, it’s thought of as normal, but it’s not normal. There is so much we can do to help these patients, ranging from conservative treatment to surgical therapies.
The connection between hormones and urethral health is true on the female side as well. As you go through menopause, the urethral tissue thins out, gets dry, gets irritated, and can cause worsening incontinence, pain with sex, and genital urinary syndrome of menopause. It’s really important.
For our primary care doctors, how should we talk about stress incontinence in men? How do we diagnose it?
Dr. Morey: It’s easy to diagnose. Just do a quick history. Find out how many pads a day they are using. You have to ask the question, and then you have them stand up and look inside their underwear. You’ll see what kind of pad they are wearing. Is it just a shield or are they actually wearing full diapers? Then I have them do a standing cough test. I stand off to the side, holding a couple of towels, and have the patient cough four times. I can tell if it’s a full stream or just a couple of drops. Is it nothing but they are wearing a pad? You match up what you see with their experience, and in an instant it tells you how severe their problem is and it helps you direct them on to further treatment, because many patients have treatment fatigue. They’ve already been through the system. They have really suffered and they don’t know which way to go. They don’t know what’s available.
Dr. Rubin: On the female side, we have pelvic floor physical therapy. We have pads and devices that you can wear, and pessaries. We have surgical options, like bulking agents into the urethra as well as urethral slings, which can be quite helpful for women. So there’s a lot of hope out there for women, and from what I learned from you at this conference, there’s a lot of hope for men as well. So talk us through treatment, from conservative to surgical options.
Dr. Morey: There hasn’t been much innovation in male incontinence treatment over the past few decades, but we’re starting to see signs of new products appearing on the horizon, so I’m very optimistic that in the next 5 or 10 years, we’ll have more. But right now it comes down to slings and artificial sphincters, which are devices with little pumps and hydraulics, and they’re very good. But they’ve been around for 50 years, and they have this other potential risk factor of the erosion of the tissue.
We don’t have a pill that we can give the patient to tighten up those muscles. We can help them with overactive bladder. But maybe the hormonal influence is a way to optimize the health of the tissue so that these surgical treatments can really deliver the best outcomes. And as I always say, and having treated so many of these patients, it’s really a game of millimeters — how much coaptation you get. If you’re off by the slightest amount, that’s an unhappy patient. So it doesn’t take much to make it a lot better.
Dr. Rubin: There’s so much hope for our patients, and this can really have an effect on sexual health. You know the benefits you see in their quality of life and sexual health when you can stop leakage.
Dr. Morey: I always take care of the waterworks first. Many of the men have both urinary problems and erectile problems. Nobody feels sexy when they’re leaking urine all over their partner. So first we take care of that. And then, in the motivated younger patients, we bring them back and talk to them about potentially having a second operation.
Dr. Rubin: And so similarly, in women with urinary incontinence, it can have a major impact on sexual health — how they show up and how they talk to their partner. So, it is really important for our primary care docs to talk to patients about urinary incontinence and not just say, “Oh, well, you’re getting older. There’s nothing that you can do.” There’s actually no age at which there is nothing that we can do. And it’s really important to refer patients to those urologists who have extra training in incontinence and sexual health, because we do care about these quality-of-life measures and there is a lot we can do, ranging from conservative to more invasive treatments. But patients really should have options.
Dr. Morey: I heard during this meeting that urinary incontinence was the number-one source of treatment regret among patients who had their prostate treated for cancer. So, this is a really big deal for our patients. And it impacts wellness, quality of life, and overall well-being.
Dr. Rubin: When we are counseling patients for cancer surgeries or cancer treatments such as radiation therapy, it’s really hard for the patients who have never had urinary incontinence to imagine what that might be like. When you’re telling them they could have a stroke or a heart attack, or they could have erectile dysfunction or urinary incontinence, it all sounds similar to them. It could happen to someone else. It’s very hard to truly counsel patients on these quality-of-life issues that they’ve never encountered before.
Dr. Morey: We have found that it takes a long time for patients to get into our office for treatment, and it’s unbelievable — often 5 years in diapers before they find us.
Dr. Rubin: Hopefully videos like this will teach our docs and our patients that there is hope out there, that you don’t need to wait through years of suffering from incontinence. So, how does somebody find a reconstructive urologist or a sexual medicine urologist?
Dr. Morey: There are a couple of good websites out there, such as fixincontinence.com and edcure.org. The device manufacturers have pretty good information for patients.
Dr. Rubin: The Sexual Medicine Society of North America (SMSNA) has a great find-a-provider website, which provides a list of urologists who are trained in both sexual health and urinary incontinence, because they both matter. Our patients deeply care about these issues.
Rachel S. Rubin, MD, has disclosed the following relevant financial relationships: Serve(d) as a speaker for Sprout; received research grant from Maternal Medical; received income in an amount equal to or greater than $250 from Absorption Pharmaceuticals, GSK, Endo.
A version of this article appeared on Medscape.com.
Does worsening metabolic syndrome increase the risk of developing cancer?
The conditions that comprise metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, China, and colleagues.
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2019 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
What Does New Study Add to Other Research on Metabolic Syndrome and Cancer Risk?
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years. The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
What Is the Takeaway Message for Clinical Practice?
The results suggest that monitoring and managing metabolic syndrome could help reduce cancer risk, the researchers concluded.
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, said in a press release accompanying the study.
More research is needed to assess the impact of these interventions on cancer risk, he noted. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he said in a statement.
The study was supported by the National Key Research and Development Program of China. The researchers had no financial conflicts to disclose.
The conditions that comprise metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, China, and colleagues.
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2019 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
What Does New Study Add to Other Research on Metabolic Syndrome and Cancer Risk?
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years. The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
What Is the Takeaway Message for Clinical Practice?
The results suggest that monitoring and managing metabolic syndrome could help reduce cancer risk, the researchers concluded.
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, said in a press release accompanying the study.
More research is needed to assess the impact of these interventions on cancer risk, he noted. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he said in a statement.
The study was supported by the National Key Research and Development Program of China. The researchers had no financial conflicts to disclose.
The conditions that comprise metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, China, and colleagues.
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2019 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
What Does New Study Add to Other Research on Metabolic Syndrome and Cancer Risk?
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years. The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
What Is the Takeaway Message for Clinical Practice?
The results suggest that monitoring and managing metabolic syndrome could help reduce cancer risk, the researchers concluded.
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, said in a press release accompanying the study.
More research is needed to assess the impact of these interventions on cancer risk, he noted. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he said in a statement.
The study was supported by the National Key Research and Development Program of China. The researchers had no financial conflicts to disclose.
FROM CANCER
Higher Prostate Cancer Rates Seen in Black Men, but Advanced Cases Similar to White Men
There was a substantial difference in prostate cancer diagnosis across ethnic groups: 25% of Black men with a raised PSA were diagnosed with prostate cancer within 1 year of being tested, compared with 20% of White men and 13% of Asian men, in the analysis of a large primary care cohort in the United Kingdom.
Incidence of advanced prostate cancer for Asian men with a raised PSA result was 4.5%, compared with 7.5% for White men and 7.0% for Black men.
Men included in the study were aged 40 and older and had no prior cancer diagnosis. Their ethnicity and PSA test result were logged in a national dataset between 2010 and 2017.
The study of more than 730,000 men, published in BMC Medicine, didn’t explore reasons for the differences, but experts offer their thoughts on what led to the findings and what these results imply.
Why the Higher Diagnosis Rates but Not More Advanced Disease in Black Men?
Lead author Liz Down, a graduate research assistant at the University of Exeter, Exeter, England, suggests the higher diagnosis rates but not more advanced disease in Black men may be linked to genetic variations.
Her team’s studies have shown that Black men in the United Kingdom and United States have higher levels of PSA. The PSA value is used to identify patients who might benefit from specialist investigation, and current guidelines in the UK and US don’t distinguish between ethnic groups.
As most men have slow-growing prostate cancer, this may lead to a disproportionately higher number of Black men being diagnosed with prostate cancer, she said.
“One possible interpretation,” Ms. Down notes, “is that prostate cancer follows a similar trajectory in Black and White men. What is different, however, is that Black men have higher PSA levels.”
As to why the advanced-cancer incidence is similar in Black and White patients in the study, Daniel George, MD, director of genitourinary oncology at Duke Cancer Institute in Durham, North Carolina, says it’s important to understand that the Black men in this study “are not necessarily representative of the Black population at large.”
