User login
Cardiovascular risks elevated in transgender youth
Cardiovascular and metabolic risk factors are increased among transgender youths, compared with youths who are not transgender. Elevations in lipid levels and body mass index (BMI) also occur in adult transgender patients, new research shows.
“This is the first study of its size in the United States of which we are aware that looks at the odds of youth with a diagnosis of gender dysphoria having medical diagnoses that relate to overall metabolic and cardiovascular health,” first author Anna Valentine, MD, of Children’s Hospital Colorado, Aurora, said in a press statement.
Although previous studies have shown that among transgender adults, BMI is higher and there is an increased risk for cardiovascular events, such as stroke or heart attack, compared with nontransgender people, research on adolescent transgender patients has been lacking.
With a recent survey showing that nearly 2% of adolescents identify as transgender, interest in health outcomes among younger patients is high.
To investigate, Dr. Valentine, and colleagues evaluated data from the PEDSnet pediatric database on 4,177 youths who had received a diagnosis of gender dysphoria. The participants had been enrolled at six sites from 2009 to 2019. The researchers compared these patients in a ratio of 1:4 with 16,664 control persons who had not been diagnosed with gender dysphoria. They reported their findings as a poster at the annual meeting of the Endocrine Society.
For the propensity-score analysis, participants were matched according to year of birth, age at last visit, site, race, ethnicity, insurance status, and duration in the database.
In both the transgender and control groups, about 66% were female at birth, 73% were White, and 9% Hispanic. For both groups, the average age was 16.2 years at the last visit. The average duration in the database was 7 years.
Study didn’t distinguish between those receiving and those not receiving gender-affirming hormones
In the retrospective study, among those who identified as transgender, the rates of diagnoses of dyslipidemia (odds ratio, 1.6; P < .0001) and metabolic syndrome (OR, 1.9; P = .0086) were significantly higher, compared with those without gender dysphoria.
Among the transgender male patients (born female) but not transgender female patients (born male), rates of diagnoses of overweight/obesity (OR, 1.7; P < .0001) and polycystic ovary syndrome were higher (OR, 1.9, P = .0006), compared with controls.
Gender-affirming hormone therapy, such as with testosterone or estradiol, is among the suspected culprits for the cardiovascular effects. However, importantly, this study did not differentiate between patients who had received estradiol or testosterone for gender affirmation and those who had not, Dr. Valentine said.
“We don’t know [whether gender-affirming hormone therapy is a cause], as we have not looked at this yet,” she said in an interview. “We are looking at that in our next analyses and will be including that in our future publication.
“We’ll also be looking at the relationship between having overweight/obesity and the other diagnoses that influence cardiovascular health (high blood pressure, liver dysfunction, and abnormal cholesterol), as that could certainly be playing a role as well,” she said.
For many transgender patients, gender-affirming hormone therapy is lifelong. One question that needs to be evaluated concerns whether the dose of such therapy has a role on cardiovascular effects and if so, whether adjustments could be made without compromising the therapeutic effect, Dr. Valentine noted.
“This is an important question, and future research is needed to evaluate whether doses [of gender-affirming hormones] are related to cardiometabolic outcomes,” she said.
Potential confounders in the study include the fact that rates of overweight and obesity are higher among youths with gender dysphoria. This can in itself can increase the risk for other disorders, Dr. Valentine noted.
Furthermore, rates of mental health comorbidities are higher among youths with gender dysphoria. One consequence of this may be that they engage in less physical activity, she said.
Hormone therapy, health care disparities, or both could explain risk
In commenting on the study, Joshua D. Safer, MD, executive director of the Center for Transgender Medicine and Surgery, the Mount Sinai Health System, New York, said that although similar cardiovascular effects are known to occur in transgender adults as well, they may or may not be hormone related. Other factors can increase the risk.
“With transgender adults, any differences in lipids or cardiac risk factors relative to cisgender people might be attributable either to hormone therapy or to health care disparities,” he said in an interview.
“The data are mixed. It may be that most differences relate to lack of access to care and to mistreatment by society,” he said. “Even studies that focus on hormones see a worsened situation for trans women versus trans men.”
Other recent research that shows potential cardiovascular effects among adult transgender men includes a study of more than 1,000 transgender men (born female) who received testosterone. That study, which was also presented at the ENDO meeting and was reported by this news organization, found an increased risk for high hematocrit levels, which could lead to a thrombotic event.
However, a study published in Pediatrics, which was also reported by this news organization, that included 611 transgender youths who had taken gender-affirming hormone therapy for more than a year found no increased risk for thrombosis, even in the presence of thrombosis risk factors, including obesity, tobacco use, and family history of thrombosis. However, the senior author of that study pointed out that the duration of follow-up in that study was relatively short, which may have been why they did not find an increased risk for thrombosis.
Dr. Safer noted that transgender youths and adults alike face a host of cultural factors that could play a role in increased cardiovascular risks.
“For adults, the major candidate explanations for worse BMI and cardiac risk factors are societal mistreatment, and for trans women specifically, progestins. For youth, the major candidate explanations are societal mistreatment and lack of access to athletics,” he said.
The authors and Dr. Safer disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Cardiovascular and metabolic risk factors are increased among transgender youths, compared with youths who are not transgender. Elevations in lipid levels and body mass index (BMI) also occur in adult transgender patients, new research shows.
“This is the first study of its size in the United States of which we are aware that looks at the odds of youth with a diagnosis of gender dysphoria having medical diagnoses that relate to overall metabolic and cardiovascular health,” first author Anna Valentine, MD, of Children’s Hospital Colorado, Aurora, said in a press statement.
Although previous studies have shown that among transgender adults, BMI is higher and there is an increased risk for cardiovascular events, such as stroke or heart attack, compared with nontransgender people, research on adolescent transgender patients has been lacking.
With a recent survey showing that nearly 2% of adolescents identify as transgender, interest in health outcomes among younger patients is high.
To investigate, Dr. Valentine, and colleagues evaluated data from the PEDSnet pediatric database on 4,177 youths who had received a diagnosis of gender dysphoria. The participants had been enrolled at six sites from 2009 to 2019. The researchers compared these patients in a ratio of 1:4 with 16,664 control persons who had not been diagnosed with gender dysphoria. They reported their findings as a poster at the annual meeting of the Endocrine Society.
For the propensity-score analysis, participants were matched according to year of birth, age at last visit, site, race, ethnicity, insurance status, and duration in the database.
In both the transgender and control groups, about 66% were female at birth, 73% were White, and 9% Hispanic. For both groups, the average age was 16.2 years at the last visit. The average duration in the database was 7 years.
Study didn’t distinguish between those receiving and those not receiving gender-affirming hormones
In the retrospective study, among those who identified as transgender, the rates of diagnoses of dyslipidemia (odds ratio, 1.6; P < .0001) and metabolic syndrome (OR, 1.9; P = .0086) were significantly higher, compared with those without gender dysphoria.
Among the transgender male patients (born female) but not transgender female patients (born male), rates of diagnoses of overweight/obesity (OR, 1.7; P < .0001) and polycystic ovary syndrome were higher (OR, 1.9, P = .0006), compared with controls.
Gender-affirming hormone therapy, such as with testosterone or estradiol, is among the suspected culprits for the cardiovascular effects. However, importantly, this study did not differentiate between patients who had received estradiol or testosterone for gender affirmation and those who had not, Dr. Valentine said.
“We don’t know [whether gender-affirming hormone therapy is a cause], as we have not looked at this yet,” she said in an interview. “We are looking at that in our next analyses and will be including that in our future publication.
“We’ll also be looking at the relationship between having overweight/obesity and the other diagnoses that influence cardiovascular health (high blood pressure, liver dysfunction, and abnormal cholesterol), as that could certainly be playing a role as well,” she said.
For many transgender patients, gender-affirming hormone therapy is lifelong. One question that needs to be evaluated concerns whether the dose of such therapy has a role on cardiovascular effects and if so, whether adjustments could be made without compromising the therapeutic effect, Dr. Valentine noted.
“This is an important question, and future research is needed to evaluate whether doses [of gender-affirming hormones] are related to cardiometabolic outcomes,” she said.
Potential confounders in the study include the fact that rates of overweight and obesity are higher among youths with gender dysphoria. This can in itself can increase the risk for other disorders, Dr. Valentine noted.
Furthermore, rates of mental health comorbidities are higher among youths with gender dysphoria. One consequence of this may be that they engage in less physical activity, she said.
Hormone therapy, health care disparities, or both could explain risk
In commenting on the study, Joshua D. Safer, MD, executive director of the Center for Transgender Medicine and Surgery, the Mount Sinai Health System, New York, said that although similar cardiovascular effects are known to occur in transgender adults as well, they may or may not be hormone related. Other factors can increase the risk.
“With transgender adults, any differences in lipids or cardiac risk factors relative to cisgender people might be attributable either to hormone therapy or to health care disparities,” he said in an interview.
“The data are mixed. It may be that most differences relate to lack of access to care and to mistreatment by society,” he said. “Even studies that focus on hormones see a worsened situation for trans women versus trans men.”
Other recent research that shows potential cardiovascular effects among adult transgender men includes a study of more than 1,000 transgender men (born female) who received testosterone. That study, which was also presented at the ENDO meeting and was reported by this news organization, found an increased risk for high hematocrit levels, which could lead to a thrombotic event.
However, a study published in Pediatrics, which was also reported by this news organization, that included 611 transgender youths who had taken gender-affirming hormone therapy for more than a year found no increased risk for thrombosis, even in the presence of thrombosis risk factors, including obesity, tobacco use, and family history of thrombosis. However, the senior author of that study pointed out that the duration of follow-up in that study was relatively short, which may have been why they did not find an increased risk for thrombosis.
Dr. Safer noted that transgender youths and adults alike face a host of cultural factors that could play a role in increased cardiovascular risks.
“For adults, the major candidate explanations for worse BMI and cardiac risk factors are societal mistreatment, and for trans women specifically, progestins. For youth, the major candidate explanations are societal mistreatment and lack of access to athletics,” he said.
The authors and Dr. Safer disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Cardiovascular and metabolic risk factors are increased among transgender youths, compared with youths who are not transgender. Elevations in lipid levels and body mass index (BMI) also occur in adult transgender patients, new research shows.
“This is the first study of its size in the United States of which we are aware that looks at the odds of youth with a diagnosis of gender dysphoria having medical diagnoses that relate to overall metabolic and cardiovascular health,” first author Anna Valentine, MD, of Children’s Hospital Colorado, Aurora, said in a press statement.
Although previous studies have shown that among transgender adults, BMI is higher and there is an increased risk for cardiovascular events, such as stroke or heart attack, compared with nontransgender people, research on adolescent transgender patients has been lacking.
With a recent survey showing that nearly 2% of adolescents identify as transgender, interest in health outcomes among younger patients is high.
To investigate, Dr. Valentine, and colleagues evaluated data from the PEDSnet pediatric database on 4,177 youths who had received a diagnosis of gender dysphoria. The participants had been enrolled at six sites from 2009 to 2019. The researchers compared these patients in a ratio of 1:4 with 16,664 control persons who had not been diagnosed with gender dysphoria. They reported their findings as a poster at the annual meeting of the Endocrine Society.
For the propensity-score analysis, participants were matched according to year of birth, age at last visit, site, race, ethnicity, insurance status, and duration in the database.
In both the transgender and control groups, about 66% were female at birth, 73% were White, and 9% Hispanic. For both groups, the average age was 16.2 years at the last visit. The average duration in the database was 7 years.
Study didn’t distinguish between those receiving and those not receiving gender-affirming hormones
In the retrospective study, among those who identified as transgender, the rates of diagnoses of dyslipidemia (odds ratio, 1.6; P < .0001) and metabolic syndrome (OR, 1.9; P = .0086) were significantly higher, compared with those without gender dysphoria.
Among the transgender male patients (born female) but not transgender female patients (born male), rates of diagnoses of overweight/obesity (OR, 1.7; P < .0001) and polycystic ovary syndrome were higher (OR, 1.9, P = .0006), compared with controls.
Gender-affirming hormone therapy, such as with testosterone or estradiol, is among the suspected culprits for the cardiovascular effects. However, importantly, this study did not differentiate between patients who had received estradiol or testosterone for gender affirmation and those who had not, Dr. Valentine said.
“We don’t know [whether gender-affirming hormone therapy is a cause], as we have not looked at this yet,” she said in an interview. “We are looking at that in our next analyses and will be including that in our future publication.
“We’ll also be looking at the relationship between having overweight/obesity and the other diagnoses that influence cardiovascular health (high blood pressure, liver dysfunction, and abnormal cholesterol), as that could certainly be playing a role as well,” she said.
For many transgender patients, gender-affirming hormone therapy is lifelong. One question that needs to be evaluated concerns whether the dose of such therapy has a role on cardiovascular effects and if so, whether adjustments could be made without compromising the therapeutic effect, Dr. Valentine noted.
“This is an important question, and future research is needed to evaluate whether doses [of gender-affirming hormones] are related to cardiometabolic outcomes,” she said.
Potential confounders in the study include the fact that rates of overweight and obesity are higher among youths with gender dysphoria. This can in itself can increase the risk for other disorders, Dr. Valentine noted.
Furthermore, rates of mental health comorbidities are higher among youths with gender dysphoria. One consequence of this may be that they engage in less physical activity, she said.
Hormone therapy, health care disparities, or both could explain risk
In commenting on the study, Joshua D. Safer, MD, executive director of the Center for Transgender Medicine and Surgery, the Mount Sinai Health System, New York, said that although similar cardiovascular effects are known to occur in transgender adults as well, they may or may not be hormone related. Other factors can increase the risk.
“With transgender adults, any differences in lipids or cardiac risk factors relative to cisgender people might be attributable either to hormone therapy or to health care disparities,” he said in an interview.
“The data are mixed. It may be that most differences relate to lack of access to care and to mistreatment by society,” he said. “Even studies that focus on hormones see a worsened situation for trans women versus trans men.”
Other recent research that shows potential cardiovascular effects among adult transgender men includes a study of more than 1,000 transgender men (born female) who received testosterone. That study, which was also presented at the ENDO meeting and was reported by this news organization, found an increased risk for high hematocrit levels, which could lead to a thrombotic event.
However, a study published in Pediatrics, which was also reported by this news organization, that included 611 transgender youths who had taken gender-affirming hormone therapy for more than a year found no increased risk for thrombosis, even in the presence of thrombosis risk factors, including obesity, tobacco use, and family history of thrombosis. However, the senior author of that study pointed out that the duration of follow-up in that study was relatively short, which may have been why they did not find an increased risk for thrombosis.
Dr. Safer noted that transgender youths and adults alike face a host of cultural factors that could play a role in increased cardiovascular risks.
“For adults, the major candidate explanations for worse BMI and cardiac risk factors are societal mistreatment, and for trans women specifically, progestins. For youth, the major candidate explanations are societal mistreatment and lack of access to athletics,” he said.
The authors and Dr. Safer disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Many unknowns on fertility preservation in transgender patients
Unknowns around the long-term effects of gender-affirming hormonal treatment on fertility in transgender individuals, especially adolescents, and what this means for fertility preservation, should be red flags for clinicians, according to one expert addressing the issue at the recent virtual ENDO 2021 meeting.
“One of the main concerns regarding fertility preservation in this population is that the decision to seek gender-affirming therapy is often made early in the reproductive lifespan, and for many patients this is well before the consideration of … child-bearing,” remarked Marie Menke, MD, an ob/gyn from University of Michigan, Ann Arbor, presenting in a session dedicated to state-of-the-art approaches to gamete preservation.
“These patients need to consider simultaneously their desire for gender-affirming therapy and their desire for child-bearing,” she added, explaining that gender-affirming therapy typically requires suppression of the hormonal axis that supports reproduction.
“This level of shared decision-making requires time and multidisciplinary involvement in the face of … limited data, and even with the best of counseling it can be quite overwhelming,” Dr. Menke stressed.
Specifically, the effects of gender-affirming therapy on both fertility and fertility preservation options in transgender individuals in comparison to the general population are areas that require much more research, she emphasized.
On the topic of adolescents specifically, she said they are “a special population,” as many seeking medical therapy for gender dysphoria have never considered long-term fertility goals or desires. Reports of such discussions during pediatric gender care vary greatly depending on the age of the patient and their geographic location.
And where such conversations have happened, “often there is no recollection by patients of such discussion prior to referral to endocrinology,” she emphasized.
Session co-moderator Irene Su, MD, a reproductive endocrinologist at the University of California, San Diego, said shared decisions with patients have to be made every day, even though data are limited.
“Little is known about both the adverse medical impact of gender-affirming hormonal therapy on fertility potential, as well as the psychosocial impact of interrupting/reversing gender-affirming hormonal therapy in the future to attempt fertility,” she told this news organization.
However, “because there are reasons to be concerned about an adverse impact on fertility, transgender individuals need access to fertility risk and preservation counseling,” she stressed.
Dr. Su has a special interest in improving reproductive health in young cancer survivors, and this involves similar discussions around fertility preservation – a medical subspecialty known as “oncofertility.”
There is a greater pool of knowledge in this field compared with fertility preservation and family planning in transgender patients, Dr. Su noted.
“While we need similar data in transgender individuals, what we’ve learned from the cancer survivor population is that they and their families want to know about known and unknown fertility risks and options, even if they ultimately do not choose to undertake fertility preservation procedures,” she explains.
Desire for future kids, but <10% currently preserve fertility
Dr. Menke said the estimated prevalence of individuals who identify as transgender is around 0.7% of the U.S. population, and she observed that, “by and large, fertility management involves tissue cryopreservation.”
She presented survey data showing that between 33%-54% of transgender and nonbinary individuals report a desire to have biological children currently, or in the future, and 94.6% are also strongly in support of transgender people having access to fertility preservation procedures.
Likewise, an online cross-sectional survey of over 1,100 people in the general population found that 76.2% agree that transgender individuals should be offered fertility preservation, and 60% support fertility preservation in minors.
Multiple professional societies support counseling in regard to options for fertility preservation and recommend that it should be offered to transgender individuals.
The American Society for Reproductive Medicine (ASRM), the American College of Obstetricians and Gynecologists (ACOG), the World Professional Association for Transgender Health (WPATH), and the Endocrine Society all advocate that individuals seeking gender-affirming medical treatment should receive multidisciplinary counseling regarding fertility preservation prior to puberty suppression in adolescents, and prior to cross-sex hormone treatment in both adolescents and adults.
But despite all of these recommendations and the survey findings, fertility preservation rates in transgender patients are low, “at less than 10%,” reported Dr. Menke.
Fertility preservation counseling and management ideally needs to begin prior to initiation of hormone therapy, stressed Dr. Menke.
Given the limited data on the long-term effects of gender-affirming therapy on fertility and its preservation, such counseling often leads to a myriad of questions, she further explained.
“Patients ask ‘What are the chances of having biological children if I don’t pursue fertility preservation?’, and ‘How likely am I to have a biological child if I do pursue fertility preservation?’, as well as issues around access to care, with patients asking, ‘Will I be able to pursue this option [of fertility preservation]?’”
“The chance of having a biological child if fertility preservation is pursued is similar to those [patients with cancer] who receive ‘oncofertility’ care, which has a good prognosis,” she explained.
However, issues around access to care, and the cost of it, can be barriers.
What does a transgender male, born female, need to do?
For transgender males, options for fertility preservation include the recommended option of cryopreservation of the eggs (oocytes), although freezing of embryos and/or ovarian tissue are also possible.
The latter would be required in a prepubertal individual if they wanted to start puberty blockers and then go straight onto cross-sex hormones, Dr. Menke noted, although she said it’s not definitively known if prepubertal ovarian tissue is capable of being stimulated in the future to produce viable mature oocytes.
In someone who has gone through puberty, the ideal time to freeze eggs is before beginning gender-affirming hormone therapy, Dr. Menke explained. This is because it is not known whether testosterone has any adverse impact on oocyte development.
“We just don’t have definitive data that long-term testosterone isn’t gonadotoxic,” she said in response to a question about this after her talk.
Assessment of the reproductive consequences of gender-affirming therapy in transgender males can also be complicated by coexisting conditions, Dr. Menke explained.
For example, up to 58% of transgender males have polycystic ovary syndrome (PCOS) prior to transitioning, she noted. PCOS itself, and/or the gender-affirming therapy, may cause histologic changes of the ovarian tissue – for example, hyperplasia of ovarian stroma – and it’s not yet known to what extent this may impact future fertility, if present, she noted.
For oocyte preservation in female-to-male transgender individuals, stimulation with gonadotropins for 2-3 weeks is needed, and the procedure is invasive, requiring repeated vaginal ultrasounds. During this period, estradiol levels are supraphysiologic, and there is potential for breast development and vaginal bleeding post-retrieval, which individuals will need to be counseled about, Dr. Menke noted.
The cost of this also needs to be factored into the equation. Depending on insurance coverage, costs may be covered – and where there is no precedent, individuals can try referring their insurance companies to the ‘oncofertility consortium access-to-care model’, Dr. Menke advised.
If there is no coverage, the average cost for one egg-freezing cycle ranges from $10,000-$17,000 in the U.S., and often two to three cycles are needed to generate sufficient oocytes to be sure of a pregnancy. In addition, there are storage costs. Plus, there will be the cost of any future intervention to achieve a pregnancy, she stressed.
