User login
Poor pregnancy outcomes seen in teens with type 2 diabetes
VANCOUVER, B.C. – Despite agreeing to use birth control and receiving frequent counseling about pregnancy avoidance, a sizable share of teens with type 2 diabetes mellitus become pregnant, and these pregnancies often have poor outcomes, researchers reported at the World Diabetes Congress.
The analysis was based on 452 female participants in the national Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study, the largest trial in youth with this form of diabetes to date and one designed to have good representation of various racial/ethnic groups.
Overall, 10% of the girls became pregnant during a period of up to 6.5 years. The majority were not using contraception and did not recall the counseling. More than one-fourth of the pregnancies ended in fetal loss or stillbirth. And one-fifth of live-born infants had major congenital anomalies.
“We need to better understand the reasons for pregnancy in youth with type 2 diabetes and why, despite counseling, they become pregnant,” commented first author Dr. Kristen J. Nadeau of the division of pediatric endocrinology, department of pediatrics, University of Colorado, Aurora.
“Best practices for metabolically unhealthy pregnancy prevention in type 2 diabetic teens also requires further study,” she added. “Long-acting contraception, we think, currently is the best method and likely the way to go in these girls who are not retaining the education and [adhering to] the behaviors that we are hoping for.”
“This study is critically important and horribly depressing,” commented session comoderator Dr. Robert E. Ratner, professor of medicine at Georgetown University and senior research scientist at the MedStar Health Research Institute, Washington, as well as chief scientific and medical officer of the American Diabetes Association, Alexandria, Va.
“It points out the difficulties of being a teenager and the even greater difficulties of being a teenager with a chronic disease,” he said in an interview, adding that there are no easy solutions.
“The combination of a teen pregnancy in someone with type 2 diabetes creates the perfect storm,” Dr. Nadeau noted. “Diabetes control is worse in adolescence than in any other time in the lifespan, and with increasing rates of type 2 diabetes in youth, increases in a teen pregnancy that are complicated by diabetes are anticipated,” she added.
At baseline, participants in TODAY were 10-17 years old, were overweight or obese, and had a diabetes duration of less than 2 years and a hemoglobin A1c level of less than 8%. They were randomized to three treatment arms (metformin alone, metformin plus rosiglitazone, or metformin plus an intensive lifestyle program).
Consent for the trial required the use of a birth control method, including abstinence; in addition, every 2-3 months, the girls received diabetes education and counseling to defer pregnancy until their HbA1c level fell below 6%. They also had regular pregnancy testing, and those with a positive result were taken off their trial medication and referred to a maternal-fetal medicine specialist.
The results reported at the meeting and simultaneously published in Diabetes Care (doi: 10.2337/dc15-1206) showed that 46 (10.2%) of the girls had 63 pregnancies. On average, they were 18 years old at the time of a first pregnancy.
Despite the counseling, only about 5% of those teens who became pregnant reported that they had been using contraception. Moreover, just 13% recalled the counseling.
The median body mass index closest to conception was 35.2 kg/m2, and the median HbA1c level was 7%. “Because of the fact that we were so heavily monitoring these girls, we had their HbA1c under better control than is typical. In our typical clinic, the mean is more like 8.5%-9%,” Dr. Nadeau noted.
Relative to peers who did not become pregnant, those who did were significantly older, were less likely to be living with both parents or their mother, and had a lower household income.
Seven of the 63 pregnancies were electively terminated. Of the 53 remaining pregnancies with data, 12 ended in pregnancy loss and 2 ended in a stillbirth.
Among the 39 live-born infants, 6 were preterm and 8 had major congenital anomalies. And among the 37 with known birth weight, 10 were either small or large for gestational age.
Girls randomized to metformin plus rosiglitazone had a higher rate of term normal births than peers in the other arms (P = .027). “Of note, none of the participants reported taking the rosiglitazone after the pregnancy was discovered, as was per the study protocol,” Dr. Nadeau commented. In contrast, neither maternal body mass index nor – surprisingly – HbA1c level was significantly associated with pregnancy outcome.
The rate of preterm birth observed in the teens studied was similar to what has been seen in adult women with diabetes, she noted. But the rate of major congenital anomalies was about four times higher.
“This potentially might be due to lower overall socioeconomic status of the girls in the TODAY study. Other reasons for the anomalies are uncertain, but might include metabolic control, smoking, or extreme obesity,” she said.
Dr. Nadeau disclosed that she had no relevant conflicts of interest.
VANCOUVER, B.C. – Despite agreeing to use birth control and receiving frequent counseling about pregnancy avoidance, a sizable share of teens with type 2 diabetes mellitus become pregnant, and these pregnancies often have poor outcomes, researchers reported at the World Diabetes Congress.
The analysis was based on 452 female participants in the national Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study, the largest trial in youth with this form of diabetes to date and one designed to have good representation of various racial/ethnic groups.
Overall, 10% of the girls became pregnant during a period of up to 6.5 years. The majority were not using contraception and did not recall the counseling. More than one-fourth of the pregnancies ended in fetal loss or stillbirth. And one-fifth of live-born infants had major congenital anomalies.
“We need to better understand the reasons for pregnancy in youth with type 2 diabetes and why, despite counseling, they become pregnant,” commented first author Dr. Kristen J. Nadeau of the division of pediatric endocrinology, department of pediatrics, University of Colorado, Aurora.
“Best practices for metabolically unhealthy pregnancy prevention in type 2 diabetic teens also requires further study,” she added. “Long-acting contraception, we think, currently is the best method and likely the way to go in these girls who are not retaining the education and [adhering to] the behaviors that we are hoping for.”
“This study is critically important and horribly depressing,” commented session comoderator Dr. Robert E. Ratner, professor of medicine at Georgetown University and senior research scientist at the MedStar Health Research Institute, Washington, as well as chief scientific and medical officer of the American Diabetes Association, Alexandria, Va.
“It points out the difficulties of being a teenager and the even greater difficulties of being a teenager with a chronic disease,” he said in an interview, adding that there are no easy solutions.
“The combination of a teen pregnancy in someone with type 2 diabetes creates the perfect storm,” Dr. Nadeau noted. “Diabetes control is worse in adolescence than in any other time in the lifespan, and with increasing rates of type 2 diabetes in youth, increases in a teen pregnancy that are complicated by diabetes are anticipated,” she added.
At baseline, participants in TODAY were 10-17 years old, were overweight or obese, and had a diabetes duration of less than 2 years and a hemoglobin A1c level of less than 8%. They were randomized to three treatment arms (metformin alone, metformin plus rosiglitazone, or metformin plus an intensive lifestyle program).
Consent for the trial required the use of a birth control method, including abstinence; in addition, every 2-3 months, the girls received diabetes education and counseling to defer pregnancy until their HbA1c level fell below 6%. They also had regular pregnancy testing, and those with a positive result were taken off their trial medication and referred to a maternal-fetal medicine specialist.
The results reported at the meeting and simultaneously published in Diabetes Care (doi: 10.2337/dc15-1206) showed that 46 (10.2%) of the girls had 63 pregnancies. On average, they were 18 years old at the time of a first pregnancy.
Despite the counseling, only about 5% of those teens who became pregnant reported that they had been using contraception. Moreover, just 13% recalled the counseling.
The median body mass index closest to conception was 35.2 kg/m2, and the median HbA1c level was 7%. “Because of the fact that we were so heavily monitoring these girls, we had their HbA1c under better control than is typical. In our typical clinic, the mean is more like 8.5%-9%,” Dr. Nadeau noted.
Relative to peers who did not become pregnant, those who did were significantly older, were less likely to be living with both parents or their mother, and had a lower household income.
Seven of the 63 pregnancies were electively terminated. Of the 53 remaining pregnancies with data, 12 ended in pregnancy loss and 2 ended in a stillbirth.
Among the 39 live-born infants, 6 were preterm and 8 had major congenital anomalies. And among the 37 with known birth weight, 10 were either small or large for gestational age.
Girls randomized to metformin plus rosiglitazone had a higher rate of term normal births than peers in the other arms (P = .027). “Of note, none of the participants reported taking the rosiglitazone after the pregnancy was discovered, as was per the study protocol,” Dr. Nadeau commented. In contrast, neither maternal body mass index nor – surprisingly – HbA1c level was significantly associated with pregnancy outcome.
The rate of preterm birth observed in the teens studied was similar to what has been seen in adult women with diabetes, she noted. But the rate of major congenital anomalies was about four times higher.
“This potentially might be due to lower overall socioeconomic status of the girls in the TODAY study. Other reasons for the anomalies are uncertain, but might include metabolic control, smoking, or extreme obesity,” she said.
Dr. Nadeau disclosed that she had no relevant conflicts of interest.
VANCOUVER, B.C. – Despite agreeing to use birth control and receiving frequent counseling about pregnancy avoidance, a sizable share of teens with type 2 diabetes mellitus become pregnant, and these pregnancies often have poor outcomes, researchers reported at the World Diabetes Congress.
The analysis was based on 452 female participants in the national Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study, the largest trial in youth with this form of diabetes to date and one designed to have good representation of various racial/ethnic groups.
Overall, 10% of the girls became pregnant during a period of up to 6.5 years. The majority were not using contraception and did not recall the counseling. More than one-fourth of the pregnancies ended in fetal loss or stillbirth. And one-fifth of live-born infants had major congenital anomalies.
“We need to better understand the reasons for pregnancy in youth with type 2 diabetes and why, despite counseling, they become pregnant,” commented first author Dr. Kristen J. Nadeau of the division of pediatric endocrinology, department of pediatrics, University of Colorado, Aurora.
“Best practices for metabolically unhealthy pregnancy prevention in type 2 diabetic teens also requires further study,” she added. “Long-acting contraception, we think, currently is the best method and likely the way to go in these girls who are not retaining the education and [adhering to] the behaviors that we are hoping for.”
“This study is critically important and horribly depressing,” commented session comoderator Dr. Robert E. Ratner, professor of medicine at Georgetown University and senior research scientist at the MedStar Health Research Institute, Washington, as well as chief scientific and medical officer of the American Diabetes Association, Alexandria, Va.
“It points out the difficulties of being a teenager and the even greater difficulties of being a teenager with a chronic disease,” he said in an interview, adding that there are no easy solutions.
“The combination of a teen pregnancy in someone with type 2 diabetes creates the perfect storm,” Dr. Nadeau noted. “Diabetes control is worse in adolescence than in any other time in the lifespan, and with increasing rates of type 2 diabetes in youth, increases in a teen pregnancy that are complicated by diabetes are anticipated,” she added.
At baseline, participants in TODAY were 10-17 years old, were overweight or obese, and had a diabetes duration of less than 2 years and a hemoglobin A1c level of less than 8%. They were randomized to three treatment arms (metformin alone, metformin plus rosiglitazone, or metformin plus an intensive lifestyle program).
Consent for the trial required the use of a birth control method, including abstinence; in addition, every 2-3 months, the girls received diabetes education and counseling to defer pregnancy until their HbA1c level fell below 6%. They also had regular pregnancy testing, and those with a positive result were taken off their trial medication and referred to a maternal-fetal medicine specialist.
The results reported at the meeting and simultaneously published in Diabetes Care (doi: 10.2337/dc15-1206) showed that 46 (10.2%) of the girls had 63 pregnancies. On average, they were 18 years old at the time of a first pregnancy.
Despite the counseling, only about 5% of those teens who became pregnant reported that they had been using contraception. Moreover, just 13% recalled the counseling.
The median body mass index closest to conception was 35.2 kg/m2, and the median HbA1c level was 7%. “Because of the fact that we were so heavily monitoring these girls, we had their HbA1c under better control than is typical. In our typical clinic, the mean is more like 8.5%-9%,” Dr. Nadeau noted.
Relative to peers who did not become pregnant, those who did were significantly older, were less likely to be living with both parents or their mother, and had a lower household income.
Seven of the 63 pregnancies were electively terminated. Of the 53 remaining pregnancies with data, 12 ended in pregnancy loss and 2 ended in a stillbirth.
Among the 39 live-born infants, 6 were preterm and 8 had major congenital anomalies. And among the 37 with known birth weight, 10 were either small or large for gestational age.
Girls randomized to metformin plus rosiglitazone had a higher rate of term normal births than peers in the other arms (P = .027). “Of note, none of the participants reported taking the rosiglitazone after the pregnancy was discovered, as was per the study protocol,” Dr. Nadeau commented. In contrast, neither maternal body mass index nor – surprisingly – HbA1c level was significantly associated with pregnancy outcome.
The rate of preterm birth observed in the teens studied was similar to what has been seen in adult women with diabetes, she noted. But the rate of major congenital anomalies was about four times higher.
“This potentially might be due to lower overall socioeconomic status of the girls in the TODAY study. Other reasons for the anomalies are uncertain, but might include metabolic control, smoking, or extreme obesity,” she said.
Dr. Nadeau disclosed that she had no relevant conflicts of interest.
AT THE WORLD DIABETES CONGRESS
Key clinical point: Pregnancies are fairly common among diabetic teens and frequently have poor outcomes.
Major finding: There were high rates of loss or stillbirth (26.4%), preterm birth (15.4%), and major congenital anomalies (20.5%).
Data source: An analysis of retrospectively collected data from a randomized controlled trial among 452 female youth with type 2 diabetes (TODAY study).
Disclosures: Dr. Nadeau disclosed that she had no relevant financial conflicts of interest.
Steroid use down, biologic use rising in pregnancies of women with rheumatic disease
Steroids and hydroxychloroquine remain the most widely prescribed treatment options for pregnant women with rheumatologic diseases, according to a study looking at prescribing patterns in a cohort of women diagnosed with systemic lupus erythematosus, rheumatoid arthritis, psoriatic arthritis, or ankylosing spondylitis.
Lead investigator Dr. Rishi J. Desai of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, and his colleagues found that the use of biologic agents during pregnancy, though still low, rose for 2,645 women from all regions of the United States covered by private insurance or Medicaid between 2001 and 2012. The investigators evaluated prescription filling records for steroids, nonbiologic disease-modifying agents, and biologics. The women in the study all had live births. Dr. Desai and his colleagues looked at scripts for individual agents filled in the 3-month period prior to each woman’s pregnancy and during her pregnancy (Arthritis Rheumatol. 2015 Nov 25. doi: 10.1002/art.39521).

Nearly two-thirds of women with psoriatic arthritis or ankylosing spondylitis stopped filling immunomodulatory prescriptions during their pregnancies, while only 26% of lupus and 34.5% of rheumatoid arthritis patients did so. In the cohort as a whole, steroids and hydroxychloroquine were the most frequently used agents in pregnancy (48.4% and 27.1%, respectively). Steroid use during pregnancy dropped over time, from 54.4 per 100 deliveries to 42.4 between 2001 and 2012, while rates for biologics increased from 5.1 per 100 to 16.6 (P less than .001 for both trends).
“More comparative research on the safety of steroids as well as disease-modifying agents used during pregnancy will be critical for providing the necessary evidence to guide treatment decisions in future,” Dr. Desai and his colleagues wrote in their analysis.
The findings also suggest, the investigators wrote, “that with availability of some reassuring data indicating absence of a major fetal adverse event after biologic use in pregnancy, physicians have become more comfortable with continuing treatment with these agents.”
Use of agents potentially harmful to a developing fetus, including methotrexate, mycophenolate mofetil, and leflunomide, was very low in the study. However, the investigators noted, because their study enrolled only women with successful pregnancies, it could have underestimated the use of some of these agents, as women using them may have chosen to terminate their pregnancies.
The study received no outside funding. Two coauthors reported financial relationships with AstraZeneca, and one of them also reported funding from Pfizer and Eli Lilly.
Steroids and hydroxychloroquine remain the most widely prescribed treatment options for pregnant women with rheumatologic diseases, according to a study looking at prescribing patterns in a cohort of women diagnosed with systemic lupus erythematosus, rheumatoid arthritis, psoriatic arthritis, or ankylosing spondylitis.
Lead investigator Dr. Rishi J. Desai of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, and his colleagues found that the use of biologic agents during pregnancy, though still low, rose for 2,645 women from all regions of the United States covered by private insurance or Medicaid between 2001 and 2012. The investigators evaluated prescription filling records for steroids, nonbiologic disease-modifying agents, and biologics. The women in the study all had live births. Dr. Desai and his colleagues looked at scripts for individual agents filled in the 3-month period prior to each woman’s pregnancy and during her pregnancy (Arthritis Rheumatol. 2015 Nov 25. doi: 10.1002/art.39521).
Nearly two-thirds of women with psoriatic arthritis or ankylosing spondylitis stopped filling immunomodulatory prescriptions during their pregnancies, while only 26% of lupus and 34.5% of rheumatoid arthritis patients did so. In the cohort as a whole, steroids and hydroxychloroquine were the most frequently used agents in pregnancy (48.4% and 27.1%, respectively). Steroid use during pregnancy dropped over time, from 54.4 per 100 deliveries to 42.4 between 2001 and 2012, while rates for biologics increased from 5.1 per 100 to 16.6 (P less than .001 for both trends).
