User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Masking in school: A battle of the op-eds
Traditionally, as the ides of August descend upon us we expect to be bombarded with advertisements encouraging parents and students to finish up their back-to-school shopping. But, this year the question on every parent and school administrator’s mind is not which color back pack will be the most popular this year but whether a mask should be a required part of the back-to-school ensemble.

The American Academy of Pediatrics has recommended that “All students older than 2 years and all school staff should wear a mask at school” (“American Academy of Pediatrics Updates Recommendations for Opening Schools in Fall 2021.” 2021 Jul 19). The academy’s statement includes a generous list of common sense caveats but it does not include a statement that masks have been shown to be protective for children in school environments. The Centers for Disease Control and Prevention “recommends” universal indoor masking along with keeping a 3-foot separation but again fails to include any references to support the effectiveness of masks (“Guidance for COVID-19 Prevention in K-12 Schools.” 2021 Aug 5).
Not surprisingly, into this void have stepped two pairs of experts – one group purporting to have evidence that masking is effective in school environments and the other warning that masks may not only be ineffective but that they also carry some significant downsides. And, where can you find these opposing positions? Not in The Lancet. Not in the New England Journal of Medicine. We don’t have time for any of that peer-reviewed monkey business. No, this is pandemic-era science where we have an abundance of opinions and paucity of facts. You will find these opposing articles on the op-ed pages of two of this country’s major newspapers.
In the Aug. 10, 2021, edition of the New York Times you will find an article (“We Studied One Million Students. This Is What We Learned About Masking”) by two pediatricians, Kanecia Zimmerman, MD, and Danny Benjamin Jr., MD, who have “studied” a million students in North Carolina school systems and tell us universal masking is “one of the most effective and efficient strategies for preventing SARS-CoV-2 transmission in schools. These investigators write that they “believe” the low rate of in school transmission they observed in North Carolina was “because of the mask-on-mask school environment.”
However, in the next paragraph the authors admit, “Because North Carolina had a mask mandate for all K-12 schools, we could not compare masked schools with unmasked schools.” They lean instead on studies from three other states with mask mandates that also had low transmission rates and a single report of an outbreak in Israel that employed neither masking nor safe distancing.
On the other side of the divide is an article in the Wall Street Journal titled “The Case Against Masks for Children” by Marty Makary, MD, and H. Cody Meissner, MD, (2021 Aug 9). The authors, one a pediatric infectious disease specialist, argue that there is “no science behind mask mandates for children.” And, observe that, of the $46 billion spent on research grants by the National Institutes of Health, “not a single grant was dedicated to studying masking in children.”
Dr. Makary and Dr. Meissner present a variety of concerns about the effects of masking including those on the development and communication skills of young children. None of their theoretical concerns of course are supported by controlled studies. They also observe that in previous studies children seem to be less likely to transmit COVID-19 than adults. Although we all know the landscape is changing with the emergence of the delta strain. In their strongest statement the authors claim, “It is abusive to force kids who struggle with them [masks] to sacrifice for the sake of unvaccinated adults.”
So there you have it. It is a situation we have come to expect over the last 2 years – plenty of opinions and too few facts supported by controlled studies. Both pairs of authors, however, agree on two things: Vaccination should continue to be considered our primary tool in prevention and control of COVID-19. and children need to be in school. Based on nothing more than a hunch and 7 decades of hunching, I tend to side with Dr. Makary and Dr. Meissner. Depending on the situation, I suggest masking but wouldn’t mandate it for children in school.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Traditionally, as the ides of August descend upon us we expect to be bombarded with advertisements encouraging parents and students to finish up their back-to-school shopping. But, this year the question on every parent and school administrator’s mind is not which color back pack will be the most popular this year but whether a mask should be a required part of the back-to-school ensemble.
The American Academy of Pediatrics has recommended that “All students older than 2 years and all school staff should wear a mask at school” (“American Academy of Pediatrics Updates Recommendations for Opening Schools in Fall 2021.” 2021 Jul 19). The academy’s statement includes a generous list of common sense caveats but it does not include a statement that masks have been shown to be protective for children in school environments. The Centers for Disease Control and Prevention “recommends” universal indoor masking along with keeping a 3-foot separation but again fails to include any references to support the effectiveness of masks (“Guidance for COVID-19 Prevention in K-12 Schools.” 2021 Aug 5).
Not surprisingly, into this void have stepped two pairs of experts – one group purporting to have evidence that masking is effective in school environments and the other warning that masks may not only be ineffective but that they also carry some significant downsides. And, where can you find these opposing positions? Not in The Lancet. Not in the New England Journal of Medicine. We don’t have time for any of that peer-reviewed monkey business. No, this is pandemic-era science where we have an abundance of opinions and paucity of facts. You will find these opposing articles on the op-ed pages of two of this country’s major newspapers.
In the Aug. 10, 2021, edition of the New York Times you will find an article (“We Studied One Million Students. This Is What We Learned About Masking”) by two pediatricians, Kanecia Zimmerman, MD, and Danny Benjamin Jr., MD, who have “studied” a million students in North Carolina school systems and tell us universal masking is “one of the most effective and efficient strategies for preventing SARS-CoV-2 transmission in schools. These investigators write that they “believe” the low rate of in school transmission they observed in North Carolina was “because of the mask-on-mask school environment.”
However, in the next paragraph the authors admit, “Because North Carolina had a mask mandate for all K-12 schools, we could not compare masked schools with unmasked schools.” They lean instead on studies from three other states with mask mandates that also had low transmission rates and a single report of an outbreak in Israel that employed neither masking nor safe distancing.
On the other side of the divide is an article in the Wall Street Journal titled “The Case Against Masks for Children” by Marty Makary, MD, and H. Cody Meissner, MD, (2021 Aug 9). The authors, one a pediatric infectious disease specialist, argue that there is “no science behind mask mandates for children.” And, observe that, of the $46 billion spent on research grants by the National Institutes of Health, “not a single grant was dedicated to studying masking in children.”
Dr. Makary and Dr. Meissner present a variety of concerns about the effects of masking including those on the development and communication skills of young children. None of their theoretical concerns of course are supported by controlled studies. They also observe that in previous studies children seem to be less likely to transmit COVID-19 than adults. Although we all know the landscape is changing with the emergence of the delta strain. In their strongest statement the authors claim, “It is abusive to force kids who struggle with them [masks] to sacrifice for the sake of unvaccinated adults.”
So there you have it. It is a situation we have come to expect over the last 2 years – plenty of opinions and too few facts supported by controlled studies. Both pairs of authors, however, agree on two things: Vaccination should continue to be considered our primary tool in prevention and control of COVID-19. and children need to be in school. Based on nothing more than a hunch and 7 decades of hunching, I tend to side with Dr. Makary and Dr. Meissner. Depending on the situation, I suggest masking but wouldn’t mandate it for children in school.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Traditionally, as the ides of August descend upon us we expect to be bombarded with advertisements encouraging parents and students to finish up their back-to-school shopping. But, this year the question on every parent and school administrator’s mind is not which color back pack will be the most popular this year but whether a mask should be a required part of the back-to-school ensemble.
The American Academy of Pediatrics has recommended that “All students older than 2 years and all school staff should wear a mask at school” (“American Academy of Pediatrics Updates Recommendations for Opening Schools in Fall 2021.” 2021 Jul 19). The academy’s statement includes a generous list of common sense caveats but it does not include a statement that masks have been shown to be protective for children in school environments. The Centers for Disease Control and Prevention “recommends” universal indoor masking along with keeping a 3-foot separation but again fails to include any references to support the effectiveness of masks (“Guidance for COVID-19 Prevention in K-12 Schools.” 2021 Aug 5).
Not surprisingly, into this void have stepped two pairs of experts – one group purporting to have evidence that masking is effective in school environments and the other warning that masks may not only be ineffective but that they also carry some significant downsides. And, where can you find these opposing positions? Not in The Lancet. Not in the New England Journal of Medicine. We don’t have time for any of that peer-reviewed monkey business. No, this is pandemic-era science where we have an abundance of opinions and paucity of facts. You will find these opposing articles on the op-ed pages of two of this country’s major newspapers.
In the Aug. 10, 2021, edition of the New York Times you will find an article (“We Studied One Million Students. This Is What We Learned About Masking”) by two pediatricians, Kanecia Zimmerman, MD, and Danny Benjamin Jr., MD, who have “studied” a million students in North Carolina school systems and tell us universal masking is “one of the most effective and efficient strategies for preventing SARS-CoV-2 transmission in schools. These investigators write that they “believe” the low rate of in school transmission they observed in North Carolina was “because of the mask-on-mask school environment.”
However, in the next paragraph the authors admit, “Because North Carolina had a mask mandate for all K-12 schools, we could not compare masked schools with unmasked schools.” They lean instead on studies from three other states with mask mandates that also had low transmission rates and a single report of an outbreak in Israel that employed neither masking nor safe distancing.
On the other side of the divide is an article in the Wall Street Journal titled “The Case Against Masks for Children” by Marty Makary, MD, and H. Cody Meissner, MD, (2021 Aug 9). The authors, one a pediatric infectious disease specialist, argue that there is “no science behind mask mandates for children.” And, observe that, of the $46 billion spent on research grants by the National Institutes of Health, “not a single grant was dedicated to studying masking in children.”
Dr. Makary and Dr. Meissner present a variety of concerns about the effects of masking including those on the development and communication skills of young children. None of their theoretical concerns of course are supported by controlled studies. They also observe that in previous studies children seem to be less likely to transmit COVID-19 than adults. Although we all know the landscape is changing with the emergence of the delta strain. In their strongest statement the authors claim, “It is abusive to force kids who struggle with them [masks] to sacrifice for the sake of unvaccinated adults.”
So there you have it. It is a situation we have come to expect over the last 2 years – plenty of opinions and too few facts supported by controlled studies. Both pairs of authors, however, agree on two things: Vaccination should continue to be considered our primary tool in prevention and control of COVID-19. and children need to be in school. Based on nothing more than a hunch and 7 decades of hunching, I tend to side with Dr. Makary and Dr. Meissner. Depending on the situation, I suggest masking but wouldn’t mandate it for children in school.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
COVID-19 mitigation measures led to shifts in typical annual respiratory virus patterns
Nonpharmaceutical interventions, such as masking, staying home, limiting travel, and social distancing, have been doing more than reducing the risk for COVID-19. They’re also having an impact on infection rates and the timing of seasonal surges of other common respiratory diseases, according to an article published July 23 in Morbidity and Mortality Weekly Report.
Typically, respiratory pathogens such as respiratory syncytial virus (RSV), common cold coronaviruses, parainfluenza viruses, and respiratory adenoviruses increase in the fall and remain high throughout winter, following the same basic patterns as influenza. Although the historically low rates of influenza remained low into spring 2021, that’s not the case for several other common respiratory viruses.
“Clinicians should be aware of increases in some respiratory virus activity and remain vigilant for off-season increases,” wrote Sonja J. Olsen, PhD, and her colleagues at the Centers for Disease Control and Prevention. She told this news organization that clinicians should use multipathogen testing to help guide treatment.
The authors also underscore the importance of fall influenza vaccination campaigns for anyone aged 6 months or older.
Timothy Brewer, MD, MPH, a professor of medicine in the Division of Infectious Diseases at the University of California, Los Angeles (UCLA), and of epidemiology at the UCLA Fielding School of Public Health, agreed that it’s important for health care professionals to consider off-season illnesses in their patients.
“Practitioners should be aware that if they see a sick child in the summer, outside of what normally might be influenza season, but they look like they have influenza, consider potentially influenza and test for it, because it might be possible that we may have disrupted that natural pattern,” Dr. Brewer told this news organization. Dr. Brewer, who was not involved in the CDC research, said it’s also “critically important” to encourage influenza vaccination as the season approaches.
The CDC researchers used the U.S. World Health Organization Collaborating Laboratories System and the CDC’s National Respiratory and Enteric Virus Surveillance System to analyze virologic data from Oct. 3, 2020, to May 22, 2021, for influenza and Jan. 4, 2020, to May 22, 2021, for other respiratory viruses. The authors compared virus circulation during these periods to circulation during the same dates from four previous years.
Data to calculate influenza and RSV hospitalization rates came from the Influenza Hospitalization Surveillance Network and RSV Hospitalization Surveillance Network.
The authors report that flu activity dropped dramatically in March 2020 to its lowest levels since 1997, the earliest season for which data are available. Only 0.2% of more than 1 million specimens tested positive for influenza; the rate of hospitalizations for lab-confirmed flu was 0.8 per 100,000 people. Flu levels remained low through the summer, fall, and on to May 2021.
A potential drawback to this low activity, however, is a more prevalent and severe upcoming flu season, the authors write. The repeated exposure to flu viruses every year often “does not lead to illness, but it does serve to boost our immune response to influenza viruses,” Dr. Olsen said in an interview. “The absence of influenza viruses in the community over the last year means that we are not getting these regular boosts to our immune system. When we finally get exposed, our body may mount a weak response, and this could mean we develop a more clinically severe illness.”
Children are most susceptible to that phenomenon because they haven’t had a lifetime of exposure to flu viruses, Dr. Olsen said.
“An immunologically naive child may be more likely to develop a severe illness than someone who has lived through several influenza seasons,” she said. “This is why it is especially important for everyone 6 months and older to get vaccinated against influenza this season.”
Rhinovirus and enterovirus infections rebounded fairly quickly after their decline in March 2020 and started increasing in May 2020 until they reached “near prepandemic seasonal levels,” the authors write.
RSV infections dropped from 15.3% of weekly positive results in January 2020 to 1.4% by April and then stayed below 1% through the end of 2020. In past years, weekly positive results climbed to 3% in October and peaked at 12.5% to 16.7% in late December. Instead, RSV weekly positive results began increasing in April 2021, rising from 1.1% to 2.8% in May.
The “unusually timed” late spring increase in RSV “is probably associated with various nonpharmaceutical measures that have been in place but are now relaxing,” Dr. Olsen stated.
The RSV hospitalization rate was 0.3 per 100,000 people from October 2020 to April 2021, compared to 27.1 and 33.4 per 100,000 people in the previous 2 years. Of all RSV hospitalizations in the past year, 76.5% occurred in April-May 2021.
Rates of illness caused by the four common human coronaviruses (OC43, NL63, 229E, and HKU1) dropped from 7.5% of weekly positive results in January 2020 to 1.3% in April 2020 and stayed below 1% through February 2021. Then they climbed to 6.6% by May 2021. Infection rates of parainfluenza viruses types 1-4 similarly dropped from 2.6% in January 2020 to 1% in March 2020 and stayed below 1% until April 2021. Since then, rates of the common coronaviruses increased to 6.6% and parainfluenza viruses to 10.9% in May 2021.
Normally, parainfluenza viruses peak in October-November and May-June, so “the current increase could represent a return to prepandemic seasonality,” the authors write.
Human pneumoviruses’ weekly positive results initially increased from 4.2% in January 2020 to 7% in March and then fell to 1.9% the second week of April and remained below 1% through May 2021. In typical years, these viruses peak from 6.2% to 7.7% in March-April. Respiratory adenovirus activity similarly dropped to historically low levels in April 2021 and then began increasing to reach 3% by May 2021, the usual level for that month.
“The different circulation patterns observed across respiratory viruses probably also reflect differences in the virus transmission routes and how effective various nonpharmaceutical measures are at stopping transmission,” Dr. Olsen said in an interview. “As pandemic mitigation measures continue to be adjusted, we expect to see more changes in the circulation of these viruses, including a return to prepandemic circulation, as seen for rhinoviruses and enteroviruses.”
Rhinovirus and enterovirus rates dropped from 14.9% in March 2020 to 3.2% in May – lower than typical – and then climbed to a peak in October 2020. The peak (21.7% weekly positive results) was, however, still lower than the usual median of 32.8%. After dropping to 9.9% in January 2021, it then rose 19.1% in May, potentially reflecting “the usual spring peak that has occurred in previous years,” the authors write.
The authors note that it’s not yet clear how the COVID-19 pandemic and related mitigation measures will continue to affect respiratory virus circulation.
The authors hypothesize that the reasons for a seeming return to seasonal activity of respiratory adenoviruses, rhinoviruses, and enteroviruses could involve “different transmission mechanisms, the role of asymptomatic transmission, and prolonged survival of these nonenveloped viruses on surfaces, all of which might make these viruses less susceptible to nonpharmaceutical interventions.”
Dr. Brewer, of UCLA, agreed.
All the viruses basically “flatline except for adenoviruses and enteroviruses, and they behave a little differently in terms of how they spread,” he said. “Enteroviruses are much more likely to be fecal-oral spread than the other viruses [in the study].”
The delayed circulation of parainfluenza and human coronaviruses may have resulted from suspension of in-person classes through late winter 2020, they write, but that doesn’t explain the relative absence of pneumovirus activity, which usually affects the same young pediatric populations as RSV.
Dr. Brewer said California is seeing a surge of RSV right now, as are many states, especially throughout in the South. He’s not surprised by RSV’s deferred season, because those most affected – children younger than 2 years – are less likely to wear masks now and were “not going to daycare, not being out in public” in 2020. “As people are doing more activities, that’s probably why RSV has been starting to go up since April,” he said.
