User login
Violence against women: Gail Robinson
Dr. Robinson is professor of psychiatry and obstetrics/gynecology and professor of equality, gender, and population at the University of Toronto. She’s also chair of GAP’s Committee on Gender & Mental Health. In this episode, Dr. Robinson delves into strategies for interacting with survivors of violence, the roots of the “Me Too” movement, as well as rising rates of maternal mortality in the United States.
Amazon
Apple Podcasts
Google Podcasts
Spotify
Dr. Robinson is professor of psychiatry and obstetrics/gynecology and professor of equality, gender, and population at the University of Toronto. She’s also chair of GAP’s Committee on Gender & Mental Health. In this episode, Dr. Robinson delves into strategies for interacting with survivors of violence, the roots of the “Me Too” movement, as well as rising rates of maternal mortality in the United States.
Amazon
Apple Podcasts
Google Podcasts
Spotify
Dr. Robinson is professor of psychiatry and obstetrics/gynecology and professor of equality, gender, and population at the University of Toronto. She’s also chair of GAP’s Committee on Gender & Mental Health. In this episode, Dr. Robinson delves into strategies for interacting with survivors of violence, the roots of the “Me Too” movement, as well as rising rates of maternal mortality in the United States.
Amazon
Apple Podcasts
Google Podcasts
Spotify
Intimate partner violence, guns, and the ObGyn
On the afternoon of November 19, 2018, Dr. Tamara O’Neal was shot and killed by her ex-fiancé outside Mercy Hospital and Medical Center in Chicago, Illinois. After killing Dr. O’Neal, the gunman ran into the hospital where he exchanged gunfire with police, killing a pharmacy resident and a police officer, before he was killed by police.1
This horrific encounter between a woman and her former partner begs for a conversation about intimate partner violence (IPV). A data brief of The National Intimate Partner and Sexual Violence Survey was published in November 2018. According to this report, 30.6% of women experienced physical violence by an intimate partner in 2015, with 21.4% of women experiencing severe physical violence. In addition, 31.0% of men experienced physical violence by an intimate partner in 2015; 14.9% of men experienced severe physical violence.2

Intimate partner violence is “our lane”
The shooting at Mercy Hospital occurred amongst a backdrop of controversy between the National Rifle Association (NRA) and the medical community. On November 7, 2018, the NRA tweeted that doctors should “stay in their lane” with regard to gun control after a position paper from the American College of Physicians on reducing firearm deaths and injuries was published in the Annals of Internal Medicine.3 Doctors from every field and from all over the country responded through social media by stating that treating bullet wounds and caring for those affected by gun violence was “their lane.”4
It is time for us as a community to recognize that gun violence affects us all. The majority of mass shooters have a history of IPV and often target their current or prior partner during the shooting.5 At this intersection of IPV and gun control, the physician has a unique role. We not only treat those affected by gun violence and advocate for better gun control but we also have a duty to screen our patients for IPV. Part of the sacred patient-physician relationship is being present for our patients when they need us most. The American College of Obstetricians and Gynecologists (ACOG) recommends that ObGyns screen patients for IPV at regular intervals and recognizes that it may take several conversations before a patient discloses her history of IPV.6 Additionally, given the increased risk of gun injuries and death, it behooves us to also screen for gun safety in the home.
Ask patients about IPV, and ask again
The shooting at Mercy Hospital was a stark reminder that IPV can affect any of us. With nearly one-third of women and more than one-quarter of men experiencing IPV in their lifetime, action must be taken. The first step is to routinely screen patients for IPV, offering support and community resources. (see “Screening for intimate partner violence). The second step is to work to decrease the access perpetrators of IPV have to weapons with which to enact violence—through legislation, community engagement, and using our physician voices.
States that have passed legislation that prohibits persons with active restraining orders or a history of IPV or domestic violence from possessing firearms has seen a decrease in IPV firearm homicide rates.7 These policies can make a profound impact on the safety of our patients. Women who are in violent relationships are 5 times more likely to die if their partner has access to a firearm.5
Continue to: #BreakTheCycle...
#BreakTheCycle
The 116th Congress convened in January. We have an opportunity to make real gun legislation reform and work to keep our communities and our patients at risk for IPV safer. Tweet your representatives with #BreakTheCycle, and be on the lookout for important legislation to enact real change.
To sign the open letter from American Healthcare Professionals to the NRA regarding their recent comments and our medical experiences with gun violence, click here. Currently, there are more than 41,000 signatures.
There are numerous verified screening tools available to assess for intimate partner violence (IPV) for both pregnant and nonpregnant patients. Many recommended tools are accessible on the Centers for Disease Control and Prevention (CDC) website: https://www.cdc.gov/violenceprevention/pdf/ipv/ipvandsvscreening.pdf. In our office, the tool most commonly used is a 3-part question assessing domestic violence and IPV. It is important to recognize IPV can affect everyone—all races and religions regardless of socioeconomic background, sexual orientation, and pregnancy status. All patients deserve screening for IPV, and it should never be assumed a patient is not at risk. During an annual gynecology visit for return and new patients or a new obstetric intake visit, we use the following script obtained from ACOG’s Committee Opinion 518 on IPV1 :
Because violence is so common in many women’s lives and because there is help available for women being abused, I now ask every patient about domestic violence:
1. Within the past year (or since you have become pregnant) have you been hit, slapped, kicked, or otherwise physically hurt by someone?
2. Are you in a relationship with a person who threatens or physically hurts you?
3. Has anyone forced you to have sexual activities that made you feel uncomfortable?
If a patient screens positive, we assess their immediate safety. If a social worker is readily available, we arrange an urgent meeting with the patient. If offices do not have immediate access to this service, online information can be provided to patients, including the National Resource Center on Domestic Violence (https://nnedv.org/) and a toll-free number to the National Domestic Violence Hotline: 1-800-799-7233. Additionally, we ask patients about any history of verbal, physical, or sexual violence with prior partners, family members, acquaintances, coworkers, etc. Although the patient might not be at immediate risk, prior experiences with abuse can cause fear and anxiety around gynecologic and obstetric exams. Acknowledging this history can help the clinician adjust his or her physical exam and support the patient during, what may be, a triggering experience.
As an additional resource, Dr. Katherine Hicks-Courant, a resident at Tufts Medical Center, in Boston, Massachusetts, created a tool kit for providers working with pregnant patients with a history of sexual assault. It can be accessed without login online under the Junior Fellow Initiative Toolkit section at http://www.acog.org.
References
1. American College of Obstetricians and Gynecologists. Committee Opinion No. 518: intimate partner violence. Obstet Gynecol. 2012;119:412-417.
If you, or someone you know, needs help, please call The National Domestic Violence Hotline at 1-800-799-7233.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Buckley M, Gorner J, Greene M. “Chicago hospital shooting: Young cop, doctor, pharmacy resident and gunman die in Mercy Hospital attack. Chicago Tribune. Nov. 20, 2018.
2. Smith SG, Zhang X, Basile KC, et al. The National Intimate Partner
and Sexual Violence Survey (NISVS): 2015 data brief – updated release. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; November 2018.
3. Butkus R, Doherty R, Bornstein SS; for the Health and Public Policy Committee of the American College of Physicians. Reducing firearm injuries and deaths in the United States: a position paper from the American College of Physicians. Ann Intern Med. 2018;169:704-707.
4. Papenfuss M. NRA Tweets Warning to Anti-Gun Doctors: ‘Stay In Your Lane’. The Huffington Post. November 8, 2018.
5. Everytown for Gun Safety website. Mass Shootings in the United States: 2009–2016. Available at https://everytownresearch.org/reports/mass-shootings-analysis/. Accessed January 17, 2019.
6. The American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 518: intimate partner violence. Obstet Gynecol. 2012;119(2 pt 1):412-417. https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Health-Care-for-Underserved-Women/Intimate-Partner-Violence.
7. Zeoli AM, McCourt A, Buggs S, et al. Analysis of the strength of legal firearms restrictions for perpetrators of domestic violence and their associations with intimate partner homicide. Am J Epidemiol. 2018;187:2365-2371.

Dr. Koniares is Resident, Department of Obstetrics and Gynecology, Tufts Medical Center, Boston, Massachusetts.
Dr. Evans is Assistant Professor, Tufts University School of Medicine; Associate Program Director, Department of Obstetrics and Gynecology, Tufts Medical Center.
The authors report no financial relationships relevant to this article.
Dr. Koniares is Resident, Department of Obstetrics and Gynecology, Tufts Medical Center, Boston, Massachusetts.
Dr. Evans is Assistant Professor, Tufts University School of Medicine; Associate Program Director, Department of Obstetrics and Gynecology, Tufts Medical Center.
The authors report no financial relationships relevant to this article.
Dr. Koniares is Resident, Department of Obstetrics and Gynecology, Tufts Medical Center, Boston, Massachusetts.
Dr. Evans is Assistant Professor, Tufts University School of Medicine; Associate Program Director, Department of Obstetrics and Gynecology, Tufts Medical Center.
The authors report no financial relationships relevant to this article.
