User login
Children and COVID: The long goodbye continues
COVID-19 continues to be a diminishing issue for U.S. children, as the number of new cases declined for the ninth consecutive week, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and CHA said in their weekly COVID report. The most recently infected children brought the total number of COVID-19 cases to just over 12.8 million since the pandemic began.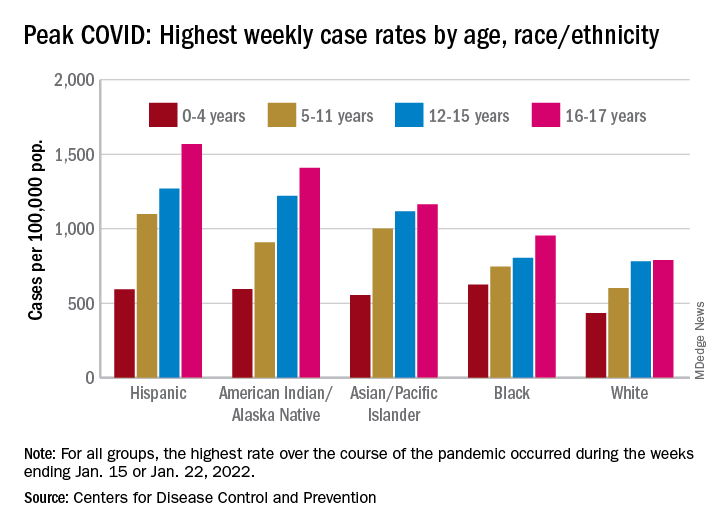
Other measures of COVID occurrence in children, such as hospital admissions and emergency department visits, also followed recent downward trends, although the sizes of the declines are beginning to decrease. Admissions dropped by 13.3% during the week ending March 26, but that followed declines of 25%, 20%, 26.5% and 24.4% for the 4 previous weeks, data from the Centers for Disease Control and Prevention show.
The slowdown in ED visits started a couple of weeks earlier, but the decline is still ongoing. As of March 25, ED visits with a confirmed COVID diagnosis represented just 0.4% of all visits for children aged 0-11 years, down from 1.1% on Feb. 25 and a peak of 14.3% on Jan. 15. For children aged 12-15, the latest figure is just 0.2%, compared with 0.5% on Feb. 25 and a peak of 14.3% on Jan. 9, the CDC reported on its COVID Data Tracker.
Although he was speaking of the nation as a whole and not specifically of children, Anthony Fauci, MD, the director of the National Institute of Allergy and Infectious Diseases, recently told the Washington Post that, “unless something changes dramatically,” another major surge isn’t on the horizon.
That sentiment, however, was not entirely shared by Moderna’s chief medical officer, Paul Burton, MD, PhD. In an interview with WebMD, he said that another COVID wave is inevitable and that it’s too soon to dismantle the vaccine infrastructure: “We’ve come so far. We’ve put so much into this to now take our foot off the gas. I think it would be a mistake for public health worldwide.”
Disparities during the Omicron surge
As the country puts Omicron in its rear view mirror, a quick look back at the CDC data shows some differences in how children were affected. At the surge’s peak in early to mid-January, Hispanic children were the most likely to get COVID-19, with incidence highest in the older groups. (See graph.)
At their peak week of Jan. 2-8, Hispanic children aged 16-17 years had a COVID rate of 1,568 cases per 100,000 population, versus 790 per 100,000 for White children, whose peak occurred a week later, from Jan. 9 to 15. Hispanic children aged 5-11 (1,098 per 100,000) and 12-15 (1,269 per 100,000) also had the highest recorded rates of the largest racial/ethnic groups, while Black children had the highest one-week rate, 625 per 100,000, among the 0- to 4-year-olds, according to the CDC.
COVID-19 continues to be a diminishing issue for U.S. children, as the number of new cases declined for the ninth consecutive week, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and CHA said in their weekly COVID report. The most recently infected children brought the total number of COVID-19 cases to just over 12.8 million since the pandemic began.
Other measures of COVID occurrence in children, such as hospital admissions and emergency department visits, also followed recent downward trends, although the sizes of the declines are beginning to decrease. Admissions dropped by 13.3% during the week ending March 26, but that followed declines of 25%, 20%, 26.5% and 24.4% for the 4 previous weeks, data from the Centers for Disease Control and Prevention show.
The slowdown in ED visits started a couple of weeks earlier, but the decline is still ongoing. As of March 25, ED visits with a confirmed COVID diagnosis represented just 0.4% of all visits for children aged 0-11 years, down from 1.1% on Feb. 25 and a peak of 14.3% on Jan. 15. For children aged 12-15, the latest figure is just 0.2%, compared with 0.5% on Feb. 25 and a peak of 14.3% on Jan. 9, the CDC reported on its COVID Data Tracker.
Although he was speaking of the nation as a whole and not specifically of children, Anthony Fauci, MD, the director of the National Institute of Allergy and Infectious Diseases, recently told the Washington Post that, “unless something changes dramatically,” another major surge isn’t on the horizon.
That sentiment, however, was not entirely shared by Moderna’s chief medical officer, Paul Burton, MD, PhD. In an interview with WebMD, he said that another COVID wave is inevitable and that it’s too soon to dismantle the vaccine infrastructure: “We’ve come so far. We’ve put so much into this to now take our foot off the gas. I think it would be a mistake for public health worldwide.”
Disparities during the Omicron surge
As the country puts Omicron in its rear view mirror, a quick look back at the CDC data shows some differences in how children were affected. At the surge’s peak in early to mid-January, Hispanic children were the most likely to get COVID-19, with incidence highest in the older groups. (See graph.)
At their peak week of Jan. 2-8, Hispanic children aged 16-17 years had a COVID rate of 1,568 cases per 100,000 population, versus 790 per 100,000 for White children, whose peak occurred a week later, from Jan. 9 to 15. Hispanic children aged 5-11 (1,098 per 100,000) and 12-15 (1,269 per 100,000) also had the highest recorded rates of the largest racial/ethnic groups, while Black children had the highest one-week rate, 625 per 100,000, among the 0- to 4-year-olds, according to the CDC.
COVID-19 continues to be a diminishing issue for U.S. children, as the number of new cases declined for the ninth consecutive week, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and CHA said in their weekly COVID report. The most recently infected children brought the total number of COVID-19 cases to just over 12.8 million since the pandemic began.
Other measures of COVID occurrence in children, such as hospital admissions and emergency department visits, also followed recent downward trends, although the sizes of the declines are beginning to decrease. Admissions dropped by 13.3% during the week ending March 26, but that followed declines of 25%, 20%, 26.5% and 24.4% for the 4 previous weeks, data from the Centers for Disease Control and Prevention show.
The slowdown in ED visits started a couple of weeks earlier, but the decline is still ongoing. As of March 25, ED visits with a confirmed COVID diagnosis represented just 0.4% of all visits for children aged 0-11 years, down from 1.1% on Feb. 25 and a peak of 14.3% on Jan. 15. For children aged 12-15, the latest figure is just 0.2%, compared with 0.5% on Feb. 25 and a peak of 14.3% on Jan. 9, the CDC reported on its COVID Data Tracker.
Although he was speaking of the nation as a whole and not specifically of children, Anthony Fauci, MD, the director of the National Institute of Allergy and Infectious Diseases, recently told the Washington Post that, “unless something changes dramatically,” another major surge isn’t on the horizon.
That sentiment, however, was not entirely shared by Moderna’s chief medical officer, Paul Burton, MD, PhD. In an interview with WebMD, he said that another COVID wave is inevitable and that it’s too soon to dismantle the vaccine infrastructure: “We’ve come so far. We’ve put so much into this to now take our foot off the gas. I think it would be a mistake for public health worldwide.”
Disparities during the Omicron surge
As the country puts Omicron in its rear view mirror, a quick look back at the CDC data shows some differences in how children were affected. At the surge’s peak in early to mid-January, Hispanic children were the most likely to get COVID-19, with incidence highest in the older groups. (See graph.)
At their peak week of Jan. 2-8, Hispanic children aged 16-17 years had a COVID rate of 1,568 cases per 100,000 population, versus 790 per 100,000 for White children, whose peak occurred a week later, from Jan. 9 to 15. Hispanic children aged 5-11 (1,098 per 100,000) and 12-15 (1,269 per 100,000) also had the highest recorded rates of the largest racial/ethnic groups, while Black children had the highest one-week rate, 625 per 100,000, among the 0- to 4-year-olds, according to the CDC.
Suicide attempts in kids ages 10-12 quadrupled over 20 years
Suicide attempts spurring calls to poison control centers more than quadrupled among U.S. children aged 10-12 years from 2000 to 2020, according to research published in JAMA Pediatrics.
The reasons for the increase in suicide attempts isn’t clear from the new study, but the researchers note that popular social media networks launched during the 20-year period, and other studies have linked spending time on social media with depression in adolescence. The COVID-19 pandemic, which began in the last year the researchers looked at, also disrupted normal life and routines for children.
For all children older than age 9, the proportion of incidents in which kids ate or drank something harmful that were deemed suicide attempts increased, while those classified as misuse or abuse of potentially poisonous substances declined. Children aged 6-9 did not have an increase in suicide attempts, the study found.
“It’s a huge problem we’re seeing in [ERs]. It’s exponentially blowing up numbers across the nation,” says David Sheridan, MD, an ER pediatric doctor at the Oregon Health and Science University, Portland, who led the study.
Adolescents or preteens who have attempted suicide can sit in ERs “for days or weeks” as they wait to be moved elsewhere in the hospital or to an outpatient facility for treatment, Dr. Sheridan says. The delays are not only unpleasant for the children, he says, but they also strain hospitals by leaving less space available for other patients coming to the ER.
“It’s really tough on the entire health care system, and most importantly, it’s really rough on the families who are going through a crisis,” Dr. Sheridan says. He noted that young people often attempt suicide by taking excessive quantities of common over-the-counter products found in many medicine cabinets – acetaminophen, ibuprofen, diphenhydramine – not items marked “poison.”
Twenty-year trend
The researchers examined phone calls to poison control centers about kids age 6 and up taking in potentially harmful substances from 2000-2020 recorded in the National Poison Data System, which is maintained by the American Association of Poison Control Centers.
Of more than 1.2 million total calls, 854,000 involved girls. A poison control data analyst determined if the call involved attempted suicide or the deliberate misuse or abuse of a potentially poisonous substance.
The researchers identified 1,005 deaths. About 70% of the total cases had either no effect or a minor effect on the child’s health.
Over the 20-year period, more than 90% of the calls involved children aged at least 13 years, with approximately 72,000 (5.7%) about children aged 10-12. Most calls for children 13 and older were for suicide attempts.
Suspected suicide attempts accounted for about 50% of the total calls to poison control centers among children aged 10-12 in 2000 – a figure that ballooned to 80% in 2020, the researchers found.
Both the number of calls and the proportion related to suicide attempts increased among children aged 10-12, Dr. Sheridan says. By 2020, the researchers found, poison control centers were fielding 4.5 times as many suicide-related calls among kids of this age group as they had in 2000. This jump was the largest such increase for any age group in the study, he says.
The reasons for such a large increase of suicide-related calls among preadolescents are unclear, the researchers note.
The increase became apparent around 2013, at the time many popular social media networks launched. Dr. Sheridan and his colleagues cite studies showing an association between spending more time on social media or watching television and depression in adolescence but said further research is needed to understand the root causes of this increase.
The latest study did not look specifically at the effect of the COVID-19 pandemic on suicide among young people. The Centers for Disease Control and Prevention earlier reported a sharp rise in suicide attempts among youth during the early months of the pandemic, especially among girls aged 12-17 years. By February 2021, suicide attempts within this group had climbed by 50%, compared with 2 years earlier.
Although suicide attempts are concerning enough, deaths by suicide are even more worrisome, experts said.
The researchers’ findings are consistent with overall recent trends in youth suicide deaths, says Jeff Bridge, PhD, an epidemiologist at Nationwide Children’s Hospital, Columbus. From 2010-2020, suicide rates increased by 50% among 13- to 18-year-olds, Dr. Bridge said, and more than doubled in children aged 10-12.
The latest study captured only calls to poison control centers, so it did not count suicide attempts that did not result in a call for help. Another limitation of the study is that poison control data are not categorized by race or ethnicity, prompting Dr. Bridge to urge researchers to look specifically at the effect of race and ethnicity on these trends.