Despite the fact that, unlike many East Asian cultures, the United States has not traditionally been a mask-wearing culture, Dr. Brewer wouldn’t be surprised if more Americans begin wearing masks during flu season. “Hopefully another thing that will come out of this is better hand hygiene, with people just getting used to washing their hands more, particularly after they come home from being out,” he added.
Dr. Brewer similarly emphasized the importance of flu vaccination for the upcoming season, especially for younger children who may have poorer natural immunity to influenza, owing to its low circulation rates in 2020-2021.
The study was funded by the CDC. Dr. Brewer and Dr. Olsen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nonpharmaceutical interventions, such as masking, staying home, limiting travel, and social distancing, have been doing more than reducing the risk for COVID-19. They’re also having an impact on infection rates and the timing of seasonal surges of other common respiratory diseases, according to an article published July 23 in Morbidity and Mortality Weekly Report.
Typically, respiratory pathogens such as respiratory syncytial virus (RSV), common cold coronaviruses, parainfluenza viruses, and respiratory adenoviruses increase in the fall and remain high throughout winter, following the same basic patterns as influenza. Although the historically low rates of influenza remained low into spring 2021, that’s not the case for several other common respiratory viruses.
“Clinicians should be aware of increases in some respiratory virus activity and remain vigilant for off-season increases,” wrote Sonja J. Olsen, PhD, and her colleagues at the Centers for Disease Control and Prevention. She told this news organization that clinicians should use multipathogen testing to help guide treatment.
The authors also underscore the importance of fall influenza vaccination campaigns for anyone aged 6 months or older.
Timothy Brewer, MD, MPH, a professor of medicine in the Division of Infectious Diseases at the University of California, Los Angeles (UCLA), and of epidemiology at the UCLA Fielding School of Public Health, agreed that it’s important for health care professionals to consider off-season illnesses in their patients.
“Practitioners should be aware that if they see a sick child in the summer, outside of what normally might be influenza season, but they look like they have influenza, consider potentially influenza and test for it, because it might be possible that we may have disrupted that natural pattern,” Dr. Brewer told this news organization. Dr. Brewer, who was not involved in the CDC research, said it’s also “critically important” to encourage influenza vaccination as the season approaches.
The CDC researchers used the U.S. World Health Organization Collaborating Laboratories System and the CDC’s National Respiratory and Enteric Virus Surveillance System to analyze virologic data from Oct. 3, 2020, to May 22, 2021, for influenza and Jan. 4, 2020, to May 22, 2021, for other respiratory viruses. The authors compared virus circulation during these periods to circulation during the same dates from four previous years.
Data to calculate influenza and RSV hospitalization rates came from the Influenza Hospitalization Surveillance Network and RSV Hospitalization Surveillance Network.
The authors report that flu activity dropped dramatically in March 2020 to its lowest levels since 1997, the earliest season for which data are available. Only 0.2% of more than 1 million specimens tested positive for influenza; the rate of hospitalizations for lab-confirmed flu was 0.8 per 100,000 people. Flu levels remained low through the summer, fall, and on to May 2021.
A potential drawback to this low activity, however, is a more prevalent and severe upcoming flu season, the authors write. The repeated exposure to flu viruses every year often “does not lead to illness, but it does serve to boost our immune response to influenza viruses,” Dr. Olsen said in an interview. “The absence of influenza viruses in the community over the last year means that we are not getting these regular boosts to our immune system. When we finally get exposed, our body may mount a weak response, and this could mean we develop a more clinically severe illness.”
Children are most susceptible to that phenomenon because they haven’t had a lifetime of exposure to flu viruses, Dr. Olsen said.
“An immunologically naive child may be more likely to develop a severe illness than someone who has lived through several influenza seasons,” she said. “This is why it is especially important for everyone 6 months and older to get vaccinated against influenza this season.”
Rhinovirus and enterovirus infections rebounded fairly quickly after their decline in March 2020 and started increasing in May 2020 until they reached “near prepandemic seasonal levels,” the authors write.
RSV infections dropped from 15.3% of weekly positive results in January 2020 to 1.4% by April and then stayed below 1% through the end of 2020. In past years, weekly positive results climbed to 3% in October and peaked at 12.5% to 16.7% in late December. Instead, RSV weekly positive results began increasing in April 2021, rising from 1.1% to 2.8% in May.
The “unusually timed” late spring increase in RSV “is probably associated with various nonpharmaceutical measures that have been in place but are now relaxing,” Dr. Olsen stated.
The RSV hospitalization rate was 0.3 per 100,000 people from October 2020 to April 2021, compared to 27.1 and 33.4 per 100,000 people in the previous 2 years. Of all RSV hospitalizations in the past year, 76.5% occurred in April-May 2021.
Rates of illness caused by the four common human coronaviruses (OC43, NL63, 229E, and HKU1) dropped from 7.5% of weekly positive results in January 2020 to 1.3% in April 2020 and stayed below 1% through February 2021. Then they climbed to 6.6% by May 2021. Infection rates of parainfluenza viruses types 1-4 similarly dropped from 2.6% in January 2020 to 1% in March 2020 and stayed below 1% until April 2021. Since then, rates of the common coronaviruses increased to 6.6% and parainfluenza viruses to 10.9% in May 2021.
Normally, parainfluenza viruses peak in October-November and May-June, so “the current increase could represent a return to prepandemic seasonality,” the authors write.
Human pneumoviruses’ weekly positive results initially increased from 4.2% in January 2020 to 7% in March and then fell to 1.9% the second week of April and remained below 1% through May 2021. In typical years, these viruses peak from 6.2% to 7.7% in March-April. Respiratory adenovirus activity similarly dropped to historically low levels in April 2021 and then began increasing to reach 3% by May 2021, the usual level for that month.
“The different circulation patterns observed across respiratory viruses probably also reflect differences in the virus transmission routes and how effective various nonpharmaceutical measures are at stopping transmission,” Dr. Olsen said in an interview. “As pandemic mitigation measures continue to be adjusted, we expect to see more changes in the circulation of these viruses, including a return to prepandemic circulation, as seen for rhinoviruses and enteroviruses.”
Rhinovirus and enterovirus rates dropped from 14.9% in March 2020 to 3.2% in May – lower than typical – and then climbed to a peak in October 2020. The peak (21.7% weekly positive results) was, however, still lower than the usual median of 32.8%. After dropping to 9.9% in January 2021, it then rose 19.1% in May, potentially reflecting “the usual spring peak that has occurred in previous years,” the authors write.
The authors note that it’s not yet clear how the COVID-19 pandemic and related mitigation measures will continue to affect respiratory virus circulation.
The authors hypothesize that the reasons for a seeming return to seasonal activity of respiratory adenoviruses, rhinoviruses, and enteroviruses could involve “different transmission mechanisms, the role of asymptomatic transmission, and prolonged survival of these nonenveloped viruses on surfaces, all of which might make these viruses less susceptible to nonpharmaceutical interventions.”
Dr. Brewer, of UCLA, agreed.
All the viruses basically “flatline except for adenoviruses and enteroviruses, and they behave a little differently in terms of how they spread,” he said. “Enteroviruses are much more likely to be fecal-oral spread than the other viruses [in the study].”
The delayed circulation of parainfluenza and human coronaviruses may have resulted from suspension of in-person classes through late winter 2020, they write, but that doesn’t explain the relative absence of pneumovirus activity, which usually affects the same young pediatric populations as RSV.
Dr. Brewer said California is seeing a surge of RSV right now, as are many states, especially throughout in the South. He’s not surprised by RSV’s deferred season, because those most affected – children younger than 2 years – are less likely to wear masks now and were “not going to daycare, not being out in public” in 2020. “As people are doing more activities, that’s probably why RSV has been starting to go up since April,” he said.
Despite the fact that, unlike many East Asian cultures, the United States has not traditionally been a mask-wearing culture, Dr. Brewer wouldn’t be surprised if more Americans begin wearing masks during flu season. “Hopefully another thing that will come out of this is better hand hygiene, with people just getting used to washing their hands more, particularly after they come home from being out,” he added.
Dr. Brewer similarly emphasized the importance of flu vaccination for the upcoming season, especially for younger children who may have poorer natural immunity to influenza, owing to its low circulation rates in 2020-2021.
The study was funded by the CDC. Dr. Brewer and Dr. Olsen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nonpharmaceutical interventions, such as masking, staying home, limiting travel, and social distancing, have been doing more than reducing the risk for COVID-19. They’re also having an impact on infection rates and the timing of seasonal surges of other common respiratory diseases, according to an article published July 23 in Morbidity and Mortality Weekly Report.
Typically, respiratory pathogens such as respiratory syncytial virus (RSV), common cold coronaviruses, parainfluenza viruses, and respiratory adenoviruses increase in the fall and remain high throughout winter, following the same basic patterns as influenza. Although the historically low rates of influenza remained low into spring 2021, that’s not the case for several other common respiratory viruses.
“Clinicians should be aware of increases in some respiratory virus activity and remain vigilant for off-season increases,” wrote Sonja J. Olsen, PhD, and her colleagues at the Centers for Disease Control and Prevention. She told this news organization that clinicians should use multipathogen testing to help guide treatment.
The authors also underscore the importance of fall influenza vaccination campaigns for anyone aged 6 months or older.
Timothy Brewer, MD, MPH, a professor of medicine in the Division of Infectious Diseases at the University of California, Los Angeles (UCLA), and of epidemiology at the UCLA Fielding School of Public Health, agreed that it’s important for health care professionals to consider off-season illnesses in their patients.
“Practitioners should be aware that if they see a sick child in the summer, outside of what normally might be influenza season, but they look like they have influenza, consider potentially influenza and test for it, because it might be possible that we may have disrupted that natural pattern,” Dr. Brewer told this news organization. Dr. Brewer, who was not involved in the CDC research, said it’s also “critically important” to encourage influenza vaccination as the season approaches.
The CDC researchers used the U.S. World Health Organization Collaborating Laboratories System and the CDC’s National Respiratory and Enteric Virus Surveillance System to analyze virologic data from Oct. 3, 2020, to May 22, 2021, for influenza and Jan. 4, 2020, to May 22, 2021, for other respiratory viruses. The authors compared virus circulation during these periods to circulation during the same dates from four previous years.
Data to calculate influenza and RSV hospitalization rates came from the Influenza Hospitalization Surveillance Network and RSV Hospitalization Surveillance Network.
The authors report that flu activity dropped dramatically in March 2020 to its lowest levels since 1997, the earliest season for which data are available. Only 0.2% of more than 1 million specimens tested positive for influenza; the rate of hospitalizations for lab-confirmed flu was 0.8 per 100,000 people. Flu levels remained low through the summer, fall, and on to May 2021.
A potential drawback to this low activity, however, is a more prevalent and severe upcoming flu season, the authors write. The repeated exposure to flu viruses every year often “does not lead to illness, but it does serve to boost our immune response to influenza viruses,” Dr. Olsen said in an interview. “The absence of influenza viruses in the community over the last year means that we are not getting these regular boosts to our immune system. When we finally get exposed, our body may mount a weak response, and this could mean we develop a more clinically severe illness.”
Children are most susceptible to that phenomenon because they haven’t had a lifetime of exposure to flu viruses, Dr. Olsen said.
“An immunologically naive child may be more likely to develop a severe illness than someone who has lived through several influenza seasons,” she said. “This is why it is especially important for everyone 6 months and older to get vaccinated against influenza this season.”
Rhinovirus and enterovirus infections rebounded fairly quickly after their decline in March 2020 and started increasing in May 2020 until they reached “near prepandemic seasonal levels,” the authors write.
RSV infections dropped from 15.3% of weekly positive results in January 2020 to 1.4% by April and then stayed below 1% through the end of 2020. In past years, weekly positive results climbed to 3% in October and peaked at 12.5% to 16.7% in late December. Instead, RSV weekly positive results began increasing in April 2021, rising from 1.1% to 2.8% in May.
The “unusually timed” late spring increase in RSV “is probably associated with various nonpharmaceutical measures that have been in place but are now relaxing,” Dr. Olsen stated.
The RSV hospitalization rate was 0.3 per 100,000 people from October 2020 to April 2021, compared to 27.1 and 33.4 per 100,000 people in the previous 2 years. Of all RSV hospitalizations in the past year, 76.5% occurred in April-May 2021.
Rates of illness caused by the four common human coronaviruses (OC43, NL63, 229E, and HKU1) dropped from 7.5% of weekly positive results in January 2020 to 1.3% in April 2020 and stayed below 1% through February 2021. Then they climbed to 6.6% by May 2021. Infection rates of parainfluenza viruses types 1-4 similarly dropped from 2.6% in January 2020 to 1% in March 2020 and stayed below 1% until April 2021. Since then, rates of the common coronaviruses increased to 6.6% and parainfluenza viruses to 10.9% in May 2021.
Normally, parainfluenza viruses peak in October-November and May-June, so “the current increase could represent a return to prepandemic seasonality,” the authors write.
Human pneumoviruses’ weekly positive results initially increased from 4.2% in January 2020 to 7% in March and then fell to 1.9% the second week of April and remained below 1% through May 2021. In typical years, these viruses peak from 6.2% to 7.7% in March-April. Respiratory adenovirus activity similarly dropped to historically low levels in April 2021 and then began increasing to reach 3% by May 2021, the usual level for that month.
“The different circulation patterns observed across respiratory viruses probably also reflect differences in the virus transmission routes and how effective various nonpharmaceutical measures are at stopping transmission,” Dr. Olsen said in an interview. “As pandemic mitigation measures continue to be adjusted, we expect to see more changes in the circulation of these viruses, including a return to prepandemic circulation, as seen for rhinoviruses and enteroviruses.”
Rhinovirus and enterovirus rates dropped from 14.9% in March 2020 to 3.2% in May – lower than typical – and then climbed to a peak in October 2020. The peak (21.7% weekly positive results) was, however, still lower than the usual median of 32.8%. After dropping to 9.9% in January 2021, it then rose 19.1% in May, potentially reflecting “the usual spring peak that has occurred in previous years,” the authors write.
The authors note that it’s not yet clear how the COVID-19 pandemic and related mitigation measures will continue to affect respiratory virus circulation.
The authors hypothesize that the reasons for a seeming return to seasonal activity of respiratory adenoviruses, rhinoviruses, and enteroviruses could involve “different transmission mechanisms, the role of asymptomatic transmission, and prolonged survival of these nonenveloped viruses on surfaces, all of which might make these viruses less susceptible to nonpharmaceutical interventions.”
Dr. Brewer, of UCLA, agreed.
All the viruses basically “flatline except for adenoviruses and enteroviruses, and they behave a little differently in terms of how they spread,” he said. “Enteroviruses are much more likely to be fecal-oral spread than the other viruses [in the study].”
The delayed circulation of parainfluenza and human coronaviruses may have resulted from suspension of in-person classes through late winter 2020, they write, but that doesn’t explain the relative absence of pneumovirus activity, which usually affects the same young pediatric populations as RSV.
Dr. Brewer said California is seeing a surge of RSV right now, as are many states, especially throughout in the South. He’s not surprised by RSV’s deferred season, because those most affected – children younger than 2 years – are less likely to wear masks now and were “not going to daycare, not being out in public” in 2020. “As people are doing more activities, that’s probably why RSV has been starting to go up since April,” he said.
Despite the fact that, unlike many East Asian cultures, the United States has not traditionally been a mask-wearing culture, Dr. Brewer wouldn’t be surprised if more Americans begin wearing masks during flu season. “Hopefully another thing that will come out of this is better hand hygiene, with people just getting used to washing their hands more, particularly after they come home from being out,” he added.
Dr. Brewer similarly emphasized the importance of flu vaccination for the upcoming season, especially for younger children who may have poorer natural immunity to influenza, owing to its low circulation rates in 2020-2021.
The study was funded by the CDC. Dr. Brewer and Dr. Olsen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Tirzepatide questions persist despite serial phase 3 success in type 2 diabetes
The streak of positive phase 3 trial results for the novel “twincretin” tirzepatide when treating patients with type 2 diabetes continued in a report in The Lancet on results from the SURPASS-3 trial, which compared weekly subcutaneous injections of tirzepatide against daily treatment with insulin degludec in patients inadequately controlled on metformin alone or on metformin plus a sodium-glucose cotransporter 2 inhibitor.
Despite positive results in SURPASS-3, as well as in four other pivotal trials that are in the process of releasing full results, the safety and efficacy picture of tirzepatide still includes several as-yet unresolved issues, including the true incidence rate of gastrointestinal adverse effects, the role these effects play in weight loss during tirzepatide treatment, and the drug’s effect on important endpoints beyond weight loss and glycemic control such as cardiovascular outcomes and renal function, said two Australian experts who coauthored a comment on the new SURPASS-3 report.
Tirzepatide is called a “twincretin” because the molecule acts as both a glucagonlike peptide–1 receptor agonist, the drug class that includes semaglutide (Ozempic, Rybelsus, Wegovy) and liraglutide (Saxenda, Victoza), and also as a glucose-dependent insulinotropic polypeptide (GIP). Trial results reported to date suggest that tirzepatide “might be more potent than available GLP-1 receptor agonists,” based on evidence of superior glycemic control it produced relative to semaglutide in results from the SURPASS-2 phase 3 trial reported in August 2021, wrote Christopher K. Rayner, MD, and Michael Horowitz, MD, in their comment.
Uncertainty about gastrointestinal adverse effects
“Limitations of SURPASS-3 include the relatively small number of Asian and Black” patients enrolled, “and an open-label design that carries a risk for bias” when tallying the incidence of gastrointestinal adverse effects, which the trial recorded based on self-reports by enrolled patients.
