User login
Class-action suit filed against ABIM over MOC
A group of internists is suing the American Board of Internal Medicine over its maintenance of certification (MOC) process, alleging that the board is monopolizing the MOC market.

The lawsuit, filed Dec. 6 in Pennsylvania district court, claims that ABIM is charging inflated monopoly prices for maintaining certification, that the organization is forcing physicians to purchase MOC, and that ABIM is inducing employers and others to require ABIM certification. The four plaintiff-physicians are asking a judge to find ABIM in violation of federal antitrust law and to bar the board from continuing its MOC process. The suit is filed as a class action on behalf of all internists and subspecialists required by ABIM to purchase MOC to maintain their ABIM certifications. The plaintiffs seek damages and injunctive relief, plus lawsuit and attorney costs arising from ABIM’s alleged antitrust violations.
In a statement, ABIM expressed disappointment at the lawsuit and said the organization will vigorously defend itself, adding that doing so will “consume resources far better dedicated to continuous improvement of its programs.”
ABIM declined to answer questions addressing specific accusations from the lawsuit. However, in an interview, ABIM President Richard Baron, MD, said that “ABIM board-certified physicians have taken the initiative to distinguish themselves. This is a credential that physicians earn. We offer certified physicians the opportunity to demonstrate to the medical community, their peers, and the public that they are current and have special expertise.”
ABIM has not yet filed a formal response to the lawsuit, which was due by Jan. 6. Court documents show that in January, ABIM entered the appearances of four attorneys that will represent the board in the case. From there, discovery and evidence gathering in the case will begin.
Katherine Murray Leisure, MD, an infectious disease specialist based in Plymouth, Mass., is one of the plaintiffs. While she said that she could not comment specifically on the lawsuit, she has written publicly about her ABIM concerns in the past.
In a 2015 letter to Dr. Baron and posted on an anti-MOC website, Dr. Murray outlined a litany of complaints against ABIM’s MOC process and called on the U.S. Congress to investigate ABIM’s financial, legal, and ethical conduct.
“[The American Board of Medical Specialties] and ABIM collected more than $10,000 in fees and lost practice hours every decade from each [diplomate] doing MOC,” Dr. Murray Leisure wrote. “MOC took weeks away from our offices, clinics, patients, families, specialty societies, and individual research. ABMS MOC removed hundreds, perhaps thousands … of America’s best, once board-certified physicians from full hospital careers and earnings whenever [diplomates] did not complete these high-stakes MOC programs. … The righteous and fast solution to such moral, ethical, scientific, and constitutional problems is to end MOC now.”
Plaintiffs Glen Dela Cruz Manalo, MD; Alexa Joshua, MD; and Gerard Kenney, MD, did not return messages seeking comment. When contacted, attorneys for the plaintiffs declined to comment.
The doctors’ 32-page lawsuit characterizes ABIM as an organization motivated by money that has made its MOC process increasingly more burdensome for physicians over the years without evidence that MOC has any beneficial impact on doctors, patients, or the public. Complying with ABIM’s MOC costs internists an average of $23,607 in financial cost and time lost over 10 years, and costs up to $40,495 for some specialists, according to the suit.
The physicians allege that ABIM controls in excess of 95% of the market for MOC of internists, in violation of federal antitrust laws, and that the organization has unlawfully obtained and maintained monopoly power for MOC services.
The board’s illegal tying of its initial certification to its MOC results in burdensome conditions, including “raising the cost of the practice of medicine, constraining the supply of internists thereby harming competition, decreasing the supply of certified internists, and increasing the cost of medical services to patients and consumers,” the suit claims.
The legal challenge details how MOC has personally and professionally impacted each of the four plaintiffs. Dr. Manalo, a gastroenterologist, lost his privileges at St. Vincent Healthcare in Billings, Mont., and was subsequently terminated after he declined to maintain his ABIM certification as a gastroenterologist. In a letter to ABIM, Dr. Manalo wrote that it was “unfair and outright discriminatory that practitioners certified on or after 1990 are the only ones required to certify,” according to the lawsuit. Dr. Manalo later took a position as staff gastroenterologist at Jonathan M. Wainwright Memorial Veterans Affairs Medical Center in Walla Walla, Wash., at a substantially reduced salary. He became unemployed in 2017.
Dr. Murray Leisure obtained an initial and lifelong board certification in internal medicine from ABIM in 1984 and an infectious disease certification in 1990. ABlM terminated Dr. Murray’s infectious diseases certification after she failed her MOC examination in 2009, which led to lost privileges at Jordan Hospital in Plymouth, Mass. The loss caused significant damage to Dr. Murray, including lost income, a tarnished reputation, and the lost opportunity to help patients, according to the lawsuit. Jordan Hospital restored her privileges after Dr. Murray passed her MOC examination in 2012.
Dr. Kenney lost a job opportunity with Mount Nittany Physicians Group in State College, Pa., after he declined to renew his ABIM certification in gastroenterology. He is currently a physician with the University of Pittsburgh Medical Center in Seneca, Pa.
That the ABIM website lists him as “not certified,” is misleading, and makes it appear that his initial certifications were revoked due to failure to pass a MOC examination or misconduct, rather than because the certifications lapsed, according to the suit. The description makes Dr. Kenney appear less qualified to patients, hospitals, insurance companies, medical corporations, other employers, and others, he claims.
Dr. Joshua could not renew her consulting and admitting privileges at Detroit Medical Center after she failed an MOC examination in 2014 and became uncertified in internal medicine, according to the suit. In addition, Blue Cross Blue Shield informed Dr. Joshua it would no longer cover her because it required ABIM certification for coverage. She unsuccessfully appealed based on her certification with the National Board of Physicians and Surgeons. As a result of her certification termination, Dr. Joshua can only practice outpatient medicine at Detroit Medical Center.
In an interview, Dr. Baron emphasized the number of modifications made to its MOC process in recent years after responding to physician concerns. This includes an overhaul of the organization’s governance structure to include more than 200 practicing physicians and opening new avenues for physicians to engage in the creation of assessment content that more closely reflects what they see in practice, he said. In addition, ABIM now surveys all specialists to contribute to the exam blueprint review and the creation of the new Item Writing Task Force.

“We take all suggestions from physicians seriously, and have used it to launch many new initiatives including: the Knowledge Check-In, a new Physician Portal, partnerships to give physicians dual credit for CME and MOC, and exploration of alternative assessment models with medical societies,” he said.
Dr. Baron acknowledged past criticism of the MOC process, but said he is proud of the work ABIM has done to address physician concerns about the choice, relevance, and convenience of its MOC program.
*This story was updated on Feb. 6, 2019.
A group of internists is suing the American Board of Internal Medicine over its maintenance of certification (MOC) process, alleging that the board is monopolizing the MOC market.
The lawsuit, filed Dec. 6 in Pennsylvania district court, claims that ABIM is charging inflated monopoly prices for maintaining certification, that the organization is forcing physicians to purchase MOC, and that ABIM is inducing employers and others to require ABIM certification. The four plaintiff-physicians are asking a judge to find ABIM in violation of federal antitrust law and to bar the board from continuing its MOC process. The suit is filed as a class action on behalf of all internists and subspecialists required by ABIM to purchase MOC to maintain their ABIM certifications. The plaintiffs seek damages and injunctive relief, plus lawsuit and attorney costs arising from ABIM’s alleged antitrust violations.
In a statement, ABIM expressed disappointment at the lawsuit and said the organization will vigorously defend itself, adding that doing so will “consume resources far better dedicated to continuous improvement of its programs.”
ABIM declined to answer questions addressing specific accusations from the lawsuit. However, in an interview, ABIM President Richard Baron, MD, said that “ABIM board-certified physicians have taken the initiative to distinguish themselves. This is a credential that physicians earn. We offer certified physicians the opportunity to demonstrate to the medical community, their peers, and the public that they are current and have special expertise.”
ABIM has not yet filed a formal response to the lawsuit, which was due by Jan. 6. Court documents show that in January, ABIM entered the appearances of four attorneys that will represent the board in the case. From there, discovery and evidence gathering in the case will begin.
Katherine Murray Leisure, MD, an infectious disease specialist based in Plymouth, Mass., is one of the plaintiffs. While she said that she could not comment specifically on the lawsuit, she has written publicly about her ABIM concerns in the past.
In a 2015 letter to Dr. Baron and posted on an anti-MOC website, Dr. Murray outlined a litany of complaints against ABIM’s MOC process and called on the U.S. Congress to investigate ABIM’s financial, legal, and ethical conduct.
“[The American Board of Medical Specialties] and ABIM collected more than $10,000 in fees and lost practice hours every decade from each [diplomate] doing MOC,” Dr. Murray Leisure wrote. “MOC took weeks away from our offices, clinics, patients, families, specialty societies, and individual research. ABMS MOC removed hundreds, perhaps thousands … of America’s best, once board-certified physicians from full hospital careers and earnings whenever [diplomates] did not complete these high-stakes MOC programs. … The righteous and fast solution to such moral, ethical, scientific, and constitutional problems is to end MOC now.”
Plaintiffs Glen Dela Cruz Manalo, MD; Alexa Joshua, MD; and Gerard Kenney, MD, did not return messages seeking comment. When contacted, attorneys for the plaintiffs declined to comment.
The doctors’ 32-page lawsuit characterizes ABIM as an organization motivated by money that has made its MOC process increasingly more burdensome for physicians over the years without evidence that MOC has any beneficial impact on doctors, patients, or the public. Complying with ABIM’s MOC costs internists an average of $23,607 in financial cost and time lost over 10 years, and costs up to $40,495 for some specialists, according to the suit.
The physicians allege that ABIM controls in excess of 95% of the market for MOC of internists, in violation of federal antitrust laws, and that the organization has unlawfully obtained and maintained monopoly power for MOC services.
The board’s illegal tying of its initial certification to its MOC results in burdensome conditions, including “raising the cost of the practice of medicine, constraining the supply of internists thereby harming competition, decreasing the supply of certified internists, and increasing the cost of medical services to patients and consumers,” the suit claims.
The legal challenge details how MOC has personally and professionally impacted each of the four plaintiffs. Dr. Manalo, a gastroenterologist, lost his privileges at St. Vincent Healthcare in Billings, Mont., and was subsequently terminated after he declined to maintain his ABIM certification as a gastroenterologist. In a letter to ABIM, Dr. Manalo wrote that it was “unfair and outright discriminatory that practitioners certified on or after 1990 are the only ones required to certify,” according to the lawsuit. Dr. Manalo later took a position as staff gastroenterologist at Jonathan M. Wainwright Memorial Veterans Affairs Medical Center in Walla Walla, Wash., at a substantially reduced salary. He became unemployed in 2017.
Dr. Murray Leisure obtained an initial and lifelong board certification in internal medicine from ABIM in 1984 and an infectious disease certification in 1990. ABlM terminated Dr. Murray’s infectious diseases certification after she failed her MOC examination in 2009, which led to lost privileges at Jordan Hospital in Plymouth, Mass. The loss caused significant damage to Dr. Murray, including lost income, a tarnished reputation, and the lost opportunity to help patients, according to the lawsuit. Jordan Hospital restored her privileges after Dr. Murray passed her MOC examination in 2012.