“This study supports screening for suicide risk as young as 10 years old,” Dr. Bridge says.
Dr. Sheridan agrees that prevention is essential: “The ER is where kids come when they’re in crisis. Trying to be more preventative by diagnosing or picking up on this earlier, I think, is really important.”
A version of this article first appeared on WebMD.com.
Suicide attempts spurring calls to poison control centers more than quadrupled among U.S. children aged 10-12 years from 2000 to 2020, according to research published in JAMA Pediatrics.
The reasons for the increase in suicide attempts isn’t clear from the new study, but the researchers note that popular social media networks launched during the 20-year period, and other studies have linked spending time on social media with depression in adolescence. The COVID-19 pandemic, which began in the last year the researchers looked at, also disrupted normal life and routines for children.
For all children older than age 9, the proportion of incidents in which kids ate or drank something harmful that were deemed suicide attempts increased, while those classified as misuse or abuse of potentially poisonous substances declined. Children aged 6-9 did not have an increase in suicide attempts, the study found.
“It’s a huge problem we’re seeing in [ERs]. It’s exponentially blowing up numbers across the nation,” says David Sheridan, MD, an ER pediatric doctor at the Oregon Health and Science University, Portland, who led the study.
Adolescents or preteens who have attempted suicide can sit in ERs “for days or weeks” as they wait to be moved elsewhere in the hospital or to an outpatient facility for treatment, Dr. Sheridan says. The delays are not only unpleasant for the children, he says, but they also strain hospitals by leaving less space available for other patients coming to the ER.
“It’s really tough on the entire health care system, and most importantly, it’s really rough on the families who are going through a crisis,” Dr. Sheridan says. He noted that young people often attempt suicide by taking excessive quantities of common over-the-counter products found in many medicine cabinets – acetaminophen, ibuprofen, diphenhydramine – not items marked “poison.”
Twenty-year trend
The researchers examined phone calls to poison control centers about kids age 6 and up taking in potentially harmful substances from 2000-2020 recorded in the National Poison Data System, which is maintained by the American Association of Poison Control Centers.
Of more than 1.2 million total calls, 854,000 involved girls. A poison control data analyst determined if the call involved attempted suicide or the deliberate misuse or abuse of a potentially poisonous substance.
The researchers identified 1,005 deaths. About 70% of the total cases had either no effect or a minor effect on the child’s health.
Over the 20-year period, more than 90% of the calls involved children aged at least 13 years, with approximately 72,000 (5.7%) about children aged 10-12. Most calls for children 13 and older were for suicide attempts.
Suspected suicide attempts accounted for about 50% of the total calls to poison control centers among children aged 10-12 in 2000 – a figure that ballooned to 80% in 2020, the researchers found.
Both the number of calls and the proportion related to suicide attempts increased among children aged 10-12, Dr. Sheridan says. By 2020, the researchers found, poison control centers were fielding 4.5 times as many suicide-related calls among kids of this age group as they had in 2000. This jump was the largest such increase for any age group in the study, he says.
The reasons for such a large increase of suicide-related calls among preadolescents are unclear, the researchers note.
The increase became apparent around 2013, at the time many popular social media networks launched. Dr. Sheridan and his colleagues cite studies showing an association between spending more time on social media or watching television and depression in adolescence but said further research is needed to understand the root causes of this increase.
The latest study did not look specifically at the effect of the COVID-19 pandemic on suicide among young people. The Centers for Disease Control and Prevention earlier reported a sharp rise in suicide attempts among youth during the early months of the pandemic, especially among girls aged 12-17 years. By February 2021, suicide attempts within this group had climbed by 50%, compared with 2 years earlier.
Although suicide attempts are concerning enough, deaths by suicide are even more worrisome, experts said.
The researchers’ findings are consistent with overall recent trends in youth suicide deaths, says Jeff Bridge, PhD, an epidemiologist at Nationwide Children’s Hospital, Columbus. From 2010-2020, suicide rates increased by 50% among 13- to 18-year-olds, Dr. Bridge said, and more than doubled in children aged 10-12.
The latest study captured only calls to poison control centers, so it did not count suicide attempts that did not result in a call for help. Another limitation of the study is that poison control data are not categorized by race or ethnicity, prompting Dr. Bridge to urge researchers to look specifically at the effect of race and ethnicity on these trends.
“This study supports screening for suicide risk as young as 10 years old,” Dr. Bridge says.
Dr. Sheridan agrees that prevention is essential: “The ER is where kids come when they’re in crisis. Trying to be more preventative by diagnosing or picking up on this earlier, I think, is really important.”
A version of this article first appeared on WebMD.com.
Suicide attempts spurring calls to poison control centers more than quadrupled among U.S. children aged 10-12 years from 2000 to 2020, according to research published in JAMA Pediatrics.
The reasons for the increase in suicide attempts isn’t clear from the new study, but the researchers note that popular social media networks launched during the 20-year period, and other studies have linked spending time on social media with depression in adolescence. The COVID-19 pandemic, which began in the last year the researchers looked at, also disrupted normal life and routines for children.
For all children older than age 9, the proportion of incidents in which kids ate or drank something harmful that were deemed suicide attempts increased, while those classified as misuse or abuse of potentially poisonous substances declined. Children aged 6-9 did not have an increase in suicide attempts, the study found.
“It’s a huge problem we’re seeing in [ERs]. It’s exponentially blowing up numbers across the nation,” says David Sheridan, MD, an ER pediatric doctor at the Oregon Health and Science University, Portland, who led the study.
Adolescents or preteens who have attempted suicide can sit in ERs “for days or weeks” as they wait to be moved elsewhere in the hospital or to an outpatient facility for treatment, Dr. Sheridan says. The delays are not only unpleasant for the children, he says, but they also strain hospitals by leaving less space available for other patients coming to the ER.
“It’s really tough on the entire health care system, and most importantly, it’s really rough on the families who are going through a crisis,” Dr. Sheridan says. He noted that young people often attempt suicide by taking excessive quantities of common over-the-counter products found in many medicine cabinets – acetaminophen, ibuprofen, diphenhydramine – not items marked “poison.”
Twenty-year trend
The researchers examined phone calls to poison control centers about kids age 6 and up taking in potentially harmful substances from 2000-2020 recorded in the National Poison Data System, which is maintained by the American Association of Poison Control Centers.
Of more than 1.2 million total calls, 854,000 involved girls. A poison control data analyst determined if the call involved attempted suicide or the deliberate misuse or abuse of a potentially poisonous substance.
The researchers identified 1,005 deaths. About 70% of the total cases had either no effect or a minor effect on the child’s health.
Over the 20-year period, more than 90% of the calls involved children aged at least 13 years, with approximately 72,000 (5.7%) about children aged 10-12. Most calls for children 13 and older were for suicide attempts.
Suspected suicide attempts accounted for about 50% of the total calls to poison control centers among children aged 10-12 in 2000 – a figure that ballooned to 80% in 2020, the researchers found.
Both the number of calls and the proportion related to suicide attempts increased among children aged 10-12, Dr. Sheridan says. By 2020, the researchers found, poison control centers were fielding 4.5 times as many suicide-related calls among kids of this age group as they had in 2000. This jump was the largest such increase for any age group in the study, he says.
The reasons for such a large increase of suicide-related calls among preadolescents are unclear, the researchers note.
The increase became apparent around 2013, at the time many popular social media networks launched. Dr. Sheridan and his colleagues cite studies showing an association between spending more time on social media or watching television and depression in adolescence but said further research is needed to understand the root causes of this increase.
The latest study did not look specifically at the effect of the COVID-19 pandemic on suicide among young people. The Centers for Disease Control and Prevention earlier reported a sharp rise in suicide attempts among youth during the early months of the pandemic, especially among girls aged 12-17 years. By February 2021, suicide attempts within this group had climbed by 50%, compared with 2 years earlier.
Although suicide attempts are concerning enough, deaths by suicide are even more worrisome, experts said.
The researchers’ findings are consistent with overall recent trends in youth suicide deaths, says Jeff Bridge, PhD, an epidemiologist at Nationwide Children’s Hospital, Columbus. From 2010-2020, suicide rates increased by 50% among 13- to 18-year-olds, Dr. Bridge said, and more than doubled in children aged 10-12.
The latest study captured only calls to poison control centers, so it did not count suicide attempts that did not result in a call for help. Another limitation of the study is that poison control data are not categorized by race or ethnicity, prompting Dr. Bridge to urge researchers to look specifically at the effect of race and ethnicity on these trends.
“This study supports screening for suicide risk as young as 10 years old,” Dr. Bridge says.
Dr. Sheridan agrees that prevention is essential: “The ER is where kids come when they’re in crisis. Trying to be more preventative by diagnosing or picking up on this earlier, I think, is really important.”
A version of this article first appeared on WebMD.com.
FROM JAMA PEDIATRICS
Virtual and in-person pediatric visits get similar family ratings
CHICAGO – Satisfaction ratings for virtual outpatient visits for pediatric orthopedic patients were similar to those for in-person office visits across most categories in an analysis of postencounter surveys completed by patients at the Cleveland Clinic.
Satisfaction ratings for both virtual and office visits were consistently higher than 85% across all measured parameters, according to the data presented at the annual meeting of the American Academy of Orthopaedic Surgeons.
Ahmed Emara, MD, a clinical research fellow in adult joint reconstruction at the Cleveland Clinic, led the study, which included data from all patients or guardians at the clinic who experienced such visits from March 2020 to March 2021.
A total of 1,686 responses were received, of which 226 (13.4%) involved virtual visits and 1,460 (86.6%) involved in-office visits. The primary endpoint was a patient-reported satisfaction score of good or excellent.
Analysis included ratings for access, care provider, telemedicine technology, and overall assessment/perception of satisfaction.
Target areas for improvement
In some areas, the virtual visits were less satisfactory than the in-office visits.
Patients had lower odds of reporting good/excellent satisfaction regarding their ability to schedule at a particularly convenient time (odds ratio, 0.1; 95% confidence interval, 0.08-0.18; P < .001). The study authors said scheduling more virtual time slots may help increase satisfaction in that area.
Satisfaction was also lower than with in-office visits with respect to providers’ explanations of patients’ conditions (OR, 0.4; 95% CI, 0.17-0.91; P = .03). Providers may need to find ways to better provide educational material in addition to the virtual consultation, the authors wrote.
No significant differences in categories of satisfaction
The researchers accounted for age, sex, traumatic etiology, and anatomic location of the complaint in multivariate regression analysis and found no significant differences between the two types of visits in the odds of getting a good/excellent rating for the following areas: patient inclusion in treatment decision (P = .562), discussion of proposed treatment (P = .222), concern by the provider (P = .189), degree of care for the patient as a person (P = .208), adequacy of teamwork in care provision (P = .053), likelihood of recommending the practice to others (P = .108), ease of receiving care at a particular practice (P = .109), ease of contacting the clinic (P = .177), and likelihood of recommending a particular provider (P = .218).
Anna Dimitriovna Vergun, MD, a pediatric orthopedist at the University of North Carolina at Chapel Hill, who was not involved in the study, said in an interview she had been conducting virtual visits even before the pandemic, when she worked for several years at a Shriner’s children’s hospital in Los Angeles, before coming to UNC. The virtual visits were necessary because the hospital offered charity care and covered an area that included several states.
She said that during the height of the pandemic, 80% of her visits at UNC were virtual; it is down to about 5% now.
Some consultations don’t need physical visits at all, Dr. Vergun noted. For example, UNC is starting a clinic for prenatal counseling in cases in which ultrasound detects a limb deformity. Without a virtual option, she said, pregnant mothers in all parts of the state may have to drive long distances when no physical exam is necessary.
And sometimes, a visit simply involves checking in with families to see whether pain is being controlled, which is done well virtually.
“Those are particularly useful for telemedicine,” Dr. Vergun said. “There’s a lot of space for this to be useful. You sometimes don’t realize it until you start doing it and getting feedback from the families that they like it.”
Other exams may be better suited to office visits, she said. These include spine and hip exams and exams in which providers need to check reflexes.
She said she sees many cases of club feet, for which an in-person exam is needed to determine flexibility.
Expert says virtual misses nuances
Ryan Fitzgerald, MD, an orthopedic expert with Children’s Orthopaedic and Scoliosis Surgery Associates in St. Petersburg, Fla., who also was not involved in the study, said in an interview he doesn’t offer the virtual option now because he thinks those visits usually miss too much.