A better design would use validated questionnaires geared to discerning gastrointestinal symptoms like the ones used in trials involving patients with functional gastrointestinal disorders, wrote Dr. Rayner, a professor of gastroenterology at the University of Adelaide, and Dr. Horowitz, a professor at the same institution and also director of the endocrine and metabolic unit at Royal Adelaide Hospital.
This approach would “allow for more robust evaluation of whether gastrointestinal symptoms are associated with increased weight loss,” they proposed, a possible partial explanation for the weight loss of some patients treated with a GLP-1 receptor agonist.
Additional outstanding questions about tirzepatide include the contribution resulting from the drug’s stimulation of the GIP receptor, as well as the role of GLP-1 receptor stimulation by tirzepatide in slowing gastric emptying. And they also cite the still-unreported effects of tirzepatide on cardiovascular events, fatty liver disease, and kidney function, and its longer-term effects with chronic treatment beyond a year.
All five of the recently completed SURPASS trials ran for 40-52 weeks.
Tirzepatide surpasses insulin degludec’s glycemic control
SURPASS-3 enrolled 1,444 patients with type 2 diabetes at 122 sites in 13 countries during 2019. The study’s primary endpoint was mean change in hemoglobin A1c from baseline after 52 weeks on treatment. The results showed that the A1c reduction with tirzepatide treatment significantly exceeded the drop produced by insulin degludec by 0.59%, 0.86%, and 1.04%, respectively, across the three tirzepatide dosages tested in a dose-response fashion, according to the recent publication.
The most common treatment-emergent adverse effects were gastrointestinal, which decreased with continued treatment, and tirzepatide produced fewer episodes of hypoglycemia, compared with insulin degludec (Tresiba).
In addition to full reports now out from SURPASS-2 and SURPASS-3, researchers also recently published full primary results from SURPASS-1. Results from SURPASS-5 appeared in a poster presented at the American Diabetes Association scientific sessions in June 2021 but have not yet been published in a full report, and the primary results from SURPASS-4are expected in a report during the European Association for the Study of Diabetes in September 2021.
SURPASS-3 and the other trials of tirzepatide were funded by Lilly, the company developing the drug. Dr. Rayner has been an adviser to Allergen and Glyscend, and has received research funding from Sanofi and Novartis. Dr. Horowitz has received symposia fees from Lilly, as well as from AstraZeneca and Boehringer Ingelheim.
The streak of positive phase 3 trial results for the novel “twincretin” tirzepatide when treating patients with type 2 diabetes continued in a report in The Lancet on results from the SURPASS-3 trial, which compared weekly subcutaneous injections of tirzepatide against daily treatment with insulin degludec in patients inadequately controlled on metformin alone or on metformin plus a sodium-glucose cotransporter 2 inhibitor.
Despite positive results in SURPASS-3, as well as in four other pivotal trials that are in the process of releasing full results, the safety and efficacy picture of tirzepatide still includes several as-yet unresolved issues, including the true incidence rate of gastrointestinal adverse effects, the role these effects play in weight loss during tirzepatide treatment, and the drug’s effect on important endpoints beyond weight loss and glycemic control such as cardiovascular outcomes and renal function, said two Australian experts who coauthored a comment on the new SURPASS-3 report.
Tirzepatide is called a “twincretin” because the molecule acts as both a glucagonlike peptide–1 receptor agonist, the drug class that includes semaglutide (Ozempic, Rybelsus, Wegovy) and liraglutide (Saxenda, Victoza), and also as a glucose-dependent insulinotropic polypeptide (GIP). Trial results reported to date suggest that tirzepatide “might be more potent than available GLP-1 receptor agonists,” based on evidence of superior glycemic control it produced relative to semaglutide in results from the SURPASS-2 phase 3 trial reported in August 2021, wrote Christopher K. Rayner, MD, and Michael Horowitz, MD, in their comment.
Uncertainty about gastrointestinal adverse effects
“Limitations of SURPASS-3 include the relatively small number of Asian and Black” patients enrolled, “and an open-label design that carries a risk for bias” when tallying the incidence of gastrointestinal adverse effects, which the trial recorded based on self-reports by enrolled patients.
A better design would use validated questionnaires geared to discerning gastrointestinal symptoms like the ones used in trials involving patients with functional gastrointestinal disorders, wrote Dr. Rayner, a professor of gastroenterology at the University of Adelaide, and Dr. Horowitz, a professor at the same institution and also director of the endocrine and metabolic unit at Royal Adelaide Hospital.
This approach would “allow for more robust evaluation of whether gastrointestinal symptoms are associated with increased weight loss,” they proposed, a possible partial explanation for the weight loss of some patients treated with a GLP-1 receptor agonist.
Additional outstanding questions about tirzepatide include the contribution resulting from the drug’s stimulation of the GIP receptor, as well as the role of GLP-1 receptor stimulation by tirzepatide in slowing gastric emptying. And they also cite the still-unreported effects of tirzepatide on cardiovascular events, fatty liver disease, and kidney function, and its longer-term effects with chronic treatment beyond a year.
All five of the recently completed SURPASS trials ran for 40-52 weeks.
Tirzepatide surpasses insulin degludec’s glycemic control
SURPASS-3 enrolled 1,444 patients with type 2 diabetes at 122 sites in 13 countries during 2019. The study’s primary endpoint was mean change in hemoglobin A1c from baseline after 52 weeks on treatment. The results showed that the A1c reduction with tirzepatide treatment significantly exceeded the drop produced by insulin degludec by 0.59%, 0.86%, and 1.04%, respectively, across the three tirzepatide dosages tested in a dose-response fashion, according to the recent publication.
The most common treatment-emergent adverse effects were gastrointestinal, which decreased with continued treatment, and tirzepatide produced fewer episodes of hypoglycemia, compared with insulin degludec (Tresiba).
In addition to full reports now out from SURPASS-2 and SURPASS-3, researchers also recently published full primary results from SURPASS-1. Results from SURPASS-5 appeared in a poster presented at the American Diabetes Association scientific sessions in June 2021 but have not yet been published in a full report, and the primary results from SURPASS-4are expected in a report during the European Association for the Study of Diabetes in September 2021.
SURPASS-3 and the other trials of tirzepatide were funded by Lilly, the company developing the drug. Dr. Rayner has been an adviser to Allergen and Glyscend, and has received research funding from Sanofi and Novartis. Dr. Horowitz has received symposia fees from Lilly, as well as from AstraZeneca and Boehringer Ingelheim.
The streak of positive phase 3 trial results for the novel “twincretin” tirzepatide when treating patients with type 2 diabetes continued in a report in The Lancet on results from the SURPASS-3 trial, which compared weekly subcutaneous injections of tirzepatide against daily treatment with insulin degludec in patients inadequately controlled on metformin alone or on metformin plus a sodium-glucose cotransporter 2 inhibitor.
Despite positive results in SURPASS-3, as well as in four other pivotal trials that are in the process of releasing full results, the safety and efficacy picture of tirzepatide still includes several as-yet unresolved issues, including the true incidence rate of gastrointestinal adverse effects, the role these effects play in weight loss during tirzepatide treatment, and the drug’s effect on important endpoints beyond weight loss and glycemic control such as cardiovascular outcomes and renal function, said two Australian experts who coauthored a comment on the new SURPASS-3 report.
Tirzepatide is called a “twincretin” because the molecule acts as both a glucagonlike peptide–1 receptor agonist, the drug class that includes semaglutide (Ozempic, Rybelsus, Wegovy) and liraglutide (Saxenda, Victoza), and also as a glucose-dependent insulinotropic polypeptide (GIP). Trial results reported to date suggest that tirzepatide “might be more potent than available GLP-1 receptor agonists,” based on evidence of superior glycemic control it produced relative to semaglutide in results from the SURPASS-2 phase 3 trial reported in August 2021, wrote Christopher K. Rayner, MD, and Michael Horowitz, MD, in their comment.
Uncertainty about gastrointestinal adverse effects
“Limitations of SURPASS-3 include the relatively small number of Asian and Black” patients enrolled, “and an open-label design that carries a risk for bias” when tallying the incidence of gastrointestinal adverse effects, which the trial recorded based on self-reports by enrolled patients.
A better design would use validated questionnaires geared to discerning gastrointestinal symptoms like the ones used in trials involving patients with functional gastrointestinal disorders, wrote Dr. Rayner, a professor of gastroenterology at the University of Adelaide, and Dr. Horowitz, a professor at the same institution and also director of the endocrine and metabolic unit at Royal Adelaide Hospital.
This approach would “allow for more robust evaluation of whether gastrointestinal symptoms are associated with increased weight loss,” they proposed, a possible partial explanation for the weight loss of some patients treated with a GLP-1 receptor agonist.
Additional outstanding questions about tirzepatide include the contribution resulting from the drug’s stimulation of the GIP receptor, as well as the role of GLP-1 receptor stimulation by tirzepatide in slowing gastric emptying. And they also cite the still-unreported effects of tirzepatide on cardiovascular events, fatty liver disease, and kidney function, and its longer-term effects with chronic treatment beyond a year.
All five of the recently completed SURPASS trials ran for 40-52 weeks.
Tirzepatide surpasses insulin degludec’s glycemic control
SURPASS-3 enrolled 1,444 patients with type 2 diabetes at 122 sites in 13 countries during 2019. The study’s primary endpoint was mean change in hemoglobin A1c from baseline after 52 weeks on treatment. The results showed that the A1c reduction with tirzepatide treatment significantly exceeded the drop produced by insulin degludec by 0.59%, 0.86%, and 1.04%, respectively, across the three tirzepatide dosages tested in a dose-response fashion, according to the recent publication.
The most common treatment-emergent adverse effects were gastrointestinal, which decreased with continued treatment, and tirzepatide produced fewer episodes of hypoglycemia, compared with insulin degludec (Tresiba).
In addition to full reports now out from SURPASS-2 and SURPASS-3, researchers also recently published full primary results from SURPASS-1. Results from SURPASS-5 appeared in a poster presented at the American Diabetes Association scientific sessions in June 2021 but have not yet been published in a full report, and the primary results from SURPASS-4are expected in a report during the European Association for the Study of Diabetes in September 2021.
SURPASS-3 and the other trials of tirzepatide were funded by Lilly, the company developing the drug. Dr. Rayner has been an adviser to Allergen and Glyscend, and has received research funding from Sanofi and Novartis. Dr. Horowitz has received symposia fees from Lilly, as well as from AstraZeneca and Boehringer Ingelheim.
FROM THE LANCET
CAG Clinical Practice Guideline: Vaccination in patients with IBD
The Canadian Association of Gastroenterology (CAG) has published a two-part clinical practice guideline for immunizing patients with inflammatory bowel disease (IBD) that covers both live and inactivated vaccines across pediatric and adult patients.
The guideline, which has been endorsed by the American Gastroenterological Association, is composed of recommendations drawn from a broader body of data than prior publications on the same topic, according to Eric I. Benchimol, MD, PhD, of the University of Ottawa and the University of Toronto, and colleagues.
“Previous guidelines on immunizations of patients with IBD considered only the limited available evidence of vaccine safety and effectiveness in IBD populations, and failed to consider the ample evidence available in the general population or in other immune-mediated inflammatory diseases when assessing the certainty of evidence or developing their recommendations,” they wrote in Gastroenterology.
Part 1: Live vaccine recommendations
The first part of the guideline includes seven recommendations for use of live vaccines in patients with IBD.
In this area, decision-making is largely dependent upon use of immunosuppressive therapy, which the investigators defined as “corticosteroids, thiopurines, biologics, small molecules such as JAK [Janus kinase] inhibitors, and combinations thereof,” with the caveat that “there is no standard definition of immunosuppression,” and “the degree to which immunosuppressive therapy causes clinically significant immunosuppression generally is dose related and varies by drug.”
Before offering specific recommendations, Dr. Benchimol and colleagues provided three general principles to abide by: 1. Clinicians should review each patient’s history of immunization and vaccine-preventable diseases at diagnosis and on a routine basis; 2. Appropriate vaccinations should ideally be given prior to starting immunosuppressive therapy; and 3. Immunosuppressive therapy (when urgently needed) should not be delayed so that immunizations can be given in advance.
“[Delaying therapy] could lead to more anticipated harms than benefits, due to the risk of progression of the inflammatory activity and resulting complications,” the investigators wrote.
Specific recommendations in the guideline address measles, mumps, and rubella (MMR); and varicella. Both vaccines are recommended for susceptible pediatric and adult patients not taking immunosuppressive therapy. In contrast, neither vaccine is recommended for immunosuppressed patients of any age. Certainty of evidence ranged from very low to moderate.
Concerning vaccination within the first 6 months of life for infants born of mothers taking biologics, the expert panel did not reach a consensus.
“[T]he group was unable to recommend for or against their routine use because the desirable and undesirable effects were closely balanced and the evidence on safety outcomes was insufficient to justify a recommendation,” wrote Dr. Benchimol and colleagues. “Health care providers should be cautious with the administration of live vaccines in the first year of life in the infants of mothers using biologics. These infants should be evaluated by clinicians with expertise in the impact of exposure to monoclonal antibody biologics in utero.”
Part 2: Inactivated vaccine recommendations
The second part of the guideline, by lead author Jennifer L. Jones, MD, of Dalhousie University, Queen Elizabeth II Health Sciences Center, Halifax, N.S., and colleagues, provides 15 recommendations for giving inactivated vaccines to patients with IBD.
The panel considered eight vaccines: Haemophilus influenzae type B (Hib); herpes zoster (HZ); hepatitis B; influenza; Streptococcus pneumoniae (pneumococcal vaccine); Neisseria meningitidis (meningococcal vaccine); human papillomavirus (HPV); and diphtheria, tetanus, and pertussis.
Generally, the above vaccines are recommended on an age-appropriate basis, regardless of immunosuppression status, albeit with varying levels of confidence. For example, the Hib vaccine is strongly recommended for pediatric patients 5 years and younger, whereas the same recommendation for older children and adults is conditional.
For several patient populations and vaccines, the guideline panel did not reach a consensus, including use of double-dose hepatitis B vaccine for immunosuppressed adults, timing seasonal flu shots with dosing of biologics, use of pneumococcal vaccines in nonimmunosuppressed patents without a risk factor for pneumococcal disease, use of meningococcal vaccines in adults not at risk for invasive meningococcal disease, and use of HPV vaccine in patients aged 27-45 years.
While immunosuppressive therapy is not a contraindication for giving inactivated vaccines, Dr. Jones and colleagues noted that immunosuppression may hinder vaccine responses.
“Given that patients with IBD on immunosuppressive therapy may have lower immune response to vaccine, further research will be needed to assess the safety and effectiveness of high-dose vs. standard-dose vaccination strategy,” they wrote, also noting that more work is needed to determine if accelerated vaccinations strategies may be feasible prior to initiation of immunosuppressive therapy.
Because of a lack of evidence, the guideline panel did not issue IBD-specific recommendations for vaccines against SARS-CoV-2; however, Dr. Jones and colleagues suggested that clinicians reference a CAG publication on the subject published earlier this year.
The guideline was supported by grants to the Canadian Association of Gastroenterology from the Canadian Institutes of Health Research’s Institute of Nutrition, Metabolism and Diabetes; and CANImmunize. Dr. Benchimol disclosed additional relationships with the Canadian Institutes of Health Research, Crohn’s and Colitis Canada; and the Canadian Child Health Clinician Scientist Program.
The Canadian Association of Gastroenterology (CAG) has published a two-part clinical practice guideline for immunizing patients with inflammatory bowel disease (IBD) that covers both live and inactivated vaccines across pediatric and adult patients.
The guideline, which has been endorsed by the American Gastroenterological Association, is composed of recommendations drawn from a broader body of data than prior publications on the same topic, according to Eric I. Benchimol, MD, PhD, of the University of Ottawa and the University of Toronto, and colleagues.
“Previous guidelines on immunizations of patients with IBD considered only the limited available evidence of vaccine safety and effectiveness in IBD populations, and failed to consider the ample evidence available in the general population or in other immune-mediated inflammatory diseases when assessing the certainty of evidence or developing their recommendations,” they wrote in Gastroenterology.
Part 1: Live vaccine recommendations
The first part of the guideline includes seven recommendations for use of live vaccines in patients with IBD.
In this area, decision-making is largely dependent upon use of immunosuppressive therapy, which the investigators defined as “corticosteroids, thiopurines, biologics, small molecules such as JAK [Janus kinase] inhibitors, and combinations thereof,” with the caveat that “there is no standard definition of immunosuppression,” and “the degree to which immunosuppressive therapy causes clinically significant immunosuppression generally is dose related and varies by drug.”
Before offering specific recommendations, Dr. Benchimol and colleagues provided three general principles to abide by: 1. Clinicians should review each patient’s history of immunization and vaccine-preventable diseases at diagnosis and on a routine basis; 2. Appropriate vaccinations should ideally be given prior to starting immunosuppressive therapy; and 3. Immunosuppressive therapy (when urgently needed) should not be delayed so that immunizations can be given in advance.
“[Delaying therapy] could lead to more anticipated harms than benefits, due to the risk of progression of the inflammatory activity and resulting complications,” the investigators wrote.
