User login
Will New Obesity Drugs Make Bariatric Surgery Obsolete?
MADRID — In spirited presentations at the annual meeting of the European Association for the Study of Diabetes, Louis J. Aronne, MD, of Weill Cornell Medicine in New York City, made a compelling case that the next generation of obesity medications will make bariatric surgery obsolete, and Francesco Rubino, MD, of King’s College London in England, made an equally compelling case that they will not.
In fact, Dr. Rubino predicted that “metabolic” surgery — new nomenclature reflecting the power of surgery to reduce not only obesity, but also other metabolic conditions, over the long term — will continue and could even increase in years to come.
‘Medical Treatment Will Dominate’
“Obesity treatment is the superhero of treating metabolic disease because it can defeat all of the bad guys at once, not just one, like the other treatments,” Dr. Aronne told meeting attendees. “If you treat somebody’s cholesterol, you’re just treating their cholesterol, and you may actually increase their risk of developing type 2 diabetes (T2D). You treat their blood pressure, you don’t treat their glucose and you don’t treat their lipids — the list goes on and on and on. But by treating obesity, if you can get enough weight loss, you can get all those things at once.”
He pointed to the SELECT trial, which showed that treating obesity with a glucagon-like peptide 1 receptor agonist reduced major adverse cardiovascular events as well as death from any cause, results in line with those from other modes of treatment for cardiovascular disease (CVD) or lipid lowering, he said. “But we get much more with these drugs, including positive effects on heart failure, chronic kidney disease, and a 73% reduction in T2D. So, we’re now on the verge of a major change in the way we manage metabolic disease.”
Dr. Aronne drew a parallel between treating obesity and the historic way of treating hypertension. Years ago, he said, “we waited too long to treat people. We waited until they had severe hypertension that in many cases was irreversible. What would you prefer to do now for obesity — have the patient lose weight with a medicine that is proven to reduce complications or wait until they develop diabetes, high blood pressure, heart disease and then have them undergo surgery to treat that?”
Looking ahead, “the trend could be to treat obesity before it gets out of hand,” he suggested. Treatment might start in people with a body mass index (BMI) of 27 kg/m2, who would be treated to a target BMI of 25. “That’s only a 10% or so change, but our goal would be to keep them in the normal range so they never go above that target. In fact, I think we’re going to be looking at people with severe obesity in a few years and saying, ‘I can’t believe someone didn’t treat that guy earlier.’ What’s going to happen to bariatric surgery if no one gets to a higher weight?”
The plethora of current weight-loss drugs and the large group on the horizon mean that if someone doesn’t respond to one drug, there will be plenty of other choices, Dr. Aronne continued. People will be referred for surgery, but possibly only after they’ve not responded to medical treatment — or just the opposite. “In the United States, it’s much cheaper to have surgery, and I bet the insurance companies are going to make people have surgery before they can get the medicines,” he acknowledged.
A recent report from Morgan Stanley suggests that the global market for the newer weight-loss drugs could increase by 15-fold over the next 5 years as their benefits expand beyond weight loss and that as much as 9% of the US population will be taking the drugs by 2035, Dr. Aronne said, adding that he thinks 9% is an underestimate. By contrast, the number of patients treated by his team’s surgical program is down about 20%.
“I think it’s very clear that medical treatment is going to dominate,” he concluded. “But, it’s also possible that surgery could go up because so many people are going to be coming for medical therapy that we may wind up referring more for surgical therapy.”
‘Surgery Is Saving Lives’
Dr. Rubino is convinced that anti-obesity drugs will not make surgery obsolete, “but it will not be business as usual,” he told meeting attendees. “In fact, I think these drugs will expedite a process that is already ongoing — a transformation of bariatric into metabolic surgery.”
“Bariatric surgery will go down in history as one of the biggest missed opportunities that we, as medical professionals, have seen over the past many years,” he said. “It has been shown beyond any doubt to reduce all-cause mortality — in other words, it saves lives,” and it’s also cost effective and improves quality of life. Yet, fewer than 1% of people globally who meet the criteria actually get the surgery.
Many clinicians don’t inform patients about the treatment and don’t refer them for it, he said. “That would be equivalent to having surgery for CVD [cardiovascular disease], cancer, or other important diseases available but not being accessed as they should be.”
A big reason for the dearth of procedures is that people have unrealistic expectations about diet and exercise interventions for weight loss, he said. His team’s survey, presented at the 26th World Congress of the International Federation for the Surgery of Obesity and Metabolic Disorders, showed that 43% of respondents believed diet and exercise was the best treatment for severe obesity (BMI > 35). A more recent survey asked which among several choices was the most effective weight-loss intervention, and again a large proportion “believed wrongly that diet and exercise is most effective — more so than drugs or surgery — despite plenty of evidence that this is not the case.”
In this context, he said, “any surgery, no matter how safe or effective, would never be very popular.” If obesity is viewed as a modifiable risk factor, patients may say they’ll think about it for 6 months. In contrast, “nobody will tell you ‘I will think about it’ if you tell them they need gallbladder surgery to get rid of gallstone pain.”
Although drugs are available to treat obesity, none of them are curative, and if they’re stopped, the weight comes back, Dr. Rubino pointed out. “Efficacy of drugs is measured in weeks or months, whereas efficacy of surgery is measured in decades of durability — in the case of bariatric surgery, 10-20 years. That’s why bariatric surgery will remain an option,” he said. “It’s not just preventing disease, it’s resolving ongoing disease.”
Furthermore, bariatric surgery is showing value for people with established T2D, whereas in the past, it was mainly considered to be a weight-loss intervention for younger, healthier patients, he said. “In my practice, we’re operating more often in people with T2D, even those at higher risk for anesthesia and surgery — eg, patients with heart failure, chronic kidney disease, on dialysis — and we’re still able to maintain the same safety with minimally invasive laparoscopic surgery that we had with healthier patients.”
A vote held at the end of the session revealed that the audience was split about half and half in favor of drugs making bariatric surgery obsolete or not.
“I think we may have to duke it out now,” Dr. Aronne quipped.
Dr. Aronne disclosed being a consultant, speaker, and adviser for and receiving research support from Altimmune, Amgen, AstraZeneca, Eli Lilly, Intellihealth, Janssen, Novo Nordisk, Pfizer, Senda, UnitedHealth Group, Versanis, and others; he has ownership interests in ERX, Intellihealth, Jamieson, Kallyope, Skye Bioscience, Veru, and others; and he is on the board of directors of ERX, Jamieson Wellness, and Intellihealth/FlyteHealth. Dr. Rubino disclosed receiving research and educational grants from Novo Nordisk, Ethicon, and Medtronic; he is on the scientific advisory board/data safety advisory board for Keyron, Morphic Medical, and GT Metabolic Solutions; he receives speaking honoraria from Medtronic, Ethicon, Novo Nordisk, and Eli Lilly; and he is president of the nonprofit Metabolic Health Institute.
A version of this article first appeared on Medscape.com.
MADRID — In spirited presentations at the annual meeting of the European Association for the Study of Diabetes, Louis J. Aronne, MD, of Weill Cornell Medicine in New York City, made a compelling case that the next generation of obesity medications will make bariatric surgery obsolete, and Francesco Rubino, MD, of King’s College London in England, made an equally compelling case that they will not.
In fact, Dr. Rubino predicted that “metabolic” surgery — new nomenclature reflecting the power of surgery to reduce not only obesity, but also other metabolic conditions, over the long term — will continue and could even increase in years to come.
‘Medical Treatment Will Dominate’
“Obesity treatment is the superhero of treating metabolic disease because it can defeat all of the bad guys at once, not just one, like the other treatments,” Dr. Aronne told meeting attendees. “If you treat somebody’s cholesterol, you’re just treating their cholesterol, and you may actually increase their risk of developing type 2 diabetes (T2D). You treat their blood pressure, you don’t treat their glucose and you don’t treat their lipids — the list goes on and on and on. But by treating obesity, if you can get enough weight loss, you can get all those things at once.”
He pointed to the SELECT trial, which showed that treating obesity with a glucagon-like peptide 1 receptor agonist reduced major adverse cardiovascular events as well as death from any cause, results in line with those from other modes of treatment for cardiovascular disease (CVD) or lipid lowering, he said. “But we get much more with these drugs, including positive effects on heart failure, chronic kidney disease, and a 73% reduction in T2D. So, we’re now on the verge of a major change in the way we manage metabolic disease.”
Dr. Aronne drew a parallel between treating obesity and the historic way of treating hypertension. Years ago, he said, “we waited too long to treat people. We waited until they had severe hypertension that in many cases was irreversible. What would you prefer to do now for obesity — have the patient lose weight with a medicine that is proven to reduce complications or wait until they develop diabetes, high blood pressure, heart disease and then have them undergo surgery to treat that?”
Looking ahead, “the trend could be to treat obesity before it gets out of hand,” he suggested. Treatment might start in people with a body mass index (BMI) of 27 kg/m2, who would be treated to a target BMI of 25. “That’s only a 10% or so change, but our goal would be to keep them in the normal range so they never go above that target. In fact, I think we’re going to be looking at people with severe obesity in a few years and saying, ‘I can’t believe someone didn’t treat that guy earlier.’ What’s going to happen to bariatric surgery if no one gets to a higher weight?”
The plethora of current weight-loss drugs and the large group on the horizon mean that if someone doesn’t respond to one drug, there will be plenty of other choices, Dr. Aronne continued. People will be referred for surgery, but possibly only after they’ve not responded to medical treatment — or just the opposite. “In the United States, it’s much cheaper to have surgery, and I bet the insurance companies are going to make people have surgery before they can get the medicines,” he acknowledged.
A recent report from Morgan Stanley suggests that the global market for the newer weight-loss drugs could increase by 15-fold over the next 5 years as their benefits expand beyond weight loss and that as much as 9% of the US population will be taking the drugs by 2035, Dr. Aronne said, adding that he thinks 9% is an underestimate. By contrast, the number of patients treated by his team’s surgical program is down about 20%.
“I think it’s very clear that medical treatment is going to dominate,” he concluded. “But, it’s also possible that surgery could go up because so many people are going to be coming for medical therapy that we may wind up referring more for surgical therapy.”
‘Surgery Is Saving Lives’
Dr. Rubino is convinced that anti-obesity drugs will not make surgery obsolete, “but it will not be business as usual,” he told meeting attendees. “In fact, I think these drugs will expedite a process that is already ongoing — a transformation of bariatric into metabolic surgery.”
“Bariatric surgery will go down in history as one of the biggest missed opportunities that we, as medical professionals, have seen over the past many years,” he said. “It has been shown beyond any doubt to reduce all-cause mortality — in other words, it saves lives,” and it’s also cost effective and improves quality of life. Yet, fewer than 1% of people globally who meet the criteria actually get the surgery.
Many clinicians don’t inform patients about the treatment and don’t refer them for it, he said. “That would be equivalent to having surgery for CVD [cardiovascular disease], cancer, or other important diseases available but not being accessed as they should be.”
A big reason for the dearth of procedures is that people have unrealistic expectations about diet and exercise interventions for weight loss, he said. His team’s survey, presented at the 26th World Congress of the International Federation for the Surgery of Obesity and Metabolic Disorders, showed that 43% of respondents believed diet and exercise was the best treatment for severe obesity (BMI > 35). A more recent survey asked which among several choices was the most effective weight-loss intervention, and again a large proportion “believed wrongly that diet and exercise is most effective — more so than drugs or surgery — despite plenty of evidence that this is not the case.”
In this context, he said, “any surgery, no matter how safe or effective, would never be very popular.” If obesity is viewed as a modifiable risk factor, patients may say they’ll think about it for 6 months. In contrast, “nobody will tell you ‘I will think about it’ if you tell them they need gallbladder surgery to get rid of gallstone pain.”
Although drugs are available to treat obesity, none of them are curative, and if they’re stopped, the weight comes back, Dr. Rubino pointed out. “Efficacy of drugs is measured in weeks or months, whereas efficacy of surgery is measured in decades of durability — in the case of bariatric surgery, 10-20 years. That’s why bariatric surgery will remain an option,” he said. “It’s not just preventing disease, it’s resolving ongoing disease.”
Furthermore, bariatric surgery is showing value for people with established T2D, whereas in the past, it was mainly considered to be a weight-loss intervention for younger, healthier patients, he said. “In my practice, we’re operating more often in people with T2D, even those at higher risk for anesthesia and surgery — eg, patients with heart failure, chronic kidney disease, on dialysis — and we’re still able to maintain the same safety with minimally invasive laparoscopic surgery that we had with healthier patients.”
A vote held at the end of the session revealed that the audience was split about half and half in favor of drugs making bariatric surgery obsolete or not.
“I think we may have to duke it out now,” Dr. Aronne quipped.
Dr. Aronne disclosed being a consultant, speaker, and adviser for and receiving research support from Altimmune, Amgen, AstraZeneca, Eli Lilly, Intellihealth, Janssen, Novo Nordisk, Pfizer, Senda, UnitedHealth Group, Versanis, and others; he has ownership interests in ERX, Intellihealth, Jamieson, Kallyope, Skye Bioscience, Veru, and others; and he is on the board of directors of ERX, Jamieson Wellness, and Intellihealth/FlyteHealth. Dr. Rubino disclosed receiving research and educational grants from Novo Nordisk, Ethicon, and Medtronic; he is on the scientific advisory board/data safety advisory board for Keyron, Morphic Medical, and GT Metabolic Solutions; he receives speaking honoraria from Medtronic, Ethicon, Novo Nordisk, and Eli Lilly; and he is president of the nonprofit Metabolic Health Institute.
A version of this article first appeared on Medscape.com.
MADRID — In spirited presentations at the annual meeting of the European Association for the Study of Diabetes, Louis J. Aronne, MD, of Weill Cornell Medicine in New York City, made a compelling case that the next generation of obesity medications will make bariatric surgery obsolete, and Francesco Rubino, MD, of King’s College London in England, made an equally compelling case that they will not.
In fact, Dr. Rubino predicted that “metabolic” surgery — new nomenclature reflecting the power of surgery to reduce not only obesity, but also other metabolic conditions, over the long term — will continue and could even increase in years to come.
‘Medical Treatment Will Dominate’
“Obesity treatment is the superhero of treating metabolic disease because it can defeat all of the bad guys at once, not just one, like the other treatments,” Dr. Aronne told meeting attendees. “If you treat somebody’s cholesterol, you’re just treating their cholesterol, and you may actually increase their risk of developing type 2 diabetes (T2D). You treat their blood pressure, you don’t treat their glucose and you don’t treat their lipids — the list goes on and on and on. But by treating obesity, if you can get enough weight loss, you can get all those things at once.”
He pointed to the SELECT trial, which showed that treating obesity with a glucagon-like peptide 1 receptor agonist reduced major adverse cardiovascular events as well as death from any cause, results in line with those from other modes of treatment for cardiovascular disease (CVD) or lipid lowering, he said. “But we get much more with these drugs, including positive effects on heart failure, chronic kidney disease, and a 73% reduction in T2D. So, we’re now on the verge of a major change in the way we manage metabolic disease.”
Dr. Aronne drew a parallel between treating obesity and the historic way of treating hypertension. Years ago, he said, “we waited too long to treat people. We waited until they had severe hypertension that in many cases was irreversible. What would you prefer to do now for obesity — have the patient lose weight with a medicine that is proven to reduce complications or wait until they develop diabetes, high blood pressure, heart disease and then have them undergo surgery to treat that?”
Looking ahead, “the trend could be to treat obesity before it gets out of hand,” he suggested. Treatment might start in people with a body mass index (BMI) of 27 kg/m2, who would be treated to a target BMI of 25. “That’s only a 10% or so change, but our goal would be to keep them in the normal range so they never go above that target. In fact, I think we’re going to be looking at people with severe obesity in a few years and saying, ‘I can’t believe someone didn’t treat that guy earlier.’ What’s going to happen to bariatric surgery if no one gets to a higher weight?”
The plethora of current weight-loss drugs and the large group on the horizon mean that if someone doesn’t respond to one drug, there will be plenty of other choices, Dr. Aronne continued. People will be referred for surgery, but possibly only after they’ve not responded to medical treatment — or just the opposite. “In the United States, it’s much cheaper to have surgery, and I bet the insurance companies are going to make people have surgery before they can get the medicines,” he acknowledged.
A recent report from Morgan Stanley suggests that the global market for the newer weight-loss drugs could increase by 15-fold over the next 5 years as their benefits expand beyond weight loss and that as much as 9% of the US population will be taking the drugs by 2035, Dr. Aronne said, adding that he thinks 9% is an underestimate. By contrast, the number of patients treated by his team’s surgical program is down about 20%.
“I think it’s very clear that medical treatment is going to dominate,” he concluded. “But, it’s also possible that surgery could go up because so many people are going to be coming for medical therapy that we may wind up referring more for surgical therapy.”
‘Surgery Is Saving Lives’
Dr. Rubino is convinced that anti-obesity drugs will not make surgery obsolete, “but it will not be business as usual,” he told meeting attendees. “In fact, I think these drugs will expedite a process that is already ongoing — a transformation of bariatric into metabolic surgery.”
“Bariatric surgery will go down in history as one of the biggest missed opportunities that we, as medical professionals, have seen over the past many years,” he said. “It has been shown beyond any doubt to reduce all-cause mortality — in other words, it saves lives,” and it’s also cost effective and improves quality of life. Yet, fewer than 1% of people globally who meet the criteria actually get the surgery.
Many clinicians don’t inform patients about the treatment and don’t refer them for it, he said. “That would be equivalent to having surgery for CVD [cardiovascular disease], cancer, or other important diseases available but not being accessed as they should be.”
A big reason for the dearth of procedures is that people have unrealistic expectations about diet and exercise interventions for weight loss, he said. His team’s survey, presented at the 26th World Congress of the International Federation for the Surgery of Obesity and Metabolic Disorders, showed that 43% of respondents believed diet and exercise was the best treatment for severe obesity (BMI > 35). A more recent survey asked which among several choices was the most effective weight-loss intervention, and again a large proportion “believed wrongly that diet and exercise is most effective — more so than drugs or surgery — despite plenty of evidence that this is not the case.”
In this context, he said, “any surgery, no matter how safe or effective, would never be very popular.” If obesity is viewed as a modifiable risk factor, patients may say they’ll think about it for 6 months. In contrast, “nobody will tell you ‘I will think about it’ if you tell them they need gallbladder surgery to get rid of gallstone pain.”
