User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
In the Future, a Robot Intensivist May Save Your Life
This transcript has been edited for clarity.
They call it the “golden hour”: 60 minutes, give or take, when the chance to save the life of a trauma victim is at its greatest. If the patient can be resuscitated and stabilized in that time window, they stand a good chance of surviving. If not, well, they don’t.
But resuscitation is complicated. It requires blood products, fluids, vasopressors — all given in precise doses in response to rapidly changing hemodynamics. To do it right takes specialized training, advanced life support (ALS). If the patient is in a remote area or an area without ALS-certified emergency medical services, or is far from the nearest trauma center, that golden hour is lost. And the patient may be as well.
But we live in the future. We have robots in factories, self-driving cars, autonomous drones. Why not an autonomous trauma doctor? If you are in a life-threatening accident, would you want to be treated ... by a robot?
Enter “resuscitation based on functional hemodynamic monitoring,” or “ReFit,” introduced in this article appearing in the journal Intensive Care Medicine Experimental.
The idea behind ReFit is straightforward. Resuscitation after trauma should be based on hitting key hemodynamic targets using the tools we have available in the field: blood, fluids, pressors. The researchers wanted to develop a closed-loop system, something that could be used by minimally trained personnel. The input to the system? Hemodynamic data, provided through a single measurement device, an arterial catheter. The output: blood, fluids, and pressors, delivered intravenously.
The body (a prototype) of the system looks like this. You can see various pumps labeled with various fluids, electronic controllers, and so forth.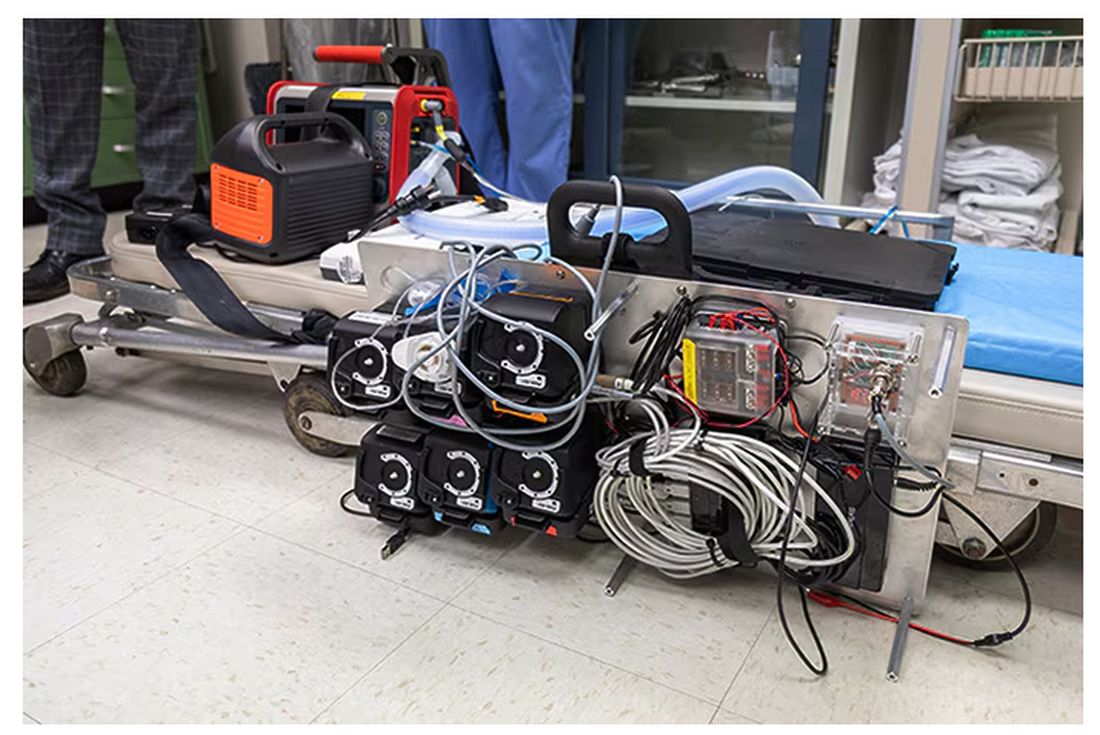
If that’s the body, then this is the brain – a ruggedized laptop interpreting a readout of that arterial catheter.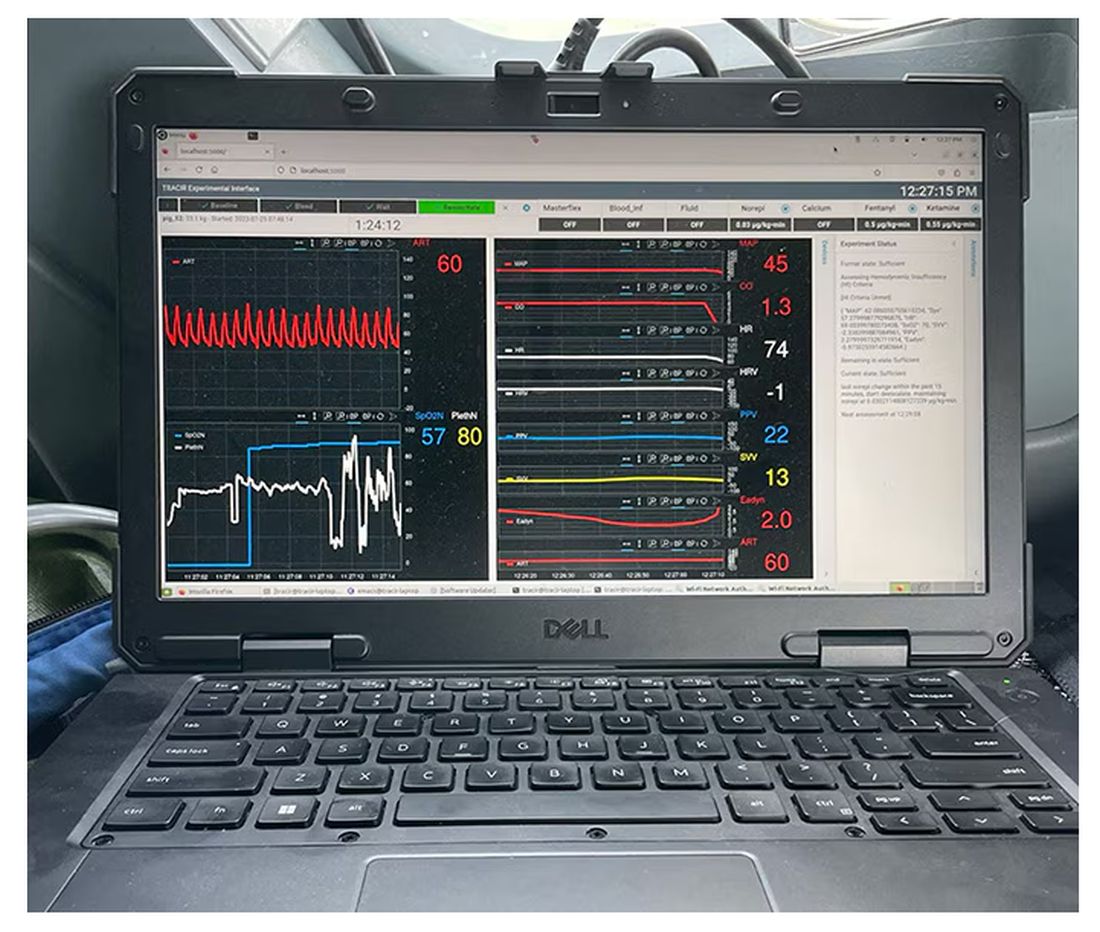
If that’s the brain, then the ReFit algorithm is the mind. The algorithm does its best to leverage all the data it can, so I want to walk through it in a bit of detail.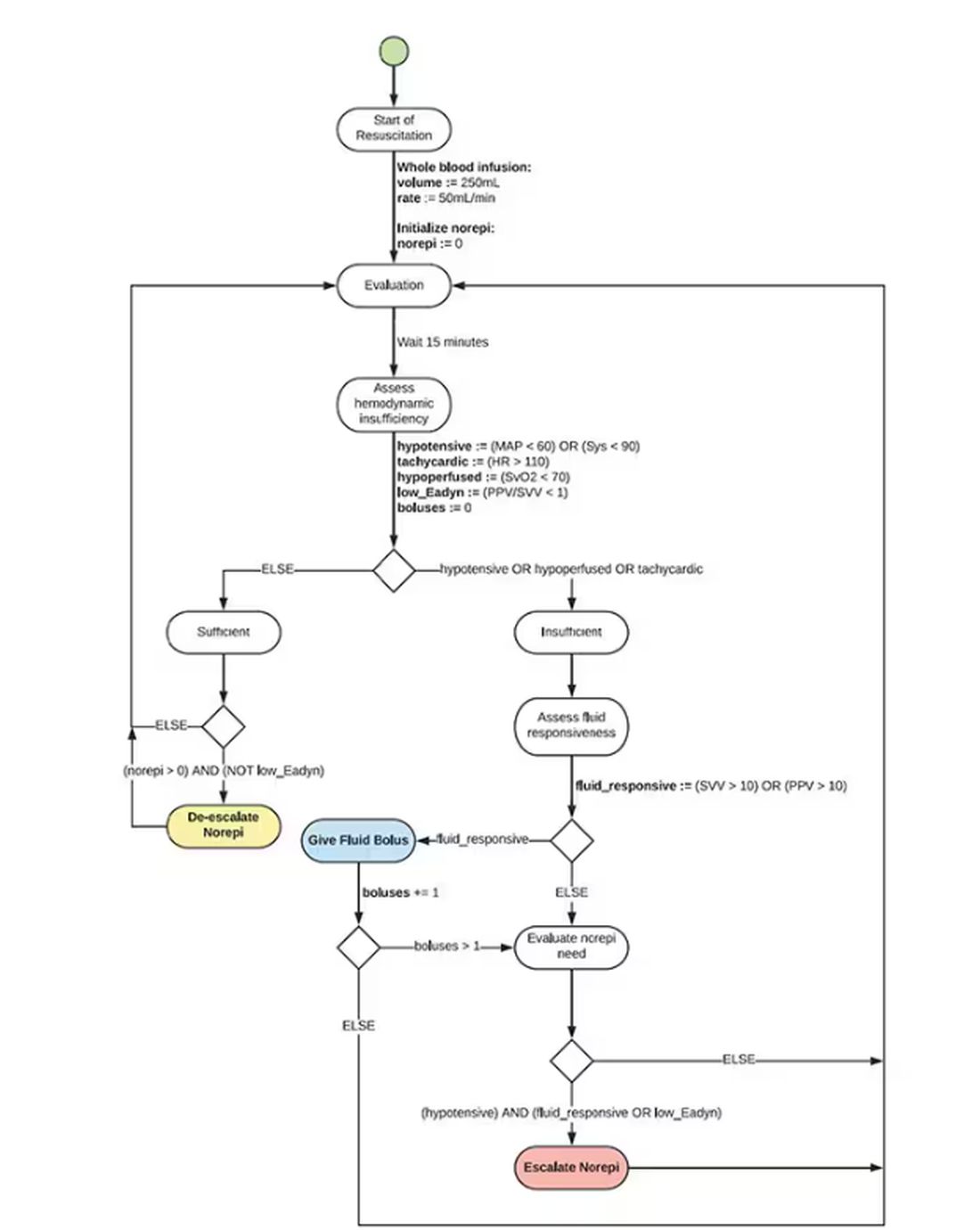
First, check to see whether the patient is stable, defined as a heart rate < 110 beats/min and a mean arterial pressure > 60 mm Hg. If not, you’re off to the races, starting with a bolus of whole blood.
Next, the algorithm gets really interesting. If the patient is still unstable, the computer assesses fluid responsiveness by giving a test dose of fluid and measuring the pulse pressure variation. Greater pulse pressure variation means more fluid responsiveness and the algorithm gives more fluid. Less pulse pressure variation leads the algorithm to uptitrate pressors — in this case, norepinephrine.
This cycle of evaluation and response keeps repeating. The computer titrates fluids and pressors up and down entirely on its own, in theory freeing the human team members to do other things, like getting the patient to a trauma center for definitive care.
So, how do you test whether something like this works? Clearly, you don’t want the trial run of a system like this to be used on a real human suffering from a real traumatic injury.
Once again, we have animals to thank for research advances — in this case, pigs. Fifteen pigs are described in the study. To simulate a severe, hemorrhagic trauma, they were anesthetized and the liver was lacerated. They were then observed passively until the mean arterial pressure had dropped to below 40 mm Hg.
This is a pretty severe injury. Three unfortunate animals served as controls, two of which died within the 3-hour time window of the study. Eight animals were plugged into the ReFit system.
For a window into what happens during this process, let’s take a look at the mean arterial pressure and heart rate readouts for one of the animals. You see that the blood pressure starts to fall precipitously after the liver laceration. The heart rate quickly picks up to compensate, raising the mean arterial pressure a bit, but this would be unsustainable with ongoing bleeding.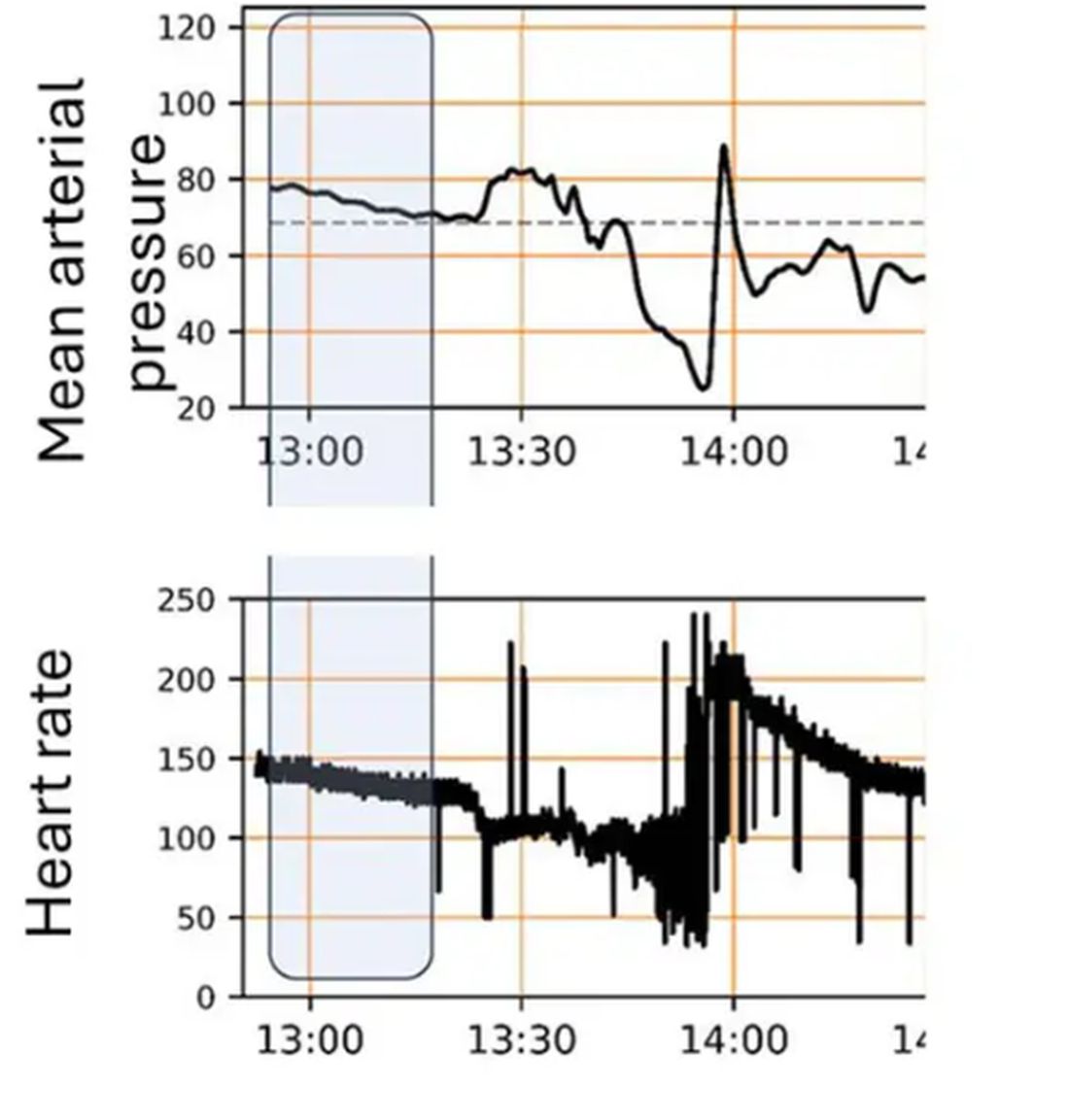
Here, the ReFit system takes over. Autonomously, the system administers two units of blood, followed by fluids, and then norepinephrine or further fluids per the protocol I described earlier. 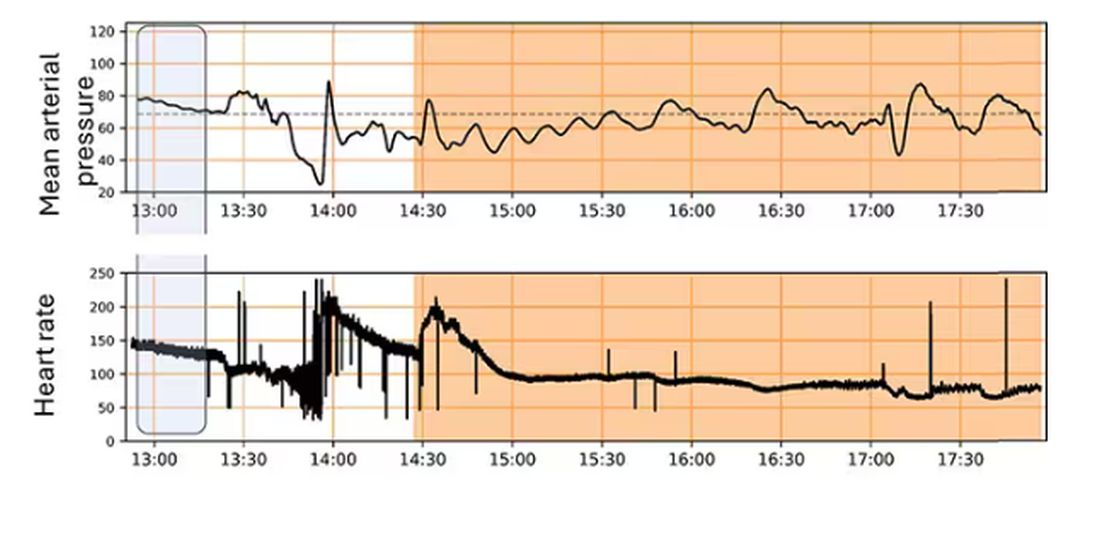
The practical upshot of all of this is stabilization, despite an as-yet untreated liver laceration.
Could an experienced ALS provider do this? Of course. But, as I mentioned before, you aren’t always near an experienced ALS provider.
This is all well and good in the lab, but in the real world, you actually need to transport a trauma patient. The researchers tried this also. To prove feasibility, four pigs were taken from the lab to the top of the University of Pittsburgh Medical Center, flown to Allegheny County Airport and back. Total time before liver laceration repair? Three hours. And all four survived.
It won’t surprise you to hear that this work was funded by the Department of Defense. You can see how a system like this, made a bit more rugged, a bit smaller, and a bit more self-contained could have real uses in the battlefield. But trauma is not unique to war, and something that can extend the time you have to safely transport a patient to definitive care — well, that’s worth its weight in golden hours.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
They call it the “golden hour”: 60 minutes, give or take, when the chance to save the life of a trauma victim is at its greatest. If the patient can be resuscitated and stabilized in that time window, they stand a good chance of surviving. If not, well, they don’t.
But resuscitation is complicated. It requires blood products, fluids, vasopressors — all given in precise doses in response to rapidly changing hemodynamics. To do it right takes specialized training, advanced life support (ALS). If the patient is in a remote area or an area without ALS-certified emergency medical services, or is far from the nearest trauma center, that golden hour is lost. And the patient may be as well.
But we live in the future. We have robots in factories, self-driving cars, autonomous drones. Why not an autonomous trauma doctor? If you are in a life-threatening accident, would you want to be treated ... by a robot?
Enter “resuscitation based on functional hemodynamic monitoring,” or “ReFit,” introduced in this article appearing in the journal Intensive Care Medicine Experimental.
The idea behind ReFit is straightforward. Resuscitation after trauma should be based on hitting key hemodynamic targets using the tools we have available in the field: blood, fluids, pressors. The researchers wanted to develop a closed-loop system, something that could be used by minimally trained personnel. The input to the system? Hemodynamic data, provided through a single measurement device, an arterial catheter. The output: blood, fluids, and pressors, delivered intravenously.
