User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Pandemic restrictions ignite innovative pivot for psychiatry
As medical school faculty members – and our students – know well, the COVID-19 pandemic forced us to become creative and shift much of our curricula online. Many hospitals chose to limit medical student rotations because of safety concerns. Students fell victim to canceled psychiatry rotations and electives during the pandemic’s early days. Privacy issues, combined with stigma tied to mental illness, made this shift to virtual instruction particularly challenging. But as a field, we persevered! And, as we learned during our shift toward telemedicine, many of the changes we made in medical education are probably here to stay.

Our team at the New York Institute of Technology College of Osteopathic Medicine (NYITCOM) was able to implement a novel curriculum that allowed our students to learn psychiatry and maintain high-quality medical school education.
We developed an online course for third-year students’ rotation in psychiatry, with several modules that focused on a variety of psychiatric topics and disorders, including the basic classifications and categories of depression, anxiety, personality disorders, and psychotic disorders. There were also video encounters available showing actual patient encounters. On completion of the online module, a faculty session was held to discuss topics of concern/confusion to the students, areas of interest, and a variety of related topics, such as professionalism in psychiatry, essentials of the mental status exam, management of diverse populations, and COVID repercussions in psychiatry.
For fourth-year students, we developed a telemedicine psychiatry elective, which allowed the students to observe psychiatric evaluations, psychiatric medication review visits, and even follow-up psychotherapy sessions, with the school’s clinical psychologists. The new method was minimally invasive, and it was accepted by patients and welcomed by the students.
During a time when hospitals were limiting onsite student rotations and discouraging patient contact, medical students still needed to experience patient interactions. As the director of the school’s Center for Behavioral Health, I designed an additional program that allowed students to participate in observing patients who presented with psychiatric complaints and symptoms. It had to be confidential in nature, accessible, and safe.
I recalled my own training in a hospital setting, where students and residents were allowed to observe a patient being evaluated by an attending, through a one-way mirror. It was a method that was acceptable at the time in a hospital, but unfortunately, not in a private office setting. As such, students and residents experienced such an interaction in acute inpatient and/or outpatient clinics of a hospital. The experience was invaluable.
The concept was simple, yet very efficient. The clinicians in the Center for Behavioral Health were seeing all patients with psychiatric needs via a HIPAA-compliant telemedicine platform. Access was granted for students – with the patient’s consent – and they “entered the session” without being seen or heard. This presented little to no distraction to the patient, and the student was able to observe a range of clinical sessions.
The course also provided online supplemental modules, including essential psychiatric topics, psychopharmacology, and a psychotherapeutic module that discussed a myriad of therapeutic interventions. In addition, the student was supervised weekly by the course director, the psychopharmacologist, and the clinical psychologist. The course director provided daily wrap-up reviews as well.
Originally, this new approach was envisioned as a temporary solution for use during the pandemic. But it has become clear that this approach would be beneficial post pandemic as well. Most of the students who participated in the course were actually interested in pursuing psychiatry as their future specialty. It allowed them to observe a population of patients firsthand that they might encounter in private practice, as opposed to only hospital settings.
Being present in a session with a patient with psychiatric symptoms and diagnoses has always been a challenge. Many patients refuse to have another medical professional in the room because of the intimate details being discussed and their associated stigma. The patients’ inability to see or hear the student during the sessions allows them to ignore the students’ presence – or at least not be intimidated by it. This, therefore, allows the students access and affords them a unique and memorable educational experience.
The pandemic curtailed and altered medical students’ traditional exposure to patients, but we found innovative ways to redefine it. As difficult as COVID-19 has been for the health care community, we have been able to use the restrictions forced by the pandemic to identify innovative ways to improve the education of our medical students.
In addition to serving as director of the Center for Behavioral Health at NYITCOM in Old Westbury, N.Y., Dr. Jarkon is assistant professor in the department of family medicine. She has no disclosures.
As medical school faculty members – and our students – know well, the COVID-19 pandemic forced us to become creative and shift much of our curricula online. Many hospitals chose to limit medical student rotations because of safety concerns. Students fell victim to canceled psychiatry rotations and electives during the pandemic’s early days. Privacy issues, combined with stigma tied to mental illness, made this shift to virtual instruction particularly challenging. But as a field, we persevered! And, as we learned during our shift toward telemedicine, many of the changes we made in medical education are probably here to stay.
Our team at the New York Institute of Technology College of Osteopathic Medicine (NYITCOM) was able to implement a novel curriculum that allowed our students to learn psychiatry and maintain high-quality medical school education.
We developed an online course for third-year students’ rotation in psychiatry, with several modules that focused on a variety of psychiatric topics and disorders, including the basic classifications and categories of depression, anxiety, personality disorders, and psychotic disorders. There were also video encounters available showing actual patient encounters. On completion of the online module, a faculty session was held to discuss topics of concern/confusion to the students, areas of interest, and a variety of related topics, such as professionalism in psychiatry, essentials of the mental status exam, management of diverse populations, and COVID repercussions in psychiatry.
For fourth-year students, we developed a telemedicine psychiatry elective, which allowed the students to observe psychiatric evaluations, psychiatric medication review visits, and even follow-up psychotherapy sessions, with the school’s clinical psychologists. The new method was minimally invasive, and it was accepted by patients and welcomed by the students.
During a time when hospitals were limiting onsite student rotations and discouraging patient contact, medical students still needed to experience patient interactions. As the director of the school’s Center for Behavioral Health, I designed an additional program that allowed students to participate in observing patients who presented with psychiatric complaints and symptoms. It had to be confidential in nature, accessible, and safe.
I recalled my own training in a hospital setting, where students and residents were allowed to observe a patient being evaluated by an attending, through a one-way mirror. It was a method that was acceptable at the time in a hospital, but unfortunately, not in a private office setting. As such, students and residents experienced such an interaction in acute inpatient and/or outpatient clinics of a hospital. The experience was invaluable.
The concept was simple, yet very efficient. The clinicians in the Center for Behavioral Health were seeing all patients with psychiatric needs via a HIPAA-compliant telemedicine platform. Access was granted for students – with the patient’s consent – and they “entered the session” without being seen or heard. This presented little to no distraction to the patient, and the student was able to observe a range of clinical sessions.
The course also provided online supplemental modules, including essential psychiatric topics, psychopharmacology, and a psychotherapeutic module that discussed a myriad of therapeutic interventions. In addition, the student was supervised weekly by the course director, the psychopharmacologist, and the clinical psychologist. The course director provided daily wrap-up reviews as well.
Originally, this new approach was envisioned as a temporary solution for use during the pandemic. But it has become clear that this approach would be beneficial post pandemic as well. Most of the students who participated in the course were actually interested in pursuing psychiatry as their future specialty. It allowed them to observe a population of patients firsthand that they might encounter in private practice, as opposed to only hospital settings.
Being present in a session with a patient with psychiatric symptoms and diagnoses has always been a challenge. Many patients refuse to have another medical professional in the room because of the intimate details being discussed and their associated stigma. The patients’ inability to see or hear the student during the sessions allows them to ignore the students’ presence – or at least not be intimidated by it. This, therefore, allows the students access and affords them a unique and memorable educational experience.
The pandemic curtailed and altered medical students’ traditional exposure to patients, but we found innovative ways to redefine it. As difficult as COVID-19 has been for the health care community, we have been able to use the restrictions forced by the pandemic to identify innovative ways to improve the education of our medical students.
In addition to serving as director of the Center for Behavioral Health at NYITCOM in Old Westbury, N.Y., Dr. Jarkon is assistant professor in the department of family medicine. She has no disclosures.
As medical school faculty members – and our students – know well, the COVID-19 pandemic forced us to become creative and shift much of our curricula online. Many hospitals chose to limit medical student rotations because of safety concerns. Students fell victim to canceled psychiatry rotations and electives during the pandemic’s early days. Privacy issues, combined with stigma tied to mental illness, made this shift to virtual instruction particularly challenging. But as a field, we persevered! And, as we learned during our shift toward telemedicine, many of the changes we made in medical education are probably here to stay.
Our team at the New York Institute of Technology College of Osteopathic Medicine (NYITCOM) was able to implement a novel curriculum that allowed our students to learn psychiatry and maintain high-quality medical school education.
We developed an online course for third-year students’ rotation in psychiatry, with several modules that focused on a variety of psychiatric topics and disorders, including the basic classifications and categories of depression, anxiety, personality disorders, and psychotic disorders. There were also video encounters available showing actual patient encounters. On completion of the online module, a faculty session was held to discuss topics of concern/confusion to the students, areas of interest, and a variety of related topics, such as professionalism in psychiatry, essentials of the mental status exam, management of diverse populations, and COVID repercussions in psychiatry.
For fourth-year students, we developed a telemedicine psychiatry elective, which allowed the students to observe psychiatric evaluations, psychiatric medication review visits, and even follow-up psychotherapy sessions, with the school’s clinical psychologists. The new method was minimally invasive, and it was accepted by patients and welcomed by the students.
During a time when hospitals were limiting onsite student rotations and discouraging patient contact, medical students still needed to experience patient interactions. As the director of the school’s Center for Behavioral Health, I designed an additional program that allowed students to participate in observing patients who presented with psychiatric complaints and symptoms. It had to be confidential in nature, accessible, and safe.
I recalled my own training in a hospital setting, where students and residents were allowed to observe a patient being evaluated by an attending, through a one-way mirror. It was a method that was acceptable at the time in a hospital, but unfortunately, not in a private office setting. As such, students and residents experienced such an interaction in acute inpatient and/or outpatient clinics of a hospital. The experience was invaluable.
The concept was simple, yet very efficient. The clinicians in the Center for Behavioral Health were seeing all patients with psychiatric needs via a HIPAA-compliant telemedicine platform. Access was granted for students – with the patient’s consent – and they “entered the session” without being seen or heard. This presented little to no distraction to the patient, and the student was able to observe a range of clinical sessions.
The course also provided online supplemental modules, including essential psychiatric topics, psychopharmacology, and a psychotherapeutic module that discussed a myriad of therapeutic interventions. In addition, the student was supervised weekly by the course director, the psychopharmacologist, and the clinical psychologist. The course director provided daily wrap-up reviews as well.
Originally, this new approach was envisioned as a temporary solution for use during the pandemic. But it has become clear that this approach would be beneficial post pandemic as well. Most of the students who participated in the course were actually interested in pursuing psychiatry as their future specialty. It allowed them to observe a population of patients firsthand that they might encounter in private practice, as opposed to only hospital settings.
Being present in a session with a patient with psychiatric symptoms and diagnoses has always been a challenge. Many patients refuse to have another medical professional in the room because of the intimate details being discussed and their associated stigma. The patients’ inability to see or hear the student during the sessions allows them to ignore the students’ presence – or at least not be intimidated by it. This, therefore, allows the students access and affords them a unique and memorable educational experience.
The pandemic curtailed and altered medical students’ traditional exposure to patients, but we found innovative ways to redefine it. As difficult as COVID-19 has been for the health care community, we have been able to use the restrictions forced by the pandemic to identify innovative ways to improve the education of our medical students.
In addition to serving as director of the Center for Behavioral Health at NYITCOM in Old Westbury, N.Y., Dr. Jarkon is assistant professor in the department of family medicine. She has no disclosures.
COVID-detecting dogs pilot first airport program
If she identifies a specific scent, she’ll let her handler know simply by sitting down. When this good girl sits, that means Cobra has detected an olfactory signal of the coronavirus, the virus that causes COVID-19.
Cobra, a Belgian Malinois, is one of two canines – her partner is One Betta, a Dutch shepherd – working this checkpoint at Miami International. They are part of a pilot program with the Global Forensic and Justice Center at Florida International University, using the detection dogs as a quick screen for people who have COVID-19.
Their detection rate is high, at more than 98%, and the program has been such a success that it’s being extended for another month at the airport.
If these two dogs continue to accurately detect COVID-19, they and other canines with similar training could be deployed to other places with lots of people coming and going at once, including other airports or even schools. In fact, COVID-sniffing dogs are in use in some university classrooms already.
But building up a big brigade of live animals as disease detectors involves some thorny issues, including where the animals retire once their careers are complete.
“When COVID first arose, we said let’s see if we can train these two dogs on either the virus or the odor of COVID-19,” says Kenneth Furton, PhD, a professor of chemistry and biochemistry, provost, and executive vice president at Florida International University.
His team had completed a study with what he calls “medical detector dogs,” animals that might be able to detect the odor of someone having a seizure. That led them to see how well the animals could detect other kinds of disorders.
Training a dog to sniff out specific odors starts with getting them to understand the task in general. Dr. Furton says that the animals first are trained to grasp that their job is to detect one odor among many. Once the dogs grasp that, they can be trained on just about any specific odor.
In fact, in addition to detecting seizures, dogs reportedly have been able to identify diabetes and even some cancers, such as ovarian cancer.
Dr. Furton says he’s not aware of any previous use of dogs to screen for infectious disease. That may simply be because nothing recently has struck with the global ferocity of COVID, driving humans to turn to their best friends for help.
Cobra and One Betta got their start learning to identify the presence of laurel wilt, a fungus that attacks avocado trees and kills them, costing Florida growers millions. With that expertise under their collars, the two dogs need only a few weeks to get good at detecting other smells assigned to them.
Training the dogs, safely
To train Cobra and One Betta on COVID-19 odors, Dr. Furton’s team first acquired mask samples from people hospitalized with COVID and people who did not have the disease. In battling the viruses, people produce certain chemicals that they exhale every time they breathe. When Dr. Furton and his colleagues compared the exhaled components trapped in the masks, they found differences between masks from people with COVID and those without.
Having confirmed that exhalations can be COVID-specific, the research team trained four dogs – Cobra, One Betta, Hubble, and Max – to detect masks from people with COVID among an assortment of mask choices. Before this step, though, the researchers made sure that any trace of active virus was destroyed by ultraviolet light so that the dogs would not be infected.
Each time the dogs accurately selected a mask from a COVID patient, their reward was access to a favorite toy: A red ball to chew on. Although all four dogs performed very well, yes, they did, Cobra and One Betta showed the most accuracy, outperforming their training colleagues. From their training scores, Cobra ranked first, with 99.45% accuracy. Despite her name, says Dr. Furton, One Betta was “not one better,” coming in second at 98.1%, which is still quite high.
Both dogs are good at their airport screening duties. If one of them sits after sniffing a mask at the checkpoint, the next step is for the mask owner to be tested.
From Aug. 23 to Sept. 8, the two canines screened 1,093 people during 8 working days, alerting on only one case, according to Greg Chin, communications director for the Miami-Dade Aviation Department. That person had tested positive for COVID 2 weeks earlier and was returning to work after quarantine, and their rapid test after the dog alerted was negative.
Dr. Furton says that there are some reports of dogs also alerting before tests can show a positive result, suggesting the dogs’ odor detection can be more precise. They hope to expand their study to see how tight the window of dog-based detection is.
For now, the detector dogs are doing so well that the program has been extended for 30 more days, Mr. Chin says.
As promising as this seems, using dogs for screening carries some logistical and ethical tangles. Training a canine army to deploy for high-volume detection points means that once the work is done, a whole lot of dogs will need a safe place to retire. In addition, the initial training takes several months, says Dr. Furton, whereas if a device were developed for screening, manufacturing could likely be ramped up quickly to meet demand.
The dogs might not need to retire right away, though.
“We envision that they could be redeployed to another type of detection for another infectious disease” if the need arises, Dr. Furton says. But in the end, when working with dogs, he says, there is “a moral connection that you don’t have to deal with using instruments.”
Although the pilot screening at Miami International is the first airport test, the dogs have also done this work in other venues, including at a state emergency operations center in Florida and in some university classrooms, says Dr. Furton.
A version of this article first appeared on WebMD.com.
If she identifies a specific scent, she’ll let her handler know simply by sitting down. When this good girl sits, that means Cobra has detected an olfactory signal of the coronavirus, the virus that causes COVID-19.
Cobra, a Belgian Malinois, is one of two canines – her partner is One Betta, a Dutch shepherd – working this checkpoint at Miami International. They are part of a pilot program with the Global Forensic and Justice Center at Florida International University, using the detection dogs as a quick screen for people who have COVID-19.
Their detection rate is high, at more than 98%, and the program has been such a success that it’s being extended for another month at the airport.
If these two dogs continue to accurately detect COVID-19, they and other canines with similar training could be deployed to other places with lots of people coming and going at once, including other airports or even schools. In fact, COVID-sniffing dogs are in use in some university classrooms already.
But building up a big brigade of live animals as disease detectors involves some thorny issues, including where the animals retire once their careers are complete.
“When COVID first arose, we said let’s see if we can train these two dogs on either the virus or the odor of COVID-19,” says Kenneth Furton, PhD, a professor of chemistry and biochemistry, provost, and executive vice president at Florida International University.
His team had completed a study with what he calls “medical detector dogs,” animals that might be able to detect the odor of someone having a seizure. That led them to see how well the animals could detect other kinds of disorders.
Training a dog to sniff out specific odors starts with getting them to understand the task in general. Dr. Furton says that the animals first are trained to grasp that their job is to detect one odor among many. Once the dogs grasp that, they can be trained on just about any specific odor.
In fact, in addition to detecting seizures, dogs reportedly have been able to identify diabetes and even some cancers, such as ovarian cancer.
Dr. Furton says he’s not aware of any previous use of dogs to screen for infectious disease. That may simply be because nothing recently has struck with the global ferocity of COVID, driving humans to turn to their best friends for help.
Cobra and One Betta got their start learning to identify the presence of laurel wilt, a fungus that attacks avocado trees and kills them, costing Florida growers millions. With that expertise under their collars, the two dogs need only a few weeks to get good at detecting other smells assigned to them.
Training the dogs, safely
To train Cobra and One Betta on COVID-19 odors, Dr. Furton’s team first acquired mask samples from people hospitalized with COVID and people who did not have the disease. In battling the viruses, people produce certain chemicals that they exhale every time they breathe. When Dr. Furton and his colleagues compared the exhaled components trapped in the masks, they found differences between masks from people with COVID and those without.
Having confirmed that exhalations can be COVID-specific, the research team trained four dogs – Cobra, One Betta, Hubble, and Max – to detect masks from people with COVID among an assortment of mask choices. Before this step, though, the researchers made sure that any trace of active virus was destroyed by ultraviolet light so that the dogs would not be infected.
Each time the dogs accurately selected a mask from a COVID patient, their reward was access to a favorite toy: A red ball to chew on. Although all four dogs performed very well, yes, they did, Cobra and One Betta showed the most accuracy, outperforming their training colleagues. From their training scores, Cobra ranked first, with 99.45% accuracy. Despite her name, says Dr. Furton, One Betta was “not one better,” coming in second at 98.1%, which is still quite high.
