User login
Official Newspaper of the American College of Surgeons
Stereotactic laser ablation found feasible for hypothalamic hamartoma
SAN DIEGO – Magnetic resonance-guided stereotactic laser ablation is a safe and effective option in the treatment of hypothalamic hamartoma, results from a multicenter pilot study showed.
At the annual meeting of the American Academy of Neurology, Dr. Daniel J. Curry reported results from 20 patients who have undergone treatment with a Food and Drug Administration–cleared neurosurgical tissue coagulation system called Visualase. Hypothalamic hamartoma (HH) is a rare disorder of pediatric epilepsy with an estimated prevalence of 1:50,000-100,000, said Dr. Curry, director of pediatric surgical epilepsy and functional neurosurgery at Texas Children’s Hospital, Houston.
"The main presentation is the mirthless laughter of gelastic seizures, but patients can have other seizure types," he said. "The diagnosis is frequently delayed, and high seizure burden in the brain can lead to epileptic encephalopathy. Seizures are notoriously resistant to medical managements necessitating surgical intervention ... open, endoscopic, or ablative."
To date, surgical intervention has been limited due to modest outcomes, with 37%-50% achieving seizure freedom. The location of HH tumors makes surgical intervention difficult, and as a result 7%-10% of patients have permanent surgical morbidity.
For the technique using the Visualase, Dr. Curry and his associates at four other medical centers in the United States performed the surgical technique through a single 4-mm incision, a 3.2-mm burr hole, and a 1.65-mm cannula trajectory with Visualase under real-time MR thermography, first with a confirmation test at about 3 W, followed by higher doses of 6-10 W for 50-120 seconds. Temperature limits were set to protect the hypothalamus and basilar artery and optic tract. The surgery had an immediate effect, and patients stayed in the hospital for a mean of 2 days.
The primary measure was seizure frequency at 1 year while the secondary measure was the complication profile of stereotactic laser ablation in epilepsy.
Of the 20 patients, 5 were adults, and the entire study population ranged in age from 22 months to 34 years. A total of 21 ablations were performed in the 20 patients. Dr. Curry reported that all but four patients were seizure free after the procedure. However, the rate of seizures diminished among the four who were not seizure free.
Seizures recurred in one of the pediatric patients. "We re-ablated him and he is now seizure free," Dr. Curry said.
Complications to date have included two missed targets, one case of IV phenytoin toxicity, one case of transient diabetes insipidus, two cases of transient hemiparesis, and one subarachnoid hemorrhage. Perioperative, temporary weight gain was detected in most patients. "With lack of hormonal disturbance, this is thought to be due to the perioperative, high-dose steroid use," Dr. Curry explained.
Postoperative interviews with parents of study participants "have revealed significant improvements in intellectual development, concentration, and interactiveness," he said. "Most families report improvement of mood, decreased behavioral disorders, and rage attacks."
To date, only two patients have completed formal postoperative neuropsychological testing. "There were no significant declines in memory in either patient," Dr. Curry said. One had improved math skills and reading comprehension while the other complained of memory dysfunction but was not below normal on testing.
"We have learned that laser ablation of hypothalamic hamartoma can be accomplished safely," Dr. Curry concluded. "More studies are needed to explain the antiepileptic effect in settings of incomplete radiologic destruction of the target and to advance thermal planning."
Dr. Curry said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Magnetic resonance-guided stereotactic laser ablation is a safe and effective option in the treatment of hypothalamic hamartoma, results from a multicenter pilot study showed.
At the annual meeting of the American Academy of Neurology, Dr. Daniel J. Curry reported results from 20 patients who have undergone treatment with a Food and Drug Administration–cleared neurosurgical tissue coagulation system called Visualase. Hypothalamic hamartoma (HH) is a rare disorder of pediatric epilepsy with an estimated prevalence of 1:50,000-100,000, said Dr. Curry, director of pediatric surgical epilepsy and functional neurosurgery at Texas Children’s Hospital, Houston.
"The main presentation is the mirthless laughter of gelastic seizures, but patients can have other seizure types," he said. "The diagnosis is frequently delayed, and high seizure burden in the brain can lead to epileptic encephalopathy. Seizures are notoriously resistant to medical managements necessitating surgical intervention ... open, endoscopic, or ablative."
To date, surgical intervention has been limited due to modest outcomes, with 37%-50% achieving seizure freedom. The location of HH tumors makes surgical intervention difficult, and as a result 7%-10% of patients have permanent surgical morbidity.
For the technique using the Visualase, Dr. Curry and his associates at four other medical centers in the United States performed the surgical technique through a single 4-mm incision, a 3.2-mm burr hole, and a 1.65-mm cannula trajectory with Visualase under real-time MR thermography, first with a confirmation test at about 3 W, followed by higher doses of 6-10 W for 50-120 seconds. Temperature limits were set to protect the hypothalamus and basilar artery and optic tract. The surgery had an immediate effect, and patients stayed in the hospital for a mean of 2 days.
The primary measure was seizure frequency at 1 year while the secondary measure was the complication profile of stereotactic laser ablation in epilepsy.
Of the 20 patients, 5 were adults, and the entire study population ranged in age from 22 months to 34 years. A total of 21 ablations were performed in the 20 patients. Dr. Curry reported that all but four patients were seizure free after the procedure. However, the rate of seizures diminished among the four who were not seizure free.
Seizures recurred in one of the pediatric patients. "We re-ablated him and he is now seizure free," Dr. Curry said.
Complications to date have included two missed targets, one case of IV phenytoin toxicity, one case of transient diabetes insipidus, two cases of transient hemiparesis, and one subarachnoid hemorrhage. Perioperative, temporary weight gain was detected in most patients. "With lack of hormonal disturbance, this is thought to be due to the perioperative, high-dose steroid use," Dr. Curry explained.
Postoperative interviews with parents of study participants "have revealed significant improvements in intellectual development, concentration, and interactiveness," he said. "Most families report improvement of mood, decreased behavioral disorders, and rage attacks."
To date, only two patients have completed formal postoperative neuropsychological testing. "There were no significant declines in memory in either patient," Dr. Curry said. One had improved math skills and reading comprehension while the other complained of memory dysfunction but was not below normal on testing.
"We have learned that laser ablation of hypothalamic hamartoma can be accomplished safely," Dr. Curry concluded. "More studies are needed to explain the antiepileptic effect in settings of incomplete radiologic destruction of the target and to advance thermal planning."
Dr. Curry said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Magnetic resonance-guided stereotactic laser ablation is a safe and effective option in the treatment of hypothalamic hamartoma, results from a multicenter pilot study showed.
At the annual meeting of the American Academy of Neurology, Dr. Daniel J. Curry reported results from 20 patients who have undergone treatment with a Food and Drug Administration–cleared neurosurgical tissue coagulation system called Visualase. Hypothalamic hamartoma (HH) is a rare disorder of pediatric epilepsy with an estimated prevalence of 1:50,000-100,000, said Dr. Curry, director of pediatric surgical epilepsy and functional neurosurgery at Texas Children’s Hospital, Houston.
"The main presentation is the mirthless laughter of gelastic seizures, but patients can have other seizure types," he said. "The diagnosis is frequently delayed, and high seizure burden in the brain can lead to epileptic encephalopathy. Seizures are notoriously resistant to medical managements necessitating surgical intervention ... open, endoscopic, or ablative."
To date, surgical intervention has been limited due to modest outcomes, with 37%-50% achieving seizure freedom. The location of HH tumors makes surgical intervention difficult, and as a result 7%-10% of patients have permanent surgical morbidity.
For the technique using the Visualase, Dr. Curry and his associates at four other medical centers in the United States performed the surgical technique through a single 4-mm incision, a 3.2-mm burr hole, and a 1.65-mm cannula trajectory with Visualase under real-time MR thermography, first with a confirmation test at about 3 W, followed by higher doses of 6-10 W for 50-120 seconds. Temperature limits were set to protect the hypothalamus and basilar artery and optic tract. The surgery had an immediate effect, and patients stayed in the hospital for a mean of 2 days.
The primary measure was seizure frequency at 1 year while the secondary measure was the complication profile of stereotactic laser ablation in epilepsy.
Of the 20 patients, 5 were adults, and the entire study population ranged in age from 22 months to 34 years. A total of 21 ablations were performed in the 20 patients. Dr. Curry reported that all but four patients were seizure free after the procedure. However, the rate of seizures diminished among the four who were not seizure free.
Seizures recurred in one of the pediatric patients. "We re-ablated him and he is now seizure free," Dr. Curry said.
Complications to date have included two missed targets, one case of IV phenytoin toxicity, one case of transient diabetes insipidus, two cases of transient hemiparesis, and one subarachnoid hemorrhage. Perioperative, temporary weight gain was detected in most patients. "With lack of hormonal disturbance, this is thought to be due to the perioperative, high-dose steroid use," Dr. Curry explained.
Postoperative interviews with parents of study participants "have revealed significant improvements in intellectual development, concentration, and interactiveness," he said. "Most families report improvement of mood, decreased behavioral disorders, and rage attacks."
To date, only two patients have completed formal postoperative neuropsychological testing. "There were no significant declines in memory in either patient," Dr. Curry said. One had improved math skills and reading comprehension while the other complained of memory dysfunction but was not below normal on testing.
"We have learned that laser ablation of hypothalamic hamartoma can be accomplished safely," Dr. Curry concluded. "More studies are needed to explain the antiepileptic effect in settings of incomplete radiologic destruction of the target and to advance thermal planning."
Dr. Curry said that he had no relevant financial conflicts to disclose.
AT THE 2013 AAN ANNUAL MEETING
Major finding: After 20 patients with hypothalamic hamartoma underwent MR-guided stereotactic laser ablation, all but 4 were seizure free.
Data source: A multicenter pilot study of 21 ablations performed in patients who ranged in age from 22 months to 34 years.
Disclosures: Dr. Curry said that he had no relevant financial conflicts to disclose.
Commentary: Friending patients on Facebook
Can we be friends? Seems innocent enough, no? Yet "friending" on Facebook is fraught with ethical and professional challenges for physicians.
What should you do if a patient wants to friend you on Facebook? Here’s what some doctors have done. According to 2011 survey in the Journal of General Internal Medicine, 58% of practicing physicians reported that they always replied "no" to friend requests from patients, while 42% said that they accepted them on a case-by-case basis (J. Gen. Intern. Med. 2011;26:1168-74).
Physicians who choose to not friend patients online are often concerned about issues including HIPAA (Health Insurance Portability and Accountability Act) violations, maintaining a separation between their personal and professional lives, and offending patients when they decline requests.
What should you do? What is the best practice for physicians friending patients online? The American Medical Association doesn’t prohibit the practice, but it urges physicians to "maintain appropriate boundaries of the patient-physician relationship in accordance with professional ethical guidelines," just as they would in any other context.
By contrast, in 2011, the British Medical Association issued a new guideline advising physicians not to accept friend requests from former and current patients because of how doctors’ personal information could be perceived and shared.
Here’s a simple solution that works well for many physicians: Create a professional Facebook page for your practice and redirect patients there. It’s easy to do: Once you log in to Facebook, go to "create a page," then choose "local business or place," fill in the information, and you’re ready to go. This strategy allows you to keep your personal Facebook account private.
Your personal account should be relegated to family and real-life personal friends. This is where you share photos of your child’s birthday party or updates on your recent kitchen remodel.
Your business page should be devoted to your professional life. This is where you share pertinent information about your practice, links to blog posts you’ve written, and other educational or useful information for your followers. You can write updates with a personal tone, but the content should remain professional and HIPAA compliant.
This two-tiered solution to Facebook friending has many benefits. When you say no to a patient friend request on your personal page, you can redirect him or her to your public page. You’re still keeping the lines of communication open. A public or business page allows anyone to like it, which benefits you and your practice; importantly, it disallows friending. This means you can share information and connect with others (including current, past, and future patients) online, without blurring the line between your professional and personal life.
Even if you do have separate Facebook pages, remember that anything you post online can be discovered. That means a picture of you and your buddies drinking beer at a bar or attending a political rally can be found by people who you might not want to find them. But you know that already.
Just as you work to protect your face-to-face reputation, you should work to protect your reputation online. After all, if your online reputation gets muddied, so will your offline one. It’s about setting boundaries, which physicians have been doing for centuries.
If we’ve met in person, and you really do like me, feel free to friend me on Facebook. If you want to take things more slowly, then follow me on Twitter, where I’m @Dermdoc. And let me know your thoughts about physicians and patients friending online.
Dr. Benabio is in private practice in San Diego. Visit his consumer health blog at http://thedermblog.com or connect with him on Twitter @Dermdoc and on Facebook (DermDoc).
Can we be friends? Seems innocent enough, no? Yet "friending" on Facebook is fraught with ethical and professional challenges for physicians.
What should you do if a patient wants to friend you on Facebook? Here’s what some doctors have done. According to 2011 survey in the Journal of General Internal Medicine, 58% of practicing physicians reported that they always replied "no" to friend requests from patients, while 42% said that they accepted them on a case-by-case basis (J. Gen. Intern. Med. 2011;26:1168-74).
Physicians who choose to not friend patients online are often concerned about issues including HIPAA (Health Insurance Portability and Accountability Act) violations, maintaining a separation between their personal and professional lives, and offending patients when they decline requests.
