User login
Concussion burden tied to later hypertension in football players
a new study suggests.
Among more than 4,000 participants, 37% had hypertension at a median of 24 years post career and reported a median concussion symptom score (CSS) of 23 on a scale of 0 to 130.
“We have long seen an incompletely explained link between football participation and later-life cardiovascular disease,” Aaron L. Baggish, MD, of Massachusetts Hospital and Harvard Medical School, Boston, told this news organization.
“This study tested [whether] concussion burden during years of active play would be a determinant of later-life hypertension, the most common cause of cardiovascular disease, and indeed found this relationship to be a strong one.”
The study was published online in Circulation.
Link to cognitive decline?
Dr. Baggish and colleagues recruited former professional American-style football (ASF) players to participate in a survey administered by the Football Players Health Study at Harvard University.
Concussion burden was quantified with respect to the occurrence and severity of common concussion symptoms – e.g., headaches, nausea, dizziness, confusion, loss of consciousness (LOC), disorientation, and feeling unsteady on one’s feet – over years of active participation.
Prevalent hypertension was determined either by the participants’ previously receiving from a clinician a recommendation for medication for “high blood pressure” or by the participants’ taking such medication at the time of survey completion. Diabetes status was determined by the participants’ receiving a prior recommendation for or prescription for “diabetes or high blood sugar” medication.
Of 15,070 invited to participate in the study, 4,168 did so. The mean age of the participants was 51.8 years; 39.4% were Black; the mean body mass index was 31.3; and 33.9% were linemen. Participants played for a mean of 6.9 seasons and were surveyed at a median 24.1 years post ASF career completion. The median CSS was 23.
A total of 1,542 participants (37.3%) had hypertension, and 8.8% had diabetes.
After adjustment for established hypertension risk factors, including smoking, race, diabetes, age, and BMI, there was a graded association between CSS category and odds of later-life hypertension and between high CSS exposure and prevalent hypertension.
Results persisted when LOC, a single highly specific severe concussion symptom, was used in isolation as a surrogate for CSS, the investigators noted.
“These results suggest that repetitive early-life brain injury may have later-life implications for cardiovascular health,” they wrote. They also noted that hypertension has been shown to independently increase the risk of cognitive decline.
While premature cognitive decline among ASF players is generally attributed to chronic traumatic encephalopathy, “data from the current study raise the possibility that some element of cognitive decline among former ASF players may be attributable to hypertension,” which is potentially treatable.
“Future studies clarifying associations and causal pathways between brain injury, hypertension, and brain health are warranted,” they concluded.
Dr. Baggish added, “We hope that clinicians will now understand that head injury is an independent risk factor for high blood pressure and will screen vulnerable populations accordingly, as this may lead to better recognition of previously underdiagnosed hypertension with subsequent opportunities for intervention.”
Close monitoring
Commenting on the study, Jonathan Kim, MD, chair-elect of the American College of Cardiology’s Sports–Cardiology Section and chief of sports cardiology at Emory University in Atlanta, said, “They clearly show an independent association, which is not causality but is a new finding that requires more research. To me, it really emphasizes that cardiovascular risk is the most important health consequence that we should be worried about in retired NFL [National Football League] players.
“There are multifactorial reasons – not just repetitive head trauma – why this athletic population is at risk for the development of high blood pressure, even among college players,” he said.
Dr. Kim’s team has shown in studies conducted in collaboration with Dr. Baggish and others that collegiate football players who gain weight and develop increased systolic blood pressure are at risk of developing a “pathologic” cardiovascular phenotype.
Other research from this group showed links between nonsteroidal anti-inflammatory drug use among high school and collegiate ASF players and increased cardiovascular risk, as well as ASF-associated hypertension and ventricular-arterial coupling.
The suggestion that late-life hypertension could play a role in premature cognitive decline among ASF players “warrants further study,” Dr. Kim said, “because we do know that hypertension in the general population can be associated with cognitive decline. So that’s an important future direction.”
He concluded: “It’s a matter of focusing on cardiac prevention.” After their careers, players should be counseled on the importance of losing weight and adopting heart-healthy habits. In addition to some of the traditional concerns that might lead to closer follow-up of these patients, “having a lot of concussions in the history could potentially be another risk factor that should warrant close monitoring of blood pressure and, of course, treatment if necessary.”
The study was supported by Harvard Catalyst/the Harvard Clinical and Translational Science Center and the NFL Players Association. Dr. Baggish and several coauthors have received funding from the NFL Players Association.
A version of this article originally appeared on Medscape.com.
a new study suggests.
Among more than 4,000 participants, 37% had hypertension at a median of 24 years post career and reported a median concussion symptom score (CSS) of 23 on a scale of 0 to 130.
“We have long seen an incompletely explained link between football participation and later-life cardiovascular disease,” Aaron L. Baggish, MD, of Massachusetts Hospital and Harvard Medical School, Boston, told this news organization.
“This study tested [whether] concussion burden during years of active play would be a determinant of later-life hypertension, the most common cause of cardiovascular disease, and indeed found this relationship to be a strong one.”
The study was published online in Circulation.
Link to cognitive decline?
Dr. Baggish and colleagues recruited former professional American-style football (ASF) players to participate in a survey administered by the Football Players Health Study at Harvard University.
Concussion burden was quantified with respect to the occurrence and severity of common concussion symptoms – e.g., headaches, nausea, dizziness, confusion, loss of consciousness (LOC), disorientation, and feeling unsteady on one’s feet – over years of active participation.
Prevalent hypertension was determined either by the participants’ previously receiving from a clinician a recommendation for medication for “high blood pressure” or by the participants’ taking such medication at the time of survey completion. Diabetes status was determined by the participants’ receiving a prior recommendation for or prescription for “diabetes or high blood sugar” medication.
Of 15,070 invited to participate in the study, 4,168 did so. The mean age of the participants was 51.8 years; 39.4% were Black; the mean body mass index was 31.3; and 33.9% were linemen. Participants played for a mean of 6.9 seasons and were surveyed at a median 24.1 years post ASF career completion. The median CSS was 23.
A total of 1,542 participants (37.3%) had hypertension, and 8.8% had diabetes.
After adjustment for established hypertension risk factors, including smoking, race, diabetes, age, and BMI, there was a graded association between CSS category and odds of later-life hypertension and between high CSS exposure and prevalent hypertension.
Results persisted when LOC, a single highly specific severe concussion symptom, was used in isolation as a surrogate for CSS, the investigators noted.
“These results suggest that repetitive early-life brain injury may have later-life implications for cardiovascular health,” they wrote. They also noted that hypertension has been shown to independently increase the risk of cognitive decline.
While premature cognitive decline among ASF players is generally attributed to chronic traumatic encephalopathy, “data from the current study raise the possibility that some element of cognitive decline among former ASF players may be attributable to hypertension,” which is potentially treatable.
“Future studies clarifying associations and causal pathways between brain injury, hypertension, and brain health are warranted,” they concluded.
Dr. Baggish added, “We hope that clinicians will now understand that head injury is an independent risk factor for high blood pressure and will screen vulnerable populations accordingly, as this may lead to better recognition of previously underdiagnosed hypertension with subsequent opportunities for intervention.”
Close monitoring
Commenting on the study, Jonathan Kim, MD, chair-elect of the American College of Cardiology’s Sports–Cardiology Section and chief of sports cardiology at Emory University in Atlanta, said, “They clearly show an independent association, which is not causality but is a new finding that requires more research. To me, it really emphasizes that cardiovascular risk is the most important health consequence that we should be worried about in retired NFL [National Football League] players.
“There are multifactorial reasons – not just repetitive head trauma – why this athletic population is at risk for the development of high blood pressure, even among college players,” he said.
Dr. Kim’s team has shown in studies conducted in collaboration with Dr. Baggish and others that collegiate football players who gain weight and develop increased systolic blood pressure are at risk of developing a “pathologic” cardiovascular phenotype.
Other research from this group showed links between nonsteroidal anti-inflammatory drug use among high school and collegiate ASF players and increased cardiovascular risk, as well as ASF-associated hypertension and ventricular-arterial coupling.
The suggestion that late-life hypertension could play a role in premature cognitive decline among ASF players “warrants further study,” Dr. Kim said, “because we do know that hypertension in the general population can be associated with cognitive decline. So that’s an important future direction.”
He concluded: “It’s a matter of focusing on cardiac prevention.” After their careers, players should be counseled on the importance of losing weight and adopting heart-healthy habits. In addition to some of the traditional concerns that might lead to closer follow-up of these patients, “having a lot of concussions in the history could potentially be another risk factor that should warrant close monitoring of blood pressure and, of course, treatment if necessary.”
The study was supported by Harvard Catalyst/the Harvard Clinical and Translational Science Center and the NFL Players Association. Dr. Baggish and several coauthors have received funding from the NFL Players Association.
A version of this article originally appeared on Medscape.com.
a new study suggests.
Among more than 4,000 participants, 37% had hypertension at a median of 24 years post career and reported a median concussion symptom score (CSS) of 23 on a scale of 0 to 130.
“We have long seen an incompletely explained link between football participation and later-life cardiovascular disease,” Aaron L. Baggish, MD, of Massachusetts Hospital and Harvard Medical School, Boston, told this news organization.
“This study tested [whether] concussion burden during years of active play would be a determinant of later-life hypertension, the most common cause of cardiovascular disease, and indeed found this relationship to be a strong one.”
The study was published online in Circulation.
Link to cognitive decline?
Dr. Baggish and colleagues recruited former professional American-style football (ASF) players to participate in a survey administered by the Football Players Health Study at Harvard University.
Concussion burden was quantified with respect to the occurrence and severity of common concussion symptoms – e.g., headaches, nausea, dizziness, confusion, loss of consciousness (LOC), disorientation, and feeling unsteady on one’s feet – over years of active participation.
Prevalent hypertension was determined either by the participants’ previously receiving from a clinician a recommendation for medication for “high blood pressure” or by the participants’ taking such medication at the time of survey completion. Diabetes status was determined by the participants’ receiving a prior recommendation for or prescription for “diabetes or high blood sugar” medication.
Of 15,070 invited to participate in the study, 4,168 did so. The mean age of the participants was 51.8 years; 39.4% were Black; the mean body mass index was 31.3; and 33.9% were linemen. Participants played for a mean of 6.9 seasons and were surveyed at a median 24.1 years post ASF career completion. The median CSS was 23.
A total of 1,542 participants (37.3%) had hypertension, and 8.8% had diabetes.
After adjustment for established hypertension risk factors, including smoking, race, diabetes, age, and BMI, there was a graded association between CSS category and odds of later-life hypertension and between high CSS exposure and prevalent hypertension.
Results persisted when LOC, a single highly specific severe concussion symptom, was used in isolation as a surrogate for CSS, the investigators noted.
“These results suggest that repetitive early-life brain injury may have later-life implications for cardiovascular health,” they wrote. They also noted that hypertension has been shown to independently increase the risk of cognitive decline.
While premature cognitive decline among ASF players is generally attributed to chronic traumatic encephalopathy, “data from the current study raise the possibility that some element of cognitive decline among former ASF players may be attributable to hypertension,” which is potentially treatable.
“Future studies clarifying associations and causal pathways between brain injury, hypertension, and brain health are warranted,” they concluded.
Dr. Baggish added, “We hope that clinicians will now understand that head injury is an independent risk factor for high blood pressure and will screen vulnerable populations accordingly, as this may lead to better recognition of previously underdiagnosed hypertension with subsequent opportunities for intervention.”
Close monitoring
Commenting on the study, Jonathan Kim, MD, chair-elect of the American College of Cardiology’s Sports–Cardiology Section and chief of sports cardiology at Emory University in Atlanta, said, “They clearly show an independent association, which is not causality but is a new finding that requires more research. To me, it really emphasizes that cardiovascular risk is the most important health consequence that we should be worried about in retired NFL [National Football League] players.
“There are multifactorial reasons – not just repetitive head trauma – why this athletic population is at risk for the development of high blood pressure, even among college players,” he said.
Dr. Kim’s team has shown in studies conducted in collaboration with Dr. Baggish and others that collegiate football players who gain weight and develop increased systolic blood pressure are at risk of developing a “pathologic” cardiovascular phenotype.
Other research from this group showed links between nonsteroidal anti-inflammatory drug use among high school and collegiate ASF players and increased cardiovascular risk, as well as ASF-associated hypertension and ventricular-arterial coupling.
The suggestion that late-life hypertension could play a role in premature cognitive decline among ASF players “warrants further study,” Dr. Kim said, “because we do know that hypertension in the general population can be associated with cognitive decline. So that’s an important future direction.”
He concluded: “It’s a matter of focusing on cardiac prevention.” After their careers, players should be counseled on the importance of losing weight and adopting heart-healthy habits. In addition to some of the traditional concerns that might lead to closer follow-up of these patients, “having a lot of concussions in the history could potentially be another risk factor that should warrant close monitoring of blood pressure and, of course, treatment if necessary.”
The study was supported by Harvard Catalyst/the Harvard Clinical and Translational Science Center and the NFL Players Association. Dr. Baggish and several coauthors have received funding from the NFL Players Association.
A version of this article originally appeared on Medscape.com.
FROM CIRCULATION
Spinal cord stimulation restores poststroke arm, hand function in two patients
The results provide “promising, albeit preliminary, evidence that spinal cord stimulation could be an assistive as well as a restorative approach for upper-limb recovery after stroke,” wrote first author Marc P. Powell, PhD, of Reach Neuro Inc., Pittsburgh, and colleagues.
The findings were published online in Nature Medicine.
Top cause of paralysis
“Stroke is the largest cause of paralysis in the world,” with nearly three-quarters of patients with stroke experiencing lasting deficits in motor control of their arm and hand, co–senior study author Marco Capogrosso, PhD, assistant professor of neurological surgery at the University of Pittsburgh, said during a press briefing.
Stroke can disrupt communication between the brain and the spinal cord, leading to motor deficits in the arm and hand. However, below the lesion, the spinal circuits that control movement remain intact and could be targeted to restore function, Dr. Capogrosso noted.
Spinal cord stimulation has shown promise in promoting long-lasting recovery of leg motor function in patients with spinal cord injury; but until now, it’s been largely unexplored for upper-limb recovery.
In this “first-in-human” study, the investigators percutaneously implanted two linear leads in the dorsolateral epidural space targeting neural circuits that control arm and hand muscles in two patients.
One of the patients was a woman (age, 31 years) who had experienced a right thalamic hemorrhagic stroke secondary to a cavernous malformation 9 years before enrolling in the pilot study.
The other patient was a woman (age, 47 years) who experienced a right ischemic middle cerebral artery (MCA) stroke secondary to a right carotid dissection, resulting in a large MCA territory infarct 3 years before entering the study.
In both patients, continuous stimulation of the targeted neural circuits led to significant and immediate improvement in arm and hand strength and dexterity. This enabled the patients to perform movements that they couldn’t perform without spinal cord stimulation.
The process also enabled fine motor skills, such as opening a lock and using utensils to eat independently – tasks that the younger woman had not been able to do for 9 years.
“Perhaps even more interesting, we found that after a few weeks of use, some of these improvements endure when the stimulation is switched off, indicating exciting avenues for the future of stroke therapies,” Dr. Capogrosso said in a news release.
No serious adverse events were reported.
‘Easily translated’
Dr. Capogrosso said that, thanks to years of preclinical research, the investigators have developed a practical, easy-to-use stimulation protocol adapting existing clinical technologies that “could be easily translated to the hospital and quickly moved from the lab to the clinic.”
The researchers noted, however, that further studies in larger cohorts will be required to validate the safety and efficacy of this approach.