Both dogs are good at their airport screening duties. If one of them sits after sniffing a mask at the checkpoint, the next step is for the mask owner to be tested.
From Aug. 23 to Sept. 8, the two canines screened 1,093 people during 8 working days, alerting on only one case, according to Greg Chin, communications director for the Miami-Dade Aviation Department. That person had tested positive for COVID 2 weeks earlier and was returning to work after quarantine, and their rapid test after the dog alerted was negative.
Dr. Furton says that there are some reports of dogs also alerting before tests can show a positive result, suggesting the dogs’ odor detection can be more precise. They hope to expand their study to see how tight the window of dog-based detection is.
For now, the detector dogs are doing so well that the program has been extended for 30 more days, Mr. Chin says.
As promising as this seems, using dogs for screening carries some logistical and ethical tangles. Training a canine army to deploy for high-volume detection points means that once the work is done, a whole lot of dogs will need a safe place to retire. In addition, the initial training takes several months, says Dr. Furton, whereas if a device were developed for screening, manufacturing could likely be ramped up quickly to meet demand.
The dogs might not need to retire right away, though.
“We envision that they could be redeployed to another type of detection for another infectious disease” if the need arises, Dr. Furton says. But in the end, when working with dogs, he says, there is “a moral connection that you don’t have to deal with using instruments.”
Although the pilot screening at Miami International is the first airport test, the dogs have also done this work in other venues, including at a state emergency operations center in Florida and in some university classrooms, says Dr. Furton.
A version of this article first appeared on WebMD.com.
If she identifies a specific scent, she’ll let her handler know simply by sitting down. When this good girl sits, that means Cobra has detected an olfactory signal of the coronavirus, the virus that causes COVID-19.
Cobra, a Belgian Malinois, is one of two canines – her partner is One Betta, a Dutch shepherd – working this checkpoint at Miami International. They are part of a pilot program with the Global Forensic and Justice Center at Florida International University, using the detection dogs as a quick screen for people who have COVID-19.
Their detection rate is high, at more than 98%, and the program has been such a success that it’s being extended for another month at the airport.
If these two dogs continue to accurately detect COVID-19, they and other canines with similar training could be deployed to other places with lots of people coming and going at once, including other airports or even schools. In fact, COVID-sniffing dogs are in use in some university classrooms already.
But building up a big brigade of live animals as disease detectors involves some thorny issues, including where the animals retire once their careers are complete.
“When COVID first arose, we said let’s see if we can train these two dogs on either the virus or the odor of COVID-19,” says Kenneth Furton, PhD, a professor of chemistry and biochemistry, provost, and executive vice president at Florida International University.
His team had completed a study with what he calls “medical detector dogs,” animals that might be able to detect the odor of someone having a seizure. That led them to see how well the animals could detect other kinds of disorders.
Training a dog to sniff out specific odors starts with getting them to understand the task in general. Dr. Furton says that the animals first are trained to grasp that their job is to detect one odor among many. Once the dogs grasp that, they can be trained on just about any specific odor.
In fact, in addition to detecting seizures, dogs reportedly have been able to identify diabetes and even some cancers, such as ovarian cancer.
Dr. Furton says he’s not aware of any previous use of dogs to screen for infectious disease. That may simply be because nothing recently has struck with the global ferocity of COVID, driving humans to turn to their best friends for help.
Cobra and One Betta got their start learning to identify the presence of laurel wilt, a fungus that attacks avocado trees and kills them, costing Florida growers millions. With that expertise under their collars, the two dogs need only a few weeks to get good at detecting other smells assigned to them.
Training the dogs, safely
To train Cobra and One Betta on COVID-19 odors, Dr. Furton’s team first acquired mask samples from people hospitalized with COVID and people who did not have the disease. In battling the viruses, people produce certain chemicals that they exhale every time they breathe. When Dr. Furton and his colleagues compared the exhaled components trapped in the masks, they found differences between masks from people with COVID and those without.
Having confirmed that exhalations can be COVID-specific, the research team trained four dogs – Cobra, One Betta, Hubble, and Max – to detect masks from people with COVID among an assortment of mask choices. Before this step, though, the researchers made sure that any trace of active virus was destroyed by ultraviolet light so that the dogs would not be infected.
Each time the dogs accurately selected a mask from a COVID patient, their reward was access to a favorite toy: A red ball to chew on. Although all four dogs performed very well, yes, they did, Cobra and One Betta showed the most accuracy, outperforming their training colleagues. From their training scores, Cobra ranked first, with 99.45% accuracy. Despite her name, says Dr. Furton, One Betta was “not one better,” coming in second at 98.1%, which is still quite high.
Both dogs are good at their airport screening duties. If one of them sits after sniffing a mask at the checkpoint, the next step is for the mask owner to be tested.
From Aug. 23 to Sept. 8, the two canines screened 1,093 people during 8 working days, alerting on only one case, according to Greg Chin, communications director for the Miami-Dade Aviation Department. That person had tested positive for COVID 2 weeks earlier and was returning to work after quarantine, and their rapid test after the dog alerted was negative.
Dr. Furton says that there are some reports of dogs also alerting before tests can show a positive result, suggesting the dogs’ odor detection can be more precise. They hope to expand their study to see how tight the window of dog-based detection is.
For now, the detector dogs are doing so well that the program has been extended for 30 more days, Mr. Chin says.
As promising as this seems, using dogs for screening carries some logistical and ethical tangles. Training a canine army to deploy for high-volume detection points means that once the work is done, a whole lot of dogs will need a safe place to retire. In addition, the initial training takes several months, says Dr. Furton, whereas if a device were developed for screening, manufacturing could likely be ramped up quickly to meet demand.
The dogs might not need to retire right away, though.
“We envision that they could be redeployed to another type of detection for another infectious disease” if the need arises, Dr. Furton says. But in the end, when working with dogs, he says, there is “a moral connection that you don’t have to deal with using instruments.”
Although the pilot screening at Miami International is the first airport test, the dogs have also done this work in other venues, including at a state emergency operations center in Florida and in some university classrooms, says Dr. Furton.
A version of this article first appeared on WebMD.com.
Surge in new-onset tics in adults tied to COVID-19 stress
, new research suggests.
Results from a large, single-center study show several cases of tic-like movements and vocalizations with abrupt onset among older adolescents and adults during the pandemic. None had a previous diagnosis of a tic disorder. Among 10 patients, two were diagnosed with a purely functional movement disorder, four with an organic tic disorder, and four with both.
“Within our movement disorders clinic specifically ... we’ve been seeing an increased number of patients with an almost explosive onset of these tic-like movements and vocalizations later in life than what is typically seen with organic tic disorders and Tourette syndrome, which is typically in school-aged children,” said study investigator Caroline Olvera, MD, Rush University Medical Center, Chicago.
“Abrupt onset of symptoms can be seen in patients with tic disorders, although this is typically quoted as less than 10%, or even 5% is more characteristic of functional neurological disorders in general and also with psychogenic tics,” she added.
The findings were presented at the International Congress of Parkinson’s Disease and Movement Disorders.
Anxiety, other psychiatric conditions
Tic disorders typically start in childhood. However, the researchers observed an increase in the number of patients with abrupt onset of tic-like movements and vocalizations later in life, which is more often characteristic of functional neurological disorders.
To examine the profile, associated conditions, and risk factors in this population, the investigators conducted a thorough chart review of patients attending movement disorder clinics between March 2020, when the COVID pandemic was officially declared, and March 2021.
Patients with acute onset of tics were identified using the International Classification of Diseases codes for behavioral tics, tic vocalizations, and Tourette syndrome.
The charts were then narrowed down to patients with no previous diagnosis of these conditions. Most patients were videotaped for assessment by the rest of the movement disorder neurologists in the practice. Since the end of the study inclusion period in March 2021, Dr. Olvera estimates that the clinic experienced a doubling or tripling of the number of similar patients.
In the study cohort of 10 patients, the median age at presentation was 19 years (range, 15-41 years), nine were female, the gender of the other one was unknown, and the duration of tics was 8 weeks (range, 1-24 weeks) by the time they were first seen in the clinic. Four patients reported having COVID infection before tic onset.
All exhibited motor tics and nine had vocal tics. Two were diagnosed with a purely functional neurologic disorder, four with only an organic tic disorder, and four with organic tics with a functional overlay.
“All patients, including those with organic tic disorders, had a history of anxiety and also reported worsening anxiety in the setting of the COVID pandemic,” Dr. Olvera said.
The majority of patients were on a psychotropic medication prior to coming to the clinic, and these were primarily for anxiety and depression. Three patients had a history of suicidality, often very severe and leading to hospitalization, she noted.
“In terms of our conclusions from the project, we feel that this phenotype of acute explosive onset of tic-like movements and vocalizations in this older population of adults, compared with typical organic tic disorders and Tourette syndrome, appears novel to the pandemic,” she said.
She cautioned that functional and organic tics share many characteristics and therefore may be difficult to differentiate.
COVID stress
Commenting on the findings, Michele Tagliati, MD, director of the movement disorders program at Cedars-Sinai Medical Center, Los Angeles, said the research highlights how clinicians’ understanding of particular diseases can be challenged during extraordinary events such as COVID-19 and the heightened stress it causes.
“I’m not surprised that these [disorders] might have had a spike during a stressful time as COVID,” he said.
Patients are “really scared and really anxious, they’re afraid to die, and they’re afraid that their life will be over. So they might express their psychological difficulty, their discomfort, with these calls for help that look like tics. But they’re not what we consider physiological or organic things,” he added.
Dr. Tagliati added that he doesn’t believe rapid tic onset in adults is not a complication of the coronavirus infection, but rather a consequence of psychological pressure brought on by the pandemic.
Treating underlying anxiety may be a useful approach, possibly with the support of psychiatrists, which in many cases is enough to relieve the conditions and overcome the symptoms, he noted.
However, at other times, it’s not that simple, he added. Sometimes patients “fall through the cracks between neurology and psychiatry,” Dr. Tagliati said.
Dr. Olvera and Dr. Tagliati have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
Results from a large, single-center study show several cases of tic-like movements and vocalizations with abrupt onset among older adolescents and adults during the pandemic. None had a previous diagnosis of a tic disorder. Among 10 patients, two were diagnosed with a purely functional movement disorder, four with an organic tic disorder, and four with both.
“Within our movement disorders clinic specifically ... we’ve been seeing an increased number of patients with an almost explosive onset of these tic-like movements and vocalizations later in life than what is typically seen with organic tic disorders and Tourette syndrome, which is typically in school-aged children,” said study investigator Caroline Olvera, MD, Rush University Medical Center, Chicago.
“Abrupt onset of symptoms can be seen in patients with tic disorders, although this is typically quoted as less than 10%, or even 5% is more characteristic of functional neurological disorders in general and also with psychogenic tics,” she added.
The findings were presented at the International Congress of Parkinson’s Disease and Movement Disorders.
Anxiety, other psychiatric conditions
Tic disorders typically start in childhood. However, the researchers observed an increase in the number of patients with abrupt onset of tic-like movements and vocalizations later in life, which is more often characteristic of functional neurological disorders.
To examine the profile, associated conditions, and risk factors in this population, the investigators conducted a thorough chart review of patients attending movement disorder clinics between March 2020, when the COVID pandemic was officially declared, and March 2021.
Patients with acute onset of tics were identified using the International Classification of Diseases codes for behavioral tics, tic vocalizations, and Tourette syndrome.
The charts were then narrowed down to patients with no previous diagnosis of these conditions. Most patients were videotaped for assessment by the rest of the movement disorder neurologists in the practice. Since the end of the study inclusion period in March 2021, Dr. Olvera estimates that the clinic experienced a doubling or tripling of the number of similar patients.
In the study cohort of 10 patients, the median age at presentation was 19 years (range, 15-41 years), nine were female, the gender of the other one was unknown, and the duration of tics was 8 weeks (range, 1-24 weeks) by the time they were first seen in the clinic. Four patients reported having COVID infection before tic onset.
All exhibited motor tics and nine had vocal tics. Two were diagnosed with a purely functional neurologic disorder, four with only an organic tic disorder, and four with organic tics with a functional overlay.
“All patients, including those with organic tic disorders, had a history of anxiety and also reported worsening anxiety in the setting of the COVID pandemic,” Dr. Olvera said.
The majority of patients were on a psychotropic medication prior to coming to the clinic, and these were primarily for anxiety and depression. Three patients had a history of suicidality, often very severe and leading to hospitalization, she noted.
“In terms of our conclusions from the project, we feel that this phenotype of acute explosive onset of tic-like movements and vocalizations in this older population of adults, compared with typical organic tic disorders and Tourette syndrome, appears novel to the pandemic,” she said.
She cautioned that functional and organic tics share many characteristics and therefore may be difficult to differentiate.
COVID stress
Commenting on the findings, Michele Tagliati, MD, director of the movement disorders program at Cedars-Sinai Medical Center, Los Angeles, said the research highlights how clinicians’ understanding of particular diseases can be challenged during extraordinary events such as COVID-19 and the heightened stress it causes.
“I’m not surprised that these [disorders] might have had a spike during a stressful time as COVID,” he said.
Patients are “really scared and really anxious, they’re afraid to die, and they’re afraid that their life will be over. So they might express their psychological difficulty, their discomfort, with these calls for help that look like tics. But they’re not what we consider physiological or organic things,” he added.
Dr. Tagliati added that he doesn’t believe rapid tic onset in adults is not a complication of the coronavirus infection, but rather a consequence of psychological pressure brought on by the pandemic.
Treating underlying anxiety may be a useful approach, possibly with the support of psychiatrists, which in many cases is enough to relieve the conditions and overcome the symptoms, he noted.
However, at other times, it’s not that simple, he added. Sometimes patients “fall through the cracks between neurology and psychiatry,” Dr. Tagliati said.
Dr. Olvera and Dr. Tagliati have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
Results from a large, single-center study show several cases of tic-like movements and vocalizations with abrupt onset among older adolescents and adults during the pandemic. None had a previous diagnosis of a tic disorder. Among 10 patients, two were diagnosed with a purely functional movement disorder, four with an organic tic disorder, and four with both.
“Within our movement disorders clinic specifically ... we’ve been seeing an increased number of patients with an almost explosive onset of these tic-like movements and vocalizations later in life than what is typically seen with organic tic disorders and Tourette syndrome, which is typically in school-aged children,” said study investigator Caroline Olvera, MD, Rush University Medical Center, Chicago.
“Abrupt onset of symptoms can be seen in patients with tic disorders, although this is typically quoted as less than 10%, or even 5% is more characteristic of functional neurological disorders in general and also with psychogenic tics,” she added.
The findings were presented at the International Congress of Parkinson’s Disease and Movement Disorders.
Anxiety, other psychiatric conditions
Tic disorders typically start in childhood. However, the researchers observed an increase in the number of patients with abrupt onset of tic-like movements and vocalizations later in life, which is more often characteristic of functional neurological disorders.
To examine the profile, associated conditions, and risk factors in this population, the investigators conducted a thorough chart review of patients attending movement disorder clinics between March 2020, when the COVID pandemic was officially declared, and March 2021.
Patients with acute onset of tics were identified using the International Classification of Diseases codes for behavioral tics, tic vocalizations, and Tourette syndrome.
The charts were then narrowed down to patients with no previous diagnosis of these conditions. Most patients were videotaped for assessment by the rest of the movement disorder neurologists in the practice. Since the end of the study inclusion period in March 2021, Dr. Olvera estimates that the clinic experienced a doubling or tripling of the number of similar patients.
In the study cohort of 10 patients, the median age at presentation was 19 years (range, 15-41 years), nine were female, the gender of the other one was unknown, and the duration of tics was 8 weeks (range, 1-24 weeks) by the time they were first seen in the clinic. Four patients reported having COVID infection before tic onset.
All exhibited motor tics and nine had vocal tics. Two were diagnosed with a purely functional neurologic disorder, four with only an organic tic disorder, and four with organic tics with a functional overlay.
“All patients, including those with organic tic disorders, had a history of anxiety and also reported worsening anxiety in the setting of the COVID pandemic,” Dr. Olvera said.
The majority of patients were on a psychotropic medication prior to coming to the clinic, and these were primarily for anxiety and depression. Three patients had a history of suicidality, often very severe and leading to hospitalization, she noted.
“In terms of our conclusions from the project, we feel that this phenotype of acute explosive onset of tic-like movements and vocalizations in this older population of adults, compared with typical organic tic disorders and Tourette syndrome, appears novel to the pandemic,” she said.
She cautioned that functional and organic tics share many characteristics and therefore may be difficult to differentiate.
COVID stress
Commenting on the findings, Michele Tagliati, MD, director of the movement disorders program at Cedars-Sinai Medical Center, Los Angeles, said the research highlights how clinicians’ understanding of particular diseases can be challenged during extraordinary events such as COVID-19 and the heightened stress it causes.
“I’m not surprised that these [disorders] might have had a spike during a stressful time as COVID,” he said.
Patients are “really scared and really anxious, they’re afraid to die, and they’re afraid that their life will be over. So they might express their psychological difficulty, their discomfort, with these calls for help that look like tics. But they’re not what we consider physiological or organic things,” he added.
Dr. Tagliati added that he doesn’t believe rapid tic onset in adults is not a complication of the coronavirus infection, but rather a consequence of psychological pressure brought on by the pandemic.
Treating underlying anxiety may be a useful approach, possibly with the support of psychiatrists, which in many cases is enough to relieve the conditions and overcome the symptoms, he noted.
However, at other times, it’s not that simple, he added. Sometimes patients “fall through the cracks between neurology and psychiatry,” Dr. Tagliati said.
Dr. Olvera and Dr. Tagliati have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM MDS VIRTUAL CONGRESS 2021
Ten lessons learned from the pandemic, and a way forward: Report
The federal government is taking “steps in the right direction” to help control this pandemic, but there have been many hard lessons learned, according to a new report from the Association of American Medical Colleges (AAMC).
This is among 10 recommendations that address what AAMC views as systemic inadequacies in the nation’s COVID-19 response that can help advise policy makers on how to better prepare for the next pandemic.
The recommendations are:
- The White House must lead the charge and ensure coordination among departments and agencies.
- The federal government must engage industry and research universities at the outset, commit to purchasing needed supplies and therapeutics in advance.
- The federal government must ensure an effective supply chain for critical goods and materials.
- Congress must appropriate needed funding to meet public health needs.
- Federal and state governments must relax regulatory restrictions on clinical care during a national emergency.