In this study, “they’re a little bit more healthcare inclined,” Dr. George notes. The study population is actively seeking the PSA test. Their socioeconomic profile might be closer to their White counterparts’, and that may make results more similar, he said.
“It’s possible that because this is a screening and not just men coming in for symptoms or cause, that we’re not seeing as much advanced disease,” he continued.
Amar Kishan, MD, chief of the genitourinary oncology service at University of California Los Angeles (UCLA) Health, says the genomic factors and environmental stressors that lead to elevated PSA counts don’t necessarily translate into aggressiveness of disease.
Why do Different Races have Different Prostate Cancer Risk?
Dr. George points out that the study also highlights that Asian men were significantly less likely to be diagnosed with prostate cancer within 1 year of the test.
The reasons for differences in prostate risk by race are complex, he notes. There are some clues that biologic factors may be at work. For instance, early puberty has a link to prostate cancer as it does to breast cancer, and height is also associated with a greater risk of prostate cancer, Dr. George said.
It’s not necessarily a racial association but there are some biological factors associated with prostate cancer later in life, he explained. “These may be enriched in certain populations, including northern Europeans and patients with African ancestries.”
The study also notes that Black men are more likely to die from prostate cancer than are White men, and Asian men are less likely than White or Black men to die from it.
Ms. Down said the difference in prostate cancer mortality between Black vs White men, in particular, may be related to a number of factors, and age, and lifetime risk of prostate cancer may play a major role, at least in the UK.
Should There Be Different ‘Normal’ PSA Levels for Different Races?
Dr. George says there is likely a need to change the system because a PSA level in one race may not signal the same risk it does in another. So medicine probably needs to standardize what a “normal” PSA is by race, he says, adding that he is a coauthor of an upcoming paper regarding that issue.
The lowest instances of prostate cancer were in Asian patients so this isn’t just a Black and White issue, Dr. George notes. “Being able to establish benchmarks by race and ethnicity is something that is probably needed in the field,” he says.
Dr. Kishan, on the other hand, says data from this study are not enough to support differentiating PSA levels based on race. He noted a limitation of the study is that it was not able to calculate the false-negative rate of PSA tests.
What are the Implications for Treating and Screening for Prostate Cancer
Dr. Kishan says there may be a role for increased intensity of screening, whether at an earlier age or with different intervals, but prostate cancer treatment should not differ by race.
“Our prior study, as well as others,” he says, “have shown that when you balance Black and White patients for every factor that might impact prognosis other than race — such as age, disease aggressiveness, etc. — Black men actually tend to have better outcomes than White men. Thus, it would mean potentially overtreating (i.e., causing unnecessary side effects) to increase treatment intensity purely based on race with the available data.”
According to the paper, prostate cancer incidence in men with higher PSA levels increases with increasing age, even when using age-adjusted thresholds.
Dr. George says we know from this study and other studies as well that Black men are more likely to be diagnosed with prostate at a younger age. “Therefore, we probably need to be thinking about screening Black men starting at a younger age. These are the men who are most likely to benefit from an intervention — patients who have life expectancies of 20 years or more.”
What are the Downsides to Overdiagnosing Prostate Cancer in Men?
“It’s one of the biggest concerns that men have in proactively seeking healthcare,” Dr. George says. “They’re more likely to undergo treatment for this disease if they’re getting screened because (clinicians are) more likely to find it.”
Some of those men, he says, are going to undergo treatment for disease that won’t ultimately kill them, but may cause complications the men shouldn’t have had at all or otherwise may have had later.
“Overtreatment is a real concern. That’s why active surveillance is so important to minimize overtreatment of patients by finding out which cancers are low risk for progression and which are becoming more aggressive,” Dr. George says.
Authors of the study write that “the potential for overdiagnosis and the subsequent psychological and physical impact of diagnosis and treatment is an important consideration.”
All authors of the new paper received financial support from Cancer Research UK, the National Institute for Health and Care Research (NIHR), and the Higgins family for the submitted work.
Dr. George reports no relevant financial relationships.
Dr. Kishan reports consulting fees and speaking honoraria from Varian Medical Systems, Janssen, and Boston Scientific; research funding from PointBioPharma, Lantheus, and Janssen; and serving on advisory boards for Lantheus, Janssen and Boston Scientific.
There was a substantial difference in prostate cancer diagnosis across ethnic groups: 25% of Black men with a raised PSA were diagnosed with prostate cancer within 1 year of being tested, compared with 20% of White men and 13% of Asian men, in the analysis of a large primary care cohort in the United Kingdom.
Incidence of advanced prostate cancer for Asian men with a raised PSA result was 4.5%, compared with 7.5% for White men and 7.0% for Black men.
Men included in the study were aged 40 and older and had no prior cancer diagnosis. Their ethnicity and PSA test result were logged in a national dataset between 2010 and 2017.
The study of more than 730,000 men, published in BMC Medicine, didn’t explore reasons for the differences, but experts offer their thoughts on what led to the findings and what these results imply.
Why the Higher Diagnosis Rates but Not More Advanced Disease in Black Men?
Lead author Liz Down, a graduate research assistant at the University of Exeter, Exeter, England, suggests the higher diagnosis rates but not more advanced disease in Black men may be linked to genetic variations.
Her team’s studies have shown that Black men in the United Kingdom and United States have higher levels of PSA. The PSA value is used to identify patients who might benefit from specialist investigation, and current guidelines in the UK and US don’t distinguish between ethnic groups.
As most men have slow-growing prostate cancer, this may lead to a disproportionately higher number of Black men being diagnosed with prostate cancer, she said.
“One possible interpretation,” Ms. Down notes, “is that prostate cancer follows a similar trajectory in Black and White men. What is different, however, is that Black men have higher PSA levels.”
As to why the advanced-cancer incidence is similar in Black and White patients in the study, Daniel George, MD, director of genitourinary oncology at Duke Cancer Institute in Durham, North Carolina, says it’s important to understand that the Black men in this study “are not necessarily representative of the Black population at large.”
In this study, “they’re a little bit more healthcare inclined,” Dr. George notes. The study population is actively seeking the PSA test. Their socioeconomic profile might be closer to their White counterparts’, and that may make results more similar, he said.
“It’s possible that because this is a screening and not just men coming in for symptoms or cause, that we’re not seeing as much advanced disease,” he continued.
Amar Kishan, MD, chief of the genitourinary oncology service at University of California Los Angeles (UCLA) Health, says the genomic factors and environmental stressors that lead to elevated PSA counts don’t necessarily translate into aggressiveness of disease.
Why do Different Races have Different Prostate Cancer Risk?
Dr. George points out that the study also highlights that Asian men were significantly less likely to be diagnosed with prostate cancer within 1 year of the test.
The reasons for differences in prostate risk by race are complex, he notes. There are some clues that biologic factors may be at work. For instance, early puberty has a link to prostate cancer as it does to breast cancer, and height is also associated with a greater risk of prostate cancer, Dr. George said.
It’s not necessarily a racial association but there are some biological factors associated with prostate cancer later in life, he explained. “These may be enriched in certain populations, including northern Europeans and patients with African ancestries.”
The study also notes that Black men are more likely to die from prostate cancer than are White men, and Asian men are less likely than White or Black men to die from it.
Ms. Down said the difference in prostate cancer mortality between Black vs White men, in particular, may be related to a number of factors, and age, and lifetime risk of prostate cancer may play a major role, at least in the UK.
Should There Be Different ‘Normal’ PSA Levels for Different Races?
Dr. George says there is likely a need to change the system because a PSA level in one race may not signal the same risk it does in another. So medicine probably needs to standardize what a “normal” PSA is by race, he says, adding that he is a coauthor of an upcoming paper regarding that issue.
The lowest instances of prostate cancer were in Asian patients so this isn’t just a Black and White issue, Dr. George notes. “Being able to establish benchmarks by race and ethnicity is something that is probably needed in the field,” he says.
Dr. Kishan, on the other hand, says data from this study are not enough to support differentiating PSA levels based on race. He noted a limitation of the study is that it was not able to calculate the false-negative rate of PSA tests.
What are the Implications for Treating and Screening for Prostate Cancer
Dr. Kishan says there may be a role for increased intensity of screening, whether at an earlier age or with different intervals, but prostate cancer treatment should not differ by race.