COSSA is a private practice that provides orthopedic services for Johns Hopkins All Children’s Hospital.
“I think physicians’ perspective versus the families’ perspective may be quite a bit different,” he said.
While families like the convenience, “a lot of what we do is watching the patient walk, looking at their hip range of motion, and virtually, that’s a really difficult thing to do,” he said.
You can instruct a family on how to turn a camera on the patient, but “it doesn’t always translate,” he said.
He said virtual visits also highlight disparities in access, because many families don’t own the hardware needed for such visits, and internet connections can be spotty or images pixelated.
Dr. Fitzgerald said virtual visits were helpful during the pandemic and would be beneficial for yearly checkups “if you know [the patient] well and it’s a fairly run-of-the-mill thing.”
However, he said, “everything we do is about human interaction, and I think that’s a downfall of the virtual platform right now. While it is helpful in situations like COVID and where it is a very basic follow-up, it still has a ways to go.”
Dr. Fitzgerald is a consultant for OrthoPediatrics, Medtronic, and Depuy Synthes. Dr. Vergun disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO – Satisfaction ratings for virtual outpatient visits for pediatric orthopedic patients were similar to those for in-person office visits across most categories in an analysis of postencounter surveys completed by patients at the Cleveland Clinic.
Satisfaction ratings for both virtual and office visits were consistently higher than 85% across all measured parameters, according to the data presented at the annual meeting of the American Academy of Orthopaedic Surgeons.
Ahmed Emara, MD, a clinical research fellow in adult joint reconstruction at the Cleveland Clinic, led the study, which included data from all patients or guardians at the clinic who experienced such visits from March 2020 to March 2021.
A total of 1,686 responses were received, of which 226 (13.4%) involved virtual visits and 1,460 (86.6%) involved in-office visits. The primary endpoint was a patient-reported satisfaction score of good or excellent.
Analysis included ratings for access, care provider, telemedicine technology, and overall assessment/perception of satisfaction.
Target areas for improvement
In some areas, the virtual visits were less satisfactory than the in-office visits.
Patients had lower odds of reporting good/excellent satisfaction regarding their ability to schedule at a particularly convenient time (odds ratio, 0.1; 95% confidence interval, 0.08-0.18; P < .001). The study authors said scheduling more virtual time slots may help increase satisfaction in that area.
Satisfaction was also lower than with in-office visits with respect to providers’ explanations of patients’ conditions (OR, 0.4; 95% CI, 0.17-0.91; P = .03). Providers may need to find ways to better provide educational material in addition to the virtual consultation, the authors wrote.
No significant differences in categories of satisfaction
The researchers accounted for age, sex, traumatic etiology, and anatomic location of the complaint in multivariate regression analysis and found no significant differences between the two types of visits in the odds of getting a good/excellent rating for the following areas: patient inclusion in treatment decision (P = .562), discussion of proposed treatment (P = .222), concern by the provider (P = .189), degree of care for the patient as a person (P = .208), adequacy of teamwork in care provision (P = .053), likelihood of recommending the practice to others (P = .108), ease of receiving care at a particular practice (P = .109), ease of contacting the clinic (P = .177), and likelihood of recommending a particular provider (P = .218).
Anna Dimitriovna Vergun, MD, a pediatric orthopedist at the University of North Carolina at Chapel Hill, who was not involved in the study, said in an interview she had been conducting virtual visits even before the pandemic, when she worked for several years at a Shriner’s children’s hospital in Los Angeles, before coming to UNC. The virtual visits were necessary because the hospital offered charity care and covered an area that included several states.
She said that during the height of the pandemic, 80% of her visits at UNC were virtual; it is down to about 5% now.
Some consultations don’t need physical visits at all, Dr. Vergun noted. For example, UNC is starting a clinic for prenatal counseling in cases in which ultrasound detects a limb deformity. Without a virtual option, she said, pregnant mothers in all parts of the state may have to drive long distances when no physical exam is necessary.
And sometimes, a visit simply involves checking in with families to see whether pain is being controlled, which is done well virtually.
“Those are particularly useful for telemedicine,” Dr. Vergun said. “There’s a lot of space for this to be useful. You sometimes don’t realize it until you start doing it and getting feedback from the families that they like it.”
Other exams may be better suited to office visits, she said. These include spine and hip exams and exams in which providers need to check reflexes.
She said she sees many cases of club feet, for which an in-person exam is needed to determine flexibility.
Expert says virtual misses nuances
Ryan Fitzgerald, MD, an orthopedic expert with Children’s Orthopaedic and Scoliosis Surgery Associates in St. Petersburg, Fla., who also was not involved in the study, said in an interview he doesn’t offer the virtual option now because he thinks those visits usually miss too much.
COSSA is a private practice that provides orthopedic services for Johns Hopkins All Children’s Hospital.
“I think physicians’ perspective versus the families’ perspective may be quite a bit different,” he said.
While families like the convenience, “a lot of what we do is watching the patient walk, looking at their hip range of motion, and virtually, that’s a really difficult thing to do,” he said.
You can instruct a family on how to turn a camera on the patient, but “it doesn’t always translate,” he said.
He said virtual visits also highlight disparities in access, because many families don’t own the hardware needed for such visits, and internet connections can be spotty or images pixelated.
Dr. Fitzgerald said virtual visits were helpful during the pandemic and would be beneficial for yearly checkups “if you know [the patient] well and it’s a fairly run-of-the-mill thing.”
However, he said, “everything we do is about human interaction, and I think that’s a downfall of the virtual platform right now. While it is helpful in situations like COVID and where it is a very basic follow-up, it still has a ways to go.”
Dr. Fitzgerald is a consultant for OrthoPediatrics, Medtronic, and Depuy Synthes. Dr. Vergun disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO – Satisfaction ratings for virtual outpatient visits for pediatric orthopedic patients were similar to those for in-person office visits across most categories in an analysis of postencounter surveys completed by patients at the Cleveland Clinic.
Satisfaction ratings for both virtual and office visits were consistently higher than 85% across all measured parameters, according to the data presented at the annual meeting of the American Academy of Orthopaedic Surgeons.
Ahmed Emara, MD, a clinical research fellow in adult joint reconstruction at the Cleveland Clinic, led the study, which included data from all patients or guardians at the clinic who experienced such visits from March 2020 to March 2021.
A total of 1,686 responses were received, of which 226 (13.4%) involved virtual visits and 1,460 (86.6%) involved in-office visits. The primary endpoint was a patient-reported satisfaction score of good or excellent.
Analysis included ratings for access, care provider, telemedicine technology, and overall assessment/perception of satisfaction.
Target areas for improvement
In some areas, the virtual visits were less satisfactory than the in-office visits.
Patients had lower odds of reporting good/excellent satisfaction regarding their ability to schedule at a particularly convenient time (odds ratio, 0.1; 95% confidence interval, 0.08-0.18; P < .001). The study authors said scheduling more virtual time slots may help increase satisfaction in that area.
Satisfaction was also lower than with in-office visits with respect to providers’ explanations of patients’ conditions (OR, 0.4; 95% CI, 0.17-0.91; P = .03). Providers may need to find ways to better provide educational material in addition to the virtual consultation, the authors wrote.
No significant differences in categories of satisfaction
The researchers accounted for age, sex, traumatic etiology, and anatomic location of the complaint in multivariate regression analysis and found no significant differences between the two types of visits in the odds of getting a good/excellent rating for the following areas: patient inclusion in treatment decision (P = .562), discussion of proposed treatment (P = .222), concern by the provider (P = .189), degree of care for the patient as a person (P = .208), adequacy of teamwork in care provision (P = .053), likelihood of recommending the practice to others (P = .108), ease of receiving care at a particular practice (P = .109), ease of contacting the clinic (P = .177), and likelihood of recommending a particular provider (P = .218).
Anna Dimitriovna Vergun, MD, a pediatric orthopedist at the University of North Carolina at Chapel Hill, who was not involved in the study, said in an interview she had been conducting virtual visits even before the pandemic, when she worked for several years at a Shriner’s children’s hospital in Los Angeles, before coming to UNC. The virtual visits were necessary because the hospital offered charity care and covered an area that included several states.
She said that during the height of the pandemic, 80% of her visits at UNC were virtual; it is down to about 5% now.
Some consultations don’t need physical visits at all, Dr. Vergun noted. For example, UNC is starting a clinic for prenatal counseling in cases in which ultrasound detects a limb deformity. Without a virtual option, she said, pregnant mothers in all parts of the state may have to drive long distances when no physical exam is necessary.
And sometimes, a visit simply involves checking in with families to see whether pain is being controlled, which is done well virtually.
“Those are particularly useful for telemedicine,” Dr. Vergun said. “There’s a lot of space for this to be useful. You sometimes don’t realize it until you start doing it and getting feedback from the families that they like it.”
Other exams may be better suited to office visits, she said. These include spine and hip exams and exams in which providers need to check reflexes.
She said she sees many cases of club feet, for which an in-person exam is needed to determine flexibility.
Expert says virtual misses nuances
Ryan Fitzgerald, MD, an orthopedic expert with Children’s Orthopaedic and Scoliosis Surgery Associates in St. Petersburg, Fla., who also was not involved in the study, said in an interview he doesn’t offer the virtual option now because he thinks those visits usually miss too much.
COSSA is a private practice that provides orthopedic services for Johns Hopkins All Children’s Hospital.
“I think physicians’ perspective versus the families’ perspective may be quite a bit different,” he said.
While families like the convenience, “a lot of what we do is watching the patient walk, looking at their hip range of motion, and virtually, that’s a really difficult thing to do,” he said.
You can instruct a family on how to turn a camera on the patient, but “it doesn’t always translate,” he said.
He said virtual visits also highlight disparities in access, because many families don’t own the hardware needed for such visits, and internet connections can be spotty or images pixelated.
Dr. Fitzgerald said virtual visits were helpful during the pandemic and would be beneficial for yearly checkups “if you know [the patient] well and it’s a fairly run-of-the-mill thing.”
However, he said, “everything we do is about human interaction, and I think that’s a downfall of the virtual platform right now. While it is helpful in situations like COVID and where it is a very basic follow-up, it still has a ways to go.”
Dr. Fitzgerald is a consultant for OrthoPediatrics, Medtronic, and Depuy Synthes. Dr. Vergun disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT AAOS 2022
ADHD link to prenatal opioid exposure shifts with other substances
Children prenatally exposed to opioids alone have an increased risk of attention-deficit/hyperactivity disorder (ADHD), but interactions between opioids and both cannabis use and alcohol use were linked to varying levels of ADHD risk as well, according to findings published March 11 in JAMA Network Open.
While many prenatal exposure studies examine associations with one substance, the results of this case-control study “suggest that it is important to consider prenatal exposure to multiple substances and the interactions between these substances when counseling women regarding substance use during pregnancy,” wrote Henri M. Garrison-Desany of the Johns Hopkins University, Baltimore, and colleagues.
Using data from children in the prospective Boston Birth Cohort between 1998 and 2019, the researchers did a secondary analysis on the 3,138 children (50.4% of whom were male) with at least 2 years of follow-up, excluding children from multiple-gestation pregnancies, in vitro fertilization pregnancies, and deliveries involving major maternal trauma or major chromosomal anomalies. Mothers answered a questionnaire within 24-72 hours of delivery regarding their demographics, substance use, pregnancy history, and health status. Among the mothers, 58.6% were Black, 22.3% were Hispanic, 7.2% were White, 1.5% were Asian, and 10.4% were other races/ethnicities.
The children’s electronic medical records were used to identify those with ADHD diagnoses. The researchers did not assess prescription opioid exposure during pregnancy, but they based opioid exposure on mothers’ reports of recreationally using heroin or oxycodone, mothers’ reports of receiving methadone treatment, or a newborn diagnosis of neonatal abstinence syndrome or neonatal opioid withdrawal syndrome.
Just under a quarter of the women (24.2%) reported using at least one substance during pregnancy. After tobacco smoking (18.5%), the next most reported substances were alcohol (8.1%), cannabis (3.9%), and opioids (1.9%). With a median 12 years of follow-up, 15.5% of the children had been diagnosed with ADHD, most of whom (71.6%) were male.