Specific recommendations in the guideline address measles, mumps, and rubella (MMR); and varicella. Both vaccines are recommended for susceptible pediatric and adult patients not taking immunosuppressive therapy. In contrast, neither vaccine is recommended for immunosuppressed patients of any age. Certainty of evidence ranged from very low to moderate.
Concerning vaccination within the first 6 months of life for infants born of mothers taking biologics, the expert panel did not reach a consensus.
“[T]he group was unable to recommend for or against their routine use because the desirable and undesirable effects were closely balanced and the evidence on safety outcomes was insufficient to justify a recommendation,” wrote Dr. Benchimol and colleagues. “Health care providers should be cautious with the administration of live vaccines in the first year of life in the infants of mothers using biologics. These infants should be evaluated by clinicians with expertise in the impact of exposure to monoclonal antibody biologics in utero.”
Part 2: Inactivated vaccine recommendations
The second part of the guideline, by lead author Jennifer L. Jones, MD, of Dalhousie University, Queen Elizabeth II Health Sciences Center, Halifax, N.S., and colleagues, provides 15 recommendations for giving inactivated vaccines to patients with IBD.
The panel considered eight vaccines: Haemophilus influenzae type B (Hib); herpes zoster (HZ); hepatitis B; influenza; Streptococcus pneumoniae (pneumococcal vaccine); Neisseria meningitidis (meningococcal vaccine); human papillomavirus (HPV); and diphtheria, tetanus, and pertussis.
Generally, the above vaccines are recommended on an age-appropriate basis, regardless of immunosuppression status, albeit with varying levels of confidence. For example, the Hib vaccine is strongly recommended for pediatric patients 5 years and younger, whereas the same recommendation for older children and adults is conditional.
For several patient populations and vaccines, the guideline panel did not reach a consensus, including use of double-dose hepatitis B vaccine for immunosuppressed adults, timing seasonal flu shots with dosing of biologics, use of pneumococcal vaccines in nonimmunosuppressed patents without a risk factor for pneumococcal disease, use of meningococcal vaccines in adults not at risk for invasive meningococcal disease, and use of HPV vaccine in patients aged 27-45 years.
While immunosuppressive therapy is not a contraindication for giving inactivated vaccines, Dr. Jones and colleagues noted that immunosuppression may hinder vaccine responses.
“Given that patients with IBD on immunosuppressive therapy may have lower immune response to vaccine, further research will be needed to assess the safety and effectiveness of high-dose vs. standard-dose vaccination strategy,” they wrote, also noting that more work is needed to determine if accelerated vaccinations strategies may be feasible prior to initiation of immunosuppressive therapy.
Because of a lack of evidence, the guideline panel did not issue IBD-specific recommendations for vaccines against SARS-CoV-2; however, Dr. Jones and colleagues suggested that clinicians reference a CAG publication on the subject published earlier this year.
The guideline was supported by grants to the Canadian Association of Gastroenterology from the Canadian Institutes of Health Research’s Institute of Nutrition, Metabolism and Diabetes; and CANImmunize. Dr. Benchimol disclosed additional relationships with the Canadian Institutes of Health Research, Crohn’s and Colitis Canada; and the Canadian Child Health Clinician Scientist Program.
The Canadian Association of Gastroenterology (CAG) has published a two-part clinical practice guideline for immunizing patients with inflammatory bowel disease (IBD) that covers both live and inactivated vaccines across pediatric and adult patients.
The guideline, which has been endorsed by the American Gastroenterological Association, is composed of recommendations drawn from a broader body of data than prior publications on the same topic, according to Eric I. Benchimol, MD, PhD, of the University of Ottawa and the University of Toronto, and colleagues.
“Previous guidelines on immunizations of patients with IBD considered only the limited available evidence of vaccine safety and effectiveness in IBD populations, and failed to consider the ample evidence available in the general population or in other immune-mediated inflammatory diseases when assessing the certainty of evidence or developing their recommendations,” they wrote in Gastroenterology.
Part 1: Live vaccine recommendations
The first part of the guideline includes seven recommendations for use of live vaccines in patients with IBD.
In this area, decision-making is largely dependent upon use of immunosuppressive therapy, which the investigators defined as “corticosteroids, thiopurines, biologics, small molecules such as JAK [Janus kinase] inhibitors, and combinations thereof,” with the caveat that “there is no standard definition of immunosuppression,” and “the degree to which immunosuppressive therapy causes clinically significant immunosuppression generally is dose related and varies by drug.”
Before offering specific recommendations, Dr. Benchimol and colleagues provided three general principles to abide by: 1. Clinicians should review each patient’s history of immunization and vaccine-preventable diseases at diagnosis and on a routine basis; 2. Appropriate vaccinations should ideally be given prior to starting immunosuppressive therapy; and 3. Immunosuppressive therapy (when urgently needed) should not be delayed so that immunizations can be given in advance.
“[Delaying therapy] could lead to more anticipated harms than benefits, due to the risk of progression of the inflammatory activity and resulting complications,” the investigators wrote.
Specific recommendations in the guideline address measles, mumps, and rubella (MMR); and varicella. Both vaccines are recommended for susceptible pediatric and adult patients not taking immunosuppressive therapy. In contrast, neither vaccine is recommended for immunosuppressed patients of any age. Certainty of evidence ranged from very low to moderate.
Concerning vaccination within the first 6 months of life for infants born of mothers taking biologics, the expert panel did not reach a consensus.
“[T]he group was unable to recommend for or against their routine use because the desirable and undesirable effects were closely balanced and the evidence on safety outcomes was insufficient to justify a recommendation,” wrote Dr. Benchimol and colleagues. “Health care providers should be cautious with the administration of live vaccines in the first year of life in the infants of mothers using biologics. These infants should be evaluated by clinicians with expertise in the impact of exposure to monoclonal antibody biologics in utero.”
Part 2: Inactivated vaccine recommendations
The second part of the guideline, by lead author Jennifer L. Jones, MD, of Dalhousie University, Queen Elizabeth II Health Sciences Center, Halifax, N.S., and colleagues, provides 15 recommendations for giving inactivated vaccines to patients with IBD.
The panel considered eight vaccines: Haemophilus influenzae type B (Hib); herpes zoster (HZ); hepatitis B; influenza; Streptococcus pneumoniae (pneumococcal vaccine); Neisseria meningitidis (meningococcal vaccine); human papillomavirus (HPV); and diphtheria, tetanus, and pertussis.
Generally, the above vaccines are recommended on an age-appropriate basis, regardless of immunosuppression status, albeit with varying levels of confidence. For example, the Hib vaccine is strongly recommended for pediatric patients 5 years and younger, whereas the same recommendation for older children and adults is conditional.
For several patient populations and vaccines, the guideline panel did not reach a consensus, including use of double-dose hepatitis B vaccine for immunosuppressed adults, timing seasonal flu shots with dosing of biologics, use of pneumococcal vaccines in nonimmunosuppressed patents without a risk factor for pneumococcal disease, use of meningococcal vaccines in adults not at risk for invasive meningococcal disease, and use of HPV vaccine in patients aged 27-45 years.
While immunosuppressive therapy is not a contraindication for giving inactivated vaccines, Dr. Jones and colleagues noted that immunosuppression may hinder vaccine responses.
“Given that patients with IBD on immunosuppressive therapy may have lower immune response to vaccine, further research will be needed to assess the safety and effectiveness of high-dose vs. standard-dose vaccination strategy,” they wrote, also noting that more work is needed to determine if accelerated vaccinations strategies may be feasible prior to initiation of immunosuppressive therapy.
Because of a lack of evidence, the guideline panel did not issue IBD-specific recommendations for vaccines against SARS-CoV-2; however, Dr. Jones and colleagues suggested that clinicians reference a CAG publication on the subject published earlier this year.
The guideline was supported by grants to the Canadian Association of Gastroenterology from the Canadian Institutes of Health Research’s Institute of Nutrition, Metabolism and Diabetes; and CANImmunize. Dr. Benchimol disclosed additional relationships with the Canadian Institutes of Health Research, Crohn’s and Colitis Canada; and the Canadian Child Health Clinician Scientist Program.
FROM GASTROENTEROLOGY
Ultraprocessed foods comprise most of the calories for youths
In the 2 decades from 1999 to 2018, ultraprocessed foods consistently accounted for the majority of energy intake by American young people, a large cross-sectional study of National Health and Nutrition Examination Survey (NHANES) data shows.
In young people aged 2-19 years, the estimated percentage of total energy from consumption of ultraprocessed foods increased from 61.4% to 67.0%, for a difference of 5.6% (95% confidence interval [CI] 3.5-7.7, P < .001 for trend), according to Lu Wang, PhD, MPH, a postdoctoral fellow at the Friedman School of Nutrition Science and Policy at Tufts University in Boston, and colleagues.
In contrast, total energy from non- or minimally processed foods decreased from 28.8% to 23.5% (difference −5.3%, 95% CI, −7.5 to −3.2, P < .001 for trend).
“The estimated percentage of energy consumed from ultraprocessed foods increased from 1999 to 2018, with an increasing trend in ready-to-heat and -eat mixed dishes and a decreasing trend in sugar-sweetened beverages,” the authors wrote. The report was published online Aug. 10 in JAMA.
The findings held regardless of the educational and socioeconomic status of the children’s parents.
Significant disparities by race and ethnicity emerged, however, with the ultraprocessed food phenomenon more marked in non-Hispanic Black youths and Mexican-American youths than in their non-Hispanic White counterparts. “Targeted marketing of junk foods toward racial/ethnic minority youths may partly contribute to such differences,” the authors wrote. “However, persistently lower consumption of ultraprocessed foods among Mexican-American youths may reflect more home cooking among Hispanic families.”
Among non-Hispanic Black youths consumption rose from 62.2% to 72.5% (difference 10.3%, 95% CI, 6.8-13.8) and among Mexican-American youths from 55.8% to 63.5% (difference 7.6%, 95% CI, 4.4-10.9). In non-Hispanic White youths intake rose from 63.4% to 68.6% (difference 5.2%, 95% CI, 2.1-8.3, P = .04 for trends).
In addition, a higher consumption of ultraprocessed foods among school-aged youths than among preschool children aged 2-5 years may reflect increased marketing, availability, and selection of ultraprocessed foods for older youths, the authors noted.
Food processing, with its potential adverse effects, may need to be considered as a food dimension in addition to nutrients and food groups in future dietary recommendations and food policies, they added.
“An increasing number of studies are showing a link between ultraprocessed food consumption and adverse health outcomes in children,” corresponding author Fang Fang Zhang, MD, PhD, Neely Family Professor and associate professor at Tufts’ Friedman School of Nutrition Science and Policy, said in an interview. “Health care providers can play a larger role in encouraging patients – and their parents – to replace unhealthy ultraprocessed foods such as ultraprocessed sweet bakery products with healthy unprocessed or minimally processed foods in their diet such as less processed whole grains. “

In Dr. Zhang’s view, teachers also have a part to play in promoting nutrition literacy. “Schools can play an important role in empowering children with knowledge and skills to make healthy food choices,” she said. “Nutrition literacy should be an integral part of the health education curriculum in all K-12 schools.”
Commenting on the study but not involved in it, Michelle Katzow, MD, a pediatrician/obesity medicine specialist and assistant professor at the Feinstein Institutes for Medical Research in Manhasset, N.Y., said the work highlights an often overlooked aspect of the modern American diet that may well be contributing to poor health outcomes in young people.

“It suggests that even as the science advances and we learn more about the adverse health effects of ultraprocessed foods, public health efforts to improve nutrition and food quality in children have not been successful,” she said in an interview. “This is because it is so hard for public health advocates to compete with the food industry, which stands to really benefit financially from hooking kids on processed foods that are not good for their health.”
Dr. Katzow added that the observed racial/ethnic disparities are not surprising in light of a growing body of evidence that racism exists in food marketing. “We need to put forward policies that regulate the food industry, particularly in relation to its most susceptible targets, our kids.”
Study details
The serial cross-sectional analysis used 24-hour dietary recall data from a nationally representative sample from 10 NHANES cycles for the range of 1999-2000 to 2017-2018. The weighted mean age of the cohort was 10.7 years and 49.1% were girls.
Among the subgroups of ultraprocessed foods, the estimated percentage of energy from ready-to-heat and ready-to-eat mixed dishes increased from 2.2% to 11.2% (difference 8.9%; 95%, CI, 7.7-10.2).
Energy from sweets and sweet snacks increased from 10.7% to 12.9% (difference 2.3%; 95% CI, 1.0-3.6), but the estimated percentage of energy decreased for sugar-sweetened beverages from 10.8% to 5.3% (difference −5.5%; 95% CI, −6.5 to −4.5).
In other categories, estimated energy intake from processed fats and oils, condiments, and sauces fell from 7.1% to 4.0% (difference −3.1%; 95% CI, −3.7 to −2.6, all P < .05 for trend).
Not surprisingly, ultraprocessed foods had an overall poorer nutrient profile than that of nonultraprocessed, although they often contained less saturated fat, and they also contained more carbohydrates, mostly from low-quality sources with added sugars and low levels of dietary fiber and protein.
And despite a higher total folate content in ultraprocessed foods because of fortification, higher-level consumers took in less total folate owing to their lower consumption of whole foods.
The authors cautioned that in addition to poor nutrient profiles, processing itself may harm health by changing the physical structure and chemical composition of food, which could lead to elevated glycemic response and reduced satiety. Furthermore, recent research has linked food additives such as emulsifiers, stabilizers, and artificial sweeteners to adverse metabolomic effects and obesity risk. Pointing to the recent success of efforts to reduce consumption of sugary beverages, Dr. Zhang said, “We need to mobilize the same energy and level of commitment when it comes to other unhealthy ultraprocessed foods such as cakes, cookies, doughnuts, and brownies.”
The trends identified by the Tufts study “are concerning and potentially have major public health significance,” according to an accompanying JAMA editorial.
“Better dietary assessment methods are needed to document trends and understand the unique role of ultraprocessed foods to inform future evidence-based policy and dietary recommendations,” wrote Katie A. Meyer, ScD, and Lindsey Smith Taillie, PhD, of the Gillings School of Global Public Health at the University of North Carolina in Chapel Hill.
The editorialists share the authors’ view that “a conceptual advancement would be to consider the level and characteristics of processing as just one of multiple dimensions (including nutrients and food groups) used to classify foods as healthy or unhealthy.” They pointed out that the Pan American Health Organization already recommends targeting products that are ultraprocessed and high in concerning add-in nutrients.
They cautioned, however, that the classification of ultraprocessed foods will not be easy because it requires data on a full list of ingredients, and the effects of processing generally cannot be separated from the composite nutrients of ultraprocessed foods.
This presents a challenge for national food consumption research “given that most large epidemiological studies rely on food frequency questionnaires that lack the information necessary to classify processing levels,” they wrote.
This study was supported by the National Institutes of Health and the São Paulo Research Foundation. Coauthor Dariush Mozaffarian, MD, a cardiologist at Tufts University, disclosed support from the Bill & Melinda Gates Foundation, the National Institutes of Health, and the Rockefeller Foundation as well as personal fees from several commercial companies. He has served on several scientific advisory boards and received royalties from UpToDate, all outside of the submitted work. Dr. Meyer reported a grant from choline manufacturer Balchem. Dr. Taillie reported funding from Bloomberg Philanthropies. Dr. Zhang had no disclosures. Dr. Katzow disclosed no competing interests.
In the 2 decades from 1999 to 2018, ultraprocessed foods consistently accounted for the majority of energy intake by American young people, a large cross-sectional study of National Health and Nutrition Examination Survey (NHANES) data shows.
In young people aged 2-19 years, the estimated percentage of total energy from consumption of ultraprocessed foods increased from 61.4% to 67.0%, for a difference of 5.6% (95% confidence interval [CI] 3.5-7.7, P < .001 for trend), according to Lu Wang, PhD, MPH, a postdoctoral fellow at the Friedman School of Nutrition Science and Policy at Tufts University in Boston, and colleagues.
In contrast, total energy from non- or minimally processed foods decreased from 28.8% to 23.5% (difference −5.3%, 95% CI, −7.5 to −3.2, P < .001 for trend).
“The estimated percentage of energy consumed from ultraprocessed foods increased from 1999 to 2018, with an increasing trend in ready-to-heat and -eat mixed dishes and a decreasing trend in sugar-sweetened beverages,” the authors wrote. The report was published online Aug. 10 in JAMA.
The findings held regardless of the educational and socioeconomic status of the children’s parents.
Significant disparities by race and ethnicity emerged, however, with the ultraprocessed food phenomenon more marked in non-Hispanic Black youths and Mexican-American youths than in their non-Hispanic White counterparts. “Targeted marketing of junk foods toward racial/ethnic minority youths may partly contribute to such differences,” the authors wrote. “However, persistently lower consumption of ultraprocessed foods among Mexican-American youths may reflect more home cooking among Hispanic families.”
Among non-Hispanic Black youths consumption rose from 62.2% to 72.5% (difference 10.3%, 95% CI, 6.8-13.8) and among Mexican-American youths from 55.8% to 63.5% (difference 7.6%, 95% CI, 4.4-10.9). In non-Hispanic White youths intake rose from 63.4% to 68.6% (difference 5.2%, 95% CI, 2.1-8.3, P = .04 for trends).
In addition, a higher consumption of ultraprocessed foods among school-aged youths than among preschool children aged 2-5 years may reflect increased marketing, availability, and selection of ultraprocessed foods for older youths, the authors noted.