On the afternoon of November 19, 2018, Dr. Tamara O’Neal was shot and killed by her ex-fiancé outside Mercy Hospital and Medical Center in Chicago, Illinois. After killing Dr. O’Neal, the gunman ran into the hospital where he exchanged gunfire with police, killing a pharmacy resident and a police officer, before he was killed by police.1
This horrific encounter between a woman and her former partner begs for a conversation about intimate partner violence (IPV). A data brief of The National Intimate Partner and Sexual Violence Survey was published in November 2018. According to this report, 30.6% of women experienced physical violence by an intimate partner in 2015, with 21.4% of women experiencing severe physical violence. In addition, 31.0% of men experienced physical violence by an intimate partner in 2015; 14.9% of men experienced severe physical violence.2
Intimate partner violence is “our lane”
The shooting at Mercy Hospital occurred amongst a backdrop of controversy between the National Rifle Association (NRA) and the medical community. On November 7, 2018, the NRA tweeted that doctors should “stay in their lane” with regard to gun control after a position paper from the American College of Physicians on reducing firearm deaths and injuries was published in the Annals of Internal Medicine.3 Doctors from every field and from all over the country responded through social media by stating that treating bullet wounds and caring for those affected by gun violence was “their lane.”4
It is time for us as a community to recognize that gun violence affects us all. The majority of mass shooters have a history of IPV and often target their current or prior partner during the shooting.5 At this intersection of IPV and gun control, the physician has a unique role. We not only treat those affected by gun violence and advocate for better gun control but we also have a duty to screen our patients for IPV. Part of the sacred patient-physician relationship is being present for our patients when they need us most. The American College of Obstetricians and Gynecologists (ACOG) recommends that ObGyns screen patients for IPV at regular intervals and recognizes that it may take several conversations before a patient discloses her history of IPV.6 Additionally, given the increased risk of gun injuries and death, it behooves us to also screen for gun safety in the home.
Ask patients about IPV, and ask again
The shooting at Mercy Hospital was a stark reminder that IPV can affect any of us. With nearly one-third of women and more than one-quarter of men experiencing IPV in their lifetime, action must be taken. The first step is to routinely screen patients for IPV, offering support and community resources. (see “Screening for intimate partner violence). The second step is to work to decrease the access perpetrators of IPV have to weapons with which to enact violence—through legislation, community engagement, and using our physician voices.
States that have passed legislation that prohibits persons with active restraining orders or a history of IPV or domestic violence from possessing firearms has seen a decrease in IPV firearm homicide rates.7 These policies can make a profound impact on the safety of our patients. Women who are in violent relationships are 5 times more likely to die if their partner has access to a firearm.5
Continue to: #BreakTheCycle...
#BreakTheCycle
The 116th Congress convened in January. We have an opportunity to make real gun legislation reform and work to keep our communities and our patients at risk for IPV safer. Tweet your representatives with #BreakTheCycle, and be on the lookout for important legislation to enact real change.
To sign the open letter from American Healthcare Professionals to the NRA regarding their recent comments and our medical experiences with gun violence, click here. Currently, there are more than 41,000 signatures.
There are numerous verified screening tools available to assess for intimate partner violence (IPV) for both pregnant and nonpregnant patients. Many recommended tools are accessible on the Centers for Disease Control and Prevention (CDC) website: https://www.cdc.gov/violenceprevention/pdf/ipv/ipvandsvscreening.pdf. In our office, the tool most commonly used is a 3-part question assessing domestic violence and IPV. It is important to recognize IPV can affect everyone—all races and religions regardless of socioeconomic background, sexual orientation, and pregnancy status. All patients deserve screening for IPV, and it should never be assumed a patient is not at risk. During an annual gynecology visit for return and new patients or a new obstetric intake visit, we use the following script obtained from ACOG’s Committee Opinion 518 on IPV1 :
Because violence is so common in many women’s lives and because there is help available for women being abused, I now ask every patient about domestic violence:
1. Within the past year (or since you have become pregnant) have you been hit, slapped, kicked, or otherwise physically hurt by someone?
2. Are you in a relationship with a person who threatens or physically hurts you?
3. Has anyone forced you to have sexual activities that made you feel uncomfortable?
If a patient screens positive, we assess their immediate safety. If a social worker is readily available, we arrange an urgent meeting with the patient. If offices do not have immediate access to this service, online information can be provided to patients, including the National Resource Center on Domestic Violence (https://nnedv.org/) and a toll-free number to the National Domestic Violence Hotline: 1-800-799-7233. Additionally, we ask patients about any history of verbal, physical, or sexual violence with prior partners, family members, acquaintances, coworkers, etc. Although the patient might not be at immediate risk, prior experiences with abuse can cause fear and anxiety around gynecologic and obstetric exams. Acknowledging this history can help the clinician adjust his or her physical exam and support the patient during, what may be, a triggering experience.
As an additional resource, Dr. Katherine Hicks-Courant, a resident at Tufts Medical Center, in Boston, Massachusetts, created a tool kit for providers working with pregnant patients with a history of sexual assault. It can be accessed without login online under the Junior Fellow Initiative Toolkit section at http://www.acog.org.
References
1. American College of Obstetricians and Gynecologists. Committee Opinion No. 518: intimate partner violence. Obstet Gynecol. 2012;119:412-417.
If you, or someone you know, needs help, please call The National Domestic Violence Hotline at 1-800-799-7233.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
On the afternoon of November 19, 2018, Dr. Tamara O’Neal was shot and killed by her ex-fiancé outside Mercy Hospital and Medical Center in Chicago, Illinois. After killing Dr. O’Neal, the gunman ran into the hospital where he exchanged gunfire with police, killing a pharmacy resident and a police officer, before he was killed by police.1
This horrific encounter between a woman and her former partner begs for a conversation about intimate partner violence (IPV). A data brief of The National Intimate Partner and Sexual Violence Survey was published in November 2018. According to this report, 30.6% of women experienced physical violence by an intimate partner in 2015, with 21.4% of women experiencing severe physical violence. In addition, 31.0% of men experienced physical violence by an intimate partner in 2015; 14.9% of men experienced severe physical violence.2
Intimate partner violence is “our lane”
The shooting at Mercy Hospital occurred amongst a backdrop of controversy between the National Rifle Association (NRA) and the medical community. On November 7, 2018, the NRA tweeted that doctors should “stay in their lane” with regard to gun control after a position paper from the American College of Physicians on reducing firearm deaths and injuries was published in the Annals of Internal Medicine.3 Doctors from every field and from all over the country responded through social media by stating that treating bullet wounds and caring for those affected by gun violence was “their lane.”4
It is time for us as a community to recognize that gun violence affects us all. The majority of mass shooters have a history of IPV and often target their current or prior partner during the shooting.5 At this intersection of IPV and gun control, the physician has a unique role. We not only treat those affected by gun violence and advocate for better gun control but we also have a duty to screen our patients for IPV. Part of the sacred patient-physician relationship is being present for our patients when they need us most. The American College of Obstetricians and Gynecologists (ACOG) recommends that ObGyns screen patients for IPV at regular intervals and recognizes that it may take several conversations before a patient discloses her history of IPV.6 Additionally, given the increased risk of gun injuries and death, it behooves us to also screen for gun safety in the home.
Ask patients about IPV, and ask again
The shooting at Mercy Hospital was a stark reminder that IPV can affect any of us. With nearly one-third of women and more than one-quarter of men experiencing IPV in their lifetime, action must be taken. The first step is to routinely screen patients for IPV, offering support and community resources. (see “Screening for intimate partner violence). The second step is to work to decrease the access perpetrators of IPV have to weapons with which to enact violence—through legislation, community engagement, and using our physician voices.
States that have passed legislation that prohibits persons with active restraining orders or a history of IPV or domestic violence from possessing firearms has seen a decrease in IPV firearm homicide rates.7 These policies can make a profound impact on the safety of our patients. Women who are in violent relationships are 5 times more likely to die if their partner has access to a firearm.5
Continue to: #BreakTheCycle...
#BreakTheCycle
The 116th Congress convened in January. We have an opportunity to make real gun legislation reform and work to keep our communities and our patients at risk for IPV safer. Tweet your representatives with #BreakTheCycle, and be on the lookout for important legislation to enact real change.
To sign the open letter from American Healthcare Professionals to the NRA regarding their recent comments and our medical experiences with gun violence, click here. Currently, there are more than 41,000 signatures.
There are numerous verified screening tools available to assess for intimate partner violence (IPV) for both pregnant and nonpregnant patients. Many recommended tools are accessible on the Centers for Disease Control and Prevention (CDC) website: https://www.cdc.gov/violenceprevention/pdf/ipv/ipvandsvscreening.pdf. In our office, the tool most commonly used is a 3-part question assessing domestic violence and IPV. It is important to recognize IPV can affect everyone—all races and religions regardless of socioeconomic background, sexual orientation, and pregnancy status. All patients deserve screening for IPV, and it should never be assumed a patient is not at risk. During an annual gynecology visit for return and new patients or a new obstetric intake visit, we use the following script obtained from ACOG’s Committee Opinion 518 on IPV1 :
Because violence is so common in many women’s lives and because there is help available for women being abused, I now ask every patient about domestic violence:
1. Within the past year (or since you have become pregnant) have you been hit, slapped, kicked, or otherwise physically hurt by someone?
2. Are you in a relationship with a person who threatens or physically hurts you?
3. Has anyone forced you to have sexual activities that made you feel uncomfortable?
If a patient screens positive, we assess their immediate safety. If a social worker is readily available, we arrange an urgent meeting with the patient. If offices do not have immediate access to this service, online information can be provided to patients, including the National Resource Center on Domestic Violence (https://nnedv.org/) and a toll-free number to the National Domestic Violence Hotline: 1-800-799-7233. Additionally, we ask patients about any history of verbal, physical, or sexual violence with prior partners, family members, acquaintances, coworkers, etc. Although the patient might not be at immediate risk, prior experiences with abuse can cause fear and anxiety around gynecologic and obstetric exams. Acknowledging this history can help the clinician adjust his or her physical exam and support the patient during, what may be, a triggering experience.
As an additional resource, Dr. Katherine Hicks-Courant, a resident at Tufts Medical Center, in Boston, Massachusetts, created a tool kit for providers working with pregnant patients with a history of sexual assault. It can be accessed without login online under the Junior Fellow Initiative Toolkit section at http://www.acog.org.
References
1. American College of Obstetricians and Gynecologists. Committee Opinion No. 518: intimate partner violence. Obstet Gynecol. 2012;119:412-417.