“Our prior study, as well as others,” he says, “have shown that when you balance Black and White patients for every factor that might impact prognosis other than race — such as age, disease aggressiveness, etc. — Black men actually tend to have better outcomes than White men. Thus, it would mean potentially overtreating (i.e., causing unnecessary side effects) to increase treatment intensity purely based on race with the available data.”
According to the paper, prostate cancer incidence in men with higher PSA levels increases with increasing age, even when using age-adjusted thresholds.
Dr. George says we know from this study and other studies as well that Black men are more likely to be diagnosed with prostate at a younger age. “Therefore, we probably need to be thinking about screening Black men starting at a younger age. These are the men who are most likely to benefit from an intervention — patients who have life expectancies of 20 years or more.”
What are the Downsides to Overdiagnosing Prostate Cancer in Men?
“It’s one of the biggest concerns that men have in proactively seeking healthcare,” Dr. George says. “They’re more likely to undergo treatment for this disease if they’re getting screened because (clinicians are) more likely to find it.”
Some of those men, he says, are going to undergo treatment for disease that won’t ultimately kill them, but may cause complications the men shouldn’t have had at all or otherwise may have had later.
“Overtreatment is a real concern. That’s why active surveillance is so important to minimize overtreatment of patients by finding out which cancers are low risk for progression and which are becoming more aggressive,” Dr. George says.
Authors of the study write that “the potential for overdiagnosis and the subsequent psychological and physical impact of diagnosis and treatment is an important consideration.”
All authors of the new paper received financial support from Cancer Research UK, the National Institute for Health and Care Research (NIHR), and the Higgins family for the submitted work.
Dr. George reports no relevant financial relationships.
Dr. Kishan reports consulting fees and speaking honoraria from Varian Medical Systems, Janssen, and Boston Scientific; research funding from PointBioPharma, Lantheus, and Janssen; and serving on advisory boards for Lantheus, Janssen and Boston Scientific.
There was a substantial difference in prostate cancer diagnosis across ethnic groups: 25% of Black men with a raised PSA were diagnosed with prostate cancer within 1 year of being tested, compared with 20% of White men and 13% of Asian men, in the analysis of a large primary care cohort in the United Kingdom.
Incidence of advanced prostate cancer for Asian men with a raised PSA result was 4.5%, compared with 7.5% for White men and 7.0% for Black men.
Men included in the study were aged 40 and older and had no prior cancer diagnosis. Their ethnicity and PSA test result were logged in a national dataset between 2010 and 2017.
The study of more than 730,000 men, published in BMC Medicine, didn’t explore reasons for the differences, but experts offer their thoughts on what led to the findings and what these results imply.
Why the Higher Diagnosis Rates but Not More Advanced Disease in Black Men?
Lead author Liz Down, a graduate research assistant at the University of Exeter, Exeter, England, suggests the higher diagnosis rates but not more advanced disease in Black men may be linked to genetic variations.
Her team’s studies have shown that Black men in the United Kingdom and United States have higher levels of PSA. The PSA value is used to identify patients who might benefit from specialist investigation, and current guidelines in the UK and US don’t distinguish between ethnic groups.
As most men have slow-growing prostate cancer, this may lead to a disproportionately higher number of Black men being diagnosed with prostate cancer, she said.
“One possible interpretation,” Ms. Down notes, “is that prostate cancer follows a similar trajectory in Black and White men. What is different, however, is that Black men have higher PSA levels.”
As to why the advanced-cancer incidence is similar in Black and White patients in the study, Daniel George, MD, director of genitourinary oncology at Duke Cancer Institute in Durham, North Carolina, says it’s important to understand that the Black men in this study “are not necessarily representative of the Black population at large.”
In this study, “they’re a little bit more healthcare inclined,” Dr. George notes. The study population is actively seeking the PSA test. Their socioeconomic profile might be closer to their White counterparts’, and that may make results more similar, he said.
“It’s possible that because this is a screening and not just men coming in for symptoms or cause, that we’re not seeing as much advanced disease,” he continued.
Amar Kishan, MD, chief of the genitourinary oncology service at University of California Los Angeles (UCLA) Health, says the genomic factors and environmental stressors that lead to elevated PSA counts don’t necessarily translate into aggressiveness of disease.
Why do Different Races have Different Prostate Cancer Risk?
Dr. George points out that the study also highlights that Asian men were significantly less likely to be diagnosed with prostate cancer within 1 year of the test.
The reasons for differences in prostate risk by race are complex, he notes. There are some clues that biologic factors may be at work. For instance, early puberty has a link to prostate cancer as it does to breast cancer, and height is also associated with a greater risk of prostate cancer, Dr. George said.
It’s not necessarily a racial association but there are some biological factors associated with prostate cancer later in life, he explained. “These may be enriched in certain populations, including northern Europeans and patients with African ancestries.”
The study also notes that Black men are more likely to die from prostate cancer than are White men, and Asian men are less likely than White or Black men to die from it.
Ms. Down said the difference in prostate cancer mortality between Black vs White men, in particular, may be related to a number of factors, and age, and lifetime risk of prostate cancer may play a major role, at least in the UK.
Should There Be Different ‘Normal’ PSA Levels for Different Races?
Dr. George says there is likely a need to change the system because a PSA level in one race may not signal the same risk it does in another. So medicine probably needs to standardize what a “normal” PSA is by race, he says, adding that he is a coauthor of an upcoming paper regarding that issue.
The lowest instances of prostate cancer were in Asian patients so this isn’t just a Black and White issue, Dr. George notes. “Being able to establish benchmarks by race and ethnicity is something that is probably needed in the field,” he says.
Dr. Kishan, on the other hand, says data from this study are not enough to support differentiating PSA levels based on race. He noted a limitation of the study is that it was not able to calculate the false-negative rate of PSA tests.
What are the Implications for Treating and Screening for Prostate Cancer
Dr. Kishan says there may be a role for increased intensity of screening, whether at an earlier age or with different intervals, but prostate cancer treatment should not differ by race.
“Our prior study, as well as others,” he says, “have shown that when you balance Black and White patients for every factor that might impact prognosis other than race — such as age, disease aggressiveness, etc. — Black men actually tend to have better outcomes than White men. Thus, it would mean potentially overtreating (i.e., causing unnecessary side effects) to increase treatment intensity purely based on race with the available data.”
According to the paper, prostate cancer incidence in men with higher PSA levels increases with increasing age, even when using age-adjusted thresholds.
Dr. George says we know from this study and other studies as well that Black men are more likely to be diagnosed with prostate at a younger age. “Therefore, we probably need to be thinking about screening Black men starting at a younger age. These are the men who are most likely to benefit from an intervention — patients who have life expectancies of 20 years or more.”
What are the Downsides to Overdiagnosing Prostate Cancer in Men?
“It’s one of the biggest concerns that men have in proactively seeking healthcare,” Dr. George says. “They’re more likely to undergo treatment for this disease if they’re getting screened because (clinicians are) more likely to find it.”
Some of those men, he says, are going to undergo treatment for disease that won’t ultimately kill them, but may cause complications the men shouldn’t have had at all or otherwise may have had later.
“Overtreatment is a real concern. That’s why active surveillance is so important to minimize overtreatment of patients by finding out which cancers are low risk for progression and which are becoming more aggressive,” Dr. George says.
Authors of the study write that “the potential for overdiagnosis and the subsequent psychological and physical impact of diagnosis and treatment is an important consideration.”
All authors of the new paper received financial support from Cancer Research UK, the National Institute for Health and Care Research (NIHR), and the Higgins family for the submitted work.
Dr. George reports no relevant financial relationships.
Dr. Kishan reports consulting fees and speaking honoraria from Varian Medical Systems, Janssen, and Boston Scientific; research funding from PointBioPharma, Lantheus, and Janssen; and serving on advisory boards for Lantheus, Janssen and Boston Scientific.
FROM BMC MEDICINE
Does Exercise Reduce Cancer Risk? It’s Just Not That Simple
“Exercise is medicine” has become something of a mantra, with good reason. There’s no doubt that regular physical activity has a broad range of health benefits. Exercise can improve circulation, help control weight, reduce stress, and boost mood — take your pick.