The body (a prototype) of the system looks like this. You can see various pumps labeled with various fluids, electronic controllers, and so forth.
If that’s the body, then this is the brain – a ruggedized laptop interpreting a readout of that arterial catheter.
If that’s the brain, then the ReFit algorithm is the mind. The algorithm does its best to leverage all the data it can, so I want to walk through it in a bit of detail.
First, check to see whether the patient is stable, defined as a heart rate < 110 beats/min and a mean arterial pressure > 60 mm Hg. If not, you’re off to the races, starting with a bolus of whole blood.
Next, the algorithm gets really interesting. If the patient is still unstable, the computer assesses fluid responsiveness by giving a test dose of fluid and measuring the pulse pressure variation. Greater pulse pressure variation means more fluid responsiveness and the algorithm gives more fluid. Less pulse pressure variation leads the algorithm to uptitrate pressors — in this case, norepinephrine.
This cycle of evaluation and response keeps repeating. The computer titrates fluids and pressors up and down entirely on its own, in theory freeing the human team members to do other things, like getting the patient to a trauma center for definitive care.
So, how do you test whether something like this works? Clearly, you don’t want the trial run of a system like this to be used on a real human suffering from a real traumatic injury.
Once again, we have animals to thank for research advances — in this case, pigs. Fifteen pigs are described in the study. To simulate a severe, hemorrhagic trauma, they were anesthetized and the liver was lacerated. They were then observed passively until the mean arterial pressure had dropped to below 40 mm Hg.
This is a pretty severe injury. Three unfortunate animals served as controls, two of which died within the 3-hour time window of the study. Eight animals were plugged into the ReFit system.
For a window into what happens during this process, let’s take a look at the mean arterial pressure and heart rate readouts for one of the animals. You see that the blood pressure starts to fall precipitously after the liver laceration. The heart rate quickly picks up to compensate, raising the mean arterial pressure a bit, but this would be unsustainable with ongoing bleeding.
Here, the ReFit system takes over. Autonomously, the system administers two units of blood, followed by fluids, and then norepinephrine or further fluids per the protocol I described earlier.
The practical upshot of all of this is stabilization, despite an as-yet untreated liver laceration.
Could an experienced ALS provider do this? Of course. But, as I mentioned before, you aren’t always near an experienced ALS provider.
This is all well and good in the lab, but in the real world, you actually need to transport a trauma patient. The researchers tried this also. To prove feasibility, four pigs were taken from the lab to the top of the University of Pittsburgh Medical Center, flown to Allegheny County Airport and back. Total time before liver laceration repair? Three hours. And all four survived.
It won’t surprise you to hear that this work was funded by the Department of Defense. You can see how a system like this, made a bit more rugged, a bit smaller, and a bit more self-contained could have real uses in the battlefield. But trauma is not unique to war, and something that can extend the time you have to safely transport a patient to definitive care — well, that’s worth its weight in golden hours.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
They call it the “golden hour”: 60 minutes, give or take, when the chance to save the life of a trauma victim is at its greatest. If the patient can be resuscitated and stabilized in that time window, they stand a good chance of surviving. If not, well, they don’t.
But resuscitation is complicated. It requires blood products, fluids, vasopressors — all given in precise doses in response to rapidly changing hemodynamics. To do it right takes specialized training, advanced life support (ALS). If the patient is in a remote area or an area without ALS-certified emergency medical services, or is far from the nearest trauma center, that golden hour is lost. And the patient may be as well.
But we live in the future. We have robots in factories, self-driving cars, autonomous drones. Why not an autonomous trauma doctor? If you are in a life-threatening accident, would you want to be treated ... by a robot?
Enter “resuscitation based on functional hemodynamic monitoring,” or “ReFit,” introduced in this article appearing in the journal Intensive Care Medicine Experimental.
The idea behind ReFit is straightforward. Resuscitation after trauma should be based on hitting key hemodynamic targets using the tools we have available in the field: blood, fluids, pressors. The researchers wanted to develop a closed-loop system, something that could be used by minimally trained personnel. The input to the system? Hemodynamic data, provided through a single measurement device, an arterial catheter. The output: blood, fluids, and pressors, delivered intravenously.
The body (a prototype) of the system looks like this. You can see various pumps labeled with various fluids, electronic controllers, and so forth.
If that’s the body, then this is the brain – a ruggedized laptop interpreting a readout of that arterial catheter.
If that’s the brain, then the ReFit algorithm is the mind. The algorithm does its best to leverage all the data it can, so I want to walk through it in a bit of detail.
First, check to see whether the patient is stable, defined as a heart rate < 110 beats/min and a mean arterial pressure > 60 mm Hg. If not, you’re off to the races, starting with a bolus of whole blood.
Next, the algorithm gets really interesting. If the patient is still unstable, the computer assesses fluid responsiveness by giving a test dose of fluid and measuring the pulse pressure variation. Greater pulse pressure variation means more fluid responsiveness and the algorithm gives more fluid. Less pulse pressure variation leads the algorithm to uptitrate pressors — in this case, norepinephrine.
This cycle of evaluation and response keeps repeating. The computer titrates fluids and pressors up and down entirely on its own, in theory freeing the human team members to do other things, like getting the patient to a trauma center for definitive care.
So, how do you test whether something like this works? Clearly, you don’t want the trial run of a system like this to be used on a real human suffering from a real traumatic injury.
Once again, we have animals to thank for research advances — in this case, pigs. Fifteen pigs are described in the study. To simulate a severe, hemorrhagic trauma, they were anesthetized and the liver was lacerated. They were then observed passively until the mean arterial pressure had dropped to below 40 mm Hg.
This is a pretty severe injury. Three unfortunate animals served as controls, two of which died within the 3-hour time window of the study. Eight animals were plugged into the ReFit system.
For a window into what happens during this process, let’s take a look at the mean arterial pressure and heart rate readouts for one of the animals. You see that the blood pressure starts to fall precipitously after the liver laceration. The heart rate quickly picks up to compensate, raising the mean arterial pressure a bit, but this would be unsustainable with ongoing bleeding.
Here, the ReFit system takes over. Autonomously, the system administers two units of blood, followed by fluids, and then norepinephrine or further fluids per the protocol I described earlier.
The practical upshot of all of this is stabilization, despite an as-yet untreated liver laceration.
Could an experienced ALS provider do this? Of course. But, as I mentioned before, you aren’t always near an experienced ALS provider.
This is all well and good in the lab, but in the real world, you actually need to transport a trauma patient. The researchers tried this also. To prove feasibility, four pigs were taken from the lab to the top of the University of Pittsburgh Medical Center, flown to Allegheny County Airport and back. Total time before liver laceration repair? Three hours. And all four survived.
It won’t surprise you to hear that this work was funded by the Department of Defense. You can see how a system like this, made a bit more rugged, a bit smaller, and a bit more self-contained could have real uses in the battlefield. But trauma is not unique to war, and something that can extend the time you have to safely transport a patient to definitive care — well, that’s worth its weight in golden hours.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Bariatric Surgery May Reduce Breast Cancer Risk for Some
TOPLINE:
.
METHODOLOGY:
- Previous research suggests that bariatric surgery is associated with a lower risk for cancer in people with obesity, as well as female-specific cancers in women with obesity, especially those with higher baseline insulin levels. But there is a need for large prospective studies with more detailed patient information.
- The current secondary analysis included 2867 matched women (mean age, 48 years) from a prospective nonrandomized Swedish trial, which recruited men and women who had obesity between 1987 and 2001.
- Overall, 1420 women underwent bariatric surgery, and 1447 received usual care.
- Median baseline insulin levels were 15.8 μIU/L. In the surgery group, 68.3% of patients had vertical banded gastroplasty, 18.3% underwent gastric banding, and 13.4% underwent gastric bypass.
- The main outcome was breast cancer incidence, as identified from Swedish National Cancer Registry.
TAKEAWAY:
- Over a median follow-up of 23.9 years, 66 breast cancer events occurred in the surgery group and 88 in the usual care group (P = .02).
- Bariatric surgery was associated with a 33% lower risk for breast cancer (adjusted hazard ratio [aHR], 0.67), after excluding cases that occurred within the first 3 years (to account for any undiagnosed breast cancer at baseline) and adjusting for age, body mass index, alcohol, and smoking status.
- Looking at the menopausal status at baseline, bariatric surgery was associated with a reduced risk for breast cancer in premenopausal women (aHR, 0.64) but not postmenopausal women (aHR, 0.84; 95% CI, 0.49-1.45; P = .54).
- Bariatric surgery was also associated with a lower risk for breast cancer in women with baseline insulin levels above the median (aHR, 0.55) than in those with baseline insulin levels below the median (aHR, 1.01).
IN PRACTICE:
“The surgical treatment benefit was predominantly seen in women with hyperinsulinemia, suggesting insulin may be used as a predictor of treatment effect,” the authors wrote. Authors of an accompanying editorial, however, cautioned that “it is not known if insulin levels or insulin resistance are true biomarkers of breast cancer risk in patients with obesity undergoing bariatric surgery” and urged further research into underlying biological mechanisms.
SOURCE:
This study, led by Felipe M. Kristensson, MD, from Institute of Medicine, Department of Molecular and Clinical Medicine, the Sahlgrenska Academy at University of Gothenburg, Gothenburg, Sweden, was published online in JAMA Surgery. The accompanying editorial was led by Swati A. Kulkarni, MD, of the Comprehensive Cancer Center, Feinberg School of Medicine, Northwestern University, Chicago.
LIMITATIONS:
The study was not randomized. Breast cancer was not a predefined outcome of the main trial. Most patients underwent vertical banded gastroplasty, which is rarely used and could limit applicability of the results; however, vertical banded gastroplasty results in weight loss similar to that observed after sleeve gastrectomy. Follow-up values for insulin and insulin resistance were not available. The researchers noted significant differences in 12 out of 17 baseline characteristics between the two groups, including a larger proportion of postmenopausal women in the usual care group.
DISCLOSURES:
This study was supported by the Swedish state, Swedish Research Council, the Health & Medical Care Committee of the Region Västra Götaland, and the Adlerbert Research Foundation. The authors did not report any conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
.
METHODOLOGY:
- Previous research suggests that bariatric surgery is associated with a lower risk for cancer in people with obesity, as well as female-specific cancers in women with obesity, especially those with higher baseline insulin levels. But there is a need for large prospective studies with more detailed patient information.
- The current secondary analysis included 2867 matched women (mean age, 48 years) from a prospective nonrandomized Swedish trial, which recruited men and women who had obesity between 1987 and 2001.
- Overall, 1420 women underwent bariatric surgery, and 1447 received usual care.
- Median baseline insulin levels were 15.8 μIU/L. In the surgery group, 68.3% of patients had vertical banded gastroplasty, 18.3% underwent gastric banding, and 13.4% underwent gastric bypass.
- The main outcome was breast cancer incidence, as identified from Swedish National Cancer Registry.
TAKEAWAY:
- Over a median follow-up of 23.9 years, 66 breast cancer events occurred in the surgery group and 88 in the usual care group (P = .02).
- Bariatric surgery was associated with a 33% lower risk for breast cancer (adjusted hazard ratio [aHR], 0.67), after excluding cases that occurred within the first 3 years (to account for any undiagnosed breast cancer at baseline) and adjusting for age, body mass index, alcohol, and smoking status.
- Looking at the menopausal status at baseline, bariatric surgery was associated with a reduced risk for breast cancer in premenopausal women (aHR, 0.64) but not postmenopausal women (aHR, 0.84; 95% CI, 0.49-1.45; P = .54).
- Bariatric surgery was also associated with a lower risk for breast cancer in women with baseline insulin levels above the median (aHR, 0.55) than in those with baseline insulin levels below the median (aHR, 1.01).
IN PRACTICE:
“The surgical treatment benefit was predominantly seen in women with hyperinsulinemia, suggesting insulin may be used as a predictor of treatment effect,” the authors wrote. Authors of an accompanying editorial, however, cautioned that “it is not known if insulin levels or insulin resistance are true biomarkers of breast cancer risk in patients with obesity undergoing bariatric surgery” and urged further research into underlying biological mechanisms.
SOURCE:
This study, led by Felipe M. Kristensson, MD, from Institute of Medicine, Department of Molecular and Clinical Medicine, the Sahlgrenska Academy at University of Gothenburg, Gothenburg, Sweden, was published online in JAMA Surgery. The accompanying editorial was led by Swati A. Kulkarni, MD, of the Comprehensive Cancer Center, Feinberg School of Medicine, Northwestern University, Chicago.
LIMITATIONS:
The study was not randomized. Breast cancer was not a predefined outcome of the main trial. Most patients underwent vertical banded gastroplasty, which is rarely used and could limit applicability of the results; however, vertical banded gastroplasty results in weight loss similar to that observed after sleeve gastrectomy. Follow-up values for insulin and insulin resistance were not available. The researchers noted significant differences in 12 out of 17 baseline characteristics between the two groups, including a larger proportion of postmenopausal women in the usual care group.
DISCLOSURES:
This study was supported by the Swedish state, Swedish Research Council, the Health & Medical Care Committee of the Region Västra Götaland, and the Adlerbert Research Foundation. The authors did not report any conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
.
METHODOLOGY:
- Previous research suggests that bariatric surgery is associated with a lower risk for cancer in people with obesity, as well as female-specific cancers in women with obesity, especially those with higher baseline insulin levels. But there is a need for large prospective studies with more detailed patient information.
- The current secondary analysis included 2867 matched women (mean age, 48 years) from a prospective nonrandomized Swedish trial, which recruited men and women who had obesity between 1987 and 2001.
- Overall, 1420 women underwent bariatric surgery, and 1447 received usual care.
- Median baseline insulin levels were 15.8 μIU/L. In the surgery group, 68.3% of patients had vertical banded gastroplasty, 18.3% underwent gastric banding, and 13.4% underwent gastric bypass.
- The main outcome was breast cancer incidence, as identified from Swedish National Cancer Registry.
TAKEAWAY:
- Over a median follow-up of 23.9 years, 66 breast cancer events occurred in the surgery group and 88 in the usual care group (P = .02).
- Bariatric surgery was associated with a 33% lower risk for breast cancer (adjusted hazard ratio [aHR], 0.67), after excluding cases that occurred within the first 3 years (to account for any undiagnosed breast cancer at baseline) and adjusting for age, body mass index, alcohol, and smoking status.
- Looking at the menopausal status at baseline, bariatric surgery was associated with a reduced risk for breast cancer in premenopausal women (aHR, 0.64) but not postmenopausal women (aHR, 0.84; 95% CI, 0.49-1.45; P = .54).
- Bariatric surgery was also associated with a lower risk for breast cancer in women with baseline insulin levels above the median (aHR, 0.55) than in those with baseline insulin levels below the median (aHR, 1.01).
IN PRACTICE:
“The surgical treatment benefit was predominantly seen in women with hyperinsulinemia, suggesting insulin may be used as a predictor of treatment effect,” the authors wrote. Authors of an accompanying editorial, however, cautioned that “it is not known if insulin levels or insulin resistance are true biomarkers of breast cancer risk in patients with obesity undergoing bariatric surgery” and urged further research into underlying biological mechanisms.
SOURCE:
This study, led by Felipe M. Kristensson, MD, from Institute of Medicine, Department of Molecular and Clinical Medicine, the Sahlgrenska Academy at University of Gothenburg, Gothenburg, Sweden, was published online in JAMA Surgery. The accompanying editorial was led by Swati A. Kulkarni, MD, of the Comprehensive Cancer Center, Feinberg School of Medicine, Northwestern University, Chicago.
LIMITATIONS:
The study was not randomized. Breast cancer was not a predefined outcome of the main trial. Most patients underwent vertical banded gastroplasty, which is rarely used and could limit applicability of the results; however, vertical banded gastroplasty results in weight loss similar to that observed after sleeve gastrectomy. Follow-up values for insulin and insulin resistance were not available. The researchers noted significant differences in 12 out of 17 baseline characteristics between the two groups, including a larger proportion of postmenopausal women in the usual care group.
DISCLOSURES:
This study was supported by the Swedish state, Swedish Research Council, the Health & Medical Care Committee of the Region Västra Götaland, and the Adlerbert Research Foundation. The authors did not report any conflicts of interest.
A version of this article appeared on Medscape.com.
Gene Tests Could Predict if a Drug Will Work for a Patient
What if there were tests that could tell you whether the following drugs were a good match for your patients: Antidepressants, statins, painkillers, anticlotting medicines, chemotherapy agents, HIV treatments, organ transplant antirejection drugs, proton pump inhibitors for heartburn, and more?
That’s quite a list. And that’s pharmacogenetics, testing patients for genetic differences that affect how well a given drug will work for them and what kind of side effects to expect.
“About 9 out of 10 people will have a genetic difference in their DNA that can impact how they respond to common medications,” said Emily J. Cicali, PharmD, a clinical associate at the University of Florida College of Pharmacy, Gainesville.
Dr. Cicali is the clinical director of UF Health’s MyRx, a virtual program that gives Florida and New Jersey residents access to pharmacogenetic (PGx) tests plus expert interpretation by the health system’s pharmacists. Genetic factors are thought to contribute to about 25% or more of inappropriate drug responses or adverse events, said Kristin Wiisanen, PharmD, dean of the College of Pharmacy at Rosalind Franklin University of Medicine and Science in North Chicago.
Dr. Cicali said.
Through a cheek swab or blood sample, the MyRx program — and a growing number of health system programs, doctors’ offices, and home tests available across the United States — gives consumers a window on inherited gene variants that can affect how their body activates, metabolizes, and clears away medications from a long list of widely used drugs.
Why PGx Tests Can Have a Big Impact
These tests work by looking for genes that control drug metabolism.
“You have several different drug-metabolizing enzymes in your liver,” Dr. Cicali explained. “Pharmacogenetic tests look for gene variants that encode for these enzymes. If you’re an ultrarapid metabolizer, you have more of the enzymes that metabolize certain drugs, and there could be a risk the drug won’t work well because it doesn’t stay in the body long enough. On the other end of the spectrum, poor metabolizers have low levels of enzymes that affect certain drugs, so the drugs hang around longer and cause side effects.”
While pharmacogenetics is still considered an emerging science, it’s becoming more mainstream as test prices drop, insurance coverage expands, and an explosion of new research boosts understanding of gene-drug interactions, Dr. Wiisanen said.
Politicians are trying to extend its reach, too. The Right Drug Dose Now Act of 2024, introduced in Congress in late March, aims to accelerate the use of PGx by boosting public awareness and by inserting PGx test results into consumers’ electronic health records. (Though a similar bill died in a US House subcommittee in 2023.)
“The use of pharmacogenetic data to guide prescribing is growing rapidly,” Dr. Wiisanen said. “It’s becoming a routine part of drug therapy for many medications.”
What the Research Shows
When researchers sequenced the DNA of more than 10,000 Mayo Clinic patients, they made a discovery that might surprise many Americans: Gene variants that affect the effectiveness and safety of widely used drugs are not rare glitches. More than 99% of study participants had at least one. And 79% had three or more.
The Mayo-Baylor RIGHT 10K Study — one of the largest PGx studies ever conducted in the United States — looked at 77 gene variants, most involved with drug metabolism in the liver. Researchers focused closely on 13 with extensively studied, gene-based prescribing recommendations for 21 drugs including antidepressants, statins, pain killers, anticlotting medications for heart conditions, HIV treatments, chemotherapy agents, and antirejection drugs for organ transplants.
When researchers added participants’ genetic data to their electronic health records, they also sent semi-urgent alerts, which are alerts with the potential for severe harm, to the clinicians of 61 study volunteers. Over half changed patients’ drugs or doses.
The changes made a difference. One participant taking the pain drug tramadol turned out to be a poor metabolizer and was having dizzy spells because blood levels of the drug stayed high for long periods. Stopping tramadol stopped the dizziness. A participant taking escitalopram plus bupropion for major depression found out that the combo was likely ineffective because they metabolized escitalopram rapidly. A switch to a higher dose of bupropion alone put their depression into full remission.
“So many factors play into how you respond to medications,” said Mayo Clinic pharmacogenomics pharmacist Jessica Wright, PharmD, BCACP, one of the study authors. “Genetics is one of those pieces. Pharmacogenetic testing can reveal things that clinicians may not have been aware of or could help explain a patient’s exaggerated side effect.”