How long frozen oocytes remain viable is also still a matter of scientific debate, although “as the technology changes from slow-freeze to vitrification,” this time period should lengthen, Dr. Menke said.
In transgender males who have not preserved oocytes or embryos prior to transitioning, it’s necessary to stop testosterone to have the best chance of harvesting viable gametes, Dr. Menke said. Furthermore, individuals undertaking this procedure need to take into account all of the above-mentioned side effects of egg harvesting.
Although there have been reports of successful pregnancies with eggs retrieved from transgender males who have temporarily stopped testosterone, fertilization and embryo development following discontinuation of testosterone still require “additional investigation,” she observed.
Furthermore, “there are case reports of oocyte stimulation and retrieval of mature oocytes while patients continue testosterone therapy, and this may be an option in the future,” she noted, again stressing that it’s not known if excess testosterone is gonadotoxic.
Other options for fertility preservation in the transgender male include embryo cryopreservation, but this still involves hormonal stimulation and invasive procedures and would require the use of a sperm donor in a person who doesn’t currently have a partner (or who has one, but not necessarily one with whom they want to create a child).
For transgender males there is also the possibility of using a surrogate mother for the pregnancy, she noted.
What about transgender women, assigned male at birth?
For those assigned male at birth who wish to take puberty blockers, fertility preservation would require cryopreservation of testicular tissue, although Dr. Menke stressed that this is still considered “experimental.”
In the postpubertal period, the simplest option is to cryopreserve semen, with this ideally being performed prior to the individual commencing gender-affirming hormone therapy, Dr. Menke said.
If this is not done prior to beginning hormonal treatment, estrogen will need to be discontinued for fertility preservation, she noted.
Return of sperm function following cessation of estrogen may be limited – “expect at least 3 months before return of reproductive function,” Dr. Menke said. And even this may not be sufficient to restore normal spermatogenesis, she cautioned. “Absent or reduced spermatogenesis or morphological changes to Sertoli cells [have been reported in transgender women].”
Also, “there are needs for multiple attempts at ejaculation and storage requirements” for this approach. Cost for freezing sperm in the U.S., if not covered by insurance, is around $400, she noted, with storage costs ranging from $100 to up to $800 a year.
“Case reports using cryopreserved sperm [in transgender individuals] are promising overall … with clinical pregnancy rates following [in vitro fertilization] (IVF) with cryopreserved sperm … equivalent to patients without evidence of male factor fertility,” Dr. Menke reported.
However, she emphasized the fact that IVF, or intracytoplasmic sperm injection (ICSI), will still be necessary for conception, with potential additional costs.
Some individuals may also need to undergo surgical removal of sperm postpuberty; this is typically performed where there is evidence of male factor infertility, for example.
Embryo cryopreservation requires a partner or use of donor oocytes and, again, will have cost implications.
In conclusion, Dr. Menke reiterated that the use of fertility preservation techniques among transgender people is low, and it is more frequently accessed by transgender females. Among the identified barriers to fertility preservation are cost, lack of information, invasiveness of procedures, and desire not to delay medical transition.
Dr. Menke has disclosed no relevant financial relationships. Dr. Su has received a speaker honorarium from Ferring Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Unknowns around the long-term effects of gender-affirming hormonal treatment on fertility in transgender individuals, especially adolescents, and what this means for fertility preservation, should be red flags for clinicians, according to one expert addressing the issue at the recent virtual ENDO 2021 meeting.
“One of the main concerns regarding fertility preservation in this population is that the decision to seek gender-affirming therapy is often made early in the reproductive lifespan, and for many patients this is well before the consideration of … child-bearing,” remarked Marie Menke, MD, an ob/gyn from University of Michigan, Ann Arbor, presenting in a session dedicated to state-of-the-art approaches to gamete preservation.
“These patients need to consider simultaneously their desire for gender-affirming therapy and their desire for child-bearing,” she added, explaining that gender-affirming therapy typically requires suppression of the hormonal axis that supports reproduction.
“This level of shared decision-making requires time and multidisciplinary involvement in the face of … limited data, and even with the best of counseling it can be quite overwhelming,” Dr. Menke stressed.
Specifically, the effects of gender-affirming therapy on both fertility and fertility preservation options in transgender individuals in comparison to the general population are areas that require much more research, she emphasized.
On the topic of adolescents specifically, she said they are “a special population,” as many seeking medical therapy for gender dysphoria have never considered long-term fertility goals or desires. Reports of such discussions during pediatric gender care vary greatly depending on the age of the patient and their geographic location.
And where such conversations have happened, “often there is no recollection by patients of such discussion prior to referral to endocrinology,” she emphasized.
Session co-moderator Irene Su, MD, a reproductive endocrinologist at the University of California, San Diego, said shared decisions with patients have to be made every day, even though data are limited.
“Little is known about both the adverse medical impact of gender-affirming hormonal therapy on fertility potential, as well as the psychosocial impact of interrupting/reversing gender-affirming hormonal therapy in the future to attempt fertility,” she told this news organization.
However, “because there are reasons to be concerned about an adverse impact on fertility, transgender individuals need access to fertility risk and preservation counseling,” she stressed.
Dr. Su has a special interest in improving reproductive health in young cancer survivors, and this involves similar discussions around fertility preservation – a medical subspecialty known as “oncofertility.”
There is a greater pool of knowledge in this field compared with fertility preservation and family planning in transgender patients, Dr. Su noted.
“While we need similar data in transgender individuals, what we’ve learned from the cancer survivor population is that they and their families want to know about known and unknown fertility risks and options, even if they ultimately do not choose to undertake fertility preservation procedures,” she explains.
Desire for future kids, but <10% currently preserve fertility
Dr. Menke said the estimated prevalence of individuals who identify as transgender is around 0.7% of the U.S. population, and she observed that, “by and large, fertility management involves tissue cryopreservation.”
She presented survey data showing that between 33%-54% of transgender and nonbinary individuals report a desire to have biological children currently, or in the future, and 94.6% are also strongly in support of transgender people having access to fertility preservation procedures.
Likewise, an online cross-sectional survey of over 1,100 people in the general population found that 76.2% agree that transgender individuals should be offered fertility preservation, and 60% support fertility preservation in minors.
Multiple professional societies support counseling in regard to options for fertility preservation and recommend that it should be offered to transgender individuals.
The American Society for Reproductive Medicine (ASRM), the American College of Obstetricians and Gynecologists (ACOG), the World Professional Association for Transgender Health (WPATH), and the Endocrine Society all advocate that individuals seeking gender-affirming medical treatment should receive multidisciplinary counseling regarding fertility preservation prior to puberty suppression in adolescents, and prior to cross-sex hormone treatment in both adolescents and adults.
But despite all of these recommendations and the survey findings, fertility preservation rates in transgender patients are low, “at less than 10%,” reported Dr. Menke.
Fertility preservation counseling and management ideally needs to begin prior to initiation of hormone therapy, stressed Dr. Menke.
Given the limited data on the long-term effects of gender-affirming therapy on fertility and its preservation, such counseling often leads to a myriad of questions, she further explained.
“Patients ask ‘What are the chances of having biological children if I don’t pursue fertility preservation?’, and ‘How likely am I to have a biological child if I do pursue fertility preservation?’, as well as issues around access to care, with patients asking, ‘Will I be able to pursue this option [of fertility preservation]?’”
“The chance of having a biological child if fertility preservation is pursued is similar to those [patients with cancer] who receive ‘oncofertility’ care, which has a good prognosis,” she explained.
However, issues around access to care, and the cost of it, can be barriers.
What does a transgender male, born female, need to do?
For transgender males, options for fertility preservation include the recommended option of cryopreservation of the eggs (oocytes), although freezing of embryos and/or ovarian tissue are also possible.
The latter would be required in a prepubertal individual if they wanted to start puberty blockers and then go straight onto cross-sex hormones, Dr. Menke noted, although she said it’s not definitively known if prepubertal ovarian tissue is capable of being stimulated in the future to produce viable mature oocytes.
In someone who has gone through puberty, the ideal time to freeze eggs is before beginning gender-affirming hormone therapy, Dr. Menke explained. This is because it is not known whether testosterone has any adverse impact on oocyte development.
“We just don’t have definitive data that long-term testosterone isn’t gonadotoxic,” she said in response to a question about this after her talk.
Assessment of the reproductive consequences of gender-affirming therapy in transgender males can also be complicated by coexisting conditions, Dr. Menke explained.
For example, up to 58% of transgender males have polycystic ovary syndrome (PCOS) prior to transitioning, she noted. PCOS itself, and/or the gender-affirming therapy, may cause histologic changes of the ovarian tissue – for example, hyperplasia of ovarian stroma – and it’s not yet known to what extent this may impact future fertility, if present, she noted.
For oocyte preservation in female-to-male transgender individuals, stimulation with gonadotropins for 2-3 weeks is needed, and the procedure is invasive, requiring repeated vaginal ultrasounds. During this period, estradiol levels are supraphysiologic, and there is potential for breast development and vaginal bleeding post-retrieval, which individuals will need to be counseled about, Dr. Menke noted.
The cost of this also needs to be factored into the equation. Depending on insurance coverage, costs may be covered – and where there is no precedent, individuals can try referring their insurance companies to the ‘oncofertility consortium access-to-care model’, Dr. Menke advised.
If there is no coverage, the average cost for one egg-freezing cycle ranges from $10,000-$17,000 in the U.S., and often two to three cycles are needed to generate sufficient oocytes to be sure of a pregnancy. In addition, there are storage costs. Plus, there will be the cost of any future intervention to achieve a pregnancy, she stressed.
How long frozen oocytes remain viable is also still a matter of scientific debate, although “as the technology changes from slow-freeze to vitrification,” this time period should lengthen, Dr. Menke said.
In transgender males who have not preserved oocytes or embryos prior to transitioning, it’s necessary to stop testosterone to have the best chance of harvesting viable gametes, Dr. Menke said. Furthermore, individuals undertaking this procedure need to take into account all of the above-mentioned side effects of egg harvesting.
Although there have been reports of successful pregnancies with eggs retrieved from transgender males who have temporarily stopped testosterone, fertilization and embryo development following discontinuation of testosterone still require “additional investigation,” she observed.
Furthermore, “there are case reports of oocyte stimulation and retrieval of mature oocytes while patients continue testosterone therapy, and this may be an option in the future,” she noted, again stressing that it’s not known if excess testosterone is gonadotoxic.
Other options for fertility preservation in the transgender male include embryo cryopreservation, but this still involves hormonal stimulation and invasive procedures and would require the use of a sperm donor in a person who doesn’t currently have a partner (or who has one, but not necessarily one with whom they want to create a child).
For transgender males there is also the possibility of using a surrogate mother for the pregnancy, she noted.
What about transgender women, assigned male at birth?
For those assigned male at birth who wish to take puberty blockers, fertility preservation would require cryopreservation of testicular tissue, although Dr. Menke stressed that this is still considered “experimental.”
In the postpubertal period, the simplest option is to cryopreserve semen, with this ideally being performed prior to the individual commencing gender-affirming hormone therapy, Dr. Menke said.
If this is not done prior to beginning hormonal treatment, estrogen will need to be discontinued for fertility preservation, she noted.
Return of sperm function following cessation of estrogen may be limited – “expect at least 3 months before return of reproductive function,” Dr. Menke said. And even this may not be sufficient to restore normal spermatogenesis, she cautioned. “Absent or reduced spermatogenesis or morphological changes to Sertoli cells [have been reported in transgender women].”
Also, “there are needs for multiple attempts at ejaculation and storage requirements” for this approach. Cost for freezing sperm in the U.S., if not covered by insurance, is around $400, she noted, with storage costs ranging from $100 to up to $800 a year.
“Case reports using cryopreserved sperm [in transgender individuals] are promising overall … with clinical pregnancy rates following [in vitro fertilization] (IVF) with cryopreserved sperm … equivalent to patients without evidence of male factor fertility,” Dr. Menke reported.
However, she emphasized the fact that IVF, or intracytoplasmic sperm injection (ICSI), will still be necessary for conception, with potential additional costs.
Some individuals may also need to undergo surgical removal of sperm postpuberty; this is typically performed where there is evidence of male factor infertility, for example.
Embryo cryopreservation requires a partner or use of donor oocytes and, again, will have cost implications.
In conclusion, Dr. Menke reiterated that the use of fertility preservation techniques among transgender people is low, and it is more frequently accessed by transgender females. Among the identified barriers to fertility preservation are cost, lack of information, invasiveness of procedures, and desire not to delay medical transition.
Dr. Menke has disclosed no relevant financial relationships. Dr. Su has received a speaker honorarium from Ferring Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Unknowns around the long-term effects of gender-affirming hormonal treatment on fertility in transgender individuals, especially adolescents, and what this means for fertility preservation, should be red flags for clinicians, according to one expert addressing the issue at the recent virtual ENDO 2021 meeting.
“One of the main concerns regarding fertility preservation in this population is that the decision to seek gender-affirming therapy is often made early in the reproductive lifespan, and for many patients this is well before the consideration of … child-bearing,” remarked Marie Menke, MD, an ob/gyn from University of Michigan, Ann Arbor, presenting in a session dedicated to state-of-the-art approaches to gamete preservation.
“These patients need to consider simultaneously their desire for gender-affirming therapy and their desire for child-bearing,” she added, explaining that gender-affirming therapy typically requires suppression of the hormonal axis that supports reproduction.
“This level of shared decision-making requires time and multidisciplinary involvement in the face of … limited data, and even with the best of counseling it can be quite overwhelming,” Dr. Menke stressed.
Specifically, the effects of gender-affirming therapy on both fertility and fertility preservation options in transgender individuals in comparison to the general population are areas that require much more research, she emphasized.
On the topic of adolescents specifically, she said they are “a special population,” as many seeking medical therapy for gender dysphoria have never considered long-term fertility goals or desires. Reports of such discussions during pediatric gender care vary greatly depending on the age of the patient and their geographic location.
And where such conversations have happened, “often there is no recollection by patients of such discussion prior to referral to endocrinology,” she emphasized.
Session co-moderator Irene Su, MD, a reproductive endocrinologist at the University of California, San Diego, said shared decisions with patients have to be made every day, even though data are limited.
“Little is known about both the adverse medical impact of gender-affirming hormonal therapy on fertility potential, as well as the psychosocial impact of interrupting/reversing gender-affirming hormonal therapy in the future to attempt fertility,” she told this news organization.
However, “because there are reasons to be concerned about an adverse impact on fertility, transgender individuals need access to fertility risk and preservation counseling,” she stressed.
Dr. Su has a special interest in improving reproductive health in young cancer survivors, and this involves similar discussions around fertility preservation – a medical subspecialty known as “oncofertility.”
There is a greater pool of knowledge in this field compared with fertility preservation and family planning in transgender patients, Dr. Su noted.
“While we need similar data in transgender individuals, what we’ve learned from the cancer survivor population is that they and their families want to know about known and unknown fertility risks and options, even if they ultimately do not choose to undertake fertility preservation procedures,” she explains.
Desire for future kids, but <10% currently preserve fertility
Dr. Menke said the estimated prevalence of individuals who identify as transgender is around 0.7% of the U.S. population, and she observed that, “by and large, fertility management involves tissue cryopreservation.”
She presented survey data showing that between 33%-54% of transgender and nonbinary individuals report a desire to have biological children currently, or in the future, and 94.6% are also strongly in support of transgender people having access to fertility preservation procedures.
Likewise, an online cross-sectional survey of over 1,100 people in the general population found that 76.2% agree that transgender individuals should be offered fertility preservation, and 60% support fertility preservation in minors.
Multiple professional societies support counseling in regard to options for fertility preservation and recommend that it should be offered to transgender individuals.
The American Society for Reproductive Medicine (ASRM), the American College of Obstetricians and Gynecologists (ACOG), the World Professional Association for Transgender Health (WPATH), and the Endocrine Society all advocate that individuals seeking gender-affirming medical treatment should receive multidisciplinary counseling regarding fertility preservation prior to puberty suppression in adolescents, and prior to cross-sex hormone treatment in both adolescents and adults.
But despite all of these recommendations and the survey findings, fertility preservation rates in transgender patients are low, “at less than 10%,” reported Dr. Menke.
Fertility preservation counseling and management ideally needs to begin prior to initiation of hormone therapy, stressed Dr. Menke.
Given the limited data on the long-term effects of gender-affirming therapy on fertility and its preservation, such counseling often leads to a myriad of questions, she further explained.
“Patients ask ‘What are the chances of having biological children if I don’t pursue fertility preservation?’, and ‘How likely am I to have a biological child if I do pursue fertility preservation?’, as well as issues around access to care, with patients asking, ‘Will I be able to pursue this option [of fertility preservation]?’”
“The chance of having a biological child if fertility preservation is pursued is similar to those [patients with cancer] who receive ‘oncofertility’ care, which has a good prognosis,” she explained.
However, issues around access to care, and the cost of it, can be barriers.
What does a transgender male, born female, need to do?
For transgender males, options for fertility preservation include the recommended option of cryopreservation of the eggs (oocytes), although freezing of embryos and/or ovarian tissue are also possible.
The latter would be required in a prepubertal individual if they wanted to start puberty blockers and then go straight onto cross-sex hormones, Dr. Menke noted, although she said it’s not definitively known if prepubertal ovarian tissue is capable of being stimulated in the future to produce viable mature oocytes.
In someone who has gone through puberty, the ideal time to freeze eggs is before beginning gender-affirming hormone therapy, Dr. Menke explained. This is because it is not known whether testosterone has any adverse impact on oocyte development.
“We just don’t have definitive data that long-term testosterone isn’t gonadotoxic,” she said in response to a question about this after her talk.
Assessment of the reproductive consequences of gender-affirming therapy in transgender males can also be complicated by coexisting conditions, Dr. Menke explained.
For example, up to 58% of transgender males have polycystic ovary syndrome (PCOS) prior to transitioning, she noted. PCOS itself, and/or the gender-affirming therapy, may cause histologic changes of the ovarian tissue – for example, hyperplasia of ovarian stroma – and it’s not yet known to what extent this may impact future fertility, if present, she noted.
For oocyte preservation in female-to-male transgender individuals, stimulation with gonadotropins for 2-3 weeks is needed, and the procedure is invasive, requiring repeated vaginal ultrasounds. During this period, estradiol levels are supraphysiologic, and there is potential for breast development and vaginal bleeding post-retrieval, which individuals will need to be counseled about, Dr. Menke noted.
The cost of this also needs to be factored into the equation. Depending on insurance coverage, costs may be covered – and where there is no precedent, individuals can try referring their insurance companies to the ‘oncofertility consortium access-to-care model’, Dr. Menke advised.
If there is no coverage, the average cost for one egg-freezing cycle ranges from $10,000-$17,000 in the U.S., and often two to three cycles are needed to generate sufficient oocytes to be sure of a pregnancy. In addition, there are storage costs. Plus, there will be the cost of any future intervention to achieve a pregnancy, she stressed.
How long frozen oocytes remain viable is also still a matter of scientific debate, although “as the technology changes from slow-freeze to vitrification,” this time period should lengthen, Dr. Menke said.
In transgender males who have not preserved oocytes or embryos prior to transitioning, it’s necessary to stop testosterone to have the best chance of harvesting viable gametes, Dr. Menke said. Furthermore, individuals undertaking this procedure need to take into account all of the above-mentioned side effects of egg harvesting.
Although there have been reports of successful pregnancies with eggs retrieved from transgender males who have temporarily stopped testosterone, fertilization and embryo development following discontinuation of testosterone still require “additional investigation,” she observed.
Furthermore, “there are case reports of oocyte stimulation and retrieval of mature oocytes while patients continue testosterone therapy, and this may be an option in the future,” she noted, again stressing that it’s not known if excess testosterone is gonadotoxic.
Other options for fertility preservation in the transgender male include embryo cryopreservation, but this still involves hormonal stimulation and invasive procedures and would require the use of a sperm donor in a person who doesn’t currently have a partner (or who has one, but not necessarily one with whom they want to create a child).
For transgender males there is also the possibility of using a surrogate mother for the pregnancy, she noted.
What about transgender women, assigned male at birth?
For those assigned male at birth who wish to take puberty blockers, fertility preservation would require cryopreservation of testicular tissue, although Dr. Menke stressed that this is still considered “experimental.”
In the postpubertal period, the simplest option is to cryopreserve semen, with this ideally being performed prior to the individual commencing gender-affirming hormone therapy, Dr. Menke said.
If this is not done prior to beginning hormonal treatment, estrogen will need to be discontinued for fertility preservation, she noted.
Return of sperm function following cessation of estrogen may be limited – “expect at least 3 months before return of reproductive function,” Dr. Menke said. And even this may not be sufficient to restore normal spermatogenesis, she cautioned. “Absent or reduced spermatogenesis or morphological changes to Sertoli cells [have been reported in transgender women].”
Also, “there are needs for multiple attempts at ejaculation and storage requirements” for this approach. Cost for freezing sperm in the U.S., if not covered by insurance, is around $400, she noted, with storage costs ranging from $100 to up to $800 a year.