Food processing, with its potential adverse effects, may need to be considered as a food dimension in addition to nutrients and food groups in future dietary recommendations and food policies, they added.
“An increasing number of studies are showing a link between ultraprocessed food consumption and adverse health outcomes in children,” corresponding author Fang Fang Zhang, MD, PhD, Neely Family Professor and associate professor at Tufts’ Friedman School of Nutrition Science and Policy, said in an interview. “Health care providers can play a larger role in encouraging patients – and their parents – to replace unhealthy ultraprocessed foods such as ultraprocessed sweet bakery products with healthy unprocessed or minimally processed foods in their diet such as less processed whole grains. “
In Dr. Zhang’s view, teachers also have a part to play in promoting nutrition literacy. “Schools can play an important role in empowering children with knowledge and skills to make healthy food choices,” she said. “Nutrition literacy should be an integral part of the health education curriculum in all K-12 schools.”
Commenting on the study but not involved in it, Michelle Katzow, MD, a pediatrician/obesity medicine specialist and assistant professor at the Feinstein Institutes for Medical Research in Manhasset, N.Y., said the work highlights an often overlooked aspect of the modern American diet that may well be contributing to poor health outcomes in young people.
“It suggests that even as the science advances and we learn more about the adverse health effects of ultraprocessed foods, public health efforts to improve nutrition and food quality in children have not been successful,” she said in an interview. “This is because it is so hard for public health advocates to compete with the food industry, which stands to really benefit financially from hooking kids on processed foods that are not good for their health.”
Dr. Katzow added that the observed racial/ethnic disparities are not surprising in light of a growing body of evidence that racism exists in food marketing. “We need to put forward policies that regulate the food industry, particularly in relation to its most susceptible targets, our kids.”
Study details
The serial cross-sectional analysis used 24-hour dietary recall data from a nationally representative sample from 10 NHANES cycles for the range of 1999-2000 to 2017-2018. The weighted mean age of the cohort was 10.7 years and 49.1% were girls.
Among the subgroups of ultraprocessed foods, the estimated percentage of energy from ready-to-heat and ready-to-eat mixed dishes increased from 2.2% to 11.2% (difference 8.9%; 95%, CI, 7.7-10.2).
Energy from sweets and sweet snacks increased from 10.7% to 12.9% (difference 2.3%; 95% CI, 1.0-3.6), but the estimated percentage of energy decreased for sugar-sweetened beverages from 10.8% to 5.3% (difference −5.5%; 95% CI, −6.5 to −4.5).
In other categories, estimated energy intake from processed fats and oils, condiments, and sauces fell from 7.1% to 4.0% (difference −3.1%; 95% CI, −3.7 to −2.6, all P < .05 for trend).
Not surprisingly, ultraprocessed foods had an overall poorer nutrient profile than that of nonultraprocessed, although they often contained less saturated fat, and they also contained more carbohydrates, mostly from low-quality sources with added sugars and low levels of dietary fiber and protein.
And despite a higher total folate content in ultraprocessed foods because of fortification, higher-level consumers took in less total folate owing to their lower consumption of whole foods.
The authors cautioned that in addition to poor nutrient profiles, processing itself may harm health by changing the physical structure and chemical composition of food, which could lead to elevated glycemic response and reduced satiety. Furthermore, recent research has linked food additives such as emulsifiers, stabilizers, and artificial sweeteners to adverse metabolomic effects and obesity risk. Pointing to the recent success of efforts to reduce consumption of sugary beverages, Dr. Zhang said, “We need to mobilize the same energy and level of commitment when it comes to other unhealthy ultraprocessed foods such as cakes, cookies, doughnuts, and brownies.”
The trends identified by the Tufts study “are concerning and potentially have major public health significance,” according to an accompanying JAMA editorial.
“Better dietary assessment methods are needed to document trends and understand the unique role of ultraprocessed foods to inform future evidence-based policy and dietary recommendations,” wrote Katie A. Meyer, ScD, and Lindsey Smith Taillie, PhD, of the Gillings School of Global Public Health at the University of North Carolina in Chapel Hill.
The editorialists share the authors’ view that “a conceptual advancement would be to consider the level and characteristics of processing as just one of multiple dimensions (including nutrients and food groups) used to classify foods as healthy or unhealthy.” They pointed out that the Pan American Health Organization already recommends targeting products that are ultraprocessed and high in concerning add-in nutrients.
They cautioned, however, that the classification of ultraprocessed foods will not be easy because it requires data on a full list of ingredients, and the effects of processing generally cannot be separated from the composite nutrients of ultraprocessed foods.
This presents a challenge for national food consumption research “given that most large epidemiological studies rely on food frequency questionnaires that lack the information necessary to classify processing levels,” they wrote.
This study was supported by the National Institutes of Health and the São Paulo Research Foundation. Coauthor Dariush Mozaffarian, MD, a cardiologist at Tufts University, disclosed support from the Bill & Melinda Gates Foundation, the National Institutes of Health, and the Rockefeller Foundation as well as personal fees from several commercial companies. He has served on several scientific advisory boards and received royalties from UpToDate, all outside of the submitted work. Dr. Meyer reported a grant from choline manufacturer Balchem. Dr. Taillie reported funding from Bloomberg Philanthropies. Dr. Zhang had no disclosures. Dr. Katzow disclosed no competing interests.
In the 2 decades from 1999 to 2018, ultraprocessed foods consistently accounted for the majority of energy intake by American young people, a large cross-sectional study of National Health and Nutrition Examination Survey (NHANES) data shows.
In young people aged 2-19 years, the estimated percentage of total energy from consumption of ultraprocessed foods increased from 61.4% to 67.0%, for a difference of 5.6% (95% confidence interval [CI] 3.5-7.7, P < .001 for trend), according to Lu Wang, PhD, MPH, a postdoctoral fellow at the Friedman School of Nutrition Science and Policy at Tufts University in Boston, and colleagues.
In contrast, total energy from non- or minimally processed foods decreased from 28.8% to 23.5% (difference −5.3%, 95% CI, −7.5 to −3.2, P < .001 for trend).
“The estimated percentage of energy consumed from ultraprocessed foods increased from 1999 to 2018, with an increasing trend in ready-to-heat and -eat mixed dishes and a decreasing trend in sugar-sweetened beverages,” the authors wrote. The report was published online Aug. 10 in JAMA.
The findings held regardless of the educational and socioeconomic status of the children’s parents.
Significant disparities by race and ethnicity emerged, however, with the ultraprocessed food phenomenon more marked in non-Hispanic Black youths and Mexican-American youths than in their non-Hispanic White counterparts. “Targeted marketing of junk foods toward racial/ethnic minority youths may partly contribute to such differences,” the authors wrote. “However, persistently lower consumption of ultraprocessed foods among Mexican-American youths may reflect more home cooking among Hispanic families.”
Among non-Hispanic Black youths consumption rose from 62.2% to 72.5% (difference 10.3%, 95% CI, 6.8-13.8) and among Mexican-American youths from 55.8% to 63.5% (difference 7.6%, 95% CI, 4.4-10.9). In non-Hispanic White youths intake rose from 63.4% to 68.6% (difference 5.2%, 95% CI, 2.1-8.3, P = .04 for trends).
In addition, a higher consumption of ultraprocessed foods among school-aged youths than among preschool children aged 2-5 years may reflect increased marketing, availability, and selection of ultraprocessed foods for older youths, the authors noted.
Food processing, with its potential adverse effects, may need to be considered as a food dimension in addition to nutrients and food groups in future dietary recommendations and food policies, they added.
“An increasing number of studies are showing a link between ultraprocessed food consumption and adverse health outcomes in children,” corresponding author Fang Fang Zhang, MD, PhD, Neely Family Professor and associate professor at Tufts’ Friedman School of Nutrition Science and Policy, said in an interview. “Health care providers can play a larger role in encouraging patients – and their parents – to replace unhealthy ultraprocessed foods such as ultraprocessed sweet bakery products with healthy unprocessed or minimally processed foods in their diet such as less processed whole grains. “
In Dr. Zhang’s view, teachers also have a part to play in promoting nutrition literacy. “Schools can play an important role in empowering children with knowledge and skills to make healthy food choices,” she said. “Nutrition literacy should be an integral part of the health education curriculum in all K-12 schools.”
Commenting on the study but not involved in it, Michelle Katzow, MD, a pediatrician/obesity medicine specialist and assistant professor at the Feinstein Institutes for Medical Research in Manhasset, N.Y., said the work highlights an often overlooked aspect of the modern American diet that may well be contributing to poor health outcomes in young people.
“It suggests that even as the science advances and we learn more about the adverse health effects of ultraprocessed foods, public health efforts to improve nutrition and food quality in children have not been successful,” she said in an interview. “This is because it is so hard for public health advocates to compete with the food industry, which stands to really benefit financially from hooking kids on processed foods that are not good for their health.”
Dr. Katzow added that the observed racial/ethnic disparities are not surprising in light of a growing body of evidence that racism exists in food marketing. “We need to put forward policies that regulate the food industry, particularly in relation to its most susceptible targets, our kids.”
Study details
The serial cross-sectional analysis used 24-hour dietary recall data from a nationally representative sample from 10 NHANES cycles for the range of 1999-2000 to 2017-2018. The weighted mean age of the cohort was 10.7 years and 49.1% were girls.
Among the subgroups of ultraprocessed foods, the estimated percentage of energy from ready-to-heat and ready-to-eat mixed dishes increased from 2.2% to 11.2% (difference 8.9%; 95%, CI, 7.7-10.2).
Energy from sweets and sweet snacks increased from 10.7% to 12.9% (difference 2.3%; 95% CI, 1.0-3.6), but the estimated percentage of energy decreased for sugar-sweetened beverages from 10.8% to 5.3% (difference −5.5%; 95% CI, −6.5 to −4.5).
In other categories, estimated energy intake from processed fats and oils, condiments, and sauces fell from 7.1% to 4.0% (difference −3.1%; 95% CI, −3.7 to −2.6, all P < .05 for trend).
Not surprisingly, ultraprocessed foods had an overall poorer nutrient profile than that of nonultraprocessed, although they often contained less saturated fat, and they also contained more carbohydrates, mostly from low-quality sources with added sugars and low levels of dietary fiber and protein.
And despite a higher total folate content in ultraprocessed foods because of fortification, higher-level consumers took in less total folate owing to their lower consumption of whole foods.
The authors cautioned that in addition to poor nutrient profiles, processing itself may harm health by changing the physical structure and chemical composition of food, which could lead to elevated glycemic response and reduced satiety. Furthermore, recent research has linked food additives such as emulsifiers, stabilizers, and artificial sweeteners to adverse metabolomic effects and obesity risk. Pointing to the recent success of efforts to reduce consumption of sugary beverages, Dr. Zhang said, “We need to mobilize the same energy and level of commitment when it comes to other unhealthy ultraprocessed foods such as cakes, cookies, doughnuts, and brownies.”
The trends identified by the Tufts study “are concerning and potentially have major public health significance,” according to an accompanying JAMA editorial.
“Better dietary assessment methods are needed to document trends and understand the unique role of ultraprocessed foods to inform future evidence-based policy and dietary recommendations,” wrote Katie A. Meyer, ScD, and Lindsey Smith Taillie, PhD, of the Gillings School of Global Public Health at the University of North Carolina in Chapel Hill.
The editorialists share the authors’ view that “a conceptual advancement would be to consider the level and characteristics of processing as just one of multiple dimensions (including nutrients and food groups) used to classify foods as healthy or unhealthy.” They pointed out that the Pan American Health Organization already recommends targeting products that are ultraprocessed and high in concerning add-in nutrients.
They cautioned, however, that the classification of ultraprocessed foods will not be easy because it requires data on a full list of ingredients, and the effects of processing generally cannot be separated from the composite nutrients of ultraprocessed foods.
This presents a challenge for national food consumption research “given that most large epidemiological studies rely on food frequency questionnaires that lack the information necessary to classify processing levels,” they wrote.
This study was supported by the National Institutes of Health and the São Paulo Research Foundation. Coauthor Dariush Mozaffarian, MD, a cardiologist at Tufts University, disclosed support from the Bill & Melinda Gates Foundation, the National Institutes of Health, and the Rockefeller Foundation as well as personal fees from several commercial companies. He has served on several scientific advisory boards and received royalties from UpToDate, all outside of the submitted work. Dr. Meyer reported a grant from choline manufacturer Balchem. Dr. Taillie reported funding from Bloomberg Philanthropies. Dr. Zhang had no disclosures. Dr. Katzow disclosed no competing interests.
FROM JAMA
Surge of new child COVID cases continues for 6th consecutive week
The current COVID-19 surge has brought new cases in children to their highest level since February, according to a new report.
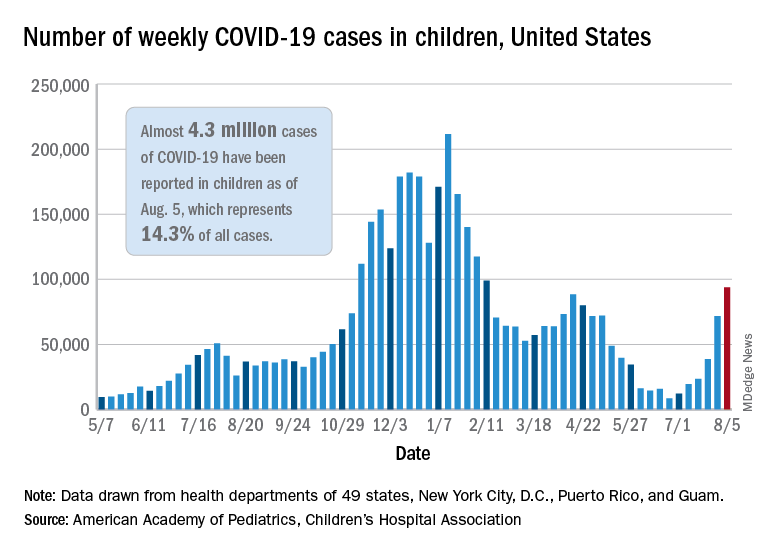
New pediatric cases rose for the 6th straight week, with almost 94,000 reported for the week ending Aug. 5.
That weekly total was up by 31% over the previous week and by over 1,000% since late June, when the new-case figure was at its lowest point (8,447) since early in the pandemic, the American Academy of Pediatrics and the Children’s Hospital Association said. COVID-related deaths – 13 for the week – were also higher than at any time since March 2021.
Almost 4.3 million children have been infected with SARS-CoV-2, which is 14.3% of all cases reported in 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. Children represented 15.0% of the new cases reported in those jurisdictions during the week ending Aug. 5, the AAP and CHA said in their weekly report.
Another measure that has been trending upward recently is vaccine initiation among 12- to 15-year-olds, although the latest weekly total is still well below the high of 1.4 million seen in May. First-time vaccinations reached almost 411,000 for the week of Aug. 3-9, marking the fourth consecutive increase in that age group, the Centers for Disease Control and Prevention said on its COVID Data Tracker. Vaccinations also increased, although more modestly, for 16- and 17-year-olds in the most recent week.
Cumulative figures for children aged 12-17 show that almost 10.4 million have received at least one dose and that 7.7 million are fully vaccinated as of Aug. 9. By age group, 42.2% of those aged 12-15 have received at least one dose, and 30.4% have completed the vaccine regimen. Among those aged 16-17 years, 52.2% have gotten their first dose, and 41.4% are fully vaccinated, according to the COVID Data Tracker.
Looking at vaccination rates on the state level shows that only 20% of children aged 12-17 in Wyoming and 21% in Mississippi have gotten at least one dose as of Aug. 4, while Massachusetts is up to 68% and Vermont reports 70%. Rates for full vaccination range from 11% in Mississippi and Alabama to 61% in Vermont, based on an AAP analysis of CDC data, which is not available for Idaho.
The current COVID-19 surge has brought new cases in children to their highest level since February, according to a new report.
New pediatric cases rose for the 6th straight week, with almost 94,000 reported for the week ending Aug. 5.
That weekly total was up by 31% over the previous week and by over 1,000% since late June, when the new-case figure was at its lowest point (8,447) since early in the pandemic, the American Academy of Pediatrics and the Children’s Hospital Association said. COVID-related deaths – 13 for the week – were also higher than at any time since March 2021.
Almost 4.3 million children have been infected with SARS-CoV-2, which is 14.3% of all cases reported in 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. Children represented 15.0% of the new cases reported in those jurisdictions during the week ending Aug. 5, the AAP and CHA said in their weekly report.
Another measure that has been trending upward recently is vaccine initiation among 12- to 15-year-olds, although the latest weekly total is still well below the high of 1.4 million seen in May. First-time vaccinations reached almost 411,000 for the week of Aug. 3-9, marking the fourth consecutive increase in that age group, the Centers for Disease Control and Prevention said on its COVID Data Tracker. Vaccinations also increased, although more modestly, for 16- and 17-year-olds in the most recent week.
Cumulative figures for children aged 12-17 show that almost 10.4 million have received at least one dose and that 7.7 million are fully vaccinated as of Aug. 9. By age group, 42.2% of those aged 12-15 have received at least one dose, and 30.4% have completed the vaccine regimen. Among those aged 16-17 years, 52.2% have gotten their first dose, and 41.4% are fully vaccinated, according to the COVID Data Tracker.