“More comparative research on the safety of steroids as well as disease-modifying agents used during pregnancy will be critical for providing the necessary evidence to guide treatment decisions in future,” Dr. Desai and his colleagues wrote in their analysis.
The findings also suggest, the investigators wrote, “that with availability of some reassuring data indicating absence of a major fetal adverse event after biologic use in pregnancy, physicians have become more comfortable with continuing treatment with these agents.”
Use of agents potentially harmful to a developing fetus, including methotrexate, mycophenolate mofetil, and leflunomide, was very low in the study. However, the investigators noted, because their study enrolled only women with successful pregnancies, it could have underestimated the use of some of these agents, as women using them may have chosen to terminate their pregnancies.
The study received no outside funding. Two coauthors reported financial relationships with AstraZeneca, and one of them also reported funding from Pfizer and Eli Lilly.
Steroids and hydroxychloroquine remain the most widely prescribed treatment options for pregnant women with rheumatologic diseases, according to a study looking at prescribing patterns in a cohort of women diagnosed with systemic lupus erythematosus, rheumatoid arthritis, psoriatic arthritis, or ankylosing spondylitis.
Lead investigator Dr. Rishi J. Desai of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, and his colleagues found that the use of biologic agents during pregnancy, though still low, rose for 2,645 women from all regions of the United States covered by private insurance or Medicaid between 2001 and 2012. The investigators evaluated prescription filling records for steroids, nonbiologic disease-modifying agents, and biologics. The women in the study all had live births. Dr. Desai and his colleagues looked at scripts for individual agents filled in the 3-month period prior to each woman’s pregnancy and during her pregnancy (Arthritis Rheumatol. 2015 Nov 25. doi: 10.1002/art.39521).
Nearly two-thirds of women with psoriatic arthritis or ankylosing spondylitis stopped filling immunomodulatory prescriptions during their pregnancies, while only 26% of lupus and 34.5% of rheumatoid arthritis patients did so. In the cohort as a whole, steroids and hydroxychloroquine were the most frequently used agents in pregnancy (48.4% and 27.1%, respectively). Steroid use during pregnancy dropped over time, from 54.4 per 100 deliveries to 42.4 between 2001 and 2012, while rates for biologics increased from 5.1 per 100 to 16.6 (P less than .001 for both trends).
“More comparative research on the safety of steroids as well as disease-modifying agents used during pregnancy will be critical for providing the necessary evidence to guide treatment decisions in future,” Dr. Desai and his colleagues wrote in their analysis.
The findings also suggest, the investigators wrote, “that with availability of some reassuring data indicating absence of a major fetal adverse event after biologic use in pregnancy, physicians have become more comfortable with continuing treatment with these agents.”
Use of agents potentially harmful to a developing fetus, including methotrexate, mycophenolate mofetil, and leflunomide, was very low in the study. However, the investigators noted, because their study enrolled only women with successful pregnancies, it could have underestimated the use of some of these agents, as women using them may have chosen to terminate their pregnancies.
The study received no outside funding. Two coauthors reported financial relationships with AstraZeneca, and one of them also reported funding from Pfizer and Eli Lilly.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point: Women with lupus and other rheumatic diseases used fewer steroids during pregnancy over a 12-year period, while use of biologic agents increased over time.
Major finding: Steroid use dropped from 54.4 per 100 deliveries to 42.4 between 2001 and 2012, while biologic use increased from 5.1 per 100 to 16.6 (P less than .001 for both).
Data source: Private and public insurance records, including prescription filling data, for 2,645 U.S. women with lupus, rheumatoid arthritis, psoriatic arthritis, or ankylosing spondylitis who gave birth between 2001 and 2012.
Disclosures: The study received no outside funding. Two coauthors reported financial relationships with pharmaceutical manufacturers.

Interpregnancy weight gain ups stillbirth risk
The risk of stillbirth increases linearly with interpregnancy weight gain, according to a Swedish population-based cohort study.
The researchers found that between-pregnancy weight gain greater than four body mass index units – about 11 kg or 24 lbs – was associated with more than a 50% increase in stillbirth risk in a second pregnancy, even after controlling for confounders such as maternal education and smoking.

The Swedish study of 456,711 women who had their first and second singleton births between 1992 and 2012 showed an increased risk of infant mortality for women who had a healthy weight in their first pregnancy and then gained weight. For those that gained between two and four body mass index (BMI) units, the relative risk was 27%, compared with stable weight women. There was a 60% increased risk of infant mortality among women who gained more than four BMI units, according to the findings published online in the Lancet on Dec. 2.
Each BMI unit corresponds to about 2.8 kg (6 lbs) in an average height woman (167 cm, or 5 feet 5 inches).
Already overweight women did not show an increased risk of infant mortality with weight gain, but did show significantly reduced infant mortality with weight loss greater than two BMI units between pregnancies (relative risk 0.49; 95% confidence interval, 0.27-0.88). But that same weight loss in healthy-weight women increased the risk of infant mortality (Lancet. 2015 Dec 2. doi: 10.1016/S0140-6736(15)00990-3).
“Obesity and weight gain are associated with inflammatory upregulation, and inflammation has been proposed as one mechanism for the associations between maternal overweight and obesity and several adverse pregnancy outcomes,” wrote Dr. Sven Cnattingius, from the Karolinska Institute, Stockholm, and Dr. Eduardo Villamor from the University of Michigan, Ann Arbor.
The study was supported by the Swedish Research Council for Health, Working Life and Welfare, and the Karolinska Institute. The researchers reported having no financial disclosures.
The risk of stillbirth increases linearly with interpregnancy weight gain, according to a Swedish population-based cohort study.
The researchers found that between-pregnancy weight gain greater than four body mass index units – about 11 kg or 24 lbs – was associated with more than a 50% increase in stillbirth risk in a second pregnancy, even after controlling for confounders such as maternal education and smoking.
The Swedish study of 456,711 women who had their first and second singleton births between 1992 and 2012 showed an increased risk of infant mortality for women who had a healthy weight in their first pregnancy and then gained weight. For those that gained between two and four body mass index (BMI) units, the relative risk was 27%, compared with stable weight women. There was a 60% increased risk of infant mortality among women who gained more than four BMI units, according to the findings published online in the Lancet on Dec. 2.
Each BMI unit corresponds to about 2.8 kg (6 lbs) in an average height woman (167 cm, or 5 feet 5 inches).
Already overweight women did not show an increased risk of infant mortality with weight gain, but did show significantly reduced infant mortality with weight loss greater than two BMI units between pregnancies (relative risk 0.49; 95% confidence interval, 0.27-0.88). But that same weight loss in healthy-weight women increased the risk of infant mortality (Lancet. 2015 Dec 2. doi: 10.1016/S0140-6736(15)00990-3).
“Obesity and weight gain are associated with inflammatory upregulation, and inflammation has been proposed as one mechanism for the associations between maternal overweight and obesity and several adverse pregnancy outcomes,” wrote Dr. Sven Cnattingius, from the Karolinska Institute, Stockholm, and Dr. Eduardo Villamor from the University of Michigan, Ann Arbor.
The study was supported by the Swedish Research Council for Health, Working Life and Welfare, and the Karolinska Institute. The researchers reported having no financial disclosures.
The risk of stillbirth increases linearly with interpregnancy weight gain, according to a Swedish population-based cohort study.
The researchers found that between-pregnancy weight gain greater than four body mass index units – about 11 kg or 24 lbs – was associated with more than a 50% increase in stillbirth risk in a second pregnancy, even after controlling for confounders such as maternal education and smoking.
The Swedish study of 456,711 women who had their first and second singleton births between 1992 and 2012 showed an increased risk of infant mortality for women who had a healthy weight in their first pregnancy and then gained weight. For those that gained between two and four body mass index (BMI) units, the relative risk was 27%, compared with stable weight women. There was a 60% increased risk of infant mortality among women who gained more than four BMI units, according to the findings published online in the Lancet on Dec. 2.
Each BMI unit corresponds to about 2.8 kg (6 lbs) in an average height woman (167 cm, or 5 feet 5 inches).
Already overweight women did not show an increased risk of infant mortality with weight gain, but did show significantly reduced infant mortality with weight loss greater than two BMI units between pregnancies (relative risk 0.49; 95% confidence interval, 0.27-0.88). But that same weight loss in healthy-weight women increased the risk of infant mortality (Lancet. 2015 Dec 2. doi: 10.1016/S0140-6736(15)00990-3).
“Obesity and weight gain are associated with inflammatory upregulation, and inflammation has been proposed as one mechanism for the associations between maternal overweight and obesity and several adverse pregnancy outcomes,” wrote Dr. Sven Cnattingius, from the Karolinska Institute, Stockholm, and Dr. Eduardo Villamor from the University of Michigan, Ann Arbor.
The study was supported by the Swedish Research Council for Health, Working Life and Welfare, and the Karolinska Institute. The researchers reported having no financial disclosures.
FROM THE LANCET
Key clinical point: The risk of stillbirth increases linearly with interpregnancy weight gain.
Major finding: Women who gained more than four BMI units after their first pregnancy had a more than 50% increased risk of stillbirth in their second pregnancy.
Data source: A population-based cohort study in 456,711 women.
Disclosures: The study was supported by the Swedish Research Council for Health, Working Life and Welfare, and the Karolinska Institute. The researchers reported having no financial disclosures.

Flu vaccines highly effective for pregnant women and their children
Administering flu vaccines to pregnant women during their second and third trimesters results in high seroprotection against all influenza strains for most women and for more than half of their newly born babies, reported Dr. M.P. Kostinov and colleagues at the I.I. Mechnikov Scientific Research Institute of Vaccines and Sera, at Ul’yanovsk State University, Moscow. The study was published in the Journal of Vaccines & Vaccination.
Researchers gave influenza vaccines (the Grippol Plus vaccine) to 27 women in their second trimesters and 21 women in their third trimesters of pregnancy during 2010-2012. Each 0.5-mL dose of the preservative-free vaccine contained antigens of the following strains: A/California/7/2009/H1N1/v-like (5 mcg), A/H3N2/(Victoria)-like (5 mcg), and B/Brisbane-like (5 mcg) flu.

Within 1 month after vaccination, the seroprotection rate against all influenza strains was above the recommended threshold level of 1:40 in more than 70% of pregnant women. A gradual decrease in the seroprotection rates against all three influenza strains was reported in the postpartum period.
In infants, protective levels of antibodies were detected within 2-3 days of delivery and ranged from 52% to 62% regardless of the trimester when the vaccination was given. Within 3 months, this seroprotection decreased, and within 6 months it disappeared. The mothers’ protective levels against vaccine strains were 46%-65% after delivery.
Read the article in the Journal of Vaccines & Vaccination (Pakhomov et al. J Vaccines Vaccin. 2015,6:5).
Administering flu vaccines to pregnant women during their second and third trimesters results in high seroprotection against all influenza strains for most women and for more than half of their newly born babies, reported Dr. M.P. Kostinov and colleagues at the I.I. Mechnikov Scientific Research Institute of Vaccines and Sera, at Ul’yanovsk State University, Moscow. The study was published in the Journal of Vaccines & Vaccination.
Researchers gave influenza vaccines (the Grippol Plus vaccine) to 27 women in their second trimesters and 21 women in their third trimesters of pregnancy during 2010-2012. Each 0.5-mL dose of the preservative-free vaccine contained antigens of the following strains: A/California/7/2009/H1N1/v-like (5 mcg), A/H3N2/(Victoria)-like (5 mcg), and B/Brisbane-like (5 mcg) flu.
Within 1 month after vaccination, the seroprotection rate against all influenza strains was above the recommended threshold level of 1:40 in more than 70% of pregnant women. A gradual decrease in the seroprotection rates against all three influenza strains was reported in the postpartum period.
In infants, protective levels of antibodies were detected within 2-3 days of delivery and ranged from 52% to 62% regardless of the trimester when the vaccination was given. Within 3 months, this seroprotection decreased, and within 6 months it disappeared. The mothers’ protective levels against vaccine strains were 46%-65% after delivery.
Read the article in the Journal of Vaccines & Vaccination (Pakhomov et al. J Vaccines Vaccin. 2015,6:5).
Administering flu vaccines to pregnant women during their second and third trimesters results in high seroprotection against all influenza strains for most women and for more than half of their newly born babies, reported Dr. M.P. Kostinov and colleagues at the I.I. Mechnikov Scientific Research Institute of Vaccines and Sera, at Ul’yanovsk State University, Moscow. The study was published in the Journal of Vaccines & Vaccination.
Researchers gave influenza vaccines (the Grippol Plus vaccine) to 27 women in their second trimesters and 21 women in their third trimesters of pregnancy during 2010-2012. Each 0.5-mL dose of the preservative-free vaccine contained antigens of the following strains: A/California/7/2009/H1N1/v-like (5 mcg), A/H3N2/(Victoria)-like (5 mcg), and B/Brisbane-like (5 mcg) flu.
Within 1 month after vaccination, the seroprotection rate against all influenza strains was above the recommended threshold level of 1:40 in more than 70% of pregnant women. A gradual decrease in the seroprotection rates against all three influenza strains was reported in the postpartum period.
In infants, protective levels of antibodies were detected within 2-3 days of delivery and ranged from 52% to 62% regardless of the trimester when the vaccination was given. Within 3 months, this seroprotection decreased, and within 6 months it disappeared. The mothers’ protective levels against vaccine strains were 46%-65% after delivery.
Read the article in the Journal of Vaccines & Vaccination (Pakhomov et al. J Vaccines Vaccin. 2015,6:5).
FROM JOURNAL OF VACCINES & VACCINATION

Should newborns at 22 or 23 weeks’ gestational age be aggressively resuscitated?
For many decades the limit of viability was believed to be approximately 24 weeks of gestation. In many medical centers, newborns delivered at less than 25 weeks are evaluated in the delivery room and the decision to resuscitate is based on the infant’s clinical response. In the past, aggressive and extended resuscitation of newborns at 22 and 23 weeks was not common because the prognosis was bleak and clinicians did not want to inflict unnecessary pain when the chances for survival were limited. Recent advances in obstetric and pediatric care, however, have resulted in the survival of some infants born at 22 weeks’ gestation, calling into question long-held beliefs about the limits of viability.
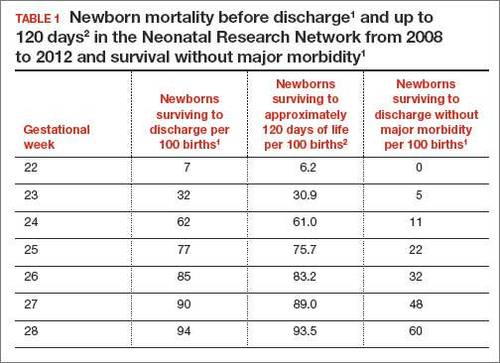
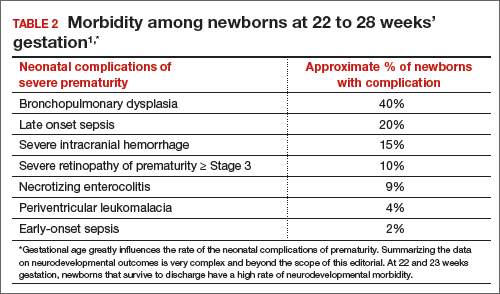
In 2 recent reports, investigators used data from the National Institute of Child Health and Human Development (NICHD) Neonatal Research Network to acquire detailed information about newborn survival and morbidity at 22 through 28 weeks’ gestation (TABLES 1 and 2).1,2 These data show that the survival of newborns at 23 through 27 weeks’ gestation is increasing, albeit slowly. Survival, without major morbidity, is gradually improving for newborns at 25 through 28 weeks.1,2 But what is the prognosis for a fetus born at 22 or 23 weeks?
There are several aspects of this issue to consider, including accurate dating of the gestational age and current viability outcomes data.
Determining the limit of viability: Accurate dating is essentialThe limit of viability is the milestone in gestation when there is a high probability of extrauterine survival. A major challenge in studies of the limit of viability for newborns is that accurate gestational dating is not always available. For example, in recent reports from the NICHD Neonatal Research Network the gestational age was determined by the best obstetric estimate, or the Ballard or Dubowitz examination, of the newborn.1,2
It is well known that ultrasound dating early in gestation is a better estimate of gestational age than last menstrual period, uterine sizing, or pediatric examination of the newborn. Hence, the available data are limited by the absence of precise gestational dating with early ultrasound. Data on the limit of viability with large numbers of births between 22 and 24 weeks with early ultrasound dating would help to refine our understanding of the limit of viability.