Although drugs are available to treat obesity, none of them are curative, and if they’re stopped, the weight comes back, Dr. Rubino pointed out. “Efficacy of drugs is measured in weeks or months, whereas efficacy of surgery is measured in decades of durability — in the case of bariatric surgery, 10-20 years. That’s why bariatric surgery will remain an option,” he said. “It’s not just preventing disease, it’s resolving ongoing disease.”
Furthermore, bariatric surgery is showing value for people with established T2D, whereas in the past, it was mainly considered to be a weight-loss intervention for younger, healthier patients, he said. “In my practice, we’re operating more often in people with T2D, even those at higher risk for anesthesia and surgery — eg, patients with heart failure, chronic kidney disease, on dialysis — and we’re still able to maintain the same safety with minimally invasive laparoscopic surgery that we had with healthier patients.”
A vote held at the end of the session revealed that the audience was split about half and half in favor of drugs making bariatric surgery obsolete or not.
“I think we may have to duke it out now,” Dr. Aronne quipped.
Dr. Aronne disclosed being a consultant, speaker, and adviser for and receiving research support from Altimmune, Amgen, AstraZeneca, Eli Lilly, Intellihealth, Janssen, Novo Nordisk, Pfizer, Senda, UnitedHealth Group, Versanis, and others; he has ownership interests in ERX, Intellihealth, Jamieson, Kallyope, Skye Bioscience, Veru, and others; and he is on the board of directors of ERX, Jamieson Wellness, and Intellihealth/FlyteHealth. Dr. Rubino disclosed receiving research and educational grants from Novo Nordisk, Ethicon, and Medtronic; he is on the scientific advisory board/data safety advisory board for Keyron, Morphic Medical, and GT Metabolic Solutions; he receives speaking honoraria from Medtronic, Ethicon, Novo Nordisk, and Eli Lilly; and he is president of the nonprofit Metabolic Health Institute.
A version of this article first appeared on Medscape.com.
FROM EASD 2024
Hot Flashes: Do They Predict CVD and Dementia?
This transcript has been edited for clarity.
I’d like to talk about a recent report in the journal Menopause linking menopausal symptoms to increased risk for cognitive impairment. I’d also like to discuss some of the recent studies that have addressed whether hot flashes are linked to increased risk for heart disease and other forms of cardiovascular disease (CVD).
Given that 75%-80% of perimenopausal and postmenopausal women have hot flashes and vasomotor symptoms, it’s undoubtedly a more complex relationship between hot flashes and these outcomes than a simple one-size-fits-all, yes-or-no question.
Increasing evidence shows that several additional factors are important, including the age at which the symptoms are occurring, the time since menopause, the severity of the symptoms, whether they co-occur with night sweats and sleep disruption, and the cardiovascular status of the woman.
Several studies suggest that women who have more severe hot flashes and vasomotor symptoms are more likely to have prevalent cardiovascular risk factors — hypertension, dyslipidemia, high body mass index, endothelial dysfunction — as measured by flow-mediated vasodilation and other measures.
It is quite plausible that hot flashes could be a marker for increased risk for cognitive impairment. But the question remains, are hot flashes associated with cognitive impairment independent of these other risk factors? It appears that the associations between hot flashes, vasomotor symptoms, and CVD, and other adverse outcomes, may be more likely when hot flashes persist after age 60 or are newly occurring in later menopause. In the Women’s Health Initiative observational study, the presence of hot flashes and vasomotor symptoms in early menopause was not linked to any increased risk for heart attack, stroke, total CVD, or all-cause mortality.
However, the onset of these symptoms, especially new onset of these symptoms after age 60 or in later menopause, was in fact linked to increased risk for CVD and all-cause mortality. With respect to cognitive impairment, if a woman is having hot flashes and night sweats with regular sleep disruption, performance on cognitive testing would not be as favorable as it would be in the absence of these symptoms.
This brings us to the new study in Menopause that included approximately 1300 Latino women in nine Latin American countries, with an average age of 55 years. Looking at the association between severe menopausal symptoms and cognitive impairment, researchers found that women with severe symptoms were more likely to have cognitive impairment.
Conversely, they found that the women who had a favorable CVD risk factor status (physically active, lower BMI, healthier) and were ever users of estrogen were less likely to have cognitive impairment.
Clearly, for estrogen therapy, we need randomized clinical trials of the presence or absence of vasomotor symptoms and cognitive and CVD outcomes. Such analyses are ongoing, and new randomized trials focused specifically on women in early menopause would be very beneficial.
At the present time, it’s important that we not alarm women about the associations seen in some of these studies because often they are not independent associations; they aren’t independent of other risk factors that are commonly linked to hot flashes and night sweats. There are many other complexities in the relationship between hot flashes and cognitive impairment.
We need to appreciate that women who have moderate to severe hot flashes (especially when associated with disrupted sleep) do have impaired quality of life. It’s important to treat these symptoms, especially in early menopause, and very effective hormonal and nonhormonal treatments are available.
For women with symptoms that persist into later menopause or who have new onset of symptoms in later menopause, it’s important to prioritize cardiovascular health. For example, be more vigilant about behavioral lifestyle counseling to lower risk, and be even more aggressive in treating dyslipidemia and diabetes.
JoAnn E. Manson, Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School; Chief, Division of Preventive Medicine, Brigham and Women’s Hospital, Boston, Massachusetts; and Past President, North American Menopause Society, 2011-2012, has disclosed the following relevant financial relationships: Received study pill donation and infrastructure support from Mars Symbioscience (for the COSMOS trial).
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’d like to talk about a recent report in the journal Menopause linking menopausal symptoms to increased risk for cognitive impairment. I’d also like to discuss some of the recent studies that have addressed whether hot flashes are linked to increased risk for heart disease and other forms of cardiovascular disease (CVD).
Given that 75%-80% of perimenopausal and postmenopausal women have hot flashes and vasomotor symptoms, it’s undoubtedly a more complex relationship between hot flashes and these outcomes than a simple one-size-fits-all, yes-or-no question.
Increasing evidence shows that several additional factors are important, including the age at which the symptoms are occurring, the time since menopause, the severity of the symptoms, whether they co-occur with night sweats and sleep disruption, and the cardiovascular status of the woman.
Several studies suggest that women who have more severe hot flashes and vasomotor symptoms are more likely to have prevalent cardiovascular risk factors — hypertension, dyslipidemia, high body mass index, endothelial dysfunction — as measured by flow-mediated vasodilation and other measures.
It is quite plausible that hot flashes could be a marker for increased risk for cognitive impairment. But the question remains, are hot flashes associated with cognitive impairment independent of these other risk factors? It appears that the associations between hot flashes, vasomotor symptoms, and CVD, and other adverse outcomes, may be more likely when hot flashes persist after age 60 or are newly occurring in later menopause. In the Women’s Health Initiative observational study, the presence of hot flashes and vasomotor symptoms in early menopause was not linked to any increased risk for heart attack, stroke, total CVD, or all-cause mortality.
However, the onset of these symptoms, especially new onset of these symptoms after age 60 or in later menopause, was in fact linked to increased risk for CVD and all-cause mortality. With respect to cognitive impairment, if a woman is having hot flashes and night sweats with regular sleep disruption, performance on cognitive testing would not be as favorable as it would be in the absence of these symptoms.
This brings us to the new study in Menopause that included approximately 1300 Latino women in nine Latin American countries, with an average age of 55 years. Looking at the association between severe menopausal symptoms and cognitive impairment, researchers found that women with severe symptoms were more likely to have cognitive impairment.
Conversely, they found that the women who had a favorable CVD risk factor status (physically active, lower BMI, healthier) and were ever users of estrogen were less likely to have cognitive impairment.
Clearly, for estrogen therapy, we need randomized clinical trials of the presence or absence of vasomotor symptoms and cognitive and CVD outcomes. Such analyses are ongoing, and new randomized trials focused specifically on women in early menopause would be very beneficial.
At the present time, it’s important that we not alarm women about the associations seen in some of these studies because often they are not independent associations; they aren’t independent of other risk factors that are commonly linked to hot flashes and night sweats. There are many other complexities in the relationship between hot flashes and cognitive impairment.
We need to appreciate that women who have moderate to severe hot flashes (especially when associated with disrupted sleep) do have impaired quality of life. It’s important to treat these symptoms, especially in early menopause, and very effective hormonal and nonhormonal treatments are available.
For women with symptoms that persist into later menopause or who have new onset of symptoms in later menopause, it’s important to prioritize cardiovascular health. For example, be more vigilant about behavioral lifestyle counseling to lower risk, and be even more aggressive in treating dyslipidemia and diabetes.
JoAnn E. Manson, Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School; Chief, Division of Preventive Medicine, Brigham and Women’s Hospital, Boston, Massachusetts; and Past President, North American Menopause Society, 2011-2012, has disclosed the following relevant financial relationships: Received study pill donation and infrastructure support from Mars Symbioscience (for the COSMOS trial).
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’d like to talk about a recent report in the journal Menopause linking menopausal symptoms to increased risk for cognitive impairment. I’d also like to discuss some of the recent studies that have addressed whether hot flashes are linked to increased risk for heart disease and other forms of cardiovascular disease (CVD).
Given that 75%-80% of perimenopausal and postmenopausal women have hot flashes and vasomotor symptoms, it’s undoubtedly a more complex relationship between hot flashes and these outcomes than a simple one-size-fits-all, yes-or-no question.
Increasing evidence shows that several additional factors are important, including the age at which the symptoms are occurring, the time since menopause, the severity of the symptoms, whether they co-occur with night sweats and sleep disruption, and the cardiovascular status of the woman.
Several studies suggest that women who have more severe hot flashes and vasomotor symptoms are more likely to have prevalent cardiovascular risk factors — hypertension, dyslipidemia, high body mass index, endothelial dysfunction — as measured by flow-mediated vasodilation and other measures.
It is quite plausible that hot flashes could be a marker for increased risk for cognitive impairment. But the question remains, are hot flashes associated with cognitive impairment independent of these other risk factors? It appears that the associations between hot flashes, vasomotor symptoms, and CVD, and other adverse outcomes, may be more likely when hot flashes persist after age 60 or are newly occurring in later menopause. In the Women’s Health Initiative observational study, the presence of hot flashes and vasomotor symptoms in early menopause was not linked to any increased risk for heart attack, stroke, total CVD, or all-cause mortality.
However, the onset of these symptoms, especially new onset of these symptoms after age 60 or in later menopause, was in fact linked to increased risk for CVD and all-cause mortality. With respect to cognitive impairment, if a woman is having hot flashes and night sweats with regular sleep disruption, performance on cognitive testing would not be as favorable as it would be in the absence of these symptoms.
This brings us to the new study in Menopause that included approximately 1300 Latino women in nine Latin American countries, with an average age of 55 years. Looking at the association between severe menopausal symptoms and cognitive impairment, researchers found that women with severe symptoms were more likely to have cognitive impairment.
Conversely, they found that the women who had a favorable CVD risk factor status (physically active, lower BMI, healthier) and were ever users of estrogen were less likely to have cognitive impairment.
Clearly, for estrogen therapy, we need randomized clinical trials of the presence or absence of vasomotor symptoms and cognitive and CVD outcomes. Such analyses are ongoing, and new randomized trials focused specifically on women in early menopause would be very beneficial.
At the present time, it’s important that we not alarm women about the associations seen in some of these studies because often they are not independent associations; they aren’t independent of other risk factors that are commonly linked to hot flashes and night sweats. There are many other complexities in the relationship between hot flashes and cognitive impairment.
We need to appreciate that women who have moderate to severe hot flashes (especially when associated with disrupted sleep) do have impaired quality of life. It’s important to treat these symptoms, especially in early menopause, and very effective hormonal and nonhormonal treatments are available.
For women with symptoms that persist into later menopause or who have new onset of symptoms in later menopause, it’s important to prioritize cardiovascular health. For example, be more vigilant about behavioral lifestyle counseling to lower risk, and be even more aggressive in treating dyslipidemia and diabetes.
JoAnn E. Manson, Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School; Chief, Division of Preventive Medicine, Brigham and Women’s Hospital, Boston, Massachusetts; and Past President, North American Menopause Society, 2011-2012, has disclosed the following relevant financial relationships: Received study pill donation and infrastructure support from Mars Symbioscience (for the COSMOS trial).
A version of this article first appeared on Medscape.com.
‘Reform School’ for Pharmacy Benefit Managers: How Might Legislation Help Patients?
The term “reform school” is a bit outdated. It used to refer to institutions where young offenders were sent instead of prison. Some argue that pharmacy benefit managers (PBMs) should bypass reform school and go straight to prison. “PBM reform” has become a ubiquitous term, encompassing any legislative or regulatory efforts aimed at curbing PBMs’ bad behavior. When discussing PBM reform, it’s crucial to understand the various segments of the healthcare system affected by PBMs. This complexity often makes it challenging to determine what these reform packages would actually achieve and who they would benefit.
Pharmacists have long been vocal critics of PBMs, and while their issues are extremely important, it is essential to remember that the ultimate victims of PBM misconduct, in terms of access to care, are patients. At some point, we will all be patients, making this issue universally relevant. It has been quite challenging to follow federal legislation on this topic as these packages attempt to address a number of bad behaviors by PBMs affecting a variety of victims. This discussion will examine those reforms that would directly improve patient’s access to available and affordable medications.
Policy Categories of PBM Reform
There are five policy categories of PBM reform legislation overall, including three that have the greatest potential to directly address patient needs. The first is patient access to medications (utilization management, copay assistance, prior authorization, etc.), followed by delinking drug list prices from PBM income and pass-through of price concessions from the manufacturer. The remaining two categories involve transparency and pharmacy-facing reform, both of which are very important. However, this discussion will revolve around the first three categories. It should be noted that many of the legislation packages addressing the categories of patient access, delinking, and pass-through also include transparency issues, particularly as they relate to pharmacy-facing issues.
Patient Access to Medications — Step Therapy Legislation
One of the major obstacles to patient access to medications is the use of PBM utilization management tools such as step therapy (“fail first”), prior authorizations, nonmedical switching, and formulary exclusions. These tools dictate when patients can obtain necessary medications and for how long patients who are stable on their current treatments can remain on them.

While many states have enacted step therapy reforms to prevent stable patients from being whip-sawed between medications that maximize PBM profits (often labeled as “savings”), these state protections apply only to state-regulated health plans. These include fully insured health plans and those offered through the Affordable Care Act’s Health Insurance Marketplace. It also includes state employees, state corrections, and, in some cases, state labor unions. State legislation does not extend to patients covered by employer self-insured health plans, called ERISA plans for the federal law that governs employee benefit plans, the Employee Retirement Income Security Act. These ERISA plans include nearly 35 million people nationwide.
This is where the Safe Step Act (S.652/H.R.2630) becomes crucial, as it allows employees to request exceptions to harmful fail-first protocols. The bill has gained significant momentum, having been reported out of the Senate HELP Committee and discussed in House markups. The Safe Step Act would mandate that an exception to a step therapy protocol must be granted if:
- The required treatment has been ineffective
- The treatment is expected to be ineffective, and delaying effective treatment would lead to irreversible consequences
- The treatment will cause or is likely to cause an adverse reaction
- The treatment is expected to prevent the individual from performing daily activities or occupational responsibilities
- The individual is stable on their current prescription drugs
- There are other circumstances as determined by the Employee Benefits Security Administration
This legislation is vital for ensuring that patients have timely access to the medications they need without unnecessary delays or disruptions.
Patient Access to Medications — Prior Authorizations
Another significant issue affecting patient access to medications is prior authorizations (PAs). According to an American Medical Association survey, nearly one in four physicians (24%) report that a PA has led to a serious adverse event for a patient in their care. In rheumatology, PAs often result in delays in care (even for those initially approved) and a significant increase in steroid usage. In particular, PAs in Medicare Advantage (MA) plans are harmful to Medicare beneficiaries.
The Improving Seniors’ Timely Access to Care Act (H.R.8702 / S.4532) aims to reform PAs used in MA plans, making the process more efficient and transparent to improve access to care for seniors. Unfortunately, it does not cover Part D drugs and may only cover Part B drugs depending on the MA plan’s benefit package. Here are the key provisions of the act:
- Electronic PA: Implementing real-time decisions for routinely approved items and services.
- Transparency: Requiring annual publication of PA information, such as the percentage of requests approved and the average response time.
- Quality and Timeliness Standards: The Centers for Medicare & Medicaid Services (CMS) will set standards for the quality and timeliness of PA determinations.
- Streamlining Approvals: Simplifying the approval process and reducing the time allowed for health plans to consider PA requests.
This bill passed the House in September 2022 but stalled in the Senate because of an unfavorable Congressional Budget Office score. CMS has since finalized portions of this bill via regulation, zeroing out the CBO score and increasing the chances of its passage.
Delinking Drug Prices from PBM Income and Pass-Through of Price Concessions
Affordability is a crucial aspect of accessibility, especially when it comes to medications. Over the years, we’ve learned that PBMs often favor placing the highest list price drugs on formularies because the rebates and various fees they receive from manufacturers are based on a percentage of the list price. In other words, the higher the medication’s price, the more money the PBM makes.
This practice is evident in both commercial and government formularies, where brand-name drugs are often preferred, while lower-priced generics are either excluded or placed on higher tiers. As a result, while major PBMs benefit from these rebates and fees, patients continue to pay their cost share based on the list price of the medication.
To improve the affordability of medications, a key aspect of PBM reform should be to disincentivize PBMs from selecting higher-priced medications and/or require the pass-through of manufacturer price concessions to patients.
Several major PBM reform bills are currently being considered that address either the delinking of price concessions from the list price of the drug or some form of pass-through of these concessions. These reforms are essential to ensure that patients can access affordable medications without being burdened by inflated costs.
The legislation includes the Pharmacy Benefit Manager Reform Act (S.1339); the Modernizing & Ensuring PBM Accountability Act (S.2973); the Better Mental Health Care, Lower Cost Drugs, and Extenders Act (S.3430); the Protecting Patients Against PBM Abuses Act (H.R. 2880); the DRUG Act (S.2474 / H.R.6283); and the Share the Savings with Seniors Act (S.2474 / H.R.5376).