Dr. Kenney lost a job opportunity with Mount Nittany Physicians Group in State College, Pa., after he declined to renew his ABIM certification in gastroenterology. He is currently a physician with the University of Pittsburgh Medical Center in Seneca, Pa.
That the ABIM website lists him as “not certified,” is misleading, and makes it appear that his initial certifications were revoked due to failure to pass a MOC examination or misconduct, rather than because the certifications lapsed, according to the suit. The description makes Dr. Kenney appear less qualified to patients, hospitals, insurance companies, medical corporations, other employers, and others, he claims.
Dr. Joshua could not renew her consulting and admitting privileges at Detroit Medical Center after she failed an MOC examination in 2014 and became uncertified in internal medicine, according to the suit. In addition, Blue Cross Blue Shield informed Dr. Joshua it would no longer cover her because it required ABIM certification for coverage. She unsuccessfully appealed based on her certification with the National Board of Physicians and Surgeons. As a result of her certification termination, Dr. Joshua can only practice outpatient medicine at Detroit Medical Center.
In an interview, Dr. Baron emphasized the number of modifications made to its MOC process in recent years after responding to physician concerns. This includes an overhaul of the organization’s governance structure to include more than 200 practicing physicians and opening new avenues for physicians to engage in the creation of assessment content that more closely reflects what they see in practice, he said. In addition, ABIM now surveys all specialists to contribute to the exam blueprint review and the creation of the new Item Writing Task Force.
“We take all suggestions from physicians seriously, and have used it to launch many new initiatives including: the Knowledge Check-In, a new Physician Portal, partnerships to give physicians dual credit for CME and MOC, and exploration of alternative assessment models with medical societies,” he said.
Dr. Baron acknowledged past criticism of the MOC process, but said he is proud of the work ABIM has done to address physician concerns about the choice, relevance, and convenience of its MOC program.
*This story was updated on Feb. 6, 2019.
A group of internists is suing the American Board of Internal Medicine over its maintenance of certification (MOC) process, alleging that the board is monopolizing the MOC market.
The lawsuit, filed Dec. 6 in Pennsylvania district court, claims that ABIM is charging inflated monopoly prices for maintaining certification, that the organization is forcing physicians to purchase MOC, and that ABIM is inducing employers and others to require ABIM certification. The four plaintiff-physicians are asking a judge to find ABIM in violation of federal antitrust law and to bar the board from continuing its MOC process. The suit is filed as a class action on behalf of all internists and subspecialists required by ABIM to purchase MOC to maintain their ABIM certifications. The plaintiffs seek damages and injunctive relief, plus lawsuit and attorney costs arising from ABIM’s alleged antitrust violations.
In a statement, ABIM expressed disappointment at the lawsuit and said the organization will vigorously defend itself, adding that doing so will “consume resources far better dedicated to continuous improvement of its programs.”
ABIM declined to answer questions addressing specific accusations from the lawsuit. However, in an interview, ABIM President Richard Baron, MD, said that “ABIM board-certified physicians have taken the initiative to distinguish themselves. This is a credential that physicians earn. We offer certified physicians the opportunity to demonstrate to the medical community, their peers, and the public that they are current and have special expertise.”
ABIM has not yet filed a formal response to the lawsuit, which was due by Jan. 6. Court documents show that in January, ABIM entered the appearances of four attorneys that will represent the board in the case. From there, discovery and evidence gathering in the case will begin.
Katherine Murray Leisure, MD, an infectious disease specialist based in Plymouth, Mass., is one of the plaintiffs. While she said that she could not comment specifically on the lawsuit, she has written publicly about her ABIM concerns in the past.
In a 2015 letter to Dr. Baron and posted on an anti-MOC website, Dr. Murray outlined a litany of complaints against ABIM’s MOC process and called on the U.S. Congress to investigate ABIM’s financial, legal, and ethical conduct.
“[The American Board of Medical Specialties] and ABIM collected more than $10,000 in fees and lost practice hours every decade from each [diplomate] doing MOC,” Dr. Murray Leisure wrote. “MOC took weeks away from our offices, clinics, patients, families, specialty societies, and individual research. ABMS MOC removed hundreds, perhaps thousands … of America’s best, once board-certified physicians from full hospital careers and earnings whenever [diplomates] did not complete these high-stakes MOC programs. … The righteous and fast solution to such moral, ethical, scientific, and constitutional problems is to end MOC now.”
Plaintiffs Glen Dela Cruz Manalo, MD; Alexa Joshua, MD; and Gerard Kenney, MD, did not return messages seeking comment. When contacted, attorneys for the plaintiffs declined to comment.
The doctors’ 32-page lawsuit characterizes ABIM as an organization motivated by money that has made its MOC process increasingly more burdensome for physicians over the years without evidence that MOC has any beneficial impact on doctors, patients, or the public. Complying with ABIM’s MOC costs internists an average of $23,607 in financial cost and time lost over 10 years, and costs up to $40,495 for some specialists, according to the suit.
The physicians allege that ABIM controls in excess of 95% of the market for MOC of internists, in violation of federal antitrust laws, and that the organization has unlawfully obtained and maintained monopoly power for MOC services.
The board’s illegal tying of its initial certification to its MOC results in burdensome conditions, including “raising the cost of the practice of medicine, constraining the supply of internists thereby harming competition, decreasing the supply of certified internists, and increasing the cost of medical services to patients and consumers,” the suit claims.
The legal challenge details how MOC has personally and professionally impacted each of the four plaintiffs. Dr. Manalo, a gastroenterologist, lost his privileges at St. Vincent Healthcare in Billings, Mont., and was subsequently terminated after he declined to maintain his ABIM certification as a gastroenterologist. In a letter to ABIM, Dr. Manalo wrote that it was “unfair and outright discriminatory that practitioners certified on or after 1990 are the only ones required to certify,” according to the lawsuit. Dr. Manalo later took a position as staff gastroenterologist at Jonathan M. Wainwright Memorial Veterans Affairs Medical Center in Walla Walla, Wash., at a substantially reduced salary. He became unemployed in 2017.
Dr. Murray Leisure obtained an initial and lifelong board certification in internal medicine from ABIM in 1984 and an infectious disease certification in 1990. ABlM terminated Dr. Murray’s infectious diseases certification after she failed her MOC examination in 2009, which led to lost privileges at Jordan Hospital in Plymouth, Mass. The loss caused significant damage to Dr. Murray, including lost income, a tarnished reputation, and the lost opportunity to help patients, according to the lawsuit. Jordan Hospital restored her privileges after Dr. Murray passed her MOC examination in 2012.
Dr. Kenney lost a job opportunity with Mount Nittany Physicians Group in State College, Pa., after he declined to renew his ABIM certification in gastroenterology. He is currently a physician with the University of Pittsburgh Medical Center in Seneca, Pa.
That the ABIM website lists him as “not certified,” is misleading, and makes it appear that his initial certifications were revoked due to failure to pass a MOC examination or misconduct, rather than because the certifications lapsed, according to the suit. The description makes Dr. Kenney appear less qualified to patients, hospitals, insurance companies, medical corporations, other employers, and others, he claims.
Dr. Joshua could not renew her consulting and admitting privileges at Detroit Medical Center after she failed an MOC examination in 2014 and became uncertified in internal medicine, according to the suit. In addition, Blue Cross Blue Shield informed Dr. Joshua it would no longer cover her because it required ABIM certification for coverage. She unsuccessfully appealed based on her certification with the National Board of Physicians and Surgeons. As a result of her certification termination, Dr. Joshua can only practice outpatient medicine at Detroit Medical Center.
In an interview, Dr. Baron emphasized the number of modifications made to its MOC process in recent years after responding to physician concerns. This includes an overhaul of the organization’s governance structure to include more than 200 practicing physicians and opening new avenues for physicians to engage in the creation of assessment content that more closely reflects what they see in practice, he said. In addition, ABIM now surveys all specialists to contribute to the exam blueprint review and the creation of the new Item Writing Task Force.
“We take all suggestions from physicians seriously, and have used it to launch many new initiatives including: the Knowledge Check-In, a new Physician Portal, partnerships to give physicians dual credit for CME and MOC, and exploration of alternative assessment models with medical societies,” he said.
Dr. Baron acknowledged past criticism of the MOC process, but said he is proud of the work ABIM has done to address physician concerns about the choice, relevance, and convenience of its MOC program.
*This story was updated on Feb. 6, 2019.

Time for single payer? ColdironCare
At a New Year’s Eve party a few years back, I noticed a man sitting nearby clutching his left upper arm. He was ashen and obviously uncomfortable. Acute coronary insufficiency, I thought, and I asked him if I could call the life squad for him. “Oh no,” he said, “I have these spells several times a day, the nitro will kick in after a minute, and this will ease off.” I listened as he explained he had a “widow maker,” a 90% plus left main occlusion, but “I am Canadian, and my government is going to pay for my bypass,” he said. “I just have to wait 6 more weeks.” The irony? He was the son of our host, and we were sitting in his mothers’ multimillion dollar home in the Florida Keys. He could be in a Miami hospital’s operating room in an hour or 2.
Wow. Click. Got it.

Fast forward to a lobbying discussion on Capitol Hill: A sympathetic U.S. senator tossed me this softball: ‘What do you think about Medicare reimbursement?” I expect he thought I was going to complain about how bad Medicare is, about its failure to keep current with inflation (currently about 30% behind), and the obtuse quality metrics it now requires. Instead, I found myself saying, “Medicare is my most reliable payer, paying on time – in 2 weeks for clean claims – and the private insurers have beaten me up badly. Medicare is one of my best payers.”
Wrong answer, but true statement.
There is much talk these days about , particularly considering all the barriers to care. (See my recent column, “Produce and Promises.”) Physicians and patients endure a mutual misery inflicted by private insurance companies.
What to do about health care in America?
First, let’s deal with the extraordinary costs of health care in the United States – 19% of our gross domestic product. About 3%-4 % of this figure is an accounting gimmick, since it includes nursing home care, which is considered “domiciliary” care rather than health care in Europe. In addition, drug costs are higher in the U.S., largely to cover the development of new drugs that cost less in the rest of the world. Wait lists are largely unheard of in the United States, and if you have such ready capacity, that means you incur the costs of idle capacity. Also, rarely is a new miracle drug flatly denied for coverage in the United States. If you persist, you will usually get your drug.
We are a commodity-driven society, and that is the real reason that health care costs so much in this country. Hence, we come to the real debate, the “R” word. How do we ration access to care? (See my 2017 column, “Why the Affordable Care Act will be Greatly Modified.”)
