User login
Neurology Reviews covers innovative and emerging news in neurology and neuroscience every month, with a focus on practical approaches to treating Parkinson's disease, epilepsy, headache, stroke, multiple sclerosis, Alzheimer's disease, and other neurologic disorders.
PML
Progressive multifocal leukoencephalopathy
Rituxan
The leading independent newspaper covering neurology news and commentary.
Sedentary lifestyle tied to increased dementia risk
The study of nearly 50,000 adults in the UK Biobank shows that dementia risk increased 8% with 10 hours of sedentary time and 63% with 12 hours. That’s particularly concerning because Americans spend an average of 9.5 hours a day sitting.
Sleep wasn’t factored into the sedentary time and how someone accumulated the 10 hours – either in one continuous block or broken up throughout the day – was irrelevant.
“Our analysis cannot determine whether there is a causal link, so prescriptive conclusions are not really possible; however. I think it is very reasonable to conclude that sitting less and moving more may help reduce risk of dementia,” lead investigator David Raichlen, PhD, professor of biological sciences and anthropology, University of Southern California, Los Angeles, said in an interview.
The findings were published online in JAMA.
A surprising find?
The study is a retrospective analysis of prospectively collected data from the UK Biobank of 49,841 adults aged 60 years or older who wore an accelerometer on their wrists 24 hours a day for a week. Participants had no history of dementia when they wore the movement monitoring device.
Investigators used machine-based learning to determine sedentary time based on readings from the accelerometers. Sleep was not included as sedentary behavior.
Over a mean follow-up of 6.72 years, 414 participants were diagnosed with dementia.
Investigators found that dementia risk rises by 8% at 10 hours a day (adjusted hazard ratio, 1.08; P < .001) and 63% at 12 hours a day (aHR, 1.63; P < .001), compared with 9.27 hours a day. Those who logged 15 hours of sedentary behavior a day had more than triple the dementia risk (aHR, 3.21; P < .001).
Although previous studies had found that breaking up sedentary periods with short bursts of activity help offset some negative health effects of sitting, that wasn’t the case here. Dementia risk was elevated whether participants were sedentary for 10 uninterrupted hours or multiple sedentary periods that totaled 10 hours over the whole day.
“This was surprising,” Dr. Raichlen said. “We expected to find that patterns of sedentary behavior would play a role in risk of dementia, but once you take into account the daily volume of time spent sedentary, how you get there doesn’t seem to matter as much.”
The study did not examine how participants spent sedentary time, but an earlier study by Dr. Raichlen found that watching TV was associated with a greater risk of dementia in older adults, compared with working on a computer.
More research welcome
Dr. Raichlen noted that the number of dementia cases in the study is low and that the view of sedentary behavior is based on 1 week of accelerometer readings. A longitudinal study is needed to determine if the findings last over a longer time period.
In a comment, Claire Sexton, DPhil, senior director of scientific programs and outreach for the Alzheimer’s Association, says that earlier studies reported an association between sedentary time and dementia, so these results aren’t “particularly surprising.”
“However, reports that did not find an association have also been published, so additional research on possible associations is welcome,” she said.
It’s also important to note that this observational study doesn’t establish a causal relationship between inactivity and cognitive function, which Dr. Sexton said means the influence of other dementia risk factors that are also exacerbated by sedentary behavior can’t be ruled out.
“Although results remained significant after adjusting for several of these factors, further research is required to better understand the various elements that may influence the observed relationship,” noted Dr. Sexton, who was not part of the study. “Reverse causality – that changes in the brain related to dementia are causing the sedentary behavior – cannot be ruled out.”
The study was funded by the National Institutes of Health, the state of Arizona, the Arizona Department of Health Services, and the McKnight Brain Research Foundation. Dr. Raichlen and Dr. Sexton report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study of nearly 50,000 adults in the UK Biobank shows that dementia risk increased 8% with 10 hours of sedentary time and 63% with 12 hours. That’s particularly concerning because Americans spend an average of 9.5 hours a day sitting.
Sleep wasn’t factored into the sedentary time and how someone accumulated the 10 hours – either in one continuous block or broken up throughout the day – was irrelevant.
“Our analysis cannot determine whether there is a causal link, so prescriptive conclusions are not really possible; however. I think it is very reasonable to conclude that sitting less and moving more may help reduce risk of dementia,” lead investigator David Raichlen, PhD, professor of biological sciences and anthropology, University of Southern California, Los Angeles, said in an interview.
The findings were published online in JAMA.
A surprising find?
The study is a retrospective analysis of prospectively collected data from the UK Biobank of 49,841 adults aged 60 years or older who wore an accelerometer on their wrists 24 hours a day for a week. Participants had no history of dementia when they wore the movement monitoring device.
Investigators used machine-based learning to determine sedentary time based on readings from the accelerometers. Sleep was not included as sedentary behavior.
Over a mean follow-up of 6.72 years, 414 participants were diagnosed with dementia.
Investigators found that dementia risk rises by 8% at 10 hours a day (adjusted hazard ratio, 1.08; P < .001) and 63% at 12 hours a day (aHR, 1.63; P < .001), compared with 9.27 hours a day. Those who logged 15 hours of sedentary behavior a day had more than triple the dementia risk (aHR, 3.21; P < .001).
Although previous studies had found that breaking up sedentary periods with short bursts of activity help offset some negative health effects of sitting, that wasn’t the case here. Dementia risk was elevated whether participants were sedentary for 10 uninterrupted hours or multiple sedentary periods that totaled 10 hours over the whole day.
“This was surprising,” Dr. Raichlen said. “We expected to find that patterns of sedentary behavior would play a role in risk of dementia, but once you take into account the daily volume of time spent sedentary, how you get there doesn’t seem to matter as much.”
The study did not examine how participants spent sedentary time, but an earlier study by Dr. Raichlen found that watching TV was associated with a greater risk of dementia in older adults, compared with working on a computer.
More research welcome
Dr. Raichlen noted that the number of dementia cases in the study is low and that the view of sedentary behavior is based on 1 week of accelerometer readings. A longitudinal study is needed to determine if the findings last over a longer time period.
In a comment, Claire Sexton, DPhil, senior director of scientific programs and outreach for the Alzheimer’s Association, says that earlier studies reported an association between sedentary time and dementia, so these results aren’t “particularly surprising.”
“However, reports that did not find an association have also been published, so additional research on possible associations is welcome,” she said.
It’s also important to note that this observational study doesn’t establish a causal relationship between inactivity and cognitive function, which Dr. Sexton said means the influence of other dementia risk factors that are also exacerbated by sedentary behavior can’t be ruled out.
“Although results remained significant after adjusting for several of these factors, further research is required to better understand the various elements that may influence the observed relationship,” noted Dr. Sexton, who was not part of the study. “Reverse causality – that changes in the brain related to dementia are causing the sedentary behavior – cannot be ruled out.”
The study was funded by the National Institutes of Health, the state of Arizona, the Arizona Department of Health Services, and the McKnight Brain Research Foundation. Dr. Raichlen and Dr. Sexton report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study of nearly 50,000 adults in the UK Biobank shows that dementia risk increased 8% with 10 hours of sedentary time and 63% with 12 hours. That’s particularly concerning because Americans spend an average of 9.5 hours a day sitting.
Sleep wasn’t factored into the sedentary time and how someone accumulated the 10 hours – either in one continuous block or broken up throughout the day – was irrelevant.
“Our analysis cannot determine whether there is a causal link, so prescriptive conclusions are not really possible; however. I think it is very reasonable to conclude that sitting less and moving more may help reduce risk of dementia,” lead investigator David Raichlen, PhD, professor of biological sciences and anthropology, University of Southern California, Los Angeles, said in an interview.
The findings were published online in JAMA.
A surprising find?
The study is a retrospective analysis of prospectively collected data from the UK Biobank of 49,841 adults aged 60 years or older who wore an accelerometer on their wrists 24 hours a day for a week. Participants had no history of dementia when they wore the movement monitoring device.
Investigators used machine-based learning to determine sedentary time based on readings from the accelerometers. Sleep was not included as sedentary behavior.
Over a mean follow-up of 6.72 years, 414 participants were diagnosed with dementia.
Investigators found that dementia risk rises by 8% at 10 hours a day (adjusted hazard ratio, 1.08; P < .001) and 63% at 12 hours a day (aHR, 1.63; P < .001), compared with 9.27 hours a day. Those who logged 15 hours of sedentary behavior a day had more than triple the dementia risk (aHR, 3.21; P < .001).
Although previous studies had found that breaking up sedentary periods with short bursts of activity help offset some negative health effects of sitting, that wasn’t the case here. Dementia risk was elevated whether participants were sedentary for 10 uninterrupted hours or multiple sedentary periods that totaled 10 hours over the whole day.
“This was surprising,” Dr. Raichlen said. “We expected to find that patterns of sedentary behavior would play a role in risk of dementia, but once you take into account the daily volume of time spent sedentary, how you get there doesn’t seem to matter as much.”
The study did not examine how participants spent sedentary time, but an earlier study by Dr. Raichlen found that watching TV was associated with a greater risk of dementia in older adults, compared with working on a computer.
More research welcome
Dr. Raichlen noted that the number of dementia cases in the study is low and that the view of sedentary behavior is based on 1 week of accelerometer readings. A longitudinal study is needed to determine if the findings last over a longer time period.
In a comment, Claire Sexton, DPhil, senior director of scientific programs and outreach for the Alzheimer’s Association, says that earlier studies reported an association between sedentary time and dementia, so these results aren’t “particularly surprising.”
“However, reports that did not find an association have also been published, so additional research on possible associations is welcome,” she said.
It’s also important to note that this observational study doesn’t establish a causal relationship between inactivity and cognitive function, which Dr. Sexton said means the influence of other dementia risk factors that are also exacerbated by sedentary behavior can’t be ruled out.
“Although results remained significant after adjusting for several of these factors, further research is required to better understand the various elements that may influence the observed relationship,” noted Dr. Sexton, who was not part of the study. “Reverse causality – that changes in the brain related to dementia are causing the sedentary behavior – cannot be ruled out.”
The study was funded by the National Institutes of Health, the state of Arizona, the Arizona Department of Health Services, and the McKnight Brain Research Foundation. Dr. Raichlen and Dr. Sexton report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA
Dusty, but still cool
When I was 16, keeping my car shiny was a priority. I washed it every weekend and waxed it once a month. I was pretty good at it and got paid to do the occasional job for a neighbor, too.

In college I was busier, and my car was back at the house, so it didn’t need to be washed as much.
In medical school I think I washed the car once a year. Residency was probably the same.
Today I realized I couldn’t remember when I last had it washed (at my age I don’t have time to do it myself). So I looked it up in Quicken: Nov. 14, 2018.
Really? I’ve gone almost 5 years without washing my car? I can’t even blame that on the pandemic.
I mean, I still like my car. It’s comfortable, has good air conditioning (in Phoenix that’s critical), and gets me where I want to go. At my age those things are what’s really important. It’s hard to believe that 40 years ago, keeping a polished car was the center of my existence. Of course, it probably still is for most guys that age.
It’s a reminder of how much things change as life goes by.
Here in my little corner of neurology, multiple sclerosis has gone from steroids for relapses, to a few injections of mild benefit, to a bunch of drugs that are, literally, game-changing for many patients. And the Big Four epilepsy drugs (Dilantin, Tegretol, Depakote, and Phenobarb) are slowly fading into the background.
But back to changing priorities – it’s the way life rewrites our plans at each step. From a freshly waxed car to good grades to mortgages to kids – and then watching as they wax their cars.
Suddenly my car looks dusty. Am I the same way? I’m certainly not 16 anymore. Realistically, the majority of my life and career are behind me now. That doesn’t mean I’m not still having fun, it’s just the truth. I try not to think about it that much, as doing so won’t change anything.
In all honesty, neither did washing my car. I mean, the car looked good, but did it make me one of the cool kids? Or get me a girlfriend? Or invited to THE parties? Not at all. Like so many things about appearances, very few of them really matter. There’s only so far that style will get you, compared with substance.
Which doesn’t change the fact that I need to wash my car. But procrastination is for another column.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
When I was 16, keeping my car shiny was a priority. I washed it every weekend and waxed it once a month. I was pretty good at it and got paid to do the occasional job for a neighbor, too.
In college I was busier, and my car was back at the house, so it didn’t need to be washed as much.
In medical school I think I washed the car once a year. Residency was probably the same.
Today I realized I couldn’t remember when I last had it washed (at my age I don’t have time to do it myself). So I looked it up in Quicken: Nov. 14, 2018.
Really? I’ve gone almost 5 years without washing my car? I can’t even blame that on the pandemic.
I mean, I still like my car. It’s comfortable, has good air conditioning (in Phoenix that’s critical), and gets me where I want to go. At my age those things are what’s really important. It’s hard to believe that 40 years ago, keeping a polished car was the center of my existence. Of course, it probably still is for most guys that age.
It’s a reminder of how much things change as life goes by.
Here in my little corner of neurology, multiple sclerosis has gone from steroids for relapses, to a few injections of mild benefit, to a bunch of drugs that are, literally, game-changing for many patients. And the Big Four epilepsy drugs (Dilantin, Tegretol, Depakote, and Phenobarb) are slowly fading into the background.
But back to changing priorities – it’s the way life rewrites our plans at each step. From a freshly waxed car to good grades to mortgages to kids – and then watching as they wax their cars.
Suddenly my car looks dusty. Am I the same way? I’m certainly not 16 anymore. Realistically, the majority of my life and career are behind me now. That doesn’t mean I’m not still having fun, it’s just the truth. I try not to think about it that much, as doing so won’t change anything.
In all honesty, neither did washing my car. I mean, the car looked good, but did it make me one of the cool kids? Or get me a girlfriend? Or invited to THE parties? Not at all. Like so many things about appearances, very few of them really matter. There’s only so far that style will get you, compared with substance.
Which doesn’t change the fact that I need to wash my car. But procrastination is for another column.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
When I was 16, keeping my car shiny was a priority. I washed it every weekend and waxed it once a month. I was pretty good at it and got paid to do the occasional job for a neighbor, too.
In college I was busier, and my car was back at the house, so it didn’t need to be washed as much.
In medical school I think I washed the car once a year. Residency was probably the same.
Today I realized I couldn’t remember when I last had it washed (at my age I don’t have time to do it myself). So I looked it up in Quicken: Nov. 14, 2018.
Really? I’ve gone almost 5 years without washing my car? I can’t even blame that on the pandemic.
I mean, I still like my car. It’s comfortable, has good air conditioning (in Phoenix that’s critical), and gets me where I want to go. At my age those things are what’s really important. It’s hard to believe that 40 years ago, keeping a polished car was the center of my existence. Of course, it probably still is for most guys that age.
It’s a reminder of how much things change as life goes by.
Here in my little corner of neurology, multiple sclerosis has gone from steroids for relapses, to a few injections of mild benefit, to a bunch of drugs that are, literally, game-changing for many patients. And the Big Four epilepsy drugs (Dilantin, Tegretol, Depakote, and Phenobarb) are slowly fading into the background.
But back to changing priorities – it’s the way life rewrites our plans at each step. From a freshly waxed car to good grades to mortgages to kids – and then watching as they wax their cars.
Suddenly my car looks dusty. Am I the same way? I’m certainly not 16 anymore. Realistically, the majority of my life and career are behind me now. That doesn’t mean I’m not still having fun, it’s just the truth. I try not to think about it that much, as doing so won’t change anything.
In all honesty, neither did washing my car. I mean, the car looked good, but did it make me one of the cool kids? Or get me a girlfriend? Or invited to THE parties? Not at all. Like so many things about appearances, very few of them really matter. There’s only so far that style will get you, compared with substance.
Which doesn’t change the fact that I need to wash my car. But procrastination is for another column.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
New European restrictions on topiramate in pregnancy
While it’s well known that topiramate can cause major congenital malformations and fetal growth restriction when used during pregnancy, recent data also suggest a possibly increased risk for neurodevelopmental disorders when topiramate is used during pregnancy, the EMA said in a statement.
The data include two observational studies that showed children born to mothers with epilepsy and who were exposed to topiramate in the womb may have a two- to threefold higher risk for neurodevelopmental disorders, in particular autism spectrum disorders (ASD), intellectual disability, or attention deficit hyperactivity disorder (ADHD), compared with children born to mothers with epilepsy not taking antiepileptic medication.
For patients using topiramate for the treatment of epilepsy, the PRAC now recommends that the medicine not be used during pregnancy unless no other suitable treatment is available.
The PRAC had also recommended a pregnancy prevention program to avoid exposure of the developing fetus to topiramate. “These measures will inform any woman or girl who is able to have children of the risks of taking topiramate during pregnancy and the need to avoid becoming pregnant while taking topiramate,” the EMA said.
Regardless of indication, the agency said topiramate should be used in women of childbearing age only when the following conditions of the pregnancy prevention program are met:
- A pregnancy test before starting treatment.
- Counseling about the risks of topiramate treatment and the need for highly effective contraception throughout treatment.
- A review of ongoing treatment at least annually by completion of a risk awareness form.
The PRAC recommends that health care professionals ensure women of childbearing age are fully aware of the risks of taking topiramate during pregnancy. The committee noted that alternative treatment options should be considered and the need for topiramate treatment should be reassessed at least annually.
The product information for topiramate-containing medicines will be updated to further highlight the risks for neurodevelopmental disorders and the additional safety measures to be taken.
Patients and health care professionals will be provided with educational materials regarding the risks of using topiramate during pregnancy, and a patient card will be provided to the patient with each medicine package. A visible warning will also be added to the outer packaging of the medicine.
The new PRAC recommendations will be sent to the Coordination Group for Mutual Recognition and Decentralised Procedures – Human (CMDh), which will adopt a position.
A version of this article first appeared on Medscape.com.
While it’s well known that topiramate can cause major congenital malformations and fetal growth restriction when used during pregnancy, recent data also suggest a possibly increased risk for neurodevelopmental disorders when topiramate is used during pregnancy, the EMA said in a statement.
The data include two observational studies that showed children born to mothers with epilepsy and who were exposed to topiramate in the womb may have a two- to threefold higher risk for neurodevelopmental disorders, in particular autism spectrum disorders (ASD), intellectual disability, or attention deficit hyperactivity disorder (ADHD), compared with children born to mothers with epilepsy not taking antiepileptic medication.
For patients using topiramate for the treatment of epilepsy, the PRAC now recommends that the medicine not be used during pregnancy unless no other suitable treatment is available.
The PRAC had also recommended a pregnancy prevention program to avoid exposure of the developing fetus to topiramate. “These measures will inform any woman or girl who is able to have children of the risks of taking topiramate during pregnancy and the need to avoid becoming pregnant while taking topiramate,” the EMA said.
Regardless of indication, the agency said topiramate should be used in women of childbearing age only when the following conditions of the pregnancy prevention program are met:
- A pregnancy test before starting treatment.
- Counseling about the risks of topiramate treatment and the need for highly effective contraception throughout treatment.
- A review of ongoing treatment at least annually by completion of a risk awareness form.
The PRAC recommends that health care professionals ensure women of childbearing age are fully aware of the risks of taking topiramate during pregnancy. The committee noted that alternative treatment options should be considered and the need for topiramate treatment should be reassessed at least annually.
The product information for topiramate-containing medicines will be updated to further highlight the risks for neurodevelopmental disorders and the additional safety measures to be taken.
Patients and health care professionals will be provided with educational materials regarding the risks of using topiramate during pregnancy, and a patient card will be provided to the patient with each medicine package. A visible warning will also be added to the outer packaging of the medicine.
The new PRAC recommendations will be sent to the Coordination Group for Mutual Recognition and Decentralised Procedures – Human (CMDh), which will adopt a position.
A version of this article first appeared on Medscape.com.
While it’s well known that topiramate can cause major congenital malformations and fetal growth restriction when used during pregnancy, recent data also suggest a possibly increased risk for neurodevelopmental disorders when topiramate is used during pregnancy, the EMA said in a statement.