Lower cancer risk is also on the list — with exercise promoted as a risk-cutting strategy in government guidelines and in recommendations from professional groups such as the American Cancer Society.
The bulk of the data hangs on less rigorous, observational studies that have linked physical activity to lower risks for certain cancers, but plenty of questions remain.
What are the cancer types where exercise makes a difference? How significant is that impact? And what, exactly, defines a physical activity pattern powerful enough to move the needle on cancer risk?
Here’s an overview of the state of the evidence.
Exercise and Cancer Types: A Mixed Bag
When it comes to cancer prevention strategies, guidelines uniformly endorse less couch time and more movement. But a deeper look at the science reveals a complex and often poorly understood connection between exercise and cancer risk.
For certain cancer types, the benefits of exercise on cancer risk seem fairly well established.
The latest edition of the Physical Activity Guidelines for Americans, published in 2018, cites “strong evidence” that regular exercise might curb the risks for breast and colon cancers as well as bladder, endometrial, esophageal, kidney, and gastric cancers. These guidelines also point to “moderate”-strength evidence of a protective association with lung cancer.
The evidence of a protective effect, however, is strongest for breast and colon cancers, said Jennifer Ligibel, MD, senior physician in the Breast Oncology Center at Dana-Farber Cancer Institute, Boston, . “But,” she pointed out, “that may be because they’re some of the most common cancers, and it’s been easier to detect an association.”
Guidelines from the American Cancer Society, published in 2020, align with the 2018 recommendations.
“We believe there’s strong evidence to suggest at least eight different types of cancer are associated with physical activity,” said Erika Rees-Punia, PhD, MPH, senior principal scientist, epidemiology and behavioral research at the American Cancer Society.
That view is not universal, however. Current recommendations from the World Cancer Research Fund and American Institute for Cancer Research, for example, are more circumspect, citing only three cancers with good evidence of a protective effect from exercise: Breast (postmenopausal), colon, and endometrial.
“We definitely can’t say exercise reduces the risk of all cancers,” said Lee Jones, PhD, head of the Exercise Oncology Program at Memorial Sloan Kettering Cancer Center in New York City. “The data suggest it’s just not that simple.”
And it’s challenging to put all the evidence together, Dr. Jones added.
The physical activity guidelines are based on published systematic reviews, meta-analyses, and pooled analyses of data from observational studies that examined the relationship between physical activity — aerobic exercise, specifically — and cancer incidence. That means the evidence comes with all the limitations observational studies entail, such as how they collect information on participants’ exercise habits — which, Dr. Jones noted, is typically done via “monster questionnaires” that gauge physical activity in broad strokes.
Pooling all those findings into a meta-analysis is tricky, Dr. Jones added, because individual studies vary in important ways — from follow-up periods to how they quantify exercise and track cancer incidence.
In a study published in February in Cancer Cell, Dr. Jones and his colleagues attempted to address some of those issues by leveraging data from the PLCO screening trial.
The PLCO was a prospective study of over 60,000 US adults that compared the effects of annual screening vs usual care on cancer mortality. At enrollment, participants completed questionnaires that included an assessment of “vigorous” exercise. Based on that, Dr. Jones and his colleagues classified 55% as “exercisers” — meaning they reported 2 or more hours of vigorous exercise per week. The remaining 45%, who were in the 0 to 1 hour per week range, were deemed non-exercisers.
Over a median of 18 years, nearly 16,000 first-time invasive cancers were diagnosed, and some interesting differences between exercisers and non-exercisers emerged. The active group had lower risks for three cancers: Head and neck, with a 26% lower risk (hazard ratio [HR], 0.74), lung (a 20% lower risk), and breast (an 11% lower risk).
What was striking, however, was the lack of connection between exercise and many cancers cited in the guidelines, including colon, gastric, bladder, endometrial, and renal cancers.
Perhaps even more surprising — exercisers had higher risks for prostate cancer (12%) and melanoma (20%). This finding, Dr. Jones said, is in line with a previous pooled analysis of data from 12 US and European prospective cohorts. In this study, the most physically active participants (90th percentile) had higher risks for melanoma and prostate cancer, compared with the least active group (10th percentile).
The melanoma findings do make sense, Dr. Jones said, given that highly active people may spend a lot of time in the sun. “My advice,” Dr. Jones said, “is, if you’re exercising outside, wear sunscreen.” The prostate cancer findings, however, are more puzzling and warrant further research, he noted.
But the bottom line is that the relationship between exercise and cancer types is mixed and far from nailed down.
How Big Is the Effect?
Even if exercise reduces the risk for only certain cancers, that’s still important, particularly when those links appear strongest for common cancer types, such as breast and colon.
But how much of a difference can exercise make?
Based on the evidence, it may only be a modest one. A 2019 systematic review by the Physical Activity Guidelines Advisory Committee provided a rough estimate: Across hundreds of epidemiological studies, people with the highest physical activity levels had a 10%-20% lower risk for the cancers cited in the 2018 exercise guidelines compared with people who were least active.
These figures, however, are probably an underestimate, said Anne McTiernan, MD, PhD, a member of the advisory committee and professor of epidemiology, at Fred Hutchinson Cancer Center, Seattle.
“This is what we usually see when a factor is not measured very well,” said Dr. McTiernan, explaining that the individual studies differed in their categories of “highest” and “lowest” physical activity, such that one study’s “highest” could be another’s mid-range.
“In other words, the effects of physical activity are likely larger” than the review found, Dr. McTiernan said.
The next logical question is whether a bigger exercise “dose” — more time or higher intensity — would have a greater impact on cancer risk. A 2019 study published in the Journal of Clinical Oncology tried to clarify that by pooling data on over 750,000 participants from nine prospective cohorts.
Overall, people meeting government recommendations for exercise — equivalent to about 2.5-5 hours of weekly moderate activity, such as a brisk walk, or about 1.25-2.5 hours of more vigorous activities, like running — had lower risks for seven of 15 cancer types studied compared with less active people.
For cancers with positive findings, being on the higher end of the recommended 2.5- to 5-hour weekly range was better. Risk reductions for breast cancer, for instance, were 6% at 2.5 hours of physical activity per week and 10% at 5 hours per week. Similar trends emerged for other cancer types, including colon (8%-14%), endometrial (10%-18%), liver cancer (18%-27%), and non-Hodgkin lymphoma in women (11%-18%).
But there may be an exercise sweet spot that maximizes the cancer risk benefit.
Among people who surpassed the recommendations — exercising for more time or more intensely — the risk reduction benefit did not necessarily improve in a linear fashion. For certain cancer types, such as colon and endometrial, the benefits of more vigorous exercise “eroded at higher levels of activity,” the authors said.
The issue here is that most studies have not dug deeply into aerobic exercise habits. Often, studies present participants with a list of activities — walking, biking, and running — and ask them to estimate how often and for what duration they do each.
Plus, “we’ve usually lumped moderate and vigorous activities together,” Dr. Rees-Punia said, which means there’s a lack of “granular data” to say whether certain intensities or frequencies of exercise are optimal and for whom.
Why Exercise May Lower Cancer Risk
Exercise habits do not, of course, exist in a vacuum. Highly active people, Dr. Ligibel said, tend to be of higher socioeconomic status, leaner, and have generally healthier lifestyles than sedentary people.
Body weight is a big confounder as well. However, Dr. Rees-Punia noted, it’s also probably a reason that exercise is linked to lower cancer risks, particularly by preventing weight gain. Still, studies have found that the association between exercise and many cancers remains significant after adjusting for body mass index.
The why remains unclear, though some studies offer clues.
“There’s been some really interesting mechanistic research, suggesting that exercise may help inhibit tumor growth or upregulate the immune system,” Dr. Ligibel said.
That includes not only lab research but small intervention studies. While these studies have largely involved people who already have cancer, some have also focused on healthy individuals.
A 2019 study from Dr. Ligibel and her colleagues, which randomly assigned 49 women newly diagnosed with breast cancer to start either an exercise program or mind-body practices ahead of surgery, found exercisers, who had been active for about a month at the time of surgery, showed signs of immune system upregulation in their tumors, while the control group did not.
Among healthy postmenopausal women, a meta-analysis of six clinical trials from Dr. McTiernan and her colleagues found that exercise plus calorie reduction can reduce levels of breast cancer-related endogenous hormones, more so than calorie-cutting alone. And a 2023 study found that high-intensity exercise boosted the ranks of certain immune cells and reduced inflammation in the colon among people at high risk for colon and endometrial cancers due to Lynch syndrome.