What should you do? What is the best practice for physicians friending patients online? The American Medical Association doesn’t prohibit the practice, but it urges physicians to "maintain appropriate boundaries of the patient-physician relationship in accordance with professional ethical guidelines," just as they would in any other context.
By contrast, in 2011, the British Medical Association issued a new guideline advising physicians not to accept friend requests from former and current patients because of how doctors’ personal information could be perceived and shared.
Here’s a simple solution that works well for many physicians: Create a professional Facebook page for your practice and redirect patients there. It’s easy to do: Once you log in to Facebook, go to "create a page," then choose "local business or place," fill in the information, and you’re ready to go. This strategy allows you to keep your personal Facebook account private.
Your personal account should be relegated to family and real-life personal friends. This is where you share photos of your child’s birthday party or updates on your recent kitchen remodel.
Your business page should be devoted to your professional life. This is where you share pertinent information about your practice, links to blog posts you’ve written, and other educational or useful information for your followers. You can write updates with a personal tone, but the content should remain professional and HIPAA compliant.
This two-tiered solution to Facebook friending has many benefits. When you say no to a patient friend request on your personal page, you can redirect him or her to your public page. You’re still keeping the lines of communication open. A public or business page allows anyone to like it, which benefits you and your practice; importantly, it disallows friending. This means you can share information and connect with others (including current, past, and future patients) online, without blurring the line between your professional and personal life.
Even if you do have separate Facebook pages, remember that anything you post online can be discovered. That means a picture of you and your buddies drinking beer at a bar or attending a political rally can be found by people who you might not want to find them. But you know that already.
Just as you work to protect your face-to-face reputation, you should work to protect your reputation online. After all, if your online reputation gets muddied, so will your offline one. It’s about setting boundaries, which physicians have been doing for centuries.
If we’ve met in person, and you really do like me, feel free to friend me on Facebook. If you want to take things more slowly, then follow me on Twitter, where I’m @Dermdoc. And let me know your thoughts about physicians and patients friending online.
Dr. Benabio is in private practice in San Diego. Visit his consumer health blog at http://thedermblog.com or connect with him on Twitter @Dermdoc and on Facebook (DermDoc).
Can we be friends? Seems innocent enough, no? Yet "friending" on Facebook is fraught with ethical and professional challenges for physicians.
What should you do if a patient wants to friend you on Facebook? Here’s what some doctors have done. According to 2011 survey in the Journal of General Internal Medicine, 58% of practicing physicians reported that they always replied "no" to friend requests from patients, while 42% said that they accepted them on a case-by-case basis (J. Gen. Intern. Med. 2011;26:1168-74).
Physicians who choose to not friend patients online are often concerned about issues including HIPAA (Health Insurance Portability and Accountability Act) violations, maintaining a separation between their personal and professional lives, and offending patients when they decline requests.
What should you do? What is the best practice for physicians friending patients online? The American Medical Association doesn’t prohibit the practice, but it urges physicians to "maintain appropriate boundaries of the patient-physician relationship in accordance with professional ethical guidelines," just as they would in any other context.
By contrast, in 2011, the British Medical Association issued a new guideline advising physicians not to accept friend requests from former and current patients because of how doctors’ personal information could be perceived and shared.
Here’s a simple solution that works well for many physicians: Create a professional Facebook page for your practice and redirect patients there. It’s easy to do: Once you log in to Facebook, go to "create a page," then choose "local business or place," fill in the information, and you’re ready to go. This strategy allows you to keep your personal Facebook account private.
Your personal account should be relegated to family and real-life personal friends. This is where you share photos of your child’s birthday party or updates on your recent kitchen remodel.
Your business page should be devoted to your professional life. This is where you share pertinent information about your practice, links to blog posts you’ve written, and other educational or useful information for your followers. You can write updates with a personal tone, but the content should remain professional and HIPAA compliant.
This two-tiered solution to Facebook friending has many benefits. When you say no to a patient friend request on your personal page, you can redirect him or her to your public page. You’re still keeping the lines of communication open. A public or business page allows anyone to like it, which benefits you and your practice; importantly, it disallows friending. This means you can share information and connect with others (including current, past, and future patients) online, without blurring the line between your professional and personal life.
Even if you do have separate Facebook pages, remember that anything you post online can be discovered. That means a picture of you and your buddies drinking beer at a bar or attending a political rally can be found by people who you might not want to find them. But you know that already.
Just as you work to protect your face-to-face reputation, you should work to protect your reputation online. After all, if your online reputation gets muddied, so will your offline one. It’s about setting boundaries, which physicians have been doing for centuries.
If we’ve met in person, and you really do like me, feel free to friend me on Facebook. If you want to take things more slowly, then follow me on Twitter, where I’m @Dermdoc. And let me know your thoughts about physicians and patients friending online.
Dr. Benabio is in private practice in San Diego. Visit his consumer health blog at http://thedermblog.com or connect with him on Twitter @Dermdoc and on Facebook (DermDoc).

Mortality after surgery for radiation-related cardiac problems unexpectedly high
Mortality is twice as high for cancer survivors undergoing cardiac surgery to correct damage done by thoracic radiation therapy as it is among matched patients who are undergoing the same procedures but who haven’t been exposed to radiotherapy, according to a report published online April 8 in Circulation.
In what they described as "the largest study to assess long-term survival in this population undergoing complex cardiac surgery and compare them to a well-matched comparison population," investigators found that mortality was 55% in the patients who had received radiation therapy, compared with 28% in the nonexposed controls. At least half of the deaths among the cancer survivors were attributed to cardiopulmonary disease, while only 5% were due to recurrent malignancy.
"Surgical intervention should be applied cautiously to patients who have had significant thoracic radiation previously," including survivors of breast, lung, hematologic, thyroid, and other cancers.
Trying to gauge mortality risk in such patients solely by using their preoperative scores on standard risk-prediction measures is inaccurate at best. In this study population, the survivors of breast, lung, hematologic, thyroid, and other cancers would have been deemed at intermediate risk for undergoing cardiac surgery, with an expected mortality of only 3%-5% based on their preoperative assessments – 10 times lower than their actual postoperative mortality, said Dr. Willis Wu and his associates at the Heart and Vascular Institute at the Cleveland Clinic.
"Our findings suggest that surgical intervention should be applied cautiously to patients who have had significant thoracic radiation previously," they wrote. Cardiac surgery that is considered conventional or even routine in most patients – including coronary artery bypass graft, valve repair, valve replacement, vascular surgery, pericardiectomy, left ventricular assist device implantation, and myectomy – may actually worsen the condition of radiation-exposed patients.
"It seems appropriate to examine other types of treatment options in patients with radiation heart disease who have significant valvular, coronary, or myocardial disease," the researchers noted.
Dr. Wu and his associates performed their retrospective observational study because of the dearth of information regarding long-term outcomes in cancer survivors who were exposed to chest irradiation. This knowledge gap makes treatment decisions "especially difficult" once radiation-related heart disease is discovered.
Such patients are known to have high rates of coronary artery, valvular, pericardial, myocardial, and conduction disease that progresses over time and may not become evident until decades after cancer treatment was completed.
Surgery is often thought necessary to effectively address these cardiac complications of prior radiation therapy. "These patients have multiple cardiac lesions and [often] have comorbidities such as pulmonary or vascular disease related to radiation," the investigators said.
They analyzed the medical records of 478 patients undergoing cardiac surgery at their tertiary care center in 2000-2003. A total of 173 had a prior history of malignancy treated with chest irradiation; the remaining 305 patients had no such history and were matched to the radiation group for age, sex, type of surgery, and date of surgery.
The patients exposed to radiation were relatively young but had advanced symptoms. Forty-five percent had obstructive proximal coronary artery disease; one-fourth had already undergone open heart surgery, including 16% who had prior coronary artery bypass graft surgery. There also was a high prevalence of valvular disease, with 51% of patients showing at least moderate mitral regurgitation, 6% showing severe mitral stenosis, 29% showing at least moderate aortic regurgitation, 23% showing severe aortic stenosis, and 34% showing at least moderate tricuspid regurgitation.
The mean interval between the current cardiac surgery and the last thoracic radiation treatment was 18 years. Approximately 53% of the study patients had survived breast cancer, 27% had survived Hodgkin’s lymphoma, 7% had survived lung cancer, 6% had survived non-Hodgkin’s lymphoma, and 8% had survived other malignancies including thyroid and testicular cancers.
Approximately 75% of both study groups were women.
During a mean follow-up of 7.6 years, overall mortality was 37%. Despite the success of the cardiac procedures, a significantly higher proportion of radiation-exposed patients died (55%), compared with the unexposed patients (28%), for a hazard ratio of 2.54, Dr. Wu and his colleagues said (Circulation 2013 April 8; doi:10.1161/CIRCULATIONAHA.13.001435).
Mortality was significantly higher across all subgroups of patients exposed to radiation. In particular, it was high among patients expected to have low mortality: 43% in patients aged younger than 65 years and 45% in those with lower preoperative risk scores. In fact, the youngest patients in the radiation group fared worse than the oldest patients in the comparison group.
Mortality also was significantly higher for the radiation-exposed patients than for controls across all types of cardiac surgery.
The cause of death was not known for a substantial proportion of subjects in this study, but cardiopulmonary causes were implicated in at least half of the deaths among radiation-exposed patients. "Why this should be the case in a group of patients who received potentially life-preserving revascularization, valve, and other procedures is unknown at present," Dr. Wu and his associates said.
In addition, patients with radiation-related heart disease had longer hospital stays, were more likely to develop atrial fibrillation after surgery, were more likely to require pacemaker implantation after surgery, had higher rates of ventricular dysfunction and of valvular regurgitation following surgery, and had higher 30-day mortality.
The finding that radiation-exposed patients "remained in hospital for a considerable period after their surgery" suggests that the procedures and postoperative courses were complicated.
"Radiation patients frequently develop pulmonary complications as a result of open heart surgery, not the least of which are recurrent pleural effusions and severe restrictive lung disease. It is our experience that respiratory complications may significantly compromise function and survival in patients with extensive prior radiation," the researchers said.
"Additionally, the presence of myocardial disease either as a result of the underlying cardiac condition (potentially exacerbated by prior chemotherapy) or as a consequence of a restrictive-type cardiomyopathy produced by the effects of radiation may play a role in impaired survival and is not necessarily improved by valvular or revascularization surgery," they said.
The radiation-exposed patients’ poor long-term survival after conventional cardiac surgery indicates that other, nonsurgical treatments may be necessary for this complex patient population, they added.
No relevant financial conflicts were reported.
There is little doubt that prior radiotherapy complicates surgery. Specifically, standard radiation used with curative intent for breast cancer, lymphoma, and a few other mediastinal/thorax malignancies, has important long-term effects.
Dr. Murthy |

These authors report on the increased complications and mortality of open heart operation following chest radiation given on average, some 20 years before. What is left out is that it is the radiotherapy itself that may be responsible for the current pathology for which many of the patients are requiring their heart operations. So you have the classic "insult-to-injury" of radiation being both the cause as well as the impediment to cure, in many of these circumstances. The caveat, of course, is that without their index radiotherapy, these patients would not have survived to now be burdened by the latent effects of ionizing radiation on the thorax.
Sudish Murthy, MD, FACS, is surgical director, Center of Major Airway Disease, The Cleveland Clinic.
There is little doubt that prior radiotherapy complicates surgery. Specifically, standard radiation used with curative intent for breast cancer, lymphoma, and a few other mediastinal/thorax malignancies, has important long-term effects.
Dr. Murthy |
These authors report on the increased complications and mortality of open heart operation following chest radiation given on average, some 20 years before. What is left out is that it is the radiotherapy itself that may be responsible for the current pathology for which many of the patients are requiring their heart operations. So you have the classic "insult-to-injury" of radiation being both the cause as well as the impediment to cure, in many of these circumstances. The caveat, of course, is that without their index radiotherapy, these patients would not have survived to now be burdened by the latent effects of ionizing radiation on the thorax.
Sudish Murthy, MD, FACS, is surgical director, Center of Major Airway Disease, The Cleveland Clinic.
There is little doubt that prior radiotherapy complicates surgery. Specifically, standard radiation used with curative intent for breast cancer, lymphoma, and a few other mediastinal/thorax malignancies, has important long-term effects.
Dr. Murthy |
These authors report on the increased complications and mortality of open heart operation following chest radiation given on average, some 20 years before. What is left out is that it is the radiotherapy itself that may be responsible for the current pathology for which many of the patients are requiring their heart operations. So you have the classic "insult-to-injury" of radiation being both the cause as well as the impediment to cure, in many of these circumstances. The caveat, of course, is that without their index radiotherapy, these patients would not have survived to now be burdened by the latent effects of ionizing radiation on the thorax.
Sudish Murthy, MD, FACS, is surgical director, Center of Major Airway Disease, The Cleveland Clinic.
Mortality is twice as high for cancer survivors undergoing cardiac surgery to correct damage done by thoracic radiation therapy as it is among matched patients who are undergoing the same procedures but who haven’t been exposed to radiotherapy, according to a report published online April 8 in Circulation.
In what they described as "the largest study to assess long-term survival in this population undergoing complex cardiac surgery and compare them to a well-matched comparison population," investigators found that mortality was 55% in the patients who had received radiation therapy, compared with 28% in the nonexposed controls. At least half of the deaths among the cancer survivors were attributed to cardiopulmonary disease, while only 5% were due to recurrent malignancy.