Pharmacogenetics is also called pharmacogenomics. The terms are often used interchangeably, even among PGx pharmacists, though the first refers to how individual genes influence drug response and the second to the effects of multiple genes, said Kelly E. Caudle, PharmD, PhD, an associate member of the Department of Pharmacy and Pharmaceutical Sciences at St. Jude Children’s Research Hospital in Memphis, Tennessee. Dr. Caudle is also co-principal investigator and director of the National Institutes of Health (NIH)-funded Clinical Pharmacogenetics Implementation Consortium (CPIC). The group creates, publishes, and posts evidence-based clinical practice guidelines for drugs with well-researched PGx influences.
By any name, PGx may help explain, predict, and sidestep unpredictable responses to a variety of drugs:
- In a 2023 multicenter study of 6944 people from seven European countries in The Lancet, those given customized drug treatments based on a 12-gene PGx panel had 30% fewer side effects than those who didn’t get this personalized prescribing. People in the study were being treated for cancer, heart disease, and mental health issues, among other conditions.
- In a 2023 from China’s Tongji University, Shanghai, of 650 survivors of strokes and transient ischemic attacks, those whose antiplatelet drugs (such as clopidogrel) were customized based on PGx testing had a lower risk for stroke and other vascular events in the next 90 days. The study was published in Frontiers in Pharmacology.
- In a University of Pennsylvania of 1944 adults with major depression, published in the Journal of the American Medical Association, those whose antidepressants were guided by PGx test results were 28% more likely to go into remission during the first 24 weeks of treatment than those in a control group. But by 24 weeks, equal numbers were in remission. A 2023 Chinese of 11 depression studies, published in BMC Psychiatry, came to a similar conclusion: PGx-guided antidepressant prescriptions may help people feel better quicker, perhaps by avoiding some of the usual trial-and-error of different depression drugs.
PGx checks are already strongly recommended or considered routine before some medications are prescribed. These include abacavir (Ziagen), an antiviral treatment for HIV that can have severe side effects in people with one gene variant.
The US Food and Drug Administration (FDA) recommends genetic testing for people with colon cancer before starting the drug irinotecan (Camptosar), which can cause severe diarrhea and raise infection risk in people with a gene variant that slows the drug’s elimination from the body.
Genetic testing is also recommended by the FDA for people with acute lymphoblastic leukemia before receiving the chemotherapy drug mercaptopurine (Purinethol) because a gene variant that affects drug processing can trigger serious side effects and raise the risk for infection at standard dosages.
“One of the key benefits of pharmacogenomic testing is in preventing adverse drug reactions,” Dr. Wiisanen said. “Testing of the thiopurine methyltransferase enzyme to guide dosing with 6-mercaptopurine or azathioprine can help prevent myelosuppression, a serious adverse drug reaction caused by lower production of blood cells in bone marrow.”
When, Why, and How to Test
“A family doctor should consider a PGx test if a patient is planning on taking a medication for which there is a CPIC guideline with a dosing recommendation,” said Teri Klein, PhD, professor of biomedical data science at Stanford University in California, and principal investigator at PharmGKB, an online resource funded by the NIH that provides information for healthcare practitioners, researchers, and consumers about PGx. Affiliated with CPIC, it’s based at Stanford University.
You might also consider it for patients already on a drug who are “not responding or experiencing side effects,” Dr. Caudle said.
Here’s how four PGx experts suggest consumers and physicians approach this option.
Find a Test
More than a dozen PGx tests are on the market — some only a provider can order, others a consumer can order after a review by their provider or by a provider from the testing company. Some of the tests (using saliva) may be administered at home, while blood tests are done in a doctor’s office or laboratory. Companies that offer the tests include ARUP Laboratories, Genomind, Labcorp, Mayo Clinic Laboratories, Myriad Neuroscience, Precision Sciences Inc., Tempus, and OneOme, but there are many others online. (Keep in mind that many laboratories offer “lab-developed tests” — created for use in a single laboratory — but these can be harder to verify. “The FDA regulates pharmacogenomic testing in laboratories,” Dr. Wiisanen said, “but many of the regulatory parameters are still being defined.”)
Because PGx is so new, there is no official list of recommended tests. So you’ll have to do a little homework. You can check that the laboratory is accredited by searching for it in the NIH Genetic Testing Laboratory Registry database. Beyond that, you’ll have to consult other evidence-based resources to confirm that the drug you’re interested in has research-backed data about specific gene variants (alleles) that affect metabolism as well as research-based clinical guidelines for using PGx results to make prescribing decisions.
The CPIC’s guidelines include dosing and alternate drug recommendations for more than 100 antidepressants, chemotherapy drugs, the antiplatelet and anticlotting drugs clopidogrel and warfarin, local anesthetics, antivirals and antibacterials, pain killers and anti-inflammatory drugs, and some cholesterol-lowering statins such as lovastatin and fluvastatin.
For help figuring out if a test looks for the right gene variants, Dr. Caudle and Dr. Wright recommended checking with the Association for Molecular Pathology’s website. The group published a brief list of best practices for pharmacogenomic testing in 2019. And it keeps a list of gene variants (alleles) that should be included in tests. Clinical guidelines from the CPIC and other groups, available on PharmGKB’s website, also list gene variants that affect the metabolism of the drug.
Consider Cost
The price tag for a test is typically several hundred dollars — but it can run as high as $1000-$2500. And health insurance doesn’t always pick up the tab.
In a 2023 University of Florida study of more than 1000 insurance claims for PGx testing, the number reimbursed varied from 72% for a pain diagnosis to 52% for cardiology to 46% for psychiatry.
Medicare covers some PGx testing when a consumer and their providers meet certain criteria, including whether a drug being considered has a significant gene-drug interaction. California’s Medi-Cal health insurance program covers PGx as do Medicaid programs in some states, including Arkansas and Rhode Island. You can find state-by-state coverage information on the Genetics Policy Hub’s website.
Understand the Results
As more insurers cover PGx, Dr. Klein and Dr. Wiisanen say the field will grow and more providers will use it to inform prescribing. But some health systems aren’t waiting.
In addition to UF Health’s MyRx, PGx is part of personalized medicine programs at the University of Pennsylvania in Philadelphia, Endeavor Health in Chicago, the Mayo Clinic, the University of California, San Francisco, Sanford Health in Sioux Falls, South Dakota, and St. Jude Children’s Research Hospital in Memphis, Tennessee.
Beyond testing, they offer a very useful service: A consult with a pharmacogenetics pharmacist to review the results and explain what they mean for a consumer’s current and future medications.
Physicians and curious consumers can also consult CPIC’s guidelines, which give recommendations about how to interpret the results of a PGx test, said Dr. Klein, a co-principal investigator at CPIC. CPIC has a grading system for both the evidence that supports the recommendation (high, moderate, or weak) and the recommendation itself (strong, moderate, or optional).
Currently, labeling for 456 prescription drugs sold in the United States includes some type of PGx information, according to the FDA’s Table of Pharmacogenomic Biomarkers in Drug Labeling and an annotated guide from PharmGKB.
Just 108 drug labels currently tell doctors and patients what to do with the information — such as requiring or suggesting testing or offering prescribing recommendations, according to PharmGKB. In contrast, PharmGKB’s online resources include evidence-based clinical guidelines for 201 drugs from CPIC and from professional PGx societies in the Netherlands, Canada, France, and elsewhere.
Consumers and physicians can also look for a pharmacist with pharmacogenetics training in their area or through a nearby medical center to learn more, Dr. Wright suggested. And while consumers can test without working with their own physician, the experts advise against it. Don’t stop or change the dose of medications you already take on your own, they say . And do work with your primary care practitioner or specialist to get tested and understand how the results fit into the bigger picture of how your body responds to your medications.
A version of this article appeared on Medscape.com.
What if there were tests that could tell you whether the following drugs were a good match for your patients: Antidepressants, statins, painkillers, anticlotting medicines, chemotherapy agents, HIV treatments, organ transplant antirejection drugs, proton pump inhibitors for heartburn, and more?
That’s quite a list. And that’s pharmacogenetics, testing patients for genetic differences that affect how well a given drug will work for them and what kind of side effects to expect.
“About 9 out of 10 people will have a genetic difference in their DNA that can impact how they respond to common medications,” said Emily J. Cicali, PharmD, a clinical associate at the University of Florida College of Pharmacy, Gainesville.
Dr. Cicali is the clinical director of UF Health’s MyRx, a virtual program that gives Florida and New Jersey residents access to pharmacogenetic (PGx) tests plus expert interpretation by the health system’s pharmacists. Genetic factors are thought to contribute to about 25% or more of inappropriate drug responses or adverse events, said Kristin Wiisanen, PharmD, dean of the College of Pharmacy at Rosalind Franklin University of Medicine and Science in North Chicago.
Dr. Cicali said.
Through a cheek swab or blood sample, the MyRx program — and a growing number of health system programs, doctors’ offices, and home tests available across the United States — gives consumers a window on inherited gene variants that can affect how their body activates, metabolizes, and clears away medications from a long list of widely used drugs.
Why PGx Tests Can Have a Big Impact
These tests work by looking for genes that control drug metabolism.
“You have several different drug-metabolizing enzymes in your liver,” Dr. Cicali explained. “Pharmacogenetic tests look for gene variants that encode for these enzymes. If you’re an ultrarapid metabolizer, you have more of the enzymes that metabolize certain drugs, and there could be a risk the drug won’t work well because it doesn’t stay in the body long enough. On the other end of the spectrum, poor metabolizers have low levels of enzymes that affect certain drugs, so the drugs hang around longer and cause side effects.”
While pharmacogenetics is still considered an emerging science, it’s becoming more mainstream as test prices drop, insurance coverage expands, and an explosion of new research boosts understanding of gene-drug interactions, Dr. Wiisanen said.
Politicians are trying to extend its reach, too. The Right Drug Dose Now Act of 2024, introduced in Congress in late March, aims to accelerate the use of PGx by boosting public awareness and by inserting PGx test results into consumers’ electronic health records. (Though a similar bill died in a US House subcommittee in 2023.)
“The use of pharmacogenetic data to guide prescribing is growing rapidly,” Dr. Wiisanen said. “It’s becoming a routine part of drug therapy for many medications.”
What the Research Shows
When researchers sequenced the DNA of more than 10,000 Mayo Clinic patients, they made a discovery that might surprise many Americans: Gene variants that affect the effectiveness and safety of widely used drugs are not rare glitches. More than 99% of study participants had at least one. And 79% had three or more.
The Mayo-Baylor RIGHT 10K Study — one of the largest PGx studies ever conducted in the United States — looked at 77 gene variants, most involved with drug metabolism in the liver. Researchers focused closely on 13 with extensively studied, gene-based prescribing recommendations for 21 drugs including antidepressants, statins, pain killers, anticlotting medications for heart conditions, HIV treatments, chemotherapy agents, and antirejection drugs for organ transplants.
When researchers added participants’ genetic data to their electronic health records, they also sent semi-urgent alerts, which are alerts with the potential for severe harm, to the clinicians of 61 study volunteers. Over half changed patients’ drugs or doses.
The changes made a difference. One participant taking the pain drug tramadol turned out to be a poor metabolizer and was having dizzy spells because blood levels of the drug stayed high for long periods. Stopping tramadol stopped the dizziness. A participant taking escitalopram plus bupropion for major depression found out that the combo was likely ineffective because they metabolized escitalopram rapidly. A switch to a higher dose of bupropion alone put their depression into full remission.
“So many factors play into how you respond to medications,” said Mayo Clinic pharmacogenomics pharmacist Jessica Wright, PharmD, BCACP, one of the study authors. “Genetics is one of those pieces. Pharmacogenetic testing can reveal things that clinicians may not have been aware of or could help explain a patient’s exaggerated side effect.”
Pharmacogenetics is also called pharmacogenomics. The terms are often used interchangeably, even among PGx pharmacists, though the first refers to how individual genes influence drug response and the second to the effects of multiple genes, said Kelly E. Caudle, PharmD, PhD, an associate member of the Department of Pharmacy and Pharmaceutical Sciences at St. Jude Children’s Research Hospital in Memphis, Tennessee. Dr. Caudle is also co-principal investigator and director of the National Institutes of Health (NIH)-funded Clinical Pharmacogenetics Implementation Consortium (CPIC). The group creates, publishes, and posts evidence-based clinical practice guidelines for drugs with well-researched PGx influences.
By any name, PGx may help explain, predict, and sidestep unpredictable responses to a variety of drugs:
- In a 2023 multicenter study of 6944 people from seven European countries in The Lancet, those given customized drug treatments based on a 12-gene PGx panel had 30% fewer side effects than those who didn’t get this personalized prescribing. People in the study were being treated for cancer, heart disease, and mental health issues, among other conditions.
- In a 2023 from China’s Tongji University, Shanghai, of 650 survivors of strokes and transient ischemic attacks, those whose antiplatelet drugs (such as clopidogrel) were customized based on PGx testing had a lower risk for stroke and other vascular events in the next 90 days. The study was published in Frontiers in Pharmacology.
- In a University of Pennsylvania of 1944 adults with major depression, published in the Journal of the American Medical Association, those whose antidepressants were guided by PGx test results were 28% more likely to go into remission during the first 24 weeks of treatment than those in a control group. But by 24 weeks, equal numbers were in remission. A 2023 Chinese of 11 depression studies, published in BMC Psychiatry, came to a similar conclusion: PGx-guided antidepressant prescriptions may help people feel better quicker, perhaps by avoiding some of the usual trial-and-error of different depression drugs.
PGx checks are already strongly recommended or considered routine before some medications are prescribed. These include abacavir (Ziagen), an antiviral treatment for HIV that can have severe side effects in people with one gene variant.
The US Food and Drug Administration (FDA) recommends genetic testing for people with colon cancer before starting the drug irinotecan (Camptosar), which can cause severe diarrhea and raise infection risk in people with a gene variant that slows the drug’s elimination from the body.
Genetic testing is also recommended by the FDA for people with acute lymphoblastic leukemia before receiving the chemotherapy drug mercaptopurine (Purinethol) because a gene variant that affects drug processing can trigger serious side effects and raise the risk for infection at standard dosages.
“One of the key benefits of pharmacogenomic testing is in preventing adverse drug reactions,” Dr. Wiisanen said. “Testing of the thiopurine methyltransferase enzyme to guide dosing with 6-mercaptopurine or azathioprine can help prevent myelosuppression, a serious adverse drug reaction caused by lower production of blood cells in bone marrow.”
When, Why, and How to Test
“A family doctor should consider a PGx test if a patient is planning on taking a medication for which there is a CPIC guideline with a dosing recommendation,” said Teri Klein, PhD, professor of biomedical data science at Stanford University in California, and principal investigator at PharmGKB, an online resource funded by the NIH that provides information for healthcare practitioners, researchers, and consumers about PGx. Affiliated with CPIC, it’s based at Stanford University.
You might also consider it for patients already on a drug who are “not responding or experiencing side effects,” Dr. Caudle said.
Here’s how four PGx experts suggest consumers and physicians approach this option.
Find a Test
More than a dozen PGx tests are on the market — some only a provider can order, others a consumer can order after a review by their provider or by a provider from the testing company. Some of the tests (using saliva) may be administered at home, while blood tests are done in a doctor’s office or laboratory. Companies that offer the tests include ARUP Laboratories, Genomind, Labcorp, Mayo Clinic Laboratories, Myriad Neuroscience, Precision Sciences Inc., Tempus, and OneOme, but there are many others online. (Keep in mind that many laboratories offer “lab-developed tests” — created for use in a single laboratory — but these can be harder to verify. “The FDA regulates pharmacogenomic testing in laboratories,” Dr. Wiisanen said, “but many of the regulatory parameters are still being defined.”)
Because PGx is so new, there is no official list of recommended tests. So you’ll have to do a little homework. You can check that the laboratory is accredited by searching for it in the NIH Genetic Testing Laboratory Registry database. Beyond that, you’ll have to consult other evidence-based resources to confirm that the drug you’re interested in has research-backed data about specific gene variants (alleles) that affect metabolism as well as research-based clinical guidelines for using PGx results to make prescribing decisions.
The CPIC’s guidelines include dosing and alternate drug recommendations for more than 100 antidepressants, chemotherapy drugs, the antiplatelet and anticlotting drugs clopidogrel and warfarin, local anesthetics, antivirals and antibacterials, pain killers and anti-inflammatory drugs, and some cholesterol-lowering statins such as lovastatin and fluvastatin.
For help figuring out if a test looks for the right gene variants, Dr. Caudle and Dr. Wright recommended checking with the Association for Molecular Pathology’s website. The group published a brief list of best practices for pharmacogenomic testing in 2019. And it keeps a list of gene variants (alleles) that should be included in tests. Clinical guidelines from the CPIC and other groups, available on PharmGKB’s website, also list gene variants that affect the metabolism of the drug.
Consider Cost
The price tag for a test is typically several hundred dollars — but it can run as high as $1000-$2500. And health insurance doesn’t always pick up the tab.
In a 2023 University of Florida study of more than 1000 insurance claims for PGx testing, the number reimbursed varied from 72% for a pain diagnosis to 52% for cardiology to 46% for psychiatry.
Medicare covers some PGx testing when a consumer and their providers meet certain criteria, including whether a drug being considered has a significant gene-drug interaction. California’s Medi-Cal health insurance program covers PGx as do Medicaid programs in some states, including Arkansas and Rhode Island. You can find state-by-state coverage information on the Genetics Policy Hub’s website.
Understand the Results
As more insurers cover PGx, Dr. Klein and Dr. Wiisanen say the field will grow and more providers will use it to inform prescribing. But some health systems aren’t waiting.
In addition to UF Health’s MyRx, PGx is part of personalized medicine programs at the University of Pennsylvania in Philadelphia, Endeavor Health in Chicago, the Mayo Clinic, the University of California, San Francisco, Sanford Health in Sioux Falls, South Dakota, and St. Jude Children’s Research Hospital in Memphis, Tennessee.
Beyond testing, they offer a very useful service: A consult with a pharmacogenetics pharmacist to review the results and explain what they mean for a consumer’s current and future medications.
Physicians and curious consumers can also consult CPIC’s guidelines, which give recommendations about how to interpret the results of a PGx test, said Dr. Klein, a co-principal investigator at CPIC. CPIC has a grading system for both the evidence that supports the recommendation (high, moderate, or weak) and the recommendation itself (strong, moderate, or optional).
Currently, labeling for 456 prescription drugs sold in the United States includes some type of PGx information, according to the FDA’s Table of Pharmacogenomic Biomarkers in Drug Labeling and an annotated guide from PharmGKB.
Just 108 drug labels currently tell doctors and patients what to do with the information — such as requiring or suggesting testing or offering prescribing recommendations, according to PharmGKB. In contrast, PharmGKB’s online resources include evidence-based clinical guidelines for 201 drugs from CPIC and from professional PGx societies in the Netherlands, Canada, France, and elsewhere.
Consumers and physicians can also look for a pharmacist with pharmacogenetics training in their area or through a nearby medical center to learn more, Dr. Wright suggested. And while consumers can test without working with their own physician, the experts advise against it. Don’t stop or change the dose of medications you already take on your own, they say . And do work with your primary care practitioner or specialist to get tested and understand how the results fit into the bigger picture of how your body responds to your medications.
A version of this article appeared on Medscape.com.
What if there were tests that could tell you whether the following drugs were a good match for your patients: Antidepressants, statins, painkillers, anticlotting medicines, chemotherapy agents, HIV treatments, organ transplant antirejection drugs, proton pump inhibitors for heartburn, and more?
That’s quite a list. And that’s pharmacogenetics, testing patients for genetic differences that affect how well a given drug will work for them and what kind of side effects to expect.
“About 9 out of 10 people will have a genetic difference in their DNA that can impact how they respond to common medications,” said Emily J. Cicali, PharmD, a clinical associate at the University of Florida College of Pharmacy, Gainesville.
Dr. Cicali is the clinical director of UF Health’s MyRx, a virtual program that gives Florida and New Jersey residents access to pharmacogenetic (PGx) tests plus expert interpretation by the health system’s pharmacists. Genetic factors are thought to contribute to about 25% or more of inappropriate drug responses or adverse events, said Kristin Wiisanen, PharmD, dean of the College of Pharmacy at Rosalind Franklin University of Medicine and Science in North Chicago.
Dr. Cicali said.
Through a cheek swab or blood sample, the MyRx program — and a growing number of health system programs, doctors’ offices, and home tests available across the United States — gives consumers a window on inherited gene variants that can affect how their body activates, metabolizes, and clears away medications from a long list of widely used drugs.
Why PGx Tests Can Have a Big Impact
These tests work by looking for genes that control drug metabolism.
“You have several different drug-metabolizing enzymes in your liver,” Dr. Cicali explained. “Pharmacogenetic tests look for gene variants that encode for these enzymes. If you’re an ultrarapid metabolizer, you have more of the enzymes that metabolize certain drugs, and there could be a risk the drug won’t work well because it doesn’t stay in the body long enough. On the other end of the spectrum, poor metabolizers have low levels of enzymes that affect certain drugs, so the drugs hang around longer and cause side effects.”
