Randomized controlled trials in oncology can make or break an investigational drug, with both patient lives and pharmaceutical company profits at stake.
These trials typically pit two options against each other, an investigational therapy and a control therapy – often a standard of care – to see which has greater benefit.
But there are ethical gray areas in trial designs that may, intentionally or inadvertently, tip the balance in favor of the experimental arm of a trial. These biases may result in substandard care for trial participants, even harm, and can invalidate or dilute scientific findings.
One major issue is whether participants in the control arm of a trial receive the standard of care or active therapy after disease progression. In clinical trial parlance, this practice is called crossover.
Patients who do not receive standard-of-care therapy after disease progression may be “unfairly disadvantaged,” experts wrote in a commentary published in late June.What’s worse, optimal crossover does not always happen, commentary author Edward R. Scheffer Cliff, MBBS, MPH, from Brigham and Women’s Hospital in Boston said in an interview.
A recent example comes from the ADAURA trial comparing adjuvant therapy with osimertinib (Tagrisso) to placebo following complete resection of localized or locally advanced stage IB-IIIA non–small cell lung cancer (NSCLC) harboring EGFR mutations.
The trial, which began in November 2015, was unblinded early and halted on the recommendation of the independent data-monitoring committee because osimertinib was associated with a nearly 80% reduction in the risk of disease recurrence or death. These data led to the Food and Drug Administration’s 2018 approval of osimertinib as first-line treatment in this setting.
The recent overall survival data from ADAURA, presented at the 2023 American Society of Clinical Oncology annual meeting, helped confirm the drug’s benefit: Osimertinib was associated with a 51% reduced risk for death, compared with placebo.
But critics of this report were troubled by the fact that, despite the reported benefits of osimertinib, only 79 of 205 patients (38.5%) in the control arm who relapsed received the drug – now considered standard of care in this setting.
The low rate of osimertinib crossover represents a serious flaw in the trial design and potentially an ethical problem.
In the commentary, Dr. Cliff, alongside colleagues Aaron S. Kesselheim, MD, JD, MPH, and William B. Feldman, MD, DPhil, MPH, detailed the ethical issues associated with substandard crossover in clinical trials.
“In the ethical design of clinical trials, patients make important sacrifices to participate, and in exchange, the academic and clinical communities owe them optimal treatment both during the intervention part of the trial and, if they progress, after progression, especially when it is directly in the control of the trial sponsor as to whether a drug that they produce is made available to a clinical trial participant,” Dr. Cliff and colleagues wrote.
The authors highlighted 10 clinical trials – including SHINE,ZUMA-7,CLL14,ALCYONE, and JAVELIN 100 – that had problematic crossover. In the SHINE trial, for instance, 39% of control arm patients with mantle cell lymphoma received BTKi therapy post progression, while in the ALCYONE trial of multiple myeloma, only 10% of control patients received daratumumab at first progression. The VISION trial had the lowest crossover rate, with only one control arm patient (0.5%) with metastatic castration-resistant prostate cancer receiving lutetium-PSMA-617 after progression.
“Depriving control arm patients access to standard-of-care post-RCT therapy also has important scientific implications,” Dr. Cliff and colleagues wrote. In oncology, “if patients in the control arm do not receive standard-of-care therapy after disease progression, then they are unfairly disadvantaged, and it becomes difficult to assess whether the intervention has indeed improved quality of life or survival.”
Clinical trials should be designed with both ethical behavior and scientific integrity in mind, Dr. Cliff told this news organization. It’s incumbent on everyone directly or peripherally involved in randomized trials to ensure that they are designed with mandatory unblinding at the time of disease progression, and that crossover is both allowed and funded by the trial sponsor and mandated by the trial investigators and FDA.
When it comes to clinical trials and the sacrifices patients make to participate, “I think everyone needs to lift their game,” Dr. Cliff said.
The commentary by Dr. Cliff and colleagues was supported by Arnold Ventures. Dr. Cliff disclosed institutional funding from the firm. Dr. Kesselheim reported reimbursement for expert testimony. Dr. Feldman reported consulting for Alosa Health and Aetion, and expert testimony on litigation.
A version of this article appeared on Medscape.com.
Randomized controlled trials in oncology can make or break an investigational drug, with both patient lives and pharmaceutical company profits at stake.
These trials typically pit two options against each other, an investigational therapy and a control therapy – often a standard of care – to see which has greater benefit.
But there are ethical gray areas in trial designs that may, intentionally or inadvertently, tip the balance in favor of the experimental arm of a trial. These biases may result in substandard care for trial participants, even harm, and can invalidate or dilute scientific findings.
One major issue is whether participants in the control arm of a trial receive the standard of care or active therapy after disease progression. In clinical trial parlance, this practice is called crossover.
Patients who do not receive standard-of-care therapy after disease progression may be “unfairly disadvantaged,” experts wrote in a commentary published in late June.What’s worse, optimal crossover does not always happen, commentary author Edward R. Scheffer Cliff, MBBS, MPH, from Brigham and Women’s Hospital in Boston said in an interview.
A recent example comes from the ADAURA trial comparing adjuvant therapy with osimertinib (Tagrisso) to placebo following complete resection of localized or locally advanced stage IB-IIIA non–small cell lung cancer (NSCLC) harboring EGFR mutations.
The trial, which began in November 2015, was unblinded early and halted on the recommendation of the independent data-monitoring committee because osimertinib was associated with a nearly 80% reduction in the risk of disease recurrence or death. These data led to the Food and Drug Administration’s 2018 approval of osimertinib as first-line treatment in this setting.
The recent overall survival data from ADAURA, presented at the 2023 American Society of Clinical Oncology annual meeting, helped confirm the drug’s benefit: Osimertinib was associated with a 51% reduced risk for death, compared with placebo.
But critics of this report were troubled by the fact that, despite the reported benefits of osimertinib, only 79 of 205 patients (38.5%) in the control arm who relapsed received the drug – now considered standard of care in this setting.
The low rate of osimertinib crossover represents a serious flaw in the trial design and potentially an ethical problem.
In the commentary, Dr. Cliff, alongside colleagues Aaron S. Kesselheim, MD, JD, MPH, and William B. Feldman, MD, DPhil, MPH, detailed the ethical issues associated with substandard crossover in clinical trials.
“In the ethical design of clinical trials, patients make important sacrifices to participate, and in exchange, the academic and clinical communities owe them optimal treatment both during the intervention part of the trial and, if they progress, after progression, especially when it is directly in the control of the trial sponsor as to whether a drug that they produce is made available to a clinical trial participant,” Dr. Cliff and colleagues wrote.
The authors highlighted 10 clinical trials – including SHINE,ZUMA-7,CLL14,ALCYONE, and JAVELIN 100 – that had problematic crossover. In the SHINE trial, for instance, 39% of control arm patients with mantle cell lymphoma received BTKi therapy post progression, while in the ALCYONE trial of multiple myeloma, only 10% of control patients received daratumumab at first progression. The VISION trial had the lowest crossover rate, with only one control arm patient (0.5%) with metastatic castration-resistant prostate cancer receiving lutetium-PSMA-617 after progression.
“Depriving control arm patients access to standard-of-care post-RCT therapy also has important scientific implications,” Dr. Cliff and colleagues wrote. In oncology, “if patients in the control arm do not receive standard-of-care therapy after disease progression, then they are unfairly disadvantaged, and it becomes difficult to assess whether the intervention has indeed improved quality of life or survival.”
Clinical trials should be designed with both ethical behavior and scientific integrity in mind, Dr. Cliff told this news organization. It’s incumbent on everyone directly or peripherally involved in randomized trials to ensure that they are designed with mandatory unblinding at the time of disease progression, and that crossover is both allowed and funded by the trial sponsor and mandated by the trial investigators and FDA.
When it comes to clinical trials and the sacrifices patients make to participate, “I think everyone needs to lift their game,” Dr. Cliff said.
The commentary by Dr. Cliff and colleagues was supported by Arnold Ventures. Dr. Cliff disclosed institutional funding from the firm. Dr. Kesselheim reported reimbursement for expert testimony. Dr. Feldman reported consulting for Alosa Health and Aetion, and expert testimony on litigation.
A version of this article appeared on Medscape.com.
Randomized controlled trials in oncology can make or break an investigational drug, with both patient lives and pharmaceutical company profits at stake.
These trials typically pit two options against each other, an investigational therapy and a control therapy – often a standard of care – to see which has greater benefit.
But there are ethical gray areas in trial designs that may, intentionally or inadvertently, tip the balance in favor of the experimental arm of a trial. These biases may result in substandard care for trial participants, even harm, and can invalidate or dilute scientific findings.
One major issue is whether participants in the control arm of a trial receive the standard of care or active therapy after disease progression. In clinical trial parlance, this practice is called crossover.
Patients who do not receive standard-of-care therapy after disease progression may be “unfairly disadvantaged,” experts wrote in a commentary published in late June.What’s worse, optimal crossover does not always happen, commentary author Edward R. Scheffer Cliff, MBBS, MPH, from Brigham and Women’s Hospital in Boston said in an interview.
A recent example comes from the ADAURA trial comparing adjuvant therapy with osimertinib (Tagrisso) to placebo following complete resection of localized or locally advanced stage IB-IIIA non–small cell lung cancer (NSCLC) harboring EGFR mutations.
The trial, which began in November 2015, was unblinded early and halted on the recommendation of the independent data-monitoring committee because osimertinib was associated with a nearly 80% reduction in the risk of disease recurrence or death. These data led to the Food and Drug Administration’s 2018 approval of osimertinib as first-line treatment in this setting.
The recent overall survival data from ADAURA, presented at the 2023 American Society of Clinical Oncology annual meeting, helped confirm the drug’s benefit: Osimertinib was associated with a 51% reduced risk for death, compared with placebo.
But critics of this report were troubled by the fact that, despite the reported benefits of osimertinib, only 79 of 205 patients (38.5%) in the control arm who relapsed received the drug – now considered standard of care in this setting.
The low rate of osimertinib crossover represents a serious flaw in the trial design and potentially an ethical problem.
In the commentary, Dr. Cliff, alongside colleagues Aaron S. Kesselheim, MD, JD, MPH, and William B. Feldman, MD, DPhil, MPH, detailed the ethical issues associated with substandard crossover in clinical trials.
“In the ethical design of clinical trials, patients make important sacrifices to participate, and in exchange, the academic and clinical communities owe them optimal treatment both during the intervention part of the trial and, if they progress, after progression, especially when it is directly in the control of the trial sponsor as to whether a drug that they produce is made available to a clinical trial participant,” Dr. Cliff and colleagues wrote.
The authors highlighted 10 clinical trials – including SHINE,ZUMA-7,CLL14,ALCYONE, and JAVELIN 100 – that had problematic crossover. In the SHINE trial, for instance, 39% of control arm patients with mantle cell lymphoma received BTKi therapy post progression, while in the ALCYONE trial of multiple myeloma, only 10% of control patients received daratumumab at first progression. The VISION trial had the lowest crossover rate, with only one control arm patient (0.5%) with metastatic castration-resistant prostate cancer receiving lutetium-PSMA-617 after progression.
“Depriving control arm patients access to standard-of-care post-RCT therapy also has important scientific implications,” Dr. Cliff and colleagues wrote. In oncology, “if patients in the control arm do not receive standard-of-care therapy after disease progression, then they are unfairly disadvantaged, and it becomes difficult to assess whether the intervention has indeed improved quality of life or survival.”
Clinical trials should be designed with both ethical behavior and scientific integrity in mind, Dr. Cliff told this news organization. It’s incumbent on everyone directly or peripherally involved in randomized trials to ensure that they are designed with mandatory unblinding at the time of disease progression, and that crossover is both allowed and funded by the trial sponsor and mandated by the trial investigators and FDA.
When it comes to clinical trials and the sacrifices patients make to participate, “I think everyone needs to lift their game,” Dr. Cliff said.
The commentary by Dr. Cliff and colleagues was supported by Arnold Ventures. Dr. Cliff disclosed institutional funding from the firm. Dr. Kesselheim reported reimbursement for expert testimony. Dr. Feldman reported consulting for Alosa Health and Aetion, and expert testimony on litigation.
A version of this article appeared on Medscape.com.
Recently published conclusions from the first interim analysis of overall survival in the IMpower010 trial of adjuvant atezolizumab for non–small cell lung cancer (NSCLC) have met with some pushback on Twitter.
Here’s why.
At a median follow-up of 45.3 months, 127 of 507 patients (25%) in the atezolizumab group and 124 of 498 (24.9%) in the best supportive care group had died.
Among all 882 patients with stage II-IIIA disease, the investigators found no significant improvement in overall survival with atezolizumab, compared with best supportive care (hazard ratio, 0.95; 95% confidence interval, 0.74-1.24).
The researchers, however, concluded that the trial showed a “positive” trend favoring atezolizumab in PD-L1 subgroup analyses.
In a subgroup of 476 patients with tumor PD-L1 expression ≥ 1%, patients who received atezolizumab exhibited a nonsignificant 29% improvement in overall survival (HR, 0.71; 95% CI, 0.49-1.03). The best results were in the subgroup of 229 patients with tumor PD-L1 expression ≥ 50% – these patients exhibited a 57% improvement in overall survival with atezolizumab (HR, 0.43; 95% CI, 0.24-0.78). Those with PD-L1 expression 1%-49%, however, demonstrated no improvement in overall survival (HR, 0.95).
In a Twitter post, H. Jack West, MD, City of Hope Comprehensive Cancer Center, Duarte, Calif., urged caution in interpreting the study data: “Let’s be clear: OS results are neg for OS benefit in PD-L1+ NSCLC. If we’re going to rely on smaller subgroups to highlight HR of 0.43 for those w/high PD-L1, we should also note HR for OS was 0.95 (i.e., NO trend for OS benefit) for those w/PD-L1 1-49%.”
The tweet continued: “With favorable results driven entirely by a 30% subgroup, it’s understandable that Roche would want to also promote benefit in broader population. But we shouldn’t perpetuate misinformation that there’s a benefit for broad group of PD-L1+, even if the effort is to market it this way.”
In an interview, Dr. West elaborated on his tweet, explaining that the way the overall survival data are presented in the paper is “disingenuous and misleading.”
The paper clearly highlights that the drug was significantly beneficial for the narrower population who had high PD-L1 expression. But the hazard ratio of 0.95 for the entire population is like “where’s Waldo in this paper. It’s almost impossible to find, but it should have been prominently included in the figure of results by subgroup,” Dr. West said.
“This is something that should have been objected to by the oncologists on the paper and by the reviews and the editors,” Dr. West said.
Two other oncologists agreed.
Joel Grossman, MD, tweeted: “Bingo. I’m not sure we need cancer ground shots or lengthy treatises on common sense, but I am damn sure we need honest interpretation of clinical trial data as Jack shows here. We can’t tolerate over-broad borderline deception that leads to poor and wasteful decision-making.”
