User login
Around 5% of US Population Diagnosed With Autoimmune Disease
TOPLINE:
In 2022, autoimmune diseases affected over 15 million individuals in the United States, with women nearly twice as likely to be affected as men and more than one third of affected individuals having more than one autoimmune condition.
METHODOLOGY:
- Researchers used electronic health record (EHR) data from six healthcare systems in the United States between 2011 and 2022 to estimate the prevalence of autoimmune diseases according to sex and age.
- They selected 105 autoimmune diseases from the textbook The Autoimmune Diseases and estimated their prevalence in more than 10 million individuals from these healthcare systems; these statistics were subsequently extrapolated to an estimated US population of 333.3 million.
- An individual was considered to have a diagnosis of an autoimmune disease if they had at least two diagnosis codes for the condition, with the codes being at least 30 days apart.
- A software program was developed to compute the prevalence of autoimmune diseases alone and in aggregate, enabling other researchers to replicate or modify the analysis over time.
TAKEAWAY:
- More than 15 million people, accounting for 4.6% of the US population, were diagnosed with at least one autoimmune disease from January 2011 to June 2022; 34% were diagnosed with more than one autoimmune disease.
- Sex-stratified analysis revealed that 63% of patients diagnosed with autoimmune disease were women, and only 37% were men, establishing a female-to-male ratio of 1.7:1; age-stratified analysis revealed increasing prevalence of autoimmune conditions with age, peaking in individuals aged ≥ 65 years.
- Among individuals with autoimmune diseases, 65% of patients had one condition, whereas 24% had two, 8% had three, and 2% had four or more autoimmune diseases (does not add to 100% due to rounding).
- Rheumatoid arthritis emerged as the most prevalent autoimmune disease, followed by psoriasis, type 1 diabetes, Grave’s disease, and autoimmune thyroiditis; 19 of the top 20 most prevalent autoimmune diseases occurred more frequently in women.
IN PRACTICE:
“Accurate data on the prevalence of autoimmune diseases as a category of disease and for individual autoimmune diseases are needed to further clinical and basic research to improve diagnosis, biomarkers, and therapies for these diseases, which significantly impact the US population,” the authors wrote.
SOURCE:
The study was led by Aaron H. Abend, Autoimmune Registry, Guilford, Connecticut, and was published online in The Journal of Clinical Investigation.
LIMITATIONS:
The use of EHR data presented several challenges, including potential inaccuracies in diagnosis codes and the possibility of missing patients with single diagnosis codes because of the two-code requirement. Certain autoimmune diseases evolve over time and involve nonspecific clinical signs and symptoms that can mimic other diseases, potentially resulting in underdiagnosis. Moreover, rare diseases lacking specific diagnosis codes may have been underrepresented.
DISCLOSURES:
The study received support from Autoimmune Registry; the National Institutes of Health National Center for Advancing Translational Sciences; the National Heart, Lung, and Blood Institute; and other sources. Information on potential conflicts of interest was not disclosed.
This article was created using several editorial tools, including artificial intelligence, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
In 2022, autoimmune diseases affected over 15 million individuals in the United States, with women nearly twice as likely to be affected as men and more than one third of affected individuals having more than one autoimmune condition.
METHODOLOGY:
- Researchers used electronic health record (EHR) data from six healthcare systems in the United States between 2011 and 2022 to estimate the prevalence of autoimmune diseases according to sex and age.
- They selected 105 autoimmune diseases from the textbook The Autoimmune Diseases and estimated their prevalence in more than 10 million individuals from these healthcare systems; these statistics were subsequently extrapolated to an estimated US population of 333.3 million.
- An individual was considered to have a diagnosis of an autoimmune disease if they had at least two diagnosis codes for the condition, with the codes being at least 30 days apart.
- A software program was developed to compute the prevalence of autoimmune diseases alone and in aggregate, enabling other researchers to replicate or modify the analysis over time.
TAKEAWAY:
- More than 15 million people, accounting for 4.6% of the US population, were diagnosed with at least one autoimmune disease from January 2011 to June 2022; 34% were diagnosed with more than one autoimmune disease.
- Sex-stratified analysis revealed that 63% of patients diagnosed with autoimmune disease were women, and only 37% were men, establishing a female-to-male ratio of 1.7:1; age-stratified analysis revealed increasing prevalence of autoimmune conditions with age, peaking in individuals aged ≥ 65 years.
- Among individuals with autoimmune diseases, 65% of patients had one condition, whereas 24% had two, 8% had three, and 2% had four or more autoimmune diseases (does not add to 100% due to rounding).
- Rheumatoid arthritis emerged as the most prevalent autoimmune disease, followed by psoriasis, type 1 diabetes, Grave’s disease, and autoimmune thyroiditis; 19 of the top 20 most prevalent autoimmune diseases occurred more frequently in women.
IN PRACTICE:
“Accurate data on the prevalence of autoimmune diseases as a category of disease and for individual autoimmune diseases are needed to further clinical and basic research to improve diagnosis, biomarkers, and therapies for these diseases, which significantly impact the US population,” the authors wrote.
SOURCE:
The study was led by Aaron H. Abend, Autoimmune Registry, Guilford, Connecticut, and was published online in The Journal of Clinical Investigation.
LIMITATIONS:
The use of EHR data presented several challenges, including potential inaccuracies in diagnosis codes and the possibility of missing patients with single diagnosis codes because of the two-code requirement. Certain autoimmune diseases evolve over time and involve nonspecific clinical signs and symptoms that can mimic other diseases, potentially resulting in underdiagnosis. Moreover, rare diseases lacking specific diagnosis codes may have been underrepresented.
DISCLOSURES:
The study received support from Autoimmune Registry; the National Institutes of Health National Center for Advancing Translational Sciences; the National Heart, Lung, and Blood Institute; and other sources. Information on potential conflicts of interest was not disclosed.
This article was created using several editorial tools, including artificial intelligence, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
In 2022, autoimmune diseases affected over 15 million individuals in the United States, with women nearly twice as likely to be affected as men and more than one third of affected individuals having more than one autoimmune condition.
METHODOLOGY:
- Researchers used electronic health record (EHR) data from six healthcare systems in the United States between 2011 and 2022 to estimate the prevalence of autoimmune diseases according to sex and age.
- They selected 105 autoimmune diseases from the textbook The Autoimmune Diseases and estimated their prevalence in more than 10 million individuals from these healthcare systems; these statistics were subsequently extrapolated to an estimated US population of 333.3 million.
- An individual was considered to have a diagnosis of an autoimmune disease if they had at least two diagnosis codes for the condition, with the codes being at least 30 days apart.
- A software program was developed to compute the prevalence of autoimmune diseases alone and in aggregate, enabling other researchers to replicate or modify the analysis over time.
TAKEAWAY:
- More than 15 million people, accounting for 4.6% of the US population, were diagnosed with at least one autoimmune disease from January 2011 to June 2022; 34% were diagnosed with more than one autoimmune disease.
- Sex-stratified analysis revealed that 63% of patients diagnosed with autoimmune disease were women, and only 37% were men, establishing a female-to-male ratio of 1.7:1; age-stratified analysis revealed increasing prevalence of autoimmune conditions with age, peaking in individuals aged ≥ 65 years.
- Among individuals with autoimmune diseases, 65% of patients had one condition, whereas 24% had two, 8% had three, and 2% had four or more autoimmune diseases (does not add to 100% due to rounding).
- Rheumatoid arthritis emerged as the most prevalent autoimmune disease, followed by psoriasis, type 1 diabetes, Grave’s disease, and autoimmune thyroiditis; 19 of the top 20 most prevalent autoimmune diseases occurred more frequently in women.
IN PRACTICE:
“Accurate data on the prevalence of autoimmune diseases as a category of disease and for individual autoimmune diseases are needed to further clinical and basic research to improve diagnosis, biomarkers, and therapies for these diseases, which significantly impact the US population,” the authors wrote.
SOURCE:
The study was led by Aaron H. Abend, Autoimmune Registry, Guilford, Connecticut, and was published online in The Journal of Clinical Investigation.
LIMITATIONS:
The use of EHR data presented several challenges, including potential inaccuracies in diagnosis codes and the possibility of missing patients with single diagnosis codes because of the two-code requirement. Certain autoimmune diseases evolve over time and involve nonspecific clinical signs and symptoms that can mimic other diseases, potentially resulting in underdiagnosis. Moreover, rare diseases lacking specific diagnosis codes may have been underrepresented.
DISCLOSURES:
The study received support from Autoimmune Registry; the National Institutes of Health National Center for Advancing Translational Sciences; the National Heart, Lung, and Blood Institute; and other sources. Information on potential conflicts of interest was not disclosed.
This article was created using several editorial tools, including artificial intelligence, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Early-Onset Asthma May Slow Memory Development
Children with asthma scored significantly lower than those without asthma on measures of episodic memory, based on longitudinal data from nearly 500 individuals.
Animal models have shown associations between asthma and memory problems, but data for children are lacking, wrote Nicholas J. Christopher-Hayes, MA, of the University of California, Davis, and colleagues.
“Asthma is very frequent among children, and there is mounting evidence from rodent models that asthma may result in neural injury in the hippocampus, which in turn may cause memory loss,” Christopher-Hayes said in an interview. “Although there is also a good amount of research with older adults, very little research has been done with children, the period that is most frequently linked to asthma onset,” he said. Therefore, the researchers leveraged a large national study on child development to examine development of memory as a function of asthma exposure.
In this study published in JAMA Network Open, the researchers conducted both a longitudinal and cross-sectional analysis of data from the Adolescent Brain Cognitive Development Study, which began in 2015. Children were enrolled at ages 9-10 years with a follow-up assessment 1-2 years later.
The participants were categorized as early childhood-onset asthma (asthma at baseline and follow-up), later childhood-onset asthma (asthma at follow-up only), or no asthma history. The primary outcome of the longitudinal analysis was episodic memory. Approximately half of the participants were boys, and slightly more than half were White.
Overall, those with early-onset asthma showed significantly lower rates of longitudinal memory improvements at follow-up compared with the comparison group (P < .01).
Developmental memory improvement in children with later-onset asthma was not significantly different from the control individuals.
Secondary outcomes included processing speed and inhibition, and attention. In a cross-sectional analysis with a larger sample of 2062 children from the same database (1031 with any asthma), those with asthma scored significantly lower on measures not only of episodic memory but also processing speed and inhibition/attention than children with no asthma, with P values of .04, .01, and .02, respectively.
The results were limited by several factors, including the reliance on parent reports for indicators of asthma and the lack of data on the potential effect of prescription corticosteroid use on neurocognitive development, the researchers noted.
The mechanism behind the association remains unclear; the inflammation associated with asthma may disrupt neural processing and manifest as cognitive dysfunction, as has been seen in rodent models of asthma, the researchers wrote. “It is possible that associations between asthma and developmental trajectories emerge earlier for memory, perhaps due to its sensitivity to subtle hippocampal injury,” they noted.
Longer follow-up studies are needed to fully understand how childhood asthma predicts memory declines or difficulties in childhood and beyond, said Christopher-Hayes. “We also need additional studies to understand why children who were diagnosed earlier and had asthma for longer seem to be particularly affected,” he said.
The results of this study were consistent with previous findings and therefore not surprising, senior author Simona Ghetti, PhD, a professor of psychology at the University of California, Davis, said in an interview. However, the finding that the extent of exposure to asthma was associated with slower memory improvement in childhood was striking, she said. That children with an earlier asthma onset who had disease indicators for a longer period showed a slower development of memory over time, suggests that asthma exposure may affect the developmental trajectory of memory, Ghetti noted.
“Recommendations to clinicians are premature because we need a better understanding of the boundary conditions, such as the minimal level of asthma exposure that might generate memory difficulties,” said Ghetti.
“Nevertheless, our results underscore the importance of looking at asthma as a potential source of cognitive difficulty in children,” she said.
Asthma’s Extensive Effect
Evidence is mounting that a diagnosis of asthma may have implications outside the pulmonary system, Diego J. Maselli, MD, professor and chief of the Division of Pulmonary Diseases & Critical Care at UT Health, San Antonio, said in an interview.
“Asthmatics may be at risk of nasal polyps, allergic rhinitis, and other allergic conditions, but there is emerging of evidence inflammation associated with asthma may affect other organ systems,” said Maselli, who was not involved in the study.
“For example, chronic inflammation in asthmatics may increase the risk of cardiovascular disease,” he said.
Although less is known about the effects of asthma on the nervous system, animal models suggest that inflammation associated with asthma may result in neuronal injury and potential effects on memory, said Maselli.
The findings of this study provide evidence of potential detrimental effects on the memory of children with asthma but should be interpreted with caution, Maselli said. “Children with chronic medical conditions may have an inherent disadvantage compared with their peers due to the burden of their disease, medication utilization and side effects, absenteeism from school, physical limitations, and other disease-specific circumstances,” he noted.
“Uncontrolled asthma, in particular, has strong links to low socioeconomic factors that are closely tied to access to adequate medical care, nutrition, educational institutions, and other relevant contributors to normal cognitive development,” Maselli said. Although the authors account for some of these socioeconomic factors by evaluating income and race, other variables may have influenced the results, he added.
Overall, this study’s findings suggested that the diagnosis of asthma in children may be associated with memory deficits and may influence neurodevelopment; however, more research is needed to determine whether the findings are replicated in other cohorts, said Maselli. “In particular, evaluating the effects of the severity of asthma and different asthma endotypes would be crucial to identify children with a higher risk of memory or cognitive deficits and confirm these associations,” he said.
This study was funded by the Memory and Plasticity Program at the University of California, Davis, and by a Learning, Memory, and Plasticity Training Program Fellowship grant from the National Institutes of Health. The researchers and Maselli had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Children with asthma scored significantly lower than those without asthma on measures of episodic memory, based on longitudinal data from nearly 500 individuals.
Animal models have shown associations between asthma and memory problems, but data for children are lacking, wrote Nicholas J. Christopher-Hayes, MA, of the University of California, Davis, and colleagues.
“Asthma is very frequent among children, and there is mounting evidence from rodent models that asthma may result in neural injury in the hippocampus, which in turn may cause memory loss,” Christopher-Hayes said in an interview. “Although there is also a good amount of research with older adults, very little research has been done with children, the period that is most frequently linked to asthma onset,” he said. Therefore, the researchers leveraged a large national study on child development to examine development of memory as a function of asthma exposure.
In this study published in JAMA Network Open, the researchers conducted both a longitudinal and cross-sectional analysis of data from the Adolescent Brain Cognitive Development Study, which began in 2015. Children were enrolled at ages 9-10 years with a follow-up assessment 1-2 years later.
The participants were categorized as early childhood-onset asthma (asthma at baseline and follow-up), later childhood-onset asthma (asthma at follow-up only), or no asthma history. The primary outcome of the longitudinal analysis was episodic memory. Approximately half of the participants were boys, and slightly more than half were White.
Overall, those with early-onset asthma showed significantly lower rates of longitudinal memory improvements at follow-up compared with the comparison group (P < .01).
Developmental memory improvement in children with later-onset asthma was not significantly different from the control individuals.
Secondary outcomes included processing speed and inhibition, and attention. In a cross-sectional analysis with a larger sample of 2062 children from the same database (1031 with any asthma), those with asthma scored significantly lower on measures not only of episodic memory but also processing speed and inhibition/attention than children with no asthma, with P values of .04, .01, and .02, respectively.
The results were limited by several factors, including the reliance on parent reports for indicators of asthma and the lack of data on the potential effect of prescription corticosteroid use on neurocognitive development, the researchers noted.
The mechanism behind the association remains unclear; the inflammation associated with asthma may disrupt neural processing and manifest as cognitive dysfunction, as has been seen in rodent models of asthma, the researchers wrote. “It is possible that associations between asthma and developmental trajectories emerge earlier for memory, perhaps due to its sensitivity to subtle hippocampal injury,” they noted.
Longer follow-up studies are needed to fully understand how childhood asthma predicts memory declines or difficulties in childhood and beyond, said Christopher-Hayes. “We also need additional studies to understand why children who were diagnosed earlier and had asthma for longer seem to be particularly affected,” he said.
The results of this study were consistent with previous findings and therefore not surprising, senior author Simona Ghetti, PhD, a professor of psychology at the University of California, Davis, said in an interview. However, the finding that the extent of exposure to asthma was associated with slower memory improvement in childhood was striking, she said. That children with an earlier asthma onset who had disease indicators for a longer period showed a slower development of memory over time, suggests that asthma exposure may affect the developmental trajectory of memory, Ghetti noted.
“Recommendations to clinicians are premature because we need a better understanding of the boundary conditions, such as the minimal level of asthma exposure that might generate memory difficulties,” said Ghetti.
“Nevertheless, our results underscore the importance of looking at asthma as a potential source of cognitive difficulty in children,” she said.
Asthma’s Extensive Effect
Evidence is mounting that a diagnosis of asthma may have implications outside the pulmonary system, Diego J. Maselli, MD, professor and chief of the Division of Pulmonary Diseases & Critical Care at UT Health, San Antonio, said in an interview.
“Asthmatics may be at risk of nasal polyps, allergic rhinitis, and other allergic conditions, but there is emerging of evidence inflammation associated with asthma may affect other organ systems,” said Maselli, who was not involved in the study.
“For example, chronic inflammation in asthmatics may increase the risk of cardiovascular disease,” he said.
Although less is known about the effects of asthma on the nervous system, animal models suggest that inflammation associated with asthma may result in neuronal injury and potential effects on memory, said Maselli.
The findings of this study provide evidence of potential detrimental effects on the memory of children with asthma but should be interpreted with caution, Maselli said. “Children with chronic medical conditions may have an inherent disadvantage compared with their peers due to the burden of their disease, medication utilization and side effects, absenteeism from school, physical limitations, and other disease-specific circumstances,” he noted.
“Uncontrolled asthma, in particular, has strong links to low socioeconomic factors that are closely tied to access to adequate medical care, nutrition, educational institutions, and other relevant contributors to normal cognitive development,” Maselli said. Although the authors account for some of these socioeconomic factors by evaluating income and race, other variables may have influenced the results, he added.
Overall, this study’s findings suggested that the diagnosis of asthma in children may be associated with memory deficits and may influence neurodevelopment; however, more research is needed to determine whether the findings are replicated in other cohorts, said Maselli. “In particular, evaluating the effects of the severity of asthma and different asthma endotypes would be crucial to identify children with a higher risk of memory or cognitive deficits and confirm these associations,” he said.
This study was funded by the Memory and Plasticity Program at the University of California, Davis, and by a Learning, Memory, and Plasticity Training Program Fellowship grant from the National Institutes of Health. The researchers and Maselli had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Children with asthma scored significantly lower than those without asthma on measures of episodic memory, based on longitudinal data from nearly 500 individuals.
Animal models have shown associations between asthma and memory problems, but data for children are lacking, wrote Nicholas J. Christopher-Hayes, MA, of the University of California, Davis, and colleagues.
“Asthma is very frequent among children, and there is mounting evidence from rodent models that asthma may result in neural injury in the hippocampus, which in turn may cause memory loss,” Christopher-Hayes said in an interview. “Although there is also a good amount of research with older adults, very little research has been done with children, the period that is most frequently linked to asthma onset,” he said. Therefore, the researchers leveraged a large national study on child development to examine development of memory as a function of asthma exposure.
In this study published in JAMA Network Open, the researchers conducted both a longitudinal and cross-sectional analysis of data from the Adolescent Brain Cognitive Development Study, which began in 2015. Children were enrolled at ages 9-10 years with a follow-up assessment 1-2 years later.
The participants were categorized as early childhood-onset asthma (asthma at baseline and follow-up), later childhood-onset asthma (asthma at follow-up only), or no asthma history. The primary outcome of the longitudinal analysis was episodic memory. Approximately half of the participants were boys, and slightly more than half were White.
Overall, those with early-onset asthma showed significantly lower rates of longitudinal memory improvements at follow-up compared with the comparison group (P < .01).
Developmental memory improvement in children with later-onset asthma was not significantly different from the control individuals.
Secondary outcomes included processing speed and inhibition, and attention. In a cross-sectional analysis with a larger sample of 2062 children from the same database (1031 with any asthma), those with asthma scored significantly lower on measures not only of episodic memory but also processing speed and inhibition/attention than children with no asthma, with P values of .04, .01, and .02, respectively.
The results were limited by several factors, including the reliance on parent reports for indicators of asthma and the lack of data on the potential effect of prescription corticosteroid use on neurocognitive development, the researchers noted.
The mechanism behind the association remains unclear; the inflammation associated with asthma may disrupt neural processing and manifest as cognitive dysfunction, as has been seen in rodent models of asthma, the researchers wrote. “It is possible that associations between asthma and developmental trajectories emerge earlier for memory, perhaps due to its sensitivity to subtle hippocampal injury,” they noted.
Longer follow-up studies are needed to fully understand how childhood asthma predicts memory declines or difficulties in childhood and beyond, said Christopher-Hayes. “We also need additional studies to understand why children who were diagnosed earlier and had asthma for longer seem to be particularly affected,” he said.
The results of this study were consistent with previous findings and therefore not surprising, senior author Simona Ghetti, PhD, a professor of psychology at the University of California, Davis, said in an interview. However, the finding that the extent of exposure to asthma was associated with slower memory improvement in childhood was striking, she said. That children with an earlier asthma onset who had disease indicators for a longer period showed a slower development of memory over time, suggests that asthma exposure may affect the developmental trajectory of memory, Ghetti noted.