Looking at vaccination rates on the state level shows that only 20% of children aged 12-17 in Wyoming and 21% in Mississippi have gotten at least one dose as of Aug. 4, while Massachusetts is up to 68% and Vermont reports 70%. Rates for full vaccination range from 11% in Mississippi and Alabama to 61% in Vermont, based on an AAP analysis of CDC data, which is not available for Idaho.
The current COVID-19 surge has brought new cases in children to their highest level since February, according to a new report.
New pediatric cases rose for the 6th straight week, with almost 94,000 reported for the week ending Aug. 5.
That weekly total was up by 31% over the previous week and by over 1,000% since late June, when the new-case figure was at its lowest point (8,447) since early in the pandemic, the American Academy of Pediatrics and the Children’s Hospital Association said. COVID-related deaths – 13 for the week – were also higher than at any time since March 2021.
Almost 4.3 million children have been infected with SARS-CoV-2, which is 14.3% of all cases reported in 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. Children represented 15.0% of the new cases reported in those jurisdictions during the week ending Aug. 5, the AAP and CHA said in their weekly report.
Another measure that has been trending upward recently is vaccine initiation among 12- to 15-year-olds, although the latest weekly total is still well below the high of 1.4 million seen in May. First-time vaccinations reached almost 411,000 for the week of Aug. 3-9, marking the fourth consecutive increase in that age group, the Centers for Disease Control and Prevention said on its COVID Data Tracker. Vaccinations also increased, although more modestly, for 16- and 17-year-olds in the most recent week.
Cumulative figures for children aged 12-17 show that almost 10.4 million have received at least one dose and that 7.7 million are fully vaccinated as of Aug. 9. By age group, 42.2% of those aged 12-15 have received at least one dose, and 30.4% have completed the vaccine regimen. Among those aged 16-17 years, 52.2% have gotten their first dose, and 41.4% are fully vaccinated, according to the COVID Data Tracker.
Looking at vaccination rates on the state level shows that only 20% of children aged 12-17 in Wyoming and 21% in Mississippi have gotten at least one dose as of Aug. 4, while Massachusetts is up to 68% and Vermont reports 70%. Rates for full vaccination range from 11% in Mississippi and Alabama to 61% in Vermont, based on an AAP analysis of CDC data, which is not available for Idaho.
Reticular Rash on the Chest
The Diagnosis: Erythema Ab Igne
Based on the clinical findings and history, a diagnosis of erythema ab igne (EAI), a skin reaction to chronic infrared radiation exposure, was made. The name of this condition translates from Latin as “redness from fire”; other names include toasted skin syndrome and fire stains. The most common presentation is reticulated hyperpigmentation, erythema, and cutaneous atrophy, as well as possible crusting, scaling, or telangiectasia. The rash also typically presents in areas of heat exposure—from heated blankets, heating pads, or the use of infrared heaters or lamps.1,2 The patient usually will have pain and pruritus over the affected areas. The diagnosis of EAI largely is clinical and based on the patient’s history of exposure; it rarely requires biopsy and histologic analysis. However, some of the common histopathologic findings include hyperkeratosis, a hyperpigmented basal layer, hemosiderin deposits, prominent melanophages, basal cell degeneration, course collagen, and elastosis.2,3 These changes are common with UV radiation exposure and thermal damage. The primary treatment in all cases is to remove or reduce the source of infrared radiation. However, EAI has been reported to be successfully treated with removal of the insult as well as topical agents such as imiquimod and 5-fluorouracil.4 Possible complications include increased risk for malignancies such as squamous cell carcinoma in the affected area.1
The possible differential for EAI includes livedo reticularis, livedo racemosa, cutis marmorata, and cutis marmorata telangiectatica congenita. All of these conditions are related to dysfunction of the cutaneous vasculature that creates a reticular, mottled, reddish purple rash. When the livedo is reversible and idiopathic, it is referred to as livedo reticularis, but when it is generalized and permanent it is referred to as livedo racemosa. Livedo racemosa can be caused by a variety of conditions, including systemic lupus erythematosus and antiphospholipid syndrome.1 Physiologic livedo reticularis that is more transient and can be reversed by warming is referred to as cutis marmorata. Finally, cutis marmorata telangiectatica congenita primarily is found in neonates, and although persistent, it usually improves with age. Erythema ab igne also is a type of livedo with a known heat exposure and localized distribution.
Our patient was educated on the etiology of the rash, specifically related to heating pad usage for multiple years, and the risk for cutaneous malignancy after longstanding EAI. It was recommended that she discontinue use of a heating pad on the affected areas to allow them to properly heal. If she found that heating pad usage was necessary, she was advised to limit use to 5 to 10 minutes with 2 to 3 hours in between applications. In addition, she was advised to apply petroleum jelly daily for assistance with wound healing as well as anti-itch sensitive lotion twice daily on the arms and back to alleviate some of the tingling pain. We explained that areas of hyperpigmentation may improve with time; however, areas of erythema/ atrophy may be long-lasting.
- Aria AB, Chen L, Silapunt S. Erythema ab igne from heating pad use: a report of three clinical cases and a differential diagnosis. Cureus. 2018;10:E2635.
- Dellavalle RP, Gillum P. Erythema ab igne following heating/cooling blanket use in the intensive care unit. Cutis. 2000;66:136-138.
- Finlayson GR, Sams WM Jr, Smith JG Jr. Erythema ab igne: a histopathological study. J Invest Dermatol. 1966;46:104-108.
- Tan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ. 2000;162:77-78.
The Diagnosis: Erythema Ab Igne
Based on the clinical findings and history, a diagnosis of erythema ab igne (EAI), a skin reaction to chronic infrared radiation exposure, was made. The name of this condition translates from Latin as “redness from fire”; other names include toasted skin syndrome and fire stains. The most common presentation is reticulated hyperpigmentation, erythema, and cutaneous atrophy, as well as possible crusting, scaling, or telangiectasia. The rash also typically presents in areas of heat exposure—from heated blankets, heating pads, or the use of infrared heaters or lamps.1,2 The patient usually will have pain and pruritus over the affected areas. The diagnosis of EAI largely is clinical and based on the patient’s history of exposure; it rarely requires biopsy and histologic analysis. However, some of the common histopathologic findings include hyperkeratosis, a hyperpigmented basal layer, hemosiderin deposits, prominent melanophages, basal cell degeneration, course collagen, and elastosis.2,3 These changes are common with UV radiation exposure and thermal damage. The primary treatment in all cases is to remove or reduce the source of infrared radiation. However, EAI has been reported to be successfully treated with removal of the insult as well as topical agents such as imiquimod and 5-fluorouracil.4 Possible complications include increased risk for malignancies such as squamous cell carcinoma in the affected area.1
The possible differential for EAI includes livedo reticularis, livedo racemosa, cutis marmorata, and cutis marmorata telangiectatica congenita. All of these conditions are related to dysfunction of the cutaneous vasculature that creates a reticular, mottled, reddish purple rash. When the livedo is reversible and idiopathic, it is referred to as livedo reticularis, but when it is generalized and permanent it is referred to as livedo racemosa. Livedo racemosa can be caused by a variety of conditions, including systemic lupus erythematosus and antiphospholipid syndrome.1 Physiologic livedo reticularis that is more transient and can be reversed by warming is referred to as cutis marmorata. Finally, cutis marmorata telangiectatica congenita primarily is found in neonates, and although persistent, it usually improves with age. Erythema ab igne also is a type of livedo with a known heat exposure and localized distribution.
Our patient was educated on the etiology of the rash, specifically related to heating pad usage for multiple years, and the risk for cutaneous malignancy after longstanding EAI. It was recommended that she discontinue use of a heating pad on the affected areas to allow them to properly heal. If she found that heating pad usage was necessary, she was advised to limit use to 5 to 10 minutes with 2 to 3 hours in between applications. In addition, she was advised to apply petroleum jelly daily for assistance with wound healing as well as anti-itch sensitive lotion twice daily on the arms and back to alleviate some of the tingling pain. We explained that areas of hyperpigmentation may improve with time; however, areas of erythema/ atrophy may be long-lasting.
The Diagnosis: Erythema Ab Igne
Based on the clinical findings and history, a diagnosis of erythema ab igne (EAI), a skin reaction to chronic infrared radiation exposure, was made. The name of this condition translates from Latin as “redness from fire”; other names include toasted skin syndrome and fire stains. The most common presentation is reticulated hyperpigmentation, erythema, and cutaneous atrophy, as well as possible crusting, scaling, or telangiectasia. The rash also typically presents in areas of heat exposure—from heated blankets, heating pads, or the use of infrared heaters or lamps.1,2 The patient usually will have pain and pruritus over the affected areas. The diagnosis of EAI largely is clinical and based on the patient’s history of exposure; it rarely requires biopsy and histologic analysis. However, some of the common histopathologic findings include hyperkeratosis, a hyperpigmented basal layer, hemosiderin deposits, prominent melanophages, basal cell degeneration, course collagen, and elastosis.2,3 These changes are common with UV radiation exposure and thermal damage. The primary treatment in all cases is to remove or reduce the source of infrared radiation. However, EAI has been reported to be successfully treated with removal of the insult as well as topical agents such as imiquimod and 5-fluorouracil.4 Possible complications include increased risk for malignancies such as squamous cell carcinoma in the affected area.1
The possible differential for EAI includes livedo reticularis, livedo racemosa, cutis marmorata, and cutis marmorata telangiectatica congenita. All of these conditions are related to dysfunction of the cutaneous vasculature that creates a reticular, mottled, reddish purple rash. When the livedo is reversible and idiopathic, it is referred to as livedo reticularis, but when it is generalized and permanent it is referred to as livedo racemosa. Livedo racemosa can be caused by a variety of conditions, including systemic lupus erythematosus and antiphospholipid syndrome.1 Physiologic livedo reticularis that is more transient and can be reversed by warming is referred to as cutis marmorata. Finally, cutis marmorata telangiectatica congenita primarily is found in neonates, and although persistent, it usually improves with age. Erythema ab igne also is a type of livedo with a known heat exposure and localized distribution.
Our patient was educated on the etiology of the rash, specifically related to heating pad usage for multiple years, and the risk for cutaneous malignancy after longstanding EAI. It was recommended that she discontinue use of a heating pad on the affected areas to allow them to properly heal. If she found that heating pad usage was necessary, she was advised to limit use to 5 to 10 minutes with 2 to 3 hours in between applications. In addition, she was advised to apply petroleum jelly daily for assistance with wound healing as well as anti-itch sensitive lotion twice daily on the arms and back to alleviate some of the tingling pain. We explained that areas of hyperpigmentation may improve with time; however, areas of erythema/ atrophy may be long-lasting.
- Aria AB, Chen L, Silapunt S. Erythema ab igne from heating pad use: a report of three clinical cases and a differential diagnosis. Cureus. 2018;10:E2635.
- Dellavalle RP, Gillum P. Erythema ab igne following heating/cooling blanket use in the intensive care unit. Cutis. 2000;66:136-138.
- Finlayson GR, Sams WM Jr, Smith JG Jr. Erythema ab igne: a histopathological study. J Invest Dermatol. 1966;46:104-108.
- Tan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ. 2000;162:77-78.
- Aria AB, Chen L, Silapunt S. Erythema ab igne from heating pad use: a report of three clinical cases and a differential diagnosis. Cureus. 2018;10:E2635.
- Dellavalle RP, Gillum P. Erythema ab igne following heating/cooling blanket use in the intensive care unit. Cutis. 2000;66:136-138.
- Finlayson GR, Sams WM Jr, Smith JG Jr. Erythema ab igne: a histopathological study. J Invest Dermatol. 1966;46:104-108.
- Tan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ. 2000;162:77-78.

A 53-year-old woman with a history of diabetes mellitus, hypertension, chronic complex regional pain syndrome type 1, and chronic prescription opiate use presented to the hospital with a pruritic rash on the chest of 15 years’ duration that started a few weeks after a left shoulder repair. The patient was using fentanyl patches and acetaminophen with oxycodone as well as a heating pad for 20 to 22 hours per day for many years to help with her chronic pain. She also described similar lesions on the abdomen and back when she used the heating pad on those areas for weeks at a time. Vital signs were within normal limits. Physical examination revealed a lacy, reticular, eroded, well-demarcated rash on the chest along with areas of cracking. Laboratory evaluation did not reveal any abnormalities.

Tackle obesity to drop risk for secondary cardiac event
Patients who had been hospitalized for heart attack or cardiovascular revascularization procedures commonly were overweight (46%) or had obesity (35%), but at a follow-up visit, few had lost weight or planned to do so, according to researchers who conduced a large European study.

The findings emphasize that obesity needs to be recognized as a disease that has to be optimally managed to lessen the risk for a secondary cardiovascular event, the authors stressed.
The study, by Dirk De Bacquer, PhD, professor, department of public health, Ghent (Belgium) University, and colleagues, was published recently in the European Heart Journal – Quality of Care and Clinical Outcomes.
The researchers analyzed data from more than 10,000 patients in the EUROASPIRE IV and V studies who were hospitalized for acute myocardial infarction (MI), coronary artery bypass graft (CABG), or percutaneous coronary intervention (PCI) and answered a survey 16 months later on average.
Although 20% of the patients with obesity had lost 5% or more of their initial weight, 16% had gained 5% or more of their initial weight.
Notably, “the discharge letter did not record the weight status in a quarter of [the patients with obesity] and a substantial proportion reported to have never been told by a healthcare professional [that they were] overweight,” the investigators wrote.
“It seems,” Dr. De Bacquer and colleagues noted, “that obesity is not considered by physicians as a serious medical problem, which requires attention, recommendations, and obvious advice on personal weight targets.”
However, “the benefits for patients who lost weight in our study, resulting in a healthier cardiovascular risk profile, are really worthwhile,” they pointed out.
Cardiovascular rehabilitation should include weight loss intervention
“The safest and most effective approach for managing body weight” in patients with coronary artery disease and obesity “is adopting a healthy eating pattern and increasing levels of physical activity,” they wrote.
Their findings that “patients who reported reducing their fat and sugar intake, consuming more fruit, vegetables, and fish and doing more regular physical activity, had significant weight loss,” support this.
Dr. De Bacquer and colleagues recommend that cardiovascular prevention and rehabilitation programs “should include weight loss intervention, including different forms of self-support, as a specific component of a comprehensive intervention to reduce total cardiovascular risk, extend life expectancy, and improve quality of life.”
Clinicians should “consider the incremental value of telehealth intervention as well as recently described pharmacological interventions,” they added, noting that the study did not look at these options or at metabolic surgery.
Invited to comment, one expert pointed out that two new observational studies of metabolic surgery in patients with obesity and coronary artery disease reported positive outcomes.
Another expert took issue with the “patient blaming” tone of the article and the lack of actionable ways to help patients lose weight.
Medical therapy or bariatric surgery as other options?
“The study demonstrated how prevalent obesity is in patients with heart disease“ and “confirmed how difficult it is to achieve weight loss, in particular, in patients with heart disease, where weight loss would be beneficial,” Erik Näslund, MD, PhD, said in an interview.
Even though “current guidelines stress weight-loss counseling, some patients actually gained weight,” observed Dr. Näslund, of Danderyd Hospital and Karolinska Institutet, Stockholm.
On the other hand, patients who lost 5% or more of their initial weight had reduced comorbidities that are associated with cardiovascular disease.
“The best way to achieve long-term weight loss in patients with severe obesity is metabolic (bariatric) surgery,” noted Dr. Näslund, who was not involved in the study. “There are now two recent papers in the journal Circulation that demonstrate that metabolic surgery has a role in the secondary prevention of cardiovascular disease in patients with severe obesity” – one study from Dr. Näslund’s group (Circulation. 2021;143:1458-67), as previously reported, and one study from researchers in Ontario, Canada (Circulation. 2021;143:1468-80).
However, those were observational studies, and the findings would need to be confirmed in a randomized clinical trial before they could be used as recommended practice of care, he cautioned. In addition, most patients in the current study would not fulfill the minimum body weight criteria for metabolic surgery.
“Therefore, there is a need for intensified medical therapy for these patients,” as another treatment option, said Dr. Näslund.
“It would be interesting,” he speculated, “to study how the new glucagon-like peptide-1 (GLP-1) receptor agonist therapies could work in this setting as a weight loss agent and perhaps have a positive independent cardiovascular benefit.”
Obesity is a disease; clinicians need to be respectful
Meanwhile, Obesity Society fellow and spokesperson Fatima Cody Stanford, MD, said in an interview that she didn’t think the language and tone of the article was respectful for patients with obesity, and the researchers “talked about the old narrative of how we support patients with obesity.”
Lifestyle modification can be at the core of treatment, but medication or bariatric surgery may be other options to “help patients get to their best selves.
“Patients with obesity deserve to be cared for and treated with respect,” said Dr. Stanford, an obesity medicine physician scientist at Massachusetts General Hospital and Harvard Medical School, Boston.
Treatment needs to be individualized and clinicians need to listen to patient concerns. For example, a patient with obesity may not be able to follow advice to walk more. “I can barely stand up,” one patient with obesity and osteoarthritis told Dr. Stanford.
And patients’ insurance may not cover cardiac rehabilitation – especially patients from racial minorities or those with lower socioeconomic status, she noted.
“My feeling has always been that it is important to be respectful to all patients,” Dr. Näslund agreed. “I do agree that we need to recognize obesity as a chronic disease, and the paper in EHJ demonstrates this, as obesity was not registered in many of the discharge notes.