While pharmacogenetics is still considered an emerging science, it’s becoming more mainstream as test prices drop, insurance coverage expands, and an explosion of new research boosts understanding of gene-drug interactions, Dr. Wiisanen said.
Politicians are trying to extend its reach, too. The Right Drug Dose Now Act of 2024, introduced in Congress in late March, aims to accelerate the use of PGx by boosting public awareness and by inserting PGx test results into consumers’ electronic health records. (Though a similar bill died in a US House subcommittee in 2023.)
“The use of pharmacogenetic data to guide prescribing is growing rapidly,” Dr. Wiisanen said. “It’s becoming a routine part of drug therapy for many medications.”
What the Research Shows
When researchers sequenced the DNA of more than 10,000 Mayo Clinic patients, they made a discovery that might surprise many Americans: Gene variants that affect the effectiveness and safety of widely used drugs are not rare glitches. More than 99% of study participants had at least one. And 79% had three or more.
The Mayo-Baylor RIGHT 10K Study — one of the largest PGx studies ever conducted in the United States — looked at 77 gene variants, most involved with drug metabolism in the liver. Researchers focused closely on 13 with extensively studied, gene-based prescribing recommendations for 21 drugs including antidepressants, statins, pain killers, anticlotting medications for heart conditions, HIV treatments, chemotherapy agents, and antirejection drugs for organ transplants.
When researchers added participants’ genetic data to their electronic health records, they also sent semi-urgent alerts, which are alerts with the potential for severe harm, to the clinicians of 61 study volunteers. Over half changed patients’ drugs or doses.
The changes made a difference. One participant taking the pain drug tramadol turned out to be a poor metabolizer and was having dizzy spells because blood levels of the drug stayed high for long periods. Stopping tramadol stopped the dizziness. A participant taking escitalopram plus bupropion for major depression found out that the combo was likely ineffective because they metabolized escitalopram rapidly. A switch to a higher dose of bupropion alone put their depression into full remission.
“So many factors play into how you respond to medications,” said Mayo Clinic pharmacogenomics pharmacist Jessica Wright, PharmD, BCACP, one of the study authors. “Genetics is one of those pieces. Pharmacogenetic testing can reveal things that clinicians may not have been aware of or could help explain a patient’s exaggerated side effect.”
Pharmacogenetics is also called pharmacogenomics. The terms are often used interchangeably, even among PGx pharmacists, though the first refers to how individual genes influence drug response and the second to the effects of multiple genes, said Kelly E. Caudle, PharmD, PhD, an associate member of the Department of Pharmacy and Pharmaceutical Sciences at St. Jude Children’s Research Hospital in Memphis, Tennessee. Dr. Caudle is also co-principal investigator and director of the National Institutes of Health (NIH)-funded Clinical Pharmacogenetics Implementation Consortium (CPIC). The group creates, publishes, and posts evidence-based clinical practice guidelines for drugs with well-researched PGx influences.
By any name, PGx may help explain, predict, and sidestep unpredictable responses to a variety of drugs:
- In a 2023 multicenter study of 6944 people from seven European countries in The Lancet, those given customized drug treatments based on a 12-gene PGx panel had 30% fewer side effects than those who didn’t get this personalized prescribing. People in the study were being treated for cancer, heart disease, and mental health issues, among other conditions.
- In a 2023 from China’s Tongji University, Shanghai, of 650 survivors of strokes and transient ischemic attacks, those whose antiplatelet drugs (such as clopidogrel) were customized based on PGx testing had a lower risk for stroke and other vascular events in the next 90 days. The study was published in Frontiers in Pharmacology.
- In a University of Pennsylvania of 1944 adults with major depression, published in the Journal of the American Medical Association, those whose antidepressants were guided by PGx test results were 28% more likely to go into remission during the first 24 weeks of treatment than those in a control group. But by 24 weeks, equal numbers were in remission. A 2023 Chinese of 11 depression studies, published in BMC Psychiatry, came to a similar conclusion: PGx-guided antidepressant prescriptions may help people feel better quicker, perhaps by avoiding some of the usual trial-and-error of different depression drugs.
PGx checks are already strongly recommended or considered routine before some medications are prescribed. These include abacavir (Ziagen), an antiviral treatment for HIV that can have severe side effects in people with one gene variant.
The US Food and Drug Administration (FDA) recommends genetic testing for people with colon cancer before starting the drug irinotecan (Camptosar), which can cause severe diarrhea and raise infection risk in people with a gene variant that slows the drug’s elimination from the body.
Genetic testing is also recommended by the FDA for people with acute lymphoblastic leukemia before receiving the chemotherapy drug mercaptopurine (Purinethol) because a gene variant that affects drug processing can trigger serious side effects and raise the risk for infection at standard dosages.
“One of the key benefits of pharmacogenomic testing is in preventing adverse drug reactions,” Dr. Wiisanen said. “Testing of the thiopurine methyltransferase enzyme to guide dosing with 6-mercaptopurine or azathioprine can help prevent myelosuppression, a serious adverse drug reaction caused by lower production of blood cells in bone marrow.”
When, Why, and How to Test
“A family doctor should consider a PGx test if a patient is planning on taking a medication for which there is a CPIC guideline with a dosing recommendation,” said Teri Klein, PhD, professor of biomedical data science at Stanford University in California, and principal investigator at PharmGKB, an online resource funded by the NIH that provides information for healthcare practitioners, researchers, and consumers about PGx. Affiliated with CPIC, it’s based at Stanford University.
You might also consider it for patients already on a drug who are “not responding or experiencing side effects,” Dr. Caudle said.
Here’s how four PGx experts suggest consumers and physicians approach this option.
Find a Test
More than a dozen PGx tests are on the market — some only a provider can order, others a consumer can order after a review by their provider or by a provider from the testing company. Some of the tests (using saliva) may be administered at home, while blood tests are done in a doctor’s office or laboratory. Companies that offer the tests include ARUP Laboratories, Genomind, Labcorp, Mayo Clinic Laboratories, Myriad Neuroscience, Precision Sciences Inc., Tempus, and OneOme, but there are many others online. (Keep in mind that many laboratories offer “lab-developed tests” — created for use in a single laboratory — but these can be harder to verify. “The FDA regulates pharmacogenomic testing in laboratories,” Dr. Wiisanen said, “but many of the regulatory parameters are still being defined.”)
Because PGx is so new, there is no official list of recommended tests. So you’ll have to do a little homework. You can check that the laboratory is accredited by searching for it in the NIH Genetic Testing Laboratory Registry database. Beyond that, you’ll have to consult other evidence-based resources to confirm that the drug you’re interested in has research-backed data about specific gene variants (alleles) that affect metabolism as well as research-based clinical guidelines for using PGx results to make prescribing decisions.
The CPIC’s guidelines include dosing and alternate drug recommendations for more than 100 antidepressants, chemotherapy drugs, the antiplatelet and anticlotting drugs clopidogrel and warfarin, local anesthetics, antivirals and antibacterials, pain killers and anti-inflammatory drugs, and some cholesterol-lowering statins such as lovastatin and fluvastatin.
For help figuring out if a test looks for the right gene variants, Dr. Caudle and Dr. Wright recommended checking with the Association for Molecular Pathology’s website. The group published a brief list of best practices for pharmacogenomic testing in 2019. And it keeps a list of gene variants (alleles) that should be included in tests. Clinical guidelines from the CPIC and other groups, available on PharmGKB’s website, also list gene variants that affect the metabolism of the drug.
Consider Cost
The price tag for a test is typically several hundred dollars — but it can run as high as $1000-$2500. And health insurance doesn’t always pick up the tab.
In a 2023 University of Florida study of more than 1000 insurance claims for PGx testing, the number reimbursed varied from 72% for a pain diagnosis to 52% for cardiology to 46% for psychiatry.
Medicare covers some PGx testing when a consumer and their providers meet certain criteria, including whether a drug being considered has a significant gene-drug interaction. California’s Medi-Cal health insurance program covers PGx as do Medicaid programs in some states, including Arkansas and Rhode Island. You can find state-by-state coverage information on the Genetics Policy Hub’s website.
Understand the Results
As more insurers cover PGx, Dr. Klein and Dr. Wiisanen say the field will grow and more providers will use it to inform prescribing. But some health systems aren’t waiting.
In addition to UF Health’s MyRx, PGx is part of personalized medicine programs at the University of Pennsylvania in Philadelphia, Endeavor Health in Chicago, the Mayo Clinic, the University of California, San Francisco, Sanford Health in Sioux Falls, South Dakota, and St. Jude Children’s Research Hospital in Memphis, Tennessee.
Beyond testing, they offer a very useful service: A consult with a pharmacogenetics pharmacist to review the results and explain what they mean for a consumer’s current and future medications.
Physicians and curious consumers can also consult CPIC’s guidelines, which give recommendations about how to interpret the results of a PGx test, said Dr. Klein, a co-principal investigator at CPIC. CPIC has a grading system for both the evidence that supports the recommendation (high, moderate, or weak) and the recommendation itself (strong, moderate, or optional).
Currently, labeling for 456 prescription drugs sold in the United States includes some type of PGx information, according to the FDA’s Table of Pharmacogenomic Biomarkers in Drug Labeling and an annotated guide from PharmGKB.
Just 108 drug labels currently tell doctors and patients what to do with the information — such as requiring or suggesting testing or offering prescribing recommendations, according to PharmGKB. In contrast, PharmGKB’s online resources include evidence-based clinical guidelines for 201 drugs from CPIC and from professional PGx societies in the Netherlands, Canada, France, and elsewhere.
Consumers and physicians can also look for a pharmacist with pharmacogenetics training in their area or through a nearby medical center to learn more, Dr. Wright suggested. And while consumers can test without working with their own physician, the experts advise against it. Don’t stop or change the dose of medications you already take on your own, they say . And do work with your primary care practitioner or specialist to get tested and understand how the results fit into the bigger picture of how your body responds to your medications.
A version of this article appeared on Medscape.com.
Florida Allows Doctors To Perform C-Sections Outside of Hospitals
Florida has become the first state to allow doctors to perform cesarean sections outside of hospitals, siding with a private equity-owned physicians group that says the change will lower costs and give pregnant women the homier birthing atmosphere that many desire.
But the hospital industry and the nation’s leading obstetricians’ association say that even though some Florida hospitals have closed their maternity wards in recent years, performing C-sections in doctor-run clinics will increase the risks for women and babies when complications arise.
“A pregnant patient that is considered low-risk in one moment can suddenly need lifesaving care in the next,” Cole Greves, an Orlando perinatologist who chairs the Florida chapter of the American College of Obstetricians and Gynecologists, said in an email to KFF Health News. The new birth clinics, “even with increased regulation, cannot guarantee the level of safety patients would receive within a hospital.”
This spring, a law was enacted allowing “advanced birth centers,” where physicians can deliver babies vaginally or by C-section to women deemed at low risk of complications. Women would be able to stay overnight at the clinics.
Women’s Care Enterprises, a private equity-owned physicians group with locations mostly in Florida along with California and Kentucky, lobbied the state legislature to make the change. BC Partners, a London-based investment firm, bought Women’s Care in 2020.
“We have patients who don’t want to deliver in a hospital, and that breaks our heart,” said Stephen Snow, who recently retired as an ob.gyn. with Women’s Care and testified before the Florida Legislature advocating for the change in 2018.
Brittany Miller, vice president of strategic initiatives with Women’s Care, said the group would not comment on the issue.
Health experts are leery.
“What this looks like is a poor substitute for quality obstetrical care effectively being billed as something that gives people more choices,” said Alice Abernathy, an assistant professor of obstetrics and gynecology at the University of Pennsylvania Perelman School of Medicine. “This feels like a bad band-aid on a chronic issue that will make outcomes worse rather than better,” Abernathy said.
Nearly one-third of U.S. births occur via C-section, the surgical delivery of a baby through an incision in the mother’s abdomen and uterus. Generally, doctors use the procedure when they believe it is safer than vaginal delivery for the parent, the baby, or both. Such medical decisions can take place months before birth, or in an emergency.
Florida state Sen. Gayle Harrell, the Republican who sponsored the birth center bill, said having a C-section outside of a hospital may seem like a radical change, but so was the opening of outpatient surgery centers in the late 1980s.
Harrell, who managed her husband’s ob.gyn. practice, said birth centers will have to meet the same high standards for staffing, infection control, and other aspects as those at outpatient surgery centers.
“Given where we are with the need, and maternity deserts across the state, this is something that will help us and help moms get the best care,” she said.
Seventeen hospitals in the state have closed their maternity units since 2019, with many citing low insurance reimbursement and high malpractice costs, according to the Florida Hospital Association.
Mary Mayhew, CEO of the Florida Hospital Association, said it is wrong to compare birth centers to ambulatory surgery centers because of the many risks associated with C-sections, such as hemorrhaging.
The Florida law requires advanced birth centers to have a transfer agreement with a hospital, but it does not dictate where the facilities can open nor their proximity to a hospital.
“We have serious concerns about the impact this model has on our collective efforts to improve maternal and infant health,” Mayhew said. “Our hospitals do not see this in the best interest of providing quality and safety in labor and delivery.”
Despite its opposition to the new birth centers, the Florida Hospital Association did not fight passage of the overall bill because it also included a major increase in the amount Medicaid pays hospitals for maternity care.
Mayhew said it is unlikely that the birth centers would help address care shortages. Hospitals are already struggling with a shortage of ob.gyns., she said, and it is unrealistic to expect advanced birth centers to open in rural areas with a large proportion of people on Medicaid, which pays the lowest reimbursement for labor and delivery care.
It is unclear whether insurers will cover the advanced birth centers, though most insurers and Medicaid cover care at midwife-run birth centers. The advanced birth centers will not accept emergency walk-ins and will treat only patients whose insurance contracts with the facilities, making them in-network.
Snow, the retired ob.gyn. with Women’s Care, said the group plans to open an advanced birth center in the Tampa or Orlando area.
The advanced birth center concept is an improvement on midwife care that enables deliveries outside of hospitals, he said, as the centers allow women to stay overnight and, if necessary, offer anesthesia and C-sections.
Snow acknowledged that, with a private equity firm invested in Women’s Care, the birth center idea is also about making money. But he said hospitals have the same profit incentive and, like midwives, likely oppose the idea of centers that can provide C-sections because they could cut into hospital revenue.
“We are trying to reduce the cost of medicine, and this would be more cost-effective and more pleasant for patients,” he said.
Kate Bauer, executive director of the American Association of Birth Centers, said patients could confuse advanced birth centers with the existing, free-standing birth centers for low-risk births that have been run by midwives for decades. There are currently 31 licensed birth centers in Florida and 411 free-standing birth centers in the United States, she said.
“This is a radical departure from the standard of care,” Bauer said. “It’s a bad idea,” she said, because it could increase risks to mom and baby.
No other state allows C-sections outside of hospitals. The only facility that offers similar care is a birth clinic in Wichita, Kansas, which is connected by a short walkway to a hospital, Wesley Medical Center.
The clinic provides “hotel-like” maternity suites where staffers deliver about 100 babies a month, compared with 500 per month in the hospital itself.
Morgan Tracy, a maternity nurse navigator at the center, said the concept works largely because the hospital and birthing suites can share staff and pharmacy access, plus patients can be quickly transferred to the main hospital if complications arise.
“The beauty is there are team members on both sides of the street,” Tracy said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Florida has become the first state to allow doctors to perform cesarean sections outside of hospitals, siding with a private equity-owned physicians group that says the change will lower costs and give pregnant women the homier birthing atmosphere that many desire.
But the hospital industry and the nation’s leading obstetricians’ association say that even though some Florida hospitals have closed their maternity wards in recent years, performing C-sections in doctor-run clinics will increase the risks for women and babies when complications arise.
“A pregnant patient that is considered low-risk in one moment can suddenly need lifesaving care in the next,” Cole Greves, an Orlando perinatologist who chairs the Florida chapter of the American College of Obstetricians and Gynecologists, said in an email to KFF Health News. The new birth clinics, “even with increased regulation, cannot guarantee the level of safety patients would receive within a hospital.”
This spring, a law was enacted allowing “advanced birth centers,” where physicians can deliver babies vaginally or by C-section to women deemed at low risk of complications. Women would be able to stay overnight at the clinics.
Women’s Care Enterprises, a private equity-owned physicians group with locations mostly in Florida along with California and Kentucky, lobbied the state legislature to make the change. BC Partners, a London-based investment firm, bought Women’s Care in 2020.
“We have patients who don’t want to deliver in a hospital, and that breaks our heart,” said Stephen Snow, who recently retired as an ob.gyn. with Women’s Care and testified before the Florida Legislature advocating for the change in 2018.
Brittany Miller, vice president of strategic initiatives with Women’s Care, said the group would not comment on the issue.
Health experts are leery.
“What this looks like is a poor substitute for quality obstetrical care effectively being billed as something that gives people more choices,” said Alice Abernathy, an assistant professor of obstetrics and gynecology at the University of Pennsylvania Perelman School of Medicine. “This feels like a bad band-aid on a chronic issue that will make outcomes worse rather than better,” Abernathy said.
Nearly one-third of U.S. births occur via C-section, the surgical delivery of a baby through an incision in the mother’s abdomen and uterus. Generally, doctors use the procedure when they believe it is safer than vaginal delivery for the parent, the baby, or both. Such medical decisions can take place months before birth, or in an emergency.
Florida state Sen. Gayle Harrell, the Republican who sponsored the birth center bill, said having a C-section outside of a hospital may seem like a radical change, but so was the opening of outpatient surgery centers in the late 1980s.
Harrell, who managed her husband’s ob.gyn. practice, said birth centers will have to meet the same high standards for staffing, infection control, and other aspects as those at outpatient surgery centers.
“Given where we are with the need, and maternity deserts across the state, this is something that will help us and help moms get the best care,” she said.
Seventeen hospitals in the state have closed their maternity units since 2019, with many citing low insurance reimbursement and high malpractice costs, according to the Florida Hospital Association.
Mary Mayhew, CEO of the Florida Hospital Association, said it is wrong to compare birth centers to ambulatory surgery centers because of the many risks associated with C-sections, such as hemorrhaging.
The Florida law requires advanced birth centers to have a transfer agreement with a hospital, but it does not dictate where the facilities can open nor their proximity to a hospital.
“We have serious concerns about the impact this model has on our collective efforts to improve maternal and infant health,” Mayhew said. “Our hospitals do not see this in the best interest of providing quality and safety in labor and delivery.”
Despite its opposition to the new birth centers, the Florida Hospital Association did not fight passage of the overall bill because it also included a major increase in the amount Medicaid pays hospitals for maternity care.
Mayhew said it is unlikely that the birth centers would help address care shortages. Hospitals are already struggling with a shortage of ob.gyns., she said, and it is unrealistic to expect advanced birth centers to open in rural areas with a large proportion of people on Medicaid, which pays the lowest reimbursement for labor and delivery care.
It is unclear whether insurers will cover the advanced birth centers, though most insurers and Medicaid cover care at midwife-run birth centers. The advanced birth centers will not accept emergency walk-ins and will treat only patients whose insurance contracts with the facilities, making them in-network.
Snow, the retired ob.gyn. with Women’s Care, said the group plans to open an advanced birth center in the Tampa or Orlando area.
The advanced birth center concept is an improvement on midwife care that enables deliveries outside of hospitals, he said, as the centers allow women to stay overnight and, if necessary, offer anesthesia and C-sections.
Snow acknowledged that, with a private equity firm invested in Women’s Care, the birth center idea is also about making money. But he said hospitals have the same profit incentive and, like midwives, likely oppose the idea of centers that can provide C-sections because they could cut into hospital revenue.
“We are trying to reduce the cost of medicine, and this would be more cost-effective and more pleasant for patients,” he said.
Kate Bauer, executive director of the American Association of Birth Centers, said patients could confuse advanced birth centers with the existing, free-standing birth centers for low-risk births that have been run by midwives for decades. There are currently 31 licensed birth centers in Florida and 411 free-standing birth centers in the United States, she said.
“This is a radical departure from the standard of care,” Bauer said. “It’s a bad idea,” she said, because it could increase risks to mom and baby.
No other state allows C-sections outside of hospitals. The only facility that offers similar care is a birth clinic in Wichita, Kansas, which is connected by a short walkway to a hospital, Wesley Medical Center.
The clinic provides “hotel-like” maternity suites where staffers deliver about 100 babies a month, compared with 500 per month in the hospital itself.
Morgan Tracy, a maternity nurse navigator at the center, said the concept works largely because the hospital and birthing suites can share staff and pharmacy access, plus patients can be quickly transferred to the main hospital if complications arise.