They are currently working with more patients with stroke to fine-tune placement of the leads and stimulation protocol, as well as determine which patients are best suited for the approach.
“Creating effective neurorehabilitation solutions for people affected by movement impairment after stroke is becoming ever more urgent,” co–senior author Elvira Pirondini, PhD, assistant professor of physical medicine and rehabilitation at the University of Pittsburgh, said in the release.
“Even mild deficits resulting from a stroke can isolate people from social and professional lives and become very debilitating, with motor impairments in the arm and hand being especially taxing and impeding simple daily activities, such as writing, eating, and getting dressed,” she added.
This research was funded by the National Institutes of Health BRAIN Initiative, with additional research support provided by the Department of Neurological Surgery and the Department of Physical Medicine and Rehabilitation at Pitt, and the Department of Mechanical Engineering and the Neuroscience Institute at Carnegie Mellon University. Three investigators have financial interests in Reach Neuro, which has an interest in the technology being evaluated in this study.
A version of this article first appeared on Medscape.com.
The results provide “promising, albeit preliminary, evidence that spinal cord stimulation could be an assistive as well as a restorative approach for upper-limb recovery after stroke,” wrote first author Marc P. Powell, PhD, of Reach Neuro Inc., Pittsburgh, and colleagues.
The findings were published online in Nature Medicine.
Top cause of paralysis
“Stroke is the largest cause of paralysis in the world,” with nearly three-quarters of patients with stroke experiencing lasting deficits in motor control of their arm and hand, co–senior study author Marco Capogrosso, PhD, assistant professor of neurological surgery at the University of Pittsburgh, said during a press briefing.
Stroke can disrupt communication between the brain and the spinal cord, leading to motor deficits in the arm and hand. However, below the lesion, the spinal circuits that control movement remain intact and could be targeted to restore function, Dr. Capogrosso noted.
Spinal cord stimulation has shown promise in promoting long-lasting recovery of leg motor function in patients with spinal cord injury; but until now, it’s been largely unexplored for upper-limb recovery.
In this “first-in-human” study, the investigators percutaneously implanted two linear leads in the dorsolateral epidural space targeting neural circuits that control arm and hand muscles in two patients.
One of the patients was a woman (age, 31 years) who had experienced a right thalamic hemorrhagic stroke secondary to a cavernous malformation 9 years before enrolling in the pilot study.
The other patient was a woman (age, 47 years) who experienced a right ischemic middle cerebral artery (MCA) stroke secondary to a right carotid dissection, resulting in a large MCA territory infarct 3 years before entering the study.
In both patients, continuous stimulation of the targeted neural circuits led to significant and immediate improvement in arm and hand strength and dexterity. This enabled the patients to perform movements that they couldn’t perform without spinal cord stimulation.
The process also enabled fine motor skills, such as opening a lock and using utensils to eat independently – tasks that the younger woman had not been able to do for 9 years.
“Perhaps even more interesting, we found that after a few weeks of use, some of these improvements endure when the stimulation is switched off, indicating exciting avenues for the future of stroke therapies,” Dr. Capogrosso said in a news release.
No serious adverse events were reported.
‘Easily translated’
Dr. Capogrosso said that, thanks to years of preclinical research, the investigators have developed a practical, easy-to-use stimulation protocol adapting existing clinical technologies that “could be easily translated to the hospital and quickly moved from the lab to the clinic.”
The researchers noted, however, that further studies in larger cohorts will be required to validate the safety and efficacy of this approach.
They are currently working with more patients with stroke to fine-tune placement of the leads and stimulation protocol, as well as determine which patients are best suited for the approach.
“Creating effective neurorehabilitation solutions for people affected by movement impairment after stroke is becoming ever more urgent,” co–senior author Elvira Pirondini, PhD, assistant professor of physical medicine and rehabilitation at the University of Pittsburgh, said in the release.
“Even mild deficits resulting from a stroke can isolate people from social and professional lives and become very debilitating, with motor impairments in the arm and hand being especially taxing and impeding simple daily activities, such as writing, eating, and getting dressed,” she added.
This research was funded by the National Institutes of Health BRAIN Initiative, with additional research support provided by the Department of Neurological Surgery and the Department of Physical Medicine and Rehabilitation at Pitt, and the Department of Mechanical Engineering and the Neuroscience Institute at Carnegie Mellon University. Three investigators have financial interests in Reach Neuro, which has an interest in the technology being evaluated in this study.
A version of this article first appeared on Medscape.com.
The results provide “promising, albeit preliminary, evidence that spinal cord stimulation could be an assistive as well as a restorative approach for upper-limb recovery after stroke,” wrote first author Marc P. Powell, PhD, of Reach Neuro Inc., Pittsburgh, and colleagues.
The findings were published online in Nature Medicine.
Top cause of paralysis
“Stroke is the largest cause of paralysis in the world,” with nearly three-quarters of patients with stroke experiencing lasting deficits in motor control of their arm and hand, co–senior study author Marco Capogrosso, PhD, assistant professor of neurological surgery at the University of Pittsburgh, said during a press briefing.
Stroke can disrupt communication between the brain and the spinal cord, leading to motor deficits in the arm and hand. However, below the lesion, the spinal circuits that control movement remain intact and could be targeted to restore function, Dr. Capogrosso noted.
Spinal cord stimulation has shown promise in promoting long-lasting recovery of leg motor function in patients with spinal cord injury; but until now, it’s been largely unexplored for upper-limb recovery.
In this “first-in-human” study, the investigators percutaneously implanted two linear leads in the dorsolateral epidural space targeting neural circuits that control arm and hand muscles in two patients.
One of the patients was a woman (age, 31 years) who had experienced a right thalamic hemorrhagic stroke secondary to a cavernous malformation 9 years before enrolling in the pilot study.
The other patient was a woman (age, 47 years) who experienced a right ischemic middle cerebral artery (MCA) stroke secondary to a right carotid dissection, resulting in a large MCA territory infarct 3 years before entering the study.
In both patients, continuous stimulation of the targeted neural circuits led to significant and immediate improvement in arm and hand strength and dexterity. This enabled the patients to perform movements that they couldn’t perform without spinal cord stimulation.
The process also enabled fine motor skills, such as opening a lock and using utensils to eat independently – tasks that the younger woman had not been able to do for 9 years.
“Perhaps even more interesting, we found that after a few weeks of use, some of these improvements endure when the stimulation is switched off, indicating exciting avenues for the future of stroke therapies,” Dr. Capogrosso said in a news release.
No serious adverse events were reported.
‘Easily translated’
Dr. Capogrosso said that, thanks to years of preclinical research, the investigators have developed a practical, easy-to-use stimulation protocol adapting existing clinical technologies that “could be easily translated to the hospital and quickly moved from the lab to the clinic.”
The researchers noted, however, that further studies in larger cohorts will be required to validate the safety and efficacy of this approach.
They are currently working with more patients with stroke to fine-tune placement of the leads and stimulation protocol, as well as determine which patients are best suited for the approach.
“Creating effective neurorehabilitation solutions for people affected by movement impairment after stroke is becoming ever more urgent,” co–senior author Elvira Pirondini, PhD, assistant professor of physical medicine and rehabilitation at the University of Pittsburgh, said in the release.
“Even mild deficits resulting from a stroke can isolate people from social and professional lives and become very debilitating, with motor impairments in the arm and hand being especially taxing and impeding simple daily activities, such as writing, eating, and getting dressed,” she added.
This research was funded by the National Institutes of Health BRAIN Initiative, with additional research support provided by the Department of Neurological Surgery and the Department of Physical Medicine and Rehabilitation at Pitt, and the Department of Mechanical Engineering and the Neuroscience Institute at Carnegie Mellon University. Three investigators have financial interests in Reach Neuro, which has an interest in the technology being evaluated in this study.
A version of this article first appeared on Medscape.com.
FROM NATURE MEDICINE
Two cups of coffee increase heart dangers with hypertension
according to researchers at Institute for Global Health Policy Research, Bureau of International Health Cooperation, National Center for Global Health and Medicine, Tokyo.
What to know
People with severely high blood pressure who drink two or more cups of caffeinated coffee each day could double their risk of dying from a heart attack, stroke, or any type of cardiovascular disease.
Too much coffee may raise blood pressure and lead to anxiety, heart palpitations, and difficulty sleeping.
An 8-ounce cup of coffee has 80-100 mg of caffeine, while an 8-ounce cup of green or black tea has 30-50 mg.
Drinking one cup of coffee a day or any amount of green tea was not associated with risk of death across any blood pressure categories, and drinking green tea was not associated with increased risk of death related to cardiovascular disease at any blood pressure level.
Frequent consumers of coffee were more likely to be younger, current smokers, current drinkers, to eat fewer vegetables, and to have higher total cholesterol levels and lower systolic blood pressure regardless of their blood pressure category.
This is a summary of the article “Coffee and Green Tea Consumption and Cardiovascular Disease Mortality Among People With and Without Hypertension,” published in the Journal of the American Heart Association.
A version of this article first appeared on Medscape.com.
according to researchers at Institute for Global Health Policy Research, Bureau of International Health Cooperation, National Center for Global Health and Medicine, Tokyo.
What to know
People with severely high blood pressure who drink two or more cups of caffeinated coffee each day could double their risk of dying from a heart attack, stroke, or any type of cardiovascular disease.
Too much coffee may raise blood pressure and lead to anxiety, heart palpitations, and difficulty sleeping.
An 8-ounce cup of coffee has 80-100 mg of caffeine, while an 8-ounce cup of green or black tea has 30-50 mg.
Drinking one cup of coffee a day or any amount of green tea was not associated with risk of death across any blood pressure categories, and drinking green tea was not associated with increased risk of death related to cardiovascular disease at any blood pressure level.
Frequent consumers of coffee were more likely to be younger, current smokers, current drinkers, to eat fewer vegetables, and to have higher total cholesterol levels and lower systolic blood pressure regardless of their blood pressure category.
This is a summary of the article “Coffee and Green Tea Consumption and Cardiovascular Disease Mortality Among People With and Without Hypertension,” published in the Journal of the American Heart Association.
A version of this article first appeared on Medscape.com.
according to researchers at Institute for Global Health Policy Research, Bureau of International Health Cooperation, National Center for Global Health and Medicine, Tokyo.
What to know
People with severely high blood pressure who drink two or more cups of caffeinated coffee each day could double their risk of dying from a heart attack, stroke, or any type of cardiovascular disease.
Too much coffee may raise blood pressure and lead to anxiety, heart palpitations, and difficulty sleeping.
An 8-ounce cup of coffee has 80-100 mg of caffeine, while an 8-ounce cup of green or black tea has 30-50 mg.
Drinking one cup of coffee a day or any amount of green tea was not associated with risk of death across any blood pressure categories, and drinking green tea was not associated with increased risk of death related to cardiovascular disease at any blood pressure level.
Frequent consumers of coffee were more likely to be younger, current smokers, current drinkers, to eat fewer vegetables, and to have higher total cholesterol levels and lower systolic blood pressure regardless of their blood pressure category.
This is a summary of the article “Coffee and Green Tea Consumption and Cardiovascular Disease Mortality Among People With and Without Hypertension,” published in the Journal of the American Heart Association.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF AMERICAN HEART ASSOCIATION
‘Quick, affordable’ test helps predict CGRP response for migraine
new research suggests.
The ictal phase refers to “sensitization occurring during a time when central trigeminovascular neurons receive massive nociceptive input from active meningeal nociceptors,” whereas the nonictal phase refers to “sensitization occurring during a time when central trigeminovascular neurons receive no or subliminal nociceptive input from meningeal nociceptors,” investigators noted.
In an observational, open-label cohort study, pretreatment nonictal cephalic allodynia identified galcanezumab responders with nearly 80% accuracy, and it identified nonresponders with nearly 85% accuracy.
“Detection of nonictal allodynia with a simplified paradigm of Quantitative Sensory Testing (QST) may provide a quick, affordable, noninvasive, and patient-friendly way to prospectively distinguish between responders and nonresponders to the prophylactic treatment of chronic and high-frequency episodic migraine with drugs that reduce CGRP signaling,” Sait Ashina, MD, of Beth Israel Deaconess Medical Center and Harvard Medical School, both in Boston, and colleagues wrote.
The findings were published online in Cephalalgia.
Immediate clinical relevance
Investigator Rami Burstein, PhD, also with Beth Israel Deaconess Medical Center and Harvard Medical School, developed the concept of predicting response to anti-CGRP treatment by testing for the presence or absence of nonictal cephalic allodynia in collaboration with the company CGRP Diagnostics.
In 43 anti–CGRP-naive patients with migraine, the researchers used a simplified QST algorithm to determine the presence/absence of cephalic or extracephalic allodynia during the nonictal phase of migraine – defined as the period from less than 12 hours after a migraine attack to less than 12 hours before the next attack.
Patients were considered to have allodynia if heat pain thresholds were between 32° C and 40° C, if cold pain thresholds were between 32° C and 20° C, or if the mechanical pain was threshold was less than 60 g.
Using these strict criteria, pretreatment nonictal cephalic allodynia was a statistically significant predictor of response to anti-CGRP therapy. It was present in 84% of the 19 nonresponders and was absent in 79% of the 24 responders, for an overall accuracy rate of 86% (P < .0001).
Nonictal cephalic allodynia was “consistently” predictive of response for patients with chronic migraine as well as for those with high-frequency episodic migraine, the researchers reported.
In contrast, they noted that assessing nonictal extracephalic allodynia with QST missed nearly 50% of the patients with allodynia among the nonresponders (accuracy rate of 42%) and added little to the assessment of allodynia among the responders.
Mark Hasleton, PhD, CEO of CGRP Diagnostics, said in an interview that the study shows it’s possible to determine response to anti-CGRP therapy and to prescribe these medications to patients who are most likely to respond.
Dr. Hasleton, who was not personally involved with the current study, noted that pretreatment testing for nonictal cephalic allodynia may also allow for earlier prescription of anti-CGRP therapy and potentially dispense without the need for the current trial-and-error approach to prescribing. He noted that if one anti-CGRP fails the patient, it is highly likely that others will also fail.
Given the “very high correlation of the presence of nonictal cephalic allodynia in responders to galcanezumab, our recommendation would be to routinely pretest all potential anti-CGRP candidates prior to prescription,” he said.
End of trial-and-error prescribing
In a comment, Shaheen Lakhan, MD, a neurologist and researcher in Boston, said this research is “very noteworthy, moving us one step closer to predictive, precision medicine and away from the practice of trial-and-error prescribing.
“The trial-and-error approach to migraine management is daunting. These are very costly therapies, and when they don’t work, there is continued tremendous suffering and loss of quality of life for patients,” said Dr. Lakhan, who was not involved in the study.
He added that the failure of drugs to benefit individual patients “may lead to distrust of the health care provider” and to the system as a whole, which in turn could lead to less access to care for other conditions or for preventive measures.
“I envision a time when these predictive measures collectively (interictal allodynia, as in this study, plus biobehavioral data) will assist us neurologists in appropriately selecting migraine therapies,” Dr. Lakhan said.
“Beyond that, we will eventually test new therapies not in cells, animals, and even humans but in silico. In the very near future, we will have solutions tailored to not people suffering a disease but to you – an individual with a unique genetic, protein, physical, developmental, psychological, and behavioral makeup,” he added.
The study was funded in part by Eli Lilly, the National Institutes of Health, and the anesthesia department at Beth Israel Deaconess Medical Center. Galcanezumab was provided by Eli Lilly. Dr. Lakhan reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
The ictal phase refers to “sensitization occurring during a time when central trigeminovascular neurons receive massive nociceptive input from active meningeal nociceptors,” whereas the nonictal phase refers to “sensitization occurring during a time when central trigeminovascular neurons receive no or subliminal nociceptive input from meningeal nociceptors,” investigators noted.