Jeff Ryckman, MD, tweeted: “Problem is, this is a routine FDA #CarteBlanche approval regardless of no benefit in PD-L1 1%-49%. This will be Rx’d to everyone.”
Regulatory ‘gamesmanship’
The results of the IMpower010 analysis were published online in Annals of Oncology. The interim overall survival data were first reported last year at the World Conference on Lung Cancer.
IMpower010 was a global, randomized, open-label trial of 1,280 patients with completely resected stage IB (tumors ≥ 4 cm) through stage IIIA NSCLC for whom tissue samples were available for PD-L1 analysis.
All patients received four cycles of chemotherapy with cisplatin plus either pemetrexed, gemcitabine, docetaxel, or vinorelbine and were randomly assigned in a 1:1 ratio to receive either 16 cycles of atezolizumab or best supportive care.
Interim disease-free survival (DFS) results from IMpower010, presented at ASCO 2021, showed that patients with PD-L1 expression ≥ 1% experienced a 34% improvement in DFS, equating to a 21% improvement across all randomly assigned patients with stage II-IIIA disease.
On the basis of DFS findings, in 2021, the U.S. Food and Drug Administration granted atezolizumab a new indication – the adjuvant treatment following resection and platinum-based chemotherapy for patients with stage II-IIIA NSCLC whose tumors have PD-L1 expression ≥ 1%.
Looking at the big picture, Dr. West noted that regulatory approval for a drug allows for a certain amount of “gamesmanship.”
“It behooves a company to work with FDA to get approval for a broader population than it should be, relative to where the true clinical benefit lies,” he explained.
To this end, Dr. West noted that progression-free survival is increasingly being used as a primary endpoint in trials, but long-term data indicate that this surrogate endpoint is often not tethered to an overall survival benefit. However, drugs are often being approved now on the basis of a progression-free survival benefit.
“Unfortunately, that’s the system we live in today, with a bias toward, ‘If it could plausibly be interpreted as beneficial, we’ll wave it through for the broadest population possible,” Dr. West said.
The IMpower010 study and Annals of Oncology manuscript were funded by F. Hoffmann-La Roche. Several authors have disclosed relationships with the company. Dr. West has a regular column on Medscape.com and reported personal fees from AstraZeneca, Genentech/Roche, Merck, and Regeneron.
A version of this article appeared on Medscape.com.
Recently published conclusions from the first interim analysis of overall survival in the IMpower010 trial of adjuvant atezolizumab for non–small cell lung cancer (NSCLC) have met with some pushback on Twitter.
Here’s why.
At a median follow-up of 45.3 months, 127 of 507 patients (25%) in the atezolizumab group and 124 of 498 (24.9%) in the best supportive care group had died.
Among all 882 patients with stage II-IIIA disease, the investigators found no significant improvement in overall survival with atezolizumab, compared with best supportive care (hazard ratio, 0.95; 95% confidence interval, 0.74-1.24).
The researchers, however, concluded that the trial showed a “positive” trend favoring atezolizumab in PD-L1 subgroup analyses.
In a subgroup of 476 patients with tumor PD-L1 expression ≥ 1%, patients who received atezolizumab exhibited a nonsignificant 29% improvement in overall survival (HR, 0.71; 95% CI, 0.49-1.03). The best results were in the subgroup of 229 patients with tumor PD-L1 expression ≥ 50% – these patients exhibited a 57% improvement in overall survival with atezolizumab (HR, 0.43; 95% CI, 0.24-0.78). Those with PD-L1 expression 1%-49%, however, demonstrated no improvement in overall survival (HR, 0.95).
In a Twitter post, H. Jack West, MD, City of Hope Comprehensive Cancer Center, Duarte, Calif., urged caution in interpreting the study data: “Let’s be clear: OS results are neg for OS benefit in PD-L1+ NSCLC. If we’re going to rely on smaller subgroups to highlight HR of 0.43 for those w/high PD-L1, we should also note HR for OS was 0.95 (i.e., NO trend for OS benefit) for those w/PD-L1 1-49%.”
The tweet continued: “With favorable results driven entirely by a 30% subgroup, it’s understandable that Roche would want to also promote benefit in broader population. But we shouldn’t perpetuate misinformation that there’s a benefit for broad group of PD-L1+, even if the effort is to market it this way.”
In an interview, Dr. West elaborated on his tweet, explaining that the way the overall survival data are presented in the paper is “disingenuous and misleading.”
The paper clearly highlights that the drug was significantly beneficial for the narrower population who had high PD-L1 expression. But the hazard ratio of 0.95 for the entire population is like “where’s Waldo in this paper. It’s almost impossible to find, but it should have been prominently included in the figure of results by subgroup,” Dr. West said.
“This is something that should have been objected to by the oncologists on the paper and by the reviews and the editors,” Dr. West said.
Two other oncologists agreed.
Joel Grossman, MD, tweeted: “Bingo. I’m not sure we need cancer ground shots or lengthy treatises on common sense, but I am damn sure we need honest interpretation of clinical trial data as Jack shows here. We can’t tolerate over-broad borderline deception that leads to poor and wasteful decision-making.”
Jeff Ryckman, MD, tweeted: “Problem is, this is a routine FDA #CarteBlanche approval regardless of no benefit in PD-L1 1%-49%. This will be Rx’d to everyone.”
Regulatory ‘gamesmanship’
The results of the IMpower010 analysis were published online in Annals of Oncology. The interim overall survival data were first reported last year at the World Conference on Lung Cancer.
IMpower010 was a global, randomized, open-label trial of 1,280 patients with completely resected stage IB (tumors ≥ 4 cm) through stage IIIA NSCLC for whom tissue samples were available for PD-L1 analysis.
All patients received four cycles of chemotherapy with cisplatin plus either pemetrexed, gemcitabine, docetaxel, or vinorelbine and were randomly assigned in a 1:1 ratio to receive either 16 cycles of atezolizumab or best supportive care.
Interim disease-free survival (DFS) results from IMpower010, presented at ASCO 2021, showed that patients with PD-L1 expression ≥ 1% experienced a 34% improvement in DFS, equating to a 21% improvement across all randomly assigned patients with stage II-IIIA disease.
On the basis of DFS findings, in 2021, the U.S. Food and Drug Administration granted atezolizumab a new indication – the adjuvant treatment following resection and platinum-based chemotherapy for patients with stage II-IIIA NSCLC whose tumors have PD-L1 expression ≥ 1%.
Looking at the big picture, Dr. West noted that regulatory approval for a drug allows for a certain amount of “gamesmanship.”
“It behooves a company to work with FDA to get approval for a broader population than it should be, relative to where the true clinical benefit lies,” he explained.
To this end, Dr. West noted that progression-free survival is increasingly being used as a primary endpoint in trials, but long-term data indicate that this surrogate endpoint is often not tethered to an overall survival benefit. However, drugs are often being approved now on the basis of a progression-free survival benefit.
“Unfortunately, that’s the system we live in today, with a bias toward, ‘If it could plausibly be interpreted as beneficial, we’ll wave it through for the broadest population possible,” Dr. West said.
The IMpower010 study and Annals of Oncology manuscript were funded by F. Hoffmann-La Roche. Several authors have disclosed relationships with the company. Dr. West has a regular column on Medscape.com and reported personal fees from AstraZeneca, Genentech/Roche, Merck, and Regeneron.
A version of this article appeared on Medscape.com.
Recently published conclusions from the first interim analysis of overall survival in the IMpower010 trial of adjuvant atezolizumab for non–small cell lung cancer (NSCLC) have met with some pushback on Twitter.
Here’s why.
At a median follow-up of 45.3 months, 127 of 507 patients (25%) in the atezolizumab group and 124 of 498 (24.9%) in the best supportive care group had died.
Among all 882 patients with stage II-IIIA disease, the investigators found no significant improvement in overall survival with atezolizumab, compared with best supportive care (hazard ratio, 0.95; 95% confidence interval, 0.74-1.24).
The researchers, however, concluded that the trial showed a “positive” trend favoring atezolizumab in PD-L1 subgroup analyses.
In a subgroup of 476 patients with tumor PD-L1 expression ≥ 1%, patients who received atezolizumab exhibited a nonsignificant 29% improvement in overall survival (HR, 0.71; 95% CI, 0.49-1.03). The best results were in the subgroup of 229 patients with tumor PD-L1 expression ≥ 50% – these patients exhibited a 57% improvement in overall survival with atezolizumab (HR, 0.43; 95% CI, 0.24-0.78). Those with PD-L1 expression 1%-49%, however, demonstrated no improvement in overall survival (HR, 0.95).
In a Twitter post, H. Jack West, MD, City of Hope Comprehensive Cancer Center, Duarte, Calif., urged caution in interpreting the study data: “Let’s be clear: OS results are neg for OS benefit in PD-L1+ NSCLC. If we’re going to rely on smaller subgroups to highlight HR of 0.43 for those w/high PD-L1, we should also note HR for OS was 0.95 (i.e., NO trend for OS benefit) for those w/PD-L1 1-49%.”
The tweet continued: “With favorable results driven entirely by a 30% subgroup, it’s understandable that Roche would want to also promote benefit in broader population. But we shouldn’t perpetuate misinformation that there’s a benefit for broad group of PD-L1+, even if the effort is to market it this way.”
In an interview, Dr. West elaborated on his tweet, explaining that the way the overall survival data are presented in the paper is “disingenuous and misleading.”
The paper clearly highlights that the drug was significantly beneficial for the narrower population who had high PD-L1 expression. But the hazard ratio of 0.95 for the entire population is like “where’s Waldo in this paper. It’s almost impossible to find, but it should have been prominently included in the figure of results by subgroup,” Dr. West said.
“This is something that should have been objected to by the oncologists on the paper and by the reviews and the editors,” Dr. West said.
Two other oncologists agreed.
Joel Grossman, MD, tweeted: “Bingo. I’m not sure we need cancer ground shots or lengthy treatises on common sense, but I am damn sure we need honest interpretation of clinical trial data as Jack shows here. We can’t tolerate over-broad borderline deception that leads to poor and wasteful decision-making.”
Jeff Ryckman, MD, tweeted: “Problem is, this is a routine FDA #CarteBlanche approval regardless of no benefit in PD-L1 1%-49%. This will be Rx’d to everyone.”
Regulatory ‘gamesmanship’
The results of the IMpower010 analysis were published online in Annals of Oncology. The interim overall survival data were first reported last year at the World Conference on Lung Cancer.
IMpower010 was a global, randomized, open-label trial of 1,280 patients with completely resected stage IB (tumors ≥ 4 cm) through stage IIIA NSCLC for whom tissue samples were available for PD-L1 analysis.
All patients received four cycles of chemotherapy with cisplatin plus either pemetrexed, gemcitabine, docetaxel, or vinorelbine and were randomly assigned in a 1:1 ratio to receive either 16 cycles of atezolizumab or best supportive care.
Interim disease-free survival (DFS) results from IMpower010, presented at ASCO 2021, showed that patients with PD-L1 expression ≥ 1% experienced a 34% improvement in DFS, equating to a 21% improvement across all randomly assigned patients with stage II-IIIA disease.
On the basis of DFS findings, in 2021, the U.S. Food and Drug Administration granted atezolizumab a new indication – the adjuvant treatment following resection and platinum-based chemotherapy for patients with stage II-IIIA NSCLC whose tumors have PD-L1 expression ≥ 1%.
Looking at the big picture, Dr. West noted that regulatory approval for a drug allows for a certain amount of “gamesmanship.”
“It behooves a company to work with FDA to get approval for a broader population than it should be, relative to where the true clinical benefit lies,” he explained.
To this end, Dr. West noted that progression-free survival is increasingly being used as a primary endpoint in trials, but long-term data indicate that this surrogate endpoint is often not tethered to an overall survival benefit. However, drugs are often being approved now on the basis of a progression-free survival benefit.
“Unfortunately, that’s the system we live in today, with a bias toward, ‘If it could plausibly be interpreted as beneficial, we’ll wave it through for the broadest population possible,” Dr. West said.
The IMpower010 study and Annals of Oncology manuscript were funded by F. Hoffmann-La Roche. Several authors have disclosed relationships with the company. Dr. West has a regular column on Medscape.com and reported personal fees from AstraZeneca, Genentech/Roche, Merck, and Regeneron.
A version of this article appeared on Medscape.com.
Irradiating a small number of metastatic lesions does not appear to improve progression-free or overall survival in patients receiving immune checkpoint inhibitor monotherapy for advanced cancer.
METHODOLOGY:
In the phase 2 CHEERS trial, 52 patients with advanced solid tumors were randomized to anti-PD-1/PD-L1 monotherapy and 47 patients to the same treatment plus stereotactic body radiotherapy (3 x 8 Gy) to a maximum of three lesions before the second or third cycle of an immune checkpoint inhibitor.
Patients had locally advanced or metastatic melanoma, renal cell carcinoma, urothelial carcinoma, non-small cell lung carcinoma, or head and neck squamous cell carcinoma and were treated at five Belgian hospitals.
Most patients had more than three lesions.
Seven patients in the experimental group did not complete radiotherapy because of early progression or intercurrent illness.
TAKEAWAY:
Over a median follow-up of 12.5 months, median progression-free survival was 4.4 months in the radiotherapy group versus 2.8 months in the control group (hazard ratio, 0.95; P = .82).
Median overall survival was not significantly better with radiotherapy, compared with the control group (14.3 vs. 11 months; HR, 0.82; P = .47), nor was the objective response rate (27% vs. 22%; P = .56).
However, a post hoc analysis demonstrated a significant association between the number of irradiated lesions and overall survival among patients receiving radiotherapy (HR, 0.31; P = .002).
The incidence of grade 3 or worse treatment-related adverse events was 18% in both groups.
IN PRACTICE:
Although the study was negative overall, the post hoc analysis coupled with “recent evidence suggests that treating all active disease sites with higher radiation doses ... may be a more promising strategy to optimize systemic disease control,” the authors concluded.
SOURCE:
The study was led by Mathieu Spaas, MD, department of radiation oncology, Ghent (Bellgium) University, and published online in JAMA Oncology.
LIMITATIONS:
There was insufficient power to detect if certain cancers benefited more from add-on radiation because of the small sample size.
More than half of patients in the control group had already received some form of radiotherapy before study inclusion, which may mean the study underestimated the benefit of radiotherapy.
DISCLOSURES:
The work was funded by Kom Op Tegen Kanker and Varian Medical Systems.
Investigators disclosed numerous industry ties, including Merck, Novartis, and Bristol Myers Squibb.
A version of this article first appeared on Medscape.com.
Irradiating a small number of metastatic lesions does not appear to improve progression-free or overall survival in patients receiving immune checkpoint inhibitor monotherapy for advanced cancer.