“Recommendations to clinicians are premature because we need a better understanding of the boundary conditions, such as the minimal level of asthma exposure that might generate memory difficulties,” said Ghetti.
“Nevertheless, our results underscore the importance of looking at asthma as a potential source of cognitive difficulty in children,” she said.
Asthma’s Extensive Effect
Evidence is mounting that a diagnosis of asthma may have implications outside the pulmonary system, Diego J. Maselli, MD, professor and chief of the Division of Pulmonary Diseases & Critical Care at UT Health, San Antonio, said in an interview.
“Asthmatics may be at risk of nasal polyps, allergic rhinitis, and other allergic conditions, but there is emerging of evidence inflammation associated with asthma may affect other organ systems,” said Maselli, who was not involved in the study.
“For example, chronic inflammation in asthmatics may increase the risk of cardiovascular disease,” he said.
Although less is known about the effects of asthma on the nervous system, animal models suggest that inflammation associated with asthma may result in neuronal injury and potential effects on memory, said Maselli.
The findings of this study provide evidence of potential detrimental effects on the memory of children with asthma but should be interpreted with caution, Maselli said. “Children with chronic medical conditions may have an inherent disadvantage compared with their peers due to the burden of their disease, medication utilization and side effects, absenteeism from school, physical limitations, and other disease-specific circumstances,” he noted.
“Uncontrolled asthma, in particular, has strong links to low socioeconomic factors that are closely tied to access to adequate medical care, nutrition, educational institutions, and other relevant contributors to normal cognitive development,” Maselli said. Although the authors account for some of these socioeconomic factors by evaluating income and race, other variables may have influenced the results, he added.
Overall, this study’s findings suggested that the diagnosis of asthma in children may be associated with memory deficits and may influence neurodevelopment; however, more research is needed to determine whether the findings are replicated in other cohorts, said Maselli. “In particular, evaluating the effects of the severity of asthma and different asthma endotypes would be crucial to identify children with a higher risk of memory or cognitive deficits and confirm these associations,” he said.
This study was funded by the Memory and Plasticity Program at the University of California, Davis, and by a Learning, Memory, and Plasticity Training Program Fellowship grant from the National Institutes of Health. The researchers and Maselli had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Dementia Risk Higher for Stroke Survivors
TOPLINE:
Risk for dementia is nearly 80% higher in stroke survivors than in those without stroke, a new study reveals. The data suggest risk declines within 1 year after stroke but remains elevated for up to 20 years.
METHODOLOGY:
- Researchers conducted a population-wide analysis of over 15 million people in Canada between 2002 and 2022. The study focused on adults hospitalized for ischemic stroke, intracerebral hemorrhage, or acute myocardial infarction (AMI).
- Of 175,980 stroke survivors, 99% were matched 1:1 to residents without stroke on the basis of age, sex, rural residence, neighborhood deprivation, and vascular comorbidities. In addition, 90% of patients were matched to those with AMI.
- Incident dementia diagnoses were tracked starting 90 days after stroke until death, emigration, or the end of the study, using a validated algorithm based on hospitalization for dementia, prescriptions for cholinesterase inhibitors, or physician claims within 2 years.
- The mean follow-up duration was 5.6 years.
TAKEAWAY:
- Among stroke survivors, 19% were diagnosed with dementia vs 12.5% in the reference population. The dementia rate per 100 person-years was higher among stroke survivors than in the reference population over the entire follow-up period (3.34 vs 1.89).
- Over the entire study period, dementia was 76% more likely among stroke patients (hazard ratio [HR], 1.76; 95% CI, 1.73-1.79) and 82% more likely in the AMI cohort (HR, 1.82; 95% CI, 1.79-1.85) than in the reference population.
- Time-varying analysis revealed that dementia risk was highest within the first year after stroke, with a > 2.5-fold increase at 6 months (HR, 2.51; 95% CI, 2.42-2.59), which decreased to a 1.5-fold increase at 5 years (HR, 1.51; 95% CI, 1.48-1.56) but remained elevated compared with the reference population even 20 years after the index stroke.
- Recurrent stroke was associated with an approximately threefold increased risk for dementia (single recurrent stroke adjusted HR, 2.64; 95% CI, 2.54-2.74; multiple recurrent strokes adjusted HR, 3.05; 95% CI, 2.81-3.33).
IN PRACTICE:
“While much research has been focused on reducing the risk of a second stroke, our findings make it clear that more research also is needed on developing interventions to help prevent dementia after stroke,” lead author Raed A. Joundi, MD, DPhil, McMaster University, Hamilton, Ontario, Canada, said in a press release.
“There is a need to accelerate the implementation of promising interventions or multipronged approaches into large randomized controlled trials to lower the risk of dementia,” the investigators wrote.
SOURCE:
The study was published online on December 4 in Neurology.
LIMITATIONS:
The study’s limitations included reliance on administrative coding without imaging data, potential underestimation of mild dementia, and lack of granular information on stroke severity, disability, and prestroke cognitive decline. While adjustments were made for healthcare contact and secondary prevention medications, residual biases may have persisted.
DISCLOSURES:
This study received funding from the Canada Brain Research Fund, Heart & Stroke Foundation of Canada, and Canadian Stroke Consortium. Two authors hold awards and positions from national organizations and academic institutions in Canada. Additional details are provided in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Risk for dementia is nearly 80% higher in stroke survivors than in those without stroke, a new study reveals. The data suggest risk declines within 1 year after stroke but remains elevated for up to 20 years.
METHODOLOGY:
- Researchers conducted a population-wide analysis of over 15 million people in Canada between 2002 and 2022. The study focused on adults hospitalized for ischemic stroke, intracerebral hemorrhage, or acute myocardial infarction (AMI).
- Of 175,980 stroke survivors, 99% were matched 1:1 to residents without stroke on the basis of age, sex, rural residence, neighborhood deprivation, and vascular comorbidities. In addition, 90% of patients were matched to those with AMI.
- Incident dementia diagnoses were tracked starting 90 days after stroke until death, emigration, or the end of the study, using a validated algorithm based on hospitalization for dementia, prescriptions for cholinesterase inhibitors, or physician claims within 2 years.
- The mean follow-up duration was 5.6 years.
TAKEAWAY:
- Among stroke survivors, 19% were diagnosed with dementia vs 12.5% in the reference population. The dementia rate per 100 person-years was higher among stroke survivors than in the reference population over the entire follow-up period (3.34 vs 1.89).
- Over the entire study period, dementia was 76% more likely among stroke patients (hazard ratio [HR], 1.76; 95% CI, 1.73-1.79) and 82% more likely in the AMI cohort (HR, 1.82; 95% CI, 1.79-1.85) than in the reference population.
- Time-varying analysis revealed that dementia risk was highest within the first year after stroke, with a > 2.5-fold increase at 6 months (HR, 2.51; 95% CI, 2.42-2.59), which decreased to a 1.5-fold increase at 5 years (HR, 1.51; 95% CI, 1.48-1.56) but remained elevated compared with the reference population even 20 years after the index stroke.
- Recurrent stroke was associated with an approximately threefold increased risk for dementia (single recurrent stroke adjusted HR, 2.64; 95% CI, 2.54-2.74; multiple recurrent strokes adjusted HR, 3.05; 95% CI, 2.81-3.33).
IN PRACTICE:
“While much research has been focused on reducing the risk of a second stroke, our findings make it clear that more research also is needed on developing interventions to help prevent dementia after stroke,” lead author Raed A. Joundi, MD, DPhil, McMaster University, Hamilton, Ontario, Canada, said in a press release.
“There is a need to accelerate the implementation of promising interventions or multipronged approaches into large randomized controlled trials to lower the risk of dementia,” the investigators wrote.
SOURCE:
The study was published online on December 4 in Neurology.
LIMITATIONS:
The study’s limitations included reliance on administrative coding without imaging data, potential underestimation of mild dementia, and lack of granular information on stroke severity, disability, and prestroke cognitive decline. While adjustments were made for healthcare contact and secondary prevention medications, residual biases may have persisted.
DISCLOSURES:
This study received funding from the Canada Brain Research Fund, Heart & Stroke Foundation of Canada, and Canadian Stroke Consortium. Two authors hold awards and positions from national organizations and academic institutions in Canada. Additional details are provided in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Risk for dementia is nearly 80% higher in stroke survivors than in those without stroke, a new study reveals. The data suggest risk declines within 1 year after stroke but remains elevated for up to 20 years.
METHODOLOGY:
- Researchers conducted a population-wide analysis of over 15 million people in Canada between 2002 and 2022. The study focused on adults hospitalized for ischemic stroke, intracerebral hemorrhage, or acute myocardial infarction (AMI).
- Of 175,980 stroke survivors, 99% were matched 1:1 to residents without stroke on the basis of age, sex, rural residence, neighborhood deprivation, and vascular comorbidities. In addition, 90% of patients were matched to those with AMI.
- Incident dementia diagnoses were tracked starting 90 days after stroke until death, emigration, or the end of the study, using a validated algorithm based on hospitalization for dementia, prescriptions for cholinesterase inhibitors, or physician claims within 2 years.
- The mean follow-up duration was 5.6 years.
TAKEAWAY:
- Among stroke survivors, 19% were diagnosed with dementia vs 12.5% in the reference population. The dementia rate per 100 person-years was higher among stroke survivors than in the reference population over the entire follow-up period (3.34 vs 1.89).
- Over the entire study period, dementia was 76% more likely among stroke patients (hazard ratio [HR], 1.76; 95% CI, 1.73-1.79) and 82% more likely in the AMI cohort (HR, 1.82; 95% CI, 1.79-1.85) than in the reference population.
- Time-varying analysis revealed that dementia risk was highest within the first year after stroke, with a > 2.5-fold increase at 6 months (HR, 2.51; 95% CI, 2.42-2.59), which decreased to a 1.5-fold increase at 5 years (HR, 1.51; 95% CI, 1.48-1.56) but remained elevated compared with the reference population even 20 years after the index stroke.
- Recurrent stroke was associated with an approximately threefold increased risk for dementia (single recurrent stroke adjusted HR, 2.64; 95% CI, 2.54-2.74; multiple recurrent strokes adjusted HR, 3.05; 95% CI, 2.81-3.33).
IN PRACTICE:
“While much research has been focused on reducing the risk of a second stroke, our findings make it clear that more research also is needed on developing interventions to help prevent dementia after stroke,” lead author Raed A. Joundi, MD, DPhil, McMaster University, Hamilton, Ontario, Canada, said in a press release.
“There is a need to accelerate the implementation of promising interventions or multipronged approaches into large randomized controlled trials to lower the risk of dementia,” the investigators wrote.
SOURCE:
The study was published online on December 4 in Neurology.
LIMITATIONS:
The study’s limitations included reliance on administrative coding without imaging data, potential underestimation of mild dementia, and lack of granular information on stroke severity, disability, and prestroke cognitive decline. While adjustments were made for healthcare contact and secondary prevention medications, residual biases may have persisted.
DISCLOSURES:
This study received funding from the Canada Brain Research Fund, Heart & Stroke Foundation of Canada, and Canadian Stroke Consortium. Two authors hold awards and positions from national organizations and academic institutions in Canada. Additional details are provided in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Can GLP-1s Reduce Alzheimer’s Disease Risk?
Tina is a lovely 67-year-old woman who was recently found to be an APOE gene carrier (a gene associated with increased risk of developing Alzheimer’s disease as well as an earlier age of disease onset), with diffused amyloid protein deposition her brain.
Her neuropsychiatric testing was consistent with mild cognitive impairment. Although Tina is not a doctor herself, her entire family consists of doctors, and she came to me under their advisement to consider semaglutide (Ozempic) for early Alzheimer’s disease prevention.
This would usually be simple, but in Tina’s case, there was a complicating factor: At 5’ and 90 pounds, she was already considerably underweight and was at risk of becoming severely undernourished.
To understand the potential role for glucagon-like peptide-1 (GLP-1) receptor agonists such as Ozempic in prevention, a quick primer on Alzheimer’s Disease is necessary.
The exact cause of Alzheimer’s disease remains elusive, but it is probably due to a combination of factors, including:
- Buildup of abnormal amyloid and tau proteins around brain cells
- Brain shrinkage, with subsequent damage to blood vessels and mitochondria, and inflammation
- Genetic predisposition
- Lifestyle factors, including obesity, high blood pressure, high cholesterol, and diabetes.
Once in the brain, they can reduce inflammation and improve functioning of the neurons. In early rodent trials, GLP-1 receptor agonists led to reduced amyloid and tau aggregation, downregulation of inflammation, and improved memory.
In 2021, multiple studies showed that liraglutide, an early GLP-1 receptor agonist, improved cognitive function and MRI volume in patients with Alzheimer’s disease.
A study recently published in Alzheimer’s & Dementia analyzed data from 1 million people with type 2 diabetes and no prior Alzheimer’s disease diagnosis. The authors compared Alzheimer’s disease occurrence in patients taking various diabetes medications, including insulin, metformin, and GLP-1 receptor agonists. The study found that participants taking semaglutide had up to a 70% reduction in Alzheimer’s risk. The results were consistent across gender, age, and weight.
Given the reassuring safety profile of GLP-1 receptor agonists and lack of other effective treatment or prophylaxis for Alzheimer’s disease, I agreed to start her on dulaglutide (Trulicity). My rationale was twofold:
1. In studies, dulaglutide has the highest uptake in the brain tissue at 68%. By contrast, there is virtually zero uptake in brain tissue for semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound). Because this class of drugs exert their effects in the brain tissue, I wanted to give her a GLP-1 receptor agonist with a high percent uptake.
2. Trulicity has a minimal effect on weight loss compared with the newer-generation GLP-1 receptor agonists. Even so, I connected Tina to my dietitian to ensure that she would receive a high-protein, high-calorie diet.
Tina has now been taking Trulicity for 6 months. Although it is certainly too early to draw firm conclusions about the efficacy of her treatment, she is not experiencing any weight loss and is cognitively stable, according to her neurologist.
The EVOKE and EVOKE+ phase 3 trials are currently underway to evaluate the efficacy of semaglutide to treat mild cognitive impairment and early Alzheimer’s in amyloid-positive patients. Results are expected in 2025, but in the meantime, I feel comforted knowing that Tina is receiving a potentially beneficial and definitively low-risk treatment.
Dr Messer, Clinical Assistant Professor, Mount Sinai School of Medicine; Associate Professor, Hofstra School of Medicine, New York, NY, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Tina is a lovely 67-year-old woman who was recently found to be an APOE gene carrier (a gene associated with increased risk of developing Alzheimer’s disease as well as an earlier age of disease onset), with diffused amyloid protein deposition her brain.
Her neuropsychiatric testing was consistent with mild cognitive impairment. Although Tina is not a doctor herself, her entire family consists of doctors, and she came to me under their advisement to consider semaglutide (Ozempic) for early Alzheimer’s disease prevention.
This would usually be simple, but in Tina’s case, there was a complicating factor: At 5’ and 90 pounds, she was already considerably underweight and was at risk of becoming severely undernourished.
To understand the potential role for glucagon-like peptide-1 (GLP-1) receptor agonists such as Ozempic in prevention, a quick primer on Alzheimer’s Disease is necessary.
The exact cause of Alzheimer’s disease remains elusive, but it is probably due to a combination of factors, including:
- Buildup of abnormal amyloid and tau proteins around brain cells
- Brain shrinkage, with subsequent damage to blood vessels and mitochondria, and inflammation
- Genetic predisposition
- Lifestyle factors, including obesity, high blood pressure, high cholesterol, and diabetes.
Once in the brain, they can reduce inflammation and improve functioning of the neurons. In early rodent trials, GLP-1 receptor agonists led to reduced amyloid and tau aggregation, downregulation of inflammation, and improved memory.
In 2021, multiple studies showed that liraglutide, an early GLP-1 receptor agonist, improved cognitive function and MRI volume in patients with Alzheimer’s disease.
A study recently published in Alzheimer’s & Dementia analyzed data from 1 million people with type 2 diabetes and no prior Alzheimer’s disease diagnosis. The authors compared Alzheimer’s disease occurrence in patients taking various diabetes medications, including insulin, metformin, and GLP-1 receptor agonists. The study found that participants taking semaglutide had up to a 70% reduction in Alzheimer’s risk. The results were consistent across gender, age, and weight.
Given the reassuring safety profile of GLP-1 receptor agonists and lack of other effective treatment or prophylaxis for Alzheimer’s disease, I agreed to start her on dulaglutide (Trulicity). My rationale was twofold:
1. In studies, dulaglutide has the highest uptake in the brain tissue at 68%. By contrast, there is virtually zero uptake in brain tissue for semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound). Because this class of drugs exert their effects in the brain tissue, I wanted to give her a GLP-1 receptor agonist with a high percent uptake.
2. Trulicity has a minimal effect on weight loss compared with the newer-generation GLP-1 receptor agonists. Even so, I connected Tina to my dietitian to ensure that she would receive a high-protein, high-calorie diet.
Tina has now been taking Trulicity for 6 months. Although it is certainly too early to draw firm conclusions about the efficacy of her treatment, she is not experiencing any weight loss and is cognitively stable, according to her neurologist.
The EVOKE and EVOKE+ phase 3 trials are currently underway to evaluate the efficacy of semaglutide to treat mild cognitive impairment and early Alzheimer’s in amyloid-positive patients. Results are expected in 2025, but in the meantime, I feel comforted knowing that Tina is receiving a potentially beneficial and definitively low-risk treatment.
Dr Messer, Clinical Assistant Professor, Mount Sinai School of Medicine; Associate Professor, Hofstra School of Medicine, New York, NY, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Tina is a lovely 67-year-old woman who was recently found to be an APOE gene carrier (a gene associated with increased risk of developing Alzheimer’s disease as well as an earlier age of disease onset), with diffused amyloid protein deposition her brain.
Her neuropsychiatric testing was consistent with mild cognitive impairment. Although Tina is not a doctor herself, her entire family consists of doctors, and she came to me under their advisement to consider semaglutide (Ozempic) for early Alzheimer’s disease prevention.
This would usually be simple, but in Tina’s case, there was a complicating factor: At 5’ and 90 pounds, she was already considerably underweight and was at risk of becoming severely undernourished.
To understand the potential role for glucagon-like peptide-1 (GLP-1) receptor agonists such as Ozempic in prevention, a quick primer on Alzheimer’s Disease is necessary.
The exact cause of Alzheimer’s disease remains elusive, but it is probably due to a combination of factors, including:
- Buildup of abnormal amyloid and tau proteins around brain cells
- Brain shrinkage, with subsequent damage to blood vessels and mitochondria, and inflammation
- Genetic predisposition
- Lifestyle factors, including obesity, high blood pressure, high cholesterol, and diabetes.
Once in the brain, they can reduce inflammation and improve functioning of the neurons. In early rodent trials, GLP-1 receptor agonists led to reduced amyloid and tau aggregation, downregulation of inflammation, and improved memory.
In 2021, multiple studies showed that liraglutide, an early GLP-1 receptor agonist, improved cognitive function and MRI volume in patients with Alzheimer’s disease.
A study recently published in Alzheimer’s & Dementia analyzed data from 1 million people with type 2 diabetes and no prior Alzheimer’s disease diagnosis. The authors compared Alzheimer’s disease occurrence in patients taking various diabetes medications, including insulin, metformin, and GLP-1 receptor agonists. The study found that participants taking semaglutide had up to a 70% reduction in Alzheimer’s risk. The results were consistent across gender, age, and weight.
Given the reassuring safety profile of GLP-1 receptor agonists and lack of other effective treatment or prophylaxis for Alzheimer’s disease, I agreed to start her on dulaglutide (Trulicity). My rationale was twofold:
1. In studies, dulaglutide has the highest uptake in the brain tissue at 68%. By contrast, there is virtually zero uptake in brain tissue for semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound). Because this class of drugs exert their effects in the brain tissue, I wanted to give her a GLP-1 receptor agonist with a high percent uptake.
2. Trulicity has a minimal effect on weight loss compared with the newer-generation GLP-1 receptor agonists. Even so, I connected Tina to my dietitian to ensure that she would receive a high-protein, high-calorie diet.
Tina has now been taking Trulicity for 6 months. Although it is certainly too early to draw firm conclusions about the efficacy of her treatment, she is not experiencing any weight loss and is cognitively stable, according to her neurologist.
The EVOKE and EVOKE+ phase 3 trials are currently underway to evaluate the efficacy of semaglutide to treat mild cognitive impairment and early Alzheimer’s in amyloid-positive patients. Results are expected in 2025, but in the meantime, I feel comforted knowing that Tina is receiving a potentially beneficial and definitively low-risk treatment.
Dr Messer, Clinical Assistant Professor, Mount Sinai School of Medicine; Associate Professor, Hofstra School of Medicine, New York, NY, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Traumatic Brain Injury May Reactivate Herpes Virus Leading to Neurodegeneration
a new study suggested.
Using a three-dimensional (3D) human brain tissue model, researchers observed that quiescent HSV-1 can be reactivated by a mechanical jolt mimicking concussion, leading to signature markers of Alzheimer’s disease, including neuroinflammation and production of amyloid beta and phosphorylated tau (p-tau) and gliosis — a phenotype made worse by repeated head injury.
“This opens the question as to whether antiviral drugs or anti-inflammatory agents might be useful as early preventive treatments after head trauma to stop HSV-1 activation in its tracks and lower the risk of Alzheimer’s disease,” lead investigator Dana Cairns, PhD, with the Department of Biomedical Engineering at Tufts University, Medford, Massachusetts, said in a statement.