- Both government and the private sector must invest in needed data infrastructure.
- Federal and state policies must increase supply and well-being of physicians and other health professionals.
- Congress must continue to commit to basic and clinical research.
- Federal government should expand and improve health insurance coverage.
- Stakeholders must commit to improving equity and patient-centered care through community engagement.
Current crisis ‘avoidable’
Although the Biden administration’s COVID-19 strategy is moving in the right direction, says Atul Grover, MD, PhD, executive director of the AAMC Research and Action Institute, the branch of the association that prepared the report, “the severity of this phase of the COVID-19 pandemic was avoidable.”
According to the report, only the federal government can provide the level of coordination that is needed across states and international borders to fight the virus successfully. “The response should not rely on a piecemeal approach that varies by locality and region.”
In the absence of clear federal leadership during the pandemic’s earlier phase, the report states, “key policies were either absent or conflicting across states, counties, and municipalities. Without federal direction and coordination, states were forced to compete against each other (and, sometimes, against the federal government) for supplies.”
As a recent Kaiser Health News report shows, the states are still falling short on the COVID-19 front: For example, at least 26 states have restricted the ability of their public health authorities to take action against COVID in various ways.
In an interview, William Schaffner, MD, a professor of preventive medicine and infectious diseases at Vanderbilt University, Nashville, Tenn., agrees on the need for the federal government to lead the COVID fight.
Noting that the cooperation of states with each other and with the national government is voluntary, Dr. Schaffner asserted that “subcontracting [the COVID response] to the states doesn’t work. That results in chaos and a crazy quilt of responses that persists to this day.”
Inadequate control of COVID effort
Within the federal government, the AAMC report maintains, the White House must be directly in charge of coordinating the fight against the pandemic. The AAMC calls for the establishment of a top-level office or a coordinating team to lead the COVID effort, similar to what was done during the 2014-2015 Ebola outbreak.
Earlier this year, President Biden appointed Jeffrey Zients as White House Coronavirus Response Coordinator, succeeding Deborah Birx, MD, in that role. Dr. Grover was asked in an interview why that doesn’t meet AAMC’s requirements.
“Jeff and his team are doing a good job,” Dr. Grover said. “But the reason I think we could be doing a better job is that the messaging has not been consistent across agencies and across the federal government.”
“Jeff may not have the authority to overrule individual decisions and to ensure that all decisions are integrated across organizations. Maybe that is happening, but it’s not clear to those of us who are not in the meetings every day. At a minimum, we’ve got to get the messaging right, and it needs to be more transparent.”
Dr. Grover cites a recent press conference by the Centers for Disease Control and Prevention about the national strategy for vaccine booster shots. “No one from the FDA was there,” he said. “Theoretically, [the] FDA has signed off on boosters, but their scientists were caught off guard. The administration’s messaging needs to be consistent, and that would be more likely if someone were in charge of these agencies overall,” Dr. Grover said.
Dr. Schaffner said he prefers not to comment on this point, “but I won’t argue with the observation.”
Supplies still not adequate
In light of the medical supply shortages that have plagued the COVID-19 response, the AAMC report recommends that the federal government ensure an effective supply chain for all critical goods and materials, starting with the Strategic National Stockpile (SNS), which was created in 1999 to supplement state and local medical supplies during public health emergencies.
“The SNS should enable the nation to support care for a minimum number of critically ill patients until the federal government can assure an adequate functional supply chain for a short period of time,” the AAMC report states.
The SNS was not replenished after the 2009 H1N1 pandemic and wasn’t prepared for the COVID-19 emergency, according to the report. “Despite having built up the supply over the last year, the nation is just one major outbreak or incident away from another monumental shortage of very basic needs such as gloves, masks, and gowns.”
Dr. Grover said the national stockpile now has more gowns and gloves than it did at the pandemic’s start. But he’s concerned about what might happen if a new type of pathogen emerged. “If we were to face the same kind of COVID surge we’re now facing in the unvaccinated communities more broadly across the U.S. – for example, if we got another variant that was even more infectious or deadly – I’m not sure we’d be prepared.”
Just-in-time purchasing
Hospitals were caught short when COVID struck because of their just-in-time supply chain approach, which relied on punctual deliveries of new supplies and equipment, the report states. Of course, when demand soared and every provider was competing for scarce supplies, that didn’t happen.
Now, Dr. Grover pointed out, there is still no central system to keep track of where PPE, ventilators, oxygen tanks, and other critical items are in the supply chains of hospitals and physician practices.
So, even if policymakers determined that the nation should use both the SNS and private locations to stockpile enough supplies to care for a certain number of patients for a period of time, there wouldn’t be any way to determine what was on hand or where it was stored.
Moreover, while hospitals have built up their stockpiles to prepare for new COVID surges, he expects them to go back to just-in-time purchasing when the pandemic wanes. Although health care organizations want to take good care of patients, they have financial and physical constraints on how many supplies they can store, Dr. Grover said.
Testing conundrum
An analogous challenge exists for companies that make COVID-19 tests, Dr. Grover said. “The testing companies don’t want to produce more than they’re going to be able to sell. They’re a for-profit industry.” Partly as a result, the nation has never had as many tests as it needs, according to the report.
To solve this problem, the report authors suggest that the federal government take an approach similar to that of the Trump administration’s Operation Warp Speed (OWS), which used advance funding and vaccine prepurchases to spur development.
“The CDC is unlikely to meet testing demands in future outbreaks and pandemics using existing public health lab partnerships, even under the best conditions. Industry was reluctant to mass produce testing kits for fear demand would fail to materialize; an OWS-like advance purchasing strategy and investment in private production could have reduced the spread of COVID-19 and will be critical in mitigating a future outbreak or pandemic.”
Public health infrastructure
The report also calls for Congress to appropriate “robust and continuous funding for public health infrastructure … Chronic underfunding of public health has hurt the nation’s emergency preparedness framework and contributes to health inequity.”
This applies not only to federal funding but also to state and local funding, which has primarily been allocated on a crisis-response basis, the report states.
Dr. Grover is glad that the fiscal 2022 budget legislation includes $15 billion to finance this infrastructure, but that’s only a start, he said.
Dr. Schaffner stresses the importance of improving the IT infrastructure of public health agencies. “We need a better, higher-quality mechanism for quickly gathering critical data from doctors’ offices and hospitals and sending that information through a public health stream so it can be gathered.”
“Today, data come in at the national level, sometimes slowly, sometimes in fragmented fashion, from different jurisdictions around the country, and it’s very difficult to make secure statements and plan effectively.”
Dr. Schaffner agrees with the report’s emphasis on the need for long-term planning to prepare for the next pandemic but is pessimistic about the odds of it occurring.
“This challenges us as Americans. We have notoriously short attention spans. And we like to put difficult things behind us and look to the future,” he said.
A version of this article first appeared on Medscape.com.
The federal government is taking “steps in the right direction” to help control this pandemic, but there have been many hard lessons learned, according to a new report from the Association of American Medical Colleges (AAMC).
This is among 10 recommendations that address what AAMC views as systemic inadequacies in the nation’s COVID-19 response that can help advise policy makers on how to better prepare for the next pandemic.
The recommendations are:
- The White House must lead the charge and ensure coordination among departments and agencies.
- The federal government must engage industry and research universities at the outset, commit to purchasing needed supplies and therapeutics in advance.
- The federal government must ensure an effective supply chain for critical goods and materials.
- Congress must appropriate needed funding to meet public health needs.
- Federal and state governments must relax regulatory restrictions on clinical care during a national emergency.
- Both government and the private sector must invest in needed data infrastructure.
- Federal and state policies must increase supply and well-being of physicians and other health professionals.
- Congress must continue to commit to basic and clinical research.
- Federal government should expand and improve health insurance coverage.
- Stakeholders must commit to improving equity and patient-centered care through community engagement.
Current crisis ‘avoidable’
Although the Biden administration’s COVID-19 strategy is moving in the right direction, says Atul Grover, MD, PhD, executive director of the AAMC Research and Action Institute, the branch of the association that prepared the report, “the severity of this phase of the COVID-19 pandemic was avoidable.”
According to the report, only the federal government can provide the level of coordination that is needed across states and international borders to fight the virus successfully. “The response should not rely on a piecemeal approach that varies by locality and region.”
In the absence of clear federal leadership during the pandemic’s earlier phase, the report states, “key policies were either absent or conflicting across states, counties, and municipalities. Without federal direction and coordination, states were forced to compete against each other (and, sometimes, against the federal government) for supplies.”
As a recent Kaiser Health News report shows, the states are still falling short on the COVID-19 front: For example, at least 26 states have restricted the ability of their public health authorities to take action against COVID in various ways.
In an interview, William Schaffner, MD, a professor of preventive medicine and infectious diseases at Vanderbilt University, Nashville, Tenn., agrees on the need for the federal government to lead the COVID fight.
Noting that the cooperation of states with each other and with the national government is voluntary, Dr. Schaffner asserted that “subcontracting [the COVID response] to the states doesn’t work. That results in chaos and a crazy quilt of responses that persists to this day.”
Inadequate control of COVID effort
Within the federal government, the AAMC report maintains, the White House must be directly in charge of coordinating the fight against the pandemic. The AAMC calls for the establishment of a top-level office or a coordinating team to lead the COVID effort, similar to what was done during the 2014-2015 Ebola outbreak.
Earlier this year, President Biden appointed Jeffrey Zients as White House Coronavirus Response Coordinator, succeeding Deborah Birx, MD, in that role. Dr. Grover was asked in an interview why that doesn’t meet AAMC’s requirements.
“Jeff and his team are doing a good job,” Dr. Grover said. “But the reason I think we could be doing a better job is that the messaging has not been consistent across agencies and across the federal government.”
“Jeff may not have the authority to overrule individual decisions and to ensure that all decisions are integrated across organizations. Maybe that is happening, but it’s not clear to those of us who are not in the meetings every day. At a minimum, we’ve got to get the messaging right, and it needs to be more transparent.”
Dr. Grover cites a recent press conference by the Centers for Disease Control and Prevention about the national strategy for vaccine booster shots. “No one from the FDA was there,” he said. “Theoretically, [the] FDA has signed off on boosters, but their scientists were caught off guard. The administration’s messaging needs to be consistent, and that would be more likely if someone were in charge of these agencies overall,” Dr. Grover said.
Dr. Schaffner said he prefers not to comment on this point, “but I won’t argue with the observation.”
Supplies still not adequate
In light of the medical supply shortages that have plagued the COVID-19 response, the AAMC report recommends that the federal government ensure an effective supply chain for all critical goods and materials, starting with the Strategic National Stockpile (SNS), which was created in 1999 to supplement state and local medical supplies during public health emergencies.
“The SNS should enable the nation to support care for a minimum number of critically ill patients until the federal government can assure an adequate functional supply chain for a short period of time,” the AAMC report states.
The SNS was not replenished after the 2009 H1N1 pandemic and wasn’t prepared for the COVID-19 emergency, according to the report. “Despite having built up the supply over the last year, the nation is just one major outbreak or incident away from another monumental shortage of very basic needs such as gloves, masks, and gowns.”
Dr. Grover said the national stockpile now has more gowns and gloves than it did at the pandemic’s start. But he’s concerned about what might happen if a new type of pathogen emerged. “If we were to face the same kind of COVID surge we’re now facing in the unvaccinated communities more broadly across the U.S. – for example, if we got another variant that was even more infectious or deadly – I’m not sure we’d be prepared.”
Just-in-time purchasing
Hospitals were caught short when COVID struck because of their just-in-time supply chain approach, which relied on punctual deliveries of new supplies and equipment, the report states. Of course, when demand soared and every provider was competing for scarce supplies, that didn’t happen.
Now, Dr. Grover pointed out, there is still no central system to keep track of where PPE, ventilators, oxygen tanks, and other critical items are in the supply chains of hospitals and physician practices.
So, even if policymakers determined that the nation should use both the SNS and private locations to stockpile enough supplies to care for a certain number of patients for a period of time, there wouldn’t be any way to determine what was on hand or where it was stored.
Moreover, while hospitals have built up their stockpiles to prepare for new COVID surges, he expects them to go back to just-in-time purchasing when the pandemic wanes. Although health care organizations want to take good care of patients, they have financial and physical constraints on how many supplies they can store, Dr. Grover said.
Testing conundrum
An analogous challenge exists for companies that make COVID-19 tests, Dr. Grover said. “The testing companies don’t want to produce more than they’re going to be able to sell. They’re a for-profit industry.” Partly as a result, the nation has never had as many tests as it needs, according to the report.
To solve this problem, the report authors suggest that the federal government take an approach similar to that of the Trump administration’s Operation Warp Speed (OWS), which used advance funding and vaccine prepurchases to spur development.
“The CDC is unlikely to meet testing demands in future outbreaks and pandemics using existing public health lab partnerships, even under the best conditions. Industry was reluctant to mass produce testing kits for fear demand would fail to materialize; an OWS-like advance purchasing strategy and investment in private production could have reduced the spread of COVID-19 and will be critical in mitigating a future outbreak or pandemic.”
Public health infrastructure
The report also calls for Congress to appropriate “robust and continuous funding for public health infrastructure … Chronic underfunding of public health has hurt the nation’s emergency preparedness framework and contributes to health inequity.”
This applies not only to federal funding but also to state and local funding, which has primarily been allocated on a crisis-response basis, the report states.
Dr. Grover is glad that the fiscal 2022 budget legislation includes $15 billion to finance this infrastructure, but that’s only a start, he said.
Dr. Schaffner stresses the importance of improving the IT infrastructure of public health agencies. “We need a better, higher-quality mechanism for quickly gathering critical data from doctors’ offices and hospitals and sending that information through a public health stream so it can be gathered.”
“Today, data come in at the national level, sometimes slowly, sometimes in fragmented fashion, from different jurisdictions around the country, and it’s very difficult to make secure statements and plan effectively.”
Dr. Schaffner agrees with the report’s emphasis on the need for long-term planning to prepare for the next pandemic but is pessimistic about the odds of it occurring.
“This challenges us as Americans. We have notoriously short attention spans. And we like to put difficult things behind us and look to the future,” he said.
A version of this article first appeared on Medscape.com.
The federal government is taking “steps in the right direction” to help control this pandemic, but there have been many hard lessons learned, according to a new report from the Association of American Medical Colleges (AAMC).
This is among 10 recommendations that address what AAMC views as systemic inadequacies in the nation’s COVID-19 response that can help advise policy makers on how to better prepare for the next pandemic.
The recommendations are:
- The White House must lead the charge and ensure coordination among departments and agencies.
- The federal government must engage industry and research universities at the outset, commit to purchasing needed supplies and therapeutics in advance.
- The federal government must ensure an effective supply chain for critical goods and materials.
- Congress must appropriate needed funding to meet public health needs.
- Federal and state governments must relax regulatory restrictions on clinical care during a national emergency.
- Both government and the private sector must invest in needed data infrastructure.
- Federal and state policies must increase supply and well-being of physicians and other health professionals.
- Congress must continue to commit to basic and clinical research.
- Federal government should expand and improve health insurance coverage.
- Stakeholders must commit to improving equity and patient-centered care through community engagement.
Current crisis ‘avoidable’
Although the Biden administration’s COVID-19 strategy is moving in the right direction, says Atul Grover, MD, PhD, executive director of the AAMC Research and Action Institute, the branch of the association that prepared the report, “the severity of this phase of the COVID-19 pandemic was avoidable.”
According to the report, only the federal government can provide the level of coordination that is needed across states and international borders to fight the virus successfully. “The response should not rely on a piecemeal approach that varies by locality and region.”
In the absence of clear federal leadership during the pandemic’s earlier phase, the report states, “key policies were either absent or conflicting across states, counties, and municipalities. Without federal direction and coordination, states were forced to compete against each other (and, sometimes, against the federal government) for supplies.”
As a recent Kaiser Health News report shows, the states are still falling short on the COVID-19 front: For example, at least 26 states have restricted the ability of their public health authorities to take action against COVID in various ways.
In an interview, William Schaffner, MD, a professor of preventive medicine and infectious diseases at Vanderbilt University, Nashville, Tenn., agrees on the need for the federal government to lead the COVID fight.
Noting that the cooperation of states with each other and with the national government is voluntary, Dr. Schaffner asserted that “subcontracting [the COVID response] to the states doesn’t work. That results in chaos and a crazy quilt of responses that persists to this day.”
Inadequate control of COVID effort
Within the federal government, the AAMC report maintains, the White House must be directly in charge of coordinating the fight against the pandemic. The AAMC calls for the establishment of a top-level office or a coordinating team to lead the COVID effort, similar to what was done during the 2014-2015 Ebola outbreak.
Earlier this year, President Biden appointed Jeffrey Zients as White House Coronavirus Response Coordinator, succeeding Deborah Birx, MD, in that role. Dr. Grover was asked in an interview why that doesn’t meet AAMC’s requirements.
“Jeff and his team are doing a good job,” Dr. Grover said. “But the reason I think we could be doing a better job is that the messaging has not been consistent across agencies and across the federal government.”
“Jeff may not have the authority to overrule individual decisions and to ensure that all decisions are integrated across organizations. Maybe that is happening, but it’s not clear to those of us who are not in the meetings every day. At a minimum, we’ve got to get the messaging right, and it needs to be more transparent.”
Dr. Grover cites a recent press conference by the Centers for Disease Control and Prevention about the national strategy for vaccine booster shots. “No one from the FDA was there,” he said. “Theoretically, [the] FDA has signed off on boosters, but their scientists were caught off guard. The administration’s messaging needs to be consistent, and that would be more likely if someone were in charge of these agencies overall,” Dr. Grover said.
Dr. Schaffner said he prefers not to comment on this point, “but I won’t argue with the observation.”
Supplies still not adequate
In light of the medical supply shortages that have plagued the COVID-19 response, the AAMC report recommends that the federal government ensure an effective supply chain for all critical goods and materials, starting with the Strategic National Stockpile (SNS), which was created in 1999 to supplement state and local medical supplies during public health emergencies.
“The SNS should enable the nation to support care for a minimum number of critically ill patients until the federal government can assure an adequate functional supply chain for a short period of time,” the AAMC report states.
The SNS was not replenished after the 2009 H1N1 pandemic and wasn’t prepared for the COVID-19 emergency, according to the report. “Despite having built up the supply over the last year, the nation is just one major outbreak or incident away from another monumental shortage of very basic needs such as gloves, masks, and gowns.”