Defining an Exercise ‘Prescription’
Despite the gaps and uncertainties in the research, government guidelines as well as those from the American Cancer Society and other medical groups are in lockstep in their exercise recommendations: Adults should strive for 150-300 minutes of moderate-intensity aerobic exercise (like brisk walking), 75-150 minutes of vigorous activity (like running), or some combination each week.
The guidelines also encourage strength training twice a week — advice that’s based on research tying those activity levels to lower risks for heart disease, diabetes, and other chronic conditions.
But there’s no “best” exercise prescription for lowering cancer risk specifically. Most epidemiological studies have examined only aerobic activity, Dr. Rees-Punia said, and there’s very little known about whether strength conditioning or other moderate heart rate-elevating activities, such as daily household chores, may reduce the risk for cancer.
Given the lack of nuance in the literature, it’s hard to say what intensities, types, or amounts of exercise are best for each individual.
Going forward, device-based measurements of physical activity could “help us sort out the effects of different intensities of exercise and possibly types,” Dr. Rees-Punia said.
But overall, Dr. McTiernan said, the data do show that the risks for several cancers are lower at the widely recommended activity levels.
“The bottom-line advice is still to exercise at least 150 minutes per week at a moderate-intensity level or greater,” Dr. McTiernan said.
Or put another way, moving beats being sedentary. It’s probably wise for everyone to sit less, noted Dr. Rees-Punia, for overall health and based on evidence tying sedentary time to the risks for certain cancers, including colon, endometrial, and lung.
There’s a practical element to consider in all of this: What physical activities will people actually do on the regular? In the big epidemiological studies, Dr. McTiernan noted, middle-aged and older adults most often report walking, suggesting that’s the preferred, or most accessible activity, for many.
“You can only benefit from the physical activity you’ll actually do,” Dr. Rees-Punia said.
Dr. Ligibel echoed that sentiment, saying she encourages patients to think about physical activity as a process: “You need to find things you like to do and work them into your daily life, in a sustainable way.
“People often talk about exercise being medicine,” Dr. Ligibel said. “But I think you could take that too far. If we get too prescriptive about it, that could take the joy away.”
A version of this article appeared on Medscape.com.
“Exercise is medicine” has become something of a mantra, with good reason. There’s no doubt that regular physical activity has a broad range of health benefits. Exercise can improve circulation, help control weight, reduce stress, and boost mood — take your pick.
Lower cancer risk is also on the list — with exercise promoted as a risk-cutting strategy in government guidelines and in recommendations from professional groups such as the American Cancer Society.
The bulk of the data hangs on less rigorous, observational studies that have linked physical activity to lower risks for certain cancers, but plenty of questions remain.
What are the cancer types where exercise makes a difference? How significant is that impact? And what, exactly, defines a physical activity pattern powerful enough to move the needle on cancer risk?
Here’s an overview of the state of the evidence.
Exercise and Cancer Types: A Mixed Bag
When it comes to cancer prevention strategies, guidelines uniformly endorse less couch time and more movement. But a deeper look at the science reveals a complex and often poorly understood connection between exercise and cancer risk.
For certain cancer types, the benefits of exercise on cancer risk seem fairly well established.
The latest edition of the Physical Activity Guidelines for Americans, published in 2018, cites “strong evidence” that regular exercise might curb the risks for breast and colon cancers as well as bladder, endometrial, esophageal, kidney, and gastric cancers. These guidelines also point to “moderate”-strength evidence of a protective association with lung cancer.
The evidence of a protective effect, however, is strongest for breast and colon cancers, said Jennifer Ligibel, MD, senior physician in the Breast Oncology Center at Dana-Farber Cancer Institute, Boston, . “But,” she pointed out, “that may be because they’re some of the most common cancers, and it’s been easier to detect an association.”
Guidelines from the American Cancer Society, published in 2020, align with the 2018 recommendations.
“We believe there’s strong evidence to suggest at least eight different types of cancer are associated with physical activity,” said Erika Rees-Punia, PhD, MPH, senior principal scientist, epidemiology and behavioral research at the American Cancer Society.
That view is not universal, however. Current recommendations from the World Cancer Research Fund and American Institute for Cancer Research, for example, are more circumspect, citing only three cancers with good evidence of a protective effect from exercise: Breast (postmenopausal), colon, and endometrial.
“We definitely can’t say exercise reduces the risk of all cancers,” said Lee Jones, PhD, head of the Exercise Oncology Program at Memorial Sloan Kettering Cancer Center in New York City. “The data suggest it’s just not that simple.”
And it’s challenging to put all the evidence together, Dr. Jones added.
The physical activity guidelines are based on published systematic reviews, meta-analyses, and pooled analyses of data from observational studies that examined the relationship between physical activity — aerobic exercise, specifically — and cancer incidence. That means the evidence comes with all the limitations observational studies entail, such as how they collect information on participants’ exercise habits — which, Dr. Jones noted, is typically done via “monster questionnaires” that gauge physical activity in broad strokes.
Pooling all those findings into a meta-analysis is tricky, Dr. Jones added, because individual studies vary in important ways — from follow-up periods to how they quantify exercise and track cancer incidence.
In a study published in February in Cancer Cell, Dr. Jones and his colleagues attempted to address some of those issues by leveraging data from the PLCO screening trial.
The PLCO was a prospective study of over 60,000 US adults that compared the effects of annual screening vs usual care on cancer mortality. At enrollment, participants completed questionnaires that included an assessment of “vigorous” exercise. Based on that, Dr. Jones and his colleagues classified 55% as “exercisers” — meaning they reported 2 or more hours of vigorous exercise per week. The remaining 45%, who were in the 0 to 1 hour per week range, were deemed non-exercisers.
Over a median of 18 years, nearly 16,000 first-time invasive cancers were diagnosed, and some interesting differences between exercisers and non-exercisers emerged. The active group had lower risks for three cancers: Head and neck, with a 26% lower risk (hazard ratio [HR], 0.74), lung (a 20% lower risk), and breast (an 11% lower risk).
What was striking, however, was the lack of connection between exercise and many cancers cited in the guidelines, including colon, gastric, bladder, endometrial, and renal cancers.
Perhaps even more surprising — exercisers had higher risks for prostate cancer (12%) and melanoma (20%). This finding, Dr. Jones said, is in line with a previous pooled analysis of data from 12 US and European prospective cohorts. In this study, the most physically active participants (90th percentile) had higher risks for melanoma and prostate cancer, compared with the least active group (10th percentile).
The melanoma findings do make sense, Dr. Jones said, given that highly active people may spend a lot of time in the sun. “My advice,” Dr. Jones said, “is, if you’re exercising outside, wear sunscreen.” The prostate cancer findings, however, are more puzzling and warrant further research, he noted.
But the bottom line is that the relationship between exercise and cancer types is mixed and far from nailed down.
How Big Is the Effect?
Even if exercise reduces the risk for only certain cancers, that’s still important, particularly when those links appear strongest for common cancer types, such as breast and colon.
But how much of a difference can exercise make?
Based on the evidence, it may only be a modest one. A 2019 systematic review by the Physical Activity Guidelines Advisory Committee provided a rough estimate: Across hundreds of epidemiological studies, people with the highest physical activity levels had a 10%-20% lower risk for the cancers cited in the 2018 exercise guidelines compared with people who were least active.
These figures, however, are probably an underestimate, said Anne McTiernan, MD, PhD, a member of the advisory committee and professor of epidemiology, at Fred Hutchinson Cancer Center, Seattle.
“This is what we usually see when a factor is not measured very well,” said Dr. McTiernan, explaining that the individual studies differed in their categories of “highest” and “lowest” physical activity, such that one study’s “highest” could be another’s mid-range.
“In other words, the effects of physical activity are likely larger” than the review found, Dr. McTiernan said.
The next logical question is whether a bigger exercise “dose” — more time or higher intensity — would have a greater impact on cancer risk. A 2019 study published in the Journal of Clinical Oncology tried to clarify that by pooling data on over 750,000 participants from nine prospective cohorts.