As with all legislation, there are limitations and compromises in each of these. However, these bills are a good first step in addressing PBM remuneration (rebates and fees) based on the list price of the drug and/or passing through to the patient the benefit of manufacturer price concessions. By focusing on key areas like utilization management, delinking drug prices from PBM income, and allowing patients to directly benefit from manufacturer price concessions, we can work toward a more equitable and efficient healthcare system. Reigning in PBM bad behavior is a challenge, but the potential benefits for patient care and access make it a crucial fight worth pursuing.
Please help in efforts to improve patients’ access to available and affordable medications by contacting your representatives in Congress to impart to them the importance of passing legislation. The CSRO’s legislative map tool can help to inform you of the latest information on these and other bills and assist you in engaging with your representatives on them.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s vice president of Advocacy and Government Affairs and its immediate past president, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. She has no relevant conflicts of interest to disclose. You can reach her at [email protected].
The term “reform school” is a bit outdated. It used to refer to institutions where young offenders were sent instead of prison. Some argue that pharmacy benefit managers (PBMs) should bypass reform school and go straight to prison. “PBM reform” has become a ubiquitous term, encompassing any legislative or regulatory efforts aimed at curbing PBMs’ bad behavior. When discussing PBM reform, it’s crucial to understand the various segments of the healthcare system affected by PBMs. This complexity often makes it challenging to determine what these reform packages would actually achieve and who they would benefit.
Pharmacists have long been vocal critics of PBMs, and while their issues are extremely important, it is essential to remember that the ultimate victims of PBM misconduct, in terms of access to care, are patients. At some point, we will all be patients, making this issue universally relevant. It has been quite challenging to follow federal legislation on this topic as these packages attempt to address a number of bad behaviors by PBMs affecting a variety of victims. This discussion will examine those reforms that would directly improve patient’s access to available and affordable medications.
Policy Categories of PBM Reform
There are five policy categories of PBM reform legislation overall, including three that have the greatest potential to directly address patient needs. The first is patient access to medications (utilization management, copay assistance, prior authorization, etc.), followed by delinking drug list prices from PBM income and pass-through of price concessions from the manufacturer. The remaining two categories involve transparency and pharmacy-facing reform, both of which are very important. However, this discussion will revolve around the first three categories. It should be noted that many of the legislation packages addressing the categories of patient access, delinking, and pass-through also include transparency issues, particularly as they relate to pharmacy-facing issues.
Patient Access to Medications — Step Therapy Legislation
One of the major obstacles to patient access to medications is the use of PBM utilization management tools such as step therapy (“fail first”), prior authorizations, nonmedical switching, and formulary exclusions. These tools dictate when patients can obtain necessary medications and for how long patients who are stable on their current treatments can remain on them.
While many states have enacted step therapy reforms to prevent stable patients from being whip-sawed between medications that maximize PBM profits (often labeled as “savings”), these state protections apply only to state-regulated health plans. These include fully insured health plans and those offered through the Affordable Care Act’s Health Insurance Marketplace. It also includes state employees, state corrections, and, in some cases, state labor unions. State legislation does not extend to patients covered by employer self-insured health plans, called ERISA plans for the federal law that governs employee benefit plans, the Employee Retirement Income Security Act. These ERISA plans include nearly 35 million people nationwide.
This is where the Safe Step Act (S.652/H.R.2630) becomes crucial, as it allows employees to request exceptions to harmful fail-first protocols. The bill has gained significant momentum, having been reported out of the Senate HELP Committee and discussed in House markups. The Safe Step Act would mandate that an exception to a step therapy protocol must be granted if:
- The required treatment has been ineffective
- The treatment is expected to be ineffective, and delaying effective treatment would lead to irreversible consequences
- The treatment will cause or is likely to cause an adverse reaction
- The treatment is expected to prevent the individual from performing daily activities or occupational responsibilities
- The individual is stable on their current prescription drugs
- There are other circumstances as determined by the Employee Benefits Security Administration
This legislation is vital for ensuring that patients have timely access to the medications they need without unnecessary delays or disruptions.
Patient Access to Medications — Prior Authorizations
Another significant issue affecting patient access to medications is prior authorizations (PAs). According to an American Medical Association survey, nearly one in four physicians (24%) report that a PA has led to a serious adverse event for a patient in their care. In rheumatology, PAs often result in delays in care (even for those initially approved) and a significant increase in steroid usage. In particular, PAs in Medicare Advantage (MA) plans are harmful to Medicare beneficiaries.
The Improving Seniors’ Timely Access to Care Act (H.R.8702 / S.4532) aims to reform PAs used in MA plans, making the process more efficient and transparent to improve access to care for seniors. Unfortunately, it does not cover Part D drugs and may only cover Part B drugs depending on the MA plan’s benefit package. Here are the key provisions of the act:
- Electronic PA: Implementing real-time decisions for routinely approved items and services.
- Transparency: Requiring annual publication of PA information, such as the percentage of requests approved and the average response time.
- Quality and Timeliness Standards: The Centers for Medicare & Medicaid Services (CMS) will set standards for the quality and timeliness of PA determinations.
- Streamlining Approvals: Simplifying the approval process and reducing the time allowed for health plans to consider PA requests.
This bill passed the House in September 2022 but stalled in the Senate because of an unfavorable Congressional Budget Office score. CMS has since finalized portions of this bill via regulation, zeroing out the CBO score and increasing the chances of its passage.
Delinking Drug Prices from PBM Income and Pass-Through of Price Concessions
Affordability is a crucial aspect of accessibility, especially when it comes to medications. Over the years, we’ve learned that PBMs often favor placing the highest list price drugs on formularies because the rebates and various fees they receive from manufacturers are based on a percentage of the list price. In other words, the higher the medication’s price, the more money the PBM makes.
This practice is evident in both commercial and government formularies, where brand-name drugs are often preferred, while lower-priced generics are either excluded or placed on higher tiers. As a result, while major PBMs benefit from these rebates and fees, patients continue to pay their cost share based on the list price of the medication.
To improve the affordability of medications, a key aspect of PBM reform should be to disincentivize PBMs from selecting higher-priced medications and/or require the pass-through of manufacturer price concessions to patients.
Several major PBM reform bills are currently being considered that address either the delinking of price concessions from the list price of the drug or some form of pass-through of these concessions. These reforms are essential to ensure that patients can access affordable medications without being burdened by inflated costs.
The legislation includes the Pharmacy Benefit Manager Reform Act (S.1339); the Modernizing & Ensuring PBM Accountability Act (S.2973); the Better Mental Health Care, Lower Cost Drugs, and Extenders Act (S.3430); the Protecting Patients Against PBM Abuses Act (H.R. 2880); the DRUG Act (S.2474 / H.R.6283); and the Share the Savings with Seniors Act (S.2474 / H.R.5376).
As with all legislation, there are limitations and compromises in each of these. However, these bills are a good first step in addressing PBM remuneration (rebates and fees) based on the list price of the drug and/or passing through to the patient the benefit of manufacturer price concessions. By focusing on key areas like utilization management, delinking drug prices from PBM income, and allowing patients to directly benefit from manufacturer price concessions, we can work toward a more equitable and efficient healthcare system. Reigning in PBM bad behavior is a challenge, but the potential benefits for patient care and access make it a crucial fight worth pursuing.
Please help in efforts to improve patients’ access to available and affordable medications by contacting your representatives in Congress to impart to them the importance of passing legislation. The CSRO’s legislative map tool can help to inform you of the latest information on these and other bills and assist you in engaging with your representatives on them.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s vice president of Advocacy and Government Affairs and its immediate past president, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. She has no relevant conflicts of interest to disclose. You can reach her at [email protected].
The term “reform school” is a bit outdated. It used to refer to institutions where young offenders were sent instead of prison. Some argue that pharmacy benefit managers (PBMs) should bypass reform school and go straight to prison. “PBM reform” has become a ubiquitous term, encompassing any legislative or regulatory efforts aimed at curbing PBMs’ bad behavior. When discussing PBM reform, it’s crucial to understand the various segments of the healthcare system affected by PBMs. This complexity often makes it challenging to determine what these reform packages would actually achieve and who they would benefit.
Pharmacists have long been vocal critics of PBMs, and while their issues are extremely important, it is essential to remember that the ultimate victims of PBM misconduct, in terms of access to care, are patients. At some point, we will all be patients, making this issue universally relevant. It has been quite challenging to follow federal legislation on this topic as these packages attempt to address a number of bad behaviors by PBMs affecting a variety of victims. This discussion will examine those reforms that would directly improve patient’s access to available and affordable medications.
Policy Categories of PBM Reform
There are five policy categories of PBM reform legislation overall, including three that have the greatest potential to directly address patient needs. The first is patient access to medications (utilization management, copay assistance, prior authorization, etc.), followed by delinking drug list prices from PBM income and pass-through of price concessions from the manufacturer. The remaining two categories involve transparency and pharmacy-facing reform, both of which are very important. However, this discussion will revolve around the first three categories. It should be noted that many of the legislation packages addressing the categories of patient access, delinking, and pass-through also include transparency issues, particularly as they relate to pharmacy-facing issues.
Patient Access to Medications — Step Therapy Legislation
One of the major obstacles to patient access to medications is the use of PBM utilization management tools such as step therapy (“fail first”), prior authorizations, nonmedical switching, and formulary exclusions. These tools dictate when patients can obtain necessary medications and for how long patients who are stable on their current treatments can remain on them.
While many states have enacted step therapy reforms to prevent stable patients from being whip-sawed between medications that maximize PBM profits (often labeled as “savings”), these state protections apply only to state-regulated health plans. These include fully insured health plans and those offered through the Affordable Care Act’s Health Insurance Marketplace. It also includes state employees, state corrections, and, in some cases, state labor unions. State legislation does not extend to patients covered by employer self-insured health plans, called ERISA plans for the federal law that governs employee benefit plans, the Employee Retirement Income Security Act. These ERISA plans include nearly 35 million people nationwide.
This is where the Safe Step Act (S.652/H.R.2630) becomes crucial, as it allows employees to request exceptions to harmful fail-first protocols. The bill has gained significant momentum, having been reported out of the Senate HELP Committee and discussed in House markups. The Safe Step Act would mandate that an exception to a step therapy protocol must be granted if:
- The required treatment has been ineffective
- The treatment is expected to be ineffective, and delaying effective treatment would lead to irreversible consequences
- The treatment will cause or is likely to cause an adverse reaction
- The treatment is expected to prevent the individual from performing daily activities or occupational responsibilities
- The individual is stable on their current prescription drugs
- There are other circumstances as determined by the Employee Benefits Security Administration
This legislation is vital for ensuring that patients have timely access to the medications they need without unnecessary delays or disruptions.
Patient Access to Medications — Prior Authorizations
Another significant issue affecting patient access to medications is prior authorizations (PAs). According to an American Medical Association survey, nearly one in four physicians (24%) report that a PA has led to a serious adverse event for a patient in their care. In rheumatology, PAs often result in delays in care (even for those initially approved) and a significant increase in steroid usage. In particular, PAs in Medicare Advantage (MA) plans are harmful to Medicare beneficiaries.
The Improving Seniors’ Timely Access to Care Act (H.R.8702 / S.4532) aims to reform PAs used in MA plans, making the process more efficient and transparent to improve access to care for seniors. Unfortunately, it does not cover Part D drugs and may only cover Part B drugs depending on the MA plan’s benefit package. Here are the key provisions of the act:
- Electronic PA: Implementing real-time decisions for routinely approved items and services.
- Transparency: Requiring annual publication of PA information, such as the percentage of requests approved and the average response time.
- Quality and Timeliness Standards: The Centers for Medicare & Medicaid Services (CMS) will set standards for the quality and timeliness of PA determinations.
- Streamlining Approvals: Simplifying the approval process and reducing the time allowed for health plans to consider PA requests.
This bill passed the House in September 2022 but stalled in the Senate because of an unfavorable Congressional Budget Office score. CMS has since finalized portions of this bill via regulation, zeroing out the CBO score and increasing the chances of its passage.
Delinking Drug Prices from PBM Income and Pass-Through of Price Concessions
Affordability is a crucial aspect of accessibility, especially when it comes to medications. Over the years, we’ve learned that PBMs often favor placing the highest list price drugs on formularies because the rebates and various fees they receive from manufacturers are based on a percentage of the list price. In other words, the higher the medication’s price, the more money the PBM makes.
This practice is evident in both commercial and government formularies, where brand-name drugs are often preferred, while lower-priced generics are either excluded or placed on higher tiers. As a result, while major PBMs benefit from these rebates and fees, patients continue to pay their cost share based on the list price of the medication.
To improve the affordability of medications, a key aspect of PBM reform should be to disincentivize PBMs from selecting higher-priced medications and/or require the pass-through of manufacturer price concessions to patients.
Several major PBM reform bills are currently being considered that address either the delinking of price concessions from the list price of the drug or some form of pass-through of these concessions. These reforms are essential to ensure that patients can access affordable medications without being burdened by inflated costs.
The legislation includes the Pharmacy Benefit Manager Reform Act (S.1339); the Modernizing & Ensuring PBM Accountability Act (S.2973); the Better Mental Health Care, Lower Cost Drugs, and Extenders Act (S.3430); the Protecting Patients Against PBM Abuses Act (H.R. 2880); the DRUG Act (S.2474 / H.R.6283); and the Share the Savings with Seniors Act (S.2474 / H.R.5376).
As with all legislation, there are limitations and compromises in each of these. However, these bills are a good first step in addressing PBM remuneration (rebates and fees) based on the list price of the drug and/or passing through to the patient the benefit of manufacturer price concessions. By focusing on key areas like utilization management, delinking drug prices from PBM income, and allowing patients to directly benefit from manufacturer price concessions, we can work toward a more equitable and efficient healthcare system. Reigning in PBM bad behavior is a challenge, but the potential benefits for patient care and access make it a crucial fight worth pursuing.
Please help in efforts to improve patients’ access to available and affordable medications by contacting your representatives in Congress to impart to them the importance of passing legislation. The CSRO’s legislative map tool can help to inform you of the latest information on these and other bills and assist you in engaging with your representatives on them.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s vice president of Advocacy and Government Affairs and its immediate past president, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. She has no relevant conflicts of interest to disclose. You can reach her at [email protected].
Stones, Bones, Groans, and Moans: Could This Be Primary Hyperparathyroidism?
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I’m Dr Matthew Frank Watto, here with my great friend and America’s primary care physician, Dr. Paul Nelson Williams.
Paul, we’re going to talk about our primary hyperparathyroidism podcast with Dr. Lindsay Kuo. It’s a topic that I feel much more clear on now.
Now, Paul, in primary care, you see a lot of calcium that is just slightly high. Can we just blame that on thiazide diuretics?
Paul N. Williams, MD: It’s a place to start. As you’re starting to think about the possible etiologies, primary hyperparathyroidism and malignancy are the two that roll right off the tongue, but it is worth going back to the patient’s medication list and making sure you’re not missing something.
Thiazides famously cause hypercalcemia, but in some of the reading I did for this episode, they may just uncover it a little bit early. Patients who are on thiazides who become hypercalcemic seem to go on to develop primary hyperthyroidism anyway. So I don’t think you can solely blame the thiazide.
Another medication that can be causative is lithium. So a good place to look first after you’ve repeated the labs and confirmed hypercalcemia is the patient’s medication list.
Dr. Watto: We’ve talked before about the basic workup for hypercalcemia, and determining whether it’s PTH dependent or PTH independent. On the podcast, we talk more about the full workup, but I wanted to talk about the classic symptoms. Our expert made the point that we don’t see them as much anymore, although we do see kidney stones. People used to present very late in the disease because they weren’t having labs done routinely.
The classic symptoms include osteoporosis and bone tumors. People can get nephrocalcinosis and kidney stones. I hadn’t really thought of it this way because we’re used to diagnosing it early now. Do you feel the same?
Dr. Williams: As labs have started routinely reporting calcium levels, this is more and more often how it’s picked up. The other aspect is that as we are screening for and finding osteoporosis, part of the workup almost always involves getting a parathyroid hormone and a calcium level. We’re seeing these lab abnormalities before we’re seeing symptoms, which is good.
But it also makes things more diagnostically thorny.
Dr. Watto: Dr. Lindsay Kuo made the point that when she sees patients before and after surgery, she’s aware of these nonclassic symptoms — the stones, bones, groans, and the psychiatric overtones that can be anything from fatigue or irritability to dysphoria.
Some people have a generalized weakness that’s very nonspecific. Dr. Kuo said that sometimes these symptoms will disappear after surgery. The patients may just have gotten used to them, or they thought these symptoms were caused by something else, but after surgery they went away.
There are these nonclassic symptoms that are harder to pin down. I was surprised by that.
Dr. Williams: She mentioned polydipsia and polyuria, which have been reported in other studies. It seems like it can be anything. You have to take a good history, but none of those things in and of themselves is an indication for operating unless the patient has the classic renal or bone manifestations.
Dr. Watto: The other thing we talked about is a normal calcium level in a patient with primary hyperparathyroidism, or the finding of a PTH level in the normal range but with a high calcium level that is inappropriate. Can you talk a little bit about those two situations?
Dr. Williams: They’re hard to say but kind of easy to manage because you treat them the same way as someone who has elevated calcium and PTH levels.
The normocalcemic patient is something we might stumble across with osteoporosis screening. Initially the calcium level is elevated, so you repeat it and it’s normal but with an elevated PTH level. You’re like, shoot. Now what?
It turns out that most endocrine surgeons say that the indications for surgery for the classic form of primary hyperparathyroidism apply to these patients as well, and it probably helps with the bone outcomes, which is one of the things they follow most closely. If you have hypercalcemia, you should have a suppressed PTH level, the so-called normohormonal hyperparathyroidism, which is not normal at all. So even if the PTH is in the normal range, it’s still relatively elevated compared with what it should be. That situation is treated in the same way as the classic elevated PTH and elevated calcium levels.
Dr. Watto: If the calcium is abnormal and the PTH is not quite what you’d expect it to be, you can always ask your friendly neighborhood endocrinologist to help you figure out whether the patient really has one of these conditions. You have to make sure that they don’t have a simple secondary cause like a low vitamin D level. In that case, you fix the vitamin D and then recheck the numbers to see if they’ve normalized. But I have found a bunch of these edge cases in which it has been helpful to confer with an endocrinologist, especially before you send someone to a surgeon to take out their parathyroid gland.
This was a really fantastic conversation. If you want to hear the full podcast episode, click here.