At 23 weeks, each day of in utero development is criticalThe importance of each additional day spent in utero during the 23rd week of gestation was demonstrated in a small cohort in 2001.4 Overall, during the 23rd week of gestation the survival of newborns to discharge was 33%.4 This finding is similar to the survival rate reported by the NICHD Neonatal Research Network in 2012.1 However, survival was vastly different early, compared with later, in the 23rd week4:
- from 23 weeks 0 days to 23 weeks 2 days: no newborn survived
- at 23 weeks 3 days and 23 weeks 4 days: 40% of newborns survived
- at 23 weeks 5 days and 23 weeks 6 days: 63% of newborns survived (a similar survival rate of 24-week gestations was reported by the NICHD Neonatal Research Network1).
The development of the fetus across the 23rd week of gestation appears to be critical to newborn survival. Hence, every day of in utero development during the 23rd week is critically important. A great challenge for obstetricians is how to approach the woman with threatened preterm birth at 22 weeks 0 days’ gestation. If the woman delivers within a few days, the likelihood of survival is minimal. However, if the pregnancy can be extended to 23 weeks and 5 days, survival rates increase significantly.
Aligning the actions of birth team, mother, and familyFactors that influence the limit of viability include:
- gestational age
- gender of the fetus (Females are more likely than males to survive.)
- treatment of the mother with glucocorticoids prior to birth
- newborn weight.
To increase the likelihood of newborn survival, obstetricians need to treat women at risk for preterm birth with antenatal glucocorticoids and antibiotics for rupture of membranes and to limit fetal stress during the birth process. Guidelines have evolved to encourage clinicians to treat women at preterm birth risk with glucocorticoids either at:
- 23 weeks’ gestation or
- 22 weeks’ gestation, if birth is anticipated to occur at 23 weeks or later.5
At birth, pediatricians are then faced with the very difficult decision of whether or not to aggressively resuscitate the severely preterm infant. Complex medical, social, and ethical issues ultimately guide pediatricians’ actions in this challenging situation. It is important for their actions to be in consensus with the obstetrician, the mother, and the mother’s family and for a consensus to be reached. Dissonant plans may increase adverse outcomes for the newborn. In one study when pediatricians and obstetricians were not aligned in their actions, the risk of death of an extremely preterm newborn significantly increased.6
Prior to birth, team meetings that include the obstetricians, pediatricians, mother, and family will help to set expectations about the course of care and, in turn, improve perceived outcomes.5 If feasible, obstetricians and pediatricians should develop joint institutional guidelines about the general approach to pregnant women when birth may occur at 22 or 23 weeks’ gestation.5
A neonatal outcomes predictor
The National Institute of Child Health and Human Development provides a Web-based tool for estimating newborn outcomes based on gestational age (22 to 25 weeks), birth weight, gender, singleton or multiple gestation, and exposure to antenatal glucocorticoid treatment. The outcomes tool provides estimates for survival and survival with severe morbidity. It uses data collected by the Neonatal Research Network to predict outcomes. To access the outcomes data assessment, visit https://www.nichd.nih.gov/about/org/der/branches/ppb/programs/epbo/Pages/epbo_case.aspx.
Is aggressive management of preterm birth and neonatal resuscitation a self-fulfilling prophecy?The beliefs and training of clinicians may influence the outcome of extremely preterm newborns. For example, if obstetricians and pediatricians focus on the fact that birth at 23 weeks is not likely to result in survival without severe morbidity, they may withhold key interventions such as antenatal glucocorticoids, antibiotics for rupture of the membranes, and aggressive newborn resuscitation.7 Consequently the likelihood of survival may be reduced.
If clinicians believe in maximal interventions for all newborns at 22 and 23 weeks’ gestation, their actions may result in a small increase in newborn survival—but at the cost of painful and unnecessary interventions in many newborns who are destined to die. Finding the right balance along the broad spectrum from expectant management to aggressive and extended resuscitation is challenging. Clearly there is no “right answer” with these extremely difficult decisions.
Future trends in the limit of viabilityIn 1963, Jacqueline Bouvier Kennedy, at 34 weeks’ gestation, went into preterm labor and delivered her son Patrick at a community hospital. Patrick developed respiratory distress syndrome and was transferred to the Boston Children’s Hospital. He died shortly thereafter.8 Would Patrick have survived if he had been delivered at an institution capable of providing high-risk obstetric and newborn services? Would such modern interventions as antenatal glucocorticoids, antibiotics for ruptured membranes, liberal use of cesarean delivery, and aggressive neonatal resuscitation have improved his chances for survival?
From our current perspective, it is surprising that a 34-week newborn died shortly after birth. With modern obstetric and pediatric care that scenario is unusual. It is possible that future advances in medical care will push the limit of viability to 22 weeks’ gestation. Future generations of clinicians may be surprised that the medicine we practice today is so limited.
However, given our current resources, it is unlikely that newborns at 22 weeks’ gestation will survive, or survive without severe morbidity. Consequently, routine aggressive resuscitation of newborns at 22 weeks should be approached with caution. At 23 weeks and later, many newborns will survive and a few will survive without severe morbidity. Given the complexity of the issues, the approach to resuscitation of infants at 22 and 23 weeks must account for the perspectives of the birth mother and her family, obstetricians, and pediatricians. Managing threatened preterm birth at 22 and 23 weeks is one of our greatest challenges as obstetricians, and we need to meet this challenge with grace and skill.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Stoll BJ, Hansen NI, Bell EF, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Trends in care practices, morbidity and mortality of extremely preterm neonates, 1993-2012. JAMA. 2015;314(10):1039–1051.
- Patel RM, Kandefer S, Walsh MC, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Causes and timing of death in extremely premature infants from 2000 through 2011. N Engl J Med. 2015;372(4):331–340.
- Donovan EF, Tyson JE, Ehrenkranz RA, et al. Inaccuracy of Ballard scores before 28 weeks’ gestation. National Institute of Child Health and Human Development Neonatal Research Network. J Pediatr. 1999;135(2 pt 1):147–152.
- McElrath TF, Robinson JN, Ecker JL, Ringer SA, Norwitz ER. Neonatal outcome of infants born at 23 weeks’ gestation. Obstet Gynecol. 2001;97(1):49–52.
- Raju TN, Mercer BM, Burchfield DJ, Joseph GF Jr. Periviable birth: executive summary of a joint workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists. Obstet Gynecol. 2014;123(5):1083–1096.
- Guinsburg R, Branco de Almeida MF, dos Santos Rodrigues Sadeck L, et al; Brazilian Network on Neonatal Research. Proactive management of extreme prematurity: disagreement between obstetricians and neonatologists. J Perinatol. 2012;32(12):913-919.
- Tucker Emonds B, McKenzie F, Farrow V, Raglan G, Schulkin J. A national survey of obstetricians’ attitudes toward and practice of periviable interventions. J Perinatol. 2015;35(5):338–343.
- Altman LK. A Kennedy baby’s life and death. New York Times. http://www.nytimes.com/2013/07/30/health/a-kennedy-babys-life-and-death.html?_r=0. Published July 29, 2013. Accessed November 19, 2015.

Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, Brigham and Women’s Hospital; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.
Dr. Barbieri reports no financial relationships relevant to this article.
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, Brigham and Women’s Hospital; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.
Dr. Barbieri reports no financial relationships relevant to this article.
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, Brigham and Women’s Hospital; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.
Dr. Barbieri reports no financial relationships relevant to this article.
For many decades the limit of viability was believed to be approximately 24 weeks of gestation. In many medical centers, newborns delivered at less than 25 weeks are evaluated in the delivery room and the decision to resuscitate is based on the infant’s clinical response. In the past, aggressive and extended resuscitation of newborns at 22 and 23 weeks was not common because the prognosis was bleak and clinicians did not want to inflict unnecessary pain when the chances for survival were limited. Recent advances in obstetric and pediatric care, however, have resulted in the survival of some infants born at 22 weeks’ gestation, calling into question long-held beliefs about the limits of viability.
In 2 recent reports, investigators used data from the National Institute of Child Health and Human Development (NICHD) Neonatal Research Network to acquire detailed information about newborn survival and morbidity at 22 through 28 weeks’ gestation (TABLES 1 and 2).1,2 These data show that the survival of newborns at 23 through 27 weeks’ gestation is increasing, albeit slowly. Survival, without major morbidity, is gradually improving for newborns at 25 through 28 weeks.1,2 But what is the prognosis for a fetus born at 22 or 23 weeks?
There are several aspects of this issue to consider, including accurate dating of the gestational age and current viability outcomes data.
Determining the limit of viability: Accurate dating is essentialThe limit of viability is the milestone in gestation when there is a high probability of extrauterine survival. A major challenge in studies of the limit of viability for newborns is that accurate gestational dating is not always available. For example, in recent reports from the NICHD Neonatal Research Network the gestational age was determined by the best obstetric estimate, or the Ballard or Dubowitz examination, of the newborn.1,2
It is well known that ultrasound dating early in gestation is a better estimate of gestational age than last menstrual period, uterine sizing, or pediatric examination of the newborn. Hence, the available data are limited by the absence of precise gestational dating with early ultrasound. Data on the limit of viability with large numbers of births between 22 and 24 weeks with early ultrasound dating would help to refine our understanding of the limit of viability.
At 23 weeks, each day of in utero development is criticalThe importance of each additional day spent in utero during the 23rd week of gestation was demonstrated in a small cohort in 2001.4 Overall, during the 23rd week of gestation the survival of newborns to discharge was 33%.4 This finding is similar to the survival rate reported by the NICHD Neonatal Research Network in 2012.1 However, survival was vastly different early, compared with later, in the 23rd week4:
- from 23 weeks 0 days to 23 weeks 2 days: no newborn survived
- at 23 weeks 3 days and 23 weeks 4 days: 40% of newborns survived
- at 23 weeks 5 days and 23 weeks 6 days: 63% of newborns survived (a similar survival rate of 24-week gestations was reported by the NICHD Neonatal Research Network1).
The development of the fetus across the 23rd week of gestation appears to be critical to newborn survival. Hence, every day of in utero development during the 23rd week is critically important. A great challenge for obstetricians is how to approach the woman with threatened preterm birth at 22 weeks 0 days’ gestation. If the woman delivers within a few days, the likelihood of survival is minimal. However, if the pregnancy can be extended to 23 weeks and 5 days, survival rates increase significantly.
Aligning the actions of birth team, mother, and familyFactors that influence the limit of viability include:
- gestational age
- gender of the fetus (Females are more likely than males to survive.)
- treatment of the mother with glucocorticoids prior to birth
- newborn weight.
To increase the likelihood of newborn survival, obstetricians need to treat women at risk for preterm birth with antenatal glucocorticoids and antibiotics for rupture of membranes and to limit fetal stress during the birth process. Guidelines have evolved to encourage clinicians to treat women at preterm birth risk with glucocorticoids either at:
- 23 weeks’ gestation or
- 22 weeks’ gestation, if birth is anticipated to occur at 23 weeks or later.5
At birth, pediatricians are then faced with the very difficult decision of whether or not to aggressively resuscitate the severely preterm infant. Complex medical, social, and ethical issues ultimately guide pediatricians’ actions in this challenging situation. It is important for their actions to be in consensus with the obstetrician, the mother, and the mother’s family and for a consensus to be reached. Dissonant plans may increase adverse outcomes for the newborn. In one study when pediatricians and obstetricians were not aligned in their actions, the risk of death of an extremely preterm newborn significantly increased.6
Prior to birth, team meetings that include the obstetricians, pediatricians, mother, and family will help to set expectations about the course of care and, in turn, improve perceived outcomes.5 If feasible, obstetricians and pediatricians should develop joint institutional guidelines about the general approach to pregnant women when birth may occur at 22 or 23 weeks’ gestation.5
A neonatal outcomes predictor
The National Institute of Child Health and Human Development provides a Web-based tool for estimating newborn outcomes based on gestational age (22 to 25 weeks), birth weight, gender, singleton or multiple gestation, and exposure to antenatal glucocorticoid treatment. The outcomes tool provides estimates for survival and survival with severe morbidity. It uses data collected by the Neonatal Research Network to predict outcomes. To access the outcomes data assessment, visit https://www.nichd.nih.gov/about/org/der/branches/ppb/programs/epbo/Pages/epbo_case.aspx.
Is aggressive management of preterm birth and neonatal resuscitation a self-fulfilling prophecy?The beliefs and training of clinicians may influence the outcome of extremely preterm newborns. For example, if obstetricians and pediatricians focus on the fact that birth at 23 weeks is not likely to result in survival without severe morbidity, they may withhold key interventions such as antenatal glucocorticoids, antibiotics for rupture of the membranes, and aggressive newborn resuscitation.7 Consequently the likelihood of survival may be reduced.
If clinicians believe in maximal interventions for all newborns at 22 and 23 weeks’ gestation, their actions may result in a small increase in newborn survival—but at the cost of painful and unnecessary interventions in many newborns who are destined to die. Finding the right balance along the broad spectrum from expectant management to aggressive and extended resuscitation is challenging. Clearly there is no “right answer” with these extremely difficult decisions.
Future trends in the limit of viabilityIn 1963, Jacqueline Bouvier Kennedy, at 34 weeks’ gestation, went into preterm labor and delivered her son Patrick at a community hospital. Patrick developed respiratory distress syndrome and was transferred to the Boston Children’s Hospital. He died shortly thereafter.8 Would Patrick have survived if he had been delivered at an institution capable of providing high-risk obstetric and newborn services? Would such modern interventions as antenatal glucocorticoids, antibiotics for ruptured membranes, liberal use of cesarean delivery, and aggressive neonatal resuscitation have improved his chances for survival?
From our current perspective, it is surprising that a 34-week newborn died shortly after birth. With modern obstetric and pediatric care that scenario is unusual. It is possible that future advances in medical care will push the limit of viability to 22 weeks’ gestation. Future generations of clinicians may be surprised that the medicine we practice today is so limited.
However, given our current resources, it is unlikely that newborns at 22 weeks’ gestation will survive, or survive without severe morbidity. Consequently, routine aggressive resuscitation of newborns at 22 weeks should be approached with caution. At 23 weeks and later, many newborns will survive and a few will survive without severe morbidity. Given the complexity of the issues, the approach to resuscitation of infants at 22 and 23 weeks must account for the perspectives of the birth mother and her family, obstetricians, and pediatricians. Managing threatened preterm birth at 22 and 23 weeks is one of our greatest challenges as obstetricians, and we need to meet this challenge with grace and skill.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
For many decades the limit of viability was believed to be approximately 24 weeks of gestation. In many medical centers, newborns delivered at less than 25 weeks are evaluated in the delivery room and the decision to resuscitate is based on the infant’s clinical response. In the past, aggressive and extended resuscitation of newborns at 22 and 23 weeks was not common because the prognosis was bleak and clinicians did not want to inflict unnecessary pain when the chances for survival were limited. Recent advances in obstetric and pediatric care, however, have resulted in the survival of some infants born at 22 weeks’ gestation, calling into question long-held beliefs about the limits of viability.
In 2 recent reports, investigators used data from the National Institute of Child Health and Human Development (NICHD) Neonatal Research Network to acquire detailed information about newborn survival and morbidity at 22 through 28 weeks’ gestation (TABLES 1 and 2).1,2 These data show that the survival of newborns at 23 through 27 weeks’ gestation is increasing, albeit slowly. Survival, without major morbidity, is gradually improving for newborns at 25 through 28 weeks.1,2 But what is the prognosis for a fetus born at 22 or 23 weeks?
There are several aspects of this issue to consider, including accurate dating of the gestational age and current viability outcomes data.
Determining the limit of viability: Accurate dating is essentialThe limit of viability is the milestone in gestation when there is a high probability of extrauterine survival. A major challenge in studies of the limit of viability for newborns is that accurate gestational dating is not always available. For example, in recent reports from the NICHD Neonatal Research Network the gestational age was determined by the best obstetric estimate, or the Ballard or Dubowitz examination, of the newborn.1,2
It is well known that ultrasound dating early in gestation is a better estimate of gestational age than last menstrual period, uterine sizing, or pediatric examination of the newborn. Hence, the available data are limited by the absence of precise gestational dating with early ultrasound. Data on the limit of viability with large numbers of births between 22 and 24 weeks with early ultrasound dating would help to refine our understanding of the limit of viability.
At 23 weeks, each day of in utero development is criticalThe importance of each additional day spent in utero during the 23rd week of gestation was demonstrated in a small cohort in 2001.4 Overall, during the 23rd week of gestation the survival of newborns to discharge was 33%.4 This finding is similar to the survival rate reported by the NICHD Neonatal Research Network in 2012.1 However, survival was vastly different early, compared with later, in the 23rd week4:
- from 23 weeks 0 days to 23 weeks 2 days: no newborn survived
- at 23 weeks 3 days and 23 weeks 4 days: 40% of newborns survived
- at 23 weeks 5 days and 23 weeks 6 days: 63% of newborns survived (a similar survival rate of 24-week gestations was reported by the NICHD Neonatal Research Network1).