Overall, people meeting government recommendations for exercise — equivalent to about 2.5-5 hours of weekly moderate activity, such as a brisk walk, or about 1.25-2.5 hours of more vigorous activities, like running — had lower risks for seven of 15 cancer types studied compared with less active people.
For cancers with positive findings, being on the higher end of the recommended 2.5- to 5-hour weekly range was better. Risk reductions for breast cancer, for instance, were 6% at 2.5 hours of physical activity per week and 10% at 5 hours per week. Similar trends emerged for other cancer types, including colon (8%-14%), endometrial (10%-18%), liver cancer (18%-27%), and non-Hodgkin lymphoma in women (11%-18%).
But there may be an exercise sweet spot that maximizes the cancer risk benefit.
Among people who surpassed the recommendations — exercising for more time or more intensely — the risk reduction benefit did not necessarily improve in a linear fashion. For certain cancer types, such as colon and endometrial, the benefits of more vigorous exercise “eroded at higher levels of activity,” the authors said.
The issue here is that most studies have not dug deeply into aerobic exercise habits. Often, studies present participants with a list of activities — walking, biking, and running — and ask them to estimate how often and for what duration they do each.
Plus, “we’ve usually lumped moderate and vigorous activities together,” Dr. Rees-Punia said, which means there’s a lack of “granular data” to say whether certain intensities or frequencies of exercise are optimal and for whom.
Why Exercise May Lower Cancer Risk
Exercise habits do not, of course, exist in a vacuum. Highly active people, Dr. Ligibel said, tend to be of higher socioeconomic status, leaner, and have generally healthier lifestyles than sedentary people.
Body weight is a big confounder as well. However, Dr. Rees-Punia noted, it’s also probably a reason that exercise is linked to lower cancer risks, particularly by preventing weight gain. Still, studies have found that the association between exercise and many cancers remains significant after adjusting for body mass index.
The why remains unclear, though some studies offer clues.
“There’s been some really interesting mechanistic research, suggesting that exercise may help inhibit tumor growth or upregulate the immune system,” Dr. Ligibel said.
That includes not only lab research but small intervention studies. While these studies have largely involved people who already have cancer, some have also focused on healthy individuals.
A 2019 study from Dr. Ligibel and her colleagues, which randomly assigned 49 women newly diagnosed with breast cancer to start either an exercise program or mind-body practices ahead of surgery, found exercisers, who had been active for about a month at the time of surgery, showed signs of immune system upregulation in their tumors, while the control group did not.
Among healthy postmenopausal women, a meta-analysis of six clinical trials from Dr. McTiernan and her colleagues found that exercise plus calorie reduction can reduce levels of breast cancer-related endogenous hormones, more so than calorie-cutting alone. And a 2023 study found that high-intensity exercise boosted the ranks of certain immune cells and reduced inflammation in the colon among people at high risk for colon and endometrial cancers due to Lynch syndrome.
Defining an Exercise ‘Prescription’
Despite the gaps and uncertainties in the research, government guidelines as well as those from the American Cancer Society and other medical groups are in lockstep in their exercise recommendations: Adults should strive for 150-300 minutes of moderate-intensity aerobic exercise (like brisk walking), 75-150 minutes of vigorous activity (like running), or some combination each week.
The guidelines also encourage strength training twice a week — advice that’s based on research tying those activity levels to lower risks for heart disease, diabetes, and other chronic conditions.
But there’s no “best” exercise prescription for lowering cancer risk specifically. Most epidemiological studies have examined only aerobic activity, Dr. Rees-Punia said, and there’s very little known about whether strength conditioning or other moderate heart rate-elevating activities, such as daily household chores, may reduce the risk for cancer.
Given the lack of nuance in the literature, it’s hard to say what intensities, types, or amounts of exercise are best for each individual.
Going forward, device-based measurements of physical activity could “help us sort out the effects of different intensities of exercise and possibly types,” Dr. Rees-Punia said.
But overall, Dr. McTiernan said, the data do show that the risks for several cancers are lower at the widely recommended activity levels.
“The bottom-line advice is still to exercise at least 150 minutes per week at a moderate-intensity level or greater,” Dr. McTiernan said.
Or put another way, moving beats being sedentary. It’s probably wise for everyone to sit less, noted Dr. Rees-Punia, for overall health and based on evidence tying sedentary time to the risks for certain cancers, including colon, endometrial, and lung.
There’s a practical element to consider in all of this: What physical activities will people actually do on the regular? In the big epidemiological studies, Dr. McTiernan noted, middle-aged and older adults most often report walking, suggesting that’s the preferred, or most accessible activity, for many.
“You can only benefit from the physical activity you’ll actually do,” Dr. Rees-Punia said.
Dr. Ligibel echoed that sentiment, saying she encourages patients to think about physical activity as a process: “You need to find things you like to do and work them into your daily life, in a sustainable way.
“People often talk about exercise being medicine,” Dr. Ligibel said. “But I think you could take that too far. If we get too prescriptive about it, that could take the joy away.”
A version of this article appeared on Medscape.com.
“Exercise is medicine” has become something of a mantra, with good reason. There’s no doubt that regular physical activity has a broad range of health benefits. Exercise can improve circulation, help control weight, reduce stress, and boost mood — take your pick.
Lower cancer risk is also on the list — with exercise promoted as a risk-cutting strategy in government guidelines and in recommendations from professional groups such as the American Cancer Society.
The bulk of the data hangs on less rigorous, observational studies that have linked physical activity to lower risks for certain cancers, but plenty of questions remain.
What are the cancer types where exercise makes a difference? How significant is that impact? And what, exactly, defines a physical activity pattern powerful enough to move the needle on cancer risk?
Here’s an overview of the state of the evidence.
Exercise and Cancer Types: A Mixed Bag
When it comes to cancer prevention strategies, guidelines uniformly endorse less couch time and more movement. But a deeper look at the science reveals a complex and often poorly understood connection between exercise and cancer risk.
For certain cancer types, the benefits of exercise on cancer risk seem fairly well established.
The latest edition of the Physical Activity Guidelines for Americans, published in 2018, cites “strong evidence” that regular exercise might curb the risks for breast and colon cancers as well as bladder, endometrial, esophageal, kidney, and gastric cancers. These guidelines also point to “moderate”-strength evidence of a protective association with lung cancer.
The evidence of a protective effect, however, is strongest for breast and colon cancers, said Jennifer Ligibel, MD, senior physician in the Breast Oncology Center at Dana-Farber Cancer Institute, Boston, . “But,” she pointed out, “that may be because they’re some of the most common cancers, and it’s been easier to detect an association.”
Guidelines from the American Cancer Society, published in 2020, align with the 2018 recommendations.
“We believe there’s strong evidence to suggest at least eight different types of cancer are associated with physical activity,” said Erika Rees-Punia, PhD, MPH, senior principal scientist, epidemiology and behavioral research at the American Cancer Society.
That view is not universal, however. Current recommendations from the World Cancer Research Fund and American Institute for Cancer Research, for example, are more circumspect, citing only three cancers with good evidence of a protective effect from exercise: Breast (postmenopausal), colon, and endometrial.
“We definitely can’t say exercise reduces the risk of all cancers,” said Lee Jones, PhD, head of the Exercise Oncology Program at Memorial Sloan Kettering Cancer Center in New York City. “The data suggest it’s just not that simple.”
And it’s challenging to put all the evidence together, Dr. Jones added.
The physical activity guidelines are based on published systematic reviews, meta-analyses, and pooled analyses of data from observational studies that examined the relationship between physical activity — aerobic exercise, specifically — and cancer incidence. That means the evidence comes with all the limitations observational studies entail, such as how they collect information on participants’ exercise habits — which, Dr. Jones noted, is typically done via “monster questionnaires” that gauge physical activity in broad strokes.
Pooling all those findings into a meta-analysis is tricky, Dr. Jones added, because individual studies vary in important ways — from follow-up periods to how they quantify exercise and track cancer incidence.
In a study published in February in Cancer Cell, Dr. Jones and his colleagues attempted to address some of those issues by leveraging data from the PLCO screening trial.
The PLCO was a prospective study of over 60,000 US adults that compared the effects of annual screening vs usual care on cancer mortality. At enrollment, participants completed questionnaires that included an assessment of “vigorous” exercise. Based on that, Dr. Jones and his colleagues classified 55% as “exercisers” — meaning they reported 2 or more hours of vigorous exercise per week. The remaining 45%, who were in the 0 to 1 hour per week range, were deemed non-exercisers.