Dr. Watto, Clinical Assistant Professor, Department of Medicine, Perelman School of Medicine at University of Pennsylvania; Internist, Department of Medicine, Hospital Medicine Section, Pennsylvania Hospital, Philadelphia, Pennsylvania, has disclosed no relevant financial relationships. Dr. Williams, Associate Professor of Clinical Medicine, Department of General Internal Medicine, Lewis Katz School of Medicine; Staff Physician, Department of General Internal Medicine, Temple Internal Medicine Associates, Philadelphia, Pennsylvania, served as a director, officer, partner, employee, adviser, consultant, or trustee for The Curbsiders, and has received income in an amount equal to or greater than $250 from The Curbsiders.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I’m Dr Matthew Frank Watto, here with my great friend and America’s primary care physician, Dr. Paul Nelson Williams.
Paul, we’re going to talk about our primary hyperparathyroidism podcast with Dr. Lindsay Kuo. It’s a topic that I feel much more clear on now.
Now, Paul, in primary care, you see a lot of calcium that is just slightly high. Can we just blame that on thiazide diuretics?
Paul N. Williams, MD: It’s a place to start. As you’re starting to think about the possible etiologies, primary hyperparathyroidism and malignancy are the two that roll right off the tongue, but it is worth going back to the patient’s medication list and making sure you’re not missing something.
Thiazides famously cause hypercalcemia, but in some of the reading I did for this episode, they may just uncover it a little bit early. Patients who are on thiazides who become hypercalcemic seem to go on to develop primary hyperthyroidism anyway. So I don’t think you can solely blame the thiazide.
Another medication that can be causative is lithium. So a good place to look first after you’ve repeated the labs and confirmed hypercalcemia is the patient’s medication list.
Dr. Watto: We’ve talked before about the basic workup for hypercalcemia, and determining whether it’s PTH dependent or PTH independent. On the podcast, we talk more about the full workup, but I wanted to talk about the classic symptoms. Our expert made the point that we don’t see them as much anymore, although we do see kidney stones. People used to present very late in the disease because they weren’t having labs done routinely.
The classic symptoms include osteoporosis and bone tumors. People can get nephrocalcinosis and kidney stones. I hadn’t really thought of it this way because we’re used to diagnosing it early now. Do you feel the same?
Dr. Williams: As labs have started routinely reporting calcium levels, this is more and more often how it’s picked up. The other aspect is that as we are screening for and finding osteoporosis, part of the workup almost always involves getting a parathyroid hormone and a calcium level. We’re seeing these lab abnormalities before we’re seeing symptoms, which is good.
But it also makes things more diagnostically thorny.
Dr. Watto: Dr. Lindsay Kuo made the point that when she sees patients before and after surgery, she’s aware of these nonclassic symptoms — the stones, bones, groans, and the psychiatric overtones that can be anything from fatigue or irritability to dysphoria.
Some people have a generalized weakness that’s very nonspecific. Dr. Kuo said that sometimes these symptoms will disappear after surgery. The patients may just have gotten used to them, or they thought these symptoms were caused by something else, but after surgery they went away.
There are these nonclassic symptoms that are harder to pin down. I was surprised by that.
Dr. Williams: She mentioned polydipsia and polyuria, which have been reported in other studies. It seems like it can be anything. You have to take a good history, but none of those things in and of themselves is an indication for operating unless the patient has the classic renal or bone manifestations.
Dr. Watto: The other thing we talked about is a normal calcium level in a patient with primary hyperparathyroidism, or the finding of a PTH level in the normal range but with a high calcium level that is inappropriate. Can you talk a little bit about those two situations?
Dr. Williams: They’re hard to say but kind of easy to manage because you treat them the same way as someone who has elevated calcium and PTH levels.
The normocalcemic patient is something we might stumble across with osteoporosis screening. Initially the calcium level is elevated, so you repeat it and it’s normal but with an elevated PTH level. You’re like, shoot. Now what?
It turns out that most endocrine surgeons say that the indications for surgery for the classic form of primary hyperparathyroidism apply to these patients as well, and it probably helps with the bone outcomes, which is one of the things they follow most closely. If you have hypercalcemia, you should have a suppressed PTH level, the so-called normohormonal hyperparathyroidism, which is not normal at all. So even if the PTH is in the normal range, it’s still relatively elevated compared with what it should be. That situation is treated in the same way as the classic elevated PTH and elevated calcium levels.
Dr. Watto: If the calcium is abnormal and the PTH is not quite what you’d expect it to be, you can always ask your friendly neighborhood endocrinologist to help you figure out whether the patient really has one of these conditions. You have to make sure that they don’t have a simple secondary cause like a low vitamin D level. In that case, you fix the vitamin D and then recheck the numbers to see if they’ve normalized. But I have found a bunch of these edge cases in which it has been helpful to confer with an endocrinologist, especially before you send someone to a surgeon to take out their parathyroid gland.
This was a really fantastic conversation. If you want to hear the full podcast episode, click here.
Dr. Watto, Clinical Assistant Professor, Department of Medicine, Perelman School of Medicine at University of Pennsylvania; Internist, Department of Medicine, Hospital Medicine Section, Pennsylvania Hospital, Philadelphia, Pennsylvania, has disclosed no relevant financial relationships. Dr. Williams, Associate Professor of Clinical Medicine, Department of General Internal Medicine, Lewis Katz School of Medicine; Staff Physician, Department of General Internal Medicine, Temple Internal Medicine Associates, Philadelphia, Pennsylvania, served as a director, officer, partner, employee, adviser, consultant, or trustee for The Curbsiders, and has received income in an amount equal to or greater than $250 from The Curbsiders.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I’m Dr Matthew Frank Watto, here with my great friend and America’s primary care physician, Dr. Paul Nelson Williams.
Paul, we’re going to talk about our primary hyperparathyroidism podcast with Dr. Lindsay Kuo. It’s a topic that I feel much more clear on now.
Now, Paul, in primary care, you see a lot of calcium that is just slightly high. Can we just blame that on thiazide diuretics?
Paul N. Williams, MD: It’s a place to start. As you’re starting to think about the possible etiologies, primary hyperparathyroidism and malignancy are the two that roll right off the tongue, but it is worth going back to the patient’s medication list and making sure you’re not missing something.
Thiazides famously cause hypercalcemia, but in some of the reading I did for this episode, they may just uncover it a little bit early. Patients who are on thiazides who become hypercalcemic seem to go on to develop primary hyperthyroidism anyway. So I don’t think you can solely blame the thiazide.
Another medication that can be causative is lithium. So a good place to look first after you’ve repeated the labs and confirmed hypercalcemia is the patient’s medication list.
Dr. Watto: We’ve talked before about the basic workup for hypercalcemia, and determining whether it’s PTH dependent or PTH independent. On the podcast, we talk more about the full workup, but I wanted to talk about the classic symptoms. Our expert made the point that we don’t see them as much anymore, although we do see kidney stones. People used to present very late in the disease because they weren’t having labs done routinely.
The classic symptoms include osteoporosis and bone tumors. People can get nephrocalcinosis and kidney stones. I hadn’t really thought of it this way because we’re used to diagnosing it early now. Do you feel the same?
Dr. Williams: As labs have started routinely reporting calcium levels, this is more and more often how it’s picked up. The other aspect is that as we are screening for and finding osteoporosis, part of the workup almost always involves getting a parathyroid hormone and a calcium level. We’re seeing these lab abnormalities before we’re seeing symptoms, which is good.
But it also makes things more diagnostically thorny.
Dr. Watto: Dr. Lindsay Kuo made the point that when she sees patients before and after surgery, she’s aware of these nonclassic symptoms — the stones, bones, groans, and the psychiatric overtones that can be anything from fatigue or irritability to dysphoria.
Some people have a generalized weakness that’s very nonspecific. Dr. Kuo said that sometimes these symptoms will disappear after surgery. The patients may just have gotten used to them, or they thought these symptoms were caused by something else, but after surgery they went away.
There are these nonclassic symptoms that are harder to pin down. I was surprised by that.
Dr. Williams: She mentioned polydipsia and polyuria, which have been reported in other studies. It seems like it can be anything. You have to take a good history, but none of those things in and of themselves is an indication for operating unless the patient has the classic renal or bone manifestations.
Dr. Watto: The other thing we talked about is a normal calcium level in a patient with primary hyperparathyroidism, or the finding of a PTH level in the normal range but with a high calcium level that is inappropriate. Can you talk a little bit about those two situations?
Dr. Williams: They’re hard to say but kind of easy to manage because you treat them the same way as someone who has elevated calcium and PTH levels.
The normocalcemic patient is something we might stumble across with osteoporosis screening. Initially the calcium level is elevated, so you repeat it and it’s normal but with an elevated PTH level. You’re like, shoot. Now what?
It turns out that most endocrine surgeons say that the indications for surgery for the classic form of primary hyperparathyroidism apply to these patients as well, and it probably helps with the bone outcomes, which is one of the things they follow most closely. If you have hypercalcemia, you should have a suppressed PTH level, the so-called normohormonal hyperparathyroidism, which is not normal at all. So even if the PTH is in the normal range, it’s still relatively elevated compared with what it should be. That situation is treated in the same way as the classic elevated PTH and elevated calcium levels.
Dr. Watto: If the calcium is abnormal and the PTH is not quite what you’d expect it to be, you can always ask your friendly neighborhood endocrinologist to help you figure out whether the patient really has one of these conditions. You have to make sure that they don’t have a simple secondary cause like a low vitamin D level. In that case, you fix the vitamin D and then recheck the numbers to see if they’ve normalized. But I have found a bunch of these edge cases in which it has been helpful to confer with an endocrinologist, especially before you send someone to a surgeon to take out their parathyroid gland.
This was a really fantastic conversation. If you want to hear the full podcast episode, click here.
Dr. Watto, Clinical Assistant Professor, Department of Medicine, Perelman School of Medicine at University of Pennsylvania; Internist, Department of Medicine, Hospital Medicine Section, Pennsylvania Hospital, Philadelphia, Pennsylvania, has disclosed no relevant financial relationships. Dr. Williams, Associate Professor of Clinical Medicine, Department of General Internal Medicine, Lewis Katz School of Medicine; Staff Physician, Department of General Internal Medicine, Temple Internal Medicine Associates, Philadelphia, Pennsylvania, served as a director, officer, partner, employee, adviser, consultant, or trustee for The Curbsiders, and has received income in an amount equal to or greater than $250 from The Curbsiders.
A version of this article first appeared on Medscape.com.
Mom’s Potato Salad
Outside of caffeine, I have very few addictions. One of them is “Midnight Diner.”
“Midnight Diner” is a quirky, sometimes funny, sometimes bittersweet, Japanese series on Netflix. It’s about a small diner in Tokyo, open only in the wee hours of the morning, its enigmatic owner/cook, and the eclectic patrons that come and go. Each is seeking a dish that means something to them.
One episode (spoiler alert, in case you’re planning to watch it) deals with the regulars realizing a fellow who frequently comes in and orders potato salad is secretly Japan’s most famous porn actor, Erect Oki. This revelation garners him the respect, awe, and envy of the other male patrons, though Mr. Oki would rather be left to his potato salad.

The jokes are there ... but as things develop, we learn he has the potato salad because it reminds him of his mother’s potato salad — and that he’s been cut off from his family for more than 20 years because of his career path. The potato salad is all he has left.
While preparing for a shoot, he learns his mother has Alzheimer’s disease, and immediately returns home. As they sit talking on the patio of a care center, she tells him about her son, who lives in Tokyo, and loves her potato salad. The show doesn’t make it clear if she ever remembers who he is.
In the darkening hallways of her mind, she asks his sister for help in making potato salad for her visitor. It’s too salty, though whether this is from the ingredients or his tears is also never stated.
The episode is a poignant reminder of how Alzheimer’s disease is a worldwide human problem. Not American. Not western. Not restricted by race, or ethnicity, or continent. It effects us all as a species, as families, and as individuals. No matter what our jobs or backgrounds are.
For those of us on this side of the desk, it’s a reminder that Yes, we have all kinds of new toys, but from a practical viewpoint it’s hard to say that we’ve made any major advances. I’m sure my drug reps will disagree with me, and I’m not saying any of the treatments of the last 28 years are worthless, but even now we’re still far from a cure, or even something that stops progression.
That’s not from lack of trying, either.
For all the jokes about his job, Mr. Oki is no different from any other children trying to hold onto their parents as the disease slowly takes them away.
I hope we have real answers, soon.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Outside of caffeine, I have very few addictions. One of them is “Midnight Diner.”
“Midnight Diner” is a quirky, sometimes funny, sometimes bittersweet, Japanese series on Netflix. It’s about a small diner in Tokyo, open only in the wee hours of the morning, its enigmatic owner/cook, and the eclectic patrons that come and go. Each is seeking a dish that means something to them.
One episode (spoiler alert, in case you’re planning to watch it) deals with the regulars realizing a fellow who frequently comes in and orders potato salad is secretly Japan’s most famous porn actor, Erect Oki. This revelation garners him the respect, awe, and envy of the other male patrons, though Mr. Oki would rather be left to his potato salad.
The jokes are there ... but as things develop, we learn he has the potato salad because it reminds him of his mother’s potato salad — and that he’s been cut off from his family for more than 20 years because of his career path. The potato salad is all he has left.
While preparing for a shoot, he learns his mother has Alzheimer’s disease, and immediately returns home. As they sit talking on the patio of a care center, she tells him about her son, who lives in Tokyo, and loves her potato salad. The show doesn’t make it clear if she ever remembers who he is.
In the darkening hallways of her mind, she asks his sister for help in making potato salad for her visitor. It’s too salty, though whether this is from the ingredients or his tears is also never stated.
The episode is a poignant reminder of how Alzheimer’s disease is a worldwide human problem. Not American. Not western. Not restricted by race, or ethnicity, or continent. It effects us all as a species, as families, and as individuals. No matter what our jobs or backgrounds are.
For those of us on this side of the desk, it’s a reminder that Yes, we have all kinds of new toys, but from a practical viewpoint it’s hard to say that we’ve made any major advances. I’m sure my drug reps will disagree with me, and I’m not saying any of the treatments of the last 28 years are worthless, but even now we’re still far from a cure, or even something that stops progression.
That’s not from lack of trying, either.
For all the jokes about his job, Mr. Oki is no different from any other children trying to hold onto their parents as the disease slowly takes them away.
I hope we have real answers, soon.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Outside of caffeine, I have very few addictions. One of them is “Midnight Diner.”
“Midnight Diner” is a quirky, sometimes funny, sometimes bittersweet, Japanese series on Netflix. It’s about a small diner in Tokyo, open only in the wee hours of the morning, its enigmatic owner/cook, and the eclectic patrons that come and go. Each is seeking a dish that means something to them.
One episode (spoiler alert, in case you’re planning to watch it) deals with the regulars realizing a fellow who frequently comes in and orders potato salad is secretly Japan’s most famous porn actor, Erect Oki. This revelation garners him the respect, awe, and envy of the other male patrons, though Mr. Oki would rather be left to his potato salad.
The jokes are there ... but as things develop, we learn he has the potato salad because it reminds him of his mother’s potato salad — and that he’s been cut off from his family for more than 20 years because of his career path. The potato salad is all he has left.
While preparing for a shoot, he learns his mother has Alzheimer’s disease, and immediately returns home. As they sit talking on the patio of a care center, she tells him about her son, who lives in Tokyo, and loves her potato salad. The show doesn’t make it clear if she ever remembers who he is.
In the darkening hallways of her mind, she asks his sister for help in making potato salad for her visitor. It’s too salty, though whether this is from the ingredients or his tears is also never stated.
The episode is a poignant reminder of how Alzheimer’s disease is a worldwide human problem. Not American. Not western. Not restricted by race, or ethnicity, or continent. It effects us all as a species, as families, and as individuals. No matter what our jobs or backgrounds are.
For those of us on this side of the desk, it’s a reminder that Yes, we have all kinds of new toys, but from a practical viewpoint it’s hard to say that we’ve made any major advances. I’m sure my drug reps will disagree with me, and I’m not saying any of the treatments of the last 28 years are worthless, but even now we’re still far from a cure, or even something that stops progression.
That’s not from lack of trying, either.
For all the jokes about his job, Mr. Oki is no different from any other children trying to hold onto their parents as the disease slowly takes them away.
I hope we have real answers, soon.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Playing the ‘Doctor’ Card: A Lesson in Three Hypotheticals
Scenario I. Let’s say you wake with a collection of symptoms. None of them is concerning, but the combination seems a bit unusual, or at least confusing. You would like to speak to your PCP, whom you have known for a long time, and ask for either reassurance or advice on whether you should make an appointment. However, your experience with the front office’s organization tells you that the quick 4-minute conversation you’re looking for is not going to happen easily.
You have that robotic phone message memorized. It begins suggesting that you think you have an emergency to call 911. Then it reminds you that if have a question about COVID to press “2,” which will take you to a recorded message and eventually link you to a triage nurse if the recording doesn’t answer your questions. If you need a prescription refill you should press “3.” If you are a doctor’s office and wish speak to the doctor press “4.” If you know you need an appointment press “5.” And finally if you have a question press “6” and leave a message and a nurse will get back to you before the end of the day.

The good news is that your PCP’s office is good to its word and will return your call the same day, but the bad news is that it is likely to be well into the afternoon. And, while you don’t consider your symptoms life-threatening, you don’t want getting an answer to be an exercise in schedule disruption.
You were a doctor before you retired and you still have an “office.” It’s really more of a combination den and studio. So, technically you are a doctor’s office wanting to speak to the doctor. And, you know that pressing “4” will get you the answer you are looking for in a matter of minutes.
Scenario II. Your spouse, or your aunt, or the elderly widow next door asks you to accompany her at an upcoming doctor’s visit because she had been having trouble understanding the physician’s plan regarding further diagnosis and possible treatment. She believes having you along as kind of an interpreter/advocate would be a big help. Do you agree and do you make any stipulations?
Scenario III. Your PCP has referred you to a specialist. You are filling out the previsit form(s). Do you list your occupation as “retired physician” or just “retired”? Or just leave it blank?
Whether you deserve it or not, graduating from medical school has conferred on you a specialness in the eyes of many people. It is assumed you are smarter than the average bear and in taking the Hippocratic oath you have joined an elite club. And, with that membership comes some special undefined privileges.
But with that specialness there are are some downsides. For example, in some states being a physician once allowed you to have a license plate with “MD” in the number sequence. Sometimes that helped you avoid the occasional parking ticket. That is until folks realized the “MD” made you a target for car thieves and drug seekers who mistakenly believe we all carry drugs in our glove compartments.