Dr. Grover said the national stockpile now has more gowns and gloves than it did at the pandemic’s start. But he’s concerned about what might happen if a new type of pathogen emerged. “If we were to face the same kind of COVID surge we’re now facing in the unvaccinated communities more broadly across the U.S. – for example, if we got another variant that was even more infectious or deadly – I’m not sure we’d be prepared.”
Just-in-time purchasing
Hospitals were caught short when COVID struck because of their just-in-time supply chain approach, which relied on punctual deliveries of new supplies and equipment, the report states. Of course, when demand soared and every provider was competing for scarce supplies, that didn’t happen.
Now, Dr. Grover pointed out, there is still no central system to keep track of where PPE, ventilators, oxygen tanks, and other critical items are in the supply chains of hospitals and physician practices.
So, even if policymakers determined that the nation should use both the SNS and private locations to stockpile enough supplies to care for a certain number of patients for a period of time, there wouldn’t be any way to determine what was on hand or where it was stored.
Moreover, while hospitals have built up their stockpiles to prepare for new COVID surges, he expects them to go back to just-in-time purchasing when the pandemic wanes. Although health care organizations want to take good care of patients, they have financial and physical constraints on how many supplies they can store, Dr. Grover said.
Testing conundrum
An analogous challenge exists for companies that make COVID-19 tests, Dr. Grover said. “The testing companies don’t want to produce more than they’re going to be able to sell. They’re a for-profit industry.” Partly as a result, the nation has never had as many tests as it needs, according to the report.
To solve this problem, the report authors suggest that the federal government take an approach similar to that of the Trump administration’s Operation Warp Speed (OWS), which used advance funding and vaccine prepurchases to spur development.
“The CDC is unlikely to meet testing demands in future outbreaks and pandemics using existing public health lab partnerships, even under the best conditions. Industry was reluctant to mass produce testing kits for fear demand would fail to materialize; an OWS-like advance purchasing strategy and investment in private production could have reduced the spread of COVID-19 and will be critical in mitigating a future outbreak or pandemic.”
Public health infrastructure
The report also calls for Congress to appropriate “robust and continuous funding for public health infrastructure … Chronic underfunding of public health has hurt the nation’s emergency preparedness framework and contributes to health inequity.”
This applies not only to federal funding but also to state and local funding, which has primarily been allocated on a crisis-response basis, the report states.
Dr. Grover is glad that the fiscal 2022 budget legislation includes $15 billion to finance this infrastructure, but that’s only a start, he said.
Dr. Schaffner stresses the importance of improving the IT infrastructure of public health agencies. “We need a better, higher-quality mechanism for quickly gathering critical data from doctors’ offices and hospitals and sending that information through a public health stream so it can be gathered.”
“Today, data come in at the national level, sometimes slowly, sometimes in fragmented fashion, from different jurisdictions around the country, and it’s very difficult to make secure statements and plan effectively.”
Dr. Schaffner agrees with the report’s emphasis on the need for long-term planning to prepare for the next pandemic but is pessimistic about the odds of it occurring.
“This challenges us as Americans. We have notoriously short attention spans. And we like to put difficult things behind us and look to the future,” he said.
A version of this article first appeared on Medscape.com.
When children and teens with cancer get COVID-19
Although most children and adolescents with cancer have mild illness from COVID-19 infection, some do experience severe disease and a small percentage even die, according to a recent analysis.
The findings, published online in Lancet Oncology, represent the first global registry data spanning different income groups to report COVID-19 outcomes in pediatric oncology patients.
“We wanted to create a global pool of evidence to answer the question: Do we see severe [COVID-19] infection [in children with cancer]?” corresponding author Sheena Mukkada, MD, St. Jude Children’s Research Hospital, Memphis, said in an interview.
In a cohort of 1,319 pediatric patients followed for 30 days, Dr. Mukkada and colleagues reported that 80% of these patients had asymptomatic to moderate disease from COVID-19, while 1 in 5 experienced severe or critical illness and almost 4% died – four times the mortality rate observed in published cohorts of general pediatric patients.
The results highlight that “children and adolescents with cancer generally recover without incident from COVID-19, but can have a severe course of infection,” the authors concluded.
And knowing that some children can get very sick, investigators wanted “to identify who these patients are so that we can prioritize and protect that group,” she added.
Echoing that sentiment, Kathy Pritchard-Jones, MD, president of the International Society of Paediatric Oncology and coauthor on the study, noted in a press release that, “by working together to create this global registry, we have enabled hospitals around the world to rapidly share and learn how COVID-19 is affecting children with cancer.”
Dr. Pritchard-Jones commented that overall these results provide reassurance that “many children can continue their cancer treatment safely, but they also highlight important clinical features that may predict a more severe clinical course and the need for greater vigilance for some patients.”
Inside the Global Registry data
The Global Registry of COVID-19 in Childhood Cancer, created jointly by St. Jude Children’s Research Hospital and SIOP, included data from 131 institutions in 45 countries. Children recruited into the registry between April 2020 and February 2021 ranged in age from infancy to 18 years old.
Most patients remained asymptomatic (35%) or experienced mild to moderate illness (45%), though 20% did develop severe or critical illness.
The investigators highlighted several factors associated with a greater risk of developing more severe illness from COVID-19, which included cancer type, intensity of therapy, age, absolute lymphocyte count, and presence of comorbidities or COVID-19 symptoms.
Notably, more than 80% of either severe or critical infections occurred in patients with hematologic malignancies – with 56% of cases in patients with acute lymphoblastic lymphoma or acute lymphoblastic leukemia – followed by extracranial solid tumors (15.8%), and central nervous system tumors (2.7%).
In patients with acute lymphoblastic leukemia or acute lymphoblastic lymphoma, severe or critical disease was most common in those receiving induction therapy (30%), relapse or refractory therapy (30%), and those in the maintenance or continuation phase of therapy (19%).
Older age was associated with a higher likelihood of having severe disease – with the lowest risk in infants (9.7%) and the highest in the 15- to 18-year-old cohort (27.3%).
Patients with lymphopenia who had an absolute lymphocyte count of 300 cells per mm3 or less and an absolute neutrophil count of 500 cells per mm3 or more also had an elevated risk of severe illness from COVID-19.
Regarding whether the presence of lymphopenia or neutropenia should change the treatment approach, Dr. Mukkada noted that, when possible, these patients should receive antiviral treatment, such as remdesivir, if the center has antivirals, or be prioritized for hospital admission.
Modifying cancer treatment might be recommended if patients are highly lymphopenic or have very low neutrophil counts, but a more effective strategy is simply to ensure that age-eligible children and adolescents with cancer or who have had a hematopoietic stem-cell transplantation have been fully vaccinated against COVID-19. For children who are not yet age-eligible, everyone around them should be vaccinated.
Pediatric patients in low- and middle-income countries were also more likely to have severe or critical outcomes from COVID-19 (41.7%), compared with patients in other income groups (23.9%).
The impact of COVID-19 “has been felt in every corner of the world, but particularly in low- and middle-income countries, compared to high-income countries,” senior author Carlos Rodriguez-Galindo, MD, global director at St. Jude, said in a statement.
In terms of the intersection of cancer treatment and COVID diagnosis, almost 83% of pediatric patients were receiving treatment for their cancer. Chemotherapy was withheld in about 45% of these patients and some modification to the treatment regimen occurred in almost 56% of participants on active therapy.
“Treatment modifications were least common in patients from upper-middle–income countries, compared with other income groups,” the authors wrote.
Although an interesting observation, Dr. Mukkada noted that the registry data could not explain why treatment modifications occurred less frequently in upper-middle income countries as opposed to high-income and lower-income countries.
U.K. Monitoring Project
Not all studies, however, have found that COVID-19 infection is significantly more severe in children with cancer. In a 2020 report from the U.K. Paediatric Coronavirus Cancer Monitoring Project, researchers evaluated all children in the United Kingdom under the age of 16 diagnosed with COVID and cancer.
“[Given that] we had complete coverage of every center in the U.K. that cares for children with cancer, we are confident that we picked up at least all the severe or critical cases,” lead author Gerard Millen, MD, honorary clinical research fellow, University of Birmingham (England), said in an interview.
Between March 2020 and July 2020, Dr. Millen and colleagues identified 54 positive cases of COVID-19, 15 (28%) of which were asymptomatic, 34 (63%) mild, and 4 (7.4%) severe or critical – more in line with the incidence of severe illness reported in the general pediatric population.
“Thankfully, we had no children with cancer in the U.K. who died from COVID-19,” Dr. Millen noted. “Overall, in the U.K., we have taken the approach that the majority of children with cancer in this country are at very low risk from COVID-19 and that we do not have good evidence to modify their treatment.”
Dr. Millen pointed out that the data in the U.K. study were “remarkably similar” to those from the high-income countries in the global St. Jude/SIOP cohort, where 7.4% of patients in that cohort had severe or critical disease, compared with 7.4% of patients from their own U.K. cohort.
“I think many of the key differences between the two cohorts reflect the fact that access to treatment in many low- to middle-income countries is more challenging with many factors contributing to overall poorer outcomes for both cancer and noncancer metrics,” Dr. Millen said.
Both the U.K. and registry studies were performed prior to vaccinations becoming available to older children, and before the emergence of certain variants, including the Delta variant, which is responsible for the most recent surge of COVID-19 infections around the world.
Data on COVID-19 vaccination in children with cancer are limited but promising so far.
As for whether the Delta variant might affect outcomes for children with cancer and COVID-19, Dr. Mukkada could only speculate, but she noted that “what we are hearing anecdotally about the [Delta] disease being more severe, even in patients who don’t have cancer, is leading us to say that we can’t close the registry yet. We are still actively enrolling children.”
The study was funded by the American Lebanese Syrian Associated Charities and the National Cancer Institute. The study authors and Dr. Millen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Although most children and adolescents with cancer have mild illness from COVID-19 infection, some do experience severe disease and a small percentage even die, according to a recent analysis.
The findings, published online in Lancet Oncology, represent the first global registry data spanning different income groups to report COVID-19 outcomes in pediatric oncology patients.
“We wanted to create a global pool of evidence to answer the question: Do we see severe [COVID-19] infection [in children with cancer]?” corresponding author Sheena Mukkada, MD, St. Jude Children’s Research Hospital, Memphis, said in an interview.
In a cohort of 1,319 pediatric patients followed for 30 days, Dr. Mukkada and colleagues reported that 80% of these patients had asymptomatic to moderate disease from COVID-19, while 1 in 5 experienced severe or critical illness and almost 4% died – four times the mortality rate observed in published cohorts of general pediatric patients.
The results highlight that “children and adolescents with cancer generally recover without incident from COVID-19, but can have a severe course of infection,” the authors concluded.
And knowing that some children can get very sick, investigators wanted “to identify who these patients are so that we can prioritize and protect that group,” she added.
Echoing that sentiment, Kathy Pritchard-Jones, MD, president of the International Society of Paediatric Oncology and coauthor on the study, noted in a press release that, “by working together to create this global registry, we have enabled hospitals around the world to rapidly share and learn how COVID-19 is affecting children with cancer.”
Dr. Pritchard-Jones commented that overall these results provide reassurance that “many children can continue their cancer treatment safely, but they also highlight important clinical features that may predict a more severe clinical course and the need for greater vigilance for some patients.”
Inside the Global Registry data
The Global Registry of COVID-19 in Childhood Cancer, created jointly by St. Jude Children’s Research Hospital and SIOP, included data from 131 institutions in 45 countries. Children recruited into the registry between April 2020 and February 2021 ranged in age from infancy to 18 years old.
Most patients remained asymptomatic (35%) or experienced mild to moderate illness (45%), though 20% did develop severe or critical illness.
The investigators highlighted several factors associated with a greater risk of developing more severe illness from COVID-19, which included cancer type, intensity of therapy, age, absolute lymphocyte count, and presence of comorbidities or COVID-19 symptoms.
Notably, more than 80% of either severe or critical infections occurred in patients with hematologic malignancies – with 56% of cases in patients with acute lymphoblastic lymphoma or acute lymphoblastic leukemia – followed by extracranial solid tumors (15.8%), and central nervous system tumors (2.7%).
In patients with acute lymphoblastic leukemia or acute lymphoblastic lymphoma, severe or critical disease was most common in those receiving induction therapy (30%), relapse or refractory therapy (30%), and those in the maintenance or continuation phase of therapy (19%).
Older age was associated with a higher likelihood of having severe disease – with the lowest risk in infants (9.7%) and the highest in the 15- to 18-year-old cohort (27.3%).
Patients with lymphopenia who had an absolute lymphocyte count of 300 cells per mm3 or less and an absolute neutrophil count of 500 cells per mm3 or more also had an elevated risk of severe illness from COVID-19.
Regarding whether the presence of lymphopenia or neutropenia should change the treatment approach, Dr. Mukkada noted that, when possible, these patients should receive antiviral treatment, such as remdesivir, if the center has antivirals, or be prioritized for hospital admission.
Modifying cancer treatment might be recommended if patients are highly lymphopenic or have very low neutrophil counts, but a more effective strategy is simply to ensure that age-eligible children and adolescents with cancer or who have had a hematopoietic stem-cell transplantation have been fully vaccinated against COVID-19. For children who are not yet age-eligible, everyone around them should be vaccinated.
Pediatric patients in low- and middle-income countries were also more likely to have severe or critical outcomes from COVID-19 (41.7%), compared with patients in other income groups (23.9%).
The impact of COVID-19 “has been felt in every corner of the world, but particularly in low- and middle-income countries, compared to high-income countries,” senior author Carlos Rodriguez-Galindo, MD, global director at St. Jude, said in a statement.
In terms of the intersection of cancer treatment and COVID diagnosis, almost 83% of pediatric patients were receiving treatment for their cancer. Chemotherapy was withheld in about 45% of these patients and some modification to the treatment regimen occurred in almost 56% of participants on active therapy.
“Treatment modifications were least common in patients from upper-middle–income countries, compared with other income groups,” the authors wrote.
Although an interesting observation, Dr. Mukkada noted that the registry data could not explain why treatment modifications occurred less frequently in upper-middle income countries as opposed to high-income and lower-income countries.
U.K. Monitoring Project
Not all studies, however, have found that COVID-19 infection is significantly more severe in children with cancer. In a 2020 report from the U.K. Paediatric Coronavirus Cancer Monitoring Project, researchers evaluated all children in the United Kingdom under the age of 16 diagnosed with COVID and cancer.
“[Given that] we had complete coverage of every center in the U.K. that cares for children with cancer, we are confident that we picked up at least all the severe or critical cases,” lead author Gerard Millen, MD, honorary clinical research fellow, University of Birmingham (England), said in an interview.
Between March 2020 and July 2020, Dr. Millen and colleagues identified 54 positive cases of COVID-19, 15 (28%) of which were asymptomatic, 34 (63%) mild, and 4 (7.4%) severe or critical – more in line with the incidence of severe illness reported in the general pediatric population.
“Thankfully, we had no children with cancer in the U.K. who died from COVID-19,” Dr. Millen noted. “Overall, in the U.K., we have taken the approach that the majority of children with cancer in this country are at very low risk from COVID-19 and that we do not have good evidence to modify their treatment.”
Dr. Millen pointed out that the data in the U.K. study were “remarkably similar” to those from the high-income countries in the global St. Jude/SIOP cohort, where 7.4% of patients in that cohort had severe or critical disease, compared with 7.4% of patients from their own U.K. cohort.
“I think many of the key differences between the two cohorts reflect the fact that access to treatment in many low- to middle-income countries is more challenging with many factors contributing to overall poorer outcomes for both cancer and noncancer metrics,” Dr. Millen said.
Both the U.K. and registry studies were performed prior to vaccinations becoming available to older children, and before the emergence of certain variants, including the Delta variant, which is responsible for the most recent surge of COVID-19 infections around the world.
Data on COVID-19 vaccination in children with cancer are limited but promising so far.
As for whether the Delta variant might affect outcomes for children with cancer and COVID-19, Dr. Mukkada could only speculate, but she noted that “what we are hearing anecdotally about the [Delta] disease being more severe, even in patients who don’t have cancer, is leading us to say that we can’t close the registry yet. We are still actively enrolling children.”
The study was funded by the American Lebanese Syrian Associated Charities and the National Cancer Institute. The study authors and Dr. Millen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Although most children and adolescents with cancer have mild illness from COVID-19 infection, some do experience severe disease and a small percentage even die, according to a recent analysis.
The findings, published online in Lancet Oncology, represent the first global registry data spanning different income groups to report COVID-19 outcomes in pediatric oncology patients.
“We wanted to create a global pool of evidence to answer the question: Do we see severe [COVID-19] infection [in children with cancer]?” corresponding author Sheena Mukkada, MD, St. Jude Children’s Research Hospital, Memphis, said in an interview.
In a cohort of 1,319 pediatric patients followed for 30 days, Dr. Mukkada and colleagues reported that 80% of these patients had asymptomatic to moderate disease from COVID-19, while 1 in 5 experienced severe or critical illness and almost 4% died – four times the mortality rate observed in published cohorts of general pediatric patients.
The results highlight that “children and adolescents with cancer generally recover without incident from COVID-19, but can have a severe course of infection,” the authors concluded.
And knowing that some children can get very sick, investigators wanted “to identify who these patients are so that we can prioritize and protect that group,” she added.
Echoing that sentiment, Kathy Pritchard-Jones, MD, president of the International Society of Paediatric Oncology and coauthor on the study, noted in a press release that, “by working together to create this global registry, we have enabled hospitals around the world to rapidly share and learn how COVID-19 is affecting children with cancer.”
Dr. Pritchard-Jones commented that overall these results provide reassurance that “many children can continue their cancer treatment safely, but they also highlight important clinical features that may predict a more severe clinical course and the need for greater vigilance for some patients.”
Inside the Global Registry data
The Global Registry of COVID-19 in Childhood Cancer, created jointly by St. Jude Children’s Research Hospital and SIOP, included data from 131 institutions in 45 countries. Children recruited into the registry between April 2020 and February 2021 ranged in age from infancy to 18 years old.
Most patients remained asymptomatic (35%) or experienced mild to moderate illness (45%), though 20% did develop severe or critical illness.
The investigators highlighted several factors associated with a greater risk of developing more severe illness from COVID-19, which included cancer type, intensity of therapy, age, absolute lymphocyte count, and presence of comorbidities or COVID-19 symptoms.
Notably, more than 80% of either severe or critical infections occurred in patients with hematologic malignancies – with 56% of cases in patients with acute lymphoblastic lymphoma or acute lymphoblastic leukemia – followed by extracranial solid tumors (15.8%), and central nervous system tumors (2.7%).