There are a plethora of proposals to fund single payer out there, none of which address rationing. And while single payer affords free universal coverage, it does not assure better care. As health economist Devon Herrick, Ph.D., wrote in his health care blog in 2016: “A single payer is not some magical entity that rains down savings from Heaven by being unconcerned about profit. Rather, an efficient single payer operates more like a predatory HMO with no competition. It is currently in vogue for hipsters to matter-of-factly announce the simple solution to health reform is single payer. Be careful what you wish for; you may end up with Medicaid for All.”
In fact, if you try to ferret out how physician income will be affected by universal health care, there would be an estimated pay cut of 11%-40%, depending on how the numbers are manipulated.
Some single-payer proposals use the term “exchange rates,” which for the uninformed means Medicaid rates. In addition, payment is usually given to the local hospital system, or “authority” to dole out. I have a very bad feeling that any small practitioner in an office-based practice would be severely shortchanged in such a system. In fact, if you cut pay for office-based physicians at all, you may begin to see them disappear.
Policy wonks argue for pay cuts for American physicians because European physicians “make less money.” Those numbers are all wrong. U.S. physicians are paid for their work, and for their practice expense. That is, how much it costs to provide the service in their office, which is around 40%-50% of published income. In Europe, almost all procedures are performed in the hospital setting, and the hospital absorbs the practice expense, which is ignored in this current health care reform debate. (See my 2015 column, “Doctor, Why DO you get paid so much?”)
The big selling point of single payer for physicians is that they might have less paperwork and get paid more for seeing Medicaid patients. Yet the paperwork will persist to avoid lawsuits, electronic medical records are now ingrained into the system, and most Medicaid patients are currently seen in the federal or hospital outpatient clinic where higher rates or other subsidies are available. The comically low Medicaid rates paid to physician offices are largely evaded or not even filed for.
Single-payer advocates are basically saying, “Yes, you will be seeing patients at a loss but you will make it up in volume.” This ignores the reality that most physicians don’t need or want more volume.
Here is my plan for single-payer health care. Call it ColdironCare.
- Set payment rates for physicians at 130% of current Medicare, about where we were 30 years ago, considering inflation. Tie the reimbursement rate to the cost of living index, same as social security. If you cut physician pay 11%-40%, you will see mass retirement and the elimination of the most efficient care, office-based practice.
- Remove the practice expense payment from government-reported physician income since this is overhead spent to provide the care.
- Let all physicians participate, and don’t pay site-of-service differentials.
- Enact national tort reform, which would decrease the paperwork, overhead, and much useless defensive medicine.
- Press the generic drug manufacturers (but not the innovators) regarding drug costs. Bite the bullet, and set national coverage standards (ration care) to be revisited every 5 years, which will eliminate step therapy and prior authorizations. Allow individuals to pay out of pocket for additional treatments they want, including that questionable additional 90 days of life they may get from the $250,000 drug for the off-label indication.
- Press the hospitals, and don’t complain when many of them close, especially rural ones.
- Allow individuals, hospitals, and physicians to contract outside of the government plan (in contrast to Canada).
- Downsize the health insurance companies, and have them sell private supplemental insurance to whomever wants it.
Finally, make all of this a constitutional amendment. If not put out of reach, in 15 years we will have the same system we have today. The politicians simply will not be able to resist degrading (reforming, improving, refunding, defunding) the original plan. Or, you could simply increase Medicaid rates to Medicare rates and call it a day.
Oh, by the way, I saw that man from the New Year’s Eve party at the airport the following Christmas. He survived to get his government bypass and is doing well.
The health care system we have is miserable, except compared with all the others.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
At a New Year’s Eve party a few years back, I noticed a man sitting nearby clutching his left upper arm. He was ashen and obviously uncomfortable. Acute coronary insufficiency, I thought, and I asked him if I could call the life squad for him. “Oh no,” he said, “I have these spells several times a day, the nitro will kick in after a minute, and this will ease off.” I listened as he explained he had a “widow maker,” a 90% plus left main occlusion, but “I am Canadian, and my government is going to pay for my bypass,” he said. “I just have to wait 6 more weeks.” The irony? He was the son of our host, and we were sitting in his mothers’ multimillion dollar home in the Florida Keys. He could be in a Miami hospital’s operating room in an hour or 2.
Wow. Click. Got it.
Fast forward to a lobbying discussion on Capitol Hill: A sympathetic U.S. senator tossed me this softball: ‘What do you think about Medicare reimbursement?” I expect he thought I was going to complain about how bad Medicare is, about its failure to keep current with inflation (currently about 30% behind), and the obtuse quality metrics it now requires. Instead, I found myself saying, “Medicare is my most reliable payer, paying on time – in 2 weeks for clean claims – and the private insurers have beaten me up badly. Medicare is one of my best payers.”
Wrong answer, but true statement.
There is much talk these days about , particularly considering all the barriers to care. (See my recent column, “Produce and Promises.”) Physicians and patients endure a mutual misery inflicted by private insurance companies.
What to do about health care in America?
First, let’s deal with the extraordinary costs of health care in the United States – 19% of our gross domestic product. About 3%-4 % of this figure is an accounting gimmick, since it includes nursing home care, which is considered “domiciliary” care rather than health care in Europe. In addition, drug costs are higher in the U.S., largely to cover the development of new drugs that cost less in the rest of the world. Wait lists are largely unheard of in the United States, and if you have such ready capacity, that means you incur the costs of idle capacity. Also, rarely is a new miracle drug flatly denied for coverage in the United States. If you persist, you will usually get your drug.
We are a commodity-driven society, and that is the real reason that health care costs so much in this country. Hence, we come to the real debate, the “R” word. How do we ration access to care? (See my 2017 column, “Why the Affordable Care Act will be Greatly Modified.”)
There are a plethora of proposals to fund single payer out there, none of which address rationing. And while single payer affords free universal coverage, it does not assure better care. As health economist Devon Herrick, Ph.D., wrote in his health care blog in 2016: “A single payer is not some magical entity that rains down savings from Heaven by being unconcerned about profit. Rather, an efficient single payer operates more like a predatory HMO with no competition. It is currently in vogue for hipsters to matter-of-factly announce the simple solution to health reform is single payer. Be careful what you wish for; you may end up with Medicaid for All.”
In fact, if you try to ferret out how physician income will be affected by universal health care, there would be an estimated pay cut of 11%-40%, depending on how the numbers are manipulated.
Some single-payer proposals use the term “exchange rates,” which for the uninformed means Medicaid rates. In addition, payment is usually given to the local hospital system, or “authority” to dole out. I have a very bad feeling that any small practitioner in an office-based practice would be severely shortchanged in such a system. In fact, if you cut pay for office-based physicians at all, you may begin to see them disappear.
Policy wonks argue for pay cuts for American physicians because European physicians “make less money.” Those numbers are all wrong. U.S. physicians are paid for their work, and for their practice expense. That is, how much it costs to provide the service in their office, which is around 40%-50% of published income. In Europe, almost all procedures are performed in the hospital setting, and the hospital absorbs the practice expense, which is ignored in this current health care reform debate. (See my 2015 column, “Doctor, Why DO you get paid so much?”)
The big selling point of single payer for physicians is that they might have less paperwork and get paid more for seeing Medicaid patients. Yet the paperwork will persist to avoid lawsuits, electronic medical records are now ingrained into the system, and most Medicaid patients are currently seen in the federal or hospital outpatient clinic where higher rates or other subsidies are available. The comically low Medicaid rates paid to physician offices are largely evaded or not even filed for.
Single-payer advocates are basically saying, “Yes, you will be seeing patients at a loss but you will make it up in volume.” This ignores the reality that most physicians don’t need or want more volume.
Here is my plan for single-payer health care. Call it ColdironCare.
- Set payment rates for physicians at 130% of current Medicare, about where we were 30 years ago, considering inflation. Tie the reimbursement rate to the cost of living index, same as social security. If you cut physician pay 11%-40%, you will see mass retirement and the elimination of the most efficient care, office-based practice.
- Remove the practice expense payment from government-reported physician income since this is overhead spent to provide the care.
- Let all physicians participate, and don’t pay site-of-service differentials.
- Enact national tort reform, which would decrease the paperwork, overhead, and much useless defensive medicine.
- Press the generic drug manufacturers (but not the innovators) regarding drug costs. Bite the bullet, and set national coverage standards (ration care) to be revisited every 5 years, which will eliminate step therapy and prior authorizations. Allow individuals to pay out of pocket for additional treatments they want, including that questionable additional 90 days of life they may get from the $250,000 drug for the off-label indication.
- Press the hospitals, and don’t complain when many of them close, especially rural ones.
- Allow individuals, hospitals, and physicians to contract outside of the government plan (in contrast to Canada).
- Downsize the health insurance companies, and have them sell private supplemental insurance to whomever wants it.
Finally, make all of this a constitutional amendment. If not put out of reach, in 15 years we will have the same system we have today. The politicians simply will not be able to resist degrading (reforming, improving, refunding, defunding) the original plan. Or, you could simply increase Medicaid rates to Medicare rates and call it a day.
Oh, by the way, I saw that man from the New Year’s Eve party at the airport the following Christmas. He survived to get his government bypass and is doing well.
The health care system we have is miserable, except compared with all the others.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
At a New Year’s Eve party a few years back, I noticed a man sitting nearby clutching his left upper arm. He was ashen and obviously uncomfortable. Acute coronary insufficiency, I thought, and I asked him if I could call the life squad for him. “Oh no,” he said, “I have these spells several times a day, the nitro will kick in after a minute, and this will ease off.” I listened as he explained he had a “widow maker,” a 90% plus left main occlusion, but “I am Canadian, and my government is going to pay for my bypass,” he said. “I just have to wait 6 more weeks.” The irony? He was the son of our host, and we were sitting in his mothers’ multimillion dollar home in the Florida Keys. He could be in a Miami hospital’s operating room in an hour or 2.
Wow. Click. Got it.
Fast forward to a lobbying discussion on Capitol Hill: A sympathetic U.S. senator tossed me this softball: ‘What do you think about Medicare reimbursement?” I expect he thought I was going to complain about how bad Medicare is, about its failure to keep current with inflation (currently about 30% behind), and the obtuse quality metrics it now requires. Instead, I found myself saying, “Medicare is my most reliable payer, paying on time – in 2 weeks for clean claims – and the private insurers have beaten me up badly. Medicare is one of my best payers.”
Wrong answer, but true statement.
There is much talk these days about , particularly considering all the barriers to care. (See my recent column, “Produce and Promises.”) Physicians and patients endure a mutual misery inflicted by private insurance companies.
What to do about health care in America?
First, let’s deal with the extraordinary costs of health care in the United States – 19% of our gross domestic product. About 3%-4 % of this figure is an accounting gimmick, since it includes nursing home care, which is considered “domiciliary” care rather than health care in Europe. In addition, drug costs are higher in the U.S., largely to cover the development of new drugs that cost less in the rest of the world. Wait lists are largely unheard of in the United States, and if you have such ready capacity, that means you incur the costs of idle capacity. Also, rarely is a new miracle drug flatly denied for coverage in the United States. If you persist, you will usually get your drug.