The data include two observational studies that showed children born to mothers with epilepsy and who were exposed to topiramate in the womb may have a two- to threefold higher risk for neurodevelopmental disorders, in particular autism spectrum disorders (ASD), intellectual disability, or attention deficit hyperactivity disorder (ADHD), compared with children born to mothers with epilepsy not taking antiepileptic medication.
For patients using topiramate for the treatment of epilepsy, the PRAC now recommends that the medicine not be used during pregnancy unless no other suitable treatment is available.
The PRAC had also recommended a pregnancy prevention program to avoid exposure of the developing fetus to topiramate. “These measures will inform any woman or girl who is able to have children of the risks of taking topiramate during pregnancy and the need to avoid becoming pregnant while taking topiramate,” the EMA said.
Regardless of indication, the agency said topiramate should be used in women of childbearing age only when the following conditions of the pregnancy prevention program are met:
- A pregnancy test before starting treatment.
- Counseling about the risks of topiramate treatment and the need for highly effective contraception throughout treatment.
- A review of ongoing treatment at least annually by completion of a risk awareness form.
The PRAC recommends that health care professionals ensure women of childbearing age are fully aware of the risks of taking topiramate during pregnancy. The committee noted that alternative treatment options should be considered and the need for topiramate treatment should be reassessed at least annually.
The product information for topiramate-containing medicines will be updated to further highlight the risks for neurodevelopmental disorders and the additional safety measures to be taken.
Patients and health care professionals will be provided with educational materials regarding the risks of using topiramate during pregnancy, and a patient card will be provided to the patient with each medicine package. A visible warning will also be added to the outer packaging of the medicine.
The new PRAC recommendations will be sent to the Coordination Group for Mutual Recognition and Decentralised Procedures – Human (CMDh), which will adopt a position.
A version of this article first appeared on Medscape.com.
Long COVID and new migraines: What’s the link?
.
“I’ve also noticed visual disturbances, like flickering lights or blurred vision, which I later learned are called auras,” the 30-year-old medical billing specialist in Seattle told this news organization.
Mr. Solomon isn’t alone. It’s estimated that 1 out of 8 people with COVID develop long COVID. Of those persons, 44% also experience headaches. Research has found that many of those headaches are migraines – and many patients who are afflicted say they had never had a migraine before. These migraines tend to persist for at least 5 or 6 months, according to data from the American Headache Society.
What’s more, other patients may suddenly have more frequent or intense versions of headaches they’ve not noticed before.
The mechanism as to how long COVID could manifest migraines is not yet fully understood, but many doctors believe that inflammation caused by the virus plays a key role.
“To understand why some patients have migraine in long COVID, we have to go back to understand the role of inflammation in COVID-19 itself,” says Emad Estemalik, MD, clinical assistant professor of neurology at Cleveland Clinic Lerner College of Medicine and section head of headache medicine at Cleveland Clinic.
In COVID-19, inflammation occurs because of a cytokine storm. Cytokines, which are proteins essential for a strong immune system, can be overproduced in a patient with COVID, which causes too much inflammation in any organ in the body, including the brain. This can result in new daily headache for some patients.
A new study from Italian researchers found that many patients who develop migraines for the first time while ill with long COVID are middle-aged women (traditionally a late point in life for a first migraine) who have a family history of migraine. Potential causes could have to do with the immune system remaining persistently activated from inflammation during long COVID, as well as the activation of the trigeminovascular system in the brain, which contains neurons that can trigger a migraine.
What treatments can work for migraines related to long COVID?
Long COVID usually causes a constellation of other symptoms at the same time as migraine.
“It’s so important for patients to take an interdisciplinary approach,” Dr. Estemalik stresses. “Patients should make sure their doctors are addressing all of their symptoms.”
When it comes to specifically targeting migraines, standard treatments can be effective.
“In terms of treating migraine in long COVID patients, we don’t do anything different or special,” says Matthew E. Fink, MD, chair of neurology at Weill Cornell Medical College and chief of the Division of Stroke and Critical Care Neurology at New York–Presbyterian Hospital/Weill Cornell Medical Center. “We treat these patients with standard migraine medications.”
Mr. Solomon is following this course of action.
“My doctor prescribed triptans, which have been somewhat effective in reducing the severity and duration of the migraines,” he says. A daily supplement of magnesium and a daily dose of aspirin can also work for some patients, according to Dr. Fink.
Lifestyle modification is also a great idea.
“Patients should keep regular sleep hours, getting up and going to bed at the same time every day,” Dr. Fink continues. “Daily exercise is also recommended.”
Mr. Solomon suggests tracking migraine triggers and patterns in a journal.
“Try to identify lifestyle changes that help, like managing stress and staying hydrated,” Mr. Solomon advises. “Seeking support from health care professionals and support groups can make a significant difference.”
The best news of all: for patients that are diligent in following these strategies, they’ve been proven to work.
“We doctors are very optimistic when it comes to good outcomes for patients with long COVID and migraine,” Dr. Fink says. “I reassure my patients by telling them, ‘You will get better long-term.’ ”
A version of this article appeared on Medscape.com.
.
“I’ve also noticed visual disturbances, like flickering lights or blurred vision, which I later learned are called auras,” the 30-year-old medical billing specialist in Seattle told this news organization.
Mr. Solomon isn’t alone. It’s estimated that 1 out of 8 people with COVID develop long COVID. Of those persons, 44% also experience headaches. Research has found that many of those headaches are migraines – and many patients who are afflicted say they had never had a migraine before. These migraines tend to persist for at least 5 or 6 months, according to data from the American Headache Society.
What’s more, other patients may suddenly have more frequent or intense versions of headaches they’ve not noticed before.
The mechanism as to how long COVID could manifest migraines is not yet fully understood, but many doctors believe that inflammation caused by the virus plays a key role.
“To understand why some patients have migraine in long COVID, we have to go back to understand the role of inflammation in COVID-19 itself,” says Emad Estemalik, MD, clinical assistant professor of neurology at Cleveland Clinic Lerner College of Medicine and section head of headache medicine at Cleveland Clinic.
In COVID-19, inflammation occurs because of a cytokine storm. Cytokines, which are proteins essential for a strong immune system, can be overproduced in a patient with COVID, which causes too much inflammation in any organ in the body, including the brain. This can result in new daily headache for some patients.
A new study from Italian researchers found that many patients who develop migraines for the first time while ill with long COVID are middle-aged women (traditionally a late point in life for a first migraine) who have a family history of migraine. Potential causes could have to do with the immune system remaining persistently activated from inflammation during long COVID, as well as the activation of the trigeminovascular system in the brain, which contains neurons that can trigger a migraine.
What treatments can work for migraines related to long COVID?
Long COVID usually causes a constellation of other symptoms at the same time as migraine.
“It’s so important for patients to take an interdisciplinary approach,” Dr. Estemalik stresses. “Patients should make sure their doctors are addressing all of their symptoms.”
When it comes to specifically targeting migraines, standard treatments can be effective.
“In terms of treating migraine in long COVID patients, we don’t do anything different or special,” says Matthew E. Fink, MD, chair of neurology at Weill Cornell Medical College and chief of the Division of Stroke and Critical Care Neurology at New York–Presbyterian Hospital/Weill Cornell Medical Center. “We treat these patients with standard migraine medications.”
Mr. Solomon is following this course of action.
“My doctor prescribed triptans, which have been somewhat effective in reducing the severity and duration of the migraines,” he says. A daily supplement of magnesium and a daily dose of aspirin can also work for some patients, according to Dr. Fink.
Lifestyle modification is also a great idea.
“Patients should keep regular sleep hours, getting up and going to bed at the same time every day,” Dr. Fink continues. “Daily exercise is also recommended.”
Mr. Solomon suggests tracking migraine triggers and patterns in a journal.
“Try to identify lifestyle changes that help, like managing stress and staying hydrated,” Mr. Solomon advises. “Seeking support from health care professionals and support groups can make a significant difference.”
The best news of all: for patients that are diligent in following these strategies, they’ve been proven to work.
“We doctors are very optimistic when it comes to good outcomes for patients with long COVID and migraine,” Dr. Fink says. “I reassure my patients by telling them, ‘You will get better long-term.’ ”
A version of this article appeared on Medscape.com.
.
“I’ve also noticed visual disturbances, like flickering lights or blurred vision, which I later learned are called auras,” the 30-year-old medical billing specialist in Seattle told this news organization.
Mr. Solomon isn’t alone. It’s estimated that 1 out of 8 people with COVID develop long COVID. Of those persons, 44% also experience headaches. Research has found that many of those headaches are migraines – and many patients who are afflicted say they had never had a migraine before. These migraines tend to persist for at least 5 or 6 months, according to data from the American Headache Society.
What’s more, other patients may suddenly have more frequent or intense versions of headaches they’ve not noticed before.
The mechanism as to how long COVID could manifest migraines is not yet fully understood, but many doctors believe that inflammation caused by the virus plays a key role.
“To understand why some patients have migraine in long COVID, we have to go back to understand the role of inflammation in COVID-19 itself,” says Emad Estemalik, MD, clinical assistant professor of neurology at Cleveland Clinic Lerner College of Medicine and section head of headache medicine at Cleveland Clinic.
In COVID-19, inflammation occurs because of a cytokine storm. Cytokines, which are proteins essential for a strong immune system, can be overproduced in a patient with COVID, which causes too much inflammation in any organ in the body, including the brain. This can result in new daily headache for some patients.
A new study from Italian researchers found that many patients who develop migraines for the first time while ill with long COVID are middle-aged women (traditionally a late point in life for a first migraine) who have a family history of migraine. Potential causes could have to do with the immune system remaining persistently activated from inflammation during long COVID, as well as the activation of the trigeminovascular system in the brain, which contains neurons that can trigger a migraine.
What treatments can work for migraines related to long COVID?
Long COVID usually causes a constellation of other symptoms at the same time as migraine.
“It’s so important for patients to take an interdisciplinary approach,” Dr. Estemalik stresses. “Patients should make sure their doctors are addressing all of their symptoms.”
When it comes to specifically targeting migraines, standard treatments can be effective.
“In terms of treating migraine in long COVID patients, we don’t do anything different or special,” says Matthew E. Fink, MD, chair of neurology at Weill Cornell Medical College and chief of the Division of Stroke and Critical Care Neurology at New York–Presbyterian Hospital/Weill Cornell Medical Center. “We treat these patients with standard migraine medications.”
Mr. Solomon is following this course of action.
“My doctor prescribed triptans, which have been somewhat effective in reducing the severity and duration of the migraines,” he says. A daily supplement of magnesium and a daily dose of aspirin can also work for some patients, according to Dr. Fink.
Lifestyle modification is also a great idea.
“Patients should keep regular sleep hours, getting up and going to bed at the same time every day,” Dr. Fink continues. “Daily exercise is also recommended.”
Mr. Solomon suggests tracking migraine triggers and patterns in a journal.
“Try to identify lifestyle changes that help, like managing stress and staying hydrated,” Mr. Solomon advises. “Seeking support from health care professionals and support groups can make a significant difference.”
The best news of all: for patients that are diligent in following these strategies, they’ve been proven to work.
“We doctors are very optimistic when it comes to good outcomes for patients with long COVID and migraine,” Dr. Fink says. “I reassure my patients by telling them, ‘You will get better long-term.’ ”
A version of this article appeared on Medscape.com.
Your patient bequeathed money to you: Can you accept it?
Michael Victoroff, MD, described the phone call he received from an attorney asking a thorny ethics question involving a patient’s gift to another physician. Dr. Victoroff, a past member of the ethics committee of the American Academy of Family Physicians, had definite thoughts about it.
“The attorney was representing the daughters of an elderly gentleman who had moved from the East Coast to Colorado to be closer to them,” said Dr. Victoroff, who teaches bioethics in the MBA program at the University of Denver and also practices at the University of Colorado School of Medicine.
“The father visited his new primary care physician frequently because he had multiple health issues.”
The patient was happy with the doctor’s medical care and over time that they developed a friendship. Dr. Victoroff emphasized that no sexual or romantic impropriety ever took place between the patient and his physician.
“But the social relationship went beyond the ordinary doctor-patient boundaries. The patient ultimately named the doctor as his health care proxy in the event that he became unable to make decisions regarding his care. He also mentioned he was going to leave her $100,000 in his will,” says Dr. Victoroff.
The physician did accept the role of proxy, “which raises a whole host of ethical issues,” says Dr. Victoroff. As it happened, she was never called upon to exercise that decision-making authority, since the patient died suddenly and was mentally competent at the time.
for her to accept such a substantial bequest from a patient, and they hired an attorney to contest the will.
No law against it
Dennis Hursh, attorney and managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, noted in an interview that, “the problem isn’t legal per se. Rather, the problem is an ethical one.”
Legally speaking, there’s no prohibition against receiving a bequest or other form of gift from a patient. “People are free to dispose of their estates in whatever way they see fit, and no law technically precludes a physician from accepting a bequest,” says Dr. Victoroff. “But this presupposes there is nothing improper going on, such as extortion, deception, coercion, or exercising undue influence.”
The issue of bequeathing money to their physician gained attention in a recent case that took place in Australia. Peter Alexakis, MD, received a whopping bequest of $24 million from a patient. The elderly patient had changed his will to name Dr. Alexakis as the sole beneficiary – after Dr. Alexakis had visited him at home 92 times during the preceding months. The original heirs filed a lawsuit in Australia’s Supreme Court against Dr. Alexakis, contesting the will.
The lawsuit was unsuccessful in court, but Dr. Alexakis was found guilty of malpractice by Australia’s Health Care Complaints Commission after being reported to the HCCC by the palliative care physicians who were treating the patient. They alleged that Dr. Alexakis had interfered with their care of the patient. The more serious allegation was that the doctor had engaged in a deliberate strategy to exploit the relationship for financial gain.
Dr. Alexakis was chastised by the HCCC for engaging in “obtuse” and “suspicious” behavior and for “blurring the boundaries of the doctor-patient relationship.”
There are three domains – legal, ethical, and practical – when it comes to accepting bequests or any gifts from patients, says Dr. Victoroff.
“[In] the legal domain, for example, if you receive a bequest from anyone, patient or otherwise, you have to know your local laws about estates and taxes and so forth and obey them,” he said.
Attorney Hursh pointed out that the Australian doctor wasn’t found guilty of wrongdoing in a court of law but rather of unethical conduct by the Australian medical licensing entity.
Patients giving gifts is often a part of a physician’s life
When Ian Schorr, MD, first started out in practice, he was surprised that patients began bringing him gifts of food to express gratitude for his care.
“I thought it was unethical to accept their gifts, so I turned them down and wouldn’t accept so much as a cookie,” Dr. Schorr, a now-retired ophthalmologist, told this news organization. “But that changed because my office staff told me that some patients were feeling disappointed and insulted. I realized that some people want to express appreciation in ways that go beyond a monetary payment.”
The next time he received a gift from a patient, he “accepted it gracefully.” And he wrote a thank you note, which he continued to do any time he received a gift from a patient.
Kenneth Prager, MD, professor of clinical medicine, director of clinical ethics and chairman of the Medical Ethics Committee at Columbia University Medical Center, New York, says, “I have literally received hundreds of gifts, the vast majority being tokens of patients’ appreciation,” he said. “I’ll get boxes of chocolate or cakes, or sometimes articles of clothing.”
Occasionally, Dr. Prager receives a “somewhat larger gift” – for example, two tickets to a baseball game. “To reject these gifts would be a slap in the face to the patient,” he says, but “where it gets more ethically cloudy is when a gift is very substantial.”
Dr. Prager has never been offered a “substantial” gift or bequest personally. “But a patient whose brother I cared for has indicated that she has left instructions in her will to endow an associate chair of ethics in my honor, and I didn’t decline that,” he said.
The AMA Code of Ethics confirms that accepting gifts offered “as an expression of gratitude or a reflection of the patient’s cultural tradition” can “enhance the patient-physician relationship.” But sometimes gifts “may signal psychological needs that require the physician’s attention.” Accepting such gifts is “likely to damage the patient-physician relationship.”
Potential damage to the therapeutic relationship applies to all physicians but especially for psychiatrists and mental health professionals. “There are more stringent ethical requirements when it comes to these disciplines, where gift-giving gets into the territory of transference or may have particular psychological meaning, and accepting the gift may muddy the therapeutic waters,” Dr. Victoroff said.
Impact on the patient’s family and on other patients
The AMA statement encourages physicians to be “sensitive to the gift’s value, relative to the patient’s or physician’s means.” Physicians should decline gifts that are “disproportionately or inappropriately large, or when the physician would be uncomfortable to have colleagues know the gift had been accepted.”
They should also decline a bequest from a patient if they have reason to believe that to accept it “would present an emotional or financial hardship to the patient’s family.”
“If Bill Gates were leaving $100,000 to his doctor, I imagine Melinda would be just fine,” Mr. Hursh said. “But under ordinary circumstances, if the patient’s family might feel the impact of the bequest, it would be unethical to accept it and could be grounds for revocation of the doctor’s license.”
The AMA statement also warns physicians that by offering a gift, some patients may be seeking to “secure or influence care or to secure preferential treatment,” which can “undermine physicians’ obligation to provide services fairly to all patients.”
For this reason, bequests are “sticky,” said Laurel Lyckholm, MD, professor of hematology and oncology at West Virginia University School of Medicine. In the case of institutions where patients or community members donate money, “we know whose names are on the plaques that hang on the hospital walls, so it’s a delicate balance. What if there’s only one bed or one ventilator? Will the wife of the donor get preferential treatment?”
Follow institutional policy
A “very small gift, such as a fruitcake, is fine,” says Dr. Lyckholm, author of an essay on accepting gifts from patients. She said there’s a dollar amount ($15) that her institution mandates, above which a gift – even food – is considered too expensive to accept. “I was a nurse before I became a physician, and people always tried to give us gifts because we were so close to the minute-by-minute care of the patients,” she said. “We were not allowed to accept money or anything lavish.”
But in the case of small gifts, “the risk-benefit analysis is that there’s much more risk not to take it and to hurt the patient’s feelings.”
Gifts above $15 are given to charity. “I explain to patients that I’m not allowed to take such a large gift, but I’d love to give it to the hospital’s Rosenbaum Family House that provides patients and their relatives with lodging, or to the homeless shelter in Morgantown.”
Dr. Lyckholm, who serves on the ethics committee at J.W. Ruby Memorial Hospital, once was offered expensive tickets and said to the patient, “This is so incredibly thoughtful and kind, but I can’t accept them. I would like to give the tickets to a charity that can auction them off.”
She advises physicians to find out their institution’s policies. Many institutions have policies about what gifts their staff – whether physicians, nurses, or other health care professionals – can accept.
Passing the ‘smell test’
Accepting a large gift from a patient could potentially make it look like you might have exercised undue influence.
“That concern brings us to the third domain, which is very practical and all about appearances and perceptions,” Dr. Victoroff said.
He noted that there is “an inherent power differential between a physician and a patient. The very nature of the relationship can create a risk of ‘undue influence’ on the doctor’s part, even if it’s not apparent to the doctor.” For this reason, it’s necessary to be utterly transparent about how the bequest came about.
He suggests that if a patient informs you that he or she would like to leave money to you, it might be wise to suggest a meeting with the patient’s family, thus establishing some transparency.
It may not be possible to meet with the patient’s family for logistical reasons or because the patient would prefer not to involve their family in their estate planning. But in any case, it’s advisable to document any conversation in the patient’s chart, Dr. Victoroff advised.
“You should make a contemporaneous note that the patient initiated the suggestion and that you counseled them about the implications, no differently than you would with an interaction of a clinical nature,” he suggests. That way, if money has been left to you and is disputed, there’s a clear record that you didn’t solicit it or use any undue influence to bring it about.
He also recommended getting advice from a trusted colleague or a member of your institution’s ethics committee. “Taking time to get a second opinion about an ethical question is a safeguard, like having a chaperone in the room during an examination.”
Ultimately, “there is no human relationship without potential conflicts of interest. Our job is to manage those as best as we can, and sunlight is the best antidote to bad appearances,” Dr. Victoroff said.
A version of this article appeared on Medscape.com.