METHODOLOGY:
In the phase 2 CHEERS trial, 52 patients with advanced solid tumors were randomized to anti-PD-1/PD-L1 monotherapy and 47 patients to the same treatment plus stereotactic body radiotherapy (3 x 8 Gy) to a maximum of three lesions before the second or third cycle of an immune checkpoint inhibitor.
Patients had locally advanced or metastatic melanoma, renal cell carcinoma, urothelial carcinoma, non-small cell lung carcinoma, or head and neck squamous cell carcinoma and were treated at five Belgian hospitals.
Most patients had more than three lesions.
Seven patients in the experimental group did not complete radiotherapy because of early progression or intercurrent illness.
TAKEAWAY:
Over a median follow-up of 12.5 months, median progression-free survival was 4.4 months in the radiotherapy group versus 2.8 months in the control group (hazard ratio, 0.95; P = .82).
Median overall survival was not significantly better with radiotherapy, compared with the control group (14.3 vs. 11 months; HR, 0.82; P = .47), nor was the objective response rate (27% vs. 22%; P = .56).
However, a post hoc analysis demonstrated a significant association between the number of irradiated lesions and overall survival among patients receiving radiotherapy (HR, 0.31; P = .002).
The incidence of grade 3 or worse treatment-related adverse events was 18% in both groups.
IN PRACTICE:
Although the study was negative overall, the post hoc analysis coupled with “recent evidence suggests that treating all active disease sites with higher radiation doses ... may be a more promising strategy to optimize systemic disease control,” the authors concluded.
SOURCE:
The study was led by Mathieu Spaas, MD, department of radiation oncology, Ghent (Bellgium) University, and published online in JAMA Oncology.
LIMITATIONS:
There was insufficient power to detect if certain cancers benefited more from add-on radiation because of the small sample size.
More than half of patients in the control group had already received some form of radiotherapy before study inclusion, which may mean the study underestimated the benefit of radiotherapy.
DISCLOSURES:
The work was funded by Kom Op Tegen Kanker and Varian Medical Systems.
Investigators disclosed numerous industry ties, including Merck, Novartis, and Bristol Myers Squibb.
A version of this article first appeared on Medscape.com.
TOPLINE:
Irradiating a small number of metastatic lesions does not appear to improve progression-free or overall survival in patients receiving immune checkpoint inhibitor monotherapy for advanced cancer.
METHODOLOGY:
In the phase 2 CHEERS trial, 52 patients with advanced solid tumors were randomized to anti-PD-1/PD-L1 monotherapy and 47 patients to the same treatment plus stereotactic body radiotherapy (3 x 8 Gy) to a maximum of three lesions before the second or third cycle of an immune checkpoint inhibitor.
Patients had locally advanced or metastatic melanoma, renal cell carcinoma, urothelial carcinoma, non-small cell lung carcinoma, or head and neck squamous cell carcinoma and were treated at five Belgian hospitals.
Most patients had more than three lesions.
Seven patients in the experimental group did not complete radiotherapy because of early progression or intercurrent illness.
TAKEAWAY:
Over a median follow-up of 12.5 months, median progression-free survival was 4.4 months in the radiotherapy group versus 2.8 months in the control group (hazard ratio, 0.95; P = .82).
Median overall survival was not significantly better with radiotherapy, compared with the control group (14.3 vs. 11 months; HR, 0.82; P = .47), nor was the objective response rate (27% vs. 22%; P = .56).
However, a post hoc analysis demonstrated a significant association between the number of irradiated lesions and overall survival among patients receiving radiotherapy (HR, 0.31; P = .002).
The incidence of grade 3 or worse treatment-related adverse events was 18% in both groups.
IN PRACTICE:
Although the study was negative overall, the post hoc analysis coupled with “recent evidence suggests that treating all active disease sites with higher radiation doses ... may be a more promising strategy to optimize systemic disease control,” the authors concluded.
SOURCE:
The study was led by Mathieu Spaas, MD, department of radiation oncology, Ghent (Bellgium) University, and published online in JAMA Oncology.
LIMITATIONS:
There was insufficient power to detect if certain cancers benefited more from add-on radiation because of the small sample size.
More than half of patients in the control group had already received some form of radiotherapy before study inclusion, which may mean the study underestimated the benefit of radiotherapy.
DISCLOSURES:
The work was funded by Kom Op Tegen Kanker and Varian Medical Systems.
Investigators disclosed numerous industry ties, including Merck, Novartis, and Bristol Myers Squibb.
A version of this article first appeared on Medscape.com.
Pembrolizumab doesn’t work as well for patients with metastatic non–small cell lung cancer (NSCLC) who have diabetes.
METHODOLOGY:
Investigators reviewed the medical records of 203 consecutive patients with metastatic NSCLC who received first-line pembrolizumab either alone or in combination with chemotherapy at a single tertiary center in Israel.
Overall, 1 in 4 patients (n = 51) had diabetes mellitus; most (n = 42) were being treated with oral hypoglycemic agents, frequently metformin, and 7 were taking insulin.
Rates of tumors with PD‐L1 expression above 50% were not significantly different among patients with diabetes and those without.
TAKEAWAY:
Overall, among patients with diabetes, median progression-free survival (PFS) was significantly shorter than among patients without diabetes (5.9 vs. 7.1 months), as was overall survival (12 vs. 21 months).
Shorter overall survival was more pronounced among those with diabetes who received pembrolizumab alone (12 vs. 27 months) in comparison with patients who received pembrolizumab plus chemotherapy (14.3 vs. 19.4 months).
After adjusting for potential confounders, multivariate analysis confirmed that diabetes was an independent risk factor for shorter PFS (hazard ratio, 1.67) and shorter overall survival (HR, 1.73) for patients with NSCLC.
In a validation cohort of 452 patients with metastatic NSCLC, only 19.6% of those with diabetes continued to take pembrolizumab at 12 months versus 31.7% of those without diabetes.
IN PRACTICE:
“As NSCLC patients with [diabetes] constitute a significant subgroup, there is an urgent need to validate our findings and explore whether outcomes in these patients can be improved by better glycemic control,” the authors said, adding that “chemotherapy may offset some of the deleterious effects” of diabetes.
SOURCE:
The study was led by Yasmin Leshem, MD, PhD, of the Tel Aviv Sourasky Medical Center, and was published in Cancer.
LIMITATIONS:
Without access to blood test results outside the hospital, the researchers could not determine whether better glycemic control might have improved outcomes.
The incidence of type 1 or 2 diabetes was not well documented.
DISCLOSURES:
No funding source was reported.
Two investigators reported receiving consulting and/or other fees from Bristol-Myers Squibb, Roche, Merck, Novartis, and Merck Sharp and Dohme.
A version of this article first appeared on Medscape.com.
Pembrolizumab doesn’t work as well for patients with metastatic non–small cell lung cancer (NSCLC) who have diabetes.
METHODOLOGY:
Investigators reviewed the medical records of 203 consecutive patients with metastatic NSCLC who received first-line pembrolizumab either alone or in combination with chemotherapy at a single tertiary center in Israel.
Overall, 1 in 4 patients (n = 51) had diabetes mellitus; most (n = 42) were being treated with oral hypoglycemic agents, frequently metformin, and 7 were taking insulin.
Rates of tumors with PD‐L1 expression above 50% were not significantly different among patients with diabetes and those without.
TAKEAWAY:
Overall, among patients with diabetes, median progression-free survival (PFS) was significantly shorter than among patients without diabetes (5.9 vs. 7.1 months), as was overall survival (12 vs. 21 months).
Shorter overall survival was more pronounced among those with diabetes who received pembrolizumab alone (12 vs. 27 months) in comparison with patients who received pembrolizumab plus chemotherapy (14.3 vs. 19.4 months).
After adjusting for potential confounders, multivariate analysis confirmed that diabetes was an independent risk factor for shorter PFS (hazard ratio, 1.67) and shorter overall survival (HR, 1.73) for patients with NSCLC.
In a validation cohort of 452 patients with metastatic NSCLC, only 19.6% of those with diabetes continued to take pembrolizumab at 12 months versus 31.7% of those without diabetes.
IN PRACTICE:
“As NSCLC patients with [diabetes] constitute a significant subgroup, there is an urgent need to validate our findings and explore whether outcomes in these patients can be improved by better glycemic control,” the authors said, adding that “chemotherapy may offset some of the deleterious effects” of diabetes.
SOURCE:
The study was led by Yasmin Leshem, MD, PhD, of the Tel Aviv Sourasky Medical Center, and was published in Cancer.
LIMITATIONS:
Without access to blood test results outside the hospital, the researchers could not determine whether better glycemic control might have improved outcomes.
The incidence of type 1 or 2 diabetes was not well documented.
DISCLOSURES:
No funding source was reported.
Two investigators reported receiving consulting and/or other fees from Bristol-Myers Squibb, Roche, Merck, Novartis, and Merck Sharp and Dohme.
A version of this article first appeared on Medscape.com.
TOPLINE:
Pembrolizumab doesn’t work as well for patients with metastatic non–small cell lung cancer (NSCLC) who have diabetes.
METHODOLOGY:
Investigators reviewed the medical records of 203 consecutive patients with metastatic NSCLC who received first-line pembrolizumab either alone or in combination with chemotherapy at a single tertiary center in Israel.
Overall, 1 in 4 patients (n = 51) had diabetes mellitus; most (n = 42) were being treated with oral hypoglycemic agents, frequently metformin, and 7 were taking insulin.
Rates of tumors with PD‐L1 expression above 50% were not significantly different among patients with diabetes and those without.
TAKEAWAY:
Overall, among patients with diabetes, median progression-free survival (PFS) was significantly shorter than among patients without diabetes (5.9 vs. 7.1 months), as was overall survival (12 vs. 21 months).
Shorter overall survival was more pronounced among those with diabetes who received pembrolizumab alone (12 vs. 27 months) in comparison with patients who received pembrolizumab plus chemotherapy (14.3 vs. 19.4 months).
After adjusting for potential confounders, multivariate analysis confirmed that diabetes was an independent risk factor for shorter PFS (hazard ratio, 1.67) and shorter overall survival (HR, 1.73) for patients with NSCLC.
In a validation cohort of 452 patients with metastatic NSCLC, only 19.6% of those with diabetes continued to take pembrolizumab at 12 months versus 31.7% of those without diabetes.
IN PRACTICE:
“As NSCLC patients with [diabetes] constitute a significant subgroup, there is an urgent need to validate our findings and explore whether outcomes in these patients can be improved by better glycemic control,” the authors said, adding that “chemotherapy may offset some of the deleterious effects” of diabetes.
SOURCE:
The study was led by Yasmin Leshem, MD, PhD, of the Tel Aviv Sourasky Medical Center, and was published in Cancer.
LIMITATIONS:
Without access to blood test results outside the hospital, the researchers could not determine whether better glycemic control might have improved outcomes.
The incidence of type 1 or 2 diabetes was not well documented.
DISCLOSURES:
No funding source was reported.
Two investigators reported receiving consulting and/or other fees from Bristol-Myers Squibb, Roche, Merck, Novartis, and Merck Sharp and Dohme.
A version of this article first appeared on Medscape.com.
Federal Practitioner and the Association of VA Hematology/Oncology (AVAHO) present the 2023 edition of Cancer Data Trends (click to view the digital edition).This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.
Federal Practitioner and the Association of VA Hematology/Oncology (AVAHO) present the 2023 edition of Cancer Data Trends (click to view the digital edition).This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.
Federal Practitioner and the Association of VA Hematology/Oncology (AVAHO) present the 2023 edition of Cancer Data Trends (click to view the digital edition).This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.
Boudreau JH et al. Chest. 2021;160(1):358-367. doi:10.1016/j.chest.2021.02.016
Maurice NM, Tanner NT. Semin Oncol. 2022;S0093-7754(22)00041-0. doi:10.1053/j.seminoncol.2022.06.001
Rusher TN et al. Fed Pract. 2022;39(suppl 2):S48-S51. doi:10.12788/fp.0269
Núñez ER et al. JAMA Netw Open. 2021;4(7):e2116233. doi:10.1001/jamanetworkopen.2021.16233
Lake M et al. BMC Cancer. 2020;20(1):561. doi:1186/s12885-020-06923-0
Author and Disclosure Information
Apar Kishor Ganti, MD, MS Doctor and Mrs. D. Leon UNMC Research Fund Chair in Internal Medicine Staff Physician, VA Nebraska-Western Iowa Health Care System Professor of Medicine, Division of Oncology-Hematology Professor (Courtesy) of Biochemistry and Molecular Biology Associate Director of Clinical Research, Fred & Pamela Buffett Cancer Center University of Nebraska Medical Center Omaha, NE
Apar Kishor Ganti, MD, MS Doctor and Mrs. D. Leon UNMC Research Fund Chair in Internal Medicine Staff Physician, VA Nebraska-Western Iowa Health Care System Professor of Medicine, Division of Oncology-Hematology Professor (Courtesy) of Biochemistry and Molecular Biology Associate Director of Clinical Research, Fred & Pamela Buffett Cancer Center University of Nebraska Medical Center Omaha, NE
Author and Disclosure Information
Apar Kishor Ganti, MD, MS Doctor and Mrs. D. Leon UNMC Research Fund Chair in Internal Medicine Staff Physician, VA Nebraska-Western Iowa Health Care System Professor of Medicine, Division of Oncology-Hematology Professor (Courtesy) of Biochemistry and Molecular Biology Associate Director of Clinical Research, Fred & Pamela Buffett Cancer Center University of Nebraska Medical Center Omaha, NE
Consolidated Pubs: Do Not Show Source Publication Logo
Use ProPublica
CFC Schedule Remove Status
Hide sidebar & use full width
render the right sidebar.
Conference Recap Checkbox
Not Conference Recap
Clinical Edge
Display the Slideshow in this Article
Article Slideshow Optional Introduction
Slideshow below.