But outside experts urged caution in drawing any firm conclusions, pending further study.
The study was published online in the journal Science Signaling.
HSV-1: A Major Alzheimer’s Disease Risk Factor?
TBI is a major risk factor for Alzheimer’s disease and dementia, but the pathways in the brain leading from TBI to dementia are unknown.
HSV-1 is found in over 80% of people; varicella zoster virus (VZV) is found in about 95%. Both viruses are known to enter the brain and lay dormant in neurons and glial cells. Prior evidence indicates that HSV-1 in the brain of APOE-ε4 carriers confers a strong risk for Alzheimer’s disease.
A number of years ago, the team created a 3D model of human brain tissue to study the link between TBI, the viruses, and dementia. The model is 6 mm wide, shaped like a donut, and made of a spongy material of silk protein and collagen saturated with neural stem cells. The cells mature into neurons, communicate with each other, and form a network that mimics the brain environment.
In an earlier study using the model quiescently infected with HSV-1, Cairns and colleagues found that subsequent exposure to VZV created the inflammatory conditions that led to reactivation of HSV-1.
This led them to wonder what would happen if they subjected the brain tissue model to a physical disruption akin to a concussion. Would HSV-1 wake up and start the process of neurodegeneration?
To investigate, they examined the effects of one or more controlled blows to the 3D human brain tissue model in the absence or presence of quiescent HSV-1 infection.
After repeated, mild controlled blows, researchers found that the latently infected 3D brain tissue displayed reactivated HSV-1 and the production and accumulation of amyloid beta and p-tau — which promotes neurodegeneration. The blows also activated gliosis, which is associated with destructive neuroinflammation.
These effects are collectively associated with Alzheimer’s disease, dementia, and chronic traumatic encephalopathy, they pointed out, and were increased with additional injury but were absent in tissue not infected with HSV-1.
“These data suggest that HSV-1 in the brain is pivotal in increasing the risk of Alzheimer’s disease, as other recent studies using cerebral organoids have suggested,” the researchers wrote.
They propose that following brain injury, “whether by infection or mechanical damage, the resulting inflammation induces HSV-1 reactivation in the brain leading to the development of Alzheimer’s disease/dementia and that HSV-1 is a major cause of the disease, especially in APOE4 carriers.”
Future studies should investigate “possible ways of mitigating or stopping the damage caused by head injury, thereby reducing subsequent development of Alzheimer’s disease by implementing efforts to prevent the reactivation of virus in brain such as anti-inflammatory and/or antiviral treatment post-injury,” researchers suggested.
Outside Experts Weigh in
Several outside experts offered perspective on the study in a statement from the UK nonprofit Science Media Centre.
Tara Spires-Jones, PhD, president of the British Neuroscience Association and group leader at the UK Dementia Research Institute, London, England, said that, while the study is interesting, there are limitations.
“The increase in Alzheimer’s-like brain changes in these latent virus-containing cells subjected to injury does not resemble the pathology that is found in the brain of people with Alzheimer’s disease,” Spires-Jones noted.
“These experiments were also in cells grown in artificial conditions without important Alzheimer’s-related factors such as age and blood vessel changes. Finally, these experiments were repeated in a small number of experimental replicates (three times per experiment), so these results will need to be confirmed in more relevant biological systems with larger studies to be sure there is a biological link between latent herpes simplex virus type 1, brain injury, and Alzheimer’s pathology,” Spires-Jones cautioned.
Robert Howard, MD, MRCPsych, University College London (UCL) Division of Psychiatry, said the study suggests a possible mechanism for the association between HSV-1, brain injury, and Alzheimer’s disease.
“However, as so often in science, it is very important to bear in mind that association does not mean causation. Much more research will be needed before this can be seriously considered a plausible mechanism for the development of dementia,” Howard cautioned.
“Avoidance of brain injuries, such as those encountered in some contact sports, is already known to be an important way to prevent dementia, and I’m unconvinced that this reflects anything more complicated than mechanical damage causing death of brain cells,” he added.
Jennifer Pocock, PhD, with UCL Queen Square Institute of Neurology, noted the role of microglia, which are activated by mild and repetitive TBI, isn’t addressed in the study.
“This paper seems to suggest that only astrocytes contribute to the reported neuroinflammation in brain tissue. Also, the inclusion of APOE3/4 is not clearly defined. Because of this, the findings are likely to represent an over interpretation for the ‘real world’ as the inclusion of microglia may negate or accentuate them, depending on the severity of the TBI,” Pocock said.
The study was funded by the US Army Research Office and Department of Defense. The authors have declared no relevant conflicts of interest. Spires-Jones and Howard had no relevant disclosures related to this study. Pocock has received research funding from AstraZeneca and Daiichi Sankyo.
A version of this article appeared on Medscape.com.
a new study suggested.
Using a three-dimensional (3D) human brain tissue model, researchers observed that quiescent HSV-1 can be reactivated by a mechanical jolt mimicking concussion, leading to signature markers of Alzheimer’s disease, including neuroinflammation and production of amyloid beta and phosphorylated tau (p-tau) and gliosis — a phenotype made worse by repeated head injury.
“This opens the question as to whether antiviral drugs or anti-inflammatory agents might be useful as early preventive treatments after head trauma to stop HSV-1 activation in its tracks and lower the risk of Alzheimer’s disease,” lead investigator Dana Cairns, PhD, with the Department of Biomedical Engineering at Tufts University, Medford, Massachusetts, said in a statement.
But outside experts urged caution in drawing any firm conclusions, pending further study.
The study was published online in the journal Science Signaling.
HSV-1: A Major Alzheimer’s Disease Risk Factor?
TBI is a major risk factor for Alzheimer’s disease and dementia, but the pathways in the brain leading from TBI to dementia are unknown.
HSV-1 is found in over 80% of people; varicella zoster virus (VZV) is found in about 95%. Both viruses are known to enter the brain and lay dormant in neurons and glial cells. Prior evidence indicates that HSV-1 in the brain of APOE-ε4 carriers confers a strong risk for Alzheimer’s disease.
A number of years ago, the team created a 3D model of human brain tissue to study the link between TBI, the viruses, and dementia. The model is 6 mm wide, shaped like a donut, and made of a spongy material of silk protein and collagen saturated with neural stem cells. The cells mature into neurons, communicate with each other, and form a network that mimics the brain environment.
In an earlier study using the model quiescently infected with HSV-1, Cairns and colleagues found that subsequent exposure to VZV created the inflammatory conditions that led to reactivation of HSV-1.
This led them to wonder what would happen if they subjected the brain tissue model to a physical disruption akin to a concussion. Would HSV-1 wake up and start the process of neurodegeneration?
To investigate, they examined the effects of one or more controlled blows to the 3D human brain tissue model in the absence or presence of quiescent HSV-1 infection.
After repeated, mild controlled blows, researchers found that the latently infected 3D brain tissue displayed reactivated HSV-1 and the production and accumulation of amyloid beta and p-tau — which promotes neurodegeneration. The blows also activated gliosis, which is associated with destructive neuroinflammation.
These effects are collectively associated with Alzheimer’s disease, dementia, and chronic traumatic encephalopathy, they pointed out, and were increased with additional injury but were absent in tissue not infected with HSV-1.
“These data suggest that HSV-1 in the brain is pivotal in increasing the risk of Alzheimer’s disease, as other recent studies using cerebral organoids have suggested,” the researchers wrote.
They propose that following brain injury, “whether by infection or mechanical damage, the resulting inflammation induces HSV-1 reactivation in the brain leading to the development of Alzheimer’s disease/dementia and that HSV-1 is a major cause of the disease, especially in APOE4 carriers.”
Future studies should investigate “possible ways of mitigating or stopping the damage caused by head injury, thereby reducing subsequent development of Alzheimer’s disease by implementing efforts to prevent the reactivation of virus in brain such as anti-inflammatory and/or antiviral treatment post-injury,” researchers suggested.
Outside Experts Weigh in
Several outside experts offered perspective on the study in a statement from the UK nonprofit Science Media Centre.
Tara Spires-Jones, PhD, president of the British Neuroscience Association and group leader at the UK Dementia Research Institute, London, England, said that, while the study is interesting, there are limitations.
“The increase in Alzheimer’s-like brain changes in these latent virus-containing cells subjected to injury does not resemble the pathology that is found in the brain of people with Alzheimer’s disease,” Spires-Jones noted.
“These experiments were also in cells grown in artificial conditions without important Alzheimer’s-related factors such as age and blood vessel changes. Finally, these experiments were repeated in a small number of experimental replicates (three times per experiment), so these results will need to be confirmed in more relevant biological systems with larger studies to be sure there is a biological link between latent herpes simplex virus type 1, brain injury, and Alzheimer’s pathology,” Spires-Jones cautioned.
Robert Howard, MD, MRCPsych, University College London (UCL) Division of Psychiatry, said the study suggests a possible mechanism for the association between HSV-1, brain injury, and Alzheimer’s disease.
“However, as so often in science, it is very important to bear in mind that association does not mean causation. Much more research will be needed before this can be seriously considered a plausible mechanism for the development of dementia,” Howard cautioned.
“Avoidance of brain injuries, such as those encountered in some contact sports, is already known to be an important way to prevent dementia, and I’m unconvinced that this reflects anything more complicated than mechanical damage causing death of brain cells,” he added.
Jennifer Pocock, PhD, with UCL Queen Square Institute of Neurology, noted the role of microglia, which are activated by mild and repetitive TBI, isn’t addressed in the study.
“This paper seems to suggest that only astrocytes contribute to the reported neuroinflammation in brain tissue. Also, the inclusion of APOE3/4 is not clearly defined. Because of this, the findings are likely to represent an over interpretation for the ‘real world’ as the inclusion of microglia may negate or accentuate them, depending on the severity of the TBI,” Pocock said.
The study was funded by the US Army Research Office and Department of Defense. The authors have declared no relevant conflicts of interest. Spires-Jones and Howard had no relevant disclosures related to this study. Pocock has received research funding from AstraZeneca and Daiichi Sankyo.
A version of this article appeared on Medscape.com.
a new study suggested.
Using a three-dimensional (3D) human brain tissue model, researchers observed that quiescent HSV-1 can be reactivated by a mechanical jolt mimicking concussion, leading to signature markers of Alzheimer’s disease, including neuroinflammation and production of amyloid beta and phosphorylated tau (p-tau) and gliosis — a phenotype made worse by repeated head injury.
“This opens the question as to whether antiviral drugs or anti-inflammatory agents might be useful as early preventive treatments after head trauma to stop HSV-1 activation in its tracks and lower the risk of Alzheimer’s disease,” lead investigator Dana Cairns, PhD, with the Department of Biomedical Engineering at Tufts University, Medford, Massachusetts, said in a statement.
But outside experts urged caution in drawing any firm conclusions, pending further study.
The study was published online in the journal Science Signaling.
HSV-1: A Major Alzheimer’s Disease Risk Factor?
TBI is a major risk factor for Alzheimer’s disease and dementia, but the pathways in the brain leading from TBI to dementia are unknown.
HSV-1 is found in over 80% of people; varicella zoster virus (VZV) is found in about 95%. Both viruses are known to enter the brain and lay dormant in neurons and glial cells. Prior evidence indicates that HSV-1 in the brain of APOE-ε4 carriers confers a strong risk for Alzheimer’s disease.
A number of years ago, the team created a 3D model of human brain tissue to study the link between TBI, the viruses, and dementia. The model is 6 mm wide, shaped like a donut, and made of a spongy material of silk protein and collagen saturated with neural stem cells. The cells mature into neurons, communicate with each other, and form a network that mimics the brain environment.
In an earlier study using the model quiescently infected with HSV-1, Cairns and colleagues found that subsequent exposure to VZV created the inflammatory conditions that led to reactivation of HSV-1.
This led them to wonder what would happen if they subjected the brain tissue model to a physical disruption akin to a concussion. Would HSV-1 wake up and start the process of neurodegeneration?
To investigate, they examined the effects of one or more controlled blows to the 3D human brain tissue model in the absence or presence of quiescent HSV-1 infection.
After repeated, mild controlled blows, researchers found that the latently infected 3D brain tissue displayed reactivated HSV-1 and the production and accumulation of amyloid beta and p-tau — which promotes neurodegeneration. The blows also activated gliosis, which is associated with destructive neuroinflammation.
These effects are collectively associated with Alzheimer’s disease, dementia, and chronic traumatic encephalopathy, they pointed out, and were increased with additional injury but were absent in tissue not infected with HSV-1.
“These data suggest that HSV-1 in the brain is pivotal in increasing the risk of Alzheimer’s disease, as other recent studies using cerebral organoids have suggested,” the researchers wrote.
They propose that following brain injury, “whether by infection or mechanical damage, the resulting inflammation induces HSV-1 reactivation in the brain leading to the development of Alzheimer’s disease/dementia and that HSV-1 is a major cause of the disease, especially in APOE4 carriers.”
Future studies should investigate “possible ways of mitigating or stopping the damage caused by head injury, thereby reducing subsequent development of Alzheimer’s disease by implementing efforts to prevent the reactivation of virus in brain such as anti-inflammatory and/or antiviral treatment post-injury,” researchers suggested.
Outside Experts Weigh in
Several outside experts offered perspective on the study in a statement from the UK nonprofit Science Media Centre.
Tara Spires-Jones, PhD, president of the British Neuroscience Association and group leader at the UK Dementia Research Institute, London, England, said that, while the study is interesting, there are limitations.
“The increase in Alzheimer’s-like brain changes in these latent virus-containing cells subjected to injury does not resemble the pathology that is found in the brain of people with Alzheimer’s disease,” Spires-Jones noted.
“These experiments were also in cells grown in artificial conditions without important Alzheimer’s-related factors such as age and blood vessel changes. Finally, these experiments were repeated in a small number of experimental replicates (three times per experiment), so these results will need to be confirmed in more relevant biological systems with larger studies to be sure there is a biological link between latent herpes simplex virus type 1, brain injury, and Alzheimer’s pathology,” Spires-Jones cautioned.
Robert Howard, MD, MRCPsych, University College London (UCL) Division of Psychiatry, said the study suggests a possible mechanism for the association between HSV-1, brain injury, and Alzheimer’s disease.
“However, as so often in science, it is very important to bear in mind that association does not mean causation. Much more research will be needed before this can be seriously considered a plausible mechanism for the development of dementia,” Howard cautioned.
“Avoidance of brain injuries, such as those encountered in some contact sports, is already known to be an important way to prevent dementia, and I’m unconvinced that this reflects anything more complicated than mechanical damage causing death of brain cells,” he added.
Jennifer Pocock, PhD, with UCL Queen Square Institute of Neurology, noted the role of microglia, which are activated by mild and repetitive TBI, isn’t addressed in the study.
“This paper seems to suggest that only astrocytes contribute to the reported neuroinflammation in brain tissue. Also, the inclusion of APOE3/4 is not clearly defined. Because of this, the findings are likely to represent an over interpretation for the ‘real world’ as the inclusion of microglia may negate or accentuate them, depending on the severity of the TBI,” Pocock said.
The study was funded by the US Army Research Office and Department of Defense. The authors have declared no relevant conflicts of interest. Spires-Jones and Howard had no relevant disclosures related to this study. Pocock has received research funding from AstraZeneca and Daiichi Sankyo.
A version of this article appeared on Medscape.com.
FROM SCIENCE SIGNALING
Improving Interprofessional Neurology Training Using Tele-Education
Improving Interprofessional Neurology Training Using Tele-Education
Neurologic disorders are major causes of death and disability. Globally, the burden of neurologic disorders continues to increase. The prevalence of disabling neurologic disorders significantly increases with age. As people live longer, health care systems will face increasing demands for treatment, rehabilitation, and support services for neurologic disorders. The scarcity of established modifiable risks for most of the neurologic burden demonstrates how new knowledge is required to develop effective prevention and treatment strategies.1
A single-center study for chronic headache at a rural institution found that, when combined with public education, clinician education not only can increase access to care but also reduce specialist overuse, hospitalizations, polypharmacy, and emergency department visits.2 A predicted shortage of neurologists has sparked increased interest in the field and individual neurology educators are helping fuel its popularity.3-5
TELE-EDUCATION
Educating the next generation of health professionals is 1 of 4 statutory missions of the US Department of Veterans Affairs (VA).6 Tele-education (also known as telelearning and distance learning) deviates from traditional in-person classroom settings, in which the lecture has been a core pedagogic method.7 Audio, video, and online technologies provide health education and can overcome geographic barriers for rural and remote clinicians.8 Recent technological improvements have allowed for inexpensive and efficient dissemination of educational materials, including video lectures, podcasts, online modules, assessment materials, and even entire curricula.9
There has been an increase in the awareness of the parallel curriculum involving self-directed and asynchronous learning opportunities. 10 Several studies report knowledge gained via tele-education is comparable to conventional classroom learning.11-13 A systematic review of e-learning perceptions among health care students suggested benefits (eg, learning flexibility, pedagogical design, online interactions, basic computer skills, and access to technology) and drawbacks (eg, limited acquisition of clinical skills, internet connection problems, and issues with using educational platforms).1
The COVID-19 pandemic forced an abrupt cessation of traditional in-person education, forcing educational institutions and medical organizations to transition to telelearning. Solutions in the education field appeared during the pandemic, such as videoconferencing, social media, and telemedicine, that effectively addressed the sudden cessation of in-person medical education.15
Graduate medical education in neurology residency programs served as an experimental set up for tele-education during the pandemic. Residents from neurology training programs outlined the benefits of a volunteer lecturer-based online didactic program that was established to meet this need, which included exposure to subspeciality topics, access to subspecialist experts not available within the department, exposure to different pedagogic methods, interaction with members of other educational institutions and training programs, career development opportunities, and the potential for forming a community of learning.16
Not all recent educational developments are technology-based. For example, instruction focused on specific patient experiences, and learning processes that emphasize problem solving and personal responsibility over specific knowledge have been successful in neurology.17,18 Departments and institutions must be creative in finding ways to fund continuing education, especially when budgets are limited.19
ANNUAL NEUROLOGY SEMINAR
An annual Veterans Health Administration (VHA) neurology seminar began in 2019 as a 1-day in-person event. Neurologists at the Michael E. DeBakey VA Medical Center in Houston presented in 50-minute sessions. Nonspecialist clinical personnel and neurology clinicians attended the event. Attendees requested making the presentations widely available and regularly repeating the seminar.
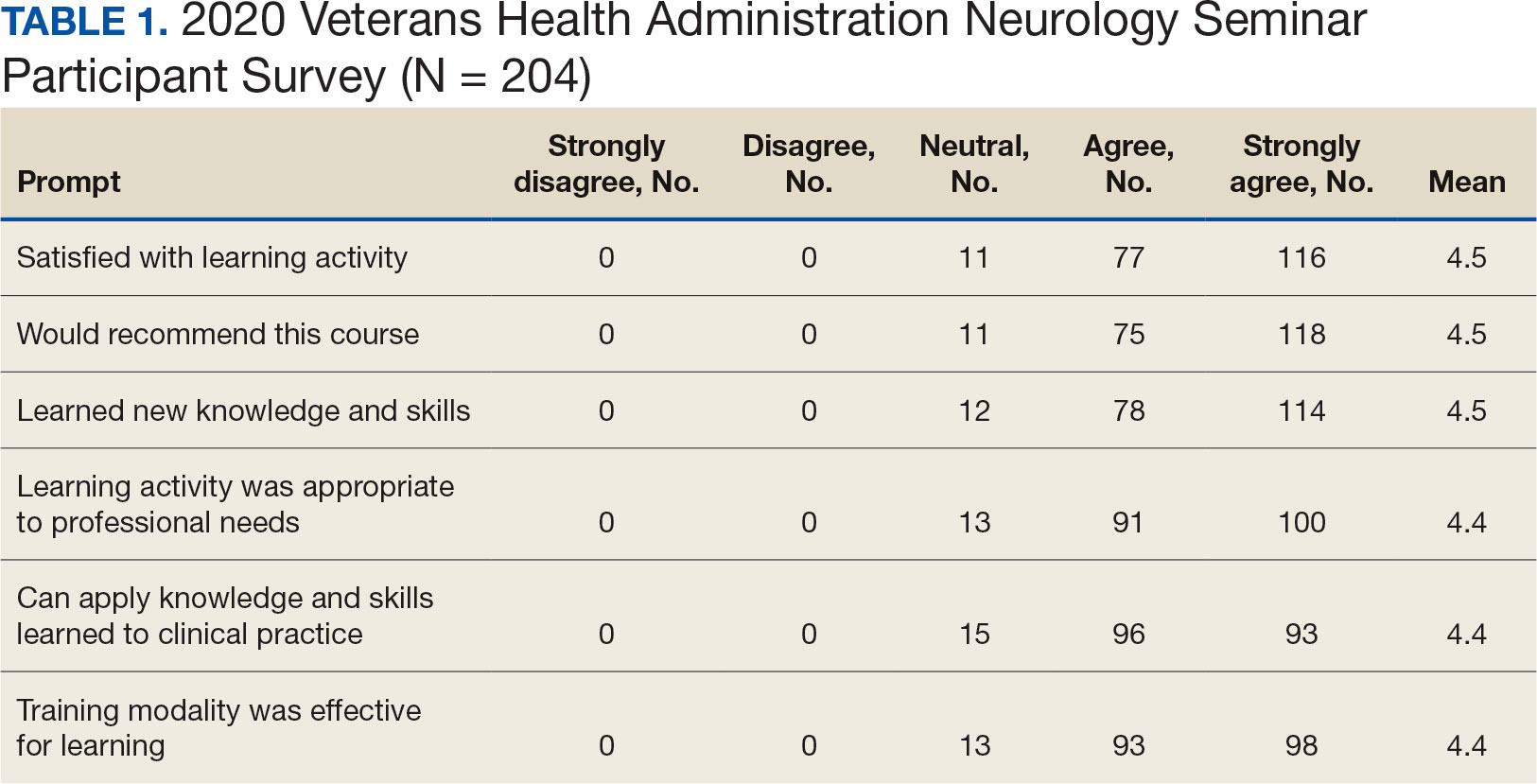
The second neurology seminar took place during the COVID-19 pandemic. It was conducted online and advertised across the Veterans Integrated Services Network (VISN) 16. The 1-day program had 204 participants who were primarily nurses (59%) and physicians (21%); 94% agreed with the program objectives (Table 1). Participants could earn CME credits for the 7 presentations primarily by VHA experts.
