User login
Pharmacomechanical thrombolysis does not reduce post-thrombotic syndrome risk
In patients with acute proximal deep vein thrombosis who were undergoing anticoagulation, adding pharmacomechanical catheter-directed thrombolysis did not reduce risk of the post-thrombotic syndrome, according to results of a phase 3, randomized, controlled trial.
Moreover, addition of pharmacomechanical thrombolysis increased risk of major bleeding risk, investigators wrote in a report published online Dec. 6 in the New England Journal of Medicine.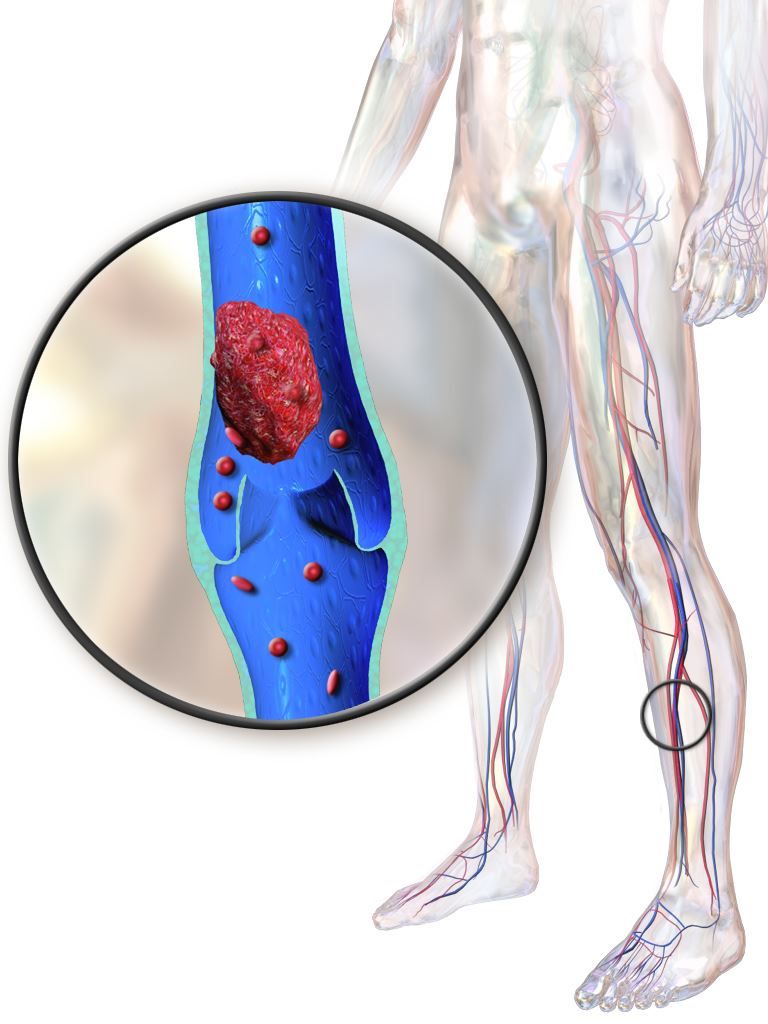
“Our trial, for uncertain reasons, did not confirm these findings,” wrote Suresh Vedantham, MD of Washington University, St. Louis, and his coauthors.
Post-thrombotic syndrome is associated with chronic limb swelling and pain, and can lead to leg ulcers, impaired quality of life, and major disability. About half of patients with proximal deep vein thrombosis (DVT) will develop the post-thrombotic syndrome within 2 years, despite use of anticoagulation therapy, Dr. Vedantham and his colleagues noted.
Pharmacomechanical thrombosis is the catheter-directed delivery of a fibrinolytic agent into the thrombus, along with aspiration or maceration of the thrombus. The goal of the treatment is to reduce the burden of thrombus, which in turn might reduce risk of the post-thrombotic syndrome.
However, in their randomized trial known as ATTRACT, which included 692 patients with an acute proximal DVT, rates of post-thrombotic syndrome between 6 to 24 months after intervention were 47% in the pharmacomechanical thrombolysis group and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56), according to the report (N Engl J Med. 2017;377:2240-52). Control group patients received no procedural intervention.
Major bleeds within 10 days of the intervention were 1.7% and 0.3% for the pharmacomechanical thrombolysis and control groups, respectively (P = .049).
By contrast, in the CAVENT trial, catheter-directed thrombolysis reduced the risk of the post-thrombotic syndrome over 5 years of follow-up (Lancet Haematol. 2016;3[2]:e64-71). Dr. Vedantham and his coauthors suggested that factors potentially explaining the difference in outcomes include the number of patients enrolled (692 in ATTRACT, versus 209 in CAVENT), or the greater use of mechanical therapies in ATTRACT versus longer recombinant tissue plasminogen activator infusions in CAVENT.
The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. Dr. Vedantham reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
In patients with acute proximal deep vein thrombosis who were undergoing anticoagulation, adding pharmacomechanical catheter-directed thrombolysis did not reduce risk of the post-thrombotic syndrome, according to results of a phase 3, randomized, controlled trial.
Moreover, addition of pharmacomechanical thrombolysis increased risk of major bleeding risk, investigators wrote in a report published online Dec. 6 in the New England Journal of Medicine.
“Our trial, for uncertain reasons, did not confirm these findings,” wrote Suresh Vedantham, MD of Washington University, St. Louis, and his coauthors.
Post-thrombotic syndrome is associated with chronic limb swelling and pain, and can lead to leg ulcers, impaired quality of life, and major disability. About half of patients with proximal deep vein thrombosis (DVT) will develop the post-thrombotic syndrome within 2 years, despite use of anticoagulation therapy, Dr. Vedantham and his colleagues noted.
Pharmacomechanical thrombosis is the catheter-directed delivery of a fibrinolytic agent into the thrombus, along with aspiration or maceration of the thrombus. The goal of the treatment is to reduce the burden of thrombus, which in turn might reduce risk of the post-thrombotic syndrome.
However, in their randomized trial known as ATTRACT, which included 692 patients with an acute proximal DVT, rates of post-thrombotic syndrome between 6 to 24 months after intervention were 47% in the pharmacomechanical thrombolysis group and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56), according to the report (N Engl J Med. 2017;377:2240-52). Control group patients received no procedural intervention.
Major bleeds within 10 days of the intervention were 1.7% and 0.3% for the pharmacomechanical thrombolysis and control groups, respectively (P = .049).
By contrast, in the CAVENT trial, catheter-directed thrombolysis reduced the risk of the post-thrombotic syndrome over 5 years of follow-up (Lancet Haematol. 2016;3[2]:e64-71). Dr. Vedantham and his coauthors suggested that factors potentially explaining the difference in outcomes include the number of patients enrolled (692 in ATTRACT, versus 209 in CAVENT), or the greater use of mechanical therapies in ATTRACT versus longer recombinant tissue plasminogen activator infusions in CAVENT.
The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. Dr. Vedantham reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
In patients with acute proximal deep vein thrombosis who were undergoing anticoagulation, adding pharmacomechanical catheter-directed thrombolysis did not reduce risk of the post-thrombotic syndrome, according to results of a phase 3, randomized, controlled trial.
Moreover, addition of pharmacomechanical thrombolysis increased risk of major bleeding risk, investigators wrote in a report published online Dec. 6 in the New England Journal of Medicine.
“Our trial, for uncertain reasons, did not confirm these findings,” wrote Suresh Vedantham, MD of Washington University, St. Louis, and his coauthors.
Post-thrombotic syndrome is associated with chronic limb swelling and pain, and can lead to leg ulcers, impaired quality of life, and major disability. About half of patients with proximal deep vein thrombosis (DVT) will develop the post-thrombotic syndrome within 2 years, despite use of anticoagulation therapy, Dr. Vedantham and his colleagues noted.
Pharmacomechanical thrombosis is the catheter-directed delivery of a fibrinolytic agent into the thrombus, along with aspiration or maceration of the thrombus. The goal of the treatment is to reduce the burden of thrombus, which in turn might reduce risk of the post-thrombotic syndrome.
However, in their randomized trial known as ATTRACT, which included 692 patients with an acute proximal DVT, rates of post-thrombotic syndrome between 6 to 24 months after intervention were 47% in the pharmacomechanical thrombolysis group and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56), according to the report (N Engl J Med. 2017;377:2240-52). Control group patients received no procedural intervention.
Major bleeds within 10 days of the intervention were 1.7% and 0.3% for the pharmacomechanical thrombolysis and control groups, respectively (P = .049).
By contrast, in the CAVENT trial, catheter-directed thrombolysis reduced the risk of the post-thrombotic syndrome over 5 years of follow-up (Lancet Haematol. 2016;3[2]:e64-71). Dr. Vedantham and his coauthors suggested that factors potentially explaining the difference in outcomes include the number of patients enrolled (692 in ATTRACT, versus 209 in CAVENT), or the greater use of mechanical therapies in ATTRACT versus longer recombinant tissue plasminogen activator infusions in CAVENT.
The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. Dr. Vedantham reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: Rates of post-thrombotic syndrome were 47% in the pharmacomechanical thrombolysis group, and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56).
Data source: A phase 3, multicenter, randomized, open-label, assessor-blinded, controlled clinical trial, including 692 patients with acute proximal deep vein thrombosis.
Disclosures: The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. First author Suresh Vedantham, MD, reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
Fremanezumab may reduce chronic migraine frequency
Subcutaneous injections of fremanezumab, a humanized monoclonal antibody, reduced headache frequency, compared with placebo, in patients with chronic migraine, according to results of a randomized, double-blind, placebo-controlled trial.
Beneficial effects of fremanezumab were seen within 4 weeks of the initial treatment, according to Stephen D. Silberstein, MD, director of the Jefferson Headache Center at Thomas Jefferson University, Philadelphia, and his coauthors.

“Expert opinion has been that patients with chronic migraine should receive preventive treatment,” they wrote. “However, these treatments may be underused, not adhered to, associated with side effects, or ineffective.”
Fremanezumab targets calcitonin gene-related peptide, which is “involved in central and peripheral pathophysiological events of migraine,” according to the investigators.
The trial comprised 1,130 patients with chronic migraine, defined as occurring at least 8 days per month and headache of any severity at least 15 days per month. They were randomly assigned to receive fremanezumab on a planned quarterly regimen (a single dose at baseline, followed by placebo injections at weeks 4 and 8), fremanezumab monthly (a single dose at baseline, followed by lower doses at weeks 4 and 8), or matching placebo.
For the 12-week period after the first dose, the average number of headache days per month dropped by 4.3 from a baseline mean of 13.2 in the group of patients receiving treatment quarterly, and by 4.6 from a baseline of 12.8 in patients on monthly treatment, compared with a reduction of only 2.5 from a baseline of 13.3 in the placebo-treated patient group (P less than .001 for both fremanezumab groups vs. placebo).