Michael Victoroff, MD, described the phone call he received from an attorney asking a thorny ethics question involving a patient’s gift to another physician. Dr. Victoroff, a past member of the ethics committee of the American Academy of Family Physicians, had definite thoughts about it.
“The attorney was representing the daughters of an elderly gentleman who had moved from the East Coast to Colorado to be closer to them,” said Dr. Victoroff, who teaches bioethics in the MBA program at the University of Denver and also practices at the University of Colorado School of Medicine.
“The father visited his new primary care physician frequently because he had multiple health issues.”
The patient was happy with the doctor’s medical care and over time that they developed a friendship. Dr. Victoroff emphasized that no sexual or romantic impropriety ever took place between the patient and his physician.
“But the social relationship went beyond the ordinary doctor-patient boundaries. The patient ultimately named the doctor as his health care proxy in the event that he became unable to make decisions regarding his care. He also mentioned he was going to leave her $100,000 in his will,” says Dr. Victoroff.
The physician did accept the role of proxy, “which raises a whole host of ethical issues,” says Dr. Victoroff. As it happened, she was never called upon to exercise that decision-making authority, since the patient died suddenly and was mentally competent at the time.
for her to accept such a substantial bequest from a patient, and they hired an attorney to contest the will.
No law against it
Dennis Hursh, attorney and managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, noted in an interview that, “the problem isn’t legal per se. Rather, the problem is an ethical one.”
Legally speaking, there’s no prohibition against receiving a bequest or other form of gift from a patient. “People are free to dispose of their estates in whatever way they see fit, and no law technically precludes a physician from accepting a bequest,” says Dr. Victoroff. “But this presupposes there is nothing improper going on, such as extortion, deception, coercion, or exercising undue influence.”
The issue of bequeathing money to their physician gained attention in a recent case that took place in Australia. Peter Alexakis, MD, received a whopping bequest of $24 million from a patient. The elderly patient had changed his will to name Dr. Alexakis as the sole beneficiary – after Dr. Alexakis had visited him at home 92 times during the preceding months. The original heirs filed a lawsuit in Australia’s Supreme Court against Dr. Alexakis, contesting the will.
The lawsuit was unsuccessful in court, but Dr. Alexakis was found guilty of malpractice by Australia’s Health Care Complaints Commission after being reported to the HCCC by the palliative care physicians who were treating the patient. They alleged that Dr. Alexakis had interfered with their care of the patient. The more serious allegation was that the doctor had engaged in a deliberate strategy to exploit the relationship for financial gain.
Dr. Alexakis was chastised by the HCCC for engaging in “obtuse” and “suspicious” behavior and for “blurring the boundaries of the doctor-patient relationship.”
There are three domains – legal, ethical, and practical – when it comes to accepting bequests or any gifts from patients, says Dr. Victoroff.
“[In] the legal domain, for example, if you receive a bequest from anyone, patient or otherwise, you have to know your local laws about estates and taxes and so forth and obey them,” he said.
Attorney Hursh pointed out that the Australian doctor wasn’t found guilty of wrongdoing in a court of law but rather of unethical conduct by the Australian medical licensing entity.
Patients giving gifts is often a part of a physician’s life
When Ian Schorr, MD, first started out in practice, he was surprised that patients began bringing him gifts of food to express gratitude for his care.
“I thought it was unethical to accept their gifts, so I turned them down and wouldn’t accept so much as a cookie,” Dr. Schorr, a now-retired ophthalmologist, told this news organization. “But that changed because my office staff told me that some patients were feeling disappointed and insulted. I realized that some people want to express appreciation in ways that go beyond a monetary payment.”
The next time he received a gift from a patient, he “accepted it gracefully.” And he wrote a thank you note, which he continued to do any time he received a gift from a patient.
Kenneth Prager, MD, professor of clinical medicine, director of clinical ethics and chairman of the Medical Ethics Committee at Columbia University Medical Center, New York, says, “I have literally received hundreds of gifts, the vast majority being tokens of patients’ appreciation,” he said. “I’ll get boxes of chocolate or cakes, or sometimes articles of clothing.”
Occasionally, Dr. Prager receives a “somewhat larger gift” – for example, two tickets to a baseball game. “To reject these gifts would be a slap in the face to the patient,” he says, but “where it gets more ethically cloudy is when a gift is very substantial.”
Dr. Prager has never been offered a “substantial” gift or bequest personally. “But a patient whose brother I cared for has indicated that she has left instructions in her will to endow an associate chair of ethics in my honor, and I didn’t decline that,” he said.
The AMA Code of Ethics confirms that accepting gifts offered “as an expression of gratitude or a reflection of the patient’s cultural tradition” can “enhance the patient-physician relationship.” But sometimes gifts “may signal psychological needs that require the physician’s attention.” Accepting such gifts is “likely to damage the patient-physician relationship.”
Potential damage to the therapeutic relationship applies to all physicians but especially for psychiatrists and mental health professionals. “There are more stringent ethical requirements when it comes to these disciplines, where gift-giving gets into the territory of transference or may have particular psychological meaning, and accepting the gift may muddy the therapeutic waters,” Dr. Victoroff said.
Impact on the patient’s family and on other patients
The AMA statement encourages physicians to be “sensitive to the gift’s value, relative to the patient’s or physician’s means.” Physicians should decline gifts that are “disproportionately or inappropriately large, or when the physician would be uncomfortable to have colleagues know the gift had been accepted.”
They should also decline a bequest from a patient if they have reason to believe that to accept it “would present an emotional or financial hardship to the patient’s family.”
“If Bill Gates were leaving $100,000 to his doctor, I imagine Melinda would be just fine,” Mr. Hursh said. “But under ordinary circumstances, if the patient’s family might feel the impact of the bequest, it would be unethical to accept it and could be grounds for revocation of the doctor’s license.”
The AMA statement also warns physicians that by offering a gift, some patients may be seeking to “secure or influence care or to secure preferential treatment,” which can “undermine physicians’ obligation to provide services fairly to all patients.”
For this reason, bequests are “sticky,” said Laurel Lyckholm, MD, professor of hematology and oncology at West Virginia University School of Medicine. In the case of institutions where patients or community members donate money, “we know whose names are on the plaques that hang on the hospital walls, so it’s a delicate balance. What if there’s only one bed or one ventilator? Will the wife of the donor get preferential treatment?”
Follow institutional policy
A “very small gift, such as a fruitcake, is fine,” says Dr. Lyckholm, author of an essay on accepting gifts from patients. She said there’s a dollar amount ($15) that her institution mandates, above which a gift – even food – is considered too expensive to accept. “I was a nurse before I became a physician, and people always tried to give us gifts because we were so close to the minute-by-minute care of the patients,” she said. “We were not allowed to accept money or anything lavish.”
But in the case of small gifts, “the risk-benefit analysis is that there’s much more risk not to take it and to hurt the patient’s feelings.”
Gifts above $15 are given to charity. “I explain to patients that I’m not allowed to take such a large gift, but I’d love to give it to the hospital’s Rosenbaum Family House that provides patients and their relatives with lodging, or to the homeless shelter in Morgantown.”
Dr. Lyckholm, who serves on the ethics committee at J.W. Ruby Memorial Hospital, once was offered expensive tickets and said to the patient, “This is so incredibly thoughtful and kind, but I can’t accept them. I would like to give the tickets to a charity that can auction them off.”
She advises physicians to find out their institution’s policies. Many institutions have policies about what gifts their staff – whether physicians, nurses, or other health care professionals – can accept.
Passing the ‘smell test’
Accepting a large gift from a patient could potentially make it look like you might have exercised undue influence.
“That concern brings us to the third domain, which is very practical and all about appearances and perceptions,” Dr. Victoroff said.
He noted that there is “an inherent power differential between a physician and a patient. The very nature of the relationship can create a risk of ‘undue influence’ on the doctor’s part, even if it’s not apparent to the doctor.” For this reason, it’s necessary to be utterly transparent about how the bequest came about.
He suggests that if a patient informs you that he or she would like to leave money to you, it might be wise to suggest a meeting with the patient’s family, thus establishing some transparency.
It may not be possible to meet with the patient’s family for logistical reasons or because the patient would prefer not to involve their family in their estate planning. But in any case, it’s advisable to document any conversation in the patient’s chart, Dr. Victoroff advised.
“You should make a contemporaneous note that the patient initiated the suggestion and that you counseled them about the implications, no differently than you would with an interaction of a clinical nature,” he suggests. That way, if money has been left to you and is disputed, there’s a clear record that you didn’t solicit it or use any undue influence to bring it about.
He also recommended getting advice from a trusted colleague or a member of your institution’s ethics committee. “Taking time to get a second opinion about an ethical question is a safeguard, like having a chaperone in the room during an examination.”
Ultimately, “there is no human relationship without potential conflicts of interest. Our job is to manage those as best as we can, and sunlight is the best antidote to bad appearances,” Dr. Victoroff said.
A version of this article appeared on Medscape.com.
Michael Victoroff, MD, described the phone call he received from an attorney asking a thorny ethics question involving a patient’s gift to another physician. Dr. Victoroff, a past member of the ethics committee of the American Academy of Family Physicians, had definite thoughts about it.
“The attorney was representing the daughters of an elderly gentleman who had moved from the East Coast to Colorado to be closer to them,” said Dr. Victoroff, who teaches bioethics in the MBA program at the University of Denver and also practices at the University of Colorado School of Medicine.
“The father visited his new primary care physician frequently because he had multiple health issues.”
The patient was happy with the doctor’s medical care and over time that they developed a friendship. Dr. Victoroff emphasized that no sexual or romantic impropriety ever took place between the patient and his physician.
“But the social relationship went beyond the ordinary doctor-patient boundaries. The patient ultimately named the doctor as his health care proxy in the event that he became unable to make decisions regarding his care. He also mentioned he was going to leave her $100,000 in his will,” says Dr. Victoroff.
The physician did accept the role of proxy, “which raises a whole host of ethical issues,” says Dr. Victoroff. As it happened, she was never called upon to exercise that decision-making authority, since the patient died suddenly and was mentally competent at the time.
for her to accept such a substantial bequest from a patient, and they hired an attorney to contest the will.
No law against it
Dennis Hursh, attorney and managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, noted in an interview that, “the problem isn’t legal per se. Rather, the problem is an ethical one.”
Legally speaking, there’s no prohibition against receiving a bequest or other form of gift from a patient. “People are free to dispose of their estates in whatever way they see fit, and no law technically precludes a physician from accepting a bequest,” says Dr. Victoroff. “But this presupposes there is nothing improper going on, such as extortion, deception, coercion, or exercising undue influence.”
The issue of bequeathing money to their physician gained attention in a recent case that took place in Australia. Peter Alexakis, MD, received a whopping bequest of $24 million from a patient. The elderly patient had changed his will to name Dr. Alexakis as the sole beneficiary – after Dr. Alexakis had visited him at home 92 times during the preceding months. The original heirs filed a lawsuit in Australia’s Supreme Court against Dr. Alexakis, contesting the will.
The lawsuit was unsuccessful in court, but Dr. Alexakis was found guilty of malpractice by Australia’s Health Care Complaints Commission after being reported to the HCCC by the palliative care physicians who were treating the patient. They alleged that Dr. Alexakis had interfered with their care of the patient. The more serious allegation was that the doctor had engaged in a deliberate strategy to exploit the relationship for financial gain.
Dr. Alexakis was chastised by the HCCC for engaging in “obtuse” and “suspicious” behavior and for “blurring the boundaries of the doctor-patient relationship.”
There are three domains – legal, ethical, and practical – when it comes to accepting bequests or any gifts from patients, says Dr. Victoroff.
“[In] the legal domain, for example, if you receive a bequest from anyone, patient or otherwise, you have to know your local laws about estates and taxes and so forth and obey them,” he said.
Attorney Hursh pointed out that the Australian doctor wasn’t found guilty of wrongdoing in a court of law but rather of unethical conduct by the Australian medical licensing entity.
Patients giving gifts is often a part of a physician’s life
When Ian Schorr, MD, first started out in practice, he was surprised that patients began bringing him gifts of food to express gratitude for his care.
“I thought it was unethical to accept their gifts, so I turned them down and wouldn’t accept so much as a cookie,” Dr. Schorr, a now-retired ophthalmologist, told this news organization. “But that changed because my office staff told me that some patients were feeling disappointed and insulted. I realized that some people want to express appreciation in ways that go beyond a monetary payment.”
The next time he received a gift from a patient, he “accepted it gracefully.” And he wrote a thank you note, which he continued to do any time he received a gift from a patient.
Kenneth Prager, MD, professor of clinical medicine, director of clinical ethics and chairman of the Medical Ethics Committee at Columbia University Medical Center, New York, says, “I have literally received hundreds of gifts, the vast majority being tokens of patients’ appreciation,” he said. “I’ll get boxes of chocolate or cakes, or sometimes articles of clothing.”
Occasionally, Dr. Prager receives a “somewhat larger gift” – for example, two tickets to a baseball game. “To reject these gifts would be a slap in the face to the patient,” he says, but “where it gets more ethically cloudy is when a gift is very substantial.”
Dr. Prager has never been offered a “substantial” gift or bequest personally. “But a patient whose brother I cared for has indicated that she has left instructions in her will to endow an associate chair of ethics in my honor, and I didn’t decline that,” he said.
The AMA Code of Ethics confirms that accepting gifts offered “as an expression of gratitude or a reflection of the patient’s cultural tradition” can “enhance the patient-physician relationship.” But sometimes gifts “may signal psychological needs that require the physician’s attention.” Accepting such gifts is “likely to damage the patient-physician relationship.”
Potential damage to the therapeutic relationship applies to all physicians but especially for psychiatrists and mental health professionals. “There are more stringent ethical requirements when it comes to these disciplines, where gift-giving gets into the territory of transference or may have particular psychological meaning, and accepting the gift may muddy the therapeutic waters,” Dr. Victoroff said.
Impact on the patient’s family and on other patients
The AMA statement encourages physicians to be “sensitive to the gift’s value, relative to the patient’s or physician’s means.” Physicians should decline gifts that are “disproportionately or inappropriately large, or when the physician would be uncomfortable to have colleagues know the gift had been accepted.”
They should also decline a bequest from a patient if they have reason to believe that to accept it “would present an emotional or financial hardship to the patient’s family.”
“If Bill Gates were leaving $100,000 to his doctor, I imagine Melinda would be just fine,” Mr. Hursh said. “But under ordinary circumstances, if the patient’s family might feel the impact of the bequest, it would be unethical to accept it and could be grounds for revocation of the doctor’s license.”
The AMA statement also warns physicians that by offering a gift, some patients may be seeking to “secure or influence care or to secure preferential treatment,” which can “undermine physicians’ obligation to provide services fairly to all patients.”
For this reason, bequests are “sticky,” said Laurel Lyckholm, MD, professor of hematology and oncology at West Virginia University School of Medicine. In the case of institutions where patients or community members donate money, “we know whose names are on the plaques that hang on the hospital walls, so it’s a delicate balance. What if there’s only one bed or one ventilator? Will the wife of the donor get preferential treatment?”
Follow institutional policy
A “very small gift, such as a fruitcake, is fine,” says Dr. Lyckholm, author of an essay on accepting gifts from patients. She said there’s a dollar amount ($15) that her institution mandates, above which a gift – even food – is considered too expensive to accept. “I was a nurse before I became a physician, and people always tried to give us gifts because we were so close to the minute-by-minute care of the patients,” she said. “We were not allowed to accept money or anything lavish.”
But in the case of small gifts, “the risk-benefit analysis is that there’s much more risk not to take it and to hurt the patient’s feelings.”
Gifts above $15 are given to charity. “I explain to patients that I’m not allowed to take such a large gift, but I’d love to give it to the hospital’s Rosenbaum Family House that provides patients and their relatives with lodging, or to the homeless shelter in Morgantown.”
Dr. Lyckholm, who serves on the ethics committee at J.W. Ruby Memorial Hospital, once was offered expensive tickets and said to the patient, “This is so incredibly thoughtful and kind, but I can’t accept them. I would like to give the tickets to a charity that can auction them off.”
She advises physicians to find out their institution’s policies. Many institutions have policies about what gifts their staff – whether physicians, nurses, or other health care professionals – can accept.
Passing the ‘smell test’
Accepting a large gift from a patient could potentially make it look like you might have exercised undue influence.
“That concern brings us to the third domain, which is very practical and all about appearances and perceptions,” Dr. Victoroff said.
He noted that there is “an inherent power differential between a physician and a patient. The very nature of the relationship can create a risk of ‘undue influence’ on the doctor’s part, even if it’s not apparent to the doctor.” For this reason, it’s necessary to be utterly transparent about how the bequest came about.
He suggests that if a patient informs you that he or she would like to leave money to you, it might be wise to suggest a meeting with the patient’s family, thus establishing some transparency.
It may not be possible to meet with the patient’s family for logistical reasons or because the patient would prefer not to involve their family in their estate planning. But in any case, it’s advisable to document any conversation in the patient’s chart, Dr. Victoroff advised.
“You should make a contemporaneous note that the patient initiated the suggestion and that you counseled them about the implications, no differently than you would with an interaction of a clinical nature,” he suggests. That way, if money has been left to you and is disputed, there’s a clear record that you didn’t solicit it or use any undue influence to bring it about.
He also recommended getting advice from a trusted colleague or a member of your institution’s ethics committee. “Taking time to get a second opinion about an ethical question is a safeguard, like having a chaperone in the room during an examination.”
Ultimately, “there is no human relationship without potential conflicts of interest. Our job is to manage those as best as we can, and sunlight is the best antidote to bad appearances,” Dr. Victoroff said.
A version of this article appeared on Medscape.com.
Abdominal fat linked to lower brain volume in midlife
In a large study of healthy middle-aged adults, greater visceral and subcutaneous abdominal fat on abdominal MRI predicted brain atrophy on imaging, especially in women.
“The study shows that excess fat is bad for the brain and worse in women, including in Alzheimer’s disease risk regions,” lead author Cyrus Raji, MD, PhD, with the Mallinckrodt Institute of Radiology, Washington University, St. Louis, Mo., said in an interview.
The study was published online in the journal Aging and Disease
Modifiable risk factor
Multiple studies have suggested a connection between body fat accumulation and increased dementia risk. But few have examined the relationship between types of fat (visceral and subcutaneous) and brain volume.
For the new study, 10,000 healthy adults aged 20-80 years (mean age, 52.9 years; 53% men) underwent a short whole-body MRI protocol. Regression analyses of abdominal fat types and normalized brain volumes were evaluated, controlling for age and sex.
The research team found that higher amounts of both visceral and subcutaneous abdominal fat predicted lower total gray and white matter volume, as well as lower volume in the hippocampus, frontal cortex, and temporal, parietal, and occipital lobes.
“The findings are quite dramatic,” Dr. Raji told this news organization. “Overall, we found that both subcutaneous and visceral fat has similar levels of negative relationships with brain volumes.”
Women had a higher burden of brain atrophy with increased visceral fat than men. However, it’s difficult to place the sex differences in context because of the lack of prior work specifically investigating visceral fat, brain volume loss, and sex differences, the researchers caution.
They also note that while statistically significant relationships were observed between visceral fat levels and gray matter volume changes, their effect sizes were generally small.
“Thus, the statistical significance of this work is influenced by the large sample size and less so by large effect size in any given set of regions,” the investigators write.
Other limitations include the cross-sectional nature of the study, which precludes conclusions about causality. The analysis also did not account for other lifestyle factors such as physical activity, diet, and genetic variables.
The researchers call for further investigation “to better elucidate underlying mechanisms and discover possible interventions targeting abdominal fat reduction as a strategy to maintain brain health.”
‘Helpful addition to the literature’
In a comment, Claire Sexton, DPhil, Alzheimer’s Association senior director of scientific programs and outreach, noted that “previous studies have linked obesity with cognitive decline and increased risk of dementia. Rather than using BMI as a proxy for body fat, the current study examined visceral and subcutaneous fat directly using imaging techniques.”