“Case reports using cryopreserved sperm [in transgender individuals] are promising overall … with clinical pregnancy rates following [in vitro fertilization] (IVF) with cryopreserved sperm … equivalent to patients without evidence of male factor fertility,” Dr. Menke reported.
However, she emphasized the fact that IVF, or intracytoplasmic sperm injection (ICSI), will still be necessary for conception, with potential additional costs.
Some individuals may also need to undergo surgical removal of sperm postpuberty; this is typically performed where there is evidence of male factor infertility, for example.
Embryo cryopreservation requires a partner or use of donor oocytes and, again, will have cost implications.
In conclusion, Dr. Menke reiterated that the use of fertility preservation techniques among transgender people is low, and it is more frequently accessed by transgender females. Among the identified barriers to fertility preservation are cost, lack of information, invasiveness of procedures, and desire not to delay medical transition.
Dr. Menke has disclosed no relevant financial relationships. Dr. Su has received a speaker honorarium from Ferring Pharmaceuticals.
A version of this article first appeared on Medscape.com.
‘Politics has no place here,’ AAP says about transgender care
The American Academy of Pediatrics (AAP) released a statement condemning state legislation introduced across the country that would prohibit the medical treatment of children who identify as transgender.
“Politics has no place here. Transgender children, like all children, just want to belong. We will fight state by state, in the courts, and on the national stage to make sure they know they do,” said the American Academy of Pediatrics, an organization that recommends that youth who identify as transgender have access to comprehensive, gender-affirming and “developmentally appropriate” health care.
There has been a lot of controversy among physicians surrounding gender-affirming care for children. In 2019, three separate groups of physicians questioned the hormonal treatment of children and adolescents with gender dysphoria, saying more research is needed to support gender-affirming care recommendations from groups such as the AAP. In addition, California-based endocrinologist Michael K. Laidlaw, MD, called the use of puberty blockers – medication used to delay or prevent the onset of puberty – an “experiment” and “public health problem.”
Some of the bills circulating would prohibit gender-affirming care for children and penalize pediatricians and other physicians for providing such care. Other bills would prevent transgender youth from participating in sports or on athletic teams according to their gender identity, requiring them to join teams aligned with the sex they were assigned at birth.
Jason Rafferty, MD, a pediatrician who authored AAP’s 2018 policy statement encouraging pediatricians to provide gender-affirmative care to children and adolescents, said in an interview that these proposed state bills are targeting a vulnerable population at a vulnerable time.
“You have this marginalized group and right in the midst of a pandemic – and [social isolation] – and you have these policies coming out that are really targeting the most vulnerable,” said Dr. Rafferty, who practices at the Adolescent Healthcare Center at Hasbro Children’s Hospital, Providence, R.I. “Some of the proposed policies would ensure that some of these transgender kids wouldn’t have access to basic medical care [or access to areas] where pediatricians are affirming these kids and creating a safe environment for them.”
M. Brett Cooper, MD, of pediatrics at UT Southwestern Medical Center, Dallas, said in an interview that the proposed state legislations are based on personal beliefs, not evidence-based care.
He said the AAP is speaking out because many of these proposed state legislatures are advancing bills that would affect gender-diverse children.
“Many of these bills are making it close to passing both chambers of a state legislature and thus sent to the governor for approval,” Dr. Cooper said. “In past legislative sessions, bills such as these have never it made out of committee in either a state House or state Senate.”
Early in March, South Dakota Governor Kristi Noem tweeted that she was “excited to sign” a bill that would prevent children who are transgender from participating in sports or on athletic teams according to their gender identity, requiring them to join teams aligned with the sex they were assigned at birth.
Meanwhile, previous studies have shown that teens whose gender identity does not align with their sex assigned at birth were more likely to report a suicide attempt, compared with cisgender youth. A 2015 study has attributed this increased risk of suicide to marginalization, social exclusion, and trauma. The bills being proposed may exacerbate this, according to Dr. Rafferty.
These bills point in the direction of approaches and models that research shows may be harmful to transgender children, he said.
“Beyond that, policies that are out there affecting participation in sports and other activities really just draw attention to these youth in unnecessary ways and really puts their physical and mental health at risk in a school environment,” he added.
“Whether it’s health care, school, community, or home [these policies] just really create a very hostile and dangerous environment toward a population that already is at significant risk,” Dr. Rafferty said.
The AAP’s clinical care guidelines for children who identify as transgender state that pediatricians who provide gender-affirmative care and speak with children and their families about gender issues help foster an environment of nurturance and support.
“Many people think that the care provided to gender diverse young people is rogue,” Dr. Cooper said. “Pediatric gender clinics are often either multidisciplinary or have a readily accessible team, including social work, mental health, and the physician. Medical care for gender diverse youth follows well-established standards of care.”
Dr. Rafferty said it is important for care providers to support children and teenagers who identify as transgender by creating a safe space and helping them identify what they need.
“There’s a lot out there that really tries to unite gender and biological sex together, saying that gender can be reduced to your anatomy,” Dr. Rafferty said. “But I think what we’re coming to appreciate is that our sense of identity is much more complex than simply our genes or biology.”
Dr. Rafferty is a member of the American Academy of Pediatrics, the Society of Adolescent Health and Medicine, and the American Academy of Child and Adolescent Psychiatry. Dr. Cooper is a columnist for Pediatric News and is on the board of trustees for the Texas Medical Association.
The American Academy of Pediatrics (AAP) released a statement condemning state legislation introduced across the country that would prohibit the medical treatment of children who identify as transgender.
“Politics has no place here. Transgender children, like all children, just want to belong. We will fight state by state, in the courts, and on the national stage to make sure they know they do,” said the American Academy of Pediatrics, an organization that recommends that youth who identify as transgender have access to comprehensive, gender-affirming and “developmentally appropriate” health care.
There has been a lot of controversy among physicians surrounding gender-affirming care for children. In 2019, three separate groups of physicians questioned the hormonal treatment of children and adolescents with gender dysphoria, saying more research is needed to support gender-affirming care recommendations from groups such as the AAP. In addition, California-based endocrinologist Michael K. Laidlaw, MD, called the use of puberty blockers – medication used to delay or prevent the onset of puberty – an “experiment” and “public health problem.”
Some of the bills circulating would prohibit gender-affirming care for children and penalize pediatricians and other physicians for providing such care. Other bills would prevent transgender youth from participating in sports or on athletic teams according to their gender identity, requiring them to join teams aligned with the sex they were assigned at birth.
Jason Rafferty, MD, a pediatrician who authored AAP’s 2018 policy statement encouraging pediatricians to provide gender-affirmative care to children and adolescents, said in an interview that these proposed state bills are targeting a vulnerable population at a vulnerable time.
“You have this marginalized group and right in the midst of a pandemic – and [social isolation] – and you have these policies coming out that are really targeting the most vulnerable,” said Dr. Rafferty, who practices at the Adolescent Healthcare Center at Hasbro Children’s Hospital, Providence, R.I. “Some of the proposed policies would ensure that some of these transgender kids wouldn’t have access to basic medical care [or access to areas] where pediatricians are affirming these kids and creating a safe environment for them.”
M. Brett Cooper, MD, of pediatrics at UT Southwestern Medical Center, Dallas, said in an interview that the proposed state legislations are based on personal beliefs, not evidence-based care.
He said the AAP is speaking out because many of these proposed state legislatures are advancing bills that would affect gender-diverse children.
“Many of these bills are making it close to passing both chambers of a state legislature and thus sent to the governor for approval,” Dr. Cooper said. “In past legislative sessions, bills such as these have never it made out of committee in either a state House or state Senate.”
Early in March, South Dakota Governor Kristi Noem tweeted that she was “excited to sign” a bill that would prevent children who are transgender from participating in sports or on athletic teams according to their gender identity, requiring them to join teams aligned with the sex they were assigned at birth.
Meanwhile, previous studies have shown that teens whose gender identity does not align with their sex assigned at birth were more likely to report a suicide attempt, compared with cisgender youth. A 2015 study has attributed this increased risk of suicide to marginalization, social exclusion, and trauma. The bills being proposed may exacerbate this, according to Dr. Rafferty.
These bills point in the direction of approaches and models that research shows may be harmful to transgender children, he said.
“Beyond that, policies that are out there affecting participation in sports and other activities really just draw attention to these youth in unnecessary ways and really puts their physical and mental health at risk in a school environment,” he added.
“Whether it’s health care, school, community, or home [these policies] just really create a very hostile and dangerous environment toward a population that already is at significant risk,” Dr. Rafferty said.
The AAP’s clinical care guidelines for children who identify as transgender state that pediatricians who provide gender-affirmative care and speak with children and their families about gender issues help foster an environment of nurturance and support.
“Many people think that the care provided to gender diverse young people is rogue,” Dr. Cooper said. “Pediatric gender clinics are often either multidisciplinary or have a readily accessible team, including social work, mental health, and the physician. Medical care for gender diverse youth follows well-established standards of care.”
Dr. Rafferty said it is important for care providers to support children and teenagers who identify as transgender by creating a safe space and helping them identify what they need.
“There’s a lot out there that really tries to unite gender and biological sex together, saying that gender can be reduced to your anatomy,” Dr. Rafferty said. “But I think what we’re coming to appreciate is that our sense of identity is much more complex than simply our genes or biology.”
Dr. Rafferty is a member of the American Academy of Pediatrics, the Society of Adolescent Health and Medicine, and the American Academy of Child and Adolescent Psychiatry. Dr. Cooper is a columnist for Pediatric News and is on the board of trustees for the Texas Medical Association.
The American Academy of Pediatrics (AAP) released a statement condemning state legislation introduced across the country that would prohibit the medical treatment of children who identify as transgender.
“Politics has no place here. Transgender children, like all children, just want to belong. We will fight state by state, in the courts, and on the national stage to make sure they know they do,” said the American Academy of Pediatrics, an organization that recommends that youth who identify as transgender have access to comprehensive, gender-affirming and “developmentally appropriate” health care.
There has been a lot of controversy among physicians surrounding gender-affirming care for children. In 2019, three separate groups of physicians questioned the hormonal treatment of children and adolescents with gender dysphoria, saying more research is needed to support gender-affirming care recommendations from groups such as the AAP. In addition, California-based endocrinologist Michael K. Laidlaw, MD, called the use of puberty blockers – medication used to delay or prevent the onset of puberty – an “experiment” and “public health problem.”
Some of the bills circulating would prohibit gender-affirming care for children and penalize pediatricians and other physicians for providing such care. Other bills would prevent transgender youth from participating in sports or on athletic teams according to their gender identity, requiring them to join teams aligned with the sex they were assigned at birth.
Jason Rafferty, MD, a pediatrician who authored AAP’s 2018 policy statement encouraging pediatricians to provide gender-affirmative care to children and adolescents, said in an interview that these proposed state bills are targeting a vulnerable population at a vulnerable time.
“You have this marginalized group and right in the midst of a pandemic – and [social isolation] – and you have these policies coming out that are really targeting the most vulnerable,” said Dr. Rafferty, who practices at the Adolescent Healthcare Center at Hasbro Children’s Hospital, Providence, R.I. “Some of the proposed policies would ensure that some of these transgender kids wouldn’t have access to basic medical care [or access to areas] where pediatricians are affirming these kids and creating a safe environment for them.”
M. Brett Cooper, MD, of pediatrics at UT Southwestern Medical Center, Dallas, said in an interview that the proposed state legislations are based on personal beliefs, not evidence-based care.
He said the AAP is speaking out because many of these proposed state legislatures are advancing bills that would affect gender-diverse children.
“Many of these bills are making it close to passing both chambers of a state legislature and thus sent to the governor for approval,” Dr. Cooper said. “In past legislative sessions, bills such as these have never it made out of committee in either a state House or state Senate.”
Early in March, South Dakota Governor Kristi Noem tweeted that she was “excited to sign” a bill that would prevent children who are transgender from participating in sports or on athletic teams according to their gender identity, requiring them to join teams aligned with the sex they were assigned at birth.
Meanwhile, previous studies have shown that teens whose gender identity does not align with their sex assigned at birth were more likely to report a suicide attempt, compared with cisgender youth. A 2015 study has attributed this increased risk of suicide to marginalization, social exclusion, and trauma. The bills being proposed may exacerbate this, according to Dr. Rafferty.
These bills point in the direction of approaches and models that research shows may be harmful to transgender children, he said.
“Beyond that, policies that are out there affecting participation in sports and other activities really just draw attention to these youth in unnecessary ways and really puts their physical and mental health at risk in a school environment,” he added.
“Whether it’s health care, school, community, or home [these policies] just really create a very hostile and dangerous environment toward a population that already is at significant risk,” Dr. Rafferty said.
The AAP’s clinical care guidelines for children who identify as transgender state that pediatricians who provide gender-affirmative care and speak with children and their families about gender issues help foster an environment of nurturance and support.
“Many people think that the care provided to gender diverse young people is rogue,” Dr. Cooper said. “Pediatric gender clinics are often either multidisciplinary or have a readily accessible team, including social work, mental health, and the physician. Medical care for gender diverse youth follows well-established standards of care.”
Dr. Rafferty said it is important for care providers to support children and teenagers who identify as transgender by creating a safe space and helping them identify what they need.
“There’s a lot out there that really tries to unite gender and biological sex together, saying that gender can be reduced to your anatomy,” Dr. Rafferty said. “But I think what we’re coming to appreciate is that our sense of identity is much more complex than simply our genes or biology.”
Dr. Rafferty is a member of the American Academy of Pediatrics, the Society of Adolescent Health and Medicine, and the American Academy of Child and Adolescent Psychiatry. Dr. Cooper is a columnist for Pediatric News and is on the board of trustees for the Texas Medical Association.
Addressing mental health for transgender patients during the pandemic
Obstetrician/gynecologists are often first-line providers in addressing mental health concerns for our patients. Routine screening for intimate partner violence, obtaining a history of sexual assault, and assessing patients for postpartum depression are among the many tools that we use to ascertain the psychological well-being of cisgender women. As transgender patients continue to seek care from ob.gyns., it is vital that we not only screen transgender patients for depression and intimate partner violence, but also assess factors relating to social support.

Mental health disorders disproportionately affect the transgender population. A large online survey showed that 41% of transgender patients had experienced suicidality, with rates among transgender youth even higher.1 While the rates of sexual violence are higher among LGBTQ patients compared with cisgender counterparts, the rate of sexual assault is as high as 47% in the transgender population.2,3 Additional surveys and studies have demonstrated that more than 70% of transgender individuals report discrimination in school (K-12), 27% have lost their jobs because of their gender identity; and 30% have experienced homelessness at some point.3 Tragically, these rates are further affected by race and ethnicity with American Indian (65%), multiracial (59%), Middle Eastern (58%), and Black (53%) respondents in the survey stating they were assaulted at some point.3
In a prepandemic world, mental health for transgender patients was influenced by several factors, such as stigmatization, health care disparities, limited access to health care, prolonged exposure to discrimination, lack of a supportive environment, and history of trauma or violence. During the pandemic, these factors have been magnified. Furthermore, many of the supportive services such as group meetings at LGBTQ centers, networking events/conferences, LGBTQ pride events, and social gatherings at bars or restaurants have been postponed, reduced to accommodate social distancing measures, or moved to virtual platforms.
While the pandemic has led to increased unemployment rates, concerns over housing and rent payments, and limiting one’s social circle in the general population, these rates are increased among LGBTQ adults. Data are limited on how significantly the pandemic has affected LGBTQ adults, but an analysis conducted by the Kaiser Family Foundation found that 56% of LGBTQ adults reported that they or someone they know lost a job, compared with 44% of non-LGBTQ adults.4 In addition, 75% of LGBTQ adults report that the pandemic has negatively affected their mental health, compared with 49% of the non-LGBTQ population.4 To my dismay, I’ve seen these statistics reflected in my own patient population.
Given this knowledge, it is even more crucial that obstetrician/gynecologists screen for depression, substance use, and intimate partner violence, in addition to assessing the patient’s social determinants for overall well-being. These often include determining a patient’s living situation, employment status, familial support, and social support. In my practice, if concerns are raised in any of these areas, we have a streamlined referral system connecting patients to a variety of therapists, psychologists, and/or social workers, with close follow-up on either a weekly or monthly basis depending on the particular issue the patient is facing. While many patients may be hesitant to go to in-office appointments or where transportation poses a barrier, telemedicine visits are useful adjuncts to assess patient’s overall well-being.
While the pandemic has been extraordinarily difficult for us all, it is important for us to be even stronger advocates for communities that have experienced further challenges as a result of this global tragedy.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Karasic D. Mental health care for the adult transgender patient. In: Ferrando CA, ed. Comprehensive Care of the Transgender Patient. Philadelphia, PA: Elsevier; 2020:8-11.
2. Black MC et al. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report. Atlanta: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2011.
3. James SE et al. The Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality; 2016.
4. Dawson L et al. The impact of the COVID-19 pandemic on LGBT people. KFF COVID-19 Vaccine Monitor. Kaiser Family Foundation. March 11, 2021.
Obstetrician/gynecologists are often first-line providers in addressing mental health concerns for our patients. Routine screening for intimate partner violence, obtaining a history of sexual assault, and assessing patients for postpartum depression are among the many tools that we use to ascertain the psychological well-being of cisgender women. As transgender patients continue to seek care from ob.gyns., it is vital that we not only screen transgender patients for depression and intimate partner violence, but also assess factors relating to social support.
Mental health disorders disproportionately affect the transgender population. A large online survey showed that 41% of transgender patients had experienced suicidality, with rates among transgender youth even higher.1 While the rates of sexual violence are higher among LGBTQ patients compared with cisgender counterparts, the rate of sexual assault is as high as 47% in the transgender population.2,3 Additional surveys and studies have demonstrated that more than 70% of transgender individuals report discrimination in school (K-12), 27% have lost their jobs because of their gender identity; and 30% have experienced homelessness at some point.3 Tragically, these rates are further affected by race and ethnicity with American Indian (65%), multiracial (59%), Middle Eastern (58%), and Black (53%) respondents in the survey stating they were assaulted at some point.3
In a prepandemic world, mental health for transgender patients was influenced by several factors, such as stigmatization, health care disparities, limited access to health care, prolonged exposure to discrimination, lack of a supportive environment, and history of trauma or violence. During the pandemic, these factors have been magnified. Furthermore, many of the supportive services such as group meetings at LGBTQ centers, networking events/conferences, LGBTQ pride events, and social gatherings at bars or restaurants have been postponed, reduced to accommodate social distancing measures, or moved to virtual platforms.
While the pandemic has led to increased unemployment rates, concerns over housing and rent payments, and limiting one’s social circle in the general population, these rates are increased among LGBTQ adults. Data are limited on how significantly the pandemic has affected LGBTQ adults, but an analysis conducted by the Kaiser Family Foundation found that 56% of LGBTQ adults reported that they or someone they know lost a job, compared with 44% of non-LGBTQ adults.4 In addition, 75% of LGBTQ adults report that the pandemic has negatively affected their mental health, compared with 49% of the non-LGBTQ population.4 To my dismay, I’ve seen these statistics reflected in my own patient population.
Given this knowledge, it is even more crucial that obstetrician/gynecologists screen for depression, substance use, and intimate partner violence, in addition to assessing the patient’s social determinants for overall well-being. These often include determining a patient’s living situation, employment status, familial support, and social support. In my practice, if concerns are raised in any of these areas, we have a streamlined referral system connecting patients to a variety of therapists, psychologists, and/or social workers, with close follow-up on either a weekly or monthly basis depending on the particular issue the patient is facing. While many patients may be hesitant to go to in-office appointments or where transportation poses a barrier, telemedicine visits are useful adjuncts to assess patient’s overall well-being.
While the pandemic has been extraordinarily difficult for us all, it is important for us to be even stronger advocates for communities that have experienced further challenges as a result of this global tragedy.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Karasic D. Mental health care for the adult transgender patient. In: Ferrando CA, ed. Comprehensive Care of the Transgender Patient. Philadelphia, PA: Elsevier; 2020:8-11.
2. Black MC et al. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report. Atlanta: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2011.
3. James SE et al. The Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality; 2016.
4. Dawson L et al. The impact of the COVID-19 pandemic on LGBT people. KFF COVID-19 Vaccine Monitor. Kaiser Family Foundation. March 11, 2021.
Obstetrician/gynecologists are often first-line providers in addressing mental health concerns for our patients. Routine screening for intimate partner violence, obtaining a history of sexual assault, and assessing patients for postpartum depression are among the many tools that we use to ascertain the psychological well-being of cisgender women. As transgender patients continue to seek care from ob.gyns., it is vital that we not only screen transgender patients for depression and intimate partner violence, but also assess factors relating to social support.
Mental health disorders disproportionately affect the transgender population. A large online survey showed that 41% of transgender patients had experienced suicidality, with rates among transgender youth even higher.1 While the rates of sexual violence are higher among LGBTQ patients compared with cisgender counterparts, the rate of sexual assault is as high as 47% in the transgender population.2,3 Additional surveys and studies have demonstrated that more than 70% of transgender individuals report discrimination in school (K-12), 27% have lost their jobs because of their gender identity; and 30% have experienced homelessness at some point.3 Tragically, these rates are further affected by race and ethnicity with American Indian (65%), multiracial (59%), Middle Eastern (58%), and Black (53%) respondents in the survey stating they were assaulted at some point.3
In a prepandemic world, mental health for transgender patients was influenced by several factors, such as stigmatization, health care disparities, limited access to health care, prolonged exposure to discrimination, lack of a supportive environment, and history of trauma or violence. During the pandemic, these factors have been magnified. Furthermore, many of the supportive services such as group meetings at LGBTQ centers, networking events/conferences, LGBTQ pride events, and social gatherings at bars or restaurants have been postponed, reduced to accommodate social distancing measures, or moved to virtual platforms.