“The beauty is there are team members on both sides of the street,” Tracy said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Florida has become the first state to allow doctors to perform cesarean sections outside of hospitals, siding with a private equity-owned physicians group that says the change will lower costs and give pregnant women the homier birthing atmosphere that many desire.
But the hospital industry and the nation’s leading obstetricians’ association say that even though some Florida hospitals have closed their maternity wards in recent years, performing C-sections in doctor-run clinics will increase the risks for women and babies when complications arise.
“A pregnant patient that is considered low-risk in one moment can suddenly need lifesaving care in the next,” Cole Greves, an Orlando perinatologist who chairs the Florida chapter of the American College of Obstetricians and Gynecologists, said in an email to KFF Health News. The new birth clinics, “even with increased regulation, cannot guarantee the level of safety patients would receive within a hospital.”
This spring, a law was enacted allowing “advanced birth centers,” where physicians can deliver babies vaginally or by C-section to women deemed at low risk of complications. Women would be able to stay overnight at the clinics.
Women’s Care Enterprises, a private equity-owned physicians group with locations mostly in Florida along with California and Kentucky, lobbied the state legislature to make the change. BC Partners, a London-based investment firm, bought Women’s Care in 2020.
“We have patients who don’t want to deliver in a hospital, and that breaks our heart,” said Stephen Snow, who recently retired as an ob.gyn. with Women’s Care and testified before the Florida Legislature advocating for the change in 2018.
Brittany Miller, vice president of strategic initiatives with Women’s Care, said the group would not comment on the issue.
Health experts are leery.
“What this looks like is a poor substitute for quality obstetrical care effectively being billed as something that gives people more choices,” said Alice Abernathy, an assistant professor of obstetrics and gynecology at the University of Pennsylvania Perelman School of Medicine. “This feels like a bad band-aid on a chronic issue that will make outcomes worse rather than better,” Abernathy said.
Nearly one-third of U.S. births occur via C-section, the surgical delivery of a baby through an incision in the mother’s abdomen and uterus. Generally, doctors use the procedure when they believe it is safer than vaginal delivery for the parent, the baby, or both. Such medical decisions can take place months before birth, or in an emergency.
Florida state Sen. Gayle Harrell, the Republican who sponsored the birth center bill, said having a C-section outside of a hospital may seem like a radical change, but so was the opening of outpatient surgery centers in the late 1980s.
Harrell, who managed her husband’s ob.gyn. practice, said birth centers will have to meet the same high standards for staffing, infection control, and other aspects as those at outpatient surgery centers.
“Given where we are with the need, and maternity deserts across the state, this is something that will help us and help moms get the best care,” she said.
Seventeen hospitals in the state have closed their maternity units since 2019, with many citing low insurance reimbursement and high malpractice costs, according to the Florida Hospital Association.
Mary Mayhew, CEO of the Florida Hospital Association, said it is wrong to compare birth centers to ambulatory surgery centers because of the many risks associated with C-sections, such as hemorrhaging.
The Florida law requires advanced birth centers to have a transfer agreement with a hospital, but it does not dictate where the facilities can open nor their proximity to a hospital.
“We have serious concerns about the impact this model has on our collective efforts to improve maternal and infant health,” Mayhew said. “Our hospitals do not see this in the best interest of providing quality and safety in labor and delivery.”
Despite its opposition to the new birth centers, the Florida Hospital Association did not fight passage of the overall bill because it also included a major increase in the amount Medicaid pays hospitals for maternity care.
Mayhew said it is unlikely that the birth centers would help address care shortages. Hospitals are already struggling with a shortage of ob.gyns., she said, and it is unrealistic to expect advanced birth centers to open in rural areas with a large proportion of people on Medicaid, which pays the lowest reimbursement for labor and delivery care.
It is unclear whether insurers will cover the advanced birth centers, though most insurers and Medicaid cover care at midwife-run birth centers. The advanced birth centers will not accept emergency walk-ins and will treat only patients whose insurance contracts with the facilities, making them in-network.
Snow, the retired ob.gyn. with Women’s Care, said the group plans to open an advanced birth center in the Tampa or Orlando area.
The advanced birth center concept is an improvement on midwife care that enables deliveries outside of hospitals, he said, as the centers allow women to stay overnight and, if necessary, offer anesthesia and C-sections.
Snow acknowledged that, with a private equity firm invested in Women’s Care, the birth center idea is also about making money. But he said hospitals have the same profit incentive and, like midwives, likely oppose the idea of centers that can provide C-sections because they could cut into hospital revenue.
“We are trying to reduce the cost of medicine, and this would be more cost-effective and more pleasant for patients,” he said.
Kate Bauer, executive director of the American Association of Birth Centers, said patients could confuse advanced birth centers with the existing, free-standing birth centers for low-risk births that have been run by midwives for decades. There are currently 31 licensed birth centers in Florida and 411 free-standing birth centers in the United States, she said.
“This is a radical departure from the standard of care,” Bauer said. “It’s a bad idea,” she said, because it could increase risks to mom and baby.
No other state allows C-sections outside of hospitals. The only facility that offers similar care is a birth clinic in Wichita, Kansas, which is connected by a short walkway to a hospital, Wesley Medical Center.
The clinic provides “hotel-like” maternity suites where staffers deliver about 100 babies a month, compared with 500 per month in the hospital itself.
Morgan Tracy, a maternity nurse navigator at the center, said the concept works largely because the hospital and birthing suites can share staff and pharmacy access, plus patients can be quickly transferred to the main hospital if complications arise.
“The beauty is there are team members on both sides of the street,” Tracy said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Suicide in Surgeons: The Heavy Toll of a High-Stakes Career
For those outside the medical profession, it took a global pandemic to finally understand how pervasive distress and suicide are among medical professionals, particularly surgeons.
For James Harrop, MD, it was made real years earlier by a colleague he’d trained alongside and worked with for decades — “one of the best surgeons I’ve ever seen” who, one day, just wasn’t there.
Lost in his own work, it wasn’t until Dr. Harrop, a professor of neurological and orthopedic surgery at Thomas Jefferson University, Philadelphia, read an article in The New England Journal of Medicine and realized his friend Michael Weinstein, MD, MPH, had been profoundly depressed for years and was hospitalized for his own safety.
Dr. Weinstein recovered and later gave grand rounds at Thomas Jefferson University, where he is an associate professor of surgery in the Acute Care Surgery Division. But the story stuck with Dr. Harrop.
“I said to Mike afterward, I’ve known you for 20 years and, retrospectively, going back, I never saw a single sign that you were depressed, sad, or had any issues, and he said to me ‘that’s because I did everything I could to make sure no one knew I had a problem,’ ” Dr. Harrop said during a talk on physician suicide on May 4 at the American Association of Neurological Surgeons (AANS) 2024 Annual Meeting.
“And that scared me because we need to help these people, we need to identify who they are.”
Surgeons at Greater Risk
Among 9175 physicians surveyed in the 2023 Medscape Physician Suicide Report, 9% had considered suicide, and 1% had attempted it. The average for US adults is 4.9% and 0.5%, respectively.
Surgeons are at particularly high risk. A 2011 survey of 7905 US surgeons found that 1 in 16 (6.3%) had considered suicide in the previous year. A post-pandemic survey of more than 600 surgeons and surgical trainees reported that one in seven had suicidal ideation.
It’s often estimated that between 300 and 400 physicians die by suicide each year in the United States, but exact numbers are not known. Recent updated estimates from the National Violent Death Reporting System put the number at 119 physician suicides annually.
Notably, that’s no better than data reported more than 50 years ago in the landmark policy paper The Sick Physician: Impairment by Psychiatric Disorders, Including Alcoholism and Drug Dependence. It sounded the alarm on poor mental health in physicians and reported that 100 doctors died by suicide annually — the equivalent of the average medical school graduating class at the time.
“If I take my med school class and double it, that’s how many physicians die each year,” Dr. Harrop said. “And here’s the bad news, it starts in medical school.”
Research shows higher rates of depression and suicidal ideation in medical students and residents than in other graduates, with rates varying by stage of training, he noted.
In a multischool study, 12% of medical students and residents had probable major depression, 9.2% mild/moderate depression, and suicidal ideation jumped from 6.6% in the first year of medical school to 9.4% in year 4.
A recent AANS survey of 346 neurosurgery residents revealed 67% had burnout, and 41% seriously considered quitting. Burnout rose to a high of 76% in the second year and decreased to 49% and 54% in years 3 and 4, respectively.
Inadequate operating room exposure, hostile faculty, and stressors outside work were tied to burnout, whereas mentorship was linked to a threefold lower likelihood of burnout.
Notably, a 2019 study conservatively estimated that the annual cost of burnout-related physician turnover and reduced clinical hours was $4.6 billion nationally and $7600 per employed physician for an organization.
“We need to be kinder to each other, to look out for each other, and to talk to each other,” Dr. Harrop told conference attendees.
‘Death by a 1000 Cuts’
A host of factors are associated with physician suicide including long work hours, delayed gratification, difficulty balancing work and home life, changing healthcare systems, lawsuits, and the unique ability to prescribe medications, said Dr. Harrop.
“In my life, I think of it as death by 1000 cuts. Every day I come in, you’ve got another person attacking you,” he said, referencing Death by 1000 Cuts: Medscape National Physician Burnout & Suicide Report 2021.
Dr. Harrop told this news organization that talking with numerous experts in this field has made him appreciate that anyone is at a risk for suicide.
“The problem is an overload of external resources crushing your existence to the point that you become paralyzed and make the irrational thought that the best solution is to end your life,” he said.
Ann Stroink, MD, immediate past president of the AANS, said in an interview that one potential trigger for burnout is the current shortage of neurosurgeons in the United States, which has led to increased workloads and potential sleep deprivation among existing neurosurgeons.
“To address this critical issue, we’ve been advocating through legislative channels for additional Medicare[-funded] slots” to train more neurosurgeons, she said. “It’s imperative that we take proactive steps to ensure that our healthcare system can sustainably meet the needs of patients, while also supporting the well-being of our neurosurgical professionals.”
The AANS is also advocating for decreased regulatory burdens associated with Medicare and insurance coverage, such as prior authorization, to help alleviate the administrative burdens that often contribute to burnout among its members, Dr. Stroink said.
A Model for Suicide Prevention
Dr. Harrop emphasized that suicide is preventable and that there is “some good news.” Turning to another high-risk profession, he noted that the US Air Force was able to reduce its suicide rate by 42.7% between 1994 and 1998 by doing three basic things.
The agency established a central surveillance database, restructured prevention services, and, more importantly, began conducting annual suicide prevention and awareness training, using gatekeepers to channel at-risk personnel to appropriate agencies and performing mental health questionnaires at enrollment and annually.
Similarly, education, screening, and access to mental health treatment are core recommendations for a national response to depression and suicide in physician trainees, said Dr. Harrop, who noted that his own hospital has started using the Patient Health Questionnaire 9-item for its staff.
Asked by this news organization how much progress has been made since The Sick Physician report, Dr. Harrop said, “we are probably doing worse” in terms of the number of physician suicides, but “on a positive note, we are better with resources and acknowledgment that a problem exists.”
He noted that the AANS, which has published a physician burnout series on its Neurosurgery Blog, has shown great interest in this topic and is working to spread the word to help neurosurgeons. “My simple talk has led to me being approached by numerous people and healthcare organizations on how to further focus resources and prevention of this problem.”
Asked the one thing he would tell his friend, Michael Weinstein, a fellow surgeon, or trainee who’s struggling, Dr. Harrop said, “I am here for you, and we will get over these temporary problems, which are not significant in the big picture of what you mean to the world.”
Dr. Harrop reported serving as an adviser for Ethicon and Spiderwort.
A version of this article appeared on Medscape.com.
For those outside the medical profession, it took a global pandemic to finally understand how pervasive distress and suicide are among medical professionals, particularly surgeons.
For James Harrop, MD, it was made real years earlier by a colleague he’d trained alongside and worked with for decades — “one of the best surgeons I’ve ever seen” who, one day, just wasn’t there.
Lost in his own work, it wasn’t until Dr. Harrop, a professor of neurological and orthopedic surgery at Thomas Jefferson University, Philadelphia, read an article in The New England Journal of Medicine and realized his friend Michael Weinstein, MD, MPH, had been profoundly depressed for years and was hospitalized for his own safety.
Dr. Weinstein recovered and later gave grand rounds at Thomas Jefferson University, where he is an associate professor of surgery in the Acute Care Surgery Division. But the story stuck with Dr. Harrop.
“I said to Mike afterward, I’ve known you for 20 years and, retrospectively, going back, I never saw a single sign that you were depressed, sad, or had any issues, and he said to me ‘that’s because I did everything I could to make sure no one knew I had a problem,’ ” Dr. Harrop said during a talk on physician suicide on May 4 at the American Association of Neurological Surgeons (AANS) 2024 Annual Meeting.
“And that scared me because we need to help these people, we need to identify who they are.”
Surgeons at Greater Risk
Among 9175 physicians surveyed in the 2023 Medscape Physician Suicide Report, 9% had considered suicide, and 1% had attempted it. The average for US adults is 4.9% and 0.5%, respectively.
Surgeons are at particularly high risk. A 2011 survey of 7905 US surgeons found that 1 in 16 (6.3%) had considered suicide in the previous year. A post-pandemic survey of more than 600 surgeons and surgical trainees reported that one in seven had suicidal ideation.
It’s often estimated that between 300 and 400 physicians die by suicide each year in the United States, but exact numbers are not known. Recent updated estimates from the National Violent Death Reporting System put the number at 119 physician suicides annually.
Notably, that’s no better than data reported more than 50 years ago in the landmark policy paper The Sick Physician: Impairment by Psychiatric Disorders, Including Alcoholism and Drug Dependence. It sounded the alarm on poor mental health in physicians and reported that 100 doctors died by suicide annually — the equivalent of the average medical school graduating class at the time.
“If I take my med school class and double it, that’s how many physicians die each year,” Dr. Harrop said. “And here’s the bad news, it starts in medical school.”
Research shows higher rates of depression and suicidal ideation in medical students and residents than in other graduates, with rates varying by stage of training, he noted.
In a multischool study, 12% of medical students and residents had probable major depression, 9.2% mild/moderate depression, and suicidal ideation jumped from 6.6% in the first year of medical school to 9.4% in year 4.
A recent AANS survey of 346 neurosurgery residents revealed 67% had burnout, and 41% seriously considered quitting. Burnout rose to a high of 76% in the second year and decreased to 49% and 54% in years 3 and 4, respectively.
Inadequate operating room exposure, hostile faculty, and stressors outside work were tied to burnout, whereas mentorship was linked to a threefold lower likelihood of burnout.
Notably, a 2019 study conservatively estimated that the annual cost of burnout-related physician turnover and reduced clinical hours was $4.6 billion nationally and $7600 per employed physician for an organization.
“We need to be kinder to each other, to look out for each other, and to talk to each other,” Dr. Harrop told conference attendees.
‘Death by a 1000 Cuts’
A host of factors are associated with physician suicide including long work hours, delayed gratification, difficulty balancing work and home life, changing healthcare systems, lawsuits, and the unique ability to prescribe medications, said Dr. Harrop.
“In my life, I think of it as death by 1000 cuts. Every day I come in, you’ve got another person attacking you,” he said, referencing Death by 1000 Cuts: Medscape National Physician Burnout & Suicide Report 2021.
Dr. Harrop told this news organization that talking with numerous experts in this field has made him appreciate that anyone is at a risk for suicide.
“The problem is an overload of external resources crushing your existence to the point that you become paralyzed and make the irrational thought that the best solution is to end your life,” he said.
Ann Stroink, MD, immediate past president of the AANS, said in an interview that one potential trigger for burnout is the current shortage of neurosurgeons in the United States, which has led to increased workloads and potential sleep deprivation among existing neurosurgeons.
“To address this critical issue, we’ve been advocating through legislative channels for additional Medicare[-funded] slots” to train more neurosurgeons, she said. “It’s imperative that we take proactive steps to ensure that our healthcare system can sustainably meet the needs of patients, while also supporting the well-being of our neurosurgical professionals.”
The AANS is also advocating for decreased regulatory burdens associated with Medicare and insurance coverage, such as prior authorization, to help alleviate the administrative burdens that often contribute to burnout among its members, Dr. Stroink said.
A Model for Suicide Prevention
Dr. Harrop emphasized that suicide is preventable and that there is “some good news.” Turning to another high-risk profession, he noted that the US Air Force was able to reduce its suicide rate by 42.7% between 1994 and 1998 by doing three basic things.
The agency established a central surveillance database, restructured prevention services, and, more importantly, began conducting annual suicide prevention and awareness training, using gatekeepers to channel at-risk personnel to appropriate agencies and performing mental health questionnaires at enrollment and annually.
Similarly, education, screening, and access to mental health treatment are core recommendations for a national response to depression and suicide in physician trainees, said Dr. Harrop, who noted that his own hospital has started using the Patient Health Questionnaire 9-item for its staff.
Asked by this news organization how much progress has been made since The Sick Physician report, Dr. Harrop said, “we are probably doing worse” in terms of the number of physician suicides, but “on a positive note, we are better with resources and acknowledgment that a problem exists.”
He noted that the AANS, which has published a physician burnout series on its Neurosurgery Blog, has shown great interest in this topic and is working to spread the word to help neurosurgeons. “My simple talk has led to me being approached by numerous people and healthcare organizations on how to further focus resources and prevention of this problem.”
Asked the one thing he would tell his friend, Michael Weinstein, a fellow surgeon, or trainee who’s struggling, Dr. Harrop said, “I am here for you, and we will get over these temporary problems, which are not significant in the big picture of what you mean to the world.”
Dr. Harrop reported serving as an adviser for Ethicon and Spiderwort.
A version of this article appeared on Medscape.com.
For those outside the medical profession, it took a global pandemic to finally understand how pervasive distress and suicide are among medical professionals, particularly surgeons.
For James Harrop, MD, it was made real years earlier by a colleague he’d trained alongside and worked with for decades — “one of the best surgeons I’ve ever seen” who, one day, just wasn’t there.
Lost in his own work, it wasn’t until Dr. Harrop, a professor of neurological and orthopedic surgery at Thomas Jefferson University, Philadelphia, read an article in The New England Journal of Medicine and realized his friend Michael Weinstein, MD, MPH, had been profoundly depressed for years and was hospitalized for his own safety.
Dr. Weinstein recovered and later gave grand rounds at Thomas Jefferson University, where he is an associate professor of surgery in the Acute Care Surgery Division. But the story stuck with Dr. Harrop.
“I said to Mike afterward, I’ve known you for 20 years and, retrospectively, going back, I never saw a single sign that you were depressed, sad, or had any issues, and he said to me ‘that’s because I did everything I could to make sure no one knew I had a problem,’ ” Dr. Harrop said during a talk on physician suicide on May 4 at the American Association of Neurological Surgeons (AANS) 2024 Annual Meeting.
“And that scared me because we need to help these people, we need to identify who they are.”
Surgeons at Greater Risk
Among 9175 physicians surveyed in the 2023 Medscape Physician Suicide Report, 9% had considered suicide, and 1% had attempted it. The average for US adults is 4.9% and 0.5%, respectively.
Surgeons are at particularly high risk. A 2011 survey of 7905 US surgeons found that 1 in 16 (6.3%) had considered suicide in the previous year. A post-pandemic survey of more than 600 surgeons and surgical trainees reported that one in seven had suicidal ideation.
It’s often estimated that between 300 and 400 physicians die by suicide each year in the United States, but exact numbers are not known. Recent updated estimates from the National Violent Death Reporting System put the number at 119 physician suicides annually.
Notably, that’s no better than data reported more than 50 years ago in the landmark policy paper The Sick Physician: Impairment by Psychiatric Disorders, Including Alcoholism and Drug Dependence. It sounded the alarm on poor mental health in physicians and reported that 100 doctors died by suicide annually — the equivalent of the average medical school graduating class at the time.
“If I take my med school class and double it, that’s how many physicians die each year,” Dr. Harrop said. “And here’s the bad news, it starts in medical school.”
Research shows higher rates of depression and suicidal ideation in medical students and residents than in other graduates, with rates varying by stage of training, he noted.
In a multischool study, 12% of medical students and residents had probable major depression, 9.2% mild/moderate depression, and suicidal ideation jumped from 6.6% in the first year of medical school to 9.4% in year 4.
A recent AANS survey of 346 neurosurgery residents revealed 67% had burnout, and 41% seriously considered quitting. Burnout rose to a high of 76% in the second year and decreased to 49% and 54% in years 3 and 4, respectively.
Inadequate operating room exposure, hostile faculty, and stressors outside work were tied to burnout, whereas mentorship was linked to a threefold lower likelihood of burnout.