In an observational, open-label cohort study, pretreatment nonictal cephalic allodynia identified galcanezumab responders with nearly 80% accuracy, and it identified nonresponders with nearly 85% accuracy.
“Detection of nonictal allodynia with a simplified paradigm of Quantitative Sensory Testing (QST) may provide a quick, affordable, noninvasive, and patient-friendly way to prospectively distinguish between responders and nonresponders to the prophylactic treatment of chronic and high-frequency episodic migraine with drugs that reduce CGRP signaling,” Sait Ashina, MD, of Beth Israel Deaconess Medical Center and Harvard Medical School, both in Boston, and colleagues wrote.
The findings were published online in Cephalalgia.
Immediate clinical relevance
Investigator Rami Burstein, PhD, also with Beth Israel Deaconess Medical Center and Harvard Medical School, developed the concept of predicting response to anti-CGRP treatment by testing for the presence or absence of nonictal cephalic allodynia in collaboration with the company CGRP Diagnostics.
In 43 anti–CGRP-naive patients with migraine, the researchers used a simplified QST algorithm to determine the presence/absence of cephalic or extracephalic allodynia during the nonictal phase of migraine – defined as the period from less than 12 hours after a migraine attack to less than 12 hours before the next attack.
Patients were considered to have allodynia if heat pain thresholds were between 32° C and 40° C, if cold pain thresholds were between 32° C and 20° C, or if the mechanical pain was threshold was less than 60 g.
Using these strict criteria, pretreatment nonictal cephalic allodynia was a statistically significant predictor of response to anti-CGRP therapy. It was present in 84% of the 19 nonresponders and was absent in 79% of the 24 responders, for an overall accuracy rate of 86% (P < .0001).
Nonictal cephalic allodynia was “consistently” predictive of response for patients with chronic migraine as well as for those with high-frequency episodic migraine, the researchers reported.
In contrast, they noted that assessing nonictal extracephalic allodynia with QST missed nearly 50% of the patients with allodynia among the nonresponders (accuracy rate of 42%) and added little to the assessment of allodynia among the responders.
Mark Hasleton, PhD, CEO of CGRP Diagnostics, said in an interview that the study shows it’s possible to determine response to anti-CGRP therapy and to prescribe these medications to patients who are most likely to respond.
Dr. Hasleton, who was not personally involved with the current study, noted that pretreatment testing for nonictal cephalic allodynia may also allow for earlier prescription of anti-CGRP therapy and potentially dispense without the need for the current trial-and-error approach to prescribing. He noted that if one anti-CGRP fails the patient, it is highly likely that others will also fail.
Given the “very high correlation of the presence of nonictal cephalic allodynia in responders to galcanezumab, our recommendation would be to routinely pretest all potential anti-CGRP candidates prior to prescription,” he said.
End of trial-and-error prescribing
In a comment, Shaheen Lakhan, MD, a neurologist and researcher in Boston, said this research is “very noteworthy, moving us one step closer to predictive, precision medicine and away from the practice of trial-and-error prescribing.
“The trial-and-error approach to migraine management is daunting. These are very costly therapies, and when they don’t work, there is continued tremendous suffering and loss of quality of life for patients,” said Dr. Lakhan, who was not involved in the study.
He added that the failure of drugs to benefit individual patients “may lead to distrust of the health care provider” and to the system as a whole, which in turn could lead to less access to care for other conditions or for preventive measures.
“I envision a time when these predictive measures collectively (interictal allodynia, as in this study, plus biobehavioral data) will assist us neurologists in appropriately selecting migraine therapies,” Dr. Lakhan said.
“Beyond that, we will eventually test new therapies not in cells, animals, and even humans but in silico. In the very near future, we will have solutions tailored to not people suffering a disease but to you – an individual with a unique genetic, protein, physical, developmental, psychological, and behavioral makeup,” he added.
The study was funded in part by Eli Lilly, the National Institutes of Health, and the anesthesia department at Beth Israel Deaconess Medical Center. Galcanezumab was provided by Eli Lilly. Dr. Lakhan reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
The ictal phase refers to “sensitization occurring during a time when central trigeminovascular neurons receive massive nociceptive input from active meningeal nociceptors,” whereas the nonictal phase refers to “sensitization occurring during a time when central trigeminovascular neurons receive no or subliminal nociceptive input from meningeal nociceptors,” investigators noted.
In an observational, open-label cohort study, pretreatment nonictal cephalic allodynia identified galcanezumab responders with nearly 80% accuracy, and it identified nonresponders with nearly 85% accuracy.
“Detection of nonictal allodynia with a simplified paradigm of Quantitative Sensory Testing (QST) may provide a quick, affordable, noninvasive, and patient-friendly way to prospectively distinguish between responders and nonresponders to the prophylactic treatment of chronic and high-frequency episodic migraine with drugs that reduce CGRP signaling,” Sait Ashina, MD, of Beth Israel Deaconess Medical Center and Harvard Medical School, both in Boston, and colleagues wrote.
The findings were published online in Cephalalgia.
Immediate clinical relevance
Investigator Rami Burstein, PhD, also with Beth Israel Deaconess Medical Center and Harvard Medical School, developed the concept of predicting response to anti-CGRP treatment by testing for the presence or absence of nonictal cephalic allodynia in collaboration with the company CGRP Diagnostics.
In 43 anti–CGRP-naive patients with migraine, the researchers used a simplified QST algorithm to determine the presence/absence of cephalic or extracephalic allodynia during the nonictal phase of migraine – defined as the period from less than 12 hours after a migraine attack to less than 12 hours before the next attack.
Patients were considered to have allodynia if heat pain thresholds were between 32° C and 40° C, if cold pain thresholds were between 32° C and 20° C, or if the mechanical pain was threshold was less than 60 g.
Using these strict criteria, pretreatment nonictal cephalic allodynia was a statistically significant predictor of response to anti-CGRP therapy. It was present in 84% of the 19 nonresponders and was absent in 79% of the 24 responders, for an overall accuracy rate of 86% (P < .0001).
Nonictal cephalic allodynia was “consistently” predictive of response for patients with chronic migraine as well as for those with high-frequency episodic migraine, the researchers reported.
In contrast, they noted that assessing nonictal extracephalic allodynia with QST missed nearly 50% of the patients with allodynia among the nonresponders (accuracy rate of 42%) and added little to the assessment of allodynia among the responders.
Mark Hasleton, PhD, CEO of CGRP Diagnostics, said in an interview that the study shows it’s possible to determine response to anti-CGRP therapy and to prescribe these medications to patients who are most likely to respond.
Dr. Hasleton, who was not personally involved with the current study, noted that pretreatment testing for nonictal cephalic allodynia may also allow for earlier prescription of anti-CGRP therapy and potentially dispense without the need for the current trial-and-error approach to prescribing. He noted that if one anti-CGRP fails the patient, it is highly likely that others will also fail.
Given the “very high correlation of the presence of nonictal cephalic allodynia in responders to galcanezumab, our recommendation would be to routinely pretest all potential anti-CGRP candidates prior to prescription,” he said.
End of trial-and-error prescribing
In a comment, Shaheen Lakhan, MD, a neurologist and researcher in Boston, said this research is “very noteworthy, moving us one step closer to predictive, precision medicine and away from the practice of trial-and-error prescribing.
“The trial-and-error approach to migraine management is daunting. These are very costly therapies, and when they don’t work, there is continued tremendous suffering and loss of quality of life for patients,” said Dr. Lakhan, who was not involved in the study.
He added that the failure of drugs to benefit individual patients “may lead to distrust of the health care provider” and to the system as a whole, which in turn could lead to less access to care for other conditions or for preventive measures.
“I envision a time when these predictive measures collectively (interictal allodynia, as in this study, plus biobehavioral data) will assist us neurologists in appropriately selecting migraine therapies,” Dr. Lakhan said.
“Beyond that, we will eventually test new therapies not in cells, animals, and even humans but in silico. In the very near future, we will have solutions tailored to not people suffering a disease but to you – an individual with a unique genetic, protein, physical, developmental, psychological, and behavioral makeup,” he added.
The study was funded in part by Eli Lilly, the National Institutes of Health, and the anesthesia department at Beth Israel Deaconess Medical Center. Galcanezumab was provided by Eli Lilly. Dr. Lakhan reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CEPHALALGIA
Adult brains contain millions of ‘silent synapses’
according to neuroscientists from the Massachusetts Institute of Technology.
What to know:
- An estimated 30% of all synapses in the brain’s cortex are silent and become active to allow the adult brain to continually form new memories and leave existing conventional synapses unmodified.
- Silent synapses are looking for new connections, and when important new information is presented, connections between the relevant neurons are strengthened to allow the brain to remember new things.
- Using the silent synapses for the new memories does not overwrite the important memories stored in more mature synapses, which are harder to change.
- The brain’s neurons display a wide range of plasticity mechanisms that account for how brains can efficiently learn new things and retain them in long-term memory.
- Flexibility of synapses is critical for acquiring new information, and stability is required to retain important information, enabling one to more easily adjust and change behaviors and habits or incorporate new information.
This is a summary of the article, “Filopodia Are a Structural Substrate for Silent Synapses in Adult Neocortex,” published in Nature Nov. 30, 2022. The full article can be found at nature.com .
A version of this article first appeared on Medscape.com.
according to neuroscientists from the Massachusetts Institute of Technology.
What to know:
- An estimated 30% of all synapses in the brain’s cortex are silent and become active to allow the adult brain to continually form new memories and leave existing conventional synapses unmodified.
- Silent synapses are looking for new connections, and when important new information is presented, connections between the relevant neurons are strengthened to allow the brain to remember new things.
- Using the silent synapses for the new memories does not overwrite the important memories stored in more mature synapses, which are harder to change.
- The brain’s neurons display a wide range of plasticity mechanisms that account for how brains can efficiently learn new things and retain them in long-term memory.
- Flexibility of synapses is critical for acquiring new information, and stability is required to retain important information, enabling one to more easily adjust and change behaviors and habits or incorporate new information.
This is a summary of the article, “Filopodia Are a Structural Substrate for Silent Synapses in Adult Neocortex,” published in Nature Nov. 30, 2022. The full article can be found at nature.com .
A version of this article first appeared on Medscape.com.
according to neuroscientists from the Massachusetts Institute of Technology.
What to know:
- An estimated 30% of all synapses in the brain’s cortex are silent and become active to allow the adult brain to continually form new memories and leave existing conventional synapses unmodified.
- Silent synapses are looking for new connections, and when important new information is presented, connections between the relevant neurons are strengthened to allow the brain to remember new things.
- Using the silent synapses for the new memories does not overwrite the important memories stored in more mature synapses, which are harder to change.
- The brain’s neurons display a wide range of plasticity mechanisms that account for how brains can efficiently learn new things and retain them in long-term memory.
- Flexibility of synapses is critical for acquiring new information, and stability is required to retain important information, enabling one to more easily adjust and change behaviors and habits or incorporate new information.
This is a summary of the article, “Filopodia Are a Structural Substrate for Silent Synapses in Adult Neocortex,” published in Nature Nov. 30, 2022. The full article can be found at nature.com .
A version of this article first appeared on Medscape.com.
Endovascular therapy benefits large infarction: ANGEL-ASPECT
The trial was stopped early because a planned interim analysis showed efficacy of endovascular therapy in this patient population.
Among patients in China with acute ischemic stroke and a large cerebral infarction, treatment with endovascular therapy within 24 hours after stroke onset “resulted in a better functional outcome at 3 months than medical management alone,” lead author Xiaochuan Huo, MD, PhD, associate chief physician, interventional neurology department, Beijing Tiantan Hospital, Capital Medical University, told this news organization.
“This trial added important evidence for the benefits of endovascular therapy,” Dr. Huo added.
The findings were presented at the International Stroke Conference and were published online in The New England Journal of Medicine. The conference was presented by the American Stroke Association, a division of the American Heart Association.
Will change practice
Commenting on the results, Tudor G. Jovin, MD, professor and chair, department of neurology, Cooper Medical School of Rowan University, Camden, N.J., said he has “little doubt” this study will change practice.
Despite previous studies showing signals of benefit from thrombectomy for patients with large-core infarcts, and some even finding a large treatment effect, “somehow the world didn’t register this,” said Dr. Jovin.
“The stroke community was perhaps reluctant to accept these signals that were there in plain sight because we have been primed for such a long time that reperfusing large infarcts was, if not detrimental, not beneficial.”
But this study, along with another study showing similar results, SELECT 2, which was also presented at this meeting and was published in the same issue of NEJM, provide “overwhelming proof” and “have finally made the community aware,” said Dr. Jovin. “This is sort of a wake-up call to say, ‘Hey, this is real; patients with large infarcts also benefit from thrombectomy.’ “
This new research suggests it’s not necessary to learn the infarct size, at least in the early time window, and doing so just wastes precious time, added Dr. Jovin.
The impact of thrombectomy on patients with “super large infarcts” is still not clear, although these are “extremely rare” in the early time window, perhaps representing only about 1% of patients, said Dr. Jovin.
The increased rate of hemorrhages in study patients receiving thrombectomy “is the price you pay” for the benefits, he said. He noted that this is not any different from the situation with tissue plasminogen activator (tPA), which is routinely used because the benefits far outweigh the risks.
ANGEL-ASPECT
As patients with large infarctions are generally excluded from studies of thrombectomy, it’s been unclear whether they benefit from this therapy, the researchers noted.
The multicenter Endovascular Therapy in Acute Anterior Circulation Large Vessel Occlusive Patients With a Large Infarct Core (ANGEL-ASPECT) trial included 455 adult patients (median age, 68 years; 38.7% women) who had a large infarct core caused by acute large-vessel occlusion in the anterior circulation (Alberta Stroke Program Early CT Score [ASPECTS] 3-5 without core volume limitations or ASPECTS 0–2 with core volume between 70 and 100 mL).
Study participants had to have a score of 6-30 on the National Institutes of Health Stroke Scale (NIHSS) and a retrospectively determined prestroke score of 0 or 1 on the Modified Rankin Scale (mRS).
The median baseline NIHSS score of study patients was 16, the median ASPECTS was 3, and the median infarct-core volume was 62 mL.
Researchers randomly assigned patients to undergo either medical management alone or medical management as well as endovascular therapy. Medical management included intravenous (IV) thrombolysis for those who were eligible.
IV thrombolysis was administered before thrombectomy for about 28% of patients in each group. Some 78.7% of all patients arrived at the hospital outside the typical 4.5-hour window and were ineligible for thrombolysis.
A greater percentage of patients in the endovascular therapy group was receiving antihypertensive medications (83.0%) than in the medical management alone group (54.0%). About 20% of patients in each group were taking an anticoagulant medication.
When the trial was halted, outcome data were available for 336 patients. An additional 120 patients had undergone randomization, and 455 had completed 90 days of follow-up.
Better functional outcome
The primary outcome was the score on the mRS at 90 days. Results showed a shift in the distribution of scores on the mRS at 90 days toward better outcomes favoring endovascular therapy over medical management alone (generalized odds ratio, 1.37; 95% confidence interval [CI], 1.11-1.69; P = .004).
The efficacy of endovascular therapy with respect to the primary outcome was similar across predefined subgroups and across all trial sites. However, the trial was not powered to allow definite conclusions based on the results of subgroup analyses.
Although patients with an ASPECT score of 0-2 (indicating very large infarct cores) are considered unlikely to benefit from endovascular treatment, the researchers did find some signals of gain for these patients.