We are a commodity-driven society, and that is the real reason that health care costs so much in this country. Hence, we come to the real debate, the “R” word. How do we ration access to care? (See my 2017 column, “Why the Affordable Care Act will be Greatly Modified.”)
There are a plethora of proposals to fund single payer out there, none of which address rationing. And while single payer affords free universal coverage, it does not assure better care. As health economist Devon Herrick, Ph.D., wrote in his health care blog in 2016: “A single payer is not some magical entity that rains down savings from Heaven by being unconcerned about profit. Rather, an efficient single payer operates more like a predatory HMO with no competition. It is currently in vogue for hipsters to matter-of-factly announce the simple solution to health reform is single payer. Be careful what you wish for; you may end up with Medicaid for All.”
In fact, if you try to ferret out how physician income will be affected by universal health care, there would be an estimated pay cut of 11%-40%, depending on how the numbers are manipulated.
Some single-payer proposals use the term “exchange rates,” which for the uninformed means Medicaid rates. In addition, payment is usually given to the local hospital system, or “authority” to dole out. I have a very bad feeling that any small practitioner in an office-based practice would be severely shortchanged in such a system. In fact, if you cut pay for office-based physicians at all, you may begin to see them disappear.
Policy wonks argue for pay cuts for American physicians because European physicians “make less money.” Those numbers are all wrong. U.S. physicians are paid for their work, and for their practice expense. That is, how much it costs to provide the service in their office, which is around 40%-50% of published income. In Europe, almost all procedures are performed in the hospital setting, and the hospital absorbs the practice expense, which is ignored in this current health care reform debate. (See my 2015 column, “Doctor, Why DO you get paid so much?”)
The big selling point of single payer for physicians is that they might have less paperwork and get paid more for seeing Medicaid patients. Yet the paperwork will persist to avoid lawsuits, electronic medical records are now ingrained into the system, and most Medicaid patients are currently seen in the federal or hospital outpatient clinic where higher rates or other subsidies are available. The comically low Medicaid rates paid to physician offices are largely evaded or not even filed for.
Single-payer advocates are basically saying, “Yes, you will be seeing patients at a loss but you will make it up in volume.” This ignores the reality that most physicians don’t need or want more volume.
Here is my plan for single-payer health care. Call it ColdironCare.
- Set payment rates for physicians at 130% of current Medicare, about where we were 30 years ago, considering inflation. Tie the reimbursement rate to the cost of living index, same as social security. If you cut physician pay 11%-40%, you will see mass retirement and the elimination of the most efficient care, office-based practice.
- Remove the practice expense payment from government-reported physician income since this is overhead spent to provide the care.
- Let all physicians participate, and don’t pay site-of-service differentials.
- Enact national tort reform, which would decrease the paperwork, overhead, and much useless defensive medicine.
- Press the generic drug manufacturers (but not the innovators) regarding drug costs. Bite the bullet, and set national coverage standards (ration care) to be revisited every 5 years, which will eliminate step therapy and prior authorizations. Allow individuals to pay out of pocket for additional treatments they want, including that questionable additional 90 days of life they may get from the $250,000 drug for the off-label indication.
- Press the hospitals, and don’t complain when many of them close, especially rural ones.
- Allow individuals, hospitals, and physicians to contract outside of the government plan (in contrast to Canada).
- Downsize the health insurance companies, and have them sell private supplemental insurance to whomever wants it.
Finally, make all of this a constitutional amendment. If not put out of reach, in 15 years we will have the same system we have today. The politicians simply will not be able to resist degrading (reforming, improving, refunding, defunding) the original plan. Or, you could simply increase Medicaid rates to Medicare rates and call it a day.
Oh, by the way, I saw that man from the New Year’s Eve party at the airport the following Christmas. He survived to get his government bypass and is doing well.
The health care system we have is miserable, except compared with all the others.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
Telemedicine not widely used
Also today, you ought to be judicious with empiric antibiotics for febrile neutropenia, home-based exercise is better than supervised treadmill exercise for peripheral arterial disease, and brain injury in sickle cell merits more attention.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, you ought to be judicious with empiric antibiotics for febrile neutropenia, home-based exercise is better than supervised treadmill exercise for peripheral arterial disease, and brain injury in sickle cell merits more attention.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, you ought to be judicious with empiric antibiotics for febrile neutropenia, home-based exercise is better than supervised treadmill exercise for peripheral arterial disease, and brain injury in sickle cell merits more attention.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Open enrollment 2019: Busiest week so far at HealthCare.gov
but the weekly and cumulative totals for plans selected continued to run below last year’s levels, according to the Centers for Medicare & Medicaid Services.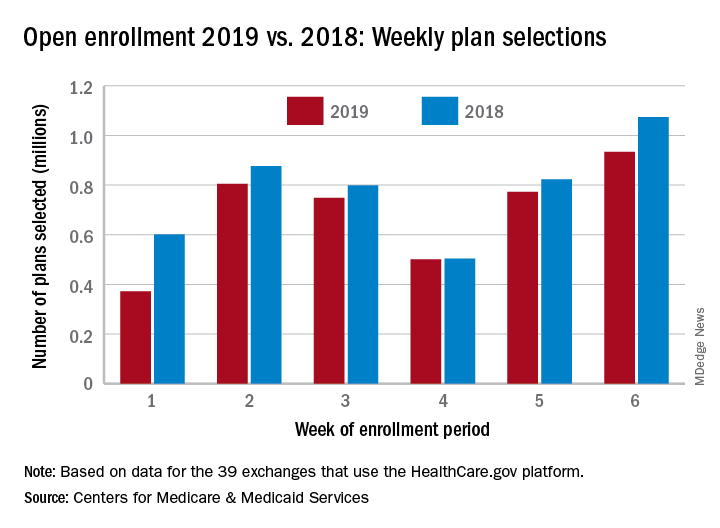
Over 934,000 plans were selected from Dec. 2 to Dec. 8, which puts the total at 4.13 million plans for the 2019 coverage year in the 39 states that use the HealthCare.gov platform, the CMS reported. Consumers renewing their coverage make up the majority of plans selected during week 6 (640,000) and cumulatively for the season (3.03 million), with new applications running at 295,000 for week 6 and 1.1 million overall.
Those numbers are down from last year, when 1.07 million plans (685,000 renewals and 389,000 new applications) were selected during week 6 of open enrollment for the 2018 coverage year, which brought the total for the season at the time to 4.68 million (3.30 million/1.38 million), CMS data show.
The deadline to enroll in a plan for 2019 is Dec. 15.
but the weekly and cumulative totals for plans selected continued to run below last year’s levels, according to the Centers for Medicare & Medicaid Services.
Over 934,000 plans were selected from Dec. 2 to Dec. 8, which puts the total at 4.13 million plans for the 2019 coverage year in the 39 states that use the HealthCare.gov platform, the CMS reported. Consumers renewing their coverage make up the majority of plans selected during week 6 (640,000) and cumulatively for the season (3.03 million), with new applications running at 295,000 for week 6 and 1.1 million overall.
Those numbers are down from last year, when 1.07 million plans (685,000 renewals and 389,000 new applications) were selected during week 6 of open enrollment for the 2018 coverage year, which brought the total for the season at the time to 4.68 million (3.30 million/1.38 million), CMS data show.
The deadline to enroll in a plan for 2019 is Dec. 15.
but the weekly and cumulative totals for plans selected continued to run below last year’s levels, according to the Centers for Medicare & Medicaid Services.
Over 934,000 plans were selected from Dec. 2 to Dec. 8, which puts the total at 4.13 million plans for the 2019 coverage year in the 39 states that use the HealthCare.gov platform, the CMS reported. Consumers renewing their coverage make up the majority of plans selected during week 6 (640,000) and cumulatively for the season (3.03 million), with new applications running at 295,000 for week 6 and 1.1 million overall.
Those numbers are down from last year, when 1.07 million plans (685,000 renewals and 389,000 new applications) were selected during week 6 of open enrollment for the 2018 coverage year, which brought the total for the season at the time to 4.68 million (3.30 million/1.38 million), CMS data show.
The deadline to enroll in a plan for 2019 is Dec. 15.
Parental leave for residents
Also today, exercise is important for patients with sickle cell, COPD patients are experiencing a risk in non-TB mycobacteria infections, and how to be an influencer on social media.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, exercise is important for patients with sickle cell, COPD patients are experiencing a risk in non-TB mycobacteria infections, and how to be an influencer on social media.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, exercise is important for patients with sickle cell, COPD patients are experiencing a risk in non-TB mycobacteria infections, and how to be an influencer on social media.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Bacterial contamination behind most cosmetics recalls
Most of the 313 cosmetic and personal care products recalled from 2002 to 2016 had problems with bacterial contamination, according to data obtained from the Food and Drug Administration.
, said Timothy M. Janetos, MD, and his associates at Northwestern University in Chicago. Bacterial contamination was by far the most common reason – 76% of the recalls over that period (11 class I, 217 class II, and 9 class II) – with unapproved ingredients and labeling problems well behind at 6%.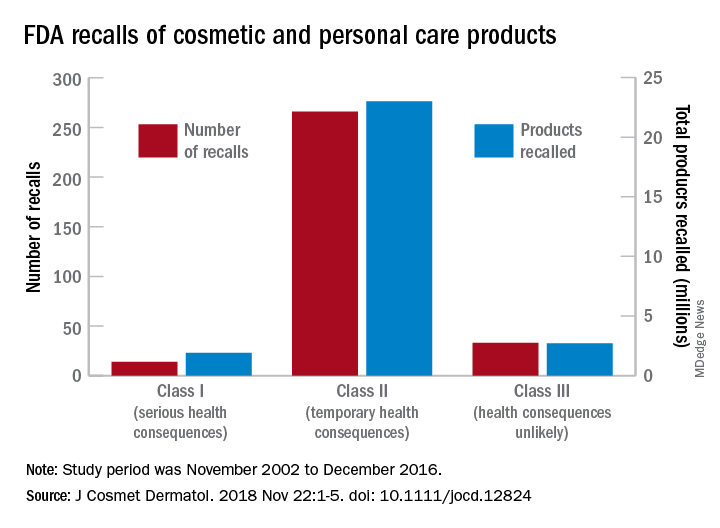
Recalls are classified by the FDA according to risk to patient safety: Class I means there is “reasonable probability of causing serious adverse health outcomes or death,” class II defines the risk as “temporary or reversible,” and class III recalls are “unlikely to cause an adverse health consequence,” they explained.
“While the number of total recalls per year was low in the context of the industry’s size and the ubiquity of cosmetic use by consumers (median: 17/year), these events involved millions of products distributed worldwide,” Dr. Janetos and his associates wrote. The class I recalls covered over 1.9 million products in distribution, the class II recalls accounted for 23 million products, and class II recalls involved over 2.7 million products.
Baby products were the category most likely to be affected, accounting for 76 (24%) of all recalls, the investigators said, with 30 involving one manufacturer of cleansing kits intended for hospital use. All but 3 of the 76 recalls resulted from bacterial contamination.