Dr. Sexton, who was not associated with this study, said the finding that increased body fat was associated with reduced brain volumes suggests “a possible mechanism to explain the previously reported associations between obesity and cognition.”
“Though some degree of atrophy and brain shrinkage is common with old age, awareness of this association is important because reduced brain volume may be associated with problems with thinking, memory, and performing everyday tasks, and because rates of obesity continue to rise in the United States, along with obesity-related conditions including heart disease, stroke, type 2 diabetes and certain types of cancer,” she added.
“While a helpful addition to the literature, the study does have important limitations. As an observational study, it cannot establish whether higher levels of body fat directly causes reduced brain volumes,” Dr. Sexton cautioned.
In addition, the study did not take into account important related factors like physical activity and diet, which may influence any relationship between body fat and brain volumes, she noted. “Overall, it is not just one factor that is important to consider when considering risk for cognitive decline and dementia, but multiple factors.
“Obesity and the location of body fat must be considered in combination with one’s total lived experience and habits, including physical activity, education, head injury, sleep, mental health, and the health of your heart/cardiovascular system and other key bodily systems,” Dr. Sexton said.
The Alzheimer’s Association is leading a 2-year clinical trial known as U.S. POINTER to see whether combining physical activity, healthy nutrition, social and intellectual challenges, and improved self-management of medical conditions can protect cognitive function in older adults who are at increased risk for cognitive decline.
This work was supported in part by Providence St. Joseph Health in Seattle; Saint John’s Health Center Foundation; Pacific Neuroscience Institute and Foundation; Will and Cary Singleton; and the McLoughlin family. Dr. Raji is a consultant for Brainreader, Apollo Health, Voxelwise, Neurevolution, Pacific Neuroscience Institute Foundation, and Icometrix. Dr. Sexton reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large study of healthy middle-aged adults, greater visceral and subcutaneous abdominal fat on abdominal MRI predicted brain atrophy on imaging, especially in women.
“The study shows that excess fat is bad for the brain and worse in women, including in Alzheimer’s disease risk regions,” lead author Cyrus Raji, MD, PhD, with the Mallinckrodt Institute of Radiology, Washington University, St. Louis, Mo., said in an interview.
The study was published online in the journal Aging and Disease
Modifiable risk factor
Multiple studies have suggested a connection between body fat accumulation and increased dementia risk. But few have examined the relationship between types of fat (visceral and subcutaneous) and brain volume.
For the new study, 10,000 healthy adults aged 20-80 years (mean age, 52.9 years; 53% men) underwent a short whole-body MRI protocol. Regression analyses of abdominal fat types and normalized brain volumes were evaluated, controlling for age and sex.
The research team found that higher amounts of both visceral and subcutaneous abdominal fat predicted lower total gray and white matter volume, as well as lower volume in the hippocampus, frontal cortex, and temporal, parietal, and occipital lobes.
“The findings are quite dramatic,” Dr. Raji told this news organization. “Overall, we found that both subcutaneous and visceral fat has similar levels of negative relationships with brain volumes.”
Women had a higher burden of brain atrophy with increased visceral fat than men. However, it’s difficult to place the sex differences in context because of the lack of prior work specifically investigating visceral fat, brain volume loss, and sex differences, the researchers caution.
They also note that while statistically significant relationships were observed between visceral fat levels and gray matter volume changes, their effect sizes were generally small.
“Thus, the statistical significance of this work is influenced by the large sample size and less so by large effect size in any given set of regions,” the investigators write.
Other limitations include the cross-sectional nature of the study, which precludes conclusions about causality. The analysis also did not account for other lifestyle factors such as physical activity, diet, and genetic variables.
The researchers call for further investigation “to better elucidate underlying mechanisms and discover possible interventions targeting abdominal fat reduction as a strategy to maintain brain health.”
‘Helpful addition to the literature’
In a comment, Claire Sexton, DPhil, Alzheimer’s Association senior director of scientific programs and outreach, noted that “previous studies have linked obesity with cognitive decline and increased risk of dementia. Rather than using BMI as a proxy for body fat, the current study examined visceral and subcutaneous fat directly using imaging techniques.”
Dr. Sexton, who was not associated with this study, said the finding that increased body fat was associated with reduced brain volumes suggests “a possible mechanism to explain the previously reported associations between obesity and cognition.”
“Though some degree of atrophy and brain shrinkage is common with old age, awareness of this association is important because reduced brain volume may be associated with problems with thinking, memory, and performing everyday tasks, and because rates of obesity continue to rise in the United States, along with obesity-related conditions including heart disease, stroke, type 2 diabetes and certain types of cancer,” she added.
“While a helpful addition to the literature, the study does have important limitations. As an observational study, it cannot establish whether higher levels of body fat directly causes reduced brain volumes,” Dr. Sexton cautioned.
In addition, the study did not take into account important related factors like physical activity and diet, which may influence any relationship between body fat and brain volumes, she noted. “Overall, it is not just one factor that is important to consider when considering risk for cognitive decline and dementia, but multiple factors.
“Obesity and the location of body fat must be considered in combination with one’s total lived experience and habits, including physical activity, education, head injury, sleep, mental health, and the health of your heart/cardiovascular system and other key bodily systems,” Dr. Sexton said.
The Alzheimer’s Association is leading a 2-year clinical trial known as U.S. POINTER to see whether combining physical activity, healthy nutrition, social and intellectual challenges, and improved self-management of medical conditions can protect cognitive function in older adults who are at increased risk for cognitive decline.
This work was supported in part by Providence St. Joseph Health in Seattle; Saint John’s Health Center Foundation; Pacific Neuroscience Institute and Foundation; Will and Cary Singleton; and the McLoughlin family. Dr. Raji is a consultant for Brainreader, Apollo Health, Voxelwise, Neurevolution, Pacific Neuroscience Institute Foundation, and Icometrix. Dr. Sexton reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large study of healthy middle-aged adults, greater visceral and subcutaneous abdominal fat on abdominal MRI predicted brain atrophy on imaging, especially in women.
“The study shows that excess fat is bad for the brain and worse in women, including in Alzheimer’s disease risk regions,” lead author Cyrus Raji, MD, PhD, with the Mallinckrodt Institute of Radiology, Washington University, St. Louis, Mo., said in an interview.
The study was published online in the journal Aging and Disease
Modifiable risk factor
Multiple studies have suggested a connection between body fat accumulation and increased dementia risk. But few have examined the relationship between types of fat (visceral and subcutaneous) and brain volume.
For the new study, 10,000 healthy adults aged 20-80 years (mean age, 52.9 years; 53% men) underwent a short whole-body MRI protocol. Regression analyses of abdominal fat types and normalized brain volumes were evaluated, controlling for age and sex.
The research team found that higher amounts of both visceral and subcutaneous abdominal fat predicted lower total gray and white matter volume, as well as lower volume in the hippocampus, frontal cortex, and temporal, parietal, and occipital lobes.
“The findings are quite dramatic,” Dr. Raji told this news organization. “Overall, we found that both subcutaneous and visceral fat has similar levels of negative relationships with brain volumes.”
Women had a higher burden of brain atrophy with increased visceral fat than men. However, it’s difficult to place the sex differences in context because of the lack of prior work specifically investigating visceral fat, brain volume loss, and sex differences, the researchers caution.
They also note that while statistically significant relationships were observed between visceral fat levels and gray matter volume changes, their effect sizes were generally small.
“Thus, the statistical significance of this work is influenced by the large sample size and less so by large effect size in any given set of regions,” the investigators write.
Other limitations include the cross-sectional nature of the study, which precludes conclusions about causality. The analysis also did not account for other lifestyle factors such as physical activity, diet, and genetic variables.
The researchers call for further investigation “to better elucidate underlying mechanisms and discover possible interventions targeting abdominal fat reduction as a strategy to maintain brain health.”
‘Helpful addition to the literature’
In a comment, Claire Sexton, DPhil, Alzheimer’s Association senior director of scientific programs and outreach, noted that “previous studies have linked obesity with cognitive decline and increased risk of dementia. Rather than using BMI as a proxy for body fat, the current study examined visceral and subcutaneous fat directly using imaging techniques.”
Dr. Sexton, who was not associated with this study, said the finding that increased body fat was associated with reduced brain volumes suggests “a possible mechanism to explain the previously reported associations between obesity and cognition.”
“Though some degree of atrophy and brain shrinkage is common with old age, awareness of this association is important because reduced brain volume may be associated with problems with thinking, memory, and performing everyday tasks, and because rates of obesity continue to rise in the United States, along with obesity-related conditions including heart disease, stroke, type 2 diabetes and certain types of cancer,” she added.
“While a helpful addition to the literature, the study does have important limitations. As an observational study, it cannot establish whether higher levels of body fat directly causes reduced brain volumes,” Dr. Sexton cautioned.
In addition, the study did not take into account important related factors like physical activity and diet, which may influence any relationship between body fat and brain volumes, she noted. “Overall, it is not just one factor that is important to consider when considering risk for cognitive decline and dementia, but multiple factors.
“Obesity and the location of body fat must be considered in combination with one’s total lived experience and habits, including physical activity, education, head injury, sleep, mental health, and the health of your heart/cardiovascular system and other key bodily systems,” Dr. Sexton said.
The Alzheimer’s Association is leading a 2-year clinical trial known as U.S. POINTER to see whether combining physical activity, healthy nutrition, social and intellectual challenges, and improved self-management of medical conditions can protect cognitive function in older adults who are at increased risk for cognitive decline.
This work was supported in part by Providence St. Joseph Health in Seattle; Saint John’s Health Center Foundation; Pacific Neuroscience Institute and Foundation; Will and Cary Singleton; and the McLoughlin family. Dr. Raji is a consultant for Brainreader, Apollo Health, Voxelwise, Neurevolution, Pacific Neuroscience Institute Foundation, and Icometrix. Dr. Sexton reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AGING AND DISEASES
The magic of music
I’m really going to miss Jimmy Buffett.
I’ve liked his music as far back as I can remember, and was lucky enough to see him in person in the mid-90s.
I’ve written about music before, but its affect on us never fails to amaze me. Songs can be background noise conducive to getting things done. They can also be in the foreground, serving as a mental vacation (or accompanying a real one). They can transport you to another place, briefly clearing your head from the daily goings-on around you. Even if it’s just during the drive home, it’s a welcome escape to a virtual beach and tropical drink.
Songs can bring back memories of certain events or people that we link them to. My dad loved anything by Neil Diamond, and nothing brings back thoughts of Dad more than when my iTunes randomly picks “I Am ... I Said.” Or John Williams’ Star Wars theme, taking me back to the summer of 1977 when I sat, spellbound, by this incredible movie whose magic is still going strong two generations later.
It’s amazing how our brain tries to make music out of nothing. Even in silence we have ear worms, the songs stuck in our head for hours to days (recently I’ve had “I Sing the Body Electric” from the 1980 movie Fame playing in there).
My office is over an MRI scanner, so I can always hear the chiller pumps softly running in the background. Sometimes my brain will turn their rhythmic chirping into a song, altering the pace of the song to fit them. The soft clicking of the ceiling fan, in my home office, does the same thing (for some reason my brain usually tries to fit “Yellow Submarine” to that one, no idea why).
Music is a part of that mysterious essence that makes us human. It touches all of us in some way, which varies between people, songs, and artists.
Jimmy Buffet’s music has a vacation vibe. Songs of the Caribbean & Keys, beaches, bars, boats, and tropical drinks. The 4:12 running time of his most well-known song, “Margaritaville,” gives a brief respite from my day when it comes on.
He passes into the beyond, to the sadness of his family, friends, and fans. But, unlike people, music can be immortal, and so he lives on through his creations. Like, Bach, Lennon, Bowie, Joplin, Sousa, and too many others to count, his work – and the enjoyment we get from it – are a gift left behind for the future.
Tight lines, Jimmy.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m really going to miss Jimmy Buffett.
I’ve liked his music as far back as I can remember, and was lucky enough to see him in person in the mid-90s.
I’ve written about music before, but its affect on us never fails to amaze me. Songs can be background noise conducive to getting things done. They can also be in the foreground, serving as a mental vacation (or accompanying a real one). They can transport you to another place, briefly clearing your head from the daily goings-on around you. Even if it’s just during the drive home, it’s a welcome escape to a virtual beach and tropical drink.
Songs can bring back memories of certain events or people that we link them to. My dad loved anything by Neil Diamond, and nothing brings back thoughts of Dad more than when my iTunes randomly picks “I Am ... I Said.” Or John Williams’ Star Wars theme, taking me back to the summer of 1977 when I sat, spellbound, by this incredible movie whose magic is still going strong two generations later.
It’s amazing how our brain tries to make music out of nothing. Even in silence we have ear worms, the songs stuck in our head for hours to days (recently I’ve had “I Sing the Body Electric” from the 1980 movie Fame playing in there).
My office is over an MRI scanner, so I can always hear the chiller pumps softly running in the background. Sometimes my brain will turn their rhythmic chirping into a song, altering the pace of the song to fit them. The soft clicking of the ceiling fan, in my home office, does the same thing (for some reason my brain usually tries to fit “Yellow Submarine” to that one, no idea why).
Music is a part of that mysterious essence that makes us human. It touches all of us in some way, which varies between people, songs, and artists.
Jimmy Buffet’s music has a vacation vibe. Songs of the Caribbean & Keys, beaches, bars, boats, and tropical drinks. The 4:12 running time of his most well-known song, “Margaritaville,” gives a brief respite from my day when it comes on.
He passes into the beyond, to the sadness of his family, friends, and fans. But, unlike people, music can be immortal, and so he lives on through his creations. Like, Bach, Lennon, Bowie, Joplin, Sousa, and too many others to count, his work – and the enjoyment we get from it – are a gift left behind for the future.
Tight lines, Jimmy.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m really going to miss Jimmy Buffett.
I’ve liked his music as far back as I can remember, and was lucky enough to see him in person in the mid-90s.
I’ve written about music before, but its affect on us never fails to amaze me. Songs can be background noise conducive to getting things done. They can also be in the foreground, serving as a mental vacation (or accompanying a real one). They can transport you to another place, briefly clearing your head from the daily goings-on around you. Even if it’s just during the drive home, it’s a welcome escape to a virtual beach and tropical drink.
Songs can bring back memories of certain events or people that we link them to. My dad loved anything by Neil Diamond, and nothing brings back thoughts of Dad more than when my iTunes randomly picks “I Am ... I Said.” Or John Williams’ Star Wars theme, taking me back to the summer of 1977 when I sat, spellbound, by this incredible movie whose magic is still going strong two generations later.
It’s amazing how our brain tries to make music out of nothing. Even in silence we have ear worms, the songs stuck in our head for hours to days (recently I’ve had “I Sing the Body Electric” from the 1980 movie Fame playing in there).
My office is over an MRI scanner, so I can always hear the chiller pumps softly running in the background. Sometimes my brain will turn their rhythmic chirping into a song, altering the pace of the song to fit them. The soft clicking of the ceiling fan, in my home office, does the same thing (for some reason my brain usually tries to fit “Yellow Submarine” to that one, no idea why).
Music is a part of that mysterious essence that makes us human. It touches all of us in some way, which varies between people, songs, and artists.
Jimmy Buffet’s music has a vacation vibe. Songs of the Caribbean & Keys, beaches, bars, boats, and tropical drinks. The 4:12 running time of his most well-known song, “Margaritaville,” gives a brief respite from my day when it comes on.
He passes into the beyond, to the sadness of his family, friends, and fans. But, unlike people, music can be immortal, and so he lives on through his creations. Like, Bach, Lennon, Bowie, Joplin, Sousa, and too many others to count, his work – and the enjoyment we get from it – are a gift left behind for the future.
Tight lines, Jimmy.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
MS drugs during pregnancy show no safety signals
AURORA, COLO. – Several drugs for multiple sclerosis (MS) that are contraindicated during pregnancy nevertheless have not shown concerning safety signals in a series of small studies presented as posters at the annual meeting of the Consortium of Multiple Sclerosis Centers. The industry-sponsored research included an assessment of pregnancy and infant outcomes for cladribine, ocrelizumab, ofatumumab, and ozanimod, all of which are not recommended during pregnancy based primarily on minimal data that suggests, but does not confirm, possible teratogenicity.
“When these new medications hit the market, maternal-fetal medicine physicians and obstetricians are left with very scant data on how to counsel patients, and it’s often based on theory, case reports, or animal studies,” said Teodora Kolarova, MD, a maternal-fetal medicine physician at the University of Washington, Seattle, who was not involved in any of the research. “Although these sample sizes seem small, the population they are sampling from – patients with MS who take immunomodulators who then experience a pregnancy – is much smaller than all pregnant patients.”
Taken together, the findings suggest no increased risk of miscarriage or congenital malformation, compared with baseline risk, Dr. Kolarova said.
“As a whole, these studies are overall reassuring with, of course, some caveats, including timing of medication exposure, limited sample size, and limited outcome data,” Dr. Kolarova said. She noted that embryonic organ formation is complete by 10 weeks gestation, by which time an unplanned pregnancy may not have been recognized yet. “In the subset of patients in the studies that were exposed during the first trimester, there was no increase in congenital malformations from a baseline risk of about 2%-3% in the general population, which is helpful for patient counseling.”
Counseling during the childbearing years
That kind of counseling is important yet absent for many people capable of pregnancy, suggests separate research also presented at the conference by Suma Shah, MD, an associate professor of neurology at Duke University, Durham, N.C. Dr. Shah gave 13-question surveys to female MS patients of all ages at her institution and presented an analysis of data from 38 completed surveys. Among those taking disease-modifying therapies, their medications included ocrelizumab, rituximab, teriflunomide, fingolimod, fumarates, interferons, natalizumab, and cladribine.
“MS disproportionately impacts women among 20 to 40 years, and that’s a really big part of their childbearing years when there are big decisions being made about whether they’re going to choose to grow family or not,” said Dr. Shah. The average age of those who completed the survey was 44. Dr. Shah noted that a lot of research has looked at the safety of older disease-modifying agents in pregnancy, but that information doesn’t appear to be filtering down to patients. “What I really wanted to look at is what do our parent patients understand about whether or not they can even think about pregnancy – and there’s a lot of work to be done.”
Just under a third of survey respondents said they did not have as many children as they would like, and a quarter said they were told they couldn’t have children if they had a diagnosis of MS.
“That was a little heartbreaking to hear because that’s not the truth,” Dr. Shah said. She said it’s necessary to have a more detailed conversation looking at tailored decisions for patients. “Both of those things – patients not being able to grow their family to the number that they desire, and not feeling like they can grow a family – I would think in 2023 we would have come farther than that, and there’s still a lot of room there to improve.”
She advised clinicians not to assume that MS patients know what their options are regarding family planning. “There’s still a lot of room for conversations,” she said. She also explicitly recommends discussing family planning and pregnancy planning with every patient, no matter their gender, early and often.
Cladribine shows no miscarriage, malformations
Dr. Kolarova noted that one of the studies, on cladribine, had a fairly robust sample size with its 180 pregnancy exposures. In that study, led by Kerstin Hellwig, MD, of Ruhr University in Bochum, Germany, data came from the global surveillance program MAPLE-MS, established to assess cladribine effects on pregnancy and infant outcomes. The researchers analyzed data from 76 mothers and 9 fathers who, at any time from 2017 to 2022, were taking cladribine during pregnancy or up to 6 months before pregnancy. Outcomes included live birth, miscarriage, stillbirth, elective abortion, ectopic pregnancy, and major congenital anomalies.
Just over half the mothers (53.9%) were exposed before pregnancy, and about a quarter (26.3%) were exposed during the first trimester. The timing was unknown for most of the other mothers (18.4%). Among the fathers, two-thirds (66.7%) were exposed before pregnancy, and one-third had unknown timing.
Among the 180 pregnancies in the maternal cohort, 42.2% had known outcomes. Nearly half the women (48.7%) taking cladribine had live births, 28.9% had elective abortions, and 21.1% had miscarriages. Only 9 of the 22 pregnancies in the paternal cohort had known outcomes, which included 88.9% live births and 11.1% miscarriages. None of the pregnancies resulted in stillbirth or in a live birth with major congenital anomalies.