Based on feedback and a needs assessment, the program expanded in 2021 and 2022. With support from the national VHA neurology office and VHA Employee Education System (EES), the Institute for Learning, Education, and Development (ILEAD), the feedback identified topics that resonate with VHA clinicians. Neurological disorders in the fields of stroke, dementia, and headache were included since veterans with these disorders regularly visit primary care, geriatrics, mental health, and other clinical offices. Updates provided in the diagnosis and treatment of common neurological disorders were well received. Almost all speakers were VHA clinicians, which allowed them to focus on topics relevant to clinical practice at the VHA.
Attendance has increased annually. In 2021, 550 clinicians registered (52% nurses) and 433 completed the postseminar survey (Table 2). In 2022, 635 participants registered and 342 completed evaluations, including attendees from other federal agencies who were invited to participate via EES TRAIN (Training Finder Real-time Affiliate Integrated Network). Forty-seven participants from other federal agencies, including the US Department of Defense, National Institute of Health, and Centers for Disease Control and Prevention, completed the feedback evaluation via TRAIN (Table 3). Participants report high levels of satisfaction each year (mean of 4.5 on a 5-point scale). Respondents preferred conventional lecture presentation and case-based discussions for the teaching format and dementia was the most requested topic for future seminars (Table 4).
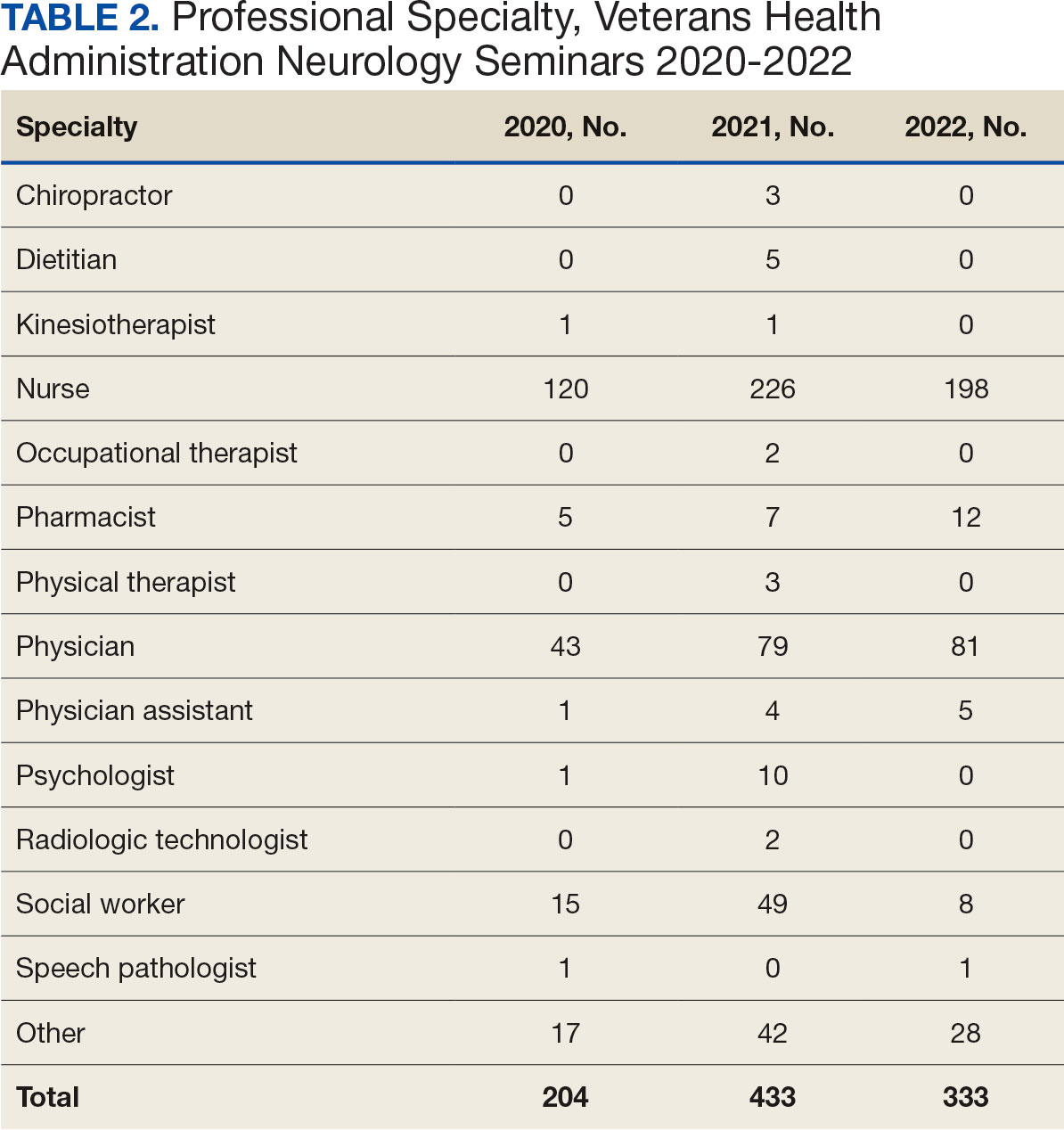

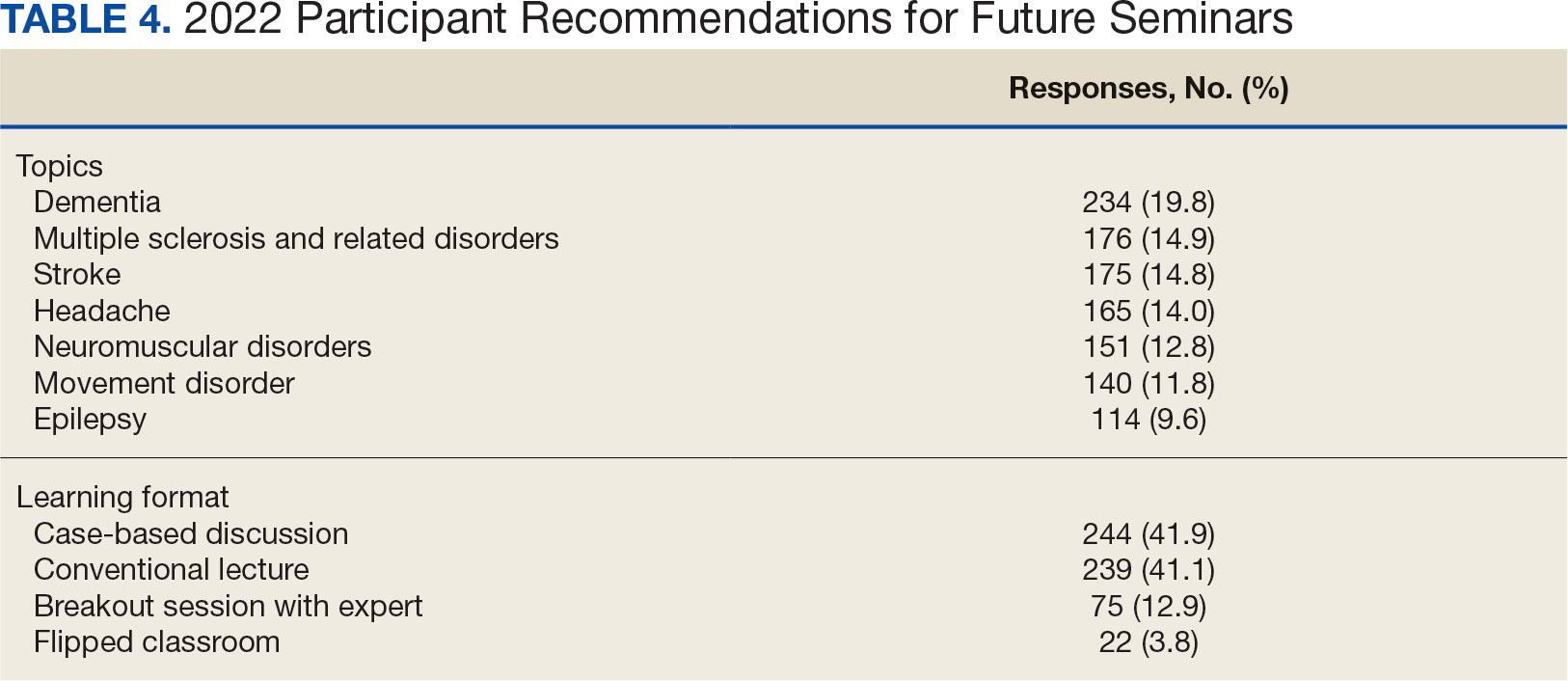
The content of each seminar was designed to include . 1 topic relevant to current clinical practice. The 2020 seminar covered topics of cerebrovascular complications of COVID- 19 and living well with neurodegenerative disease in the COVID-19 era. In 2021, the seminar included COVID-19 and neurologic manifestations. In 2022, topics included trends in stroke rehabilitation. In addition, ≥ 1 session addressed neurologic issues within the VHA. In 2020, the VA Deputy National Director of Neurology presented on the VHA stroke systems of care. In 2021, there was a presentation on traumatic brain injury (TBI) in the military. In 2022, sessions covered long term neurologic consequences of TBI and use of telemedicine for neurologic disorders. Feedback on the sessions were positive (eAppendix, available at doi:10.12788/fp.0545).
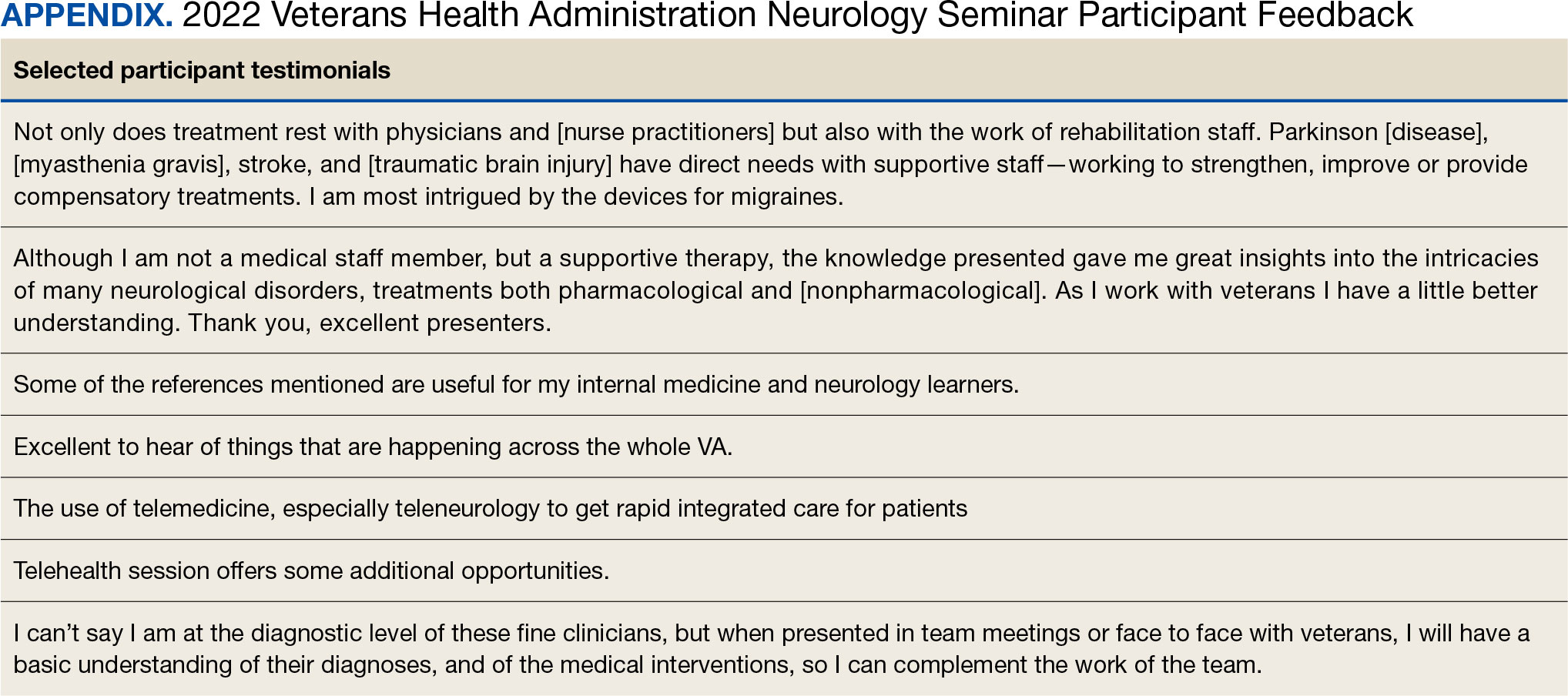
At the request of the participants, individual presentations were shared via email by the course director and speakers. In collaboration with the EES, each session was recorded and the 2022 seminar was made available to registrants in TMS and EES TRAIN and via the VHA Neurology SharePoint.
DISCUSSION
The annual VHA neurology seminar is a 1-day neurology conference that provides education to general neurologists and other clinicians caring for patients with neurologic disorders. It is the first of its kind neurology education program in the VHA covering most subspecialties in neurology and aims at improving neurologic patient care and access through education. Sessions have covered stroke, epilepsy, sleep, amyotrophic lateral sclerosis, neuropathy, dementia, movement disorders and Parkinson disease, headaches, multiple sclerosis, neurorehabilitation, and telehealth.
The seminar has transitioned from an inperson meeting to a virtual format, making neurology education more convenient and accessible. The virtual format provides the means to increase educational collaborations and share lecture platforms with other federal agencies. The program offers CME credits at no cost to government employees. Recorded lectures can also be asynchronously viewed from the Neurology SharePoint without the ability to earn CME credits. These recordings may be used to educate trainees as well.
The seminar aims to educate all health care professionals caring for patients with neurologic disorders. It aims to eliminate neurophobia, the fear of neural sciences and clinical neurology, and help general practitioners, especially in rural areas, take care of patients with neurologic disorders. The seminars introduce general practitioners to VHA neurology experts; the epilepsy, headache multiple sclerosis, and Parkinson disease centers of excellence; and the national programs for telestroke and teleneurology.
Education Support in the VHA
The EES/ILEAD provides a wide variety of learning opportunities to VHA employees on a broad range of topics, making it one of the largest medical education programs in the country. Pharmacists, social workers, psychologists, therapists, nurses, physician assistants, and physicians have access to certified training opportunities to gain knowledge and skills needed to provide high-quality, veteran-centered care.
A review of geriatrics learning activities through the EES found > 15,000 lectures from 1999 to 2009 for > 300,000 attendees.20 To our knowledge, a review of neurology-related learning activities offered by the EES/ILEAD has not been completed, but the study on geriatrics shows that a similar review would be feasible, given the integrated education system, and helpful in identifying what topics are covered, formats are used, and participants are engaged in neurology education at the VHA. This is a future project planned by the neurology education workgroup.
The EES/ILEAD arranged CME credit for the VHA Neurology Seminar and assisted in organizing an online event with > 500 attendees. Technology support and tools provided by EES during the virtual seminar, such as polling and chat features, kept the audience engaged. Other specialties may similarly value a virtual, all-day seminar format that is efficient and can encourage increased participation from practitioners, nurses, and clinicians.
Future Growth
We plan to increase future participation in the annual neurology seminar with primary care, geriatrics, neurology, and other specialties by instituting an improved and earlier marketing strategy. This includes working with the VHA neurology office to inform neurology practitioners as well as other program offices in the VHA. We intend to host the seminar the same day every year to make it easy for attendees to plan accordingly. In the future we may consider hybrid in-person and virtual modalities if feasible. We plan to focus on reaching out to other government agencies through platforms like TRAIN and the American Academy of Neurology government sections. Securing funding, administrative staff, and protected time in the future may help expand the program further.
Limitations
While a virtual format offers several advantages, using it removes the feel of an in-person meeting, which could be viewed by some attendees as a limitation. The other challenges and drawbacks of transitioning to the virtual platform for a national meeting are similar to those reported in the literature: time zone differences, internet issues, and participants having difficulty using certain online platforms. Attendance could also be limited by scheduling conflicts.16 Despite a large audience attending the seminar, many clinicians do not get protected time from their institutions. Institutional and leadership support at national and local levels will likely improve participation and help participants earn CME credits. While we are still doing a preliminary needs assessment, a formal needs assessment across federal governmental organizations will be helpful.
CONCLUSIONS
The annual VHA neurology seminar promotes interprofessional education, introduces neurology subspecialty centers of excellence, improves access to renowned neurology experts, and provides neurology-related updates through a VHA lens. The program not only provides educational updates to neurology clinicians, but also increases the confidence of non-neurology clinicians called to care for veterans with neurological disorders in their respective clinics.
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990- 2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459-480. doi:10.1016/S1474-4422(18)30499-X
- Baker V, Hack N. Improving access to care for patients with migraine in a remote Pacific population. Neurol Clin Pract. 2020;10(5):444-448. doi:10.1212/CPJ.0000000000000774
- Gutmann L, Cahill C, Jordan JT, et al. Characteristics of graduating US allopathic medical students pursuing a career in neurology. Neurology. 2019;92(17):e2051-e2063. doi:10.1212/WNL.0000000000007369
- Jordan JT, Cahill C, Ostendorf T, et al. Attracting neurology’s next generation: a qualitative study of specialty choice and perceptions. Neurology. 2020;95(8):e1080- e1090. doi:10.1212/WNL.0000000000009461
- Minen MT, Kaplan K, Akter S, et al. Understanding how to strengthen the neurology pipeline with insights from undergraduate neuroscience students. Neurology 2022;98(8):314-323. doi:10.1212/WNL.0000000000013259
- US Department of Veterans Affairs, Office of Academic Affiliations. To Educate for VA and the Nation. Updated August 1, 2024. Accessed August 15, 2024. https://www.va.gov/oaa/
- Schaefer SM, Dominguez M, Moeller JJ. The future of the lecture in neurology education. Semin Neurol. 2018;38(4):418-427. doi:10.1055/s-0038-1667042
- Curran VR. Tele-education. J Telemed Telecare. 2006;12(2):57-63. doi:10.1258/135763306776084400
- Lau KHV, Lakhan SE, Achike F. New media, technology and neurology education. Semin Neurol. 2018;38(4):457- 464. doi:10.1055/s-0038-1666985
- Quirk M, Chumley H. The adaptive medical curriculum: a model for continuous improvement. Med Teach. 2018;40(8):786-790. doi:10.1080/0142159X.2018.1484896
- Brockfeld T, Müller B, de Laffolie J. Video versus live lecture courses: a comparative evaluation of lecture types and results. Med Educ Online. 2018;23(1):1555434. doi:10.1080/10872981.2018.1555434
- Davis J, Crabb S, Rogers E, Zamora J, Khan K. Computer-based teaching is as good as face to face lecture-based teaching of evidence based medicine: a randomized controlled trial. Med Teach. 2008;30(3):302-307. doi:10.1080/01421590701784349
- Markova T, Roth LM, Monsur J. Synchronous distance learning as an effective and feasible method for delivering residency didactics. Fam Med. 2005;37(8):570-575.