"Surgical intervention should be applied cautiously to patients who have had significant thoracic radiation previously," including survivors of breast, lung, hematologic, thyroid, and other cancers.
Trying to gauge mortality risk in such patients solely by using their preoperative scores on standard risk-prediction measures is inaccurate at best. In this study population, the survivors of breast, lung, hematologic, thyroid, and other cancers would have been deemed at intermediate risk for undergoing cardiac surgery, with an expected mortality of only 3%-5% based on their preoperative assessments – 10 times lower than their actual postoperative mortality, said Dr. Willis Wu and his associates at the Heart and Vascular Institute at the Cleveland Clinic.
"Our findings suggest that surgical intervention should be applied cautiously to patients who have had significant thoracic radiation previously," they wrote. Cardiac surgery that is considered conventional or even routine in most patients – including coronary artery bypass graft, valve repair, valve replacement, vascular surgery, pericardiectomy, left ventricular assist device implantation, and myectomy – may actually worsen the condition of radiation-exposed patients.
"It seems appropriate to examine other types of treatment options in patients with radiation heart disease who have significant valvular, coronary, or myocardial disease," the researchers noted.
Dr. Wu and his associates performed their retrospective observational study because of the dearth of information regarding long-term outcomes in cancer survivors who were exposed to chest irradiation. This knowledge gap makes treatment decisions "especially difficult" once radiation-related heart disease is discovered.
Such patients are known to have high rates of coronary artery, valvular, pericardial, myocardial, and conduction disease that progresses over time and may not become evident until decades after cancer treatment was completed.
Surgery is often thought necessary to effectively address these cardiac complications of prior radiation therapy. "These patients have multiple cardiac lesions and [often] have comorbidities such as pulmonary or vascular disease related to radiation," the investigators said.
They analyzed the medical records of 478 patients undergoing cardiac surgery at their tertiary care center in 2000-2003. A total of 173 had a prior history of malignancy treated with chest irradiation; the remaining 305 patients had no such history and were matched to the radiation group for age, sex, type of surgery, and date of surgery.
The patients exposed to radiation were relatively young but had advanced symptoms. Forty-five percent had obstructive proximal coronary artery disease; one-fourth had already undergone open heart surgery, including 16% who had prior coronary artery bypass graft surgery. There also was a high prevalence of valvular disease, with 51% of patients showing at least moderate mitral regurgitation, 6% showing severe mitral stenosis, 29% showing at least moderate aortic regurgitation, 23% showing severe aortic stenosis, and 34% showing at least moderate tricuspid regurgitation.
The mean interval between the current cardiac surgery and the last thoracic radiation treatment was 18 years. Approximately 53% of the study patients had survived breast cancer, 27% had survived Hodgkin’s lymphoma, 7% had survived lung cancer, 6% had survived non-Hodgkin’s lymphoma, and 8% had survived other malignancies including thyroid and testicular cancers.
Approximately 75% of both study groups were women.
During a mean follow-up of 7.6 years, overall mortality was 37%. Despite the success of the cardiac procedures, a significantly higher proportion of radiation-exposed patients died (55%), compared with the unexposed patients (28%), for a hazard ratio of 2.54, Dr. Wu and his colleagues said (Circulation 2013 April 8; doi:10.1161/CIRCULATIONAHA.13.001435).
Mortality was significantly higher across all subgroups of patients exposed to radiation. In particular, it was high among patients expected to have low mortality: 43% in patients aged younger than 65 years and 45% in those with lower preoperative risk scores. In fact, the youngest patients in the radiation group fared worse than the oldest patients in the comparison group.
Mortality also was significantly higher for the radiation-exposed patients than for controls across all types of cardiac surgery.
The cause of death was not known for a substantial proportion of subjects in this study, but cardiopulmonary causes were implicated in at least half of the deaths among radiation-exposed patients. "Why this should be the case in a group of patients who received potentially life-preserving revascularization, valve, and other procedures is unknown at present," Dr. Wu and his associates said.
In addition, patients with radiation-related heart disease had longer hospital stays, were more likely to develop atrial fibrillation after surgery, were more likely to require pacemaker implantation after surgery, had higher rates of ventricular dysfunction and of valvular regurgitation following surgery, and had higher 30-day mortality.
The finding that radiation-exposed patients "remained in hospital for a considerable period after their surgery" suggests that the procedures and postoperative courses were complicated.
"Radiation patients frequently develop pulmonary complications as a result of open heart surgery, not the least of which are recurrent pleural effusions and severe restrictive lung disease. It is our experience that respiratory complications may significantly compromise function and survival in patients with extensive prior radiation," the researchers said.
"Additionally, the presence of myocardial disease either as a result of the underlying cardiac condition (potentially exacerbated by prior chemotherapy) or as a consequence of a restrictive-type cardiomyopathy produced by the effects of radiation may play a role in impaired survival and is not necessarily improved by valvular or revascularization surgery," they said.
The radiation-exposed patients’ poor long-term survival after conventional cardiac surgery indicates that other, nonsurgical treatments may be necessary for this complex patient population, they added.
No relevant financial conflicts were reported.
Mortality is twice as high for cancer survivors undergoing cardiac surgery to correct damage done by thoracic radiation therapy as it is among matched patients who are undergoing the same procedures but who haven’t been exposed to radiotherapy, according to a report published online April 8 in Circulation.
In what they described as "the largest study to assess long-term survival in this population undergoing complex cardiac surgery and compare them to a well-matched comparison population," investigators found that mortality was 55% in the patients who had received radiation therapy, compared with 28% in the nonexposed controls. At least half of the deaths among the cancer survivors were attributed to cardiopulmonary disease, while only 5% were due to recurrent malignancy.
"Surgical intervention should be applied cautiously to patients who have had significant thoracic radiation previously," including survivors of breast, lung, hematologic, thyroid, and other cancers.
Trying to gauge mortality risk in such patients solely by using their preoperative scores on standard risk-prediction measures is inaccurate at best. In this study population, the survivors of breast, lung, hematologic, thyroid, and other cancers would have been deemed at intermediate risk for undergoing cardiac surgery, with an expected mortality of only 3%-5% based on their preoperative assessments – 10 times lower than their actual postoperative mortality, said Dr. Willis Wu and his associates at the Heart and Vascular Institute at the Cleveland Clinic.
"Our findings suggest that surgical intervention should be applied cautiously to patients who have had significant thoracic radiation previously," they wrote. Cardiac surgery that is considered conventional or even routine in most patients – including coronary artery bypass graft, valve repair, valve replacement, vascular surgery, pericardiectomy, left ventricular assist device implantation, and myectomy – may actually worsen the condition of radiation-exposed patients.
"It seems appropriate to examine other types of treatment options in patients with radiation heart disease who have significant valvular, coronary, or myocardial disease," the researchers noted.
Dr. Wu and his associates performed their retrospective observational study because of the dearth of information regarding long-term outcomes in cancer survivors who were exposed to chest irradiation. This knowledge gap makes treatment decisions "especially difficult" once radiation-related heart disease is discovered.
Such patients are known to have high rates of coronary artery, valvular, pericardial, myocardial, and conduction disease that progresses over time and may not become evident until decades after cancer treatment was completed.
Surgery is often thought necessary to effectively address these cardiac complications of prior radiation therapy. "These patients have multiple cardiac lesions and [often] have comorbidities such as pulmonary or vascular disease related to radiation," the investigators said.
They analyzed the medical records of 478 patients undergoing cardiac surgery at their tertiary care center in 2000-2003. A total of 173 had a prior history of malignancy treated with chest irradiation; the remaining 305 patients had no such history and were matched to the radiation group for age, sex, type of surgery, and date of surgery.
The patients exposed to radiation were relatively young but had advanced symptoms. Forty-five percent had obstructive proximal coronary artery disease; one-fourth had already undergone open heart surgery, including 16% who had prior coronary artery bypass graft surgery. There also was a high prevalence of valvular disease, with 51% of patients showing at least moderate mitral regurgitation, 6% showing severe mitral stenosis, 29% showing at least moderate aortic regurgitation, 23% showing severe aortic stenosis, and 34% showing at least moderate tricuspid regurgitation.
The mean interval between the current cardiac surgery and the last thoracic radiation treatment was 18 years. Approximately 53% of the study patients had survived breast cancer, 27% had survived Hodgkin’s lymphoma, 7% had survived lung cancer, 6% had survived non-Hodgkin’s lymphoma, and 8% had survived other malignancies including thyroid and testicular cancers.
Approximately 75% of both study groups were women.
During a mean follow-up of 7.6 years, overall mortality was 37%. Despite the success of the cardiac procedures, a significantly higher proportion of radiation-exposed patients died (55%), compared with the unexposed patients (28%), for a hazard ratio of 2.54, Dr. Wu and his colleagues said (Circulation 2013 April 8; doi:10.1161/CIRCULATIONAHA.13.001435).
Mortality was significantly higher across all subgroups of patients exposed to radiation. In particular, it was high among patients expected to have low mortality: 43% in patients aged younger than 65 years and 45% in those with lower preoperative risk scores. In fact, the youngest patients in the radiation group fared worse than the oldest patients in the comparison group.
Mortality also was significantly higher for the radiation-exposed patients than for controls across all types of cardiac surgery.
The cause of death was not known for a substantial proportion of subjects in this study, but cardiopulmonary causes were implicated in at least half of the deaths among radiation-exposed patients. "Why this should be the case in a group of patients who received potentially life-preserving revascularization, valve, and other procedures is unknown at present," Dr. Wu and his associates said.
In addition, patients with radiation-related heart disease had longer hospital stays, were more likely to develop atrial fibrillation after surgery, were more likely to require pacemaker implantation after surgery, had higher rates of ventricular dysfunction and of valvular regurgitation following surgery, and had higher 30-day mortality.
The finding that radiation-exposed patients "remained in hospital for a considerable period after their surgery" suggests that the procedures and postoperative courses were complicated.
"Radiation patients frequently develop pulmonary complications as a result of open heart surgery, not the least of which are recurrent pleural effusions and severe restrictive lung disease. It is our experience that respiratory complications may significantly compromise function and survival in patients with extensive prior radiation," the researchers said.
"Additionally, the presence of myocardial disease either as a result of the underlying cardiac condition (potentially exacerbated by prior chemotherapy) or as a consequence of a restrictive-type cardiomyopathy produced by the effects of radiation may play a role in impaired survival and is not necessarily improved by valvular or revascularization surgery," they said.
The radiation-exposed patients’ poor long-term survival after conventional cardiac surgery indicates that other, nonsurgical treatments may be necessary for this complex patient population, they added.
No relevant financial conflicts were reported.
FROM CIRCULATION
Major Finding: Despite the success of the cardiac procedures, a significantly higher proportion of radiation-exposed patients died during follow-up (55%), compared with the unexposed patients (28%).
Data Source: A retrospective, single-center, observational study involving 173 cancer survivors who were previously exposed to thoracic radiotherapy and 305 matched controls who underwent cardiac surgery in 2000-2003 and were followed for approximately 7 years.
Disclosures: No relevant financial conflicts were reported.
Money Troubles: The Policy & Practice Podcast
In a few days, President Obama will offer up his proposed federal budget for fiscal year 2014. His plan comes out at the same time that physicians and patients are grappling with the fall-out of the sequestration cuts and some shortfalls in coverage under the Affordable Care Act (ACA).
On Capitol Hill this week, Rep. Michael Burgess (R-Texas) took the administration to task after a program designed to insure adults with preexisting health conditions ran out of money. Rep. Burgess, a physician, said the Obama administration was at fault for underestimating the need.

Some cancer patients are feeling the effects of sequestration. As of April 1, Medicare began the sequestration process, which cut Medicare physician pay by 2%. It also cut the fees paid for administering cancer drugs. As a result, some community oncologists are being forced to turn Medicare patients away.
And don’t forget about the looming 24% cut to Medicare physician fees, which is scheduled to take effect on Jan. 1, 2014. That cut, called for under the Sustainable Growth Rate (SGR) formula, can only be averted through action by Congress. Two of the House committees that oversee Medicare are working on a plan and are seeking physician comment. The preliminary plan would eliminate the SGR and phase in a new payment scheme that would base part of a physician’s pay on quality of care. Alternative payment models that get physician away from the fee-for-service system are also part of the plan.
Hear about all these issues and more in this week’s Policy and Practice podcast. And stay tuned next week for a detailed assessment of the President’s budget and how it will affect physicians.
In a few days, President Obama will offer up his proposed federal budget for fiscal year 2014. His plan comes out at the same time that physicians and patients are grappling with the fall-out of the sequestration cuts and some shortfalls in coverage under the Affordable Care Act (ACA).
On Capitol Hill this week, Rep. Michael Burgess (R-Texas) took the administration to task after a program designed to insure adults with preexisting health conditions ran out of money. Rep. Burgess, a physician, said the Obama administration was at fault for underestimating the need.
Some cancer patients are feeling the effects of sequestration. As of April 1, Medicare began the sequestration process, which cut Medicare physician pay by 2%. It also cut the fees paid for administering cancer drugs. As a result, some community oncologists are being forced to turn Medicare patients away.
And don’t forget about the looming 24% cut to Medicare physician fees, which is scheduled to take effect on Jan. 1, 2014. That cut, called for under the Sustainable Growth Rate (SGR) formula, can only be averted through action by Congress. Two of the House committees that oversee Medicare are working on a plan and are seeking physician comment. The preliminary plan would eliminate the SGR and phase in a new payment scheme that would base part of a physician’s pay on quality of care. Alternative payment models that get physician away from the fee-for-service system are also part of the plan.