In the United States and among veterans, lung cancer has the highest rate of cancer-related mortality. Earlier detection and increased screening of high-risk individuals can improve the overall survival rate.1 With the broadening of the USPSTF lung cancer screening guidelines, in 2020 an estimated 15 million people in the United States—including at least 900,000 veterans—were eligible for lung cancer screening by CT.2,3 However, only 5% of those eligible were screened.4,5 One reason for this vast discrepancy is uneven access. Estimates in 2021 were that <20% of eligible veterans have undergone lung cancer screening because of problems accessing it in rural areas.6
Implementing the expanded USPSTF guidelines is key to maximizing screening among underserved populations, such as those in rural areas who may lack access to nearby health care, as well as racial and ethnic minorities.1 A study of one VAMCs standardization of screening practices found that radiologists were more likely to adapt to these changes than primary care clinicians, suggesting a need to better understand differences in health care professional practices and priorities to universally improve screening rates across the VA.1
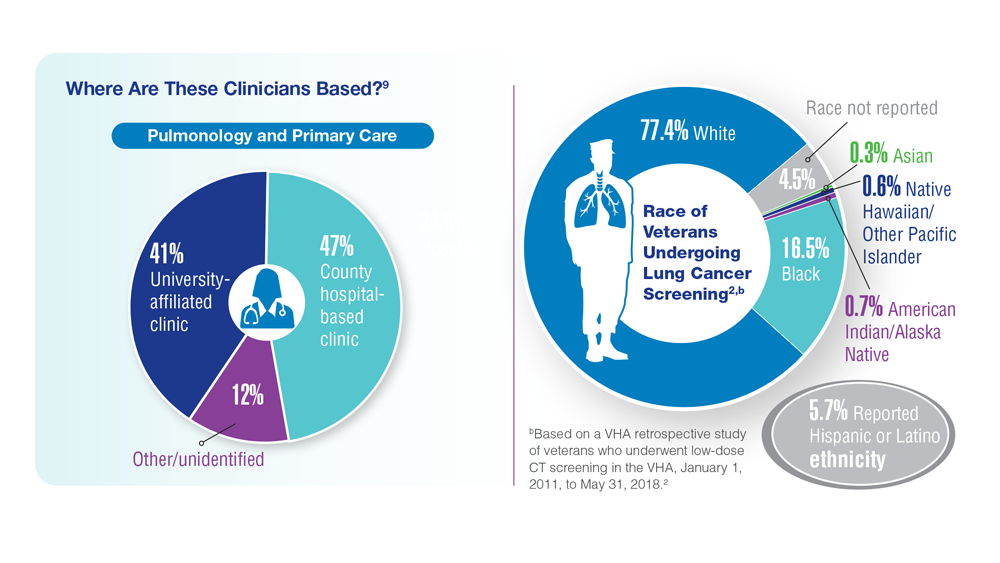
An important question will always be how many high-risk veterans are being screened for lung cancer?1 To ensure proper care, it is important to understand the characteristics of clinicians who provide screening based on setting and clinical areas of expertise. Where are they, who are they, and how do our most vulnerable populations gain access? Access is critical, particularly among clinicians who typically provide screening to those underserved populations.
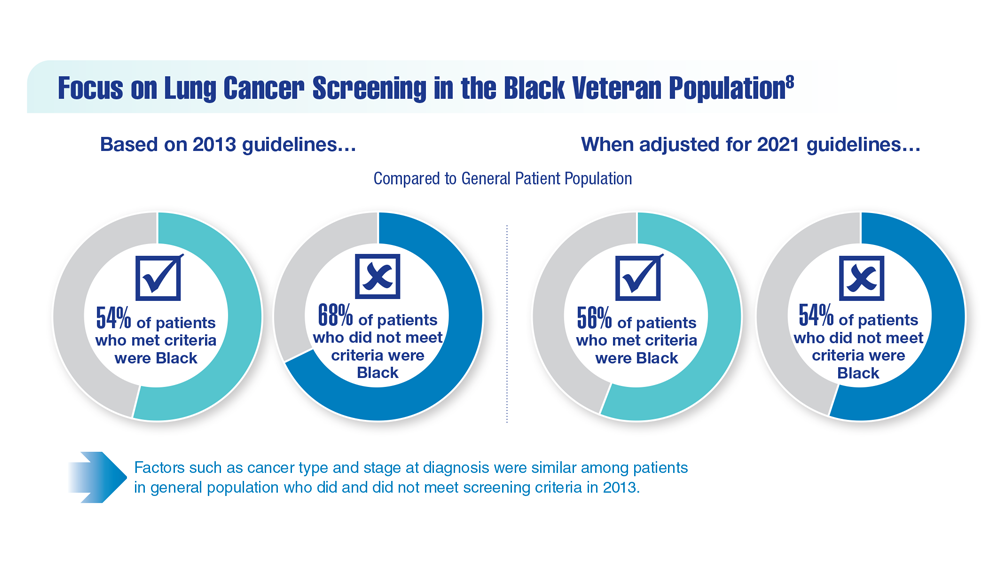
Although lung cancer screening rates have increased over the years, overall, utilization remains low, even though data show a 20% reduction in lung cancer mortality with adherence to yearly CT screening.7 Looking at these rates helps us understand the need to intervene to increase lung cancer screening rates.8 Guidelines have been an essential component when it comes to outcomes related to screenings. Through programs implemented by the VHA, the goal is to improve the uptake and quality of lung cancer screening and optimize the practice and access for all veterans.9 For clinicians, future work should evaluate lung cancer screening programs with high vs low rates of adherence to identify and publicize best practices for timely, appropriate follow-up.9 Although adherence rates remain low regardless of race, further research, particularly among Black veterans, is encouraged to address delayed follow-up and to create culturally competent and inclusive lung cancer screening programs.10
Small-cell lung cancer (SCLC) occurs almost exclusively in cigarette smokers. Veterans are particularly vulnerable to SCLC because of their prevalent smoking history and exposures to carcinogens, including Agent Orange.
SCLC is characterized by the early development of widespread metastases, including liver, bone, and brain.
Unlike, non–-small cell lung cancer, which has seen great improvement in survival from the introduction of immunotherapy and targeted agents, there has been relatively little improvement in SCLC.
Patients generally are classified into limited- and extensive-stage disease, but platinum-based chemotherapy is almost always the standard first-line treatment. Unfortunately, most patients relapse within a year.
In this ReCAP, Dr Shadia Jalal, of Indiana University Melvin and Bren Simon Comprehensive Cancer Center, discusses second-line treatment options for SCLC patients who relapse after chemotherapy. She also discusses four subtypes of SCLC categorized on the basis of specific transcription regulators, which may offer the potential of targeted therapies for this patient population.
--
Shadia Jalal, MD, Associate Professor of Medicine, Physician, Indiana University Melvin and Bren Simon Comprehensive Cancer Center, Indianapolis, Indiana
Shadia Jalal, MD, has disclosed no relevant financial relationships.
Small-cell lung cancer (SCLC) occurs almost exclusively in cigarette smokers. Veterans are particularly vulnerable to SCLC because of their prevalent smoking history and exposures to carcinogens, including Agent Orange.
SCLC is characterized by the early development of widespread metastases, including liver, bone, and brain.
Unlike, non–-small cell lung cancer, which has seen great improvement in survival from the introduction of immunotherapy and targeted agents, there has been relatively little improvement in SCLC.
Patients generally are classified into limited- and extensive-stage disease, but platinum-based chemotherapy is almost always the standard first-line treatment. Unfortunately, most patients relapse within a year.
In this ReCAP, Dr Shadia Jalal, of Indiana University Melvin and Bren Simon Comprehensive Cancer Center, discusses second-line treatment options for SCLC patients who relapse after chemotherapy. She also discusses four subtypes of SCLC categorized on the basis of specific transcription regulators, which may offer the potential of targeted therapies for this patient population.
--
Shadia Jalal, MD, Associate Professor of Medicine, Physician, Indiana University Melvin and Bren Simon Comprehensive Cancer Center, Indianapolis, Indiana
Shadia Jalal, MD, has disclosed no relevant financial relationships.
Small-cell lung cancer (SCLC) occurs almost exclusively in cigarette smokers. Veterans are particularly vulnerable to SCLC because of their prevalent smoking history and exposures to carcinogens, including Agent Orange.
SCLC is characterized by the early development of widespread metastases, including liver, bone, and brain.
Unlike, non–-small cell lung cancer, which has seen great improvement in survival from the introduction of immunotherapy and targeted agents, there has been relatively little improvement in SCLC.
Patients generally are classified into limited- and extensive-stage disease, but platinum-based chemotherapy is almost always the standard first-line treatment. Unfortunately, most patients relapse within a year.
In this ReCAP, Dr Shadia Jalal, of Indiana University Melvin and Bren Simon Comprehensive Cancer Center, discusses second-line treatment options for SCLC patients who relapse after chemotherapy. She also discusses four subtypes of SCLC categorized on the basis of specific transcription regulators, which may offer the potential of targeted therapies for this patient population.
--
Shadia Jalal, MD, Associate Professor of Medicine, Physician, Indiana University Melvin and Bren Simon Comprehensive Cancer Center, Indianapolis, Indiana
Shadia Jalal, MD, has disclosed no relevant financial relationships.
Rajwanth Veluswamy, MD, MSCR
Adenosquamous carcinoma (ASC) of the lung is a rare, biphasic type of non-small cell lung cancer (NSCLC) that accounts for 2% to 4% of all lung cancers.1 According to the World Health Organization (WHO) classification, the composition of ASC includes both adenocarcinoma (AC) and squamous cell carcinoma (SCC) histologies, with each subtype comprising at least 10% of the tumor.2 As with other lung cancers, the average age at ASC diagnosis is about 70 years of age, it affects more men than women, and most patients are current or former smokers.3,4 Despite these similarities, mounting evidence suggests that the molecular and genomic features of ASC are unique and they remain poorly understood.5-8
Perhaps owing to the distinct genomics of these tumors, ASC of the lung is reported to be relatively aggressive compared to typical AC and SCC tumors. Studies indicate that ASCs at diagnosis have higher rates of lymph node invasion, metastasize rapidly, and carry a generally poor prognosis. Accordingly, the overall survival (OS) of patients with these tumors is relatively short compared to other NSCLC subtypes.2,3,8-10 In a 2022 population-based study of the SEER database, 5-year postsurgical survival rates for early-stage cancers were reportedly 65% for ASC vs 69% for SCC P=0.003 and 77% for AC P<0.001.3 While it is clear that underlying biology driving ASC differs from more typical NSCLC subtypes, there is a lack of effective treatment options specific to ASC and a paucity of clinical research available to support therapeutic decisions for patients with ASC histology. Current management of NSCLC is based primarily on the stage of the tumor, and clinical features of the patient. In a more personalized era of targeted treatments, tumor histology is used only to predict the presence of actionable mutations in adenocarcinomas.7,8 However, optimal treatment strategies for ASC remain a significant unmet need in lung cancer.
Diagnosis: Complex but Critically Important
Given the mixed histologies that characterize ASC of the lung, intratumoral heterogeneity often hinders and may delay diagnosis. Studies suggest that ASC is misdiagnosed as AC or SCC in at least half of biopsies prior to surgical pathology confirming an ASC diagnosis.11 In one retrospective study, nearly all ASC cases (98%) were either misdiagnosed or undiagnosed preoperatively.12 What’s more is that different types of biopsy samples may yield different results. One case report of a patient eventually diagnosed with ASC described 3 different results on workup: SCC on bronchial lavage and bronchial biopsy, AC on immunohistochemistry, and NSCLC undifferentiated on pleural effusion cytology.13 While a diagnosis can be made using biopsy and cytology samples, a definitive diagnosis may require larger samples (ie, several core biopsies or complete surgical resections) to fully evaluate all components of the tumor lesion.
Comprehensively evaluating entire tumor specimens can aid in further characterization ASC of the lung. ASCs may be sub-classified according to the proportions of AC and SCC histology components present. Tumors with either AC or SCC components comprising at least 60% of the tumor are referred to as AC- or SCC-predominant ASC, respectively. Those with a more even split of AC and SCC histologies (40% to 60% of each) are referred to as structure-balanced ASC and have been reported to have a better prognosis than either of the more imbalanced subtypes.9,14
Adding to the complexity of diagnosing ASC of the lung is its unclear histologic origin and the transitional nature of these tumors over time. Some studies have pointed to possible precursor lesions, including AC with squamous metaplasia, collision tumor, and high-grade mucoepidermoid tumors.15 Reports have also shown that the molecular and histological features of the primary tumor can differ from that of metastases/recurrences.16,17 In one case report, a patient with a resected ASC harboring an epidermal growth factor receptor (EGFR)-sensitizing mutation recurred several months later as SCC in the brain with the same EGFR mutation. A later recurrence in the lung was diagnosed as an AC and had the same EGFR mutation.16 In this example, if only the SCC component had been diagnosed, molecular testing would likely have never been ordered and the potentially actionable EGFR mutation would have been left undetected. Therefore, careful and accurate diagnosis of ASC is critically important in guiding testing for driver mutations, as well as in informing treatment choices in ASC.
Genomics
Studies indicate that ASC of the lung exhibits genomic features of both AC and SCC, with standard immunohistochemical profiles represented in each component. As expected, TTF1 positivity is common in the AC component while p63 and CK5/6 are expressed in the SCC component.18 However, evidence also indicates that ASC of the lung is a distinct entity rather than being a simple hybrid of AC and SCC histologies. That is, despite the seemingly dichotomous nature of ASC, this type of tumor is thought to have unique molecular and genomic features that have not yet been fully identified.5-8
While the genomics of AC and SCC of the lung have been well studied, the inherent intratumoral heterogeneity that defines ASC, together with its relative rarity, complicates its analysis. There is a paucity of data available, but several groups have conducted molecular testing to better understand the genotype of ASC and potentially discover predictors about prognosis and treatment. To date, most studies on ASC lung samples have been small, and while some groups have reported overlapping results, other findings contrast with one another. In one of the most recent and comprehensive studies published on the topic, Wang et al. used next-generation sequencing (NGS) to identify a wide range of somatic mutations in 124 Chinese patients with ASC of the lung, including TP53 (66.9%), CDKN2A (21%), TERT (21%), and LRP1B (18.5%).6 Importantly, they found high rates of EGFR mutations (54.8%), of which 45.6% were EGFR 19del, 38.2% were EGFR L858R and 29.4% were EGFR amplifications.
Notably, not all studies have found such a strikingly increased rate of EGFR mutations in ASC versus AC of the lung.19 Other actionable mutations were found in the analysis by Wang and colleagues, including ALK and ROS1 fusions. Regarding known predictors of immunogenicity in these tumors, a subset of patients were associated with high tumor mutational burden (TMB), which was correlated with mutations in ARID2, BRCA1, and KEAP1. Immunohistochemical analyses demonstrated half of patients were positive for PD-L1 (≥ 1% tumor proportion score [TPS]).6 Interestingly, another study showed that PD-L1 expression in ASC differed between SCC (30% to 40%) and AC (11% to 15%) components.20
Actionable mutation rates (ie, EGFR, ALK) in AC are known to vary between Asian and White patients, a finding that seems to be similar in ASC of the lung as well, although it is less clear given the limited sample size of ASC studies. Vassella et al. performed NGS and fluorescence in situ hybridization (FISH) on ASC samples from 16 White patients and found that 30% had EGFR mutations, while Tochigi et al reported an EGFR mutation rate of 13% in a study of 23 Western patients.5,12,21 In their analysis, Vassella and colleagues also found a high rate of mutations in the PI3K pathway (25%), but no KRAS mutations, which are the most common molecular driver in typical AC (30%), and thus supporting the notion that ASC has its own molecular genomic profile, distinct from AC or SCC.5,21 Also of interest in this study was the finding that classifier miR-205 expression was intermediate between that of classical AC and SCC, suggesting that ASC of the lung may alternatively represent a transitional stage between these tumor types rather than an unrelated entity.5 These findings, along with others that have been reported on the genomic landscape of ASC, have advanced our understanding of the underlying biology of this malignancy, but also highlight the unmet need for more research to improve our ability to personalize treatment for ASCs.