If you, or someone you know, needs help, please call The National Domestic Violence Hotline at 1-800-799-7233.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Buckley M, Gorner J, Greene M. “Chicago hospital shooting: Young cop, doctor, pharmacy resident and gunman die in Mercy Hospital attack. Chicago Tribune. Nov. 20, 2018.
2. Smith SG, Zhang X, Basile KC, et al. The National Intimate Partner
and Sexual Violence Survey (NISVS): 2015 data brief – updated release. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; November 2018.
3. Butkus R, Doherty R, Bornstein SS; for the Health and Public Policy Committee of the American College of Physicians. Reducing firearm injuries and deaths in the United States: a position paper from the American College of Physicians. Ann Intern Med. 2018;169:704-707.
4. Papenfuss M. NRA Tweets Warning to Anti-Gun Doctors: ‘Stay In Your Lane’. The Huffington Post. November 8, 2018.
5. Everytown for Gun Safety website. Mass Shootings in the United States: 2009–2016. Available at https://everytownresearch.org/reports/mass-shootings-analysis/. Accessed January 17, 2019.
6. The American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 518: intimate partner violence. Obstet Gynecol. 2012;119(2 pt 1):412-417. https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Health-Care-for-Underserved-Women/Intimate-Partner-Violence.
7. Zeoli AM, McCourt A, Buggs S, et al. Analysis of the strength of legal firearms restrictions for perpetrators of domestic violence and their associations with intimate partner homicide. Am J Epidemiol. 2018;187:2365-2371.
1. Buckley M, Gorner J, Greene M. “Chicago hospital shooting: Young cop, doctor, pharmacy resident and gunman die in Mercy Hospital attack. Chicago Tribune. Nov. 20, 2018.
2. Smith SG, Zhang X, Basile KC, et al. The National Intimate Partner
and Sexual Violence Survey (NISVS): 2015 data brief – updated release. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; November 2018.
3. Butkus R, Doherty R, Bornstein SS; for the Health and Public Policy Committee of the American College of Physicians. Reducing firearm injuries and deaths in the United States: a position paper from the American College of Physicians. Ann Intern Med. 2018;169:704-707.
4. Papenfuss M. NRA Tweets Warning to Anti-Gun Doctors: ‘Stay In Your Lane’. The Huffington Post. November 8, 2018.
5. Everytown for Gun Safety website. Mass Shootings in the United States: 2009–2016. Available at https://everytownresearch.org/reports/mass-shootings-analysis/. Accessed January 17, 2019.
6. The American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 518: intimate partner violence. Obstet Gynecol. 2012;119(2 pt 1):412-417. https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Health-Care-for-Underserved-Women/Intimate-Partner-Violence.
7. Zeoli AM, McCourt A, Buggs S, et al. Analysis of the strength of legal firearms restrictions for perpetrators of domestic violence and their associations with intimate partner homicide. Am J Epidemiol. 2018;187:2365-2371.

Revised ACA premium calculator could up uninsured rate
– changes that critics caution could leave more people uninsured.

But the Centers for Medicare & Medicaid Services says the changes would lower premiums and give enrollees the option to choose a plan that doesn’t offer abortion services.
The CMS released the proposed rule online Jan. 17, and it’s expected to be published in the Federal Register Jan. 24. (A fact sheet highlighting the changes can be found here.)
Under one of the proposals, the CMS would alter the risk-adjustment model used to determine premium growth beginning in 2020.
But the proposed rule’s regulatory impact statement notes that the risk-adjustment change could reduce enrollment in health insurance products through the federal exchanges by 100,000 people in each of the years from 2020 through 2023. And the revised risk-adjustment model could reduce federal spending on premium tax credits by $900 million in both 2020 and 2021, and by $1 billion in 2022 and 2023.
“Some of the 100,000 individuals estimated to enroll in exchange coverage as a result of the proposed change ... may purchase short-term, limited-duration insurance, though a majority is likely to become uninsured,” the CMS stated in its proposed rule. “Either transition may result in greater exposure to health care costs, which previous research suggests reduces utilization of health care services.”
Matt Fiedler, fellow at the Brookings Institution’s Center for Health Policy, highlighted the potential effect a drop in premium tax credits could have on potential enrollees.
According to Mr. Fiedler, a single person at 300% of the federal poverty level (FPL) would lose $92 per year in premium tax credits. And a family of four at 300% of FPL would lose $189 per year in premium tax credits, he calculated. He predicted “smaller effects at lower income levels and larger effects at higher income levels.”
The proposed rule would also require issuers of qualified health plans that offer abortion services to provide at least one “mirror” plan that omits abortion coverage. That could lead insurers to drop abortion coverage in their qualified health plans, the CMS noted, but it didn’t estimate how many issuers are expected to drop abortion coverage.
The agency said the proposed requirement “would increase consumer choice by offering additional plan options to potential enrollees who may refuse to enroll in, or may be discouraged from enrolling in, qualified health plans because the plans in their service area cover non-Hyde abortion services.” The CMS conceded that the existence of two such plans could confuse consumers, and “research has shown that offering consumers additional health plan options may result in consumers opting to not purchase a plan at all.”
The CMS also is seeking comment on changes to the automatic re-enrollment policy.
“Most current enrollees receive significant government subsidies, making them potentially less sensitive to premiums and premium changes,” the agency stated in the proposed rule. “Some consumers who are automatically re-enrolled in their current plan may be shielded from changes to their coverage, which may result in consumers being less aware of their options from year to year.”
Comments on the proposed rule are due by Feb. 19.
– changes that critics caution could leave more people uninsured.
But the Centers for Medicare & Medicaid Services says the changes would lower premiums and give enrollees the option to choose a plan that doesn’t offer abortion services.
The CMS released the proposed rule online Jan. 17, and it’s expected to be published in the Federal Register Jan. 24. (A fact sheet highlighting the changes can be found here.)
Under one of the proposals, the CMS would alter the risk-adjustment model used to determine premium growth beginning in 2020.
But the proposed rule’s regulatory impact statement notes that the risk-adjustment change could reduce enrollment in health insurance products through the federal exchanges by 100,000 people in each of the years from 2020 through 2023. And the revised risk-adjustment model could reduce federal spending on premium tax credits by $900 million in both 2020 and 2021, and by $1 billion in 2022 and 2023.
“Some of the 100,000 individuals estimated to enroll in exchange coverage as a result of the proposed change ... may purchase short-term, limited-duration insurance, though a majority is likely to become uninsured,” the CMS stated in its proposed rule. “Either transition may result in greater exposure to health care costs, which previous research suggests reduces utilization of health care services.”
Matt Fiedler, fellow at the Brookings Institution’s Center for Health Policy, highlighted the potential effect a drop in premium tax credits could have on potential enrollees.
According to Mr. Fiedler, a single person at 300% of the federal poverty level (FPL) would lose $92 per year in premium tax credits. And a family of four at 300% of FPL would lose $189 per year in premium tax credits, he calculated. He predicted “smaller effects at lower income levels and larger effects at higher income levels.”
The proposed rule would also require issuers of qualified health plans that offer abortion services to provide at least one “mirror” plan that omits abortion coverage. That could lead insurers to drop abortion coverage in their qualified health plans, the CMS noted, but it didn’t estimate how many issuers are expected to drop abortion coverage.
The agency said the proposed requirement “would increase consumer choice by offering additional plan options to potential enrollees who may refuse to enroll in, or may be discouraged from enrolling in, qualified health plans because the plans in their service area cover non-Hyde abortion services.” The CMS conceded that the existence of two such plans could confuse consumers, and “research has shown that offering consumers additional health plan options may result in consumers opting to not purchase a plan at all.”
The CMS also is seeking comment on changes to the automatic re-enrollment policy.
“Most current enrollees receive significant government subsidies, making them potentially less sensitive to premiums and premium changes,” the agency stated in the proposed rule. “Some consumers who are automatically re-enrolled in their current plan may be shielded from changes to their coverage, which may result in consumers being less aware of their options from year to year.”
Comments on the proposed rule are due by Feb. 19.
– changes that critics caution could leave more people uninsured.
But the Centers for Medicare & Medicaid Services says the changes would lower premiums and give enrollees the option to choose a plan that doesn’t offer abortion services.
The CMS released the proposed rule online Jan. 17, and it’s expected to be published in the Federal Register Jan. 24. (A fact sheet highlighting the changes can be found here.)
Under one of the proposals, the CMS would alter the risk-adjustment model used to determine premium growth beginning in 2020.
But the proposed rule’s regulatory impact statement notes that the risk-adjustment change could reduce enrollment in health insurance products through the federal exchanges by 100,000 people in each of the years from 2020 through 2023. And the revised risk-adjustment model could reduce federal spending on premium tax credits by $900 million in both 2020 and 2021, and by $1 billion in 2022 and 2023.
“Some of the 100,000 individuals estimated to enroll in exchange coverage as a result of the proposed change ... may purchase short-term, limited-duration insurance, though a majority is likely to become uninsured,” the CMS stated in its proposed rule. “Either transition may result in greater exposure to health care costs, which previous research suggests reduces utilization of health care services.”
Matt Fiedler, fellow at the Brookings Institution’s Center for Health Policy, highlighted the potential effect a drop in premium tax credits could have on potential enrollees.
According to Mr. Fiedler, a single person at 300% of the federal poverty level (FPL) would lose $92 per year in premium tax credits. And a family of four at 300% of FPL would lose $189 per year in premium tax credits, he calculated. He predicted “smaller effects at lower income levels and larger effects at higher income levels.”
The proposed rule would also require issuers of qualified health plans that offer abortion services to provide at least one “mirror” plan that omits abortion coverage. That could lead insurers to drop abortion coverage in their qualified health plans, the CMS noted, but it didn’t estimate how many issuers are expected to drop abortion coverage.