Hear about all these issues and more in this week’s Policy and Practice podcast. And stay tuned next week for a detailed assessment of the President’s budget and how it will affect physicians.
In a few days, President Obama will offer up his proposed federal budget for fiscal year 2014. His plan comes out at the same time that physicians and patients are grappling with the fall-out of the sequestration cuts and some shortfalls in coverage under the Affordable Care Act (ACA).
On Capitol Hill this week, Rep. Michael Burgess (R-Texas) took the administration to task after a program designed to insure adults with preexisting health conditions ran out of money. Rep. Burgess, a physician, said the Obama administration was at fault for underestimating the need.
Some cancer patients are feeling the effects of sequestration. As of April 1, Medicare began the sequestration process, which cut Medicare physician pay by 2%. It also cut the fees paid for administering cancer drugs. As a result, some community oncologists are being forced to turn Medicare patients away.
And don’t forget about the looming 24% cut to Medicare physician fees, which is scheduled to take effect on Jan. 1, 2014. That cut, called for under the Sustainable Growth Rate (SGR) formula, can only be averted through action by Congress. Two of the House committees that oversee Medicare are working on a plan and are seeking physician comment. The preliminary plan would eliminate the SGR and phase in a new payment scheme that would base part of a physician’s pay on quality of care. Alternative payment models that get physician away from the fee-for-service system are also part of the plan.
Hear about all these issues and more in this week’s Policy and Practice podcast. And stay tuned next week for a detailed assessment of the President’s budget and how it will affect physicians.

Early surgical menopause linked to cognitive decline
SAN DIEGO – Earlier age at surgical menopause may be associated with a steeper decline in cognitive function and increased Alzheimer’s disease–related neuropathologic scores, preliminary results from two longitudinal studies have shown.
"Our findings support a growing literature on the impact of surgical menopause on cognitive function, and add granularity to these outcome measures," Dr. Riley M. Bove said at the annual meeting of the American Academy of Neurology. "In light of the sometimes conflicting and sometimes controversial findings related to modifying factors such as hormone replacement therapy [HRT], we believe that ongoing investigations are warranted."

In an effort to determine the impact of reproductive decline on the spectrum of cognitive decline, Dr. Bove, a neurologist at Brigham and Women’s Hospital, Boston, and her associates studied 1,884 women enrolled in two ongoing longitudinal studies: the Memory and Aging Project (MAP), a study of older men and women in assisted living facilities that was launched in 1997, and the Religious Orders Study (ROS), a study of Catholic priests, nuns, and brothers that was launched in 1994.
"Observational studies have noted that the loss of estrogen associated with menopause, including surgical menopause, may be associated with cognitive decline," Dr. Bove said. "In animal models estrogen has been found to be neuroprotective. However, in humans the evidence is a lot more complex. The results of the Womens Health Initiative Memory Study a decade ago did find adverse effects of hormone replacement therapy initiated in women in their 60s. Since then a window of opportunity hypothesis has emerged, according to which HRT perimenopausally may be protective, but following this window, it may be neutral or even harmful. We aimed to look at longitudinal changes in cognition, risk of an Alzheimer’s diagnosis, and neuropathologic measures related to Alzheimer’s disease. Our hypothesis was that earlier surgical menopause is associated with earlier risk of cognitive decline."
Study participants, who have been followed for up to 19 years, underwent a baseline clinical and reproductive history, annual clinical and cognitive evaluations, and annual blood draws. The researchers examined the association between age at menarche and menopause, number of cycling years, and ever use and duration of HRT.
During annual cognitive tests, the researchers evaluated five composite domains that were weighted toward memory and categorized by factor analysis. The domains include episodic memory (seven tests), semantic memory (three tests), working memory (three tests), perceptual speed (two tests), and visuospatial ability (two tests). They also established a global cognition composite score, which was a sum of the 17 individual tests.
Dr. Bove and her associates considered a clinical diagnosis of Alzheimer’s based on clinical criteria and neuropathologic measures. The three Alzheimer’s disease–associated measures were neuritic plaques, neurofibrillary tangles, and diffuse plaques, as well as a global AD pathology score, which was an average of these three measures. Age at menopause was a continuous variable. All models controlled for age, smoking, and years of education.
Of the total women studied, all were free of dementia at enrollment, their mean age was 78 years, and 91% were non-Hispanic white. On average, compared with women in the ROS study, those in the MAP study were older (79.6 vs. 75.9 years, respectively); were less educated (14.1 vs. 17.9 years); were more likely to smoke (38% vs. 8%); had an earlier age at menarche (12.8 vs. 13.1); had a later age at menopause (47.3 vs. 46.6); and had a slightly higher number of cycling years (34.5 vs. 33.4).
Of the 1,884 women, 1,277 reported having natural menopause, and 607 reported having surgical menopause. More women in the surgical menopause group reported HRT use (53% vs. 27%, respectively). "Approximately 90% of HRT use was oral, so we collapsed all of the different forms of HRT use into one group," she explained.
Among women who had undergone surgical menopause, early age at menopause was associated with a faster decline in global cognition (P = .0007), as well as faster declines in episodic memory (P = .0003) and semantic memory (P = .0022). "We did not find the similar association in the natural menopause group," Dr. Bove said.
However, the researchers observed no significant association between age at surgical menopause and risk of clinical Alzheimer’s (P = .093) nor in the pathologic diagnosis of Alzheimer’s (P = .053). Early age at surgical menopause was associated with significantly lower scores in global AD pathology (P = .038) and neuritic plaques (P = .013) but not in neurofibrillary tangles (P = .138) or diffuse plaques (P = .490).
Dr. Bove also reported that there were no associations between HRT use ever vs. never in any of the outcomes examined, "even when HRT use was stratified according to its timing of initiation relative to menopause. Additionally, we did not find a significant association between duration of HRT use and any of the neurologic outcomes."
She acknowledged certain limitations of the study, including the fact that study participants were required to be nondemented at baseline. "This may have led to exclusion bias if there were early effects of menopause on cognitive function," Dr. Bove said. "The cognitive outcomes were weighted toward memory, and the reproductive histories were patient reported and retrospective, so there’s a limited definition of surgical menopause. We don’t have any information as to whether the oophorectomies were unilateral or bilateral, or the indication for the surgeries. There was also limited data about HRT use."
Dr. Bove said that she had no relevant financial disclosures.
SAN DIEGO – Earlier age at surgical menopause may be associated with a steeper decline in cognitive function and increased Alzheimer’s disease–related neuropathologic scores, preliminary results from two longitudinal studies have shown.
"Our findings support a growing literature on the impact of surgical menopause on cognitive function, and add granularity to these outcome measures," Dr. Riley M. Bove said at the annual meeting of the American Academy of Neurology. "In light of the sometimes conflicting and sometimes controversial findings related to modifying factors such as hormone replacement therapy [HRT], we believe that ongoing investigations are warranted."
In an effort to determine the impact of reproductive decline on the spectrum of cognitive decline, Dr. Bove, a neurologist at Brigham and Women’s Hospital, Boston, and her associates studied 1,884 women enrolled in two ongoing longitudinal studies: the Memory and Aging Project (MAP), a study of older men and women in assisted living facilities that was launched in 1997, and the Religious Orders Study (ROS), a study of Catholic priests, nuns, and brothers that was launched in 1994.
"Observational studies have noted that the loss of estrogen associated with menopause, including surgical menopause, may be associated with cognitive decline," Dr. Bove said. "In animal models estrogen has been found to be neuroprotective. However, in humans the evidence is a lot more complex. The results of the Womens Health Initiative Memory Study a decade ago did find adverse effects of hormone replacement therapy initiated in women in their 60s. Since then a window of opportunity hypothesis has emerged, according to which HRT perimenopausally may be protective, but following this window, it may be neutral or even harmful. We aimed to look at longitudinal changes in cognition, risk of an Alzheimer’s diagnosis, and neuropathologic measures related to Alzheimer’s disease. Our hypothesis was that earlier surgical menopause is associated with earlier risk of cognitive decline."
Study participants, who have been followed for up to 19 years, underwent a baseline clinical and reproductive history, annual clinical and cognitive evaluations, and annual blood draws. The researchers examined the association between age at menarche and menopause, number of cycling years, and ever use and duration of HRT.
During annual cognitive tests, the researchers evaluated five composite domains that were weighted toward memory and categorized by factor analysis. The domains include episodic memory (seven tests), semantic memory (three tests), working memory (three tests), perceptual speed (two tests), and visuospatial ability (two tests). They also established a global cognition composite score, which was a sum of the 17 individual tests.
Dr. Bove and her associates considered a clinical diagnosis of Alzheimer’s based on clinical criteria and neuropathologic measures. The three Alzheimer’s disease–associated measures were neuritic plaques, neurofibrillary tangles, and diffuse plaques, as well as a global AD pathology score, which was an average of these three measures. Age at menopause was a continuous variable. All models controlled for age, smoking, and years of education.
Of the total women studied, all were free of dementia at enrollment, their mean age was 78 years, and 91% were non-Hispanic white. On average, compared with women in the ROS study, those in the MAP study were older (79.6 vs. 75.9 years, respectively); were less educated (14.1 vs. 17.9 years); were more likely to smoke (38% vs. 8%); had an earlier age at menarche (12.8 vs. 13.1); had a later age at menopause (47.3 vs. 46.6); and had a slightly higher number of cycling years (34.5 vs. 33.4).
Of the 1,884 women, 1,277 reported having natural menopause, and 607 reported having surgical menopause. More women in the surgical menopause group reported HRT use (53% vs. 27%, respectively). "Approximately 90% of HRT use was oral, so we collapsed all of the different forms of HRT use into one group," she explained.
Among women who had undergone surgical menopause, early age at menopause was associated with a faster decline in global cognition (P = .0007), as well as faster declines in episodic memory (P = .0003) and semantic memory (P = .0022). "We did not find the similar association in the natural menopause group," Dr. Bove said.
However, the researchers observed no significant association between age at surgical menopause and risk of clinical Alzheimer’s (P = .093) nor in the pathologic diagnosis of Alzheimer’s (P = .053). Early age at surgical menopause was associated with significantly lower scores in global AD pathology (P = .038) and neuritic plaques (P = .013) but not in neurofibrillary tangles (P = .138) or diffuse plaques (P = .490).
Dr. Bove also reported that there were no associations between HRT use ever vs. never in any of the outcomes examined, "even when HRT use was stratified according to its timing of initiation relative to menopause. Additionally, we did not find a significant association between duration of HRT use and any of the neurologic outcomes."
She acknowledged certain limitations of the study, including the fact that study participants were required to be nondemented at baseline. "This may have led to exclusion bias if there were early effects of menopause on cognitive function," Dr. Bove said. "The cognitive outcomes were weighted toward memory, and the reproductive histories were patient reported and retrospective, so there’s a limited definition of surgical menopause. We don’t have any information as to whether the oophorectomies were unilateral or bilateral, or the indication for the surgeries. There was also limited data about HRT use."
Dr. Bove said that she had no relevant financial disclosures.
SAN DIEGO – Earlier age at surgical menopause may be associated with a steeper decline in cognitive function and increased Alzheimer’s disease–related neuropathologic scores, preliminary results from two longitudinal studies have shown.
"Our findings support a growing literature on the impact of surgical menopause on cognitive function, and add granularity to these outcome measures," Dr. Riley M. Bove said at the annual meeting of the American Academy of Neurology. "In light of the sometimes conflicting and sometimes controversial findings related to modifying factors such as hormone replacement therapy [HRT], we believe that ongoing investigations are warranted."
In an effort to determine the impact of reproductive decline on the spectrum of cognitive decline, Dr. Bove, a neurologist at Brigham and Women’s Hospital, Boston, and her associates studied 1,884 women enrolled in two ongoing longitudinal studies: the Memory and Aging Project (MAP), a study of older men and women in assisted living facilities that was launched in 1997, and the Religious Orders Study (ROS), a study of Catholic priests, nuns, and brothers that was launched in 1994.
"Observational studies have noted that the loss of estrogen associated with menopause, including surgical menopause, may be associated with cognitive decline," Dr. Bove said. "In animal models estrogen has been found to be neuroprotective. However, in humans the evidence is a lot more complex. The results of the Womens Health Initiative Memory Study a decade ago did find adverse effects of hormone replacement therapy initiated in women in their 60s. Since then a window of opportunity hypothesis has emerged, according to which HRT perimenopausally may be protective, but following this window, it may be neutral or even harmful. We aimed to look at longitudinal changes in cognition, risk of an Alzheimer’s diagnosis, and neuropathologic measures related to Alzheimer’s disease. Our hypothesis was that earlier surgical menopause is associated with earlier risk of cognitive decline."
Study participants, who have been followed for up to 19 years, underwent a baseline clinical and reproductive history, annual clinical and cognitive evaluations, and annual blood draws. The researchers examined the association between age at menarche and menopause, number of cycling years, and ever use and duration of HRT.
During annual cognitive tests, the researchers evaluated five composite domains that were weighted toward memory and categorized by factor analysis. The domains include episodic memory (seven tests), semantic memory (three tests), working memory (three tests), perceptual speed (two tests), and visuospatial ability (two tests). They also established a global cognition composite score, which was a sum of the 17 individual tests.