While the pandemic has led to increased unemployment rates, concerns over housing and rent payments, and limiting one’s social circle in the general population, these rates are increased among LGBTQ adults. Data are limited on how significantly the pandemic has affected LGBTQ adults, but an analysis conducted by the Kaiser Family Foundation found that 56% of LGBTQ adults reported that they or someone they know lost a job, compared with 44% of non-LGBTQ adults.4 In addition, 75% of LGBTQ adults report that the pandemic has negatively affected their mental health, compared with 49% of the non-LGBTQ population.4 To my dismay, I’ve seen these statistics reflected in my own patient population.
Given this knowledge, it is even more crucial that obstetrician/gynecologists screen for depression, substance use, and intimate partner violence, in addition to assessing the patient’s social determinants for overall well-being. These often include determining a patient’s living situation, employment status, familial support, and social support. In my practice, if concerns are raised in any of these areas, we have a streamlined referral system connecting patients to a variety of therapists, psychologists, and/or social workers, with close follow-up on either a weekly or monthly basis depending on the particular issue the patient is facing. While many patients may be hesitant to go to in-office appointments or where transportation poses a barrier, telemedicine visits are useful adjuncts to assess patient’s overall well-being.
While the pandemic has been extraordinarily difficult for us all, it is important for us to be even stronger advocates for communities that have experienced further challenges as a result of this global tragedy.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Karasic D. Mental health care for the adult transgender patient. In: Ferrando CA, ed. Comprehensive Care of the Transgender Patient. Philadelphia, PA: Elsevier; 2020:8-11.
2. Black MC et al. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report. Atlanta: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2011.
3. James SE et al. The Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality; 2016.
4. Dawson L et al. The impact of the COVID-19 pandemic on LGBT people. KFF COVID-19 Vaccine Monitor. Kaiser Family Foundation. March 11, 2021.
‘I think I’m transgender’: A clinician’s guide to next steps
A 16-year-old patient sits in front of you and says, “I think I’m transgender.”
![]()
What do you do?
Whether you are an endocrinologist, family physician, pediatrician, or emergency physician, it’s probably a situation for which medical school education did not sufficiently prepare you. What you know is that you want to do your best to guide your patient and offer every resource necessary for a healthy and happy life. The good news is that your patient trusted you enough to disclose this information to you.
Sadly, this isn’t always the case. About 23% of transgender adults responding to the 2015 U.S. Transgender Survey put off necessary health care because they fear being mistreated or disrespected. Nearly one-third (31%) of survey respondents reported that none of their health care providers knew they were transgender.
Now that your patient feels comfortable enough with you to share this information, you must make sure you do everything in your power to continue to earn your patient’s trust.
Language matters
First, make sure that you are respectful with your terminology. Ask the patient for their name, pronouns, and gender identity. For example: “My name is Dr. Pine, and my pronouns are she/her. What are your pronouns? How do you describe your gender identity?” Each person may have terminology that is specific to their own experience, so allowing people to use their own language is the most respectful method.
People may identify as male, female, transwoman, transman, gender fluid, nonbinary, agender, neutrois, pangender, two-spirit, or other options not listed here. Physicians can be supportive by ensuring that their paperwork or electronic medical systems are sensitive to the needs of the transgender community. Having an option for the patient’s chosen name is courteous to all patients, regardless of gender identity; not everyone uses their legal name in everyday conversation.
Paperwork and electronic medical systems should ask for gender identity and sex assigned at birth, allow write-in options for issues of gender and sexual orientation, and ask for an anatomical inventory or organ inventory so that cancer screening can be conducted for the appropriate body parts.
Questions to ask
Ask patients about their gender journey: How long have they felt this way? How did they come to understand themselves and their gender? When did they start to disclose their experience with others? With pediatric patients, I ask if they have discussed this with their parents/guardians, and if they would like to have that conversation together.
Ask how you can support the patient on their journey. Are they interested in therapy, puberty blockers, hormones, or surgery? People may seek therapy for help coping with internalized transphobia, family rejection, or stigma. They may also want information or support with accessing hormones or surgery. In addition to individual therapy, there are numerous support groups for children, individuals, parents/guardians, and partners, such as PFLAG.org and Genderspectrum.org.
If you are the right kind of doctor and ready to prescribe, you can begin counseling. If not, you should know how to find local resources. The World Professional Association for Transgender Health has a directory of providers, and there are other resources listed below.
What does gender transitioning entail?
There are many components to gender transition. Some transitions may consist primarily of a social transition, with people using a different name, pronouns, and external expression, such as hairstyle and clothing. For others, there may be a medical component.
Mental health care is also an important component of gender transition for children, adolescents, adults, and family members. Mental health concerns are significantly greater in transgender and gender-nonconforming people, with higher rates of depression, anxiety, suicidal ideation, self-harm, substance abuse, eating disorders, and neurodiversity on the autism spectrum. In a study of more than 6,400 transgender people in the United States, 41% reported attempting suicide – a rate 25 times higher than that of the general population. Numerous studies show that hormonal treatment decreases depression, suicidal ideation, and anxiety, and also improves quality of life.
One common misperception, especially when working with children, is that youth transition involves a “sex change” (an outdated term) or any type of surgery. In reality, the main intervention before puberty is psychological support and social transition. The use of a chosen name at school, home, work, and with friends was shown to be associated with lower depression, suicidal ideation, and suicidal behavior. Another study demonstrated that children supported in their identities have mental health similar to that of cisgender siblings and peers.
When puberty approaches, if there is distress around natal pubertal development, then gonadotropin-releasing hormone agonists or “puberty blockers” may be used to temporarily pause the pubertal process, but only after Tanner stage II-III is reached. These medications have been safely used for decades for patients with central precocious puberty. Access to puberty-blocking medication in adolescence (when desired) has been associated with lower rates of suicidal ideation in adulthood and can truly be a lifesaving intervention.
When teens are older, they may choose to take gender-affirming hormone therapy to go through the puberty that is concordant with their affirmed gender. Adults who decide to transition medically may decide to take hormone therapy and may have gender-confirmation surgery, if desired, to align the body with their gender identity and alleviate gender dysphoria. Overall, access to medical care and hormone therapy have been shown to decrease depression, anxiety, and suicidality, and improve quality of life.
Sexuality and fertility
It is important to understand that sexuality is separate from gender identity, and that attraction and sexual activity cannot be assumed. Take a sensitive romantic and sexual history from your patient to get the information necessary to counsel patients about safe relationships and sexual practices. It is important not to make assumptions; a patient who is asexual may still be having sex, and a transgender man may be having receptive vaginal intercourse and may need information about contraception and family planning.
Also, be careful about using clinical language. Some people may want to use anatomical terms, but others may be uncomfortable or triggered by them. For instance, a transgender man may use “chest” for breasts, or “genital canal,” and “junk,” “dick,” or “front hole” for the vagina. Ask patients what terms they prefer to use.
It is also important to consider the impact that medical and surgical interventions may have on fertility, especially when discussing the topic with children and adolescents who may not have spent much time thinking about family planning. Be careful not to make assumptions about plans for parenthood, and remember that there are many paths to becoming a parent.
What does the patient need right now?
When I was a fourth-year medical student on my outpatient child psychiatry rotation, a 5-year-old child assigned male at birth was guarded and frightened of me until their mother said: “It’s okay, Dr. Elyse likes girl things too,” at which point the child became animated and happy while chatting with me about Barbie dolls. My patient had already endured teasing about gender nonconformity, starting in kindergarten; it was unclear to my patient whether I would be a safe person or a bully.
The mother was kind and affirming, but she also wanted answers. Would her child grow up to be a gay man? Or a transgender woman? Would her child be able to live freely, or would they always be quiet around others, scared of what people might say? Would her child be safe?
We can’t predict the future, but as doctors, we want to use all of our knowledge and tools to help our patients live healthy lives. In this case, it meant helping the mother know how to support her child’s identity, how to advocate for a safe school and community, where to connect with other gender-creative children, and how to tolerate ambiguity and celebrate the child she has, not the child she expected.
We know that people with higher support and higher self-esteem can have greater resilience and greater success. This family may need medical resources for puberty blockers, hormone therapy, and even surgery someday, but reassurance is what was needed in the moment. When your patient comes out to you, they are trusting you. It is your obligation and privilege as a medical professional to help them begin a journey to an authentic life.
A version of this article first appeared on Medscape.com.
A 16-year-old patient sits in front of you and says, “I think I’m transgender.”
![]()
What do you do?
Whether you are an endocrinologist, family physician, pediatrician, or emergency physician, it’s probably a situation for which medical school education did not sufficiently prepare you. What you know is that you want to do your best to guide your patient and offer every resource necessary for a healthy and happy life. The good news is that your patient trusted you enough to disclose this information to you.
Sadly, this isn’t always the case. About 23% of transgender adults responding to the 2015 U.S. Transgender Survey put off necessary health care because they fear being mistreated or disrespected. Nearly one-third (31%) of survey respondents reported that none of their health care providers knew they were transgender.
Now that your patient feels comfortable enough with you to share this information, you must make sure you do everything in your power to continue to earn your patient’s trust.
Language matters
First, make sure that you are respectful with your terminology. Ask the patient for their name, pronouns, and gender identity. For example: “My name is Dr. Pine, and my pronouns are she/her. What are your pronouns? How do you describe your gender identity?” Each person may have terminology that is specific to their own experience, so allowing people to use their own language is the most respectful method.
People may identify as male, female, transwoman, transman, gender fluid, nonbinary, agender, neutrois, pangender, two-spirit, or other options not listed here. Physicians can be supportive by ensuring that their paperwork or electronic medical systems are sensitive to the needs of the transgender community. Having an option for the patient’s chosen name is courteous to all patients, regardless of gender identity; not everyone uses their legal name in everyday conversation.
Paperwork and electronic medical systems should ask for gender identity and sex assigned at birth, allow write-in options for issues of gender and sexual orientation, and ask for an anatomical inventory or organ inventory so that cancer screening can be conducted for the appropriate body parts.
Questions to ask
Ask patients about their gender journey: How long have they felt this way? How did they come to understand themselves and their gender? When did they start to disclose their experience with others? With pediatric patients, I ask if they have discussed this with their parents/guardians, and if they would like to have that conversation together.
Ask how you can support the patient on their journey. Are they interested in therapy, puberty blockers, hormones, or surgery? People may seek therapy for help coping with internalized transphobia, family rejection, or stigma. They may also want information or support with accessing hormones or surgery. In addition to individual therapy, there are numerous support groups for children, individuals, parents/guardians, and partners, such as PFLAG.org and Genderspectrum.org.
If you are the right kind of doctor and ready to prescribe, you can begin counseling. If not, you should know how to find local resources. The World Professional Association for Transgender Health has a directory of providers, and there are other resources listed below.
What does gender transitioning entail?
There are many components to gender transition. Some transitions may consist primarily of a social transition, with people using a different name, pronouns, and external expression, such as hairstyle and clothing. For others, there may be a medical component.
Mental health care is also an important component of gender transition for children, adolescents, adults, and family members. Mental health concerns are significantly greater in transgender and gender-nonconforming people, with higher rates of depression, anxiety, suicidal ideation, self-harm, substance abuse, eating disorders, and neurodiversity on the autism spectrum. In a study of more than 6,400 transgender people in the United States, 41% reported attempting suicide – a rate 25 times higher than that of the general population. Numerous studies show that hormonal treatment decreases depression, suicidal ideation, and anxiety, and also improves quality of life.
One common misperception, especially when working with children, is that youth transition involves a “sex change” (an outdated term) or any type of surgery. In reality, the main intervention before puberty is psychological support and social transition. The use of a chosen name at school, home, work, and with friends was shown to be associated with lower depression, suicidal ideation, and suicidal behavior. Another study demonstrated that children supported in their identities have mental health similar to that of cisgender siblings and peers.
When puberty approaches, if there is distress around natal pubertal development, then gonadotropin-releasing hormone agonists or “puberty blockers” may be used to temporarily pause the pubertal process, but only after Tanner stage II-III is reached. These medications have been safely used for decades for patients with central precocious puberty. Access to puberty-blocking medication in adolescence (when desired) has been associated with lower rates of suicidal ideation in adulthood and can truly be a lifesaving intervention.
When teens are older, they may choose to take gender-affirming hormone therapy to go through the puberty that is concordant with their affirmed gender. Adults who decide to transition medically may decide to take hormone therapy and may have gender-confirmation surgery, if desired, to align the body with their gender identity and alleviate gender dysphoria. Overall, access to medical care and hormone therapy have been shown to decrease depression, anxiety, and suicidality, and improve quality of life.
Sexuality and fertility
It is important to understand that sexuality is separate from gender identity, and that attraction and sexual activity cannot be assumed. Take a sensitive romantic and sexual history from your patient to get the information necessary to counsel patients about safe relationships and sexual practices. It is important not to make assumptions; a patient who is asexual may still be having sex, and a transgender man may be having receptive vaginal intercourse and may need information about contraception and family planning.
Also, be careful about using clinical language. Some people may want to use anatomical terms, but others may be uncomfortable or triggered by them. For instance, a transgender man may use “chest” for breasts, or “genital canal,” and “junk,” “dick,” or “front hole” for the vagina. Ask patients what terms they prefer to use.
It is also important to consider the impact that medical and surgical interventions may have on fertility, especially when discussing the topic with children and adolescents who may not have spent much time thinking about family planning. Be careful not to make assumptions about plans for parenthood, and remember that there are many paths to becoming a parent.
What does the patient need right now?
When I was a fourth-year medical student on my outpatient child psychiatry rotation, a 5-year-old child assigned male at birth was guarded and frightened of me until their mother said: “It’s okay, Dr. Elyse likes girl things too,” at which point the child became animated and happy while chatting with me about Barbie dolls. My patient had already endured teasing about gender nonconformity, starting in kindergarten; it was unclear to my patient whether I would be a safe person or a bully.
The mother was kind and affirming, but she also wanted answers. Would her child grow up to be a gay man? Or a transgender woman? Would her child be able to live freely, or would they always be quiet around others, scared of what people might say? Would her child be safe?
We can’t predict the future, but as doctors, we want to use all of our knowledge and tools to help our patients live healthy lives. In this case, it meant helping the mother know how to support her child’s identity, how to advocate for a safe school and community, where to connect with other gender-creative children, and how to tolerate ambiguity and celebrate the child she has, not the child she expected.
We know that people with higher support and higher self-esteem can have greater resilience and greater success. This family may need medical resources for puberty blockers, hormone therapy, and even surgery someday, but reassurance is what was needed in the moment. When your patient comes out to you, they are trusting you. It is your obligation and privilege as a medical professional to help them begin a journey to an authentic life.
A version of this article first appeared on Medscape.com.
A 16-year-old patient sits in front of you and says, “I think I’m transgender.”
![]()
What do you do?
Whether you are an endocrinologist, family physician, pediatrician, or emergency physician, it’s probably a situation for which medical school education did not sufficiently prepare you. What you know is that you want to do your best to guide your patient and offer every resource necessary for a healthy and happy life. The good news is that your patient trusted you enough to disclose this information to you.
Sadly, this isn’t always the case. About 23% of transgender adults responding to the 2015 U.S. Transgender Survey put off necessary health care because they fear being mistreated or disrespected. Nearly one-third (31%) of survey respondents reported that none of their health care providers knew they were transgender.
Now that your patient feels comfortable enough with you to share this information, you must make sure you do everything in your power to continue to earn your patient’s trust.
Language matters
First, make sure that you are respectful with your terminology. Ask the patient for their name, pronouns, and gender identity. For example: “My name is Dr. Pine, and my pronouns are she/her. What are your pronouns? How do you describe your gender identity?” Each person may have terminology that is specific to their own experience, so allowing people to use their own language is the most respectful method.
People may identify as male, female, transwoman, transman, gender fluid, nonbinary, agender, neutrois, pangender, two-spirit, or other options not listed here. Physicians can be supportive by ensuring that their paperwork or electronic medical systems are sensitive to the needs of the transgender community. Having an option for the patient’s chosen name is courteous to all patients, regardless of gender identity; not everyone uses their legal name in everyday conversation.
Paperwork and electronic medical systems should ask for gender identity and sex assigned at birth, allow write-in options for issues of gender and sexual orientation, and ask for an anatomical inventory or organ inventory so that cancer screening can be conducted for the appropriate body parts.
Questions to ask
Ask patients about their gender journey: How long have they felt this way? How did they come to understand themselves and their gender? When did they start to disclose their experience with others? With pediatric patients, I ask if they have discussed this with their parents/guardians, and if they would like to have that conversation together.
Ask how you can support the patient on their journey. Are they interested in therapy, puberty blockers, hormones, or surgery? People may seek therapy for help coping with internalized transphobia, family rejection, or stigma. They may also want information or support with accessing hormones or surgery. In addition to individual therapy, there are numerous support groups for children, individuals, parents/guardians, and partners, such as PFLAG.org and Genderspectrum.org.
If you are the right kind of doctor and ready to prescribe, you can begin counseling. If not, you should know how to find local resources. The World Professional Association for Transgender Health has a directory of providers, and there are other resources listed below.
What does gender transitioning entail?
There are many components to gender transition. Some transitions may consist primarily of a social transition, with people using a different name, pronouns, and external expression, such as hairstyle and clothing. For others, there may be a medical component.
Mental health care is also an important component of gender transition for children, adolescents, adults, and family members. Mental health concerns are significantly greater in transgender and gender-nonconforming people, with higher rates of depression, anxiety, suicidal ideation, self-harm, substance abuse, eating disorders, and neurodiversity on the autism spectrum. In a study of more than 6,400 transgender people in the United States, 41% reported attempting suicide – a rate 25 times higher than that of the general population. Numerous studies show that hormonal treatment decreases depression, suicidal ideation, and anxiety, and also improves quality of life.
One common misperception, especially when working with children, is that youth transition involves a “sex change” (an outdated term) or any type of surgery. In reality, the main intervention before puberty is psychological support and social transition. The use of a chosen name at school, home, work, and with friends was shown to be associated with lower depression, suicidal ideation, and suicidal behavior. Another study demonstrated that children supported in their identities have mental health similar to that of cisgender siblings and peers.
When puberty approaches, if there is distress around natal pubertal development, then gonadotropin-releasing hormone agonists or “puberty blockers” may be used to temporarily pause the pubertal process, but only after Tanner stage II-III is reached. These medications have been safely used for decades for patients with central precocious puberty. Access to puberty-blocking medication in adolescence (when desired) has been associated with lower rates of suicidal ideation in adulthood and can truly be a lifesaving intervention.
When teens are older, they may choose to take gender-affirming hormone therapy to go through the puberty that is concordant with their affirmed gender. Adults who decide to transition medically may decide to take hormone therapy and may have gender-confirmation surgery, if desired, to align the body with their gender identity and alleviate gender dysphoria. Overall, access to medical care and hormone therapy have been shown to decrease depression, anxiety, and suicidality, and improve quality of life.
Sexuality and fertility
It is important to understand that sexuality is separate from gender identity, and that attraction and sexual activity cannot be assumed. Take a sensitive romantic and sexual history from your patient to get the information necessary to counsel patients about safe relationships and sexual practices. It is important not to make assumptions; a patient who is asexual may still be having sex, and a transgender man may be having receptive vaginal intercourse and may need information about contraception and family planning.
Also, be careful about using clinical language. Some people may want to use anatomical terms, but others may be uncomfortable or triggered by them. For instance, a transgender man may use “chest” for breasts, or “genital canal,” and “junk,” “dick,” or “front hole” for the vagina. Ask patients what terms they prefer to use.
It is also important to consider the impact that medical and surgical interventions may have on fertility, especially when discussing the topic with children and adolescents who may not have spent much time thinking about family planning. Be careful not to make assumptions about plans for parenthood, and remember that there are many paths to becoming a parent.
What does the patient need right now?
When I was a fourth-year medical student on my outpatient child psychiatry rotation, a 5-year-old child assigned male at birth was guarded and frightened of me until their mother said: “It’s okay, Dr. Elyse likes girl things too,” at which point the child became animated and happy while chatting with me about Barbie dolls. My patient had already endured teasing about gender nonconformity, starting in kindergarten; it was unclear to my patient whether I would be a safe person or a bully.
The mother was kind and affirming, but she also wanted answers. Would her child grow up to be a gay man? Or a transgender woman? Would her child be able to live freely, or would they always be quiet around others, scared of what people might say? Would her child be safe?
We can’t predict the future, but as doctors, we want to use all of our knowledge and tools to help our patients live healthy lives. In this case, it meant helping the mother know how to support her child’s identity, how to advocate for a safe school and community, where to connect with other gender-creative children, and how to tolerate ambiguity and celebrate the child she has, not the child she expected.