Before considering interaction of different substances, children exposed to opioids had a little over twice the risk of ADHD (hazard ratio [HR], 2.19) compared to those with no prenatal substance exposure. Although neither cannabis nor alcohol was independently associated with ADHD, smoking had a 40% increased risk, and researchers found a 21% increase in risk of ADHD with each additional substance mothers used during pregnancy. The researchers had adjusted these findings for maternal age, race/ethnicity, marital status, educational level, annual household income, parity, number of perinatal visits, and general stress during pregnancy, based on a structured interview.
When the researchers considered all the substances together, opioid exposure increased risk of ADHD by 60% (HR, 1.6), opioids with cannabis increased risk by 42%, opioids with alcohol increased risk by 15%, and opioids with smoking increased risk by 17%.
”Our findings suggest opioids may interact with other substances (including cannabis), which may be particularly deleterious,” the researchers reported. “It is not clear whether this interaction is owing to biological or environmental factors, such as whether individuals with illicit polysubstance use are more likely to use more substances or whether they have other characteristics that may impact child development.”
The authors noted that cannabis exposure has been linked to other neurodevelopmental outcomes, including reduced executive and motor function in infants. ”Notably, although we did not find a significant independent association between cannabis exposure and ADHD, children exposed to both cannabis and opioids had a 23% greater risk than expected from either exposure individually,” they reported.
The researchers suggest that their findings provide data for considering harm reduction approaches that reduce use of any single substance during pregnancy. “Focusing on the most obviously harmful exposures may be a useful way to reduce the risk of ADHD,” they wrote. “Further work is needed to directly investigate this hypothesis and examine whether reduction in the use of any substance among those with polysubstance use could be acceptable compared with abstinence.”
In an invited commentary, Angela Lupattelli, PhD, and Nhung T. H. Trinh, PhD, both of the department of pharmacy at the University of Oslo, noted the methodological challenges of assessing exposures and associations from multiple different substances during pregnancy.
“First, how can we disentangle the consequences of individual and/or combined substance exposures during pregnancy from the underlying risks?” they asked. In addition to differences in baseline characteristic between those who use opioids or cannabis, Dr. Lupattelli and Dr. Trinh noted that other important unmeasured factors, such as genetics and family environment, may confound the effect size estimates for ADHD.
They also noted the need to consider intensity, dose, duration, and timing of substance use during pregnancy.
“Understanding the longer-term safety of substance use during pregnancy is paramount to inform prevention policy and shape counseling strategies. Observational studies, despite their limitations, are a necessary piece of the puzzle,” they wrote. “However, the study findings should be interpreted with caution, as the use of advanced analytical methods cannot overcome the unavailability of some important confounding factors and exposure information.”
The research was funded by the U.S. Department of Health and Human Services and the National Institutes of Health. The authors had no industry-related disclosures.
Children prenatally exposed to opioids alone have an increased risk of attention-deficit/hyperactivity disorder (ADHD), but interactions between opioids and both cannabis use and alcohol use were linked to varying levels of ADHD risk as well, according to findings published March 11 in JAMA Network Open.
While many prenatal exposure studies examine associations with one substance, the results of this case-control study “suggest that it is important to consider prenatal exposure to multiple substances and the interactions between these substances when counseling women regarding substance use during pregnancy,” wrote Henri M. Garrison-Desany of the Johns Hopkins University, Baltimore, and colleagues.
Using data from children in the prospective Boston Birth Cohort between 1998 and 2019, the researchers did a secondary analysis on the 3,138 children (50.4% of whom were male) with at least 2 years of follow-up, excluding children from multiple-gestation pregnancies, in vitro fertilization pregnancies, and deliveries involving major maternal trauma or major chromosomal anomalies. Mothers answered a questionnaire within 24-72 hours of delivery regarding their demographics, substance use, pregnancy history, and health status. Among the mothers, 58.6% were Black, 22.3% were Hispanic, 7.2% were White, 1.5% were Asian, and 10.4% were other races/ethnicities.
The children’s electronic medical records were used to identify those with ADHD diagnoses. The researchers did not assess prescription opioid exposure during pregnancy, but they based opioid exposure on mothers’ reports of recreationally using heroin or oxycodone, mothers’ reports of receiving methadone treatment, or a newborn diagnosis of neonatal abstinence syndrome or neonatal opioid withdrawal syndrome.
Just under a quarter of the women (24.2%) reported using at least one substance during pregnancy. After tobacco smoking (18.5%), the next most reported substances were alcohol (8.1%), cannabis (3.9%), and opioids (1.9%). With a median 12 years of follow-up, 15.5% of the children had been diagnosed with ADHD, most of whom (71.6%) were male.
Before considering interaction of different substances, children exposed to opioids had a little over twice the risk of ADHD (hazard ratio [HR], 2.19) compared to those with no prenatal substance exposure. Although neither cannabis nor alcohol was independently associated with ADHD, smoking had a 40% increased risk, and researchers found a 21% increase in risk of ADHD with each additional substance mothers used during pregnancy. The researchers had adjusted these findings for maternal age, race/ethnicity, marital status, educational level, annual household income, parity, number of perinatal visits, and general stress during pregnancy, based on a structured interview.
When the researchers considered all the substances together, opioid exposure increased risk of ADHD by 60% (HR, 1.6), opioids with cannabis increased risk by 42%, opioids with alcohol increased risk by 15%, and opioids with smoking increased risk by 17%.
”Our findings suggest opioids may interact with other substances (including cannabis), which may be particularly deleterious,” the researchers reported. “It is not clear whether this interaction is owing to biological or environmental factors, such as whether individuals with illicit polysubstance use are more likely to use more substances or whether they have other characteristics that may impact child development.”
The authors noted that cannabis exposure has been linked to other neurodevelopmental outcomes, including reduced executive and motor function in infants. ”Notably, although we did not find a significant independent association between cannabis exposure and ADHD, children exposed to both cannabis and opioids had a 23% greater risk than expected from either exposure individually,” they reported.
The researchers suggest that their findings provide data for considering harm reduction approaches that reduce use of any single substance during pregnancy. “Focusing on the most obviously harmful exposures may be a useful way to reduce the risk of ADHD,” they wrote. “Further work is needed to directly investigate this hypothesis and examine whether reduction in the use of any substance among those with polysubstance use could be acceptable compared with abstinence.”
In an invited commentary, Angela Lupattelli, PhD, and Nhung T. H. Trinh, PhD, both of the department of pharmacy at the University of Oslo, noted the methodological challenges of assessing exposures and associations from multiple different substances during pregnancy.
“First, how can we disentangle the consequences of individual and/or combined substance exposures during pregnancy from the underlying risks?” they asked. In addition to differences in baseline characteristic between those who use opioids or cannabis, Dr. Lupattelli and Dr. Trinh noted that other important unmeasured factors, such as genetics and family environment, may confound the effect size estimates for ADHD.
They also noted the need to consider intensity, dose, duration, and timing of substance use during pregnancy.
“Understanding the longer-term safety of substance use during pregnancy is paramount to inform prevention policy and shape counseling strategies. Observational studies, despite their limitations, are a necessary piece of the puzzle,” they wrote. “However, the study findings should be interpreted with caution, as the use of advanced analytical methods cannot overcome the unavailability of some important confounding factors and exposure information.”
The research was funded by the U.S. Department of Health and Human Services and the National Institutes of Health. The authors had no industry-related disclosures.
Children prenatally exposed to opioids alone have an increased risk of attention-deficit/hyperactivity disorder (ADHD), but interactions between opioids and both cannabis use and alcohol use were linked to varying levels of ADHD risk as well, according to findings published March 11 in JAMA Network Open.
While many prenatal exposure studies examine associations with one substance, the results of this case-control study “suggest that it is important to consider prenatal exposure to multiple substances and the interactions between these substances when counseling women regarding substance use during pregnancy,” wrote Henri M. Garrison-Desany of the Johns Hopkins University, Baltimore, and colleagues.
Using data from children in the prospective Boston Birth Cohort between 1998 and 2019, the researchers did a secondary analysis on the 3,138 children (50.4% of whom were male) with at least 2 years of follow-up, excluding children from multiple-gestation pregnancies, in vitro fertilization pregnancies, and deliveries involving major maternal trauma or major chromosomal anomalies. Mothers answered a questionnaire within 24-72 hours of delivery regarding their demographics, substance use, pregnancy history, and health status. Among the mothers, 58.6% were Black, 22.3% were Hispanic, 7.2% were White, 1.5% were Asian, and 10.4% were other races/ethnicities.
The children’s electronic medical records were used to identify those with ADHD diagnoses. The researchers did not assess prescription opioid exposure during pregnancy, but they based opioid exposure on mothers’ reports of recreationally using heroin or oxycodone, mothers’ reports of receiving methadone treatment, or a newborn diagnosis of neonatal abstinence syndrome or neonatal opioid withdrawal syndrome.
Just under a quarter of the women (24.2%) reported using at least one substance during pregnancy. After tobacco smoking (18.5%), the next most reported substances were alcohol (8.1%), cannabis (3.9%), and opioids (1.9%). With a median 12 years of follow-up, 15.5% of the children had been diagnosed with ADHD, most of whom (71.6%) were male.
Before considering interaction of different substances, children exposed to opioids had a little over twice the risk of ADHD (hazard ratio [HR], 2.19) compared to those with no prenatal substance exposure. Although neither cannabis nor alcohol was independently associated with ADHD, smoking had a 40% increased risk, and researchers found a 21% increase in risk of ADHD with each additional substance mothers used during pregnancy. The researchers had adjusted these findings for maternal age, race/ethnicity, marital status, educational level, annual household income, parity, number of perinatal visits, and general stress during pregnancy, based on a structured interview.
When the researchers considered all the substances together, opioid exposure increased risk of ADHD by 60% (HR, 1.6), opioids with cannabis increased risk by 42%, opioids with alcohol increased risk by 15%, and opioids with smoking increased risk by 17%.
”Our findings suggest opioids may interact with other substances (including cannabis), which may be particularly deleterious,” the researchers reported. “It is not clear whether this interaction is owing to biological or environmental factors, such as whether individuals with illicit polysubstance use are more likely to use more substances or whether they have other characteristics that may impact child development.”
The authors noted that cannabis exposure has been linked to other neurodevelopmental outcomes, including reduced executive and motor function in infants. ”Notably, although we did not find a significant independent association between cannabis exposure and ADHD, children exposed to both cannabis and opioids had a 23% greater risk than expected from either exposure individually,” they reported.
The researchers suggest that their findings provide data for considering harm reduction approaches that reduce use of any single substance during pregnancy. “Focusing on the most obviously harmful exposures may be a useful way to reduce the risk of ADHD,” they wrote. “Further work is needed to directly investigate this hypothesis and examine whether reduction in the use of any substance among those with polysubstance use could be acceptable compared with abstinence.”
In an invited commentary, Angela Lupattelli, PhD, and Nhung T. H. Trinh, PhD, both of the department of pharmacy at the University of Oslo, noted the methodological challenges of assessing exposures and associations from multiple different substances during pregnancy.
“First, how can we disentangle the consequences of individual and/or combined substance exposures during pregnancy from the underlying risks?” they asked. In addition to differences in baseline characteristic between those who use opioids or cannabis, Dr. Lupattelli and Dr. Trinh noted that other important unmeasured factors, such as genetics and family environment, may confound the effect size estimates for ADHD.
They also noted the need to consider intensity, dose, duration, and timing of substance use during pregnancy.
“Understanding the longer-term safety of substance use during pregnancy is paramount to inform prevention policy and shape counseling strategies. Observational studies, despite their limitations, are a necessary piece of the puzzle,” they wrote. “However, the study findings should be interpreted with caution, as the use of advanced analytical methods cannot overcome the unavailability of some important confounding factors and exposure information.”
The research was funded by the U.S. Department of Health and Human Services and the National Institutes of Health. The authors had no industry-related disclosures.
FROM JAMA NETWORK OPEN
‘Don’t say gay’: The politicization of gender-diverse youth
The past several weeks have been rather tumultuous for LGBTQ Americans, particularly transgender youth. The Texas attorney general penned a legal opinion stating that hormone therapy and puberty blockers for transgender youth constitute “child abuse” under Texas law. Following the statement, Texas governor Greg Abbott swiftly issued a directive to protective services to launch investigations into families providing such services to their children. Almost simultaneously, the Florida Senate approved the Parental Rights in Education bill (dubbed the “Don’t Say Gay” bill by opponents), which limits how sexual orientation and gender identity are taught in the classroom.