”Robust conclusions cannot be made about the risks of adverse pregnancy outcomes with cladribine tablets, but no increase has been signaled thus far,” the researchers reported. ”It is necessary to counsel patients to prevent pregnancy and to use effective contraception during cladribine tablets intake and for at least 6 months after the last cladribine tablet intake in each treatment year.”
Emily Evans, MD, MBE, medical director at U.S. Neurology and Immunology in Rockland, Mass., speaking on behalf of the findings, said they were fairly encouraging.
“Of course, we don’t encourage patients to get pregnant within 6 months of their last dose of cladribine tablets,” Dr. Evans said, but “within those individuals who have gotten pregnant within 6 months of their last dose of cladribine, or who have fathered a child within 6 months of their last dose of cladribine tablets, we’re seeing overall encouraging outcomes. We’re specifically not seeing any differences in the rates of spontaneous abortions, and we’re not seeing any differences in the rates of congenital malformations.”
Ocrelizumab and ofatumumab: No infections so far
Current recommendations for ocrelizumab are to avoid pregnancy for 6 months after the last infusion and stop any breastfeeding during therapy. Yet these recommendations are only because of insufficient data rather than evidence of risk, according to Lana Zhovtis Ryerson, MD, of the NYU Multiple Sclerosis Comprehensive Care Center in New York. She and her colleagues identified all women of childbearing age who had received ocrelizumab within 1 year of pregnancy at their NYU institution. A retrospective chart review found 18 women, with an average age of 35, an average 11 years of an MS diagnosis, and an average 11 months taking ocrelizumab.
Among the 18 pregnancies, four women had a first trimester miscarriage, one had a second trimester miscarriage, and one had an abortion. The miscarriage rate could have been partly influenced by the older maternal population, the authors noted. Of the remaining 12 live births, one infant was premature at 34 weeks, and three infants stayed in NICU but were discharged within 2 weeks.
One patient experienced an MS relapse postpartum, despite receiving ocrelizumab within 45 days of delivery. Of the 16 women who agreed to participate in a Pregnancy Assessment Monitoring System (PRAMS) developed by the CDC, two women chose to breastfeed, and seven said their neurologist recommended against breastfeeding. None of the children’s pediatricians advised delaying vaccinations.
“This small sample observational study has not identified a potential additional risk with ocrelizumab for an adverse pregnancy outcome,” the authors concluded, but they added that ongoing studies, MINORE and SOPRANINO, can help guide future recommendations.
Though still limited, slightly more data exists on ofatumumab during pregnancy, including transient B-cell depletion and lymphopenia in infants whose mothers received anti-CD20 antibodies during pregnancy. However, research has found minimal IgG transfer in the first trimester, though it begins rising in the second trimester, and in utero ofatumumab exposure did not lead to any maternal toxicity or adverse prenatal or postnatal developmental effects in cynomolgus monkeys.
Riley Love, MD, of the University of California, San Francisco, Weill Institute for Neuroscience, and her colleagues both prospectively and retrospectively examined pregnancy and infant outcomes for up to 1 year post partum in women with MS who took ofatumumab during pregnancy or in the 6 months leading up to pregnancy. Their population included 104 prospective cases, most of which (84%) included first trimester exposure, and 14 retrospective cases. One in five of the prospective cases occurred during a clinical trial, while the remaining 80% occurred in postmarketing surveillance.
The prospectively followed women were an average 32 years old and were an average 7 weeks pregnant at the time of reporting. Among the 106 fetuses (including two twin pregnancies), only 30 outcomes had data at the cutoff time, including 16 live births, 9 abortions, and 5 miscarriages. None of the live births had congenital anomalies or serious infections. Another 30 pregnancies were lost to follow-up, and 46 were ongoing.
In the 14 retrospective cases, 57% of women were exposed in the first trimester, and 43% were exposed leading up to pregnancy. Half the cases occurred during clinical trials, and half in postmarketing surveillance. The women were an average 32 years old and were an average 10 weeks pregnant at reporting. Among the 14 pregnancies, nine were miscarriages, one was aborted, and four were born live with no congenital anomalies.
The authors did not draw any conclusions from the findings; they cited too little data and an ongoing study by Novartis to investigate ofatumumab in pregnancy.
“Therapies such as ofatumumab and ocrelizumab can lead to increased risk of infection due to transient B-cell depletion in neonates, but the two studies looking at this did not demonstrate increased infectious morbidity for these infants,” Dr. Kolarova said. “As with all poster presentations, I look forward to reading the full papers once they are published as they will often include a lot more detail about when during pregnancy medication exposure occurred and more detailed outcome data that was assessed.”
Ozanimod outcomes within general population’s ‘expected ranges’
The final study looked at outcomes of pregnancies in people taking ozanimod and in the partners of people taking ozanimod in a clinical trial setting. The findings show low rates of miscarriage, preterm birth, and congenital anomalies that the authors concluded were within the typical range expected for the general population.
“While pregnancy should be avoided when taking and for 3 months after stopping ozanimod to allow for drug elimination, there is no evidence to date of increased occurrence of adverse pregnancy outcomes with ozanimod exposure during early pregnancy,” wrote Anthony Krakovich, of Bristol Myers Squibb in Princeton, N.J., and his associates.
Ozanimod is an oral sphingosine 1-phosphate (S1P) receptor 1 and 5 modulator whose therapeutic mechanism is not fully understood “but may involve the reduction of lymphocyte migration into the central nervous system and intestine,” the authors wrote. S1P receptors are involved in vascular formation during embryogenesis, and animal studies in rats and rabbits have shown toxicity to the embryo and fetus from S1P receptor modulators, including death and malformations. S1P receptor modulator labels therefore note potential fetal risk and the need for effective contraception while taking the drug.
The study prospectively tracked clinical trial participants taking ozanimod as healthy volunteers or for relapsing MS, ulcerative colitis, or Crohn’s disease. Most of the participants who became pregnant (73%) had relapsing MS, while 18% had ulcerative colitis and 8% had Crohn’s disease.
In female patients receiving ozanimod, 78 pregnancies resulted in 12 miscarriages (including one twin), 15 abortions, and 42 live births, with 6 pregnancies ongoing at the time of reporting and no data available for the remaining 4 pregnancies. Among the 42 live births, 4 were premature but otherwise healthy, 1 had a duplex kidney, and the other 37 infants were typical with no apparent health concerns. These rates of miscarriage, preterm birth, and congenital anomalies were within the expected ranges for the general population, the researchers wrote.
The researchers also assessed pregnancy outcomes for partners of male participants taking ozanimod. The 29 partner pregnancies resulted in 21 live births and one miscarriage, with one pregnancy ongoing and no information available for the other seven. The live births included 5 premature infants (including twins), 13 typical and healthy infants, 1 with Hirschsprung’s disease, 1 with a congenital hydrocele, and 1 with a partial atrioventricular septal defect. Again, the researchers concluded that these rates were within the typical range for the general population and that “no teratogenicity was observed.”
“We often encourage patients with MS, regardless of disease activity and therapies, to seek preconception evaluations with Maternal-Fetal Medicine and their neurologists in order to make plans for pregnancy and postpartum care,” Dr. Kolarova said. “That being said, access to subspecialized health care is not available to all, and pregnancy prior to such consultation does occur. These studies provide novel information that we have not had access to in the past and can improve patient counseling regarding their risks and options.”
The study on cladribine was funded by Merck KGaA, at which two authors are employed. Dr. Hellwig reported consulting, speaker, and/or research support from Bayer, Biogen, Teva, Novartis, Roche, Sanofi, Schering Healthcare, Serono, and Merck, and one author is a former employee of EMD Serono. The study on ocrelizumab was funded by Genentech. Dr. Zhovtis Ryerson reported personal fees from Biogen, Genentech, and Novartis, and research grants from Biogen, Genentech, and CMSC. The other authors had no disclosures. The study on ofatumumab was funded by Novartis. Dr. Bove has received research funds from Biogen, Novartis, and Roche Genentech, and consulting fees from EMD Serono, Horizon, Janssen, and TG Therapeutics; she has an ownership interest in Global Consult MD. Five authors are Novartis employees. Her coauthors, including Dr. Hellwig, reported advisory, consulting, research, speaking, or traveling fees from Alexion, Bayer, Biogen, Celgene BMS, EMD Serono, Horizon, Janssen, Lundbeck, Merck, Pfizer, Roche Genentech, Sanofi Genzyme, Schering Healthcare, Teva, TG Therapeutics, and Novartis. The study on ozanimod was funded by Bristol Myers Squibb. Dr. Krakovich and another author are employees and/or shareholders of Bristol Myers Squibb. The other authors reported consulting, speaking, advisory board, and/or research fees from AbbVie, Almirall, Arena, Biogen, Boehringer Ingelhei, Celgene, Celltrion, EXCEMED, Falk Benelux, Ferring, Forward Pharma, Genentech, Genzyme, Gilead, Janssen, Lilly, Merck, Novartis, Ono Pharma, Pfizer, Prometheus Labs, Protagonist, Roche, Sanofi, Synthon, Takeda, and Teva. Dr. Kolarova had no disclosures. Dr. Shah has received research support from Biogen and VeraSci.
AURORA, COLO. – Several drugs for multiple sclerosis (MS) that are contraindicated during pregnancy nevertheless have not shown concerning safety signals in a series of small studies presented as posters at the annual meeting of the Consortium of Multiple Sclerosis Centers. The industry-sponsored research included an assessment of pregnancy and infant outcomes for cladribine, ocrelizumab, ofatumumab, and ozanimod, all of which are not recommended during pregnancy based primarily on minimal data that suggests, but does not confirm, possible teratogenicity.
“When these new medications hit the market, maternal-fetal medicine physicians and obstetricians are left with very scant data on how to counsel patients, and it’s often based on theory, case reports, or animal studies,” said Teodora Kolarova, MD, a maternal-fetal medicine physician at the University of Washington, Seattle, who was not involved in any of the research. “Although these sample sizes seem small, the population they are sampling from – patients with MS who take immunomodulators who then experience a pregnancy – is much smaller than all pregnant patients.”
Taken together, the findings suggest no increased risk of miscarriage or congenital malformation, compared with baseline risk, Dr. Kolarova said.
“As a whole, these studies are overall reassuring with, of course, some caveats, including timing of medication exposure, limited sample size, and limited outcome data,” Dr. Kolarova said. She noted that embryonic organ formation is complete by 10 weeks gestation, by which time an unplanned pregnancy may not have been recognized yet. “In the subset of patients in the studies that were exposed during the first trimester, there was no increase in congenital malformations from a baseline risk of about 2%-3% in the general population, which is helpful for patient counseling.”
Counseling during the childbearing years
That kind of counseling is important yet absent for many people capable of pregnancy, suggests separate research also presented at the conference by Suma Shah, MD, an associate professor of neurology at Duke University, Durham, N.C. Dr. Shah gave 13-question surveys to female MS patients of all ages at her institution and presented an analysis of data from 38 completed surveys. Among those taking disease-modifying therapies, their medications included ocrelizumab, rituximab, teriflunomide, fingolimod, fumarates, interferons, natalizumab, and cladribine.
“MS disproportionately impacts women among 20 to 40 years, and that’s a really big part of their childbearing years when there are big decisions being made about whether they’re going to choose to grow family or not,” said Dr. Shah. The average age of those who completed the survey was 44. Dr. Shah noted that a lot of research has looked at the safety of older disease-modifying agents in pregnancy, but that information doesn’t appear to be filtering down to patients. “What I really wanted to look at is what do our parent patients understand about whether or not they can even think about pregnancy – and there’s a lot of work to be done.”
Just under a third of survey respondents said they did not have as many children as they would like, and a quarter said they were told they couldn’t have children if they had a diagnosis of MS.
“That was a little heartbreaking to hear because that’s not the truth,” Dr. Shah said. She said it’s necessary to have a more detailed conversation looking at tailored decisions for patients. “Both of those things – patients not being able to grow their family to the number that they desire, and not feeling like they can grow a family – I would think in 2023 we would have come farther than that, and there’s still a lot of room there to improve.”
She advised clinicians not to assume that MS patients know what their options are regarding family planning. “There’s still a lot of room for conversations,” she said. She also explicitly recommends discussing family planning and pregnancy planning with every patient, no matter their gender, early and often.
Cladribine shows no miscarriage, malformations
Dr. Kolarova noted that one of the studies, on cladribine, had a fairly robust sample size with its 180 pregnancy exposures. In that study, led by Kerstin Hellwig, MD, of Ruhr University in Bochum, Germany, data came from the global surveillance program MAPLE-MS, established to assess cladribine effects on pregnancy and infant outcomes. The researchers analyzed data from 76 mothers and 9 fathers who, at any time from 2017 to 2022, were taking cladribine during pregnancy or up to 6 months before pregnancy. Outcomes included live birth, miscarriage, stillbirth, elective abortion, ectopic pregnancy, and major congenital anomalies.
Just over half the mothers (53.9%) were exposed before pregnancy, and about a quarter (26.3%) were exposed during the first trimester. The timing was unknown for most of the other mothers (18.4%). Among the fathers, two-thirds (66.7%) were exposed before pregnancy, and one-third had unknown timing.
Among the 180 pregnancies in the maternal cohort, 42.2% had known outcomes. Nearly half the women (48.7%) taking cladribine had live births, 28.9% had elective abortions, and 21.1% had miscarriages. Only 9 of the 22 pregnancies in the paternal cohort had known outcomes, which included 88.9% live births and 11.1% miscarriages. None of the pregnancies resulted in stillbirth or in a live birth with major congenital anomalies.
”Robust conclusions cannot be made about the risks of adverse pregnancy outcomes with cladribine tablets, but no increase has been signaled thus far,” the researchers reported. ”It is necessary to counsel patients to prevent pregnancy and to use effective contraception during cladribine tablets intake and for at least 6 months after the last cladribine tablet intake in each treatment year.”
Emily Evans, MD, MBE, medical director at U.S. Neurology and Immunology in Rockland, Mass., speaking on behalf of the findings, said they were fairly encouraging.
“Of course, we don’t encourage patients to get pregnant within 6 months of their last dose of cladribine tablets,” Dr. Evans said, but “within those individuals who have gotten pregnant within 6 months of their last dose of cladribine, or who have fathered a child within 6 months of their last dose of cladribine tablets, we’re seeing overall encouraging outcomes. We’re specifically not seeing any differences in the rates of spontaneous abortions, and we’re not seeing any differences in the rates of congenital malformations.”
Ocrelizumab and ofatumumab: No infections so far
Current recommendations for ocrelizumab are to avoid pregnancy for 6 months after the last infusion and stop any breastfeeding during therapy. Yet these recommendations are only because of insufficient data rather than evidence of risk, according to Lana Zhovtis Ryerson, MD, of the NYU Multiple Sclerosis Comprehensive Care Center in New York. She and her colleagues identified all women of childbearing age who had received ocrelizumab within 1 year of pregnancy at their NYU institution. A retrospective chart review found 18 women, with an average age of 35, an average 11 years of an MS diagnosis, and an average 11 months taking ocrelizumab.
Among the 18 pregnancies, four women had a first trimester miscarriage, one had a second trimester miscarriage, and one had an abortion. The miscarriage rate could have been partly influenced by the older maternal population, the authors noted. Of the remaining 12 live births, one infant was premature at 34 weeks, and three infants stayed in NICU but were discharged within 2 weeks.
One patient experienced an MS relapse postpartum, despite receiving ocrelizumab within 45 days of delivery. Of the 16 women who agreed to participate in a Pregnancy Assessment Monitoring System (PRAMS) developed by the CDC, two women chose to breastfeed, and seven said their neurologist recommended against breastfeeding. None of the children’s pediatricians advised delaying vaccinations.
“This small sample observational study has not identified a potential additional risk with ocrelizumab for an adverse pregnancy outcome,” the authors concluded, but they added that ongoing studies, MINORE and SOPRANINO, can help guide future recommendations.
Though still limited, slightly more data exists on ofatumumab during pregnancy, including transient B-cell depletion and lymphopenia in infants whose mothers received anti-CD20 antibodies during pregnancy. However, research has found minimal IgG transfer in the first trimester, though it begins rising in the second trimester, and in utero ofatumumab exposure did not lead to any maternal toxicity or adverse prenatal or postnatal developmental effects in cynomolgus monkeys.
Riley Love, MD, of the University of California, San Francisco, Weill Institute for Neuroscience, and her colleagues both prospectively and retrospectively examined pregnancy and infant outcomes for up to 1 year post partum in women with MS who took ofatumumab during pregnancy or in the 6 months leading up to pregnancy. Their population included 104 prospective cases, most of which (84%) included first trimester exposure, and 14 retrospective cases. One in five of the prospective cases occurred during a clinical trial, while the remaining 80% occurred in postmarketing surveillance.
The prospectively followed women were an average 32 years old and were an average 7 weeks pregnant at the time of reporting. Among the 106 fetuses (including two twin pregnancies), only 30 outcomes had data at the cutoff time, including 16 live births, 9 abortions, and 5 miscarriages. None of the live births had congenital anomalies or serious infections. Another 30 pregnancies were lost to follow-up, and 46 were ongoing.
In the 14 retrospective cases, 57% of women were exposed in the first trimester, and 43% were exposed leading up to pregnancy. Half the cases occurred during clinical trials, and half in postmarketing surveillance. The women were an average 32 years old and were an average 10 weeks pregnant at reporting. Among the 14 pregnancies, nine were miscarriages, one was aborted, and four were born live with no congenital anomalies.
The authors did not draw any conclusions from the findings; they cited too little data and an ongoing study by Novartis to investigate ofatumumab in pregnancy.
“Therapies such as ofatumumab and ocrelizumab can lead to increased risk of infection due to transient B-cell depletion in neonates, but the two studies looking at this did not demonstrate increased infectious morbidity for these infants,” Dr. Kolarova said. “As with all poster presentations, I look forward to reading the full papers once they are published as they will often include a lot more detail about when during pregnancy medication exposure occurred and more detailed outcome data that was assessed.”
Ozanimod outcomes within general population’s ‘expected ranges’
The final study looked at outcomes of pregnancies in people taking ozanimod and in the partners of people taking ozanimod in a clinical trial setting. The findings show low rates of miscarriage, preterm birth, and congenital anomalies that the authors concluded were within the typical range expected for the general population.
“While pregnancy should be avoided when taking and for 3 months after stopping ozanimod to allow for drug elimination, there is no evidence to date of increased occurrence of adverse pregnancy outcomes with ozanimod exposure during early pregnancy,” wrote Anthony Krakovich, of Bristol Myers Squibb in Princeton, N.J., and his associates.
Ozanimod is an oral sphingosine 1-phosphate (S1P) receptor 1 and 5 modulator whose therapeutic mechanism is not fully understood “but may involve the reduction of lymphocyte migration into the central nervous system and intestine,” the authors wrote. S1P receptors are involved in vascular formation during embryogenesis, and animal studies in rats and rabbits have shown toxicity to the embryo and fetus from S1P receptor modulators, including death and malformations. S1P receptor modulator labels therefore note potential fetal risk and the need for effective contraception while taking the drug.
The study prospectively tracked clinical trial participants taking ozanimod as healthy volunteers or for relapsing MS, ulcerative colitis, or Crohn’s disease. Most of the participants who became pregnant (73%) had relapsing MS, while 18% had ulcerative colitis and 8% had Crohn’s disease.
In female patients receiving ozanimod, 78 pregnancies resulted in 12 miscarriages (including one twin), 15 abortions, and 42 live births, with 6 pregnancies ongoing at the time of reporting and no data available for the remaining 4 pregnancies. Among the 42 live births, 4 were premature but otherwise healthy, 1 had a duplex kidney, and the other 37 infants were typical with no apparent health concerns. These rates of miscarriage, preterm birth, and congenital anomalies were within the expected ranges for the general population, the researchers wrote.