Migraine days also declined significantly more among patients receiving quarterly and monthly fremanezumab by 12 weeks (from a mean of 16.2 to 11.3 and from 16.0 to 11.0, respectively) when compared with placebo (from 16.4 to 13.2; P less than .001 for both comparisons).
The number of patients experiencing a reduction of at least 50% in average number of headache days was higher in both fremanezumab groups at 38% for the quarterly dosing and 41% for monthly dosing, compared with placebo at 18% (P less than .001 for comparisons of fremanezumab to placebo).
Injection site pain was the most common adverse event in the trial, occurring in 30% and 26% of the fremanezumab quarterly and monthly groups, respectively, and 28% of the placebo group, according to the reported data.
Serious adverse events occurred in 1% of patients in the quarterly treatment group, 2% of the monthly group, and 2% of the placebo group, the data showed.
An ongoing extension of the trial will provide “further insights” on the safety and efficacy of treating chronic migraine with fremanezumab over a longer term, the investigators said.
Teva Pharmaceuticals funded the study. Dr. Silberstein and some of his coauthors reported receiving consulting fees from Teva and others. Many coauthors were employees of Teva.
Subcutaneous injections of fremanezumab, a humanized monoclonal antibody, reduced headache frequency, compared with placebo, in patients with chronic migraine, according to results of a randomized, double-blind, placebo-controlled trial.
Beneficial effects of fremanezumab were seen within 4 weeks of the initial treatment, according to Stephen D. Silberstein, MD, director of the Jefferson Headache Center at Thomas Jefferson University, Philadelphia, and his coauthors.
“Expert opinion has been that patients with chronic migraine should receive preventive treatment,” they wrote. “However, these treatments may be underused, not adhered to, associated with side effects, or ineffective.”
Fremanezumab targets calcitonin gene-related peptide, which is “involved in central and peripheral pathophysiological events of migraine,” according to the investigators.
The trial comprised 1,130 patients with chronic migraine, defined as occurring at least 8 days per month and headache of any severity at least 15 days per month. They were randomly assigned to receive fremanezumab on a planned quarterly regimen (a single dose at baseline, followed by placebo injections at weeks 4 and 8), fremanezumab monthly (a single dose at baseline, followed by lower doses at weeks 4 and 8), or matching placebo.
For the 12-week period after the first dose, the average number of headache days per month dropped by 4.3 from a baseline mean of 13.2 in the group of patients receiving treatment quarterly, and by 4.6 from a baseline of 12.8 in patients on monthly treatment, compared with a reduction of only 2.5 from a baseline of 13.3 in the placebo-treated patient group (P less than .001 for both fremanezumab groups vs. placebo).
Migraine days also declined significantly more among patients receiving quarterly and monthly fremanezumab by 12 weeks (from a mean of 16.2 to 11.3 and from 16.0 to 11.0, respectively) when compared with placebo (from 16.4 to 13.2; P less than .001 for both comparisons).
The number of patients experiencing a reduction of at least 50% in average number of headache days was higher in both fremanezumab groups at 38% for the quarterly dosing and 41% for monthly dosing, compared with placebo at 18% (P less than .001 for comparisons of fremanezumab to placebo).
Injection site pain was the most common adverse event in the trial, occurring in 30% and 26% of the fremanezumab quarterly and monthly groups, respectively, and 28% of the placebo group, according to the reported data.
Serious adverse events occurred in 1% of patients in the quarterly treatment group, 2% of the monthly group, and 2% of the placebo group, the data showed.
An ongoing extension of the trial will provide “further insights” on the safety and efficacy of treating chronic migraine with fremanezumab over a longer term, the investigators said.
Teva Pharmaceuticals funded the study. Dr. Silberstein and some of his coauthors reported receiving consulting fees from Teva and others. Many coauthors were employees of Teva.
Subcutaneous injections of fremanezumab, a humanized monoclonal antibody, reduced headache frequency, compared with placebo, in patients with chronic migraine, according to results of a randomized, double-blind, placebo-controlled trial.
Beneficial effects of fremanezumab were seen within 4 weeks of the initial treatment, according to Stephen D. Silberstein, MD, director of the Jefferson Headache Center at Thomas Jefferson University, Philadelphia, and his coauthors.
“Expert opinion has been that patients with chronic migraine should receive preventive treatment,” they wrote. “However, these treatments may be underused, not adhered to, associated with side effects, or ineffective.”
Fremanezumab targets calcitonin gene-related peptide, which is “involved in central and peripheral pathophysiological events of migraine,” according to the investigators.
The trial comprised 1,130 patients with chronic migraine, defined as occurring at least 8 days per month and headache of any severity at least 15 days per month. They were randomly assigned to receive fremanezumab on a planned quarterly regimen (a single dose at baseline, followed by placebo injections at weeks 4 and 8), fremanezumab monthly (a single dose at baseline, followed by lower doses at weeks 4 and 8), or matching placebo.
For the 12-week period after the first dose, the average number of headache days per month dropped by 4.3 from a baseline mean of 13.2 in the group of patients receiving treatment quarterly, and by 4.6 from a baseline of 12.8 in patients on monthly treatment, compared with a reduction of only 2.5 from a baseline of 13.3 in the placebo-treated patient group (P less than .001 for both fremanezumab groups vs. placebo).
Migraine days also declined significantly more among patients receiving quarterly and monthly fremanezumab by 12 weeks (from a mean of 16.2 to 11.3 and from 16.0 to 11.0, respectively) when compared with placebo (from 16.4 to 13.2; P less than .001 for both comparisons).
The number of patients experiencing a reduction of at least 50% in average number of headache days was higher in both fremanezumab groups at 38% for the quarterly dosing and 41% for monthly dosing, compared with placebo at 18% (P less than .001 for comparisons of fremanezumab to placebo).
Injection site pain was the most common adverse event in the trial, occurring in 30% and 26% of the fremanezumab quarterly and monthly groups, respectively, and 28% of the placebo group, according to the reported data.
Serious adverse events occurred in 1% of patients in the quarterly treatment group, 2% of the monthly group, and 2% of the placebo group, the data showed.
An ongoing extension of the trial will provide “further insights” on the safety and efficacy of treating chronic migraine with fremanezumab over a longer term, the investigators said.
Teva Pharmaceuticals funded the study. Dr. Silberstein and some of his coauthors reported receiving consulting fees from Teva and others. Many coauthors were employees of Teva.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: The average number of headache days was reduced by 4.3 and 4.6 for fremanezumab quarterly and monthly, respectively, compared with 2.5 for placebo (P less than .001 for both comparisons of fremanezumab to placebo).
Data source: A randomized, double-blind, placebo-controlled, parallel-group study of 1,130 patients with chronic migraine who received 12 weeks of treatment.
Disclosures: Teva Pharmaceuticals funded the study. Dr. Silberstein and some of his coauthors reported receiving consulting fees from Teva and others. Many coauthors were employees of Teva.
Vasopressin stimulates red blood cell production
The hormone vasopressin, well known for its antidiuretic effects, also appears to stimulate proliferation and differentiation of red blood cell (RBC) precursors, results of a series of preclinical investigations suggest.
Treating anemic mice with an arginine vasopressin (AVP) receptor agonist increased hematocrit and reticulocyte counts significantly, compared with controls, according to the results published in Science Translational Medicine (2017 Nov 29;9:eaao1632).
That finding could have implications for the development of new treatments designed to stimulate RBC production after bleeding, chemotherapy, or drug toxicity, according to the investigators.
“Currently, EPO is the only agent that is used clinically to stimulate erythropoiesis, but there are patients who do not respond to EPO or who cannot take the drug because it stimulates tumor growth,” the investigators wrote. “AVP appears to be an EPO-independent, fast-acting agent that increases RBC numbers after anemia.”
Dr. Mayer and his colleagues initially asked whether AVP might play a role in RBC production after observing that patients with central diabetes insipidus (CDI), who lack the antidiuretic hormone, are frequently anemic. A review of patient records from an NIH database revealed that 60% of CDI patients were anemic despite treatment with desmopressin.
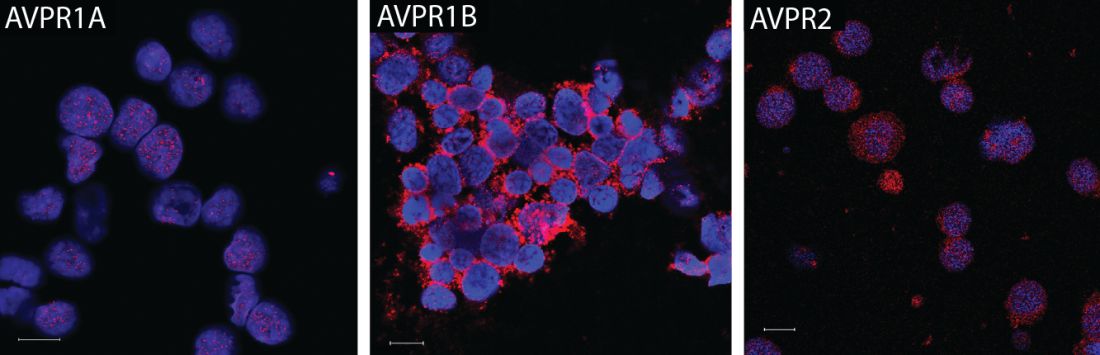
They subsequently found that all three AVP receptor subtypes are expressed in human and mouse hematopoietic stem and progenitor cells. In particular, the AVPR1B subtype appeared to play the most important role in regulating erythropoiesis.
Accordingly, they tested the ability of both AVP and a AVPR1B-specific agonist to stimulate production of RBCs in mice that had anemia induced by bleeding or irradiation. They found significant improvements in both hematocrit and reticulocyte numbers as early as 2 days after treatment started.
Subsequent experiments were designed to determine whether the effect of AVP on RBC production was caused by EPO release. In fact, the effects of AVP occurred “long before an effect of EPO was observed,” investigators wrote.
The research was supported by the NIH. Some of the study authors are listed as inventors on a patent application held by the U.S. Department of Health and Human Services covering methods for modulating erythropoiesis with arginine vasopressin receptor 1b molecules.
The hormone vasopressin, well known for its antidiuretic effects, also appears to stimulate proliferation and differentiation of red blood cell (RBC) precursors, results of a series of preclinical investigations suggest.
Treating anemic mice with an arginine vasopressin (AVP) receptor agonist increased hematocrit and reticulocyte counts significantly, compared with controls, according to the results published in Science Translational Medicine (2017 Nov 29;9:eaao1632).
That finding could have implications for the development of new treatments designed to stimulate RBC production after bleeding, chemotherapy, or drug toxicity, according to the investigators.
“Currently, EPO is the only agent that is used clinically to stimulate erythropoiesis, but there are patients who do not respond to EPO or who cannot take the drug because it stimulates tumor growth,” the investigators wrote. “AVP appears to be an EPO-independent, fast-acting agent that increases RBC numbers after anemia.”