“The FDA currently has no authority to order a cosmetics manufacturer to recall a product,” they wrote, and “inspectors are only capable of inspecting 0.3% of foreign-imported products yearly,” so underreporting of such problems is likely. “Dermatologists are often the first to encounter [adverse events] related to cosmetic products and can help strengthen public safety by actively reporting these events and advocating for recalls,” said Dr. Janetos and his associates, who did not declare any conflicts of interest.
Information on reporting cosmetic-related complaints to the FDA is available on the FDA website at: https://www.fda.gov/Cosmetics/ComplianceEnforcement/AdverseEventReporting/default.htm.
[email protected]
SOURCE: Janetos TM et al. J Cosmet Dermatol. 2018 Nov 22:1-5. doi: 10.1111/jocd.12824.
Most of the 313 cosmetic and personal care products recalled from 2002 to 2016 had problems with bacterial contamination, according to data obtained from the Food and Drug Administration.
, said Timothy M. Janetos, MD, and his associates at Northwestern University in Chicago. Bacterial contamination was by far the most common reason – 76% of the recalls over that period (11 class I, 217 class II, and 9 class II) – with unapproved ingredients and labeling problems well behind at 6%.
Recalls are classified by the FDA according to risk to patient safety: Class I means there is “reasonable probability of causing serious adverse health outcomes or death,” class II defines the risk as “temporary or reversible,” and class III recalls are “unlikely to cause an adverse health consequence,” they explained.
“While the number of total recalls per year was low in the context of the industry’s size and the ubiquity of cosmetic use by consumers (median: 17/year), these events involved millions of products distributed worldwide,” Dr. Janetos and his associates wrote. The class I recalls covered over 1.9 million products in distribution, the class II recalls accounted for 23 million products, and class II recalls involved over 2.7 million products.
Baby products were the category most likely to be affected, accounting for 76 (24%) of all recalls, the investigators said, with 30 involving one manufacturer of cleansing kits intended for hospital use. All but 3 of the 76 recalls resulted from bacterial contamination.
“The FDA currently has no authority to order a cosmetics manufacturer to recall a product,” they wrote, and “inspectors are only capable of inspecting 0.3% of foreign-imported products yearly,” so underreporting of such problems is likely. “Dermatologists are often the first to encounter [adverse events] related to cosmetic products and can help strengthen public safety by actively reporting these events and advocating for recalls,” said Dr. Janetos and his associates, who did not declare any conflicts of interest.
Information on reporting cosmetic-related complaints to the FDA is available on the FDA website at: https://www.fda.gov/Cosmetics/ComplianceEnforcement/AdverseEventReporting/default.htm.
[email protected]
SOURCE: Janetos TM et al. J Cosmet Dermatol. 2018 Nov 22:1-5. doi: 10.1111/jocd.12824.
Most of the 313 cosmetic and personal care products recalled from 2002 to 2016 had problems with bacterial contamination, according to data obtained from the Food and Drug Administration.
, said Timothy M. Janetos, MD, and his associates at Northwestern University in Chicago. Bacterial contamination was by far the most common reason – 76% of the recalls over that period (11 class I, 217 class II, and 9 class II) – with unapproved ingredients and labeling problems well behind at 6%.
Recalls are classified by the FDA according to risk to patient safety: Class I means there is “reasonable probability of causing serious adverse health outcomes or death,” class II defines the risk as “temporary or reversible,” and class III recalls are “unlikely to cause an adverse health consequence,” they explained.
“While the number of total recalls per year was low in the context of the industry’s size and the ubiquity of cosmetic use by consumers (median: 17/year), these events involved millions of products distributed worldwide,” Dr. Janetos and his associates wrote. The class I recalls covered over 1.9 million products in distribution, the class II recalls accounted for 23 million products, and class II recalls involved over 2.7 million products.
Baby products were the category most likely to be affected, accounting for 76 (24%) of all recalls, the investigators said, with 30 involving one manufacturer of cleansing kits intended for hospital use. All but 3 of the 76 recalls resulted from bacterial contamination.
“The FDA currently has no authority to order a cosmetics manufacturer to recall a product,” they wrote, and “inspectors are only capable of inspecting 0.3% of foreign-imported products yearly,” so underreporting of such problems is likely. “Dermatologists are often the first to encounter [adverse events] related to cosmetic products and can help strengthen public safety by actively reporting these events and advocating for recalls,” said Dr. Janetos and his associates, who did not declare any conflicts of interest.
Information on reporting cosmetic-related complaints to the FDA is available on the FDA website at: https://www.fda.gov/Cosmetics/ComplianceEnforcement/AdverseEventReporting/default.htm.
[email protected]
SOURCE: Janetos TM et al. J Cosmet Dermatol. 2018 Nov 22:1-5. doi: 10.1111/jocd.12824.
FROM THE JOURNAL OF COSMETIC DERMATOLOGY
Fewer insured may have helped slow health spending growth in 2017
Health care spending as a percentage of gross domestic product remained relatively stable in 2017, despite a slowdown in the growth of spending.

Total health care spending in the United States was $3.5 trillion in 2017, an increase of 3.9% from 2016, according to data released Dec. 6 by the Centers for Medicare & Medicaid Services.
The growth rate was down from that of 2016 (4.8%) but similar to growth rates experienced during 2008-2013, according to the research article in Health Affairs.
“The slower growth in health care spending in 2017 resulted primarily from slower growth in hospital care, physician and clinical services, and retail prescription drugs, with residual use and intensity of these goods and services contributing substantially to the trend,” Anne B. Martin, an economist in the CMS Office of the Actuary’s National Health Statistics Group, and her colleagues wrote.
The report notes that slower growth in the use and intensity of health care goods and services in 2017 “may have been affected by slower growth in overall health insurance enrollment, as the insured share of the population fell from 91.1% in 2016 to 90.9% in 2017.”
Spending on hospital care increased 4.6% to $1.1 trillion in 2017 and accounted for 33% of total health care spending; however, growth was slower than in the previous year (5.6%). Ms. Martin and her colleagues noted that growth in outpatient visits slowed while growth in inpatient days increased at about the same rate and prices in hospital care grew in 2017 to 1.7% from 1.2% in the previous year.
Spending on physician and clinical services grew 4.2% in 2017 to $694.3 billion and accounted for 20% of total health care spending. The growth rate is down from the previous year (5.6%) and a recent peak of 6% in 2015.
“Although spending growth for both physician services and clinical services slowed in 2017, the growth rate for the latter (5.0%) continued to out pace the rate for the former (3.9%), as spending for most types of outpatient care centers contributed to the stronger growth in spending for clinical services,” Ms. Martin and her colleagues reported.
They attributed the slowdown to non-price factors, such as slower growth in the use and intensity of physician and clinical services, although price growth for physician and clinical services increased 0.4% in 2017, up from 0.2% in 2016.
Spending on retail prescription drugs grew 0.4% in 2017 to $333.4 billion and accounted for 10% of total national health spending. It is the slowest growth rate increase since 2012, a year that saw a number of blockbuster drugs lose patent protection. This was down from a growth rate of 2.3% in 2016 and down from recent rates of 12.4% in 2014 and 8.9% in 2015.
“Slower growth in non-price factors, such as the use and mix of retail prescription drugs – and, to a lesser extent, in retail prescription drug prices – contributed to the slower overall growth in retail prescription drug spending in 2017,” according to the authors. Key factors included slower growth in the number of prescriptions dispensed, the continued shift to lower-cost generics, and slower growth in the volume of high-cost drugs, particularly those used to treat hepatitis C. Price decreases in generics and lower increases for existing brand-name drugs also contributed to the lower spending growth in 2017.
Ms. Martin and her colleagues highlighted the slower growth rate in the number of prescriptions (1.8% in 2017, down from 2.3% in 2016) “resulted in large part from a decline in the number of prescriptions dispensed for drugs used to treat pain.”
Medicare spending, which represents 20% of all national health care spending in 2017 ($705.9 billion), grew 4.2%, a slight decline from the 4.3% growth in 2016. Enrollment growth slowed slightly to 2.5% in 2017 from 2.7% in the previous year, while in the same time frame, per-enrollee expenditures increased slightly to 1.7% from 1.6%. Slower growth in fee-for-service Medicare spending was offset by faster growth in spending by Medicare private health plans.
Medicaid spending reached $581.9 billion (17% of national health care spending), and the growth rate slowed for the third straight year, increasing 2.9% in 2017 versus 4.2% in 2016. The slower growth “was influenced by a deceleration in enrollment growth and a reduction in the Medicaid net cost of health insurance as the federal government recovered payments from managed care organizations based on their favorable prior-period experience,” the authors stated. Enrollment growth has been decelerating following a peak of growth of 11.9% in 2014 because of states that elected to expand Medicaid eligibility, which was followed by 3 years of slower growth rates of 4.9%, 3.0% and 2.0% in 2015, 2016, and 2017, respectively. Per-enrollee spending also slowed to 0.9% growth in 2017 from a rate of 1.2% in 2016, attributed to “the decline in government administration and the net cost of insurance.”
SOURCE: Martin A et al. Health Aff. 2018. doi: 10.1377/hlthaff.2018.05085.
Health care spending as a percentage of gross domestic product remained relatively stable in 2017, despite a slowdown in the growth of spending.
Total health care spending in the United States was $3.5 trillion in 2017, an increase of 3.9% from 2016, according to data released Dec. 6 by the Centers for Medicare & Medicaid Services.
The growth rate was down from that of 2016 (4.8%) but similar to growth rates experienced during 2008-2013, according to the research article in Health Affairs.
“The slower growth in health care spending in 2017 resulted primarily from slower growth in hospital care, physician and clinical services, and retail prescription drugs, with residual use and intensity of these goods and services contributing substantially to the trend,” Anne B. Martin, an economist in the CMS Office of the Actuary’s National Health Statistics Group, and her colleagues wrote.
The report notes that slower growth in the use and intensity of health care goods and services in 2017 “may have been affected by slower growth in overall health insurance enrollment, as the insured share of the population fell from 91.1% in 2016 to 90.9% in 2017.”
Spending on hospital care increased 4.6% to $1.1 trillion in 2017 and accounted for 33% of total health care spending; however, growth was slower than in the previous year (5.6%). Ms. Martin and her colleagues noted that growth in outpatient visits slowed while growth in inpatient days increased at about the same rate and prices in hospital care grew in 2017 to 1.7% from 1.2% in the previous year.
Spending on physician and clinical services grew 4.2% in 2017 to $694.3 billion and accounted for 20% of total health care spending. The growth rate is down from the previous year (5.6%) and a recent peak of 6% in 2015.
“Although spending growth for both physician services and clinical services slowed in 2017, the growth rate for the latter (5.0%) continued to out pace the rate for the former (3.9%), as spending for most types of outpatient care centers contributed to the stronger growth in spending for clinical services,” Ms. Martin and her colleagues reported.
They attributed the slowdown to non-price factors, such as slower growth in the use and intensity of physician and clinical services, although price growth for physician and clinical services increased 0.4% in 2017, up from 0.2% in 2016.