Treatment
Owing to the heterogeneity of ASC of the lung, as well as its complex and incompletely characterized genomic landscape, treating patients with these tumors is challenging. In general, stage-based treatment approaches are used to manage ASC. The current treatment paradigm of all NSCLC has dramatically changed in recent years, with increasing incorporation of targeted treatments and immunotherapies across all stages and histologic types. Considering ASCs are composed of glandular cell components, they can contain substantial levels of relevant actionable driver mutations as described above. Therefore, if ASC is diagnosed or if a SCC has a glandular component,molecular testing is recommended and supported by guidelines, even on surgical specimens where EGFR may be targeted as adjuvant treatment.23 However, while targeting actionable mutations and the PD1/PDL1 axis has been studied extensively in AC and SCC in all stages, the impact of these markers in ASC is unknown because patients with this histologic subtype are frequently excluded from clinical trials.
For patients with ASC and actionable mutations, EGFR inhibitors have been perhaps the best-studied targeted therapies. EGFR inhibitors have yielded responses in ASC, but the benefit has been highly variable in small case series and generally inferior to outcomes in patients with AC alone.19 Ongoing clinical trials are aiming to better understand the effects of EGFR inhibitors in ASC. As one example, first-line almonertinib is being compared to paclitaxel/carboplatin in the phase 2 ARISE clinical trial, which is specifically enrolling patients with EGFR mutation-positive locally advanced or metastatic pulmonary ASC (Clinicaltrials.gov NCT04354961). Most other reported studies are case studies or retrospective in nature.
Given that outcomes are usually reported from single patients or a group of only a few patients, contradictory findings are not uncommon. For example, crizotinib, a multi-kinase inhibitor approved for the treatment of advanced or metastatic ALK-positive and ROS1-positive NSCLC, was reported to have a clinical response in an ASC in a patient with recurrent ALK-positive disease which lasted for just over one year.24 However, the response to second-line crizotinib in a case report of female non-smoking patient with ROS1-positive ASC was only 4 months.25 Newer, more specific kinase inhibitors are currently in clinical practice and trials of ALK and ROS1 NSCLCs; however, their efficacy is ASC remains unclear.
In the absence of driver mutations, the optimal choice of chemotherapy (often given with immunotherapy) for neo-/adjuvant therapy or for metastatic disease has not yet been identified. While the AC component might typically be treated with pemetrexed plus a platinum agent, the SCC component may be better treated with taxane plus a platinum agent.23 Especially in cases where neither histologic subtype is predominant, it can be difficult to decide which combination may be suitable for an individual patient. Whether the relative proportion of AC and SCC components affect treatment outcomes is not yet known. Outcomes of pemetrexed-based chemotherapy have been reported in a case study of 2 patients with relapsed disease harboring ALK and ROS1 mutations, pemetrexed alone or as part of a combination regimen (with pembrolizumab and carboplatin) was able to maintain stable disease for at least a year.26
While immune checkpoint inhibitors, either as monotherapy or in combination with chemotherapy, are currently recommended for patients with NSCLC23, few studies have reported outcomes of patients with ASC specifically. One recent real-world analysis by Li et al. evaluated the effect of immunotherapy in 46 patients with ASC, of which 18 (39%) did not contain actionable driver mutations and 18 (39%) had unknown mutational status.27 In this study, 28% of the overall cohort responded to checkpoint inhibitors, the median progression-free survival was 6 months, and the median OS was 24.7 months. Notably, similar efficacy was observed in the 20 patients receiving immunotherapy monotherapy vs 26 patients who received combination immunotherapy plus chemotherapy.27 Among 4 patients with EGFR mutations, 2 received immunotherapy monotherapy and progressed immediately compared to the other 2 receiving combination immunotherapy with chemotherapy achieving disease control and improved OS (18 months).
As exemplified by the select few cases summarized above, conventional treatments used in NSCLC have achieved only modest responses in ASC, most with a shorter response duration. The lack of specific treatment strategies for ASC, based on our understanding of underlying tumor biology, limits optimal treatment outcomes for this increasingly common diagnosis. Novel therapies are sorely needed. A consensus should be developed to either study novel treatments specifically in this subtype or allow for the incorporation of ASCs into future NSCLC clinical trials.
Ruffini E, Rena O, Oliaro A, Filosso PL, Bongiovanni M, Arslanian A, Papalia E, Maggi G. Lung tumors with mixed histologic pattern. Clinico-pathologic characteristics and prognostic significance. Eur J Cardiothorac Surg. 2002; 22:701–707. doi:10.1016/s1010-7940(02)00481-5
Almonertinib versus paclitaxel plus carboplatin as first-line treatment in patients with EGFR mutation positive locally advanced or metastatic pulmonary adenosquamous carcinoma (ARISE). ClinicalTrials.gov website. Accessed March 7, 2023. https://clinicaltrials.gov/ct2/show/NCT0435496
Maeda H, Matsumura A, Kawabata T, et al. Adenosquamous carcinoma of the lung: surgical results as compared with squamous cell and adeno¬carcinoma cases. Eur J Cardiothorac Surg. 2012;41:357–361. doi:10.1016/j.ejcts.2011.05.050
Wang T, Zhou J, Wang Y, et al. Clinicopathological characteristics and prognosis of resectable lung adenosquamous carcinoma: a population-based study of the SEER database. Jpn J Clin Oncol. 2022;52:1191-1200. doi:10.1093/jjco/hyac096
Vassella E, Langsch S, Dettmer MS, et al. Molecular profiling of lung adenosquamous carcinoma: a hybrid or genuine type? Oncotarget. 2015;6:23905-23916. doi:10.18632/oncotarget.4163
Wang H, Liu J, Zhu S, et al. Comprehensive analyses of genomic features and mutational signatures in adenosquamous carcinoma of the lung. Front Oncol. 2022;12:945843. doi:10.3389/fonc.2022.945843
Li C, Lu H. Adenosquamous carcinoma of the lung. Onco Targets Ther. 2018;11:4829-4835. doi:10.2147/OTT.S164574
Wang J, Wang Y, Tong M, Pan H, Li D. Research progress of the clinicopathologic features of lung adenosquamous carcinoma. Onco Targets Ther. 2018;11:7011-7017. doi:10.2147/OTT.S179904
Gawrychowski J, Brulinski K, Malinowski E, Papla B. Prognosis and survival after radical resection of primary adenosquamous lung carcinoma. Eur J Cardiothorac Surg. 2005; 27:686–692. doi:10.1016/j.ejcts.2004.12.030
Cooke DT, Nguyen DV, Yang Y, Chen SL, Yu C, Calhoun RF. Survival comparison of adenosquamous, squamous cell, and adenocarcinoma of the lung after lobectomy. Annal Thorac Surg. 2010; 90:943–948. doi:10.1016/j.athoracsur.2010.05.025
Damadoglu E, Aybatli A, Yalçinsoy M, et al. Adenosquamous carcinoma of the lung (an analysis of 13 cases). Tuberk Toraks. 2005;53:161–166. https://pubmed.ncbi.nlm.nih.gov/16100653/
Mordant P, Grand B, Cazes A, et al. Adenosquamous carcinoma of the lung: surgical management, pathologic characteristics, and prognostic implications. Ann Thorac Surg. 2013;95:1189–1195. doi:10.1016/j.athoracsur.2012.12.037
Shelton DA, Rana DN, Holbrook M, Taylor P, Bailey S. Adenosquamous carcinoma of the lung diagnosed by cytology? A diagnostic dilemma. Diagn Cytopathol. 2012;40:830–833. doi:10.1002/dc.21664
Zhao H, Yang H, Yao F, et al. Improved survival associated with a balanced structure between adenomatous and squamous components in patients with adenosquamous carcinoma of the lung. Eur J Surg Oncol. 2016;42:1699–1706. doi:10.1016/j.ejso.2016.05.009
Shimizu J,Oda M,Hayashi Y,Nonomura A,Watanabe YA. Clinicopathological Study of resected cases of adenosquamous carcinoma of the lung. Chest. 1996; 109: 989-994. doi:10.1378/chest.109.4.989
Burkart J, Shilo K, Zhao W, Ozkan E, Ajam A, Otterson GA. Metastatic squamous cell carcinoma component from an adenosquamous carcinoma of the lung with Identical epidermal growth factor receptor mutations. Case Rep Pulmonol. 2015;2015:283875. doi:10.1155/2015/283875
Du C, Li Z, Wang Z, Wang L, Tian YU. Stereotactic aspiration combined with gamma knife radiosurgery for the treatment of cystic brainstem metastasis originating from lung adenosquamous carcinoma: A case report. Oncol Lett. 2015;9:1607–1613. doi:10.3892/ol.2015.2968
Mukhopadhyay S, Katzenstein ALA. Subclassification of non-small cell lung carcinomas lacking morphologic differentiation on biopsy specimens: Utility of an immuno-histochemical panel containing TTF-1, napsin A, p63, and CK5/6. Am J Surg Pathol. 2011; 35:15–25. doi:10.1097/PAS.0b013e3182036d05
Song X, Wang Z. Clinical efficacy evaluation of tyrosine kinase inhibitors for nonadenocarcinoma lung cancer patients harboring EGFR-sensitizing mutations. Onco Targets Ther. 2017;10:3119-3122. doi:10.2147/OTT.S134523
Shi X, Wu S, Sun J, Liu Y, Zeng X, Liang Z. PD-L1 expression in lung adenosquamous carcinomas compared with the more common variants of non-small cell lung cancer. Sci Rep. 2017;7:46209. doi:10.1038/srep46209
Cancer Genome Atlas Research N. Comprehensive molec¬ular profiling of lung adenocarcinoma. Nature. 2014; 511:543–550. doi:10.1038/nature13385
Tochigi N, Dacic S, Nikiforova M, Cieply KM, Yousem SA. Adenosquamous carcinoma of the lung: a microdissection study of KRAS and EGFR mutational and amplification status in a western patient population. Am J Clin Pathol. 2011; 135:783–789. doi:10.1309/AJCP08IQZAOGYLFL
National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Non-small cell lung cancer. Version 2.2023. February 17, 2023. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed March 7, 2023.
Chaft JE, Rekhtman N, Ladanyi M, Riely GJ. ALK-rearranged lung cancer: adenosquamous lung cancer masquerading as pure squamous carcinoma. J Thorac Oncol. 2012;7:768–769. doi:10.1097/JTO.0b013e31824c9485
Cheng Y, Yang J, Wang D, Yan D. ROS1 fusion lung adenosquamous carcinoma patient with short-term clinical benefit after crizotinib treatment: a case report. Ann Transl Med. 2022;10:157. doi:10.21037/atm-21-6754
Patil J, Nie Y, Aisner DL, Camidge DR. Case report: significant clinical benefit from pemetrexed-based therapy in ROS-1 and ALK-rearranged lung cancer with adenosquamous histology. Front Oncol. 2022;11:788245. doi:10.3389/fonc.2021.788245
Li C, Zheng X, Li P, et al. Heterogeneity of tumor immune microenvironment and real-world analysis of immunotherapy efficacy in lung adenosquamous carcinoma. Front Immunol. 2022;13:944812. doi:10.3389/fimmu.2022.944812
Author and Disclosure Information
Rajwanth Veluswamy, MD, MSCR Assistant Professor of Medicine, Hematology and Medical Oncology Icahn School of Medicine at Mount Sinai New York, NY
Rajwanth R. Veluswamy, MD, MSCR, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Boehringer Ingelheim; Merus; Novocure; Merck; Regeneron; Beigene; G1 Therapeutics; Novartis; BerGenBio.
Serve(d) as a speaker or a member of a speakers bureau for: AstraZeneca
Received research grant from: Bristol-Myers Squibb; Onconova; AstraZeneca; Boehringer Ingelheim
Rajwanth Veluswamy, MD, MSCR Assistant Professor of Medicine, Hematology and Medical Oncology Icahn School of Medicine at Mount Sinai New York, NY
Rajwanth R. Veluswamy, MD, MSCR, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Boehringer Ingelheim; Merus; Novocure; Merck; Regeneron; Beigene; G1 Therapeutics; Novartis; BerGenBio.
Serve(d) as a speaker or a member of a speakers bureau for: AstraZeneca
Received research grant from: Bristol-Myers Squibb; Onconova; AstraZeneca; Boehringer Ingelheim
Author and Disclosure Information
Rajwanth Veluswamy, MD, MSCR Assistant Professor of Medicine, Hematology and Medical Oncology Icahn School of Medicine at Mount Sinai New York, NY
Rajwanth R. Veluswamy, MD, MSCR, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Boehringer Ingelheim; Merus; Novocure; Merck; Regeneron; Beigene; G1 Therapeutics; Novartis; BerGenBio.
Serve(d) as a speaker or a member of a speakers bureau for: AstraZeneca
Received research grant from: Bristol-Myers Squibb; Onconova; AstraZeneca; Boehringer Ingelheim
Rajwanth Veluswamy, MD, MSCR
Adenosquamous carcinoma (ASC) of the lung is a rare, biphasic type of non-small cell lung cancer (NSCLC) that accounts for 2% to 4% of all lung cancers.1 According to the World Health Organization (WHO) classification, the composition of ASC includes both adenocarcinoma (AC) and squamous cell carcinoma (SCC) histologies, with each subtype comprising at least 10% of the tumor.2 As with other lung cancers, the average age at ASC diagnosis is about 70 years of age, it affects more men than women, and most patients are current or former smokers.3,4 Despite these similarities, mounting evidence suggests that the molecular and genomic features of ASC are unique and they remain poorly understood.5-8
Perhaps owing to the distinct genomics of these tumors, ASC of the lung is reported to be relatively aggressive compared to typical AC and SCC tumors. Studies indicate that ASCs at diagnosis have higher rates of lymph node invasion, metastasize rapidly, and carry a generally poor prognosis. Accordingly, the overall survival (OS) of patients with these tumors is relatively short compared to other NSCLC subtypes.2,3,8-10 In a 2022 population-based study of the SEER database, 5-year postsurgical survival rates for early-stage cancers were reportedly 65% for ASC vs 69% for SCC P=0.003 and 77% for AC P<0.001.3 While it is clear that underlying biology driving ASC differs from more typical NSCLC subtypes, there is a lack of effective treatment options specific to ASC and a paucity of clinical research available to support therapeutic decisions for patients with ASC histology. Current management of NSCLC is based primarily on the stage of the tumor, and clinical features of the patient. In a more personalized era of targeted treatments, tumor histology is used only to predict the presence of actionable mutations in adenocarcinomas.7,8 However, optimal treatment strategies for ASC remain a significant unmet need in lung cancer.