The development of the fetus across the 23rd week of gestation appears to be critical to newborn survival. Hence, every day of in utero development during the 23rd week is critically important. A great challenge for obstetricians is how to approach the woman with threatened preterm birth at 22 weeks 0 days’ gestation. If the woman delivers within a few days, the likelihood of survival is minimal. However, if the pregnancy can be extended to 23 weeks and 5 days, survival rates increase significantly.
Aligning the actions of birth team, mother, and familyFactors that influence the limit of viability include:
- gestational age
- gender of the fetus (Females are more likely than males to survive.)
- treatment of the mother with glucocorticoids prior to birth
- newborn weight.
To increase the likelihood of newborn survival, obstetricians need to treat women at risk for preterm birth with antenatal glucocorticoids and antibiotics for rupture of membranes and to limit fetal stress during the birth process. Guidelines have evolved to encourage clinicians to treat women at preterm birth risk with glucocorticoids either at:
- 23 weeks’ gestation or
- 22 weeks’ gestation, if birth is anticipated to occur at 23 weeks or later.5
At birth, pediatricians are then faced with the very difficult decision of whether or not to aggressively resuscitate the severely preterm infant. Complex medical, social, and ethical issues ultimately guide pediatricians’ actions in this challenging situation. It is important for their actions to be in consensus with the obstetrician, the mother, and the mother’s family and for a consensus to be reached. Dissonant plans may increase adverse outcomes for the newborn. In one study when pediatricians and obstetricians were not aligned in their actions, the risk of death of an extremely preterm newborn significantly increased.6
Prior to birth, team meetings that include the obstetricians, pediatricians, mother, and family will help to set expectations about the course of care and, in turn, improve perceived outcomes.5 If feasible, obstetricians and pediatricians should develop joint institutional guidelines about the general approach to pregnant women when birth may occur at 22 or 23 weeks’ gestation.5
A neonatal outcomes predictor
The National Institute of Child Health and Human Development provides a Web-based tool for estimating newborn outcomes based on gestational age (22 to 25 weeks), birth weight, gender, singleton or multiple gestation, and exposure to antenatal glucocorticoid treatment. The outcomes tool provides estimates for survival and survival with severe morbidity. It uses data collected by the Neonatal Research Network to predict outcomes. To access the outcomes data assessment, visit https://www.nichd.nih.gov/about/org/der/branches/ppb/programs/epbo/Pages/epbo_case.aspx.
Is aggressive management of preterm birth and neonatal resuscitation a self-fulfilling prophecy?The beliefs and training of clinicians may influence the outcome of extremely preterm newborns. For example, if obstetricians and pediatricians focus on the fact that birth at 23 weeks is not likely to result in survival without severe morbidity, they may withhold key interventions such as antenatal glucocorticoids, antibiotics for rupture of the membranes, and aggressive newborn resuscitation.7 Consequently the likelihood of survival may be reduced.
If clinicians believe in maximal interventions for all newborns at 22 and 23 weeks’ gestation, their actions may result in a small increase in newborn survival—but at the cost of painful and unnecessary interventions in many newborns who are destined to die. Finding the right balance along the broad spectrum from expectant management to aggressive and extended resuscitation is challenging. Clearly there is no “right answer” with these extremely difficult decisions.
Future trends in the limit of viabilityIn 1963, Jacqueline Bouvier Kennedy, at 34 weeks’ gestation, went into preterm labor and delivered her son Patrick at a community hospital. Patrick developed respiratory distress syndrome and was transferred to the Boston Children’s Hospital. He died shortly thereafter.8 Would Patrick have survived if he had been delivered at an institution capable of providing high-risk obstetric and newborn services? Would such modern interventions as antenatal glucocorticoids, antibiotics for ruptured membranes, liberal use of cesarean delivery, and aggressive neonatal resuscitation have improved his chances for survival?
From our current perspective, it is surprising that a 34-week newborn died shortly after birth. With modern obstetric and pediatric care that scenario is unusual. It is possible that future advances in medical care will push the limit of viability to 22 weeks’ gestation. Future generations of clinicians may be surprised that the medicine we practice today is so limited.
However, given our current resources, it is unlikely that newborns at 22 weeks’ gestation will survive, or survive without severe morbidity. Consequently, routine aggressive resuscitation of newborns at 22 weeks should be approached with caution. At 23 weeks and later, many newborns will survive and a few will survive without severe morbidity. Given the complexity of the issues, the approach to resuscitation of infants at 22 and 23 weeks must account for the perspectives of the birth mother and her family, obstetricians, and pediatricians. Managing threatened preterm birth at 22 and 23 weeks is one of our greatest challenges as obstetricians, and we need to meet this challenge with grace and skill.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Stoll BJ, Hansen NI, Bell EF, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Trends in care practices, morbidity and mortality of extremely preterm neonates, 1993-2012. JAMA. 2015;314(10):1039–1051.
- Patel RM, Kandefer S, Walsh MC, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Causes and timing of death in extremely premature infants from 2000 through 2011. N Engl J Med. 2015;372(4):331–340.
- Donovan EF, Tyson JE, Ehrenkranz RA, et al. Inaccuracy of Ballard scores before 28 weeks’ gestation. National Institute of Child Health and Human Development Neonatal Research Network. J Pediatr. 1999;135(2 pt 1):147–152.
- McElrath TF, Robinson JN, Ecker JL, Ringer SA, Norwitz ER. Neonatal outcome of infants born at 23 weeks’ gestation. Obstet Gynecol. 2001;97(1):49–52.
- Raju TN, Mercer BM, Burchfield DJ, Joseph GF Jr. Periviable birth: executive summary of a joint workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists. Obstet Gynecol. 2014;123(5):1083–1096.
- Guinsburg R, Branco de Almeida MF, dos Santos Rodrigues Sadeck L, et al; Brazilian Network on Neonatal Research. Proactive management of extreme prematurity: disagreement between obstetricians and neonatologists. J Perinatol. 2012;32(12):913-919.
- Tucker Emonds B, McKenzie F, Farrow V, Raglan G, Schulkin J. A national survey of obstetricians’ attitudes toward and practice of periviable interventions. J Perinatol. 2015;35(5):338–343.
- Altman LK. A Kennedy baby’s life and death. New York Times. http://www.nytimes.com/2013/07/30/health/a-kennedy-babys-life-and-death.html?_r=0. Published July 29, 2013. Accessed November 19, 2015.
- Stoll BJ, Hansen NI, Bell EF, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Trends in care practices, morbidity and mortality of extremely preterm neonates, 1993-2012. JAMA. 2015;314(10):1039–1051.
- Patel RM, Kandefer S, Walsh MC, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Causes and timing of death in extremely premature infants from 2000 through 2011. N Engl J Med. 2015;372(4):331–340.
- Donovan EF, Tyson JE, Ehrenkranz RA, et al. Inaccuracy of Ballard scores before 28 weeks’ gestation. National Institute of Child Health and Human Development Neonatal Research Network. J Pediatr. 1999;135(2 pt 1):147–152.
- McElrath TF, Robinson JN, Ecker JL, Ringer SA, Norwitz ER. Neonatal outcome of infants born at 23 weeks’ gestation. Obstet Gynecol. 2001;97(1):49–52.
- Raju TN, Mercer BM, Burchfield DJ, Joseph GF Jr. Periviable birth: executive summary of a joint workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists. Obstet Gynecol. 2014;123(5):1083–1096.
- Guinsburg R, Branco de Almeida MF, dos Santos Rodrigues Sadeck L, et al; Brazilian Network on Neonatal Research. Proactive management of extreme prematurity: disagreement between obstetricians and neonatologists. J Perinatol. 2012;32(12):913-919.
- Tucker Emonds B, McKenzie F, Farrow V, Raglan G, Schulkin J. A national survey of obstetricians’ attitudes toward and practice of periviable interventions. J Perinatol. 2015;35(5):338–343.
- Altman LK. A Kennedy baby’s life and death. New York Times. http://www.nytimes.com/2013/07/30/health/a-kennedy-babys-life-and-death.html?_r=0. Published July 29, 2013. Accessed November 19, 2015.

Patient denies consent to endometriosis treatment

Patient denies consent to endometriosis treatment
A woman underwent laparoscopic surgery to remove an ovarian cyst. During surgery, the gynecologist found endometriosis and used electrosurgery to destroy the implants. Following extensive electrosurgery, a hemorrhage occurred. The gynecologist placed 5 large clips to control bleeding. The patient was discharged. When she returned to the hospital in pain, she was sent home again. She visited another emergency department (ED), where a clip was found to have blocked a ureter. She underwent ureteroneocystostomy to repair the damage. The patient now reports incontinence, a ligated ureter, and extensive scar tissue, which may keep her from being able to become pregnant.
Patient’s claim She only consented to ovarian cyst removal, not to any other procedures. The gynecologist was negligent in performing electrosurgery and placing the clips. A urologist should have checked for injury.
Physician’s defense When a patient agrees to laparoscopic surgery, she also agrees to exploratory abdominal surgery. The gynecologist performs electrosurgery to treat endometriosis in 30% to 60% of her surgical cases. Electrosurgery was essential to stop the patient’s pain. The clips were carefully placed when treating the hemorrhage.
Verdict A $206,886 California verdict was returned against the gynecologist.
Eclampsia, death: $6.9M settlement
A mother delivered a healthy baby on May 21. Twice in the week following delivery, she returned to the ED reporting shortness of breath, swollen legs, and elevated blood pressure. Pulmonary embolism was excluded both times. After the second visit, she was discharged with a diagnosis of shortness of breath of unknown etiology. The patient’s ObGyn was not contacted nor was urinalysis performed. On June 1, she suffered seizures and brain injury; she died on June 10.
Estate’s claim The ED physicians failed to diagnose and treat eclampsia.
Defendant’s defense The case was settled early in the trial.
Verdict A $6.9 million Illinois settlement was reached with the hospital.
Child has CP: $8M settlement
At 40 1/7 weeks’ gestation, labor was induced in an obese woman who had a heart condition. Over the next 36 hours, dinoprostone and oxytocin were administered, but her cervix only dilated to 2 cm. Two days later, the fetal heart rate reached 160 bpm. The ObGyn ordered terbutaline in anticipation of cesarean delivery, but he did not come to the hospital. The fetal heart rate continued to rise and then bradycardia occurred. When notified, the ObGyn came to the hospital for an emergency cesarean delivery. The child was severely depressed at birth with Apgar scores of 0, 1, and 2 at 1, 5, and 10 minutes, respectively. Magnetic resonance imaging at 23 days showed distinct hypoxic ischemic injury in the infant. Cerebral palsy was later diagnosed. The child is nonambulatory with significant cognitive impairment.
Parents’ claim Failure to perform cesarean delivery in a timely manner caused injury to the child.
Defendant’s defense The case was settled during the trial.
Verdict An $8 million Wisconsin settlement was reached with the medical center and physician group.
Infant has a stroke: $3M settlement
A 26-year-old diabetic woman was referred to a maternal-fetal medicine (MFM) specialist. She had been hospitalized for nausea and dehydration several times during her pregnancy, but it appeared that fetal development was normal.
As labor progressed, fetal distress was diagnosed in the setting of low blood pressure. When notified, the MFM immediately ordered an emergency cesarean delivery. A few days after birth, it was determined that the child had a stroke in utero.
Parents’ claim Emergency cesarean delivery should have been performed earlier. Hospital staff did not communicate fetal distress to the MFM in a timely manner.
Defendant’s defense The case was settled at trial.
Verdict A $3 million Connecticut settlement was reached with the hospital.
Patient denies consent to endometriosis treatment
A woman underwent laparoscopic surgery to remove an ovarian cyst. During surgery, the gynecologist found endometriosis and used electrosurgery to destroy the implants. Following extensive electrosurgery, a hemorrhage occurred. The gynecologist placed 5 large clips to control bleeding. The patient was discharged. When she returned to the hospital in pain, she was sent home again. She visited another emergency department (ED), where a clip was found to have blocked a ureter. She underwent ureteroneocystostomy to repair the damage. The patient now reports incontinence, a ligated ureter, and extensive scar tissue, which may keep her from being able to become pregnant.
Patient’s claim She only consented to ovarian cyst removal, not to any other procedures. The gynecologist was negligent in performing electrosurgery and placing the clips. A urologist should have checked for injury.
Physician’s defense When a patient agrees to laparoscopic surgery, she also agrees to exploratory abdominal surgery. The gynecologist performs electrosurgery to treat endometriosis in 30% to 60% of her surgical cases. Electrosurgery was essential to stop the patient’s pain. The clips were carefully placed when treating the hemorrhage.
Verdict A $206,886 California verdict was returned against the gynecologist.
Eclampsia, death: $6.9M settlement
A mother delivered a healthy baby on May 21. Twice in the week following delivery, she returned to the ED reporting shortness of breath, swollen legs, and elevated blood pressure. Pulmonary embolism was excluded both times. After the second visit, she was discharged with a diagnosis of shortness of breath of unknown etiology. The patient’s ObGyn was not contacted nor was urinalysis performed. On June 1, she suffered seizures and brain injury; she died on June 10.
Estate’s claim The ED physicians failed to diagnose and treat eclampsia.
Defendant’s defense The case was settled early in the trial.
Verdict A $6.9 million Illinois settlement was reached with the hospital.
Child has CP: $8M settlement
At 40 1/7 weeks’ gestation, labor was induced in an obese woman who had a heart condition. Over the next 36 hours, dinoprostone and oxytocin were administered, but her cervix only dilated to 2 cm. Two days later, the fetal heart rate reached 160 bpm. The ObGyn ordered terbutaline in anticipation of cesarean delivery, but he did not come to the hospital. The fetal heart rate continued to rise and then bradycardia occurred. When notified, the ObGyn came to the hospital for an emergency cesarean delivery. The child was severely depressed at birth with Apgar scores of 0, 1, and 2 at 1, 5, and 10 minutes, respectively. Magnetic resonance imaging at 23 days showed distinct hypoxic ischemic injury in the infant. Cerebral palsy was later diagnosed. The child is nonambulatory with significant cognitive impairment.
Parents’ claim Failure to perform cesarean delivery in a timely manner caused injury to the child.
Defendant’s defense The case was settled during the trial.
Verdict An $8 million Wisconsin settlement was reached with the medical center and physician group.
Infant has a stroke: $3M settlement
A 26-year-old diabetic woman was referred to a maternal-fetal medicine (MFM) specialist. She had been hospitalized for nausea and dehydration several times during her pregnancy, but it appeared that fetal development was normal.
As labor progressed, fetal distress was diagnosed in the setting of low blood pressure. When notified, the MFM immediately ordered an emergency cesarean delivery. A few days after birth, it was determined that the child had a stroke in utero.
Parents’ claim Emergency cesarean delivery should have been performed earlier. Hospital staff did not communicate fetal distress to the MFM in a timely manner.
Defendant’s defense The case was settled at trial.
Verdict A $3 million Connecticut settlement was reached with the hospital.
Patient denies consent to endometriosis treatment
A woman underwent laparoscopic surgery to remove an ovarian cyst. During surgery, the gynecologist found endometriosis and used electrosurgery to destroy the implants. Following extensive electrosurgery, a hemorrhage occurred. The gynecologist placed 5 large clips to control bleeding. The patient was discharged. When she returned to the hospital in pain, she was sent home again. She visited another emergency department (ED), where a clip was found to have blocked a ureter. She underwent ureteroneocystostomy to repair the damage. The patient now reports incontinence, a ligated ureter, and extensive scar tissue, which may keep her from being able to become pregnant.
Patient’s claim She only consented to ovarian cyst removal, not to any other procedures. The gynecologist was negligent in performing electrosurgery and placing the clips. A urologist should have checked for injury.
Physician’s defense When a patient agrees to laparoscopic surgery, she also agrees to exploratory abdominal surgery. The gynecologist performs electrosurgery to treat endometriosis in 30% to 60% of her surgical cases. Electrosurgery was essential to stop the patient’s pain. The clips were carefully placed when treating the hemorrhage.
Verdict A $206,886 California verdict was returned against the gynecologist.
Eclampsia, death: $6.9M settlement
A mother delivered a healthy baby on May 21. Twice in the week following delivery, she returned to the ED reporting shortness of breath, swollen legs, and elevated blood pressure. Pulmonary embolism was excluded both times. After the second visit, she was discharged with a diagnosis of shortness of breath of unknown etiology. The patient’s ObGyn was not contacted nor was urinalysis performed. On June 1, she suffered seizures and brain injury; she died on June 10.
Estate’s claim The ED physicians failed to diagnose and treat eclampsia.
Defendant’s defense The case was settled early in the trial.
Verdict A $6.9 million Illinois settlement was reached with the hospital.