Despite the benefits of gender-affirming care for gender-diverse youth, 22 states have introduced legislation that bans the provision of gender-affirming medical care under the age of 18, even with the consent of parents or legal guardians.1 Unfortunately, gender-diverse youth are more likely than are their cisgender peers to experience poverty, homelessness, depression, suicide, and violence.1 As a result of ongoing stigma, many gender-diverse patients are hesitant to seek out professional medical care, which includes mental health care, routine health care, and gender-affirming therapies. The positive effects of gender-affirming care for transgender youth are clear, and life saving for many. Gender-affirming medical interventions improve social and mental health outcomes, such as decreased suicidal ideation, depression, and improved peer relations that last until adulthood.1

As with all aspects in medicine, providers and families of gender-diverse youth need to balance the four ethical principles that guide decision-making and informed consent. For practitioners working with the pediatric/adolescent populations, the age at which pediatric or adolescent patients can truly provide consent or assent is still not determined.2 This presents a unique set of challenges in the realm of gender-affirming care particularly when children/adolescents and their parents have differing perspectives on proposed treatment plans. For example, when discussing fertility preservation, a 16-year-old patient is much more likely to understand implications of future fertility than a 9-year-old patient. Furthermore, providers must find the delicate balance between maximizing treatment benefits (beneficence) while minimizing harm (nonmaleficence), while also discussing the uncertainty about the long-term risks of gender-affirming treatments.2 The final obligation for health care providers is ensuring all patients have equitable access to care (justice) – which is why we must all oppose legislation that criminalizes treatment for gender-diverse youth, regardless of our individual opinions on gender-affirming care for patients.
Opponents of gender-affirming care for transgender youth often cite concern about permanent effects or psychological distress if a child begins gender-affirming therapy and then chooses to discontinue. While the medical community should be, and is alarmed about patients who detransition, the solution to limiting the number of patients who experience regret or detransition is most certainly not criminalizing or universally banning gender-affirming care for all patients.3 Experts in transgender medicine and surgery (some of whom are transgender themselves) have expressed apprehension regarding the evaluation of gender-diverse children and youth. The concern is not whether gender-diverse youth should receive gender-affirming treatments, but rather they questioned the assessments made by providers who may be less fully qualified to deliver treatment and who deviate from well-established standards of care.4 The logical solution would be to further improve upon the current standards of care, ensure providers have appropriate training, and to expand multidisciplinary models of gender-affirming centers for youth.
If politicians were truly worried about the welfare of gender-diverse children, there would be a shift in the allocation of funds or resources to improve research endeavors and establish effective multidisciplinary clinics to meet the needs of this marginalized patient population. While the medical community should carefully examine gender-affirming care in transgender youth, criminalizing care is unconscionable. Our community needs more evidence-based research, providers, and centers, not politics.
The LGBTQ community and providers are rightfully fearful of the repercussions of such legislation. And the politicians and supporters of such bills should be equally apprehensive of the negative consequences this legislation will have on the mental health of transgender youth.
While the model for gender-affirming medicine and surgery needs continual assessment to ensure all patients, regardless of age and goals of transition, are receiving evidence-based, quality care, these discussions and subsequent decision-making should occur among medical professionals, not among politicians and the lay press.4
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Hughes LD et al. ‘These laws will be devastating’: Provider perspectives on legislation banning gender-affirming care for transgender adolescents. J Adol Health;2021;69:976-82.
2. Kimberly LL et al. Ethical issues in gender-affirming care for youth. Pediatrics. Pediatrics;018;142(6)e20181537.
3. Ashley F. Psychol Sexual Orient Gender Divers. APA PsycNet. 2021.
4. Ault A. Transgender docs warn about gender-affirmative care for youth. WebMD. 2021 Nov. Accessed March 14, 2022.
The past several weeks have been rather tumultuous for LGBTQ Americans, particularly transgender youth. The Texas attorney general penned a legal opinion stating that hormone therapy and puberty blockers for transgender youth constitute “child abuse” under Texas law. Following the statement, Texas governor Greg Abbott swiftly issued a directive to protective services to launch investigations into families providing such services to their children. Almost simultaneously, the Florida Senate approved the Parental Rights in Education bill (dubbed the “Don’t Say Gay” bill by opponents), which limits how sexual orientation and gender identity are taught in the classroom.
Despite the benefits of gender-affirming care for gender-diverse youth, 22 states have introduced legislation that bans the provision of gender-affirming medical care under the age of 18, even with the consent of parents or legal guardians.1 Unfortunately, gender-diverse youth are more likely than are their cisgender peers to experience poverty, homelessness, depression, suicide, and violence.1 As a result of ongoing stigma, many gender-diverse patients are hesitant to seek out professional medical care, which includes mental health care, routine health care, and gender-affirming therapies. The positive effects of gender-affirming care for transgender youth are clear, and life saving for many. Gender-affirming medical interventions improve social and mental health outcomes, such as decreased suicidal ideation, depression, and improved peer relations that last until adulthood.1
As with all aspects in medicine, providers and families of gender-diverse youth need to balance the four ethical principles that guide decision-making and informed consent. For practitioners working with the pediatric/adolescent populations, the age at which pediatric or adolescent patients can truly provide consent or assent is still not determined.2 This presents a unique set of challenges in the realm of gender-affirming care particularly when children/adolescents and their parents have differing perspectives on proposed treatment plans. For example, when discussing fertility preservation, a 16-year-old patient is much more likely to understand implications of future fertility than a 9-year-old patient. Furthermore, providers must find the delicate balance between maximizing treatment benefits (beneficence) while minimizing harm (nonmaleficence), while also discussing the uncertainty about the long-term risks of gender-affirming treatments.2 The final obligation for health care providers is ensuring all patients have equitable access to care (justice) – which is why we must all oppose legislation that criminalizes treatment for gender-diverse youth, regardless of our individual opinions on gender-affirming care for patients.
Opponents of gender-affirming care for transgender youth often cite concern about permanent effects or psychological distress if a child begins gender-affirming therapy and then chooses to discontinue. While the medical community should be, and is alarmed about patients who detransition, the solution to limiting the number of patients who experience regret or detransition is most certainly not criminalizing or universally banning gender-affirming care for all patients.3 Experts in transgender medicine and surgery (some of whom are transgender themselves) have expressed apprehension regarding the evaluation of gender-diverse children and youth. The concern is not whether gender-diverse youth should receive gender-affirming treatments, but rather they questioned the assessments made by providers who may be less fully qualified to deliver treatment and who deviate from well-established standards of care.4 The logical solution would be to further improve upon the current standards of care, ensure providers have appropriate training, and to expand multidisciplinary models of gender-affirming centers for youth.
If politicians were truly worried about the welfare of gender-diverse children, there would be a shift in the allocation of funds or resources to improve research endeavors and establish effective multidisciplinary clinics to meet the needs of this marginalized patient population. While the medical community should carefully examine gender-affirming care in transgender youth, criminalizing care is unconscionable. Our community needs more evidence-based research, providers, and centers, not politics.
The LGBTQ community and providers are rightfully fearful of the repercussions of such legislation. And the politicians and supporters of such bills should be equally apprehensive of the negative consequences this legislation will have on the mental health of transgender youth.
While the model for gender-affirming medicine and surgery needs continual assessment to ensure all patients, regardless of age and goals of transition, are receiving evidence-based, quality care, these discussions and subsequent decision-making should occur among medical professionals, not among politicians and the lay press.4
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Hughes LD et al. ‘These laws will be devastating’: Provider perspectives on legislation banning gender-affirming care for transgender adolescents. J Adol Health;2021;69:976-82.
2. Kimberly LL et al. Ethical issues in gender-affirming care for youth. Pediatrics. Pediatrics;018;142(6)e20181537.
3. Ashley F. Psychol Sexual Orient Gender Divers. APA PsycNet. 2021.
4. Ault A. Transgender docs warn about gender-affirmative care for youth. WebMD. 2021 Nov. Accessed March 14, 2022.
The past several weeks have been rather tumultuous for LGBTQ Americans, particularly transgender youth. The Texas attorney general penned a legal opinion stating that hormone therapy and puberty blockers for transgender youth constitute “child abuse” under Texas law. Following the statement, Texas governor Greg Abbott swiftly issued a directive to protective services to launch investigations into families providing such services to their children. Almost simultaneously, the Florida Senate approved the Parental Rights in Education bill (dubbed the “Don’t Say Gay” bill by opponents), which limits how sexual orientation and gender identity are taught in the classroom.
Despite the benefits of gender-affirming care for gender-diverse youth, 22 states have introduced legislation that bans the provision of gender-affirming medical care under the age of 18, even with the consent of parents or legal guardians.1 Unfortunately, gender-diverse youth are more likely than are their cisgender peers to experience poverty, homelessness, depression, suicide, and violence.1 As a result of ongoing stigma, many gender-diverse patients are hesitant to seek out professional medical care, which includes mental health care, routine health care, and gender-affirming therapies. The positive effects of gender-affirming care for transgender youth are clear, and life saving for many. Gender-affirming medical interventions improve social and mental health outcomes, such as decreased suicidal ideation, depression, and improved peer relations that last until adulthood.1
As with all aspects in medicine, providers and families of gender-diverse youth need to balance the four ethical principles that guide decision-making and informed consent. For practitioners working with the pediatric/adolescent populations, the age at which pediatric or adolescent patients can truly provide consent or assent is still not determined.2 This presents a unique set of challenges in the realm of gender-affirming care particularly when children/adolescents and their parents have differing perspectives on proposed treatment plans. For example, when discussing fertility preservation, a 16-year-old patient is much more likely to understand implications of future fertility than a 9-year-old patient. Furthermore, providers must find the delicate balance between maximizing treatment benefits (beneficence) while minimizing harm (nonmaleficence), while also discussing the uncertainty about the long-term risks of gender-affirming treatments.2 The final obligation for health care providers is ensuring all patients have equitable access to care (justice) – which is why we must all oppose legislation that criminalizes treatment for gender-diverse youth, regardless of our individual opinions on gender-affirming care for patients.
Opponents of gender-affirming care for transgender youth often cite concern about permanent effects or psychological distress if a child begins gender-affirming therapy and then chooses to discontinue. While the medical community should be, and is alarmed about patients who detransition, the solution to limiting the number of patients who experience regret or detransition is most certainly not criminalizing or universally banning gender-affirming care for all patients.3 Experts in transgender medicine and surgery (some of whom are transgender themselves) have expressed apprehension regarding the evaluation of gender-diverse children and youth. The concern is not whether gender-diverse youth should receive gender-affirming treatments, but rather they questioned the assessments made by providers who may be less fully qualified to deliver treatment and who deviate from well-established standards of care.4 The logical solution would be to further improve upon the current standards of care, ensure providers have appropriate training, and to expand multidisciplinary models of gender-affirming centers for youth.
If politicians were truly worried about the welfare of gender-diverse children, there would be a shift in the allocation of funds or resources to improve research endeavors and establish effective multidisciplinary clinics to meet the needs of this marginalized patient population. While the medical community should carefully examine gender-affirming care in transgender youth, criminalizing care is unconscionable. Our community needs more evidence-based research, providers, and centers, not politics.
The LGBTQ community and providers are rightfully fearful of the repercussions of such legislation. And the politicians and supporters of such bills should be equally apprehensive of the negative consequences this legislation will have on the mental health of transgender youth.
While the model for gender-affirming medicine and surgery needs continual assessment to ensure all patients, regardless of age and goals of transition, are receiving evidence-based, quality care, these discussions and subsequent decision-making should occur among medical professionals, not among politicians and the lay press.4
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Hughes LD et al. ‘These laws will be devastating’: Provider perspectives on legislation banning gender-affirming care for transgender adolescents. J Adol Health;2021;69:976-82.
2. Kimberly LL et al. Ethical issues in gender-affirming care for youth. Pediatrics. Pediatrics;018;142(6)e20181537.
3. Ashley F. Psychol Sexual Orient Gender Divers. APA PsycNet. 2021.
4. Ault A. Transgender docs warn about gender-affirmative care for youth. WebMD. 2021 Nov. Accessed March 14, 2022.
Neurodevelopmental disorders prevalent with extremely preterm birth
A large registry-based cohort study in Sweden has revealed that 75% of children born before 24 weeks of gestation had neurodevelopmental disorders, including intellectual disabilities and autism, and required habilitative services.