In patients with acute lymphoblastic leukemia or acute lymphoblastic lymphoma, severe or critical disease was most common in those receiving induction therapy (30%), relapse or refractory therapy (30%), and those in the maintenance or continuation phase of therapy (19%).
Older age was associated with a higher likelihood of having severe disease – with the lowest risk in infants (9.7%) and the highest in the 15- to 18-year-old cohort (27.3%).
Patients with lymphopenia who had an absolute lymphocyte count of 300 cells per mm3 or less and an absolute neutrophil count of 500 cells per mm3 or more also had an elevated risk of severe illness from COVID-19.
Regarding whether the presence of lymphopenia or neutropenia should change the treatment approach, Dr. Mukkada noted that, when possible, these patients should receive antiviral treatment, such as remdesivir, if the center has antivirals, or be prioritized for hospital admission.
Modifying cancer treatment might be recommended if patients are highly lymphopenic or have very low neutrophil counts, but a more effective strategy is simply to ensure that age-eligible children and adolescents with cancer or who have had a hematopoietic stem-cell transplantation have been fully vaccinated against COVID-19. For children who are not yet age-eligible, everyone around them should be vaccinated.
Pediatric patients in low- and middle-income countries were also more likely to have severe or critical outcomes from COVID-19 (41.7%), compared with patients in other income groups (23.9%).
The impact of COVID-19 “has been felt in every corner of the world, but particularly in low- and middle-income countries, compared to high-income countries,” senior author Carlos Rodriguez-Galindo, MD, global director at St. Jude, said in a statement.
In terms of the intersection of cancer treatment and COVID diagnosis, almost 83% of pediatric patients were receiving treatment for their cancer. Chemotherapy was withheld in about 45% of these patients and some modification to the treatment regimen occurred in almost 56% of participants on active therapy.
“Treatment modifications were least common in patients from upper-middle–income countries, compared with other income groups,” the authors wrote.
Although an interesting observation, Dr. Mukkada noted that the registry data could not explain why treatment modifications occurred less frequently in upper-middle income countries as opposed to high-income and lower-income countries.
U.K. Monitoring Project
Not all studies, however, have found that COVID-19 infection is significantly more severe in children with cancer. In a 2020 report from the U.K. Paediatric Coronavirus Cancer Monitoring Project, researchers evaluated all children in the United Kingdom under the age of 16 diagnosed with COVID and cancer.
“[Given that] we had complete coverage of every center in the U.K. that cares for children with cancer, we are confident that we picked up at least all the severe or critical cases,” lead author Gerard Millen, MD, honorary clinical research fellow, University of Birmingham (England), said in an interview.
Between March 2020 and July 2020, Dr. Millen and colleagues identified 54 positive cases of COVID-19, 15 (28%) of which were asymptomatic, 34 (63%) mild, and 4 (7.4%) severe or critical – more in line with the incidence of severe illness reported in the general pediatric population.
“Thankfully, we had no children with cancer in the U.K. who died from COVID-19,” Dr. Millen noted. “Overall, in the U.K., we have taken the approach that the majority of children with cancer in this country are at very low risk from COVID-19 and that we do not have good evidence to modify their treatment.”
Dr. Millen pointed out that the data in the U.K. study were “remarkably similar” to those from the high-income countries in the global St. Jude/SIOP cohort, where 7.4% of patients in that cohort had severe or critical disease, compared with 7.4% of patients from their own U.K. cohort.
“I think many of the key differences between the two cohorts reflect the fact that access to treatment in many low- to middle-income countries is more challenging with many factors contributing to overall poorer outcomes for both cancer and noncancer metrics,” Dr. Millen said.
Both the U.K. and registry studies were performed prior to vaccinations becoming available to older children, and before the emergence of certain variants, including the Delta variant, which is responsible for the most recent surge of COVID-19 infections around the world.
Data on COVID-19 vaccination in children with cancer are limited but promising so far.
As for whether the Delta variant might affect outcomes for children with cancer and COVID-19, Dr. Mukkada could only speculate, but she noted that “what we are hearing anecdotally about the [Delta] disease being more severe, even in patients who don’t have cancer, is leading us to say that we can’t close the registry yet. We are still actively enrolling children.”
The study was funded by the American Lebanese Syrian Associated Charities and the National Cancer Institute. The study authors and Dr. Millen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 causes major interruption in global HIV progress
“We’ve been set back by COVID but we’ve seen remarkable resilience, a lot of innovation and creativity,” Siobhan Crowley MD, head of HIV at the Global Fund, said in an interview.
“If you consider that 21.9 million people are getting antiretrovirals at this point through the Global Fund, I think that needs to be appreciated. Ten years ago, that wouldn’t have been the case; all of those people would have disappeared into the ethers,” she said.
Through close partnerships with the U.S. Agency for International Development, the U.S. President’s Emergency Plan for AIDS Relief, and other Western countries and organizations, the Global Fund has invested $22.7 billion in programs to prevent and treat HIV and AIDS, and $3.8 billion in tuberculosis (TB)/HIV programs, according to the organization’s 2021 Results Report.
But the report also underscores the significant effect that the COVID-19 pandemic has had on funded countries’ progress toward achieving renewed 90-90-90 targets for HIV testing/diagnosis, treatment, and viral suppression by 2030.
The setbacks have been challenging and have touched nearly every service from prevention to treatment. According to the report, between 2019 and 2020:
- Voluntary male circumcision declined by 27%.
- Numbers reached by HIV prevention programs fell by 11%.
- 4.5% fewer mothers received medications to prevent HIV transmission to their babies.
- HIV testing services, including initiation, decreased by 22%.
The numbers tell only a part of the story, according to Dr. Crowley.
“We put in place an emergency mechanism to make funds available for countries to do everything except vaccines in support of COVID,” Dr. Crowley explained. (As of August 2021, these funds had been allocated to 107 countries and 16 multicountry programs.)
Countries were advised that they could use the emergency funds three different ways: 1) for COVID-specific purposes (e.g., diagnostics, oxygen, personal protective equipment; 2) to support mitigation strategies geared toward protecting existing HIV, tuberculosis, and malaria programs and getting them back on track; and 3) for so-called “health system fixes,” such as investing in data systems to track COVID, HIV, and other core diseases, as well as the community workforce.
With regard to HIV, each country supported by the Global Fund was asked to ensure that multimonth (3-6 months) dispensing was implemented and/or accelerated so that patients could avoid congested facilities, and, wherever possible, that drugs were delivered or accessed outside the facility. One example of the success of this effort was found in South Africa, where the number of people on antiretrovirals increased almost threefold, from 1.2 million to 4.2 million people.
Countries also were asked to adapt HIV testing procedures by, for example, moving organized testing out of the facilities and into neighborhoods to meet people where they are. Rapid diagnostic testing and triage care linkage using technologies such as WhatsApp were the result, as were opportunities for home testing which, Dr. Crowley noted, remains a critical component of the overall strategy.
“The self-test is important for two reasons, not just because you are trying to find people with HIV, but also, when people know that they’re negative, they know what they can or should do to stay negative,” she said. “It’s quite a powerful motivator.”
Self-testing might also help countries motivate the 6 million people who know that they have HIV but are not on treatment. But there are still 4.1 million residing in these countries who aren’t aware that they are infected, according to the report. This figure is especially troubling, considering that some may also be harboring TB coinfections, including multidrug-resistant TB (MDR-TB).
The imperfect storm globally and in the U.S.
“One of the things that was striking in the report was the decline in the number of people reached with testing and prevention services,” Chris Beyrer, MD, MPH, the Desmond M. Tutu Professor of Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health in Baltimore, said in an interview. Dr. Beyrer was not involved in the report’s development.
“You know, a 10% decline in 1 year to reach people in need is substantial,” he said. “Let’s say it continues; many people are predicting that we won’t have reasonable coverage for low-income countries with COVID until 2023. That adds up to a substantial decline in people reached with these services.”
Dr. Beyrer also expressed concern about the convergence of HIV and TB in already overburdened, fragile health care systems. “Globally, the No. 1 cause of death for people living with HIV is TB, and of course, it’s highly transmissible. So, in many high-burden countries, children are exposed, typically from household members early on, and so the number of people with latent TB infection is just enormous.
“If you look at the report, the worst outcomes are MDR-TB. Those multidrug-resistant and extensively-drug-resistant strains are really a threat to everybody,” Dr. Beyrer said.
But it’s not time for U.S. providers to rest on their laurels either. Dr. Beyrer noted that the 22% decline in HIV testing reported by the Global Fund is similar to what has been happening in the United States with elective procedures such as HIV testing and even preventive procedures like medical male circumcision.
“It’s very clear here in the Global Fund data that the majority of new infections worldwide are in key populations [that] include gay and bisexual men, men who have sex with men, transgender women who have sex with men, people who inject drugs, and sex workers of all genders. Those are people who already faced barriers to health care access and were made worse by COVID.”
Dr. Beyrer noted that, according to the Centers for Disease Control and Prevention, in 2019 in the United States, 68% of new HIV infections occurred in gay and bisexual men, and the effect that COVID-19 will have is still unknown. He also noted the similarity between the most marginalized populations in the Global Fund report and African American men, who have not realized the same increase in the use of preexposure prophylaxis or the same decline in new infections as have their White counterparts.
“It’s also where we are seeing the worst of COVID, low immunization coverage, and high rates of hospitalization and death. ... It’s a dark, dark time for many,” Dr. Crowley said. “And there has also been some amazing resilience and adaptation. The weird thing is, the HIV platform is a natural platform; I mean, if we can keep 21.9 million people on treatment, we can probably deliver them a COVID test and a vaccine.”
Dr. Crowley and Dr. Beyrer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We’ve been set back by COVID but we’ve seen remarkable resilience, a lot of innovation and creativity,” Siobhan Crowley MD, head of HIV at the Global Fund, said in an interview.
“If you consider that 21.9 million people are getting antiretrovirals at this point through the Global Fund, I think that needs to be appreciated. Ten years ago, that wouldn’t have been the case; all of those people would have disappeared into the ethers,” she said.
Through close partnerships with the U.S. Agency for International Development, the U.S. President’s Emergency Plan for AIDS Relief, and other Western countries and organizations, the Global Fund has invested $22.7 billion in programs to prevent and treat HIV and AIDS, and $3.8 billion in tuberculosis (TB)/HIV programs, according to the organization’s 2021 Results Report.
But the report also underscores the significant effect that the COVID-19 pandemic has had on funded countries’ progress toward achieving renewed 90-90-90 targets for HIV testing/diagnosis, treatment, and viral suppression by 2030.
The setbacks have been challenging and have touched nearly every service from prevention to treatment. According to the report, between 2019 and 2020:
- Voluntary male circumcision declined by 27%.
- Numbers reached by HIV prevention programs fell by 11%.
- 4.5% fewer mothers received medications to prevent HIV transmission to their babies.
- HIV testing services, including initiation, decreased by 22%.
The numbers tell only a part of the story, according to Dr. Crowley.
“We put in place an emergency mechanism to make funds available for countries to do everything except vaccines in support of COVID,” Dr. Crowley explained. (As of August 2021, these funds had been allocated to 107 countries and 16 multicountry programs.)
Countries were advised that they could use the emergency funds three different ways: 1) for COVID-specific purposes (e.g., diagnostics, oxygen, personal protective equipment; 2) to support mitigation strategies geared toward protecting existing HIV, tuberculosis, and malaria programs and getting them back on track; and 3) for so-called “health system fixes,” such as investing in data systems to track COVID, HIV, and other core diseases, as well as the community workforce.
With regard to HIV, each country supported by the Global Fund was asked to ensure that multimonth (3-6 months) dispensing was implemented and/or accelerated so that patients could avoid congested facilities, and, wherever possible, that drugs were delivered or accessed outside the facility. One example of the success of this effort was found in South Africa, where the number of people on antiretrovirals increased almost threefold, from 1.2 million to 4.2 million people.
Countries also were asked to adapt HIV testing procedures by, for example, moving organized testing out of the facilities and into neighborhoods to meet people where they are. Rapid diagnostic testing and triage care linkage using technologies such as WhatsApp were the result, as were opportunities for home testing which, Dr. Crowley noted, remains a critical component of the overall strategy.
“The self-test is important for two reasons, not just because you are trying to find people with HIV, but also, when people know that they’re negative, they know what they can or should do to stay negative,” she said. “It’s quite a powerful motivator.”
Self-testing might also help countries motivate the 6 million people who know that they have HIV but are not on treatment. But there are still 4.1 million residing in these countries who aren’t aware that they are infected, according to the report. This figure is especially troubling, considering that some may also be harboring TB coinfections, including multidrug-resistant TB (MDR-TB).
The imperfect storm globally and in the U.S.
“One of the things that was striking in the report was the decline in the number of people reached with testing and prevention services,” Chris Beyrer, MD, MPH, the Desmond M. Tutu Professor of Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health in Baltimore, said in an interview. Dr. Beyrer was not involved in the report’s development.
“You know, a 10% decline in 1 year to reach people in need is substantial,” he said. “Let’s say it continues; many people are predicting that we won’t have reasonable coverage for low-income countries with COVID until 2023. That adds up to a substantial decline in people reached with these services.”
Dr. Beyrer also expressed concern about the convergence of HIV and TB in already overburdened, fragile health care systems. “Globally, the No. 1 cause of death for people living with HIV is TB, and of course, it’s highly transmissible. So, in many high-burden countries, children are exposed, typically from household members early on, and so the number of people with latent TB infection is just enormous.
“If you look at the report, the worst outcomes are MDR-TB. Those multidrug-resistant and extensively-drug-resistant strains are really a threat to everybody,” Dr. Beyrer said.
But it’s not time for U.S. providers to rest on their laurels either. Dr. Beyrer noted that the 22% decline in HIV testing reported by the Global Fund is similar to what has been happening in the United States with elective procedures such as HIV testing and even preventive procedures like medical male circumcision.
“It’s very clear here in the Global Fund data that the majority of new infections worldwide are in key populations [that] include gay and bisexual men, men who have sex with men, transgender women who have sex with men, people who inject drugs, and sex workers of all genders. Those are people who already faced barriers to health care access and were made worse by COVID.”
Dr. Beyrer noted that, according to the Centers for Disease Control and Prevention, in 2019 in the United States, 68% of new HIV infections occurred in gay and bisexual men, and the effect that COVID-19 will have is still unknown. He also noted the similarity between the most marginalized populations in the Global Fund report and African American men, who have not realized the same increase in the use of preexposure prophylaxis or the same decline in new infections as have their White counterparts.
“It’s also where we are seeing the worst of COVID, low immunization coverage, and high rates of hospitalization and death. ... It’s a dark, dark time for many,” Dr. Crowley said. “And there has also been some amazing resilience and adaptation. The weird thing is, the HIV platform is a natural platform; I mean, if we can keep 21.9 million people on treatment, we can probably deliver them a COVID test and a vaccine.”
Dr. Crowley and Dr. Beyrer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We’ve been set back by COVID but we’ve seen remarkable resilience, a lot of innovation and creativity,” Siobhan Crowley MD, head of HIV at the Global Fund, said in an interview.
“If you consider that 21.9 million people are getting antiretrovirals at this point through the Global Fund, I think that needs to be appreciated. Ten years ago, that wouldn’t have been the case; all of those people would have disappeared into the ethers,” she said.
Through close partnerships with the U.S. Agency for International Development, the U.S. President’s Emergency Plan for AIDS Relief, and other Western countries and organizations, the Global Fund has invested $22.7 billion in programs to prevent and treat HIV and AIDS, and $3.8 billion in tuberculosis (TB)/HIV programs, according to the organization’s 2021 Results Report.
But the report also underscores the significant effect that the COVID-19 pandemic has had on funded countries’ progress toward achieving renewed 90-90-90 targets for HIV testing/diagnosis, treatment, and viral suppression by 2030.
The setbacks have been challenging and have touched nearly every service from prevention to treatment. According to the report, between 2019 and 2020:
- Voluntary male circumcision declined by 27%.
- Numbers reached by HIV prevention programs fell by 11%.
- 4.5% fewer mothers received medications to prevent HIV transmission to their babies.
- HIV testing services, including initiation, decreased by 22%.
The numbers tell only a part of the story, according to Dr. Crowley.
“We put in place an emergency mechanism to make funds available for countries to do everything except vaccines in support of COVID,” Dr. Crowley explained. (As of August 2021, these funds had been allocated to 107 countries and 16 multicountry programs.)
Countries were advised that they could use the emergency funds three different ways: 1) for COVID-specific purposes (e.g., diagnostics, oxygen, personal protective equipment; 2) to support mitigation strategies geared toward protecting existing HIV, tuberculosis, and malaria programs and getting them back on track; and 3) for so-called “health system fixes,” such as investing in data systems to track COVID, HIV, and other core diseases, as well as the community workforce.
With regard to HIV, each country supported by the Global Fund was asked to ensure that multimonth (3-6 months) dispensing was implemented and/or accelerated so that patients could avoid congested facilities, and, wherever possible, that drugs were delivered or accessed outside the facility. One example of the success of this effort was found in South Africa, where the number of people on antiretrovirals increased almost threefold, from 1.2 million to 4.2 million people.
Countries also were asked to adapt HIV testing procedures by, for example, moving organized testing out of the facilities and into neighborhoods to meet people where they are. Rapid diagnostic testing and triage care linkage using technologies such as WhatsApp were the result, as were opportunities for home testing which, Dr. Crowley noted, remains a critical component of the overall strategy.
“The self-test is important for two reasons, not just because you are trying to find people with HIV, but also, when people know that they’re negative, they know what they can or should do to stay negative,” she said. “It’s quite a powerful motivator.”
Self-testing might also help countries motivate the 6 million people who know that they have HIV but are not on treatment. But there are still 4.1 million residing in these countries who aren’t aware that they are infected, according to the report. This figure is especially troubling, considering that some may also be harboring TB coinfections, including multidrug-resistant TB (MDR-TB).
The imperfect storm globally and in the U.S.
“One of the things that was striking in the report was the decline in the number of people reached with testing and prevention services,” Chris Beyrer, MD, MPH, the Desmond M. Tutu Professor of Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health in Baltimore, said in an interview. Dr. Beyrer was not involved in the report’s development.
“You know, a 10% decline in 1 year to reach people in need is substantial,” he said. “Let’s say it continues; many people are predicting that we won’t have reasonable coverage for low-income countries with COVID until 2023. That adds up to a substantial decline in people reached with these services.”
Dr. Beyrer also expressed concern about the convergence of HIV and TB in already overburdened, fragile health care systems. “Globally, the No. 1 cause of death for people living with HIV is TB, and of course, it’s highly transmissible. So, in many high-burden countries, children are exposed, typically from household members early on, and so the number of people with latent TB infection is just enormous.