Over a median of 18 years, nearly 16,000 first-time invasive cancers were diagnosed, and some interesting differences between exercisers and non-exercisers emerged. The active group had lower risks for three cancers: Head and neck, with a 26% lower risk (hazard ratio [HR], 0.74), lung (a 20% lower risk), and breast (an 11% lower risk).
What was striking, however, was the lack of connection between exercise and many cancers cited in the guidelines, including colon, gastric, bladder, endometrial, and renal cancers.
Perhaps even more surprising — exercisers had higher risks for prostate cancer (12%) and melanoma (20%). This finding, Dr. Jones said, is in line with a previous pooled analysis of data from 12 US and European prospective cohorts. In this study, the most physically active participants (90th percentile) had higher risks for melanoma and prostate cancer, compared with the least active group (10th percentile).
The melanoma findings do make sense, Dr. Jones said, given that highly active people may spend a lot of time in the sun. “My advice,” Dr. Jones said, “is, if you’re exercising outside, wear sunscreen.” The prostate cancer findings, however, are more puzzling and warrant further research, he noted.
But the bottom line is that the relationship between exercise and cancer types is mixed and far from nailed down.
How Big Is the Effect?
Even if exercise reduces the risk for only certain cancers, that’s still important, particularly when those links appear strongest for common cancer types, such as breast and colon.
But how much of a difference can exercise make?
Based on the evidence, it may only be a modest one. A 2019 systematic review by the Physical Activity Guidelines Advisory Committee provided a rough estimate: Across hundreds of epidemiological studies, people with the highest physical activity levels had a 10%-20% lower risk for the cancers cited in the 2018 exercise guidelines compared with people who were least active.
These figures, however, are probably an underestimate, said Anne McTiernan, MD, PhD, a member of the advisory committee and professor of epidemiology, at Fred Hutchinson Cancer Center, Seattle.
“This is what we usually see when a factor is not measured very well,” said Dr. McTiernan, explaining that the individual studies differed in their categories of “highest” and “lowest” physical activity, such that one study’s “highest” could be another’s mid-range.
“In other words, the effects of physical activity are likely larger” than the review found, Dr. McTiernan said.
The next logical question is whether a bigger exercise “dose” — more time or higher intensity — would have a greater impact on cancer risk. A 2019 study published in the Journal of Clinical Oncology tried to clarify that by pooling data on over 750,000 participants from nine prospective cohorts.
Overall, people meeting government recommendations for exercise — equivalent to about 2.5-5 hours of weekly moderate activity, such as a brisk walk, or about 1.25-2.5 hours of more vigorous activities, like running — had lower risks for seven of 15 cancer types studied compared with less active people.
For cancers with positive findings, being on the higher end of the recommended 2.5- to 5-hour weekly range was better. Risk reductions for breast cancer, for instance, were 6% at 2.5 hours of physical activity per week and 10% at 5 hours per week. Similar trends emerged for other cancer types, including colon (8%-14%), endometrial (10%-18%), liver cancer (18%-27%), and non-Hodgkin lymphoma in women (11%-18%).
But there may be an exercise sweet spot that maximizes the cancer risk benefit.
Among people who surpassed the recommendations — exercising for more time or more intensely — the risk reduction benefit did not necessarily improve in a linear fashion. For certain cancer types, such as colon and endometrial, the benefits of more vigorous exercise “eroded at higher levels of activity,” the authors said.
The issue here is that most studies have not dug deeply into aerobic exercise habits. Often, studies present participants with a list of activities — walking, biking, and running — and ask them to estimate how often and for what duration they do each.
Plus, “we’ve usually lumped moderate and vigorous activities together,” Dr. Rees-Punia said, which means there’s a lack of “granular data” to say whether certain intensities or frequencies of exercise are optimal and for whom.
Why Exercise May Lower Cancer Risk
Exercise habits do not, of course, exist in a vacuum. Highly active people, Dr. Ligibel said, tend to be of higher socioeconomic status, leaner, and have generally healthier lifestyles than sedentary people.
Body weight is a big confounder as well. However, Dr. Rees-Punia noted, it’s also probably a reason that exercise is linked to lower cancer risks, particularly by preventing weight gain. Still, studies have found that the association between exercise and many cancers remains significant after adjusting for body mass index.
The why remains unclear, though some studies offer clues.
“There’s been some really interesting mechanistic research, suggesting that exercise may help inhibit tumor growth or upregulate the immune system,” Dr. Ligibel said.
That includes not only lab research but small intervention studies. While these studies have largely involved people who already have cancer, some have also focused on healthy individuals.
A 2019 study from Dr. Ligibel and her colleagues, which randomly assigned 49 women newly diagnosed with breast cancer to start either an exercise program or mind-body practices ahead of surgery, found exercisers, who had been active for about a month at the time of surgery, showed signs of immune system upregulation in their tumors, while the control group did not.
Among healthy postmenopausal women, a meta-analysis of six clinical trials from Dr. McTiernan and her colleagues found that exercise plus calorie reduction can reduce levels of breast cancer-related endogenous hormones, more so than calorie-cutting alone. And a 2023 study found that high-intensity exercise boosted the ranks of certain immune cells and reduced inflammation in the colon among people at high risk for colon and endometrial cancers due to Lynch syndrome.
Defining an Exercise ‘Prescription’
Despite the gaps and uncertainties in the research, government guidelines as well as those from the American Cancer Society and other medical groups are in lockstep in their exercise recommendations: Adults should strive for 150-300 minutes of moderate-intensity aerobic exercise (like brisk walking), 75-150 minutes of vigorous activity (like running), or some combination each week.
The guidelines also encourage strength training twice a week — advice that’s based on research tying those activity levels to lower risks for heart disease, diabetes, and other chronic conditions.
But there’s no “best” exercise prescription for lowering cancer risk specifically. Most epidemiological studies have examined only aerobic activity, Dr. Rees-Punia said, and there’s very little known about whether strength conditioning or other moderate heart rate-elevating activities, such as daily household chores, may reduce the risk for cancer.
Given the lack of nuance in the literature, it’s hard to say what intensities, types, or amounts of exercise are best for each individual.
Going forward, device-based measurements of physical activity could “help us sort out the effects of different intensities of exercise and possibly types,” Dr. Rees-Punia said.
But overall, Dr. McTiernan said, the data do show that the risks for several cancers are lower at the widely recommended activity levels.
“The bottom-line advice is still to exercise at least 150 minutes per week at a moderate-intensity level or greater,” Dr. McTiernan said.
Or put another way, moving beats being sedentary. It’s probably wise for everyone to sit less, noted Dr. Rees-Punia, for overall health and based on evidence tying sedentary time to the risks for certain cancers, including colon, endometrial, and lung.
There’s a practical element to consider in all of this: What physical activities will people actually do on the regular? In the big epidemiological studies, Dr. McTiernan noted, middle-aged and older adults most often report walking, suggesting that’s the preferred, or most accessible activity, for many.
“You can only benefit from the physical activity you’ll actually do,” Dr. Rees-Punia said.
Dr. Ligibel echoed that sentiment, saying she encourages patients to think about physical activity as a process: “You need to find things you like to do and work them into your daily life, in a sustainable way.
“People often talk about exercise being medicine,” Dr. Ligibel said. “But I think you could take that too far. If we get too prescriptive about it, that could take the joy away.”
A version of this article appeared on Medscape.com.
Nivolumab Wins First-Line Indication in Metastatic Urothelial Carcinoma
Approval was based on the CHECKMATE-901 trial in 608 patients randomized equally to either cisplatin and gemcitabine for ≤ six cycles or nivolumab plus cisplatin and gemcitabine for ≤ six cycles, followed by nivolumab alone for ≤ 2 years.
Median overall survival was 21.7 months with nivolumab add-on vs 18.9 months with cisplatin/gemcitabine alone (hazard ratio [HR], 0.78; P = .0171). The nivolumab group had a slightly higher median progression-free survival of 7.9 months vs 7.6 months in the cisplatin and gemcitabine group (HR, 0.72; P = .0012).
The most common adverse events, occurring in ≥ 15% of nivolumab patients, were nausea, fatigue, musculoskeletal pain, constipation, decreased appetite, rash, vomiting, peripheral neuropathy, urinary tract infection, diarrhea, edema, hypothyroidism, and pruritus.