Dr. Bove and her associates considered a clinical diagnosis of Alzheimer’s based on clinical criteria and neuropathologic measures. The three Alzheimer’s disease–associated measures were neuritic plaques, neurofibrillary tangles, and diffuse plaques, as well as a global AD pathology score, which was an average of these three measures. Age at menopause was a continuous variable. All models controlled for age, smoking, and years of education.
Of the total women studied, all were free of dementia at enrollment, their mean age was 78 years, and 91% were non-Hispanic white. On average, compared with women in the ROS study, those in the MAP study were older (79.6 vs. 75.9 years, respectively); were less educated (14.1 vs. 17.9 years); were more likely to smoke (38% vs. 8%); had an earlier age at menarche (12.8 vs. 13.1); had a later age at menopause (47.3 vs. 46.6); and had a slightly higher number of cycling years (34.5 vs. 33.4).
Of the 1,884 women, 1,277 reported having natural menopause, and 607 reported having surgical menopause. More women in the surgical menopause group reported HRT use (53% vs. 27%, respectively). "Approximately 90% of HRT use was oral, so we collapsed all of the different forms of HRT use into one group," she explained.
Among women who had undergone surgical menopause, early age at menopause was associated with a faster decline in global cognition (P = .0007), as well as faster declines in episodic memory (P = .0003) and semantic memory (P = .0022). "We did not find the similar association in the natural menopause group," Dr. Bove said.
However, the researchers observed no significant association between age at surgical menopause and risk of clinical Alzheimer’s (P = .093) nor in the pathologic diagnosis of Alzheimer’s (P = .053). Early age at surgical menopause was associated with significantly lower scores in global AD pathology (P = .038) and neuritic plaques (P = .013) but not in neurofibrillary tangles (P = .138) or diffuse plaques (P = .490).
Dr. Bove also reported that there were no associations between HRT use ever vs. never in any of the outcomes examined, "even when HRT use was stratified according to its timing of initiation relative to menopause. Additionally, we did not find a significant association between duration of HRT use and any of the neurologic outcomes."
She acknowledged certain limitations of the study, including the fact that study participants were required to be nondemented at baseline. "This may have led to exclusion bias if there were early effects of menopause on cognitive function," Dr. Bove said. "The cognitive outcomes were weighted toward memory, and the reproductive histories were patient reported and retrospective, so there’s a limited definition of surgical menopause. We don’t have any information as to whether the oophorectomies were unilateral or bilateral, or the indication for the surgeries. There was also limited data about HRT use."
Dr. Bove said that she had no relevant financial disclosures.
AT THE 2013 AAN ANNUAL MEETING
Major finding: Among women who had undergone surgical menopause, early age at menopause was associated with a faster decline in global cognition (P = .0007) as well as faster declines in episodic memory (P = .0003) and semantic memory (P = .0022).
Data source: Findings from 1,884 women enrolled in two ongoing longitudinal studies: the Memory and Aging Project (MAP), a study of older men and women in assisted living facilities that was launched in 1997, and the Religious Orders Study (ROS), a study of Catholic priests, nuns, and brothers that was launched in 1994.
Disclosures: Dr. Bove said she had no relevant financial disclosures.

High CRP augurs worse outcomes from palliative surgery for cancer
NATIONAL HARBOR, MD. – Elevated levels of C-reactive protein may be a marker for poor response to palliative surgery, Dr. Andrew M. Blakely said at the annual Society of Surgical Oncology Cancer Symposium.
In a study of 50 patients who underwent elective palliative procedures for various cancer-related symptoms, elevated C-reactive protein (CRP), but not fatigue scores or performance status, was associated with a nearly fourfold risk for worse overall survival, reported Dr. Blakely, a surgery resident at Alpert Medical School, Brown University, Providence, R.I.

Elevated CRP, defined as levels greater than 8 mg/L, was also associated with increased overall and tumor-grade specific complications.
"This is important, because these complications are poorly tolerated by advanced cancer patients, and they serve to greatly diminish the potential benefit of palliative surgery," Dr. Blakely said.
He and colleagues at Brown and the Rhode Island Hospital, also in Providence, looked at potential prognostic factors in patients who chose surgery to relieve symptoms of advanced cancers such as gastrointestinal obstruction, or local-regional control of tumor-related pain or bleeding.
Malignancies treated included gastric, pancreatic, colon, melanoma, sarcomas, breast cancer, hepatobiliary and ovarian cancer, and squamous cell carcinomas.
They found that 44 patients (88%) stated that the surgery "was worth it," and 37 patients (74%) reported symptom resolution or improvement following surgery.
At 1-month follow-up, the complication rate was 44%, and 10% of patients had died. Although there was no association between CRP levels and morbidity or mortality among all patients, 11 of 27 patients with low-grade (grade 1 or 2) complications had elevated CRP (P = .001), as did all 6 patients with high-grade (grade 3 or 4) malignancies (P = .010), and 4 of 5 patients who died (P =.007).
In univariate analysis, factors significantly associated with major complications included elevated CRP (P = .005) and National Cancer Institute (NCI) fatigue score of 1 or greater (P = .001). Factors associated with overall survival were elevated CRP (P less than .0001), and NCI fatigue score (P = .04).
But in multivariate analysis controlling for those factors and for male sex, low albumin levels, significant weight loss, no previous cancer therapy, and hemoglobin less than 10.5 g/dL, only elevated CRP was associated with poor overall survival, with a hazard ratio of 3.6 (P = .0003).
The authors speculate that elevated CRP is a marker for systemic inflammation that may be associated with a higher risk for postoperative complications and for poorer overall survival among patients with advanced cancer.
"Even in this highly selected population, there was 44% morbidity and 10% mortality, illustrating the difficulty in patient selection," Dr. Blakely said.
CRP testing is a simple, low-cost, and objective test that can be easily added on to preoperative evaluation of candidates for palliative surgery, and it may be a useful element in patient selection and counseling, he said.
The study was internally funded. Dr. Blakely reported having no financial disclosures.
NATIONAL HARBOR, MD. – Elevated levels of C-reactive protein may be a marker for poor response to palliative surgery, Dr. Andrew M. Blakely said at the annual Society of Surgical Oncology Cancer Symposium.
In a study of 50 patients who underwent elective palliative procedures for various cancer-related symptoms, elevated C-reactive protein (CRP), but not fatigue scores or performance status, was associated with a nearly fourfold risk for worse overall survival, reported Dr. Blakely, a surgery resident at Alpert Medical School, Brown University, Providence, R.I.
Elevated CRP, defined as levels greater than 8 mg/L, was also associated with increased overall and tumor-grade specific complications.
"This is important, because these complications are poorly tolerated by advanced cancer patients, and they serve to greatly diminish the potential benefit of palliative surgery," Dr. Blakely said.
He and colleagues at Brown and the Rhode Island Hospital, also in Providence, looked at potential prognostic factors in patients who chose surgery to relieve symptoms of advanced cancers such as gastrointestinal obstruction, or local-regional control of tumor-related pain or bleeding.
Malignancies treated included gastric, pancreatic, colon, melanoma, sarcomas, breast cancer, hepatobiliary and ovarian cancer, and squamous cell carcinomas.
They found that 44 patients (88%) stated that the surgery "was worth it," and 37 patients (74%) reported symptom resolution or improvement following surgery.
At 1-month follow-up, the complication rate was 44%, and 10% of patients had died. Although there was no association between CRP levels and morbidity or mortality among all patients, 11 of 27 patients with low-grade (grade 1 or 2) complications had elevated CRP (P = .001), as did all 6 patients with high-grade (grade 3 or 4) malignancies (P = .010), and 4 of 5 patients who died (P =.007).
In univariate analysis, factors significantly associated with major complications included elevated CRP (P = .005) and National Cancer Institute (NCI) fatigue score of 1 or greater (P = .001). Factors associated with overall survival were elevated CRP (P less than .0001), and NCI fatigue score (P = .04).
But in multivariate analysis controlling for those factors and for male sex, low albumin levels, significant weight loss, no previous cancer therapy, and hemoglobin less than 10.5 g/dL, only elevated CRP was associated with poor overall survival, with a hazard ratio of 3.6 (P = .0003).
The authors speculate that elevated CRP is a marker for systemic inflammation that may be associated with a higher risk for postoperative complications and for poorer overall survival among patients with advanced cancer.
"Even in this highly selected population, there was 44% morbidity and 10% mortality, illustrating the difficulty in patient selection," Dr. Blakely said.
CRP testing is a simple, low-cost, and objective test that can be easily added on to preoperative evaluation of candidates for palliative surgery, and it may be a useful element in patient selection and counseling, he said.
The study was internally funded. Dr. Blakely reported having no financial disclosures.
NATIONAL HARBOR, MD. – Elevated levels of C-reactive protein may be a marker for poor response to palliative surgery, Dr. Andrew M. Blakely said at the annual Society of Surgical Oncology Cancer Symposium.
In a study of 50 patients who underwent elective palliative procedures for various cancer-related symptoms, elevated C-reactive protein (CRP), but not fatigue scores or performance status, was associated with a nearly fourfold risk for worse overall survival, reported Dr. Blakely, a surgery resident at Alpert Medical School, Brown University, Providence, R.I.
Elevated CRP, defined as levels greater than 8 mg/L, was also associated with increased overall and tumor-grade specific complications.
"This is important, because these complications are poorly tolerated by advanced cancer patients, and they serve to greatly diminish the potential benefit of palliative surgery," Dr. Blakely said.
He and colleagues at Brown and the Rhode Island Hospital, also in Providence, looked at potential prognostic factors in patients who chose surgery to relieve symptoms of advanced cancers such as gastrointestinal obstruction, or local-regional control of tumor-related pain or bleeding.
Malignancies treated included gastric, pancreatic, colon, melanoma, sarcomas, breast cancer, hepatobiliary and ovarian cancer, and squamous cell carcinomas.
They found that 44 patients (88%) stated that the surgery "was worth it," and 37 patients (74%) reported symptom resolution or improvement following surgery.
At 1-month follow-up, the complication rate was 44%, and 10% of patients had died. Although there was no association between CRP levels and morbidity or mortality among all patients, 11 of 27 patients with low-grade (grade 1 or 2) complications had elevated CRP (P = .001), as did all 6 patients with high-grade (grade 3 or 4) malignancies (P = .010), and 4 of 5 patients who died (P =.007).
In univariate analysis, factors significantly associated with major complications included elevated CRP (P = .005) and National Cancer Institute (NCI) fatigue score of 1 or greater (P = .001). Factors associated with overall survival were elevated CRP (P less than .0001), and NCI fatigue score (P = .04).
But in multivariate analysis controlling for those factors and for male sex, low albumin levels, significant weight loss, no previous cancer therapy, and hemoglobin less than 10.5 g/dL, only elevated CRP was associated with poor overall survival, with a hazard ratio of 3.6 (P = .0003).
The authors speculate that elevated CRP is a marker for systemic inflammation that may be associated with a higher risk for postoperative complications and for poorer overall survival among patients with advanced cancer.
"Even in this highly selected population, there was 44% morbidity and 10% mortality, illustrating the difficulty in patient selection," Dr. Blakely said.
CRP testing is a simple, low-cost, and objective test that can be easily added on to preoperative evaluation of candidates for palliative surgery, and it may be a useful element in patient selection and counseling, he said.
The study was internally funded. Dr. Blakely reported having no financial disclosures.
AT SSO 2013
Major finding: The hazard ratio for worse survival after palliative surgery among advanced cancer patients with elevated C-reactive protein was 3.6 (P = .0003).
Data source: Retrospective review of a prospective single-center database.
Disclosures: The study was internally funded. Dr. Blakely reported having no financial disclosures.

What's for dessert?
Hemingway once remarked: “Retirement is the ugliest word in the language.” Since most surgeons as well as many others would agree with his assessment, I believe it is time to retire the word retirement and look to another, more positive means of depicting the twilight years of our lives. Shakespeare, writing several centuries before Hemingway, considered the world a stage on which the days of our existence are played out.
<[stk 3]>My rather simplistic view of the surgeon’s life is that of a three-act play or a three-course meal. Act I, the appetizer, represents a surgeon’s approximately 33 years of education and may be, at least in the early years, in part directed by his parents. Act II, the main course and also 33 years give or take a few, is our vocational phase during which we deliver surgical care to our patients. Act III, the dessert, and for symmetry’s sake, can also approach 33 years, is what we formerly called retirement. With appropriate planning and foresight, each of these acts can be and should be gratifying and fulfilling. <[etk]>
<[stk 3]>For most of us a great deal of thought and meticulous planning are responsible for whatever success and satisfaction we have gained from Acts I and II. Unfortunately, such is not the case for Act III, that can be suddenly thrust upon us because of illness or disability. The pundits recommend careful preparation for Act III but their counsel is usually limited to financial considerations. This is an important aspect of Act III, but we all know that a secure economic future does not guarantee happiness or fulfillment. <[etk]>
So what can one do during Act II to make it more likely that the years of Act III are filled with contentment and purpose rather than frustration and regret? Realizing that no formula for Act III fits all, some recommendations and observations may be helpful. Most economic considerations for Act III are obvious and well documented. In nearly all situations, it is wise to never live to or beyond one’s income, to maximize retirement contributions, and to allow carefully chosen professionals rather than ourselves to manage our finances. If too much is consumed during the main course, little will be left for dessert.