- Naciri A, Radid M, Kharbach A, Chemsi G. E-learning in health professions education during the COVID-19 pandemic: a systematic review. J Educ Eval Health Prof. 2021;18:27. doi:10.3352/jeehp.2021.18.27
- Dedeilia A, Sotiropoulos MG, Hanrahan JG, Janga D, Dedeilias P, Sideris M. Medical and surgical education challenges and innovations in the COVID-19 era: a systematic review. In Vivo. 2020;34(3 Suppl):1603-1611. doi:10.21873/invivo.11950
- Weber DJ, Albert DVF, Aravamuthan BR, Bernson-Leung ME, Bhatti D, Milligan TA. Training in neurology: rapid implementation of cross-institutional neurology resident education in the time of COVID-19. Neurology. 2020;95(19):883-886. doi:10.1212/WNL.0000000000010753
- Frey J, Neeley B, Umer A, et al. Training in neurology: neuro day: an innovative curriculum connecting medical students with patients. Neurology. 2021;96(10):e1482- e1486. doi:10.1212/WNL.0000000000010859
- Schwartzstein RM, Dienstag JL, King RW, et al. The Harvard Medical School Pathways Curriculum: reimagining developmentally appropriate medical education for contemporary learners. Acad Med. 2020;95(11):1687-1695. doi:10.1097/ACM.0000000000003270
- Greer DM, Moeller J, Torres DR, et al. Funding the educational mission in neurology. Neurology. 2021;96(12):574- 582. doi:10.1212/WNL.0000000000011635
- Thielke S, Tumosa N, Lindenfeld R, Shay K. Geriatric focused educational offerings in the Department of Veterans Affairs from 1999 to 2009. Gerontol Geriatr Educ. 2011;32(1):38-53. doi:10.1080/02701960.2011.550214
Neurologic disorders are major causes of death and disability. Globally, the burden of neurologic disorders continues to increase. The prevalence of disabling neurologic disorders significantly increases with age. As people live longer, health care systems will face increasing demands for treatment, rehabilitation, and support services for neurologic disorders. The scarcity of established modifiable risks for most of the neurologic burden demonstrates how new knowledge is required to develop effective prevention and treatment strategies.1
A single-center study for chronic headache at a rural institution found that, when combined with public education, clinician education not only can increase access to care but also reduce specialist overuse, hospitalizations, polypharmacy, and emergency department visits.2 A predicted shortage of neurologists has sparked increased interest in the field and individual neurology educators are helping fuel its popularity.3-5
TELE-EDUCATION
Educating the next generation of health professionals is 1 of 4 statutory missions of the US Department of Veterans Affairs (VA).6 Tele-education (also known as telelearning and distance learning) deviates from traditional in-person classroom settings, in which the lecture has been a core pedagogic method.7 Audio, video, and online technologies provide health education and can overcome geographic barriers for rural and remote clinicians.8 Recent technological improvements have allowed for inexpensive and efficient dissemination of educational materials, including video lectures, podcasts, online modules, assessment materials, and even entire curricula.9
There has been an increase in the awareness of the parallel curriculum involving self-directed and asynchronous learning opportunities. 10 Several studies report knowledge gained via tele-education is comparable to conventional classroom learning.11-13 A systematic review of e-learning perceptions among health care students suggested benefits (eg, learning flexibility, pedagogical design, online interactions, basic computer skills, and access to technology) and drawbacks (eg, limited acquisition of clinical skills, internet connection problems, and issues with using educational platforms).1
The COVID-19 pandemic forced an abrupt cessation of traditional in-person education, forcing educational institutions and medical organizations to transition to telelearning. Solutions in the education field appeared during the pandemic, such as videoconferencing, social media, and telemedicine, that effectively addressed the sudden cessation of in-person medical education.15
Graduate medical education in neurology residency programs served as an experimental set up for tele-education during the pandemic. Residents from neurology training programs outlined the benefits of a volunteer lecturer-based online didactic program that was established to meet this need, which included exposure to subspeciality topics, access to subspecialist experts not available within the department, exposure to different pedagogic methods, interaction with members of other educational institutions and training programs, career development opportunities, and the potential for forming a community of learning.16
Not all recent educational developments are technology-based. For example, instruction focused on specific patient experiences, and learning processes that emphasize problem solving and personal responsibility over specific knowledge have been successful in neurology.17,18 Departments and institutions must be creative in finding ways to fund continuing education, especially when budgets are limited.19
ANNUAL NEUROLOGY SEMINAR
An annual Veterans Health Administration (VHA) neurology seminar began in 2019 as a 1-day in-person event. Neurologists at the Michael E. DeBakey VA Medical Center in Houston presented in 50-minute sessions. Nonspecialist clinical personnel and neurology clinicians attended the event. Attendees requested making the presentations widely available and regularly repeating the seminar.
The second neurology seminar took place during the COVID-19 pandemic. It was conducted online and advertised across the Veterans Integrated Services Network (VISN) 16. The 1-day program had 204 participants who were primarily nurses (59%) and physicians (21%); 94% agreed with the program objectives (Table 1). Participants could earn CME credits for the 7 presentations primarily by VHA experts.
Based on feedback and a needs assessment, the program expanded in 2021 and 2022. With support from the national VHA neurology office and VHA Employee Education System (EES), the Institute for Learning, Education, and Development (ILEAD), the feedback identified topics that resonate with VHA clinicians. Neurological disorders in the fields of stroke, dementia, and headache were included since veterans with these disorders regularly visit primary care, geriatrics, mental health, and other clinical offices. Updates provided in the diagnosis and treatment of common neurological disorders were well received. Almost all speakers were VHA clinicians, which allowed them to focus on topics relevant to clinical practice at the VHA.
Attendance has increased annually. In 2021, 550 clinicians registered (52% nurses) and 433 completed the postseminar survey (Table 2). In 2022, 635 participants registered and 342 completed evaluations, including attendees from other federal agencies who were invited to participate via EES TRAIN (Training Finder Real-time Affiliate Integrated Network). Forty-seven participants from other federal agencies, including the US Department of Defense, National Institute of Health, and Centers for Disease Control and Prevention, completed the feedback evaluation via TRAIN (Table 3). Participants report high levels of satisfaction each year (mean of 4.5 on a 5-point scale). Respondents preferred conventional lecture presentation and case-based discussions for the teaching format and dementia was the most requested topic for future seminars (Table 4).
The content of each seminar was designed to include . 1 topic relevant to current clinical practice. The 2020 seminar covered topics of cerebrovascular complications of COVID- 19 and living well with neurodegenerative disease in the COVID-19 era. In 2021, the seminar included COVID-19 and neurologic manifestations. In 2022, topics included trends in stroke rehabilitation. In addition, ≥ 1 session addressed neurologic issues within the VHA. In 2020, the VA Deputy National Director of Neurology presented on the VHA stroke systems of care. In 2021, there was a presentation on traumatic brain injury (TBI) in the military. In 2022, sessions covered long term neurologic consequences of TBI and use of telemedicine for neurologic disorders. Feedback on the sessions were positive (eAppendix, available at doi:10.12788/fp.0545).
At the request of the participants, individual presentations were shared via email by the course director and speakers. In collaboration with the EES, each session was recorded and the 2022 seminar was made available to registrants in TMS and EES TRAIN and via the VHA Neurology SharePoint.
DISCUSSION
The annual VHA neurology seminar is a 1-day neurology conference that provides education to general neurologists and other clinicians caring for patients with neurologic disorders. It is the first of its kind neurology education program in the VHA covering most subspecialties in neurology and aims at improving neurologic patient care and access through education. Sessions have covered stroke, epilepsy, sleep, amyotrophic lateral sclerosis, neuropathy, dementia, movement disorders and Parkinson disease, headaches, multiple sclerosis, neurorehabilitation, and telehealth.
The seminar has transitioned from an inperson meeting to a virtual format, making neurology education more convenient and accessible. The virtual format provides the means to increase educational collaborations and share lecture platforms with other federal agencies. The program offers CME credits at no cost to government employees. Recorded lectures can also be asynchronously viewed from the Neurology SharePoint without the ability to earn CME credits. These recordings may be used to educate trainees as well.
The seminar aims to educate all health care professionals caring for patients with neurologic disorders. It aims to eliminate neurophobia, the fear of neural sciences and clinical neurology, and help general practitioners, especially in rural areas, take care of patients with neurologic disorders. The seminars introduce general practitioners to VHA neurology experts; the epilepsy, headache multiple sclerosis, and Parkinson disease centers of excellence; and the national programs for telestroke and teleneurology.
Education Support in the VHA
The EES/ILEAD provides a wide variety of learning opportunities to VHA employees on a broad range of topics, making it one of the largest medical education programs in the country. Pharmacists, social workers, psychologists, therapists, nurses, physician assistants, and physicians have access to certified training opportunities to gain knowledge and skills needed to provide high-quality, veteran-centered care.
A review of geriatrics learning activities through the EES found > 15,000 lectures from 1999 to 2009 for > 300,000 attendees.20 To our knowledge, a review of neurology-related learning activities offered by the EES/ILEAD has not been completed, but the study on geriatrics shows that a similar review would be feasible, given the integrated education system, and helpful in identifying what topics are covered, formats are used, and participants are engaged in neurology education at the VHA. This is a future project planned by the neurology education workgroup.
The EES/ILEAD arranged CME credit for the VHA Neurology Seminar and assisted in organizing an online event with > 500 attendees. Technology support and tools provided by EES during the virtual seminar, such as polling and chat features, kept the audience engaged. Other specialties may similarly value a virtual, all-day seminar format that is efficient and can encourage increased participation from practitioners, nurses, and clinicians.
Future Growth
We plan to increase future participation in the annual neurology seminar with primary care, geriatrics, neurology, and other specialties by instituting an improved and earlier marketing strategy. This includes working with the VHA neurology office to inform neurology practitioners as well as other program offices in the VHA. We intend to host the seminar the same day every year to make it easy for attendees to plan accordingly. In the future we may consider hybrid in-person and virtual modalities if feasible. We plan to focus on reaching out to other government agencies through platforms like TRAIN and the American Academy of Neurology government sections. Securing funding, administrative staff, and protected time in the future may help expand the program further.
Limitations
While a virtual format offers several advantages, using it removes the feel of an in-person meeting, which could be viewed by some attendees as a limitation. The other challenges and drawbacks of transitioning to the virtual platform for a national meeting are similar to those reported in the literature: time zone differences, internet issues, and participants having difficulty using certain online platforms. Attendance could also be limited by scheduling conflicts.16 Despite a large audience attending the seminar, many clinicians do not get protected time from their institutions. Institutional and leadership support at national and local levels will likely improve participation and help participants earn CME credits. While we are still doing a preliminary needs assessment, a formal needs assessment across federal governmental organizations will be helpful.
CONCLUSIONS
The annual VHA neurology seminar promotes interprofessional education, introduces neurology subspecialty centers of excellence, improves access to renowned neurology experts, and provides neurology-related updates through a VHA lens. The program not only provides educational updates to neurology clinicians, but also increases the confidence of non-neurology clinicians called to care for veterans with neurological disorders in their respective clinics.
Neurologic disorders are major causes of death and disability. Globally, the burden of neurologic disorders continues to increase. The prevalence of disabling neurologic disorders significantly increases with age. As people live longer, health care systems will face increasing demands for treatment, rehabilitation, and support services for neurologic disorders. The scarcity of established modifiable risks for most of the neurologic burden demonstrates how new knowledge is required to develop effective prevention and treatment strategies.1
A single-center study for chronic headache at a rural institution found that, when combined with public education, clinician education not only can increase access to care but also reduce specialist overuse, hospitalizations, polypharmacy, and emergency department visits.2 A predicted shortage of neurologists has sparked increased interest in the field and individual neurology educators are helping fuel its popularity.3-5
TELE-EDUCATION
Educating the next generation of health professionals is 1 of 4 statutory missions of the US Department of Veterans Affairs (VA).6 Tele-education (also known as telelearning and distance learning) deviates from traditional in-person classroom settings, in which the lecture has been a core pedagogic method.7 Audio, video, and online technologies provide health education and can overcome geographic barriers for rural and remote clinicians.8 Recent technological improvements have allowed for inexpensive and efficient dissemination of educational materials, including video lectures, podcasts, online modules, assessment materials, and even entire curricula.9
There has been an increase in the awareness of the parallel curriculum involving self-directed and asynchronous learning opportunities. 10 Several studies report knowledge gained via tele-education is comparable to conventional classroom learning.11-13 A systematic review of e-learning perceptions among health care students suggested benefits (eg, learning flexibility, pedagogical design, online interactions, basic computer skills, and access to technology) and drawbacks (eg, limited acquisition of clinical skills, internet connection problems, and issues with using educational platforms).1
The COVID-19 pandemic forced an abrupt cessation of traditional in-person education, forcing educational institutions and medical organizations to transition to telelearning. Solutions in the education field appeared during the pandemic, such as videoconferencing, social media, and telemedicine, that effectively addressed the sudden cessation of in-person medical education.15
Graduate medical education in neurology residency programs served as an experimental set up for tele-education during the pandemic. Residents from neurology training programs outlined the benefits of a volunteer lecturer-based online didactic program that was established to meet this need, which included exposure to subspeciality topics, access to subspecialist experts not available within the department, exposure to different pedagogic methods, interaction with members of other educational institutions and training programs, career development opportunities, and the potential for forming a community of learning.16
Not all recent educational developments are technology-based. For example, instruction focused on specific patient experiences, and learning processes that emphasize problem solving and personal responsibility over specific knowledge have been successful in neurology.17,18 Departments and institutions must be creative in finding ways to fund continuing education, especially when budgets are limited.19
ANNUAL NEUROLOGY SEMINAR
An annual Veterans Health Administration (VHA) neurology seminar began in 2019 as a 1-day in-person event. Neurologists at the Michael E. DeBakey VA Medical Center in Houston presented in 50-minute sessions. Nonspecialist clinical personnel and neurology clinicians attended the event. Attendees requested making the presentations widely available and regularly repeating the seminar.
The second neurology seminar took place during the COVID-19 pandemic. It was conducted online and advertised across the Veterans Integrated Services Network (VISN) 16. The 1-day program had 204 participants who were primarily nurses (59%) and physicians (21%); 94% agreed with the program objectives (Table 1). Participants could earn CME credits for the 7 presentations primarily by VHA experts.
Based on feedback and a needs assessment, the program expanded in 2021 and 2022. With support from the national VHA neurology office and VHA Employee Education System (EES), the Institute for Learning, Education, and Development (ILEAD), the feedback identified topics that resonate with VHA clinicians. Neurological disorders in the fields of stroke, dementia, and headache were included since veterans with these disorders regularly visit primary care, geriatrics, mental health, and other clinical offices. Updates provided in the diagnosis and treatment of common neurological disorders were well received. Almost all speakers were VHA clinicians, which allowed them to focus on topics relevant to clinical practice at the VHA.
Attendance has increased annually. In 2021, 550 clinicians registered (52% nurses) and 433 completed the postseminar survey (Table 2). In 2022, 635 participants registered and 342 completed evaluations, including attendees from other federal agencies who were invited to participate via EES TRAIN (Training Finder Real-time Affiliate Integrated Network). Forty-seven participants from other federal agencies, including the US Department of Defense, National Institute of Health, and Centers for Disease Control and Prevention, completed the feedback evaluation via TRAIN (Table 3). Participants report high levels of satisfaction each year (mean of 4.5 on a 5-point scale). Respondents preferred conventional lecture presentation and case-based discussions for the teaching format and dementia was the most requested topic for future seminars (Table 4).
The content of each seminar was designed to include . 1 topic relevant to current clinical practice. The 2020 seminar covered topics of cerebrovascular complications of COVID- 19 and living well with neurodegenerative disease in the COVID-19 era. In 2021, the seminar included COVID-19 and neurologic manifestations. In 2022, topics included trends in stroke rehabilitation. In addition, ≥ 1 session addressed neurologic issues within the VHA. In 2020, the VA Deputy National Director of Neurology presented on the VHA stroke systems of care. In 2021, there was a presentation on traumatic brain injury (TBI) in the military. In 2022, sessions covered long term neurologic consequences of TBI and use of telemedicine for neurologic disorders. Feedback on the sessions were positive (eAppendix, available at doi:10.12788/fp.0545).
At the request of the participants, individual presentations were shared via email by the course director and speakers. In collaboration with the EES, each session was recorded and the 2022 seminar was made available to registrants in TMS and EES TRAIN and via the VHA Neurology SharePoint.
DISCUSSION
The annual VHA neurology seminar is a 1-day neurology conference that provides education to general neurologists and other clinicians caring for patients with neurologic disorders. It is the first of its kind neurology education program in the VHA covering most subspecialties in neurology and aims at improving neurologic patient care and access through education. Sessions have covered stroke, epilepsy, sleep, amyotrophic lateral sclerosis, neuropathy, dementia, movement disorders and Parkinson disease, headaches, multiple sclerosis, neurorehabilitation, and telehealth.
The seminar has transitioned from an inperson meeting to a virtual format, making neurology education more convenient and accessible. The virtual format provides the means to increase educational collaborations and share lecture platforms with other federal agencies. The program offers CME credits at no cost to government employees. Recorded lectures can also be asynchronously viewed from the Neurology SharePoint without the ability to earn CME credits. These recordings may be used to educate trainees as well.
The seminar aims to educate all health care professionals caring for patients with neurologic disorders. It aims to eliminate neurophobia, the fear of neural sciences and clinical neurology, and help general practitioners, especially in rural areas, take care of patients with neurologic disorders. The seminars introduce general practitioners to VHA neurology experts; the epilepsy, headache multiple sclerosis, and Parkinson disease centers of excellence; and the national programs for telestroke and teleneurology.
Education Support in the VHA
The EES/ILEAD provides a wide variety of learning opportunities to VHA employees on a broad range of topics, making it one of the largest medical education programs in the country. Pharmacists, social workers, psychologists, therapists, nurses, physician assistants, and physicians have access to certified training opportunities to gain knowledge and skills needed to provide high-quality, veteran-centered care.
A review of geriatrics learning activities through the EES found > 15,000 lectures from 1999 to 2009 for > 300,000 attendees.20 To our knowledge, a review of neurology-related learning activities offered by the EES/ILEAD has not been completed, but the study on geriatrics shows that a similar review would be feasible, given the integrated education system, and helpful in identifying what topics are covered, formats are used, and participants are engaged in neurology education at the VHA. This is a future project planned by the neurology education workgroup.
The EES/ILEAD arranged CME credit for the VHA Neurology Seminar and assisted in organizing an online event with > 500 attendees. Technology support and tools provided by EES during the virtual seminar, such as polling and chat features, kept the audience engaged. Other specialties may similarly value a virtual, all-day seminar format that is efficient and can encourage increased participation from practitioners, nurses, and clinicians.
Future Growth
We plan to increase future participation in the annual neurology seminar with primary care, geriatrics, neurology, and other specialties by instituting an improved and earlier marketing strategy. This includes working with the VHA neurology office to inform neurology practitioners as well as other program offices in the VHA. We intend to host the seminar the same day every year to make it easy for attendees to plan accordingly. In the future we may consider hybrid in-person and virtual modalities if feasible. We plan to focus on reaching out to other government agencies through platforms like TRAIN and the American Academy of Neurology government sections. Securing funding, administrative staff, and protected time in the future may help expand the program further.
Limitations
While a virtual format offers several advantages, using it removes the feel of an in-person meeting, which could be viewed by some attendees as a limitation. The other challenges and drawbacks of transitioning to the virtual platform for a national meeting are similar to those reported in the literature: time zone differences, internet issues, and participants having difficulty using certain online platforms. Attendance could also be limited by scheduling conflicts.16 Despite a large audience attending the seminar, many clinicians do not get protected time from their institutions. Institutional and leadership support at national and local levels will likely improve participation and help participants earn CME credits. While we are still doing a preliminary needs assessment, a formal needs assessment across federal governmental organizations will be helpful.
CONCLUSIONS
The annual VHA neurology seminar promotes interprofessional education, introduces neurology subspecialty centers of excellence, improves access to renowned neurology experts, and provides neurology-related updates through a VHA lens. The program not only provides educational updates to neurology clinicians, but also increases the confidence of non-neurology clinicians called to care for veterans with neurological disorders in their respective clinics.
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990- 2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459-480. doi:10.1016/S1474-4422(18)30499-X
- Baker V, Hack N. Improving access to care for patients with migraine in a remote Pacific population. Neurol Clin Pract. 2020;10(5):444-448. doi:10.1212/CPJ.0000000000000774
- Gutmann L, Cahill C, Jordan JT, et al. Characteristics of graduating US allopathic medical students pursuing a career in neurology. Neurology. 2019;92(17):e2051-e2063. doi:10.1212/WNL.0000000000007369
- Jordan JT, Cahill C, Ostendorf T, et al. Attracting neurology’s next generation: a qualitative study of specialty choice and perceptions. Neurology. 2020;95(8):e1080- e1090. doi:10.1212/WNL.0000000000009461
- Minen MT, Kaplan K, Akter S, et al. Understanding how to strengthen the neurology pipeline with insights from undergraduate neuroscience students. Neurology 2022;98(8):314-323. doi:10.1212/WNL.0000000000013259
- US Department of Veterans Affairs, Office of Academic Affiliations. To Educate for VA and the Nation. Updated August 1, 2024. Accessed August 15, 2024. https://www.va.gov/oaa/
- Schaefer SM, Dominguez M, Moeller JJ. The future of the lecture in neurology education. Semin Neurol. 2018;38(4):418-427. doi:10.1055/s-0038-1667042
- Curran VR. Tele-education. J Telemed Telecare. 2006;12(2):57-63. doi:10.1258/135763306776084400
- Lau KHV, Lakhan SE, Achike F. New media, technology and neurology education. Semin Neurol. 2018;38(4):457- 464. doi:10.1055/s-0038-1666985
- Quirk M, Chumley H. The adaptive medical curriculum: a model for continuous improvement. Med Teach. 2018;40(8):786-790. doi:10.1080/0142159X.2018.1484896
- Brockfeld T, Müller B, de Laffolie J. Video versus live lecture courses: a comparative evaluation of lecture types and results. Med Educ Online. 2018;23(1):1555434. doi:10.1080/10872981.2018.1555434
- Davis J, Crabb S, Rogers E, Zamora J, Khan K. Computer-based teaching is as good as face to face lecture-based teaching of evidence based medicine: a randomized controlled trial. Med Teach. 2008;30(3):302-307. doi:10.1080/01421590701784349
- Markova T, Roth LM, Monsur J. Synchronous distance learning as an effective and feasible method for delivering residency didactics. Fam Med. 2005;37(8):570-575.