The agency said the proposed requirement “would increase consumer choice by offering additional plan options to potential enrollees who may refuse to enroll in, or may be discouraged from enrolling in, qualified health plans because the plans in their service area cover non-Hyde abortion services.” The CMS conceded that the existence of two such plans could confuse consumers, and “research has shown that offering consumers additional health plan options may result in consumers opting to not purchase a plan at all.”
The CMS also is seeking comment on changes to the automatic re-enrollment policy.
“Most current enrollees receive significant government subsidies, making them potentially less sensitive to premiums and premium changes,” the agency stated in the proposed rule. “Some consumers who are automatically re-enrolled in their current plan may be shielded from changes to their coverage, which may result in consumers being less aware of their options from year to year.”
Comments on the proposed rule are due by Feb. 19.
Ezetimibe effective as primary prevention
Also today, the FDA says that the benefits of paclitaxel-coated devices outweigh risks for peripheral arterial disease, flu activity is down for the second consecutive week, and a look at homelessness among LGBT youth in the United States.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, the FDA says that the benefits of paclitaxel-coated devices outweigh risks for peripheral arterial disease, flu activity is down for the second consecutive week, and a look at homelessness among LGBT youth in the United States.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, the FDA says that the benefits of paclitaxel-coated devices outweigh risks for peripheral arterial disease, flu activity is down for the second consecutive week, and a look at homelessness among LGBT youth in the United States.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Cyberbullied by anti-vaxxers: Monique Tello Part I
Dr. Tell wrote about her experience in a blog post where she opened up about how difficult the process has been, and how she has found support in a community of her colleagues.
Apple Podcasts
Google Podcasts
Spotify
Dr. Tell wrote about her experience in a blog post where she opened up about how difficult the process has been, and how she has found support in a community of her colleagues.
Apple Podcasts
Google Podcasts
Spotify
Dr. Tell wrote about her experience in a blog post where she opened up about how difficult the process has been, and how she has found support in a community of her colleagues.
Apple Podcasts
Google Podcasts
Spotify

Survey: Government shutdown is affecting patient health
A majority of U.S. health care professionals report that their patients have been negatively affected by the federal government’s partial shutdown, according to a survey conducted Jan. 11 by health care market research company InCrowd.
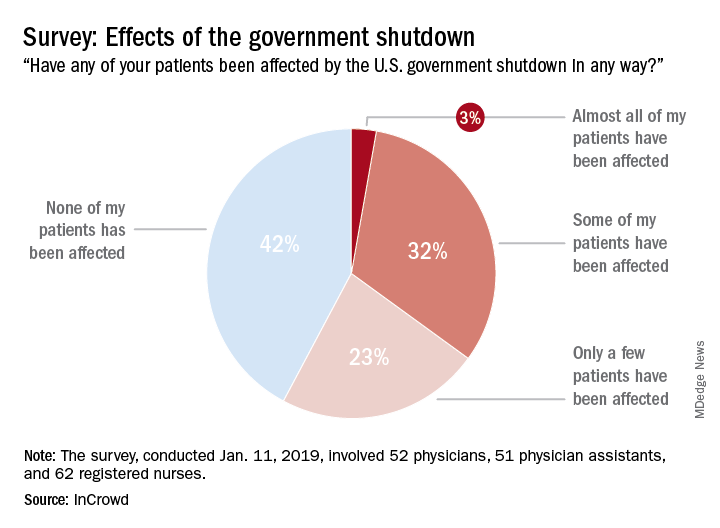
The results showed that 58% of the 165 respondents (52 primary care physicians, 51 physician assistants, and 63 registered nurses) surveyed believe that their patents have been affected in some way by the shutdown: Three percent said that almost all of their patients have been affected, 32% said that some have been affected, and 23% said that only a few patients have been affected. The largest share of clinicians (42%), however, believes that none of their patients have experienced any effects from the shutdown, InCrowd reported Jan. 17.
That distribution changes considerably, however, when looking at the physicians only: 4% (almost all), 39% (some), 31% (a few), and 26% (none). Registered nurses (50%) and physician assistants (45%) were much more likely to say that none of their patients had been affected, InCrowd reported.
“Patient access to care and compliance issues due to financial concerns and loss of benefits are already being observed by respondents. Forty percent of respondents reported a high degree of both issues with patients affording medicine and incidences where patient avoided treatments and appointments all together,” the InCrowd investigators said.
This article was updated 1/18/19.
A majority of U.S. health care professionals report that their patients have been negatively affected by the federal government’s partial shutdown, according to a survey conducted Jan. 11 by health care market research company InCrowd.
The results showed that 58% of the 165 respondents (52 primary care physicians, 51 physician assistants, and 63 registered nurses) surveyed believe that their patents have been affected in some way by the shutdown: Three percent said that almost all of their patients have been affected, 32% said that some have been affected, and 23% said that only a few patients have been affected. The largest share of clinicians (42%), however, believes that none of their patients have experienced any effects from the shutdown, InCrowd reported Jan. 17.
That distribution changes considerably, however, when looking at the physicians only: 4% (almost all), 39% (some), 31% (a few), and 26% (none). Registered nurses (50%) and physician assistants (45%) were much more likely to say that none of their patients had been affected, InCrowd reported.
“Patient access to care and compliance issues due to financial concerns and loss of benefits are already being observed by respondents. Forty percent of respondents reported a high degree of both issues with patients affording medicine and incidences where patient avoided treatments and appointments all together,” the InCrowd investigators said.
This article was updated 1/18/19.
A majority of U.S. health care professionals report that their patients have been negatively affected by the federal government’s partial shutdown, according to a survey conducted Jan. 11 by health care market research company InCrowd.
The results showed that 58% of the 165 respondents (52 primary care physicians, 51 physician assistants, and 63 registered nurses) surveyed believe that their patents have been affected in some way by the shutdown: Three percent said that almost all of their patients have been affected, 32% said that some have been affected, and 23% said that only a few patients have been affected. The largest share of clinicians (42%), however, believes that none of their patients have experienced any effects from the shutdown, InCrowd reported Jan. 17.
That distribution changes considerably, however, when looking at the physicians only: 4% (almost all), 39% (some), 31% (a few), and 26% (none). Registered nurses (50%) and physician assistants (45%) were much more likely to say that none of their patients had been affected, InCrowd reported.
“Patient access to care and compliance issues due to financial concerns and loss of benefits are already being observed by respondents. Forty percent of respondents reported a high degree of both issues with patients affording medicine and incidences where patient avoided treatments and appointments all together,” the InCrowd investigators said.
This article was updated 1/18/19.
Mandatory reporting laws
Question: You are moonlighting in the emergency department and have just finished treating a 5-year-old boy with an apparent Colles’ fracture, who was accompanied by his mother with bruises on her face. Her exam revealed additional bruises over her abdominal wall. The mother said they accidentally tripped and fell down the stairs, and spontaneously denied any acts of violence in the family.
Given this scenario, which of the following is best?
A. You suspect both child and spousal abuse, but lack sufficient evidence to report the incident.
B. Failure to report based on reasonable suspicion alone may amount to a criminal offense punishable by possible imprisonment.
C. You may face a potential malpractice lawsuit if subsequent injuries caused by abuse could have been prevented had you reported.
D. Mandatory reporting laws apply not only to abuse of children and spouses, but also of the elderly and other vulnerable adults.
E. All are correct except A.
Answer: E. All doctors, especially those working in emergency departments, treat injuries on a regular basis. Accidents probably account for the majority of these injuries, but the most pernicious are those caused by willful abuse or neglect. Such conduct, believed to be widespread and underrecognized, victimizes children, women, the elderly, and other vulnerable groups.

Mandatory reporting laws arose from the need to identify and prevent these activities that cause serious harm and loss of lives. Physicians and other health care workers are in a prime position to diagnose or raise the suspicion of abuse and neglect. This article focuses on laws that mandate physician reporting of such behavior. Not addressed are other reportable situations such as certain infectious diseases, gunshot wounds, threats to third parties, and so on.
Child abuse
The best-known example of a mandatory reporting law relates to child abuse, which is broadly defined as when a parent or caretaker emotionally, physically, or sexually abuses, neglects, or abandons a child. Child abuse laws are intended to protect children from serious harm without abridging parental discipline of their children.
Cases of child abuse are pervasive; four or five children are tragically killed by abuse or neglect every day, and each year, some 6 million children are reported as victims of child abuse. Henry Kempe’s studies on the “battered child syndrome” in 1962 served to underscore the physician’s role in exposing child maltreatment, and 1973 saw the enactment of the Child Abuse Prevention and Treatment Act, which set standards for mandatory reporting as a condition for federal funding.
All U.S. states have statutes identifying persons who are required to report suspected child maltreatment to an appropriate agency, such as child protective services. Reasonable suspicion, without need for proof, is sufficient to trigger the mandatory reporting duty. A summary of the general reporting requirements, as well as each state’s key statutory features, are available at Child Welfare Information Gateway.1
Bruises, fractures, and burns are recurring examples of injuries resulting from child abuse, but there are many others, including severe emotional harm, which is an important consequence. Clues to abuse include a child’s fearful and anxious demeanor, wearing clothes to hide injuries, and inappropriate sexual conduct.2 The perpetrators and/or complicit parties typically blame an innocent home accident for the victim’s injuries to mislead the health care provider.
Elder abuse
Elder abuse is broadly construed to include physical, sexual, and psychological abuse, as well as financial exploitation and caregiver neglect.3 It is a serious problem in the United States, estimated in 2008 to affect 1 in 10 elders. The figure is likely an underestimate, because many elderly victims are afraid or unwilling to lodge a complaint against the abuser whom they love and may depend upon.4
The law, which protects the “elderly” (e.g., those aged 62 years or older in Hawaii), may also be extended to other younger vulnerable adults, who because of an impairment, are unable to 1) communicate or make responsible decisions to manage one’s own care or resources, 2) carry out or arrange for essential activities of daily living, or 3) protect one’s self from abuse.5
The law mandates reporting where there is reason to believe abuse has occurred or the vulnerable adult is in danger of abuse if immediate action is not taken. Reporting statutes for elder abuse vary somewhat on the identity of mandated reporters (health care providers are always included), the victim’s mental capacity, dwelling place (home or in an assisted-living facility), and type of purported activity that warrants reporting.