So what about that first scenario? Do you press “4” to jump yourself to the head of the queue and avoid the inconvenience of having to wait for a reasonably timely response from your PCP? After all, you are fellow physicians and you’ve known her for a decade or two. If you are retired is your time any more valuable than that of her other patients? If you are still in active practice you can argue that getting special attention will benefit your patients. But, if it’s a weekend and you are off it’s a bit harder to rationalize special treatment. Playing the doctor card in this situation is your own decision but you must be prepared to shoulder the perceptions by your PCP and her staff as well as your own sense of fairness.
The other two scenarios are much different. In neither are you risking the impression that you are asking for a favor. But, they each have their downsides. In the second scenario you are doing someone a favor to act as an interpreter. How could this have downside? Unfortunately, what happens too often in situations like this is that when the patient’s physician learns that you are a fellow physician, the rest of the visit becomes a dialogue in doctor-speak between the two physicians with the patient sitting by as an observer. In the end this discussion may benefit the patient by creating a treatment plan that the patient can understand either because they overheard it or more likely because you eventually explained it to them.
On the other the hand, this doctor-to-doctor chat has done nothing to build a doctor-patient relationship that had obviously been lacking something. In situations like this it is probably better to keep the doctor card up your sleeve to be played at the end of the visit or maybe not at all. Before agreeing to be an interpreter/advocate, ask the patient to avoid mentioning that you are a physician. Instead, ask that she introduce you as a friend or relative that she has asked to come along to serve as a memory bank. During the visit it may be helpful to occasionally interject and suggest that the patient ask a question that hasn’t been adequately addressed. While some physicians may be upset when they belatedly find you have not revealed up front that you are a physician, I find this a harmless omission that has the benefit of improving patient care.
The final scenario — in which you are the patient — is likely to occur more often as you get older. When filling out a previsit form, I often simply put retired or leave it blank. But, how I answer the question often seems to be irrelevant because I have learned that physicians and their staff read those boilerplate forms so cursorily that even when I report my status as “retired physician” everyone seems surprised if and when it later comes to light.
My rationale in keeping the doctor card close to my vest in these situations is that I want to be addressed without any assumptions regarding my medical knowledge, which in my situation is well over half a century old and spotty at best. I don’t want my physicians to say “I’m sure you understand.” Because I often don’t. I would like them to learn about who I am just as I hope they would other patients. I won’t be offended if they “talk down” to me. If this specialist is as good as I’ve heard she is, I want to hear her full performance, not one edited for fellow and former physicians.
It doesn’t arrive gold edged with a list of special privileges. If it comes with any extras, they are risks that must be avoided.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Scenario I. Let’s say you wake with a collection of symptoms. None of them is concerning, but the combination seems a bit unusual, or at least confusing. You would like to speak to your PCP, whom you have known for a long time, and ask for either reassurance or advice on whether you should make an appointment. However, your experience with the front office’s organization tells you that the quick 4-minute conversation you’re looking for is not going to happen easily.
You have that robotic phone message memorized. It begins suggesting that you think you have an emergency to call 911. Then it reminds you that if have a question about COVID to press “2,” which will take you to a recorded message and eventually link you to a triage nurse if the recording doesn’t answer your questions. If you need a prescription refill you should press “3.” If you are a doctor’s office and wish speak to the doctor press “4.” If you know you need an appointment press “5.” And finally if you have a question press “6” and leave a message and a nurse will get back to you before the end of the day.
The good news is that your PCP’s office is good to its word and will return your call the same day, but the bad news is that it is likely to be well into the afternoon. And, while you don’t consider your symptoms life-threatening, you don’t want getting an answer to be an exercise in schedule disruption.
You were a doctor before you retired and you still have an “office.” It’s really more of a combination den and studio. So, technically you are a doctor’s office wanting to speak to the doctor. And, you know that pressing “4” will get you the answer you are looking for in a matter of minutes.
Scenario II. Your spouse, or your aunt, or the elderly widow next door asks you to accompany her at an upcoming doctor’s visit because she had been having trouble understanding the physician’s plan regarding further diagnosis and possible treatment. She believes having you along as kind of an interpreter/advocate would be a big help. Do you agree and do you make any stipulations?
Scenario III. Your PCP has referred you to a specialist. You are filling out the previsit form(s). Do you list your occupation as “retired physician” or just “retired”? Or just leave it blank?
Whether you deserve it or not, graduating from medical school has conferred on you a specialness in the eyes of many people. It is assumed you are smarter than the average bear and in taking the Hippocratic oath you have joined an elite club. And, with that membership comes some special undefined privileges.
But with that specialness there are are some downsides. For example, in some states being a physician once allowed you to have a license plate with “MD” in the number sequence. Sometimes that helped you avoid the occasional parking ticket. That is until folks realized the “MD” made you a target for car thieves and drug seekers who mistakenly believe we all carry drugs in our glove compartments.
So what about that first scenario? Do you press “4” to jump yourself to the head of the queue and avoid the inconvenience of having to wait for a reasonably timely response from your PCP? After all, you are fellow physicians and you’ve known her for a decade or two. If you are retired is your time any more valuable than that of her other patients? If you are still in active practice you can argue that getting special attention will benefit your patients. But, if it’s a weekend and you are off it’s a bit harder to rationalize special treatment. Playing the doctor card in this situation is your own decision but you must be prepared to shoulder the perceptions by your PCP and her staff as well as your own sense of fairness.
The other two scenarios are much different. In neither are you risking the impression that you are asking for a favor. But, they each have their downsides. In the second scenario you are doing someone a favor to act as an interpreter. How could this have downside? Unfortunately, what happens too often in situations like this is that when the patient’s physician learns that you are a fellow physician, the rest of the visit becomes a dialogue in doctor-speak between the two physicians with the patient sitting by as an observer. In the end this discussion may benefit the patient by creating a treatment plan that the patient can understand either because they overheard it or more likely because you eventually explained it to them.
On the other the hand, this doctor-to-doctor chat has done nothing to build a doctor-patient relationship that had obviously been lacking something. In situations like this it is probably better to keep the doctor card up your sleeve to be played at the end of the visit or maybe not at all. Before agreeing to be an interpreter/advocate, ask the patient to avoid mentioning that you are a physician. Instead, ask that she introduce you as a friend or relative that she has asked to come along to serve as a memory bank. During the visit it may be helpful to occasionally interject and suggest that the patient ask a question that hasn’t been adequately addressed. While some physicians may be upset when they belatedly find you have not revealed up front that you are a physician, I find this a harmless omission that has the benefit of improving patient care.
The final scenario — in which you are the patient — is likely to occur more often as you get older. When filling out a previsit form, I often simply put retired or leave it blank. But, how I answer the question often seems to be irrelevant because I have learned that physicians and their staff read those boilerplate forms so cursorily that even when I report my status as “retired physician” everyone seems surprised if and when it later comes to light.
My rationale in keeping the doctor card close to my vest in these situations is that I want to be addressed without any assumptions regarding my medical knowledge, which in my situation is well over half a century old and spotty at best. I don’t want my physicians to say “I’m sure you understand.” Because I often don’t. I would like them to learn about who I am just as I hope they would other patients. I won’t be offended if they “talk down” to me. If this specialist is as good as I’ve heard she is, I want to hear her full performance, not one edited for fellow and former physicians.
It doesn’t arrive gold edged with a list of special privileges. If it comes with any extras, they are risks that must be avoided.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Scenario I. Let’s say you wake with a collection of symptoms. None of them is concerning, but the combination seems a bit unusual, or at least confusing. You would like to speak to your PCP, whom you have known for a long time, and ask for either reassurance or advice on whether you should make an appointment. However, your experience with the front office’s organization tells you that the quick 4-minute conversation you’re looking for is not going to happen easily.
You have that robotic phone message memorized. It begins suggesting that you think you have an emergency to call 911. Then it reminds you that if have a question about COVID to press “2,” which will take you to a recorded message and eventually link you to a triage nurse if the recording doesn’t answer your questions. If you need a prescription refill you should press “3.” If you are a doctor’s office and wish speak to the doctor press “4.” If you know you need an appointment press “5.” And finally if you have a question press “6” and leave a message and a nurse will get back to you before the end of the day.
The good news is that your PCP’s office is good to its word and will return your call the same day, but the bad news is that it is likely to be well into the afternoon. And, while you don’t consider your symptoms life-threatening, you don’t want getting an answer to be an exercise in schedule disruption.
You were a doctor before you retired and you still have an “office.” It’s really more of a combination den and studio. So, technically you are a doctor’s office wanting to speak to the doctor. And, you know that pressing “4” will get you the answer you are looking for in a matter of minutes.
Scenario II. Your spouse, or your aunt, or the elderly widow next door asks you to accompany her at an upcoming doctor’s visit because she had been having trouble understanding the physician’s plan regarding further diagnosis and possible treatment. She believes having you along as kind of an interpreter/advocate would be a big help. Do you agree and do you make any stipulations?
Scenario III. Your PCP has referred you to a specialist. You are filling out the previsit form(s). Do you list your occupation as “retired physician” or just “retired”? Or just leave it blank?
Whether you deserve it or not, graduating from medical school has conferred on you a specialness in the eyes of many people. It is assumed you are smarter than the average bear and in taking the Hippocratic oath you have joined an elite club. And, with that membership comes some special undefined privileges.
But with that specialness there are are some downsides. For example, in some states being a physician once allowed you to have a license plate with “MD” in the number sequence. Sometimes that helped you avoid the occasional parking ticket. That is until folks realized the “MD” made you a target for car thieves and drug seekers who mistakenly believe we all carry drugs in our glove compartments.
So what about that first scenario? Do you press “4” to jump yourself to the head of the queue and avoid the inconvenience of having to wait for a reasonably timely response from your PCP? After all, you are fellow physicians and you’ve known her for a decade or two. If you are retired is your time any more valuable than that of her other patients? If you are still in active practice you can argue that getting special attention will benefit your patients. But, if it’s a weekend and you are off it’s a bit harder to rationalize special treatment. Playing the doctor card in this situation is your own decision but you must be prepared to shoulder the perceptions by your PCP and her staff as well as your own sense of fairness.
The other two scenarios are much different. In neither are you risking the impression that you are asking for a favor. But, they each have their downsides. In the second scenario you are doing someone a favor to act as an interpreter. How could this have downside? Unfortunately, what happens too often in situations like this is that when the patient’s physician learns that you are a fellow physician, the rest of the visit becomes a dialogue in doctor-speak between the two physicians with the patient sitting by as an observer. In the end this discussion may benefit the patient by creating a treatment plan that the patient can understand either because they overheard it or more likely because you eventually explained it to them.
On the other the hand, this doctor-to-doctor chat has done nothing to build a doctor-patient relationship that had obviously been lacking something. In situations like this it is probably better to keep the doctor card up your sleeve to be played at the end of the visit or maybe not at all. Before agreeing to be an interpreter/advocate, ask the patient to avoid mentioning that you are a physician. Instead, ask that she introduce you as a friend or relative that she has asked to come along to serve as a memory bank. During the visit it may be helpful to occasionally interject and suggest that the patient ask a question that hasn’t been adequately addressed. While some physicians may be upset when they belatedly find you have not revealed up front that you are a physician, I find this a harmless omission that has the benefit of improving patient care.
The final scenario — in which you are the patient — is likely to occur more often as you get older. When filling out a previsit form, I often simply put retired or leave it blank. But, how I answer the question often seems to be irrelevant because I have learned that physicians and their staff read those boilerplate forms so cursorily that even when I report my status as “retired physician” everyone seems surprised if and when it later comes to light.
My rationale in keeping the doctor card close to my vest in these situations is that I want to be addressed without any assumptions regarding my medical knowledge, which in my situation is well over half a century old and spotty at best. I don’t want my physicians to say “I’m sure you understand.” Because I often don’t. I would like them to learn about who I am just as I hope they would other patients. I won’t be offended if they “talk down” to me. If this specialist is as good as I’ve heard she is, I want to hear her full performance, not one edited for fellow and former physicians.
It doesn’t arrive gold edged with a list of special privileges. If it comes with any extras, they are risks that must be avoided.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Old, Frail Patients: Study More, Intervene Less?
Lessons From SENIOR-RITA
The ability to save cardiac muscle during an acute coronary syndrome with percutaneous coronary intervention (PCI) made cardiology one of the most popular fields in medicine.
But acute coronary syndromes come in different categories. While rapid PCI clearly benefits patients with ST-segment elevation myocardial infarction (STEMI), the best use of angiography and PCI for patients with non–ST-segment elevation myocardial infarction (NSTEMI) is more complex.
There have been many trials and meta-analyses, and generally, outcomes are similar with either approach. Perhaps if one looks with enough optimism, there is a benefit for the more aggressive approach in higher-risk patients.
Despite the similar outcomes with the two strategies, most patients are treated with the early invasive approach. Early and invasive fit the spirit of modern cardiology.
Yet, older patients with acute coronary syndromes present a different challenge. NSTEMI trials, like most trials, enrolled mostly younger adults.
Whether evidence obtained in young people applies to older patients is one of the most common and important questions in all of medical practice. Older patients may be at higher risk for a primary outcome, but they also have greater risks for harm from therapy as well as more competing causes of morbidity and mortality.
Only a handful of smaller trials have enrolled older patients with NSTEMI. These trials have produced little evidence that an early invasive approach should be preferred.
The SENIOR-RITA Trial
At ESC, Vijay Kunadian, MD, from Newcastle, England, presented results of SENIOR-RITA, a large trial comparing an invasive vs conservative strategy in NSTEMI patients 75 years of age or older.
In the conservative arm, coronary angiography was allowed if the patient deteriorated and the procedure was clinically indicated in the judgment of the treating physicians.
Slightly more than 1500 patients with NSTEMI were randomly assigned to either strategy in 48 centers in the United Kingdom. Their mean age was 82 years, nearly half were women, and about a third were frail.
Over 4 years of follow-up, the primary outcome of cardiovascular (CV) death or MI occurred at a similar rate in both arms: 25.6% vs 26.3% for invasive vs conservative, respectively (HR, 0.94; 95% CI, 0.77-1.14; P =.53).
Rates of CV death were also not significantly different (15.8% vs 14.2%; HR, 1.11; 95% CI, 0.86-1.44).
The rate of nonfatal MI was slightly lower in the invasive arm (11.7% vs 15.0%; HR, 0.75; 95% CI, 0.57-0.99).
Some other notable findings: Fewer than half of patients in the invasive arm underwent revascularization. Coronary angiography was done in about a quarter of patients in the conservative arm, and revascularization in only 14%.
Comments
Because medicine has improved and patients live longer, cardiologists increasingly see older adults with frailty. It’s important to study these patients.
The authors tell us that 1 in 5 patients screened were enrolled, and those not enrolled were similar in age and were treated nearly equally with either strategy. Not all trials offer this information; it’s important because knowing that patients in a trial are representative helps us translate evidence to our actual patients.
Another positive was the investigators’ smart choice of cardiovascular death and MI as their primary outcome. Strategy trials are usually open label. If they had included an outcome that requires a decision from a clinician, such as unplanned revascularization, then bias becomes a possibility when patients and clinicians are aware of the treatment assignment. (I wrote about poor endpoint choice in the ABYSS trial.)
The most notable finding in SENIOR-RITA was that approximately 76% of patients in the conservative arm did not have a coronary angiogram and 86% were not revascularized.
Yet, the rate of CV death and MI were similar during 4 years of follow-up. This observation is nearly identical to the findings in chronic stable disease, seen in the ISCHEMIA trial. (See Figure 6a in the paper’s supplement.)
I take two messages from this consistent observation: One is that medical therapy is quite good at treating coronary artery disease not associated with acute vessel closure in STEMI.
The other is that using coronary angiography and revascularization as a bailout, in only a fraction of cases, achieves the same result, so the conservative strategy should be preferred.
I am not sure that the SENIOR-RITA researchers see it this way. They write in their discussion that “clinicians are often reluctant to offer an invasive strategy to frail older adults.” They then remind readers that modern PCI techniques (radial approach) have low rates of adverse events.
Perhaps I misread their message, but that paragraph seemed like it was reinforcing our tendency to offer invasive approaches to patients with NSTEMI.
I feel differently. When a trial reports similar outcomes with two strategies, I think we should favor the one with less intervention. I feel even more strongly about this philosophy in older patients with frailty.
Are we not in the business of helping people with the least amount of intervention?
The greatest challenge for the cardiologist of today is not a lack of treatment options, but whether we should use all options in older, frailer adults.
Good on the SENIOR-RITA investigators, for they have shown that we can avoid intervention in the vast majority of older adults presenting with NSTEMI.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Kentucky, and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Lessons From SENIOR-RITA
Lessons From SENIOR-RITA
The ability to save cardiac muscle during an acute coronary syndrome with percutaneous coronary intervention (PCI) made cardiology one of the most popular fields in medicine.
But acute coronary syndromes come in different categories. While rapid PCI clearly benefits patients with ST-segment elevation myocardial infarction (STEMI), the best use of angiography and PCI for patients with non–ST-segment elevation myocardial infarction (NSTEMI) is more complex.
There have been many trials and meta-analyses, and generally, outcomes are similar with either approach. Perhaps if one looks with enough optimism, there is a benefit for the more aggressive approach in higher-risk patients.
Despite the similar outcomes with the two strategies, most patients are treated with the early invasive approach. Early and invasive fit the spirit of modern cardiology.
Yet, older patients with acute coronary syndromes present a different challenge. NSTEMI trials, like most trials, enrolled mostly younger adults.
Whether evidence obtained in young people applies to older patients is one of the most common and important questions in all of medical practice. Older patients may be at higher risk for a primary outcome, but they also have greater risks for harm from therapy as well as more competing causes of morbidity and mortality.
Only a handful of smaller trials have enrolled older patients with NSTEMI. These trials have produced little evidence that an early invasive approach should be preferred.
The SENIOR-RITA Trial
At ESC, Vijay Kunadian, MD, from Newcastle, England, presented results of SENIOR-RITA, a large trial comparing an invasive vs conservative strategy in NSTEMI patients 75 years of age or older.
In the conservative arm, coronary angiography was allowed if the patient deteriorated and the procedure was clinically indicated in the judgment of the treating physicians.
Slightly more than 1500 patients with NSTEMI were randomly assigned to either strategy in 48 centers in the United Kingdom. Their mean age was 82 years, nearly half were women, and about a third were frail.