Dr. Mayer and his colleagues initially asked whether AVP might play a role in RBC production after observing that patients with central diabetes insipidus (CDI), who lack the antidiuretic hormone, are frequently anemic. A review of patient records from an NIH database revealed that 60% of CDI patients were anemic despite treatment with desmopressin.
They subsequently found that all three AVP receptor subtypes are expressed in human and mouse hematopoietic stem and progenitor cells. In particular, the AVPR1B subtype appeared to play the most important role in regulating erythropoiesis.
Accordingly, they tested the ability of both AVP and a AVPR1B-specific agonist to stimulate production of RBCs in mice that had anemia induced by bleeding or irradiation. They found significant improvements in both hematocrit and reticulocyte numbers as early as 2 days after treatment started.
Subsequent experiments were designed to determine whether the effect of AVP on RBC production was caused by EPO release. In fact, the effects of AVP occurred “long before an effect of EPO was observed,” investigators wrote.
The research was supported by the NIH. Some of the study authors are listed as inventors on a patent application held by the U.S. Department of Health and Human Services covering methods for modulating erythropoiesis with arginine vasopressin receptor 1b molecules.
The hormone vasopressin, well known for its antidiuretic effects, also appears to stimulate proliferation and differentiation of red blood cell (RBC) precursors, results of a series of preclinical investigations suggest.
Treating anemic mice with an arginine vasopressin (AVP) receptor agonist increased hematocrit and reticulocyte counts significantly, compared with controls, according to the results published in Science Translational Medicine (2017 Nov 29;9:eaao1632).
That finding could have implications for the development of new treatments designed to stimulate RBC production after bleeding, chemotherapy, or drug toxicity, according to the investigators.
“Currently, EPO is the only agent that is used clinically to stimulate erythropoiesis, but there are patients who do not respond to EPO or who cannot take the drug because it stimulates tumor growth,” the investigators wrote. “AVP appears to be an EPO-independent, fast-acting agent that increases RBC numbers after anemia.”
Dr. Mayer and his colleagues initially asked whether AVP might play a role in RBC production after observing that patients with central diabetes insipidus (CDI), who lack the antidiuretic hormone, are frequently anemic. A review of patient records from an NIH database revealed that 60% of CDI patients were anemic despite treatment with desmopressin.
They subsequently found that all three AVP receptor subtypes are expressed in human and mouse hematopoietic stem and progenitor cells. In particular, the AVPR1B subtype appeared to play the most important role in regulating erythropoiesis.
Accordingly, they tested the ability of both AVP and a AVPR1B-specific agonist to stimulate production of RBCs in mice that had anemia induced by bleeding or irradiation. They found significant improvements in both hematocrit and reticulocyte numbers as early as 2 days after treatment started.
Subsequent experiments were designed to determine whether the effect of AVP on RBC production was caused by EPO release. In fact, the effects of AVP occurred “long before an effect of EPO was observed,” investigators wrote.
The research was supported by the NIH. Some of the study authors are listed as inventors on a patent application held by the U.S. Department of Health and Human Services covering methods for modulating erythropoiesis with arginine vasopressin receptor 1b molecules.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point:
Major finding: In anemic mice, treatment with a vasopressin or a vasopressin receptor agonist significantly increased hematocrit and reticulocyte number vs. controls.
Data source: A series of in vitro and in vivo experiments, plus a retrospective review of anemia incidence data in patients with central diabetes insipidus.
Disclosures: The research was supported by the National Institutes of Health. Some of the study authors are listed as inventors on a patent application held by the U.S. Department of Health and Human Services covering methods for modulating erythropoiesis with arginine vasopressin receptor 1b molecules.
Radiofrequency ablation improves stent patency in malignant biliary strictures
In patients with malignant biliary strictures, radiofrequency ablation may improve stent patency and prolong survival, according to results of a recent meta-analysis.
Radiofrequency ablation was also safe and well tolerated. The report appears in Gastrointestinal Endoscopy (2017. doi: 10.1016/j.gie.2017.10.029).
Although the data to date are limited and mostly observational, radiofrequency ablation “may be a promising adjuvant therapy in patients with malignant biliary obstruction who otherwise have dismal outcomes with current standard of therapy,” wrote Aijaz Ahmed Sofi, MD, of the department of gastroenterology, Arizona Center for Digestive Health, Gilbert, and coauthors.
Use of radiofrequency ablation is thought to improve the patency of biliary stents placed as a palliative measure in patients with unresectable malignant biliary strictures. However, several studies evaluating this and other endpoints have produced “variable results,” the authors said in the report.
In a comprehensive literature search, Dr. Sofi and colleagues identified nine studies including 505 patients. Only one of the studies was randomized and controlled, and results from it were preliminary, they noted.
Combined results showed a 50.6-day pooled weighted mean difference in stent patency (95% confidence interval, 32.83-68.48) in favor of radiofrequency ablation, according to reported data. In addition, there was a significant difference in survival favoring use of radiofrequency ablation (hazard ratio, 1.395; 95% confidence interval, 1.145-1.7; P less than .001).
While there was no difference between groups in risk of cholangitis, pancreatitis, hemobilia, and acute cholecystitis, abdominal pain after the procedure was more frequent in the radiofrequency ablation group (31% vs. 20%, P = .003).
This is the first systematic review and meta-analysis evaluating radiofrequency ablation as an adjuvant therapy in patients who receive biliary stents for malignant biliary obstruction, according to the investigators.
Despite the findings, Dr. Sofi and colleagues were careful to emphasize the limitations of the analysis, writing that it provides “very low quality evidence” in favor of radiofrequency ablation therapy for management of malignant biliary strictures.
“The results of currently ongoing controlled studies examining the role of RFA [radiofrequency ablation] in malignant biliary obstruction are keenly awaited,” they wrote.
Dr. Sofi and colleagues reported no potential conflicts of interest associated with the study.
In patients with malignant biliary strictures, radiofrequency ablation may improve stent patency and prolong survival, according to results of a recent meta-analysis.
Radiofrequency ablation was also safe and well tolerated. The report appears in Gastrointestinal Endoscopy (2017. doi: 10.1016/j.gie.2017.10.029).
Although the data to date are limited and mostly observational, radiofrequency ablation “may be a promising adjuvant therapy in patients with malignant biliary obstruction who otherwise have dismal outcomes with current standard of therapy,” wrote Aijaz Ahmed Sofi, MD, of the department of gastroenterology, Arizona Center for Digestive Health, Gilbert, and coauthors.
Use of radiofrequency ablation is thought to improve the patency of biliary stents placed as a palliative measure in patients with unresectable malignant biliary strictures. However, several studies evaluating this and other endpoints have produced “variable results,” the authors said in the report.
In a comprehensive literature search, Dr. Sofi and colleagues identified nine studies including 505 patients. Only one of the studies was randomized and controlled, and results from it were preliminary, they noted.
Combined results showed a 50.6-day pooled weighted mean difference in stent patency (95% confidence interval, 32.83-68.48) in favor of radiofrequency ablation, according to reported data. In addition, there was a significant difference in survival favoring use of radiofrequency ablation (hazard ratio, 1.395; 95% confidence interval, 1.145-1.7; P less than .001).
While there was no difference between groups in risk of cholangitis, pancreatitis, hemobilia, and acute cholecystitis, abdominal pain after the procedure was more frequent in the radiofrequency ablation group (31% vs. 20%, P = .003).
This is the first systematic review and meta-analysis evaluating radiofrequency ablation as an adjuvant therapy in patients who receive biliary stents for malignant biliary obstruction, according to the investigators.
Despite the findings, Dr. Sofi and colleagues were careful to emphasize the limitations of the analysis, writing that it provides “very low quality evidence” in favor of radiofrequency ablation therapy for management of malignant biliary strictures.
“The results of currently ongoing controlled studies examining the role of RFA [radiofrequency ablation] in malignant biliary obstruction are keenly awaited,” they wrote.
Dr. Sofi and colleagues reported no potential conflicts of interest associated with the study.
In patients with malignant biliary strictures, radiofrequency ablation may improve stent patency and prolong survival, according to results of a recent meta-analysis.
Radiofrequency ablation was also safe and well tolerated. The report appears in Gastrointestinal Endoscopy (2017. doi: 10.1016/j.gie.2017.10.029).
Although the data to date are limited and mostly observational, radiofrequency ablation “may be a promising adjuvant therapy in patients with malignant biliary obstruction who otherwise have dismal outcomes with current standard of therapy,” wrote Aijaz Ahmed Sofi, MD, of the department of gastroenterology, Arizona Center for Digestive Health, Gilbert, and coauthors.
Use of radiofrequency ablation is thought to improve the patency of biliary stents placed as a palliative measure in patients with unresectable malignant biliary strictures. However, several studies evaluating this and other endpoints have produced “variable results,” the authors said in the report.
In a comprehensive literature search, Dr. Sofi and colleagues identified nine studies including 505 patients. Only one of the studies was randomized and controlled, and results from it were preliminary, they noted.
Combined results showed a 50.6-day pooled weighted mean difference in stent patency (95% confidence interval, 32.83-68.48) in favor of radiofrequency ablation, according to reported data. In addition, there was a significant difference in survival favoring use of radiofrequency ablation (hazard ratio, 1.395; 95% confidence interval, 1.145-1.7; P less than .001).
While there was no difference between groups in risk of cholangitis, pancreatitis, hemobilia, and acute cholecystitis, abdominal pain after the procedure was more frequent in the radiofrequency ablation group (31% vs. 20%, P = .003).
This is the first systematic review and meta-analysis evaluating radiofrequency ablation as an adjuvant therapy in patients who receive biliary stents for malignant biliary obstruction, according to the investigators.
Despite the findings, Dr. Sofi and colleagues were careful to emphasize the limitations of the analysis, writing that it provides “very low quality evidence” in favor of radiofrequency ablation therapy for management of malignant biliary strictures.
“The results of currently ongoing controlled studies examining the role of RFA [radiofrequency ablation] in malignant biliary obstruction are keenly awaited,” they wrote.
Dr. Sofi and colleagues reported no potential conflicts of interest associated with the study.
FROM GASTROINTESTINAL ENDOSCOPY
Key clinical point: Although data to date are limited and mostly observational, radiofrequency ablation appears to improve stent patency and may prolong survival in patients with malignant biliary strictures.
Major finding: There was a significant difference in survival (P less than .001) and 50.6-day pooled weighted mean difference in stent patency (95% CI, 32.83-68.48) in favor of radiofrequency ablation.
Data source: A meta-analysis of 505 patients from nine studies that were identified through a comprehensive literature search.
Disclosures: There was no funding source for the study. The authors reported no potential conflicts of interest.
Mutations influence prognostic value of tumor location in stage III colon cancer
Among patients with resected stage III colon cancer, the prognostic value of primary tumor location varied according to patients’ BRAF or RAS mutational status, according to a post hoc analysis of patients in the Pan-European Trials in Alimentary Tract Cancer (PETACC)-8 trial.