Domestic violence
As defined by the National Coalition Against Domestic Violence, “Domestic violence is the willful intimidation, physical assault, battery, sexual assault, and/or other abusive behavior as part of a systematic pattern of power and control perpetrated by one intimate partner against another. ... The frequency and severity of domestic violence can vary dramatically; however, the one constant component of domestic violence is one partner’s consistent efforts to maintain power and control over the other.”6 Domestic violence is said to have reached epidemic proportions, with one in four women experiencing it at some point in her life.
Virtually all states mandate the reporting of domestic violence by health care providers if there is a reasonable suspicion that observed patient injuries are the result of physical abuse.7 California, for example, requires the provider to call local law enforcement as soon as possible or to send in a written report within 48 hours.
There may be exceptions to required reporting, as when an adult victim withholds consent but accepts victim referral services. State laws encourage but do not always require that the health care provider inform the patient about the report, but federal law dictates otherwise unless this puts the patient at risk. Hawaii’s domestic violence laws were originally enacted to deter spousal abuse, but they now also protect other household members.8
Any individual who assumes a duty or responsibility pursuant to all of these reporting laws is immunized from criminal or civil liability. On the other hand, a mandated reporter who knowingly fails to report an incident or who willfully prevents another person from reporting such an incident commits a criminal offence.
In the case of a physician, there is the added risk of a malpractice lawsuit based on “violation of statute” (breach of a legal duty), should another injury occur down the road that was arguably preventable by his or her failure to report.
Experts generally believe that mandatory reporting laws are important in identifying child maltreatment. However, it has been asserted that despite a 5-decade history of mandatory reporting, no clear endpoints attest to the efficacy of this approach, and it is argued that no data exist to demonstrate that incremental increases in reporting have contributed to child safety.
Particularly challenging are attempts at impact comparisons between states with different policies. A number of countries, including the United Kingdom, do not have mandatory reporting laws and regulate reporting by professional societies.9
In addition, some critics of mandatory reporting raise concerns surrounding law enforcement showing up at the victim’s house to question the family about abuse, or to make an arrest or issue warnings. They posit that when the behavior of an abuser is under scrutiny, this can paradoxically create a potentially more dangerous environment for the patient-victim, whom the perpetrator now considers to have betrayed his or her trust. Others bemoan that revealing patient confidences violates the physician’s ethical code.
However, the intolerable incidence of violence against the vulnerable has properly made mandatory reporting the law of the land. Although the criminal penalty is currently light for failure to report, there is a move toward increasing its severity. Hawaii, for example, recently introduced Senate Bill 2477 that makes nonreporting by those required to do so a Class C felony punishable by up to 5 years in prison. The offense currently is a petty misdemeanor punishable by up to 30 days in jail.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Child Welfare Information Gateway (2016). Mandatory reporters of child abuse and neglect. Washington, D.C.: U.S. Department of Health and Human Services, Children’s Bureau. Available at www.childwelfare.gov; email: [email protected]; phone: 800-394-3366.
2. Available at www.childwelfare.gov/topics/can.
3. Available at www.justice.gov/elderjustice/elder-justice-statutes-0.
4. Available at www.cdc.gov/violenceprevention/elderabuse/index.html.
5. Hawaii Revised Statutes, Sec. 346-222, 346-224, 346-250, 412:3-114.5.
6. Available at ncadv.org.
7. Ann Emerg Med. 2002 Jan;39(1):56-60.
8. Hawaii Revised Statutes, Sec. 709-906.
9. Pediatrics. 2017 Apr;139(4). pii: e20163511.
Question: You are moonlighting in the emergency department and have just finished treating a 5-year-old boy with an apparent Colles’ fracture, who was accompanied by his mother with bruises on her face. Her exam revealed additional bruises over her abdominal wall. The mother said they accidentally tripped and fell down the stairs, and spontaneously denied any acts of violence in the family.
Given this scenario, which of the following is best?
A. You suspect both child and spousal abuse, but lack sufficient evidence to report the incident.
B. Failure to report based on reasonable suspicion alone may amount to a criminal offense punishable by possible imprisonment.
C. You may face a potential malpractice lawsuit if subsequent injuries caused by abuse could have been prevented had you reported.
D. Mandatory reporting laws apply not only to abuse of children and spouses, but also of the elderly and other vulnerable adults.
E. All are correct except A.
Answer: E. All doctors, especially those working in emergency departments, treat injuries on a regular basis. Accidents probably account for the majority of these injuries, but the most pernicious are those caused by willful abuse or neglect. Such conduct, believed to be widespread and underrecognized, victimizes children, women, the elderly, and other vulnerable groups.
Mandatory reporting laws arose from the need to identify and prevent these activities that cause serious harm and loss of lives. Physicians and other health care workers are in a prime position to diagnose or raise the suspicion of abuse and neglect. This article focuses on laws that mandate physician reporting of such behavior. Not addressed are other reportable situations such as certain infectious diseases, gunshot wounds, threats to third parties, and so on.
Child abuse
The best-known example of a mandatory reporting law relates to child abuse, which is broadly defined as when a parent or caretaker emotionally, physically, or sexually abuses, neglects, or abandons a child. Child abuse laws are intended to protect children from serious harm without abridging parental discipline of their children.
Cases of child abuse are pervasive; four or five children are tragically killed by abuse or neglect every day, and each year, some 6 million children are reported as victims of child abuse. Henry Kempe’s studies on the “battered child syndrome” in 1962 served to underscore the physician’s role in exposing child maltreatment, and 1973 saw the enactment of the Child Abuse Prevention and Treatment Act, which set standards for mandatory reporting as a condition for federal funding.
All U.S. states have statutes identifying persons who are required to report suspected child maltreatment to an appropriate agency, such as child protective services. Reasonable suspicion, without need for proof, is sufficient to trigger the mandatory reporting duty. A summary of the general reporting requirements, as well as each state’s key statutory features, are available at Child Welfare Information Gateway.1
Bruises, fractures, and burns are recurring examples of injuries resulting from child abuse, but there are many others, including severe emotional harm, which is an important consequence. Clues to abuse include a child’s fearful and anxious demeanor, wearing clothes to hide injuries, and inappropriate sexual conduct.2 The perpetrators and/or complicit parties typically blame an innocent home accident for the victim’s injuries to mislead the health care provider.
Elder abuse
Elder abuse is broadly construed to include physical, sexual, and psychological abuse, as well as financial exploitation and caregiver neglect.3 It is a serious problem in the United States, estimated in 2008 to affect 1 in 10 elders. The figure is likely an underestimate, because many elderly victims are afraid or unwilling to lodge a complaint against the abuser whom they love and may depend upon.4
The law, which protects the “elderly” (e.g., those aged 62 years or older in Hawaii), may also be extended to other younger vulnerable adults, who because of an impairment, are unable to 1) communicate or make responsible decisions to manage one’s own care or resources, 2) carry out or arrange for essential activities of daily living, or 3) protect one’s self from abuse.5
The law mandates reporting where there is reason to believe abuse has occurred or the vulnerable adult is in danger of abuse if immediate action is not taken. Reporting statutes for elder abuse vary somewhat on the identity of mandated reporters (health care providers are always included), the victim’s mental capacity, dwelling place (home or in an assisted-living facility), and type of purported activity that warrants reporting.
Domestic violence
As defined by the National Coalition Against Domestic Violence, “Domestic violence is the willful intimidation, physical assault, battery, sexual assault, and/or other abusive behavior as part of a systematic pattern of power and control perpetrated by one intimate partner against another. ... The frequency and severity of domestic violence can vary dramatically; however, the one constant component of domestic violence is one partner’s consistent efforts to maintain power and control over the other.”6 Domestic violence is said to have reached epidemic proportions, with one in four women experiencing it at some point in her life.
Virtually all states mandate the reporting of domestic violence by health care providers if there is a reasonable suspicion that observed patient injuries are the result of physical abuse.7 California, for example, requires the provider to call local law enforcement as soon as possible or to send in a written report within 48 hours.
There may be exceptions to required reporting, as when an adult victim withholds consent but accepts victim referral services. State laws encourage but do not always require that the health care provider inform the patient about the report, but federal law dictates otherwise unless this puts the patient at risk. Hawaii’s domestic violence laws were originally enacted to deter spousal abuse, but they now also protect other household members.8
Any individual who assumes a duty or responsibility pursuant to all of these reporting laws is immunized from criminal or civil liability. On the other hand, a mandated reporter who knowingly fails to report an incident or who willfully prevents another person from reporting such an incident commits a criminal offence.
In the case of a physician, there is the added risk of a malpractice lawsuit based on “violation of statute” (breach of a legal duty), should another injury occur down the road that was arguably preventable by his or her failure to report.
Experts generally believe that mandatory reporting laws are important in identifying child maltreatment. However, it has been asserted that despite a 5-decade history of mandatory reporting, no clear endpoints attest to the efficacy of this approach, and it is argued that no data exist to demonstrate that incremental increases in reporting have contributed to child safety.
Particularly challenging are attempts at impact comparisons between states with different policies. A number of countries, including the United Kingdom, do not have mandatory reporting laws and regulate reporting by professional societies.9
In addition, some critics of mandatory reporting raise concerns surrounding law enforcement showing up at the victim’s house to question the family about abuse, or to make an arrest or issue warnings. They posit that when the behavior of an abuser is under scrutiny, this can paradoxically create a potentially more dangerous environment for the patient-victim, whom the perpetrator now considers to have betrayed his or her trust. Others bemoan that revealing patient confidences violates the physician’s ethical code.