The researchers also assessed pregnancy outcomes for partners of male participants taking ozanimod. The 29 partner pregnancies resulted in 21 live births and one miscarriage, with one pregnancy ongoing and no information available for the other seven. The live births included 5 premature infants (including twins), 13 typical and healthy infants, 1 with Hirschsprung’s disease, 1 with a congenital hydrocele, and 1 with a partial atrioventricular septal defect. Again, the researchers concluded that these rates were within the typical range for the general population and that “no teratogenicity was observed.”
“We often encourage patients with MS, regardless of disease activity and therapies, to seek preconception evaluations with Maternal-Fetal Medicine and their neurologists in order to make plans for pregnancy and postpartum care,” Dr. Kolarova said. “That being said, access to subspecialized health care is not available to all, and pregnancy prior to such consultation does occur. These studies provide novel information that we have not had access to in the past and can improve patient counseling regarding their risks and options.”
The study on cladribine was funded by Merck KGaA, at which two authors are employed. Dr. Hellwig reported consulting, speaker, and/or research support from Bayer, Biogen, Teva, Novartis, Roche, Sanofi, Schering Healthcare, Serono, and Merck, and one author is a former employee of EMD Serono. The study on ocrelizumab was funded by Genentech. Dr. Zhovtis Ryerson reported personal fees from Biogen, Genentech, and Novartis, and research grants from Biogen, Genentech, and CMSC. The other authors had no disclosures. The study on ofatumumab was funded by Novartis. Dr. Bove has received research funds from Biogen, Novartis, and Roche Genentech, and consulting fees from EMD Serono, Horizon, Janssen, and TG Therapeutics; she has an ownership interest in Global Consult MD. Five authors are Novartis employees. Her coauthors, including Dr. Hellwig, reported advisory, consulting, research, speaking, or traveling fees from Alexion, Bayer, Biogen, Celgene BMS, EMD Serono, Horizon, Janssen, Lundbeck, Merck, Pfizer, Roche Genentech, Sanofi Genzyme, Schering Healthcare, Teva, TG Therapeutics, and Novartis. The study on ozanimod was funded by Bristol Myers Squibb. Dr. Krakovich and another author are employees and/or shareholders of Bristol Myers Squibb. The other authors reported consulting, speaking, advisory board, and/or research fees from AbbVie, Almirall, Arena, Biogen, Boehringer Ingelhei, Celgene, Celltrion, EXCEMED, Falk Benelux, Ferring, Forward Pharma, Genentech, Genzyme, Gilead, Janssen, Lilly, Merck, Novartis, Ono Pharma, Pfizer, Prometheus Labs, Protagonist, Roche, Sanofi, Synthon, Takeda, and Teva. Dr. Kolarova had no disclosures. Dr. Shah has received research support from Biogen and VeraSci.
AURORA, COLO. – Several drugs for multiple sclerosis (MS) that are contraindicated during pregnancy nevertheless have not shown concerning safety signals in a series of small studies presented as posters at the annual meeting of the Consortium of Multiple Sclerosis Centers. The industry-sponsored research included an assessment of pregnancy and infant outcomes for cladribine, ocrelizumab, ofatumumab, and ozanimod, all of which are not recommended during pregnancy based primarily on minimal data that suggests, but does not confirm, possible teratogenicity.
“When these new medications hit the market, maternal-fetal medicine physicians and obstetricians are left with very scant data on how to counsel patients, and it’s often based on theory, case reports, or animal studies,” said Teodora Kolarova, MD, a maternal-fetal medicine physician at the University of Washington, Seattle, who was not involved in any of the research. “Although these sample sizes seem small, the population they are sampling from – patients with MS who take immunomodulators who then experience a pregnancy – is much smaller than all pregnant patients.”
Taken together, the findings suggest no increased risk of miscarriage or congenital malformation, compared with baseline risk, Dr. Kolarova said.
“As a whole, these studies are overall reassuring with, of course, some caveats, including timing of medication exposure, limited sample size, and limited outcome data,” Dr. Kolarova said. She noted that embryonic organ formation is complete by 10 weeks gestation, by which time an unplanned pregnancy may not have been recognized yet. “In the subset of patients in the studies that were exposed during the first trimester, there was no increase in congenital malformations from a baseline risk of about 2%-3% in the general population, which is helpful for patient counseling.”
Counseling during the childbearing years
That kind of counseling is important yet absent for many people capable of pregnancy, suggests separate research also presented at the conference by Suma Shah, MD, an associate professor of neurology at Duke University, Durham, N.C. Dr. Shah gave 13-question surveys to female MS patients of all ages at her institution and presented an analysis of data from 38 completed surveys. Among those taking disease-modifying therapies, their medications included ocrelizumab, rituximab, teriflunomide, fingolimod, fumarates, interferons, natalizumab, and cladribine.
“MS disproportionately impacts women among 20 to 40 years, and that’s a really big part of their childbearing years when there are big decisions being made about whether they’re going to choose to grow family or not,” said Dr. Shah. The average age of those who completed the survey was 44. Dr. Shah noted that a lot of research has looked at the safety of older disease-modifying agents in pregnancy, but that information doesn’t appear to be filtering down to patients. “What I really wanted to look at is what do our parent patients understand about whether or not they can even think about pregnancy – and there’s a lot of work to be done.”
Just under a third of survey respondents said they did not have as many children as they would like, and a quarter said they were told they couldn’t have children if they had a diagnosis of MS.
“That was a little heartbreaking to hear because that’s not the truth,” Dr. Shah said. She said it’s necessary to have a more detailed conversation looking at tailored decisions for patients. “Both of those things – patients not being able to grow their family to the number that they desire, and not feeling like they can grow a family – I would think in 2023 we would have come farther than that, and there’s still a lot of room there to improve.”
She advised clinicians not to assume that MS patients know what their options are regarding family planning. “There’s still a lot of room for conversations,” she said. She also explicitly recommends discussing family planning and pregnancy planning with every patient, no matter their gender, early and often.
Cladribine shows no miscarriage, malformations
Dr. Kolarova noted that one of the studies, on cladribine, had a fairly robust sample size with its 180 pregnancy exposures. In that study, led by Kerstin Hellwig, MD, of Ruhr University in Bochum, Germany, data came from the global surveillance program MAPLE-MS, established to assess cladribine effects on pregnancy and infant outcomes. The researchers analyzed data from 76 mothers and 9 fathers who, at any time from 2017 to 2022, were taking cladribine during pregnancy or up to 6 months before pregnancy. Outcomes included live birth, miscarriage, stillbirth, elective abortion, ectopic pregnancy, and major congenital anomalies.
Just over half the mothers (53.9%) were exposed before pregnancy, and about a quarter (26.3%) were exposed during the first trimester. The timing was unknown for most of the other mothers (18.4%). Among the fathers, two-thirds (66.7%) were exposed before pregnancy, and one-third had unknown timing.
Among the 180 pregnancies in the maternal cohort, 42.2% had known outcomes. Nearly half the women (48.7%) taking cladribine had live births, 28.9% had elective abortions, and 21.1% had miscarriages. Only 9 of the 22 pregnancies in the paternal cohort had known outcomes, which included 88.9% live births and 11.1% miscarriages. None of the pregnancies resulted in stillbirth or in a live birth with major congenital anomalies.
”Robust conclusions cannot be made about the risks of adverse pregnancy outcomes with cladribine tablets, but no increase has been signaled thus far,” the researchers reported. ”It is necessary to counsel patients to prevent pregnancy and to use effective contraception during cladribine tablets intake and for at least 6 months after the last cladribine tablet intake in each treatment year.”
Emily Evans, MD, MBE, medical director at U.S. Neurology and Immunology in Rockland, Mass., speaking on behalf of the findings, said they were fairly encouraging.
“Of course, we don’t encourage patients to get pregnant within 6 months of their last dose of cladribine tablets,” Dr. Evans said, but “within those individuals who have gotten pregnant within 6 months of their last dose of cladribine, or who have fathered a child within 6 months of their last dose of cladribine tablets, we’re seeing overall encouraging outcomes. We’re specifically not seeing any differences in the rates of spontaneous abortions, and we’re not seeing any differences in the rates of congenital malformations.”
Ocrelizumab and ofatumumab: No infections so far
Current recommendations for ocrelizumab are to avoid pregnancy for 6 months after the last infusion and stop any breastfeeding during therapy. Yet these recommendations are only because of insufficient data rather than evidence of risk, according to Lana Zhovtis Ryerson, MD, of the NYU Multiple Sclerosis Comprehensive Care Center in New York. She and her colleagues identified all women of childbearing age who had received ocrelizumab within 1 year of pregnancy at their NYU institution. A retrospective chart review found 18 women, with an average age of 35, an average 11 years of an MS diagnosis, and an average 11 months taking ocrelizumab.
Among the 18 pregnancies, four women had a first trimester miscarriage, one had a second trimester miscarriage, and one had an abortion. The miscarriage rate could have been partly influenced by the older maternal population, the authors noted. Of the remaining 12 live births, one infant was premature at 34 weeks, and three infants stayed in NICU but were discharged within 2 weeks.
One patient experienced an MS relapse postpartum, despite receiving ocrelizumab within 45 days of delivery. Of the 16 women who agreed to participate in a Pregnancy Assessment Monitoring System (PRAMS) developed by the CDC, two women chose to breastfeed, and seven said their neurologist recommended against breastfeeding. None of the children’s pediatricians advised delaying vaccinations.
“This small sample observational study has not identified a potential additional risk with ocrelizumab for an adverse pregnancy outcome,” the authors concluded, but they added that ongoing studies, MINORE and SOPRANINO, can help guide future recommendations.
Though still limited, slightly more data exists on ofatumumab during pregnancy, including transient B-cell depletion and lymphopenia in infants whose mothers received anti-CD20 antibodies during pregnancy. However, research has found minimal IgG transfer in the first trimester, though it begins rising in the second trimester, and in utero ofatumumab exposure did not lead to any maternal toxicity or adverse prenatal or postnatal developmental effects in cynomolgus monkeys.
Riley Love, MD, of the University of California, San Francisco, Weill Institute for Neuroscience, and her colleagues both prospectively and retrospectively examined pregnancy and infant outcomes for up to 1 year post partum in women with MS who took ofatumumab during pregnancy or in the 6 months leading up to pregnancy. Their population included 104 prospective cases, most of which (84%) included first trimester exposure, and 14 retrospective cases. One in five of the prospective cases occurred during a clinical trial, while the remaining 80% occurred in postmarketing surveillance.
The prospectively followed women were an average 32 years old and were an average 7 weeks pregnant at the time of reporting. Among the 106 fetuses (including two twin pregnancies), only 30 outcomes had data at the cutoff time, including 16 live births, 9 abortions, and 5 miscarriages. None of the live births had congenital anomalies or serious infections. Another 30 pregnancies were lost to follow-up, and 46 were ongoing.
In the 14 retrospective cases, 57% of women were exposed in the first trimester, and 43% were exposed leading up to pregnancy. Half the cases occurred during clinical trials, and half in postmarketing surveillance. The women were an average 32 years old and were an average 10 weeks pregnant at reporting. Among the 14 pregnancies, nine were miscarriages, one was aborted, and four were born live with no congenital anomalies.
The authors did not draw any conclusions from the findings; they cited too little data and an ongoing study by Novartis to investigate ofatumumab in pregnancy.
“Therapies such as ofatumumab and ocrelizumab can lead to increased risk of infection due to transient B-cell depletion in neonates, but the two studies looking at this did not demonstrate increased infectious morbidity for these infants,” Dr. Kolarova said. “As with all poster presentations, I look forward to reading the full papers once they are published as they will often include a lot more detail about when during pregnancy medication exposure occurred and more detailed outcome data that was assessed.”
Ozanimod outcomes within general population’s ‘expected ranges’
The final study looked at outcomes of pregnancies in people taking ozanimod and in the partners of people taking ozanimod in a clinical trial setting. The findings show low rates of miscarriage, preterm birth, and congenital anomalies that the authors concluded were within the typical range expected for the general population.
“While pregnancy should be avoided when taking and for 3 months after stopping ozanimod to allow for drug elimination, there is no evidence to date of increased occurrence of adverse pregnancy outcomes with ozanimod exposure during early pregnancy,” wrote Anthony Krakovich, of Bristol Myers Squibb in Princeton, N.J., and his associates.
Ozanimod is an oral sphingosine 1-phosphate (S1P) receptor 1 and 5 modulator whose therapeutic mechanism is not fully understood “but may involve the reduction of lymphocyte migration into the central nervous system and intestine,” the authors wrote. S1P receptors are involved in vascular formation during embryogenesis, and animal studies in rats and rabbits have shown toxicity to the embryo and fetus from S1P receptor modulators, including death and malformations. S1P receptor modulator labels therefore note potential fetal risk and the need for effective contraception while taking the drug.
The study prospectively tracked clinical trial participants taking ozanimod as healthy volunteers or for relapsing MS, ulcerative colitis, or Crohn’s disease. Most of the participants who became pregnant (73%) had relapsing MS, while 18% had ulcerative colitis and 8% had Crohn’s disease.
In female patients receiving ozanimod, 78 pregnancies resulted in 12 miscarriages (including one twin), 15 abortions, and 42 live births, with 6 pregnancies ongoing at the time of reporting and no data available for the remaining 4 pregnancies. Among the 42 live births, 4 were premature but otherwise healthy, 1 had a duplex kidney, and the other 37 infants were typical with no apparent health concerns. These rates of miscarriage, preterm birth, and congenital anomalies were within the expected ranges for the general population, the researchers wrote.
The researchers also assessed pregnancy outcomes for partners of male participants taking ozanimod. The 29 partner pregnancies resulted in 21 live births and one miscarriage, with one pregnancy ongoing and no information available for the other seven. The live births included 5 premature infants (including twins), 13 typical and healthy infants, 1 with Hirschsprung’s disease, 1 with a congenital hydrocele, and 1 with a partial atrioventricular septal defect. Again, the researchers concluded that these rates were within the typical range for the general population and that “no teratogenicity was observed.”
“We often encourage patients with MS, regardless of disease activity and therapies, to seek preconception evaluations with Maternal-Fetal Medicine and their neurologists in order to make plans for pregnancy and postpartum care,” Dr. Kolarova said. “That being said, access to subspecialized health care is not available to all, and pregnancy prior to such consultation does occur. These studies provide novel information that we have not had access to in the past and can improve patient counseling regarding their risks and options.”
The study on cladribine was funded by Merck KGaA, at which two authors are employed. Dr. Hellwig reported consulting, speaker, and/or research support from Bayer, Biogen, Teva, Novartis, Roche, Sanofi, Schering Healthcare, Serono, and Merck, and one author is a former employee of EMD Serono. The study on ocrelizumab was funded by Genentech. Dr. Zhovtis Ryerson reported personal fees from Biogen, Genentech, and Novartis, and research grants from Biogen, Genentech, and CMSC. The other authors had no disclosures. The study on ofatumumab was funded by Novartis. Dr. Bove has received research funds from Biogen, Novartis, and Roche Genentech, and consulting fees from EMD Serono, Horizon, Janssen, and TG Therapeutics; she has an ownership interest in Global Consult MD. Five authors are Novartis employees. Her coauthors, including Dr. Hellwig, reported advisory, consulting, research, speaking, or traveling fees from Alexion, Bayer, Biogen, Celgene BMS, EMD Serono, Horizon, Janssen, Lundbeck, Merck, Pfizer, Roche Genentech, Sanofi Genzyme, Schering Healthcare, Teva, TG Therapeutics, and Novartis. The study on ozanimod was funded by Bristol Myers Squibb. Dr. Krakovich and another author are employees and/or shareholders of Bristol Myers Squibb. The other authors reported consulting, speaking, advisory board, and/or research fees from AbbVie, Almirall, Arena, Biogen, Boehringer Ingelhei, Celgene, Celltrion, EXCEMED, Falk Benelux, Ferring, Forward Pharma, Genentech, Genzyme, Gilead, Janssen, Lilly, Merck, Novartis, Ono Pharma, Pfizer, Prometheus Labs, Protagonist, Roche, Sanofi, Synthon, Takeda, and Teva. Dr. Kolarova had no disclosures. Dr. Shah has received research support from Biogen and VeraSci.
FROM CMSC 2023
Domestic violence in health care is real and underreported
To protect survivors’ identities, some names have been changed or shortened.
Natasha Abadilla, MD, met the man who would become her abuser while working abroad for a public health nonprofit. When he began emotionally and physically abusing her, she did everything she could to hide it.
“My coworkers knew nothing of the abuse. I became an expert in applying makeup to hide the bruises,” recalls Dr. Abadilla, now a second-year resident and pediatric neurologist at Lucile Packard Children’s Hospital at Stanford.
Dr. Abadilla says she strongly identifies as a hard worker and – to this day – hopes her work did not falter despite her partner’s constant drain on her. But the impact of the abuse continued to affect her for years. Like many survivors of domestic violence, she struggled with PTSD and depression.
Health care workers are often the first point of contact for survivors of domestic violence. Experts and advocates continue to push for more training for clinicians to identify and respond to signs among their patients. Often missing from this conversation is the reality that those tasked with screening can also be victims of intimate partner violence themselves.
What’s more: The very strengths that medical professionals often pride themselves on – perfectionism, empathy, grit – can make it harder for them to identify abuse in their own relationships and push through humiliation and shame to seek help.
Dr. Abadilla is exceptional among survivors in the medical field. Rather than keep her experience quiet, she has shared it publicly.
Awareness, she believes, can save lives.
An understudied problem in an underserved group
The majority of research on health care workers in this area has focused on workplace violence, which 62% experience worldwide. But intimate partner violence remains understudied and underdiscussed. Some medical professionals are even saddled with a “double burden,” facing trauma at work and at home, note the authors of a 2022 meta-analysis published in the journal Trauma, Violence, & Abuse.
The problem has had dire consequences. In recent years, many health care workers have been killed by their abusers:
- In 2016, Casey M. Drawert, MD, a Texas-based critical care anesthesiologist, was fatally shot by her husband in a murder-suicide.
- In 2018, Tamara O’Neal, MD, an ER physician, and Dayna Less, a first-year pharmacy resident, were killed by Dr. O’Neal’s ex-fiancé at Mercy Hospital in Chicago.
- In 2019, Sarah Hawley, MD, a first-year University of Utah resident, was fatally shot by her boyfriend in a murder-suicide.
- In 2021, Moria Kinsey, a nurse practitioner in Tahlequah, Okla., was murdered by a physician.
- In July of 2023, Gwendolyn Lavonne Riddick, DO, an ob.gyn. in North Carolina, was fatally shot by the father of her 3-year-old son.
There are others.
In the wake of these tragedies, calls for health care workers to screen each other as well as patients have grown. But for an untold number of survivors, breaking the silence is still not possible due to concerns about their reputation, professional consequences, the threat of harassment from abusers who are often in the same field, a medical culture of selfless endurance, and a lack of appropriate resources.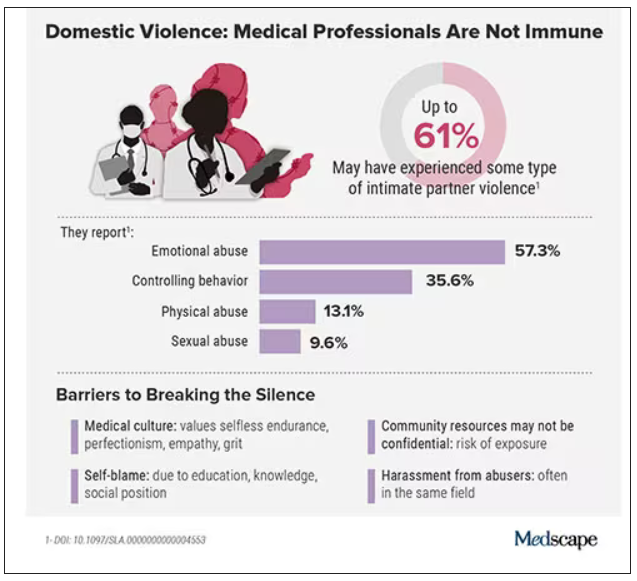
While the vast majority have stayed silent, those who have spoken out say there’s a need for targeted interventions to educate medical professionals as well as more supportive policies throughout the health care system.