Specifically, in patients with BRAF or RAS mutations, disease-free survival (DFS) was better in right-sided vs. left-sided tumors, while in patients with RAS and BRAF double wild type, DFS was worse in right-sided vs. left-sided tumors, authors of the study reported in JAMA Oncology.
Right-sided tumor location has been associated with poor survival in previous studies of patients with metastatic colorectal cancer. However, for patients with stage III disease, such as those in this study, little is known about how tumor sidedness affects outcomes, the investigators wrote (JAMA Oncol. 2017 Nov 22. doi: 10.1001/jamaoncol.2017.3695).
“Although primary tumor location does not seem to be associated with DFS in the whole study population, opposite sidedness prognostic values are observed for RAS and BRAF wild-type and mutant tumors,” wrote Julien Taieb, MD, PhD, Department of Hepatogastroenterology and GI Oncology, Hôpital Européen Georges-Pompidou, Paris, and his coauthors.
The post hoc analysis included 1,869 resected stage III colon cancer patients with full information on primary tumor location in the PETACC-8 phase 3 randomized trial. The primary objective of the trial was to evaluate adjuvant treatment with the FOLFOX regimen with or without cetuximab.
Forty percent of the patients had a right-sided tumor, data show.
Right-sided tumor location was not prognostic for DFS for all patients, though it was associated with shorter survival after relapse (hazard ratio, 1.54; 95% confidence interval, 1.23-1.93; P = .001) and overall survival (HR, 1.25; 95%CI, 1.02-1.54; P = .03).
However, when looking at different molecular subgroups, Dr. Taieb and his colleagues found that DFS was better in right-sided vs. left-sided tumors in patients with RAS mutations (HR, 0.80; 95% CI, 0.64-1.00; P = .046), and similar findings were seen in BRAF-mutated tumors.
Conversely, DFS was worse in right-sided vs. left-sided tumors among those patients with RAS and BRAF double wild type (HR, 1.39; 95% CI, 1.01-1.92; P = .04), the investigators reported.
Investigators also sought to evaluate whether tumor location predicted the benefit of cetuximab.
However, “no benefit of adding cetuximab to FOLFOX was observed in our population of patients with stage III left-sided tumors, nor was any detrimental effect of adding cetuximab observed in right-sided tumors,” Dr. Taieb and his coauthors wrote.
PETACC-8 was sponsored by the Fédération Francophone de Cancérologie Digestive with some support from Merck KGaA and Sanofi-Aventis. Dr. Taieb reported participating in consulting or advisory boards for Merck KGaA, Sanofi, Roche/Genentech, Pfizer, and Amgen.
Among patients with resected stage III colon cancer, the prognostic value of primary tumor location varied according to patients’ BRAF or RAS mutational status, according to a post hoc analysis of patients in the Pan-European Trials in Alimentary Tract Cancer (PETACC)-8 trial.
Specifically, in patients with BRAF or RAS mutations, disease-free survival (DFS) was better in right-sided vs. left-sided tumors, while in patients with RAS and BRAF double wild type, DFS was worse in right-sided vs. left-sided tumors, authors of the study reported in JAMA Oncology.
Right-sided tumor location has been associated with poor survival in previous studies of patients with metastatic colorectal cancer. However, for patients with stage III disease, such as those in this study, little is known about how tumor sidedness affects outcomes, the investigators wrote (JAMA Oncol. 2017 Nov 22. doi: 10.1001/jamaoncol.2017.3695).
“Although primary tumor location does not seem to be associated with DFS in the whole study population, opposite sidedness prognostic values are observed for RAS and BRAF wild-type and mutant tumors,” wrote Julien Taieb, MD, PhD, Department of Hepatogastroenterology and GI Oncology, Hôpital Européen Georges-Pompidou, Paris, and his coauthors.
The post hoc analysis included 1,869 resected stage III colon cancer patients with full information on primary tumor location in the PETACC-8 phase 3 randomized trial. The primary objective of the trial was to evaluate adjuvant treatment with the FOLFOX regimen with or without cetuximab.
Forty percent of the patients had a right-sided tumor, data show.
Right-sided tumor location was not prognostic for DFS for all patients, though it was associated with shorter survival after relapse (hazard ratio, 1.54; 95% confidence interval, 1.23-1.93; P = .001) and overall survival (HR, 1.25; 95%CI, 1.02-1.54; P = .03).
However, when looking at different molecular subgroups, Dr. Taieb and his colleagues found that DFS was better in right-sided vs. left-sided tumors in patients with RAS mutations (HR, 0.80; 95% CI, 0.64-1.00; P = .046), and similar findings were seen in BRAF-mutated tumors.
Conversely, DFS was worse in right-sided vs. left-sided tumors among those patients with RAS and BRAF double wild type (HR, 1.39; 95% CI, 1.01-1.92; P = .04), the investigators reported.
Investigators also sought to evaluate whether tumor location predicted the benefit of cetuximab.
However, “no benefit of adding cetuximab to FOLFOX was observed in our population of patients with stage III left-sided tumors, nor was any detrimental effect of adding cetuximab observed in right-sided tumors,” Dr. Taieb and his coauthors wrote.
PETACC-8 was sponsored by the Fédération Francophone de Cancérologie Digestive with some support from Merck KGaA and Sanofi-Aventis. Dr. Taieb reported participating in consulting or advisory boards for Merck KGaA, Sanofi, Roche/Genentech, Pfizer, and Amgen.
Among patients with resected stage III colon cancer, the prognostic value of primary tumor location varied according to patients’ BRAF or RAS mutational status, according to a post hoc analysis of patients in the Pan-European Trials in Alimentary Tract Cancer (PETACC)-8 trial.
Specifically, in patients with BRAF or RAS mutations, disease-free survival (DFS) was better in right-sided vs. left-sided tumors, while in patients with RAS and BRAF double wild type, DFS was worse in right-sided vs. left-sided tumors, authors of the study reported in JAMA Oncology.
Right-sided tumor location has been associated with poor survival in previous studies of patients with metastatic colorectal cancer. However, for patients with stage III disease, such as those in this study, little is known about how tumor sidedness affects outcomes, the investigators wrote (JAMA Oncol. 2017 Nov 22. doi: 10.1001/jamaoncol.2017.3695).
“Although primary tumor location does not seem to be associated with DFS in the whole study population, opposite sidedness prognostic values are observed for RAS and BRAF wild-type and mutant tumors,” wrote Julien Taieb, MD, PhD, Department of Hepatogastroenterology and GI Oncology, Hôpital Européen Georges-Pompidou, Paris, and his coauthors.
The post hoc analysis included 1,869 resected stage III colon cancer patients with full information on primary tumor location in the PETACC-8 phase 3 randomized trial. The primary objective of the trial was to evaluate adjuvant treatment with the FOLFOX regimen with or without cetuximab.
Forty percent of the patients had a right-sided tumor, data show.
Right-sided tumor location was not prognostic for DFS for all patients, though it was associated with shorter survival after relapse (hazard ratio, 1.54; 95% confidence interval, 1.23-1.93; P = .001) and overall survival (HR, 1.25; 95%CI, 1.02-1.54; P = .03).
However, when looking at different molecular subgroups, Dr. Taieb and his colleagues found that DFS was better in right-sided vs. left-sided tumors in patients with RAS mutations (HR, 0.80; 95% CI, 0.64-1.00; P = .046), and similar findings were seen in BRAF-mutated tumors.
Conversely, DFS was worse in right-sided vs. left-sided tumors among those patients with RAS and BRAF double wild type (HR, 1.39; 95% CI, 1.01-1.92; P = .04), the investigators reported.
Investigators also sought to evaluate whether tumor location predicted the benefit of cetuximab.
However, “no benefit of adding cetuximab to FOLFOX was observed in our population of patients with stage III left-sided tumors, nor was any detrimental effect of adding cetuximab observed in right-sided tumors,” Dr. Taieb and his coauthors wrote.
PETACC-8 was sponsored by the Fédération Francophone de Cancérologie Digestive with some support from Merck KGaA and Sanofi-Aventis. Dr. Taieb reported participating in consulting or advisory boards for Merck KGaA, Sanofi, Roche/Genentech, Pfizer, and Amgen.
FROM JAMA ONCOLOGY
Key clinical point: In patients with resected stage III colon cancer, prognosis associated with right-sided vs. left-sided tumors appears to vary according to RAS and BRAF mutational status.
Major finding: In patients with RAS mutations, DFS was better in right-sided vs. left-sided tumors (HR, 0.80; 95% CI, 0.64-1.00; P = .046), while in patients with RAS and BRAF double wild type, DFS was worse in right-sided vs. left-sided tumors (HR, 1.39; 95% CI, 1.01-1.92; P = .04).
Data source: A post hoc analysis of 1,869 patients in the Pan-European Trials in Alimentary Tract Cancer (PETACC)-8 phase 3 randomized trial with available tumor blocks of resected stage III colon adenocarcinoma.
Disclosures: PETACC-8 was sponsored by the Fédération Francophone de Cancérologie Digestive with some support from Merck KGaA and Sanofi-Aventis. Study authors reported various disclosures; first author Julien Taieb, MD, PhD reported participating in consulting or advisory boards for Merck KGaA, Sanofi, Roche/Genentech, Pfizer, and Amgen.
Does incretin therapy increase pancreatic cancer risk?
Risk of pancreatic cancer doubled among diabetes patients on incretin therapy in a recent retrospective cohort study, although it is unlikely that the drugs actually caused the increase, according to investigators.
, wrote Dr. Mathieu Boniol, vice president of statistics, International Prevention Research Institute, Lyon, France, and colleagues.
The study was sparked by concerns about a possible increased risk of cancer among patients prescribed incretin drugs, which include glucagonlike peptide receptor–1 (GLP-1R) agonists and dipeptidyl peptidase 4 (DPP-4) inhibitors, authors said.
Results of the retrospective cohort analysis are based on two European public health insurance databases, comprising 33,292 diabetes patients treated with incretin drugs and 525,733 treated with other noninsulin antidiabetic drugs.
The risk of pancreatic cancer doubled for patients receiving incretin treatment (adjusted hazard ratio, 2.14; 95% confidence interval, 1.71-2.67), compared with patients receiving other noninsulin drugs, after adjusting for age, sex, and whether or not patients subsequently received an insulin prescription, investigators reported.
However, risk of pancreatic cancer decreased over time in patients on incretin therapy, according to further analyses by Dr. Boniol and colleagues.
That finding of diminishing risk over time argues against concluding that incretin drugs cause pancreatic cancer, according to investigators.
“A direct causal effect could be suspected if a steadily increasing risk of pancreatic cancer was associated with a steadily longer exposure to incretin drugs,” they said.
In the first 3 months after the first incretin prescription, risk of pancreatic cancer was 3.35 times greater (95% CI, 2.32-4.84), which “gradually diminished” to 1.69 (95% CI, 1.12-2.55) a year after the first prescription, the investigators said in the report.