However, the intolerable incidence of violence against the vulnerable has properly made mandatory reporting the law of the land. Although the criminal penalty is currently light for failure to report, there is a move toward increasing its severity. Hawaii, for example, recently introduced Senate Bill 2477 that makes nonreporting by those required to do so a Class C felony punishable by up to 5 years in prison. The offense currently is a petty misdemeanor punishable by up to 30 days in jail.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Child Welfare Information Gateway (2016). Mandatory reporters of child abuse and neglect. Washington, D.C.: U.S. Department of Health and Human Services, Children’s Bureau. Available at www.childwelfare.gov; email: [email protected]; phone: 800-394-3366.
2. Available at www.childwelfare.gov/topics/can.
3. Available at www.justice.gov/elderjustice/elder-justice-statutes-0.
4. Available at www.cdc.gov/violenceprevention/elderabuse/index.html.
5. Hawaii Revised Statutes, Sec. 346-222, 346-224, 346-250, 412:3-114.5.
6. Available at ncadv.org.
7. Ann Emerg Med. 2002 Jan;39(1):56-60.
8. Hawaii Revised Statutes, Sec. 709-906.
9. Pediatrics. 2017 Apr;139(4). pii: e20163511.
Question: You are moonlighting in the emergency department and have just finished treating a 5-year-old boy with an apparent Colles’ fracture, who was accompanied by his mother with bruises on her face. Her exam revealed additional bruises over her abdominal wall. The mother said they accidentally tripped and fell down the stairs, and spontaneously denied any acts of violence in the family.
Given this scenario, which of the following is best?
A. You suspect both child and spousal abuse, but lack sufficient evidence to report the incident.
B. Failure to report based on reasonable suspicion alone may amount to a criminal offense punishable by possible imprisonment.
C. You may face a potential malpractice lawsuit if subsequent injuries caused by abuse could have been prevented had you reported.
D. Mandatory reporting laws apply not only to abuse of children and spouses, but also of the elderly and other vulnerable adults.
E. All are correct except A.
Answer: E. All doctors, especially those working in emergency departments, treat injuries on a regular basis. Accidents probably account for the majority of these injuries, but the most pernicious are those caused by willful abuse or neglect. Such conduct, believed to be widespread and underrecognized, victimizes children, women, the elderly, and other vulnerable groups.
Mandatory reporting laws arose from the need to identify and prevent these activities that cause serious harm and loss of lives. Physicians and other health care workers are in a prime position to diagnose or raise the suspicion of abuse and neglect. This article focuses on laws that mandate physician reporting of such behavior. Not addressed are other reportable situations such as certain infectious diseases, gunshot wounds, threats to third parties, and so on.
Child abuse
The best-known example of a mandatory reporting law relates to child abuse, which is broadly defined as when a parent or caretaker emotionally, physically, or sexually abuses, neglects, or abandons a child. Child abuse laws are intended to protect children from serious harm without abridging parental discipline of their children.
Cases of child abuse are pervasive; four or five children are tragically killed by abuse or neglect every day, and each year, some 6 million children are reported as victims of child abuse. Henry Kempe’s studies on the “battered child syndrome” in 1962 served to underscore the physician’s role in exposing child maltreatment, and 1973 saw the enactment of the Child Abuse Prevention and Treatment Act, which set standards for mandatory reporting as a condition for federal funding.
All U.S. states have statutes identifying persons who are required to report suspected child maltreatment to an appropriate agency, such as child protective services. Reasonable suspicion, without need for proof, is sufficient to trigger the mandatory reporting duty. A summary of the general reporting requirements, as well as each state’s key statutory features, are available at Child Welfare Information Gateway.1
Bruises, fractures, and burns are recurring examples of injuries resulting from child abuse, but there are many others, including severe emotional harm, which is an important consequence. Clues to abuse include a child’s fearful and anxious demeanor, wearing clothes to hide injuries, and inappropriate sexual conduct.2 The perpetrators and/or complicit parties typically blame an innocent home accident for the victim’s injuries to mislead the health care provider.
Elder abuse
Elder abuse is broadly construed to include physical, sexual, and psychological abuse, as well as financial exploitation and caregiver neglect.3 It is a serious problem in the United States, estimated in 2008 to affect 1 in 10 elders. The figure is likely an underestimate, because many elderly victims are afraid or unwilling to lodge a complaint against the abuser whom they love and may depend upon.4
The law, which protects the “elderly” (e.g., those aged 62 years or older in Hawaii), may also be extended to other younger vulnerable adults, who because of an impairment, are unable to 1) communicate or make responsible decisions to manage one’s own care or resources, 2) carry out or arrange for essential activities of daily living, or 3) protect one’s self from abuse.5
The law mandates reporting where there is reason to believe abuse has occurred or the vulnerable adult is in danger of abuse if immediate action is not taken. Reporting statutes for elder abuse vary somewhat on the identity of mandated reporters (health care providers are always included), the victim’s mental capacity, dwelling place (home or in an assisted-living facility), and type of purported activity that warrants reporting.
Domestic violence
As defined by the National Coalition Against Domestic Violence, “Domestic violence is the willful intimidation, physical assault, battery, sexual assault, and/or other abusive behavior as part of a systematic pattern of power and control perpetrated by one intimate partner against another. ... The frequency and severity of domestic violence can vary dramatically; however, the one constant component of domestic violence is one partner’s consistent efforts to maintain power and control over the other.”6 Domestic violence is said to have reached epidemic proportions, with one in four women experiencing it at some point in her life.
Virtually all states mandate the reporting of domestic violence by health care providers if there is a reasonable suspicion that observed patient injuries are the result of physical abuse.7 California, for example, requires the provider to call local law enforcement as soon as possible or to send in a written report within 48 hours.
There may be exceptions to required reporting, as when an adult victim withholds consent but accepts victim referral services. State laws encourage but do not always require that the health care provider inform the patient about the report, but federal law dictates otherwise unless this puts the patient at risk. Hawaii’s domestic violence laws were originally enacted to deter spousal abuse, but they now also protect other household members.8
Any individual who assumes a duty or responsibility pursuant to all of these reporting laws is immunized from criminal or civil liability. On the other hand, a mandated reporter who knowingly fails to report an incident or who willfully prevents another person from reporting such an incident commits a criminal offence.
In the case of a physician, there is the added risk of a malpractice lawsuit based on “violation of statute” (breach of a legal duty), should another injury occur down the road that was arguably preventable by his or her failure to report.
Experts generally believe that mandatory reporting laws are important in identifying child maltreatment. However, it has been asserted that despite a 5-decade history of mandatory reporting, no clear endpoints attest to the efficacy of this approach, and it is argued that no data exist to demonstrate that incremental increases in reporting have contributed to child safety.
Particularly challenging are attempts at impact comparisons between states with different policies. A number of countries, including the United Kingdom, do not have mandatory reporting laws and regulate reporting by professional societies.9
In addition, some critics of mandatory reporting raise concerns surrounding law enforcement showing up at the victim’s house to question the family about abuse, or to make an arrest or issue warnings. They posit that when the behavior of an abuser is under scrutiny, this can paradoxically create a potentially more dangerous environment for the patient-victim, whom the perpetrator now considers to have betrayed his or her trust. Others bemoan that revealing patient confidences violates the physician’s ethical code.
However, the intolerable incidence of violence against the vulnerable has properly made mandatory reporting the law of the land. Although the criminal penalty is currently light for failure to report, there is a move toward increasing its severity. Hawaii, for example, recently introduced Senate Bill 2477 that makes nonreporting by those required to do so a Class C felony punishable by up to 5 years in prison. The offense currently is a petty misdemeanor punishable by up to 30 days in jail.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Child Welfare Information Gateway (2016). Mandatory reporters of child abuse and neglect. Washington, D.C.: U.S. Department of Health and Human Services, Children’s Bureau. Available at www.childwelfare.gov; email: [email protected]; phone: 800-394-3366.
2. Available at www.childwelfare.gov/topics/can.
3. Available at www.justice.gov/elderjustice/elder-justice-statutes-0.
4. Available at www.cdc.gov/violenceprevention/elderabuse/index.html.
5. Hawaii Revised Statutes, Sec. 346-222, 346-224, 346-250, 412:3-114.5.
6. Available at ncadv.org.
7. Ann Emerg Med. 2002 Jan;39(1):56-60.
8. Hawaii Revised Statutes, Sec. 709-906.
9. Pediatrics. 2017 Apr;139(4). pii: e20163511.
Rural suicidality and resilience
Overall U.S. life expectancy decreased from 78.7 years to 78.6 years from 2016 to 2017. Researchers from the Centers for Disease Control and Prevention noted that, along with drug overdose deaths, suicide also drove the decrease in average lifespan over that time period. Addressing suicide in rural communities presents unique challenges.
Dr. Bonham is vice chair of community behavioral health in the department of psychiatry and behavioral sciences at the University of New Mexico, Albuquerque. Dr. Kriechman is a child, adolescent and family psychiatrist at the university, where he serves as principal investigator on ASPYR – Alliance-building for Suicide Prevention & Youth Resilience.
You can hear more on resilience and suicide from the MDedge Psychcast in these past episodes:
- Find the MDedge Psychcast where ever you listen:
Overall U.S. life expectancy decreased from 78.7 years to 78.6 years from 2016 to 2017. Researchers from the Centers for Disease Control and Prevention noted that, along with drug overdose deaths, suicide also drove the decrease in average lifespan over that time period. Addressing suicide in rural communities presents unique challenges.
Dr. Bonham is vice chair of community behavioral health in the department of psychiatry and behavioral sciences at the University of New Mexico, Albuquerque. Dr. Kriechman is a child, adolescent and family psychiatrist at the university, where he serves as principal investigator on ASPYR – Alliance-building for Suicide Prevention & Youth Resilience.