Over 4 years of follow-up, the primary outcome of cardiovascular (CV) death or MI occurred at a similar rate in both arms: 25.6% vs 26.3% for invasive vs conservative, respectively (HR, 0.94; 95% CI, 0.77-1.14; P =.53).
Rates of CV death were also not significantly different (15.8% vs 14.2%; HR, 1.11; 95% CI, 0.86-1.44).
The rate of nonfatal MI was slightly lower in the invasive arm (11.7% vs 15.0%; HR, 0.75; 95% CI, 0.57-0.99).
Some other notable findings: Fewer than half of patients in the invasive arm underwent revascularization. Coronary angiography was done in about a quarter of patients in the conservative arm, and revascularization in only 14%.
Comments
Because medicine has improved and patients live longer, cardiologists increasingly see older adults with frailty. It’s important to study these patients.
The authors tell us that 1 in 5 patients screened were enrolled, and those not enrolled were similar in age and were treated nearly equally with either strategy. Not all trials offer this information; it’s important because knowing that patients in a trial are representative helps us translate evidence to our actual patients.
Another positive was the investigators’ smart choice of cardiovascular death and MI as their primary outcome. Strategy trials are usually open label. If they had included an outcome that requires a decision from a clinician, such as unplanned revascularization, then bias becomes a possibility when patients and clinicians are aware of the treatment assignment. (I wrote about poor endpoint choice in the ABYSS trial.)
The most notable finding in SENIOR-RITA was that approximately 76% of patients in the conservative arm did not have a coronary angiogram and 86% were not revascularized.
Yet, the rate of CV death and MI were similar during 4 years of follow-up. This observation is nearly identical to the findings in chronic stable disease, seen in the ISCHEMIA trial. (See Figure 6a in the paper’s supplement.)
I take two messages from this consistent observation: One is that medical therapy is quite good at treating coronary artery disease not associated with acute vessel closure in STEMI.
The other is that using coronary angiography and revascularization as a bailout, in only a fraction of cases, achieves the same result, so the conservative strategy should be preferred.
I am not sure that the SENIOR-RITA researchers see it this way. They write in their discussion that “clinicians are often reluctant to offer an invasive strategy to frail older adults.” They then remind readers that modern PCI techniques (radial approach) have low rates of adverse events.
Perhaps I misread their message, but that paragraph seemed like it was reinforcing our tendency to offer invasive approaches to patients with NSTEMI.
I feel differently. When a trial reports similar outcomes with two strategies, I think we should favor the one with less intervention. I feel even more strongly about this philosophy in older patients with frailty.
Are we not in the business of helping people with the least amount of intervention?
The greatest challenge for the cardiologist of today is not a lack of treatment options, but whether we should use all options in older, frailer adults.
Good on the SENIOR-RITA investigators, for they have shown that we can avoid intervention in the vast majority of older adults presenting with NSTEMI.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Kentucky, and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The ability to save cardiac muscle during an acute coronary syndrome with percutaneous coronary intervention (PCI) made cardiology one of the most popular fields in medicine.
But acute coronary syndromes come in different categories. While rapid PCI clearly benefits patients with ST-segment elevation myocardial infarction (STEMI), the best use of angiography and PCI for patients with non–ST-segment elevation myocardial infarction (NSTEMI) is more complex.
There have been many trials and meta-analyses, and generally, outcomes are similar with either approach. Perhaps if one looks with enough optimism, there is a benefit for the more aggressive approach in higher-risk patients.
Despite the similar outcomes with the two strategies, most patients are treated with the early invasive approach. Early and invasive fit the spirit of modern cardiology.
Yet, older patients with acute coronary syndromes present a different challenge. NSTEMI trials, like most trials, enrolled mostly younger adults.
Whether evidence obtained in young people applies to older patients is one of the most common and important questions in all of medical practice. Older patients may be at higher risk for a primary outcome, but they also have greater risks for harm from therapy as well as more competing causes of morbidity and mortality.
Only a handful of smaller trials have enrolled older patients with NSTEMI. These trials have produced little evidence that an early invasive approach should be preferred.
The SENIOR-RITA Trial
At ESC, Vijay Kunadian, MD, from Newcastle, England, presented results of SENIOR-RITA, a large trial comparing an invasive vs conservative strategy in NSTEMI patients 75 years of age or older.
In the conservative arm, coronary angiography was allowed if the patient deteriorated and the procedure was clinically indicated in the judgment of the treating physicians.
Slightly more than 1500 patients with NSTEMI were randomly assigned to either strategy in 48 centers in the United Kingdom. Their mean age was 82 years, nearly half were women, and about a third were frail.
Over 4 years of follow-up, the primary outcome of cardiovascular (CV) death or MI occurred at a similar rate in both arms: 25.6% vs 26.3% for invasive vs conservative, respectively (HR, 0.94; 95% CI, 0.77-1.14; P =.53).
Rates of CV death were also not significantly different (15.8% vs 14.2%; HR, 1.11; 95% CI, 0.86-1.44).
The rate of nonfatal MI was slightly lower in the invasive arm (11.7% vs 15.0%; HR, 0.75; 95% CI, 0.57-0.99).
Some other notable findings: Fewer than half of patients in the invasive arm underwent revascularization. Coronary angiography was done in about a quarter of patients in the conservative arm, and revascularization in only 14%.
Comments
Because medicine has improved and patients live longer, cardiologists increasingly see older adults with frailty. It’s important to study these patients.
The authors tell us that 1 in 5 patients screened were enrolled, and those not enrolled were similar in age and were treated nearly equally with either strategy. Not all trials offer this information; it’s important because knowing that patients in a trial are representative helps us translate evidence to our actual patients.
Another positive was the investigators’ smart choice of cardiovascular death and MI as their primary outcome. Strategy trials are usually open label. If they had included an outcome that requires a decision from a clinician, such as unplanned revascularization, then bias becomes a possibility when patients and clinicians are aware of the treatment assignment. (I wrote about poor endpoint choice in the ABYSS trial.)
The most notable finding in SENIOR-RITA was that approximately 76% of patients in the conservative arm did not have a coronary angiogram and 86% were not revascularized.
Yet, the rate of CV death and MI were similar during 4 years of follow-up. This observation is nearly identical to the findings in chronic stable disease, seen in the ISCHEMIA trial. (See Figure 6a in the paper’s supplement.)
I take two messages from this consistent observation: One is that medical therapy is quite good at treating coronary artery disease not associated with acute vessel closure in STEMI.
The other is that using coronary angiography and revascularization as a bailout, in only a fraction of cases, achieves the same result, so the conservative strategy should be preferred.
I am not sure that the SENIOR-RITA researchers see it this way. They write in their discussion that “clinicians are often reluctant to offer an invasive strategy to frail older adults.” They then remind readers that modern PCI techniques (radial approach) have low rates of adverse events.
Perhaps I misread their message, but that paragraph seemed like it was reinforcing our tendency to offer invasive approaches to patients with NSTEMI.
I feel differently. When a trial reports similar outcomes with two strategies, I think we should favor the one with less intervention. I feel even more strongly about this philosophy in older patients with frailty.
Are we not in the business of helping people with the least amount of intervention?
The greatest challenge for the cardiologist of today is not a lack of treatment options, but whether we should use all options in older, frailer adults.
Good on the SENIOR-RITA investigators, for they have shown that we can avoid intervention in the vast majority of older adults presenting with NSTEMI.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Kentucky, and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Navigating Ethical and Clinical Considerations Relating to Percutaneous Gastrostomy (PEG) Tubes
Cases
Consults for percutaneous gastrostomy (PEG) tube placement for a patient ...
- With dysphagia after stroke: A 70-year-old female with a history of hypertension presented to the hospital with altered mental status and left-sided weakness. She was previously active and independently living. MRI of the brain revealed a right basal ganglia infarct. As a result, she developed dysphagia. She was evaluated by speech and language pathology and underwent a modified barium swallow. Given concerns for aspiration, the recommendation was made for gastroenterology (GI) consultation to place PEG tube for nutrition and medication administration.
- With advanced dementia: An 85-year-old male with an extensive medical history including advanced dementia was admitted from his nursing home for decreased oral intake. His baseline mental status is awake and alert, but he is nonverbal and does not follow commands. Upon 72-hour calorie count, the nutrition consultants determined that he cannot independently meet his nutrition goals. His family wants “everything done” and are asking about a “feeding tube.” The primary team has now consulted GI for PEG tube placement.
- Who is being discharged to a long-term care facility: A 45-year-old male was admitted to the ICU after a heroin overdose. CPR was initiated in the field and return of spontaneous circulation was obtained after 25 minutes. The patient has minimal brainstem reflexes. He is ventilator dependent. He has no family, and now is status-post tracheostomy placement by two-physician consent. The patient is ready for discharge to a long-term care facility that will not accept patients with nasogastric tubes. GI is consulted for PEG tube placement.
Discussion
Gastroenterologists are often consulted for PEG tube placement. However, This is rooted in the fact that, as one expert wrote, “feeding, unlike any other medical treatment, has a moral and emotional significance derived from culture.”1 Understanding the evidence, ethical considerations, and team dynamic behind PEG tube placement is critical for every gastroenterologist. Herein we review these topics and offer guidelines for having patient-centered conversations involving these fundamental concepts.

First, the gastroenterologist should understand the evidence to debunk myths and clarify truths surrounding PEG tube placement. While PEG tubes may help patients with amyotrophic lateral sclerosis stabilize their weight and can even be prophylactically placed in select patients with head and neck cancer,2,3 they are not always appropriate in patients in early recovery from stroke and have not been shown to improve outcomes in patients with advanced dementia. At least 50% of stroke-related dysphagia resolves within 1-2 weeks, and so the American Heart Association Stroke Council recommends continuing nasogastric tube feeding for 2-3 weeks in patients such as the one presented in case 1 before considering PEG tube placement.4
In situations of advanced dementia such as in case,2 several studies demonstrate that PEG tubes do not reduce or prevent aspiration pneumonia, prevent consequences of malnutrition, prolong life, reduce pressure ulcers, reduce urinary of gastrointestinal tract infections, lead to functional improvement, mitigate decline, or even improve comfort or quality of life for patients or their caregivers.5-7 Despite this evidence, as demonstrated in case,3 it is true that many American skilled nursing facilities will not accept a patient without a PEG if enteral feeding is needed. This restriction may vary by state: One study found that skilled nursing facilities in New York City are much less likely to accept patients with nasogastric feeding tubes than randomly selected skilled nursing facilities throughout the country.6 Nonetheless, gastroenterologists should look to the literature to understand the outcomes of populations of patients after PEG tube placement and use that data to guide decision-making.

Secondly, the five ethical principles that inform all medical decision making – autonomy, beneficence, nonmaleficence, justice, and futility – should also inform the gastroenterologist’s rationale in offering PEG placement.8
Autonomy implies that the medical team has determined who is able to make the decision regarding PEG tube placement for the patient. Beneficence connects the patient’s medical diagnosis and technical parameters of PEG tube placement with his or her goals of care. Nonmaleficence ensures the decision-making party understands the benefits and risks of the procedure, including anticipatory guidance on possible PEG tube management, complications, risks, and need for replacement. Justice incorporates the context of the patient’s life, including family dynamics, religious, cultural, and financial factors. Futility connects the patient’s prognosis with practical aspects of having a PEG tube.
The complexity of PEG placement lies in the fact that these ethical principles are often at odds with each other. For example, case 2 highlights the conflicting principles of autonomy and futility for elderly dementia patients: While PEG tube placements do not improve comfort or quality of life in advanced dementia (futility), the family representing the patient has stated they want everything done for his care, including PEG tube placement (autonomy). Navigating these ethical principles can be difficult, but having a framework to organize the different factors offers sound guidance for the gastroenterologist.
Finally, the gastroenterologist should recognize the roles of the multidisciplinary team members, including the patient and their representatives, regarding PEG tube placement consults. While gastroenterologists can be viewed as the technicians consulted to simply “place the tube,” they must seek to understand the members of the team representing the patient to be stewards of their skill set. Consulting team physicians carry great responsibility in organizing the medical and psychosocial aspects of each patient’s care, and their proper goals to relieve suffering and prevent death may color their judgment regarding who they believe is a candidate for a PEG tube. Nutritionists, speech therapists, and case managers can help provide objective data on the practicality and feasibility of a PEG tube in their patients. The healthcare system may influence the decision to consult heavily, as seen in the rules of the long-term care facility in case.3 While it is the job of the multidisciplinary medical team to explain the evidence and ethical considerations of PEG tube placement in a patient-centered manner, ultimately the decision belongs to the patient and their family or representatives.
The moral burden of not pursuing PEG placement may supersede the medical advice in many situations. There is an emotionally taxing perception that withholding nutrition via PEG is “starving the patient,” despite literature showing many terminally ill patients do not experience thirst or hunger, and those who do have alleviation of these symptoms with small amounts of food or liquid, not with PEG placement.5 As every patient is unique, PEG tube consultation guidelines created with input from all stakeholders have been utilized to ensure that patients are medically optimized for PEG tube placement and that evidence and ethics-based considerations are evaluated by the multidisciplinary team. An example of such a guideline is shown in Figure 1.
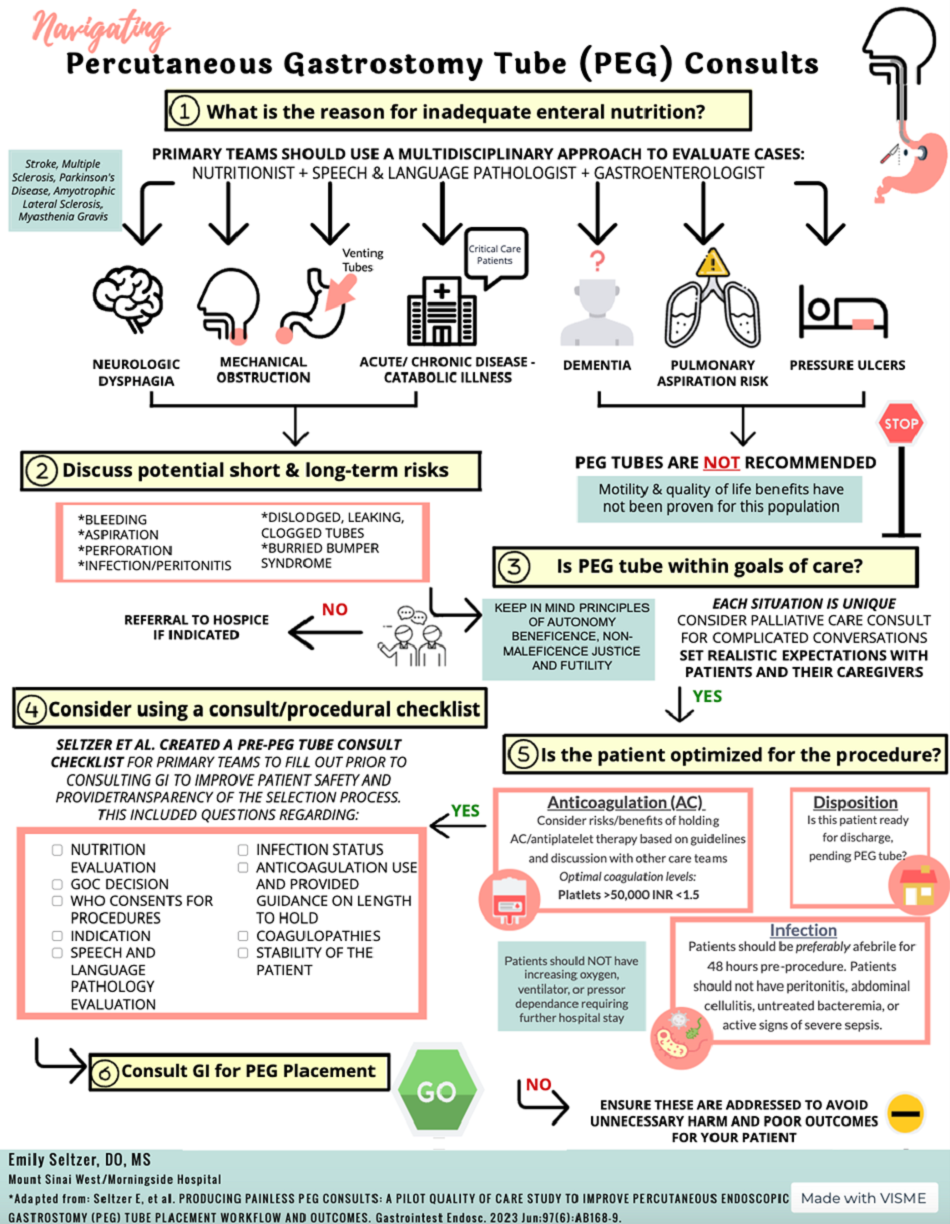
If the gastroenterologist encounters more contentious consultations, there are ways to build consensus to both alleviate patient and family suffering as well as elevate the discussions between teams.
First, identify the type of consult that is repeatedly bringing differing viewpoints and differing ethical principles into play. Second, get representatives from teams together in a neutral environment to understand stakeholders needs. New data suggest, in stroke cases like case 1, there may be dramatic benefit in long-term ability to recover if patients can get early intensive rehabilitation.9 This intense daily rehabilitation is not available within the hospital setting at many locations, and facilitation of discharge may be requested earlier than usually advised tube placement. Third, build a common language for requests and responses between teams. For instance, neurologists can identify and document which patients have less likelihood of early spontaneous recovery, and this can allow gastroenterologists to understand that those patients with little potential for early swallowing recovery can safely be targeted for PEG earlier during the hospital course. Other patients described as having a potential for spontaneous improvement should be given time to recover before an intervention is considered.10 Having a common understanding of goals and a better-informed decision pathway helps each team member feel fulfilled and rewarded, which will ultimately help reduce compassion fatigue and moral burden on providers.

In conclusion, PEG tube placement can be a challenging consultation for gastroenterologists because of the clinical, social, and ethical ramifications at stake for the patient. Even when PEG tube placement is technically feasible, the gastroenterologist should feel empowered to address the evidence-based outcomes of PEG tube placement, discuss the ethical principles of the decision-making process, and communicate with a multidisciplinary team using guidelines as set forth by this paper to best serve the patient.