We know that people with higher support and higher self-esteem can have greater resilience and greater success. This family may need medical resources for puberty blockers, hormone therapy, and even surgery someday, but reassurance is what was needed in the moment. When your patient comes out to you, they are trusting you. It is your obligation and privilege as a medical professional to help them begin a journey to an authentic life.
A version of this article first appeared on Medscape.com.
ACOG advises on care for transgender patients
Transgender patients have unique needs regarding obstetric and gynecologic care as well as preventive care, and ob.gyns. can help by providing support, education, and understanding, according to new guidance from the American College of Obstetricians and Gynecologists.
“The American College of Obstetricians and Gynecologists opposes discrimination on the basis of gender identity, urges public and private health insurance plans to cover necessary services for individuals with gender dysphoria, and advocates for inclusive, thoughtful, and affirming care for transgender individuals,” according to the committee opinion, published in the March issue of Obstetrics & Gynecology. The opinion was developed jointly by ACOG’s Committee on Gynecologic Practice and Committee on Health Care for Underserved Women, led by Beth Cronin, MD, of Brown University, Providence, R.I., and Colleen K, Stockdale, MD, of the University of Iowa, Iowa City.
“Lack of awareness, knowledge, and sensitivity, as well as bias from health care professionals leads to inadequate access to, underuse of, and inequities within the health care system for transgender patients,” the authors wrote.
The committee opinion provides guidance for ob.gyns. on topics including inclusivity, routine screening, fertility and reproductive issues, hormone therapy, medication use, and surgery.
“One of the most incredible things about being an ob.gyn. is that this field is a hybrid of primary care and surgical practice,” said K. Ashley Brandt, DO, in an interview. “Many patients seek out care from ob.gyns. for routine screening such as a Pap test, for initiation of hormone therapy, or for postoperative management,” said Dr. Brandt, an ob.gyn. and a plastic surgeon at Reading Hospital/Tower Health System in West Reading, Pa. “Many of my colleagues are starting to see an increase in transgender and gender-nonconforming individuals and do not know where to access resources or information on basic care needs. I think ACOG issuing this guidance is a great first step in providing an overview for the ob.gyn., who otherwise haven’t had formal training in transgender medicine,” she emphasized.
Dr. Brandt said she was not surprised by any of the recommendations. “These recommendations, while evolving and updating as new data emerge, have been in place by WPATH (the World Professional Association for Transgender Health) and the Endocrine Society for quite some time,” she noted. “However, this updated committee opinion is a summary of recommendations that are relevant to the clinical practice of an ob.gyn.”
“Since the publication of Care for Transgender Adolescents (2017) and Healthcare for Transgender Individuals (2011), there has been an exponential increase in data that have helped to improve and guide best practices for this patient population including better defining risks, needs, therapy, and follow-up,” said Nancy Sokkary, MD, a specialist in pediatric and adolescent gynecology in Macon, Ga., in an interview. “This document also served as an opportunity for ACOG to educate ob.gyns. about health inequities and emphasize need for gender-affirming and inclusive care,” she said.
“These recommendations are consistent with literature that has been published over the last several years,” she added. “It is certainly important for ob.gyns. to have a document unequivocally supporting hysterectomies and bilateral salpingo-oophorectomy as medically necessary for transgender patients that desire these procedures for their transition.”
Inclusive environment
Approximately 1.4 million adults and 150,000 youth aged 13-17 years in the United States identify as transgender, but these individuals are often marginalized socially and economically, which can lead to worse health outcomes, according to the committee. “Creating a safe and affirming health care environment for all patients, including transgender individuals, is essential,” the authors said. Steps to create a supportive office setting include educating staff to avoid assumptions about sex and gender, and ask appropriately about choice of pronouns and orientation. Use patient forms that reflect a full range of options and places for patients to write in a response. Also, use electronic medical records to track information on use of names other than legal names. “Ob.gyns. play an important role in caring for gender-nonconforming people,” said Dr. Sokkary. “Ob.gyn. providers may have varying levels of participation in gender-affirming hormone or surgery provision, but they can universally conduct routine health maintenance, contraceptive and fertility counseling, and obstetric care in a respectful and inclusive environment,” she said.
Track transition issues
The opinion notes that many gender-transition medications can be prescribed not only by ob.gyns., but by a range of health care professionals with training and education. When it comes to medication and surgery, neither medication nor surgery is required for legally changing one’s name or gender, but patient desires vary from those seeking only letters of support for such legal changes to those who want to pursue hormone therapy or procedures such as chest surgery, hysterectomy, or phalloplasty.
Transgender patients seeking care from ob.gyns. include transmasculine and transfeminine individuals who are seeking various degrees of masculinizing or feminizing therapies.
Masculinizing therapies may result in development of facial hair, deepening voice, and changes in muscle mass, but patients undergoing masculinizing therapies should be reminded of the potential for continued ovulation, according to the opinion. “The only absolute contraindications to masculinizing hormone therapy are current pregnancy, unstable coronary artery disease, and polycythemia (hematocrit greater than 55%),” the authors wrote.
Feminizing therapies have no absolute contraindications, but “risks include venous thromboembolism (VTE), hypertriglyceridemia, development of gallstones, and elevated liver enzymes,” they noted.
Talk about sex and fertility
Clinicians treating transgender patients should discuss fertility and parenting early in the process of any gender transition, ideally before the patient undergoes hormone therapy or surgery, according to the opinion. Fertility preservation options for transgender patients are the same as for cisgender patients who wish to preserve fertility for various reasons, and include “sperm banking, oocyte preservation, embryo preservation, and in some cases, ovarian or testicular tissue cryopreservation,” the authors noted.
However, patients who do not desire pregnancy but may have the potential to become pregnant or impregnate others should be counseled on contraceptive options and reminded that gender-affirming hormone therapy alone does not provide effective contraception, they emphasized. In addition, “all patients should be counseled on barrier use for prevention of sexually transmitted diseases,” they said.
Consistent routine screening and preventive care
The committee opinion also states that transgender patients should undergo routine screening for any anatomical structures that are present, such as breast cancer screening for transmasculine individuals with breast tissue, and cervical cancer screening for those with a cervix. Transfeminine individuals should undergo prostate cancer screening in accordance with the recommendations for cisgender men, the authors said.
“As for all patients, transgender individuals should be counseled about the importance of routine preventive health care,” according to the opinion. “All individuals should be routinely screened for intimate partner violence, depression, substance use, cancer, and other health care needs and should be screened for sexually transmitted infections and counseled about appropriate immunizations based on age and risk factors, including HPV vaccination,” the authors said.
“We continue to see patient discrimination and discomfort with the medical system as a barrier to preventive care among gender-nonconforming individuals,” said Dr. Sokkary. “[Ensuring] that your clinic is a safe, inclusive place is a good start. Also, having providers such as ob.gyns. and family medicine physicians provide gender-affirming care in addition to routine screening and testing is helpful,” she said.
One of the ongoing challenges of counseling transgender patients across a range of age groups, from youth through menopause, is a lack of data on the long-term effects of hormone therapy or surgical intervention, Dr. Brandt noted. “Since there is a paucity of this information, many of the screening recommendations fall in line with that of cisgender patients; however, this is not always the case as screening is determined by hormonal usage, risk factors, and surgical state. It is important for clinicians to be aware of evolutions in screening that will continue to occur as more evidence becomes available,” she emphasized.
In addition, “This document did not include specific guidance for transgender and gender-diverse adolescents, and there are many factors and recommendations that are unique to this population,” Dr. Sokkary said.
Barriers and overcoming them
The main barrier to care with transgender and gender-nonconfirming patients is access to care and finding providers who are competent in gender-affirming health, Dr. Brandt noted. “Another significant barrier involves caring for transgender male patients in a traditionally ‘women’s health’ specialty,” she said. “While the office of an ob.gyn. can be very affirming for transgender women, it has the potential to exacerbate discomfort in transgender male patients,” she noted. “Having gender-affirming posters and pamphlets in the waiting area are ways to make patients feel more at ease. Another of the ways to overcome this barrier is education of the staff and health care providers,” added Dr. Brandt. “Fortunately, this is starting to occur at medical school and residency levels. For ob.gyns. already in practice, articles such as this committee opinion can serve as a resource for providers seeking to understand health care needs of this community,” she said.
“Cost and insurance coverage continue to be barriers, but this has improved immensely: There are now several local and national resources that can help with this depending on the issue,” said Dr. Sokkary. “Additionally, we still lack robust data that define cancer risk among transgender individuals, and until we have more evidence-based recommendations providers should follow screening outlined in this document,” she said.
Use the ACOG opinion as a starting point
“This committee opinion is a great introduction and summary for ob.gyns. seeking to understand basic care needs for gender-nonconforming individuals,” said Dr. Brandt. “However, I strongly encourage ob.gyns. who wish to truly incorporate gender-affirming care as part of their routine clinical practice to participate in continuing education, read the WPATH standards of care among many of the resources provided in the committee opinion, and attend conferences that are specific to transgender health and medicine,” she said.
The opinion received no outside funding. The authors were vetted by ACOG and had no relevant financial conflicts to disclose. Dr. Brandt had no financial conflicts to disclose. Dr. Sokkary had no financial conflicts to disclose.
Transgender patients have unique needs regarding obstetric and gynecologic care as well as preventive care, and ob.gyns. can help by providing support, education, and understanding, according to new guidance from the American College of Obstetricians and Gynecologists.
“The American College of Obstetricians and Gynecologists opposes discrimination on the basis of gender identity, urges public and private health insurance plans to cover necessary services for individuals with gender dysphoria, and advocates for inclusive, thoughtful, and affirming care for transgender individuals,” according to the committee opinion, published in the March issue of Obstetrics & Gynecology. The opinion was developed jointly by ACOG’s Committee on Gynecologic Practice and Committee on Health Care for Underserved Women, led by Beth Cronin, MD, of Brown University, Providence, R.I., and Colleen K, Stockdale, MD, of the University of Iowa, Iowa City.
“Lack of awareness, knowledge, and sensitivity, as well as bias from health care professionals leads to inadequate access to, underuse of, and inequities within the health care system for transgender patients,” the authors wrote.
The committee opinion provides guidance for ob.gyns. on topics including inclusivity, routine screening, fertility and reproductive issues, hormone therapy, medication use, and surgery.
“One of the most incredible things about being an ob.gyn. is that this field is a hybrid of primary care and surgical practice,” said K. Ashley Brandt, DO, in an interview. “Many patients seek out care from ob.gyns. for routine screening such as a Pap test, for initiation of hormone therapy, or for postoperative management,” said Dr. Brandt, an ob.gyn. and a plastic surgeon at Reading Hospital/Tower Health System in West Reading, Pa. “Many of my colleagues are starting to see an increase in transgender and gender-nonconforming individuals and do not know where to access resources or information on basic care needs. I think ACOG issuing this guidance is a great first step in providing an overview for the ob.gyn., who otherwise haven’t had formal training in transgender medicine,” she emphasized.
Dr. Brandt said she was not surprised by any of the recommendations. “These recommendations, while evolving and updating as new data emerge, have been in place by WPATH (the World Professional Association for Transgender Health) and the Endocrine Society for quite some time,” she noted. “However, this updated committee opinion is a summary of recommendations that are relevant to the clinical practice of an ob.gyn.”
“Since the publication of Care for Transgender Adolescents (2017) and Healthcare for Transgender Individuals (2011), there has been an exponential increase in data that have helped to improve and guide best practices for this patient population including better defining risks, needs, therapy, and follow-up,” said Nancy Sokkary, MD, a specialist in pediatric and adolescent gynecology in Macon, Ga., in an interview. “This document also served as an opportunity for ACOG to educate ob.gyns. about health inequities and emphasize need for gender-affirming and inclusive care,” she said.
“These recommendations are consistent with literature that has been published over the last several years,” she added. “It is certainly important for ob.gyns. to have a document unequivocally supporting hysterectomies and bilateral salpingo-oophorectomy as medically necessary for transgender patients that desire these procedures for their transition.”
Inclusive environment
Approximately 1.4 million adults and 150,000 youth aged 13-17 years in the United States identify as transgender, but these individuals are often marginalized socially and economically, which can lead to worse health outcomes, according to the committee. “Creating a safe and affirming health care environment for all patients, including transgender individuals, is essential,” the authors said. Steps to create a supportive office setting include educating staff to avoid assumptions about sex and gender, and ask appropriately about choice of pronouns and orientation. Use patient forms that reflect a full range of options and places for patients to write in a response. Also, use electronic medical records to track information on use of names other than legal names. “Ob.gyns. play an important role in caring for gender-nonconforming people,” said Dr. Sokkary. “Ob.gyn. providers may have varying levels of participation in gender-affirming hormone or surgery provision, but they can universally conduct routine health maintenance, contraceptive and fertility counseling, and obstetric care in a respectful and inclusive environment,” she said.
Track transition issues
The opinion notes that many gender-transition medications can be prescribed not only by ob.gyns., but by a range of health care professionals with training and education. When it comes to medication and surgery, neither medication nor surgery is required for legally changing one’s name or gender, but patient desires vary from those seeking only letters of support for such legal changes to those who want to pursue hormone therapy or procedures such as chest surgery, hysterectomy, or phalloplasty.
Transgender patients seeking care from ob.gyns. include transmasculine and transfeminine individuals who are seeking various degrees of masculinizing or feminizing therapies.
Masculinizing therapies may result in development of facial hair, deepening voice, and changes in muscle mass, but patients undergoing masculinizing therapies should be reminded of the potential for continued ovulation, according to the opinion. “The only absolute contraindications to masculinizing hormone therapy are current pregnancy, unstable coronary artery disease, and polycythemia (hematocrit greater than 55%),” the authors wrote.
Feminizing therapies have no absolute contraindications, but “risks include venous thromboembolism (VTE), hypertriglyceridemia, development of gallstones, and elevated liver enzymes,” they noted.
Talk about sex and fertility
Clinicians treating transgender patients should discuss fertility and parenting early in the process of any gender transition, ideally before the patient undergoes hormone therapy or surgery, according to the opinion. Fertility preservation options for transgender patients are the same as for cisgender patients who wish to preserve fertility for various reasons, and include “sperm banking, oocyte preservation, embryo preservation, and in some cases, ovarian or testicular tissue cryopreservation,” the authors noted.
However, patients who do not desire pregnancy but may have the potential to become pregnant or impregnate others should be counseled on contraceptive options and reminded that gender-affirming hormone therapy alone does not provide effective contraception, they emphasized. In addition, “all patients should be counseled on barrier use for prevention of sexually transmitted diseases,” they said.
Consistent routine screening and preventive care
The committee opinion also states that transgender patients should undergo routine screening for any anatomical structures that are present, such as breast cancer screening for transmasculine individuals with breast tissue, and cervical cancer screening for those with a cervix. Transfeminine individuals should undergo prostate cancer screening in accordance with the recommendations for cisgender men, the authors said.
“As for all patients, transgender individuals should be counseled about the importance of routine preventive health care,” according to the opinion. “All individuals should be routinely screened for intimate partner violence, depression, substance use, cancer, and other health care needs and should be screened for sexually transmitted infections and counseled about appropriate immunizations based on age and risk factors, including HPV vaccination,” the authors said.
“We continue to see patient discrimination and discomfort with the medical system as a barrier to preventive care among gender-nonconforming individuals,” said Dr. Sokkary. “[Ensuring] that your clinic is a safe, inclusive place is a good start. Also, having providers such as ob.gyns. and family medicine physicians provide gender-affirming care in addition to routine screening and testing is helpful,” she said.
One of the ongoing challenges of counseling transgender patients across a range of age groups, from youth through menopause, is a lack of data on the long-term effects of hormone therapy or surgical intervention, Dr. Brandt noted. “Since there is a paucity of this information, many of the screening recommendations fall in line with that of cisgender patients; however, this is not always the case as screening is determined by hormonal usage, risk factors, and surgical state. It is important for clinicians to be aware of evolutions in screening that will continue to occur as more evidence becomes available,” she emphasized.
In addition, “This document did not include specific guidance for transgender and gender-diverse adolescents, and there are many factors and recommendations that are unique to this population,” Dr. Sokkary said.
Barriers and overcoming them
The main barrier to care with transgender and gender-nonconfirming patients is access to care and finding providers who are competent in gender-affirming health, Dr. Brandt noted. “Another significant barrier involves caring for transgender male patients in a traditionally ‘women’s health’ specialty,” she said. “While the office of an ob.gyn. can be very affirming for transgender women, it has the potential to exacerbate discomfort in transgender male patients,” she noted. “Having gender-affirming posters and pamphlets in the waiting area are ways to make patients feel more at ease. Another of the ways to overcome this barrier is education of the staff and health care providers,” added Dr. Brandt. “Fortunately, this is starting to occur at medical school and residency levels. For ob.gyns. already in practice, articles such as this committee opinion can serve as a resource for providers seeking to understand health care needs of this community,” she said.
“Cost and insurance coverage continue to be barriers, but this has improved immensely: There are now several local and national resources that can help with this depending on the issue,” said Dr. Sokkary. “Additionally, we still lack robust data that define cancer risk among transgender individuals, and until we have more evidence-based recommendations providers should follow screening outlined in this document,” she said.
Use the ACOG opinion as a starting point
“This committee opinion is a great introduction and summary for ob.gyns. seeking to understand basic care needs for gender-nonconforming individuals,” said Dr. Brandt. “However, I strongly encourage ob.gyns. who wish to truly incorporate gender-affirming care as part of their routine clinical practice to participate in continuing education, read the WPATH standards of care among many of the resources provided in the committee opinion, and attend conferences that are specific to transgender health and medicine,” she said.
The opinion received no outside funding. The authors were vetted by ACOG and had no relevant financial conflicts to disclose. Dr. Brandt had no financial conflicts to disclose. Dr. Sokkary had no financial conflicts to disclose.
Transgender patients have unique needs regarding obstetric and gynecologic care as well as preventive care, and ob.gyns. can help by providing support, education, and understanding, according to new guidance from the American College of Obstetricians and Gynecologists.
“The American College of Obstetricians and Gynecologists opposes discrimination on the basis of gender identity, urges public and private health insurance plans to cover necessary services for individuals with gender dysphoria, and advocates for inclusive, thoughtful, and affirming care for transgender individuals,” according to the committee opinion, published in the March issue of Obstetrics & Gynecology. The opinion was developed jointly by ACOG’s Committee on Gynecologic Practice and Committee on Health Care for Underserved Women, led by Beth Cronin, MD, of Brown University, Providence, R.I., and Colleen K, Stockdale, MD, of the University of Iowa, Iowa City.
“Lack of awareness, knowledge, and sensitivity, as well as bias from health care professionals leads to inadequate access to, underuse of, and inequities within the health care system for transgender patients,” the authors wrote.
The committee opinion provides guidance for ob.gyns. on topics including inclusivity, routine screening, fertility and reproductive issues, hormone therapy, medication use, and surgery.
“One of the most incredible things about being an ob.gyn. is that this field is a hybrid of primary care and surgical practice,” said K. Ashley Brandt, DO, in an interview. “Many patients seek out care from ob.gyns. for routine screening such as a Pap test, for initiation of hormone therapy, or for postoperative management,” said Dr. Brandt, an ob.gyn. and a plastic surgeon at Reading Hospital/Tower Health System in West Reading, Pa. “Many of my colleagues are starting to see an increase in transgender and gender-nonconforming individuals and do not know where to access resources or information on basic care needs. I think ACOG issuing this guidance is a great first step in providing an overview for the ob.gyn., who otherwise haven’t had formal training in transgender medicine,” she emphasized.
Dr. Brandt said she was not surprised by any of the recommendations. “These recommendations, while evolving and updating as new data emerge, have been in place by WPATH (the World Professional Association for Transgender Health) and the Endocrine Society for quite some time,” she noted. “However, this updated committee opinion is a summary of recommendations that are relevant to the clinical practice of an ob.gyn.”
“Since the publication of Care for Transgender Adolescents (2017) and Healthcare for Transgender Individuals (2011), there has been an exponential increase in data that have helped to improve and guide best practices for this patient population including better defining risks, needs, therapy, and follow-up,” said Nancy Sokkary, MD, a specialist in pediatric and adolescent gynecology in Macon, Ga., in an interview. “This document also served as an opportunity for ACOG to educate ob.gyns. about health inequities and emphasize need for gender-affirming and inclusive care,” she said.
“These recommendations are consistent with literature that has been published over the last several years,” she added. “It is certainly important for ob.gyns. to have a document unequivocally supporting hysterectomies and bilateral salpingo-oophorectomy as medically necessary for transgender patients that desire these procedures for their transition.”
Inclusive environment
Approximately 1.4 million adults and 150,000 youth aged 13-17 years in the United States identify as transgender, but these individuals are often marginalized socially and economically, which can lead to worse health outcomes, according to the committee. “Creating a safe and affirming health care environment for all patients, including transgender individuals, is essential,” the authors said. Steps to create a supportive office setting include educating staff to avoid assumptions about sex and gender, and ask appropriately about choice of pronouns and orientation. Use patient forms that reflect a full range of options and places for patients to write in a response. Also, use electronic medical records to track information on use of names other than legal names. “Ob.gyns. play an important role in caring for gender-nonconforming people,” said Dr. Sokkary. “Ob.gyn. providers may have varying levels of participation in gender-affirming hormone or surgery provision, but they can universally conduct routine health maintenance, contraceptive and fertility counseling, and obstetric care in a respectful and inclusive environment,” she said.