In addition, somatic disorders such as asthma and failure to thrive/short stature were diagnosed in 88% of the cohort. The findings, published in Acta Paediatrica, emphasize the need for further study of this population, especially as survival rates continue to increase.
“The primary aim of this large, retrospective, national study was to report clinical diagnoses registered after children born before 24 weeks were discharged from neonatal care,” explained lead author Eva Morsing, MD, PhD, of Lund (Sweden) University, and colleagues.
Data on diagnoses of neurodevelopmental disorders and selected somatic diagnoses were obtained from national Swedish registries. Study participants’ individual medical files were also examined by the researchers.
Results
The study cohort comprised 383 infants born at a median of 23.3 weeks of gestation (range, 21.9-23.9 weeks). The median birthweight of participants was 565 grams (range, 340-874 grams), with a median birthweight standard deviation (SD) of −0.40 (range, −3.63–3.17).
The majority (75%) of infants had a neurodevelopmental disorder, including speech disorders (52%), intellectual disabilities (40%), attention-deficit/hyperactivity disorder (30%), autism spectrum disorder (24%), visual impairment (22%), cerebral palsy (17%), epilepsy (10%), and hearing impairment (5%).
With respect to gender, a greater number of boys than girls born at 23 weeks had intellectual disabilities (45% vs. 27%; P < .01) and visual impairment (25% vs. 14%; P < .01). Moreover, 55% of the participants were referred for habilitative services.
With respect to somatic diagnoses, failure to thrive/short stature was diagnosed in 39% of the cohort, and it occurred more often in those born at 21 and 22 weeks than in those born at 23 weeks (49% vs. 36%; P < .05).
In addition, asthma and childhood bronchopulmonary dysplasia, pulmonary hypertension, and vocal cord paresis were diagnosed in 63%, 12%, and 13% of participants, respectively.
“Several studies have reported higher rates of preterm morbidities, and poor neurodevelopmental outcomes after extremely preterm birth in boys rather than girls,” study author Ann Hellström, MD, PhD, of the University of Gothenburg, Sweden, said in an interview.
“While the reasons for this were not studied in the present paper, reports in the literature suggest that boys have a higher average growth rate than girls and appear to be more sensitive to suboptimal neonatal nutrition than girls,” Dr. Hellström explained.
“We also know that sex steroids differ in relation to intrauterine life depending on the sex after preterm birth,” Dr. Hellström added.
In an accompanying editorial, Neil Marlow, MD, of University College London, wrote, “One headline from this study [that is interesting] is the high prevalence of autistic spectrum disorders recorded.
“This is a particular finding in extremely preterm cohorts from Sweden, who record more diagnoses than in other longitudinal studies,” Dr. Marlow added. “It certainly warrants further investigation and understanding.”
The researchers acknowledged that a key limitation of the study was the broad age range at the most recent follow-up visit, which ranged from 2 to 13 years, explaining that some diagnoses may occur later in childhood.
“Neonatal clinical practice needs to adopt a long-term perspective and clinicians treating children and adults should be aware of the complicated health problems of children born before 24 weeks,” they concluded.
This study was supported by the Swedish Medical Research Council, the Gothenburg Medical Society, and by grant funding from the Swedish government. The authors reported no relevant disclosures.
A large registry-based cohort study in Sweden has revealed that 75% of children born before 24 weeks of gestation had neurodevelopmental disorders, including intellectual disabilities and autism, and required habilitative services.
In addition, somatic disorders such as asthma and failure to thrive/short stature were diagnosed in 88% of the cohort. The findings, published in Acta Paediatrica, emphasize the need for further study of this population, especially as survival rates continue to increase.
“The primary aim of this large, retrospective, national study was to report clinical diagnoses registered after children born before 24 weeks were discharged from neonatal care,” explained lead author Eva Morsing, MD, PhD, of Lund (Sweden) University, and colleagues.
Data on diagnoses of neurodevelopmental disorders and selected somatic diagnoses were obtained from national Swedish registries. Study participants’ individual medical files were also examined by the researchers.
Results
The study cohort comprised 383 infants born at a median of 23.3 weeks of gestation (range, 21.9-23.9 weeks). The median birthweight of participants was 565 grams (range, 340-874 grams), with a median birthweight standard deviation (SD) of −0.40 (range, −3.63–3.17).
The majority (75%) of infants had a neurodevelopmental disorder, including speech disorders (52%), intellectual disabilities (40%), attention-deficit/hyperactivity disorder (30%), autism spectrum disorder (24%), visual impairment (22%), cerebral palsy (17%), epilepsy (10%), and hearing impairment (5%).
With respect to gender, a greater number of boys than girls born at 23 weeks had intellectual disabilities (45% vs. 27%; P < .01) and visual impairment (25% vs. 14%; P < .01). Moreover, 55% of the participants were referred for habilitative services.
With respect to somatic diagnoses, failure to thrive/short stature was diagnosed in 39% of the cohort, and it occurred more often in those born at 21 and 22 weeks than in those born at 23 weeks (49% vs. 36%; P < .05).
In addition, asthma and childhood bronchopulmonary dysplasia, pulmonary hypertension, and vocal cord paresis were diagnosed in 63%, 12%, and 13% of participants, respectively.
“Several studies have reported higher rates of preterm morbidities, and poor neurodevelopmental outcomes after extremely preterm birth in boys rather than girls,” study author Ann Hellström, MD, PhD, of the University of Gothenburg, Sweden, said in an interview.
“While the reasons for this were not studied in the present paper, reports in the literature suggest that boys have a higher average growth rate than girls and appear to be more sensitive to suboptimal neonatal nutrition than girls,” Dr. Hellström explained.
“We also know that sex steroids differ in relation to intrauterine life depending on the sex after preterm birth,” Dr. Hellström added.
In an accompanying editorial, Neil Marlow, MD, of University College London, wrote, “One headline from this study [that is interesting] is the high prevalence of autistic spectrum disorders recorded.
“This is a particular finding in extremely preterm cohorts from Sweden, who record more diagnoses than in other longitudinal studies,” Dr. Marlow added. “It certainly warrants further investigation and understanding.”
The researchers acknowledged that a key limitation of the study was the broad age range at the most recent follow-up visit, which ranged from 2 to 13 years, explaining that some diagnoses may occur later in childhood.
“Neonatal clinical practice needs to adopt a long-term perspective and clinicians treating children and adults should be aware of the complicated health problems of children born before 24 weeks,” they concluded.
This study was supported by the Swedish Medical Research Council, the Gothenburg Medical Society, and by grant funding from the Swedish government. The authors reported no relevant disclosures.
A large registry-based cohort study in Sweden has revealed that 75% of children born before 24 weeks of gestation had neurodevelopmental disorders, including intellectual disabilities and autism, and required habilitative services.
In addition, somatic disorders such as asthma and failure to thrive/short stature were diagnosed in 88% of the cohort. The findings, published in Acta Paediatrica, emphasize the need for further study of this population, especially as survival rates continue to increase.
“The primary aim of this large, retrospective, national study was to report clinical diagnoses registered after children born before 24 weeks were discharged from neonatal care,” explained lead author Eva Morsing, MD, PhD, of Lund (Sweden) University, and colleagues.
Data on diagnoses of neurodevelopmental disorders and selected somatic diagnoses were obtained from national Swedish registries. Study participants’ individual medical files were also examined by the researchers.
Results
The study cohort comprised 383 infants born at a median of 23.3 weeks of gestation (range, 21.9-23.9 weeks). The median birthweight of participants was 565 grams (range, 340-874 grams), with a median birthweight standard deviation (SD) of −0.40 (range, −3.63–3.17).
The majority (75%) of infants had a neurodevelopmental disorder, including speech disorders (52%), intellectual disabilities (40%), attention-deficit/hyperactivity disorder (30%), autism spectrum disorder (24%), visual impairment (22%), cerebral palsy (17%), epilepsy (10%), and hearing impairment (5%).
With respect to gender, a greater number of boys than girls born at 23 weeks had intellectual disabilities (45% vs. 27%; P < .01) and visual impairment (25% vs. 14%; P < .01). Moreover, 55% of the participants were referred for habilitative services.
With respect to somatic diagnoses, failure to thrive/short stature was diagnosed in 39% of the cohort, and it occurred more often in those born at 21 and 22 weeks than in those born at 23 weeks (49% vs. 36%; P < .05).
In addition, asthma and childhood bronchopulmonary dysplasia, pulmonary hypertension, and vocal cord paresis were diagnosed in 63%, 12%, and 13% of participants, respectively.
“Several studies have reported higher rates of preterm morbidities, and poor neurodevelopmental outcomes after extremely preterm birth in boys rather than girls,” study author Ann Hellström, MD, PhD, of the University of Gothenburg, Sweden, said in an interview.
“While the reasons for this were not studied in the present paper, reports in the literature suggest that boys have a higher average growth rate than girls and appear to be more sensitive to suboptimal neonatal nutrition than girls,” Dr. Hellström explained.
“We also know that sex steroids differ in relation to intrauterine life depending on the sex after preterm birth,” Dr. Hellström added.
In an accompanying editorial, Neil Marlow, MD, of University College London, wrote, “One headline from this study [that is interesting] is the high prevalence of autistic spectrum disorders recorded.
“This is a particular finding in extremely preterm cohorts from Sweden, who record more diagnoses than in other longitudinal studies,” Dr. Marlow added. “It certainly warrants further investigation and understanding.”
The researchers acknowledged that a key limitation of the study was the broad age range at the most recent follow-up visit, which ranged from 2 to 13 years, explaining that some diagnoses may occur later in childhood.
“Neonatal clinical practice needs to adopt a long-term perspective and clinicians treating children and adults should be aware of the complicated health problems of children born before 24 weeks,” they concluded.
This study was supported by the Swedish Medical Research Council, the Gothenburg Medical Society, and by grant funding from the Swedish government. The authors reported no relevant disclosures.
FROM ACTA PAEDIATRICA
Moderna reports positive COVID-19 vaccine response in kids down to 6 months
Moderna on March 23 released interim results indicating that its mRNA-1273 COVID vaccine produced “robust” neutralizing antibody titers in children aged 6 months to 6 years – levels similar to those seen in adults.
Vaccine efficacy against infection was 43.7% in children aged 6 months to 2 years and 37.5% among children aged 2-6 years, the new data from its phase 2/3 KidCOVE study show.
The company explained the lower efficacy numbers by noting that its study involving these younger children was conducted during the Omicron wave. The same decrease in efficacy against infection was reported in adults during the Omicron surge.
A majority of COVID-19 cases were mild in the approximately 6,900 children aged 6 months to 6 years in the study. No severe COVID-19 cases, hospitalizations, or deaths were reported.
The primary series of two 25-mcg doses of the vaccine given 28 days apart was generally well tolerated. Most adverse events were mild to moderate. For example, temperature greater than 38° C (>100.4° F) was reported for 17.0% of the 6-month-old to 2-year-old group and for 14.6% of the 2- to 6-year-old group. A few children, 0.2% of each group, experienced a temperature greater than 40° C (>104° F).
Moderna plans to include these response, efficacy, and safety data in an application to the Food and Drug Administration for emergency use authorization (EUA) of the vaccine in these younger children in the coming weeks.
“We now have clinical data on the performance of our vaccine from infants 6 months of age through older adults,” Moderna CEO Stephane Bancel said in a news release. He described the interim results as “good news for parents of children under 6 years of age.”
In other news
Moderna also announced that it began the FDA EUA submission process for a 50-μg two-dose primary series for children aged 6-12 years.
The company is also updating its EUA submission for a 100-mcg two-dose primary series for children and adolescents aged 12-18 years.
Similar to its booster research in adults, Moderna plans to evaluate the potential of a booster dose for all pediatric populations, including those aged 6 months to 6 years, 6-12 years, and adolescents. The company is evaluating both a booster dose of mRNA-1273 and its bivalent booster candidate (mRNA1273.214), which includes an Omicron variant booster and mRNA-1273.
A version of this article first appeared on Medscape.com.
Moderna on March 23 released interim results indicating that its mRNA-1273 COVID vaccine produced “robust” neutralizing antibody titers in children aged 6 months to 6 years – levels similar to those seen in adults.