Child has CP: $8M settlement
At 40 1/7 weeks’ gestation, labor was induced in an obese woman who had a heart condition. Over the next 36 hours, dinoprostone and oxytocin were administered, but her cervix only dilated to 2 cm. Two days later, the fetal heart rate reached 160 bpm. The ObGyn ordered terbutaline in anticipation of cesarean delivery, but he did not come to the hospital. The fetal heart rate continued to rise and then bradycardia occurred. When notified, the ObGyn came to the hospital for an emergency cesarean delivery. The child was severely depressed at birth with Apgar scores of 0, 1, and 2 at 1, 5, and 10 minutes, respectively. Magnetic resonance imaging at 23 days showed distinct hypoxic ischemic injury in the infant. Cerebral palsy was later diagnosed. The child is nonambulatory with significant cognitive impairment.
Parents’ claim Failure to perform cesarean delivery in a timely manner caused injury to the child.
Defendant’s defense The case was settled during the trial.
Verdict An $8 million Wisconsin settlement was reached with the medical center and physician group.
Infant has a stroke: $3M settlement
A 26-year-old diabetic woman was referred to a maternal-fetal medicine (MFM) specialist. She had been hospitalized for nausea and dehydration several times during her pregnancy, but it appeared that fetal development was normal.
As labor progressed, fetal distress was diagnosed in the setting of low blood pressure. When notified, the MFM immediately ordered an emergency cesarean delivery. A few days after birth, it was determined that the child had a stroke in utero.
Parents’ claim Emergency cesarean delivery should have been performed earlier. Hospital staff did not communicate fetal distress to the MFM in a timely manner.
Defendant’s defense The case was settled at trial.
Verdict A $3 million Connecticut settlement was reached with the hospital.
In this Article
- Eclampsia, death: $6.9M settlement
- Child has CP: $8M settlement
- Infant has a stroke: $3M settlement

Expert panel issues guidelines for treatment of hematologic cancers in pregnancy
Consensus guidelines for the perinatal management of hematologic malignancies detected during pregnancy have been issued by a panel of international experts.
The guidelines, published online in the Journal of Clinical Oncology, aim to ensure that timely treatment of the cancers is not delayed in pregnant women (doi: 10.1200/JCO.2015.62.4445).
While rare, hematologic malignancies in pregnancy introduce clinical, social, ethical, and moral dilemmas. Evidence-based data are scarce, according to the researchers, who note the International Network on Cancer, Infertility and Pregnancy registers all cancers occurring during gestation.
“Patient accrual is ongoing and essential, because registration of new cases and long-term follow-up will improve clinical knowledge and increase the level of evidence,” Dr. Michael Lishner of Tel Aviv University and Meir Medical Center, Kfar Saba, Israel, and his fellow panelists wrote.
Hodgkin lymphoma
The researchers note that Hodgkin lymphoma is the most common hematologic cancer in pregnancy, and the prognosis for these patients is excellent. When diagnosed during the first trimester, a regimen based on vinblastine monotherapy has been used. ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) therapy can be used postpartum and has been used in cases of progression during pregnancy, the panelists wrote.
“The limited data available suggest that ABVD may be administered safely and effectively during the latter phases of pregnancy,” the panel wrote. “Although it may be associated with prematurity and lower birth weights, studies have not reported significant disadvantages.”
Non-Hodgkin lymphoma
The second most common cancer in pregnancy is non-Hodgkin lymphoma. In the case of indolent disease, watchful waiting is possible, with the intent to treat with monoclonal antibodies – with or without chemotherapy – if symptoms or evidence of disease progression are noted. Steroids can be administered during the first trimester as a bridge to the second trimester, when chemotherapy can be used with relatively greater safety, the panelists noted.
Aggressive lymphomas diagnosed before 20 weeks’ gestation warrant pregnancy termination and treatment, they recommend. When diagnosed after 20 weeks, therapy should be comparable to that given a nonpregnant woman, including monoclonal antibodies (R-CHOP).
Chronic myeloid leukemia
Chronic myeloid leukemia occurs in approximately 1 in 100,000 pregnancies and is typically diagnosed during routine blood testing in an asymptomatic patient. As a result, treatment may not be needed until the patient’s white count or platelet count have risen to levels associated with the onset of symptoms. An approximate guideline is a white cell count greater than 100 X 109/L and a platelet count greater than 500 X 109/L.
Therapeutic approaches in pregnancy include interferon-a (INF-a), which does not inhibit DNA synthesis or readily cross the placenta, and leukapheresis, which is frequently required two to three times per week during the first and second trimesters. Counts tend to drop during the third trimester, allowing less frequent intervention.
Consideration should be given to adding aspirin or low-molecular-weight heparin (LMWH) when the platelet count exceeds 1,000 X 109/L.
Myeloproliferative neoplasms
The most common myeloproliferative neoplasm seen in women of childbearing age is essential thrombocytosis.
“A large meta-analysis of pregnant women with essential thrombocytosis reported a live birth rate of 50%-70%, first trimester loss in 25%-40%, late pregnancy loss in 10%, placental abruption in 3.6%, and intrauterine growth restriction in 4.5%. Maternal morbidity is rare, but stroke has been reported,” according to the panelists.
Limited literature suggests similar outcomes for pregnant women with polycythemia vera and primary myelofibrosis.
In low-risk pregnancies, aspirin (75 mg/day) should be offered unless clearly contraindicated. For women with polycythemia vera, venesection may be continued when tolerated to maintain the hematocrit within the gestation-appropriate range.
Fetal ultrasound scans should be performed at 20, 26, and 34 weeks of gestation and uterine artery Doppler should be performed at 20 weeks’ gestation. If the mean pulsatility index exceeds 1.4, the pregnancy may be considered high risk, and treatment and monitoring should be increased.
In high-risk pregnancies, additional treatment includes cytoreductive therapy with or without LMWH. If cytoreductive therapy is required, INF-a should be titrated to maintain a platelet count of less than 400 X 109/L and hematocrit within appropriate range.
Local protocols regarding interruption of LMWH should be adhered to during labor, and dehydration should be avoided. Platelet count and hematocrit may increase postpartum, requiring cytoreductive therapy. Thromboprophylaxis should be considered at 6 weeks’ postpartum because of the increased risk of thrombosis, the guidelines note.
Acute leukemia
“The remarkable anemia, thrombocytopenia, and neutropenia that characterize acute myeloid and lymphoblastic leukemia” require prompt treatment. Leukapheresis in the presence of clinically significant evidence of leukostasis can be considered, regardless of gestational stage. When patients are diagnosed with acute myeloid leukemia during the first trimester, pregnancy termination followed by conventional induction therapy (cytarabine/anthracycline) is recommended.
Those diagnosed later in pregnancy can receive conventional induction therapy, although this seems to be associated with increased risk of fetal growth restriction and even fetal loss. “Notably, neonates rarely experience neutropenia and cardiac impairment unless exposed to lipophilic idarubicin, which should not be used,” the panelists wrote.
When acute promyelocytic leukemia is diagnosed in the first trimester, pregnancy termination is recommended before initiating conventional ATRA-anthracycline therapy. Later in pregnancy, the regimen demonstrates low teratogenicity and can be used in women diagnosed after that stage. Arsenic treatment is highly teratogenic and is prohibited throughout gestation.
Acute lymphocytic leukemia (ALL) requires prophylactic CNS therapy, including methotrexate and L-asparaginase, which are fetotoxic. Methotrexate interferes with organogenesis and is prohibited before week 20 of gestation. L-asparaginase may increase the high risk for thromboembolic events attributed to the combination of pregnancy and malignancy.
Notably, tyrosine kinase inhibitors, essential for patients with Philadelphia chromosome–positive ALL, are teratogenic. Given these limitations, women diagnosed with ALL before 20 weeks’ gestation should undergo termination of the pregnancy and start conventional treatment. After week 20, conventional chemotherapy can be administered during pregnancy. Tyrosine kinase inhibitors can be initiated postpartum.
The guidelines also contain recommendations on diagnostic testing and radiotherapy, maternal supportive care, and perinatal and pediatric aspects of hematologic malignancies in pregnancy. An online appendix offers recommendations on the treatment of rare hematologic malignancies, including hairy cell leukemia, multiple myeloma, and myelodysplastic syndromes.
Dr. Lishner and nine of his coauthors had no financial relationships to disclose. Three coauthors received honoraria and research funding or are consultants to a wide variety of drug makers.
On Twitter @maryjodales
Consensus guidelines for the perinatal management of hematologic malignancies detected during pregnancy have been issued by a panel of international experts.
The guidelines, published online in the Journal of Clinical Oncology, aim to ensure that timely treatment of the cancers is not delayed in pregnant women (doi: 10.1200/JCO.2015.62.4445).
While rare, hematologic malignancies in pregnancy introduce clinical, social, ethical, and moral dilemmas. Evidence-based data are scarce, according to the researchers, who note the International Network on Cancer, Infertility and Pregnancy registers all cancers occurring during gestation.
“Patient accrual is ongoing and essential, because registration of new cases and long-term follow-up will improve clinical knowledge and increase the level of evidence,” Dr. Michael Lishner of Tel Aviv University and Meir Medical Center, Kfar Saba, Israel, and his fellow panelists wrote.
Hodgkin lymphoma
The researchers note that Hodgkin lymphoma is the most common hematologic cancer in pregnancy, and the prognosis for these patients is excellent. When diagnosed during the first trimester, a regimen based on vinblastine monotherapy has been used. ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) therapy can be used postpartum and has been used in cases of progression during pregnancy, the panelists wrote.
“The limited data available suggest that ABVD may be administered safely and effectively during the latter phases of pregnancy,” the panel wrote. “Although it may be associated with prematurity and lower birth weights, studies have not reported significant disadvantages.”
Non-Hodgkin lymphoma
The second most common cancer in pregnancy is non-Hodgkin lymphoma. In the case of indolent disease, watchful waiting is possible, with the intent to treat with monoclonal antibodies – with or without chemotherapy – if symptoms or evidence of disease progression are noted. Steroids can be administered during the first trimester as a bridge to the second trimester, when chemotherapy can be used with relatively greater safety, the panelists noted.
Aggressive lymphomas diagnosed before 20 weeks’ gestation warrant pregnancy termination and treatment, they recommend. When diagnosed after 20 weeks, therapy should be comparable to that given a nonpregnant woman, including monoclonal antibodies (R-CHOP).
Chronic myeloid leukemia
Chronic myeloid leukemia occurs in approximately 1 in 100,000 pregnancies and is typically diagnosed during routine blood testing in an asymptomatic patient. As a result, treatment may not be needed until the patient’s white count or platelet count have risen to levels associated with the onset of symptoms. An approximate guideline is a white cell count greater than 100 X 109/L and a platelet count greater than 500 X 109/L.
Therapeutic approaches in pregnancy include interferon-a (INF-a), which does not inhibit DNA synthesis or readily cross the placenta, and leukapheresis, which is frequently required two to three times per week during the first and second trimesters. Counts tend to drop during the third trimester, allowing less frequent intervention.
Consideration should be given to adding aspirin or low-molecular-weight heparin (LMWH) when the platelet count exceeds 1,000 X 109/L.
Myeloproliferative neoplasms
The most common myeloproliferative neoplasm seen in women of childbearing age is essential thrombocytosis.
“A large meta-analysis of pregnant women with essential thrombocytosis reported a live birth rate of 50%-70%, first trimester loss in 25%-40%, late pregnancy loss in 10%, placental abruption in 3.6%, and intrauterine growth restriction in 4.5%. Maternal morbidity is rare, but stroke has been reported,” according to the panelists.
Limited literature suggests similar outcomes for pregnant women with polycythemia vera and primary myelofibrosis.
In low-risk pregnancies, aspirin (75 mg/day) should be offered unless clearly contraindicated. For women with polycythemia vera, venesection may be continued when tolerated to maintain the hematocrit within the gestation-appropriate range.
Fetal ultrasound scans should be performed at 20, 26, and 34 weeks of gestation and uterine artery Doppler should be performed at 20 weeks’ gestation. If the mean pulsatility index exceeds 1.4, the pregnancy may be considered high risk, and treatment and monitoring should be increased.
In high-risk pregnancies, additional treatment includes cytoreductive therapy with or without LMWH. If cytoreductive therapy is required, INF-a should be titrated to maintain a platelet count of less than 400 X 109/L and hematocrit within appropriate range.
Local protocols regarding interruption of LMWH should be adhered to during labor, and dehydration should be avoided. Platelet count and hematocrit may increase postpartum, requiring cytoreductive therapy. Thromboprophylaxis should be considered at 6 weeks’ postpartum because of the increased risk of thrombosis, the guidelines note.
Acute leukemia
“The remarkable anemia, thrombocytopenia, and neutropenia that characterize acute myeloid and lymphoblastic leukemia” require prompt treatment. Leukapheresis in the presence of clinically significant evidence of leukostasis can be considered, regardless of gestational stage. When patients are diagnosed with acute myeloid leukemia during the first trimester, pregnancy termination followed by conventional induction therapy (cytarabine/anthracycline) is recommended.
Those diagnosed later in pregnancy can receive conventional induction therapy, although this seems to be associated with increased risk of fetal growth restriction and even fetal loss. “Notably, neonates rarely experience neutropenia and cardiac impairment unless exposed to lipophilic idarubicin, which should not be used,” the panelists wrote.
When acute promyelocytic leukemia is diagnosed in the first trimester, pregnancy termination is recommended before initiating conventional ATRA-anthracycline therapy. Later in pregnancy, the regimen demonstrates low teratogenicity and can be used in women diagnosed after that stage. Arsenic treatment is highly teratogenic and is prohibited throughout gestation.
Acute lymphocytic leukemia (ALL) requires prophylactic CNS therapy, including methotrexate and L-asparaginase, which are fetotoxic. Methotrexate interferes with organogenesis and is prohibited before week 20 of gestation. L-asparaginase may increase the high risk for thromboembolic events attributed to the combination of pregnancy and malignancy.
Notably, tyrosine kinase inhibitors, essential for patients with Philadelphia chromosome–positive ALL, are teratogenic. Given these limitations, women diagnosed with ALL before 20 weeks’ gestation should undergo termination of the pregnancy and start conventional treatment. After week 20, conventional chemotherapy can be administered during pregnancy. Tyrosine kinase inhibitors can be initiated postpartum.
The guidelines also contain recommendations on diagnostic testing and radiotherapy, maternal supportive care, and perinatal and pediatric aspects of hematologic malignancies in pregnancy. An online appendix offers recommendations on the treatment of rare hematologic malignancies, including hairy cell leukemia, multiple myeloma, and myelodysplastic syndromes.
Dr. Lishner and nine of his coauthors had no financial relationships to disclose. Three coauthors received honoraria and research funding or are consultants to a wide variety of drug makers.
On Twitter @maryjodales
Consensus guidelines for the perinatal management of hematologic malignancies detected during pregnancy have been issued by a panel of international experts.
The guidelines, published online in the Journal of Clinical Oncology, aim to ensure that timely treatment of the cancers is not delayed in pregnant women (doi: 10.1200/JCO.2015.62.4445).
While rare, hematologic malignancies in pregnancy introduce clinical, social, ethical, and moral dilemmas. Evidence-based data are scarce, according to the researchers, who note the International Network on Cancer, Infertility and Pregnancy registers all cancers occurring during gestation.
“Patient accrual is ongoing and essential, because registration of new cases and long-term follow-up will improve clinical knowledge and increase the level of evidence,” Dr. Michael Lishner of Tel Aviv University and Meir Medical Center, Kfar Saba, Israel, and his fellow panelists wrote.
Hodgkin lymphoma
The researchers note that Hodgkin lymphoma is the most common hematologic cancer in pregnancy, and the prognosis for these patients is excellent. When diagnosed during the first trimester, a regimen based on vinblastine monotherapy has been used. ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) therapy can be used postpartum and has been used in cases of progression during pregnancy, the panelists wrote.
“The limited data available suggest that ABVD may be administered safely and effectively during the latter phases of pregnancy,” the panel wrote. “Although it may be associated with prematurity and lower birth weights, studies have not reported significant disadvantages.”
Non-Hodgkin lymphoma
The second most common cancer in pregnancy is non-Hodgkin lymphoma. In the case of indolent disease, watchful waiting is possible, with the intent to treat with monoclonal antibodies – with or without chemotherapy – if symptoms or evidence of disease progression are noted. Steroids can be administered during the first trimester as a bridge to the second trimester, when chemotherapy can be used with relatively greater safety, the panelists noted.
Aggressive lymphomas diagnosed before 20 weeks’ gestation warrant pregnancy termination and treatment, they recommend. When diagnosed after 20 weeks, therapy should be comparable to that given a nonpregnant woman, including monoclonal antibodies (R-CHOP).
Chronic myeloid leukemia
Chronic myeloid leukemia occurs in approximately 1 in 100,000 pregnancies and is typically diagnosed during routine blood testing in an asymptomatic patient. As a result, treatment may not be needed until the patient’s white count or platelet count have risen to levels associated with the onset of symptoms. An approximate guideline is a white cell count greater than 100 X 109/L and a platelet count greater than 500 X 109/L.