A<[stk 3]>ll surgeons have spent much of their lives in service to others, and it is important for most of us that this continue after laying aside our scalpels. For some, this need is met by medical missionary work here or abroad or by service in one or more volunteer organizations. Funding a family foundation during the higher income years of Act II permits you to be a substantial player in philanthropy throughout the years of Act III. If this is done fairly early, even rather modest contributions will grow to an impressive sum by the time Act III arrives, permitting you to make a significant difference in a worthy agency or institution or in the lives of people in need.<[etk]>
<[stk -3]>Life as a surgeon can be all-consuming. An essential activity during Act II is to develop interests, even passions, outside of surgery. It is tempting to put this off until one has more leisure time, but this can be a fatal mistake. Suddenly or even gradually confronting Act III with no appealing substitutes for the many hours spent in the clinic and operating room can lead to an unfulfilling existence. Ideally one or more of these interests should be initiated during Act II, but if that is not possible because of time restrictions, ideas should be carefully recorded as they come to mind so they are not forgotten when the time for action arrives. Preferably some of these should be relevant to the significant other in your life to solidify a relationship that may have suffered from years of separation caused by a demanding work schedule. <[etk]>
<[stk -3]>The most difficult aspect of the transition to Act III can be the loss of identity as a surgeon. Nurturing new interests and passions provides the opportunity to reinvent yourself in a new and exciting way that may be just as satisfying as your former professional life. <[etk]>
Most would agree that nothing in life is more important than relationships. Those with friends and especially family can be stressed and even frayed during the rigorous years of training and work as a surgeon. These must be repaired before or during Act III.
One of the joys that can occupy these later years is the luxury of meaningful time spent with your mate, adult children, grandchildren, and friends. If romance with that important person in your life has waned during the harried years of surgery, Act III is the time to reinvigorate it and bring it to a new and refreshing pinnacle.
<[stk 3]>Finally, a key consideration is timing. When is it time to end your life as a surgeon? Should it be done abruptly or gradually? Gradually is often a challenge as many partnerships are not prone to include a part-time surgeon who does not participate in the call schedule. Again, no size fits all, but it is far preferable to quit when one is near the peak of his/her skills than when associates notice decline that may or may not be verbalized. <[etk]>
<[stk 3]>Rather than emphasizing the ending, in my opinion it is advantageous, even essential, to highlight a new beginning – one in which the skills and talents gained during a life in surgery can be redirected toward novel pursuits and opportunities to help society in new and exciting ways. To get there requires careful planning. As we all know, dessert can be delicious and enjoyable, but it all depends on what w<[ker -3]>e order. <[etk]>
Dr. Rikkers is Editor in Chief of Surgery News.
Hemingway once remarked: “Retirement is the ugliest word in the language.” Since most surgeons as well as many others would agree with his assessment, I believe it is time to retire the word retirement and look to another, more positive means of depicting the twilight years of our lives. Shakespeare, writing several centuries before Hemingway, considered the world a stage on which the days of our existence are played out.
<[stk 3]>My rather simplistic view of the surgeon’s life is that of a three-act play or a three-course meal. Act I, the appetizer, represents a surgeon’s approximately 33 years of education and may be, at least in the early years, in part directed by his parents. Act II, the main course and also 33 years give or take a few, is our vocational phase during which we deliver surgical care to our patients. Act III, the dessert, and for symmetry’s sake, can also approach 33 years, is what we formerly called retirement. With appropriate planning and foresight, each of these acts can be and should be gratifying and fulfilling. <[etk]>
<[stk 3]>For most of us a great deal of thought and meticulous planning are responsible for whatever success and satisfaction we have gained from Acts I and II. Unfortunately, such is not the case for Act III, that can be suddenly thrust upon us because of illness or disability. The pundits recommend careful preparation for Act III but their counsel is usually limited to financial considerations. This is an important aspect of Act III, but we all know that a secure economic future does not guarantee happiness or fulfillment. <[etk]>
So what can one do during Act II to make it more likely that the years of Act III are filled with contentment and purpose rather than frustration and regret? Realizing that no formula for Act III fits all, some recommendations and observations may be helpful. Most economic considerations for Act III are obvious and well documented. In nearly all situations, it is wise to never live to or beyond one’s income, to maximize retirement contributions, and to allow carefully chosen professionals rather than ourselves to manage our finances. If too much is consumed during the main course, little will be left for dessert.
A<[stk 3]>ll surgeons have spent much of their lives in service to others, and it is important for most of us that this continue after laying aside our scalpels. For some, this need is met by medical missionary work here or abroad or by service in one or more volunteer organizations. Funding a family foundation during the higher income years of Act II permits you to be a substantial player in philanthropy throughout the years of Act III. If this is done fairly early, even rather modest contributions will grow to an impressive sum by the time Act III arrives, permitting you to make a significant difference in a worthy agency or institution or in the lives of people in need.<[etk]>
<[stk -3]>Life as a surgeon can be all-consuming. An essential activity during Act II is to develop interests, even passions, outside of surgery. It is tempting to put this off until one has more leisure time, but this can be a fatal mistake. Suddenly or even gradually confronting Act III with no appealing substitutes for the many hours spent in the clinic and operating room can lead to an unfulfilling existence. Ideally one or more of these interests should be initiated during Act II, but if that is not possible because of time restrictions, ideas should be carefully recorded as they come to mind so they are not forgotten when the time for action arrives. Preferably some of these should be relevant to the significant other in your life to solidify a relationship that may have suffered from years of separation caused by a demanding work schedule. <[etk]>
<[stk -3]>The most difficult aspect of the transition to Act III can be the loss of identity as a surgeon. Nurturing new interests and passions provides the opportunity to reinvent yourself in a new and exciting way that may be just as satisfying as your former professional life. <[etk]>
Most would agree that nothing in life is more important than relationships. Those with friends and especially family can be stressed and even frayed during the rigorous years of training and work as a surgeon. These must be repaired before or during Act III.
One of the joys that can occupy these later years is the luxury of meaningful time spent with your mate, adult children, grandchildren, and friends. If romance with that important person in your life has waned during the harried years of surgery, Act III is the time to reinvigorate it and bring it to a new and refreshing pinnacle.
<[stk 3]>Finally, a key consideration is timing. When is it time to end your life as a surgeon? Should it be done abruptly or gradually? Gradually is often a challenge as many partnerships are not prone to include a part-time surgeon who does not participate in the call schedule. Again, no size fits all, but it is far preferable to quit when one is near the peak of his/her skills than when associates notice decline that may or may not be verbalized. <[etk]>
<[stk 3]>Rather than emphasizing the ending, in my opinion it is advantageous, even essential, to highlight a new beginning – one in which the skills and talents gained during a life in surgery can be redirected toward novel pursuits and opportunities to help society in new and exciting ways. To get there requires careful planning. As we all know, dessert can be delicious and enjoyable, but it all depends on what w<[ker -3]>e order. <[etk]>
Dr. Rikkers is Editor in Chief of Surgery News.
Hemingway once remarked: “Retirement is the ugliest word in the language.” Since most surgeons as well as many others would agree with his assessment, I believe it is time to retire the word retirement and look to another, more positive means of depicting the twilight years of our lives. Shakespeare, writing several centuries before Hemingway, considered the world a stage on which the days of our existence are played out.
<[stk 3]>My rather simplistic view of the surgeon’s life is that of a three-act play or a three-course meal. Act I, the appetizer, represents a surgeon’s approximately 33 years of education and may be, at least in the early years, in part directed by his parents. Act II, the main course and also 33 years give or take a few, is our vocational phase during which we deliver surgical care to our patients. Act III, the dessert, and for symmetry’s sake, can also approach 33 years, is what we formerly called retirement. With appropriate planning and foresight, each of these acts can be and should be gratifying and fulfilling. <[etk]>
<[stk 3]>For most of us a great deal of thought and meticulous planning are responsible for whatever success and satisfaction we have gained from Acts I and II. Unfortunately, such is not the case for Act III, that can be suddenly thrust upon us because of illness or disability. The pundits recommend careful preparation for Act III but their counsel is usually limited to financial considerations. This is an important aspect of Act III, but we all know that a secure economic future does not guarantee happiness or fulfillment. <[etk]>
So what can one do during Act II to make it more likely that the years of Act III are filled with contentment and purpose rather than frustration and regret? Realizing that no formula for Act III fits all, some recommendations and observations may be helpful. Most economic considerations for Act III are obvious and well documented. In nearly all situations, it is wise to never live to or beyond one’s income, to maximize retirement contributions, and to allow carefully chosen professionals rather than ourselves to manage our finances. If too much is consumed during the main course, little will be left for dessert.
A<[stk 3]>ll surgeons have spent much of their lives in service to others, and it is important for most of us that this continue after laying aside our scalpels. For some, this need is met by medical missionary work here or abroad or by service in one or more volunteer organizations. Funding a family foundation during the higher income years of Act II permits you to be a substantial player in philanthropy throughout the years of Act III. If this is done fairly early, even rather modest contributions will grow to an impressive sum by the time Act III arrives, permitting you to make a significant difference in a worthy agency or institution or in the lives of people in need.<[etk]>
<[stk -3]>Life as a surgeon can be all-consuming. An essential activity during Act II is to develop interests, even passions, outside of surgery. It is tempting to put this off until one has more leisure time, but this can be a fatal mistake. Suddenly or even gradually confronting Act III with no appealing substitutes for the many hours spent in the clinic and operating room can lead to an unfulfilling existence. Ideally one or more of these interests should be initiated during Act II, but if that is not possible because of time restrictions, ideas should be carefully recorded as they come to mind so they are not forgotten when the time for action arrives. Preferably some of these should be relevant to the significant other in your life to solidify a relationship that may have suffered from years of separation caused by a demanding work schedule. <[etk]>
<[stk -3]>The most difficult aspect of the transition to Act III can be the loss of identity as a surgeon. Nurturing new interests and passions provides the opportunity to reinvent yourself in a new and exciting way that may be just as satisfying as your former professional life. <[etk]>
Most would agree that nothing in life is more important than relationships. Those with friends and especially family can be stressed and even frayed during the rigorous years of training and work as a surgeon. These must be repaired before or during Act III.
One of the joys that can occupy these later years is the luxury of meaningful time spent with your mate, adult children, grandchildren, and friends. If romance with that important person in your life has waned during the harried years of surgery, Act III is the time to reinvigorate it and bring it to a new and refreshing pinnacle.
<[stk 3]>Finally, a key consideration is timing. When is it time to end your life as a surgeon? Should it be done abruptly or gradually? Gradually is often a challenge as many partnerships are not prone to include a part-time surgeon who does not participate in the call schedule. Again, no size fits all, but it is far preferable to quit when one is near the peak of his/her skills than when associates notice decline that may or may not be verbalized. <[etk]>
<[stk 3]>Rather than emphasizing the ending, in my opinion it is advantageous, even essential, to highlight a new beginning – one in which the skills and talents gained during a life in surgery can be redirected toward novel pursuits and opportunities to help society in new and exciting ways. To get there requires careful planning. As we all know, dessert can be delicious and enjoyable, but it all depends on what w<[ker -3]>e order. <[etk]>
Dr. Rikkers is Editor in Chief of Surgery News.

Do surgical residents need ethics teaching?
Recently, I was invited to present surgical grand rounds on an ethics topic. After the talk, a senior surgeon, now retired, who was in the audience confided to me that in all of his years of residency, he had never had a lecture on ethics. This off-hand comment raised a question that demands consideration in the contemporary era of increasingly limited time available for teaching in surgical residencies. Do we need ethics teaching in surgery residencies?
As someone who spent significant time in the last few years in ethics teaching activities, my reflex answer is “Yes.” However, it is worthwhile to explore the reasons why, in the education of contemporary surgeons, it is important to focus dedicated attention on the ethical issues that arise in the practice of surgery.
Certainly, it is not true that ethics was previously unimportant in surgery. In 1915 when the early organizers of the American College of Surgeons were first writing down the qualifications for membership, they emphasized the importance of ethics: “The moral and ethical fitness of the candidates shall be determined by the reports of surgeons whose names are submitted by the candidate himself, and by such other reports and data as the Credentials Committee and the administration of the College may obtain.”[i] Thus, the early founders of the College considered “ethical fitness” to be essential to their members. Since there were clearly ethical and unethical ways to practice surgery, why has the focused emphasis on ethics teaching only occurred in recent decades?
I believe that there are three changes that have occurred in surgical care and surgical education that have led to the importance of this recent focus on ethics education in contemporary surgical training programs: the limitations on work hours for surgical residents, the increasing shift to outpatient care, and the increasing number of options for surgical patients brought about by improvements in surgical technology.
To begin with, surgical residents today spend significantly less time in the hospital every week than did surgical residents in years past. Although one could debate the actual educational value the additional time that I and my surgical predecessors spent in the hospital, there is no question that the significant shortening of the amount of time that surgical residents spend with surgical faculty has resulted in fewer opportunities for learning through role modeling. These many additional hours in the hospital for surgical residents in the past resulted in greater opportunities for residents to see how their faculty dealt with the challenges of managing ethically complex cases. Although these interactions were not often thought of as “ethical role modeling” in prior years, there is no question that significant ethical teaching occurred in this informal curriculum.