Diagnosis: Complex but Critically Important
Given the mixed histologies that characterize ASC of the lung, intratumoral heterogeneity often hinders and may delay diagnosis. Studies suggest that ASC is misdiagnosed as AC or SCC in at least half of biopsies prior to surgical pathology confirming an ASC diagnosis.11 In one retrospective study, nearly all ASC cases (98%) were either misdiagnosed or undiagnosed preoperatively.12 What’s more is that different types of biopsy samples may yield different results. One case report of a patient eventually diagnosed with ASC described 3 different results on workup: SCC on bronchial lavage and bronchial biopsy, AC on immunohistochemistry, and NSCLC undifferentiated on pleural effusion cytology.13 While a diagnosis can be made using biopsy and cytology samples, a definitive diagnosis may require larger samples (ie, several core biopsies or complete surgical resections) to fully evaluate all components of the tumor lesion.
Comprehensively evaluating entire tumor specimens can aid in further characterization ASC of the lung. ASCs may be sub-classified according to the proportions of AC and SCC histology components present. Tumors with either AC or SCC components comprising at least 60% of the tumor are referred to as AC- or SCC-predominant ASC, respectively. Those with a more even split of AC and SCC histologies (40% to 60% of each) are referred to as structure-balanced ASC and have been reported to have a better prognosis than either of the more imbalanced subtypes.9,14
Adding to the complexity of diagnosing ASC of the lung is its unclear histologic origin and the transitional nature of these tumors over time. Some studies have pointed to possible precursor lesions, including AC with squamous metaplasia, collision tumor, and high-grade mucoepidermoid tumors.15 Reports have also shown that the molecular and histological features of the primary tumor can differ from that of metastases/recurrences.16,17 In one case report, a patient with a resected ASC harboring an epidermal growth factor receptor (EGFR)-sensitizing mutation recurred several months later as SCC in the brain with the same EGFR mutation. A later recurrence in the lung was diagnosed as an AC and had the same EGFR mutation.16 In this example, if only the SCC component had been diagnosed, molecular testing would likely have never been ordered and the potentially actionable EGFR mutation would have been left undetected. Therefore, careful and accurate diagnosis of ASC is critically important in guiding testing for driver mutations, as well as in informing treatment choices in ASC.
Genomics
Studies indicate that ASC of the lung exhibits genomic features of both AC and SCC, with standard immunohistochemical profiles represented in each component. As expected, TTF1 positivity is common in the AC component while p63 and CK5/6 are expressed in the SCC component.18 However, evidence also indicates that ASC of the lung is a distinct entity rather than being a simple hybrid of AC and SCC histologies. That is, despite the seemingly dichotomous nature of ASC, this type of tumor is thought to have unique molecular and genomic features that have not yet been fully identified.5-8
While the genomics of AC and SCC of the lung have been well studied, the inherent intratumoral heterogeneity that defines ASC, together with its relative rarity, complicates its analysis. There is a paucity of data available, but several groups have conducted molecular testing to better understand the genotype of ASC and potentially discover predictors about prognosis and treatment. To date, most studies on ASC lung samples have been small, and while some groups have reported overlapping results, other findings contrast with one another. In one of the most recent and comprehensive studies published on the topic, Wang et al. used next-generation sequencing (NGS) to identify a wide range of somatic mutations in 124 Chinese patients with ASC of the lung, including TP53 (66.9%), CDKN2A (21%), TERT (21%), and LRP1B (18.5%).6 Importantly, they found high rates of EGFR mutations (54.8%), of which 45.6% were EGFR 19del, 38.2% were EGFR L858R and 29.4% were EGFR amplifications.
Notably, not all studies have found such a strikingly increased rate of EGFR mutations in ASC versus AC of the lung.19 Other actionable mutations were found in the analysis by Wang and colleagues, including ALK and ROS1 fusions. Regarding known predictors of immunogenicity in these tumors, a subset of patients were associated with high tumor mutational burden (TMB), which was correlated with mutations in ARID2, BRCA1, and KEAP1. Immunohistochemical analyses demonstrated half of patients were positive for PD-L1 (≥ 1% tumor proportion score [TPS]).6 Interestingly, another study showed that PD-L1 expression in ASC differed between SCC (30% to 40%) and AC (11% to 15%) components.20
Actionable mutation rates (ie, EGFR, ALK) in AC are known to vary between Asian and White patients, a finding that seems to be similar in ASC of the lung as well, although it is less clear given the limited sample size of ASC studies. Vassella et al. performed NGS and fluorescence in situ hybridization (FISH) on ASC samples from 16 White patients and found that 30% had EGFR mutations, while Tochigi et al reported an EGFR mutation rate of 13% in a study of 23 Western patients.5,12,21 In their analysis, Vassella and colleagues also found a high rate of mutations in the PI3K pathway (25%), but no KRAS mutations, which are the most common molecular driver in typical AC (30%), and thus supporting the notion that ASC has its own molecular genomic profile, distinct from AC or SCC.5,21 Also of interest in this study was the finding that classifier miR-205 expression was intermediate between that of classical AC and SCC, suggesting that ASC of the lung may alternatively represent a transitional stage between these tumor types rather than an unrelated entity.5 These findings, along with others that have been reported on the genomic landscape of ASC, have advanced our understanding of the underlying biology of this malignancy, but also highlight the unmet need for more research to improve our ability to personalize treatment for ASCs.
Treatment
Owing to the heterogeneity of ASC of the lung, as well as its complex and incompletely characterized genomic landscape, treating patients with these tumors is challenging. In general, stage-based treatment approaches are used to manage ASC. The current treatment paradigm of all NSCLC has dramatically changed in recent years, with increasing incorporation of targeted treatments and immunotherapies across all stages and histologic types. Considering ASCs are composed of glandular cell components, they can contain substantial levels of relevant actionable driver mutations as described above. Therefore, if ASC is diagnosed or if a SCC has a glandular component,molecular testing is recommended and supported by guidelines, even on surgical specimens where EGFR may be targeted as adjuvant treatment.23 However, while targeting actionable mutations and the PD1/PDL1 axis has been studied extensively in AC and SCC in all stages, the impact of these markers in ASC is unknown because patients with this histologic subtype are frequently excluded from clinical trials.
For patients with ASC and actionable mutations, EGFR inhibitors have been perhaps the best-studied targeted therapies. EGFR inhibitors have yielded responses in ASC, but the benefit has been highly variable in small case series and generally inferior to outcomes in patients with AC alone.19 Ongoing clinical trials are aiming to better understand the effects of EGFR inhibitors in ASC. As one example, first-line almonertinib is being compared to paclitaxel/carboplatin in the phase 2 ARISE clinical trial, which is specifically enrolling patients with EGFR mutation-positive locally advanced or metastatic pulmonary ASC (Clinicaltrials.gov NCT04354961). Most other reported studies are case studies or retrospective in nature.
Given that outcomes are usually reported from single patients or a group of only a few patients, contradictory findings are not uncommon. For example, crizotinib, a multi-kinase inhibitor approved for the treatment of advanced or metastatic ALK-positive and ROS1-positive NSCLC, was reported to have a clinical response in an ASC in a patient with recurrent ALK-positive disease which lasted for just over one year.24 However, the response to second-line crizotinib in a case report of female non-smoking patient with ROS1-positive ASC was only 4 months.25 Newer, more specific kinase inhibitors are currently in clinical practice and trials of ALK and ROS1 NSCLCs; however, their efficacy is ASC remains unclear.
In the absence of driver mutations, the optimal choice of chemotherapy (often given with immunotherapy) for neo-/adjuvant therapy or for metastatic disease has not yet been identified. While the AC component might typically be treated with pemetrexed plus a platinum agent, the SCC component may be better treated with taxane plus a platinum agent.23 Especially in cases where neither histologic subtype is predominant, it can be difficult to decide which combination may be suitable for an individual patient. Whether the relative proportion of AC and SCC components affect treatment outcomes is not yet known. Outcomes of pemetrexed-based chemotherapy have been reported in a case study of 2 patients with relapsed disease harboring ALK and ROS1 mutations, pemetrexed alone or as part of a combination regimen (with pembrolizumab and carboplatin) was able to maintain stable disease for at least a year.26
While immune checkpoint inhibitors, either as monotherapy or in combination with chemotherapy, are currently recommended for patients with NSCLC23, few studies have reported outcomes of patients with ASC specifically. One recent real-world analysis by Li et al. evaluated the effect of immunotherapy in 46 patients with ASC, of which 18 (39%) did not contain actionable driver mutations and 18 (39%) had unknown mutational status.27 In this study, 28% of the overall cohort responded to checkpoint inhibitors, the median progression-free survival was 6 months, and the median OS was 24.7 months. Notably, similar efficacy was observed in the 20 patients receiving immunotherapy monotherapy vs 26 patients who received combination immunotherapy plus chemotherapy.27 Among 4 patients with EGFR mutations, 2 received immunotherapy monotherapy and progressed immediately compared to the other 2 receiving combination immunotherapy with chemotherapy achieving disease control and improved OS (18 months).
As exemplified by the select few cases summarized above, conventional treatments used in NSCLC have achieved only modest responses in ASC, most with a shorter response duration. The lack of specific treatment strategies for ASC, based on our understanding of underlying tumor biology, limits optimal treatment outcomes for this increasingly common diagnosis. Novel therapies are sorely needed. A consensus should be developed to either study novel treatments specifically in this subtype or allow for the incorporation of ASCs into future NSCLC clinical trials.
Rajwanth Veluswamy, MD, MSCR
Adenosquamous carcinoma (ASC) of the lung is a rare, biphasic type of non-small cell lung cancer (NSCLC) that accounts for 2% to 4% of all lung cancers.1 According to the World Health Organization (WHO) classification, the composition of ASC includes both adenocarcinoma (AC) and squamous cell carcinoma (SCC) histologies, with each subtype comprising at least 10% of the tumor.2 As with other lung cancers, the average age at ASC diagnosis is about 70 years of age, it affects more men than women, and most patients are current or former smokers.3,4 Despite these similarities, mounting evidence suggests that the molecular and genomic features of ASC are unique and they remain poorly understood.5-8
Perhaps owing to the distinct genomics of these tumors, ASC of the lung is reported to be relatively aggressive compared to typical AC and SCC tumors. Studies indicate that ASCs at diagnosis have higher rates of lymph node invasion, metastasize rapidly, and carry a generally poor prognosis. Accordingly, the overall survival (OS) of patients with these tumors is relatively short compared to other NSCLC subtypes.2,3,8-10 In a 2022 population-based study of the SEER database, 5-year postsurgical survival rates for early-stage cancers were reportedly 65% for ASC vs 69% for SCC P=0.003 and 77% for AC P<0.001.3 While it is clear that underlying biology driving ASC differs from more typical NSCLC subtypes, there is a lack of effective treatment options specific to ASC and a paucity of clinical research available to support therapeutic decisions for patients with ASC histology. Current management of NSCLC is based primarily on the stage of the tumor, and clinical features of the patient. In a more personalized era of targeted treatments, tumor histology is used only to predict the presence of actionable mutations in adenocarcinomas.7,8 However, optimal treatment strategies for ASC remain a significant unmet need in lung cancer.
Diagnosis: Complex but Critically Important
Given the mixed histologies that characterize ASC of the lung, intratumoral heterogeneity often hinders and may delay diagnosis. Studies suggest that ASC is misdiagnosed as AC or SCC in at least half of biopsies prior to surgical pathology confirming an ASC diagnosis.11 In one retrospective study, nearly all ASC cases (98%) were either misdiagnosed or undiagnosed preoperatively.12 What’s more is that different types of biopsy samples may yield different results. One case report of a patient eventually diagnosed with ASC described 3 different results on workup: SCC on bronchial lavage and bronchial biopsy, AC on immunohistochemistry, and NSCLC undifferentiated on pleural effusion cytology.13 While a diagnosis can be made using biopsy and cytology samples, a definitive diagnosis may require larger samples (ie, several core biopsies or complete surgical resections) to fully evaluate all components of the tumor lesion.
Comprehensively evaluating entire tumor specimens can aid in further characterization ASC of the lung. ASCs may be sub-classified according to the proportions of AC and SCC histology components present. Tumors with either AC or SCC components comprising at least 60% of the tumor are referred to as AC- or SCC-predominant ASC, respectively. Those with a more even split of AC and SCC histologies (40% to 60% of each) are referred to as structure-balanced ASC and have been reported to have a better prognosis than either of the more imbalanced subtypes.9,14
Adding to the complexity of diagnosing ASC of the lung is its unclear histologic origin and the transitional nature of these tumors over time. Some studies have pointed to possible precursor lesions, including AC with squamous metaplasia, collision tumor, and high-grade mucoepidermoid tumors.15 Reports have also shown that the molecular and histological features of the primary tumor can differ from that of metastases/recurrences.16,17 In one case report, a patient with a resected ASC harboring an epidermal growth factor receptor (EGFR)-sensitizing mutation recurred several months later as SCC in the brain with the same EGFR mutation. A later recurrence in the lung was diagnosed as an AC and had the same EGFR mutation.16 In this example, if only the SCC component had been diagnosed, molecular testing would likely have never been ordered and the potentially actionable EGFR mutation would have been left undetected. Therefore, careful and accurate diagnosis of ASC is critically important in guiding testing for driver mutations, as well as in informing treatment choices in ASC.
Genomics
Studies indicate that ASC of the lung exhibits genomic features of both AC and SCC, with standard immunohistochemical profiles represented in each component. As expected, TTF1 positivity is common in the AC component while p63 and CK5/6 are expressed in the SCC component.18 However, evidence also indicates that ASC of the lung is a distinct entity rather than being a simple hybrid of AC and SCC histologies. That is, despite the seemingly dichotomous nature of ASC, this type of tumor is thought to have unique molecular and genomic features that have not yet been fully identified.5-8
While the genomics of AC and SCC of the lung have been well studied, the inherent intratumoral heterogeneity that defines ASC, together with its relative rarity, complicates its analysis. There is a paucity of data available, but several groups have conducted molecular testing to better understand the genotype of ASC and potentially discover predictors about prognosis and treatment. To date, most studies on ASC lung samples have been small, and while some groups have reported overlapping results, other findings contrast with one another. In one of the most recent and comprehensive studies published on the topic, Wang et al. used next-generation sequencing (NGS) to identify a wide range of somatic mutations in 124 Chinese patients with ASC of the lung, including TP53 (66.9%), CDKN2A (21%), TERT (21%), and LRP1B (18.5%).6 Importantly, they found high rates of EGFR mutations (54.8%), of which 45.6% were EGFR 19del, 38.2% were EGFR L858R and 29.4% were EGFR amplifications.