Vaccine efficacy against infection was 43.7% in children aged 6 months to 2 years and 37.5% among children aged 2-6 years, the new data from its phase 2/3 KidCOVE study show.
The company explained the lower efficacy numbers by noting that its study involving these younger children was conducted during the Omicron wave. The same decrease in efficacy against infection was reported in adults during the Omicron surge.
A majority of COVID-19 cases were mild in the approximately 6,900 children aged 6 months to 6 years in the study. No severe COVID-19 cases, hospitalizations, or deaths were reported.
The primary series of two 25-mcg doses of the vaccine given 28 days apart was generally well tolerated. Most adverse events were mild to moderate. For example, temperature greater than 38° C (>100.4° F) was reported for 17.0% of the 6-month-old to 2-year-old group and for 14.6% of the 2- to 6-year-old group. A few children, 0.2% of each group, experienced a temperature greater than 40° C (>104° F).
Moderna plans to include these response, efficacy, and safety data in an application to the Food and Drug Administration for emergency use authorization (EUA) of the vaccine in these younger children in the coming weeks.
“We now have clinical data on the performance of our vaccine from infants 6 months of age through older adults,” Moderna CEO Stephane Bancel said in a news release. He described the interim results as “good news for parents of children under 6 years of age.”
In other news
Moderna also announced that it began the FDA EUA submission process for a 50-μg two-dose primary series for children aged 6-12 years.
The company is also updating its EUA submission for a 100-mcg two-dose primary series for children and adolescents aged 12-18 years.
Similar to its booster research in adults, Moderna plans to evaluate the potential of a booster dose for all pediatric populations, including those aged 6 months to 6 years, 6-12 years, and adolescents. The company is evaluating both a booster dose of mRNA-1273 and its bivalent booster candidate (mRNA1273.214), which includes an Omicron variant booster and mRNA-1273.
A version of this article first appeared on Medscape.com.
Moderna on March 23 released interim results indicating that its mRNA-1273 COVID vaccine produced “robust” neutralizing antibody titers in children aged 6 months to 6 years – levels similar to those seen in adults.
Vaccine efficacy against infection was 43.7% in children aged 6 months to 2 years and 37.5% among children aged 2-6 years, the new data from its phase 2/3 KidCOVE study show.
The company explained the lower efficacy numbers by noting that its study involving these younger children was conducted during the Omicron wave. The same decrease in efficacy against infection was reported in adults during the Omicron surge.
A majority of COVID-19 cases were mild in the approximately 6,900 children aged 6 months to 6 years in the study. No severe COVID-19 cases, hospitalizations, or deaths were reported.
The primary series of two 25-mcg doses of the vaccine given 28 days apart was generally well tolerated. Most adverse events were mild to moderate. For example, temperature greater than 38° C (>100.4° F) was reported for 17.0% of the 6-month-old to 2-year-old group and for 14.6% of the 2- to 6-year-old group. A few children, 0.2% of each group, experienced a temperature greater than 40° C (>104° F).
Moderna plans to include these response, efficacy, and safety data in an application to the Food and Drug Administration for emergency use authorization (EUA) of the vaccine in these younger children in the coming weeks.
“We now have clinical data on the performance of our vaccine from infants 6 months of age through older adults,” Moderna CEO Stephane Bancel said in a news release. He described the interim results as “good news for parents of children under 6 years of age.”
In other news
Moderna also announced that it began the FDA EUA submission process for a 50-μg two-dose primary series for children aged 6-12 years.
The company is also updating its EUA submission for a 100-mcg two-dose primary series for children and adolescents aged 12-18 years.
Similar to its booster research in adults, Moderna plans to evaluate the potential of a booster dose for all pediatric populations, including those aged 6 months to 6 years, 6-12 years, and adolescents. The company is evaluating both a booster dose of mRNA-1273 and its bivalent booster candidate (mRNA1273.214), which includes an Omicron variant booster and mRNA-1273.
A version of this article first appeared on Medscape.com.
Children and COVID: CDC gives perspective on hospitalizations
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.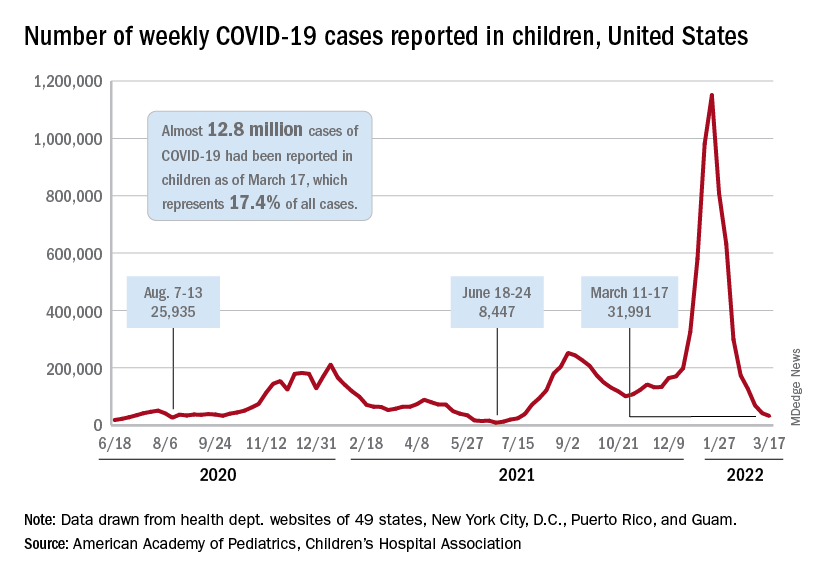
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
Racial disparities seen in pediatric postoperative mortality rates
Among Black and White children, higher socioeconomic status (SES) was associated with lower pediatric postoperative mortality, according to a cohort study published in JAMA Network Open. However, this association was not equitable when comparing Black and White children.
The results showed that postoperative mortality rates were significantly higher in Black children in the highest income category, compared with White children in the same category.
“[We] assessed whether increasing family SES is associated with lower pediatric postoperative mortality and, if so, whether this association is equitable among Black and White children,” Brittany L. Willer, MD, of Nationwide Children’s Hospital in Columbus, Ohio, and colleagues wrote.
The researchers retrospectively analyzed data from 51 pediatric tertiary care hospitals apart of the Children’s Hospital Association Pediatric Health Information System. The cohort included children younger than 18 years who underwent inpatient surgical procedures between January 2004 and December 2020.
The exposures of interest were race and parental income quartile; the primary endpoint was risk-adjusted in-hospital mortality rates by race and parental income quartile.
Results
The study cohort included 1,378,111 participants, including 248,464 (18.0%) Black and 1,129,647 (82.0%) White children, respectively.
The overall mortality rate was 1.2%, and rates decreased as income quartile increased (1.4% in quartile 1 [lowest income]; 1.3% in quartile 2; 1.0% in quartile 3; and 0.9% in quartile 4 [highest income]; P < .001).
Among participants in the three lowest income quartiles, Black children had 33% greater odds of postoperative death versus White children (adjusted odds ratio, 1.33; 95% confidence interval, 1.27-1.39; P < .001). This difference persisted in children in the highest income quartile (aOR, 1.39; 95% CI, 1.25-1.54; P < .001).
In addition, postoperative mortality rates in Black children in the highest income quartile (1.30%; 95% CI, 1.19%-1.42%) were similar to those of White children in the lowest income quartile (1.20%; 95% CI, 1.16%-1.25%).
“These findings suggest that increasing family SES did not provide equitable advantage to Black, compared with White children, and interventions that target socioeconomic inequities alone may not fully address persistent racial disparities in pediatric postoperative mortality,” wrote Dr. Willer and colleagues. “A multifaceted approach that includes dismantling of socioeconomic barriers, equitable availability of comprehensive pediatric surgical care, and personalized care for children of all races is needed.”
The researchers acknowledged that a potential limitation of the study was the use of zip code–level median household income as a proxy for family SES.
A perspective
In an interview, Timothy Joos, MD, a Seattle internist and pediatrician in private practice, said “there is a fair dose of racism and classism inside all of us – recognizing and coming to terms with it are steps toward improving equity issues.
“As providers, we have to remind ourselves to give our most prompt and thorough care to the patients with the most acute and severe illnesses,” Dr. Joos said. “As organizations, we have to pursue feedback from all our clients, but with special outreach to those that are used to not having their voices heard.”
No funding sources were reported. The authors reported no relevant disclosures. Dr. Joos is a member of the Pediatric News editorial advisory board but had no other disclosures.
Among Black and White children, higher socioeconomic status (SES) was associated with lower pediatric postoperative mortality, according to a cohort study published in JAMA Network Open. However, this association was not equitable when comparing Black and White children.
The results showed that postoperative mortality rates were significantly higher in Black children in the highest income category, compared with White children in the same category.
“[We] assessed whether increasing family SES is associated with lower pediatric postoperative mortality and, if so, whether this association is equitable among Black and White children,” Brittany L. Willer, MD, of Nationwide Children’s Hospital in Columbus, Ohio, and colleagues wrote.
The researchers retrospectively analyzed data from 51 pediatric tertiary care hospitals apart of the Children’s Hospital Association Pediatric Health Information System. The cohort included children younger than 18 years who underwent inpatient surgical procedures between January 2004 and December 2020.
The exposures of interest were race and parental income quartile; the primary endpoint was risk-adjusted in-hospital mortality rates by race and parental income quartile.
Results
The study cohort included 1,378,111 participants, including 248,464 (18.0%) Black and 1,129,647 (82.0%) White children, respectively.
The overall mortality rate was 1.2%, and rates decreased as income quartile increased (1.4% in quartile 1 [lowest income]; 1.3% in quartile 2; 1.0% in quartile 3; and 0.9% in quartile 4 [highest income]; P < .001).
Among participants in the three lowest income quartiles, Black children had 33% greater odds of postoperative death versus White children (adjusted odds ratio, 1.33; 95% confidence interval, 1.27-1.39; P < .001). This difference persisted in children in the highest income quartile (aOR, 1.39; 95% CI, 1.25-1.54; P < .001).
In addition, postoperative mortality rates in Black children in the highest income quartile (1.30%; 95% CI, 1.19%-1.42%) were similar to those of White children in the lowest income quartile (1.20%; 95% CI, 1.16%-1.25%).
“These findings suggest that increasing family SES did not provide equitable advantage to Black, compared with White children, and interventions that target socioeconomic inequities alone may not fully address persistent racial disparities in pediatric postoperative mortality,” wrote Dr. Willer and colleagues. “A multifaceted approach that includes dismantling of socioeconomic barriers, equitable availability of comprehensive pediatric surgical care, and personalized care for children of all races is needed.”
The researchers acknowledged that a potential limitation of the study was the use of zip code–level median household income as a proxy for family SES.
A perspective
In an interview, Timothy Joos, MD, a Seattle internist and pediatrician in private practice, said “there is a fair dose of racism and classism inside all of us – recognizing and coming to terms with it are steps toward improving equity issues.
“As providers, we have to remind ourselves to give our most prompt and thorough care to the patients with the most acute and severe illnesses,” Dr. Joos said. “As organizations, we have to pursue feedback from all our clients, but with special outreach to those that are used to not having their voices heard.”
No funding sources were reported. The authors reported no relevant disclosures. Dr. Joos is a member of the Pediatric News editorial advisory board but had no other disclosures.
Among Black and White children, higher socioeconomic status (SES) was associated with lower pediatric postoperative mortality, according to a cohort study published in JAMA Network Open. However, this association was not equitable when comparing Black and White children.
The results showed that postoperative mortality rates were significantly higher in Black children in the highest income category, compared with White children in the same category.
“[We] assessed whether increasing family SES is associated with lower pediatric postoperative mortality and, if so, whether this association is equitable among Black and White children,” Brittany L. Willer, MD, of Nationwide Children’s Hospital in Columbus, Ohio, and colleagues wrote.
The researchers retrospectively analyzed data from 51 pediatric tertiary care hospitals apart of the Children’s Hospital Association Pediatric Health Information System. The cohort included children younger than 18 years who underwent inpatient surgical procedures between January 2004 and December 2020.
The exposures of interest were race and parental income quartile; the primary endpoint was risk-adjusted in-hospital mortality rates by race and parental income quartile.
Results
The study cohort included 1,378,111 participants, including 248,464 (18.0%) Black and 1,129,647 (82.0%) White children, respectively.