“If we as healthcare workers measured a weight of our patients the same way that we take a blood pressure,” he said, “perhaps the [stigma] of obesity would be reduced.”
Study findings
The researchers examined pooled data from EUROASPIRE IV (2012-13) and EUROASPIRE V (2016-17) surveys of patients who were overweight or had obesity who had been discharged from hospital after MI, CABG, or PCI to determine if they had received lifestyle advice for weight loss, if they had acted on this advice, and if losing weight altered their cardiovascular disease risk factors.
They identified 10,507 adult patients in 29 mainly European countries who had complete survey data.
The mean age of the patients was 63 at the time of their hospitalization; 25% were women. Many had hypertension (66%-88%), dyslipidemia (69%-80%), or diabetes (16%-37%).
The prevalence of obesity varied from 8% to 46% in men and from 18% to 57% in women, in different countries. Patients with obesity had a mean body weight of 97 kg (213 pounds).
One of the most “striking” findings was the “apparent lack of motivation” to lose weight, Dr. De Bacquer and colleagues wrote. Half of the patients with obesity had not attempted to lose weight in the month before the follow-up visit and most did not plan to do so in the following month.
Goal setting is an important aspect of behavior modification techniques, they wrote, yet 7% of the patients did not know their body weight and 21% did not have an optimal weight target.
Half of the patients had been advised to follow a cardiac rehabilitation program and two-thirds had been advised to follow dietary recommendations and move more.
Those who made positive dietary changes and were more physically active were more likely to lose at least 5% of their weight.
And patients who lost at least 5% of their initial weight were less likely to have hypertension, dyslipidemia, or diabetes compared with patients who had gained this much weight, which “is likely to translate into improved prognosis on the long term,” the authors wrote.
EUROASPIRE IV and V were supported through research grants to the European Society of Cardiology from Amgen, AstraZeneca, Bristol-Myers Squibb/Emea Sarl, GlaxoSmithKline, Hoffmann-La Roche, and Merck, Sharp & Dohme (EUROASPIRE IV) and Amarin, Amgen, Daiichi Sankyo, Eli Lilly, Pfizer, Sanofi, Ferrer, and Novo Nordisk (EUROASPIRE V). Dr. De Bacquer, Dr. Näslund, and Dr. Stanford have no disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients who had been hospitalized for heart attack or cardiovascular revascularization procedures commonly were overweight (46%) or had obesity (35%), but at a follow-up visit, few had lost weight or planned to do so, according to researchers who conduced a large European study.
The findings emphasize that obesity needs to be recognized as a disease that has to be optimally managed to lessen the risk for a secondary cardiovascular event, the authors stressed.
The study, by Dirk De Bacquer, PhD, professor, department of public health, Ghent (Belgium) University, and colleagues, was published recently in the European Heart Journal – Quality of Care and Clinical Outcomes.
The researchers analyzed data from more than 10,000 patients in the EUROASPIRE IV and V studies who were hospitalized for acute myocardial infarction (MI), coronary artery bypass graft (CABG), or percutaneous coronary intervention (PCI) and answered a survey 16 months later on average.
Although 20% of the patients with obesity had lost 5% or more of their initial weight, 16% had gained 5% or more of their initial weight.
Notably, “the discharge letter did not record the weight status in a quarter of [the patients with obesity] and a substantial proportion reported to have never been told by a healthcare professional [that they were] overweight,” the investigators wrote.
“It seems,” Dr. De Bacquer and colleagues noted, “that obesity is not considered by physicians as a serious medical problem, which requires attention, recommendations, and obvious advice on personal weight targets.”
However, “the benefits for patients who lost weight in our study, resulting in a healthier cardiovascular risk profile, are really worthwhile,” they pointed out.
Cardiovascular rehabilitation should include weight loss intervention
“The safest and most effective approach for managing body weight” in patients with coronary artery disease and obesity “is adopting a healthy eating pattern and increasing levels of physical activity,” they wrote.
Their findings that “patients who reported reducing their fat and sugar intake, consuming more fruit, vegetables, and fish and doing more regular physical activity, had significant weight loss,” support this.
Dr. De Bacquer and colleagues recommend that cardiovascular prevention and rehabilitation programs “should include weight loss intervention, including different forms of self-support, as a specific component of a comprehensive intervention to reduce total cardiovascular risk, extend life expectancy, and improve quality of life.”
Clinicians should “consider the incremental value of telehealth intervention as well as recently described pharmacological interventions,” they added, noting that the study did not look at these options or at metabolic surgery.
Invited to comment, one expert pointed out that two new observational studies of metabolic surgery in patients with obesity and coronary artery disease reported positive outcomes.
Another expert took issue with the “patient blaming” tone of the article and the lack of actionable ways to help patients lose weight.
Medical therapy or bariatric surgery as other options?
“The study demonstrated how prevalent obesity is in patients with heart disease“ and “confirmed how difficult it is to achieve weight loss, in particular, in patients with heart disease, where weight loss would be beneficial,” Erik Näslund, MD, PhD, said in an interview.
Even though “current guidelines stress weight-loss counseling, some patients actually gained weight,” observed Dr. Näslund, of Danderyd Hospital and Karolinska Institutet, Stockholm.
On the other hand, patients who lost 5% or more of their initial weight had reduced comorbidities that are associated with cardiovascular disease.
“The best way to achieve long-term weight loss in patients with severe obesity is metabolic (bariatric) surgery,” noted Dr. Näslund, who was not involved in the study. “There are now two recent papers in the journal Circulation that demonstrate that metabolic surgery has a role in the secondary prevention of cardiovascular disease in patients with severe obesity” – one study from Dr. Näslund’s group (Circulation. 2021;143:1458-67), as previously reported, and one study from researchers in Ontario, Canada (Circulation. 2021;143:1468-80).
However, those were observational studies, and the findings would need to be confirmed in a randomized clinical trial before they could be used as recommended practice of care, he cautioned. In addition, most patients in the current study would not fulfill the minimum body weight criteria for metabolic surgery.
“Therefore, there is a need for intensified medical therapy for these patients,” as another treatment option, said Dr. Näslund.
“It would be interesting,” he speculated, “to study how the new glucagon-like peptide-1 (GLP-1) receptor agonist therapies could work in this setting as a weight loss agent and perhaps have a positive independent cardiovascular benefit.”
Obesity is a disease; clinicians need to be respectful
Meanwhile, Obesity Society fellow and spokesperson Fatima Cody Stanford, MD, said in an interview that she didn’t think the language and tone of the article was respectful for patients with obesity, and the researchers “talked about the old narrative of how we support patients with obesity.”
Lifestyle modification can be at the core of treatment, but medication or bariatric surgery may be other options to “help patients get to their best selves.
“Patients with obesity deserve to be cared for and treated with respect,” said Dr. Stanford, an obesity medicine physician scientist at Massachusetts General Hospital and Harvard Medical School, Boston.
Treatment needs to be individualized and clinicians need to listen to patient concerns. For example, a patient with obesity may not be able to follow advice to walk more. “I can barely stand up,” one patient with obesity and osteoarthritis told Dr. Stanford.
And patients’ insurance may not cover cardiac rehabilitation – especially patients from racial minorities or those with lower socioeconomic status, she noted.
“My feeling has always been that it is important to be respectful to all patients,” Dr. Näslund agreed. “I do agree that we need to recognize obesity as a chronic disease, and the paper in EHJ demonstrates this, as obesity was not registered in many of the discharge notes.
“If we as healthcare workers measured a weight of our patients the same way that we take a blood pressure,” he said, “perhaps the [stigma] of obesity would be reduced.”
Study findings
The researchers examined pooled data from EUROASPIRE IV (2012-13) and EUROASPIRE V (2016-17) surveys of patients who were overweight or had obesity who had been discharged from hospital after MI, CABG, or PCI to determine if they had received lifestyle advice for weight loss, if they had acted on this advice, and if losing weight altered their cardiovascular disease risk factors.
They identified 10,507 adult patients in 29 mainly European countries who had complete survey data.
The mean age of the patients was 63 at the time of their hospitalization; 25% were women. Many had hypertension (66%-88%), dyslipidemia (69%-80%), or diabetes (16%-37%).
The prevalence of obesity varied from 8% to 46% in men and from 18% to 57% in women, in different countries. Patients with obesity had a mean body weight of 97 kg (213 pounds).
One of the most “striking” findings was the “apparent lack of motivation” to lose weight, Dr. De Bacquer and colleagues wrote. Half of the patients with obesity had not attempted to lose weight in the month before the follow-up visit and most did not plan to do so in the following month.
Goal setting is an important aspect of behavior modification techniques, they wrote, yet 7% of the patients did not know their body weight and 21% did not have an optimal weight target.
Half of the patients had been advised to follow a cardiac rehabilitation program and two-thirds had been advised to follow dietary recommendations and move more.
Those who made positive dietary changes and were more physically active were more likely to lose at least 5% of their weight.
And patients who lost at least 5% of their initial weight were less likely to have hypertension, dyslipidemia, or diabetes compared with patients who had gained this much weight, which “is likely to translate into improved prognosis on the long term,” the authors wrote.
EUROASPIRE IV and V were supported through research grants to the European Society of Cardiology from Amgen, AstraZeneca, Bristol-Myers Squibb/Emea Sarl, GlaxoSmithKline, Hoffmann-La Roche, and Merck, Sharp & Dohme (EUROASPIRE IV) and Amarin, Amgen, Daiichi Sankyo, Eli Lilly, Pfizer, Sanofi, Ferrer, and Novo Nordisk (EUROASPIRE V). Dr. De Bacquer, Dr. Näslund, and Dr. Stanford have no disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients who had been hospitalized for heart attack or cardiovascular revascularization procedures commonly were overweight (46%) or had obesity (35%), but at a follow-up visit, few had lost weight or planned to do so, according to researchers who conduced a large European study.
The findings emphasize that obesity needs to be recognized as a disease that has to be optimally managed to lessen the risk for a secondary cardiovascular event, the authors stressed.
The study, by Dirk De Bacquer, PhD, professor, department of public health, Ghent (Belgium) University, and colleagues, was published recently in the European Heart Journal – Quality of Care and Clinical Outcomes.
The researchers analyzed data from more than 10,000 patients in the EUROASPIRE IV and V studies who were hospitalized for acute myocardial infarction (MI), coronary artery bypass graft (CABG), or percutaneous coronary intervention (PCI) and answered a survey 16 months later on average.
Although 20% of the patients with obesity had lost 5% or more of their initial weight, 16% had gained 5% or more of their initial weight.
Notably, “the discharge letter did not record the weight status in a quarter of [the patients with obesity] and a substantial proportion reported to have never been told by a healthcare professional [that they were] overweight,” the investigators wrote.
“It seems,” Dr. De Bacquer and colleagues noted, “that obesity is not considered by physicians as a serious medical problem, which requires attention, recommendations, and obvious advice on personal weight targets.”
However, “the benefits for patients who lost weight in our study, resulting in a healthier cardiovascular risk profile, are really worthwhile,” they pointed out.
Cardiovascular rehabilitation should include weight loss intervention
“The safest and most effective approach for managing body weight” in patients with coronary artery disease and obesity “is adopting a healthy eating pattern and increasing levels of physical activity,” they wrote.
Their findings that “patients who reported reducing their fat and sugar intake, consuming more fruit, vegetables, and fish and doing more regular physical activity, had significant weight loss,” support this.
Dr. De Bacquer and colleagues recommend that cardiovascular prevention and rehabilitation programs “should include weight loss intervention, including different forms of self-support, as a specific component of a comprehensive intervention to reduce total cardiovascular risk, extend life expectancy, and improve quality of life.”
Clinicians should “consider the incremental value of telehealth intervention as well as recently described pharmacological interventions,” they added, noting that the study did not look at these options or at metabolic surgery.
Invited to comment, one expert pointed out that two new observational studies of metabolic surgery in patients with obesity and coronary artery disease reported positive outcomes.
Another expert took issue with the “patient blaming” tone of the article and the lack of actionable ways to help patients lose weight.
Medical therapy or bariatric surgery as other options?
“The study demonstrated how prevalent obesity is in patients with heart disease“ and “confirmed how difficult it is to achieve weight loss, in particular, in patients with heart disease, where weight loss would be beneficial,” Erik Näslund, MD, PhD, said in an interview.
Even though “current guidelines stress weight-loss counseling, some patients actually gained weight,” observed Dr. Näslund, of Danderyd Hospital and Karolinska Institutet, Stockholm.
On the other hand, patients who lost 5% or more of their initial weight had reduced comorbidities that are associated with cardiovascular disease.
“The best way to achieve long-term weight loss in patients with severe obesity is metabolic (bariatric) surgery,” noted Dr. Näslund, who was not involved in the study. “There are now two recent papers in the journal Circulation that demonstrate that metabolic surgery has a role in the secondary prevention of cardiovascular disease in patients with severe obesity” – one study from Dr. Näslund’s group (Circulation. 2021;143:1458-67), as previously reported, and one study from researchers in Ontario, Canada (Circulation. 2021;143:1468-80).
However, those were observational studies, and the findings would need to be confirmed in a randomized clinical trial before they could be used as recommended practice of care, he cautioned. In addition, most patients in the current study would not fulfill the minimum body weight criteria for metabolic surgery.
“Therefore, there is a need for intensified medical therapy for these patients,” as another treatment option, said Dr. Näslund.
“It would be interesting,” he speculated, “to study how the new glucagon-like peptide-1 (GLP-1) receptor agonist therapies could work in this setting as a weight loss agent and perhaps have a positive independent cardiovascular benefit.”
Obesity is a disease; clinicians need to be respectful
Meanwhile, Obesity Society fellow and spokesperson Fatima Cody Stanford, MD, said in an interview that she didn’t think the language and tone of the article was respectful for patients with obesity, and the researchers “talked about the old narrative of how we support patients with obesity.”
Lifestyle modification can be at the core of treatment, but medication or bariatric surgery may be other options to “help patients get to their best selves.
“Patients with obesity deserve to be cared for and treated with respect,” said Dr. Stanford, an obesity medicine physician scientist at Massachusetts General Hospital and Harvard Medical School, Boston.
Treatment needs to be individualized and clinicians need to listen to patient concerns. For example, a patient with obesity may not be able to follow advice to walk more. “I can barely stand up,” one patient with obesity and osteoarthritis told Dr. Stanford.
And patients’ insurance may not cover cardiac rehabilitation – especially patients from racial minorities or those with lower socioeconomic status, she noted.
“My feeling has always been that it is important to be respectful to all patients,” Dr. Näslund agreed. “I do agree that we need to recognize obesity as a chronic disease, and the paper in EHJ demonstrates this, as obesity was not registered in many of the discharge notes.
“If we as healthcare workers measured a weight of our patients the same way that we take a blood pressure,” he said, “perhaps the [stigma] of obesity would be reduced.”
Study findings
The researchers examined pooled data from EUROASPIRE IV (2012-13) and EUROASPIRE V (2016-17) surveys of patients who were overweight or had obesity who had been discharged from hospital after MI, CABG, or PCI to determine if they had received lifestyle advice for weight loss, if they had acted on this advice, and if losing weight altered their cardiovascular disease risk factors.
They identified 10,507 adult patients in 29 mainly European countries who had complete survey data.
The mean age of the patients was 63 at the time of their hospitalization; 25% were women. Many had hypertension (66%-88%), dyslipidemia (69%-80%), or diabetes (16%-37%).
The prevalence of obesity varied from 8% to 46% in men and from 18% to 57% in women, in different countries. Patients with obesity had a mean body weight of 97 kg (213 pounds).
One of the most “striking” findings was the “apparent lack of motivation” to lose weight, Dr. De Bacquer and colleagues wrote. Half of the patients with obesity had not attempted to lose weight in the month before the follow-up visit and most did not plan to do so in the following month.
Goal setting is an important aspect of behavior modification techniques, they wrote, yet 7% of the patients did not know their body weight and 21% did not have an optimal weight target.
Half of the patients had been advised to follow a cardiac rehabilitation program and two-thirds had been advised to follow dietary recommendations and move more.
Those who made positive dietary changes and were more physically active were more likely to lose at least 5% of their weight.
And patients who lost at least 5% of their initial weight were less likely to have hypertension, dyslipidemia, or diabetes compared with patients who had gained this much weight, which “is likely to translate into improved prognosis on the long term,” the authors wrote.
EUROASPIRE IV and V were supported through research grants to the European Society of Cardiology from Amgen, AstraZeneca, Bristol-Myers Squibb/Emea Sarl, GlaxoSmithKline, Hoffmann-La Roche, and Merck, Sharp & Dohme (EUROASPIRE IV) and Amarin, Amgen, Daiichi Sankyo, Eli Lilly, Pfizer, Sanofi, Ferrer, and Novo Nordisk (EUROASPIRE V). Dr. De Bacquer, Dr. Näslund, and Dr. Stanford have no disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Plant-based lignan intake linked to lower CHD risk
Consumption of a plant-based diet rich in lignans is associated with a lower risk of coronary heart disease (CHD), new research suggests.

In a prospective cohort study that followed almost 214,108 men and women who were free of CHD and cancer at baseline, increased long-term intake of lignans, polyphenolic substances produced by plants, was associated with significantly lower risk of total CHD in both men and women.