Notably, not all studies have found such a strikingly increased rate of EGFR mutations in ASC versus AC of the lung.19 Other actionable mutations were found in the analysis by Wang and colleagues, including ALK and ROS1 fusions. Regarding known predictors of immunogenicity in these tumors, a subset of patients were associated with high tumor mutational burden (TMB), which was correlated with mutations in ARID2, BRCA1, and KEAP1. Immunohistochemical analyses demonstrated half of patients were positive for PD-L1 (≥ 1% tumor proportion score [TPS]).6 Interestingly, another study showed that PD-L1 expression in ASC differed between SCC (30% to 40%) and AC (11% to 15%) components.20
Actionable mutation rates (ie, EGFR, ALK) in AC are known to vary between Asian and White patients, a finding that seems to be similar in ASC of the lung as well, although it is less clear given the limited sample size of ASC studies. Vassella et al. performed NGS and fluorescence in situ hybridization (FISH) on ASC samples from 16 White patients and found that 30% had EGFR mutations, while Tochigi et al reported an EGFR mutation rate of 13% in a study of 23 Western patients.5,12,21 In their analysis, Vassella and colleagues also found a high rate of mutations in the PI3K pathway (25%), but no KRAS mutations, which are the most common molecular driver in typical AC (30%), and thus supporting the notion that ASC has its own molecular genomic profile, distinct from AC or SCC.5,21 Also of interest in this study was the finding that classifier miR-205 expression was intermediate between that of classical AC and SCC, suggesting that ASC of the lung may alternatively represent a transitional stage between these tumor types rather than an unrelated entity.5 These findings, along with others that have been reported on the genomic landscape of ASC, have advanced our understanding of the underlying biology of this malignancy, but also highlight the unmet need for more research to improve our ability to personalize treatment for ASCs.
Treatment
Owing to the heterogeneity of ASC of the lung, as well as its complex and incompletely characterized genomic landscape, treating patients with these tumors is challenging. In general, stage-based treatment approaches are used to manage ASC. The current treatment paradigm of all NSCLC has dramatically changed in recent years, with increasing incorporation of targeted treatments and immunotherapies across all stages and histologic types. Considering ASCs are composed of glandular cell components, they can contain substantial levels of relevant actionable driver mutations as described above. Therefore, if ASC is diagnosed or if a SCC has a glandular component,molecular testing is recommended and supported by guidelines, even on surgical specimens where EGFR may be targeted as adjuvant treatment.23 However, while targeting actionable mutations and the PD1/PDL1 axis has been studied extensively in AC and SCC in all stages, the impact of these markers in ASC is unknown because patients with this histologic subtype are frequently excluded from clinical trials.
For patients with ASC and actionable mutations, EGFR inhibitors have been perhaps the best-studied targeted therapies. EGFR inhibitors have yielded responses in ASC, but the benefit has been highly variable in small case series and generally inferior to outcomes in patients with AC alone.19 Ongoing clinical trials are aiming to better understand the effects of EGFR inhibitors in ASC. As one example, first-line almonertinib is being compared to paclitaxel/carboplatin in the phase 2 ARISE clinical trial, which is specifically enrolling patients with EGFR mutation-positive locally advanced or metastatic pulmonary ASC (Clinicaltrials.gov NCT04354961). Most other reported studies are case studies or retrospective in nature.
Given that outcomes are usually reported from single patients or a group of only a few patients, contradictory findings are not uncommon. For example, crizotinib, a multi-kinase inhibitor approved for the treatment of advanced or metastatic ALK-positive and ROS1-positive NSCLC, was reported to have a clinical response in an ASC in a patient with recurrent ALK-positive disease which lasted for just over one year.24 However, the response to second-line crizotinib in a case report of female non-smoking patient with ROS1-positive ASC was only 4 months.25 Newer, more specific kinase inhibitors are currently in clinical practice and trials of ALK and ROS1 NSCLCs; however, their efficacy is ASC remains unclear.
In the absence of driver mutations, the optimal choice of chemotherapy (often given with immunotherapy) for neo-/adjuvant therapy or for metastatic disease has not yet been identified. While the AC component might typically be treated with pemetrexed plus a platinum agent, the SCC component may be better treated with taxane plus a platinum agent.23 Especially in cases where neither histologic subtype is predominant, it can be difficult to decide which combination may be suitable for an individual patient. Whether the relative proportion of AC and SCC components affect treatment outcomes is not yet known. Outcomes of pemetrexed-based chemotherapy have been reported in a case study of 2 patients with relapsed disease harboring ALK and ROS1 mutations, pemetrexed alone or as part of a combination regimen (with pembrolizumab and carboplatin) was able to maintain stable disease for at least a year.26
While immune checkpoint inhibitors, either as monotherapy or in combination with chemotherapy, are currently recommended for patients with NSCLC23, few studies have reported outcomes of patients with ASC specifically. One recent real-world analysis by Li et al. evaluated the effect of immunotherapy in 46 patients with ASC, of which 18 (39%) did not contain actionable driver mutations and 18 (39%) had unknown mutational status.27 In this study, 28% of the overall cohort responded to checkpoint inhibitors, the median progression-free survival was 6 months, and the median OS was 24.7 months. Notably, similar efficacy was observed in the 20 patients receiving immunotherapy monotherapy vs 26 patients who received combination immunotherapy plus chemotherapy.27 Among 4 patients with EGFR mutations, 2 received immunotherapy monotherapy and progressed immediately compared to the other 2 receiving combination immunotherapy with chemotherapy achieving disease control and improved OS (18 months).
As exemplified by the select few cases summarized above, conventional treatments used in NSCLC have achieved only modest responses in ASC, most with a shorter response duration. The lack of specific treatment strategies for ASC, based on our understanding of underlying tumor biology, limits optimal treatment outcomes for this increasingly common diagnosis. Novel therapies are sorely needed. A consensus should be developed to either study novel treatments specifically in this subtype or allow for the incorporation of ASCs into future NSCLC clinical trials.
Ruffini E, Rena O, Oliaro A, Filosso PL, Bongiovanni M, Arslanian A, Papalia E, Maggi G. Lung tumors with mixed histologic pattern. Clinico-pathologic characteristics and prognostic significance. Eur J Cardiothorac Surg. 2002; 22:701–707. doi:10.1016/s1010-7940(02)00481-5
Almonertinib versus paclitaxel plus carboplatin as first-line treatment in patients with EGFR mutation positive locally advanced or metastatic pulmonary adenosquamous carcinoma (ARISE). ClinicalTrials.gov website. Accessed March 7, 2023. https://clinicaltrials.gov/ct2/show/NCT0435496
Maeda H, Matsumura A, Kawabata T, et al. Adenosquamous carcinoma of the lung: surgical results as compared with squamous cell and adeno¬carcinoma cases. Eur J Cardiothorac Surg. 2012;41:357–361. doi:10.1016/j.ejcts.2011.05.050
Wang T, Zhou J, Wang Y, et al. Clinicopathological characteristics and prognosis of resectable lung adenosquamous carcinoma: a population-based study of the SEER database. Jpn J Clin Oncol. 2022;52:1191-1200. doi:10.1093/jjco/hyac096
Vassella E, Langsch S, Dettmer MS, et al. Molecular profiling of lung adenosquamous carcinoma: a hybrid or genuine type? Oncotarget. 2015;6:23905-23916. doi:10.18632/oncotarget.4163
Wang H, Liu J, Zhu S, et al. Comprehensive analyses of genomic features and mutational signatures in adenosquamous carcinoma of the lung. Front Oncol. 2022;12:945843. doi:10.3389/fonc.2022.945843
Li C, Lu H. Adenosquamous carcinoma of the lung. Onco Targets Ther. 2018;11:4829-4835. doi:10.2147/OTT.S164574
Wang J, Wang Y, Tong M, Pan H, Li D. Research progress of the clinicopathologic features of lung adenosquamous carcinoma. Onco Targets Ther. 2018;11:7011-7017. doi:10.2147/OTT.S179904
Gawrychowski J, Brulinski K, Malinowski E, Papla B. Prognosis and survival after radical resection of primary adenosquamous lung carcinoma. Eur J Cardiothorac Surg. 2005; 27:686–692. doi:10.1016/j.ejcts.2004.12.030
Cooke DT, Nguyen DV, Yang Y, Chen SL, Yu C, Calhoun RF. Survival comparison of adenosquamous, squamous cell, and adenocarcinoma of the lung after lobectomy. Annal Thorac Surg. 2010; 90:943–948. doi:10.1016/j.athoracsur.2010.05.025
Damadoglu E, Aybatli A, Yalçinsoy M, et al. Adenosquamous carcinoma of the lung (an analysis of 13 cases). Tuberk Toraks. 2005;53:161–166. https://pubmed.ncbi.nlm.nih.gov/16100653/
Mordant P, Grand B, Cazes A, et al. Adenosquamous carcinoma of the lung: surgical management, pathologic characteristics, and prognostic implications. Ann Thorac Surg. 2013;95:1189–1195. doi:10.1016/j.athoracsur.2012.12.037
Shelton DA, Rana DN, Holbrook M, Taylor P, Bailey S. Adenosquamous carcinoma of the lung diagnosed by cytology? A diagnostic dilemma. Diagn Cytopathol. 2012;40:830–833. doi:10.1002/dc.21664
Zhao H, Yang H, Yao F, et al. Improved survival associated with a balanced structure between adenomatous and squamous components in patients with adenosquamous carcinoma of the lung. Eur J Surg Oncol. 2016;42:1699–1706. doi:10.1016/j.ejso.2016.05.009
Shimizu J,Oda M,Hayashi Y,Nonomura A,Watanabe YA. Clinicopathological Study of resected cases of adenosquamous carcinoma of the lung. Chest. 1996; 109: 989-994. doi:10.1378/chest.109.4.989
Burkart J, Shilo K, Zhao W, Ozkan E, Ajam A, Otterson GA. Metastatic squamous cell carcinoma component from an adenosquamous carcinoma of the lung with Identical epidermal growth factor receptor mutations. Case Rep Pulmonol. 2015;2015:283875. doi:10.1155/2015/283875
Du C, Li Z, Wang Z, Wang L, Tian YU. Stereotactic aspiration combined with gamma knife radiosurgery for the treatment of cystic brainstem metastasis originating from lung adenosquamous carcinoma: A case report. Oncol Lett. 2015;9:1607–1613. doi:10.3892/ol.2015.2968
Mukhopadhyay S, Katzenstein ALA. Subclassification of non-small cell lung carcinomas lacking morphologic differentiation on biopsy specimens: Utility of an immuno-histochemical panel containing TTF-1, napsin A, p63, and CK5/6. Am J Surg Pathol. 2011; 35:15–25. doi:10.1097/PAS.0b013e3182036d05
Song X, Wang Z. Clinical efficacy evaluation of tyrosine kinase inhibitors for nonadenocarcinoma lung cancer patients harboring EGFR-sensitizing mutations. Onco Targets Ther. 2017;10:3119-3122. doi:10.2147/OTT.S134523
Shi X, Wu S, Sun J, Liu Y, Zeng X, Liang Z. PD-L1 expression in lung adenosquamous carcinomas compared with the more common variants of non-small cell lung cancer. Sci Rep. 2017;7:46209. doi:10.1038/srep46209
Cancer Genome Atlas Research N. Comprehensive molec¬ular profiling of lung adenocarcinoma. Nature. 2014; 511:543–550. doi:10.1038/nature13385
Tochigi N, Dacic S, Nikiforova M, Cieply KM, Yousem SA. Adenosquamous carcinoma of the lung: a microdissection study of KRAS and EGFR mutational and amplification status in a western patient population. Am J Clin Pathol. 2011; 135:783–789. doi:10.1309/AJCP08IQZAOGYLFL
National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Non-small cell lung cancer. Version 2.2023. February 17, 2023. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed March 7, 2023.