“If you look at the report, the worst outcomes are MDR-TB. Those multidrug-resistant and extensively-drug-resistant strains are really a threat to everybody,” Dr. Beyrer said.
But it’s not time for U.S. providers to rest on their laurels either. Dr. Beyrer noted that the 22% decline in HIV testing reported by the Global Fund is similar to what has been happening in the United States with elective procedures such as HIV testing and even preventive procedures like medical male circumcision.
“It’s very clear here in the Global Fund data that the majority of new infections worldwide are in key populations [that] include gay and bisexual men, men who have sex with men, transgender women who have sex with men, people who inject drugs, and sex workers of all genders. Those are people who already faced barriers to health care access and were made worse by COVID.”
Dr. Beyrer noted that, according to the Centers for Disease Control and Prevention, in 2019 in the United States, 68% of new HIV infections occurred in gay and bisexual men, and the effect that COVID-19 will have is still unknown. He also noted the similarity between the most marginalized populations in the Global Fund report and African American men, who have not realized the same increase in the use of preexposure prophylaxis or the same decline in new infections as have their White counterparts.
“It’s also where we are seeing the worst of COVID, low immunization coverage, and high rates of hospitalization and death. ... It’s a dark, dark time for many,” Dr. Crowley said. “And there has also been some amazing resilience and adaptation. The weird thing is, the HIV platform is a natural platform; I mean, if we can keep 21.9 million people on treatment, we can probably deliver them a COVID test and a vaccine.”
Dr. Crowley and Dr. Beyrer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA approves topical ruxolitinib for atopic dermatitis, first JAK inhibitor for this indication in the U.S.
The , making it the first topical JAK inhibitor approved for AD – and the first JAK inhibitor approved for this indication – in the United States.

The approval is limited to patients whose AD is not adequately controlled with topical prescription therapies, or when those therapies are not advisable.
“Approval of topical ruxolitinib fills a major gap in the treatment of atopic dermatitis: a safe, effective, and tolerable non-steroidal topical therapy,” Eric L. Simpson, MD, professor of dermatology and director of the Oregon Health & Science University Dermatology Clinical Research Center, Portland, told this news organization. “This approval will allow for long-term treatment without the concern of steroid side effects. From earlier studies, ruxolitinib cream appears to be as effective as a medium-potency topical steroid. These efficacy levels and low incidence of burning will be a welcome addition to our current nonsteroidal therapies.”
The drug’s approval was based on results from two phase 3, randomized studies of identical design involving 1,249 patients aged 12 years and older with AD: TRuE-AD1 and TRuE-AD2. In these studies, ruxolitinib cream demonstrated anti-inflammatory activity, with rapid and sustained antipruritic action, compared with vehicle. In the trials, patients with an Investigator’s Global Assessment (IGA) score of 2 or 3 and 3%-20% of affected body surface area (BSA) were randomized (2:2:1) to twice-daily 0.75% ruxolitinib cream, 1.5% ruxolitinib cream, or vehicle cream for 8 continuous weeks. The 1.5% concentration was approved by the FDA.
A study first published in May of 2021 found that significantly more patients in TRuE-AD1 and TRuE-AD2 achieved IGA treatment success with 0.75% (50% vs. 39%, respectively) and 1.5% ruxolitinib cream (53.8% vs. 51.3%), compared with vehicle (15.1% vs. 7.6%; P < .0001) at week 8. In addition, significant reductions in itch, compared with vehicle, were reported within 12 hours of first applying 1.5% ruxolitinib cream (P < .05).
More key findings from TRuE-AD1 and TRuE-AD2 are scheduled to be presented during the upcoming European Academy of Dermatology and Venereology meeting Sept. 29-Oct. 2, but during the Revolutionizing Atopic Dermatitis Symposium on June 13, Kim Papp, MD, PhD, presented long-term safety data of ruxolitinib cream in patients who were followed for an additional 44 weeks. Dr. Papp, a dermatologist and founder of Probity Medical Research, Waterloo, Ont., reported that 543 patients from TRuE-AD1 and 530 from TRuE-AD2 entered the long-term analysis and that about 78% of these patients completed the study. From weeks 12 to 52, the proportion of patients with an IGA score of 0 or 1 with 0.75% and 1.5% ruxolitinib cream ranged from 62%-77% and 67%-77%, respectively, in TRuE-AD1, to 60%-77% and 72%-80% in TRuE-AD2.
The measured mean total affected BSA was less than 3% throughout the follow-up period in the 1.5% ruxolitinib cream arm in TRuE-AD1 and TRuE-AD2 and was less than 3% in the 0.75% ruxolitinib cream arm during most of the study period.
In a pooled safety analysis, treatment-emergent adverse events (TEAEs) were reported in 60% and 54% of patients who applied 0.75% and 1.5% ruxolitinib cream, respectively, over 44 weeks. The frequency of application-site reactions remained low. Specifically, treatment-related adverse events were reported in 5% of patients who applied 0.75% ruxolitinib cream and in 3% of patients who applied 1.5% ruxolitinib cream; none were serious. TEAEs led to discontinuation in 2% of patients in the 0.75% ruxolitinib cream group, and no patients in the 1.5% ruxolitinib cream group.
Dr. Papp and his colleagues observed that the most common treatment adverse events were upper respiratory tract infections and nasopharyngitis. According to Incyte’s press release, the most common treatment-emergent adverse reactions in patients treated with ruxolitinib during clinical trials were nasopharyngitis, diarrhea, bronchitis, ear infection, eosinophil count increases, urticaria, folliculitis, tonsillitis, and rhinorrhea. The labeling includes boxed warnings for serious infections, mortality, malignancy, major adverse cardiovascular events, and thrombosis, seen with oral JAK inhibitors for inflammatory conditions.
Incyte will market ruxolitinib under the trade name Opzelura.
Dr. Simpson disclosed that he is a consultant to and/or an investigator for several pharmaceutical companies, including Incyte, Regeneron/Sanofi, Eli Lilly and Company, AbbVie, and Pfizer.
Dr. Papp disclosed that he has received honoraria or clinical research grants as a consultant, speaker, scientific officer, advisory board member, and/or steering committee member for several pharmaceutical companies, including Incyte.
Commentary by Robert Sidbury, MD, MPH
Another nonsteroidal topical medication approved for atopic dermatitis (AD)? Thank goodness. Topical ruxolitinib 1.5% cream twice daily for mild to moderate AD demonstrated excellent efficacy vs. placebo in duplicative trials (53.8/51.3% vs. 15.1%/7.6%; P < .001), with a reassuring safety profile. Application site reactions were uncommon, though past experience with other new nonsteroidal agents suggests judgment be reserved on that score. More compelling was the fact that no patients discontinued therapy in the 1.5% arm, and adverse events were mild and self-limited such as nasopharyngitis and diarrhea. This stands in contradistinction to the boxed warning attached to JAK inhibitors (topical and systemic) against a daunting list of destructive possibilities: malignancy, infection, cardiovascular disease, and blood clots. None of these things was seen in these topical ruxolitinib trials.
Dr. Sidbury is chief of dermatology at Seattle Children's Hospital and professor, department of pediatrics, University of Washington, Seattle. He is a site principal investigator for dupilumab trials, for which the hospital has a contract with Regeneron.
This article was updated 6/16/22.
The , making it the first topical JAK inhibitor approved for AD – and the first JAK inhibitor approved for this indication – in the United States.
The approval is limited to patients whose AD is not adequately controlled with topical prescription therapies, or when those therapies are not advisable.
“Approval of topical ruxolitinib fills a major gap in the treatment of atopic dermatitis: a safe, effective, and tolerable non-steroidal topical therapy,” Eric L. Simpson, MD, professor of dermatology and director of the Oregon Health & Science University Dermatology Clinical Research Center, Portland, told this news organization. “This approval will allow for long-term treatment without the concern of steroid side effects. From earlier studies, ruxolitinib cream appears to be as effective as a medium-potency topical steroid. These efficacy levels and low incidence of burning will be a welcome addition to our current nonsteroidal therapies.”
The drug’s approval was based on results from two phase 3, randomized studies of identical design involving 1,249 patients aged 12 years and older with AD: TRuE-AD1 and TRuE-AD2. In these studies, ruxolitinib cream demonstrated anti-inflammatory activity, with rapid and sustained antipruritic action, compared with vehicle. In the trials, patients with an Investigator’s Global Assessment (IGA) score of 2 or 3 and 3%-20% of affected body surface area (BSA) were randomized (2:2:1) to twice-daily 0.75% ruxolitinib cream, 1.5% ruxolitinib cream, or vehicle cream for 8 continuous weeks. The 1.5% concentration was approved by the FDA.
A study first published in May of 2021 found that significantly more patients in TRuE-AD1 and TRuE-AD2 achieved IGA treatment success with 0.75% (50% vs. 39%, respectively) and 1.5% ruxolitinib cream (53.8% vs. 51.3%), compared with vehicle (15.1% vs. 7.6%; P < .0001) at week 8. In addition, significant reductions in itch, compared with vehicle, were reported within 12 hours of first applying 1.5% ruxolitinib cream (P < .05).
More key findings from TRuE-AD1 and TRuE-AD2 are scheduled to be presented during the upcoming European Academy of Dermatology and Venereology meeting Sept. 29-Oct. 2, but during the Revolutionizing Atopic Dermatitis Symposium on June 13, Kim Papp, MD, PhD, presented long-term safety data of ruxolitinib cream in patients who were followed for an additional 44 weeks. Dr. Papp, a dermatologist and founder of Probity Medical Research, Waterloo, Ont., reported that 543 patients from TRuE-AD1 and 530 from TRuE-AD2 entered the long-term analysis and that about 78% of these patients completed the study. From weeks 12 to 52, the proportion of patients with an IGA score of 0 or 1 with 0.75% and 1.5% ruxolitinib cream ranged from 62%-77% and 67%-77%, respectively, in TRuE-AD1, to 60%-77% and 72%-80% in TRuE-AD2.
The measured mean total affected BSA was less than 3% throughout the follow-up period in the 1.5% ruxolitinib cream arm in TRuE-AD1 and TRuE-AD2 and was less than 3% in the 0.75% ruxolitinib cream arm during most of the study period.
In a pooled safety analysis, treatment-emergent adverse events (TEAEs) were reported in 60% and 54% of patients who applied 0.75% and 1.5% ruxolitinib cream, respectively, over 44 weeks. The frequency of application-site reactions remained low. Specifically, treatment-related adverse events were reported in 5% of patients who applied 0.75% ruxolitinib cream and in 3% of patients who applied 1.5% ruxolitinib cream; none were serious. TEAEs led to discontinuation in 2% of patients in the 0.75% ruxolitinib cream group, and no patients in the 1.5% ruxolitinib cream group.
Dr. Papp and his colleagues observed that the most common treatment adverse events were upper respiratory tract infections and nasopharyngitis. According to Incyte’s press release, the most common treatment-emergent adverse reactions in patients treated with ruxolitinib during clinical trials were nasopharyngitis, diarrhea, bronchitis, ear infection, eosinophil count increases, urticaria, folliculitis, tonsillitis, and rhinorrhea. The labeling includes boxed warnings for serious infections, mortality, malignancy, major adverse cardiovascular events, and thrombosis, seen with oral JAK inhibitors for inflammatory conditions.
Incyte will market ruxolitinib under the trade name Opzelura.
Dr. Simpson disclosed that he is a consultant to and/or an investigator for several pharmaceutical companies, including Incyte, Regeneron/Sanofi, Eli Lilly and Company, AbbVie, and Pfizer.
Dr. Papp disclosed that he has received honoraria or clinical research grants as a consultant, speaker, scientific officer, advisory board member, and/or steering committee member for several pharmaceutical companies, including Incyte.
Commentary by Robert Sidbury, MD, MPH
Another nonsteroidal topical medication approved for atopic dermatitis (AD)? Thank goodness. Topical ruxolitinib 1.5% cream twice daily for mild to moderate AD demonstrated excellent efficacy vs. placebo in duplicative trials (53.8/51.3% vs. 15.1%/7.6%; P < .001), with a reassuring safety profile. Application site reactions were uncommon, though past experience with other new nonsteroidal agents suggests judgment be reserved on that score. More compelling was the fact that no patients discontinued therapy in the 1.5% arm, and adverse events were mild and self-limited such as nasopharyngitis and diarrhea. This stands in contradistinction to the boxed warning attached to JAK inhibitors (topical and systemic) against a daunting list of destructive possibilities: malignancy, infection, cardiovascular disease, and blood clots. None of these things was seen in these topical ruxolitinib trials.
Dr. Sidbury is chief of dermatology at Seattle Children's Hospital and professor, department of pediatrics, University of Washington, Seattle. He is a site principal investigator for dupilumab trials, for which the hospital has a contract with Regeneron.
This article was updated 6/16/22.
The , making it the first topical JAK inhibitor approved for AD – and the first JAK inhibitor approved for this indication – in the United States.
The approval is limited to patients whose AD is not adequately controlled with topical prescription therapies, or when those therapies are not advisable.
“Approval of topical ruxolitinib fills a major gap in the treatment of atopic dermatitis: a safe, effective, and tolerable non-steroidal topical therapy,” Eric L. Simpson, MD, professor of dermatology and director of the Oregon Health & Science University Dermatology Clinical Research Center, Portland, told this news organization. “This approval will allow for long-term treatment without the concern of steroid side effects. From earlier studies, ruxolitinib cream appears to be as effective as a medium-potency topical steroid. These efficacy levels and low incidence of burning will be a welcome addition to our current nonsteroidal therapies.”
The drug’s approval was based on results from two phase 3, randomized studies of identical design involving 1,249 patients aged 12 years and older with AD: TRuE-AD1 and TRuE-AD2. In these studies, ruxolitinib cream demonstrated anti-inflammatory activity, with rapid and sustained antipruritic action, compared with vehicle. In the trials, patients with an Investigator’s Global Assessment (IGA) score of 2 or 3 and 3%-20% of affected body surface area (BSA) were randomized (2:2:1) to twice-daily 0.75% ruxolitinib cream, 1.5% ruxolitinib cream, or vehicle cream for 8 continuous weeks. The 1.5% concentration was approved by the FDA.
A study first published in May of 2021 found that significantly more patients in TRuE-AD1 and TRuE-AD2 achieved IGA treatment success with 0.75% (50% vs. 39%, respectively) and 1.5% ruxolitinib cream (53.8% vs. 51.3%), compared with vehicle (15.1% vs. 7.6%; P < .0001) at week 8. In addition, significant reductions in itch, compared with vehicle, were reported within 12 hours of first applying 1.5% ruxolitinib cream (P < .05).
More key findings from TRuE-AD1 and TRuE-AD2 are scheduled to be presented during the upcoming European Academy of Dermatology and Venereology meeting Sept. 29-Oct. 2, but during the Revolutionizing Atopic Dermatitis Symposium on June 13, Kim Papp, MD, PhD, presented long-term safety data of ruxolitinib cream in patients who were followed for an additional 44 weeks. Dr. Papp, a dermatologist and founder of Probity Medical Research, Waterloo, Ont., reported that 543 patients from TRuE-AD1 and 530 from TRuE-AD2 entered the long-term analysis and that about 78% of these patients completed the study. From weeks 12 to 52, the proportion of patients with an IGA score of 0 or 1 with 0.75% and 1.5% ruxolitinib cream ranged from 62%-77% and 67%-77%, respectively, in TRuE-AD1, to 60%-77% and 72%-80% in TRuE-AD2.
The measured mean total affected BSA was less than 3% throughout the follow-up period in the 1.5% ruxolitinib cream arm in TRuE-AD1 and TRuE-AD2 and was less than 3% in the 0.75% ruxolitinib cream arm during most of the study period.
In a pooled safety analysis, treatment-emergent adverse events (TEAEs) were reported in 60% and 54% of patients who applied 0.75% and 1.5% ruxolitinib cream, respectively, over 44 weeks. The frequency of application-site reactions remained low. Specifically, treatment-related adverse events were reported in 5% of patients who applied 0.75% ruxolitinib cream and in 3% of patients who applied 1.5% ruxolitinib cream; none were serious. TEAEs led to discontinuation in 2% of patients in the 0.75% ruxolitinib cream group, and no patients in the 1.5% ruxolitinib cream group.
Dr. Papp and his colleagues observed that the most common treatment adverse events were upper respiratory tract infections and nasopharyngitis. According to Incyte’s press release, the most common treatment-emergent adverse reactions in patients treated with ruxolitinib during clinical trials were nasopharyngitis, diarrhea, bronchitis, ear infection, eosinophil count increases, urticaria, folliculitis, tonsillitis, and rhinorrhea. The labeling includes boxed warnings for serious infections, mortality, malignancy, major adverse cardiovascular events, and thrombosis, seen with oral JAK inhibitors for inflammatory conditions.
Incyte will market ruxolitinib under the trade name Opzelura.
Dr. Simpson disclosed that he is a consultant to and/or an investigator for several pharmaceutical companies, including Incyte, Regeneron/Sanofi, Eli Lilly and Company, AbbVie, and Pfizer.
Dr. Papp disclosed that he has received honoraria or clinical research grants as a consultant, speaker, scientific officer, advisory board member, and/or steering committee member for several pharmaceutical companies, including Incyte.
Commentary by Robert Sidbury, MD, MPH
Another nonsteroidal topical medication approved for atopic dermatitis (AD)? Thank goodness. Topical ruxolitinib 1.5% cream twice daily for mild to moderate AD demonstrated excellent efficacy vs. placebo in duplicative trials (53.8/51.3% vs. 15.1%/7.6%; P < .001), with a reassuring safety profile. Application site reactions were uncommon, though past experience with other new nonsteroidal agents suggests judgment be reserved on that score. More compelling was the fact that no patients discontinued therapy in the 1.5% arm, and adverse events were mild and self-limited such as nasopharyngitis and diarrhea. This stands in contradistinction to the boxed warning attached to JAK inhibitors (topical and systemic) against a daunting list of destructive possibilities: malignancy, infection, cardiovascular disease, and blood clots. None of these things was seen in these topical ruxolitinib trials.
Dr. Sidbury is chief of dermatology at Seattle Children's Hospital and professor, department of pediatrics, University of Washington, Seattle. He is a site principal investigator for dupilumab trials, for which the hospital has a contract with Regeneron.
This article was updated 6/16/22.
Nurses ‘at the breaking point,’ consider quitting due to COVID issues: Survey
In the best of times, critical care nurses have one of the most difficult and stressful jobs in health care. The COVID-19 pandemic has made that immeasurably worse. As hospitals have been flooded with critically ill patients, nurses have been overwhelmed.