Spending on retail prescription drugs grew 0.4% in 2017 to $333.4 billion and accounted for 10% of total national health spending. It is the slowest growth rate increase since 2012, a year that saw a number of blockbuster drugs lose patent protection. This was down from a growth rate of 2.3% in 2016 and down from recent rates of 12.4% in 2014 and 8.9% in 2015.
“Slower growth in non-price factors, such as the use and mix of retail prescription drugs – and, to a lesser extent, in retail prescription drug prices – contributed to the slower overall growth in retail prescription drug spending in 2017,” according to the authors. Key factors included slower growth in the number of prescriptions dispensed, the continued shift to lower-cost generics, and slower growth in the volume of high-cost drugs, particularly those used to treat hepatitis C. Price decreases in generics and lower increases for existing brand-name drugs also contributed to the lower spending growth in 2017.
Ms. Martin and her colleagues highlighted the slower growth rate in the number of prescriptions (1.8% in 2017, down from 2.3% in 2016) “resulted in large part from a decline in the number of prescriptions dispensed for drugs used to treat pain.”
Medicare spending, which represents 20% of all national health care spending in 2017 ($705.9 billion), grew 4.2%, a slight decline from the 4.3% growth in 2016. Enrollment growth slowed slightly to 2.5% in 2017 from 2.7% in the previous year, while in the same time frame, per-enrollee expenditures increased slightly to 1.7% from 1.6%. Slower growth in fee-for-service Medicare spending was offset by faster growth in spending by Medicare private health plans.
Medicaid spending reached $581.9 billion (17% of national health care spending), and the growth rate slowed for the third straight year, increasing 2.9% in 2017 versus 4.2% in 2016. The slower growth “was influenced by a deceleration in enrollment growth and a reduction in the Medicaid net cost of health insurance as the federal government recovered payments from managed care organizations based on their favorable prior-period experience,” the authors stated. Enrollment growth has been decelerating following a peak of growth of 11.9% in 2014 because of states that elected to expand Medicaid eligibility, which was followed by 3 years of slower growth rates of 4.9%, 3.0% and 2.0% in 2015, 2016, and 2017, respectively. Per-enrollee spending also slowed to 0.9% growth in 2017 from a rate of 1.2% in 2016, attributed to “the decline in government administration and the net cost of insurance.”
SOURCE: Martin A et al. Health Aff. 2018. doi: 10.1377/hlthaff.2018.05085.
Health care spending as a percentage of gross domestic product remained relatively stable in 2017, despite a slowdown in the growth of spending.
Total health care spending in the United States was $3.5 trillion in 2017, an increase of 3.9% from 2016, according to data released Dec. 6 by the Centers for Medicare & Medicaid Services.
The growth rate was down from that of 2016 (4.8%) but similar to growth rates experienced during 2008-2013, according to the research article in Health Affairs.
“The slower growth in health care spending in 2017 resulted primarily from slower growth in hospital care, physician and clinical services, and retail prescription drugs, with residual use and intensity of these goods and services contributing substantially to the trend,” Anne B. Martin, an economist in the CMS Office of the Actuary’s National Health Statistics Group, and her colleagues wrote.
The report notes that slower growth in the use and intensity of health care goods and services in 2017 “may have been affected by slower growth in overall health insurance enrollment, as the insured share of the population fell from 91.1% in 2016 to 90.9% in 2017.”
Spending on hospital care increased 4.6% to $1.1 trillion in 2017 and accounted for 33% of total health care spending; however, growth was slower than in the previous year (5.6%). Ms. Martin and her colleagues noted that growth in outpatient visits slowed while growth in inpatient days increased at about the same rate and prices in hospital care grew in 2017 to 1.7% from 1.2% in the previous year.
Spending on physician and clinical services grew 4.2% in 2017 to $694.3 billion and accounted for 20% of total health care spending. The growth rate is down from the previous year (5.6%) and a recent peak of 6% in 2015.
“Although spending growth for both physician services and clinical services slowed in 2017, the growth rate for the latter (5.0%) continued to out pace the rate for the former (3.9%), as spending for most types of outpatient care centers contributed to the stronger growth in spending for clinical services,” Ms. Martin and her colleagues reported.
They attributed the slowdown to non-price factors, such as slower growth in the use and intensity of physician and clinical services, although price growth for physician and clinical services increased 0.4% in 2017, up from 0.2% in 2016.
Spending on retail prescription drugs grew 0.4% in 2017 to $333.4 billion and accounted for 10% of total national health spending. It is the slowest growth rate increase since 2012, a year that saw a number of blockbuster drugs lose patent protection. This was down from a growth rate of 2.3% in 2016 and down from recent rates of 12.4% in 2014 and 8.9% in 2015.
“Slower growth in non-price factors, such as the use and mix of retail prescription drugs – and, to a lesser extent, in retail prescription drug prices – contributed to the slower overall growth in retail prescription drug spending in 2017,” according to the authors. Key factors included slower growth in the number of prescriptions dispensed, the continued shift to lower-cost generics, and slower growth in the volume of high-cost drugs, particularly those used to treat hepatitis C. Price decreases in generics and lower increases for existing brand-name drugs also contributed to the lower spending growth in 2017.
Ms. Martin and her colleagues highlighted the slower growth rate in the number of prescriptions (1.8% in 2017, down from 2.3% in 2016) “resulted in large part from a decline in the number of prescriptions dispensed for drugs used to treat pain.”
Medicare spending, which represents 20% of all national health care spending in 2017 ($705.9 billion), grew 4.2%, a slight decline from the 4.3% growth in 2016. Enrollment growth slowed slightly to 2.5% in 2017 from 2.7% in the previous year, while in the same time frame, per-enrollee expenditures increased slightly to 1.7% from 1.6%. Slower growth in fee-for-service Medicare spending was offset by faster growth in spending by Medicare private health plans.
Medicaid spending reached $581.9 billion (17% of national health care spending), and the growth rate slowed for the third straight year, increasing 2.9% in 2017 versus 4.2% in 2016. The slower growth “was influenced by a deceleration in enrollment growth and a reduction in the Medicaid net cost of health insurance as the federal government recovered payments from managed care organizations based on their favorable prior-period experience,” the authors stated. Enrollment growth has been decelerating following a peak of growth of 11.9% in 2014 because of states that elected to expand Medicaid eligibility, which was followed by 3 years of slower growth rates of 4.9%, 3.0% and 2.0% in 2015, 2016, and 2017, respectively. Per-enrollee spending also slowed to 0.9% growth in 2017 from a rate of 1.2% in 2016, attributed to “the decline in government administration and the net cost of insurance.”
SOURCE: Martin A et al. Health Aff. 2018. doi: 10.1377/hlthaff.2018.05085.
FROM HEALTH AFFAIRS
Key clinical point: National health care spending growth slowed to 3.9% in 2017.
Major finding: The $3.5 trillion in national health care spending represents 17.9% of GDP.
Study details: Annual analysis of national health expenditures conducted by federal actuaries.
Disclosures: Analysis conducted by the Centers for Medicaid & Medicare Services Office of the Actuary; the authors have no relevant financial conflicts of interest.
Source: Martin A et al. Health Affairs. 2018. doi: 10.1377/hlthaff.2018.05085.
Action on HealthCare.gov picked up during week 5
Activity during week 5 of open enrollment on HealthCare.gov was up by more than 50% over the previous week, but the total number of plans selected for the 2019 coverage year remains lower than it was last year, according to the Centers for Medicare & Medicaid Services.
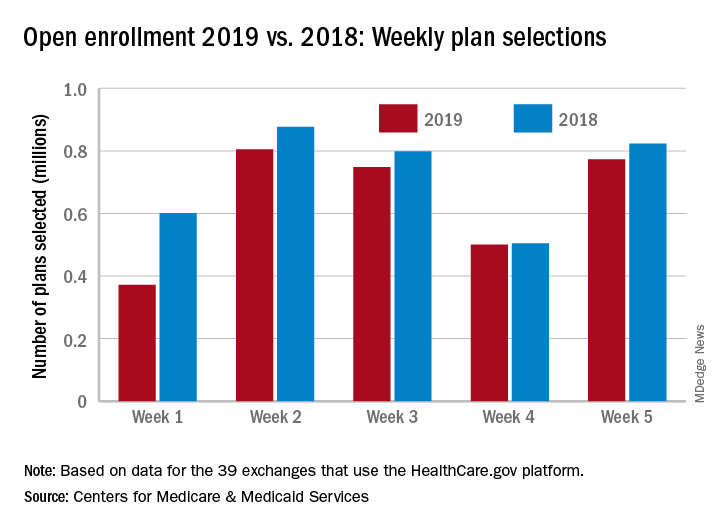
The 773,000 plans selected during week 5 (Nov. 25 – Dec. 1) of the 2019 open enrollment season were an increase of 54% over week 4, CMS data show for the 39 states that use the HealthCare.gov platform, with the cumulative total now at 3.2 million. By comparison, week-5 selections in last year’s open enrollment totaled 823,000, and the cumulative figure was 3.6 million.
The deadline for applying for 2019 coverage on HealthCare.gov is Dec. 15.
Activity during week 5 of open enrollment on HealthCare.gov was up by more than 50% over the previous week, but the total number of plans selected for the 2019 coverage year remains lower than it was last year, according to the Centers for Medicare & Medicaid Services.
The 773,000 plans selected during week 5 (Nov. 25 – Dec. 1) of the 2019 open enrollment season were an increase of 54% over week 4, CMS data show for the 39 states that use the HealthCare.gov platform, with the cumulative total now at 3.2 million. By comparison, week-5 selections in last year’s open enrollment totaled 823,000, and the cumulative figure was 3.6 million.
The deadline for applying for 2019 coverage on HealthCare.gov is Dec. 15.
Activity during week 5 of open enrollment on HealthCare.gov was up by more than 50% over the previous week, but the total number of plans selected for the 2019 coverage year remains lower than it was last year, according to the Centers for Medicare & Medicaid Services.
The 773,000 plans selected during week 5 (Nov. 25 – Dec. 1) of the 2019 open enrollment season were an increase of 54% over week 4, CMS data show for the 39 states that use the HealthCare.gov platform, with the cumulative total now at 3.2 million. By comparison, week-5 selections in last year’s open enrollment totaled 823,000, and the cumulative figure was 3.6 million.
The deadline for applying for 2019 coverage on HealthCare.gov is Dec. 15.
The Gift and the Thought Both Count
It is that time of year when federal compliance officers, clinical ethicists, and staff counsels are flooded with queries about the legal and ethical acceptability of gifts. And no wonder, all the winter holidays often involve giving gifts. The simple and spontaneous acts of giving and receiving gifts become more complicated and deliberative in the federal health care system. Both legal rules and ethical values bear upon who can offer and accept what gift to whom upon what occasion and in what amount. The “Standards of Ethical Conduct for Employees of the Executive Branch” devotes 2 entire subparts to the subject of gifts.1 We will examine a small section of the document that can become a big issue for federal practitioners during that holiday—gifts from patients.