“Although no conclusions can be drawn because the trial was not powered for this analysis and the confidence interval for the odds ratio between the trial groups included 1, there may have been a benefit with endovascular therapy in this subgroup,” the authors wrote. “More trials are warranted to determine if this benefit is valid.”
As for secondary outcomes, the percentage of patients with a score of 0-2 on the mRS at 90 days was 30.0% in the endovascular therapy group and 11.6% in the medical management group (relative risk [RR], 2.62; 95% CI, 1.69-4.06).
The percentage of patients with a score of 0-3 on the mRS at 90 days was 47.0% in the endovascular therapy group and 33.3% in the medical management group (RR, 1.50; 95% CI, 1.17-1.91).
The primary safety outcome was symptomatic intracranial hemorrhage within 48 hours, which occurred in 6.1% of the endovascular therapy group, compared to 2.7% in the medical management group (RR, 2.07; 95% CI, 0.79-5.41; P = .12)
Mortality within 90 days was 21.7% in the endovascular therapy group and 20.0% in the medical management group. Other serious adverse events occurred in 40.0% in the endovascular therapy group and 38.2% in the medical management group (P = .70).
The percentage of patients receiving IV thrombolysis was relatively low, which may have affected outcomes in the medical management group. Another potential limitation was that urokinase rather than alteplase, which is probably more effective, was used for thrombolysis in a small percentage of patients.
Further, the study did not include patients older than 80 years or those with an ASPECT value greater than 5 and infarct core volume of 70-100 mL, and it included only Chinese patients, so the results may not be generalizable, the researchers noted.
These findings will likely change clinical practice, said Dr. Huo, who noted that the current guideline doesn’t provide “a high-level recommendation” for [endovascular therapy] in patients with a low ASPECT score.
“These new results will change the guideline” to suggest endovascular therapy for large-core patients, he said.
Welcome news
An accompanying editorial by Pierre Fayad, MD, department of neurological sciences, division of vascular neurology and stroke, University of Nebraska Medical Center, Omaha, welcomed results from this and other recent related studies.
From these new results, “it is reasonable to suggest that endovascular thrombectomy be offered to patients with large strokes” if they arrive in a timely fashion at a center capable of performing the procedure and have an ASPECT value of 3-5 or an ischemic-core volume of 50 mL or greater, he wrote.
“The improved chance of independent walking and the ability to perform other daily activities in patients with the most severe strokes is welcome news for patients and for the field of stroke treatment.”
The study received funding from Covidien Healthcare International Trading (Shanghai), Johnson & Johnson MedTech, Genesis MedTech (Shanghai), and Shanghai HeartCare Medical Technology. Dr. Huo and Dr. Jovin report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The trial was stopped early because a planned interim analysis showed efficacy of endovascular therapy in this patient population.
Among patients in China with acute ischemic stroke and a large cerebral infarction, treatment with endovascular therapy within 24 hours after stroke onset “resulted in a better functional outcome at 3 months than medical management alone,” lead author Xiaochuan Huo, MD, PhD, associate chief physician, interventional neurology department, Beijing Tiantan Hospital, Capital Medical University, told this news organization.
“This trial added important evidence for the benefits of endovascular therapy,” Dr. Huo added.
The findings were presented at the International Stroke Conference and were published online in The New England Journal of Medicine. The conference was presented by the American Stroke Association, a division of the American Heart Association.
Will change practice
Commenting on the results, Tudor G. Jovin, MD, professor and chair, department of neurology, Cooper Medical School of Rowan University, Camden, N.J., said he has “little doubt” this study will change practice.
Despite previous studies showing signals of benefit from thrombectomy for patients with large-core infarcts, and some even finding a large treatment effect, “somehow the world didn’t register this,” said Dr. Jovin.
“The stroke community was perhaps reluctant to accept these signals that were there in plain sight because we have been primed for such a long time that reperfusing large infarcts was, if not detrimental, not beneficial.”
But this study, along with another study showing similar results, SELECT 2, which was also presented at this meeting and was published in the same issue of NEJM, provide “overwhelming proof” and “have finally made the community aware,” said Dr. Jovin. “This is sort of a wake-up call to say, ‘Hey, this is real; patients with large infarcts also benefit from thrombectomy.’ “
This new research suggests it’s not necessary to learn the infarct size, at least in the early time window, and doing so just wastes precious time, added Dr. Jovin.
The impact of thrombectomy on patients with “super large infarcts” is still not clear, although these are “extremely rare” in the early time window, perhaps representing only about 1% of patients, said Dr. Jovin.
The increased rate of hemorrhages in study patients receiving thrombectomy “is the price you pay” for the benefits, he said. He noted that this is not any different from the situation with tissue plasminogen activator (tPA), which is routinely used because the benefits far outweigh the risks.
ANGEL-ASPECT
As patients with large infarctions are generally excluded from studies of thrombectomy, it’s been unclear whether they benefit from this therapy, the researchers noted.
The multicenter Endovascular Therapy in Acute Anterior Circulation Large Vessel Occlusive Patients With a Large Infarct Core (ANGEL-ASPECT) trial included 455 adult patients (median age, 68 years; 38.7% women) who had a large infarct core caused by acute large-vessel occlusion in the anterior circulation (Alberta Stroke Program Early CT Score [ASPECTS] 3-5 without core volume limitations or ASPECTS 0–2 with core volume between 70 and 100 mL).
Study participants had to have a score of 6-30 on the National Institutes of Health Stroke Scale (NIHSS) and a retrospectively determined prestroke score of 0 or 1 on the Modified Rankin Scale (mRS).
The median baseline NIHSS score of study patients was 16, the median ASPECTS was 3, and the median infarct-core volume was 62 mL.
Researchers randomly assigned patients to undergo either medical management alone or medical management as well as endovascular therapy. Medical management included intravenous (IV) thrombolysis for those who were eligible.
IV thrombolysis was administered before thrombectomy for about 28% of patients in each group. Some 78.7% of all patients arrived at the hospital outside the typical 4.5-hour window and were ineligible for thrombolysis.
A greater percentage of patients in the endovascular therapy group was receiving antihypertensive medications (83.0%) than in the medical management alone group (54.0%). About 20% of patients in each group were taking an anticoagulant medication.
When the trial was halted, outcome data were available for 336 patients. An additional 120 patients had undergone randomization, and 455 had completed 90 days of follow-up.
Better functional outcome
The primary outcome was the score on the mRS at 90 days. Results showed a shift in the distribution of scores on the mRS at 90 days toward better outcomes favoring endovascular therapy over medical management alone (generalized odds ratio, 1.37; 95% confidence interval [CI], 1.11-1.69; P = .004).
The efficacy of endovascular therapy with respect to the primary outcome was similar across predefined subgroups and across all trial sites. However, the trial was not powered to allow definite conclusions based on the results of subgroup analyses.
Although patients with an ASPECT score of 0-2 (indicating very large infarct cores) are considered unlikely to benefit from endovascular treatment, the researchers did find some signals of gain for these patients.
“Although no conclusions can be drawn because the trial was not powered for this analysis and the confidence interval for the odds ratio between the trial groups included 1, there may have been a benefit with endovascular therapy in this subgroup,” the authors wrote. “More trials are warranted to determine if this benefit is valid.”
As for secondary outcomes, the percentage of patients with a score of 0-2 on the mRS at 90 days was 30.0% in the endovascular therapy group and 11.6% in the medical management group (relative risk [RR], 2.62; 95% CI, 1.69-4.06).
The percentage of patients with a score of 0-3 on the mRS at 90 days was 47.0% in the endovascular therapy group and 33.3% in the medical management group (RR, 1.50; 95% CI, 1.17-1.91).
The primary safety outcome was symptomatic intracranial hemorrhage within 48 hours, which occurred in 6.1% of the endovascular therapy group, compared to 2.7% in the medical management group (RR, 2.07; 95% CI, 0.79-5.41; P = .12)
Mortality within 90 days was 21.7% in the endovascular therapy group and 20.0% in the medical management group. Other serious adverse events occurred in 40.0% in the endovascular therapy group and 38.2% in the medical management group (P = .70).
The percentage of patients receiving IV thrombolysis was relatively low, which may have affected outcomes in the medical management group. Another potential limitation was that urokinase rather than alteplase, which is probably more effective, was used for thrombolysis in a small percentage of patients.
Further, the study did not include patients older than 80 years or those with an ASPECT value greater than 5 and infarct core volume of 70-100 mL, and it included only Chinese patients, so the results may not be generalizable, the researchers noted.
These findings will likely change clinical practice, said Dr. Huo, who noted that the current guideline doesn’t provide “a high-level recommendation” for [endovascular therapy] in patients with a low ASPECT score.
“These new results will change the guideline” to suggest endovascular therapy for large-core patients, he said.
Welcome news
An accompanying editorial by Pierre Fayad, MD, department of neurological sciences, division of vascular neurology and stroke, University of Nebraska Medical Center, Omaha, welcomed results from this and other recent related studies.
From these new results, “it is reasonable to suggest that endovascular thrombectomy be offered to patients with large strokes” if they arrive in a timely fashion at a center capable of performing the procedure and have an ASPECT value of 3-5 or an ischemic-core volume of 50 mL or greater, he wrote.
“The improved chance of independent walking and the ability to perform other daily activities in patients with the most severe strokes is welcome news for patients and for the field of stroke treatment.”
The study received funding from Covidien Healthcare International Trading (Shanghai), Johnson & Johnson MedTech, Genesis MedTech (Shanghai), and Shanghai HeartCare Medical Technology. Dr. Huo and Dr. Jovin report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The trial was stopped early because a planned interim analysis showed efficacy of endovascular therapy in this patient population.
Among patients in China with acute ischemic stroke and a large cerebral infarction, treatment with endovascular therapy within 24 hours after stroke onset “resulted in a better functional outcome at 3 months than medical management alone,” lead author Xiaochuan Huo, MD, PhD, associate chief physician, interventional neurology department, Beijing Tiantan Hospital, Capital Medical University, told this news organization.
“This trial added important evidence for the benefits of endovascular therapy,” Dr. Huo added.
The findings were presented at the International Stroke Conference and were published online in The New England Journal of Medicine. The conference was presented by the American Stroke Association, a division of the American Heart Association.
Will change practice
Commenting on the results, Tudor G. Jovin, MD, professor and chair, department of neurology, Cooper Medical School of Rowan University, Camden, N.J., said he has “little doubt” this study will change practice.
Despite previous studies showing signals of benefit from thrombectomy for patients with large-core infarcts, and some even finding a large treatment effect, “somehow the world didn’t register this,” said Dr. Jovin.
“The stroke community was perhaps reluctant to accept these signals that were there in plain sight because we have been primed for such a long time that reperfusing large infarcts was, if not detrimental, not beneficial.”
But this study, along with another study showing similar results, SELECT 2, which was also presented at this meeting and was published in the same issue of NEJM, provide “overwhelming proof” and “have finally made the community aware,” said Dr. Jovin. “This is sort of a wake-up call to say, ‘Hey, this is real; patients with large infarcts also benefit from thrombectomy.’ “
This new research suggests it’s not necessary to learn the infarct size, at least in the early time window, and doing so just wastes precious time, added Dr. Jovin.
The impact of thrombectomy on patients with “super large infarcts” is still not clear, although these are “extremely rare” in the early time window, perhaps representing only about 1% of patients, said Dr. Jovin.
The increased rate of hemorrhages in study patients receiving thrombectomy “is the price you pay” for the benefits, he said. He noted that this is not any different from the situation with tissue plasminogen activator (tPA), which is routinely used because the benefits far outweigh the risks.
ANGEL-ASPECT
As patients with large infarctions are generally excluded from studies of thrombectomy, it’s been unclear whether they benefit from this therapy, the researchers noted.
The multicenter Endovascular Therapy in Acute Anterior Circulation Large Vessel Occlusive Patients With a Large Infarct Core (ANGEL-ASPECT) trial included 455 adult patients (median age, 68 years; 38.7% women) who had a large infarct core caused by acute large-vessel occlusion in the anterior circulation (Alberta Stroke Program Early CT Score [ASPECTS] 3-5 without core volume limitations or ASPECTS 0–2 with core volume between 70 and 100 mL).
Study participants had to have a score of 6-30 on the National Institutes of Health Stroke Scale (NIHSS) and a retrospectively determined prestroke score of 0 or 1 on the Modified Rankin Scale (mRS).
The median baseline NIHSS score of study patients was 16, the median ASPECTS was 3, and the median infarct-core volume was 62 mL.
Researchers randomly assigned patients to undergo either medical management alone or medical management as well as endovascular therapy. Medical management included intravenous (IV) thrombolysis for those who were eligible.
IV thrombolysis was administered before thrombectomy for about 28% of patients in each group. Some 78.7% of all patients arrived at the hospital outside the typical 4.5-hour window and were ineligible for thrombolysis.
A greater percentage of patients in the endovascular therapy group was receiving antihypertensive medications (83.0%) than in the medical management alone group (54.0%). About 20% of patients in each group were taking an anticoagulant medication.
When the trial was halted, outcome data were available for 336 patients. An additional 120 patients had undergone randomization, and 455 had completed 90 days of follow-up.
Better functional outcome
The primary outcome was the score on the mRS at 90 days. Results showed a shift in the distribution of scores on the mRS at 90 days toward better outcomes favoring endovascular therapy over medical management alone (generalized odds ratio, 1.37; 95% confidence interval [CI], 1.11-1.69; P = .004).
The efficacy of endovascular therapy with respect to the primary outcome was similar across predefined subgroups and across all trial sites. However, the trial was not powered to allow definite conclusions based on the results of subgroup analyses.
Although patients with an ASPECT score of 0-2 (indicating very large infarct cores) are considered unlikely to benefit from endovascular treatment, the researchers did find some signals of gain for these patients.
“Although no conclusions can be drawn because the trial was not powered for this analysis and the confidence interval for the odds ratio between the trial groups included 1, there may have been a benefit with endovascular therapy in this subgroup,” the authors wrote. “More trials are warranted to determine if this benefit is valid.”
As for secondary outcomes, the percentage of patients with a score of 0-2 on the mRS at 90 days was 30.0% in the endovascular therapy group and 11.6% in the medical management group (relative risk [RR], 2.62; 95% CI, 1.69-4.06).
The percentage of patients with a score of 0-3 on the mRS at 90 days was 47.0% in the endovascular therapy group and 33.3% in the medical management group (RR, 1.50; 95% CI, 1.17-1.91).
The primary safety outcome was symptomatic intracranial hemorrhage within 48 hours, which occurred in 6.1% of the endovascular therapy group, compared to 2.7% in the medical management group (RR, 2.07; 95% CI, 0.79-5.41; P = .12)
Mortality within 90 days was 21.7% in the endovascular therapy group and 20.0% in the medical management group. Other serious adverse events occurred in 40.0% in the endovascular therapy group and 38.2% in the medical management group (P = .70).
The percentage of patients receiving IV thrombolysis was relatively low, which may have affected outcomes in the medical management group. Another potential limitation was that urokinase rather than alteplase, which is probably more effective, was used for thrombolysis in a small percentage of patients.
Further, the study did not include patients older than 80 years or those with an ASPECT value greater than 5 and infarct core volume of 70-100 mL, and it included only Chinese patients, so the results may not be generalizable, the researchers noted.
These findings will likely change clinical practice, said Dr. Huo, who noted that the current guideline doesn’t provide “a high-level recommendation” for [endovascular therapy] in patients with a low ASPECT score.
“These new results will change the guideline” to suggest endovascular therapy for large-core patients, he said.
Welcome news
An accompanying editorial by Pierre Fayad, MD, department of neurological sciences, division of vascular neurology and stroke, University of Nebraska Medical Center, Omaha, welcomed results from this and other recent related studies.