Notably, a 2019 study conservatively estimated that the annual cost of burnout-related physician turnover and reduced clinical hours was $4.6 billion nationally and $7600 per employed physician for an organization.
“We need to be kinder to each other, to look out for each other, and to talk to each other,” Dr. Harrop told conference attendees.
‘Death by a 1000 Cuts’
A host of factors are associated with physician suicide including long work hours, delayed gratification, difficulty balancing work and home life, changing healthcare systems, lawsuits, and the unique ability to prescribe medications, said Dr. Harrop.
“In my life, I think of it as death by 1000 cuts. Every day I come in, you’ve got another person attacking you,” he said, referencing Death by 1000 Cuts: Medscape National Physician Burnout & Suicide Report 2021.
Dr. Harrop told this news organization that talking with numerous experts in this field has made him appreciate that anyone is at a risk for suicide.
“The problem is an overload of external resources crushing your existence to the point that you become paralyzed and make the irrational thought that the best solution is to end your life,” he said.
Ann Stroink, MD, immediate past president of the AANS, said in an interview that one potential trigger for burnout is the current shortage of neurosurgeons in the United States, which has led to increased workloads and potential sleep deprivation among existing neurosurgeons.
“To address this critical issue, we’ve been advocating through legislative channels for additional Medicare[-funded] slots” to train more neurosurgeons, she said. “It’s imperative that we take proactive steps to ensure that our healthcare system can sustainably meet the needs of patients, while also supporting the well-being of our neurosurgical professionals.”
The AANS is also advocating for decreased regulatory burdens associated with Medicare and insurance coverage, such as prior authorization, to help alleviate the administrative burdens that often contribute to burnout among its members, Dr. Stroink said.
A Model for Suicide Prevention
Dr. Harrop emphasized that suicide is preventable and that there is “some good news.” Turning to another high-risk profession, he noted that the US Air Force was able to reduce its suicide rate by 42.7% between 1994 and 1998 by doing three basic things.
The agency established a central surveillance database, restructured prevention services, and, more importantly, began conducting annual suicide prevention and awareness training, using gatekeepers to channel at-risk personnel to appropriate agencies and performing mental health questionnaires at enrollment and annually.
Similarly, education, screening, and access to mental health treatment are core recommendations for a national response to depression and suicide in physician trainees, said Dr. Harrop, who noted that his own hospital has started using the Patient Health Questionnaire 9-item for its staff.
Asked by this news organization how much progress has been made since The Sick Physician report, Dr. Harrop said, “we are probably doing worse” in terms of the number of physician suicides, but “on a positive note, we are better with resources and acknowledgment that a problem exists.”
He noted that the AANS, which has published a physician burnout series on its Neurosurgery Blog, has shown great interest in this topic and is working to spread the word to help neurosurgeons. “My simple talk has led to me being approached by numerous people and healthcare organizations on how to further focus resources and prevention of this problem.”
Asked the one thing he would tell his friend, Michael Weinstein, a fellow surgeon, or trainee who’s struggling, Dr. Harrop said, “I am here for you, and we will get over these temporary problems, which are not significant in the big picture of what you mean to the world.”
Dr. Harrop reported serving as an adviser for Ethicon and Spiderwort.
A version of this article appeared on Medscape.com.
How Physician Mortgage Loans Work for Doctors With Debt
Tell someone you’re a doctor, and the reaction is often: “You must be rich.” But physicians who are just finishing medical school or are in their early careers might feel far from it. The average medical school debt is more than $200,000, with total debts including undergrad climbing well north of $250,000.
That leaves house-hunting physicians in a predicament. A key factor for lending institutions is the “debt to income” ratio, a calculation which indicates if you already have too much debt to pay your mortgage. That single equation could eliminate you from lenders’ mortgage requirements.
But young doctors are also in a unique situation. Yes, they carry above-average levels of debt, but they are on a path to substantial income in future years. That’s where the physician mortgage loan (PML) becomes a useful option.
What Is a Physician Mortgage Loan?
, according to Stephen Chang, MD, a radiologist, and a managing director at Acts Financial Advisors in McLean, Virginia.
The key features, according to James M. Dahle, MD, an emergency physician and founder of The White Coat Investor, include:
- No required down payment, which is typically 20% with a conventional loan.
- No private mortgage insurance (PMI). This is often a requirement of traditional loans, designed to protect the lender if the buyer misses payments. PMLs don’t involve PMI even if you don’t put down 20%.
- No pay stubs. With a conventional loan, pay stubs are often required to prove income level and reliability. PMLs will often allow an employment contract in place of those.
- Different consideration of the student loan burden.
Those are the upsides, of course, but there may be downsides. Dr. Dahle said a PML might involve slightly higher rates and fees than a conventional mortgage does but not always.
Who Is Best Suited for a Physician Mortgage Loan?
Financial advisers caution that everyone should first consider their full financial picture before applying for a mortgage, PML or otherwise. “If you don’t have the money saved for a down payment, one can ask if you are financially prepared to purchase a home,” says Cobin Soelberg, MD, an anesthesiologist and owner of Greeley Wealth Management, a financial planning firm serving physician families in Bend, Oregon.
If your savings are slim, you might need to build those accounts further before pursuing home ownership and the expenses that come along with it.
Your credit score can contribute to the equation. “With any loan product, we always recommend working to optimize your personal credit score as soon as possible before applying for a loan,” said Mark P. Eid, MD, a dermatologist and co–managing director (with Dr. Chang) at Act Financial Advisors. “Once you get into the high 700s, you’ve typically qualified for the best interest rates, so while that perfect 850 is nice to achieve, it’s by no means necessary.”
Also, assess your reasons for purchasing a home and whether it will fit your lifestyle in the coming years. “The main reason that [my wife and I] wanted to buy a home was for stability,” said Jordan Frey, MD, founder of The Prudent Plastic Surgeon. “After living in apartments for years, we wanted a place that was truly our own. We definitely felt disappointed and frustrated when worrying that our student debt may limit our ability to do this.”
Like many physicians, Dr. Frey had taken on a huge amount of debt, to the tune of half a million dollars in student loans and credit card debt when he finished training in 2020. The question Dr. Frey and his wife wrestled with was: “How much debt should we take on in addition to what we already have?”
What Are the Risks? What’s in the Fine Print?
The eased limitations of PMLs come with potential pitfalls, and physicians should not imagine that they have unlimited buying power.
“Many physicians buy more expensive or bigger houses than they need simply because banks are willing to lend physicians money,” Dr. Soelberg warns. “So, the doctor gets locked into a large mortgage and cannot build wealth, save for retirement, and repay their student loans.”
As you shop around, beware of omissions and scams. When meeting with lenders, Dr. Frey recalled that some didn’t even present PMLs as an option, and others presented them with unfavorable terms. He was careful to look for disadvantages hidden in the fine print, such as a potential “big hike in the rate a year later.”
But sometimes, a scam is not outright deception but is more like temptation. So it’s important to have your own best interests in mind without relying on lenders’ advice.
“When we were shopping around, some mortgage lenders would [offer] $1.5 million, and we thought ‘that makes no sense,’ ” said Dr. Frey. “[Physicians] have big future income, which makes us attractive to these lenders. No one in their right mind would give a mortgage like this to anyone else. They aren’t worried about whether it’s a smart decision for you or not.”
What Other Red Flags Should You Look Out for?
Dr. Frey recommends medical professionals beware of these red flags when shopping for PMLs:
- A request for any type of collateral, including your medical practice
- A rate that is much higher than others
- A lender is pushing you to borrow a higher amount than you’re comfortable with
- A lender attempts to influence your decision about the size of your down payment
Remember, if you are choosing an adjustable-rate mortgage (ARM), your rate will recalibrate on the basis of the market’s rates — for better or worse. This means that your payment might be higher or lower, taking current interest rates into account, based on the market.
Looking back, Dr. Frey said he might reconsider his decision to use a 10-year ARM. He and his wife chose it because the rate was low at the time, and they planned to pay off the mortgage quickly or move before it went up. But the uncertainty added an element of pressure.
How Can PMLs Contribute to Overall Financial Health?
Dr. Frey says his physician mortgage was “a huge advantage,” allowing him and his wife to put 0% down on their home without PMI. But most importantly, it fit within their overall financial plan, which included investing. “The money that we would have potentially used for a down payment, we used to buy a rental property, which then got us more income,” he says.
Of course, buying a rental property is not the only path to financial health and freedom. Many people approach a home as an investment that will eventually become fully their own. Others might put that down payment toward building a safety net of savings accounts.
Used strategically and intentionally, PMLs can put you on a more predictable financial path. And with less money stress, buying a home can be an exciting milestone as you plan your future and put down roots in a community.
A version of this article appeared on Medscape.com.
Tell someone you’re a doctor, and the reaction is often: “You must be rich.” But physicians who are just finishing medical school or are in their early careers might feel far from it. The average medical school debt is more than $200,000, with total debts including undergrad climbing well north of $250,000.
That leaves house-hunting physicians in a predicament. A key factor for lending institutions is the “debt to income” ratio, a calculation which indicates if you already have too much debt to pay your mortgage. That single equation could eliminate you from lenders’ mortgage requirements.
But young doctors are also in a unique situation. Yes, they carry above-average levels of debt, but they are on a path to substantial income in future years. That’s where the physician mortgage loan (PML) becomes a useful option.
What Is a Physician Mortgage Loan?
, according to Stephen Chang, MD, a radiologist, and a managing director at Acts Financial Advisors in McLean, Virginia.
The key features, according to James M. Dahle, MD, an emergency physician and founder of The White Coat Investor, include:
- No required down payment, which is typically 20% with a conventional loan.
- No private mortgage insurance (PMI). This is often a requirement of traditional loans, designed to protect the lender if the buyer misses payments. PMLs don’t involve PMI even if you don’t put down 20%.
- No pay stubs. With a conventional loan, pay stubs are often required to prove income level and reliability. PMLs will often allow an employment contract in place of those.
- Different consideration of the student loan burden.
Those are the upsides, of course, but there may be downsides. Dr. Dahle said a PML might involve slightly higher rates and fees than a conventional mortgage does but not always.
Who Is Best Suited for a Physician Mortgage Loan?
Financial advisers caution that everyone should first consider their full financial picture before applying for a mortgage, PML or otherwise. “If you don’t have the money saved for a down payment, one can ask if you are financially prepared to purchase a home,” says Cobin Soelberg, MD, an anesthesiologist and owner of Greeley Wealth Management, a financial planning firm serving physician families in Bend, Oregon.
If your savings are slim, you might need to build those accounts further before pursuing home ownership and the expenses that come along with it.
Your credit score can contribute to the equation. “With any loan product, we always recommend working to optimize your personal credit score as soon as possible before applying for a loan,” said Mark P. Eid, MD, a dermatologist and co–managing director (with Dr. Chang) at Act Financial Advisors. “Once you get into the high 700s, you’ve typically qualified for the best interest rates, so while that perfect 850 is nice to achieve, it’s by no means necessary.”
Also, assess your reasons for purchasing a home and whether it will fit your lifestyle in the coming years. “The main reason that [my wife and I] wanted to buy a home was for stability,” said Jordan Frey, MD, founder of The Prudent Plastic Surgeon. “After living in apartments for years, we wanted a place that was truly our own. We definitely felt disappointed and frustrated when worrying that our student debt may limit our ability to do this.”
Like many physicians, Dr. Frey had taken on a huge amount of debt, to the tune of half a million dollars in student loans and credit card debt when he finished training in 2020. The question Dr. Frey and his wife wrestled with was: “How much debt should we take on in addition to what we already have?”
What Are the Risks? What’s in the Fine Print?
The eased limitations of PMLs come with potential pitfalls, and physicians should not imagine that they have unlimited buying power.
“Many physicians buy more expensive or bigger houses than they need simply because banks are willing to lend physicians money,” Dr. Soelberg warns. “So, the doctor gets locked into a large mortgage and cannot build wealth, save for retirement, and repay their student loans.”
As you shop around, beware of omissions and scams. When meeting with lenders, Dr. Frey recalled that some didn’t even present PMLs as an option, and others presented them with unfavorable terms. He was careful to look for disadvantages hidden in the fine print, such as a potential “big hike in the rate a year later.”
But sometimes, a scam is not outright deception but is more like temptation. So it’s important to have your own best interests in mind without relying on lenders’ advice.
“When we were shopping around, some mortgage lenders would [offer] $1.5 million, and we thought ‘that makes no sense,’ ” said Dr. Frey. “[Physicians] have big future income, which makes us attractive to these lenders. No one in their right mind would give a mortgage like this to anyone else. They aren’t worried about whether it’s a smart decision for you or not.”
What Other Red Flags Should You Look Out for?
Dr. Frey recommends medical professionals beware of these red flags when shopping for PMLs:
- A request for any type of collateral, including your medical practice
- A rate that is much higher than others
- A lender is pushing you to borrow a higher amount than you’re comfortable with
- A lender attempts to influence your decision about the size of your down payment
Remember, if you are choosing an adjustable-rate mortgage (ARM), your rate will recalibrate on the basis of the market’s rates — for better or worse. This means that your payment might be higher or lower, taking current interest rates into account, based on the market.
Looking back, Dr. Frey said he might reconsider his decision to use a 10-year ARM. He and his wife chose it because the rate was low at the time, and they planned to pay off the mortgage quickly or move before it went up. But the uncertainty added an element of pressure.
How Can PMLs Contribute to Overall Financial Health?
Dr. Frey says his physician mortgage was “a huge advantage,” allowing him and his wife to put 0% down on their home without PMI. But most importantly, it fit within their overall financial plan, which included investing. “The money that we would have potentially used for a down payment, we used to buy a rental property, which then got us more income,” he says.
Of course, buying a rental property is not the only path to financial health and freedom. Many people approach a home as an investment that will eventually become fully their own. Others might put that down payment toward building a safety net of savings accounts.
Used strategically and intentionally, PMLs can put you on a more predictable financial path. And with less money stress, buying a home can be an exciting milestone as you plan your future and put down roots in a community.
A version of this article appeared on Medscape.com.
Tell someone you’re a doctor, and the reaction is often: “You must be rich.” But physicians who are just finishing medical school or are in their early careers might feel far from it. The average medical school debt is more than $200,000, with total debts including undergrad climbing well north of $250,000.
That leaves house-hunting physicians in a predicament. A key factor for lending institutions is the “debt to income” ratio, a calculation which indicates if you already have too much debt to pay your mortgage. That single equation could eliminate you from lenders’ mortgage requirements.
But young doctors are also in a unique situation. Yes, they carry above-average levels of debt, but they are on a path to substantial income in future years. That’s where the physician mortgage loan (PML) becomes a useful option.
What Is a Physician Mortgage Loan?
, according to Stephen Chang, MD, a radiologist, and a managing director at Acts Financial Advisors in McLean, Virginia.
The key features, according to James M. Dahle, MD, an emergency physician and founder of The White Coat Investor, include:
- No required down payment, which is typically 20% with a conventional loan.
- No private mortgage insurance (PMI). This is often a requirement of traditional loans, designed to protect the lender if the buyer misses payments. PMLs don’t involve PMI even if you don’t put down 20%.
- No pay stubs. With a conventional loan, pay stubs are often required to prove income level and reliability. PMLs will often allow an employment contract in place of those.
- Different consideration of the student loan burden.
Those are the upsides, of course, but there may be downsides. Dr. Dahle said a PML might involve slightly higher rates and fees than a conventional mortgage does but not always.
Who Is Best Suited for a Physician Mortgage Loan?
Financial advisers caution that everyone should first consider their full financial picture before applying for a mortgage, PML or otherwise. “If you don’t have the money saved for a down payment, one can ask if you are financially prepared to purchase a home,” says Cobin Soelberg, MD, an anesthesiologist and owner of Greeley Wealth Management, a financial planning firm serving physician families in Bend, Oregon.
If your savings are slim, you might need to build those accounts further before pursuing home ownership and the expenses that come along with it.
Your credit score can contribute to the equation. “With any loan product, we always recommend working to optimize your personal credit score as soon as possible before applying for a loan,” said Mark P. Eid, MD, a dermatologist and co–managing director (with Dr. Chang) at Act Financial Advisors. “Once you get into the high 700s, you’ve typically qualified for the best interest rates, so while that perfect 850 is nice to achieve, it’s by no means necessary.”
Also, assess your reasons for purchasing a home and whether it will fit your lifestyle in the coming years. “The main reason that [my wife and I] wanted to buy a home was for stability,” said Jordan Frey, MD, founder of The Prudent Plastic Surgeon. “After living in apartments for years, we wanted a place that was truly our own. We definitely felt disappointed and frustrated when worrying that our student debt may limit our ability to do this.”
Like many physicians, Dr. Frey had taken on a huge amount of debt, to the tune of half a million dollars in student loans and credit card debt when he finished training in 2020. The question Dr. Frey and his wife wrestled with was: “How much debt should we take on in addition to what we already have?”
What Are the Risks? What’s in the Fine Print?
The eased limitations of PMLs come with potential pitfalls, and physicians should not imagine that they have unlimited buying power.
“Many physicians buy more expensive or bigger houses than they need simply because banks are willing to lend physicians money,” Dr. Soelberg warns. “So, the doctor gets locked into a large mortgage and cannot build wealth, save for retirement, and repay their student loans.”
As you shop around, beware of omissions and scams. When meeting with lenders, Dr. Frey recalled that some didn’t even present PMLs as an option, and others presented them with unfavorable terms. He was careful to look for disadvantages hidden in the fine print, such as a potential “big hike in the rate a year later.”
But sometimes, a scam is not outright deception but is more like temptation. So it’s important to have your own best interests in mind without relying on lenders’ advice.
“When we were shopping around, some mortgage lenders would [offer] $1.5 million, and we thought ‘that makes no sense,’ ” said Dr. Frey. “[Physicians] have big future income, which makes us attractive to these lenders. No one in their right mind would give a mortgage like this to anyone else. They aren’t worried about whether it’s a smart decision for you or not.”
What Other Red Flags Should You Look Out for?
Dr. Frey recommends medical professionals beware of these red flags when shopping for PMLs:
- A request for any type of collateral, including your medical practice
- A rate that is much higher than others
- A lender is pushing you to borrow a higher amount than you’re comfortable with
- A lender attempts to influence your decision about the size of your down payment
Remember, if you are choosing an adjustable-rate mortgage (ARM), your rate will recalibrate on the basis of the market’s rates — for better or worse. This means that your payment might be higher or lower, taking current interest rates into account, based on the market.
Looking back, Dr. Frey said he might reconsider his decision to use a 10-year ARM. He and his wife chose it because the rate was low at the time, and they planned to pay off the mortgage quickly or move before it went up. But the uncertainty added an element of pressure.
How Can PMLs Contribute to Overall Financial Health?
Dr. Frey says his physician mortgage was “a huge advantage,” allowing him and his wife to put 0% down on their home without PMI. But most importantly, it fit within their overall financial plan, which included investing. “The money that we would have potentially used for a down payment, we used to buy a rental property, which then got us more income,” he says.
Of course, buying a rental property is not the only path to financial health and freedom. Many people approach a home as an investment that will eventually become fully their own. Others might put that down payment toward building a safety net of savings accounts.
Used strategically and intentionally, PMLs can put you on a more predictable financial path. And with less money stress, buying a home can be an exciting milestone as you plan your future and put down roots in a community.
A version of this article appeared on Medscape.com.
‘Big Breakthrough’: New Low-Field MRI Is Safer and Easier
For years, researchers and medical companies have explored low-field MRI systems (those with a magnetic field strength of less than 1 T) — searching for a feasible alternative to the loud, expensive machines requiring special rooms with shielding to block their powerful magnetic field.
Most low-field scanners in development are for brain scans only. In 2022, the US Food and Drug Administration (FDA) cleared the first portable MRI system — Hyperfine’s Swoop, designed for use at a patient’s bedside — for head and brain scans. But the technology has not been applied to whole-body MRI — until now.
In a new study published in Science, researchers from Hong Kong described a whole-body, ultra low–field MRI.
The device uses a 0.05 T magnet — one sixtieth the magnetic field strength of the standard 3 T MRI model common in hospitals today, said lead author Ed Wu, PhD, professor of biomedical engineering at The University of Hong Kong.
Because the field strength is so low, no protective shielding is needed. Patients and bystanders can safely use smart phones . And the scanner is safe for patients with implanted devices, like a cochlear implant or pacemaker, or any metal on their body or clothes. No hearing protection is required, either, because the machine is so quiet.
If all goes well, the technology could be commercially available in as little as a few years, Dr. Wu said.
But first, funding and FDA approval would be needed. “A company is going to have to come along and say, ‘This looks fantastic. We’re going to commercialize this, and we’re going to go through this certification process,’ ” said Andrew Webb, PhD, professor of radiology and the founding director of the C.J. Gorter MRI Center at the Leiden University Medical Center, Leiden, the Netherlands. (Dr. Webb was not involved in the study.)