- Naciri A, Radid M, Kharbach A, Chemsi G. E-learning in health professions education during the COVID-19 pandemic: a systematic review. J Educ Eval Health Prof. 2021;18:27. doi:10.3352/jeehp.2021.18.27
- Dedeilia A, Sotiropoulos MG, Hanrahan JG, Janga D, Dedeilias P, Sideris M. Medical and surgical education challenges and innovations in the COVID-19 era: a systematic review. In Vivo. 2020;34(3 Suppl):1603-1611. doi:10.21873/invivo.11950
- Weber DJ, Albert DVF, Aravamuthan BR, Bernson-Leung ME, Bhatti D, Milligan TA. Training in neurology: rapid implementation of cross-institutional neurology resident education in the time of COVID-19. Neurology. 2020;95(19):883-886. doi:10.1212/WNL.0000000000010753
- Frey J, Neeley B, Umer A, et al. Training in neurology: neuro day: an innovative curriculum connecting medical students with patients. Neurology. 2021;96(10):e1482- e1486. doi:10.1212/WNL.0000000000010859
- Schwartzstein RM, Dienstag JL, King RW, et al. The Harvard Medical School Pathways Curriculum: reimagining developmentally appropriate medical education for contemporary learners. Acad Med. 2020;95(11):1687-1695. doi:10.1097/ACM.0000000000003270
- Greer DM, Moeller J, Torres DR, et al. Funding the educational mission in neurology. Neurology. 2021;96(12):574- 582. doi:10.1212/WNL.0000000000011635
- Thielke S, Tumosa N, Lindenfeld R, Shay K. Geriatric focused educational offerings in the Department of Veterans Affairs from 1999 to 2009. Gerontol Geriatr Educ. 2011;32(1):38-53. doi:10.1080/02701960.2011.550214
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990- 2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459-480. doi:10.1016/S1474-4422(18)30499-X
- Baker V, Hack N. Improving access to care for patients with migraine in a remote Pacific population. Neurol Clin Pract. 2020;10(5):444-448. doi:10.1212/CPJ.0000000000000774
- Gutmann L, Cahill C, Jordan JT, et al. Characteristics of graduating US allopathic medical students pursuing a career in neurology. Neurology. 2019;92(17):e2051-e2063. doi:10.1212/WNL.0000000000007369
- Jordan JT, Cahill C, Ostendorf T, et al. Attracting neurology’s next generation: a qualitative study of specialty choice and perceptions. Neurology. 2020;95(8):e1080- e1090. doi:10.1212/WNL.0000000000009461
- Minen MT, Kaplan K, Akter S, et al. Understanding how to strengthen the neurology pipeline with insights from undergraduate neuroscience students. Neurology 2022;98(8):314-323. doi:10.1212/WNL.0000000000013259
- US Department of Veterans Affairs, Office of Academic Affiliations. To Educate for VA and the Nation. Updated August 1, 2024. Accessed August 15, 2024. https://www.va.gov/oaa/
- Schaefer SM, Dominguez M, Moeller JJ. The future of the lecture in neurology education. Semin Neurol. 2018;38(4):418-427. doi:10.1055/s-0038-1667042
- Curran VR. Tele-education. J Telemed Telecare. 2006;12(2):57-63. doi:10.1258/135763306776084400
- Lau KHV, Lakhan SE, Achike F. New media, technology and neurology education. Semin Neurol. 2018;38(4):457- 464. doi:10.1055/s-0038-1666985
- Quirk M, Chumley H. The adaptive medical curriculum: a model for continuous improvement. Med Teach. 2018;40(8):786-790. doi:10.1080/0142159X.2018.1484896
- Brockfeld T, Müller B, de Laffolie J. Video versus live lecture courses: a comparative evaluation of lecture types and results. Med Educ Online. 2018;23(1):1555434. doi:10.1080/10872981.2018.1555434
- Davis J, Crabb S, Rogers E, Zamora J, Khan K. Computer-based teaching is as good as face to face lecture-based teaching of evidence based medicine: a randomized controlled trial. Med Teach. 2008;30(3):302-307. doi:10.1080/01421590701784349
- Markova T, Roth LM, Monsur J. Synchronous distance learning as an effective and feasible method for delivering residency didactics. Fam Med. 2005;37(8):570-575.
- Naciri A, Radid M, Kharbach A, Chemsi G. E-learning in health professions education during the COVID-19 pandemic: a systematic review. J Educ Eval Health Prof. 2021;18:27. doi:10.3352/jeehp.2021.18.27
- Dedeilia A, Sotiropoulos MG, Hanrahan JG, Janga D, Dedeilias P, Sideris M. Medical and surgical education challenges and innovations in the COVID-19 era: a systematic review. In Vivo. 2020;34(3 Suppl):1603-1611. doi:10.21873/invivo.11950
- Weber DJ, Albert DVF, Aravamuthan BR, Bernson-Leung ME, Bhatti D, Milligan TA. Training in neurology: rapid implementation of cross-institutional neurology resident education in the time of COVID-19. Neurology. 2020;95(19):883-886. doi:10.1212/WNL.0000000000010753
- Frey J, Neeley B, Umer A, et al. Training in neurology: neuro day: an innovative curriculum connecting medical students with patients. Neurology. 2021;96(10):e1482- e1486. doi:10.1212/WNL.0000000000010859
- Schwartzstein RM, Dienstag JL, King RW, et al. The Harvard Medical School Pathways Curriculum: reimagining developmentally appropriate medical education for contemporary learners. Acad Med. 2020;95(11):1687-1695. doi:10.1097/ACM.0000000000003270
- Greer DM, Moeller J, Torres DR, et al. Funding the educational mission in neurology. Neurology. 2021;96(12):574- 582. doi:10.1212/WNL.0000000000011635
- Thielke S, Tumosa N, Lindenfeld R, Shay K. Geriatric focused educational offerings in the Department of Veterans Affairs from 1999 to 2009. Gerontol Geriatr Educ. 2011;32(1):38-53. doi:10.1080/02701960.2011.550214
Improving Interprofessional Neurology Training Using Tele-Education
Improving Interprofessional Neurology Training Using Tele-Education
Gestational Eclampsia Linked to Fivefold Epilepsy Risk
Gestational hypertension, preeclampsia, or eclampsia is associated with a significantly higher risk for neurologic disorders such as migraine or epilepsy in the years following a first pregnancy, new research suggests.
The risk was highest in those with gestational eclampsia, who had a 70% increased chance of developing a neurologic disorder, including a fivefold increased risk for epilepsy, investigators found.
“When consulting women with new-onset neurological disorders, it’s important to inquire about their pregnancy history, as pregnancy complications such as gestational hypertension, preeclampsia, and eclampsia have been associated with an increased risk of neurological disorders later in life.” Therese Friis, MD, PhD student, Department of Women’s and Children’s Health, Uppsala University in Sweden, said in an interview.
The findings were published online in JAMA Neurology.
Most studies of maternal outcomes after gestational hypertension, preeclampsia, or eclampsia have focused on long-term risks for cardiovascular disease or neurologic complications such as stroke, dementia, and cognitive impairment. And many of these studies were relatively small and based on interviews or questionnaires.
“We wanted to investigate whether women with a hypertensive disorder of pregnancy also had a risk of other neurological complications, closer in time to the pregnancy,” said Friis.
The new study included 648,385 women (mean age, 28.5 years) whose first pregnancy occurred between 2005 and 2018. Of these, 94% had a normotensive pregnancy, 2% had gestational hypertension, 4% had preeclampsia without eclampsia, and 0.1% had eclampsia.
Gestational hypertension was defined as new-onset systolic blood pressure of ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg; preeclampsia was defined as gestational hypertension accompanied by proteinuria; and eclampsia was defined as tonic-clonic seizures without other etiology accompanied by preeclampsia.
Researchers used linked Swedish national registries that collect data on pregnancies, births, and infant and maternal characteristics. Among other things, they controlled for maternal age, early pregnancy body mass index, education level, and pregestational and gestational diabetes.
The primary outcome was a composite of five new-onset neurologic diagnoses: Migraine, headache, epilepsy, sleep disorder, and mental fatigue (neurasthenia), although one diagnosis was sufficient, from 42 days to 15 years after childbirth. Mean follow-up was 7.7 years.
Fivefold Epilepsy Risk
Compared with normotensive pregnancies, the risk for the primary outcome was 70% greater in those with eclampsia (adjusted hazard ratio [aHR], 1.70; 95% CI, 1.16-2.50), 27% higher for gestational hypertension (aHR, 1.27; 95% CI, 1.12-1.45), and 32% for preeclampsia (aHR, 1.32; 95% CI, 1.22-1.42).
Researchers also looked at the risk for individual neurologic disorders. There were too few neurasthenia events to generate meaningful results, so this diagnosis was omitted from the analysis.
Here, the study found women with eclampsia had five times the risk for epilepsy (aHR, 5.31; 95% CI, 2.85-9.89) compared with women with normotensive pregnancies.
The underlying mechanism for this association is unclear. However, said Friis, eclampsia and epilepsy share common pathways, such as neuroinflammation, and women with epilepsy before pregnancy run an increased risk for eclampsia.
“So common underlying pathways might increase the risk both for eclampsia in cases of a seizure disorder and a future seizure disorder after eclampsia,” she said.
In addition, preeclampsia and, in particular, eclampsia can cause irreversible subclinical cerebral infarcts found in areas of cerebral edema, she added. “These infarcts or scarring of brain tissue could potentially serve as foci for later epileptic activity.”
Researchers separated women with preeclampsia (with or without eclampsia) into those with preterm (less than 37 weeks; 21%) and term (79%) deliveries. As Friis explained, women with preterm preeclampsia have a higher risk for acute complications and long-term cardiovascular outcomes than those with term preeclampsia.
Compared with those with normotensive pregnancies, investigators found an increased risk for the composite neurologic outcome among women with preterm preeclampsia (aHR, 1.54; 95% CI, 1.34-1.79), but also for those with term preeclampsia (aHR, 1.27; 95% CI, 1.17-1.38).
Common Vascular Component
The study also showed gestational hypertension and preeclampsia were associated with a later diagnosis of migraine, suggesting a possible common underlying vascular component.
“The increased risk of migraine following preeclampsia could be linked to endothelial damage at the blood-brain barrier level and alterations in cerebral blood flow and arterial vasospasm found in eclampsia, but this is only speculation,” said Friis.
The analysis also found an association between preeclampsia and a later diagnosis of headache. But this result likely encompasses several headache diagnoses, including migraine, so “it’s challenging to draw conclusions about the underlying mechanisms,” Friis added.
The study didn’t consider diagnoses from primary healthcare, which resulted in relatively few outcomes. The authors explained they could only identify the most severe cases; for example, women referred to specialized care.
Another potential study limitation is that Swedish registers don’t include information on race or ethnicity. Evidence shows there are racial differences in the risk for cardiovascular outcomes after preeclampsia.
This area of research is important as most women will experience at least one pregnancy in their lifetime, and preeclampsia affects 3%-5% of pregnancies. Further research is needed to understand the underlying pathophysiological mechanisms and the long-term consequences of this disorder, said Friis.
She added she hopes more therapeutic options will be available in the future for neuroprotective treatment for women with gestational hypertensive disorders.
Asked to comment, Thomas Vidic, MD, clinical professor of neurology, Indiana University School of Medicine, South Bend, said in an interview that this is an important study that includes robust data.
In his opinion, the most significant study finding is the marked increase in epilepsy risk after gestational eclampsia.
“In women who have new-onset epilepsy of unknown cause, asking about having eclampsia or preeclampsia during pregnancy is definitely a worthwhile question,” he said.
Confirming an etiology paints “a better picture” for patients wondering why they’re experiencing seizures, he added.
As with any registry-based study, this one had some acknowledged limitations, “but at the same time, the authors were able to have such a large database that I think this study is very worthwhile,” said Vidic.
The study received support from the Swedish Research Council. Neither Friis nor Vidic had relevant conflicts of interest.
A version of this article appeared on Medscape.com.
Gestational hypertension, preeclampsia, or eclampsia is associated with a significantly higher risk for neurologic disorders such as migraine or epilepsy in the years following a first pregnancy, new research suggests.
The risk was highest in those with gestational eclampsia, who had a 70% increased chance of developing a neurologic disorder, including a fivefold increased risk for epilepsy, investigators found.
“When consulting women with new-onset neurological disorders, it’s important to inquire about their pregnancy history, as pregnancy complications such as gestational hypertension, preeclampsia, and eclampsia have been associated with an increased risk of neurological disorders later in life.” Therese Friis, MD, PhD student, Department of Women’s and Children’s Health, Uppsala University in Sweden, said in an interview.
The findings were published online in JAMA Neurology.
Most studies of maternal outcomes after gestational hypertension, preeclampsia, or eclampsia have focused on long-term risks for cardiovascular disease or neurologic complications such as stroke, dementia, and cognitive impairment. And many of these studies were relatively small and based on interviews or questionnaires.
“We wanted to investigate whether women with a hypertensive disorder of pregnancy also had a risk of other neurological complications, closer in time to the pregnancy,” said Friis.
The new study included 648,385 women (mean age, 28.5 years) whose first pregnancy occurred between 2005 and 2018. Of these, 94% had a normotensive pregnancy, 2% had gestational hypertension, 4% had preeclampsia without eclampsia, and 0.1% had eclampsia.
Gestational hypertension was defined as new-onset systolic blood pressure of ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg; preeclampsia was defined as gestational hypertension accompanied by proteinuria; and eclampsia was defined as tonic-clonic seizures without other etiology accompanied by preeclampsia.
Researchers used linked Swedish national registries that collect data on pregnancies, births, and infant and maternal characteristics. Among other things, they controlled for maternal age, early pregnancy body mass index, education level, and pregestational and gestational diabetes.
The primary outcome was a composite of five new-onset neurologic diagnoses: Migraine, headache, epilepsy, sleep disorder, and mental fatigue (neurasthenia), although one diagnosis was sufficient, from 42 days to 15 years after childbirth. Mean follow-up was 7.7 years.
Fivefold Epilepsy Risk
Compared with normotensive pregnancies, the risk for the primary outcome was 70% greater in those with eclampsia (adjusted hazard ratio [aHR], 1.70; 95% CI, 1.16-2.50), 27% higher for gestational hypertension (aHR, 1.27; 95% CI, 1.12-1.45), and 32% for preeclampsia (aHR, 1.32; 95% CI, 1.22-1.42).
Researchers also looked at the risk for individual neurologic disorders. There were too few neurasthenia events to generate meaningful results, so this diagnosis was omitted from the analysis.
Here, the study found women with eclampsia had five times the risk for epilepsy (aHR, 5.31; 95% CI, 2.85-9.89) compared with women with normotensive pregnancies.
The underlying mechanism for this association is unclear. However, said Friis, eclampsia and epilepsy share common pathways, such as neuroinflammation, and women with epilepsy before pregnancy run an increased risk for eclampsia.
“So common underlying pathways might increase the risk both for eclampsia in cases of a seizure disorder and a future seizure disorder after eclampsia,” she said.
In addition, preeclampsia and, in particular, eclampsia can cause irreversible subclinical cerebral infarcts found in areas of cerebral edema, she added. “These infarcts or scarring of brain tissue could potentially serve as foci for later epileptic activity.”
Researchers separated women with preeclampsia (with or without eclampsia) into those with preterm (less than 37 weeks; 21%) and term (79%) deliveries. As Friis explained, women with preterm preeclampsia have a higher risk for acute complications and long-term cardiovascular outcomes than those with term preeclampsia.
Compared with those with normotensive pregnancies, investigators found an increased risk for the composite neurologic outcome among women with preterm preeclampsia (aHR, 1.54; 95% CI, 1.34-1.79), but also for those with term preeclampsia (aHR, 1.27; 95% CI, 1.17-1.38).
Common Vascular Component
The study also showed gestational hypertension and preeclampsia were associated with a later diagnosis of migraine, suggesting a possible common underlying vascular component.
“The increased risk of migraine following preeclampsia could be linked to endothelial damage at the blood-brain barrier level and alterations in cerebral blood flow and arterial vasospasm found in eclampsia, but this is only speculation,” said Friis.
The analysis also found an association between preeclampsia and a later diagnosis of headache. But this result likely encompasses several headache diagnoses, including migraine, so “it’s challenging to draw conclusions about the underlying mechanisms,” Friis added.
The study didn’t consider diagnoses from primary healthcare, which resulted in relatively few outcomes. The authors explained they could only identify the most severe cases; for example, women referred to specialized care.
Another potential study limitation is that Swedish registers don’t include information on race or ethnicity. Evidence shows there are racial differences in the risk for cardiovascular outcomes after preeclampsia.
This area of research is important as most women will experience at least one pregnancy in their lifetime, and preeclampsia affects 3%-5% of pregnancies. Further research is needed to understand the underlying pathophysiological mechanisms and the long-term consequences of this disorder, said Friis.
She added she hopes more therapeutic options will be available in the future for neuroprotective treatment for women with gestational hypertensive disorders.
Asked to comment, Thomas Vidic, MD, clinical professor of neurology, Indiana University School of Medicine, South Bend, said in an interview that this is an important study that includes robust data.
In his opinion, the most significant study finding is the marked increase in epilepsy risk after gestational eclampsia.
“In women who have new-onset epilepsy of unknown cause, asking about having eclampsia or preeclampsia during pregnancy is definitely a worthwhile question,” he said.
Confirming an etiology paints “a better picture” for patients wondering why they’re experiencing seizures, he added.
As with any registry-based study, this one had some acknowledged limitations, “but at the same time, the authors were able to have such a large database that I think this study is very worthwhile,” said Vidic.
The study received support from the Swedish Research Council. Neither Friis nor Vidic had relevant conflicts of interest.
A version of this article appeared on Medscape.com.
Gestational hypertension, preeclampsia, or eclampsia is associated with a significantly higher risk for neurologic disorders such as migraine or epilepsy in the years following a first pregnancy, new research suggests.
The risk was highest in those with gestational eclampsia, who had a 70% increased chance of developing a neurologic disorder, including a fivefold increased risk for epilepsy, investigators found.
“When consulting women with new-onset neurological disorders, it’s important to inquire about their pregnancy history, as pregnancy complications such as gestational hypertension, preeclampsia, and eclampsia have been associated with an increased risk of neurological disorders later in life.” Therese Friis, MD, PhD student, Department of Women’s and Children’s Health, Uppsala University in Sweden, said in an interview.
The findings were published online in JAMA Neurology.
Most studies of maternal outcomes after gestational hypertension, preeclampsia, or eclampsia have focused on long-term risks for cardiovascular disease or neurologic complications such as stroke, dementia, and cognitive impairment. And many of these studies were relatively small and based on interviews or questionnaires.
“We wanted to investigate whether women with a hypertensive disorder of pregnancy also had a risk of other neurological complications, closer in time to the pregnancy,” said Friis.
The new study included 648,385 women (mean age, 28.5 years) whose first pregnancy occurred between 2005 and 2018. Of these, 94% had a normotensive pregnancy, 2% had gestational hypertension, 4% had preeclampsia without eclampsia, and 0.1% had eclampsia.
Gestational hypertension was defined as new-onset systolic blood pressure of ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg; preeclampsia was defined as gestational hypertension accompanied by proteinuria; and eclampsia was defined as tonic-clonic seizures without other etiology accompanied by preeclampsia.
Researchers used linked Swedish national registries that collect data on pregnancies, births, and infant and maternal characteristics. Among other things, they controlled for maternal age, early pregnancy body mass index, education level, and pregestational and gestational diabetes.
The primary outcome was a composite of five new-onset neurologic diagnoses: Migraine, headache, epilepsy, sleep disorder, and mental fatigue (neurasthenia), although one diagnosis was sufficient, from 42 days to 15 years after childbirth. Mean follow-up was 7.7 years.
Fivefold Epilepsy Risk
Compared with normotensive pregnancies, the risk for the primary outcome was 70% greater in those with eclampsia (adjusted hazard ratio [aHR], 1.70; 95% CI, 1.16-2.50), 27% higher for gestational hypertension (aHR, 1.27; 95% CI, 1.12-1.45), and 32% for preeclampsia (aHR, 1.32; 95% CI, 1.22-1.42).
Researchers also looked at the risk for individual neurologic disorders. There were too few neurasthenia events to generate meaningful results, so this diagnosis was omitted from the analysis.
Here, the study found women with eclampsia had five times the risk for epilepsy (aHR, 5.31; 95% CI, 2.85-9.89) compared with women with normotensive pregnancies.
The underlying mechanism for this association is unclear. However, said Friis, eclampsia and epilepsy share common pathways, such as neuroinflammation, and women with epilepsy before pregnancy run an increased risk for eclampsia.
“So common underlying pathways might increase the risk both for eclampsia in cases of a seizure disorder and a future seizure disorder after eclampsia,” she said.
In addition, preeclampsia and, in particular, eclampsia can cause irreversible subclinical cerebral infarcts found in areas of cerebral edema, she added. “These infarcts or scarring of brain tissue could potentially serve as foci for later epileptic activity.”
Researchers separated women with preeclampsia (with or without eclampsia) into those with preterm (less than 37 weeks; 21%) and term (79%) deliveries. As Friis explained, women with preterm preeclampsia have a higher risk for acute complications and long-term cardiovascular outcomes than those with term preeclampsia.
Compared with those with normotensive pregnancies, investigators found an increased risk for the composite neurologic outcome among women with preterm preeclampsia (aHR, 1.54; 95% CI, 1.34-1.79), but also for those with term preeclampsia (aHR, 1.27; 95% CI, 1.17-1.38).
Common Vascular Component
The study also showed gestational hypertension and preeclampsia were associated with a later diagnosis of migraine, suggesting a possible common underlying vascular component.