From these new results, “it is reasonable to suggest that endovascular thrombectomy be offered to patients with large strokes” if they arrive in a timely fashion at a center capable of performing the procedure and have an ASPECT value of 3-5 or an ischemic-core volume of 50 mL or greater, he wrote.
“The improved chance of independent walking and the ability to perform other daily activities in patients with the most severe strokes is welcome news for patients and for the field of stroke treatment.”
The study received funding from Covidien Healthcare International Trading (Shanghai), Johnson & Johnson MedTech, Genesis MedTech (Shanghai), and Shanghai HeartCare Medical Technology. Dr. Huo and Dr. Jovin report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ISC 2023
Similar effect of early, late BP reduction in stroke: CATIS-2
in the CATIS-2 trial.
The trial was presented by Liping Liu, MD, Beijing Tiantan Hospital, at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
“Antihypertensive treatment can be delayed for at least 7 days following ischemic stroke onset, unless there are severe acute comorbidities that demand emergency blood pressure reduction to prevent serious complications,” Dr. Liu concluded.
But he acknowledged that the optimal BP management strategy in these patients remains uncertain and should be the focus of future research.
Discussing the trial at an ISC 2023 Highlights session, Lauren Sansing, MD, Yale University, New Haven, Conn., and ISC program vice chair, said: “These results seem to support waiting for a week or so before treating blood pressure in these patients.”
But Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., and ISC program chair, countered: “To me, it’s kind of a neutral result, so what I take home from this is that you don’t necessarily have to wait.”
Dr. Jovin continued: “We used to think that it was mandatory not to treat blood pressure early because of the risk of deceasing the perfusion pressure, but this trial suggests the effects are neutral and there is probably as much benefit from lowering blood pressure for other reasons that offsets the potential harm.
“I think these are good data to rely on when we make these kinds of treatment decisions. Personally, I am a bit more aggressive with early blood pressure management and it’s good to see that you don’t get punished for that,” he added.
In his presentation, Dr. Liu explained that increased BP is common in acute stroke and is strongly associated with poor functional outcome and recurrence of ischemic stroke, but the optimal blood pressure management strategy in acute ischemic stroke remains controversial.
In the first CATIS trial (China Antihypertensive Trial in Acute Ischemic Stroke), which compared antihypertensive treatment within 48 hours of stroke onset with no antihypertensive treatment in ischemic stroke patients not receiving thrombolysis, the main results suggested that BP reduction with antihypertensive medications did not reduce the likelihood of death and major disability at 14 days or hospital discharge. But a subgroup analysis found that initiating antihypertensive treatment between 24 and 48 hours of stroke onset showed a beneficial effect on reducing death or major disability.
Current AHA/ASA guidelines suggest that, in patients with BP greater than 220/120 mm Hg who have not received thrombolysis or thrombectomy and have no comorbid conditions requiring urgent antihypertensive treatment, the benefit of initiating or reinitiating antihypertensive treatment within the first 48-72 hours is uncertain, although the guidelines say it might be reasonable to lower BP by around 15% during the first 24 hours after stroke onset, Dr. Liu noted.
The CATIS-2 trial was a multicenter, randomized, open-label, blinded-endpoints trial conducted at 106 centers in China that enrolled 4810 patients within 24-48 hours of onset of acute ischemic stroke who had elevated BP. Patients had not received thrombolytic therapy or mechanical thrombectomy.
Patients were randomly assigned to early antihypertensive therapy (initiated after randomization and aiming for a 10%-20% reduction in systolic BP) or delayed antihypertensive therapy (restarted antihypertensive therapy on day 8 of randomization, aiming for a BP of < 140/90 mm Hg).
The median age of the patients was 64 years, 65% were male, 80% had a history of hypertension, and the median National Institutes of Health Stroke Scale score was 3. Baseline BP averaged 163/92 mm Hg in both groups. The median time from stroke onset to antihypertensive treatment was 1.5 days in the early group and 8.5 days in the delayed group.
BP results showed that, at 24 hours after randomization, mean systolic pressure was reduced by 16.4 mm Hg (9.7%) in the early-treatment group and by 8.6 mm Hg (4.9%) in the delayed-treatment group (difference, –7.8 mm Hg; P < .0001).
At day 7, mean systolic pressure was 139.1 mm Hg in the early-treatment group, compared with 150.9 mm Hg in the delayed-treatment group, with a net difference in systolic BP of –11.9 mm Hg (P < .0001).
The primary outcome was the composite of death and major disability (modified Rankin Scale ≥ 3) at 3 months. This did not differ between the groups, occurring in 12.1% in the early antihypertensive treatment group versus 10.5% in the delayed antihypertensive treatment group (risk ratio, 1.15; P = .08).
There was also no difference in the major secondary outcome of shift in scores of mRS at 3 months, with a common odds ratio of 1.05 (95% confidence interval, 0.95-1.17).
There was no interaction with the composite outcome of death or major disability at 90 days in the prespecified subgroups.
Dr. Liu pointed out several limitations of the study. These included an observed primary outcome rate substantially lower than expected; the BP reduction seen within the first 7 days in the early-treatment group was moderate; and the results of the study cannot be applied to patients treated with thrombolysis or thrombectomy.
Dr. Liu has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
in the CATIS-2 trial.
The trial was presented by Liping Liu, MD, Beijing Tiantan Hospital, at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
“Antihypertensive treatment can be delayed for at least 7 days following ischemic stroke onset, unless there are severe acute comorbidities that demand emergency blood pressure reduction to prevent serious complications,” Dr. Liu concluded.
But he acknowledged that the optimal BP management strategy in these patients remains uncertain and should be the focus of future research.
Discussing the trial at an ISC 2023 Highlights session, Lauren Sansing, MD, Yale University, New Haven, Conn., and ISC program vice chair, said: “These results seem to support waiting for a week or so before treating blood pressure in these patients.”
But Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., and ISC program chair, countered: “To me, it’s kind of a neutral result, so what I take home from this is that you don’t necessarily have to wait.”
Dr. Jovin continued: “We used to think that it was mandatory not to treat blood pressure early because of the risk of deceasing the perfusion pressure, but this trial suggests the effects are neutral and there is probably as much benefit from lowering blood pressure for other reasons that offsets the potential harm.
“I think these are good data to rely on when we make these kinds of treatment decisions. Personally, I am a bit more aggressive with early blood pressure management and it’s good to see that you don’t get punished for that,” he added.
In his presentation, Dr. Liu explained that increased BP is common in acute stroke and is strongly associated with poor functional outcome and recurrence of ischemic stroke, but the optimal blood pressure management strategy in acute ischemic stroke remains controversial.
In the first CATIS trial (China Antihypertensive Trial in Acute Ischemic Stroke), which compared antihypertensive treatment within 48 hours of stroke onset with no antihypertensive treatment in ischemic stroke patients not receiving thrombolysis, the main results suggested that BP reduction with antihypertensive medications did not reduce the likelihood of death and major disability at 14 days or hospital discharge. But a subgroup analysis found that initiating antihypertensive treatment between 24 and 48 hours of stroke onset showed a beneficial effect on reducing death or major disability.
Current AHA/ASA guidelines suggest that, in patients with BP greater than 220/120 mm Hg who have not received thrombolysis or thrombectomy and have no comorbid conditions requiring urgent antihypertensive treatment, the benefit of initiating or reinitiating antihypertensive treatment within the first 48-72 hours is uncertain, although the guidelines say it might be reasonable to lower BP by around 15% during the first 24 hours after stroke onset, Dr. Liu noted.
The CATIS-2 trial was a multicenter, randomized, open-label, blinded-endpoints trial conducted at 106 centers in China that enrolled 4810 patients within 24-48 hours of onset of acute ischemic stroke who had elevated BP. Patients had not received thrombolytic therapy or mechanical thrombectomy.
Patients were randomly assigned to early antihypertensive therapy (initiated after randomization and aiming for a 10%-20% reduction in systolic BP) or delayed antihypertensive therapy (restarted antihypertensive therapy on day 8 of randomization, aiming for a BP of < 140/90 mm Hg).
The median age of the patients was 64 years, 65% were male, 80% had a history of hypertension, and the median National Institutes of Health Stroke Scale score was 3. Baseline BP averaged 163/92 mm Hg in both groups. The median time from stroke onset to antihypertensive treatment was 1.5 days in the early group and 8.5 days in the delayed group.
BP results showed that, at 24 hours after randomization, mean systolic pressure was reduced by 16.4 mm Hg (9.7%) in the early-treatment group and by 8.6 mm Hg (4.9%) in the delayed-treatment group (difference, –7.8 mm Hg; P < .0001).
At day 7, mean systolic pressure was 139.1 mm Hg in the early-treatment group, compared with 150.9 mm Hg in the delayed-treatment group, with a net difference in systolic BP of –11.9 mm Hg (P < .0001).
The primary outcome was the composite of death and major disability (modified Rankin Scale ≥ 3) at 3 months. This did not differ between the groups, occurring in 12.1% in the early antihypertensive treatment group versus 10.5% in the delayed antihypertensive treatment group (risk ratio, 1.15; P = .08).
There was also no difference in the major secondary outcome of shift in scores of mRS at 3 months, with a common odds ratio of 1.05 (95% confidence interval, 0.95-1.17).
There was no interaction with the composite outcome of death or major disability at 90 days in the prespecified subgroups.
Dr. Liu pointed out several limitations of the study. These included an observed primary outcome rate substantially lower than expected; the BP reduction seen within the first 7 days in the early-treatment group was moderate; and the results of the study cannot be applied to patients treated with thrombolysis or thrombectomy.
Dr. Liu has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
in the CATIS-2 trial.
The trial was presented by Liping Liu, MD, Beijing Tiantan Hospital, at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
“Antihypertensive treatment can be delayed for at least 7 days following ischemic stroke onset, unless there are severe acute comorbidities that demand emergency blood pressure reduction to prevent serious complications,” Dr. Liu concluded.
But he acknowledged that the optimal BP management strategy in these patients remains uncertain and should be the focus of future research.
Discussing the trial at an ISC 2023 Highlights session, Lauren Sansing, MD, Yale University, New Haven, Conn., and ISC program vice chair, said: “These results seem to support waiting for a week or so before treating blood pressure in these patients.”
But Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., and ISC program chair, countered: “To me, it’s kind of a neutral result, so what I take home from this is that you don’t necessarily have to wait.”
Dr. Jovin continued: “We used to think that it was mandatory not to treat blood pressure early because of the risk of deceasing the perfusion pressure, but this trial suggests the effects are neutral and there is probably as much benefit from lowering blood pressure for other reasons that offsets the potential harm.
“I think these are good data to rely on when we make these kinds of treatment decisions. Personally, I am a bit more aggressive with early blood pressure management and it’s good to see that you don’t get punished for that,” he added.
In his presentation, Dr. Liu explained that increased BP is common in acute stroke and is strongly associated with poor functional outcome and recurrence of ischemic stroke, but the optimal blood pressure management strategy in acute ischemic stroke remains controversial.
In the first CATIS trial (China Antihypertensive Trial in Acute Ischemic Stroke), which compared antihypertensive treatment within 48 hours of stroke onset with no antihypertensive treatment in ischemic stroke patients not receiving thrombolysis, the main results suggested that BP reduction with antihypertensive medications did not reduce the likelihood of death and major disability at 14 days or hospital discharge. But a subgroup analysis found that initiating antihypertensive treatment between 24 and 48 hours of stroke onset showed a beneficial effect on reducing death or major disability.
Current AHA/ASA guidelines suggest that, in patients with BP greater than 220/120 mm Hg who have not received thrombolysis or thrombectomy and have no comorbid conditions requiring urgent antihypertensive treatment, the benefit of initiating or reinitiating antihypertensive treatment within the first 48-72 hours is uncertain, although the guidelines say it might be reasonable to lower BP by around 15% during the first 24 hours after stroke onset, Dr. Liu noted.
The CATIS-2 trial was a multicenter, randomized, open-label, blinded-endpoints trial conducted at 106 centers in China that enrolled 4810 patients within 24-48 hours of onset of acute ischemic stroke who had elevated BP. Patients had not received thrombolytic therapy or mechanical thrombectomy.
Patients were randomly assigned to early antihypertensive therapy (initiated after randomization and aiming for a 10%-20% reduction in systolic BP) or delayed antihypertensive therapy (restarted antihypertensive therapy on day 8 of randomization, aiming for a BP of < 140/90 mm Hg).
The median age of the patients was 64 years, 65% were male, 80% had a history of hypertension, and the median National Institutes of Health Stroke Scale score was 3. Baseline BP averaged 163/92 mm Hg in both groups. The median time from stroke onset to antihypertensive treatment was 1.5 days in the early group and 8.5 days in the delayed group.
BP results showed that, at 24 hours after randomization, mean systolic pressure was reduced by 16.4 mm Hg (9.7%) in the early-treatment group and by 8.6 mm Hg (4.9%) in the delayed-treatment group (difference, –7.8 mm Hg; P < .0001).
At day 7, mean systolic pressure was 139.1 mm Hg in the early-treatment group, compared with 150.9 mm Hg in the delayed-treatment group, with a net difference in systolic BP of –11.9 mm Hg (P < .0001).
The primary outcome was the composite of death and major disability (modified Rankin Scale ≥ 3) at 3 months. This did not differ between the groups, occurring in 12.1% in the early antihypertensive treatment group versus 10.5% in the delayed antihypertensive treatment group (risk ratio, 1.15; P = .08).
There was also no difference in the major secondary outcome of shift in scores of mRS at 3 months, with a common odds ratio of 1.05 (95% confidence interval, 0.95-1.17).
There was no interaction with the composite outcome of death or major disability at 90 days in the prespecified subgroups.
Dr. Liu pointed out several limitations of the study. These included an observed primary outcome rate substantially lower than expected; the BP reduction seen within the first 7 days in the early-treatment group was moderate; and the results of the study cannot be applied to patients treated with thrombolysis or thrombectomy.
Dr. Liu has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ISC 2023
Thrombolysis not necessary in mild nondisabling stroke: ARAMIS
in the ARAMIS trial.
The trial was presented by Thanh Nguyen, MD, Boston Medical Center, at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
“Given the ease of administration, less intensive monitoring, low cost, and safety profile of dual antiplatelet therapy, the current findings support the use of dual antiplatelet in this population,” Dr. Nguyen concluded.
In a comment on the trial, Pooja Khatri, MD, professor of neurology at the University of Cincinnati, and lead investigator of the previous PRISMS study of tissue plasminogen activator (tPA) or alteplase in mild stroke, said the results reinforced the current recommendations of giving dual antiplatelet therapy but not alteplase to these patients.
Noting that the standard of care is now to give dual antiplatelet therapy to these patients, Dr. Khatri said: “These data reassure that this remains the right way to go.”
She added that her take-home message from the study would be: “Keep giving dual antiplatelet therapy, and we may be doing more harm than good with alteplase in this patient population.”
Introducing her presentation, Dr. Nguyen explained that mild ischemic stroke, defined as having a National Institutes of Health Stroke Scale (NIHSS) score of 5 or less, comprises half of ischemic stroke patients in the United States. But the benefit of thrombolysis in patients with minor ischemic stroke that is not disabling is unknown.
A subgroup analysis of one of the major thrombolysis trials (IST-3) found that a higher proportion of patients with mild ischemic stroke who were treated within 3 hours of symptom onset were alive and independent at 6 months if they had been given thrombolysis (84%), compared to 65% in the control group who received standard medical treatment.