Dr. Seltzer is based in the Department of Internal Medicine, Mount Sinai Morningside-West, New York City. Dr. Pusateri is based in the Division of Gastroenterology, Hepatology and Nutrition, Ohio State University Wexner Medical Center, Columbus. Dr. Nguyen is based in the Division of Gastroenterology and Center for Esophageal Diseases, Baylor Scott & White Health, Dallas, Texas. Dr. Stein is based in the Division of Gastroenterology, Robert Wood Johnson University Hospital, Rutgers University, New Brunswick, New Jersey. All authors contributed equally to this manuscript, and have no disclosures related to this article.
References
1. Mackie S. Gastroenterol Nurs. 2001 May-Jun;24(3):138-42.
2. Miller RG et al. Neurology. 2009 Oct. doi: 10.1212/WNL.0b013e3181bc0141.
3. Colevas AD et al. J Natl Compr Canc Netw. 2018 May. doi: 10.6004/jnccn.2018.0026.
4. Holloway RG et al. Stroke. 2014 Jun. doi: 10.1161/STR.0000000000000015.
5. Finucane TE et al. JAMA. 1999 Oct. doi: 10.1001/jama.282.14.1365.
6. Burgermaster M et al. Nutr Clin Pract. 2016 Jun. doi: 10.1177/0884533616629636.
7. American Geriatrics Society Ethics C, Clinical P, Models of Care C. J Am Geriatr Soc. 2014 Aug. doi: 10.1111/jgs.12924.
8. Beauchamp TL. Principlism in Bioethics. In: Serna P, eds. Bioethical Decision Making and Argumentation. International Library of Ethics, Law, and the New Medicine, vol 70. Springer; Cham. 2016 Sept:1-16. doi: 10.1007/978-3-319-43419-3_1.
9. Powers WJ et al. Stroke. 2019 Oct. doi: 10.1161/STR.0000000000000211.
10. Galovic M et al. JAMA Neurol. 2019 May. doi: 10.1001/jamaneurol.2018.4858.
Cases
Consults for percutaneous gastrostomy (PEG) tube placement for a patient ...
- With dysphagia after stroke: A 70-year-old female with a history of hypertension presented to the hospital with altered mental status and left-sided weakness. She was previously active and independently living. MRI of the brain revealed a right basal ganglia infarct. As a result, she developed dysphagia. She was evaluated by speech and language pathology and underwent a modified barium swallow. Given concerns for aspiration, the recommendation was made for gastroenterology (GI) consultation to place PEG tube for nutrition and medication administration.
- With advanced dementia: An 85-year-old male with an extensive medical history including advanced dementia was admitted from his nursing home for decreased oral intake. His baseline mental status is awake and alert, but he is nonverbal and does not follow commands. Upon 72-hour calorie count, the nutrition consultants determined that he cannot independently meet his nutrition goals. His family wants “everything done” and are asking about a “feeding tube.” The primary team has now consulted GI for PEG tube placement.
- Who is being discharged to a long-term care facility: A 45-year-old male was admitted to the ICU after a heroin overdose. CPR was initiated in the field and return of spontaneous circulation was obtained after 25 minutes. The patient has minimal brainstem reflexes. He is ventilator dependent. He has no family, and now is status-post tracheostomy placement by two-physician consent. The patient is ready for discharge to a long-term care facility that will not accept patients with nasogastric tubes. GI is consulted for PEG tube placement.
Discussion
Gastroenterologists are often consulted for PEG tube placement. However, This is rooted in the fact that, as one expert wrote, “feeding, unlike any other medical treatment, has a moral and emotional significance derived from culture.”1 Understanding the evidence, ethical considerations, and team dynamic behind PEG tube placement is critical for every gastroenterologist. Herein we review these topics and offer guidelines for having patient-centered conversations involving these fundamental concepts.
First, the gastroenterologist should understand the evidence to debunk myths and clarify truths surrounding PEG tube placement. While PEG tubes may help patients with amyotrophic lateral sclerosis stabilize their weight and can even be prophylactically placed in select patients with head and neck cancer,2,3 they are not always appropriate in patients in early recovery from stroke and have not been shown to improve outcomes in patients with advanced dementia. At least 50% of stroke-related dysphagia resolves within 1-2 weeks, and so the American Heart Association Stroke Council recommends continuing nasogastric tube feeding for 2-3 weeks in patients such as the one presented in case 1 before considering PEG tube placement.4
In situations of advanced dementia such as in case,2 several studies demonstrate that PEG tubes do not reduce or prevent aspiration pneumonia, prevent consequences of malnutrition, prolong life, reduce pressure ulcers, reduce urinary of gastrointestinal tract infections, lead to functional improvement, mitigate decline, or even improve comfort or quality of life for patients or their caregivers.5-7 Despite this evidence, as demonstrated in case,3 it is true that many American skilled nursing facilities will not accept a patient without a PEG if enteral feeding is needed. This restriction may vary by state: One study found that skilled nursing facilities in New York City are much less likely to accept patients with nasogastric feeding tubes than randomly selected skilled nursing facilities throughout the country.6 Nonetheless, gastroenterologists should look to the literature to understand the outcomes of populations of patients after PEG tube placement and use that data to guide decision-making.
Secondly, the five ethical principles that inform all medical decision making – autonomy, beneficence, nonmaleficence, justice, and futility – should also inform the gastroenterologist’s rationale in offering PEG placement.8
Autonomy implies that the medical team has determined who is able to make the decision regarding PEG tube placement for the patient. Beneficence connects the patient’s medical diagnosis and technical parameters of PEG tube placement with his or her goals of care. Nonmaleficence ensures the decision-making party understands the benefits and risks of the procedure, including anticipatory guidance on possible PEG tube management, complications, risks, and need for replacement. Justice incorporates the context of the patient’s life, including family dynamics, religious, cultural, and financial factors. Futility connects the patient’s prognosis with practical aspects of having a PEG tube.
The complexity of PEG placement lies in the fact that these ethical principles are often at odds with each other. For example, case 2 highlights the conflicting principles of autonomy and futility for elderly dementia patients: While PEG tube placements do not improve comfort or quality of life in advanced dementia (futility), the family representing the patient has stated they want everything done for his care, including PEG tube placement (autonomy). Navigating these ethical principles can be difficult, but having a framework to organize the different factors offers sound guidance for the gastroenterologist.
Finally, the gastroenterologist should recognize the roles of the multidisciplinary team members, including the patient and their representatives, regarding PEG tube placement consults. While gastroenterologists can be viewed as the technicians consulted to simply “place the tube,” they must seek to understand the members of the team representing the patient to be stewards of their skill set. Consulting team physicians carry great responsibility in organizing the medical and psychosocial aspects of each patient’s care, and their proper goals to relieve suffering and prevent death may color their judgment regarding who they believe is a candidate for a PEG tube. Nutritionists, speech therapists, and case managers can help provide objective data on the practicality and feasibility of a PEG tube in their patients. The healthcare system may influence the decision to consult heavily, as seen in the rules of the long-term care facility in case.3 While it is the job of the multidisciplinary medical team to explain the evidence and ethical considerations of PEG tube placement in a patient-centered manner, ultimately the decision belongs to the patient and their family or representatives.
The moral burden of not pursuing PEG placement may supersede the medical advice in many situations. There is an emotionally taxing perception that withholding nutrition via PEG is “starving the patient,” despite literature showing many terminally ill patients do not experience thirst or hunger, and those who do have alleviation of these symptoms with small amounts of food or liquid, not with PEG placement.5 As every patient is unique, PEG tube consultation guidelines created with input from all stakeholders have been utilized to ensure that patients are medically optimized for PEG tube placement and that evidence and ethics-based considerations are evaluated by the multidisciplinary team. An example of such a guideline is shown in Figure 1.
If the gastroenterologist encounters more contentious consultations, there are ways to build consensus to both alleviate patient and family suffering as well as elevate the discussions between teams.
First, identify the type of consult that is repeatedly bringing differing viewpoints and differing ethical principles into play. Second, get representatives from teams together in a neutral environment to understand stakeholders needs. New data suggest, in stroke cases like case 1, there may be dramatic benefit in long-term ability to recover if patients can get early intensive rehabilitation.9 This intense daily rehabilitation is not available within the hospital setting at many locations, and facilitation of discharge may be requested earlier than usually advised tube placement. Third, build a common language for requests and responses between teams. For instance, neurologists can identify and document which patients have less likelihood of early spontaneous recovery, and this can allow gastroenterologists to understand that those patients with little potential for early swallowing recovery can safely be targeted for PEG earlier during the hospital course. Other patients described as having a potential for spontaneous improvement should be given time to recover before an intervention is considered.10 Having a common understanding of goals and a better-informed decision pathway helps each team member feel fulfilled and rewarded, which will ultimately help reduce compassion fatigue and moral burden on providers.
In conclusion, PEG tube placement can be a challenging consultation for gastroenterologists because of the clinical, social, and ethical ramifications at stake for the patient. Even when PEG tube placement is technically feasible, the gastroenterologist should feel empowered to address the evidence-based outcomes of PEG tube placement, discuss the ethical principles of the decision-making process, and communicate with a multidisciplinary team using guidelines as set forth by this paper to best serve the patient.
Dr. Seltzer is based in the Department of Internal Medicine, Mount Sinai Morningside-West, New York City. Dr. Pusateri is based in the Division of Gastroenterology, Hepatology and Nutrition, Ohio State University Wexner Medical Center, Columbus. Dr. Nguyen is based in the Division of Gastroenterology and Center for Esophageal Diseases, Baylor Scott & White Health, Dallas, Texas. Dr. Stein is based in the Division of Gastroenterology, Robert Wood Johnson University Hospital, Rutgers University, New Brunswick, New Jersey. All authors contributed equally to this manuscript, and have no disclosures related to this article.
References
1. Mackie S. Gastroenterol Nurs. 2001 May-Jun;24(3):138-42.
2. Miller RG et al. Neurology. 2009 Oct. doi: 10.1212/WNL.0b013e3181bc0141.
3. Colevas AD et al. J Natl Compr Canc Netw. 2018 May. doi: 10.6004/jnccn.2018.0026.
4. Holloway RG et al. Stroke. 2014 Jun. doi: 10.1161/STR.0000000000000015.
5. Finucane TE et al. JAMA. 1999 Oct. doi: 10.1001/jama.282.14.1365.
6. Burgermaster M et al. Nutr Clin Pract. 2016 Jun. doi: 10.1177/0884533616629636.
7. American Geriatrics Society Ethics C, Clinical P, Models of Care C. J Am Geriatr Soc. 2014 Aug. doi: 10.1111/jgs.12924.
8. Beauchamp TL. Principlism in Bioethics. In: Serna P, eds. Bioethical Decision Making and Argumentation. International Library of Ethics, Law, and the New Medicine, vol 70. Springer; Cham. 2016 Sept:1-16. doi: 10.1007/978-3-319-43419-3_1.
9. Powers WJ et al. Stroke. 2019 Oct. doi: 10.1161/STR.0000000000000211.
10. Galovic M et al. JAMA Neurol. 2019 May. doi: 10.1001/jamaneurol.2018.4858.
Cases
Consults for percutaneous gastrostomy (PEG) tube placement for a patient ...
- With dysphagia after stroke: A 70-year-old female with a history of hypertension presented to the hospital with altered mental status and left-sided weakness. She was previously active and independently living. MRI of the brain revealed a right basal ganglia infarct. As a result, she developed dysphagia. She was evaluated by speech and language pathology and underwent a modified barium swallow. Given concerns for aspiration, the recommendation was made for gastroenterology (GI) consultation to place PEG tube for nutrition and medication administration.
- With advanced dementia: An 85-year-old male with an extensive medical history including advanced dementia was admitted from his nursing home for decreased oral intake. His baseline mental status is awake and alert, but he is nonverbal and does not follow commands. Upon 72-hour calorie count, the nutrition consultants determined that he cannot independently meet his nutrition goals. His family wants “everything done” and are asking about a “feeding tube.” The primary team has now consulted GI for PEG tube placement.
- Who is being discharged to a long-term care facility: A 45-year-old male was admitted to the ICU after a heroin overdose. CPR was initiated in the field and return of spontaneous circulation was obtained after 25 minutes. The patient has minimal brainstem reflexes. He is ventilator dependent. He has no family, and now is status-post tracheostomy placement by two-physician consent. The patient is ready for discharge to a long-term care facility that will not accept patients with nasogastric tubes. GI is consulted for PEG tube placement.
Discussion
Gastroenterologists are often consulted for PEG tube placement. However, This is rooted in the fact that, as one expert wrote, “feeding, unlike any other medical treatment, has a moral and emotional significance derived from culture.”1 Understanding the evidence, ethical considerations, and team dynamic behind PEG tube placement is critical for every gastroenterologist. Herein we review these topics and offer guidelines for having patient-centered conversations involving these fundamental concepts.
First, the gastroenterologist should understand the evidence to debunk myths and clarify truths surrounding PEG tube placement. While PEG tubes may help patients with amyotrophic lateral sclerosis stabilize their weight and can even be prophylactically placed in select patients with head and neck cancer,2,3 they are not always appropriate in patients in early recovery from stroke and have not been shown to improve outcomes in patients with advanced dementia. At least 50% of stroke-related dysphagia resolves within 1-2 weeks, and so the American Heart Association Stroke Council recommends continuing nasogastric tube feeding for 2-3 weeks in patients such as the one presented in case 1 before considering PEG tube placement.4
In situations of advanced dementia such as in case,2 several studies demonstrate that PEG tubes do not reduce or prevent aspiration pneumonia, prevent consequences of malnutrition, prolong life, reduce pressure ulcers, reduce urinary of gastrointestinal tract infections, lead to functional improvement, mitigate decline, or even improve comfort or quality of life for patients or their caregivers.5-7 Despite this evidence, as demonstrated in case,3 it is true that many American skilled nursing facilities will not accept a patient without a PEG if enteral feeding is needed. This restriction may vary by state: One study found that skilled nursing facilities in New York City are much less likely to accept patients with nasogastric feeding tubes than randomly selected skilled nursing facilities throughout the country.6 Nonetheless, gastroenterologists should look to the literature to understand the outcomes of populations of patients after PEG tube placement and use that data to guide decision-making.
Secondly, the five ethical principles that inform all medical decision making – autonomy, beneficence, nonmaleficence, justice, and futility – should also inform the gastroenterologist’s rationale in offering PEG placement.8
Autonomy implies that the medical team has determined who is able to make the decision regarding PEG tube placement for the patient. Beneficence connects the patient’s medical diagnosis and technical parameters of PEG tube placement with his or her goals of care. Nonmaleficence ensures the decision-making party understands the benefits and risks of the procedure, including anticipatory guidance on possible PEG tube management, complications, risks, and need for replacement. Justice incorporates the context of the patient’s life, including family dynamics, religious, cultural, and financial factors. Futility connects the patient’s prognosis with practical aspects of having a PEG tube.
The complexity of PEG placement lies in the fact that these ethical principles are often at odds with each other. For example, case 2 highlights the conflicting principles of autonomy and futility for elderly dementia patients: While PEG tube placements do not improve comfort or quality of life in advanced dementia (futility), the family representing the patient has stated they want everything done for his care, including PEG tube placement (autonomy). Navigating these ethical principles can be difficult, but having a framework to organize the different factors offers sound guidance for the gastroenterologist.
Finally, the gastroenterologist should recognize the roles of the multidisciplinary team members, including the patient and their representatives, regarding PEG tube placement consults. While gastroenterologists can be viewed as the technicians consulted to simply “place the tube,” they must seek to understand the members of the team representing the patient to be stewards of their skill set. Consulting team physicians carry great responsibility in organizing the medical and psychosocial aspects of each patient’s care, and their proper goals to relieve suffering and prevent death may color their judgment regarding who they believe is a candidate for a PEG tube. Nutritionists, speech therapists, and case managers can help provide objective data on the practicality and feasibility of a PEG tube in their patients. The healthcare system may influence the decision to consult heavily, as seen in the rules of the long-term care facility in case.3 While it is the job of the multidisciplinary medical team to explain the evidence and ethical considerations of PEG tube placement in a patient-centered manner, ultimately the decision belongs to the patient and their family or representatives.
The moral burden of not pursuing PEG placement may supersede the medical advice in many situations. There is an emotionally taxing perception that withholding nutrition via PEG is “starving the patient,” despite literature showing many terminally ill patients do not experience thirst or hunger, and those who do have alleviation of these symptoms with small amounts of food or liquid, not with PEG placement.5 As every patient is unique, PEG tube consultation guidelines created with input from all stakeholders have been utilized to ensure that patients are medically optimized for PEG tube placement and that evidence and ethics-based considerations are evaluated by the multidisciplinary team. An example of such a guideline is shown in Figure 1.
If the gastroenterologist encounters more contentious consultations, there are ways to build consensus to both alleviate patient and family suffering as well as elevate the discussions between teams.
First, identify the type of consult that is repeatedly bringing differing viewpoints and differing ethical principles into play. Second, get representatives from teams together in a neutral environment to understand stakeholders needs. New data suggest, in stroke cases like case 1, there may be dramatic benefit in long-term ability to recover if patients can get early intensive rehabilitation.9 This intense daily rehabilitation is not available within the hospital setting at many locations, and facilitation of discharge may be requested earlier than usually advised tube placement. Third, build a common language for requests and responses between teams. For instance, neurologists can identify and document which patients have less likelihood of early spontaneous recovery, and this can allow gastroenterologists to understand that those patients with little potential for early swallowing recovery can safely be targeted for PEG earlier during the hospital course. Other patients described as having a potential for spontaneous improvement should be given time to recover before an intervention is considered.10 Having a common understanding of goals and a better-informed decision pathway helps each team member feel fulfilled and rewarded, which will ultimately help reduce compassion fatigue and moral burden on providers.
In conclusion, PEG tube placement can be a challenging consultation for gastroenterologists because of the clinical, social, and ethical ramifications at stake for the patient. Even when PEG tube placement is technically feasible, the gastroenterologist should feel empowered to address the evidence-based outcomes of PEG tube placement, discuss the ethical principles of the decision-making process, and communicate with a multidisciplinary team using guidelines as set forth by this paper to best serve the patient.
Dr. Seltzer is based in the Department of Internal Medicine, Mount Sinai Morningside-West, New York City. Dr. Pusateri is based in the Division of Gastroenterology, Hepatology and Nutrition, Ohio State University Wexner Medical Center, Columbus. Dr. Nguyen is based in the Division of Gastroenterology and Center for Esophageal Diseases, Baylor Scott & White Health, Dallas, Texas. Dr. Stein is based in the Division of Gastroenterology, Robert Wood Johnson University Hospital, Rutgers University, New Brunswick, New Jersey. All authors contributed equally to this manuscript, and have no disclosures related to this article.