Therapeutic approaches in pregnancy include interferon-a (INF-a), which does not inhibit DNA synthesis or readily cross the placenta, and leukapheresis, which is frequently required two to three times per week during the first and second trimesters. Counts tend to drop during the third trimester, allowing less frequent intervention.
Consideration should be given to adding aspirin or low-molecular-weight heparin (LMWH) when the platelet count exceeds 1,000 X 109/L.
Myeloproliferative neoplasms
The most common myeloproliferative neoplasm seen in women of childbearing age is essential thrombocytosis.
“A large meta-analysis of pregnant women with essential thrombocytosis reported a live birth rate of 50%-70%, first trimester loss in 25%-40%, late pregnancy loss in 10%, placental abruption in 3.6%, and intrauterine growth restriction in 4.5%. Maternal morbidity is rare, but stroke has been reported,” according to the panelists.
Limited literature suggests similar outcomes for pregnant women with polycythemia vera and primary myelofibrosis.
In low-risk pregnancies, aspirin (75 mg/day) should be offered unless clearly contraindicated. For women with polycythemia vera, venesection may be continued when tolerated to maintain the hematocrit within the gestation-appropriate range.
Fetal ultrasound scans should be performed at 20, 26, and 34 weeks of gestation and uterine artery Doppler should be performed at 20 weeks’ gestation. If the mean pulsatility index exceeds 1.4, the pregnancy may be considered high risk, and treatment and monitoring should be increased.
In high-risk pregnancies, additional treatment includes cytoreductive therapy with or without LMWH. If cytoreductive therapy is required, INF-a should be titrated to maintain a platelet count of less than 400 X 109/L and hematocrit within appropriate range.
Local protocols regarding interruption of LMWH should be adhered to during labor, and dehydration should be avoided. Platelet count and hematocrit may increase postpartum, requiring cytoreductive therapy. Thromboprophylaxis should be considered at 6 weeks’ postpartum because of the increased risk of thrombosis, the guidelines note.
Acute leukemia
“The remarkable anemia, thrombocytopenia, and neutropenia that characterize acute myeloid and lymphoblastic leukemia” require prompt treatment. Leukapheresis in the presence of clinically significant evidence of leukostasis can be considered, regardless of gestational stage. When patients are diagnosed with acute myeloid leukemia during the first trimester, pregnancy termination followed by conventional induction therapy (cytarabine/anthracycline) is recommended.
Those diagnosed later in pregnancy can receive conventional induction therapy, although this seems to be associated with increased risk of fetal growth restriction and even fetal loss. “Notably, neonates rarely experience neutropenia and cardiac impairment unless exposed to lipophilic idarubicin, which should not be used,” the panelists wrote.
When acute promyelocytic leukemia is diagnosed in the first trimester, pregnancy termination is recommended before initiating conventional ATRA-anthracycline therapy. Later in pregnancy, the regimen demonstrates low teratogenicity and can be used in women diagnosed after that stage. Arsenic treatment is highly teratogenic and is prohibited throughout gestation.
Acute lymphocytic leukemia (ALL) requires prophylactic CNS therapy, including methotrexate and L-asparaginase, which are fetotoxic. Methotrexate interferes with organogenesis and is prohibited before week 20 of gestation. L-asparaginase may increase the high risk for thromboembolic events attributed to the combination of pregnancy and malignancy.
Notably, tyrosine kinase inhibitors, essential for patients with Philadelphia chromosome–positive ALL, are teratogenic. Given these limitations, women diagnosed with ALL before 20 weeks’ gestation should undergo termination of the pregnancy and start conventional treatment. After week 20, conventional chemotherapy can be administered during pregnancy. Tyrosine kinase inhibitors can be initiated postpartum.
The guidelines also contain recommendations on diagnostic testing and radiotherapy, maternal supportive care, and perinatal and pediatric aspects of hematologic malignancies in pregnancy. An online appendix offers recommendations on the treatment of rare hematologic malignancies, including hairy cell leukemia, multiple myeloma, and myelodysplastic syndromes.
Dr. Lishner and nine of his coauthors had no financial relationships to disclose. Three coauthors received honoraria and research funding or are consultants to a wide variety of drug makers.
On Twitter @maryjodales
FROM JOURNAL OF CLINICAL ONCOLOGY
C-section target rates may be set too low
Countries with a cesarean delivery rate as high as 19% have lower maternal and neonatal mortality, compared with countries that have higher c-section rates, according to a report published online Dec. 1 in JAMA.
The findings suggest that the current World Health Organization (WHO) recommendation that national rates of cesarean delivery shouldn’t exceed 10%-15% of live births may be setting the target rate too low, according to Dr. George Molina of Ariadne Labs at Brigham and Women’s Hospital and the Harvard T.H. Chan School of Public Health, Boston, and his associates.
“The WHO recommendation that population level cesarean delivery rates should not exceed 10%-15% was a consensus opinion based on the observation that some countries with the lowest perinatal mortality rates had cesarean delivery rates that were less than 10/100 live births,” the researchers wrote. “Prior studies suggesting that lower cesarean delivery rate thresholds were optimal for maternal and neonatal mortality were incomplete because they examined data from limited sets of countries and often examined outcomes in wealthier countries.”

The researchers estimated that globally, the number of cesarean deliveries was 22.9 million in 2012 for a global cesarean delivery rate of 19.4/100 live births.
Cesarean delivery rates of up to 19.1/100 live births were inversely correlated with the maternal mortality ratio at the country level, and cesarean delivery rates of up to 19.4/100 live births were inversely correlated with the neonatal mortality ratio.
Dr. Molina and his colleagues analyzed the most recent information concerning modes of delivery, per capita health expenditures, life expectancy, and numerous other related factors using several multinational health databases. The goal was to estimate national rates of cesarean delivery and relate those figures to maternal and neonatal mortality for as many countries as possible, focusing on the most recent single year (2012) for which adequate data were available.
A sensitivity analysis of the 76 countries with the highest-quality cesarean delivery rate information showed that cesarean delivery rates greater than 6.9 to 20.1 per 100 live births were inversely correlated with the maternal mortality ratio. Cesarean delivery rates of 12.6 to 24.0 per 100 live births were inversely correlated with neonatal mortality (JAMA. 2015 Dec 1;314[21]:2263-70. doi: 10.1001/jama.2015.15553).
The researchers noted that they focused solely on mortality and did not assess other health outcomes. This means that they could not address the many possible benefits of cesarean delivery, such as reduced morbidity from complicated vaginal delivery or from prolonged obstructed labor.
In a separate report, a different research group found that children born by planned cesarean delivery, as compared with vaginal delivery, had a slightly increased risk of asthma requiring hospital admission, of needing a prescription for a salbutamol inhaler at age 5 years, and of all-cause mortality by age 21 years.
Dr. Mairead Blackof the University of Aberdeen (England) and her associates examined the relationship between planned cesarean delivery and chronic illness and death among the offspring. They assessed outcomes in 321,287 singleton live births to first-time mothers that occurred in Scotland in 1993-2007; the children were followed until January 2015, for a mean follow-up of 14.8 years.
In this cohort, 12,355 children (3.8%) were born by planned cesarean delivery, 56,015 (17.5%) by unscheduled cesarean, and 252,917 (78.7%) by vaginal delivery.
Children born by planned C-sections were slightly, but significantly more likely than were those born vaginally to develop asthma requiring hospital admission (3.73% vs. 3.41%; hazard ratio, 1.22).
Compared with children delivered vaginally, those delivered by planned cesarean section also were slightly, but significantly more likely to require a prescription for a salbutamol inhaler at age 5 years (10.34% vs. 9.62%; HR, 1.13) and to die before the age of 21 years(0.40% vs. 0.32%; HR, 1.41).
However, there were no significant differences between the two study groups in risk of developing inflammatory bowel disease (0.11% vs. 0.13%) or cancer (0.23% vs 0.21%), they noted (JAMA. 2015 Dec 1;314[21]:2271-9. doi: 10.1001/jama.2015.16176).
These findings “suggest that avoidance of vaginal birth may be an important early-life factor in the growing global burden of asthma, although absolute increase in risk to individuals is low,” Dr. Black and her associates wrote.
The researchers in both studies reported having no relevant financial disclosures. Dr. Black’s study was supported in part by the Wellcome Trust.
The findings of Molina et al. challenge a 30-year-old recommendation that a cesarean delivery rate of less than 15% should be a target for all health care institutions.
The study results also highlight the enormous variation in cesarean rates around the world and the need for the international obstetric community to evaluate this important health care issue. There is no one-size-fits-all optimal level of cesarean delivery that applies to all institutions, all health care systems, or all countries. The goal should be to identify meaningful ranges of risk-adjusted rates of cesarean deliveries for different populations and practices.
Dr. Mary E. D’Alton and Dr. Mark P. Hehir are in the department of obstetrics and gynecology at New York Presbyterian Hospital and Columbia University, New York. They reported having no relevant financial disclosures. These comments are adapted from an editorial accompanying the reports by Dr. Molina and Dr. Black (JAMA. 2015 Dec 1;314[21]:2238-40).
The findings of Molina et al. challenge a 30-year-old recommendation that a cesarean delivery rate of less than 15% should be a target for all health care institutions.
The study results also highlight the enormous variation in cesarean rates around the world and the need for the international obstetric community to evaluate this important health care issue. There is no one-size-fits-all optimal level of cesarean delivery that applies to all institutions, all health care systems, or all countries. The goal should be to identify meaningful ranges of risk-adjusted rates of cesarean deliveries for different populations and practices.
Dr. Mary E. D’Alton and Dr. Mark P. Hehir are in the department of obstetrics and gynecology at New York Presbyterian Hospital and Columbia University, New York. They reported having no relevant financial disclosures. These comments are adapted from an editorial accompanying the reports by Dr. Molina and Dr. Black (JAMA. 2015 Dec 1;314[21]:2238-40).
The findings of Molina et al. challenge a 30-year-old recommendation that a cesarean delivery rate of less than 15% should be a target for all health care institutions.
The study results also highlight the enormous variation in cesarean rates around the world and the need for the international obstetric community to evaluate this important health care issue. There is no one-size-fits-all optimal level of cesarean delivery that applies to all institutions, all health care systems, or all countries. The goal should be to identify meaningful ranges of risk-adjusted rates of cesarean deliveries for different populations and practices.
Dr. Mary E. D’Alton and Dr. Mark P. Hehir are in the department of obstetrics and gynecology at New York Presbyterian Hospital and Columbia University, New York. They reported having no relevant financial disclosures. These comments are adapted from an editorial accompanying the reports by Dr. Molina and Dr. Black (JAMA. 2015 Dec 1;314[21]:2238-40).
Countries with a cesarean delivery rate as high as 19% have lower maternal and neonatal mortality, compared with countries that have higher c-section rates, according to a report published online Dec. 1 in JAMA.
The findings suggest that the current World Health Organization (WHO) recommendation that national rates of cesarean delivery shouldn’t exceed 10%-15% of live births may be setting the target rate too low, according to Dr. George Molina of Ariadne Labs at Brigham and Women’s Hospital and the Harvard T.H. Chan School of Public Health, Boston, and his associates.
“The WHO recommendation that population level cesarean delivery rates should not exceed 10%-15% was a consensus opinion based on the observation that some countries with the lowest perinatal mortality rates had cesarean delivery rates that were less than 10/100 live births,” the researchers wrote. “Prior studies suggesting that lower cesarean delivery rate thresholds were optimal for maternal and neonatal mortality were incomplete because they examined data from limited sets of countries and often examined outcomes in wealthier countries.”
The researchers estimated that globally, the number of cesarean deliveries was 22.9 million in 2012 for a global cesarean delivery rate of 19.4/100 live births.
Cesarean delivery rates of up to 19.1/100 live births were inversely correlated with the maternal mortality ratio at the country level, and cesarean delivery rates of up to 19.4/100 live births were inversely correlated with the neonatal mortality ratio.
Dr. Molina and his colleagues analyzed the most recent information concerning modes of delivery, per capita health expenditures, life expectancy, and numerous other related factors using several multinational health databases. The goal was to estimate national rates of cesarean delivery and relate those figures to maternal and neonatal mortality for as many countries as possible, focusing on the most recent single year (2012) for which adequate data were available.
A sensitivity analysis of the 76 countries with the highest-quality cesarean delivery rate information showed that cesarean delivery rates greater than 6.9 to 20.1 per 100 live births were inversely correlated with the maternal mortality ratio. Cesarean delivery rates of 12.6 to 24.0 per 100 live births were inversely correlated with neonatal mortality (JAMA. 2015 Dec 1;314[21]:2263-70. doi: 10.1001/jama.2015.15553).
The researchers noted that they focused solely on mortality and did not assess other health outcomes. This means that they could not address the many possible benefits of cesarean delivery, such as reduced morbidity from complicated vaginal delivery or from prolonged obstructed labor.
In a separate report, a different research group found that children born by planned cesarean delivery, as compared with vaginal delivery, had a slightly increased risk of asthma requiring hospital admission, of needing a prescription for a salbutamol inhaler at age 5 years, and of all-cause mortality by age 21 years.
Dr. Mairead Blackof the University of Aberdeen (England) and her associates examined the relationship between planned cesarean delivery and chronic illness and death among the offspring. They assessed outcomes in 321,287 singleton live births to first-time mothers that occurred in Scotland in 1993-2007; the children were followed until January 2015, for a mean follow-up of 14.8 years.
In this cohort, 12,355 children (3.8%) were born by planned cesarean delivery, 56,015 (17.5%) by unscheduled cesarean, and 252,917 (78.7%) by vaginal delivery.
Children born by planned C-sections were slightly, but significantly more likely than were those born vaginally to develop asthma requiring hospital admission (3.73% vs. 3.41%; hazard ratio, 1.22).
Compared with children delivered vaginally, those delivered by planned cesarean section also were slightly, but significantly more likely to require a prescription for a salbutamol inhaler at age 5 years (10.34% vs. 9.62%; HR, 1.13) and to die before the age of 21 years(0.40% vs. 0.32%; HR, 1.41).
However, there were no significant differences between the two study groups in risk of developing inflammatory bowel disease (0.11% vs. 0.13%) or cancer (0.23% vs 0.21%), they noted (JAMA. 2015 Dec 1;314[21]:2271-9. doi: 10.1001/jama.2015.16176).
These findings “suggest that avoidance of vaginal birth may be an important early-life factor in the growing global burden of asthma, although absolute increase in risk to individuals is low,” Dr. Black and her associates wrote.
The researchers in both studies reported having no relevant financial disclosures. Dr. Black’s study was supported in part by the Wellcome Trust.
Countries with a cesarean delivery rate as high as 19% have lower maternal and neonatal mortality, compared with countries that have higher c-section rates, according to a report published online Dec. 1 in JAMA.
The findings suggest that the current World Health Organization (WHO) recommendation that national rates of cesarean delivery shouldn’t exceed 10%-15% of live births may be setting the target rate too low, according to Dr. George Molina of Ariadne Labs at Brigham and Women’s Hospital and the Harvard T.H. Chan School of Public Health, Boston, and his associates.
“The WHO recommendation that population level cesarean delivery rates should not exceed 10%-15% was a consensus opinion based on the observation that some countries with the lowest perinatal mortality rates had cesarean delivery rates that were less than 10/100 live births,” the researchers wrote. “Prior studies suggesting that lower cesarean delivery rate thresholds were optimal for maternal and neonatal mortality were incomplete because they examined data from limited sets of countries and often examined outcomes in wealthier countries.”
The researchers estimated that globally, the number of cesarean deliveries was 22.9 million in 2012 for a global cesarean delivery rate of 19.4/100 live births.
Cesarean delivery rates of up to 19.1/100 live births were inversely correlated with the maternal mortality ratio at the country level, and cesarean delivery rates of up to 19.4/100 live births were inversely correlated with the neonatal mortality ratio.
Dr. Molina and his colleagues analyzed the most recent information concerning modes of delivery, per capita health expenditures, life expectancy, and numerous other related factors using several multinational health databases. The goal was to estimate national rates of cesarean delivery and relate those figures to maternal and neonatal mortality for as many countries as possible, focusing on the most recent single year (2012) for which adequate data were available.
A sensitivity analysis of the 76 countries with the highest-quality cesarean delivery rate information showed that cesarean delivery rates greater than 6.9 to 20.1 per 100 live births were inversely correlated with the maternal mortality ratio. Cesarean delivery rates of 12.6 to 24.0 per 100 live births were inversely correlated with neonatal mortality (JAMA. 2015 Dec 1;314[21]:2263-70. doi: 10.1001/jama.2015.15553).
The researchers noted that they focused solely on mortality and did not assess other health outcomes. This means that they could not address the many possible benefits of cesarean delivery, such as reduced morbidity from complicated vaginal delivery or from prolonged obstructed labor.