Track transition issues
The opinion notes that many gender-transition medications can be prescribed not only by ob.gyns., but by a range of health care professionals with training and education. When it comes to medication and surgery, neither medication nor surgery is required for legally changing one’s name or gender, but patient desires vary from those seeking only letters of support for such legal changes to those who want to pursue hormone therapy or procedures such as chest surgery, hysterectomy, or phalloplasty.
Transgender patients seeking care from ob.gyns. include transmasculine and transfeminine individuals who are seeking various degrees of masculinizing or feminizing therapies.
Masculinizing therapies may result in development of facial hair, deepening voice, and changes in muscle mass, but patients undergoing masculinizing therapies should be reminded of the potential for continued ovulation, according to the opinion. “The only absolute contraindications to masculinizing hormone therapy are current pregnancy, unstable coronary artery disease, and polycythemia (hematocrit greater than 55%),” the authors wrote.
Feminizing therapies have no absolute contraindications, but “risks include venous thromboembolism (VTE), hypertriglyceridemia, development of gallstones, and elevated liver enzymes,” they noted.
Talk about sex and fertility
Clinicians treating transgender patients should discuss fertility and parenting early in the process of any gender transition, ideally before the patient undergoes hormone therapy or surgery, according to the opinion. Fertility preservation options for transgender patients are the same as for cisgender patients who wish to preserve fertility for various reasons, and include “sperm banking, oocyte preservation, embryo preservation, and in some cases, ovarian or testicular tissue cryopreservation,” the authors noted.
However, patients who do not desire pregnancy but may have the potential to become pregnant or impregnate others should be counseled on contraceptive options and reminded that gender-affirming hormone therapy alone does not provide effective contraception, they emphasized. In addition, “all patients should be counseled on barrier use for prevention of sexually transmitted diseases,” they said.
Consistent routine screening and preventive care
The committee opinion also states that transgender patients should undergo routine screening for any anatomical structures that are present, such as breast cancer screening for transmasculine individuals with breast tissue, and cervical cancer screening for those with a cervix. Transfeminine individuals should undergo prostate cancer screening in accordance with the recommendations for cisgender men, the authors said.
“As for all patients, transgender individuals should be counseled about the importance of routine preventive health care,” according to the opinion. “All individuals should be routinely screened for intimate partner violence, depression, substance use, cancer, and other health care needs and should be screened for sexually transmitted infections and counseled about appropriate immunizations based on age and risk factors, including HPV vaccination,” the authors said.
“We continue to see patient discrimination and discomfort with the medical system as a barrier to preventive care among gender-nonconforming individuals,” said Dr. Sokkary. “[Ensuring] that your clinic is a safe, inclusive place is a good start. Also, having providers such as ob.gyns. and family medicine physicians provide gender-affirming care in addition to routine screening and testing is helpful,” she said.
One of the ongoing challenges of counseling transgender patients across a range of age groups, from youth through menopause, is a lack of data on the long-term effects of hormone therapy or surgical intervention, Dr. Brandt noted. “Since there is a paucity of this information, many of the screening recommendations fall in line with that of cisgender patients; however, this is not always the case as screening is determined by hormonal usage, risk factors, and surgical state. It is important for clinicians to be aware of evolutions in screening that will continue to occur as more evidence becomes available,” she emphasized.
In addition, “This document did not include specific guidance for transgender and gender-diverse adolescents, and there are many factors and recommendations that are unique to this population,” Dr. Sokkary said.
Barriers and overcoming them
The main barrier to care with transgender and gender-nonconfirming patients is access to care and finding providers who are competent in gender-affirming health, Dr. Brandt noted. “Another significant barrier involves caring for transgender male patients in a traditionally ‘women’s health’ specialty,” she said. “While the office of an ob.gyn. can be very affirming for transgender women, it has the potential to exacerbate discomfort in transgender male patients,” she noted. “Having gender-affirming posters and pamphlets in the waiting area are ways to make patients feel more at ease. Another of the ways to overcome this barrier is education of the staff and health care providers,” added Dr. Brandt. “Fortunately, this is starting to occur at medical school and residency levels. For ob.gyns. already in practice, articles such as this committee opinion can serve as a resource for providers seeking to understand health care needs of this community,” she said.
“Cost and insurance coverage continue to be barriers, but this has improved immensely: There are now several local and national resources that can help with this depending on the issue,” said Dr. Sokkary. “Additionally, we still lack robust data that define cancer risk among transgender individuals, and until we have more evidence-based recommendations providers should follow screening outlined in this document,” she said.
Use the ACOG opinion as a starting point
“This committee opinion is a great introduction and summary for ob.gyns. seeking to understand basic care needs for gender-nonconforming individuals,” said Dr. Brandt. “However, I strongly encourage ob.gyns. who wish to truly incorporate gender-affirming care as part of their routine clinical practice to participate in continuing education, read the WPATH standards of care among many of the resources provided in the committee opinion, and attend conferences that are specific to transgender health and medicine,” she said.
The opinion received no outside funding. The authors were vetted by ACOG and had no relevant financial conflicts to disclose. Dr. Brandt had no financial conflicts to disclose. Dr. Sokkary had no financial conflicts to disclose.
Large study finds trans men on testosterone at risk for blood clots
Over 10% of transgender men (females transitioning to male) who take testosterone develop high hematocrit levels that could put them at greater risk for a thrombotic event, and the largest increase in levels occurs in the first year after starting therapy, a new Dutch study indicates.
Erythrocytosis, defined as a hematocrit greater than 0.50 L/L, is a potentially serious side effect of testosterone therapy, say Milou Cecilia Madsen, MD, and colleagues in their article published online Feb. 18, 2021, in the Journal of Clinical Endocrinology & Metabolism.
When hematocrit was measured twice, 11.1% of the cohort of 1073 trans men had levels in excess of 0.50 L/L over a 20-year follow-up.
“Erythrocytosis is common in transgender men treated with testosterone, especially in those who smoke, have [a] high BMI [body mass index], and [who] use testosterone injections,” Dr. Madsen, of the VU University Medical Center Amsterdam, said in a statement from the Endocrine Society.
“A reasonable first step in the care of transgender men with high red blood cells while on testosterone is to advise them to quit smoking, switch injectable testosterone to gel, and, if BMI is high, to lose weight,” she added.
First large study of testosterone in trans men with 20-year follow-up
Transgender men often undergo testosterone therapy as part of gender-affirming treatment.
Secondary erythrocytosis, a condition where the body makes too many red blood cells, is a common side effect of testosterone therapy that can increase the risk of thrombolic events, heart attack, and stroke, Dr. Madsen and colleagues explained.
This is the first study of a large cohort of trans men taking testosterone therapy followed for up to 20 years. Because of the large sample size, statistical analysis with many determinants could be performed. And because of the long follow-up, a clear time relation between initiation of testosterone therapy and hematocrit could be studied, they noted.
Participants were part of the Amsterdam Cohort of Gender Dysphoria study, a large cohort of individuals seen at the Center of Expertise on Gender Dysphoria at Amsterdam University Medical Center between 1972 and 2015.
Laboratory measurements taken between 2004 and 2018 were available for analysis. Trans men visited the center every 3-6 months during their first year of testosterone therapy and were then monitored every year or every other year.
Long-acting undecanoate injection was associated with the highest risk of a hematocrit level greater than 0.50 L/L, and the risk of erythrocytosis in those who took long-acting intramuscular injections was about threefold higher, compared with testosterone gel (adjusted odds ratio, 3.1).
In contrast, short-acting ester injections and oral administration of testosterone had a similar risk for erythrocytosis, as did testosterone gel.
Other determinants of elevated hematocrit included smoking, medical history of a number of comorbid conditions, and older age on initiation of testosterone.
In contrast, “higher testosterone levels per se were not associated with an increased odds of hematocrit greater than 0.50 L/L”, the authors noted.
Current advice for trans men based on old guidance for hypogonadism
The authors said that current advice for trans men is based on recommendations for testosterone-treated hypogonadal cis men (those assigned male at birth) from 2008, which advises a hematocrit greater than 0.50 L/L has a moderate to high risk of adverse outcome. For levels greater than 0.54 L/L, cessation of testosterone therapy, a dose reduction, or therapeutic phlebotomy to reduce the risk of adverse events is advised. For levels 0.50-0.54 L/L, no clear advice is given.
But questions remain as to whether these guidelines are applicable to trans men because the duration of testosterone therapy is much longer in trans men and hormone treatment often cannot be discontinued without causing distress.
Meanwhile, hematology guidelines indicate an upper limit for hematocrit for cis females of 0.48 L/L.
“It could be argued that the upper limit for cis females should be applied, as trans men are born with female genetics,” the authors said. “This is a subject for further research.”
Duration of testosterone therapy impacts risk of erythrocytosis
In the study, the researchers found that longer duration of testosterone therapy increased the risk of developing hematocrit levels greater than 0.50 L/L. For example, after 1 year, the cumulative incidence of erythrocytosis was 8%; after 10 years, it was 38%; and after 14 years, it was 50%.
Until more specific guidance is developed for trans men, if hematocrit levels rise to 0.50-0.54 L/L, the researchers suggested taking “reasonable” steps to prevent a further increase:
- Consider switching patients who use injectable testosterone to transdermal products.
- Advise patients with a BMI greater than 25 kg/m2 to lose weight to attain a BMI of 18.5-25.
- Advise patients to stop smoking.
- Pursue treatment optimization for chronic lung disease or sleep apnea.
The study had no external funding. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Over 10% of transgender men (females transitioning to male) who take testosterone develop high hematocrit levels that could put them at greater risk for a thrombotic event, and the largest increase in levels occurs in the first year after starting therapy, a new Dutch study indicates.
Erythrocytosis, defined as a hematocrit greater than 0.50 L/L, is a potentially serious side effect of testosterone therapy, say Milou Cecilia Madsen, MD, and colleagues in their article published online Feb. 18, 2021, in the Journal of Clinical Endocrinology & Metabolism.
When hematocrit was measured twice, 11.1% of the cohort of 1073 trans men had levels in excess of 0.50 L/L over a 20-year follow-up.
“Erythrocytosis is common in transgender men treated with testosterone, especially in those who smoke, have [a] high BMI [body mass index], and [who] use testosterone injections,” Dr. Madsen, of the VU University Medical Center Amsterdam, said in a statement from the Endocrine Society.
“A reasonable first step in the care of transgender men with high red blood cells while on testosterone is to advise them to quit smoking, switch injectable testosterone to gel, and, if BMI is high, to lose weight,” she added.
First large study of testosterone in trans men with 20-year follow-up
Transgender men often undergo testosterone therapy as part of gender-affirming treatment.
Secondary erythrocytosis, a condition where the body makes too many red blood cells, is a common side effect of testosterone therapy that can increase the risk of thrombolic events, heart attack, and stroke, Dr. Madsen and colleagues explained.
This is the first study of a large cohort of trans men taking testosterone therapy followed for up to 20 years. Because of the large sample size, statistical analysis with many determinants could be performed. And because of the long follow-up, a clear time relation between initiation of testosterone therapy and hematocrit could be studied, they noted.
Participants were part of the Amsterdam Cohort of Gender Dysphoria study, a large cohort of individuals seen at the Center of Expertise on Gender Dysphoria at Amsterdam University Medical Center between 1972 and 2015.
Laboratory measurements taken between 2004 and 2018 were available for analysis. Trans men visited the center every 3-6 months during their first year of testosterone therapy and were then monitored every year or every other year.
Long-acting undecanoate injection was associated with the highest risk of a hematocrit level greater than 0.50 L/L, and the risk of erythrocytosis in those who took long-acting intramuscular injections was about threefold higher, compared with testosterone gel (adjusted odds ratio, 3.1).
In contrast, short-acting ester injections and oral administration of testosterone had a similar risk for erythrocytosis, as did testosterone gel.
Other determinants of elevated hematocrit included smoking, medical history of a number of comorbid conditions, and older age on initiation of testosterone.
In contrast, “higher testosterone levels per se were not associated with an increased odds of hematocrit greater than 0.50 L/L”, the authors noted.
Current advice for trans men based on old guidance for hypogonadism
The authors said that current advice for trans men is based on recommendations for testosterone-treated hypogonadal cis men (those assigned male at birth) from 2008, which advises a hematocrit greater than 0.50 L/L has a moderate to high risk of adverse outcome. For levels greater than 0.54 L/L, cessation of testosterone therapy, a dose reduction, or therapeutic phlebotomy to reduce the risk of adverse events is advised. For levels 0.50-0.54 L/L, no clear advice is given.
But questions remain as to whether these guidelines are applicable to trans men because the duration of testosterone therapy is much longer in trans men and hormone treatment often cannot be discontinued without causing distress.
Meanwhile, hematology guidelines indicate an upper limit for hematocrit for cis females of 0.48 L/L.
“It could be argued that the upper limit for cis females should be applied, as trans men are born with female genetics,” the authors said. “This is a subject for further research.”
Duration of testosterone therapy impacts risk of erythrocytosis
In the study, the researchers found that longer duration of testosterone therapy increased the risk of developing hematocrit levels greater than 0.50 L/L. For example, after 1 year, the cumulative incidence of erythrocytosis was 8%; after 10 years, it was 38%; and after 14 years, it was 50%.
Until more specific guidance is developed for trans men, if hematocrit levels rise to 0.50-0.54 L/L, the researchers suggested taking “reasonable” steps to prevent a further increase:
- Consider switching patients who use injectable testosterone to transdermal products.
- Advise patients with a BMI greater than 25 kg/m2 to lose weight to attain a BMI of 18.5-25.
- Advise patients to stop smoking.
- Pursue treatment optimization for chronic lung disease or sleep apnea.
The study had no external funding. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Over 10% of transgender men (females transitioning to male) who take testosterone develop high hematocrit levels that could put them at greater risk for a thrombotic event, and the largest increase in levels occurs in the first year after starting therapy, a new Dutch study indicates.
Erythrocytosis, defined as a hematocrit greater than 0.50 L/L, is a potentially serious side effect of testosterone therapy, say Milou Cecilia Madsen, MD, and colleagues in their article published online Feb. 18, 2021, in the Journal of Clinical Endocrinology & Metabolism.
When hematocrit was measured twice, 11.1% of the cohort of 1073 trans men had levels in excess of 0.50 L/L over a 20-year follow-up.
“Erythrocytosis is common in transgender men treated with testosterone, especially in those who smoke, have [a] high BMI [body mass index], and [who] use testosterone injections,” Dr. Madsen, of the VU University Medical Center Amsterdam, said in a statement from the Endocrine Society.
“A reasonable first step in the care of transgender men with high red blood cells while on testosterone is to advise them to quit smoking, switch injectable testosterone to gel, and, if BMI is high, to lose weight,” she added.
First large study of testosterone in trans men with 20-year follow-up
Transgender men often undergo testosterone therapy as part of gender-affirming treatment.
Secondary erythrocytosis, a condition where the body makes too many red blood cells, is a common side effect of testosterone therapy that can increase the risk of thrombolic events, heart attack, and stroke, Dr. Madsen and colleagues explained.
This is the first study of a large cohort of trans men taking testosterone therapy followed for up to 20 years. Because of the large sample size, statistical analysis with many determinants could be performed. And because of the long follow-up, a clear time relation between initiation of testosterone therapy and hematocrit could be studied, they noted.
Participants were part of the Amsterdam Cohort of Gender Dysphoria study, a large cohort of individuals seen at the Center of Expertise on Gender Dysphoria at Amsterdam University Medical Center between 1972 and 2015.
Laboratory measurements taken between 2004 and 2018 were available for analysis. Trans men visited the center every 3-6 months during their first year of testosterone therapy and were then monitored every year or every other year.
Long-acting undecanoate injection was associated with the highest risk of a hematocrit level greater than 0.50 L/L, and the risk of erythrocytosis in those who took long-acting intramuscular injections was about threefold higher, compared with testosterone gel (adjusted odds ratio, 3.1).
In contrast, short-acting ester injections and oral administration of testosterone had a similar risk for erythrocytosis, as did testosterone gel.
Other determinants of elevated hematocrit included smoking, medical history of a number of comorbid conditions, and older age on initiation of testosterone.
In contrast, “higher testosterone levels per se were not associated with an increased odds of hematocrit greater than 0.50 L/L”, the authors noted.
Current advice for trans men based on old guidance for hypogonadism
The authors said that current advice for trans men is based on recommendations for testosterone-treated hypogonadal cis men (those assigned male at birth) from 2008, which advises a hematocrit greater than 0.50 L/L has a moderate to high risk of adverse outcome. For levels greater than 0.54 L/L, cessation of testosterone therapy, a dose reduction, or therapeutic phlebotomy to reduce the risk of adverse events is advised. For levels 0.50-0.54 L/L, no clear advice is given.
But questions remain as to whether these guidelines are applicable to trans men because the duration of testosterone therapy is much longer in trans men and hormone treatment often cannot be discontinued without causing distress.
Meanwhile, hematology guidelines indicate an upper limit for hematocrit for cis females of 0.48 L/L.
“It could be argued that the upper limit for cis females should be applied, as trans men are born with female genetics,” the authors said. “This is a subject for further research.”
Duration of testosterone therapy impacts risk of erythrocytosis
In the study, the researchers found that longer duration of testosterone therapy increased the risk of developing hematocrit levels greater than 0.50 L/L. For example, after 1 year, the cumulative incidence of erythrocytosis was 8%; after 10 years, it was 38%; and after 14 years, it was 50%.
Until more specific guidance is developed for trans men, if hematocrit levels rise to 0.50-0.54 L/L, the researchers suggested taking “reasonable” steps to prevent a further increase:
- Consider switching patients who use injectable testosterone to transdermal products.
- Advise patients with a BMI greater than 25 kg/m2 to lose weight to attain a BMI of 18.5-25.
- Advise patients to stop smoking.
- Pursue treatment optimization for chronic lung disease or sleep apnea.