As such, these new data do not help prove or disprove a causal link between incretin use and pancreatic cancer, continued Dr. Hellman, a past president of the American Association of Clinical Endocrinologists.
“I think, right now, we don’t have the data,” he said in an interview. “It’s a question that makes us nervous, because of what we know about the laboratory effects of the drugs, but we don’t have the answer yet. We need longer studies with larger numbers of people to answer that question.”
The study, funded by Sanofi, was conducted at the request of the European Medicines Agency to assess risk of pancreatic cancer associated with lixisenatide. However, the study covers a period prior to use of lixisenatide in the general population because the approval of the GLP-1R agonist was “too recent,” the study authors wrote.
The analyses in the study were conducted in 2015 and 2016 for two cohorts of subjects: one in Belgium, for which data had been collected from 2008 to 2013, and one in Italy, with data from 2000 to 2012.
Further studies are needed to assess how long-term use of incretin drugs may affect risk of pancreatic cancer, the authors said.
The analysis was conducted as part of a postauthorization safety study requested by the European Medicines Agency and funded by Sanofi. One study author reported receiving grants from Roche, Amgen, and Bristol-Myers Squibb outside the submitted work; the remaining investigators had no relevant financial disclosures.
Risk of pancreatic cancer doubled among diabetes patients on incretin therapy in a recent retrospective cohort study, although it is unlikely that the drugs actually caused the increase, according to investigators.
, wrote Dr. Mathieu Boniol, vice president of statistics, International Prevention Research Institute, Lyon, France, and colleagues.
The study was sparked by concerns about a possible increased risk of cancer among patients prescribed incretin drugs, which include glucagonlike peptide receptor–1 (GLP-1R) agonists and dipeptidyl peptidase 4 (DPP-4) inhibitors, authors said.
Results of the retrospective cohort analysis are based on two European public health insurance databases, comprising 33,292 diabetes patients treated with incretin drugs and 525,733 treated with other noninsulin antidiabetic drugs.
The risk of pancreatic cancer doubled for patients receiving incretin treatment (adjusted hazard ratio, 2.14; 95% confidence interval, 1.71-2.67), compared with patients receiving other noninsulin drugs, after adjusting for age, sex, and whether or not patients subsequently received an insulin prescription, investigators reported.
However, risk of pancreatic cancer decreased over time in patients on incretin therapy, according to further analyses by Dr. Boniol and colleagues.
That finding of diminishing risk over time argues against concluding that incretin drugs cause pancreatic cancer, according to investigators.
“A direct causal effect could be suspected if a steadily increasing risk of pancreatic cancer was associated with a steadily longer exposure to incretin drugs,” they said.
In the first 3 months after the first incretin prescription, risk of pancreatic cancer was 3.35 times greater (95% CI, 2.32-4.84), which “gradually diminished” to 1.69 (95% CI, 1.12-2.55) a year after the first prescription, the investigators said in the report.
As such, these new data do not help prove or disprove a causal link between incretin use and pancreatic cancer, continued Dr. Hellman, a past president of the American Association of Clinical Endocrinologists.
“I think, right now, we don’t have the data,” he said in an interview. “It’s a question that makes us nervous, because of what we know about the laboratory effects of the drugs, but we don’t have the answer yet. We need longer studies with larger numbers of people to answer that question.”
The study, funded by Sanofi, was conducted at the request of the European Medicines Agency to assess risk of pancreatic cancer associated with lixisenatide. However, the study covers a period prior to use of lixisenatide in the general population because the approval of the GLP-1R agonist was “too recent,” the study authors wrote.
The analyses in the study were conducted in 2015 and 2016 for two cohorts of subjects: one in Belgium, for which data had been collected from 2008 to 2013, and one in Italy, with data from 2000 to 2012.
Further studies are needed to assess how long-term use of incretin drugs may affect risk of pancreatic cancer, the authors said.
The analysis was conducted as part of a postauthorization safety study requested by the European Medicines Agency and funded by Sanofi. One study author reported receiving grants from Roche, Amgen, and Bristol-Myers Squibb outside the submitted work; the remaining investigators had no relevant financial disclosures.
Risk of pancreatic cancer doubled among diabetes patients on incretin therapy in a recent retrospective cohort study, although it is unlikely that the drugs actually caused the increase, according to investigators.
, wrote Dr. Mathieu Boniol, vice president of statistics, International Prevention Research Institute, Lyon, France, and colleagues.
The study was sparked by concerns about a possible increased risk of cancer among patients prescribed incretin drugs, which include glucagonlike peptide receptor–1 (GLP-1R) agonists and dipeptidyl peptidase 4 (DPP-4) inhibitors, authors said.
Results of the retrospective cohort analysis are based on two European public health insurance databases, comprising 33,292 diabetes patients treated with incretin drugs and 525,733 treated with other noninsulin antidiabetic drugs.
The risk of pancreatic cancer doubled for patients receiving incretin treatment (adjusted hazard ratio, 2.14; 95% confidence interval, 1.71-2.67), compared with patients receiving other noninsulin drugs, after adjusting for age, sex, and whether or not patients subsequently received an insulin prescription, investigators reported.
However, risk of pancreatic cancer decreased over time in patients on incretin therapy, according to further analyses by Dr. Boniol and colleagues.
That finding of diminishing risk over time argues against concluding that incretin drugs cause pancreatic cancer, according to investigators.
“A direct causal effect could be suspected if a steadily increasing risk of pancreatic cancer was associated with a steadily longer exposure to incretin drugs,” they said.
In the first 3 months after the first incretin prescription, risk of pancreatic cancer was 3.35 times greater (95% CI, 2.32-4.84), which “gradually diminished” to 1.69 (95% CI, 1.12-2.55) a year after the first prescription, the investigators said in the report.
As such, these new data do not help prove or disprove a causal link between incretin use and pancreatic cancer, continued Dr. Hellman, a past president of the American Association of Clinical Endocrinologists.
“I think, right now, we don’t have the data,” he said in an interview. “It’s a question that makes us nervous, because of what we know about the laboratory effects of the drugs, but we don’t have the answer yet. We need longer studies with larger numbers of people to answer that question.”
The study, funded by Sanofi, was conducted at the request of the European Medicines Agency to assess risk of pancreatic cancer associated with lixisenatide. However, the study covers a period prior to use of lixisenatide in the general population because the approval of the GLP-1R agonist was “too recent,” the study authors wrote.
The analyses in the study were conducted in 2015 and 2016 for two cohorts of subjects: one in Belgium, for which data had been collected from 2008 to 2013, and one in Italy, with data from 2000 to 2012.
Further studies are needed to assess how long-term use of incretin drugs may affect risk of pancreatic cancer, the authors said.
The analysis was conducted as part of a postauthorization safety study requested by the European Medicines Agency and funded by Sanofi. One study author reported receiving grants from Roche, Amgen, and Bristol-Myers Squibb outside the submitted work; the remaining investigators had no relevant financial disclosures.
FROM DIABETES CARE
Key clinical point: Incretin therapy was associated with increased pancreatic cancer risk, but possibly because of occult pancreatic cancer that aggravates diabetes.
Major finding: Patients receiving incretin drugs had a doubling of pancreatic cancer risk (aHR 2.14 (95% CI, 1.71-2.67).
Data source: Retrospective cohort analysis of public health insurance databases including 33,292 diabetes patients treated with incretin drugs and 525,733 treated with another noninsulin antidiabetic drug.
Disclosures: The analysis was conducted as part of a postauthorization safety study requested by the European Medicines Agency and funded by Sanofi. One study author reported receiving grants from Roche, Amgen, and Bristol-Myers Squibb outside the submitted work; the remaining investigators had no relevant financial disclosures.
Late-breaking abstracts highlight treatment advances in CLL, myeloma, and more
.
In a preplanned interim analysis of data from 389 patients in the randomized phase III Murano trial, venetoclax and rituximab therapy proved “superior to the standard of care and well tolerated, and a major advance in the management of [relapsed/refractory] CLL,” ASH President Kenneth C. Anderson, MD said during a premeeting preview session for the media.
In Murano, venetoclax plus rituximab bettered bendamustine plus rituximab in progression-free survival, overall survival, overall and complete response rates, and number of patients achieving minimal residual disease (MRD) negativity, said Dr. Anderson, who is also director of the Lebow Institute for Myeloma Therapeutics and Jerome Lipper Myeloma Center at Dana-Farber Cancer Institute, Boston.
The results were consistent in all risk subsets, including patients who had high-risk disease by virtue of chromosome 17p deletion, according Dr. Anderson.
In another late-breaking randomized phase III study, known as ALCYONE, adding the CD38-targeting monoclonal antibody daratumumab to standard therapy with bortezomib, melphalan, and prednisone (VMP) resulted in a “doubling” of progression-free survival in patients who had newly diagnosed multiple myeloma and were ineligible for transplantation, he reported.
In the trial of more than 700 patients, daratumumab plus VMP as initial treatment for nontransplant patients was well tolerated and improved outcomes, including overall response rate and the percent of patients who achieved MRD negative status.
“As we saw in CLL, so it’s true in this abstract in myeloma: this is a very major advance,” Dr. Anderson said.
Also during the preview session, ASH Secretary Robert A. Brodsky, MD, discussed the randomized, phase III HERCULES study results, which showed that patients with acquired thrombotic thrombocytopenic purpura (TTP) may benefit when caplacizumab is added to standard therapy. Caplacizumab targets the A1 domain of von Willebrand factor, which inhibits interaction between ultra-large von Willebrand factor and platelets.
In the trial, 145 patients were randomized to receive either plasma exchange alone or plasma exchange and caplacizumab.
Preliminary results suggest “this was a very positive trial” with a primary endpoint of time to platelet response that “greatly favored the caplacizumab arm,” said Dr. Brodsky, professor of medicine and oncology and director of the division of hematology at Johns Hopkins University, Baltimore. “Even the secondary composite endpoint of death, recurrence, and/or major thromboembolic events was much improved with caplacizumab, so this is a very positive trial and potentially a game-changing drug for the management of TTP, which can be very challenging.”
Dr. Brodsky also discussed the Hokusai VTE-Cancer Study, a randomized, open-label, blinded outcome assessment trial that showed the oral factor Xa inhibitor edoxaban was noninferior to subcutaneous dalteparin for the prevention of cancer-associated venous thromboembolism.
With more than 1,000 patients enrolled in 114 centers, the Hokusai VTE-Cancer Study had a primary outcome of the composite of the first recurrent VTE or major bleeding event during follow-up. The primary outcome occurred in 12.8% of patients in the edoxaban group, compared with 13.5% of patients in the dalteparin group (P = .0056 for noninferiority), according to the preliminary published results.
The key question addressed by the trial is whether a newer oral anticoagulant, edoxaban, can substitute for the older, subcutaneously administered low-molecular-weight heparin, dalteparin. The results “confirmed that a newer oral anticoagulant is at least as good and as safe as the low molecular weight heparin,” allowing patients the convenience of an oral therapy, Dr. Brodsky noted.