The overall mortality rate was 1.2%, and rates decreased as income quartile increased (1.4% in quartile 1 [lowest income]; 1.3% in quartile 2; 1.0% in quartile 3; and 0.9% in quartile 4 [highest income]; P < .001).
Among participants in the three lowest income quartiles, Black children had 33% greater odds of postoperative death versus White children (adjusted odds ratio, 1.33; 95% confidence interval, 1.27-1.39; P < .001). This difference persisted in children in the highest income quartile (aOR, 1.39; 95% CI, 1.25-1.54; P < .001).
In addition, postoperative mortality rates in Black children in the highest income quartile (1.30%; 95% CI, 1.19%-1.42%) were similar to those of White children in the lowest income quartile (1.20%; 95% CI, 1.16%-1.25%).
“These findings suggest that increasing family SES did not provide equitable advantage to Black, compared with White children, and interventions that target socioeconomic inequities alone may not fully address persistent racial disparities in pediatric postoperative mortality,” wrote Dr. Willer and colleagues. “A multifaceted approach that includes dismantling of socioeconomic barriers, equitable availability of comprehensive pediatric surgical care, and personalized care for children of all races is needed.”
The researchers acknowledged that a potential limitation of the study was the use of zip code–level median household income as a proxy for family SES.
A perspective
In an interview, Timothy Joos, MD, a Seattle internist and pediatrician in private practice, said “there is a fair dose of racism and classism inside all of us – recognizing and coming to terms with it are steps toward improving equity issues.
“As providers, we have to remind ourselves to give our most prompt and thorough care to the patients with the most acute and severe illnesses,” Dr. Joos said. “As organizations, we have to pursue feedback from all our clients, but with special outreach to those that are used to not having their voices heard.”
No funding sources were reported. The authors reported no relevant disclosures. Dr. Joos is a member of the Pediatric News editorial advisory board but had no other disclosures.
FROM JAMA NETWORK OPEN
Get the science right
Get the science right. I have spent years researching and reflecting on what makes the best physicians, the best medicine, the optimal organized medical system, and the best medical ethics and law to support all of it. I have traveled to almost innumerable conferences to discuss these topics with colleagues who have similar goals. Time and time again, I come back to the conclusion that, in the modern era, the second-most important thing to do is to get the science right.
The practice of medicine in my Western world can be traced back to Hippocrates and earlier. The practice of nursing has other milestones. The healing arts have different points of origin in other cultures, such as China. In a modern world of mass communication, these various historical paths are converging on scientific evidence. The science to support medicine has always had flaws, but it has fared better than the other options. Sometimes, the science was so sketchy that the key was to believe in whatever the shaman was providing. But for the past 100 years, science, rather than tradition and hierarchy, has been relied upon to guide policy and action. For the past 50 years, evidence-based medicine has ascended. Have we become better than the snake oil salesmen of the late 19th century?

Modern health care is far from perfect. The pandemic has been a major stressor to the health care system. The pandemic has revealed flaws and weaknesses, including inequity in access to care, health illiteracy, and a shaky moral compass balancing individual liberty and social good. Overall, despite multiple mistakes dealing with a novel threat, I think the institutions promoting science have performed well during the pandemic, especially when compared with the moral and governmental institutions encouraging ethical behavior and making policies to promote justice.
My highest praise would be for the professionalism of health care workers. Nurses and physicians have staffed the hospitals and clinics caring for people when the hallways were overflowing for days without end. Without the commitment, the teamwork, and the courage to provide that care, the death toll would have been much higher and the suffering unimaginable. My observation is that these people were not motivated by an abstract primum non nocere, first do no harm. It was the commitment to love one’s neighbor and care for the sick. This dedication is the first most important thing in professionalism.
Part of what fuels that commitment is a belief that what they are doing makes a difference. The belief is stronger when there is measurable, scientific evidence that a difference is being made. The scientific decisions have not been perfect, but at this point the evidence is clear that the shutdown flattened the curve. Vaccines saved lives and will continue to do so. Masks saved lives. Nursing care, particularly intensive care, reduced the case fatality rate and assuaged suffering and grief.
What lessons about training new providers can be gleaned from the past 2 years? Those who teach professionalism for physicians, nurses, and other health care workers should strengthen the common value systems that undergird the commitment people have to the patients and the professions. In the face of postmodern nihilism and relativism, virtues need to be clarified and reinforced. In the face of political polarization which seeks to make a political affiliation the locus of loyalty and commitment, emphasize the fellowship of the health care professions.
To me as a scientist, a key lesson is that we need to be better at getting the science right. Two years ago I was wiping some groceries with alcohol and quarantining cans in shopping bags in the corner of the kitchen for 24 hours before shelving them. I still push elevator buttons with my knuckles. The Centers for Disease Control and Prevention needs to revamp their policy making procedures.
Institutions must work to reestablish the public trust in science. That is a challenge because while many amazing scientific advances have occurred (i.e., my MRI last week showed far more going on than my orthopedist and physical therapist detected based on clinical exam). Imaging such as MR and ultrasound have been major advances in diagnostic medicine, but there are also repeated examples demonstrating where medicine has been wrong. In the past 6 months I have read new guidelines for ear tubes, for neonatal jaundice, for newborn sepsis, and for newborn hypoglycemia. All indicate to me that my training 30 years ago was on target and the interval “improvements” in practice have been worthless Brownian motion based on false scientific discoveries. My recommendation would be that pediatrics do one-third as much research but do that research three times better and get it right.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
Get the science right. I have spent years researching and reflecting on what makes the best physicians, the best medicine, the optimal organized medical system, and the best medical ethics and law to support all of it. I have traveled to almost innumerable conferences to discuss these topics with colleagues who have similar goals. Time and time again, I come back to the conclusion that, in the modern era, the second-most important thing to do is to get the science right.
The practice of medicine in my Western world can be traced back to Hippocrates and earlier. The practice of nursing has other milestones. The healing arts have different points of origin in other cultures, such as China. In a modern world of mass communication, these various historical paths are converging on scientific evidence. The science to support medicine has always had flaws, but it has fared better than the other options. Sometimes, the science was so sketchy that the key was to believe in whatever the shaman was providing. But for the past 100 years, science, rather than tradition and hierarchy, has been relied upon to guide policy and action. For the past 50 years, evidence-based medicine has ascended. Have we become better than the snake oil salesmen of the late 19th century?
Modern health care is far from perfect. The pandemic has been a major stressor to the health care system. The pandemic has revealed flaws and weaknesses, including inequity in access to care, health illiteracy, and a shaky moral compass balancing individual liberty and social good. Overall, despite multiple mistakes dealing with a novel threat, I think the institutions promoting science have performed well during the pandemic, especially when compared with the moral and governmental institutions encouraging ethical behavior and making policies to promote justice.
My highest praise would be for the professionalism of health care workers. Nurses and physicians have staffed the hospitals and clinics caring for people when the hallways were overflowing for days without end. Without the commitment, the teamwork, and the courage to provide that care, the death toll would have been much higher and the suffering unimaginable. My observation is that these people were not motivated by an abstract primum non nocere, first do no harm. It was the commitment to love one’s neighbor and care for the sick. This dedication is the first most important thing in professionalism.
Part of what fuels that commitment is a belief that what they are doing makes a difference. The belief is stronger when there is measurable, scientific evidence that a difference is being made. The scientific decisions have not been perfect, but at this point the evidence is clear that the shutdown flattened the curve. Vaccines saved lives and will continue to do so. Masks saved lives. Nursing care, particularly intensive care, reduced the case fatality rate and assuaged suffering and grief.
What lessons about training new providers can be gleaned from the past 2 years? Those who teach professionalism for physicians, nurses, and other health care workers should strengthen the common value systems that undergird the commitment people have to the patients and the professions. In the face of postmodern nihilism and relativism, virtues need to be clarified and reinforced. In the face of political polarization which seeks to make a political affiliation the locus of loyalty and commitment, emphasize the fellowship of the health care professions.
To me as a scientist, a key lesson is that we need to be better at getting the science right. Two years ago I was wiping some groceries with alcohol and quarantining cans in shopping bags in the corner of the kitchen for 24 hours before shelving them. I still push elevator buttons with my knuckles. The Centers for Disease Control and Prevention needs to revamp their policy making procedures.
Institutions must work to reestablish the public trust in science. That is a challenge because while many amazing scientific advances have occurred (i.e., my MRI last week showed far more going on than my orthopedist and physical therapist detected based on clinical exam). Imaging such as MR and ultrasound have been major advances in diagnostic medicine, but there are also repeated examples demonstrating where medicine has been wrong. In the past 6 months I have read new guidelines for ear tubes, for neonatal jaundice, for newborn sepsis, and for newborn hypoglycemia. All indicate to me that my training 30 years ago was on target and the interval “improvements” in practice have been worthless Brownian motion based on false scientific discoveries. My recommendation would be that pediatrics do one-third as much research but do that research three times better and get it right.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
Get the science right. I have spent years researching and reflecting on what makes the best physicians, the best medicine, the optimal organized medical system, and the best medical ethics and law to support all of it. I have traveled to almost innumerable conferences to discuss these topics with colleagues who have similar goals. Time and time again, I come back to the conclusion that, in the modern era, the second-most important thing to do is to get the science right.
The practice of medicine in my Western world can be traced back to Hippocrates and earlier. The practice of nursing has other milestones. The healing arts have different points of origin in other cultures, such as China. In a modern world of mass communication, these various historical paths are converging on scientific evidence. The science to support medicine has always had flaws, but it has fared better than the other options. Sometimes, the science was so sketchy that the key was to believe in whatever the shaman was providing. But for the past 100 years, science, rather than tradition and hierarchy, has been relied upon to guide policy and action. For the past 50 years, evidence-based medicine has ascended. Have we become better than the snake oil salesmen of the late 19th century?
Modern health care is far from perfect. The pandemic has been a major stressor to the health care system. The pandemic has revealed flaws and weaknesses, including inequity in access to care, health illiteracy, and a shaky moral compass balancing individual liberty and social good. Overall, despite multiple mistakes dealing with a novel threat, I think the institutions promoting science have performed well during the pandemic, especially when compared with the moral and governmental institutions encouraging ethical behavior and making policies to promote justice.
My highest praise would be for the professionalism of health care workers. Nurses and physicians have staffed the hospitals and clinics caring for people when the hallways were overflowing for days without end. Without the commitment, the teamwork, and the courage to provide that care, the death toll would have been much higher and the suffering unimaginable. My observation is that these people were not motivated by an abstract primum non nocere, first do no harm. It was the commitment to love one’s neighbor and care for the sick. This dedication is the first most important thing in professionalism.
Part of what fuels that commitment is a belief that what they are doing makes a difference. The belief is stronger when there is measurable, scientific evidence that a difference is being made. The scientific decisions have not been perfect, but at this point the evidence is clear that the shutdown flattened the curve. Vaccines saved lives and will continue to do so. Masks saved lives. Nursing care, particularly intensive care, reduced the case fatality rate and assuaged suffering and grief.
What lessons about training new providers can be gleaned from the past 2 years? Those who teach professionalism for physicians, nurses, and other health care workers should strengthen the common value systems that undergird the commitment people have to the patients and the professions. In the face of postmodern nihilism and relativism, virtues need to be clarified and reinforced. In the face of political polarization which seeks to make a political affiliation the locus of loyalty and commitment, emphasize the fellowship of the health care professions.
To me as a scientist, a key lesson is that we need to be better at getting the science right. Two years ago I was wiping some groceries with alcohol and quarantining cans in shopping bags in the corner of the kitchen for 24 hours before shelving them. I still push elevator buttons with my knuckles. The Centers for Disease Control and Prevention needs to revamp their policy making procedures.
Institutions must work to reestablish the public trust in science. That is a challenge because while many amazing scientific advances have occurred (i.e., my MRI last week showed far more going on than my orthopedist and physical therapist detected based on clinical exam). Imaging such as MR and ultrasound have been major advances in diagnostic medicine, but there are also repeated examples demonstrating where medicine has been wrong. In the past 6 months I have read new guidelines for ear tubes, for neonatal jaundice, for newborn sepsis, and for newborn hypoglycemia. All indicate to me that my training 30 years ago was on target and the interval “improvements” in practice have been worthless Brownian motion based on false scientific discoveries. My recommendation would be that pediatrics do one-third as much research but do that research three times better and get it right.
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].