The benefit was increased in participants with a greater intake of fiber, suggesting that synergistic effects between the two might exist in relation to CHD reduction.
The results were published online in the Journal of the American College of Cardiology.
“Lignan is an estrogen-like molecule, so it exerts some estrogenic effects which are cardioprotective. It also has anti-inflammatory properties,” first author Yang Hu, ScD, a research fellow at the Harvard School of Public Health, Boston, said in an interview.
“Our results that showed an inverse association between lignan consumption and heart disease risk were expected, because it is known that lignans, which are predominantly from plant-based foods, like whole grains, fruit, vegetables, red wine, and coffee, are all associated with lower CHD risk,” Dr. Hu said.
What is novel about the current study is that it established a threshold for lignan consumption, above which there is no CHD benefit, he said.
“It is not a matter of the more you consume, the lower your risk. There is a certain amount of lignan you have to reach, after which there is no more benefit,” Dr. Hu said.
Dr. Hu and associates prospectively followed 214,108 men and women in three cohorts who did not have cardiovascular disease or cancer at baseline. The cohorts were the Health Professionals Follow-Up Study, Nurses’ Health Study, and Nurses’ Health Study II.
Diets were assessed using the Food Frequency Questionnaire every 2-4 years at follow-up visits.
During 5.5 million person-years of follow-up, Dr. Hu and associates documented 10,244 CHD cases, including 6,283 nonfatal myocardial infarctions and 3,961 fatal CHD cases.
The results showed that higher total lignan intake, and all individual lignan intake as well, were associated with significantly lower risk of total CHD.
Participants with higher total lignan intake were older and had more favorable health and lifestyle profiles including lower body mass index, lower prevalence of hypertension and hypercholesterolemia, high levels of physical activity, and better diet quality.
Overall, the pooled hazard ratios of CHD were 0.85 (95% confidence interval, 0.79-0.92) for total lignans, 0.76 (95% CI, 0.71-0.82) for matairesinol, 0.87 (95% CI, 0.81-0.93) for secoisolariciresinol, 0.89 (95% CI, 0.83-0.95) for pinoresinol, and 0.89 (95% CI: 0.83- 0.95) for lariciresinol (all P values for trend ≤ .003).
In addition, nonlinear relationships were found for total lignan, matairesinol, and secoisolariciresinol: The risk reduction plateaued at intakes above approximately 300 mcg/d for total lignan; 10 mcg/d for matairesinol, and 100 mcg/d for secoisolariciresinol.
The inverse associations for total lignan intake were more apparent among participants with higher total fiber intake.
In addition, lignan intake was more strongly associated with plasma concentrations of enterolactone when fiber intake was higher.
Dr. Hu said a next avenue of research will explore the synergistic association between lignans and fiber in further lowering CHD risk.
Lignans are exclusively metabolized by gut microbiota, Dr. Hu noted. “This opens another avenue of research because we can take further steps to see how the gut microbiota compositions and fiber interact with the production of lignans and how these might affect disease risk for other conditions, such as diabetes.”
An important study
“The evidence is building that there is an association between polyphenol intake and chronic disease, especially for CVD [cardiovascular disease],” David J.A. Jenkins, MD, PhD, and colleagues wrote in an accompanying editorial.
“Plant polyphenols may be important components of healthy plant-based diets that contribute to freedom from chronic diseases such as CVD, diabetes, and possibly cancer and so are associated with a reduction in all-cause mortality,” they wrote.
“I think this is an important study even though the results are not unexpected,” Dr. Jenkins, professor in the departments of medicine and nutritional sciences at the University of Toronto, said in an interview.
“We do know that plant polyphenols are important sources of antioxidants and may have many protective roles in preventing destruction of proteins and DNA destruction, so the results here reinforce very strongly the concept of plant foods and their importance in the diet,” he said.
The data reaffirmed the value of eating a variety of plant foods and eating them in a less processed form, because they have higher amounts of their phenolic compounds, Dr. Jenkins said.
“Things like wheat, oats, barley, [and] whole grain foods will have more phenolic components with them, as do fruits and vegetables,” he said.
Dr. Hu and Dr. Jenkins disclosed no relevant financial relationships.
Aversion of this article first appeared on Medscape.com.
Consumption of a plant-based diet rich in lignans is associated with a lower risk of coronary heart disease (CHD), new research suggests.
In a prospective cohort study that followed almost 214,108 men and women who were free of CHD and cancer at baseline, increased long-term intake of lignans, polyphenolic substances produced by plants, was associated with significantly lower risk of total CHD in both men and women.
The benefit was increased in participants with a greater intake of fiber, suggesting that synergistic effects between the two might exist in relation to CHD reduction.
The results were published online in the Journal of the American College of Cardiology.
“Lignan is an estrogen-like molecule, so it exerts some estrogenic effects which are cardioprotective. It also has anti-inflammatory properties,” first author Yang Hu, ScD, a research fellow at the Harvard School of Public Health, Boston, said in an interview.
“Our results that showed an inverse association between lignan consumption and heart disease risk were expected, because it is known that lignans, which are predominantly from plant-based foods, like whole grains, fruit, vegetables, red wine, and coffee, are all associated with lower CHD risk,” Dr. Hu said.
What is novel about the current study is that it established a threshold for lignan consumption, above which there is no CHD benefit, he said.
“It is not a matter of the more you consume, the lower your risk. There is a certain amount of lignan you have to reach, after which there is no more benefit,” Dr. Hu said.
Dr. Hu and associates prospectively followed 214,108 men and women in three cohorts who did not have cardiovascular disease or cancer at baseline. The cohorts were the Health Professionals Follow-Up Study, Nurses’ Health Study, and Nurses’ Health Study II.
Diets were assessed using the Food Frequency Questionnaire every 2-4 years at follow-up visits.
During 5.5 million person-years of follow-up, Dr. Hu and associates documented 10,244 CHD cases, including 6,283 nonfatal myocardial infarctions and 3,961 fatal CHD cases.
The results showed that higher total lignan intake, and all individual lignan intake as well, were associated with significantly lower risk of total CHD.
Participants with higher total lignan intake were older and had more favorable health and lifestyle profiles including lower body mass index, lower prevalence of hypertension and hypercholesterolemia, high levels of physical activity, and better diet quality.
Overall, the pooled hazard ratios of CHD were 0.85 (95% confidence interval, 0.79-0.92) for total lignans, 0.76 (95% CI, 0.71-0.82) for matairesinol, 0.87 (95% CI, 0.81-0.93) for secoisolariciresinol, 0.89 (95% CI, 0.83-0.95) for pinoresinol, and 0.89 (95% CI: 0.83- 0.95) for lariciresinol (all P values for trend ≤ .003).
In addition, nonlinear relationships were found for total lignan, matairesinol, and secoisolariciresinol: The risk reduction plateaued at intakes above approximately 300 mcg/d for total lignan; 10 mcg/d for matairesinol, and 100 mcg/d for secoisolariciresinol.
The inverse associations for total lignan intake were more apparent among participants with higher total fiber intake.
In addition, lignan intake was more strongly associated with plasma concentrations of enterolactone when fiber intake was higher.
Dr. Hu said a next avenue of research will explore the synergistic association between lignans and fiber in further lowering CHD risk.
Lignans are exclusively metabolized by gut microbiota, Dr. Hu noted. “This opens another avenue of research because we can take further steps to see how the gut microbiota compositions and fiber interact with the production of lignans and how these might affect disease risk for other conditions, such as diabetes.”
An important study
“The evidence is building that there is an association between polyphenol intake and chronic disease, especially for CVD [cardiovascular disease],” David J.A. Jenkins, MD, PhD, and colleagues wrote in an accompanying editorial.
“Plant polyphenols may be important components of healthy plant-based diets that contribute to freedom from chronic diseases such as CVD, diabetes, and possibly cancer and so are associated with a reduction in all-cause mortality,” they wrote.
“I think this is an important study even though the results are not unexpected,” Dr. Jenkins, professor in the departments of medicine and nutritional sciences at the University of Toronto, said in an interview.
“We do know that plant polyphenols are important sources of antioxidants and may have many protective roles in preventing destruction of proteins and DNA destruction, so the results here reinforce very strongly the concept of plant foods and their importance in the diet,” he said.
The data reaffirmed the value of eating a variety of plant foods and eating them in a less processed form, because they have higher amounts of their phenolic compounds, Dr. Jenkins said.
“Things like wheat, oats, barley, [and] whole grain foods will have more phenolic components with them, as do fruits and vegetables,” he said.
Dr. Hu and Dr. Jenkins disclosed no relevant financial relationships.
Aversion of this article first appeared on Medscape.com.
Consumption of a plant-based diet rich in lignans is associated with a lower risk of coronary heart disease (CHD), new research suggests.
In a prospective cohort study that followed almost 214,108 men and women who were free of CHD and cancer at baseline, increased long-term intake of lignans, polyphenolic substances produced by plants, was associated with significantly lower risk of total CHD in both men and women.
The benefit was increased in participants with a greater intake of fiber, suggesting that synergistic effects between the two might exist in relation to CHD reduction.
The results were published online in the Journal of the American College of Cardiology.
“Lignan is an estrogen-like molecule, so it exerts some estrogenic effects which are cardioprotective. It also has anti-inflammatory properties,” first author Yang Hu, ScD, a research fellow at the Harvard School of Public Health, Boston, said in an interview.
“Our results that showed an inverse association between lignan consumption and heart disease risk were expected, because it is known that lignans, which are predominantly from plant-based foods, like whole grains, fruit, vegetables, red wine, and coffee, are all associated with lower CHD risk,” Dr. Hu said.
What is novel about the current study is that it established a threshold for lignan consumption, above which there is no CHD benefit, he said.
“It is not a matter of the more you consume, the lower your risk. There is a certain amount of lignan you have to reach, after which there is no more benefit,” Dr. Hu said.
Dr. Hu and associates prospectively followed 214,108 men and women in three cohorts who did not have cardiovascular disease or cancer at baseline. The cohorts were the Health Professionals Follow-Up Study, Nurses’ Health Study, and Nurses’ Health Study II.
Diets were assessed using the Food Frequency Questionnaire every 2-4 years at follow-up visits.
During 5.5 million person-years of follow-up, Dr. Hu and associates documented 10,244 CHD cases, including 6,283 nonfatal myocardial infarctions and 3,961 fatal CHD cases.
The results showed that higher total lignan intake, and all individual lignan intake as well, were associated with significantly lower risk of total CHD.
Participants with higher total lignan intake were older and had more favorable health and lifestyle profiles including lower body mass index, lower prevalence of hypertension and hypercholesterolemia, high levels of physical activity, and better diet quality.
Overall, the pooled hazard ratios of CHD were 0.85 (95% confidence interval, 0.79-0.92) for total lignans, 0.76 (95% CI, 0.71-0.82) for matairesinol, 0.87 (95% CI, 0.81-0.93) for secoisolariciresinol, 0.89 (95% CI, 0.83-0.95) for pinoresinol, and 0.89 (95% CI: 0.83- 0.95) for lariciresinol (all P values for trend ≤ .003).
In addition, nonlinear relationships were found for total lignan, matairesinol, and secoisolariciresinol: The risk reduction plateaued at intakes above approximately 300 mcg/d for total lignan; 10 mcg/d for matairesinol, and 100 mcg/d for secoisolariciresinol.
The inverse associations for total lignan intake were more apparent among participants with higher total fiber intake.
In addition, lignan intake was more strongly associated with plasma concentrations of enterolactone when fiber intake was higher.
Dr. Hu said a next avenue of research will explore the synergistic association between lignans and fiber in further lowering CHD risk.
Lignans are exclusively metabolized by gut microbiota, Dr. Hu noted. “This opens another avenue of research because we can take further steps to see how the gut microbiota compositions and fiber interact with the production of lignans and how these might affect disease risk for other conditions, such as diabetes.”
An important study
“The evidence is building that there is an association between polyphenol intake and chronic disease, especially for CVD [cardiovascular disease],” David J.A. Jenkins, MD, PhD, and colleagues wrote in an accompanying editorial.
“Plant polyphenols may be important components of healthy plant-based diets that contribute to freedom from chronic diseases such as CVD, diabetes, and possibly cancer and so are associated with a reduction in all-cause mortality,” they wrote.
“I think this is an important study even though the results are not unexpected,” Dr. Jenkins, professor in the departments of medicine and nutritional sciences at the University of Toronto, said in an interview.
“We do know that plant polyphenols are important sources of antioxidants and may have many protective roles in preventing destruction of proteins and DNA destruction, so the results here reinforce very strongly the concept of plant foods and their importance in the diet,” he said.
The data reaffirmed the value of eating a variety of plant foods and eating them in a less processed form, because they have higher amounts of their phenolic compounds, Dr. Jenkins said.
“Things like wheat, oats, barley, [and] whole grain foods will have more phenolic components with them, as do fruits and vegetables,” he said.
Dr. Hu and Dr. Jenkins disclosed no relevant financial relationships.
Aversion of this article first appeared on Medscape.com.
He Needs More Than Lip Service for This Lesion
ANSWER
The correct answer is all of the above (choice “g”).
DISCUSSION
Squamous cell carcinoma (SCC) of the lip—almost always the lower lip—is quite common and appears to be caused by several factors. These can include exposure to ultraviolet light, ionizing radiation, arsenic (through contaminated groundwater or certain medications), tobacco, and human papillomavirus.
Early on in its manifestation, this patient’s SCC could have been excised with margins, producing an excellent prognosis. But with the extended delay in diagnosis and apparent related adenopathy, the patient’s future looked much less certain. At the very least, he would face extensive surgery, possible lymph node dissection, and maybe chemo and radiation therapies. Metastasis to the brain and lung(s) were very real possibilities.
The history associated with this case is far from uncommon, since these cancers are often mistaken for infection, which further delays correct diagnosis and treatment. Compounding this problem—and for reasons unclear to this author—affected patients are often referred to the wrong specialist. The critical missing piece of information was a diagnosis, which could only have been obtained through an incisional biopsy. Only then could the patient be referred appropriately.
Fortunately, in this case, the patient ended up under the care of a head and neck surgeon who planned to address this tumor after imaging of the head, neck, and lungs was completed.
ANSWER
The correct answer is all of the above (choice “g”).
DISCUSSION
Squamous cell carcinoma (SCC) of the lip—almost always the lower lip—is quite common and appears to be caused by several factors. These can include exposure to ultraviolet light, ionizing radiation, arsenic (through contaminated groundwater or certain medications), tobacco, and human papillomavirus.
Early on in its manifestation, this patient’s SCC could have been excised with margins, producing an excellent prognosis. But with the extended delay in diagnosis and apparent related adenopathy, the patient’s future looked much less certain. At the very least, he would face extensive surgery, possible lymph node dissection, and maybe chemo and radiation therapies. Metastasis to the brain and lung(s) were very real possibilities.
The history associated with this case is far from uncommon, since these cancers are often mistaken for infection, which further delays correct diagnosis and treatment. Compounding this problem—and for reasons unclear to this author—affected patients are often referred to the wrong specialist. The critical missing piece of information was a diagnosis, which could only have been obtained through an incisional biopsy. Only then could the patient be referred appropriately.
Fortunately, in this case, the patient ended up under the care of a head and neck surgeon who planned to address this tumor after imaging of the head, neck, and lungs was completed.
ANSWER
The correct answer is all of the above (choice “g”).
DISCUSSION
Squamous cell carcinoma (SCC) of the lip—almost always the lower lip—is quite common and appears to be caused by several factors. These can include exposure to ultraviolet light, ionizing radiation, arsenic (through contaminated groundwater or certain medications), tobacco, and human papillomavirus.
Early on in its manifestation, this patient’s SCC could have been excised with margins, producing an excellent prognosis. But with the extended delay in diagnosis and apparent related adenopathy, the patient’s future looked much less certain. At the very least, he would face extensive surgery, possible lymph node dissection, and maybe chemo and radiation therapies. Metastasis to the brain and lung(s) were very real possibilities.
The history associated with this case is far from uncommon, since these cancers are often mistaken for infection, which further delays correct diagnosis and treatment. Compounding this problem—and for reasons unclear to this author—affected patients are often referred to the wrong specialist. The critical missing piece of information was a diagnosis, which could only have been obtained through an incisional biopsy. Only then could the patient be referred appropriately.
Fortunately, in this case, the patient ended up under the care of a head and neck surgeon who planned to address this tumor after imaging of the head, neck, and lungs was completed.

Several years ago, the patient developed what he thought was a cold sore, which waxed and waned but never quite healed. It grew considerably over time but caused no pain, so the patient and his wife assumed it was benign. A few times over the years, his primary care provider (PCP) prescribed oral antibiotics, then later acyclovir, to treat the lesion. When it became large enough to interfere with normal speech, the patient’s PCP referred him to a dentist, who in turn arranged an urgent consultation with dermatology.
The patient was retired but had spent more than 50 years working and recreating outdoors without any protection. For 40 of those adult years, he had smoked. His health was good in other respects.
The 3-cm warty mass on the vermillion surface of the lower lip, just to the left of center, was focally eroded and quite firm to touch. Palpation of local nodal locations revealed several fixed nontender nodes, most notably in the submental area. His sun-exposed skin was quite sun damaged, with stellate scarring, abundant dyschromia, telangiectasias, and marked solar atrophy.
A 5-mm punch biopsy was performed, showing poorly differentiated squamous cell carcinoma.