In a separate report, a different research group found that children born by planned cesarean delivery, as compared with vaginal delivery, had a slightly increased risk of asthma requiring hospital admission, of needing a prescription for a salbutamol inhaler at age 5 years, and of all-cause mortality by age 21 years.
Dr. Mairead Blackof the University of Aberdeen (England) and her associates examined the relationship between planned cesarean delivery and chronic illness and death among the offspring. They assessed outcomes in 321,287 singleton live births to first-time mothers that occurred in Scotland in 1993-2007; the children were followed until January 2015, for a mean follow-up of 14.8 years.
In this cohort, 12,355 children (3.8%) were born by planned cesarean delivery, 56,015 (17.5%) by unscheduled cesarean, and 252,917 (78.7%) by vaginal delivery.
Children born by planned C-sections were slightly, but significantly more likely than were those born vaginally to develop asthma requiring hospital admission (3.73% vs. 3.41%; hazard ratio, 1.22).
Compared with children delivered vaginally, those delivered by planned cesarean section also were slightly, but significantly more likely to require a prescription for a salbutamol inhaler at age 5 years (10.34% vs. 9.62%; HR, 1.13) and to die before the age of 21 years(0.40% vs. 0.32%; HR, 1.41).
However, there were no significant differences between the two study groups in risk of developing inflammatory bowel disease (0.11% vs. 0.13%) or cancer (0.23% vs 0.21%), they noted (JAMA. 2015 Dec 1;314[21]:2271-9. doi: 10.1001/jama.2015.16176).
These findings “suggest that avoidance of vaginal birth may be an important early-life factor in the growing global burden of asthma, although absolute increase in risk to individuals is low,” Dr. Black and her associates wrote.
The researchers in both studies reported having no relevant financial disclosures. Dr. Black’s study was supported in part by the Wellcome Trust.
FROM JAMA
Key clinical point: Countries in which the national rate of cesarean deliveries is up to 19% have lower maternal and neonatal mortality.
Major finding: Cesarean delivery rates of up to 19.1/100 live births were inversely correlated with the maternal mortality ratio at the country level, and cesarean delivery rates of up 19.4/100 live births were inversely correlated with the neonatal mortality ratio.
Data source: A cross-sectional ecologic study estimating the 2012 rate of cesarean delivery in 194 World Health Organization member nations.
Disclosures: The researchers reported having no relevant financial disclosures.

“Where is it safe to practice obstetrics?” is a broader question
“SHOULD THE 30-MINUTE RULE FOR EMERGENT CESAREAN DELIVERY BE APPLIED UNIVERSALLY?”
“Where is it safe to practice obstetrics?” is a broader question Drs. Chauhan and Mendez-Figueroa presented a thoughtful series of case studies. Unfortunately, the cases were intended for the considerate ObGyn—the one who can appreciate that every case has a differing set of variables—and did not account for the context and legal environment in which we practice. In the theater that is our malpractice reality, these cases would carry little weight with a jury that is empathizing with a child with cerebral palsy, often years after the event.
“Where is it safe to practice obstetrics?” is a broader, and perhaps more interesting, question. And a more relevant case would involve a smaller hospital, perhaps in a rural area, that does not have in-house anesthesia available for 30-minute starts.
Daniel R. Szekely, MD, PhD
Tacoma, Washington
We are hoisted on a petard of our own makingThere is absolutely no justification for ObGyns being held to this so-called “standard of care.” The evidence is scant or lacking that delivery in a 30-minute timeframe has any significant bearing on the neonatal outcome. Despite this, the lay public and medical-legal community see this as an absolute rule to be followed. If there is a less-than-perfect outcome, we are hoisted on this petard of our own making.
We as a group (that is, the American College of Obstetricians and
Gynecologists) need to work to right this unfortunate wrong!
William H. Deschner, MD
Seattle, Washington
Practicing is downright scary The “30-minute rule” is no help to ObGyns in the field. At a community hospital, where surgical teams are called in from home (we cannot afford to do otherwise), it is often impossible to meet this standard. University-level care even cannot meet the measure at times. We never should have been painted into this corner. Now, any attempts to loosen the rule will be seen as trying to practice defensive medicine.
People who do not do what we do for a living have no concept of the anxiety and sleep loss we incur while seeking the best outcomes for our patients. I long for the soon-to-come day when I retire. Due to the litigious environment, I am saddened that I cannot heartily recommend the field to young doctors.
James Nunn, MD
Chicago, Illinois
“UPDATE ON VAGINAL HYSTERECTOMY”
BARBARA S. LEVY, MD (SEPTEMBER 2015)
Why has TAH remained the dominant hysterectomy route for generations?I read with great interest Dr. Levy’s recent comments on the benefits of new technology to improve the vaginal hysterectomy (VH) rate. Thank you and Dr. Levy for all the work you have done to advance the care of our patients. I have some other fundamental concerns about the future of hysterectomy.
Why has total abdominal hysterectomy (TAH) remained the dominant route of hysterectomy for generations? Why have past efforts to minimize TAH met with limited results?
Dr. Levy maintains in her article that, “the biggest barrier to widespread use [of VH] may simply be the lack of industry support.” What industry has supported TAH in a manner not also applicable to VH?
What do the techniques in Dr. Levy’s article and the efforts by ACOG and other authorities1 offer that will materially increase the adoption of VH? What evidence is there that the use of such devices as VITOM system will overcome the low rate of VH? How much training is required before a surgeon can realize patient-centered benefit from using the VITOM or other new devices during VH?
The lack of evidence-based training and implementation of robotic surgery has resulted in well-deserved criticism of robotics, centered, in part, around complications. Will the complication rate rise as those who do not perform VH transition to its adoption using VITOM and other devices?
I hope that the generations-long failure of all efforts to raise the VH rate is overcome with evidence-based educational protocols.
Antonio R. Pizarro, MD
Shreveport, Louisiana
Reference
1. Bosworth T. ACOG taking steps to increase vaginal hysterectomy rates. Ob.Gyn. News. http://www.obgynnews.com/?id=11146&tx_ttnews[tt_news]=392609&cHash=d78b8bea4aa3483c10dc5d843207d211. Posted April 6, 2015. Accessed October 2, 2015.
The problem: lack of trainingSadly, lack of training is the problem in this best approach to removing the benign uterus. These tools are helpful and should be in the surgeon’s armamentarium. We need experienced vaginal surgeons to teach this procedure. In some ways, just as much skill and dexterity are needed as with laparoscopic or robotic methods.
William H. Deschner, MD
Seattle, Washington
Dr. Levy respondsI appreciate the insightful comments of Drs. Pizarro and Deschner. Clearly, as the volume of hysterectomies has decreased and the number of techniques we must teach our residents has expanded, we are challenged to provide robust training in all hysterectomy routes. TAH, as the status quo, has not required the development of new equipment and technology, whereas assisting gynecologic surgeons to convert open procedures to minimally invasive approaches has been advanced and driven by our industry partners.
I totally agree with the concern that we cannot rely on historic data to determine the safest and most cost-effective route for hysterectomy. I encourage all of us to track and publically report our outcomes and monitor the complication rates of gynecologic surgical procedures. Our ongoing commitment to delivering the best care for our patients requires nothing less.
Structured business methods will improve outcomesDr. Barbieri’s call for getting organized and breaking down health care silos while establishing multidisciplinary teams is of great importance. Most providers have not witnessed a maternal mortality in their careers and many are not aware of the near misses. Incorporating foundations of established business methods has been advocated to reduce waste, improve collaboration, decrease variance, and improve patient safety.
If we view the adverse outcomes through this lens, then the increase in maternal mortality and morbidity are lagging indicators in the structured analysis methods (such as Six Sigma and Lean Six Sigma). These methods lead us to focus and measure the leading indicators of input and process (prenatal care and pregnancy management). Our reliance on lagging indicators often comes too late to make any change effective.
Around 1973, several important processes were introduced into obstetric practice: fetal heart-rate monitoring; ultrasonography; and a reduction of the use of forceps with an increase in the use of vacuum extraction. Safety rates improved, but we witnessed the 8% cesarean delivery rate in 1973 rise to 32% in 2013.1,2 The maternal mortality rate reported in 2013 is now the same as it was in 1973. A corresponding increase in the cesarean delivery rate over this time frame could be inferred.
By focusing on analysis and management of variables in pregnancy and implementing standardization of care based on good evidence from all disciplines involved in patient safety, we can improve maternal mortality. Simulations and debriefings are critical instruments to enhance management of all aspects of prenatal management, particularly emergent care.
As leaders in improving maternal quality, ObGyns must implement structured business methods (input and process analysis) to improve outcomes. A culture also can be positively altered if the mission and vision are clearly elucidated. Transparent, dynamic, granular, accurate, and reliable data will facilitate “buy-in” of the caregivers and provide more successful solutions. Decreased variance is critical. Expect resistance due to provider autonomy. The alteration in culture of the multidisciplinary team takes time, but a reduction in cesarean delivery rates should be number one on the list to reduce maternal mortality. The unintended consequences of all interventions and monitoring methods also should be pursued.
Robert A. Knuppel, MD, MPH, MBA
Naples, Florida
Judith Withers, RN, MN, MBA
San Diego, California
References
1. Blanchette E. The rising cesarean delivery rate in America. Obstet Gynecol. 2011;118(3):687–690.
2. Knuppel RA. Personal review of Centers for Disease Control and Prevention, National Vital Statistics Reports, 1973–2015.
Dr. Barbieri respondsI wholeheartedly agree with Dr. Knuppel and Ms. Withers: increasing the use of high reliability clinical processes is critically important in our quest to reduce maternal mortality. In addition to decreasing the cesarean delivery rate, I would prioritize ensuring the use of highly effective contraceptives by women with serious medical comorbidities that increase their risk of maternal mortality.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“SHOULD THE 30-MINUTE RULE FOR EMERGENT CESAREAN DELIVERY BE APPLIED UNIVERSALLY?”
“Where is it safe to practice obstetrics?” is a broader question Drs. Chauhan and Mendez-Figueroa presented a thoughtful series of case studies. Unfortunately, the cases were intended for the considerate ObGyn—the one who can appreciate that every case has a differing set of variables—and did not account for the context and legal environment in which we practice. In the theater that is our malpractice reality, these cases would carry little weight with a jury that is empathizing with a child with cerebral palsy, often years after the event.
“Where is it safe to practice obstetrics?” is a broader, and perhaps more interesting, question. And a more relevant case would involve a smaller hospital, perhaps in a rural area, that does not have in-house anesthesia available for 30-minute starts.
Daniel R. Szekely, MD, PhD
Tacoma, Washington
We are hoisted on a petard of our own makingThere is absolutely no justification for ObGyns being held to this so-called “standard of care.” The evidence is scant or lacking that delivery in a 30-minute timeframe has any significant bearing on the neonatal outcome. Despite this, the lay public and medical-legal community see this as an absolute rule to be followed. If there is a less-than-perfect outcome, we are hoisted on this petard of our own making.
We as a group (that is, the American College of Obstetricians and
Gynecologists) need to work to right this unfortunate wrong!
William H. Deschner, MD
Seattle, Washington
Practicing is downright scary The “30-minute rule” is no help to ObGyns in the field. At a community hospital, where surgical teams are called in from home (we cannot afford to do otherwise), it is often impossible to meet this standard. University-level care even cannot meet the measure at times. We never should have been painted into this corner. Now, any attempts to loosen the rule will be seen as trying to practice defensive medicine.
People who do not do what we do for a living have no concept of the anxiety and sleep loss we incur while seeking the best outcomes for our patients. I long for the soon-to-come day when I retire. Due to the litigious environment, I am saddened that I cannot heartily recommend the field to young doctors.
James Nunn, MD
Chicago, Illinois
“UPDATE ON VAGINAL HYSTERECTOMY”
BARBARA S. LEVY, MD (SEPTEMBER 2015)
Why has TAH remained the dominant hysterectomy route for generations?I read with great interest Dr. Levy’s recent comments on the benefits of new technology to improve the vaginal hysterectomy (VH) rate. Thank you and Dr. Levy for all the work you have done to advance the care of our patients. I have some other fundamental concerns about the future of hysterectomy.
Why has total abdominal hysterectomy (TAH) remained the dominant route of hysterectomy for generations? Why have past efforts to minimize TAH met with limited results?
Dr. Levy maintains in her article that, “the biggest barrier to widespread use [of VH] may simply be the lack of industry support.” What industry has supported TAH in a manner not also applicable to VH?
What do the techniques in Dr. Levy’s article and the efforts by ACOG and other authorities1 offer that will materially increase the adoption of VH? What evidence is there that the use of such devices as VITOM system will overcome the low rate of VH? How much training is required before a surgeon can realize patient-centered benefit from using the VITOM or other new devices during VH?
The lack of evidence-based training and implementation of robotic surgery has resulted in well-deserved criticism of robotics, centered, in part, around complications. Will the complication rate rise as those who do not perform VH transition to its adoption using VITOM and other devices?
I hope that the generations-long failure of all efforts to raise the VH rate is overcome with evidence-based educational protocols.
Antonio R. Pizarro, MD
Shreveport, Louisiana
Reference
1. Bosworth T. ACOG taking steps to increase vaginal hysterectomy rates. Ob.Gyn. News. http://www.obgynnews.com/?id=11146&tx_ttnews[tt_news]=392609&cHash=d78b8bea4aa3483c10dc5d843207d211. Posted April 6, 2015. Accessed October 2, 2015.
The problem: lack of trainingSadly, lack of training is the problem in this best approach to removing the benign uterus. These tools are helpful and should be in the surgeon’s armamentarium. We need experienced vaginal surgeons to teach this procedure. In some ways, just as much skill and dexterity are needed as with laparoscopic or robotic methods.
William H. Deschner, MD
Seattle, Washington
Dr. Levy respondsI appreciate the insightful comments of Drs. Pizarro and Deschner. Clearly, as the volume of hysterectomies has decreased and the number of techniques we must teach our residents has expanded, we are challenged to provide robust training in all hysterectomy routes. TAH, as the status quo, has not required the development of new equipment and technology, whereas assisting gynecologic surgeons to convert open procedures to minimally invasive approaches has been advanced and driven by our industry partners.
I totally agree with the concern that we cannot rely on historic data to determine the safest and most cost-effective route for hysterectomy. I encourage all of us to track and publically report our outcomes and monitor the complication rates of gynecologic surgical procedures. Our ongoing commitment to delivering the best care for our patients requires nothing less.
Structured business methods will improve outcomesDr. Barbieri’s call for getting organized and breaking down health care silos while establishing multidisciplinary teams is of great importance. Most providers have not witnessed a maternal mortality in their careers and many are not aware of the near misses. Incorporating foundations of established business methods has been advocated to reduce waste, improve collaboration, decrease variance, and improve patient safety.
If we view the adverse outcomes through this lens, then the increase in maternal mortality and morbidity are lagging indicators in the structured analysis methods (such as Six Sigma and Lean Six Sigma). These methods lead us to focus and measure the leading indicators of input and process (prenatal care and pregnancy management). Our reliance on lagging indicators often comes too late to make any change effective.
Around 1973, several important processes were introduced into obstetric practice: fetal heart-rate monitoring; ultrasonography; and a reduction of the use of forceps with an increase in the use of vacuum extraction. Safety rates improved, but we witnessed the 8% cesarean delivery rate in 1973 rise to 32% in 2013.1,2 The maternal mortality rate reported in 2013 is now the same as it was in 1973. A corresponding increase in the cesarean delivery rate over this time frame could be inferred.
By focusing on analysis and management of variables in pregnancy and implementing standardization of care based on good evidence from all disciplines involved in patient safety, we can improve maternal mortality. Simulations and debriefings are critical instruments to enhance management of all aspects of prenatal management, particularly emergent care.
As leaders in improving maternal quality, ObGyns must implement structured business methods (input and process analysis) to improve outcomes. A culture also can be positively altered if the mission and vision are clearly elucidated. Transparent, dynamic, granular, accurate, and reliable data will facilitate “buy-in” of the caregivers and provide more successful solutions. Decreased variance is critical. Expect resistance due to provider autonomy. The alteration in culture of the multidisciplinary team takes time, but a reduction in cesarean delivery rates should be number one on the list to reduce maternal mortality. The unintended consequences of all interventions and monitoring methods also should be pursued.
Robert A. Knuppel, MD, MPH, MBA
Naples, Florida
Judith Withers, RN, MN, MBA
San Diego, California
References
1. Blanchette E. The rising cesarean delivery rate in America. Obstet Gynecol. 2011;118(3):687–690.
2. Knuppel RA. Personal review of Centers for Disease Control and Prevention, National Vital Statistics Reports, 1973–2015.
Dr. Barbieri respondsI wholeheartedly agree with Dr. Knuppel and Ms. Withers: increasing the use of high reliability clinical processes is critically important in our quest to reduce maternal mortality. In addition to decreasing the cesarean delivery rate, I would prioritize ensuring the use of highly effective contraceptives by women with serious medical comorbidities that increase their risk of maternal mortality.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“SHOULD THE 30-MINUTE RULE FOR EMERGENT CESAREAN DELIVERY BE APPLIED UNIVERSALLY?”