Improving Access to MRI
One hope for this technology is to bring MRI to more people worldwide. Africa has less than one MRI scanner per million residents, whereas the United States has about 40.
While a new 3 T machine can cost about $1 million, the low-field version is much cheaper — only about $22,000 in materials cost per scanner, according to Dr. Wu.
A low magnetic field means less electricity, too — the machine can be plugged into a standard wall outlet. And because a fully shielded room isn’t needed, that could save another $100,000 in materials, Dr. Webb said.
Its ease of use could improve accessibility in countries with limited training, Dr. Webb pointed out.
“To be a technician is 2-3 years training for a regular MRI machine, a lot of it to do safety, a lot of it to do very subtle planning,” said Webb. “These [low-field] systems are much simpler.”
Challenges and the Future
The prototype weighs about 1.5 tons or 3000 lb. (A 3 T MRI can weigh between 6 and 13 tons or 12,000 and 26,000 lb.) That might sound like a lot, but it’s comparable to a mobile CT scanner, which is designed to be moved from room to room. Plus, “its weight can be substantially reduced if further optimized,” Dr. Wu said.
One challenge with low-field MRIs is image quality, which tends to be not as clear and detailed as those from high-power machines. To address this, the research team used deep learning (artificial intelligence) to enhance the image quality. “Computing power and large-scale data underpin our success, which tackles the physics and math problems that are traditionally considered intractable in existing MRI methodology,” Dr. Wu said.
Dr. Webb said he was impressed by the image quality shown in the study. They “look much higher quality than you would expect from such a low-field system,” he said. Still, only healthy volunteers were scanned. The true test will be using it to view subtle pathologies, Dr. Webb said.
That’s what Dr. Wu and his team are working on now — taking scans to diagnose various medical conditions. His group’s brain-only version of the low-field MRI has been used for diagnosis, he noted.
A version of this article appeared on Medscape.com.
For years, researchers and medical companies have explored low-field MRI systems (those with a magnetic field strength of less than 1 T) — searching for a feasible alternative to the loud, expensive machines requiring special rooms with shielding to block their powerful magnetic field.
Most low-field scanners in development are for brain scans only. In 2022, the US Food and Drug Administration (FDA) cleared the first portable MRI system — Hyperfine’s Swoop, designed for use at a patient’s bedside — for head and brain scans. But the technology has not been applied to whole-body MRI — until now.
In a new study published in Science, researchers from Hong Kong described a whole-body, ultra low–field MRI.
The device uses a 0.05 T magnet — one sixtieth the magnetic field strength of the standard 3 T MRI model common in hospitals today, said lead author Ed Wu, PhD, professor of biomedical engineering at The University of Hong Kong.
Because the field strength is so low, no protective shielding is needed. Patients and bystanders can safely use smart phones . And the scanner is safe for patients with implanted devices, like a cochlear implant or pacemaker, or any metal on their body or clothes. No hearing protection is required, either, because the machine is so quiet.
If all goes well, the technology could be commercially available in as little as a few years, Dr. Wu said.
But first, funding and FDA approval would be needed. “A company is going to have to come along and say, ‘This looks fantastic. We’re going to commercialize this, and we’re going to go through this certification process,’ ” said Andrew Webb, PhD, professor of radiology and the founding director of the C.J. Gorter MRI Center at the Leiden University Medical Center, Leiden, the Netherlands. (Dr. Webb was not involved in the study.)
Improving Access to MRI
One hope for this technology is to bring MRI to more people worldwide. Africa has less than one MRI scanner per million residents, whereas the United States has about 40.
While a new 3 T machine can cost about $1 million, the low-field version is much cheaper — only about $22,000 in materials cost per scanner, according to Dr. Wu.
A low magnetic field means less electricity, too — the machine can be plugged into a standard wall outlet. And because a fully shielded room isn’t needed, that could save another $100,000 in materials, Dr. Webb said.
Its ease of use could improve accessibility in countries with limited training, Dr. Webb pointed out.
“To be a technician is 2-3 years training for a regular MRI machine, a lot of it to do safety, a lot of it to do very subtle planning,” said Webb. “These [low-field] systems are much simpler.”
Challenges and the Future
The prototype weighs about 1.5 tons or 3000 lb. (A 3 T MRI can weigh between 6 and 13 tons or 12,000 and 26,000 lb.) That might sound like a lot, but it’s comparable to a mobile CT scanner, which is designed to be moved from room to room. Plus, “its weight can be substantially reduced if further optimized,” Dr. Wu said.
One challenge with low-field MRIs is image quality, which tends to be not as clear and detailed as those from high-power machines. To address this, the research team used deep learning (artificial intelligence) to enhance the image quality. “Computing power and large-scale data underpin our success, which tackles the physics and math problems that are traditionally considered intractable in existing MRI methodology,” Dr. Wu said.
Dr. Webb said he was impressed by the image quality shown in the study. They “look much higher quality than you would expect from such a low-field system,” he said. Still, only healthy volunteers were scanned. The true test will be using it to view subtle pathologies, Dr. Webb said.
That’s what Dr. Wu and his team are working on now — taking scans to diagnose various medical conditions. His group’s brain-only version of the low-field MRI has been used for diagnosis, he noted.
A version of this article appeared on Medscape.com.
For years, researchers and medical companies have explored low-field MRI systems (those with a magnetic field strength of less than 1 T) — searching for a feasible alternative to the loud, expensive machines requiring special rooms with shielding to block their powerful magnetic field.
Most low-field scanners in development are for brain scans only. In 2022, the US Food and Drug Administration (FDA) cleared the first portable MRI system — Hyperfine’s Swoop, designed for use at a patient’s bedside — for head and brain scans. But the technology has not been applied to whole-body MRI — until now.
In a new study published in Science, researchers from Hong Kong described a whole-body, ultra low–field MRI.
The device uses a 0.05 T magnet — one sixtieth the magnetic field strength of the standard 3 T MRI model common in hospitals today, said lead author Ed Wu, PhD, professor of biomedical engineering at The University of Hong Kong.
Because the field strength is so low, no protective shielding is needed. Patients and bystanders can safely use smart phones . And the scanner is safe for patients with implanted devices, like a cochlear implant or pacemaker, or any metal on their body or clothes. No hearing protection is required, either, because the machine is so quiet.
If all goes well, the technology could be commercially available in as little as a few years, Dr. Wu said.
But first, funding and FDA approval would be needed. “A company is going to have to come along and say, ‘This looks fantastic. We’re going to commercialize this, and we’re going to go through this certification process,’ ” said Andrew Webb, PhD, professor of radiology and the founding director of the C.J. Gorter MRI Center at the Leiden University Medical Center, Leiden, the Netherlands. (Dr. Webb was not involved in the study.)
Improving Access to MRI
One hope for this technology is to bring MRI to more people worldwide. Africa has less than one MRI scanner per million residents, whereas the United States has about 40.
While a new 3 T machine can cost about $1 million, the low-field version is much cheaper — only about $22,000 in materials cost per scanner, according to Dr. Wu.
A low magnetic field means less electricity, too — the machine can be plugged into a standard wall outlet. And because a fully shielded room isn’t needed, that could save another $100,000 in materials, Dr. Webb said.
Its ease of use could improve accessibility in countries with limited training, Dr. Webb pointed out.
“To be a technician is 2-3 years training for a regular MRI machine, a lot of it to do safety, a lot of it to do very subtle planning,” said Webb. “These [low-field] systems are much simpler.”
Challenges and the Future
The prototype weighs about 1.5 tons or 3000 lb. (A 3 T MRI can weigh between 6 and 13 tons or 12,000 and 26,000 lb.) That might sound like a lot, but it’s comparable to a mobile CT scanner, which is designed to be moved from room to room. Plus, “its weight can be substantially reduced if further optimized,” Dr. Wu said.
One challenge with low-field MRIs is image quality, which tends to be not as clear and detailed as those from high-power machines. To address this, the research team used deep learning (artificial intelligence) to enhance the image quality. “Computing power and large-scale data underpin our success, which tackles the physics and math problems that are traditionally considered intractable in existing MRI methodology,” Dr. Wu said.
Dr. Webb said he was impressed by the image quality shown in the study. They “look much higher quality than you would expect from such a low-field system,” he said. Still, only healthy volunteers were scanned. The true test will be using it to view subtle pathologies, Dr. Webb said.
That’s what Dr. Wu and his team are working on now — taking scans to diagnose various medical conditions. His group’s brain-only version of the low-field MRI has been used for diagnosis, he noted.
A version of this article appeared on Medscape.com.
Crossing State Lines: PA Licensure Compact Coming Soon
For decades, physicians and nurses who ventured across state lines to practice, particularly in locum tenens roles, have reaped the benefits of medical licensure compacts. Yet, the same courtesy has eluded physician assistants (PAs), until now.
In April, Virginia Governor Glenn Youngkin signed the bill enacting the PA Compact making Virginia the seventh state to join. The legislation opens a cross-state agreement with seven states and finally allows locum tenens PAs to practice across these state’s borders.
How the PA Compact Works
The interstate arrangement recognizes valid, unencumbered PA licenses issued by other states in the compact. PAs working within the seven states won’t need a separate license from any of those states to practice.
The states include Delaware, Nebraska, Utah, Washington, West Virginia, Wisconsin, and Virginia. While the compact has been approved, the American Academy of Physician Associates said it could take an additional 18-24 months for the states to execute it, giving PAs the access they need to work in the compact states.
How the PA Compact Helps
The PA Compact holds the promise of alleviating some of the travel barriers that PAs often encounter, especially when they work locum tenens or in telehealth and must traverse state lines to deliver essential healthcare. This agreement not only enhances healthcare access but also empowers facilities to recruit new PAs, thereby bridging gaps in their healthcare staffing and addressing public health emergencies more effectively.
PAs will also gain increased flexibility and additional opportunities to earn and benefit from the right to practice in more states without requiring a time-consuming and expensive licensure from each state.
One motivating factor behind developing an interstate compact for physician assistants is that the same types of compacts for physicians and nurses are highly successful. The Nurse Licensure Compact and the Interstate Medical Licensure Compact for physicians encompass 37 and 41 states, respectively. While the seven-state PA Compact is in its earliest stages, it will likely be equally beneficial for PAs.
A survey by Barton Associates found that 95% of PAs said they would be more likely to consider working in a different state if the PA Compact made it more accessible.
Other states have begun legislation to enact a PA Compact, including Colorado, New Hampshire, Maine, Michigan New York, Ohio, Oklahoma, Rhode Island, Tennessee, and Vermont.
If your state still needs to enact a compact or file for compact legislation, let your elected officials know that the PAs in your state want to join a compact.
A version of this article appeared on Medscape.com .
For decades, physicians and nurses who ventured across state lines to practice, particularly in locum tenens roles, have reaped the benefits of medical licensure compacts. Yet, the same courtesy has eluded physician assistants (PAs), until now.
In April, Virginia Governor Glenn Youngkin signed the bill enacting the PA Compact making Virginia the seventh state to join. The legislation opens a cross-state agreement with seven states and finally allows locum tenens PAs to practice across these state’s borders.
How the PA Compact Works
The interstate arrangement recognizes valid, unencumbered PA licenses issued by other states in the compact. PAs working within the seven states won’t need a separate license from any of those states to practice.
The states include Delaware, Nebraska, Utah, Washington, West Virginia, Wisconsin, and Virginia. While the compact has been approved, the American Academy of Physician Associates said it could take an additional 18-24 months for the states to execute it, giving PAs the access they need to work in the compact states.
How the PA Compact Helps
The PA Compact holds the promise of alleviating some of the travel barriers that PAs often encounter, especially when they work locum tenens or in telehealth and must traverse state lines to deliver essential healthcare. This agreement not only enhances healthcare access but also empowers facilities to recruit new PAs, thereby bridging gaps in their healthcare staffing and addressing public health emergencies more effectively.
PAs will also gain increased flexibility and additional opportunities to earn and benefit from the right to practice in more states without requiring a time-consuming and expensive licensure from each state.
One motivating factor behind developing an interstate compact for physician assistants is that the same types of compacts for physicians and nurses are highly successful. The Nurse Licensure Compact and the Interstate Medical Licensure Compact for physicians encompass 37 and 41 states, respectively. While the seven-state PA Compact is in its earliest stages, it will likely be equally beneficial for PAs.
A survey by Barton Associates found that 95% of PAs said they would be more likely to consider working in a different state if the PA Compact made it more accessible.
Other states have begun legislation to enact a PA Compact, including Colorado, New Hampshire, Maine, Michigan New York, Ohio, Oklahoma, Rhode Island, Tennessee, and Vermont.
If your state still needs to enact a compact or file for compact legislation, let your elected officials know that the PAs in your state want to join a compact.
A version of this article appeared on Medscape.com .
For decades, physicians and nurses who ventured across state lines to practice, particularly in locum tenens roles, have reaped the benefits of medical licensure compacts. Yet, the same courtesy has eluded physician assistants (PAs), until now.
In April, Virginia Governor Glenn Youngkin signed the bill enacting the PA Compact making Virginia the seventh state to join. The legislation opens a cross-state agreement with seven states and finally allows locum tenens PAs to practice across these state’s borders.
How the PA Compact Works
The interstate arrangement recognizes valid, unencumbered PA licenses issued by other states in the compact. PAs working within the seven states won’t need a separate license from any of those states to practice.
The states include Delaware, Nebraska, Utah, Washington, West Virginia, Wisconsin, and Virginia. While the compact has been approved, the American Academy of Physician Associates said it could take an additional 18-24 months for the states to execute it, giving PAs the access they need to work in the compact states.
How the PA Compact Helps
The PA Compact holds the promise of alleviating some of the travel barriers that PAs often encounter, especially when they work locum tenens or in telehealth and must traverse state lines to deliver essential healthcare. This agreement not only enhances healthcare access but also empowers facilities to recruit new PAs, thereby bridging gaps in their healthcare staffing and addressing public health emergencies more effectively.
PAs will also gain increased flexibility and additional opportunities to earn and benefit from the right to practice in more states without requiring a time-consuming and expensive licensure from each state.
One motivating factor behind developing an interstate compact for physician assistants is that the same types of compacts for physicians and nurses are highly successful. The Nurse Licensure Compact and the Interstate Medical Licensure Compact for physicians encompass 37 and 41 states, respectively. While the seven-state PA Compact is in its earliest stages, it will likely be equally beneficial for PAs.
A survey by Barton Associates found that 95% of PAs said they would be more likely to consider working in a different state if the PA Compact made it more accessible.
Other states have begun legislation to enact a PA Compact, including Colorado, New Hampshire, Maine, Michigan New York, Ohio, Oklahoma, Rhode Island, Tennessee, and Vermont.
If your state still needs to enact a compact or file for compact legislation, let your elected officials know that the PAs in your state want to join a compact.
A version of this article appeared on Medscape.com .
Follow-Up Outcomes Data Often Missing for FDA Drug Approvals Based on Surrogate Markers
Over the past few decades, the US Food and Drug Administration (FDA) has increasingly relied on surrogate measures such as blood tests instead of clinical outcomes for medication approvals. But critics say the agency lacks consistent standards to ensure the surrogate aligns with clinical outcomes that matter to patients — things like improvements in symptoms and gains in function.
Sometimes those decisions backfire. Consider: In July 2021, the FDA approved aducanumab for the treatment of Alzheimer’s disease, bucking the advice of an advisory panel for the agency that questioned the effectiveness of the medication. Regulators relied on data from the drugmaker, Biogen, showing the monoclonal antibody could reduce levels of amyloid beta plaques in blood — a surrogate marker officials hoped would translate to clinical benefit.
The FDA’s decision triggered significant controversy, and Biogen in January announced it is pulling it from the market this year, citing disappointing sales.
Although the case of aducanumab might seem extreme, given the stakes — Alzheimer’s remains a disease without an effective treatment — it’s far from unusual.
“When we prescribe a drug, there is an underlying assumption that the FDA has done its due diligence to confirm the drug is safe and of benefit,” said Reshma Ramachandran, MD, MPP, MHS, a researcher at Yale School of Medicine, New Haven, Connecticut, and a coauthor of a recent review of surrogate outcomes. “In fact, we found either no evidence or low-quality evidence.” Such markers are associated with clinical outcomes. “We just don’t know if they work meaningfully to treat the patient’s condition. The results were pretty shocking for us,” she said.
The FDA in 2018 released an Adult Surrogate Endpoint Table listing markers that can be used as substitutes for clinical outcomes to more quickly test, review, and approve new therapies. The analysis found the majority of these endpoints lacked subsequent confirmations, defined as published meta-analyses of clinical studies to validate the association between the marker and a clinical outcome important to patients.
In a paper published in JAMA, Dr. Ramachandran and her colleagues looked at 37 surrogate endpoints for nearly 3 dozen nononcologic diseases in the table.
Approval with surrogate markers implies responsibility for postapproval or validation studies — not just lab measures or imaging findings but mortality, morbidity, or improved quality of life, said Joshua D. Wallach, PhD, MS, assistant professor in the department of epidemiology at the Emory Rollins School of Public Health in Atlanta and lead author of the JAMA review.
Dr. Wallach said surrogate markers are easier to measure and do not require large and long trials. But the FDA has not provided clear rules for what makes a surrogate marker valid in clinical trials.
“They’ve said that at a minimum, it requires meta-analytical evidence from studies that have looked at the correlation or the association between the surrogate and the clinical outcome,” Dr. Wallach said. “Our understanding was that if that’s a minimum expectation, we should be able to find those studies in the literature. And the reality is that we were unable to find evidence from those types of studies supporting the association between the surrogate and the clinical outcome.”
Physicians generally do not receive training about the FDA approval process and the difference between biomarkers, surrogate markers, and clinical endpoints, Dr. Ramachandran said. “Our study shows that things are much more uncertain than we thought when it comes to the prescribing of new drugs,” she said.
Surrogate Markers on the Rise
Dr. Wallach’s group looked for published meta-analyses compiling randomized controlled trials reporting surrogate endpoints for more than 3 dozen chronic nononcologic conditions, including type 2 diabetes, Alzheimer’s, kidney disease, HIV, gout, and lupus. They found no meta-analyses at all for 59% of the surrogate markers, while for those that were studied, few reported high-strength evidence of an association with clinical outcomes.
The findings echo previous research. In a 2020 study in JAMA Network Open, researchers tallied primary endpoints for all FDA approvals of new drugs and therapies during three 3-year periods: 1995-1997, 2005-2007, and 2015-2017. The proportion of products whose approvals were based on the use of clinical endpoints decreased from 43.8% in 1995-1997 to 28.4% in 2005-2007 to 23.3% in 2015-2017. The share based on surrogate endpoints rose from 43.3% to roughly 60% over the same interval.
A 2017 study in the Journal of Health Economics found the use of “imperfect” surrogate endpoints helped support the approval of an average of 16 new drugs per year between 2010 and 2014 compared with six per year from 1998 to 2008.
Similar concerns about weak associations between surrogate markers and drugs used to treat cancer have been documented before, including in a 2020 study published in eClinicalMedicine. The researchers found the surrogate endpoints in the FDA table either were not tested or were tested but proven to be weak surrogates.
“And yet the FDA considered these as good enough not only for accelerated approval but also for regular approval,” said Bishal Gyawali, MD, PhD, associate professor in the department of oncology at Queen’s University, Kingston, Ontario, Canada, who led the group.
The use of surrogate endpoints is also increasing in Europe, said Huseyin Naci, MHS, PhD, associate professor of health policy at the London School of Economics and Political Science in England. He cited a cohort study of 298 randomized clinical trials (RCTs) in JAMA Oncology suggesting “contemporary oncology RCTs now largely measure putative surrogate endpoints.” Dr. Wallach called the FDA’s surrogate table “a great first step toward transparency. But a key column is missing from that table, telling us what is the basis for which the FDA allows drug companies to use the recognized surrogate markers. What is the evidence they are considering?”
If the agency allows companies the flexibility to validate surrogate endpoints, postmarketing studies designed to confirm the clinical utility of those endpoints should follow.
“We obviously want physicians to be guided by evidence when they’re selecting treatments, and they need to be able to interpret the clinical benefits of the drug that they’re prescribing,” he said. “This is really about having the research consumer, patients, and physicians, as well as industry, understand why certain markers are considered and not considered.”
Dr. Wallach reported receiving grants from the FDA (through the Yale University — Mayo Clinic Center of Excellence in Regulatory Science and Innovation), National Institute on Alcohol Abuse and Alcoholism (1K01AA028258), and Johnson & Johnson (through the Yale University Open Data Access Project); and consulting fees from Hagens Berman Sobol Shapiro LLP and Dugan Law Firm APLC outside the submitted work. Dr. Ramachandran reported receiving grants from the Stavros Niarchos Foundation and FDA; receiving consulting fees from ReAct Action on Antibiotic Resistance strategy policy program outside the submitted work; and serving in an unpaid capacity as chair of the FDA task force for the nonprofit organization Doctors for America and in an unpaid capacity as board president for Universities Allied for Essential Medicines North America.