This year’s late-breaking abstracts at ASH are:
LBA-1 Results of the Randomized, Double-Blind, Placebo-Controlled, Phase III Hercules Study of Caplacizumab in Patients with Acquired Thrombotic Thrombocytopenic Purpura.
LBA-2 Venetoclax Plus Rituximab Is Superior to Bendamustine Plus Rituximab in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia - Results from Pre-Planned Interim Analysis of the Randomized Phase III Murano Study.
LBA-3 Mutations in SRP54 Gene Cause Severe Primary Neutropenia As Well As Shwachman-Diamond-like Syndrome.
LBA-4 Phase III Randomized Study of Daratumumab Plus Bortezomib, Melphalan, and Prednisone (D-VMP) Versus Bortezomib, Melphalan, and Prednisone (VMP) in Newly Diagnosed Multiple Myeloma (NDMM) Patients (Pts) Ineligible for Transplant (ALCYONE).
LBA-5 Prospective Molecular MRD Detection By NGS: A Powerful Independent Predictor for Relapse and Survival in Adults with Newly Diagnosed AML.
LBA-6 A Randomized, Open-Label, Blinded Outcome Assessment Trial Evaluating the Efficacy and Safety of LMWH/Edoxaban Versus Dalteparin for Venous Thromboembolism Associated with Cancer: Hokusai VTE-Cancer Study
.
In a preplanned interim analysis of data from 389 patients in the randomized phase III Murano trial, venetoclax and rituximab therapy proved “superior to the standard of care and well tolerated, and a major advance in the management of [relapsed/refractory] CLL,” ASH President Kenneth C. Anderson, MD said during a premeeting preview session for the media.
In Murano, venetoclax plus rituximab bettered bendamustine plus rituximab in progression-free survival, overall survival, overall and complete response rates, and number of patients achieving minimal residual disease (MRD) negativity, said Dr. Anderson, who is also director of the Lebow Institute for Myeloma Therapeutics and Jerome Lipper Myeloma Center at Dana-Farber Cancer Institute, Boston.
The results were consistent in all risk subsets, including patients who had high-risk disease by virtue of chromosome 17p deletion, according Dr. Anderson.
In another late-breaking randomized phase III study, known as ALCYONE, adding the CD38-targeting monoclonal antibody daratumumab to standard therapy with bortezomib, melphalan, and prednisone (VMP) resulted in a “doubling” of progression-free survival in patients who had newly diagnosed multiple myeloma and were ineligible for transplantation, he reported.
In the trial of more than 700 patients, daratumumab plus VMP as initial treatment for nontransplant patients was well tolerated and improved outcomes, including overall response rate and the percent of patients who achieved MRD negative status.
“As we saw in CLL, so it’s true in this abstract in myeloma: this is a very major advance,” Dr. Anderson said.
Also during the preview session, ASH Secretary Robert A. Brodsky, MD, discussed the randomized, phase III HERCULES study results, which showed that patients with acquired thrombotic thrombocytopenic purpura (TTP) may benefit when caplacizumab is added to standard therapy. Caplacizumab targets the A1 domain of von Willebrand factor, which inhibits interaction between ultra-large von Willebrand factor and platelets.
In the trial, 145 patients were randomized to receive either plasma exchange alone or plasma exchange and caplacizumab.
Preliminary results suggest “this was a very positive trial” with a primary endpoint of time to platelet response that “greatly favored the caplacizumab arm,” said Dr. Brodsky, professor of medicine and oncology and director of the division of hematology at Johns Hopkins University, Baltimore. “Even the secondary composite endpoint of death, recurrence, and/or major thromboembolic events was much improved with caplacizumab, so this is a very positive trial and potentially a game-changing drug for the management of TTP, which can be very challenging.”
Dr. Brodsky also discussed the Hokusai VTE-Cancer Study, a randomized, open-label, blinded outcome assessment trial that showed the oral factor Xa inhibitor edoxaban was noninferior to subcutaneous dalteparin for the prevention of cancer-associated venous thromboembolism.
With more than 1,000 patients enrolled in 114 centers, the Hokusai VTE-Cancer Study had a primary outcome of the composite of the first recurrent VTE or major bleeding event during follow-up. The primary outcome occurred in 12.8% of patients in the edoxaban group, compared with 13.5% of patients in the dalteparin group (P = .0056 for noninferiority), according to the preliminary published results.
The key question addressed by the trial is whether a newer oral anticoagulant, edoxaban, can substitute for the older, subcutaneously administered low-molecular-weight heparin, dalteparin. The results “confirmed that a newer oral anticoagulant is at least as good and as safe as the low molecular weight heparin,” allowing patients the convenience of an oral therapy, Dr. Brodsky noted.
This year’s late-breaking abstracts at ASH are:
LBA-1 Results of the Randomized, Double-Blind, Placebo-Controlled, Phase III Hercules Study of Caplacizumab in Patients with Acquired Thrombotic Thrombocytopenic Purpura.
LBA-2 Venetoclax Plus Rituximab Is Superior to Bendamustine Plus Rituximab in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia - Results from Pre-Planned Interim Analysis of the Randomized Phase III Murano Study.
LBA-3 Mutations in SRP54 Gene Cause Severe Primary Neutropenia As Well As Shwachman-Diamond-like Syndrome.
LBA-4 Phase III Randomized Study of Daratumumab Plus Bortezomib, Melphalan, and Prednisone (D-VMP) Versus Bortezomib, Melphalan, and Prednisone (VMP) in Newly Diagnosed Multiple Myeloma (NDMM) Patients (Pts) Ineligible for Transplant (ALCYONE).
LBA-5 Prospective Molecular MRD Detection By NGS: A Powerful Independent Predictor for Relapse and Survival in Adults with Newly Diagnosed AML.
LBA-6 A Randomized, Open-Label, Blinded Outcome Assessment Trial Evaluating the Efficacy and Safety of LMWH/Edoxaban Versus Dalteparin for Venous Thromboembolism Associated with Cancer: Hokusai VTE-Cancer Study
.
In a preplanned interim analysis of data from 389 patients in the randomized phase III Murano trial, venetoclax and rituximab therapy proved “superior to the standard of care and well tolerated, and a major advance in the management of [relapsed/refractory] CLL,” ASH President Kenneth C. Anderson, MD said during a premeeting preview session for the media.
In Murano, venetoclax plus rituximab bettered bendamustine plus rituximab in progression-free survival, overall survival, overall and complete response rates, and number of patients achieving minimal residual disease (MRD) negativity, said Dr. Anderson, who is also director of the Lebow Institute for Myeloma Therapeutics and Jerome Lipper Myeloma Center at Dana-Farber Cancer Institute, Boston.
The results were consistent in all risk subsets, including patients who had high-risk disease by virtue of chromosome 17p deletion, according Dr. Anderson.
In another late-breaking randomized phase III study, known as ALCYONE, adding the CD38-targeting monoclonal antibody daratumumab to standard therapy with bortezomib, melphalan, and prednisone (VMP) resulted in a “doubling” of progression-free survival in patients who had newly diagnosed multiple myeloma and were ineligible for transplantation, he reported.
In the trial of more than 700 patients, daratumumab plus VMP as initial treatment for nontransplant patients was well tolerated and improved outcomes, including overall response rate and the percent of patients who achieved MRD negative status.
“As we saw in CLL, so it’s true in this abstract in myeloma: this is a very major advance,” Dr. Anderson said.
Also during the preview session, ASH Secretary Robert A. Brodsky, MD, discussed the randomized, phase III HERCULES study results, which showed that patients with acquired thrombotic thrombocytopenic purpura (TTP) may benefit when caplacizumab is added to standard therapy. Caplacizumab targets the A1 domain of von Willebrand factor, which inhibits interaction between ultra-large von Willebrand factor and platelets.
In the trial, 145 patients were randomized to receive either plasma exchange alone or plasma exchange and caplacizumab.
Preliminary results suggest “this was a very positive trial” with a primary endpoint of time to platelet response that “greatly favored the caplacizumab arm,” said Dr. Brodsky, professor of medicine and oncology and director of the division of hematology at Johns Hopkins University, Baltimore. “Even the secondary composite endpoint of death, recurrence, and/or major thromboembolic events was much improved with caplacizumab, so this is a very positive trial and potentially a game-changing drug for the management of TTP, which can be very challenging.”
Dr. Brodsky also discussed the Hokusai VTE-Cancer Study, a randomized, open-label, blinded outcome assessment trial that showed the oral factor Xa inhibitor edoxaban was noninferior to subcutaneous dalteparin for the prevention of cancer-associated venous thromboembolism.
With more than 1,000 patients enrolled in 114 centers, the Hokusai VTE-Cancer Study had a primary outcome of the composite of the first recurrent VTE or major bleeding event during follow-up. The primary outcome occurred in 12.8% of patients in the edoxaban group, compared with 13.5% of patients in the dalteparin group (P = .0056 for noninferiority), according to the preliminary published results.
The key question addressed by the trial is whether a newer oral anticoagulant, edoxaban, can substitute for the older, subcutaneously administered low-molecular-weight heparin, dalteparin. The results “confirmed that a newer oral anticoagulant is at least as good and as safe as the low molecular weight heparin,” allowing patients the convenience of an oral therapy, Dr. Brodsky noted.
This year’s late-breaking abstracts at ASH are:
LBA-1 Results of the Randomized, Double-Blind, Placebo-Controlled, Phase III Hercules Study of Caplacizumab in Patients with Acquired Thrombotic Thrombocytopenic Purpura.
LBA-2 Venetoclax Plus Rituximab Is Superior to Bendamustine Plus Rituximab in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia - Results from Pre-Planned Interim Analysis of the Randomized Phase III Murano Study.
LBA-3 Mutations in SRP54 Gene Cause Severe Primary Neutropenia As Well As Shwachman-Diamond-like Syndrome.
LBA-4 Phase III Randomized Study of Daratumumab Plus Bortezomib, Melphalan, and Prednisone (D-VMP) Versus Bortezomib, Melphalan, and Prednisone (VMP) in Newly Diagnosed Multiple Myeloma (NDMM) Patients (Pts) Ineligible for Transplant (ALCYONE).
LBA-5 Prospective Molecular MRD Detection By NGS: A Powerful Independent Predictor for Relapse and Survival in Adults with Newly Diagnosed AML.
LBA-6 A Randomized, Open-Label, Blinded Outcome Assessment Trial Evaluating the Efficacy and Safety of LMWH/Edoxaban Versus Dalteparin for Venous Thromboembolism Associated with Cancer: Hokusai VTE-Cancer Study
FROM ASH 2017
Squamous cell carcinoma linked to 25% increase in all-cause mortality
FROM JAAD
Squamous cell carcinomas (SCC), but not basal cell carcinomas (BCC), were associated with a risk of death from any cause that was 25% higher than that seen in the general population, based on a systematic literature review and meta-analysis published in the Journal of American Academy of Dermatology (2017. doi: 10.1016/j.jaad.2017.11.026).