The study had no external funding. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The importance of family acceptance for LGBTQ youth
It is well established that LGBTQ individuals experience more health disparities compared with their cisgender, heterosexual counterparts. In general, LGBTQ adolescents and young adults have higher levels of depression, suicide attempts, and substance use than those of their heterosexual peers. However, a key protective factor is family acceptance and support. By encouraging families to modify and change behaviors that are experienced by their LGBTQ children as rejecting and to engage in supportive and affirming behaviors, providers can help families to decrease risk and promote healthy outcomes for LGBTQ youth and young adults. 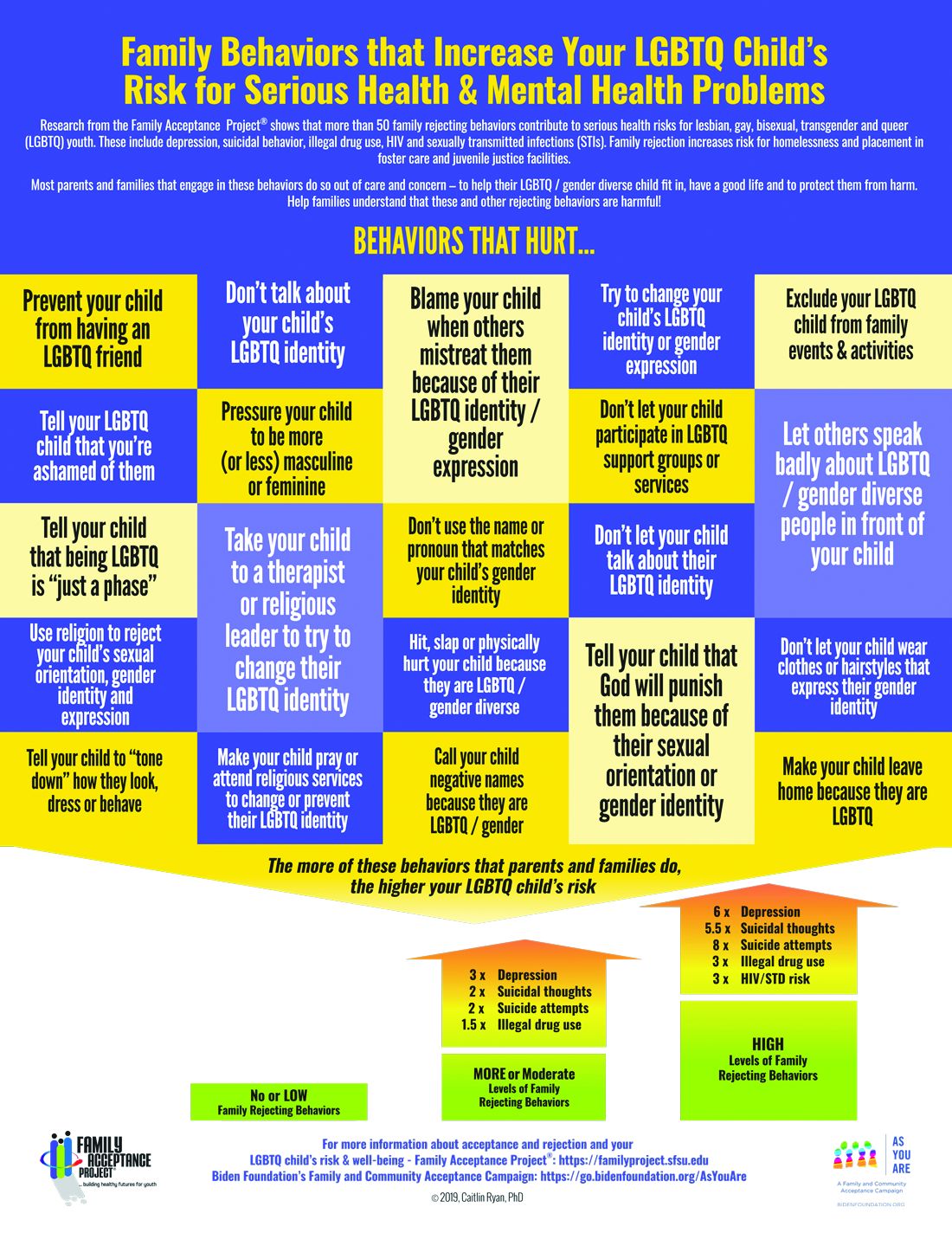
We all know that a supportive family can make a difference for any child, but this is especially true for LGBTQ youth and is critical during a pandemic when young people are confined with families and separated from peers and supportive adults outside the home. Several research studies show that family support can improve outcomes related to suicide, depression, homelessness, drug use, and HIV in LGBTQ young people. Family acceptance improves health outcomes, while rejection undermines family relationships and worsens both health and other serious outcomes such as homelessness and placement in custodial care. Pediatricians can help their patients by educating parents and caregivers with LGBTQ children about the critical role of family support – both those who see themselves as accepting and those who believe that being gay or transgender is wrong and are struggling with parenting a child who identifies as LGBTQ or who is gender diverse.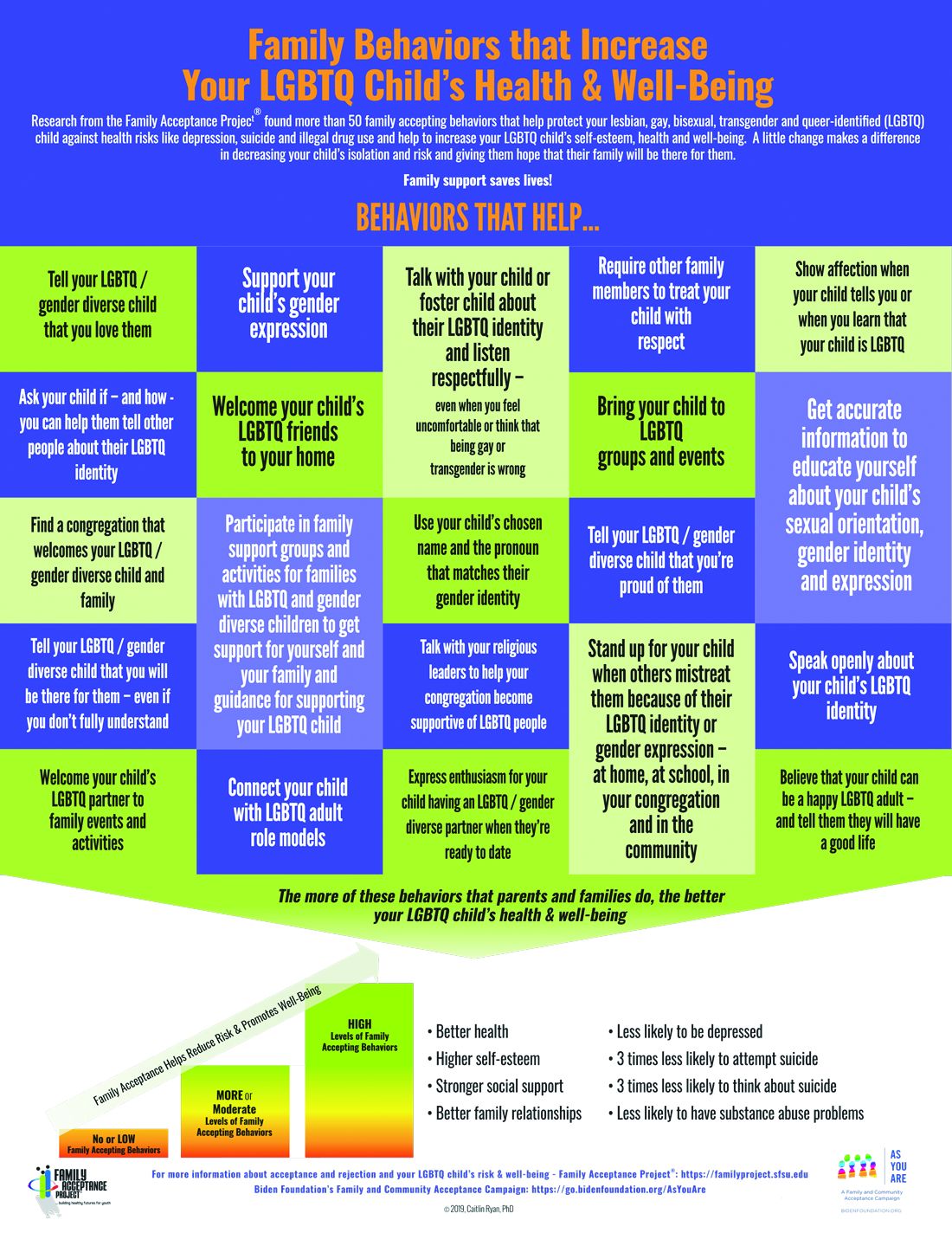
The Family Acceptance Project (FAP) at San Francisco State University conducted the first research on LGBTQ youth and families, developed the first evidence-informed family support model, and has published a range of studies and evidence-based resources that demonstrate the harm caused by family rejection, validate the importance of family acceptance, and provide guidance to increase family support. FAP’s research found that parents and caregivers that engage in rejecting behaviors are typically motivated by care and concern and by trying to protect their children from harm. They believe such behaviors will help their LGBTQ children fit in, have a good life, meet cultural and religious expectations, and be respected by others.1 FAP’s research identified and measured more than 50 rejecting behaviors that parents and caregivers use to respond to their LGBTQ children. Some of these commonly expressed rejecting behaviors include ridiculing and making disparaging comments about their child and other LGBTQ people; excluding them from family activities; blaming their child when others mistreat them because they are LGBTQ; blocking access to LGBTQ resources including friends, support groups, and activities; and trying to change their child’s sexual orientation and gender identity.2 LGBTQ youth experience these and other such behaviors as hurtful, harmful, and traumatic and may feel that they need to hide or repress their identity which can affect their self-esteem, increase isolation, depression, and risky behaviors.3 Providers working with families of LGBTQ youth should focus on shared goals, such as reducing risk and having a happy, healthy child. Most parents love their children and fear for their well-being. However, many are uninformed about their child’s gender identity and sexual orientation and don’t know how to nurture and support them.
In FAP’s initial study, LGB young people who reported higher levels of family rejection had substantially higher rates of attempted suicide, depression, illegal drug use, and unprotected sex.4 These rates were even more significant among Latino gay and bisexual men.4 Those who are rejected by family are less likely to want to have a family or to be parents themselves5 and have lower educational and income levels.6

To reduce risk, pediatricians should ask LGBTQ patients about family rejecting behaviors and help parents and caregivers to identify and understand the effect of such behaviors to reduce health risks and conflict that can lead to running away, expulsion, and removal from the home. Even decreasing rejecting behaviors to moderate levels can significantly improve negative outcomes.5
Caitlin Ryan, PhD, and her team also identified and measured more than 50 family accepting behaviors that help protect against risk and promote well-being. They found that young adults who experience high levels of family acceptance during adolescence report significantly higher levels of self-esteem, social support, and general health with much lower levels of depression, suicidality, and substance abuse.7 Family accepting and supportive behaviors include talking with the child about their LGBTQ identity; advocating for their LGBTQ child when others mistreat them; requiring other family members to treat their LGBTQ child with respect; and supporting their child’s gender identity.5 FAP has developed an evidence-informed family support model and multilingual educational resources for families, providers, youth and religious leaders to decrease rejection and increase family support. These are available in print copies and for download at familyproject.sfsu.edu.
In addition, Dr. Ryan and colleagues1,4,8 recommend the following guidance for providers:
- Ask LGBTQ adolescents about family reactions to their sexual orientation, gender identity, and expression, and refer to LGBTQ community support programs and for supportive counseling, as needed.
- Identify LGBTQ community support programs and online resources to educate parents about how to help their children. Parents need culturally relevant peer support to help decrease rejection and increase family support.
- Advise parents that negative reactions to their adolescent’s LGBTQ identity may negatively impact their child’s health and mental health while supportive and affirming reactions promote well-being.
- Advise parents and caregivers to modify and change family rejecting behaviors that increase their child’s risk for suicide, depression, substance abuse ,and risky sexual behaviors.
- Expand anticipatory guidance to include information on the need for support and the link between family rejection and negative health problems.
- Provide guidance on sexual orientation and gender identity as part of normative child development during well-baby and early childhood care.
- Use FAP’s multilingual family education booklets and Healthy Futures poster series in family and patient education and provide these materials in clinical and community settings. FAP’s Healthy Futures posters include a poster guidance, a version on family acceptance, a version on family rejection and a family acceptance version for conservative families and settings. They are available in camera-ready art in four sizes in English and Spanish and are forthcoming in five Asian languages: familyproject.sfsu.edu/poster.
Dr. Lawlis is assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures.
Resources
• Family Acceptance Project – consultation and training; evidence-based educational materials for families, providers, religious leaders and youth.
• PFLAG – peer support for parents and friends with LGBTQ children in all states and several other countries.
References
1. Ryan C. Generating a revolution in prevention, wellness & care for LGBT children & youth. Temple Political & Civil Rights Law Review. 2014;23(2):331-44.
2. Ryan C. Healthy Futures Poster Series – Family Accepting & Rejecting Behaviors That Impact LGBTQ Children’s Health & Well-Being. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2019.
3. Ryan C. Family Acceptance Project: Culturally grounded framework for supporting LGBTQ children and youth. J Am Acad Child Adolesc Psychiatr. 2019;58(10):S58-9.
4. Ryan C et al. Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346-52.
5. Ryan C. Supportive families, healthy children: Helping families with lesbian, gay, bisexual & transgender children. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2009.
6. Ryan C et al. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J Homosexuality. 2020;67(2):159-73.
7. Ryan C et al. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nursing. 2010;23(4):205-13. 8. Substance Abuse and Mental Health Services Administration. A Practitioner’s Guide: Helping Families to Support Their LGBT Children. In: Administration SAaMhS, ed. Vol PEP14-LGBTKIDS. Rockville, MD: HHS Publication; 2014.
It is well established that LGBTQ individuals experience more health disparities compared with their cisgender, heterosexual counterparts. In general, LGBTQ adolescents and young adults have higher levels of depression, suicide attempts, and substance use than those of their heterosexual peers. However, a key protective factor is family acceptance and support. By encouraging families to modify and change behaviors that are experienced by their LGBTQ children as rejecting and to engage in supportive and affirming behaviors, providers can help families to decrease risk and promote healthy outcomes for LGBTQ youth and young adults.
We all know that a supportive family can make a difference for any child, but this is especially true for LGBTQ youth and is critical during a pandemic when young people are confined with families and separated from peers and supportive adults outside the home. Several research studies show that family support can improve outcomes related to suicide, depression, homelessness, drug use, and HIV in LGBTQ young people. Family acceptance improves health outcomes, while rejection undermines family relationships and worsens both health and other serious outcomes such as homelessness and placement in custodial care. Pediatricians can help their patients by educating parents and caregivers with LGBTQ children about the critical role of family support – both those who see themselves as accepting and those who believe that being gay or transgender is wrong and are struggling with parenting a child who identifies as LGBTQ or who is gender diverse.
The Family Acceptance Project (FAP) at San Francisco State University conducted the first research on LGBTQ youth and families, developed the first evidence-informed family support model, and has published a range of studies and evidence-based resources that demonstrate the harm caused by family rejection, validate the importance of family acceptance, and provide guidance to increase family support. FAP’s research found that parents and caregivers that engage in rejecting behaviors are typically motivated by care and concern and by trying to protect their children from harm. They believe such behaviors will help their LGBTQ children fit in, have a good life, meet cultural and religious expectations, and be respected by others.1 FAP’s research identified and measured more than 50 rejecting behaviors that parents and caregivers use to respond to their LGBTQ children. Some of these commonly expressed rejecting behaviors include ridiculing and making disparaging comments about their child and other LGBTQ people; excluding them from family activities; blaming their child when others mistreat them because they are LGBTQ; blocking access to LGBTQ resources including friends, support groups, and activities; and trying to change their child’s sexual orientation and gender identity.2 LGBTQ youth experience these and other such behaviors as hurtful, harmful, and traumatic and may feel that they need to hide or repress their identity which can affect their self-esteem, increase isolation, depression, and risky behaviors.3 Providers working with families of LGBTQ youth should focus on shared goals, such as reducing risk and having a happy, healthy child. Most parents love their children and fear for their well-being. However, many are uninformed about their child’s gender identity and sexual orientation and don’t know how to nurture and support them.
In FAP’s initial study, LGB young people who reported higher levels of family rejection had substantially higher rates of attempted suicide, depression, illegal drug use, and unprotected sex.4 These rates were even more significant among Latino gay and bisexual men.4 Those who are rejected by family are less likely to want to have a family or to be parents themselves5 and have lower educational and income levels.6
To reduce risk, pediatricians should ask LGBTQ patients about family rejecting behaviors and help parents and caregivers to identify and understand the effect of such behaviors to reduce health risks and conflict that can lead to running away, expulsion, and removal from the home. Even decreasing rejecting behaviors to moderate levels can significantly improve negative outcomes.5
Caitlin Ryan, PhD, and her team also identified and measured more than 50 family accepting behaviors that help protect against risk and promote well-being. They found that young adults who experience high levels of family acceptance during adolescence report significantly higher levels of self-esteem, social support, and general health with much lower levels of depression, suicidality, and substance abuse.7 Family accepting and supportive behaviors include talking with the child about their LGBTQ identity; advocating for their LGBTQ child when others mistreat them; requiring other family members to treat their LGBTQ child with respect; and supporting their child’s gender identity.5 FAP has developed an evidence-informed family support model and multilingual educational resources for families, providers, youth and religious leaders to decrease rejection and increase family support. These are available in print copies and for download at familyproject.sfsu.edu.
In addition, Dr. Ryan and colleagues1,4,8 recommend the following guidance for providers:
- Ask LGBTQ adolescents about family reactions to their sexual orientation, gender identity, and expression, and refer to LGBTQ community support programs and for supportive counseling, as needed.
- Identify LGBTQ community support programs and online resources to educate parents about how to help their children. Parents need culturally relevant peer support to help decrease rejection and increase family support.
- Advise parents that negative reactions to their adolescent’s LGBTQ identity may negatively impact their child’s health and mental health while supportive and affirming reactions promote well-being.
- Advise parents and caregivers to modify and change family rejecting behaviors that increase their child’s risk for suicide, depression, substance abuse ,and risky sexual behaviors.
- Expand anticipatory guidance to include information on the need for support and the link between family rejection and negative health problems.
- Provide guidance on sexual orientation and gender identity as part of normative child development during well-baby and early childhood care.
- Use FAP’s multilingual family education booklets and Healthy Futures poster series in family and patient education and provide these materials in clinical and community settings. FAP’s Healthy Futures posters include a poster guidance, a version on family acceptance, a version on family rejection and a family acceptance version for conservative families and settings. They are available in camera-ready art in four sizes in English and Spanish and are forthcoming in five Asian languages: familyproject.sfsu.edu/poster.
Dr. Lawlis is assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures.
Resources
• Family Acceptance Project – consultation and training; evidence-based educational materials for families, providers, religious leaders and youth.
• PFLAG – peer support for parents and friends with LGBTQ children in all states and several other countries.
References
1. Ryan C. Generating a revolution in prevention, wellness & care for LGBT children & youth. Temple Political & Civil Rights Law Review. 2014;23(2):331-44.
2. Ryan C. Healthy Futures Poster Series – Family Accepting & Rejecting Behaviors That Impact LGBTQ Children’s Health & Well-Being. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2019.
3. Ryan C. Family Acceptance Project: Culturally grounded framework for supporting LGBTQ children and youth. J Am Acad Child Adolesc Psychiatr. 2019;58(10):S58-9.
4. Ryan C et al. Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346-52.
5. Ryan C. Supportive families, healthy children: Helping families with lesbian, gay, bisexual & transgender children. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2009.
6. Ryan C et al. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J Homosexuality. 2020;67(2):159-73.
7. Ryan C et al. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nursing. 2010;23(4):205-13. 8. Substance Abuse and Mental Health Services Administration. A Practitioner’s Guide: Helping Families to Support Their LGBT Children. In: Administration SAaMhS, ed. Vol PEP14-LGBTKIDS. Rockville, MD: HHS Publication; 2014.
It is well established that LGBTQ individuals experience more health disparities compared with their cisgender, heterosexual counterparts. In general, LGBTQ adolescents and young adults have higher levels of depression, suicide attempts, and substance use than those of their heterosexual peers. However, a key protective factor is family acceptance and support. By encouraging families to modify and change behaviors that are experienced by their LGBTQ children as rejecting and to engage in supportive and affirming behaviors, providers can help families to decrease risk and promote healthy outcomes for LGBTQ youth and young adults.
We all know that a supportive family can make a difference for any child, but this is especially true for LGBTQ youth and is critical during a pandemic when young people are confined with families and separated from peers and supportive adults outside the home. Several research studies show that family support can improve outcomes related to suicide, depression, homelessness, drug use, and HIV in LGBTQ young people. Family acceptance improves health outcomes, while rejection undermines family relationships and worsens both health and other serious outcomes such as homelessness and placement in custodial care. Pediatricians can help their patients by educating parents and caregivers with LGBTQ children about the critical role of family support – both those who see themselves as accepting and those who believe that being gay or transgender is wrong and are struggling with parenting a child who identifies as LGBTQ or who is gender diverse.
The Family Acceptance Project (FAP) at San Francisco State University conducted the first research on LGBTQ youth and families, developed the first evidence-informed family support model, and has published a range of studies and evidence-based resources that demonstrate the harm caused by family rejection, validate the importance of family acceptance, and provide guidance to increase family support. FAP’s research found that parents and caregivers that engage in rejecting behaviors are typically motivated by care and concern and by trying to protect their children from harm. They believe such behaviors will help their LGBTQ children fit in, have a good life, meet cultural and religious expectations, and be respected by others.1 FAP’s research identified and measured more than 50 rejecting behaviors that parents and caregivers use to respond to their LGBTQ children. Some of these commonly expressed rejecting behaviors include ridiculing and making disparaging comments about their child and other LGBTQ people; excluding them from family activities; blaming their child when others mistreat them because they are LGBTQ; blocking access to LGBTQ resources including friends, support groups, and activities; and trying to change their child’s sexual orientation and gender identity.2 LGBTQ youth experience these and other such behaviors as hurtful, harmful, and traumatic and may feel that they need to hide or repress their identity which can affect their self-esteem, increase isolation, depression, and risky behaviors.3 Providers working with families of LGBTQ youth should focus on shared goals, such as reducing risk and having a happy, healthy child. Most parents love their children and fear for their well-being. However, many are uninformed about their child’s gender identity and sexual orientation and don’t know how to nurture and support them.
In FAP’s initial study, LGB young people who reported higher levels of family rejection had substantially higher rates of attempted suicide, depression, illegal drug use, and unprotected sex.4 These rates were even more significant among Latino gay and bisexual men.4 Those who are rejected by family are less likely to want to have a family or to be parents themselves5 and have lower educational and income levels.6
To reduce risk, pediatricians should ask LGBTQ patients about family rejecting behaviors and help parents and caregivers to identify and understand the effect of such behaviors to reduce health risks and conflict that can lead to running away, expulsion, and removal from the home. Even decreasing rejecting behaviors to moderate levels can significantly improve negative outcomes.5
Caitlin Ryan, PhD, and her team also identified and measured more than 50 family accepting behaviors that help protect against risk and promote well-being. They found that young adults who experience high levels of family acceptance during adolescence report significantly higher levels of self-esteem, social support, and general health with much lower levels of depression, suicidality, and substance abuse.7 Family accepting and supportive behaviors include talking with the child about their LGBTQ identity; advocating for their LGBTQ child when others mistreat them; requiring other family members to treat their LGBTQ child with respect; and supporting their child’s gender identity.5 FAP has developed an evidence-informed family support model and multilingual educational resources for families, providers, youth and religious leaders to decrease rejection and increase family support. These are available in print copies and for download at familyproject.sfsu.edu.
In addition, Dr. Ryan and colleagues1,4,8 recommend the following guidance for providers:
- Ask LGBTQ adolescents about family reactions to their sexual orientation, gender identity, and expression, and refer to LGBTQ community support programs and for supportive counseling, as needed.
- Identify LGBTQ community support programs and online resources to educate parents about how to help their children. Parents need culturally relevant peer support to help decrease rejection and increase family support.