First, veterans (patients) are “prohibited sources” in section 5 CFR §2635.203 (d).1 And since VA employees are subject to restrictions on accepting gifts from sources outside the government, unless an exception applies, federal employees may not accept a gift because of their official position (eg, Federal Practitioner, editor-in-chief) or a gift from a patient (prohibited source; [5 CFR §2635.201]).
It might seem like this is going to be a very short column this month, as gifts from patients are forbidden. Yet, a Christmas card or homemade fudge isn’t really a gift, is it?
5 CFR §2635.203 (b) defines what is and is not a gift: For example, minor items of food or items like a thank-you card are specifically excluded in section (b) 1-10.
Is Christmas an exception or are just types of gifts excluded?
There are exceptions to the general regulation about accepting gifts from prohibited sources. Many staff will recall hearing about the “$20 rule,” which is actually the “$20-50” rule stating that a federal employee may accept a gift from a patient (prohibited source) if the value of said gift is under $20 and the employee does not accept more than $50 from any single source in a calendar year. §2635.204 lists the exceptions. However, starting in 2017, the regulations changed to require that federal employees also consider not just whether they could accept a gift but—ethically—they should take the gift even if it was permitted under the law. The Office of Government Ethics made this change because it wanted to emphasize the importance of considering not just how things are but how things appear to be. The regulations contain detailed descriptions of what employees should think about and stipulates that the decisions will not be further scrutinized (5 CFR §2635.201[b]).1
Based on this new emphasis on appearances, ethically, no doctor or nurse should accept the keys to a new BMW from a patient who owns a luxury car dealership. But what about more prosaic and probable presents: the holiday cookies a single father made with his children for the nurse practitioner who has been his primary care practitioner for years; the birdhouse a Vietnam veteran made in her crafts class for the surgeon who removed her gallbladder; or even the store-bought but no less heartfelt tin of popcorn from an elderly veteran for the hospitalist who saw him through a rough bought of pneumonia?
Related: Happy Federal New Year
The rules about practitioners accepting patient gifts are rational and unambiguous: It is the values conflict surrounding patient gifts that is often emotion driven and muddled; it may be easier and safer to adopt the “just say no” policy. And yet, while this might seem the most unassailable position to avoid a conflict of interest, could this possibly be a more practitioner- than patient-centered standard? Authoritative sources in the ethics literature are equally divided and ambivalent on the question.2,3 The American College of Physicians Ethics Manual states: “In deciding whether to accept a gift from a patient, the physician should consider the nature of the gift and its value to the patient, the potential implications for the patient-physician relationship of accepting or refusing it, and the patient’s probable intention and expectations.”4 A small gift as a token of appreciation is not ethically problematic. Favored treatment as a result of acceptance of any gift is problematic, undermines professionalism, and may interfere with objectivity in the care of the patient.4
Related: Am I My Brother’s/Sister’s Keeper?
Many an ethics commentator have cautioned, “beware of patients bearing gifts.”5 In making an ethical assessment of whether or not to accept the gift, a key question a practitioner needs to ask him or herself is about the patient’s motive. Even the patient may be unaware of the reasons behind their giving, and the wise practitioner will take a mindful moment to think about the context and timing of the gift and the nature of his or her relationship to the patient. Sadly, many of our patients are lonely especially at this family time of year and on some level may hope the gift will help slide the professional relationship toward a more personal one. Some patients may think a gift might earn them preferential treatment. Finally, a few patients may have a romantic or sexual attraction toward a clinician.
Often in the latter 2 cases, a pattern will develop that discloses the patient’s true intent. Very expensive gifts, monetary gifts, excessively personal gifts, or frequent gifts should alert the practitioner that more may be going on. A kind reminder to the patient that providing good care is the only reward needed may be sufficient. For practitioners whose ethical code does not permit them to accept gifts, then a genuine thank you and an explanation of the rules and/or values behind the refusal may be necessary. There are other times when the practitioner or a supervisor/advisor may need to reset the boundaries or even to transfer the patient to another practitioner. The norms in mental health care and psychotherapy are more stringent because of the intimacy of the relationship and the potential vulnerability of patients.6
For gifts that seem genuine and generous or cost a trivial amount, then there is an ethical argument to be made for accepting them with gratitude. In many cultures, hospitality is a tradition, and expressing appreciation a virtue, so when a practitioner refuses to graciously take a small gift, they risk offending the patient. Rejection of a gift can be seen as disrespectful and could cause a rupture in an otherwise sound practitioner-patient relationship. Other patients experience strong feelings of gratitude and admiration for their practitioners, stronger than most of us recognize. The ability for a patient to give their practitioner a holiday gift, particularly one they invested time and energy in creating or choosing, can enhance their sense of self-worth and individual agency. These gifts are not so much an attempt to diminish the professional power differential but to close the gap between 2 human beings in an unequal relationship that is yet one of shared decision making. All practitioners should be aware of the often underappreciated social power of a gift to influence decisions.
Related: Caring Under a Microscope
At the same time, clinicians can strive to be sensitively attuned to the reality that, sometimes the cookie is just a cookie so eat and enjoy, just remember to share with your group. External judgments are often cited as practical rules of thumb for determining the ethical acceptability of a gift: Would you want your mother, newspaper, or colleague to know you took the present? I prefer an internal moral compass that steers always to the true north of is accepting this gift really in the patient’s best interest?
1. Standards of ethical conduct for employees of the executive branch. Fed Regist. 2016;81(223):81641-81657. To be codified at 5 CFR §2635.
2. Spence SA. Patients bearing gifts: are there strings attached. BMJ. 2005;331.
3. American Medical Association. American Medical Association Code of Medical Ethics Opinion 1.2.8. https://www.ama-assn.org/delivering-care/code-medical-ethics-patient-physician-relationships. Accessed November 27, 2018.
4. Snyder L; Ethics, Professionalism, and Human Rights Committee. American College of Physicians Ethics Manual, 6th ed. Ann Intern Med. 2012;156(1, Part 2):73-104.
5. Levine A, Valeriote T. Beware the patient bearing gifts. http://epmonthly.com/article/beware-patient-bearing-gifts. Published December 14, 2016. Accessed November 27, 2018.
6. Brendel DH, Chu J, Radden J, et al. The price of a gift: an approach to receiving gifts from psychiatric patients. Harv Rev Psychiatry. 2007;15(2):43-51.
It is that time of year when federal compliance officers, clinical ethicists, and staff counsels are flooded with queries about the legal and ethical acceptability of gifts. And no wonder, all the winter holidays often involve giving gifts. The simple and spontaneous acts of giving and receiving gifts become more complicated and deliberative in the federal health care system. Both legal rules and ethical values bear upon who can offer and accept what gift to whom upon what occasion and in what amount. The “Standards of Ethical Conduct for Employees of the Executive Branch” devotes 2 entire subparts to the subject of gifts.1 We will examine a small section of the document that can become a big issue for federal practitioners during that holiday—gifts from patients.
First, veterans (patients) are “prohibited sources” in section 5 CFR §2635.203 (d).1 And since VA employees are subject to restrictions on accepting gifts from sources outside the government, unless an exception applies, federal employees may not accept a gift because of their official position (eg, Federal Practitioner, editor-in-chief) or a gift from a patient (prohibited source; [5 CFR §2635.201]).
It might seem like this is going to be a very short column this month, as gifts from patients are forbidden. Yet, a Christmas card or homemade fudge isn’t really a gift, is it?
5 CFR §2635.203 (b) defines what is and is not a gift: For example, minor items of food or items like a thank-you card are specifically excluded in section (b) 1-10.
Is Christmas an exception or are just types of gifts excluded?
There are exceptions to the general regulation about accepting gifts from prohibited sources. Many staff will recall hearing about the “$20 rule,” which is actually the “$20-50” rule stating that a federal employee may accept a gift from a patient (prohibited source) if the value of said gift is under $20 and the employee does not accept more than $50 from any single source in a calendar year. §2635.204 lists the exceptions. However, starting in 2017, the regulations changed to require that federal employees also consider not just whether they could accept a gift but—ethically—they should take the gift even if it was permitted under the law. The Office of Government Ethics made this change because it wanted to emphasize the importance of considering not just how things are but how things appear to be. The regulations contain detailed descriptions of what employees should think about and stipulates that the decisions will not be further scrutinized (5 CFR §2635.201[b]).1
Based on this new emphasis on appearances, ethically, no doctor or nurse should accept the keys to a new BMW from a patient who owns a luxury car dealership. But what about more prosaic and probable presents: the holiday cookies a single father made with his children for the nurse practitioner who has been his primary care practitioner for years; the birdhouse a Vietnam veteran made in her crafts class for the surgeon who removed her gallbladder; or even the store-bought but no less heartfelt tin of popcorn from an elderly veteran for the hospitalist who saw him through a rough bought of pneumonia?
Related: Happy Federal New Year
The rules about practitioners accepting patient gifts are rational and unambiguous: It is the values conflict surrounding patient gifts that is often emotion driven and muddled; it may be easier and safer to adopt the “just say no” policy. And yet, while this might seem the most unassailable position to avoid a conflict of interest, could this possibly be a more practitioner- than patient-centered standard? Authoritative sources in the ethics literature are equally divided and ambivalent on the question.2,3 The American College of Physicians Ethics Manual states: “In deciding whether to accept a gift from a patient, the physician should consider the nature of the gift and its value to the patient, the potential implications for the patient-physician relationship of accepting or refusing it, and the patient’s probable intention and expectations.”4 A small gift as a token of appreciation is not ethically problematic. Favored treatment as a result of acceptance of any gift is problematic, undermines professionalism, and may interfere with objectivity in the care of the patient.4
Related: Am I My Brother’s/Sister’s Keeper?
Many an ethics commentator have cautioned, “beware of patients bearing gifts.”5 In making an ethical assessment of whether or not to accept the gift, a key question a practitioner needs to ask him or herself is about the patient’s motive. Even the patient may be unaware of the reasons behind their giving, and the wise practitioner will take a mindful moment to think about the context and timing of the gift and the nature of his or her relationship to the patient. Sadly, many of our patients are lonely especially at this family time of year and on some level may hope the gift will help slide the professional relationship toward a more personal one. Some patients may think a gift might earn them preferential treatment. Finally, a few patients may have a romantic or sexual attraction toward a clinician.