“The increased risk of migraine following preeclampsia could be linked to endothelial damage at the blood-brain barrier level and alterations in cerebral blood flow and arterial vasospasm found in eclampsia, but this is only speculation,” said Friis.
The analysis also found an association between preeclampsia and a later diagnosis of headache. But this result likely encompasses several headache diagnoses, including migraine, so “it’s challenging to draw conclusions about the underlying mechanisms,” Friis added.
The study didn’t consider diagnoses from primary healthcare, which resulted in relatively few outcomes. The authors explained they could only identify the most severe cases; for example, women referred to specialized care.
Another potential study limitation is that Swedish registers don’t include information on race or ethnicity. Evidence shows there are racial differences in the risk for cardiovascular outcomes after preeclampsia.
This area of research is important as most women will experience at least one pregnancy in their lifetime, and preeclampsia affects 3%-5% of pregnancies. Further research is needed to understand the underlying pathophysiological mechanisms and the long-term consequences of this disorder, said Friis.
She added she hopes more therapeutic options will be available in the future for neuroprotective treatment for women with gestational hypertensive disorders.
Asked to comment, Thomas Vidic, MD, clinical professor of neurology, Indiana University School of Medicine, South Bend, said in an interview that this is an important study that includes robust data.
In his opinion, the most significant study finding is the marked increase in epilepsy risk after gestational eclampsia.
“In women who have new-onset epilepsy of unknown cause, asking about having eclampsia or preeclampsia during pregnancy is definitely a worthwhile question,” he said.
Confirming an etiology paints “a better picture” for patients wondering why they’re experiencing seizures, he added.
As with any registry-based study, this one had some acknowledged limitations, “but at the same time, the authors were able to have such a large database that I think this study is very worthwhile,” said Vidic.
The study received support from the Swedish Research Council. Neither Friis nor Vidic had relevant conflicts of interest.
A version of this article appeared on Medscape.com.
FROM JAMA NEUROLOGY
Donepezil Shows Promise in TBI Recovery
TOPLINE:
Donepezil was associated with improved verbal memory and enhanced recall and processing speed, compared with placebo, in patients with severe traumatic brain injury (TBI), with a favorable safety profile despite mild to moderate gastrointestinal side effects.
METHODOLOGY:
- A four-site, randomized, parallel-group, double-blind, placebo-controlled, 10-week clinical trial (MEMRI-TBI-D) was conducted between 2013 and 2019 to evaluate the efficacy of donepezil for verbal memory impairments following severe TBI.
- 75 adults (75% men; mean age, 37 years) with complicated mild, moderate, or severe nonpenetrating TBI at least 6 months prior to study participation were included and randomly assigned to receive donepezil (n = 37) or placebo (n = 38).
- Participants received 5 mg donepezil daily or matching placebo for 2 weeks, then donepezil at 10 mg daily or matching placebo for 8 weeks; treatment was discontinued at 10 weeks, with an additional 4-week observation period.
- Verbal memory was assessed using the Hopkins Verbal Learning Test–Revised (HVLT-R). The primary outcome measure was verbal learning, evaluated through the HVLT-R total recall (ie, Total Trials 1-3) score.
TAKEAWAY:
- Compared with placebo, donepezil was associated with significantly greater improvements in verbal learning in both modified intent-to-treat and per-protocol analyses (P = .034 and .036, respectively).
- Treatment-responder rates were significantly higher in the donepezil group than in the placebo group (42 vs 18%; P = .03), with donepezil responders showing significant improvements in delayed recall and processing speed.
- Although there were no serious adverse events in either group, treatment-emergent adverse events were significantly more common in the donepezil group vs placebo (46% vs 8%; P < .001). No serious adverse events occurred in either group.
- Diarrhea and nausea were significantly more common in the donepezil group than in the placebo group (Fisher’s exact test: diarrhea, P = .03; nausea, P = .01).
IN PRACTICE:
“This study demonstrates the efficacy of donepezil on severe, persistent verbal memory impairments after predominantly severe TBI, with significant benefit for a subset of persons with such injuries, as well as a relatively favorable safety and tolerability profile,” the investigators wrote.
SOURCE:
The study was led by David B. Arciniegas, MD, University of Colorado School of Medicine, Aurora. It was published online in The Journal of Neuropsychiatry and Clinical Neurosciences.
LIMITATIONS:
The study included a relatively small sample with predominantly severe TBI requiring hospitalization and inpatient rehabilitation. The sample characteristics limit the generalizability of the findings to persons with other severities of TBI, other types of memory impairments, or more complex neuropsychiatric presentations. The study population had an average of 14 years of education, making generalizability to individuals with lower education levels uncertain. Additionally, while measures of information processing speed and immediate auditory attention were included, specific measures of sustained or selective attention were not, making it difficult to rule out improvements in higher-level attention as potential contributors to the observed verbal memory performance improvements.
DISCLOSURES:
The study was funded by the National Institute on Disability, Independent Living, and Rehabilitation Research, with in-kind support from TIRR Memorial Hermann. Four authors disclosed various financial and professional affiliations, including advisory roles with pharmaceutical and diagnostic companies, support from institutional awards, and involvement in programs funded by external organizations. One author served as the editor of The Journal of Neuropsychiatry and Clinical Neurosciences, with an independent editor overseeing the review and publication process for this article.
This article was created using several editorial tools, including artificial intelligence, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Donepezil was associated with improved verbal memory and enhanced recall and processing speed, compared with placebo, in patients with severe traumatic brain injury (TBI), with a favorable safety profile despite mild to moderate gastrointestinal side effects.
METHODOLOGY:
- A four-site, randomized, parallel-group, double-blind, placebo-controlled, 10-week clinical trial (MEMRI-TBI-D) was conducted between 2013 and 2019 to evaluate the efficacy of donepezil for verbal memory impairments following severe TBI.
- 75 adults (75% men; mean age, 37 years) with complicated mild, moderate, or severe nonpenetrating TBI at least 6 months prior to study participation were included and randomly assigned to receive donepezil (n = 37) or placebo (n = 38).
- Participants received 5 mg donepezil daily or matching placebo for 2 weeks, then donepezil at 10 mg daily or matching placebo for 8 weeks; treatment was discontinued at 10 weeks, with an additional 4-week observation period.
- Verbal memory was assessed using the Hopkins Verbal Learning Test–Revised (HVLT-R). The primary outcome measure was verbal learning, evaluated through the HVLT-R total recall (ie, Total Trials 1-3) score.
TAKEAWAY:
- Compared with placebo, donepezil was associated with significantly greater improvements in verbal learning in both modified intent-to-treat and per-protocol analyses (P = .034 and .036, respectively).
- Treatment-responder rates were significantly higher in the donepezil group than in the placebo group (42 vs 18%; P = .03), with donepezil responders showing significant improvements in delayed recall and processing speed.
- Although there were no serious adverse events in either group, treatment-emergent adverse events were significantly more common in the donepezil group vs placebo (46% vs 8%; P < .001). No serious adverse events occurred in either group.
- Diarrhea and nausea were significantly more common in the donepezil group than in the placebo group (Fisher’s exact test: diarrhea, P = .03; nausea, P = .01).
IN PRACTICE:
“This study demonstrates the efficacy of donepezil on severe, persistent verbal memory impairments after predominantly severe TBI, with significant benefit for a subset of persons with such injuries, as well as a relatively favorable safety and tolerability profile,” the investigators wrote.
SOURCE:
The study was led by David B. Arciniegas, MD, University of Colorado School of Medicine, Aurora. It was published online in The Journal of Neuropsychiatry and Clinical Neurosciences.
LIMITATIONS:
The study included a relatively small sample with predominantly severe TBI requiring hospitalization and inpatient rehabilitation. The sample characteristics limit the generalizability of the findings to persons with other severities of TBI, other types of memory impairments, or more complex neuropsychiatric presentations. The study population had an average of 14 years of education, making generalizability to individuals with lower education levels uncertain. Additionally, while measures of information processing speed and immediate auditory attention were included, specific measures of sustained or selective attention were not, making it difficult to rule out improvements in higher-level attention as potential contributors to the observed verbal memory performance improvements.
DISCLOSURES:
The study was funded by the National Institute on Disability, Independent Living, and Rehabilitation Research, with in-kind support from TIRR Memorial Hermann. Four authors disclosed various financial and professional affiliations, including advisory roles with pharmaceutical and diagnostic companies, support from institutional awards, and involvement in programs funded by external organizations. One author served as the editor of The Journal of Neuropsychiatry and Clinical Neurosciences, with an independent editor overseeing the review and publication process for this article.
This article was created using several editorial tools, including artificial intelligence, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Donepezil was associated with improved verbal memory and enhanced recall and processing speed, compared with placebo, in patients with severe traumatic brain injury (TBI), with a favorable safety profile despite mild to moderate gastrointestinal side effects.
METHODOLOGY:
- A four-site, randomized, parallel-group, double-blind, placebo-controlled, 10-week clinical trial (MEMRI-TBI-D) was conducted between 2013 and 2019 to evaluate the efficacy of donepezil for verbal memory impairments following severe TBI.
- 75 adults (75% men; mean age, 37 years) with complicated mild, moderate, or severe nonpenetrating TBI at least 6 months prior to study participation were included and randomly assigned to receive donepezil (n = 37) or placebo (n = 38).
- Participants received 5 mg donepezil daily or matching placebo for 2 weeks, then donepezil at 10 mg daily or matching placebo for 8 weeks; treatment was discontinued at 10 weeks, with an additional 4-week observation period.
- Verbal memory was assessed using the Hopkins Verbal Learning Test–Revised (HVLT-R). The primary outcome measure was verbal learning, evaluated through the HVLT-R total recall (ie, Total Trials 1-3) score.
TAKEAWAY:
- Compared with placebo, donepezil was associated with significantly greater improvements in verbal learning in both modified intent-to-treat and per-protocol analyses (P = .034 and .036, respectively).
- Treatment-responder rates were significantly higher in the donepezil group than in the placebo group (42 vs 18%; P = .03), with donepezil responders showing significant improvements in delayed recall and processing speed.
- Although there were no serious adverse events in either group, treatment-emergent adverse events were significantly more common in the donepezil group vs placebo (46% vs 8%; P < .001). No serious adverse events occurred in either group.
- Diarrhea and nausea were significantly more common in the donepezil group than in the placebo group (Fisher’s exact test: diarrhea, P = .03; nausea, P = .01).
IN PRACTICE:
“This study demonstrates the efficacy of donepezil on severe, persistent verbal memory impairments after predominantly severe TBI, with significant benefit for a subset of persons with such injuries, as well as a relatively favorable safety and tolerability profile,” the investigators wrote.
SOURCE:
The study was led by David B. Arciniegas, MD, University of Colorado School of Medicine, Aurora. It was published online in The Journal of Neuropsychiatry and Clinical Neurosciences.
LIMITATIONS:
The study included a relatively small sample with predominantly severe TBI requiring hospitalization and inpatient rehabilitation. The sample characteristics limit the generalizability of the findings to persons with other severities of TBI, other types of memory impairments, or more complex neuropsychiatric presentations. The study population had an average of 14 years of education, making generalizability to individuals with lower education levels uncertain. Additionally, while measures of information processing speed and immediate auditory attention were included, specific measures of sustained or selective attention were not, making it difficult to rule out improvements in higher-level attention as potential contributors to the observed verbal memory performance improvements.
DISCLOSURES:
The study was funded by the National Institute on Disability, Independent Living, and Rehabilitation Research, with in-kind support from TIRR Memorial Hermann. Four authors disclosed various financial and professional affiliations, including advisory roles with pharmaceutical and diagnostic companies, support from institutional awards, and involvement in programs funded by external organizations. One author served as the editor of The Journal of Neuropsychiatry and Clinical Neurosciences, with an independent editor overseeing the review and publication process for this article.
This article was created using several editorial tools, including artificial intelligence, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Brain Changes in Youth Who Use Substances: Cause or Effect?
A widely accepted assumption in the addiction field is that neuroanatomical changes observed in young people who use alcohol or other substances are largely the consequence of exposure to these substances.
But a new study suggests that neuroanatomical features in children, including greater whole brain and cortical volumes, are evident before exposure to any substances.
The investigators, led by Alex P. Miller, PhD, assistant professor, Department of Psychiatry, Indiana University, Indianapolis, noted that the findings add to a growing body of work that suggests
The findings were published online in JAMA Network Open.
Neuroanatomy a Predisposing Risk Factor?
Earlier research showed that substance use is associated with lower gray matter volume, thinner cortex, and less white matter integrity. While it has been widely thought that these changes were induced by the use of alcohol or illicit drugs, recent longitudinal and genetic studies suggest that the neuroanatomical changes may also be predisposing risk factors for substance use.
To better understand the issue, investigators analyzed data on 9804 children (mean baseline age, 9.9 years; 53% men; 76% White) at 22 US sites enrolled in the Adolescent Brain Cognitive Development (ABCD) Study that’s examining brain and behavioral development from middle childhood to young adulthood.
The researchers collected information on the use of alcohol, nicotine, cannabis, and other illicit substances from in-person interviews at baseline and years 1, 2, and 3, as well as interim phone interviews at 6, 18, and 30 months. MRI scans provided extensive brain structural data, including global and regional cortical volume, thickness, surface area, sulcal depth, and subcortical volume.
Of the total, 3460 participants (35%) initiated substance use before age 15, with 90% reporting alcohol use initiation. There was considerable overlap between initiation of alcohol, nicotine, and cannabis.
The researchers tested whether baseline neuroanatomical variability was associated with any substance use initiation before or up to 3 years following initial neuroimaging scans. Study covariates included baseline age, sex, pubertal status, familial relationship (eg, sibling or twin), and prenatal substance exposures. Researchers didn’t control for sociodemographic characteristics as these could influence associations.
Significant Brain Differences
Compared with no substance use initiation, any substance use initiation was associated with larger global neuroanatomical indices, including whole brain (beta = 0.05; P = 2.80 × 10–8), total intracranial (beta = 0.04; P = 3.49 × 10−6), cortical (beta = 0.05; P = 4.31 × 10–8), and subcortical volumes (beta = 0.05; P = 4.39 × 10–8), as well as greater total cortical surface area (beta = 0.04; P = 6.05 × 10–7).
The direction of associations between cortical thickness and substance use initiation was regionally specific; any substance use initiation was characterized by thinner cortex in all frontal regions (eg, rostral middle frontal gyrus, beta = −0.03; P = 6.99 × 10–6), but thicker cortex in all other lobes. It was also associated with larger regional brain volumes, deeper regional sulci, and differences in regional cortical surface area.
The authors noted total cortical thickness peaks at age 1.7 years and steadily declines throughout life. By contrast, subcortical volumes peak at 14.4 years of age and generally remain stable before steep later life declines.
Secondary analyses compared initiation of the three most commonly used substances in early adolescence (alcohol, nicotine, and cannabis) with no substance use.
Findings for alcohol largely mirrored those for any substance use. However, the study uncovered additional significant associations, including greater left lateral occipital volume and bilateral para-hippocampal gyri cortical thickness and less bilateral superior frontal gyri cortical thickness.
Nicotine use was associated with lower right superior frontal gyrus volume and deeper left lateral orbitofrontal cortex sulci. And cannabis use was associated with thinner left precentral gyrus and lower right inferior parietal gyrus and right caudate volumes.
The authors noted results for nicotine and cannabis may not have had adequate statistical power, and small effects suggest these findings aren’t clinically informative for individuals. However, they wrote, “They do inform and challenge current theoretical models of addiction.”
Associations Precede Substance Use
A post hoc analysis further challenges current models of addiction. When researchers looked only at the 1203 youth who initiated substance use after the baseline neuroimaging session, they found most associations preceded substance use.
“That regional associations may precede substance use initiation, including less cortical thickness in the right rostral middle frontal gyrus, challenges predominant interpretations that these associations arise largely due to neurotoxic consequences of exposure and increases the plausibility that these features may, at least partially, reflect markers of predispositional risk,” wrote the authors.
A study limitation was that unmeasured confounders and undetected systemic differences in missing data may have influenced associations. Sociodemographic, environmental, and genetic variables that were not included as covariates are likely associated with both neuroanatomical variability and substance use initiation and may moderate associations between them, said the authors.
The ABCD Study provides “a robust and large database of longitudinal data” that goes beyond previous neuroimaging research “to understand the bidirectional relationship between brain structure and substance use,” Miller said in a press release.
“The hope is that these types of studies, in conjunction with other data on environmental exposures and genetic risk, could help change how we think about the development of substance use disorders and inform more accurate models of addiction moving forward,” Miller said.
Reevaluating Causal Assumptions
In an accompanying editorial, Felix Pichardo, MA, and Sylia Wilson, PhD, from the Institute of Child Development, University of Minnesota, Minneapolis, suggested that it may be time to “reevaluate the causal assumptions that underlie brain disease models of addiction” and the mechanisms by which it develops, persists, and becomes harmful.
Neurotoxic effects of substances are central to current brain disease models of addiction, wrote Pichardo and Wilson. “Substance exposure is thought to affect cortical and subcortical regions that support interrelated systems, resulting in desensitization of reward-related processing, increased stress that prompts cravings, negative emotions when cravings are unsated, and weakening of cognitive control abilities that leads to repeated returns to use.”
The editorial writers praised the ABCD Study for its large sample size for providing a level of precision, statistical accuracy, and ability to identify both larger and smaller effects, which are critical for addiction research.
Unlike most addiction research that relies on cross-sectional designs, the current study used longitudinal assessments, which is another of its strengths, they noted.
“Longitudinal study designs like in the ABCD Study are fundamental for establishing temporal ordering across constructs, which is important because establishing temporal precedence is a key step in determining causal links and underlying mechanisms.”
The inclusion of several genetically informative components, such as the family study design, nested twin subsamples, and DNA collection, “allows researchers to extend beyond temporal precedence toward increased causal inference and identification of mechanisms,” they added.
The study received support from the National Institutes of Health. The study authors and editorial writers had no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
A widely accepted assumption in the addiction field is that neuroanatomical changes observed in young people who use alcohol or other substances are largely the consequence of exposure to these substances.
But a new study suggests that neuroanatomical features in children, including greater whole brain and cortical volumes, are evident before exposure to any substances.
The investigators, led by Alex P. Miller, PhD, assistant professor, Department of Psychiatry, Indiana University, Indianapolis, noted that the findings add to a growing body of work that suggests
The findings were published online in JAMA Network Open.
Neuroanatomy a Predisposing Risk Factor?
Earlier research showed that substance use is associated with lower gray matter volume, thinner cortex, and less white matter integrity. While it has been widely thought that these changes were induced by the use of alcohol or illicit drugs, recent longitudinal and genetic studies suggest that the neuroanatomical changes may also be predisposing risk factors for substance use.
To better understand the issue, investigators analyzed data on 9804 children (mean baseline age, 9.9 years; 53% men; 76% White) at 22 US sites enrolled in the Adolescent Brain Cognitive Development (ABCD) Study that’s examining brain and behavioral development from middle childhood to young adulthood.
The researchers collected information on the use of alcohol, nicotine, cannabis, and other illicit substances from in-person interviews at baseline and years 1, 2, and 3, as well as interim phone interviews at 6, 18, and 30 months. MRI scans provided extensive brain structural data, including global and regional cortical volume, thickness, surface area, sulcal depth, and subcortical volume.
Of the total, 3460 participants (35%) initiated substance use before age 15, with 90% reporting alcohol use initiation. There was considerable overlap between initiation of alcohol, nicotine, and cannabis.
The researchers tested whether baseline neuroanatomical variability was associated with any substance use initiation before or up to 3 years following initial neuroimaging scans. Study covariates included baseline age, sex, pubertal status, familial relationship (eg, sibling or twin), and prenatal substance exposures. Researchers didn’t control for sociodemographic characteristics as these could influence associations.
Significant Brain Differences
Compared with no substance use initiation, any substance use initiation was associated with larger global neuroanatomical indices, including whole brain (beta = 0.05; P = 2.80 × 10–8), total intracranial (beta = 0.04; P = 3.49 × 10−6), cortical (beta = 0.05; P = 4.31 × 10–8), and subcortical volumes (beta = 0.05; P = 4.39 × 10–8), as well as greater total cortical surface area (beta = 0.04; P = 6.05 × 10–7).
The direction of associations between cortical thickness and substance use initiation was regionally specific; any substance use initiation was characterized by thinner cortex in all frontal regions (eg, rostral middle frontal gyrus, beta = −0.03; P = 6.99 × 10–6), but thicker cortex in all other lobes. It was also associated with larger regional brain volumes, deeper regional sulci, and differences in regional cortical surface area.
The authors noted total cortical thickness peaks at age 1.7 years and steadily declines throughout life. By contrast, subcortical volumes peak at 14.4 years of age and generally remain stable before steep later life declines.
Secondary analyses compared initiation of the three most commonly used substances in early adolescence (alcohol, nicotine, and cannabis) with no substance use.
Findings for alcohol largely mirrored those for any substance use. However, the study uncovered additional significant associations, including greater left lateral occipital volume and bilateral para-hippocampal gyri cortical thickness and less bilateral superior frontal gyri cortical thickness.
Nicotine use was associated with lower right superior frontal gyrus volume and deeper left lateral orbitofrontal cortex sulci. And cannabis use was associated with thinner left precentral gyrus and lower right inferior parietal gyrus and right caudate volumes.
The authors noted results for nicotine and cannabis may not have had adequate statistical power, and small effects suggest these findings aren’t clinically informative for individuals. However, they wrote, “They do inform and challenge current theoretical models of addiction.”