Chaft JE, Rekhtman N, Ladanyi M, Riely GJ. ALK-rearranged lung cancer: adenosquamous lung cancer masquerading as pure squamous carcinoma. J Thorac Oncol. 2012;7:768–769. doi:10.1097/JTO.0b013e31824c9485
Cheng Y, Yang J, Wang D, Yan D. ROS1 fusion lung adenosquamous carcinoma patient with short-term clinical benefit after crizotinib treatment: a case report. Ann Transl Med. 2022;10:157. doi:10.21037/atm-21-6754
Patil J, Nie Y, Aisner DL, Camidge DR. Case report: significant clinical benefit from pemetrexed-based therapy in ROS-1 and ALK-rearranged lung cancer with adenosquamous histology. Front Oncol. 2022;11:788245. doi:10.3389/fonc.2021.788245
Li C, Zheng X, Li P, et al. Heterogeneity of tumor immune microenvironment and real-world analysis of immunotherapy efficacy in lung adenosquamous carcinoma. Front Immunol. 2022;13:944812. doi:10.3389/fimmu.2022.944812
References
Ruffini E, Rena O, Oliaro A, Filosso PL, Bongiovanni M, Arslanian A, Papalia E, Maggi G. Lung tumors with mixed histologic pattern. Clinico-pathologic characteristics and prognostic significance. Eur J Cardiothorac Surg. 2002; 22:701–707. doi:10.1016/s1010-7940(02)00481-5
Almonertinib versus paclitaxel plus carboplatin as first-line treatment in patients with EGFR mutation positive locally advanced or metastatic pulmonary adenosquamous carcinoma (ARISE). ClinicalTrials.gov website. Accessed March 7, 2023. https://clinicaltrials.gov/ct2/show/NCT0435496
Maeda H, Matsumura A, Kawabata T, et al. Adenosquamous carcinoma of the lung: surgical results as compared with squamous cell and adeno¬carcinoma cases. Eur J Cardiothorac Surg. 2012;41:357–361. doi:10.1016/j.ejcts.2011.05.050
Wang T, Zhou J, Wang Y, et al. Clinicopathological characteristics and prognosis of resectable lung adenosquamous carcinoma: a population-based study of the SEER database. Jpn J Clin Oncol. 2022;52:1191-1200. doi:10.1093/jjco/hyac096
Vassella E, Langsch S, Dettmer MS, et al. Molecular profiling of lung adenosquamous carcinoma: a hybrid or genuine type? Oncotarget. 2015;6:23905-23916. doi:10.18632/oncotarget.4163
Wang H, Liu J, Zhu S, et al. Comprehensive analyses of genomic features and mutational signatures in adenosquamous carcinoma of the lung. Front Oncol. 2022;12:945843. doi:10.3389/fonc.2022.945843
Li C, Lu H. Adenosquamous carcinoma of the lung. Onco Targets Ther. 2018;11:4829-4835. doi:10.2147/OTT.S164574
Wang J, Wang Y, Tong M, Pan H, Li D. Research progress of the clinicopathologic features of lung adenosquamous carcinoma. Onco Targets Ther. 2018;11:7011-7017. doi:10.2147/OTT.S179904
Gawrychowski J, Brulinski K, Malinowski E, Papla B. Prognosis and survival after radical resection of primary adenosquamous lung carcinoma. Eur J Cardiothorac Surg. 2005; 27:686–692. doi:10.1016/j.ejcts.2004.12.030
Cooke DT, Nguyen DV, Yang Y, Chen SL, Yu C, Calhoun RF. Survival comparison of adenosquamous, squamous cell, and adenocarcinoma of the lung after lobectomy. Annal Thorac Surg. 2010; 90:943–948. doi:10.1016/j.athoracsur.2010.05.025
Damadoglu E, Aybatli A, Yalçinsoy M, et al. Adenosquamous carcinoma of the lung (an analysis of 13 cases). Tuberk Toraks. 2005;53:161–166. https://pubmed.ncbi.nlm.nih.gov/16100653/
Mordant P, Grand B, Cazes A, et al. Adenosquamous carcinoma of the lung: surgical management, pathologic characteristics, and prognostic implications. Ann Thorac Surg. 2013;95:1189–1195. doi:10.1016/j.athoracsur.2012.12.037
Shelton DA, Rana DN, Holbrook M, Taylor P, Bailey S. Adenosquamous carcinoma of the lung diagnosed by cytology? A diagnostic dilemma. Diagn Cytopathol. 2012;40:830–833. doi:10.1002/dc.21664
Zhao H, Yang H, Yao F, et al. Improved survival associated with a balanced structure between adenomatous and squamous components in patients with adenosquamous carcinoma of the lung. Eur J Surg Oncol. 2016;42:1699–1706. doi:10.1016/j.ejso.2016.05.009
Shimizu J,Oda M,Hayashi Y,Nonomura A,Watanabe YA. Clinicopathological Study of resected cases of adenosquamous carcinoma of the lung. Chest. 1996; 109: 989-994. doi:10.1378/chest.109.4.989
Burkart J, Shilo K, Zhao W, Ozkan E, Ajam A, Otterson GA. Metastatic squamous cell carcinoma component from an adenosquamous carcinoma of the lung with Identical epidermal growth factor receptor mutations. Case Rep Pulmonol. 2015;2015:283875. doi:10.1155/2015/283875
Du C, Li Z, Wang Z, Wang L, Tian YU. Stereotactic aspiration combined with gamma knife radiosurgery for the treatment of cystic brainstem metastasis originating from lung adenosquamous carcinoma: A case report. Oncol Lett. 2015;9:1607–1613. doi:10.3892/ol.2015.2968
Mukhopadhyay S, Katzenstein ALA. Subclassification of non-small cell lung carcinomas lacking morphologic differentiation on biopsy specimens: Utility of an immuno-histochemical panel containing TTF-1, napsin A, p63, and CK5/6. Am J Surg Pathol. 2011; 35:15–25. doi:10.1097/PAS.0b013e3182036d05
Song X, Wang Z. Clinical efficacy evaluation of tyrosine kinase inhibitors for nonadenocarcinoma lung cancer patients harboring EGFR-sensitizing mutations. Onco Targets Ther. 2017;10:3119-3122. doi:10.2147/OTT.S134523
Shi X, Wu S, Sun J, Liu Y, Zeng X, Liang Z. PD-L1 expression in lung adenosquamous carcinomas compared with the more common variants of non-small cell lung cancer. Sci Rep. 2017;7:46209. doi:10.1038/srep46209
Cancer Genome Atlas Research N. Comprehensive molec¬ular profiling of lung adenocarcinoma. Nature. 2014; 511:543–550. doi:10.1038/nature13385
Tochigi N, Dacic S, Nikiforova M, Cieply KM, Yousem SA. Adenosquamous carcinoma of the lung: a microdissection study of KRAS and EGFR mutational and amplification status in a western patient population. Am J Clin Pathol. 2011; 135:783–789. doi:10.1309/AJCP08IQZAOGYLFL
National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Non-small cell lung cancer. Version 2.2023. February 17, 2023. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed March 7, 2023.
Chaft JE, Rekhtman N, Ladanyi M, Riely GJ. ALK-rearranged lung cancer: adenosquamous lung cancer masquerading as pure squamous carcinoma. J Thorac Oncol. 2012;7:768–769. doi:10.1097/JTO.0b013e31824c9485
Cheng Y, Yang J, Wang D, Yan D. ROS1 fusion lung adenosquamous carcinoma patient with short-term clinical benefit after crizotinib treatment: a case report. Ann Transl Med. 2022;10:157. doi:10.21037/atm-21-6754
Patil J, Nie Y, Aisner DL, Camidge DR. Case report: significant clinical benefit from pemetrexed-based therapy in ROS-1 and ALK-rearranged lung cancer with adenosquamous histology. Front Oncol. 2022;11:788245. doi:10.3389/fonc.2021.788245
Li C, Zheng X, Li P, et al. Heterogeneity of tumor immune microenvironment and real-world analysis of immunotherapy efficacy in lung adenosquamous carcinoma. Front Immunol. 2022;13:944812. doi:10.3389/fimmu.2022.944812
Katie Kowalski, MPH
For nearly 40 years, the National Organization for Rare Disorders (NORD) has worked to drive meaningful and enduring impact so that people living with rare diseases, including rare cancers, can live their best lives. We are proud to collaborate with MDedge to deliver timely information about rare cancers to healthcare professionals. Rare cancers are those that affect fewer than 40,000 people per year in the United States. While the incidence of each rare cancer may be low, collectively, they make up a significant proportion (27%) of all cancers.1 Moreover, rare cancers present unique challenges: they are difficult to identify and often diagnosed at later stages when they are harder to treat. Patients often have trouble finding specialists who are familiar with their rare cancer. Additionally, the availability of effective drugs to treat rare cancers is limited and enrollment in rare cancer clinical trials is challenging due to small, and often not diverse, study populations. Currently, the 5-year survival rate for rare cancers in adults (48.5%) is worse than for common cancers (63.4%).2
While people living with rare cancers continue to face daunting obstacles, progress is being made, and there are reasons to hope for a better future. Advances in genomic testing and precision medicine provide increasing evidence that rare cancers can be more efficiently and effectively diagnosed and treated. Genomic tests examine tumor DNA to identify mutations that are unique to an individual’s cancer. This genetic information enables a more precise diagnosis and targeted treatment approach. Jim Palma, Co-Lead of the NORD Rare Cancer Coalition, said “There is promise for rare cancer patients due to increased legislative efforts to cover the costs of genomic testing coupled by an increase in FDA approvals for targeted and tissue agnostic therapies.”
In 2019, the National Cancer Institute established MyPART, a vast pediatric and adult rare tumor network that aims to bolster patient involvement in research and develop effective therapies through tumor sample collection, shared data, shared samples, new methods to test treatments, and new trial designs. In 2022, MyPART welcomed NORD’s Rare Cancer Coalition as an advocacy partner.
Meanwhile, advocacy organizations are giving rare cancer a rising voice. NORD’s Rare Cancer Coalition unites rare cancer patient advocacy organizations and helps them drive progress together. The coalition promotes research and awareness through its annual Rare Cancer Day (September 30) campaign. Additionally, NORD has produced over 22 continuing medical education modules on rare cancers in collaboration with PlatformQ Health, providing updates on new therapies and treatment approaches. NORD also offers rare disease reports and educational videos on rare cancers, sessions inclusive of rare cancer topics at the annual NORD Summit, and a quarterly e-newsletter, “Caring for Rare” for healthcare professionals. Please visit us at rarediseases.org to access these resources.
Much work on rare cancers remains to be done, but the progress over recent years points to better outcomes moving forward. We are grateful for the work you do and your dedication to your patients, including those with rare cancers and other rare conditions. We hope you will find the information in this special issue useful for your clinical practice.
– Katie Kowalski, MPH Associate Director of Education National Organization for Rare Disorders
Gatta G, Capocaccia R, Botta L, et al. Burden and centralized treatment in Europe of rare tumours: Results of RARECAREnet-a population-based study. Lancet Oncol. 2017,18(8):1022–1039. doi:10.1016/S1470-2045(17)30445-X
Katie Kowalski, MPH
For nearly 40 years, the National Organization for Rare Disorders (NORD) has worked to drive meaningful and enduring impact so that people living with rare diseases, including rare cancers, can live their best lives. We are proud to collaborate with MDedge to deliver timely information about rare cancers to healthcare professionals. Rare cancers are those that affect fewer than 40,000 people per year in the United States. While the incidence of each rare cancer may be low, collectively, they make up a significant proportion (27%) of all cancers.1 Moreover, rare cancers present unique challenges: they are difficult to identify and often diagnosed at later stages when they are harder to treat. Patients often have trouble finding specialists who are familiar with their rare cancer. Additionally, the availability of effective drugs to treat rare cancers is limited and enrollment in rare cancer clinical trials is challenging due to small, and often not diverse, study populations. Currently, the 5-year survival rate for rare cancers in adults (48.5%) is worse than for common cancers (63.4%).2
While people living with rare cancers continue to face daunting obstacles, progress is being made, and there are reasons to hope for a better future. Advances in genomic testing and precision medicine provide increasing evidence that rare cancers can be more efficiently and effectively diagnosed and treated. Genomic tests examine tumor DNA to identify mutations that are unique to an individual’s cancer. This genetic information enables a more precise diagnosis and targeted treatment approach. Jim Palma, Co-Lead of the NORD Rare Cancer Coalition, said “There is promise for rare cancer patients due to increased legislative efforts to cover the costs of genomic testing coupled by an increase in FDA approvals for targeted and tissue agnostic therapies.”
In 2019, the National Cancer Institute established MyPART, a vast pediatric and adult rare tumor network that aims to bolster patient involvement in research and develop effective therapies through tumor sample collection, shared data, shared samples, new methods to test treatments, and new trial designs. In 2022, MyPART welcomed NORD’s Rare Cancer Coalition as an advocacy partner.
Meanwhile, advocacy organizations are giving rare cancer a rising voice. NORD’s Rare Cancer Coalition unites rare cancer patient advocacy organizations and helps them drive progress together. The coalition promotes research and awareness through its annual Rare Cancer Day (September 30) campaign. Additionally, NORD has produced over 22 continuing medical education modules on rare cancers in collaboration with PlatformQ Health, providing updates on new therapies and treatment approaches. NORD also offers rare disease reports and educational videos on rare cancers, sessions inclusive of rare cancer topics at the annual NORD Summit, and a quarterly e-newsletter, “Caring for Rare” for healthcare professionals. Please visit us at rarediseases.org to access these resources.
Much work on rare cancers remains to be done, but the progress over recent years points to better outcomes moving forward. We are grateful for the work you do and your dedication to your patients, including those with rare cancers and other rare conditions. We hope you will find the information in this special issue useful for your clinical practice.
– Katie Kowalski, MPH Associate Director of Education National Organization for Rare Disorders
Katie Kowalski, MPH
For nearly 40 years, the National Organization for Rare Disorders (NORD) has worked to drive meaningful and enduring impact so that people living with rare diseases, including rare cancers, can live their best lives. We are proud to collaborate with MDedge to deliver timely information about rare cancers to healthcare professionals. Rare cancers are those that affect fewer than 40,000 people per year in the United States. While the incidence of each rare cancer may be low, collectively, they make up a significant proportion (27%) of all cancers.1 Moreover, rare cancers present unique challenges: they are difficult to identify and often diagnosed at later stages when they are harder to treat. Patients often have trouble finding specialists who are familiar with their rare cancer. Additionally, the availability of effective drugs to treat rare cancers is limited and enrollment in rare cancer clinical trials is challenging due to small, and often not diverse, study populations. Currently, the 5-year survival rate for rare cancers in adults (48.5%) is worse than for common cancers (63.4%).2
While people living with rare cancers continue to face daunting obstacles, progress is being made, and there are reasons to hope for a better future. Advances in genomic testing and precision medicine provide increasing evidence that rare cancers can be more efficiently and effectively diagnosed and treated. Genomic tests examine tumor DNA to identify mutations that are unique to an individual’s cancer. This genetic information enables a more precise diagnosis and targeted treatment approach. Jim Palma, Co-Lead of the NORD Rare Cancer Coalition, said “There is promise for rare cancer patients due to increased legislative efforts to cover the costs of genomic testing coupled by an increase in FDA approvals for targeted and tissue agnostic therapies.”
In 2019, the National Cancer Institute established MyPART, a vast pediatric and adult rare tumor network that aims to bolster patient involvement in research and develop effective therapies through tumor sample collection, shared data, shared samples, new methods to test treatments, and new trial designs. In 2022, MyPART welcomed NORD’s Rare Cancer Coalition as an advocacy partner.
Meanwhile, advocacy organizations are giving rare cancer a rising voice. NORD’s Rare Cancer Coalition unites rare cancer patient advocacy organizations and helps them drive progress together. The coalition promotes research and awareness through its annual Rare Cancer Day (September 30) campaign. Additionally, NORD has produced over 22 continuing medical education modules on rare cancers in collaboration with PlatformQ Health, providing updates on new therapies and treatment approaches. NORD also offers rare disease reports and educational videos on rare cancers, sessions inclusive of rare cancer topics at the annual NORD Summit, and a quarterly e-newsletter, “Caring for Rare” for healthcare professionals. Please visit us at rarediseases.org to access these resources.
Much work on rare cancers remains to be done, but the progress over recent years points to better outcomes moving forward. We are grateful for the work you do and your dedication to your patients, including those with rare cancers and other rare conditions. We hope you will find the information in this special issue useful for your clinical practice.
– Katie Kowalski, MPH Associate Director of Education National Organization for Rare Disorders
Gatta G, Capocaccia R, Botta L, et al. Burden and centralized treatment in Europe of rare tumours: Results of RARECAREnet-a population-based study. Lancet Oncol. 2017,18(8):1022–1039. doi:10.1016/S1470-2045(17)30445-X
Gatta G, Capocaccia R, Botta L, et al. Burden and centralized treatment in Europe of rare tumours: Results of RARECAREnet-a population-based study. Lancet Oncol. 2017,18(8):1022–1039. doi:10.1016/S1470-2045(17)30445-X
This edition of Rare Diseases Report: Cancers highlights the latest breakthroughs and remaining unmet needs in the management of rare cancers. In addition to celebrating the great progress that has been made in recent years, we also discuss new challenges, such as how the healthcare system can prepare to manage the growing number of rare cancer survivors who are living longer due to improvements in disease management.
This edition of Rare Diseases Report: Cancers highlights the latest breakthroughs and remaining unmet needs in the management of rare cancers. In addition to celebrating the great progress that has been made in recent years, we also discuss new challenges, such as how the healthcare system can prepare to manage the growing number of rare cancer survivors who are living longer due to improvements in disease management.
This edition of Rare Diseases Report: Cancers highlights the latest breakthroughs and remaining unmet needs in the management of rare cancers. In addition to celebrating the great progress that has been made in recent years, we also discuss new challenges, such as how the healthcare system can prepare to manage the growing number of rare cancer survivors who are living longer due to improvements in disease management.