“Where is it safe to practice obstetrics?” is a broader question Drs. Chauhan and Mendez-Figueroa presented a thoughtful series of case studies. Unfortunately, the cases were intended for the considerate ObGyn—the one who can appreciate that every case has a differing set of variables—and did not account for the context and legal environment in which we practice. In the theater that is our malpractice reality, these cases would carry little weight with a jury that is empathizing with a child with cerebral palsy, often years after the event.
“Where is it safe to practice obstetrics?” is a broader, and perhaps more interesting, question. And a more relevant case would involve a smaller hospital, perhaps in a rural area, that does not have in-house anesthesia available for 30-minute starts.
Daniel R. Szekely, MD, PhD
Tacoma, Washington
We are hoisted on a petard of our own makingThere is absolutely no justification for ObGyns being held to this so-called “standard of care.” The evidence is scant or lacking that delivery in a 30-minute timeframe has any significant bearing on the neonatal outcome. Despite this, the lay public and medical-legal community see this as an absolute rule to be followed. If there is a less-than-perfect outcome, we are hoisted on this petard of our own making.
We as a group (that is, the American College of Obstetricians and
Gynecologists) need to work to right this unfortunate wrong!
William H. Deschner, MD
Seattle, Washington
Practicing is downright scary The “30-minute rule” is no help to ObGyns in the field. At a community hospital, where surgical teams are called in from home (we cannot afford to do otherwise), it is often impossible to meet this standard. University-level care even cannot meet the measure at times. We never should have been painted into this corner. Now, any attempts to loosen the rule will be seen as trying to practice defensive medicine.
People who do not do what we do for a living have no concept of the anxiety and sleep loss we incur while seeking the best outcomes for our patients. I long for the soon-to-come day when I retire. Due to the litigious environment, I am saddened that I cannot heartily recommend the field to young doctors.
James Nunn, MD
Chicago, Illinois
“UPDATE ON VAGINAL HYSTERECTOMY”
BARBARA S. LEVY, MD (SEPTEMBER 2015)
Why has TAH remained the dominant hysterectomy route for generations?I read with great interest Dr. Levy’s recent comments on the benefits of new technology to improve the vaginal hysterectomy (VH) rate. Thank you and Dr. Levy for all the work you have done to advance the care of our patients. I have some other fundamental concerns about the future of hysterectomy.
Why has total abdominal hysterectomy (TAH) remained the dominant route of hysterectomy for generations? Why have past efforts to minimize TAH met with limited results?
Dr. Levy maintains in her article that, “the biggest barrier to widespread use [of VH] may simply be the lack of industry support.” What industry has supported TAH in a manner not also applicable to VH?
What do the techniques in Dr. Levy’s article and the efforts by ACOG and other authorities1 offer that will materially increase the adoption of VH? What evidence is there that the use of such devices as VITOM system will overcome the low rate of VH? How much training is required before a surgeon can realize patient-centered benefit from using the VITOM or other new devices during VH?
The lack of evidence-based training and implementation of robotic surgery has resulted in well-deserved criticism of robotics, centered, in part, around complications. Will the complication rate rise as those who do not perform VH transition to its adoption using VITOM and other devices?
I hope that the generations-long failure of all efforts to raise the VH rate is overcome with evidence-based educational protocols.
Antonio R. Pizarro, MD
Shreveport, Louisiana
Reference
1. Bosworth T. ACOG taking steps to increase vaginal hysterectomy rates. Ob.Gyn. News. http://www.obgynnews.com/?id=11146&tx_ttnews[tt_news]=392609&cHash=d78b8bea4aa3483c10dc5d843207d211. Posted April 6, 2015. Accessed October 2, 2015.
The problem: lack of trainingSadly, lack of training is the problem in this best approach to removing the benign uterus. These tools are helpful and should be in the surgeon’s armamentarium. We need experienced vaginal surgeons to teach this procedure. In some ways, just as much skill and dexterity are needed as with laparoscopic or robotic methods.
William H. Deschner, MD
Seattle, Washington
Dr. Levy respondsI appreciate the insightful comments of Drs. Pizarro and Deschner. Clearly, as the volume of hysterectomies has decreased and the number of techniques we must teach our residents has expanded, we are challenged to provide robust training in all hysterectomy routes. TAH, as the status quo, has not required the development of new equipment and technology, whereas assisting gynecologic surgeons to convert open procedures to minimally invasive approaches has been advanced and driven by our industry partners.
I totally agree with the concern that we cannot rely on historic data to determine the safest and most cost-effective route for hysterectomy. I encourage all of us to track and publically report our outcomes and monitor the complication rates of gynecologic surgical procedures. Our ongoing commitment to delivering the best care for our patients requires nothing less.
Structured business methods will improve outcomesDr. Barbieri’s call for getting organized and breaking down health care silos while establishing multidisciplinary teams is of great importance. Most providers have not witnessed a maternal mortality in their careers and many are not aware of the near misses. Incorporating foundations of established business methods has been advocated to reduce waste, improve collaboration, decrease variance, and improve patient safety.
If we view the adverse outcomes through this lens, then the increase in maternal mortality and morbidity are lagging indicators in the structured analysis methods (such as Six Sigma and Lean Six Sigma). These methods lead us to focus and measure the leading indicators of input and process (prenatal care and pregnancy management). Our reliance on lagging indicators often comes too late to make any change effective.
Around 1973, several important processes were introduced into obstetric practice: fetal heart-rate monitoring; ultrasonography; and a reduction of the use of forceps with an increase in the use of vacuum extraction. Safety rates improved, but we witnessed the 8% cesarean delivery rate in 1973 rise to 32% in 2013.1,2 The maternal mortality rate reported in 2013 is now the same as it was in 1973. A corresponding increase in the cesarean delivery rate over this time frame could be inferred.
By focusing on analysis and management of variables in pregnancy and implementing standardization of care based on good evidence from all disciplines involved in patient safety, we can improve maternal mortality. Simulations and debriefings are critical instruments to enhance management of all aspects of prenatal management, particularly emergent care.
As leaders in improving maternal quality, ObGyns must implement structured business methods (input and process analysis) to improve outcomes. A culture also can be positively altered if the mission and vision are clearly elucidated. Transparent, dynamic, granular, accurate, and reliable data will facilitate “buy-in” of the caregivers and provide more successful solutions. Decreased variance is critical. Expect resistance due to provider autonomy. The alteration in culture of the multidisciplinary team takes time, but a reduction in cesarean delivery rates should be number one on the list to reduce maternal mortality. The unintended consequences of all interventions and monitoring methods also should be pursued.
Robert A. Knuppel, MD, MPH, MBA
Naples, Florida
Judith Withers, RN, MN, MBA
San Diego, California
References
1. Blanchette E. The rising cesarean delivery rate in America. Obstet Gynecol. 2011;118(3):687–690.
2. Knuppel RA. Personal review of Centers for Disease Control and Prevention, National Vital Statistics Reports, 1973–2015.
Dr. Barbieri respondsI wholeheartedly agree with Dr. Knuppel and Ms. Withers: increasing the use of high reliability clinical processes is critically important in our quest to reduce maternal mortality. In addition to decreasing the cesarean delivery rate, I would prioritize ensuring the use of highly effective contraceptives by women with serious medical comorbidities that increase their risk of maternal mortality.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
ACR: Don’t stop TNFis during rheumatoid arthritis pregnancy
SAN FRANCISCO – It might be best to keep women with rheumatoid arthritis on their tumor necrosis factor blockers during pregnancy, according to German investigators.
They found that women are likely to flare without them and need more prednisolone, which is associated with preterm birth and other problems, while an increasing body of evidence suggests that tumor necrosis factor inhibitors (TNFis) are relatively safe during pregnancy.
“We should” rethink discontinuing TNFis during pregnancy, as recommended in some quarters. “We do not want women to flare during pregnancy,” said investigator Dr. Rebecca Fischer-Betz of the department of rheumatology at Heinrich Heine University in Düsseldorf.

She and her colleagues compared birth outcomes in 18 rheumatoid arthritis (RA) patients who discontinued TNFi treatment shortly after they got pregnant against those of 24 women with RA who were never exposed to a TNFi because, in general, they had less severe disease.
Twelve of the women (75%) in the TNFi group flared, versus four women (17%) in the control group. Although patients in both groups started with a mean 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP) below 3.0, women in the TNFi group had a rise in activity to a mean of about 3.5 in the second trimester, while disease activity in control patients remained stable.
Compared with controls, women who stopped TNFis were also far more likely to flare (odds ratio, 10.0; 95% confidence interval, 2.3-42.8; P = .002), even after adjusting for age, DAS28-CRP at conception, rheumatoid factor and cyclic citrullinated peptide status, and other potential confounders. They also relied more heavily on prednisolone, taking, for example, a mean dose of 13 mg in the second trimester versus 8 mg in the control group. Perhaps not surprisingly, the mean duration of pregnancy was 37 weeks in the TNFi group, with six women (33%) delivering at or before 37 weeks; women in the control group delivered, on average, at 39 weeks, with four (17%) delivering at or before week 37.
The investigators found that the risk of preterm birth increased with every cumulative milligram of prednisolone (OR, 1.08; 95% CI, 1.02-1.15; P less than .01).
“Women with RA who discontinue TNFis at conception face a high risk for flares during pregnancy, independently of known risk factors like seropositivity. Flares are usually treated with prednisolone. We found a dose-dependent, significant increased risk for preterm birth associated with prednisolone. In this era of treat-to-target management of RA, our paradigm for RA pregnancy management may need adjusting. By controlling RA activity with medications considered relatively safe in pregnancy, we may be able to improve both the pregnancy experience and pregnancy outcomes,” the investigators concluded.
The women were 33 years old on average, and all had live births; four early miscarriages were excluded from analysis. All the pregnancies were planned, with methotrexate discontinued at least 3 months before conception. There was no statistical difference in the rate of seropositivity between the groups, “which is interesting because we know seropositivity is a risk factor for staying active during pregnancy,” Dr. Fischer-Betz said.
Two boys born to women who took TNFis had minor malformations, one with nasal bone aplasia, retrognathia, and hydronephrosis, and the other with hypospadias. Both of their mothers had taken etanercept (Enbrel) in the first trimester. There was one malformation in the control group, a girl born with hydronephrosis.
There was no outside funding for the work, and the investigators have no disclosures.
SAN FRANCISCO – It might be best to keep women with rheumatoid arthritis on their tumor necrosis factor blockers during pregnancy, according to German investigators.
They found that women are likely to flare without them and need more prednisolone, which is associated with preterm birth and other problems, while an increasing body of evidence suggests that tumor necrosis factor inhibitors (TNFis) are relatively safe during pregnancy.
“We should” rethink discontinuing TNFis during pregnancy, as recommended in some quarters. “We do not want women to flare during pregnancy,” said investigator Dr. Rebecca Fischer-Betz of the department of rheumatology at Heinrich Heine University in Düsseldorf.
She and her colleagues compared birth outcomes in 18 rheumatoid arthritis (RA) patients who discontinued TNFi treatment shortly after they got pregnant against those of 24 women with RA who were never exposed to a TNFi because, in general, they had less severe disease.
Twelve of the women (75%) in the TNFi group flared, versus four women (17%) in the control group. Although patients in both groups started with a mean 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP) below 3.0, women in the TNFi group had a rise in activity to a mean of about 3.5 in the second trimester, while disease activity in control patients remained stable.
Compared with controls, women who stopped TNFis were also far more likely to flare (odds ratio, 10.0; 95% confidence interval, 2.3-42.8; P = .002), even after adjusting for age, DAS28-CRP at conception, rheumatoid factor and cyclic citrullinated peptide status, and other potential confounders. They also relied more heavily on prednisolone, taking, for example, a mean dose of 13 mg in the second trimester versus 8 mg in the control group. Perhaps not surprisingly, the mean duration of pregnancy was 37 weeks in the TNFi group, with six women (33%) delivering at or before 37 weeks; women in the control group delivered, on average, at 39 weeks, with four (17%) delivering at or before week 37.
The investigators found that the risk of preterm birth increased with every cumulative milligram of prednisolone (OR, 1.08; 95% CI, 1.02-1.15; P less than .01).
“Women with RA who discontinue TNFis at conception face a high risk for flares during pregnancy, independently of known risk factors like seropositivity. Flares are usually treated with prednisolone. We found a dose-dependent, significant increased risk for preterm birth associated with prednisolone. In this era of treat-to-target management of RA, our paradigm for RA pregnancy management may need adjusting. By controlling RA activity with medications considered relatively safe in pregnancy, we may be able to improve both the pregnancy experience and pregnancy outcomes,” the investigators concluded.
The women were 33 years old on average, and all had live births; four early miscarriages were excluded from analysis. All the pregnancies were planned, with methotrexate discontinued at least 3 months before conception. There was no statistical difference in the rate of seropositivity between the groups, “which is interesting because we know seropositivity is a risk factor for staying active during pregnancy,” Dr. Fischer-Betz said.
Two boys born to women who took TNFis had minor malformations, one with nasal bone aplasia, retrognathia, and hydronephrosis, and the other with hypospadias. Both of their mothers had taken etanercept (Enbrel) in the first trimester. There was one malformation in the control group, a girl born with hydronephrosis.
There was no outside funding for the work, and the investigators have no disclosures.
SAN FRANCISCO – It might be best to keep women with rheumatoid arthritis on their tumor necrosis factor blockers during pregnancy, according to German investigators.
They found that women are likely to flare without them and need more prednisolone, which is associated with preterm birth and other problems, while an increasing body of evidence suggests that tumor necrosis factor inhibitors (TNFis) are relatively safe during pregnancy.
“We should” rethink discontinuing TNFis during pregnancy, as recommended in some quarters. “We do not want women to flare during pregnancy,” said investigator Dr. Rebecca Fischer-Betz of the department of rheumatology at Heinrich Heine University in Düsseldorf.
She and her colleagues compared birth outcomes in 18 rheumatoid arthritis (RA) patients who discontinued TNFi treatment shortly after they got pregnant against those of 24 women with RA who were never exposed to a TNFi because, in general, they had less severe disease.
Twelve of the women (75%) in the TNFi group flared, versus four women (17%) in the control group. Although patients in both groups started with a mean 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP) below 3.0, women in the TNFi group had a rise in activity to a mean of about 3.5 in the second trimester, while disease activity in control patients remained stable.
Compared with controls, women who stopped TNFis were also far more likely to flare (odds ratio, 10.0; 95% confidence interval, 2.3-42.8; P = .002), even after adjusting for age, DAS28-CRP at conception, rheumatoid factor and cyclic citrullinated peptide status, and other potential confounders. They also relied more heavily on prednisolone, taking, for example, a mean dose of 13 mg in the second trimester versus 8 mg in the control group. Perhaps not surprisingly, the mean duration of pregnancy was 37 weeks in the TNFi group, with six women (33%) delivering at or before 37 weeks; women in the control group delivered, on average, at 39 weeks, with four (17%) delivering at or before week 37.
The investigators found that the risk of preterm birth increased with every cumulative milligram of prednisolone (OR, 1.08; 95% CI, 1.02-1.15; P less than .01).
“Women with RA who discontinue TNFis at conception face a high risk for flares during pregnancy, independently of known risk factors like seropositivity. Flares are usually treated with prednisolone. We found a dose-dependent, significant increased risk for preterm birth associated with prednisolone. In this era of treat-to-target management of RA, our paradigm for RA pregnancy management may need adjusting. By controlling RA activity with medications considered relatively safe in pregnancy, we may be able to improve both the pregnancy experience and pregnancy outcomes,” the investigators concluded.
The women were 33 years old on average, and all had live births; four early miscarriages were excluded from analysis. All the pregnancies were planned, with methotrexate discontinued at least 3 months before conception. There was no statistical difference in the rate of seropositivity between the groups, “which is interesting because we know seropositivity is a risk factor for staying active during pregnancy,” Dr. Fischer-Betz said.
Two boys born to women who took TNFis had minor malformations, one with nasal bone aplasia, retrognathia, and hydronephrosis, and the other with hypospadias. Both of their mothers had taken etanercept (Enbrel) in the first trimester. There was one malformation in the control group, a girl born with hydronephrosis.
There was no outside funding for the work, and the investigators have no disclosures.
AT THE ACR ANNUAL MEETING
Key clinical point: Stopping a TNFi during pregnancy comes at the cost of increased reliance on prednisolone.
Major finding: Compared with controls, women who stopped a TNFi during pregnancy were far more likely to flare (OR, 10.0; 95% CI, 2.3-42.8; P = .002).
Data source: Birth outcomes in 42 women with rheumatoid arthritis.
Disclosures: There was no outside funding for the work, and the investigators have no disclosures.