“Because these tumors often occur in the same patients and are both often caused by exposure to ultraviolet radiation, patients with BCC and SCC are often grouped together,” Mackenzie R. Wehner, MD, of the University of Pennsylvania, Philadelphia, and co-authors wrote. “Our data contributes to the argument that the carcinogenesis of these tumors and long-term outcomes for patients with these tumors may be distinct.”
Patients with SCC “may need additional education and age-appropriate screening to prevent deaths from major diseases,” the authors concluded.
Dr. Wehner and colleagues systematically searched the medical literature and found four studies encompassing a total of 175,849 patients with SCC and 464,230 patients with BCC.

Relative to the general population, mortality for those with an SCC was 1.25 (95% CI, 1.17-1.32). At 0.92 (95% CI 0.83-1.02), there was no significant difference in mortality for patients with a BCC.
Collectively and individually, the studies found a statistically significant increased relative mortality for having SCC.
There are clear distinctions between BCC and SCC with regard to histology, pathophysiology, survival, and other parameters, the study authors said. “While many patients get both BCC and SCC, future research should take into account that these cancers may have different long-term risks and outcomes.”
FROM JAAD
Squamous cell carcinomas (SCC), but not basal cell carcinomas (BCC), were associated with a risk of death from any cause that was 25% higher than that seen in the general population, based on a systematic literature review and meta-analysis published in the Journal of American Academy of Dermatology (2017. doi: 10.1016/j.jaad.2017.11.026).
“Because these tumors often occur in the same patients and are both often caused by exposure to ultraviolet radiation, patients with BCC and SCC are often grouped together,” Mackenzie R. Wehner, MD, of the University of Pennsylvania, Philadelphia, and co-authors wrote. “Our data contributes to the argument that the carcinogenesis of these tumors and long-term outcomes for patients with these tumors may be distinct.”
Patients with SCC “may need additional education and age-appropriate screening to prevent deaths from major diseases,” the authors concluded.
Dr. Wehner and colleagues systematically searched the medical literature and found four studies encompassing a total of 175,849 patients with SCC and 464,230 patients with BCC.
Relative to the general population, mortality for those with an SCC was 1.25 (95% CI, 1.17-1.32). At 0.92 (95% CI 0.83-1.02), there was no significant difference in mortality for patients with a BCC.
Collectively and individually, the studies found a statistically significant increased relative mortality for having SCC.
There are clear distinctions between BCC and SCC with regard to histology, pathophysiology, survival, and other parameters, the study authors said. “While many patients get both BCC and SCC, future research should take into account that these cancers may have different long-term risks and outcomes.”
FROM JAAD
Squamous cell carcinomas (SCC), but not basal cell carcinomas (BCC), were associated with a risk of death from any cause that was 25% higher than that seen in the general population, based on a systematic literature review and meta-analysis published in the Journal of American Academy of Dermatology (2017. doi: 10.1016/j.jaad.2017.11.026).
“Because these tumors often occur in the same patients and are both often caused by exposure to ultraviolet radiation, patients with BCC and SCC are often grouped together,” Mackenzie R. Wehner, MD, of the University of Pennsylvania, Philadelphia, and co-authors wrote. “Our data contributes to the argument that the carcinogenesis of these tumors and long-term outcomes for patients with these tumors may be distinct.”
Patients with SCC “may need additional education and age-appropriate screening to prevent deaths from major diseases,” the authors concluded.
Dr. Wehner and colleagues systematically searched the medical literature and found four studies encompassing a total of 175,849 patients with SCC and 464,230 patients with BCC.
Relative to the general population, mortality for those with an SCC was 1.25 (95% CI, 1.17-1.32). At 0.92 (95% CI 0.83-1.02), there was no significant difference in mortality for patients with a BCC.
Collectively and individually, the studies found a statistically significant increased relative mortality for having SCC.
There are clear distinctions between BCC and SCC with regard to histology, pathophysiology, survival, and other parameters, the study authors said. “While many patients get both BCC and SCC, future research should take into account that these cancers may have different long-term risks and outcomes.”
FDA authorizes next-generation sequencing test for tumor profiling
The Food and Drug Administration has authorized a new tumor profiling test that can identify a larger number of genetic mutations than available in any other test previously reviewed, the agency has announced.
The tumor profiling test, developed at Memorial Sloan Kettering Cancer Center and known as MSK-IMPACT (Integrated Mutation Profiling of Actionable Cancer Targets), is a custom targeted sequencing platform that uses exon capture and sequencing, so-called next-generation sequencing, to identify point mutations, small insertions and deletions, and microsatellite instability in tumor specimens. The assay involves hybridization capture and deep sequencing of all protein coding exons of 468 cancer-associated genes, as well as molecular changes in a tumor’s genomic makeup, according to the FDA announcement.
Unlike cancer diagnostic tests designed to determine the presence of one cancer biomarker for use with a single drug, the IMPACT test compares tumor tissue to a “normal” tissue or cell sample from the same patient to find genetic alterations that could potentially guide treatment options. However, the FDA said, the results of IMPACT are “not conclusive” for choosing a corresponding treatment.
Next-generation sequencing technologies can examine “hundreds, if not millions, of DNA variants at a time,” Jeffrey Shuren, MD, director of the FDA’s Center for Devices and Radiological Health, said in the announcement. “We are only at the beginning of realizing the true potential for these devices to assist patients and their health care providers in learning about the genetic underpinnings of their disease.”
Evaluations of IMPACT suggest the assay is “highly accurate” with a greater than 99% capability of detecting a mutation at a frequency of approximately 5%, according to the FDA.
In addition, detection of molecular changes, including microsatellite instability, were concordant more than 92% of the time when compared with traditional detection methods, the agency said.
Along with the marketing authorization for IMPACT, which was granted to Memorial Sloan Kettering Cancer Center, the agency announced that the New York State Department of Health has been accredited as an FDA third-party reviewer of in vitro diagnostics similar to IMPACT.
That action “paves the way” for efficient review and availability of other next-generation sequencing–based cancer profiling tools.
Allowing third parties to review next-generation sequencing–based tumor profiling tests will “reduce the burden on test developers and streamline the regulatory assessment of these types of innovative products,” FDA Commissioner Scott Gottlieb, MD, said in the announcement.
The Food and Drug Administration has authorized a new tumor profiling test that can identify a larger number of genetic mutations than available in any other test previously reviewed, the agency has announced.
The tumor profiling test, developed at Memorial Sloan Kettering Cancer Center and known as MSK-IMPACT (Integrated Mutation Profiling of Actionable Cancer Targets), is a custom targeted sequencing platform that uses exon capture and sequencing, so-called next-generation sequencing, to identify point mutations, small insertions and deletions, and microsatellite instability in tumor specimens. The assay involves hybridization capture and deep sequencing of all protein coding exons of 468 cancer-associated genes, as well as molecular changes in a tumor’s genomic makeup, according to the FDA announcement.
Unlike cancer diagnostic tests designed to determine the presence of one cancer biomarker for use with a single drug, the IMPACT test compares tumor tissue to a “normal” tissue or cell sample from the same patient to find genetic alterations that could potentially guide treatment options. However, the FDA said, the results of IMPACT are “not conclusive” for choosing a corresponding treatment.
Next-generation sequencing technologies can examine “hundreds, if not millions, of DNA variants at a time,” Jeffrey Shuren, MD, director of the FDA’s Center for Devices and Radiological Health, said in the announcement. “We are only at the beginning of realizing the true potential for these devices to assist patients and their health care providers in learning about the genetic underpinnings of their disease.”
Evaluations of IMPACT suggest the assay is “highly accurate” with a greater than 99% capability of detecting a mutation at a frequency of approximately 5%, according to the FDA.
In addition, detection of molecular changes, including microsatellite instability, were concordant more than 92% of the time when compared with traditional detection methods, the agency said.
Along with the marketing authorization for IMPACT, which was granted to Memorial Sloan Kettering Cancer Center, the agency announced that the New York State Department of Health has been accredited as an FDA third-party reviewer of in vitro diagnostics similar to IMPACT.
That action “paves the way” for efficient review and availability of other next-generation sequencing–based cancer profiling tools.
Allowing third parties to review next-generation sequencing–based tumor profiling tests will “reduce the burden on test developers and streamline the regulatory assessment of these types of innovative products,” FDA Commissioner Scott Gottlieb, MD, said in the announcement.
The Food and Drug Administration has authorized a new tumor profiling test that can identify a larger number of genetic mutations than available in any other test previously reviewed, the agency has announced.
The tumor profiling test, developed at Memorial Sloan Kettering Cancer Center and known as MSK-IMPACT (Integrated Mutation Profiling of Actionable Cancer Targets), is a custom targeted sequencing platform that uses exon capture and sequencing, so-called next-generation sequencing, to identify point mutations, small insertions and deletions, and microsatellite instability in tumor specimens. The assay involves hybridization capture and deep sequencing of all protein coding exons of 468 cancer-associated genes, as well as molecular changes in a tumor’s genomic makeup, according to the FDA announcement.
Unlike cancer diagnostic tests designed to determine the presence of one cancer biomarker for use with a single drug, the IMPACT test compares tumor tissue to a “normal” tissue or cell sample from the same patient to find genetic alterations that could potentially guide treatment options. However, the FDA said, the results of IMPACT are “not conclusive” for choosing a corresponding treatment.
Next-generation sequencing technologies can examine “hundreds, if not millions, of DNA variants at a time,” Jeffrey Shuren, MD, director of the FDA’s Center for Devices and Radiological Health, said in the announcement. “We are only at the beginning of realizing the true potential for these devices to assist patients and their health care providers in learning about the genetic underpinnings of their disease.”
Evaluations of IMPACT suggest the assay is “highly accurate” with a greater than 99% capability of detecting a mutation at a frequency of approximately 5%, according to the FDA.
In addition, detection of molecular changes, including microsatellite instability, were concordant more than 92% of the time when compared with traditional detection methods, the agency said.
Along with the marketing authorization for IMPACT, which was granted to Memorial Sloan Kettering Cancer Center, the agency announced that the New York State Department of Health has been accredited as an FDA third-party reviewer of in vitro diagnostics similar to IMPACT.
That action “paves the way” for efficient review and availability of other next-generation sequencing–based cancer profiling tools.
Allowing third parties to review next-generation sequencing–based tumor profiling tests will “reduce the burden on test developers and streamline the regulatory assessment of these types of innovative products,” FDA Commissioner Scott Gottlieb, MD, said in the announcement.