You can hear more on resilience and suicide from the MDedge Psychcast in these past episodes:
- Find the MDedge Psychcast where ever you listen:
Overall U.S. life expectancy decreased from 78.7 years to 78.6 years from 2016 to 2017. Researchers from the Centers for Disease Control and Prevention noted that, along with drug overdose deaths, suicide also drove the decrease in average lifespan over that time period. Addressing suicide in rural communities presents unique challenges.
Dr. Bonham is vice chair of community behavioral health in the department of psychiatry and behavioral sciences at the University of New Mexico, Albuquerque. Dr. Kriechman is a child, adolescent and family psychiatrist at the university, where he serves as principal investigator on ASPYR – Alliance-building for Suicide Prevention & Youth Resilience.
You can hear more on resilience and suicide from the MDedge Psychcast in these past episodes:
- Find the MDedge Psychcast where ever you listen:
Courts block Trump from eroding contraceptive mandate
Federal judges have blocked the Trump administration from weakening the Affordable Care Act’s contraceptive mandate in two separate orders that bar the President from letting more entities claim exemptions.
On Jan. 14, U.S. District Court Judge Wendy Beetlestone for the Eastern District of Pennsylvania issued a temporary nationwide ban on two rules that would have allowed an expanded group of employers and insurers to object to providing contraception coverage on either religious or moral grounds. The regulations, announced Nov. 7, 2018, were scheduled to take effect Jan. 14. The day before, U.S. District Judge Haywood Gilliam for the Northern District of California issued a similar temporary ban, but his order applied only to the 13 plaintiff states in the case, plus the District of Columbia.

While Pennsylvania and New Jersey are the only plaintiffs in the Judge Beetlestone case, she wrote that a nationwide injunction is required to protect numerous citizens from losing contraceptive coverage and resulting in “significant, direct, and proprietary harm” to states in the form of increased state-funded contraceptive services and increased costs associated with unintended pregnancies. Judge Gilliam provided similar reasoning in his Jan. 13 order, writing that the 13 plaintiff states have proven that rules promulgated by the U.S. Department of Health and Human Services would cause women to lose employer-sponsored contraceptive coverage, resulting in economic harm to the states.
California Attorney General Xavier Becerra, a plaintiff in the second case, said Judge Gilliam’s ruling will stop the Trump administration from denying millions of women and families access to co-pay birth control guaranteed by the Affordable Care Act.
“The law couldn’t be clearer – employers have no business interfering in women’s health care decisions,” Mr. Becerra said in the statement. “[The] court ruling stops another attempt by the Trump administration to trample on women’s access to basic reproductive care.”
At press time, the Trump administration officials had responded publicly to the court orders. The administration previously said the new policies would “better balance the government’s interest in promoting coverage for contraceptive and sterilization services with the government’s interests in providing conscience protections for entities with sincerely held moral convictions.” HHS estimated that the rules would affect no more than 200 employers.
Mark Rienzi, president of the Becket Fund for Religious Liberty, a legal institute that defends religious freedoms, expressed disappointment at the court orders. Becket represents the Little Sisters of the Poor, an organization that has been fighting for several years for an exemption to the contraceptive mandate.
“Government bureaucrats should not be allowed to threaten the rights of the Little Sisters of the Poor to serve according to their Catholic beliefs,” Mr. Rienzi said in a statement. “Now the nuns are forced to keep fighting this unnecessary lawsuit to protect their ability to focus on caring for the poor. We are confident these decisions will be overturned.”
The ACA initially required all employers to cover birth control for employees with no copayments, except for group health plans of religious employers, which were deemed exempt. Those religious employers were primarily churches and other houses of worship. After a number of complaints and legal challenges, the Obama administration created a workaround for nonprofit religious employers to opt out of the mandate.
However, critics argued the process itself was a violation of their religious freedom. The issue led to the case of Zubik v. Burwell, a legal challenge over the mandate exemption that went before the U.S. Supreme Court in March 2016. The issue was never resolved. In May 2016, the Supreme Court vacated the lower court rulings related to Zubik v. Burwell and remanded the case back to the four appeals courts that had originally ruled on the issue.
The Trump administration then announced new rules aimed at broadening exemptions to the ACA’s contraceptive mandate to entities that object to services covered by the mandate on the basis of sincerely held religious beliefs. A second rule would protect nonprofit organizations and small businesses that have nonreligious moral convictions that oppose services covered by the mandate. The religious and moral exemptions would apply to institutions of education, issuers, and individuals, but not to governmental entities.
Thirteen states and the District of Columbia then sued the Trump administration over the rules as well as Pennsylvania and New Jersey in a separate case.
The nationwide ban against the rules will remain in effect while the cases continue through the court system.
Federal judges have blocked the Trump administration from weakening the Affordable Care Act’s contraceptive mandate in two separate orders that bar the President from letting more entities claim exemptions.
On Jan. 14, U.S. District Court Judge Wendy Beetlestone for the Eastern District of Pennsylvania issued a temporary nationwide ban on two rules that would have allowed an expanded group of employers and insurers to object to providing contraception coverage on either religious or moral grounds. The regulations, announced Nov. 7, 2018, were scheduled to take effect Jan. 14. The day before, U.S. District Judge Haywood Gilliam for the Northern District of California issued a similar temporary ban, but his order applied only to the 13 plaintiff states in the case, plus the District of Columbia.
While Pennsylvania and New Jersey are the only plaintiffs in the Judge Beetlestone case, she wrote that a nationwide injunction is required to protect numerous citizens from losing contraceptive coverage and resulting in “significant, direct, and proprietary harm” to states in the form of increased state-funded contraceptive services and increased costs associated with unintended pregnancies. Judge Gilliam provided similar reasoning in his Jan. 13 order, writing that the 13 plaintiff states have proven that rules promulgated by the U.S. Department of Health and Human Services would cause women to lose employer-sponsored contraceptive coverage, resulting in economic harm to the states.
California Attorney General Xavier Becerra, a plaintiff in the second case, said Judge Gilliam’s ruling will stop the Trump administration from denying millions of women and families access to co-pay birth control guaranteed by the Affordable Care Act.
“The law couldn’t be clearer – employers have no business interfering in women’s health care decisions,” Mr. Becerra said in the statement. “[The] court ruling stops another attempt by the Trump administration to trample on women’s access to basic reproductive care.”
At press time, the Trump administration officials had responded publicly to the court orders. The administration previously said the new policies would “better balance the government’s interest in promoting coverage for contraceptive and sterilization services with the government’s interests in providing conscience protections for entities with sincerely held moral convictions.” HHS estimated that the rules would affect no more than 200 employers.
Mark Rienzi, president of the Becket Fund for Religious Liberty, a legal institute that defends religious freedoms, expressed disappointment at the court orders. Becket represents the Little Sisters of the Poor, an organization that has been fighting for several years for an exemption to the contraceptive mandate.
“Government bureaucrats should not be allowed to threaten the rights of the Little Sisters of the Poor to serve according to their Catholic beliefs,” Mr. Rienzi said in a statement. “Now the nuns are forced to keep fighting this unnecessary lawsuit to protect their ability to focus on caring for the poor. We are confident these decisions will be overturned.”
The ACA initially required all employers to cover birth control for employees with no copayments, except for group health plans of religious employers, which were deemed exempt. Those religious employers were primarily churches and other houses of worship. After a number of complaints and legal challenges, the Obama administration created a workaround for nonprofit religious employers to opt out of the mandate.
However, critics argued the process itself was a violation of their religious freedom. The issue led to the case of Zubik v. Burwell, a legal challenge over the mandate exemption that went before the U.S. Supreme Court in March 2016. The issue was never resolved. In May 2016, the Supreme Court vacated the lower court rulings related to Zubik v. Burwell and remanded the case back to the four appeals courts that had originally ruled on the issue.
The Trump administration then announced new rules aimed at broadening exemptions to the ACA’s contraceptive mandate to entities that object to services covered by the mandate on the basis of sincerely held religious beliefs. A second rule would protect nonprofit organizations and small businesses that have nonreligious moral convictions that oppose services covered by the mandate. The religious and moral exemptions would apply to institutions of education, issuers, and individuals, but not to governmental entities.
Thirteen states and the District of Columbia then sued the Trump administration over the rules as well as Pennsylvania and New Jersey in a separate case.
The nationwide ban against the rules will remain in effect while the cases continue through the court system.
Federal judges have blocked the Trump administration from weakening the Affordable Care Act’s contraceptive mandate in two separate orders that bar the President from letting more entities claim exemptions.
On Jan. 14, U.S. District Court Judge Wendy Beetlestone for the Eastern District of Pennsylvania issued a temporary nationwide ban on two rules that would have allowed an expanded group of employers and insurers to object to providing contraception coverage on either religious or moral grounds. The regulations, announced Nov. 7, 2018, were scheduled to take effect Jan. 14. The day before, U.S. District Judge Haywood Gilliam for the Northern District of California issued a similar temporary ban, but his order applied only to the 13 plaintiff states in the case, plus the District of Columbia.
While Pennsylvania and New Jersey are the only plaintiffs in the Judge Beetlestone case, she wrote that a nationwide injunction is required to protect numerous citizens from losing contraceptive coverage and resulting in “significant, direct, and proprietary harm” to states in the form of increased state-funded contraceptive services and increased costs associated with unintended pregnancies. Judge Gilliam provided similar reasoning in his Jan. 13 order, writing that the 13 plaintiff states have proven that rules promulgated by the U.S. Department of Health and Human Services would cause women to lose employer-sponsored contraceptive coverage, resulting in economic harm to the states.
California Attorney General Xavier Becerra, a plaintiff in the second case, said Judge Gilliam’s ruling will stop the Trump administration from denying millions of women and families access to co-pay birth control guaranteed by the Affordable Care Act.