Among numerous other oncology indications, nivolumab was previously approved for adjuvant treatment following urothelial carcinoma resection and for locally advanced or metastatic urothelial carcinoma that progresses during or following platinum-containing chemotherapy.
A version of this article appeared on Medscape.com .
Approval was based on the CHECKMATE-901 trial in 608 patients randomized equally to either cisplatin and gemcitabine for ≤ six cycles or nivolumab plus cisplatin and gemcitabine for ≤ six cycles, followed by nivolumab alone for ≤ 2 years.
Median overall survival was 21.7 months with nivolumab add-on vs 18.9 months with cisplatin/gemcitabine alone (hazard ratio [HR], 0.78; P = .0171). The nivolumab group had a slightly higher median progression-free survival of 7.9 months vs 7.6 months in the cisplatin and gemcitabine group (HR, 0.72; P = .0012).
The most common adverse events, occurring in ≥ 15% of nivolumab patients, were nausea, fatigue, musculoskeletal pain, constipation, decreased appetite, rash, vomiting, peripheral neuropathy, urinary tract infection, diarrhea, edema, hypothyroidism, and pruritus.
Among numerous other oncology indications, nivolumab was previously approved for adjuvant treatment following urothelial carcinoma resection and for locally advanced or metastatic urothelial carcinoma that progresses during or following platinum-containing chemotherapy.
A version of this article appeared on Medscape.com .
Approval was based on the CHECKMATE-901 trial in 608 patients randomized equally to either cisplatin and gemcitabine for ≤ six cycles or nivolumab plus cisplatin and gemcitabine for ≤ six cycles, followed by nivolumab alone for ≤ 2 years.
Median overall survival was 21.7 months with nivolumab add-on vs 18.9 months with cisplatin/gemcitabine alone (hazard ratio [HR], 0.78; P = .0171). The nivolumab group had a slightly higher median progression-free survival of 7.9 months vs 7.6 months in the cisplatin and gemcitabine group (HR, 0.72; P = .0012).
The most common adverse events, occurring in ≥ 15% of nivolumab patients, were nausea, fatigue, musculoskeletal pain, constipation, decreased appetite, rash, vomiting, peripheral neuropathy, urinary tract infection, diarrhea, edema, hypothyroidism, and pruritus.
Among numerous other oncology indications, nivolumab was previously approved for adjuvant treatment following urothelial carcinoma resection and for locally advanced or metastatic urothelial carcinoma that progresses during or following platinum-containing chemotherapy.
A version of this article appeared on Medscape.com .
First Denosumab Biosimilar Approved in Two Different Formulations
The US Food and Drug Administration (FDA) has approved the first biosimilar to denosumab, denosumab-bddz (Wyost/Jubbonti).
The biosimilar was also granted interchangeability status, which allows pharmacists to substitute the biosimilar for the reference product without involving the prescribing clinician (according to state law). Sandoz announced the approval on March 5, 2024. The lower dosage of denosumab-bddz, marketed as Jubbonti, was also approved by Health Canada in February.
The FDA approval “is based on robust clinical studies and accompanied by labeling with safety warnings,” according to the press release. Like the reference products Prolia and Xgeva, denosumab-bddz is approved for two indications at separate doses.
Wyost (120-mg/1.7-mL injection) is approved to:
- Prevent skeletal-related events in patients with multiple myeloma and in patients with bone metastases from solid tumors
- Treat adults and skeletally mature adolescents with giant cell tumor of bone that is unresectable or where surgical resection is likely to result in severe morbidity
- Treat hypercalcemia of cancer that is refractory to bisphosphonate therapy
Jubbonti (60-mg/1-mL injection) is approved to:
- Treat postmenopausal women with osteoporosis who are at high risk for fracture
- Increase bone mass in men with osteoporosis who are at high risk for fracture
- Treat glucocorticoid-induced osteoporosis in men and women who are at high risk for fracture
- Increase bone mass in men who are at high risk for fracture who are receiving androgen deprivation therapy for nonmetastatic prostate cancer
- Increase bone mass in women who are at high risk for fracture who are receiving adjuvant aromatase inhibitor therapy for breast cancer.
Both doses are contraindicated for hypocalcemia and known clinically significant hypersensitivity to denosumab products. Exposure to denosumab products during pregnancy can cause fetal harm, so women of reproductive potential should be advised to use effective contraception during therapy and for at least 5 months after the last dose of denosumab-bddz.
Sandoz did not provide information on US launch details, citing “ongoing patent litigation around these products.”
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved the first biosimilar to denosumab, denosumab-bddz (Wyost/Jubbonti).
The biosimilar was also granted interchangeability status, which allows pharmacists to substitute the biosimilar for the reference product without involving the prescribing clinician (according to state law). Sandoz announced the approval on March 5, 2024. The lower dosage of denosumab-bddz, marketed as Jubbonti, was also approved by Health Canada in February.
The FDA approval “is based on robust clinical studies and accompanied by labeling with safety warnings,” according to the press release. Like the reference products Prolia and Xgeva, denosumab-bddz is approved for two indications at separate doses.
Wyost (120-mg/1.7-mL injection) is approved to:
- Prevent skeletal-related events in patients with multiple myeloma and in patients with bone metastases from solid tumors
- Treat adults and skeletally mature adolescents with giant cell tumor of bone that is unresectable or where surgical resection is likely to result in severe morbidity
- Treat hypercalcemia of cancer that is refractory to bisphosphonate therapy
Jubbonti (60-mg/1-mL injection) is approved to:
- Treat postmenopausal women with osteoporosis who are at high risk for fracture
- Increase bone mass in men with osteoporosis who are at high risk for fracture
- Treat glucocorticoid-induced osteoporosis in men and women who are at high risk for fracture
- Increase bone mass in men who are at high risk for fracture who are receiving androgen deprivation therapy for nonmetastatic prostate cancer
- Increase bone mass in women who are at high risk for fracture who are receiving adjuvant aromatase inhibitor therapy for breast cancer.
Both doses are contraindicated for hypocalcemia and known clinically significant hypersensitivity to denosumab products. Exposure to denosumab products during pregnancy can cause fetal harm, so women of reproductive potential should be advised to use effective contraception during therapy and for at least 5 months after the last dose of denosumab-bddz.
Sandoz did not provide information on US launch details, citing “ongoing patent litigation around these products.”
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved the first biosimilar to denosumab, denosumab-bddz (Wyost/Jubbonti).
The biosimilar was also granted interchangeability status, which allows pharmacists to substitute the biosimilar for the reference product without involving the prescribing clinician (according to state law). Sandoz announced the approval on March 5, 2024. The lower dosage of denosumab-bddz, marketed as Jubbonti, was also approved by Health Canada in February.
The FDA approval “is based on robust clinical studies and accompanied by labeling with safety warnings,” according to the press release. Like the reference products Prolia and Xgeva, denosumab-bddz is approved for two indications at separate doses.
Wyost (120-mg/1.7-mL injection) is approved to:
- Prevent skeletal-related events in patients with multiple myeloma and in patients with bone metastases from solid tumors
- Treat adults and skeletally mature adolescents with giant cell tumor of bone that is unresectable or where surgical resection is likely to result in severe morbidity
- Treat hypercalcemia of cancer that is refractory to bisphosphonate therapy
Jubbonti (60-mg/1-mL injection) is approved to:
- Treat postmenopausal women with osteoporosis who are at high risk for fracture
- Increase bone mass in men with osteoporosis who are at high risk for fracture
- Treat glucocorticoid-induced osteoporosis in men and women who are at high risk for fracture
- Increase bone mass in men who are at high risk for fracture who are receiving androgen deprivation therapy for nonmetastatic prostate cancer
- Increase bone mass in women who are at high risk for fracture who are receiving adjuvant aromatase inhibitor therapy for breast cancer.
Both doses are contraindicated for hypocalcemia and known clinically significant hypersensitivity to denosumab products. Exposure to denosumab products during pregnancy can cause fetal harm, so women of reproductive potential should be advised to use effective contraception during therapy and for at least 5 months after the last dose of denosumab-bddz.
Sandoz did not provide information on US launch details, citing “ongoing patent litigation around these products.”
A version of this article appeared on Medscape.com.