- Advise parents that negative reactions to their adolescent’s LGBTQ identity may negatively impact their child’s health and mental health while supportive and affirming reactions promote well-being.
- Advise parents and caregivers to modify and change family rejecting behaviors that increase their child’s risk for suicide, depression, substance abuse ,and risky sexual behaviors.
- Expand anticipatory guidance to include information on the need for support and the link between family rejection and negative health problems.
- Provide guidance on sexual orientation and gender identity as part of normative child development during well-baby and early childhood care.
- Use FAP’s multilingual family education booklets and Healthy Futures poster series in family and patient education and provide these materials in clinical and community settings. FAP’s Healthy Futures posters include a poster guidance, a version on family acceptance, a version on family rejection and a family acceptance version for conservative families and settings. They are available in camera-ready art in four sizes in English and Spanish and are forthcoming in five Asian languages: familyproject.sfsu.edu/poster.
Dr. Lawlis is assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures.
Resources
• Family Acceptance Project – consultation and training; evidence-based educational materials for families, providers, religious leaders and youth.
• PFLAG – peer support for parents and friends with LGBTQ children in all states and several other countries.
References
1. Ryan C. Generating a revolution in prevention, wellness & care for LGBT children & youth. Temple Political & Civil Rights Law Review. 2014;23(2):331-44.
2. Ryan C. Healthy Futures Poster Series – Family Accepting & Rejecting Behaviors That Impact LGBTQ Children’s Health & Well-Being. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2019.
3. Ryan C. Family Acceptance Project: Culturally grounded framework for supporting LGBTQ children and youth. J Am Acad Child Adolesc Psychiatr. 2019;58(10):S58-9.
4. Ryan C et al. Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346-52.
5. Ryan C. Supportive families, healthy children: Helping families with lesbian, gay, bisexual & transgender children. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2009.
6. Ryan C et al. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J Homosexuality. 2020;67(2):159-73.
7. Ryan C et al. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nursing. 2010;23(4):205-13. 8. Substance Abuse and Mental Health Services Administration. A Practitioner’s Guide: Helping Families to Support Their LGBT Children. In: Administration SAaMhS, ed. Vol PEP14-LGBTKIDS. Rockville, MD: HHS Publication; 2014.
First monthly injectable HIV treatment approved by FDA
Cabenuva (cabotegravir and rilpivirine, a once-per-month injectable formulation) was approved by the Food and Drug Administration as a complete regimen for treatment of HIV-1 infection in adults. It is intended to replace current antiretroviral regimens in those patients who are virologically suppressed with no history of treatment failure and with no known or suspected resistance to either of the two component drugs.
Cabenuva is the first FDA-approved monthly injectable, complete regimen for HIV-infected adults, according to the agency’s announcement.
In addition, the FDA-approved Vocabria (cabotegravir, tablet formulation), a preparatory treatment intended to be taken in combination with oral rilpivirine (Edurant) for 1 month prior to starting treatment with Cabenuva to ensure the medications are well tolerated before switching to the extended-release injectable formulation. The FDA granted the approval of Cabenuva and Vocabria to ViiV Healthcare.
Cabotegravir is as an integrase strand transfer inhibitor that blocks HIV integrase by attaching to the active integrase site and inhibiting retroviral DNA integration, which is necessary in order for HIV to replicate. In contrast, rilpivirine acts as a diarylpyrimidine nonnucleoside reverse transcriptase inhibitor of HIV-1.
Approval of Cabenuva was based upon two randomized, open-label, controlled clinical trials in 1,182 HIV-infected adults who were virologically suppressed (HIV-1 RNA less than 50 copies/mL) before initiation of treatment with Cabenuva. The two pivotal phase three clinical studies were: Antiretroviral Therapy as Long-Acting Suppression (ATLAS; NCT02951052) and First Long-Acting Injectable Regimen (FLAIR; NCT02938520). Patients in both trials continued to show virologic suppression at the conclusion of each study, and no clinically relevant change from baseline in CD4+ cell counts was observed, according to the FDA announcement.
Adverse reactions with Cabenuva included injection-site reactions, fever, fatigue, headache, musculoskeletal pain, nausea, sleep disorders, dizziness, and rash. The FDA warned that Cabenuva should not be used if there is a known previous hypersensitivity reaction to cabotegravir or rilpivirine, or in patients who are not virally suppressed (HIV-1 RNA greater than 50 copies/mL).
Cabenuva and Vocabria were granted Fast Track and Priority Review designation by the FDA. Prescribing information for Cabenuva is available on the ViiV Healthcare website.
Cabenuva (cabotegravir and rilpivirine, a once-per-month injectable formulation) was approved by the Food and Drug Administration as a complete regimen for treatment of HIV-1 infection in adults. It is intended to replace current antiretroviral regimens in those patients who are virologically suppressed with no history of treatment failure and with no known or suspected resistance to either of the two component drugs.
Cabenuva is the first FDA-approved monthly injectable, complete regimen for HIV-infected adults, according to the agency’s announcement.
In addition, the FDA-approved Vocabria (cabotegravir, tablet formulation), a preparatory treatment intended to be taken in combination with oral rilpivirine (Edurant) for 1 month prior to starting treatment with Cabenuva to ensure the medications are well tolerated before switching to the extended-release injectable formulation. The FDA granted the approval of Cabenuva and Vocabria to ViiV Healthcare.
Cabotegravir is as an integrase strand transfer inhibitor that blocks HIV integrase by attaching to the active integrase site and inhibiting retroviral DNA integration, which is necessary in order for HIV to replicate. In contrast, rilpivirine acts as a diarylpyrimidine nonnucleoside reverse transcriptase inhibitor of HIV-1.
Approval of Cabenuva was based upon two randomized, open-label, controlled clinical trials in 1,182 HIV-infected adults who were virologically suppressed (HIV-1 RNA less than 50 copies/mL) before initiation of treatment with Cabenuva. The two pivotal phase three clinical studies were: Antiretroviral Therapy as Long-Acting Suppression (ATLAS; NCT02951052) and First Long-Acting Injectable Regimen (FLAIR; NCT02938520). Patients in both trials continued to show virologic suppression at the conclusion of each study, and no clinically relevant change from baseline in CD4+ cell counts was observed, according to the FDA announcement.
Adverse reactions with Cabenuva included injection-site reactions, fever, fatigue, headache, musculoskeletal pain, nausea, sleep disorders, dizziness, and rash. The FDA warned that Cabenuva should not be used if there is a known previous hypersensitivity reaction to cabotegravir or rilpivirine, or in patients who are not virally suppressed (HIV-1 RNA greater than 50 copies/mL).
Cabenuva and Vocabria were granted Fast Track and Priority Review designation by the FDA. Prescribing information for Cabenuva is available on the ViiV Healthcare website.
Cabenuva (cabotegravir and rilpivirine, a once-per-month injectable formulation) was approved by the Food and Drug Administration as a complete regimen for treatment of HIV-1 infection in adults. It is intended to replace current antiretroviral regimens in those patients who are virologically suppressed with no history of treatment failure and with no known or suspected resistance to either of the two component drugs.
Cabenuva is the first FDA-approved monthly injectable, complete regimen for HIV-infected adults, according to the agency’s announcement.
In addition, the FDA-approved Vocabria (cabotegravir, tablet formulation), a preparatory treatment intended to be taken in combination with oral rilpivirine (Edurant) for 1 month prior to starting treatment with Cabenuva to ensure the medications are well tolerated before switching to the extended-release injectable formulation. The FDA granted the approval of Cabenuva and Vocabria to ViiV Healthcare.
Cabotegravir is as an integrase strand transfer inhibitor that blocks HIV integrase by attaching to the active integrase site and inhibiting retroviral DNA integration, which is necessary in order for HIV to replicate. In contrast, rilpivirine acts as a diarylpyrimidine nonnucleoside reverse transcriptase inhibitor of HIV-1.
Approval of Cabenuva was based upon two randomized, open-label, controlled clinical trials in 1,182 HIV-infected adults who were virologically suppressed (HIV-1 RNA less than 50 copies/mL) before initiation of treatment with Cabenuva. The two pivotal phase three clinical studies were: Antiretroviral Therapy as Long-Acting Suppression (ATLAS; NCT02951052) and First Long-Acting Injectable Regimen (FLAIR; NCT02938520). Patients in both trials continued to show virologic suppression at the conclusion of each study, and no clinically relevant change from baseline in CD4+ cell counts was observed, according to the FDA announcement.
Adverse reactions with Cabenuva included injection-site reactions, fever, fatigue, headache, musculoskeletal pain, nausea, sleep disorders, dizziness, and rash. The FDA warned that Cabenuva should not be used if there is a known previous hypersensitivity reaction to cabotegravir or rilpivirine, or in patients who are not virally suppressed (HIV-1 RNA greater than 50 copies/mL).
Cabenuva and Vocabria were granted Fast Track and Priority Review designation by the FDA. Prescribing information for Cabenuva is available on the ViiV Healthcare website.
NEWS FROM THE FDA
TRANSforming gynecology: An introduction to hormone therapy for the obstetrician/gynecologist
Incorporating gender-nonconforming patients into practice can seem like a daunting task at first. However, obstetricians/gynecologists, midwives, and other advanced women’s health care practitioners can provide quality care for both transgender men and women. Basic preventative services such as routine health and cancer screening and testing for sexually transmitted infections does not require specialized training in transgender health. In fact, administration of hormonal therapy and some surgical interventions are well within the scope of practice of the general obstetrician/gynecologist, as long as the provider has undergone appropriate training to achieve expertise. For example, organizations such as the World Professional Association for Transgender Health (WPATH) not only provides standards of care regarding the treatment of transgender individuals, but they also have training and educational opportunities targeted at providers who wish to become certified in more advanced care of the transgender patient. If an obstetrician/gynecologist is interested in prescribing hormone therapy, seeking further training within the field is a must.
It is important to remember that the process by which transgender individuals express their gender is a spectrum. Not all patients who identify as transgender will seek hormone therapy or surgical procedures. However, even if a provider has not undergone more specific training to administer hormone therapy, it is still very important to have a basic understanding of the hormones, routes of administration, and side effects.
While cross-sex hormone therapy does differ in practice, compared with hormone replacement therapy in cisgender counterparts, the principles are relatively similar. Testosterone therapy is the mainstay treatment for transgender men who desire medical transition.1,2 The overall goal of therapy is to achieve testosterone levels within the cisgender male physiologic range (300-1000 ng/dL). While the most common route of administration is subcutaneous or intramuscular injections in weekly, biweekly, or quarterly intervals, other routes may include daily transdermal patches and gels or oral formulations.1 Within the first few months of use, patients will notice signs of masculinization such as increased facial and body hair, increased muscle mass, increased libido, and amenorrhea. Other changes include male-pattern hair loss, clitoromegaly, redistribution of fat, voice deepening, and mood changes.1
Hormone therapy for transgender women is a bit more complicated as estrogen alone will often not achieve feminizing characteristics that are satisfying for patients.3 Estrogen therapy can include oral formulations of 17-beta estradiol or conjugated estrogens, although the latter is typically avoided because of the marked increase in thromboembolic events. Estrogens can also be administered in sublingual, intramuscular, or transdermal forms. Antiandrogens are often required to help decrease endogenous testosterone levels to cisgender female levels (30-100 ng/dL).3 Spironolactone is most commonly prescribed as an adjunct to estrogen therapy. Finasteride and GnRH agonists like leuprolide acetate can also be added if spironolactone is not effective or not tolerated by the patient. Feminizing effects of estrogen can take several months and most commonly include decreased spontaneous erections, decreased libido, breast growth, redistribution of fat to the waist and hips, decreased skin oiliness, and softening of the skin.3
Overall, hormone therapy for both transgender men and women is considered effective, safe, and well tolerated.4 Monitoring is typically performed every 3 months within the first year after initiating hormone therapy, and then continued every 6-12 months thereafter. Routine screening for all organs and tissues present (e.g. prostate, breast) should be undertaken.3 While this simply highlights the therapy and surveillance for patients, it is important to remember that many transgender men and women will see an obstetrician/gynecologist at some interval during their transition. Ultimately, it is paramount that we as obstetricians/gynecologists have a basic understanding of the treatments available so we can provide our patients with competent and compassionate care.
Dr. Brandt is an obstetrician/gynecologist and a plastic surgeon at Reading Hospital/Tower Health System in West Reading, Pa., where she has developed a gender-affirming medical and surgical clinic for ob.gyn. residents and plastic surgeon fellows.
References
1. World Professional Association for Transgender Health. Standards of care for the health of transsexual, transgender, and gender nonconforming people. 7th version. Accessed 10/15/20.
2. Joint meeting of the International Society of Endocrinology and the Endocrine Society 2014; ICE/ENDO 2014, Paper 14354. Accessed 01/08/16.
3. Qian R, Safer JD. Hormone treatment for the adult transgender patient, in “Comprehensive Care of the Transgender Patient,” 1st ed. Philadelphia: Elsevier, 2020, pp. 34-6.
4. Weinand JD and Safer JD. Hormone therapy in transgender adults is safe with provider supervision: A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol. 2015;2(2):55-60.
Incorporating gender-nonconforming patients into practice can seem like a daunting task at first. However, obstetricians/gynecologists, midwives, and other advanced women’s health care practitioners can provide quality care for both transgender men and women. Basic preventative services such as routine health and cancer screening and testing for sexually transmitted infections does not require specialized training in transgender health. In fact, administration of hormonal therapy and some surgical interventions are well within the scope of practice of the general obstetrician/gynecologist, as long as the provider has undergone appropriate training to achieve expertise. For example, organizations such as the World Professional Association for Transgender Health (WPATH) not only provides standards of care regarding the treatment of transgender individuals, but they also have training and educational opportunities targeted at providers who wish to become certified in more advanced care of the transgender patient. If an obstetrician/gynecologist is interested in prescribing hormone therapy, seeking further training within the field is a must.
It is important to remember that the process by which transgender individuals express their gender is a spectrum. Not all patients who identify as transgender will seek hormone therapy or surgical procedures. However, even if a provider has not undergone more specific training to administer hormone therapy, it is still very important to have a basic understanding of the hormones, routes of administration, and side effects.
While cross-sex hormone therapy does differ in practice, compared with hormone replacement therapy in cisgender counterparts, the principles are relatively similar. Testosterone therapy is the mainstay treatment for transgender men who desire medical transition.1,2 The overall goal of therapy is to achieve testosterone levels within the cisgender male physiologic range (300-1000 ng/dL). While the most common route of administration is subcutaneous or intramuscular injections in weekly, biweekly, or quarterly intervals, other routes may include daily transdermal patches and gels or oral formulations.1 Within the first few months of use, patients will notice signs of masculinization such as increased facial and body hair, increased muscle mass, increased libido, and amenorrhea. Other changes include male-pattern hair loss, clitoromegaly, redistribution of fat, voice deepening, and mood changes.1
Hormone therapy for transgender women is a bit more complicated as estrogen alone will often not achieve feminizing characteristics that are satisfying for patients.3 Estrogen therapy can include oral formulations of 17-beta estradiol or conjugated estrogens, although the latter is typically avoided because of the marked increase in thromboembolic events. Estrogens can also be administered in sublingual, intramuscular, or transdermal forms. Antiandrogens are often required to help decrease endogenous testosterone levels to cisgender female levels (30-100 ng/dL).3 Spironolactone is most commonly prescribed as an adjunct to estrogen therapy. Finasteride and GnRH agonists like leuprolide acetate can also be added if spironolactone is not effective or not tolerated by the patient. Feminizing effects of estrogen can take several months and most commonly include decreased spontaneous erections, decreased libido, breast growth, redistribution of fat to the waist and hips, decreased skin oiliness, and softening of the skin.3
Overall, hormone therapy for both transgender men and women is considered effective, safe, and well tolerated.4 Monitoring is typically performed every 3 months within the first year after initiating hormone therapy, and then continued every 6-12 months thereafter. Routine screening for all organs and tissues present (e.g. prostate, breast) should be undertaken.3 While this simply highlights the therapy and surveillance for patients, it is important to remember that many transgender men and women will see an obstetrician/gynecologist at some interval during their transition. Ultimately, it is paramount that we as obstetricians/gynecologists have a basic understanding of the treatments available so we can provide our patients with competent and compassionate care.
Dr. Brandt is an obstetrician/gynecologist and a plastic surgeon at Reading Hospital/Tower Health System in West Reading, Pa., where she has developed a gender-affirming medical and surgical clinic for ob.gyn. residents and plastic surgeon fellows.
References
1. World Professional Association for Transgender Health. Standards of care for the health of transsexual, transgender, and gender nonconforming people. 7th version. Accessed 10/15/20.
2. Joint meeting of the International Society of Endocrinology and the Endocrine Society 2014; ICE/ENDO 2014, Paper 14354. Accessed 01/08/16.
3. Qian R, Safer JD. Hormone treatment for the adult transgender patient, in “Comprehensive Care of the Transgender Patient,” 1st ed. Philadelphia: Elsevier, 2020, pp. 34-6.
4. Weinand JD and Safer JD. Hormone therapy in transgender adults is safe with provider supervision: A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol. 2015;2(2):55-60.
Incorporating gender-nonconforming patients into practice can seem like a daunting task at first. However, obstetricians/gynecologists, midwives, and other advanced women’s health care practitioners can provide quality care for both transgender men and women. Basic preventative services such as routine health and cancer screening and testing for sexually transmitted infections does not require specialized training in transgender health. In fact, administration of hormonal therapy and some surgical interventions are well within the scope of practice of the general obstetrician/gynecologist, as long as the provider has undergone appropriate training to achieve expertise. For example, organizations such as the World Professional Association for Transgender Health (WPATH) not only provides standards of care regarding the treatment of transgender individuals, but they also have training and educational opportunities targeted at providers who wish to become certified in more advanced care of the transgender patient. If an obstetrician/gynecologist is interested in prescribing hormone therapy, seeking further training within the field is a must.
It is important to remember that the process by which transgender individuals express their gender is a spectrum. Not all patients who identify as transgender will seek hormone therapy or surgical procedures. However, even if a provider has not undergone more specific training to administer hormone therapy, it is still very important to have a basic understanding of the hormones, routes of administration, and side effects.
While cross-sex hormone therapy does differ in practice, compared with hormone replacement therapy in cisgender counterparts, the principles are relatively similar. Testosterone therapy is the mainstay treatment for transgender men who desire medical transition.1,2 The overall goal of therapy is to achieve testosterone levels within the cisgender male physiologic range (300-1000 ng/dL). While the most common route of administration is subcutaneous or intramuscular injections in weekly, biweekly, or quarterly intervals, other routes may include daily transdermal patches and gels or oral formulations.1 Within the first few months of use, patients will notice signs of masculinization such as increased facial and body hair, increased muscle mass, increased libido, and amenorrhea. Other changes include male-pattern hair loss, clitoromegaly, redistribution of fat, voice deepening, and mood changes.1
Hormone therapy for transgender women is a bit more complicated as estrogen alone will often not achieve feminizing characteristics that are satisfying for patients.3 Estrogen therapy can include oral formulations of 17-beta estradiol or conjugated estrogens, although the latter is typically avoided because of the marked increase in thromboembolic events. Estrogens can also be administered in sublingual, intramuscular, or transdermal forms. Antiandrogens are often required to help decrease endogenous testosterone levels to cisgender female levels (30-100 ng/dL).3 Spironolactone is most commonly prescribed as an adjunct to estrogen therapy. Finasteride and GnRH agonists like leuprolide acetate can also be added if spironolactone is not effective or not tolerated by the patient. Feminizing effects of estrogen can take several months and most commonly include decreased spontaneous erections, decreased libido, breast growth, redistribution of fat to the waist and hips, decreased skin oiliness, and softening of the skin.3
Overall, hormone therapy for both transgender men and women is considered effective, safe, and well tolerated.4 Monitoring is typically performed every 3 months within the first year after initiating hormone therapy, and then continued every 6-12 months thereafter. Routine screening for all organs and tissues present (e.g. prostate, breast) should be undertaken.3 While this simply highlights the therapy and surveillance for patients, it is important to remember that many transgender men and women will see an obstetrician/gynecologist at some interval during their transition. Ultimately, it is paramount that we as obstetricians/gynecologists have a basic understanding of the treatments available so we can provide our patients with competent and compassionate care.
Dr. Brandt is an obstetrician/gynecologist and a plastic surgeon at Reading Hospital/Tower Health System in West Reading, Pa., where she has developed a gender-affirming medical and surgical clinic for ob.gyn. residents and plastic surgeon fellows.
References
1. World Professional Association for Transgender Health. Standards of care for the health of transsexual, transgender, and gender nonconforming people. 7th version. Accessed 10/15/20.
2. Joint meeting of the International Society of Endocrinology and the Endocrine Society 2014; ICE/ENDO 2014, Paper 14354. Accessed 01/08/16.
3. Qian R, Safer JD. Hormone treatment for the adult transgender patient, in “Comprehensive Care of the Transgender Patient,” 1st ed. Philadelphia: Elsevier, 2020, pp. 34-6.
4. Weinand JD and Safer JD. Hormone therapy in transgender adults is safe with provider supervision: A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol. 2015;2(2):55-60.