Associations Precede Substance Use
A post hoc analysis further challenges current models of addiction. When researchers looked only at the 1203 youth who initiated substance use after the baseline neuroimaging session, they found most associations preceded substance use.
“That regional associations may precede substance use initiation, including less cortical thickness in the right rostral middle frontal gyrus, challenges predominant interpretations that these associations arise largely due to neurotoxic consequences of exposure and increases the plausibility that these features may, at least partially, reflect markers of predispositional risk,” wrote the authors.
A study limitation was that unmeasured confounders and undetected systemic differences in missing data may have influenced associations. Sociodemographic, environmental, and genetic variables that were not included as covariates are likely associated with both neuroanatomical variability and substance use initiation and may moderate associations between them, said the authors.
The ABCD Study provides “a robust and large database of longitudinal data” that goes beyond previous neuroimaging research “to understand the bidirectional relationship between brain structure and substance use,” Miller said in a press release.
“The hope is that these types of studies, in conjunction with other data on environmental exposures and genetic risk, could help change how we think about the development of substance use disorders and inform more accurate models of addiction moving forward,” Miller said.
Reevaluating Causal Assumptions
In an accompanying editorial, Felix Pichardo, MA, and Sylia Wilson, PhD, from the Institute of Child Development, University of Minnesota, Minneapolis, suggested that it may be time to “reevaluate the causal assumptions that underlie brain disease models of addiction” and the mechanisms by which it develops, persists, and becomes harmful.
Neurotoxic effects of substances are central to current brain disease models of addiction, wrote Pichardo and Wilson. “Substance exposure is thought to affect cortical and subcortical regions that support interrelated systems, resulting in desensitization of reward-related processing, increased stress that prompts cravings, negative emotions when cravings are unsated, and weakening of cognitive control abilities that leads to repeated returns to use.”
The editorial writers praised the ABCD Study for its large sample size for providing a level of precision, statistical accuracy, and ability to identify both larger and smaller effects, which are critical for addiction research.
Unlike most addiction research that relies on cross-sectional designs, the current study used longitudinal assessments, which is another of its strengths, they noted.
“Longitudinal study designs like in the ABCD Study are fundamental for establishing temporal ordering across constructs, which is important because establishing temporal precedence is a key step in determining causal links and underlying mechanisms.”
The inclusion of several genetically informative components, such as the family study design, nested twin subsamples, and DNA collection, “allows researchers to extend beyond temporal precedence toward increased causal inference and identification of mechanisms,” they added.
The study received support from the National Institutes of Health. The study authors and editorial writers had no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
A widely accepted assumption in the addiction field is that neuroanatomical changes observed in young people who use alcohol or other substances are largely the consequence of exposure to these substances.
But a new study suggests that neuroanatomical features in children, including greater whole brain and cortical volumes, are evident before exposure to any substances.
The investigators, led by Alex P. Miller, PhD, assistant professor, Department of Psychiatry, Indiana University, Indianapolis, noted that the findings add to a growing body of work that suggests
The findings were published online in JAMA Network Open.
Neuroanatomy a Predisposing Risk Factor?
Earlier research showed that substance use is associated with lower gray matter volume, thinner cortex, and less white matter integrity. While it has been widely thought that these changes were induced by the use of alcohol or illicit drugs, recent longitudinal and genetic studies suggest that the neuroanatomical changes may also be predisposing risk factors for substance use.
To better understand the issue, investigators analyzed data on 9804 children (mean baseline age, 9.9 years; 53% men; 76% White) at 22 US sites enrolled in the Adolescent Brain Cognitive Development (ABCD) Study that’s examining brain and behavioral development from middle childhood to young adulthood.
The researchers collected information on the use of alcohol, nicotine, cannabis, and other illicit substances from in-person interviews at baseline and years 1, 2, and 3, as well as interim phone interviews at 6, 18, and 30 months. MRI scans provided extensive brain structural data, including global and regional cortical volume, thickness, surface area, sulcal depth, and subcortical volume.
Of the total, 3460 participants (35%) initiated substance use before age 15, with 90% reporting alcohol use initiation. There was considerable overlap between initiation of alcohol, nicotine, and cannabis.
The researchers tested whether baseline neuroanatomical variability was associated with any substance use initiation before or up to 3 years following initial neuroimaging scans. Study covariates included baseline age, sex, pubertal status, familial relationship (eg, sibling or twin), and prenatal substance exposures. Researchers didn’t control for sociodemographic characteristics as these could influence associations.
Significant Brain Differences
Compared with no substance use initiation, any substance use initiation was associated with larger global neuroanatomical indices, including whole brain (beta = 0.05; P = 2.80 × 10–8), total intracranial (beta = 0.04; P = 3.49 × 10−6), cortical (beta = 0.05; P = 4.31 × 10–8), and subcortical volumes (beta = 0.05; P = 4.39 × 10–8), as well as greater total cortical surface area (beta = 0.04; P = 6.05 × 10–7).
The direction of associations between cortical thickness and substance use initiation was regionally specific; any substance use initiation was characterized by thinner cortex in all frontal regions (eg, rostral middle frontal gyrus, beta = −0.03; P = 6.99 × 10–6), but thicker cortex in all other lobes. It was also associated with larger regional brain volumes, deeper regional sulci, and differences in regional cortical surface area.
The authors noted total cortical thickness peaks at age 1.7 years and steadily declines throughout life. By contrast, subcortical volumes peak at 14.4 years of age and generally remain stable before steep later life declines.
Secondary analyses compared initiation of the three most commonly used substances in early adolescence (alcohol, nicotine, and cannabis) with no substance use.
Findings for alcohol largely mirrored those for any substance use. However, the study uncovered additional significant associations, including greater left lateral occipital volume and bilateral para-hippocampal gyri cortical thickness and less bilateral superior frontal gyri cortical thickness.
Nicotine use was associated with lower right superior frontal gyrus volume and deeper left lateral orbitofrontal cortex sulci. And cannabis use was associated with thinner left precentral gyrus and lower right inferior parietal gyrus and right caudate volumes.
The authors noted results for nicotine and cannabis may not have had adequate statistical power, and small effects suggest these findings aren’t clinically informative for individuals. However, they wrote, “They do inform and challenge current theoretical models of addiction.”
Associations Precede Substance Use
A post hoc analysis further challenges current models of addiction. When researchers looked only at the 1203 youth who initiated substance use after the baseline neuroimaging session, they found most associations preceded substance use.
“That regional associations may precede substance use initiation, including less cortical thickness in the right rostral middle frontal gyrus, challenges predominant interpretations that these associations arise largely due to neurotoxic consequences of exposure and increases the plausibility that these features may, at least partially, reflect markers of predispositional risk,” wrote the authors.
A study limitation was that unmeasured confounders and undetected systemic differences in missing data may have influenced associations. Sociodemographic, environmental, and genetic variables that were not included as covariates are likely associated with both neuroanatomical variability and substance use initiation and may moderate associations between them, said the authors.
The ABCD Study provides “a robust and large database of longitudinal data” that goes beyond previous neuroimaging research “to understand the bidirectional relationship between brain structure and substance use,” Miller said in a press release.
“The hope is that these types of studies, in conjunction with other data on environmental exposures and genetic risk, could help change how we think about the development of substance use disorders and inform more accurate models of addiction moving forward,” Miller said.
Reevaluating Causal Assumptions
In an accompanying editorial, Felix Pichardo, MA, and Sylia Wilson, PhD, from the Institute of Child Development, University of Minnesota, Minneapolis, suggested that it may be time to “reevaluate the causal assumptions that underlie brain disease models of addiction” and the mechanisms by which it develops, persists, and becomes harmful.
Neurotoxic effects of substances are central to current brain disease models of addiction, wrote Pichardo and Wilson. “Substance exposure is thought to affect cortical and subcortical regions that support interrelated systems, resulting in desensitization of reward-related processing, increased stress that prompts cravings, negative emotions when cravings are unsated, and weakening of cognitive control abilities that leads to repeated returns to use.”
The editorial writers praised the ABCD Study for its large sample size for providing a level of precision, statistical accuracy, and ability to identify both larger and smaller effects, which are critical for addiction research.
Unlike most addiction research that relies on cross-sectional designs, the current study used longitudinal assessments, which is another of its strengths, they noted.
“Longitudinal study designs like in the ABCD Study are fundamental for establishing temporal ordering across constructs, which is important because establishing temporal precedence is a key step in determining causal links and underlying mechanisms.”
The inclusion of several genetically informative components, such as the family study design, nested twin subsamples, and DNA collection, “allows researchers to extend beyond temporal precedence toward increased causal inference and identification of mechanisms,” they added.
The study received support from the National Institutes of Health. The study authors and editorial writers had no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
FROM JAMA NETWORK OPEN
AI Shows Early Promise in Detecting Infantile Spasms
LOS ANGELES — according to a new study.
Infants with the condition can have poor outcomes with even small delays in diagnosis and ensuing treatment, potentially leading to intellectual disability, autism, and worse epilepsy. “It’s super important to start the treatment early, but oftentimes, these symptoms are just misrecognized by primary care or ER physicians. It takes a long time to diagnose,” said Gadi Miron, MD, who presented the study at the American Epilepsy Society (AES) 78th Annual Meeting 2024.
What Is This? What Should I Do?
Parents who observe unusual behavior often seek advice from friends and family members and receive false reassurance that such behavior isn’t unusual. Even physicians may contribute if they are unaware of infantile spasms, which is a rare disorder. “And then again, they get false reassurance, and because of that false reassurance, you get a diagnostic delay,” said Shaun Hussain, MD, who was asked to comment on the study.
The timing and frequency of infantile spasms create challenges for diagnosis. They only last about 1 second, and they tend to cluster in the morning. By the time a caregiver brings an infant to a healthcare provider, they may have trouble describing the behavior. “Parents are struggling to describe what they saw, and it often just does not resonate, or doesn’t make the healthcare provider think about infantile spasms,” said Hussain.
The idea to employ AI came from looking at videos of infants on YouTube and the realization that many patients upload them in an effort to seek advice. “So many parents upload these videos and ask in the comments, ‘What is this? What should I do? Can somebody help me?’ said Miron, who is a neurologist and researcher at Charité — Universitätsmedizin Berlin in Germany.
AI and Video Can Aid Diagnosis
The researchers built a model that they trained to recognize epileptic spasms using openly available YouTube videos, including 141 infants, 991 recorded seizures, and 597 non-seizure video segments, along with a non-seizure cohort of 127 infants with an accompanying 1385 video segments.
Each video segment was reviewed by two specialists, and they had to agree for it to be counted as an epileptic spasm.
The model detected epileptic seizures with an area under the curve (AUC) of 0.96. It had a sensitivity of 82%, specificity of 90%, and accuracy of 85% when applied to the training set.
The researchers then tested it against three validation sets. In the first, a smartphone-based set retrieved from TikTok of 26 infants with 70 epileptic spasms and 31 non-seizure 5-second video segments, the model had an AUC of 0.98, a sensitivity of 89%, a specificity of 100%, and an accuracy of 92%.
A second smartphone-based set of 67 infants, drawn from YouTube, showed a false detection rate of 0.75% (five detections out of 666 video segments). A third dataset collected from in-hospital EEG monitoring of 21 infants without seizures revealed a false-positive rate of 3.4% (365 of 10,860 video segments).
The group is now developing an app that will allow parents to upload videos that can be analyzed using the model. Physicians can then view the video and determine if there is suspicion of a seizure.
Miron also believes that this approach could find use in other types of seizures and populations, including older children and adults. “We have actually built some models for detection of seizures for videos in adults as well. Looking more towards the future, I’m sure AI will be used to analyze videos of other neurological disorders with motor symptoms [such as] movement disorders and gait,” he said.
Encouraging Early Research
Hussain, who is a professor of pediatrics at UCLA Health, lauded the work generally but emphasized that it is still in the early stage. “Their comparison was a relatively easy one. They’re just comparing normal versus infantile spasms, and they’re looking at the seizure versus normal behavior. Usually, the distinction is much harder in that there are kids who are having behaviors that are maybe other types of seizures, which is much harder to distinguish from infantile spasms, in contrast to just normal behaviors. The other mimic of infantile spasms is things like infant heartburn. Those kids will often have some posturing, and they often will be in pain. They might cry. That’s something that infantile spasms will often generate, so that’s why there’s a lot of confusion between those two,” said Hussain.
He noted that there have been efforts to raise awareness of infantile spasms among physicians and the general public, but that hasn’t reduced the increased detection.
Another Resource
In fact, parents with suspicions often go to social media sites like YouTube and a Facebook group dedicated to infantile spasms. “You can Google infantile spasms, and you’ll see examples of weird behaviors, and then you’ll look in the comments, and you’ll see this commenter said: ‘These could be infantile spasms. You should go to a children’s hospital. Don’t leave until you get an EEG to make sure that these are not seizures. There’s all kinds of great advice there, and it really shouldn’t be the situation where to get the best care, you need to go on YouTube,’ ” said Hussain.
Miron and Hussain had no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
LOS ANGELES — according to a new study.
Infants with the condition can have poor outcomes with even small delays in diagnosis and ensuing treatment, potentially leading to intellectual disability, autism, and worse epilepsy. “It’s super important to start the treatment early, but oftentimes, these symptoms are just misrecognized by primary care or ER physicians. It takes a long time to diagnose,” said Gadi Miron, MD, who presented the study at the American Epilepsy Society (AES) 78th Annual Meeting 2024.
What Is This? What Should I Do?
Parents who observe unusual behavior often seek advice from friends and family members and receive false reassurance that such behavior isn’t unusual. Even physicians may contribute if they are unaware of infantile spasms, which is a rare disorder. “And then again, they get false reassurance, and because of that false reassurance, you get a diagnostic delay,” said Shaun Hussain, MD, who was asked to comment on the study.
The timing and frequency of infantile spasms create challenges for diagnosis. They only last about 1 second, and they tend to cluster in the morning. By the time a caregiver brings an infant to a healthcare provider, they may have trouble describing the behavior. “Parents are struggling to describe what they saw, and it often just does not resonate, or doesn’t make the healthcare provider think about infantile spasms,” said Hussain.
The idea to employ AI came from looking at videos of infants on YouTube and the realization that many patients upload them in an effort to seek advice. “So many parents upload these videos and ask in the comments, ‘What is this? What should I do? Can somebody help me?’ said Miron, who is a neurologist and researcher at Charité — Universitätsmedizin Berlin in Germany.
AI and Video Can Aid Diagnosis
The researchers built a model that they trained to recognize epileptic spasms using openly available YouTube videos, including 141 infants, 991 recorded seizures, and 597 non-seizure video segments, along with a non-seizure cohort of 127 infants with an accompanying 1385 video segments.
Each video segment was reviewed by two specialists, and they had to agree for it to be counted as an epileptic spasm.
The model detected epileptic seizures with an area under the curve (AUC) of 0.96. It had a sensitivity of 82%, specificity of 90%, and accuracy of 85% when applied to the training set.
The researchers then tested it against three validation sets. In the first, a smartphone-based set retrieved from TikTok of 26 infants with 70 epileptic spasms and 31 non-seizure 5-second video segments, the model had an AUC of 0.98, a sensitivity of 89%, a specificity of 100%, and an accuracy of 92%.
A second smartphone-based set of 67 infants, drawn from YouTube, showed a false detection rate of 0.75% (five detections out of 666 video segments). A third dataset collected from in-hospital EEG monitoring of 21 infants without seizures revealed a false-positive rate of 3.4% (365 of 10,860 video segments).
The group is now developing an app that will allow parents to upload videos that can be analyzed using the model. Physicians can then view the video and determine if there is suspicion of a seizure.
Miron also believes that this approach could find use in other types of seizures and populations, including older children and adults. “We have actually built some models for detection of seizures for videos in adults as well. Looking more towards the future, I’m sure AI will be used to analyze videos of other neurological disorders with motor symptoms [such as] movement disorders and gait,” he said.
Encouraging Early Research
Hussain, who is a professor of pediatrics at UCLA Health, lauded the work generally but emphasized that it is still in the early stage. “Their comparison was a relatively easy one. They’re just comparing normal versus infantile spasms, and they’re looking at the seizure versus normal behavior. Usually, the distinction is much harder in that there are kids who are having behaviors that are maybe other types of seizures, which is much harder to distinguish from infantile spasms, in contrast to just normal behaviors. The other mimic of infantile spasms is things like infant heartburn. Those kids will often have some posturing, and they often will be in pain. They might cry. That’s something that infantile spasms will often generate, so that’s why there’s a lot of confusion between those two,” said Hussain.
He noted that there have been efforts to raise awareness of infantile spasms among physicians and the general public, but that hasn’t reduced the increased detection.
Another Resource
In fact, parents with suspicions often go to social media sites like YouTube and a Facebook group dedicated to infantile spasms. “You can Google infantile spasms, and you’ll see examples of weird behaviors, and then you’ll look in the comments, and you’ll see this commenter said: ‘These could be infantile spasms. You should go to a children’s hospital. Don’t leave until you get an EEG to make sure that these are not seizures. There’s all kinds of great advice there, and it really shouldn’t be the situation where to get the best care, you need to go on YouTube,’ ” said Hussain.
Miron and Hussain had no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
LOS ANGELES — according to a new study.
Infants with the condition can have poor outcomes with even small delays in diagnosis and ensuing treatment, potentially leading to intellectual disability, autism, and worse epilepsy. “It’s super important to start the treatment early, but oftentimes, these symptoms are just misrecognized by primary care or ER physicians. It takes a long time to diagnose,” said Gadi Miron, MD, who presented the study at the American Epilepsy Society (AES) 78th Annual Meeting 2024.
What Is This? What Should I Do?
Parents who observe unusual behavior often seek advice from friends and family members and receive false reassurance that such behavior isn’t unusual. Even physicians may contribute if they are unaware of infantile spasms, which is a rare disorder. “And then again, they get false reassurance, and because of that false reassurance, you get a diagnostic delay,” said Shaun Hussain, MD, who was asked to comment on the study.
The timing and frequency of infantile spasms create challenges for diagnosis. They only last about 1 second, and they tend to cluster in the morning. By the time a caregiver brings an infant to a healthcare provider, they may have trouble describing the behavior. “Parents are struggling to describe what they saw, and it often just does not resonate, or doesn’t make the healthcare provider think about infantile spasms,” said Hussain.
The idea to employ AI came from looking at videos of infants on YouTube and the realization that many patients upload them in an effort to seek advice. “So many parents upload these videos and ask in the comments, ‘What is this? What should I do? Can somebody help me?’ said Miron, who is a neurologist and researcher at Charité — Universitätsmedizin Berlin in Germany.
AI and Video Can Aid Diagnosis
The researchers built a model that they trained to recognize epileptic spasms using openly available YouTube videos, including 141 infants, 991 recorded seizures, and 597 non-seizure video segments, along with a non-seizure cohort of 127 infants with an accompanying 1385 video segments.
Each video segment was reviewed by two specialists, and they had to agree for it to be counted as an epileptic spasm.
The model detected epileptic seizures with an area under the curve (AUC) of 0.96. It had a sensitivity of 82%, specificity of 90%, and accuracy of 85% when applied to the training set.
The researchers then tested it against three validation sets. In the first, a smartphone-based set retrieved from TikTok of 26 infants with 70 epileptic spasms and 31 non-seizure 5-second video segments, the model had an AUC of 0.98, a sensitivity of 89%, a specificity of 100%, and an accuracy of 92%.
A second smartphone-based set of 67 infants, drawn from YouTube, showed a false detection rate of 0.75% (five detections out of 666 video segments). A third dataset collected from in-hospital EEG monitoring of 21 infants without seizures revealed a false-positive rate of 3.4% (365 of 10,860 video segments).
The group is now developing an app that will allow parents to upload videos that can be analyzed using the model. Physicians can then view the video and determine if there is suspicion of a seizure.
Miron also believes that this approach could find use in other types of seizures and populations, including older children and adults. “We have actually built some models for detection of seizures for videos in adults as well. Looking more towards the future, I’m sure AI will be used to analyze videos of other neurological disorders with motor symptoms [such as] movement disorders and gait,” he said.
Encouraging Early Research
Hussain, who is a professor of pediatrics at UCLA Health, lauded the work generally but emphasized that it is still in the early stage. “Their comparison was a relatively easy one. They’re just comparing normal versus infantile spasms, and they’re looking at the seizure versus normal behavior. Usually, the distinction is much harder in that there are kids who are having behaviors that are maybe other types of seizures, which is much harder to distinguish from infantile spasms, in contrast to just normal behaviors. The other mimic of infantile spasms is things like infant heartburn. Those kids will often have some posturing, and they often will be in pain. They might cry. That’s something that infantile spasms will often generate, so that’s why there’s a lot of confusion between those two,” said Hussain.
He noted that there have been efforts to raise awareness of infantile spasms among physicians and the general public, but that hasn’t reduced the increased detection.
Another Resource
In fact, parents with suspicions often go to social media sites like YouTube and a Facebook group dedicated to infantile spasms. “You can Google infantile spasms, and you’ll see examples of weird behaviors, and then you’ll look in the comments, and you’ll see this commenter said: ‘These could be infantile spasms. You should go to a children’s hospital. Don’t leave until you get an EEG to make sure that these are not seizures. There’s all kinds of great advice there, and it really shouldn’t be the situation where to get the best care, you need to go on YouTube,’ ” said Hussain.
Miron and Hussain had no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
FROM AES 2024