Rituximab key to survival after transplant for mantle cell lymphoma
The study, which outlines the experience across a variety of different treatment patterns at City of Hope National Medical Center, Duarte, Calif., between January 1997 and November 2013, suggests a “large benefit” of adding rituximab, wrote Matthew G. Mei, MD, of the center’s department of hematology and hematopoietic cell transplantation, and his colleagues. Further, maintenance rituximab was associated with improved survival outcomes in patients with positron emission tomography (PET)-negative status at first complete remission.
The benefit of rituximab “stands out, and adds to the increasing body of evidence supporting this practice for all MCL patients after ASCT, regardless of age and frontline induction regimens,” wrote Dr. Mei and his colleagues (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.07.006). This was the case even with improvements in early diagnosis and supportive care, and the incorporation of novel agents such as bortezomib, lenalidomide, and ibrutinib, they wrote, noting significantly better outcomes for patients who underwent ASCT after 2007.
In multivariate analysis, maintenance rituximab therapy after ASCT was the single most important factor associated with improvement in progression-free survival (relative risk [RR], .25; 95% confidence interval, .14-.44) and overall survival (RR, .17; 95% CI, .07-.38).
Positron emission tomography scans were done prior to ASCT for 133 patients; after ASCT, 105 (79%) were found to be in a PET-negative complete remission. All but one of the patients with PET-negative disease received rituximab before ASCT. For that PET-negative subset, maintenance rituximab was significantly associated with improvements in progression-free survival (RR, .20; 95% CI, .09-.43) and overall survival (RR, .17; 95% CI, .05-.59).
This study represents one of the largest single-center reports to date on MCL patients who have undergone ASCT, according to the authors. “This study also sets the stage for prospective investigation aiming at optimization of maintenance therapy following ASCT.”
Dr. Mei reported no disclosures, and senior author Lihua E. Budde, MD, PhD, reported being a member of the Lymphoma Research Foundation MCL consortium. The study was supported by research funding from the National Cancer Institute.
This study confirms the value of maintenance rituximab for a large cohort of patients with mantle cell lymphoma who have undergone high-dose chemotherapy and autologous stem cell transplantation outside of clinical trials.
The findings also affirm results of a recent phase 3 randomized trial (LyMa) suggesting that in previously untreated MCL patients who have undergone ASCT, rituximab maintenance is superior to observation in improving overall survival and progression-free survival.
However, the most interesting aspect of this study is the positron emission tomography data. Namely, the benefit of rituximab maintenance was apparent in patients regardless of whether they were in a PET-positive or PET-negative first complete remission at ASCT. “This important finding implies that the benefit of rituximab maintenance after ASCT is present for low- and high-risk MCL patients.”
Despite these confirmatory findings, the treatment landscape for MCL has changed significantly in recent years, particularly with the introduction of treatments such as ibrutinib.
In a clinical trial currently underway, the European Mantle Cell Lymphoma Network is evaluating ibrutinib as an upfront treatment for young and fit patients. Specifically, the study compares first-line ASCT and rituximab maintenance, ASCT with ibrutinib maintenance, or a transplant-free approach with ibrutinib and chemotherapy.
Unless and until the data from this study “redefine the value of ASCT in the ibrutinib era, ASCT and rituximab maintenance should be recommended as the standard treatment after ASCT for transplant-eligible patients with MCL.”
Tobias Roider, MD, and Sascha Dietrich, MD, are with the Department of Medicine V, University of Heidelberg, Germany. Their comments are in an editorial (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.09.008). The authors reported no financial disclosures or conflicts of interest.
This study confirms the value of maintenance rituximab for a large cohort of patients with mantle cell lymphoma who have undergone high-dose chemotherapy and autologous stem cell transplantation outside of clinical trials.
The findings also affirm results of a recent phase 3 randomized trial (LyMa) suggesting that in previously untreated MCL patients who have undergone ASCT, rituximab maintenance is superior to observation in improving overall survival and progression-free survival.
However, the most interesting aspect of this study is the positron emission tomography data. Namely, the benefit of rituximab maintenance was apparent in patients regardless of whether they were in a PET-positive or PET-negative first complete remission at ASCT. “This important finding implies that the benefit of rituximab maintenance after ASCT is present for low- and high-risk MCL patients.”
Despite these confirmatory findings, the treatment landscape for MCL has changed significantly in recent years, particularly with the introduction of treatments such as ibrutinib.
In a clinical trial currently underway, the European Mantle Cell Lymphoma Network is evaluating ibrutinib as an upfront treatment for young and fit patients. Specifically, the study compares first-line ASCT and rituximab maintenance, ASCT with ibrutinib maintenance, or a transplant-free approach with ibrutinib and chemotherapy.
Unless and until the data from this study “redefine the value of ASCT in the ibrutinib era, ASCT and rituximab maintenance should be recommended as the standard treatment after ASCT for transplant-eligible patients with MCL.”
Tobias Roider, MD, and Sascha Dietrich, MD, are with the Department of Medicine V, University of Heidelberg, Germany. Their comments are in an editorial (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.09.008). The authors reported no financial disclosures or conflicts of interest.
This study confirms the value of maintenance rituximab for a large cohort of patients with mantle cell lymphoma who have undergone high-dose chemotherapy and autologous stem cell transplantation outside of clinical trials.
The findings also affirm results of a recent phase 3 randomized trial (LyMa) suggesting that in previously untreated MCL patients who have undergone ASCT, rituximab maintenance is superior to observation in improving overall survival and progression-free survival.
However, the most interesting aspect of this study is the positron emission tomography data. Namely, the benefit of rituximab maintenance was apparent in patients regardless of whether they were in a PET-positive or PET-negative first complete remission at ASCT. “This important finding implies that the benefit of rituximab maintenance after ASCT is present for low- and high-risk MCL patients.”
Despite these confirmatory findings, the treatment landscape for MCL has changed significantly in recent years, particularly with the introduction of treatments such as ibrutinib.
In a clinical trial currently underway, the European Mantle Cell Lymphoma Network is evaluating ibrutinib as an upfront treatment for young and fit patients. Specifically, the study compares first-line ASCT and rituximab maintenance, ASCT with ibrutinib maintenance, or a transplant-free approach with ibrutinib and chemotherapy.
Unless and until the data from this study “redefine the value of ASCT in the ibrutinib era, ASCT and rituximab maintenance should be recommended as the standard treatment after ASCT for transplant-eligible patients with MCL.”
Tobias Roider, MD, and Sascha Dietrich, MD, are with the Department of Medicine V, University of Heidelberg, Germany. Their comments are in an editorial (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.09.008). The authors reported no financial disclosures or conflicts of interest.
The study, which outlines the experience across a variety of different treatment patterns at City of Hope National Medical Center, Duarte, Calif., between January 1997 and November 2013, suggests a “large benefit” of adding rituximab, wrote Matthew G. Mei, MD, of the center’s department of hematology and hematopoietic cell transplantation, and his colleagues. Further, maintenance rituximab was associated with improved survival outcomes in patients with positron emission tomography (PET)-negative status at first complete remission.
The benefit of rituximab “stands out, and adds to the increasing body of evidence supporting this practice for all MCL patients after ASCT, regardless of age and frontline induction regimens,” wrote Dr. Mei and his colleagues (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.07.006). This was the case even with improvements in early diagnosis and supportive care, and the incorporation of novel agents such as bortezomib, lenalidomide, and ibrutinib, they wrote, noting significantly better outcomes for patients who underwent ASCT after 2007.
In multivariate analysis, maintenance rituximab therapy after ASCT was the single most important factor associated with improvement in progression-free survival (relative risk [RR], .25; 95% confidence interval, .14-.44) and overall survival (RR, .17; 95% CI, .07-.38).
Positron emission tomography scans were done prior to ASCT for 133 patients; after ASCT, 105 (79%) were found to be in a PET-negative complete remission. All but one of the patients with PET-negative disease received rituximab before ASCT. For that PET-negative subset, maintenance rituximab was significantly associated with improvements in progression-free survival (RR, .20; 95% CI, .09-.43) and overall survival (RR, .17; 95% CI, .05-.59).
This study represents one of the largest single-center reports to date on MCL patients who have undergone ASCT, according to the authors. “This study also sets the stage for prospective investigation aiming at optimization of maintenance therapy following ASCT.”
Dr. Mei reported no disclosures, and senior author Lihua E. Budde, MD, PhD, reported being a member of the Lymphoma Research Foundation MCL consortium. The study was supported by research funding from the National Cancer Institute.
The study, which outlines the experience across a variety of different treatment patterns at City of Hope National Medical Center, Duarte, Calif., between January 1997 and November 2013, suggests a “large benefit” of adding rituximab, wrote Matthew G. Mei, MD, of the center’s department of hematology and hematopoietic cell transplantation, and his colleagues. Further, maintenance rituximab was associated with improved survival outcomes in patients with positron emission tomography (PET)-negative status at first complete remission.
The benefit of rituximab “stands out, and adds to the increasing body of evidence supporting this practice for all MCL patients after ASCT, regardless of age and frontline induction regimens,” wrote Dr. Mei and his colleagues (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.07.006). This was the case even with improvements in early diagnosis and supportive care, and the incorporation of novel agents such as bortezomib, lenalidomide, and ibrutinib, they wrote, noting significantly better outcomes for patients who underwent ASCT after 2007.
In multivariate analysis, maintenance rituximab therapy after ASCT was the single most important factor associated with improvement in progression-free survival (relative risk [RR], .25; 95% confidence interval, .14-.44) and overall survival (RR, .17; 95% CI, .07-.38).
Positron emission tomography scans were done prior to ASCT for 133 patients; after ASCT, 105 (79%) were found to be in a PET-negative complete remission. All but one of the patients with PET-negative disease received rituximab before ASCT. For that PET-negative subset, maintenance rituximab was significantly associated with improvements in progression-free survival (RR, .20; 95% CI, .09-.43) and overall survival (RR, .17; 95% CI, .05-.59).
This study represents one of the largest single-center reports to date on MCL patients who have undergone ASCT, according to the authors. “This study also sets the stage for prospective investigation aiming at optimization of maintenance therapy following ASCT.”
Dr. Mei reported no disclosures, and senior author Lihua E. Budde, MD, PhD, reported being a member of the Lymphoma Research Foundation MCL consortium. The study was supported by research funding from the National Cancer Institute.
FROM BIOLOGY OF BLOOD AND MARROW TRANSPLANTATION
Key clinical point: Over time and in many different patterns, rituximab maintenance therapy stood out as the prominent factor influencing survival in patients with mantle cell lymphoma who undergo autologous stem cell transplant.
Major finding: Maintenance rituximab was significantly associated with superior progression-free survival (relative risk, .25; 95% confidence interval, .14-.44) and overall survival (RR, .17; 95% CI, .07-.38).
Data source: Retrospective analysis of data for 191 patients with MCL who underwent ASCT at a medical center in California between January 1997 and November 2013.
Disclosures: The study was supported by research funding from the National Cancer Institute. Senior author Lihua E. Budde, MD, PhD, reported being a member of the Lymphoma Research Foundation MCL consortium.