Second, and closely related to the reduction in surgical resident work hours, has been the significant shift to outpatient surgical care. This shift has meant that surgical residents whose time is focused on what happens in the hospital have even fewer opportunities to witness faculty engaging in many central aspects of the ethical care of surgical patients (e.g., obtaining informed consent for complex surgical procedures, communicating bad news to patients and families, or weighing risks and benefits of high risk elective surgical procedures).
Perhaps most importantly, today there are more options for surgical therapies than ever before. The central question for a surgeon in 1913 when the American College of Surgeons was formed was, “What can be done for this patient?” Today, in caring for the most complex and critically ill patients, the question that is foremost for surgeons is often “What should be done?” This question is not a purely surgical question, but also an ethical question. Consider a patient who has developed multisystem organ failure after complications from surgery. Because of the advances in critical care, such a patient might be able to be kept alive with technologies such as mechanical ventilation, augmented cardiac output with a ventricular assist device, and hemodialysis. These therapies cannot be judged to be appropriate or not without thoughtful consideration of an individual patient’s overall goals and values. In such a case, weighing values and probabilities for success or failure relative to a particular patient’s goals moves beyond purely scientific surgical decision making into the realm of ethics.
For all of these reasons, I believe that although surgeons have practiced in an ethical fashion for countless generations, the contemporary education of surgeons should include focused attention on ethics and the ethical implications of the surgical interventions that we recommend for our patients. Some might argue that the ultimate goal of surgical education should be to fully integrate the ethical considerations into the surgical care rendered to patients. However, there is so much surgical science to be learned in residency, that in order for consideration of the ethical implications to not be lost, I believe that there must be dedicated attention to ethics teaching.
Although it is an artificial separation to think about distinguishing the ethical considerations from the surgical decision making for a particular patient, the separation is valuable to emphasize the differences between surgical science and surgical ethics. The former is dependent on anatomy, physiology, and surgical technique; whereas the latter is dependent on relationships, communication, and patient values. Although we can train surgical residents to be excellent technicians with a focus purely on surgical science, we can only educate great doctors who are also surgeons by expanding the discussions of optimal surgical care to include the considerations central to surgical ethics.
[1] This important historical background is courtesy of David Nahrwold, MD.
Dr. Angelos is an ACS Fellow, the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, chief, endocrine surgery, and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Recently, I was invited to present surgical grand rounds on an ethics topic. After the talk, a senior surgeon, now retired, who was in the audience confided to me that in all of his years of residency, he had never had a lecture on ethics. This off-hand comment raised a question that demands consideration in the contemporary era of increasingly limited time available for teaching in surgical residencies. Do we need ethics teaching in surgery residencies?
As someone who spent significant time in the last few years in ethics teaching activities, my reflex answer is “Yes.” However, it is worthwhile to explore the reasons why, in the education of contemporary surgeons, it is important to focus dedicated attention on the ethical issues that arise in the practice of surgery.
Certainly, it is not true that ethics was previously unimportant in surgery. In 1915 when the early organizers of the American College of Surgeons were first writing down the qualifications for membership, they emphasized the importance of ethics: “The moral and ethical fitness of the candidates shall be determined by the reports of surgeons whose names are submitted by the candidate himself, and by such other reports and data as the Credentials Committee and the administration of the College may obtain.”[i] Thus, the early founders of the College considered “ethical fitness” to be essential to their members. Since there were clearly ethical and unethical ways to practice surgery, why has the focused emphasis on ethics teaching only occurred in recent decades?
I believe that there are three changes that have occurred in surgical care and surgical education that have led to the importance of this recent focus on ethics education in contemporary surgical training programs: the limitations on work hours for surgical residents, the increasing shift to outpatient care, and the increasing number of options for surgical patients brought about by improvements in surgical technology.
To begin with, surgical residents today spend significantly less time in the hospital every week than did surgical residents in years past. Although one could debate the actual educational value the additional time that I and my surgical predecessors spent in the hospital, there is no question that the significant shortening of the amount of time that surgical residents spend with surgical faculty has resulted in fewer opportunities for learning through role modeling. These many additional hours in the hospital for surgical residents in the past resulted in greater opportunities for residents to see how their faculty dealt with the challenges of managing ethically complex cases. Although these interactions were not often thought of as “ethical role modeling” in prior years, there is no question that significant ethical teaching occurred in this informal curriculum.
Second, and closely related to the reduction in surgical resident work hours, has been the significant shift to outpatient surgical care. This shift has meant that surgical residents whose time is focused on what happens in the hospital have even fewer opportunities to witness faculty engaging in many central aspects of the ethical care of surgical patients (e.g., obtaining informed consent for complex surgical procedures, communicating bad news to patients and families, or weighing risks and benefits of high risk elective surgical procedures).
Perhaps most importantly, today there are more options for surgical therapies than ever before. The central question for a surgeon in 1913 when the American College of Surgeons was formed was, “What can be done for this patient?” Today, in caring for the most complex and critically ill patients, the question that is foremost for surgeons is often “What should be done?” This question is not a purely surgical question, but also an ethical question. Consider a patient who has developed multisystem organ failure after complications from surgery. Because of the advances in critical care, such a patient might be able to be kept alive with technologies such as mechanical ventilation, augmented cardiac output with a ventricular assist device, and hemodialysis. These therapies cannot be judged to be appropriate or not without thoughtful consideration of an individual patient’s overall goals and values. In such a case, weighing values and probabilities for success or failure relative to a particular patient’s goals moves beyond purely scientific surgical decision making into the realm of ethics.
For all of these reasons, I believe that although surgeons have practiced in an ethical fashion for countless generations, the contemporary education of surgeons should include focused attention on ethics and the ethical implications of the surgical interventions that we recommend for our patients. Some might argue that the ultimate goal of surgical education should be to fully integrate the ethical considerations into the surgical care rendered to patients. However, there is so much surgical science to be learned in residency, that in order for consideration of the ethical implications to not be lost, I believe that there must be dedicated attention to ethics teaching.
Although it is an artificial separation to think about distinguishing the ethical considerations from the surgical decision making for a particular patient, the separation is valuable to emphasize the differences between surgical science and surgical ethics. The former is dependent on anatomy, physiology, and surgical technique; whereas the latter is dependent on relationships, communication, and patient values. Although we can train surgical residents to be excellent technicians with a focus purely on surgical science, we can only educate great doctors who are also surgeons by expanding the discussions of optimal surgical care to include the considerations central to surgical ethics.
[1] This important historical background is courtesy of David Nahrwold, MD.
Dr. Angelos is an ACS Fellow, the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, chief, endocrine surgery, and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Recently, I was invited to present surgical grand rounds on an ethics topic. After the talk, a senior surgeon, now retired, who was in the audience confided to me that in all of his years of residency, he had never had a lecture on ethics. This off-hand comment raised a question that demands consideration in the contemporary era of increasingly limited time available for teaching in surgical residencies. Do we need ethics teaching in surgery residencies?
As someone who spent significant time in the last few years in ethics teaching activities, my reflex answer is “Yes.” However, it is worthwhile to explore the reasons why, in the education of contemporary surgeons, it is important to focus dedicated attention on the ethical issues that arise in the practice of surgery.
Certainly, it is not true that ethics was previously unimportant in surgery. In 1915 when the early organizers of the American College of Surgeons were first writing down the qualifications for membership, they emphasized the importance of ethics: “The moral and ethical fitness of the candidates shall be determined by the reports of surgeons whose names are submitted by the candidate himself, and by such other reports and data as the Credentials Committee and the administration of the College may obtain.”[i] Thus, the early founders of the College considered “ethical fitness” to be essential to their members. Since there were clearly ethical and unethical ways to practice surgery, why has the focused emphasis on ethics teaching only occurred in recent decades?
I believe that there are three changes that have occurred in surgical care and surgical education that have led to the importance of this recent focus on ethics education in contemporary surgical training programs: the limitations on work hours for surgical residents, the increasing shift to outpatient care, and the increasing number of options for surgical patients brought about by improvements in surgical technology.
To begin with, surgical residents today spend significantly less time in the hospital every week than did surgical residents in years past. Although one could debate the actual educational value the additional time that I and my surgical predecessors spent in the hospital, there is no question that the significant shortening of the amount of time that surgical residents spend with surgical faculty has resulted in fewer opportunities for learning through role modeling. These many additional hours in the hospital for surgical residents in the past resulted in greater opportunities for residents to see how their faculty dealt with the challenges of managing ethically complex cases. Although these interactions were not often thought of as “ethical role modeling” in prior years, there is no question that significant ethical teaching occurred in this informal curriculum.
Second, and closely related to the reduction in surgical resident work hours, has been the significant shift to outpatient surgical care. This shift has meant that surgical residents whose time is focused on what happens in the hospital have even fewer opportunities to witness faculty engaging in many central aspects of the ethical care of surgical patients (e.g., obtaining informed consent for complex surgical procedures, communicating bad news to patients and families, or weighing risks and benefits of high risk elective surgical procedures).
Perhaps most importantly, today there are more options for surgical therapies than ever before. The central question for a surgeon in 1913 when the American College of Surgeons was formed was, “What can be done for this patient?” Today, in caring for the most complex and critically ill patients, the question that is foremost for surgeons is often “What should be done?” This question is not a purely surgical question, but also an ethical question. Consider a patient who has developed multisystem organ failure after complications from surgery. Because of the advances in critical care, such a patient might be able to be kept alive with technologies such as mechanical ventilation, augmented cardiac output with a ventricular assist device, and hemodialysis. These therapies cannot be judged to be appropriate or not without thoughtful consideration of an individual patient’s overall goals and values. In such a case, weighing values and probabilities for success or failure relative to a particular patient’s goals moves beyond purely scientific surgical decision making into the realm of ethics.
For all of these reasons, I believe that although surgeons have practiced in an ethical fashion for countless generations, the contemporary education of surgeons should include focused attention on ethics and the ethical implications of the surgical interventions that we recommend for our patients. Some might argue that the ultimate goal of surgical education should be to fully integrate the ethical considerations into the surgical care rendered to patients. However, there is so much surgical science to be learned in residency, that in order for consideration of the ethical implications to not be lost, I believe that there must be dedicated attention to ethics teaching.
Although it is an artificial separation to think about distinguishing the ethical considerations from the surgical decision making for a particular patient, the separation is valuable to emphasize the differences between surgical science and surgical ethics. The former is dependent on anatomy, physiology, and surgical technique; whereas the latter is dependent on relationships, communication, and patient values. Although we can train surgical residents to be excellent technicians with a focus purely on surgical science, we can only educate great doctors who are also surgeons by expanding the discussions of optimal surgical care to include the considerations central to surgical ethics.
[1] This important historical background is courtesy of David Nahrwold, MD.
Dr. Angelos is an ACS Fellow, the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, chief, endocrine surgery, and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Designer T cells take aim at liver metastases
NATIONAL HARBOR, MD – Designer T cells used in immunotherapy for the treatment of liver metastases are well tolerated and reduced tumor burden in a small phase I study, reported an investigator at the annual Society of Surgical Oncology Cancer Symposium.
But the biggest barrier to the success of the therapy may lie in the liver itself, said Dr. Steven C. Katz, a surgical oncologist at the Roger Williams Cancer Center in Providence, R.I.
"Thinking long term, we’re going to have to address the suppressive forces that exist in the liver. I don’t think this is really going to succeed clinically until we find a way to do that," he said.
Genetically modified, designer T-cell technology allows translational science researchers to manufacture and deliver highly potent, specific agents to invoke a desired antitumor response, rather than trying to boost a general host immune response through, say, a vaccine, Dr. Katz said.
The technology has the potential to act against a variety of tumor types, and has been demonstrated to have activity against chronic lymphocytic leukemia, synovial sarcoma, and melanoma, he said.
The technique involves harvesting T cells from patients, activating them in culture, and then transfecting them with a retrovirus to get them to express a highly specific chimeric antigen receptor (CAR).
Dr. Katz and his colleagues are developing a CAR with an immunoglobulin fragment directed against carcinoembryonic antigen (CEA).
"A T cell that expresses this anti-CEA CAR, when it encounters a CEA-positive tumor, ... is activated to divide [and] produce cytokines and is poised to lyse and kill tumor cells in a highly specific fashion, and we demonstrated this in vitro, as have several other groups," he said.
But getting the antigen to the target – CEA-positive liver metastases – is just part of the challenge, he added. Delivering the CAR into the hepatic arterial circulation appears to be the optimal approach for confining the therapy to the target area, thus avoiding possible complications such as colitis that can occur when anti-CEA is delivered systemically.
A second barrier to the therapy is that the liver contains high numbers of suppressive immune cells such as regulatory T cells and myeloid-derived suppressor cells. Coinfusion of cytokines such as interleukin-2 (IL-2) appears to be a necessary step for preventing intrahepatic suppression of therapy, Dr. Katz said.
The investigators have initiated a phase I safety and intrapatient dose-escalation trial of the technology. Patients with CEA-positive liver metastases are given percutaneous infusions of their modified T cells through a femoral artery puncture directly into the hepatic artery. Embolization of the gastroduodenal and right gastric arteries is performed to prevent or limit extrahepatic infusion of the modified cells.
The patients all have unresectable, histologically confirmed CEA-positive liver metastases from colorectal, hepatobiliary, ampullary, or gastric primary tumors; have no extrahepatic disease beyond the lungs; and have had failure of one or more lines of standard systemic chemotherapy.
The first three patients have been treated in a dose-escalation fashion without cytokines. A second cohort of three patients is receiving both designer T cells and a continuous systemic infusion of IL-2 at a relatively low dose of 75,000 IU/kg per day to suppress the liver’s immune response.