This led to the first randomized trial (PRISMS) dedicated to patients with mild nondisabling stroke, which found that alteplase given within 3 hours of symptom onset did not increase the likelihood of a good functional outcome at 90 days in comparison with single-agent aspirin. The study was unfortunately terminated early for administrative reasons, and no definitive conclusions could be drawn on the basis of these results, Dr. Nguyen reported.
In 2018, the American Heart Association/American Stroke Association guidelines indicated that for patients who present within 3 hours of symptom onset with mild ischemic stroke that was judged to be nondisabling, thrombolysis with intravenous alteplase could be considered, she noted.
In the meantime, dual antiplatelet therapy was shown to be safe and effective in the POINT and CHANCE trials in patients presenting with minor stroke within 12 or 24 hours, and the CHANCE trial also found a benefit in reducing recurrent stroke that was most effective in the first 2 weeks.
The current ARAMIS trial was therefore conducted to evaluate dual antiplatelet therapy in comparison with thrombolysis for patients with acute minor stroke (NIHSS 5 or less) who presented within 4.5 hours of symptom onset and were without clearly disabling deficit.
The trial was conducted in 38 hospitals in China and included 760 patients (median NIHSS score of 2) who were randomly assigned to receive intravenous alteplase at the standard dose of 0.9 mg/kg, followed by guideline-based antiplatelet treatment, or dual antiplatelet therapy (clopidogrel 300 mg plus 100 mg aspirin loading dose followed by 10 to 14 days of aspirin 100 mg and clopidogrel 75 mg).
The trial was designed to assess noninferiority of dual antiplatelet therapy to alteplase with noninferiority margin of –4.5%.
In the modified intention-to-treat analysis, which included 722 patients, the primary outcome (excellent functional outcome, defined as a Modified Rankin Scale score of 0 or 1 at 90 days) occurred in 93.8% of patients in the dual antiplatelet therapy group and in 91.4% of the alteplase group. This gave a difference of 2.4%, which fell within the limits for noninferiority (P = .0002 for noninferiority test).
“Therefore, this was a positive trial,” Dr. Nguyen stated.
About 20% of patients crossed over from the dual antiplatelet group to the thrombolysis group, and about 16% of patients crossed over from the thrombolysis group to the dual antiplatelet group. But a per-protocol and an “as treated” analysis showed results similar to those of the main intention-to-treat analysis.
Secondary outcomes were largely similar between the two groups other than early neurologic deterioration, which was less common in the dual antiplatelet therapy group.
In terms of safety, symptomatic intracranial hemorrhage occurred in 0.3% (1/369) in the dual antiplatelet group and in 0.9% (3/350) in the alteplase group, a nonsignificant difference.
Events of “any bleeding” occurred in more patients in the thrombolysis group (5.4%) than in the dual antiplatelet therapy group (1.6%), and this difference was significant (P = .01).
Subgroup analysis showed a trend toward benefit of alteplase for patients with higher NIHSS score at baseline (NIHSS > 3). Otherwise, the other subgroups looked similar to the main results.
Dr. Nguyen pointed out one limitation of the study – that dual antiplatelet therapy was updated to standard treatment in this target population in the 2019 AHA/ASA guidelines.
In her discussion of the study, Dr. Khatri suggested that the ARAMIS results were what might have been expected.
“Dual antiplatelet therapy is designed to prevent stroke. Even in the POINT trial, dual antiplatelet therapy showed no effect on 90-day functional outcome. It was really about prevention. The PRISMS trial suggested that alteplase was also unlikely to improve 90-day functional outcome in this population of patients with mild and not clearly disabling stroke. So, it is not surprising that dual antiplatelet therapy was noninferior to alteplase for 90-day functional outcome for both those reasons,” she explained.
“That being said, while designed as a noninferiority study, it is interesting to note that alteplase again showed no evidence of treatment effect compared to antiplatelet therapy, affirming what was observed in the prematurely terminated PRISMS trial,” Dr. Khatri added.
In a discussion of the study at an ISC 2023 highlights session, ISC program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., said: “This is very important data and it’s actually the first completed trial that examines this question.”
But, he added, “I think we need to refine our knowledge about what a nondisabling stroke actually is. You could argue that every stroke is disabling. I think we need more clarity on this definition, as in practice, many clinicians still give tPA on account of these mild strokes still being disabling.”
The ARAMIS trial was funded by the National Key R&D Program of China and the Science and Technology Project Plan of Liaoning Province. Dr. Nguyen reports research support from Medtronic that was not related to the current study.
A version of this article first appeared on Medscape.com.
in the ARAMIS trial.
The trial was presented by Thanh Nguyen, MD, Boston Medical Center, at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
“Given the ease of administration, less intensive monitoring, low cost, and safety profile of dual antiplatelet therapy, the current findings support the use of dual antiplatelet in this population,” Dr. Nguyen concluded.
In a comment on the trial, Pooja Khatri, MD, professor of neurology at the University of Cincinnati, and lead investigator of the previous PRISMS study of tissue plasminogen activator (tPA) or alteplase in mild stroke, said the results reinforced the current recommendations of giving dual antiplatelet therapy but not alteplase to these patients.
Noting that the standard of care is now to give dual antiplatelet therapy to these patients, Dr. Khatri said: “These data reassure that this remains the right way to go.”
She added that her take-home message from the study would be: “Keep giving dual antiplatelet therapy, and we may be doing more harm than good with alteplase in this patient population.”
Introducing her presentation, Dr. Nguyen explained that mild ischemic stroke, defined as having a National Institutes of Health Stroke Scale (NIHSS) score of 5 or less, comprises half of ischemic stroke patients in the United States. But the benefit of thrombolysis in patients with minor ischemic stroke that is not disabling is unknown.
A subgroup analysis of one of the major thrombolysis trials (IST-3) found that a higher proportion of patients with mild ischemic stroke who were treated within 3 hours of symptom onset were alive and independent at 6 months if they had been given thrombolysis (84%), compared to 65% in the control group who received standard medical treatment.
This led to the first randomized trial (PRISMS) dedicated to patients with mild nondisabling stroke, which found that alteplase given within 3 hours of symptom onset did not increase the likelihood of a good functional outcome at 90 days in comparison with single-agent aspirin. The study was unfortunately terminated early for administrative reasons, and no definitive conclusions could be drawn on the basis of these results, Dr. Nguyen reported.
In 2018, the American Heart Association/American Stroke Association guidelines indicated that for patients who present within 3 hours of symptom onset with mild ischemic stroke that was judged to be nondisabling, thrombolysis with intravenous alteplase could be considered, she noted.
In the meantime, dual antiplatelet therapy was shown to be safe and effective in the POINT and CHANCE trials in patients presenting with minor stroke within 12 or 24 hours, and the CHANCE trial also found a benefit in reducing recurrent stroke that was most effective in the first 2 weeks.
The current ARAMIS trial was therefore conducted to evaluate dual antiplatelet therapy in comparison with thrombolysis for patients with acute minor stroke (NIHSS 5 or less) who presented within 4.5 hours of symptom onset and were without clearly disabling deficit.
The trial was conducted in 38 hospitals in China and included 760 patients (median NIHSS score of 2) who were randomly assigned to receive intravenous alteplase at the standard dose of 0.9 mg/kg, followed by guideline-based antiplatelet treatment, or dual antiplatelet therapy (clopidogrel 300 mg plus 100 mg aspirin loading dose followed by 10 to 14 days of aspirin 100 mg and clopidogrel 75 mg).
The trial was designed to assess noninferiority of dual antiplatelet therapy to alteplase with noninferiority margin of –4.5%.
In the modified intention-to-treat analysis, which included 722 patients, the primary outcome (excellent functional outcome, defined as a Modified Rankin Scale score of 0 or 1 at 90 days) occurred in 93.8% of patients in the dual antiplatelet therapy group and in 91.4% of the alteplase group. This gave a difference of 2.4%, which fell within the limits for noninferiority (P = .0002 for noninferiority test).
“Therefore, this was a positive trial,” Dr. Nguyen stated.
About 20% of patients crossed over from the dual antiplatelet group to the thrombolysis group, and about 16% of patients crossed over from the thrombolysis group to the dual antiplatelet group. But a per-protocol and an “as treated” analysis showed results similar to those of the main intention-to-treat analysis.
Secondary outcomes were largely similar between the two groups other than early neurologic deterioration, which was less common in the dual antiplatelet therapy group.
In terms of safety, symptomatic intracranial hemorrhage occurred in 0.3% (1/369) in the dual antiplatelet group and in 0.9% (3/350) in the alteplase group, a nonsignificant difference.
Events of “any bleeding” occurred in more patients in the thrombolysis group (5.4%) than in the dual antiplatelet therapy group (1.6%), and this difference was significant (P = .01).
Subgroup analysis showed a trend toward benefit of alteplase for patients with higher NIHSS score at baseline (NIHSS > 3). Otherwise, the other subgroups looked similar to the main results.
Dr. Nguyen pointed out one limitation of the study – that dual antiplatelet therapy was updated to standard treatment in this target population in the 2019 AHA/ASA guidelines.
In her discussion of the study, Dr. Khatri suggested that the ARAMIS results were what might have been expected.
“Dual antiplatelet therapy is designed to prevent stroke. Even in the POINT trial, dual antiplatelet therapy showed no effect on 90-day functional outcome. It was really about prevention. The PRISMS trial suggested that alteplase was also unlikely to improve 90-day functional outcome in this population of patients with mild and not clearly disabling stroke. So, it is not surprising that dual antiplatelet therapy was noninferior to alteplase for 90-day functional outcome for both those reasons,” she explained.
“That being said, while designed as a noninferiority study, it is interesting to note that alteplase again showed no evidence of treatment effect compared to antiplatelet therapy, affirming what was observed in the prematurely terminated PRISMS trial,” Dr. Khatri added.
In a discussion of the study at an ISC 2023 highlights session, ISC program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., said: “This is very important data and it’s actually the first completed trial that examines this question.”
But, he added, “I think we need to refine our knowledge about what a nondisabling stroke actually is. You could argue that every stroke is disabling. I think we need more clarity on this definition, as in practice, many clinicians still give tPA on account of these mild strokes still being disabling.”
The ARAMIS trial was funded by the National Key R&D Program of China and the Science and Technology Project Plan of Liaoning Province. Dr. Nguyen reports research support from Medtronic that was not related to the current study.
A version of this article first appeared on Medscape.com.
in the ARAMIS trial.
The trial was presented by Thanh Nguyen, MD, Boston Medical Center, at the International Stroke Conference presented by the American Stroke Association, a division of the American Heart Association.
“Given the ease of administration, less intensive monitoring, low cost, and safety profile of dual antiplatelet therapy, the current findings support the use of dual antiplatelet in this population,” Dr. Nguyen concluded.
In a comment on the trial, Pooja Khatri, MD, professor of neurology at the University of Cincinnati, and lead investigator of the previous PRISMS study of tissue plasminogen activator (tPA) or alteplase in mild stroke, said the results reinforced the current recommendations of giving dual antiplatelet therapy but not alteplase to these patients.
Noting that the standard of care is now to give dual antiplatelet therapy to these patients, Dr. Khatri said: “These data reassure that this remains the right way to go.”
She added that her take-home message from the study would be: “Keep giving dual antiplatelet therapy, and we may be doing more harm than good with alteplase in this patient population.”
Introducing her presentation, Dr. Nguyen explained that mild ischemic stroke, defined as having a National Institutes of Health Stroke Scale (NIHSS) score of 5 or less, comprises half of ischemic stroke patients in the United States. But the benefit of thrombolysis in patients with minor ischemic stroke that is not disabling is unknown.
A subgroup analysis of one of the major thrombolysis trials (IST-3) found that a higher proportion of patients with mild ischemic stroke who were treated within 3 hours of symptom onset were alive and independent at 6 months if they had been given thrombolysis (84%), compared to 65% in the control group who received standard medical treatment.
This led to the first randomized trial (PRISMS) dedicated to patients with mild nondisabling stroke, which found that alteplase given within 3 hours of symptom onset did not increase the likelihood of a good functional outcome at 90 days in comparison with single-agent aspirin. The study was unfortunately terminated early for administrative reasons, and no definitive conclusions could be drawn on the basis of these results, Dr. Nguyen reported.
In 2018, the American Heart Association/American Stroke Association guidelines indicated that for patients who present within 3 hours of symptom onset with mild ischemic stroke that was judged to be nondisabling, thrombolysis with intravenous alteplase could be considered, she noted.
In the meantime, dual antiplatelet therapy was shown to be safe and effective in the POINT and CHANCE trials in patients presenting with minor stroke within 12 or 24 hours, and the CHANCE trial also found a benefit in reducing recurrent stroke that was most effective in the first 2 weeks.
The current ARAMIS trial was therefore conducted to evaluate dual antiplatelet therapy in comparison with thrombolysis for patients with acute minor stroke (NIHSS 5 or less) who presented within 4.5 hours of symptom onset and were without clearly disabling deficit.
The trial was conducted in 38 hospitals in China and included 760 patients (median NIHSS score of 2) who were randomly assigned to receive intravenous alteplase at the standard dose of 0.9 mg/kg, followed by guideline-based antiplatelet treatment, or dual antiplatelet therapy (clopidogrel 300 mg plus 100 mg aspirin loading dose followed by 10 to 14 days of aspirin 100 mg and clopidogrel 75 mg).
The trial was designed to assess noninferiority of dual antiplatelet therapy to alteplase with noninferiority margin of –4.5%.
In the modified intention-to-treat analysis, which included 722 patients, the primary outcome (excellent functional outcome, defined as a Modified Rankin Scale score of 0 or 1 at 90 days) occurred in 93.8% of patients in the dual antiplatelet therapy group and in 91.4% of the alteplase group. This gave a difference of 2.4%, which fell within the limits for noninferiority (P = .0002 for noninferiority test).
“Therefore, this was a positive trial,” Dr. Nguyen stated.
About 20% of patients crossed over from the dual antiplatelet group to the thrombolysis group, and about 16% of patients crossed over from the thrombolysis group to the dual antiplatelet group. But a per-protocol and an “as treated” analysis showed results similar to those of the main intention-to-treat analysis.
Secondary outcomes were largely similar between the two groups other than early neurologic deterioration, which was less common in the dual antiplatelet therapy group.
In terms of safety, symptomatic intracranial hemorrhage occurred in 0.3% (1/369) in the dual antiplatelet group and in 0.9% (3/350) in the alteplase group, a nonsignificant difference.
Events of “any bleeding” occurred in more patients in the thrombolysis group (5.4%) than in the dual antiplatelet therapy group (1.6%), and this difference was significant (P = .01).
Subgroup analysis showed a trend toward benefit of alteplase for patients with higher NIHSS score at baseline (NIHSS > 3). Otherwise, the other subgroups looked similar to the main results.
Dr. Nguyen pointed out one limitation of the study – that dual antiplatelet therapy was updated to standard treatment in this target population in the 2019 AHA/ASA guidelines.
In her discussion of the study, Dr. Khatri suggested that the ARAMIS results were what might have been expected.
“Dual antiplatelet therapy is designed to prevent stroke. Even in the POINT trial, dual antiplatelet therapy showed no effect on 90-day functional outcome. It was really about prevention. The PRISMS trial suggested that alteplase was also unlikely to improve 90-day functional outcome in this population of patients with mild and not clearly disabling stroke. So, it is not surprising that dual antiplatelet therapy was noninferior to alteplase for 90-day functional outcome for both those reasons,” she explained.
“That being said, while designed as a noninferiority study, it is interesting to note that alteplase again showed no evidence of treatment effect compared to antiplatelet therapy, affirming what was observed in the prematurely terminated PRISMS trial,” Dr. Khatri added.
In a discussion of the study at an ISC 2023 highlights session, ISC program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry Hill, N.J., said: “This is very important data and it’s actually the first completed trial that examines this question.”