A version of this article appeared on Medscape.com.
Over the past few decades, the US Food and Drug Administration (FDA) has increasingly relied on surrogate measures such as blood tests instead of clinical outcomes for medication approvals. But critics say the agency lacks consistent standards to ensure the surrogate aligns with clinical outcomes that matter to patients — things like improvements in symptoms and gains in function.
Sometimes those decisions backfire. Consider: In July 2021, the FDA approved aducanumab for the treatment of Alzheimer’s disease, bucking the advice of an advisory panel for the agency that questioned the effectiveness of the medication. Regulators relied on data from the drugmaker, Biogen, showing the monoclonal antibody could reduce levels of amyloid beta plaques in blood — a surrogate marker officials hoped would translate to clinical benefit.
The FDA’s decision triggered significant controversy, and Biogen in January announced it is pulling it from the market this year, citing disappointing sales.
Although the case of aducanumab might seem extreme, given the stakes — Alzheimer’s remains a disease without an effective treatment — it’s far from unusual.
“When we prescribe a drug, there is an underlying assumption that the FDA has done its due diligence to confirm the drug is safe and of benefit,” said Reshma Ramachandran, MD, MPP, MHS, a researcher at Yale School of Medicine, New Haven, Connecticut, and a coauthor of a recent review of surrogate outcomes. “In fact, we found either no evidence or low-quality evidence.” Such markers are associated with clinical outcomes. “We just don’t know if they work meaningfully to treat the patient’s condition. The results were pretty shocking for us,” she said.
The FDA in 2018 released an Adult Surrogate Endpoint Table listing markers that can be used as substitutes for clinical outcomes to more quickly test, review, and approve new therapies. The analysis found the majority of these endpoints lacked subsequent confirmations, defined as published meta-analyses of clinical studies to validate the association between the marker and a clinical outcome important to patients.
In a paper published in JAMA, Dr. Ramachandran and her colleagues looked at 37 surrogate endpoints for nearly 3 dozen nononcologic diseases in the table.
Approval with surrogate markers implies responsibility for postapproval or validation studies — not just lab measures or imaging findings but mortality, morbidity, or improved quality of life, said Joshua D. Wallach, PhD, MS, assistant professor in the department of epidemiology at the Emory Rollins School of Public Health in Atlanta and lead author of the JAMA review.
Dr. Wallach said surrogate markers are easier to measure and do not require large and long trials. But the FDA has not provided clear rules for what makes a surrogate marker valid in clinical trials.
“They’ve said that at a minimum, it requires meta-analytical evidence from studies that have looked at the correlation or the association between the surrogate and the clinical outcome,” Dr. Wallach said. “Our understanding was that if that’s a minimum expectation, we should be able to find those studies in the literature. And the reality is that we were unable to find evidence from those types of studies supporting the association between the surrogate and the clinical outcome.”
Physicians generally do not receive training about the FDA approval process and the difference between biomarkers, surrogate markers, and clinical endpoints, Dr. Ramachandran said. “Our study shows that things are much more uncertain than we thought when it comes to the prescribing of new drugs,” she said.
Surrogate Markers on the Rise
Dr. Wallach’s group looked for published meta-analyses compiling randomized controlled trials reporting surrogate endpoints for more than 3 dozen chronic nononcologic conditions, including type 2 diabetes, Alzheimer’s, kidney disease, HIV, gout, and lupus. They found no meta-analyses at all for 59% of the surrogate markers, while for those that were studied, few reported high-strength evidence of an association with clinical outcomes.
The findings echo previous research. In a 2020 study in JAMA Network Open, researchers tallied primary endpoints for all FDA approvals of new drugs and therapies during three 3-year periods: 1995-1997, 2005-2007, and 2015-2017. The proportion of products whose approvals were based on the use of clinical endpoints decreased from 43.8% in 1995-1997 to 28.4% in 2005-2007 to 23.3% in 2015-2017. The share based on surrogate endpoints rose from 43.3% to roughly 60% over the same interval.
A 2017 study in the Journal of Health Economics found the use of “imperfect” surrogate endpoints helped support the approval of an average of 16 new drugs per year between 2010 and 2014 compared with six per year from 1998 to 2008.
Similar concerns about weak associations between surrogate markers and drugs used to treat cancer have been documented before, including in a 2020 study published in eClinicalMedicine. The researchers found the surrogate endpoints in the FDA table either were not tested or were tested but proven to be weak surrogates.
“And yet the FDA considered these as good enough not only for accelerated approval but also for regular approval,” said Bishal Gyawali, MD, PhD, associate professor in the department of oncology at Queen’s University, Kingston, Ontario, Canada, who led the group.
The use of surrogate endpoints is also increasing in Europe, said Huseyin Naci, MHS, PhD, associate professor of health policy at the London School of Economics and Political Science in England. He cited a cohort study of 298 randomized clinical trials (RCTs) in JAMA Oncology suggesting “contemporary oncology RCTs now largely measure putative surrogate endpoints.” Dr. Wallach called the FDA’s surrogate table “a great first step toward transparency. But a key column is missing from that table, telling us what is the basis for which the FDA allows drug companies to use the recognized surrogate markers. What is the evidence they are considering?”
If the agency allows companies the flexibility to validate surrogate endpoints, postmarketing studies designed to confirm the clinical utility of those endpoints should follow.
“We obviously want physicians to be guided by evidence when they’re selecting treatments, and they need to be able to interpret the clinical benefits of the drug that they’re prescribing,” he said. “This is really about having the research consumer, patients, and physicians, as well as industry, understand why certain markers are considered and not considered.”
Dr. Wallach reported receiving grants from the FDA (through the Yale University — Mayo Clinic Center of Excellence in Regulatory Science and Innovation), National Institute on Alcohol Abuse and Alcoholism (1K01AA028258), and Johnson & Johnson (through the Yale University Open Data Access Project); and consulting fees from Hagens Berman Sobol Shapiro LLP and Dugan Law Firm APLC outside the submitted work. Dr. Ramachandran reported receiving grants from the Stavros Niarchos Foundation and FDA; receiving consulting fees from ReAct Action on Antibiotic Resistance strategy policy program outside the submitted work; and serving in an unpaid capacity as chair of the FDA task force for the nonprofit organization Doctors for America and in an unpaid capacity as board president for Universities Allied for Essential Medicines North America.
A version of this article appeared on Medscape.com.
Over the past few decades, the US Food and Drug Administration (FDA) has increasingly relied on surrogate measures such as blood tests instead of clinical outcomes for medication approvals. But critics say the agency lacks consistent standards to ensure the surrogate aligns with clinical outcomes that matter to patients — things like improvements in symptoms and gains in function.
Sometimes those decisions backfire. Consider: In July 2021, the FDA approved aducanumab for the treatment of Alzheimer’s disease, bucking the advice of an advisory panel for the agency that questioned the effectiveness of the medication. Regulators relied on data from the drugmaker, Biogen, showing the monoclonal antibody could reduce levels of amyloid beta plaques in blood — a surrogate marker officials hoped would translate to clinical benefit.
The FDA’s decision triggered significant controversy, and Biogen in January announced it is pulling it from the market this year, citing disappointing sales.
Although the case of aducanumab might seem extreme, given the stakes — Alzheimer’s remains a disease without an effective treatment — it’s far from unusual.
“When we prescribe a drug, there is an underlying assumption that the FDA has done its due diligence to confirm the drug is safe and of benefit,” said Reshma Ramachandran, MD, MPP, MHS, a researcher at Yale School of Medicine, New Haven, Connecticut, and a coauthor of a recent review of surrogate outcomes. “In fact, we found either no evidence or low-quality evidence.” Such markers are associated with clinical outcomes. “We just don’t know if they work meaningfully to treat the patient’s condition. The results were pretty shocking for us,” she said.
The FDA in 2018 released an Adult Surrogate Endpoint Table listing markers that can be used as substitutes for clinical outcomes to more quickly test, review, and approve new therapies. The analysis found the majority of these endpoints lacked subsequent confirmations, defined as published meta-analyses of clinical studies to validate the association between the marker and a clinical outcome important to patients.
In a paper published in JAMA, Dr. Ramachandran and her colleagues looked at 37 surrogate endpoints for nearly 3 dozen nononcologic diseases in the table.
Approval with surrogate markers implies responsibility for postapproval or validation studies — not just lab measures or imaging findings but mortality, morbidity, or improved quality of life, said Joshua D. Wallach, PhD, MS, assistant professor in the department of epidemiology at the Emory Rollins School of Public Health in Atlanta and lead author of the JAMA review.
Dr. Wallach said surrogate markers are easier to measure and do not require large and long trials. But the FDA has not provided clear rules for what makes a surrogate marker valid in clinical trials.
“They’ve said that at a minimum, it requires meta-analytical evidence from studies that have looked at the correlation or the association between the surrogate and the clinical outcome,” Dr. Wallach said. “Our understanding was that if that’s a minimum expectation, we should be able to find those studies in the literature. And the reality is that we were unable to find evidence from those types of studies supporting the association between the surrogate and the clinical outcome.”
Physicians generally do not receive training about the FDA approval process and the difference between biomarkers, surrogate markers, and clinical endpoints, Dr. Ramachandran said. “Our study shows that things are much more uncertain than we thought when it comes to the prescribing of new drugs,” she said.
Surrogate Markers on the Rise
Dr. Wallach’s group looked for published meta-analyses compiling randomized controlled trials reporting surrogate endpoints for more than 3 dozen chronic nononcologic conditions, including type 2 diabetes, Alzheimer’s, kidney disease, HIV, gout, and lupus. They found no meta-analyses at all for 59% of the surrogate markers, while for those that were studied, few reported high-strength evidence of an association with clinical outcomes.
The findings echo previous research. In a 2020 study in JAMA Network Open, researchers tallied primary endpoints for all FDA approvals of new drugs and therapies during three 3-year periods: 1995-1997, 2005-2007, and 2015-2017. The proportion of products whose approvals were based on the use of clinical endpoints decreased from 43.8% in 1995-1997 to 28.4% in 2005-2007 to 23.3% in 2015-2017. The share based on surrogate endpoints rose from 43.3% to roughly 60% over the same interval.
A 2017 study in the Journal of Health Economics found the use of “imperfect” surrogate endpoints helped support the approval of an average of 16 new drugs per year between 2010 and 2014 compared with six per year from 1998 to 2008.
Similar concerns about weak associations between surrogate markers and drugs used to treat cancer have been documented before, including in a 2020 study published in eClinicalMedicine. The researchers found the surrogate endpoints in the FDA table either were not tested or were tested but proven to be weak surrogates.
“And yet the FDA considered these as good enough not only for accelerated approval but also for regular approval,” said Bishal Gyawali, MD, PhD, associate professor in the department of oncology at Queen’s University, Kingston, Ontario, Canada, who led the group.
The use of surrogate endpoints is also increasing in Europe, said Huseyin Naci, MHS, PhD, associate professor of health policy at the London School of Economics and Political Science in England. He cited a cohort study of 298 randomized clinical trials (RCTs) in JAMA Oncology suggesting “contemporary oncology RCTs now largely measure putative surrogate endpoints.” Dr. Wallach called the FDA’s surrogate table “a great first step toward transparency. But a key column is missing from that table, telling us what is the basis for which the FDA allows drug companies to use the recognized surrogate markers. What is the evidence they are considering?”
If the agency allows companies the flexibility to validate surrogate endpoints, postmarketing studies designed to confirm the clinical utility of those endpoints should follow.
“We obviously want physicians to be guided by evidence when they’re selecting treatments, and they need to be able to interpret the clinical benefits of the drug that they’re prescribing,” he said. “This is really about having the research consumer, patients, and physicians, as well as industry, understand why certain markers are considered and not considered.”
Dr. Wallach reported receiving grants from the FDA (through the Yale University — Mayo Clinic Center of Excellence in Regulatory Science and Innovation), National Institute on Alcohol Abuse and Alcoholism (1K01AA028258), and Johnson & Johnson (through the Yale University Open Data Access Project); and consulting fees from Hagens Berman Sobol Shapiro LLP and Dugan Law Firm APLC outside the submitted work. Dr. Ramachandran reported receiving grants from the Stavros Niarchos Foundation and FDA; receiving consulting fees from ReAct Action on Antibiotic Resistance strategy policy program outside the submitted work; and serving in an unpaid capacity as chair of the FDA task force for the nonprofit organization Doctors for America and in an unpaid capacity as board president for Universities Allied for Essential Medicines North America.
A version of this article appeared on Medscape.com.
FROM JAMA
Arthroscopy Doesn’t Delay Total Knee Replacement in Knee Osteoarthritis
TOPLINE:
Adding arthroscopic surgery to nonoperative management neither delays nor accelerates the timing of total knee arthroplasty (TKA) in patients with knee osteoarthritis (OA).
METHODOLOGY:
- Some case series show that arthroscopic surgery for knee OA may delay more invasive procedures, such as TKA or osteotomy, while longitudinal cohort studies often contradict this. Current OA guidelines are yet to address this issue.
- This secondary analysis of a randomized trial compared the long-term incidence of TKA in 178 patients (mean age, 59 years; 64.3% women) with knee OA who were referred for potential arthroscopic surgery at a tertiary care center in Canada.
- The patients received nonoperative care with or without additional arthroscopic surgery.
- Patients in the arthroscopic surgery group had specific knee procedures (resection of degenerative knee tissues) along with nonoperative management (physical therapy plus medications as required), while the control group received nonoperative management alone.
- The primary outcome was TKA on the knee being studied, and the secondary outcome was TKA or osteotomy on either knee.
TAKEAWAY:
- During a median follow-up of 13.8 years, 37.6% of patients underwent TKA, with comparable proportions of patients in the arthroscopic surgery and control groups undergoing TKA (adjusted hazard ratio [aHR], 0.85; 95% CI, 0.52-1.40).
- The rates of TKA or osteotomy on either knee were similar in both groups (aHR, 0.91; 95% CI, 0.59-1.41).
- A time-stratified analysis done for 0-5 years, 5-10 years, and beyond 10 years of follow-up also showed a consistent interpretation.
- When patients with crossover to arthroscopic surgery during the follow-up were included, the results remained similar for both the primary (HR, 0.88; 95% CI, 0.53-1.44) and secondary (HR, 1.08; 95% CI, 0.69-1.68) outcomes.
IN PRACTICE:
“Our study findings do not support the use of arthroscopic surgery for OA of the knee.” “Arthroscopic surgery does not provide additional benefit to nonoperative management for improving pain, stiffness, and function and is likely not cost-effective at 2 years of follow-up,” the authors wrote.
SOURCE:
This study was led by Trevor B. Birmingham, PhD, Fowler Kennedy Sport Medicine Clinic, University of Western Ontario, London, Ontario, Canada. It was published online in JAMA Network Open
LIMITATIONS:
The study was designed to assess differences in 2-year patient-reported outcomes rather than long-term TKA incidence. Factors influencing decisions to undergo TKA or osteotomy were not considered. Moreover, the effects observed in this study should be evaluated considering the estimated confidence intervals.
DISCLOSURES:
This study was supported by the ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. Some authors declared consulting, performing contracted services, or receiving grant funding, royalties, and nonfinancial support from various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
Adding arthroscopic surgery to nonoperative management neither delays nor accelerates the timing of total knee arthroplasty (TKA) in patients with knee osteoarthritis (OA).
METHODOLOGY:
- Some case series show that arthroscopic surgery for knee OA may delay more invasive procedures, such as TKA or osteotomy, while longitudinal cohort studies often contradict this. Current OA guidelines are yet to address this issue.
- This secondary analysis of a randomized trial compared the long-term incidence of TKA in 178 patients (mean age, 59 years; 64.3% women) with knee OA who were referred for potential arthroscopic surgery at a tertiary care center in Canada.
- The patients received nonoperative care with or without additional arthroscopic surgery.
- Patients in the arthroscopic surgery group had specific knee procedures (resection of degenerative knee tissues) along with nonoperative management (physical therapy plus medications as required), while the control group received nonoperative management alone.
- The primary outcome was TKA on the knee being studied, and the secondary outcome was TKA or osteotomy on either knee.
TAKEAWAY:
- During a median follow-up of 13.8 years, 37.6% of patients underwent TKA, with comparable proportions of patients in the arthroscopic surgery and control groups undergoing TKA (adjusted hazard ratio [aHR], 0.85; 95% CI, 0.52-1.40).
- The rates of TKA or osteotomy on either knee were similar in both groups (aHR, 0.91; 95% CI, 0.59-1.41).
- A time-stratified analysis done for 0-5 years, 5-10 years, and beyond 10 years of follow-up also showed a consistent interpretation.
- When patients with crossover to arthroscopic surgery during the follow-up were included, the results remained similar for both the primary (HR, 0.88; 95% CI, 0.53-1.44) and secondary (HR, 1.08; 95% CI, 0.69-1.68) outcomes.
IN PRACTICE:
“Our study findings do not support the use of arthroscopic surgery for OA of the knee.” “Arthroscopic surgery does not provide additional benefit to nonoperative management for improving pain, stiffness, and function and is likely not cost-effective at 2 years of follow-up,” the authors wrote.
SOURCE:
This study was led by Trevor B. Birmingham, PhD, Fowler Kennedy Sport Medicine Clinic, University of Western Ontario, London, Ontario, Canada. It was published online in JAMA Network Open
LIMITATIONS:
The study was designed to assess differences in 2-year patient-reported outcomes rather than long-term TKA incidence. Factors influencing decisions to undergo TKA or osteotomy were not considered. Moreover, the effects observed in this study should be evaluated considering the estimated confidence intervals.
DISCLOSURES:
This study was supported by the ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. Some authors declared consulting, performing contracted services, or receiving grant funding, royalties, and nonfinancial support from various sources.
A version of this article appeared on Medscape.com.
TOPLINE:
Adding arthroscopic surgery to nonoperative management neither delays nor accelerates the timing of total knee arthroplasty (TKA) in patients with knee osteoarthritis (OA).
METHODOLOGY:
- Some case series show that arthroscopic surgery for knee OA may delay more invasive procedures, such as TKA or osteotomy, while longitudinal cohort studies often contradict this. Current OA guidelines are yet to address this issue.
- This secondary analysis of a randomized trial compared the long-term incidence of TKA in 178 patients (mean age, 59 years; 64.3% women) with knee OA who were referred for potential arthroscopic surgery at a tertiary care center in Canada.
- The patients received nonoperative care with or without additional arthroscopic surgery.
- Patients in the arthroscopic surgery group had specific knee procedures (resection of degenerative knee tissues) along with nonoperative management (physical therapy plus medications as required), while the control group received nonoperative management alone.
- The primary outcome was TKA on the knee being studied, and the secondary outcome was TKA or osteotomy on either knee.
TAKEAWAY:
- During a median follow-up of 13.8 years, 37.6% of patients underwent TKA, with comparable proportions of patients in the arthroscopic surgery and control groups undergoing TKA (adjusted hazard ratio [aHR], 0.85; 95% CI, 0.52-1.40).
- The rates of TKA or osteotomy on either knee were similar in both groups (aHR, 0.91; 95% CI, 0.59-1.41).
- A time-stratified analysis done for 0-5 years, 5-10 years, and beyond 10 years of follow-up also showed a consistent interpretation.
- When patients with crossover to arthroscopic surgery during the follow-up were included, the results remained similar for both the primary (HR, 0.88; 95% CI, 0.53-1.44) and secondary (HR, 1.08; 95% CI, 0.69-1.68) outcomes.
IN PRACTICE:
“Our study findings do not support the use of arthroscopic surgery for OA of the knee.” “Arthroscopic surgery does not provide additional benefit to nonoperative management for improving pain, stiffness, and function and is likely not cost-effective at 2 years of follow-up,” the authors wrote.
SOURCE:
This study was led by Trevor B. Birmingham, PhD, Fowler Kennedy Sport Medicine Clinic, University of Western Ontario, London, Ontario, Canada. It was published online in JAMA Network Open
LIMITATIONS:
The study was designed to assess differences in 2-year patient-reported outcomes rather than long-term TKA incidence. Factors influencing decisions to undergo TKA or osteotomy were not considered. Moreover, the effects observed in this study should be evaluated considering the estimated confidence intervals.
DISCLOSURES:
This study was supported by the ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. Some authors declared consulting, performing contracted services, or receiving grant funding, royalties, and nonfinancial support from various sources.
A version of this article appeared on Medscape.com.