References
1. Mackie S. Gastroenterol Nurs. 2001 May-Jun;24(3):138-42.
2. Miller RG et al. Neurology. 2009 Oct. doi: 10.1212/WNL.0b013e3181bc0141.
3. Colevas AD et al. J Natl Compr Canc Netw. 2018 May. doi: 10.6004/jnccn.2018.0026.
4. Holloway RG et al. Stroke. 2014 Jun. doi: 10.1161/STR.0000000000000015.
5. Finucane TE et al. JAMA. 1999 Oct. doi: 10.1001/jama.282.14.1365.
6. Burgermaster M et al. Nutr Clin Pract. 2016 Jun. doi: 10.1177/0884533616629636.
7. American Geriatrics Society Ethics C, Clinical P, Models of Care C. J Am Geriatr Soc. 2014 Aug. doi: 10.1111/jgs.12924.
8. Beauchamp TL. Principlism in Bioethics. In: Serna P, eds. Bioethical Decision Making and Argumentation. International Library of Ethics, Law, and the New Medicine, vol 70. Springer; Cham. 2016 Sept:1-16. doi: 10.1007/978-3-319-43419-3_1.
9. Powers WJ et al. Stroke. 2019 Oct. doi: 10.1161/STR.0000000000000211.
10. Galovic M et al. JAMA Neurol. 2019 May. doi: 10.1001/jamaneurol.2018.4858.
ANA Testing: When to Tap the Brakes
This transcript has been edited for clarity.
There are five reasons you do not want to order that notorious antinuclear antibody (ANA) test — when a patient comes into your office and you say, “Let’s just run a wellness check” and you order the ANA test, or the patient comes in and says, “Hey doc, order everything, okay?” — without really thinking these things through.
1. I’m sure you know that the ANA test, if positive, does not exclude other conditions. For instance, older women could have a positive ANA test; it’s very common in this group.
2. There’s a high false-positive rate for an ANA test. For instance, cancers and viral infections can cause an ANA test to be positive, and certain medications can cause a false-positive ANA test.
3. Context matters. If you have a patient that has particular symptoms, joint swelling, a strong family history of autoimmune disease, a luminal rash that you can’t understand, hair loss, those kind of things, then yes, when you order that ANA test, it’s going to be valuable. If the patient does not have those symptoms, you are just running down this rabbit hole that causes worry for you and your patient.
4. The ANA test on its own is not helpful until you order the subtypes. Double-stranded DNA and anti-SSA or anti-SSB antibodies are just a few examples of the subtypes of the ANA test that really help you understand what you ordered.
5. The elephant in the room: What is the pretest probability of your diagnostic test — all the symptoms, the hair loss, the malar rash, the sores in the mouth, the joint swelling, the blood in the urine? Fluid around the heart, pericarditis, pleurisy, those kinds of symptoms, right? When you have those symptoms and you order an ANA test, then you have basically put directions into your GPS. So now you know that if the test is positive, these are the things you’re going to do with the test going forward.
I hope that these five things have told you: Hey, before you order that ANA test, let’s make sure that we’re not causing unnecessary stress for our patients and also minimizing unnecessary testing.
Dr. Dada, CEO, Overlake Arthritis and Osteoporosis Center, Bellevue, Washington, disclosed ties with Horizon Pharmaceuticals.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There are five reasons you do not want to order that notorious antinuclear antibody (ANA) test — when a patient comes into your office and you say, “Let’s just run a wellness check” and you order the ANA test, or the patient comes in and says, “Hey doc, order everything, okay?” — without really thinking these things through.
1. I’m sure you know that the ANA test, if positive, does not exclude other conditions. For instance, older women could have a positive ANA test; it’s very common in this group.
2. There’s a high false-positive rate for an ANA test. For instance, cancers and viral infections can cause an ANA test to be positive, and certain medications can cause a false-positive ANA test.
3. Context matters. If you have a patient that has particular symptoms, joint swelling, a strong family history of autoimmune disease, a luminal rash that you can’t understand, hair loss, those kind of things, then yes, when you order that ANA test, it’s going to be valuable. If the patient does not have those symptoms, you are just running down this rabbit hole that causes worry for you and your patient.
4. The ANA test on its own is not helpful until you order the subtypes. Double-stranded DNA and anti-SSA or anti-SSB antibodies are just a few examples of the subtypes of the ANA test that really help you understand what you ordered.
5. The elephant in the room: What is the pretest probability of your diagnostic test — all the symptoms, the hair loss, the malar rash, the sores in the mouth, the joint swelling, the blood in the urine? Fluid around the heart, pericarditis, pleurisy, those kinds of symptoms, right? When you have those symptoms and you order an ANA test, then you have basically put directions into your GPS. So now you know that if the test is positive, these are the things you’re going to do with the test going forward.
I hope that these five things have told you: Hey, before you order that ANA test, let’s make sure that we’re not causing unnecessary stress for our patients and also minimizing unnecessary testing.
Dr. Dada, CEO, Overlake Arthritis and Osteoporosis Center, Bellevue, Washington, disclosed ties with Horizon Pharmaceuticals.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There are five reasons you do not want to order that notorious antinuclear antibody (ANA) test — when a patient comes into your office and you say, “Let’s just run a wellness check” and you order the ANA test, or the patient comes in and says, “Hey doc, order everything, okay?” — without really thinking these things through.
1. I’m sure you know that the ANA test, if positive, does not exclude other conditions. For instance, older women could have a positive ANA test; it’s very common in this group.
2. There’s a high false-positive rate for an ANA test. For instance, cancers and viral infections can cause an ANA test to be positive, and certain medications can cause a false-positive ANA test.
3. Context matters. If you have a patient that has particular symptoms, joint swelling, a strong family history of autoimmune disease, a luminal rash that you can’t understand, hair loss, those kind of things, then yes, when you order that ANA test, it’s going to be valuable. If the patient does not have those symptoms, you are just running down this rabbit hole that causes worry for you and your patient.
4. The ANA test on its own is not helpful until you order the subtypes. Double-stranded DNA and anti-SSA or anti-SSB antibodies are just a few examples of the subtypes of the ANA test that really help you understand what you ordered.
5. The elephant in the room: What is the pretest probability of your diagnostic test — all the symptoms, the hair loss, the malar rash, the sores in the mouth, the joint swelling, the blood in the urine? Fluid around the heart, pericarditis, pleurisy, those kinds of symptoms, right? When you have those symptoms and you order an ANA test, then you have basically put directions into your GPS. So now you know that if the test is positive, these are the things you’re going to do with the test going forward.
I hope that these five things have told you: Hey, before you order that ANA test, let’s make sure that we’re not causing unnecessary stress for our patients and also minimizing unnecessary testing.
Dr. Dada, CEO, Overlake Arthritis and Osteoporosis Center, Bellevue, Washington, disclosed ties with Horizon Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Diabetes Increases Injury Risk: A Troubling Trend
In 2024, a record number of people are celebrating their 65th birthdays. Increasing age is associated with a higher risk for falls, fractures, and other injuries that may require hospitalization.
In older adults with type 1 and type 2 diabetes, the risk for falls is double that seen in older people without these conditions. Increased clinician awareness of the many factors that result in this higher risk in people with diabetes, and timely implementation of strategies to prevent falls, are essential.
The annual incidence of falls in people with diabetes older than 65 years is about 39%, compared with 19% among those without diabetes. People with diabetes on insulin face an even greater increased risk for falls compared with those who are not using insulin (94% vs 27% increased risk).
Many well-known aspects of diabetes contribute to this greater risk. These include decreased sensorimotor function, musculoskeletal and neuromuscular deficits, foot and body pain, poor vision, hypoglycemic episodes, pharmacologic complications, and problems with hearing and balance.
Optimal management of diabetes and its complications is essential, and the American Diabetes Association has developed clear guidelines for clinicians to follow to reduce the risk for diabetes related complications and manage these conditions.
The prevalence of diabetic peripheral neuropathy increases with age and duration of diabetes. People with diabetic peripheral neuropathy and diminished sensation on their feet are at increased risk for loss of postural control. Loss of proprioceptive feedback (the ability to sense movement, action and location) during standing and walking leads increases the risk for falls.
In addition, less physical activity, impaired muscle strength, and suboptimal postural control all influence gait patterns and increase the risk for falling. Adults with diabetes have a two to three times higher risk for sarcopenia (decreased muscle strength and muscle mass). They also have low plantar flexion strength, causing increased displacement of their center of gravity, which in turn reduces their maximum forward stride and may result in falls and injury.
Many people with diabetes experience neuropathic foot and body pain, requiring psychotropic and other medications that may exacerbate the risk, such as amitriptyline and duloxetine. Furthermore, older adults with diabetes are more likely to take more prescription medications and may be more sensitive to effects of multiple medications than are individuals without diabetes.
A hazard of managing diabetes, particularly with insulin, is the increased risk for unexpected low blood glucose levels. These episodes can also occur in patients taking certain kinds of oral diabetes medications, but they are more common in those on insulin. Low blood glucose can cause dizziness, confusion, and postural instability, increasing the risk for falling.
Diabetic eye complications include retinopathy, macular edema, cataracts, and glaucoma. In a study of close to 10,000 middle-aged and older adults with diabetes, those with moderate eye complications had almost double the risk of falls as those without eye complications.
Another concern with diabetes is its effect on nerves and blood vessels in the inner ear, leading to a negative effect on balance and hearing loss, both of which are also associated with a higher risk for falling and injury.
Clinicians can reduce the risk for falls in patients by taking measures to improve diabetes control and reduce the risk for microvascular disease affecting the nerves, eyes, and ears.
In addition, exercises that optimize muscle mass, bone strength, gait, and balance, and use of specialized footwear in people with neuropathy, may reduce fall risk. Chair yoga and tai chi have also been shown to be helpful. Clinicians can also advise patients on commonsense strategies to implement in their homes, such as ensuring proper lighting, reducing, clutter and minimizing the use of floor rugs.
The risk for falls and the associated risk for fracture and possible hospitalization are of significant concern in older adults — particularly those with diabetes, and even more so in those with diabetes who are on insulin. It is our responsibility as clinicians to implement strategies to optimize diabetes control in our patients and monitor them for microvascular and other complications that may increase this risk, and manage them appropriately if and when these complications occur.
Madhusmita Misra, Professor, Chair, Physician-in-Chief, Department of Pediatrics, University of Virginia and UVA Health Children’s, Charlottesville, has disclosed being a key opinion leader for Lumos Pharma. Sidhartha Pani, Assistant Professor, Department of Internal Medicine, UVA School of Medicine; Medical Director, Department of General Medicine, Same Day Care Clinic, Charlottesville, disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In 2024, a record number of people are celebrating their 65th birthdays. Increasing age is associated with a higher risk for falls, fractures, and other injuries that may require hospitalization.
In older adults with type 1 and type 2 diabetes, the risk for falls is double that seen in older people without these conditions. Increased clinician awareness of the many factors that result in this higher risk in people with diabetes, and timely implementation of strategies to prevent falls, are essential.
The annual incidence of falls in people with diabetes older than 65 years is about 39%, compared with 19% among those without diabetes. People with diabetes on insulin face an even greater increased risk for falls compared with those who are not using insulin (94% vs 27% increased risk).
Many well-known aspects of diabetes contribute to this greater risk. These include decreased sensorimotor function, musculoskeletal and neuromuscular deficits, foot and body pain, poor vision, hypoglycemic episodes, pharmacologic complications, and problems with hearing and balance.
Optimal management of diabetes and its complications is essential, and the American Diabetes Association has developed clear guidelines for clinicians to follow to reduce the risk for diabetes related complications and manage these conditions.
The prevalence of diabetic peripheral neuropathy increases with age and duration of diabetes. People with diabetic peripheral neuropathy and diminished sensation on their feet are at increased risk for loss of postural control. Loss of proprioceptive feedback (the ability to sense movement, action and location) during standing and walking leads increases the risk for falls.
In addition, less physical activity, impaired muscle strength, and suboptimal postural control all influence gait patterns and increase the risk for falling. Adults with diabetes have a two to three times higher risk for sarcopenia (decreased muscle strength and muscle mass). They also have low plantar flexion strength, causing increased displacement of their center of gravity, which in turn reduces their maximum forward stride and may result in falls and injury.
Many people with diabetes experience neuropathic foot and body pain, requiring psychotropic and other medications that may exacerbate the risk, such as amitriptyline and duloxetine. Furthermore, older adults with diabetes are more likely to take more prescription medications and may be more sensitive to effects of multiple medications than are individuals without diabetes.
A hazard of managing diabetes, particularly with insulin, is the increased risk for unexpected low blood glucose levels. These episodes can also occur in patients taking certain kinds of oral diabetes medications, but they are more common in those on insulin. Low blood glucose can cause dizziness, confusion, and postural instability, increasing the risk for falling.
Diabetic eye complications include retinopathy, macular edema, cataracts, and glaucoma. In a study of close to 10,000 middle-aged and older adults with diabetes, those with moderate eye complications had almost double the risk of falls as those without eye complications.
Another concern with diabetes is its effect on nerves and blood vessels in the inner ear, leading to a negative effect on balance and hearing loss, both of which are also associated with a higher risk for falling and injury.
Clinicians can reduce the risk for falls in patients by taking measures to improve diabetes control and reduce the risk for microvascular disease affecting the nerves, eyes, and ears.
In addition, exercises that optimize muscle mass, bone strength, gait, and balance, and use of specialized footwear in people with neuropathy, may reduce fall risk. Chair yoga and tai chi have also been shown to be helpful. Clinicians can also advise patients on commonsense strategies to implement in their homes, such as ensuring proper lighting, reducing, clutter and minimizing the use of floor rugs.
The risk for falls and the associated risk for fracture and possible hospitalization are of significant concern in older adults — particularly those with diabetes, and even more so in those with diabetes who are on insulin. It is our responsibility as clinicians to implement strategies to optimize diabetes control in our patients and monitor them for microvascular and other complications that may increase this risk, and manage them appropriately if and when these complications occur.
Madhusmita Misra, Professor, Chair, Physician-in-Chief, Department of Pediatrics, University of Virginia and UVA Health Children’s, Charlottesville, has disclosed being a key opinion leader for Lumos Pharma. Sidhartha Pani, Assistant Professor, Department of Internal Medicine, UVA School of Medicine; Medical Director, Department of General Medicine, Same Day Care Clinic, Charlottesville, disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In 2024, a record number of people are celebrating their 65th birthdays. Increasing age is associated with a higher risk for falls, fractures, and other injuries that may require hospitalization.
In older adults with type 1 and type 2 diabetes, the risk for falls is double that seen in older people without these conditions. Increased clinician awareness of the many factors that result in this higher risk in people with diabetes, and timely implementation of strategies to prevent falls, are essential.
The annual incidence of falls in people with diabetes older than 65 years is about 39%, compared with 19% among those without diabetes. People with diabetes on insulin face an even greater increased risk for falls compared with those who are not using insulin (94% vs 27% increased risk).
Many well-known aspects of diabetes contribute to this greater risk. These include decreased sensorimotor function, musculoskeletal and neuromuscular deficits, foot and body pain, poor vision, hypoglycemic episodes, pharmacologic complications, and problems with hearing and balance.
Optimal management of diabetes and its complications is essential, and the American Diabetes Association has developed clear guidelines for clinicians to follow to reduce the risk for diabetes related complications and manage these conditions.
The prevalence of diabetic peripheral neuropathy increases with age and duration of diabetes. People with diabetic peripheral neuropathy and diminished sensation on their feet are at increased risk for loss of postural control. Loss of proprioceptive feedback (the ability to sense movement, action and location) during standing and walking leads increases the risk for falls.
In addition, less physical activity, impaired muscle strength, and suboptimal postural control all influence gait patterns and increase the risk for falling. Adults with diabetes have a two to three times higher risk for sarcopenia (decreased muscle strength and muscle mass). They also have low plantar flexion strength, causing increased displacement of their center of gravity, which in turn reduces their maximum forward stride and may result in falls and injury.
Many people with diabetes experience neuropathic foot and body pain, requiring psychotropic and other medications that may exacerbate the risk, such as amitriptyline and duloxetine. Furthermore, older adults with diabetes are more likely to take more prescription medications and may be more sensitive to effects of multiple medications than are individuals without diabetes.
A hazard of managing diabetes, particularly with insulin, is the increased risk for unexpected low blood glucose levels. These episodes can also occur in patients taking certain kinds of oral diabetes medications, but they are more common in those on insulin. Low blood glucose can cause dizziness, confusion, and postural instability, increasing the risk for falling.
Diabetic eye complications include retinopathy, macular edema, cataracts, and glaucoma. In a study of close to 10,000 middle-aged and older adults with diabetes, those with moderate eye complications had almost double the risk of falls as those without eye complications.
Another concern with diabetes is its effect on nerves and blood vessels in the inner ear, leading to a negative effect on balance and hearing loss, both of which are also associated with a higher risk for falling and injury.
Clinicians can reduce the risk for falls in patients by taking measures to improve diabetes control and reduce the risk for microvascular disease affecting the nerves, eyes, and ears.
In addition, exercises that optimize muscle mass, bone strength, gait, and balance, and use of specialized footwear in people with neuropathy, may reduce fall risk. Chair yoga and tai chi have also been shown to be helpful. Clinicians can also advise patients on commonsense strategies to implement in their homes, such as ensuring proper lighting, reducing, clutter and minimizing the use of floor rugs.
The risk for falls and the associated risk for fracture and possible hospitalization are of significant concern in older adults — particularly those with diabetes, and even more so in those with diabetes who are on insulin. It is our responsibility as clinicians to implement strategies to optimize diabetes control in our patients and monitor them for microvascular and other complications that may increase this risk, and manage them appropriately if and when these complications occur.
Madhusmita Misra, Professor, Chair, Physician-in-Chief, Department of Pediatrics, University of Virginia and UVA Health Children’s, Charlottesville, has disclosed being a key opinion leader for Lumos Pharma. Sidhartha Pani, Assistant Professor, Department of Internal Medicine, UVA School of Medicine; Medical Director, Department of General Medicine, Same Day Care Clinic, Charlottesville, disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.