But, he added, “I think we need to refine our knowledge about what a nondisabling stroke actually is. You could argue that every stroke is disabling. I think we need more clarity on this definition, as in practice, many clinicians still give tPA on account of these mild strokes still being disabling.”
The ARAMIS trial was funded by the National Key R&D Program of China and the Science and Technology Project Plan of Liaoning Province. Dr. Nguyen reports research support from Medtronic that was not related to the current study.
A version of this article first appeared on Medscape.com.
FROM ISC 2023
Diabetes drug tied to lower dementia risk
new research suggests.
Overall, in a large cohort study from South Korea, patients who took pioglitazone were 16% less likely to develop dementia over an average of 10 years than peers who did not take the drug.
However, the dementia risk reduction was 54% among those with ischemic heart disease and 43% among those with a history of stroke.
“Our study was to see the association between pioglitazone use and incidence of dementia, not how (with what mechanisms) this drug can suppress dementia pathology,” coinvestigator Eosu Kim, MD, PhD, Yonsei University, Seoul, South Korea, said in an interview.
However, “as we found this drug is more effective in diabetic patients who have blood circulation problems in the heart or brain than in those without such problems, we speculate that pioglitazone’s antidementia action may be related to improving blood vessel’s health,” Dr. Kim said.
This finding suggests that pioglitazone could be used as a personalized treatment approach for dementia prevention in this subgroup of patients with diabetes, the researchers noted.
The results were published online in Neurology.
Dose-response relationship
Risk for dementia is doubled in adults with T2DM, the investigators wrote. Prior studies have suggested that pioglitazone may protect against dementia, as well as a first or recurrent stroke, in patients with T2DM.
This led Dr. Kim and colleagues to examine the effects of pioglitazone on dementia risk overall and in relation to stroke and ischemic heart disease.
Using the national Korean health database, the researchers identified 91,218 adults aged 50 and older with new-onset T2DM who did not have dementia. A total of 3,467 were treated with pioglitazone.
Pioglitazone exposure was defined as a total cumulative daily dose of 90 or more calculated from all dispensations during 4 years after T2DM diagnosis, with outcomes assessed after this period.
Over an average of 10 years, 8.3% of pioglitazone users developed dementia, compared with 10.0% of nonusers.
There was a statistically significant 16% lower risk for developing all-cause dementia among pioglitazone users than among nonusers (adjusted hazard ratio, 0.84; 95% confidence interval, 0.75-0.95).
A dose-response relationship was evident; pioglitazone users who received the highest cumulative daily dose were at lower risk for dementia (aHR, 0.72; 95% CI, 0.55-0.94).
Several limitations
The reduced risk for dementia was more pronounced among patients who used pioglitazone for 4 years in comparison with patients who did not use the drug (aHR, 0.63; 95% CI, 0.44-0.90).
The apparent protective effect of pioglitazone with regard to dementia was greater among those with a history of ischemic heart disease (aHR, 0.46; 95% CI, 0.24-0.90) or stroke (aHR, 0.57; 95% CI, 0.38-0.86) before diabetes diagnosis.
The incidence of stroke was also reduced with pioglitazone use (aHR, 0.81; 95% CI, 0.66-1.0).
“These results provide valuable information on who could potentially benefit from pioglitazone use for prevention of dementia,” Dr. Kim said in a news release.
However, “the risk and benefit balance of long-term use of this drug to prevent dementia should be prospectively assessed,” he said in an interview.
The researchers cautioned that the study was observational; hence, the reported associations cannot address causal relationships. Also, because of the use of claims data, drug compliance could not be guaranteed, and exposure may have been overestimated.
There is also the potential for selection bias, and no information on apolipoprotein E was available, they noted.
More data needed
In an accompanying editorial, Colleen J. Maxwell, PhD, University of Waterloo (Ont.), and colleagues wrote that the results “not only support previous studies showing the potential cognitive benefit of pioglitazone but also extend our understanding of this benefit through the mediating effect of reducing ischemic stroke.”
However, because of their associated risks, which include fractures, weight gain, heart failure, and bladder cancer, thiazolidinediones are not currently favored in diabetes management guidelines – and their use has significantly declined since the mid to late 2000s, the editorialists noted.
They agreed that it will be important to reassess the risk-benefit profile of pioglitazone in T2DM as additional findings emerge.
They also noted that sodium-glucose cotransporter-2 inhibitors, which have significant cardiovascular and renal benefits and minimal side effects, may also lower the risk for dementia.
“As both pioglitazone and SGLT-2 inhibitors are second-line options for physicians, the current decision would easily be in favor of SGLT-2 inhibitors given their safety profile,” Dr. Maxwell and colleagues wrote.
For now, pioglitazone “should not be used to prevent dementia in patients with T2DM,” they concluded.
The study was supported by grants from the National Research Foundation of Korea funded by the Korean government and the Ministry of Health and Welfare. The investigators and editorialists report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests.
Overall, in a large cohort study from South Korea, patients who took pioglitazone were 16% less likely to develop dementia over an average of 10 years than peers who did not take the drug.
However, the dementia risk reduction was 54% among those with ischemic heart disease and 43% among those with a history of stroke.
“Our study was to see the association between pioglitazone use and incidence of dementia, not how (with what mechanisms) this drug can suppress dementia pathology,” coinvestigator Eosu Kim, MD, PhD, Yonsei University, Seoul, South Korea, said in an interview.
However, “as we found this drug is more effective in diabetic patients who have blood circulation problems in the heart or brain than in those without such problems, we speculate that pioglitazone’s antidementia action may be related to improving blood vessel’s health,” Dr. Kim said.
This finding suggests that pioglitazone could be used as a personalized treatment approach for dementia prevention in this subgroup of patients with diabetes, the researchers noted.
The results were published online in Neurology.
Dose-response relationship
Risk for dementia is doubled in adults with T2DM, the investigators wrote. Prior studies have suggested that pioglitazone may protect against dementia, as well as a first or recurrent stroke, in patients with T2DM.
This led Dr. Kim and colleagues to examine the effects of pioglitazone on dementia risk overall and in relation to stroke and ischemic heart disease.
Using the national Korean health database, the researchers identified 91,218 adults aged 50 and older with new-onset T2DM who did not have dementia. A total of 3,467 were treated with pioglitazone.
Pioglitazone exposure was defined as a total cumulative daily dose of 90 or more calculated from all dispensations during 4 years after T2DM diagnosis, with outcomes assessed after this period.
Over an average of 10 years, 8.3% of pioglitazone users developed dementia, compared with 10.0% of nonusers.
There was a statistically significant 16% lower risk for developing all-cause dementia among pioglitazone users than among nonusers (adjusted hazard ratio, 0.84; 95% confidence interval, 0.75-0.95).
A dose-response relationship was evident; pioglitazone users who received the highest cumulative daily dose were at lower risk for dementia (aHR, 0.72; 95% CI, 0.55-0.94).
Several limitations
The reduced risk for dementia was more pronounced among patients who used pioglitazone for 4 years in comparison with patients who did not use the drug (aHR, 0.63; 95% CI, 0.44-0.90).
The apparent protective effect of pioglitazone with regard to dementia was greater among those with a history of ischemic heart disease (aHR, 0.46; 95% CI, 0.24-0.90) or stroke (aHR, 0.57; 95% CI, 0.38-0.86) before diabetes diagnosis.
The incidence of stroke was also reduced with pioglitazone use (aHR, 0.81; 95% CI, 0.66-1.0).
“These results provide valuable information on who could potentially benefit from pioglitazone use for prevention of dementia,” Dr. Kim said in a news release.
However, “the risk and benefit balance of long-term use of this drug to prevent dementia should be prospectively assessed,” he said in an interview.
The researchers cautioned that the study was observational; hence, the reported associations cannot address causal relationships. Also, because of the use of claims data, drug compliance could not be guaranteed, and exposure may have been overestimated.
There is also the potential for selection bias, and no information on apolipoprotein E was available, they noted.
More data needed
In an accompanying editorial, Colleen J. Maxwell, PhD, University of Waterloo (Ont.), and colleagues wrote that the results “not only support previous studies showing the potential cognitive benefit of pioglitazone but also extend our understanding of this benefit through the mediating effect of reducing ischemic stroke.”
However, because of their associated risks, which include fractures, weight gain, heart failure, and bladder cancer, thiazolidinediones are not currently favored in diabetes management guidelines – and their use has significantly declined since the mid to late 2000s, the editorialists noted.
They agreed that it will be important to reassess the risk-benefit profile of pioglitazone in T2DM as additional findings emerge.
They also noted that sodium-glucose cotransporter-2 inhibitors, which have significant cardiovascular and renal benefits and minimal side effects, may also lower the risk for dementia.
“As both pioglitazone and SGLT-2 inhibitors are second-line options for physicians, the current decision would easily be in favor of SGLT-2 inhibitors given their safety profile,” Dr. Maxwell and colleagues wrote.
For now, pioglitazone “should not be used to prevent dementia in patients with T2DM,” they concluded.
The study was supported by grants from the National Research Foundation of Korea funded by the Korean government and the Ministry of Health and Welfare. The investigators and editorialists report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests.
Overall, in a large cohort study from South Korea, patients who took pioglitazone were 16% less likely to develop dementia over an average of 10 years than peers who did not take the drug.
However, the dementia risk reduction was 54% among those with ischemic heart disease and 43% among those with a history of stroke.
“Our study was to see the association between pioglitazone use and incidence of dementia, not how (with what mechanisms) this drug can suppress dementia pathology,” coinvestigator Eosu Kim, MD, PhD, Yonsei University, Seoul, South Korea, said in an interview.
However, “as we found this drug is more effective in diabetic patients who have blood circulation problems in the heart or brain than in those without such problems, we speculate that pioglitazone’s antidementia action may be related to improving blood vessel’s health,” Dr. Kim said.
This finding suggests that pioglitazone could be used as a personalized treatment approach for dementia prevention in this subgroup of patients with diabetes, the researchers noted.
The results were published online in Neurology.
Dose-response relationship
Risk for dementia is doubled in adults with T2DM, the investigators wrote. Prior studies have suggested that pioglitazone may protect against dementia, as well as a first or recurrent stroke, in patients with T2DM.
This led Dr. Kim and colleagues to examine the effects of pioglitazone on dementia risk overall and in relation to stroke and ischemic heart disease.
Using the national Korean health database, the researchers identified 91,218 adults aged 50 and older with new-onset T2DM who did not have dementia. A total of 3,467 were treated with pioglitazone.
Pioglitazone exposure was defined as a total cumulative daily dose of 90 or more calculated from all dispensations during 4 years after T2DM diagnosis, with outcomes assessed after this period.
Over an average of 10 years, 8.3% of pioglitazone users developed dementia, compared with 10.0% of nonusers.
There was a statistically significant 16% lower risk for developing all-cause dementia among pioglitazone users than among nonusers (adjusted hazard ratio, 0.84; 95% confidence interval, 0.75-0.95).
A dose-response relationship was evident; pioglitazone users who received the highest cumulative daily dose were at lower risk for dementia (aHR, 0.72; 95% CI, 0.55-0.94).
Several limitations
The reduced risk for dementia was more pronounced among patients who used pioglitazone for 4 years in comparison with patients who did not use the drug (aHR, 0.63; 95% CI, 0.44-0.90).
The apparent protective effect of pioglitazone with regard to dementia was greater among those with a history of ischemic heart disease (aHR, 0.46; 95% CI, 0.24-0.90) or stroke (aHR, 0.57; 95% CI, 0.38-0.86) before diabetes diagnosis.
The incidence of stroke was also reduced with pioglitazone use (aHR, 0.81; 95% CI, 0.66-1.0).
“These results provide valuable information on who could potentially benefit from pioglitazone use for prevention of dementia,” Dr. Kim said in a news release.
However, “the risk and benefit balance of long-term use of this drug to prevent dementia should be prospectively assessed,” he said in an interview.
The researchers cautioned that the study was observational; hence, the reported associations cannot address causal relationships. Also, because of the use of claims data, drug compliance could not be guaranteed, and exposure may have been overestimated.
There is also the potential for selection bias, and no information on apolipoprotein E was available, they noted.
More data needed
In an accompanying editorial, Colleen J. Maxwell, PhD, University of Waterloo (Ont.), and colleagues wrote that the results “not only support previous studies showing the potential cognitive benefit of pioglitazone but also extend our understanding of this benefit through the mediating effect of reducing ischemic stroke.”
However, because of their associated risks, which include fractures, weight gain, heart failure, and bladder cancer, thiazolidinediones are not currently favored in diabetes management guidelines – and their use has significantly declined since the mid to late 2000s, the editorialists noted.
They agreed that it will be important to reassess the risk-benefit profile of pioglitazone in T2DM as additional findings emerge.
They also noted that sodium-glucose cotransporter-2 inhibitors, which have significant cardiovascular and renal benefits and minimal side effects, may also lower the risk for dementia.
“As both pioglitazone and SGLT-2 inhibitors are second-line options for physicians, the current decision would easily be in favor of SGLT-2 inhibitors given their safety profile,” Dr. Maxwell and colleagues wrote.
For now, pioglitazone “should not be used to prevent dementia in patients with T2DM,” they concluded.
The study was supported by grants from the National Research Foundation of Korea funded by the Korean government and the Ministry of Health and Welfare. The investigators and editorialists report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM NEUROLOGY
Immunodeficiencies tied to psychiatric disorders in offspring
new research suggests.
Results from a cohort study of more than 4.2 million individuals showed that offspring of mothers with PIDs had a 17% increased risk for a psychiatric disorder and a 20% increased risk for suicidal behavior, compared with their peers with mothers who did not have PIDs.
The risk was more pronounced in offspring of mothers with both PIDs and autoimmune diseases. These risks remained after strictly controlling for different covariates, such as the parents’ psychiatric history, offspring PIDs, and offspring autoimmune diseases.
The investigators, led by Josef Isung, MD, PhD, Centre for Psychiatry Research, department of clinical neuroscience, Karolinska Institutet, Stockholm, noted that they could not “pinpoint a precise causal mechanism” underlying these findings.
Still, “the results add to the existing literature suggesting that the intrauterine immune environment may have implications for fetal neurodevelopment and that a compromised maternal immune system during pregnancy may be a risk factor for psychiatric disorders and suicidal behavior in their offspring in the long term,” they wrote.
The findings were published online in JAMA Psychiatry.
‘Natural experiment’
Maternal immune activation (MIA) is “an overarching term for aberrant and disrupted immune activity in the mother during gestation [and] has long been of interest in relation to adverse health outcomes in the offspring,” Dr. Isung noted.
“In relation to negative psychiatric outcomes, there is an abundance of preclinical evidence that has shown a negative impact on offspring secondary to MIA. And in humans, there are several observational studies supporting this link,” he said in an interview.
Dr. Isung added that PIDs are “rare conditions” known to be associated with repeated infections and high rates of autoimmune diseases, causing substantial disability.
“PIDs represent an interesting ‘natural experiment’ for researchers to understand more about the association between immune system dysfunctions and mental health,” he said.
Dr. Isung’s group previously showed that individuals with PIDs have increased odds of psychiatric disorders and suicidal behavior. The link was more pronounced in women with PIDs – and was even more pronounced in those with both PIDs and autoimmune diseases.
In the current study, “we wanted to see whether offspring of individuals were differentially at risk of psychiatric disorders and suicidal behavior, depending on being offspring of mothers or fathers with PIDs,” Dr. Isung said.
“Our hypothesis was that mothers with PIDs would have an increased risk of having offspring with neuropsychiatric outcomes, and that this risk could be due to MIA,” he added.