Are health care workers more at risk?
Although more studies are needed, research indicates health care workers experience domestic violence at rates comparable to those of other populations, whereas some data suggest rates may be higher.
In the United States, more than one in three women and one in four men experience some form of intimate partner violence in their lifetime. Similarly, a 2020 study found that 24% of 400 physicians responding to a survey reported a history of domestic violence, with 15% reporting verbal abuse, 8% reporting physical violence, 4% reporting sexual abuse, and 4% reporting stalking.
Meanwhile, in an anonymous survey completed by 882 practicing surgeons and trainees in the United States from late 2018 to early 2019, more than 60% reported experiencing some type of intimate partner violence, most commonly emotional abuse.
Recent studies in the United Kingdom, Australia, and elsewhere show that significant numbers of medical professionals are fighting this battle. A 2019 study of more than 2,000 nurses, midwives, and health care assistants in the United Kingdom found that nurses were three times more likely to experience domestic violence than the average person.
What would help solve this problem: More study of health care worker-survivors as a unique group with unique risk factors. In general, domestic violence is most prevalent among women and people in marginalized groups. But young adults, such as medical students and trainees, can face an increased risk due to economic strain. Major life changes, such as relocating for residency, can also drive up stress and fray social connections, further isolating victims.
Why it’s so much harder for medical professionals to reveal abuse
For medical professionals accustomed to being strong and forging on, identifying as a victim of abuse can seem like a personal contradiction. It can feel easier to separate their personal and professional lives rather than face a complex reality.
In a personal essay on KevinMD.com, medical student Chloe N. L. Lee describes this emotional turmoil. “As an aspiring psychiatrist, I questioned my character judgment (how did I end up with a misogynistic abuser?) and wondered if I ought to have known better. I worried that my colleagues would deem me unfit to care for patients. And I thought that this was not supposed to happen to women like me,” Ms. Lee writes.
Kimberly, a licensed therapist, experienced a similar pattern of self-blame when her partner began exhibiting violent behavior. “For a long time, I felt guilty because I said to myself, You’re a therapist. You’re supposed to know this,” she recalls. At the same time, she felt driven to help him and sought couples therapy as his violence escalated.
Whitney, a pharmacist, recognized the “hallmarks” of abuse in her relationship, but she coped by compartmentalizing. Whitney says she was vulnerable to her abuser as a young college student who struggled financially. As he showered her with gifts, she found herself waving away red flags like aggressiveness or overprotectiveness.
After Whitney graduated, her partner’s emotional manipulation escalated into frequent physical assaults. When he gave her a black eye, she could not bring herself to go into work. She quit her job without notice. Despite a spotless record, none of her coworkers ever reached out to investigate her sudden departure.
It would take 8 years for Whitney to acknowledge the abuse and seize a moment to escape. She fled with just her purse and started over in a new city, rebuilding her life in the midst of harassment and threats from her ex. She says she’s grateful to be alive.
An imperfect system doesn’t help
Health care workers rarely ask for support or disclose abuse at work. Some have cited stigma, a lack of confidentiality (especially when the abuser is also in health care), fears about colleagues’ judgment, and a culture that doesn’t prioritize self-care.
Sometimes policies get in the way: In a 2021 qualitative study of interviews with 21 female physician-survivors in the United Kingdom, many said that despite the intense stress of abuse and recovery, they were unable to take any time off.
Of 180 UK-based midwife-survivors interviewed in a 2018 study, only 60 sought support at work and 30 received it. Many said their supervisors pressured them to report the abuse and get back to work, called social services behind their back, or reported them to their professional regulator. “I was treated like the perpetrator,” one said. Barbara Hernandez, PhD, a researcher who studies physician-survivors and director of physician vitality at Loma Linda University in southern California, says workplace violence and mistreatment from patients or colleagues – and a poor institutional response – can make those in health care feel like they have to “shut up and put up,” priming them to also tolerate abuse at home.
When survivors do reach out, there can be a disconnect between the resources they need and those they’re offered, Dr. Hernandez adds. In a recent survey of 400 physicians she conducted, respondents typically said they would advise a physician-survivor to “get to a shelter quickly.” But when roles were reversed, they admitted going to a shelter was the least feasible option. Support groups can also be problematic in smaller communities where physicians might be recognized or see their own patients.
Complicating matters further, the violence often comes from within the medical community. This can lead to particularly malicious abuse tactics like sending false accusations to a victim’s regulatory college or board; prolonged court and custody battles to drain them of all resources and their ability to hold a job; or even sabotage, harassment, or violence at work. The sheen of the abuser’s public persona, on the other hand, can guard them from any accountability.
For example, one physician-survivor said her ex-partner, a psychiatrist, coerced her into believing she was mentally ill, claimed she was “psychotic” in order to take back their children after she left, and had numerous colleagues serve as character witnesses in court for him, “saying he couldn’t have done any of these things, how great he is, and what a wonderful father he is.”
Slow progress is still progress
After Sherilyn M. Gordon-Burroughs, MD, a Texas-based transplant surgeon, mother, and educator, was killed by her husband in a murder-suicide in 2017, her friends Barbara Lee Bass, MD, president of the American College of Surgeons, and Patricia L. Turner, MD, were spurred into action. Together, they founded the ACS Intimate Partner Violence Task Force. Their mission is to educate surgeons to identify the signs of intimate partner violence (IPV) in themselves and their colleagues and connect them with resources.
“There is a concerted effort to close that gap,” says D’Andrea K. Joseph, MD, cochair of the task force and chief of trauma and acute care surgery at NYU Langone in New York. In the future, Dr. Joseph predicts, “making this a part of the curriculum, that it’s standardized for residents and trainees, that there is a safe place for victims ... and that we can band together and really recognize and assist our colleagues who are in trouble.”
Resources created by the ACS IPV task force, such as the toolkit and curriculum, provide a model for other health care leaders. But there have been few similar initiatives aimed at increasing IPV intervention within the medical system.
What you can do in your workplace
In her essay, Ms. Lee explains that a major turning point came when a physician friend explicitly asked if she was experiencing abuse. He then gently confirmed she was, and asked without judgment how he could support her, an approach that mirrors advice from the National Domestic Violence Hotline.
“Having a physician validate that this was, indeed, an abusive situation helped enormously ... I believe it may have saved my life,” she writes.
That validation can be crucial, and Dr. Abadilla urges other physicians to regularly check in with colleagues, especially those who seem particularly positive with a go-getter attitude and yet may not seem themselves. That was how she presented when she was struggling the most.
Supporting systemic changes within your organization and beyond is also important. The authors of the 2022 meta-analysis stress the need for domestic violence training, legislative changes, paid leave, and union support.
Finding strength in recovery
Over a decade after escaping her abuser, Whitney says she’s only just begun to share her experience, but what she’s learned has made her a better pharmacist. She says she’s more attuned to subtle signs something could be off with patients and coworkers. When someone makes comments about feeling anxious or that they can’t do anything right, it’s important to ask why, she says.
Recently, Kimberly has opened up to her mentor and other therapists, many of whom have shared that they’re also survivors.
“The last thing I said to [my abuser] is you think you’ve won and you’re hurting me, but what you’ve done to me – I’m going to utilize this and I’m going to help other people,” Kimberly says. “This pain that I have will go away, and I’m going to save the lives of others.”
A version of this article first appeared on Medscape.com.
To protect survivors’ identities, some names have been changed or shortened.
Natasha Abadilla, MD, met the man who would become her abuser while working abroad for a public health nonprofit. When he began emotionally and physically abusing her, she did everything she could to hide it.
“My coworkers knew nothing of the abuse. I became an expert in applying makeup to hide the bruises,” recalls Dr. Abadilla, now a second-year resident and pediatric neurologist at Lucile Packard Children’s Hospital at Stanford.
Dr. Abadilla says she strongly identifies as a hard worker and – to this day – hopes her work did not falter despite her partner’s constant drain on her. But the impact of the abuse continued to affect her for years. Like many survivors of domestic violence, she struggled with PTSD and depression.
Health care workers are often the first point of contact for survivors of domestic violence. Experts and advocates continue to push for more training for clinicians to identify and respond to signs among their patients. Often missing from this conversation is the reality that those tasked with screening can also be victims of intimate partner violence themselves.
What’s more: The very strengths that medical professionals often pride themselves on – perfectionism, empathy, grit – can make it harder for them to identify abuse in their own relationships and push through humiliation and shame to seek help.
Dr. Abadilla is exceptional among survivors in the medical field. Rather than keep her experience quiet, she has shared it publicly.
Awareness, she believes, can save lives.
An understudied problem in an underserved group
The majority of research on health care workers in this area has focused on workplace violence, which 62% experience worldwide. But intimate partner violence remains understudied and underdiscussed. Some medical professionals are even saddled with a “double burden,” facing trauma at work and at home, note the authors of a 2022 meta-analysis published in the journal Trauma, Violence, & Abuse.
The problem has had dire consequences. In recent years, many health care workers have been killed by their abusers:
- In 2016, Casey M. Drawert, MD, a Texas-based critical care anesthesiologist, was fatally shot by her husband in a murder-suicide.
- In 2018, Tamara O’Neal, MD, an ER physician, and Dayna Less, a first-year pharmacy resident, were killed by Dr. O’Neal’s ex-fiancé at Mercy Hospital in Chicago.
- In 2019, Sarah Hawley, MD, a first-year University of Utah resident, was fatally shot by her boyfriend in a murder-suicide.
- In 2021, Moria Kinsey, a nurse practitioner in Tahlequah, Okla., was murdered by a physician.
- In July of 2023, Gwendolyn Lavonne Riddick, DO, an ob.gyn. in North Carolina, was fatally shot by the father of her 3-year-old son.
There are others.
In the wake of these tragedies, calls for health care workers to screen each other as well as patients have grown. But for an untold number of survivors, breaking the silence is still not possible due to concerns about their reputation, professional consequences, the threat of harassment from abusers who are often in the same field, a medical culture of selfless endurance, and a lack of appropriate resources.
While the vast majority have stayed silent, those who have spoken out say there’s a need for targeted interventions to educate medical professionals as well as more supportive policies throughout the health care system.
Are health care workers more at risk?
Although more studies are needed, research indicates health care workers experience domestic violence at rates comparable to those of other populations, whereas some data suggest rates may be higher.
In the United States, more than one in three women and one in four men experience some form of intimate partner violence in their lifetime. Similarly, a 2020 study found that 24% of 400 physicians responding to a survey reported a history of domestic violence, with 15% reporting verbal abuse, 8% reporting physical violence, 4% reporting sexual abuse, and 4% reporting stalking.
Meanwhile, in an anonymous survey completed by 882 practicing surgeons and trainees in the United States from late 2018 to early 2019, more than 60% reported experiencing some type of intimate partner violence, most commonly emotional abuse.
Recent studies in the United Kingdom, Australia, and elsewhere show that significant numbers of medical professionals are fighting this battle. A 2019 study of more than 2,000 nurses, midwives, and health care assistants in the United Kingdom found that nurses were three times more likely to experience domestic violence than the average person.
What would help solve this problem: More study of health care worker-survivors as a unique group with unique risk factors. In general, domestic violence is most prevalent among women and people in marginalized groups. But young adults, such as medical students and trainees, can face an increased risk due to economic strain. Major life changes, such as relocating for residency, can also drive up stress and fray social connections, further isolating victims.
Why it’s so much harder for medical professionals to reveal abuse
For medical professionals accustomed to being strong and forging on, identifying as a victim of abuse can seem like a personal contradiction. It can feel easier to separate their personal and professional lives rather than face a complex reality.
In a personal essay on KevinMD.com, medical student Chloe N. L. Lee describes this emotional turmoil. “As an aspiring psychiatrist, I questioned my character judgment (how did I end up with a misogynistic abuser?) and wondered if I ought to have known better. I worried that my colleagues would deem me unfit to care for patients. And I thought that this was not supposed to happen to women like me,” Ms. Lee writes.
Kimberly, a licensed therapist, experienced a similar pattern of self-blame when her partner began exhibiting violent behavior. “For a long time, I felt guilty because I said to myself, You’re a therapist. You’re supposed to know this,” she recalls. At the same time, she felt driven to help him and sought couples therapy as his violence escalated.
Whitney, a pharmacist, recognized the “hallmarks” of abuse in her relationship, but she coped by compartmentalizing. Whitney says she was vulnerable to her abuser as a young college student who struggled financially. As he showered her with gifts, she found herself waving away red flags like aggressiveness or overprotectiveness.
After Whitney graduated, her partner’s emotional manipulation escalated into frequent physical assaults. When he gave her a black eye, she could not bring herself to go into work. She quit her job without notice. Despite a spotless record, none of her coworkers ever reached out to investigate her sudden departure.
It would take 8 years for Whitney to acknowledge the abuse and seize a moment to escape. She fled with just her purse and started over in a new city, rebuilding her life in the midst of harassment and threats from her ex. She says she’s grateful to be alive.
An imperfect system doesn’t help
Health care workers rarely ask for support or disclose abuse at work. Some have cited stigma, a lack of confidentiality (especially when the abuser is also in health care), fears about colleagues’ judgment, and a culture that doesn’t prioritize self-care.
Sometimes policies get in the way: In a 2021 qualitative study of interviews with 21 female physician-survivors in the United Kingdom, many said that despite the intense stress of abuse and recovery, they were unable to take any time off.
Of 180 UK-based midwife-survivors interviewed in a 2018 study, only 60 sought support at work and 30 received it. Many said their supervisors pressured them to report the abuse and get back to work, called social services behind their back, or reported them to their professional regulator. “I was treated like the perpetrator,” one said. Barbara Hernandez, PhD, a researcher who studies physician-survivors and director of physician vitality at Loma Linda University in southern California, says workplace violence and mistreatment from patients or colleagues – and a poor institutional response – can make those in health care feel like they have to “shut up and put up,” priming them to also tolerate abuse at home.
When survivors do reach out, there can be a disconnect between the resources they need and those they’re offered, Dr. Hernandez adds. In a recent survey of 400 physicians she conducted, respondents typically said they would advise a physician-survivor to “get to a shelter quickly.” But when roles were reversed, they admitted going to a shelter was the least feasible option. Support groups can also be problematic in smaller communities where physicians might be recognized or see their own patients.
Complicating matters further, the violence often comes from within the medical community. This can lead to particularly malicious abuse tactics like sending false accusations to a victim’s regulatory college or board; prolonged court and custody battles to drain them of all resources and their ability to hold a job; or even sabotage, harassment, or violence at work. The sheen of the abuser’s public persona, on the other hand, can guard them from any accountability.
For example, one physician-survivor said her ex-partner, a psychiatrist, coerced her into believing she was mentally ill, claimed she was “psychotic” in order to take back their children after she left, and had numerous colleagues serve as character witnesses in court for him, “saying he couldn’t have done any of these things, how great he is, and what a wonderful father he is.”
Slow progress is still progress
After Sherilyn M. Gordon-Burroughs, MD, a Texas-based transplant surgeon, mother, and educator, was killed by her husband in a murder-suicide in 2017, her friends Barbara Lee Bass, MD, president of the American College of Surgeons, and Patricia L. Turner, MD, were spurred into action. Together, they founded the ACS Intimate Partner Violence Task Force. Their mission is to educate surgeons to identify the signs of intimate partner violence (IPV) in themselves and their colleagues and connect them with resources.
“There is a concerted effort to close that gap,” says D’Andrea K. Joseph, MD, cochair of the task force and chief of trauma and acute care surgery at NYU Langone in New York. In the future, Dr. Joseph predicts, “making this a part of the curriculum, that it’s standardized for residents and trainees, that there is a safe place for victims ... and that we can band together and really recognize and assist our colleagues who are in trouble.”
Resources created by the ACS IPV task force, such as the toolkit and curriculum, provide a model for other health care leaders. But there have been few similar initiatives aimed at increasing IPV intervention within the medical system.
What you can do in your workplace
In her essay, Ms. Lee explains that a major turning point came when a physician friend explicitly asked if she was experiencing abuse. He then gently confirmed she was, and asked without judgment how he could support her, an approach that mirrors advice from the National Domestic Violence Hotline.
“Having a physician validate that this was, indeed, an abusive situation helped enormously ... I believe it may have saved my life,” she writes.
That validation can be crucial, and Dr. Abadilla urges other physicians to regularly check in with colleagues, especially those who seem particularly positive with a go-getter attitude and yet may not seem themselves. That was how she presented when she was struggling the most.
Supporting systemic changes within your organization and beyond is also important. The authors of the 2022 meta-analysis stress the need for domestic violence training, legislative changes, paid leave, and union support.
Finding strength in recovery
Over a decade after escaping her abuser, Whitney says she’s only just begun to share her experience, but what she’s learned has made her a better pharmacist. She says she’s more attuned to subtle signs something could be off with patients and coworkers. When someone makes comments about feeling anxious or that they can’t do anything right, it’s important to ask why, she says.
Recently, Kimberly has opened up to her mentor and other therapists, many of whom have shared that they’re also survivors.
“The last thing I said to [my abuser] is you think you’ve won and you’re hurting me, but what you’ve done to me – I’m going to utilize this and I’m going to help other people,” Kimberly says. “This pain that I have will go away, and I’m going to save the lives of others.”
A version of this article first appeared on Medscape.com.
To protect survivors’ identities, some names have been changed or shortened.
Natasha Abadilla, MD, met the man who would become her abuser while working abroad for a public health nonprofit. When he began emotionally and physically abusing her, she did everything she could to hide it.
“My coworkers knew nothing of the abuse. I became an expert in applying makeup to hide the bruises,” recalls Dr. Abadilla, now a second-year resident and pediatric neurologist at Lucile Packard Children’s Hospital at Stanford.
Dr. Abadilla says she strongly identifies as a hard worker and – to this day – hopes her work did not falter despite her partner’s constant drain on her. But the impact of the abuse continued to affect her for years. Like many survivors of domestic violence, she struggled with PTSD and depression.
Health care workers are often the first point of contact for survivors of domestic violence. Experts and advocates continue to push for more training for clinicians to identify and respond to signs among their patients. Often missing from this conversation is the reality that those tasked with screening can also be victims of intimate partner violence themselves.
What’s more: The very strengths that medical professionals often pride themselves on – perfectionism, empathy, grit – can make it harder for them to identify abuse in their own relationships and push through humiliation and shame to seek help.
Dr. Abadilla is exceptional among survivors in the medical field. Rather than keep her experience quiet, she has shared it publicly.
Awareness, she believes, can save lives.
An understudied problem in an underserved group
The majority of research on health care workers in this area has focused on workplace violence, which 62% experience worldwide. But intimate partner violence remains understudied and underdiscussed. Some medical professionals are even saddled with a “double burden,” facing trauma at work and at home, note the authors of a 2022 meta-analysis published in the journal Trauma, Violence, & Abuse.
The problem has had dire consequences. In recent years, many health care workers have been killed by their abusers:
- In 2016, Casey M. Drawert, MD, a Texas-based critical care anesthesiologist, was fatally shot by her husband in a murder-suicide.
- In 2018, Tamara O’Neal, MD, an ER physician, and Dayna Less, a first-year pharmacy resident, were killed by Dr. O’Neal’s ex-fiancé at Mercy Hospital in Chicago.
- In 2019, Sarah Hawley, MD, a first-year University of Utah resident, was fatally shot by her boyfriend in a murder-suicide.
- In 2021, Moria Kinsey, a nurse practitioner in Tahlequah, Okla., was murdered by a physician.
- In July of 2023, Gwendolyn Lavonne Riddick, DO, an ob.gyn. in North Carolina, was fatally shot by the father of her 3-year-old son.
There are others.
In the wake of these tragedies, calls for health care workers to screen each other as well as patients have grown. But for an untold number of survivors, breaking the silence is still not possible due to concerns about their reputation, professional consequences, the threat of harassment from abusers who are often in the same field, a medical culture of selfless endurance, and a lack of appropriate resources.
While the vast majority have stayed silent, those who have spoken out say there’s a need for targeted interventions to educate medical professionals as well as more supportive policies throughout the health care system.