"We know that IL-2 is going to be essential for these T cells to survive and do what we want them to do in vivo," Dr. Katz said.
Of the first six patients enrolled, two have been withdrawn from the study: one who had disease progression within the lungs following a second infusion of designer T cells, and one whose designer T cells were discovered to be infected with West Nile virus.
There have been no serious grade 3 or 4 adverse events to date. Adverse events have included grade 2 fevers, a grade 1 fever, and a rash. There has been no significant elevation over baseline in liver enzymes or bilirubin, Dr. Katz said.
Flow cytometry in early testing has shown that the modified T cells appear to be confined to the normal liver and metastatic sites, and have not been detected in significant numbers in peripheral circulation.
To date, only one patient has been treated with designer T cells and IL-2 support; this patient has thus far had a "very favorable" course, with a 40% decrease in tumor burden, although these results are still too early for clinical conclusions to be drawn.
The investigators are exploring additional strategies to circumvent intrahepatic suppression of the therapy by blocking the action of myeloid-derived suppressor cells.
The study was supported by a Society of Surgical Oncology Clinical Investigator Award, an education grant from Genentech, the National Institutes of Health, and the Rhode Island Foundation. Dr. Katz reported having no relevant financial disclosures.
NATIONAL HARBOR, MD – Designer T cells used in immunotherapy for the treatment of liver metastases are well tolerated and reduced tumor burden in a small phase I study, reported an investigator at the annual Society of Surgical Oncology Cancer Symposium.
But the biggest barrier to the success of the therapy may lie in the liver itself, said Dr. Steven C. Katz, a surgical oncologist at the Roger Williams Cancer Center in Providence, R.I.
"Thinking long term, we’re going to have to address the suppressive forces that exist in the liver. I don’t think this is really going to succeed clinically until we find a way to do that," he said.
Genetically modified, designer T-cell technology allows translational science researchers to manufacture and deliver highly potent, specific agents to invoke a desired antitumor response, rather than trying to boost a general host immune response through, say, a vaccine, Dr. Katz said.
The technology has the potential to act against a variety of tumor types, and has been demonstrated to have activity against chronic lymphocytic leukemia, synovial sarcoma, and melanoma, he said.
The technique involves harvesting T cells from patients, activating them in culture, and then transfecting them with a retrovirus to get them to express a highly specific chimeric antigen receptor (CAR).
Dr. Katz and his colleagues are developing a CAR with an immunoglobulin fragment directed against carcinoembryonic antigen (CEA).
"A T cell that expresses this anti-CEA CAR, when it encounters a CEA-positive tumor, ... is activated to divide [and] produce cytokines and is poised to lyse and kill tumor cells in a highly specific fashion, and we demonstrated this in vitro, as have several other groups," he said.
But getting the antigen to the target – CEA-positive liver metastases – is just part of the challenge, he added. Delivering the CAR into the hepatic arterial circulation appears to be the optimal approach for confining the therapy to the target area, thus avoiding possible complications such as colitis that can occur when anti-CEA is delivered systemically.
A second barrier to the therapy is that the liver contains high numbers of suppressive immune cells such as regulatory T cells and myeloid-derived suppressor cells. Coinfusion of cytokines such as interleukin-2 (IL-2) appears to be a necessary step for preventing intrahepatic suppression of therapy, Dr. Katz said.
The investigators have initiated a phase I safety and intrapatient dose-escalation trial of the technology. Patients with CEA-positive liver metastases are given percutaneous infusions of their modified T cells through a femoral artery puncture directly into the hepatic artery. Embolization of the gastroduodenal and right gastric arteries is performed to prevent or limit extrahepatic infusion of the modified cells.
The patients all have unresectable, histologically confirmed CEA-positive liver metastases from colorectal, hepatobiliary, ampullary, or gastric primary tumors; have no extrahepatic disease beyond the lungs; and have had failure of one or more lines of standard systemic chemotherapy.
The first three patients have been treated in a dose-escalation fashion without cytokines. A second cohort of three patients is receiving both designer T cells and a continuous systemic infusion of IL-2 at a relatively low dose of 75,000 IU/kg per day to suppress the liver’s immune response.
"We know that IL-2 is going to be essential for these T cells to survive and do what we want them to do in vivo," Dr. Katz said.
Of the first six patients enrolled, two have been withdrawn from the study: one who had disease progression within the lungs following a second infusion of designer T cells, and one whose designer T cells were discovered to be infected with West Nile virus.
There have been no serious grade 3 or 4 adverse events to date. Adverse events have included grade 2 fevers, a grade 1 fever, and a rash. There has been no significant elevation over baseline in liver enzymes or bilirubin, Dr. Katz said.
Flow cytometry in early testing has shown that the modified T cells appear to be confined to the normal liver and metastatic sites, and have not been detected in significant numbers in peripheral circulation.
To date, only one patient has been treated with designer T cells and IL-2 support; this patient has thus far had a "very favorable" course, with a 40% decrease in tumor burden, although these results are still too early for clinical conclusions to be drawn.
The investigators are exploring additional strategies to circumvent intrahepatic suppression of the therapy by blocking the action of myeloid-derived suppressor cells.
The study was supported by a Society of Surgical Oncology Clinical Investigator Award, an education grant from Genentech, the National Institutes of Health, and the Rhode Island Foundation. Dr. Katz reported having no relevant financial disclosures.
NATIONAL HARBOR, MD – Designer T cells used in immunotherapy for the treatment of liver metastases are well tolerated and reduced tumor burden in a small phase I study, reported an investigator at the annual Society of Surgical Oncology Cancer Symposium.
But the biggest barrier to the success of the therapy may lie in the liver itself, said Dr. Steven C. Katz, a surgical oncologist at the Roger Williams Cancer Center in Providence, R.I.
"Thinking long term, we’re going to have to address the suppressive forces that exist in the liver. I don’t think this is really going to succeed clinically until we find a way to do that," he said.
Genetically modified, designer T-cell technology allows translational science researchers to manufacture and deliver highly potent, specific agents to invoke a desired antitumor response, rather than trying to boost a general host immune response through, say, a vaccine, Dr. Katz said.
The technology has the potential to act against a variety of tumor types, and has been demonstrated to have activity against chronic lymphocytic leukemia, synovial sarcoma, and melanoma, he said.
The technique involves harvesting T cells from patients, activating them in culture, and then transfecting them with a retrovirus to get them to express a highly specific chimeric antigen receptor (CAR).
Dr. Katz and his colleagues are developing a CAR with an immunoglobulin fragment directed against carcinoembryonic antigen (CEA).
"A T cell that expresses this anti-CEA CAR, when it encounters a CEA-positive tumor, ... is activated to divide [and] produce cytokines and is poised to lyse and kill tumor cells in a highly specific fashion, and we demonstrated this in vitro, as have several other groups," he said.
But getting the antigen to the target – CEA-positive liver metastases – is just part of the challenge, he added. Delivering the CAR into the hepatic arterial circulation appears to be the optimal approach for confining the therapy to the target area, thus avoiding possible complications such as colitis that can occur when anti-CEA is delivered systemically.
A second barrier to the therapy is that the liver contains high numbers of suppressive immune cells such as regulatory T cells and myeloid-derived suppressor cells. Coinfusion of cytokines such as interleukin-2 (IL-2) appears to be a necessary step for preventing intrahepatic suppression of therapy, Dr. Katz said.
The investigators have initiated a phase I safety and intrapatient dose-escalation trial of the technology. Patients with CEA-positive liver metastases are given percutaneous infusions of their modified T cells through a femoral artery puncture directly into the hepatic artery. Embolization of the gastroduodenal and right gastric arteries is performed to prevent or limit extrahepatic infusion of the modified cells.
The patients all have unresectable, histologically confirmed CEA-positive liver metastases from colorectal, hepatobiliary, ampullary, or gastric primary tumors; have no extrahepatic disease beyond the lungs; and have had failure of one or more lines of standard systemic chemotherapy.
The first three patients have been treated in a dose-escalation fashion without cytokines. A second cohort of three patients is receiving both designer T cells and a continuous systemic infusion of IL-2 at a relatively low dose of 75,000 IU/kg per day to suppress the liver’s immune response.
"We know that IL-2 is going to be essential for these T cells to survive and do what we want them to do in vivo," Dr. Katz said.
Of the first six patients enrolled, two have been withdrawn from the study: one who had disease progression within the lungs following a second infusion of designer T cells, and one whose designer T cells were discovered to be infected with West Nile virus.
There have been no serious grade 3 or 4 adverse events to date. Adverse events have included grade 2 fevers, a grade 1 fever, and a rash. There has been no significant elevation over baseline in liver enzymes or bilirubin, Dr. Katz said.
Flow cytometry in early testing has shown that the modified T cells appear to be confined to the normal liver and metastatic sites, and have not been detected in significant numbers in peripheral circulation.
To date, only one patient has been treated with designer T cells and IL-2 support; this patient has thus far had a "very favorable" course, with a 40% decrease in tumor burden, although these results are still too early for clinical conclusions to be drawn.
The investigators are exploring additional strategies to circumvent intrahepatic suppression of the therapy by blocking the action of myeloid-derived suppressor cells.
The study was supported by a Society of Surgical Oncology Clinical Investigator Award, an education grant from Genentech, the National Institutes of Health, and the Rhode Island Foundation. Dr. Katz reported having no relevant financial disclosures.
AT SSO 2013
Major finding: One patient who received designer T cells and interleukin-2 has had a 40% decrease in liver metastases.
Data source: Early report of a phase I safety and dose-escalation trial of T-cell immunotherapy for unresectable liver metastases.
Disclosures: The study was supported by a Society of Surgical Oncology Investigator Award, an educational grant from Genentech, the National Institutes of Health, and the Rhode Island Foundation. Dr. Katz reported having no relevant financial disclosures.
Physicians' spouses/partners satisfied with relationships
Almost 87% of physicians’ spouses or partners said that they were satisfied with their relationships, according to a survey of 891 individuals.
More than 55% of the spouses and partners of physicians who responded said that they were "extremely satisfied" with their relationships and more than 31% said they were "somewhat satisfied," reported Dr. Tait D. Shanafelt of the Mayo Clinic, Rochester, Minn., and his associates.
Almost 81% of the respondents said that, knowing what they know now, they would choose a physician spouse or partner again, the investigators noted (Mayo Clin. Proc. 2013;88:216-25).
Approximately 73% of the respondents were women, but the men who responded were more likely to be employed outside the home: 73% vs. 51% of female spouses/partners. About 10% of respondents who worked outside the home were physicians themselves, and almost 31% were nonphysician health care professionals, Dr. Shanafelt and his associates said.
The survey, conducted from Aug. 17 to Sept. 11, 2011, involved a national sample of physicians from all specialties taken from the American Medical Association’s Physician Masterfile. The study was funded by the AMA and the Mayo Clinic’s Program on Physician Well-Being.
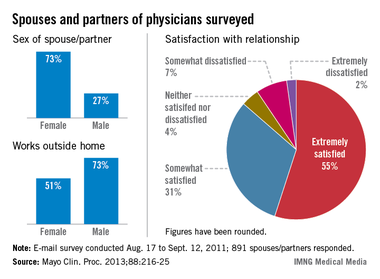
Almost 87% of physicians’ spouses or partners said that they were satisfied with their relationships, according to a survey of 891 individuals.
More than 55% of the spouses and partners of physicians who responded said that they were "extremely satisfied" with their relationships and more than 31% said they were "somewhat satisfied," reported Dr. Tait D. Shanafelt of the Mayo Clinic, Rochester, Minn., and his associates.
Almost 81% of the respondents said that, knowing what they know now, they would choose a physician spouse or partner again, the investigators noted (Mayo Clin. Proc. 2013;88:216-25).
Approximately 73% of the respondents were women, but the men who responded were more likely to be employed outside the home: 73% vs. 51% of female spouses/partners. About 10% of respondents who worked outside the home were physicians themselves, and almost 31% were nonphysician health care professionals, Dr. Shanafelt and his associates said.
The survey, conducted from Aug. 17 to Sept. 11, 2011, involved a national sample of physicians from all specialties taken from the American Medical Association’s Physician Masterfile. The study was funded by the AMA and the Mayo Clinic’s Program on Physician Well-Being.
Almost 87% of physicians’ spouses or partners said that they were satisfied with their relationships, according to a survey of 891 individuals.
More than 55% of the spouses and partners of physicians who responded said that they were "extremely satisfied" with their relationships and more than 31% said they were "somewhat satisfied," reported Dr. Tait D. Shanafelt of the Mayo Clinic, Rochester, Minn., and his associates.
Almost 81% of the respondents said that, knowing what they know now, they would choose a physician spouse or partner again, the investigators noted (Mayo Clin. Proc. 2013;88:216-25).
Approximately 73% of the respondents were women, but the men who responded were more likely to be employed outside the home: 73% vs. 51% of female spouses/partners. About 10% of respondents who worked outside the home were physicians themselves, and almost 31% were nonphysician health care professionals, Dr. Shanafelt and his associates said.
The survey, conducted from Aug. 17 to Sept. 11, 2011, involved a national sample of physicians from all specialties taken from the American Medical Association’s Physician Masterfile. The study was funded by the AMA and the Mayo Clinic’s Program on Physician Well-Being.
FROM MAYO CLINIC PROCEEDINGS