“The law couldn’t be clearer – employers have no business interfering in women’s health care decisions,” Mr. Becerra said in the statement. “[The] court ruling stops another attempt by the Trump administration to trample on women’s access to basic reproductive care.”
At press time, the Trump administration officials had responded publicly to the court orders. The administration previously said the new policies would “better balance the government’s interest in promoting coverage for contraceptive and sterilization services with the government’s interests in providing conscience protections for entities with sincerely held moral convictions.” HHS estimated that the rules would affect no more than 200 employers.
Mark Rienzi, president of the Becket Fund for Religious Liberty, a legal institute that defends religious freedoms, expressed disappointment at the court orders. Becket represents the Little Sisters of the Poor, an organization that has been fighting for several years for an exemption to the contraceptive mandate.
“Government bureaucrats should not be allowed to threaten the rights of the Little Sisters of the Poor to serve according to their Catholic beliefs,” Mr. Rienzi said in a statement. “Now the nuns are forced to keep fighting this unnecessary lawsuit to protect their ability to focus on caring for the poor. We are confident these decisions will be overturned.”
The ACA initially required all employers to cover birth control for employees with no copayments, except for group health plans of religious employers, which were deemed exempt. Those religious employers were primarily churches and other houses of worship. After a number of complaints and legal challenges, the Obama administration created a workaround for nonprofit religious employers to opt out of the mandate.
However, critics argued the process itself was a violation of their religious freedom. The issue led to the case of Zubik v. Burwell, a legal challenge over the mandate exemption that went before the U.S. Supreme Court in March 2016. The issue was never resolved. In May 2016, the Supreme Court vacated the lower court rulings related to Zubik v. Burwell and remanded the case back to the four appeals courts that had originally ruled on the issue.
The Trump administration then announced new rules aimed at broadening exemptions to the ACA’s contraceptive mandate to entities that object to services covered by the mandate on the basis of sincerely held religious beliefs. A second rule would protect nonprofit organizations and small businesses that have nonreligious moral convictions that oppose services covered by the mandate. The religious and moral exemptions would apply to institutions of education, issuers, and individuals, but not to governmental entities.
Thirteen states and the District of Columbia then sued the Trump administration over the rules as well as Pennsylvania and New Jersey in a separate case.
The nationwide ban against the rules will remain in effect while the cases continue through the court system.
New or existing drugs? Both fuel price inflation
Inflation in existing drugs’ prices and the debut of new drugs are both contributing to the overall rising costs of pharmaceuticals.

.
For oral and injectable specialty drugs, costs increased 20.6% and 12.5%, respectively, with 71.1% and 52.4% attributable to new drugs. Costs of oral and injectable generic drugs grew by 4.4% and 7.3%, also driven by entrants into the market.
Researchers looked at monthly wholesale acquisition costs of 24,877 National Drug Codes for oral drugs and 3,049 injectable drugs from 2005 to 2016. They compared them with pharmacy claims from the UPMC Health Plan, which offers insurance products to more than 3.2 million members across the spectrum of private and public arenas.
“Our analyses yielded three main findings,” explained Inmaculada Hernandez, PharmD, PhD, University of Pittsburgh, and her colleagues in a report published in the January 2019 issue of Health Affairs.
“First, costs increased considerably faster than inflation across all drug classes, and increases were highest for oral specialty drugs and lowest for oral generics,” Dr. Hernandez and her colleagues wrote.
“Second, rising costs of brand-name drugs were driven by inflation in the prices of widely used existing drugs,” they added. A combination of new products and price inflation in existing drugs drove the rising costs of specialty drugs, with new drugs accounting for a larger share of the price increases.
Third, “existing generics tended to decrease the average cost of generic drugs,” Dr. Hernandez noted. However, new generic products cost more than those already on the market, which fueled the annual increases in average costs.
The authors noted that their estimates demonstrate the role of inflation on pharmaceutical cost increases and support policy efforts to control that inflation.
“In the current value-based landscape, increasing drug costs attributable to new products can sometimes be justified on the basis of improved outcomes,” Dr. Hernandez and colleagues stated. “However, rising costs due to inflation do not reflect improved value for patients.”
The researchers noted that the data are limited by the lack of rebate information, which is generally proprietary. Thus, “the contribution of existing drugs may have been lower than we estimated,” they noted. In addition, “because the magnitude of rebates has increased in the past decade, our findings likely overestimated cost increases for brand-name drugs.” The researchers also didn’t examine the effect of drugs transitioning from brand to generic offerings.
The authors provided no disclosures.
SOURCE: Hernandez I et al. Health Aff (Millwood). 2019 Jan 2019. doi: 10.1377/hlthaff.2018.05147.
Inflation in existing drugs’ prices and the debut of new drugs are both contributing to the overall rising costs of pharmaceuticals.
.
For oral and injectable specialty drugs, costs increased 20.6% and 12.5%, respectively, with 71.1% and 52.4% attributable to new drugs. Costs of oral and injectable generic drugs grew by 4.4% and 7.3%, also driven by entrants into the market.
Researchers looked at monthly wholesale acquisition costs of 24,877 National Drug Codes for oral drugs and 3,049 injectable drugs from 2005 to 2016. They compared them with pharmacy claims from the UPMC Health Plan, which offers insurance products to more than 3.2 million members across the spectrum of private and public arenas.
“Our analyses yielded three main findings,” explained Inmaculada Hernandez, PharmD, PhD, University of Pittsburgh, and her colleagues in a report published in the January 2019 issue of Health Affairs.
“First, costs increased considerably faster than inflation across all drug classes, and increases were highest for oral specialty drugs and lowest for oral generics,” Dr. Hernandez and her colleagues wrote.
“Second, rising costs of brand-name drugs were driven by inflation in the prices of widely used existing drugs,” they added. A combination of new products and price inflation in existing drugs drove the rising costs of specialty drugs, with new drugs accounting for a larger share of the price increases.
Third, “existing generics tended to decrease the average cost of generic drugs,” Dr. Hernandez noted. However, new generic products cost more than those already on the market, which fueled the annual increases in average costs.
The authors noted that their estimates demonstrate the role of inflation on pharmaceutical cost increases and support policy efforts to control that inflation.
“In the current value-based landscape, increasing drug costs attributable to new products can sometimes be justified on the basis of improved outcomes,” Dr. Hernandez and colleagues stated. “However, rising costs due to inflation do not reflect improved value for patients.”
The researchers noted that the data are limited by the lack of rebate information, which is generally proprietary. Thus, “the contribution of existing drugs may have been lower than we estimated,” they noted. In addition, “because the magnitude of rebates has increased in the past decade, our findings likely overestimated cost increases for brand-name drugs.” The researchers also didn’t examine the effect of drugs transitioning from brand to generic offerings.
The authors provided no disclosures.
SOURCE: Hernandez I et al. Health Aff (Millwood). 2019 Jan 2019. doi: 10.1377/hlthaff.2018.05147.
Inflation in existing drugs’ prices and the debut of new drugs are both contributing to the overall rising costs of pharmaceuticals.
.
For oral and injectable specialty drugs, costs increased 20.6% and 12.5%, respectively, with 71.1% and 52.4% attributable to new drugs. Costs of oral and injectable generic drugs grew by 4.4% and 7.3%, also driven by entrants into the market.
Researchers looked at monthly wholesale acquisition costs of 24,877 National Drug Codes for oral drugs and 3,049 injectable drugs from 2005 to 2016. They compared them with pharmacy claims from the UPMC Health Plan, which offers insurance products to more than 3.2 million members across the spectrum of private and public arenas.
“Our analyses yielded three main findings,” explained Inmaculada Hernandez, PharmD, PhD, University of Pittsburgh, and her colleagues in a report published in the January 2019 issue of Health Affairs.
“First, costs increased considerably faster than inflation across all drug classes, and increases were highest for oral specialty drugs and lowest for oral generics,” Dr. Hernandez and her colleagues wrote.
“Second, rising costs of brand-name drugs were driven by inflation in the prices of widely used existing drugs,” they added. A combination of new products and price inflation in existing drugs drove the rising costs of specialty drugs, with new drugs accounting for a larger share of the price increases.
Third, “existing generics tended to decrease the average cost of generic drugs,” Dr. Hernandez noted. However, new generic products cost more than those already on the market, which fueled the annual increases in average costs.
The authors noted that their estimates demonstrate the role of inflation on pharmaceutical cost increases and support policy efforts to control that inflation.
“In the current value-based landscape, increasing drug costs attributable to new products can sometimes be justified on the basis of improved outcomes,” Dr. Hernandez and colleagues stated. “However, rising costs due to inflation do not reflect improved value for patients.”
The researchers noted that the data are limited by the lack of rebate information, which is generally proprietary. Thus, “the contribution of existing drugs may have been lower than we estimated,” they noted. In addition, “because the magnitude of rebates has increased in the past decade, our findings likely overestimated cost increases for brand-name drugs.” The researchers also didn’t examine the effect of drugs transitioning from brand to generic offerings.
The authors provided no disclosures.
SOURCE: Hernandez I et al. Health Aff (Millwood). 2019 Jan 2019. doi: 10.1377/hlthaff.2018.05147.
FROM HEALTH AFFAIRS
Key clinical point: Price inflation in existing drugs and new product introductions are driving increases in pharmaceutical costs.
Major finding: 71% of oral specialty drug price increases during 2005-2019 are attributable to new products.
Study details: Researchers analyzed the wholesale acquisition prices of 24,877 oral drugs and 3,049 injectable drugs and compared them with pharmacy claims across all public and private insurance products offered by the UPMC Health Plan.
Disclosures: The authors provided no disclosures.
Source: Hernandez I et al. Health Aff (Millwood). 2019 Jan. doi: 10.1377/hlthaff.2018.05147.