“What we’re hearing from our nurses is really shocking,” Amanda Bettencourt, PhD, APRN, CCRN-K, president-elect of the American Association of Critical-Care Nurses (AACN), told this news organization. “They’re saying they’re at the breaking point.”
Between August 26 and August 30, the AACN surveyed more than 6,000 critical care nurses, zeroing in on four key questions regarding the pandemic and its impact on nursing. The results were alarming – not only with regard to individual nurses but also for the nursing profession and the future of health care. A full 66% of those surveyed said their experiences during the pandemic have caused them to consider leaving nursing. The respondents’ take on their colleagues was even more concerning. Ninety-two percent agreed with the following two statements: “I believe the pandemic has depleted nurses at my hospital. Their careers will be shorter than they intended.”
“This puts the entire health care system at risk,” says Dr. Bettencourt, who is assistant professor in the department of family and community health at the University of Pennsylvania School of Nursing, Philadelphia. Intensive care unit (ICU) nurses are highly trained and are skilled in caring for critically ill patients with complex medical needs. “It’s not easy to replace a critical care nurse when one leaves,” she says.
And when nurses leave, patients suffer, says Beth Wathen, MSN, RN, CCRN-K, president of the ACCN and frontline nurse at Children’s Hospital Colorado, Aurora. “Hospitals can have all the beds and all the rooms and all the equipment they want, but without nurses and others at the front lines to provide that essential care, none of it really matters, whether we’re talking about caring for COVID patients or caring for patients with other health ailments.”
Heartbreak of the unvaccinated
The problem is not just overwork because of the flood of COVID-19 patients. The emotional strain is enormous as well. “What’s demoralizing for us is not that patients are sick and that it’s physically exhausting to take care of sick patients. We’re used to that,” says Dr. Bettencourt.
But few nurses have experienced the sheer magnitude of patients caused by this pandemic. “The past 18 months have been grueling,” says Ms. Wathen. “The burden on frontline caregivers and our nurses at the front line has been immense.”
The situation is made worse by how unnecessary much of the suffering is at this point. Seventy-six percent of the survey’s respondents agreed with the following statement: “People who hold out on getting vaccinated undermine nurses’ physical and mental well-being.” That comment doesn’t convey the nature or extent of the effect on caregivers’ well-being. “That 9 out of 10 of the people we’re seeing in ICU right now are unvaccinated just adds to the sense of heartbreak and frustration,” says Ms. Wathen. “These deaths don’t have to be happening right now. And that’s hard to bear witness to.”
The politicization of public health has also taken a toll. “That’s been the hard part of this entire pandemic,” says Ms. Wathen. “This really isn’t at all about politics. This is about your health; this is about my health. This is about our collective health as a community and as a country.”
Like the rest of the world, nurses are also concerned about their own loved ones. The survey statement, “I fear taking care of patients with COVID puts my family’s health at risk,” garnered 67% agreement. Ms. Wathen points out that nurses take the appropriate precautions but still worry about taking infection home to their families. “This disease is a tricky one,” she says. She points out that until this pandemic is over, in addition to being vaccinated, nurses and the public still need to be vigilant about wearing masks, social distancing, and taking other precautions to ensure the safety of us all. “Our individual decisions don’t just affect ourselves. They affect our family, the people in our circle, and the people in our community,” she says.
Avoiding a professional exodus
It’s too early yet to have reliable national data on how many nurses have already left their jobs because of COVID-19, but it is clear that there are too few nurses of all kinds. Earlier this month, the American Nurses Association sent a letter to the U.S. Secretary of Health and Human Services urging the agency to declare the nursing shortage a crisis and to take immediate steps to find solutions.
The nursing shortage predates the pandemic, and COVID-19 has brought a simmering problem to a boil. Nurses are calling on the public and the health care system for help. From inside the industry, the needs are pretty much what they were before the pandemic. Dr. Bettencourt and Ms. Wathen point to the need for supportive leadership, healthy work environments, sufficient staffing to meet patients’ needs, and a voice in decisions, such as decisions about staffing, that affect nurses and their patients. Nurses want to be heard and appreciated. “It’s not that these are new things,” says Dr. Bettencourt. “We just need them even more now because we’re stressed even more than we were before.”
Critical care nurses have a different request of the public. They’re asking – pleading, actually – with the public to get vaccinated, wear masks in public, practice social distancing, and bring this pandemic to an end.
“COVID kills, and it’s a really difficult, tragic, and lonely death,” says Ms. Wathen. “We’ve witnessed hundreds of thousands of those deaths. But now we have a way to stop it. If many more people get vaccinated, we can stop this pandemic. And hopefully that will stop this current trend of nurses leaving.”
A version of this article first appeared on Medscape.com.
In the best of times, critical care nurses have one of the most difficult and stressful jobs in health care. The COVID-19 pandemic has made that immeasurably worse. As hospitals have been flooded with critically ill patients, nurses have been overwhelmed.
“What we’re hearing from our nurses is really shocking,” Amanda Bettencourt, PhD, APRN, CCRN-K, president-elect of the American Association of Critical-Care Nurses (AACN), told this news organization. “They’re saying they’re at the breaking point.”
Between August 26 and August 30, the AACN surveyed more than 6,000 critical care nurses, zeroing in on four key questions regarding the pandemic and its impact on nursing. The results were alarming – not only with regard to individual nurses but also for the nursing profession and the future of health care. A full 66% of those surveyed said their experiences during the pandemic have caused them to consider leaving nursing. The respondents’ take on their colleagues was even more concerning. Ninety-two percent agreed with the following two statements: “I believe the pandemic has depleted nurses at my hospital. Their careers will be shorter than they intended.”
“This puts the entire health care system at risk,” says Dr. Bettencourt, who is assistant professor in the department of family and community health at the University of Pennsylvania School of Nursing, Philadelphia. Intensive care unit (ICU) nurses are highly trained and are skilled in caring for critically ill patients with complex medical needs. “It’s not easy to replace a critical care nurse when one leaves,” she says.
And when nurses leave, patients suffer, says Beth Wathen, MSN, RN, CCRN-K, president of the ACCN and frontline nurse at Children’s Hospital Colorado, Aurora. “Hospitals can have all the beds and all the rooms and all the equipment they want, but without nurses and others at the front lines to provide that essential care, none of it really matters, whether we’re talking about caring for COVID patients or caring for patients with other health ailments.”
Heartbreak of the unvaccinated
The problem is not just overwork because of the flood of COVID-19 patients. The emotional strain is enormous as well. “What’s demoralizing for us is not that patients are sick and that it’s physically exhausting to take care of sick patients. We’re used to that,” says Dr. Bettencourt.
But few nurses have experienced the sheer magnitude of patients caused by this pandemic. “The past 18 months have been grueling,” says Ms. Wathen. “The burden on frontline caregivers and our nurses at the front line has been immense.”
The situation is made worse by how unnecessary much of the suffering is at this point. Seventy-six percent of the survey’s respondents agreed with the following statement: “People who hold out on getting vaccinated undermine nurses’ physical and mental well-being.” That comment doesn’t convey the nature or extent of the effect on caregivers’ well-being. “That 9 out of 10 of the people we’re seeing in ICU right now are unvaccinated just adds to the sense of heartbreak and frustration,” says Ms. Wathen. “These deaths don’t have to be happening right now. And that’s hard to bear witness to.”
The politicization of public health has also taken a toll. “That’s been the hard part of this entire pandemic,” says Ms. Wathen. “This really isn’t at all about politics. This is about your health; this is about my health. This is about our collective health as a community and as a country.”
Like the rest of the world, nurses are also concerned about their own loved ones. The survey statement, “I fear taking care of patients with COVID puts my family’s health at risk,” garnered 67% agreement. Ms. Wathen points out that nurses take the appropriate precautions but still worry about taking infection home to their families. “This disease is a tricky one,” she says. She points out that until this pandemic is over, in addition to being vaccinated, nurses and the public still need to be vigilant about wearing masks, social distancing, and taking other precautions to ensure the safety of us all. “Our individual decisions don’t just affect ourselves. They affect our family, the people in our circle, and the people in our community,” she says.
Avoiding a professional exodus
It’s too early yet to have reliable national data on how many nurses have already left their jobs because of COVID-19, but it is clear that there are too few nurses of all kinds. Earlier this month, the American Nurses Association sent a letter to the U.S. Secretary of Health and Human Services urging the agency to declare the nursing shortage a crisis and to take immediate steps to find solutions.
The nursing shortage predates the pandemic, and COVID-19 has brought a simmering problem to a boil. Nurses are calling on the public and the health care system for help. From inside the industry, the needs are pretty much what they were before the pandemic. Dr. Bettencourt and Ms. Wathen point to the need for supportive leadership, healthy work environments, sufficient staffing to meet patients’ needs, and a voice in decisions, such as decisions about staffing, that affect nurses and their patients. Nurses want to be heard and appreciated. “It’s not that these are new things,” says Dr. Bettencourt. “We just need them even more now because we’re stressed even more than we were before.”
Critical care nurses have a different request of the public. They’re asking – pleading, actually – with the public to get vaccinated, wear masks in public, practice social distancing, and bring this pandemic to an end.
“COVID kills, and it’s a really difficult, tragic, and lonely death,” says Ms. Wathen. “We’ve witnessed hundreds of thousands of those deaths. But now we have a way to stop it. If many more people get vaccinated, we can stop this pandemic. And hopefully that will stop this current trend of nurses leaving.”
A version of this article first appeared on Medscape.com.
In the best of times, critical care nurses have one of the most difficult and stressful jobs in health care. The COVID-19 pandemic has made that immeasurably worse. As hospitals have been flooded with critically ill patients, nurses have been overwhelmed.
“What we’re hearing from our nurses is really shocking,” Amanda Bettencourt, PhD, APRN, CCRN-K, president-elect of the American Association of Critical-Care Nurses (AACN), told this news organization. “They’re saying they’re at the breaking point.”
Between August 26 and August 30, the AACN surveyed more than 6,000 critical care nurses, zeroing in on four key questions regarding the pandemic and its impact on nursing. The results were alarming – not only with regard to individual nurses but also for the nursing profession and the future of health care. A full 66% of those surveyed said their experiences during the pandemic have caused them to consider leaving nursing. The respondents’ take on their colleagues was even more concerning. Ninety-two percent agreed with the following two statements: “I believe the pandemic has depleted nurses at my hospital. Their careers will be shorter than they intended.”
“This puts the entire health care system at risk,” says Dr. Bettencourt, who is assistant professor in the department of family and community health at the University of Pennsylvania School of Nursing, Philadelphia. Intensive care unit (ICU) nurses are highly trained and are skilled in caring for critically ill patients with complex medical needs. “It’s not easy to replace a critical care nurse when one leaves,” she says.
And when nurses leave, patients suffer, says Beth Wathen, MSN, RN, CCRN-K, president of the ACCN and frontline nurse at Children’s Hospital Colorado, Aurora. “Hospitals can have all the beds and all the rooms and all the equipment they want, but without nurses and others at the front lines to provide that essential care, none of it really matters, whether we’re talking about caring for COVID patients or caring for patients with other health ailments.”
Heartbreak of the unvaccinated
The problem is not just overwork because of the flood of COVID-19 patients. The emotional strain is enormous as well. “What’s demoralizing for us is not that patients are sick and that it’s physically exhausting to take care of sick patients. We’re used to that,” says Dr. Bettencourt.
But few nurses have experienced the sheer magnitude of patients caused by this pandemic. “The past 18 months have been grueling,” says Ms. Wathen. “The burden on frontline caregivers and our nurses at the front line has been immense.”
The situation is made worse by how unnecessary much of the suffering is at this point. Seventy-six percent of the survey’s respondents agreed with the following statement: “People who hold out on getting vaccinated undermine nurses’ physical and mental well-being.” That comment doesn’t convey the nature or extent of the effect on caregivers’ well-being. “That 9 out of 10 of the people we’re seeing in ICU right now are unvaccinated just adds to the sense of heartbreak and frustration,” says Ms. Wathen. “These deaths don’t have to be happening right now. And that’s hard to bear witness to.”
The politicization of public health has also taken a toll. “That’s been the hard part of this entire pandemic,” says Ms. Wathen. “This really isn’t at all about politics. This is about your health; this is about my health. This is about our collective health as a community and as a country.”
Like the rest of the world, nurses are also concerned about their own loved ones. The survey statement, “I fear taking care of patients with COVID puts my family’s health at risk,” garnered 67% agreement. Ms. Wathen points out that nurses take the appropriate precautions but still worry about taking infection home to their families. “This disease is a tricky one,” she says. She points out that until this pandemic is over, in addition to being vaccinated, nurses and the public still need to be vigilant about wearing masks, social distancing, and taking other precautions to ensure the safety of us all. “Our individual decisions don’t just affect ourselves. They affect our family, the people in our circle, and the people in our community,” she says.
Avoiding a professional exodus
It’s too early yet to have reliable national data on how many nurses have already left their jobs because of COVID-19, but it is clear that there are too few nurses of all kinds. Earlier this month, the American Nurses Association sent a letter to the U.S. Secretary of Health and Human Services urging the agency to declare the nursing shortage a crisis and to take immediate steps to find solutions.
The nursing shortage predates the pandemic, and COVID-19 has brought a simmering problem to a boil. Nurses are calling on the public and the health care system for help. From inside the industry, the needs are pretty much what they were before the pandemic. Dr. Bettencourt and Ms. Wathen point to the need for supportive leadership, healthy work environments, sufficient staffing to meet patients’ needs, and a voice in decisions, such as decisions about staffing, that affect nurses and their patients. Nurses want to be heard and appreciated. “It’s not that these are new things,” says Dr. Bettencourt. “We just need them even more now because we’re stressed even more than we were before.”
Critical care nurses have a different request of the public. They’re asking – pleading, actually – with the public to get vaccinated, wear masks in public, practice social distancing, and bring this pandemic to an end.
“COVID kills, and it’s a really difficult, tragic, and lonely death,” says Ms. Wathen. “We’ve witnessed hundreds of thousands of those deaths. But now we have a way to stop it. If many more people get vaccinated, we can stop this pandemic. And hopefully that will stop this current trend of nurses leaving.”
A version of this article first appeared on Medscape.com.
Decline in child COVID may signal end of latest surge
A second consecutive week of falling COVID-19 cases in children, along with continued declines in new admissions, may indicate that the latest surge has peaked.
Children made up over 25% of all new cases each week over that 3-week period covering the end of August and the first half of September, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.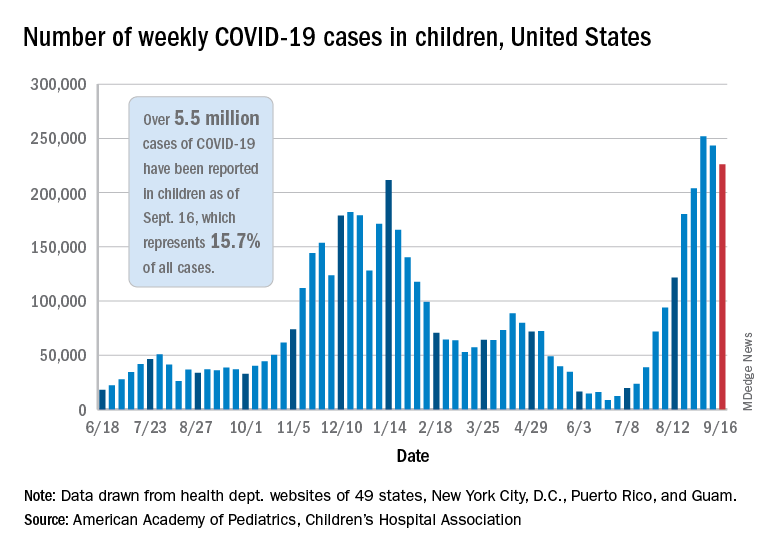
New hospitalizations in children aged 0-17 years peaked on Sept. 4 – when the rate reached 0.51 per 100,000 population – and were down to 0.47 as of Sept. 11, the latest date for which data should be considered reliable, the Centers for Disease Control and Prevention said.
The CDC’s data largely agree with the AAP/CHA report, showing that cases peaked during the week of Aug. 22-28. Cases per 100,000 for children that week looked like this: 154.7 (age 0-4 years), 276.6 (5-11 years), 320.0 (12-15), and 334.1 (16-17). The highest rates that week among adults were 288.6 per 100,000 in 30- to 39-year-olds and 286.5 for those aged 18-29, the CDC said on its COVID Data Tracker.
By the week of Sept. 5-11 – reporting delays can affect more recent data – the rates in children were down more than 20% in each of the four age groups, according to the CDC.
Vaccinations among children, unfortunately, continue to decline. Vaccine initiations for 12- to 15-year-olds slipped from 199,000 (Sept. 7-13) to 179,000 during the week of Sept. 14-20, while the 16- to 17-year-olds went from almost 83,000 down to 75,000. Initiations have dropped for 6 straight weeks in both age groups, based on the CDC data.
Despite those declines, however, the 16- and 17-year-olds just passed a couple of vaccination milestones. More than 60% – 60.9%, to be exact – have now received at least one dose of COVID vaccine, and 50.3% can be considered fully vaccinated. For those aged 12-15, the corresponding figures are 53.1% and 42.0%, the CDC reported.
When children under age 12 years are included – through clinical trial involvement or incorrect birth dates – the CDC data put the total count of Americans under age 18 who have received at least one dose of vaccine at almost 12.8 million, with vaccination complete in 10.3 million.
Total cases, as calculated by the APA and CHA, are now over 5.5 million, although that figure includes cases in individuals as old as 20 years, since many states differ from the CDC on the age range for a child. The CDC’s COVID Data Tracker put the total for children aged 0-17 at nearly 4.6 million.
The total number of COVID-related deaths in children is 480 as of Sept. 16, the AAP and CHA said, based on data from 45 states, New York, City, Puerto Rico, and Guam, but the CDC provides a higher number, 548, since the pandemic began. Children aged 0-4 years represent the largest share (32.3%) of those 548 deaths, followed by the 12- to 15-year-olds (26.5%), based on the CDC data.
A second consecutive week of falling COVID-19 cases in children, along with continued declines in new admissions, may indicate that the latest surge has peaked.
Children made up over 25% of all new cases each week over that 3-week period covering the end of August and the first half of September, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
New hospitalizations in children aged 0-17 years peaked on Sept. 4 – when the rate reached 0.51 per 100,000 population – and were down to 0.47 as of Sept. 11, the latest date for which data should be considered reliable, the Centers for Disease Control and Prevention said.