Often in the latter 2 cases, a pattern will develop that discloses the patient’s true intent. Very expensive gifts, monetary gifts, excessively personal gifts, or frequent gifts should alert the practitioner that more may be going on. A kind reminder to the patient that providing good care is the only reward needed may be sufficient. For practitioners whose ethical code does not permit them to accept gifts, then a genuine thank you and an explanation of the rules and/or values behind the refusal may be necessary. There are other times when the practitioner or a supervisor/advisor may need to reset the boundaries or even to transfer the patient to another practitioner. The norms in mental health care and psychotherapy are more stringent because of the intimacy of the relationship and the potential vulnerability of patients.6
For gifts that seem genuine and generous or cost a trivial amount, then there is an ethical argument to be made for accepting them with gratitude. In many cultures, hospitality is a tradition, and expressing appreciation a virtue, so when a practitioner refuses to graciously take a small gift, they risk offending the patient. Rejection of a gift can be seen as disrespectful and could cause a rupture in an otherwise sound practitioner-patient relationship. Other patients experience strong feelings of gratitude and admiration for their practitioners, stronger than most of us recognize. The ability for a patient to give their practitioner a holiday gift, particularly one they invested time and energy in creating or choosing, can enhance their sense of self-worth and individual agency. These gifts are not so much an attempt to diminish the professional power differential but to close the gap between 2 human beings in an unequal relationship that is yet one of shared decision making. All practitioners should be aware of the often underappreciated social power of a gift to influence decisions.
Related: Caring Under a Microscope
At the same time, clinicians can strive to be sensitively attuned to the reality that, sometimes the cookie is just a cookie so eat and enjoy, just remember to share with your group. External judgments are often cited as practical rules of thumb for determining the ethical acceptability of a gift: Would you want your mother, newspaper, or colleague to know you took the present? I prefer an internal moral compass that steers always to the true north of is accepting this gift really in the patient’s best interest?
It is that time of year when federal compliance officers, clinical ethicists, and staff counsels are flooded with queries about the legal and ethical acceptability of gifts. And no wonder, all the winter holidays often involve giving gifts. The simple and spontaneous acts of giving and receiving gifts become more complicated and deliberative in the federal health care system. Both legal rules and ethical values bear upon who can offer and accept what gift to whom upon what occasion and in what amount. The “Standards of Ethical Conduct for Employees of the Executive Branch” devotes 2 entire subparts to the subject of gifts.1 We will examine a small section of the document that can become a big issue for federal practitioners during that holiday—gifts from patients.
First, veterans (patients) are “prohibited sources” in section 5 CFR §2635.203 (d).1 And since VA employees are subject to restrictions on accepting gifts from sources outside the government, unless an exception applies, federal employees may not accept a gift because of their official position (eg, Federal Practitioner, editor-in-chief) or a gift from a patient (prohibited source; [5 CFR §2635.201]).
It might seem like this is going to be a very short column this month, as gifts from patients are forbidden. Yet, a Christmas card or homemade fudge isn’t really a gift, is it?
5 CFR §2635.203 (b) defines what is and is not a gift: For example, minor items of food or items like a thank-you card are specifically excluded in section (b) 1-10.
Is Christmas an exception or are just types of gifts excluded?
There are exceptions to the general regulation about accepting gifts from prohibited sources. Many staff will recall hearing about the “$20 rule,” which is actually the “$20-50” rule stating that a federal employee may accept a gift from a patient (prohibited source) if the value of said gift is under $20 and the employee does not accept more than $50 from any single source in a calendar year. §2635.204 lists the exceptions. However, starting in 2017, the regulations changed to require that federal employees also consider not just whether they could accept a gift but—ethically—they should take the gift even if it was permitted under the law. The Office of Government Ethics made this change because it wanted to emphasize the importance of considering not just how things are but how things appear to be. The regulations contain detailed descriptions of what employees should think about and stipulates that the decisions will not be further scrutinized (5 CFR §2635.201[b]).1
Based on this new emphasis on appearances, ethically, no doctor or nurse should accept the keys to a new BMW from a patient who owns a luxury car dealership. But what about more prosaic and probable presents: the holiday cookies a single father made with his children for the nurse practitioner who has been his primary care practitioner for years; the birdhouse a Vietnam veteran made in her crafts class for the surgeon who removed her gallbladder; or even the store-bought but no less heartfelt tin of popcorn from an elderly veteran for the hospitalist who saw him through a rough bought of pneumonia?
Related: Happy Federal New Year
The rules about practitioners accepting patient gifts are rational and unambiguous: It is the values conflict surrounding patient gifts that is often emotion driven and muddled; it may be easier and safer to adopt the “just say no” policy. And yet, while this might seem the most unassailable position to avoid a conflict of interest, could this possibly be a more practitioner- than patient-centered standard? Authoritative sources in the ethics literature are equally divided and ambivalent on the question.2,3 The American College of Physicians Ethics Manual states: “In deciding whether to accept a gift from a patient, the physician should consider the nature of the gift and its value to the patient, the potential implications for the patient-physician relationship of accepting or refusing it, and the patient’s probable intention and expectations.”4 A small gift as a token of appreciation is not ethically problematic. Favored treatment as a result of acceptance of any gift is problematic, undermines professionalism, and may interfere with objectivity in the care of the patient.4
Related: Am I My Brother’s/Sister’s Keeper?
Many an ethics commentator have cautioned, “beware of patients bearing gifts.”5 In making an ethical assessment of whether or not to accept the gift, a key question a practitioner needs to ask him or herself is about the patient’s motive. Even the patient may be unaware of the reasons behind their giving, and the wise practitioner will take a mindful moment to think about the context and timing of the gift and the nature of his or her relationship to the patient. Sadly, many of our patients are lonely especially at this family time of year and on some level may hope the gift will help slide the professional relationship toward a more personal one. Some patients may think a gift might earn them preferential treatment. Finally, a few patients may have a romantic or sexual attraction toward a clinician.
Often in the latter 2 cases, a pattern will develop that discloses the patient’s true intent. Very expensive gifts, monetary gifts, excessively personal gifts, or frequent gifts should alert the practitioner that more may be going on. A kind reminder to the patient that providing good care is the only reward needed may be sufficient. For practitioners whose ethical code does not permit them to accept gifts, then a genuine thank you and an explanation of the rules and/or values behind the refusal may be necessary. There are other times when the practitioner or a supervisor/advisor may need to reset the boundaries or even to transfer the patient to another practitioner. The norms in mental health care and psychotherapy are more stringent because of the intimacy of the relationship and the potential vulnerability of patients.6
For gifts that seem genuine and generous or cost a trivial amount, then there is an ethical argument to be made for accepting them with gratitude. In many cultures, hospitality is a tradition, and expressing appreciation a virtue, so when a practitioner refuses to graciously take a small gift, they risk offending the patient. Rejection of a gift can be seen as disrespectful and could cause a rupture in an otherwise sound practitioner-patient relationship. Other patients experience strong feelings of gratitude and admiration for their practitioners, stronger than most of us recognize. The ability for a patient to give their practitioner a holiday gift, particularly one they invested time and energy in creating or choosing, can enhance their sense of self-worth and individual agency. These gifts are not so much an attempt to diminish the professional power differential but to close the gap between 2 human beings in an unequal relationship that is yet one of shared decision making. All practitioners should be aware of the often underappreciated social power of a gift to influence decisions.
Related: Caring Under a Microscope
At the same time, clinicians can strive to be sensitively attuned to the reality that, sometimes the cookie is just a cookie so eat and enjoy, just remember to share with your group. External judgments are often cited as practical rules of thumb for determining the ethical acceptability of a gift: Would you want your mother, newspaper, or colleague to know you took the present? I prefer an internal moral compass that steers always to the true north of is accepting this gift really in the patient’s best interest?
1. Standards of ethical conduct for employees of the executive branch. Fed Regist. 2016;81(223):81641-81657. To be codified at 5 CFR §2635.
2. Spence SA. Patients bearing gifts: are there strings attached. BMJ. 2005;331.
3. American Medical Association. American Medical Association Code of Medical Ethics Opinion 1.2.8. https://www.ama-assn.org/delivering-care/code-medical-ethics-patient-physician-relationships. Accessed November 27, 2018.
4. Snyder L; Ethics, Professionalism, and Human Rights Committee. American College of Physicians Ethics Manual, 6th ed. Ann Intern Med. 2012;156(1, Part 2):73-104.
5. Levine A, Valeriote T. Beware the patient bearing gifts. http://epmonthly.com/article/beware-patient-bearing-gifts. Published December 14, 2016. Accessed November 27, 2018.
6. Brendel DH, Chu J, Radden J, et al. The price of a gift: an approach to receiving gifts from psychiatric patients. Harv Rev Psychiatry. 2007;15(2):43-51.
1. Standards of ethical conduct for employees of the executive branch. Fed Regist. 2016;81(223):81641-81657. To be codified at 5 CFR §2635.
2. Spence SA. Patients bearing gifts: are there strings attached. BMJ. 2005;331.
3. American Medical Association. American Medical Association Code of Medical Ethics Opinion 1.2.8. https://www.ama-assn.org/delivering-care/code-medical-ethics-patient-physician-relationships. Accessed November 27, 2018.
4. Snyder L; Ethics, Professionalism, and Human Rights Committee. American College of Physicians Ethics Manual, 6th ed. Ann Intern Med. 2012;156(1, Part 2):73-104.
5. Levine A, Valeriote T. Beware the patient bearing gifts. http://epmonthly.com/article/beware-patient-bearing-gifts. Published December 14, 2016. Accessed November 27, 2018.
6. Brendel DH, Chu J, Radden J, et al. The price of a gift: an approach to receiving gifts from psychiatric patients. Harv Rev Psychiatry. 2007;15(2):43-51.

Jack Drescher: Sexual Conversion Therapy
Dr. Drescher is a psychiatrist and psychoanalyst in private practice in New York City. In this episode he explains issues with the therapy as well as how to treat patients who have undergone this “therapy.”
In 2016, Dr. Drescher and his colleagues authored a report that reviews the history of conversion therapy and offers guidelines for government regulations as well as for other regulatory bodies.
He and his colleagues wrote that “peer-reviewed literature from multiple professional organizations, including the American Psychiatric Association and the American Psychological Association, have found no evidence that conversion therapy treatments result in changes in sexual orientation.” They also noted that there is evidence suggesting that these treatments are harmful.
Dr. Drescher is a psychiatrist and psychoanalyst in private practice in New York City. In this episode he explains issues with the therapy as well as how to treat patients who have undergone this “therapy.”
In 2016, Dr. Drescher and his colleagues authored a report that reviews the history of conversion therapy and offers guidelines for government regulations as well as for other regulatory bodies.
He and his colleagues wrote that “peer-reviewed literature from multiple professional organizations, including the American Psychiatric Association and the American Psychological Association, have found no evidence that conversion therapy treatments result in changes in sexual orientation.” They also noted that there is evidence suggesting that these treatments are harmful.
Dr. Drescher is a psychiatrist and psychoanalyst in private practice in New York City. In this episode he explains issues with the therapy as well as how to treat patients who have undergone this “therapy.”
In 2016, Dr. Drescher and his colleagues authored a report that reviews the history of conversion therapy and offers guidelines for government regulations as well as for other regulatory bodies.
He and his colleagues wrote that “peer-reviewed literature from multiple professional organizations, including the American Psychiatric Association and the American Psychological Association, have found no evidence that conversion therapy treatments result in changes in sexual orientation.” They also noted that there is evidence suggesting that these treatments are harmful.