Are health care workers more at risk?
Although more studies are needed, research indicates health care workers experience domestic violence at rates comparable to those of other populations, whereas some data suggest rates may be higher.
In the United States, more than one in three women and one in four men experience some form of intimate partner violence in their lifetime. Similarly, a 2020 study found that 24% of 400 physicians responding to a survey reported a history of domestic violence, with 15% reporting verbal abuse, 8% reporting physical violence, 4% reporting sexual abuse, and 4% reporting stalking.
Meanwhile, in an anonymous survey completed by 882 practicing surgeons and trainees in the United States from late 2018 to early 2019, more than 60% reported experiencing some type of intimate partner violence, most commonly emotional abuse.
Recent studies in the United Kingdom, Australia, and elsewhere show that significant numbers of medical professionals are fighting this battle. A 2019 study of more than 2,000 nurses, midwives, and health care assistants in the United Kingdom found that nurses were three times more likely to experience domestic violence than the average person.
What would help solve this problem: More study of health care worker-survivors as a unique group with unique risk factors. In general, domestic violence is most prevalent among women and people in marginalized groups. But young adults, such as medical students and trainees, can face an increased risk due to economic strain. Major life changes, such as relocating for residency, can also drive up stress and fray social connections, further isolating victims.
Why it’s so much harder for medical professionals to reveal abuse
For medical professionals accustomed to being strong and forging on, identifying as a victim of abuse can seem like a personal contradiction. It can feel easier to separate their personal and professional lives rather than face a complex reality.
In a personal essay on KevinMD.com, medical student Chloe N. L. Lee describes this emotional turmoil. “As an aspiring psychiatrist, I questioned my character judgment (how did I end up with a misogynistic abuser?) and wondered if I ought to have known better. I worried that my colleagues would deem me unfit to care for patients. And I thought that this was not supposed to happen to women like me,” Ms. Lee writes.
Kimberly, a licensed therapist, experienced a similar pattern of self-blame when her partner began exhibiting violent behavior. “For a long time, I felt guilty because I said to myself, You’re a therapist. You’re supposed to know this,” she recalls. At the same time, she felt driven to help him and sought couples therapy as his violence escalated.
Whitney, a pharmacist, recognized the “hallmarks” of abuse in her relationship, but she coped by compartmentalizing. Whitney says she was vulnerable to her abuser as a young college student who struggled financially. As he showered her with gifts, she found herself waving away red flags like aggressiveness or overprotectiveness.
After Whitney graduated, her partner’s emotional manipulation escalated into frequent physical assaults. When he gave her a black eye, she could not bring herself to go into work. She quit her job without notice. Despite a spotless record, none of her coworkers ever reached out to investigate her sudden departure.
It would take 8 years for Whitney to acknowledge the abuse and seize a moment to escape. She fled with just her purse and started over in a new city, rebuilding her life in the midst of harassment and threats from her ex. She says she’s grateful to be alive.
An imperfect system doesn’t help
Health care workers rarely ask for support or disclose abuse at work. Some have cited stigma, a lack of confidentiality (especially when the abuser is also in health care), fears about colleagues’ judgment, and a culture that doesn’t prioritize self-care.
Sometimes policies get in the way: In a 2021 qualitative study of interviews with 21 female physician-survivors in the United Kingdom, many said that despite the intense stress of abuse and recovery, they were unable to take any time off.
Of 180 UK-based midwife-survivors interviewed in a 2018 study, only 60 sought support at work and 30 received it. Many said their supervisors pressured them to report the abuse and get back to work, called social services behind their back, or reported them to their professional regulator. “I was treated like the perpetrator,” one said. Barbara Hernandez, PhD, a researcher who studies physician-survivors and director of physician vitality at Loma Linda University in southern California, says workplace violence and mistreatment from patients or colleagues – and a poor institutional response – can make those in health care feel like they have to “shut up and put up,” priming them to also tolerate abuse at home.
When survivors do reach out, there can be a disconnect between the resources they need and those they’re offered, Dr. Hernandez adds. In a recent survey of 400 physicians she conducted, respondents typically said they would advise a physician-survivor to “get to a shelter quickly.” But when roles were reversed, they admitted going to a shelter was the least feasible option. Support groups can also be problematic in smaller communities where physicians might be recognized or see their own patients.
Complicating matters further, the violence often comes from within the medical community. This can lead to particularly malicious abuse tactics like sending false accusations to a victim’s regulatory college or board; prolonged court and custody battles to drain them of all resources and their ability to hold a job; or even sabotage, harassment, or violence at work. The sheen of the abuser’s public persona, on the other hand, can guard them from any accountability.
For example, one physician-survivor said her ex-partner, a psychiatrist, coerced her into believing she was mentally ill, claimed she was “psychotic” in order to take back their children after she left, and had numerous colleagues serve as character witnesses in court for him, “saying he couldn’t have done any of these things, how great he is, and what a wonderful father he is.”
Slow progress is still progress
After Sherilyn M. Gordon-Burroughs, MD, a Texas-based transplant surgeon, mother, and educator, was killed by her husband in a murder-suicide in 2017, her friends Barbara Lee Bass, MD, president of the American College of Surgeons, and Patricia L. Turner, MD, were spurred into action. Together, they founded the ACS Intimate Partner Violence Task Force. Their mission is to educate surgeons to identify the signs of intimate partner violence (IPV) in themselves and their colleagues and connect them with resources.
“There is a concerted effort to close that gap,” says D’Andrea K. Joseph, MD, cochair of the task force and chief of trauma and acute care surgery at NYU Langone in New York. In the future, Dr. Joseph predicts, “making this a part of the curriculum, that it’s standardized for residents and trainees, that there is a safe place for victims ... and that we can band together and really recognize and assist our colleagues who are in trouble.”
Resources created by the ACS IPV task force, such as the toolkit and curriculum, provide a model for other health care leaders. But there have been few similar initiatives aimed at increasing IPV intervention within the medical system.
What you can do in your workplace
In her essay, Ms. Lee explains that a major turning point came when a physician friend explicitly asked if she was experiencing abuse. He then gently confirmed she was, and asked without judgment how he could support her, an approach that mirrors advice from the National Domestic Violence Hotline.
“Having a physician validate that this was, indeed, an abusive situation helped enormously ... I believe it may have saved my life,” she writes.
That validation can be crucial, and Dr. Abadilla urges other physicians to regularly check in with colleagues, especially those who seem particularly positive with a go-getter attitude and yet may not seem themselves. That was how she presented when she was struggling the most.
Supporting systemic changes within your organization and beyond is also important. The authors of the 2022 meta-analysis stress the need for domestic violence training, legislative changes, paid leave, and union support.
Finding strength in recovery
Over a decade after escaping her abuser, Whitney says she’s only just begun to share her experience, but what she’s learned has made her a better pharmacist. She says she’s more attuned to subtle signs something could be off with patients and coworkers. When someone makes comments about feeling anxious or that they can’t do anything right, it’s important to ask why, she says.
Recently, Kimberly has opened up to her mentor and other therapists, many of whom have shared that they’re also survivors.
“The last thing I said to [my abuser] is you think you’ve won and you’re hurting me, but what you’ve done to me – I’m going to utilize this and I’m going to help other people,” Kimberly says. “This pain that I have will go away, and I’m going to save the lives of others.”
A version of this article first appeared on Medscape.com.
One in five doctors with long COVID can no longer work: Survey
Crippling symptoms, lost careers, and eroded incomes: This is the harsh reality for doctors suffering with long COVID, according to the first major survey of physicians with the condition.
The survey, conducted by the British Medical Association and the Long COVID Doctors for Action support group, sheds light on the lingering effects of long COVID on more than 600 chronically ill and disabled doctors with the condition. It also spotlights what they describe as a lack of medical and financial support from their government and employers at the National Health Service.
“We feel betrayed and abandoned,” said Kelly Fearnley, MBChB, chair and cofounder of Long COVID Doctors for Action. “At a time of national crisis, when health care workers were asked to step up, we did. When the nation needed us, we stepped up. We put our lives on the line. We put our families’ lives on the line. And now that we are injured after knowingly being unprotected and deliberately and repeatedly exposed to a level 3 biohazard, we now find ourselves in this position.”
Dr. Fearnley fell ill while working in a hospital’s COVID ward in November 2020. She is one of an estimated 2 million people in the United Kingdom – including thousands of NHS employees – with long COVID. She hasn’t been able to return to work in nearly 3 years.
Long COVID affects more than 65 million people worldwide. It is estimated that 1 in 10 people infected with the virus develop long-term symptoms. In the United Kingdom, health care and social care workers are seven times more likely to have had severe COVID-19 than other types of employees.
Doctors responding to the BMA survey reported a wide range of long COVID symptoms, including fatigue, headaches, muscular pain, nerve damage, joint pain, and respiratory problems.
Among the survey’s key findings, 60% of doctors said long COVID has affected their ability to carry out day-to-day tasks on a regular basis. Almost one in five (18%) said they were no longer able to work, while fewer than one in three (31%) were working full time. This compares with more than half (57%) of respondents working full time before the onset of their COVID illness – a decline of 46%.
Nearly half (48%) of respondents said they have experienced some form of loss of earnings as a result of long COVID, and almost half of the doctors were never referred to an NHS long COVID clinic. The survey included the following first-person accounts from doctors living with the condition.
- One doctor said: “I nearly lost my life, my home, my partner and my career. I have received little support to help keep these. The impact on my mental health nearly cost [me] my life again.”
- A senior consulting physician commented: “Life is absolutely miserable. Every day is a struggle. I wake up exhausted, the insomnia and night terrors are horrendous as I live through my worst fears every night. Any activity such as eating meals, washing, etc., will mean I have to go to bed for a few hours. I am unable to look after myself or my child, exercise or maintain social relationships. I have no financial security. Long COVID has totally destroyed my life.”
- A salaried general practitioner said: “I can no longer work, finances are ruined. I didn’t have employment protection so am now unemployed and penniless.”
Calls for action from the BMA include the following:
- Financial support for doctors and health care staff with long COVID.
- The recognition of long COVID as an occupational disease among health care workers, along with a definition of the condition that covers all of the debilitating disease’s symptoms.
- Improved access to physical and mental health services to help comprehensive assessment, investigations, and treatment.
- Greater workplace protection for health care staff who risk their lives for others.
- Better support for long COVID sufferers to return to work safely if they can, including a flexible approach to the use of workplace adjustments.
“One would think, given the circumstances under which we fell ill and current workforce shortages, NHS employers would be eager to do everything to facilitate the return to work of people with long COVID,” said Dr. Fearnley. “However, NHS employers are legally required to implement only ‘reasonable adjustments,’ and so things such as extended phased return or adjustments to shift patterns are not always being facilitated. Instead, an increasing number of employers are choosing to terminate contracts.”
Raymond Agius, the BMA’s occupational medicine committee cochair, also put the blame on inadequate safety measures for doctors. Those inadequate measures persist to this day, inasmuch as U.K. hospitals have dropped masking requirements.
“During the COVID-19 pandemic, doctors were left exposed and unprotected at work,” he said in a BMA press release. “They often did not have access to the right PPE. ... Too many risk assessments of workplaces and especially of vulnerable doctors were not undertaken.”
A small minority of doctors who were surveyed said they had access to respiratory protective equipment about the time they contracted COVID-19. Only 11% had access to an FFP2 respirator (the equivalent of an N95 mask); 16% had an FFP3 respirator (the equivalent of an N99 mask).
To date, the British government hasn’t issued much of a response to the survey, saying only that it has invested more than ₤50 million to better understand long COVID.
A version of this article first appeared on Medscape.com.
Crippling symptoms, lost careers, and eroded incomes: This is the harsh reality for doctors suffering with long COVID, according to the first major survey of physicians with the condition.
The survey, conducted by the British Medical Association and the Long COVID Doctors for Action support group, sheds light on the lingering effects of long COVID on more than 600 chronically ill and disabled doctors with the condition. It also spotlights what they describe as a lack of medical and financial support from their government and employers at the National Health Service.
“We feel betrayed and abandoned,” said Kelly Fearnley, MBChB, chair and cofounder of Long COVID Doctors for Action. “At a time of national crisis, when health care workers were asked to step up, we did. When the nation needed us, we stepped up. We put our lives on the line. We put our families’ lives on the line. And now that we are injured after knowingly being unprotected and deliberately and repeatedly exposed to a level 3 biohazard, we now find ourselves in this position.”
Dr. Fearnley fell ill while working in a hospital’s COVID ward in November 2020. She is one of an estimated 2 million people in the United Kingdom – including thousands of NHS employees – with long COVID. She hasn’t been able to return to work in nearly 3 years.
Long COVID affects more than 65 million people worldwide. It is estimated that 1 in 10 people infected with the virus develop long-term symptoms. In the United Kingdom, health care and social care workers are seven times more likely to have had severe COVID-19 than other types of employees.
Doctors responding to the BMA survey reported a wide range of long COVID symptoms, including fatigue, headaches, muscular pain, nerve damage, joint pain, and respiratory problems.
Among the survey’s key findings, 60% of doctors said long COVID has affected their ability to carry out day-to-day tasks on a regular basis. Almost one in five (18%) said they were no longer able to work, while fewer than one in three (31%) were working full time. This compares with more than half (57%) of respondents working full time before the onset of their COVID illness – a decline of 46%.
Nearly half (48%) of respondents said they have experienced some form of loss of earnings as a result of long COVID, and almost half of the doctors were never referred to an NHS long COVID clinic. The survey included the following first-person accounts from doctors living with the condition.
- One doctor said: “I nearly lost my life, my home, my partner and my career. I have received little support to help keep these. The impact on my mental health nearly cost [me] my life again.”
- A senior consulting physician commented: “Life is absolutely miserable. Every day is a struggle. I wake up exhausted, the insomnia and night terrors are horrendous as I live through my worst fears every night. Any activity such as eating meals, washing, etc., will mean I have to go to bed for a few hours. I am unable to look after myself or my child, exercise or maintain social relationships. I have no financial security. Long COVID has totally destroyed my life.”
- A salaried general practitioner said: “I can no longer work, finances are ruined. I didn’t have employment protection so am now unemployed and penniless.”
Calls for action from the BMA include the following:
- Financial support for doctors and health care staff with long COVID.
- The recognition of long COVID as an occupational disease among health care workers, along with a definition of the condition that covers all of the debilitating disease’s symptoms.
- Improved access to physical and mental health services to help comprehensive assessment, investigations, and treatment.
- Greater workplace protection for health care staff who risk their lives for others.
- Better support for long COVID sufferers to return to work safely if they can, including a flexible approach to the use of workplace adjustments.
“One would think, given the circumstances under which we fell ill and current workforce shortages, NHS employers would be eager to do everything to facilitate the return to work of people with long COVID,” said Dr. Fearnley. “However, NHS employers are legally required to implement only ‘reasonable adjustments,’ and so things such as extended phased return or adjustments to shift patterns are not always being facilitated. Instead, an increasing number of employers are choosing to terminate contracts.”
Raymond Agius, the BMA’s occupational medicine committee cochair, also put the blame on inadequate safety measures for doctors. Those inadequate measures persist to this day, inasmuch as U.K. hospitals have dropped masking requirements.
“During the COVID-19 pandemic, doctors were left exposed and unprotected at work,” he said in a BMA press release. “They often did not have access to the right PPE. ... Too many risk assessments of workplaces and especially of vulnerable doctors were not undertaken.”
A small minority of doctors who were surveyed said they had access to respiratory protective equipment about the time they contracted COVID-19. Only 11% had access to an FFP2 respirator (the equivalent of an N95 mask); 16% had an FFP3 respirator (the equivalent of an N99 mask).
To date, the British government hasn’t issued much of a response to the survey, saying only that it has invested more than ₤50 million to better understand long COVID.
A version of this article first appeared on Medscape.com.
Crippling symptoms, lost careers, and eroded incomes: This is the harsh reality for doctors suffering with long COVID, according to the first major survey of physicians with the condition.
The survey, conducted by the British Medical Association and the Long COVID Doctors for Action support group, sheds light on the lingering effects of long COVID on more than 600 chronically ill and disabled doctors with the condition. It also spotlights what they describe as a lack of medical and financial support from their government and employers at the National Health Service.
“We feel betrayed and abandoned,” said Kelly Fearnley, MBChB, chair and cofounder of Long COVID Doctors for Action. “At a time of national crisis, when health care workers were asked to step up, we did. When the nation needed us, we stepped up. We put our lives on the line. We put our families’ lives on the line. And now that we are injured after knowingly being unprotected and deliberately and repeatedly exposed to a level 3 biohazard, we now find ourselves in this position.”
Dr. Fearnley fell ill while working in a hospital’s COVID ward in November 2020. She is one of an estimated 2 million people in the United Kingdom – including thousands of NHS employees – with long COVID. She hasn’t been able to return to work in nearly 3 years.
Long COVID affects more than 65 million people worldwide. It is estimated that 1 in 10 people infected with the virus develop long-term symptoms. In the United Kingdom, health care and social care workers are seven times more likely to have had severe COVID-19 than other types of employees.
Doctors responding to the BMA survey reported a wide range of long COVID symptoms, including fatigue, headaches, muscular pain, nerve damage, joint pain, and respiratory problems.
Among the survey’s key findings, 60% of doctors said long COVID has affected their ability to carry out day-to-day tasks on a regular basis. Almost one in five (18%) said they were no longer able to work, while fewer than one in three (31%) were working full time. This compares with more than half (57%) of respondents working full time before the onset of their COVID illness – a decline of 46%.
Nearly half (48%) of respondents said they have experienced some form of loss of earnings as a result of long COVID, and almost half of the doctors were never referred to an NHS long COVID clinic. The survey included the following first-person accounts from doctors living with the condition.
- One doctor said: “I nearly lost my life, my home, my partner and my career. I have received little support to help keep these. The impact on my mental health nearly cost [me] my life again.”
- A senior consulting physician commented: “Life is absolutely miserable. Every day is a struggle. I wake up exhausted, the insomnia and night terrors are horrendous as I live through my worst fears every night. Any activity such as eating meals, washing, etc., will mean I have to go to bed for a few hours. I am unable to look after myself or my child, exercise or maintain social relationships. I have no financial security. Long COVID has totally destroyed my life.”
- A salaried general practitioner said: “I can no longer work, finances are ruined. I didn’t have employment protection so am now unemployed and penniless.”
Calls for action from the BMA include the following:
- Financial support for doctors and health care staff with long COVID.
- The recognition of long COVID as an occupational disease among health care workers, along with a definition of the condition that covers all of the debilitating disease’s symptoms.
- Improved access to physical and mental health services to help comprehensive assessment, investigations, and treatment.
- Greater workplace protection for health care staff who risk their lives for others.
- Better support for long COVID sufferers to return to work safely if they can, including a flexible approach to the use of workplace adjustments.
“One would think, given the circumstances under which we fell ill and current workforce shortages, NHS employers would be eager to do everything to facilitate the return to work of people with long COVID,” said Dr. Fearnley. “However, NHS employers are legally required to implement only ‘reasonable adjustments,’ and so things such as extended phased return or adjustments to shift patterns are not always being facilitated. Instead, an increasing number of employers are choosing to terminate contracts.”
Raymond Agius, the BMA’s occupational medicine committee cochair, also put the blame on inadequate safety measures for doctors. Those inadequate measures persist to this day, inasmuch as U.K. hospitals have dropped masking requirements.
“During the COVID-19 pandemic, doctors were left exposed and unprotected at work,” he said in a BMA press release. “They often did not have access to the right PPE. ... Too many risk assessments of workplaces and especially of vulnerable doctors were not undertaken.”
A small minority of doctors who were surveyed said they had access to respiratory protective equipment about the time they contracted COVID-19. Only 11% had access to an FFP2 respirator (the equivalent of an N95 mask); 16% had an FFP3 respirator (the equivalent of an N99 mask).
To date, the British government hasn’t issued much of a response to the survey, saying only that it has invested more than ₤50 million to better understand long COVID.
A version of this article first appeared on Medscape.com.