The CDC’s data largely agree with the AAP/CHA report, showing that cases peaked during the week of Aug. 22-28. Cases per 100,000 for children that week looked like this: 154.7 (age 0-4 years), 276.6 (5-11 years), 320.0 (12-15), and 334.1 (16-17). The highest rates that week among adults were 288.6 per 100,000 in 30- to 39-year-olds and 286.5 for those aged 18-29, the CDC said on its COVID Data Tracker.
By the week of Sept. 5-11 – reporting delays can affect more recent data – the rates in children were down more than 20% in each of the four age groups, according to the CDC.
Vaccinations among children, unfortunately, continue to decline. Vaccine initiations for 12- to 15-year-olds slipped from 199,000 (Sept. 7-13) to 179,000 during the week of Sept. 14-20, while the 16- to 17-year-olds went from almost 83,000 down to 75,000. Initiations have dropped for 6 straight weeks in both age groups, based on the CDC data.
Despite those declines, however, the 16- and 17-year-olds just passed a couple of vaccination milestones. More than 60% – 60.9%, to be exact – have now received at least one dose of COVID vaccine, and 50.3% can be considered fully vaccinated. For those aged 12-15, the corresponding figures are 53.1% and 42.0%, the CDC reported.
When children under age 12 years are included – through clinical trial involvement or incorrect birth dates – the CDC data put the total count of Americans under age 18 who have received at least one dose of vaccine at almost 12.8 million, with vaccination complete in 10.3 million.
Total cases, as calculated by the APA and CHA, are now over 5.5 million, although that figure includes cases in individuals as old as 20 years, since many states differ from the CDC on the age range for a child. The CDC’s COVID Data Tracker put the total for children aged 0-17 at nearly 4.6 million.
The total number of COVID-related deaths in children is 480 as of Sept. 16, the AAP and CHA said, based on data from 45 states, New York, City, Puerto Rico, and Guam, but the CDC provides a higher number, 548, since the pandemic began. Children aged 0-4 years represent the largest share (32.3%) of those 548 deaths, followed by the 12- to 15-year-olds (26.5%), based on the CDC data.
A second consecutive week of falling COVID-19 cases in children, along with continued declines in new admissions, may indicate that the latest surge has peaked.
Children made up over 25% of all new cases each week over that 3-week period covering the end of August and the first half of September, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
New hospitalizations in children aged 0-17 years peaked on Sept. 4 – when the rate reached 0.51 per 100,000 population – and were down to 0.47 as of Sept. 11, the latest date for which data should be considered reliable, the Centers for Disease Control and Prevention said.
The CDC’s data largely agree with the AAP/CHA report, showing that cases peaked during the week of Aug. 22-28. Cases per 100,000 for children that week looked like this: 154.7 (age 0-4 years), 276.6 (5-11 years), 320.0 (12-15), and 334.1 (16-17). The highest rates that week among adults were 288.6 per 100,000 in 30- to 39-year-olds and 286.5 for those aged 18-29, the CDC said on its COVID Data Tracker.
By the week of Sept. 5-11 – reporting delays can affect more recent data – the rates in children were down more than 20% in each of the four age groups, according to the CDC.
Vaccinations among children, unfortunately, continue to decline. Vaccine initiations for 12- to 15-year-olds slipped from 199,000 (Sept. 7-13) to 179,000 during the week of Sept. 14-20, while the 16- to 17-year-olds went from almost 83,000 down to 75,000. Initiations have dropped for 6 straight weeks in both age groups, based on the CDC data.
Despite those declines, however, the 16- and 17-year-olds just passed a couple of vaccination milestones. More than 60% – 60.9%, to be exact – have now received at least one dose of COVID vaccine, and 50.3% can be considered fully vaccinated. For those aged 12-15, the corresponding figures are 53.1% and 42.0%, the CDC reported.
When children under age 12 years are included – through clinical trial involvement or incorrect birth dates – the CDC data put the total count of Americans under age 18 who have received at least one dose of vaccine at almost 12.8 million, with vaccination complete in 10.3 million.
Total cases, as calculated by the APA and CHA, are now over 5.5 million, although that figure includes cases in individuals as old as 20 years, since many states differ from the CDC on the age range for a child. The CDC’s COVID Data Tracker put the total for children aged 0-17 at nearly 4.6 million.
The total number of COVID-related deaths in children is 480 as of Sept. 16, the AAP and CHA said, based on data from 45 states, New York, City, Puerto Rico, and Guam, but the CDC provides a higher number, 548, since the pandemic began. Children aged 0-4 years represent the largest share (32.3%) of those 548 deaths, followed by the 12- to 15-year-olds (26.5%), based on the CDC data.
Nurses ‘at the breaking point,’ consider quitting due to COVID issues: Survey
As hospitals have been flooded with critically ill patients, nurses have been overwhelmed.
“What we’re hearing from our nurses is really shocking,” Amanda Bettencourt, PhD, APRN, CCRN-K, president-elect of the American Association of Critical-Care Nurses (AACN), said in an interview. “They’re saying they’re at the breaking point.”
Between Aug. 26 and Aug. 30, the AACN surveyed more than 6,000 critical care nurses, zeroing in on four key questions regarding the pandemic and its impact on nursing. The results were alarming – not only with regard to individual nurses but also for the nursing profession and the future of health care. A full 66% of those surveyed said their experiences during the pandemic have caused them to consider leaving nursing. The respondents’ take on their colleagues was even more concerning. Ninety-two percent agreed with the following two statements: “I believe the pandemic has depleted nurses at my hospital. Their careers will be shorter than they intended.”
“This puts the entire health care system at risk,” says Dr. Bettencourt, assistant professor in the department of family and community health at the University of Pennsylvania School of Nursing, Philadelphia. Intensive care unit (ICU) nurses are highly trained and are skilled in caring for critically ill patients with complex medical needs. “It’s not easy to replace a critical care nurse when one leaves,” she said.
And when nurses leave, patients suffer, said Beth Wathen, MSN, RN, CCRN-K, president of the ACCN and frontline nurse at Children’s Hospital Colorado, in Aurora. “Hospitals can have all the beds and all the rooms and all the equipment they want, but without nurses and others at the front lines to provide that essential care, none of it really matters, whether we’re talking about caring for COVID patients or caring for patients with other health ailments.”
Heartbreak of the unvaccinated
The problem is not just overwork because of the flood of COVID-19 patients. The emotional strain is enormous as well. “What’s demoralizing for us is not that patients are sick and that it’s physically exhausting to take care of sick patients. We’re used to that,” said Dr. Bettencourt.
But few nurses have experienced the sheer magnitude of patients caused by this pandemic. “The past 18 months have been grueling,” says Ms. Wathen. “The burden on frontline caregivers and our nurses at the front line has been immense.”
The situation is made worse by how unnecessary much of the suffering is at this point. Seventy-six percent of the survey’s respondents agreed with the following statement: “People who hold out on getting vaccinated undermine nurses’ physical and mental well-being.” That comment doesn’t convey the nature or extent of the effect on caregivers’ well-being. “That 9 out of 10 of the people we’re seeing in ICU right now are unvaccinated just adds to the sense of heartbreak and frustration,” says Ms. Wathen. “These deaths don’t have to be happening right now. And that’s hard to bear witness to.”
The politicization of public health has also taken a toll. “That’s been the hard part of this entire pandemic,” says Ms. Wathen. “This really isn’t at all about politics. This is about your health; this is about my health. This is about our collective health as a community and as a country.”
Like the rest of the world, nurses are also concerned about their own loved ones. The survey statement, “I fear taking care of patients with COVID puts my family’s health at risk,” garnered 67% agreement. Ms. Wathen points out that nurses take the appropriate precautions but still worry about taking infection home to their families. “This disease is a tricky one,” she says. She points out that until this pandemic is over, in addition to being vaccinated, nurses and the public still need to be vigilant about wearing masks, social distancing, and taking other precautions to ensure the safety of us all. “Our individual decisions don’t just affect ourselves. They affect our family, the people in our circle, and the people in our community,” she said.
Avoiding a professional exodus
It’s too early yet to have reliable national data on how many nurses have already left their jobs because of COVID-19, but it is clear that there are too few nurses of all kinds. The American Nurses Association sent a letter to the U.S. Secretary of Health and Human Services urging the agency to declare the nursing shortage a crisis and to take immediate steps to find solutions.
The nursing shortage predates the pandemic, and COVID-19 has brought a simmering problem to the boil. Nurses are calling on the public and the health care system for help. From inside the industry, the needs are pretty much what they were before the pandemic. Dr. Bettencourt and Ms. Wathen point to the need for supportive leadership, healthy work environments, sufficient staffing to meet patients’ needs, and a voice in decisions, such as decisions about staffing, that affect nurses and their patients. Nurses want to be heard and appreciated. “It’s not that these are new things,” said Dr. Bettencourt. “We just need them even more now because we’re stressed even more than we were before.”
Critical care nurses have a different request of the public. They’re asking – pleading, actually – with the public to get vaccinated, wear masks in public, practice social distancing, and bring this pandemic to an end.
“COVID kills, and it’s a really difficult, tragic, and lonely death,” said Ms. Wathen. “We’ve witnessed hundreds of thousands of those deaths. But now we have a way to stop it. If many more people get vaccinated, we can stop this pandemic. And hopefully that will stop this current trend of nurses leaving.”
A version of this article first appeared on Medscape.com.
As hospitals have been flooded with critically ill patients, nurses have been overwhelmed.
“What we’re hearing from our nurses is really shocking,” Amanda Bettencourt, PhD, APRN, CCRN-K, president-elect of the American Association of Critical-Care Nurses (AACN), said in an interview. “They’re saying they’re at the breaking point.”
Between Aug. 26 and Aug. 30, the AACN surveyed more than 6,000 critical care nurses, zeroing in on four key questions regarding the pandemic and its impact on nursing. The results were alarming – not only with regard to individual nurses but also for the nursing profession and the future of health care. A full 66% of those surveyed said their experiences during the pandemic have caused them to consider leaving nursing. The respondents’ take on their colleagues was even more concerning. Ninety-two percent agreed with the following two statements: “I believe the pandemic has depleted nurses at my hospital. Their careers will be shorter than they intended.”
“This puts the entire health care system at risk,” says Dr. Bettencourt, assistant professor in the department of family and community health at the University of Pennsylvania School of Nursing, Philadelphia. Intensive care unit (ICU) nurses are highly trained and are skilled in caring for critically ill patients with complex medical needs. “It’s not easy to replace a critical care nurse when one leaves,” she said.
And when nurses leave, patients suffer, said Beth Wathen, MSN, RN, CCRN-K, president of the ACCN and frontline nurse at Children’s Hospital Colorado, in Aurora. “Hospitals can have all the beds and all the rooms and all the equipment they want, but without nurses and others at the front lines to provide that essential care, none of it really matters, whether we’re talking about caring for COVID patients or caring for patients with other health ailments.”
Heartbreak of the unvaccinated
The problem is not just overwork because of the flood of COVID-19 patients. The emotional strain is enormous as well. “What’s demoralizing for us is not that patients are sick and that it’s physically exhausting to take care of sick patients. We’re used to that,” said Dr. Bettencourt.
But few nurses have experienced the sheer magnitude of patients caused by this pandemic. “The past 18 months have been grueling,” says Ms. Wathen. “The burden on frontline caregivers and our nurses at the front line has been immense.”
The situation is made worse by how unnecessary much of the suffering is at this point. Seventy-six percent of the survey’s respondents agreed with the following statement: “People who hold out on getting vaccinated undermine nurses’ physical and mental well-being.” That comment doesn’t convey the nature or extent of the effect on caregivers’ well-being. “That 9 out of 10 of the people we’re seeing in ICU right now are unvaccinated just adds to the sense of heartbreak and frustration,” says Ms. Wathen. “These deaths don’t have to be happening right now. And that’s hard to bear witness to.”
The politicization of public health has also taken a toll. “That’s been the hard part of this entire pandemic,” says Ms. Wathen. “This really isn’t at all about politics. This is about your health; this is about my health. This is about our collective health as a community and as a country.”
Like the rest of the world, nurses are also concerned about their own loved ones. The survey statement, “I fear taking care of patients with COVID puts my family’s health at risk,” garnered 67% agreement. Ms. Wathen points out that nurses take the appropriate precautions but still worry about taking infection home to their families. “This disease is a tricky one,” she says. She points out that until this pandemic is over, in addition to being vaccinated, nurses and the public still need to be vigilant about wearing masks, social distancing, and taking other precautions to ensure the safety of us all. “Our individual decisions don’t just affect ourselves. They affect our family, the people in our circle, and the people in our community,” she said.
Avoiding a professional exodus
It’s too early yet to have reliable national data on how many nurses have already left their jobs because of COVID-19, but it is clear that there are too few nurses of all kinds. The American Nurses Association sent a letter to the U.S. Secretary of Health and Human Services urging the agency to declare the nursing shortage a crisis and to take immediate steps to find solutions.
The nursing shortage predates the pandemic, and COVID-19 has brought a simmering problem to the boil. Nurses are calling on the public and the health care system for help. From inside the industry, the needs are pretty much what they were before the pandemic. Dr. Bettencourt and Ms. Wathen point to the need for supportive leadership, healthy work environments, sufficient staffing to meet patients’ needs, and a voice in decisions, such as decisions about staffing, that affect nurses and their patients. Nurses want to be heard and appreciated. “It’s not that these are new things,” said Dr. Bettencourt. “We just need them even more now because we’re stressed even more than we were before.”
Critical care nurses have a different request of the public. They’re asking – pleading, actually – with the public to get vaccinated, wear masks in public, practice social distancing, and bring this pandemic to an end.
“COVID kills, and it’s a really difficult, tragic, and lonely death,” said Ms. Wathen. “We’ve witnessed hundreds of thousands of those deaths. But now we have a way to stop it. If many more people get vaccinated, we can stop this pandemic. And hopefully that will stop this current trend of nurses leaving.”
A version of this article first appeared on Medscape.com.
As hospitals have been flooded with critically ill patients, nurses have been overwhelmed.
“What we’re hearing from our nurses is really shocking,” Amanda Bettencourt, PhD, APRN, CCRN-K, president-elect of the American Association of Critical-Care Nurses (AACN), said in an interview. “They’re saying they’re at the breaking point.”
Between Aug. 26 and Aug. 30, the AACN surveyed more than 6,000 critical care nurses, zeroing in on four key questions regarding the pandemic and its impact on nursing. The results were alarming – not only with regard to individual nurses but also for the nursing profession and the future of health care. A full 66% of those surveyed said their experiences during the pandemic have caused them to consider leaving nursing. The respondents’ take on their colleagues was even more concerning. Ninety-two percent agreed with the following two statements: “I believe the pandemic has depleted nurses at my hospital. Their careers will be shorter than they intended.”
“This puts the entire health care system at risk,” says Dr. Bettencourt, assistant professor in the department of family and community health at the University of Pennsylvania School of Nursing, Philadelphia. Intensive care unit (ICU) nurses are highly trained and are skilled in caring for critically ill patients with complex medical needs. “It’s not easy to replace a critical care nurse when one leaves,” she said.
And when nurses leave, patients suffer, said Beth Wathen, MSN, RN, CCRN-K, president of the ACCN and frontline nurse at Children’s Hospital Colorado, in Aurora. “Hospitals can have all the beds and all the rooms and all the equipment they want, but without nurses and others at the front lines to provide that essential care, none of it really matters, whether we’re talking about caring for COVID patients or caring for patients with other health ailments.”
Heartbreak of the unvaccinated
The problem is not just overwork because of the flood of COVID-19 patients. The emotional strain is enormous as well. “What’s demoralizing for us is not that patients are sick and that it’s physically exhausting to take care of sick patients. We’re used to that,” said Dr. Bettencourt.
But few nurses have experienced the sheer magnitude of patients caused by this pandemic. “The past 18 months have been grueling,” says Ms. Wathen. “The burden on frontline caregivers and our nurses at the front line has been immense.”
The situation is made worse by how unnecessary much of the suffering is at this point. Seventy-six percent of the survey’s respondents agreed with the following statement: “People who hold out on getting vaccinated undermine nurses’ physical and mental well-being.” That comment doesn’t convey the nature or extent of the effect on caregivers’ well-being. “That 9 out of 10 of the people we’re seeing in ICU right now are unvaccinated just adds to the sense of heartbreak and frustration,” says Ms. Wathen. “These deaths don’t have to be happening right now. And that’s hard to bear witness to.”
The politicization of public health has also taken a toll. “That’s been the hard part of this entire pandemic,” says Ms. Wathen. “This really isn’t at all about politics. This is about your health; this is about my health. This is about our collective health as a community and as a country.”
Like the rest of the world, nurses are also concerned about their own loved ones. The survey statement, “I fear taking care of patients with COVID puts my family’s health at risk,” garnered 67% agreement. Ms. Wathen points out that nurses take the appropriate precautions but still worry about taking infection home to their families. “This disease is a tricky one,” she says. She points out that until this pandemic is over, in addition to being vaccinated, nurses and the public still need to be vigilant about wearing masks, social distancing, and taking other precautions to ensure the safety of us all. “Our individual decisions don’t just affect ourselves. They affect our family, the people in our circle, and the people in our community,” she said.
Avoiding a professional exodus
It’s too early yet to have reliable national data on how many nurses have already left their jobs because of COVID-19, but it is clear that there are too few nurses of all kinds. The American Nurses Association sent a letter to the U.S. Secretary of Health and Human Services urging the agency to declare the nursing shortage a crisis and to take immediate steps to find solutions.
The nursing shortage predates the pandemic, and COVID-19 has brought a simmering problem to the boil. Nurses are calling on the public and the health care system for help. From inside the industry, the needs are pretty much what they were before the pandemic. Dr. Bettencourt and Ms. Wathen point to the need for supportive leadership, healthy work environments, sufficient staffing to meet patients’ needs, and a voice in decisions, such as decisions about staffing, that affect nurses and their patients. Nurses want to be heard and appreciated. “It’s not that these are new things,” said Dr. Bettencourt. “We just need them even more now because we’re stressed even more than we were before.”
Critical care nurses have a different request of the public. They’re asking – pleading, actually – with the public to get vaccinated, wear masks in public, practice social distancing, and bring this pandemic to an end.
“COVID kills, and it’s a really difficult, tragic, and lonely death,” said Ms. Wathen. “We’ve witnessed hundreds of thousands of those deaths. But now we have a way to stop it. If many more people get vaccinated, we can stop this pandemic. And hopefully that will stop this current trend of nurses leaving.”
A version of this article first appeared on Medscape.com.