The researchers turned to Swedish nationwide health and administrative registers. They analyzed data on all individuals with diagnoses of PIDs identified between 1973 and 2013. Offspring born prior to 2003 were included, and parent-offspring pairs in which both parents had a history of PIDs were excluded.
The final study sample consisted of 4,294,169 offspring (51.4% boys). Of these participants, 7,270 (0.17%) had a parent with PIDs.
The researchers identified lifetime records of 10 psychiatric disorders: obsessive-compulsive disorder, ADHD, autism spectrum disorders, schizophrenia and other psychotic disorders, bipolar disorders, major depressive disorder and other mood disorders, anxiety and stress-related disorders, eating disorders, substance use disorders, and Tourette syndrome and chronic tic disorders.
The investigators included parental birth year, psychopathology, suicide attempts, suicide deaths, and autoimmune diseases as covariates, as well as offsprings’ birth year and gender.
Elucidation needed
Results showed that, of the 4,676 offspring of mothers with PID, 17.1% had a psychiatric disorder versus 12.7% of offspring of mothers without PIDs. This translated “into a 17% increased risk for offspring of mothers with PIDs in the fully adjusted model,” the investigators reported.
The risk was even higher for offspring of mothers who had not only PIDs but also one of six of the individual psychiatric disorders, with incident rate ratios ranging from 1.15 to 1.71.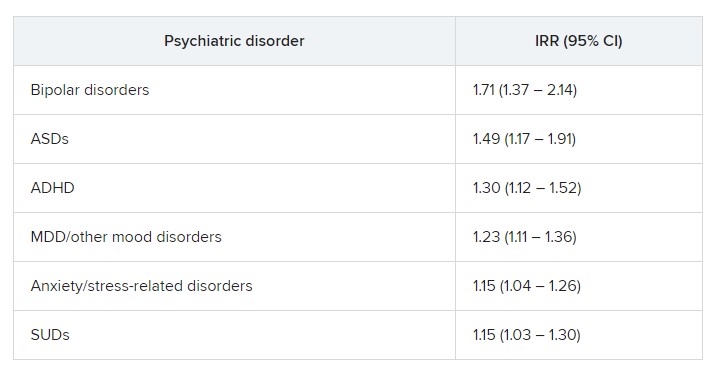
“In fully adjusted models, offspring of mothers with PIDs had an increased risk of any psychiatric disorder, while no such risks were observed in offspring of fathers with PIDs” (IRR, 1.17 vs. 1.03; P < .001), the researchers reported.
A higher risk for suicidal behavior was also observed among offspring of mothers with PIDS, in contrast to those of fathers with PIDs (IRR, 1.2 vs. 1.1; P = .01).
The greatest risk for any psychiatric disorder, as well as suicidal behavior, was found in offspring of mothers who had both PIDs and autoimmune diseases (IRRs, 1.24 and 1.44, respectively).
“The results could be seen as substantiating the hypothesis that immune disruption may be important in the pathophysiology of psychiatric disorders and suicidal behavior,” Dr. Isung said.
“Furthermore, the fact that only offspring of mothers and not offspring of fathers with PIDs had this association would align with our hypothesis that MIA is of importance,” he added.
However, he noted that “the specific mechanisms are most likely multifactorial and remain to be elucidated.”
Important piece of the puzzle?
In a comment, Michael Eriksen Benros, MD, PhD, professor of immunopsychiatry, department of immunology and microbiology, health, and medical sciences, University of Copenhagen, said this was a “high-quality study” that used a “rich data source.”
Dr. Benros, who is also head of research (biological and precision psychiatry) at the Copenhagen Research Centre for Mental Health, Copenhagen University Hospital, was not involved with the current study.
He noted that prior studies, including some conducted by his own group, have shown that maternal infections overall did not seem to be “specifically linked to mental disorders in the offspring.”
However, “specific maternal infections or specific brain-reactive antibodies during the pregnancy period have been shown to be associated with neurodevelopmental outcomes among the children,” such as intellectual disability, he said.
Regarding direct clinical implications of the study, “it is important to note that the increased risk of psychiatric disorders and suicidality in the offspring of mothers with PID were small,” Dr. Benros said.
“However, it adds an important part to the scientific puzzle regarding the role of maternal immune activation during pregnancy and the risk of mental disorders,” he added.
The study was funded by the Söderström König Foundation and the Fredrik and Ingrid Thuring Foundation. Neither Dr. Isung nor Dr. Benros reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests.
Results from a cohort study of more than 4.2 million individuals showed that offspring of mothers with PIDs had a 17% increased risk for a psychiatric disorder and a 20% increased risk for suicidal behavior, compared with their peers with mothers who did not have PIDs.
The risk was more pronounced in offspring of mothers with both PIDs and autoimmune diseases. These risks remained after strictly controlling for different covariates, such as the parents’ psychiatric history, offspring PIDs, and offspring autoimmune diseases.
The investigators, led by Josef Isung, MD, PhD, Centre for Psychiatry Research, department of clinical neuroscience, Karolinska Institutet, Stockholm, noted that they could not “pinpoint a precise causal mechanism” underlying these findings.
Still, “the results add to the existing literature suggesting that the intrauterine immune environment may have implications for fetal neurodevelopment and that a compromised maternal immune system during pregnancy may be a risk factor for psychiatric disorders and suicidal behavior in their offspring in the long term,” they wrote.
The findings were published online in JAMA Psychiatry.
‘Natural experiment’
Maternal immune activation (MIA) is “an overarching term for aberrant and disrupted immune activity in the mother during gestation [and] has long been of interest in relation to adverse health outcomes in the offspring,” Dr. Isung noted.
“In relation to negative psychiatric outcomes, there is an abundance of preclinical evidence that has shown a negative impact on offspring secondary to MIA. And in humans, there are several observational studies supporting this link,” he said in an interview.
Dr. Isung added that PIDs are “rare conditions” known to be associated with repeated infections and high rates of autoimmune diseases, causing substantial disability.
“PIDs represent an interesting ‘natural experiment’ for researchers to understand more about the association between immune system dysfunctions and mental health,” he said.
Dr. Isung’s group previously showed that individuals with PIDs have increased odds of psychiatric disorders and suicidal behavior. The link was more pronounced in women with PIDs – and was even more pronounced in those with both PIDs and autoimmune diseases.
In the current study, “we wanted to see whether offspring of individuals were differentially at risk of psychiatric disorders and suicidal behavior, depending on being offspring of mothers or fathers with PIDs,” Dr. Isung said.
“Our hypothesis was that mothers with PIDs would have an increased risk of having offspring with neuropsychiatric outcomes, and that this risk could be due to MIA,” he added.
The researchers turned to Swedish nationwide health and administrative registers. They analyzed data on all individuals with diagnoses of PIDs identified between 1973 and 2013. Offspring born prior to 2003 were included, and parent-offspring pairs in which both parents had a history of PIDs were excluded.
The final study sample consisted of 4,294,169 offspring (51.4% boys). Of these participants, 7,270 (0.17%) had a parent with PIDs.
The researchers identified lifetime records of 10 psychiatric disorders: obsessive-compulsive disorder, ADHD, autism spectrum disorders, schizophrenia and other psychotic disorders, bipolar disorders, major depressive disorder and other mood disorders, anxiety and stress-related disorders, eating disorders, substance use disorders, and Tourette syndrome and chronic tic disorders.
The investigators included parental birth year, psychopathology, suicide attempts, suicide deaths, and autoimmune diseases as covariates, as well as offsprings’ birth year and gender.
Elucidation needed
Results showed that, of the 4,676 offspring of mothers with PID, 17.1% had a psychiatric disorder versus 12.7% of offspring of mothers without PIDs. This translated “into a 17% increased risk for offspring of mothers with PIDs in the fully adjusted model,” the investigators reported.
The risk was even higher for offspring of mothers who had not only PIDs but also one of six of the individual psychiatric disorders, with incident rate ratios ranging from 1.15 to 1.71.
“In fully adjusted models, offspring of mothers with PIDs had an increased risk of any psychiatric disorder, while no such risks were observed in offspring of fathers with PIDs” (IRR, 1.17 vs. 1.03; P < .001), the researchers reported.
A higher risk for suicidal behavior was also observed among offspring of mothers with PIDS, in contrast to those of fathers with PIDs (IRR, 1.2 vs. 1.1; P = .01).
The greatest risk for any psychiatric disorder, as well as suicidal behavior, was found in offspring of mothers who had both PIDs and autoimmune diseases (IRRs, 1.24 and 1.44, respectively).
“The results could be seen as substantiating the hypothesis that immune disruption may be important in the pathophysiology of psychiatric disorders and suicidal behavior,” Dr. Isung said.
“Furthermore, the fact that only offspring of mothers and not offspring of fathers with PIDs had this association would align with our hypothesis that MIA is of importance,” he added.
However, he noted that “the specific mechanisms are most likely multifactorial and remain to be elucidated.”
Important piece of the puzzle?
In a comment, Michael Eriksen Benros, MD, PhD, professor of immunopsychiatry, department of immunology and microbiology, health, and medical sciences, University of Copenhagen, said this was a “high-quality study” that used a “rich data source.”
Dr. Benros, who is also head of research (biological and precision psychiatry) at the Copenhagen Research Centre for Mental Health, Copenhagen University Hospital, was not involved with the current study.
He noted that prior studies, including some conducted by his own group, have shown that maternal infections overall did not seem to be “specifically linked to mental disorders in the offspring.”
However, “specific maternal infections or specific brain-reactive antibodies during the pregnancy period have been shown to be associated with neurodevelopmental outcomes among the children,” such as intellectual disability, he said.
Regarding direct clinical implications of the study, “it is important to note that the increased risk of psychiatric disorders and suicidality in the offspring of mothers with PID were small,” Dr. Benros said.
“However, it adds an important part to the scientific puzzle regarding the role of maternal immune activation during pregnancy and the risk of mental disorders,” he added.
The study was funded by the Söderström König Foundation and the Fredrik and Ingrid Thuring Foundation. Neither Dr. Isung nor Dr. Benros reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new research suggests.
Results from a cohort study of more than 4.2 million individuals showed that offspring of mothers with PIDs had a 17% increased risk for a psychiatric disorder and a 20% increased risk for suicidal behavior, compared with their peers with mothers who did not have PIDs.
The risk was more pronounced in offspring of mothers with both PIDs and autoimmune diseases. These risks remained after strictly controlling for different covariates, such as the parents’ psychiatric history, offspring PIDs, and offspring autoimmune diseases.
The investigators, led by Josef Isung, MD, PhD, Centre for Psychiatry Research, department of clinical neuroscience, Karolinska Institutet, Stockholm, noted that they could not “pinpoint a precise causal mechanism” underlying these findings.
Still, “the results add to the existing literature suggesting that the intrauterine immune environment may have implications for fetal neurodevelopment and that a compromised maternal immune system during pregnancy may be a risk factor for psychiatric disorders and suicidal behavior in their offspring in the long term,” they wrote.
The findings were published online in JAMA Psychiatry.
‘Natural experiment’
Maternal immune activation (MIA) is “an overarching term for aberrant and disrupted immune activity in the mother during gestation [and] has long been of interest in relation to adverse health outcomes in the offspring,” Dr. Isung noted.
“In relation to negative psychiatric outcomes, there is an abundance of preclinical evidence that has shown a negative impact on offspring secondary to MIA. And in humans, there are several observational studies supporting this link,” he said in an interview.
Dr. Isung added that PIDs are “rare conditions” known to be associated with repeated infections and high rates of autoimmune diseases, causing substantial disability.
“PIDs represent an interesting ‘natural experiment’ for researchers to understand more about the association between immune system dysfunctions and mental health,” he said.
Dr. Isung’s group previously showed that individuals with PIDs have increased odds of psychiatric disorders and suicidal behavior. The link was more pronounced in women with PIDs – and was even more pronounced in those with both PIDs and autoimmune diseases.
In the current study, “we wanted to see whether offspring of individuals were differentially at risk of psychiatric disorders and suicidal behavior, depending on being offspring of mothers or fathers with PIDs,” Dr. Isung said.
“Our hypothesis was that mothers with PIDs would have an increased risk of having offspring with neuropsychiatric outcomes, and that this risk could be due to MIA,” he added.
The researchers turned to Swedish nationwide health and administrative registers. They analyzed data on all individuals with diagnoses of PIDs identified between 1973 and 2013. Offspring born prior to 2003 were included, and parent-offspring pairs in which both parents had a history of PIDs were excluded.
The final study sample consisted of 4,294,169 offspring (51.4% boys). Of these participants, 7,270 (0.17%) had a parent with PIDs.
The researchers identified lifetime records of 10 psychiatric disorders: obsessive-compulsive disorder, ADHD, autism spectrum disorders, schizophrenia and other psychotic disorders, bipolar disorders, major depressive disorder and other mood disorders, anxiety and stress-related disorders, eating disorders, substance use disorders, and Tourette syndrome and chronic tic disorders.
The investigators included parental birth year, psychopathology, suicide attempts, suicide deaths, and autoimmune diseases as covariates, as well as offsprings’ birth year and gender.
Elucidation needed
Results showed that, of the 4,676 offspring of mothers with PID, 17.1% had a psychiatric disorder versus 12.7% of offspring of mothers without PIDs. This translated “into a 17% increased risk for offspring of mothers with PIDs in the fully adjusted model,” the investigators reported.
The risk was even higher for offspring of mothers who had not only PIDs but also one of six of the individual psychiatric disorders, with incident rate ratios ranging from 1.15 to 1.71.
“In fully adjusted models, offspring of mothers with PIDs had an increased risk of any psychiatric disorder, while no such risks were observed in offspring of fathers with PIDs” (IRR, 1.17 vs. 1.03; P < .001), the researchers reported.
A higher risk for suicidal behavior was also observed among offspring of mothers with PIDS, in contrast to those of fathers with PIDs (IRR, 1.2 vs. 1.1; P = .01).
The greatest risk for any psychiatric disorder, as well as suicidal behavior, was found in offspring of mothers who had both PIDs and autoimmune diseases (IRRs, 1.24 and 1.44, respectively).
“The results could be seen as substantiating the hypothesis that immune disruption may be important in the pathophysiology of psychiatric disorders and suicidal behavior,” Dr. Isung said.
“Furthermore, the fact that only offspring of mothers and not offspring of fathers with PIDs had this association would align with our hypothesis that MIA is of importance,” he added.
However, he noted that “the specific mechanisms are most likely multifactorial and remain to be elucidated.”
Important piece of the puzzle?
In a comment, Michael Eriksen Benros, MD, PhD, professor of immunopsychiatry, department of immunology and microbiology, health, and medical sciences, University of Copenhagen, said this was a “high-quality study” that used a “rich data source.”
Dr. Benros, who is also head of research (biological and precision psychiatry) at the Copenhagen Research Centre for Mental Health, Copenhagen University Hospital, was not involved with the current study.
He noted that prior studies, including some conducted by his own group, have shown that maternal infections overall did not seem to be “specifically linked to mental disorders in the offspring.”
However, “specific maternal infections or specific brain-reactive antibodies during the pregnancy period have been shown to be associated with neurodevelopmental outcomes among the children,” such as intellectual disability, he said.
Regarding direct clinical implications of the study, “it is important to note that the increased risk of psychiatric disorders and suicidality in the offspring of mothers with PID were small,” Dr. Benros said.
“However, it adds an important part to the scientific puzzle regarding the role of maternal immune activation during pregnancy and the risk of mental disorders,” he added.
The study was funded by the Söderström König Foundation and the Fredrik and Ingrid Thuring Foundation. Neither Dr. Isung nor Dr. Benros reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM JAMA PSYCHIATRY